
Neuroimaging Correlates of Traumatic Brain Injury and Suicidal Behavior
14
J Head Trauma Rehabil Vol. 26, No. 4, pp. 276–289 Copyright c 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins Neuroimaging Correlates of Traumatic Brain Injury and Suicidal Behavior Deborah A. Yurgelun-Todd, PhD; C. Elliott Bueler, BA; Erin C. McGlade, PhD; John C. Churchwell, PhD; Lisa A. Brenner, PhD; Melissa P. Lopez-Larson, MD Introduction: There is an urgent need to define the neurobiological and cognitive underpinnings of suicidal ideation and behavior in veterans with traumatic brain injury (TBI). Separate studies implicate frontal white matter systems in the pathophysiology of TBI, suicidality, and impulsivity. We examined the relationship between the integrity of major frontal white matter (WM) systems on measures of impulsivity and suicidality in veterans with TBI. Methods: Fifteen male veterans with TBI and 17 matched healthy controls (HC) received clinical ratings, measures of impulsivity and MRI scans on a 3T magnet. Diffusion tensor imaging (DTI) data for the genu and cingulum were analyzed using Freesurfer and FSL. Correlations were performed for fractional anisotropy (FA) (DTI) values and measures of suicidality and impulsivity for veterans with TBI. Results: Significantly decreased in FA values in the left cingulum (P = 0.02), and left (P = 0.02) and total genu (P = 0.01) were observed in the TBI group relative to controls. Measures of impulsivity were significantly greater for the TBI group and total and right cingulum FA positively correlated with current suicidal ideation and measures of impulsivity (P <0.03). Conclusion: These data demonstrate a significant reduction in FA in frontal WM tracts in veterans with mild TBI that was associated with both impulsivity and suicidality. These findings may reflect a neurobiological vulnerability to suicidal risk related to white matter microstructure. Keywords: diffusion tensor imaging, magnetic resonance imaging, suicide, TBI E FFORTS at understanding the neurobiological cor- relates of traumatic brain injury (TBI), prefrontal function, and suicidal ideation have thus far provided in- conclusive results. Concussion and primary blast-related TBI are common in returning veterans and appear to produce neurophysiological changes that resemble dif- fuse axonal injury (DAI). Standard magnetic resonance imaging (MRI) may not be sensitive to these brain alterations, 1 but they may be detectable with newer dif- fusion tensor imaging (DTI) methods. 2 Although DTI imaging methods have begun to identify alterations in white matter associated with TBI, there is a paucity of data accounting for the link between TBI and the in- Author Affiliations: The Brain Institute, University of Utah, Salt Lake City, Utah (Drs Yurgelun-Todd, McGlade, Churchwell, and Lopez-Larson, and Mr Bueler); University of Utah School of Medicine, Salt Lake City, Utah (Drs Yurgelun-Todd and Lopez-Larson); VA VISN 19 Mental Illness Research, Education and Clinical Center (MIRREC), Salt Lake City, Utah (Drs Yurgelun-Todd, McGlade, and Lopez-Larson); VA VISN 19 MIRECC, Denver, Colorado (Dr Brenner); Department of Psychiatry, University of Colorado Denver, School of Medicine, Denver, Colorado (Dr Brenner); Department of Physical Medicine and Rehabilitation, University of Colorado Denver, School of Medicine, Denver, Colorado (Dr Brenner); and Department of Neurology, University of Colorado Denver, School of Medicine, Denver, Colorado (Dr Brenner). This work was supported by research grants from Merit review 5I01CX000253–02 and VISN 19 MIRECC. Corresponding Author: Deborah A. Yurgelun-Todd, PhD, The Brain Insti- tute, 383 Colorow Dr, Salt Lake City, UT 84108 (deborah.yurgelun-todd@ hsc.utah.edu). DOI: 10.1097/HTR.0b013e31822251dc creased risk for suicide among veteran populations. It has been theorized that an important mediating fac- tor between the postinjury onset of psychiatric disorder and the presence of suicidal ideation is an increase in impulsivity, which may impair higher-order cognitive functions. 3 Disruptions in brain neural circuits that sup- port cognitive processing in individuals with TBI may result in deficits in inhibitory function resulting in in- creased impulsivity and poor decision-making capacity. Further, it has been proposed that impulsivity may serve as a marker for suicide risk and several studies have reported that individuals who have attempted suicide demonstrate greater impulsivity. 4,5 Overall, these find- ings indicate the importance of examining alterations in white matter microstructure in prefrontal and frontolim- bic circuits as they relate to impulsivity and suicidal risk. A number of investigations have highlighted the cor- relation of mild to severe TBI from various causes such as falls, motor vehicle accidents, and assaults with elevated risk for suicide. 6,7 The importance of understanding the short- and long-term behavioral and neuropsychological sequelae of mild to severe TBI events cannot be over- stated. One recent study of 16 civilian participants with severe and diffuse TBI as a result of a motor or bicycle accident reported reductions in mental speed, decreased attentional capacity, and reduced mental efficiency. 8 Furthermore, individuals with TBI have been shown to have increased impulsivity, irritability, and frustration as well. 8,9 As noted earlier, growing evidence suggests a significant connection between impulsivity and suicidal Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 276
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Neuroimaging Correlates of Traumatic Brain Injury and Suicidal Behavior

J Head Trauma RehabilVol. 26, No. 4, pp. 276–289Copyright c© 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins
Neuroimaging Correlates of TraumaticBrain Injury and Suicidal Behavior
Deborah A. Yurgelun-Todd, PhD; C. Elliott Bueler, BA; Erin C. McGlade, PhD;John C. Churchwell, PhD; Lisa A. Brenner, PhD; Melissa P. Lopez-Larson, MD
Introduction: There is an urgent need to define the neurobiological and cognitive underpinnings of suicidal ideationand behavior in veterans with traumatic brain injury (TBI). Separate studies implicate frontal white matter systemsin the pathophysiology of TBI, suicidality, and impulsivity. We examined the relationship between the integrityof major frontal white matter (WM) systems on measures of impulsivity and suicidality in veterans with TBI.Methods: Fifteen male veterans with TBI and 17 matched healthy controls (HC) received clinical ratings, measuresof impulsivity and MRI scans on a 3T magnet. Diffusion tensor imaging (DTI) data for the genu and cingulumwere analyzed using Freesurfer and FSL. Correlations were performed for fractional anisotropy (FA) (DTI) valuesand measures of suicidality and impulsivity for veterans with TBI. Results: Significantly decreased in FA values inthe left cingulum (P = 0.02), and left (P = 0.02) and total genu (P = 0.01) were observed in the TBI group relativeto controls. Measures of impulsivity were significantly greater for the TBI group and total and right cingulum FApositively correlated with current suicidal ideation and measures of impulsivity (P <0.03). Conclusion: These datademonstrate a significant reduction in FA in frontal WM tracts in veterans with mild TBI that was associated withboth impulsivity and suicidality. These findings may reflect a neurobiological vulnerability to suicidal risk relatedto white matter microstructure. Keywords: diffusion tensor imaging, magnetic resonance imaging, suicide, TBI
EFFORTS at understanding the neurobiological cor-relates of traumatic brain injury (TBI), prefrontal
function, and suicidal ideation have thus far provided in-conclusive results. Concussion and primary blast-relatedTBI are common in returning veterans and appear toproduce neurophysiological changes that resemble dif-fuse axonal injury (DAI). Standard magnetic resonanceimaging (MRI) may not be sensitive to these brainalterations,1 but they may be detectable with newer dif-fusion tensor imaging (DTI) methods.2 Although DTIimaging methods have begun to identify alterations inwhite matter associated with TBI, there is a paucity ofdata accounting for the link between TBI and the in-
Author Affiliations: The Brain Institute, University of Utah, Salt LakeCity, Utah (Drs Yurgelun-Todd, McGlade, Churchwell, andLopez-Larson, and Mr Bueler); University of Utah School of Medicine,Salt Lake City, Utah (Drs Yurgelun-Todd and Lopez-Larson); VA VISN19 Mental Illness Research, Education and Clinical Center (MIRREC),Salt Lake City, Utah (Drs Yurgelun-Todd, McGlade, and Lopez-Larson);VA VISN 19 MIRECC, Denver, Colorado (Dr Brenner); Department ofPsychiatry, University of Colorado Denver, School of Medicine, Denver,Colorado (Dr Brenner); Department of Physical Medicine andRehabilitation, University of Colorado Denver, School of Medicine,Denver, Colorado (Dr Brenner); and Department of Neurology, Universityof Colorado Denver, School of Medicine, Denver, Colorado (Dr Brenner).
This work was supported by research grants from Merit review5I01CX000253–02 and VISN 19 MIRECC.
Corresponding Author: Deborah A. Yurgelun-Todd, PhD, The Brain Insti-tute, 383 Colorow Dr, Salt Lake City, UT 84108 ([email protected]).
DOI: 10.1097/HTR.0b013e31822251dc
creased risk for suicide among veteran populations. Ithas been theorized that an important mediating fac-tor between the postinjury onset of psychiatric disorderand the presence of suicidal ideation is an increase inimpulsivity, which may impair higher-order cognitivefunctions.3 Disruptions in brain neural circuits that sup-port cognitive processing in individuals with TBI mayresult in deficits in inhibitory function resulting in in-creased impulsivity and poor decision-making capacity.Further, it has been proposed that impulsivity may serveas a marker for suicide risk and several studies havereported that individuals who have attempted suicidedemonstrate greater impulsivity.4,5 Overall, these find-ings indicate the importance of examining alterations inwhite matter microstructure in prefrontal and frontolim-bic circuits as they relate to impulsivity and suicidal risk.
A number of investigations have highlighted the cor-relation of mild to severe TBI from various causes such asfalls, motor vehicle accidents, and assaults with elevatedrisk for suicide.6,7 The importance of understanding theshort- and long-term behavioral and neuropsychologicalsequelae of mild to severe TBI events cannot be over-stated. One recent study of 16 civilian participants withsevere and diffuse TBI as a result of a motor or bicycleaccident reported reductions in mental speed, decreasedattentional capacity, and reduced mental efficiency.8
Furthermore, individuals with TBI have been shown tohave increased impulsivity, irritability, and frustrationas well.8,9 As noted earlier, growing evidence suggests asignificant connection between impulsivity and suicidal
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
276

Neuroimaging Correlates of TBI and Suicide 277
behavior. Using the Test of Variable Attention, a con-tinuous performance measure sensitive to impulsivity,Horesh5 found that commission and omission errorsdifferentiated individuals who have attempted suicidefrom nonattempters. This report is consistent with re-sults from a study by Gorlyn,4 which found that indi-viduals who have attempted suicide scored higher onlaboratory measures of impulsivity. These findings lendfurther support for an association between impulsivityand suicide and suggest that both self-report and labo-ratory measures of impulsivity may have predictive va-lidity relative to suicidal behavior. Similarly, in a groupof affectively ill patients followed naturalistically for upto 14 years, Maser et al10 found that individuals whohave attempted and completed suicide shared a num-ber of core characteristics, including impulsivity. More-over, impulsivity was again found to be one of the bestprospective predictors of completed suicides. Together,these findings support previously held notions that im-pulsivity is indeed a risk factor for suicidality.
Impulsivity may also play a role in other cognitiveimpairments seen in suicidal behavior, such as impairedmental flexibility and reduced problem solving abil-ity. For example, deficits in problem solving have beenwidely implicated in the onset and perpetuation of sui-cidal ideation and suicide attempts.11 Decision mak-ing involves the evaluation of gains and losses associ-ated with choice outcomes among possible alternatives.Problem solving and decision making require multiplesteps including establishing a preference among alterna-tives, response selection, and the experience of choiceoutcome.12 Impulsivity may contribute to poor deci-sion making ability by reducing deliberative processingtime, decreasing one’s ability to attend to alternativesand by decreasing response control resulting in behav-ioral disinhibition. Thus, increased impulsivity may bedisruptive at multiple points within the decision makingprocess. Recent studies have implicated specific neuro-biological processes in problem solving and decisionmaking that may link them to structural brain changesseen in TBI. In particular, TBI may result in increasedbehavioral dyscontrol13 and behavioral disinhibition,14
which may increase risk for self-injury and suicide.15
Behavioral disinhibition has been associated with poorexecutive functioning, which is supported by the pre-frontal cortex, a brain region that has been shown tobe especially vulnerable to mild, moderate, and severeTBI.16–18 These findings suggest that neurobiologicalunderpinnings of suicidal ideation and behavior in veter-ans with TBI may be associated with changes in frontallymediated executive function. Diffusion tensor imagingprovides a sensitive technique for exploring frontal brainchanges as they relate to behavioral risk for suicide.
Conventional MRI allows for adequate visualizationof brain structures; however, white matter tracts are
not readily distinguishable. Using standard techniques,white matter tracts appear homogenous, without anysuggestion of the actual complex arrangement of thefiber tracts themselves. Diffusion tensor imaging (DT-MRI) is a modality designed to measure differencesin constraints on water diffusion in various types oftissue.19 There are 2 primary DTI metrics used to as-sess white matter integrity—fractional anisotropy (FA)and apparent diffusion coefficient (ADC). Fractionalanisotropy is a measurement from 0 to 1, where 0 rep-resents maximal isotropic diffusion of water (eg, freediffusion in perfect sphere) and 1 represents maximalanisotropic diffusion(ie, diffusion of water in a singledirection).20 Apparent diffusion coefficient, or mean dif-fusivity (MD), serves as an index of the rate of diffusionaveraged over all directions.21 Elevated FA beyond nor-mal values have been reported even in mild TBI and mayreflect an inflammatory response such as axonal swellingor cytotoxic edema.22–26 For example, in a study of pa-tients with TBI observed within 6 days postinjury (meantime postinjury <3 days), Wu et al24 found that, com-pared with controls, patients exhibited increased FA inthe cingulum bundle bilaterally. In contrast, lower FA,which has also been reported in mild TBI, may indi-cate axonal degradation and disruption with excess wa-ter between tracts or in periventricular spaces.27 Recentfindings from Hartikainen et al28 are consistent with evi-dence suggesting an acute increase in FA following mildto moderate head injury indicative of axonal swellingand then a long-term decrease in FA.
Diffusion tensor imaging has proven effective in ob-serving the relationship between behavioral traits andstructural connectivity within the brain. For example,studies of non-TBI populations have reported abnormalwhite matter and/or reduced FA in frontal regions thatare associated with measures of impulsivity. In a studyof patients with attention-deficit/hyperactivity disorder,DTI measures of frontal FA were reported to correlatewith impulsivity.29 Using the Stroop Task as a measureof inhibition in methamphetamine abusers, Salo andcolleagues30 reported FA values within the genu cor-related significantly with measures of cognitive control.In cocaine-dependent subjects, Moeller and colleagues31
also reported a significant negative correlation betweenFA in the anterior corpus callosum and measures ofimpulsivity as well as a positive correlation betweenFA and measures of discriminability. Furthermore, ina recent study, Matsuo and colleagues32 examined therelationship among corpus callosum (CC) areas, impul-sivity, and suicidality in participants with bipolar dis-order. The suicidal BD participants had a significantinverse correlation between anterior genu area and theBIS total, motor and nonplanning scores indicating re-duced frontal volume in this regions was associated withincreased impulsivity.32 Taken together, these findings
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

278 JOURNAL OF HEAD TRAUMA REHABILITATION/JULY–AUGUST 2011
TABLE 1 Subject demographics and clinical information (TBI and controls)
Healthy controls Veterans with TBIVariable (x) (N = 17) (N = 15) P
Age ( ± SD), y 34.00 ± 10.59 34.93 ± 9.71 0.797Sex, Male/Female 17/0 15/0 -Handedness, Right/Left 17/0 15/0 -Education, years 16.18 ± 2.35 13.80 ± 1.86 0.003Global Assessment of Functioning (GAF) 85.41 ± 5.05 60.33 ± 9.96 0.000Hollingshead Socioeconomic Scale 41.27 ± 15.92 29.53 ± 11.84 0.030Hamilton Anxiety Scale (HAM-A) 4.82 ± 5.19 15.13 ± 9.77 0.001Hamilton Depression Scale (HAM-D) 3.29 ± 3.70 12.27 ± 6.96 0.000Profile of Mood States (POMS) 4.24 ± 17.72 39.27 ± 31.87 0.001SI Composite—Current Suicidal Ideation – 1.40 ± 1.64 0.000SI Composite—Most Severe Past History of Suicidal Ideation – 4.07 ± 3.37 0.000Barratt Impulsivity Scale (BIS)a
Attention 18.00 ± 4.02 22.07 ± 3.56 0.012Motor 21.25 ± 4.33 23.53 ± 5.30 0.230Planning 25.08 ± 5.42 27.07 ± 4.64 0.325Total 64.17 ± 10.13 72.67 ± 10.10 0.040
aIncludes BIS data for 12 controls.
suggest that behavioral measures of impulsivity and sui-cidality may be associated with changes in frontal whitematter integrity in veterans with TBI.
DTI measures of white matter integrity have alsobeen studied in TBI within the context of behavioraltraits and cognitive performance.2 In one study, 20mild, 17 moderate to severe TBI, and 18 controlswere administered neuropsychological testing andunderwent DTI scanning. Kraus and colleagues2 foundthat white matter load (a measure of the total numberof regions with reduced FA) was negatively correlatedwith all cognitive domains, providing evidence thatcognition is dependent upon the integrity of connec-tive white matter tissue in maintaining performance.The relationship between white matter integrity andcognition has also been observed to be altered by illicitdrug use.31 For example, one study administered testsof impulsivity and immediate and delayed memory inaddition to DT-MRI scanning to 18 cocaine-dependentsubjects and 18 healthy controls. Within the cocaine-dependent cohort, Moeller and colleagues31 founda significant negative correlation between FA in theanterior corpus callosum and measures of impulsivityas well as a positive correlation between FA andmeasures of discriminability. Overall, these findingssuggest that the application of DT-MRI to detect whitematter–associated behavioral changes in individualswith TBI, impulsivity, and suicide will be informative.
To date, no DTI study of veterans with TBI has ex-amined the relationship between white matter integrityand measures of both impulsivity and suicidal intent.Thus, the objective of the current DTI study was to testthe hypothesis that TBI status has a significant influenceon frontal lobe FA, and that this measure of microstruc-
tural integrity would be associated with suicidality andimpulsivity.
METHODS
Subjects
The institutional review boards at the University ofUtah and the George E. Whalen Department of Veter-ans Affairs (VA) Medical Center approved this study. Allsubjects provided written informed consent prior to par-ticipation in this study. A total of 15 male veterans withTBI and 17 male healthy controls (HC) were recruitedfrom the George E. Whalen VA Medical Center andthe community via local advertisements and by wordof mouth. Inclusion criteria for all participants in thisanalysis were: ages 18 to 55 years. Demographic infor-mation on the diagnostic groups is shown in Table 1.Ten of the HC were civilians and 6 were veterans. Vet-erans were considered to have a TBI if they reportedan injury event to the head followed by an alterationor loss of consciousness.33 The Ohio State University—TBI Identification Method (OSU-TBI) was administeredduring clinical evaluation to quantify presence, number,and severity of lifetime TBI injuries.34 Mild brain injuryevents were defined as a loss of consciousness for 30minutes or less. A brain injury event was defined asmoderate to severe if loss of consciousness was greaterthan 30 minutes. All TBI participants suffered a closedhead injury with 13 of the 15 participants reporting atleast one blast-related injury. Other injuries reported bythe TBI participants included motor vehicle accidents,falls, and blows to the head from an object (See Table 2for further details).
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Neuroimaging Correlates of TBI and Suicide 279
TABLE 2 Brain injury characteristics and psychotropic usage in the TBI veteranparticipants
Most Total number ofsevere Total number of TBI that were Type of brain
Participant TBI lifetime TBI moderate/severe Medications injury
001 Moderate/severe
3 1 Antidepressant, moodstabilizer/anticonvulsant,antipsychotics
Fall
LOC > 30min
Multiple IEDs
002 Moderate/severeLOC >30 min
1 1 Antidepressant,hypnotic/sedative,moodstabilizer/anticonvulsant, antipsychotic
IED + MVA
003 Moderate/severeLOC >30 min
2 2 Mood stabilizer/anticonvul sants,anxiolytic
Blow to the headfrom object
IED + Fall004 Mild 1 0 Antidepressant IED
LOC <5min
005 Mild 2 0 None Blow to headwith object
LOC 5-30min
IED
006 Mild 2 0 Mood stabilizer/anticonvulsants,anxiolytics
Blow to headwith object ×2
LOC <5min
007 Mild 3 0 None Fall × 2no LOC IED
008 Mild 2 0 None Blow to headwith object
no LOC IED009 Mild 4 0 Mood stabilizer/
anticonvulsantsFall ultiple IEDs
LOC 5-30min
010 Mild 1 0 Hypnotic/sedative Multiple IEDsno LOC
011 Mild 3 0 Antidepressant,Hypnotic/sedative
Blow to headwith object
LOC 5–30min
Multiple IEDs
012 Mild 6 0 Antidepressant,anxiolytic,hypnotic/sedative
MVA
LOC <5min
Multiple IEDs
013 Mild 10 0 Antidepressants,hypnotic/sedative
Multiple Blows tohead withobject
(continues)
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com
280 JOURNAL OF HEAD TRAUMA REHABILITATION/JULY–AUGUST 2011
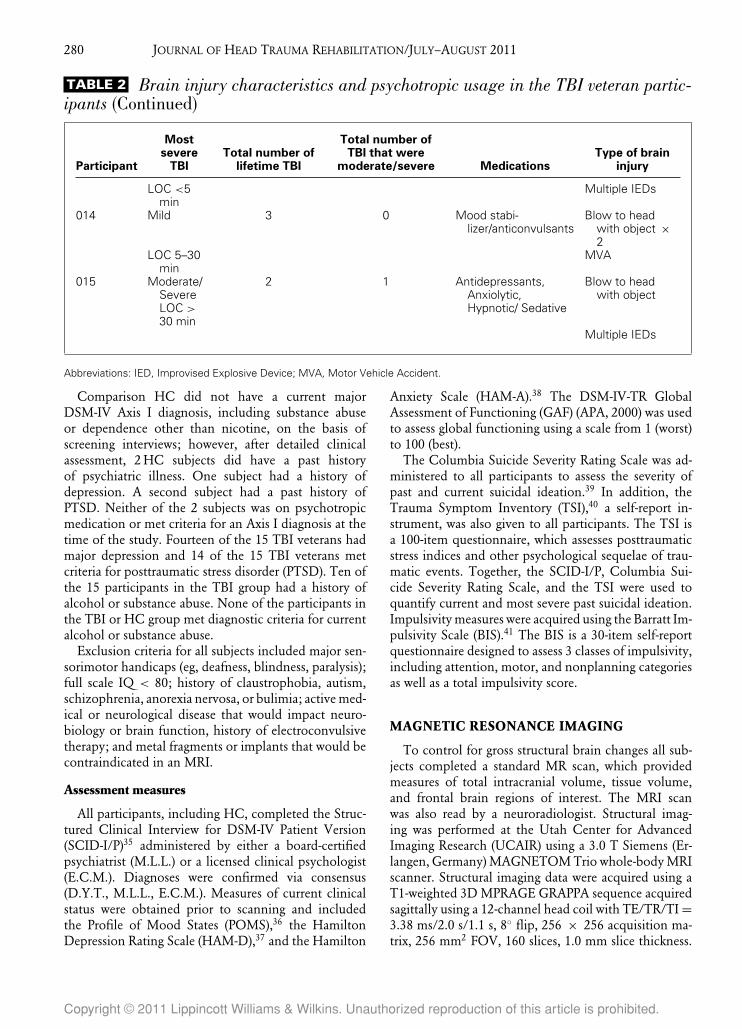
TABLE 2 Brain injury characteristics and psychotropic usage in the TBI veteran partic-ipants (Continued)
Most Total number ofsevere Total number of TBI that were Type of brain
Participant TBI lifetime TBI moderate/severe Medications injury
LOC <5min
Multiple IEDs
014 Mild 3 0 Mood stabi-lizer/anticonvulsants
Blow to headwith object ×2
LOC 5–30min
MVA
015 Moderate/SevereLOC >30 min
2 1 Antidepressants,Anxiolytic,Hypnotic/ Sedative
Blow to headwith object
Multiple IEDs
Abbreviations: IED, Improvised Explosive Device; MVA, Motor Vehicle Accident.
Comparison HC did not have a current majorDSM-IV Axis I diagnosis, including substance abuseor dependence other than nicotine, on the basis ofscreening interviews; however, after detailed clinicalassessment, 2 HC subjects did have a past historyof psychiatric illness. One subject had a history ofdepression. A second subject had a past history ofPTSD. Neither of the 2 subjects was on psychotropicmedication or met criteria for an Axis I diagnosis at thetime of the study. Fourteen of the 15 TBI veterans hadmajor depression and 14 of the 15 TBI veterans metcriteria for posttraumatic stress disorder (PTSD). Ten ofthe 15 participants in the TBI group had a history ofalcohol or substance abuse. None of the participants inthe TBI or HC group met diagnostic criteria for currentalcohol or substance abuse.
Exclusion criteria for all subjects included major sen-sorimotor handicaps (eg, deafness, blindness, paralysis);full scale IQ < 80; history of claustrophobia, autism,schizophrenia, anorexia nervosa, or bulimia; active med-ical or neurological disease that would impact neuro-biology or brain function, history of electroconvulsivetherapy; and metal fragments or implants that would becontraindicated in an MRI.
Assessment measures
All participants, including HC, completed the Struc-tured Clinical Interview for DSM-IV Patient Version(SCID-I/P)35 administered by either a board-certifiedpsychiatrist (M.L.L.) or a licensed clinical psychologist(E.C.M.). Diagnoses were confirmed via consensus(D.Y.T., M.L.L., E.C.M.). Measures of current clinicalstatus were obtained prior to scanning and includedthe Profile of Mood States (POMS),36 the HamiltonDepression Rating Scale (HAM-D),37 and the Hamilton
Anxiety Scale (HAM-A).38 The DSM-IV-TR GlobalAssessment of Functioning (GAF) (APA, 2000) was usedto assess global functioning using a scale from 1 (worst)to 100 (best).
The Columbia Suicide Severity Rating Scale was ad-ministered to all participants to assess the severity ofpast and current suicidal ideation.39 In addition, theTrauma Symptom Inventory (TSI),40 a self-report in-strument, was also given to all participants. The TSI isa 100-item questionnaire, which assesses posttraumaticstress indices and other psychological sequelae of trau-matic events. Together, the SCID-I/P, Columbia Sui-cide Severity Rating Scale, and the TSI were used toquantify current and most severe past suicidal ideation.Impulsivity measures were acquired using the Barratt Im-pulsivity Scale (BIS).41 The BIS is a 30-item self-reportquestionnaire designed to assess 3 classes of impulsivity,including attention, motor, and nonplanning categoriesas well as a total impulsivity score.
MAGNETIC RESONANCE IMAGING
To control for gross structural brain changes all sub-jects completed a standard MR scan, which providedmeasures of total intracranial volume, tissue volume,and frontal brain regions of interest. The MRI scanwas also read by a neuroradiologist. Structural imag-ing was performed at the Utah Center for AdvancedImaging Research (UCAIR) using a 3.0 T Siemens (Er-langen, Germany) MAGNETOM Trio whole-body MRIscanner. Structural imaging data were acquired using aT1-weighted 3D MPRAGE GRAPPA sequence acquiredsagittally using a 12-channel head coil with TE/TR/TI =3.38 ms/2.0 s/1.1 s, 8◦ flip, 256 × 256 acquisition ma-trix, 256 mm2 FOV, 160 slices, 1.0 mm slice thickness.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Neuroimaging Correlates of TBI and Suicide 281
A DT-MRI GRAPPA sequence was also obtained utiliz-ing 64 directions, 2 diffusion weightings: b = 0, 1000s/mm2, TE/TR = 88 millisecond/9 s; matrix = 128 ×128 on 256 × 256 FOV; 2 × 2 × 2 isotropic voxels,slice thickness = 2.0 mm with 0 gap, and 70 slices). Theoriginal imaging data were transferred from the scannerin the DICOM format and coded.
Morphometry
Brain volume measurements for each participant werecalculated within the FreeSurfer image analysis envi-ronment, which is documented and freely available fordownload online (http://surfer.nmr.mgh.harvard.edu/).A description of morphometric processing tailored tothe needs of this study is extracted from the written de-scription of morphometric procedures provided at theFreeSurfer Web site. This processing includes motioncorrection, removal of nonbrain tissue using a hybridwatershed/surface deformation procedure,42 automatedTalairach transformation, segmentation of the subcorti-cal white matter and deep gray matter volumetric struc-tures (including hippocampus, amygdala, caudate, puta-men, ventricles),43,44 intensity normalization,45 tessel-lation of the gray matter white matter boundary, au-tomated topology correction,46,47 and surface deforma-tion following intensity gradients to optimally place thegray/white and gray/cerebrospinal fluid borders at thelocation where the greatest shift in intensity defines thetransition to the other tissue class.48–50 Once the corticalmodels are complete, the cerebral cortex is parcellatedinto units on the basis of gyral and sulcal structure.51,52
Freesurfer morphometric procedures have been demon-strated to show good test-retest reliability across scannermanufacturers and across field strengths.53 Volumetricmeasures were obtained for intracranial volume; whitematter; and a priori regions of interest, including thecingulate gyrus and frontal lobe.
Following the FreeSurfer processing stream, each sub-ject was checked for resulting errors by visually in-specting pial and white matter surface boundaries. Tomaintain the reliability of the dataset, subjects con-taining obvious pial surface or white matter boundaryabnormalities were excluded from the study. One vet-eran participant with a TBI was excluded from furtheranalysis secondary to difficulties within the Freesurferprocessing stream. No pial or white matter surfacechanges were made to subjects included in this study.The rationale behind this decision includes a greaterconfidence in error estimation as correcting subject im-ages, slice by slice and voxel by voxel, is too proneto variability and any small errors left in the pial sur-face following the recon-all processing stream would bemaintained throughout the data set. White matter cor-rections were not made because of the nature of our
cohort. Subjects who have endured TBI are more likelyto have white matter lesions, and as this is an area that isbeing measured, correcting for lesions would alter whitematter volume results. During the FreeSurfer processingstream, each subject’s scan data are registered to the Ta-lairach atlas. As part of the FreeSurfer processing stream,subject’s cortex is automatically parcellated into a 34 re-gions of interest as detailed by Desikan et al (2006).51
Desikan and colleagues51 also specify which of the 34regions of interest are included in each lobe; this des-ignation was utilized when compiling our compositedata. Volume measurements were taken from the asegstatistical file generated by FreeSurfer, which includesubcortical volume measurements.
Diffusion tensor imaging
The diffusion weighted imaging data were analyzedusing FSL’s FDT (FMRIB’s Diffusion Toolbox) (Pleasesee Web site for detailed methods and reference list:http://www.fmrib.ox.ac.uk/fsl).54–56 The DTI data werevisually inspected for significant distortion, motion, andeddy artifact before processing and post processing toensure data integrity. One HC participant was excludedfrom further analyses secondary to significant head mo-tion. Then the data were processed with tools withinFDT, including eddy current and motion correction,brain extraction,57 and fitting a tensor model to theraw diffusion data. These steps resulted in extraction offractional anisotropy (FA) and mean diffusivity (MD).All subjects’ FA data were then aligned into a commonspace using the nonlinear registration tool FNIRT,58,59
which uses a b-spline representation of the registrationwarp field.60 The target image used in the registrationswas chosen to be the most “typical” subject in the studyto generate a study-specific FA target image. This targetimage was then affine-aligned into MNI152 standardspace. All participants’ images were then transformedinto 1 × 1 × 1 mm MNI152 space by combiningthe nonlinear transform to the target FA image with theaffine transform from that target to MNI152 space. Thisresults in a standard-space version of each subject’s FAimage, which is next merged into a single FA 4D imagecontaining all participants. For mean diffusivity images,the FA images were utilized to achieve the same non-linear registration for MD images. All subject’s warpedMD data were then merged in a 4D file.
White matter regions of interest
Given the study hypotheses, regions of interest formajor white matter tracts were created for the genu andthe cingulum utilizing the Johns Hopkins University(JHU)-White Matter Labels (1 mm) Atlas61,62 (Figure 1).The JHU-White Matter Label Atlas was overlaid ontothe mean FA map that was created for the study group.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

282 JOURNAL OF HEAD TRAUMA REHABILITATION/JULY–AUGUST 2011
Figure 1. JHU white matter label atlas—1mm superimposedover the group mean fractional anisotropy image.
The sagittal slice in which the largest white matter re-gion could be found for the genu and cingulum wasidentified. Next, utilizing the JHU-White Matter tem-plate, ROIs were drawn for the genu and cingulum forthe right and left hemisphere separately. These ROIswere then projected onto the FA and MD maps foreach individual and mean FA and MD were obtained(Figure 2).
Statistics
Independent Student t tests and χ2 tests were per-formed for demographic and clinical data. Univariateanalyses were performed for brain volume measures,utilizing total intracranial volume as a covariate. Inde-
Figure 2. Cingulum and Genu regions of interest overlaid onthe group mean fractional anisotropy image. The Cingulum isshown in green and the Genu in red.
pendent t tests were performed for FA and MD data toanalyze between group differences. Pearson correlationswere performed between mean FA and clinical variablesincluding measures of suicidal ideation, impulsivity, andtime from injury measures. Effect sizes were computedfor both the volumetric data and the DTI data. Cohen dwas calculated for DTI data and Cohen f was performedfor volumetric data as we utilized total intracranial vol-ume as a covariate.63 Because we had specific a priorihypotheses regarding 2 brain regions, the cingulum andgenu for the DTI FA analyses, corrections for multiplecomparisons were not performed.
RESULTS
We acquired data from 15 male, right-handed vet-erans with TBI (mean age 34.9 ± 9.7 years), and 17male HCs matched for age, sex, and handedness (meanage 34.0 ± 10.6 years). All TBI participants reportedat least 1 injury event to the head followed by an alter-ation of consciousness or loss of consciousness, whilecontrols reported no head injuries. Of the TBI partici-pants, 3 reported their most severe TBI as mild withoutloss of consciousness. Four TBI participants reportedtheir most severe injury event as mild with loss of con-sciousness for less than 5 minutes and 4 reported a mildinjury event with loss of consciousness between 5 and30 minutes. Another 4 TBI participants reported a mod-erate to severe TBI event with loss of consciousnessgreater than 30 minutes. Only one TBI participant suf-fered from more than 1 moderate to severe TBI event.Twelve participants had more than 1 TBI event. Theaverage number of TBI events was 3 with a range of 1 to10 events. Each study subject completed an MRI scanread by a clinical neuroradiologist. Fourteen of the 15TBI scans were read as within normal limits. The scanfor the fifteenth subject indicated a history of congeni-tal cyst, which was not thought to have current clinicalsignificance. TBI veterans reported an average of 13.8years of education, while controls reported an averageof 16.2 years of education (p = 0.003). In addition,controls had higher socioeconomic status (41.3 ± 15.9on the Hollingshead Socioeconomic Scale)64 comparedwith TBI veterans (29.5 ± 11.8) and significantly higherGlobal Assessment of Functioning (GAF) scores (TBI:60.33 ± 9.96; HC: 85.41 ± 5.05; P = 0.000), as ratedby the interviewing clinician during a structured clinicaldiagnostic assessment. Demographic and clinical char-acteristics of the diagnostic groups are shown in Tables 1and 2.
At the time of scanning, veterans with TBI reportedsignificantly more depressive and anxious symptomscompared with controls (TBI HAM-A: 15.13 ± 9.77,HC HAM-A: 4.82 ± 5.19, P = 0.001; TBI HAM-D:12.27 ± 6.96, HC HAM-D: 3.29 ± 3.70, P = 0.000).
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Neuroimaging Correlates of TBI and Suicide 283
TABLE 3 Total and lobar brain volumes for participants with traumatic brain injury andhealthy controls (cm3)
TBI Healthy controls Effect sizeRegion (N = 14) (N = 17) Pa (Cohen f)
Intracranial volume 1485.19 ± 136.39 1468.09 ± 161.79 NS 0.06Total lateral ventricle 10.73 ± 5.16 14.01 ± 9.32 NS 0.22Left frontal lobe 85.86 ± 6.68 89.87 ± 1.10 0.10 0.22Right frontal lobe 85.80 ± 6.64 90.52 ± 10.20 0.05 0.28Total frontal lobe 171.65 ± 13.22 180.39 ± 21.06 0.07 0.25Left cingulate cortex 10.04 ± 1.21 10.69 ± 1.62 NS 0.23Right cingulate cortex 9.98 ± 1.59 10.29 ± 1.33 NS 0.11Total cingulate cortex 20.03 ± 2.55 20.99 ± 2.68 NS 0.19Left hemisphere white matter volume 254.18 ± 24.87 259.62 ± 21.12 NS 0.12Right hemisphere white matter volume 254.99 ± 25.64 258.38 ± 20.79 NS 0.07Total white matter volume 509.18 ± 50.38 517.99 ± 41.82 NS 0.10
aUnivariate analysis with total intracranial volume as a covariate.
Fourteen of the 15 TBI veterans had Major Depressionand 14 of the15 TBI veterans met criteria for posttrau-matic stress disorder (PTSD). All 15 veterans with TBIhad at least one Axis I diagnosis. Twelve of the 15TBI veterans were also taking medications. The mostfrequent medications reported were antidepressants (7),mood stabilizer/anticonvulsants (5), antipsychotics (2),hypnotic/sedatives (6), and anxiolytics (4).
Composite scores where created to measure “cur-rent suicidal ideation” utilizing information from theColumbia Suicide Severity Rating Scale, the SCID-I/P,and 3 items on the Trauma Severity Inventory (TSI).These items included “Threatening or attempting sui-cide,” “Wishing you were dead,” and “Feeling like lifewasn’t worth living. Participants were given a score from0 to 3 for each of these items and a total compositesuicidality score was obtained by summing the scoresfrom these 3 items. Possible scores ranged from 0 to9, with 9 representing highest endorsement of suicidalideation. The same composite score was also generatedfor history of most severe suicidal ideation for each ofthe 15 subjects. Composite suicidality scores for currentsuicidal ideation for veterans with TBI ranged from 0 to5 with a mean of 1.40, while those for history of mostsevere suicidal ideation ranged from 0 to 9 with a meanof 4.07. A composite BIS score was also calculated to as-sess overall impulsivity for study participants, althoughcomparisons were also made for each subscale. Veteranswith TBI reported significantly higher scores for atten-tion (TBI: 22.07 ± 3.56; HC: 18.00 ± 4.02; P = 0.012)and total BIS (TBI: 72.67 ± 10.10; HC: 64.17 ± 10.13;P = 0.040). No statistically significant between-groupdifferences were observed for scores on the motor andplanning subcategories (See Table 1). Time from first in-jury after the age of 6 years, time from most severe injuryand time from most recent injury for the TBI group were
191.2 ± 127.1, 104.5 ± 111.0, 95.4 ± 110.5 months,respectively.
Morphometric Analysis
Univariate analyses with total intracranial volume as acovariate were performed for a priori regions of interestincluding lateral ventricle volume, frontal lobe, cingu-late cortex, and white matter volume on 14 participantswith TBI and 17 HC. Participants with TBI showed atrend for reduction in total frontal lobe volume (F2,30 =3.53, P = 0.07) in the left frontal lobe (F2,30 = 2.8, P =0.10) and in the right frontal lobe (F2,30 = 4.13, P = 0.05)compared with healthy controls. No significant differ-ences were found in white matter or ventricular volumebetween groups (see Table 3 for total and lobar brainvolume means and effect size).
Fractional anisotropy
Independent sample t tests were conducted for FAvalues for major white matter tracts including the cingu-lum and genu for 15 participants with TBI and 16 HC.Results indicate significantly decreased FA values in theTBI group relative to controls in the left cingulum (t29
= 2.5; P = 0.02), left genu (t29 = 2.6; P = 0.02), andbilateral genu (t29 = 2.8; P = 0.01). Other areas of in-terest failed to reach significance (Table 4). Measuresof Mean Diffusivity (MD) did not show significant be-tween group differences for the regions examined.
Correlations with impulsivity and suicidality
To examine the relationship between FA and mea-sures of impulsivity and suicide within group corre-lations were completed for veterans with TBI. Frac-tional Anisotropy of the total cingulum (r13 = 0.567,
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

284 JOURNAL OF HEAD TRAUMA REHABILITATION/JULY–AUGUST 2011
TABLE 4 Mean fractional anisotropy (FA) and mean diffusivity (MD) values for majorwhite matter tracts in veterans with traumatic brain injury (TBI) relative to healthycontrols (HC)
TBI (n = 15) HC (n = 16)Between
groupMean (STD) Mean (STD) significance Effect size (d)
FATotal cingulum 0.381 (0.028) 0.397 (0.024) 0.116 0.60Left cingulum 0.349 (0.032) 0.377 (0.029) 0.019 0.92Right cingulum 0.413 (0.035) 0.416 (0.028) 0.787 0.10Total genu 0.514 (0.018) 0.536 (0.025) 0.010 1.03Left genu 0.473 (0.029) 0.505 (0.039) 0.015 0.96Right genu 0.555 (0.022) 0.567 (0.026) 0.171 0.52
MDa
Total cingulum 0.748 (0.024) 0.746 (0.030) 0.885 0.05Left cingulum 0.781 (0.026) 0.772 (0.034) 0.398 0.32Right cingulum 0.714 (0.033) 0.720 (0.029) 0.561 0.22Total genu 0.882 (0.036) 0.872 (0.040) 0.495 0.26Left genu 0.897 (0.046) 0.885 (0.059) 0.545 0.23Right genu 0.867 (0.043) 0.860 (0.045) 0.653 0.17
aConsistent with convention, values are reported in 10–3 mm2/s.
P = 0.028) and right cingulum (r13 = 0.588, P = 0.021)were found to positively correlate with current suicidalideation. Fractional anisotropy of the total cingulumwas also positively correlated with the BIS total score(r13 = 0.605, P = 0.017) and the BIS attention subscale(r13 = 0.550, P = 0.033). The right cingulum was foundto be positively correlated with BIS total score (r13 =0.592, P = 0.020). The right genu positively correlatedwith the BIS total score (r13 = 0.552, P = 0.033) andthe BIS attention (r 13 = 0.637, P = 0.011) and planning(r13 = 0.637, P = 0.011) subscales.
Current suicidal ideation was positively correlatedwith BIS attention (r13 = 0.551, P = 0.052), BIS motor(r13 = 0.549, P = 0.034), BIS planning (r13 = 0.494, P =0.061), and BIS total (r13 = 0.694, P = 0.004). Finally, weexamined whether current depression, measured by theHAM-D and POMS, or current anxiety, measured byHAM-A were associated with FA and found no signifi-cant correlation for these behavioral measures. BecauseMD did not show significant between group differencesfor any brain region, correlations with clinical character-istics were not performed.
Correlations with time of injury
To evaluate the effect of time of injury on DTI FA,correlations were performed for time from first injury,time from most severe injury and time from most re-cent injury for brain regions with significant FA differ-ences for the veteran TBI group. There were no signifi-cant correlations found for DTI FA and time of injurymeasures.
DISCUSSION
The current findings are consistent with previous DTIstudies demonstrating decreased frontal FA in individ-uals with postacute mild TBI.21,65 Relative to controls,the veteran TBI cohort showed reduced FA in the leftcingulum, the left genu, and total genu. These changesin white matter microstructure were evident despite thefact there were no significant differences between thestudy groups for intracranial volume, or total wholebrain white matter volume. Measures of mean diffu-sivity for the same fiber tract regions also did not showbetween group differences. Veterans with TBI producedsignificantly higher Total BIS scores and attention sub-scale scores, and reported more suicidal ideation relativeto comparison subjects. As hypothesized, measures ofFA within the TBI group correlated with both currentsuicidal ideation and BIS measures of impulsivity. Ourresults suggest that while current depression or anxietydid not correlate with FA, increased impulsivity, andsuicidality were associated with altered white matter mi-crostructure in our veterans with TBI.
There is limited data on structural differences in sui-cidal individuals on the basis of conventional MR tech-niques. Several investigations have reported gray mat-ter (GM) hyperintensities and volume abnormalities,most commonly observed in the orbitofrontal cortex(OFC). Moreover, most investigations to date have ex-amined suicidal intent or history in individuals witha concurrent psychiatric disorder. For example, vol-umetric changes in GM were found in a group ofpatients with late-onset depression with a history of
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Neuroimaging Correlates of TBI and Suicide 285
suicide when compared with a depressed group with-out a history of suicide attempts. Reduced GM volumeswere detected in the frontal, parietal, and temporal re-gions as well as the insula, lentiform nucleus, midbrain,and the cerebellum.66 Gray matter density reductionwas also found in a group of patients with schizophre-nia and a history of past suicide attempts compared withan age-, treatment-, and illness duration–matched groupwith schizophrenia without a history of past suicide at-tempts. Using whole-brain voxel-based morphometrytechniques, researchers found that the left OFC andleft superior temporal gyrus were reduced in the pa-tients who had a history of a suicide attempt.67 Monkuland colleagues68 also reported OFC abnormalities in asample of female suicidal patients with major depressivedisorder. These individuals showed smaller right andleft OFC gray matter volumes and larger right amygdalavolumes than nonsuicidal patients. In a study of MRIhyperintensities in patients with unipolar depressionwith and without a history of suicide attempts, Ahearnand colleagues69 found that unipolar patients with ahistory of suicide attempts showed significantly moresubcortical gray matter hyperintensities and a trend to-ward more periventricular white matter hyperintensities,which were linked to the onset of mood disorders. Al-though these findings indicate a potential role for struc-tural brain changes in patients with a history of suicidalbehavior, these MR methods are unlikely to provideoptimal discrimination in measuring cortical changessecondary to TBI.
Mild TBI, which may be experienced by soldiers, of-ten results in acceleration/deceleration forces causingdiffuse axonal injury (DAI), contusion, and subduralhemorrhage.70 In the case of DAI, these forces can causeshaking, twisting, and shearing of axonal fibers, whichmay eventually lead to cell death and tissue loss. Themost common locations for this type of injury are thecorticomedullary (GM–white matter) junction (particu-larly frontotemporal), internal capsule, deep GM, andcorpus callosum. The corpus callosum forms the largestcommissural white matter bundle in the brain. Its genuconnects orbitofrontal and frontal cortices, whereas itsbody and splenium connect temporal, parietal, and oc-cipital regions.71 Our findings are consistent with brainregions reportedly affected by mild TBI although find-ings have varied depending on the type of imaging thathas been used. Diffusion tensor imaging (DTI), whichcan assess the microstructural integrity of white matterpathways, has therefore been proposed to be a highlysensitive means of detecting brain changes associatedwith TBI.65
It has been shown that traumatic brain injury can re-sult in long-lasting central nervous system impairmentsas measured by DTI, MRI, and fMRI.72 For example,a recent morphometric study of TBI, which included
severe TBI, demonstrated continued brain atrophyover the course of 1 year postinjury. Furthermore,this percent change in brain volume postinjury wasfound to predict long-term functional status.73 In amultivariate analysis of 12 patients with TBI, Avants etal74 used T1 structural MRI and DTI to show that TBIsignificantly reduces brain volume and increases MD inthe thalamus and hippocampus. Kim and colleagues75
used tensor-based morphometry in 29 civilians diag-nosed with TBI after suffering a closed head injury andfound widespread volume reductions in neocorticalgray and white matter and in subcortical nuclei andalso found an increase in volume in ventricle regions.Similarly, decreased GM volume has been observed inmild to severe TBI across a range of structures includingthe frontal and temporal cortices, cingulate gyrus, sub-cortical gray matter, and cerebellum with gray matterloss correlated with performance on tasks requiringattention.76 Traumatic brain injury resulting in diffuseaxonal injury (DAI) may cause acute neurologicalchanges,77 some of which have been shown to persistmonths postinjury, as evidenced by decreased FAvalues in the corpus callosum that remain significantlylow even during the chronic phase of injury.78 In thecurrent study, the time from first TBI ranged from 48to 456 months, indicating that no individual was in anacute recovery phase. Exploratory correlation analysesof DTI FA data and time of injury measures found noassociation between time of injury and FA. It is notpossible with the current cross sectional study designto identify the changes associated with TBI or the timecourse of any brain changes. Nevertheless, our mild TBIsample demonstrated decreased FA in frontal regionshypothesized to be associated with impulsivity.
Our findings of reduced FA in the genu and the fron-tolimbic white matter tract, the cingulum, are also con-sistent with prior MRI studies showing lower FA in thewhite matter of the frontal cortex and the cingulum in in-dividuals with depression.79–84 For instance, Nobuharaand colleagues81 found reduced FA in the white mat-ter of the right ACC, bilateral superior frontal gyri, andleft middle frontal gyrus in depressed participants. Fur-thermore, the authors reported that the white matterFA in frontal regions was inversely related to severity ofdepression.81 However, in the current study, genu andcingulum FA measures were not found to correlate withcurrent state measures of depression or anxiety. Jia andcolleagues85 also found that individuals with depressionand have attempted suicide had lower FA in the whitematter of the right frontal lobe relative to healthy com-parison subjects; however, they reported subgyral frontalwhite matter abnormality in comparison to our findingsof cingulum abnormalities associated with suicidality.
Current literature supports the role of the prefron-tolimbic circuit in the pathophysiology of depression.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

286 JOURNAL OF HEAD TRAUMA REHABILITATION/JULY–AUGUST 2011
Both functional and structural abnormalities within thiscircuit may result in a similar manifestation of symp-toms. However, in individuals where the disconnectionin the network was thought to be structural, such as inTBI, worsened outcomes have been reported includingpoor treatment response and lasting cognitive deficits.86
Several DTI studies of depression have found that re-duced FA in frontal white matter is associated with treat-ment resistance. For example, Alexopoulos et al79 re-ported lower FA in frontal regions to low antidepressantremission rate. In addition, Taylor and colleagues82 re-ported that individuals with depression were more likelyto respond to treatment if they had higher FA valuesin the superior frontal gyri and anterior cingulate cor-tices. These findings suggest that a dysfunction of theprefrontolimbic network may produce depression by anumber of different mechanisms, which will have im-portant implications for designing treatment protocols.In this investigation, it is not possible to disambiguatethe onset of psychiatric illness, the impact of mild TBIand the onset of white matter microstructural changes.As can be seen in Tables 1 and 2, the study partici-pants were being treated with multiple medications atthe time of imaging and given the high rates of currentmood and anxiety symptoms, could be viewed as treat-ment refractory. Interestingly, our genu and cingulumFA measures were not found to correlate with currentstate measures, suggesting our imaging findings are notstate-based markers of psychiatric illness.
Comparison between the study groups on BIS mea-sures of impulsivity showed that veterans with mild TBIreported significantly more impulsive behavior than thecomparison group. Given that healthy control subjectshad minimal psychiatric illness by definition, the mildTBI group also reported more current and past suici-dal ideation. Within group correlations showed that forthe mild TBI veterans current suicidal ideation was pos-itively correlated with impulsivity measures and withfrontal DTI measures of FA. While previous studies havereported a relationship between FA and impulsivity29,30
and impulsivity and suicidal ideation.4,87 this is thefirst study to examine suicidal ideation, impulsivity, andfrontal FA in veterans with TBI. Our findings suggest ab-normal FA in frontal WM tracts may be associated withincreased risk for both impulsivity and suicidality. Theseoutcomes may be the result of a structural disconnectionin frontal pathways that mediate behavioral inhibition,problem solving and decision making.12,13,15 Additionalstudies with larger sample sizes will be needed to test thisperspective.
There are a number of factors that must be consid-ered when interpreting these study findings. First, theclassification of TBI subjects is an area of ongoing de-bate and the application of different classification cri-teria can impact study results. TBI subjects have of-
ten been categorized as mild, moderate, or severe onthe basis of the Glasgow Coma Scale (GCS).88 How-ever, concerns have been raised that this instrumentmay be too coarse for research purposes. The devel-opment of more refined approaches for assessing andclassifying TBI for study purposes has recently been ad-dressed and it has been proposed that a pathoanatomicstrategy may be optimal.89 Headway toward develop-ing a uniform system for assessing TBI has been sup-ported by efforts to improve consistency in data collec-tion through the implementation of a library of datacollection instruments.90 However, no new assessmentstrategies have emerged and uniform data collection isyet to be widely implemented. Our categorization wason the basis of subject self-report using a structured in-terview (OSU-TBI), a method that is less sensitive thandirect medical documentation. However, given that ourstudy focused on returned veterans and not active dutypersonnel, this assessment was feasible and provided anobjective quantifiable method for examining TBI. Fur-thermore, our TBI sample was well characterized withcurrent and lifetime history of psychiatric symptomsdocumented. The presence of comorbid TBI and psy-chiatric disorders in our veteran TBI group precludescausal inferences regarding the observed changes in FA.It is also unknown what impact current and past his-tory of medication may play in our study findings. Thusfar, reports on the effects of medication on DTI mea-sures appear inconsistent, although some studies sug-gest that FA measures may be impacted by medication.For example, white matter FA has been found to beinversely related with mood stabilizer load in bipolarsubjects,91 antipsychotic dose positively correlated withFA in schizophrenic subjects,92 and antidepressant treat-ment has been related to significant increases in FA insubjects with obsessive compulsive disorder.93 However,other studies have found no relationship between psy-chotropic medications, including antidepressants, moodstabilizers, antipsychotics, and benzodiazepines, and FAin psychiatric disorders.94–98 Additional limitations thatshould be considered when interpreting the findings ofthis study include group differences in education andSES, the use of a combined civilian and military con-trol group, the modest sample size, the heterogeneity inbrain injury event(s) and severity and time postinjury.
In summary, this is one of the first studies to evalu-ate structural and microstructural brain changes as mea-sured by FA and diffusivity using DTI and morphometryusing MRI in veterans with TBI and history of suici-dal behavior. The present results suggest that veteranswith TBI had reduced FA, increased self- reported im-pulsivity, and increased suicidal ideation. A significantassociation was found for decreased white matter in-tegrity (FA) and both impulsivity and suicidal ideation.These findings are consistent with previous evidence
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Neuroimaging Correlates of TBI and Suicide 287
indicating that increased suicide may be associated withbehavioral disinhibition and frontal-limbic dysfunctionand suggest a neurobiologic mechanism that may in-crease vulnerability to suicide. One potential applica-tion of these findings may be identifying individualsat-risk for suicide. Further evaluation of these key whitematter tracts through the use of statistical classificationalgorithms is warranted to ascertain whether or not in-dividuals can be classified as “at-risk” vs “not at risk”
utilizing DTI FA data for the genu and cingulum aloneand in combination with measures of impulsivity.
ACKNOWLEDGMENTS
This research was carried out with assistance fromMelody Johnson, Radiological Technologist, and HenryBuswell, MRI Research Manager—Utah Center for Ad-vanced Imaging Research (UCAIR).
REFERENCES
1. Taber KH, Hurley RA. Traumatic axonal injury: atlas of majorpathways. J Neuropsychiatry Clin Neurosci. Spring 2007;19(2):iv–104.
2. Kraus MF, Susmaras T, Caughlin BP, Walker CJ, Sweeney JA,Little DM. White matter integrity and cognition in chronic trau-matic brain injury: a diffusion tensor imaging study. Brain. Oct2007;130(pt 10):2508–2519.
3. Tate RMP, Simpson GB, Flanagan SM, Coffey M. Completedsuicide after traumatic brain injury. Journal of Head Trauma Reha-bilitation. 1997;12(6):16–28.
4. Gorlyn M. Impulsivity in the prediction of suicidal behavior inadolescent populations. Int J Adolesc Med Health. 2005;17(3):205–209.
5. Horesh N. Self-report vs. computerized measures of impulsivityas a correlate of suicidal behavior. Crisis. 2001;22(1):27–31.
6. Teasdale TW, Engberg AW. Suicide after traumatic brain injury:a population study. J Neurol Neurosurg Psychiatry. 2001;71(4):436–440.
7. Simpson G, Tate R. Suicidality after traumatic brain in-jury: demographic, injury and clinical correlates. Psychol Med.2002;32(4):687–697.
8. Leclercq M, Couillet J, Azouvi P, et al. Dual task performanceafter severe diffuse traumatic brain injury or vascular prefrontaldamage. J Clin Exp Neuropsychol. 2000;22(3):339–350.
9. Parker RS. Recommendations for the revision of DSM-IV diag-nostic categories for co-morbid posttraumatic stress disorder andtraumatic brain injury. Neurorehabilitation. 2002;17(2):131–143.
10 Maser JD, Akiskal HS, Schettler P, et al. Can temperament identifyaffectively ill patients who engage in lethal or near-lethal suicidalbehavior? A 14-year prospective study. Suicide Life Threat Behav.2002;32(1):10–32.
11. McAuliffe C, Corcoran P, Hickey P, McLeavey BC. Optionalthinking ability among hospital-treated deliberate self-harm pa-tients: a 1-year follow-up study. Br J Clin Psychol. 2008;47(pt 1):43–58.
12. Paulus MP. Decision-making dysfunctions in psychiatry—alteredhomeostatic processing? Science. 2007;318(5850):602–606.
13. Lux WE. A neuropsychiatric perspective on traumatic brain injury.J Rehabil Res Dev. 2007;44(7):951–962.
14. Kim E. Agitation, aggression, and disinhibition syndromes aftertraumatic brain injury. Neurorehabilitation. 2002;17(4):297–310.
15. Karol RL. Neuropsychological Intervention: The Practical Treatment ofSevere Behavioral Dyscontrol After Acquired Brain Injury. Boca Raton,FL: CRC Press; 2003.
16. Luria AG. Higher Cortical Functions in Man. 2nd ed. New York, NY:Basic Books; 1980.
17. Perlstein WM, Cole MA, Demery JA, et al. Parametric manip-ulation of working memory load in traumatic brain injury: be-havioral and neural correlates. J Int Neuropsychol Soc. 2004;10(5):724–741.
18. Witt ST, Lovejoy DW, Pearlson GD, Stevens MC. Decreasedprefrontal cortex activity in mild traumatic brain injury duringperformance of an auditory oddball task. Brain Imaging Behav.2010;4(3/4):232–247.
19. Kennedy KM, Raz N. Aging white matter and cognition: dif-ferential effects of regional variations in diffusion propertieson memory, executive functions, and speed. Neuropsychologia.2009;47(3):916–927.
20. Bigler ED, Bazarian JJ. Diffusion tensor imaging: a biomarker formild traumatic brain injury? Neurology. 23 2010;74(8):626–627.
21. Niogi SN, Mukherjee P. Diffusion tensor imaging of mildtraumatic brain injury. J Head Trauma Rehabil. 2010;25(4):241–255.
22. Bazarian JJ, Zhong J, Blyth B, Zhu T, Kavcic V, Peterson D. Dif-fusion tensor imaging detects clinically important axonal damageafter mild traumatic brain injury: a pilot study. J Neurotrauma.2007;24(9):1447–1459.
23. Chu Z, Wilde EA, Hunter JV, et al. Voxel-based analysis of diffu-sion tensor imaging in mild traumatic brain injury in adolescents.AJNR Am J Neuroradiol. 2009;31(2):340–346.
24. Wu TC, Wilde EA, Bigler ED, et al. Evaluating the relationship be-tween memory functioning and cingulum bundles in acute mildtraumatic brain injury using diffusion tensor imaging. J Neuro-trauma. 2010;27(2):303–307.
25. Wilde EA, McCauley SR, Hunter JV, et al. Diffusion tensor imag-ing of acute mild traumatic brain injury in adolescents. Neurology.2008;70(12):948–955.
26. Mayer AR, Ling J, Mannell MV, et al. A prospective diffusiontensor imaging study in mild traumatic brain injury. Neurology.2010;74(8):643–650.
27. Lipton ML, Gulko E, Zimmerman ME, et al. Diffusion-tensorimaging implicates prefrontal axonal injury in executive functionimpairment following very mild traumatic brain injury. Radiology.2009;252(3):816–824.
28. Hartikainen KM, Waljas M, Isoviita T, et al. Persistent symptomsin mild to moderate traumatic brain injury associated with execu-tive dysfunction. J Clin Exp Neuropsychol. 2010;32(7):1–8.
29. Konrad A, Dielentheis TF, El Masri D, et al. Disturbed structuralconnectivity is related to inattention and impulsivity in adult atten-tion deficit hyperactivity disorder. Eur J Neurosci. 2010;31(5):912–919.
30. Salo R, Nordahl TE, Buonocore MH, et al. Cognitive controland white matter callosal microstructure in methamphetamine-dependent subjects: a diffusion tensor imaging study. Biol Psychi-atry. 2009;65(2):122–128.
31. Moeller FG, Hasan KM, Steinberg JL, et al. Reduced ante-rior corpus callosum white matter integrity is related to in-creased impulsivity and reduced discriminability in cocaine-dependent subjects: diffusion tensor imaging. Neuropsychopharma-cology. 2005;30(3):610–617.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

288 JOURNAL OF HEAD TRAUMA REHABILITATION/JULY–AUGUST 2011
32. Matsuo K, Nielsen N, Nicoletti MA, et al. Anterior genu corpuscallosum and impulsivity in suicidal patients with bipolar disorder.Neurosci Lett. 2010;469(1):75–80.
33. Belanger HG, Uomoto JM, Vanderploeg RD. The Veterans HealthAdministration’s (VHA’s) Polytrauma System of Care for mildtraumatic brain injury: costs, benefits, and controversies. J HeadTrauma Rehabil. 2009;24(1):4–13.
34. Corrigan JD, Bogner J. Initial reliability and validity of the OhioState University TBI Identification Method. J Head Trauma Rehabil.2007;22(6):318–329.
35. First M, Spitzer R, Gibbon M, Williams J. Structured Clinical Inter-view for the DSM-IV Axis I Disorders. Washington, DC: US Depart-ment of Veterans Affairs; 1996.
36. McNair DM, Lorr M, Droppleman LF. Revised Manual for the Profileof Mood States. San Diego, CA: Educational and Industrial TestingServices; 1992.
37. Hamilton M. A rating scale for depression. J Neurol NeurosurgPsychiatry. 1960;23:56–62.
38. Hamilton A. Diagnosis and rating of anxiety. British Journal ofPsychiatry. 1969; (3):76–79.
39. Oquendo M, Halberstam B, Mann JJ. Risk factors for suicidalbehavior: utility and limitations of research instruments. In: FirstMB, ed. Standardized Evaluation in Clinical Practice 2003:103–130.
40. Briere J. Trauma Symptom Inventory Professional Manual. Odessa,FL: Psychological Assessment Resources; 1995.
41. Patton JH, Stanford MS, Barratt ES. Factor structure of the BarrattImpulsiveness Scale. Journal of Clinical Psychology. 1995; (51):768–774.
42. Segonne F, Dale AM, Busa E, et al. A hybrid approach to the skullstripping problem in MRI. Neuroimage. 2004;22(3):1060–1075.
43. Fischl B, Salat DH, Busa E, et al. Whole brain segmentation:automated labeling of neuroanatomical structures in the humanbrain. Neuron. 2002;33(3):341–355.
44. Fischl B, Salat DH, van der Kouwe AJ, et al. Sequence-independent segmentation of magnetic resonance images. Neu-roimage. 2004;23(suppl 1):S69–S84.
45. Sled JG, Zijdenbos AP, Evans AC. A nonparametric method for au-tomatic correction of intensity nonuniformity in MRI data. IEEETrans Med Imaging. 1998;17(1):87–97.
46. Segonne F, Pacheco J, Fischl B. Geometrically accurate topology-correction of cortical surfaces using nonseparating loops. IEEETrans Med Imaging. 2007;26(4):518–529.
47. Fischl B, Liu A, Dale AM. Automated manifold surgery: construct-ing geometrically accurate and topologically correct models of thehuman cerebral cortex. IEEE Trans Med Imaging. 2001;20(1):70–80.
48. Dale AM, Fischl B, Sereno MI. Cortical surface-based anal-ysis. I. Segmentation and surface reconstruction. Neuroimage.1999;9(2):179–194.
49. Fischl B, Dale AM. Measuring the thickness of the human cerebralcortex from magnetic resonance images. Proc Natl Acad Sci U S A.2000;97(20):11050–11055.
50. Dale AM, Sereno MI. Improved localization of cortical activ-ity by combining EEG, and MEG with MRI cortical surface re-construction: a linear approach. Journal of Cognitive Neuroscience.1993;5:162–176.
51. Desikan RS, Segonne F, Fischl B, et al. An automated labelingsystem for subdividing the human cerebral cortex on MRI scansinto gyral based regions of interest. Neuroimage. 2006;31(3):968–980.
52. Fischl B, van der Kouwe A, Destrieux C, et al. Automaticallyparcellating the human cerebral cortex. Cereb Cortex. 2004;14(1):11–22.
53. Han X, Jovicich J, Salat D, et al. Reliability of MRI-derived mea-surements of human cerebral cortical thickness: the effects of
field strength, scanner upgrade and manufacturer. Neuroimage.2006;32(1):180–194.
54. Woolrich MW, Jbabdi S, Patenaude B, et al. Bayesian analy-sis of neuroimaging data in FSL. Neuroimage. Mar 2009;45(1suppl):S173–S186.
55. Smith SM, Jenkinson M, Woolrich MW, et al. Advances in func-tional and structural MR image analysis and implementation asFSL. Neuroimage. 2004;23(suppl 1):S208–S219.
56. Smith SM, Jenkinson M, Johansen-Berg H, et al. Tract-based spa-tial statistics: voxelwise analysis of multi-subject diffusion data.Neuroimage. 2006;31(4):1487–1505.
57. Smith SM. Fast robust automated brain extraction. Hum BrainMapp. 2002;17(3):143–155.
58. Andersson JLR, Jenkinson M, Smith S. Non-linear optimisation.2007. FMRIB technical report TR07JA1. www.fmrib.ox.ac.uk/analysis/techrep. Accessed May 31, 2011.
59. Andersson JLR, Jenkinson M, Smith S. Non-linear registration,aka spatial normalisation. FMRIB technical report TR07JA2.www.fmrib.ox.ac.uk/analysis/techrep. Accessed May 31, 2011.
60. Rueckert D, Sonoda LI, Hayes C, Hill DL, Leach MO, Hawkes DJ.Nonrigid registration using free-form deformations: applicationto breast MR images. IEEE Trans Med Imaging. 1999;18(8):712–721.
61. Wakana S, Caprihan A, Panzenboeck MM, et al. Reproducibilityof quantitative tractography methods applied to cerebral whitematter. Neuroimage. 2007;36(3):630–644.
62. Mori S, Wakana S, Nagae-Poetscher L, van Zijl P. MRI Atlas of Hu-man White Matter. 1st ed. Amsterdam, The Netherlands: Elsevier;2005.
63. Cohen J. A power primer. Psychol Bull. 1992;112(1):155–159.64. Cirino PT, Chin CE, Sevcik RA, Wolf M, Lovett M, Morris RD.
Measuring socioeconomic status: reliability and preliminary valid-ity for different approaches. Assessment. 2002;9:145–155.
65. Arfanakis K, Haughton VM, Carew JD, Rogers BP, Dempsey RJ,Meyerand ME. Diffusion tensor MR imaging in diffuse axonalinjury. AJNR Am J Neuroradiol. 2002;23(5):794–802.
66. Hwang JP, Lee TW, Tsai SJ, et al. Cortical and subcortical abnor-malities in late-onset depression with history of suicide attemptsinvestigated with MRI and voxel-based morphometry. J GeriatrPsychiatry Neurol. 2010;23(3):171–184.
67. Aguilar EJ, Garcia-Marti G, Marti-Bonmati L, et al. Left or-bitofrontal and superior temporal gyrus structural changes asso-ciated to suicidal behavior in patients with schizophrenia. ProgNeuropsychopharmacol Biol Psychiatry. 2008;32(7):1673–1676.
68. Monkul ES, Hatch JP, Nicoletti MA, et al. Fronto-limbic brainstructures in suicidal and non-suicidal female patients with majordepressive disorder. Mol Psychiatry. 2007;12(4):360–366.
69. Ahearn EP, Jamison KR, Steffens DC, et al. MRI correlates ofsuicide attempt history in unipolar depression. Biol Psychiatry.2001;50(4):266–270.
70. Taber KH, Warden DL, Hurley RA. Blast-related traumaticbrain injury: what is known? J Neuropsychiatry Clin Neurosci.2006;18(2):141–145.
71. Abe O, Masutani Y, Aoki S, et al. Topography of the humancorpus callosum using diffusion tensor tractography. J ComputAssist Tomogr. 2004;28(4):533–539.
72. Robertson IH. Traumatic brain injury: recovery, prediction, andthe clinician. Arch Phys Med Rehabil. 2008;89(12 suppl):S1–S2.
73. Sidaros A, Skimminge A, Liptrot MG, et al. Long-term global andregional brain volume changes following severe traumatic braininjury: a longitudinal study with clinical correlates. Neuroimage.2009;44(1):1–8.
74. Avants B, Duda JT, Kim J, et al. Multivariate analysis of struc-tural and diffusion imaging in traumatic brain injury. Acad Radiol.2008;15(11):1360–1375.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Neuroimaging Correlates of TBI and Suicide 289
75. Kim J, Avants B, Patel S, et al. Structural consequences of dif-fuse traumatic brain injury: a large deformation tensor-based mor-phometry study. Neuroimage. 2008;39(3):1014–1026.
76. Gale SD, Baxter L, Roundy N, Johnson SC. Traumatic brain in-jury and grey matter concentration: a preliminary voxel based mor-phometry study. J Neurol Neurosurg Psychiatry. 2005;76(7):984–988.
77. Wei CW, Tharmakulasingam J, Crawley A, et al. Use of diffusion-tensor imaging in traumatic spinal cord injury to identifyconcomitant traumatic brain injury. Arch Phys Med Rehabil.2008;89(12 suppl):S85–S91.
78. Ljungqvist J, Nilsson D, Ljungberg M, et al. Longitudinal study ofthe diffusion tensor imaging properties of the corpus callosum inacute and chronic diffuse axonal injury. Brain Inj. 2011;25(4):370–378.
79. Alexopoulos GS, Kiosses DN, Choi SJ, Murphy CF, Lim KO.Frontal white matter microstructure and treatment responseof late-life depression: a preliminary study. Am J Psychiatry.2002;159(11):1929–1932.
80. Alexopoulos GS, Murphy CF, Gunning-Dixon FM, et al. Mi-crostructural white matter abnormalities and remission of geriatricdepression. Am J Psychiatry. 2008;165(2):238–244.
81. Nobuhara K, Okugawa G, Sugimoto T, et al. Frontal white matteranisotropy and symptom severity of late-life depression: a mag-netic resonance diffusion tensor imaging study. J Neurol NeurosurgPsychiatry. 2006;77(1):120–122.
82. Taylor WD, MacFall JR, Payne ME, et al. Late-life depressionand microstructural abnormalities in dorsolateral prefrontal cortexwhite matter. Am J Psychiatry. 2004;161(7):1293–1296.
83. Li L, Ma N, Li Z, et al. Prefrontal white matter abnormalities inyoung adult with major depressive disorder: a diffusion tensorimaging study. Brain Res. 2007;1168:124–128.
84. Yang Q, Huang X, Hong N, Yu X. White matter microstruc-tural abnormalities in late-life depression. Int Psychogeriatr.2007;19(4):757–766.
85. Jia Z, Huang X, Wu Q, et al. High-field magnetic resonance imag-ing of suicidality in patients with major depressive disorder. Am JPsychiatry. 2010;167(11):1381–1390.
86. Maller JJ, Thomson RH, Lewis PM, Rose SE, Pannek K, FitzgeraldPB. Traumatic brain injury, major depression, and diffusion tensorimaging: making connections. Brain Res Rev. 2010;64(1):213–240.
87. Bender TW, Gordon KH, Bresin K, Joiner TE, Jr. Impulsivity
and suicidality: the mediating role of painful and provocativeexperiences. J Affect Disord. 2010;129(1/3):301–307.
88. Teasdale G, Jennett B. Assessment of coma and impaired con-sciousness. A practical scale. Lancet. 1974;2(7872):81–84.
89. Saatman KE, Duhaime AC, Bullock R, Maas AI, Valadka A, Man-ley GT. Classification of traumatic brain injury for targeted thera-pies. J Neurotrauma. 2008;25(7):719–738.
90. Whyte J, Vasterling J, Manley GT. Common data elements forresearch on traumatic brain injury and psychological health:current status and future development. Arch Phys Med Rehabil.2010;91(11):1692–1696.
91. Versace A, Almeida JR, Hassel S, et al. Elevated left and reducedright orbitomedial prefrontal fractional anisotropy in adults withbipolar disorder revealed by tract-based spatial statistics. Arch GenPsychiatry. 2008;65(9):1041–1052.
92. Minami T, Nobuhara K, Okugawa G, et al. Diffusion tensor mag-netic resonance imaging of disruption of regional white matter inschizophrenia. Neuropsychobiology. 2003;47(3):141–145.
93. Yoo SY, Jang JH, Shin YW, et al. White matter abnormalitiesin drug-naive patients with obsessive-compulsive disorder: a dif-fusion tensor study before and after citalopram treatment. ActaPsychiatr Scand. 2007;116(3):211–219.
94. Zanetti MV, Jackowski MP, Versace A, et al. State-dependent mi-crostructural white matter changes in bipolar I depression. EurArch Psychiatry Clin Neurosci. 2009;259(6):316–328.
95. Versace A, Almeida JR, Quevedo K, et al. Right orbitofrontalcorticolimbic and left corticocortical white matter connectiv-ity differentiate bipolar and unipolar depression. Biol Psychiatry.2010;68(6):560–567.
96. Barnea-Goraly N, Chang KD, Karchemskiy A, Howe ME, ReissAL. Limbic and corpus callosum aberrations in adolescents withbipolar disorder: a tract-based spatial statistics analysis. Biol Psychi-atry. 2009;66(3):238–244.
97. Wessa M, Houenou J, Leboyer M, et al. Microstructuralwhite matter changes in euthymic bipolar patients: a whole-brain diffusion tensor imaging study. Bipolar Disord. 2009;11(5):504–514.
98. Yurgelun-Todd DA, Silveri MM, Gruber SA, Rohan ML, Pi-mentel PJ. White matter abnormalities observed in bipolar dis-order: a diffusion tensor imaging study. Bipolar Disord. 2007;9(5):504–512.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com




















