Fine Tuning of Traumatic Brain Injury Management in ...
13
REVIEW published: 24 February 2021 doi: 10.3389/fneur.2021.638132 Frontiers in Neurology | www.frontiersin.org 1 February 2021 | Volume 12 | Article 638132 Edited by: Jian Hai, Tongji Hospital Affiliated to Tongji University, China Reviewed by: Marek Czosnyka, University of Cambridge, United Kingdom Danilo Cardim, University of Texas Southwestern Medical Center, United States *Correspondence: Teodor M. Svedung Wettervik teodor.svedung-wettervik@ neuro.uu.se Specialty section: This article was submitted to Neurotrauma, a section of the journal Frontiers in Neurology Received: 05 December 2020 Accepted: 20 January 2021 Published: 24 February 2021 Citation: Svedung Wettervik TM, Lewén A and Enblad P (2021) Fine Tuning of Traumatic Brain Injury Management in Neurointensive Care—Indicative Observations and Future Perspectives. Front. Neurol. 12:638132. doi: 10.3389/fneur.2021.638132 Fine Tuning of Traumatic Brain Injury Management in Neurointensive Care—Indicative Observations and Future Perspectives Teodor M. Svedung Wettervik*, Anders Lewén and Per Enblad Department of Neuroscience, Section of Neurosurgery, Uppsala University, Uppsala, Sweden Neurointensive care (NIC) has contributed to great improvements in clinical outcomes for patients with severe traumatic brain injury (TBI) by preventing, detecting, and treating secondary insults and thereby reducing secondary brain injury. Traditional NIC management has mainly focused on generally applicable escalated treatment protocols to avoid high intracranial pressure (ICP) and to keep the cerebral perfusion pressure (CPP) at sufficiently high levels. However, TBI is a very heterogeneous disease regarding the type of injury, age, comorbidity, secondary injury mechanisms, etc. In recent years, the introduction of multimodality monitoring, including, e.g., pressure autoregulation, brain tissue oxygenation, and cerebral energy metabolism, in addition to ICP and CPP, has increased the understanding of the complex pathophysiology and the physiological effects of treatments in this condition. In this article, we will present some potential future approaches for more individualized patient management and fine-tuning of NIC, taking advantage of multimodal monitoring to further improve outcome after severe TBI. Keywords: multimodality monitoring, secondary brain injury, secondary insults, neurointensive care, traumatic brain injury INTRODUCTION In the later decades of the twentieth century, the understanding of the critical factors responsible for neurological deterioration after traumatic brain injury (TBI) increased (1). It became clear that although the primary brain injury after TBI cannot be cured, secondary insults leading to further brain injury can be avoided by vigilant monitoring with attentive prevention and early treatment of such insults. This led to the development of standardized management protocols for severe TBI at specialized neurointensive care (NIC) units, resulting in significant improvements in the clinical outcome for these patients (2, 3). The concept of NIC, to avoid secondary brain injury by intensive monitoring and aggressive treatment of emerging secondary insults, is still the fundamental basis for modern NIC. The purpose of this presentation was to give an overview of potential directions toward the NIC of the future. The structure of this review is based on the critical steps to achieve sufficient cerebral energy metabolism for neuronal survival in relation to multimodality monitoring (Figure 1).
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Fine Tuning of Traumatic Brain Injury Management in ...

REVIEWpublished: 24 February 2021
doi: 10.3389/fneur.2021.638132
Frontiers in Neurology | www.frontiersin.org 1 February 2021 | Volume 12 | Article 638132
Edited by:
Jian Hai,
Tongji Hospital Affiliated to Tongji
University, China
Reviewed by:
Marek Czosnyka,
University of Cambridge,
United Kingdom
Danilo Cardim,
University of Texas Southwestern
Medical Center, United States
*Correspondence:
Teodor M. Svedung Wettervik
teodor.svedung-wettervik@
neuro.uu.se
Specialty section:
This article was submitted to
Neurotrauma,
a section of the journal
Frontiers in Neurology
Received: 05 December 2020
Accepted: 20 January 2021
Published: 24 February 2021
Citation:
Svedung Wettervik TM, Lewén A and
Enblad P (2021) Fine Tuning of
Traumatic Brain Injury Management in
Neurointensive Care—Indicative
Observations and Future
Perspectives.
Front. Neurol. 12:638132.
doi: 10.3389/fneur.2021.638132
Fine Tuning of Traumatic Brain InjuryManagement in NeurointensiveCare—Indicative Observations andFuture PerspectivesTeodor M. Svedung Wettervik*, Anders Lewén and Per Enblad
Department of Neuroscience, Section of Neurosurgery, Uppsala University, Uppsala, Sweden
Neurointensive care (NIC) has contributed to great improvements in clinical outcomes
for patients with severe traumatic brain injury (TBI) by preventing, detecting, and
treating secondary insults and thereby reducing secondary brain injury. Traditional NIC
management has mainly focused on generally applicable escalated treatment protocols
to avoid high intracranial pressure (ICP) and to keep the cerebral perfusion pressure
(CPP) at sufficiently high levels. However, TBI is a very heterogeneous disease regarding
the type of injury, age, comorbidity, secondary injury mechanisms, etc. In recent years,
the introduction of multimodality monitoring, including, e.g., pressure autoregulation,
brain tissue oxygenation, and cerebral energy metabolism, in addition to ICP and CPP,
has increased the understanding of the complex pathophysiology and the physiological
effects of treatments in this condition. In this article, we will present some potential future
approaches for more individualized patient management and fine-tuning of NIC, taking
advantage of multimodal monitoring to further improve outcome after severe TBI.
Keywords: multimodality monitoring, secondary brain injury, secondary insults, neurointensive care, traumatic
brain injury
INTRODUCTION
In the later decades of the twentieth century, the understanding of the critical factors responsiblefor neurological deterioration after traumatic brain injury (TBI) increased (1). It became clear thatalthough the primary brain injury after TBI cannot be cured, secondary insults leading to furtherbrain injury can be avoided by vigilant monitoring with attentive prevention and early treatmentof such insults. This led to the development of standardized management protocols for severe TBIat specialized neurointensive care (NIC) units, resulting in significant improvements in the clinicaloutcome for these patients (2, 3).
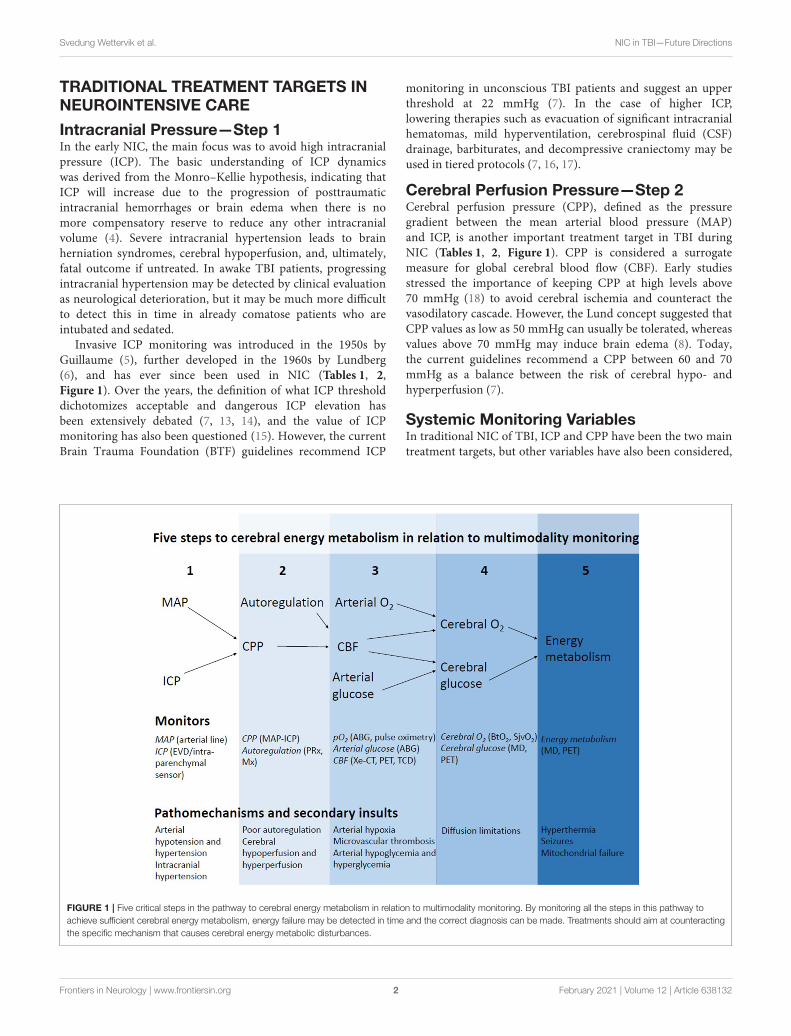
The concept of NIC, to avoid secondary brain injury by intensive monitoring and aggressivetreatment of emerging secondary insults, is still the fundamental basis for modern NIC. Thepurpose of this presentation was to give an overview of potential directions toward the NIC ofthe future. The structure of this review is based on the critical steps to achieve sufficient cerebralenergy metabolism for neuronal survival in relation to multimodality monitoring (Figure 1).
Svedung Wettervik et al. NIC in TBI—Future Directions
TRADITIONAL TREATMENT TARGETS INNEUROINTENSIVE CARE
Intracranial Pressure—Step 1In the early NIC, the main focus was to avoid high intracranialpressure (ICP). The basic understanding of ICP dynamicswas derived from the Monro–Kellie hypothesis, indicating thatICP will increase due to the progression of posttraumaticintracranial hemorrhages or brain edema when there is nomore compensatory reserve to reduce any other intracranialvolume (4). Severe intracranial hypertension leads to brainherniation syndromes, cerebral hypoperfusion, and, ultimately,fatal outcome if untreated. In awake TBI patients, progressingintracranial hypertension may be detected by clinical evaluationas neurological deterioration, but it may be much more difficultto detect this in time in already comatose patients who areintubated and sedated.
Invasive ICP monitoring was introduced in the 1950s byGuillaume (5), further developed in the 1960s by Lundberg(6), and has ever since been used in NIC (Tables 1, 2,Figure 1). Over the years, the definition of what ICP thresholddichotomizes acceptable and dangerous ICP elevation hasbeen extensively debated (7, 13, 14), and the value of ICPmonitoring has also been questioned (15). However, the currentBrain Trauma Foundation (BTF) guidelines recommend ICP
FIGURE 1 | Five critical steps in the pathway to cerebral energy metabolism in relation to multimodality monitoring. By monitoring all the steps in this pathway to
achieve sufficient cerebral energy metabolism, energy failure may be detected in time and the correct diagnosis can be made. Treatments should aim at counteracting
the specific mechanism that causes cerebral energy metabolic disturbances.
monitoring in unconscious TBI patients and suggest an upperthreshold at 22 mmHg (7). In the case of higher ICP,lowering therapies such as evacuation of significant intracranialhematomas, mild hyperventilation, cerebrospinal fluid (CSF)drainage, barbiturates, and decompressive craniectomy may beused in tiered protocols (7, 16, 17).
Cerebral Perfusion Pressure—Step 2Cerebral perfusion pressure (CPP), defined as the pressuregradient between the mean arterial blood pressure (MAP)and ICP, is another important treatment target in TBI duringNIC (Tables 1, 2, Figure 1). CPP is considered a surrogatemeasure for global cerebral blood flow (CBF). Early studiesstressed the importance of keeping CPP at high levels above70 mmHg (18) to avoid cerebral ischemia and counteract thevasodilatory cascade. However, the Lund concept suggested thatCPP values as low as 50 mmHg can usually be tolerated, whereasvalues above 70 mmHg may induce brain edema (8). Today,the current guidelines recommend a CPP between 60 and 70mmHg as a balance between the risk of cerebral hypo- andhyperperfusion (7).
Systemic Monitoring VariablesIn traditional NIC of TBI, ICP and CPP have been the two maintreatment targets, but other variables have also been considered,
Frontiers in Neurology | www.frontiersin.org 2 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
TABLE 1 | Multimodality monitoring—a selection of methods and their benefits and limitations.
Physiological
variable
Monitoring method Continuous/Intermittent Global/Focal Benefits Limitations
ICP EVD Continuous Global Both monitoring and
treatment of ICP by CSF
drainage.
Infection risk. Impossible
when compressed ventricles.
Risk of invalid ICP monitoring
in case of slit ventricle.
Intraparenchymal sensor Continuous Global Possible also when
compressed ventricles.
Invalid ICP monitoring due
to slit ventricle is not a
problem.
Does not offer ICP treatment
with CSF drainage.
CPP ICP device and arterial line
for continuous systemic
ABP.
Continuous Global Feasible, continuous
global CBF surrogate.
Unreliable surrogate, does
not consider cerebrovascular
resistance.
CBF autoregulation PRx (ICP and ABP) Continuous with time
window
Global Feasible measure of the
global autoregulatory
status.
Low signal-to-noise ratio.
Does not take into account
focal asymmetries.
CPPopt (PRx and CPP) Continuous with time
window
Global Feasible, continuous
global CBF surrogate.
Frequent absence of
U-shaped curves. Does not
take into account focal
asymmetries. Requires
advanced software.
Mx (TCD and CPP) Intermittent Global and focal May detect regional
autoregulatory differences.
User-dependent. Poor
evaluation of the posterior
circulation.
Cerebral blood flow Radiology (Xe-CT, PET,
MRI)
Intermittent Global and focal Both global and focal. Difficult to transport unstable
patients to the radiology
department.
TCD Intermittent Global and focal Feasible and may be used
bedside.
Measures velocity.
User-dependent. Poor
evaluation of the posterior
circulation.
Intraparenchymal thermal
diffusion probe
Continuous Focal Feasible and continuous
CBF measure.
Unreliable. Focal, does not
take into account variabilty in
CBF between brain regions.
Brain tissue
oxygenation
Jugular bulb catheter
(SjvO2)
Continuous Global Continuous and feasible
global measure.
Low sensitivity for focal
ischemia.
Intraparenchymal device
(BtO2)
Continuous Focal Continuous and feasible
focal measure.
Variabilty in oxygenation
between brain regions.
NIRS Continuous Focal Non-invasive. Unreliable. Does not evaluate
the posterior circulation.
Cerebral energy
metabolism
MD Continuous Focal Feasible for continuous
evaluation.
Variability in energy
metabolism between brain
regions.
PET Intermittent Global and focal Possible to investigate
complex aspects of
energy metabolism.
Difficult to transport unstable
patients to the radiology
department.
ABP, Arterial blood pressure; CBF, Cerebral blood flow; CSF, Cerebrospinal fluid; EVD, external ventricular drain; ICP, Intracranial pressure; MD, Microdialysis; Mx, Mean flow inex; NIRS,
Near infrared spectroscopy; PET, Positron emission tomography; PRx, Pressure reactivity index; TCD, Transcranial Doppler; Xe-CT, Xenon-enhanced computed tomography.
e.g., to maintain sufficient arterial oxygenation (pO2 ≥ 12kPa), to avoid systemic hyperthermia (T < 38◦C), and to keeparterial glucose within normal limits (5–10mM) (2, 19). Figure 2demonstrates the Uppsala standardized TBI managementprotocol as an example of a local escalated ICP-orientedmanagement protocol with a focus on avoiding secondary insults(2, 11, 19).
INDICATIVE OBSERVATIONS AND FUTUREPERSPECTIVES
Multimodality Monitoring of the ComplexPathophysiology in Traumatic Brain InjuryThe traditional NIC treatment targets in TBI, ICP, and CPP, aretwo important surrogate measures of the cerebral environment,
Frontiers in Neurology | www.frontiersin.org 3 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
TABLE 2 | Monitoring variables, target intervals, and treatments.
Variable Target interval Treatment
ICP BTF: ICP ≤ 22mm Hg (7)
Uppsala: ICP ≤ 20mm Hg (2)
Head elevation
Hematoma evacuation
Hyperventilation
CSF drainage
Sedation
Barbiturates
Decompressive craniectomy
CPP BTF: 60 to 70mm Hg (7)
Uppsala: CPP ≥ 60mm Hg
(2)
Lund concept: CPP 50 to
70mm Hg (8)
Autoregulatory management:
CPP close to CPPopt (9)
ICP control (above)
Intravenous fluids
Vasopressors
CBF pressure
autoregulation
BTF: No target (7)
Uppsala: No target (2)
CPP optimum
Hyperventilation
Hyperoxia
Body temperature control
Arterial glucose and
lactate management
CBF BTF: No target (7)
Uppsala: No target (2)
CPP and
autoregulationmanagement
Arterial
oxygenation
BTF: No target (7)
Uppsala: pO2 > 12 kPa and
Hgb > 100 g/L (2)
Respiratory optimization
Red blood cell traunsfusion
Arterial
glucose
BTF: No target (7)
Uppsala: 5–10mM (2)
Tight glycemic control:
4.4–6.1mM (10)
Intravenous glucose
Insulin injection/infusion
Cerebral
oxygenation
BTF: No target (7)
Uppsala: No target (2)
CBF and arterial
oxygenation management
Cerebral
glucose
BTF: No target (7)
Uppsala: No target, but
clinical evaluation if cerebral
glucose < 0.5mM (MD) (11)
MD consensus meeting 2014:
Cerebral glucose >
0.2–0.8mM (12)
CBF and arterial
glucose management
Cerebral
energy
metabolism
BTF: No target (7)
Uppsala: No target, but
clinical evaluation if cerebral
LPR > 40 (MD) (11)
MD consensus meeting 2014:
Cerebral LPR < 25–40 (12)
Optimize the
variables above.
BTF, Brain Trauma Foundation; CBF, Cerebral blood flow; CPP, Cerebral perfusion
pressure; CPPopt, Optimal CPP; CSF, Cerebrospinal fluid; ICP, Intracranial pressure; LPR,
Lactate-/pyruvate ratio; MD, Microdialysis.
but many other variables are also crucial steps in the pathwayto achieve an optimal cerebral energy metabolic state (Figure 1).CBF delivers oxygen and glucose to the injured brain. Theautoregulation of CBF by the cerebral vessels is often disturbedafter TBI and focal CBF disturbances may occur despitenormal ICP and CPP (20–24). In addition, systemic traumaticinjuries could precipitate for arterial hypoxia with secondarybrain tissue hypoxia despite normal CBF in the large cerebralvessels. Furthermore, microvascular thrombosis and diffusionlimitations from brain edema may limit oxygen delivery in
the microvascular circulation despite normal macrovascularCBF and arterial oxygenation (25, 26). However, even if braintissue oxygenation and the level of energy metabolites are atadequate levels, cerebral energy failure may still occur due tomitochondrial dysfunction (26–28). In addition, mechanismssuch as seizures and hyperthermia increase energy consumptionand may be detrimental if the compensatory cerebral energyreserve is compromised (29–33).
Multimodality monitoring makes it possible to continuouslysurveil the different steps in the pathway to cerebral energymetabolism (Tables 1, 2 and Figure 1). The methods used areboth global and focal, as well as continuous and intermittent.Some methods give direct information about the crucialparameters for the energy metabolism and others provideindirect measures. The complete picture is obtained by anintegrated analysis of all measures. The future direction of NICis a more detailed analysis of each of the crucial pathwaysfor cerebral energy metabolism using multimodality monitoringin order to identify the correct cause of energy metabolicdisturbances (Table 3) (34). This may in turn lead to a moretimely and cause-specific treatment. The following sectionswill review the background and potential future applicationsof some monitoring techniques for the fine-tuning of next-generation NIC.
CBF Pressure Autoregulation and CPPManagement—Step 2Global and regional CBF can be measured intermittently withdifferent imaging techniques, and regional CBF can also bemeasured continuously by means of an intraparenchymal probe(Table 1). It would be advantageous to continuously monitorglobal CBF, but there is, at present, no feasible way. CPP iscurrently the best surrogate measure for global CBF, but thisconcept leaves the cerebrovascular reactivity out of the equation,and there is an interest to find better surrogate measures of CBFthat takes both CPP and the cerebrovascular status into account.
Lassen described the cerebral autoregulation in 1959 ashe demonstrated that CBF is maintained over a wide rangeof MAPs (35, 36). The autoregulatory capacity may becomederanged following TBI, which is strongly associated with pooroutcome (14, 21, 37). Several methods to monitor the cerebralautoregulation in the NIC have been introduced (Table 1),such as the mean flow index (Mx) and the pressure reactivityindex (PRx). PRx has received the greatest interest and iscontinuously measured as the correlation coefficient betweenMAP and ICP over 5min (37). Negative index values indicateintact pressure autoregulation, such as when an increase inMAP leads to cerebral vasoconstriction to maintain normalCBF with a corresponding reduction in CBV and ICP. Positiveindex values indicate disturbed pressure autoregulation, such aswhen an increase in MAP leads to passive cerebral vasodilationwith corresponding increases in CBF, CBV, and ICP (37–39).The clinical utility of PRx is still under development. However,as low PRx values are associated with better clinical outcome,autoregulatory-oriented management that aims at improvingPRx has been suggested, as outlined below.
Frontiers in Neurology | www.frontiersin.org 4 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
FIGURE 2 | The Uppsala standardized traumatic brain injury (TBI) management protocol as an example of a local escalated intracranial pressure (ICP)-oriented
management protocol with a focus on avoiding secondary insults. The figure demonstrates an example of a local ICP-oriented management protocol (2). The
therapeutic intensity is gradually increased by starting with ICP-lowering treatments that carry a lower risk of complications and escalating to treatments with greater
risks if the ICP target cannot otherwise be controlled. Decompressive craniectomy may be performed both on a primary indication (first surgical procedure, i.e., the
fourth step is used as the first step) in the case of severe brain edema in the early course, but chiefly on a secondary indication (when all other treatments are
exhausted).
Autoregulatory management aims at giving the patienttreatments that improve the autoregulatory capacity. Particularly,the association between pressure autoregulation and CPP hasreceived interest. In a first attempt to consider autoregulationin CPP management, patients were classified as either pressureactive or pressure passive, and the absolute autoregulatory statuswas suggested to determine whether the patient would benefitfrom high or low CPP (40). It was then demonstrated in anobservational study including two centers with different CPPphilosophy (Uppsala and Edinburgh) that patients with pressure-passive cerebral vessels (high PRx) had better outcomes if treatedwith ICP-oriented therapy with relatively lower CPP targets,whereas pressure-active patients (low PRx) benefitted from CPP-oriented treatment with relatively higher CPP targets (41). Inthe next attempt, it was found that PRx varies with CPP in aU-shaped way and that the CPP with the concurrently lowestPRx could be targeted where autoregulation works best (22),as demonstrated in Figure 3. Several studies have supportedthat deviation of the absolute CPP above and below theoptimal (CPPopt) is associated with poor outcomes (24, 42–45).Furthermore, brain tissue oxygenation reaches a plateau whenCPP approaches CPPopt, indicating optimal CBF (46). These
findings support that CPPopt may be a better CBF surrogate thattakes into account both the absolute CPP and the cerebrovascularstatus for the individual patient.
However, despite these promising findings, several concernshave been raised regarding CPPopt that need to be addressedin future trials. The U-shaped association between CPP andPRx is absent during ∼40% of the monitoring time (47), whichlimits the feasibility of CPPopt as a target (48). Secondly, theappearance of the U-shaped curvemay vary from flat to steep andthe absolute PRx at CPPopt may vary from negative to positivevalues (Figure 3). The necessity to keeping CPP close to CPPoptprobably depends on the curve shape and the absolute PRx (42).For example, if CPPopt is high, the absolute PRx is negative, andthe U-shaped curve is relatively flat, the Lassen plateau phaseof autoregulation should be acceptably wide and a much lowerabsolute CPP below CPPopt could then be allowed since highertargets are otherwise associated with complications such as acuterespiratory distress syndrome (49). On the contrary, it could bemore critical to keep CPP close to CPPopt if the curve is steepand PRx is high. Thirdly, although patients that spontaneouslyhad CPP values close to CPPopt had better clinical outcomein retrospective studies (43), CPPopt as an active treatment
Frontiers in Neurology | www.frontiersin.org 5 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
target has so far not been sufficiently investigated prospectively(50). Particularly, CPPopt is often above 70 mmHg, i.e., abovethe upper fixed threshold according to the BTF guidelines (7),but using vasopressors to achieve such high targets could carryadverse effects. The safety and feasibility of CPPopt as a treatmenttarget is investigated in a multicenter randomized controlled trial(COGiTATE) (9). The results of this trial will determine thefuture directions of CPP research and management in TBI care.
TABLE 3 | Secondary brain injury conditions, multimodality monitoring patterns
and potential cause-specific treatments.
Condition Multimodality monitoring
pattern
Potential treatments
Intracranial
hypertension
High ICP, low CPP, brain tissue
hypoxia, and high LPR
ICP lowering treatments
Arterial
hypotension
Normal ICP, low ABP/CPP, brain
tissue hypoxia, and high LPR.
Address cause for arterial
hypotension, give
intravenous fluids and
vasopressors. Arterial
hyperoxia treatment?
Autoregulatory
disturbances
Normal to high ICP, low to high
CPP, high PRx, brain tissue
hypoxia, and high LPR.
Target CPPopt, treat high
ICP, keep arterial glucose,
pO2 and pCO2 within
optimal intervals.
Oxygen diffusion
limitation
Normal ICP, normal CPP, brain
tissue hypoxia, and high LPR.
Arterial hyperoxia
treatment.
Cerebral
hypermetabolism
Normal ICP, normal CPP, possibly
brain tissue hypoxia, low cerebral
glucose and pyruvate, and high
LPR.
Body temperature and
seizure control. Sedation.
Arterial hyperoxia
treatment?
Mitochondrial
dysfunction
Normal ICP, normal CPP, normal
brain tissue oxygenation, normal
cerebral glucose and pyruvate,
and high LPR.
Arterial hyperoxia?
Cyclosporin A?
The table illustrates different multimodality monitoring patterns for different clinical
conditions, including e.g., cerebral ischemia with delivery failure of cerebral energy
metabolites, as well as when the cerebral energy metabolic state is compromised due
to hypermetabolism or poor mitochondrial function.
Autoregulatory Management and SystemicPhysiology—Step 2In addition to CPP, several other variables that controlthe cerebrovascular resistance are associated with pressureautoregulation and could potentially be targeted in an integratedautoregulatory protocol. Arterial hyperglycemia may disturbthe endothelial and myogenic function of the cerebral vessels(51, 52). In line with these findings, we and others havedemonstrated that arterial hyperglycemia is independentlyassociated with a higher PRx (53, 54), indicating that a tighterglycemic control at least below 10mM could be beneficialfrom an autoregulatory point of view. Furthermore, lactateis a cerebral vasodilator and higher systemic levels mayincrease CBF (55). However, we have found that a higherarterial lactate is independently associated with a higher PRx(33), and it is possible that the corresponding increase inCBF (55) represents dysregulated hyperemia. This calls forcaution in clinical TBI trials on lactate-based fluids as a wayof increasing the delivery of an alternative energy fuel tothe brain due to the possible negative effect of lactate onpressure autoregulation. Hyperthermia could induce cerebralvasodilation, and some findings support an association betweena higher body temperature and a higher PRx (56), whereasother studies have found no such association (33). Arterialhypoxia also leads to cerebral vasodilation in order to increaseCBF to maintain normal brain tissue oxygenation (57), whereashigher oxygen levels may increase the cerebrovascular tone.We have found that higher arterial oxygen levels above12 kPa are associated with lower PRx, i.e., better pressureautoregulation (58). Similarly, increased cerebrovascular tone byhyperventilation is associated with better pressure autoregulation(56, 59, 60).
Hence, several systemic variables, in addition to CPP,could potentially be targeted in an integrated autoregulatoryprotocol including, e.g., temperature management,glycemic control, and respiratory targets to optimize pO2
and pCO2.
FIGURE 3 | Optimal cerebral perfusion pressure (CPPopt)—differences in curve shape. The CPPopt curves may vary over time and between patients, as illustrated in
these three different curves. There are questions on how the curve shape and the absolute pressure reactivity index (PRx) are relevant in CPPopt management.
Patients with a steeper CPPopt curve may, in theory, be more vulnerable to changes in CPP.
Frontiers in Neurology | www.frontiersin.org 6 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
Arterial and Brain Oxygenation—Steps 3and 4Ischemic and hypoxic secondary brain injuries are common afterTBI (61), and treatment aims at maintaining adequate CBF andarterial oxygen content for aerobic energy metabolism. Arterialoxygen content is monitored with repeated arterial blood gasanalyses of hemoglobin (Hgb) and pO2 and continuously withpulse oximetry (SpO2). The arterial oxygen content is, to a greatextent, dependent on the level of oxygen-binding Hgb, whereasdissolved oxygen only constitutes a fraction of the total arterialoxygen content under normal conditions (62). There is greatcontroversy regarding the definition of clinically relevant anemiafor cerebral oxygen delivery, but an Hgb below 9 g/dl maydiscriminate when the risk of cerebral hypoxia is significantlyincreased (63). Although red blood cell transfusion (RBCT) couldimprove cerebral oxygen delivery (64), adverse effects such asa worsening in pressure autoregulation (65) and an increasedrisk of thromboembolic events have been described (66). Clinicalstudies on liberal vs. restricted RBCT based on Hgb thresholds(e.g., 10 vs. 7 g/dl) indicate a neutral to negative effect on clinicaloutcomes with the liberal approach (64, 66–69). The observationsthat both anemia and RBCT are independently associated withpoor outcomes make the clinical management difficult, but it ispossible that the indication for RBCT could be guided by meansof multimodal monitoring. Despite, or because, the controversyin this matter, there is currently no BTF guidelines on RBCT insevere TBI (7).
There is also limited knowledge and lack of guidelinesregarding specific arterial oxygen thresholds (7), but pO2
levels above 12 kPa and SaO2 above 95% may be targeted(2). Additionally, brain tissue oxygenation can be monitoredglobally with a jugular vein bulb (SjvO2) and focally withan intraparenchymal probe (BtO2) (Table 1). BTF currentlyrecommends SjvO2 monitoring and avoiding ischemic SjvO2
levels below 50% (7). There is no BTF recommendation on BtO2
monitoring (7), but focal brain tissue hypoxia below 20 mmHghas been associated with poor clinical outcomes (70).
Although there is only a small fraction of free and dissolvedpO2 in the blood (62), an increase in pO2 to hyperoxic levelscould still be beneficial in TBI. Increasing the fraction of theinspired oxygen (FiO2), i.e., normobaric hyperoxia (NBO), hasbeen proven to increase arterial and brain tissue oxygenation(71). NBOmay then compensate for ischemic hypoxia, overcomediffusion barriers, and improve mitochondrial function (62).Hyperoxia reduces cerebral glycolytic enzymes and therebydecreases pyruvate and lactate (57, 71, 72), but there are questionswhether cerebral oxidative energy metabolism improves. A PETstudy found that hyperoxia improves energy metabolism inischemic brain regions (73), and microdialysis (MD) studiessupport true energy metabolic improvements in the case ofpoor substrate supply (58) or anaerobic energy metabolism (74).On the other end, some studies suggest that hyperoxia inducesdetrimental reactive oxygen species that negatively affect cerebraltissue survival, although this may only occur to a small extentin a limited number of patients (75). Brain tissue oxygen-guidedtreatment protocols have been introduced, in which low brain
tissue oxygenation may be treated with an increase in FiO2.However, there is still clinical equipoise of this approach dueto small positive to neutral effects on clinical outcomes inprospective trials (76–78).
Delivery of Cerebral Energy Metabolites,Cerebral Energy Metabolism,Neurochemical Monitoring, andTreatments—Steps 3, 4, and 5Cerebral nutrients, such as glucose and lactate, are delivered bythe CBF. The arterial levels may be monitored with repeatedarterial blood gases to ensure sufficient arterial content. Thecerebral energy metabolites, glucose, pyruvate, and lactate, aswell as the rate of oxidative energy metabolism (lactate/pyruvateratio, LPR) may be evaluated with hourly measures by meansof cerebral MD, i.e., a double-lumen, semi-permeable catheterthat is perfused with artificial CSF (79, 80). The catheter caneither be placed in macroscopically normal-appearing braintissue to estimate global cerebral energy metabolism or in peri-contusional areas to estimate focal cerebral energy metabolismin “tissue-at-risk” (81). Recently, the new MD system (Loke)has been introduced, which measures cerebral glucose, pyruvate,and lactate minute by minute. This may reveal the complexexplanatory variables for cerebral energy metabolism in higherresolution. The cerebral energymetabolismmay also be evaluatedwith radiological snapshots using PET (Table 1).
Glucose is the main cerebral energy fuel. The arterial glucoselevel and CBF determine cerebral glucose delivery, but thecerebral glucose level also depends on the cerebral energymetabolic rate. Arterial and cerebral glucose are normallycorrelated, but this association may be disturbed after TBI(33, 54, 82–84) as the CBF and cerebral energy metabolic ratecould have greater influence on cerebral glucose levels. Theimmediate effects of TBI include a sympathetic stress responsethat, among other things, gives rise to a surge in arterial glucose(85). This is beneficial since it is necessary to avoid arterialhypoglycemia and neuroglycopenia for the vulnerable brain, butarterial hyperglycemia is also associated with worse outcomesafter TBI (86–88). Although the latter association could reflectmore severe underlying traumatic injuries, hyperglycemia could,per se, induce secondary brain injury by causing disturbancesin cerebral autoregulation and mitochondrial function (54, 89).Since both too low and too high arterial glucose could exert anegative effect on the brain, tight glycemic control with intensiveinsulin therapy (IIT) management has been suggested in TBIcare. IIT showed promising results in general ICU patients at anearly stage (10, 90, 91), but recent studies show that IIT causesan increased burden of arterial hypoglycemia that outweighsthe benefits of avoiding hyperglycemia, resulting in a neutral tonegative net effect on outcomes in various ICU populations aswell as in TBI (92–97). Specifically, TBI patients treated withIIT developed more severe energy metabolic disturbances withreductions in cerebral glucose and oxidative energy metabolismthan those treated with conventional glycemic control (95, 98).Hence, a narrow arterial glucose interval is appealing in theory,
Frontiers in Neurology | www.frontiersin.org 7 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
but is currently not feasible due to the risk of overtreatment. BTFdoes not have any recommendation on optimal glucose levelsor management in TBI (7). Due to the lack of clear evidenceof benefits for IIT in the NIC setting, a looser glycemic controlis mostly applied, e.g., between 5 and 10mM (99). CerebralMD glucose below 0.2–0.8mM is considered dangerously low,and such thresholds could aid in guiding treatment for whenthe termination of insulin treatment or infusion of glucose iswarranted (12).
The understanding of arterial lactate as an additional cerebralenergy substrate (100) has increased in the last years. However,the arterial contribution to cerebral lactate is only 10% whenthe arterial lactate concentration is 1mM, but increases to60% at 5mM (101). An increased consumption of lactateas an energy fuel may, in turn, spare cerebral glucose (55,102, 103). Higher lactate decreases the cerebrovascular tone,induces vasodilation, and increases CBF (55, 104), but possiblyat the expense of a worsened pressure autoregulation (33).Exogenous, hypertonic lactate may exert anti-edematous effectsand alleviate intracranial hypertension (102). Animal TBI studiessupport a reduction in lesion volume after exogenous lactateinfusion (105). Clinical trials also indicate that exogenous lactateimproves outcomes (106), although a higher endogenous arteriallactate is independently associated with worse outcomes afterTBI (33). Future studies are needed to determine the roleof intravenous lactate supplement in TBI care. Nevertheless,high endogenous levels of cerebral lactate above 4mM indicateanaerobic energymetabolism and are associated with unfavorableclinical outcomes (12, 107).
Furthermore, high cerebral MD LPRs above 25–40 indicatedisturbed cerebral energy metabolism (12, 107). The etiologyfor LPR elevations may differ. A high LPR with concurrentlylow cerebral glucose and pyruvate has been suggested to reflectcerebral ischemia/substrate delivery failure, whereas a high LPRwith concurrently normal/high cerebral glucose and pyruvatehas been suggested to reflect mitochondrial dysfunction (26).Substrate delivery could, in theory, be improved by a higherCPP, improved pressure autoregulation, and higher arterialsubstrate content (Table 3). The importance of mitochondrialdysfunction has gained increased interest and understanding inrecent years. There is currently no treatment for this condition,but cyclosporine A, which is an immunosuppressant, improvesthe mitochondrial function in animal TBI models and hasdemonstrated some promise in preliminary human trials, butlarger studies are needed to evaluate its efficacy (108, 109).
MD may also aid in monitoring more complex dynamicpathophysiological processes in the brain following TBI.Neuroinflammation after TBI may exert both beneficial andnegative effects on the brain, depending on the time windowafter injury and the specific mechanisms (110). MD can beused to evaluate neuroinflammatory biomarkers bedside in orderto better understand the neuroinflammatory mechanisms, theirrelation to the dynamic clinical course, secondary insults, andclinical outcomes in TBI (111, 112). This may aid in thedevelopment of optimal neuroprotective agents, as outlinedbelow, and the cerebral MD biomarkers could potentially be usedto improve the indication for such treatments.
Neuroprotective AgentsIn addition to the secondary physiological insults, there is acascade of injurymechanisms on the cellular andmolecular levelsafter the primary brain injury, e.g., toxic release of excitatoryneurotransmitters, apoptotic pathways, neuroinflammation, andmitochondrial dysfunction (113). Many neuroprotective agentshave been developed to counteract these pathomechanisms,but there has so far been limited success in translation fromanimal to clinical studies (113). For example, N-methyl-D-aspartate (NMDA) receptor antagonists and calcium channelantagonists both reduce excitotoxicity in animal TBI models,but their efficacy in human TBI trials has been limited (114,115). Human TBI trials on immunomodulating agents have alsobeen disappointing. Progesterone had a neutral effect (116),whereas corticosteroids even worsened clinical outcomes (117).As outlined above, cyclosporine A has demonstrated somepromise in preliminary human trials, but larger studies areneeded to evaluate its efficacy (108, 109).
One reason for the so far disappointing results ofneuroprotective drugs in humans may be that the therapeutictime window is limited, and it may be difficult to administerthe treatments within the right time in the clinical setting.Furthermore, TBI in humans is very heterogeneous, and thesubtype may be of importance for the therapeutic effect. Animaltrials are often based on relatively homogenous TBI models,while the clinical trials often have included all types of TBIpatients. Many pharmacological trials have also been donein the dawn of NIC, when secondary insults were not yet asefficiently surveyed and managed as today, and the relativeimportance of these agents might have been less significantin that setting. In conclusion, despite the limited effect of theneuroprotective agents shown in human TBI trials, it is possiblethat neuroprotective agents with a more optimal treatmenttiming, better understanding of the injury processes, and animproved patient selection in a high-quality NIC setting couldyield improved outcomes. Future studies that take these aspectsinto account are needed.
Multimodality Monitoring and PrecisionMedicineThemultimodality monitoring patternmay reveal the underlyingetiology of cerebral energy failure following TBI so that cause-specific treatments may be initiated (Table 3). For example, incases of intracranial hypertension, low CPP, brain tissue hypoxia,and cerebral energy failure, treatments should aim at loweringICP to improve the cerebral environment. In other cases withnormal ICP, CPP within optimal targets, and normal arterialoxygenation, but poor brain tissue oxygenation and concurrentcerebral energy metabolic failure (Figure 4), arterial hyperoxiacould be used to possibly overcome cerebral diffusion barriers.In cases where all variables such as ICP, CPP, and brain tissueoxygenation are within the targeted intervals, except for theenergy metabolic state (LPR), mitochondrial dysfunction is aplausible explanation. There is currently no treatment for thiscondition, but there are ongoing trials for, e.g., neuroprotectiveagents that may relieve mitochondrial dysfunction.
Frontiers in Neurology | www.frontiersin.org 8 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
FIGURE 4 | Illustrative patient case with multimodal monitoring. The figure demonstrates the temporal evolution of cerebral physiology over ∼2 days. Although
intracranial pressure (ICP), cerebral perfusion pressure (CPP), pressure reactivity index (PRx), and oxygen saturation (SpO2) were within adequate intervals, the patient
developed brain tissue hypoxia and cerebral energy failure (high lactate/pyruvate ratio). The pathophysiology may include microvascular thrombosis and/or increased
diffusion limitations from cerebral edema.
Cerebral Monitoring in a Resource-LimitedSettingHigh-resolution multimodal monitoring offers the best methodto fully evaluate the cerebral environment after TBI, but suchtools may be limited to a few research-minded academic centers.There is, hence, also an interest inmore feasible monitoring tools.PRx and CPPopt both require high-resolution data and advancedsoftware. However, low-frequency autoregulation index (LAx)and the corresponding LAx-derived CPPopt are based onminute-by-minute data, require less advance software, and maybe a fair substitute for centers without access to PRx andCPPopt (118). Transcranial Doppler is also a feasible noninvasiveand accessible method to assess cerebral blood flow velocity,particularly in the absence of CPP and advanced radiologicalimaging, and could be used to guide blood pressure management.
CONCLUDING REMARKS
Traditional NIC has focused on reducing secondary braininjury by treating elevated ICP and maintaining the CPPsufficiently high to avoid cerebral ischemia. However, recentfindings support that the TBI pathophysiology is muchmore complex and cerebral energy failure frequently occursin the absence of intracranial hypertension and low CPP.
Particularly, the roles of pathomechanisms such as disturbancesin pressure autoregulation, microvascular thrombosis, oxygendiffusion limitations, and mitochondrial dysfunction have gainedincreased understanding. By multimodal monitoring, cerebralenergy metabolic failure may be detected earlier and its etiologycould be better diagnosed. This may, in turn, lead to precisionmedicine with more cause-specific treatments to avoid secondarybrain injury for these patients. Future studies are needed toelaborate on the strengths and limitations of certain monitoringtools and their role in guiding cause-specific treatments in NICof severe TBI.
AUTHOR CONTRIBUTIONS
TS: conceptualization, writing–original draft. AL:conceptualization, writing–review and editing. PE:conceptualization, supervision, writing–review and editing.All authors contributed to the article and approved thesubmitted version.
FUNDING
The research was supported by the Department ofNeuroscience/Neurosurgery, Uppsala University, Sweden.
Frontiers in Neurology | www.frontiersin.org 9 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
REFERENCES
1. Rose J, Valtonen S, Jennett B. Avoidable factors contributing to death after
head injury. Br Med J. (1977) 2:615–8. doi: 10.1136/bmj.2.6087.615
2. Elf K, Nilsson P, Enblad P. Outcome after traumatic brain
injury improved by an organized secondary insult program
and standardized neurointensive care. Crit Care Med. (2002)
30:2129–34. doi: 10.1097/00003246-200209000-00029
3. Patel HC, Menon DK, Tebbs S, Hawker R, Hutchinson PJ, Kirkpatrick PJ.
Specialist neurocritical care and outcome from head injury. Int Care Med.
(2002) 28:547–53. doi: 10.1007/s00134-002-1235-4
4. Mokri B. The Monro-Kellie hypothesis applications in CSF volume
depletion. Neurology. (2001) 56:1746–8. doi: 10.1212/WNL.56.12.1746
5. Guillaume J, Janny P. Continuous intracranial manometry; physiopathologic
and clinical significance of the method. La Presse medicale. (1951) 59:953–5.
6. Lundberg N, Troupp H, Lorin H. Continuous recording of
the ventricular-fluid pressure in patients with severe acute
traumatic brain injury. A preliminary report. J Neurosurg. (1965)
22:581–90. doi: 10.3171/jns.1965.22.6.0581
7. Carney N, Totten AM, O’Reilly C, Ullman JS, Hawryluk GW, Bell MJ, et al.
Guidelines for the management of severe traumatic brain injury, fourth
edition.Neurosurgery. (2017) 80:6–15. doi: 10.1227/NEU.0000000000001432
8. Grande PO. Critical evaluation of the lund concept for treatment of severe
traumatic head injury, 25 years after its introduction. Front Neurol. (2017)
8:315. doi: 10.3389/fneur.2017.00315
9. Beqiri E, Smielewski P, Robba C, Czosnyka M, Cabeleira MT, Tas
J, et al. Feasibility of individualised severe traumatic brain injury
management using an automated assessment of optimal cerebral perfusion
pressure: the COGiTATE phase II study protocol. BMJ Open. (2019)
9:e030727. doi: 10.1136/bmjopen-2019-030727
10. van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz
M, et al. Intensive insulin therapy in critically ill patients. N Engl J Med.
(2001) 345:1359–67. doi: 10.1056/NEJMoa011300
11. Svedung Wettervik T. Aspects on Mechanisms, Treatment and
Outcome in Severe Traumatic Brain Injury. Uppsala: Acta Universitatis
Upsaliensis (2020).
12. Hutchinson PJ, Jalloh I, Helmy A, Carpenter KL, Rostami E, Bellander BM,
et al. Consensus statement from the 2014 International Microdialysis Forum.
Int Care Med. (2015) 41:1517–28. doi: 10.1007/s00134-015-3930-y
13. Bratton SL, Chestnut RM, Ghajar J, McConnell Hammond FF, Harris OA,
Hartl R, et al. Guidelines for the management of severe traumatic brain
injury. IX. Cerebral perfusion thresholds. J Neurotrauma. (2007) 24 Suppl
1:S59–64. doi: 10.1089/neu.2007.9987
14. Sorrentino E, Diedler J, Kasprowicz M, Budohoski KP, Haubrich
C, Smielewski P, et al. Critical thresholds for cerebrovascular
reactivity after traumatic brain injury. Neurocritical Care. (2012)
16:258–66. doi: 10.1007/s12028-011-9630-8
15. Chesnut RM, Temkin N, Carney N, Dikmen S, Rondina C, Videtta W, et al.
A trial of intracranial-pressure monitoring in traumatic brain injury. N Engl
J Med. (2012) 367:2471–81. doi: 10.1056/NEJMoa1207363
16. Hawryluk GWJ, Aguilera S, Buki A, Bulger E, Citerio G, Cooper
DJ, et al. A management algorithm for patients with intracranial
pressure monitoring: the Seattle International Severe Traumatic Brain
Injury Consensus Conference (SIBICC). Int Care Med. (2019) 45:1783–
94. doi: 10.1007/s00134-019-05805-9
17. Hawryluk GWJ, Rubiano AM, Totten AM, O’Reilly C, Ullman JS, Bratton SL,
et al. Guidelines for the Management of Severe Traumatic Brain Injury: 2020
update of the decompressive craniectomy recommendations. Neurosurgery.
(2020) 87:427–34. doi: 10.1093/neuros/nyaa278
18. Rosner MJ, Rosner SD, Johnson AH. Cerebral perfusion pressure:
management protocol and clinical results. J Neurosurg. (1995) 83:949–
62. doi: 10.3171/jns.1995.83.6.0949
19. Wettervik TS, Lenell S, Nyholm L, Howells T, Lewen A, Enblad
P. Decompressive craniectomy in traumatic brain injury: usage and
clinical outcome in a single centre. Acta Neurochirurg. (2018) 160:229–
37. doi: 10.1007/s00701-017-3418-3
20. Paulson OB, Strandgaard S, Edvinsson L. Cerebral autoregulation.
Cerebrovasc Brain Metab Rev. (1990) 2:161–92.
21. Czosnyka M, Smielewski P, Kirkpatrick P, Menon DK, Pickard JD.
Monitoring of cerebral autoregulation in head-injured patients. Stroke.
(1996) 27:1829–34. doi: 10.1161/01.STR.27.10.1829
22. Czosnyka M, Smielewski P, Piechnik S, Steiner LA, Pickard JD.
Cerebral autoregulation following head injury. J Neurosurg. (2001)
95:756–63. doi: 10.3171/jns.2001.95.5.0756
23. Zeiler FA, Ercole A, Czosnyka M, Smielewski P, Hawryluk G,
Hutchinson PJA, et al. Continuous cerebrovascular reactivity
monitoring in moderate/severe traumatic brain injury: a narrative
review of advances in neurocritical care. Br J Anaesth. (2020)
124:440–53. doi: 10.1016/j.bja.2019.11.031
24. Svedung Wettervik TM, Howells T, Enblad P, Lewén A. Temporal
neurophysiological dynamics in traumatic brain injury-the role of pressure
reactivity and optimal cerebral perfusion pressure for predicting outcome. J
Neurotr. (2019) 36:1818–27. doi: 10.1089/neu.2018.6157
25. Veenith TV, Carter EL, Geeraerts T, Grossac J, Newcombe VF,
Outtrim J, et al. Pathophysiologic mechanisms of cerebral ischemia
and diffusion hypoxia in traumatic brain injury. JAMA Neurol. (2016)
73:542–50. doi: 10.1001/jamaneurol.2016.0091
26. Lazaridis C. Cerebral oxidative metabolism failure in traumatic brain injury:
“Brain shock”. J Crit Care. (2017) 37:230–3. doi: 10.1016/j.jcrc.2016.09.027
27. Vespa P, Bergsneider M, Hattori N, Wu HM, Huang SC, Martin NA, et al.
Metabolic crisis without brain ischemia is common after traumatic brain
injury: a combined microdialysis and positron emission tomography study. J
Cereb Blood Flow Metab. (2005) 25:763–74. doi: 10.1038/sj.jcbfm.9600073
28. Verweij BH, Muizelaar JP, Vinas FC, Peterson PL, Xiong Y, Lee CP. Impaired
cerebral mitochondrial function after traumatic brain injury in humans. J
Neurosurg. (2000) 93:815–20. doi: 10.3171/jns.2000.93.5.0815
29. Mrozek S, Vardon F, Geeraerts T. Brain temperature: physiology
and pathophysiology after brain injury. Anesthesiol Res Prac. (2012)
2012:989487. doi: 10.1155/2012/989487
30. Stocchetti N, Rossi S, Zanier ER, Colombo A, Beretta L, Citerio G. Pyrexia
in head-injured patients admitted to intensive care. Int Care Med. (2002)
28:1555–62. doi: 10.1007/s00134-002-1513-1
31. Rossi S, Zanier ER, Mauri I, Columbo A, Stocchetti N. Brain temperature,
body core temperature, and intracranial pressure in acute cerebral damage. J
Neurol Neurosurg Psychiatry. (2001) 71:448–54. doi: 10.1136/jnnp.71.4.448
32. Wang CX, Stroink A, Casto JM, Kattner K. Hyperthermia
exacerbates ischaemic brain injury. Int J Stroke. (2009) 4:274–
84. doi: 10.1111/j.1747-4949.2009.00317.x
33. Svedung Wettervik TM, Engquist H, Lenell S, Howells T, Hillered
L, Rostami E, et al. Systemic hyperthermia in traumatic brain
injury-relation to intracranial pressure dynamics, cerebral energy
metabolism, and clinical outcome. J Neurosurg Anesthesiol. (2020).
doi: 10.1097/ANA.0000000000000695. [Epub ahead of print].
34. Le Roux P, Menon DK, Citerio G, Vespa P, Bader MK, Brophy GM,
et al. Consensus summary statement of the international multidisciplinary
consensus conference on multimodality monitoring in neurocritical care.
Neurocritical care. (2014) 21:1–26. doi: 10.1007/s12028-014-0041-5
35. Lassen N. Autoregulation of cerebral blood flow. Circ Res. (1964)
15 Suppl:201.
36. Lassen NA. Cerebral blood flow and oxygen consumption in man. Physiol
Rev. (1959) 39:183–238. doi: 10.1152/physrev.1959.39.2.183
37. Czosnyka M, Smielewski P, Kirkpatrick P, Laing RJ, Menon D, Pickard JD.
Continuous assessment of the cerebral vasomotor reactivity in head injury.
Neurosurgery. (1997) 41:11–9. doi: 10.1097/00006123-199707000-00005
38. Brady KM, Lee JK, Kibler KK, Easley RB, Koehler RC, Shaffner DH.
Continuous measurement of autoregulation by spontaneous fluctuations
in cerebral perfusion pressure: comparison of 3 methods. Stroke. (2008)
39:2531–7. doi: 10.1161/STROKEAHA.108.514877
39. Zeiler FA, Donnelly J, Calviello L, Lee JK, Smielewski P, Brady K, et al.
Validation of pressure reactivity and pulse amplitude indices against the
lower limit of autoregulation, part I: experimental intracranial hypertension.
J Neurotrauma. (2018) 35:2803–11. doi: 10.1089/neu.2017.5603
40. Lang EW, Chesnut RM. A bedside method for investigating the
integrity and critical thresholds of cerebral pressure autoregulation in
severe traumatic brain injury patients. Br J Neurosurg. (2000) 14:117–
26. doi: 10.1080/02688690050004534
Frontiers in Neurology | www.frontiersin.org 10 February 2021 | Volume 12 | Article 638132
Svedung Wettervik et al. NIC in TBI—Future Directions
41. Howells T, Elf K, Jones PA, Ronne-Engstrom E, Piper I, Nilsson P, et al.
Pressure reactivity as a guide in the treatment of cerebral perfusion
pressure in patients with brain trauma. J Neurosurg. (2005) 102:311–
7. doi: 10.3171/jns.2005.102.2.0311
42. Donnelly J, Czosnyka M, Adams H, Robba C, Steiner LA, Cardim D,
et al. Individualizing thresholds of cerebral perfusion pressure using
estimated limits of autoregulation. Crit Care Med. (2017) 45:1464–
71. doi: 10.1097/CCM.0000000000002575
43. Steiner LA, Czosnyka M, Piechnik SK, Smielewski P, Chatfield D,
Menon DK, et al. Continuous monitoring of cerebrovascular pressure
reactivity allows determination of optimal cerebral perfusion pressure
in patients with traumatic brain injury. Crit Care Med. (2002) 30:733–
8. doi: 10.1097/00003246-200204000-00002
44. Aries MJ, Czosnyka M, Budohoski KP, Steiner LA, Lavinio A, Kolias
AG, et al. Continuous determination of optimal cerebral perfusion
pressure in traumatic brain injury. Crit Care Med. (2012) 40:2456–
63. doi: 10.1097/CCM.0b013e3182514eb6
45. Svedung Wettervik T, Howells T, Lewén A, Enblad P. Blood
pressure variability and optimal cerebral perfusion pressure-new
therapeutic targets in traumatic brain injury. Neurosurgery. (2020)
86:E300–e9. doi: 10.1093/neuros/nyz515
46. Jaeger M, Dengl M, Meixensberger J, Schuhmann MU. Effects of
cerebrovascular pressure reactivity-guided optimization of cerebral
perfusion pressure on brain tissue oxygenation after traumatic brain injury.
Crit Care Med. (2010) 38:1343–7. doi: 10.1097/CCM.0b013e3181d45530
47. Howells T, Smielewski P, Donnelly J, Czosnyka M, Hutchinson PJA,
Menon DK, et al. Optimal cerebral perfusion pressure in centers
with different treatment protocols. Crit Care Med. (2018) 46:e235–
e41. doi: 10.1097/CCM.0000000000002930
48. Weersink CS, Aries MJ, Dias C, Liu MX, Kolias AG, Donnelly J, et al.
Clinical and physiological events that contribute to the success rate of finding
“optimal” cerebral perfusion pressure in severe brain trauma patients. Crit
Care Med. (2015) 43:1952–63. doi: 10.1097/CCM.0000000000001165
49. Robertson CS, Valadka AB, Hannay HJ, Contant CF, Gopinath SP, Cormio
M, et al. Prevention of secondary ischemic insults after severe head injury.
Crit Care Med. (1999) 27:2086–95. doi: 10.1097/00003246-199910000-00002
50. Dias C, Silva MJ, Pereira E, Monteiro E, Maia I, Barbosa S, et al. Optimal
cerebral perfusion pressure management at bedside: a single-center pilot
study.Neurocritical Care. (2015) 23:92–102. doi: 10.1007/s12028-014-0103-8
51. Lott ME, Hogeman C, Herr M, Gabbay R, Sinoway LI. Effects
of an oral glucose tolerance test on the myogenic response in
healthy individuals. Am J Physiol Heart Circ Physiol. (2007)
292:H304–H10. doi: 10.1152/ajpheart.00940.2005
52. Ward ME, Yan L, Angle MR. Modulation of rat pial arteriolar
responses to flow by glucose. Anesthesiology. (2002) 97:471–
7. doi: 10.1097/00000542-200208000-00026
53. Donnelly J, Czosnyka M, Sudhan N, Varsos GV, Nasr N, Jalloh I, et al.
Increased blood glucose is related to disturbed cerebrovascular pressure
reactivity after traumatic brain injury. Neurocritical Care. (2015) 22:20–
5. doi: 10.1007/s12028-014-0042-4
54. Svedung Wettervik T, Howells T, Ronne-Engstrom E, Hillered L, Lewen
A, Enblad P, et al. High arterial glucose is associated with poor pressure
autoregulation, high cerebral lactate/pyruvate ratio and poor outcome
following traumatic brain injury. Neurocritical Care. (2019) 31:526–
33. doi: 10.1007/s12028-019-00743-2
55. Carteron L, Solari D, Patet C, Quintard H, Miroz JP, Bloch J,
et al. Hypertonic lactate to improve cerebral perfusion and glucose
availability after acute brain injury. Crit Care Med. (2018) 46:1649–
55. doi: 10.1097/CCM.0000000000003274
56. Zeiler FA, Ercole A, Beqiri E, Cabeleira M, Aries M, Zoerle T, et al.
Cerebrovascular reactivity is not associated with therapeutic intensity in
adult traumatic brain injury: a CENTER-TBI analysis. Acta Neuroch. (2019)
161:1955–64. doi: 10.1007/s00701-019-03980-8
57. Menzel M, Doppenberg EM, Zauner A, Soukup J, Reinert MM, Bullock
R. Increased inspired oxygen concentration as a factor in improved
brain tissue oxygenation and tissue lactate levels after severe human
head injury. J Neurosurg. (1999) 91:1–10. doi: 10.3171/jns.1999.91.
1.0001
58. Wettervik TS, Engquist H, Howells T, Lenell S, Rostami E, Hillered L,
et al. Arterial oxygenation in traumatic brain injury-relation to cerebral
energy metabolism, autoregulation, and clinical outcome. J Inten Care Med.
(2020). doi: 10.1177/0885066620944097. [Epub ahead of print].
59. Svedung Wettervik T, Howells T, Hillered L, Nilsson P, Engquist H, Lewen
A, et al. Mild hyperventilation in traumatic brain injury-relation to cerebral
energy metabolism, pressure autoregulation, and clinical outcome. World
Neurosurg. (2020) 133:e567–e75. doi: 10.1016/j.wneu.2019.09.099
60. Steiner LA, Balestreri M, Johnston AJ, Coles JP, Chatfield DA, Pickard
JD, et al. Effects of moderate hyperventilation on cerebrovascular
pressure-reactivity after head injury. Acta Neuroch. (2005)
95:17–20. doi: 10.1007/3-211-32318-X_4
61. Graham DI, Adams JH. Ischaemic brain damage in fatal head injuries.
Lancet. (1971) 1:265–6. doi: 10.1016/S0140-6736(71)91003-8
62. Diringer MN, Zazulia AR, Powers WJ. Does ischemia contribute
to energy failure in severe TBI? Transl Stroke Res. (2011) 2:517–
23. doi: 10.1007/s12975-011-0119-8
63. Oddo M, Levine JM, Kumar M, Iglesias K, Frangos S, Maloney-Wilensky E,
et al. Anemia and brain oxygen after severe traumatic brain injury. Int Care
Med. (2012) 38:1497–504. doi: 10.1007/s00134-012-2593-1
64. Yamal JM, Rubin ML, Benoit JS, Tilley BC, Gopinath S, Hannay HJ, et al.
Effect of hemoglobin transfusion threshold on cerebral hemodynamics and
oxygenation. J Neurotrauma. (2015) 32:1239–45. doi: 10.1089/neu.2014.3752
65. Sekhon MS, Griesdale DE, Czosnyka M, Donnelly J, Liu X, Aries MJ,
et al. The effect of red blood cell transfusion on cerebral autoregulation
in patients with severe traumatic brain injury. Neurocritical care. (2015)
23:210–6. doi: 10.1007/s12028-015-0141-x
66. Robertson CS, Hannay HJ, Yamal JM, Gopinath S, Goodman JC, Tilley BC,
et al. Effect of erythropoietin and transfusion threshold on neurological
recovery after traumatic brain injury: a randomized clinical trial. JAMA.
(2014) 312:36–47. doi: 10.1001/jama.2014.6490
67. Utter GH, Shahlaie K, Zwienenberg-Lee M, Muizelaar JP. Anemia in the
setting of traumatic brain injury: the arguments for and against liberal
transfusion. J Neurotrauma. (2011) 28:155–65. doi: 10.1089/neu.2010.1451
68. Gobatto ALN, Link MA, Solla DJ, Bassi E, Tierno PF, Paiva W, et al.
Transfusion requirements after head trauma: a randomized feasibility
controlled trial. Crit Care. (2019) 23:89. doi: 10.1186/s13054-018-2273-9
69. Salim A, Hadjizacharia P, DuBose J, Brown C, Inaba K, Chan L, et al.
Role of anemia in traumatic brain injury. J Am Coll Surg. (2008) 207:398–
406. doi: 10.1016/j.jamcollsurg.2008.03.013
70. Chang JJ, Youn TS, Benson D, Mattick H, Andrade N, Harper CR,
et al. Physiologic and functional outcome correlates of brain tissue
hypoxia in traumatic brain injury. Crit Care Med. (2009) 37:283–
90. doi: 10.1097/CCM.0b013e318192fbd7
71. Tolias CM, Reinert M, Seiler R, Gilman C, Scharf A, Bullock MR.
Normobaric hyperoxia–induced improvement in cerebral metabolism and
reduction in intracranial pressure in patients with severe head injury: a
prospective historical cohort-matched study. J Neurosurg. (2004) 101:435–
44. doi: 10.3171/jns.2004.101.3.0435
72. Reinert M, Schaller B, Widmer HR, Seiler R, Bullock R. Influence of oxygen
therapy on glucose-lactate metabolism after diffuse brain injury. J Neurosurg.
(2004) 101:323–9. doi: 10.3171/jns.2004.101.2.0323
73. Nortje J, Coles JP, Timofeev I, Fryer TD, Aigbirhio FI, Smielewski P, et al.
Effect of hyperoxia on regional oxygenation and metabolism after severe
traumatic brain injury: preliminary findings. Crit Care Med. (2008) 36:273–
81. doi: 10.1097/01.CCM.0000292014.60835.15
74. Vilalta A, Sahuquillo J, Merino MA, Poca MA, Garnacho A, Martinez-
Valverde T, et al. Normobaric hyperoxia in traumatic brain injury: does
brain metabolic state influence the response to hyperoxic challenge? J
Neurotrauma. (2011) 28:1139–48. doi: 10.1089/neu.2010.1720
75. Vidal-Jorge M, Sánchez-Guerrero A, Mur-Bonet G, Castro L, Radoi A,
Riveiro M, et al. Does normobaric hyperoxia cause oxidative stress in the
injured brain? A microdialysis study using 8-iso-prostaglandin F2α as a
biomarker. J Neurotrauma. (2017) 34:2731–42. doi: 10.1089/neu.2017.4992
76. Spiotta AM, Stiefel MF, Gracias VH, Garuffe AM, Kofke WA, Maloney-
Wilensky E, et al. Brain tissue oxygen-directed management and outcome
in patients with severe traumatic brain injury. J Neurosurg. (2010) 113:571–
80. doi: 10.3171/2010.1.JNS09506
Frontiers in Neurology | www.frontiersin.org 11 February 2021 | Volume 12 | Article 638132
Svedung Wettervik et al. NIC in TBI—Future Directions
77. Martini RP, Deem S, Yanez ND, Chesnut RM, Weiss NS, Daniel S, et al.
Management guided by brain tissue oxygen monitoring and outcome
following severe traumatic brain injury. J Neurosurg. (2009) 111:644–
9. doi: 10.3171/2009.2.JNS08998
78. Okonkwo DO, Shutter LA, Moore C, Temkin NR, Puccio AM, Madden
CJ, et al. Brain oxygen optimization in severe traumatic brain injury
phase-II: a phase II randomized trial. Crit Care Med. (2017) 45:1907–
14. doi: 10.1097/CCM.0000000000002619
79. Ungerstedt U, Pycock C. Functional correlates of dopamine
neurotransmission. Bull Schw Akad Med Wis. (1974) 30:44.
80. Persson L, Hillered L. Chemical monitoring of neurosurgical intensive
care patients using intracerebral microdialysis. J Neurosurg. (1992) 76:72–
80. doi: 10.3171/jns.1992.76.1.0072
81. Engstrom M, Polito A, Reinstrup P, Romner B, Ryding E,
Ungerstedt U, et al. Intracerebral microdialysis in severe brain
trauma: the importance of catheter location. J Neurosurg. (2005)
102:460–9. doi: 10.3171/jns.2005.102.3.0460
82. Rostami E, Bellander BM. Monitoring of glucose in brain, adipose tissue,
and peripheral blood in patients with traumatic brain injury: a microdialysis
study. J Diab Sci Tech. (2011) 5:596–604. doi: 10.1177/193229681100500314
83. Diaz-Parejo P, Ståhl N, Xu W, Reinstrup P, Ungerstedt U, Nordström
CH. Cerebral energy metabolism during transient hyperglycemia in
patients with severe brain trauma. Int Care Med. (2003) 29:544–
50. doi: 10.1007/s00134-003-1669-3
84. Magnoni S, Tedesco C, Carbonara M, Pluderi M, Colombo A, Stocchetti
N. Relationship between systemic glucose and cerebral glucose is preserved
in patients with severe traumatic brain injury, but glucose delivery to
the brain may become limited when oxidative metabolism is impaired:
implications for glycemic control. Crit Care Med. (2012) 40:1785–
91. doi: 10.1097/CCM.0b013e318246bd45
85. Rosner MJ, Newsome HH, Becker DP. Mechanical brain
injury: the sympathoadrenal response. J Neurosurg. (1984)
61:76–86. doi: 10.3171/jns.1984.61.1.0076
86. Jeremitsky E, Omert LA, DunhamCM,Wilberger J, Rodriguez A. The impact
of hyperglycemia on patients with severe brain injury. J Trauma. (2005)
58:47–50. doi: 10.1097/01.TA.0000135158.42242.B1
87. LamAM,WinnHR, Cullen BF, Sundling N. Hyperglycemia and neurological
outcome in patients with head injury. J Neurosurg. (1991) 75:545–
51. doi: 10.3171/jns.1991.75.4.0545
88. Young B, Ott L, Dempsey R, Haack D, Tibbs P. Relationship
between admission hyperglycemia and neurologic outcome
of severely brain-injured patients. Ann Surg. (1989) 210:466–
72. doi: 10.1097/00000658-198910000-00007
89. Russell JW, Golovoy D, Vincent AM, Mahendru P, Olzmann JA, Mentzer A,
et al. High glucose-induced oxidative stress and mitochondrial dysfunction
in neurons. FASEB J. (2002) 16:1738–48. doi: 10.1096/fj.01-1027com
90. Krinsley JS. Effect of an intensive glucose management protocol on the
mortality of critically ill adult patients. Mayo Clinic Proc. (2004) 79:992–
1000. doi: 10.4065/79.8.992
91. Van den Berghe G, Wilmer A, Hermans G, Meersseman W, Wouters PJ,
Milants I, et al. Intensive insulin therapy in the medical ICU. N Engl J Med.
(2006) 354:449–61. doi: 10.1056/NEJMoa052521
92. Bilotta F, Caramia R, Cernak I, Paoloni FP, Doronzio A,
Cuzzone V, et al. Intensive insulin therapy after severe traumatic
brain injury: a randomized clinical trial. Neurocrit Care. (2008)
9:159–66. doi: 10.1007/s12028-008-9084-9
93. Coester A, Neumann CR, Schmidt MI. Intensive insulin therapy in severe
traumatic brain injury: a randomized trial. J Traum Acute Care Surg.
(2010) 68:904–11. doi: 10.1097/TA.0b013e3181c9afc2
94. Meier R, Béchir M, Ludwig S, Sommerfeld J, Keel M, Steiger P, et al.
Differential temporal profile of lowered blood glucose levels (3.5 to 6.5
mmol/l versus 5 to 8 mmol/l) in patients with severe traumatic brain injury.
Crit Care. (2008) 12:R98. doi: 10.1186/cc6974
95. Vespa P, Boonyaputthikul R, McArthur DL, Miller C, Etchepare M,
Bergsneider M, et al. Intensive insulin therapy reduces microdialysis
glucose values without altering glucose utilization or improving the
lactate/pyruvate ratio after traumatic brain injury. Crit Care Med. (2006)
34:850–6. doi: 10.1097/01.CCM.0000201875.12245.6F
96. Finfer S, Liu B, Chittock DR, Norton R, Myburgh JA, McArthur C, et al.
Hypoglycemia and risk of death in critically ill patients.N Engl J Med. (2012)
367:1108–18. doi: 10.1056/NEJMoa1204942
97. Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, et al. Intensive
versus conventional glucose control in critically ill patients. N Engl J Med.
(2009) 360:1283–97. doi: 10.1056/NEJMoa0810625
98. Oddo M, Schmidt JM, Carrera E, Badjatia N, Connolly ES, Presciutti M,
et al. Impact of tight glycemic control on cerebral glucose metabolism after
severe brain injury: a microdialysis study. Crit Care Med. (2008) 36:3233–
8. doi: 10.1097/CCM.0b013e31818f4026
99. Rostami E. Glucose and the injured brain-monitored in the neurointensive
care unit. Front Neurol. (2014) 5:91. doi: 10.3389/fneur.2014.00091
100. Pellerin L, Magistretti PJ. Glutamate uptake into astrocytes
stimulates aerobic glycolysis: a mechanism coupling neuronal
activity to glucose utilization. Proc Natl Acad Sci USA. (1994)
91:10625–9. doi: 10.1073/pnas.91.22.10625
101. Boumezbeur F, Petersen KF, Cline GW, Mason GF, Behar KL, Shulman GI,
et al. The contribution of blood lactate to brain energymetabolism in humans
measured by dynamic 13C nuclear magnetic resonance spectroscopy. J
Neurosci. (2010) 30:13983–91. doi: 10.1523/JNEUROSCI.2040-10.2010
102. Bouzat P, Sala N, Suys T, Zerlauth JB, Marques-Vidal P,
Feihl F, et al. Cerebral metabolic effects of exogenous lactate
supplementation on the injured human brain. Int Care Med. (2014)
40:412–21. doi: 10.1007/s00134-013-3203-6
103. Quintard H, Patet C, Zerlauth JB, Suys T, Bouzat P, Pellerin
L, et al. Improvement of neuroenergetics by hypertonic lactate
therapy in patients with traumatic brain injury is dependent on
baseline cerebral lactate/pyruvate ratio. J Neurotrauma. (2016)
33:681–7. doi: 10.1089/neu.2015.4057
104. Attwell D, Buchan AM, Charpak S, Lauritzen M, Macvicar BA, Newman
EA. Glial and neuronal control of brain blood flow. Nature. (2010) 468:232–
43. doi: 10.1038/nature09613
105. Alessandri B, Schwandt E, Kamada Y, Nagata M, Heimann A, Kempski O.
The neuroprotective effect of lactate is not due to improved glutamate uptake
after controlled cortical impact in rats. J Neurotrauma. (2012) 29:2181–
91. doi: 10.1089/neu.2011.2067
106. Patet C, Suys T, Carteron L, Oddo M. Cerebral lactate metabolism
after traumatic brain injury. Curr Neurol Neurosci Rep. (2016)
16:31. doi: 10.1007/s11910-016-0638-5
107. Timofeev I, Carpenter KL, Nortje J, Al-Rawi PG, O’Connell MT, Czosnyka
M, et al. Cerebral extracellular chemistry and outcome following traumatic
brain injury: a microdialysis study of 223 patients. Brain. (2011) 134(Pt
2):484–94. doi: 10.1093/brain/awq353
108. Sánchez-Aguilar M, Tapia-Pérez JH, Sánchez-Rodríguez JJ, Viñas-Ríos JM,
Martínez-Pérez P, de la Cruz-Mendoza E, et al. Effect of rosuvastatin
on cytokines after traumatic head injury. J Neurosurg. (2013) 118:669–
75. doi: 10.3171/2012.12.JNS121084
109. Kelsen J, Karlsson M, Hansson MJ, Yang Z, Fischer W, Hugerth
M, et al. Copenhagen head injury ciclosporin study: a phase IIA
safety, pharmacokinetics, and biomarker study of ciclosporin in
severe traumatic brain injury patients. J Neurotrauma. (2019)
36:3253–63. doi: 10.1089/neu.2018.6369
110. Simon DW, McGeachy MJ, Bayir H, Clark RS, Loane DJ, Kochanek PM. The
far-reaching scope of neuroinflammation after traumatic brain injury. Nat
Rev Neurol. (2017) 13:171. doi: 10.1038/nrneurol.2017.13
111. Dyhrfort P, Shen Q, Clausen F, Thulin M, Enblad P, Kamali-Moghaddam
M, et al. Monitoring of protein biomarkers of inflammation in human
traumatic brain injury using microdialysis and proximity extension assay
technology in neurointensive care. J Neurotrauma. (2019) 36:2872–
85. doi: 10.1089/neu.2018.6320
112. Hillered L, Dahlin AP, Clausen F, Chu J, Bergquist J, Hjort K,
et al. Cerebral microdialysis for protein biomarker monitoring in the
neurointensive care setting-a technical approach. Front Neurol. (2014)
5:245. doi: 10.3389/fneur.2014.00245
113. McConeghy KW, Hatton J, Hughes L, Cook AM. A review
of neuroprotection pharmacology and therapies in patients
with acute traumatic brain injury. CNS Drugs. (2012) 26:613–
36. doi: 10.2165/11634020-000000000-00000
Frontiers in Neurology | www.frontiersin.org 12 February 2021 | Volume 12 | Article 638132

Svedung Wettervik et al. NIC in TBI—Future Directions
114. Murray GD, Teasdale GM, Schmitz H. Nimodipine in traumatic
subarachnoid haemorrhage: a re-analysis of the HIT I and HIT II trials. Acta
Neuroch. (1996) 138:1163–7. doi: 10.1007/BF01809745
115. Ikonomidou C, Turski L. Why did NMDA receptor antagonists fail clinical
trials for stroke and traumatic brain injury? Lancet Neurol. (2002) 1:383–
6. doi: 10.1016/S1474-4422(02)00164-3
116. Skolnick BE, Maas AI, Narayan RK, van der Hoop RG, MacAllister T, Ward
JD, et al. A clinical trial of progesterone for severe traumatic brain injury. N
Engl J Med. (2014) 371:2467–76. doi: 10.1056/NEJMoa1411090
117. Roberts I, Yates D, Sandercock P, Farrell B, Wasserberg J, Lomas G,
et al. Effect of intravenous corticosteroids on death within 14 days
in 10008 adults with clinically significant head injury (MRC CRASH
trial): randomised placebo-controlled trial. Lancet. (2004) 364:1321–
8. doi: 10.1016/S0140-6736(04)17188-2
118. Depreitere B, Güiza F, Van den Berghe G, Schuhmann MU, Maier G,
Piper I, et al. Pressure autoregulation monitoring and cerebral perfusion
pressure target recommendation in patients with severe traumatic brain
injury based on minute-by-minute monitoring data. J Neurosurg. (2014)
120:1451–7. doi: 10.3171/2014.3.JNS131500
Conflict of Interest: The authors declare that the research was conducted in the
absence of any commercial or financial relationships that could be construed as a
potential conflict of interest.
Copyright © 2021 Svedung Wettervik, Lewén and Enblad. This is an open-access
article distributed under the terms of the Creative Commons Attribution License (CC
BY). The use, distribution or reproduction in other forums is permitted, provided
the original author(s) and the copyright owner(s) are credited and that the original
publication in this journal is cited, in accordance with accepted academic practice.
No use, distribution or reproduction is permitted which does not comply with these
terms.
Frontiers in Neurology | www.frontiersin.org 13 February 2021 | Volume 12 | Article 638132