
Interne kontrole na primjeru poduzeća adidas Croatia d.o.o. ...
Upload
khangminh22Category
view
1download
0
19
UDK 616-036.88:796Original scientific paperReceived: 9 september 2011Accepted: 14 December 2011
Corresponding author: Zijad Durakoviće-mail: [email protected]
SUDDEN CARDIAC DEATH DUE TO PHYSICAL EXERCISE IN CROATIA IN A 27-YEAR PERIOD
Zijad Duraković1, Marjeta Mišigoj Duraković2, Josip Škavić3
1Department of Medical Anthropology and Epidemiology, Institute for Anthropological Research, Zagreb, Croatia;
2Department of Kinesiological Anthropology and Methodology, Faculty of Kinesiology, Zagreb, Croatia;
3Department of Forensic Medicine and Criminology, Medical Faculty University of Zagreb, Croatia
Dedicated to the memory of our teacher professor Radovan Medved, MD, PhD, the founder of the Croatian Sports Medicine, a corresponding member of the Croatian Academy of Sciences and Arts.
SummaryIn a period of 27 years: from January 1, 1984 to December 31, 2010 we noticed
69 sudden and unexpected cardiac deaths during physical exercise in Croatia. There were 6 sudden cardiac deaths in male athletes. At the autopsy, an athletic runner aged 21, had an acute myocardial infarction with normal coronaries and left ventricular wall thickened. A professional soccer player aged 17, had hypoplastic right coronary artery and narrowed ascending aorta, bacterial tonsillitis and subacute myocarditis. A student rugby player aged 29, and a school boy-basketball player aged 15, had hypertrophic cardiomyopathy. The arrhythmogenic right ventricular dysplasia was a cause of death in two athletes. The first was a short trails runner, and the second was a soccer player.
The hypertrophic cardiomyopathy was a cause of death in 3 athletes and 2 persons during recreational exercise. An acute myopericarditis was a cause of death in 2 pro-fessional soccer players, and in one who died during swimming. One had subacute di-ffuse myopericarditis, bacterial tonsillitis and narrowed ascending aorta of 10 mm. The other had chronic myopericarditis and cardiac aneurysm of the left ventricle. The third

Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
20
had fibrinous pericarditis, hyperthropic cardiomyopathy, hypoplastic ascending aorta, bilateral bronchopneumonia and cerebral contusion with edema.
Sudden cardiac deaths appeared in 10 school boys. Two of them had been engaged in physical exercise at school, the third was a professional soccer player, the fourth was engaged in recreational swimming, and the fifth had just finished secondary school and was working at the site recreatively. In 3 of them congenital cardiovascular diseases was found: in 2 hypoplastic coronary arteries and in 2 hypertrophic cardiomyopathy. The fourth had normal heart findings including coronaries, but had bilateral pneumonia with a non-cardiogenic pulmonary edema. The fifth had a chronic myopericarditis with an aneurysm of the left ventricle.
Pneumonia was a cause of death in 3 male teenagers aged 18-19. The first was wor-king at the site recreatively, the second was engaged in soccer recreatively and the third was professional soccer player. One died suddenly during physical exercise at the field and 2 died in the hospital. The first had bilateral bacterial pneumonia, non-cardiogenic pulmonary edema and cerebral edema. The second had bilateral bacterial pneumonia, adult respiratory distress syndrome, disseminated intravascular coagulation, cerebral edema, hypoplastic right coronary artery and myocardial fibrosis. The third had bila-teral bacterial pneumonia, fibrinous pericarditis, and cerebral contusion with edema, thickening of the left ventricle 20 mm and hypoplastic ascending aorta.
We noticed 5 sudden death among Croatian male physicians, during or after recre-ational exercise: swimming, soccer, tennis and jogging; 3 were autopsied, and all had coronary heart disease. Two physicians who were not been autopsied, had possible an alcohol cardiomyopathy. Fifteen “elderly” men, died suddenly during exercise: 6 in swimming, 4 in playing tennis, one ridded, one was jogging, 2 bowling and one died during sexual act. At autopsy, 14 had coronary heart disease: 5 critical coronary artery stenosis, and 2 had signs of recent myocardial infarctions, 3 had left descending coro-nary artery occluded, and one with acute myocardial infarction of the anterior wall, 12 had myocardial scars due to previous myocardial infarctions and one signs of diffuse myocardial fibrosis. Twelve of them had left ventricular hypertrophy.
In Croatia the death rate among athletes reached 0.19/100 000 yearly (p=0.00005), in the male population aged 15-40 years, engaged in sports and recreational physical exercise: 0.71/100 0000 (p=0.00001), in the total male population aged 15-64 enga-ged in sport and recreational exercise 0.96/100 000 (p=0.00001), in arrhythmogenic right ventricular dysplasia reached 0.06/100.000 (p=0.00000), in teenagers suffered of hypertrophic cardiomyopathy 0.10/100 000 (p=0.00000), in myopericarditis it was 0.11/100,000 (p=0.00000), in pneumonia 0.11/100 000 (p=0.00000), in teenagers 0.37/100 000 (p=0.00226), in physician-specialists reached 24.8/100 000 (p=0.00000), in elders reached 2.99/100 000 (p=0.00001).
Keywords: men; athletes; recreational physical exercise; sudden death

21
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
IntroductIon
In trained and functionally fit athletes with a healthy heart, acute cardiovas-cular incidents due to training are very scarce. Regular physical exercise, contro-lled and adapted to physical conditions has beneficial effects surpassing hazards. If the principles of physical training are considered, possible complications could be avoided. In persons aged under 30, who died during or immediately after physical exercise, the most common reasons for lethal events is a congenital heart disease: hypertrophic cardiomyopathy, congenital coronary artery anomalies (including an abnormal origin of coronary artery, hypoplastic coronary artery, myocardial brid-ging), aortic stenosis, aortic dissection (often associated with Marfan,s syndrome), myocarditis - higher than expected [1], an idiopathic dilated cardiomyopathy, mitral valve prolapsed, idiopathic cardiac hypertrophy, infiltrating cardiomiopathies (f.e. amyloidosis), right ventricular dysplasia [2,3] , long Q-T interval syndrome, the Bru-gada syndrome: right bundle branch block, right precordial ST-segment elevation associated with ventricular tachycardia [4]. Risk factors for sudden death include positive familial history for conditions associated with sudden death, recurrent or exercise-induced non-neurogenic syncope, anginal chest pain, palpitations, dys-pnea, cardiovascular diseases, seizure activity, and athletic competition [5]. That is why a medical check-up before exercise is essential, as well as medical controls in persons taking exercise [5-9].
Among cardiovascular disease leading to sudden death [8,10-15], arrhythmoge-nic right ventricular dysplasia or cardiopathy (ARVD/C) by some authors reached 2-5% of all sudden deaths in young persons, with a higher death rate during exercise [16]. ARVD is primary myocardial diseases caused of genetic defect of desmoso-mes, i.e. area in myocardium which links together the myocardial myofibrils. Those desmosomes are composed of several proteins. In this disease we are facing with changes of cell adhesion proteins: plakoglobulin, plakophilin-2, desmoglein-2, de-smoplakin [17,18]. Many of those proteins can have harmful mutations. ARVD is very often biventricular disease involving the right ventricular myocardium and typically the subepicardial region of the left ventricle characterized of myocyte vacuolization. It is replaced with fibro fatty tissue in the right ventricle leading to myocardial atrophy and with more fibrosis than fibro fatty infiltration in the left ventricle [16,19]. It could be connected with a high risk of ventricular instability and malignant ventricular arrhythmias. Sudden cardiac death could be the only mani-festation of the disease, especially in young athletes [16].
Hypertrophic cardiomyopathy (HCM) is the most common cause of sudden car-diac death in young competitive athletes [20,21]. HCM means thickened and not
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
22
dilated left ventricular wall, without any other disease leading to left ventricular hypertrophy (LVH). The etiology of HCM is unknown. Teare [22] was the first who described it, as an asymmetrical heart hypertrophy. HCM is a primary myocardi-al disease [23] with 450 different mutations identified in 13 genes, in which three genes are responsible for more than 50% of all genotype cases: cardiac troponin-T (chromosome 1), myosin-binding protein C (chromosome 11) and beta-myosin he-avy chain (chromosome 14). In HCM, LVH is asymmetric and could be concentric, localized in the basal anterior septum, posterior septum, anterolateral wall, posteri-or wall or in the apex. The consequence of HCM could be sudden cardiac death due to decrease of a cardiac output leading to dyspnea during exercise, postural arterial hypotension, palpitations or syncope, myocardial ischemia with typical or atypical angina chest pain during exercise and with a high risk of ventricular instability and a malignant ventricular arrhythmias. LVH increases the risk of sudden cardiac death by promoting subendocardial ischemia [24].
Myopericarditis is at the third place among the causes of sudden cardiac dea-th in young persons engaged in sport and recreational exercise and the incidence being higher than expected [7,8,10,25-31]. Risk factors for sudden death associated with exercise include positive familial history for conditions associated with sudden death, cardiovascular diseases and symptoms suggesting them: syncope recurrent, exercise-induced, and non-neurogenic in nature, angina chest pain, palpitations, dyspnea, and seizure activity (5,32-34]. Adolescents with these risk factors should be referred to a cardiologist for diagnostic and therapeutic interventions.
Acute respiratory tract infections are the most frequent reasons of morbidity and inability for exercise [7,8,11,17,31]. Their frequency reached over 65 per cent of all infections. Several epidemiological studies point out the increased risk of morbi-dity from the respiratory tract infections in athletes during the intensive indurance training sessions [13]. Athletes in periods of intensive training and after highly stre-nous training are more often affected by respiratory tract infections. But in those engaged in recreative physical exercise consider that such regular activities protect them from these infections [7,31,35].
Physicians engaged in physical exercise have specific problems because they very often underestimate their own physical condition. Complications, during or af-ter exercise, might occur both in persons who suffer from heart disease and in those who are „free“ from disease as physician very often are [25,36-41].
Elderly people are specific group with regard to physical exercise, because nu-merous changes occur in the human organism with advancing age. Elderly people regularly engaged in recreational physical exercise have lower risk for cardiovascu-lar complications than inactive persons [11,42-46].

23
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
The aim of this study is to analyze the prevalence of sudden cardiac death in males due or immediately after sports or recreational physical exercise in regard to reasons and other specific consequences in Croatia.
Sample and methodS
According to the register of a population from 2001 year, from the Croatian De-partment of Statistics, in Croatia it were 4 437 460 inhabitants, of which it was 2 135 900 males. There were 1 484 625 males aged 15 to 65 years, and 265 108 males aged >65 years, and 7% of them practicing physical exercise (18 558). In a group of persons aged 15 to 65 years, there were 97 940 school boys and 116 056 athletes, who were practicing physical exercise (213 996). Of other males aged 15 to 65 years (1 270 629), 10% were practicing physical exercise (127 063). So we are coming to the number of 359 617 males older than 15 years, who were practicing physical exercise.
The data presented here are part of a large retrospective study dealing with 69 sudden and unexpected deaths during or immediately after physical exercise in men of all ages (and no women) in a 27-year period in Croatia: from January 1, 1984 to De-cember 31, 2010. All of them were autopsied. The data of deceased persons were found from the Public Health Registry, Sports Clubs and Services of Forensic Medicine in Croatia. The cases of sudden cardiac death who were autopsied are presented accor-ding to the age of victims, type of physical activity-exercise-sport during which death occurs as well as in a subgroup of physically active physicians who died suddenly. Special attention is paid to the cases of fatal cardiac events in 6 athletes and 13 teena-gers, 15 elderly persons engaged in physical exercise, and in a subgroup of 5 physici-ans. These cases are presented in detail as well as the cases with underlying HCM in 5 adolescents, ARVD in 2 athletes, myopericarditis in 3, and bronchopneumonia in 3 adolescents. The total prevalence as well as the prevalence of sudden cardiac death in males during or immediately after physical exercise in groups regarding chronologi-cal age and with regard to the possible cause of death was calculated as a number of cases per 100 000 persons engaged in such physical activities.
Statistical differences between deceased groups regarding the chronological age and underlying deseases in relation to all male inhabitants engaged in sports and recreative physical exercise in Croatia, was calculated using the Chi-square test and Poisson rates.
reSultS
In a period of 27 years, 69 sudden cardiac death due to physical exercise were registered. The age of of victims was between 13 to 82 years and all of them were
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
24
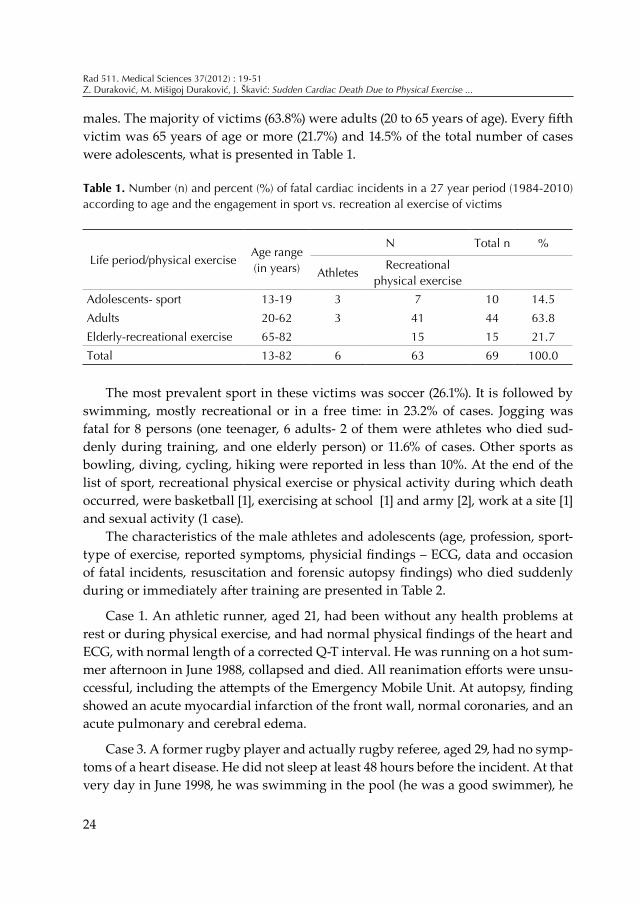
Table 1. Number (n) and percent (%) of fatal cardiac incidents in a 27 year period (1984-2010) according to age and the engagement in sport vs. recreation al exercise of victims
Life period/physical exercise Age range(in years)
N Total n %
Athletes Recreational
physical exercise Adolescents- sport 13-19 3 7 10 14.5Adults 20-62 3 41 44 63.8Elderly-recreational exercise 65-82 15 15 21.7Total 13-82 6 63 69 100.0
males. The majority of victims (63.8%) were adults (20 to 65 years of age). Every fifth victim was 65 years of age or more (21.7%) and 14.5% of the total number of cases were adolescents, what is presented in Table 1.
The most prevalent sport in these victims was soccer (26.1%). It is followed by swimming, mostly recreational or in a free time: in 23.2% of cases. Jogging was fatal for 8 persons (one teenager, 6 adults- 2 of them were athletes who died sud-denly during training, and one elderly person) or 11.6% of cases. Other sports as bowling, diving, cycling, hiking were reported in less than 10%. At the end of the list of sport, recreational physical exercise or physical activity during which death occurred, were basketball [1], exercising at school [1] and army [2], work at a site [1] and sexual activity (1 case).
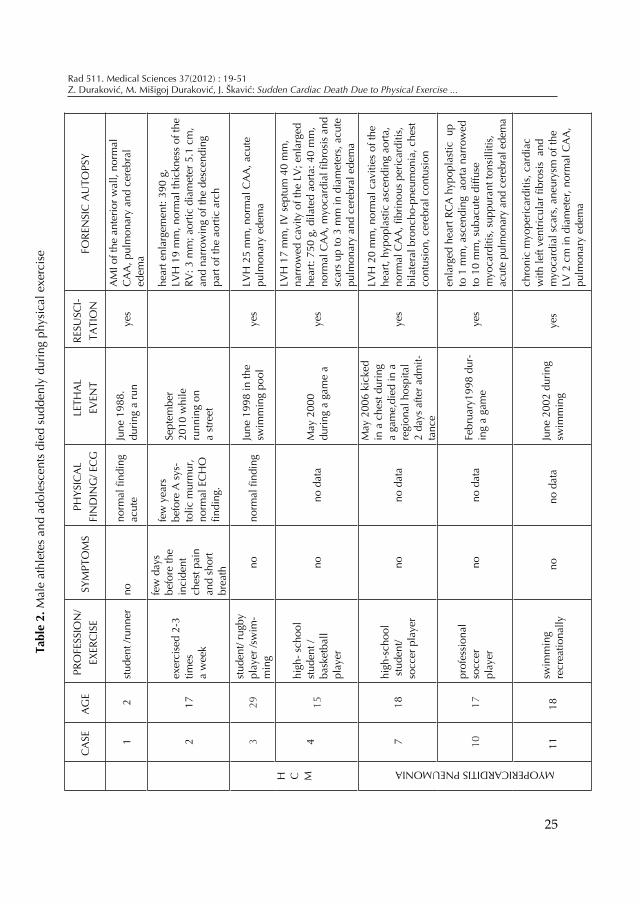
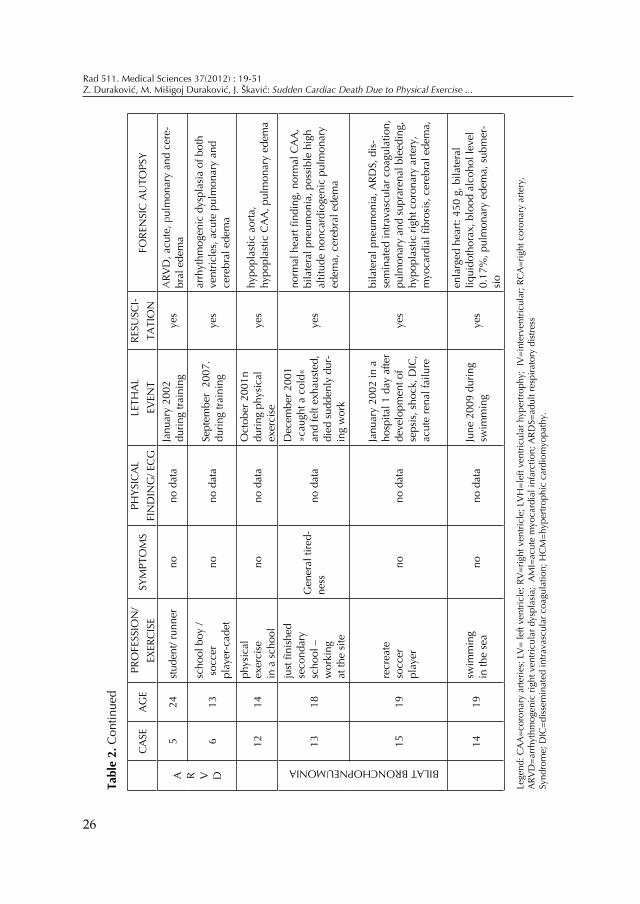
The characteristics of the male athletes and adolescents (age, profession, sport-type of exercise, reported symptoms, physicial findings – ECG, data and occasion of fatal incidents, resuscitation and forensic autopsy findings) who died suddenly during or immediately after training are presented in Table 2.
Case 1. An athletic runner, aged 21, had been without any health problems at rest or during physical exercise, and had normal physical findings of the heart and ECG, with normal length of a corrected Q-T interval. He was running on a hot sum-mer afternoon in June 1988, collapsed and died. All reanimation efforts were unsu-ccessful, including the attempts of the Emergency Mobile Unit. At autopsy, finding showed an acute myocardial infarction of the front wall, normal coronaries, and an acute pulmonary and cerebral edema.
Case 3. A former rugby player and actually rugby referee, aged 29, had no symp-toms of a heart disease. He did not sleep at least 48 hours before the incident. At that very day in June 1998, he was swimming in the pool (he was a good swimmer), he
25
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
Tabl
e 2.
Mal
e at
hlet
es a
nd a
dole
scen
ts d
ied
sudd
enly
dur
ing
phys
ical
exe
rcis
e
CA
SEA
gE
PRO
FESS
ION
/Ex
ERC
ISE
SyM
PTO
MS
PhyS
ICA
L FI
ND
INg
/ EC
gLE
ThA
L Ev
ENT
RESu
SCI-
TATI
ON
FORE
NSI
C A
uTO
PSy
12
stud
ent /
runn
erno
norm
al fi
ndin
g ac
ute
June
198
8.
durin
g a
run
yes
AM
I of t
he a
nter
ior w
all,
norm
al
CA
A, p
ulm
onar
y an
d ce
rebr
al
edem
a
217
exer
cise
d 2-
3tim
es
a w
eek
few
day
s be
fore
the
inci
dent
ch
est p
ain
and
shor
t br
eath
few
yea
rs
befo
re A
sys
-to
lic m
urm
ur,
norm
al E
Ch
O
findi
ng.
Sept
embe
r 20
10 w
hile
ru
nnin
g on
a
stre
et
hear
t enl
arge
men
t: 39
0 g,
Lvh
19
mm
, nor
mal
thic
knes
s of
the
Rv: 3
mm
; aor
tic d
iam
eter
5.1
cm
, an
d na
rrow
ing
of th
e de
scen
ding
pa
rt of
the
aorti
c ar
ch
h C M
329
stud
ent/
rugb
y pl
ayer
/sw
im-
min
gno
norm
al fi
ndin
gJu
ne 1
998
in th
e sw
imm
ing
pool
yes
Lvh
25
mm
, nor
mal
CA
A, a
cute
pu
lmon
ary
edem
a
415
high
- sch
ool
stud
ent /
ba
sket
ball
play
er
nono
dat
aM
ay 2
000
durin
g a
gam
e a
yes
Lvh
17
mm
, Iv
sep
tum
40
mm
, na
rrow
ed c
avity
of t
he L
v; e
nlar
ged
hear
t: 75
0 g,
dila
ted
aorta
: 40
mm
, no
rmal
CA
A, m
yoca
rdia
l fibr
osis
and
sc
ars
up to
3 m
m in
dia
met
ers,
acu
te
pulm
onar
y an
d ce
rebr
al e
dem
a
718
high
-sch
ool
stu
dent
/ so
ccer
pla
yer
nono
dat
a
May
200
6 ki
cked
in
a c
hest
dur
ing
a ga
me,
died
in a
re
gion
al h
ospi
tal
2 da
ys a
fter a
dmit-
tanc
e
yes
Lvh
20
mm
, nor
mal
cav
ities
of t
he
hear
t, hy
popl
astic
asc
endi
ng a
orta
, no
rmal
CA
A, fi
brin
ous
peric
ardi
tis,
bila
tera
l bro
ncho
-pne
umon
ia, c
hest
co
ntus
ion,
cer
ebra
l con
tusi
on
1017
prof
essi
onal
so
ccer
pl
ayer
no
no d
ata
Febr
uary
1998
dur
-in
g a
gam
e ye
s
enla
rged
hea
rt RC
A h
ypop
last
ic u
p to
1 m
m, a
scen
ding
aor
ta n
arro
wed
to
10
mm
, sub
acut
e di
ffuse
myo
card
itis,
sup
pura
nt to
nsill
itis,
ac
ute
pulm
onar
y an
d ce
rebr
al e
dem
a
1118
swim
min
g re
crea
tiona
llyno
no d
ata
June
200
2 du
ring
sw
imm
ing
yes
chro
nic
myo
peric
ardi
tis, c
ardi
ac
with
left
vent
ricul
ar fi
bros
is a
nd
myo
card
ial s
cars
, ane
urys
m o
f the
Lv
2 c
m in
dia
met
er, n
orm
al C
AA
, pu
lmon
ary
edem
a
MyOPERICARDITIS PNEuMONIA
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
26
CA
SEA
gE
PRO
FESS
ION
/Ex
ERC
ISE
SyM
PTO
MS
PhyS
ICA
L FI
ND
INg
/ EC
gLE
ThA
L Ev
ENT
RESu
SCI-
TATI
ON
FORE
NSI
C A
uTO
PSy
A R v D
524
stud
ent/
runn
erno
no d
ata
Janu
ary
2002
du
ring
train
ing
yes
ARv
D, a
cute
, pul
mon
ary
and
cere
-br
al e
dem
a
613
scho
ol b
oy /
soc
cer
play
er-c
adet
nono
dat
aSe
ptem
ber
2007
. du
ring
train
ing
yes
arrh
ythm
ogen
ic d
yspl
asia
of b
oth
vent
ricle
s, a
cute
pul
mon
ary
and
cere
bral
ede
ma
1214
phys
ical
ex
erci
se
in a
sch
ool
nono
dat
aO
ctob
er 2
001n
du
ring
phys
ical
ex
erci
seye
shy
popl
astic
aor
ta,
hypo
plas
tic C
AA
, pul
mon
ary
edem
a
1318
just
fini
shed
se
cond
ary
scho
ol –
w
orki
ng
at th
e si
te
gen
eral
tire
d-ne
ss
no d
ata
Dec
embe
r 200
1 »c
augh
t a c
old«
an
d fe
lt ex
haus
ted,
di
ed s
udde
nly
dur-
ing
wor
k
yes
norm
al h
eart
findi
ng, n
orm
al C
AA
, bi
late
ral p
neum
onia
, pos
sibl
e hi
gh
altit
ude
nonc
ardi
ogen
ic p
ulm
onar
y ed
ema,
cer
ebra
l ede
ma
1519
recr
eate
so
ccer
pl
ayer
no
no d
ata
Janu
ary
2002
in a
ho
spita
l 1 d
ay a
fter
deve
lopm
ent o
f se
psis
, sho
ck, D
IC,
acut
e re
nal f
ailu
re
yes
bila
tera
l pne
umon
ia, A
RDS,
dis
-se
min
ated
intra
vasc
ular
coa
gula
tion,
pu
lmon
ary
and
supr
aren
al b
leed
ing,
hy
popl
astic
righ
t cor
onar
y ar
tery
, m
yoca
rdia
l fibr
osis
, cer
ebra
l ede
ma,
1419
swim
min
g in
the
sea
nono
dat
aJu
ne 2
009
durin
g sw
imm
ing
yes
enla
rged
hea
rt: 4
50 g
, bila
tera
l liq
uido
thor
ax, b
lood
alc
ohol
leve
l 0.
17%
, pul
mon
ary
edem
a, s
ubm
er-
sio
BILAT BRONChOPNEuMONIA
Lege
nd: C
AA
=cor
onar
y ar
terie
s; L
v=
left
vent
ricle
; Rv
=rig
ht v
entri
cle;
Lv
h=l
eft v
entri
cula
r hyp
ertro
phy;
Iv
=int
erve
ntric
ular
; RC
A=r
ight
cor
onar
y ar
tery
, A
RvD
=arr
hyth
mog
enic
righ
t ven
tricu
lar d
yspl
asia
; A
MI=
acut
e m
yoca
rdia
l inf
arct
ion;
ARD
S=ad
ult r
espi
rato
ry d
istre
ssSy
ndro
me;
DIC
=dis
sem
inat
ed in
trava
scul
ar c
oagu
latio
n; h
CM
=hyp
ertro
phic
car
diom
yopa
thy.
Tabl
e 2.
Con
tinue
d
27
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
felt increased tiredness, stopped to swim for a few minutes, then swimmed once again, and then felt increased tiredness, collapsed and died. All reanimation efforts were unsuccessful including a Mobile Emergency Medical Unit. At the autopsy he had hypertrophic cardiomyopathy: by the criteria of gross pathological changes of cardiomegaly, left ventricular hypertrophy: 25 mm, with normal cavities of the who-le heart and normal coronary arteries. Histological findings of myocardium showed diffuse interstitial and replacement fibrosis, dysplasia of the tunica media of small vessels and contraction band and coagulate necrosis. He had acute pulmonary and cerebral edema.
Case 4. A basketball player-school boy aged 15, during a game in May 2000, he felt exhausted, and was standing at the site, watching the others playing basketball. Then he resumed training, jumped suddenly, put the hand on his chest, collapsed and died. All reanimation attempts were unsuccessful including attempts at the Re-gional University Hospital. A forensic autopsy finding showed hypertrophic cardi-omyopathy with interventricular septum of 40 mm and left ventricular wall of 17 mm. The left ventricle was not dilated. He had an acute pulmonary and cerebral edema.
Two young men: cases 5 and 6, suffered of arrhythmogenic right ventricular dysplasia.
Case 5. A male high degree short trails runner for years, aged 24, referred no cardiovascular or any other symptoms. During an athletic training in the morning in January 2002 he was running due to training and after short time suddenly co-llapsed and died. He was intubated and ventilated mechanically immediately by a physician at the field, and after that he was resuscitated by a medical team of the Re-animation Unit all the time during transport, to the Regional University Hospital. At the admittance he was unconscious,with anisocoric pupils, with no respirations, no heard heart sounds, with central cyanosis, and with flat line on an ECG monitor all the time during long unsuccessful resuscitation. The clinical diagnoses were: reanimatio facta, haemorrhagia cerebri suspecta, cardiomyopathia hypertrophica suspecta, sanguinatio ex ore, ventilatio mechanica, implantatio electrostimulatori cordis facta, dissociatio electromechanica. At the autopsy, the size of the whole he-art was 11 x 11 x 6.5 cm, the left ventricle wall reached 15 mm; both ventricles were dilated, with normal mitral, aortal, tricuspid and pulmonary valves and no signs of coronary or aortal atherosclerosis. Histological finding of the right ventricle wall showed abundant subepicardial accumulation of an adipose tissue with infiltration between myocardial bundles. The finding of the lungs and of the brain showed acu-te edema. The autopsy diagnoses were: dysplasia arrhythmogenes ventriculi dextri

Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
28
cordis, dilatatio cordis totius, oedema pulmonum et cerebri acutum, cyanosis uni-versalis.
Case 6. A soccer player as a cadet, aged 13, without any previous physical dis-comfort, suddenly collapsed and died during soccer training in the middle of Janu-ary 2002. He was resuscitated at the field by a coach and after that by a medical team of the Reanimation Unit, with no success. At autopsy, the size of the whole heart was 10 x 10 x 5 cm, the left ventricle wall reached 10 mm, the right ventricle wall 3 mm, both ventricles were dilated, with normal mitral, aortal, tricuspid and pulmonary valves and with no signs of coronary or aortal atherosclerosis. Histological finding of the myocardium showed abundant subepicardial accumulation of adipose and fibrotic tissues with segmental lymphocyte infiltration between bundles of both ventricles. The findings of the lungs and the brain showed acute edema. The autop-sy diagnoses were: dysplasia arrhythmogenes ventriculi dextri et ventriculi sinistri cordis, oedema cerebri grave, oedema pulmonum, cyanosis universalis.
In athletes died during training or during to competitive game in Croatia, the death rate is 0.19/100 000 yearly, in male population aged 15-40 who practiced physi-cal exercise 0.71/100 000, in total male population aged 15-64 who practice physical exercise reached 0.96/100 000.
The death rate of an arrhythmogenic right ventricular dysplasia what was a cause of death in two athletes reached 0.06/100 000.
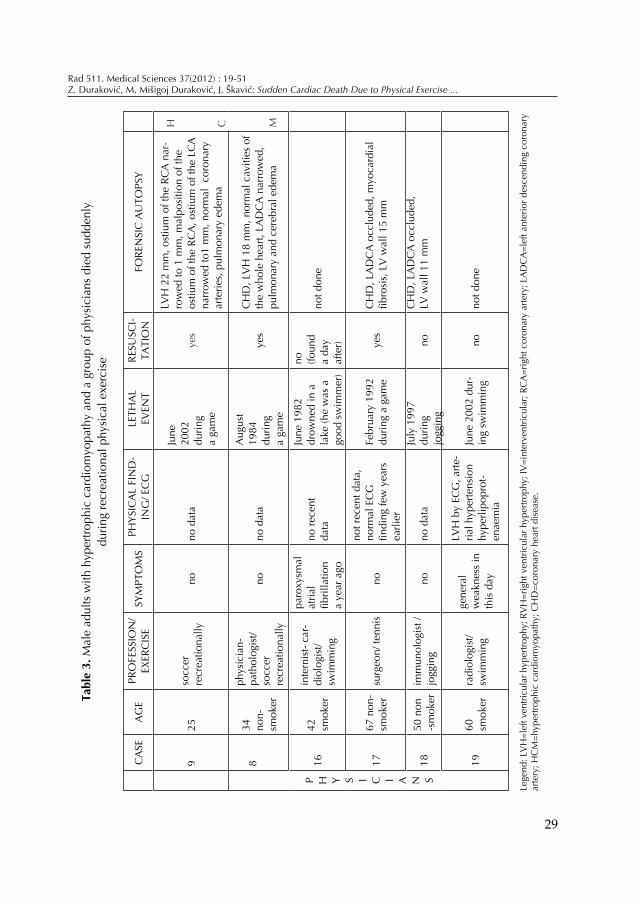
Five young men died because of hypertrophic cardiomyopathy, of which cases 3, 4 and 7 are presented in the Table 2, and cases, 8 and 9 in the Table 3. The death rate reached 0.10/100 000.
Case 7 (Table 2). The third athlete aged 18 was a school boy and professional soccer player. During a soccer game in May 2006 one player kicked his head with a ball. He felt general weakness with a short breath and he felt down. He was tran-sferred to the nearest University Hospital where he have been cured because of bilateral bacterial pneumonia, and died two days after admittance in a state of a septic shock, in spite of all therapeutic efforts. The autopsy showed hypoplastic as-cedenting aorta and biventricular hypertrophy. The left ventricular wall reached 20 mm, and normal cavities of the heart. The heart weight was amounting to 450 g. He had a large bilateral bacterial pneumonia, fibrinous pericarditis, cerebral contusions with edema and pointed bleeding.
Case 8 (Table 3) The fourth was a physician, cardiovascular pathologist aged 34, who played soccer twice a week recreationally. He was without any physical discomfort during physical exercise. In the evening in August 1984 during a soccer game, he did not feel well, went to a car and drived few hundred meters, than sto-
29
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
Tabl
e 3.
Mal
e ad
ults
with
hyp
ertro
phic
car
diom
yopa
thy
and
a gr
oup
of p
hysi
cian
s di
ed s
udde
nly
durin
g re
crea
tiona
l phy
sica
l exe
rcis
e
CA
SEA
gE
PRO
FESS
ION
/Ex
ERC
ISE
SyM
PTO
MS
PhyS
ICA
L FI
ND
-IN
g/ E
Cg
LETh
AL
EvEN
TRE
SuSC
I-TA
TIO
NFO
REN
SIC
Au
TOPS
y
925
socc
er
recr
eatio
nally
nono
dat
a
June
20
02
durin
g a
gam
e
yes
Lvh
22
mm
, ost
ium
of t
he R
CA
nar
-ro
wed
to 1
mm
, mal
posi
tion
of th
e os
tium
of t
he R
CA
, ost
ium
of t
he L
CA
na
rrow
ed to
1 m
m, n
orm
al c
oron
ary
arte
ries,
pul
mon
ary
edem
a
h C M
P h y S I C I A N S
834
no
n-
smok
er
phys
icia
n-pa
thol
ogis
t/ so
ccer
re
crea
tiona
lly
nono
dat
a
Aug
ust
1984
du
ring
a ga
me
yes
Ch
D, L
vh
18
mm
, nor
mal
cav
ities
of
the
who
le h
eart,
LA
DC
A n
arro
wed
,pu
lmon
ary
and
cere
bral
ede
ma
1642
sm
oker
inte
rnis
t- ca
r-di
olog
ist/
swim
min
g
paro
xysm
al
atria
l fib
rilla
tion
a ye
ar a
go
no re
cent
da
ta
June
198
2
drow
ned
in a
la
ke (h
e w
as a
go
od s
wim
mer
)
no (foun
d a
day
afte
r)
not d
one
1767
non
- sm
oker
surg
eon/
tenn
isno
not r
ecen
t dat
a,
norm
al E
Cg
fin
ding
few
yea
rs
earli
er
Febr
uary
199
2 du
ring
a ga
me
yes
Ch
D, L
AD
CA
occ
lude
d, m
yoca
rdia
l fib
rosi
s, L
V w
all 1
5 m
m
1850
non
-s
mok
erim
mun
olog
ist /
jogg
ing
nono
dat
aJu
ly 1
997
durin
g jo
ggin
gno
Ch
D, L
AD
CA
occ
lude
d,
Lv w
all 1
1 m
m
1960
sm
oker
radi
olog
ist/
swim
min
g
gene
ral
wea
knes
s in
th
is d
ay
Lvh
by
ECg
, arte
-ria
l hyp
erte
nsio
n hy
perli
popr
ot-
enae
mia
June
200
2 du
r-in
g sw
imm
ing
nono
t don
e
Lege
nd: L
vh
=lef
t ven
tricu
lar h
yper
troph
y; R
vh
=rig
ht v
entri
cula
r hyp
ertro
phy;
Iv=i
nter
vent
ricul
ar; R
CA
=rig
ht c
oron
ary
arte
ry; L
AD
CA
=lef
t ant
erio
r des
cend
ing
coro
nary
ar
tery
; hC
M=h
yper
troph
ic c
ardi
omyo
path
y; C
hD
=cor
onar
y he
art d
isea
se.

Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
30
pped, step out from a car, collapsed and died. All reanimation efforts were unsucce-ssful, including reanimation attempts in a nearest hospital – Regional Army Hos-pital. The forensic autopsy finding showed left ventricular hypertrophy of 18 mm, with no dilatation of the left ventricular cavity. Left descending coronary artery was narrowed. He had an acute pulmonary and cerebral edema.
Case 9 (Table 3). The fifth aged 25, played soccer recreationally. During an eve-ning game in January 2005 in a sport hall, he suddenly collapsed and died. All reanimation attempts at the field were unsuccessful including a Mobile Emergency Medical Unit. The autopsy showed left ventricular hypertrophy of 22 mm and right ventricular hypertrophy of 7 mm, with normal cavities of the whole heart. The left and the right coronary arteries were narrowed at the ostial places to 1 mm (hypo-plastia ostii arteriarum coronariarum cordis with malposition of the ostium of the right coronary artery). He had emphysema of the left pulmonary wing. He had an acute pulmonary and cerebral edema.
The data of three cases suffered of myopericarditis: two athletes and one engaged in recreative physical exercise are presented in Table 2 (case 7, case 10 and case 11).
Case 7. A school boy, aged 18, died suddenly during swimming is presented abo-ve as he had HCM, but also fibrinous pericarditis and large bilateral pneumonia.
Case 10. A professional soccer player, aged 17, was without symptoms. During regular training in February 1998 in a training hall, he suddenly collapsed and died. All reanimation attempts, including electrical defibrillation due to ventricular fi-brillation repeated many times, were unsuccessful. An autopsy finding showed an enlargement of the whole heart hypoplastic right coronary artery, narrowed ascen-ding aorta of 10 mm (normal finding at the ascending aorta reached 3.09 ± 0.41 cm), the thickness of the left ventricular wall was 18 mm, acute bacterial tonsillitis, and subacute diffuse myopericarditis.
Case 11. A school boy, aged 18 died suddenly during swimming. Resuscitation attempts were unsuccessful. An autopsy showed chronic myopericarditis and car-diac aneurysm of the left ventricle.
In this group of persons suffered of myopericarditis the death rate reached 0.10/100 000.
Ten teenagers-school boys who died during sports or recreative physical exercise are presented in theTable 2. Three of them presented before, died during sports acti-vities: cases 4, 6 and 10. Seven teenagers died suddenly during recreational physical activities: cases 2, 7, 11, 12, 13, 14 and 15. The first was a school boy aged 17 (case 2) who was doing recreational physical exercise few times a week, without any com-

31
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
plaints. Few years before the incident, by the data of his family, a systolic murmur above the heart was discovered, with no written data about it. They told that the cardiac echosonography showed normal finding. Few days before the incident he has had a chest pain and a short breath. On a day of the incident in September 2010 he was running on a street, felt down and died. He was resuscitated on a street unsuccessfully. The forensic autopsy showed an enlargement of the heart reached 390 grams, thickening of the left ventricular wall of 19 mm (normal finding up to 12 mm), with normal thickness of the right ventricle: 3 mm, the aortic diameters were wide and reached 5.1 cm, and narrowing of the descending part of the aortic arch.
The second was a boy aged 14, who was engaged in regular physical activities in a school and died suddenly during exercise: a hypoplastic aorta and hypoplastic coronary arteries were found (case 12).
The third was 15 years old boy who died while playing basketball in school had hypertrophic cardiomyopathy, (case 4, presented above). The fourth victim, the 18 years old adolescent (case 13), had normal heart finding, bilateral pneumonia and possible high altitude noncardiogenic pulmonary edema. He was hospitalized in an Intensive Care Unit and dying after 24 hours. The fifth boy, aged 18, who died during recreational swimming, had signs of chronic myopericarditis with an ane-urysm of the left ventricle (case 11). The mechanism for the lethal event in all five cases was probably malignant ventricular arrhythmia. The sixth boy – soccer player recreationally, aged 18, with hypoplastic ascending aorta, has been kicked in a chest during a game and died in a hospital due to bronchopneumonia (case 7). The se-venth teenager aged 19, had cardiomegaly and sunk probably as a consequence of alcohol drink intake (case 14).
In male school boys in Croatia the death rate during physical exercise reached 0.37/100 000 yearly.
Three teenagers died during physical exercise of pneumonia. The first aged 18, smoker, just finished a secondary school and started to work recreatively at the site (case 13). The second aged 19 was a student who played soccer recreatively (case 15). In January 2002 he played soccer and few hours after a game he felt several pains in his left hip and leg and he developed high body temperature: 40oC. He left to the hospital at the other day. At the admittance he was septic and died one day later in spite of all therapeutic effort including antibiotics, inotropic drugs, fresh frozen plasma, coagulation factors, mechanic ventilation etc. The clinical diagnoses were: septic shock, adult respiratory distress syndrome, disseminated intravascular coa-gulation, acute renal failure. The forensic autopsy showed adult respiratory distress syndrome, disseminated intravascular coagulation, multiple pulmonary and supra-renal bleeding, hypoplastic right coronary artery, myocardial fibrosis and acute ce-

Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
32
rebral edema. Histological finding showed bilateral bacterial pneumonia. The third aged 18 was a school boy and professional soccer player. He didn’t com-
plain of any discomfort during physical exercise (case 7). In this period, five physicians specialists (one younger, three middle aged and one
elderly) died suddenly during recreational physical exercise. In three of them a fo-rensic autopsy was performed. All three had coronary heart disease; two of them left ventricular hypertrophy also. In all three left descending anterior coronary ar-tery was atherosclerotic, with stenosis in one and occlusion in two. In one of them myocardial scars of two past myocardial infarctions were found. In no one acute myocardial infarction was found, so that obviously malignant ventricular arrhyt-hmia was a cause of death. Two of them had a thickness of the left ventricle 15 and 18 mm. The main characteristics of them are presented in Table 3.
If 15% of male physicians specialists in Croatia are involved in recreate physical exercise (out of a total number of 4.957), the death rate reached 24.8/100 000.
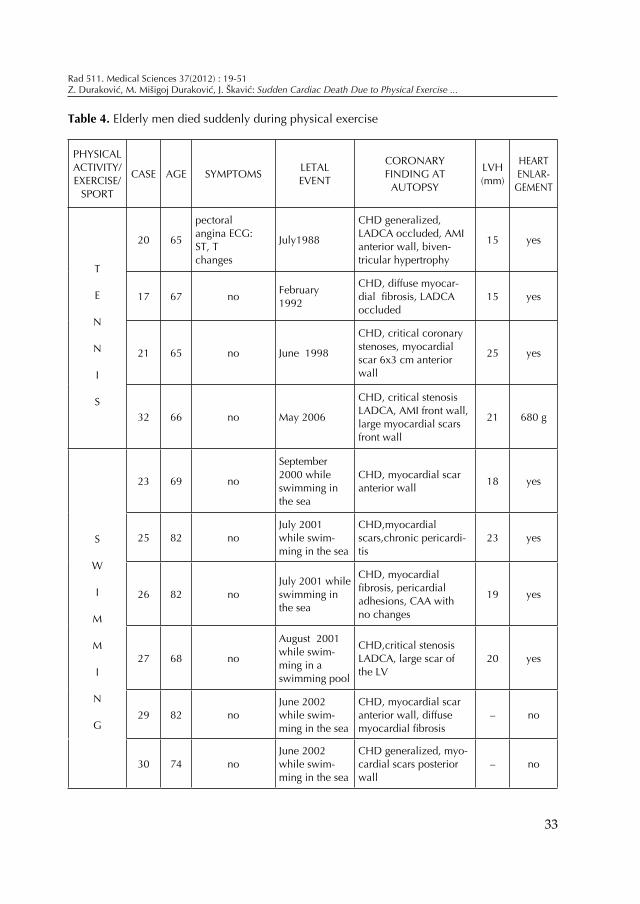
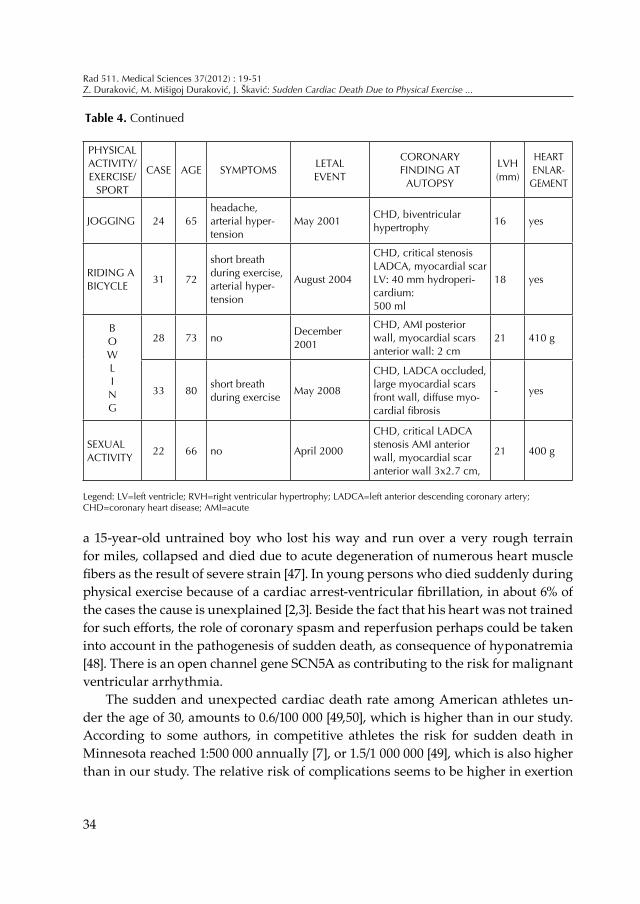
Fifteen men aged 65 to 82 years, died due to physical exercise: 6 were engaged in swimming, 4 in tennis, one ridded, one was jogging, 2 bowling and one died during sexual act. One had symptoms of pectoral angina, 2 suffered from arterial hyper-tension, one accompanied by headache, and 2 had short breath during exercise due to congestive heart failure. Eleven were without symptoms. At autopsy, 14 had coro-nary heart disease, 5 had critical coronary artery stenosis, and 2 of them had signs of recent myocardial infarction, 3 had occluded left descending anterior coronary artery, one with acute myocardial infarction of the anterior wall, 12 had scars due to previous myocardial infarctions and one signs of diffuse myocardial fibrosis. In 12 of them left ventricular wall reached 15-23 mm. The characteristics of elderly men who died suddenly during or immediately after recreational physical exercise are presented in Table 4.
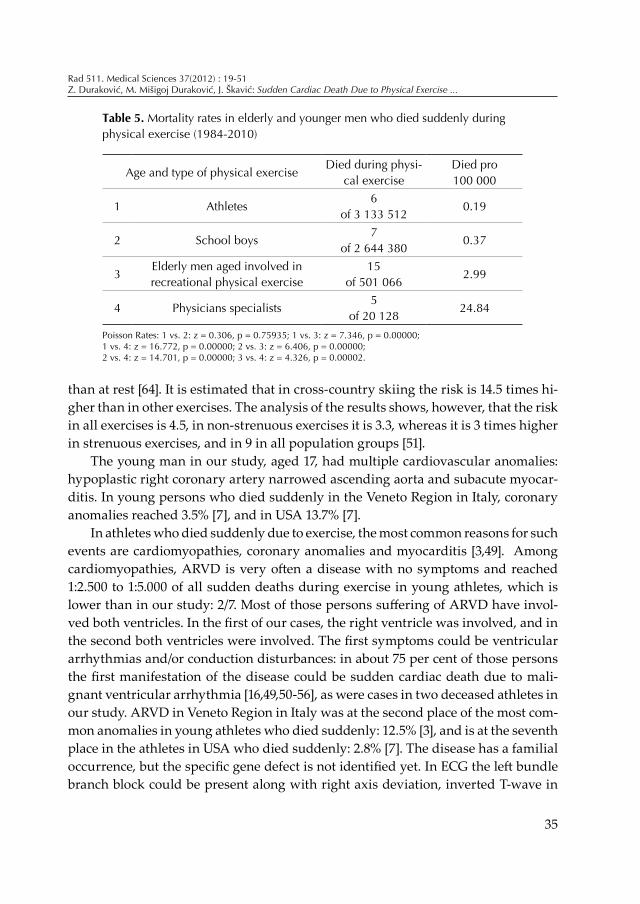
The mortality rates in elderly and younger men died suddenly during physi-cal exercise are presented in Table 5. The reported deaths show that recreational physical exercise in elders reached 2.99/100 000, a higher incidence than the entire male population aged 15-64, engaged in recreational physical exercise: 0.96/100 000 (p=0.00001). That is a higher incidence than in the male population aged 15-40 enga-ged in physical exercise: 0.71/100.0000 (p=0.00001). This incidence is higher than in young athletes: 0.19/100 000 (p=0.00000).
dIScuSSIon
Sport activities have protecting effect on human organism. Sudden death in ap-parently healthy persons engaged in physical exercise is very rare. One subject was
33
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
Table 4. Elderly men died suddenly during physical exercise
PhySICAL ACTIvITy/ExERCISE/
SPORT
CASE AgE SyMPTOMS LETAL EvENT
CORONARy FINDINg AT
AuTOPSy
Lvh(mm)
hEART ENLAR-
gEMENT
T
E
N
N
I
S
20 65
pectoral angina ECg: ST, T changes
July1988
ChD generalized, LADCA occluded, AMI anterior wall, biven-tricular hypertrophy
15 yes
17 67 no February1992
ChD, diffuse myocar-dial fibrosis, LADCA occluded
15 yes
21 65 no June 1998
ChD, critical coronary stenoses, myocardial scar 6x3 cm anterior wall
25 yes
32 66 no May 2006
ChD, critical stenosis LADCA, AMI front wall, large myocardial scars front wall
21 680 g
S
W
I
M
M
I
N
g
23 69 no
September 2000 while swimming in the sea
ChD, myocardial scar anterior wall 18 yes
25 82 noJuly 2001while swim-ming in the sea
ChD,myocardial scars,chronic pericardi-tis
23 yes
26 82 noJuly 2001 while swimming in the sea
ChD, myocardial fibrosis, pericardial adhesions, CAA with no changes
19 yes
27 68 no
August 2001while swim-ming in a swimming pool
ChD,critical stenosis LADCA, large scar of the Lv
20 yes
29 82 noJune 2002 while swim-ming in the sea
ChD, myocardial scar anterior wall, diffuse myocardial fibrosis
– no
30 74 noJune 2002 while swim-ming in the sea
ChD generalized, myo-cardial scars posterior wall
– no
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
34
a 15-year-old untrained boy who lost his way and run over a very rough terrain for miles, collapsed and died due to acute degeneration of numerous heart muscle fibers as the result of severe strain [47]. In young persons who died suddenly during physical exercise because of a cardiac arrest-ventricular fibrillation, in about 6% of the cases the cause is unexplained [2,3]. Beside the fact that his heart was not trained for such efforts, the role of coronary spasm and reperfusion perhaps could be taken into account in the pathogenesis of sudden death, as consequence of hyponatremia [48]. There is an open channel gene SCN5A as contributing to the risk for malignant ventricular arrhythmia.
The sudden and unexpected cardiac death rate among American athletes un-der the age of 30, amounts to 0.6/100 000 [49,50], which is higher than in our study. According to some authors, in competitive athletes the risk for sudden death in Minnesota reached 1:500 000 annually [7], or 1.5/1 000 000 [49], which is also higher than in our study. The relative risk of complications seems to be higher in exertion
PhySICAL ACTIvITy/ExERCISE/
SPORT
CASE AgE SyMPTOMS LETAL EvENT
CORONARy FINDINg AT
AuTOPSy
Lvh(mm)
hEART ENLAR-
gEMENT
JOggINg 24 65headache, arterial hyper-tension
May 2001 ChD, biventricular hypertrophy 16 yes
RIDINg A BICyCLE 31 72
short breath during exercise, arterial hyper-tension
August 2004
ChD, critical stenosis LADCA, myocardial scar Lv: 40 mm hydroperi-cardium:500 ml
18 yes
BOWLINg
28 73 no December 2001
ChD, AMI posterior wall, myocardial scars anterior wall: 2 cm
21 410 g
33 80 short breath during exercise May 2008
ChD, LADCA occluded, large myocardial scars front wall, diffuse myo-cardial fibrosis
- yes
SExuAL ACTIvITy 22 66 no April 2000
ChD, critical LADCA stenosis AMI anterior wall, myocardial scar anterior wall 3x2.7 cm,
21 400 g
Table 4. Continued
Legend: Lv=left ventricle; Rvh=right ventricular hypertrophy; LADCA=left anterior descending coronary artery; ChD=coronary heart disease; AMI=acute
35
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
than at rest [64]. It is estimated that in cross-country skiing the risk is 14.5 times hi-gher than in other exercises. The analysis of the results shows, however, that the risk in all exercises is 4.5, in non-strenuous exercises it is 3.3, whereas it is 3 times higher in strenuous exercises, and in 9 in all population groups [51].
The young man in our study, aged 17, had multiple cardiovascular anomalies: hypoplastic right coronary artery narrowed ascending aorta and subacute myocar-ditis. In young persons who died suddenly in the Veneto Region in Italy, coronary anomalies reached 3.5% [7], and in USA 13.7% [7].
In athletes who died suddenly due to exercise, the most common reasons for such events are cardiomyopathies, coronary anomalies and myocarditis [3,49]. Among cardiomyopathies, ARVD is very often a disease with no symptoms and reached 1:2.500 to 1:5.000 of all sudden deaths during exercise in young athletes, which is lower than in our study: 2/7. Most of those persons suffering of ARVD have invol-ved both ventricles. In the first of our cases, the right ventricle was involved, and in the second both ventricles were involved. The first symptoms could be ventricular arrhythmias and/or conduction disturbances: in about 75 per cent of those persons the first manifestation of the disease could be sudden cardiac death due to mali-gnant ventricular arrhythmia [16,49,50-56], as were cases in two deceased athletes in our study. ARVD in Veneto Region in Italy was at the second place of the most com-mon anomalies in young athletes who died suddenly: 12.5% [3], and is at the seventh place in the athletes in USA who died suddenly: 2.8% [7]. The disease has a familial occurrence, but the specific gene defect is not identified yet. In ECG the left bundle branch block could be present along with right axis deviation, inverted T-wave in
Table 5. Mortality rates in elderly and younger men who died suddenly during physical exercise (1984-2010)
Age and type of physical exerciseDied during physi-
cal exercise Died pro100 000
1 Athletes6
of 3 133 5120.19
2 School boys7
of 2 644 3800.37
3Elderly men aged involved in recreational physical exercise
15of 501 066
2.99
4 Physicians specialists5
of 20 12824.84
Poisson Rates: 1 vs. 2: z = 0.306, p = 0.75935; 1 vs. 3: z = 7.346, p = 0.00000; 1 vs. 4: z = 16.772, p = 0.00000; 2 vs. 3: z = 6.406, p = 0.00000; 2 vs. 4: z = 14.701, p = 0.00000; 3 vs. 4: z = 4.326, p = 0.00002.
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
36
the right precordial leads and with ventricular premature beats, and after that with ventricular tachycardia. The right ventricular enlargement could be present, and the left ventricular enlargement is present in 50%. The right ventricular wall is rela-tively thin, and that is why in ARVD a subepicardial process is sometimes difficult to diagnose in vivo. Pathological anatomy finding depends on the stage of the dise-ase and show changes in the myocardium including thinning in the some areas of the right ventricle with fibro-fatty changes [16,19,53,56-58]. Sometimes we are facing with an aneurysm of the right ventricle in a small number of these cases.
The etiology of ARVD is unknown. We are facing very often with a presence with inflammatory myocardial infiltrates and progression from myocarditis to ARVD, and also with the discovery of the mutation in genes related to desmosomes. There is an open question: could it be an inflammatory process modified by genetic influence in desmosome-related proteins [16]. This is an autosomal dominant hereditary disease in almost 50 per cent of all cases with variable penetrance [20], and could be located to various chromosomes [17,18], the first to chromosome 14q23-q24.
ARVD is uncommon under ten years of age, and rare appeared in the elderly [57,58]. By the Task Force criteria of this disease [32], the following criteria are neces-sary for definitive diagnosis of this disease: two major, or one major plus two minor, or 4 minor criteria; the borderline diagnosis consists of one major plus one minor, or three minor criteria; the possible diagnosis consists one major, or two minor criteria from different categories. The ECG showing an epsilon wave indicating ARVD, whi-ch is presented in only 33 per cent of patients suffering of ARVD [18,59,60]. Our two present young athletes we could not use the mentioned criteria, because they were without symptoms and died suddenly at the field during training.
Among cardiomyopathies by some data, HCM reached 0.2% of population [31]. HCM has variable thickening of the septum and the left ventricular wall and dif-ferent clinical presentations. It could be obstructive forms of HCM (in about 30%) and non-obstructive forms (in about 60%), and in additional 10%, obstruction could be presented due to vigorous physical exercise [61]. There is no strong correlation between the degree of HCM and subjective symptoms [62-64]. Sometimes it is not easy to clinically distinguish physiological myocardial hypertrophy from HCM in athletes. Ventricular thickness more than 18 mm (sometimes 15), implies criteria for HCM.
The HCM reached 5% in the young in the Veneto Region in Italy [65], and it is at the first place of all causes of death during physical exercise in young athletes in USA: 26.4% [7]. It reached 0.1-0.2% in the population in USA, but it is a cause of sudden and unexpected cardiac death of competitive athletes in more than 50% [63]. The disease could be asymptomatic and the first manifestation could be sudden
37
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
cardiac death. These data were present in 2 athletes in our study and the death rate reached 0.06/100 000.
It is known that a magnitude of left ventricular or septal hypertrophy leads to high risk for sudden cardiac death and is a strong independent predictor to progno-sis. The risk of sudden cardiac death raised progressively with left ventricular wall thickness: if LVH reached up to 19 mm, a risk for sudden death is low, but LVH of 30 mm or more doubled the risk of sudden cardiac death [66]. In those five presented cases of HCM in our study, a heavy obstructive form of HCM was seen in a school boy aged 15, with no previous symptoms, who died suddenly, i.v. septum reached 40 mm. It confirms the rule that extreme LVH are seen in the youngest with mild or no symptoms [66]. In other two athletes died suddenly, LVH reached 20 and 25 mm. In two of our persons engaged in physical activities recreationally and died suddenly, LVH reached 18-22 mm, in spite of the opinions that in persons with mild or moderate LVH the risk is low.
A sudden cardiac death due to physical exercise in young athletes in Croatia suf-fered of HCM reached 0.06/100.000 yearly (p=0.00000), in all young athletes suffered of other heart diseases reached 0.19/100 000 (p=0.00000), and in the total male popu-lation aged 15-40 engaged in sports and recreational physical exercise: 0.71/100.0000. In preparticipation screening for HCM, a familial history data have to be included especially to sudden cardiac death (it could be negative), personal symptoms in-cluding recurrent exertion syncope, physical examination by physician (it could be normal finding in most of these patients), an ECG (it could be non-specific), LVH by echocardiography (<19 mm=low risk, >30 mm=high risk), and 24 h ECG- Holter (malignant ventricular arrhythmias).
The article deals with the aspects of interrelationship between physical exercise and different types of myopericarditis in young male athletes. In the Veneto Region, myocarditis was at the third place as the cause of death in athletes during physical exercise reaching up to 7.5% [65]. In our study the rate was 0.11/100 000 compared to 0.19/100 000 in young athletes [11] who died due to all cardiac reasons during exercise.
Myocarditis reached 7.5% in the Veneto Region [65], and was at the 3-rd place as a cause of death rate in athletes during physical exercise, in our study: 0.11 /100 000. In general Croatian population aged 15-40 who practice physical exercise, the death rate reached 0.71/100 000. This means that athletes obviously are protected from cardiovascular events.
Myopericarditis could lead to malignant ventricular arrhythmia and sudden cardiac death. Acute viral infections of the upper respiratory tract can diminish iso-metric myocardial strength for 15% [31,49]. In such cases, diminution of enzymatic

Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
38
myocardial activity [46] and abnormality of myocardial structure could be detected by electronic microscopy in samples of repeated myocardial biopsies. In Croatia, Medved et al. [67] were the first who described a case report dealing with a sudden cardiac death due to chronic myopericarditis in athlete, aged 29, a professional so-ccer player who had clinical signs of heart enlargement and frequent left ventricular premature beats. He refused to follow the physicians’ advices to stop with compe-titive matches. During a game, he suddenly felt ill, suddenly collapsed and died in spring 1973. He was resuscitated, transferred to the nearest hospital but died in transit. Forensic autopsy showed chronic myopericarditis, LVH of 15 mm, the right ventricle wall reached 5 mm; the initial part of the aorta was narrowed, and with enlargement of the whole heart.
Physical exercise is contraindicated in different types of myopericarditis for at least six months. When to restart training depends on the disappearance of subjecti-ve symptoms, on the normalization of clinical state and biochemical parameters, i.e. double viral titers, on the normalization of electrocardiographic finding in a 24-hour electrocardiogram, and on electrocardiographic and echocardiography scans at rest and during exercise (stress). Sometimes in specific cases other procedures are needed: radionuclide studies, cardiac catheterization and magnetic resonance imaging.
Many possibilities exist in defining an exertion-related sudden cardiac death. The time period needed for the cardiovascular system to return to resting steady state varies with many factors such as the type, intensity and duration of the activi-ty, and the health status and physical condition of the individual. Thus, it is not easy to define exactly what are an exertion- related death and especially a sudden death caused by exercise. Some researchers count only deaths during or immediately after the cessation of exercise as exercise-related deaths, while some authors include also deaths that had occurred 30 minutes, 60 minutes or even more after the exercise [51,68]. According to our data the rate of sudden and unexpected death during or after recreational physical exercise was 0.37/100 000 per year in boys in or immedi-ately after secondary schools in Croatia. This is lower incidence than in other age groups in Croatia. For example the rate of sudden and unexpected death during or after physical exercise in male physicians-specialists was much higher than in adolescents: 24.8/100 000, and also higher than in men aged 15-40: 0.71/100 000 per year in Croatia, in men aged 15-64 years: 0.96/100 000 per year, and in the elderly: 2.99/100,000 per year [8]. Although the incidence of sudden unexpected death in the school boys was low, our findings bring up once again the question, whether some or all of these incidents could have been prevented. None of the boys had reported any noticeable symptoms at exertion. However, all of them suffered from chronic or acute cardiac or other diseases: two had congenital hypoplasia of the coronary

39
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
arteries, one together with narrowing of the ascending aorta and subacute myocar-ditis, one had HCM, one had a chronic myopericarditis with a left ventricular ane-urysm. In one young man the heart findings were normal, but there was bilateral pneumonia and possible non-cardiogenic pulmonary and cerebral edema. This 18 years old adolescent was badly nourished, skinny, exhausted because of flu, and possibly dehydrated. The possible cause of death might have been hyponatremic en-cephalopathy with consecutive non-cardiogenic pulmonary edema during bilateral pneumonia. Non-cardiogenic pulmonary edema could be a clinical manifestation of hyponatremic encephalopathy [48]. The most common abnormalities of young per-sons who have died suddenly during or after physical exercise have been found to be hypertrophic cardiomyopathy (especially in young competitive athletes, 36%) or congenital coronary anomalies [6,69,70]. In Italy (Veneto region) in a 17-year period (1979–1996) among 49 competitive young athletes (44 male and 5 female) who died suddenly, hypertrophic cardiomyopathy was observed in only one subject or 2% in autopsy [71], and coronary anomalies in 18% of the victims. In a Swedish study [2], in a period of 14 years, 16 sudden and unexpected cardiac deaths among young orienteer’s aged 18–27 years (15 male and one female) were found. Six had acute myocarditis, four ARVD, and two had healed myocarditis. This data demonstrates that the causes of sudden death of young athletes at exertion can vary greatly in di-fferent countries and athletic populations. The most common mechanism for lethal event is ventricular fibrillation. The most difficult problem is that cardiac disease in young persons is usually not recognized prior to death, as was the case also in our study. An American study [7] suggests that a person can begin a gradual exercise program without consulting a physician, if the answer is no to the following que-stions: 1) history of heart trouble; 2) heart murmur, 3) heart attack, 4) arterial hyper-tension; 5) diabetes mellitus, 6) arthritis; 7) family history of premature coronary heart disease; 8) exercise-related shortness of breath, faintness, dizziness, or pain or pressure in the chest, neck, shoulder or arm. In order to give reliable answers to these questions, information from prior medical examinations are often needed [16]. Carefully collected anamnestic data with special attention to personal and familial (parental sudden death) cardiovascular history, personal physical examination, an electrocardiogram at rest, and especially an echocardiography study on the basis of other information are essential in every potential athlete or in suspicious cases.
Echocardiography is today a standard non-invasive cardiac investigation especi-ally in screening of congenital heart diseases. A 12-lead electrocardiogram is the most valuable preparticipation cardiovascular modality of these three mentioned methods at the beginning, and an echocardiography is a superior method for detecting con-genital cardiovascular anomalies. However, it cannot be considered as a large-scale
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
40
screening examination of symptomless individuals because of the equipment and expertness needed and also because of diagnostic uncertainties. Echocardiography can give a false positive finding e.g. in borderline thickness of the left ventricle or in dilated heart cavities. A false negative finding can occur in cases of HCM which might not be detectable until the adolescent period [7]. Detection of premonitory cardiac symptoms such as shortness of breath, history of exertion syncope or chest pain, has to lead to diagnostic procedures such as ergometry, thallium stress test, ec-hocardiography and coronarography especially in competitive athletes [6]. Physical exercise is contraindicated in a case of acute infection, especially a respiratory one. In this report the cause of death was an acute respiratory infection, in one previously healthy adolescent. In another boy with hypoplastic aorta and coronaries and suba-cute myocarditis, a respiratory infection probably was a trigger. Thus, examination of the anamnestic and autopsy findings in the six cases of this data suggests that avoidance of heavy exertion at the time of respiratory infection (cases 7 and 10) and thorough preparticipation physical examination and indicated diagnostic tests (cases 3 and possibly 5) could have helped in avoiding the fatal event.
This study deals also with the aspects of the interrelationship between physical exercise and acute respiratory tract infections in young male athletes also. All three presented teenagers athletes suffered of bacterial pneumonia. Two of them had car-diovascular diseases: one aged 19 had hypoplastic right coronary artery and myo-cardial fibrosis and the other aged 18 had HCM and hypoplastic ascending aorta. Pneumonia as a cause of sudden cardiac death during physical exercise is very rare [11]. In Swedish study during 14 years, 15 young men and one young woman died during exercise [1]. By some authors HCM is the most frequent causes of death in yo-unger subjects [49,72]. HCM was an uncommon cause of death in young competitive athletes: in Veneto region in Italy, 49 sudden death in athletes were registered from 1979-1996, of which 12.2% had anomalous origin of a coronary artery and only 2.0% had HCM [3]. In distinguishing physiological myocardial hypertrophy from HCM, we are facing with the next criteria: normal values of ventricular thickness reached 11 mm, borderline values between 11-13 mm and thickness for HCM above 15 mm. These data was present in one athlete in our study.
Two of presented cases had multiple cardiovascular anomalies and acute bacte-rial pneumonia at the same time. One had hypoplastic aorta with subacute diffuse myopericarditis. The other had hypoplastic right coronary artery. Coronary artery hypoplasia is an infrequent disease and could be associated with sudden cardiac death as could be narrowness of the ascending aorta or hypoplastic aorta. These result differ by different authors: in young persons who died suddenly in the Veneto Region in Italy, coronary anomalies reached 3.5% [7], and in 13.7% in USA [7].

41
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
Myocarditis possibly related to exercise during the febrile phase of a viral illness could be the reason for sudden death [49,72], especially when it is connected with the narrowing of the ascending aorta as was the case in one teenager in our study.
In Croatia the death rate including all reasons among athletes reached 0.19/100 000. The sudden and unexpected cardiac death rate among USA athletes below age of 30 amounts 1.6/100 000, which is higher than in our study. In Minnesota that rate reached 0.2/100 000 or 0.46/100 000 annually which is also higher than in our study [6,9].
From a study in USA [9], 122 sudden death due to physical exercise were descri-bed among 21.481 male physicians or 41/7.176 every four years, which is also higher than in our study.
The relative risk of cardiovascular complications is higher in exercise than at rest: cross-country skiing is 14.5 times higher than in other exercises. The risk in strenuous exercise is 4.5 times higher than in non-strenuous exercise [51]. In litera-ture we were unable to find data of mortality rate during bacterial pneumonia in athletes during training. Physical exercise is contraindicated in acute respiratory tract infections. In all three present cases acute bacterial pneumonia had been a cause of death. When to start with physical training after pneumonia depends on disappearing of clinical signs of pneumonia, normalization of body temperature, disappearing of pulmonary infiltrate by chest X-ray or local signs of tonsillitis and regional physical finding i.e. an enlargement of lymphatic nodes, of C-reactive pro-tein and erythrocyte sedimentation rate, and normalization of white cell count.
A medical checkup before recreational physical exercise is essential including a clinical examination, a serum concentration of risk factors and other risk factors, an electrocardiogram at rest, a stress test and echocardiography studies in clinical indi-cation, and medical controls in persons taking exercise. It has to be done every three years in that aged 40 and more who are without symptoms. It has to be done every two years in those aged 35 and more with one or more risk factors for atherosclerosis – coronary heart disease, in persons with suspect cardiac, pulmonary or metabolic disease. A medical check-up has to be done once a year in those with known cardiac, pulmonary or metabolic disease or with positive stress test previously regardless of their age [41,66,69,71]. This study shows that medical evaluation is important becau-se of the underlying problems such as sudden death during exercise. In non-trained persons and in the elderly a physical exercise should be recommended of a gradu-ally intensity, which could not exceed 6 METs (1 MET = 3.5 ml O2/kg/min).
In this study the aspects of the interrelationship between recreational physical exercise and cardiovascular risks in five physicians are presented. Three of them were autopsied and in all coronary heart disease was found, with no signs of an

Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
42
acute myocardial infarction. In two a LVH was found which could be an important risk factor for a malignant arrhythmia. In two who were not been autopsied, an alcohol cardiomyopathy was probably a reason for malignant arrhythmia. One had atrial fibrillation one year before sudden death. The other had arterial hypertension also, an excessive hyperlipoproteinaemia, and probably a silent myocardial ische-mia due to coronary heart disease. Atherosclerosis is silent until critical stenosis, coronary thrombosis (observed in three physicians in this study); embolus or coro-nary dissection or aneurysm supervenes. Sudden cardiac death could sometimes be the first sign of coronary disease (in over 25 per cent), precipitated by excessive physical exercise, what was observed in five presented physicians. LVH, presented in two of three autopsied physicians, is often connected with arterial hypertension. In LVH there is also an imbalance between myocardial supply and requirements. This disease is very often a silent cardiovascular risk factor and could have impor-tant prognostic implications [25,41,51].
Sudden death in apparently healthy persons who are engaged in physical exer-cise is extremely rare. When cardiovascular incidents occur during exercise, the most frequent cause is an organic heart or vascular disease [25,36-40,51,73-76]. One should always bear in mind the fact that a great number of persons with coronary disease engage in physical exercise, and only a few have any discomfort. These data are supported by the analysis of the health- related condition of the Croatian population [25,36-41]: the so-called healthy persons of both genders aged 65–84 have 6 diagnoses on the range 0–17, including cardiovascular diseases. The relati-ve risk of cardiovascular complications seems to be higher in exertion than at rest [25,36-41,51]. The relative risk of sudden death during up to 30 minutes of vigorous exercise reached 16.9, and absolute risk is low: 1/1,510,000.
Fifteen of 69 died persons from this study were aged 65 or over. Eleven of those persons did not have any previous cardiovascular symptoms, and they had not had any medical record in the recent years before the accident. In this group, in all but one coronary heart disease was the cause of death. In accordance with the literature, when cardiovascular incidents occur during physical exercise in elders, the most frequent cause of sudden death is coronary heart disease [11,42,75,76].
People engaged in physical exercise have a lower risk of cardiovascular compli-cations than inactive persons. Exercise is thus an important component of healthy living for the senior citizens. It has been evidenced that physical exercise positively affects maintenance and promotion of health. Physical activity should be controlled, regular and adapted to the health condition [6]. The medical check-ups before exer-cise are essential, as well as medical control over persons taking exercise [76-80].

43
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
Physical exercise of an biologically elderly person may make a heart less sta-ble; could actually increase chances for arrhythmia; it does bring protection aga-inst heart attack, but this protection is gained and lost rapidly. In elderly it is ne-cessary to have an activity plan for preventive and therapeutic recommendations [11]. Most of the elderly could be active physically. In most of the elderly capable to exercise recommendations is moderate aerobic physical exercise for 30 minutes, 5 times a week, or vigorous activity (such as jogging) for 20 minutes three times a week [79,80].
In Croatia, about 7 per cent of the entire male population undertakes recreatio-nal physical exercise. The reported deaths reveal that low or moderate recreational physical exercise in elders reached 2.99/100 000, a higher incidence than the entire male population aged 15-64 engaged in recreational physical exercise: 0.96/100 000 yearly. That is a higher incidence than in the total male population aged 15-40, en-gaged in physical exercise in Croatia: 0.71/100.0000, with the significant difference (p=0.00001). It is also a higher incidence than in athletes suffering from acute bacte-rial pneumonia or suppurant tonsillitis, a higher incidence than in young athletes: 0.19/100 000 [17], and the difference is significant (p=0.00005). LVH of 15-25 mm was found in 12/15 indicating an underlying risk of untoward cardiovascular events in elderly persons without symptoms.
The prevalence of sudden death almost exclusively in males is probably con-sequence of two factors: males are doing heavier physical exercise than women, and coronary heart disease is more frequently presented in males.
By the recommendations of the American College of Sports Medicine and the American Heart Association [78], the exercise test is not necessary for asymptomatic persons before starting with a low or moderate level of physical exercise and there is no need for an examination of a physician. Persons with symptoms or with diagno-sed cardiovascular disease(s), arterial hypertension, diabetes mellitus or some other chronic disease, have to consult a physician before physical exercise especially vigo-rous one. But our results does not go to this direction: by our experiences only 4 out of 15 elderly men who practiced low or moderate physical exercise had symptoms of cardiovascular disease. When cardiovascular incidents occur during physical exer-cise in elders, the most frequent cause of sudden death is coronary heart disease. In 14 out of 15 presented elderly men who died suddenly during or immediately after recreational physical exercise, coronary heart disease was found. In four of them a recent myocardial infarction was observed, five had critical coronary stenosis, three had occluded one coronary artery and thirteen had scars of previous myocardial infarction(s). That is why by our opinion, since preparticipation medical screening cannot ensure safety of exercise completely, physical condition check before exerci-
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
44
se is necessary to avoid possible harmful effect of physical exercise. Our data show that the usual underlying cause of sudden cardiac death during or immediately after physical exercise is coronary heart disease in elders. More than 50% of elders have at least one risk factor and about 10% of them have more than two risk factors for atherosclerosis. More efficient medical screening systems will be needed to cope with the increasing numbers of participants in exercise [56].
These findings suggest that medical examination of all elderly persons has to be done before recreational physical exercise and their health has to be monitored by clinical examination, searching for risk factors for atherosclerosis, performing ECG at rest, stress ECG, and echocardiography, because of the potential presence of an underlying disease that could result in acute cardiovascular complications during exercise.
In 37 deceased males who are not presented here in details, 32 of them suffered of coronary heart disease, 7 of them with signs of an acute myocardial infarction, 19 with signs of myocardial fibrosis or myocardial scars, and 18 with signs of left ventricular hypertrophy were observed.
references
[1] Wesslen L, Pahlson C, Lindquist O, Hjelm E, Gnarpe J, Larsson R. An increase in sudden unexpected death among young Swedish orienteers during 1979-1992. Europ Heart J 1996; 17: 902-910.
[2] Corrado D, Basso C, Buja G, Nava A, Rossi L, Thienne G. Right bundle branch block, right precordial S-T segment elevation and sudden death in young peo-ple. Circulation 2001; 103: 710-717.
[3] Corrado D, Basso C, Schiavon M, Thienne G. Screening for hypertrophic cardio-myopathy in young athletes. N Engl J Med 1998; 339: 364-369.
[4] Roguin N, Wishniak A. Anomalous origin of the main stem of the coronary artery associated with sudden death in a young athlete. Cardiol Young 2000; 10: 669.
[5] Walsh CA. Syncope and sudden death in the adolescent. Adolesc Med 2001; 12: 105-132.
[6] Basso C, Maron BJ, Corrado D, Thienne G. Clinical profile of congenital coronary artery anomalies with origin wrong aortic sinus leading to sudden cardiac death in young competitive athletes. J Am Coll Cardiol 2000; 35: 1493-1501.
[7] Maron BJ. Sudden death in young athletes. N Engl J Med 2003; 49: 1064-1075.[8] Duraković Z, Mišigoj Duraković M, Škavić J. Sudden death due to recreational
exercise in physicians. Coll Antropol 2002; 26: 509-513.[9] Duraković Z, Mišigoj Duraković M, Škavić J. Sudden cardiac death due to recre-
ational exercise in the elderly. Coll Antropol 2002; 26: 239-243.
45
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
[10] Duraković Z, Mišigoj Duraković M, Vuori I, Čorović N, Kuvalja S, Kuvalja D, Škavić J, Definis Gojanović M. Acute cardiovascular complications due to physical exer-cise in male teenagers. Coll Antropol 2004; 28: 271-276.
[11] Durakovic Z, Misigoj-Durakovic M, Vuori I, Skavic J, Belicza M. Sudden cardiac death due to physical exercise in male competitive athletes. A report of six cases. J Sports Med Phys Fitness 2005; 45(4): 532-536.
[12] Duraković Z, Mišigoj Duraković M, Škavić J, Tomljenović A. Myopericarditis and sudden cardiac death due to physical exercise in male athletes. Coll Antropol 2008; 32: 399-401.
[13] Duraković Z, Mišigoj Duraković M, Škavić J, Duraković L. Physical exercise and car-diac death due to pneumonia in male teenagers. Coll Antropol 2009; 33: 387-390.
[14] Duraković Z, Mišigoj Duraković M. Suppurative tonsillitis and sudden cardiac death due to physical training in a young soccer player. Coll Antropol 2010; 34(4): 159-161.
[15] Duraković Z, Mišigoj Duraković M, Škavić J, Definis Gojanović M. Physical activity and sudden cardiac death in elders: A Croatian study. Coll Antropol 2011; 35(1): 103-106.
[16] Burke AP. Arrhythmogenic right ventricular cardiomyopathy http://emedicine medscape.com/article/1612324-overview, updated Aug.23,2010.
[17] Rampazzo A, Nava A, Malacrida S, Beffagna G, Bauce B, Rossi V, Zimbello R, Simio-nati B, Basso C, Thiene G, Towbin JA, Danieli GA. Mutation in human desmoplakin domain binding to plakoglobin causes a dominant form of arrhythmogenic ri-ght ventricular cardiomyopathy. Am J Hum Genet 2002; 71(5): 1200-6.
[18] Corrado D, Thiene G. Corrado D, Thiene G. Arrhythmogenic right ventricular car-diomyopathy/dysplasia: clinical impact of molecular genetic studies. Circula-tion. 2006; 113 (13): 1634
[19] Gemayel C, Pellicia A, Thompson PD, Gemayel C, Pellicia A, Thompson PD. Arrhyth-mogenic right ventricular cardiomyopathy. J Am Coll Cardiol 2001; 38: 1773-1781.
[20] Duraković Z, Mišigoj Duraković M, Škavić J. Arrhythmogenic right ventricular dysplasia and sudden cardiac death in Croatians, young athletes in 25 years. Coll Antropol 2011; 35(3): 793-796
[21] Maron BJ. Distinguishing hypertrophic cardiomyopathy from athlete,s heart: a clinical problem of increasing magnitude and significance. Heart 2005; 91(11): 1380-1382.
[22] Teare D. Asymmetrical hypertrophy of the heart in young adults. Brit Heart J 1958; 20: 1-8.
[23] Frenneaux MP. Assessing the risk of sudden cardiac death in a patient with hypertrophic cardiomyopathy. Heart 2004; 90(5): 570-575.
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
46
[24] McNally EM. Hypertrophic cardiomyopathy. Circulation Res 2006; 98: 443-445.[25] Duraković Z, Mišigoj Duraković M, Medved R, Škavić J. Cardiovascular risks dur-
ing physical exercise – sudden death. Kinesiology 1999; 31: 68-73.[26] Podewils LJ, Guallar E. Mens sana in corpore sano. Ann Intern Med 2006; 144:
135-136. [27] Duraković Z, Mišigoj Duraković M. Some aspects of modern medical diagnostics
in estimating of ability to physical exercise (in Croatian). Medix 2001; 35: 76-80.[28] Duraković Z, Mišigoj Duraković M , Medved R, Škavić J. Physical exercise and cardio-
vascular risks – sudden death. Proceedings of the European Conference: Health related physical activity and adults. Poreč, Croatia, June 22-25, 2000, pp. 1-6.
[29] Mišigoj Duraković M, Duraković Z, Baršić B. To exercise or not to exercise in acute upper respiratory tract infections. Kinesiology 2005; 37: 5-12.
[30] Medved R, Duraković Z, Mišigoj Duraković M. Cardiovascular system and sport (in Croatian). Liječ Vjesn 1998; 120: 228-236.
[31] Maron BJ, Thompson PD, Puffer JC, McGrew CA, Strong WB, Douglas PS, Clark LT, Mitten MJ, Crawford MH, Atkins DL, Driscoll DJ, Epstein AE. Cardiovascular pre-participation screening of competitive athletes. Circulation 1996; 94: 850-856.
[32] Wesslen L, Pahlson C, Lindquist O, Hjelm E, Gnarpe J, Larsson E, Baandrup U, Eriks-son L, Fohlman J, Engstrand L, Linglof T, Nystromrosander C, Gnarpe H, MagniusL, Rolf C, Friman G. An increase in sudden unexpected cardiac deaths among young Swedish orienteers during 1979-1992. Europ Heart J 1996; 17: 902-910.
[33] Gussak I, Antzelevitch C, Bjerregaard P, Towbin JA, Chaitman BR. The Brugada syndrome: clinical, electrophysiologic and genetic aspects. J Am Coll Cardiol. 1999; 33: 5-15.
[34] Pfister GC, Puffer JC, Maron BJ. Preparticipation cardiovascular screening for US collegiate student-athletes. JAMA 2000; 283: 1597-1599.
[35] Maron BJ, Douglas PS, Graham TP, Nishimura RA, Thompson PD. Task force 1: preparticipation screening and diagnosis of cardiovascular disease in athletes. J Am Coll Cardiol 2005; 45: 1322-1326.
[36] Duraković Z, Mišigoj Duraković M, Škavić J. Hypertrophic cardiomyopathy and sudden cardiac death due to physical exercise in Croatia in a 27-year period, Collegium Antropologicum 2011; 35(4): 1051-1054.
[37] Duraković Z, Mišigoj Duraković M, Čorović N, Čubrilo Turek M, Turek S, Manitašević A. Hospitalization of older and younger patients in a Department of internal medicine: variety of reasons and outcome. Coll Antropol 1996; 20: 213-220.
[38] Čorović N, Duraković Z. A prospective study of changes in the electrocardiogram in a middle-aged population of Croatia during a 13 year period. Coll Antropol 1996; 20: 193-199.
47
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
[39] Duraković Z. The high plasma digoxin level: comparison with clinical symptoms and an electrocardiogram in the elderly and younger patients. Coll Antropol 1992; 16: 371-376.
[40] Duraković Z, Mišigoj Duraković M, Čorović N, Pezerović Dž, Gašparović V, Čubrilo Turek M, Turek S, Đurek M, Naumovski Mihalić S, De Syo D. Hypothermia and acute renal failure in the elderly. Coll Antropol 1998; 22: 135-140.
[41] Mišigoj Duraković M. Exercise and health (in Croatian). Grafos, Zagreb, 1999, and Kinesiological Faculty University of Zagreb and Fakulteta for Sport (in Slo-venian), Ljubljana, Slovenia 2003.
[42] Durakovic Z, Misigoj Durakovic M, Skavic J. Sudden cardiac death associated with recreational physical exercise in elderly men. Europ J Geriatr 2000; 6: 135-139.
[43] McGinnis JM. A vision for health in our new century. Am J Health Promot 2003; 18: 146-150.
[44] Vuori I. Physical inactivity is a cause and physical activity is a remedy for maior public health problems. Kinesiology 2004; 2: 123-153.
[45] Ajisaka R. Principle of Medical Screening for Participation in exercise in resi-dents in the community. Int J Sports Health Sci 2006; 4: 370-379.
[46] Chodzko-Zajko WJ, Proctor DN, Flatarone MA, Minson CT, Nigg CH, Salem GJ, Skin-ner JS. Exercise and physical activity for older adults. Medicine & Science in Sporst & Exercise, the Am Coll Sports Med 2009, pp.1510-1529.
[47] Connor RCR. Sudden death after exertion in an apparently healthy boy. Br Med J 1969; 4: 30-31.
[48] Ayus JC, Varon J, Arieff AI. Hyponatremia, cerebral edema, and non-cardiogenic pulmonary edema in marathon runners. Ann Intern Med 2000; 132: 711-174.
[49] Futterman LG, Myerburg R. Sudden death in athletes: an update. Sports Med 1998; 26: 335-350.
[50] McCaffrey FM, Braden DS, Strong WB: Sudden cardiac death in young athletes: a review. Am J Dis Child 1991;145:177-183.
[51] Vuori I. The cardiovascular risk of physical activity. Acta Med Scand 1986;sup-pl.711:205-214.
[52] Maron BJ. Hyperthrophic cardiomyopathy. Circulation 2002; 106: 2419-2421. [53] Calkins H. Arrhythmogenic right ventricular dysplasia. Trans Am Clin Climatol
Assoc 2008; 119: 273-286.[54] Heidbuchel H, Hoogsteen J, Fagard R, Vanhees L, Ector H, Willems R, Van Lierde J.
High prevalence of right ventricular involvement in endurance athletes with ventricular arrhythmias. Role of an electrophysiologic study in risk stratifica-tion http://euroheart.oxfordjournals.org/content/24/16/1473.full http//www.fac.org.ar/cvirtual/cvirteng
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
48
[55] Pellicia A. Athlete,s heart and cardiomyopathy. http://www.fac.org.ar/cvirtual/cvirteng/cienteng/ceeng/cen3901i/pellic/ipellic.htm.2011
[56] Thiene G, Corrado D, Basso C. Arrhythmogenic right ventricular Cardiomyopa-thy/dysplasia. Orphanet J Rare Dis 2007; http/www.ncbi. nlm.nih. gov/pmc/ar-ticles/PMC2222049.
[57] Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, Bluemke DA, Calkins H, Cor-rado D, Cox MG, Daubert JP, Fontaine G, Gear K, Hauer R, Nava A, Picard MH, Protonotarios N, Saffitz JE, Sanborn DM, Steinberg JS, Tandri H, Thiene G, Towbin JA, Tsatsopoulou A, Wichter T, Zareba W. Diagnosis of arrhythmogenic right ven-tricular cardiomyopathy/dysplasia: proposed modification of the task force cri-teria. Circulation 2010; 121: 1533-1541.
[58] Hamid MS, Norman M, Quraishi A, Firoozi S, Thaman R, Gimeno JR, Sachdev B, Rowland E, Elliott PM, McKenna WJ. Prospective evaluation of relatives for fa-milial arrhythmogenic right ventricular cardiomyopathy/dysplasia. J Am Coll Cardiol 2002; 40: 1445-1450.
[59] http://en.ecqpedia.org/wiki/File:Epsilon wave.png, 2011.[60] Nasir K, Bomma C, Tandri H, Roguin A, Dalal D, Prakasa K, Tichnell C, James C,
Jspevak P, Marcus F, Calkins H. Electrocardiographic features of arrhythmogenic right ventricular dysplasia/cardiomyopathy according to disease severity: a need to broaden diagnostic criteria. Circulation 2004, 110: 1527-1534.
[61] http://www.cardiomyopathy.org/Exercise-in-hypertrophic cardiomyopathy Html. 2011[62] Dimitrow PP, Chojnowska L, Rudzinski T, Piotrowski W, Ziolkowska L, Wojtarowisz
A, Wycisk A, Dabrowska Kugacka A, Nowalany Kozielska E, Sobkowicz B, Wrobel W, Alescewicz Baranowska J, Rynkiewicz A, Loboz, Grudzień K, Marchel M, Wysokinsi A. Sudden death in hypertrophic cardiomyopathy. Old risk factors re-assessed in a new model of maximalized follow-up. Europ Heart J 2010; 31[24): 3084-3093.
[63] Hypertrophic cardiomyopathy. American Heart Association http://www.heart.org/groups/heart-public/@hcm -/documents/downloadable/ucm–312225.pdf.Ac-cessed Dec. 7, 2010.
[64] Elliot PM. Clinical manifestations of hypertrophic cardiomyopathy. http://www.uptodate.com/home/index.html. Accessed Dec. 7, 2010.
[65] Basso C, Corrado D, Thienne G. Cardiovascular causes of sudden death in young individuals including athletes. Cardiol Rev 1999;7:127-135.
[66] Spirito P, Bellone P, Harris KM, Bernabo P, Bruzzi P, Maron BJ. Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyo-pathy. N Engl J Med 2000; 342: 1778-1785.
[67] Medved R , Volarić B, Pavišić Medved V. Sudden death of a top-level football play-er. Proceedings of the XVIII-th World Congress of Sports Medicine, Oxford Sep-tember 6-11,1970., Br J Sports Med 1973;1-2.
49
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
[68] Pigozzi F, Rizzo M. Sudden death in competitive athletes. Clinics Sports Med 2008; 27: 153-181.
[69] Papadakis M, Sharma S, Cox S, Sheppard MN, Panoulas VF, Behr ER. The magni-tude of sudden cardiac death in the young: a death certificate-based review in England and Wales. Europace 2009; 11 [10): 1353-1358.
[70] Duraković Z, Mišigoj Duraković M, Medved R, Škavić J. Physical exercise and cardio-vascular risks – sudden death. Proceedings of the European Conference: Health related physical activity and adults. Poreč, Croatia June 22-5, 2000, pp. 1-6.
[71] Basso C, Corrado D, Thiene G. Review causes of sudden death in competitive athletes. Cardiol Rev 1999; 7: 127-135.
[72] Oakley D. The athlete,s heart. Heart 2001; 86: 722-726.[73] Pearson TA, Blair SN, Daniels SR, Eckel RH, Fair JM, Fortmann SP, Franklin BA, Gold-
stein LB, Greenland P, Grundy SM, Hong Y, Miller NH, Lauer RM, Ockene IS, Sacco RL, Sallis JF, Smith SC, Stone NJ, Taubert KA. AHA Guidelines for Primary Preven-tion of Cardiovascular Disease and Stroke: 2002 Update: Consensus Panel Guide to Comprehensive Risk Reduction for Adult Patients Without Coronary or Other Atherosclerotic Vascular Diseases. American Heart Association Science Advisory and Coordinating Committee.” Circulation. 2002; 106[3): 388-91.
[74] Albert CM, Mittleman MM, Chou CU, Lee IM, Henneken CH, Manson JE. Sudden death from cardiac causes by vigorous exertion N Engl J Med 2000; 343: 1355-1361.
[75] Shah CP, Thakur RK, Ip JH, Xie B. Cardiac arrhythmias in the elderly. Cardiac Electrophys Rev 2004;1: 283-286.
[76] Exercise does not make heart grow younger. www.medicalnewstoday.com (Aug 18,2007).
[77] Podewils LJ, Guallar E. Mens sana in corpora sano. Ann Intern Med 2006; 144: 135-136.
[78] Haskell WL, Lee I-M, Pate RR, Powell KE, Blair SN, Franklin BA, Macera CA, Heath GW, Thompson PD, Bauman A. Physical activity and public health, Update rec-ommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007; 116: 1081-1093.
[79] Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, Macera CA, Cas-taneda-Sceppa C. Physical activity and public health in older adults: recommen-dation from the American College of Sports Medicine and the American Heart Association. Circulation 2007; 116: 1094-1105.
[80] DHHS. Physical Activity Guidelines Advisory Committee Report. Rockville, MD; U.S. Department of Health and Human Services 2008.
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
50
Sažetak
Nagla kardijalna smrt tijekom tjelesne aktivnosti u Hrvatskoj u 27-godišnjem razdoblju
Prikazane su nagle kardijalne smrti za vrijeme treninga u hrvatskoj kao dio retrospektivnog istraživanja 69 muškaraca naglo i neočekivano umrlih za vrijeme tjelovježbe u Hrvatskoj od 1. siječnja 1984. do 31. prosinca 2010. i u svih je provedena sudsko-medicinska obdukcija.
U sportaša je bilo šest naglih i neočekivanih smrtnih ishoda. Obdukcijom trkača u dobi 21 godine otkriven je akutni infarkt miokarda s normalnim vjenačnim arterijama i hipertrofijom lijeve klijetke. U drugog, u dobi 17 godina, vjenačne arterije bile su hipoplastične a silazna aorta sužena te su bili prisutni gnojni tonzilitis i subakutni miokarditis. Dva su sportaša umrla tijekom treninga zbog aritmogene displazije desne klijetke. Prvi je bio trkač na kratke pruge, a drugi no-gometaš. U Hrvatskoj stopa nagle smrti u sportaša iznosi 0.19/100 000 godišnje (p = 0.00005); zbog aritmogene displazije desne klijetke ta stopa iznosi 0.06/100 000 (p = 0.00000), u svih mladih sportaša koji su bolovali od drugih bolesti srca ona iznosi 0.10/100 000 (p = 0.00000), u ukupnoj populaciji muškaraca u dobi 15 – 40 g. koji su uključeni u takmičarsku ili rekreacijsku tjelovježbu ta stopa iznosi 0.71/100 000 godišnje (p = 0.00001), a u svih muškaraca u dobi 15 – 64 g. 0.96/100 000 (p = 0.00000).
Pet sportaša preminulo je zbog hipertrofijske kardiomiopatije: trojica za vrijeme treninga i dvojica za vrijeme rekreacijske tjelovježbe. Jedan je imao opstrukcijsku hipertrofijsku kardiomio-patiju, a ostali su imali neopstrukcijski oblik. Prvi sportaš naglo je preminuo za vrijeme treninga trčanja, a drugi i treći sportaš bili su košarkaši. Dvojica su preminula za vrijeme nogometne igre. Nagla kardijalna smrt zbog hipertrofijske kardiomiopatije za vrijeme rekreacijske tjelovježbe u mladih sportaša u Hrvatskoj iznosi 0.10/100 000 (p = 0.00000).
Dogodila su se tri nagla i neočekivana smrtna ishoda zbog mioperikarditisa, i to kod dvojice nogometaša te jednog plivača. Obdukcijom je otkriveno da je prvi bolovao od subakutnog difu-znog mioperikarditisa, gnojnog tonzilitisa i sužene uzlazne aorte, drugi od kroničnog mioperikar-ditisa i aneurizmatskog proširenja lijeve klijetke, a treći od fibrinoznog perikarditisa, zadebljanja lijeve klijetke od 20 mm, hipoplastične uzlazne aorte, obostrane bronhopneumonije i kontuzije mozga s edemom. U Hrvatskoj u tjelovježbača stopa smrtnog ishoda zbog mioperikarditisa izno-si 0.11/100 000 (p = 0.00000).
Stenoza aorte ustanovljena je u dva adolescenta. Prvi je bio učenik i košarkaš u dobi 17 g. Obdukcijom je otkriveno povećanje cijelog srca, suženje uzlazne aorte, zadeljana stijenka lijeve klijetke, bakterijski tonzilitis i subakutni difuzni miokarditis. Drugi učenik preminuo je naglo za vrijeme trčanja. Nalaz obdukcije upućivao je na povećanje cijelog srca, zadebljanje stijenke lijeve klijetke i suženje silazne aorte.
Malformacije vjenačnih arterija ustanovljene su u trojice mladića. U nogometaša koji je na-glo preminuo tijekom utakmice postojala je hipoplazija desne vjenačne arterije, suženje uzlazne aorte, akutni bakterijski tonzilitis i subakutni miokarditis. U dječaka koji je preminuo za vrijeme tjelovježbe ustanovljene su hipoplastične vjenačne arterije. U mladića koji je povremeno re-kreacijski igrao nogomet i preminuo za vrijeme utakmice desna i lijeva vjenačna arterija bile su sužena ušća od 1 mm.
Među adolescentima bilo je 10 naglih i neočekivanih smrti tijekom ili nakon tjelovježbe. Obdukcijski je kod četvorice ustanovljena prirođena bolest srca. Dvojica su imala hipoplastične koronarne arterije, jedan uz to i bakterijsku upalu tonzila, suženu aortu i subakutni miokardi-tis. Treći je imao hipertrofijsku kardiomiopatiju. Četvrti je bolovao od obostrane upale pluća s nekardiogenim edemom pluća. Peti je imao aneurizmu lijeve klijetke. Šesti je igrao nogomet
51
Rad 511. Medical Sciences 37(2012) : 19-51Z. Duraković, M. Mišigoj Duraković, J. Škavić: Sudden Cardiac Death Due to Physical Exercise ...
rekreacijski i preminuo je zbog obostrane upale pluća, a imao je i fibrinozni perikarditis. Sedmi je imao kardiomegaliju, obostrani hidrotoraks i etanol u krvi (0.17%). Stopa smrti za vrijeme ili neposredno nakon tjelovježbe u adolescenata u Hrvatskoj iznosi 0.37/100 000 (p = 0.00226). Zbila su se tri nagla i neočekivana smrtna ishoda zbog pneumonije u mladića. Jedan je radio rekreacijski na gradilištu, drugi se bavio rekreacijski nogometom, treći je bio profesionalni no-gometaš. Nalaz obdukcije u prvog upućivao je na obostranu bakterijsku upalu pluća, mogući nekardiogeni edem pluća i edem mozga. U drugog je nalaz upućivao na obostranu bakterijsku upalu pluća, respiracijski distresni sindrom odraslih, diseminiranu intravaskularnu koagulaciju, krvarenje u nadbubrežne žlijezde, hipoplastičnu desnu koronarnu arteriju i fibrozu miokarda. U trećeg je nalaz upućivao na obostranu bakterijsku upalu pluća, fibrinozni perikarditis, cerebralnu kontuziju s edemom, zadebljanje lijeve klijetke i hipoplastičnu uzlaznu aortu. Stopa smrtnosti u adolescenata zbog pneumonije u hrvatskoj iznosi 0.11/100 000 (p = 0.00000).
Mladi nogometaš bez prethodnih zdravstvenih tegoba preminuo je naglo i neočekivano ti-jekom treninga. Obdukcijom je ustanovljena bakterijska upala tonzila, subakutni mioperikarditis i sužena uzlazna aorta.
Pet je liječnika specijalista naglo i neočekivano umrlo tijekom ili neposredno nakon rekre-acijskog tjelesnog vježbanja: plivanja, nogometa, tenisa i trčanja. U trojice koja nisu imala pret-hodne simptome te su bila nepušači obdukcijom je ustanovljena koronarna bolest srca: u jednog je ustanovljena stenoza, u dvojice okluzija prednje silazne koronarne krvne žile, u jednog su ustanovljeni ožiljci miokarda od dva ranije preboljela infarkta miokarda, u dva hipertrofija lijeve klijetke. U dvojice koja nisu obducirana radilo se o mogućoj alkoholnoj kardiomiopatiji. Obojica su bila pušači. U jednog je zabilježena fibrilacija atrija godinu prije nagle smrti. U drugog se vjerojatno radilo o bolesti vjenčanih arterija, uz arterijsku hipertenziju i hiperlipoproteinemiju. U Hrvatskoj je 4.957 liječnika specijalista muškaraca, a u njih stopa naglih smrti za vrijeme tjelo-vježbe iznosi 24.8/100 000 godišnje (p = 0.00000).
Petnaest „starijih” muškaraca naglo je umrlo za vrijeme različitih oblika tjelovježbe: plivanja u moru, tenisa, kuglanja, rekreacijskog trčanja. Obdukcijom je otkriveno da ih je 14 imalo bolest vjenačnih krvnih žila: petorica kritično vjenačno suženje, dvojica uz recentni infarkt mišića srca prednje stijenke, trojica začepljenu prednju silaznu vjenačnu arteriju, jedan od njih uz to i akutni infarkt prednje stijenke srca, dvanaestorica ožiljke nakon preboljelih infarkta srca, jedan je imao difuznu fibrozu miokarda. Dvanaestorica su imala zadebljanje lijeve klijetke. U Hrvatskoj se oko 7% muškaraca starije dobi bavi rekreacijskom tjelovježbom, a u njih stopa smrtnosti iznosi 2.99/100 000 (p = 0.00001).
Ključne riječi: muškarci; sportaši; rekreativna tjelesna aktivnost; iznenadna smrt

Copyright © 2022 FDOKUMEN




















