
Systematic Review of the Clinical Course, Natural History, and Prognosis for Pediatric Mild...
9
REVIEW ARTICLE Psychosocial Consequences of Mild Traumatic Brain Injury in Children: Results of a Systematic Review by the International Collaboration on Mild Traumatic Brain Injury Prognosis Michelle L. Keightley, PhD, CPsych, a,b Pierre Co ˆte ´, DC, PhD, c,d,e,f Peter Rumney, MD, g,h Ryan Hung, MD, MSc, g,h Linda J. Carroll, PhD, i Carol Cancelliere, DC, MPH, e,j J. David Cassidy, PhD, DrMedSc e,f,j,k From the a Bloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, Toronto, Ontario, Canada; b Departments of Occupational Science and Occupational Therapy, Psychology and Graduate Department of Rehabilitation Science, University of Toronto, Toronto, Ontario, Canada; c Faculty of Health Sciences, University of Ontario Institute of Technology, Oshawa, Ontario, Canada; d UOIT- CMCC Centre for the Study of Disability Prevention and Rehabilitation, Toronto, Ontario, Canada; e Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Canada; f Division of Epidemiology, Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario, Canada; g Department of Rehabilitation and Complex Continuing Care, Holland Bloorview Kids Rehabilitation Hospital, Toronto, Ontario, Canada; h Department of Pediatrics, University of Toronto, Toronto, Ontario, Canada; i School of Public Health and Alberta Centre for Injury Control and Research, University of Alberta, Edmonton, Alberta, Canada; j Division of Health Care and Outcomes Research, Toronto Western Research Institute, University Health Network, University of Toronto, Toronto, Ontario, Canada; and k Institute of Sports Science and Clinical Biomechanics, Faculty of Health, University of Southern Denmark, Odense, Denmark. Abstract Objective: To synthesize the best available evidence regarding psychosocial consequences of mild traumatic brain injury (MTBI) in children. Data Sources: MEDLINE, Embase, CINAHL, PsycINFO, and SPORTDiscus were searched (2001e2012). Inclusion criteria included published peer-reviewed reports in English, French, Norwegian, Spanish, Swedish, and Danish. References were also identified from relevant reviews and meta-analyses, and the bibliographies of eligible articles. Study Selection: This article presents an update of a previous review with a much larger scope, of which this topic is a small subset of the questions addressed by that review. Controlled trials and cohort and case-control studies were selected according to predefined criteria. Two independent reviewers used modified Scottish Intercollegiate Guidelines Network criteria to critically appraise eligible studies. A total of 77,914 records were screened; 101 of these articles were deemed scientifically admissible, of which 6 investigated the psychosocial consequences of MTBI in children. Data Extraction: Two reviewers independently extracted data from accepted studies into evidence tables. Data Synthesis: We conducted a best-evidence synthesis by linking our conclusions to the evidence tables. Most accepted studies were exploratory rather than confirmatory. Preliminary evidence suggests that most children recover within 3 months post-MTBI. After 1 year, the prevalence of postconcussion symptoms and syndrome is similar between children with MTBI and children with orthopedic injuries. The Supported by the Ontario Neurotrauma Foundation (grant no. 2010-ABI-MTBIWHO-871). The funder was not involved in the design or preparation of the study protocol, or in the management of the project, analysis or interpretation of data, or the preparation of the final article. No commercial party having a direct financial interest in the results of the research supporting this article has conferred or will confer a benefit on the authors or on any organization with which the authors are associated. The findings and conclusions in this research are those of the authors alone and do not necessarily represent the official views or policies of the Centers for Disease Control and Prevention or any agency of the United States government. Inclusion of individuals, programs, or organizations in this article does not constitute endorsement by the United States government. 0003-9993/14/$36 - see front matter ª 2014 by the American Congress of Rehabilitation Medicine http://dx.doi.org/10.1016/j.apmr.2013.12.018 Archives of Physical Medicine and Rehabilitation journal homepage: www.archives-pmr.org Archives of Physical Medicine and Rehabilitation 2014;95(3 Suppl 2):S192-200
Transcript of Systematic Review of the Clinical Course, Natural History, and Prognosis for Pediatric Mild...
REVIEW ARTICLE
Psychosocial Consequences of Mild Traumatic BrainInjury in Children: Results of a Systematic Review bythe International Collaboration on Mild TraumaticBrain Injury Prognosis
Michelle L. Keightley, PhD, CPsych,a,b Pierre Cote, DC, PhD,c,d,e,f Peter Rumney, MD,g,h
Ryan Hung, MD, MSc,g,h Linda J. Carroll, PhD,i Carol Cancelliere, DC, MPH,e,j
J. David Cassidy, PhD, DrMedSce,f,j,k
From the aBloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, Toronto, Ontario, Canada; bDepartments ofOccupational Science and Occupational Therapy, Psychology and Graduate Department of Rehabilitation Science, University of Toronto,Toronto, Ontario, Canada; cFaculty of Health Sciences, University of Ontario Institute of Technology, Oshawa, Ontario, Canada; dUOIT-CMCC Centre for the Study of Disability Prevention and Rehabilitation, Toronto, Ontario, Canada; eInstitute of Health Policy, Managementand Evaluation, University of Toronto, Toronto, Ontario, Canada; fDivision of Epidemiology, Dalla Lana School of Public Health,University of Toronto, Toronto, Ontario, Canada; gDepartment of Rehabilitation and Complex Continuing Care, Holland Bloorview KidsRehabilitation Hospital, Toronto, Ontario, Canada; hDepartment of Pediatrics, University of Toronto, Toronto, Ontario, Canada; iSchool ofPublic Health and Alberta Centre for Injury Control and Research, University of Alberta, Edmonton, Alberta, Canada; jDivision of HealthCare and Outcomes Research, Toronto Western Research Institute, University Health Network, University of Toronto, Toronto, Ontario,Canada; and kInstitute of Sports Science and Clinical Biomechanics, Faculty of Health, University of Southern Denmark, Odense,Denmark.
AbstractObjective: To synthesize the best available evidence regarding psychosocial consequences of mild traumatic brain injury (MTBI) in children.Data Sources: MEDLINE, Embase, CINAHL, PsycINFO, and SPORTDiscus were searched (2001e2012). Inclusion criteria included publishedpeer-reviewed reports in English, French, Norwegian, Spanish, Swedish, and Danish. References were also identified from relevant reviews andmeta-analyses, and the bibliographies of eligible articles.Study Selection: This article presents an update of a previous review with a much larger scope, of which this topic is a small subset of thequestions addressed by that review. Controlled trials and cohort and case-control studies were selected according to predefined criteria. Twoindependent reviewers used modified Scottish Intercollegiate Guidelines Network criteria to critically appraise eligible studies. A total of 77,914records were screened; 101 of these articles were deemed scientifically admissible, of which 6 investigated the psychosocial consequences ofMTBI in children.Data Extraction: Two reviewers independently extracted data from accepted studies into evidence tables.Data Synthesis: We conducted a best-evidence synthesis by linking our conclusions to the evidence tables. Most accepted studies wereexploratory rather than confirmatory. Preliminary evidence suggests that most children recover within 3 months post-MTBI. After 1 year, theprevalence of postconcussion symptoms and syndrome is similar between children with MTBI and children with orthopedic injuries. The
Supported by the Ontario Neurotrauma Foundation (grant no. 2010-ABI-MTBIWHO-871). The funder was not involved in the design or preparation of the study protocol, or in the management of the
project, analysis or interpretation of data, or the preparation of the final article.
No commercial party having a direct financial interest in the results of the research supporting this article has conferred or will confer a benefit on the authors or on any organization with which the
authors are associated.
The findings and conclusions in this research are those of the authors alone and do not necessarily represent the official views or policies of the Centers for Disease Control and Prevention or any agency
of the United States government. Inclusion of individuals, programs, or organizations in this article does not constitute endorsement by the United States government.
0003-9993/14/$36 - see front matter ª 2014 by the American Congress of Rehabilitation Medicinehttp://dx.doi.org/10.1016/j.apmr.2013.12.018
Archives of Physical Medicine and Rehabilitationjournal homepage: www.archives-pmr.org
Archives of Physical Medicine and Rehabilitation 2014;95(3 Suppl 2):S192-200

functional status of children with MTBI improves over a 30-month follow-up period, but further research is needed to investigate the possibilitythat children with MTBI experience greater rates of psychiatric illness during the 3 years after their injury.Conclusions: The prognosis of MTBI is favorable in children. Most appear to recover functionally from a physical and psychological perspective.However, future research should investigate the risk for psychiatric illness.Archives of Physical Medicine and Rehabilitation 2014;95(3 Suppl 2):S192-200
ª 2014 by the American Congress of Rehabilitation Medicine
Mild traumatic brain injury (MTBI), or concussion, is a prevalentinjury in children and youth younger than 19 years (see casedefinition of MTBI below). Determining the true incidence ofpediatric MTBI has historically proven difficult; however, it isestimated that 1 in 220 pediatric emergency department visits isthe result of an MTBI.1 Recent statistics from the Centers forDisease Control and Prevention (CDC) indicate that an estimated3.8 million concussions occur annually in the United States, themajority in children and young adults.2
Similar to adults, youth may experience a range of neuro-behavioral deficits after concussion that can include combinationsof somatic, cognitive, and emotional/behavioral postconcussionsymptoms.3 These deficits can affect psychosocial functioning viaparticipation restrictions in daily activities (eg, sport, school,family, social). Because childhood and adolescence are the periodsduring which the greatest plasticity and growth occurs in thebrain,4,5 it is thought that the young brain may be more vulnerableto the effects of MTBI,6,7 resulting in delayed recovery8 and thepotential for persisting functional deficits that may influencepsychological outcomes. While it has been suggested that in-dividuals with MTBI typically recover within 1 to 2 weeks,9,10
symptoms and related performance deficits persisting for severalweeks to months postinjury have been reported.11 Similarly, ad-olescents have been reported to be more susceptible to short-termneuropsychological and neurophysiological deficits after concus-sion than younger children and adults.12 However, the long-termimpact of MTBI in children remains to be examined, in partic-ular, how short-term MTBI-related psychological deficits influ-ence long-term psychosocial outcomes.
In its 2004 systematic review13 of MTBI prognosis, the WorldHealth Organization (WHO) Collaborating Centre for Neuro-trauma Prevention, Management, and Rehabilitation Task Forcereported that the prognosis is favorable for children with MTBI.The WHO Collaborating Centre Task Force found that post-concussion symptoms were generally transient, usually resolvingwithin 3 months, and resembled symptoms experienced by chil-dren who had sustained other types of injuries (ie, orthopedic). Theevidence available at the time also suggested that few childrenexperienced short- or long-term cognitive deficits and that childrenwith MTBI did not subsequently have higher rates of behavioral orschool problems than children with other types of injuries.13
Little information exists specific to the psychosocial outcomesof MTBI in children. The term psychosocial was first coined byErikson in the 1950s and is generally used to refer to the broadcategory of behavioral/psychological and social determinants oroutcomes. The medical and research communities have prioritizedresearch focused onMTBI in children and youth because of its highprevalence in this population and the potentially disabling conse-quences of the injury.8 The purpose of this systematic review is tosynthesize the best available evidence in order to describe thepsychosocial consequences of MTBI in children, including psy-chosocial outcomes such as behavioral, emotional, psychological,or psychiatric outcomes or family functioning. This article is anupdate of a previous WHO review13 but is focused only on psy-chosocial issues in children. The previousWHO review included allprognostic issues in all age groups. We have done this to providegreater detail on this issue. Other focused prognostic updates arereported in companion articles in this journal supplement.
Methods
Protocol registration
We conducted a systematic review and best-evidence synthesis inorder to update the findings of theWHOCollaborating Task Force.13
The review was conducted and reported in compliance with thePreferred Reporting Items for Systematic Reviews and Meta-Analyses statement.14 In accordance with the statement, oursystematic review protocol was registered in the InternationalProspective Register of Systematic Reviews15 on July 11, 2011, andwas last updated on November 2, 2012 (registration no.CRD42011001410).We also published the protocol for our review.16
Search strategy
The literature search and critical review strategy is outlined indetail elsewhere.17 Briefly, the electronic databases MEDLINE,PsycINFO, Embase, CINAHL, and SPORTDiscus were system-atically searched from January 1, 2001, to June 30, 2011. Thesesearches were updated on February 10, 2012. The search termsincluded “craniocerebral trauma,” ”prognosis,” and ”mental dis-orders” among others. The reference lists of all reviews and meta-analyses related to MTBI, and articles meeting the eligibilitycriteria were screened for additional articles that may have beenmissed by our electronic searches. International Collaboration onMTBI Prognosis (ICoMP) members also provided informationabout studies that they had knowledge of but were not found in thedatabases or reference lists.
Selection of articles
Articles were screened for eligibility according to predefined in-clusion and exclusion criteria. Inclusion criteria included original,
List of abbreviations:CDC Centers for Disease Control and Prevention
CI confidence intervalICoMP International Collaboration on MTBI PrognosisMTBI mild traumatic brain injuryPTSD posttraumatic stress disorderSIGN Scottish Intercollegiate Guidelines NetworkTBI traumatic brain injury
WHO World Health Organization
Psychosocial consequences of mild TBI in children S193
www.archives-pmr.org
published peer-reviewed research reports in English, French,Swedish, Norwegian, Danish, and Spanish. To be included in thisreport on psychosocial outcomes of MTBI in children, studies hadto have a minimum of 30 MTBI pediatric cases and had to assesschildhood psychosocial outcomes such as psychiatric illness,family functioning, or broad indicators of childhood behavior,health, and quality of life. Thus, this article presents a subset ofthe results from the larger review on MTBI prognosis, whichappears in this same journal supplement.
Eligible study designs were controlled trials and cohort andcase-control studies. Exclusion criteria included cross-sectionalstudies, case reports and series, cadaveric studies, biomechanicalstudies, and laboratory studies. While we screened all relevantreviews and meta-analyses to locate primary studies, we did not
critically review them, and they are not included in this best-evidence synthesis.
Case definition
MTBI was defined according to the definitions endorsed by theWHO Collaborating Centre Task Force and the CDC. The WHOTask Force defines MTBI as “an acute brain injury resulting frommechanical energy to the head from external physical forces.Operational criteria for clinical identification include: (i) one ormore of the following: confusion or disorientation, loss of con-sciousness for 30 minutes or less, post-traumatic amnesia for lessthan 24 hours, and/or other transient neurological abnormalities
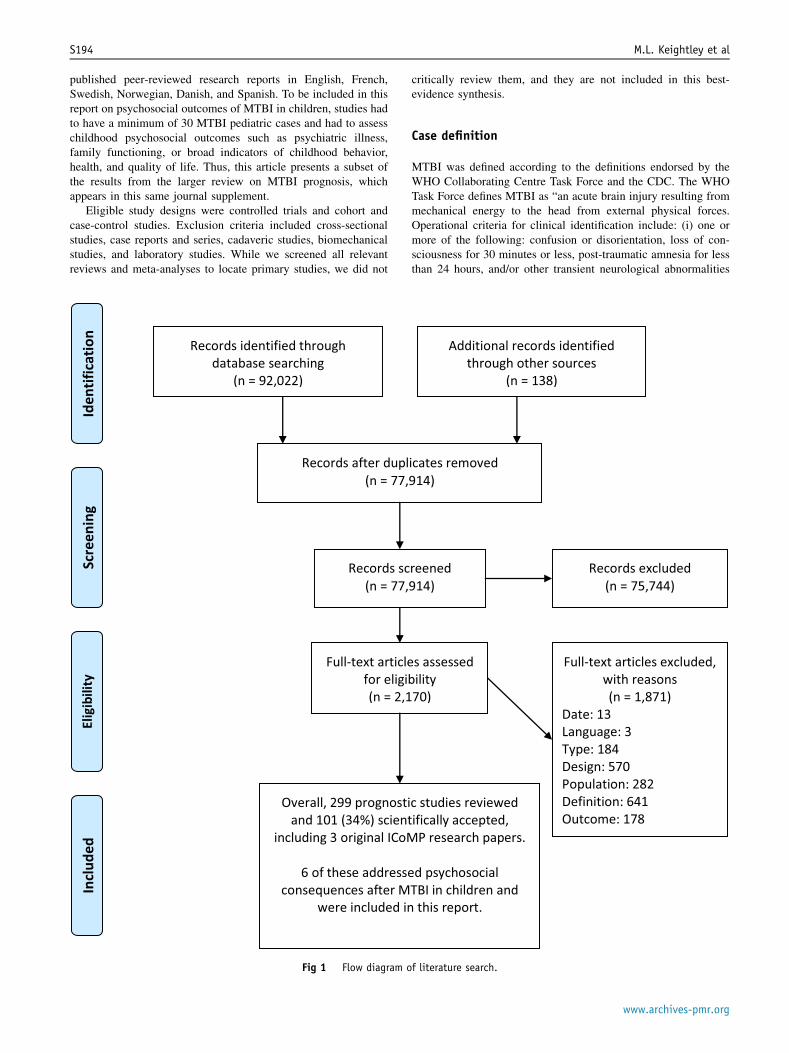
Fig 1 Flow diagram of literature search.
S194 M.L. Keightley et al
www.archives-pmr.org

Table 1 Evidence table of accepted studies on psychosocial outcomes in children with MTBI
Author, Year, CountrySource Population, Study Size,Participation, F/U Inclusion/Exclusion Criteria MTBI Case Definition Prognostic Factors/Outcomes Findings
Course of recoveryAnderson et al,6 2001;Australia
Phase I cohort study
Pediatric admissions to RoyalChildren’s Hospital,Victoria, Australia, becauseof TBI (nZ42)
F/U: 30mo
Age of injury 3 <13 plussubgroup of children aged<3y at time of injury;admission to hospital;ability to completecognitive evaluations;completion of acute, 12-moand 30-mo evaluations
Exclusions: penetrating headinjury, previous TBI; TBI asa result of abuse;preexisting physical,neurologic, psychiatric, ordevelopmental disorder
Admission GCS score, 13e15;documented evidence ofTBI including period ofaltered consciousness; noCT/MRI abnormality, noneurologic deficits
Outcomes: at 30mo, parentsadministered the VinelandAdaptive Behavior Scale;Rowe Behavioral RatingInventory (ages 8e12y)and Personality Inventoryfor Children (ages <8y);Family Functioning Scales;Family Burden of Injury.Resolved and at 30mopostinjury
Improvement was observed inall outcome measures at30mo post-MTBI.
At admission, 83.3% had nodeficits, 14.3% had 1deficit, and 2.4% had 2deficits in functionaldomains. At 30mo, 90.5%had no deficits, 9.5% had 1deficit, and no individualshad 2 deficits.
Hajek, et al,23 2010; UnitedStates
Phase I cohort study
Children (aged 8e15y)recruited from 2 Ohio EDs
MTBI: eligible (nZ393); 48%participated (nZ186); onlyanalyzed those whocompleted all F/Uassessments (nZ167)
Unexposed: OIgroupdeligible (nZ286);35% participated (nZ99);84 were analyzed.
F/U: 2wk, 3mo, 12mo
Inclusion for MTBI group:MTBI.
Inclusion for unexposed (OI):fracture with AIS !3 withno head injury
Exclusion for exposed andunexposed: injury-relatedsurgery, hypoxia or shockpostinjury, previous TBIwith admission, priorneurologic disorder, severepsychiatric disorderrequiring hospitalization;associated injuries with AIS>3; injuries hinderingneuropsychologicalassessment; injuries relatedto child abuse or drug/alcohol use
LOC <30min, GCS score 13e14, "2 symptoms of MTBIreported by ED physicians.Evidence of CT skull fractureor intracranial lesion stillincluded
Course: postconcussivesymptoms, assessed by PCS-I, HBI, posttraumatic stresssymptoms as assessed byPCL-C/PR
Psychosocial outcome:posttraumatic stresssymptoms
Prevalence of PTSD amongpatients with MTBIdecreased from 8% atbaseline to 2% at 12mo.Prevalence of PTSDremained stable at 7% inpatients with OIs.Prevalence ofpostconcussion symptomsamong patients with MTBIand OI decreased frombaseline to 12mo: 51% to19% (for MTBI) and 30% to19% (for OI), respectively.No clinically importantdifference inpostconcussive symptomsand PTSD between MTBI andOI groups
Kenardy et al,22 2012;Australia
Phase I cohort study
Children and adolescents(aged 6e15y) assessed inthe ED of 3 tertiaryhospitals for MTBI (nZ94).
F/U: 2, 3, 6, 12, and 18mo
Inclusion: childhood TBI withdocumented LOC; consentfrom parents; and forchildren aged "10y, assentto participate
GCS score between 13 and 15;absence of neurologic orradiologic abnormalities
Outcomes: Parent Report ChildHealth Questionnaire (CHQ-PF50). Physical (CHQ-Ph50)and psychological (CHQ-PsS)
Children with MTBI recoveredwithin the first 3mo post-MTBI.
(continued on next page)
Psychosocialconsequences
ofmild
TBIin
childrenS195
www.archives-pm
r.org
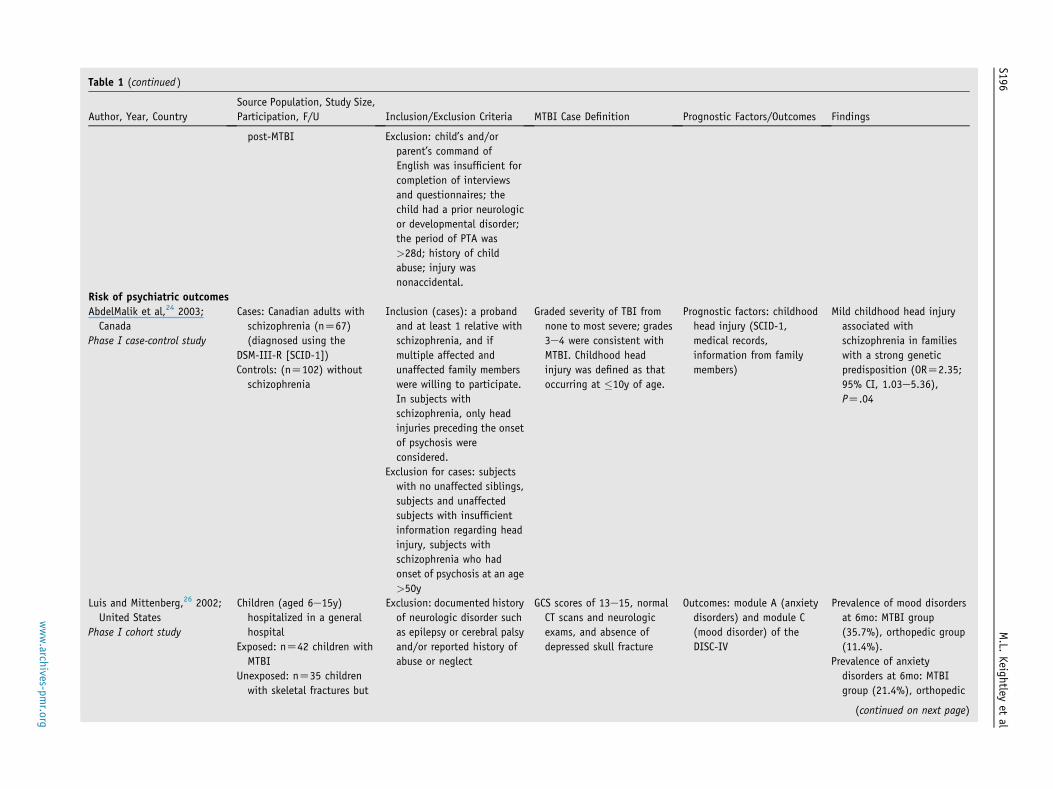
Table 1 (continued )
Author, Year, CountrySource Population, Study Size,Participation, F/U Inclusion/Exclusion Criteria MTBI Case Definition Prognostic Factors/Outcomes Findings
post-MTBI Exclusion: child’s and/orparent’s command ofEnglish was insufficient forcompletion of interviewsand questionnaires; thechild had a prior neurologicor developmental disorder;the period of PTA was>28d; history of childabuse; injury wasnonaccidental.
Risk of psychiatric outcomesAbdelMalik et al,24 2003;Canada
Phase I case-control study
Cases: Canadian adults withschizophrenia (nZ67)(diagnosed using the
DSM-III-R [SCID-1])Controls: (nZ102) withoutschizophrenia
Inclusion (cases): a probandand at least 1 relative withschizophrenia, and ifmultiple affected andunaffected family memberswere willing to participate.In subjects withschizophrenia, only headinjuries preceding the onsetof psychosis wereconsidered.
Exclusion for cases: subjectswith no unaffected siblings,subjects and unaffectedsubjects with insufficientinformation regarding headinjury, subjects withschizophrenia who hadonset of psychosis at an age>50y
Graded severity of TBI fromnone to most severe; grades3e4 were consistent withMTBI. Childhood headinjury was defined as thatoccurring at !10y of age.
Prognostic factors: childhoodhead injury (SCID-1,medical records,information from familymembers)
Mild childhood head injuryassociated withschizophrenia in familieswith a strong geneticpredisposition (ORZ2.35;95% CI, 1.03e5.36),PZ.04
Luis and Mittenberg,26 2002;United States
Phase I cohort study
Children (aged 6e15y)hospitalized in a generalhospital
Exposed: nZ42 children withMTBI
Unexposed: nZ35 childrenwith skeletal fractures but
Exclusion: documented historyof neurologic disorder suchas epilepsy or cerebral palsyand/or reported history ofabuse or neglect
GCS scores of 13e15, normalCT scans and neurologicexams, and absence ofdepressed skull fracture
Outcomes: module A (anxietydisorders) and module C(mood disorder) of theDISC-IV
Prevalence of mood disordersat 6mo: MTBI group(35.7%), orthopedic group(11.4%).
Prevalence of anxietydisorders at 6mo: MTBIgroup (21.4%), orthopedic
(continued on next page)
S196M.L.
Keightleyet
al
www.archives-pm
r.org

Table 1 (continued )
Author, Year, CountrySource Population, Study Size,Participation, F/U Inclusion/Exclusion Criteria MTBI Case Definition Prognostic Factors/Outcomes Findings
no head traumaF/U: 6mo
group (2.8%)
Massagli et al,25 2004; UnitedStates
Phase III cohort study
Exposed: children (aged!14y) with MTBI assessedin ED, hospital andoutpatient clinics in a largehealth maintenanceorganization (nZ490)
Unexposed: children matchedby sex, age, and enrollmentat the time of injury(nZ1470)
F/U: 3y
Inclusion: enrolled in GroupHealth Cooperative of PugetSound on the referencedate, with an ICD-9-CMdiagnosis of TBI
Exclusion: ICD-9-CM TBIdiagnosis in the year prior
CDC criteria: ICD-9-CM codesindicate brief (<1h) LOC orno LOC; no intracraniallesions
Outcomes: psychiatricdiagnoses, psychiatricmedication prescription,and utilization ofpsychiatric services
The 3-y cumulative incidenceof psychiatric illness was30% in MTBI patients vs20% in unexposed children.
Among those with no historyof psychiatric illness, the3-y incidence of psychiatricillness was 26% in MTBIpatients and 16% inunexposed.
Incidence of psychiatricdiagnoses peaked in thefirst year; most commondisorders were thefollowing: other orunspecified mental disorder(13%); hyperactivity(10%); and adjustmentreaction (6%).
Children with MTBI aged 10e14y without a history ofpsychiatric illness weremore likely (RRZ2.3, 95%CI, 1.7e3.2) than childrenaged 0e4y to have apsychiatric illnessdiagnosed.
Abbreviations: AIS, Abbreviated Injury Scale; CHQ, Child Health Questionnaire; CT, computed tomography; DISC-IV, Diagnostic Interview Schedule for ChildreneFourth Edition; DSM-III-R, Diagnostic andStatistical Manual of Mental Disorders, Revised Third Edition; ED, emergency department; F/U, follow-up; GCS, Glasgow Coma Scale; HBI, Health and Behavior Inventory; ICD-9-CM, International Classification ofDiseases, 9th Revision, Clinical Modification; LOC, loss of consciousness; MRI, magnetic resonance imaging; OI, orthopedic injury; OR, odds ratio; PCL-C/PR, PTSD Checklist for Children/Parent Report; PCS-I,Postconcussive Symptom Interview; PTA, posttraumatic amnesia; RR, relative risk; SCID, Structured Clinical Interview.
Psychosocialconsequences
ofmild
TBIin
childrenS197
www.archives-pm
r.org

such as focal signs, seizure, and intracranial lesion not requiringsurgery; and (ii) Glasgow Coma Scale score of 13e15 after 30minutes postinjury or later upon presentation for healthcare. Thesemanifestations of MTBI must not be due to drugs, alcohol, med-ications, caused by other injuries or treatment for other injuries,(eg, systemic injuries, facial injuries or intubation), caused byother problems (eg, psychological trauma, language barrier orcoexisting medical conditions) or caused by penetrating cranio-cerebral injury.”13 Persons with fractured skulls were included ifthey fit this case definition. The CDC provides an additionaldefinition that can be derived from clinical records. According tothe CDC, MTBI is present if an Abbreviated Injury Severity Scalescore of 2 for the head region is documented.18 An administrativedata definition for surveillance or research is also provided.18
Specifically, cases of MTBI are recognized among persons whoare assigned certain International Classification of Diseases, NinthRevision, Clinical Modification diagnostic codes.16
Assessment of methodological quality
The critical appraisal process is reported in detail elsewhere.Briefly, all eligible articles were critically appraised using amodification of the Scottish Intercollegiate Guidelines Network(SIGN) criteria.19 Two reviewers performed independent, in-depthreviews of each eligible study to appraise the methodologicalquality of the articles and assess the impact of selection bias, in-formation bias, and confounding on the results. A third reviewerwas consulted for disagreements. Similarly, 2 reviewers inde-pendently extracted data from scientifically admissible articlesinto evidence tables to inform our results.
Synthesis of evidence
We performed a best-evidence synthesis by extracting data fromaccepted studies (ie, those with a low risk of bias) into evidencetables and linking these to our findings.16 The steps includesearching the literature, evaluating the quality of the studies,extracting findings from the low-risk-of-bias articles into tables, andsynthesizing this best evidence into conclusions about the topic. Ourassessment of bias was completed before tabling the evidence, anddata extracted into the evidence table included author, year andcountry of publication; source population, study size, participation,and follow-up; inclusion/exclusion criteria; MTBI case definition(as originally published); prognostic factors/outcomes; and find-ings.16 We used evidence that was restricted to psychosocial con-sequences after MTBI in children. The data from studies thatincluded a range of severity of TBI were excluded unless the resultswere stratified to present MTBI-specific findings. We also catego-rized the evidence on relevant prognostic factors as exploratory orconfirmatory, using the phases of study framework described byCote et al.20 Phase I studies are hypothesis-generating investigationsthat explore the associations between potential prognostic factorsand disease outcomes in a descriptive or univariate way. Phase IIstudies are extensive exploratory analyses that focus on particularsets of prognostic factors, or attempt to discover which factors havethe highest prognostic value. Phase I and phase II studies providepreliminary evidence. Lastly, phase III studies are large confirma-tory studies of explicit prestated hypotheses that allow for a focusedexamination of the strength, direction, and independence of theproposed relationship between a prognostic factor and the outcomeof interest. Information from accepted phase III studies is
considered the strongest evidence, followed by evidence fromaccepted phase II studies. Phase I studies do not consider con-founding factors and are considered more limited evidence.
Results
This article reports on the subset of articles of MTBI prognosisthat relate to psychosocial outcomes in children after MTBI. Forthe larger entire ICoMP review addressing MTBI prognosis, atotal of 77,914 records were screened, and 299 met the eligibilitycriteria. Of these, 101 were accepted as scientifically admissible(ie, low risk of bias according to SIGN criteria) (fig 1).17 Of the101 accepted articles for the entire MTBI prognosis review, 6 wererelated to psychosocial prognosis in children after MTBI and wereincluded in this article (table 1).
Most of the evidence on the psychosocial consequences of MTBIin children is preliminary. Of the 6 accepted studies, 5 were phase Istudies and 1 was a phase III study.21-26 Three studies23-26 were con-ducted in theUnitedStates, 2 studieswere conducted inAustralia,21,22
and 1 study24 was conducted in Canada. Most participants wereyounger than 15 years and recruited from hospital emergency de-partments. Follow-up periods varied from 12 to 30 months.
Course of recovery of psychosocial outcomes after MTBI
Three studies, all phase I exploratory studies, report on recovery ofpsychosocial functioning after MTBI. One study suggests that ac-cording to parents’ reports, most children aged 6 to 15 years withMTBI recruited from emergency departments in Australia recovertheir physical, psychological, and social functioning within 3months of their injury.22 In the United States, the point prevalenceof postconcussion symptoms was assessed at baseline (within 3wkof injury), at 3 months, and again 1 year after the injury in children(aged 8e15y) with MTBI and in children with orthopedic in-juries.23 At baseline, the prevalence of these symptoms was higherin the MTBI group (52% vs 30%), but by 3 months the prevalencewas no different between groups, and at 1 year the prevalence ofpostconcussion symptoms was 19% in both groups. However, in thesame population, posttraumatic stress disorder (PTSD) developedin a small number of children; the point prevalence of PTSDassessed 1 year after the injury was higher in children with ortho-pedic injuries (7%) than those with MTBI (2%).23 Finally, 2studies21,22 of Australian children recruited from hospitals suggestthat the functional status of children with MTBI improves steadilyover the first 6 to 12 months postinjury and does not appear todeteriorate over a 30-month follow-up.
Risk of psychiatric illness and utilization of psychiatricservices
Three studies (2 phase I studies and 1 phase III cohort study)investigated the association between MTBI in children and sub-sequent psychiatric illness.24-26
AbdelMalik et al24 studied the association between MTBI andschizophrenia in a family-matched case-control study of familieswith a strong genetic disposition for schizophrenia (phase I study).The authors found a positive association (odds ratio, 2.35; 95%confidence interval [CI], 1.03e5.36) between MTBI and schizo-phrenia (diagnosed according to the Diagnostic and StatisticalManual of Mental Disorders, Revised Third Edition [StructuredClinical Interview] criteria). However, the majority of participants
S198 M.L. Keightley et al
www.archives-pmr.org

were reporting on an MTBI that had occurred decades earlier,which may have compromised the validity of the study.
Luis and Mittenberg26 compared 42 children with MTBI and35 children with skeletal fractures without head trauma who wereadmitted to a general hospital (phase I cohort study). The preva-lence of mood disorders assessed 6 months after onset was higherin the MTBI group (35.7%) than in the orthopedic group (11.4%),as was the prevalence of anxiety disorders (21.4% for MTBI vs2.8% for the orthopedic group).
Another study ofU.S. children (phase III cohort) investigated theincidence of psychiatric diagnoses, psychiatric medication pre-scription, and utilization of psychiatric services for children (age!14y) with diagnosed MTBI compared with unexposed sex- andage-matched children from the same health maintenance organi-zation.25 Children with a prior history of psychiatric illness,regardless of whether they had sustained an MTBI, were atincreased risk for a subsequent psychiatric disorder, and MTBI didnot increase that risk. However, for those children with no priorpsychiatric diagnosis during the year before their injury, thosechildren with MTBI were more likely to have a psychiatric illnessdiagnosed in the 3 years postinjury compared with the non-MTBI-injured controls (relative risk, 1.62; 95% CI, 1.0e2.7).25 Thisincreased risk in children with MTBI was observed especially for adiagnosis of hyperactivity during the first year postinjury comparedwith controls (relative risk, 7.59; 95% CI, 2.7e21.6).25 However,that associationwas no longer present by the second year postinjury.
Discussion
Clearly, there is a lack of attention to the psychosocial consequencesafter MTBI in children within the available literature. Despite suchlimited evidence, our review is the first of its kind to focus uniquelyon psychosocial outcomes afterMTBI in children. The best availableevidence fromour review suggests that for childrenwithMTBI,mostsymptoms resolve within 3 months of the injury,22,23 and theirfunctional status improves steadily over the first 6 to 12 monthspostinjury without obvious deterioration over a 30-month follow-upperiod.21,22 In 2004, the WHO Collaborating Centre Task Force onMTBI found that the prognosis formost children afterMTBI is good,with quick resolution of symptoms and little evidence of residualcognitive, behavioral, or academic deficits.13 However, we alsofound 3 studies24-26 (1 phase III, 2 phase I) that focused on psychi-atric illness and utilization of psychiatric services, and all indicated apositive association between childhood MTBI and subsequent psy-chiatric diagnoses, including mood and hyperactivity disorderswithin the following 3 years postinjury. Only 125 of these studieswasa phase III study, and although it was a large study with a strongdesign, the age- and sex-matched control group did not have aninjury. However, 124 of the other phase I studies, which did includecontrols with other injuries, also found an MTBI-related increasedrisk of psychiatric illness. Although these findings need to beconfirmed in future research, they suggest increased concern aboutMTBI exposures in children. We recommend that more, better-designed, confirmatory studies be done in the very near future.
We were disappointed to find so few high-quality studiesaddressing this important topic. The reviewed literature was small,and several methodological issues limit its validity. For instance,most study participants were recruited from hospital emergencydepartments that may have included a select group of patients withmore severe injuries. This limits the generalizability of the findings,given that many youth who experience a milder MTBI may not
present to a hospital. In addition, because of the limited number ofstudies, the findings reflect a fairly narrow scope of psychosocialoutcomes. Psychosocial health in children represents amuch broaderrealmof function, and the lack of studies focusing on other importantoutcomes, such as overall childhood quality of life, represents asignificant limitation. Future studies should measure different psy-chosocial factors in a hierarchical fashion, combining specific familyand childhood indicators and history with persisting posttraumasymptomatology, psychiatric behaviors, and diagnoses with quality-of-life outcomes in order to better understand their interactions withoutcomes. Furthermore, the longest time frame for follow-up was 30months, and this should be expanded, especially given the broad ageranges captured in most MTBI participant samples. For example, itwould be worthwhile to systematically evaluate how sex or age atonset might influence psychosocial outcomes in early adulthood andbeyond. Finally, the research did not address the possibility for earlyintervention (ie, within the first year) for those youth with a pre-morbid psychiatric disturbance or vulnerability, as well as MTBI-related PTSD, in order to influence outcome.25 Although speculativeat this point, research could certainly be conducted to investigate thevalue of cognitive behavioral or trauma-specific therapies with thissubset of the MTBI pediatric population.
To summarize, there is a great need for well-designed, long-term confirmatory studies that consider potential confounders, tobetter understand psychosocial outcomes after childhood MTBI.Potential confounders that were not well explored across thestudies include sex, age at onset of injury, family socioeconomicstatus, prior health and functioning, and the general impact ofinjuries in children. Furthermore, future studies should considerthe impact of MTBI on broader measures of psychosocial functionsuch as childhood quality of life.
Study limitations
Our review has limitations.27 Publication bias is possible since weonly reviewed studies that were published in peer-reviewed journalsand in specific languages. Therefore, potentially relevant studiesmay have been missed. Several different review teams assessedstudies for eligibility and quality. There is a certain amount ofsubjectivity involved with this process. As such, some teams mayhave rejected articles that others would have deemed admissible andvice versa. Similarly, certain studies could have been excluded thatother teams may have deemed eligible. However, we tried to guardagainst these problems by having 2 reviewers independently assessstudies using explicit criteria for inclusion and exclusion, as well asreview the evidence using the SIGN criteria. Furthermore, it shouldbe noted that the articles reviewed on MTBI in children sometimesincluded intracranial lesions, as long as the other criteria for MTBI(usually Glasgow Coma Scale, loss of consciousness, and post-traumatic amnesia) were satisfied. This was not our case definition,but those from the best available studies.16
Our findings are also limited by the quality of studies availablein the literature.
Biases could still exist in the studies we accepted for our best-evidence synthesis. Selection bias is a major concern and refers todifferences in the baseline characteristics of individuals indifferent groups such as can occur when the groups being studiedare not selected from the same source population and are thus notcomparable. Ascertaining a study’s risk for selection bias was attimes difficult because of inadequate reporting. Selection bias isalso a major threat if differential and nonrandom attrition occurs
Psychosocial consequences of mild TBI in children S199
www.archives-pmr.org

in a study. Information bias is also a major concern, especiallywhen participants are asked to recall a past exposure of MTBI thatmay have occurred decades before data collection.
Conclusions
Overall, there is a dearth of literature focusing on psychosocialoutcomes after MTBI in children and youth. Those studies thatwere reviewed contained a number of methodological weaknessesand biases. Furthermore, the shortage of confirmatory studies(phase III)20 regarding prognosis after pediatric MTBI preventsfirm conclusions. Three studies described a positive associationbetween childhood MTBI and the risk of subsequent psychiatricdiagnoses, but this finding needs to be confirmed in additional,well-designed phase III studies. Future research in this area needsto improve to address the shortcomings that we have identified.This will help to develop better evidence-based guidelines forfollow-up care and treatment in children and youth with MTBI,and could have particular importance for those youth with pre-morbid psychiatric, familial, and behavioral dysfunction.
Keywords
Brain injuries; Craniocerebral trauma; Pediatric; Psychologicaloutcomes; Recovery of function; Rehabilitation
Corresponding author
Correspondence to Michelle L. Keightley, PhD, CPsych, HollandBloorview Kids Rehabilitation Hospital, Room 2W355, 150 Kil-gour Rd, Toronto, ON, M4G 1R8. E-mail address: [email protected].
Acknowledgments
We thank the other members of ICoMPdJean-Luc af Geijerstam,Jorgen Borg, Eleanor Boyle, Victor G. Coronado, James Donovan,Alison K. Godbolt, Jan Hartvigsen, Cesar A. Hincapie, Lena W.Holm, Vicki L. Kristman, Alvin Li, Connie Marras, CatharinaNygren-de Boussard, and Britt-Marie Stalnacke; Panos Lambiris,Information Scientist, University Health Network, for assisting indeveloping, testing, and updating the search strategies; and MeijiaZhou for assistance with retrieving and screening articles.
References
1. Meehan WP III, Mannix R. Pediatric concussions in United Statesemergency departments in the years 2002 to 2006. J Pediatr 2010;157:889-93.
2. Langlois JA, Rutland-Brown W, Wald MM. The epidemiology andimpact of traumatic brain injury: a brief overview. J Head TraumaRehabil 2006;21:375-8.
3. Kirkwood MW, Yeates KO, Wilson PE. Pediatric sport-relatedconcussion: a review of the clinical management of an oft-neglectedpopulation. Pediatrics 2006;117:1359-71.
4. Giedd JN, Blumenthal J, Jeffries NO, et al. Brain development duringchildhood and adolescence: a longitudinal MRI study. Nat Neurosci1999;2:861-3.
5. Sowell ER, Thompson PM, Holmes CJ, Batth R, Jernigan TL,Toga AW. Localizing age-related changes in brain structure betweenchildhood and adolescence using statistical parametric mapping.Neuroimage 1999;9(6 Pt 1):587-97.
6. Anderson V, Catroppa C, Morse S, Haritou F, Rosenfeld J. Outcomefrom mild head injury in young children: a prospective study. J ClinExp Neuropsychol 2001;23:705-17.
7. McCrory P, Collie A, Anderson V, Davis G. Can we manage sportrelated concussion in children the same as in adults? Br J Sports Med2004;38:516-9.
8. McCrory P, Meeuwisse W, Johnston K, et al. Consensus statement onconcussion in sport 3rd InternationalConference onConcussion in Sportheld in Zurich, November 2008. Clin J Sport Med 2009;19:185-200.
9. Lovell MR, Collins MW, Iverson GL, et al. Recovery from mildconcussion in high school athletes. J Neurosurg 2003;98:296-301.
10. McCrea M, Guskiewicz KM, Marshall SW, et al. Acute effects andrecovery time following concussion in collegiate football players: theNCAA Concussion Study. JAMA 2003;290:2556-63.
11. Gagnon I, Galli C, Friedman D, Grilli L, Iverson GL. Active reha-bilitation for children who are slow to recover following sport-relatedconcussion. Brain Inj 2009;23:956-64.
12. Baillargeon A, Lassonde M, Leclerc S, Ellemberg D. Neuropsycho-logical and neurophysiological assessment of sport concussion inchildren, adolescents and adults. Brain Inj 2012;26:211-20.
13. Carroll LJ, Cassidy JD, Peloso PM, et al. Prognosis for mild traumaticbrain injury: results of the WHO Collaborating Centre Task Force onMild Traumatic Brain Injury. J RehabilMed 2004;36(43 Suppl):84-105.
14. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group.Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. PLoS Med 2009;6:e1000097.
15. International prospective register of systematic reviews (PROSPERO).Available at: http://www.crd.york.ac.uk/prospero/. Accessed 2011.
16. Cancelliere C, Cassidy JD, Cote P, et al. Protocol for a systematicreview of prognosis after mild traumatic brain injury: an update of theWHO Collaborating Centre Task Force findings. Syst Rev 2012;1:17.
17. Cancelliere C, Cassidy JD, Li A, Donovan J, Cote P, Hincapie CA.Systematic search and review procedures: results of the InternationalCollaboration on MTBI Prognosis. Arch Phys Med Rehabil 2014;95(3 Supplement 2):S101-31.
18. National Center for Injury Prevention and Control. Report to Congresson mild traumatic brain injury in the United States: steps to prevent aserious public health problem. Atlanta: Centers for Disease Controland Prevention; 2003.
19. Scottish Intercollegiate Guidelines Network (SIGN). Available at:http://www.sign.ac.uk/. Accessed 2011.
20. Cote P, Cassidy JD, Carroll L, Frank JW, Bombardier C. A systematicreview of the prognosis of acute whiplash and a new conceptualframework to synthesize the literature. Spine (Phila Pa 1976) 2001;26:E445-58.
21. Anderson VA, Catroppa C, Haritou F, Morse S, Rosenfeld JV. Identifyingfactors contributing to child and family outcome 30months after traumaticbrain injury in children. J Neurol Neurosurg Psychiatry 2005;76:401-8.
22. Kenardy J, Le Brocque R, Hendrikz J, Iselin G, Anderson V,McKinlay L. Impact of posttraumatic stress disorder and injuryseverity on recovery in children with traumatic brain injury. J ClinChild Adolesc Psychol 2012;41:5-14.
23. Hajek CA, Yeates KO, Gerry Taylor H, et al. Relationships amongpost-concussive symptoms and symptoms of PTSD in childrenfollowing mild traumatic brain injury. Brain Inj 2010;24:100-9.
24. AbdelMalik P, Husted J, Chow EWC, Bassett AS. Childhood headinjury and expression of schizophrenia in multiply affected families.Arch Gen Psychiatry 2003;60:231-6.
25. Massagli TL, Fann JR, Burington BE, Jaffe KM, Katon WJ,Thompson RS. Psychiatric illness after mild traumatic brain injury inchildren. Arch Phys Med Rehabil 2004;85:1428-34.
26. Luis CA, Mittenberg W. Mood and anxiety disorders following pe-diatric traumatic brain injury: a prospective study. J Clin Exp Neu-ropsychol 2002;24:270-9.
27. Kristman VL, Borg J, Godbolt AK, et al. Methodological issues andresearch recommendations for prognosis after mild traumatic braininjury: results of the InternationalCollaborationonMildTraumaticBrainInjury Prognosis. Arch Phys Med Rehab 2014;95(3 Suppl 2):S265-77.
S200 M.L. Keightley et al
www.archives-pmr.org




















