The effect of light curing units and modes on cytotoxicity of resin-core systems
Upload
independentCategory
view
1download
0
Dental Materials Journal 2009; 28(3): 253–260
Original Paper�Temperature rise induced by various light curing units through human dentin�
Arife DOGAN1, Ihsan HUBBEZOGLU2, Orhan Murat DOGAN3, Giray BOLAYIR3 and Hakan DEMIR3
1Department of Prosthodontics, Faculty of Dentistry, Gazi University, Ankara, Turkey2Department of Endodontics, Faculty of Dentistry, Cumhuriyet University, Sivas, Turkey3Department of Prosthodontics, Faculty of Dentistry, Cumhuriyet University, Sivas, TurkeyCorresponding author, Arife DOGAN; E-mail: [email protected]; [email protected]
�This�study�investigated�temperature�rises�caused�by�different�light�curing�units�(LCUs)�in�dentin�of�different�thicknesses.��The�different�LCUs�tested�in�this�study�were�namely:�quartz-tungsten-halogen�(QTH)�(Heliolux�DLX)�LCU,�plasma�arc�(PAC)�(Apollo�95E�Elite)�LCU,�and�light�emitting�diode�(LED)�(Mini�LED)�in�standard�curing�mode�as�well�as�pulse�and�soft-start�modes.��One�hundred�and�forty�dentin�disks�of�0.5,�1,�1.5,�and�2�mm�thickness�were�prepared�from�mandibular�molars�(n=7).��Temperatures�were�recorded�using�a�L-type�thermocouple�in�direct�contact�with�the�light�guide�tip.� �For�all�curing�units/modes, dentin thickness was inversely proportional to temperature rise and that QTH light gave significantly higher values compared�to�PAC�and�LED�in�all�the�test�conditions.��The�highest�temperature�rise�was�observed�under�0.5-mm-thick�dentin�disk�with�QTH,�whereas�the�lowest�temperature�rise�was�registered�with�LED�light�in�pulse�mode�under�2-mm-thick�dentin.
Keywords:�Light�curing�units,�Temperature�rise,�Dentin�
Received Jul 14, 2008: Accepted Sep 29, 2008
INTRODUCTION
In� recent� developments� for� visible� light� curing,� the�use� of� visible� light� to� cure� dental� materials� has�widely� expanded� to� cover� a� vast� array� of� products�including�composite�resins1).� �With�light-cured�dental�restorative� materials,� they� set� via� an� additional�polymerization� process� due� to� exposure� to� light� of� a�requisite� wavelength� and� intensity,� whereby� the�latter� initiates� the� generation� of� free� radicals� to�propagate�the�polymerization2).
For� many� years,� quartz-tungsten-halogen� light�curing� units� (QTH� LCUs)� have� been� used� to�polymerize� resin� composites.� � Typically,� these� light�sources�need� to� emit�500� to�800�mW/cm2�of� light� for�30�to�40�seconds�to�polymerize�composites�at�a�depth�of� 2� mm3).� � The� main� radiant� output� from� a�conventional� QTH� source� is� infra-red� energy,� which�is�absorbed�by�resin�composites�and�which�results�in�increased� molecular� vibration� and� heat� generation.��Thus,� conventional� QTH� LCUs� require� heat-absorbing filters to reduce the passage of infra-red energy�from�the�light�source�to�the�tooth4-6).��However,�the LCU’s bulb, reflector, and filter degrade over time due to high operating temperatures, and unfiltered infra-red�energy�can�result� in�heat�generation�in�the�pulp�chamber3,7-11).
Of�late,�the�light�emitting�diode�(LED)�technology�has� been� introduced� to� the� dental� profession� as� an�alternative� to� conventional� halogen� technology.� � As�opposed to the hot filaments used in halogen bulbs,
LEDs� use� doped� semiconductor� junctions� (p-n�junctions)� to�generate�and�emit� light.� �Under�proper�forward� bias� conditions,� the� injected� electrons� and�holes� recombine� at� a� p-n� junction� and� thereby� emit�light;� in� the�case�of�gallium�nitride�LEDs,�blue� light�is� emitted.� � Additionally,� a� small� polymer� lens� is�included� in� front� of� the� p-n� junction� to� produce� a�partially�collimated�light3,8,11).
On� the� comparison� between� LED� and� QTH�LCUs,� previous� studies� have� reported� on� a� slew� of�advantages� that� the� former�wield�over� the� latter.� � It�has been reported that LEDs are more efficient than QTH� lamps� in� converting� energy� to� light� and� that�the� wavelength� of� light� emitted� by� LEDs� closely�matches�the�absorption�spectrum�of�camphorquinone�(CQ),� a� photoinitiator� widely� used� in� light-activated�dental� resins3,8-10,12,13).� � Unlike� QTH� light� sources,�LEDs�do�not�generate�infra-red�rays�—�which�means�that� they� have� a� constant� light� output� and� a� longer�lamp� life� expectancy3,5,7,10).� � Heating� of� irradiated�objects� by� LED� lights� is� also� expected� to� be�minimal14).� �Furthermore,�most�of� the�available�LED�LCUs�offer�a�user-programmable�curing�time�ranging�from�5�to�60�seconds.��This�provision�arguably�augers�well�for�the�trend�toward�shorter�curing�times�in�the�polymerization�of�dental�composites15).
The� plasma� arc� (PAC)� curing� light� is� also�designed for high-speed curing of composite filling materials�in�direct�resin�restorations.��A�high-energy,�high-pressure� ionized� gas� in� the� presence� of� an�electrical�current�is�used�to�create�a�high-temperature�

Dent Mater J 2009; 28(3): 253–260254
light�source�strong�enough�to�increase�the�curing�rate�of�resin�composites16).��With�the�development�of�xenon�PAC�lights,�much�higher�light� intensities�(2000�mW/cm2)� are� currently� employed� to� polymerize� dental�composites� within� a� curing� time� of� merely� 3�seconds17,18).
On� the� other� hand,� rapid� polymerization� may�result� in� the� formation� of� short� polymer� chains� and�shorten� the� pre-gel� phase� such� that� the� material� is�unable� to� adequately� absorb� polymerization�contraction�stresses2).� �With�a�view�to�controlling�the�effect� of� polymerization� shrinkage� stemming� from�polymerization� contraction� stresses19),� recent�developments� have� focused� on� various� irradiations�protocols� such� as� soft-start� polymerization� or� pulse�curing.� �Soft-start�polymerization�is�characterized�by�using� an� initial� low� power� intensity� of� the� curing�light� followed� by� a� higher� power� intensity12,19,20).� � As�for pulse curing, it is initiated by a short flash of light� followed� by� a� relaxing� time� of� several� minutes�before final cure is performed10).� � These� techniques�allow the composite resin to flow from the tooth surface,� reduce� stress,� and� potentially� improve� the�marginal� integrity� of� the� restoration10,12,14,21).��However,� if� soft-start� mode� were� to� be� used� for� the�polymerization�of�resin�composites�in�order�to�realize�these� advantages,� prolonged� curing� time� is�necessary15),� and� this� may� lead� to� increased� pulpal�temperatures.
The� increase� in� pulpal� temperature� has� been�attributed� to� two� main� sources:� radiation� energy�emitted�by�the�LCU�and�the�polymerization�exotherm�of� resin� composites2,4,16,17,20,22,23).� � It� has� been� reported�that� photopolymerization� with� high� energy� output�curing units caused significantly higher pulp chamber temperature�changes�as�compared�to�the�conventional�curing�units16,19,24-26).
Besides the influential role of light curing units on� the� effect� of� heat� experienced� by� the� pulp,� some�factors�such�as�dentin�thickness�and�proximity�of�the�material� to� the� pulp� may� also� play� a� role2,4).��Damaging�effects�of�temperature�increase�on�the�pulp�during� resin� composite� polymerization� has� been�widely� investigated.� � However,� the� increased� power�of recently developed LCUs (≥1500 mW/cm2)� has�renewed�concerns�about�the�biological�safety�of�these�curing� units,� especially� when� they� are� used� in� deep�cavities�with�minimal�remaining�dentin�thickness.
To� date,� thermal� emission� from� these� recently�developed,�high-power�LCUs�has�not�been�thoroughly�and�fully�evaluated.� �To�gain�a�better�understanding�on� the� response� of� dentin� to� these� latest� changes� in�light� intensity,�this�study�examined�the�temperature�rise� in� dentin� of� different� thicknesses� caused� by�halogen,�LED,�and�PAC�LCUs.��Temperature�changes�associated� with� various� curing� modes� of� LED� LCU�were�also�compared.
MATERIALS AND METHODS
Preparation of dentin disksDentin�disks�of�0.5,�1,�1.5,�and�2�mm�thickness�were�prepared� from� freshly� extracted,� caries-free�mandibular molars embedded in Teflon molds with epoxy�resin.��These�disks�were�obtained�by�sectioning�perpendicular� to� the� long� axis� of� the� tooth� with� a�water-cooled� saw� (Isomet,� Buehler� Ltd.,� Lake� Bluff,�IL,� USA)� and� kept� in� distilled� water� until� use.� � For�each� dentin� thickness,� 35� specimens� were� obtained�for�the�different�curing�light�protocols�(n=7).��A�mylar�strip�was�placed�over�each�dentin�disk�and�the�latter�was� irradiated� from� the� top� through� the� strip� using�one�of�the�LCUs�tested.
Light curing units (LCUs)The�light�curing�units� (LCUs)�selected�for�this�study�included� a� conventional� quartz-tungsten-halogen�(QTH;� Heliolux� DLX,� Ivoclar-Vivadent,� Schaan,�Liechtenstein)� LCU,� a� plasma� arc� (PAC;� Apollo� 95E�Elite,� Dental� Medical� Technology� Systems� Inc.,�Orange,� CA,� USA)� LCU,� and� a� blue� light� emitting�diode� (LED;� Mini� LED,� Satelec,� Merignac,� France)�LCU.��Besides�the�standard�mode�of�these�LCUs,�the�soft-start� and� pulse� modes� of� LED� LCU� were� also�evaluated.� � Table� 1� shows� the� details� of� the� LCUs�and�their�curing�modes.
Temperature measurementThermal�emission�of�the�LCUs�was�measured�using�a�type�L� thermocouple� (Fe-Const.�Elimko�Co.,�Ankara,�Turkey)� connected� to� a� data� logger� (E-680,� Elimko�Co.,�Ankara,�Turkey).��E-680�series�of�universal�data�loggers/scanners� were� advanced,� new-generation�microcontroller-based� industrial� instruments�compatible� with� IEC� 668� standards.� � Data� were�collected�using�a�data�logging�software�(Data�Logger,�5.1�ver.,�Elimko�Co.,�Ankara,�Turkey)�and�stored�in�a�centrally�located�PC.
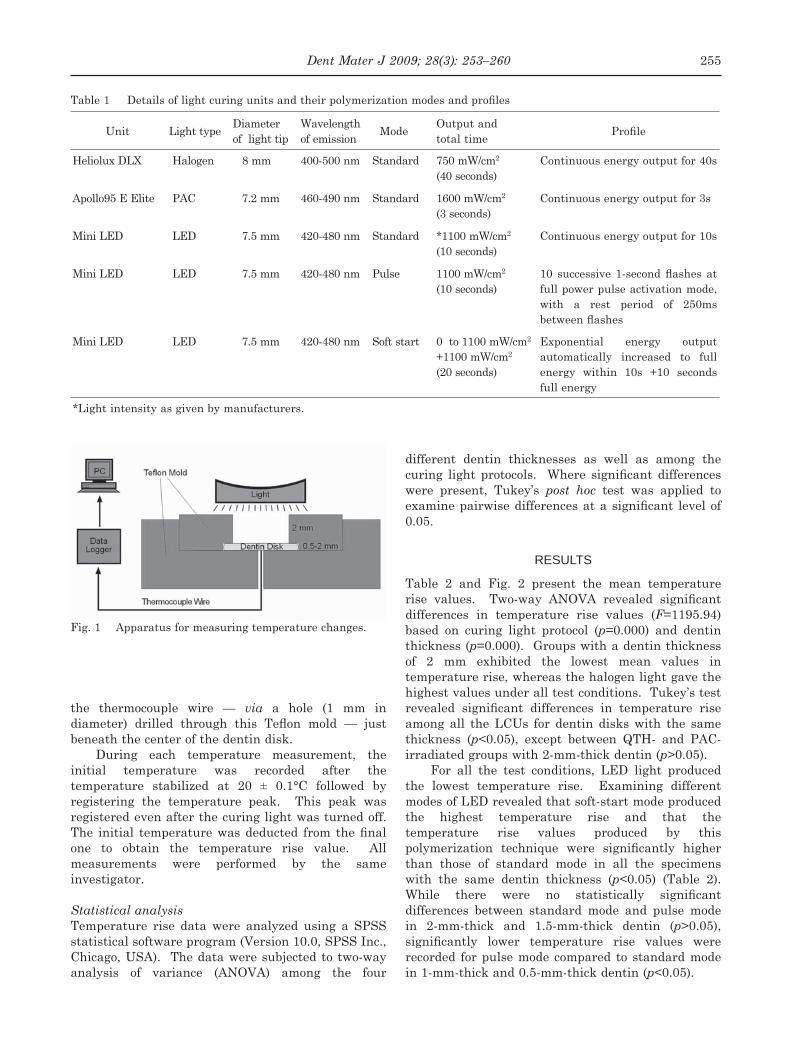
To� standardize� the� temperature� rise�measurements,� an� apparatus� was� specially� devised�for this study. It comprised two Teflon mold cylinders constructed from polytetrafluoroethylene. The movable top Teflon mold cylinder included a central�aperture�(6�mm�diameter,�2�mm�depth)�which�was� located� exactly� over� the� test� specimen.� � It� was�available� in� different� sizes� (8� mm� diameter,� 0.5,� 1,�1.5,�and�2�mm�depth)�so�as�to� form�the� lateral�walls�of�the�dentin�disks�placed�at�the�bottom�(Fig.�1).��The�light� tip� of� the� LCU� was� positioned� at� the� center� of�the Teflon mold and in direct contact with the mold, thus�standardizing�the�distance�between�the�light�tip�of� the� LCU� and� the� dentin� disks� in� each� test�condition. Apart from the movable top Teflon mold, the� entire� apparatus� was� surrounded� by� another�Teflon mold cylinder which provided an entrance for
Dent Mater J 2009; 28(3): 253–260 255
the� thermocouple� wire� —� via� a� hole� (1� mm� in�diameter) drilled through this Teflon mold — just beneath�the�center�of�the�dentin�disk.
During� each� temperature� measurement,� the�initial� temperature� was� recorded� after� the�temperature� stabilized� at� 20� ±� 0.1°C� followed� by�registering� the� temperature� peak.� � This� peak� was�registered�even�after�the�curing�light�was�turned�off.��The initial temperature was deducted from the final one� to� obtain� the� temperature� rise� value.� � All�measurements� were� performed� by� the� same�investigator.
Statistical analysisTemperature� rise� data� were� analyzed� using� a� SPSS�statistical�software�program�(Version�10.0,�SPSS�Inc.,�Chicago,�USA).� �The�data�were�subjected�to�two-way�analysis� of� variance� (ANOVA)� among� the� four�
different� dentin� thicknesses� as� well� as� among� the�curing light protocols. Where significant differences were� present,� Tukey’s� post hoc� test� was� applied� to�examine pairwise differences at a significant level of 0.05.
RESULTS
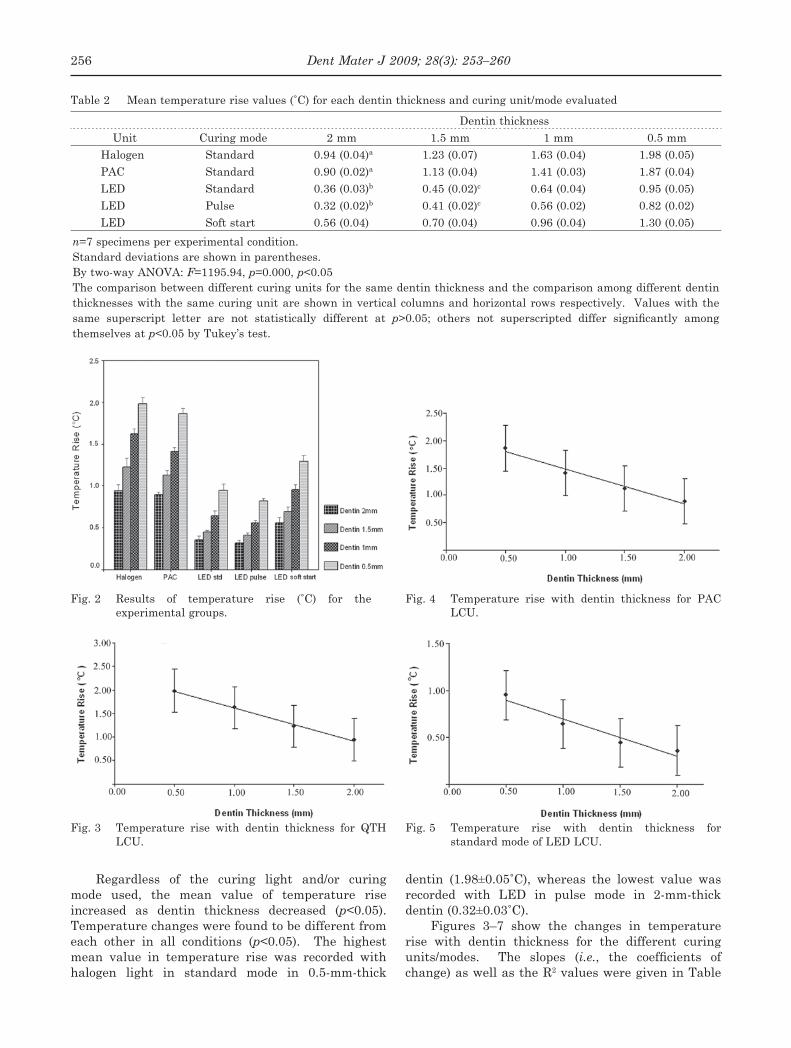
Table� 2� and� Fig.� 2� present� the� mean� temperature�rise values. Two-way ANOVA revealed significant differences� in� temperature� rise� values� (F=1195.94)�based� on� curing� light� protocol� (p=0.000)� and� dentin�thickness�(p=0.000).� �Groups�with�a�dentin�thickness�of� 2� mm� exhibited� the� lowest� mean� values� in�temperature�rise,�whereas�the�halogen�light�gave�the�highest�values�under�all�test�conditions.��Tukey’s�test�revealed significant differences in temperature rise among� all� the� LCUs� for� dentin� disks� with� the� same�thickness� (p<0.05),� except� between� QTH-� and� PAC-irradiated�groups�with�2-mm-thick�dentin�(p>0.05).
For� all� the� test� conditions,� LED� light� produced�the� lowest� temperature� rise.� � Examining� different�modes�of�LED�revealed�that�soft-start�mode�produced�the� highest� temperature� rise� and� that� the�temperature� rise� values� produced� by� this�polymerization technique were significantly higher than� those� of� standard� mode� in� all� the� specimens�with� the� same� dentin� thickness� (p<0.05)� (Table� 2).��While there were no statistically significant differences� between� standard� mode� and� pulse� mode�in� 2-mm-thick� and� 1.5-mm-thick� dentin� (p>0.05),�significantly lower temperature rise values were recorded� for�pulse�mode�compared� to�standard�mode�in�1-mm-thick�and�0.5-mm-thick�dentin�(p<0.05).
Table 1 Details of light curing units and their polymerization modes and profiles
Unit Light�type Diameter�of��light�tip
Wavelength�of�emission Mode Output�and�
total�time Profile
Heliolux�DLX Halogen 8�mm 400-500�nm� Standard 750�mW/cm2
(40�seconds)Continuous�energy�output�for�40s
Apollo95�E�Elite PAC 7.2�mm 460-490�nm Standard� 1600�mW/cm2
(3�seconds)Continuous�energy�output�for�3s
Mini�LED LED 7.5�mm 420-480�nm Standard *1100�mW/cm2
(10�seconds)Continuous�energy�output�for�10s
Mini�LED LED 7.5�mm 420-480�nm Pulse 1100�mW/cm2
(10�seconds)10 successive 1-second flashes at full�power�pulse�activation�mode,�with� a� rest� period� of� 250ms�between flashes
Mini�LED LED 7.5�mm 420-480�nm Soft�start 0��to�1100�mW/cm2
+1100�mW/cm2
(20�seconds)
Exponential� energy� output�automatically� increased� to� full�energy� within� 10s� +10� seconds�full�energy
*Light�intensity�as�given�by�manufacturers.
Fig.�1� Apparatus�for�measuring�temperature�changes.
Dent Mater J 2009; 28(3): 253–260256
Regardless� of� the� curing� light� and/or� curing�mode� used,� the� mean� value� of� temperature� rise�increased� as� dentin� thickness� decreased� (p<0.05).��Temperature�changes�were�found�to�be�different�from�each� other� in� all� conditions� (p<0.05).� � The� highest�mean� value� in� temperature� rise� was� recorded� with�halogen� light� in� standard� mode� in� 0.5-mm-thick�
dentin (1.98±0.05˚C), whereas the lowest value was recorded� with� LED� in� pulse� mode� in� 2-mm-thick�dentin (0.32±0.03˚C).
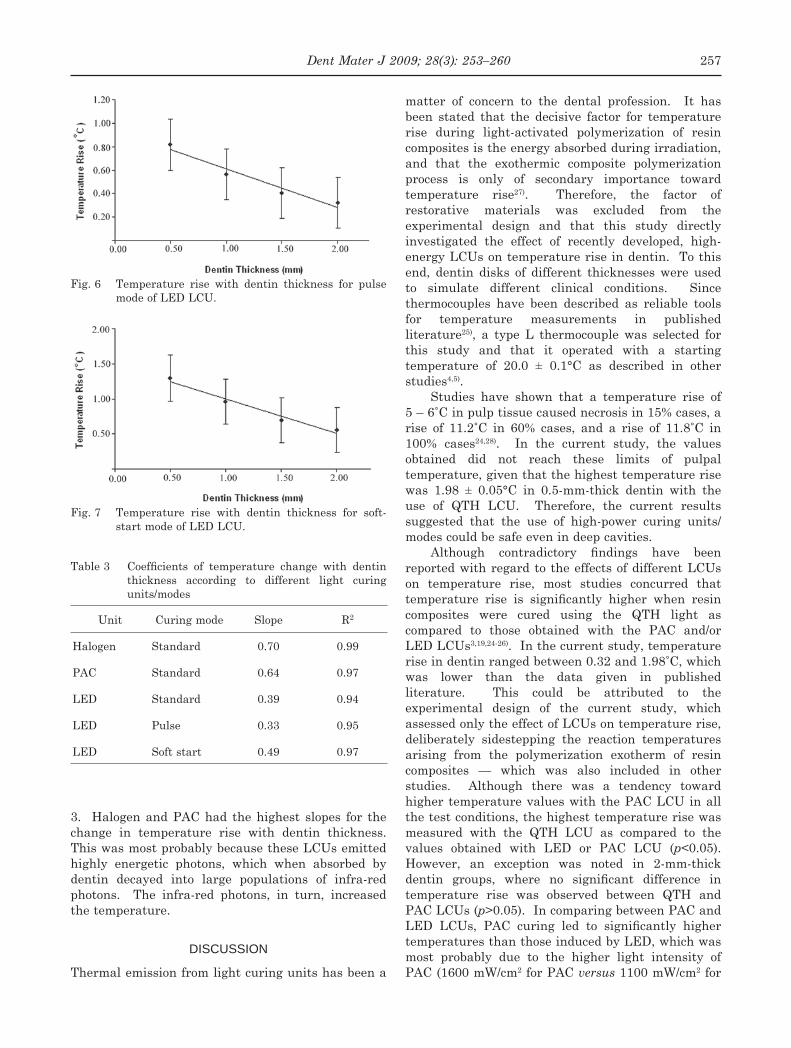
Figures� 3–7� show� the� changes� in� temperature�rise� with� dentin� thickness� for� the� different� curing�units/modes.� � The� slopes� (i.e., the coefficients of change)�as�well�as�the�R2�values�were�given�in�Table�
Table 2 Mean temperature rise values (˚C) for each dentin thickness and curing unit/mode evaluated
Dentin�thicknessUnit Curing�mode 2�mm 1.5�mm 1�mm 0.5�mm
Halogen Standard 0.94�(0.04)a 1.23�(0.07) 1.63�(0.04) 1.98�(0.05)PAC Standard 0.90�(0.02)a 1.13�(0.04) 1.41�(0.03) 1.87�(0.04)LED Standard 0.36�(0.03)b 0.45�(0.02)c 0.64�(0.04) 0.95�(0.05)LED Pulse 0.32�(0.02)b 0.41�(0.02)c 0.56�(0.02) 0.82�(0.02)LED Soft�start 0.56�(0.04) 0.70�(0.04) 0.96�(0.04) 1.30�(0.05)
n=7�specimens�per�experimental�condition.Standard�deviations�are�shown�in�parentheses.By�two-way�ANOVA:�F=1195.94,�p=0.000,�p<0.05The�comparison�between�different�curing�units�for�the�same�dentin�thickness�and�the�comparison�among�different�dentin�thicknesses�with�the�same�curing�unit�are�shown�in�vertical�columns�and�horizontal�rows�respectively.� �Values�with�the�same� superscript� letter� are� not� statistically� different� at� p>0.05; others not superscripted differ significantly among themselves�at�p<0.05�by�Tukey’s�test.
Fig. 2 Results of temperature rise (˚C) for the experimental�groups.
Fig.�4� Temperature� rise� with� dentin� thickness� for� PAC�LCU.
Fig.�5� Temperature� rise� with� dentin� thickness� for�standard�mode�of�LED�LCU.
Fig.�3� Temperature� rise� with� dentin� thickness� for� QTH�LCU.
Dent Mater J 2009; 28(3): 253–260 257
3.� � Halogen� and� PAC� had� the� highest� slopes� for� the�change� in� temperature� rise� with� dentin� thickness.��This�was�most�probably�because�these�LCUs�emitted�highly� energetic� photons,� which� when� absorbed� by�dentin� decayed� into� large� populations� of� infra-red�photons.� � The� infra-red� photons,� in� turn,� increased�the�temperature.
DISCUSSION
Thermal�emission�from�light�curing�units�has�been�a�
matter� of� concern� to� the� dental� profession.� � It� has�been� stated� that� the� decisive� factor� for� temperature�rise� during� light-activated� polymerization� of� resin�composites�is�the�energy�absorbed�during�irradiation,�and� that� the� exothermic� composite� polymerization�process� is� only� of� secondary� importance� toward�temperature� rise27).� � Therefore,� the� factor� of�restorative� materials� was� excluded� from� the�experimental� design� and� that� this� study� directly�investigated� the� effect� of� recently� developed,� high-energy�LCUs�on�temperature�rise�in�dentin.� �To�this�end,� dentin� disks� of� different� thicknesses� were� used�to� simulate� different� clinical� conditions.� � Since�thermocouples� have� been� described� as� reliable� tools�for� temperature� measurements� in� published�literature25),� a� type� L� thermocouple� was� selected� for�this� study� and� that� it� operated� with� a� starting�temperature� of� 20.0� ±� 0.1°C� as� described� in� other�studies4,5).
Studies� have� shown� that� a� temperature� rise� of��5 – 6˚C in pulp tissue caused necrosis in 15% cases, a rise of 11.2˚C in 60% cases, and a rise of 11.8˚C in 100% cases24,28).� � In� the� current� study,� the� values�obtained� did� not� reach� these� limits� of� pulpal�temperature,�given�that�the�highest�temperature�rise�was� 1.98� ±� 0.05°C� in� 0.5-mm-thick� dentin� with� the�use� of� QTH� LCU.� � Therefore,� the� current� results�suggested� that� the� use� of� high-power� curing� units/modes�could�be�safe�even�in�deep�cavities.
Although contradictory findings have been reported�with�regard�to�the�effects�of�different�LCUs�on� temperature� rise,� most� studies� concurred� that�temperature rise is significantly higher when resin composites� were� cured� using� the� QTH� light� as�compared� to� those� obtained� with� the� PAC� and/or�LED�LCUs3,19,24-26).��In�the�current�study,�temperature�rise in dentin ranged between 0.32 and 1.98˚C, which was� lower� than� the� data� given� in� published�literature.� � This� could� be� attributed� to� the�experimental� design� of� the� current� study,� which�assessed�only�the�effect�of�LCUs�on�temperature�rise,�deliberately� sidestepping� the� reaction� temperatures�arising� from� the� polymerization� exotherm� of� resin�composites� —� which� was� also� included� in� other�studies.� � Although� there� was� a� tendency� toward�higher� temperature�values�with� the�PAC�LCU�in�all�the�test�conditions,�the�highest�temperature�rise�was�measured� with� the� QTH� LCU� as� compared� to� the�values� obtained� with� LED� or� PAC� LCU� (p<0.05).��However,� an� exception� was� noted� in� 2-mm-thick�dentin groups, where no significant difference in temperature� rise� was� observed� between� QTH� and�PAC�LCUs�(p>0.05).��In�comparing�between�PAC�and�LED LCUs, PAC curing led to significantly higher temperatures�than�those�induced�by�LED,�which�was�most� probably� due� to� the� higher� light� intensity� of�PAC�(1600�mW/cm2�for�PAC�versus�1100�mW/cm2�for�
Fig.�6� Temperature� rise� with� dentin� thickness� for� pulse�mode�of�LED�LCU.
Fig.�7� Temperature� rise� with� dentin� thickness� for� soft-start�mode�of�LED�LCU.
Table 3 Coefficients of temperature change with dentin thickness� according� to� different� light� curing�units/modes
Unit Curing�mode Slope R2
Halogen Standard 0.70 0.99
PAC Standard 0.64 0.97
LED Standard 0.39 0.94
LED Pulse 0.33 0.95
LED Soft�start 0.49 0.97
Dent Mater J 2009; 28(3): 253–260258
LED).Yap� and� Soh19)� have� concluded� that� LED� curing�
lights emitted significantly less heat from their light guides� than� QTH� lights.� � This� assertion� could� be�accepted, given that the filtered emission spectrum of a�QTH�lamp�is�broader�than�that�of�a�LED�and�that�it�includes�wavelengths�of�light�capable�of�generating�a� higher� quantity� of� heat6).� � According� to� Lloyd� et al.29), the most significant factor that increased pulpal temperature� during� light� curing� is� the� energy�absorbed� from� irradiation.� � This� might� well� explain�the�observation� that� irradiation�with�QTH�LCU�was�associated� with� higher� temperature� rise� in�comparison�with�PAC�or�LED�LCU.� �The�QTH�LCU�used�in�this�experiment�had�a�lower�light�intensity�of�750� mW/cm2� but� produced� a� higher� total� energy� (30�J/cm2)�due�to� its�40-second�curing�time,�as�compared�with� PAC� (4.8� J/cm2� for� 3� seconds)� and� LED� (11��J/cm2�for�10�seconds).� �This�result�seemed�to�suggest�that temperature rise was influenced by total energy rather�than�light�intensity�in�the�case�of�QTH�LCU.
According� to� our� results,� it� could� be� concluded�that� in�order� to�attain� temperature� rises� lower� than�the� critical� value� which� causes� pulpal� injury,� the�high-power� LED� LCU� seemed� to� be� a� plausible�option.� � Among� the� three� different� modes� of� LED�used,� the� soft-start� mode� registered� the� highest�temperature� rise� (p<0.05)� in� all� the� test� conditions.��The� difference� in� total� energy� produced� by� these�three� modes� of� LED� could� have� also� accounted� for�the�different�temperature�changes.� �The�total�energy�produced�with�soft-start�mode�was�22�J/cm2,�whereas�it�was�11�J/cm2�for�the�other�two�modes.��From�these�results,� it�could�be�suggested�that�the�standard�and/or�pulse�modes�of�LED�LCU�might�reduce�the�risk�of�pulpal� injury� even� in� the� case� of� thin� dentin� tissue.��This�was�because�the�standard�and/or�pulse�modes�of�LED� LCU� produced� a� lower� temperature� rise� not�only� when� compared� with� the� soft-start� mode,� but�also� against� the� standard� curing� mode� of� QTH� and�PAC� LCUs� used� in� this� study.� � In� some� clinical�conditions,� the�use�of� soft-start�polymerization� could�be� a� solution� for� decreasing� stress� during�polymerization,� thereby� improving� the� marginal�sealing�of�the�restoration�and�reducing�microleakage.��However,� this� curing� mode� requires� a� longer� curing�time�and�consequently�raises� the�temperature�of� the�resin� composite� and� the� surrounding� dentin21,30).��Therefore,� especially� in� deep� cavities,� this� technique�should�be�used�with�caution.
In� this� study,� another� temperature� rise-determining�factor�that�was�taken�into�consideration�was� the� thickness� of� residual� dentin.� � According� to�Loney� and� Price31),� a� thicker� dentin� substrate� can�reduce� the� temperature� because� of� low� thermal�conductibility� of� this� substrate.� � The� present� study�confirmed this assertion. For all the light curing
units/modes� tested,� there� was� an� exponential�increase� in� temperature� rise� as� dentin� thickness�decreased� and� that� all� the� differences� were�significant.
Figures� 3–7� show� the� changes� in� temperature�with� dentin� thickness� for� the� different� curing� light�protocols,� whilst� Table� 3� gives� the� slopes� (i.e.,�coefficients of change, indicating how fast the temperature�changed�with�dentin�thickness)�and�the�R2�values.��The�last�column�of�Table�3�shows�that�the�lowest� R2� value� is� 0.94,� hence� indicating� the� high�reproducibility� of� data.� � Further,� Table� 3� revealed�that� the� slope� for� pulse� mode� of� LED� ranked� the�lowest,� whereas� that� of� QTH� LCU� ranked� the�highest.� � Photons� emitted� from� the� LED� source� are�not� energetic,� which� thus� explained� why� the� slopes�for�all�the�curing�modes�of�LED�were�lower�compared�to� those� of� QTH� and� PAC� LCUs.� � In� comparing�among� the� curing� modes� of� LED,� intermittent�irradiation�(i.e.,�pulse�mode�of�LED)�naturally�yielded�a� smaller� slope� (0.33)� than� in� the� continuous� case�(i.e.,� standard�mode� of�LED,� slope:� 0.39).� �Moreover,�extension� of� curing� time� from� 10� seconds� to� 20�seconds� increased� the� slope� from� 0.39� to� 0.49.� � This�was�because�the�energy�deposited�on�dentin�could�not�diffuse�out�easily�from�the�material,�and�thus�created�a�steeper�slope�for�the�soft-start�mode.
PAC� LCU� probably� emitted� more� energetic�photons� than� blue� LED,� causing� higher� energy�deposition.� � QTH� LCU� also� emitted� highly� energetic�photons,� thus� yielding� the� steepest� slope� of� 0.70� as�seen� from� Table� 3.� � However,� the� output� energy� of�PAC�was�1600�mW/cm2�while�that�of�QTH�LCU�was�750� mW/cm2� (Table� 1).� � In� other� words,� not� all�photons�were�absorbed�by�dentin.� �This�was�because�the absorption coefficient of a material usually depends� on� the� wavelength� of� light,� which� means�that� materials� preferentially� absorb� certain�wavelengths�of�light.
Another� point� is� that� not� all� absorbed� light�energy�directly�converts�into�heat.��Depending�on�the�excitation� modes� of� the� absorber,� some� excited�photons�decay�into�some�other�forms�of�photons�with�lower frequencies. If the photon final state after decay�is�in�the�infra-red�region,�it�will�usually�result�in�higher�temperature�rise�since�infra-red�absorption�causes� thermal� agitation.� � In� the� case� of� QTH� and�PAC� LCUs,� photons� with� high� frequencies� were�absorbed� according� to� Einstein’s� equation� (i.e.,�Energy�E=hv,�where�h� is�Planck’s�constant,�and�v� is�frequency).��Therefore,�they�degraded�into�low�energy�photons with increased population, finally causing thermal�agitation.
In� summary,� the� current� study� indicated� that�the� three� commonly� used� dental� photocuring� light�sources�—�namely,�QTH,�PAC,�and�LED�LCUs�—�did�not� reach� the� critical� temperature� rise� which� would�
Dent Mater J 2009; 28(3): 253–260 259
cause�pulpal�injury,�as�reported�by�Zach�and�Cohen28).��However,�the�extrapolation�of�temperatures�obtained�in� this� in vitro� study� cannot� be� directly� applied� to�temperature�changes�in situ�because�of�these�clinical�factors: blood circulation in the pulp chamber, fluid motion� in� the� dentinal� tubules,� as� well� as� the�dynamics� of� surrounding� periodontal� tissue16).� � In�addition,�the�experimental�setup�of�this�study�did�not�consider� heat� conduction� through� composite� resin�polymerization�—�which�could�be�a�weighty�factor�in�clinical�conditions.� �Therefore,� further� in vivo�and� in vitro� investigations�are�needed�to�assess�the�effect�of�exothermic� reaction� of� resin� composites� on�temperature�changes�in�dentin�when�different�curing�methods�are�used.
CONCLUSIONS
Within�the� limitations�of� this� in vitro� study,� it�could�be�concluded�that:
1.� Using� the� irradiation� times� as� recommended�by�the�manufacturers,�the�QTH�LCU�produced�significantly higher temperature rises than did LED�and�PAC�LCUs�in�all�the�test�conditions.
2.� The� standard� and� pulse� modes� of� LED� LCU�showed�lower�mean�values�in�temperature�rise�than�the�soft-start�mode.
3.� Dentin�thickness�was�inversely�proportional�to�temperature�rise.
ACKNOWLEDGMENTS
Special�thanks�to�Prof.�Güngör�Gündüz,�Department�of� Chemical� Engineering,� Middle� East� Technical�University,� for� his� invaluable� contributions� in�explaining the correlation coefficient of the relationship� between� dentin� thickness� and�temperature�rise.
This work was supported by Scientific Research Unit� of� Cumhuriyet� University� (CUBAP),� Project�Number:�DIS-043.
REFERENCES
1) Martin FE. A survey of the efficiency of visible light curing�units.��J�Dent�1998;�26:�239-243.
2)� Deb� S,� Sehmi� H.� � A� comparative� study� of� the�properties� of� dental� resin� composites� polymerized�with� plasma� and� halogen� light.� � Dent� Mater� 2003;�19:�517-522.
3)� Bouillaguet�S,�Caillot�G,�Forchelet�J,�Cattani-Lorente�M,� Wataha� JC,� Krejci� I.� � Thermal� risks� from� LED-�and� high-intensity� QTH-curing� units� during�polymerization�of�dental�resins.��J�Biomed�Mater�Res�Part�B:�Appl�Biomater�2005;�72B:�260-267.
4)� Schneider�LFJ,�Consani�S,�Sinhoreti�MAC,�Sobrinho�LC,� Milan� FM.� � Temperature� change� and� hardness�with� different� resin� composites� and� photo-activation�
methods.��Oper�Dent�2005;�30:�516-521.5)� Schneider�LF,�Consani�S,�Correr-Sobrinho�L,�Correr�
AB,�Sinhoreti�MA.��Halogen�and�LED�light�curing�of�composite:� temperature� increase� and� Knoop�hardness.��Clin�Oral�Invest�2006;�10:�66-71.
6)� Vandewalle� KS,� Roberts� HW,� Tiba� A,� Charlton� DG.��Thermal emission and curing efficiency of LED and halogen�curing�lights.��Oper�Dent�2005;�30:�257-264.
7)� Kurachi� C,� Tuboy� AM,� Magalhães� DV,� Bagnato� VS.��Hardness� evaluation� of� a� dental� composite�polymerized� with� experimental� LED-based� devices.��Dent�Mater�2001;�17:�309-315.
8)� Jandt� KD,� Mills� RW,� Blackwell� GB,� Ashworth� SH.��Depth� of� cure� and� compressive� strength� of� dental�composites� cured� with� blue� light� emitting� diodes�(LEDs).��Dent�Mater�2000;�16:�41-47.
9)� Mills� RW,� Jandt� KD,� Ashworth� SH.� � Dental�composite�depth�of� cure�with�halogen�and�blue� light�emitting�diode�technology.��Br�Dent�J�1999;�186:�388-391.
10)� Moon� HJ,� Lee� YK,� Lim� BS,� Kim� CW.� � Effects� of�various� light� curing� methods� on� the� leachability� of�uncured� substances� and� hardness� of� a� composite�resin.��J�Oral�Rehabil�2004;�31:�258-264.
11)� Oberholzer�TG,�Du�Preez�IC,�Kidd�M.��Effect�of�LED�curing�on�the�microleakage,�shear�bond�strength�and�surface� hardness� of� a� resin-based� composite�restoration.��Biomaterials�2005;�26:�3981-3986.
12) Awliya WY. The influence of temperature on the efficacy of polymerization of composite resin. J Contemp�Dent�Pract�2007;�8:�9-16.
13)� Uhl� A,� Mills� RW,� Jandt� KD.� � Polymerization� and�light-induced� heat� of� dental� composites� cured� with�LED�and�halogen�technology.��Biomaterials�2003;�24:�1809-1820.
14)� Hofmann�N,�Hugo�B,�Klaiber�B.��Effect�of�irradiation�type� (LED� or� QTH)� on� photo-activated� composite�shrinkage� strain� kinetics,� temperature� rise,� and�hardness.��Eur�J�Oral�Sci�2002;�110:�471-479.
15)� Uhl� A,� Mills� RW,� Jandt� KD.� � Photoinitiator�dependent� composite� depth� of� cure� and� Knoop�hardness� with� halogen� and� LED� light� curing� units.��Biomaterials�2003;�24:�1787-1795.
16)� Hannig� M,� Bott� B.� � In-vitro� pulp� chamber�temperature� rise� during� composite� resin�polymerization� with� various� light-curing� sources.��Dent�Mater�1999;�15:�275-281.
17) Kleverlaan CJ, de Gee AJ. Curing efficiency and heat� generation� of� various� resin� composites� cured�with� high-intensity� halogen� lights.� � Eur� J� Oral� Sci�2004;�112:�84-88.
18)� Lovell� LG,� Newman� SM,� Donaldson� MM,� Bowman�CN.� � The� effect� of� light� intensity� on� double� bond�conversion and flexural strength of a model, unfilled dental�resin.��Dent�Mater�2003;�19:�458-465.
19)� Yap� AU,� Soh� MS.� � Thermal� emission� by� different�light-curing�units.��Oper�Dent�2003;�28:�260-266.
20)� Shortall�AC,�Harrington�E.��Temperature�rise�during�polymerization�of�light-activated�resin�composites.� �J�Oral�Rehabil�1998;�25:�908-913.
21)� Mehl� A,� Hickel� R,� Kunzelmann� KH.� � Physical�properties� and� gap� formation� of� light-cured�composites� with� and� without� “soft-start�

Dent Mater J 2009; 28(3): 253–260260
polymerization”.��J�Dent�1997;�25:�321-330.22)� Al-Qudah�AA,�Mitchell�CA,�Biagioni�PA,�Hussey�DL.��
Effect� of� composite� shade,� increment� thickness� and�curing�light�on�temperature�rise�during�photocuring.��J�Dent�2007;�35:�238-245.
23)� Hubbezoglu� I,� Dogan� A,� Dogan� OM,� Bolayir� G,� Bek�B.��Effect�of�light�curing�modes�and�resin�composites�on�temperature�rise�under�human�dentin:�an�in vitro�study.��Dent�Mater�J�2008;�27:�581-589.
24)� Knezevic� A,� Tarle� Z,� Meniga� A,� Sutalo� J,� Pichler� G.��Influence of light intensity from different curing units� upon� composite� temperature� rise.� � J� Oral�Rehabil�2005;�32:�362-367.
25)� Martins�GR,�Cavalcanti�BN,�Rode�SM.� � Increases� in�intrapulpal� temperature� during� polymerization� of�composite�resin.��J�Prosthet�Dent�2006;�96:�328-331.
26)� Ozturk�B,�Ozturk�AN,�Usumez�A,�Usumez�S,�Özer�F.��Temperature� rise� during� adhesive� and� resin�composite� polymerization� with� various� light� curing�sources.��Oper�Dent�2004;�29:�325-332.
27)� Danesh� G,� Davids� H,� Duda� S,� Kaup� M,� Ott� K,�Schafer� E.� � Temperature� rise� in� the� pulp� chamber�induced� by� a� conventional� halogen� light-curing�source�and�a�plasma�arc�lamp.��Am�J�Dent�2004;�17:�203-208.
28)� Zach� L,� Cohen� G.� � Pulp� response� to� externally�applied�heat.��Oral�Surg�Oral�Med�Oral�Pathol�1965;�19:�515-530.
29)� Lloyd� CH,� Joshi� A,� McGlynn� E.� � Temperature� rises�produced� by� light� sources� and� composites� during�curing.��Dent�Mater�1986;�2:�170-174.
30)� Aguiar� FHB,� Barros� GKP,� Santos� AJS,� Ambrosano�GMB,� Lovadino� JR.� � Effect� of� polymerization� modes�and� resin� composite� on� the� temperature� rise� of�human� dentin� of� different� thickneses:� an� in vitro�study.��Oper�Dent�2005;�30:�602-607.
31)� Loney� RW,� Price� RB.� � Temperature� transmission� of�high-output� light-curing�units�through�dentin.� �Oper�Dent�2001;�26:�516-520.
Copyright © 2022 FDOKUMEN