SUDDEN FALLS DUE TO SEIZURE-INDUCED CARDIAC ASYSTOLE IN DRUG-RESISTANT FOCAL EPILEPSY
7
DOI: 10.1212/01.wnl.0000289193.89796.83 2008;70;1933-1935; originally published online Feb 6, 2008; Neurology Riguzzi, C. A. Tassinari and P. Tinuper G. Rubboli, F. Bisulli, R. Michelucci, S. Meletti, M. A. Ribani, P. Cortelli, I. Naldi, P. DRUG-RESISTANT FOCAL EPILEPSY SUDDEN FALLS DUE TO SEIZURE-INDUCED CARDIAC ASYSTOLE IN This information is current as of May 13, 2008 http://www.neurology.org/cgi/content/full/70/20/1933 located on the World Wide Web at: The online version of this article, along with updated information and services, is All rights reserved. Print ISSN: 0028-3878. Online ISSN: 1526-632X. since 1951, it is now a weekly with 48 issues per year. Copyright © 2008 by AAN Enterprises, Inc. ® is the official journal of the American Academy of Neurology. Published continuously Neurology at CENTRO PER LA VALUT CEVEAS on May 13, 2008 www.neurology.org Downloaded from
Transcript of SUDDEN FALLS DUE TO SEIZURE-INDUCED CARDIAC ASYSTOLE IN DRUG-RESISTANT FOCAL EPILEPSY

DOI: 10.1212/01.wnl.0000289193.89796.83 2008;70;1933-1935; originally published online Feb 6, 2008; Neurology
Riguzzi, C. A. Tassinari and P. Tinuper G. Rubboli, F. Bisulli, R. Michelucci, S. Meletti, M. A. Ribani, P. Cortelli, I. Naldi, P.
DRUG-RESISTANT FOCAL EPILEPSYSUDDEN FALLS DUE TO SEIZURE-INDUCED CARDIAC ASYSTOLE IN
This information is current as of May 13, 2008
http://www.neurology.org/cgi/content/full/70/20/1933located on the World Wide Web at:
The online version of this article, along with updated information and services, is
All rights reserved. Print ISSN: 0028-3878. Online ISSN: 1526-632X. since 1951, it is now a weekly with 48 issues per year. Copyright © 2008 by AAN Enterprises, Inc.
® is the official journal of the American Academy of Neurology. Published continuouslyNeurology
at CENTRO PER LA VALUT CEVEAS on May 13, 2008 www.neurology.orgDownloaded from

Clinical/ScientificNotes
G. Rubboli, MDF. Bisulli, MD, PhDR. Michelucci, MD,PhD
S. Meletti, MD, PhDM.A. Ribani, MDP. Cortelli, MD, PhDI. Naldi, MDP. Riguzzi, MDC.A. Tassinari, MDP. Tinuper, MD
SUDDEN FALLS DUE TO SEIZURE-INDUCEDCARDIAC ASYSTOLE IN DRUG-RESISTANTFOCAL EPILEPSY
Sudden, abrupt falls to the ground during focalseizures, without any associated major motormanifestations, are a well-known althoughpoorly investigated phenomenon.1 Pathophysio-logic mechanisms may include bitemporal orfrontal involvement with subsequent bilateralspread of the epileptic discharge.2,3 Seizure-related cardiac arrhythmias (i.e., bradycardia orasystole4,5) may result in syncope but may not al-ways be considered in the etiology of ictal suddenfalls. We describe three patients with drug-resistantfocal epilepsy undergoing presurgical evaluation inwhom sudden falls during focal seizures resultedfrom seizure-related cardiac asystole.
Case reports. Case 1. Since age 29 years, this 52-year-old man had had seizures with loss of con-tact, paleness, and oroalimentary automatisms.At 49 years, seizure frequency increased, in spiteof several antiepileptic treatments, and about50% of episodes were associated with abrupt fallsto the ground. Brain MRI demonstrated right me-sial temporal sclerosis. During long-term video-polygraphic monitoring three stereotypicalseizures were collected, characterized by psy-chomotor arrest and fall, followed by oroalimen-tary and right hand automatisms (figure, and video1 on the Neurology® Web site at www.neurology.org). Ictal EEG-EKG recording showed a right tem-poral rhythmic theta discharge associated with 7 to8 seconds asystole; the fall of the patient occurred atthe end of the asystole (figure). After right an-teromesial temporal lobectomy (follow-up 19months), neither focal seizures nor sudden fall to theground have been reported.
Case 2. Since age 15 years, this 39-year-oldwoman had had seizures characterized by visualhallucinations, loss of consciousness, and occa-sionally secondary generalization. At 30 years ofage, seizure frequency increased, the visual auradisappeared, and a sudden fall could occur. BrainMRI was unremarkable. During long-term video-
polygraphic monitoring, a seizure characterizedby psychomotor arrest, loss of consciousness, andfall was recorded (figure e-1 and video 2). IctalEEG showed left side and vertex rhythmic thetaactivity; subsequent bilateral propagation of theEEG discharge was associated with heart rateslowing and repeated 3 to 4 seconds sinus pauses;the fall occurred at the end of a 3-second pause(figure e-1). Surgical treatment was not consid-ered feasible and pacemaker implantation wasadvised; this option has been refused by the pa-tient.
Case 3. This 35-year-old woman started topresent, at the age of 7 years, episodes of loss ofconsciousness, occasionally followed by fall tothe ground and confusion, diagnosed as syncope.Subsequently the episodes were characterized alsoby experiential phenomena (fear, deja vecu),autonomic symptoms (pallor, nausea), andoroalimentary automatisms. Their frequencyprogressively increased and, at the age of 30, adiagnostic workup demonstrated the epileptic or-igin. Brain MRI showed left mesial temporal scle-rosis. Prolonged video-polygraphic monitoringdocumented seizures characterized by earlyoroalimentary automatisms, nausea, pallor, thenloss of consciousness (figure e-2, video 3). IctalEEG showed a right temporal theta discharge, as-sociated with heart rate slowing; pallor and lossof consciousness coincided with an asystole last-ing about 5 seconds (figure e-2). Evidence of sei-zure onset from both sides ruled out surgicaltreatment, therefore a cardiac demand stimulatorwas implanted. Since pacemaker implantation(follow-up: 22 months), the patient’s seizures arecharacterized by deja vu and automatisms, with-out pallor or loss of consciousness.
Discussion. Our report shows that severe brady-arrhythmias triggered by a focal epileptic dis-charges can result in transient asystole, andthereby can lead to sudden falls during focal sei-zures. This is a possible pathophysiologic mecha-nism of ictal falls, an alternative to those usuallyconsidered, including tonic or atonic seizures, bi-temporal involvement, or frontal origin with bi-
Supplemental data atwww.neurology.org
Editorial, page 1874
Neurology 70 May 13, 2008 1933 at CENTRO PER LA VALUT CEVEAS on May 13, 2008 www.neurology.orgDownloaded from

lateral spread.2,3 Seizure-induced asystole andsyncope may be difficult to distinguish solely onclinical grounds due to the similar symptom-atology (such as loss of consciousness, clonicjerks, salivation, and postictal fatigue). Inci-dence of ictal asystole is probably under-estimated; in fact, its diagnosis requiresdocumentation of bradycardia/asystole andEEG evidence of an associated seizure. The useof long-term video-EEG/EKG recording is oftennecessary to make the diagnosis, and to avoidmisdiagnosis that may occur when paroxysmalbradyarrhythmias are studied only from a car-diac perspective without simultaneous EEG-EKG monitoring.
A correct diagnosis can be of paramount im-portance in the management of patients with
epilepsy, since cardiac arrhythmias are consid-ered to play a role in sudden death in epilep-sy.5,6 Indeed, cardiac pacemaker implantation isadvised in patients with seizure-related brady-cardia/asystole. Further, a diagnosis of ictalsyncope with seizures should prompt a re-evaluation of the use of potentially arrhythmo-genic antiepileptic drugs, such as carbamazepine,which can lengthen the EKG Q-T interval andmight thereby increase the arrhythmic effects ofepileptic seizures.7 We suggest that sudden fallsoccurring during focal seizures should be prop-erly investigated by EEG-EKG recording of theictal events.
e-Pub ahead of print on February 6, 2008, at www.neurology.org.
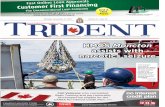
Figure At seizure onset (seizure shown in video 1), the appearance in the EEG of rhythmic theta activity in theright temporal leads is associated in the EKG with asystolic periods whose duration can range from 3to 8 seconds
The backward fall of the patient occurs when the heart rate is starting to recover. Then, the right temporal discharge slowsdown progressively, remaining confined to the right temporal channels, clinically associated with oroalimentary and right handautomatisms.
1934 Neurology 70 May 13, 2008 at CENTRO PER LA VALUT CEVEAS on May 13, 2008 www.neurology.orgDownloaded from

From the Neurology Unit, Department of Neurosciences(G.R., R.M., P.R., C.A.T.), and Cardiology Unit (M.A.R.),Bellaria Hospital; Department of Neurosciences, Universityof Modena and Reggio Emilia (S.M.); and Institute of Neu-rology (F.B., P.C., I.N., P.T.), Department of NeurologicalSciences, University of Bologna, Italy.
Disclosure: The authors report no conflicts of interest.
Received February 26, 2007. Accepted in final form August23, 2007.
Address correspondence and reprint requests to Dr. GuidoRubboli, Neurology Unit, Department of Neurosciences,Bellaria Hospital, Via Altura, 3–40139 Bologna, Italy;[email protected]
Copyright © 2008 by AAN Enterprises, Inc.
ACKNOWLEDGMENTThe authors thank Dr. Andrea Rubboli of the Cardiology Unit, Mag-
giore Hospital, Bologna, for helpful suggestions. They also thank Lara
Alvisi and Giorgio Barletta for technical assistance in performing poly-
graphic study and Elena Zoni for help in editing the manuscript.
1. Tassinari CA, Michelucci R, Shigematsu H, Seino M.Atonic and falling seizures. In: Engel J, Pedley T, eds.Epilepsy: A comprehensive textbook. Philadelphia:Lippincott-Raven; 1997:605–616.
2. Tinuper P, Cerullo A, Marini C, et al. Epileptic dropattacks in partial epilepsy: clinical features, evolutionand prognosis. J Neurol Neurosurg Psychiatry 1998;64:231–237.
3. Leung H, Schindler K, Kwan P, Elger C. Asystole in-duced by electrical stimulation of the left cingulate gy-rus. Epileptic Dis 2007;9:77–81.
4. Tinuper P, Bisulli F, Cerullo A, et al. Ictal bradycardia inpartial epileptic seizures: autonomic investigation in threecases and literature review. Brain 2001;124:2361–2371.
5. Britton JW, Benarroch E. Seizures and syncope: ana-tomic basis and diagnostic considerations. Clin AutonRes 2006;16:18–28.
6. Schraeder PL, Lathers CM. Paroxysmal autonomicdysfunction, epileptogenic activity and sudden death.Epilepsy Res 1989;3:55–62.
7. Timmings PL. Sudden unexpected death in epilepsy: iscarbamazepine implicated? Seizure 1998;7:289–291.
ACOUSTIC SLEEP STARTS WITH SLEEP-ONSET INSOMNIA RELATED TO ABRAINSTEM LESIONSensory sleep starts are variants of the more com-mon motor sleep starts (hypnic jerks).1 Thoughsensory sleep starts may lead to repeated awaken-ings resulting in sleep-onset insomnia, theircourse is usually benign and no cerebral lesion hasyet been described as being pathogenetically in-volved. Here we report a case of acoustic sleepstarts (“exploding head syndrome”) which con-tests this latter assertion because their onset coin-cided with the occurrence of a brainstem lesion.
Case report. A 64-year-old woman reported onproblems initiating sleep related to the impressionof a cracking sound of average loudness. Up to 15times during the first hours after going to bed thissound occurred shortly after losing full conscious-ness, followed by an experience of jerking in allfour limbs and a brief sensation of fear leading tofull wakefulness.
The patient, who had been healthy until then,noticed her sleep problem for the first time 12years ago, coinciding with the diagnosis of pul-monary and extrapulmonary sarcoidosis. Corti-costeroids were instituted under which no furtherprogression of sarcoidosis occurred, even whensteroids were tapered. Over this period the pa-tient’s sleep problem was waxing and waning inintensity. Treatment with doxepin, citalopram,trimipramine, and amitriptyline led to no im-provement. Only bromazepam (6 mg/day, 8weeks) instantly led to unhampered sleep. Succes-
sive MRI scans of the brain (figure, A and B) re-vealed an unchanging, nonenhancing, singular,symmetric T2-hyperintense pontomesencephaliclesion around the periaquaductal gray reachinginto the tegmentum.
Neurologic examination was normal. Upon 3nights of polysomnography the hypnograms (fig-ure, C) were fragmented in the beginning of thesleep period, because she experienced a crackingsound four times, always accompanied by a sen-sation of startling. Recordings revealed arousalsfrom non-REM1/2 (figure D), but without muscleactivity in muscles normally involved in a startleresponse. Because of absent EMG activity, pro-priospinal myoclonus could be ruled out. The di-agnosis of acoustic sleep starts (“exploding headsyndrome”) was established and clonazepam at0.5 mg at night was begun, which has led to un-disturbed sleep since its institution 8 months ago.Twice, discontinuation of clonazepam led to im-mediate relapse of symptoms.
Discussion. Sleep starts can be accompanied bysensory experiences (acoustic, pain)2 and fear.The exploding head syndrome1 is a sensory para-somnia that seems to be a variant of sleep starts ininstances when acoustic sensations figure promi-nently.3 Phenomenologically, patients with acous-tic sleep starts experience a startle response,though the acoustic stimulus leading to the startleresponse is not external, but induced by NREMsleep. As presented in this case, the specific expe-rience of the sleep-induced startle may be accom-panied by an absence of muscle activity and thus
Farid Salih, MDRandolf Klingebiel,MD
Rolf Zschenderlein,MD
Pascal Grosse, MD
Neurology 70 May 13, 2008 1935 at CENTRO PER LA VALUT CEVEAS on May 13, 2008 www.neurology.orgDownloaded from

represent hallucinatory motor parasomnia. Inwakefulness, acoustic and other stimuli (tactile,vestibular) can produce a startle response throughcircuits between the cochlear (trigeminal, vestibu-lar) nuclei and the gigantocellular nuclei in theventrocaudal part of the medulla oblongata,which are connected to spinal motoneuronsthrough the reticulospinal system.4 As sleep startsshare with the startle response a preference forproximal and axial muscles,5 it seems plausiblethat they are also mediated through the reticu-lospinal pathway. It could be argued that muscleactivity can be suppressed, as it happens physio-logically in sleep through inhibitory circuits be-tween neurons in the brainstem and muscle, thusproviding the anatomic basis of this hallucinatoryparasomnia.
No model has been proposed to explain theoccurrence of sleep-induced acoustic sensations.Successful treatment with serotonergic drugs insome patients argues in favor of deficient seroto-nergic transmission.6 However, in our patientGABAergic medication was effective. Recently,evidence has been gathered in naturally sleepingrats that glycinergic and GABAergic inhibitoryneurons in the brainstem are responsible for thecharacteristic decrease in the firing rate of seroto-nergic neurons of the dorsal raphe nucleus in thetransition from wakefulness to non-REM sleep asa precondition for stable sleep initiation. Glycin-ergic neurons targeting the dorsal raphe nucleusare predominantly located in pontine ventralperiaquaductal gray and the lateral paragiganto-cellular nucleus, while GABAergic neurons arefound in the pontine ventral periaquaductal gray.7
The patient’s lesion in the ventral and central por-tion of the mesencephalic–pontine region makesit seem reasonable that this lesion is pathogeneti-cally involved in the sleep disorder. However, it isnot possible to precisely relate the lesion to anystructures at the level of nuclei. But the patient’sprevailing negative responses to serotonergicdrugs and positive responses to GABAergic drugsargue for compromised GABAergic transmission,presumably that to the dorsal raphe nucleus. Be-cause of its stationary character over 8 years andits signal intensities, the lesion appears to repre-sent gliosis. Etiologically, it is possibly related tothe patient’s sarcoidosis as residual sarcoid le-sions occur preferentially adjacent to CSF spaces.
From the Department of Neurology (F.S., R.Z., P.G.), Interdis-ciplinary Sleep Disorders Centre (F.S., P.G.), and Departmentof Neuroradiology (R.K.), Charite-Universitatsmedizin Berlin,Germany.
Figure MRI scans, hypnogram, and polysomnography
(A, B) T2-weighted cranial MRI, transverse (A) and midsagittal (B) plane. A singular hyperin-tense mesencephalic lesion (arrows) is depicted, indicative of brainstem gliosis. (C) Hypno-gram showing repetitive arousals due to a cracking sound (arrows) with shorter andprolonged periods of wakefulness. The patient was instructed to press a button next to herbed every time the characteristic cracking sound occurred and she awakened. These arous-als were unrelated to preceding apneas (not shown) or limb movements. Note that not allarousals are accompanied by acoustic sleep starts. EEG showed no epileptic discharges inany sleep recording. Average polysomnographic data: total sleep time was 181 minutes,waking periods during sleep time was 166 minutes; percentage of non-REM 1 was 19.3%, ofnon-REM 2 36.7%, of non-REM 3/4, and of REM 6.4%; respiratory disturbance index (RDI)was 13.6/hour (obstructive: 2/hour; central: 5.3/hour; mixed: 6.3/hour), periodic limb move-ment index (PLM-I) was 1.7/hour, REM sleep muscle atonia was preserved. (D) Polysomnogra-phy of one single arousal (arrow) following non-REM 2 induced by a loud cracking sound and asensation of startling. Muscle tone in recorded muscle was present, but no muscle shows acontraction before the patient fully wakes up and moves. LOC � left eye; ROC � right eye;LSCM � left sternocleidomastoid; RSCM � right sternocleidomastoid; ldeltoid � left deltoid;rdeltoid � right deltoid; L1DI � left first dorsal interosseus; R1DI � right first dorsal interos-seus; LTA � left tibialis anterior; RTA � right tibialis anterior.
1936 Neurology 70 May 13, 2008 at CENTRO PER LA VALUT CEVEAS on May 13, 2008 www.neurology.orgDownloaded from

Disclosure: The authors report no disclosures.
Received May 23, 2007. Accepted in final form October 5,2007.
Address correspondence and reprint requests to Dr. FaridSalih, Neurologische Klinik und Poliklinik, Charite-Universitatsmedizin Berlin, Campus Virchow-Klinikum, Au-gustenburger Platz 1, 13353 Berlin, Germany; e-mail:[email protected]
1. American Academy of Sleep Medicine. The Interna-tional Classification of Sleep Disorders. 2nd ed.Westchester, IL: 2005.
2. Sander HW, Geisse H, Quinto C, Sachdeo R, Chokro-verty S. Sensory sleep starts. J Neurol Neurosurg Psy-chiatry 1998;64:690.
3. Pearce JMS. Clinical features of the exploding headsyndrome. J Neurol Neurosurg Psychiatry 1989;52:907–910.
4. Yeomans JS, Li L, Scott BW, Frankland PW. Tactile,acoustic and vestibular systems sum to elicit the startlereflex. Neurosci Biobehav Rev 2002;26:1–11.
5. Montagna P, Liguori R, Zucconi M, et al. Physiologi-cal hypnic myoclonus. Electroencephalogr Clin Neuro-physiol 1988;70:172–176.
6. Sachs C, Svanborg E. The exploding head syndrome:polysomnographic recordings and therapeutic sugges-tions. Sleep 1991;14:263–266.
7. Gervasoni D, Peyron C, Rampon C, et al. Role andorigin of the GABAergic innervation of dorsal rapheserotonergic neurons. J Neurosci 2000;20:4217–4225.
Activate Your Online SubscriptionAtwww.neurology.org, subscribers can nowaccess the full text of the current issue ofNeurology®
and back issues. Select the “Login instructions” link that is provided on the Help screen. Here youwill be guided through a step-by-step activation process.
Neurology® online offers:
• e-Pub ahead of print
• Extensive search capabilities
• Complete online Information for Authors
• Access to Journal content in both Adobe Acrobat PDF and HTML formats
• Links to PubMed
• Examinations on designated articles for CME credit
• Resident & Fellow section
• Patient Page
• Access to in-depth supplementary scientific data
Neurology 70 May 13, 2008 1937 at CENTRO PER LA VALUT CEVEAS on May 13, 2008 www.neurology.orgDownloaded from

DOI: 10.1212/01.wnl.0000289193.89796.83 2008;70;1933-1935; originally published online Feb 6, 2008; Neurology
Riguzzi, C. A. Tassinari and P. Tinuper G. Rubboli, F. Bisulli, R. Michelucci, S. Meletti, M. A. Ribani, P. Cortelli, I. Naldi, P.
DRUG-RESISTANT FOCAL EPILEPSYSUDDEN FALLS DUE TO SEIZURE-INDUCED CARDIAC ASYSTOLE IN
This information is current as of May 13, 2008
& ServicesUpdated Information
http://www.neurology.org/cgi/content/full/70/20/1933including high-resolution figures, can be found at:
Related Articles http://www.neurology.org/cgi/content/full/70/20/1874
A related article has been published:
Supplementary Material
96.83/DC1http://www.neurology.org/cgi/content/full/01.wnl.0000289193.897Supplementary material can be found at:
Permissions & Licensing
http://www.neurology.org/misc/Permissions.shtmlor in its entirety can be found online at: Information about reproducing this article in parts (figures, tables)
Reprints http://www.neurology.org/misc/reprints.shtml
Information about ordering reprints can be found online:
at CENTRO PER LA VALUT CEVEAS on May 13, 2008 www.neurology.orgDownloaded from