
tenosynovial giant cell tumours
334
TENOSYNOVIAL GIANT CELL TUMOURS Monique J.L. Mastboom
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of tenosynovial giant cell tumours

tenosynovial giant
cell tumours
monique J.l. mastboom

tenosynovial giant
cell tumours
monique J.l. mastboom


Although it’s rare, it still needs care

PROEFSCHRIFT
ter verkrijging van
de graad van Doctor aan de Universiteit van Leiden,
op gezag van Rector Magnificus prof. mr. C.J.J.M. Stolker,
volgens besluit van het College voor Promoties
te verdedigen op dinsdag 13 november 2018
klokke 16.15 uur
door
Monique J.L. Mastboom
geboren op 19 oktober 1988
te Nijmegen, Nederland
tenosynovial giant cell
tumours
Cover design and thesis layout Lisanne de Koster
ISBN 978-94-9301-479-4
Printed by Gildeprint, Enschede, the Netherlands
Copyright © 2018 by Monique Mastboom
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means
without permission in writing from the author. The copyright of the articles has been transferred to the
respective journals.
The conduction of the research included in this thesis was carried out at the Department of Orthopaedics of
the Leiden University Medical Centre, Leiden, the Netherlands.
The printing of this thesis was financially supported by Universiteit Leiden, Daiichi Sankyo, Implantcast
Benelux, Anna-Fonds, ChipSoft, MoElBaDa, Consul-TENT, Bedrijfestijn. All funding is gratefully acknowledged.

Promotores
Prof. dr. P.D.S. Dijkstra
Prof. dr. A.J. Gelderblom
Co-promotor
Dr. M.A.J. van de Sande
Leden promotiecommissie
Prof. dr. J.V.M.G. Bovee
Prof. dr. W.T.A. van der Graaf The Royal Marsden NHS Foundation Trust, London
Dr. I.C.M. van der Geest Radboud Universitair Medisch Centrum, Nijmegen

General introduction and outline of this thesis
Incidence
Higher incidence rates than previously known in Tenosynovial Giant Cell Tumours
M.J.L. Mastboom, F.G.M. Verspoor, A.J. Verschoor, D. Uittenbogaard, B. Nemeth, W.J.B.
Mastboom, J.V.M.G. Bovee, P.D.S. Dijkstra, H.W.B. Schreuder, H. Gelderblom, M.A.J. van
de Sande, TGCT study group.
Acta Orthop. 2017 Dec;88(6):688-694
Diagnostics
Does CSF1 over-expression or rearrangement influence biological behaviour
in Tenosynovial Giant Cell Tumours of the knee?
M.J.L. Mastboom, D.M. Hoek, J.V.M.G. Bovee, M.A.J. van de Sande*, K. Szuhai* (*Shared
last authorship).
Histopathology 2018 Aug. doi: 10.1111/his.13744
Disease severity
Severity classification of Tenosynovial Giant Cell Tumours on MR imaging
M.J.L. Mastboom*, F.G.M. Verspoor*, D.F. Hanff, M.G.J. Gademan, P.D.S. Dijkstra, H.W.B.
Schreuder, J.L. Bloem, R.J.P. van der Wal, M.A.J. van de Sande (*Shared first authorship).
Surg Oncol. 2018 Sept;27(3):544-550
Hormones
Can increased symptoms of Tenosynovial Giant Cell Tumours during
pregnancy be explained by a change in female sex hormones?
M.J.L. Mastboom, F.G.M. Verspoor, R. Planje, H.W.B. Schreuder, M.A.J. van de Sande.
Submitted
table of contents
11
28
48
70
94
Chapter 1.
Chapter 2.
Chapter 3.
Chapter 4.
Chapter 5.

114
134
162
190
Chapter 6.
Chapter 7.
Chapter 8.
Chapter 9.
Children
Tenosynovial Giant Cell Tumours in children: a similar entity compared with adults
M.J.L. Mastboom, F.G.M. Verspoor, D. Uittenbogaard, G.R. Schaap, P.C. Jutte, H.W.B.
Schreuder, M.A.J. van de Sande.
Clin Orthop Relat Res. 2018 Sept;476(9):1803-1812
Localized-TGCT
Surgical treatment of localized-type Tenosynovial Giant Cell tumours of large joints
M.J.L. Mastboom, E. Staals, F.G.M. Verspoor, A.J. Rueten-Budde, S. Stacchiotti, E.
Palmerini, G.R. Schaap, P.C. Jutte, W. Aston, A. Leithner, D. Dammerer, A. Takeuchi, Q.
Thio, X. Niu, J.S. Wunder, TGCT study group, M.A.J. van de Sande.
Submitted
Diffuse-TGCT
Outcome of surgical treatment for patients with diffuse-type Tenosynovial
Giant Cell Tumours
M.J.L. Mastboom, E. Palmerini, F.G.M. Verspoor, A.J. Rueten-Budde, S. Stacchiotti, E.
Staals, G.R. Schaap, P.C. Jutte, W. Aston, H. Gelderblom, A. Leithner, D. Dammerer, A.
Takeuchi, Q. Thio, X. Niu, J.S. Wunder, TGCT study group, M.A.J. van de Sande.
Submitted
Treatment
Long-term efficacy of imatinib mesylate in patients with advanced
Tenosynovial Giant Cell Tumour
M.J.L. Mastboom*, F.G.M. Verspoor*, G. Hannink, R.G. Maki, A. Wagner, E. Bompas, J. Desai,
A. Italiano, B.M. Seddon, W.T.A. van der Graaf, J.Y. Blay, M. Brahmi, L. Eberst, S. Stacchiotti,
O. Mir, M.A.J. van de Sande, H. Gelderblom, P.A. Cassier (*Shared first authorship).
Submitted
Quality of life
The effect of surgery in Tenosynovial Giant Cell Tumours as measured by
patient reported outcomes on quality of life and joint function
M.J.L. Mastboom*, F.G.M. Verspoor*, G. Hannink, W.T.A. van der Graaf, M.A.J. van de
Sande, H.W.B. Schreuder (*Shared first authorship).
Accepted in Bone Joint J
Impact on daily living
The patient perspective on the impact of Tenosynovial Giant Cell Tumours
on daily living: Crowdsourcing study on physical function and quality of life
M.J.L. Mastboom, R. Planje, M.A.J. van de Sande.
Interact J Med Res. 2018 Feb 23;7(1):e4.
Limb amputation
Limb amputation after multiple treatments of Tenosynovial Giant Cell
Tumour: Series of 4 Dutch cases
M.J.L. Mastboom, F.G.M. Verspoor, H. Gelderblom, M.A.J. van de Sande.
Case Rep Orthop. 2017;7402570.
Summary of this thesis
General discussion & Future perspectives
Summary in Dutch (Nederlandse samenvatting)
Appendices
List of publications
Acknowledgements
Curriculum vitae
208
232
258
274
284
304
316
Chapter 10.
Chapter 11.
Chapter 12.
Chapter 13.
Chapter 14.
Chapter 15.
Chapter 16.

general introduction
and outlineof this thesis intr
oduc
tionch
apte
r on
e

14
Chapter one
Background
Tenosynovial Giant Cell Tumour (TGCT) is an orphan, mono-articular disease, arising from
the synovial lining of joints, bursae or tendon sheaths1, 2. TGCT is divided into a lobulated
well circumscribed lesion (localized-type) and a more locally aggressive lesion (diffuse-type)
(figure 1). In general, the disease is considered a benign entity, but the diffuse-type can invade
surrounding tissues and is regarded as locally invasive1, 2. The best treatment modality for this
disease is a highly discussed topic. Literature about this disease is scarce. However, the impact
of the disease can be severe: a deteriorated joint function threatens the quality of life in the
relatively young patient population3-5. Therefore, it is of upmost importance to gain insight in
the pathophysiology and severity of the disease to improve treatment strategies.
Historical vignette
In the 2013 WHO classification, giant cell tumour of the tendon sheath and pigmented villonodular
synovitis (PVNS) were unified in one overarching name: tenosynovial giant cell tumours (TGCT)
(table 1)1, 2. Historically, different terms have been used for this entity, including synovial
xanthoma, xanthogranuloma, synovial fibroendothelioma or endothelioma, xanthomatous
giant cell tumour of the tendon sheath, myeloplaxoma, chronic haemorrhagic villous synovitis,
giant cell fibrohaemangioma, fibrohaemosideric sarcoma, sarcoma fusigiganocellulare, benign
or malignant polymorphocellular tumour of the synovial membrane, and fibrous xanthoma of
the synovial membrane6-9.
In 1852, Chassaignac reported a nodular lesion of the synovial membrane affecting the flexor
tendons of the fingers10. Simon was the first to describe the localized form11 and Moser the
first to define the diffuse form affecting the knee12. At that time, the disorder was considered a
malignant condition. Dowd was the first person to question this13. Jaffe elucidated the clinical,
radiological and pathological characteristics of the yellow-brown tumor-like tenosynovial
lesions and suggested a reactive or inflammatory origin of the disease as both nodular
synovitis and pigmented villonodular synovitis (PVNS) showed similar histological features
and both showed a benign course6. The authors also merged both localized- and diffuse-forms
to PVNS. However, the condition was considered neoplastic after the discovery of numerical

General introduction and outline of this thesis
15
1
Figure 1 A 65-year-old female patient with a large medical history, consisting of multiple mutilating
diffuse-type TGCT-related surgeries of her right knee. a. Swollen right knee in bonnet position. On the
posterior, medial side is TGCT growing outside the operation-scar (arrow-head). b. Sagittal Short-TI
Inversion Recovery metal clear MR image, revealing extensive tumour growth, also extending superficially
into the skin (arrow-head). Characteristic TGCT blooming effect is seen attributed to scattered areas of low
signal intensity, typical for iron deposition. c. Positron emission tomography–computed tomography (PET-
CT): enhancement around total knee replacement, suspect for recurrent TGCT. d. Macroscopic aspect of
this tumour after surgical removal, including the typical red-brownish colours and villous appearance. This
section shows the extensive TGCT with a polypus bulge growing into the skin (arrow-head).
a b
dc

16
Chapter one
and structural chromosomal aberrations14-20. At present, an inflammatory disease component
remains, as only a small part of TGCT encompassing cells are considered neoplastic or tumour
cells (2-16%). These neoplastic cells express elevated levels of CSF1, resulting in an increase of
neoplastic cells by an autocrine-loop as well as the recruitment of multiple non-neoplastic cells
by a paracrine Ioop. This phenomenon is coined as ‘the landscape effect’21, 22.
aetiology
Chromosomal aberrations, in both localized- and
diffuse-TGCT, include trisomy for chromosomes 5
and 7 and translocations involving 1p11-13, most
commonly partnering with 2q37 emerging in a
t(1;2)(p13,q37) translocation (figure 2). At the 1p13
breakpoint, the Colony Stimulating Factor 1 (CSF1)
gene is located. In both TGCT subtypes, CSF1 is
fused to the collagen 6A3 (COL6A3) promotor. As
a result, the fusion leads to deregulated expression
of CSF121 (figure 3).
1 #
#
2
Figure 2 Systemic partial karyotype showing
characteristic TGCT translocation t(1;2)(p13;q37).
Source: CyDAS Online Analysis Site,
http://www.cydas.org/OnlineAnalysis/

General introduction and outline of this thesis
17
1Figure 3 Etiopathogenesis of
TGCT, neoplastic cells carrying
the translocation (t(1;2)
(p13;q37)), express elevated
levels of CSF1 (red triangles).
This results in an increase of
neoplastic cells through an
autocrine loop. In addition, the
recruitment of inflammatory cells
of the monocyte/macrophage
lineage expressing the CSF1
receptor (paracrine loop), results
in the tumour-landscape effect.
Source: permission obtained from
designer drs. D.M. Hoek
18
Chapter one
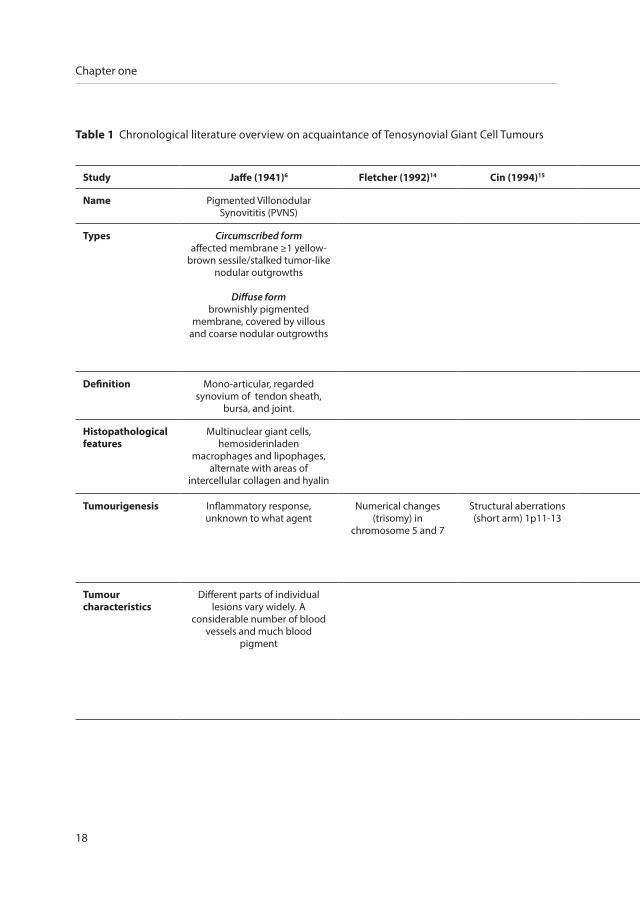
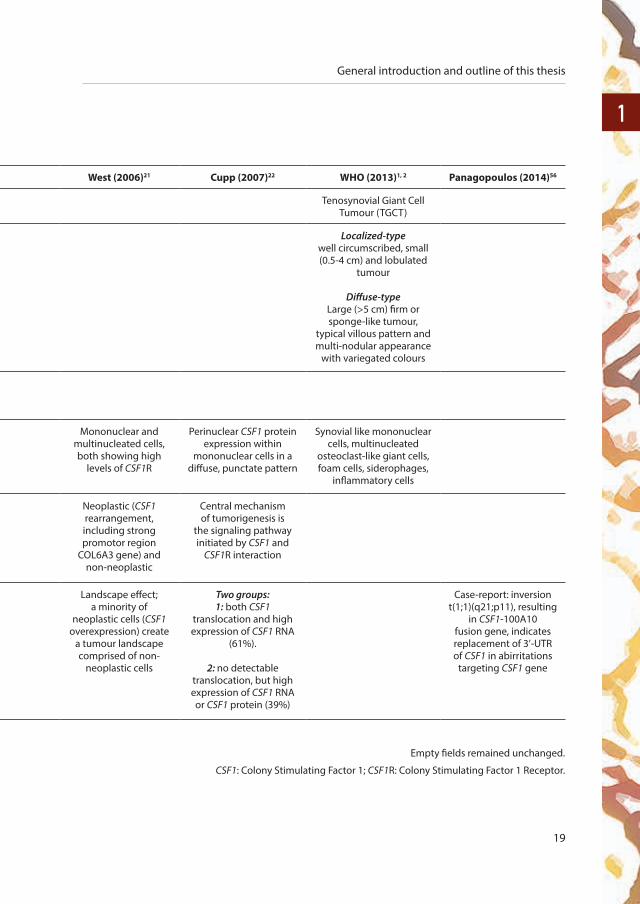
Table 1 Chronological literature overview on acquaintance of Tenosynovial Giant Cell Tumours
Study Jaffe (1941)6 Fletcher (1992)14 Cin (1994)15 West (2006)21 Cupp (2007)22 WHO (2013)1, 2 Panagopoulos (2014)56
Name Pigmented Villonodular Synovititis (PVNS)
Tenosynovial Giant Cell Tumour (TGCT)
Types Circumscribed formaffected membrane ≥1 yellow-
brown sessile/stalked tumor-like nodular outgrowths
Diffuse form brownishly pigmented
membrane, covered by villous and coarse nodular outgrowths
Localized-typewell circumscribed, small (0.5-4 cm) and lobulated
tumour
Diffuse-typeLarge (>5 cm) firm or sponge-like tumour,
typical villous pattern and multi-nodular appearance
with variegated colours
Definition Mono-articular, regarded synovium of tendon sheath,
bursa, and joint.
Histopathological features
Multinuclear giant cells, hemosiderinladen
macrophages and lipophages,alternate with areas of
intercellular collagen and hyalin
Mononuclear and multinucleated cells, both showing high
levels of CSF1R
Perinuclear CSF1 protein expression within
mononuclear cells in a diffuse, punctate pattern
Synovial like mononuclear cells, multinucleated
osteoclast-like giant cells, foam cells, siderophages,
inflammatory cells
Tumourigenesis Inflammatory response, unknown to what agent
Numerical changes (trisomy) in
chromosome 5 and 7
Structural aberrations (short arm) 1p11-13
Neoplastic (CSF1 rearrangement, including strong promotor region
COL6A3 gene) and non-neoplastic
Central mechanism of tumorigenesis is
the signaling pathway initiated by CSF1 and
CSF1R interaction
Tumour characteristics
Different parts of individual lesions vary widely. A
considerable number of blood vessels and much blood
pigment
Landscape effect; a minority of
neoplastic cells (CSF1 overexpression) create
a tumour landscape comprised of non-
neoplastic cells
Two groups:1: both CSF1
translocation and high expression of CSF1 RNA
(61%).
2: no detectable translocation, but high expression of CSF1 RNA or CSF1 protein (39%)
Case-report: inversion t(1;1)(q21;p11), resulting
in CSF1-100A10 fusion gene, indicates replacement of 3’-UTR of CSF1 in abirritations
targeting CSF1 gene
General introduction and outline of this thesis
19
1Table 1 Chronological literature overview on acquaintance of Tenosynovial Giant Cell Tumours
Study Jaffe (1941)6 Fletcher (1992)14 Cin (1994)15 West (2006)21 Cupp (2007)22 WHO (2013)1, 2 Panagopoulos (2014)56
Name Pigmented Villonodular Synovititis (PVNS)
Tenosynovial Giant Cell Tumour (TGCT)
Types Circumscribed formaffected membrane ≥1 yellow-
brown sessile/stalked tumor-like nodular outgrowths
Diffuse form brownishly pigmented
membrane, covered by villous and coarse nodular outgrowths
Localized-typewell circumscribed, small (0.5-4 cm) and lobulated
tumour
Diffuse-typeLarge (>5 cm) firm or sponge-like tumour,
typical villous pattern and multi-nodular appearance
with variegated colours
Definition Mono-articular, regarded synovium of tendon sheath,
bursa, and joint.
Histopathological features
Multinuclear giant cells, hemosiderinladen
macrophages and lipophages,alternate with areas of
intercellular collagen and hyalin
Mononuclear and multinucleated cells, both showing high
levels of CSF1R
Perinuclear CSF1 protein expression within
mononuclear cells in a diffuse, punctate pattern
Synovial like mononuclear cells, multinucleated
osteoclast-like giant cells, foam cells, siderophages,
inflammatory cells
Tumourigenesis Inflammatory response, unknown to what agent
Numerical changes (trisomy) in
chromosome 5 and 7
Structural aberrations (short arm) 1p11-13
Neoplastic (CSF1 rearrangement, including strong promotor region
COL6A3 gene) and non-neoplastic
Central mechanism of tumorigenesis is
the signaling pathway initiated by CSF1 and
CSF1R interaction
Tumour characteristics
Different parts of individual lesions vary widely. A
considerable number of blood vessels and much blood
pigment
Landscape effect; a minority of
neoplastic cells (CSF1 overexpression) create
a tumour landscape comprised of non-
neoplastic cells
Two groups:1: both CSF1
translocation and high expression of CSF1 RNA
(61%).
2: no detectable translocation, but high expression of CSF1 RNA or CSF1 protein (39%)
Case-report: inversion t(1;1)(q21;p11), resulting
in CSF1-100A10 fusion gene, indicates replacement of 3’-UTR of CSF1 in abirritations
targeting CSF1 gene
Empty fields remained unchanged.
CSF1: Colony Stimulating Factor 1; CSF1R: Colony Stimulating Factor 1 Receptor.
20
Chapter one
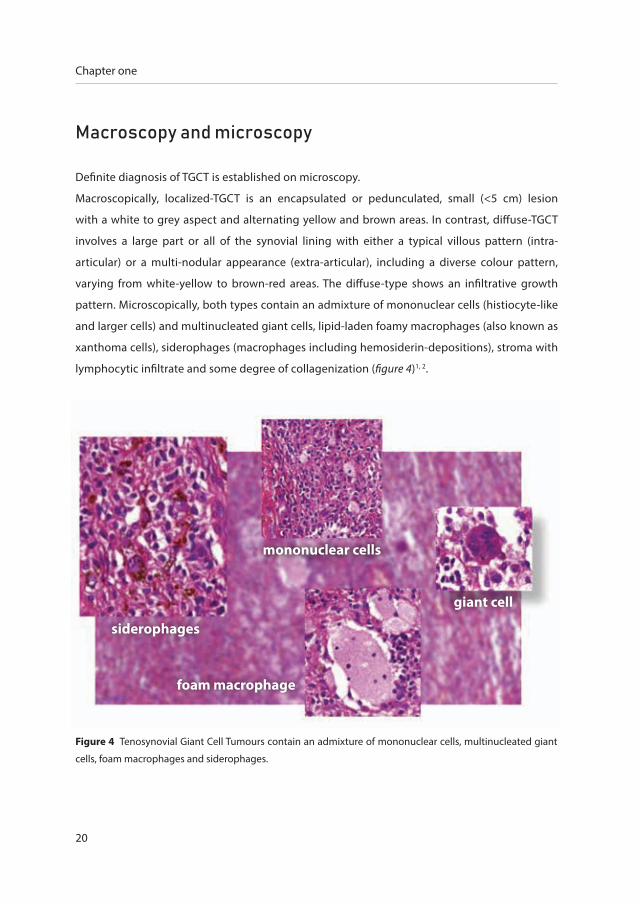
macroscopy and microscopy
Definite diagnosis of TGCT is established on microscopy.
Macroscopically, localized-TGCT is an encapsulated or pedunculated, small (<5 cm) lesion
with a white to grey aspect and alternating yellow and brown areas. In contrast, diffuse-TGCT
involves a large part or all of the synovial lining with either a typical villous pattern (intra-
articular) or a multi-nodular appearance (extra-articular), including a diverse colour pattern,
varying from white-yellow to brown-red areas. The diffuse-type shows an infiltrative growth
pattern. Microscopically, both types contain an admixture of mononuclear cells (histiocyte-like
and larger cells) and multinucleated giant cells, lipid-laden foamy macrophages (also known as
xanthoma cells), siderophages (macrophages including hemosiderin-depositions), stroma with
lymphocytic infiltrate and some degree of collagenization (figure 4)1, 2.
Figure 4 Tenosynovial Giant Cell Tumours contain an admixture of mononuclear cells, multinucleated giant
cells, foam macrophages and siderophages.
siderophages
mononuclear cells
giant cell
foam macrophage

General introduction and outline of this thesis
21
1clinical presentation
TGCT affecting small joints, both fingers and toes, usually presents as localized-TGCT. In large
joints, excluding digits, both localized- and diffuse-TGCT are seen. The diffuse-type mainly
affects weight-bearing joints, predominantly the knee (75%)1, 2, 4. TGCT incidence is based on one
single US-county study in 1980, that reported an incidence of 9 and 2 per million person-years
for localized- (including digits) and diffuse-TGCT, respectively23. Male:female ratio is about 1:1.5
for both types. The mean age at the time of diagnosis lies between 30 and 50 years1, 2, 4. Typically,
patients primarily present with pain and swelling of the associated joint (figure 1a). Additional
symptoms might be limited range of motion, stiffness, instability, giving way and locking
complaints5. Time to definitive diagnosis is often prolonged, on average 4.4 years, due to these
unspecific symptoms and the rarity of the disease4, 24, 25. As TGCT is not lethal, overall survival
is similar to the general population. Diffuse-TGCT frequently becomes a debilitating chronic
illness; therefore joint function and quality of life should be assessed as disease-outcome3, 5, 26, 27.
radiology
In daily practice, an X-ray imaging of the affected joint is frequently performed as a first line
imaging. Degenerative changes and effusion may be present but are nonspecific, and could
also be noticed on computed tomography (CT). Magnetic resonance (MR) imaging is the most
distinctive imaging technique7, 8, 28-30. MR imaging reveals nodular (localized-type) or villous
(diffuse-type) proliferation of synovium, including associated joint effusion. On T1- and T2-
weighted fast spin echo and other fluid sensitive sequences, lesions demonstrate predominantly
intermediate to low signal intensity (dark). After intravenous administration of Gadolinium-
chelate, TGCT shows heterogeneous enhancement. Hemosiderin deposits are frequently seen,
but occur also in other entities31. This degraded hemoglobin deposits cause local changes in
susceptibility (‘blooming effect’) on gradient echo sequences, resulting in low signal intensity
areas that are larger than the anatomical substrate (figure 1b). No substantial change in signal
intensity is detected when comparing the localized- and diffuse-types7, 28. Differential diagnosis
based on MR imaging includes hemophilia, synovial hemangioma, rheumatoid pannus, amyloid
arthrophy and desmoid fibromatosis.

22
Chapter one
treatment modalities
The current standard of care is still surgical resection of the tumour, either arthroscopically
or with an open resection (figure 5), in order to: 1. reduce pain, stiffness, and joint destruction
caused by the disease process; 2. improve function; and 3. minimize the risk of recurrence.
Depending on the extensiveness of the disease, complete resection is frequently impossible,
especially in diffuse-TGCT. Some reports consider arthroscopic management of TGCT superior to
open surgery, because of less morbidity and a shorter recovery period32-36. Standard arthroscopy
of the knee using the anteromedial and anterolateral approaches however, does not allow
surgical access to all areas where diseased tissue could be present. A systematic review showed
lower recurrence rates for open synovectomy (average 14%, maximum 67%) compared to
arthroscopic synovectomy (average 40%, maximum 92%) in diffuse-TGCT37. A randomized
controlled trial for arthroscopic synovectomy versus open synovectomy or surgical treatment
versus targeted therapy is not (yet) performed.
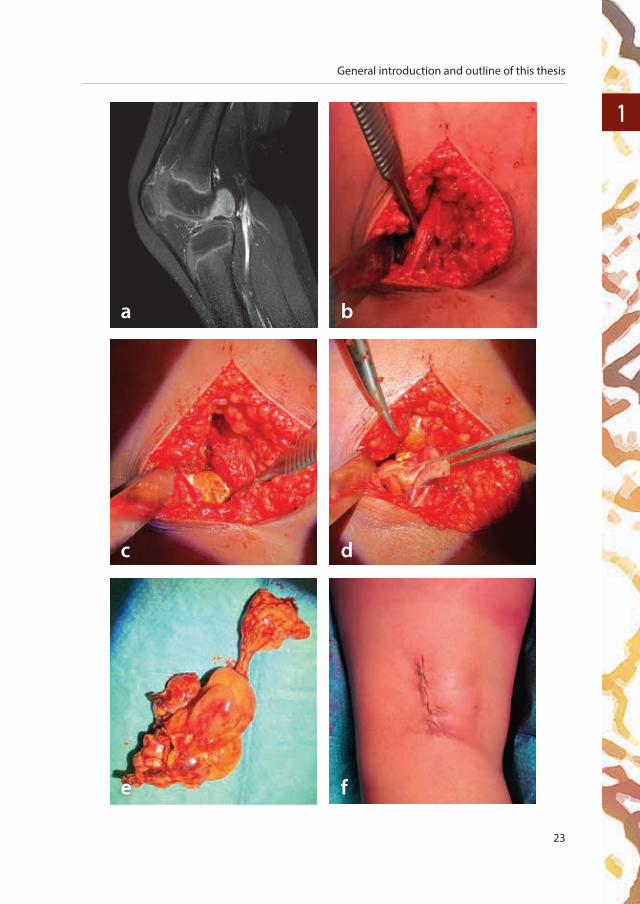
Figure 5 (right page) Example of the surgical technique of an open synovectomy in localized-
TGCT. An 8-year-old boy presented at the outpatient clinic with intermittent complaints of pain and
swelling of his left knee of more than 12 months. These progressive debilitating symptoms were
not sufficiently reduced by paracetamol and have led to school absenteeism. In the outpatient
clinic, swelling was not objectified without limitation in range of motion and palpation was diffusely
pressure painful. X-ray imaging did not show abnormalities. a. A sagittal T1-weighted MR imaging
after intravenous administration of Gadolinium-chelate, revealed a well-circumscribed lesion
on the posterior knee compartment. The T1-weighted and Proton Density MR scan (not shown
here) revealed a lesion of low intensity. Despite the young age of the boy, a localized-TGCT was
suspected. An open resection was planned, because of debilitating symptoms. b. A small lazy-C-
incision was performed on the posterior, lateral side of the left knee. This approach and surgical
window was chosen because of the lateral tumour localization. After opening the crural fascia,
the saphena parva vene, the suralis cutaneous medius nerve, the tibialis nerve and the peroneus
nerve were identified. Lateral gastrocnemius muscle was partially released, because of lateral
localization of the tumour, without compromising the neurovascular bundle. c & d. The capsule
overlying the tumour was partially released. A yellow-brown tumourous aspect showed and
could be resected en bloc from the posterior cruciate ligament where it generally pedicles from.
e. The entire localized-TGCT was excised. f. Minimal invasive techniques can be used to prevent post-
operative complaints such as stiffness. After histological examination, TGCT diagnosis was confirmed.
General introduction and outline of this thesis
23
1
a b
c d
e f
24
Chapter one
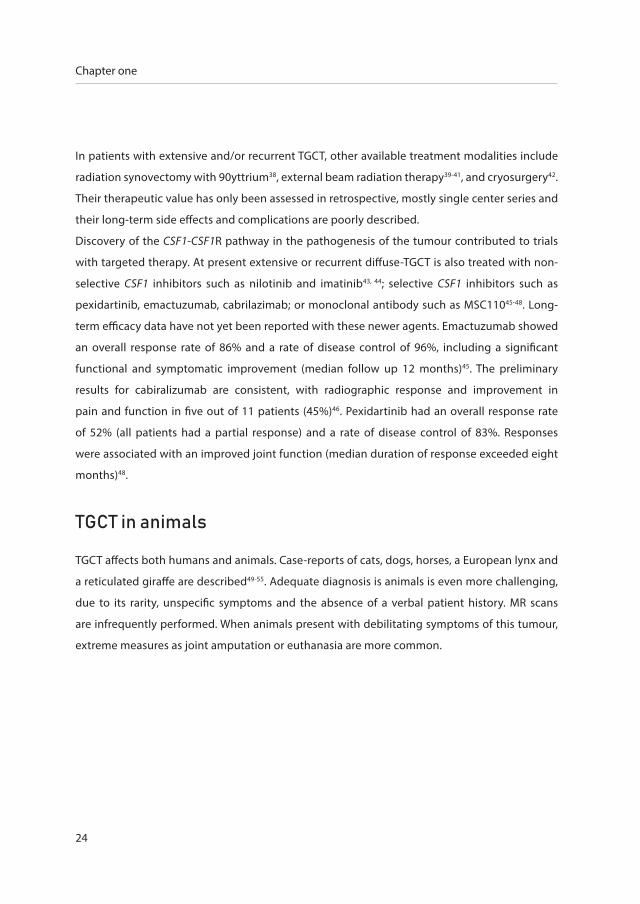
In patients with extensive and/or recurrent TGCT, other available treatment modalities include
radiation synovectomy with 90yttrium38, external beam radiation therapy39-41, and cryosurgery42.
Their therapeutic value has only been assessed in retrospective, mostly single center series and
their long-term side effects and complications are poorly described.
Discovery of the CSF1-CSF1R pathway in the pathogenesis of the tumour contributed to trials
with targeted therapy. At present extensive or recurrent diffuse-TGCT is also treated with non-
selective CSF1 inhibitors such as nilotinib and imatinib43, 44; selective CSF1 inhibitors such as
pexidartinib, emactuzumab, cabrilazimab; or monoclonal antibody such as MSC11045-48. Long-
term efficacy data have not yet been reported with these newer agents. Emactuzumab showed
an overall response rate of 86% and a rate of disease control of 96%, including a significant
functional and symptomatic improvement (median follow up 12 months)45. The preliminary
results for cabiralizumab are consistent, with radiographic response and improvement in
pain and function in five out of 11 patients (45%)46. Pexidartinib had an overall response rate
of 52% (all patients had a partial response) and a rate of disease control of 83%. Responses
were associated with an improved joint function (median duration of response exceeded eight
months)48.
tgct in animals
TGCT affects both humans and animals. Case-reports of cats, dogs, horses, a European lynx and
a reticulated giraffe are described49-55. Adequate diagnosis is animals is even more challenging,
due to its rarity, unspecific symptoms and the absence of a verbal patient history. MR scans
are infrequently performed. When animals present with debilitating symptoms of this tumour,
extreme measures as joint amputation or euthanasia are more common.

General introduction and outline of this thesis
25
1aim of thesis
Treatment of the often debilitating chronic illness, tenosynovial giant cell tumours (TGCT) of
large joints, is challenging. This thesis aims to find better treatment modalities for this disease
by evaluating the pathophysiology, biological behavior, diagnosis and quality of life. Sufficient
data for evaluation of the rare disease TGCT was established through collaboration with the
RadboudUMC and additionally with 31 international sarcoma centers.
Foremost, this thesis aims to create awareness for TGCT and to improve medical care. It evaluates
different aspects of this heterogeneous neoplasm and addresses currently existing lacunas
concerning disease incidence, histopathologic- and hormonal characteristics, disease severity
stratification and pediatric disease burden. Moreover, this thesis addresses long-term effects
of systemic targeted treatment and assessment of health-related quality of life after treatment
in TGCT patients. Lastly, this thesis presents the largest global individual data study of TGCT for
both localized- and diffuse-type TGCT.
outline of thesis
In chapter 2 we performed nationwide incidence calculations upon TGCT, since no incidence
study was reported past 1980. Radiologically and clinically, localized- and diffuse-TGCT are two
different entities. However, genetically and histopathologically they are identical. Chapter 3
correlates the biological behaviour of TGCT in the knee at a molecular level.
In the patient-population of localized- and diffuse-TGCT, different disease extent exist. Therefore,
chapter 4 focuses on the establishment of a TGCT severity classification, sub-classifying both
localized- and diffuse-type TGCT into two more distinct subtypes.
The clinical behaviour between TGCT patients differs greatly. In chapter 5 we explore the
influence of female sex hormones on the experienced TGCT-related symptoms.
Many case-series of TGCT in adults are described, whereas TGCT is only incidentally reported in
children. Chapter 6 evaluates differences in TGCT presentation between adults and children.
Relatively small and heterogeneous case-series emphasize the importance of a large-scaled study.
In chapter 7 and chapter 8, an international multicentre study in 31 international sarcoma
centres is described. This study explores risk factors for TGCT of large joints in 941 localized- and
26
Chapter one
1192 diffuse-type TGCT patients. Results of this study are crucial to the treatment possibilities
and prognosis of this rare entity.
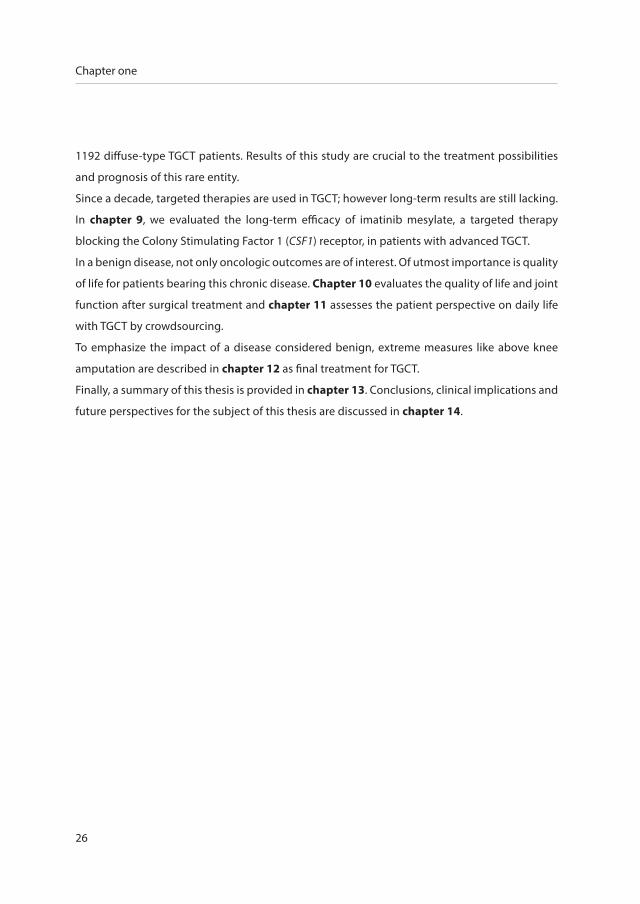
Since a decade, targeted therapies are used in TGCT; however long-term results are still lacking.
In chapter 9, we evaluated the long-term efficacy of imatinib mesylate, a targeted therapy
blocking the Colony Stimulating Factor 1 (CSF1) receptor, in patients with advanced TGCT.
In a benign disease, not only oncologic outcomes are of interest. Of utmost importance is quality
of life for patients bearing this chronic disease. Chapter 10 evaluates the quality of life and joint
function after surgical treatment and chapter 11 assesses the patient perspective on daily life
with TGCT by crowdsourcing.
To emphasize the impact of a disease considered benign, extreme measures like above knee
amputation are described in chapter 12 as final treatment for TGCT.
Finally, a summary of this thesis is provided in chapter 13. Conclusions, clinical implications and
future perspectives for the subject of this thesis are discussed in chapter 14.
General introduction and outline of this thesis
27
1references
1. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4 ed2013. p. 100-1.
2. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, diffuse type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 52013. p. 102-3.
3. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical
treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J.
2014;96-B(8):1111-8.
4. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review
and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
5. Gelhorn HL, Tong S, McQuarrie K, Vernon C, Hanlon J, Maclaine G, et al. Patient-reported Symptoms of Tenosynovial Giant
Cell Tumors. Clin Ther. 2016;38(4):778-93.
6. Jaffe HL, Lichtenstein L, Sutro CJ: Pigmented villonodular synovitis, bursitis, tenosynovitis. Arch Pathol 1941; 31:731-65.
7. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis:
radiologic-pathologic correlation. Radiographics. 2008;28(5):1493-518.
8. Hughes TH, Sartoris DJ, Schweitzer ME, Resnick DL. Pigmented villonodular synovitis: MRI characteristics. Skeletal
radiology. 1995;24(1):7-12.
9. Flandry F, Hughston JC. Pigmented villonodular synovitis. J Bone Joint Surg Am. 1987;69(6):942-9.
10. Chassaignac EP. Cancer de la gaîne des tendons. Gazette des hôpitaux civils et militairs 1852; 185-6. French
11. Simon G. Exstirpation einer sehr grossen, mit dickem Stiele angewachsenen Kniegelenkmaus mit glücklichem Erfolge.
Arch Klin Chirurgie. 1865;6:573.
12. Moser E. Primares sarkom der fussgelenkkapsel. Deutsche Ztschr f Chir. 1909;98:306-10.
13. Dowd CN. Villous arthritis of the knee (Sarcoma). Annals of Surgery. 1912;56:363.
14. Fletcher JA, Henkle C, Atkins L, Rosenberg AE, Morton CC. Trisomy 5 and trisomy 7 are nonrandom aberrations in
pigmented villonodular synovitis: confirmation of trisomy 7 in uncultured cells. Genes, chromosomes & cancer.
1992;4(3):264-6.
15. Dal Cin P, Sciot R, Samson I, De Smet L, De Wever I, Van Damme B, et al. Cytogenetic characterization of tenosynovial giant
cell tumors (nodular tenosynovitis). Cancer research. 1994;54(15):3986-7.
16. Mertens F, Orndal C, Mandahl N, Heim S, Bauer HF, Rydholm A, et al. Chromosome aberrations in tenosynovial giant cell
tumors and nontumorous synovial tissue. Genes, chromosomes & cancer. 1993;6(4):212-7.
17. Ohjimi Y, Iwasaki H, Ishiguro M, Kaneko Y, Tashiro H, Emoto G, et al. Short arm of chromosome 1 aberration recurrently
found in pigmented villonodular synovitis. Cancer genetics and cytogenetics. 1996;90(1):80-5.
18. Sciot R, Rosai J, Dal Cin P, de Wever I, Fletcher CD, Mandahl N, et al. Analysis of 35 cases of localized and diffuse tenosynovial
giant cell tumor: a report from the Chromosomes and Morphology (CHAMP) study group. Modern pathology : an official
journal of the United States and Canadian Academy of Pathology, Inc. 1999;12(6):576-9.
19. Nilsson M, Hoglund M, Panagopoulos I, Sciot R, Dal Cin P, Debiec-Rychter M, et al. Molecular cytogenetic mapping of
recurrent chromosomal breakpoints in tenosynovial giant cell tumors. Virchows Archiv : an international journal of
pathology. 2002;441(5):475-80.
20. Brandal P, Bjerkehagen B, Heim S. Molecular cytogenetic characterization of tenosynovial giant cell tumors. Neoplasia.
2004;6(5):578-83.

28
Chapter one
21. West RB, Rubin BP, Miller MA, Subramanian S, Kaygusuz G, Montgomery K, et al. A landscape effect in tenosynovial
giant-cell tumor from activation of CSF1 expression by a translocation in a minority of tumor cells. Proc Natl Acad Sci U
S A. 2006;103(3):690-5.
22. Cupp JS, Miller MA, Montgomery KD, Nielsen TO, O’Connell JX, Huntsman D, et al. Translocation and expression of CSF1
in pigmented villonodular synovitis, tenosynovial giant cell tumor, rheumatoid arthritis and other reactive synovitides.
The American journal of surgical pathology. 2007;31(6):970-6.
23. Myers BW, Masi AT. Pigmented villonodular synovitis and tenosynovitis: a clinical epidemiologic study of 166 cases and
literature review. Medicine (Baltimore). 1980;59(3):223-38.
24. Bhimani MA, Wenz JF, Frassica FJ. Pigmented villonodular synovitis: keys to early diagnosis. Clin Orthop Relat Res.
2001(386):197-202.
25. Cotten A, Flipo RM, Chastanet P, Desvigne-Noulet MC, Duquesnoy B, Delcambre B. Pigmented villonodular synovitis of
the hip: review of radiographic features in 58 patients. Skeletal radiology. 1995;24(1):1-6.
26. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
27. van der Heijden L, Piner SR, van de Sande MA. Pigmented villonodular synovitis: a crowdsourcing study of two hundred
and seventy two patients. Int Orthop. 2016;40(12):2459-68.
28. Poletti SC, Gates HS, 3rd, Martinez SM, Richardson WJ. The use of magnetic resonance imaging in the diagnosis of
pigmented villonodular synovitis. Orthopedics. 1990;13(2):185-90.
29. Nordemar D, Oberg J, Brosjo O, Skorpil M. Intra-Articular Synovial Sarcomas: Incidence and Differentiating Features from
Localized Pigmented Villonodular Synovitis. Sarcoma. 2015;2015:903873.
30. Wang C, Song RR, Kuang PD, Wang LH, Zhang MM. Giant cell tumor of the tendon sheath: Magnetic resonance imaging
findings in 38 patients. Oncology letters. 2017;13(6):4459-62.
31. Barile A, Sabatini M, Iannessi F, Di Cesare E, Splendiani A, Calvisi V, et al. Pigmented villonodular synovitis (PVNS) of the
knee joint: magnetic resonance imaging (MRI) using standard and dynamic paramagnetic contrast media. Report of 52
cases surgically and histologically controlled. La Radiologia medica. 2004;107(4):356-66.
32. de Carvalho LH, Jr., Soares LF, Goncalves MB, Temponi EF, de Melo Silva O, Jr. Long-term success in the treatment of
diffuse pigmented villonodular synovitis of the knee with subtotal synovectomy and radiotherapy. Arthroscopy.
2012;28(9):1271-4.
33. Kubat O, Mahnik A, Smoljanovic T, Bojanic I. Arthroscopic treatment of localized and diffuse pigmented villonodular
synovitis of the knee. Collegium antropologicum. 2010;34(4):1467-72.
34. Loriaut P, Djian P, Boyer T, Bonvarlet JP, Delin C, Makridis KG. Arthroscopic treatment of localized pigmented villonodular
synovitis of the knee. Knee Surg Sports Traumatol Arthrosc. 2012;20(8):1550-3.
35. Rhee PC, Sassoon AA, Sayeed SA, Stuart MS, Dahm DL. Arthroscopic treatment of localized pigmented villonodular
synovitis: long-term functional results. American journal of orthopedics. 2010;39(9):E90-4.
36. Noailles T, Brulefert K, Briand S, Longis PM, Andrieu K, Chalopin A, et al. Giant cell tumor of tendon sheath: Open surgery
or arthroscopic synovectomy? A systematic review of the literature. Orthop Traumatol Surg Res. 2017;103(5):809-14.
37. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
38. Gortzak Y, Vitenberg M, Frenkel Rutenberg T, Kollender Y, Dadia S, Sternheim A, et al. Inconclusive benefit of adjuvant
(90)Yttrium hydroxyapatite to radiosynovectomy for diffuse-type tenosynovial giant-cell tumour of the knee. Bone Joint
J. 2018;100-B(7):984-8.

General introduction and outline of this thesis
29
139. Heyd R, Seegenschmiedt MH, Micke O. The role of external beam radiation therapy in the adjuvant treatment of
pigmented villonodular synovitis. Zeitschrift fur Orthopadie und Unfallchirurgie. 2011;149(6):677-82.
40. Mollon B, Lee A, Busse JW, Griffin AM, Ferguson PC, Wunder JS, et al. The effect of surgical synovectomy and radiotherapy
on the rate of recurrence of pigmented villonodular synovitis of the knee: an individual patient meta-analysis. Bone Joint
J. 2015;97-B(4):550-7.
41. Griffin AM, Ferguson PC, Catton CN, Chung PW, White LM, Wunder JS, et al. Long-term outcome of the treatment of
high-risk tenosynovial giant cell tumor/pigmented villonodular synovitis with radiotherapy and surgery. Cancer.
2012;118(19):4901-9.
42. Verspoor FG, Scholte A, van der Geest IC, Hannink G, Schreuder HW. Cryosurgery as Additional Treatment in Tenosynovial
Giant Cell Tumors. Sarcoma. 2016:3072135.
43. Gelderblom H, Cropet C, Chevreau C, Boyle R, Tattersall M, Stacchiotti S, et al. Nilotinib in locally advanced pigmented
villonodular synovitis: a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2018.
44. Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, et al. Efficacy of imatinib mesylate for the
treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis.
Cancer. 2012;118(6):1649-55.
45. Cassier PA, Italiano A, Gomez-Roca CA, Le Tourneau C, Toulmonde M, Cannarile MA, et al. CSF1R inhibition with
emactuzumab in locally advanced diffuse-type tenosynovial giant cell tumours of the soft tissue: a dose-escalation and
dose-expansion phase 1 study. Lancet Oncol. 2015;16(8):949-56.
46. Sankhala KK, Blay JY, Ganjoo KN, Italiano A, Hassan AB, Kim TM, et al. A phase I/II dose escalation and expansion study
of cabiralizumab (cabira; FPA-008), an anti-CSF1R antibody, in tenosynovial giant cell tumor (TGCT, diffuse pigmented
villonodular synovitis D-PVNS). ASCO conference 2017. 35 (15 Supplement 1).
47. Brahmi M, Vinceneux A, Cassier PA. Current Systemic Treatment Options for Tenosynovial Giant Cell Tumor/Pigmented
Villonodular Synovitis: Targeting the CSF1/CSF1R Axis. Current treatment options in oncology. 2016;17(2):10.
48. Tap WD, Gelderblom H, Stacchiotti S, Palmerini E, Ferrari S, Desai J, et al. Final results of ENLIVEN: A global, double-blind,
randomized, placebo-controlled, phase 3 study of pexidartinib in advanced tenosynovial giant cell tumor (TGCT). ASCO
conference Chicago 2018.
49. Ihms EA, Rivas A, Bronson E, Mangus LM. Pigmented Villonodular Synovitis in a Reticulated Giraffe (Giraffa
Camelopardalis). Journal of zoo and wildlife medicine : official publication of the American Association of Zoo
Veterinarians. 2017;48(2):573-7.
50. Malatesta D, Cuomo A, Mara M, Di Guardo G, Gentile L, Macolino A, et al. Benign giant cell tumour of tendon sheaths in a
European Lynx (Lynx lynx). Journal of veterinary medicine A, Physiology, pathology, clinical medicine. 2005;52(3):125-30.
51. Akerblom S, Sjostrom L. Villonodular synovitis in the dog: a report of four cases. Veterinary and comparative orthopaedics
and traumatology: VCOT. 2006;19(2):87-92.
52. Dempsey LM, Maddox TW, Meiring T, Wustefeld-Janssens B, Comerford EJ. Computed Tomography Findings of
Pigmented Villonodular Synovitis in a Dog. Veterinary and comparative orthopaedics and traumatology: VCOT. 2018.
53. Cotchin E. Further observations on neoplasms in dogs, with particular reference to site of origin and malignancy. Brit
Vet J 1954;110:274-86.
54. Hulse EV. A benign giant-cell synovioma in a cat. The Journal of pathology and bacteriology. 1966;91(1):269-71.
55. Davies JD, Little NR. Synovioma in a cat. The Journal of small animal practice. 1972;13(3):127-33.
56. Panagopoulos I, Brandal P, Gorunova L, Bjerkehagen B, Heim S. Novel CSF1-S100A10 fusion gene and CSF1 transcript
identified by RNA sequencing in tenosynovial giant cell tumors. International journal of oncology. 2014;44(5):1425-32.


inci
den
ce Higher incidence
rates than previously known
in tenosynovial giant cell tumours
chap
ter
two
a nationwide study in the netherlandsM.J.L. Mastboom1, F.G.M. Verspoor2, A.J. Verschoor3, D.
Uittenbogaard1, B. Nemeth4, W.J.B. Mastboom5, J.V.M.G. Bovée6, P.D.S. Dijkstra1, H.W.B. Schreuder2, H. Gelderblom3,
M.A.J. van de Sande1, TGCT study-group*Acta Orthop. 2017 Dec;88(6):688-694

1 Orthopaedic Surgery, Leiden University Medical Centre, Leiden, the Netherlands
2 Orthopaedic Surgery, Radboud University Medical Centre, Nijmegen, the Netherlands
3 Medical Oncology, Leiden University Medical Centre, Leiden, the Netherlands
4 Clinical Epidemiology, Leiden University Medical Centre, Leiden, the Netherlands
5 Oncology Surgery, Medical Spectrum Twente, Enschede, the Netherlands
6 Pathology, Leiden University Medical Centre, Leiden, the Netherlands
*TGCT study-group:
G.R. Schaap, W.J. Kleyn Molekamp, S.T. Hokwerda, P. van der Woude, M. Henket, S.E. Brandt, J. van de Breevaart
Bravenboer, L.A. Lisowski, P. van der Zwaal, J.M.G.T. Jenner, J.A. Jansen, A. de Gast, H.J. Noten, D.E. Meuffels, T. Gosens,
R. Krips, D.T. Mensch, P.H.J. Bullens, R. Onstenk, F.L. Van Erp Taalman Kip, A.P. van Noort-Suijdendorp, C.H. Geerdink,
D.M.J. Dorleijn, H.H. Kaptijn, M.W. Bloembergen, O.P.P. Temmerman, W.P. Zijlstra, T.D. Berendes, M. van den Besselaar,
U.T. Timur, M.A. Witlox, M.R. Krijnen, P.C. Konings, B.R. Chander, F.C.W. Slootmans, D.J. Wever, D. Haverkamp, R.E.A.M.
Zwartelé, E.M. Nelissen, K.G. Auw Yang, R. de Haan, P.C. Jutte, D.B.F. Saris, S.F. de Boer, R.J. de Raadt, C.P. Schönhuth,
J.G.A. Amaya, R.J. Hillen, A.J.H. Vochteloo, B.G.W. Daalmans, P.C. Kaijser Bots, W.L.W. van Hemert

Incidence rates in tenosynovial giant cell tumours
33
2abstract
Background and purpose
Tenosynovial Giant Cell Tumours (TGCT) are rare, benign tumours, arising in synovial lining of
joints, tendon sheaths or bursae. 2 Types are distinguished: localized-, either digits or extremity,
and diffuse lesions. Current TGCT incidence is based on 1 single US-county study in 1980, with
an incidence of 9 and 2 per million person-year in localized- (including digits) and diffuse-
TGCT, respectively. We aim to determine nationwide and worldwide incidence rates (IR) in TGCT
affecting digits, TGCT localized-extremity and TGCT diffuse-type.
Material and methods
Over a 5-year period, the Dutch Pathology Registry (PALGA) identified 4503 pathology reports on
TGCT. Reports affecting digits were solely used for IR-calculations. Reports affecting extremities,
were clinically evaluated. Dutch IRs were converted to world population IRs.
Results
2815 (68%) digits, 933 (23%) localized-extremity and 390 (9%) diffuse-type TGCT were identified.
Dutch IR in digits, localized extremity and diffuse-type was 34 (95% CI 33-35), 11 (95% CI 11-
12) and 5 (95% CI 4-5) per million person-years, respectively. All 3 groups showed a female
predilection and highest number of new cases in age-category 40-59 years. Knee-joint was
most often affected: localized-extremity (46%) and diffuse-type (64%), mostly treated with
open-resection: localized (65%) and diffuse (49%). Reoperation rate due to local recurrence for
localized-extremity was 9%, diffuse-TGCT 23%.
Interpretation
This first nationwide study and detailed analyses of IRs in TGCT estimated a worldwide IR in
digits, localized-extremity and diffuse-TGCT of 29, 10 and 4 per million person-years, respectively.
Recurrence rate in diffuse-type is 2.6 times higher, compared with localized-extremity. TGCT is
still considered a rare disease; however, it is more common than previously understood.

34
Chapter two
Background
Tenosynovial Giant Cell Tumours (TGCT) are a rare entity, affecting generally young patients
(below the age of 40 years), with an equal sex distribution. The World Health Organisation (WHO)
classification of Tumours of Soft Tissue and Bone (2013) distinguishes 2 TGCT-types: localized and
diffuse lesions1, 13. Microscopically the 2 types show no clear difference. However, on Magnetic
Resonance Imaging (MRI) discrimination between these types is made2.
The localized-type was previously described as Giant Cell Tumour of Tendon Sheath, nodular synovitis
or localized Pigmented VilloNodular Synovitis (PVNS). The typical macroscopic aspect is a well
circumscribed, small (among 0.5 to 4 centimetres) usually lobulated lesion, with white to grey, yellow
and brown mottled areas1. Based on anatomical site of the localized-type tumour, differentiation is
made into a group affecting digits and a group occurring in and around larger joints3, 4. TGCT affecting
digits is defined as a localization distal to metacarpal or metatarsal bones; localized TGCT-extremity is
defined as all sites near joints proximal and including metacarpal- and metatarsal-joints.
In localized-TGCT, most lesions are found in the digits of hand and feet (Figure 1). The majority
of these lesions arise from the tendon sheath and less frequently from synovial lining of digital
joints. Common treatment is marginal excision5, 6. A systematic review showed a recurrence rate
of 15%, after an average follow-up of 37 to 79 months7. Fewer localized TGCT lesions are found
around larger joints, they originate from synovial lining, tendon sheaths or bursae (Figure 2). The
preferred treatment of these lesions is marginal excision by an arthroscopic or by open approach5,
6. A systematic review reported an average recurrence rate of 6% after arthroscopic resection and
4% after open resection (with variable follow-up)8.
The diffuse-type TGCT; previously called diffuse Pigmented VilloNodular Synovitis (PVNS) or
Synovitis (Villo)nodularis Pigmentosa (SVP), is a more destructive and locally aggressive tumour
(figure 3). Diffuse-TGCT is defined by the presence of an infiltrative soft tissue mass along synovial
lining, showing villous projections of the proliferated synovial membrane, with or without
involvement of the adjacent joint or other structures. Macroscopically, the diffuse-type affects a
large part of synovial lining and has a multinodular, multi-coloured appearance, including white,
yellow and rust-coloured areas1. 75% are located around the knee-joint8. Current treatment
Incidence rates in tenosynovial giant cell tumours
35
2
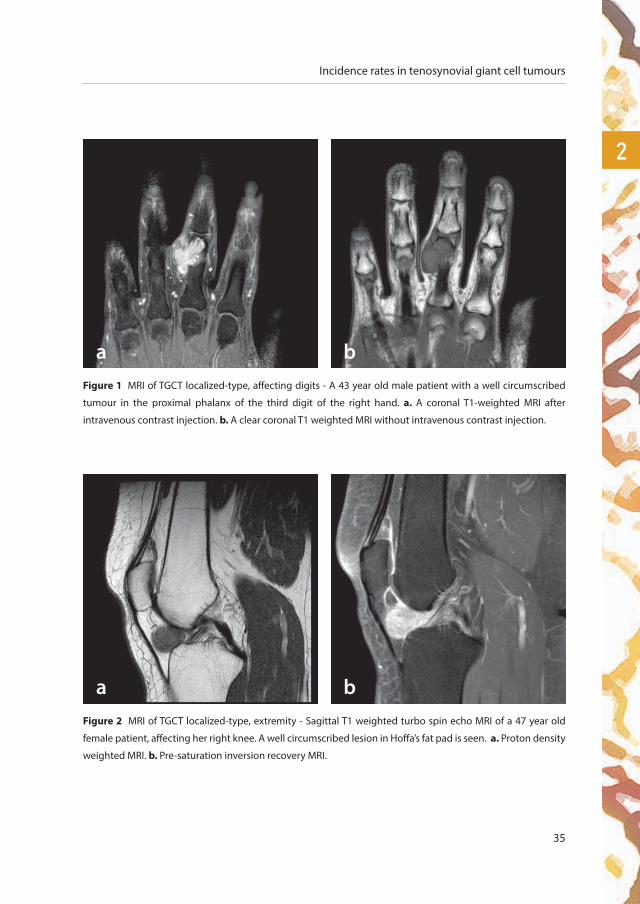
Figure 1 MRI of TGCT localized-type, affecting digits - A 43 year old male patient with a well circumscribed
tumour in the proximal phalanx of the third digit of the right hand. a. A coronal T1-weighted MRI after
intravenous contrast injection. b. A clear coronal T1 weighted MRI without intravenous contrast injection.
a b
Figure 2 MRI of TGCT localized-type, extremity - Sagittal T1 weighted turbo spin echo MRI of a 47 year old
female patient, affecting her right knee. A well circumscribed lesion in Hoffa’s fat pad is seen. a. Proton density
weighted MRI. b. Pre-saturation inversion recovery MRI.
a b

36
Chapter two
is surgical excision5, 6, 9. However, it is often difficult to perform a marginal excision. Average
recurrence rates after arthroscopy are 40% and after open resection 14%, with variable follow-up
times8. In extensive disease, peri-operative radiotherapy might reduce recurrence rate10, 11. Patients
with (multiple) recurrences experience impaired quality of life12.
According to the WHO-classification of 2002 and 2013, the Incidence Rate (IR) in TGCT is not exactly
known1, 13. Current TGCT IRs are based on 1 single US-county study completed in 1980, with an IR
of 9 and 2 per million person-year in localized- (including digits) and diffuse-TGCT, respectively14.
Verschoor et al. (2015) performed the initial nationwide registry based study on giant cell
containing tumours and calculated an overall IR for TGCT of 50 per million per year. Discrimination
between localized and diffuse disease was not possible as additional clinical information was
lacking. The difference in biological behaviour, however, demands for further stratification of this
general IR in the 3 different TGCT-groups. Therefore, we aimed to estimate the worldwide (WHO-
standardized) TGCT IR by investigating clinical data of affected joints, sex differences, 10 year age
specific categories, initial treatments, follow-up and recurrences rate at individual patient level
through extensive additional data collection at participating hospitals.
Figure 3 MRI of TGCT diffuse-type. A 23 year old male patient with an extensive proliferative synovial process
around both cruciate ligaments, dominating the anterior and posterior knee compartments, intra- and extra-
articular. Inside suprapatellar pouch and Baker’s cyst a blooming villonodular aspect shows typical iron
depositions. a. Sagittal proton density weighted turbo spin echo MRI. b. Sagittal T2 weighted fast field echo MRI.
a b
Incidence rates in tenosynovial giant cell tumours
37
2material and methods
A search in PALGA, the non-profit nationwide network and registry of histo- and cytopathology
in The Netherlands was performed15. To find all patients with Tenosynovial Giant Cell Tumours,
between January 2009 and January 2014, search terms ‘Tenosynovial Giant Cell Tumour’, ‘Pigmented
Villonodular Synovitis’ and a variety of synonyms were used, either as a code or as free text16, see
supplementary data. Received pathology-reports provided limited and anonymous information
on sex, age, date of tissue removal and conclusion of the pathology report. In these reports,
definitive diagnosis was frequently provided, however information on (localized/diffuse) type and
affected joint was only sparsely available. Therefore, further investigation of additional clinical and
radiological data was necessary. Reports with TGCT affecting digits were solely used for calculating
incidence rate (for TGCT-digits) and not further investigated clinically. PALGA interlinked 1941
pathology-reports to 95 original Dutch hospitals. Departments of pathology received a request to
collaborate in this nationwide study. After approval, personal hospital identifiers were obtained and
concerned departments (mostly orthopaedics and general surgery) were invited to confirm TGCT
diagnosis and add detailed information on TGCT-type, affected joint, sex, age at first histologically
proven TGCT, primary treatment, total surgeries related to TGCT, date of last follow-up and follow-up
status. Clinical and radiographic data were derived from medical files. Data were kept anonymously.
75 of 95 attributed hospitals collaborated, including all specialized and academic centres.
Clinical evaluation started with 1941 eligible TGCT cases. In 1576 (81%) cases, diagnosis was
confirmed. 253 Reports were determined to be in digits and amended in digits-group. For included
TGCT extremity cases (n 1323), incomplete evaluated clinical data were imputed for unknown
data on TGCT-type (n=393), affected joint (n=101), sex (n=52), age (n=54) and treatment (n=484),
using multiple imputation techniques. 10 Datasets were imputed, results were pooled according
to standard Rubin’s rules17. All imputed data were checked for errors. Finally, 1323 patients with
histological proven TGCT were included (figure 4).
In addition to the 2562 patients with TGCT affecting digits which were already identified based on
the pathology reports, 253 additional patients with TGCT affecting digits were discovered during
clinical data evaluation. 2815 TGCT patients affecting digits were identified (2649 fingers, 119 toes,
47 finger or toe), but not investigated in detail.

38
Chapter two
Reoperation rate due to local recurrence was defined as surgery for recurrent TGCT, based on
additional pathology reports in the same patient, at least 6 months after initial surgery until
January 2015 (date of PALGA-search).
Statistics
The Statistical Package for Social Sciences statistics (SPSS) version 23 was used for analyses.
The IR was separately estimated for TGCT localized-, either digits or extremity, and diffuse-type
TGCT per year, by using the number of histologically proven TGCT as numerator and the sum
of individual person-years for The Netherlands as the denominator. IRs were reported for the
overall study period, by calendar year, and stratified on type, affected joints, sex and 10-years age
categories (age at TGCT diagnosis). The Central Bureau of Statistics (CBS) provided information
on Dutch population during the examined period.
Overall worldwide IRs were obtained by standardizing Dutch IRs to global IRs by using the
direct method, applying age-specific IRs in each 10-year age group to the world WHO standard
population (http://seer.cancer.gov). Estimates of IRs were reported with 95% Confidence
Intervals (CI). Patient demographics were reported as counts and percentages for categorical
variables and as medians and interquartile ranges (IQR) for continuous variables. The Kaplan
Meier method was used to evaluate reoperation due to local recurrence free survival at 2- and
at 5-year.
Ethics, funding, and potential conflict of interest
Research is performed in accordance with the ethical standards in the 1964 Declaration of
Helsinki. As this study does not involve subject-related research, it is not covered by Dutch law on
human subjects research. This study is approved by the Institutional review board (CME) from our
institution (registration number G16.024, 22 April 2016). In collaboration of physicians of the TGCT
study group, and in special collaboration with Radboud University Medical Centre and Medical
Spectrum Twente, data collection was performed. Data capturing and analyses was performed
in the Leiden University Medical Centre. No funding or benefits were received, by none of the
authors. There is no conflict of interest by any of the authors regarding this manuscript.
Incidence rates in tenosynovial giant cell tumours
39
2
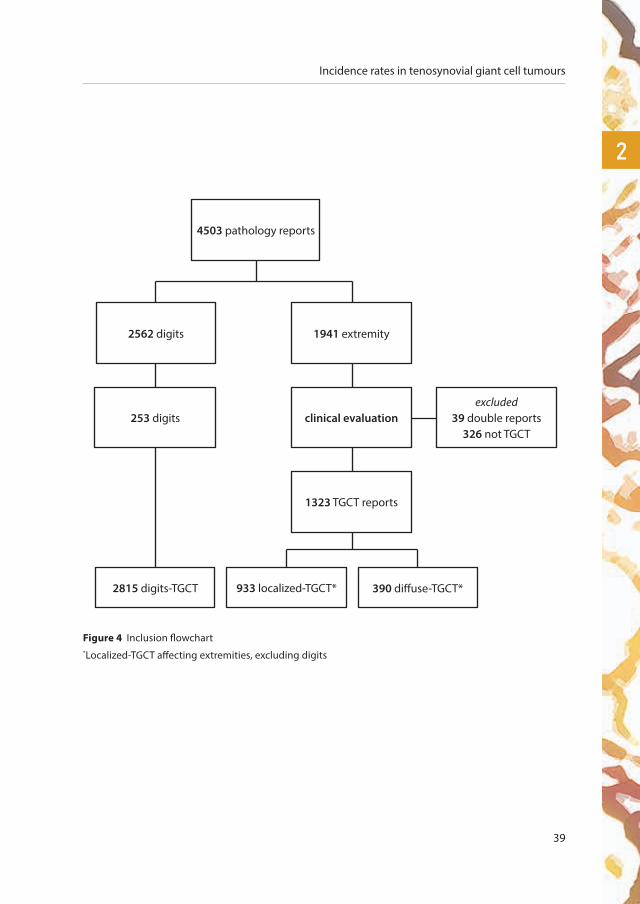
Figure 4 Inclusion flowchart *Localized-TGCT affecting extremities, excluding digits
2562 digits
4503 pathology reports
1941 extremity
clinical evaluation253 digitsexcluded
39 double reports326 not TGCT
1323 TGCT reports
2815 digits-TGCT 933 localized-TGCT* 390 diffuse-TGCT*

40
Chapter two
Table 1 Incidence rates (IRs) of localized- and diffuse-type TGCT in The Netherlands:
overall, by calendar year 2009-2013, sex and age-categories.
Person-years
Localized TGCT – digits Localized TGCT – extremity Diffuse TGCT
New cases* IR** New cases* IR** New cases* IR**
Overall 83,226,498 2815 33.8 (33 - 35) 933 11.2 (11 - 12) 390 4.7 (4 - 5)
Calendar year
2009 16,485,787 578 35.1 (32 - 38) 192 11.7 (10 - 13) 73 4.4 (4 - 6)
2010 16,574,989 561 33.8 (31 - 37) 183 11.0 (10 - 13) 82 5.0 (4 - 6)
2011 16,655,799 580 34.8 (32 - 38) 176 10.6 (9 - 12) 78 4.7 (4 - 6)
2012 16,730,348 563 33.6 (31 - 37) 188 11.2 (10 - 13) 77 4.6 (4 - 6)
2013 16,779,575 533 31.8 (29 - 35) 194 11.6 (10 - 13) 80 4.8 (4 - 6)
Sex
Female 42,032,934 1698 (60) 40.4 (39 - 42) 544 (58) 12.9 (12 - 14) 236 (61) 5.6 (5 - 6)
Male 41,193,564 1117 (40) 27.1 (26 - 29) 389 (42) 9.4 (9 - 10) 154 (39) 3.7 (3 - 4)
Age at diagnosis
0-9 9,528,271 13 (0) 1.4 (1 - 2) 6 (1) 0.6 (0 - 1) 2 (0) 0.2 (0 - 1)
10-19 10,012,994 98 (3) 9.8 (8 - 12) 57 (6) 5.7 (4 - 7) 26 (7) 2.6 (2 - 4)
20-29 10,178,289 259 (9) 25.4 (23 - 29) 108 (11) 10.6 (9 - 13) 49 (13) 4.8 (4 - 6)
30-39 10,673,194 411 (15) 38.5 (35 - 42) 169 (18) 15.8 (14 - 18) 62 (16) 5.8 (5 - 7)
40-49 12,894,743 650 (23) 50.4 (47 - 54) 211 (23) 16.4 (14 - 19) 70 (18) 5.4 (4 - 7)
50-59 11,456,662 704 (25) 61.5 (57 - 66) 193 (21) 16.9 (15 - 19) 71 (18) 6.2 (5 - 8)
60-69 9,466,681 503 (18) 53.1 (49 - 58) 133 (14) 14.0 (12 - 17) 58 (15) 6.1 (5 - 8)
70-79 5,680,080 155 (6) 27.3 (23 - 32) 41 (4) 7.2 (5 - 10) 37 (9) 6.5 (5 - 9)
80-89 2,860,556 22 (1) 7.7 (5 - 12) 15 (2) 5.2 (3 - 9) 15 (4) 5.2 (3 - 9)
*New cases: number of cases, %. **IR: Incidence rate per million person-years (95% CI).

Incidence rates in tenosynovial giant cell tumours
41
2Table 1 Incidence rates (IRs) of localized- and diffuse-type TGCT in The Netherlands:
overall, by calendar year 2009-2013, sex and age-categories.
Person-years
Localized TGCT – digits Localized TGCT – extremity Diffuse TGCT
New cases* IR** New cases* IR** New cases* IR**
Overall 83,226,498 2815 33.8 (33 - 35) 933 11.2 (11 - 12) 390 4.7 (4 - 5)
Calendar year
2009 16,485,787 578 35.1 (32 - 38) 192 11.7 (10 - 13) 73 4.4 (4 - 6)
2010 16,574,989 561 33.8 (31 - 37) 183 11.0 (10 - 13) 82 5.0 (4 - 6)
2011 16,655,799 580 34.8 (32 - 38) 176 10.6 (9 - 12) 78 4.7 (4 - 6)
2012 16,730,348 563 33.6 (31 - 37) 188 11.2 (10 - 13) 77 4.6 (4 - 6)
2013 16,779,575 533 31.8 (29 - 35) 194 11.6 (10 - 13) 80 4.8 (4 - 6)
Sex
Female 42,032,934 1698 (60) 40.4 (39 - 42) 544 (58) 12.9 (12 - 14) 236 (61) 5.6 (5 - 6)
Male 41,193,564 1117 (40) 27.1 (26 - 29) 389 (42) 9.4 (9 - 10) 154 (39) 3.7 (3 - 4)
Age at diagnosis
0-9 9,528,271 13 (0) 1.4 (1 - 2) 6 (1) 0.6 (0 - 1) 2 (0) 0.2 (0 - 1)
10-19 10,012,994 98 (3) 9.8 (8 - 12) 57 (6) 5.7 (4 - 7) 26 (7) 2.6 (2 - 4)
20-29 10,178,289 259 (9) 25.4 (23 - 29) 108 (11) 10.6 (9 - 13) 49 (13) 4.8 (4 - 6)
30-39 10,673,194 411 (15) 38.5 (35 - 42) 169 (18) 15.8 (14 - 18) 62 (16) 5.8 (5 - 7)
40-49 12,894,743 650 (23) 50.4 (47 - 54) 211 (23) 16.4 (14 - 19) 70 (18) 5.4 (4 - 7)
50-59 11,456,662 704 (25) 61.5 (57 - 66) 193 (21) 16.9 (15 - 19) 71 (18) 6.2 (5 - 8)
60-69 9,466,681 503 (18) 53.1 (49 - 58) 133 (14) 14.0 (12 - 17) 58 (15) 6.1 (5 - 8)
70-79 5,680,080 155 (6) 27.3 (23 - 32) 41 (4) 7.2 (5 - 10) 37 (9) 6.5 (5 - 9)
80-89 2,860,556 22 (1) 7.7 (5 - 12) 15 (2) 5.2 (3 - 9) 15 (4) 5.2 (3 - 9)
*New cases: number of cases, %. **IR: Incidence rate per million person-years (95% CI).
42
Chapter two
results
During a 5-year period; 2815 (68%) digits, 933 (23%) localized-extremity and 390 (9%) diffuse-type
TGCT were identified. TGCT affected digits 3 and 7 times more often compared to localized-extremity
and diffuse-TGCT, respectively. Dutch TGCT IRs were 34 (CI 33 - 35) in TGCT affecting digits, 11 (CI 11
- 12) in localized-type extremity TGCT and 5 (CI 4 - 5) in diffuse-type TGCT per million person-years.
Median age for TGCT affecting digits was 49 (IQR 38-59) years, for localized-extremity type 45 (IQR
34-56) years and diffuse-TGCT 47 (IQR 32-61) years. Male-female ratio was about 1:1.5 for any type.
Table 1 shows IRs per million person-years by calendar years 2009 up to and including 2013, sex
and 10 year age-specific categories of the 3 different TGCT-groups. In these 3 groups: IRs over
disaggregated years were quiet similar, female IR were slightly higher compared to male IRs and the
majority of new cases were seen in age-categories 40-49 and 50-59 years.
In 2015, The Netherlands counted 16,900,726 inhabitants. According to calculated IR; 571 new TGCT
affecting digits, 189 new localized-extremity and 79 new diffuse-TGCT patients were diagnosed
in 2015. The estimated standardized worldwide IRs were 29, 10 and 4 per million person-years for
respectively localized-digits, localized-extremity and diffuse-TGCT.
As TGCT affecting digits were not clinically investigated, following results were based on localized-
extremity and diffuse-type. The majority of TGCT cases affected the knee-joint; 46% and 64% in localized-
and diffuse-TGCT respectively (figure 5), followed by the hand- and wrist-joint in localized-type and the
ankle- and hip-joint in diffuse-type TGCT. Sex distribution per affected joint was comparable.
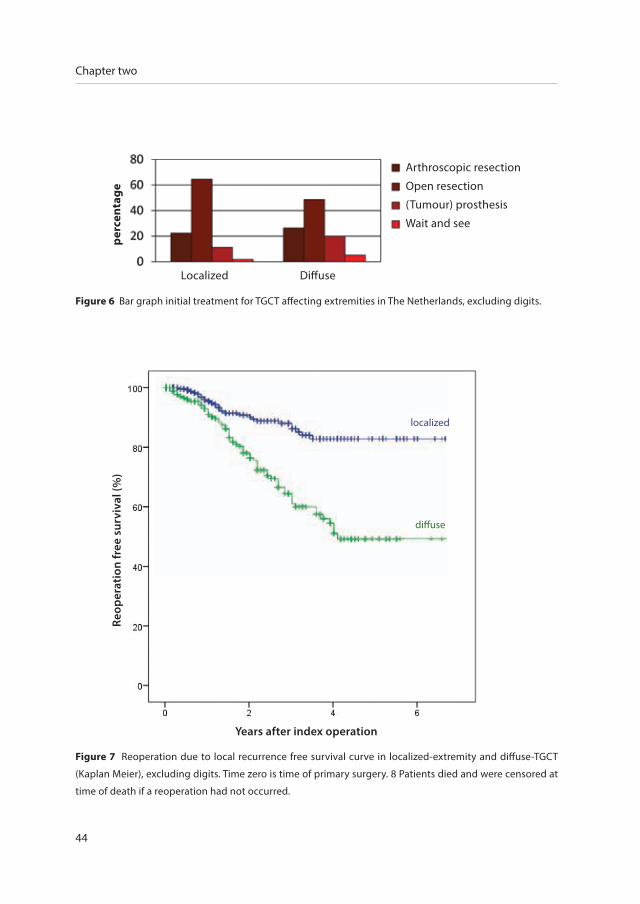
The initial TGCT treatment plan was open resection in 65% and 49% in localized- and diffuse-
lesions, respectively (figure 6). TGCT was reported as an incidental finding during endoprosthetic
replacement in 60 procedures.
According to the clinical charts, the majority of patients were lost to follow-up in both types (71%
in localized- and 55% in diffuse-TGCT). Therefore, we decided to base recurrence rates on additional
surgeries (defined by a second pathology report documenting recurrence of TGCT in PALGA). By
evaluating the municipal personal records database (Gemeentelijke BasisAdministratie (GBA)) for

Incidence rates in tenosynovial giant cell tumours
43
2all patients, 8 patients (7 localized- and 1 diffuse-TGCT) deceased at time of evaluation and were
censored at time of death when no second surgery was performed.
Reoperation rate due to local recurrence, calculated as a percentage from all TGCT patients, in localized-
TGCT was 9% and in diffuse-TGCT 23%. Reoperation free survival curves for localized- and diffuse-TGCT are
shown in figure 7. In localized-extremity, reoperation free survival at 2- and at 5-years was 90% and 83%,
respectively. In diffuse-type, reoperation free survival at 2- and at 5-years was 77% and 49%, respectively.
Only a minority (12%) of TGCT patients were primarily treated in a tertiary oncology centre: 9% of
localized-type (excluding digits) and 18% of diffuse-type.
1%
2%
1%12%24%
46%
5%
6%
localized-TGCT diffuse-TGCT
3%
2%
9%5%2%
64%
10%
4%
Figure 5 Skeleton, showing affected TGCT localization (fingers and toes excluded).
3% in localized-type and 1% in diffuse-type is classified as ‘other’ .
44
Chapter two
Figure 7 Reoperation due to local recurrence free survival curve in localized-extremity and diffuse-TGCT
(Kaplan Meier), excluding digits. Time zero is time of primary surgery. 8 Patients died and were censored at
time of death if a reoperation had not occurred.
Figure 6 Bar graph initial treatment for TGCT affecting extremities in The Netherlands, excluding digits.
Localized
perc
enta
ge
Diffuse
Years after index operation
Reop
erat
ion
free
sur
viva
l (%
)
Arthroscopic resection
Open resection
(Tumour) prosthesis
Wait and see
localized
diffuse

Incidence rates in tenosynovial giant cell tumours
45
2discussion Microscopically localized-extremity and diffuse-TGCT are identical1. A distinction is made
between localized-digits and localized-extremity, based on anatomical location and histological
differences3, 4. TGCT affecting digits are characterized as multiple, small (average 1 centimetres)
nodules surrounded by a thin fibrous capsule, originating in synovial tissue of tendon sheaths or
small joints of digits, with a small number of cleft-like spaces and thick bundles of collagenous
tissue, showing rarely inflammatory cells. On the contrary, TGCT localized-extremity lesions are
typically single, relatively large (average 2 centimetres) lesions covered by 1 or more layers of
synovial cells, intra-articular, showing large or numerous pseudoglandular spaces sometimes
filled with foam cells and showing more inflammatory cells than digits3.
Because of the rarity of the disease, current TGCT literature contains predominantly retrospective,
relatively small cohort studies, including heterogeneous data4. 2 previous studies described
TGCT incidence: Myers and Masi (1980) reported 117 new cases of localized- (including digits)
and 49 new cases of diffuse-type TGCT between 1960 and 1976, resulting in an IR of 9 per million
person-years for localized- and 2 per million person years for diffuse-type TGCT. A single hospital
study was performed by Monoghan et al. (2001) and showed an IR of 20 new cases per million
per year between 1990 and 1997 for localized-type TGCT (including digits). Compared to the
initial US-county study14, our study showed a 5-fold higher IR in localized-type (combining
localized-digits and localized-extremity), and a more than 2.6 fold higher IR in diffuse-type. This
difference could be attributed to our nationwide coverage, our registry based-clinically verified
character and because of increased knowledge about the disease.
Localized- and diffuse-lesions are distinguished clinically and on MRI. To investigate these
lesions separately, clinical and radiological confirmation is of utmost importance. Treatment
in localized-TGCT affecting digits or extremity is mostly 1 single excision. In contrast, multiple
mutilating surgeries are often required for diffuse-type TGCT, with a continuous risk of
recurrences. In an effort to find all TGCT patients, our search included specific pathology codes
for TGCT and both TGCT and synonyms of TGCT as free text (Appendix). Therefore, cases with
‘synovitis’ or differential diagnostic TGCT were represented in our search. In addition, PALGA
data is based on input of physicians and sometimes lacks specificity. For instance affected joint:
46
Chapter two
‘upper extremity’, ‘hand’ or ‘wrist’ could all turn out, after clinical evaluation, to be affected digits.
In our search, 1941 patients were clinically evaluated and 1323 ascertained histologically proven
TGCT extremity cases were included. Consequently, only 68% of eligible TGCT patients had
histologically proven TGCT of the large joints. Without clinical TGCT-confirmation, the estimated
IR would have been much higher.
Despite our large number of patients with lack of follow-up, reoperation rates due to local
recurrence were described, based on additional surgeries, defined by a second pathology
report documenting recurrence of TGCT in PALGA (up to January 2015, date PALGA-search
was performed). Recurrences without treatment (no additional pathology report) were not
included, therefore reoperation rate due to recurrence is not identical to recurrence rate.
However, compared to literature, we found comparable average recurrence rates for localized-
TGCT-extremity (9%) and for diffuse-type (23%)8. As local recurrence might develop years after
initial surgery18, and PALGA provided pathology reports with a maximum of 7 years after initial
surgery, underestimation of the true recurrence free survival is likely.
There are some limitations to this study. Determined IR may be exposed to under- or
overestimation. Primarily, our calculated IR could be slightly underestimated, because our study
is based on a search in PALGA, the nationwide network and registry of histo- and cytopathology
in The Netherlands15. TGCT patients without a biopsy or treatment are not represented in this
pathology based cohort.
Second, our IR in localized-extremity and diffuse-type could be marginally over- or
underestimated, because 21% of eligible TGCT patients was not clinically evaluated and
therefore imputed. Analyses with and without imputed data were comparable. PALGA identified
1941 eligible TGCT patients, scattered over 95 Dutch hospitals. Regarding different hospital-
boards, different concerning departments (pathology, orthopaedics, general surgery) and
different local legislations, it was challenging to evaluate all eligible TGCT patients.
Third, clinical distinction between localized-extremity and diffuse-type TGCT is difficult,
especially for clinicians not familiar with this rare disease19.
Subsequently, an overestimation of IR in TGCT localized-digits might be present. IR of digits is
solely based on PALGA-registry numbers, in contrast to localized-extremity and diffuse-TGCT IRs

Incidence rates in tenosynovial giant cell tumours
47
2which were clinically evaluated.
Global IRs were estimated by using a direct standardization approach (http://seer.cancer.gov).
Even though this is a widely accepted method, there is no adjustment for other influences in
global structure or possible risk factors in TGCT.
To calculate prevalence rates, follow-up time and status is important. Majority of our investigated
patients lacked in clinical chart follow-up. It seemed unfair to estimate TGCT prevalence rates as
the proportion of TGCT patients alive at the end of 2013 and diagnosed with TGCT: this assumes
TGCT to not resolve and not to be cured.
In The Netherlands, traditionally, larger orthopaedic clinics have been treating TGCT or diagnosed
TGCT as an incidental finding during arthroscopy or endoprosthetic replacement. When (severe)
complaints occur, patients are commonly referred to specialized tertiary sarcoma centres. In this
study, we investigated primary patients to calculate incidence rate. No centralization of care
of TGCT in these primary patients is shown, with only a minority of 12% primarily treated in a
tertiary oncology centre. Remarkably, only 18% of diffuse-TGCT was primarily treated in tertiary
oncology centres.
In summary, this study is the first nationwide study and detailed analyses of IRs in TGCT. IRs
for TGCT of digits, localized-type-extremity and diffuse-type were calculated using additional
hospital record evaluation of patients originally selected from a nationwide pathology registry.
The worldwide estimated incidence rate in digits, localized-extremity and diffuse-TGCT is 29,
10 and 4 per million person-years, respectively. Despite high clinical variability in localized-
extremity and diffuse-lesions, both types show a predilection for the knee-joint, slight
predisposition in female patients, median age around 47 years at first treatment and primarily
treated with an open resection. Recurrence rate in diffuse-type is 2.6 times higher, compared to
localized-type extremity. TGCT is still considered a rare disease, however, more common than
previously understood.
Supplementary data
An appendix is available as supplementary data in the online version of this article,
http://dx.doi.org/10.1080/17453674.2017.1361126
48
Chapter two
references
1. de St. Aubain Somerhausen N, van de Rijn M. Tenosynovial giant cell tumour, localized type/diffuse type. In: Fletcher
CD, Bridge JA, Hogendoorn PC, Mertens F, editors. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4th ed.
Lyon: IARC Press; 2013. p. 100-3.
2. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis:
radiologic-pathologic correlation. Radiographics. 2008;28(5):1493-518.
3. Ushijima M, Hashimoto H, Tsuneyoshi M, Enjoji M. Giant cell tumor of the tendon sheath (nodular tenosynovitis). A
study of 207 cases to compare the large joint group with the common digit group. Cancer. 1986;57(4):875-84.
4. Chiari C, Pirich C, Brannath W, Kotz R, Trieb K. What affects the recurrence and clinical outcome of pigmented
villonodular synovitis? Clin Orthop Relat Res. 2006;450:172-8.
5. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review
and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
6. Verspoor FG, van der Geest IC, Vegt E, Veth RP, van der Graaf WT, Schreuder HW. Pigmented villonodular synovitis:
current concepts about diagnosis and management. Future oncology. 2013;9(10):1515-31.
7. Fotiadis E, Papadopoulos A, Svarnas T, Akritopoulos P, Sachinis NP, Chalidis BE. Giant cell tumour of tendon sheath of
the digits. A systematic review. Hand (N Y). 2011;6(3):244-9.
8. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach
to giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg
Oncol. 2013;107(4):433-45.
9. Gonzalez Della Valle A, Piccaluga F, Potter HG, Salvati EA, Pusso R. Pigmented villonodular synovitis of the hip: 2- to
23-year followup study. Clin Orthop Relat Res. 2001(388):187-99.
10. Mollon B, Lee A, Busse JW, Griffin AM, Ferguson PC, Wunder JS, et al. The effect of surgical synovectomy and
radiotherapy on the rate of recurrence of pigmented villonodular synovitis of the knee: an individual patient meta-
analysis. Bone Joint J. 2015;97-B(4):550-7.
11. Griffin AM, Ferguson PC, Catton CN, Chung PW, White LM, Wunder JS, et al. Long-term outcome of the treatment
of high-risk tenosynovial giant cell tumor/pigmented villonodular synovitis with radiotherapy and surgery. Cancer.
2012;118(19):4901-9.
12. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the
surgical treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone
Joint J. 2014;96-B(8):1111-8.
13. de St. Aubain Somerhausen N, Dal Cin P. Gaint cell tumour of tendon sheath/Diffuse-type giant cell tumour. In:
Fletcher CD, Unni KK, Mertens F, editors. World Health Organization Classification of Tumours Pathology and Genetics
of Tumours of Soft Tissue and Bone. Lyon: IARC Press; 2002. p. 109-14.
14. Myers BW, Masi AT. Pigmented villonodular synovitis and tenosynovitis: a clinical epidemiologic study of 166 cases
and literature review. Medicine (Baltimore). 1980;59(3):223-38.
15. Casparie M, Tiebosch AT, Burger G, Blauwgeers H, van de Pol A, van Krieken JH, et al. Pathology databanking and
biobanking in The Netherlands, a central role for PALGA, the nationwide histopathology and cytopathology data
network and archive. Cell Oncol. 2007;29(1):19-24.
16. Verschoor A, Bovee J, van de Sande M, Gelderblom H. Incidence and demographics of giant cell containing tumors
in the Netherlands: a nationwide pathology database study. Annual Meeting of the Connective Tissue Oncology
Society; November 4-7; Salt Lake City, Utah, USA2015.
Incidence rates in tenosynovial giant cell tumours
49
217. Rubin DB. Multiple imputation after 18+ years. Journal of the American Statistical Association. 1996;91(434):473-89.
18. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
19. Flandry F, Hughston JC, McCann SB, Kurtz DM. Diagnostic features of diffuse pigmented villonodular synovitis of the
knee. Clinical orthopaedics and related research. 1994(298):212-20.

diag
nos
tics
does csF1 over-expression
or rearrangement influence
biological behaviour in
tenosynovial giant cell tumours of the knee?
chap
ter
thre
e
M.J.L. Mastboom1, D.M. Hoek2, J.V.M.G. Bovee3, M.A.J. van de Sande*1, K. Szuhai*2
Histopathology 2018 Aug. doi: 10.1111/his.13744

1 Orthopaedic Surgery, Leiden University Medical Center, Leiden, the Netherlands
2 Cell and Chemical biology, Leiden University Medical Center, Leiden, the Netherlands
3 Pathology, Leiden University Medical Center, Leiden, the Netherlands
*Authors contributed equally to this work.

CSF1 in tenosynovial giant cell tumours
53
3
abstract
Introduction
Localized- and diffuse-type tenosynovial giant cell tumours (TGCT) are regarded different
clinical and radiological TGCT-types. However, genetically and histopathologically they seem
indistinguishable. We aimed to correlate CSF1-expression and CSF1-rearrangement with the
biological behaviour of different TGCT-types with clinical outcome (recurrence).
Methods
Along a continuum of extremes, therapy naïve knee TGCT patients with >3 year follow-up, mean
age 43(range 6-71)years and 56% female were selected. Nine localized-(two recurrences), 16
diffuse-type(nine recurrences) and four synovitis as control were included. Rearrangement of
the CSF1-locus was evaluated with split-apart Fluorescence In Situ Hybridization (FISH) probes.
Regions were selected to score after identifying CSF1-expressing regions, using mRNA ISH with
the help of digital correlative microscopy. CSF1-rearrangement was considered positive in samples
containing >2 split signals/100 nuclei.
Results
Irrespective of TGCT-subtype, all cases showed CSF1-expression and in 76% CSF1-rearrangement
was detected. Quantification of CSF1-expressing cells was not informative, due to the extensive
intra tumour heterogeneity. Of the four synovitis cases, two also showed CSF1-expression, without
CSF1-rearrangement. No correlation between CSF1-expression or rearrangement with clinical
subtype and local recurrence was detected. Both localized- and diffuse-TGCT cases showed a
scattered distribution in the tissue of CSF1-expressing cells.
Conclusion
In diagnosing TGCT, CSF1 mRNA-ISH in combination with CSF1 split-apart FISH; using digital
correlative microscopy, is an auxiliary diagnostic tool to identify rarely occurring neoplastic cells.
This combined approach allowed us to detect CSF1-rearrangement in 76% of the TGCT-cases.
Neither CSF1-expression nor presence of CSF1-rearrangement could be associated with the
difference in biological behaviour of TGCT.

54
Chapter three
introduction
Tenosynovial giant cell tumour (TGCT), previously known as pigmented villonodular synovitis (PVNS)
and giant cell tumour of tendon sheath, is a rare, neoplastic lesion arising from the synovial lining of
joints, bursae or tendon sheaths in predominantly young adults. Excluding digits, this mono-articular
disease is most commonly diagnosed around the knee or other weight bearing joints1-3.
Initially, TGCT was believed to be an inflammatory disease4. After genomic aberrations were
discovered, TGCT was evidently considered neoplastic5-10. Chromosomal aberrations include
trisomy for chromosomes 5 and 7 and translocations involving the short arm of chromosome 1p11-
13, most commonly translocated to chromosome 2q37 region. At the 1p13 breakpoint, Colony
Stimulating Factor 1 (CSF1) gene is located. The translocation leads to a classical promoter fusion
event in which collagen 6A3 (COL6A3) promoter element is fused to CSF1. As a result, the fusion
leads to deregulated expression of CSF111. The excessive CSF1 secretion attracts inflammatory cells
that express the CSF1 receptor (CSF1R) (i.e. monocytes and macrophages). Consequently, in TGCT
tissue, only a small percentage of cells (2-16%) are neoplastic, carrying the t(1;2) translocation.
This phenomenon is coined as “the landscape effect”11, 12. Based on CSF1 rearrangements
(translocation), two groups are described. The first group is defined by both CSF1 over-expression
and CSF1 translocation, whereas the second group lacks the classical translocation. The latter
group likely carries other rearrangements altering CSF1 regulation leading to high CSF1 mRNA
and CSF1 protein levels12.
According to the 2013 WHO classification, TGCT is subdivided in a lobulated well circumscribed
lesion (localized-type) and a more locally aggressive lesion, involving a large part or all of the
synovial lining (diffuse-type)1, 2, 13 (figure 1). Standard choice of treatment was surgical resection of
the lesional tissue, either arthroscopically or with an open resection14-17. The localized-type TGCT is
known with a favourable course after resection (average recurrence rates <6%), while the diffuse-
type TGCT generally causes significant morbidity due to the high risk of local recurrence (>50%
depending on surgical procedure and follow-up time)15, 18, 19. Therefore, at present diffuse-type
TGCT is also treated with CSF1 inhibitors, such as nilotinib, imatinib, pexidartinib, emactuzumab,
cabrilazimab and MSC11020. Long term efficacy data have not yet been reported with these newer
agents.

CSF1 in tenosynovial giant cell tumours
55
3
Recurrent TGCT is rarely lethal, but a chronic illness with substantial morbidity to the joint leading
to functional and quality of life impairment, caused by the course of the disease itself and multiple
treatments21. Clinically, localized- and diffuse-TGCT are clearly two very different diseases. However,
histopathologically they seem indistinguishable with both subtypes containing an admixture of
mononuclear cells (histiocyte-like and larger cells) and multinucleated giant cells, lipid-laden foamy
macrophages (also known as xanthoma cells), siderophages (macrophages including hemosiderin-
depositions), stroma with lymphocytic infiltrate and some degree of collagenisation1, 2.
It remains unclear why localized- and diffuse-TGCT are microscopically and genetically identical,
but clinically distinct. Moreover, predictors for progressive disease or local recurrence are lacking.
In this study, we investigate whether CSF1 over-expression and rearrangement are correlated
with tumour characteristics (localized-/diffuse-TGCT) and clinical outcome (recurrence). We
hypothesize that diffuse-type TGCT, compared with localized-type TGCT, would have a higher load
of neoplastic cells. We expect that a higher tumour load is associated with recurrent disease.
Figure 1 Localized- and diffuse-TGCT sagittal T1-weighted MR image after intravenous contrast injection with
fat suppression. Tumour region enhances by contrast injection. a. A localized-TGCT involving Hoffa’s fat pad
in the anterior part of the left knee in a 55-year-old female patient (L4835). b. Left knee in a 61-year-old male
patient with extensive recurrent diffuse-TGCT located intra- and extra-articular with an additional posterior
large Baker’s cyst including tumour (L3496).

56
Chapter three
methods
Case acquisition and study design
Subtypes of TGCT (localized- or diffuse) were defined based on clinical features and radiological
imaging according to 2013 WHO1, 2. Along a continuum of extremes, 25 patients with TGCT
affecting the knee were carefully selected: patients with small or very large localized or diffuse
lesions, with and without recurrent disease. All cases showed all characteristic histological features
of TGCT (mononuclear cells, giant cells, macrophages, siderophages, foam cells or lymphocyte-
clusters). Included patients were therapy naïve (one diagnostic arthroscopy elsewhere was
allowed) and treated with open synovectomy at the Leiden University Medical Centre (LUMC).
A clinical follow-up of at least three years was required for inclusion. For comparison, we used
tissue specimens of four patients with non-TGCT synovitis. Written informed consent was
obtained from all patients. This study was performed in accordance with the Code of Conduct
for responsible use in The Netherlands (Dutch Federation of Medical Scientific Societies) and
approved by the local medical ethical committee (P13.029).
Inclusion selected cases and tissue specimens
Nine localized- and 16 diffuse-type TGCT patients were included, mean age at surgery of 43
(range 6-71) years, mean follow-up of 57 (range 36-121) months (table 1), with a slight female
predominance (56%). Two localized- and nine diffuse-type TGCT patients had recurrent disease,
after mean 26 (range 14-53) months. The mean age at surgery of the four patients with non-TGCT
synovitis was 53 (range 44-65) years, including two (50%) females.
For each patient, multiple formalin-fixed paraffin-embedded (FFPE) tissue blocks and
corresponding Haematoxylin and Eosin stained (H&E) 4 μm slides of the primary resected
specimen were reviewed by an expert bone and soft tissue pathologist (JVMGB) to confirm TGCT
diagnosis and to select representative areas of the tumour with highest proportion of suspected
neoplastic cells.
A large tissue heterogeneity was observed between the different blocks. As a control for the
landscaped CSF1 mRNA expression, multiple blocks were selected for three cases (L4046, L3496
and L4954) representing various tissue compositions.
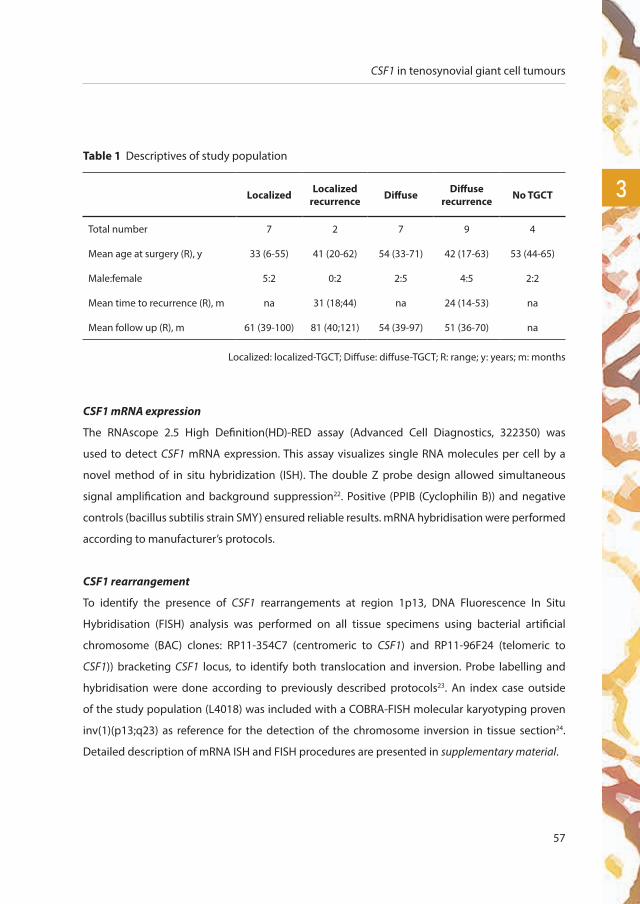
CSF1 in tenosynovial giant cell tumours
57
3
CSF1 mRNA expression
The RNAscope 2.5 High Definition(HD)-RED assay (Advanced Cell Diagnostics, 322350) was
used to detect CSF1 mRNA expression. This assay visualizes single RNA molecules per cell by a
novel method of in situ hybridization (ISH). The double Z probe design allowed simultaneous
signal amplification and background suppression22. Positive (PPIB (Cyclophilin B)) and negative
controls (bacillus subtilis strain SMY) ensured reliable results. mRNA hybridisation were performed
according to manufacturer’s protocols.
CSF1 rearrangement
To identify the presence of CSF1 rearrangements at region 1p13, DNA Fluorescence In Situ
Hybridisation (FISH) analysis was performed on all tissue specimens using bacterial artificial
chromosome (BAC) clones: RP11-354C7 (centromeric to CSF1) and RP11-96F24 (telomeric to
CSF1)) bracketing CSF1 locus, to identify both translocation and inversion. Probe labelling and
hybridisation were done according to previously described protocols23. An index case outside
of the study population (L4018) was included with a COBRA-FISH molecular karyotyping proven
inv(1)(p13;q23) as reference for the detection of the chromosome inversion in tissue section24.
Detailed description of mRNA ISH and FISH procedures are presented in supplementary material.
Table 1 Descriptives of study population
Localized Localized recurrence Diffuse Diffuse
recurrence No TGCT
Total number 7 2 7 9 4
Mean age at surgery (R), y 33 (6-55) 41 (20-62) 54 (33-71) 42 (17-63) 53 (44-65)
Male:female 5:2 0:2 2:5 4:5 2:2
Mean time to recurrence (R), m na 31 (18;44) na 24 (14-53) na
Mean follow up (R), m 61 (39-100) 81 (40;121) 54 (39-97) 51 (36-70) na
Localized: localized-TGCT; Diffuse: diffuse-TGCT; R: range; y: years; m: months

58
Chapter three
Scoring and correlative analysis
All slides were scanned in brightfield and/or fluorescence on a Pannoramic P250 or MIDI digital scanner
(3DHistech, Budapest, Hungary). Scanned images were visualized using the Pannoramic Viewer (V2.1;
3DHistech). Interpretation was performed manually by a senior FISH expert (KS), blinded towards TGCT-
type and clinical outcome. Because CSF1 expressing regions were expected to contain neoplastic cells,
three of these regions were selected. With the use of digital correlative microscopy, regions with CSF1
mRNA expressing (supposed neoplastic) cells were identified and the same areas were scored after
FISH analysis. If the distance between the two signals was larger than the size of a single hybridization
signal, cells were recorded CSF1 split positive. All nuclei within the selected area with a complete set of
signals were evaluated. Nuclei with an incomplete set of signals were excluded from counting. Samples
containing >2/100 nuclei with a CSF1 split were considered CSF1 split positive.
results
CSF1 mRNA expression
Specimens of all localized- and diffuse-TGCT cases showed a scattered, tissue infiltrating distribution of
CSF1 expressing cells (figure 2). Corresponding to the landscape effect, heterogeneous distribution of
CSF1 expressing cells were observed when sections from multiple bock were analysed, meaning that
regions completely devoid CSF1 expressing cells were seen in regions containing large proportion of
foam cells or regions with lymphocytic infiltrates. CSF1 mRNA pattern expression was not observed in
multinucleate giant cells, siderophages or foam cells. Consequently, due to the great heterogeneity
between different blocks derived from one tumour and within regions in one section, quantification
of CSF1 expressing cells, meaning the expression of the proportion of CSF1 positive cells, was not
informative and was not further analysed (supplementary material figure 1). Selecting the block with
the highest possible neoplastic cell component, we did not observe a clear difference in distribution
of CSF1 between different TGCT cases. Cells with CSF1 mRNA expression were distributed diffusely
and showed an infiltrating scattered pattern throughout the sections with some clustering at various
regions within a tissue element (figure 2, supplementary material figure 2 and 3).
For the control cases, two of the four cases with synovitis showed expression of CSF1 (L5619, L5620).
However, in these two cases CSF1 expression was restricted to cells localised in the synovial lining,
which was different from the scattered distribution seen in TGCT (figure 3). The other two cases with
synovitis showed no expression of CSF1 (L3715, L5622).
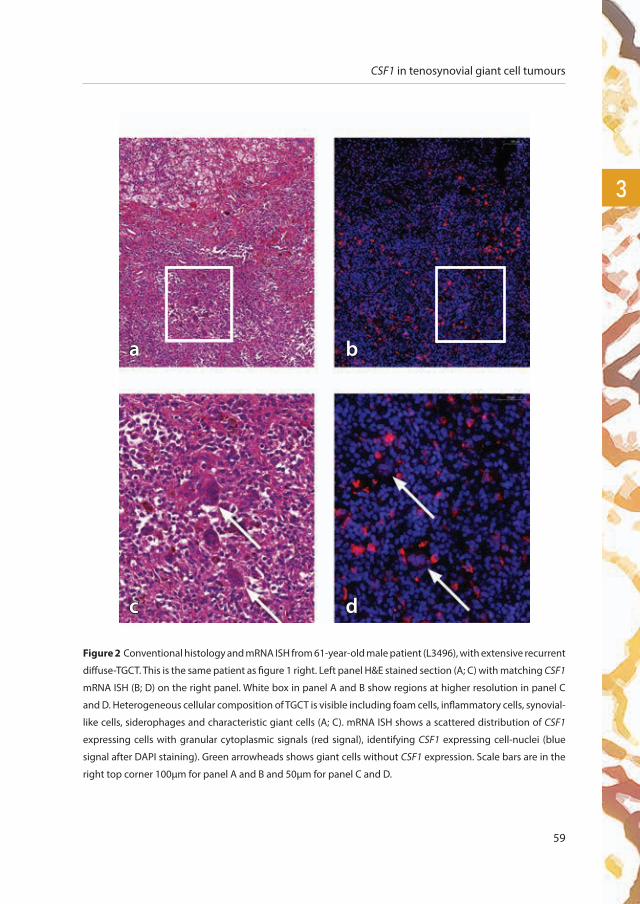
CSF1 in tenosynovial giant cell tumours
59
3
Figure 2 Conventional histology and mRNA ISH from 61-year-old male patient (L3496), with extensive recurrent
diffuse-TGCT. This is the same patient as figure 1 right. Left panel H&E stained section (A; C) with matching CSF1
mRNA ISH (B; D) on the right panel. White box in panel A and B show regions at higher resolution in panel C
and D. Heterogeneous cellular composition of TGCT is visible including foam cells, inflammatory cells, synovial-
like cells, siderophages and characteristic giant cells (A; C). mRNA ISH shows a scattered distribution of CSF1
expressing cells with granular cytoplasmic signals (red signal), identifying CSF1 expressing cell-nuclei (blue
signal after DAPI staining). Green arrowheads shows giant cells without CSF1 expression. Scale bars are in the
right top corner 100µm for panel A and B and 50µm for panel C and D.
a b
c d
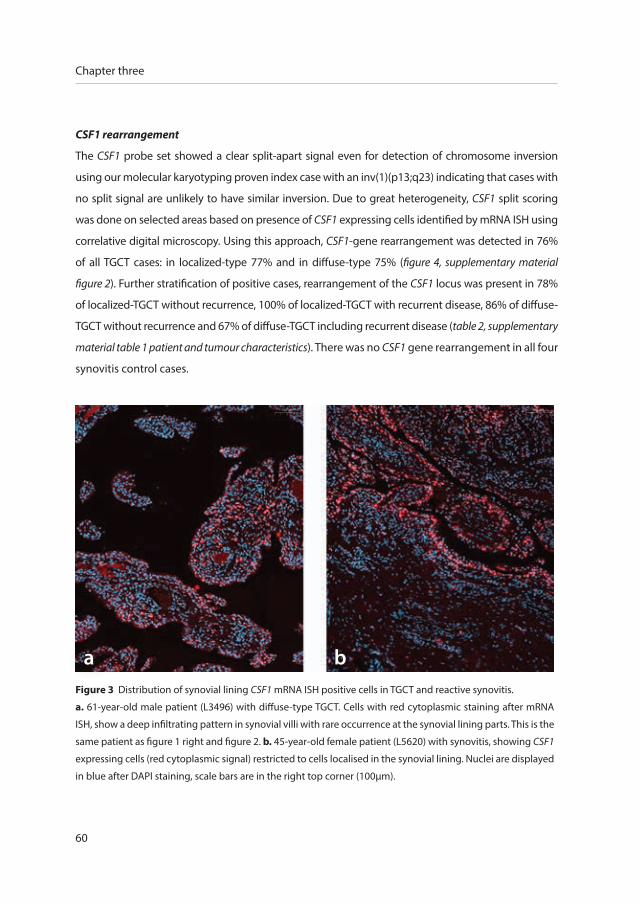
60
Chapter three
CSF1 rearrangement
The CSF1 probe set showed a clear split-apart signal even for detection of chromosome inversion
using our molecular karyotyping proven index case with an inv(1)(p13;q23) indicating that cases with
no split signal are unlikely to have similar inversion. Due to great heterogeneity, CSF1 split scoring
was done on selected areas based on presence of CSF1 expressing cells identified by mRNA ISH using
correlative digital microscopy. Using this approach, CSF1-gene rearrangement was detected in 76%
of all TGCT cases: in localized-type 77% and in diffuse-type 75% (figure 4, supplementary material
figure 2). Further stratification of positive cases, rearrangement of the CSF1 locus was present in 78%
of localized-TGCT without recurrence, 100% of localized-TGCT with recurrent disease, 86% of diffuse-
TGCT without recurrence and 67% of diffuse-TGCT including recurrent disease (table 2, supplementary
material table 1 patient and tumour characteristics). There was no CSF1 gene rearrangement in all four
synovitis control cases.
a bFigure 3 Distribution of synovial lining CSF1 mRNA ISH positive cells in TGCT and reactive synovitis.
a. 61-year-old male patient (L3496) with diffuse-type TGCT. Cells with red cytoplasmic staining after mRNA
ISH, show a deep infiltrating pattern in synovial villi with rare occurrence at the synovial lining parts. This is the
same patient as figure 1 right and figure 2. b. 45-year-old female patient (L5620) with synovitis, showing CSF1
expressing cells (red cytoplasmic signal) restricted to cells localised in the synovial lining. Nuclei are displayed
in blue after DAPI staining, scale bars are in the right top corner (100µm).
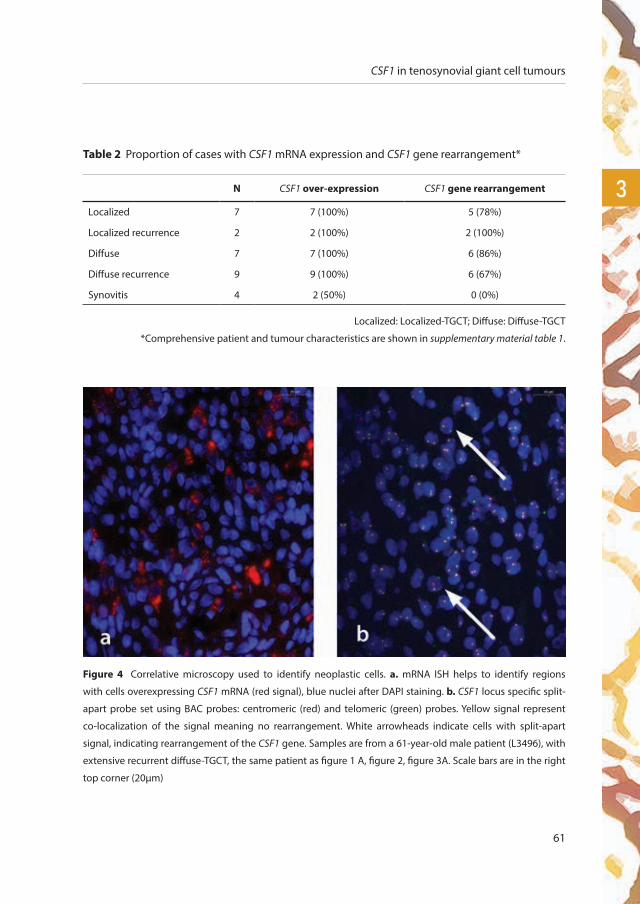
CSF1 in tenosynovial giant cell tumours
61
3
Table 2 Proportion of cases with CSF1 mRNA expression and CSF1 gene rearrangement*
N CSF1 over-expression CSF1 gene rearrangement
Localized 7 7 (100%) 5 (78%)
Localized recurrence 2 2 (100%) 2 (100%)
Diffuse 7 7 (100%) 6 (86%)
Diffuse recurrence 9 9 (100%) 6 (67%)
Synovitis 4 2 (50%) 0 (0%)
Localized: Localized-TGCT; Diffuse: Diffuse-TGCT
*Comprehensive patient and tumour characteristics are shown in supplementary material table 1.
Figure 4 Correlative microscopy used to identify neoplastic cells. a. mRNA ISH helps to identify regions
with cells overexpressing CSF1 mRNA (red signal), blue nuclei after DAPI staining. b. CSF1 locus specific split-
apart probe set using BAC probes: centromeric (red) and telomeric (green) probes. Yellow signal represent
co-localization of the signal meaning no rearrangement. White arrowheads indicate cells with split-apart
signal, indicating rearrangement of the CSF1 gene. Samples are from a 61-year-old male patient (L3496), with
extensive recurrent diffuse-TGCT, the same patient as figure 1 A, figure 2, figure 3A. Scale bars are in the right
top corner (20µm)

62
Chapter three
Figure 5 Proposed workflow
for molecular pathology w
ork up of TGC
T cases
Num
bers represent TGC
T cases in this study
CSF1, Colony Stimulating Factor1; m
RNA
ISH, m
RNA
In Situ Hybridization; D
NA
FISH, D
NA
Fluorescence In Situ Hybridisation

CSF1 in tenosynovial giant cell tumours
63
3
discussion
Localized- and diffuse-type TGCT are histopathologically identical and carry the same chromosomal
translocation, leading to uncontrolled over-expression of CSF1 due to a gene fusion between
COL6A3 and CSF1 genes. Undeniably, localized- and diffuse-type TGCT are clinically different
diseases. In a well-defined TGCT population with >3 years follow-up, molecular differences in
primary resected tissue between both subtypes and clinical outcome (recurrence) were evaluated.
We were unable to find a clear association between CSF1 over-expression or CSF1 rearrangement
and the biological behaviour in TGCT of the knee.
In this study, 76% CSF1 rearrangement was detected when lumping all our 25 cases together,
compared with 61% of the evaluated cases by Cupp et al.12. Further subdivided, our study revealed
no difference in CSF1 rearrangement for localized-TGCT (77%) and diffuse-TGCT (75%). On the
contrary, West et al. reported a large difference between these two types; 87% rearrangement
in localized- and 35% in diffuse-TGCT11. The relatively high percentage of rearrangement in our
study, could be attributed to our scoring on preselected areas, based on high CSF1 expression.
In addition, our DNA FISH analysis, using bacterial artificial chromosome (BAC) clones (RP11-
354C7 and RP11-96F24) bracketing CSF1 locus, identifies not only a translocation, but also an
inversion for CSF1 rearrangements. Panagopoulous et al. revealed a CSF1-S100A10 fusion gene,
with translocation t(1;1)(q21;p11) as the sole karyotypic abnormality25. Nilsson et al. found that
30% of the TGCT specimens did not have a rearrangement involving the 1p13 locus, where CSF1
is located using split-apart interphase FISH approach, similar to ours8. Next to the translocation,
Panagopoulos et al. reported the replacement of the 3’-UTR of CSF1, resulting in over-expression
or a longer lifetime of CSF1 mRNA due to loss of the 3-UTR controlling region25. Similar cryptic
changes leading to loss of smaller gene region involving the 3’-UTR segment of CSF1 are beyond
the detection level of our FISH probes. Next to this, other, yet not identified alterations leading to
deregulated CSF1 expression cannot be ruled out in cases with CSF1 mRNA expression without
CSF1 rearrangement of the CSF1 locus.
Up to date, clinically reliable antibodies working on FFPE tissue sections to detect CSF1 or CSF1R
are lacking. Therefore, mRNA ISH was the best regarded option to identify CSF1 over-expressing
cells. Consistent with previous reports, all 25 evaluated cases showed CSF1 up-regulation11. Exact

64
Chapter three
determination of the proportion of CSF1 expressing cells was considered not meaningful, since in
all tumours considerable intratumoural heterogeneity was observed between selected blocks and
with individual tissue sections, reflecting the “landscape effect”11. This heterogeneity prevents any
conclusion on the true neoplastic cell load in the tumour and a possible correlation to clinical outcome.
Deregulated CSF1 expression is believed to be the central mechanism of tumourigenesis for TGCT.
CSF1, also called macrophage colony-stimulating factor, is a cytokine, produced by many different
cell types including macrophages, fibroblasts, endothelial cells and osteoblasts (and other cancer
types, especially in bone metastasis)26. CSF1 is expressed in neoplastic cells infiltrating throughout
the lesion. Secreted CSF1 recruits non-neoplastic macrophages into the tumour. By binding to
its receptor CSF1R (type III receptor tyrosine kinase), CSF1 promotes survival, proliferation and
differentiation of cells of the mononuclear phagocyte lineage (e.g. monocytes, macrophages and
osteoclasts)27, 28. Besides its general biological function, CSF1 is also involved in inflammatory or
reactive synovitis (rheumatoid arthritis, chronic artritis) and cancer (breast, endometrial, ovarian,
lung, kidney)12, 27. When CSF1 is expressed in reactive synovitis, its expression is restricted to cells in
the synovial lining12, 29, as was confirmed in our synovitis control cases.
Inhibition of signalling between CSF1 and CSF1R targets the underlying cause of the disease29,
30. The involvement of this pathway contributed to the introduction of systemic therapies for
extensive diffuse-TGCT20. Primarily, imatinib31 or related drugs as nilotinib32 showed efficacy
in the treatment. Recently, new CSF1R blockers were developed and are investigated in clinical
trials; Emactuzumab and Cabiralizumab (FPA008) both monoclonal antibodies directed against
CSF1R33-35; Pexidartinib (PLX3397; retains CSF1R in inactive state)29, and MSC110 (an antagonist of
the CSF1 ligand)35. Emactuzumab (N=29) showed an overall response rate of 86% (two patients
with a complete response) and a rate of disease control of 96%, including a significant functional
and symptomatic improvement (median follow up 12 months)33. The preliminary results for
cabiralizumab (N=22) are consistent, with radiographic response and improvement in pain and
function in five out of 11 patients (45%)34. In a randomized, placebo-controlled phase 3 study,
pexidartinib showed an improved overall response rate by RECIST: 39% in the pexidartinib-group
(N=61) and 0% of placebo-group (N=59), after median six months follow-up36. However, long term
results still need to be evaluated with these newer agents.

CSF1 in tenosynovial giant cell tumours
65
3
Within our well-defined patient cohort, all patients had a minimum follow-up of three years.
However, patients without recurrent disease at the time of analysis could still develop this in due
course, since it is known that local recurrence might develop years after initial surgery1, 2, 15, 19, 37.
Verspoor et al. calculated an overall recurrence rate of 72% in 75 patients with diffuse-TGCT of the
knee with a mean follow-up from index treatment of 13.9 years. They suggested a trend towards
the longer the follow-up, the greater the number of recurrences19.
In conclusion, DNA FISH analysis, using bacterial artificial chromosome (BAC) clones (RP11-354C7
and RP11-96F24) bracketing CSF1 locus, can identify both chromosomal rearrangement caused
translocation or inversion of the CSF1 locus. Figure 5 summarizes the workflow in the current
study and the proposed workflow for molecular pathology work up of TGCT cases. The use of CSF1
mRNA ISH in combination with CSF1 split-apart FISH is an auxiliary diagnostic tool to confirm the
diagnosis of TGCT. This combined approach allowed us to detect CSF1-gene rearrangement in 76%
of the TGCT cases. At the molecular level, localized- and diffuse-type TGCT are indistinguishable
when evaluating CSF1 expression and the presence of the pathognomonic translocation involving
the CSF1 gene.
Supplementary data
Supplementary data are available in the online version of this article, doi: 10.1111/his.13744

66
Chapter three
Supplementary figure 1 Low power magnification overview of TGCT case from a 61-year-old male patient
(L3496), the same patient as figure 1 A, figure 2, figure 3A, figure 4. a. Hematoxyllin-eosin staining. b. CSF1
mRNA ISH (red) of the same case depicting identical regions, nuclei are stained with DAPI (blue). White
arrowheads indicate blood vessels with erythrocytes, giving a strong red fluorescing signal. A heterogeneous
distribution of CSF1 expressing cells with remarkable variation in their distribution in the tissue is clearly visible.
White squared inset, indicates regions in high power magnification shown in details in figure 2. Scale bars are
in the right top corner (500 µm).
Supplementary figure 2 (right page) Overview of TGCT localized case without
recurrence from a 55-year-old female patient (L4385), presented in figure 1A. a
& b. Hematoxillin-eosin staining low and high power overview. b & d. CSF1 mRNA
ISH (red) of the same case depicting identical regions, nuclei are stained with DAPI
(blue). In panel B a white squared inset indicate the region shown in high power
magnification in panel D. e. Using correlative microscope areas with more neoplastic
cells (mRNA ISH positive cells) were identified and scored for CSF1 locus specific
split-apart probe set using BAC probes. Yellow signal represent co-localization
of the signal meaning no rearrangement. White arrowheads indicate cells with
split-apart signal, indicating rearrangement of the CSF1 gene. Scale bars are at the
bottom left corners and 500 and 20 µm for low and high power images, respectively.
a b

CSF1 in tenosynovial giant cell tumours
67
3
a b
c d
e

68
Chapter three
Supplementary figure 3 Correlative microscope image comparing sections after hematoxillin-eosin staining
(a) and CSF1 mRNA ISH (b) of a diffuse, non-recurrent TGCT case from a 50-year-old male patient (L3697).
Diffuse infiltrating CSF1 expressing cells are present throughout the section. Scale bars are at the left bottom
corner (200 µm).
a
b

CSF1 in tenosynovial giant cell tumours
69
3
references
1. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4 ed2013. p. 100-1.
2. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, diffuse type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 52013. p. 102-3.
3. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence rates
than previously known in tenosynovial giant cell tumors. Acta orthopaedica. 2017:1-7.
4. Jaffe HL LL, Sutro CJ. Pigmented Villonodular Synovitis, Bursitis and Tenosynovitis. Arch Pathol. 1941(31):731-65.
5. Fletcher JA, Henkle C, Atkins L, Rosenberg AE, Morton CC. Trisomy 5 and trisomy 7 are nonrandom aberrations in
pigmented villonodular synovitis: confirmation of trisomy 7 in uncultured cells. Genes, chromosomes & cancer.
1992;4(3):264-6.
6. Mertens F, Orndal C, Mandahl N, Heim S, Bauer HF, Rydholm A, et al. Chromosome aberrations in tenosynovial giant cell
tumors and nontumorous synovial tissue. Genes, chromosomes & cancer. 1993;6(4):212-7.
7. Ohjimi Y, Iwasaki H, Ishiguro M, Kaneko Y, Tashiro H, Emoto G, et al. Short arm of chromosome 1 aberration recurrently
found in pigmented villonodular synovitis. Cancer genetics and cytogenetics. 1996;90(1):80-5.
8. Nilsson M, Hoglund M, Panagopoulos I, Sciot R, Dal Cin P, Debiec-Rychter M, et al. Molecular cytogenetic mapping of
recurrent chromosomal breakpoints in tenosynovial giant cell tumors. Virchows Archiv : an international journal of
pathology. 2002;441(5):475-80.
9. Sciot R, Rosai J, Dal Cin P, de Wever I, Fletcher CD, Mandahl N, et al. Analysis of 35 cases of localized and diffuse tenosynovial
giant cell tumor: a report from the Chromosomes and Morphology (CHAMP) study group. Modern pathology : an official
journal of the United States and Canadian Academy of Pathology, Inc. 1999;12(6):576-9.
10. Brandal P, Bjerkehagen B, Heim S. Molecular cytogenetic characterization of tenosynovial giant cell tumors. Neoplasia.
2004;6(5):578-83.
11. West RB, Rubin BP, Miller MA, Subramanian S, Kaygusuz G, Montgomery K, et al. A landscape effect in tenosynovial
giant-cell tumor from activation of CSF1 expression by a translocation in a minority of tumor cells. Proc Natl Acad Sci U
S A. 2006;103(3):690-5.
12. Cupp JS, Miller MA, Montgomery KD, Nielsen TO, O’Connell JX, Huntsman D, et al. Translocation and expression of CSF1
in pigmented villonodular synovitis, tenosynovial giant cell tumor, rheumatoid arthritis and other reactive synovitides.
The American journal of surgical pathology. 2007;31(6):970-6.
13. Mastboom MJL, Verspoor FGM, Hanff DF, Gademan MGJ, Dijkstra PDS, Schreuder HWB, Bloem JL, van der Wal RJP, van de
Sande MAJ. Severity classification of Tenosynovial Giant Cell Tumours on MR imaging. Surg Oncol. 2018;27(3):544-550.
14. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review
and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
15. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.
16. Patel KH, Gikas PD, Pollock RC, Carrington RW, Cannon SR, Skinner JA, et al. Pigmented villonodular synovitis of the knee:
A retrospective analysis of 214 cases at a UK tertiary referral centre. Knee. 2017;24(4):808-15.
17. Griffin AM, Ferguson PC, Catton CN, Chung PW, White LM, Wunder JS, et al. Long-term outcome of the treatment of
high-risk tenosynovial giant cell tumor/pigmented villonodular synovitis with radiotherapy and surgery. Cancer.
2012;118(19):4901-9.
70
Chapter three
18. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
19. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
20. Brahmi M, Vinceneux A, Cassier PA. Current Systemic Treatment Options for Tenosynovial Giant Cell Tumor/Pigmented
Villonodular Synovitis: Targeting the CSF1/CSF1R Axis. Current treatment options in oncology. 2016;17(2):10.
21. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical
treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J.
2014;96-B(8):1111-8.
22. Wang F, Flanagan J, Su N, Wang LC, Bui S, Nielson A, et al. RNAscope: a novel in situ RNA analysis platform for formalin-
fixed, paraffin-embedded tissues. The Journal of molecular diagnostics : JMD. 2012;14(1):22-9.
23. Szuhai K, Bezrookove V, Wiegant J, Vrolijk J, Dirks RW, Rosenberg C, et al. Simultaneous molecular karyotyping and
mapping of viral DNA integration sites by 25-color COBRA-FISH. Genes, chromosomes & cancer. 2000;28(1):92-7.
24. Szuhai K, Tanke HJ. COBRA: combined binary ratio labeling of nucleic-acid probes for multi-color fluorescence in situ
hybridization karyotyping. Nature protocols. 2006;1(1):264-75.
25. Panagopoulos I, Brandal P, Gorunova L, Bjerkehagen B, Heim S. Novel CSF1-S100A10 fusion gene and CSF1 transcript
identified by RNA sequencing in tenosynovial giant cell tumors. International journal of oncology. 2014;44(5):1425-32.
26. Hung JY, Horn D, Woodruff K, Prihoda T, LeSaux C, Peters J, et al. Colony-stimulating factor 1 potentiates lung cancer
bone metastasis. Laboratory investigation; a journal of technical methods and pathology. 2014;94(4):371-81.
27. Achkova D, Maher J. Role of the colony-stimulating factor (CSF)/CSF-1 receptor axis in cancer. Biochemical Society
transactions. 2016;44(2):333-41.
28. Barreda DR, Hanington PC, Belosevic M. Regulation of myeloid development and function by colony stimulating factors.
Developmental and comparative immunology. 2004;28(5):509-54.
29. Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, et al. Structure-Guided Blockade of CSF1R Kinase in
Tenosynovial Giant-Cell Tumor. The New England journal of medicine. 2015;373(5):428-37.
30. Peyraud F, Cousin S, Italiano A. CSF-1R Inhibitor Development: Current Clinical Status. Current oncology reports.
2017;19(11):70.
31. Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, et al. Efficacy of imatinib mesylate for the
treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis.
Cancer. 2012;118(6):1649-55.
32. Gelderblom H, Cropet C, Chevreau C, Boyle R, Tattersall M, Stacchiotti S, et al. Nilotinib in locally advanced pigmented
villonodular synovitis: a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2018.
33. Cassier PA, Italiano A, Gomez-Roca CA, Le Tourneau C, Toulmonde M, Cannarile MA, et al. CSF1R inhibition with
emactuzumab in locally advanced diffuse-type tenosynovial giant cell tumours of the soft tissue: a dose-escalation and
dose-expansion phase 1 study. Lancet Oncol. 2015;16(8):949-56.

CSF1 in tenosynovial giant cell tumours
71
334. Sankhala KK, Blay JY, Ganjoo KN, Italiano A, Hassan AB, Kim TM, Ravi V, Cassier PA, Rutkowski P, Sankar N, Qazi I, Sikorski RS,
Collins H, Zhang C, Shocron E, Gelderblom H. A phase I/II dose escalation and expansion study of cabiralizumab (cabira;
FPA-008), an anti-CSF1R antibody, in tenosynovial giant cell tumor (TGCT, diffuse pigmented villonodular synovitis
D-PVNS). Am. Soc. Clin. Oncol. 2017;Conference: 2017 Annual Meeting ASCO. United States. 35 (15 Supplement 1).
35. Hung M, Stuart AR, Higgins TF, Saltzman CL, Kubiak EN. Computerized Adaptive Testing Using the PROMIS Physical
Function Item Bank Reduces Test Burden With Less Ceiling Effects Compared With the Short Musculoskeletal Function
Assessment in Orthopaedic Trauma Patients. Journal of orthopaedic trauma. 2014;28(8):439-43.
36. Tap WD, Gelderblom H, Stacchiotti S, Palmerini E, Ferrari S, Desai J, et al. Final results of ENLIVEN: A global, double-blind,
randomized, placebo-controlled, phase 3 study of pexidartinib in advanced tenosynovial giant cell tumor (TGCT). ASCO
conference; 2018; Chicago.
37. Mastboom MJL, Verspoor FGM, Gelderblom H, van de Sande MAJ. Limb Amputation after Multiple Treatments of
Tenosynovial Giant Cell Tumour: Series of 4 Dutch Cases. Case reports in orthopedics. 2017;2017:7402570.


sev
erit
yseverity
classification of tenosynovial
giant cell tumours on mr imaging
chap
ter
four
M.J.L. Mastboom*1, F.G.M. Verspoor*2, D.F. Hanff3, M.G.J. Gademan4, P.D.S. Dijkstra1, H.W.B. Schreuder2, J.L. Bloem3,
R.J.P. van der Wal1, M.A.J. van de Sande1
Surgical oncology. 2018 Sept;27(3):544-550

1 Orthopaedic Surgery, Leiden University Medical Centre, Leiden, the Netherlands
2 Orthopaedic Surgery, Radboud University Medical Centre, Nijmegen, the Netherlands
3 Radiology, Leiden University Medical Centre, Leiden, the Netherlands
4 Clinical Epidemiology, Leiden University Medical Centre, Leiden, the Netherlands
*Authors contributed equally to this work.
Severity classification of tenosynovial giant cell tumours
75
4
abstract
Aim
Current development of novel systemic agents requires identification and monitoring of extensive
Tenosynovial Giant Cell Tumours (TGCT). This study defines TGCT extension on MR imaging to
classify severity.
Methods
In part one, six MR parameters were defined by field-experts to assess disease extension on MR
images: type of TGCT, articular involvement, cartilage-covered bone invasion, and involvement of
muscular/tendinous tissue, ligaments or neurovascular structures. Inter- and intra-rater agreement
were calculated using 118 TGCT MR scans. In part two, the previously defined MR parameters were
evaluated in 174 consecutive, not previously used, MR-scans. TGCT severity classification was
established based on highest to lowest Hazard Ratios (HR) on first recurrence.
Results
In part one, all MR parameters showed good inter- and intra-rater agreement (Kappa≥0.66). In
part two, cartilage-covered bone invasion and neurovascular involvement were rarely appreciated
(<13%) and therefore excluded for additional analyses. Univariate analyses for recurrent disease
yielded positive associations for type of TGCT HR12.84(95%CI4.60-35.81), articular involvement
HR6.00(95%CI2.14-16.80), muscular/tendinous tissue involvement HR3.50(95%CI1.75-7.01) and
ligament-involvement HR4.59(95%CI2.23-9.46). With these, a TGCT severity classification was
constructed with four distinct severity-stages. Recurrence free survival at 4 years (log rank p<0.0001)
was 94% in mild localized (n56, 1 recurrence), 88% in severe localized (n31, 3 recurrences), 59% in
moderate diffuse (n32, 12 recurrences) and 36% in severe diffuse (n55, 33 recurrences).
Conclusion
The proposed TGCT severity classification informs physicians and patients on disease extent and
risk for recurrence after surgical treatment. Definition of the most severe subgroup attributes to a
universal identification of eligible patients for systemic therapy or trials for novel agents.

76
Chapter four
introduction
Tenosynovial Giant Cell Tumour (TGCT) affecting large joints is an orphan, mono-articular,
potentially locally aggressive disease with high recurrence rates. According to the 2013 WHO
classification of tumours of soft tissue and bone, at the base of growth pattern, a radiological
distinction is made between single nodule (localized-TGCT) and multiple lesions (diffuse-TGCT).
These types differ in their clinical presentation, response to treatment and prognosis, but
histologically, they seem identical1-4.
Localized-type TGCT is classified as a circumscribed benign small (between 0.5 and 4 cm) mass1,
5. Standard treatment of choice is excision. Subsequently, overall reported recurrence rates are
relatively low: 0-6%6. On the contrary, diffuse-type TGCT, previously named Pigmented VilloNodular
Synovitis (PVNS), extensively involves the synovial membrane and infiltrates adjacent structures6,
7. Reported recurrence rates of diffuse-TGCT following open synovectomy are 14% up till 67% and
after arthroscopic synovectomy 40% up till 92%6. Recurrent or residual disease, frequently requiring
multiple, sometimes mutilating operations, may result in total joint arthroplasties, morbidity and
loss of quality of life8-12. With this large variety in disease presentation and recurrence rates, a
more comprehensive and outcome-based classification is asked for. The emerging era of systemic
targeted and multimodality therapies (available in trial settings) increases the need for a method
to select eligible patients in order to create comparable patient cohorts13-15.
In diagnosing and treating TGCT, magnetic resonance (MR) imaging is the most distinctive imaging
technique4, 16-19. MR imaging reveals conspicuous nodular (localized-type) or villous proliferation of
synovium (diffuse-type). However, current literature lacks specific MR discriminating features to
describe or quantify tumour extent in relation to clinical outcome. Uniform MR descriptions are
of utmost importance for clinical and research purposes. Therefore this study aims to sub-classify
tumour severity especially in diffuse-type TGCT. First, a group of radiologists and orthopaedic
surgeons identified and defined potentially distinguishing parameters. Second, these MR
parameters were applied on a different study-population to establish TGCT severity subgroups.
Severity classification of tenosynovial giant cell tumours
77
4
methods
Part I: Identification and evaluation of TGCT specific MR parameters
Using case discussions in expert meetings with two dedicated musculoskeletal radiologists and
three oncological orthopaedic surgeons, six MR parameters were selected in relation to anatomical
or surgical landmarks. These parameters were 1 type of TGCT (based on 2013 WHO classification1, 2),
2 articular involvement, 3 cartilage-covered bone invasion, 4 involvement of muscular/tendinous
tissue, 5 involvement of ligaments and 6 involvement of neurovascular structures (figure 1)
(Appendix).
To evaluate usability and reproducibility, 118 MR scans of TGCT patients, treated at the Leiden
University Medical Centre (LUMC), were randomly retrieved (MM). The six MR parameters were
evaluated in a heterogeneous group of TGCT cases as scans included cases of various large
joints (knee (79; 67%), ankle (13; 11%), foot (10; 9%)), severity subtypes and treatment phases.
MR scans were conducted using a 1.5 or 3.0 Tesla unit Philips (Best, The Netherlands) Ingenia MR
with dedicated coils. Standard musculoskeletal scan-protocol included: T1- and T2-weighted fast
spin echo, T1-weighted fat-suppressed post Gd-chelate contrast and optionally T2* gradient-
echo sequences in two planes (transversal and either sagittal or coronal). To assess inter- and
intra-rater agreement, all MR scans were evaluated by one dedicated musculoskeletal radiologist
(DH) and by two dedicated orthopaedic surgeons (RW, MS). MR evaluation was blinded to patient
characteristics.
Inter-rater agreement and accompanying 95% confidence interval (95% CI) between three
physicians was calculated for all 118 cases by Fleiss-Kappa (dichotomous outcomes in all parameters,
except for articular involvement with three outcomes). To evaluate intra-rater agreement with the
accompanying 95% CI (linear weighted kappa), 36 randomly chosen MR scans (31%) were again
evaluated three months after initial evaluation by the senior orthopaedic surgeon (MS).
Part II: Application of TGCT MR parameter
None of the MR scans in part I were used in part II. The combined TGCT-database of two sarcoma
centres in The Netherlands (LUMC and Radboud University Medical Centre (RUMC)) was used to
include consecutive MR scans conducted between 2005 and 2015 (n=283). MR scan inclusion
criteria were: pre-treatment MR scan of histologically proven TGCT of large joints, conducted in
two planes (transversal and either sagittal or coronal), and open resection as primary treatment
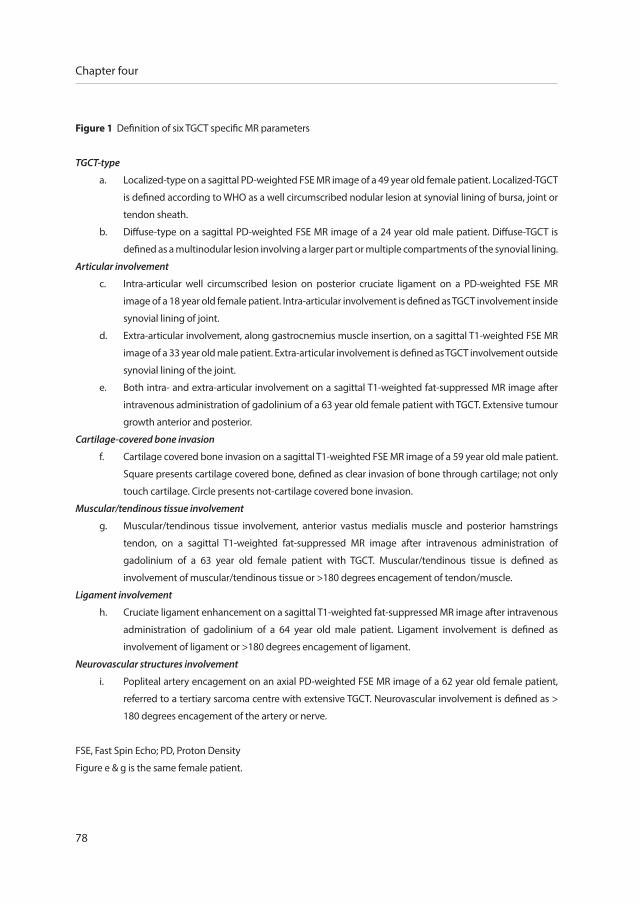
78
Chapter four
Figure 1 Definition of six TGCT specific MR parameters
TGCT-type
a. Localized-type on a sagittal PD-weighted FSE MR image of a 49 year old female patient. Localized-TGCT
is defined according to WHO as a well circumscribed nodular lesion at synovial lining of bursa, joint or
tendon sheath.
b. Diffuse-type on a sagittal PD-weighted FSE MR image of a 24 year old male patient. Diffuse-TGCT is
defined as a multinodular lesion involving a larger part or multiple compartments of the synovial lining.
Articular involvement
c. Intra-articular well circumscribed lesion on posterior cruciate ligament on a PD-weighted FSE MR
image of a 18 year old female patient. Intra-articular involvement is defined as TGCT involvement inside
synovial lining of joint.
d. Extra-articular involvement, along gastrocnemius muscle insertion, on a sagittal T1-weighted FSE MR
image of a 33 year old male patient. Extra-articular involvement is defined as TGCT involvement outside
synovial lining of the joint.
e. Both intra- and extra-articular involvement on a sagittal T1-weighted fat-suppressed MR image after
intravenous administration of gadolinium of a 63 year old female patient with TGCT. Extensive tumour
growth anterior and posterior.
Cartilage-covered bone invasion
f. Cartilage covered bone invasion on a sagittal T1-weighted FSE MR image of a 59 year old male patient.
Square presents cartilage covered bone, defined as clear invasion of bone through cartilage; not only
touch cartilage. Circle presents not-cartilage covered bone invasion.
Muscular/tendinous tissue involvement
g. Muscular/tendinous tissue involvement, anterior vastus medialis muscle and posterior hamstrings
tendon, on a sagittal T1-weighted fat-suppressed MR image after intravenous administration of
gadolinium of a 63 year old female patient with TGCT. Muscular/tendinous tissue is defined as
involvement of muscular/tendinous tissue or >180 degrees encagement of tendon/muscle.
Ligament involvement
h. Cruciate ligament enhancement on a sagittal T1-weighted fat-suppressed MR image after intravenous
administration of gadolinium of a 64 year old male patient. Ligament involvement is defined as
involvement of ligament or >180 degrees encagement of ligament.
Neurovascular structures involvement
i. Popliteal artery encagement on an axial PD-weighted FSE MR image of a 62 year old female patient,
referred to a tertiary sarcoma centre with extensive TGCT. Neurovascular involvement is defined as >
180 degrees encagement of the artery or nerve.
FSE, Fast Spin Echo; PD, Proton Density
Figure e & g is the same female patient.

Severity classification of tenosynovial giant cell tumours
79
4
a b c
d e f
g h i
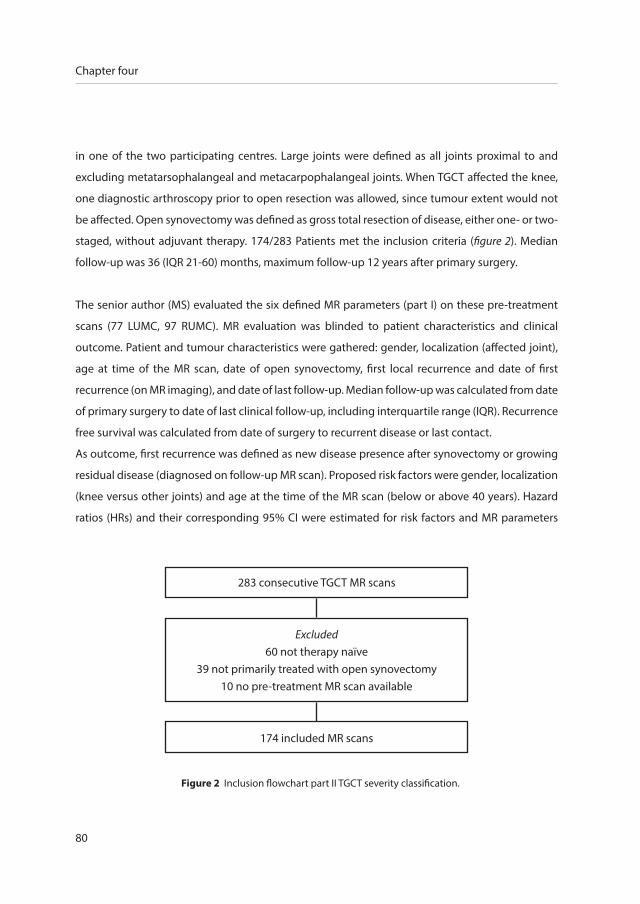
80
Chapter four
in one of the two participating centres. Large joints were defined as all joints proximal to and
excluding metatarsophalangeal and metacarpophalangeal joints. When TGCT affected the knee,
one diagnostic arthroscopy prior to open resection was allowed, since tumour extent would not
be affected. Open synovectomy was defined as gross total resection of disease, either one- or two-
staged, without adjuvant therapy. 174/283 Patients met the inclusion criteria (figure 2). Median
follow-up was 36 (IQR 21-60) months, maximum follow-up 12 years after primary surgery.
The senior author (MS) evaluated the six defined MR parameters (part I) on these pre-treatment
scans (77 LUMC, 97 RUMC). MR evaluation was blinded to patient characteristics and clinical
outcome. Patient and tumour characteristics were gathered: gender, localization (affected joint),
age at time of the MR scan, date of open synovectomy, first local recurrence and date of first
recurrence (on MR imaging), and date of last follow-up. Median follow-up was calculated from date
of primary surgery to date of last clinical follow-up, including interquartile range (IQR). Recurrence
free survival was calculated from date of surgery to recurrent disease or last contact.
As outcome, first recurrence was defined as new disease presence after synovectomy or growing
residual disease (diagnosed on follow-up MR scan). Proposed risk factors were gender, localization
(knee versus other joints) and age at the time of the MR scan (below or above 40 years). Hazard
ratios (HRs) and their corresponding 95% CI were estimated for risk factors and MR parameters
Figure 2 Inclusion flowchart part II TGCT severity classification.
283 consecutive TGCT MR scans
Excluded60 not therapy naïve
39 not primarily treated with open synovectomy10 no pre-treatment MR scan available
174 included MR scans

Severity classification of tenosynovial giant cell tumours
81
4
(part I) by univariate and multivariate Cox regression analyses to estimate the relation on recurrent
disease. Since estimating HR is unreliable for rarely present MR parameters, only parameters with
an adequate number of presence (minimum of 20%) were used for additional analyses. Recurrence
free survival close to median time of follow-up was calculated by Kaplan Meier analyses and log
rank test. Time zero was defined as date of primary open synovectomy.
At the base of HRs with positive associations of risk factors and MR parameters on first recurrences,
the TGCT severity classification was established. The TGCT subgroup flow chart started with the
MR parameter with highest HR, followed by descending HRs. Statistical Package for Social Statistics
(SPSS) version 23 was used for analyses.
Ethical statement
This study was approved by the institutional review board from our institution (registration
number P13.029). No funding was received.
results
Part I: Evaluation of TGCT specific MR parameters
Inter-rater agreements for type of TGCT, articular involvement, cartilage-covered bone invasion,
and involvement of muscular/tendinous tissue, ligaments or neurovascular structures were 0.71;
0.68; 0.66; 0.67; 0.75 and 0.73, respectively. Intra-rater agreements for these parameters were
between 0.72 and 1.00 (table 1). Since inter- and intra-rater agreements were good20 for these six
MR features, all parameters were considered viable to use for TGCT subgroup analyses.
Part II: Application of TGCT MR parameters
Out of 174 MR scans, the knee was affected most (122; 70%), followed by the ankle (20; 12%)
(table 2). In univariate analyses, none of the proposed risk factors were associated with recurrent
disease (p>0.37) (table 3) and consequently not used for further analyses. Both MR parameters
cartilage-covered bone invasion and involvement of neurovascular structures were rarely seen on
MR images (< 13%) and in accordance with our exclusion criteria not used for additional analyses.
In univariate analyses, the remaining four MR parameters were associated with recurrent disease
(p<0.002) (table 3); strongest association was seen in diffuse-type compared with localized-type

82
Chapter four
Table 1 Inter- and intra-rater agreement (kappa) in six M
R parameters
Agreem
entType of TG
CTA
rticular involvem
entCartilage-covered
bone invasion
Muscular/
tendinous tissue involvem
ent
Ligament
involvement
Neurovascular
involvement
Inter-rater0.71 (0.60-0.81)
0.68 (0.58-0.78)0.66 (0.56-0.76)
0.67 (0.56-0.77)0.75 (0.57-0.93)
0.73 (0.62-0.83)
Intra-rater0.94 (0.82-1.06)
0.89 (0.74-1.04)0.79 (0.39-1.19)
0.72 (0.50-0.94)0.86 (0.68-1.04)
1.00 (1.00-1.00)
Inter-rater, Agreement betw
een three physicians (one musculoskeletal radiologist, tw
o orthopaedic surgeons).
Intra-rater, Agreement for 31%
of MR scans initially evaluated and re-evaluated 3 m
onths thereafter by the senior orthopaedic surgeon.
Interpretation of inter- and intra-rater agreement (K-value) 20
Agreem
ent value Strength of agreem
ent
< 0.20
Poor
0.21 - 0.40 Fair
0.41 - 0.60 M
oderate
0.61 - 0.80 G
ood
0.81 - 1.00 Very good

Severity classification of tenosynovial giant cell tumours
83
4
(HR 12.84 (95%CI 4.60-35.81)), subsequently intra- and extra-articular involvement compared
with extra-articular (HR 6.00 (95%CI 2.14-16.80)) and involvement of muscular/tendinous tissue or
ligaments compared with no involvement (HR 3.50 (95%CI 1.75-7.01), HR 4.59 (95%CI 2.23-9.46),
respectively).
Multivariate analyses for MR parameters did not show individual positive association, except for
parameter type of TGCT (supplementary material I).
Four TGCT severity subtypes were established using a flowchart that begins with the parameters
with highest HR (parameter type of TGCT), followed by parameters with descending HRs. These
four subtypes showed a clinically relevant or significant prognostic value for recurrent disease
and were classified as: mild localized (n56, 1 recurrence), severe localized (n31, 3 recurrences),
moderate diffuse (n32, 12 recurrences) and severe diffuse (n55, 33 recurrences).
1. Mild localized contained localized-type, either intra- or extra-articular involvement
without involvement of muscular/tendinous tissue/ligaments.
2. Severe localized included localized-type, either intra- or extra-articular lesions and
either or both involvement of muscular/tendinous tissue/ligaments.
3. Moderate diffuse comprised diffuse-type with intra- and/or extra-articular disease
without involvement of muscular/tendinous tissue/ligaments.
4. Severe diffuse was diffuse-type including intra- and extra-articular involvement
and involvement of at least one of the three structures (muscular/tendinous tissue/
ligaments) (figure 3).
Recurrence free survival at 4 years (close to median follow-up diffuse-type) for the four patient
groups according to the new MR subtypes descended from 94% in mild localized, to 88% in severe
localized, to 59% in moderate diffuse and to 36% in the least favorable subtype, severe diffuse.
Median time to local recurrence in moderate diffuse and severe diffuse subtypes was 29.5 (IQR
14.5-48.0) and 22.0 (IQR 11.8-33.5) months, respectively. Majority of recurrent disease cases were
already treated with a re-operation (32/49, 65%). One patient, classified as severe diffuse, died of
another disease, after four months and was censored at that time. Novel MR based TGCT severity
and associated Kaplan Meier survival curves presented significant difference between the four
patient groups (log rank p<0.0001) and additional differentiation compared with solely sub-
classifying in localized- and diffuse-TGCT (figure 4 and supplementary material II).
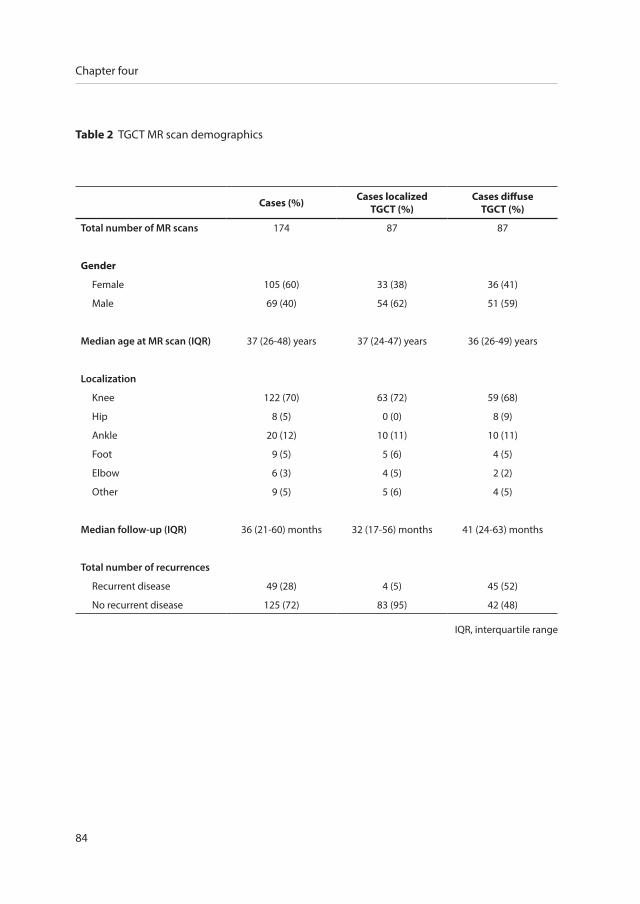
84
Chapter four
Table 2 TGCT MR scan demographics
Cases (%) Cases localizedTGCT (%)
Cases diffuseTGCT (%)
Total number of MR scans 174 87 87
Gender
Female 105 (60) 33 (38) 36 (41)
Male 69 (40) 54 (62) 51 (59)
Median age at MR scan (IQR) 37 (26-48) years 37 (24-47) years 36 (26-49) years
Localization
Knee 122 (70) 63 (72) 59 (68)
Hip 8 (5) 0 (0) 8 (9)
Ankle 20 (12) 10 (11) 10 (11)
Foot 9 (5) 5 (6) 4 (5)
Elbow 6 (3) 4 (5) 2 (2)
Other 9 (5) 5 (6) 4 (5)
Median follow-up (IQR) 36 (21-60) months 32 (17-56) months 41 (24-63) months
Total number of recurrences
Recurrent disease 49 (28) 4 (5) 45 (52)
No recurrent disease 125 (72) 83 (95) 42 (48)
IQR, interquartile range

Severity classification of tenosynovial giant cell tumours
85
4
Table 3 Risk of recurrence on MR imaging;
univariate analyses in proposed risk factors and four MR parameters.
n (%) Hazard ratio (95% CI) P
Gender
Male 69 (40) 1.29 (0.74-2.27) 0.37
Female 105 (60) 1
Age
<40 years 91 (52) 1.15 (0.66-2.02) 0.63
>40 years 83 (48) 1
Localization
Knee 122 (70) 1.15 (0.63-2.12) 0.65
Other joint 52 (30) 1
TGCT-type
Diffuse 87 (50) 12.84 (4.60-35.81) <0.000
Localized 87 (50) 1
Articular involvement
Intra-articular 59 (34) 1.11 (0.31-3.95) 0.87
Intra- and extra-articular 75 (43) 6.00 (2.14-16.80) 0.001
Extra-articular 40 (23) 1
Muscular/tendinous tissue involvement
Yes 90 (52) 3.50 (1.75-7.01) <0.000
No 84 (48) 1
Ligament involvement
Yes 86 (49) 4.59 (2.23-9.46) <0.000
No 88 (51) 1
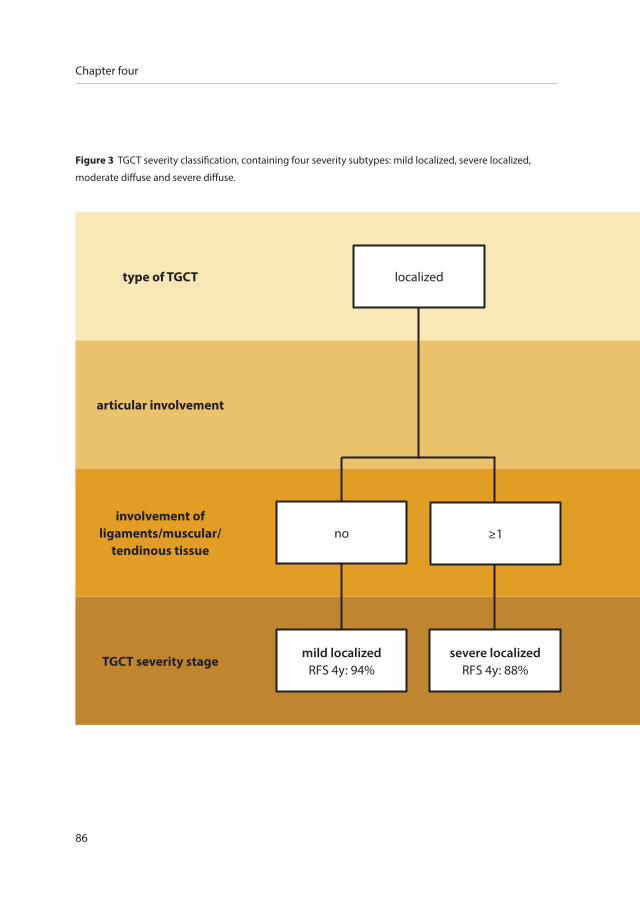
86
Chapter four
Figure 3 TGCT severity classification, containing four severity subtypes: mild localized, severe localized,
moderate diffuse and severe diffuse.
no ≥1
mild localizedRFS 4y: 94%
severe localizedRFS 4y: 88%
type of TGCT
articular involvement
involvement of ligaments/muscular/
tendinous tissue
TGCT severity stage
localized
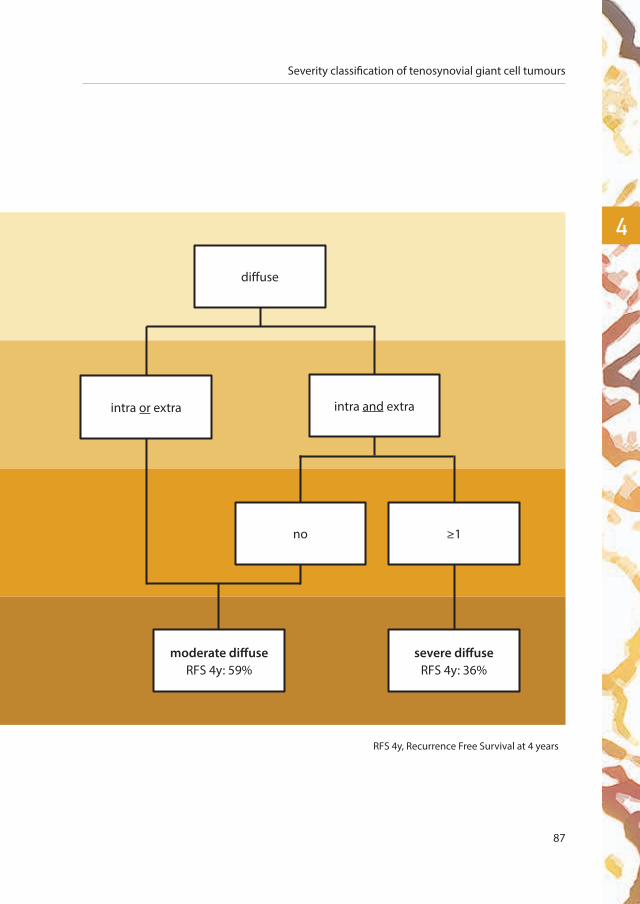
Severity classification of tenosynovial giant cell tumours
87
4
RFS 4y, Recurrence Free Survival at 4 years
diffuse
intra or extra intra and extra
no ≥1
moderate diffuseRFS 4y: 59%
severe diffuseRFS 4y: 36%

88
Chapter four
Time (years) 0 2 4 6 8
Number at risk 174 105 51 24 10
Figure 4 TGCT recurrence free survival curve for four TGCT severity subtypes, affecting large joints, estimated
with Kaplan Meier method. Time zero was date of primary open synovectomy. One patient, classified as severe
diffuse died of another disease after 4 months and was censored at that time.
Follow-up time (years)
Cum
ulat
ive
recu
rren
t TG
CT
severe diffuse
moderate diffuse
1.0
0.8
0.6
0.4
0.2
0 2 4 6 8
0.0
mild localized
severe localized
Severity classification of tenosynovial giant cell tumours
89
4
discussion
This is the first study to define severity subtypes in Tenosynovial Giant Cell Tumours (TGCT) based
on a combination of four MR imaging parameters. These subtypes correlate with a spectrum of
disease severity ranging from low to high risk of local recurrence after surgical intervention.
Within this present era of systemic targeted and multimodality therapies (available in trial settings)
in TGCT, standalone surgical resection cannot be regarded the gold standard anymore for more
severe cases21. Because of the lack of clear-cut boundaries in diffuse-TGCT, complete resection is
difficult and at times technically impossible or undesirable with joint function preservation and
quality of life in mind. In patients with locally advanced TGCT or (multiple) recurrence(s), systemic
therapies targeting the CSF1/CSF1R axis have been investigated; less potent drugs as nilotinib and
imatinib22, 23, and more specific inhibitors as emactuzumab (RG7155), pexidartinib (PLX3397) and
cabiralizumab (FPA008). Emactuzumab (N=29) had an overall response rate of 86% (two patients
with a complete response) and a rate of disease control of 96%, including a significant functional
and symptomatic improvement (median follow up 12 months)24. In a randomized, placebo-
controlled phase 3 study, pexidartinib showed an improved overall response rate by RECIST:
39% in the pexidartinib-group (N=61) and 0% of placebo-group (N=59), after median six months
follow-up25. The preliminary results with cabiralizumab (N=22) are consistent, with radiographic
response and improvement in pain and function in five out of 11 patients 2815. However, long term
efficacy data have not yet been reported with these newer agents.
Patient inclusion for these trials is very heterogeneous. A strict patient selection is desirable, to
accurately evaluate effect of these treatments. At present, patient selection for trial inclusion
is established by preference of treating physician and might differ per centre. Defining more
aggressive TGCT subtypes and including these uniformly defined patients into trials would more
adequately investigate the effect and toxicities of treatment26. In this study, we propose to include
patients defined with ‘severe diffuse’ TGCT subtype. Monitoring the effect of systemic therapy also
benefits from clear agreements on parameters.
Uniform MR descriptions are of utmost importance for clinical and research purposes. Thus far,
no well-defined tumour parameters exist. Definition of unambiguous MR criteria is challenging,

90
Chapter four
because of the rarity of the tumour and small number of heterogeneous cases, variety of joints
involved, different disease severity as well as several treatment modalities2, 27. So far, MR imaging
has shown to be the best discriminating method to evaluate TGCT4, 28. In our study, six objective
clinically relevant MR parameters were defined in relation to anatomical or surgical landmarks.
According to our exclusion criteria for the development of the severity classification, parameters
cartilage covered bone invasion and neurovascular involvement showed inadequate number of
presence and were therefore not used. However, in larger case series these two parameters might
correlate with more aggressive disease and hence a higher recurrence rate.
To date, no radiology-based TGCT severity classification exists. Subdividing between localized-
and diffuse-TGCT seems an oversimplification that fails to estimate differences in recurrent rates
for individual patients. Murphey et al. presented an extensive review of different TGCT features
on several imaging techniques, without relating these features to disease severity, treatment or
recurrences4. Van der Heijden et al. further sub-classified diffuse-TGCT affecting the knee in 30
patients into mild or severe, without linking to recurrent disease. Mild diffuse-TGCT was defined as
involvement of either anterior or posterior compartment of the knee, with the cruciate ligaments
as boundary. Severe diffuse-TGCT was defined as involvement of both compartments, with or
without extra-articular extension9. In contrast to most literature, we selected a homogeneously
treated patient population to develop four severity subtypes, by only including patients initially
treated with an open synovectomy.
In line with most papers, especially papers on trial medication, and based on clinical practice,
we included all large joints to sub-classify disease severity for TGCT. Prior research did not
show a (significant) difference in recurrence rates for both localized and diffuse disease when
comparing the knee with other joints6, 27, 29, 30. A recent TGCT incidence calculation study showed
a predominance of the knee in 46% in localized- and 64% in diffuse-type (excluding digits)5, in
line with our overrepresentation of the knee of 70%. In the future, a TGCT severity classification
focused on the knee would contain more detailed knee-specific MR parameters and equal
treatment approaches.
Limitations to this study: primary, the resulting HRs had wide confidence intervals, indicating low

Severity classification of tenosynovial giant cell tumours
91
4
precision in the estimates. This is likely related to the relatively small sample size, given that the
patients were divided into several groups based on the MR parameters. Secondly, because of the
relatively small number of recurrences in severity subtypes mild localized (n 1) and severe localized
(n 3), Hazard Ratios may be unreliable. Therefore, it was not feasible to estimate a cox model and to
generate a true prediction model. Additionally, localized-TGCT is known to have few recurrences
and often remains without clinical complaints after resection. In both sarcoma centres, patients
are therefore discharged from follow-up after the first follow-up post-surgery and requested to
return again when clinical complaints present. In our analyses, 31 localized-type patients were
censored at date of last clinical follow-up within the first two years in survival curve (figure 4). Less
often, patients with diffuse-type have also lacked follow-up (13 censored first two years). It could
be assumed that these patients did not have complaints and recurrent disease. Furthermore, in
study part two (establishing TGCT subtypes), newest included MR scans originated from 2015.
These cases had a maximum follow-up of two years. Since it is known that local recurrence might
develop years after initial surgery2, 11, 29, in our study a median of 29.5 in moderate diffuse and
22.0 months in severe diffuse-TGCT subtypes, underestimation of recurrence free survival could be
present. Finally, even though quite a large number of MR scans (174) were used in development of
the severity classification, in larger case-series including long follow-up time, it might be possible
to differentiate further in disease severity and assess additional subtypes.
To conclude, in reporting TGCT affecting large joints on MR imaging, six parameters are helpful
in discriminating disease extent. Patients can be accurately monitored by using these MR
parameters. With respect to recurrence, a combination of four MR parameters classifies patients
into one of four severity subtypes, presented with distinct recurrence free survival rates. In the era
of personalized medicine, treatment is individualized for each patient depending on the extent of
disease. Because histopathological prognostic factors are lacking, sub-classification of TGCT on MR
imaging is a potential tool to stratify future patient prognosis and identify candidates for targeted
therapies, thereby aiding with the decision in daily practice.
Supplementary data
Supplementary data related to this article can be found at
https://doi.org/10.1016/j.suronc.2018.07.002
92
Chapter four
appendix
TGCT MR parameters, affecting large joints, in therapy naïve primary TGCT patients
Agreement:
Involvement of a structure: when signal intensity is changed to TGCT signal intensity,
this structure is considered to be involved with TGCT and to be scored.
When involvement of a structure is unclear: choose ‘structure involved’ (when in
doubt; over-scoring, not under-scoring).
MI parameters
1. TGCT-type
Localized-type†: well circumscribed nodular lesion at synovial lining of bursa,
joint or tendon sheath
Diffuse-type††: multinodular lesion involving a larger part or all of the synovial
lining
2. Articular involvement
Intra-articular$: inside synovial lining of joint
Extra-articular$$: outside synovial lining of joint
Both intra- and extra-articular
3. Cartilage-covered bone invasion
Yes: clear invasion of bone invading cartilage; not only touch cartilage
No: no bone invasion or solely bone-usuration or bone invasion not cartilage-
covered
4. Muscular/tendinous tissue involvement*
Yes: involvement of muscular/tendinous tissue or >180 degrees encasement
of tendon/muscle
No: no involvement or encasement of tendon/muscle
5. Ligament involvement**
Yes: involvement of ligament or >180 degrees encasement of ligament
No: no involvement or encasement of ligament
Severity classification of tenosynovial giant cell tumours
93
4
6. Neurovascular structure involvement#
Yes: encasement >180 degrees of important nerves and/or vessels
No: no encasement of nerves or vessels
† Localized-type: be careful to always classify one nodular lesion as localized-type. Also when one
nodular lesion is reeved by another structure (it might seem like additional nodules).†† Diffuse-type: be careful to always classify diffuse-type when two or more tendon sheaths or
muscles are involved. Do not classify these cases as one large nodule.$ Intra-articular: concerning the knee: cruciate ligaments are counted as intra-articular structures
as the synovial lining of the ligaments should be considered intra-articular.$$ Extra-articular: concerning the knee: Hoffa
* Muscular/tendinous tissue involvement: concerning the knee: also account parameter when
solely popliteus muscle involvement is present.
** Ligament involvement: TGCT involvement of ligament, in hand or foot: account parameter
when intra-tarsal/digital ligaments, ankle syndesmose and plantar fascia are involved. TGCT
concerning the knee with ligament involvement: anterior and/or posterior cruciate ligament,
and/or medial/lateral collateral ligament.# Neurovascular involvement: in hand or foot: also digital or sensible nerves

94
Chapter four
references
1. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4 ed2013. p. 100-1.
2. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, diffuse type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 52013. p. 102-3.
3. Frassica FJ, Khanna JA, McCarthy EF. The role of MR imaging in soft tissue tumor evaluation: perspective of the orthopedic
oncologist and musculoskeletal pathologist. Magnetic resonance imaging clinics of North America. 2000;8(4):915-27.
4. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis:
radiologic-pathologic correlation. Radiographics. 2008;28(5):1493-518.
5. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence rates
than previously known in tenosynovial giant cell tumors. Acta orthopaedica. 2017:1-7.
6. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
7. Tyler WK, Vidal AF, Williams RJ, Healey JH. Pigmented villonodular synovitis. The Journal of the American Academy of
Orthopaedic Surgeons. 2006;14(6):376-85.
8. Mastboom MJL, Verspoor FGM, Gelderblom H, van de Sande MAJ. Limb Amputation after Multiple Treatments of
Tenosynovial Giant Cell Tumour: Series of 4 Dutch Cases. Case reports in orthopedics. 2017;2017:7402570.
9. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical
treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J.
2014;96-B(8):1111-8.
10. Verspoor FG, Hannink G, Scholte A, Van Der Geest IC, Schreuder HW. Arthroplasty for tenosynovial giant cell tumors. Acta
orthopaedica. 2016;87(5):497-503.
11. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
12. Griffin AM, Ferguson PC, Catton CN, Chung PW, White LM, Wunder JS, et al. Long-term outcome of the treatment of
high-risk tenosynovial giant cell tumor/pigmented villonodular synovitis with radiotherapy and surgery. Cancer.
2012;118(19):4901-9.
13. Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, et al. Structure-Guided Blockade of CSF1R Kinase in
Tenosynovial Giant-Cell Tumor. The New England journal of medicine. 2015;373(5):428-37.
14. Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, et al. Targeting tumor-associated macrophages with anti-CSF-
1R antibody reveals a strategy for cancer therapy. Cancer cell. 2014;25(6):846-59.
15. Sankhala KK, Blay JY, Ganjoo KN, Italiano A, Hassan AB, Kim TM, et al. A phase I/II dose escalation and expansion study
of cabiralizumab (cabira; FPA-008), an anti-CSF1R antibody, in tenosynovial giant cell tumor (TGCT, diffuse pigmented
villonodular synovitis D-PVNS). ASCO conference 2017. 35 (15 Supplement 1).
16. Hughes TH, Sartoris DJ, Schweitzer ME, Resnick DL. Pigmented villonodular synovitis: MRI characteristics. Skeletal
radiology. 1995;24(1):7-12.
17. Nordemar D, Oberg J, Brosjo O, Skorpil M. Intra-Articular Synovial Sarcomas: Incidence and Differentiating Features from
Localized Pigmented Villonodular Synovitis. Sarcoma. 2015;2015:903873.
Severity classification of tenosynovial giant cell tumours
95
4
18. Poletti SC, Gates HS, 3rd, Martinez SM, Richardson WJ. The use of magnetic resonance imaging in the diagnosis of
pigmented villonodular synovitis. Orthopedics. 1990;13(2):185-90.
19. Wang C, Song RR, Kuang PD, Wang LH, Zhang MM. Giant cell tumor of the tendon sheath: Magnetic resonance imaging
findings in 38 patients. Oncology letters. 2017;13(6):4459-62.
20. Altman D. Practical Statistics for Medical Research. Hall/CRC Ca, editor 1990.
21. Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and
future perspectives. Eur J Cancer. 2016;63:34-40.
22. Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, et al. Efficacy of imatinib mesylate for the
treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis.
Cancer. 2012;118(6):1649-55.
23. Gelderblom H, Cropet C, Chevreau C, Boyle R, Tattersall M, Stacchiotti S, et al. Nilotinib in locally advanced pigmented
villonodular synovitis: a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2018.
24. Cassier PA, Italiano A, Gomez-Roca CA, Le Tourneau C, Toulmonde M, Cannarile MA, et al. CSF1R inhibition with
emactuzumab in locally advanced diffuse-type tenosynovial giant cell tumours of the soft tissue: a dose-escalation and
dose-expansion phase 1 study. Lancet Oncol. 2015;16(8):949-56.
25. Tap WD GH, Stacchiotti S, Palmerini P, Ferrari S, Desai J, Bauer S, Blay JY, Alcindor T, Ganjoo KN, Martin Broto J, Ryan CW,
Edward Shuster DE, Zhang L, Wang Q, Hsu H, Lin PS, Tong S, Wagner AJ, editor Final results of ENLIVEN: A global, double-
blind, randomized, placebo-controlled, phase 3 study of pexidartinib in advanced tenosynovial giant cell tumor (TGCT).
ASCO conference; 2018; Chicago.
26. Gounder MM, Thomas DM, Tap WD. Locally Aggressive Connective Tissue Tumors. Journal of clinical oncology : official
journal of the American Society of Clinical Oncology. 2018;36(2):202-9.
27. Chiari C, Pirich C, Brannath W, Kotz R, Trieb K. What affects the recurrence and clinical outcome of pigmented villonodular
synovitis? Clin Orthop Relat Res. 2006;450:172-8.
28. Gouin F, Noailles T. Localized and diffuse forms of tenosynovial giant cell tumor (formerly giant cell tumor of the tendon
sheath and pigmented villonodular synovitis). Orthop Traumatol Surg Res. 2017;103(1S):S91-S7.
29. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.
30. Barile A, Sabatini M, Iannessi F, Di Cesare E, Splendiani A, Calvisi V, et al. Pigmented villonodular synovitis (PVNS) of the
knee joint: magnetic resonance imaging (MRI) using standard and dynamic paramagnetic contrast media. Report of 52
cases surgically and histologically controlled. La Radiologia medica. 2004;107(4):356-6.

Ho
rm
on
escan increased
symptoms of tenosynovial giant
cell tumours during pregnancy be explained by a change in female
sex hormones?
chap
ter
five
M.J.L. Mastboom1, F.G.M. Verspoor2, R. Planje1, H.W.B. Schreuder2, M.A.J. van de Sande1
Submitted.

98
Chapter five
1 Orthopaedic Surgery, Leiden University Medical Centre, Leiden, the Netherlands
2 Orthopaedic Surgery, Radboud University Medical Centre, Nijmegen, the Netherlands

Female sex hormones in TGCT
99
5
abstract
Objective
Tenosynovial Giant Cell Tumours (TGCT), both localized- and diffuse-type, are rare, mono-articular
neoplasms, with a slight female predominance. The clinical behaviour between patients differs
greatly. This study aims to evaluate the increase in TGCT-related symptoms during pregnancy and
the influence of female sex hormones thereon.
Methods
In a prospective-cohort-study, TGCT-related symptoms before and during pregnancy were
evaluated in two Dutch centres and by use of the largest online TGCT patient-support group.
Second, as a proxy for disease activity the combined TGCT-database of two sarcoma-centres
in the Netherlands (N=455) was used to compare recurrence free survival rates between the
sexes (during and after fertile-age). Finally, female hormonal receptor status was evaluated with
immunohistochemistry on TGCT-specimens from eight women (18-50 years).
Results
Forty percent (8/20) of women with diffuse-TGCT of lower extremity reported an increase in
TGCT-related symptoms during pregnancy, predominantly an increase in swelling (62%). Mean
VAS-score on symptoms increased between 5.9 (SD 2.1) before pregnancy to 6.6 (SD 1.7) during
pregnancy. Similar results were reported in the patient-support group.
No differences were found in recurrence free survival rates, between both sexes, (localized-
(p=0.206 ≤50 years, p=0.935 >50 years); diffuse-type (p=0.664 ≤50 years, p=0.140 >50 years)),
neither in pre- versus post-menopausal women (localized- (p=0.106); diffuse-type(p=0.666)). In
all examined localized- and diffuse-TGCT tissue-samples, oestrogen or progesterone hormone-
receptor staining was negative.
Conclusion
An increase in TGCT-related symptoms during pregnancy was reported. This could not directly be
linked to female sex hormones as hormone receptors were missing histopathologically. Recurrence
free survival rates were comparable, making a relation with female sex hormones improbable.

100
Chapter five
Background
Tenosynovial Giant Cell Tumour (TGCT), previously known as Pigmented Villonodular Synovitis
(PVNS), is a rare, benign neoplasm arising from synovial joints, tendon sheaths and bursae. It
affects a relatively young population aged 30-50 years and has a slight female predominance
(male:female 1:1.5)1-3. Two subtypes are distinguished. The localized-type is defined as a single
nodule, affecting only a distinct area of the synovium with an incidence rate of 10.2 per million
person-years (excluding digits). The diffuse-type is known to be more aggressive and involves a
larger part or the entire synovial lining. It has an incidence rate of 4.1 per million person-years4, 5.
TGCT is a mono-articular disease predominantly affecting weight-bearing joints; knee (46% and
64%), hip (1% and 9%), and ankle (5% and 10%) for localized- and diffuse-type, respectively3, 4.
Pain, swelling, limited range of motion and stiffness of the affected joint are the most common
symptoms6-9. Rapid diagnosis is difficult due to these unspecific symptoms and since most
physicians are unfamiliar with the disease5, 10-12. Arthroscopic or open synovectomy is the standard
of care1, 2, 5, 8. After surgical treatment, localized-type in the knee generally follows a favourable
course with an average recurrence rate of 4 to 6% after resection (with variable follow-up). In
contrast, diffuse-type in the knee presents with multiple recurrences, on average 14% to 40% after
surgical treatment5.
In TGCT, answers on everyday questions are lacking: e.g. do hormone-based anticonceptiva
influence my disease? Does pregnancy influence the clinical behaviour of TGCT? In the outpatient
clinic and on online TGCT patient fora, an increase in TGCT-related symptoms during pregnancy
is observed. In healthy pregnant women, joint pain in the knee and hip are frequently reported13,
14. This pain is not only attributed to the additional weight. Elevated female sex hormones
(oestrogen, progesterone and the oestrogen-dependent relaxin) are known to weaken soft
tissue structures, resulting in increased joint laxity during pregnancy, joint instability and lower
extremity dysfunction13, 15, 16. To our knowledge, only two case-reports of two pregnant women
with both localized-TGCT exist (supplementary material). The first case report described a patient
diagnosed with TGCT six months after pregnancy completion, as the patient was misdiagnosed
with chondromalacia patellae17. The second patient presented with an acute onset of knee pain
during first semester of pregnancy. It was hypothesized that pregnancy-related changes triggered
torsion or bleeding of the tumour, leading to this acute presentation18. Elevated levels of oestrogen

Female sex hormones in TGCT
101
5
and progesterone receptors have been identified in giant cell tumour of bone, dermatofibroma
protuberans and malignancies of breast, endometrium, ovary, prostate, colon. Hormone receptor
positive tumours show a better prognosis19-24. The presence of female sex hormone receptors in
TGCT is unknown.
This study aims to evaluate patient reported TGCT-related symptoms before and during pregnancy
in two different patient populations. Influences of sex specific hormones and female fertile life
phase specific hormones are determined by comparing recurrence free survival rates between
the sexes and pre- versus post-menopausal women. Finally, presence of female sex hormonal
receptor-status in available tumour tissue is assessed.
methods
Questionnaires in two sarcoma centres and a patient-support group
Patients with diffuse-TGCT were included, since diffuse-TGCT is a more widespread and extensive
disease, including more clinical complaints and higher recurrence rates, compared with localized-TGCT.
Two sarcoma centres
One-hundred sixty-two female patients with histopathologically proven diffuse-TGCT were
extracted from the combined Dutch TGCT-database (Leiden University Medical Centre (LUMC)
N=92 and Radboud University Medical Centre (RUMC) N=70) (figure 1)25. Excluded were seventy-
four patients <18 years or >50 years, non-weight bearing upper-extremity TGCT (elbow, wrist) or
temporomandibular localization. The remaining 88 patients were invited to complete the TGCT-
questionnaire. Incomplete questionnaires were unsuitable for analysis (N=26). Finally, sixty-two
questionnaires of patients with diffuse-TGCT of lower extremities were included.
The comprehensive TGCT-hormone questionnaire contained questions on patient- and tumour-
characteristics, initial TGCT-symptoms (prior to primary treatment), current TGCT-symptoms
(symptoms at time of questionnaire completion) and TGCT-symptoms before and during
pregnancy. To quantify TGCT-related symptoms, Visual Analogue Scale (VAS) questions were
included, ranging from 0 (no symptoms) to 10 (worst symptoms) (supplementary material). The
pregnancy questions were completed for the first pregnancy (>6 months) after TGCT-diagnosis

102
Chapter five
and questions were answered regarding the TGCT affected joint.
Patient-support group
Previously, an international crowdsourcing study was conducted in 337 patients to evaluate
impact of TGCT on daily living26. An e-survey was distributed in the largest, online support group
for TGCT-patients: the closed Facebook group ‘PVNS is pants!!’. This study contained 129 women
with diffuse-TGCT of lower extremity, aged between 18 and 50 years (figure 2). Besides patient-
and tumour characteristics, the e-survey contained validated questionnaires on physical function
and quality of life. Furthermore, questions on TGCT-related symptoms and intensity of symptoms,
pregnant at time of TGCTN=20
not pregnant at time of TGCT
N=42
RUMCN=70
Excluded (N=74)• <18 or >50 years, N=70• upper-extremity, N=3• Temporomandibular, N=1
LUMCN=92
diffuse-TGCTN=162
eligible for questionnaireN=88
Excluded (N=26)• incomplete questionnaire
or duplicate entries, N=26completed questionnaires
N=62
Figure 1 Inclusion flowchart of diffuse-TGCT women, treated in one of two sarcoma centres.
RUMC, Radboud University Medical Centre; LUMC, Leiden University Medical Centre.
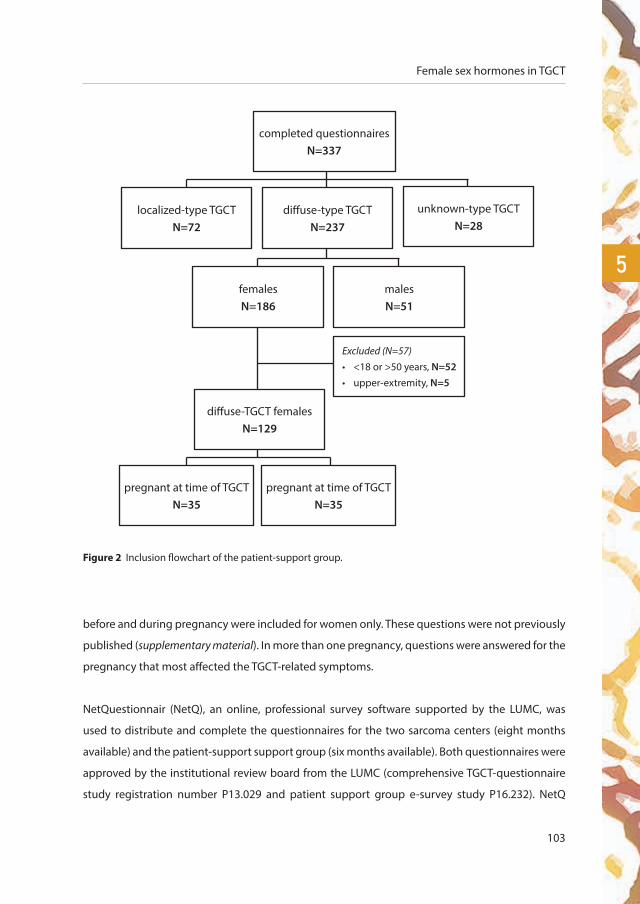
Female sex hormones in TGCT
103
5
before and during pregnancy were included for women only. These questions were not previously
published (supplementary material). In more than one pregnancy, questions were answered for the
pregnancy that most affected the TGCT-related symptoms.
NetQuestionnair (NetQ), an online, professional survey software supported by the LUMC, was
used to distribute and complete the questionnaires for the two sarcoma centers (eight months
available) and the patient-support support group (six months available). Both questionnaires were
approved by the institutional review board from the LUMC (comprehensive TGCT-questionnaire
study registration number P13.029 and patient support group e-survey study P16.232). NetQ
Figure 2 Inclusion flowchart of the patient-support group.
completed questionnairesN=337
diffuse-type TGCTN=237
localized-type TGCTN=72
unknown-type TGCTN=28
femalesN=186
malesN=51
Excluded (N=57)• <18 or >50 years, N=52• upper-extremity, N=5
diffuse-TGCT femalesN=129
pregnant at time of TGCTN=35
pregnant at time of TGCTN=35

104
Chapter five
automatically captured questionnaire-answers into an SPSS 23 file (Statistical Package for Social
Sciences statistics (SPSS®) Version 23 (Chicago, IL, USA)), only accessible to TGCT researchers.
Unique site visitors were determined by IP addresses. When duplicate entries were detected,
the most recent one was included. Statistical analyses were mainly descriptive. To verify that
diffuse-type women with increased TGCT-symptoms during pregnancy were comparable with
diffuse-type women not pregnant during TGCT in the patient support group, chi-square tests
were used for TGCT localization (knee versus hip, ankle and foot), initial surgery (arthroscopy
versus open synovectomy), recurrence (yes versus no) and total number of surgeries (1 surgery
versus ≥2 surgeries). Independent t-tests were used to compare continuous scores of validated
questionnaires on physical function and quality of life.
Comparison of recurrence free survival rates
Recurrence was defined as new disease presence after synovectomy or growing residual disease
(diagnosed on follow-up MR scan). To determine influences of sex specific hormones and female
fertile life phase specific hormones, recurrence free survival rates between the sexes and pre-
versus post-menopausal in women were assessed as a proxy. The combined database of two
sarcoma centres (LUMC and RUMC) in The Netherlands (N=455, 262 diffuse-TGCT) was used25.
This dataset contained all consecutive patients surgically treated for histopathologically proven
TGCT between 1990 to 2017. Fertile life phase was defined between 16 and ≤50 years at primary
diagnosis, since median age at natural menopause ranges between 49 and 52 years27.
Using SPSS®, recurrence free survival rate after index operation was calculated through Kaplan-
Meier survival method and log rank test in male and female patients ≤50 years and >50 years for
localized- and diffuse-type separately. Similarly, recurrence free survival rates in pre- versus post-
menopausal women were compared.
Female hormone-receptors in TGCT
Immunohistochemistry was performed on paraffin-embedded pathological specimens of
histopathologically proven TGCT tissue, obtained from eight randomly selected women between
18 and 50 years to determine female hormone receptor status. All samples were of primary
resected localized- (N=4) or diffuse-TGCT (N=4), located in the lower extremity (hip, knee, ankle).
Monoclonal Rabbit Anti-Human Oestrogen receptor α and monoclonal mouse anti-human

Female sex hormones in TGCT
105
5
progesterone receptor were used (supplementary material). Hormone receptor status was assessed
in the LUMC by a dedicated pathologist, specialized in bone and soft tissue tumours. Slides were
verified with positive controls of women with oestrogen or progesterone receptor positive breast
cancer.
results
Questionnaires in two sarcoma centres and a patient-support group
Two sarcoma centres
Sixty-two women with diffuse-TGCT of the lower extremities ((knee 50 (81%), hip 6 (9%) and ankle/
foot 6 (9%)) with a median age at diagnosis of 30 (IQR 25-38) years completed the comprehensive
Dutch questionnaire (Table 1). Twenty (32%) patients were pregnant after being diagnosed with
TGCT. Eight (40%) of these patients self-reported an increase, two (10%) a decrease of symptoms and
10 (50%) continued at the same level (Table 2). TGCT-related symptoms included pain, swelling and
limited range of motion of the affected joint, swelling was predominantly increased (62%) (Table 3). In
patients with increasing symptoms, mostly during second or third trimester (5/8 (63%)) of pregnancy,
mean VAS score increased from 5.9 (SD 2.1) before pregnancy to 6.6 (SD 1.7) during pregnancy.
Patient-support group
In 129 women, median age at time of diagnosis was 30 (IQR 24-39) years and TGCT was mostly
located in the knee (93 (72%)) (Table 1). Thirty-five (27%) women had TGCT during pregnancy.
Twenty-three (66%) pregnant women stated an increase, 3/35 (9%) a decrease and 9/35 (26%) did
not experience a difference in symptoms during pregnancy. Of all reported symptoms, swelling
(57%) of the associated joint increased the most. Additional symptoms included pain, limited
range of motion and stiffness (Table 3). Self-reported intensity of TGCT-related symptoms after
pregnancy was compared with reported intensity of symptoms before pregnancy; in 10/26 (38%)
intensity increased, 6/26 (23%) intensity decreased and in 10/26 (38%) intensity continued at a
comparable level. No differences were detected in patient- and tumour-characteristics in women
with increased TGCT-symptoms during pregnancy compared with women not pregnant during
TGCT (Supplementary material; Table 1).
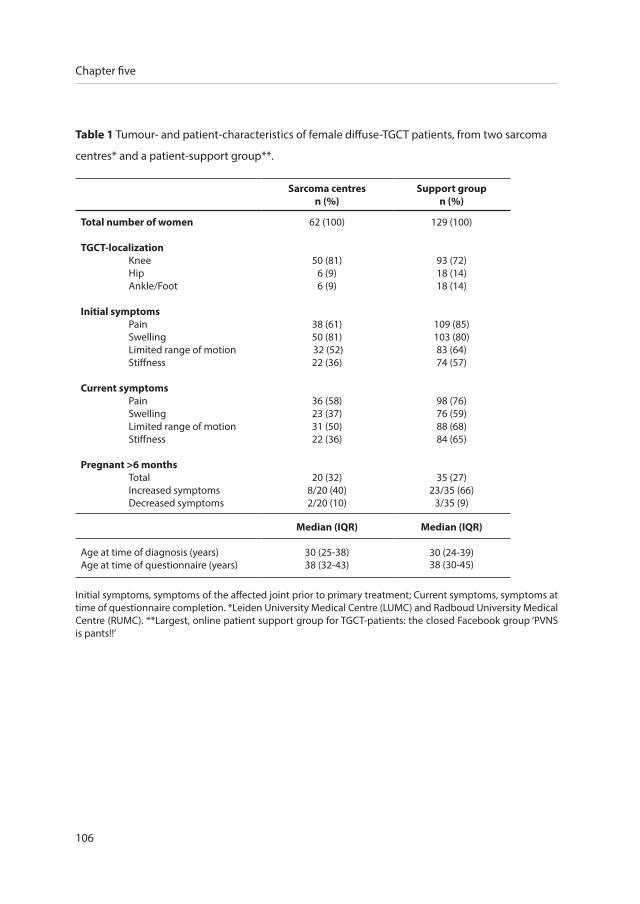
106
Chapter five
Table 1 Tumour- and patient-characteristics of female diffuse-TGCT patients, from two sarcoma
centres* and a patient-support group**.
Sarcoma centresn (%)
Support groupn (%)
Total number of women
TGCT-localizationKneeHipAnkle/Foot
Initial symptoms PainSwellingLimited range of motionStiffness
Current symptoms PainSwellingLimited range of motionStiffness
Pregnant >6 months TotalIncreased symptomsDecreased symptoms
62 (100)
50 (81)6 (9)6 (9)
38 (61)50 (81) 32 (52)22 (36)
36 (58)23 (37)31 (50)22 (36)
20 (32)8/20 (40)2/20 (10)
129 (100)
93 (72)18 (14)18 (14)
109 (85)103 (80)83 (64)74 (57)
98 (76)76 (59)88 (68)84 (65)
35 (27)23/35 (66)
3/35 (9)
Median (IQR) Median (IQR)
Age at time of diagnosis (years)Age at time of questionnaire (years)
30 (25-38)38 (32-43)
30 (24-39)38 (30-45)
Initial symptoms, symptoms of the affected joint prior to primary treatment; Current symptoms, symptoms at time of questionnaire completion. *Leiden University Medical Centre (LUMC) and Radboud University Medical Centre (RUMC). **Largest, online patient support group for TGCT-patients: the closed Facebook group ‘PVNS is pants!!’
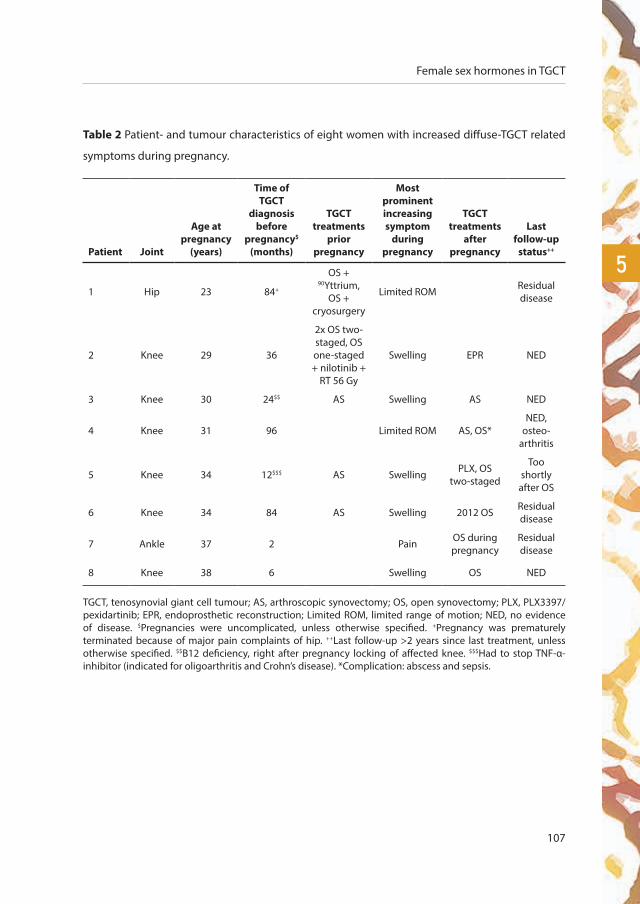
Female sex hormones in TGCT
107
5
Table 2 Patient- and tumour characteristics of eight women with increased diffuse-TGCT related
symptoms during pregnancy.
Patient Joint
Age at pregnancy
(years)
Time of TGCT
diagnosis before
pregnancy$ (months)
TGCT treatments
prior pregnancy
Most prominent increasing symptom
during pregnancy
TGCT treatments
after pregnancy
Last follow-up
status++
1 Hip 23 84+
OS + 90Yttrium,
OS + cryosurgery
Limited ROM Residual disease
2 Knee 29 36
2x OS two-staged, OS one-staged + nilotinib +
RT 56 Gy
Swelling EPR NED
3 Knee 30 24$$ AS Swelling AS NED
4 Knee 31 96 Limited ROM AS, OS*NED,
osteo-arthritis
5 Knee 34 12$$$ AS Swelling PLX, OS two-staged
Too shortly
after OS
6 Knee 34 84 AS Swelling 2012 OS Residual disease
7 Ankle 37 2 Pain OS during pregnancy
Residual disease
8 Knee 38 6 Swelling OS NED
TGCT, tenosynovial giant cell tumour; AS, arthroscopic synovectomy; OS, open synovectomy; PLX, PLX3397/pexidartinib; EPR, endoprosthetic reconstruction; Limited ROM, limited range of motion; NED, no evidence of disease. $Pregnancies were uncomplicated, unless otherwise specified. +Pregnancy was prematurely terminated because of major pain complaints of hip. ++Last follow-up >2 years since last treatment, unless otherwise specified. $$B12 deficiency, right after pregnancy locking of affected knee. $$$Had to stop TNF-α-inhibitor (indicated for oligoarthritis and Crohn’s disease). *Complication: abscess and sepsis.

108
Chapter five
Table 3 Most prominent increased TGCT-related symptoms during pregnancy.
Sarcoma centresn (%)
Support groupn (%)
Pain 1 (13) 5 (22)
Swelling 5 (62) 13 (57)
Limited range of motion 2 (25) 3 (13)
Stiffness 0 2 (8)
Total increased symptoms 8 (100) 23 (100)
All patients were requested to indicate which TGCT-symptom increased most during pregnancy. This table presents self-reported increased symptoms in 8/20 (40%) and 23/35 (66%) women with diffuse-TGCT from two Dutch sarcoma centres and the patient-support group, respectively. In both populations swelling was the most prominent symptom.
Figure 3 Recurrence free survival curve in 155 diffuse-TGCT patients ≤50 years* (p=0.664).
*Age at primary diagnosis
Years after index operation
male 71 49 32 20 12 8 6
female 84 51 34 25 18 11 9
numbers at risk
Recu
rren
ce fr
ee s
urvi
val
male
female

Female sex hormones in TGCT
109
5
Figure 3 (continued) Recurrence free survival curve in 107 diffuse-TGCT patients >50 years* (p=0.140).
*Age at primary diagnosis
Years after index operation
male 42 30 17 13 10 10 9
female 65 47 37 28 21 13 11
numbers at risk
Recu
rren
ce fr
ee s
urvi
val
male
female

110
Chapter five
Comparison of recurrence free survival rates
Female recurrence free survival rates were comparable to male rates for localized-type (log rank
p=0.206 ≤50 years, p=0.935 >50 years) and diffuse-type (log rank p=0.664 ≤50 years, p=0.140 >50
years) (figure 3). Similarly, in women during and after fertile age, recurrence free survival rates were
comparable for localized-type (log rank p=0.106) and diffuse-type (log rank p=0.666).
Female hormone-receptors in TGCT
All eight localized- and diffuse-TGCT tissue samples were oestrogen or progesterone hormone
receptor negative. Further evaluation of additional patient samples was therefore deemed
unnecessary.
discussion
This is the first study to evaluate hormonal influences on the clinical presentation of Tenosynovial
Giant Cell Tumour (TGCT). An increase in TGCT-related symptoms during pregnancy was reported,
in particular swelling of the affected joint. Recurrence free survival rates were comparable for both
sexes as well as for pre- versus postmenopausal women. Oestrogen and progesterone-receptors
were not present with immunohistochemistry in TGCT tissue.
In the current study, 56% (31/55) of pregnant patients reported an increase in TGCT-related
symptoms and a minority reported a decrease in these symptoms (9%; 5/55). Swelling of the
affected joint was self-reported as the most prominent symptom during pregnancy. Since TGCT
is a mono-articular disease, this swelling is not comparable with the clinical (bilateral) oedema
accompanying a majority of (healthy) pregnancies14. The increase in symptoms was mainly present
during second and third trimester of pregnancy. Similar, healthy pregnancy is associated with an
increase in lower extremity symptoms during these trimesters14. A valid question would be why
an increase in mono-articular TGCT swelling during pregnancy would present in these later stages
of pregnancy. Since growth hormone is already present five weeks after conception, the question
is whether growth hormone influences TGCT-related joint swelling. The experienced increase in
disease burden might be caused by progressive disease, but is more likely based on increased
effusion. Although pregnancy seems to provoke an increase in TGCT-related symptoms, this might
be coincidental according to subjective complaints, recall bias and focus on the affected joint.

Female sex hormones in TGCT
111
5
In general, a multifactorial aetiology is responsible for lower-extremity symptoms during healthy
pregnancy28. First; biomechanical changes, including the anterior shift of the center of gravity13,
the extra bodyweight29 and a different gait-pattern due to an increased pressure on the lateral
side of the foot30, are responsible for lower limb and functional knee pain in pregnant women. As
a consequence, a decrease in physical functioning is reported during progression of pregnancy,
also in healthy women15. Second; relaxation of joints is a physiologic process associated with
pregnancy. This increased joint-laxity and weakened soft tissue structures is mainly based on the
pregnancy initiated elevated levels of the hormone relaxin31. Third; discontinuation of medication
considered unsafe for the unborn child, for instance non-steroidal anti-inflammatory drugs
(NSAID’s) or tumour necrosis factor-blockers (TNF-α-inhibitors), might affect the experience of
TGCT-symptoms. Additional factors of possible influence on TGCT-related symptoms are nausea/
fatigue, stress, emotional/personal problems and anxiousness for additional tasks after pregnancy.
The increased TGCT-related symptoms during pregnancy might also be attributed to this
multifactorial aetiology for lower extremity symptoms during healthy pregnancy. One (1/8(13%))
patient with increased symptoms interrupted her TNF-α-inhibitor (indicated for oligoarthritis and
Crohn’s disease) (Table 2; patient 5).
To test the hypothesis that female sex hormones influence TGCT, we compared recurrence rates
for both sexes. Since oestrogen and progesterone in women decline after fertile age, recurrence
free survival rate analyses were performed for both sexes ≤50 and >50 years, without revealing
a difference. In accordance with literature no differences in recurrence rates between male and
female TGCT-patients were found32. To our knowledge, pre- versus post-menopausal analyses had
not been performed before and yielded also no difference.
In all eight primary resected TGCT-tissues, oestrogen or progesterone receptors were completely
absent. This is a small sample size, although it is unlikely that positive female sex hormone status
will be detected by evaluating additional specimens. Hormone-based anticonceptica or female
hormone based treatments do not seem to influence the clinical behaviour of TGCT. Future
research is recommended to find the cause of increased symptoms in TGCT during pregnancy
and to contribute to possible new treatment modalities, e.g. growth-factor, ED-A fibronectin
(expressed during embryogenesis) or changes in the auto-immune system.

112
Chapter five
Evaluation of hormonal influences in TGCT is challenging because of the rarity of the tumour
and the heterogeneous patient population. Main limitation in our two questionnaire studies
was participant recall bias. Information provided on a recall basis diminishes the accuracy of
results. Preferably, an observational study would be performed, including a control group and
radiographic evaluation of tumour severity before and after pregnancy. Furthermore, answers from
the e-survey in the patient support group could be influenced by multicultural differences. Finally,
while previous surgeries provoke deteriorated clinical outcome, treatments before pregnancy and
treatment phase during pregnancy were not taken into consideration.
conclusion
In conclusion, an increase in TGCT-related symptoms during pregnancy was reported in two
different patient cohorts. This could not directly be linked to female sex hormones as hormone
receptors were missing histopathologically. Recurrence free survival rates between both sexes and
between pre- versus post-menopausal women were also comparable, making a causal relation
with female sex hormones even more unlikely.
Female sex hormones in TGCT
113
5
references
1. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4 ed2013. p. 100-1.
2. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, diffuse type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 52013. p. 102-3.
3. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis:
radiologic-pathologic correlation. Radiographics. 2008;28(5):1493-518.
4. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence rates
than previously known in tenosynovial giant cell tumors. Acta orthopaedica. 2017:1-7.
5. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
6. Gelhorn HL, Tong S, McQuarrie K, Vernon C, Hanlon J, Maclaine G, et al. Patient-reported Symptoms of Tenosynovial Giant
Cell Tumors. Clin Ther. 2016;38(4):778-93.
7. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
8. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review
and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
9. Zvijac JE, Lau AC, Hechtman KS, Uribe JW, Tjin ATEW. Arthroscopic treatment of pigmented villonodular synovitis of the
knee. Arthroscopy. 1999;15(6):613-7.
10. Hufeland M, Gesslein M, Perka C, Schroder JH. Long-term outcome of pigmented villonodular synovitis of the hip after
joint preserving therapy. Arch Orthop Trauma Surg. 2017.
11. Vastel L, Lambert P, De Pinieux G, Charrois O, Kerboull M, Courpied JP. Surgical treatment of pigmented villonodular
synovitis of the hip. J Bone Joint Surg Am. 2005;87(5):1019-24.
12. Gonzalez Della Valle A, Piccaluga F, Potter HG, Salvati EA, Pusso R. Pigmented villonodular synovitis of the hip: 2- to 23-
year followup study. Clin Orthop Relat Res. 2001(388):187-99.
13. Marnach ML, Ramin KD, Ramsey PS, Song SW, Stensland JJ, An KN. Characterization of the relationship between joint
laxity and maternal hormones in pregnancy. Obstet Gynecol. 2003;101(2):331-5.
14. Vullo VJ, Richardson JK, Hurvitz EA. Hip, knee, and foot pain during pregnancy and the postpartum period. J Fam Pract.
1996;43(1):63-8.
15. Ostensen M, Fuhrer L, Mathieu R, Seitz M, Villiger PM. A prospective study of pregnant patients with rheumatoid arthritis
and ankylosing spondylitis using validated clinical instruments. Ann Rheum Dis. 2004;63(10):1212-7.
16. Bridges AJ, Smith E, Reid J. Joint hypermobility in adults referred to rheumatology clinics. Ann Rheum Dis. 1992;51(6):793-
6.
17. Edwards MR, Tibrewal S. Patello-femoral joint pain due to unusual location of localised pigmented villonodular
synovitis-a case report. Knee. 2004;11(4):327-9.
18. Uslu M, Cetik O, Atasoy P, Eksioglu F, Engin M. Localized pigmented villonodular synovitis of the knee: acute onset in
pregnancy. Rheumatol Int. 2006;26(11):1054-6.
19. Berger U, McClelland RA, Wilson P, Greene GL, Haussler MR, Pike JW, et al. Immunocytochemical determination of
estrogen receptor, progesterone receptor, and 1,25-dihydroxyvitamin D3 receptor in breast cancer and relationship to
prognosis. Cancer research. 1991;51(1):239-44.
114
Chapter five
20. Campbell-Thompson M, Lynch IJ, Bhardwaj B. Expression of estrogen receptor (ER) subtypes and ERbeta isoforms in
colon cancer. Cancer research. 2001;61(2):632-40.
21. Ciocca DR, Puy LA, Fasoli LC. Study of estrogen receptor, progesterone receptor, and the estrogen-regulated Mr 24,000
protein in patients with carcinomas of the endometrium and cervix. Cancer research. 1989;49(15):4298-304.
22. Demertzis N, Kotsiandri F, Giotis I, Apostolikas N. Giant-cell tumors of bone and progesterone receptors. Orthopedics.
2003;26(12):1209-12.
23. Kieback DG, Press MF, Atkinson EN, Edwards GL, Mobus VJ, Runnebaum IB, et al. Prognostic significance of estrogen
receptor expression in ovarian cancer. Immunoreactive Score (IRS) vs. Composition Adjusted Receptor Level (CARL).
Anticancer research. 1993;13(6b):2489-96.
24. Parlette LE, Smith CK, Germain LM, Rolfe CA, Skelton H. Accelerated growth of dermatofibrosarcoma protuberans during
pregnancy. Journal of the American Academy of Dermatology. 1999;41(5 Pt 1):778-83.
25. Mastboom MJL, Verspoor FGM, Uittenbogaard D, Schaap GR, Jutte PCH, Schreuder HWB, et al. Tenosynovial Giant Cell
Tumors in Children: A Similar Entity Compared With Adults. Clinical Orthopaedics and Related Research. 2018.
26. Mastboom MJL, Planje R, van de Sande MAJ. The patient perspective on the impact of Tenosynovial Giant Cell Tumors on
daily living. Crowdsourcing study on physical function and quality of life in 337 patients from 30 countries. Interactive
Journal of Medical Research. 2018.
27. Morabia A, Costanza MC. International variability in ages at menarche, first livebirth, and menopause. World Health
Organization Collaborative Study of Neoplasia and Steroid Contraceptives. Am J Epidemiol. 1998;148(12):1195-205.
28. Ponnapula P, Boberg JS. Lower extremity changes experienced during pregnancy. J Foot Ankle Surg. 2010;49(5):452-8.
29. Spahn G, Lesser A, Hofmann GO, Schiele R. [Knee-related Pain Problems during Pregnancy Correlate with an Increase in
Body Weight. Results of a Prospective Study]. Z Geburtshilfe Neonatol. 2015;219(5):213-9.
30. Nyska M, Sofer D, Porat A, Howard CB, Levi A, Meizner I. Planter foot pressures in pregnant women. Isr J Med Sci.
1997;33(2):139-46.
31. MacLennan AH, Nicolson R, Green RC, Bath M. Serum relaxin and pelvic pain of pregnancy. Lancet. 1986;2(8501):243-5.
32. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.

Female sex hormones in TGCT
115
5

cH
ild
ren
tenosynovial giant cell tumours
in children
chap
ter
six
a similar entity compared with adults
M.J.L. Mastboom1, F.G.M. Verspoor2, D. Uittenbogaard1, G.R. Schaap3, P.C. Jutte4, H.W.B. Schreuder2, M.A.J. van de Sande1
Clin Orthop Relat Res. 2018 Sept;476(9):1803-1812

1 Orthopaedic Surgery, Leiden University Medical Centre, Leiden, the Netherlands
2 Orthopaedic Surgery, Radboud University Medical Centre, Radboud, the Netherlands
3 Orthopaedic Surgery, Academic Medical Centre Amsterdam, Amsterdam, the Netherlands
4 Orthopaedics Surgery, University Medical Centre, Groningen, Groningen, the Netherlands
Tenosynovial giant cell tumours in children
119
6
abstract
Background
Tenosynovial Giant Cell Tumour (TGCT) is a rare, benign, monoarticular entity. Many case-series
in adults are described, whereas TGCT is only incidentally reported in children. Therefore, its
incidence rate and natural history in children are unknown.
Questions/purposes
(1) How many cases have been reported of this condition, and what were their characteristics?
(2) What is the standardized paediatric incidence rate for TGCT?
(3) Is there a clinical difference in TGCT between children and adults?
(4) What is the risk of recurrence after open resection in children compared with adults?
Methods
Data were derived from three sources: (1) a systematic review on TGCT in children, seeking
sources published between 1990 and 2016, included 17 heterogeneous, small case-series; (2) the
nationwide TGCT incidence study: the Dutch paediatric incidence rate was extracted from this
nationwide study by including patients younger than 18 years of age. This registry-based study,
in which eligible patients with TGCT were clinically verified, calculated Dutch incidence rates for
localized and diffuse-type TGCT in a 5-year timeframe. Standardized paediatric incidence rates
were obtained by using the direct method; (3) from our nationwide bone and soft tissue tumour
data registry, a clinical data set was derived. Fifty-seven children with histologically proven TGCT of
large joints, diagnosed and treated between 1995 and 2015, in all four tertiary sarcoma centres in
The Netherlands, were included. These clinically collected data were compared with a retrospective
database of 423 adults with TGCT. Chi square test and independent t-test were used to compare
children and adults for TGCT type, sex, localization, symptoms before diagnosis, first treatment,
recurrent disease, followup status, duration of symptoms, and time to followup. The Kaplan-Meier
method was used to evaluate recurrence-free survival at 2.5 years.

120
Chapter six
Results
TGCT is seldom reported because only 76 paediatric patients (39 female), 29 localized, 38 diffuse,
and nine unknown type, were identified from our systematic review. The standardized paediatric
TGCT incidence rate of large joints was 2.42 and 1.09 per million person-years in localized and
diffuse types, respectively. From our clinical data set, symptoms both in children and adults were
swelling, pain, and limited ROM with a median time before diagnosis of 12 months (range, 1-72
months). With the numbers available, we did not observe differences in presentation between
children and adults in terms of sex, symptoms before diagnosis, first treatment, recurrent disease,
followup status, or median time to followup. The 2.5-year recurrence-free TGCT survival rate after
open resection was not different with the numbers available between children and adults: 85%
(95% confidence interval [CI], 67%-100%) versus 89% (95% CI, 83%-96%) in localized, respectively
(p = 0.527) and 53% (95% CI, 35%-79%) versus 56% (95% CI, 49%-64%) in diffuse type, respectively
(p = 0.691).
Conclusions
Although the incidence of paediatric TGCT is low, it should be considered in the differential
diagnosis in children with chronic monoarticular joint effusions. Recurrent disease after surgical
treatment of this orphan disease seems comparable between children and adults. With targeted
therapies being developed, future research should define the most effective treatment strategies
for this heterogeneous disease.
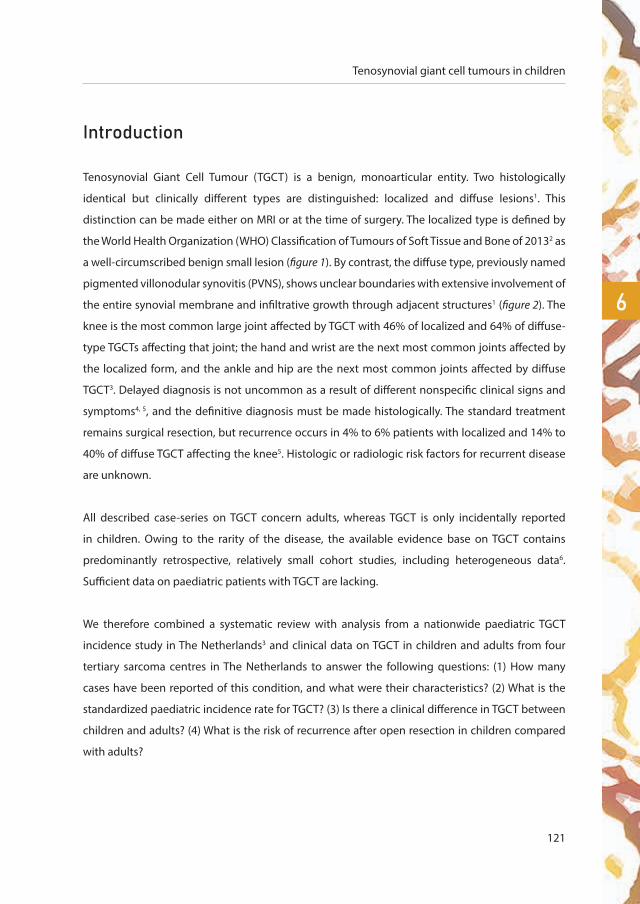
Tenosynovial giant cell tumours in children
121
6
introduction
Tenosynovial Giant Cell Tumour (TGCT) is a benign, monoarticular entity. Two histologically
identical but clinically different types are distinguished: localized and diffuse lesions1. This
distinction can be made either on MRI or at the time of surgery. The localized type is defined by
the World Health Organization (WHO) Classification of Tumours of Soft Tissue and Bone of 20132 as
a well-circumscribed benign small lesion (figure 1). By contrast, the diffuse type, previously named
pigmented villonodular synovitis (PVNS), shows unclear boundaries with extensive involvement of
the entire synovial membrane and infiltrative growth through adjacent structures1 (figure 2). The
knee is the most common large joint affected by TGCT with 46% of localized and 64% of diffuse-
type TGCTs affecting that joint; the hand and wrist are the next most common joints affected by
the localized form, and the ankle and hip are the next most common joints affected by diffuse
TGCT3. Delayed diagnosis is not uncommon as a result of different nonspecific clinical signs and
symptoms4, 5, and the definitive diagnosis must be made histologically. The standard treatment
remains surgical resection, but recurrence occurs in 4% to 6% patients with localized and 14% to
40% of diffuse TGCT affecting the knee5. Histologic or radiologic risk factors for recurrent disease
are unknown.
All described case-series on TGCT concern adults, whereas TGCT is only incidentally reported
in children. Owing to the rarity of the disease, the available evidence base on TGCT contains
predominantly retrospective, relatively small cohort studies, including heterogeneous data6.
Sufficient data on paediatric patients with TGCT are lacking.
We therefore combined a systematic review with analysis from a nationwide paediatric TGCT
incidence study in The Netherlands3 and clinical data on TGCT in children and adults from four
tertiary sarcoma centres in The Netherlands to answer the following questions: (1) How many
cases have been reported of this condition, and what were their characteristics? (2) What is the
standardized paediatric incidence rate for TGCT? (3) Is there a clinical difference in TGCT between
children and adults? (4) What is the risk of recurrence after open resection in children compared
with adults?

122
Chapter six
Patients and methods
Children were defined as patients younger than 18 years at presentation. Large joints were defined
as all joints proximal to the metatarsophalangeal and metacarpophalangeal joints. Data were
derived from three sources: a systematic review, the nationwide TGCT incidence study, and from
our bone and soft tissue tumour data registry.
A systematic review on TGCT in children was performed, seeking sources published between
1990 and 2016. Search terms and MeSh headings were “tenosynovial giant cell”, “diffuse type
giant cell”, “giant cell tumors”, “PVNS”, “pigmented villonodular synovitis”, and “synovitis, pigmented
villonodular” combined with “infant”, “child”, “neonat”, “pediatric”, “paediatric”, “toddler”, “teen”,
“teenager”, “juvenile”, “adolescent”, “girl”, and “boy”. A total of 619 articles were identified in PubMed,
Figure 1 Localized type TGCT: MRI of a 6-year-old boy with TGCT in his left knee. a. Sagittal T1-weighted
image showing a well-circumscribed nodular lesion at the synovial lining of the anterior knee compartment.
b. Sagittal T1-weighted spectral presaturation with inversion recovery (SPIR) image after IV gadolinium
administration shows heterogeneous enhancement.
a b
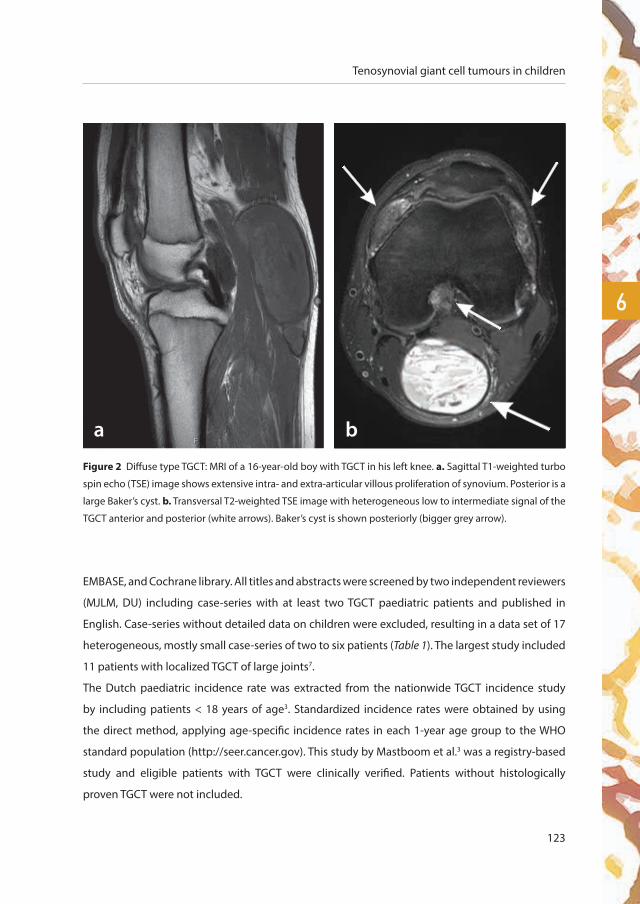
Tenosynovial giant cell tumours in children
123
6
Figure 2 Diffuse type TGCT: MRI of a 16-year-old boy with TGCT in his left knee. a. Sagittal T1-weighted turbo
spin echo (TSE) image shows extensive intra- and extra-articular villous proliferation of synovium. Posterior is a
large Baker’s cyst. b. Transversal T2-weighted TSE image with heterogeneous low to intermediate signal of the
TGCT anterior and posterior (white arrows). Baker’s cyst is shown posteriorly (bigger grey arrow).
a b
EMBASE, and Cochrane library. All titles and abstracts were screened by two independent reviewers
(MJLM, DU) including case-series with at least two TGCT paediatric patients and published in
English. Case-series without detailed data on children were excluded, resulting in a data set of 17
heterogeneous, mostly small case-series of two to six patients (Table 1). The largest study included
11 patients with localized TGCT of large joints7.
The Dutch paediatric incidence rate was extracted from the nationwide TGCT incidence study
by including patients < 18 years of age3. Standardized incidence rates were obtained by using
the direct method, applying age-specific incidence rates in each 1-year age group to the WHO
standard population (http://seer.cancer.gov). This study by Mastboom et al.3 was a registry-based
study and eligible patients with TGCT were clinically verified. Patients without histologically
proven TGCT were not included.

124
Chapter six
From our national bone and soft tissue tumour data registry (PALGA), a clinical data set was derived,
including 57 patients < 18 years with (histologically proven) TGCT in large joints, treated between
1995 and 2015, in one of the four tertiary sarcoma centres in The Netherlands. Clinical, biologic,
and imaging data on TGCT type, sex, localization, age at diagnosis, symptoms before diagnosis,
treatment(s), recurrence(s), and followup were collected.
A combined retrospective database of two tertiary oncology centres (Leiden University Medical
Centre and Radboud University Medical Centre) in The Netherlands has recorded all patients with
TGCT since 1990 (455 patients). TGCT data on children were compared with TGCT data on 423
adults (32 children within this database were excluded from the adult group).
Statistical analyses, for our clinical data set, were predominantly descriptive. Chi square test was
used to compare children and adults on TGCT type, sex (male versus female), localization (knee
versus other large joints), symptoms before diagnosis (pain, swelling, and loss of function: yes
versus no), first treatment (arthroscopic resection versus open resection), recurrent disease (no
recurrence versus recurrence), and followup status. Independent t-test was used to compare
median duration of symptoms and median time to followup. All reported p values were two-
tailed. Statistical significance level was defined at p < 0.05. The recurrence-free survival curve was
assessed with Kaplan-Meier methods.
This study was approved by the institutional review board from the Leiden University Medical
Centre (medical ethical approved protocol P13.029). Data capturing and analyses were performed
at Leiden University Medical Centre. SPSS Version 23 (Chicago, IL, USA) was used for analyses.
results
Our systematic review identified 17 case-series involving 76 children (39 female) with TGCT, 29
localized, 38 diffuse, and nine unknown type (Table 1). The paediatric group ranged from 3 to 18
years of age. The knee was most frequently affected (44 [58%]). Swelling, pain, and limited ROM were
described symptoms before diagnosis (mean duration, 15 months). The majority of patients were
primarily treated with synovectomy, either arthroscopic or open. Recurrent disease was described
in 10 patients (13%). Only five paediatric studies described function or quality of life after treatment.
Patients with (multiple) recurrences experienced impaired function and quality of life, according to
van der Heijden et al.22. Five children with diffuse TGCT, described by de Visser et al.13, had fair to

Tenosynovial giant cell tumours in children
125
6
excellent results on the Musculoskeletal Tumour Society (MSTS) score after surgical treatment (MSTS
by Enneking). Gholve et al.7 described 11 children with surgically treated localized TGCT without
disabling joint function according to a telephone questionnaire survey. Seven surgically treated
children, described by Baroni et al.4, recovered full ROM and two patients showed impaired joint
movement with occasional mild to moderate pain in four children with localized and five children
with diffuse type. Nakahara et al.21 showed three children with diffuse disease of the knee with almost
maximum Knee Society Scores and improved postoperative ROM of at least 0° to 145°.
The standardized paediatric TGCT incidence rate of large joints was 2.42 and 1.09 per million person-
years in localized and diffuse types, respectively3. Between 2009 and 2013, 53 children with localized
TGCT (excluding digits) and 24 children with diffuse TGCT were diagnosed in The Netherlands. This
resulted in a Dutch incidence rate of 2.86 per million person-years for localized TGCT (excluding digits)
and 1.30 per million person-years for diffuse TGCT; this was converted to standardized incidence
rates (Supplemental Table 1 [Supplemental materials are available with the online version of CORR®.]). In
both localized and diffuse types, the knee was most commonly affected (Figure 3).
Clinical data of TGCT in children from the four Dutch tertiary sarcoma centres seemed similar to those
observed in the combined two Dutch retrospective adult databases (Table 2). Fifty-seven children
(median age at diagnosis, 16 years; range, 4-18 years) with TGCT of large joints were identified (Table
2). Symptoms before diagnosis were swelling, pain, and limited ROM with a median duration of 12
months (range, 1-72 months). These symptoms and the diagnostic delay seemed similar to those
observed in adults (Table 2). Children showed a localized diffuse ratio of one to one; the knee was
predominantly affected (13 of 28 [46%] localized, 19 of 29 [66%] diffuse) and there was a predilection
for females (15 of 28 [54%] localized, 18 of 29 [62%] diffuse). In 423 adults, the localized:diffuse ratio
was 1:1.6; the knee was predominantly affected (121 of 172 [70%] localized, 189 of 251 [75%] diffuse)
with a predilection for females (107 of 172 [62%] localized, 142 of 251 [57%] diffuse).
Recurrence-free survival curves were not different with the numbers available between children
and adults at the four involved tumour centres (Figure 4). The 2.5-year recurrence-free survival,
after surgical treatment, in paediatric patients compared with adults was 85% (95% confidence
interval [CI], 67%-100%) versus 89% (95% CI, 83%-96%; p = 0.527) in localized and 53% (95%

126
Chapter six
Table 1 Literature overview on TGCT affecting all joints in children, including at least two
TGCT cases (1990-2016, English language)*
Study Year Number Sex Mean age (years; range)
Symptoms before
diagnosis
Mean duration of symptoms
(months; range)TGCT type Joint Primary
surgeriesRecurrent
diseaseMean followup
(months; range)
Givon8 1991 2 1 M, 1 F 7 (7-7) S, W, LROM 60 (both patients) 1 L, 1 D 2 knee 1 AS, 1 US 0 24 (12-36)
Rosenberg† 9 2001 2 2 M 12 (10-14) S NA 1 L, 1 D 2 knee 1 OS, 1 US NA NA
Neubauer|| 10 2007 5 3 M, 2 F 12 (8-15) S,P 10 (2-24) 5 unknown 4 knee, 1 ankle 5 AS 1 36 (12-84)
Gholve et al.|| 7 2007 11 6 M, 5 F 12 (7-16) S, P 10 (1-24) 11 L 2 knee, 3 ankle, 4 foot, 1 hand, 1 wrist 11 OS 0 54 (15-130)
Pannier† 11 2008 6 2 M, 4 F 12‡ NA NA 2 L, 4 D 5 knee, 1 ankle 5 US, 1 MT 2 58‡
Baroni et al. 4 2010 9 4 M, 5 F 11 (7-15)¶ S, P, LROM 18 (2-48) 4 L, 5 D 9 knee 4 AS, 5 OS 0 82 (46-143)
Current 2017 57 24 M, 33 F 14 (4-18) S, P, LROM 16 (1-72) 28 L, 29 D 32 knee, 11 ankle, 5 foot, 4 hip, 2 hand, 2 other, 1 wrist 9 AS, 47 OS, 1 WS 23 55 (0-260)
Also adult cases included
Abdul-Karim 12 1992 2 2 M 10 (10-10) S, P NA 2 D 1 foot, 1 ankle 1 US, 1 AP 0 132 (108-156)
de Visser et al. 13 1999 5 4 M, 1 F 16 (12-18) NA NA 5 D 4 knee, 1 ankle 4 US, 1 RS 5 residual disease 30 (21-75)
Perka 14 2000 2 2 F 12 (8-16) S, P, LROM 12‡ 2 L 2 knee 2 US 0 NA
Somerhausen 15 2000 4 3 M, 1 F 14 (3-18) S 7 (6-8) 4 D 1 knee, 1 foot, 1 buttock, 1 thigh 4 US 0/1 NA 44.5 (0-114)
Gibbons 16 2002 3 1 M, 2 F 11 (8-15) S 28 (6-96)§ 3 L 3 foot 3 US 0 NA
Bisbinas 17 2004 5 5 F 14 (12-15) S 2‡ 5 L 5 ankle 5 OS 0 46 (12-150)
Brien 18 2004 3 1 M, 2 F 13 (12-15) S, P 7 (1-24)§ 3 D 2 foot, 1 ankle 3 US 2 NA
Sharma 19 2006 4 2 M, 2 F 14 (8-17) S, P 2‡ 4 unknown 4 ankle 4 US 0 37.5 (19-65)
Sharma 20 2007 3 2 M, 1 F 17 (16-18) S, P 5 (2-9) 3 D 3 knee 3 OS 1 96 (54-138)
Nakahara et al. 21 2012 3 2 M, 1 F 11 (8-13) NA NA 3 D 3 knee 3 OS 0 29 (20-36)
van der Heijden 22 2014 7 2 M, 5 F 14 (6-18) NA NA 7 D 7 knee 4 AS, 3 OS 4 95 (24-212)
Total 133 57 L, 67 D, 9 unknown
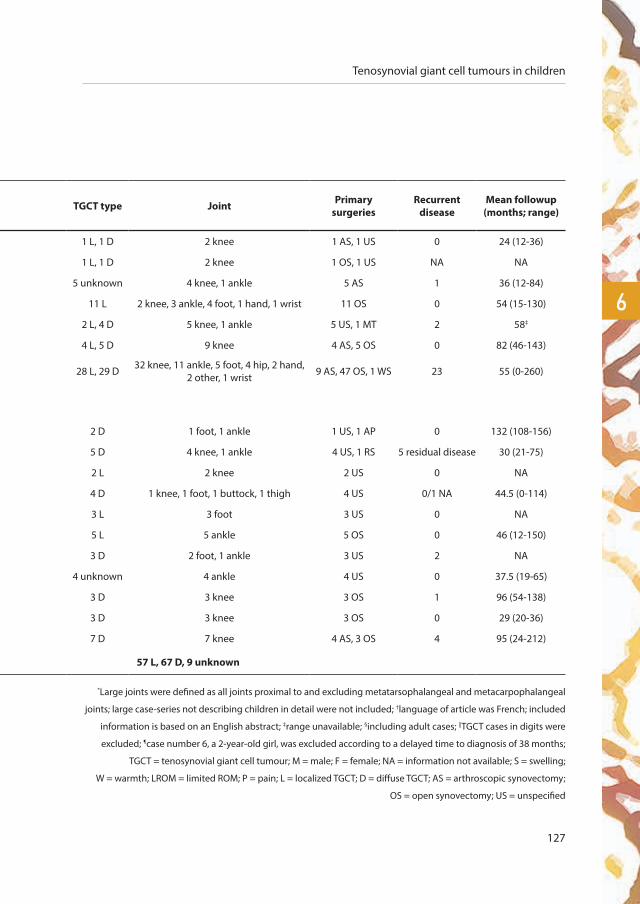
Tenosynovial giant cell tumours in children
127
6
Table 1 Literature overview on TGCT affecting all joints in children, including at least two
TGCT cases (1990-2016, English language)*
Study Year Number Sex Mean age (years; range)
Symptoms before
diagnosis
Mean duration of symptoms
(months; range)TGCT type Joint Primary
surgeriesRecurrent
diseaseMean followup
(months; range)
Givon8 1991 2 1 M, 1 F 7 (7-7) S, W, LROM 60 (both patients) 1 L, 1 D 2 knee 1 AS, 1 US 0 24 (12-36)
Rosenberg† 9 2001 2 2 M 12 (10-14) S NA 1 L, 1 D 2 knee 1 OS, 1 US NA NA
Neubauer|| 10 2007 5 3 M, 2 F 12 (8-15) S,P 10 (2-24) 5 unknown 4 knee, 1 ankle 5 AS 1 36 (12-84)
Gholve et al.|| 7 2007 11 6 M, 5 F 12 (7-16) S, P 10 (1-24) 11 L 2 knee, 3 ankle, 4 foot, 1 hand, 1 wrist 11 OS 0 54 (15-130)
Pannier† 11 2008 6 2 M, 4 F 12‡ NA NA 2 L, 4 D 5 knee, 1 ankle 5 US, 1 MT 2 58‡
Baroni et al. 4 2010 9 4 M, 5 F 11 (7-15)¶ S, P, LROM 18 (2-48) 4 L, 5 D 9 knee 4 AS, 5 OS 0 82 (46-143)
Current 2017 57 24 M, 33 F 14 (4-18) S, P, LROM 16 (1-72) 28 L, 29 D 32 knee, 11 ankle, 5 foot, 4 hip, 2 hand, 2 other, 1 wrist 9 AS, 47 OS, 1 WS 23 55 (0-260)
Also adult cases included
Abdul-Karim 12 1992 2 2 M 10 (10-10) S, P NA 2 D 1 foot, 1 ankle 1 US, 1 AP 0 132 (108-156)
de Visser et al. 13 1999 5 4 M, 1 F 16 (12-18) NA NA 5 D 4 knee, 1 ankle 4 US, 1 RS 5 residual disease 30 (21-75)
Perka 14 2000 2 2 F 12 (8-16) S, P, LROM 12‡ 2 L 2 knee 2 US 0 NA
Somerhausen 15 2000 4 3 M, 1 F 14 (3-18) S 7 (6-8) 4 D 1 knee, 1 foot, 1 buttock, 1 thigh 4 US 0/1 NA 44.5 (0-114)
Gibbons 16 2002 3 1 M, 2 F 11 (8-15) S 28 (6-96)§ 3 L 3 foot 3 US 0 NA
Bisbinas 17 2004 5 5 F 14 (12-15) S 2‡ 5 L 5 ankle 5 OS 0 46 (12-150)
Brien 18 2004 3 1 M, 2 F 13 (12-15) S, P 7 (1-24)§ 3 D 2 foot, 1 ankle 3 US 2 NA
Sharma 19 2006 4 2 M, 2 F 14 (8-17) S, P 2‡ 4 unknown 4 ankle 4 US 0 37.5 (19-65)
Sharma 20 2007 3 2 M, 1 F 17 (16-18) S, P 5 (2-9) 3 D 3 knee 3 OS 1 96 (54-138)
Nakahara et al. 21 2012 3 2 M, 1 F 11 (8-13) NA NA 3 D 3 knee 3 OS 0 29 (20-36)
van der Heijden 22 2014 7 2 M, 5 F 14 (6-18) NA NA 7 D 7 knee 4 AS, 3 OS 4 95 (24-212)
Total 133 57 L, 67 D, 9 unknown
*Large joints were defined as all joints proximal to and excluding metatarsophalangeal and metacarpophalangeal
joints; large case-series not describing children in detail were not included; †language of article was French; included
information is based on an English abstract; ‡range unavailable; §including adult cases; ||TGCT cases in digits were
excluded; ¶case number 6, a 2-year-old girl, was excluded according to a delayed time to diagnosis of 38 months;
TGCT = tenosynovial giant cell tumour; M = male; F = female; NA = information not available; S = swelling;
W = warmth; LROM = limited ROM; P = pain; L = localized TGCT; D = diffuse TGCT; AS = arthroscopic synovectomy;
OS = open synovectomy; US = unspecified

128
Chapter six
CI, 35%-79%) versus 56% (95% CI, 49%-64%; p = 0.691) in diffuse type, respectively. In the four
involved sarcoma centres, most children and adults alike were primarily surgically treated by open
resection: localized TGCT in 25 of 28 children (89%) were thus treated compared with 142 of 172
adults (85%; p = 0.486); for diffuse TGCT in children, the proportion was 22 of 29 (76%) compared
with 188 of 251 in adults (75%; p = 0.289). Recurrence risk in children and adults was likewise not
different with the numbers available: two of 28 (7%) compared with 22 of 172 (13%; p = 0.365)
in localized type and 11 of 29 (38%) compared with 119 of 251 (47%; p = 0.921) in diffuse type,
respectively.
Figure 3 Skeleton showing TGCT
localization in children extracted
from a Dutch incidence study,
excluding digits3. In diffuse
TGCT, one patient was classified
as “other”; he was treated for
TGCT in his vertebral column.
6%
17%
8%
47%
13%
9%
localized-TGCT diffuse-TGCT
4%
8%
4%
50%
25%
4%
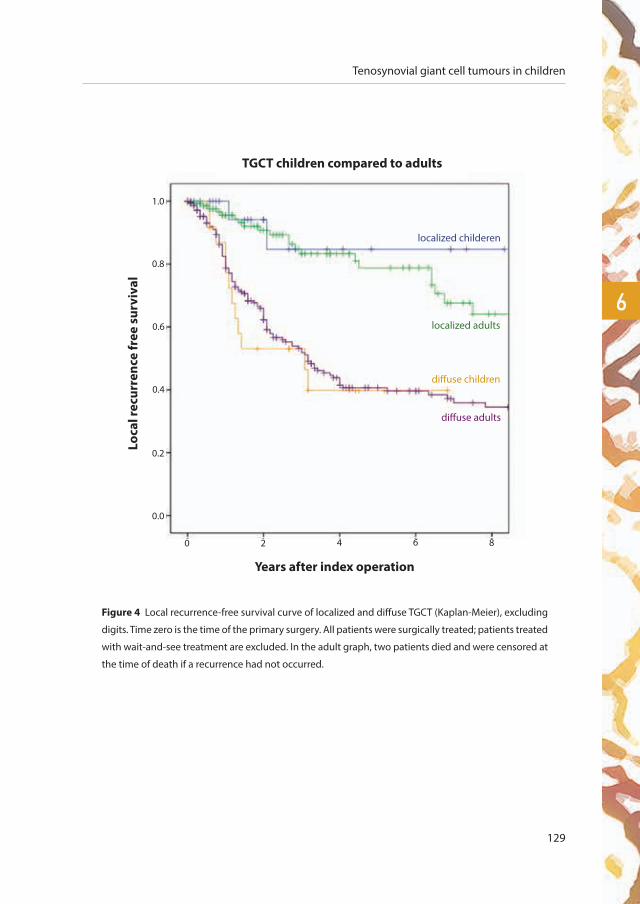
Tenosynovial giant cell tumours in children
129
6
Figure 4 Local recurrence-free survival curve of localized and diffuse TGCT (Kaplan-Meier), excluding
digits. Time zero is the time of the primary surgery. All patients were surgically treated; patients treated
with wait-and-see treatment are excluded. In the adult graph, two patients died and were censored at
the time of death if a recurrence had not occurred.
Years after index operation
Loca
l rec
urre
nce
free
sur
viva
l
TGCT children compared to adults
diffuse adults
diffuse children
localized childeren
localized adults
1.0
0.8
0.6
0.4
0.2
0 2 4 6 8
0.0

130
Chapter six
Table 2 Details of patients with TGCT of large joints in children versus adults,
including sex, localization, age, symptoms, first treatment, recurrent disease, and followup†
Children Adults Children versus adults
Patient variables Localized TGCT Diffuse TGCT Localized TGCT Diffuse TGCT p value localized TGCT
p value diffuse TGCT
Total number of patients 28 29 172 251
Sex 0.285 0.434
Male:female ratio 13:15 (1:1.2) 11:18 (1:1.6) 65:107 (1:1.6) 109:142 (1:1.3)
Localization 0.019 0.207
Knee 13 (46%) 19 (66%) 121 (70%) 189 (75%)
Other joints 15 (54%) 10 (34%) 51 (30%) 62 (25%)
Age
Median age at diagnosis (years; range) 16 (4-18) 16 (11-18) 42 (19-82) 38 (19-72)
Symptoms before diagnosis
Swelling 24 (86%) 21 (72%) 106 (62%) 163 (65%) 0.010 0.510
Pain 12 (43%) 17 (59%) 103 (60%) 157 (63%) 0.129 0.558
Limited ROM 3 (11%) 4 (14%) 13 (8%) 49 (20%) 0.608 0.486
Median duration of symptoms (months; range) 9 (1-48) 18 (1-72) 12 (1-240) 24 (1-300) 0.176 0.153
First treatment 0.486+ 0.289+
Arthroscopic resection 3 (11%) 6 (21%) 7 (4%) 37 (15%)
Open resection 25 (89%) 22 (76%) 147 (85%) 188 (75%)
Wait and see 0 1 (3%) 18 (11%) 26 (10%)
Recurrent disease† N = 28 N = 28 N = 154 N = 225 0.280 0.407
No recurrence 26 (93%) 17 (61%) 132 (86%) 106 (47%)
≥ 1 recurrence 2 (7%) 11 (39%) 22 (14%) 119 (53%)
Followup status 0.840 0.768
Disease-free 19 (68%) 16 (55%) 110 (64%) 121 (48%)
Alive with disease‡ 4 (14%) 9 (31%) 19 (11%) 94 (37%)
Death of other disease 0 0 0 2 (1%)
Lost to followup‡ 5 (18%) 4 (14%) 43 (25%) 34 (14%)
Median time to followup (months; range)* 25 (7-100) 77 (7-144) 36 (6-301) 54 (6-350) 0.127 0.780
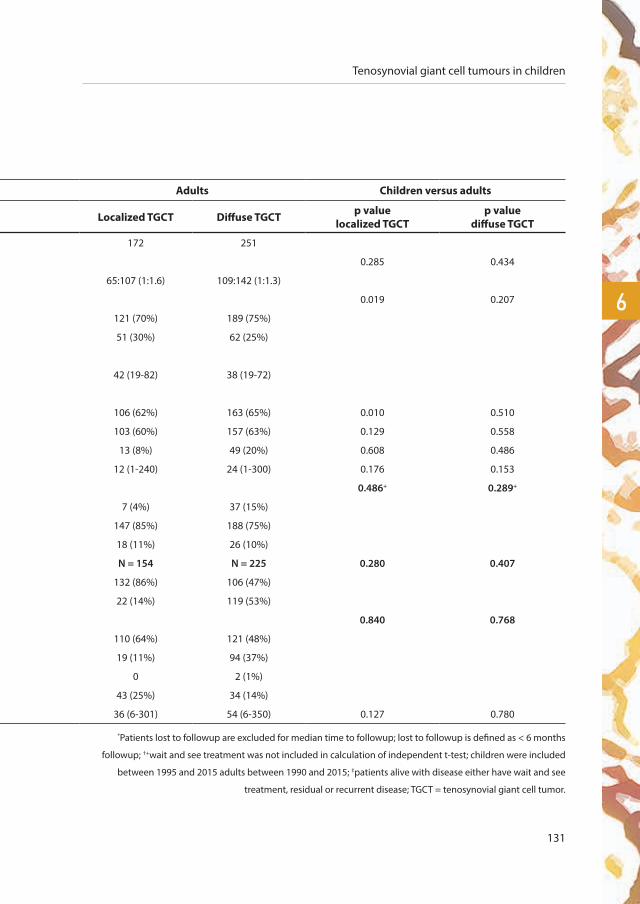
Tenosynovial giant cell tumours in children
131
6
Table 2 Details of patients with TGCT of large joints in children versus adults,
including sex, localization, age, symptoms, first treatment, recurrent disease, and followup†
Children Adults Children versus adults
Patient variables Localized TGCT Diffuse TGCT Localized TGCT Diffuse TGCT p value localized TGCT
p value diffuse TGCT
Total number of patients 28 29 172 251
Sex 0.285 0.434
Male:female ratio 13:15 (1:1.2) 11:18 (1:1.6) 65:107 (1:1.6) 109:142 (1:1.3)
Localization 0.019 0.207
Knee 13 (46%) 19 (66%) 121 (70%) 189 (75%)
Other joints 15 (54%) 10 (34%) 51 (30%) 62 (25%)
Age
Median age at diagnosis (years; range) 16 (4-18) 16 (11-18) 42 (19-82) 38 (19-72)
Symptoms before diagnosis
Swelling 24 (86%) 21 (72%) 106 (62%) 163 (65%) 0.010 0.510
Pain 12 (43%) 17 (59%) 103 (60%) 157 (63%) 0.129 0.558
Limited ROM 3 (11%) 4 (14%) 13 (8%) 49 (20%) 0.608 0.486
Median duration of symptoms (months; range) 9 (1-48) 18 (1-72) 12 (1-240) 24 (1-300) 0.176 0.153
First treatment 0.486+ 0.289+
Arthroscopic resection 3 (11%) 6 (21%) 7 (4%) 37 (15%)
Open resection 25 (89%) 22 (76%) 147 (85%) 188 (75%)
Wait and see 0 1 (3%) 18 (11%) 26 (10%)
Recurrent disease† N = 28 N = 28 N = 154 N = 225 0.280 0.407
No recurrence 26 (93%) 17 (61%) 132 (86%) 106 (47%)
≥ 1 recurrence 2 (7%) 11 (39%) 22 (14%) 119 (53%)
Followup status 0.840 0.768
Disease-free 19 (68%) 16 (55%) 110 (64%) 121 (48%)
Alive with disease‡ 4 (14%) 9 (31%) 19 (11%) 94 (37%)
Death of other disease 0 0 0 2 (1%)
Lost to followup‡ 5 (18%) 4 (14%) 43 (25%) 34 (14%)
Median time to followup (months; range)* 25 (7-100) 77 (7-144) 36 (6-301) 54 (6-350) 0.127 0.780
*Patients lost to followup are excluded for median time to followup; lost to followup is defined as < 6 months
followup; †+wait and see treatment was not included in calculation of independent t-test; children were included
between 1995 and 2015 adults between 1990 and 2015; ‡patients alive with disease either have wait and see
treatment, residual or recurrent disease; TGCT = tenosynovial giant cell tumor.

132
Chapter six
discussion
TGCT is most commonly seen in adults in the third and fourth decades of life, but this study confirms
that it also affects paediatric patients. The paediatric incidence rate for both localized and diffuse
type suggests that it is rare, but we believe it is still common enough to include in the differential
diagnosis of both children and adults with nonspecific symptoms like swelling, pain, and limited
ROM. We found no differences with the numbers available between children and adults in terms
of presenting symptoms, treatments used in the few available case-series, and recurrence-free
survival rates. In the era of personalized medicine, future research should define the most effective
treatment for TGCT, with its various clinical scenarios, both in children and adults.
There are some limitations to this study. In our systematic review, many case-series included data from
children with TGCT in embedded studies that also contained adults’ data. When data on children was
not separately described, these children were not included in the overview (Table 1). The determined
incidence rate is a conservative estimate, because our search was based on the nationwide network
and registry of histo- and cytopathology in The Netherlands23. Patients with TGCT without a biopsy
or treatment were not represented in this pathology-based cohort. By standardizing incidence rates,
they could be extrapolated to other populations. However, generalizability of the standardized
incidence rate depends on the age-specific population structure of the country compared with the
WHO population. Included patients had histologically proven TGCT by a dedicated musculoskeletal
pathologist (UF, HB, AS, JB). However, patients were not centrally reviewed for this study. Neither
functional outcome nor quality of life was evaluated. For TGCT treatment, only surgical treatment
was evaluated. Future, comparative studies on treatments should determine what should be done for
patients (children and adults) with TGCT. Although surgery is the mainstay, other treatments are used,
and future research needs to define what the best approaches are for the various clinical scenarios in
which this disease presents. In our patients, children with the localized type frequently lacked longer
term followup, mainly as a result of absence of clinical symptoms (17 censored in the first 2.5 years;
Figure 4). Smaller patient numbers with the diffuse type sometimes lacked longer followup (nine
censored in the first 2.5 years).
TGCT does not seem to be an adults-only disease and should be considered in the differential
diagnosis in children with (chronic) monoarticular joint effusion. Our systematic review identified
mainly small, heterogeneous TGCT case-series in children. Future studies might consider including
children with TGCT to allow for optimalization of the treatment protocol in both children and adults.

Tenosynovial giant cell tumours in children
133
6
The standardized paediatric TGCT incidence rate of large joints was 2.42 and 1.09 per million
person-years compared with an overall incidence rate of 10.2 and 4.1 per million person-years
in localized and diffuse types, respectively3. To date, the incidence rate for chronic monoarthritis
in children and adolescents is unknown. Savolainen et al. calculated an incidence rate of 64
per 100,000 for all types of arthritis in children (< 16 years) in a defined population in Finland24.
Although TGCT in children probably accounts for only a small percentage of all types of arthritis, it
should still be considered in the differential diagnosis.
Symptoms in children seemed similar to those in adults (Table 1). Nonspecific symptoms
accompanied by pain and diffuse joint swelling with thickening of the synovial capsule and/or
joint effusion resulted in limited movement in approximately half of the patients. Studies in adults
add mechanical symptoms, instability, and stiffness5, 25.
A systematic review (without age limitations) in 20135 reported average recurrence rates for
localized TGCT in the knee after open resection (4%) and after arthroscopic resection (6%) in
contrast to diffuse type after open resection (14%) and after arthroscopic resection (40%) at a
mean followup of 108 months. Patel et al.25 presented 214 patients with knee TGCT of all ages with
a recurrence rate of 9% in 100 localized patients and 48% in 114 patients with diffuse TGCT after a
mean followup of 25 months (range, 1-168 months). Palmerini et al.26 reported 294 patients with
TGCT of all ages in all joints with a local failure rate of 14% in localized and 36% in diffuse type after
a median followup of 4.4 years (range, 1-20 years). The sole primary disease or patients with a first
relapse were included. The current paediatric case-series showed comparable recurrence rates of
7% in localized and 39% in diffuse type after a mean followup of 55 months (range, 7-350 months).
TGCT is a rare condition in adults and it is even less common in children. Nonspecific symptoms
often contribute to a delay in establishing a diagnosis. TGCT should be considered in chronic
monoarthritis both in adults and in children. Recurrent disease after surgical treatment of this
orphan disease seems comparable between children and adults. With targeted therapies now
being developed27, future research should define the most effective treatment strategies for this
heterogeneous disease.
Supplementary data
Supplementary data are available in the online version of this article:
https://dx.doi.org/10.1007/s11999.0000000000000102

134
Chapter six
references
1. de St. Aubain Somerhausen N, van de Rijn M. Tenosynovial giant cell tumour, localized type/diffuse type. In: Fletcher CD,
Bridge JA, Hogendoorn PC, Mertens F, editors. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4th ed. Lyon:
IARC Press; 2013. p. 100-3.
2. Fletcher CDM. WHO Classification of Tumours of Soft Tissue and Bone: IARC Press; 2013.
3. Mastboom MJL, Verspoor, FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, Bovée JVMG, Dijkstra PDS,
Schreuder HWB, Gelderblom H, Sande van de MAJ, TGCT study group. Higher incidence rates than previously known in
tenosynovial giant cell tumors. Acta Orthopaedica. 2017;88.
4. Baroni E, Russo BD, Masquijo JJ, Bassini O, Miscione H. Pigmented villonodular synovitis of the knee in skeletally
immature patients. Journal of children’s orthopaedics. 2010;4(2):123-7.
5. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
6. Chiari C, Pirich C, Brannath W, Kotz R, Trieb K. What affects the recurrence and clinical outcome of pigmented villonodular
synovitis? Clin Orthop Relat Res. 2006;450:172-8.
7. Gholve PA, Hosalkar HS, Kreiger PA, Dormans JP. Giant cell tumor of tendon sheath: largest single series in children.
Journal of pediatric orthopedics. 2007;27(1):67-74.
8. Givon U, Ganel A, Heim M. Pigmented villonodular synovitis. Archives of disease in childhood. 1991;66(12):1449-50.
9. Rosenberg D, Kohler R, Chau E, Bouvier R, Pouillaude JM, David L. [Pigmented villonodular synovitis. Diffuse and localized
forms in children]. Archives de pediatrie : organe officiel de la Societe francaise de pediatrie. 2001;8(4):381-4.
10. Neubauer P, Weber AK, Miller NH, McCarthy EF. Pigmented villonodular synovitis in children: a report of six cases and
review of the literature. The Iowa orthopaedic journal. 2007;27:90-4.
11. Pannier S, Odent T, Milet A, Lambot-Juhan K, Glorion C. [Pigmented villonodular synovitis in children: review of six cases].
Revue de chirurgie orthopedique et reparatrice de l’appareil moteur. 2008;94(1):64-72.
12. Abdul-Karim FW, el-Naggar AK, Joyce MJ, Makley JT, Carter JR. Diffuse and localized tenosynovial giant cell tumor
and pigmented villonodular synovitis: a clinicopathologic and flow cytometric DNA analysis. Human pathology.
1992;23(7):729-35.
13. de Visser E, Veth RP, Pruszczynski M, Wobbes T, Van de Putte LB. Diffuse and localized pigmented villonodular synovitis:
evaluation of treatment of 38 patients. Archives of orthopaedic and trauma surgery. 1999;119(7-8):401-4.
14. Perka C, Labs K, Zippel H, Buttgereit F. Localized pigmented villonodular synovitis of the knee joint: neoplasm or reactive
granuloma? A review of 18 cases. Rheumatology (Oxford, England). 2000;39(2):172-8.
15. Somerhausen NS, Fletcher CD. Diffuse-type giant cell tumor: clinicopathologic and immunohistochemical analysis of 50
cases with extraarticular disease. The American journal of surgical pathology. 2000;24(4):479-92.
16. Gibbons CL, Khwaja HA, Cole AS, Cooke PH, Athanasou NA. Giant-cell tumour of the tendon sheath in the foot and ankle.
The Journal of bone and joint surgery British volume. 2002;84(7):1000-3.
17. Bisbinas I, De Silva U, Grimer RJ. Pigmented villonodular synovitis of the foot and ankle: a 12-year experience from a
tertiary orthopedic Oncology Unit. The Journal of foot and ankle surgery : official publication of the American College of
Foot and Ankle Surgeons. 2004;43(6):407-11.
18. Brien EW, Sacoman DM, Mirra JM. Pigmented villonodular synovitis of the foot and ankle. Foot & ankle international.
2004;25(12):908-13.
Tenosynovial giant cell tumours in children
135
6
19. Sharma H, Jane MJ, Reid R. Pigmented villonodular synovitis of the foot and ankle: Forty years of experience from the
Scottish bone tumor registry. The Journal of foot and ankle surgery : official publication of the American College of Foot
and Ankle Surgeons. 2006;45(5):329-36.
20. Sharma H, Rana B, Mahendra A, Jane MJ, Reid R. Outcome of 17 pigmented villonodular synovitis (PVNS) of the knee at
6 years mean follow-up. The Knee. 2007;14(5):390-4.
21. Nakahara H, Matsuda S, Harimaya K, Sakamoto A, Matsumoto Y, Okazaki K, et al. Clinical results of open synovectomy
for treatment of diffuse pigmented villonodular synovitis of the knee: case series and review of literature. The Knee.
2012;19(5):684-7.
22. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical
treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J.
2014;96-B(8):1111-8.
23. Casparie M, Tiebosch AT, Burger G, Blauwgeers H, van de Pol A, van Krieken JH, et al. Pathology databanking and
biobanking in The Netherlands, a central role for PALGA, the nationwide histopathology and cytopathology data
network and archive. Cell Oncol. 2007;29(1):19-24.
24. Savolainen E, Kaipiainen-Seppanen O, Kroger L, Luosujarvi R. Total incidence and distribution of inflammatory
joint diseases in a defined population: results from the Kuopio 2000 arthritis survey. The Journal of rheumatology.
2003;30(11):2460-8.
25. Patel KH, Gikas PD, Pollock RC, Carrington RW, Cannon SR, Skinner JA, et al. Pigmented villonodular synovitis of the knee:
A retrospective analysis of 214 cases at a UK tertiary referral centre. Knee. 2017;24(4):808-15.
26. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.
27. Brahmi M, Vinceneux A, Cassier PA. Current Systemic Treatment Options for Tenosynovial Giant Cell Tumor/Pigmented
Villonodular Synovitis: Targeting the CSF1/CSF1R Axis. Current treatment options in oncology. 2016;17(2):10.


loca
lize
dsurgical treatment
of localized-type tenosynovial giant
cell tumours of large joints
chap
ter
seve
n
a multicentre-pooled database of 31 international sarcoma centres
M.J.L. Mastboom1, E.L. Staals2, F.G.M. Verspoor3, A.J. Rueten-Budde4, S. Stacchiotti5, E. Palmerini6, G.R. Schaap7, P.C. Jutte8,
W. Aston9, A. Leithner10, D. Dammerer11, A. Takeuchi12, Q. Thio13, X. Niu14, J.S. Wunder15, TGCT study-group*, M.A.J. van de Sande1
Submitted.

1 Orthopaedic Surgery, Leiden University Medical Center, Leiden, The Netherlands
2 Orthopaedic Surgery, Musculoskeletal Oncology Department, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy
3 Orthopaedic Surgery, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands
4 Mathematical institute, Leiden University, Leiden, The Netherlands
5 Medical Oncology, Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy
6 Medical Oncology, Musculoskeletal Oncology Department, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy
7 Orthopaedic Surgery, Academic Medical Center, Amsterdam, The Netherlands
8 Department of Orthopaedics, University Medical Center, University of Groningen, Groningen, The Netherlands
9 Orthopedic surgery, Royal National Orthopedic Hospital, London, the United Kingdom
10 Department of Orthopaedic Surgery, Medical University Graz, Graz, Austria
11 Orthopedic surgery, Medical University of Innsbruck, Innsbruck, Austria
12 Orthopaedic surgery, Kanazawa University Graduate School of Medical Sciences, Kanazawa, Japan
13 Orthopedic surgery, Massachusetts General Hospital Harvard, Boston, United States of America
14 Department of Orthopedic Oncology, Beijing Jishuitan Hospital, Beijing, 100035, China
15 University Musculoskeletal Oncology Unit, Mount Sinai Hospital, Toronto, Canada
*TGCT study-group:
M. Fiocco, H. Gelderblom, P.D.S. Dijkstra, R.J.P. van der Wal, P.A. Daolio, P. Picci, A. Gronchi, S. Ferrari, H. Özger, R.G.
Maki, H.W.B. Schreuder, I.C.M. van der Geest, J.A.M. Bramer, M. Boffano, E. Goldenitsch, D. Campanacci, P. Cuomo,
P.C. Ferguson, A.M. Griffin, Y. Sun, T. Schubert, K. Patel, M.S.J. Aranguren, A. Blancheton, F. Gouin, H.R. Dürr, C.F.
Capellen, J. Schwab, S. Iwata, O. Vyrva, W. Weschenfelder, E.H.M. Wang, M. Wook Joo, Y.K. Kang, Y.G. Chung, W.
Ebeid, J. Bruns, T. Ueda

Localized-type tenosynovial giant cell tumours
139
7
abstract
Background
Localized-type Tenosynovial Giant Cell Tumour (TGCT) is a rare, neoplastic disease with only limited
data supporting treatment protocols. A multicentre-pooled collection of individual patient data
resulted in the largest global retrospective cohort of localized-TGCT patients to date. We describe
treatment protocols and evaluate their oncological outcome, complications and functional results.
A secondary study aim was to identify risk factors for local recurrence after surgical treatment.
Methods
Patients with histologically proven localized-TGCT of large joints were included if treated between
1990-2017 in one of 31 tertiary sarcoma centres. In 941 patients with localized-TGCT, 62% were female,
median age at initial treatment was 39 years with a median follow-up of 37 months. 67% affected the
knee and the primary treatment at a tertiary centre was one-staged open resection in 73%. Proposed
risk factors were tested in a univariate analysis and significant factors subsequently included for
multivariate analysis, with an endpoint of first local recurrence after treatment in a tertiary centre.
Results
Recurrent disease developed in 12% of all cases, with local recurrence free survival rates at 3, 5
and 10 years of 88%, 83% and 79%, respectively. The strongest risk factor for recurrent disease was
prior recurrence (p<0.001). Complications were noted in 4% after surgical treatment of localized-
TGCT. Initial symptoms of pain and swelling improved after surgical treatment(s) in 71% and
85%, respectively. For therapy naïve cases, univariate and multivariate analyses yielded positive
associations with local recurrence for tumour size ≥5 cm vs <5 cm (HR 2.50; 95%CI 1.32-4.74; p=0.005)
and initial treatment with arthroscopy vs open resection (HR 2.18; 95%CI0.98-4.84; p=0.056).
Conclusions
Risk factors for recurrent disease after resection of localized-type TGCT were larger tumour size
and initial treatment with arthroscopy. Relatively low complication rates and good functional
outcome warrant an open approach with complete resection when possible, to reduce recurrence
rates in high risk patients.

140
Chapter seven
introduction
In 2013 the WHO defined Tenosynovial Giant Cell Tumours (TGCT), after unification of Giant
Cell Tumour of the Tendon Sheath and Pigmented Villonodular Synovitis (PVNS), as a benign
mono-articular disease, arising from the synovial lining of joints, bursae or tendon sheaths in
predominantly young adults1, 2.
Clinically and radiographically, TGCT is subdivided into a lobulated often well-bordered lesion
(localized-type) that does not involve the surrounding (teno-)synovial lining and a more
aggressive lesion, involving a large part or all of the synovial lining (diffuse-type)1-3. Despite
sharing the same histopathology and genetics, the natural course of disease in localized- and
diffuse-TGCT is incomparable and necessitate a separate assessment of treatment protocol and
surgical outcome. Based on anatomical site of the localized-type tumour, differentiation is made
between disease affecting digits and disease occurring in and about larger joints4-6. The present
study focuses on localized-TGCT of large joints (figure 1), most commonly affecting the knee or
other weight bearing joints1, 2, 6, 7.
The macroscopic appearance of localized-TGCT is typically a well-circumscribed lobulated lesion,
with white to grey, yellow and brown mottled areas. According to the WHO, localized-TGCT is a
small lesion, with a size range of 0.5 to 4 cm1, 2. However, according to the authors’ experience, the
largest size can frequently exceed 4 cm, especially when compressed in relatively tight joints (e.g.
foot and ankle) or situated in the anterior or posterior aspect of the knee.
The main patients complaints related to localized-TGCT include pain, joint effusion, stiffness,
locking and limited range of motion8, 9. The predominant standard of care for localized-TGCT is
surgical resection of the tumour, in order to: (1) reduce debilitating symptoms and prevent joint
destruction caused by local compression of cartilage; (2) improve limb function; and (3) minimize
the risk of local recurrence. Clinical and oncological outcomes following surgery depend on
multiple factors including the localization and extent of disease and possibly the technical
experience of the surgeons3, 7, 10-12.
The current literature mainly consists of relatively small, or larger but heterogeneous case-series,

Localized-type tenosynovial giant cell tumours
141
7
as localized-TGCT of large joints is an orphan disease, with an incidence of 10.2 per million person-
years6. A systematic review, including predominantly small case-series up to ten patients, showed
comparable recurrence rates after arthroscopic and open resection of the knee (6% versus 4%,
respectively)13. However, studies included in this review had different follow-up times ranging
from not available to 18, up till 112 months. Complications and functional outcomes after surgical
treatment are only sparsely reported and surgical treatment by arthroscopic or open resection for
localized-TGCT at present remains a matter of debate7-9, 14-16.
Evaluation of a large number of individual patients is preferred to evaluate the best treatment
strategy and possibly identify risk-factors for recurrent disease. Individual participant data meta-
analysis offers advantages, above a meta-analyses, as missing data can be accounted for at the
individual level, subgroup analyses can be performed (e.g. per affected joint) and follow-up
information can be updated17. Therefore, we aimed to collaborate with tertiary sarcoma centres all
over the world to include individual participant data of TGCT affecting large joints.
The primary aim of this international multicentre cohort study is to provide comprehensive and
up to date insights on TGCT surgical treatment as well as oncologic and functional outcomes
and complications in this largest global retrospective cohort of patients with localized-TGCT.
Secondarily, risk factors for local recurrence after surgical treatment are identified.
methods
Recruitment and inclusion criteria
Patients with histologically proven TGCT of large joints were included if treated between 1990 and
2017 in one of 31 sarcoma centres globally (supplementary material). Large joints were defined as
all joints proximal to the metatarsophalangeal and metacarpophalangeal joints. Identification and
collection of TGCT cases was performed in the centres of origin and data were collected based on
the initial treatment at tertiary centres. Data were encrypted and transferred to the international
multicentre database at the Leiden University Medical Centre (LUMC). Patient accrual occurred
between May 2016 until May 2018.

142
Chapter seven
Figure 1 Intra-articular localized-TGCT in the posterior part of the left knee in a 19 year old female. a. Sagittal
T1-weighted Magnetic Resonance (MR) imaging after intravenous contrast injection with fat suppression. TGCT
shows marked enhancement after contrast injection. b. TGCT shows an intermediate to low signal intensity on
a sagittal T2-weighted MR scan. c. On a sagittal proton-density weighted MR imaging, localized-TGCT presents
with low signal intensity. d. Macroscopic aspect of a well-circumscribed localized-TGCT after complete open
resection. Arrow shows brownish areas, representing hemosiderin depositions. On the ruler, 1 block equals 1 cm.
a b
c d
Localized-type tenosynovial giant cell tumours
143
7
Study parameters
Collected patient-, tumour- and treatment characteristics with corresponding definitions are
shown in appendix table 1. Complete data on core criteria was necessary for reliable analyses. The
following characteristics were defined as core criteria: TGCT-type, admission status, date and type
of initial treatment at tertiary centre and first local recurrence.
Patient-, tumour- and treatment characteristics
Thirty-one specialized sarcoma centres spread throughout Europe, North America, Canada and Asia
collaborated to provide a total of 2169 TGCT cases. The present study focuses on localized-TGCT (table
1), therefore patients with diffuse-TGCT (N=1192) or unknown type TGCT (N=36) were excluded.
Statistical analyses
The endpoint for statistical analysis was local recurrence free survival after initial treatment in a tertiary
centre. Recurrent disease was defined as new disease presence after resection performed in a tertiary centre
or progressive residual disease (as diagnosed on repeated follow-up Magnetic Resonance (MR) imaging).
To investigate the effect of risk factors on outcome, univariate analyses were performed and
significant factors (p<0.05) were subsequently included in a multivariate analysis. Proposed
risk factors were admission status (therapy-naïve versus recurrent disease), sex (male versus
female), age (≤35 years versus >35 years), localization (knee versus hip versus foot and ankle
versus upper extremity), bone-involvement (present versus absent), surgical technique (open
versus arthroscopic) and size (<5 cm versus ≥5 cm). Patients with treatment ‘wait and see’ or
‘endoprosthetic reconstruction’ were excluded from statistical analyses (N=85).
Observed recurrence free survival probabilities at 3, 5, and 10 years were computed for all cases
and subgroups based on admission status and localization.
All data were selected for completeness on core criteria (appendix table 1 and figure 1). Statistical
analyses were carried out using R version 3.4.1. Exact survival information and statistical methods
are shown in supplementary material.
Purposefully, an estimate of the median time to recurrence was not provided. Calculating such
a median, based on patients for whom a recurrence was recorded, would assume that all other
patients could not experience a recurrence in the future. The extent of this so-called immortal time
bias is unknown. For this reason, such an estimate will always be an underestimation of the true
time to recurrence.

144
Chapter seven
^Therapy-naïve or primary admission at tertiary centre are considered similar. ^^≥1 Surgery elsewhere
or recurrent admission are considered similar. *Digits are excluded. #Symptoms were defined as either
pain, swelling, stiffness or limited range of motion (table 8-9). $Wait and see or conservative treatment are
considered similar. +Endoprosthetic reconstruction or wait and see as initial treatment are excluded for
risk and survival analyses. &Resection not specified is considered either arthroscopic- or open resection.
Table 1 Patient-, tumour- and treatment characteristics
Characteristics Overall (%)
Total number 941 (100)
Admission status (N=941) Therapy naïve^
≥1 Surgery elsewhere^^897 (95)
44 (5)Sex (N=941) Male Female
360 (38)581 (62)
Median age at initial treatment years (N=882) IQR ≤35 years >35 years
3927-50
374 (42)508 (58)
Localization (N=941) (figure 2) Knee Hip Ankle Foot* Shoulder Elbow Wrist Hand* Other
633 (67)37 (4)
119 (13)58 (6)9 (1)
14 (2)24 (3)33 (4)14 (2)
Bone involvement (N=689) Present Absent
57 (8) 632 (92)
Median duration of symptoms# months (N=571) IQR
94-24
Type of (surgical) treatment at tertiary centre (N=930) Arthroscopic resection One-staged open resection Endoprosthetic reconstruction+
Wait and see$,+
Resection not specified&
140 (15)675 (73)
21 (2)64 (7)30 (3)
Median tumour size initial treatment in cm (N=637) IQR <5 cm ≥5 cm
3.02.0-4.5
496 (78)141 (22)
Adjuvant therapy initial treatment (N=787) External beam radiotherapy 90Yttrium Systemic targeted therapy Other None
8 (1)21 (3)2 (0.3)11 (1)
745 (95)
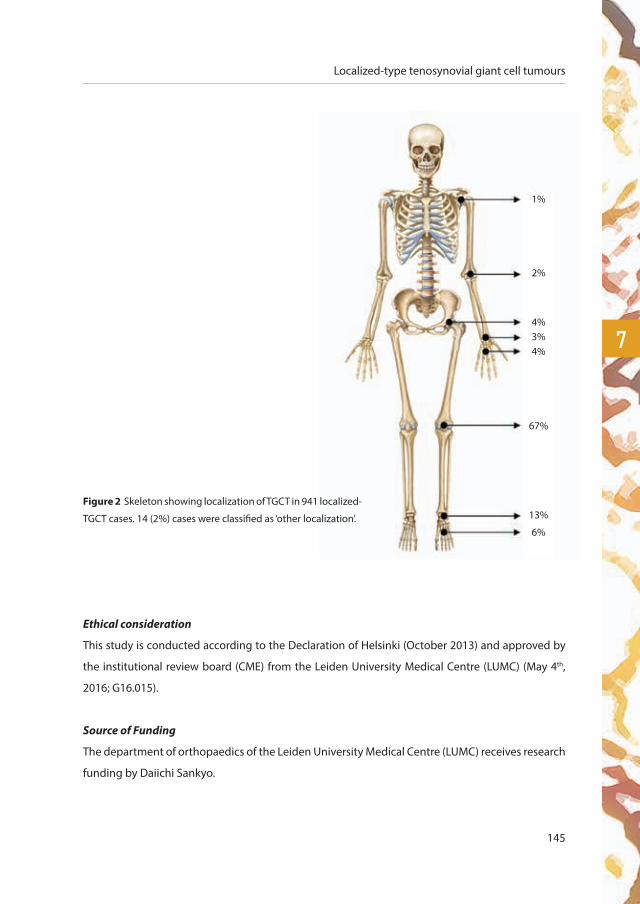
Localized-type tenosynovial giant cell tumours
145
7
Ethical consideration
This study is conducted according to the Declaration of Helsinki (October 2013) and approved by
the institutional review board (CME) from the Leiden University Medical Centre (LUMC) (May 4th,
2016; G16.015).
Source of Funding
The department of orthopaedics of the Leiden University Medical Centre (LUMC) receives research
funding by Daiichi Sankyo.
1%
2%
4%3%4%
67%
13%
6%
Figure 2 Skeleton showing localization of TGCT in 941 localized-
TGCT cases. 14 (2%) cases were classified as ‘other localization’.
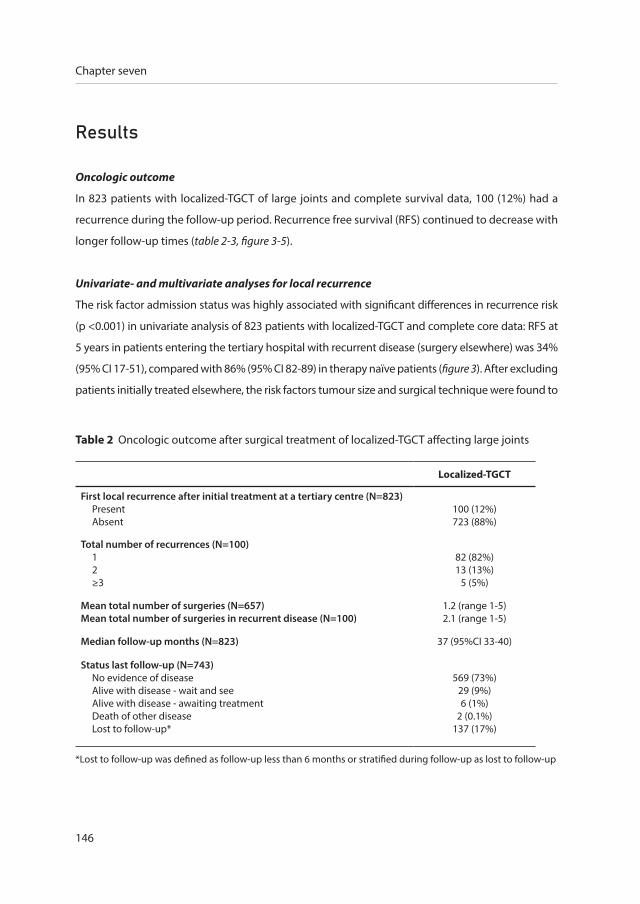
146
Chapter seven
results
Oncologic outcome
In 823 patients with localized-TGCT of large joints and complete survival data, 100 (12%) had a
recurrence during the follow-up period. Recurrence free survival (RFS) continued to decrease with
longer follow-up times (table 2-3, figure 3-5).
Univariate- and multivariate analyses for local recurrence
The risk factor admission status was highly associated with significant differences in recurrence risk
(p <0.001) in univariate analysis of 823 patients with localized-TGCT and complete core data: RFS at
5 years in patients entering the tertiary hospital with recurrent disease (surgery elsewhere) was 34%
(95% CI 17-51), compared with 86% (95% CI 82-89) in therapy naïve patients (figure 3). After excluding
patients initially treated elsewhere, the risk factors tumour size and surgical technique were found to
Table 2 Oncologic outcome after surgical treatment of localized-TGCT affecting large joints
Localized-TGCT
First local recurrence after initial treatment at a tertiary centre (N=823) Present Absent
100 (12%) 723 (88%)
Total number of recurrences (N=100) 1 2 ≥3
82 (82%)13 (13%)
5 (5%)
Mean total number of surgeries (N=657)Mean total number of surgeries in recurrent disease (N=100)
1.2 (range 1-5)2.1 (range 1-5)
Median follow-up months (N=823) 37 (95%CI 33-40)
Status last follow-up (N=743) No evidence of disease Alive with disease - wait and see Alive with disease - awaiting treatment Death of other disease Lost to follow-up*
569 (73%)29 (9%)6 (1%)
2 (0.1%)137 (17%)
*Lost to follow-up was defined as follow-up less than 6 months or stratified during follow-up as lost to follow-up

Localized-type tenosynovial giant cell tumours
147
7be positively associated with first local recurrence (table 4-5, figure 3-5). Younger patients ≤35 years
also had fewer recurrences than older patients (82% vs 88%, p=0.04). Similar results were calculated
in a subgroup analysis in therapy naïve patients with localized-TGCT affecting the knee.
Observed recurrence free survival according to admission status and localization
As arthroscopic resection is less common in the hip, foot/ankle and upper extremity, arthroscopic
and open resection were compared for TGCT affecting the knee (figure 5). The highest recurrence
rates occurred in therapy naïve patients with tumours located within the knee joint who were
initially treated with an arthroscopic resection (18%) (figure 6).
When comparing therapy naïve patients with patients initially treated elsewhere, a declining RFS
was observed at 3, 5 and 10 years in subgroup analyses of patients with tumours located in the
knee, foot/ankle and upper extremity (table 6).
Complications
A total of 34 (4%) complications after surgical treatment of localized-TGCT were reported (table
7). The majority of these complications presented after open resection (30/34; 88%). Following
arthroscopic resection, two complications were reported (6%).
Functional outcome
Prior to surgical treatment, the majority of patients had symptoms of pain (73%) and swelling (66%)
(table 8). After surgical treatment, at final follow-up, symptoms of pain, swelling, joint stiffness and
limited range of motion were absent in the majority of cases.
Table 3 Localized-TGCT recurrence free survival (RFS) of all patients and therapy naïve patients treated at a tertiary centre
Year N all % RFS all (95%CI) N therapy naïve % RFS therapy naïve (95%CI)
3 388 88 (85-91) 372 90 (88-93)
5 231 83 (80-87) 223 86 (82-89)
10 66 79 (75-84) 63 82 (78-87)
N is number of patients at risk at 3, 5, and 10 years

148
Chapter seven
Figure 3 Local recurrence free survival curve in localized-TGCT stratified for admission status (p<0.001)
Time zero was date of initial resection at tertiary centre. Primary: patient with therapy-naïve disease initially
treated at tertiary centre, recurrent: patient initially treated elsewhere
Years since surgery
Prob
abili
ty o
f RFS
primary 791 490 298 172 99 53
recurrent 32 14 10 8 5 1
years 0 2 4 6 8 10
number at risk
strata: primary recurrent

Localized-type tenosynovial giant cell tumours
149
7
Table 4 Univariate analyses in 791 patients with therapy naïve localized-TGCT
Variable N % RFS at 5 years 95%CI P value
Age
≤35 years 343 82 77-88 0.04
>35 years 447 88 84-92
Sex
male 292 88 82-93 0.56
female 499 85 80-89
Localization
knee 529 85 81-89 0.71
foot/ankle 156 84 76-93
upper extremity 82 90 81-98
Size
<5 cm 454 89 85-94 0.009
≥5 cm 124 76 66-87
Bone involvement
absent 543 85 81-89 0.70
present 50 74 57-91
Surgical technique
open 629 87 83-91 0.04
arthroscopic 132 80 72-88
RFS: Recurrence free survival, 95%CI: 95% Confidence interval
Table 5 Multivariate analyses in 554 patients with therapy naïve localized-TGCT
Variable Hazard ratio 95% CI P value
Age per year 0.99 0.97-1.01 0.425
Size <5 cm 1
≥5 cm 2.50 1.32-4.74 0.005
Surgical technique open 1
arthroscopic 2.18 0.98-4.84 0.056
95%CI: 95% Confidence interval
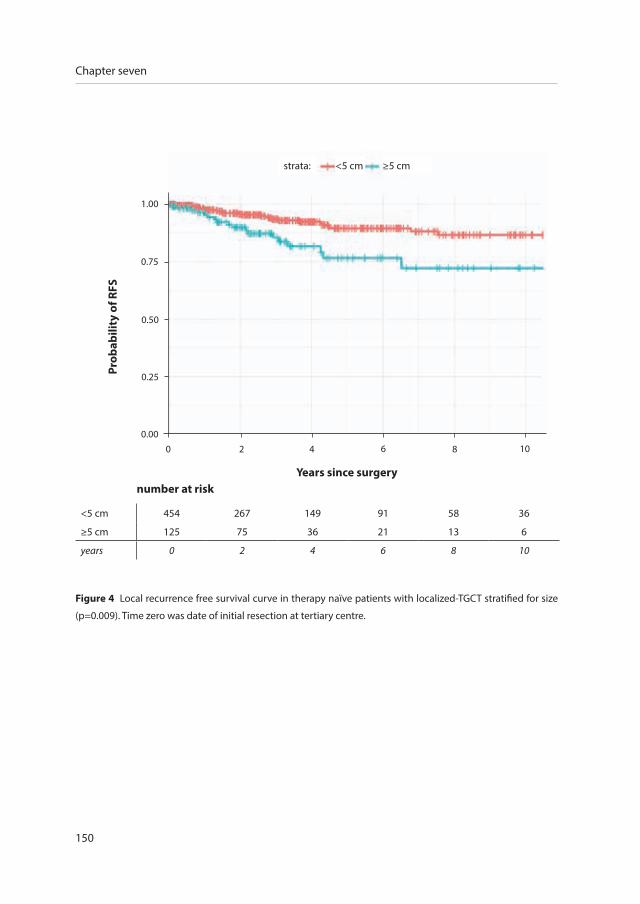
150
Chapter seven
Years since surgery
<5 cm 454 267 149 91 58 36
≥5 cm 125 75 36 21 13 6
years 0 2 4 6 8 10
number at risk
strata: <5 cm ≥5 cm
Prob
abili
ty o
f RFS
Figure 4 Local recurrence free survival curve in therapy naïve patients with localized-TGCT stratified for size
(p=0.009). Time zero was date of initial resection at tertiary centre.
1.00
0.75
0.50
0.25
0.000 2 4 6 8 10
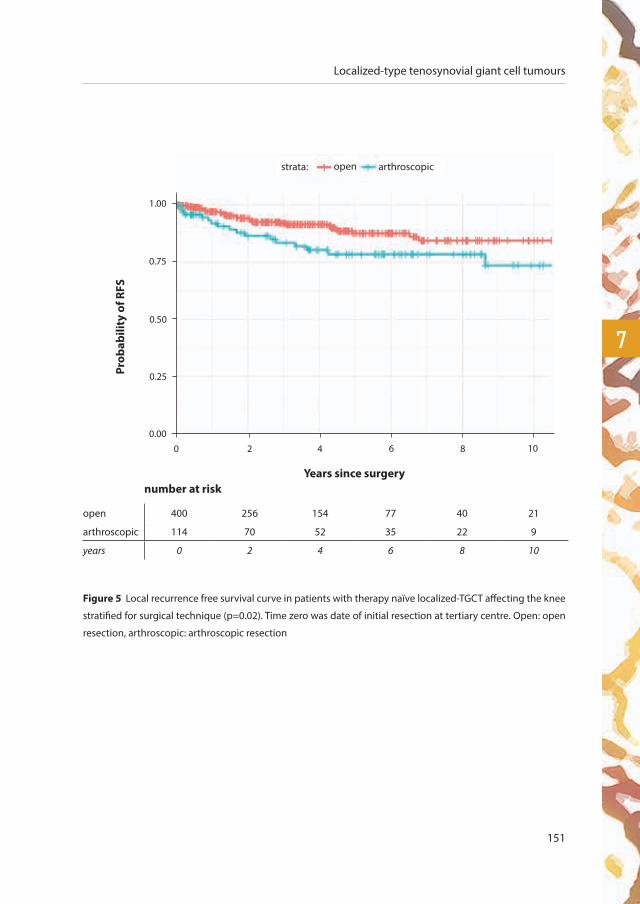
Localized-type tenosynovial giant cell tumours
151
7
Figure 5 Local recurrence free survival curve in patients with therapy naïve localized-TGCT affecting the knee
stratified for surgical technique (p=0.02). Time zero was date of initial resection at tertiary centre. Open: open
resection, arthroscopic: arthroscopic resection
Years since surgery
open 400 256 154 77 40 21
arthroscopic 114 70 52 35 22 9
years 0 2 4 6 8 10
number at risk
strata: open arthroscopic
Prob
abili
ty o
f RFS
1.00
0.75
0.50
0.25
0.000 2 4 6 8 10

152
Chapter seven
For a mean of 501 (53%) patients with localized-TGCT, complete data were available both prior to
treatment and at last follow-up (table 9). The majority of patients experienced pain and swelling
prior to initial treatment, of which 71% and 85% were resolved after surgery at final follow-up.
Swelling or stiffness might coincide with recurrent disease as 34% (21/61) and 40% (8/20) of
patients with swelling and joint stiffness respectively at final follow-up had recurrent disease. In
contrast to pain, limited range of motion or chronic use of analgesics, as 20% (25/124), 30% (8/27)
and 29% (7/24), respectively, had recurrent disease.
Chronic analgesic treatment versus complications
Two of 26 patients (8%) with a complication used chronic analgesic treatment compared to five of
429 (3%) patients without a complication.
Figure 6 Flowchart localized-TGCT. Primary: patient was first seen at tertiary centre with therapy-naïve
disease, recurrent: patient initially treated elsewhere, AR: Arthroscopic resection, OR: Open resection, SR:
Surgical resection (either arthroscopic or open resection). Treatments other than surgical resections were not
included in this flowchart (e.g. endoprosthetic reconstruction, wait and see treatment or adjuvant therapy).
Upper extremity includes shoulder, elbow, wrist and hand. Other localization (N=14) were not included in this
flowchart.
897 primary
35 hip
164 ankle/foot
73 upper extremity
24 SR
155 SR
69 SR
0 recurrences
14 recurrences (9%)
7 recurrences (10%)
611 knee114 AR
400 OR
20 recurrences (18%)
34 recurrences (9%)
44 recurrent
941 localized-TGCT

Localized-type tenosynovial giant cell tumours
153
7
Table 6 Recurrence free survival (RFS) probabilities for localized-TGCT
Admissionstatus Localization N+ %RFS at
3 years 95% CI %RFS at 5 years 95% CI %RFS at
10 years 95% CI
primary knee 529 89 87-93 85 81-89 81 76-87
primary foot/ankle 156 90 84-96 84 76-93 81 71-91
primary upper extremity* 82 93 86-100 90 81-98 86 74-97
recurrent knee 16 44 19-68 44 19-68 **
recurrent foot/ankle 11 30 3-57 18 0-41 18 0-41
recurrent upper extremity* 3 67 13-100 67 13-100 67 13-100
Since the hip was affected sporadically (primary N=24; recurrent N=2) without recurrent disease during follow-up,
reliable analyses were not possible. +N: number at baseline (time point = 0), *Upper extremity including other localization,
**Survival estimates of recurrent knee patients at 10 years could not be estimated (due to lack of follow-up information).
Primary: patient was first seen at tertiary centre with therapy-naïve disease, recurrent: patient initially treated elsewhere,
95%CI: 95% Confidence interval.
Table 7 Complications after surgical treatment at tertiary centre (N=763)
Complications after surgical treatment N (%)
Superficial wound infection 11 (1)
Deep wound infection 1 (0.1)
Joint stiffness$ 5 (0.7)
Haemorrhage 1 (0.1)
Neurovascular damage 3 (0.4)
Thrombosis 3 (0.4)
Other+ 10 (1)
As osteoarthritis is either caused by extensive disease or by (multiple) treatments, this was not taken into account for
complications. $Joint stiffness requiring manipulation under anaesthesia. +Other surgical complications after initial
treatment included: joint subluxation (hip), compartment syndrome, ligament incision during surgery, complex
regional pain syndrome, tourniquet blistering, tendinitis.
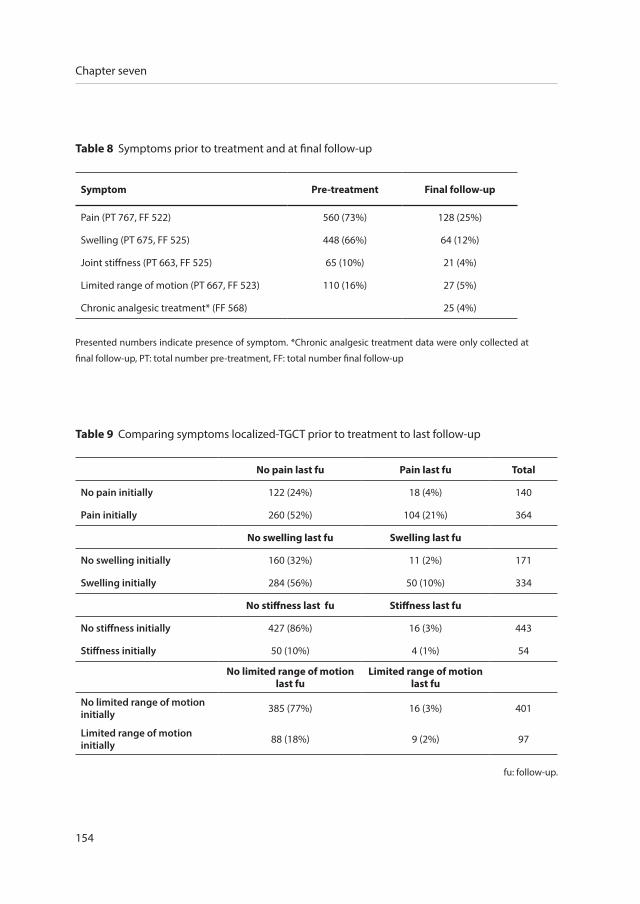
154
Chapter seven
Table 8 Symptoms prior to treatment and at final follow-up
Symptom Pre-treatment Final follow-up
Pain (PT 767, FF 522) 560 (73%) 128 (25%)
Swelling (PT 675, FF 525) 448 (66%) 64 (12%)
Joint stiffness (PT 663, FF 525) 65 (10%) 21 (4%)
Limited range of motion (PT 667, FF 523) 110 (16%) 27 (5%)
Chronic analgesic treatment* (FF 568) 25 (4%)
Presented numbers indicate presence of symptom. *Chronic analgesic treatment data were only collected at
final follow-up, PT: total number pre-treatment, FF: total number final follow-up
Table 9 Comparing symptoms localized-TGCT prior to treatment to last follow-up
No pain last fu Pain last fu Total
No pain initially 122 (24%) 18 (4%) 140
Pain initially 260 (52%) 104 (21%) 364
No swelling last fu Swelling last fu
No swelling initially 160 (32%) 11 (2%) 171
Swelling initially 284 (56%) 50 (10%) 334
No stiffness last fu Stiffness last fu
No stiffness initially 427 (86%) 16 (3%) 443
Stiffness initially 50 (10%) 4 (1%) 54
No limited range of motion last fu
Limited range of motion last fu
No limited range of motion initially 385 (77%) 16 (3%) 401
Limited range of motion initially 88 (18%) 9 (2%) 97
fu: follow-up.

Localized-type tenosynovial giant cell tumours
155
7
discussion
The results of this international multicentre study offer reliable insight into the outcome of the
treatment of patients with the orphan and heterogeneous disease localized-type Tenosynovial
Giant Cell Tumour (TGCT). We evaluated oncologic results, complications and functional results
after surgical treatment. The greatest strength of this dataset is that it represents the largest
collection of localized-TGCTs of large joints in the scientific literature, including a subgroup of
patients with long follow-up (>10 years).
Oncologic outcome
Surgical resection of TGCT has been the treatment of choice by either an arthroscopic or open
technique, based on the preference of the patient and treating physician, and might also differ by
centre. Physicians in favour of arthroscopic resection claim faster recovery, a lower complication
rate and less joint morbidity23-30. However, opponents of arthroscopic resection point out the risk
of inadequate excision, higher recurrence rates and a theoretical risk of joint seeding and portal
contamination13, 16.
In the current study, we identified higher recurrence rates after arthroscopic (18%) compares to
open resection (9%) of therapy naïve localized-TGCT affecting the knee joint. This is also presented
in the systematic review of van der Heijden et al. (6% after arthroscopic and 4% after open
resection)13. These higher recurrence rates may be explained by the longer follow-up times on
average and the larger sample size of localized-TGCT cases (table 4-5, figure 3-5). The single most
important and significant risk factor for local recurrence is recurrent disease at presentation. In a
subgroup analysis of patients with primary disease treated in a tertiary centre, the greatest risk for
first local recurrence was associated with tumour size ≥5 cm and arthroscopic resection at initial
treatment. This could be attributed to the fact that arthroscopic en bloc and complete resection
is likely only possible in a small percentage of cases with small/pedunculated and accessible
lesions, whereas in most cases intralesional removal would be performed arthroscopically thereby
potentially leaving residual disease in the joint. Several other studies reported higher rates of
recurrences after incomplete resections10, 23, 31, 32.

156
Chapter seven
Complications
All surgical treatments are associated with complications and data following resection of TGCT are
currently lacking in recent literature. The present study reported a complication rate of 4% after
surgical treatment for localized-TGCT. The most common complication in localized-TGCT was a
superficial wound infection after open resection.
Functional outcome
TGCT related symptoms are mainly joint pain, swelling, stiffness and limited range of motion, but
these occur with great variability in extent and severity. Gelhorn et al. concluded that not all patients
experience all symptoms to the same extent (e.g. swelling but no pain, or pain and swelling but no
stiffness or limited range of motion)9. Symptoms prior to initial treatment at a tertiary centre were
compared with symptoms at last follow-up. Initial symptoms of pain and swelling improved after
surgical treatment(s) in 71-85% of patients. This is comparable with a crowdsourcing study in 337
TGCT patients originating from 30 countries8. Stiffness and limited range of motion seemed not
to be debilitating symptoms in the majority of patients, either initially or at last follow-up. There
was no relationship between symptoms at last follow-up and recurrent disease. Symptoms are
subjective for each patient and not all patients were included with complete data. Nevertheless,
the main initial TGCT-related complaints are pain and swelling and these could potentially improve
after surgical treatment(s).
Joint specific analyses
In daily practise, TGCT patients present as a heterogeneous group. To provide reliable results,
homogeneous subgroup analyses are essential. This was possible with our individual participant
data meta-analysis. Even though quite a large number of TGCT cases were collected, complete risk
factor subgroup analyses were only feasible for TGCT affecting the knee (67%).
Limitations
As a result of increased awareness about TGCT, more patients are now being referred to (tertiary)
orthopaedic oncological referral centres as new targeted therapies are being examined in on-
going RCTs33-35. However, data on patients treated at non-specialized centres are lacking in both
the literature and within the present study. Therewith, selection (referral) bias is induced. The

Localized-type tenosynovial giant cell tumours
157
7
degree of selection bias according to affected joints is negligible, as similar percentages of affected
localizations (figure 2) were reported in a recent incidence calculation study with nationwide
coverage6. Non-specialized centres that resect smaller tumours without local recurrence were not
present, possibly introducing an overestimation of LR for localized-TGCT in general.
As data were collected by local investigators or physicians according to the multicentre study
design, data quality depended on data registry on site. Only data available in the source data file
of the patients could be retrieved. In addition, interpretation of individual parameters could differ.
No central histopathological review was performed, as it was assumed that each centre provided
the correct diagnosis as set by their histopathology department.
Recurrence rates could either be over-estimated or under-estimated. Over-estimation since
date of a second operation or follow-up status ‘alive with disease’ was classified as recurrence
(if recurrence data was missing). On the contrary, under-estimation could be present if patients
with recurrent disease did not return at all or did not return to their original centre. It should
be noted that patients with recurrent disease had a longer follow-up compared with patients
without recurrent disease. This could be explained by the fact that patients without symptoms
and (assumed) without recurrent disease were dismissed from follow-up and therefore presented
with shorter follow-up times. Plausibly, patients without symptoms are not experiencing recurrent
disease. In addition, if treatments were recently performed, patients also had shorter follow-up
times and are still at risk of recurrence.
conclusion
We present the largest international study that evaluated the clinical profile, management and
outcome for patients with TGCT. Localized-TGCT remains a heterogeneous and orphan disease,
with an overall recurrence free survival of 83% at 5 years. Risk factors for recurrent disease were
larger tumours, primary treatment with arthroscopy and initial surgical treatment outside of a
tertiary centre. Relatively low complication rates and good functional outcomes warrant complete
resection, most commonly accomplished by an open surgical approach, to reduce recurrence
rates in high risk patients.

158
Chapter seven
references
1. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4 ed2013. p. 100-1.
2. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, diffuse type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 52013. p. 102-3.
3. Mastboom MJL, Verspoor FGM, Hanff DF, Gademan MGJ, Dijkstra PDS, Schreuder HWB, Bloem JL, van der Wal RJP, van
de Sande MAJ. Severity classification of Tenosynovial Giant Cell Tumours on MR imaging. Surg Oncol. 2018;27:544-50.
4. Ushijima M, Hashimoto H, Tsuneyoshi M, Enjoji M. Giant cell tumor of the tendon sheath (nodular tenosynovitis). A study
of 207 cases to compare the large joint group with the common digit group. Cancer. 1986;57(4):875-84.
5. Chiari C, Pirich C, Brannath W, Kotz R, Trieb K. What affects the recurrence and clinical outcome of pigmented villonodular
synovitis? Clin Orthop Relat Res. 2006;450:172-8.
6. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence rates
than previously known in tenosynovial giant cell tumors. Acta orthopaedica. 2017:1-7.
7. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review
and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
8. Mastboom MJ, Planje R, van de Sande MA. The Patient Perspective on the Impact of Tenosynovial Giant Cell Tumors
on Daily Living: Crowdsourcing Study on Physical Function and Quality of Life. Interactive journal of medical research.
2018;7(1):e4.
9. Gelhorn HL, Tong S, McQuarrie K, Vernon C, Hanlon J, Maclaine G, et al. Patient-reported Symptoms of Tenosynovial Giant
Cell Tumors. Clin Ther. 2016;38(4):778-93.
10. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.
11. Patel KH, Gikas PD, Pollock RC, Carrington RW, Cannon SR, Skinner JA, et al. Pigmented villonodular synovitis of the knee:
A retrospective analysis of 214 cases at a UK tertiary referral centre. Knee. 2017;24(4):808-15.
12. Griffin AM, Ferguson PC, Catton CN, Chung PW, White LM, Wunder JS, et al. Long-term outcome of the treatment of
high-risk tenosynovial giant cell tumor/pigmented villonodular synovitis with radiotherapy and surgery. Cancer.
2012;118(19):4901-9.
13. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
14. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical
treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J.
2014;96-B(8):1111-8.
15. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
16. Verspoor FG, van der Geest IC, Vegt E, Veth RP, van der Graaf WT, Schreuder HW. Pigmented villonodular synovitis: current
concepts about diagnosis and management. Future oncology. 2013;9(10):1515-31.
17. Riley RD, Lambert PC, Abo-Zaid G. Meta-analysis of individual participant data: rationale, conduct, and reporting. Bmj.
2010;340:c221.
18. Honaker J, King G, Blackwell M. Amelia II: a program for missing data. J Stat Softw. 2011;45:1-54.
19. Rubin DB. Multiple imputation after 18+ years. J Am Stat Assoc. 1996;91:473-89.

Localized-type tenosynovial giant cell tumours
159
7
20. Fay MP, Shaw PA. Exact and Asymptotic Weighted Logrank Tests for Interval Censored Data: The interval R package.
Journal of statistical software. 2010;36(2).
21. Sun J. A non-parametric test for interval-censored failure time data with application to AIDS studies. Statistics in
medicine. 1996;15(13):1387-95.
22. Anderson-Bergman C. icenReg: Regression Models for Interval Censored Data in R. J Stat Softw. 2017;81(12):1-23.
23. Ogilvie-Harris DJ, McLean J, Zarnett ME. Pigmented villonodular synovitis of the knee. The results of total arthroscopic
synovectomy, partial, arthroscopic synovectomy, and arthroscopic local excision. J Bone Joint Surg Am. 1992;74(1):119-
23.
24. De Ponti A, Sansone V, Malchere M. Result of arthroscopic treatment of pigmented villonodular synovitis of the knee.
Arthroscopy. 2003;19(6):602-7.
25. Jain JK, Vidyasagar JV, Sagar R, Patel H, Chetan ML, Bajaj A. Arthroscopic synovectomy in pigmented villonodular
synovitis of the knee: clinical series and outcome. Int Orthop. 2013;37(12):2363-9.
26. de Carvalho LH, Jr., Soares LF, Goncalves MB, Temponi EF, de Melo Silva O, Jr. Long-term success in the treatment of
diffuse pigmented villonodular synovitis of the knee with subtotal synovectomy and radiotherapy. Arthroscopy.
2012;28(9):1271-4.
27. Kubat O, Mahnik A, Smoljanovic T, Bojanic I. Arthroscopic treatment of localized and diffuse pigmented villonodular
synovitis of the knee. Collegium antropologicum. 2010;34(4):1467-72.
28. Loriaut P, Djian P, Boyer T, Bonvarlet JP, Delin C, Makridis KG. Arthroscopic treatment of localized pigmented villonodular
synovitis of the knee. Knee Surg Sports Traumatol Arthrosc. 2012;20(8):1550-3.
29. Rhee PC, Sassoon AA, Sayeed SA, Stuart MS, Dahm DL. Arthroscopic treatment of localized pigmented villonodular
synovitis: long-term functional results. American journal of orthopedics. 2010;39(9):E90-4.
30. Noailles T, Brulefert K, Briand S, Longis PM, Andrieu K, Chalopin A, et al. Giant cell tumor of tendon sheath: Open surgery
or arthroscopic synovectomy? A systematic review of the literature. Orthop Traumatol Surg Res. 2017;103(5):809-14.
31. Schwartz HS, Unni KK, Pritchard DJ. Pigmented villonodular synovitis. A retrospective review of affected large joints. Clin
Orthop Relat Res. 1989(247):243-55.
32. Chin KR, Barr SJ, Winalski C, Zurakowski D, Brick GW. Treatment of advanced primary and recurrent diffuse pigmented
villonodular synovitis of the knee. J Bone Joint Surg Am. 2002;84-A(12):2192-202.
33. Tap WD, Gelderblom H, Stacchiotti S, Palmerini E, Ferrari S, Desai J, et al. Final results of ENLIVEN: A global, double-blind,
randomized, placebo-controlled, phase 3 study of pexidartinib in advanced tenosynovial giant cell tumor (TGCT). ASCO
conference. 2018.
34. Sankhala KK, Blay JY, Ganjoo KN, Italiano A, Hassan AB, Kim TM, et al. A phase I/II dose escalation and expansion study
of cabiralizumab (cabira; FPA-008), an anti-CSF1R antibody, in tenosynovial giant cell tumor (TGCT, diffuse pigmented
villonodular synovitis D-PVNS). ASCO conference 2017. 35 (15 Supplement 1).
35. Cassier PA, Italiano A, Gomez-Roca CA, Le Tourneau C, Toulmonde M, Cannarile MA, et al. CSF1R inhibition with
emactuzumab in locally advanced diffuse-type tenosynovial giant cell tumours of the soft tissue: a dose-escalation and
dose-expansion phase 1 study. Lancet Oncol. 2015;16(8):949-56.

160
Chapter seven
appendix
Table 1 Collected patient and tumour characteristics with corresponding definitions.
Characteristic Definition
TGCT-type Localized-/diffuse-TGCT as defined by the 2013 WHO1, 2
Admission status Previously treated*
Sex Male/female
Age at initial treatment Age at initial treatment
Side Left/right
Localization TGCT affected joint
Bone involvement Discontinuation of cortex by tumour ingrowth*
Date first diagnosis Date first diagnosis
Duration of symptoms Duration of symptoms in months
Pain, swelling, stiffness and limited range of motion prior to initial treatment and at last follow-up
(Clinically relevant) Pain, swelling, stiffness+ and limited range of motion prior to initial treatment* and at last follow-up
Total number surgeries All surgeries related to TGCT, including re-operations for complications
Date initial treatment** Date initial treatment at tertiary centre and date(s) of consecutive treat-ment(s)
Initial treatment**Type of initial treatment and consecutive treatment(s): arthroscopic re-section, one-staged open resection, two-staged open resection, (tumour)prosthesis, amputation, wait and see++, synovectomy not specified
Tumour size Largest size in any dimension (cm), according to the 2013 WHO classifica-tion1, 2, <5 and ≥5 cm were compared
Adjuvant therapy Nothing, radiotherapy, 90Yttrium, targeted therapy, cryosurgery, other
Date complication Date complication related to surgical treatment
Complication Type of complication related to surgical treatment: no complication, super-ficial wound infection, deep wound infection, joint stiffness+, haemorrhage, neurovascular damage, thrombosis, other, unknown
Total number recurrences Total number local recurrences
Date final follow-up Date final follow-up
Status last follow-upNo evidence of disease, alive with disease wait and see, alive with disease planned surgery of adjuvant therapy, death of disease, death of other dis-ease, lost (<6 months follow-up)
Chronic analgesic treat-ment at last follow-up Chronic analgesic treatment at last follow-up
Characteristics in bold were core criteria. *These parameters were answered by present or absent. **(Date) initial treatment, initial treatment in tertiary centre is not necessarily first treatment of the patient. +Stiffness requiring manipulation under anaesthesia. ++Wait and see and conservative treatment are considered similar.
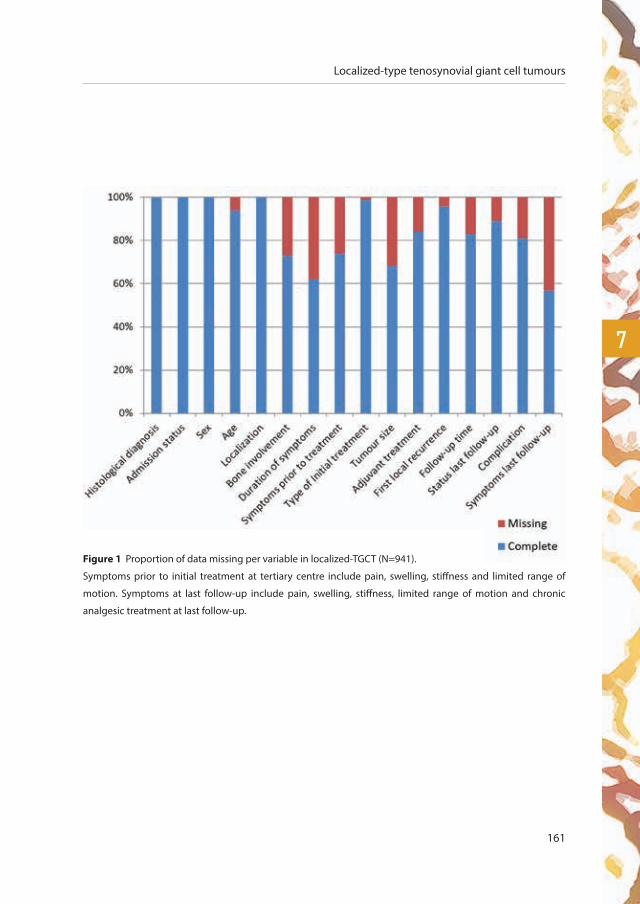
Localized-type tenosynovial giant cell tumours
161
7
Figure 1 Proportion of data missing per variable in localized-TGCT (N=941).
Symptoms prior to initial treatment at tertiary centre include pain, swelling, stiffness and limited range of
motion. Symptoms at last follow-up include pain, swelling, stiffness, limited range of motion and chronic
analgesic treatment at last follow-up.
162
Chapter seven
Supplementary material participating international sarcoma reference centres
1. Leiden University Medical Center, Leiden, The Netherlands
2. Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands
3. IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy
4. Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy
5. Istituto Ortopedico Gaetano Pini, Milano, Italy
6. Mount Sinai School of Medicine, New York, USA
7. Medical University Graz, Graz, Austria
8. Halen İstanbul Üniversitesi, Istanbul, Turkey
9. AOU Città della Salute e della Scienza, Torino, Italy
10. Orthopedic Hospital Gersthof, Vienna, Austria
11. Careggi University-Hospital, Firenze, Italy
12. University Medical Center Groningen, Groningen, The Netherlands
13. Academic Medical Center, Amsterdam, The Netherlands
14. Mount Sinai Hospital, Toronto, Canada
15. Beijing Jishuitan Hospital, Beijing, 100035, China
16. Institut Roi Albert II, Brussels, Belgium
17. Royal National Orthopedic Hospital, London, the United Kingdom
18. Hospital de Navarra, Pamplona, Spain
19. Centre hospitalier universitaire de Nantes, Nantes, France
20. Ludwig-Maximilians-University Munich, Munich, Germany
21. Medical University of Innsbruck, Innsbruck, Austria
22. Massachusetts General Hospital Harvard, Boston, United States of America
23. Chiba Cancer Center, Chiba, Japan
24. National Cancer Center, Tokyo, Japan
25. Kanazawa University Graduate School of Medical Sciences, Kanazawa, Japan
26. Sytenko Institute of Spine and Joint Pathology, Kharkiv, Ukraine
27. Universitätsklinikum Jena, Jena, Germany
28. University of the Phil-Phil General Hospital, Manila, Philippines
29. Catholic University of Korea, Seoul, Korea
30. Cairo University, Cairo, Egypt
31. Wilhelmsburger Krankenhaus Groß Sand, Hamburg, Germany

Localized-type tenosynovial giant cell tumours
163
7
Supplementary material exact survival information and statistical methods
For some cases exact survival information was not available (appendix figure 1). In 7 out of 61 cases,
we could recover the missing recurrence indicator: in 2 cases patients had a second treatment and
in 5 cases patients had follow-up status ‘alive with disease’ and were classified as recurrent disease.
If the exact time of recurrence was not recorded, an approximation was sometimes possible. If
the date of surgery to treat a local recurrence was known, this was used instead (N=33). If this
information was missing as well, then the date of last recurrence was used as an upper bound
(N=5). Otherwise the date of last recorded follow-up was used as an upper bound (N=69). If data
on recurrence status or date of recurrence was missing and could not be recovered as described,
patients were excluded for risk- and survival analyses (N=64).
Some centres did not record follow-up time in patients without recurrent disease. To prevent
exclusion of these patients, we imputed their follow-up time (N=97). Multiple imputation
technique was applied and 5 complete data sets were imputed using the R-package Amelia II18.
Statistical analyses were conducted on all data sets and the results were then pooled following
Rubin’s rule19.
As a consequence of the approximation of the time of recurrence by upper bounds in some cases,
common survival methods (Kaplan-Meier estimate, log rank test) were substituted by methods
that allow interval censoring. Observed survival curves and probabilities were computed using
non-parametric maximum likelihood estimates for interval censored data with the R-package
interval20. P-values for the univariate analyses were calculated with the score test of Sun (1996)21.
Covariates that were found to have a significant association with local recurrence free survival in
the univariate analysis were included in a multivariate Cox regression analysis using the icenReg
R-package, which allows for interval censored data22.


diF
Fuse
outcome of surgical treatment
for patients with diffuse-type
tenosynovial giant cell tumours
chap
ter
eigh
t
largest cohort of individual participant data meta-analysis of 31 international sarcoma centres
M.J.L. Mastboom1, E. Palmerini2, F.G.M. Verspoor3, A.J. Rueten-Budde4, S. Stacchiotti5, E.L. Staals6,
G.R. Schaap7, P.C. Jutte8, W. Aston9, H. Gelderblom10, A. Leithner11, D. Dammerer12, A. Takeuchi13, Q. Thio14, X. Niu15,
J.S. Wunder16, TGCT-study group*, M.A.J. van de Sande1
Submitted.
166
Chapter eight
1 Orthopaedic Surgery, Leiden University Medical Center, Leiden, the Netherlands
2 Medical Oncology, Musculoskeletal Oncology Department, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy
3 Orthopaedic Surgery, Radboud University Nijmegen Medical Center, Nijmegen, the Netherlands
4 Department of Medical Statistics and Bioinformatics, Leiden University Medical Center, Leiden, the Netherlands
5 Medical Oncology, Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy
6 Orthopaedic Surgery, Musculoskeletal Oncology Department, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy
7 Orthopaedic Surgery, Academic Medical Center, Amsterdam, the Netherlands
8 Department of Orthopaedics, University Medical Center, University of Groningen, Groningen, the Netherlands
9 Orthopedic surgery, Royal National Orthopedic Hospital, London, the United Kingdom
10 Medical Oncology, Leiden University Medical Center, Leiden, the Netherlands
11 Department of Orthopaedic Surgery, Medical University Graz, Graz, Austria
12 Orthopedic surgery, Medical University of Innsbruck, Innsbruck, Austria
13 Orthopaedic surgery, Kanazawa University Graduate School of Medical Sciences, Kanazawa, Japan
14 Orthopedic surgery, Massachusetts General Hospital Harvard, Boston, United States of America
15 Department of Orthopedic Oncology, Beijing Jishuitan Hospital, Beijing, 100035, China
16 University Musculoskeletal Oncology Unit, Mount Sinai Hospital, Toronto, Canada
*TGCT study-group
M. Fiocco, P.D.S. Dijkstra, R.J.P. van der Wal, P.A. Daolio, P. Picci, A. Gronchi, S. Ferrari, H. Özger, R.G. Maki, H.W.B.
Schreuder, I.C.M. van der Geest, J.A.M. Bramer, M. Boffano, E. Goldenitsch, D. Campanacci, P. Cuomo, P.C.
Ferguson, A.M. Griffin, Y. Sun, T. Schubert, K. Patel, M.S.J. Aranguren, A. Blancheton, F. Gouin, H.R. Dürr, C.F.
Capellen, J. Schwab, S. Iwata, O. Vyrva, W. Weschenfelder, E.H.M. Wang, M. Wook Joo, Y.K. Kang, Y.G. Chung, W.
Ebeid, J. Bruns, T. Ueda

Diffuse-type tenosynovial giant cell tumours
167
8
abstract
Objective
Diffuse-type Tenosynovial Giant Cell Tumour (TGCT) is a rare, locally aggressive and difficult to treat
disease. An international multicentre-pooled retrospective study of individual patient data was developed
to describe global treatment protocols, evaluate oncological outcome, complications and functional
results. A secondary study aim was to identify risk factors for local recurrence after surgical treatment.
Methods
Patients treated in 31 sarcoma reference centres between 1990 and 2017, with histologically proven diffuse-
TGCT of large joints were included. Of 1192 cases of diffuse-TGCT, 58% were female with a median age
35 years. 64% affected the knee and in 54% primary treatment was one-staged open synovectomy. Risk
factors were tested in a univariate analysis and significant factors subsequently included for multivariate
analysis, with first local recurrence after surgical treatment in a tertiary centre as the primary outcome.
Results
At a median follow-up of 54 (95%CI 50-58) months, recurrent disease developed in 44% of all
surgically treated cases, with local recurrence free survival (RFS) at 3, 5, 10 years of 62%, 55%
and 40%, respectively. The strongest risk factor for recurrent disease was prior recurrence (HR
3.5 95%CI 2.8-4.4, p<0.001) with a 5-year RFS of 64% in surgery naïve patients compared with
25% in patients operated for recurrent disease. Complications were noted in 12% of patients. Pain
and swelling improved after surgical treatment(s) in 59% and 72% of patients respectively. In a
subgroup analysis including only naïve cases affecting the knee, neither sex (male;female), age
(≤35years;>35years), bone-involvement (present;absent), surgical technique (open;arthroscopic)
nor tumour size (<5cm;≥5cm) yielded an association with the first local recurrence.
Conclusion
This largest international individual data study of patients with diffuse-TGCT, provides a comprehensive
and up to date disease overview, evaluating the clinical profile and management of the disease. Since
complete resection of diffuse-TGCT could be regarded as nearly impossible and recurrence rates are
unacceptably high after both arthroscopy and open synovectomy in the knee, even in specialized
centres, a multimodality approach in this disease, including adjuvant treatments, is warranted.

168
Chapter eight
introduction
In the most recent WHO classification (2013), giant cell tumour of the tendon sheath and
pigmented villonodular synovitis (PVNS) were unified by one overarching term: tenosynovial
giant cell tumours (TGCT). This rare, mono-articular disease arises from the synovial lining of
joints, bursae or tendon sheaths in predominantly young adults1, 2. Excluding digits, TGCT is most
commonly diagnosed around the knee and can be found in other weight bearing joints as well1-4.
Two clinically and radiographically distinct subtypes of TGCT are defined with different natural
courses of disease. The localized-type is defined as a well-circumscribed nodule. On the contrary,
the diffuse-type is known as an ill-circumscribed, locally aggressive and invasive tumour (figure 1,
chapter 1, page 13)1, 2, 5. Even though histopathology and genetics seem identical, the biological
behaviour of both subtypes is incomparable and therefore necessitates separate evaluations,
analyses and treatments. The current study focuses on diffuse-TGCT of large joints.
Macroscopically, diffuse-type TGCT involves a large part or even the complete synovial lining of
a joint with either a typical villous pattern (intra-articular) or a multi-nodular appearance (extra-
articular), including a diverse colour pattern, varying from white-yellow to brown-red areas. This
subtype shows an infiltrative growth pattern. Definite diagnosis is established on microscopy by
an admixture of mononuclear cells (histiocyte-like and larger cells) and multinucleated giant cells,
lipid-laden foamy macrophages (also known as xanthoma cells), siderophages (macrophages
including hemosiderin-depositions), stroma with lymphocytic infiltrate and some degree of
collagenisation. Molecular analysis is generally not required to confirm the diagnosis.
Pain, (haemorrhagic) joint effusion, stiffness and limited range of motion are the main
clinical complaints6. These non-specific symptoms frequently cause a delay in diagnosis7. The
predominant standard of care is surgical resection of diffuse-TGCT, either arthroscopically or
with an open resection or a combination of both, in order to: (1) reduce debilitating symptoms
and joint destruction caused by the disease process; (2) improve limb function; and (3) minimize
the risk of local recurrence. Clinical and oncological outcomes following surgery largely depend
on multiple factors including preoperative diagnostic evaluation, the localization and extent of
disease and possibly the choice of treatment modalities by orthopaedic surgeons3, 5, 8-10. Diffuse-
Diffuse-type tenosynovial giant cell tumours
169
8
TGCT frequently causes significant morbidity due to the invasiveness of the surgical resection
and the high rate of local recurrence (14-40% depending on surgical procedure and follow-up
time), with deteriorated health-related quality of life6, 8, 9, 11-14. Therefore, treatment of diffuse-TGCT
may include adjuvant or multimodality treatment such as external beam radiation therapy10, 15, 16,
radiation synovectomy with 90Yttrium17 or CSF1 inhibitors, such as nilotinib, imatinib, pexidartinib,
emactuzumab, cabrilazimab and MSC11018-22. Of note, so far none of these agents have been
formally approved for use in the disease, and long-term efficacy is unknown.
The incidence of diffuse-TGCT of large joints is 4.1 per million person-years4. Therefore, the current
literature mainly consists of relatively small, or larger but heterogeneous case-series. Risk-factors for
recurrent disease in individual patients need to be identified by evaluating outcomes of different
treatment strategies. Since (larger) randomized controlled trials on the role of surgery in TGCT are
lacking, individual participant data meta-analysis is currently the highest achievable evidence. It
offers advantages above a meta-analyses, including: (1) missing data can be accounted for at an
individual patient level, (2) subgroup analyses can be performed (e.g. per affected joint) and (3)
follow-up information can be updated23. Therefore, we aimed to collaborate with tertiary sarcoma
centres across the globe to include individual patient data in this investigation.
The main aim of this international multicentre cohort study is to provide comprehensive and
up to date insights on the surgical treatment and outcome for patients with diffuse-type TGCT.
Oncologic results, complications and functional results are described. In addition, risk factors for
local recurrence after surgical treatment are identified.

170
Chapter eight
methods
Recruitment and patient inclusion criteria
Patients of any age treated between January 1990 and December 2017 in one of 31 international
sarcoma centres (supplementary material: participating international sarcoma reference centres,
page 160) with histologically proven TGCT of large joints were retrospectively included. Large
joints were defined as all joints proximal to the metatarsophalangeal and metacarpophalangeal
joints. Identification and collection of the patients was performed in the centres of origin and data
were analysed from initial treatment at these tertiary centres. Data were encrypted and transferred
to the international multicentre database at the Leiden University Medical Centre (LUMC), with
patient collection ending as of May 2018.
Study parameters
Collected patient-, tumour- and treatment characteristics with corresponding definitions are
shown in appendix table 1 (chapter 7, page 158). The following characteristics were defined as
core criteria: TGCT-type (localized-; diffuse-; unknown-type), admission status (therapy-naïve; 1st
recurrence; 2nd recurrence; 3rd recurrence; etc.) date and type of initial treatment at a tertiary centre
(arthroscopic synovectomy; one-staged synovectomy; two-staged synovectomy; synovectomy
not specified; (tumour)prosthesis; amputation; wait and see); and first local recurrence after
treatment (yes; no) in a tertiary centre. Complete data on these core criteria were necessary for
reliable analyses.
Patient-, tumour- and treatment characteristics
Thirty-one specialized sarcoma centres spread throughout Europe, North America, Canada and
Asia collaborated to provide a total of 1192 diffuse-TGCT cases (table 1). As per entry criteria,
patients with localized-TGCT (N=941) and unknown type TGCT (N=36) were excluded.
Statistical analyses
The primary endpoint was local recurrence free survival (RFS) after initial treatment in a tertiary
centre. Recurrent disease was defined as the presence of new disease after resection (and
synovectomy) performed in a tertiary centre or progressive residual disease (as diagnosed by local
investigators on repeated follow-up Magnetic Resonance (MR) imaging).

Diffuse-type tenosynovial giant cell tumours
171
8
Table 1 Patient-, tumour- and treatment characteristics
Characteristics Overall (%)
Total number 1192 (100)
Admission status (N=1192) Therapy naïve^
≥1 Surgery elsewhere^^910 (76)282 (24)
Sex (N=1192) Male Female
499 (42)693 (58)
Median age at initial treatment years (N=1122) IQR
3526-48
Localization (N=1192) Knee Hip Ankle Foot* Shoulder Elbow Wrist Hand* Other
758 (64)124 (10)162 (14)
63 (5)15 (1)17 (1)25 (2)13 (1)15 (1)
Bone involvement (N=847) Present Absent
259 (30) 588 (70)
Median duration of symptoms# months (N=744) IQR
186-36
Type of surgical treatment at tertiary centre (N=1163) Arthroscopic synovectomy One-staged open synovectomy Two -staged open synovectomy##
(Tumour)prosthesis+,¥
Amputation¥
Wait and see$,¥
Synovectomy not specified
159 (14)628 (54)187 (16)
63 (5)3 (0.3)76 (7)47 (4)
Median tumour size initial treatment in cm (N=701) IQR <5 cm ≥5 cm
5.43.0-8.8
297 (42)404 (58)
Adjuvant therapy initial treatment (N=1033) External beam radiotherapy 90Yttrium Systemic/molecular targeted treatment Other None
58 (6)60 (6)15 (1)11 (1)
889 (86)
IQR, Interquartile Range; ^Therapy-naïve or primary admission status at tertiary centre are considered similar; ^^≥1 Surgery elsewhere or recurrent admission status are considered similar; *Digits are excluded; #Symptoms were defined as either pain, swelling, stiffness or limited range of motion (table 7-8); ##A two-stage synovectomy is defined as two synovectomies within six months; +An arthrodesis is classified as (tumour)prosthesis; $Wait and see and conservative treatment are considered similar; ¥(Tumour)prosthesis, amputation or wait and see as initial treatment are excluded for risk and survival analyses.

172
Chapter eight
To investigate the effect of risk factors on the outcome, univariate analyses were performed and
significant factors (p<0.05) were subsequently included into a multivariate analysis. Proposed risk
factors were admission status (therapy-naïve versus recurrent disease), sex (male versus female), age
(≤35 years versus >35 years), localization (knee versus hip versus foot/ankle versus upper extremity),
bone-involvement (present versus absent), surgical technique (open versus arthroscopic) and
tumour size (<5 cm versus ≥5cm). Patients with a wait and see policy or as initial treatment (tumour)
prosthesis surgery or an amputation were excluded from statistical analysis (N=142).
Observed RFS probabilities at 3, 5, and 10 years were computed for all cases and subgroups based
on admission status and localization.
Figure 2 Skeleton showing localization of TGCT
in 1192 diffuse-TGCT cases. 15 diffuse-TGCT cases
were classified as ‘other localization’
1%
1%
10%2%1%
64%
14%
5%
Diffuse-type tenosynovial giant cell tumours
173
8
For some patients exact survival information was not available (appendix: proportion of data
missing per variable). In 34 out of 107 cases, we could recover the missing recurrence indicator:
9 patients had a second treatment and 25 patients had follow-up status ‘alive with disease’ and
were classified as having recurrent disease. When the exact time of recurrence was not recorded,
an approximation was applied where possible. When the date of surgery to treat a recurrence was
known, this was used as the date of local recurrence instead (N=177). When this information was
missing as well, the date of last recurrence was used as an upper bound (N=58). Otherwise the
date of last recorded follow-up was used as an upper bound (N=69). When data on recurrence
status or date of recurrence was missing and could not be recovered as described, patients were
excluded for risk- and survival analyses (N=84).
Some centres did not record follow-up time for patients without recurrent disease. To prevent
exclusion of these patients, we imputed their follow-up time (N=79). Multiple imputation technique
was applied and 5 complete data sets were imputed using the R-package Amelia II24. Statistical
analyses were conducted on all data sets and the results were then pooled following Rubin’s rule25.
As a consequence of the approximation of the time of recurrent disease by upper bounds in some
cases, common survival methods (Kaplan-Meier estimate, logrank test) were substituted by methods
that allow for interval censoring. Observed survival curves and probabilities were computed using
non-parametric maximum likelihood estimates for interval censored data with the R-package
interval26. P-values for the univariate analyses were calculated with the score test of Sun (1996)27.
Covariates that were found to have a significant association with local recurrence free survival in
the univariate analysis were included in a multivariate Cox regression analysis using the icenReg
R-package, which allows for interval censored data28.
All data were selected for completeness on core criteria (appendix, chapter 7, page 158). Statistical
analyses were carried out using R version 3.4.1.
On purpose, an estimate of the median time to recurrence was not provided. Calculating such a
median based on patients for whom a recurrence was recorded, would assume that all other patients
could not experience a recurrence in the future. The extent of this so-called immortal time bias is
unknown. For this reason, such an estimate will be an underestimation of the true time to recurrence.
174
Chapter eight
Ethical consideration
This study is conducted according to the Declaration of Helsinki (October 2013) and approved by the
institutional review board (CME) from the Leiden University Medical Center (LUMC) (May 4th, 2016; G16.015).
results
Oncologic outcome
In 966 patients with surgically treated diffuse-TGCT and complete survival data, 425 (44%) had a
tumour recurrence following treatment. The recurrence free survival (RFS) continued to decrease
with longer follow-up times (table 2-3, figure 3).
Univariate- and multivariate analyses for local recurrence
In univariate analysis of 966 patients with surgically treated diffuse-TGCT and complete core data,
the risk factor admission status was found to be significantly associated with recurrence: 5-year
RFS was 64% for therapy naïve patients (95% CI 60-68) compared to 25% for patients entering the
tertiary hospital with recurrent disease (95% CI 19-31; p <0.001). This difference was confirmed by
multivariate analysis (HR 3.5 95% CI 2.8-4.4, p<0.001).
After excluding patients admitted with recurrent disease, surgical technique was also positively
associated with first local recurrence (table 4). This result was confirmed by cox regression analysis
(HR 1.407; 95% CI 1.02-1.95, p=0.04). In a subgroup analysis of therapy naïve patients with diffuse-
TGCT affecting the knee, surgical technique was not found to be associated with first local
recurrence (p=0.113).
Observed recurrence free survival according to admission status and localization
Highest recurrence rates are report in TGCT affecting the knee; 43% after arthroscopic synovectomy
and 37% after open synovectomy (figure 4). A progressively declining RFS was seen at 3, 5 and 10
years in a subgroup analysis of the knee, hip, foot/ankle and upper extremity locations in patients
either admitted with therapy naïve TGCT or patients admitted with recurrent TGCT (table 5). After
10 years follow-up, patients with therapy naïve disease affecting the knee were found to have
the lowest RFS rates of all sites (46%, 95% CI 39-54). All patients entering a tertiary hospital with
recurrent disease exhibited very low RFS at 10 years (figure 3a).
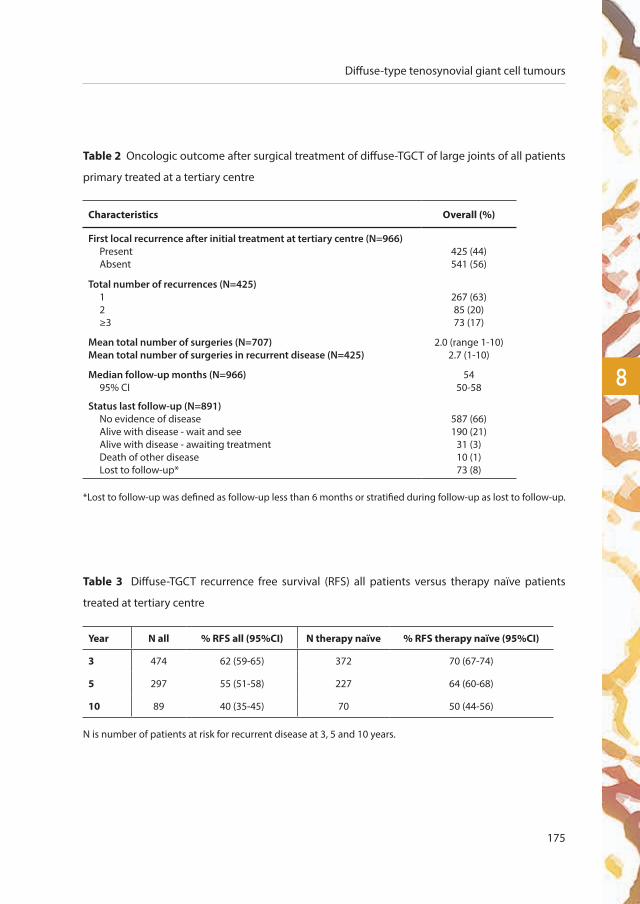
Diffuse-type tenosynovial giant cell tumours
175
8
Table 2 Oncologic outcome after surgical treatment of diffuse-TGCT of large joints of all patients
primary treated at a tertiary centre
Characteristics Overall (%)
First local recurrence after initial treatment at tertiary centre (N=966) Present Absent
425 (44)541 (56)
Total number of recurrences (N=425) 1 2 ≥3
267 (63)85 (20)73 (17)
Mean total number of surgeries (N=707)Mean total number of surgeries in recurrent disease (N=425)
2.0 (range 1-10)2.7 (1-10)
Median follow-up months (N=966) 95% CI
54 50-58
Status last follow-up (N=891) No evidence of disease Alive with disease - wait and see Alive with disease - awaiting treatment Death of other disease Lost to follow-up*
587 (66)190 (21)
31 (3)10 (1)73 (8)
*Lost to follow-up was defined as follow-up less than 6 months or stratified during follow-up as lost to follow-up.
Table 3 Diffuse-TGCT recurrence free survival (RFS) all patients versus therapy naïve patients
treated at tertiary centre
Year N all % RFS all (95%CI) N therapy naïve % RFS therapy naïve (95%CI)
3 474 62 (59-65) 372 70 (67-74)
5 297 55 (51-58) 227 64 (60-68)
10 89 40 (35-45) 70 50 (44-56)
N is number of patients at risk for recurrent disease at 3, 5 and 10 years.

176
Chapter eight
Years since surgery
Prob
abili
ty o
f RFS
primary 758 506 310 170 97 63
recurrent 208 128 88 53 30 18
years 0 2 4 6 8 10
number at risk
strata: primary recurrent
Figure 3a Local recurrence free survival curve in diffuse-TGCT stratified for admission status (p<0.001).
Time zero was date of initial resection at tertiary centre. Primary: patient with therapy-naïve disease initially
treated at tertiary centre, recurrent: patient initially treated elsewhere.
1.00
0.75
0.50
0.25
0.000 2 4 6 8 10
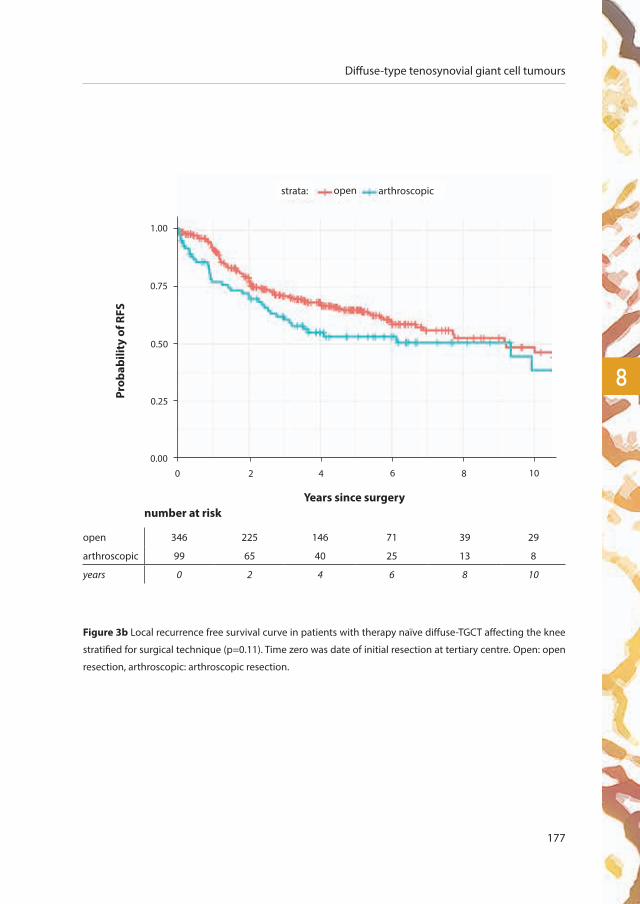
Diffuse-type tenosynovial giant cell tumours
177
8
Figure 3b Local recurrence free survival curve in patients with therapy naïve diffuse-TGCT affecting the knee
stratified for surgical technique (p=0.11). Time zero was date of initial resection at tertiary centre. Open: open
resection, arthroscopic: arthroscopic resection.
Years since surgery
open 346 225 146 71 39 29
arthroscopic 99 65 40 25 13 8
years 0 2 4 6 8 10
number at risk
strata: open arthroscopic
Prob
abili
ty o
f RFS
1.00
0.75
0.50
0.25
0.000 2 4 6 8 10

178
Chapter eight
Figure 4 Flowchart of diffuse-TGCT patients with treatments and recurrences for each affected joint.
Primary: patient was first seen at tertiary centre with therapy-naïve disease, recurrent: patient initially treated
elsewhere, AS: Arthroscopic synovectomy, OS: Open synovectomy. Treatments other than AS and OS were not
included in this flowchart (e.g. (tumour)prosthesis, amputation, wait and see treatment).
910 primary
96 AS
358 OS
41 recurrences (43%)
132 recurrences (37%)
282 recurrent
1192 diffuse-TGCT
3 AS
64 OS
1 recurrence (33%)
20 recurrences (31%)
9 AS
135 OS
3 recurrences (33%)
33 recurrences (24%)
4 AS
42 OS
3 recurrences (75%)
14 recurrences (33%)
105 hip
127 ankle/foot
55 upper extremity
559 knee
Complications
A total of 105 (12%) complications occurred following surgical treatment of diffuse-TGCT (table
6). The majority of these complications developed after one- or two-staged open synovectomy
(86/105; 82%). In comparison, 12 complications (11%) were reported following arthroscopic
synovectomy.
Functional outcome
Prior to surgical treatment, the majority of patients had symptoms of pain (76%) and swelling
(75%) (table 7). After surgical treatment, at final follow-up, these symptoms largely disappeared,
although 37% and 24% of patients respectively were still symptomatic. Joint stiffness and limited
range of motion were only present in 21% and 27% of cases, respectively, and these symptoms
improved slightly after treatment (17% and 19% at final follow-up).
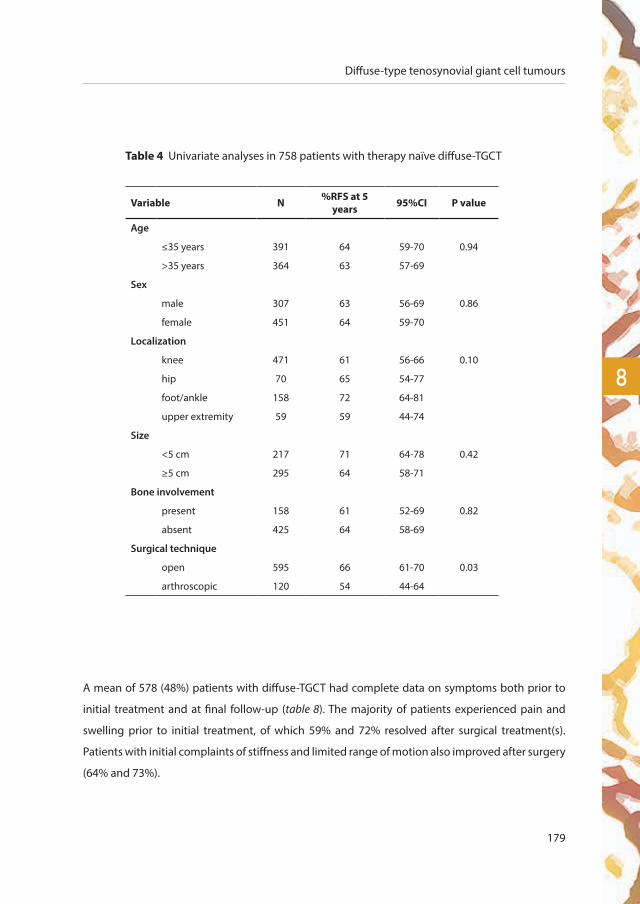
Diffuse-type tenosynovial giant cell tumours
179
8
Table 4 Univariate analyses in 758 patients with therapy naïve diffuse-TGCT
Variable N %RFS at 5 years 95%CI P value
Age
≤35 years 391 64 59-70 0.94
>35 years 364 63 57-69
Sex
male 307 63 56-69 0.86
female 451 64 59-70
Localization
knee 471 61 56-66 0.10
hip 70 65 54-77
foot/ankle 158 72 64-81
upper extremity 59 59 44-74
Size
<5 cm 217 71 64-78 0.42
≥5 cm 295 64 58-71
Bone involvement
present 158 61 52-69 0.82
absent 425 64 58-69
Surgical technique
open 595 66 61-70 0.03
arthroscopic 120 54 44-64
A mean of 578 (48%) patients with diffuse-TGCT had complete data on symptoms both prior to
initial treatment and at final follow-up (table 8). The majority of patients experienced pain and
swelling prior to initial treatment, of which 59% and 72% resolved after surgical treatment(s).
Patients with initial complaints of stiffness and limited range of motion also improved after surgery
(64% and 73%).
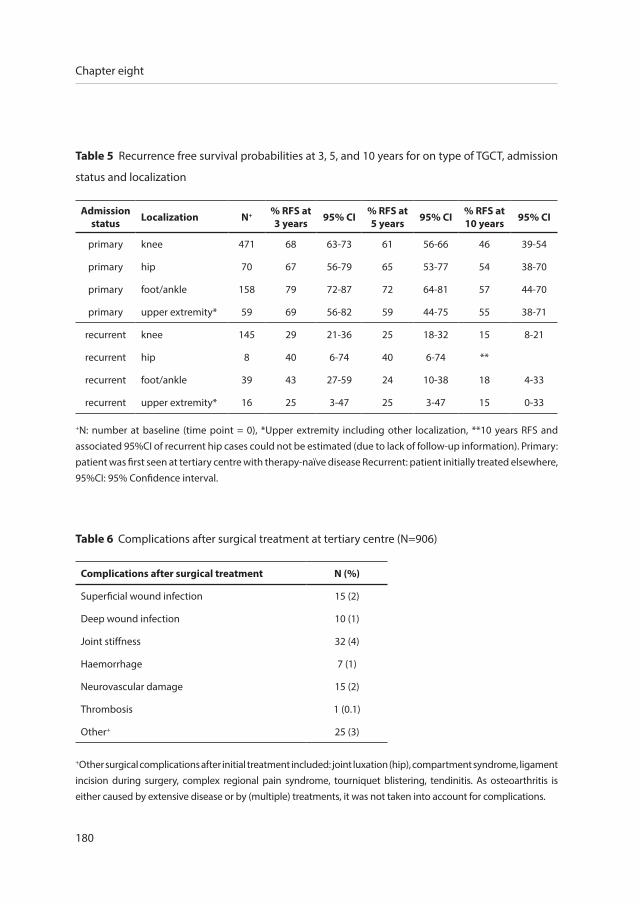
180
Chapter eight
Table 6 Complications after surgical treatment at tertiary centre (N=906)
Complications after surgical treatment N (%)
Superficial wound infection 15 (2)
Deep wound infection 10 (1)
Joint stiffness 32 (4)
Haemorrhage 7 (1)
Neurovascular damage 15 (2)
Thrombosis 1 (0.1)
Other+ 25 (3)
+Other surgical complications after initial treatment included: joint luxation (hip), compartment syndrome, ligament incision during surgery, complex regional pain syndrome, tourniquet blistering, tendinitis. As osteoarthritis is either caused by extensive disease or by (multiple) treatments, it was not taken into account for complications.
Table 5 Recurrence free survival probabilities at 3, 5, and 10 years for on type of TGCT, admission
status and localization
Admissionstatus Localization N+ % RFS at
3 years 95% CI % RFS at 5 years 95% CI % RFS at
10 years 95% CI
primary knee 471 68 63-73 61 56-66 46 39-54
primary hip 70 67 56-79 65 53-77 54 38-70
primary foot/ankle 158 79 72-87 72 64-81 57 44-70
primary upper extremity* 59 69 56-82 59 44-75 55 38-71
recurrent knee 145 29 21-36 25 18-32 15 8-21
recurrent hip 8 40 6-74 40 6-74 **
recurrent foot/ankle 39 43 27-59 24 10-38 18 4-33
recurrent upper extremity* 16 25 3-47 25 3-47 15 0-33
+N: number at baseline (time point = 0), *Upper extremity including other localization, **10 years RFS and associated 95%CI of recurrent hip cases could not be estimated (due to lack of follow-up information). Primary: patient was first seen at tertiary centre with therapy-naïve disease Recurrent: patient initially treated elsewhere, 95%CI: 95% Confidence interval.
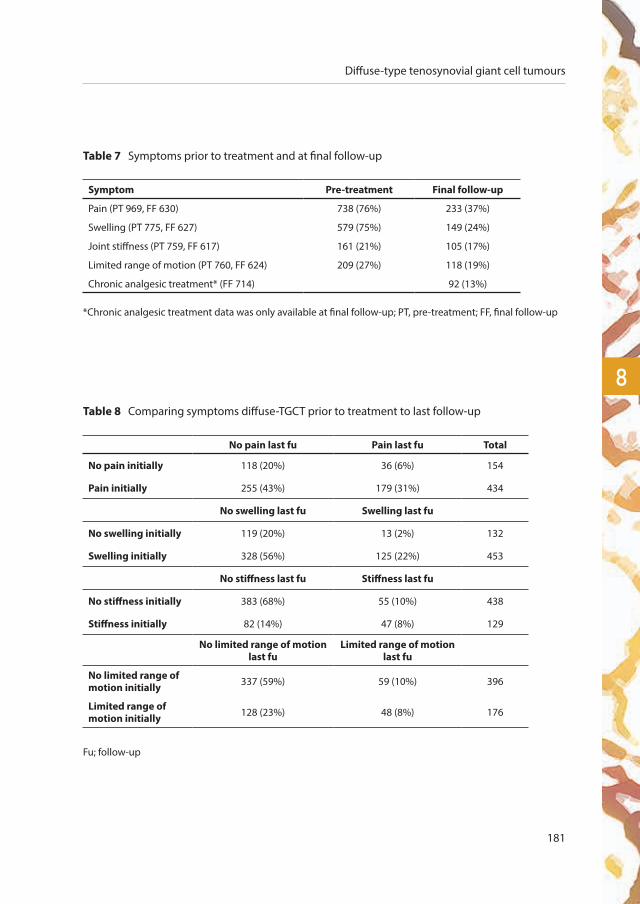
Diffuse-type tenosynovial giant cell tumours
181
8
Table 7 Symptoms prior to treatment and at final follow-up
Symptom Pre-treatment Final follow-up
Pain (PT 969, FF 630) 738 (76%) 233 (37%)
Swelling (PT 775, FF 627) 579 (75%) 149 (24%)
Joint stiffness (PT 759, FF 617) 161 (21%) 105 (17%)
Limited range of motion (PT 760, FF 624) 209 (27%) 118 (19%)
Chronic analgesic treatment* (FF 714) 92 (13%)
*Chronic analgesic treatment data was only available at final follow-up; PT, pre-treatment; FF, final follow-up
Table 8 Comparing symptoms diffuse-TGCT prior to treatment to last follow-up
No pain last fu Pain last fu Total
No pain initially 118 (20%) 36 (6%) 154
Pain initially 255 (43%) 179 (31%) 434
No swelling last fu Swelling last fu
No swelling initially 119 (20%) 13 (2%) 132
Swelling initially 328 (56%) 125 (22%) 453
No stiffness last fu Stiffness last fu
No stiffness initially 383 (68%) 55 (10%) 438
Stiffness initially 82 (14%) 47 (8%) 129
No limited range of motion last fu
Limited range of motion last fu
No limited range of motion initially 337 (59%) 59 (10%) 396
Limited range of motion initially 128 (23%) 48 (8%) 176
Fu; follow-up
182
Chapter eight
Local recurrence versus symptoms final follow-up
A higher percentage of patients with pain, swelling, stiffness and limited range of motion at final
follow-up had recurrent disease (pain; 55% recurrence versus 45% no recurrence, swelling; 66%
versus 34%, stiffness; 51% versus 49%, limited range of motion; 56% versus 44%).
More patients with recurrent disease 21% (64/300) used chronic analgesic treatment at last follow-
up compared to patients 6% (24/388) without recurrent disease.
Surgical technique versus functional outcome at last follow-up
Surgical technique did not influence functional outcome at last follow-up (pain: 41% symptoms
after AS versus 37% after OS, swelling: 29% versus 22%, stiffness: 13% versus 18%, limited range of
motion: 16% versus 21%, chronic analgesic treatment: 18% versus 12%).
Chronic analgesic treatment versus complications
24% (16/67) of patients using chronic analgesic treatment had a complication, compared with
10% (50/482) of patients without a complication.
Diffuse-type tenosynovial giant cell tumours
183
8
discussion
This international multicentre study offers new insights into the outcome of patients with the
orphan and heterogeneous disease diffuse-type Tenosynovial Giant Cell Tumour (TGCT). The
greatest strength of this dataset is that it represents the largest collection of surgically treated
diffuse-TGCT patients in the scientific literature, including RFS estimates for the knee, hip, foot/
ankle and upper extremity locations with long-term follow-up (>10 years). Oncologic results,
complications and functional results after surgical treatment are evaluated.
Oncologic outcome diffuse-TGCT
The fundamental question of whether curative treatment is necessary, or should be attempted in
non-lethal diffuse-TGCT often arises in literature. Debilitating symptoms and (progressive) joint
destruction commonly result from untreated diffuse-TGCT but can also occur following treatment.
At present, the choice of treatment is established by the preference of the patient, treating
physician and might differ by treatment centre. Surgical treatment for the locally aggressive diffuse-
TGCT is challenging, as pathologic tissue can be widely spread throughout the joint and may be
technically difficult to access and remove. In extensive disease, less than radical or only partial
resection could be preferred to improve symptoms with joint preservation in mind. However,
higher rates of recurrence have been described after macroscopically incomplete resections8, 29-31.
Some reports consider arthroscopic management of TGCT superior to open surgery, because of
less morbidity and a shorter recovery period32-36. Standard arthroscopy of the knee using only
anteromedial and anterolateral approaches however, does not allow surgical access to remove all
areas where diseased tissue is likely to be present. Therefore Blanco et al. and Mollon et al. used
multiple portals including posteromedial and posterolateral in arthroscopic synovectomy37-39. Chin
et al. stated that knee arthroscopy alone is an inferior treatment for extra-articular TGCT40. Open
synovectomy, either one- or two-staged, seems to be the preferred surgical approach to diffuse-
TGCT in most centres, because of tumour visibility and reported lower short-term recurrence
rates11, 41, 42. The disadvantage of a one- or two-staged open resection, could be deteriorated joint
function accompanied with decreased patient health-related quality of life13. A systematic review
showed lower recurrence rates for open synovectomy (average 14%, maximum 67%) compared
to arthroscopic synovectomy (average 40%, maximum 92%) in diffuse-TGCT11. Patel et al. (N=214)

184
Chapter eight
reported a statistically significant higher risk of recurrence in diffuse-type TGCT with arthroscopic
compared to open synovectomy (83.3% vs 44.8%, RR = 1.86 95% CI 1.32–2.62, P = 0.0004)9.
Palmerini et al. (N=206) did not find a difference in recurrence based on surgical technique for
localized- and diffuse-TGCT combined8.
A combined anterior arthroscopic- and posterior open synovectomy in the knee might be a
viable option, but is only incidentally reported. Mollon et al. described the combined approach
of a multiportal anterior and posterior arthroscopy and a posterior open synovectomy largely for
resection of extra-articular popliteal disease, and reported two recurrences in 15 patients38. Colman
et al. retrospectively evaluated 11 diffuse-TGCT patients treated by the combined approach and
also reported relatively low short-term recurrence rates (9%)43. A randomized controlled trial for
arthroscopic synovectomy versus open synovectomy has not been performed.
The present study calculated recurrence free survival rates for diffuse-TGTC at 3, 5 and 10 years
of 62%, 55% and 40%, respectively. This clearly underlines that with longer follow-up, recurrence
rates continue to increase (table 2-3, figure 3). The greatest risk factor for local recurrence is recurrent
disease at presentation in a tertiary centre (HR 3.5 95% CI 2.8-4.4 in multivariate analyses). In
therapy naïve patients with primary treatment in a tertiary centre, the largest risk factor for local
recurrence was arthroscopic synovectomy. The suspicion arises that more (macroscopic) tumour
tissue remains after arthroscopic synovectomy; however this largely depends on the extend of the
arthroscopy performed, whether multiple and posterior portals were used to access and remove
disease throughout the knee joint, and whether this approach is combined with an open approach
to remove residual intra-articular disease and/or extra-articular disease extension. However, none
of the assumed risk factors yielded significant differences when the analysis was performed in a
subgroup of therapy naïve patients with diffuse-TGCT affecting the knee. This could be attributed
to the near impossibility of achieving a complete macroscopic resection in widely spread, ill-
defined diffuse-TGCT patients and the impossibility of an R0 resection: macroscopically and
microscopically complete resection, neither with an arthroscopic- nor open resection.

Diffuse-type tenosynovial giant cell tumours
185
8
Multimodality treatment
Within the current era of systemic targeted and multimodality therapies (some only available
in trial settings) in TGCT, standalone surgical resection can no longer be regarded as the only
treatment for more severe diffuse forms of the disease. Surgery has been considered the treatment
of choice for decades, and the current study which included patients from 1990 onwards, consists
mainly of patients treated with a surgical procedure.
High recurrence rates, as confirmed by the present study, indicate the need for adjuvant therapies
to improve treatment outcomes for patients with diffuse-TGCT. Nonetheless, Gortzak et al. reported
no significant differences in residual disease, complication rates and overall physical and mental
health scores between patients surgically treated for TGCT of the knee with (N=34) or without (N=22)
adjuvant 90Yttrium, after a mean follow-up of 7.3 years17. Verspoor et al. evaluated 12 patients treated
with surgical synovectomy and additional cryosurgery. They did not find better results compared
to surgical resection alone44. Griffin et al. reported on 49 patients with diffuse-TGCT, most of whom
had both intra- and extra-articular and recurrent disease. They reported 3 (6%) recurrences following
synovectomy and radiation10. A meta-analysis suggested that open synovectomy (N=19 studies,
N=448) or synovectomy combined with perioperative radiotherapy (11 studies, N=123) is associated
with a reduced rate of recurrence16. Mollon et al. reserved the use of external beam radiation for
patients at high risk for local recurrence, if they had the following characteristics: multiple episodes
of recurrent intra-articular disease, extra-articular extension, or gross residual disease remaining
following surgery38. Currently, sufficient data including adequate patient numbers is lacking to
support the use of external beam radiation in primary cases, however the authors feel it should only
be performed in specific instances such as extensive or recurrent diffuse-TGCT cases.
In patients with locally advanced TGCT or (multiple) recurrence(s), systemic therapies targeting
the CSF1/CSF1R axis have been recently investigated including nilotinib, imatinib, pexidartinib
(PLX3397), emactuzumab (RG7155) and cabiralizumab (FPA008). Some systemic treatments for
TGCT have been proven to be effective18, 19, and novel and potentially more potent agents are
under investigation20-22. The disadvantages of adjuvant or targeted therapies are acute and long-
term side-effects of different degrees. Therefore, additional long-term follow-up studies in this
field remain indicated.

186
Chapter eight
Patients with aggressive disease accompanied with a high risk of recurrence following surgery
alone should be selected for (new) systemic and (neo)adjuvant treatment modalities. Diffuse-
TGCT presents as a heterogeneous disease with different disease severities. Some patients present
with tumours that are surgically relatively easy to access and these patients might not require
(neo)adjuvant therapies. Mastboom et al. defined the most severe diffuse-TGCT subgroup on MR
imaging as having diffuse-type TGCT including intra- and extra-articular disease and involvement
of at least one of the following three tissues: muscle, tendon or ligament)5. These patients seem
most eligible for multimodality or (neo)adjuvant strategies.
Complications
The literature on TGCT frequently lacks descriptions of complications after surgical treatment.
This study reported a complication rate of 12% following surgical management of patients with
diffuse-TGCT, predominantly after open resection (82%). The most common complication was joint
stiffness after open synovectomy, which might be difficult to prevent after the surgical treatment
of extensive disease. The true complication rate might be even higher, since it is suspected that
not all complications are scored.
Symptoms
TGCT related symptoms are mainly pain, swelling, stiffness and limited range of motion, but these
are reported with a great variability in degree and severity. Gelhorn et al. concluded that not
all patients experience all symptoms to the same extent (e.g. swelling but no pain, or pain and
swelling but no stiffness or limited range of motion)6. Symptoms prior to initial treatment at a
tertiary centre were compared for each patient with symptoms at last follow-up. Initial symptoms
of pain and swelling improved following treatment(s) in 43-56% of patients. This is comparable
with a crowdsourcing study in 337 TGCT patients originating from 31 countries14. In the majority
of patients, stiffness and limited range of motion did not seem to be principal symptoms either
initially, or at last follow-up. These symptoms are subjective for each patient and not all patients
were included with complete data. Nevertheless, pain and swelling are the main TGCT-related
complaints initially and frequently improve after surgical treatment(s).
Diffuse-type tenosynovial giant cell tumours
187
8
As expected, diffuse-TGCT patients with recurrent disease demonstrated higher rates of symptoms
at final follow-up, including a 3.5-fold higher rate of chronic analgesic use, compared to patients
without local recurrence at last follow-up. Also, patients using chronic analgesics had a higher rate
of complications.
Interestingly, after arthroscopic synovectomy in diffuse-TGCT, patients exhibited more pain,
swelling and a higher use of chronic analgesics, compared with open synovectomy. On the
contrary, open synovectomy was associated with higher rates of stiffness and limited range of
motion, which can be attributed to the larger surgical procedure resulting in additional scar tissue.
Joint specific analyses
Within this individual participant data meta-analysis, a homogeneous subgroup analysis for
diffuse-TGCT affecting the knee of therapy naïve patients was performed (figure 3b). Despite the
large number of patients in this study with diffuse-TGCT cases, the numbers in other joint locations
were too small to allow analysis of those specific groups.
Limitations
The main limitation of this study is selection (referral) bias, since data on patients treated at non-
specialized centres was lacking. Selection bias of affected joints seems absent when comparing
percentages of affected joints (table 1, figure 2) with a recent incidence calculation study including
nationwide coverage (in both studies 64% of diffuse-TGCT affects the knee)4.
Even though TGCT is a benign disease, particularly diffuse-TGCT can become a chronic illness
with substantial morbidity to the joint leading to functional and patient health-related quality
of life impairment, caused by the course of the disease itself and multiple treatments13. As data
were collected by local investigators or physicians according to the multicentre study design, data
quality depended on data registry on site. Only data available in the source data file of the patients
could be retrieved. In addition, interpretation of individual parameters could differ. No central
histopathological review was performed, as it was assumed that each centre provided the correct
diagnosis as set by their histopathology department. Within our study we did not collect which
patient had multiportal arthroscopy or standard anterior portal arthroscopy.

188
Chapter eight
Recurrence rates could either be over-estimated or under-estimated. Over-estimation could occur
because the follow-up status ‘alive with disease’ was classified as recurrence (if recurrence data
were missing). On the contrary, under-estimation could be present if patients with recurrent
disease, did not return at all or did not return to their original centre. It should be noted that
patients with recurrent disease had a longer follow-up compared to patients without recurrent
disease. The explanation could be that patients without symptoms and (assumed) without
recurrent disease were dismissed from follow-up and therefore had shorter follow-up times. In
addition, if treatments were recently performed, patients also had shorter follow-up times and are
still at risk of recurrence.
conclusion
This is the largest global individual data study on patients with diffuse-type TGCT and provides a
comprehensive and up to date disease overview, evaluating the clinical profile and management
of TGCT. Our study demonstrated that surgery is by far the most frequently performed treatment in
tertiary referral hospitals. However, even in specialised centres, local control of this heterogeneous
orphan disease, remains a major issue, with overall recurrence free survival of 55% at 5 years.
Since complete resection of diffuse-TGCT is often impossible and recurrence rates are high after
both arthroscopy and open synovectomy of the knee, the optimal surgical approach should be
left to the discretion of an experienced surgical and multidisciplinary team. However, in the era
of multimodality therapy, standalone surgical resection can no longer be regarded as the only
effective treatment for patients with diffuse-TGCT and alternative or combined approaches should
be considered.
Diffuse-type tenosynovial giant cell tumours
189
8
references
1. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4 ed2013. p. 100-1.
2. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, diffuse type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 52013. p. 102-3.
3. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review
and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
4. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence rates
than previously known in tenosynovial giant cell tumors. Acta orthopaedica. 2017:1-7.
5. Mastboom MJL, Verspoor FGM, Hanff DF, Gademan MGJ, Dijkstra PDS, Schreuder HWB, Bloem JL, van der Wal RJP, van
de Sande MAJ. Severity classification of Tenosynovial Giant Cell Tumours on MR imaging. Surg Oncol. 2018;27:544-50.
6. Gelhorn HL, Tong S, McQuarrie K, Vernon C, Hanlon J, Maclaine G, et al. Patient-reported Symptoms of Tenosynovial Giant
Cell Tumors. Clin Ther. 2016;38(4):778-93.
7. Bhimani MA, Wenz JF, Frassica FJ. Pigmented villonodular synovitis: keys to early diagnosis. Clin Orthop Relat Res.
2001(386):197-202.
8. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.
9. Patel KH, Gikas PD, Pollock RC, Carrington RW, Cannon SR, Skinner JA, et al. Pigmented villonodular synovitis of the knee:
A retrospective analysis of 214 cases at a UK tertiary referral centre. Knee. 2017;24(4):808-15.
10. Griffin AM, Ferguson PC, Catton CN, Chung PW, White LM, Wunder JS, et al. Long-term outcome of the treatment of
high-risk tenosynovial giant cell tumor/pigmented villonodular synovitis with radiotherapy and surgery. Cancer.
2012;118(19):4901-9.
11. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
12. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
13. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical
treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J.
2014;96-B(8):1111-8.
14. Mastboom MJ, Planje R, van de Sande MA. The Patient Perspective on the Impact of Tenosynovial Giant Cell Tumors
on Daily Living: Crowdsourcing Study on Physical Function and Quality of Life. Interactive journal of medical research.
2018;7(1):e4.
15. Heyd R, Seegenschmiedt MH, Micke O. [The role of external beam radiation therapy in the adjuvant treatment of
pigmented villonodular synovitis]. Zeitschrift fur Orthopadie und Unfallchirurgie. 2011;149(6):677-82.
16. Mollon B, Lee A, Busse JW, Griffin AM, Ferguson PC, Wunder JS, et al. The effect of surgical synovectomy and radiotherapy
on the rate of recurrence of pigmented villonodular synovitis of the knee: an individual patient meta-analysis. Bone Joint
J. 2015;97-B(4):550-7.
17. Gortzak Y, Vitenberg M, Frenkel Rutenberg T, Kollender Y, Dadia S, Sternheim A, et al. Inconclusive benefit of adjuvant
(90)Yttrium hydroxyapatite to radiosynovectomy for diffuse-type tenosynovial giant-cell tumour of the knee. Bone Joint
J. 2018;100-B(7):984-8.

190
Chapter eight
18. Gelderblom H, Cropet C, Chevreau C, Boyle R, Tattersall M, Stacchiotti S, et al. Nilotinib in locally advanced pigmented
villonodular synovitis: a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2018.
19. Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, et al. Efficacy of imatinib mesylate for the
treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis.
Cancer. 2012;118(6):1649-55.
20. Cassier PA, Italiano A, Gomez-Roca CA, Le Tourneau C, Toulmonde M, Cannarile MA, et al. CSF1R inhibition with
emactuzumab in locally advanced diffuse-type tenosynovial giant cell tumours of the soft tissue: a dose-escalation and
dose-expansion phase 1 study. Lancet Oncol. 2015;16(8):949-56.
21. Sankhala KK, Blay JY, Ganjoo KN, Italiano A, Hassan AB, Kim TM, et al. A phase I/II dose escalation and expansion study
of cabiralizumab (cabira; FPA-008), an anti-CSF1R antibody, in tenosynovial giant cell tumor (TGCT, diffuse pigmented
villonodular synovitis D-PVNS). ASCO conference 2017. 35 (15 Supplement 1).
22. Tap WD, Gelderblom H, Stacchiotti S, Palmerini E, Ferrari S, Desai J, et al. Final results of ENLIVEN: A global, double-blind,
randomized, placebo-controlled, phase 3 study of pexidartinib in advanced tenosynovial giant cell tumor (TGCT). ASCO
conference. 2018.
23. Riley RD, Lambert PC, Abo-Zaid G. Meta-analysis of individual participant data: rationale, conduct, and reporting. Bmj.
2010;340:c221.
24. Honaker J, King G, Blackwell M. Amelia II: a program for missing data. J Stat Softw. 2011;45:1-54.
25. Rubin DB. Multiple imputation after 18+ years. J Am Stat Assoc. 1996;91:473-89.
26. Fay MP, Shaw PA. Exact and Asymptotic Weighted Logrank Tests for Interval Censored Data: The interval R package.
Journal of statistical software. 2010;36(2).
27. Sun J. A non-parametric test for interval-censored failure time data with application to AIDS studies. Statistics in
medicine. 1996;15(13):1387-95.
28. Anderson-Bergman C. icenReg: Regression Models for Interval Censored Data in R. J Stat Softw. 2017;81(12):1-23.
29. Schwartz HS, Unni KK, Pritchard DJ. Pigmented villonodular synovitis. A retrospective review of affected large joints. Clin
Orthop Relat Res. 1989(247):243-55.
30. Ogilvie-Harris DJ, McLean J, Zarnett ME. Pigmented villonodular synovitis of the knee. The results of total arthroscopic
synovectomy, partial, arthroscopic synovectomy, and arthroscopic local excision. J Bone Joint Surg Am. 1992;74(1):119-
23.
31. Chin KR, Barr SJ, Winalski C, Zurakowski D, Brick GW. Treatment of advanced primary and recurrent diffuse pigmented
villonodular synovitis of the knee. J Bone Joint Surg Am. 2002;84-A(12):2192-202.
32. de Carvalho LH, Jr., Soares LF, Goncalves MB, Temponi EF, de Melo Silva O, Jr. Long-term success in the treatment of
diffuse pigmented villonodular synovitis of the knee with subtotal synovectomy and radiotherapy. Arthroscopy.
2012;28(9):1271-4.
33. Kubat O, Mahnik A, Smoljanovic T, Bojanic I. Arthroscopic treatment of localized and diffuse pigmented villonodular
synovitis of the knee. Collegium antropologicum. 2010;34(4):1467-72.
34. Loriaut P, Djian P, Boyer T, Bonvarlet JP, Delin C, Makridis KG. Arthroscopic treatment of localized pigmented villonodular
synovitis of the knee. Knee Surg Sports Traumatol Arthrosc. 2012;20(8):1550-3.
35. Rhee PC, Sassoon AA, Sayeed SA, Stuart MS, Dahm DL. Arthroscopic treatment of localized pigmented villonodular
synovitis: long-term functional results. American journal of orthopedics. 2010;39(9):E90-4.

Diffuse-type tenosynovial giant cell tumours
191
8
36. Noailles T, Brulefert K, Briand S, Longis PM, Andrieu K, Chalopin A, et al. Giant cell tumor of tendon sheath: Open surgery
or arthroscopic synovectomy? A systematic review of the literature. Orthop Traumatol Surg Res. 2017;103(5):809-14.
37. Blanco CE, Leon HO, Guthrie TB. Combined partial arthroscopic synovectomy and radiation therapy for diffuse pigmented
villonodular synovitis of the knee. Arthroscopy. 2001;17(5):527-31.
38. Mollon B, Griffin AM, Ferguson PC, Wunder JS, Theodoropoulos J. Combined arthroscopic and open synovectomy for
diffuse pigmented villonodular synovitis of the knee. Knee Surg Sports Traumatol Arthrosc. 2016;24(1):260-6.
39. Chang JS, Higgins JP, Kosy JD, Theodoropoulos J. Systematic Arthroscopic Treatment of Diffuse Pigmented Villonodular
Synovitis in the Knee. Arthroscopy techniques. 2017;6(5):e1547-e51.
40. Chin KR, Brick GW. Extraarticular pigmented villonodular synovitis: a cause for failed knee arthroscopy. Clin Orthop Relat
Res. 2002(404):330-8.
41. Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM. Surgical treatment of diffuse pigmented
villonodular synovitis of the knee. Clin Orthop Relat Res. 1994(300):183-92.
42. Sharma V, Cheng EY. Outcomes after excision of pigmented villonodular synovitis of the knee. Clin Orthop Relat Res.
2009;467(11):2852-8.
43. Colman MW, Ye J, Weiss KR, Goodman MA, McGough RL, 3rd. Does combined open and arthroscopic synovectomy for
diffuse PVNS of the knee improve recurrence rates? Clin Orthop Relat Res. 2013;471(3):883-90.
44. Verspoor FG, Scholte A, van der Geest IC, Hannink G, Schreuder HW. Cryosurgery as Additional Treatment in Tenosynovial
Giant Cell Tumors. Sarcoma. 2016;2016:3072135.


trea
tmen
tlong-term efficacy of
imatinib mesylate in patients
with advanced tenosynovial giant
cell tumour
chap
ter
nine
M.J.L. Mastboom*1, F.G.M. Verspoor*2, G. Hannink2, R.G. Maki3, A. Wagner4, E. Bompas5, J. Desai 6, A. Italiano7, B.M. Seddon8, W.T.A.
van der Graaf9, J.-Y. Blay10, M. Brahmi10, L. Eberst10, S. Stacchiotti11, O. Mir12, M.A.J. van de Sande1, H. Gelderblom13, P. A. Cassier10
Submitted.
international, multicentre study

194
Chapter nine
1 Orthopaedic Surgery, Leiden University Medical Centre, Leiden, the Netherlands
2 Orthopaedic Surgery, Radboud University Medical Centre, Nijmegen, the Netherlands
3 Medical Oncology, Monter Cancer Centre & Cold Spring Harbor Laboratory, Long Island, NY, USA
4 Medical Oncology, Dana Farber Cancer Institute, Boston, USA
5 Medical Oncology, Institut de Cancérologie de l’Ouest, Nantes, France
6 Medical Oncology, Peter Mac Callum Cancer Centre, Melbourne, Australia
7 Medical Oncology, Institut Bergonié, Bordeaux, France
8 Medical Oncology, University College Hospital, London, United Kingdom
9 Medical Oncology, Radboud University Medical Centre, Nijmegen, the Netherlands
10 Medical Oncology, Centre Léon Bérard, Lyon, France
11 Medical Oncology, Istituto Nazionale Tumori, Milano, Italy
12 Medical Oncology, Gustave Roussy Institute, Villejuif, France
13 Medical Oncology, Leiden University Medical Centre, Leiden, the Netherlands
*Authors contributed equally to this work.
Imatinib in tenosynovial giant cell tumours
195
9
abstract
Background
Tenosynovial Giant Cell Tumours (TGCT), are rare colony stimulating factor-1(CSF-1)-driven
proliferative disorders affecting joints. Diffuse-type TGCT often causes significant morbidity due
to local recurrences necessitating multiple surgeries. Imatinib mesylate (IM) blocks CSF-1 receptor.
This study investigated the long term effects of IM in TGCT.
Methods
We conducted an international multi-institutional retrospective study to assess the activity of
IM: data was collected anonymously from individual patients with locally advanced, recurrent or
metastatic TGCT.
Results
Sixty-two patients from 12 institutions across Europe, Australia and the United States were
identified. Thirty-nine patients were female (63%), median age at treatment start was 45 (range
20-80) years, with a median time from diagnose to treatment of 3.5 (range 0-38,2) years. Median
follow-up after treatment start was 52 (IQR 18-83) months. Four patients with metastatic TGCT
progressed rapidly on IM and were excluded for further analyses. Seventeen of 58 evaluable
patients achieved CR or PR. One- and five-year progression-free survival rates were 71% and 48%,
respectively. Thirty-eight (66%) patients discontinued IM after a median of 7 (range 1-80) months.
Reported adverse events in 45 (78%) patients were among other edema (48%) and fatigue (50%),
mostly grade 1-2 (89%). Five patients experienced grade 3-4 toxicities.
Conclusion
This study confirms, with additional follow-up, the efficacy of IM in TGCT. In responding cases we
confirmed prolonged IM activity on TGCT symptoms even after discontinuation, but with high
rates of treatment interruption and additional treatments.

196
Chapter nine
introduction
Tenosynovial giant-cell tumour (TGCT), historically known as pigmented villonodular synovitis
(PVNS), is a rare, at times locally aggressive neoplasm affecting the joints or tendon sheaths in
young adults. It is most common around large joints such as the knees, ankles and hips1, 2. Known
subtypes are localized and diffuse TGCT. The localized subtype comprises a single nodule and has
a favourable course while the diffuse subtype involves the synovial lining as well as surrounding
structures and is associated with a significant risk of recurrence (>50% depending on follow up
times), despite being a benign neoplasm2-4. Metastatic forms have been described, but seem to
occur very rarely5, 6.
Surgical resection is the primary treatment for both subtypes. However, diffuse TGCT is difficult to
remove completely and often requires a total synovectomy, or at time a joint replacement, or rarely
even amputation1, 2, 7. In patients with extensive and/or recurrent TGCT, other available treatment
modalities include radiation synovectomy8, external beam radiation therapy9, and cryosurgery10.
Their therapeutic value has only been assessed in retrospective, in most cases single centre series
and their long term side effects and complications are poorly described11.
Recurrent TGCT is rarely lethal, but frequently becomes a debilitating chronic illness with
substantial morbidity to the joints and quality of life impairment, caused by the disease itself and
the multiple treatments2, 12.
In TGCT, a neoplastic clone constitutes a subpopulation (2-16%)13 of cells that overexpress colony-
stimulating factor-1 (CSF-1). A t(1;2) translocation that links the CSF1 gene on chromosome 1p13
to the COL6A3 gene on chromosome 2q35 has been described and is believed to be responsible
for the overproduction of CSF1 by neoplastic cells13, 14. Inhibition of CSF1/CSF-1 receptor (CSF-1R)
signaling has shown efficacy in the treatment of locally advanced and recurrent diffuse TGCT15-17.
Imatinib mesylate (IM) inhibits the CSF-1R kinase among other kinases17. We have previously
reported on the efficacy of IM in TGCT. In the present study we provide long term follow-up on
these initial patients and data on 33 additional consecutive patients.

Imatinib in tenosynovial giant cell tumours
197
9
methods
This retrospective study was conducted at 12 referral centres across Europe (9 institutions), the
United States of America (2 institutions), and Australia (1 institution). The file of all patients with
locally advanced, recurrent or metastatic TGCT, treated with IM were reviewed. Patients information
were extracted from individual patients’ files at each institution by the local investigators and was
provided in an anonymous form for final analyses. Histopathologic examination was performed
at centre of origin by pathologists with extensive experience in mesenchymal tumours. Response
was measured using version 1.0 of Response Evaluation Criteria in Solid Tumours (RECIST). Data
were described using percentages for qualitative variables and medians with ranges for continuous
variables. Patients were not treated on a research protocol. They provided informed consent to
treatment with a ‘off-label’ medical treatment, and treatment decision was left to the treating
physician. This retrospective analysis was approved by the Ethics Committee in Lyon (Committee
for the Protection of Individuals, Sud-Est IV, Lyon, France – L10-153 dated 9 December 2010).
Survival was plotted using the Kaplan-Meier method. Progression-free survival (PFS) was
calculated from the date IM was started to the date of disease progression or death. The time to
treatment failure (TTF) was calculated from the date IM was started to the date it was stopped
because of toxicity, disease progression, or death, whichever occurred first. For patients with a
surgical resection or other additional therapy after treatment with IM, PFS and TTF were censored
at the time of surgery. Disease specific survival was calculated from the date IM was started to the
date of death due to TGCT. Symptomatic response was defined as improvement of pain and/or
joint function in patients who had symptoms at baseline. All statistical analyses were performed
using R version 3.4.0 (R Foundation, Vienna, Austria).
results
Patients
A total of 62 patients with histopathologically proven TGCT treated with imatinib were identified,
their main characteristics are described in Table 1. Briefly, median age at diagnosis was 39 (IQR
31-53) years and 45 (IQR 36-56) years at start of treatment with IM, the majority of patients were
female (N=39, 63%), and the knee (N=35, 56%) was the most commonly affected joint (Table 1). At
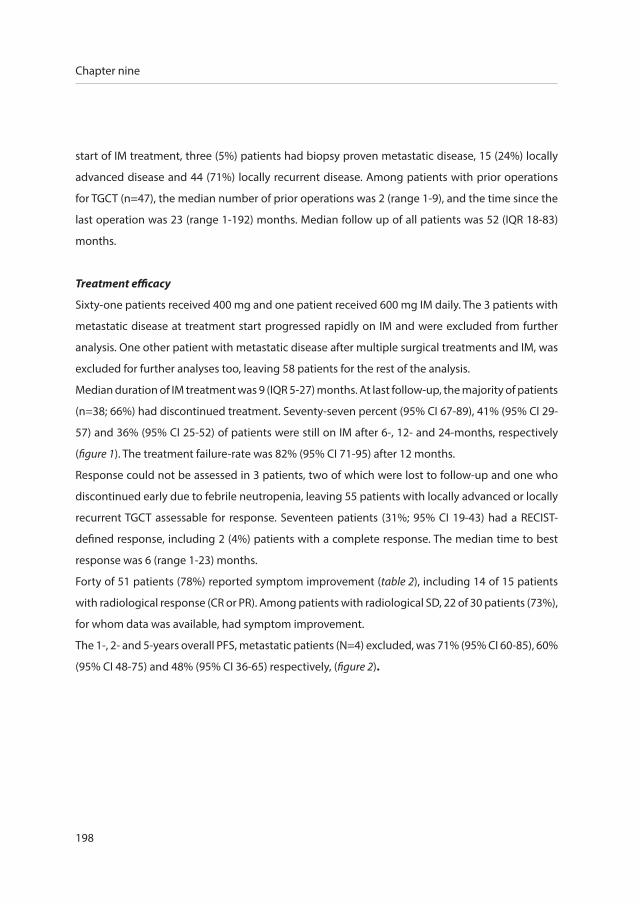
198
Chapter nine
start of IM treatment, three (5%) patients had biopsy proven metastatic disease, 15 (24%) locally
advanced disease and 44 (71%) locally recurrent disease. Among patients with prior operations
for TGCT (n=47), the median number of prior operations was 2 (range 1-9), and the time since the
last operation was 23 (range 1-192) months. Median follow up of all patients was 52 (IQR 18-83)
months.
Treatment efficacy
Sixty-one patients received 400 mg and one patient received 600 mg IM daily. The 3 patients with
metastatic disease at treatment start progressed rapidly on IM and were excluded from further
analysis. One other patient with metastatic disease after multiple surgical treatments and IM, was
excluded for further analyses too, leaving 58 patients for the rest of the analysis.
Median duration of IM treatment was 9 (IQR 5-27) months. At last follow-up, the majority of patients
(n=38; 66%) had discontinued treatment. Seventy-seven percent (95% CI 67-89), 41% (95% CI 29-
57) and 36% (95% CI 25-52) of patients were still on IM after 6-, 12- and 24-months, respectively
(figure 1). The treatment failure-rate was 82% (95% CI 71-95) after 12 months.
Response could not be assessed in 3 patients, two of which were lost to follow-up and one who
discontinued early due to febrile neutropenia, leaving 55 patients with locally advanced or locally
recurrent TGCT assessable for response. Seventeen patients (31%; 95% CI 19-43) had a RECIST-
defined response, including 2 (4%) patients with a complete response. The median time to best
response was 6 (range 1-23) months.
Forty of 51 patients (78%) reported symptom improvement (table 2), including 14 of 15 patients
with radiological response (CR or PR). Among patients with radiological SD, 22 of 30 patients (73%),
for whom data was available, had symptom improvement.
The 1-, 2- and 5-years overall PFS, metastatic patients (N=4) excluded, was 71% (95% CI 60-85), 60%
(95% CI 48-75) and 48% (95% CI 36-65) respectively, (figure 2).

Imatinib in tenosynovial giant cell tumours
199
9
Figu
re 1
Dur
atio
n of
imat
inib
mes
ylat
e tr
eatm
ent a
nd p
rogr
essi
on fr
ee s
urvi
val o
f thi
s tr
eatm
ent i
n pa
tient
s w
ith
loca
lly a
dvan
ced
or re
curr
ent d
iffus
e-ty
pe T
GC
T.
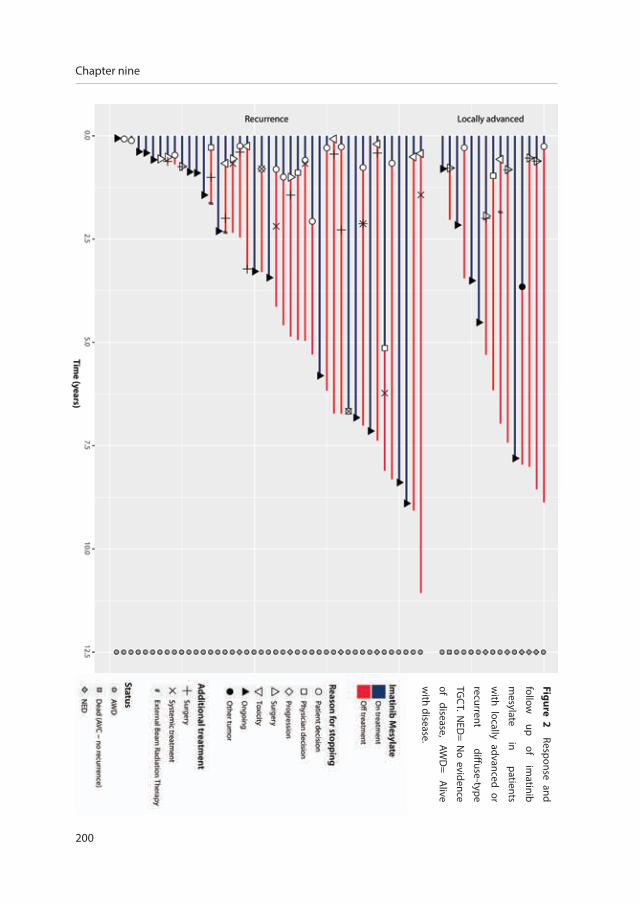
200
Chapter nine
Figure 2 Response and
follow
up of
imatinib
mesylate
in patients
with locally advanced or
recurrent diffuse-type
TGC
T. NED
= No evidence
of disease,
AWD
= A
live
with disease.

Imatinib in tenosynovial giant cell tumours
201
9
Table 1 Descriptive of diffuse-type TGCT patients receiving imatinib mesylate treatment
Patients N (%)
Total 62 (100)
Median age at diagnosis (IQR), yrs 39 (31-53)
Median time from diagnosis to start IM (IQR), yrs 3.5 (1-8)
Sex
Male 23 (37)
Female 39 (63)
Tumour location
Knee 35 (56)
Ankle 11 (18)
Hip 6 (10)
Foot 4 (6)
Shoulder 1 (2)
Elbow 1 (2)
Head and Neck 2 (3)
Wrist 2 (3)
Surgery before start IM
None 15 (24)
1-2 24 (39)
3-4 13 (21)
>4 10 (16)
Median N of surgeries (range) 2 (1-9)
Median time since last surgery (range), mo 23 (1-192)
Disease status
Locally advanced 20 (32)
Recurrence after surgery 39 (63)*
Metastatic disease 3 (5)
Abbreviations: TGCT= Tenosynovial Giant Cell tumour, IM= imatinib mesylate, N= Number of patients,
mo=months, yrs= years. *One of the locally recurrent patients progressed to metastatic disease.

202
Chapter nine
Follow-up
Overall 38/58 patients (66%), metastatic patients (N=4) excluded, eventually discontinued IM after
a median of 7.0 (range 1-80 months). the most common reason for treatment discontinuation
was patient decision to stop (n=14, which possibly reflect low grade chronic toxicity), followed
by planned surgery (n=10), toxicity (n=7), physician’s decision (n=5) and progression (n=1). One
patient discontinued IM because of the diagnosis of another tumour requiring therapy. Among
the 27 patients who discontinued treatment for reasons other than surgery or progression,
progression (either radiological progression or requirement for another line of therapy – i.e.
surgery, other medical therapy or radiotherapy) eventually occurred 17 patients after a median of
12 (range 4-84) months, while 10 patients never progressed (nor required additional therapy) after
a median follow-up to 78 (range 1-109) months, suggesting that IM was able to provide prolonged
symptomatic relief at least in a proportion of patients.
Table 2 Summary of imatinib mesylate efficacy in patients with locally advanced or recurrent
diffuse-type TGCT
Parameter Patients N (%)
RECIST best response*
Complete remission 2 (4)
Partial response 15 (27)
Stable disease 36 (65)
Progressive disease 2 (4)
Overall response rate 17 (31)
Rate of disease control 53 (96)
Symptomatic response 40 (78)**
Median IM treatment duration (IQR), mo 9.3 (5-26)
Median PFS (IQR), mo 18 (8-55)
Abbreviations: TGCT= Tenosynovial Giant Cell tumour, IM= imatinib mesylate, N= Number of patients,
mo=months, yrs= years, IQR= inter quartile range. Overall response rate includes complete remission and
partial response; Rate of disease control includes complete remission, partial response and stable disease;
Symptomatic response was indicated as present or not (40/51=78%). Metastatic patients (n=4) were excluded.
*N=3 RECIST best response not available; **N=9 symptomatic response not available.
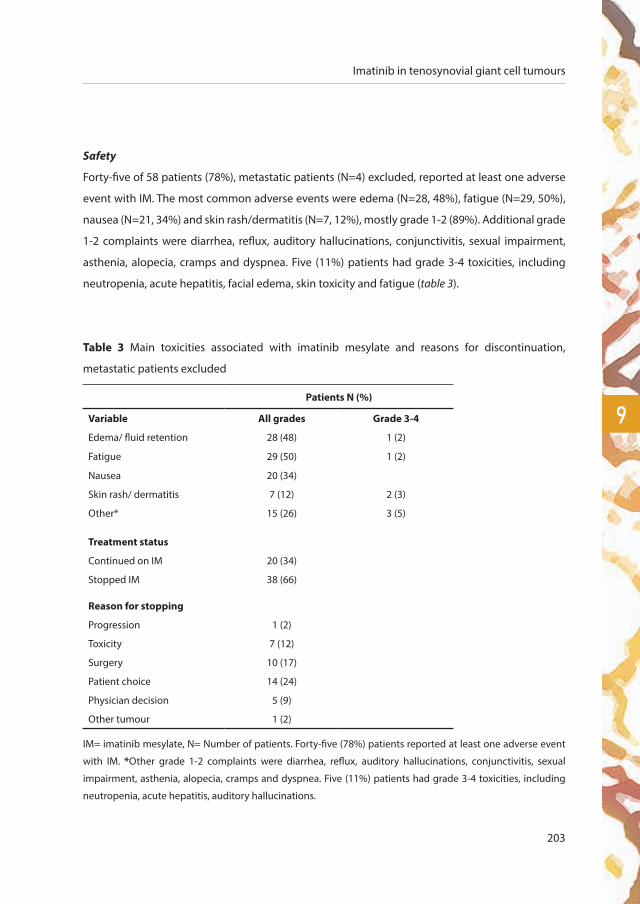
Imatinib in tenosynovial giant cell tumours
203
9
Safety
Forty-five of 58 patients (78%), metastatic patients (N=4) excluded, reported at least one adverse
event with IM. The most common adverse events were edema (N=28, 48%), fatigue (N=29, 50%),
nausea (N=21, 34%) and skin rash/dermatitis (N=7, 12%), mostly grade 1-2 (89%). Additional grade
1-2 complaints were diarrhea, reflux, auditory hallucinations, conjunctivitis, sexual impairment,
asthenia, alopecia, cramps and dyspnea. Five (11%) patients had grade 3-4 toxicities, including
neutropenia, acute hepatitis, facial edema, skin toxicity and fatigue (table 3).
Table 3 Main toxicities associated with imatinib mesylate and reasons for discontinuation,
metastatic patients excluded
Patients N (%)
Variable All grades Grade 3-4
Edema/ fluid retention 28 (48) 1 (2)
Fatigue 29 (50) 1 (2)
Nausea 20 (34)
Skin rash/ dermatitis 7 (12) 2 (3)
Other* 15 (26) 3 (5)
Treatment status
Continued on IM 20 (34)
Stopped IM 38 (66)
Reason for stopping
Progression 1 (2)
Toxicity 7 (12)
Surgery 10 (17)
Patient choice 14 (24)
Physician decision 5 (9)
Other tumour 1 (2)
IM= imatinib mesylate, N= Number of patients. Forty-five (78%) patients reported at least one adverse event
with IM. *Other grade 1-2 complaints were diarrhea, reflux, auditory hallucinations, conjunctivitis, sexual
impairment, asthenia, alopecia, cramps and dyspnea. Five (11%) patients had grade 3-4 toxicities, including
neutropenia, acute hepatitis, auditory hallucinations.

204
Chapter nine
discussion
To our knowledge, this retrospective study provides the largest case series, with long follow-
up, of patients with locally advanced, recurrent or metastatic diffuse-type TGCT treated with IM.
We confirmed that IM has activity in TGCT with an overall response rate of 31% in patients with
locally advanced/recurrent TGCT. Interestingly all patients with metastatic TGCT progressed on IM,
suggesting that metastatic TGCT is either a different disease or loses its dependency on the CSF1/
CSF1R axis during malignant transformation. The main issue, is the drop-off rate, with more than
half of the patients discontinuing therapy within a year of therapy (59%; 95% CI 29-57), in most
cases for unclear reasons (patients decision, physician’s decision) suggesting an unfavourable
efficacy/toxicity balance. Eleven percent of patients reported grade 3-4 toxicities, which is
consistent with the rates reported with IM for adjuvant gastrointestinal stromal tumours (GIST) or
chronic myeloid leukaemia (CML)18-21.
To date, surgical resection remains the treatment of choice for diffuse-type TGCT, but is associated
with high recurrence rates and multiple additional surgeries11. It is challenging to balance between
increased morbidity of multiples or invasive surgeries12, 22, alternative therapeutic options, and daily
symptoms of the tumour. A more aggressive resection or other multimodality treatments, such as
external beam radiation therapy, radiosynovectomy and cryosurgery, may adversely affect joint
function, quality of life and development of osteoarthrosis, which, given the young age group, are
relevant factors2, 23. This would justify a less invasive approach, using systemic therapy, provided
those are associated with tumour shrinkage and, most importantly, symptomatic improvements24.
In the present study, age, localization and gender distribution were consistent with the literature10,
23, 25. The extent of disease in our patient group is emphasized by an disease specific survival of 90%
including four metastatic patients and 49% of patients had three or more surgeries before start
IM. Similar to previous case-series, we calculated a 1- and 5-years PFS of 71% and 48%, metastatic
patients excluded, respectively10, 23, 25. Because of heterogeneity of patients and a variety of
treatments, it is debatable to compare these numbers.
The overall response rate appears higher compared to nilotinib (6% (95% CI unknown), a different
tyrosine kinase inhibitor, with similar potency against CSF1R26. Our overall response rate (31%
(95% CI 19-43, metastatic patients (N=4) excluded) was consistent with our previous report on the
Imatinib in tenosynovial giant cell tumours
205
9
short term results of IM (19% (95% CI 4-34) with similar disease control rate (96% versus 93%)17.
In the present study, 38 (66%) patients discontinued IM; 14 (37%) without subsequent treatment,
of which ten patients had stable disease at final follow up. Thirteen (62%) patients eventually
progressed, after discontinuing IM for toxicity or non-specific medical reason (N=21, 55%). Both
stable and progressive patients can be a result of discontinuing IM treatment or the natural course
of disease.
Newer, more specific inhibitors of CSF1R, currently only available in trial-setting such as
emactuzumab (RG7155)27, pexidartinib (PLX3397)15, and cabiralizumab28 (FPA008, Five-Prime),
have shown promising clinical activity on similar groups of diffuse TGCT patients in prospective
clinical studies with more formal criteria and timelines for response assessment than this
retrospective series. Emactuzumab (N=29)16 had an overall response rate of 86% (two patients
with a complete response) and a rate of disease control of 96%, including a significant functional
and symptomatic improvement (median follow up 12 months). Pexidartinib showed (N=23)15 an
overall response rate of 52% (all patients had a partial response) and a rate of disease control of
83%. Responses were associated with an improved joint function (median duration of response
exceeded eight months). The preliminary results with cabiralizumab (N=22) are consistent, with
radiographic response and improvement in pain and function in five out of 11 patients28. However,
long term efficacy data have not yet been reported with these newer agents.
Virtually all patients treated with IM for either CML or GISTs, experience29 at least one mild or
moderate adverse effect (grade 1-2). Toxicities of IM are determined by the disease stage and
the doses used, advanced disease and higher doses result in more frequent and severe toxicities.
Most side effects occur early in the course of treatment and tend to decrease in frequency and
intensity in time29. We consider a 10-15% rate of grade 3-4 toxicities in a generally benign but
locally aggressive disease, such as diffuse TGCT, too high. Only 22% of patients did not experience
any side effects.
Although target anti-cancer therapies are described as ‘well tolerated’, the perception of tolerability
may vary in the context of a, most often, benign condition. Understanding, monitoring and
managing the side effects will be important to optimize systemic therapy for patients with TGCT.

206
Chapter nine
Discontinuation of treatment due to toxicities was seen for IM (this series), emactuzumab15 and
pexidartinib16 in 12%, 20% and 9% patients, respectively. TGCT patients might be less willing to
cope with adverse event-related and study-related procedures. Here, we report prolonged clinical
benefit and symptomatic relief, even after discontinuation of treatment. A similarly persistent
effect was observed was also observed with monoclonal antibodies and more specific CSF1R
tyrosine kinase inhibitors this24. This suggest that intermittent treatment administration may be
an option to improve long term tolerability.
The place of systemic treatment in a benign, locally aggressive disease, such as TGCT, and how to
optimally deliver this treatment, remains unclear. More specifically, the role of CSF1R inhibitors
in the peri-operative setting still needs to be explored: the number of patients who underwent
operation after IM in our series is too low to draw any conclusions. Despite limitations related to
its retrospective nature, this study adds to the knowledge of targeting the CSF-1/CSF-1R pathway
in patients with TGCT. An optimal treatment strategy should be developed for the patient group
that benefits most from systemic therapy. The combination of a short period of treatment and the
durable effect after discontinuation, should be pursued. It is challenging to maintain compliance
for years, especially with, even “minor”, toxicities, in the context of a non-life-threatening disease.
A limitation of all, including this, clinical TGCT studies is the lack of a control group and the
absence of specific and validated patient-reported outcome measures to document treatment-
induced symptomatic, functional and economic (back to work) improvement16. Quality of life and
functional forms should be implemented. These measures are critical endpoints in demonstrating
clinical relevance and impact of treatments for benign diseases in which death is not a relevant
outcome variable30. Clinical benefit necessitates objective measures to correlate with tumour
reduction.
Imatinib in tenosynovial giant cell tumours
207
9
conclusion
Identification of a biologic aggressive subgroup of diffuse TGCT, at risk of increased surgical
morbidity or recurrent disease, should aid to decide which patients benefit most of systemic
treatments. With the advent of more potent CSF-1R inhibitors, such as emactuzumab, pexidartinib
and cabiralizumab, the role of IM in extensive TGCT might weaken, but may be balanced by the
favourable safety profile of IM. Availability of these new compounds, both in terms of registration
and reimbursement, will ultimately define the prescribed drug in daily practice.
208
Chapter nine
references
1. Ottaviani S, Ayral X, Dougados M, Gossec L. Pigmented Villonodular Synovitis: A Retrospective Single-Centre
Study of 122 Cases and Review of the Literature. Seminars in Arthritis and Rheumatism. 2011;40 (6):539-46.
2. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary
and recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
3. Ravi V, Wang WL, Lewis VO. Treatment of tenosynovial giant cell tumor and pigmented villonodular synovitis. Curr
Opin Oncol. 2011.
4. de saint Aubain Somerhausen N, van de Rijn M. Tenosynovial giant cell tumour, diffuse/localized type. In: Fletcher
CD, Bridge JA, Hogedoorn PC, Mertens F, eds. WHO classification of tumours of Soft Tissue and Bone. 2013;5(4th
ed. Lyon: IARC Press).
5. Yoon HJ, Cho YA, Lee JI, Hong SP, Hong SD. Malignant pigmented villonodular synovitis of the temporomandibular
joint with lung metastasis: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 2011;111(5):e30-6.
6. Righi A, Gambarotti M, Sbaraglia M, Frisoni T, Donati D, Vanel D, et al. Metastasizing tenosynovial giant cell tumour,
diffuse type/pigmented villonodular synovitis. Clin Sarcoma Res. 2015;5:15.
7. Mastboom MJL, Verspoor FGM, Gelderblom H, van de Sande MAJ. Limb Amputation after Multiple Treatments of
Tenosynovial Giant Cell Tumour: Series of 4 Dutch Cases. Case reports in orthopedics. 2017;2017:7402570.
8. Shabat S, Kollender Y, Merimsky O, Isakov J, Flusser G, Nyska M, et al. The use of surgery and yttrium 90 in the
management of extensive and diffuse pigmented villonodular synovitis of large joints. Rheumatology. 2002;41
(10):1113-8.
9. Heyd R, Seegenschmiedt MH, Micke O. [The Role of External Beam Radiation Therapy in the Adjuvant Treatment of
Pigmented Villonodular Synovitis.]. Z Orthop Unfall. 2011.
10. Verspoor FG, Scholte A, van der Geest IC, Hannink G, Schreuder HW. Cryosurgery as Additional Treatment in
Tenosynovial Giant Cell Tumors. Sarcoma. 2016;2016:3072135.
11. Verspoor FG, van der Geest IC, Vegt E, Veth RP, van der Graaf WT, Schreuder HW. Pigmented villonodular synovitis:
current concepts about diagnosis and management. Future Oncol. 2013;9(10):1515-31.
12. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the
surgical treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone
Joint J. 2014;96-B(8):1111-8.
13. West RB, Rubin BP, Miller MA, Subramanian S, Kaygusuz G, Montgomery K, et al. A landscape effect in tenosynovial
giant-cell tumor from activation of CSF1 expression by a translocation in a minority of tumor cells. Proceedings of
the National Academy of Sciences of the United States of America. 2006;103 (3):690-5.
14. Cupp JS, Miller MA, Montgomery KD, Nielsen TO, O’Connell JX, Huntsman D, et al. Translocation and expression of
CSF1 in pigmented villonodular synovitis, tenosynovial giant cell tumor, rheumatoid arthritis and other reactive
synovitides. American Journal of Surgical Pathology. 2007;31 (6):970-6.
15. Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, et al. Structure-Guided Blockade of CSF1R
Kinase in Tenosynovial Giant-Cell Tumor. The New England journal of medicine. 2015;373(5):428-37.
16. Cassier PA, Italiano A, Gomez-Roca CA, Le Tourneau C, Toulmonde M, Cannarile MA, et al. CSF1R inhibition
with emactuzumab in locally advanced diffuse-type tenosynovial giant cell tumours of the soft tissue: a dose-
escalation and dose-expansion phase 1 study. Lancet Oncol. 2015;16(8):949-56.
Imatinib in tenosynovial giant cell tumours
209
9
17. Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, et al. Efficacy of imatinib mesylate for the
treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis.
Cancer. 2012;118(6):1649-55.
18. Casali PG, Le Cesne A, Poveda Velasco A, Kotasek D, Rutkowski P, Hohenberger P, et al. Time to Definitive Failure to
the First Tyrosine Kinase Inhibitor in Localized GI Stromal Tumors Treated With Imatinib As an Adjuvant: A European
Organisation for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group Intergroup Randomized
Trial in Collaboration With the Australasian Gastro-Intestinal Trials Group, UNICANCER, French Sarcoma Group,
Italian Sarcoma Group, and Spanish Group for Research on Sarcomas. J Clin Oncol. 2015;33(36):4276-83.
19. Essat M, Cooper K. Imatinib as adjuvant therapy for gastrointestinal stromal tumors: a systematic review. Int J
Cancer. 2011;128(9):2202-14.
20. Joensuu H, Trent JC, Reichardt P. Practical management of tyrosine kinase inhibitor-associated side effects in GIST.
Cancer Treat Rev. 2011;37(1):75-88.
21. Kalmanti L, Saussele S, Lauseker M, Muller MC, Dietz CT, Heinrich L, et al. Safety and efficacy of imatinib in CML over
a period of 10 years: data from the randomized CML-study IV. Leukemia. 2015;29(5):1123-32.
22. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive
Review and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
23. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.
24. Brahmi M, Vinceneux A, Cassier PA. Current Systemic Treatment Options for Tenosynovial Giant Cell Tumor/
Pigmented Villonodular Synovitis: Targeting the CSF1/CSF1R Axis. Current treatment options in oncology.
2016;17(2):10.
25. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence
rates than previously known in tenosynovial giant cell tumors. Acta orthopaedica. 2017:1-7.
26. Gelderblom H, Pérol D, Chevreau C, Tattersall MNH, Stacchiotti S, Casali PG. An open-label international multicentric
phase II study of nilotinib in progressive pigmented villo-nodular synovitis (PVNS) not amenable to a conservative
surgical treatment. Proc Am Soc Clin Oncol. 2013;31 (suppl)(abstr 10516).
27. Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, et al. Targeting tumor-associated macrophages with
anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer cell. 2014;25(6):846-59.
28. Sankhala KK, Blay J-Y, Ganjoo KN, Italiano A, Hassan AB, Kim TM, et al. A phase I/II dose escalation and expansion
study of cabiralizumab (cabira; FPA-008), an anti-CSF1R antibody, in tenosynovial giant cell tumor (TGCT, diffuse
pigmented villonodular synovitis D-PVNS). . American Society of Clinical Oncology. 2017;Conference: 2017 Annual
Meeting ASCO. United States. 35 (15 Supplement 1).
29. Thanopoulou E, Judson I. The safety profile of imatinib in CML and GIST: long-term considerations. Arch Toxicol.
2012;86(1):1-12.
30. Gelhorn HL, Tong S, McQuarrie K, Vernon C, Hanlon J, Maclaine G, et al. Patient-reported Symptoms of Tenosynovial
Giant Cell Tumors. Clin Ther. 2016;38(4):778-93.

qual
ity
oF l
iFe
the effect of surgery in
tenosynovial giant cell tumours
as measured by patient reported
outcomes on quality of life and
joint function
chap
ter
ten
M.J.L. Mastboom*1, F.G.M. Verspoor*2, G. Hannink2, W.T.A. van der Graaf3 , M.A.J. van de Sande1, H.W.B Schreuder2
Accepted in Bone Joint J.

212
Chapter ten
1 Orthopaedic Surgery, Leiden University Medical Centre, Leiden, the Netherlands
2 Orthopaedic Surgery, Radboud University Medical Centre, Nijmegen, the Netherlands
3 Medical Oncology, Radboud University Medical Centre, Nijmegen, the Netherlands
*Authors contributed equally to this work.
Quality of life and joint function in tenosynovial giant cell tumours
213
10
abstract
Aim
To evaluate health-related quality of life (HRQoL) and joint function in TGCT patients before and
after surgical treatment.
Patients and methods
This prospective cohort study run in two Dutch referral centres, assessed patient-reported outcome
measures (SF-36, VAS and WOMAC) in 359 consecutive patients with localized- and diffuse-type
TGCT of large joints. Patients with recurrent disease (N=121) and a wait-and-see policy (N=32)
were excluded. Collected data were analysed at specified time intervals pre-(baseline) and/or
postoperatively up to 5 years.
Results
In total 206, 108 localized- and 98 diffuse-type, TGCT patients were analysed. Median age at
diagnosis of localized- and diffuse-type was 41 (IQR 29-49) and 37 (IQR 27-47) years, respectively.
SF-36 analyses showed statistically significant and clinically relevant deteriorated preoperative-
and direct postoperative scores compared with general population means, depending on subscale
and TGCT subtype. After 6 months of follow up, these scores improved to general population
means and continued to be fairly stable the following years. VAS scores, for both-subtypes,
showed no clinically relevant differences pre- or postoperatively. Pain experience varied hugely
between patients and also over time. WOMAC scores, for both TGCT subtypes, showed no clinically
relevant differences pre- versus postoperatively. However, in diffuse-type patients WOMAC pain
and physical function scores showed a trend towards improvement postoperatively.
Conclusion
Patients report a significant better HRQoL after surgery in TGCT whereas joint function showed
a trend towards improvement. Pain scores –which vary hugely between patients and in patients
over time- did not improve. A disease specific patient-reported outcome measure would help to
decipher impact of TGCT on patients’ daily life and functioning in more detail.

214
Chapter ten
introduction
Tenosynovial giant cell tumours (TGCT) of large joints, historically known as pigmented villonodular
synovitis (PVNS), are rare colony stimulating factor-1 (CSF-1)-driven proliferative, mono-articular
disorders. They affect the joints or tendon sheaths at all ages, however mostly at young adulthood. It
most commonly affects large, weight bearing joints such as knees, ankles and hips1, 2. The incidence
rate of localized-extremity (excluding digits) and diffuse-type TGCT is 10 and 4 per million person
years, respectively3. Localized-type comprises a single nodule and has a favourable course after
surgical treatment. Diffuse-type involves the synovial lining as well as surrounding structures. It
can behave locally aggressive and is challenging to remove completely. There is a significant risk of
recurrence after surgical treatment (>50% depending on follow up times)2, 4, 5.
Diffuse-type TGCT often requires one or multiple synovectomies, or at times a joint replacement,
and rarely even amputation1, 2, 6. In patients with extensive and/or recurrent TGCT, other available
treatment modalities include radiation synovectomy7, external beam radiation therapy8, and
cryosurgery9 of which the effects are controversial10. More recently, systemic therapy has been
introduced, targeting the CSF-1 receptor. At first treatment with the multi targeting tyrosine
kinase inhibitor imatinib started, very recently more promising data of a CSF-1 specific targeting
agent were presented11-13. Systemic treatment may need to be given for one to several years, but
the optimal treatment duration has still to be determined. Despite the variety of treatments, it is
unclear which one is the most effective with the least impact on quality of life.
A limitation of most clinical TGCT studies is the absence of disease specific and validated patient-
reported outcome measures (PROMs) to document disease and treatment related functioning and
symptomatology. Overall survival is the primary endpoint in oncologic clinical trials, however this
is not appropriate for TGCT, which is rarely lethal14. Alternate treatment endpoints in TGCT include
response rates, progression free survival, and avoidance of morbid therapies. As indicated, quality
of life (QoL) and functional scores are of utmost importance, but they are mostly not reported
or only described for small, heterogeneous patient groups2, 15. The impact of therapies and the
relevance of treatment outcomes to patients’ quality of life is therefore essential especially in a
benign but locally aggressive disease16,17.

Quality of life and joint function in tenosynovial giant cell tumours
215
10
The aim of our study is to investigate HRQoL, pain and joint function in surgically treated non-
recurrent TGCT patients, pre- and/ or postoperatively over time.
methods
This prospective cohort study was conducted at two Dutch referral centres; Radboud University
Medical Centre (RadboudUMC) and Leiden University Medical Centre (LUMC). Between 2011 until
2018 patients diagnosed with primary therapy-naïve or recurrent TGCT (magnetic resonance
imaging (MRI) and histological confirmed) of large joints, were asked to participate. Large
joints were defined as all joints except the digits. Three hundred and fifty-nine consecutive
patients were identified; 136 (38%) with localized TGCT, 223 (62%) with diffuse TGCT. During
regular outpatient clinic visits, patients who consented were requested to complete PROMs
questionnaires. To further reduce heterogeneity of the group, patients with recurrent disease at
presentation, treated conservatively (wait-and-see policy) and patients in absence of QoL and
function scores after primary surgery, were excluded from this analysis (figure 1). Also, if patients
developed relapse after surgical treatment, they were excluded from this time on. Hundred-and-
eight localized- and 98 diffuse-type therapy-naïve patients were used for final analyses (figure 1).
The study protocol (RadboudUMC (file number CMO 2012/555) and LUMC (file number CMO
P13.029)) was approved by the local institutional ethical review boards and was carried out in
the Netherlands in accordance with the applicable rules concerning the review of research ethics
committees and informed consent. Patients provided written informed consent when they
completed questionnaires (SF 36, VAS and WOMAC).
The used PROMs included the Dutch translation of a generic HRQoL instrument, the 36-item
Short Form Health Survey (SF-36)18, a Visual Analog Scale (VAS) for pain and the Western Ontario
and McMaster Universities Osteoarthritis Index (WOMAC). SF-36 is an instrument for measuring
general health, including eight subscales: Physical functioning (PF), Social functioning (SF),
Role limitations due to physical problems (RP), Role limitations due to emotional problems (RE),
General mental health (MH), Vitality (VT), Bodily pain (BP) and General health (GH). SF-36 scores
were computed by summing the item scores and transforming the scores onto a 100-point scale
(0= “worst health” and 100= “best health”). VAS for worst pain was used to estimate patients pain

216
Chapter ten
Figure 1 Flowchart of consecutive patients with TGCT, included for quality of life analyses.
*Additional cryosurgery in two localized- and five diffuse-type TGCT patients
evaluated TGCT patientsN=359
therapy naive patientslocalized, N=127diffuse, N=142
ExcludedRecurrent TGCT
localized, N=9diffuse, N=81
Localized-TGCTN=108
Diffuse-TGCTN=98
arthoscopic synovectomy, N=3
one-staged synovectomy, N=103*
prosthesis, N=2
arthoscopic synovectomy, N=3
one-staged synovectomy, N=75*
two-staged synovectomy, N=18*
prosthesis, N=2
ExcludedNo PROMS available prior to first recurrens
localized, N=6diffuse, N=25
Excluded’Wait and see policy’
localized, N=13diffuse, N=19

Quality of life and joint function in tenosynovial giant cell tumours
217
10
intensity of the affected joint for the past 24 hours, using a series of 0- to 10-point (0= “no pain”
and 10= ”pain as bad as you can imagine”)19. The Western Ontario and McMaster Universities
Osteoarthritis Index (WOMAC) was used to evaluate affected joint function20. The WOMAC is a
24-item instrument assessing pain, stiffness and difficulty performing daily activities originally
designed for osteoarthritis. All items are measured on a 5 point scale; ranging from “no” up to
“worst imaginable”. The WOMAC data were standardized to a range of values from 0-100, for which
lower values indicate more pain, more stiffness, or worse physical functioning. Gelhorn et al. 16
used a modified version of WOMAC for TGCT patients.
Patient demographics and clinical, histological, radiological, treatment and follow-up data were extracted
from individual patients’ files at each institution by the local investigator (FGMV or MJLM) and were
provided in an anonymous form for analyses. Definitive histological diagnosis was performed at the centre
of origin by dedicated pathologists with extensive experience in mesenchymal tumours. Recurrences
and PROMs were analysed according to TGCT subtype. Data were described using percentages for
qualitative variables and medians with interquartile ranges (IQR) for continuous variables.
As patient questionnaires were completed at different points in time they were categorized in the
following time intervals: pre-surgery (=0 or baseline), post-surgery after 0-3, 3-6, 6-12, 12-24, 24-36,
36-48, 48-60 months. At final analyses we did not have questionnaires in all time intervals for each
individual patient, some had solely pre- or post-operative scores. In case of recurrent disease after
primary treatment in a therapy-naïve patient, QoL and functions scores were used up to recurrence
development, confirmed on MR imaging. Follow-up time was defined as the period between first TGCT
confirmation (MR imaging and histologic) and most recent patient contact. Time to recurrence was
calculated as time from first treatment until proven (MR imaging and histologic) first recurrent disease.
Differences between QoL scores (SF-36, VAS, WOMAC) were tested using t-tests. SF-36 scores were
compared with Dutch general population scores18, and WOMAC and VAS baseline (preoperative)
scores were compared with postoperative scores.
To estimate the clinical relevance, the mean differences were compared with the minimal clinically
important difference (MCID). MCID is a QoL measure that represents the smallest difference or
change beyond statistical significance in an outcome measure score that would be considered
clinically relevant by the value patients place on change21. The MCID for SF-36 has been estimated

218
Chapter ten
at to be 10 points by Escobar et al.22 in patients undergoing total knee replacement. For VAS pain
a MCID of 2 was used23. The MCID for standardized WOMAC values has been estimated at around
15-20 points22, with relative improvements of 21-41% for its subscales23-25. We used a MCID for
WOMAC of 20 points based on consensus in the project team and the study of van der Wees et al.26
All statistical analyses were performed using R version 3.4.0 (R Foundation for Statistical Computing,
Vienna, Austria). P-values <0.05 were considered statistically significant.
results
Patients
After exclusion of patients with recurrent disease (N=121) and patients with a wait-and-see policy
(N=32), 206 patients remained for further analyses (figure 1). Median age at diagnosis of localized-
(N=108) and diffuse-type (N=98) TGCT was 41 (IQR 29-49) and 37(IQR 27-47) years, respectively. The
majority of patients were female (localized N=62 (57%)), had diffuse-type TGCT N=64 (65%)), and had
the knee as the most common affected joint in both subtypes (localized N=84 (78%)) and diffuse N=72
(74%)). Pain (localized N=61 (57%) and diffuse N=58 (60%)) and swelling (localized N=66 (61%) and
diffuse N=65 (67%)) were the most prevalent clinical symptoms at diagnosis for both subtypes (table 1).
Treatments
As primary treatment, three (3%) localized-type patients were treated with arthroscopic
synovectomy, 103 (95%) with one-staged synovectomy and two (2%) with (endo-)prosthesis. Seven
patients (6%) had a first recurrence after median 2.9 (2.1-5.6) years. Overall median follow up of
localized therapy-naïve patients was 2.0 (IQR 0.7-4.6) years. At final follow up, 104 (96%) patients
had no evidence of disease, 4 (4%) patients were alive with disease, without planned treatment.
Diffuse-type patients were treated with arthroscopic (N=3 (3%)), one-staged (N=75 (76%)) or two-
staged (N=18 (19%)) synovectomy. Two patients received an (endo-) prosthesis. Twenty-seven
patients (28%) had a first recurrence after median 1.3 (1-3) years, thereafter they were excluded
from further analyses. Overall median follow up of diffuse-type patients was 2.7 (IQR 1.4-4.9) years.
At final follow up, 70 (71%) patients had no evidence of disease, 27 (28%) patients were alive with
disease and one patient died of another disease.
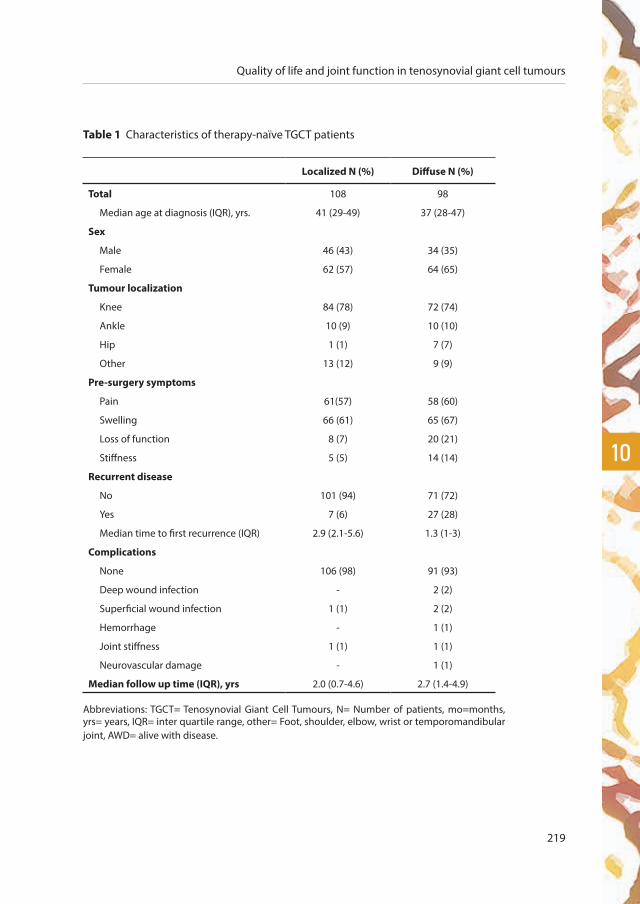
Quality of life and joint function in tenosynovial giant cell tumours
219
10
Table 1 Characteristics of therapy-naïve TGCT patients
Localized N (%) Diffuse N (%)
Total 108 98
Median age at diagnosis (IQR), yrs. 41 (29-49) 37 (28-47)
Sex
Male 46 (43) 34 (35)
Female 62 (57) 64 (65)
Tumour localization
Knee 84 (78) 72 (74)
Ankle 10 (9) 10 (10)
Hip 1 (1) 7 (7)
Other 13 (12) 9 (9)
Pre-surgery symptoms
Pain 61(57) 58 (60)
Swelling 66 (61) 65 (67)
Loss of function 8 (7) 20 (21)
Stiffness 5 (5) 14 (14)
Recurrent disease
No 101 (94) 71 (72)
Yes 7 (6) 27 (28)
Median time to first recurrence (IQR) 2.9 (2.1-5.6) 1.3 (1-3)
Complications
None 106 (98) 91 (93)
Deep wound infection - 2 (2)
Superficial wound infection 1 (1) 2 (2)
Hemorrhage - 1 (1)
Joint stiffness 1 (1) 1 (1)
Neurovascular damage - 1 (1)
Median follow up time (IQR), yrs 2.0 (0.7-4.6) 2.7 (1.4-4.9)
Abbreviations: TGCT= Tenosynovial Giant Cell Tumours, N= Number of patients, mo=months, yrs= years, IQR= inter quartile range, other= Foot, shoulder, elbow, wrist or temporomandibular joint, AWD= alive with disease.

220
Chapter ten
HR Quality of life
Compared to Dutch general population means18, localized-type patients preoperatively scored
significantly lower on PF(13.2(95%CI 6.0-20.5)), SF(18.7(95%CI 10.3-27.2)), RP(25.8(95%CI 11.9-39.8)),
RE(20.6(95%CI 7.3-34.0)) and BP(21.2(95%CI 12.7-29.8)). These differences were also clinically relevant
(mean difference> MCID 10). This effect lasted up to 3 months postoperatively on RP(40.1(95%CI
16.7-63.5)) and BP(17.2(95%CI 2.2-32.1)). Thereafter, these means improved to general population
means and continued fairly stable during the following years (figure 2a, table 2b).
Figure 2a SF-36 scores of localized-type, therapy-naïve, TGCT patients.
Spider plot showing SF-36 scores preoperative (baseline), 6-12 months postoperatively and of Dutch general
population means18: physical functioning (PF), social functioning (SF), role limitations due to physical problems
(RP), role limitations due to emotional problems (RE), general mental health (MH), vitality (VT), bodily pain (BP)
and general health (GH).

Quality of life and joint function in tenosynovial giant cell tumours
221
10
Figure 2b SF-36 scores of diffuse-type, therapy-naïve, TGCT patients.
Spider plot showing SF-36 scores preoperative (baseline), 6-12 months postoperatively and of Dutch general
population means18: physical functioning (PF), social functioning (SF), role limitations due to physical problems
(RP), role limitations due to emotional problems (RE), general mental health (MH), vitality (VT), bodily pain (BP)
and general health (GH).
Diffuse-type patients preoperatively scored statistically significant and clinically relevant (mean
difference> MCID 10) lower on PF(23.7 (95% CI 16.7-30.8)), SF (15.6 (95% CI 8.8-22.5)), RP (37.4
(95% CI 25.3-49.5)), VT (10.0 (95% CI 3.5-16.4)) and BP (21.6 (95% CI 14.7-28.5)) compared to
general population means. This difference with the general population remained significant for
up to 3 months postoperatively on PF (21.9 (95% CI 5.0-38.8)), SF (19.9 (95% CI 3.0-36.9)), RP (40.1
(95% CI 16.2-64.1)), VT (13.0 (95% CI 1.5-24.5)) and BP (22.4 (95% CI 5.3-39.4)) and up to 6 months
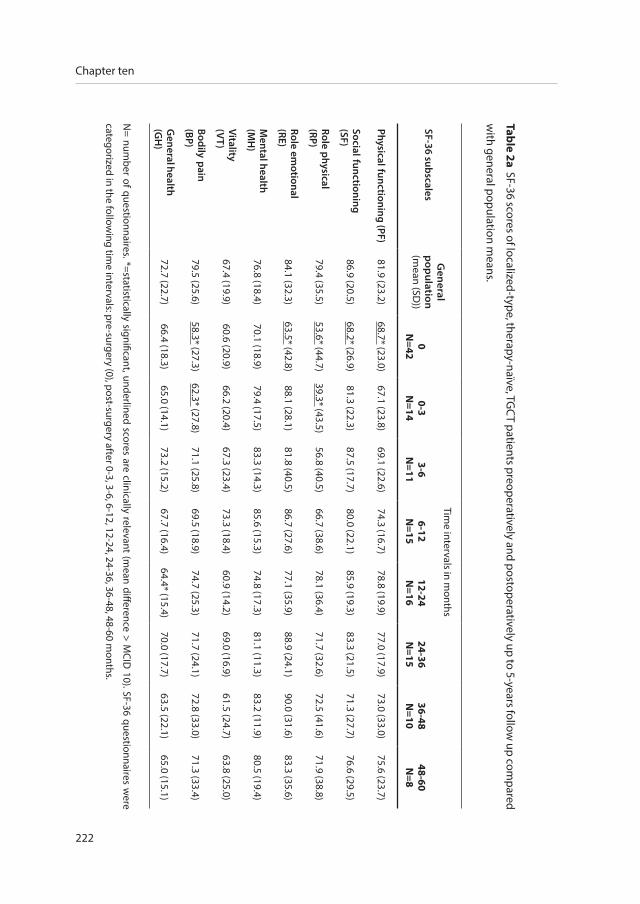
222
Chapter ten
Table 2a SF-36 scores of localized-type, therapy-naïve, TGC
T patients preoperatively and postoperatively up to 5-years follow up com
pared
with general population m
eans.
SF-36 subscalesG
eneral p
opulation
(mean (SD
))
Time intervals in m
onths
0N
=420-3
N=14
3-6N
=116-12
N=15
12-24N
=1624-36N
=1536-48N
=1048-60N
=8
Physical functioning (PF)81.9 (23.2)
68.7* (23.0)67.1 (23.8)
69.1 (22.6)74.3 (16.7)
78.8 (19.9)77.0 (17.9)
73.0 (33.0)75.6 (23.7)
Social functioning(SF)
86.9 (20.5)68.2* (26.9)
81.3 (22.3)87.5 (17.7)
80.0 (22.1)85.9 (19.3)
83.3 (21.5)71.3 (27.7)
76.6 (29.5)
Role physical(RP)
79.4 (35.5)53.6* (44.7)
39.3* (43.5)56.8 (40.5)
66.7 (38.6)78.1 (36.4)
71.7 (32.6)72.5 (41.6)
71.9 (38.8)
Role emotional
(RE)84.1 (32.3)
63.5* (42.8)88.1 (28.1)
81.8 (40.5)86.7 (27.6)
77.1 (35.9)88.9 (24.1)
90.0 (31.6)83.3 (35.6)
Mental health
(MH
)76.8 (18.4)
70.1 (18.9)79.4 (17.5)
83.3 (14.3)85.6 (15.3)
74.8 (17.3)81.1 (11.3)
83.2 (11.9)80.5 (19.4)
Vitality(V
T)67.4 (19.9)
60.6 (20.9)66.2 (20.4)
67.3 (23.4)73.3 (18.4)
60.9 (14.2)69.0 (16.9)
61.5 (24.7)63.8 (25.0)
Bodily pain(BP)
79.5 (25.6)58.3* (27.3)
62.3* (27.8)71.1 (25.8)
69.5 (18.9)74.7 (25.3)
71.7 (24.1)72.8 (33.0)
71.3 (33.4)
General health
(GH
)72.7 (22.7)
66.4 (18.3)65.0 (14.1)
73.2 (15.2)67.7 (16.4)
64.4* (15.4)70.0 (17.7)
63.5 (22.1)65.0 (15.1)
N= num
ber of questionnaires. *=statistically significant, underlined scores are clinically relevant (mean difference > M
CID 10). SF-36 questionnaires w
ere
categorized in the following tim
e intervals: pre-surgery (0), post-surgery after 0-3, 3-6, 6-12, 12-24, 24-36, 36-48, 48-60 months.
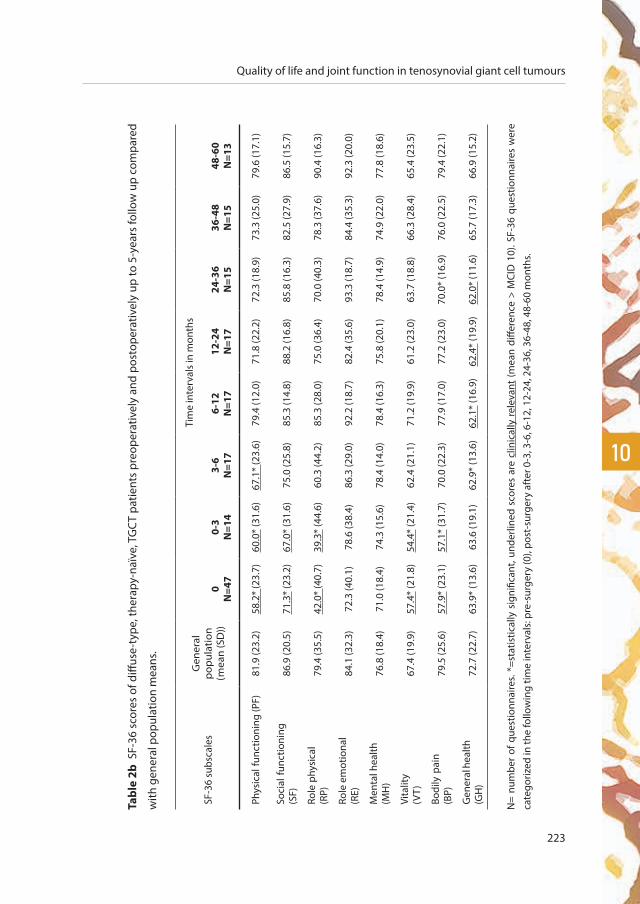
Quality of life and joint function in tenosynovial giant cell tumours
223
10
Tabl
e 2b
SF-
36 s
core
s of
diff
use-
type
, the
rapy
-naï
ve, T
GC
T pa
tient
s pr
eope
rativ
ely
and
post
oper
ativ
ely
up to
5-y
ears
follo
w u
p co
mpa
red
with
gen
eral
pop
ulat
ion
mea
ns.
SF-3
6 su
bsca
les
Gen
eral
po
pula
tion
(mea
n (S
D))
Tim
e in
terv
als
in m
onth
s
0N
=47
0-3
N=1
43-
6N
=17
6-12
N=1
712
-24
N=1
724
-36
N=1
536
-48
N=1
548
-60
N=1
3
Phys
ical
func
tioni
ng (P
F)81
.9 (2
3.2)
58.2
* (2
3.7)
60.0
* (3
1.6)
67.1
* (2
3.6)
79.4
(12.
0)71
.8 (2
2.2)
72.3
(18.
9)73
.3 (2
5.0)
79.6
(17.
1)
Soci
al fu
nctio
ning
(SF)
86.9
(20.
5)71
.3*
(23.
2)67
.0*
(31.
6)75
.0 (2
5.8)
85.3
(14.
8)88
.2 (1
6.8)
85.8
(16.
3)82
.5 (2
7.9)
86.5
(15.
7)
Role
phy
sica
l(R
P)79
.4 (3
5.5)
42.0
* (4
0.7)
39.3
* (4
4.6)
60.3
(44.
2)85
.3 (2
8.0)
75.0
(36.
4)70
.0 (4
0.3)
78.3
(37.
6)90
.4 (1
6.3)
Role
em
otio
nal
(RE)
84.1
(32.
3)72
.3 (4
0.1)
78.6
(38.
4)86
.3 (2
9.0)
92.2
(18.
7)82
.4 (3
5.6)
93.3
(18.
7)84
.4 (3
5.3)
92.3
(20.
0)
Men
tal h
ealth
(MH
)76
.8 (1
8.4)
71.0
(18.
4)74
.3 (1
5.6)
78.4
(14.
0)78
.4 (1
6.3)
75.8
(20.
1)78
.4 (1
4.9)
74.9
(22.
0)77
.8 (1
8.6)
Vita
lity
(VT)
67.4
(19.
9)57
.4*
(21.
8)54
.4*
(21.
4)62
.4 (2
1.1)
71.2
(19.
9)61
.2 (2
3.0)
63.7
(18.
8)66
.3 (2
8.4)
65.4
(23.
5)
Bodi
ly p
ain
(BP)
79.5
(25.
6)57
.9*
(23.
1)57
.1*
(31.
7)70
.0 (2
2.3)
77.9
(17.
0)77
.2 (2
3.0)
70.0
* (1
6.9)
76.0
(22.
5)79
.4 (2
2.1)
Gen
eral
hea
lth
(GH
)72
.7 (2
2.7)
63.9
* (1
3.6)
63.6
(19.
1)62
.9*
(13.
6)62
.1*
(16.
9)62
.4*
(19.
9)62
.0*
(11.
6)65
.7 (1
7.3)
66.9
(15.
2)
N=
num
ber
of q
uest
ionn
aire
s. *=
stat
istic
ally
sig
nific
ant,
unde
rline
d sc
ores
are
clin
ical
ly r
elev
ant
(mea
n di
ffere
nce
> M
CID
10)
. SF-
36 q
uest
ionn
aire
s w
ere
cate
goriz
ed in
the
follo
win
g tim
e in
terv
als:
pre
-sur
gery
(0),
post
-sur
gery
aft
er 0
-3, 3
-6, 6
-12,
12-
24, 2
4-36
, 36-
48, 4
8-60
mon
ths.

224
Chapter ten
postoperatively on PF (14.8 (95% CI 3.3-26.4)). Thereafter, the mean SF-36 scores of diffuse-type
patients improved to Dutch general population means and continued fairly stable the following
years. Compared to general population means diffuse-type patients scored statistically significant
and clinically relevant lower on GH 3-6 months (10.6 (95% CI 9.8-23.2)), 6-12 months (10.3 (95% CI
2.3-18.9)) and 24-36 months (10.7 (95% CI 4.5-16.9)) postoperatively (figure 2b, table 2b).
Visual analog scale for pain
No statistical significant nor clinical relevant difference in pain scores were found in localized-type
patients preoperatively (median VAS score 4, IQR 1-6) versus 3 months postoperatively (median
VAS score 3.5, IQR 1-5), which in fact remained the same up to five years follow up. Median VAS
scores in diffuse-type patients showed no clinical relevant difference preoperatively (median VAS
score 4, IQR 2-6) versus 3 months postoperatively (median VAS score 2, IQR 1-4), and also here the
scores remained the same up to five years follow up. Pain experience in both subtypes TGCT varied
widely between and within patients over time (range 0-7 years follow up).
Joint function
Mean WOMAC scores on pain, stiffness and physical functioning for both localized- and diffuse-
type patients showed no significant differences pre-(baseline) versus postoperatively. Patients
of both subtypes scored significantly better at some postoperative time intervals compared to
baseline scores, however mostly clinically irrelevant (mean difference< 20) (table 3a and b).
In diffuse-type patients (table 3b) WOMAC pain and physical function scores showed a trend
towards improvement in scores from preoperatively (baseline) to postoperative up to 5 years
follow-up.
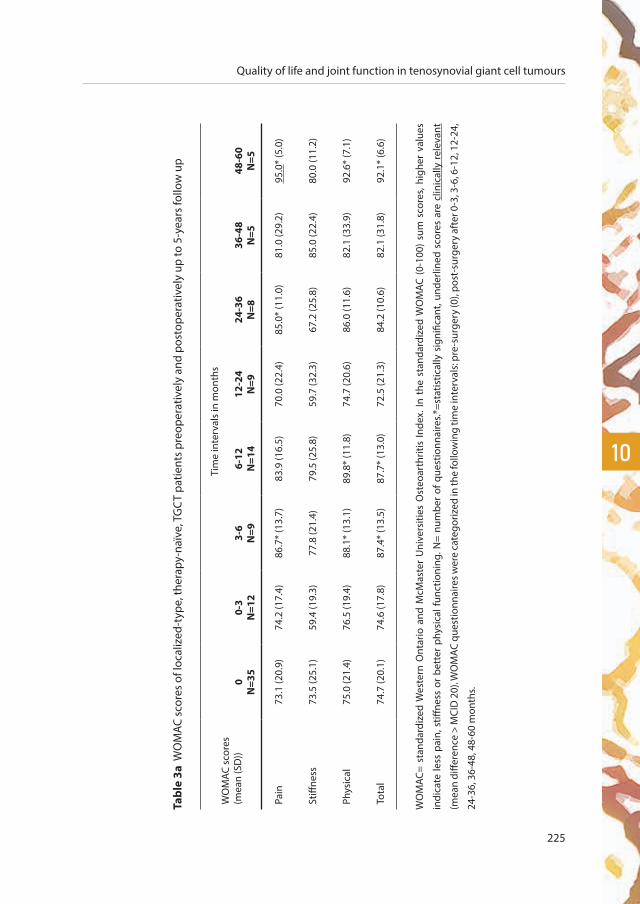
Quality of life and joint function in tenosynovial giant cell tumours
225
10
Tabl
e 3a
WO
MAC
sco
res
of lo
caliz
ed-t
ype,
ther
apy-
naïv
e, T
GC
T pa
tient
s pr
eope
rativ
ely
and
post
oper
ativ
ely
up to
5-y
ears
follo
w u
p
WO
MAC
sco
res
(mea
n (S
D))
Tim
e in
terv
als
in m
onth
s
0N
=35
0-3
N=1
23-
6N
=96-
12N
=14
12-2
4N
=924
-36
N=8
36-4
8N
=548
-60
N=5
Pain
73.1
(20.
9)74
.2 (1
7.4)
86.7
* (1
3.7)
83.9
(16.
5)70
.0 (2
2.4)
85.0
* (1
1.0)
81.0
(29.
2)95
.0*
(5.0
)
Stiff
ness
73.5
(25.
1)59
.4 (1
9.3)
77.8
(21.
4)79
.5 (2
5.8)
59.7
(32.
3)67
.2 (2
5.8)
85.0
(22.
4)80
.0 (1
1.2)
Phys
ical
75.0
(21.
4)76
.5 (1
9.4)
88.1
* (1
3.1)
89.8
* (1
1.8)
74.7
(20.
6)86
.0 (1
1.6)
82.1
(33.
9)92
.6*
(7.1
)
Tota
l74
.7 (2
0.1)
74.6
(17.
8)87
.4*
(13.
5)87
.7*
(13.
0)72
.5 (2
1.3)
84.2
(10.
6)82
.1 (3
1.8)
92.1
* (6
.6)
WO
MAC
= st
anda
rdiz
ed W
este
rn O
ntar
io a
nd M
cMas
ter
Uni
vers
ities
Ost
eoar
thrit
is In
dex.
In t
he s
tand
ardi
zed
WO
MAC
(0-
100)
sum
sco
res,
high
er v
alue
s
indi
cate
less
pai
n, s
tiffne
ss o
r be
tter
phy
sica
l fun
ctio
ning
. N=
num
ber
of q
uest
ionn
aire
s.*=s
tatis
tical
ly s
igni
fican
t, un
derli
ned
scor
es a
re c
linic
ally
rel
evan
t
(mea
n di
ffere
nce
> M
CID
20)
. WO
MAC
que
stio
nnai
res w
ere
cate
goriz
ed in
the
follo
win
g tim
e in
terv
als:
pre
-sur
gery
(0),
post
-sur
gery
aft
er 0
-3, 3
-6, 6
-12,
12-
24,
24-3
6, 3
6-48
, 48-
60 m
onth
s.
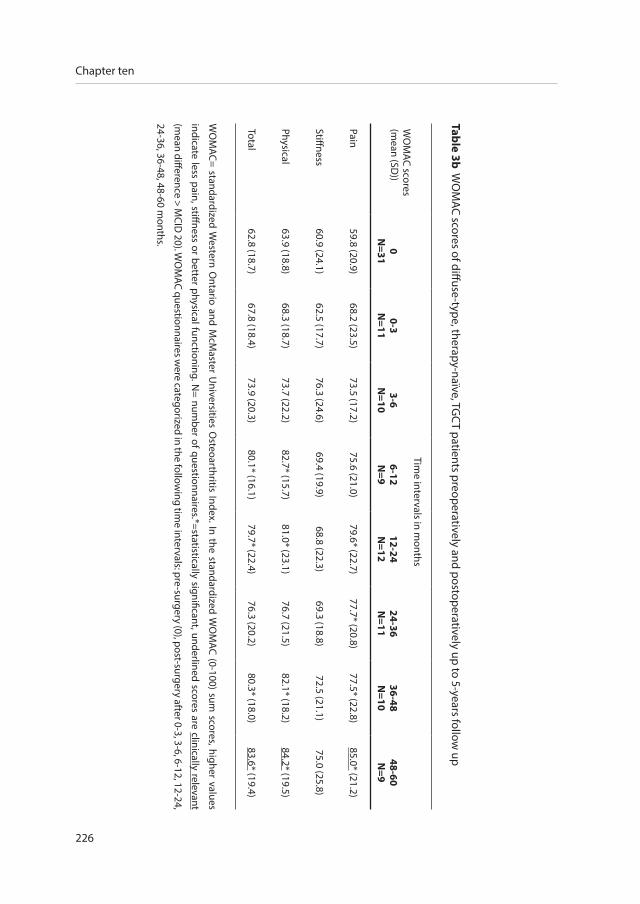
226
Chapter ten
Table 3b WO
MAC scores of diffuse-type, therapy-naïve, TG
CT patients preoperatively and postoperatively up to 5-years follow
up
WO
MAC scores
(mean (SD
))
Time intervals in m
onths
0N
=310-3
N=11
3-6N
=106-12N
=912-24N
=1224-36N
=1136-48N
=1048-60N
=9
Pain59.8 (20.9)
68.2 (23.5)73.5 (17.2)
75.6 (21.0)79.6* (22.7)
77.7* (20.8)77.5* (22.8)
85.0* (21.2)
Stiffness60.9 (24.1)
62.5 (17.7)76.3 (24.6)
69.4 (19.9)68.8 (22.3)
69.3 (18.8)72.5 (21.1)
75.0 (25.8)
Physical63.9 (18.8)
68.3 (18.7)73.7 (22.2)
82.7* (15.7)81.0* (23.1)
76.7 (21.5)82.1* (18.2)
84.2* (19.5)
Total62.8 (18.7)
67.8 (18.4)73.9 (20.3)
80.1* (16.1)79.7* (22.4)
76.3 (20.2)80.3* (18.0)
83.6* (19.4)
WO
MAC= standardized W
estern Ontario and M
cMaster U
niversities Osteoarthritis Index. In the standardized W
OM
AC (0-100) sum scores, higher values
indicate less pain, stiffness or better physical functioning. N= num
ber of questionnaires.*=statistically significant, underlined scores are clinically relevant
(mean difference > M
CID 20). W
OM
AC questionnaires were categorized in the follow
ing time intervals: pre-surgery (0), post-surgery after 0-3, 3-6, 6-12, 12-24,
24-36, 36-48, 48-60 months.

Quality of life and joint function in tenosynovial giant cell tumours
227
10
discussion
To our knowledge, this study provides the largest prospective cohort, including longest follow up
time, to report on PROMs in therapy-naïve patients with localized- and diffuse-type TGCT of large
joints followed up until relapse of disease or end of study. In both TGCT subtypes HRQoL (SF-36)
was statistically significant and clinically relevant decreased before surgical treatment on the main
physical domains (RP, PF, BP) and some mental domains (SF, RE, VT) compared to general population
means. These low scores lasted for up to 6 months postoperatively depending on TGCT subtype and
SF-36 subscale. Thereafter, all SF-36 subscales improved to general population means and continued
fairly stable the following years. Pain experience (VAS) in both subtypes varied widely between and
within patients over time. Mean function (WOMAC) scores on pain, stiffness and physical functioning
for both subtypes TGCT showed no clinically relevant difference pre-(baseline) versus postoperatively.
However, in diffuse-type patients WOMAC pain and physical function scores showed a trend towards
improvement in scores from preoperatively(baseline) to postoperatively up to five years follow-up.
TGCT can behave locally aggressive causing joint destruction and provoke significant pain, swelling,
decrease in range of motion, and stiffness11. This morbidity can lead to impairment of HRQoL and
function because of pain, medication use, disability, the knowledge of having a tumour (despite
its benign character), and loss of working hours16. To improve these consequences, treatments are
performed, which –unfortunately- might contribute to further joint destruction10. The prolonged
course of the disease and the need for multiple surgeries has been reported to result in a worse
joint function for many patients27. In addition to the physical and financial burden for the patient,
TGCT also involves high healthcare burden28. Finding an efficient treatment is important.
This study reported on the loss of HRQoL in patients with TGCT compared to general population
means. The improvements in HRQoL after surgical resections were present 3-6 months after surgery.
This could be explained by the morbidity of an operation and the associated recovery time.
We did not find statistically significant and clinically relevant differences in pain experience. This
might be explained by a variability in symptom experience as described by Gelhorn et al.16 They
found that not all patients experience all symptoms and there was variability in how patients
experienced symptoms within and among days.
228
Chapter ten
The statistically significant but lack of clinically relevant improvement in joint function (WOMAC)
could be explained by the destruction the disease already caused, or by the small number of
questionnaires left after exclusion of many patients to optimize the homogeneity of the patient
group. The lack of disease specific instruments to evaluate adequate PROMs for TGCT, may have
led to underreporting disease specific issues.
SF-36 was developed to get more general insight into patients’ health and as a means of making
comparisons across conditions29. VAS was developed as a pain assessment tool used for cancer
patients19. The WOMAC was originally developed to evaluate the outcome of a total knee
replacement in patients with osteoarthritis.20 SF-36, VAS and WOMAC are a good start in assessing
the patients perspective in TGCT, since they are validated, easy to apply and globally known. These
measures are frequently used for other diseases, allowing to compare TGCT patients with other
patient groups, for example patients with joint replacements for osteoarthrosis30,22, 31. Gelhorn et
al. investigated ‘patient-reported symptoms of TGCT’. They concluded that pain (VAS), swelling,
stiffness and impaired joint function (WOMAC) are important PROMs.
Van der Heijden et al. 15 evaluated 30 patients with therapy-naïve and recurrent diffuse-type TGCT
at a mean of 8 (range 2-32) years after diagnosis. HRQoL impairment (SF-36) was seen in all patients
initially treated with arthroscopic synovectomy (62 range 26-94) and an open synovectomy (80
range 63-98), compared to healthy controls15. The patient population was small and heterogeneous,
in which outcome measures were assessed at different time points after treatment. In the study of
Verspoor at al.2, which experienced similar limitations, HRQoL (SF-36) scores were not significantly
different between localized- and diffuse-type TGCT. However, both patient groups had impaired
HRQoL compared to general population means one the general health subscale. Diffuse patients
also scored significantly lower on other subscales (PF, MH and VT). The current study, with a more
homogenous, larger patient cohort and measurements at categorized time intervals, showed a
similar impairment in therapy-naïve patients on PF preoperatively for both subtypes and up to
6 months postoperatively in diffuse-type patients who generally need more extensive surgery
compared to localized-type TGCT.

Quality of life and joint function in tenosynovial giant cell tumours
229
10
Case series reporting on joint function before treatment often included both subtypes, various
localizations, a mixture of therapy-naïve and recurrent TGCT including multiple treatments15, 27,
32-34. Therefore, it is extremely challenging to perform a meta-analysis to prove treatment effect(s)
in the rare disease TGCT. Through the emergence of systemic treatments for TGCT, attention for
additional outcome measures besides recurrences has been raised, such as HRQoL and joint
function. International cooperation has been initiated, resulting in large registries including QoL
and joint function35. In the recent years targeted therapy has been added to the armamentarium.
At ASCO 2018 results of pexidartinib (PLX3397)12, a selective inhibitor of CSF-1 receptor, KIT,
and FLT3-ITD, were promising in a randomized, placebo controlled, phase 3 study. Pexidartinib
compared to placebo resulted in an significantly improved overall response rate (39.3% vs 0%) and
PROMIS physical function (4.06 vs 0.89), after a median 6 months follow up12. In this study range of
motion, PROMIS physical function, worst stiffness and pain response were secondary endpoints12.
The joint localization of TGCT might influence physical function36, 37. Therefore, a sensitivity analysis
was performed on our patients with TGCT affecting the knee, which showed similar results to our
primary analysis. In a univariate analyses on TGCT locations with recurrent disease as outcome,
Palmerini et al.38 did not find a difference between knees, hips and ankles.
Two crowdsourcing studies39, 40, using an online patient support-group, reported on physical
function and HRQoL in TGCT patients. In patients with diffuse-type TGCT, recurrences requiring
repeated surgery and joint replacement were reported to have a lower HRQoL and functional
outcome39, 40. Because of selection bias, it is possible that severe cases including (additional)
recurrences were more likely to be online to complete the e-survey. However, all studies, including
the current one suggest an impaired effect on HRQoL and function in patients with TGCT. The
challenge remains to find the exact quantification method.
This study has some limitations that need to be discussed. Because of the rarity of TGCT, it
is challenging to perform a prospective study with adequate patient numbers. To reduce
heterogeneity of the patient group, we chose to exclude recurrent patients, at the expense of
decreasing patient numbers. Still, heterogeneity in severity and duration of illness remained.

230
Chapter ten
Selection bias should be taken into account, because this study only contains patients from two
tertiary Dutch referral centres. Overrepresentation of extensive disease, could have resulted in an
overestimation of the impact on HRQoL and joint function. Also, patients with complaints more
often visit the outpatient clinic completing questionnaires. These patients might have more
extended, metastatic, disease. By excluding patients with recurrent TGCT, this possible bias was
reduced. On the contrary, patients who do well, like localized-type TGCT patients, were discharged
early reducing their follow up time and number of questionnaires.
It should be noticed that HRQoL and function scores were taken at variable points after treatment
for individual patients, which reduced numbers at some specific time points. Not all patients
had preoperatively and postoperative available measures, causing an increase in the range of
these outcome measures. Furthermore, it is preferred to adjust SF-36 measures for age, because
of physiologically declined HRQoL and joint function decrease in ageing18, 41. In the current study
correction for age could not be achieved by differences in ages per time interval and the age
distribution within time intervals.
Patients with localized-type TGCT generally do not have a high burden of their disease. The
question is whether PROMs are essential in patients with localized disease, who can generally be
treated curatively with a radical excision and are not eligible for systemic therapy. To date, surgical
resection remains the treatment of choice for TGCT, but is associated with high recurrence rates and
multiple additional surgeries in diffuse-type disease.10 The balance between increased morbidity
of multiple or invasive surgeries15, 42, alternative therapeutic options, and daily symptoms of the
tumour is challenging. A more aggressive resection or other multimodality treatments, such as
external beam radiation therapy, may adversely affect QoL, joint function and the development of
osteoarthrosis, which are, given the young adult age group, factors of major importance2, 38. Use
of a control group and of specific and validated PROMs will better document treatment-induced
symptomatic, functional and economic (back to work) consequences of these treatments16.
When systemic treatments show tumour growth arrest and symptomatic improvements, a less
invasive approach would be justified11. The recent studies on targeted therapy used a control
group and as secondary outcome measure PROMIS physical function12.
Quality of life and joint function in tenosynovial giant cell tumours
231
10
These measures are critical endpoints in demonstrating clinical relevance and impact of treatments
for benign diseases in which death is no outcome variable.16 Clinical benefit necessitates objective
measures to correlate with tumour reduction. When significant changes in TGCT specific
developed outcome measures are found, one should try to specify if this is the consequence of the
disease itself, of the ‘multiple’ treatment(s) received, or of other factors, such as comorbidities, the
knowledge of having a tumour or issues not related to disease.
conclusion
Patients report a significant better HRQoL after surgery in TGCT whereas joint function showed
a trend towards improvement. Pain scores –which vary hugely between patients and in patients
over time- did not improve. A disease specific patient-reported outcome measure would help to
decipher impact of TGCT on patients’ daily life and functioning in more detail.

232
Chapter ten
references
1. Ottaviani S, Ayral X, Dougados M, Gossec L. Pigmented Villonodular Synovitis: A Retrospective Single-Centre
Study of 122 Cases and Review of the Literature. Seminars in Arthritis and Rheumatism. 2011;40 (6):539-46.
2. Verspoor FGM, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of
primary and recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
3. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence
rates than previously known in tenosynovial giant cell tumors. Acta orthopaedica. 2017:1-7.
4. Ravi V, Wang WL, Lewis VO. Treatment of tenosynovial giant cell tumor and pigmented villonodular synovitis. Curr
Opin Oncol. 2011.
5. de saint Aubain Somerhausen N, van de Rijn M. Tenosynovial giant cell tumour, diffuse/localized type. In: Fletcher CD, Bridge
JA, Hogedoorn PC, Mertens F, eds. WHO classification of tumours of Soft Tissue and Bone. 2013;5(4th ed. Lyon: IARC Press).
6. Mastboom MJL, Verspoor FGM, Gelderblom H, van de Sande MAJ. Limb Amputation after Multiple Treatments of
Tenosynovial Giant Cell Tumour: Series of 4 Dutch Cases. Case reports in orthopedics. 2017;2017:7402570.
7. Shabat S, Kollender Y, Merimsky O, Isakov J, Flusser G, Nyska M, et al. The use of surgery and yttrium 90 in the management
of extensive and diffuse pigmented villonodular synovitis of large joints. Rheumatology. 2002;41 (10):1113-8.
8. Heyd R, Seegenschmiedt MH, Micke O. [The Role of External Beam Radiation Therapy in the Adjuvant Treatment of
Pigmented Villonodular Synovitis.]. Z Orthop Unfall. 2011.
9. Verspoor FG, Scholte A, van der Geest IC, Hannink G, Schreuder HW. Cryosurgery as Additional Treatment in
Tenosynovial Giant Cell Tumors. Sarcoma. 2016;2016:3072135.
10. Verspoor FG, van der Geest IC, Vegt E, Veth RP, van der Graaf WT, Schreuder HW. Pigmented villonodular synovitis:
current concepts about diagnosis and management. Future Oncol. 2013;9(10):1515-31.
11. Brahmi M, Vinceneux A, Cassier PA. Current Systemic Treatment Options for Tenosynovial Giant Cell Tumor/Pigmented
Villonodular Synovitis: Targeting the CSF1/CSF1R Axis. Current treatment options in oncology. 2016;17(2):10.
12. Tap WD, Gelderblom H, Stacchiotti S, Palmerini E, Ferrari S, Desai J, et al. Final results of ENLIVEN: A global, double-
blind, randomized, placebo-controlled, phase 3 study of pexidartinib in advanced tenosynovial giant cell tumor
(TGCT). ASCO Annual Meeting. 2018.
13. Giustini N, Bernthal NM, Bukata SV, Singh AS. Tenosynovial giant cell tumor: case report of a patient effectively
treated with pexidartinib (PLX3397) and review of the literature. Clin Sarcoma Res. 2018;8:14.
14. Gounder MM, Thomas DM, Tap WD. Locally Aggressive Connective Tissue Tumors. J Clin Oncol. 2018;36(2):202-9.
15. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the
surgical treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone
Joint J. 2014;96-B(8):1111-8.
16. Gelhorn HL, Tong S, McQuarrie K, Vernon C, Hanlon J, Maclaine G, et al. Patient-reported Symptoms of Tenosynovial
Giant Cell Tumors. Clin Ther. 2016;38(4):778-93.
17. Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, et al. Structure-Guided Blockade of CSF1R
Kinase in Tenosynovial Giant-Cell Tumor. The New England journal of medicine. 2015;373(5):428-37.
18. VanderZee KI, Sanderman R, Heyink JW, de Haes H. Psychometric qualities of the RAND 36-Item Health Survey 1.0:
a multidimensional measure of general health status. Int J Behav Med. 1996;3(2):104-22.
19. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994;23(2):129-38.
20. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status
instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in
patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15(12):1833-40.
21. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important
difference. Control Clin Trials. 1989;10(4):407-15.
22. Escobar A, Quintana JM, Bilbao A, Arostegui I, Lafuente I, Vidaurreta I. Responsiveness and clinically important

Quality of life and joint function in tenosynovial giant cell tumours
233
10
differences for the WOMAC and SF-36 after total knee replacement. Osteoarthritis Cartilage. 2007;15(3):273-80.
23. Tubach F, Ravaud P, Baron G, Falissard B, Logeart I, Bellamy N, et al. Evaluation of clinically relevant changes in
patient reported outcomes in knee and hip osteoarthritis: the minimal clinically important improvement. Ann
Rheum Dis. 2005;64(1):29-33.
24. Angst F, Ewert T, Lehmann S, Aeschlimann A, Stucki G. The factor subdimensions of the Western Ontario and
McMaster Universities Osteoarthritis Index (WOMAC) help to specify hip and knee osteoarthritis. a prospective
evaluation and validation study. J Rheumatol. 2005;32(7):1324-30.
25. White DK, Keysor JJ, Lavalley MP, Lewis CE, Torner JC, Nevitt MC, et al. Clinically important improvement in function
is common in people with or at high risk of knee OA: the MOST study. J Rheumatol. 2010;37(6):1244-51.
26. van der Wees PJ, Wammes JJ, Akkermans RP, Koetsenruijter J, Westert GP, van Kampen A, et al. Patient-reported
health outcomes after total hip and knee surgery in a Dutch University Hospital Setting: results of twenty years
clinical registry. BMC Musculoskelet Disord. 2017;18(1):97.
27. Chiari C, Pirich C, Brannath W, Kotz R, Trieb K. What affects the recurrence and clinical outcome of pigmented
villonodular synovitis? Clin Orthop Relat Res. 2006;450:172-8.
28. Burton TM, Ye X, Parker ED, Bancroft T, Healey J. Burden of Illness Associated with Tenosynovial Giant Cell Tumors.
Clin Ther. 2018;40(4):593-602 e1.
29. Brazier JE, Harper R, Munro J, Walters SJ, Snaith ML. Generic and condition-specific outcome measures for people
with osteoarthritis of the knee. Rheumatology (Oxford). 1999;38(9):870-7.
30. Verspoor FG, Hannink G, Scholte A, Van Der Geest IC, Schreuder HW. Arthroplasty for tenosynovial giant cell
tumors. Acta orthopaedica. 2016;87(5):497-503.
31. Veenhof C, Bijlsma JW, van den Ende CH, van Dijk GM, Pisters MF, Dekker J. Psychometric evaluation of osteoarthritis
questionnaires: a systematic review of the literature. Arthritis Rheum. 2006;55(3):480-92.
32. Griffin AM, Ferguson PC, Catton CN, Chung PW, White LM, Wunder JS, et al. Long-term outcome of the treatment of
high-risk tenosynovial giant cell tumor/pigmented villonodular synovitis with radiotherapy and surgery. Cancer.
2012;118(19):4901-9.
33. Ozturk H, Bulut O, Oztemur Z, Bulut S. Pigmented villonodular synovitis managed by Yttrium 90 after debulking
surgery. Saudi Medical Journal. 2008;29 (8):1197-200.
34. Wu CC, Pritsch T, Bickels J, Wienberg T, Malawer MM. Two incision synovectomy and radiation treatment for diffuse
pigmented villonodular synovitis of the knee with extra-articular component. Knee. 2007;14 (2):99-106.
35. Mastboom M, Verspoor F, Rüeten-budde A, Gelderblom H, Stacchiotti S, Daolio P, et al. Risk factors in Tenosynovial
Giant Cell Tumours, evaluated in 17 international sarcoma centres. 2018(99).
36. Della Valle AG, Piccaluga F, Potter HG, Salvati EA, Pusso R. Pigmented villonodular synovitis of the hip: 2- to 23-year
followup study. Clinical Orthopaedics and Related Research. 2001;(388):187-99.
37. Schwartz GB, Coleman DA. Pigmented villonodular synovitis of the wrist and adjacent bones. Orthopaedic Review.
1986;15 (8):526-30.
38. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.
39. van der Heijden L, Piner SR, van de Sande MA. Pigmented villonodular synovitis: a crowdsourcing study of two
hundred and seventy two patients. Int Orthop. 2016;40(12):2459-68.
40. Mastboom MJ, Planje R, van de Sande MA. The Patient Perspective on the Impact of Tenosynovial Giant Cell Tumors
on Daily Living: Crowdsourcing Study on Physical Function and Quality of Life. Interact J Med Res. 2018;7(1):e4.
41. Aaronson NK, Muller M, Cohen PD, Essink-Bot ML, Fekkes M, Sanderman R, et al. Translation, validation, and
norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations.
J Clin Epidemiol. 1998;51(11):1055-68.
42. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive
Review and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).

da
ily
liv
ing
the patient perspective on
the impact of tenosynovial giant
cell tumours on daily living
chap
ter
elev
en
M.J.L. Mastboom1, R. Planje1, M.A.J. van de Sande1
Interact J Med Res. 2018 Feb 23;7(1):e4.
crowdsourcing study on physical function and quality of life
1 Orthopaedic Surgery, Leiden University Medical Centre, Leiden, the Netherlands

237
11
Impact of tenosynovial giant cell tumours on daily living
abstract
Background
Tenosynovial Giant Cell Tumour (TGCT) is a rare, benign lesion affecting the synovial lining of
joints, bursae, and tendon sheaths. It is generally characterized as a locally aggressive and often
recurring tumour. A distinction is made between localized- and diffuse-type. The impact of TGCT
on daily living is currently ill-described.
Objective
The aim of this crowdsourcing study was to evaluate the impact of TGCT on physical function,
daily activities, societal participation (work, sports, and hobbies), and overall quality of life from
a patient perspective. The secondary aim was to define risk factors for deteriorated outcome in
TGCT.
Methods
Members of the largest known TGCT Facebook community, PVNS is Pants!!, were invited to an
e-survey, partially consisting of validated questionnaires, for 6 months. To confirm disease
presence and TGCT-type, patients were requested to share histological or radiological proof of
TGCT. Unpaired t tests and chi-square tests were used to compare groups with and without proof
and to define risk factors for deteriorated outcome.
Results
Three hundred thirty-seven questionnaires, originating from 30 countries, were completed.
Median age at diagnosis was 33 (interquartile range [IQR]=25-42) years, majority was female (79.8%
[269/337]), diffuse TGCT (70.3% [237/337]), and affected lower extremities (knee 70.9% [239/337]
and hip 9.5% [32/337]). In 299 lower-extremity TGCT patients (32.4% [97/299]) with disease
confirmation, recurrence rate was 36% and 69.5% in localized and diffuse type, respectively. For
both types, pain and swelling decreased after treatment; in contrast, stiffness and range of motion
worsened. Patients were limited in their employment (localized 13% [8/61]; diffuse 11.0% [21/191])
and sport-activities (localized 58% [40/69]; diffuse 63.9% [147/230]). Compared with general US
population, all patients showed lower Patient-Reported Outcomes Measurements Information
System-Physical Function (PROMIS-PF), Short Form-12 (SF-12), and EuroQoL 5 Dimensions 5

238
Chapter eleven
Levels (EQ5D-5L) scores, considered clinically relevant, according to estimated minimal important
difference (MID). Diffuse versus localized type scored almost 0.5 standard deviation lower for
PROMIS-PF (P<.001) and demonstrated a utility score of 5% lower for EQ-5D-5L (P=.03). In localized
TGCT, recurrent disease and ≥2 surgeries negatively influenced scores of Visual Analog Scale (VAS)-
pain/stiffness, SF-12, and EQ-5D-5L (P<.05). In diffuse type, recurrence resulted in lower score for
VAS, PROMIS-PF, SF-12, and EQ-5D-5L (P<.05). In both types, patients with treatment ≤1year had
significantly lower SF-12.
Conclusions
TGCT has a major impact on daily living in a relatively young and working population. Patients
with diffuse type, recurrent disease, and ≥2 surgeries represent lowest functional and quality of
life outcomes. Physicians should be aware that TGCT patients frequently continue to experience
declined health-related quality of life and physical function and often remain limited in daily life,
even after treatment(s).
introduction
Tenosynovial Giant Cell Tumour (TGCT), previously pigmented villonodular synovitis (PVNS), is a rare,
proliferative neoplasm affecting the synovial lining of joints, bursae, and tendons sheaths. According
to growth pattern, a radiological distinction is made between a well-circumscribed lesion (localized
type) and a locally more aggressive lesion (diffuse type)1, 2. The incidence rate reveals its rarity: for
localized type (excluding digits), 10.2 per million person-years and for diffuse type, 4.1 per million
person-years. TGCT is a monoarticular disease, concerning large joints, typically about the knee: 46%
in localized-type and 64% to 75% in diffuse-type. Male-female ratio is about 1:1.5 for both types, with
a median age at the time of TGCT diagnosis of 30 to 50 years1-3. Most common initial symptoms are
pain, stiffness, and swelling. Additional symptoms might be limited range of motion, instability, giving
way, and locking complaints4. Due to these unspecific signs and the rarity of the disease, patients
frequently experience a delay of years in diagnosis3, 5, 6. To treat these symptoms, current treatment
of choice is surgical excision, either by arthroscopic or open synovectomy7. After surgical resection,
high recurrence rates are known, with the localized type up to 50% and the diffuse type up to 92%6.
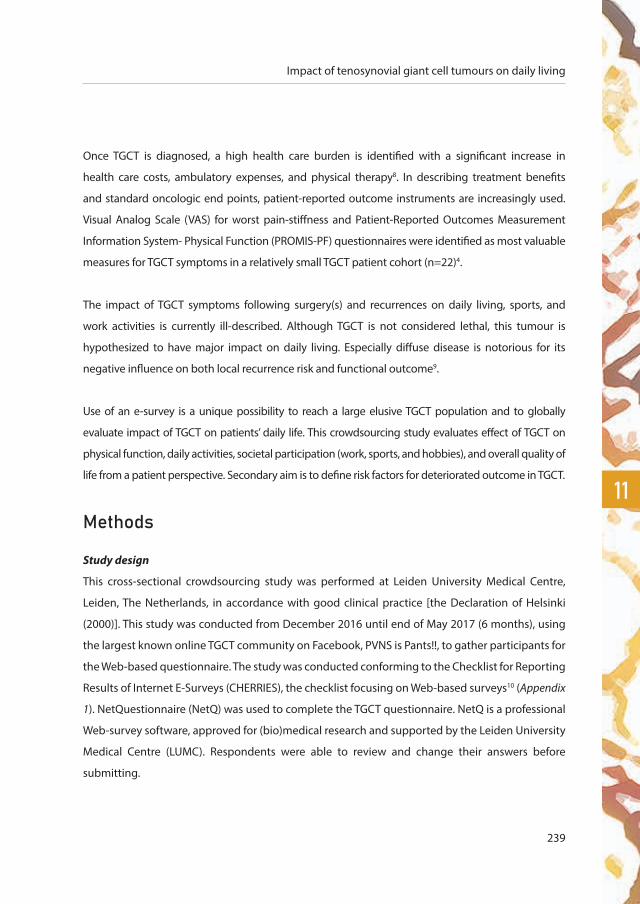
239
11
Impact of tenosynovial giant cell tumours on daily living
Once TGCT is diagnosed, a high health care burden is identified with a significant increase in
health care costs, ambulatory expenses, and physical therapy8. In describing treatment benefits
and standard oncologic end points, patient-reported outcome instruments are increasingly used.
Visual Analog Scale (VAS) for worst pain-stiffness and Patient-Reported Outcomes Measurement
Information System- Physical Function (PROMIS-PF) questionnaires were identified as most valuable
measures for TGCT symptoms in a relatively small TGCT patient cohort (n=22)4.
The impact of TGCT symptoms following surgery(s) and recurrences on daily living, sports, and
work activities is currently ill-described. Although TGCT is not considered lethal, this tumour is
hypothesized to have major impact on daily living. Especially diffuse disease is notorious for its
negative influence on both local recurrence risk and functional outcome9.
Use of an e-survey is a unique possibility to reach a large elusive TGCT population and to globally
evaluate impact of TGCT on patients’ daily life. This crowdsourcing study evaluates effect of TGCT on
physical function, daily activities, societal participation (work, sports, and hobbies), and overall quality of
life from a patient perspective. Secondary aim is to define risk factors for deteriorated outcome in TGCT.
methods
Study design
This cross-sectional crowdsourcing study was performed at Leiden University Medical Centre,
Leiden, The Netherlands, in accordance with good clinical practice [the Declaration of Helsinki
(2000)]. This study was conducted from December 2016 until end of May 2017 (6 months), using
the largest known online TGCT community on Facebook, PVNS is Pants!!, to gather participants for
the Web-based questionnaire. The study was conducted conforming to the Checklist for Reporting
Results of Internet E-Surveys (CHERRIES), the checklist focusing on Web-based surveys10 (Appendix
1). NetQuestionnaire (NetQ) was used to complete the TGCT questionnaire. NetQ is a professional
Web-survey software, approved for (bio)medical research and supported by the Leiden University
Medical Centre (LUMC). Respondents were able to review and change their answers before
submitting.

240
Chapter eleven
Patients and Recruitment
Members of PVNS is Pants!! were requested to participate in our international crowdsourcing
study “Evaluation of Tenosynovial Giant Cell Tumour on daily living” (Appendix 2). At the time of
writing (December, 2016), this closed Facebook community contained 2179 members. A patient-
friendly TGCT-research-related message was posted in the Facebook community every 4 weeks
to encourage TGCT patients to complete the questionnaire. Additional study updates and easily
understandable information on TGCT were posted on the page of a newly designed TGCT study
Facebook account11.
All members of the Facebook community had access to the questionnaire. Solely patients
with TGCT diagnosis were requested to participate in this study. To achieve a higher level of
evidence, confirmation of TGCT (histological or radiological) was requested after completing the
questionnaire. Sending (anonymized) medical reports to our protected email account was highly
desirable but left to the discretion of the participant.
Members of Facebook community PVNS is Pants!! have been notified that (research-minded)
doctors are members of this closed Facebook community for several years. Participation in this
study was voluntary, and no incentives were offered. Informed consent was given by completing
the survey. This study was approved by the Institutional Review Board (CME) from our institution
(registration number P16.232, December 5, 2016).
Unique site visitors were determined by Internet protocol (IP) addresses. When duplicate entries
were detected, the most recent one was included in the analyses. All password-protected
documents were only accessible to TGCT researchers and saved on the secured departmental
drive of our hospital. Data of participants were anonymized when medical proof was received or
when the participant did not respond to our third request for medical confirmation. To ascertain
TGCT diagnosis and TGCT type, all medical reports were verified by 2 TGCT researchers (MJLM, RP).
When in disagreement, medical reports were checked by the senior orthopaedic surgeon (MAJS)
for final conclusion.

241
11
Impact of tenosynovial giant cell tumours on daily living
Questionnaire
On the very active Facebook community PVNS is Pants!!, several patient-initiated questionnaires
and polls were performed, for instance, about treatments, coping strategies, daily limitations, and
emotional struggles. Members expressed their desire for studies regarding these topics, since the
majority of TGCT studies concern physical function and recurrent disease as outcome parameters.
Therefore, a Web-based questionnaire, using mostly validated questionnaires, was composed to
describe impact of TGCT on health-related outcome and daily living from a patient perspective. A
prerequisite was that the questionnaire would be relevant for the heterogeneous TGCT population:
for different large joints, different ages, males or females, localized or diffuse type, and for patients
at different treatment stages.
To assess relevance and completeness of our questionnaire, a pilot test with the composed
questionnaire was performed. One dedicated orthopaedic oncologic surgeon (MAJS), 2 medical
doctors (MJLM, RP), and 5 TGCT patients in our outpatient clinic, all fluent in written and spoken English
language, tested the e-survey. Validated questionnaires were used as published by the owners. After
the pilot test, a few nonvalidated questions were added or rephrased (Appendix 3).
Nonvalidated questions concerned patient and tumour characteristics, medical history, TGCT symptoms,
performed treatments, recurrences, employment status, sports, and number of visits to general
practitioner and orthopaedic surgeon. The majority of questions had a multiple-choice character,
including a not applicable or other answer option. The exact number of nonvalidated questions
depended on given answers. For instance, patients with an extensive TGCT-related history were asked
additional questions on their history, in contrast to the patients awaiting their initial treatment.
Validated questionnaires on physical function and quality of life included: VAS for worst pain and
stiffness in the last 24 hours, PROMIS-PF items, Short Form-12 Health Survey (SF-12), and EuroQoL
EQ-5D-5L (EQ-5D-5L Descriptive System and EQ-5D-5L VAS). A total of 32 validated questions were
included. VAS for pain and stiffness was used to estimate patient’s pain and stiffness intensity for
the past 24 hours: no pain/stiffness at all (0) and worst pain/stiffness imaginable (10).

242
Chapter eleven
PROMIS-PF instruments were used to measure self-reported capability of physical activities. In
this study, short forms of physical functioning for lower and upper extremity were used with 5
response options: without any difficulty (5), with a little difficulty (4), with some difficulty (3), with
much difficulty (2), and unable to do (1). Raw score was calculated by summing up the values of
the response to each question and was converted into a T score by the Assessment Centre from
PROMIS-PF. A mean of a standardized T score of 50 with a standard deviation of 10 reflects the
general US population12.
The SF-12, a generic measure of health status, functioned as a shorter alternative for the SF-36.
Number of answer options differed per question. Physical component summary (PCS) score and
mental component summary (MCS) score were calculated. Similar to PROMIS-PF, the general US
population had a mean of 50 with a standard deviation of 1013.
The EQ-5D-5L is one of the most commonly used generic health status measures in the world.
Its descriptive system comprises 5 dimensions of health: mobility, self-care, usual activities, pain
or discomfort, and anxiety or depression, with the following 5 levels of problems per dimension:
no problems (1), slight problems (2), moderate problems (3), severe problems (4), and extreme
problems (5)14. For each participant, answers per dimension were combined into an EQ-5D-5L
health state. This health state was converted into a single index value (so-called utility score) for
quality of life, by using the Crosswalk Index Value Calculator version 1.0 from the EuroQoL Group15.
Utility scores were measured on an ordinal scale of 0 to 1, with 0 indicating death and 1 indicating
full health16. Crosswalk valuation set for US population was used for all participants, since majority
of the patients originated from the United States (42.7% [144/377]). A specific analysis, called
sensitivity analysis, was performed using the valuation set for UK population, the second largest
patient population (20.2% [68/337]) in this study. Scores calculated with US valuation set were
compared with scores obtained by using UK valuation set to assess representativeness of the
scores from validated questionnaires14 (Appendix 4).
Statistical Analysis
NetQ automatically captured questionnaire answers into an SPSS 23 file. Evaluation of TGCT on
daily living was mainly descriptive.

243
11
Impact of tenosynovial giant cell tumours on daily living
Chi-square tests were used to compare patient groups with and without medical proof regarding
gender (male vs female), TGCT localization (knee vs other large lower extremity joints [hip, ankle,
and foot]), initial surgery (arthroscopy vs [one- or two-staged] open synovectomy), recurrence (yes
vs no), total number of surgeries (1 surgery vs ≥2 surgeries), and time since last treatment for TGCT
(≤1 year ago vs >1 year ago) (Appendix 5).
Independent t tests were used to compare the mean age at the time of diagnosis and continuous
scores of validated questionnaires. All reported P values were two-tailed. Statistical significance
level was defined at P<.05.
Effect size, as a quantitative measure of the strength of a phenomenon, was calculated for both
PROMIS-PF and SF-12 scores in localized- and diffuse-type patients, compared with general US
population score. Effect size, or Cohen d, is the ratio of difference between two means divided by
the standard deviation, expressed in standard deviation units. An effect size between 0.2 and 0.5
is considered small, 0.5 and 0.8 medium, and above 0.8 large17.
The minimal important difference (MID), a quality of life measure, represents the smallest
difference or change beyond statistical significance in an outcome measure score that would
be considered clinically relevant by the value patients place on change. MID for EQ-5D-5L Index
Scores is estimated between .037 and .069, based on the simulation-based instrument-defined
MID estimates18. MID for PROMIS-PF was determined by Yost et al. in advanced-stage cancer
patients19. Differences in T scores between 4.0 and 6.0 were considered clinical relevant. MID for
SF-12 PCS and MCS scores were calculated by Díaz-Arribas et al. in >450 patients with low back
pain and were stated at >3.29 for PCS and >3.77 for MCS20.
results
The TGCT questionnaire was initiated by 445 participants within a time frame of 6 months. For the
present analysis, only fully completed, unique questionnaires (337) were included (Figure 1). The
majority of incomplete questionnaires were early dropouts with a great lack of information and
therefore unsuitable for analysis.

244
Chapter eleven
Most patients were female (79.8% [269/337]) and median age at diagnosis was 33 (interquartile
range [IQR]=25-42) years. Patients originated from 30 different countries (United States: 42.7%
[144/337]; United Kingdom: 20.2% [68/337]; and the Netherlands: 12.8% [43/337]). TGCT was
typically located in lower extremities: knee (70.9% [239/337]), hip (9.5% [32/337]), ankle (11.0%
[37/337]), and foot (3.0% [10/337]). Diffuse TGCT was diagnosed in 237 of 337 (70.3%) patients
(Table 1). According to few TGCT patients with TGCT located in the upper extremity, 12 out of 337
patients (3.6%) were excluded for further analyses. Additionally, 26 out of 337 lower-extremity
Figure 1 Flowchart Tenosynovial Giant Cell Tumour (TGCT) questionnaire.
Q: Questionnaires; L: Localized-TGCT; D: Diffuse-TGCT; U: Unknown-type TGCT
455 questionnaires
excluded14 double Q
104 incomplete Q
3 L 7 D 2 U 230 D
299 L/D-TGCTof lower-extremities
337 fully completed,unique Q
325 lower-extremity
69 L 26 U
12 upper-extremity

245
11
Impact of tenosynovial giant cell tumours on daily living
Table 1 Patient and tumour characteristics (N=337)
Characteristics Value
Age at time of questionnaire (years), median (IQRa) 41 (32-50)
Age at time of TGCT diagnosis (years), median (IQR) 33 (25-42)
Total, N (%) 337 (100)
Gender, n (%)
Male 68 (20.2)
Female 269 (79.8)
Country of residence, n (%)
United States of America 144 (42.7)
United Kingdom 68 (20.2)
The Netherlands 43 (12.8)
Australia 22 (6.5)
Canada 14 (4.2)
Other 46 (13.6)
TGCTb localization, n (%)
Knee 239 (70.9)
Hip 32 (9.5)
Ankle 37 (11.0)
Foot 10 (3.0)
Shoulder 4 (1.2)
Elbow 6 (1.8)
Wrist 2 (0.6)
Otherc 7 (2.1)
TGCT type, n (%)
Localized 72 (21.4)
Diffuse 237 (70.3)
Unknown 28 (8.3)
aIQR: interquartile range (25-75%)bTGCT: tenosynovial giant cell tumour
cOther included multiple TGCT locations (all in lower extremity)
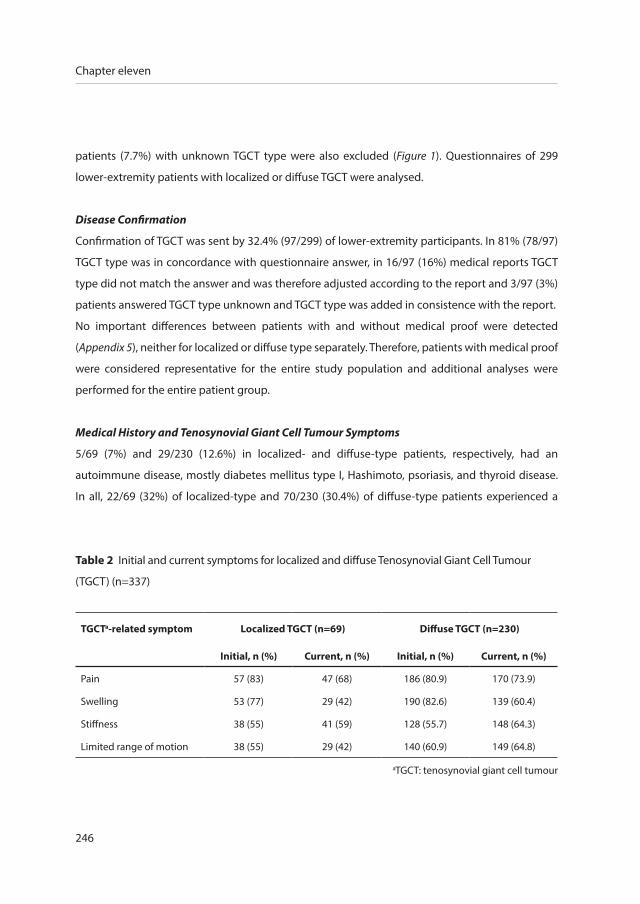
246
Chapter eleven
patients (7.7%) with unknown TGCT type were also excluded (Figure 1). Questionnaires of 299
lower-extremity patients with localized or diffuse TGCT were analysed.
Disease Confirmation
Confirmation of TGCT was sent by 32.4% (97/299) of lower-extremity participants. In 81% (78/97)
TGCT type was in concordance with questionnaire answer, in 16/97 (16%) medical reports TGCT
type did not match the answer and was therefore adjusted according to the report and 3/97 (3%)
patients answered TGCT type unknown and TGCT type was added in consistence with the report.
No important differences between patients with and without medical proof were detected
(Appendix 5), neither for localized or diffuse type separately. Therefore, patients with medical proof
were considered representative for the entire study population and additional analyses were
performed for the entire patient group.
Medical History and Tenosynovial Giant Cell Tumour Symptoms
5/69 (7%) and 29/230 (12.6%) in localized- and diffuse-type patients, respectively, had an
autoimmune disease, mostly diabetes mellitus type I, Hashimoto, psoriasis, and thyroid disease.
In all, 22/69 (32%) of localized-type and 70/230 (30.4%) of diffuse-type patients experienced a
Table 2 Initial and current symptoms for localized and diffuse Tenosynovial Giant Cell Tumour
(TGCT) (n=337)
TGCTa-related symptom Localized TGCT (n=69) Diffuse TGCT (n=230)
Initial, n (%) Current, n (%) Initial, n (%) Current, n (%)
Pain 57 (83) 47 (68) 186 (80.9) 170 (73.9)
Swelling 53 (77) 29 (42) 190 (82.6) 139 (60.4)
Stiffness 38 (55) 41 (59) 128 (55.7) 148 (64.3)
Limited range of motion 38 (55) 29 (42) 140 (60.9) 149 (64.8)
aTGCT: tenosynovial giant cell tumour
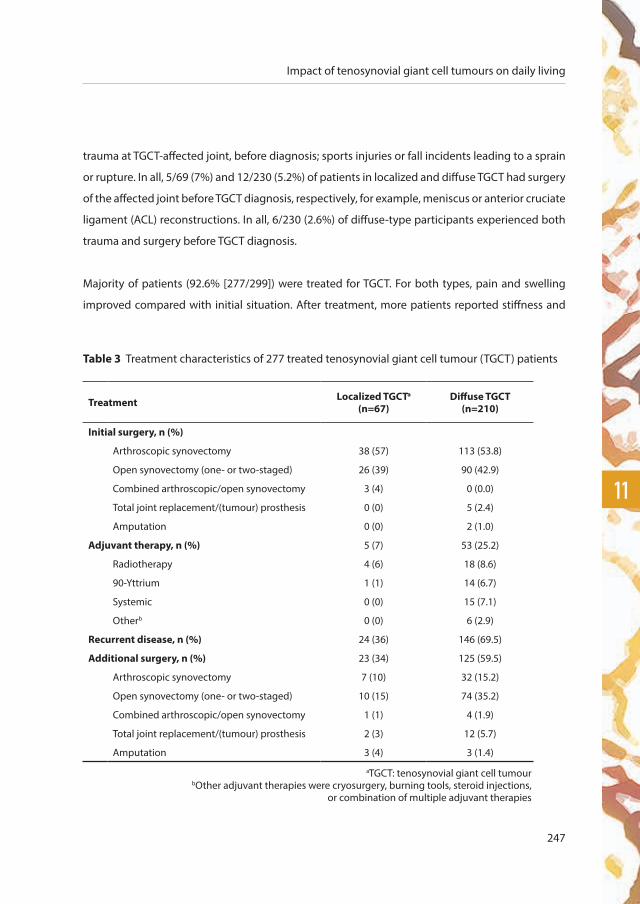
247
11
Impact of tenosynovial giant cell tumours on daily living
trauma at TGCT-affected joint, before diagnosis; sports injuries or fall incidents leading to a sprain
or rupture. In all, 5/69 (7%) and 12/230 (5.2%) of patients in localized and diffuse TGCT had surgery
of the affected joint before TGCT diagnosis, respectively, for example, meniscus or anterior cruciate
ligament (ACL) reconstructions. In all, 6/230 (2.6%) of diffuse-type participants experienced both
trauma and surgery before TGCT diagnosis.
Majority of patients (92.6% [277/299]) were treated for TGCT. For both types, pain and swelling
improved compared with initial situation. After treatment, more patients reported stiffness and
Table 3 Treatment characteristics of 277 treated tenosynovial giant cell tumour (TGCT) patients
Treatment Localized TGCTa (n=67)
Diffuse TGCT (n=210)
Initial surgery, n (%)
Arthroscopic synovectomy 38 (57) 113 (53.8)
Open synovectomy (one- or two-staged) 26 (39) 90 (42.9)
Combined arthroscopic/open synovectomy 3 (4) 0 (0.0)
Total joint replacement/(tumour) prosthesis 0 (0) 5 (2.4)
Amputation 0 (0) 2 (1.0)
Adjuvant therapy, n (%) 5 (7) 53 (25.2)
Radiotherapy 4 (6) 18 (8.6)
90-Yttrium 1 (1) 14 (6.7)
Systemic 0 (0) 15 (7.1)
Otherb 0 (0) 6 (2.9)
Recurrent disease, n (%) 24 (36) 146 (69.5)
Additional surgery, n (%) 23 (34) 125 (59.5)
Arthroscopic synovectomy 7 (10) 32 (15.2)
Open synovectomy (one- or two-staged) 10 (15) 74 (35.2)
Combined arthroscopic/open synovectomy 1 (1) 4 (1.9)
Total joint replacement/(tumour) prosthesis 2 (3) 12 (5.7)
Amputation 3 (4) 3 (1.4)
aTGCT: tenosynovial giant cell tumourbOther adjuvant therapies were cryosurgery, burning tools, steroid injections,
or combination of multiple adjuvant therapies
248
Chapter eleven
limited range of motion (Table 2). A minority of the patients (<6%) currently experienced additional
symptoms, including instability, buckling, hyperextension and/or hypermobility, clicking or
locking or popping of joint, numbness, electric shocks, tingling, dull ache, heat of the affected
joint, or hematoma.
Treatment(s)
Most performed initial surgery was arthroscopic synovectomy (57% [38/67] localized, 53.8%
[113/210] diffuse) and open synovectomy, one- or two-staged (39% [26/67] localized, 42.9% [90/210]
diffuse). In all, 5/67 (7%) localized-type and 53/210 (25.2%) diffuse-type patients had adjuvant
therapies after initial surgery, mainly radiotherapy and 90-Yttrium. In all, 24/67 (36%) of localized
type had recurrent disease after 1.5 (range 1-6) years, in contrast to 146/210 (69.5%) of diffuse type
after 2.2 (range 1-23) years (table 3). Additional surgery was performed in 23/67 (34%) of localized
type and 125/210 (59.5%) of diffuse type, predominantly open synovectomy (one- or two-staged).
Impact of Tenosynovial Giant Cell Tumour on Daily Life
Due to TGCT, 8/61 (13%) and 21/191 (11.0%) of working population in localized and diffuse TGCT,
respectively, was currently not able to (fully) perform their employment. Of these patients, 4/8 (50%)
localized patients and 17/21 (81%) diffuse patients had recurrent disease. Majority of patients, 40/69
(58%) of localized and 147/230 (63.9%) of diffuse type, were unable to perform sport activities. In
these patients, recurrent disease presented in 15/40 (38%) of localized type and 94/147 (63.9%)
of diffuse type. Disease burden was estimated by mean number of visits to general practitioner
(5.6 [range 1-50] visits for localized type, 7.1 [range 1-60] visits for diffuse type), and orthopaedic
surgeon (8.3 [range 1-97] visits for localized type, 11.9 [range 1-100] visits for diffuse type). Results
of validated questionnaires are shown in Table 4 (localized vs diffuse type), Table 5 (localized type),
and Table 6 (diffuse type). Results with positive association are described in the text.
Worst Pain and Stiffness in Last 24 Hours: Visual Analog Scale Score
For localized type, best VAS pain score was 2.76 and VAS stiffness score was 2.80. In diffuse type,
best scores for pain and stiffness were 3.04 and 3.08, respectively. Patients with recurrence of TGCT
had deteriorated VAS score for pain and stiffness (P=.01 localized type and P<.001 diffuse type). In
localized type, patients with ≥2 surgeries had higher VAS score for pain (P=.02) and stiffness (P=.01).

249
11
Impact of tenosynovial giant cell tumours on daily living
Tabl
e 4
Ris
k fa
ctor
com
paris
on o
f 69
loca
lized
ver
sus
230
diffu
se te
nosy
novi
al g
iant
cel
l tum
our (
TGC
T) o
f low
er e
xtre
miti
es
TGCT
a -typ
e
Wor
st p
ain
VASb s
core
, 0
best
sco
re a
nd
10 w
orst
sco
re
Wor
st s
tiffne
ss
VAS
scor
e, 0
be
st s
core
and
10
wor
st s
core
PRO
MIS
-PFc T
sco
re,
mea
n 50
(SD
10)
, MID
d 4.
0–6.
0
SF-1
2e , PCS
f sco
re, m
ean
50 (S
D 1
0), M
ID >3
.29
SF-1
2, M
CSg
scor
e, m
ean
50 (S
D 1
0), M
ID >3
.77
EQ-5
D-5
L D
Sh
utili
ty s
core
, 0
deat
h an
d 1
full
heal
th, M
ID
.037
–.06
9
Mea
nPi
Mea
nPi
Mea
nd j
PiM
ean
d jPi
Mea
nd j
PiM
ean
Pi
Loca
lized
3.36
.24
3.46
.14
44.5
0.55
<.00
140
.50.
95.0
847
.50.
25.4
00.
76.0
3
Diff
use
3.79
4.01
41.3
0.87
38.1
1.19
46.3
0.38
0.72
a TGC
T: te
nosy
novi
al g
iant
cel
l tum
our
b VAS:
Vis
ual A
nalo
gue
Scal
ec PR
OM
IS-P
F: P
atie
nt-R
epor
ted
Out
com
es M
easu
rem
ent I
nfor
mat
ion
Syst
em-P
hysi
cal F
unct
ioni
ngd M
ID: m
inim
al im
port
ant d
iffer
ence
repr
esen
ts th
e sm
alle
st d
iffer
ence
or c
hang
e be
yond
sta
tistic
al s
igni
fican
ce in
an
outc
ome
mea
sure
sco
re th
at w
ould
be
cons
ider
ed im
port
ant b
y th
e va
lue
patie
nts
plac
e on
cha
nge18
-20
e SF: S
hort
-For
mf PC
S: p
hysi
cal c
ompo
nent
sum
mar
yg M
CS: m
enta
l com
pone
nt s
umm
ary
h DS:
des
crip
tive
syst
emi P:
P v
alue
j d: C
ohen
d o
r effe
ct s
ize,
ratio
of d
iffer
ence
bet
wee
n 2
mea
ns d
ivid
ed b
y th
e st
anda
rd d
evia
tion

250
Chapter eleven
Table 5
Risk factor comparison of 69 localized tenosynovial giant cell tumour (TGCT) of lower extremities.
Risk-factors
Worst pain VASa score, 0 best score
and 10 worst score
Worst stiffness
VAS score, 0 best
score and 10 worst
score
PROMIS-PFb T
score, mean 50 (SD 10),
MIDc 4.0-6.0
SF-12d, PCSe score,
mean 50 (SD 10),
MID >3.29
SF-12, MCSf score,
mean 50 (SD 10),
MID >3.77
EQ-5D-5L DSg utility
score, 0 death
and 1 full health, MID
.037-.069
score Pi score Pi score Pi score Pi score Pi score Pi
Gender
Male (n=14) 2.93 .53 3.29 .79 48.5 .04 43.3 .23 49.4 .42 .81 .18
Female (n=55) 3.47 3.51 43.5 39.8 47.0 .75
Age of diagnosis
<35 years (n=36) 3.36 .997 3.39 .82 44.1 .63 40.1 .74 45.4 .07 .76 .95
≥35 years (n=33) 3.36 3.55 45.0 40.9 49.8 .77
TGCT localization
Knee (n=53) 3.04 .08 3.13 .07 44.2 .57 41.0 .43 47.2 .63 .77 .41
Hip, ankle, foot, other (n=16) 4.44 4.56 45.5 38.8 48.6 .74
Initial surgery
Arthroscopy (n=38) 3.45 .58 3.26 .63 44.2 .52 40.7 .96 47.2 .73 .76 .92
Open surgeryh (n=26) 3.04 3.62 45.6 40.8 48.0 .77
Recurrence
Yes (n=24) 4.50 .01 4.71 .01 42.8 .20 38.3 .17 45.7 .27 .70 .01
No (n=45) 2.76 2.80 45.4 41.7 48.5 .80
Total no. of surgeries
1 surgery (n=44) 2.77 .02 2.86 .01 45.4 .20 42.2 .03 48.4 .19 .79 .02
≥2 surgeries (n=23) 4.48 4.65 42.6 36.7 45.0 .71
Last treatment for TGCT
≤1 year ago (n=31) 3.77 .26 3.81 .38 42.4 .06 37.6 .04 46.0 .34 .74 .29
>1 year ago (n=36) 3.00 3.19 46.1 42.6 48.3 .78
aVAS: Visual Analogue Scale. bPROMIS-PF: Patient-Reported Outcomes Measurement Information System-Physical Functioning. cMID: minimal important difference represents the smallest difference or change beyond statistical significance in an outcome measure score that would be considered important by the value patients place on change18-20 . dSF: Short-Form. ePCS: physical component summary. fMCS: mental component summary. gDS: descriptive system. hOne- or two staged open synovectomy. iP: P value
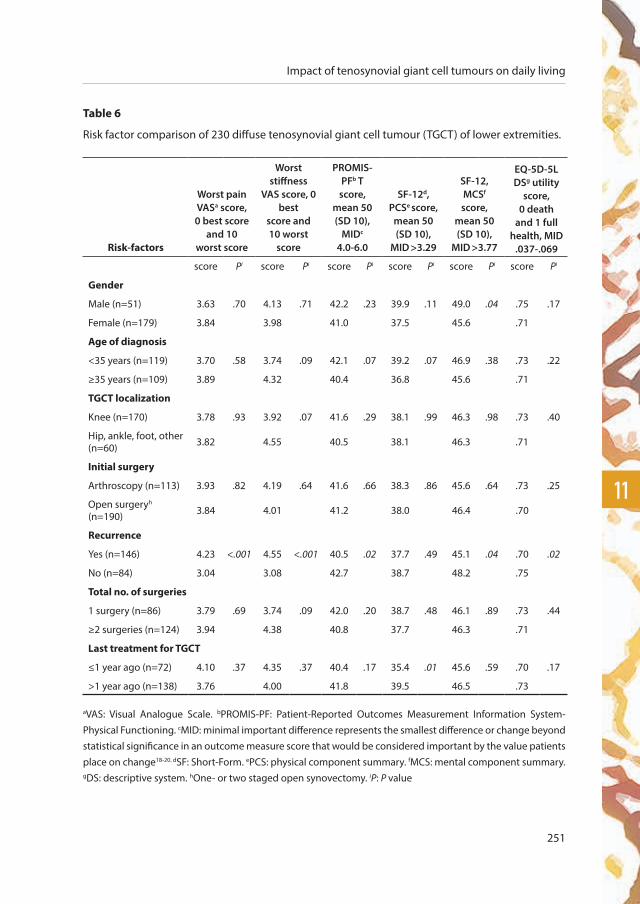
251
11
Impact of tenosynovial giant cell tumours on daily living
Table 6
Risk factor comparison of 230 diffuse tenosynovial giant cell tumour (TGCT) of lower extremities.
Risk-factors
Worst pain VASa score, 0 best score
and 10 worst score
Worst stiffness
VAS score, 0 best
score and 10 worst
score
PROMIS-PFb T
score, mean 50 (SD 10),
MIDc
4.0-6.0
SF-12d, PCSe score,
mean 50 (SD 10),
MID >3.29
SF-12, MCSf score,
mean 50 (SD 10),
MID >3.77
EQ-5D-5L DSg utility
score, 0 death
and 1 full health, MID
.037-.069
score Pi score Pi score Pi score Pi score Pi score Pi
Gender
Male (n=51) 3.63 .70 4.13 .71 42.2 .23 39.9 .11 49.0 .04 .75 .17
Female (n=179) 3.84 3.98 41.0 37.5 45.6 .71
Age of diagnosis
<35 years (n=119) 3.70 .58 3.74 .09 42.1 .07 39.2 .07 46.9 .38 .73 .22
≥35 years (n=109) 3.89 4.32 40.4 36.8 45.6 .71
TGCT localization
Knee (n=170) 3.78 .93 3.92 .07 41.6 .29 38.1 .99 46.3 .98 .73 .40
Hip, ankle, foot, other(n=60) 3.82 4.55 40.5 38.1 46.3 .71
Initial surgery
Arthroscopy (n=113) 3.93 .82 4.19 .64 41.6 .66 38.3 .86 45.6 .64 .73 .25
Open surgeryh (n=190) 3.84 4.01 41.2 38.0 46.4 .70
Recurrence
Yes (n=146) 4.23 <.001 4.55 <.001 40.5 .02 37.7 .49 45.1 .04 .70 .02
No (n=84) 3.04 3.08 42.7 38.7 48.2 .75
Total no. of surgeries
1 surgery (n=86) 3.79 .69 3.74 .09 42.0 .20 38.7 .48 46.1 .89 .73 .44
≥2 surgeries (n=124) 3.94 4.38 40.8 37.7 46.3 .71
Last treatment for TGCT
≤1 year ago (n=72) 4.10 .37 4.35 .37 40.4 .17 35.4 .01 45.6 .59 .70 .17
>1 year ago (n=138) 3.76 4.00 41.8 39.5 46.5 .73
aVAS: Visual Analogue Scale. bPROMIS-PF: Patient-Reported Outcomes Measurement Information System-Physical Functioning. cMID: minimal important difference represents the smallest difference or change beyond statistical significance in an outcome measure score that would be considered important by the value patients place on change18-20. dSF: Short-Form. ePCS: physical component summary. fMCS: mental component summary. gDS: descriptive system. hOne- or two staged open synovectomy. iP: P value

252
Chapter eleven
Patient-Reported Outcomes Measurements Information System-Physical Function: T Score
All TGCT patients had clinically relevant impaired T scores (44.5 and 41.3 for localized and diffuse
type, respectively) compared with the general US population (T score of 50). Corresponding effect
size was medium for localized type (d=0.55) and large for diffuse type (d=0.87). When comparing
both types, diffuse-type patients scored lower (P<.001). In localized type, female patients scored
lower (P=.04). Diffuse-type recurrent patients had decreased scores (P=.02).
Short Form-12 Health Survey: Physical and Mental Component Summary Score
In comparison with general US population (score of 50), both types had impaired PCS (40.5 localized
and 38.1 diffuse type) and MSC scores (47.5 localized and 46.3 diffuse type). In all patients in all
compared groups, PCS score was clinically relevant declined, in contrast to MCS score which did
not transcend the MID threshold in majority of patient groups. A large effect size was calculated
for mean PCS scores (0.95 and 1.19 for localized and diffuse type, respectively) and a medium
effect size (0.25 and 0.38 for localized and diffuse type, respectively) for MCS scores. In localized
type, higher number of surgeries (≥2) affected PCS score negatively (P=.03). Localized- and diffuse-
type patients who underwent treatment for TGCT ≤1 year ago, showed lower PCS score (P=.04
localized, P=.01 diffuse). In diffuse type, female patients demonstrated a decreased MCS score
(P=.04), as well as patients with recurrence of TGCT (P=.04).
EuroQoL 5 Dimensions 5 Levels Health Questionnaire: Index Value
All patients, in all groups (Tables 4-6), presented declined EQ5D-5L utility scores compared with
full health (1), and all scores transcended MID threshold. Overall, utility score was lower in diffuse
patients compared with localized patients (P=.03). In localized type, participants with recurrence
of TGCT and ≥2 surgeries scored lower (P=.01 and P=.02, respectively). Similarly, diffuse patients
with recurrence had decreased scores (P=.02). Median health question VAS score was 75 (IQR 65-
85) for localized and 75 (IQR 56.5-85) for diffuse type. No differences between scores calculated
with US and UK valuation sets were detected in sensitivity analysis (Appendix 4).

253
11
Impact of tenosynovial giant cell tumours on daily living
discussion
Principal Findings
The name of the largest online community of patients with TGCT, PVNS is pants!!, suggests impact
on quality of life. One of the community members motivated the name: “Pants is British slang for
crap or garbage.” To date, it is unknown what the effect of TGCT on daily living is. A questionnaire
was composed in consultation with TGCT patients to determine functional, socioeconomic, and
health burden for TGCT patients. We intended to evaluate TGCT in the real world and concluded
that TGCTs have a large impact on daily living, with declined health-related quality of life and
limitations in daily activities, sports, work, and hobbies: especially the diffuse type of lower
extremities and recurrent disease including multiple surgeries.
Limitations
The most important limitation to this study is selection bias. By using crowdsourcing to gather data,
it is likely to have a higher number of patients with severe or recurrent diseases21. Consequently,
when extrapolating these results to generally described populations of TGCT patients in literature,
care should be taken not to overestimate the decreased physical function and additional
socioeconomic limitations. TGCT usually affects young adults. Since younger patients are more
likely to be on the World Wide Web, and our included patient population had a median age of
33 (25-42) years at time of diagnosis, also in concordance with the WHO classification1, 2 and
Mastboom et al.3, we considered our participants representative for the heterogeneous disease
TGCT. Additionally, the CHERRIES was completed. This checklist provides an understanding of the
sample (self-)selection and its possible differences from a representative sample10 (Appendix 1).
An additional limitation to this study is that patients in different stages of different treatments
were included. To assess comparability within study population, we compared patients who had
treatment less than a year ago with performed treatment over a year ago. No positive associations
were discovered, except for the SF-12 PCS score in both types. This underlines the postoperative
limitations during the first year of follow-up after treatment. As we set out to evaluate impact of
TGCT on daily living in the real world heterogeneous TGCT population, the inclusion of patients
in different treatment stages matched intention of our study. Furthermore, a known disadvantage
of quality of life questionnaires (eg, SF-12) is the generalizability of the questions. Impaired
overall quality of life could be attributed to TGCT but also to additional physical abnormalities or

254
Chapter eleven
psychological problems. Also questionnaires may be completed by patients that have been ill-
informed on their disease. In all, 28 patients filled out unknown type of TGCT, and 16% of patients
who confirmed TGCT with medical proof filled out localized TGCT instead of diffuse TGCT or
vice versa. Undeniably, differentiating in localized and diffuse TGCT is challenging even for (un)
specialized physicians. The relatively high recurrence rate in this study could also be reflected by
unawareness of disease specifics. Recurrence rates in our study were 36% and 70% for localized
and diffuse type, compared with on average 4% to 6% (up to a maximum of 50%) and 14% to 40%
(up to a maximum of 92%) according to van der Heijden et al.6, respectively. It is conceivable that
residual disease or clinical symptoms were filled out as recurrent disease.
The use of self-reported questionnaires harbours the risk of incorrectly answered questions. One
could argue that all patients should have been analysed together, not subdividing into localized
and diffuse type. However, differences between two types are major, and therefore separate
analyses were necessary for a realistic view of impact of TGCT on daily living.
Crowdsourcing
The presumed definition of crowdsourcing is the practice of obtaining services, ideas, or content
by collecting contributions from a comprehensive group from an online community rather
than from traditional data suppliers9. However, the exact definition for crowdsourcing remains
controversial, as 40 definitions originating from 32 unique articles, published between 2006 and
2011, were described by Estellés-Arolas22. It is therefore challenging to well define crowdsourcing
coherently. After analyses of the 40 (sometimes contrasting) definitions, 8 characteristics common
to any given crowdsourcing initiative were found: the crowd, the task at hand, the recompense
obtained, the crowdsourcer or initiator of the crowdsourcing activity, what is obtained by them
following the crowdsourcing process, the type of process, the call to participate, and the medium.
First, in our study, the crowd is presented by patients with TGCT (preferably confirmed by medical
reports). Second, the task at hand is completing a questionnaire about the effect of TGCT on
daily living. Third, participating in this study was voluntary, therefore no recompenses were
offered. Fourth, the initiators of this study are members of the Facebook group PVNS is Pants!!
accompanied with the executors, known as the authors of this paper. Fifth, the researchers and
subsequently the participants and TGCT patients gain more knowledge on the impact of TGCT on

255
11
Impact of tenosynovial giant cell tumours on daily living
daily living. Sixth, the type of process is an evaluation process, aiming to evaluate effect of TGCT on
daily living. Seventh, all patients with TGCT, fluent in English language, were invited to complete
the questionnaire. Lastly, the medium Facebook was used to broadcast the questionnaire.
Facebook is the best applicable social network site for survey research, because it is continuously
growing, internationally known and exceeds 2 billion users globally (June 2017). The Facebook
community PVNS is Pants!!, created in 2009, is the largest TGCT online support group and mainly
consists citizens of the United States. On this very active, closed Facebook community, patients are
daily updating experiences on their disease, ask for advice from fellow TGCT patients, and comment
on other posts to provide their knowledge or sympathy. By actively posting and commenting on
research proposals, patients expressed their willingness to participate in research on TGCT. From
these posts, we learned that adequate patient information on TGCT is lacking. Our crowdsourcing
study stimulated patients’ involvement in research and was an opportunity to align research
questions with the public’s interest23, 24. TGCT is a rare disease and time to definitive diagnosis is
prolonged due to unspecific symptoms and unfamiliarity of the disease5. A challenge in studying
a rare disease is the lack of big data. Crowdsourcing is an effective and low-cost alternative to
traditional methods of participant recruitment due to the possibility to reach large groups of
individuals in a relatively short time frame25. Van der Heijden et al.9 concluded that crowdsourcing
is a promising way for evaluation of rare diseases. Czajka et al.21 used crowdsourcing to efficiently
recruit a global cohort and is the largest study on patients with multiple hereditary exostoses.
Crosier et al.26 used Facebook to recruit patients with auditory hallucinations; within 6 weeks, over
250 patients had completed this survey. Pohlig et al.27 concluded that enrollment of patients in
prospective studies is time-consuming and could be facilitated by use of crowdsourcing.
To obtain a higher level of scientific value, patients were requested for medical proof to
ascertain TGCT diagnosis. To our knowledge, no other crowdsourcing studies considered disease
confirmation. Patient data and outcome for validated questionnaires were comparable for
patients with and without medical proof. Patients were not uniformly diagnosed and treated as
they originated from 30 different countries globally. Neither was distinguished between treatment
in peripheral or tertiary referral centres. Nevertheless, we consider our study group a reflection
of the current worldwide situation and believe that declined impact on daily living is clinically
256
Chapter eleven
relevant for all patients. In contrast to malignant diseases, survival rates are not of interest for
TGCT with its benign character. According to high recurrence rates, quality of life (prior and after
treatment) is essential to evaluate.
Patient-Reported Outcome Measures
Patient reported outcome measures (PROMs) are increasingly used in health policy, patient-
centred care, and shared clinical decision making28. In the era of personalized medicine, patient
involvement is increasing in shared decision making for different treatment strategies with
functional outcome and quality of life. In our study, members of the largest online TGCT community
were involved in establishing the questionnaire Evaluation of TGCT on daily living.
Functional outcome and health-related quality of life are only spars reported for TGCT. Four studies
have reported on standardized PROMS4, 9, 29, 30. Currently, validated PROMS for TGCT patients do
not exist. In accordance with Gelhorn et al.4, VAS for worst pain and stiffness and PROMIS-PF
questionnaires were used. Conform van der Heijden et al.9, 29 and Verspoor et al.30, the SF-12, a
quality of life questionnaire, was included, known as the shorter version of the SF-36. One study
identified a high health care burden with a significant increase in health care costs, ambulatory
costs, and physical therapy in 9328 TGCT patients8.
In benign diseases, including TGCT, death is not an outcome variable. Besides tumour reduction,
critical endpoint measures are clinical relevance and impact of treatment. Currently, clinical
TGCT studies lack specific and validated PROMs to document treatment-induced symptomatic,
functional, and economic (back to work) improvement31. To obtain an impression of physical
function and quality of life in TGCT patients, participants in our study were requested to complete
different validated questionnaires. In our experience, PROMIS-PF was most useful in determining
these functional factors. To minimize the multitude of questions and include the most important
components for clinical TGCT studies, we would propose a combination of PROMIS-PF and a short
quality of life questionnaire, for instance EQ5D5L, in clinical practice.

257
11
Impact of tenosynovial giant cell tumours on daily living
Risk Factors for Deteriorated Outcome
Risk factors for deteriorated outcome in our study were diffuse-type TGCT, recurrent disease,
and ≥2 surgeries performed. This is in concordance with current literature on risk factors for a
high recurrence rate. According to the necessity of mutilating surgeries to treat recurrences, we
considered risk factors for recurrent disease comparable to risk factors for deteriorated outcome.
Higher recurrence rate in diffuse TGCT compared with localized TGCT is exuberant described1, 5-7, 30,
32-34. Bruns et al.34 described 173 patients treated in 10 orthopaedic departments in Germany and
Austria and reported higher recurrence rates in institutions treating less than 20 cases for TGCT, in
diffuse disease, in the hip joint and after arthroscopy. Schwartz et al.35 described 99 patients with TGCT
in the knee, hip, elbow, or shoulder. They concluded that localization in the knee, previous surgical
procedures, and incomplete synovectomy were related significantly to higher number of subsequent
recurrences. On the basis of current literature and to investigate possible risk factors for recurrent
disease thoroughly, gender, age at time of diagnosis, TGCT localization, initial surgery, presence of
recurrence, total number of surgeries, and time since last treatment for TGCT, were compared.
conclusions
TGCTs have major impact on daily living in a relatively young, working population (median age at
diagnosis, 33 years). Majority of symptoms improve after treatment, however, symptoms remain
in about half of the TGCT patients; especially in patients with diffuse type, recurrent disease, and
≥2 surgeries. The high recurrence rate in diffuse TGCT results in clinically important deteriorated
outcome in physical function and health-related quality of life. In preventing recurrent disease, and
its deteriorated outcome, an extensive mutilating surgery might be necessary. Physicians should
be aware that TGCT patients frequently experience symptoms and limitations in daily life and
societal participation (work, sports, and hobbies), even after treatment(s). We deem it important
for future research to evaluate treatment, including its effectiveness on improving quality of
daily living. With this study, we hope to increase knowledge on TGCT among treating physicians,
highlight the importance of quality of life, and to offer research-based information to patients.
Supplementary data
Supplementary data are available in the online version of this article: http://www.i-jmr.org/2018/1/e4

258
Chapter eleven
references
1. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, diffuse type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 52013. p. 102-3.
2. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4 ed2013. p. 100-1.
3. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence rates
than previously known in tenosynovial giant cell tumors. Acta orthopaedica. 2017:1-7.
4. Gelhorn HL, Tong S, McQuarrie K, Vernon C, Hanlon J, Maclaine G, et al. Patient-reported Symptoms of Tenosynovial Giant
Cell Tumors. Clin Ther. 2016;38(4):778-93.
5. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review
and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
6. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
7. Gouin F, Noailles T. Localized and diffuse forms of tenosynovial giant cell tumor (formerly giant cell tumor of the tendon
sheath and pigmented villonodular synovitis). Orthop Traumatol Surg Res. 2017;103(1S):S91-S7.
8. Burton T, Ye X, Parker E, Bancroft T, Healey JH. Burden of Illness in Patients With Tenosynovial Giant Cell Tumors. ISPOR
(International Society for Pharmacoeconomics and Outcomes Research) 22nd Annual International Meeting; Boston,
MA, USA2017.
9. van der Heijden L, Piner SR, van de Sande MA. Pigmented villonodular synovitis: a crowdsourcing study of two hundred
and seventy two patients. Int Orthop. 2016;40(12):2459-68.
10. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES).
J Med Internet Res. 2004;6(3):e34.
11. Study T. TGCT Study Facebook Webpage https://www.facebook.com/profile.php?id=1000132659555822016.
12. HealthMeasures. PROMIS (Patient-Reported Outcomes Measurement Information System) Physical Function Scoring
Manual [Manual]. www.healthmeasures.net2017.
13. Ware JE, Kosinski M, Keller SD. SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales. 1995.
14. van Reenen M, Janssen B. EQ-5D-5L User Guide. In: Group E, editor. Basic information on how to use the EQ-5D-5L
instrument. Version 2.1 ed2015.
15. van Hout B, Janssen MF, Feng YS, Kohlmann T, Busschbach J, Golicki D, et al. Interim scoring for the EQ-5D-5L: mapping
the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708-15.
16. Whitehead SJ, Ali S. Health outcomes in economic evaluation: the QALY and utilities. Br Med Bull. 2010;96:5-21.
17. Sawilowsky SS. New Effect Size Rules of Thumb. Journal of Modern Applied Statistical Methods. 2009;8(2):597-9.
18. McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for
EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-50.
19. Yost KJ, Eton DT, Garcia SF, Cella D. Minimally important differences were estimated for six Patient-Reported Outcomes
Measurement Information System-Cancer scales in advanced-stage cancer patients. J Clin Epidemiol. 2011;64(5):507-16.
20. Diaz-Arribas MJ, Fernandez-Serrano M, Royuela A, Kovacs FM, Gallego-Izquierdo T, Ramos-Sanchez M, et al. Minimal
Clinically Important Difference in Quality of Life for Patients with Low Back Pain. Spine (Phila Pa 1976). 2017.
259
11
Impact of tenosynovial giant cell tumours on daily living
21. Czajka CM, DiCaprio MR. What is the Proportion of Patients With Multiple Hereditary Exostoses Who Undergo Malignant
Degeneration? Clin Orthop Relat Res. 2015;473(7):2355-61.
22. Estellés-Arolas E, González-Ladrón-de-Guevara F. Towards an integrated crowdsourcing definition. J Inf Sci.
2012;38(2):189-200.
23. Truitt AR, Monsell SE, Avins AL, Nerenz DR, Lawrence SO, Bauer Z, et al. Prioritizing research topics: a comparison of
crowdsourcing and patient registry. Quality of life Research. 2017.
24. Bartek MA, Truitt AR, Widmer-Rodriguez S, Tuia J, Bauer ZA, Comstock BA, et al. The Promise and Pitfalls of Using
Crowdsourcing in Research Prioritization for Back Pain: Cross-Sectional Surveys. J Med Internet Res. 2017;19(10):e341.
25. Kuang J, Argo L, Stoddard G, Bray BE, Zeng-Treitler Q. Assessing Pictograph Recognition: A Comparison of Crowdsourcing
and Traditional Survey Approaches. J Med Internet Res. 2015;17(12):e281.
26. Crosier BS, Brian RM, Ben-Zeev D. Using Facebook to Reach People Who Experience Auditory Hallucinations. J Med
Internet Res. 2016;18(6):e160.
27. Pohlig F, Lenze U, Muhlhofer HML, Lenze FW, Schauwecker J, Knebel C, et al. IT-based Psychosocial Distress Screening
in Patients with Sarcoma and Parental Caregivers via Disease-specific Online Social Media Communities. In Vivo.
2017;31(3):443-50.
28. Gagnier JJ. Patient reported outcomes in orthopaedics. J Orthop Res. 2017;35(10):2098-108.
29. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical
treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J.
2014;96-B(8):1111-8.
30. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
31. Cassier PA, Italiano A, Gomez-Roca CA, Le Tourneau C, Toulmonde M, Cannarile MA, et al. CSF1R inhibition with
emactuzumab in locally advanced diffuse-type tenosynovial giant cell tumours of the soft tissue: a dose-escalation and
dose-expansion phase 1 study. Lancet Oncol. 2015;16(8):949-56.
32. Chiari C, Pirich C, Brannath W, Kotz R, Trieb K. What affects the recurrence and clinical outcome of pigmented villonodular
synovitis? Clin Orthop Relat Res. 2006;450:172-8.
33. Ehrenstein V, Andersen SL, Qazi I, Sankar N, Pedersen AB, Sikorski R, et al. Tenosynovial Giant Cell Tumor: Incidence,
Prevalence, Patient Characteristics, and Recurrence. A Registry-based Cohort Study in Denmark. The Journal of
rheumatology. 2017;44(10):1476-83.
34. Bruns J, Ewerbeck V, Dominkus M, Windhager R, Hassenpflug J, Windhagen H, et al. Pigmented villo-nodular synovitis
and giant-cell tumor of tendon sheaths: a binational retrospective study. Arch Orthop Trauma Surg. 2013;133(8):1047-53.
35. Schwartz HS, Unni KK, Pritchard DJ. Pigmented villonodular synovitis. A retrospective review of affected large joints. Clin
Orthop Relat Res. 1989(247):243-55.


am
Puta
tio
nlimb amputation
after multiple treatments of
tenosynovial giant cell tumour
chap
ter
twel
ve
M.J.L. Mastboom1, F.G.M. Verspoor2, H. Gelderblom3, M.A.J. van de Sande1
Case Rep Orthop. 2017;7402570.
series of 4 dutch cases

1 Orthopaedic Surgery, Leiden University Medical Centre, Leiden, the Netherlands
2 Orthopaedic Surgery, Radboud University Medical Centre, Nijmegen, the Netherlands
3 Medical Oncology, Leiden University Medical Centre, Leiden, the Netherlands

Limb amputation in tenosynovial giant cell tumours
263
12
summary
In Tenosynovial Giant Cell Tumours (TGCT), previously named Pigmented Villonodular Synovitis
(PVNS), a distinction is made between a single nodule (localized-type) and multiple nodules
(diffuse-type). Diffuse-type is considered locally aggressive. Onset and extermination of this
orphan disease remain unclear. Surgical resection is the most commonly performed treatment.
Unfortunately, recurrences often occur (up to 92%), necessitating reoperations and adjuvant
treatments. Once all treatments fail or if severe complications occur; limb-amputation may become
unavoidable. We describe four cases of above knee amputation after TGCT diagnosis.
Background
Tenosynovial Giant Cell Tumour (TGCT) is considered an orphan, mono-articular, locally aggressive
neoplasm1. TGCT patients complain of continued pain, swelling and a decreased range of motion
of the affected joint2. Typically, younger patients (below the age of 40 years) are affected. Time
to definitive diagnosis usually takes several years1. TGCT develops along the synovial lining of
joints, tendon sheaths and bursae1, 3. Two extremes along a continuum of one disease process
are described: a single nodule (localized-type) and multiple nodules (diffuse-type)1, 2, 4. These two
subtypes differ in their clinical and radiological presentation, response to treatment and prognosis.
Histologically, no differences are detected1, 5. Exact onset remains unclear. Current findings are
pleading for both a reactive inflammatory disorder and a clonal neoplastic proliferation, provoking
a CSF1 overexpression; suggesting the tumour-landscaping effect6. The localized-type (Giant Cell
Tumour of Tendon Sheath) is defined as a demarcated benign mass, most commonly occurring
in fingers (85%). Lesions are small (between 0.5 and 4 cm), typically lobulated and white to grey
along with yellow and brown areas1, 2, 4. Reported recurrences ensuing surgical treatment are
relatively low: 0-6%4. On the contrary, the diffuse-type (Diffuse-type Giant Cell Tumour (Dt-GCT),
previously named Pigmented VilloNodular Synovitis (PVNS)), shows extensive involvement of the
entire synovial membrane and tends to have the capability to grow infiltrative through adjacent
structures2, 4. Dt-GCT affects mostly weight-bearing joints: predominantly the knee-joint (75%),
followed by the hip-joint (15%). At present, surgery remains the gold standard, while systemic
targeted treatments are only available in trial-settings7. Recurrence rates for Dt-GCT is 14% (up-to
67) after open synovectomy and 40% (up-to 92) after arthroscopic synovectomy4. Recurrent or

264
Chapter twelve
resistant disease, frequently necessitate multiple mutilating surgeries, end occasionally inevitably
in total joint arthroplasties8. Once all treatments fail or severe complications occur: limb-amputation
may become unavoidable. To our knowledge, current literature lacks reports of limb-amputation
in TGCT patients, but patient groups often discuss the possibility on online fora (“PVNS is pants”
closed Facebook community; https://www.facebook.com/groups/91851410592/?ref=ts&fref=ts)9.
To underline potentially aggressiveness of TGCT, four patient history scenarios are described.
Case presentation
Case 1
A female, aged 46, was diagnosed with TGCT. Initial TGCT treatment consisted of three arthroscopic
synovectomies. First synovectomy was supplemented with low-dose radiation, consecutive two
synovectomies with intra-articular 90Yttrium. Fourteen years later, an Magnetic Resonance Imaging
(MRI) scan revealed recurrent TGCT, including bone-involvement. A total knee replacement (TKR)
was performed. Four years later, her knee started to hurt and swell again. Infection parameters were
elevated, MRI showed extensive synovitis and a PET-CT showed enhancement around her TKR, suspect
for recurrent TGCT. Her range of motion was impaired, with a flexion-extension of 50-20-0. Twenty-
three years after initial diagnosis, she was referred to our tertiary orthopaedic oncologic centre. TGCT
re-excision was not an option, as a result of extensive tumour growth (Figure 1a, Figure 1b). Imatinib (a
tyrosine kinase inhibitor with activity against CSF1R) was started for four months. Besides the tumour
growing outwards from her operation-scar, a nearby fistula revealed and started leaking. She was
admitted with malaise, fever, elevated infection parameters, a red swollen right leg and not able to
mobilize. During four weeks of admission she was treated with several blood transfusions attributed
to persistent anaemia, intravenous antibiotics and analgesics. After an investigational tyrosine-
kinase-inhibitor (TKI) in compassionate use was started, she was discharged. After a fall, a few days
after she was discharged, her condition worsened. She was readmitted and treated with intravenous
antibiotics for an acute Staphylococcus aureus infection, provoked by TGCT growing outside the
operation scar composing a direct connection to the TKR. To avoid septic shock: an urgent above
knee amputation seemed a live-saving procedure. Within one month, signs of osteomyelitis revealed.
Treatment with debridement, antibiotics and irrigation stabilized the patient. At one year follow-up,
there were no signs of local recurrence or infection and her phantom pain was decreasing.
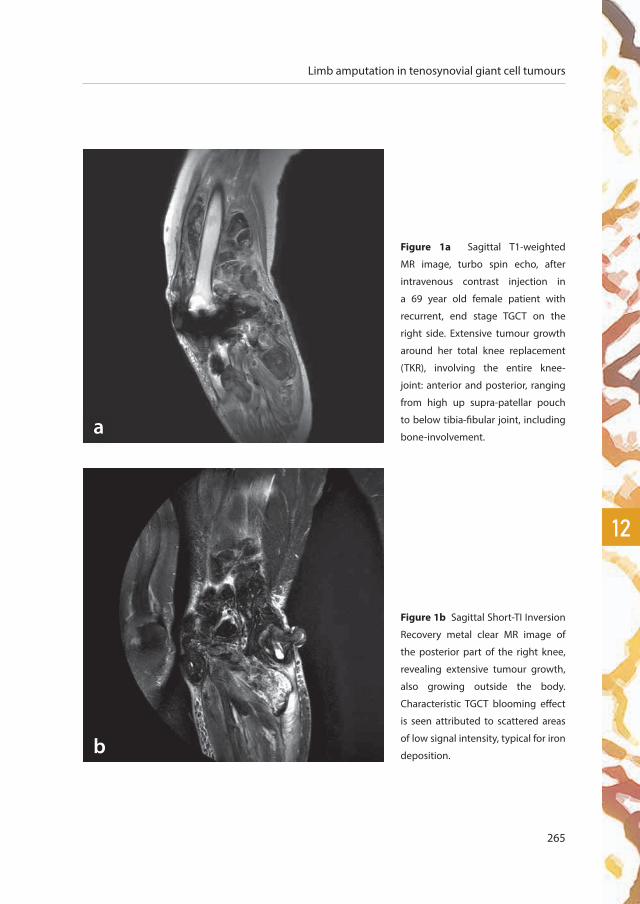
Limb amputation in tenosynovial giant cell tumours
265
12
Figure 1a Sagittal T1-weighted
MR image, turbo spin echo, after
intravenous contrast injection in
a 69 year old female patient with
recurrent, end stage TGCT on the
right side. Extensive tumour growth
around her total knee replacement
(TKR), involving the entire knee-
joint: anterior and posterior, ranging
from high up supra-patellar pouch
to below tibia-fibular joint, including
bone-involvement.
Figure 1b Sagittal Short-TI Inversion
Recovery metal clear MR image of
the posterior part of the right knee,
revealing extensive tumour growth,
also growing outside the body.
Characteristic TGCT blooming effect
is seen attributed to scattered areas
of low signal intensity, typical for iron
deposition.
a
b

266
Chapter twelve
Figure 2a Left knee sagittal
T1-weighted MR image after
intravenous contrast injection with
fat suppression in a 61-year old male
patient with extensive recurrent
Dt-GCT, showing characteristic
blooming effect. a
b
Figure 2b Sagittal turbo-spin echo
proton density-weighted MR image
presents Dt-GCT located intra- and
extra-articular, posterior a large
Baker’s cyst including tumour
involvement.

Limb amputation in tenosynovial giant cell tumours
267
12
Case 2
A 63-year old male was referred to our tertiary hospital with recurrent Dt-GCT of his left knee.
Two years prior to referral, Dt-GCT was diagnosed and (partial) arthroscopically removed
elsewhere. MRI showed a diffuse TGCT growth-pattern involving all compartments of the entire
knee-joint, including a Bakers cyst (Figure 2a, Figure 2b). Consequently, a two-staged anterior
and posterior synovectomy in two tempi was performed; macroscopically all pathological tissue
was removed. There was chondromalacia grade 3-4. A few months later, the patient suffered
progressive knee pain again. Recurrent Dt-GCT lesions, including bone-involvement and
progressive osteoarthritis were seen on X-ray and MRI. A transarticular distal femoral resection
and resection of all Dt-GCT tissue was performed. The knee joint was reconstructed using an
EndoProsthetic-Reconstruction (EPR). Thereafter patient’s knee function seemed to improve.
However, several months later, swelling and increasing knee pain developed. C-reactive protein
(CRP) and erythrocyte sedimentation rate were elevated, nevertheless cultures of aspirated
knee fluid were negative. Along with general deterioration of the patient, wound debridement,
antibiotics, irrigation, and retention (DAIR) was performed. Two out of six cultures, showed
coagulase negative staphylococci without a sign of recurrent TGCT. Despite the DAIR procedure,
his EPR had to be replaced with a gentamicin loaded spacer. Because of the difficulty to treat the
low-grade infection, his spacer was replaced with a gentamicin and vancomycin loaded spacer.
Thereafter, patient’s condition improved, his infection parameters declined and cultures of an
open biopsy were negative. The EPR was re-implanted. Unfortunately the low grade infection
recurred again. After two additional DAIR procedures the patient preferred an above-knee
amputation over another DAIR procedure, life-long antibiotics or a third 2-stage revision. At
present he is pain-free and ambulatory with an above knee prosthetic leg.

268
Chapter twelve
Case 3
A 67 year old male had a TKR after years of indistinct progressive knee-pain. Peroperatively a
benign tumour with few giant cells was diagnosed as a coincidental finding. A few months later
a supra-patellar biopsy showed a mixed malignant appearance, including TGCT components.
Unexpectedly, lymphadenopathy on his groin, did not show malignant cells, but reactive
cells. The patient suffered of systemic symptoms: night sweats, weight loss and infection like
symptoms (not specified). Both for the lymphadenopathy and his painful right knee he received
radiotherapy (70 Gy on both locations, treatment for uncontrollable pain). Histopathologic
revision, by a tertiary specialized pathologist in a reference centre, showed a Dt-GCT. Aggressive
tumour progression, including bone-involvement provoked TKR failure (Figure 3, Figure 4a, Figure
4b). Within one year, several histologically proven Dt-GCT lung metastases were discovered.
Molecular research revealed a t(1;6)(p13;q27) translocation (Supplementary materials), this is
not the typical t(1;2)(p13,q33) translocation, however literature shows different variants on this
translocation. Final diagnosis through FISH technique confirmed Dt-GCT. Discomforting pulmonal
symptoms expressed multiple lung, pleural and costal metastases. Inside the thorax, numerous
suspected lymph nodes were seen. When he developed pulmonary symptoms; an investigational
TKI was started, which had an effect on his lung-metastases, but not on his irradiated painful
lymphademic leg (Figure 5a, Figure 5b). Complaints of tiredness, disguise, a very oedematous right
leg with a leaking protuberance and persisting anaemia provided discomfort. Attributed to the
TKI, pulmonary symptoms disappeared and his lung metastases stabilized. However, a hospital
admission due to pneumonia on both sides and pulmonary embolisms caused a repercussion. As
a last resort, the primary-tumour was resected by amputation, complicated with 4 Litres blood loss
and desaturation (until 90%), necessitating admission to the intensive care unit. Histopathology
confirmed Dt-GCT without malignant cells, however margins were not disease free. Residual and
recurrent disease was seen on MRI three months post-operatively and clinically observed. After
six months, a debulking procedure was performed on his amputated stump. The TKI did not show
effect on the metastases anymore and was discontinued after one year of compassionate use.
Currently, his phantom pain is acceptable.

Limb amputation in tenosynovial giant cell tumours
269
12
Figure 3 Metal artefact reducing
sequelae sagittal T2 weighted turbo
inversion recovery MR image of the right
knee of a 67 year old male patient, with a
TKR in situ. Extensive tumour progression
around TKR and bone invasion is shown.
Figure 4 a & b X-rays (anterior-posterior and sagittal) of failing total knee replacement, attributed to aggressive
TGCT progression including bone-involvement, after radiotherapy treatment.
a b

270
Chapter twelve
Figure 5 a&b PET CT-scan showing extensive TGCT around the right knee-joint and multiple lung, pleural and
costal metastases. When pulmonary symptoms developed; an investigational tyrosine-kinase-inhibitor (TKI)
was started (a. prior to treatment, b. after treatment), which had an effect on his pulmonary-metastases, but
not on his irradiated painful lymphademic leg.

Limb amputation in tenosynovial giant cell tumours
271
12
Case 4
After years of indistinct knee-complaints, a biopsy proved Dt-GCT in a 17 year old male. Intra-
articular 90Yttrium was not effective. After a partial open synovectomy, Dt-GCT recurred. A two-
staged anterior and posterior synovectomy in two tempi (complicated by haemorrhage) was
performed at a tertiary oncology centre. During the following 13 years, the patient underwent a total
of seven surgeries in an effort to treat Dt-GCT, including a knee-arthrodesis using a compression
plate and screws (Figure 6). Osteosynthesis was removed several years later because of a low
grade osteomyelitis and persisting anaemia. Subsequently, a two-staged anterior and posterior
debulking synovectomy was performed (Figure 7 shows MRI prior to debulking). After another
debulking procedure, local tumour control did not seem feasible. An above knee amputation was
performed at the age of 30. Histopathological revision proved Dt-GCT, without malignant cells.
After several years of painless walking with an external prosthesis, pulmonary symptoms occurred.
Imatinib, an investigational TKI, chemotherapy and radiotherapy had no effect on pulmonary and
lymph node metastases. Despite all efforts, deterioration of the patient seemed irreversible. The
patient deceased at the age of 35 years.
Figure 6 Knee-arthrodesis after multiple
Dt-GCT surgeries in a 26 year old man,
using a compression plate and screws.
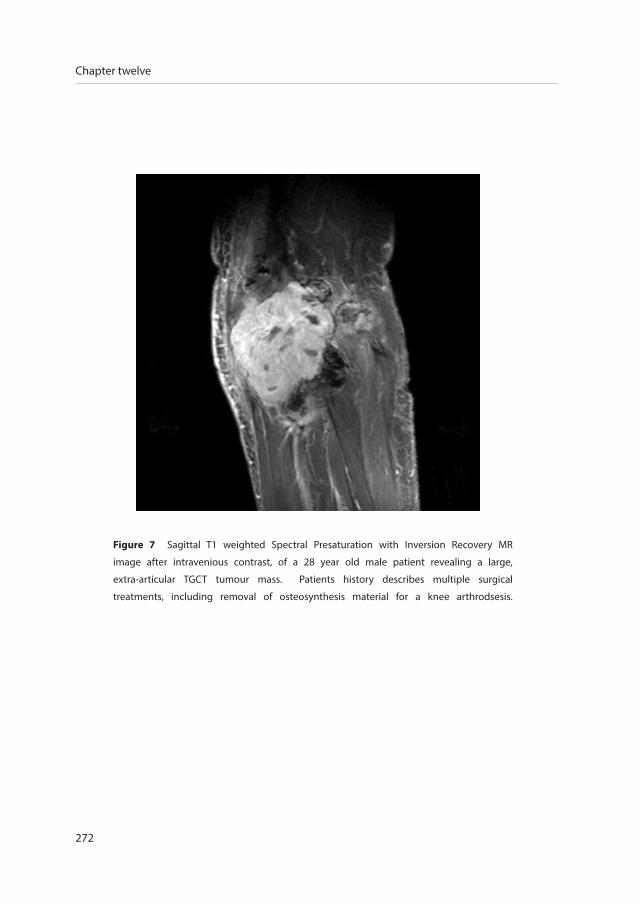
272
Chapter twelve
Figure 7 Sagittal T1 weighted Spectral Presaturation with Inversion Recovery MR
image after intravenious contrast, of a 28 year old male patient revealing a large,
extra-articular TGCT tumour mass. Patients history describes multiple surgical
treatments, including removal of osteosynthesis material for a knee arthrodsesis.

Limb amputation in tenosynovial giant cell tumours
273
12
discussion
TGCT onset is typically slow and patients present with unspecified complaints1. Pain, swelling and
stiffness in the involved joint might be misinterpreted as osteoarthritis, rheumatoid arthritis, a
meniscal tear or other ligamentous injury2. Because of the rarity of the disease, definitive diagnosis
may take several years and patients present with extensive disease. Frequently, patients are referred
to a tertiary hospital, after several arthroscopic or open synovectomies and even radiotherapy
(case number 1)10, 11. Besides declined functional outcome and quality of life10, these patients are
at risk of repeated recurrences and extensive resistant disease7. Multiple surgeries increase the risk
of infection. Continued inflammation, joint usuration and bone involvement may lead to articular
destruction that might worsen (pre-existing) osteoarthritis2. A total joint replacement or even an
endoprosthetic-reconstruction may become inevitable8, 12. Occasionally, total joint arthroplasty
is the primary procedure performed in TGCT8. Only seldom, an above-knee amputation as a last
resort in treatment of TGCT is mentioned13-16.
Is an above knee amputation justified in an essentially benign, but locally aggressive disease? After
(major) complications, for example periprosthetic infections, in primary total knee arthroplasties,
above knee amputations are performed17, 18. Our amputation cases also attributed to severe
prosthetic infections (case 1 and 2). Radiotherapy, applied in case 1 (in a non-specialized hospital)
and 3 (in order to decrease severe pain-complaints), increases risk of prosthetic failure, infection
and wound healing. The overall prevalence of above-the-knee amputation after TKA is estimated
at 0.36%17. When severe pain, a swollen joint, limited range of motion and stiffness impair range
of motion: an above-knee amputation might increase patients mobility17, 19. Therefore, we feel
amputation is justified in extreme TGCT cases.
TGCT is a heterogeneous disease. Some cases are instantly diffusely spread intra- and extra-
articular or even show malignant characteristics. Metastases in histologically benign TGCT are
extremely rare, called an implantation phenomenon and conservatively treatment is suggested14.
Symptomatic free metastases in case 3 were conservatively treated. Physicians should be aware
of the potentially aggressive course of TGCT. Multiple mutilating surgeries decline functional
outcome and quality of life10. Expert centres need to cooperate on these rare cases to understand
the biology underlying these different clinical behaviours.

274
Chapter twelve
West et al. discovered a central role for CSF1 in the pathogenesis of TGCT6. Multiple trials with
systemic therapies targeting CSF-1 receptor, show promising results as novel treatment method
for diffuse-TGCT7. Emactuzumab (RG7155) (a monoclonal antibody against CSF1R) showed an
objective response in 26 of 28 (86 %) TGCT patients20. Prolonged tumour regression is described
in patients, treated with tyrosine kinase inhibitor PLX339721. (Serious) adverse events in
emactuzumab and PLX3397 are investigated. Currently, two studies are recruiting patients with
recurrent or unresectable TGCT diffuse-type: MCS110 (a CSF1-directed monoclonal antibody,
NCT01643850) and FPA008 (an anti-CSF1R monoclonal antibody, NCT02471716). In the near
future, if these systemic treatments are approved, multiple surgeries and final limb amputation,
hopefully, will become obsolete.
To our knowledge, this is the first case-series focussing on limb-amputation after multiple
treatments of TGCT. In order to prevent extensive final treatments, like amputations, further
investigation of TGCT risk factors for recurrences is essential in proper primary-treatment planning.
In the orphan TGCT, knowledge of disease impact can be improved. Patients suffering extensive
disease including patients after multiple mutilating surgeries, might experience higher quality of
life once they feel in control of their own life again. Performing an above-knee amputation may
therefore be considered in extreme and extensive TGCT cases.
conclusion
Frequently, TGCT is successfully treated with radical surgical excision. In a substantial percentage
of cases, it presents as an aggressive and extensive disease that requires complex treatments,
and, in extreme cases, can even lead to limb-sacrificing surgery. Quick diagnosis and adequate
treatment of this rare condition are important factors for outcome. Therefore, it is essential that
these patients get referred to specialized centres at an early stage. We described four extensive
Dt-GCT cases, treated with an above-knee amputation as final treatment.
Limb amputation in tenosynovial giant cell tumours
275
12
references
1. de St. Aubain Somerhausen N, van de Rijn M. Tenosynovial giant cell tumour, localized type/diffuse type. In: Fletcher CD, Bridge JA,
Hogendoorn PC, Mertens F, editors. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4th ed. Lyon: IARC Press; 2013. p. 100-3.
2. Tyler WK, Vidal AF, Williams RJ, Healey JH. Pigmented villonodular synovitis. The Journal of the American Academy of
Orthopaedic Surgeons. 2006;14(6):376-85.
3. Mankin H, Trahan C, Hornicek F. Pigmented villonodular synovitis of joints. Journal of surgical oncology. 2011;103(5):386-9.
4. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to giant cell
tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol. 2013;107(4):433-45.
5. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-
pathologic correlation. Radiographics. 2008;28(5):1493-518.
6. West RB, Rubin BP, Miller MA, Subramanian S, Kaygusuz G, Montgomery K, et al. A landscape effect in tenosynovial giant-cell tumor
from activation of CSF1 expression by a translocation in a minority of tumor cells. Proc Natl Acad Sci U S A. 2006;103(3):690-5.
7. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review and
Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
8. Verspoor FG, Hannink G, Scholte A, Van Der Geest IC, Schreuder HW. Arthroplasty for tenosynovial giant cell tumors. Acta
orthopaedica. 2016:1-7.
9. van der Heijden L, Piner SR, van de Sande MA. Pigmented villonodular synovitis: a crowdsourcing study of two hundred and
seventy two patients. Int Orthop. 2016;40(12):2459-68.
10. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical treatment
for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J. 2014;96-B(8):1111-8.
11. Flandry F, Hughston JC, McCann SB, Kurtz DM. Diagnostic features of diffuse pigmented villonodular synovitis of the knee.
Clinical orthopaedics and related research. 1994(298):212-20.
12. Gonzalez Della Valle A, Piccaluga F, Potter HG, Salvati EA, Pusso R. Pigmented villonodular synovitis of the hip: 2- to 23-year
followup study. Clin Orthop Relat Res. 2001(388):187-99.
13. Layfield LJ, Meloni-Ehrig A, Liu K, Shepard R, Harrelson JM. Malignant giant cell tumor of synovium (malignant pigmented
villonodular synovitis). Archives of pathology & laboratory medicine. 2000;124(11):1636-41.
14. Asano N, Yoshida A, Kobayashi E, Yamaguchi T, Kawai A. Multiple metastases from histologically benign intraarticular diffuse-
type tenosynovial giant cell tumor: a case report. Human pathology. 2014;45(11):2355-8.
15. Hamlin BR, Duffy GP, Trousdale RT, Morrey BF. Total knee arthroplasty in patients who have pigmented villonodular synovitis.
The Journal of bone and joint surgery American volume. 1998;80(1):76-82.
16. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
17. Sierra RJ, Trousdale RT, Pagnano MW. Above-the-knee amputation after a total knee replacement: prevalence, etiology, and
functional outcome. The Journal of bone and joint surgery American volume. 2003;85-a(6):1000-4.
18. Khanna V, Tushinski DM, Soever LJ, Vincent AD, Backstein DJ. Above knee amputation following total knee arthroplasty: when
enough is enough. The Journal of arthroplasty. 2015;30(4):658-62.
19. Fedorka CJ, Chen AF, McGarry WM, Parvizi J, Klatt BA. Functional ability after above-the-knee amputation for infected total
knee arthroplasty. Clinical orthopaedics and related research. 2011;469(4):1024-32.
20. Cassier PA, Italiano A, Gomez-Roca CA et al., CSF1R inhibition with emactuzumab in locally advanced diffuse-type tenosynovial giant cell
tumours of the soft tissue: A doseescalation and dose-expansion phase 1 study, The Lancet Oncology, vol. 16, no. 8, pp. 949–956, 2015.
21. Tap WD, Wainberg ZA, Anthony SP et al., “Structureguided blockade of CSF1R kinase in tenosynovial giant-cell tumor,” New
England Journal of Medicine, vol. 373, no. 5, pp. 428–437, 2015.

su
mm
ar
ych
apte
r th
irte
en
summaryof this thesis
278
Chapter thirteen
summary of thesis
Both localized- and diffuse-type tenosynovial giant cell tumours (TGCT) are defined a benign
disease as metastases or lethal outcome very rarely occur. Diffuse-type TGCTs are regarded
more challenging to treat because they have an infiltrating growth pattern and lack anatomical
boundaries which make complete resection difficult and at times technically impossible or
undesirable with joint function preservation and health-related quality of life in mind. Within
this present era of systemic targeted and multimodality therapies (available in trial settings),
standalone surgical resection cannot be regarded as the gold standard anymore for all cases.
This thesis aims to unravel the heterogeneity of TGCT, to improve oncologic results and maintain
joint functionality and health-related quality of life, by addressing several disease aspects.
Patient selection for different treatment options is improved by translational research, risk factor
identification, treatment outcome evaluation and disease severity stratification.
Up to date incidence calculations are necessary for diagnostic purposes. Therefore, chapter 2
determined worldwide incidence rates in TGCT affecting digits, TGCT localized-extremity and
TGCT diffuse-type. Previous incidence rate calculations originated from 1980, in which a US county
study calculated an incidence rate of 9 and 2 per million person-year in localized- (including digits)
and diffuse-TGCT, respectively (Myers 1980). By use of PALGA, the non-profit nationwide network
and registry of histo- and cytopathology in The Netherlands, a search was performed for TGCT in
a 5-year time frame. Subsequently these data were clinically verified in the corresponding Dutch
hospitals. Dutch TGCT incidence calculations were converted to world population incidence rates.
Finally, incidence rates of TGCT affecting digits was 29, localized-type extremity TGCT 10 and
diffuse-type TGCT 4 per million person-years. All three groups showed a female predilection and
highest number of new cases in age-category 40 to 59 years. The knee was most often affected:
localized-extremity (46%) and diffuse-type (64%), mostly treated with open-resection: localized
(65%) and diffuse (49%). Reoperation rate due to local recurrence for localized-extremity was 9%,
diffuse-TGCT 23%. Compared to the initial US-county study, our study showed a 5-fold higher
incidence rate in localized-type (combining localized-digits and localized-extremity), and a more
than 2.6 fold higher incidence rate in diffuse-type. This difference could be attributed to our
nationwide coverage and because of increased awareness about the disease.

Summary of this thesis
279
13
The controversy that localized- and diffuse-type TGCT are clinically and radiologically two different
types, while histopathologically they seem indistinguishable is evaluated in chapter 3. Abundant
expression of Colony Stimulating Factor1 (CSF1), due to genomic rearrangements, is believed to
be the driver mechanism in tumour formation. This study aimed to correlate CSF1-expression
and CSF1-rearrangement with the biological behaviour of different TGCT-types and with clinical
outcome (recurrence). Along a continuum of extremes, therapy naïve knee TGCT patients with
>3-year follow-up, mean age 43 (range 6-71) years, 56% female were selected. Nine localized- (two
recurrences), 16 diffuse-type (nine recurrences) and four synovitis as control were included. The
use of CSF1 split-apart FISH, consecutive to mRNA ISH, showed to be an auxiliary diagnostic tool,
with 76% of TGCT harbouring CSF1-gene rearrangement. A clear association was not revealed
between CSF1 over-expression or CSF1 rearrangement and the biological behaviour of different
TGCT-characteristics (e.g. localized-/diffuse-type and clinical outcome (recurrence)) of the knee.
Since localized- and diffuse-TGCT differ clinically, chapter 4 established a severity classification
to stratify different disease severity stages. This classification may aid to identify eligible patients
for systemic targeted therapy or trials for novel agents. Parameters were defined by field-experts
to assess disease extension on MR images. Type of TGCT, articular involvement, involvement of
muscular/tendinous tissue and ligaments showed good inter- and intra-rater agreement (Kappa
≥0.66), had adequate number of presence (minimum of 20%) and yielded positive association
on first recurrence. Ranging from highest to lowest hazard ratios these four MR parameters
constructed the TGCT severity classification for all large joints, including four distinct severity-
stages. Recurrence free survival at 4 years (log rank p<0.0001) was 94% in mild localized, 88% in
severe localized, 59% in moderate diffuse and 36% in severe diffuse. The TGCT severity classification
informs physicians and patients on disease extent and risk for first local recurrence after surgical
treatment.
As the clinical behaviour of TGCT is very heterogeneous and probably multifactorial, chapter 5
evaluated the unexplored influence of female sex hormones on symptoms in TGCT. Female sex
hormones (oestrogen and progesterone) elevate during pregnancy. Since an increase in TGCT-
related symptoms during pregnancy is observed in the outpatient clinic and on online TGCT
280
Chapter thirteen
patient fora, we hypothesized that these increased symptoms were influenced by female sex
hormones. Fifty-six percent of pregnant patients reported an increase in TGCT-related symptoms,
predominantly swelling of the affected joint. Influences of sex specific hormones and female
fertile life phase specific hormones were determined by comparing recurrence free survival
rates between the sexes and pre- versus post-menopausal women. No differences were found
in recurrence free survival rates, between both sexes, (localized- (p=0.206 ≤50 years, p=0.935
>50 years); diffuse-type (p=0.664 ≤50 years, p=0.140 >50 years)), neither in pre- versus post-
menopausal women (localized- (p=0.106); diffuse-type (p=0.666)). This makes a causal relation
with female sex hormones unlikely. Finally, presence of female sex hormonal receptor-status in
available tumour tissue was assessed. In all examined localized- and diffuse-TGCT tissue-samples,
oestrogen or progesterone hormone-receptor staining was negative and could therewith not be
linked to the increased TGCT-related symptoms.
Many case-series in adults are described, whereas only 76 pediatric patients with TGCT were
reported, according to our systematic review, presented in chapter 6. This study compared TGCT
in children with TGCT in adults, calculated incidence rate and evaluated clinical behavior of TGCT
in children. The standardized pediatric TGCT incidence rate of large joints was 2.42 and 1.09 per
million person-years in localized and diffuse types, respectively. In 57 children diagnosed and
treated between 1995 and 2015, in one of the four tertiary sarcoma centers in The Netherlands,
symptoms were swelling, pain, and limited range of motion with a median time before diagnosis
of 12 (range 1-72) months. With the numbers available, differences in presentation between
children and adults were not observed in terms of sex, symptoms before diagnosis, first treatment,
recurrent disease, follow-up status, or median time to follow-up. The 2.5-year recurrence-free TGCT
survival rate after open resection was similar between children and adults: 85% (95%CI 67%-100%)
versus 89% (95%CI 83%-96%) in localized, respectively (p=0.527) and 53% (95%CI 35%-79%)
versus 56% (95%CI 49%-64%) in diffuse type, respectively (p=0.691). Although the incidence of
pediatric TGCT is low, it should be considered in the differential diagnosis in children with chronic
mono-articular joint effusions. Recurrent disease after surgical treatment of this orphan disease
was comparable between children and adults.
Summary of this thesis
281
13
In the literature, chapter 7 and chapter 8 presented the largest series of both localized- and
diffuse-type TGCT. Two-thousand one-hundred and sixty-nine (941 localized-, 1192 diffuse-, 36
unknown-type) histologically proven TGCT cases of large joints were included, treated between
1990-2017 in one of 31 collaborating sarcoma centers globally.
In localized-TGCT (chapter 7), 62% was female with median age at first treatment of 39 years and
median follow-up of 37 months. 67% affected the knee and primary treatment at tertiary center
was one-staged open resection in 71%. Total number of recurrent disease was 13% with local
recurrence free survival at 3, 5 and 10 years of 88%, 83% and 79% respectively. The largest risk
factor for recurrent disease was prior recurrence (p<0.001). Complications were noted in 4% after
surgical treatment of localized-TGCT. Initial symptoms of pain and swelling improved after surgical
treatment(s) in 71% and 85%. Only including therapy naïve cases, tumour size ≥5 cm versus
<5cm HR 2.50(95%CI 1.32-4.74;p=0.005) and initial treatment with arthroscopy versus open HR
2.18(95%CI0.98-4.84;p=0.056) yielded positive association with local recurrence in both univariate
and multivariate analyses. Relatively low complication rates and good functional outcome warrant
an open approach with complete resection in localized-TGCT, to reduce recurrence rates in high
risk patients.
In diffuse-TGCT (chapter 8), 58% was female, median age 35 years and median follow-up 54
months. 64% affected the knee and in 53% primary treatment was one-staged open synovectomy.
45% had first local recurrence, accompanied with local recurrence free survival at 3, 5 and 10 years
of 62%, 55% and 40%, respectively. Largest risk factor for recurrent disease was prior recurrence
(HR 3.5 95%CI 2.8-4.4, p<0.001) with a 5 years RFS in therapy naïve patients compared with
patients treated elsewhere of 64% and 25%, respectively. Complications were noted in 12%.
Initial symptoms of pain and swelling improved after surgical treatment(s) in 59% and 72% of
patients respectively. In a subgroup analyses including therapy naïve cases affecting the knee,
neither sex (male;female), age (≤35years;>35years), bone-involvement (present;absent), surgical
technique (open;arthroscopic) nor tumour size (<5cm;≥5cm) yielded an association with first local
recurrence. Since complete resection of diffuse-TGCT could be regarded as nearly impossible and
recurrence rates are unacceptably high after both arthroscopy and open synovectomy in the knee,
even in specialized centres, standalone surgical resection cannot be regarded the gold standard
anymore in the era of multimodality therapies.

282
Chapter thirteen
Chapter 9 described long term effects of imatinib mesylate, a non-selective CSF1 inhibitor, in
TGCT. Sixty-two patients from 12 institutions across Europe, Australia and the United States used
imatinib as treatment. Thirty-nine patients were female (63%), median age at treatment start was
45 years, with a median time from diagnose to treatment of 3.5 years. Median follow-up after
treatment start was 52 months. Four patients with metastatic TGCT progressed rapidly on imatinib
mesylate and were excluded for further analyses. Seventeen (29%) of 58 evaluable patients
achieved complete or partial response. One- and five-year progression-free survival rates were
71% and 48%, respectively. Thirty-eight (66%) patients discontinued imatinib after a median of 7
months. Reported adverse events in 45 (78%) patients were mostly grade 1-2 (89%) (e.g. edema
(48%) and fatigue (50%)). Five patients experienced grade 3-4 toxicities, including neutropenia,
acute hepatitis, facial edema, skin toxicity and fatigue. This study confirmed the known efficacy
of imatinib in TGCT. In responding cases, prolonged activity of imatinib on TGCT symptoms
was confirmed, even after discontinuation, but with high rates of treatment interruption and
additional treatments. Limitations of this study are related to the retrospective study design,
the lack of a control group and the absence of patient reported outcome measures. To evaluate
patients reported outcome measures, chapter 10 focused on joint function and health-related
quality of life outcome after surgical treatment in a prospective cohort study. Patient-reported
outcome measures (Short Form (SF)-36, Visual Analogue Scale (VAS) and Western Ontario and
McMaster Universities Osteoarthritis Index (WOMAC)) were assessed in a homogeneous group
of 206 consecutive patients with localized- (N=108) and diffuse-type (N=98) TGCT of large joints,
initially treated with (arthroscopic/open) synovectomy at either Leiden University Medical
Center or Radboud University Medical Center. In particular, the physical component of SF-36
subscales showed significant and clinically relevant deteriorated scores preoperative- and direct
postoperative compared with general population means, in both localized- and diffuse-TGCT. Six
months after surgery, SF-36 scores improved to general population means and continued fairly
stable the following years. Median pain (VAS) scores, for both-subtypes, showed no clinically relevant
difference pre- or postoperatively. Pain experience differed tremendously between patients and
over time. Mean function (WOMAC) scores, for both TGCT subtypes, showed no clinically relevant
differences (effect size < MCID 20) pre- versus postoperatively. However, in diffuse-type patients
WOMAC pain and physical function scores showed a trend toward improved preoperative versus
postoperative scores. To conclude, patients report a significant better health-related quality

Summary of this thesis
283
13
of life after surgery in TGCT whereas joint function showed a trend towards improvement. To
evaluate patient reported outcomes in an even larger group of patients, chapter 11 conducted a
crowdsourcing study in the largest TGCT patient support group. To evaluate the impact of TGCT
on daily living; physical function, daily activities, societal participation (work, sports and hobbies)
and overall health-related quality of life was assessed. Secondary aim was to define risk factors
for deteriorated outcome in TGCT with the use of validated questionnaires (VAS for worst pain
and stiffness, Patient Reported Outcomes Measurement Information System-physical functioning
(PROMIS-PF), SF-12 and EuroQoL (EQ-5D-5L)). In a timeframe of six months, TGCT patients were
invited to complete the online questionnaire. To confirm disease presence and TGCT-type, patients
were requested to share histological- or radiological-proof of TGCT. Three-hundred thirty-seven
questionnaires (32% with disease confirmation), originating from 30 countries, were completed.
Median age at diagnosis was 33 (IQR 25-42) years, majority was female (80%), diffuse-TGCT (70%)
and affected lower extremities: knee (71%) and hip (10%). In 299 lower extremity TGCT-patients,
recurrence-rate was 36% and 70% in localized- and diffuse-type, respectively. Due to TGCT, 13%
of localized- and 11% of diffuse-type was unable to (fully) perform their employment and 58%
of localized- and 64% of diffuse-type was unable to practice sport-activities. For both types, pain
and swelling decreased after treatment, but stiffness worsened and range of motion decreased.
This could be attributed to (multiple) surgical treatments, inducing scar tissue, cartilage wear
and adhesions. Compared with general United States population, all patients showed declined,
clinically relevant, PROMIS-PF scores, SF-12 physical and mental scores and EQ-5D-5L utility-score.
When comparing localized- and diffuse-TGCT, diffuse-type scored almost 0.5 standard-deviation
lower for PROMIS-PF (p<0.001) and 5% lower for EQ-5D-5L (p=0.03). In localized-TGCT, recurrent
disease and ≥2 surgeries negatively influenced scores of VAS-pain/stiffness, SF-12 physical and EQ-
5D-5L (p<0.05). In diffuse-type, recurrence resulted in lower score for VAS-pain/stiffness, PROMIS-
PF, SF-12 mental and EQ-5D-5L (p<0.05). In both types, patients with treatment ≤1 year ago scored
significantly lower on SF-12 physical. This study demonstrated that TGCT has major impact on
daily living in a relatively young and working population. Physicians and other relevant health
care providers (e.g. physiotherapists) should be aware that TGCT patients frequently continue to
experience declined health-related quality of life and physical function and often remain limited
in daily activities, employment and sports, even after treatment(s).
284
Chapter thirteen
Extreme final treatment measures in TGCT, an above knee amputation, are presented in chapter
12. High recurrence rates are known in diffuse-TGCT (up to 92%), necessitating reoperations and
adjuvant treatments. Once all treatments fail or if severe complications occur, limb amputation
may become unavoidable. Four cases treated with this last resort treatment for TGCT, an above-
knee amputation, were described.
Conclusions, clinical implications and future perspectives for the subject of this thesis are discussed
in chapter 14.
Summary of this thesis
285
13

dis
cuss
ion
chap
ter
four
teen
general discussion
& Future perspectives

288
Chapter fourteen
general discussion
In the 2013 WHO classification of tumours of soft tissue and bone, giant cell tumour of the tendon
sheath and pigmented villonodular synovitis (PVNS) were unified in one overarching name:
tenosynovial giant cell tumours (TGCT)1, 2. To date, among most treating physicians, the disease
still remains best known with the term PVNS3. With this thesis, we want to create disease awareness
and update knowledge on disease and treatment outcome.
TGCT is a rare heterogeneous disease (chapter 2) with a wide clinical spectrum; patients of all ages
are affected (chapter 5 and 6), including different joints (both small and large), various disease
stages and severities. This heterogeneity challenges research initiatives, as current literature mainly
consists of relatively small single centre observational case-series that often compare apples to
oranges. Frequently, series have a retrospective design and level of evidence is not exceeding level
III-IV. To achieve solutions on unmet medical needs, we need to set up research projects that reach
higher levels of evidence through thorough (inter)national, multicentre collaborative studies.
1. Translational research
The translocation (1;2)(p13;q35) that is responsible for overexpression of Colony Stimulating Factor
1 (CSF1), is thought to be the driver mechanism of this disease4, 5. It remains unclear when and
why this translocation forms, but it remains a ‘local problem’ as TGCT is a mono-articular disease.
An unravelled clinical question is how to differentiate the biological behaviour of different TGCT-
types with clinical outcome (recurrence). All TGCT cases show CSF1 over-expression. By the use of
correlative microscopy for CSF1 mRNA ISH and consecutive CSF1 split-apart FISH, we were able to
detect CSF1-gene rearrangement in 76% of the TGCT cases; 77% for localized-TGCT and 75% for
diffuse-TGCT. The relatively high percentage of rearrangement in our study could be attributed to
our scoring on preselected areas, based on high CSF1 expression. In addition, our DNA FISH analysis,
using bacterial artificial chromosome (BAC) clones (RP11-354C7 and RP11-96F24) bracketing
CSF1 locus, identified not only a translocation, but also an inversion for CSF1 rearrangements. In
diagnosing TGCT, CSF1 mRNA-ISH in combination with CSF1 split-apart FISH; using digital correlative
microscopy, is an auxiliary diagnostic tool to identify rarely occurring neoplastic cells. Although this
helps the diagnostic process, in chapter 3 we were unable to use this technique and differentiate for
biological behaviour of TGCT by evaluating CSF1 over-expression or rearrangement.

General discussion & Future perspectives
289
14
2. Individually tailored treatment
Physical joint examination is generally nonspecific in the clinical diagnosis of TGCT. A specialized
musculoskeletal radiologist can however diagnose TGCT on magnetic resonance (MR) imaging,
which is the most distinctive imaging technique6-10. MR imaging can also be a differentiating tool
to determine tumour severity staging and for evaluation of disease extent during follow-up. The
TGCT severity classification in chapter 4 defines TGCT extension on MR imaging to classify disease
severity. This classification, including four distinct severity-stages, could attribute to a treatment
strategy flowchart and improve the homogeneity in clinical studies. Definitive diagnosis however
is established by histopathology, either by biopsy or surgical resection.
The fundamental question whether curation is necessary in a locally aggressive disease often
arises in literature. Debilitating symptoms and (progressive) joint destruction commonly
result in treatment of the diseased tissue. At present, the choice of treatment is established by
preference of the patient, treating physician and might differ per centre. Most common performed
treatment is surgical excision, aiming for local tumour control. Localized-TGCT presents as a well
circumscribed lesion and recurrence rates after arthroscopic and open synovectomy are reported
similar (6% after arthroscopic and 4% after open synovectomy)11. Surgical treatment for the
locally aggressive diffuse-TGCT is more challenging, as pathologic tissue can be widely spread
and technically difficult to reach. In extensive disease (chapter 4, severe diffuse stage), irradical
resection could be preferred with joint preservation in mind. However, higher rates of recurrences
are described after macroscopically incomplete resections12-15. As primary treatment for diffuse-
TGCT, either an arthroscopic- or (one- or two staged) open synovectomy or a combination of these
two treatments is performed. Physicians in favour of arthroscopic resection claim fast recovery,
a lower complication rate and less joint morbidity13, 16-22. However, frequently at the cost of
inadequate excision, high recurrence rates (on average 40% in diffuse-TGCT) and a theoretical risk
of joint seeding and portal contamination11, 23. A complete synovectomy is generally impossible
with traditional arthroscopy, therefore Blanco et al. and Mollon et al. used multiple portals in
arthroscopic synovectomy24, 25. Chin et al. stated that knee arthroscopy is an inferior treatment
for extra-articular TGCT26. Nowadays, open synovectomy, either one- or two-staged, is the
preferred surgical therapy in most centres, because of clear tumour visibility and lower short term
recurrence rates (on average 14% in diffuse-TGCT)11, 27, 28. The disadvantage of a one- or two-staged

290
Chapter fourteen
open resection, could be deteriorated joint function accompanied with decreased health-related
quality of life (chapter 9)29. A combined anterior arthroscopic- and posterior open synovectomy
in the knee is only incidentally reported. Mollon et al. described the combined approach of an
anterior arthroscopy and posterior open synovectomy (N=15 patients), with low recurrence
rates25. Colman et al. retrospectively subdivided 48 diffuse-TGCT patients in three groups; either
treatment with an arthroscopy, the combined approach or an open approach. They concluded
that the combined approach is a feasible option because of relatively low short term recurrence
rates (9%)30. Chapter 7 revealed that the longer the follow-up, the higher the recurrence rates.
Localized-TGCT had a recurrence rate of 21% and diffuse-TGCT 69% after initial surgical resection
at a tertiary oncology centre with a follow-up of more than 10 years. The suspicion arouses that
most patients will develop a recurrence when you wait long enough. The main question remains:
is the recurrent disease accompanied by debilitating symptoms or joint destruction?
In general, all surgical treatments harbour the risk of complications. Literature frequently lacks
descriptions of complications. Chapter 7 reports a complication rate of 4% in localized-TGCT and
12% in diffuse-TGCT after initial surgical treatment at a tertiary centre. Most common complication
in diffuse-TGCT was joint stiffness, which might be difficult to prevent in surgical treatment of
extensive disease.
In extensive diffuse disease, radical excision is next to impossible as residual tumour cells (micro- R1
or macroscopically R2) may persist. In diffuse-TGCT, joint destruction and secondary osteoarthritis
is frequently present. When chronic symptoms persist, joint arthroplasty might become inevitable,
especially in large joints with tight capsules including a higher risk of bone involvement, such as
the hip and ankle29, 31, 32.
A combination of surgery and external beam radiation is considered in extensive or recurrent
diffuse-TGCT. Radiotherapy may kill residual tumour cells, but possibly at the cost of increased
(delayed) complications, especially in re-operation, and impaired functional outcome15, 33-35. Blanco
et al. reported that partial arthroscopic synovectomy of the knee combined with external beam
radiation might reduce the risk of recurrence (N=22 patients)24. A meta-analysis suggested that
open synovectomy (N=19 studies) or synovectomy combined with perioperative radiotherapy
(N=11 studies) is associated with a reduced rate of recurrence34. Mollon et al. reserved additional
General discussion & Future perspectives
291
14
external beam radiation for patients at high risk for local recurrence, if they had the following
characteristics: multiple recurrent intra-articular disease, extra-articular extension, or gross
residual disease remaining following surgery25. Currently, sufficient data including adequate
patient numbers is lacking to support the additional value of external beam radiation in primary
cases and should only be performed in specific extensive or recurrent diffuse-TGCT cases.
Additional reported treatment modalities include radiation synovectomy with 90yttrium36 and
cryosurgery37, 38, for which the therapeutic value is inconclusive and their long-term side effects
and complications are unknown. Bickels et al. treated seven patients with diffuse-TGCT of the
ankle with subtotal synovectomy and intra-articular 90yttrium and warned not to use 90yttrium
as additional treatment because of unacceptable high rate of serious complications39. Gortzak et
al. reported no significant differences in residual disease, complication rate and overall physical
and mental health scores between patients surgically treated for TGCT of the knee with (N=34) or
without (N=22) adjuvant 90Yttrium, after a mean follow-up of 7.3 years36. Chin et al. subdivided
patients, after surgical resection without disease eradication, into three groups: group I
combined arthroscopic and open synovectomy (five patients), group II combined synovectomy in
combination with intra-articular radiation synovectomy (dysprosium-165) (30 patients), and group
III combined resection and three months postoperatively external beam radiation (five patients).
They concluded that group I and Group II showed similar increases in postoperative flexion
compared with group III15. Verspoor et al. evaluated 12 patients treated with surgical synovectomy
and additional cryosurgery. They did not find better results compared to surgical resection alone37.
Diffuse-TGCT grows locally aggressive. Therefore, systemic therapy, with possible (severe) side
effects, seems justified in this benign but debilitating disease. Colony Stimulating Factor1 (CSF1),
due to genomic rearrangements, is believed to be the driver mechanism in tumour formation. By
a paracrine loop, the CSF1 excreting tumour cells, attract non-neoplastic cells, carrying the CSF1
receptor. Interruption of this pathway is the aim of systemic targeted therapies. Targeted therapy
might be used as treatment independently or to primarily down-stage the disease and facilitate
consecutive surgical resection. Non-selective CSF1 inhibitor therapies with nilotinib40 or imatinib
(chapter 8) and newer, more potent selective CSF1 inhibitors such as pexidartinib41, emactuzumab42,
cabiralizumab43; or a monoclonal antibody such as MSC110 (clinicaltrial.gov) seem promising.

292
Chapter fourteen
Results are usually tumour-centric presented, using Response Evaluation Criteria in Solid Tumors
(RECIST); complete response, partial response, stable disease and progressive disease; and patient
centric, using symptom improvement evaluation. In a randomized, placebo-controlled phase 3
study, pexidartinib showed an improved overall response rate (complete response and partial
response merged) of 39% in the pexidartinib-group (N=61) and 0% of placebo-group (N=59), after
median six months follow-up. PROMIS physical function, worst stiffness and pain response was
significantly better in patients treated with pexidartinib41. Emactuzumab (N=29) had an overall
response rate of 86% and a rate of disease control of 96%, including a significant functional and
symptomatic improvement (median follow up 12 months)42. Preliminary results of cabiralizumab
showed partial response in 5 out of 11 patients and positive functional status improvements by
Ogilvie-Harris score (from 2 to 7)43. Ogilvie-Harris score combines pain, synovitis, range of motion
and functional capacity on a scale of 0 to 12.
Complete response was reported in a total of four patients; two patients treated with
emactuzumab42 and two patients treated with imatinib, presented in chapter 8.
Reported mild side effects include edema, change of hair colour, fatigue, nausea and skin rash/
dermatitis, but also moderate to severe side effects such as neutropenia, acute hepatitis, facial
edema, skin toxicity and fatigue. Despite these side effects, in selected patients with extensive and
recurrent diffuse-TGCT, CSF1 inhibitors might offer a solution. Treatment optimization is yet to be
established; optimal agent, therapy duration, timing of surgery, toxicity profile and mechanism of
resistance.
A challenging rare subgroup of soft tissue sarcoma patients, comprises multifocal, malignant or
metastatic disease resembling TGCT (four patients with metastatic TGCT in chapter 8 and two
patients in chapter 11). These patients are incidentally reported in case-series44. The largest series
of Li et al. included seven patients with malignant TGCT and concluded that these tumours should
be regarded as a distinct sarcoma with considerable morphologic variability, metastatic propensity,
and lethality45. As specialized centres see these patients extremely rare, upcoming research should
reveal whether TGCT is capable of malignant transformation or whether this malignant tumour
should be regarded a different (malignant) entity.

General discussion & Future perspectives
293
14
To summarize, several treatment modalities in the heterogeneous disease TGCT are available.
Current literature fails to specify patient characteristics per treatment modality and lacks
randomized controlled trials, impeding definitive treatment of choice for each individual, based
on efficacy and safety. A solution for the difficulty of performing a randomized controlled trial
might be the so called stepped wedge cluster design. This is a special form of a randomised study
in which an intervention at group level is implemented in stages46. To contribute to personalized
treatment, careful evaluation of health-related quality of life and functional outcome (chapter 9
and 10), not just local recurrence and complications, should be included in patient follow-up. In
addition, large scaled studies based on individual participant data meta-analysis provide a higher
form of evidence in comparison with small heterogeneous case series. Advantages include that
missing data can be accounted for at the individual level, subgroup analyses can be performed
(e.g. per affected joint) and up to date disease status or follow-up information can be updated
continuously (chapter 7)47.
3. Centralized treatment in a multidisciplinary team
TGCT onset is typically slow and patients present with unspecified symptoms1, 2, 48, 49. Pain, swelling,
and stiffness of the involved joint might be misinterpreted as osteoarthritis, rheumatoid arthritis, a
meniscal tear, or other ligamentous injury50. Because of the rarity of the disease, definitive diagnosis
may take several years and patients present with extensive disease11, 51, 52. After several (arthroscopic
or open) synovectomies and even radiotherapy, patients are still referred to a tertiary hospital.
Besides declined functional outcome and health-related quality of life, these patients are at risk
of repeated recurrences, therapy resistant disease and higher risk of complications29. Continued
inflammation, joint usuration and bone involvement may lead to articular destruction that might
worsen (pre-existing) osteoarthritis50. By creating more public awareness, involving relevant
dedicated health care providers (e.g. rheumatologists, general practitioners, physiotherapists),
delay of diagnosis should be reduced by referring patients to specialized centres at an early
stage to provide optimal treatment(s)53. Specialized centres treat multiple patients with TGCT
and this rare disease is considered daily practice. Therefore, all members of the multidisciplinary
team are highly trained to recognize disease specifics. Members of the multidisciplinary TGCT
team include dedicated physicians with experience in musculoskeletal oncology in the field of
pathology, radiology, orthopaedic oncology, arthroscopic orthopaedics, radiotherapy, medical
294
Chapter fourteen
oncology and if necessary paediatric orthopaedics. To prevent end stage treatment options, such
as limb amputation (chapter 11), centralization of treatment should become state of the art.
Two examples of advantages of centralization of treatment are provided by the tertiary oncology
centre in Leiden (LUMC). Every half year a patient centred newsletter is send to all patients with
TGCT. This newsletter includes information on recent literature and (new) studies at patient level.
In addition, the TGCT-team of the LUMC is active on Facebook, with their own up to date Facebook
page (‘TGCT study’) and within the closed Facebook-group ‘PVNS is pants’ (chapter 10).
4. Patient-centred outcome measures
Outcome of TGCT treatments should be measured on how the patient is feeling. The mantra
for patient-centred treatment is: don’t make the treatment worse than the problem. Perhaps a
debilitating operation costs more than the disease itself in the view of health-related quality of life and
joint function preservation. Taking the factor time into account is necessary, as short term satisfying
results could emerge into deteriorated outcome in the long run. Defining specific treatment options
for each individual patient is of utmost importance. Would this individual patient benefit more from
conservative treatment or side effects of targeted therapy? Mild side effects might be considered
acceptable, however moderate to severe side effects seem less justifiable in a non-lethal disease.
Assessment of health-related quality of life and functional outcome in TGCT is necessary. However,
specific patient reported outcome instruments have yet to be defined. A few studies, including
chapter 9 and 10, have reported disease outcome from a patient perspective15, 25, 29, 36, 48, 54, 55. Used
validated questionnaires included worst pain and worst stiffness numeric rating scale (NRS), short
form (SF) health survey-12 and SF-36, Euroqol 5 (EQ5D5L), knee-injury osteoarthritis outcome
score (KOOS), hip disability osteoarthritis outcome score (HOOS), Toronto extremity salvage score
(TESS), musculoskeletal tumour society (MSTS) score, patient reported outcomes measurement
information system physical function (PROMIS-PF) and Western Ontario and McMaster Universities
Osteoarthritis Index (WOMAC). None of these patient reported outcome instruments are specifically
designed for rarely lethal, but morbid musculoskeletal tumours. Gelhorn et al. performed research
interviews regarding symptom experience to test the relevance and content validity of several
existing patient reported outcome instruments. They recommended PROMIS-PF as most suitable
questionnaire48. PROMIS-PF is subdivided in an upper- (11 questions) and lower-extremity part (13
General discussion & Future perspectives
295
14
questions). Since TGCT affects all joints, measurements eligible for all these locations would be the
aim. In addition, general health-related quality of life measures are important to compare TGCT
with other musculoskeletal disorders.
A major disadvantage of standardized questionnaires is that they include questions not applicable
for each individual participant. Therefore, the item response theory (IRT) and Computer Adaptive
Testing (CAT) are developed. IRT examines the response characteristics of individual items and
the relationship between responses to individual items and the responses to each other item
in a domain. By using IRT, CAT is a method that selects subsequent questions (from the item
bank) based on the responses until predetermined termination criteria are met. Hereby only
relevant questions are asked and the amount of questions is greatly reduced. This ensures a
higher amount of patients willing to complete the questionnaire56. Relevant questions could be
extracted from the PROMIS databank, including over 300 measures of physical, mental, and social
health for use with the general population and with individuals living with chronic conditions
(http://www.healthmeasures.net). For future self-reported outcome evaluations in TGCT, we
would propose the CAT method by use of the PROMIS item bank.
Besides well-defined subjective outcome measures, objective outcome measures also need to be
determined to structure clinical evaluation. The timed up and go test provides information on
physical strength by measuring the time (seconds) to rise from and return to a chair with three
meters walking in between57. Another functional measure is the six-minute walk test, not just
determining joint range of motion, but looking at performance of the individual58.
5. Limitations
This thesis consists of multiple cohort studies. At times, patients are present in several cohorts.
Patients treated in the RadboudUMC or LUMC, were also present in the PALGA search to calculate
the incidence (chapter 2). In the evaluation of impact on daily living (chapter 11), a Facebook
cohort is used in which Dutch patients were present, which were also registered with the PALGA
search. This overlap of patients in the cohort studies could have influenced the results. However,
since each study had a unique research question to evaluate different aspects of the disease, this
influence is considered minimal.
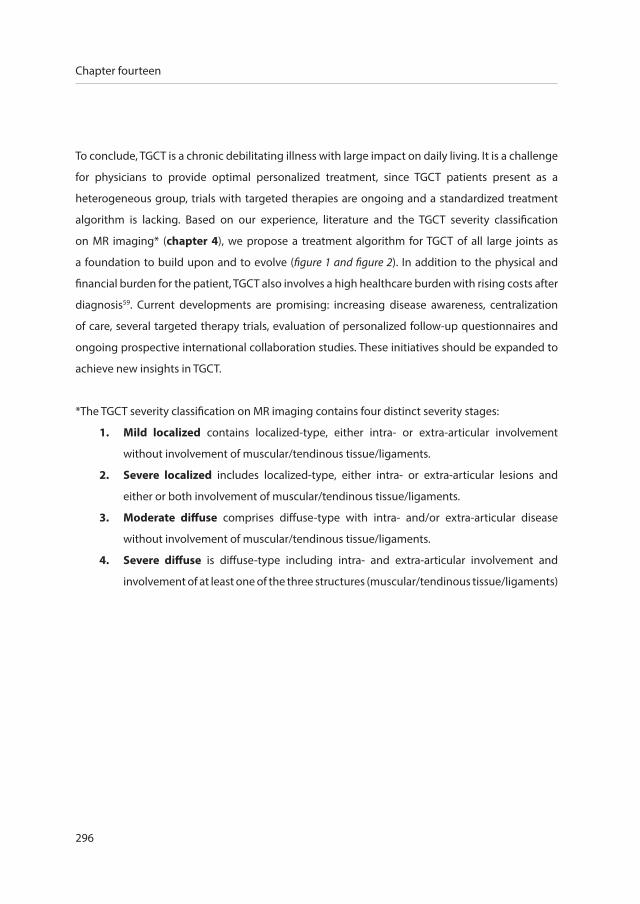
296
Chapter fourteen
To conclude, TGCT is a chronic debilitating illness with large impact on daily living. It is a challenge
for physicians to provide optimal personalized treatment, since TGCT patients present as a
heterogeneous group, trials with targeted therapies are ongoing and a standardized treatment
algorithm is lacking. Based on our experience, literature and the TGCT severity classification
on MR imaging* (chapter 4), we propose a treatment algorithm for TGCT of all large joints as
a foundation to build upon and to evolve (figure 1 and figure 2). In addition to the physical and
financial burden for the patient, TGCT also involves a high healthcare burden with rising costs after
diagnosis59. Current developments are promising: increasing disease awareness, centralization
of care, several targeted therapy trials, evaluation of personalized follow-up questionnaires and
ongoing prospective international collaboration studies. These initiatives should be expanded to
achieve new insights in TGCT.
*The TGCT severity classification on MR imaging contains four distinct severity stages:
1. Mild localized contains localized-type, either intra- or extra-articular involvement
without involvement of muscular/tendinous tissue/ligaments.
2. Severe localized includes localized-type, either intra- or extra-articular lesions and
either or both involvement of muscular/tendinous tissue/ligaments.
3. Moderate diffuse comprises diffuse-type with intra- and/or extra-articular disease
without involvement of muscular/tendinous tissue/ligaments.
4. Severe diffuse is diffuse-type including intra- and extra-articular involvement and
involvement of at least one of the three structures (muscular/tendinous tissue/ligaments)

General discussion & Future perspectives
297
14
Future perspectives
1. Translational research
The driver mechanism in TGCT tumour formation seems to be over-expression of CSF1. Only
a minority (2-16%) of cells in the tumorous tissue harbour the CSF1 rearrangement4, 5. Despite
the few tumour cells, they disrupt the entire surrounding area in different degrees of extent. We
expect the neoplastic cell to be a synovial like mononuclear cell, as was proposed by West et
al.4 They reported that CSF1 expressing cells also express CD68, without CD163 co-expression,
and therefore expect CSF1 expressing neoplastic cells to be derived from synovial-lining cells.
Identification of this neoplastic cell could attribute in investigations of new treatment modalities.
Dynamic contrast-enhanced MR imaging and histopathology research revealed high vascularization
in both localized- and diffuse-TGCT, showing marked enhancement on T1-weighted images with
a delayed wash-out60, 61. Angiogenesis is induced by CSF1 through vascular endothelial growth
factor (VEGF)62. Formation of blood vessels is fundamental for tumour development. A possible
therapeutic target would be to control this increased vascularity by inhibiting VEGF, for example
with Bevacizumab (Avastin)63.
2. Individually tailored treatment
It is unclear whether curation of diffuse-TGCT is possible at present, since residual tumour cells
(micro- R1 or macroscopically R2) remain after surgical resection, optimal targeted therapy is
under investigation and treatment with other therapies is inconclusive. A common question
arises: is wait and see or conservative treatment justified in the locally aggressive diffuse-TGCT?
Forthcoming research should provide answers on degree of joint destruction and (impaired)
health-related quality of life in a wait and see or conservative treatment course.
Currently, data on tumour progression after quitting targeted therapy treatment is lacking. Future
investigations should focus hereon. Also, several experimental studies with targeted therapy can
be thought of, for example investigation of intermittent use (drug holidays), the possibility of intra-
articular injection and the option of isolated limb perfusion with CSF1 blockers/inhibitors.
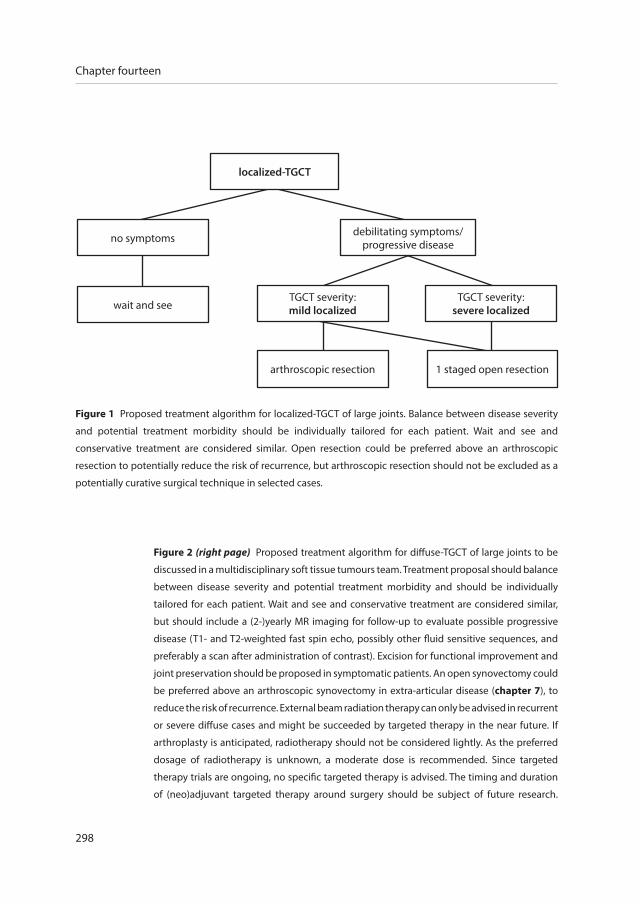
298
Chapter fourteen
Figure 2 (right page) Proposed treatment algorithm for diffuse-TGCT of large joints to be
discussed in a multidisciplinary soft tissue tumours team. Treatment proposal should balance
between disease severity and potential treatment morbidity and should be individually
tailored for each patient. Wait and see and conservative treatment are considered similar,
but should include a (2-)yearly MR imaging for follow-up to evaluate possible progressive
disease (T1- and T2-weighted fast spin echo, possibly other fluid sensitive sequences, and
preferably a scan after administration of contrast). Excision for functional improvement and
joint preservation should be proposed in symptomatic patients. An open synovectomy could
be preferred above an arthroscopic synovectomy in extra-articular disease (chapter 7), to
reduce the risk of recurrence. External beam radiation therapy can only be advised in recurrent
or severe diffuse cases and might be succeeded by targeted therapy in the near future. If
arthroplasty is anticipated, radiotherapy should not be considered lightly. As the preferred
dosage of radiotherapy is unknown, a moderate dose is recommended. Since targeted
therapy trials are ongoing, no specific targeted therapy is advised. The timing and duration
of (neo)adjuvant targeted therapy around surgery should be subject of future research.
Figure 1 Proposed treatment algorithm for localized-TGCT of large joints. Balance between disease severity
and potential treatment morbidity should be individually tailored for each patient. Wait and see and
conservative treatment are considered similar. Open resection could be preferred above an arthroscopic
resection to potentially reduce the risk of recurrence, but arthroscopic resection should not be excluded as a
potentially curative surgical technique in selected cases.
no symptoms
wait and seeTGCT severity:
severe localizedTGCT severity:mild localized
arthroscopic resection 1 staged open resection
localized-TGCT
debilitating symptoms/progressive disease
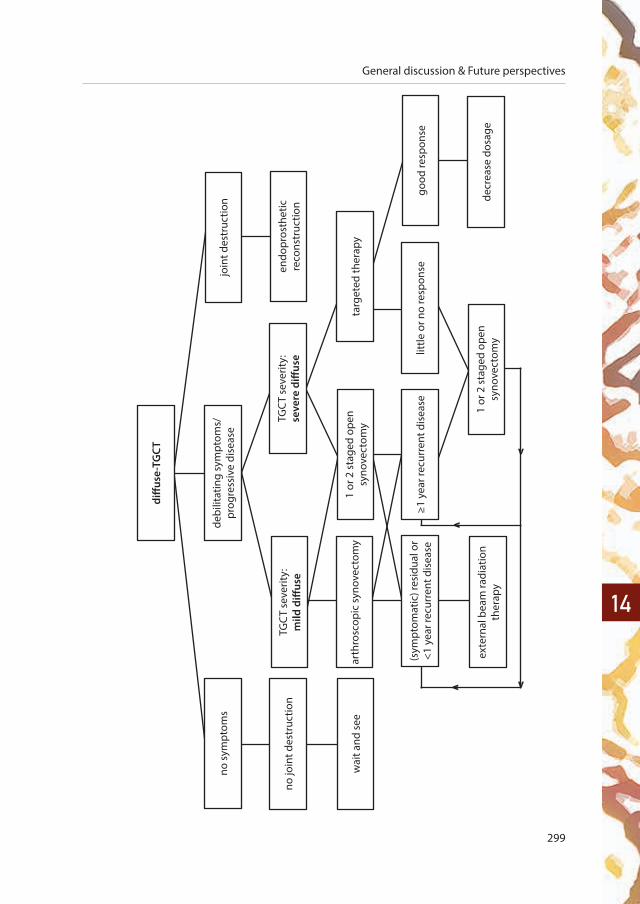
General discussion & Future perspectives
299
14
v
v
vv
diff
use-
TGCT
no s
ympt
oms
wai
t and
see
no jo
int d
estr
uctio
nTG
CT
seve
rity:
mild
diff
use
TGC
T se
verit
y:se
vere
diff
use
debi
litat
ing
sym
ptom
s/pr
ogre
ssiv
e di
seas
ejo
int d
estr
uctio
n
endo
pros
thet
ic
reco
nstr
uctio
n
arth
rosc
opic
syn
ovec
tom
yta
rget
ed th
erap
y1
or 2
sta
ged
open
sy
nove
ctom
y
(sym
ptom
atic
) res
idua
l or
<1 y
ear r
ecur
rent
dis
ease
exte
rnal
bea
m ra
diat
ion
ther
apy
1 or
2 s
tage
d op
en
syno
vect
omy
little
or n
o re
spon
sego
od re
spon
se
decr
ease
dos
age
≥1 y
ear r
ecur
rent
dis
ease

300
Chapter fourteen
Future treatment studies should combine current knowledge into new studies to improve
treatment modalities. Recurrent disease, (short- and long-term) complications, health-related
quality of life and joint function should be evaluated as outcome. Patients could be stratified by the
TGCT severity classification (chapter 4), that may be improved by using biological differentiation
using next generation sequencing or new MR imaging techniques. In a prospective cohort study,
several different treatment groups could be evaluated and compared:
Wait and see/conservative treatment in case of mild symptoms
Surgical treatment (open versus arthroscopic resection, one versus two-staged
synovectomy)
Neoadjuvant targeted therapy + surgical treatment
Surgical treatment + adjuvant targeted therapy
Neoadjuvant external beam radiation + surgical treatment
Surgical treatment + adjuvant external beam radiation
The intervention at group level could be implemented in stages, by use of the stepped wedge
cluster design46. Best modality to monitor response of tumour activity is yet to be established.
There might also be a role for dynamic contrast-enhanced MR imaging or fluorodeoxyglucose-
positron emission tomography (FDG-PET), as TGCT shows high FDG update64.
Evaluation of different treatment modalities, patient characteristics, disease severity and biological
behaviour could result in a prediction model. This prediction model should predict individual risk
profiles, that can then be linked to recommended treatment strategies and should take patient
characteristics, affected joint, volume of disease, disease extent, performed treatment(s) and
possibly histopathologic or genetic features into account.
3. Centralized treatment in a multidisciplinary team
The current trend in rare diseases is centralization of treatment that necessitates (highly) specialized
expertise. Diffuse-TGCT treatment should sail along this trend. In addition, centralization of diffuse-
TGCT treatment could be realized by creating more public awareness and easy available reliable
information.

General discussion & Future perspectives
301
14
4. Patient-centred outcome measures
For future self-reported outcome evaluations in TGCT, the CAT method by use of the PROMIS item
bank could be used. Preferably in the form of an easy accessible application on a mobile device. A
new feature could be to not only link the application to the electronic patient dossier, but to also
provide feedback to each individual patient personally, on how they are performing in the field of
physical, mental and social health compared with themselves at specified time periods previously.
As TGCT is known with recurrent disease developing years after initial surgical treatment, patients
are more likely to continue completing questionnaires if they are short and simple.
302
Chapter fourteen
references
1. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, diffuse type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 52013. p. 102-3.
2. de St. Aubain S, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM BJ, Hogendoorn PCW,
Mertens F, editor. WHO Classification of Tumours of Soft Tissue and Bone. 5. 4 ed2013. p. 100-1.
3. Patel KH, Gikas PD, Pollock RC, Carrington RW, Cannon SR, Skinner JA, et al. Pigmented villonodular synovitis of the knee:
A retrospective analysis of 214 cases at a UK tertiary referral centre. Knee. 2017;24(4):808-15.
4. West RB, Rubin BP, Miller MA, Subramanian S, Kaygusuz G, Montgomery K, et al. A landscape effect in tenosynovial giant-
cell tumor from activation of CSF1 expression by a translocation in a minority of tumor cells. Proc Natl Acad Sci U S A.
2006;103(3):690-5.
5. Cupp JS, Miller MA, Montgomery KD, Nielsen TO, O’Connell JX, Huntsman D, et al. Translocation and expression of CSF1
in pigmented villonodular synovitis, tenosynovial giant cell tumor, rheumatoid arthritis and other reactive synovitides.
The American journal of surgical pathology. 2007;31(6):970-6.
6. Poletti SC, Gates HS, 3rd, Martinez SM, Richardson WJ. The use of magnetic resonance imaging in the diagnosis of
pigmented villonodular synovitis. Orthopedics. 1990;13(2):185-90.
7. Hughes TH, Sartoris DJ, Schweitzer ME, Resnick DL. Pigmented villonodular synovitis: MRI characteristics. Skeletal
radiology. 1995;24(1):7-12.
8. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis:
radiologic-pathologic correlation. Radiographics. 2008;28(5):1493-518.
9. Nordemar D, Oberg J, Brosjo O, Skorpil M. Intra-Articular Synovial Sarcomas: Incidence and Differentiating Features from
Localized Pigmented Villonodular Synovitis. Sarcoma. 2015;2015:903873.
10. Wang C, Song RR, Kuang PD, Wang LH, Zhang MM. Giant cell tumor of the tendon sheath: Magnetic resonance imaging
findings in 38 patients. Oncology letters. 2017;13(6):4459-62.
11. van der Heijden L, Gibbons CL, Hassan AB, Kroep JR, Gelderblom H, van Rijswijk CS, et al. A multidisciplinary approach to
giant cell tumors of tendon sheath and synovium--a critical appraisal of literature and treatment proposal. J Surg Oncol.
2013;107(4):433-45.
12. Schwartz HS, Unni KK, Pritchard DJ. Pigmented villonodular synovitis. A retrospective review of affected large joints. Clin
Orthop Relat Res. 1989(247):243-55.
13. Ogilvie-Harris DJ, McLean J, Zarnett ME. Pigmented villonodular synovitis of the knee. The results of total arthroscopic
synovectomy, partial, arthroscopic synovectomy, and arthroscopic local excision. J Bone Joint Surg Am. 1992;74(1):119-23.
14. Palmerini E, Staals EL, Maki RG, Pengo S, Cioffi A, Gambarotti M, et al. Tenosynovial giant cell tumour/pigmented
villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210-7.
15. Chin KR, Barr SJ, Winalski C, Zurakowski D, Brick GW. Treatment of advanced primary and recurrent diffuse pigmented
villonodular synovitis of the knee. J Bone Joint Surg Am. 2002;84-A(12):2192-202.
16. De Ponti A, Sansone V, Malchere M. Result of arthroscopic treatment of pigmented villonodular synovitis of the knee.
Arthroscopy. 2003;19(6):602-7.
17. Jain JK, Vidyasagar JV, Sagar R, Patel H, Chetan ML, Bajaj A. Arthroscopic synovectomy in pigmented villonodular
synovitis of the knee: clinical series and outcome. Int Orthop. 2013;37(12):2363-9.
18. de Carvalho LH, Jr., Soares LF, Goncalves MB, Temponi EF, de Melo Silva O, Jr. Long-term success in the treatment of
diffuse pigmented villonodular synovitis of the knee with subtotal synovectomy and radiotherapy. Arthroscopy.
2012;28(9):1271-4.
General discussion & Future perspectives
303
14
19. Kubat O, Mahnik A, Smoljanovic T, Bojanic I. Arthroscopic treatment of localized and diffuse pigmented villonodular
synovitis of the knee. Collegium antropologicum. 2010;34(4):1467-72.
20. Loriaut P, Djian P, Boyer T, Bonvarlet JP, Delin C, Makridis KG. Arthroscopic treatment of localized pigmented villonodular
synovitis of the knee. Knee Surg Sports Traumatol Arthrosc. 2012;20(8):1550-3.
21. Rhee PC, Sassoon AA, Sayeed SA, Stuart MS, Dahm DL. Arthroscopic treatment of localized pigmented villonodular
synovitis: long-term functional results. American journal of orthopedics. 2010;39(9):E90-4.
22. Noailles T, Brulefert K, Briand S, Longis PM, Andrieu K, Chalopin A, et al. Giant cell tumor of tendon sheath: Open surgery
or arthroscopic synovectomy? A systematic review of the literature. Orthop Traumatol Surg Res. 2017;103(5):809-14.
23. Verspoor FG, van der Geest IC, Vegt E, Veth RP, van der Graaf WT, Schreuder HW. Pigmented villonodular synovitis: current
concepts about diagnosis and management. Future oncology. 2013;9(10):1515-31.
24. Blanco CE, Leon HO, Guthrie TB. Combined partial arthroscopic synovectomy and radiation therapy for diffuse pigmented
villonodular synovitis of the knee. Arthroscopy. 2001;17(5):527-31.
25. Mollon B, Griffin AM, Ferguson PC, Wunder JS, Theodoropoulos J. Combined arthroscopic and open synovectomy for
diffuse pigmented villonodular synovitis of the knee. Knee Surg Sports Traumatol Arthrosc. 2016;24(1):260-6.
26. Chin KR, Brick GW. Extraarticular pigmented villonodular synovitis: a cause for failed knee arthroscopy. Clin Orthop Relat
Res. 2002(404):330-8.
27. Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM. Surgical treatment of diffuse pigmented
villonodular synovitis of the knee. Clin Orthop Relat Res. 1994(300):183-92.
28. Sharma V, Cheng EY. Outcomes after excision of pigmented villonodular synovitis of the knee. Clin Orthop Relat Res.
2009;467(11):2852-8.
29. van der Heijden L, Mastboom MJ, Dijkstra PD, van de Sande MA. Functional outcome and quality of life after the surgical
treatment for diffuse-type giant-cell tumour around the knee: a retrospective analysis of 30 patients. Bone Joint J.
2014;96-B(8):1111-8.
30. Colman MW, Ye J, Weiss KR, Goodman MA, McGough RL, 3rd. Does combined open and arthroscopic synovectomy for
diffuse PVNS of the knee improve recurrence rates? Clin Orthop Relat Res. 2013;471(3):883-90.
31. Verspoor FG, Hannink G, Scholte A, Van Der Geest IC, Schreuder HW. Arthroplasty for tenosynovial giant cell tumors. Acta
orthopaedica. 2016;87(5):497-503.
32. Hamlin BR, Duffy GP, Trousdale RT, Morrey BF. Total knee arthroplasty in patients who have pigmented villonodular
synovitis. J Bone Joint Surg Am. 1998;80(1):76-82.
33. Heyd R, Seegenschmiedt MH, Micke O. The role of external beam radiation therapy in the adjuvant treatment of
pigmented villonodular synovitis. Zeitschrift fur Orthopadie und Unfallchirurgie. 2011;149(6):677-82.
34. Mollon B, Lee A, Busse JW, Griffin AM, Ferguson PC, Wunder JS, et al. The effect of surgical synovectomy and radiotherapy
on the rate of recurrence of pigmented villonodular synovitis of the knee: an individual patient meta-analysis. Bone Joint
J. 2015;97-B(4):550-7.
35. Griffin AM, Ferguson PC, Catton CN, Chung PW, White LM, Wunder JS, et al. Long-term outcome of the treatment of
high-risk tenosynovial giant cell tumor/pigmented villonodular synovitis with radiotherapy and surgery. Cancer.
2012;118(19):4901-9.
36. Gortzak Y, Vitenberg M, Frenkel Rutenberg T, Kollender Y, Dadia S, Sternheim A, et al. Inconclusive benefit of adjuvant
(90)Yttrium hydroxyapatite to radiosynovectomy for diffuse-type tenosynovial giant-cell tumour of the knee. Bone Joint
J. 2018;100-B(7):984-8.

304
Chapter fourteen
37. Verspoor FG, Scholte A, van der Geest IC, Hannink G, Schreuder HW. Cryosurgery as Additional Treatment in Tenosynovial
Giant Cell Tumors. Sarcoma. 2016;2016:3072135.
38. Mohler DG, Kessler BD. Open synovectomy with cryosurgical adjuvant for treatment of diffuse pigmented villonodular
synovitis of the knee. Bulletin. 2000;59(2):99-105.
39. Bickels J, Isaakov J, Kollender Y, Meller I. Unacceptable complications following intra-articular injection of yttrium 90 in
the ankle joint for diffuse pigmented villonodular synovitis. J Bone Joint Surg Am. 2008;90(2):326-8.
40. Gelderblom H, Cropet C, Chevreau C, Boyle R, Tattersall M, Stacchiotti S, et al. Nilotinib in locally advanced pigmented
villonodular synovitis: a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2018.
41. Tap WD, Gelderblom H, Stacchiotti S, Palmerini E, Ferrari S, Desai J, et al. Final results of ENLIVEN: A global, double-blind,
randomized, placebo-controlled, phase 3 study of pexidartinib in advanced tenosynovial giant cell tumor (TGCT). ASCO
conference 2018.
42. Cassier PA, Italiano A, Gomez-Roca CA, Le Tourneau C, Toulmonde M, Cannarile MA, et al. CSF1R inhibition with
emactuzumab in locally advanced diffuse-type tenosynovial giant cell tumours of the soft tissue: a dose-escalation and
dose-expansion phase 1 study. Lancet Oncol. 2015;16(8):949-56.
43. Sankhala KK, Blay JY, Ganjoo KN, Italiano A, Hassan AB, Kim TM, et al. A phase I/II dose escalation and expansion study
of cabiralizumab (cabira; FPA-008), an anti-CSF1R antibody, in tenosynovial giant cell tumor (TGCT, diffuse pigmented
villonodular synovitis D-PVNS). ASCO conference 2017. 35 (15 Supplement 1).
44. Sistla R, J VSV, Afroz T. Malignant Pigmented Villonodular Synovitis-A Rare Entity. Journal of orthopaedic case reports.
2014;4(4):9-11.
45. Li CF, Wang JW, Huang WW, Hou CC, Chou SC, Eng HL, et al. Malignant diffuse-type tenosynovial giant cell tumors:
a series of 7 cases comparing with 24 benign lesions with review of the literature. The American journal of surgical
pathology. 2008;32(4):587-99.
46. Dekkers OM. The stepped wedge design. Nederlands tijdschrift voor geneeskunde. 2012;156(9):A4069.
47. Riley RD, Lambert PC, Abo-Zaid G. Meta-analysis of individual participant data: rationale, conduct, and reporting. Bmj.
2010;340:c221.
48. Gelhorn HL, Tong S, McQuarrie K, Vernon C, Hanlon J, Maclaine G, et al. Patient-reported Symptoms of Tenosynovial Giant
Cell Tumors. Clin Ther. 2016;38(4):778-93.
49. Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented Villonodular Synovitis: A Comprehensive Review
and Proposed Treatment Algorithm. JBJS Rev. 2016;4(7).
50. Tyler WK, Vidal AF, Williams RJ, Healey JH. Pigmented villonodular synovitis. The Journal of the American Academy of
Orthopaedic Surgeons. 2006;14(6):376-85.
51. Hufeland M, Gesslein M, Perka C, Schroder JH. Long-term outcome of pigmented villonodular synovitis of the hip after
joint preserving therapy. Arch Orthop Trauma Surg. 2017.
52. Gonzalez Della Valle A, Piccaluga F, Potter HG, Salvati EA, Pusso R. Pigmented villonodular synovitis of the hip: 2- to 23-
year followup study. Clin Orthop Relat Res. 2001(388):187-99.
53. Ogura K, Yasunaga H, Horiguchi H, Ohe K, Shinoda Y, Tanaka S, et al. Impact of hospital volume on postoperative
complications and in-hospital mortality after musculoskeletal tumor surgery: analysis of a national administrative
database. J Bone Joint Surg Am. 2013;95(18):1684-91.
54. van der Heijden L, Piner SR, van de Sande MA. Pigmented villonodular synovitis: a crowdsourcing study of two hundred
and seventy two patients. Int Orthop. 2016;40(12):2459-68.

General discussion & Future perspectives
305
14
55. Verspoor FG, Zee AA, Hannink G, van der Geest IC, Veth RP, Schreuder HW. Long-term follow-up results of primary and
recurrent pigmented villonodular synovitis. Rheumatology (Oxford). 2014;53(11):2063-70.
56. Hung M, Stuart AR, Higgins TF, Saltzman CL, Kubiak EN. Computerized Adaptive Testing Using the PROMIS Physical
Function Item Bank Reduces Test Burden With Less Ceiling Effects Compared With the Short Musculoskeletal Function
Assessment in Orthopaedic Trauma Patients. Journal of orthopaedic trauma. 2014;28(8):439-43.
57. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. Journal of the
American Geriatrics Society. 1991;39(2):142-8.
58. Demers C, McKelvie RS, Negassa A, Yusuf S, Investigators RPS. Reliability, validity, and responsiveness of the six-minute
walk test in patients with heart failure. American heart journal. 2001;142(4):698-703.
59. Burton T, Ye X, Parker E, Bancroft T, Healey JH. Burden of Illness in Patients With Tenosynovial Giant Cell Tumors. ISPOR
(International Society for Pharmacoeconomics and Outcomes Research) 22nd Annual International Meeting; Boston,
MA, USA2017.
60. Dale K, Smith HJ, Paus AC, Refsum SB. Dynamic MR-imaging in the diagnosis of pigmented villonodular synovitis of the
knee. Scandinavian journal of rheumatology. 2000;29(5):336-9.
61. Barile A, Sabatini M, Iannessi F, Di Cesare E, Splendiani A, Calvisi V, et al. Pigmented villonodular synovitis (PVNS) of the
knee joint: magnetic resonance imaging (MRI) using standard and dynamic paramagnetic contrast media. Report of 52
cases surgically and histologically controlled. La Radiologia medica. 2004;107(4):356-66.
62. Curry JM, Eubank TD, Roberts RD, Wang Y, Pore N, Maity A, et al. M-CSF signals through the MAPK/ERK pathway via Sp1
to induce VEGF production and induces angiogenesis in vivo. PloS one. 2008;3(10):e3405.
63. Nissen MJ, Boucher A, Brulhart L, Menetrey J, Gabay C. Efficacy of intra-articular bevacizumab for relapsing diffuse-type
giant cell tumour. Ann Rheum Dis. 2014;73(5):947-8.
64. Amber IB, Clark BJ, Greene GS. Pigmented villonodular synovitis: dedicated PET imaging findings. BMJ case reports.
2013;2013.

sam
enva
ttin
gch
apte
r fif
teen
summary in dutch
(nederlandse samenvatting)

308
Chapter fifteen
nederlandse samenvatting
Tenosynoviale reusceltumoren (tenosynovial giant cell tumours, TGCT) zijn zeldzame goedaardige
tumoren. Deze aandoening werd voorheen pigmented villonodular synovitis (PVNS) genoemd.
De tumoren ontstaan vanuit het synoviale membraan van een gewricht – het membraan
dat de gewrichtsvloeistof aanmaakt, vanuit de peesschede of de slijmbeurs. Een TGCT kan
gewrichtsklachten geven als pijn, zwelling, stijfheid of bewegingsbeperking in verschillende mate
van ernst. Hierdoor kan de tumor een hoge morbiditeit veroorzaken in een relatief jonge, werkende
populatie. Op grond van klinische en radiologische kenmerken worden twee typen onderscheiden:
het gelokaliseerde type dat zich uit als een goed afgrensbare nodus, en het diffuse type dat lokaal
invasief is. TGCT kan behandeld worden met een operatie, een medicijn in onderzoeksverband en
eventueel aanvullend radiotherapie. Het is nog niet bekend welke behandeling het meest effectief
is. Het vaststellen van de meest geschikte behandeling is uitdagend doordat de tumor zo zeldzaam
is, patiënten erg van elkaar verschillen en elke behandeling andere nadelen (bijwerkingen,
recidieven, complicaties) kent.
Het doel van dit proefschrift was de kennis te verbeteren van de pathofysiologie en het biologisch
gedrag van TGCT, van het diagnostisch proces bij deze aandoening en van de kwaliteit van leven
bij TGCT-patiënten, om betere behandelmethoden te vinden. Door bewustzijn te creëren en
publiciteit te genereren, wordt bijgedragen aan de verbetering van de medische behandeling
van TGCT. In dit proefschrift worden verscheidene kennishiaten gedicht op het gebied van de
incidentie, histopathologische en hormonale karakteristieken, stratificatie van ziekte-ernst en
ziektelast bij kinderen. Daarnaast zijn de langetermijneffecten van systemische doelgerichte
therapie en de kwaliteit van leven na chirurgische behandeling onderzocht. Tenslotte wordt in
dit proefschrift de grootst bekende, wereldwijde studie gepresenteerd met individuele data van
patiënten met gelokaliseerde of diffuse TGCT.
Actuele incidentieberekeningen zijn noodzakelijk voor het diagnostisch proces. In hoofdstuk
2 is het wereldwijde incidentiecijfer berekend voor TGCT in vingers en/of tenen, gelokaliseerde
TGCT van de grote gewrichten, en voor diffuse TGCT. De tot nu toe gehanteerde TGCT-incidentie,
gebaseerd op een provinciale Amerikaanse studie uit 1980, is 9,2 voor het gelokaliseerde type
(inclusief vingers en tenen), en 1,8 per miljoen persoonsjaren voor het diffuse type (Myers 1980).
Summary in Dutch
309
15
Door middel van het Pathologisch Anatomisch Landelijk Geautomatiseerd Archief (PALGA)
werden alle mogelijke TGCT-patiënten in Nederland geïdentificeerd, die in een periode van vijf
jaar waren gediagnosticeerd. De diagnose werd geverifieerd op basis van de klinische data in de
lokale ziekenhuizen. De Nederlandse incidentiecijfers zijn op basis van leeftijdsopbouw omgezet
naar wereldwijde incidentiecijfers. De hiermee berekende incidentie is voor TGCT van vingers en
tenen 29, voor het gelokaliseerde type van grote gewrichten 10, en voor het diffuse type 4 per
miljoen persoonsjaren. In alle drie de groepen waren vrouwen oververtegenwoordigd en was de
incidentie het hoogst in de leeftijdscategorie 40 tot 59 jaar. De knie was het vaakst aangedaan: bij
65% van de patiënten met gelokaliseerd type TGCT en bij 49% van de patiënten met diffuus type.
Het aantal heroperaties vanwege een lokaal recidief was 9% bij gelokaliseerde en 23% bij diffuse
TGCT. Vergeleken met de oorspronkelijke incidentiestudie uit Amerika, toont deze studie een 5 keer
verhoogde incidentie voor gelokaliseerde type (vingers, tenen en grote gewrichten gecombineerd)
en een 2,6 keer zo hoge incidentie voor diffuus type TGCT. Deze hogere incidentie zou verklaard
kunnen worden door onze landelijke dekking en vanwege groeiende bekendheid met de ziekte.
Het onderzoek beschreven in hoofdstuk 3 is gericht op de tegenstrijdigheid dat gelokaliseerd
en diffuus type TGCT klinisch en radiologisch verschillend zijn, maar histopathologisch niet
te onderscheiden zouden zijn. De belangrijkste stimulans voor tumorformatie in TGCT is
een overvloedige expressie van de Colony Stimulating Factor 1 (CSF1), veroorzaakt door een
genetische translocatie. Deze studie onderzocht of er een correlatie bestond tussen de expressie
en genetische herstructurering van CSF-1, en het biologisch gedrag en klinische uitkomst van
beide TGCT-subtypes – waarbij klinische uitkomst werd gedefinieerd als lokaal recidief. Langs
een continuüm van uitersten werden patiënten geselecteerd die niet eerder behandeld waren
voor TGCT van hun knie en een follow-up van minstens 3 jaar hadden. Negen patiënten met
gelokaliseerde (2 recidieven), 15 met diffuse TGCT (9 recidieven) en 4 patiënten met synovitis (als
controle) werden geïncludeerd. De gemiddelde leeftijd was 43 (spreiding 6-71) jaar en 56% was
vrouw. De combinatie van de technieken CSF1-split apart-FISH (fluorescence in situ hybridization)
na mRNA-in situ hybridization bleek een diagnostisch hulpmiddel. Hiermee werd in 76% van
de tumoren genetische herstructurering van CSF-1 gedetecteerd. Concluderend, er werd geen
duidelijk verband gevonden tussen CSF1-expressie en CSF1-herstructurering met biologisch
gedrag en klinische uitkomst.

310
Chapter fifteen
Binnen het gelokaliseerde en diffuse type TGCT bestaat een grote verscheidenheid in ziekte-ernst.
Daarom is in hoofdstuk 4 een classificatie ontwikkeld gebaseerd op ziekte-uitgebreidheid, om
te kunnen stratificeren tussen verschillende ziektestadia. Als eerste hebben experts parameters
gedefinieerd om de uitgebreidheid van ziekte te beschrijven op basis van een MRI scan. Vier
parameters kwamen vaker dan 20% voor op MRI, toonden goede overeenkomst binnen en tussen
beoordelaars (kappa ≥0.66) en toonden een positieve correlatie met een lokaal recidief: 1. het
TGCT-type, 2. betrokkenheid van het gewricht, 3. betrokkenheid van spier- of pees-weefsel; en
4. betrokkenheid van ligament(en). Vervolgens werd de TGCT severity classificatie voor grote
gewrichten geconstrueerd. Op basis van hazard ratio’s van de vier genoemde parameters,
aflopend van hoog naar laag, werd een classificatie met vier onderscheidende ziektestadia
gemaakt. De recidiefvrije overleving na 4 jaar (log rank p<0.0001) was 94% voor het mild localized-
stadium, 88% voor severe localized, 59% voor moderate diffuse en 36% voor het severe diffuse-
stadium. Met deze TGCT severity classificatie wordt zowel de arts als de patiënt geïnformeerd over
ziekte-uitgebreidheid en het risico op een eerste, lokaal recidief na chirurgische behandeling.
Deze classificatie kan bijdragen aan de identificatie van geschikte patiënten voor systemische
doelgerichte therapie of voor trials met nieuwe medicijnen. Daarnaast kan het toepassen van deze
classificatie, door de data meer objectiveerbaar te maken, de uitkomsten van wetenschappelijk
onderzoek naar TGCT vergelijkbaarder maken.
Patiënten rapporteren een toename van TGCT-gerelateerde klachten tijdens zwangerschap, zowel
bij polikliniekbezoeken als op online TGCT-patiëntenfora. Onze hypothese was dat dit veroorzaakt
wordt door veranderingen in vrouwelijke geslachtshormonen. Geslachtshormonen (oestrogeen
en progesteron) stijgen tijdens de zwangerschap. Hoofdstuk 5 beschrijft het eerste onderzoek
naar de invloed van vrouwelijke geslachtshormonen op symptomen van TGCT. Vijfenzestig procent
van de onderzochte zwangeren rapporteerden middels een vragenlijst een toename van TGCT-
gerelateerde symptomen, voornamelijk zwelling van het aangedane gewricht. De invloed van
geslachtspecifieke hormonen en van de vrouwelijke vruchtbare leeftijdsfasen werden beoordeeld
door het vergelijken van de recidiefvrije overleving tussen mannen en vrouwen, en tussen pre-
en postmenopauzale vrouwen. Er werd geen verschil gevonden in recidiefvrije overleving voor
geslacht (gelokaliseerd type TGCT (p=0.206 ≤50 jaar, p=0.935 >50 jaar; diffuse type (p=0.664 ≤50
jaar, p=0.140 >50 jaar)) en ook niet tussen pre- versus postmenopauzale vrouwen (gelokaliseerde

Summary in Dutch
311
15
type (p=0.106); diffuse type (p=0.666)). Dit resultaat maakt een causale relatie tussen vrouwelijke
geslachtshormonen en lokaal recidief erg onwaarschijnlijk. Daarnaast werd de oestrogeen- en
progesteronreceptor status onderzocht in TGCT-weefsel van zowel het diffuse als gelokaliseerde
type. Deze receptoren bleken afwezig. Dus ook op histopathologisch niveau werd geen verband
gevonden tussen toename van vrouwelijke hormonen en de toename van de TGCT-gerelateerde
klachten tijdens zwangerschap.
Medische publicaties over TGCT bij kinderen zijn zeldzaam: na onze systematische review blijkt
slechts over 76 kinderen met TGCT gepubliceerd te zijn. In hoofdstuk 6 worden de klinische
kenmerken en beloop van TGCT bij kinderen vergeleken met die bij volwassenen. Daarnaast wordt
de incidentie op de kinderleeftijd berekend. De gestandaardiseerde pediatrische TGCT-incidentie
van grote gewrichten was 2,42 en 1,09 per miljoen persoonsjaren in respectievelijk gelokaliseerde
en diffuse TGCT. In vier tertiaire sarcoom-centra in Nederland zijn 57 kinderen gediagnosticeerd
en behandeld tussen 1995 en 2001. Gerapporteerde symptomen waren pijn, zwelling en beperkte
bewegingsuitslag met een mediane duur van symptomen van 12 (range 1-72) maanden. Er
was geen verschil tussen kinderen en volwassenen ten aanzien van geslacht, symptomen voor
diagnose, gelokaliseerde of diffuse type, eerste behandeling, percentage lokaal recidief, follow-
upstatus of follow-upduur. De 2.5 jaar recidiefvrije overleving na open resectie was vergelijkbaar
tussen kinderen en volwassenen: respectievelijk 85% (95%CI 67%-100%) versus 89% (95%CI 83%-
96%) bij het gelokaliseerde type (p=0.527) en respectievelijk 53% (95%CI 35%-79%) versus 56%
(95%CI 49%-64%) bij het diffuse type (p=0.691). Ondanks de lage pediatrische incidentie zou TGCT
in de differentiaaldiagnose moeten staan bij kinderen met langdurige zwelling van één gewricht.
De kans op recidief-ziekte na chirurgische behandeling van deze aandoening is vergelijkbaar voor
kinderen en volwassenen.
In hoofdstuk 7 en hoofdstuk 8 wordt de tot nu toe grootste serie patiënten beschreven met
gelokaliseerd of diffuus type TGCT. Er werden 2169 patiënten geïncludeerd (941 gelokaliseerd,
1192 diffuus en 36 onbekend type) met histologisch bewezen TGCT van grote gewrichten,
behandeld tussen 1990 en 2017 in één van de 31 deelnemende internationale sarcoomcentra.
Van de patiënten met gelokaliseerd type TGCT (hoofdstuk 7) was 62% vrouw, met een mediane
leeftijd tijdens eerste behandeling van 39 jaar, en een mediane follow-up van 37 maanden. De

312
Chapter fifteen
knie was aangedaan in 67% en de initiële behandeling in een tertiair centrum was open resectie
in 71% van de patiënten. In totaal kreeg 13% van de patiënten een recidief, met een recidiefvrije
overleving op 3, 5 en 10 jaar van respectievelijk 88%, 83% en 79%. De grootste risicofactor voor
een lokaal recidief was het hebben van een eerder recidief (p<0.001). In 4% van alle chirurgisch
behandelde patiënten met gelokaliseerde TGCT werd een complicatie geregistreerd. Initiële
symptomen van pijn en zwelling verbeterden na chirurgische behandeling bij respectievelijk 71%
en 85% van de patiënten. Wanneer alleen niet eerder behandelde patiënten werden geïncludeerd,
werd een positieve associatie gevonden met een lokaal recidief bij een tumor grootte ≥5 cm (versus
<5cm [HR 2.50(95%CI 1.32-4.74;p=0.005)]) en na behandeling met arthroscopie (versus open
[HR 2.18(95%CI0.98-4.84;p=0.056)]). Deze associatie bleek zowel uit univariate als multivariate
analyses. Het relatief lage complicatierisico en de goede functionele uitkomsten ondersteunen de
keuze voor een open, complete resectie bij patiënten met een gelokaliseerde TGCT en een hoog
risico op recidieven, met als doel recidiefpercentages verder te verlagen.
Van de patiënten met een diffuus type TGCT (hoofdstuk 8) was 58% vrouw, met een mediane
leeftijd van 35 jaar en een mediane follow-up van 54 maanden. Het kniegewricht was aangedaan
in 64%; en 53% van de patiënten onderging als initiële behandeling een one-staged open
synovectomie in een tertiair centrum. In totaal kreeg 45% van de patiënten een lokaal recidief,
met een recidiefvrije overleving op 3, 5 en 10 jaar van respectievelijk 62%, 55% en 40%. Het
eerder hebben gehad van een recidief bleek de grootste risicofactor voor recidief van de ziekte
(HR 3.5 95%CI 2.8-4.4, p<0.001), met een 5 jaar recidiefvrije overleving van 64% in niet eerder
behandelde patiënten, vergeleken met 25% bij patiënten die elders behandeld waren en met een
recidief naar een tertiair centrum werden verwezen. 12% van de patiënten had een complicatie
als gevolg van de chirurgische behandeling. Initiële symptomen van pijn en zwelling verbeterden
na operatie bij respectievelijk 59% en 72% van de patiënten. In een subgroepanalyse van niet
eerder behandelde patiënten met TGCT in de knie, behandeld in een tertiair centrum, werd geen
verband gevonden tussen het optreden van een lokaal recidief en de volgende factoren: geslacht,
leeftijd (jonger dan 35 jaar of 35 en ouder) bot-betrokkenheid (wel of niet), chirurgische techniek
(open of arthroscopisch) en tumor grootte (kleiner dan 5cm of 5cm en groter). Onze conclusie
is dat een op zichzelf staande chirurgische behandeling niet langer de gouden standaard moet
zijn, gezien het relatief hoge complicatierisico en het zeer hoge recidiefrisico, zeker in dit tijdperk

Summary in Dutch
313
15
van multimodale therapieën. De onmogelijkheid van het uitvoeren van een radicale resectie van
diffuse TGCT, verklaart waarschijnlijk het onacceptabel hoge recidief percentage na zowel open als
arthroscopische resectie, zelfs in gespecialiseerde centra.
Hoofdstuk 9 beschrijft de lange termijneffecten van het gebruik van imatinib mesylaat, een niet-
selectieve CSF1-remmer, bij patiënten met diffuus type TGCT. In totaal 62 patiënten uit 12 centra
in Europa, Australië en de Verenigde Staten van Amerika gebruikten imatinib als behandeling. In
deze groep waren 39 patiënten vrouw (63%), met een mediane leeftijd van 45 jaar ten tijde van de
start van de behandeling en een mediane duur vanaf diagnose tot start van de behandeling van
3,5 jaar. De mediane follow-up vanaf start van de behandeling was 52 maanden. Vier patiënten
met metastasen van TGCT werden geëxcludeerd uit de analyses wegens ernstige ziekteprogressie,
ondanks behandeling met imatinib. Van de overgebleven 58 patiënten bereikten 17 gehele of
gedeeltelijke respons (29%). De progressievrije overleving van de gehele groep na 1 en 5 jaar
waren respectievelijk 71% en 48%. 38 patiënten stopten met gebruik van imatinib na 7 maanden
(66%). Gerapporteerde bijwerkingen in 45 (78%) patiënten waren voornamelijk graad 1-2 (89%)
(zoals oedeem (48%) en moeheid (50%)). Vijf patiënten ervaarden graad 3-4 toxiciteit, inclusief
neutropenie, acute hepatitis, gezichtsoedeem, huidtoxiciteit en moeheid.
Deze studie bevestigt de werkzaamheid van een tyrosinekinaseremmer zoals imatinib in
TGCT. Zelfs na staking van de behandeling werd effect gezien, echter met hoge percentages
behandelonderbrekingen en additionele behandelingen (zoals operaties). Deze resultaten geven
richting aan het effect van imatinib, met als beperking het retrospectieve studie karakter, het
ontbreken van een controlegroep en het ontbreken van patiëntgerapporteerde uitkomstmaten.
Hoofdstuk 10 beschrijft een prospectieve cohortstudie naar gewrichtsfunctie en
gezondheidgerelateerde kwaliteit van leven-uitkomsten na chirurgische behandeling, om de
patiëntgerapporteerde uitkomstmaten te evalueren. In totaal 206 opeenvolgende patiënten
met gelokaliseerd (N=108) en diffuus type (N=98) TGCT van grote gewrichten, behandeld met
arthroscopische of open synovectomie in het Leids Universitair Medisch Centrum of Radboud
Universitair Medisch Centrum, werden geïncludeerd. Patiënten rapporteerden middels het
Short Form 36 (SF-36), de Visual Analogue Scale (VAS) en de Western Ontario and McMaster
Universities Osteoarthritis Index (WOMAC). Bij zowel gelokaliseerde als diffuse TGCT scoorden

314
Chapter fifteen
de patiënten vooral op de fysieke component van de SF-36-subschalen significant en klinisch
relevant slechter pre-operatief en direct postoperatief vergeleken met de algemene bevolking.
Zes maanden na chirurgische behandeling verbeterden de SF-36 scores naar de gemiddelden
van de algemene populatie; deze bleven de volgende jaren tamelijk stabiel. Mediane pijnscores,
gemeten middels de VAS, vertoonden geen klinisch relevant verschil pre- of postoperatief, in geen
van beide subtypes. Pijnbeleving verschilde enorm tussen patiënten en in de tijd. Gemiddelde
functiescores (WOMAC) vertoonden in beide subtypes geen klinisch relevant verschil (effect size
< MCID 20) pre- versus postoperatief. Echter, bij diffuse TGCT-patiënten toonden pijnscores en
fysieke functiescores uit de WOMAC een trend richting verbetering pre- versus postoperatieve
scores. Op alle drie de onderzochte schalen rapporteerden patiënten een significant betere
gezondheidgerelateerde kwaliteit van leven na chirurgie voor hun TGCT, en een trend richting
verbetering van gewrichtsfunctie.
In de grootst bekende TGCT-patiënten groep werd in hoofdstuk 11 de impact van TGCT op het
dagelijks leven onderzocht. De volgende aspecten werden geëvalueerd: fysieke functie, dagelijkse
activiteiten, sociale participatie (werk, sport en hobby’s) en gezondheidgerelateerde kwaliteit
van leven. Een tweede doel was het definiëren van risicofactoren voor verslechterde uitkomsten
bij TGCT, door middel van vier gevalideerde vragenlijsten: VAS worst pain and stiffness; Patient
Reported Outcomes Measurement Information System for Physical Function (PROMIS-PF); SF-12
en EuroQoL (EQ-5D-5L). Gedurende zes maanden werden TGCT-patiënten uitgenodigd om de
online vragenlijsten in te vullen. Patiënten werden verzocht om histologisch of radiologisch bewijs
van TGCT te delen om ziekteaanwezigheid en TGCT-subtype te bevestigen. In totaal werden 337
vragenlijsten volledig ingevuld (32% met ziektebevestiging), door patiënten afkomstig uit 30
landen. De mediane leeftijd tijdens de diagnose was 33 (IQR 25-42) jaar, en de meerderheid was
vrouw (80%) en had een tumor van het diffuse type (70%) in een van de onderste ledematen: knie
(71%) en heup (10%). Het recidiefpercentage was 36% bij gelokaliseerde en 70% bij diffuse TGCT,
van in totaal 299 patiënten met TGCT in een onderste extremiteit. Ruim 1 op de 10 patiënten was
door de TGCT niet in staat om zijn of haar werk (volledig) uit te voeren (gelokaliseerde 13%, diffuse
type 11%). Meer dan de helft van de patiënten was niet in staat om sportactiviteiten te beoefenen
(gelokaliseerde type 58%; diffuse type 64%). In beide subtypes verminderden pijn en zwelling na
een chirurgische behandeling, maar stijfheid en bewegingsbeperking namen toe. Littekenweefsel,

Summary in Dutch
315
15
kraakbeenslijtage en verklevingen, veroorzaakt door (meerdere) chirurgische behandelingen,
kunnen de toegenomen stijfheid en bewegingsbeperking verklaren. Vergeleken met de algemene
Amerikaanse bevolking toonden alle patiënten een klinisch relevant lagere PROMIS-PF-scores,
fysieke en mentale scores op de SF-12 en EQ-5D-5L-utiliteitscores. Wanneer het gelokaliseerde
en het diffuse type met elkaar vergeleken worden, scoorden patiënten met het diffuse type bijna
0,5 standaarddeviatie lager op de PROMIS-PF (p<0,001), en 5% lager op de EQ-5D-5L (p=0,03).
Bij patiënten met het gelokaliseerde type had de aanwezigheid van een recidief en 2 of meer
operaties een negatieve invloed op de pijn- en stijfheidscores op de VAS, fysieke scores op SF-12
en EQ-5D-5L-scores (p<0,05). In diffuse-type resulteerde recidief ziekte in lagere VAS-pijn/stijfheid,
PROMIS-PF, SF12 mentaal en EQ-5D-5L scores (p<0,05). In beide types scoorden patiënten met
behandeling korter dan 1 jaar geleden significant lager op de fysieke component van de SF-12.
Deze studie toont aan dat TGCT een grote impact heeft op het dagelijks leven in een relatief
jonge werkende patiëntenpopulatie. Artsen en andere betrokken zorgverleners, bijvoorbeeld
fysiotherapeuten, dienen zich ervan bewust te zijn dat TGCT-patiënten frequent een verminderde
kwaliteit van leven en beperkingen in hun fysiek functioneren ervaren en dat ze gehinderd blijven
in dagelijkse activiteiten zoals werk en sportactiviteiten, zelfs na behandeling(en).
Hoofdstuk 12 beschrijft een extreme, definitieve behandelingsmaatregel bij TGCT: een
bovenbeenamputatie. Bij diffuse TGCT is er zeer vaak sprake van recidieven (tot wel 92%
beschreven), die heroperaties en aanvullende behandelingen noodzakelijk maken. Als alle
behandelingen falen of ernstige complicaties optreden, kan amputatie onvermijdelijk zijn. Dit
hoofdstuk beschrijft vier ziektegeschiedenissen waarin een amputatie van het bovenbeen het
laatste redmiddel bleek.
Concluderend, TGCT is een chronische ziekte met een grote impact op het dagelijks leven. Voor
artsen is het uitdagend om de optimale gepersonaliseerde behandeling te bewerkstelligen, omdat
TGCT patiënten erg van elkaar verschillen, trials met doelgerichte therapie nog gaande zijn en er
geen gestandaardiseerd behandel algoritme bestaat. Als fundament en om verder te ontwikkelen
wordt een behandel algoritme voorgesteld voor TGCT van alle grote gewrichten in hoofdstuk
14. Dit algoritme is gebaseerd op onze ervaring, de literatuur en de TGCT severity classificatie op
MRI scans (hoofdstuk 4). Naast de fysieke en financiële last voor de patiënt zorgt TGCT ook voor
316
Chapter fifteen
stijgende medische kosten na diagnose. Huidige ontwikkelingen zijn veelbelovend: groeiend
bewustzijn, centralisatie van zorg, verscheidene doelgerichte therapie trials, evaluatie van
gepersonaliseerde follow-up vragenlijsten en lopende prospectieve internationale samenwerking
studies. Deze initiatieven moeten uitgebreid worden om nieuwe inzichten te krijgen in TGCT.
De discussie, klinische implicaties en toekomstperspectieven over het onderwerp van dit
proefschrift worden besproken in hoofdstuk 14.
Summary in Dutch
317
15


aPP
end
ices
chap
ter
sixt
een
320
Chapter sixteen
list of publications
Appendices
321
16
scientific articles
Outcome of surgical treatment for patients with diffuse-type Tenosynovial Giant Cell Tumours
M.J.L. Mastboom, E. Palmerini, F.G.M. Verspoor, A.J. Rueten-Budde, S. Stacchiotti, E. Staals, G.
Schaap, P.C. Jutte, W. Aston, H. Gelderblom, A. Leithner, D. Dammerer, A. Takeuchi, Q. Thio, X. Niu,
J.S. Wunder, TGCT study group & M.A.J. van de Sande
Submitted
Surgical treatment of localized-type Tenosynovial Giant Cell tumours of large joints
M.J.L. Mastboom, E. Staals, F.G.M. Verspoor, A.J. Rueten-Budde, S. Stacchiotti, E. Palmerini, G.
Schaap, P.C. Jutte, W. Aston, A. Leithner, D. Dammerer, A. Takeuchi, Q. Thio, X. Niu, J.S. Wunder, TGCT
study group & M.A.J. van de Sande
Submitted
Can increased symptoms of Tenosynovial Giant Cell Tumours during pregnancy be explained by a
change in female sex hormones?
M.J.L. Mastboom, F.G.M. Verspoor, R. Planje, H.W.B. Schreuder, M.A.J. van de Sande
Submitted
Long-term efficacy of imatinib mesylate in patients with advanced Tenosynovial Giant Cell Tumour
M.J.L. Mastboom*, F.G.M. Verspoor*, G. Hannink, R.G. Maki, A. Wagner, E. Bompas, J. Desai, A.
Italiano, B.M. Seddon, W.T.A. van der Graaf, J.Y. Blay, M. Brahmi, L. Eberst, S. Stacchiotti, O. Mir, M.A.J.
van de Sande, H. Gelderblom, P.A. Cassier (*Shared first authorship)
Submitted
Outcome after 52 Salto Ankle prostheses implanted by a single surgeon
F.W.M. Faber, M.J.L. Mastboom, S.T. van Vliet-Koppert, I.C.E. Bouman, P.M. van Kampen
Adv Orthopedics. 2018 Aug;2735634 doi: 10.1155/2018/2735634
322
Chapter sixteen
The effect of surgery in Tenosynovial Giant Cell Tumours as measured by patient reported
outcomes on quality of life and joint function
M.J.L. Mastboom*, F.G.M. Verspoor*, G. Hannink, W.T.A. van der Graaf, M.A.J. van de Sande, H.W.B.
Schreuder (*Shared first authorship)
Accepted in Bone Joint J
Does CSF1 over-expression or rearrangement influence biological behaviour in tenosynovial giant
cell tumours of the knee?
M.J.L. Mastboom, D.M. Hoek, J.V.M.G. Bovée, M.A.J. van de Sande, K. Szuhai
Histopathology. 2018 Aug; doi: 10.1111/his.13744
Severity classification of Tenosynovial Giant Cell Tumours on MR imaging
M.J.L. Mastboom*, F.G.M. Verspoor*, D.F. Hanff, M.G.J. Gademan, P.D.S. Dijkstra, H.W.B. Schreuder,
J.L. Bloem, R.J.P. van der Wal, M.A.J. van de Sande (*Shared first authorship)
Surg Oncol. 2018 Sept;27(3):544-550. doi.org/10.1016/j.suronc.2018.07.002
Incidence and Demographics of Giant Cell Tumor of Bone in The Netherlands: First Nationwide
Pathology Registry Study
A.J. Verschoor, J.V.M.G. Bovée, M.J.L. Mastboom, P.D.S. Dijkstra, M.A.J. van de Sande, H. Gelderblom
Acta Orthop. 2018 Jul 10:1-5. doi: 10.1080/17453674.2018.1490987
Tenosynovial Giant Cell Tumors in Children: A Similar Entity Compared With Adults
M.J.L. Mastboom, F.G.M. Verspoor, D. Uittenbogaard, G.R. Schaap, P.C. Jutte, H.W.B. Schreuder,
M.A.J. van de Sande
Clin Orthop Relat Res. 2018 Sept;476(9):1803-1812
The Patient Perspective on the Impact of Tenosynovial Giant Cell Tumors on Daily Living:
Crowdsourcing Study on Physical Function and Quality of Life.
M.J.L. Mastboom, R. Planje, M.A.J. van de Sande
Interact J Med Res. 2018 Feb 23. doi: 10.2196/ijmr.9325

Appendices
323
16
Treatments of Tenosynovial Giant Cell Tumors of the Temperomandibular joint -Report of three
cases and a review of literature
F.G.M. Verspoor, M.J.L. Mastboom, W.L.J. Weijs, A.C. Koetsveld, H.W.B. Schreuder, U. Flucke
Int J of Oral Maxillofac Surg. 2018 april doi.org/10.1016/j.ijom.2018.04.001
Higher incidence rates than previously known in tenosynovial giant cell tumors.
Mastboom M.J.L., Verspoor, F.G.M., Verschoor A.J., Uittenbogaard D., Nemeth B., Mastboom W.J.B.,
Bovée J.V.M.G., Dijkstra P.D.S., Schreuder H.W.B., Gelderblom H., Sande van de M.A.J., TGCT study group.
Acta Orthop. 2017 Aug 8:1-8. doi: 10.1080/17453674.2017.1361126
Limb Amputation after Multiple Treatments of Tenosynovial Giant Cell Tumour: Series of 4 Dutch Cases.
Mastboom M.J.L., Verspoor F.G.M., Gelderblom H., van de Sande M.A.J.
Case Rep Orthop 2017 Jun 28. doi: 10.1155/2017/7402570
Functional outcome and quality of life after the surgical treatment for diffuse-type giant-cell
tumour around the knee: a retrospective analysis of 30 patients.
van der Heijden L., Mastboom M.J.L., Dijkstra P.D.S., van de Sande M.A.J.
Bone Joint J 2014 Aug;96-B(8):1111-8. doi: 10.1302/0301-620X.96B8.33608
oral presentations
Tenosynovial Giant Cell Tumours: surgery or targeted therapy?
EMSOS 2018 Amsterdam, The Netherlands
Riskfactors in Tenosynovial Giant Cell Tumours
EMSOS 2018 Amsterdam, The Netherlands; BOOS 2018 Edinburgh, Scotland; MSTS 2018 NYC, USA;
CTOS 2018 Rome, Italy
Role of CSF1 in Tenosynovial Giant Cell Tumours
EMSOS 2018 Amsterdam, The Netherlands; BOOS 2018 Edinburgh, Schotland
324
Chapter sixteen
The patient perspective on the impact of Tenosynovial Giant Cell Tumors on daily living
EMSOS 2018 Amsterdam, The Netherlands
Severity classification of Tenosynovial Giant Cell Tumours on MR imaging
BOOS 2018 Edinburgh, Scotland; EMSOS 2017 Budapest, Hungary; CTOS 2017 Hawaii, USA
Tenosynovial Giant Cell Tumours affecting large joints in Children
ISOLS 2017 Kanazawa, Japan; EPOS 2018 Oslo, Norway
A nationwide study on Tenosynovial Giant Cell Tumours in the Netherlands
ISOLS 2017 Kanazawa, Japan; EMSOS 2017 Budapest, Hungary; NOV 2017 Den Bosch, The Netherlands
Preliminary results on the international multicenter retrospective Tenosynovial Giant Cell Tumour Study
EMSOS 2016 La Baule, France; MSTS 2016 Detroit, USA; CTOS 2016 Lisbon, Portugal
Tenosynovial Giant Cell Tumours Observational Platform Project (TOPP)
ESMO 2016 Copenhagen, Denmark
Heeft pre-operatief een 3T-MRI nut bij chronische polsklachten?
NOV 2015 Den Bosch, The Netherlands; scientific meeting LUMC, Leiden, The Netherlands
Functional outcome and quality of life after the surgical treatment for diffuse-type giant-cell tumours
ISOLS 2013, Bologna, Italy; ISCOMS 2013, Groningen, The Netherlands
Poster presentations
Prospective multicenter study in diffuse-type Tenosynovial Giant Cell Tumours
EMSOS 2018 Amsterdam, The Netherlands; ASCO 2018 Chicago, USA
Severity classification of Tenosynovial Giant Cell Tumours on MR imaging
MSTS 2018 NYS, USA
CSF1 over-expression and CSF1 split do not predict clinical outcome in Tenosynovial giant cell tumours
CTOS 2017 Hawaii, USA; MSTS 2018 NYC, USA; CTOS 2018 Rome, Italy
Appendices
325
16
The effect of Tenosynovial Giant Cell Tumours on daily living; an online cross-sectional analysis of
functionality and quality of life in 337 patients
CTOS 2017 Hawaii, USA
First results of the international multicenter retrospective Tenosynovial Giant Cell Tumour Study
ISOLS 2017 Kanazawa, Japan
Consider Tenosynovial Giant Cell Tumours in chronic mono-arthritis in children
EMSOS 2017 Budapest, Hungary
Limb amputation as a result of Tenosynovial Giant Cell Tumour
EMSOS 2016 La Baule, France
What is the use of 3T-MRI in chronic wrist complaints?
Haga scientific day and nurse evening 2015, The Hague + SEOHS 2015, Leiden, The Netherlands
Functional results and quality of life after open synovectomy for giant cell tumors of synovium in
the knee
CTOS 2013 New York City, USA + EMSOS 2013 Gothenburg, Sweden
awards and honors
Best Oral Talk award. BOOS Edinburgh, Schotland, 2018
Young Investigator award. CTOS Hawaii, USA, 2017
Nomination Best Paper award. ISOLS Kanazawa, Japan, 2017
Young Investigator award. MSTS Detroit, USA, 2016
326
Chapter sixteen
acknowledgements
Appendices
327
16
Met behulp van dit proefschrift hebben we een bijdrage kunnen leveren aan het verder ontrafelen
van de mysteriën omtrent een ongelooflijk interessant ziektebeeld: tenosynoviale reusceltumoren.
Veel dank aan alle nationale en internationale TGCT-patiënten die bereid zijn geweest hun
persoonlijke ervaringen te delen, zowel op de poli, als op Facebook, als via hun artsen.
Dankzij de hulp, de adviezen en het geduld van velen, is dit proefschrift tot stand gekomen.
Hiervoor wil ik onderstaande personen heel hartelijk bedanken:
Dr. M.A.J. van de Sande, ik voel me zeer vereerd om een van jouw eerste promovenda te mogen
zijn. Jouw enthousiasme werkt zo aanstekelijk dat ik in een mum van tijd een recordaantal
projecten was gestart, in samenwerking met verschillende afdelingen en ziekenhuizen. Gelukkig
heb ik het merendeel, mede dankzij jouw volhardendheid, weten af te ronden. Jouw talent voor
multi-tasken is bewonderenswaardig. Ik heb altijd kunnen rekenen op 100% toewijding en zeer
snelle feedback. Dankzij jou heb ik het belang van (internationale) samenwerking ingezien en écht
onderzoek leren doen. Bedankt voor de sturing en het vertrouwen en alle kansen in zowel binnen-
en buitenland.
Prof. Dr. P.D.S. Dijkstra, inspirerend hoe jij kliniek en wetenschap weet te combineren en hoe de
patiënt daarin altijd centraal staat. Bedankt voor je inzet en enthousiasme, de begeleiding van mijn
wetenschappelijke carrière, de kritische noot zo nodig, het mentorschap en de deur die altijd openstaat.
Prof. Dr. H. Gelderblom, bedankt voor de introductie in de medische oncologie. Door de vrijheid
en ruimte die ik kreeg, waarbij ik altijd binnen kon lopen voor een discussie, heb ik me verder
kunnen ontplooien.
Prof. Dr. R.G.H.H. Nelissen en stafleden orthopaedie, bedankt voor alle mogelijkheden en kansen
die ik heb gekregen op de afdeling orthopaedie, welke ik altijd graag met beide handen aangreep.
Prof. Dr. H.W.B. Schreuder, zonder de intensieve samenwerking met Nijmegen was dit boek niet
half zo mooi geworden. Door onze samenwerking kwamen er veel gedegen studie-initiatieven,
werden alle data verdubbeld, kritisch geëvalueerd en uiteindelijk afgerond middels een presentatie
en publicatie. Bedankt voor deze solide basis.

328
Chapter sixteen
Dr. F.G.M. Verspoor, dankzij onze power-samenwerking, duidelijke afspraken, heftige discussies
en zorgvuldige werken zijn onze beider proefschriften naar een hoger niveau gebracht. Tijdens
onze (langdurige) telefoongesprekken ontstonden altijd weer nieuwe initiatieven en ideeën of
juist oplossingen voor bestaande problemen. Samen hebben wij bijgedragen aan het verder
ontrafelen van deze interessante, soms ongrijpbare ziekte. Ik ben erg trots dat we dit samen
hebben gedaan!
Alle collaborating centers, co-auteurs in binnen- en buitenland: veel dank. Door gedegen
samenwerking wordt er steeds meer bekend over deze eerder zo ongrijpbare ziekte. Breaking borders!
Dear co-authors from all over the world, thank you for your collaboration in our national and
international studies: I greatly appreciate it.
Collegae van de C3 en later C2, zonder jullie relativeringsvermogen en humor was dit traject niet
zo bruisend geweest!
Medische studenten Daniël, Rosa, Willemijn, Femke en Marijn, jullie enthousiasme en frisse blik
hebben enorm bijgedragen aan dit proefschrift.
Secretaresses van de orthopaedie, Anika, Saskia en Marisa, altijd erg fijn dat jullie snel en
adequaat regelen wat er geregeld moest worden.
Maartje en Britta, mijn keuze voor jullie als mijn paranimfen was snel gemaakt. Sinds de
middelbare school zijn we een onafscheidelijk drietal, ook al zijn we soms duizenden kilometers
van elkaar verwijderd. Ik hou niet van verrassingen, alleen van die van jullie!
Masque en QQ, vooral ProzaQQ, bedankt voor de betrokkenheid en zeer welkome afleiding.
Lieve Gerritje en Marieke: de leuksten, dat blijven we!
Appendices
329
16
Marja en Romy, erg fijn om tegelijkertijd in ‘hetzelfde schuitje’ te zitten.
Lisanne, bedankt voor je niet aflatende interesse in mijn onderzoek en je inspirerende design
skills: ik ben heel trots op de omslag en lay-out van dit proefschrift. Voor ons is geen berg te hoog ;)
Hardloopbuddy’s, LUHV Currimus vooral Dave, Jan G, Jan vR, Bart en Chris, jullie geven me altijd
veel energie.
Mam, bedankt voor je geduld en dat je altijd naar mijn nog-net-niet-affe presentaties wilde
luisteren. Pap, bedankt voor je inhoudelijke discussies als ik vastgelopen was. Elvire, Bas, Daphne
en Joost, verstand op nul is het allerleukst met jullie.
Liefste Leander, mijn altijd aanwezige steun en toeverlaat, naar jou gaat de meeste dank uit.
Jouw robuuste vertrouwen in mij, geeft mij kracht en energie om hoge(re) doelen te bereiken.
Jouw relativeringsvermogen heeft sterk bijgedragen aan de afronding van dit proefschrift en het
feestelijke etentje bij iedere publicatie houden we erin. Wij samen zijn een super-team!
Alle anderen die op enigerlei wijze hebben bijgedragen aan de totstandkoming van dit proefschrift
wil ik hiervoor hartelijk danken.
330
Chapter sixteen
curriculum vitae

Appendices
331
16
Monique Josephine Leonie Mastboom was born in Nijmegen on October 19th 1988 and grew up
in a family of six in Enschede, The Netherlands. In 2004-2005 she spent a year as exchange student
in Bloomfield Hills, Michigan, USA, where she played ice-hockey and ran cross-country in the varsity
team. Two years after high school graduation in the USA, she also graduated from VWO profile
nature & health at Bonhoeffer college, Enschede. In that same year she started medical school in the
LUMC, Leiden. In 2008 she founded the Leids Universitaire Hardloopvereniging (LUHV) Currimus,
with which she organized and attended multiple relay races and cross-country tournaments.
Between 2009 and 2010 joined the board of the Enige Leidse Commissie Introductie Dagen (EL CID),
to organize the introduction week for new students. While joining several medical missions in the
Amazon jungle of Peru in 2011, she assisted during large traumatic, orthopaedic and reconstructive
surgeries and her interest in the functioning of the musculoskeletal system was enlarged.
After graduating from Medical School, she started working as ANIOS Orthopaedics in the Haga
Hospital, The Hague. In 2016 her research internship on Tenosynovial Giant Cell Tumours at the
department of Orthopaedic Surgery at the LUMC, Leiden was started. During this internship she
visited 95 hospitals in The Netherlands for an incidence calculation study, collaborated with the
other three Dutch orthopaedic oncologic centres (Prof. Dr. H.W.B. Schreuder, Drs. F.G.M. Verspoor, Dr.
G.R. Schaap, Dr. P.C. Jutte), collaborated with 30 international sarcoma centres and worked together
with seven different departments in the LUMC. This research resulted in a series of translational,
clinical and multicentre studies that formed the base of this PhD-thesis (Prof. Dr. P.D.S. Dijkstra, Prof.
Dr. A.J. Gelderblom, Dr. M.A.J. van de Sande). Most studies were presented at international scientific
meetings, awarded at the annual MSTS conference in Detroit 2016 with the young investigator
award, at the bi-annual ISOLS conference in Kanazawa 2017 with a nomination for the best paper
award, at the annual CTOS conference in Hawaii 2017 with the young investigator award and at the
annual BOOS conference in Edinburgh 2018 with the best oral talk award. Monique will continue
her orthopaedic career in Regionale Opleiding Groep Orthopaedie Oost.
During her medical training and research internship she ran four marathons (New York 2013, Tokyo
2015, Valencia 2015, Amsterdam 2017) and three running climbs during the Alpe d’HuZes (2017).
Monique lives together with Leander Lignac in Amsterdam. They are expecting their first child in
February 2019.

Although it’s rare, it still needs care !






















