
Endovascular treatment of cerebrovascular diseases and intracranial neoplasms
Upload
independentCategory
view
0download
0
A
OiaPopRtsc(sal(roCfar©
K
1
dgrb
0d
Clinical Neurology and Neurosurgery 110 (2008) 674–681
Surgical management of giant intracranial aneurysmsBhawani Shankar Sharma a,∗, Aditya Gupta a, Faiz Uddin Ahmad a,
Ashish Suri a, Veer Singh Mehta b
a Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi 110029, Indiab Paras Hospital, Sushant Lok, Gurgaon, Haryana, India
Received 16 August 2007; received in revised form 29 March 2008; accepted 5 April 2008
bstract
bjectives: The natural history of giant intracranial aneurysms is generally morbid. Mortality and morbidity associated with giant aneurysmss also higher than for smaller aneurysms. This study was carried out to assess the demographic profile, presenting features, complications,nd outcome after surgical treatment of giant intracranial aneurysms.atients and methods: A retrospective review of the medical records of all patients with giant intracranial aneurysms treated in the Departmentf Neurosurgery, Neurosciences Centre, All India Institute of Medical Sciences, New Delhi, from January 1995 through June 2007 waserformed. The demographic profiles, presenting features, radiological findings, surgical treatments, and outcomes were assessed.esults: A total of 1412 patients harboring 1675 aneurysms were treated. Out of these, 222 patients had 229 (13.7%) giant aneurysms, and of
hose, 181 aneurysms in 177 patients were managed surgically while 48 were treated with endovascular therapy. In the patients treated withurgery, common clinical presentations included subarachnoid hemorrhage (SAH) in 110 (62%) cases followed by mass effect in 57 (32%)ases. In patients who presented with SAH, the Hunt and Hess SAH grading was: grade I in 43 (39%), grade II in 40 (36%), grade III in 2321%), grade IV in two (2%), and grade V in 2 (2%) patients. One hundred and seven aneurysms (in 103 patients) were treated using directurgical clipping. Forty-six patients with good collateral circulation were treated by gradual occlusion and ligation of the internal carotidrtery (ICA) in the neck with a Silverstone clamp. Another nine patients with good collateral circulation, but persisting symptoms after ICAigation, required trapping for obliteration of the aneurysm. Eleven patients with poor collateral circulation required extracranial–intracranialEC–IC) bypass before proximal ICA ligation. A post-operative digital subtraction angiography (DSA) was performed in 118 patients andevealed well-obliterated aneurysm in 106 patients. The total treatment mortality rate was 9%. In the last 5 years, 117 patients were operatedn with four operative deaths. Overall, the outcome was excellent in 131 (74.0%), good in 22 (12.4%), and poor in eight (4.5%) cases.onclusions: It is concluded that 14% of all intracranial aneurysms are giant. The most common clinical presentation is SAH followed by
eatures of an intracranial mass lesion. The cavernous ICA is the most common portion of the ICA affected. Direct surgical clipping is a safend effective method of treatment and should be considered the first line of treatment whenever possible. With proper case selection, optimaladiological evaluation, and appropriate surgical strategy, it is possible to achieve a favorable outcome in almost 90% of the cases.
2008 Elsevier B.V. All rights reserved.
eywords: Intracranial aneurysm; Giant; Surgery; Management; Subarachnoid hemorrhage
flsp
. Introduction
Intracranial aneurysms larger than 25 mm in maximumiameter are classified as giant [1]. The natural history of
iant intracranial aneurysms (GIAs) is generally morbid as aesult of hemorrhage, neural compression, and thromboem-olic episodes. Left untreated, the majority of patients suffer∗ Corresponding author. Tel.: +91 9868398232; fax: +91 11 26588641.E-mail address: [email protected] (B.S. Sharma).
i
aaAp
303-8467/$ – see front matter © 2008 Elsevier B.V. All rights reserved.oi:10.1016/j.clineuro.2008.04.001
rom ruptures of these aneurysms. Once ruptured, the cumu-ative frequency of rebleed at 14 days is 18.4%. It has beenhown that mortality is above 60% within 2 years and 80% ofatients with untreated symptomatic GIAs are dead or totallyncapacitated within 5 years of diagnosis [2–4].
When an aneurysm grows to giant size, the neck widens
nd may incorporate the efferent arteries. The lumen usu-lly contains a thrombus and the wall may become calcified.ll of these features alone or in combination preclude sim-le surgical clipping. Endovascular treatment for GIAs is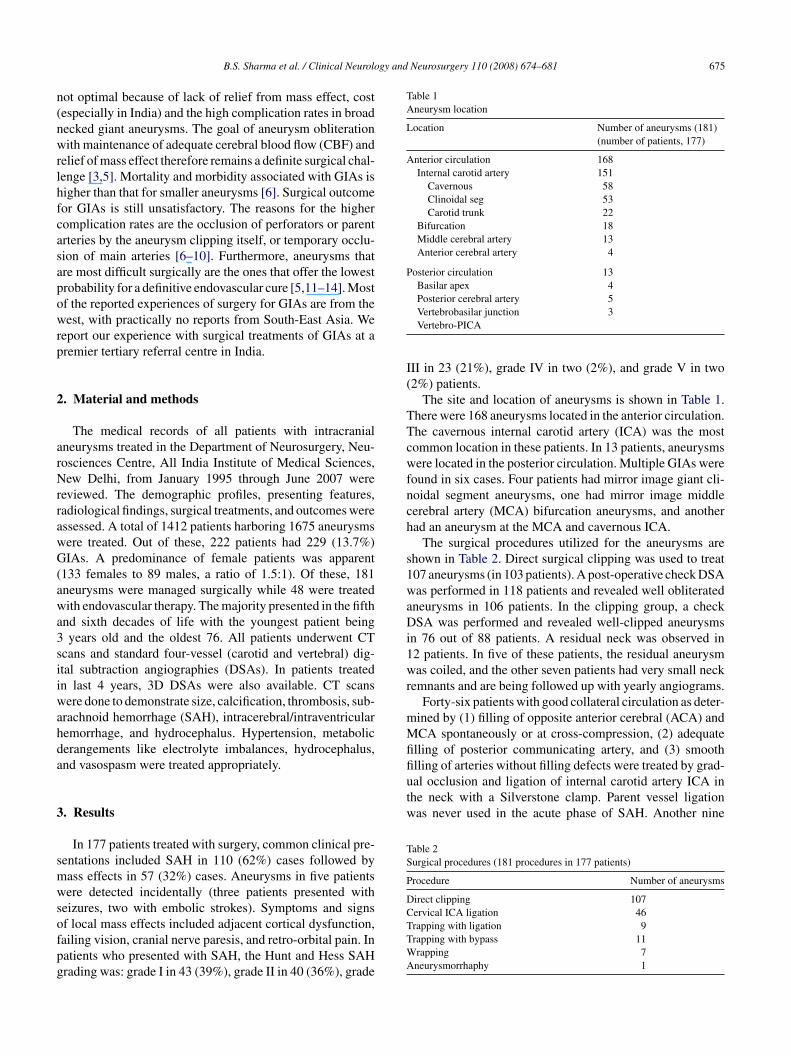
gy and Neurosurgery 110 (2008) 674–681 675
n(nwrlhfcasapowrp
2
arNrrawG(awa3siiwahda
3
smwsofpg
Table 1Aneurysm location
Location Number of aneurysms (181)(number of patients, 177)
Anterior circulation 168Internal carotid artery 151
Cavernous 58Clinoidal seg 53Carotid trunk 22
Bifurcation 18Middle cerebral artery 13Anterior cerebral artery 4
Posterior circulation 13Basilar apex 4Posterior cerebral artery 5
I(
TTcwfnch
s1waDi1wr
mMfifiual occlusion and ligation of internal carotid artery ICA inthe neck with a Silverstone clamp. Parent vessel ligationwas never used in the acute phase of SAH. Another nine
Table 2Surgical procedures (181 procedures in 177 patients)
Procedure Number of aneurysms
Direct clipping 107Cervical ICA ligation 46
B.S. Sharma et al. / Clinical Neurolo
ot optimal because of lack of relief from mass effect, costespecially in India) and the high complication rates in broadecked giant aneurysms. The goal of aneurysm obliterationith maintenance of adequate cerebral blood flow (CBF) and
elief of mass effect therefore remains a definite surgical chal-enge [3,5]. Mortality and morbidity associated with GIAs isigher than that for smaller aneurysms [6]. Surgical outcomeor GIAs is still unsatisfactory. The reasons for the higheromplication rates are the occlusion of perforators or parentrteries by the aneurysm clipping itself, or temporary occlu-ion of main arteries [6–10]. Furthermore, aneurysms thatre most difficult surgically are the ones that offer the lowestrobability for a definitive endovascular cure [5,11–14]. Mostf the reported experiences of surgery for GIAs are from theest, with practically no reports from South-East Asia. We
eport our experience with surgical treatments of GIAs at aremier tertiary referral centre in India.
. Material and methods
The medical records of all patients with intracranialneurysms treated in the Department of Neurosurgery, Neu-osciences Centre, All India Institute of Medical Sciences,ew Delhi, from January 1995 through June 2007 were
eviewed. The demographic profiles, presenting features,adiological findings, surgical treatments, and outcomes weressessed. A total of 1412 patients harboring 1675 aneurysmsere treated. Out of these, 222 patients had 229 (13.7%)IAs. A predominance of female patients was apparent
133 females to 89 males, a ratio of 1.5:1). Of these, 181neurysms were managed surgically while 48 were treatedith endovascular therapy. The majority presented in the fifth
nd sixth decades of life with the youngest patient beingyears old and the oldest 76. All patients underwent CT
cans and standard four-vessel (carotid and vertebral) dig-tal subtraction angiographies (DSAs). In patients treatedn last 4 years, 3D DSAs were also available. CT scansere done to demonstrate size, calcification, thrombosis, sub-
rachnoid hemorrhage (SAH), intracerebral/intraventricularemorrhage, and hydrocephalus. Hypertension, metabolicerangements like electrolyte imbalances, hydrocephalus,nd vasospasm were treated appropriately.
. Results
In 177 patients treated with surgery, common clinical pre-entations included SAH in 110 (62%) cases followed byass effects in 57 (32%) cases. Aneurysms in five patientsere detected incidentally (three patients presented with
eizures, two with embolic strokes). Symptoms and signs
f local mass effects included adjacent cortical dysfunction,ailing vision, cranial nerve paresis, and retro-orbital pain. Inatients who presented with SAH, the Hunt and Hess SAHrading was: grade I in 43 (39%), grade II in 40 (36%), gradeTTWA
Vertebrobasilar junction 3Vertebro-PICA
II in 23 (21%), grade IV in two (2%), and grade V in two2%) patients.
The site and location of aneurysms is shown in Table 1.here were 168 aneurysms located in the anterior circulation.he cavernous internal carotid artery (ICA) was the mostommon location in these patients. In 13 patients, aneurysmsere located in the posterior circulation. Multiple GIAs were
ound in six cases. Four patients had mirror image giant cli-oidal segment aneurysms, one had mirror image middleerebral artery (MCA) bifurcation aneurysms, and anotherad an aneurysm at the MCA and cavernous ICA.
The surgical procedures utilized for the aneurysms arehown in Table 2. Direct surgical clipping was used to treat07 aneurysms (in 103 patients). A post-operative check DSAas performed in 118 patients and revealed well obliterated
neurysms in 106 patients. In the clipping group, a checkSA was performed and revealed well-clipped aneurysms
n 76 out of 88 patients. A residual neck was observed in2 patients. In five of these patients, the residual aneurysmas coiled, and the other seven patients had very small neck
emnants and are being followed up with yearly angiograms.Forty-six patients with good collateral circulation as deter-
ined by (1) filling of opposite anterior cerebral (ACA) andCA spontaneously or at cross-compression, (2) adequate
lling of posterior communicating artery, and (3) smoothlling of arteries without filling defects were treated by grad-
rapping with ligation 9rapping with bypass 11rapping 7neurysmorrhaphy 1
6 gy and Neurosurgery 110 (2008) 674–681
ptocbpb
apac
bcNac(wiirorl
tcetewcG1vg
4
a[d
TC
C
IVMSTR
Table 4Patient outcomes
Treatment Number Excellent Good Poor Died
Clipping 103 77 10 5 11ICA lig 46 39 4 2 1Trap with bypass 11 4 4 – 3Trapping 9 5 3 – 1Wrapping 7 6 1 – –Aneurysmorrhaphy 1 – – 1 –
Total 177 131 22 8 16
Nt
uas[pwoidHpps
cacsvwha
t(saii
76 B.S. Sharma et al. / Clinical Neurolo
atients with good collateral circulation and persisting symp-oms after ICA ligation required trapping for obliterationf the aneurysm. Eleven patients with poor collateral cir-ulation required extracranial–intracranial (EC–IC) bypassefore proximal ICA ligation. A check angiogram in fouratients who had neurological deficits following EC–ICypass showed blockade and/or patent bypass.
Fifteen (8.3%) aneurysms ruptured during clipping. Allneurysms were punctured after clipping, and those thatresented with mass effects were resected (61 resectedneurysms in all). The average duration of stay in intensiveare units was 7 days.
Complications that occurred in our surgical series haveeen discussed in the text. Ten patients developed hydro-ephalus after treatment, five of whom required shunts.ine patients developed meningitis and were managed with
n intravenous antibiotic combination of third generationephalosporin, aminoglycosides, and intrathecal antibioticsvancomycion or gentamycin). We diagnosed vasospasmith transcranial Doppler in the post-operative period in the
ntensive care unit. This is treated at our centre with nimodip-ne, triple-H therapy, intrathecal papavarine and, whenequired, with endovascular therapy. Twelve patients devel-ped infarcts in the post-operative period and three of theseequired a decompressive craniectomy and duraplasty/partialobectomy.
There were 16 deaths, resulting in a total treatment mor-ality rate of 9% in the surgical group of 177 patients. Theauses of death are given in Table 3. Eleven of these wereither due to vasospasm or infarction secondary to prolongedemporary clip application or kinking of the parent artery ormbolus. In the last 5 years, 117 patients were operated onith four operative deaths. The outcome according to surgi-
al procedure performed is indicated in Table 4. We used thelasgow outcome score (GOS) to evaluate outcome (GOS= excellent, 2 = good, 3/4 = poor, and 5 = dead). Of the sur-iving patients, the outcome was excellent in 131 (74.0%),ood in 22 (12.4%), and poor in 8 (4.5%) cases.
. Discussion
Giant aneurysms constitute 3–13.5% of all intracranialneurysms, with an incidence averaging 5% in various series1,6,8,10,15–17]. Here, we observed a slightly higher inci-ence of nearly 14%. However, in a series of 602 cases of
able 3auses of mortality
ause Number of patients
nfarction 8asospasm 3eningitis 2
pontaneous cerebellar hematoma 1ransfusion reaction 1upture of contralateral aneurysm 1
rtetfomWattags
ote: in patients on whom more than one surgical procedure was performed,he second procedure is taken into account while assessing outcome.
nruptured intracranial aneurysms reported by Solomon etl. 24% were GIAs [18]. The most common clinical pre-entation mentioned in previous reports is local mass effect19,17,20,21]. It has been observed that 25–40% of GIAsresent initially with SAH [2,15,10,20]. In our series, SAHas the most common presenting feature, found in two-thirdsf the cases. This is in contrast to some previous reports, buts consistent with the report by Gewirtz et al. [22], whichescribed 68% patients presenting with SAH. In a review,osobuchi [17] found that 30–80% of patients with GIAsresent with SAH. Unruptured giant aneurysms have a higherrobability of subsequent rupture and thrombosis, and giantize does not preclude rupture [2,15,16,23].
Intracranial giant aneurysms have a propensity to occur atertain locations. Our observation that 90% of all aneurysmsre located in the anterior circulation and the single mostommon site of rupture of GIAs is the paraclinoid ICA is con-istent with previous findings [2,8,19,24]. Drake [15] foundertebro-basilar aneurysms to be most common, a findinghich can be explained by selective referrals according tois expertise and a special interest in posterior circulationneurysms.
A complete diagnostic workup is invaluable for properherapeutic decision-making. The CT scan, MRI, and DSAwith different projections as indicated) are essential. A CTcan is better for detecting calcification, skull base erosion,nd size evaluation of the aneurysm as well as the extent of thentramural clot [10,21,25]. MR imaging evaluates associatedschemia, perianeurysmal hemorrhage, and the aneurysm inelation to surrounding neurovascular and other critical struc-ures, such as the brainstem [26]. We have found 3D DSAspecially useful in planning surgery, as it permits visualiza-ion of the entire aneurysm (i.e., sac, neck, and parent vessel)rom all directions. A virtual endoscopic view can also bebtained. This clearly demonstrates the extent of involve-ent of the parent artery and defines the residual neck [27].e have obtained digital subtraction angiography in almost
ll of our patients, as it gives good anatomic pictures and sta-us of collateral circulation. We have recently used Computed
omographic angiography (CTA) and magnetic resonancengiography (MRA) in many of our patients, which provideood images of most aneurysms and in selected cases allowurgical planning and execution without the need for catheter
gy and
aap
timctfcotvvs
ap
dabac
ismtiaaao
Faio
B.S. Sharma et al. / Clinical Neurolo
ngiography. We believe that in the future, these may obvi-te the need for performing catheter angiography in manyatients.
The treatment strategy at our centre is decided jointly by aeam consisting of Neurosurgeons and Neuroradiologists. Its imperative to carefully consider multiple factors before the
ode of treatment is decided upon for an individual patient:linical presentation, age of the patient, comorbid conditions,he location, morphology, and type of aneurysm (saccular,usiform, mycotic, or traumatic), hemodynamic factors, andirculation within the normal brain. Pre-operative evaluationf cross-filling of anterior circulation, size, and patency ofhe posterior communicating artery, patency of the oppositeertebral artery, and appreciation of any anomaly or anatomicariation in circle of willis is important in planning a sound
urgical strategy.The goals of aneurysm surgery are to eliminate theneurysm from the intracranial circulation and maintainatency of the parent vessel and its branches. In our series,
cfrp
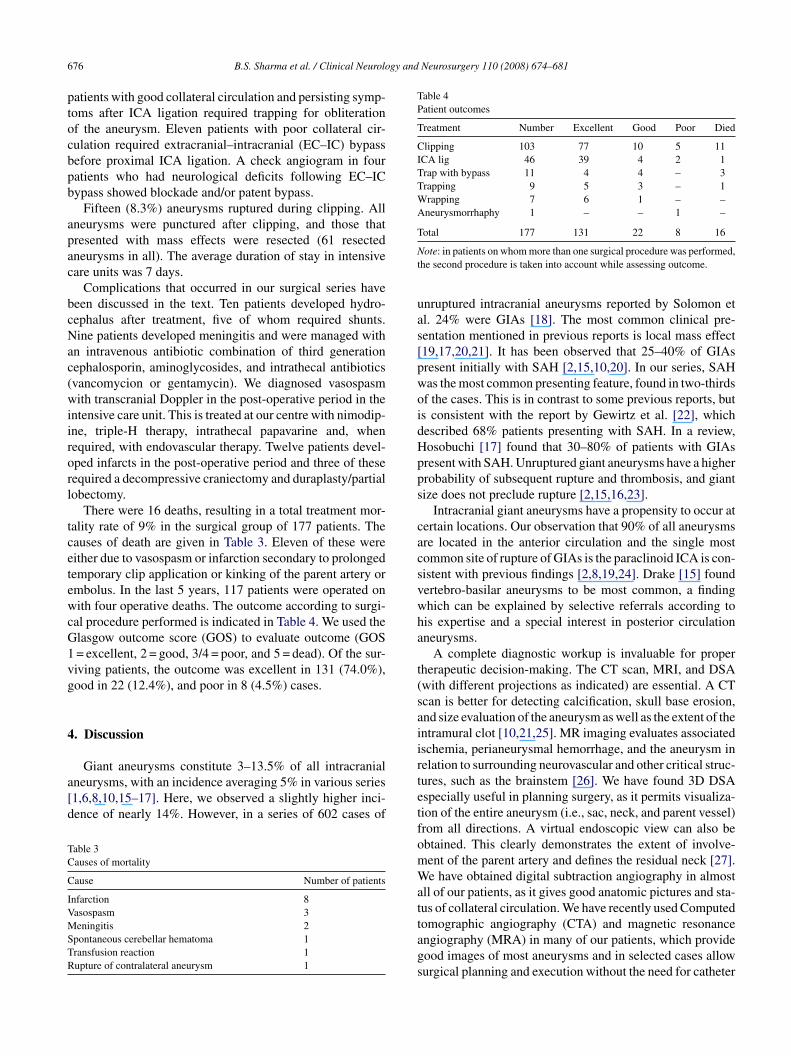
ig. 1. A 46-year-old male presented with a sudden severe headache and left hemnd right temporal hematoma. Digital subtraction angiography (DSA) revealed anferiorly and anteriorly, with a pseudolobule (B, AP view; C, lateral view). 3D recbliterated aneurysm and patent MCA branches. The patient had no focal deficits a
Neurosurgery 110 (2008) 674–681 677
irect surgical clipping was typically performed as soons possible, once all medical issues of the patient hadeen addressed and stabilized. The direct obliteration of theneurysm with clipping was possible in the majority of ourases as in other series (see Figs. 1 and 2) [3,10,21,20,28].
Selection of the optimal surgical approach and early prox-mal and distal vascular control are critical to successfulurgical treatment. The surgical approach chosen aims toaximize the operative exposure and depends upon the loca-
ion of the aneurysm. Skull base approaches such as thosenvolving medial petrosectomy, orbitozymatic osteotomy,nd condylar resection allow visualization of the parent arterynd its branches with minimal retraction [12]. Wide oper-tive exposure using orbitozygomatic osteotomy, incisionf the dural ring, resection of the lateral wall of the optic
anal, optic strut, and the anterior clinoid process are use-ul in proximal ICA aneurysms [30,31]. Giant aneurysmsequire adequate deflation of the aneurysm sac prior to clip-ing (see Figs. 1 and 2) [20]. The aneurysm wall is dissectediparesis. A non-contrast CT scan (A) revealed a subarachnoid hemorrhagegiant partially thrombosed MCA bifurcation aneurysm pointing laterally,onstruction image from the post-operative angiography (D) showed a wellt the 2-year follow-up.
678 B.S. Sharma et al. / Clinical Neurology and Neurosurgery 110 (2008) 674–681
F s of conh iant mev The poo
ataoitucoicG
att5ta
dlaei(atbww
tcP
ig. 2. A 6-year-old boy presented with a sudden severe headache and losemorrhage and a rounded opacity in suprasellar cistern. DSA revealed a giew). The patient was operated and the aneurysm was clipped and excised.f ICA branches.
nd exposed generously. The aneurysm is trapped, and thehrombus is evacuated from the neck and the clip is thenpplied. When there is a risk of mass effect, GIAs may requirepening and thrombus evacuation after they have been elim-nated completely from circulation (see Fig. 2) [20]. Specialechniques, such as temporary clipping, serial clipping, evac-ation of intraluminal thrombus, tandem or serial fenestratedlipping, clip reconstruction, booster or reinforcing clips areften required. Circumferential excision of the fundus, leav-ng a 1-cm margin distal to the neck to provide an adequateuff for subsequent reconstruction, may be required for someIAs.Temporary proximal clipping softens the aneurysm,
voids premature rupture, permits visualization of perfora-ors, and allows readjustment of the clip or multiple clips in
andem or parallel [3,5,32]. Temporary clipping was used in2 patients in our series. In our experience, occlusion for lesshan 15 min and the use of barbiturates and phenytoin usu-lly did not produce sequelae. Presence of flow in the arteriesrsdt
sciousness. A CT scan (A) revealed diffuse Fisher grade III subarachnoiddially pointing left superior hypophyseal aneurysm (B, AP view; C, lateralst-operative angiogram (D) revealed no residual aneurysm and good filling
istal to the trapped aneurysm on intraoperative microvascu-ar Doppler suggested good collateral circulation. The parentrtery occlusion time in such cases may be prolonged. How-ver, in the absence of good collateral circulation, when theschemic interval anticipated is 15–20 min, mild hypothermia32–33 ◦C) was used in addition to mannitol, barbiturates,nd phenytoin. In one patient with a giant ICA aneurysm, aemporary clip had to be applied for more than 30 min, butecause of good collateral circulation, there were no unto-ard sequelae. In all other patients, the temporary clip timeas less then 15 min.A post-surgery CT scan was done on all patients within
hree days of surgery, or earlier depending upon the clini-al situation. Many patients benefited from these CT scans.ost-operative hematomas, hydrocephalus, and infarcts were
eadily visualized on the CT scan. Five patients underwent VPhunts for post-operative hydrocephalus and three underwentecompressive craniectomy and duraplasty/partial lobec-omy for large infarcts causing mass effect. In patients with
gy and
wa
pwpnw
rapndf
[opfaiscspa
FoEccv
B.S. Sharma et al. / Clinical Neurolo
ell-established infarcts, triple-H therapy was stopped tovoid their hemorrhagic transformation or swelling.
For ICA aneurysms, the surgical options are direct clip-ing, parent artery ligation, trapping with or without bypass,rapping, or aneurysmorhaphy. For all other aneurysms, clip-ing is usually the first choice. Some aneurysms which areot clippable due to incorporation of branches can be treatedith wrapping or trapping and a bypass procedure.A parent artery occlusion study at the time of angiog-
aphy should be done to evaluate the collateral circulationnd the possible need for EC–IC bypass, as prolonged tem-
orary clipping may be required or the parent vessel mayeed permanent occlusion if the aneurysm cannot be clippedirectly. In the absence of adequate collateral circulation, weavor revascularization procedures to restore CBF (see Fig. 3)g
bc
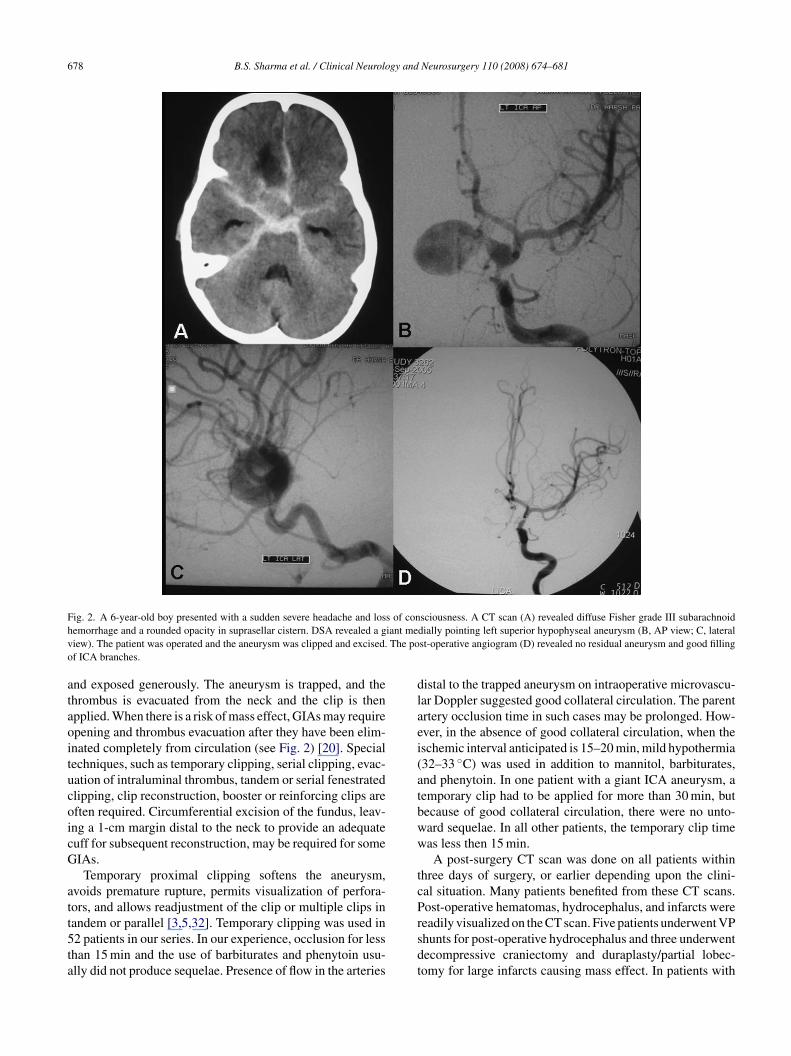
ig. 3. Left ICA angiogram, lateral view (A) showing a giant, bilobed aneurysm inphthalmic artery was arising from the superior lobule of the aneurysm. This 35-yeaCA (ascending pharyngeal branch)-to-MCA (superior branch) bypass grafting usinommunicating artery, followed by ICA ligation. The post-operative CT scan (B) shoheck angiogram revealed good patency of the radial artery graft (C) and good fillinisualized. At the 2-month follow-up, the patient had no neurological deficits.
Neurosurgery 110 (2008) 674–681 679
20,28]. In complex fusiform aneurysms, the saphenous veinr radial artery interposition graft, STA-MCA bypass or reim-lantation of branches onto the parent artery may be requiredor preservation of CBF [3,30,33]. An indirect procedure tochieve aneurysm exclusion from the circulation is requiredn 20–40% of cases, which was also observed in the presenteries [20,28]. We treat giant cavernous ICA aneurysms witharotid ligation with/without bypass [20]. As seen in ourtudy, internal carotid occlusion is a safe and effective thera-eutic method in selected patients with adequate collateralsnd should also be considered as an alternative to direct sur-
ical clipping when the latter is deemed too risky [35].Trapping allows decompression of the thrombus responsi-le for symptoms in cavernous carotid aneurysms with severeranial neuropathy that are unresponsive to proximal occlu-
volving cavernous, clinoidal and ophthalmic segments of the left ICA. Ther-old woman underwent a left orbito-zygomatic craniotomy, an end-to-sideg radial artery graft, and trapping of the aneurysm proximal to the posteriorwed artifacts from the clip on ICA and radial artery graft. The post-operativeg of MCA branches from the bypass graft (D). The aneurysm was no longer

6 gy and
sss
[aorrwt[pctg
aognalEsit[
5
glmcbWaf
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
80 B.S. Sharma et al. / Clinical Neurolo
ion or in complex distal vertebral artery aneurysms withevere brainstem compression [5]. Twenty patients in ourtudy underwent trapping of aneurysms with good results.
Surgical mortality rates vary from 4–21%8–10,15–17,20–22,28,29,34,36,37,39], averaging 10%, andre inversely proportional to the expertise and experiencef the surgeon and operating team. The surgical mortalityate of 9% observed in our series is lower than the averageeported in the literature. The most common complicationas ischemia [8,10,15]. Excellent/good results in surgically
reated patients have been reported in 63–85% of cases9,16]. The slightly more favorable outcome in 86% ofatients observed in our series probably reflects properase selection, use of good diagnostic and neurosurgicalechniques, an experienced surgical team, and a good clinicalrade of patients at admission.
Endovascular techniques are increasing in importances alternative therapeutic options in patients with failedperative intervention, poor medical condition, and in sur-ically difficult (such as those with a heavily calcifiedeck) or inaccessible GIAs. However, the aneurysms thatre most difficult surgically are the ones that offer theeast possibility of a definitive endovascular cure [5,11–14].ndovascular techniques may be used complementary tourgery, and integration of evolving endovascular technologynto the microsurgical techniques, including revasculariza-ion, can yield the best results in complex giant aneurysms4,24,37,38,40–42].
. Conclusion
It is concluded that 14% of all intracranial aneurysms areiant. SAH is the most common clinical presentation fol-owed by features of a mass lesion. The cavernous ICA is the
ost commonly affected portion of the ICA. Direct surgicallipping is a safe and effective method of treatment and shoulde considered the first line of treatment whenever possible.ith proper case selection, optimal radiological evaluation
nd appropriate surgical strategy, it is possible to achieve aavorable outcome in almost 90% of cases.
eferences
[1] Locksley HB. Report on the cooperative study of intracranial aneurysmsand subarachnoid hemorrhage, section V, Part II. Natural history ofsubarachnoid hemorrhage, intracranial aneurysms and arteriovenousmalformations: based on 6368 cases in the cooperative study. J Neuro-surg 1996;25:321–68.
[2] Khurana VG, Piepgras DG, Whisnant JP. Ruptured giant intracranialaneurysms. I. A study of rebleeding. J Neurosurg 1998;88:425–9.
[3] Lawton MT, Spetzler RF. Surgical management of giant intracra-nial aneurysms: experience with 171 patients. Clin Neurosurg1995;42:245–66.
[4] Choi IS, David C. Giant intracranial aneurysms: development, clinicalpresentation and treatment. Eur J Radiol 2003;46:178–94.
[
Neurosurgery 110 (2008) 674–681
[5] Batjer HH, Kopitnik Jr TA, Purdy PD, Matthews D, Walker B, SamsonDS, et al. Giant intracranial aneurysms. In: Wilkins RH, RengachariSS, editors. Neurosurgery, vol. 2, 2nd ed. New York: McGraw Hill;1996. p. 2361–76.
[6] Yasargil MG. Giant intracranial aneurysms. Microneurosurgery, vol. 2.New York: Springer-Verlag; 1984. p. 296–304.
[7] Khanna RK, Malik GM, Qureshi M. Predicting outcome followingsurgical treatment of unruptured IC Aneurysms: a proposed gradingsystem. J Neurosurg 1996;84:49–54.
[8] Barrow DL, Cawley C. Surgical management of complex intracranialaneurysms. Neurol India 2004;52:156–62.
[9] Sundt Jr TM, Piepgras DG. Surgical management of giant intracranialaneurysms. Nishimura: Kikuchi; 1986. pp. 324–35.
10] Choi IS, David C. Giant intracranial aneurysms: development. Clinicalpresentation and treatment. Eur J Radiol 2003;46:178–94.
11] Fernandez Zubilaga A, Guglielmi G, Vinuela F, Duckwiler GR.Endovascular occlusion of intracranial aneurysms with electricallydetachable coils: correlation of aneurysm neck size and treatmentresults. AJNR 1994;15:815–20.
12] Barrow DL, Cauley CM. Surgical management of complex intracranialaneurysms. Neurol India 2004;52:156–62.
13] Malisch TW, Guglielimi G, Vinuela F, Duckwiler G, GobinYP, Martin NA, et al. Intracranial aneurysms 390 treated withthe Gugllielmi detachable coils. Mid term clinical 391 resultsin a consecutive series of 100 patients. J Neurosurg 1997;87:176–83.
14] Murayama Y, Nien YL, Duckweiler G, Gobin YP, Jahan R, Frazee J, etal. Guglielmi detachable coil embolization of cerebral aneurysms: 11year’s experience. J Neurosurg 2003;98:959–66.
15] Drake CG. Giant intracranial aneurysms: experience with surgical treat-ment in 174 patients. Clin Neurosurg 1979;26:12–96.
16] Heros RG. Giant aneurysms. In: Ojemann, et al., editors. Surgical man-agement of neurovascular disease. 3rd ed. Baltimore: Williams andWillkins; 1995. p. 323.
17] Hosobuchi Y. Giant intracranial aneurysms. In: Wilkinson RH, Ren-gachari SS, editors. Neurosurgery. 2nd ed. New York: McGraw-Hill;1985. p. 1404–14.
18] Solomon RA, Fink ME, Pile-Spellman J. Surgical management ofunruptured intracranial aneurysms. J Neurosurg 1994;80:440–6.
19] Hosobuchi Y. Direct surgical treatment of giant intracranial aneurysms.J Neurosurg 1979;51:743–56.
20] Ausman JI, Diaz FG, Sadasivan B, Gonzeles-Portillo Jr M, Malik GM,Deopujari CE. Giant intracranial aneurysm surgery: the role microvas-cular reconstruction. Surg Neurol 1990;34:8–15.
21] Salary M, Quigley MR, Wilberger Jr JE. Relation among neurysmsize, amount of subarachnoid blood and clinical outcome. J Neurosurg2007;107:13–7.
22] Gewirtz RJ, Awad IA. Giant Aneurysms of the anterior circle of willis: management outcome of open microsurgical treatment. Surg Neurol1996;45:409–20.
23] Nagahiro S, Takada A, Goto S, Kai Y, Ushio Y. Thrombosed grow-ing giant aneurysms of the vertebral artery: growth mechanism andmanagement. J Neurosurg 1995;82:796–801.
24] Lawton MT, Quinones-Hinojosa A, Sanai N, Malek JY, Dowd CF.Combined microsurgical and endovascular management of complexintracranial aneurysms. Neurosurgery 2003;52(2):274–5, 263–74; dis-cussion.
25] Fisher A, Som PM, Mosesson RE. Giant intracranial aneurysms withskull base erosion and extracranial masses: CT and MR findings. JComput Assist Tomogr 1994;18:939–42.
26] Tang PH, Hui F, Sitoh YY. Intracranial aneurysm detection with3T magnetic resonance angiography. Ann Acad Med Singapore
2007;36:388–93.27] Lewis AI, Scalzo D, Tew Jr JM, Smith RR. Surgical management ofgiant aneurysms of the anterior circulation. In: Schmidek HH, Sweet W,editors. Operative neurosurgical techniques, vol. I, 4th ed. Philadephia:WB Saunders; 2000. p. 1205–20.
gy and
[
[
[
[
[
[
[
[
[
[
[
[
[
[
B.S. Sharma et al. / Clinical Neurolo
28] Piepgras DG, Khurana VG, Whisnant JP. Ruptured giant intracranialaneurysms. Part II. A retrospective analysis of timing and outcome ofsurgical treatment. J Neurosurg 1998;88:430–5.
29] Sundt Jr TM, Piepgras DG, Fode NC, Meyer FB. Giant intracranialaneurysms. Clin Neurosurg 1991;37:116–54.
30] Lawton MT, Spetzler RF. Surgical strategies for giant intracranialaneurysms. Neurosurg Clin N Am 1998:725–42.
31] Sekhar LN, Kalia KK, Yonas H, Wright DC, Ching H. Cranial baseapproaches to intracranial aneurysms in the subarachnoid space. Neu-rosurgery 1994;35:472–83.
32] Yu CL, Tan PP, Wu CT, Hsu JC, Chen JF, Wang YL, et al. Anaesthesiawith deep hypothermic circulatory arrest for giant basilar aneurysmsurgery. Acta Anaesthesiol 2000;38:47–51.
33] Jafar JJ, Russell SM, Woo HH. Treatment of giant intracranialaneurysms with saphenous vein extracranial intracranial bypass graft-ing: indications, operative technique, and results in 29 patients.Neurosurgery 2002;51:138–44.
34] Lownie SP, Drake CG, Peerless SJ, Ferguson GG, Pelz DM. Clinicalpresentation and management of giant anterior communicating arteryregion aneurysms. J Neurosurg 2000;92:267–77.
35] Kai Y, Hamada J, Morioka M, Yano S, Mizuno T, Kuroda J, et al.Treatment strategy for giant aneurysms in the cavernous portion of theinternal carotid artery. Surg Neurol 2007;67:148–55.
36] Mack WJ, Ducruet AF, Angevine PD, Komotar RJ, Shrebnick DB,Edwards NM, et al. Deep hypothermic circulatory arrest for com-
[
Neurosurgery 110 (2008) 674–681 681
plex cerebral aneurysms: lessons learned. Neurosurgery 2007;60:815–27.
37] Coplan ME, Sekerci Z, Cakamakci E, Donmez T, Oral N, MogulDJ. Virtual endoscope-assisted intracranial aneurysm surgery: evalu-ation of fifty-eight surgical cases. Minim Invasive Neurosurg 2007;50:27–32.
38] Chen L, Kato Y, Sano H, Watanabe S, Yoneda M, Hayakawa M, et al.Management of complex, surgically intractable intracranial aneurysms:the option for intentional reconstruction of aneurysm neck followed byendovascular coiling. Cerebrovasc Dis 2007;23:381–7.
39] Parkinson RJ, Eddleman CS, Batjer HH, Bendok BR. Giant intracranialaneurysms: endovascular challenges. Neurosurgery 2006;59(5 Suppl.3):S103–12.
40] Higashida RT, Halbach VV, Barnwell SL, Dowd C, Dormandy B, Bell J,et al. Treatment of intracranial aneurysms with preservation of the par-ent vessel: results of percutaneous balloon embolization in 84 patients.AJNR 1990;11:633–41.
41] HohBL, PutmanCM, BudzikRF, Carter BS, Ogilvy CS. Combined sur-gical and endovascular techniques of flow alteration to treat fusiformand complex wide necked intracranial aneurysms that are unsuitable
for clipping or coil embolization. J Neurosurg 2001;95:24–35.42] Chen L, Kato Y, Sano H, Watanabe S, Yoneda M, Hayakawa M. Man-agement of complex, surgically intractable intracranial aneurysms: theoption for intentional reconstruction of aneurysm neck followed byendovascular coiling. Cerebrovasc Dis 2007;23:381–7.
Copyright © 2022 FDOKUMEN




















