
Procedural discourse following traumatic brain injury
22
This article was downloaded by: [Monash University Library] On: 20 April 2013, At: 22:35 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Aphasiology Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/paph20 Procedural discourse following traumatic brain injury Pamela Snow a , Jacinta Douglas a & Jennie Ponsford b a La Trobe University, Melbourne, Australia b Bethesda Hospital, Melbourne, Australia Version of record first published: 29 May 2007. To cite this article: Pamela Snow , Jacinta Douglas & Jennie Ponsford (1997): Procedural discourse following traumatic brain injury, Aphasiology, 11:10, 947-967 To link to this article: http://dx.doi.org/10.1080/02687039708249421 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Procedural discourse following traumatic brain injury

This article was downloaded by: [Monash University Library]On: 20 April 2013, At: 22:35Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office:Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
AphasiologyPublication details, including instructions for authors and subscriptioninformation:http://www.tandfonline.com/loi/paph20
Procedural discourse following traumaticbrain injuryPamela Snow a , Jacinta Douglas a & Jennie Ponsford ba La Trobe University, Melbourne, Australiab Bethesda Hospital, Melbourne, AustraliaVersion of record first published: 29 May 2007.
To cite this article: Pamela Snow , Jacinta Douglas & Jennie Ponsford (1997): Procedural discourse followingtraumatic brain injury, Aphasiology, 11:10, 947-967
To link to this article: http://dx.doi.org/10.1080/02687039708249421
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantialor systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that thecontents will be complete or accurate or up to date. The accuracy of any instructions, formulae,and drug doses should be independently verified with primary sources. The publisher shall notbe liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever orhowsoever caused arising directly or indirectly in connection with or arising out of the use of thismaterial.

APHASIOLOGY, 1997, VOL. 11, NO. 10, 947-967
Procedural discourse following traumatic brain injury
P A M E L A S N O W , J A C I N T A D O U G L A S and J E N N I E PONSFORDt La Trobe University, Melbourne, Australia t Bethesda Hospital, Melbourne, Australia
(Received 17 Jarmay 1997; accepted 7 April 1997)
Abstract
Procedural discourse is a monologue discourse task concerned with explaining to a listener how a particular activity is carried out. The study reported here is part of a series of investigations into discourse abilities following severe traumatic brain injury (TBI). The aim of this study was to compare the procedural discourse skills of a group of 26 TBI speakers, with those of two demographically distinct control groups. The first control group comprised 26 non-TBI orthopaedic patients, and the second control group comprised 26 university students. These control groups were selected because of the hypothesis that premorbid demographic factors could influence sociolinguistic skills, and hence performance on a procedural discourse task. The TBI group was systematically compared with the control groups on content, productivity, and pragmatic measures. They were not significantly different from orthopaedic patients on measures relating to content and productivity ; however, they did differ significantly from the university students on these measures. The TBI group differed significantly from both control groups with respect to the production of pragmatic errors, and these were predominantly concerned with information transfer. The results are discussed in relation to issues in selecting control groups for discourse research following TBI, together with the clinical implications of the findings.
Introduction
Impairments of discourse abilities following traumatic brain injury (TBI) have been described by several workers in recent years (e.g. Coehlo 1995, Hagen 1984, Hartley 1995, McDonald 1993, Mentis and Prutting 1991, Snow and Ponsford 1995, Snow e t al. 1997). The term ‘discourse’ encompasses a number of genres, which may be broadly divided into two categories : interactive (i.e. conversation) and non-interactive (i.e. monologue). When using conversational discourse the individual must observe a variety of subtle interpersonal conventions such as turn- taking and topic shift rules, use of appropriate eye contact, and maintenance of an acceptable distance from the other speaker. Monologue genres (such as narrative and procedural discourse) are not, however, inextricably tied to these rules of interpersonal behaviour. Although narrative and procedural discourse may be incorporated into conversation, they are conventionally studied in isolation for
Address correspondence to : Pamela Snow, School of Human Communication Sciences, La Trobe University, Bundoora, Victoria 3083, Australia.
026&7038/97 $1200 0 1997 Taylor & Francis Ltd
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

948 P. Snow et al.
experimental purposes. Discourse difficulties which have been described following TBI include poor topic maintenance, difficulty meeting the informational needs of the listener, difficulty making contributions which sustain and extend an interaction, poor cohesion, and reduced communicative efficiency (e.g. Coehlo 1995, Hagen 1984, Hartley 1995, McDonald 1993, Mentis and Prutting 1991, Snow and Ponsford 1995, Snoi- e t a/. 1997).
Because TBI is typically associated with diffuse axonal injury, together with focal injury to the frontal and temporal regions (Ponsford 1995), these discourse changes are generally considered to reflect neurobehavioural impairment, rather than aphasia. That is, TBI is thought to be associated predominantly with a disturbance of language use, rather than language form. A number of workers have emphasized the relationship between discourse impairment and underlying cognitive dys- function (Coehlo e t a/. 1994, 1996, Hagen 1981, Hartley 1995, McDonald and Pearce 1995, McDonald and van Sommers 1993). Deficits in areas such as attention/concentration, mental flexibility, planning/organization, and self-regu- lation, have been implicated as being substantially, if not entirely, responsible for difficulties using discourse appropriately in everyday settings.
Procedural discourse is a goal-oriented monologue genre which is concerned with explaining to a listener how something is done. According to Ulatowska e t a / . (1 990) the principal difference between narrative and procedural discourse is that while the primary function of a narrative is to entertain, the main purpose of procedural discourse is t o inform or instruct. Ulatowska e t a/. observed that the procedural genre therefore makes greater demands on the speaker’s ability to be precise and explicit in conveying information. Procedural discourse comprises information units known as steps (Cannito eta/. 1988, Ulatowska e t al. 1983). These are said to be organized hierarchically into essential, optional, (may be either auxiliary or substeps), and target steps. According to Ulatowska and co-workers (1981, 1990), essential steps contain the information which must be understood by the listener in order to know what actions are required to complete the task in question. Optional steps, on the other hand, provide clarification and/or extra detail about information contained in the essential steps. The target step indicates that the procedure is complete.
Coehlo (1995) noted that, because discourse may break down at a number of different levels, samples should be analysed at multiple levels of performance, e.g. cohesion, productivity, and content. There is evidence that different discourse genres place different cognitive and/or linguistic demands on a speaker, regardless of the presence of brain damage (Coehlo e t a/. 1991a, Hartley and Jensen 1991, Shadden etal. 1991, Clatowska e ta f . 1990). Non-brain-damaged controls have been found to produce longer monologues (both temporally and in terms of the number of utterances) when producing narratives than when producing procedures. Also, speakers tend to use more complex sentences when producing narratives. Hartley and Jensen (1 991) reported that control subjects displayed greater difficulties with clarity of reference when producing procedural discourse, than when producing narratives.
While few workers have examined the procedural genre in the TBI population, it has been examined in some depth in people who have had left hemisphere strokes, right hemisphere strokes, and dementia of the Alzheimer type (DAT) (e.g. Ulatowska eta/. 1983,1990). Procedures which have been selected for use in studies of aphasic and DAT subjects include making a sandwich (Ulatowska et a/. 1988,
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

Procedural discoztrse following TBI 949
1990), changing a light bulb (Ulatowska e t al. 1988), addressing and mailing a letter (Ulatowska e t al. 1988) and changing a tyre (Cannito e t al. 1988). Mildly aphasic subjects have been shown to have relatively well preserved procedural discourse, in spite of some sentence-level breakdown. Moderately to severely impaired aphasics, however, have been shown to display breakdowns at both the sentential and discourse levels when producing procedures (Ulatowska e t al. 1990). Because aphasics might generally be said to display impaired linguistic abilities, against a background of relatively intact cognitive skills, the extent to which the findings from aphasia studies can be generalized to the TBI population is limited. Of interest, however, are the findings derived from studies of individuals with DAT, because of the diffuse pathology, and vulnerability of the frontal and temporal lobes thought to be associated with this condition (Bayles 1994). Moderately impaired DAT patients have been found to produce more irrelevant and non- specific information, and to use more exophoric reference (i.e. reference to the extralinguistic context) than controls, when producing procedural discourse (Ulatowska e t al. 1988).
A number of techniques have been used to elicit procedural discourse from TBI speakers. These include requests for descriptions of some aspect of the person’s treatment programme or work (e.g. Mentis and Prutting, 1987), explaining a novel procedure to a nai‘ve listener (e.g. McDonald 1993), or outlining the steps in a routine daily task, such as buying groceries in an American supermarket (Hartley and Jensen 1991), withdrawing money from a bank account (Snow e t al. 1995), or changing a tyre, mailing a letter, or making a sandwich (Coppens 1995). When producing procedural discourse, people who have sustained TBI have been found to display difficulty observing so-called ‘ Gricean maxims’ (Grice 1975) (e.g. McDonald 1993), show an overall reduction in communicative efficiency, together with reduced use of reference, and also produced fewer target content units (Hartley and Jensen 1991).
McDonald (1993) used a procedural discourse task to compare two TBI speakers with nine demographically matched controls. Particular strengths of this study were : (a) that the listener could be said to be truly nahe about the information to be conveyed by the speaker, and (b) the speaker could not draw on ‘old’ knowledge, as he/she did not have past experience with the particular task. The speaker, therefore, could not rely on an assumption of shared world knowledge, as is the case with most tasks that have been described in the literature (e.g. making a sandwich, writing a letter). Listener nai’vett was achieved by having the subjects explain the rules of a novel board game to a blindfolded listener who was unfamiliar with the game or its rules. McDonald found that, while there were not significant differences between measures of cohesive harmony between the TBI and non-injured subjects, the TBI subjects both made inappropriate use of exophoric reference. This occurred when their utterances contained ambiguous information, or information which they erroneously assumed the listener was privy to. McDonald also adapted Grice’s (1975) conversational maxims to develop a set of five seven-point rating scales, examining repetitiveness, detail, clarity, organiz- ation, and effectiveness. When written transcripts were evaluated by a panel of speech pathologists and psychologists, the discourse of the TBI subjects was found to be inadequate in meeting the informational needs of the listener. Discourse errors occurred predominantly in Grice’s quantity and manner categories, resulting in explanations which were judged as confusing and disorganized.
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

950 P. Snow et al.
There is broad consensus that individuals who have sustained TBI commonly display discourse behaviour which is, in one way or another, disordered. Enormous deficiencies exist, however, in the tools available to define, much less measwe, what listener judges perceive in everyday discourse. One of the key methodological issues pervading this field is heterogeneity. Workers such as Patry and Nespoulos (1990) have stressed the level of normal individual variation in discourse style which will be found in a given group, regardless of the presence of brain damage. The role of heterogeneity in obscuring group differences was also stressed by Ruff and Camenzuli (1991), who cited injury-related phenomena, together with wide variability in premorbid emotional, cognitive, psychosocial, vocational, and financial parameters. Premorbid factors are of particular relevance to the question of heterogeneity, given that those most at risk of sustaining TBI are young males in the 17-30-year age group (Anderson and McLaurin 1980). Further, it has been noted that individuals with a history of learning disability, limited vocational achievement, and o r drug/alcohol abuse are disproportionately represented in TBI samples (Haas e t al. 1987, Rime1 ef al. 1990). This ‘premorbid profile’ of the individual at risk of sustaining a TBI raises the important question of socio- linguistics. Hudson (1980), for example, has suggested that ‘speech has a social function, both as a means of communication and also as a way of identifying social groups, and to study speech without reference to the society which uses it is to exclude the possibility of finding social explanations €or the structures that are used’ (p. 4). It is important, therefore, that careful consideration is given to the selection of control groups for use in discourse research with the TBI population. McKinlay and Brooks (1984) suggested that orthopaedic patients constitute appropriate controls to employ in TBI research, as these individuals have similar demographic characteristics to the TBI group and, like the brain-injured, have recently experienced major trauma, followed by prolonged hospitalization. Unfortunately, with few exceptions (e.g. Jordan and Murdoch 1990, Snow e t al. 1995, 1997, Spence and Godfrey 1993), orthopaedic patients have not been employed as controls in TBI discourse research. Instead, hospital workers and university students (Coehlo e t al. 1991b, Liles ef a/. 1989, McDonald and Pearce 1995), and/or less adequately described control groups have been employed (Mentis and Prutting 1987). In some cases no controls at all were included (Linscott e t al. 1996, Parsons e t al. 1989).
Procedural discourse might be said to possess good ‘face’ validity as a measure of verbal ability following TBI. It appears to require the individual to select, retrieve, and sequence information contained in steps. Given the commonly reported neurobehavioural difficulties associated with TBI (Sloan and Ponsford 1995), it might be expected that difficulties in planning, organizing, self- monitoring, and taking the perspective of the listener, might impact negatively on TBI subjects’ ability to produce procedural discourse. Because it is a monologue task the speaker must rely entirely on his/her own organizational abilities, with no assistance from repair strategies offered by the listener.
Unfortunately, however, a number of methodological problems exist with respect to the analysis of procedural discourse. In particular, the distinction between essential and optional steps appears to be an arbitrary one. Ulatowska e t a/. (1983), for example, provided a list of what they deemed to be the essential steps involved in changing a light bulb, making a sandwich, making scrambled eggs, and going shopping at the supermarket. Similarly, Canniro e t al. (1988), provided a list
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

Procedural discourse following TBI 951
of what they determined were the essential steps involved in changing a tyre. Ulatowska e t al. (1 983), based their differentiation between essential and optional steps on the degree to which they judged the information is explicit or implicit. They asserted, for example, that in describing how to make scrambled eggs, the step ‘break the eggs into a bowl’ contains within it an implicit assumption that the eggs have been removed from the refrigerator. This latter step, then, because it is said to be implied, is classified as an optional step, Ulatowska e t al. further asserted that optional steps could be subclassified into auxiliary and substeps. An auxiliary step was said to be at the same hierarchical level as the essential step, because it introduces new information. The substep, however, was said to be at a subordinate level to the essential and auxiliary steps, because it provides ‘finer detail’ about steps which have already been produced. This classification implies that the bulk of what a speaker says during procedural discourse is devoted to the production of essential steps, while less speaking time would be devoted to the production of optional information.
Although this system of classifying the elements of procedural discourse is attractively simple as a basis for analysis, it does not appear to have been subjected to scrutiny with respect to the discourse of normal speakers. In particular it is not known whether normal speakers make a hierarchical distinction between types of steps and, if so, whether the presumed differentiation between essential and auxiliary steps is borne out in the way in which normal speakers organize procedural discourse. Further, it is not known to what extent this hypothetical structure can be generalized across levels of task complexity, e.g. with respect to the number of steps involved, speaker familiarity with the task, and the presumed nayvet6 of the listener. Some tasks involve more steps (essential or otherwise) than others; those described by Ulatowska e t al. (1983), for example, ranged from four to six essential steps. It is not known to what extent the variable of task length influences the detail and organization of steps. Speaker familiarity with the task is relevant in that when describing to a listener how to perform routine daily tasks such as making a sandwich, the speaker might be expected to assume a degree of shared ‘world knowledge ’ with the listener, and this may result in an assumption that optional or auxiliary steps do not need to be overtly stated.
In summary, although procedural discourse seems to possess good face validity as a measure of verbal skills after TBI, a number of theoretical and methodological questions need to be addressed in order for this genre to be assessed in a valid and reliable way in the clinical setting. The present study was conducted in an effort to address issues relating to selection of control groups, as a basis for eliciting demographically appropriate normative data. In view of the relative paucity of data on procedural discourse after TBI (as compared to narrative discourse and conversation), this study also addresses questions concerning the appropriateness of making hierarchical distinctions between ‘essential ’ and ‘ optional’ steps in 9rocedural discourse tasks.
Aims
The major aim of this study was to determine whether content, productivity, and/or pragmatic measures can be used to differentiate between severely injured TBI participants and two demographically distinct control groups, on performance of a procedural discourse task. It was hypothesized that, although these measures
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

952 P. Snow et al.
might differentiate the TBI group from a demographically distinct group, this would not necessarily be the case when the TBI group was compared to a demographically similar group. The study reported here is one of a series of detailed investigations into discourse after severe TBI. The conversational characteristics of the groups described here have been reported previously (Snow e t al. 1997).
Methods
Partiripants
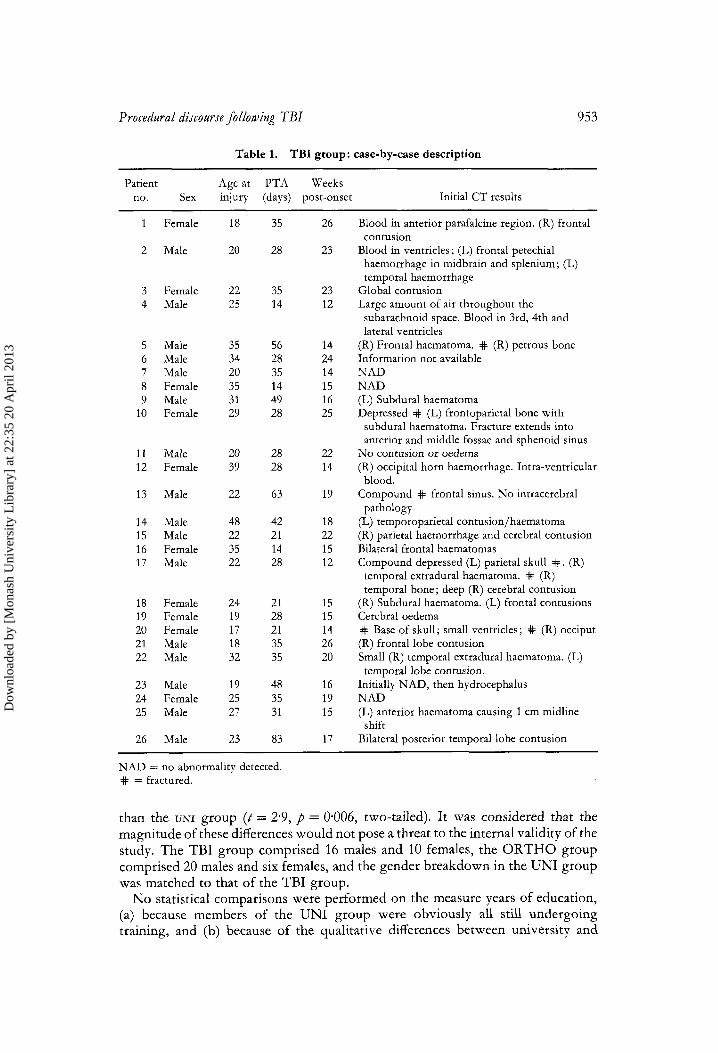
There were 78 participants in the study. These comprised 26 TBI participants, 26 non-TBI orthopaedic patients (ORTHO), and 26 university students (UNI). All participants were required to have completed the majority of their schooling in an English-speaking country, and people with a past history of hearing, neurological, or psychiatric disability were not included. Members of the TBI group were undergoing rehabilitation at either Bethesda Hospital, or the Victorian Re- habilitation Centre, Melbourne, Australia. All TBI participants had sustained a severe injury to the brain (defined as a period of post-traumatic amnesia (PTA) of 14 days or more) in a motor vehicle accident. Duration of PTA was measured using the Westmead PTA scale (Shores e t al. 1986). In order to control for time post- onset the TBI participants were all seen between 3 and 6 months post-injury. All TBI participants were outpatients at the time of inclusion in the study, and were seen a minimum of 4 weeks after emergence from PTA (A4 = 13.2, SD = 4-75, range = 5.2N5.8). Participants with clinical evidence of motor speech disturbances (as determined by a speechblanguage pathologist on the basis of anatomical and functional evaluation) were not included. Brain computerized tomography reports were available on 25 of the TBI participants, and in 21 trauma-related pathology was reported. This information is summarized in Table 1.
The ORTHO group comprised 26 individuals who had sustained orthopaedic injuries in motor-vehicle (n = 24) or workplace (n = 2) accidents, with no impairment of consciousness. This was verified via examination of medical records for documentation that impairment of consciousness had not occurred following injury, and interview with the participants. ORTHO participants who could not recall their accidents were excluded from the study. All members of this group were attending Bethesda Hospital, Melbourne, for outpatient physiotherapy.
The UNI group comprised undergraduates in a variety of disciplines, pre- dominantly in the health sciences (e.g. orthoptics and occupational therapy). These participants were included because they are considered to be demographically distinct from the two patient groups in terms of educational background, and hence verbal behaviour. Given the exploratory nature of this study, it was considered important to include a control group which could be regarded as demographically (and hence sociolinguistically) distinct from the two patient groups. It was hoped that this would facilitate the exploration of group trends in relation to variability in discourse behaviours within and between groups. Table 2 displavs the age and injury characteristics of the groups, and Table 3 gives a breakdown of the educational backgrounds of the two patient groups. The TBI group was, on average, 5.5 years younger than the ORTHO controls (t = -2.34, p = 0-023, two-tailed); however the ranges in the two groups were similar (17-48, and 18-52, respectively). Similarly, the TBI group was on average 5 years older
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13
Procedural discourse following TBI 953
Table 1. TBI group: case-by-case description
Patient Age at PTA Weeks no. Sex injury (days) post-onset Initial CT results
1 Female
2 Male
3 Female 4 Male
5 Male 6 Male 7 Male 8 Female 9 Male
10 Female
11 Male 12 Female
13 Male
14 Male 15 Male 16 Female 17 Male
18 Female 19 Female 20 Female 21 Male 22 Male
23 Male 24 Female 25 Male
26 Male
18
20
22 25
35 34 20 35 31 29
20 39
22
48 22 35 22
24 19 17 18 32
19 25 27
23
35
28
35 14
56 28 35 14 49 28
28 28
63
42 21 14 28
21 28 21 35 35
48 35 31
83
26
23
23 12
14 24 14 15 16 25
22 14
19
18 22 15 12
15 15 14 26 20
16 19 15
17
Blood in anterior parafalcine region. (R) frontal
Blood in ventricles; (L) frontal petechial contusion
haemorrhage in midbrain and splenium; (L) temporal haemorrhage
Global contusion Large amount of air throughout the subarachnoid space. Blood in 3rd, 4th and lateral ventricles
(R) Frontal haematoma. # (R) petrous bone Information not available NAD NAD (L) Subdural haematoma Depressed # (L) frontoparietal bone with
subdural haematoma. Fracture extends into anterior and middle fossae and sphenoid sinus
No contusion or oedema (R) occipital horn haemorrhage. Intra-ventricular
Compound # frontal sinus. No intracerebral
(L) temporoparietal contusion/haematoma (R) parietal haemorrhage and cerebral contusion Bilateral frontal haematomas Compound depressed (L) parietal skull # . (R)
temporal extradural haematoma. # (R) temporal bone; deep (R) cerebral contusion
blood.
pathology
(R) Subdural haematoma. (L) frontal contusions Cerebral oedema # Base of skull; small ventricles; # (R) occiput (R) frontal lobe contusion Small (R) temporal extradural haematoma. (L) temporal lobe contusion.
Initially NAD, then hydrocephalus NAD (L) anterior haematoma causing 1 cm midline
shift Bilateral posterior temporal lobe contusion
NAD = no abnormality detected. # = fractured.
than the UNI group (t = 2.9, p = 0.006, two-tailed). It was considered that the magnitude of these differences would not pose a threat to the internal validity of the study. The TBI group comprised 16 males and 10 females, the ORTHO group comprised 20 males and six females, and the gender breakdown in the UNI group was matched to that of the TBI group.
No statistical comparisons were performed on the measure years of education, (a) because members of the UNI group were obviously all still undergoing training, and (b) because of the qualitative differences between university and
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

954 P. Snow et al.
Table 2. Participant characteristics (all groups), time post injury (TBI & ORTHO) and PTA (TBI)
Group
TBI O R T H O UNI
SD Range A\f SD Range M SD Range
Age (years) 26.2 7.8 17-48 31.2 9.1 18-52 21.2 41 17-35 Education (years) 12.4 1.6 10-16 12.7 2.3 9-17 13.7 1.4 12-16
- _ - PTA (days) 34 15.7 14-83 - ~
-
Time post-injury (weeks) 17.8 4.2 12-26 22.3 23.2 3-108 - -
TBI = traumatic brain iniury group, O R T H O = orthopaedic patient control group, UNI = university student control group.
Table 3. Educational characteristics: TBI and ORTHO groups
Group
Type of education TBI O R T H O completed (4 (4 Less than high school 8 9
High school graduation 4 3 Trade (not completed) 3 0
University degree 4 3
Uni\ ersitr degree 2 5
graduationt
Trade (completed) 5 6
(not completed)
(completed)
+High school graduation refers to 12 years of schooling.
trade-school education. As shown in Table 3, however, the two patient groups were similar with respect to the type of educational training they had undertaken. In particular, it can be seen that approximately one third of both groups had not completed secondary schooling. It should be noted that five of the TBI participants had their education interrupted by their injuries, and this was the case for four of the ORTHO participants.
Procedure
All participants were seen individually by the same speech-language pathologist (P.S.) in a hospital office, or a clinic room in the School of Human Communication Sciences at La Trobe University. All sessions were videotaped using a Panasonic NV-M40 camera, which was either wall-mounted, or mounted on a tripod in the same room as the interactants. With their consent, details regarding the TBI and ORTHO participants' injuries and current medical status were obtained from the hospital medical record.
Each participant completed the following four discourse tasks : conversation,
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

Procedural discourse following TBI 955
procedural discourse, and two narratives. This paper is concerned only with the procedural discourse task. Each participant was asked by the examiner to ‘Tell me all the steps involved in withdrawing money from a bank account, as if I had never done it before.’ No restrictions were applied as to whether participants should describe this procedure as it applies to an automatic teller machine, or as it applies to withdrawing money in the bank itself.
Participants’ videotaped responses were then transcribed orthographically. Every effort was made to include all sound, syllable, and word repetitions, together with occurrences of fillers, such as ‘urn’. The groups were then compared on the following measures :
Total number of essential steps produced
This was included as a content measure. Operational definitions of ‘essential’ and ‘ optional’ steps were obtained by asking 20 speech-language pathologists to complete a written form of the task, and to classify their steps as ‘essential’ or ‘optional’. To assist with this classification task they were provided with Ulatowska e t al.’s (1983) definitions of these terms. For the purposes of this study a step was said to be ‘essential’, if it was so classified by 80% of the clinicians. Remaining steps were classified as ‘optional’. Appendix A lists the ‘essential’ and ‘optional’ steps derived for both ways of withdrawing money (via an automatic teller machine [ATM], and over-the-counter [OTC]). As can be seen, there were six essential steps for the OTC method, and eight for the ATM method. For this reason participants’ scores were converted to a percentage proportion of the clinicians’ totals.
Percentage yllables in ‘ on-target’ output
Because of concerns about the theoretical validity of a hierarchical distinction between so-called ‘essential’ and ‘ optional’ steps, a fundamental and descriptive approach was taken to the analysis of these data. This analysis required every syllable in the transcripts to be classified into one of four categories, in order that a broad distinction could be made between discourse which was ‘on-target ’ (i.e. relevant to the task of how to withdraw money from a bank account), and that which was in some way ‘ off-target ’ (i.e. not contributing to information transfer about the task). These four categories were as follows:
1. Syllables which conveyed so-called ‘ essential ’ information. 2. Syllables which conveyed so-called ‘ optional’ information. 3. Syllables in mazes. 4. Syllables which conveyed ‘low content’ output, i.e. conveying repeated or
The ‘ essential’ and ‘ optional’ steps which were derived from the clinicians’ responses (see Appendix A) were used for categories 1 and 2. A ‘maze’ has been defined as ‘a series of words or initial parts of words which do not add up, either to meaningful communication or to structural units of communication.. . They are unattached fragments which do not constitute a communication unit, and are not necessary to the communication unit’ (Loban 1963). This category was included in an effort to account for behaviours associated with reduced communicative efficiency. The final category accounted for syllables which were produced in the
irrelevant output.
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13
956 P. Snow et al.
course of repeating information already stated, or in relating irrelevant material. Syllables conveying non-specific vocabulary (e.g. ‘you know what I mean’) were also included in this category.
A modified ijersion of Damico’s (1985) Clinical Discourse Anahsis (CDA) , the C D A - ill (Snow et al. 1997)
This measure has emerged out of the conversation component of this study (Snow e t a/. 1997), and reflects all CDA (Damico 1985) discourse errors outside those occurring in the following three parameters : non-specific vocabulary, linguistic non- fluency, and revision behaviour. These behaviours were found to occur with similar frequency across the three groups included in this study. Behaviours which are included in the CDX-M include, for example, informational redundancy, insufficient information bits, failure to structure discourse, and poor topic maintenance (see Appendix B).
Analysis of data
The TBI group was compared with each of the control groups on three measures of interest (proportion of ‘essential ’ steps present, percentage syllables in ‘on- target’ output, and CDA-M). In order to control for an inflated Type I error rate with multiple comparisons (independent t-tests), modified Bonferroni adjusted (Keppell 1991) was used for the third of the three planned comparisons. This yielded an adjusted alpha-level of p = 0.025. Because the between-groups degrees of freedom was equal to 2, an alpha-level of 0.05 was employed for the first two comparisons. Where the parametric statistical assumption of homogeneity of variance was violated, non-parametric analyses were performed.
Reliability
Transcription
Point-to-point inter-rater reliability was calculated on 18 (25 YO) of the tran- scriptions carried out independently by two speech-language pathologists. Mean syllable-to-syllable agreement was 95.1 YO (SD = 1.2).
Percentage gllables in ‘ on-target ’ output
Inter-rater reliability for this measure was calculated on the same 18 samples using a Pearson product-moment correlation coefficient. This yielded a correlation of r = 0.84 (p = 0.000 [two-tailed]).
CDAL1I
Point-to-point agreement was also calculated on two speech-language pathologists’ independent ratings of 25% of samples, using the CDA-M. Mean percentage agreement across the three groups was 82.2%. Mean agreement within the TBI group was 96.7 %, within the ORTHO group 100 %, and within the UNI group 57.1 %. It should be noted that agreement within the UNI group was 100% for
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

Procedural discourse following TBI 957
four participants, but lack of agreement over single errors in the remaining three transcripts resulted in 0 % agreement on those samples.
Results
The results are presented in three sections : proportion of essential steps, percentage syllables in ‘on-target’ output, and CDA-M scores.
The measure totalsyllablesproduced was included as a control variable, in order to ensure that group differences on breakdown of syllables were not accounted for by differences in the amount of discourse provided. This measure was not related to a specific hypothesis. Independent two-tailed t-tests were used to compare the TBI group with each of the control groups on this measure, and no significant differences were found (TBI-ORTHO: t = 0.22, d.f. = 49, p = 0.82; TBI-UNI: t = -0.50, d.f. = 50, p = 0.62). The means, standard deviations, and ranges on this measure are included in Table 4.
Proportion of ‘ essential’ steps produced
Because the analysis was based on eight ‘essential’ steps for the ATM method, and six for the OTC method, scores were converted to a percentage proportion of the arbitrary totals. It should be noted that data are available on only 25 of the 26 ORTHO participants, as one member of this group declined to attempt the task, on the grounds that he does not do the banking in his household.
The descriptive statistics pertaining to this measure are summarized in Table 5. The TBI group was not found to differ significantly from the ORTHO group on this measure (t = -0.23, d.f. = 49, p = 0.82). A Mann-Whitney U-test was performed to compare the TBI and UNI groups. This difference was statistically significant (U = 231, 7 = - 1-98, p = 0.04).
speakers in each group
Percentage yllables in ‘ on-target ’ output
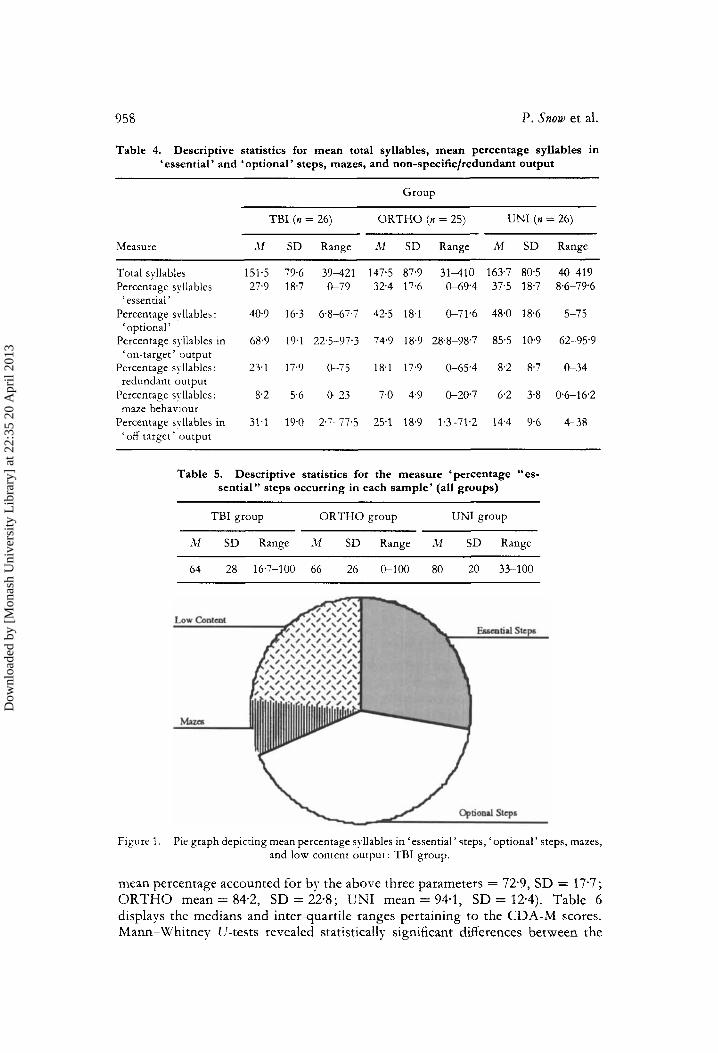
Table 4 summarizes the descriptive statistics for the measure, percentage syllables in ‘on-target’ output, and Figures 1, 2, and 3 depict pie charts of the syllable breakdowns derived from each of the groups. As can be seen, all groups produced a higher mean percentage syllables in producing so-called ‘optional ’ information, than so-called ‘ essential ’ information. A series of dependent (within-groups) t-tests indicated, however that this difference was significant only for the TBI group (t = -2.19, d.f. = 25, p = 0.04, two-tailed). When the ‘essential’ and ‘optional’ categories were combined, to form the measure percentage syllables in ‘ on-target ’ output, the TBI group was found to differ significantly from the UNI group (U = 152.0, a = -0*4[corrected for ties], p = 0.0007, two-tailed), but not from the ORTHO group (t = -0.98, d.f. = 49, p = 0.28, two-tailed).
CD A- M scores
As with the results of the conversation task completed by these groups (Snow e t al. 1997), the three parameters non-specific vocabular_y, linguistic non-juenq, and revisian behaviour accounted for the bulk of the discourse errors made by all groups (TBI
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13
958 P. Snow et al.
Table 4. Descriptive statistics for mean total syllables, mean percentage syllables in ‘essential’ and ‘optional’ steps, mazes, and non-specific/redundant output
Measure
Group
O R T H O (n = 25) TBI (n = 26) UNI (n = 26)
‘11 SD Range it1 SD Range M SD Range
Total syllables 151.5 79.6 39-421 147.5 87.9 31-410 163.7 80.5 40-419 Percentage syllables 27.9 18.7 G 7 9 32.4 17.6 0-69’4 37.5 18.7 8.6-794 ‘ essential ’
‘optional’
‘ on-target ’ output
redundant output
maze behaviour
‘ off-target ’ output
Percentage syllables: 40.9 16.3 6.8-67.7 42.5 18.1 G71.6 48.0 18.6 5-75
Percentage syllables in 68.9 19.1 22.5-97.3 74.9 18.9 28.8-98.7 85.5 10.9 62-95.9
Percentage s!-llables: 23.1 17.9 G 7 5 18.1 17.9 0-65.4 8.2 8.7 G 3 4
Percentage syllables: 8.2 5.6 0.~~23 7.0 4.9 0-20.7 6.2 3.8 06-16.2
Percentage syllables in 31.1 19.0 2.7-77.5 25.1 18.9 1.3-71.2 14.4 9.6 4-38
Table 5. Descriptive statistics for the measure ‘percentage “es- sential” steps occurring in each sample’ (all groups)
TBI group O R T H O group UNl group
SD Range ill SD Range M SD Range
64 28 16.7-100 66 26 0-100 80 20 33-100
Figure 1. Pie graph depicting mean percentage syllables in ‘essential’ steps, ‘optional’ steps, mazes, and low content output: TBI group.
mean percentage accounted for by the above three parameters = 72.9, SD = 17-7; ORTHO mean = 84.2, SD = 22.8; CNI mean = 94-1, SD = 12.4). Table 6 displays the medians and inter-quartile ranges pertaining to the CDA-M scores. Mann-Whitney U-tests revealed statistically significant differences between the
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13
Procedural discourse following TBI 959
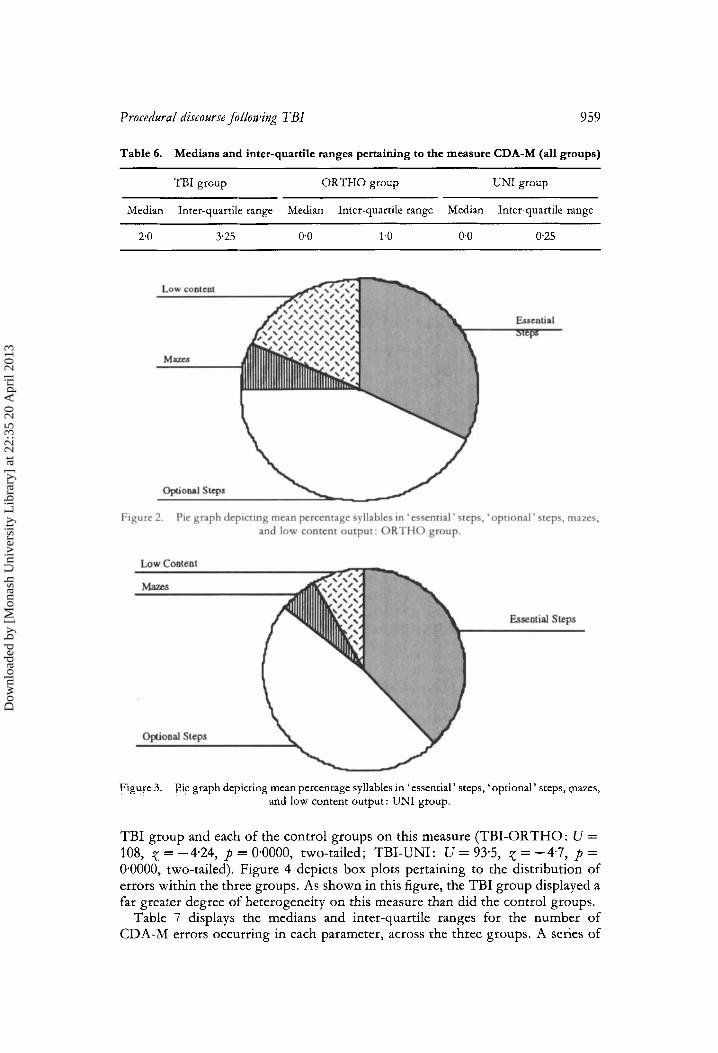
Table 6. Medians and inter-quartile ranges pertaining to the measure CDA-M (all groups)
TBI group ___
ORTHO group UNI group
Median Inter-quartile range Median Inter-quartile range Median Inter-quartile range
2.0 3.25 0 0 1.0 0 0 0.25
Figure 3. l?ie graph depicting mean percentage syllables in ‘essential’ steps, ‘optional’ steps, mazes, and low content output: UNI group.
TBI group and each of the control groups on this measure (TBI-ORTHO: U = 108, p = -4.24, p = 0.0000, two-tailed; TBI-UNI: U = 93.5, p = -4.7, p = 0.0000, two-tailed). Figure 4 depicts box plots pertaining to the distribution of errors within the three groups. As shown in this figure, the TBI group displayed a far greater degree of heterogeneity on this measure than did the control groups.
Table 7 displays the medians and inter-quartile ranges for the number of CDA-M errors occurring in each parameter, across the three groups. A series of
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

960
12
10
81
6
4
P. Snow et al.
*
8 0
1 A-
GROUP Figure 4. Box plots of procedural discourse CDA-&I scores: all groups. The box contains the 50%
of cases between the 25th and 75th percentiles, while the ‘whiskers’ extend between the lowest and highest scores, excluding outliers. Symbols and *represent odiers (value between 1.5 and 3 box-lengths from upper o r lower box edge) and extremes (a value more than 3 box- lengths from the upper or lower edge of the box), respectively.
Kruskal--Wallis AKOVAs was performed, in order to determine whether any group differences existed on the CDA-M parameters. These analyses indicated that the TBI group made significantly more errors than either control group on each of the following parameters : (1) insufficient information bits, (2) poor topic maintenance, and (3) information redundancy. Differences were not statistically significant on the remaining three categories. It is noted, however, that the only individuals who made errors in the inability to structure and message inaccuray parameters were members of the TBI group. Further, no member of the UNI group made errors in the poor topic maintenance parameter.
Discussion
This paper has described an examination of procedural discourse following severe TBI, with particular reference to the need to examine discourse with premorbid sociolinguistic behaviour as a focus. Although group differences were not found with respect to the number of syllables produced, the TBl group was found to differ significantly from a demographically distinct control group (university students) with respect to (a) the amount of content provided (defined as the percentage of a predetermined total number of essential steps present in their discourse samples), and (b) percentage syllables in ‘ on-target ’ discourse (i.e. discourse concerned with conveying both so-called ‘essential ’ and ‘ optional’ information). Significant differences on these measures were not found, however, between the TBI group and a demographically similar control group (non-TBI orthopaedic patients). Finally, the TBI group was found to differ significantly from both control groups on the CDA-M, a measure of pragmatic abiIities. In particular the TBI group’s errors reflected poor topic maintenance, and difficulties with information transfer (i.e. information redundancy and insufficient information bits).
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

k s
Tab
le 7
. M
edia
ns a
nd in
ter-
qu
arti
le ra
nges
for
raw
sco
res
on p
roce
dura
l dis
cou
rse
CD
A-M
par
amet
ers
(all
gro
up
s)
G
TB
I gr
oup
OR
TH
O g
roup
U
NI
grou
p (n =
26)
(n
= 2
5)
(n =
26)
Inte
r-qu
artil
e In
ter-
quar
tile
Inte
r-qu
artil
e ra
nge
Med
ian
rang
e M
edia
n ra
nge
XZ
P C
DA
-M p
aram
eter
M
edia
n
Insu
ffic
ient
info
rmat
ion
1 ,o
20
0.
0 1.
0 0.
0 0.
0 27
.7
o~oo
oot
N/*
Po
or t
opic
mai
nten
ance
0
0
1.0
00
0.
0 N
/A
Inab
ility
to s
truc
ture
0
0
0.0
00
0
0
00
N
/*
Inap
prop
riat
e re
spon
se
00
0.
0 N
/A
N/A
N
/A
Mes
sage
inac
cura
cy
0.0
00
N
/A
N/*
N
/A
N/A
Info
rmat
iona
l re
dund
ancy
0.
0 1.
0 0.
0 0
0
00
0.
0 6.
3 0.
04-f
9.4
0009
t 1.
9 n.
s.
3.97
n
s.
3.9
00
n.s.
N/A
ref
ers
to th
e fa
ct th
at a
ll m
embe
rs o
f th
e gr
oup
mad
e ze
ro e
rror
s in
thi
s pa
ram
eter
. t T
wo-
taile
d p-
valu
es.
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

962 P. Snow et al.
It should be noted that there is some overlap in the behaviours included in the ‘off-target ’ category, and certain parameters of the CDA-M. Mazes, for example, consist largely of linguistic non-fluencies, and revision behaviours. Mean percentage syllables in mazes was not related to a specific hypothesis in this study; however, it is interesting to note that, just as the number of errors in the linguistic non-fluency and revision behaviour parameters failed to differentiate TBIs from controls on this task, visual inspection of mean percentage syllables in mazes (see Table 4) does not suggest the presence of group differences. This is also consistent with the conversational data derived from these groups (Snow e t a/. 1997). Similarly, the ‘ low content’ category includes not only information which is irrelevant or being repeated (similar to the CDA-M parameters ‘poor topic maintenance ’ and ‘ informational redundancy ’), but also episodes of non-specific vocabulary. The fact that the measure mean percentage yllables in ‘ of-target’ output includes some behaviours which have been shown to have poor discriminability between TBI speakers and controls may account for the absence of a significant difference between the TBI and ORTHO groups in this study.
These results appear to lend support to the hypothesis that sociolinguistic factors exert an important influence on the way speakers produce procedural discourse. The TBI group was similar to the O R T H O group with respect to the amount of content (‘essential steps’) produced, and also the amount of what we have termed ‘off-target ’ behaviour (e.g. mazes, redundant, and/or irrelevant output). These findings seem to support McKinlay and Brooks’ (1984) contention that control groups need to be selected carefully for the study of neurobehavioural impairment after TBI. The inclusion of only the UNI group as controls would have resulted in Type 1 errors with respect to content and productivity measures. This could, in turn, lead to inappropriate recommendations about which behaviours need to be targeted in therapy.
The performance of the TBI participants clearly indicated that they are able to select and provide information in so-called ‘steps’. In doing so, however, they made a number of pragmatic errors, and performed significantly more poorly than both of the control groups in this respect. Although the frequency in absolute terms of such errors might be regarded as low, it must be noted that these errors may have a disproportionately negative impact on listeners. The low overall frequency of such errors also needs to be considered with respect to the brevity of the task. Because these errors were concerned with staying on topic, and providing appropriate amounts of information, they could be expected to have a negative impact on listeners. The ability to provide accurate, relevant procedural information in a succinct manner is possibly an important skill for TBI survivors attempting to resume paid employment. These results lend support to Hartley and Jensen’s (1 991) observation that deficiencies displayed by TBI speakers when producing procedural discourse reflect ‘pragmatic difficulties in taking the perspective of the listener and problems in monitoring performance for purposes of clarity’ (p. 281). In this context it is interesting to note the findings of a study by Brooks e t a/. (1987), who reported that the presence of what they termed ‘ conversational ’ difficulties was highly predictive of failure to return to work after severe TBI. Workers who have difficulty staying on topic, and/or who provide insufficient or excessive information, are likely to cause frustration and annoyance at best, and serious mis-communications at worst. Situations in which the speaker cannot assume shared world knowledge with the listener are likely to arise in
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

Procedural discourse following TBI 963
everyday settings (particularly in the workplace), and it may be that it is under these circumstances that the brain-injured individual’s ability to utilize procedural discourse is most compromised.
Procedural discourse has not been as thoroughly researched as conversation and narratives in adult neurological populations. In spite of this it appears to be a commonly used assessment task in clinical settings. A number of theoretical considerations have arisen out of this study. First, the results reported here suggest that hierarchical notions of ‘ essential’ and ‘ optional ’, while attractive from a theoretical perspective, may be difficult to apply to both ‘normal’ and TBI samples. This stems from the fact that there appears to be a wide amount of individual variability with respect to what a speaker judges as ‘implicit’ (and therefore not needing to be overtly stated), and ‘explicit’ information. Because the task employed in this study did not imply listener nalvett, it is reasonable to presume that at least some speakers made as~zimptions about shared world knowledge, and therefore omitted certain details. Instead of notions of ‘essential’ and ‘optional’, therefore, it may be more appropriate to consider procedural discourse in terms of the relevance of the information provided. Listener judges may, in fact, make a qualitative distinction between speakers on the basis of the amount of overall ‘ on- target ’ information provided. This remains to be investigated in future studies. Further, valid differences may exist between speakers with respect to what are ‘ essential’ components of a procedure. Adjusting the viewing screen, for example, may be a high priority to someone of short stature, but may not be something that a person of average height is even conscious of doing. Similarly, someone whose account is always in credit may not consider requesting an account balance, whereas this may be deemed ‘essential’ by someone who regularly withdraws amounts close to the account balance.
Finally, the conceptual complexity of the task employed needs to be considered in relation to the findings of this study. Because the banking procedure is probably a well-learned and familiar sequence, participants may have been ‘ reciting ’ from procedural memory, rather than actively selecting and ordering novel output. Ulatowska e t al. (1983) pointed out that ‘Most instructions.. . are verbalizations of memories of past actions’ (p. 317). When describing a new task, with which the speaker had no previous experience (as in McDonald’s 1993 study described above), the speaker may not be able to draw on procedural memory as an aid in producing and organizing information in steps. There is evidence that procedural memory may be relatively spared following TBI (Richardson 1990, Ewert e t al. 1989), and this may be relevant to the way in which TBI speakers approach procedural, as opposed to narrative, or conversational discourse.
Clinicians are constantly being exhorted to use connected discourse as a more ‘ functional’ means of assessing individuals who have sustained TBI, than test- based measures. Evaluation is, however, severely constrained by the fact that the theoretical understanding of procedural discourse is currently in its infancy. Further, there is a dearth of normative data on this genre, particularly that which is applicable to different sociolinguistic subgroups within a given population. Caution needs to be exercised, therefore, in the use of procedural discourse tasks in clinical settings. In spite of their brevity and face validity there seems to be scope for false-positives in the application of ratings of content or productivity, and these may have serious implications for the selection of rehabilitation goals. Notwithstanding this, the results of this study suggest that TBI individuals do
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

P. Snow et al.
display significant pragmatic difficulties when producing procedural discourse. This finding, together with the potential importance of procedural discourse in the work setting, highlights the need for continued detailed examination of this discourse genre.
Acknowledgements
We thank the speech pathology staff at Bethesda Hospital, and the Victorian Rehabilitation Centre for assistance in recruiting TBI participants for this study. Thanks also go to Margaret Mealings for assistance with transcription, and the establishment of inter-rater reliability.
References
ANDERSON, D. W. and McLaL-RIs, R. L. (Eds) (1980) Report on the national head and spinal cord injury survey. Journal of SeurasurgeT, 53 (Supplement).
BAYLES, C. (1 994) hfanagement of neurogenic communication disorders associated with dementia. In R. Chapey (Ed.) Language Intemenfion Strategies in Aduit Aphasia, 3rd edn (Williams & Wilkins, Baltimore, MD), pp. 535-545.
BROOKS, D. N., MCKINLAY, K’., SYMINGTOS, C., BEATTIE, A. and CAMPSIE, L. (1987) Return to work within the first seven years of severe head injur Brain Injury, 1, 5-19.
C.%SNITO, 3f. I?., HAYASHI, M. M. and L‘LATOU’SKA, H. . (1988) Discourse in normal and pathologic ageing : background and assessment strategies. Seminars in Speech and Language, 9, 117-134.
COEHLO, C. A . (1995) Discourse production deficits following traumatic brain injury: a critical review of the recent literature. AphasioloD, 9, 409-429.
COEHLO, C. A., LILES, B. Z. and DUFFY, R. J. (1991a) The use of discourse analyses for the evaluation of higher level traumatically brain-injured adults. Brain Injury, 5, 381-391.
COEHLO, C. A , , LILES, B. Z . and DCFFY, R. J. (1991b). Discourse analyses with closed head injured adults : Evidence for differing patterns of deficits. A4rchi~les ofPhysicalhledicine and Rehabilitation,
COEHLO, C. .I., LILES, B. Z . and DL‘FFY, R. J. (1994) Cognitive framework: A description of discourse abilities in traumatically brain-injured adults. In R. L. Bloom, L: K. Obler, S. De Santi and J. S. Ehrlich (Eds) Discourse Anahsis and d4pplzcations. Studies in Adult Clinical Poptdations (Lawrence Erlbaum, Hillsdale, N J), pp. 95-1 10.
COEHLO, C. A , , DERUYTER, F. and STEIN, M. (1 996) Treatment efficacy: cognitive-communicative disorders resulting from traumatic brain injury. Journal of Speech and Hearing Research, 39, Supplement on Treatment Efficacy, Part 1, S5-17.
COPPENS, P. (1995) Subpopulations in closed-head injury : preliminary results. Bruin Injuy, 9,195-208. DAMICO, J. S. (1985) Clinical discourse analysis: a functional approach to language assessment. In C.
S. Simon (Ed.) Communication Skills and Classroom Success (Taylor & Francis, London), pp.
EWERT, J., LEVIN, H. S. , WATSON, M. G. and KALISKY, Z . (1989) Procedural memory during post- traumatic amnesia in survivors of severe closed head injury. Archioes of Neurology, 46,911-916.
GRICE, H. P. (1975) Logic in conversation. In P. Cole and J . Morgan (Eds) Studies in Syntax and Semantics, Vol. 3 (Academic Press, New York), pp. 41-58.
HAAS, J. F., COPE, D. N. and HALL, K. (1987) Premorbid prevalence of poor premorbid academic performance in severe head injury. Journal of Xeurology, Neurosurgery and Pychiatry, 50, 52-56.
HAGEN, C. (1981) Language disorders secondary to closed head injury: diagnosis and treatment. Topics i n Language Disorders, September, 73-87.
HAGEN, C. (1984) Langauge disorders in head trauma. In A. Holland (Ed.) Language Disorders in A d d t s (San Diego, CA: College-Hill Press), pp. 245-280.
HARTLEY, L. L. (1995) CognitiiiP-Communicatit.e Abilities Following Brain I n j q (Singular Publishing Co., San Diego, CA).
HARTLEY, I,. L. and JENSEN, P. J . (1991) Narrative and procedural discourse after closed head injury. Brain Iyury, 5, 267-285.
HCDSON, R. A. (1980) Sociolinguistics (Cambridge University Press, Cambridge).
72, 465-468.
165-203.
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

Procedural discourse following TBI 965
JORDAN, F. and MURDOCH, B. (1990) A comparison of the conversational skills of closed head injured children and normal adults. Australian fournal of Hnman Communication Disorders, 18, 69-82.
KEPPELL, G. (1991) Design and AnaCysis. A researcher’shandbook, 3rd edn (Prentice-Hall, Englewood Cliffs, NJ),
LILES, B. Z., COEHLO, C. A., DUFFY, R. J. and ZALAGENS, M. R. (1989) Effects of elicitation procedures on the narratives of normal and closed head-injured adults. Journal of Speech and Hearing Disorders, 54, 356-366.
LINSCOTT, R. J., KNIGHT, R. G. and GODFREY, H. P. D. (1996) The profile of functional impairment in communication. Brain Injury, 10, 3987-412.
LOBAN, W. (1963) The language of elementary school children. National Council of Teachers of English Report No. 1 (NCTE, IL).
MCDONALD, S. (1993) Pragmatic language skills after closed head injury: ability to meet the informational needs of the listener. Brain and Language, 44, 28-46,
MCDONALD, S. and PEARCE, S. (1995) The ‘dice’ game: a new test of pragmatic language skills after closed-head injury. Brain Injury, 9, 255-271.
MCDONALD, S. and VAN SOMMERS, P. (1 993) Pragmatic language skills after closed head injury : ability to negotiate requests. Cognitive Neuropsychology, 10, 297-315.
MCKINLEY, W. W. and BnooKs, D. N. (1984) Methodological problems in assessing psychosocial recovery following severe closed head injury. Journal of Clinical Neuropsychology, 6, 87-89.
MENTIS, M. and PRUTTING, C. A. (1987) Cohesion in the discourse of normal and head injured adults. ]ournal of Speech and Hearing Research, 30, 88-98.
PARSONS, C. L., LAMBIER, J., SNOW, P., COUCH, D. and MOONEY, L. (1989) Conversational skills in closed head injury: Part 1. Australian Journal of Human Communication Disorders, 17, 37-46.
PATRY, R. and NESPOULOUS, J. L. (1990) Discourse analysis in linguistics: historical and theoretical background. In Y. Joanette and H. H. Brownell (Eds) Discourse Ability and Brain Damage (Springer-Verlag, New York), pp. 3-27.
RICHARDSON, J. T. E. (1990) Clinical and neuropsychological aspects o f closed head injury (Lawrence Erlbaum Associates Ltd., Hove, UK).
RIMEL, R. W., JANE, J. A. and BOND, M. R. (1990) Characteristics of the head injured patient. In M. Rosenthal, E. R. Griffith, M. R. Bond and J. D. Miller (Eds) Rehabilitation of the Adult and Child with Traumatic Brain I n j q (F. A. Davis, Philadelphia, PA), pp. 8-16.
RUFF, R. M. and CAMENZULI, L. F. (1991) Research challenges for behavioural rehabilitation. Searching for solutions. In J. S. Kreutzer and P. H. Wehman (Eds) Cognitive Rehabilitation for Persons with Traumatic Brain Injury. A Functional Approach. (Paul H. Brookes, Baltimore, MD),
SHADDEN, B. B., BunNETTE, R. B., EIKENBERRY, B. R. and DIBREZZO, R. (1991) All discourse tasks are not created equal. In T. E. Prescott (Ed.) Clinical Aphasiology, vol. 20 (Pro-Ed., Austin,
SHORES, E. A., MAnOSSZEKY, J. E., SANDANAM, J. and BATCHELOR, J. (1986) Preliminary validation of a scale for measuring the duration of post-traumatic amnesia. Medical Journal of Australia,
SLOAN, S. and PONSFORD, J. (1995) Assessment of cognitive difficulties following TBI. In J. Ponsford with S. Sloan and P. Snow, Traumatic Brain Injury. Rehabilitation for Everyday Adaptive Living (Lawrence Erlbaum, London), pp. 65-101.
SNOW, P. and PONSFORD, J. (1995) Assessing and managing changes in communication and interpersonal skills following TBI. In J. Ponsford with S. Sloan and P. Snow, Traumatic Brain Injury. Rehabilitation for Everydq Adaptive Living (Lawrence Erlbaum, London), pp. 137-1 64.
SNOW, P., DOUGLAS, J. and PONSFORD, J. (1995) Discourse assessment following traumatic brain injury : a pilot study examining some demographic and methodological issues. Aphasiology, 9,
SNOW, P., DOUGLAS, 1. and PONSFORD, J. (1 997) Conversational assessment following traumatic brain injury: a cornparison across two control groups. Brain Iykry, 11, 409429.
SPENCE, S. E., GODFREY, H. P. D., KNIGHT, R. G. and BISHARA, S. N. (1993) First impressions count: A controlled investigation of social skill following closed head injury. British Journal of Clinical Psychology, 32, 309-31 8.
ULATOWSKA, H. K., ALLARD, L. and CHAPMAN, S. B. (1990) Narrative and procedurat discourse in aphasia. In Y . Joanette and H. H. Brownell (Eds) Discourse Ab i l io and Brain Damage: theoretical and empirical perspectives (Springer-Verlag, New York), pp. 180-198.
pp. 23-34.
TX), pp. 327-341.
144, 569-572.
365-380.
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

P. Snow et al. 966
ULATOWSKA, H. K., ALLARD, L., DONNELL, A., BRISTOW, J., HAYNES, S. M., FLOWER, A. and NORTH, A. J . (1988) Discourse performance in subjects with dementia of the Alzheimer type. In H. rl . Whitaker (Ed.) Neuropsychological Studies of Nonfocal Brain Damage (Springer-Verlag, New York), pp. 108-131.
ULATOWSKA, H., NORTH, A. J . and MACALVSO HAYXES, S. M. (1981) Production of discourse and communicative competence in aphasia. In R. H. Brookshire (Ed.) Clinical Aphasiology Conference Proceedingr, vol. 17 (BRK, Minneapolis, MN), pp. 75-82.
ULATOWSKA, H. K., WEISS DOYEL, A, FREEDMAN STERN, R. and MACALUSO HAYES, S. (1983) Production of procedural discourse in aphasia. Brain and Language, 18, 315-341.
Appendix A: Designated ‘essential’ and ‘optional’ steps
Essential steps
A T M Method 1. Locate/go to ATM machine 2. Insert card in machine 3. Enter PIN (personal identification number) 4. Select account 5. Enter amount to withdraw 6. Remove receipt 7. Remove money 8. Remove card
OTC Method 1. Complete withdrawal slip 2. Join queue 3. Wait until the next teller is available 4. Hand book/card/slip to teller 5. Wait while teller processes withdrawal 6. Receive cash
Optional steps These have been designated as ‘ optional’ by virtue of the fact that fewer than 80 YO of clinicians deemed them to be ‘essential’.
A T M Method 1. Decide which bank 2. Check that you have your card in your wallet 3. Join the queue at the ATM 4. Make sure the machine is onlworking 5. Decide how much to withdraw 6. Open purse/wallet 7. Remove card from purse/wallet 8. Check directions re. orientation of card for insertion 9. Adjust viewing shield
10. Read instructions on screen 11. Recall PIN 12. Press enter/OK after each instruction 13. Selection function 14. Request account balance 15. Check that sufficient funds are available
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13

Procedural discourse following TBI 967
16. Press OK or change after the selected amount is displayed on the screen 17. Select denominations 18. Ensure that the amount desired can be dispensed by the machine 19. Wait while the transaction is being processed 20. Indicate whether or not you want a receipt 21. Check that the amount provided is correct 22. Place money in wallet 23. Place card in wallet 24. Terminate transaction 25. Leave
0 TC Method 1. Enter bank 2. Go to desk/table 3. Take withdrawal slip 4. Nominate account 5. Remove keycard from wallet 6. Tell the teller how much you want 7. Request an account balance 8. Pass identification-check 9. Select denominations
10. Check that the amount received is correct 11. Place money in bag/wallet 12. Leave bank
Appendix B : Clinical discourse analysis (Damico 1985)
Utterance no./ Parameter Category /quality no. of utterances
Quant ip Insufficient information bits -- Non-specific vocabulary __-
Need for repetition --
Q u a l i p Message inaccuracy -- Relation Poor topic maintenance _-
Inability to ask relevant questions Situational inappropriateness - Inappropriate speech style - Linguistic non-fluency L_
Delay before responding (> 5 seconds)
Difficulty with turn-taking --
Informational redundancy
Inappropriate responses - --
Revision behaviour __
Inability to structure discourse __
Inefficient attention to and use of gaze __ Inappropriate intonational contours
_-
Manner
Summary Total utterances --
Total discourse errors -- Total utterances with errors Percentage utterances with errors __
Dow
nloa
ded
by [
Mon
ash
Uni
vers
ity L
ibra
ry]
at 2
2:35
20
Apr
il 20
13




















