The Cross-cultural Importance Of Satisfying Vital Needs
11
THE CROSS-CULTURAL IMPORTANCE OF SATISFYING VITAL NEEDSALLEN ANDREW A. ALVAREZ Keywords vital needs, basic healthcare, health resource allocation, extreme scarcity, basic agency, preintrinsic value ABSTRACT Ethical beliefs may vary across cultures but there are things that must be valued as preconditions to any cultural practice. Physical and mental abili- ties vital to believing, valuing and practising a culture are such precon- ditions and it is always important to protect them. If one is to practise a distinct culture, she must at least have these basic abilities. Access to basic healthcare is one way to ensure that vital abilities are protected. John Rawls argued that access to all-purpose primary goods must be ensured. Amartya Sen and Martha Nussbaum claim that universal capa- bilities are what resources are meant to enable. Len Doyal and Ian Gough identify physical health and autonomy as basic needs of every person in every culture. When we disagree on what to prioritize, when resources to satisfy competing demands are scarce, our common needs can provide a point of normative convergence. Need-based rationing, however, has been criticized for being too indeterminate to give guidance for deciding which healthcare services to prioritize and for tending to create a bottomless-pit problem. But there is a difference between needing something (first-order need) and needing to have the ability to need (second-order need). Even if we disagree about which first-order need to prioritize, we must accept the importance of satisfying our second-order need to have the ability to value things. We all have a second-order need for basic healthcare as a means to protect our vital abilities even if we differ in what our cultures consider to be particular first-order needs. INTRODUCTION The WHO Commission on the Social Determinants of Health recently lamented the tragic health inequities observed within and between countries. 1 It laments the fact that girls born in Japan and Sweden can expect to live more than 80 years, while girls born in several African countries can expect to live only fewer than 50. The Com- mission asserts that ‘there is no necessary biological reason’ for this and that these inequities can be remedied if the necessary social, political and economic actions are taken. The Commission advocates universal healthcare coverage that is not dependent on people’s ability to pay. 2 The reason for trying to remedy health inequities need not only be the egalitarian moral intuition that individu- als should be regarded with equal concern and respect, as it is commonly held in the Western societies. Concern for equality is not the only reason to support universal access 1 CSDH. 2008. Closing the gap in a generation: health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health. World Health Orga- nization. Available at: http://whqlibdoc.who.int/publications/2008/ 9789241563703_eng.pdf [Accessed 28 Aug 2008]. 2 While recognizing that health status is determined largely by other social determinants, the Commission affirms that ‘maldistribution of health care – not delivering care to those who most need it – is one of the social determinants of health.’ It even states that ‘Health-care systems 8 [preventive, curative and palliative interventions, whether directed to individuals or to populations] are a vital determinant of health.’ Ibid: 1, 94, 100. Address for correspondence: Allen Andrew A. Alvarez, University of the Philippines Diliman, Philosophy Department, Faculty Center 3031 U.P. Campus, 1101 Diliman, Quezon City, Philippines. Email: [email protected] or [email protected] Bioethics ISSN 0269-9702 (print); 1467-8519 (online) doi:10.1111/j.1467-8519.2009.01761.x Volume 23 Number 9 2009 pp 486–496 © 2009 Blackwell Publishing Ltd., 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA.
Transcript of The Cross-cultural Importance Of Satisfying Vital Needs

THE CROSS-CULTURAL IMPORTANCE OF SATISFYING VITAL NEEDSbioe_1761 486..496
ALLEN ANDREW A. ALVAREZ
Keywordsvital needs,basic healthcare,health resource allocation,extreme scarcity,basic agency,preintrinsic value
ABSTRACTEthical beliefs may vary across cultures but there are things that must bevalued as preconditions to any cultural practice. Physical and mental abili-ties vital to believing, valuing and practising a culture are such precon-ditions and it is always important to protect them. If one is to practise adistinct culture, she must at least have these basic abilities. Access tobasic healthcare is one way to ensure that vital abilities are protected.John Rawls argued that access to all-purpose primary goods must beensured. Amartya Sen and Martha Nussbaum claim that universal capa-bilities are what resources are meant to enable. Len Doyal and IanGough identify physical health and autonomy as basic needs of everyperson in every culture. When we disagree on what to prioritize, whenresources to satisfy competing demands are scarce, our common needscan provide a point of normative convergence. Need-based rationing,however, has been criticized for being too indeterminate to give guidancefor deciding which healthcare services to prioritize and for tending tocreate a bottomless-pit problem. But there is a difference betweenneeding something (first-order need) and needing to have the ability toneed (second-order need). Even if we disagree about which first-orderneed to prioritize, we must accept the importance of satisfying oursecond-order need to have the ability to value things. We all have asecond-order need for basic healthcare as a means to protect our vitalabilities even if we differ in what our cultures consider to be particularfirst-order needs.
INTRODUCTION
The WHO Commission on the Social Determinants ofHealth recently lamented the tragic health inequitiesobserved within and between countries.1 It laments thefact that girls born in Japan and Sweden can expect to livemore than 80 years, while girls born in several Africancountries can expect to live only fewer than 50. The Com-mission asserts that ‘there is no necessary biologicalreason’ for this and that these inequities can be remedied
if the necessary social, political and economic actions aretaken. The Commission advocates universal healthcarecoverage that is not dependent on people’s ability to pay.2
The reason for trying to remedy health inequities neednot only be the egalitarian moral intuition that individu-als should be regarded with equal concern and respect, asit is commonly held in the Western societies. Concern forequality is not the only reason to support universal access
1 CSDH. 2008. Closing the gap in a generation: health equity throughaction on the social determinants of health. Final Report of theCommission on Social Determinants of Health. World Health Orga-nization. Available at: http://whqlibdoc.who.int/publications/2008/9789241563703_eng.pdf [Accessed 28 Aug 2008].
2 While recognizing that health status is determined largely by othersocial determinants, the Commission affirms that ‘maldistribution ofhealth care – not delivering care to those who most need it – is one of thesocial determinants of health.’ It even states that ‘Health-care systems8
[preventive, curative and palliative interventions, whether directed toindividuals or to populations] are a vital determinant of health.’ Ibid: 1,94, 100.
Address for correspondence: Allen Andrew A. Alvarez, University of the Philippines Diliman, Philosophy Department, Faculty Center 3031 U.P.Campus, 1101 Diliman, Quezon City, Philippines. Email: [email protected] or [email protected]
Bioethics ISSN 0269-9702 (print); 1467-8519 (online) doi:10.1111/j.1467-8519.2009.01761.xVolume 23 Number 9 2009 pp 486–496
© 2009 Blackwell Publishing Ltd., 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA.

to basic healthcare. There are other plausible reasons(that are non-comparative and enabling) for wanting toimprove poor health status that merits support acrosscultures.
Every individual has a vital need 3 to protect her basicability to feel, desire, value, choose, and act on thechoices she makes. People may differ on particularbeliefs, values, and preferences but they have a commonvital need to protect their basic abilities to have thesedispositions. The importance of their common enablingvital needs precedes the importance of particular thingsthey value since they won’t be able to do this in the firstplace without having basic abilities that vital needs satis-faction protects. The importance of vital needs satisfac-tion cannot be trumped by particular valued thingswithin a culture without contradicting the need for theability to value such things. We can disagree about therightness or wrongness of particular cultural practicesbut we cannot disagree about the fundamental impor-tance of the ability to practise a tradition, especially theability to evaluate it as wrong or right. The practice ofculture and its evaluation both require some basic physi-cal and mental abilities. It is pointless to ask which of ourcompeting values are more important if the bases of ourability to value these are threatened by deprivation ofour vital needs. We undermine the importance of ourbasic abilities when we pit the importance of our access toresources that satisfy our vital needs against resources weneed only to satisfy our preferences relative to our owncultural values. The importance of vital needs satisfactioncannot be trumped by particular preference-based needsshaped by particular cultures. It must be given a specialplace in discussing ethics of health resource allocationthat can be appreciated even when the discussants come
from different cultures. This we must do if we are to avoidthe inconsistency of prioritizing what we will not be ableto enjoy when we set aside vital enabling needs. This iswhat I mean when I refer to the idea of cross-culturalimportance of satisfying vital needs. To explore this idea,I proceed as follows. First, I discuss why I think the ideaof the importance of vital needs satisfaction is differentfrom the much discussed and often discredited account ofthe moral force of basic needs. I situate the discussion inthe context of health resource allocation and distributivejustice. I argue that the difference depends on whether theneeds in question are assumed to be above the bottomfloor of vital enablement or not. The vital-needs accountstipulates a definite universal level of needs satisfactionthat must be achieved first before one could value otherneeds, desires and preferences. Secondly, I discuss whatvital needs satisfaction means, its relation to basicagency, and the value it affords in relation to valuingitself. Then finally, I suggest what role vital needs satis-faction can play in developing a cross-cultural frameworkfor discussing the ethics of health resource allocation,especially in countries that suffer from extremely tighthealth budgets. For example, such framework canprovide multicultural societies, such as the Philippines,4
with a point of consensus that proponents of competingvalues can support.
WHAT IS THE DIFFERENCE BETWEENBASIC NEEDS AND VITAL NEEDS?
It is difficult to decide which needs, in general, are legiti-mate because needs tend to be dependent on the value ofwhat they are needed for.5 Another difficulty is that thevalue of health as a need depends on the satisfaction ofother more basic needs, without which health matters
3 I use the term ‘vital needs’ to emphasize what is necessary for basicagency. The term has been used extensively in environmental ethics toemphasize the kind of human needs that are strong enough to trumpneeds of other life forms. Knut Erik Tranøy, in his 1975 article, con-trasts vital needs with non-vital but legitimate needs. The very title ofTranøy’s article, especially the word ‘can’, apparently implies that ‘vitalneeds’ is related to basic agency. See K.E. Tranøy. Ought’implies ‘can’:A bridge from fact to norm? Part II. Ratio 1975; 17: 147–175. Tranøywrites that ‘prolonged or definitive frustration’ of vital needs ‘kills ordisables [emphasis added]’ (p. 155) suggesting that human basic abilityis undermined whenever vital needs are not satisfied. David Wigginsexplicitly makes a distinction between basic and vital needs: a need isbasic ‘just if what excludes futures in which y remains unharmed despitehis not having x are laws of nature, unalterable and invariable environ-mental facts, or facts about human constitution’; a need is vital if it isurgent, grave, entrenched, and non-substitutable. D. Wiggins. 1998.Needs, values, truth: essays in the philosophy of value. Oxford: ClarendonPress: xii, 14–17, 22–23, 39–40. Cf. D. Wiggins. 1985. Claims of Need.In Morality and objectivity: a tribute to J L Mackie. T. Honderich, ed.London: Routledge and Kegan Paul: 149–202. Although I share thepriority Tranøy and Wiggins give to vital needs versus other needs, myemphasis is on characteristics of vital needs that make agency possible.Cf. A. Sen. 1999. Development as freedom. Oxford: Oxford UniversityPress.
4 A.J. Romualdez. 2008. State of the Nation’s Health. Available at:http://centennial.lectures.upm.edu.ph/UP_Centennial_Lecture_Series/romualdez.html [Accessed 24 Nov 2008]. Since annual health expendi-tures in the Philippines fall below the 5% of GDP minimum set by theWorld Health Organization (WHO), scaling up basic healthcare provi-sion to a level sufficient to satisfy vital needs would enable many poorFilipinos to contribute to the economic and political life of the country.Such policy could also work in other countries, especially in these timesof global economic crisis. Expanding universal health insurance cover-age in the US, for example, could stimulate the economy because it hasbeen found to increase spending on other consumer goods. J. Gruber &A. Yelowitz. Public Health Insurance and Private Savings. J Polit Econ1999; 107: 1249–1274: 1271. If people spend more on healthcare, theywon’t be able to spend for other consumer goods anymore. Provisionrather than deprivation of vital needs is the way to enable people tocontribute in solving the causes of scarcity. Cf. J. Gruber. UniversalHealth Insurance Coverage or Economic Relief – A False Choice. NEngl J Med 2009; 360: 437–439.5 B. Barry. 1990. Political argument: a reissue with a new introduction.Berkeley, CA: University of California Press.
The Cross-Cultural Importance of Satisfying Vital Needs 487
© 2009 Blackwell Publishing Ltd.

less.6 Also, although it seems easy to claim that needshave priority over mere preferences, needs in general aretoo indeterminate to provide guidance in choosing whatmust be prioritized when resources are scarce.7 Whenneeds are used to determine what healthcare should beprovided, it tends to impose limitless demands forresources.8 These worries may be relevant to basic needsthat are shaped by particular cultures, but not to vitalneeds that are universally enabling across cultures. Whilethe basic needs required for the practice of a particularculture may not be as basic in other cultures, vital needsare so fundamental that their deprivation will disablepersons from practising any cultural tradition, even theleast demanding ones. Moderate scarcity may allow us tosatisfy basic needs that are not vital, but extreme scarcitycould undermine our capacity to satisfy even our vitalneeds.
Some objections to the moral force of needs
Brian Barry wrote a series of brief notes on needs wherehe argues that the value of needs is derivative and thatneeds don’t have independent justification. Needs alwaysoccur in the derivative formula: A needs x in order to y.9
The justification of the need for x is derived from theimportance of what comes after the phrase ‘in order to’.This formula implies that needs are important only if thepurpose for needing it is important. My response to this isthat even if most needs have derivative value, it is notnecessarily the case with needs that are vital. The impor-tance of the vital need for protection from ability-harming or agency-harming conditions (e.g. physicaland mental infirmities) is not necessarily derivative.Satisfaction of vital needs, ceteris paribus, is a precondi-tion to having ends to value.10 However, Barry furtherargues that although claims connected with ‘core’ basichuman needs do not usually demand that the purpose bestated (as it is with needs in general) ‘. . . it is still deriva-tive and the only interesting questions arise in connection
with the ends.’11 But we may ask, ‘Whose ends should itbe?’ Is it not the case that it only makes sense to talkabout ends when they are owned by someone (whetherthe owner herself or her proxy)? By recognizing thatpurpose must be owned, we reveal that Barry’s insistence,that even ‘core’ basic needs (or vital needs) are derivative,involves an assumption that the vital needs of purposeowners have already been sufficiently satisfied for them tobe able to have ends in the first place. If Barry does notassume such vital needs satisfaction, then he must at leastassume that there are others, say evaluators,12 whoalready have the ability to conceive and value ends as aproxy owners of the need in question. Even a proxy has avital need for the ability to conceive and value ends. Vitalneeds satisfaction is a precondition13 to having ends. Allevaluators of ends have a vital need for the ability to haveends, so that when the one in need is not able, anotherevaluator should be able to talk about such connectionbetween need and the supposed end it serves.14 In short,for Barry to be correct that even ‘core’ basic needs havederivative value, someone needs to have at least theability to make the connection between that basic needand the purpose from which its value is derived. Thisviciously leads to requiring an enabled evaluator forevery level of derivation. To avoid this viciousness, wecould just simply recognize that satisfaction of vital needsis a precondition to having the vital ability to have ends.If we must refer to protecting our ability to have ends asan end, we must not classify it as a type of end belongingto the same set of ends we are able to have. Otherwise itwould imply that we could choose between valuing theability to have ends and valuing the ends that we areenabled to have as if these ends were of the same type.Thus, it is not correct to say that all needs are derivativebecause we must differentiate the importance of vitalneeds from the importance of non-vital needs that dependon specific ends to be valuable. Vital needs are those thatmust be satisfied in order to have ends in the first place.The idea of derivative importance does not apply yet tothe vital need for ‘the ability to have ends’ as it does toneeding something for ‘a particular end’ that we alreadyhave.15 The non-derivative value of the vital need to
6 J. Griffin. 1986. Well-being: its meaning, measurement, and moralimportance. Oxford: Oxford University Press: 52.7 E.J. Emanuel. 1991. The ends of human life: medical ethics in a liberal
polity. Cambridge, Mass.: Harvard University Press: 110.8 Ibid: 110–112.9 Barry, op. cit. note 5, pp. 47–49, lxiv–lxix. Barry asserts this about
needs to avoid the ‘danger of treating it as an independent justificatoryprinciple’ (p. 49). This view is similar to Alan White’s position in A.R.White. 1975. Modal thinking. Oxford: Blackwell: 102–123.10 Barry counters that it is not the case that everybody’s welfare isvaluable. If the welfare of evil individuals like Hitler is disvalued, theduty of Hitler’s physician to meet his needs becomes weaker. See Barry,op. cit. note 5, p. lxvii. Barry seems to dismiss the physician’s duty to dono harm without justification. Even without saying that primum nonnocere is beyond argument, it must be shown to be false before it can bedismissed in favor of other values.
11 Ibid: 49.12 Or perhaps, ideal rational observers.13 I use the term ‘precondition’ as Len Doyal and Ian Gough used it inexplaining their idea of survival as ‘precondition for human action andinteraction’. L. Doyal & I. Gough. 1991. A theory of human need. NewYork: Guilford Press: 50–55.14 That second evaluator (when not able herself) will in turn needanother evaluator to talk about her own need-end connection, so onand so forth.15 Some needs and ends have instrumental/derivative value with respectto other ends they serve while other needs or ends may have intrinsicvalue when these are pursued for their own sake. The value of vitalneeds, however, is preintrinsic because the satisfaction of these needs isessential to being able to have ends in the first place, including those
488 Allen Andrew A. Alvarez
© 2009 Blackwell Publishing Ltd.

protect basic abilities that make having valued ends pos-sible gives moral force to the necessity of its satisfaction.
James Griffin16 claims that health is an example of aneed that can matter less when deprivation of other needs(e.g. liberty and minimum material provision) makes lifenot worth living. He contends that the importance ofhealth as a basic need depends ‘upon the level of satisfac-tion of other basic needs; if my needs for liberty andminimum material provision are not met, and are sounlikely ever to be met that life is not worth living, thenhealth must matter less too.’17 It seems that Griffinassumes that ‘health’ refers to a physical condition that isbetter than normal and not the kind of normal conditionthat material provision and liberty enable. But if hemeans that an agent will not be able to value anything inlife without the satisfaction of her basic needs, then it isstrange that he thinks health would matter less. It shouldhave been the opposite. Health as having basic abilitiesshould matter more, not less, because basic health is nec-essary to enable anyone to do basic things, e.g. providefor oneself, acquire liberty, defend one’s freedom, oracquire more freedom. The point of Griffin’s broaderargument is, roughly, that an agent’s informed desiredetermines her good. He may be correct in pointing outthat satisfaction of some basic needs is important forwhat basic needs enable. Its effectiveness is indeedaffected by satisfaction of other needs. He is not quitecorrect, however, in citing health as an example of a basicneed that depends on other basic needs. It cannot be thateven health must matter less than desires when the pos-sibility of having desires depends of the fact that one is atleast healthy enough to desire things. Health to Griffin –in certain respects – seems to be merely a kind of physicalfitness that is a result of exercising,18 so that its impor-tance diminishes when life is no longer worth living.19 Heargues that it would be ‘far too strong’ a claim to set asidethe desires for libraries or schools in favour of the needfor exercise equipment for keeping oneself fit. It is cer-tainly far too strong in the case of exercise equipment but
not in the case of health or healthcare. The demands foreducation and health are not mutually exclusive. The factis, not having either of these two can affect the other. It isnot uncommon to see evidence showing that receivingeducation improves health.20 But in order to receive edu-cation one must at least have the necessary ability tostudy. One must be ‘healthy’ enough to go to school orreceive education.21 The one who desires to be educatedcan only benefit from going to school if she is at leasthealthy enough to study, i.e. if she has a sufficient level ofmental and physical health that would enable her to enjoythe benefits of attending universities or going to libraries.The more flexible conception of need Griffin proposes22
must apply only to needs that are not vital. It should notapply to the vital need for health as a broad category ofabilities that include the ability to desire and value.Apparent basic needs can only be trumped by apparentmere desires when the latter are actually vital needs (e.g.the desire to be healthy). The value of health, if under-stood in a more fundamental way, makes avoidabledeprivation of vital needs unacceptable. It is alwaysimportant to satisfy the vital need for health preciselybecause it is needed for enabling persons to live a humanlife.
Ezekiel Emanuel worries that the idea of providingeverything we need to restore normal functioning couldjustify ‘unlimited demands on social resources’, if so, it is‘ipso facto unacceptable’.23 This worry need not lead torejecting the use of any conception of need. He is right toqualify that ‘deviations from normal human functioningand wholeness . . . are not medical needs for matters ofjustice’ and that treating ‘some diseases is more urgentthan treating others’ because ‘not every medical need is acitizens’ need.’24 Society is only obliged to provide themost urgent minimum of basic healthcare needed by itscitizens. Still, Emanuel worries that the idea of minimumbasic healthcare ‘cannot specify the particular servicesthat are actually covered and those interventions that areexcluded’ and such indeterminacy is again ‘likely to leadto unlimited demands for resources’.25 In the end, citizens
with final or intrinsic value. To claim that vital needs are not derivative(contrary to what Barry claims about all needs) does not mean thatthese needs have intrinsic value. The value of vital needs has a differentsense of fundamentality, thus I refer to such value as preintrinsic.16 Griffin, op. cit. note 6, p. 52.17 Ibid. This view has some similarity to Abraham Maslow’s view thatunless the more basic needs in the hierarchy of needs are met, therewon’t be any cognitive drive for the higher needs (as there won’t be aGriffinian desire for higher needs), thus, life won’t be worth living(because the agent won’t be driven to live that life in the absence ofpotent desire). Griffin implies that the basic need for liberty andminimum material provisions must be satisfied first before higher needsfor [above normal] health will become desirable.18 He compares the need for physical fitness (as health) with the desirefor constructing libraries or universities (as non-need), then claims thatdesires are sometimes more important than needs. See his discussion onpp. 45–46 concerning books versus exercise equipments. Ibid.19 Ibid: 49.
20 M. Marmot. Achieving Health Equity: from Root Causes to FairOutcomes. The Lancet 2007; 370: 1153–1163. See especially Figure 3, p.1154, where it is shown that life expectancy in Russia increased as higherlevels of education were attained.21 Exercise equipment, of course, is not something that one needs inorder to be healthy enough to study. It is therefore not something thatcan be considered a vital need as are basic healthcare and proper nutri-tion. Furthermore, having libraries may be something that is merelydesirable but not the need for education that libraries and universitiescould satisfy. There are no strong reasons to exclude the benefit ofeducation provided by universities and libraries from the category ofbasic needs.22 Griffin, op. cit. note 6, pp. 51–55.23 Emanuel, op. cit. note 7, pp. 110–114.24 Ibid: 112.25 Ibid: 116–117.
The Cross-Cultural Importance of Satisfying Vital Needs 489
© 2009 Blackwell Publishing Ltd.

have to choose particular conceptions of the good lifethat will be deliberated upon in society and that thisdeliberation will hopefully produce a reasonable consen-sus that will guide their decisions about what to includeor exclude in the list of basic healthcare they will collec-tively guarantee.26 The variety of conceptions of the goodmay be daunting but the necessity of enabling people todevelop conceptions, engage in public debate, and nego-tiate and implement the results of social and politicalagreements, is inescapable. We may not be able toprovide every kind of healthcare that may be needed toprotect all abilities, but we must at least provide the mostbasic healthcare that is vital for protecting the basicability of citizens to participate in the political process. Ifnot, then we will be left to rely on a few sufficiently ablelegislators to deliberate what should be good for themany and what basic healthcare services must be guar-anteed. This is not a legitimate process if we agree thatcitizens have to make their own choice. We must there-fore, at least, allow satisfaction of vital needs that isessential in sufficiently enabling the most number of citi-zens to participate.
Vital need satisfaction is a precondition to being ableto have valued ends that general needs are instrumentalfor. In saying this, it seems that objections to the moralforce of general needs do not apply to the importance ofvital needs because such objections presuppose that thosein need already have the vital ability to have ends andthe vital ability to value such ends. When vital needsare deprived, vital abilities are diminished. The accountof the cross-cultural importance of vital needs that Ipropose makes the need for vital enablement explicit.Vital needs satisfaction is a prerequisite to a coherentdiscussion of the value of particular ends. A person mustat least be healthy enough to be able to value particularthings in life before particular values can even be debated.The positive thesis I wish to defend is that satisfaction ofvital needs will enable persons to be agents that have thevital ability to feel, value, choose, and pursue a culturalpractice. The reason for claiming this is that humanpersons can only be moral agents above a definite bottomfloor of enabling satisfaction of vital needs. To deprivesatisfaction of vital needs undermines vital abilities tothink and act, including the important ability to valuethings in life. My negative thesis pertains to what theimportance of vital needs implies to the problem of healthresource allocation when resources are scarce: distribu-tive schemes presupposing that resources for health areonly moderately scarce are not appropriate in extremescarcity. To use a distribution scheme based on presumedmoderate scarcity, even when resources are extremelyscarce, would only result in deprivation of the vital needsof the losers in the distribution game. This will also be
unjustly legitimized by the wrong assumption about thekind of scarcity in effect. A distribution scheme is unjustif it avoidably deprives losers of their vital needs. It isunjust because to deprive people of their vital needswould cause their preventable disablement. Such depri-vation and disablement is unjust no matter how legiti-mate the distribution scheme might seem.
Needs, moderate scarcity, and extremescarcity
There are several contending solutions to the problem ofscarcity of resources for health. Such scarcity is usuallyconceived in terms of competing health needs in moder-ate scarcity, so that under an ideally optimal distributionscheme all vital healthcare needs would be met eventhough other non-vital needs might be deprived. Thecontending solutions include: (1) distributing resourcesequally to meet health needs or trying to mobilize healthresources to achieve equality of health status amongpopulations, (2) prioritizing those who are worse off, (3)allocating and spending health resources to the most costeffective health programs that produce the best outcomeper resources spent, and (4) if there are intractable dis-agreements about which distributive scheme should befollowed or how resources should be properly distrib-uted, resorting to fair procedures that guarantee equalityof opportunity. Consider the case of distributingresources based on the ideal of equality under moderatescarcity. When access to health resources for one is morethan enough and for another is only slightly below thebottom threshold of sufficiency, optimal redistribution ofresources under such condition results in sufficient accessto health sustenance and protection for all. Sufficientaccess to health resources would probably improve thehealth status of the previously worse off individual morethan when access is insufficient. Resources are extremelyscarce when vital needs of at least some individuals aredeprived, no matter how resources are distributed. Againconsider the case of the equality based distributionscheme under extreme scarcity. When access to healthresources for one is only barely sufficient and the accessfor another is way below the bottom threshold of suffi-ciency, redistributing resources from the well off to theworse off to achieve equality results in both individualsfalling below the threshold, with one individual remain-ing under the threshold and the other getting worse. Thisis because the total resources available are not enough forall to have their vital needs satisfied and achieve sufficienthealth.27
26 Ibid: 144–154.
27 Distributing equally in extreme scarcity can only make recipientsequally worse. The same happens when we prioritize the worse-off –everyone else will end up equally worse because resources have to betaken away from the better-off, who are actually just barely above the
490 Allen Andrew A. Alvarez
© 2009 Blackwell Publishing Ltd.

Standard solutions to the problem of allocating healthresources tend to presuppose some kind of moderatescarcity and thus may miss out on some important moralconsiderations when dealing with the allocation problemin extreme scarcity. One important weakness is the pre-supposition that access to vital enabling resources issecure, so that the result of any distribution scheme islegitimate and morally acceptable. Most standard solu-tions miss out the fact that in extreme scarcity, any dis-tribution scheme would result in shares that fall belowthe bottom floor of vital enablement. Such distributionschemes cannot function to legitimize depriving out-comes in extreme scarcity, as it does in moderate scarcity,because of the disabling results it tends to tolerate.
VITAL NEEDS SATISFACTION ANDBASIC AGENCY
Substantive approaches to health resource allocation inmoderate scarcity lack relevance in extreme scarcitybecause the problem of securing the basic abilities ofpeople through the satisfaction of their vital needs is nottaken seriously. Even procedural approaches tend tooverlook the fact that procedural solutions also requirea significant amount of resources (e.g. those needed foreducating citizens, equipping institutions, etc.). Theresources that procedures require seem too demandingfor societies with extremely scarce resources. In con-trast, an approach that pays attention to agency,enabling the satisfaction of vital needs can be useful inboth moderate and extreme scarcity because it differen-tiates the level of abilities required for achieving ends:from the very basic to the most complex. Those whobarely live at the level of subsistence are enabled (ordisabled) in significantly different ways compared withthose whose vital needs are secure. They differ not onlyin the variety of choices available to them but also inthe sufficiency of means relevant to having preferencesabove mere survival. There are inevitable disagreementsthat arise when deciding which among various needs(even those instrumental to the most valuable ends)must be given moral priority. Nevertheless, the primacyof vital needs satisfaction that enable agency should bebasic. Unless the disablement of a person’s basic agencyis irreparably terminal, there are no consistent reasonsto refrain from protecting, repairing, or sustaining suchbasic agency within a reasonable lifetime. Basic agencyis a necessary component of experiencing and valuing
things. Anything, be it desire, happiness, or pleasure,can only matter for a person when she has the vitalability to experience and value such things.28 Deprivinga person of the means to sustain her basic agency as anoutcome of rationing is tragic. Resources for basicenablement should be made available to secure at leastsufficient protection of vital abilities. Minimal access togoods and services that secure vital abilities should notbe taken away from those who already enjoy them.Only resources in excess of what has been allocated forthe satisfaction of vital needs should be up for distribu-tion. A threshold-sensitive approach to health resourceallocation – that involves prioritizing and incrementallyimproving access to the most basic health services – isa more relevant way to deal with extreme scarcity.29
Needs beyond subsistence are important but they canonly begin to matter when people are at least minimallyhealthy and posses the basic ability to need them.30
If ought implies can,31 then mutual moral obligationsof persons in society imply a corresponding basic collec-tive duty to provide sufficient means to the obligated sothey can carry out what they are obligated to do. Peoplemay disagree as to what must be the manner and extent ofsuch enabling provision. Provision could be as minimalas being sufficient for physical health with enough mentalability to make basic decisions. Provision could be asextensive as enabling optimal participation in social life,even flourishing or perfection. The necessity of a particu-lar amount of enabling provision depends on howdemanding the ends to be pursued are. Some ends aremore demanding than others.32 Lists of basic needsusually consist of both physiological and social needsfrom nourishment needs and health needs to needs for
threshold of the satisfaction of their vital needs. This is not the case inmoderate scarcity. Resources are moderately scarce when optimal dis-tribution results in sufficient satisfaction of the vital needs of everyone.For a more detailed discussion see A.A.A. Alvarez. Threshold Consid-erations in Fair Allocation of Health Resources: Justice Beyond Scar-city. Bioethics 2007; 21: 426–438.
28 I recognize that in extreme cases one can be unwillingly made to giveup basic agency, with or without the expectation of getting somethingelse in its place (perhaps, to be relieved from pain). Basic agency is givenup only because the alternative is expected to be better than having basicagency. Admittedly, a painful feeling could be so unbearable that one isforced to give up all ability to feel anything altogether just to be relievedfrom suffering, as if in the absence of all ability to feel, one could stillretain her ability to feel relief from pain. In contrast, what I claim simplyis that one cannot consistently value other things more than the veryability to value those things.29 Among the two ways to construe thresholds: provision threshold(upward) and deprivation threshold (downward), I focus on deprivationthreshold since my account deals with setting limits to deprivation inextreme scarcity. It pertains to deciding the extent of deprivation thatwe may morally allow. In contrast, limit setting viewed upward, perhapsin affluence, concerns deciding what extent of provision should be givenso that resources are put to maximum use.20 Here, we can include rational/informed desires as needs but the samereasoning applies: rational/informed desires only matter when peoplehave, at least, the basic ability to desire and be informed.31 As suggested by the title of Tranøy’s paper. Tranøy, op. cit. note 3.32 Perhaps the more complex ends and required enabling provisions are,the greater disagreements can be expected. Likewise, the more basic andvital the goals and required enabling provisions are, the more reason-able it is to expect agreement.
The Cross-Cultural Importance of Satisfying Vital Needs 491
© 2009 Blackwell Publishing Ltd.
self respect and social participation. What is missing,however, in most accounts of basic needs is the explicitrecognition of the vital abilities required to make thelisted needs needable.33 For example, for education34 to bea need the student-to-be must at least be able to study, i.e.she has to have the sufficient mental and physical powersthat make learning possible; or for happiness35 (orwelfare, or well-being) to be a need, one must have suffi-cient physical and mental ability to experience happiness,pleasure, or wellness. Being well educated is desirable andit can promote well-being aside from enabling a person tohave better opportunities in life. However, we can onlyhave these complex abilities (e.g. being able to securebetter opportunities) when we at least have basic abilities(e.g. desiring, choosing, valuing) because our vital needsare satisfied.36
Basic and complex agency
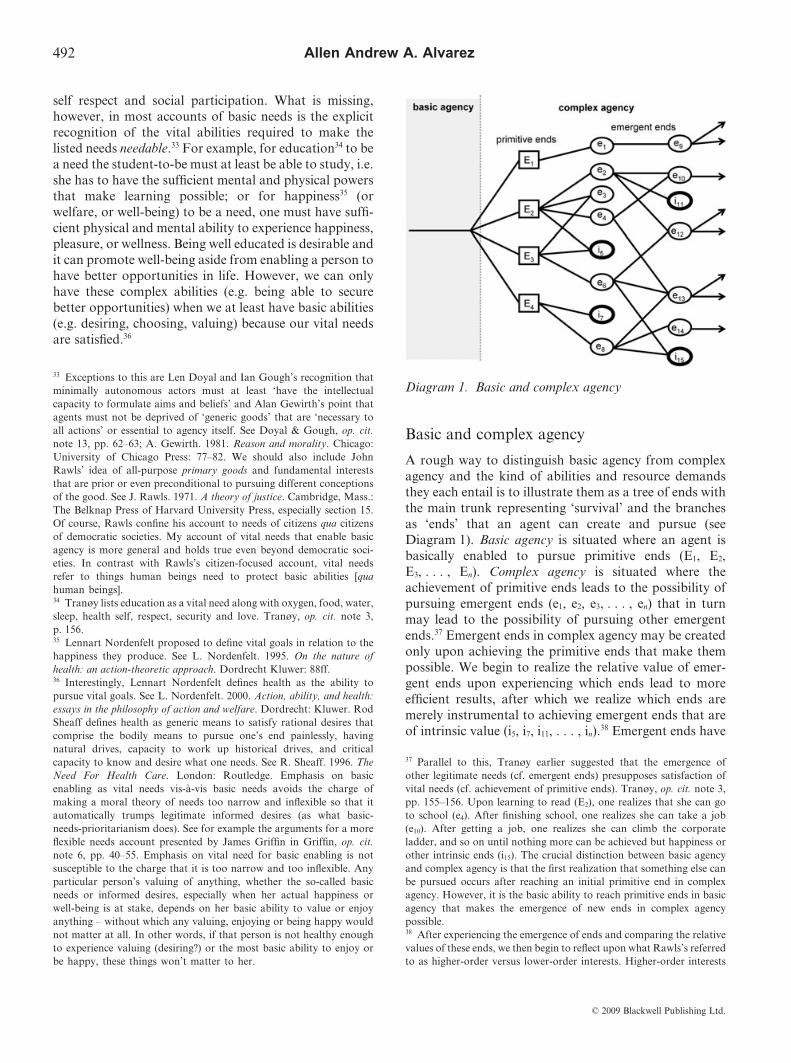
A rough way to distinguish basic agency from complexagency and the kind of abilities and resource demandsthey each entail is to illustrate them as a tree of ends withthe main trunk representing ‘survival’ and the branchesas ‘ends’ that an agent can create and pursue (seeDiagram 1). Basic agency is situated where an agent isbasically enabled to pursue primitive ends (E1, E2,E3, . . . , En). Complex agency is situated where theachievement of primitive ends leads to the possibility ofpursuing emergent ends (e1, e2, e3, . . . , en) that in turnmay lead to the possibility of pursuing other emergentends.37 Emergent ends in complex agency may be createdonly upon achieving the primitive ends that make thempossible. We begin to realize the relative value of emer-gent ends upon experiencing which ends lead to moreefficient results, after which we realize which ends aremerely instrumental to achieving emergent ends that areof intrinsic value (i5, i7, i11, . . . , in).38 Emergent ends have
33 Exceptions to this are Len Doyal and Ian Gough’s recognition thatminimally autonomous actors must at least ‘have the intellectualcapacity to formulate aims and beliefs’ and Alan Gewirth’s point thatagents must not be deprived of ‘generic goods’ that are ‘necessary toall actions’ or essential to agency itself. See Doyal & Gough, op. cit.note 13, pp. 62–63; A. Gewirth. 1981. Reason and morality. Chicago:University of Chicago Press: 77–82. We should also include JohnRawls’ idea of all-purpose primary goods and fundamental intereststhat are prior or even preconditional to pursuing different conceptionsof the good. See J. Rawls. 1971. A theory of justice. Cambridge, Mass.:The Belknap Press of Harvard University Press, especially section 15.Of course, Rawls confine his account to needs of citizens qua citizensof democratic societies. My account of vital needs that enable basicagency is more general and holds true even beyond democratic soci-eties. In contrast with Rawls’s citizen-focused account, vital needsrefer to things human beings need to protect basic abilities [quahuman beings].34 Tranøy lists education as a vital need along with oxygen, food, water,sleep, health self, respect, security and love. Tranøy, op. cit. note 3,p. 156.35 Lennart Nordenfelt proposed to define vital goals in relation to thehappiness they produce. See L. Nordenfelt. 1995. On the nature ofhealth: an action-theoretic approach. Dordrecht Kluwer: 88ff.36 Interestingly, Lennart Nordenfelt defines health as the ability topursue vital goals. See L. Nordenfelt. 2000. Action, ability, and health:essays in the philosophy of action and welfare. Dordrecht: Kluwer. RodSheaff defines health as generic means to satisfy rational desires thatcomprise the bodily means to pursue one’s end painlessly, havingnatural drives, capacity to work up historical drives, and criticalcapacity to know and desire what one needs. See R. Sheaff. 1996. TheNeed For Health Care. London: Routledge. Emphasis on basicenabling as vital needs vis-à-vis basic needs avoids the charge ofmaking a moral theory of needs too narrow and inflexible so that itautomatically trumps legitimate informed desires (as what basic-needs-prioritarianism does). See for example the arguments for a moreflexible needs account presented by James Griffin in Griffin, op. cit.note 6, pp. 40–55. Emphasis on vital need for basic enabling is notsusceptible to the charge that it is too narrow and too inflexible. Anyparticular person’s valuing of anything, whether the so-called basicneeds or informed desires, especially when her actual happiness orwell-being is at stake, depends on her basic ability to value or enjoyanything – without which any valuing, enjoying or being happy wouldnot matter at all. In other words, if that person is not healthy enoughto experience valuing (desiring?) or the most basic ability to enjoy orbe happy, these things won’t matter to her.
37 Parallel to this, Tranøy earlier suggested that the emergence ofother legitimate needs (cf. emergent ends) presupposes satisfaction ofvital needs (cf. achievement of primitive ends). Tranøy, op. cit. note 3,pp. 155–156. Upon learning to read (E2), one realizes that she can goto school (e4). After finishing school, one realizes she can take a job(e10). After getting a job, one realizes she can climb the corporateladder, and so on until nothing more can be achieved but happiness orother intrinsic ends (i15). The crucial distinction between basic agencyand complex agency is that the first realization that something else canbe pursued occurs after reaching an initial primitive end in complexagency. However, it is the basic ability to reach primitive ends in basicagency that makes the emergence of new ends in complex agencypossible.38 After experiencing the emergence of ends and comparing the relativevalues of these ends, we then begin to reflect upon what Rawls’s referredto as higher-order versus lower-order interests. Higher-order interests
Diagram 1. Basic and complex agency
492 Allen Andrew A. Alvarez
© 2009 Blackwell Publishing Ltd.

intrinsic value when we can no longer have further endsto achieve upon reaching them. Emergent ends haveinstrumental value when we only pursue them so as toachieve other ends that we value. The desire to pursueends emerges when our vital needs for having basic abili-ties are satisfied. We can only pursue primitive ends whenour vital needs are satisfied and we are enabled to con-ceive and fulfill our further ends and further extend ourabilities, say, through enhancing basic health andenhancing basic mental abilities. If one does not have thevital ability to move, she cannot engage in physical activi-ties (a primitive end) to develop her body in order toengage in sports (an emergent end) that involve morecomplex movements. If one does not have the basicability to sense things, think about ideas, represent ideasinto symbols and manipulate these symbols for commu-nication, she will not be able to study (as a primitive end)and go to school to pursue basic and higher education (asan emergent end) that involve more complex thinkingskills. The value of learning or enjoying knowledge asends can be intrinsic, but the value of satisfaction of thevital need for basic cognitive abilities to pursue and enjoysuch intrinsic good is preintrinsic.
Having at least the ability to reach primitive endsmust be ensured if we are to consider a person to be anagent at all. The normative force of the requirement tohave, at least, basic agency is a point where reasonableagreement should be expected. Of course people couldstill disagree about how basic agency is to be effectivelyattained, say, whether through ensuring provision ofbasic income or through a highly efficient free marketsystem that tend to distribute welfare equitably. Rea-sonable disagreement about which of the emergent endsshould be pursued is expected, especially when theneeded resources for these are only moderately scarceand basic agency is already widely achieved. We maytolerate such disagreements and even the distributivedecisions that could result from our negotiations. Whenresources are scarce and we must deprive some demandsto satisfy others, the bottom floor of deprivation mustat least allow sufficient provision of what is vitally
needed to secure basic agency.39 Basic agency consistsof: (1) the ability to sustain sufficient physical andmental health through a reasonable period of time (say,a normal life span), (2) the ability to feel, value, and usethings and ideas that will allow oneself to conceivegoals/ends worth pursuing, make informed/reasonedchoice between goals/ends, pursue chosen goals/ends(and possibly succeed). Satisfaction of vital needs thatenable and sustain basic agency should be secured ifmoral agency and obligations are to hold in any soci-ety.40 Basic agency enablement should be sufficient forpersons to further enhance their agency so as to makesociety more stable and conducive for the basic agencyof its members to flourish.
Basic agency and vital needs
Some need theorists41 have cited Immanuel Kant’s idea ofautonomy with the idea of basic needs as precondition tohuman action (and interaction), in particular the ideathat physical and mental capacity are essential to thepossibility of human action. Survival and mental compe-tence are obviously needed for humans to be able to acton their goals, indeed to even act at all. Even the concep-tion of goals depends on the satisfaction of these basicneeds. Autonomy or freedom can be conceived as one ofthe higher levels of abilities and the most basic level as the
are interests about things that make lower-order interests possible. Forexample, the higher-order interest to develop the moral capacity for asense of justice (the ability and desire to conduct oneself in accordancewith justice) makes it possible to pursue lower-order interests (e.g. acareer, higher education, etc.) by creating a stable society conducive tosuch particular pursuits. The higher-order interest to develop the moralcapacity for a conception of the good makes the lower-order interest ofpursuing a particular conception (e.g. a religious life, an advocacy)possible. Likewise, primitive ends of basic agency make the derivativeends of complex agency possible. The primitive end of developing thebasic ability to communicate makes the derivative end of successfulparticipation in a debate possible. Debating requires complex agencyinvolving knowledge, listening skills, strategic skills, persuasive skills,etc.
39 David Wiggins tests the truth of need statements by surveying andcomparing the different levels of moral and political thresholds ofacceptable deprivations and harms that result from such deprivations.Wiggins. op. cit. note 3, pp. 14–15.40 Len Doyal and Ian Gough attributes this line of reasoning to Kant’sidea of having a reason for acting as the basis of moral responsibilitywhich is only possible if an individual has the physical and mentalcapacity to do so. Doyal & Gough, op. cit. note 13, pp. 52–53. HarryLesser earlier wrote on survival as a basic need by stating that ‘theexistence of moral agents is a necessary precondition of moral activity.’R. Plant et al. 1980. Political philosophy and social welfare: essays on thenormative basis of welfare provision. London: Routledge & Kegan Paul:38. Following this Kantian line of reasoning, Barbara Herman wrote:‘Ends . . . that are necessary to sustain oneself as a rational beingcannot (on rational grounds) be given up. Insofar as one has ends at all,one has already willed the continued exercise of one’s agency as arational being.’ B. Herman. 1993. The practice of moral judgment. Cam-bridge, Mass.: Harvard University Press: 55. Kant makes a strongerclaim in The Metaphysics of Morals:
When it is said that it is in itself a duty for a human being to make hisend the perfection belonging to a human being as such (properlyspeaking to humanity) this perfection must be put in what can resultfrom his deeds, not in mere gifts that he must be indebted to nature;for otherwise it would not be a duty. This duty can therefore consistsonly in cultivating one’s faculties (or natural predispositions), thehighest of which is understanding . . . (Ak 6: 386.30-387.2)
I. Kant. 1996. The Metaphysics of Morals. Translated and edited byMary Gregor. Cambridge: Cambridge University Press: 150.41 Doyal & Gough, op. cit. note 13, pp. 52–53.
The Cross-Cultural Importance of Satisfying Vital Needs 493
© 2009 Blackwell Publishing Ltd.

point where human agency begins.42 Agency can bebroadly defined as the ability to act but I will use the termhere to refer to the vital ability of human persons to feel,to value, to choose, to conceive goals and to pursue thosegoals, among other things. Using means to pursue goalsis a property of personal action and we only refer tonon-person entities using means to ends as a manner ofspeaking, personifying them as it were. One cannot usemeans to achieve ends unless she is an agent, i.e. unlessshe has the vital ability to think and act as enabled by thesatisfaction of her vital needs. It goes without saying thatagency (or continuing agency) depends on continuingsurvival. The succeeding levels of abilities build on thepreceding ones so that without basic agency, complexabilities are not possible. As one sustains basic agencythrough the sustained satisfaction of her vital needs, shecan opt to develop her abilities further, say to interactwith others thereby being further enabled to the level ofsociability. After securing basic agency, some other needsremain important, such as being able to interact socially,being able to flourish, etc., depending also on howbroadly human existence should be construed. The thingsnecessary to achieve these higher abilities are basic needsbut only those things necessary to achieve basic agencyare vital needs.43 The ability to act and the ability tointeract are important in defining human agency but theyare not necessarily the end point of enhancing humanabilities. One could further enhance her abilities so as toachieve some degree of autonomy. Basic agency is notnecessarily autonomous as pointed out recently byfeminist thinkers.44 Thus, it makes sense to talk about
autonomous agency as distinct from basic agency.45
Perhaps, flourishing and autonomous agency providebroader categories of abilities. I will mention these con-cepts as higher levels of abilities in the next diagrams thatI will present.
To illustrate what satisfaction of vital needs could be,consider Diagram 2. Here, levels of human enablementare plotted against normal life years from birth to adult-hood. It starts from the most basic ability to act (basicagency), continues with abilities necessary for interactingwith other persons (sociability) followed by a broad cat-egory of further expansion of abilities (flourishing) whereabilities are further expanded, perhaps, even developingto full autonomous agency or perfection, as Kant calls it.Abilities normally develop through the course of normalhuman development. Diagram 2 illustrates how basicagency would ideally emerge from birth to childhood asvital needs are satisfied. The length of time for the emer-gence may vary from one individual to another but itshould reach the level of basic agency as basic mental andphysical abilities become sufficiently developed. Thedevelopment of abilities ends in death after a full life hasbeen lived within the length of time possible for humans.Basic agency marks the bottom floor of the least abilities
42 Andrew Jason Cohen refers to an initial agential choice where thenormativity of choice enters in. He also explicitly defends the claim that‘the agent can reject rationality and autonomy’ against Kant’s strongerclaim that this is impossible. A.J. Cohen. Existentialist Voluntarism asa Source of Normativity. Philosophical Papers 2008; 37: 89–129.43 Soran Reader, in her defence of the basic needs approach againstcriticism of its silence about the substantive content of positive ends,offers reasons that are useful for defending any basic agency-centeredaccount of vital needs, namely: (1) ‘the substantive conception of thepositive state beyond need is an essentially contestable matter for socialnegotiation. Any attempt to stipulate what its content must be willobstruct the process of political negotiation and prevent community-building consensus-formation from taking place, thereby imposingexternal values on the needy rather than helping them’; (2) ‘framework’is intended to describe actions that are morally required . . . Once needsare met, although further ends might morally permissibly be sought,there is no obligation on agents of justice to seek them. There is nomoral obligation to expand anything . . . Human beings are beings whonaturally define and seek their own ends’. S. Reader. Does a BasicNeeds Approach Need Capabilities? J Polit Philos 2006; 14: 337–350:341–342.44 Some feminist thinkers talked about autonomous agency as not only‘uncoerced but the circumstances that structure that choice are also freeof the coercive dimension of oppression’. Susan Sherwin, for example,distinguishes agency from autonomy. Agency is used to refer toinformed choice while autonomy is a more comprehensive notion offreedom ‘where not only is the immediate choice uncoerced but the
circumstances that structure that choice are also free of the coercivedimension of oppression.’ S. Sherwin, ed. 1998. The Politics of Women’sHealth: Exploring Agency and Autonomy. S. Sherwin, ed.: Philadelphia:Temple University Press: 1–18:12, 19–47; C. Mackenzie & N. Stoljar.2000. Relational autonomy: feminist perspectives on automony, agency,and the social self. New York: Oxford University Press. Bevir seems toaffirm the distinction between basic and autonomous agency and yet,following Michel Focault, rejects the possibility of autonomous agency.M. Bevir. Foucault and Critique: Deploying Agency againstAutonomy. Political Theory 1999; 27: 65–84: 67.45 The idea that autonomy is a higher agential ability seems to be in linewith Kant’s idea of one’s own perfection (eigene Vollkommenheit). SeeAk 6: 386–387. Kant, op. cit. note 40, p. 150.
Diagram 2. Ideal development of abilities
494 Allen Andrew A. Alvarez
© 2009 Blackwell Publishing Ltd.
that one could possess; below this bottom floor, anyability to think and act is absent or severely diminished.
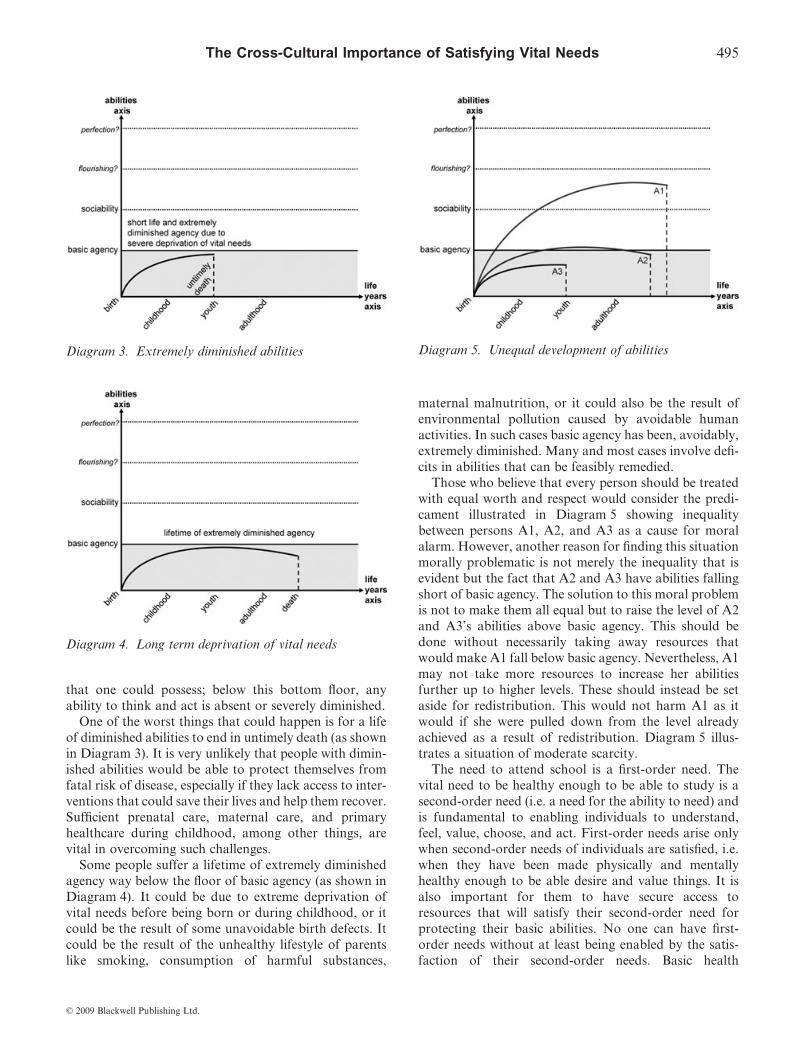
One of the worst things that could happen is for a lifeof diminished abilities to end in untimely death (as shownin Diagram 3). It is very unlikely that people with dimin-ished abilities would be able to protect themselves fromfatal risk of disease, especially if they lack access to inter-ventions that could save their lives and help them recover.Sufficient prenatal care, maternal care, and primaryhealthcare during childhood, among other things, arevital in overcoming such challenges.
Some people suffer a lifetime of extremely diminishedagency way below the floor of basic agency (as shown inDiagram 4). It could be due to extreme deprivation ofvital needs before being born or during childhood, or itcould be the result of some unavoidable birth defects. Itcould be the result of the unhealthy lifestyle of parentslike smoking, consumption of harmful substances,
maternal malnutrition, or it could also be the result ofenvironmental pollution caused by avoidable humanactivities. In such cases basic agency has been, avoidably,extremely diminished. Many and most cases involve defi-cits in abilities that can be feasibly remedied.
Those who believe that every person should be treatedwith equal worth and respect would consider the predi-cament illustrated in Diagram 5 showing inequalitybetween persons A1, A2, and A3 as a cause for moralalarm. However, another reason for finding this situationmorally problematic is not merely the inequality that isevident but the fact that A2 and A3 have abilities fallingshort of basic agency. The solution to this moral problemis not to make them all equal but to raise the level of A2and A3’s abilities above basic agency. This should bedone without necessarily taking away resources thatwould make A1 fall below basic agency. Nevertheless, A1may not take more resources to increase her abilitiesfurther up to higher levels. These should instead be setaside for redistribution. This would not harm A1 as itwould if she were pulled down from the level alreadyachieved as a result of redistribution. Diagram 5 illus-trates a situation of moderate scarcity.
The need to attend school is a first-order need. Thevital need to be healthy enough to be able to study is asecond-order need (i.e. a need for the ability to need) andis fundamental to enabling individuals to understand,feel, value, choose, and act. First-order needs arise onlywhen second-order needs of individuals are satisfied, i.e.when they have been made physically and mentallyhealthy enough to be able desire and value things. It isalso important for them to have secure access toresources that will satisfy their second-order need forprotecting their basic abilities. No one can have first-order needs without at least being enabled by the satis-faction of their second-order needs. Basic health
Diagram 3. Extremely diminished abilities
Diagram 4. Long term deprivation of vital needs
Diagram 5. Unequal development of abilities
The Cross-Cultural Importance of Satisfying Vital Needs 495
© 2009 Blackwell Publishing Ltd.

protection – as an enabling good – is important in thesecond-order sense of needing.
THE FUNDAMENTAL IMPORTANCE OFVITAL NEEDS SATISFACTION ACROSSCULTURES
The vital needs satisfaction account emphasizes the fun-damental importance of the second-order conception ofneed as criterion for health resource allocation. It showswhat practitioners of culture need to protect their abilityto practise their culture. It is also a standpoint fromwhere first-order needs can be evaluated as to whetherany of these first-order needs tend to undermine second-order needs.46 Although the way vital needs are satisfiedby health protection may vary across cultures, sufficientsatisfaction of vital needs is of cross-cultural moralimportance. Vital enablement is the universal base onwhich the practice and evaluation of culture is madepossible.
There are two policy implications that the vital needsaccount engenders. First, resources for health in low-income countries should be mobilized to secure, at least,minimal access to goods and services that sustain andprotect vital abilities. Second, minimal access to goodsand services in low-income countries should not be takenaway from those who already enjoy them because thesegoods and services protect and sustain their vital abilities.In the Philippines, as a lower middle-income country withhealth expenditures less than 5% of its GDP, these policyimplications must take the form of increasing tax-basedand insurance-based financing and resource allocationfor health that benefits/enables the poor, to reduce theirout-of-pocket health expenditures. This has been the kindof recommendation firmly held by those who have closelyinvestigated and managed the national health system oflow-income countries. For example, former health secre-
tary of the Philippines Alberto Romualdez claims that heis convinced that in the face of declining capacity ofgovernment to allocate resources to social services, evenprecisely because of this, increasing healthcare provisionto the poor are ‘required and can catalyze further changestowards greater equity in health’.47
CONCLUSION
Even if people from different cultures do not share thevalue of equality, they should at least recognize the valueof satisfying the vital needs on which their ability topractise any culture is based. The value of vital needssatisfaction is always consistent with any cultural tradi-tion even in cultures where people do not subscribe toegalitarian or liberal values. Vital needs satisfactionoffers a relevant cross-cultural reason for wanting toremedy poor health status through improving access tobasic healthcare. It can strengthen our call for globalhealth equity regardless of whether or not we agree ininvoking principle of equality.
Acknowledgements
I wish to thank the organizers of the 9th World Congress of Bioethics inRijeka, Croatia for the opportunity to present an initial version of thispaper in one of the sessions of the conference. I also thank those whohave commented on the initial version as well as the anonymous review-ers of the journal. This paper was written while I was on a scholarshipat the University of Bergen. Thanks also to Professor Reidar K. Lie forthe help he extended in making my participation at the Rijeka IABCongress possible.
Allen Andrew A. Alvarez is Assistant Professor of Philosophy at theUniversity of the Philippines in Diliman and Research Fellow in Phi-losophy at the University of Bergen. His doctoral dissertation deals withthe issue of ethics of healthcare rationing in extreme scarcity. He haswritten an encyclopedia entry on rationing and has published articles onempirical ethics, Filipino concepts of disease and illness, and researchethics.
46 The same reasoning is given in attempts to discount ethical relativismby searching for universal criteria by which to evaluate cultural prac-tices. ‘If a cultural practice produces manifest suffering or produceslifelong physical disability, there are good grounds for judging thatpractice to be ethically wrong.’ R. Macklin. 1999. Against Relativism:Cultural Diversity and the Search for Ethical Universals in Medicine.New York: Oxford University Press: 24.
47 Romualdez, op. cit. note 4, p. 2. In a similar way, Jonathan Gruber,an economist from MIT, concludes that even in the face of economiccrisis facing the US (and precisely because of it) the government shouldnow implement, rather than postpone, universal health insurance cov-erage as the correct way to enable more people to participate in stimu-lating the economy. Citing previous studies on expanding Medicaid,Gruber is convinced that ‘universal health insurance coverage . . . canimprove both individual health and the economy’s health, both todayand in the long run.’ Gruber, op. cit. note 4, pp. 437, 430.
496 Allen Andrew A. Alvarez
© 2009 Blackwell Publishing Ltd.