
Oblique Ulnar Shortening Osteotomy With a New Plate and Compression System
Upload
khangminh22Category
view
0download
0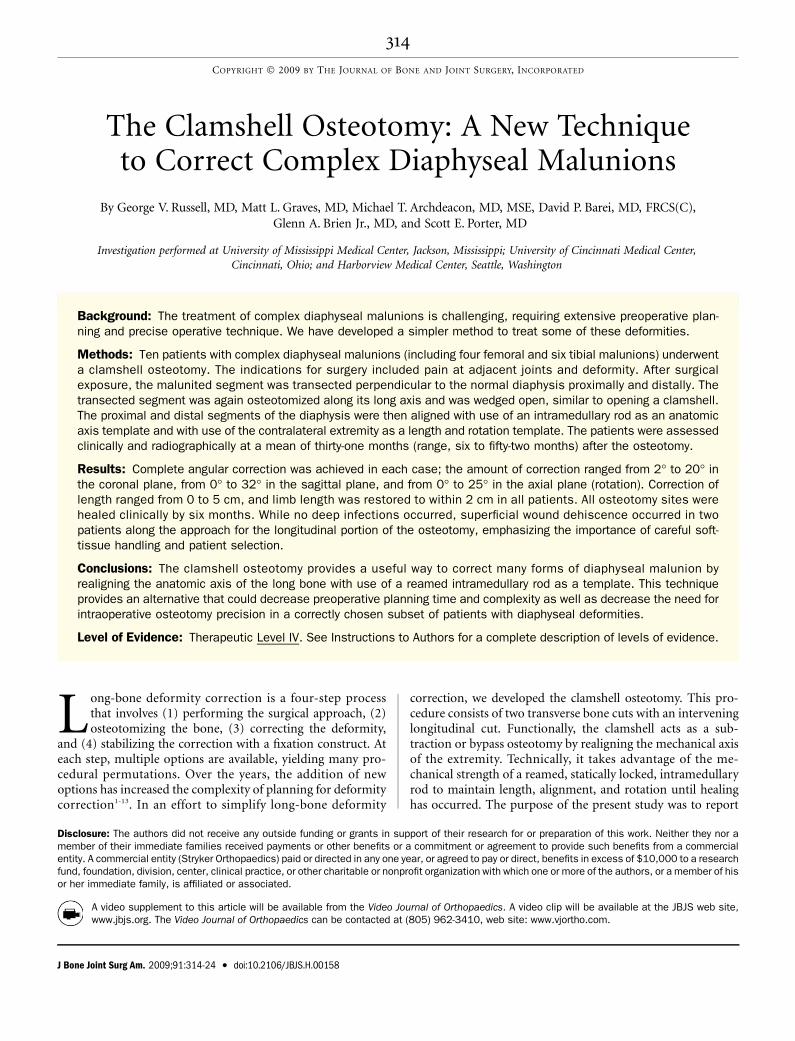
The Clamshell Osteotomy: A New Techniqueto Correct Complex Diaphyseal Malunions
By George V. Russell, MD, Matt L. Graves, MD, Michael T. Archdeacon, MD, MSE, David P. Barei, MD, FRCS(C),Glenn A. Brien Jr., MD, and Scott E. Porter, MD
Investigation performed at University of Mississippi Medical Center, Jackson, Mississippi; University of Cincinnati Medical Center,Cincinnati, Ohio; and Harborview Medical Center, Seattle, Washington
Background: The treatment of complex diaphyseal malunions is challenging, requiring extensive preoperative plan-ning and precise operative technique. We have developed a simpler method to treat some of these deformities.
Methods: Ten patients with complex diaphyseal malunions (including four femoral and six tibial malunions) underwenta clamshell osteotomy. The indications for surgery included pain at adjacent joints and deformity. After surgicalexposure, the malunited segment was transected perpendicular to the normal diaphysis proximally and distally. Thetransected segment was again osteotomized along its long axis and was wedged open, similar to opening a clamshell.The proximal and distal segments of the diaphysis were then aligned with use of an intramedullary rod as an anatomicaxis template and with use of the contralateral extremity as a length and rotation template. The patients were assessedclinically and radiographically at a mean of thirty-one months (range, six to fifty-two months) after the osteotomy.
Results: Complete angular correction was achieved in each case; the amount of correction ranged from 2� to 20� inthe coronal plane, from 0� to 32� in the sagittal plane, and from 0� to 25� in the axial plane (rotation). Correction oflength ranged from 0 to 5 cm, and limb length was restored to within 2 cm in all patients. All osteotomy sites werehealed clinically by six months. While no deep infections occurred, superficial wound dehiscence occurred in twopatients along the approach for the longitudinal portion of the osteotomy, emphasizing the importance of careful soft-tissue handling and patient selection.
Conclusions: The clamshell osteotomy provides a useful way to correct many forms of diaphyseal malunion byrealigning the anatomic axis of the long bone with use of a reamed intramedullary rod as a template. This techniqueprovides an alternative that could decrease preoperative planning time and complexity as well as decrease the need forintraoperative osteotomy precision in a correctly chosen subset of patients with diaphyseal deformities.
Level of Evidence: Therapeutic Level IV. See Instructions to Authors for a complete description of levels of evidence.
Long-bone deformity correction is a four-step processthat involves (1) performing the surgical approach, (2)osteotomizing the bone, (3) correcting the deformity,
and (4) stabilizing the correction with a fixation construct. Ateach step, multiple options are available, yielding many pro-cedural permutations. Over the years, the addition of newoptions has increased the complexity of planning for deformitycorrection1-13. In an effort to simplify long-bone deformity
correction, we developed the clamshell osteotomy. This pro-cedure consists of two transverse bone cuts with an interveninglongitudinal cut. Functionally, the clamshell acts as a sub-traction or bypass osteotomy by realigning the mechanical axisof the extremity. Technically, it takes advantage of the me-chanical strength of a reamed, statically locked, intramedullaryrod to maintain length, alignment, and rotation until healinghas occurred. The purpose of the present study was to report
Disclosure: The authors did not receive any outside funding or grants in support of their research for or preparation of this work. Neither they nor amember of their immediate families received payments or other benefits or a commitment or agreement to provide such benefits from a commercialentity. A commercial entity (Stryker Orthopaedics) paid or directed in any one year, or agreed to pay or direct, benefits in excess of $10,000 to a researchfund, foundation, division, center, clinical practice, or other charitable or nonprofit organization with which one or more of the authors, or a member of hisor her immediate family, is affiliated or associated.
A video supplement to this article will be available from the Video Journal of Orthopaedics. A video clip will be available at the JBJS web site,www.jbjs.org. The Video Journal of Orthopaedics can be contacted at (805) 962-3410, web site: www.vjortho.com.
314
COPYRIGHT � 2009 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2009;91:314-24 d doi:10.2106/JBJS.H.00158
the preliminary experience with the clamshell osteotomy atthree institutions.
Materials and MethodsInclusion and Exclusion Criteria
Aprotocol for the prospective evaluation of patients withdiaphyseal deformities was begun in January 2003 and was
approved by the institutional review boards at three centers. Theinclusion criteria for the osteotomy were (1) a diaphysealmalunion of the femur or tibia, (2) patient dissatisfaction withboth the aesthetic appearance and the functional performanceof the limb, and (3) a patient description of progressive pain inadjacent joints14. The exclusion criteria were (1) metaphysealdeformities, (2) deformities not thought to be amenable to acutecorrection secondary to shortening of >5 cm, (3) a soft-tissueenvelope preventing a surgical approach to the malunited seg-ment, and (4) evidence of active infection.
Preoperative EvaluationPreoperative evaluation included a standard musculoskeletalexamination, with lower extremity length discrepancies beingmeasured with use of a tape measure placed from the anteriorsuperior iliac spine to the tip of the medial malleolus. Tofurther assist with length measurements, blocks of differingheights were used to level the pelvis in double-limb stance.When limb-length inequalities measured >2.5 cm, radio-graphic scanograms were made. Soft-tissue changes resultingfrom previous procedures or traumatic open wounds werenoted, with specific attention being paid to the soft-tissue zoneover the segment of the deformity. Range of motion and jointstability proximal and distal to the deformity were noted. Therotational profile was judged according to the supine restingposture of the extremity, a thigh-foot axis determination fortibial torsion, and the rotatory hip range of motion arc in thesupine and prone positions for femoral deformity. Radio-graphic evaluation included characterization of the malunionwith biplanar radiographs, an evaluation of joint status prox-imal and distal to the deformity with standard radiographs,
and standing hip-to-ankle radiographs in the patella-forwardposition.
A summary of the deformity characteristics is presentedin Table I. A brief history of each case along with a descriptionof the deformity characteristics are provided in a table in theAppendix. Coronal and sagittal plane angulation was deter-mined by drawing the angle formed by the intersection of theanatomic axis of the most distal segment with that of the mostproximal segment of the bone involved. Rotation and trans-lation were referenced according to the standard practice ofdescribing the distal segment with respect to the proximalsegment. The amount of translation in the coronal and sagittalplanes was estimated on the basis of the perpendicular distancebetween the anatomic axis of the proximal segment and theanatomic axis of the distal segment when both a translational andangular deformity were present. Such deformity characterizationprovided an improved understanding of the preoperative situa-tion. Although all characteristics were taken into account, the twomost important questions were (1) Does the soft-tissue envelopeprovide a safe surgical passage to create the longitudinal osteo-tomy? and (2) Can an acute correction occur with limited risk ofpathologically stretching the neurovascular structures?
Operative TechniqueAntegrade Femoral Rod FixationThree of the four patients with a femoral malunion weremanaged with antegrade femoral rod fixation. For this pro-cedure, the patient was placed in the supine position on afracture table with boot traction. A piriformis starting pointand anatomic axis entrance angle were used. The proximalfemoral segment was sequentially reamed to allow for easymanipulation of the ball-tipped guide rod. An incision wasthen made on the lateral part of the thigh, spanning the lengthof the malunited segment. The iliotibial band was identifiedand incised to reveal the vastus lateralis fascia. The vastus lat-eralis muscle was then elevated from the posterior part of thefemur, extraperiosteally exposing the malunited segment. Anatraumatic soft-tissue technique was emphasized. The proxi-
TABLE I Deformity Characteristics
CaseSite of
MalunionCoronal Plane
AngulationSagittal Plane
Angulation RotationCoronal Plane
TranslationSagittal Plane
TranslationAxial PlaneTranslation
1 Left tibia 12� varus — — — 1 cm posterior —
2 Right tibia 2� valgus — — 1.5 cm lateral — —
3 Right tibia 13� varus 2� apex posterior — — — —
4 Left tibia 6� varus 2� apex posterior 25� internal rotation 1.7 cm medial — 0.5 cm short
5 Left femur 12� varus — 10� external rotation — 2 cm posterior 2.5 cm short
6 Right femur 12� varus 13� apex anterior 20� external rotation — — 5 cm short
7 Right femur 18� varus 32� apex posterior — — — —
8 Left tibia 10� varus — 5� internal rotation — 5 cm posterior 1 cm short
9 Right tibia 14� varus — — — 1.7 cm posterior 1.5 cm short
10 Left femur 20� varus — — — 2 cm posterior —
315
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S
mal and distal extents of the malunion were verified with use offluoroscopy. A 3.2-mm drill-bit was then used to drill multiplebicortical holes along the long axis of the malunited segment.The goal was to create a uniform line of stress-risers. A 1-in(2.54-cm) straight osteotome was used to osteotomize thesegment through the near cortex only with use of the drill-holes as a guide. The femur was then transected perpendicularto the normal portions of the diaphysis just proximal and distalto the malunited segment with use of a sagittal saw, creating afree intercalary segment of bone. The free intercalary segmentwas wedged open initially with a 1-in (2.54-cm) osteotome andsubsequently with a lamina spreader. The lateral cortex wasseparated widely to ensure that the medial cortex was alsoseparated. This step of the procedure has been likened toopening a clamshell. Occasionally, separate fracture lines were
accidentally propagated within the osteotomized segmentduring the opening of the clamshell. These were ignored, andthe technique was continued.
After realignment of the proximal and distal femoralsegments with use of indirect reduction techniques, a guide rodwas placed from the center of the anatomic axis of the proximalsegment through the osteotomized segment to the center of thedistal femoral segment, with careful attention being paid to theentrance angle into the distal segment15. The vastus lateralis wasthen allowed to drape over the exposed segment in order toretain bone fragments produced by subsequent reaming.Medullary reaming was carried out in the proximal segmentuntil the osteotomized segment was encountered. The reamerwas then pushed through the osteotomy zone until the intactdistal femoral fragment was encountered. Reaming of the
Fig. 1-A Fig. 1-B
Figs. 1-A through 1-F Case 5. Fig. 1-A Preoperative anteroposterior radiograph showing a femoral deformity with 12� of varus. Fig. 1-B
Preoperative lateral radiograph demonstrating 2 cm of posterior translation of the distal segment.
316
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S

distal fragment was then performed. A femoral rod measuring1 mm less in diameter than the final reamer was then im-planted. Interlocking bolts were placed in the proximal fem-oral fragment in the static position with use of the jig. Finallength and rotational corrections were performed at this timeon the basis of preoperative measurements, and then inter-locking through the distal femoral segment with the freehandperfect circle technique was accomplished.
The vastus lateralis was then retracted to expose theosteotomy zone. The secondary gaps created by the restorationof length, alignment, and rotation were then inspected. Thebone fragments produced by reaming generally filled theosteotomy gaps. In the cases of three patients, it was thoughtthat the bone fragments produced by reaming may have beeninsufficient to adequately bridge the osteotomy gaps anddemineralized bone matrix (DBX; Synthes, Paoli, Pennsyl-vania) was used to supplement the bone fragments producedby reaming. The iliotibial band and skin were then closed. Acase example is presented in Figures 1-A through 1-F.
Retrograde Femoral Rod FixationOne patient with a femoral malunion was managed with ret-rograde femoral rod fixation. For this procedure, the patientwas placed in the supine position on a radiolucent operatingtable with both of the lower extremities included in the surgicalfield. The involved lower extremity was placed atop a radio-lucent triangular positioning device, allowing the knee to beflexed approximately 45�. A medial parapatellar approach wasused to gain access to the starting point. The starting point andthe entrance angle into the distal segment were confirmedradiographically, followed by distal segment reaming. Themalunited femoral segment was then treated exactly as de-
scribed above with the antegrade rodding technique. Thereaming rod was placed through the distal femoral segment,through the osteotomy segment, and up to the piriformis fossain the proximal segment, with care being taken to ensure anappropriate entrance angle and ending point in the proximalsegment15. Before sequential reaming, provisional alignmentwas achieved in all planes with use of indirect reduction ma-neuvers. After reaming, a retrograde femoral rod was placedand distal interlocking bolts were placed through the jig. Finallength and rotational adjustments were performed with use ofthe contralateral lower extremity as a template, and thenproximal interlocking bolts were placed.
Tibial Rod FixationThe patient was positioned supine on the operating room tablewith both lower extremities in the surgical field. A lateral in-cision was created along the fibular shaft at the planned level ofthe proximal transverse component of the tibial osteotomy. Anoblique osteotomy was created in the fibula to allow for alarger surface area for contact and healing. A medial para-patellar entrance to the previously defined safe zone for thetibial rod starting point was used16. With use of fluoroscopy,care was taken to ensure an appropriate entrance angle into theproximal tibial segment during reaming. A longitudinal incisionwas made over the anterior compartment, one fingerbreadthlateral to the tibial crest along the proposed longitudinal os-teotomy site. The anterior compartment musculature wastranslated posteriorly, allowing for an extraperiosteal exposureof the lateral aspect of the malunited segment. An atraumaticsoft-tissue technique was emphasized. The positions of theproximal and distal transverse osteotomies were localized withradiographic guidance. Unlike the coronal plane clamshell
Fig. 1-C Fig. 1-D
Fig. 1-C Drawing depicting the deformity. The malunited segment is outlined by the dashed lines, which represent the proposed transverse
osteotomy cuts. Fig. 1-D Drawing depicting the completed osteotomy and correction. The close-up view (center) shows the clamshell shape of
the osteotomized segment.
317
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S
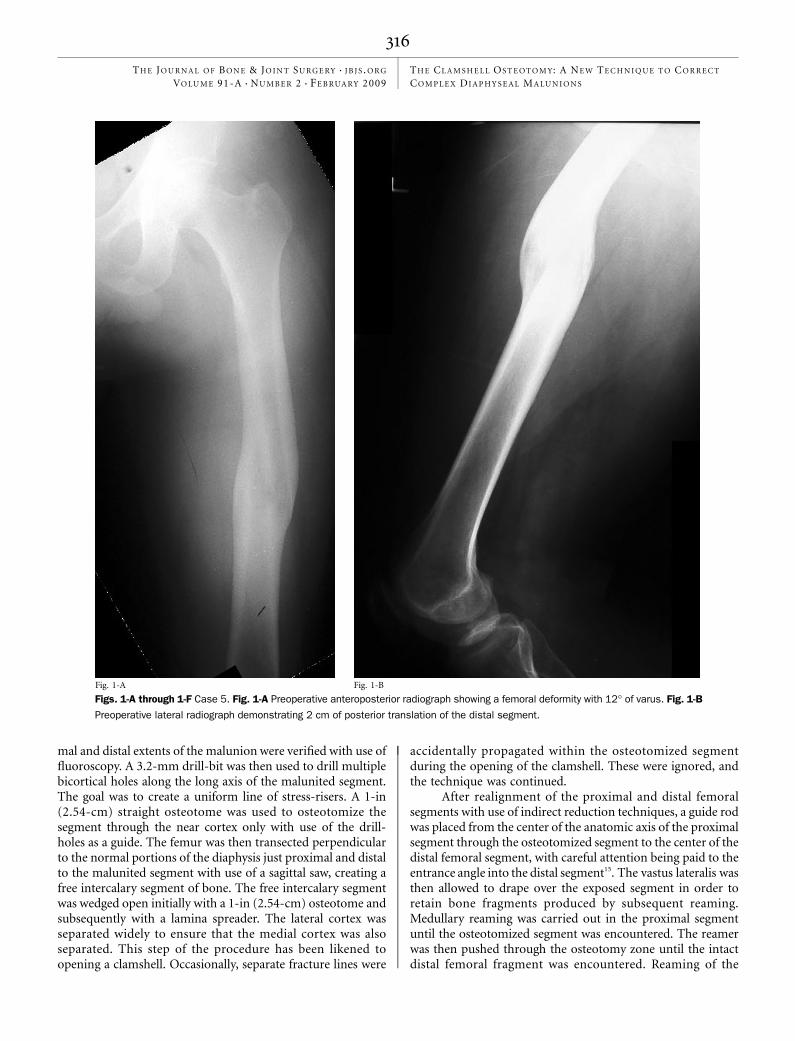
osteotomy that was performed in the femur, the clamshellcomponent of the osteotomy was created parallel to the medialtibial face (Fig. 2). A 2.5-mm drill-bit was used to create thepath for the longitudinal osteotomy with the goal of creating a
bicortical uniform plane of stress-risers. Completion of theosteotomy of the near cortex only was accomplished with anosteotome with use of the drill-holes as a guide. A sagittal sawwas used to create the transverse proximal and distal oste-
Fig. 1-E Fig. 1-F
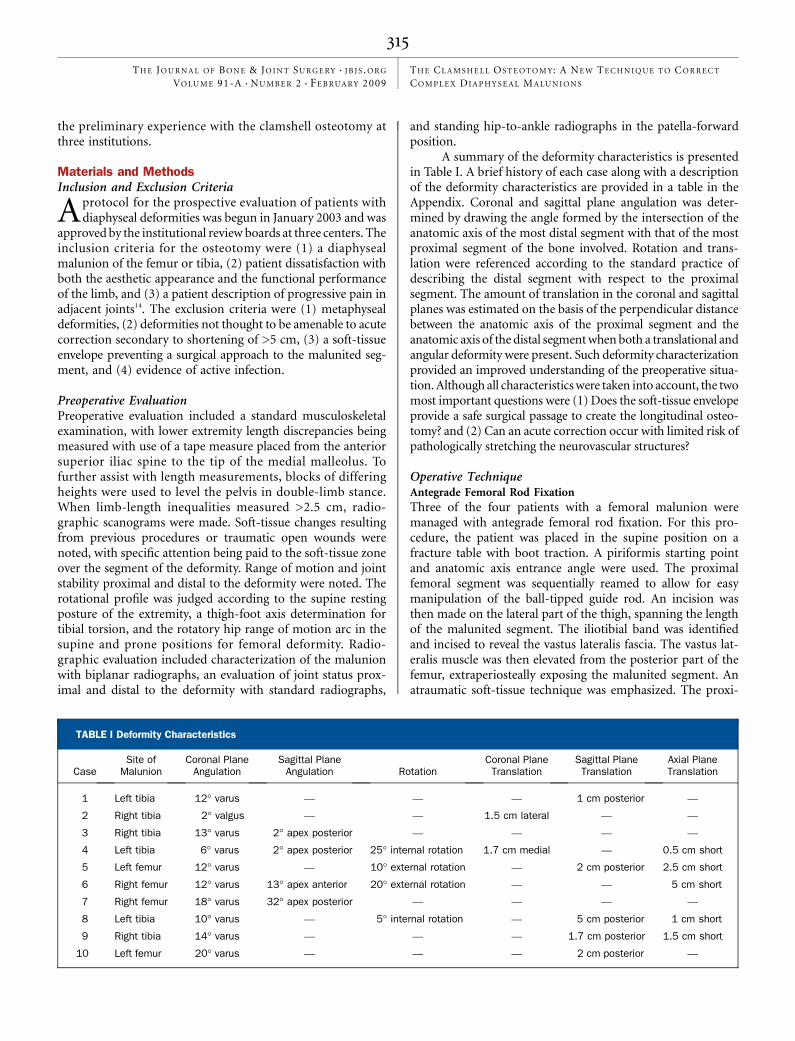
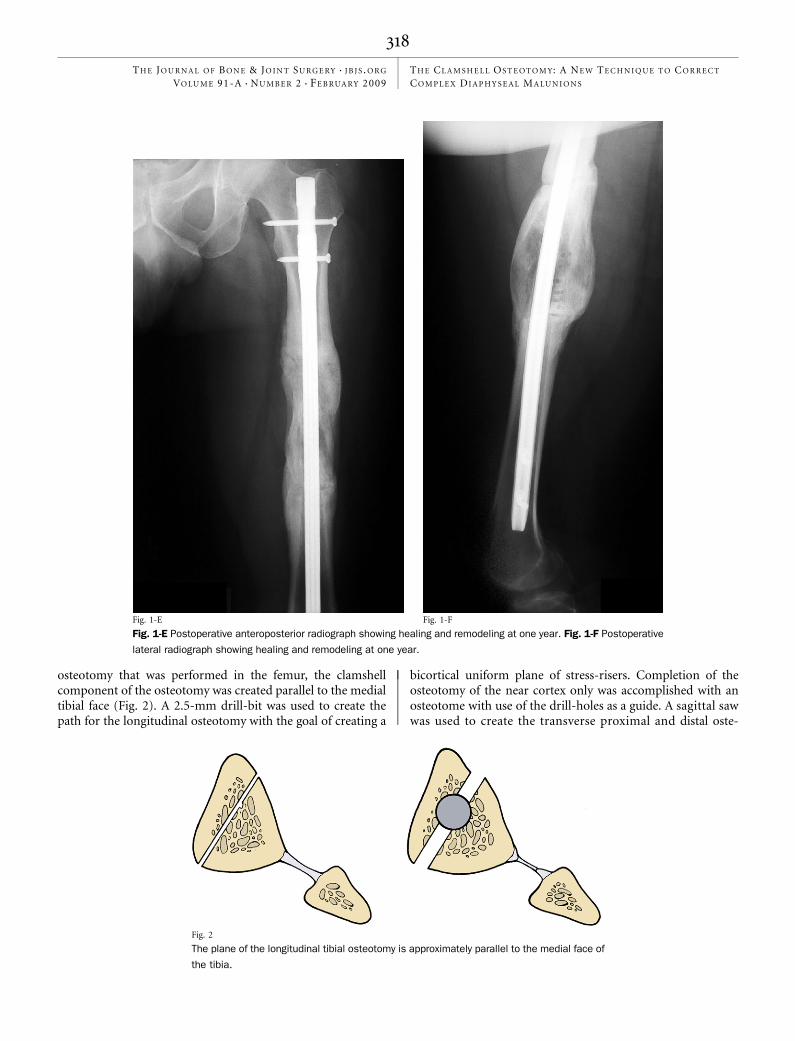
Fig. 1-E Postoperative anteroposterior radiograph showing healing and remodeling at one year. Fig. 1-F Postoperative
lateral radiograph showing healing and remodeling at one year.
Fig. 2
The plane of the longitudinal tibial osteotomy is approximately parallel to the medial face of
the tibia.
318
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S

otomies. The far cortex of the osteotomized segment was splitparallel to the medial face with use of an osteotome and alamina spreader. The limb was placed over a radiolucent tri-angle. The guide rod was passed from the proximal segmentthrough the osteotomized segment into the distal tibialsegment under fluoroscopy. Care was taken to ensure that theentrance angle and the ending point in the distal segment wereappropriate15. The anterior compartment was allowed to drapeover the cortex to preserve the bone fragments produced bysubsequent reaming at the osteotomy sites. The proximal anddistal segments were reamed sequentially until cortical chatter
was noted. The reamer was pushed through the clamshellsegment to protect the neurovascular structures. The tibial rodwas then passed, and standard proximal interlocking was ac-complished. The leg was removed from the positioning pillowand was placed flat on the operating table. The other leg wasused as a control for final length and rotational alignment,followed by distal interlocking. The anterior compartmentmusculature was retracted posteriorly from the lateral part ofthe tibia to allow for inspection of the osteotomy sites. Thebone fragments produced by intramedullary reaming usuallyfilled the osteotomy site. For gaps of ‡1 cm, demineralized
Fig. 3-A Fig. 3-B
Figs. 3-A through 3-F Case 8. Fig. 3-A Preoperative anteroposterior radiograph
demonstrating 10� of varus. Fig. 3-B Preoperative lateral radiograph demonstrating
5 cm of posterior translation.
319
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S

Fig. 3C
Fig. 3-D
Fig. 3-C Drawing depicting deformity correction in the coronal plane. Fig. 3-D Drawing
depicting deformity correction in the sagittal plane.
320
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S

bone matrix (DBX; Synthes) was used. Closure of the extensileapproach to the malunited segment was achieved with use ofthe Allgower modification of the Donati technique17, empha-sizing careful soft-tissue handling. A case example is presentedin Figures 3-A through 3-F.
Postoperative ProtocolAll patients were admitted to the hospital, where patient-controlled analgesia as well as oral narcotics were used for paincontrol. Intravenous cefazolin was administered for twenty-
four hours postoperatively. Mobilization began on the firstpostoperative day, with the patient using crutches with toe-touch weight-bearing under the direction of a licensed physicaltherapist. Weight-bearing was advanced incrementally as os-teotomy site healing progressed, with a goal of full weight-bearing by twelve weeks. Prophylaxis against thromboembolicdisease was provided by the use of support stockings, se-quential compression devices, and low-molecular-weightheparin. The patients were followed in an outpatient settingbeginning two weeks postoperatively. Postoperative evaluation
Fig. 3-E Fig. 3-F
Figs. 3-E and 3-F Anteroposterior (Fig. 3-E) and lateral (Fig. 3-F) radiographs, made one year after
deformity correction, showing healing.
321
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S

included clinical and radiographic evaluation at two weeks, sixweeks, three months, six months, nine months, one year, andtwo years. Clinical evaluation included a standard extremity-based musculoskeletal examination with a focus on motion ofthe joints proximal and distal to the correction, the strengthof the muscles around the previous deformity, gait pattern,and peripheral nerve status. The postoperative radiographsincluded biplanar views of the previously malunited bone.The radiographs were evaluated for progression of healingand maintenance of the anatomic axis alignment that hadbeen achieved at the time of surgery. Biplanar radiographs ofthe joints proximal and distal to the correction and standinghip-to-ankle radiographs were made after healing and wereused to search for signs of degenerative arthritis and to evaluatethe lower extremity mechanical axes with respect to those onthe contralateral, uninjured side.
Source of FundingThere was no external funding source for this study.
Results
Between January 2003 and August 2006, ten patients (in-cluding seven male patients and three female patients)
with diaphyseal malunions (including four femoral malunionsand six tibial malunions) who met the inclusion criteria un-derwent a clamshell osteotomy. These procedures were com-pleted at three separate institutions. The average age at the timeof the procedure was forty-one years (range, fourteen toseventy-one years). Five patients had involvement of the rightlower extremity, and five had involvement of the left. Onepatient had chronic obstructive pulmonary disease and hy-pertension, and the others had an unremarkable medicalhistory. The mean duration of follow-up after surgery wasthirty-one months (range, six to fifty-two months). All de-formities were posttraumatic. The average duration of thedeformity before correction was approximately eighteen years(range, one to fifty years). Treatment of previous fractures hadincluded traction, casting, and external fixation. Three frac-tures were initially open. Two of the three open fractures weresecondary to blunt trauma and were classified as Gustilo andAnderson type IIIA, whereas the third was a low-velocityballistic fracture. The remaining fractures were closed and weresecondary to blunt trauma. Although not an exclusion crite-rion, none of the patients in the present series had retention ofinternal fixation devices. None of the patients had had previ-ous internal fixation, and two had been managed with externalfixation devices. Three of the ten patients smoked tobaccoproducts.
Correction of Deformity and UnionAll osteotomy sites were healed clinically by the six-monthfollow-up visit. In addition, all but one of the osteotomy siteswere thought to be healed radiographically (with bridgingbone across three of four cortices) by the six-month follow-upvisit. The remaining patient had bridging of two of four cor-tices, but no clinical symptoms, and had returned to full duty
at work. In all cases, evaluation of the postoperative radio-graphs revealed correction of coronal and sagittal plane an-gulations to within 4�, complete correction of translation,and complete correction of joint-line orientation angleswhen compared with population averages4. Clinical evaluationrevealed correction of limb-length inequalities to within 2 cmin all cases, as judged with both a tape measure and blocks forpelvic leveling. The correction of length ranged from 0 to 5 cm.The rotational profile also appeared to be fully corrected asjudged on the basis of the supine resting posture of the ex-tremity, thigh-foot axis determination in the patients with atibial deformity, and symmetric range of rotation of the hips inboth the supine and the prone position in the patients with afemoral deformity.
ComplicationsHardware failure in the form of broken interlocking screwswas noted in one case. One tibial nail was dynamized at fourmonths to treat a delayed union, and the osteotomy site wenton to heal uneventfully. Despite the loss of interlocking screwstability in both of these cases, loss of angular correction didnot occur and one leg shortened approximately 3 mm duringthe healing process. One patient had postoperative deliriumtremens, which resolved with symptomatic care. Two patientshad a superficial wound dehiscence along the direct approachfor the longitudinal component of the osteotomy. One of thesepatients was managed with local wound care, and the woundhealed uneventfully. The second patient required operativedebridement and reapproximation of the skin edges. The incisionand the osteotomy sites subsequently healed without furthercomplication. One of the two patients with wound problemssmoked. No neurovascular complications were noted.
Discussion
We designed this osteotomy in an attempt to simplify thecorrection of combined angular and translational mal-
unions of the diaphyses of the femur and tibia. The concept ofthe clamshell osteotomy evolved from an extension of theexperience of one of the authors (G.V.R.) with intramedullarytechniques for comminuted diaphyseal fractures and knowl-edge of the Sofield technique5. Conceptually, the osteotomy iseasy to understand. Simply stated, the clamshell osteotomy canbe thought of as a comminuted diaphyseal fracture that onewould treat with an intramedullary rod, with the rod acting asan anatomic axis reduction template. The concerns aboutlength, alignment, and rotation are similar and are treated in afashion similar to acute fracture fixation.
The present study and the described technique do havepotential limitations. First, as with other observational studies,biases could be present secondary to the study design and themethods of data collection. The inclusion and exclusion cri-teria were set at the beginning of the study on the basis of whatwere thought to be appropriate indications for this technique.These criteria were very specific, and great care should be takenwhen evaluating patients with diaphyseal malunions who donot meet these criteria. Independent observers were not used
322
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S

consistently in this study to judge deformity correction andpostoperative outcome scores. Although patient satisfactionwas voiced when specifically sought (with one institution ac-counting for five patients) and radiographs revealed correctionof the deformity and healing of the osteotomy sites, functionaloutcomes were not assessed.
Second, the osteotomy site has no inherent stability;therefore, the rod initially serves as a load-bearing device.Minimizing soft-tissue and periosteal damage is important topromote early callus formation, thereby providing implantprotection through load-sharing. Despite the lack of inherentstability, partial weight-bearing was allowed immediately. Todate, there has been no evidence of hardware failure leading toloss of reduction of anything other than 3 mm of length.Delayed union requiring dynamization was noted in one case.Presently, we add demineralized bone matrix to the transverseosteotomy sites if there appears to be inadequate bone contactachieved with the bone fragments produced by reaming. Thissituation has only occurred when lengthening was required toequalize leg lengths.
Third, certain preoperative deformity characteristics mustbe closely evaluated. Extensive shortening of the bone cannotbe corrected safely through the malunion site in the acutesetting. Correction of no more than 5 cm of shortening in thefemur and 3 cm in the tibia has been attempted. Correction ofshortening clearly differs from acute fracture treatment inwhich the soft-tissue envelope has only been shortened tran-siently. Appropriate caution must be taken with respect tostretching the neurovascular structures during this procedure.An understanding of the potential need for soft-tissue coverageafter deformity correction should be present preoperatively.This warning is consistent with all types of acute deformitycorrection requiring an incision and is not specific to thistechnique.
Fourth, a poor soft-tissue envelope preventing a surgicalapproach to the malunion site is a clear contraindication to thetechnique. Percutaneous transverse osteotomies are possible atthe extremes of the malunited segment, but the longitudinalosteotomy requires an extensile approach. This is most likely toaffect the treatment of tibial deformities as the muscular envelopeis more limited. Previous trauma leading to marginal soft tissueslikely affected the result in one patient who initially had sustaineda type-IIIA open fracture and had a postoperative wound de-hiscence. Every attempt should be made to create the longitu-dinal incision over the anterior or superficial posteriorcompartment of the leg in case dehiscence does occur. Anatraumatic soft-tissue approach must be a priority, and thedegree of soft-tissue dissection should be minimized. On thebasis of the present case series, we do not know the applicabilityof this technique in patients with retained or previous in-ternal fixation.
With use of our inclusion and exclusion criteria, this oste-otomy compares favorably to other techniques2,6,8,9,18. Some ad-vantages of the osteotomy are clear: there is limited preoperativeplanning, and there is some leniency in the precision of theosteotomy itself. In addition, this technique can be used to
manage certain patients who have an acute diaphyseal fractureproximal or distal to a diaphyseal malunion. This was suc-cessfully accomplished twice in the present series by using theacute fracture as one of the transverse limbs of the osteotomy.Our high union rate without loss of reduction, despite thecreation of multiple diaphyseal healing sites, is comparablewith or better than the findings associated with other pub-lished techniques2,6,8,9,18. On the other hand, problems withinterlocking screw failure occurred in one patient, and prob-lems with incision healing occurred in two patients. The needfor an atraumatic soft-tissue technique is consistent withmalunion correction with plate fixation8,10 but is a relativeweakness when compared with correction of malunions with amultiplanar external fixator1.
One clear advantage of the fixation device is early weight-bearing, which can be permitted because of the inherentstrength of the intramedullary rod. Early weight-bearing is alsocommonly allowed with circular frame treatment1. The realadvantages of the intramedullary rod as compared with thecircular frame are related to cost and the absence of pin-trackconcerns in association with the intramedullary rod1. Non-locking plate fixation is another option, but early weight-bearing is usually discouraged with that technique8,9. In addition,osteotomy precision is generally more important and preop-erative planning is generally more demanding when usingplate fixation in order to protect the implant by creatingcongruent surfaces for compression.
In this small series of patients, the clamshell osteotomyproved to be a useful technique that can simplify complexlower extremity deformity correction. With appropriate pa-tient selection, a good understanding of intramedullary rodfixation techniques, and careful soft-tissue handling, complexdeformity correction can be achieved with a minimum ofpreoperative planning in properly selected patients.
AppendixA table showing details on all ten patients is availablewith the electronic versions of this article, on our web
site at jbjs.org (go to the article citation and click on ‘‘Sup-plementary Material’’) and on our quarterly CD/DVD (callour subscription department, at 781-449-9780, to order theCD or DVD). n
George V. Russell, MDMatt L. Graves, MDGlenn A. Brien Jr., MDScott E. Porter, MDDepartment of Orthopaedic Surgery and Rehabilitation,University of Mississippi Medical Center,2500 North State Street,Jackson, MS 39216.E-mail address for M.L. Graves: [email protected]
Michael T. Archdeacon, MD, MSEDepartment of Orthopaedic Surgery,
323
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S

University of Cincinnati,College of Medicine, P.O. Box 670212, 231 Albert Sabin Way,Cincinnati, OH 45267-0212
David P. Barei, MD, FRCS(C)Department of Orthopaedic Surgery, Harborview Medical Center,P.O. Box 359798, 325 9th Avenue, Seattle, WA 98104-2499
References
1. Feldman DS, Shin SS, Madan S, Koval KJ. Correction of tibial malunion andnonunion with six-axis analysis deformity correction using the Taylor Spatial Frame.J Orthop Trauma. 2003;17:549-54.
2. Farquharson-Roberts MA. Corrective osteotomy for combined shortening androtational malunion of the femur. J Bone Joint Surg Br. 1995;77:979-80.
3. Heijens E, Gladbach B, Pfeil J. Definition, quantification, and correction oftranslation deformities using long leg, frontal plane radiography. J Pediatr Orthop B.1999;8:285-91.
4. Paley D, Herzenberg JE, Tetsworth K, McKie J, Bhave A. Deformity planning forfrontal and sagittal plane corrective osteotomies. Orthop Clin North Am.1994;25:425-65.
5. Sofield H, Millar EA. Fragmentation, realignment, and intramedullary rod fixation ofdeformities of the long bones in children. J Bone Joint Surg Am. 1959;41:1371-91.
6. Marsh DR, Shah S, Elliott J, Kurdy N. The Ilizarov method in nonunion, malunionand infection of fractures. J Bone Joint Surg Br. 1997;79:273-9.
7. Kempf I, Grosse A, Abalo C. Locked intramedullary nailing. Its application tofemoral and tibial axial, rotational, lengthening, and shortening osteotomies. ClinOrthop Relat Res. 1986;212:165-73.
8. Sangeorzan BJ, Sangeorzan BP, Hansen ST Jr, Judd RP. Mathematically di-rected single-cut osteotomy for correction of tibial malunion. J Orthop Trauma.1989;3:267-75.
9. Johnson EE. Multiplane correctional osteotomy of the tibia for diaphyseal mal-union. Clin Orthop Relat Res. 1987;215:223-32.
10. Sanders R, Anglen JO, Mark JB. Oblique osteotomy for the correction of tibialmalunion. J Bone Joint Surg Am. 1995;77:240-6.
11. Yamamoto T, Hashimoto Y, Mizuno K. Oblique wedge osteotomy for femoraldiaphyseal deformity in fibrous dysplasia: a case report. Clin Orthop Relat Res.2001;384:245-9.
12. Milch H. Osteotomy of the long bones. Springfield: Charles C Thomas;1947.
13. Mast JW, Teitge RA, Gowda M. Preoperative planning for the treatment ofnonunions and the correction of malunions of the long bones. Orthop Clin NorthAm. 1990;21:693-714.
14. Hierholzer G. Indications for corrective osteotomy after malunited fractures. In:Hierholzer G, editor. Corrective osteotomies of the lower extremity after trauma.Berlin: Springer-Verlag; 1985. p 9-28.
15. Freedman EL, Johnson EE. Radiographic analysis of tibial fracture malalign-ment following intramedullary nailing. Clin Orthop Relat Res. 1995;315:25-33.
16. McConnell T, Tornetta P 3rd, Tilzey J, Casey D. Tibial portal placement: theradiographic correlate of the anatomic safe zone. J Orthop Trauma. 2001;15:207-9.
17. Sagi HC, Papp S, Dipasquale T. The effect of suture pattern and tension oncutaneous blood flow as assessed by laser Doppler flowmetry in a pig model.J Orthop Trauma. 2008;22:171-5.
18. Mayo KA, Benirschke SK. Treatment of tibial malunions and nonunions withreamed intramedullary nails. Orthop Clin North Am. 1990;21:715-24.
324
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 91-A d NU M B E R 2 d F E B RUA RY 2009TH E CL A M S H E L L OS T E O T O M Y: A NE W TE C H N I Q U E T O C O R R E C T
CO M P L E X DI A P H Y S E A L M A LU N I O N S
Copyright © 2022 FDOKUMEN




















