Segmentation and Compression of Pharynx and Esophagus Fluoroscopic Images
Upload
independentCategory
view
0download
0
Stepwise circumferential and focal ablation ofBarrett’s esophagus with high−grade dysplasia:results of the first prospective series of 11 patients
Authors J. J. Gondrie1, R. E. Pouw1, C. M. T. Sondermeijer1, F. P. Peters1, W. L. Curvers1, W. D. Rosmolen1, K. K. Krishnadath1,F. Ten Kate2, P. Fockens1, J. J. Bergman1
Institutions 1 Department of Gastroenterology, Academic Medical Center, Amsterdam, the Netherlands2 Department of Pathology, Academic Medical Center, Amsterdam, the Netherlands
submitted 7 December 2007accepted after revision23 January 2008
BibliographyDOI 10.1055/s−2007−995567Published online12 March 2008Endoscopy 2008; 40:359±369 � Georg ThiemeVerlag KG Stuttgart ´ New YorkISSN 0013−726X
Corresponding authorJ. J. Bergman, MDDepartment ofGastroenterology andHepatologyAcademic Medical CenterMeibergdreef 91105 AZ, AmsterdamThe NetherlandsFax: +31−20−[email protected]
Original article 359
Introduction!
In patients with Barrett’s esophagus containingearly neoplasia (i. e. high−grade dysplasia [HGD]or intramucosal cancer [IMC]) endoscopic treat−ment has been reported as a safe and effectivetreatment strategy in selected patients [1 ± 7].Endoscopic therapy of early Barrett’s neoplasiacan be divided into two distinct categories: endo−scopic resection techniques and endoscopic abla−tive techniques. Endoscopic resection of focal le−sions may result in their complete removal andallows for histological assessment [5,8, 9]. Thisenables proper patient selection, with patientsshowing submucosal invasion being referred forsubsequent surgery, and those with mucosalneoplasia being amendable for additional endo−scopic management. Endoscopic resection, how−
ever, only removes a focal area from the Barrett’sesophagus keeping the patient at risk for meta−chronous lesions during follow−up [1,5, 7]. Step−wise radical endoscopic resection (SRER) hasbeen investigated as endoscopic treatment ofthe whole Barrett’s esophagus segment contain−ing HGD/IMC [2,10]. In SRER, the complete Bar−rett’s mucosa is radically resected in consecutivesessions with complete histological correlationand removal of all genetic alterations associatedwith Barrett’s esophagus [11]. Unfortunately,SRER is technically demanding and is associatedwith a symptomatic stenosis rate of 38%. In addi−tion, only patients with a Barrett’s length of< 5 cm appear amendable for this approach[2,10].Endoscopic resection can be combined with abla−tive therapy to remove any residual dysplasia as
Background and study aims: Stepwise circum−ferential and focal ablation of nondysplastic Bar−rett’s esophagus has proven safe and effective.This study assessed the efficacy and safety of ab−lation for Barrett’s esophagus with high−gradedysplasia (HGD), and residual Barrett’s esopha−gus with dysplasia after prior endoscopic resec−tion for visible lesions.Patients and methods: This was a prospectivecohort study. All visible abnormalities were re−sected prior to ablation. Persistence of dysplasiaand absence of invasive cancer was confirmedwith biopsies after endoscopic resection. A bal−loon−based electrode was used for primary cir−cumferential ablation and an endoscope−mount−ed electrode was used for secondary focal abla−tion. Eradication of dysplasia and Barrett’s esoph−agus was the main outcome measure.Results: Eleven patients (eight men; median age60 years) were treated (median Barrett’s length5 cm). Visible abnormalities were removed withendoscopic resection in six patients. The worstpathological grade of residual Barrett’s esopha−
gus after endoscopic resection and prior to abla−tion was LGD (n = 2) and HGD (n = 9). Patients un−derwent a median of two circumferential andtwo focal ablation sessions. Complete remissionof dysplasia and complete endoscopic and histo−logical removal of Barrett’s esophagus wasachieved in 11/11 patients (100%). There wereno adverse events or strictures, and in none ofthe 473 biopsies of neo−squamous mucosa wassubsquamous Barrett’s esophagus (“buried Bar−rett’s”) observed. During a median follow−upperiod of 14 months after the last treatment ses−sion and a median number of two follow−up en−doscopies, none of the patients showed recur−rence of dysplasia or endoscopic signs of recur−rent Barrett’s mucosa.Conclusions: Stepwise circumferential and focalablation appears to be a safe and effective treat−ment for complete removal of Barrett’s esopha−gus containing HGD, and can be safely performedafter prior endoscopic resection for endoscopi−cally visible abnormalities.
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369

well as any remaining nondysplastic Barrett’s mucosa. Photody−namic therapy (PDT) and, to a lesser extent, argon plasma coag−ulation (APC) historically have been the most widely used tech−niques in this respect [3, 4, 6,12± 15]. Studies on the efficacy ofthese techniques for the eradication of Barrett’s esophagus dys−plasia have shown conflicting results. A multicenter randomizedstudy comparing Photofrin−PDT (Axcan Pharma Inc., Mont−Saint−Hilaire, Quebec, Canada) with a sham treatment in pa−tients with HGD, showed that PDT led to a reduction of the num−ber of cancers occurring during follow−up (13 % vs. 28% progres−sion), but complete and persistent removal of HGD was achievedin only 59 % of patients and Barrett’s esophagus persisted inmore than 50 % of ablated patients [4]. In Europe, some groupshave published excellent results for treatment of HGD with PDTusing 5−aminolevulinic acid (5−ALA) as photosensitizer [3]. Ourgroup has investigated the efficacy of 5−ALA−PDT for the sameindication and found that only 50 % of patients had sustained re−mission of HGD [13].In addition to these conflicting results, both PDT and APC havesignificant drawbacks. First, they often do not result in completeablation of the whole Barrett’s segment [3,4,12,13]. Secondly,foci of intestinal metaplasia may be hidden underneath theneo−squamous mucosa after treatment (“buried Barrett’s”), andsome investigators fear that these areas may progress to cancerwithout being detected endoscopically due to their “hidden” na−ture [16± 18]. Thirdly, studies have shown that oncogenetic al−terations present in Barrett’s esophagus prior to PDT and APC,can still be found in the areas of residual Barrett’s and thesemay be associated with recurrences of HGD or IMC during fol−low−up [19, 20]. Lastly, APC and PDT are associated with compli−cations, of which esophageal stenosis is the most relevant, oc−curring in 20 % to 36 % of cases [4, 21].Circumferential and focal ablation using the HALO ablation sys−tem is a new endoscopic ablation technique that appears not tobe associated with the aforementioned drawbacks of PDT andAPC. The Barrett’s esophagus is ablated by radiofrequency ener−gy delivered through a specially designed balloon (HALO360),which contains multiple electrodes encircling its outer surface.For focal ablation of residual areas of Barrett’s esophagus, an en−doscope−mounted, articulated, cap−based electrode using thesame technology is used (HALO90). Studies have shown that thistype of ablation allows for effective controlled removal of theBarrett’s mucosa without the occurrence of esophageal stenosisor buried Barrett’s [22]. Radiofrequency ablation, however, hasonly been investigated in patients with nondysplastic Barrett’sesophagus and patients with LGD, both more arbitrary indica−tions for endoscopic ablation therapy [23]. No reports are avail−able on the use of ablation for treatment of HGD or its use afterendoscopic resection of focal areas with HGD or IMC, which wasthe aim of the current study.
Patients and methods!
Inclusion and exclusion criteriaPatients were eligible if they met all of the following inclusioncriteria:1. Barrett’s esophagus, defined as a columnar lined esophagus
on endoscopy showing intestinal metaplasia upon biopsy,with a maximum length between 2 and 10 cm;
2. HGD or IMC on two separate endoscopies, confirmed by anindependent review of slides by an experienced gastrointes−tinal pathologist (FtK);
3. in case of visible endoscopic abnormalities on high−resolu−tion endoscopy: focal endoscopic resection prior to ablation;
4. in case of prior endoscopic resection: documented presenceof residual LGD or HGD in biopsies obtained after endoscopicresection,
5. age between 18 and 85 years;6. written informed consent.Patients were excluded if any one of the following exclusioncriteria was present:1. in case of a prior endoscopic resection: vertical resection
margin positive for cancer, submucosal invading cancer,poorly differentiated cancer, or presence of lymphatic/vascular invasion;
2. significant esophageal stenosis (either related to prior endo−scopic resection or prior esophagitis), defined as resistance inpassing a therapeutic endoscope (Olympus ITQ160 or IT140,Olympus Europe, Hamburg, Germany, outer diameter 11.3mm);
3. visible abnormalities after endoscopic resection, but prior toablation;
4. invasive cancer in any biopsy obtained after endoscopicresection, but prior to ablation;
5. absence of residual dysplasia (i. e. LGD or HGD) after endo−scopic resection, but prior to ablation.
Endoscopic work−up and management prior to ablationPrior to inclusion in the study, patients underwent at least twoseparate endoscopic procedures for thorough mapping of theBarrett’s segment. Procedures were performed with high−reso−lution endoscopes with narrow band imaging (NBI) facilities,either the Olympus GIF−Q240FZ in conjunction with the Lucera260 system (Olympus, Tokyo, Japan) or the Olympus GIF−H180in conjunction with the Exera II−system and a high−definitionmonitor (Olympus Europe, Hamburg, Germany).The length of the Barrett’s esophagus was determined accordingthe Prague C&M classification [24]. In addition, the location ofthe diaphragmatic pinch and the presence of a hiatal herniawere recorded. The maximum proximal extent of the Barrett’smucosa (i. e. including islands) was also documented, as isolatedislands are not categorized in the Prague system. Visible lesionswere classified according to the Japanese Classification of EarlyGastric Carcinoma [25] and targeted for biopsies or endoscopicresection. Subsequently, random 4−quadrant biopsies were tak−en at 1 cm intervals.All patients underwent endoscopic ultrasonography (EUS) (Alo−ka SSD−5000 ProSound, Aloka, Meerbusch, Germany) using elec−tronic radial endoscopes (GF−UE160, Olympus GmbH, Hamburg,Germany). All patients with endoscopically visible abnormal−ities had the lesions removed by focal endoscopic resection fordiagnostic purposes prior to ablation and to ensure that ablationwas performed on an endoscopically flat mucosa without cancer.Endoscopic resection was performed with the cap−technique orwith the multiband mucosectomy technique [8, 26]. After endo−scopic resection, all resection specimens were collected for his−topathological analysis. High−resolution endoscopy was per−formed 6 weeks after endoscopic resection to exclude the pres−ence of persistent visible abnormalities prior to ablation, and toobtain biopsies (random 4−quadrant biopsies at 1 cm intervals)to confirm the presence of residual dysplasia in the remaining
Original article360
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369
Barrett’s esophagus. Ablation was performed within 3 monthsafter the last mapping endoscopy and at least 6 weeks after en−doscopic resection.
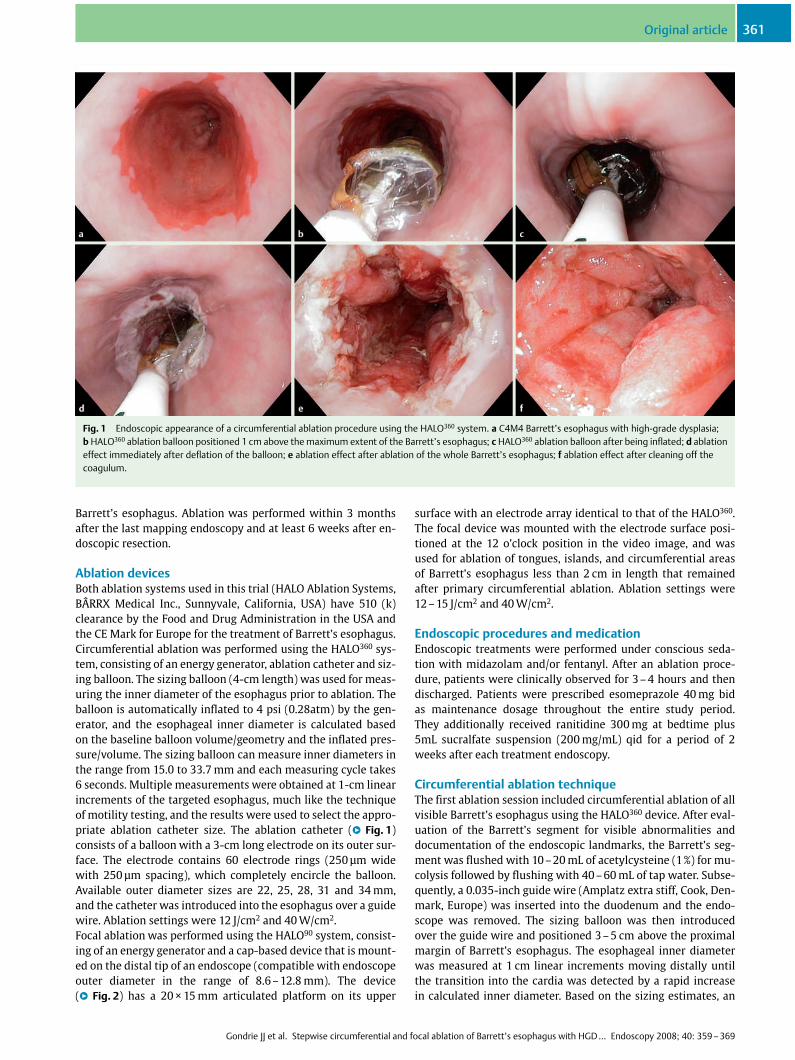
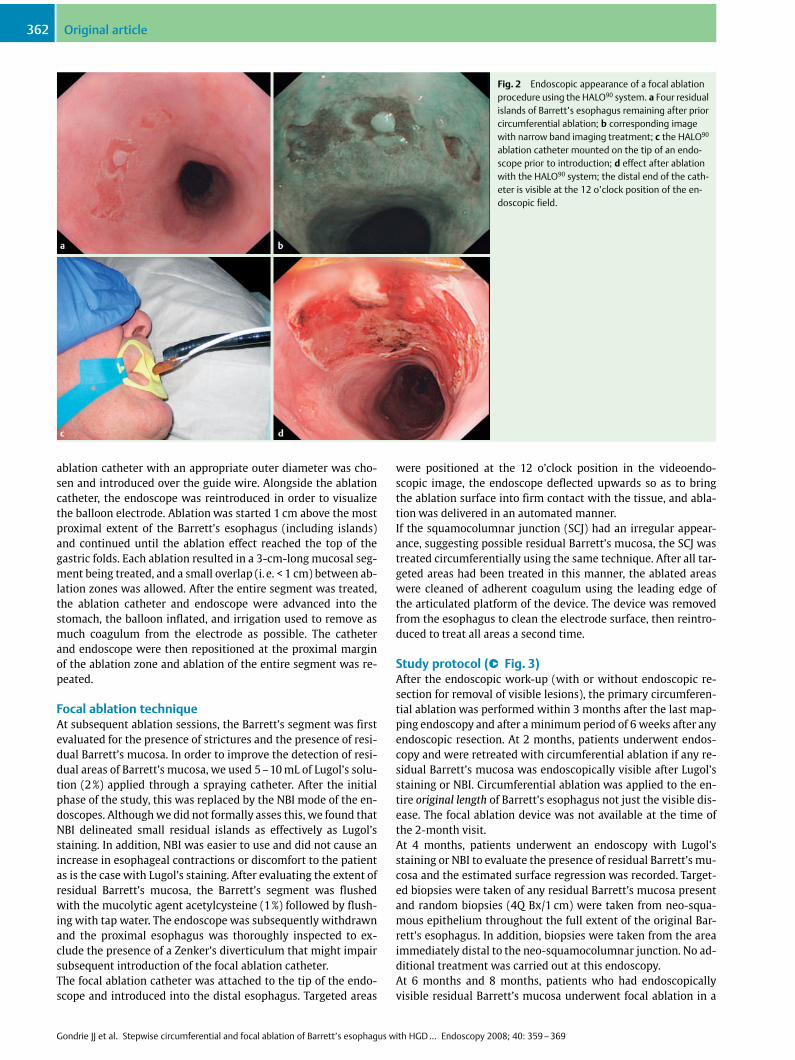
Ablation devicesBoth ablation systems used in this trial (HALO Ablation Systems,B�RRX Medical Inc., Sunnyvale, California, USA) have 510 (k)clearance by the Food and Drug Administration in the USA andthe CE Mark for Europe for the treatment of Barrett’s esophagus.Circumferential ablation was performed using the HALO360 sys−tem, consisting of an energy generator, ablation catheter and siz−ing balloon. The sizing balloon (4−cm length) was used for meas−uring the inner diameter of the esophagus prior to ablation. Theballoon is automatically inflated to 4 psi (0.28atm) by the gen−erator, and the esophageal inner diameter is calculated basedon the baseline balloon volume/geometry and the inflated pres−sure/volume. The sizing balloon can measure inner diameters inthe range from 15.0 to 33.7 mm and each measuring cycle takes6 seconds. Multiple measurements were obtained at 1−cm linearincrements of the targeted esophagus, much like the techniqueof motility testing, and the results were used to select the appro−priate ablation catheter size. The ablation catheter (l" Fig. 1)consists of a balloon with a 3−cm long electrode on its outer sur−face. The electrode contains 60 electrode rings (250 �m widewith 250 �m spacing), which completely encircle the balloon.Available outer diameter sizes are 22, 25, 28, 31 and 34 mm,and the catheter was introduced into the esophagus over a guidewire. Ablation settings were 12 J/cm2 and 40 W/cm2.Focal ablation was performed using the HALO90 system, consist−ing of an energy generator and a cap−based device that is mount−ed on the distal tip of an endoscope (compatible with endoscopeouter diameter in the range of 8.6 ± 12.8 mm). The device(l" Fig. 2) has a 20 � 15 mm articulated platform on its upper
surface with an electrode array identical to that of the HALO360.The focal device was mounted with the electrode surface posi−tioned at the 12 o’clock position in the video image, and wasused for ablation of tongues, islands, and circumferential areasof Barrett’s esophagus less than 2 cm in length that remainedafter primary circumferential ablation. Ablation settings were12± 15 J/cm2 and 40 W/cm2.
Endoscopic procedures and medicationEndoscopic treatments were performed under conscious seda−tion with midazolam and/or fentanyl. After an ablation proce−dure, patients were clinically observed for 3± 4 hours and thendischarged. Patients were prescribed esomeprazole 40 mg bidas maintenance dosage throughout the entire study period.They additionally received ranitidine 300 mg at bedtime plus5mL sucralfate suspension (200 mg/mL) qid for a period of 2weeks after each treatment endoscopy.
Circumferential ablation techniqueThe first ablation session included circumferential ablation of allvisible Barrett’s esophagus using the HALO360 device. After eval−uation of the Barrett’s segment for visible abnormalities anddocumentation of the endoscopic landmarks, the Barrett’s seg−ment was flushed with 10 ±20 mL of acetylcysteine (1%) for mu−colysis followed by flushing with 40 ± 60 mL of tap water. Subse−quently, a 0.035−inch guide wire (Amplatz extra stiff, Cook, Den−mark, Europe) was inserted into the duodenum and the endo−scope was removed. The sizing balloon was then introducedover the guide wire and positioned 3± 5 cm above the proximalmargin of Barrett’s esophagus. The esophageal inner diameterwas measured at 1 cm linear increments moving distally untilthe transition into the cardia was detected by a rapid increasein calculated inner diameter. Based on the sizing estimates, an
Fig. 1 Endoscopic appearance of a circumferential ablation procedure using the HALO360 system. a C4M4 Barrett’s esophagus with high−grade dysplasia;b HALO360 ablation balloon positioned 1 cm above the maximum extent of the Barrett’s esophagus; c HALO360 ablation balloon after being inflated; d ablationeffect immediately after deflation of the balloon; e ablation effect after ablation of the whole Barrett’s esophagus; f ablation effect after cleaning off thecoagulum.
Original article 361
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369
ablation catheter with an appropriate outer diameter was cho−sen and introduced over the guide wire. Alongside the ablationcatheter, the endoscope was reintroduced in order to visualizethe balloon electrode. Ablation was started 1 cm above the mostproximal extent of the Barrett’s esophagus (including islands)and continued until the ablation effect reached the top of thegastric folds. Each ablation resulted in a 3−cm−long mucosal seg−ment being treated, and a small overlap (i. e. < 1 cm) between ab−lation zones was allowed. After the entire segment was treated,the ablation catheter and endoscope were advanced into thestomach, the balloon inflated, and irrigation used to remove asmuch coagulum from the electrode as possible. The catheterand endoscope were then repositioned at the proximal marginof the ablation zone and ablation of the entire segment was re−peated.
Focal ablation techniqueAt subsequent ablation sessions, the Barrett’s segment was firstevaluated for the presence of strictures and the presence of resi−dual Barrett’s mucosa. In order to improve the detection of resi−dual areas of Barrett’s mucosa, we used 5 ±10 mL of Lugol’s solu−tion (2%) applied through a spraying catheter. After the initialphase of the study, this was replaced by the NBI mode of the en−doscopes. Although we did not formally asses this, we found thatNBI delineated small residual islands as effectively as Lugol’sstaining. In addition, NBI was easier to use and did not cause anincrease in esophageal contractions or discomfort to the patientas is the case with Lugol’s staining. After evaluating the extent ofresidual Barrett’s mucosa, the Barrett’s segment was flushedwith the mucolytic agent acetylcysteine (1%) followed by flush−ing with tap water. The endoscope was subsequently withdrawnand the proximal esophagus was thoroughly inspected to ex−clude the presence of a Zenker’s diverticulum that might impairsubsequent introduction of the focal ablation catheter.The focal ablation catheter was attached to the tip of the endo−scope and introduced into the distal esophagus. Targeted areas
were positioned at the 12 o’clock position in the videoendo−scopic image, the endoscope deflected upwards so as to bringthe ablation surface into firm contact with the tissue, and abla−tion was delivered in an automated manner.If the squamocolumnar junction (SCJ) had an irregular appear−ance, suggesting possible residual Barrett’s mucosa, the SCJ wastreated circumferentially using the same technique. After all tar−geted areas had been treated in this manner, the ablated areaswere cleaned of adherent coagulum using the leading edge ofthe articulated platform of the device. The device was removedfrom the esophagus to clean the electrode surface, then reintro−duced to treat all areas a second time.
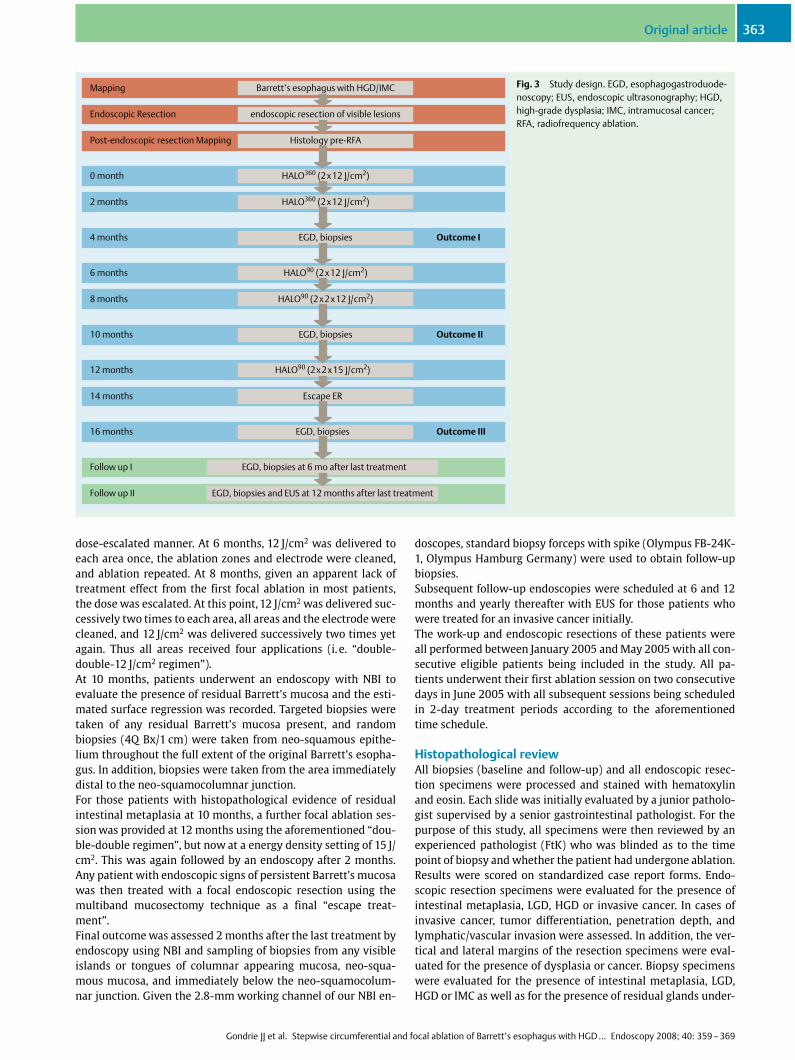
Study protocol (l" Fig. 3)After the endoscopic work−up (with or without endoscopic re−section for removal of visible lesions), the primary circumferen−tial ablation was performed within 3 months after the last map−ping endoscopy and after a minimum period of 6 weeks after anyendoscopic resection. At 2 months, patients underwent endos−copy and were retreated with circumferential ablation if any re−sidual Barrett’s mucosa was endoscopically visible after Lugol’sstaining or NBI. Circumferential ablation was applied to the en−tire original length of Barrett’s esophagus not just the visible dis−ease. The focal ablation device was not available at the time ofthe 2−month visit.At 4 months, patients underwent an endoscopy with Lugol’sstaining or NBI to evaluate the presence of residual Barrett’s mu−cosa and the estimated surface regression was recorded. Target−ed biopsies were taken of any residual Barrett’s mucosa presentand random biopsies (4Q Bx/1 cm) were taken from neo−squa−mous epithelium throughout the full extent of the original Bar−rett’s esophagus. In addition, biopsies were taken from the areaimmediately distal to the neo−squamocolumnar junction. No ad−ditional treatment was carried out at this endoscopy.At 6 months and 8 months, patients who had endoscopicallyvisible residual Barrett’s mucosa underwent focal ablation in a
Fig. 2 Endoscopic appearance of a focal ablationprocedure using the HALO90 system. a Four residualislands of Barrett’s esophagus remaining after priorcircumferential ablation; b corresponding imagewith narrow band imaging treatment; c the HALO90
ablation catheter mounted on the tip of an endo−scope prior to introduction; d effect after ablationwith the HALO90 system; the distal end of the cath−eter is visible at the 12 o’clock position of the en−doscopic field.
Original article362
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369
dose−escalated manner. At 6 months, 12 J/cm2 was delivered toeach area once, the ablation zones and electrode were cleaned,and ablation repeated. At 8 months, given an apparent lack oftreatment effect from the first focal ablation in most patients,the dose was escalated. At this point, 12 J/cm2 was delivered suc−cessively two times to each area, all areas and the electrode werecleaned, and 12 J/cm2 was delivered successively two times yetagain. Thus all areas received four applications (i. e. “double−double−12 J/cm2 regimen”).At 10 months, patients underwent an endoscopy with NBI toevaluate the presence of residual Barrett’s mucosa and the esti−mated surface regression was recorded. Targeted biopsies weretaken of any residual Barrett’s mucosa present, and randombiopsies (4Q Bx/1 cm) were taken from neo−squamous epithe−lium throughout the full extent of the original Barrett’s esopha−gus. In addition, biopsies were taken from the area immediatelydistal to the neo−squamocolumnar junction.For those patients with histopathological evidence of residualintestinal metaplasia at 10 months, a further focal ablation ses−sion was provided at 12 months using the aforementioned “dou−ble−double regimen”, but now at a energy density setting of 15 J/cm2. This was again followed by an endoscopy after 2 months.Any patient with endoscopic signs of persistent Barrett’s mucosawas then treated with a focal endoscopic resection using themultiband mucosectomy technique as a final “escape treat−ment”.Final outcome was assessed 2 months after the last treatment byendoscopy using NBI and sampling of biopsies from any visibleislands or tongues of columnar appearing mucosa, neo−squa−mous mucosa, and immediately below the neo−squamocolum−nar junction. Given the 2.8−mm working channel of our NBI en−
doscopes, standard biopsy forceps with spike (Olympus FB−24K−1, Olympus Hamburg Germany) were used to obtain follow−upbiopsies.Subsequent follow−up endoscopies were scheduled at 6 and 12months and yearly thereafter with EUS for those patients whowere treated for an invasive cancer initially.The work−up and endoscopic resections of these patients wereall performed between January 2005 and May 2005 with all con−secutive eligible patients being included in the study. All pa−tients underwent their first ablation session on two consecutivedays in June 2005 with all subsequent sessions being scheduledin 2−day treatment periods according to the aforementionedtime schedule.
Histopathological reviewAll biopsies (baseline and follow−up) and all endoscopic resec−tion specimens were processed and stained with hematoxylinand eosin. Each slide was initially evaluated by a junior patholo−gist supervised by a senior gastrointestinal pathologist. For thepurpose of this study, all specimens were then reviewed by anexperienced pathologist (FtK) who was blinded as to the timepoint of biopsy and whether the patient had undergone ablation.Results were scored on standardized case report forms. Endo−scopic resection specimens were evaluated for the presence ofintestinal metaplasia, LGD, HGD or invasive cancer. In cases ofinvasive cancer, tumor differentiation, penetration depth, andlymphatic/vascular invasion were assessed. In addition, the ver−tical and lateral margins of the resection specimens were eval−uated for the presence of dysplasia or cancer. Biopsy specimenswere evaluated for the presence of intestinal metaplasia, LGD,HGD or IMC as well as for the presence of residual glands under−
Mapping Barrett’s esophagus with HGD/IMC
Endoscopic Resection endoscopic resection of visible lesions
Post-endoscopic resection Mapping Histology pre-RFA
0 month HALO360 (2 x12 J/cm2)
2 months HALO360 (2 x12 J/cm2)
4 months EGD, biopsies Outcome I
6 months HALO90 (2 x12 J/cm2)
8 months HALO90 (2 x2x12 J/cm2)
10 months EGD, biopsies Outcome II
12 months HALO90 (2 x2x15 J/cm2)
14 months Escape ER
16 months EGD, biopsies Outcome III
Follow up I EGD, biopsies at 6 mo after last treatment
Follow up II EGD, biopsies and EUS at 12 months after last treatment
Fig. 3 Study design. EGD, esophagogastroduode−noscopy; EUS, endoscopic ultrasonography; HGD,high−grade dysplasia; IMC, intramucosal cancer;RFA, radiofrequency ablation.
Original article 363
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369
neath neo−squamous epithelium (buried Barrett’s) irrespectiveof whether these communicated with the surface or not.
Post−ablation symptom assessmentAblation−related symptoms were assessed for 14 days after eachablation procedure, including dysphagia, odynophagia, throatpain, abdominal pain, and chest pain. We used a standardizedpatient diary that queried each symptom using a 100−mm visualanalog scale (VAS), with extremes of “0” (no symptoms) and“100” (severe symptoms). The need for pain medication was re−corded as well. The patient completed the questionnaire prior toablation, immediately before being discharged after the proce−dure, and on a daily basis after each procedure for 14 days.
Outcome measuresThe following primary endpoints were defined:1. rate of complete histological clearance of dysplasia and can−
cer;2. rate of complete endoscopic and histological eradication of
intestinal metaplasia (including biopsies obtained from neo−squamous mucosa and below the neo−squamocolumnarjunction).
Secondary endpoints were:1. acute and late complications of ablation;2. estimated percentage of surface regression of Barrett’s mu−
cosa;3. the number of treatment sessions required;4. the patients’ symptoms as recorded on pre− and post−treat−
ment diary.These endpoints were assessed at 4 months (after two circum−ferential ablation sessions), at 10 months (after two circumfer−ential and maximum 1±2 focal ablation sessions), and at 2months after escape treatment with an additional focal ablationsession at 15J/cm2 supplemented with an endoscopic resectionwhen necessary (l" Fig. 3).
Ethical considerations, sample size, and statisticsThe study was approved by the medical ethics committee of ourinstitute, and written informed consent was obtained from allparticipants.As no data were available on the efficacy of this ablation tech−nique with or without prior endoscopic resection for the primaryendpoint of the study (eradication of neoplasia), and becausethis was the first ablation study performed for this indication,we did not perform a formal sample size calculation. This studywas initially planned to include 10 patients and then to evaluatethe results, anticipating that this would lead to an adjustment ofthe treatment protocol. We included eleven patients because weanticipated a drop−out rate of 10%.Data were analyzed using SPSS statistical software package(SPSS Inc., Chicago, USA). For descriptive statistics, the mean (�SD) was used in case of a normal distribution of variables, andthe median (25 %±75 %) was used for variables with a skeweddistribution. Where appropriate, the Wilcoxon rank sum testand Fisher exact test were used.
Results!
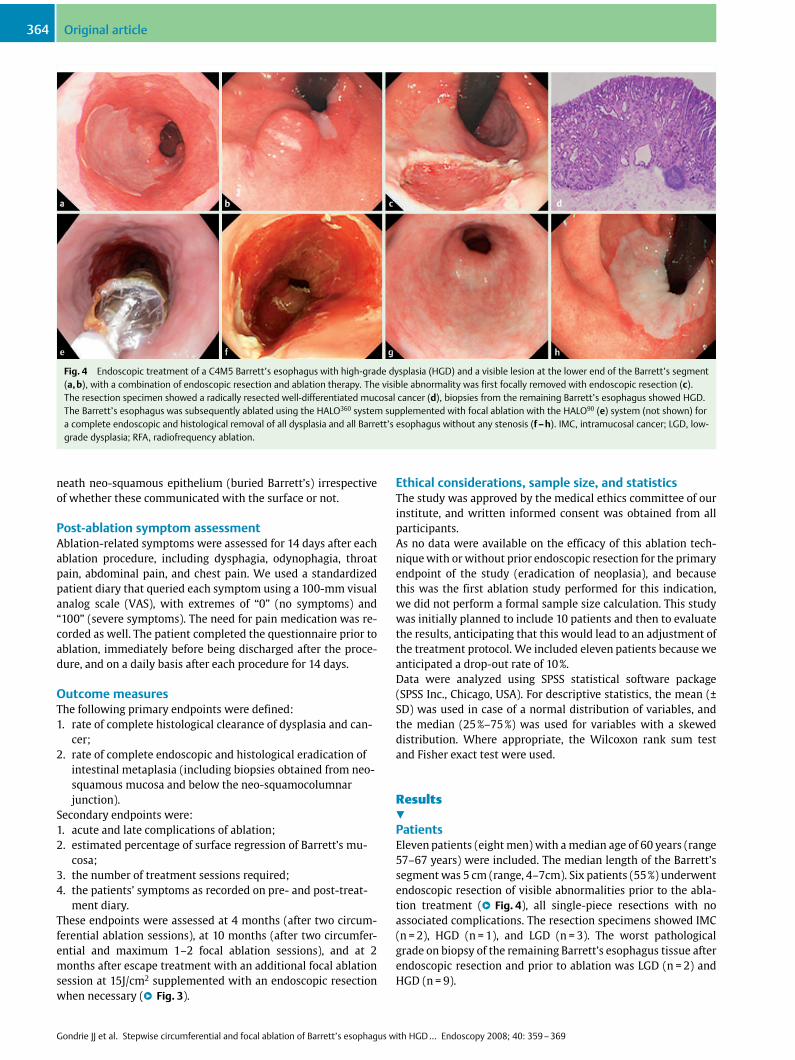
PatientsEleven patients (eight men) with a median age of 60 years (range57±67 years) were included. The median length of the Barrett’ssegment was 5 cm (range, 4±7cm). Six patients (55 %) underwentendoscopic resection of visible abnormalities prior to the abla−tion treatment (l" Fig. 4), all single−piece resections with noassociated complications. The resection specimens showed IMC(n = 2), HGD (n = 1), and LGD (n = 3). The worst pathologicalgrade on biopsy of the remaining Barrett’s esophagus tissue afterendoscopic resection and prior to ablation was LGD (n = 2) andHGD (n = 9).
Fig. 4 Endoscopic treatment of a C4M5 Barrett’s esophagus with high−grade dysplasia (HGD) and a visible lesion at the lower end of the Barrett’s segment(a, b), with a combination of endoscopic resection and ablation therapy. The visible abnormality was first focally removed with endoscopic resection (c).The resection specimen showed a radically resected well−differentiated mucosal cancer (d), biopsies from the remaining Barrett’s esophagus showed HGD.The Barrett’s esophagus was subsequently ablated using the HALO360 system supplemented with focal ablation with the HALO90 (e) system (not shown) fora complete endoscopic and histological removal of all dysplasia and all Barrett’s esophagus without any stenosis (f ± h). IMC, intramucosal cancer; LGD, low−grade dysplasia; RFA, radiofrequency ablation.
Original article364
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369
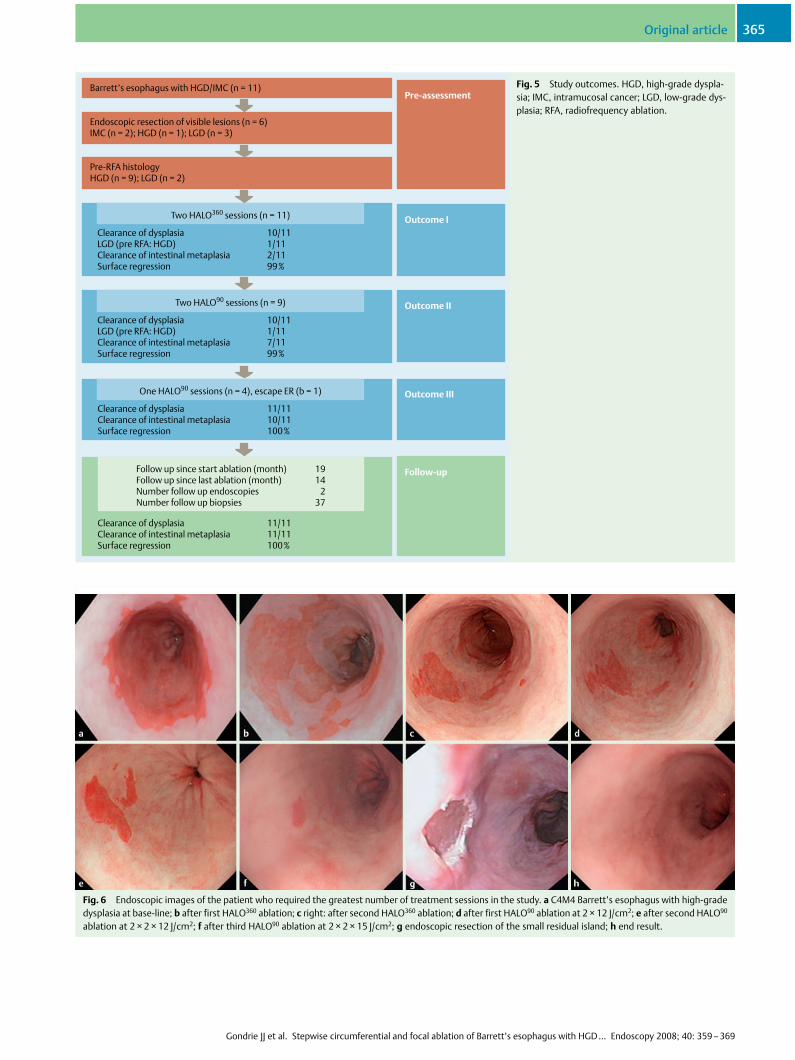
Barrett’s esophagus with HGD/IMC (n = 11)
Endoscopic resection of visible lesions (n = 6)IMC (n = 2); HGD (n = 1); LGD (n = 3)
Pre-RFA histologyHGD (n = 9); LGD (n = 2)
Clearance of dysplasia 10/11LGD (pre RFA: HGD) 1/11Clearance of intestinal metaplasia 2/11Surface regression 99%
Two HALO360 sessions (n = 11)
Clearance of dysplasia 10/11LGD (pre RFA: HGD) 1/11Clearance of intestinal metaplasia 7/11Surface regression 99%
Two HALO90 sessions (n = 9)
Clearance of dysplasia 11/11Clearance of intestinal metaplasia 10/11Surface regression 100%
One HALO90 sessions (n = 4), escape ER (b = 1)
Clearance of dysplasia 11/11Clearance of intestinal metaplasia 11/11Surface regression 100%
Follow up since start ablation (month) 19Follow up since last ablation (month) 14Number follow up endoscopies 2Number follow up biopsies 37
Pre-assessment
Outcome I
Outcome II
Outcome III
Follow-up
Fig. 5 Study outcomes. HGD, high−grade dyspla−sia; IMC, intramucosal cancer; LGD, low−grade dys−plasia; RFA, radiofrequency ablation.
Fig. 6 Endoscopic images of the patient who required the greatest number of treatment sessions in the study. a C4M4 Barrett’s esophagus with high−gradedysplasia at base−line; b after first HALO360 ablation; c right: after second HALO360 ablation; d after first HALO90 ablation at 2 � 12 J/cm2; e after second HALO90
ablation at 2 � 2 � 12 J/cm2; f after third HALO90 ablation at 2 � 2 � 15 J/cm2; g endoscopic resection of the small residual island; h end result.
Original article 365
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369
Clearance of dysplasia and intestinal metaplasia(l" Fig. 5)Complete histological eradication of dysplasia was achieved inall eleven patients (100%). This endpoint was reached at 4months (i. e. after two circumferential ablation sessions) in 10/11 (91%) patients. The patient with persisting dysplasia at 4months was downgraded from HGD to LGD. After subsequent fo−cal ablation in this one patient, the surface area of the residualBarrett’s mucosa diminished but was still found to contain LGDat 10 months. He underwent a single focal endoscopic resectionof the remaining 8−mm island, and achieved complete clearanceof dysplasia and intestinal metaplasia (l" Fig. 6).All eleven patients had complete resolution of endoscopicallyvisible columnar−lined epithelium, and complete histologicaleradication of intestinal metaplasia (including biopsies obtainedfrom neo−squamous mucosa and below the neo−squamocolum−nar junction) was achieved in all eleven patients as well (100%;l" Fig. 5). At 4 months (i. e. after two circumferential ablationsessions) only 2/11 patients had complete clearance of intestinalmetaplasia (18 %) but remaining Barrett’s mucosa typically con−sisted of small residual islands; the median percentage surfaceregression being 99 % (IQR 97 ±99). At 10 months (i. e. after twosubsequent focal ablation sessions) the rate of complete clear−ance of intestinal metaplasia increased to 7/11 patients (mediansurface regression 99% (IQR 99± 100)). Four patients underwenta final focal ablation session at 15J/cm2 followed by an escapeendoscopic resection in one patient to achieve complete clear−ance of intestinal metaplasia in all patients.During a median follow−up period of 19 months (IQR 18 ± 22)after the first ablation session and 14 months (IQR 9 ± 14) afterachieving complete endoscopic removal of all Barrett’s esopha−gus, and a median number of two follow−up endoscopies, noneof the patients showed recurrence of dysplasia or endoscopicsigns of recurrent Barrett’s mucosa. One patient had focal intes−tinal metaplasia diagnosed in a biopsy obtained immediatelydistal to an endoscopically normal appearing neo−squamoco−lumnar junction. A total number of eight biopsies were obtainedfrom this location at two different follow−up endoscopies in thispatient, with only a single biopsy showing focal intestinal meta−plasia.A total of 473 biopsies were obtained from normal appearingneo−squamous mucosa (median number per patient 37 [IQR35± 54]). There was no evidence of intestinal metaplasia in any
of these 473 biopsy fragments, and by definition, no evidence ofburied glandular mucosa.
Number of treatment sessions and complicationsAccording to the study protocol, all patients underwent two cir−cumferential ablation sessions. Patients subsequently under−went a median of two focal ablation sessions (IQR 2 ±3): therewere two patients with one focal ablation session; five patientswith two focal ablation sessions, and four patients with three fo−cal ablation sessions. One patient was treated with a single focalendoscopic resection as escape treatment (l" Fig. 6).All ablation treatment sessions were carried out as outpatientprocedures. There were no severe complications. One patientwas readmitted 6 hours after a circumferential ablation sessionwith fever and chest pain, which resolved with conservativetreatment. He was discharged after 2 days. One patient had ret−rosternal pain 5 hours after circumferential ablation, promptingprovision of additional analgesic medication, which resulted inresolution of discomfort.No other complications occurred during the treatment protocolor follow−up period. Of particular note, there were no symptomsof dysphagia and no signs of esophageal stricture formation atany follow−up endoscopy
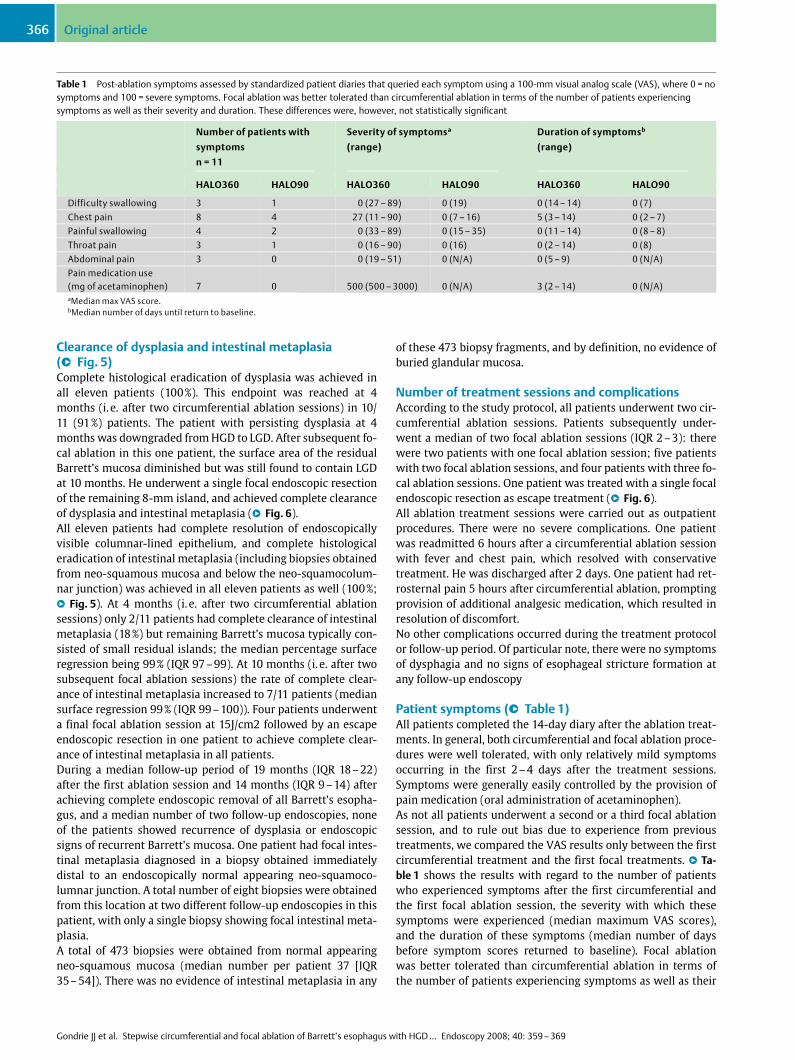
Patient symptoms (l" Table 1)All patients completed the 14−day diary after the ablation treat−ments. In general, both circumferential and focal ablation proce−dures were well tolerated, with only relatively mild symptomsoccurring in the first 2 ±4 days after the treatment sessions.Symptoms were generally easily controlled by the provision ofpain medication (oral administration of acetaminophen).As not all patients underwent a second or a third focal ablationsession, and to rule out bias due to experience from previoustreatments, we compared the VAS results only between the firstcircumferential treatment and the first focal treatments. l" Ta−ble 1 shows the results with regard to the number of patientswho experienced symptoms after the first circumferential andthe first focal ablation session, the severity with which thesesymptoms were experienced (median maximum VAS scores),and the duration of these symptoms (median number of daysbefore symptom scores returned to baseline). Focal ablationwas better tolerated than circumferential ablation in terms ofthe number of patients experiencing symptoms as well as their
Table 1 Post−ablation symptoms assessed by standardized patient diaries that queried each symptom using a 100−mm visual analog scale (VAS), where 0 = nosymptoms and 100 = severe symptoms. Focal ablation was better tolerated than circumferential ablation in terms of the number of patients experiencingsymptoms as well as their severity and duration. These differences were, however, not statistically significant
Number of patients with
symptoms
n = 11
Severity of symptomsa
(range)
Duration of symptomsb
(range)
HALO360 HALO90 HALO360 HALO90 HALO360 HALO90
Difficulty swallowing 3 1 0 (27 ± 89) 0 (19) 0 (14 ± 14) 0 (7)
Chest pain 8 4 27 (11 ± 90) 0 (7 ± 16) 5 (3 ± 14) 0 (2 ± 7)
Painful swallowing 4 2 0 (33 ± 89) 0 (15 ± 35) 0 (11 ± 14) 0 (8 ± 8)
Throat pain 3 1 0 (16 ± 90) 0 (16) 0 (2 ± 14) 0 (8)
Abdominal pain 3 0 0 (19 ± 51) 0 (N/A) 0 (5 ± 9) 0 (N/A)
Pain medication use(mg of acetaminophen) 7 0 500 (500 ± 3000) 0 (N/A) 3 (2 ± 14) 0 (N/A)aMedian max VAS score.bMedian number of days until return to baseline.
Original article366
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369

severity and duration. These differences were, however, not sta−tistically significant.
Discussion!
This is the first prospective study evaluating the use of stepwisecircumferential and focal ablation using the HALO system in Bar−rett’s patients with either HGD or with residual HGD/LGD afterprior endoscopic resection for HGD or IMC. Removal of visible le−sions with endoscopic resection not only allowed for optimalstaging of the patients but also ensured that ablation was ap−plied only on flat mucosa, preventing possible inadvertent treat−ment of patients with deeper invading lesions.In order to guarantee that only patients with “true” HGD/IMCentered the study, the histopathological diagnosis made by thepathologist of the referring hospital (for patients primarily diag−nosed elsewhere) or a junior pathologist supervised by a seniorpathologist (for patients primarily diagnosed at our unit) wasconfirmed by the study pathologist who was blinded to previousevaluations and independently reviewed all specimens. Patientswere only included if the study pathologist confirmed the initialdiagnosis of the other pathologists. More importantly, the histo−pathological diagnosis had to be made at two separate endosco−pies prior to inclusion in the study, and materials from both pro−cedures were read as mentioned above.Ablation was found to be highly effective: all patients had com−plete clearance of dysplasia, complete endoscopic and histologi−cal removal of intestinal metaplasia without recurrence of dys−plasia or endoscopic signs of Barrett’s mucosa during a medianfollow−up of 19 months. Furthermore, all ablation sessions werecarried out as outpatient procedures, there were no severe com−plications, and post−ablation symptoms were generally mild andof short duration.Despite the circumferential extent of the ablation, no patientwas diagnosed with post−ablation esophageal stenosis or suf−fered from dysphagia. The absence of ablation−related esopha−geal stenosis is a remarkable advantage compared with other ab−lation techniques, such as APC, PDT, or extensive endoscopic re−section [2± 4, 6, 21]. Earlier studies in the porcine esophagus andin humans prior to esophagectomy have shown that circumfer−ential ablation at 8 ± 12 J/cm2 results in complete epithelial abla−tion without submucosal injury or stricture formation [27,28].These findings are also in accordance with the US multicenterstudy in which 102 patients underwent ablation of intestinalmetaplasia (AIM study) and no esophageal strictures were en−countered [22]. The AIM study used an energy density of 10 J/cm2 for ablation of nondysplastic Barrett’s esophagus, whereasin the present study ablation was performed at an energy settingof 12 J/cm2 to ablate dysplastic Barrett’s esophagus. Apart from ahigher energy setting, more than half of our patients had under−gone a prior endoscopic resection, suggesting that ablation canbe applied safely after a prior endoscopic resection. It should benoted, however, that the endoscopic resections performed in ourpatients were relatively small in size, and thus we can not ex−clude the possibility that the combination of more extensive re−sections and ablation may be associated with esophageal steno−sis.Another remarkable finding was the absence of areas of intes−tinal metaplasia buried underneath the neo−squamous mucosa(buried Barrett’s) in 473 biopsies. In the US AIM study, over4000 biopsies were evaluated and again no buried Barrett’s was
detected [22]. Other ablation techniques in Barrett’s esophagushave invariably shown the occurrence of buried Barrett’s, andsome fear that these areas may progress to cancer without beingdetected endoscopically due to their “hidden” nature [16 ± 18].Although the current data do not provide absolute proof of ab−sence of buried Barrett’s after the HALO ablation technique, it atleast suggests that the frequency with which these are observedis significantly less than known of other ablation techniques. Ourresults suggest that ablation with the HALO ablation system isthe first ablation technique to find the right trade−off betweeneffectiveness (achieving complete removal of dysplasia andintestinal metaplasia without buried Barrett’s) and the avoid−ance of damage to the deeper esophageal layers causing compli−cations, such as stricture formation.As this was the first prospective study using this ablation tech−nique in patients with Barrett’s esophagus with HGD/IMC, thenumber of ablation sessions was not set beforehand. A relativelyhigh number of ablation procedures were required to achievethe rather impressive success rate in the present study: patientsunderwent a median number of two circumferential and two fo−cal ablation sessions. There are, however, reasons to expect thatfewer sessions will be required to achieve the same results in thefuture. First, while all patients underwent two circumferentialablations, 10 of the 11 only had small residual islands of Barrett’smucosa left after their first session. Although focal ablationwould have been a more logical choice, all patients had a secondcircumferential ablation as the focal device was not yet availableat that time. Second, this was the first study in which the focalablation device was used, which required us to dose−escalateduring the study period. Future studies are required to deter−mine which combination of number of applications and energydensity is the optimum for improving the efficacy of focal abla−tion. It can be expected, however, that with a more optimized fo−cal ablation regimen, a lower number of treatment sessions willsuffice in future studies.After ablation it may be difficult to assess if the neo−squamoco−lumnar junction is really at the top of the gastric folds or wheth−er a small rim of columnar−lined esophagus is still remaining.Further treatment may be guided by obtaining biopsies fromthis mucosa but negative biopsies do not exclude the presenceof residual intestinal metaplasia given its focal nature. This wasillustrated by one of our patients who, although having no endo−scopic signs of recurrence of Barrett’s esophagus, did show focalintestinal metaplasia in one of the eight biopsies obtained distalto the neo−squamocolumnar junction during follow−up. Theintestinal metaplasia was discovered at the first follow−up en−doscopy, whereas biopsies obtained at the second follow−up en−doscopy were negative. In our opinion this reflects sampling er−ror of pre−existing intestinal metaplasia which might imply thatthe patient was in fact incompletely treated. From a methodolo−gical standpoint this may be a problem, as it will be difficult todistinguish treatment failures from recurrences during follow−up. This might be solved by arbitrarily defining complete remov−al as the absence of intestinal metaplasia in all biopsies (includ−ing random biopsies distal to the neo−squamocolumnar junc−tion, at two consecutive follow−up endoscopies). From a clinicalstandpoint, however, the relevance of finding focal intestinalmetaplasia distal to a normal−appearing neo−squamocolumnarjunction may be debated. One may argue that complete histolo−gical removal of all intestinal metaplasia in patients with priorHGD or IMC is necessary to consider them to be completelycured from their underlying disease. On the other hand, intes−
Original article 367
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369

tinal metaplasia of the cardia can be detected in up to 25% of pa−tients with a normal−appearing squamocolumnar junction andis not considered a premalignant condition in those cases [29].In our opinion, finding focal intestinal metaplasia of the cardiaafter successful ablation does not justify additional treatment,as the risk of malignant degeneration is unknown. We do notfeel that the prior ablation increases the patient’s risk for malig−nant degeneration beyond that of their pre−existing conditionand given their prior diagnosis of HGD or IMC, all patients willcontinue to undergo surveillance endoscopies. In addition, theefficacy of additional treatment of focal intestinal metaplasiadistal to a normal−appearing neo−squamocolumnar junctionwill be difficult to assess given the patchy nature of this histolo−gical findingIn addition to the aforementioned patient with focal intestinalmetaplasia of the cardia during follow−up, one may argue thatablation also failed in the patient who required an escape endo−scopic resection of an island of Barrett’s containing LGD. Again,this is mainly a methodological issue: if success is defined asthe treatment effect after ablation only, the success rate of eradi−cation of dysplasia of the current study is 91% (10/11 patients).From a clinical perspective, this is rather arbitrary: a crucial as−pect of our treatment protocol was the removal of all visible le−sions by endoscopic resection prior to ablation, and in six of our11 patients the final treatment outcome was actually a result ofthe combined treatment of endoscopic resection and ablation.The fact that one patient required an endoscopic resection forcomplete removal of dysplasia after instead of prior to ablationfits within that treatment protocol. It also illustrates an impor−tant advantage of ablation with the HALO ablation system overother ablation techniques: although the patient had undergonea total of five ablative treatments, an endoscopic resection ofthe target area was easily performed using the multiband muco−sectomy technique without the need for submucosal lifting.Other ablation techniques, such as PDT or APC, generally resultin significant scarring of the esophageal wall making it difficultto perform additional endoscopic resections in case of treatmentfailure.This study has several limitations that need to be addressed.First, this study was conducted at a tertiary referral center withextensive experience in the endoscopic detection and treatmentof early Barrett’s neoplasia. All visible lesions were first removedby endoscopic resection to ensure that patients were properlystaged and that ablation was applied only on flat mucosa, pre−venting inadvertent treatment of patients with deeper invadinglesions. In centers with less experience in this field the outcomesof ablation treatment may be different. In our opinion, ablationshould only be used after meticulous endoscopic inspection ofthe Barrett’s segment has excluded the presence of visible le−sions, and that endoscopically visible abnormalities, no matterhow subtle, are removed by endoscopic resection prior to abla−tion.Secondly, only a limited number of patients were included andthe duration of follow−up was relatively short. A larger group ofpatients need to be treated to further prove the safety and effica−cy of the technique, and longer follow−up is required to showthat complete eradication of dysplasia and intestinal metaplasiaactually persists. It may not be realistic to expect that futurestudies will show complete removal of dysplasia and intestinalmetaplasia in all cases, as in the present study. As mentionedabove, some patients may have residual intestinal metaplasia ofthe cardia for which the clinical relevance is unclear, and some
patients may require the use of additional treatment modalities(such as endoscopic resection) to achieve complete eradicationof dysplasia and intestinal metaplasia. Nevertheless, given theknown drawbacks of alternative treatment options (e. g. esopha−gectomy, PDT or widespread endoscopic resection) our currentresults suggest that this newer ablation technique is an impor−tant breakthrough in the endoscopic management of patientswith early Barrett’s neoplasia.In summary, this is the first prospective study of the use of step−wise circumferential and focal ablation for treatment of bothHGD and residual HGD/LGD after prior endoscopic resection forHGD or IMC. All eleven patients had complete clearance of dys−plasia as well as complete endoscopic and histological clearanceof all Barrett’s mucosa. None of the patients developed esopha−geal stenosis and no buried Barrett’s was detected in nearly 500biopsies obtained from neo−squamous mucosa. These resultssuggest that this circumferential and focal ablation is a safe andeffective treatment for early Barrett’s neoplasia and that it canbe safely performed after prior endoscopic resection of endo−scopically visible abnormalities.
Competing interests: J. J. Bergman has received research supportin the form of grants and materials for conducting studies for thefollowing companies: B�RRX Medical, Sunnyvale, CA, USA;Olympus Endoscopy Tokyo Japan; and Wilson−Cook, Limerick,Ireland.
References1 Peters FP, Kara MA, Rosmolen WD et al. Endoscopic treatment of high−
grade dysplasia and early stage cancer in Barrett’s esophagus. Gastro−intest Endosc 2005; 61: 506± 514
2 Peters FP, Kara MA, Rosmolen WD et al. Stepwise radical endoscopic re−section is effective for complete removal of Barrett’s esophagus withearly neoplasia: a prospective study. Am J Gastroenterol 2006; 101:1449 ± 1457
3 Pech O, Gossner L, May A et al. Long−term results of photodynamictherapy with 5−aminolevulinic acid for superficial Barrett’s cancerand high−grade intraepithelial neoplasia. Gastrointest Endosc 2005;62: 24± 30
4 Overholt BF, Lightdale CJ, Wang KK et al. Photodynamic therapy withporfimer sodium for ablation of high−grade dysplasia in Barrett’sesophagus: international, partially blinded, randomized phase IIItrial. Gastrointest Endosc 2005; 62: 488± 498
5 Ell C, May A, Pech O et al. Curative endoscopic resection of early esoph−ageal adenocarcinomas (Barrett’s cancer). Gastrointest Endosc 2007;65: 3± 10
6 Prasad GA, Wang KK, Buttar NS et al. Long−term survival following en−doscopic and surgical treatment of high−grade dysplasia in Barrett’sesophagus. Gastroenterology 2007; 132: 1226 ± 1233
7 May A, Gossner L, Pech O et al. Local endoscopic therapy for intraepi−thelial high−grade neoplasia and early adenocarcinoma in Barrett’soesophagus: acute−phase and intermediate results of a new treat−ment approach. Eur J Gastroenterol Hepatol 2002; 14: 1085 ± 1091
8 Bergman JJ. Endoscopic treatment of high−grade intraepithelial neo−plasia and early cancer in Barrett’s oesophagus. Best Pract Res ClinGastroenterol 2005; 19: 889 ± 907
9 Bergman JJ. Endoscopic resection for treatment of mucosal Barrett’scancer: time to swing the pendulum. Gastrointest Endosc 2007; 65:11 ± 13
10 Seewald S, Akaraviputh T, Seitz U et al. Circumferential EMR and com−plete removal of Barrett’s epithelium: a new approach to manage−ment of Barrett’s esophagus containing high−grade intraepithelialneoplasia and intramucosal carcinoma. Gastrointest Endosc 2003;57: 854 ± 859
11 Peters FP, Krishnadath KK, Rygiel AM et al. Stepwise radical endoscopicresection of the complete Barrett’s esophagus with early neoplasiasuccessfully eradicates pre−existing genetic abnormalities. Am J Gas−troenterol 2007; 102: 1853 ± 1861
Original article368
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369

12 Ackroyd R, Brown NJ, Davis MF et al. Photodynamic therapy for dys−plastic Barrett’s oesophagus: a prospective, double blind, randomised,placebo controlled trial. Gut 2000; 47: 612± 617
13 Peters F, Kara M, Rosmolen W et al. Poor results of 5−aminolevulinicacid−photodynamic therapy for residual high−grade dysplasia and ear−ly cancer in barrett esophagus after endoscopic resection. Endoscopy2005; 37: 418 ± 424
14 Ackroyd R, Tam W, Schoeman M et al. Prospective randomized con−trolled trial of argon plasma coagulation ablation vs. endoscopic sur−veillance of patients with Barrett’s esophagus after antireflux surgery.Gastrointest Endosc 2004; 59: 1± 7
15 Dulai GS, Jensen DM, Cortina G et al. Randomized trial of argon plasmacoagulation vs. multipolar electrocoagulation for ablation of Barrett’sesophagus. Gastrointest Endosc 2005; 61: 232 ± 240
16 Overholt BF, Panjehpour M, Halberg DL. Photodynamic therapy for Bar−rett’s esophagus with dysplasia and/or early stage carcinoma: long−term results. Gastrointest Endosc 2003; 58: 183± 188
17 Hornick JL, Blount PL, Sanchez CA et al. Biologic properties of columnarepithelium underneath reepithelialized squamous mucosa in Bar−rett’s esophagus. Am J Surg Pathol 2005; 29: 372± 380
18 Van Laethem JL, Peny MO, Salmon I et al. Intramucosal adenocarcinomaarising under squamous re−epithelialisation of Barrett’s oesophagus.Gut 2000; 46: 574 ± 577
19 Hage M, Siersema PD, Vissers KJ et al. Genomic analysis of Barrett’sesophagus after ablative therapy: persistence of genetic alterationsat tumor suppressor loci. Int J Cancer 2006; 118: 155 ± 160
20 Krishnadath KK, Wang KK, Taniguchi K et al. Persistent genetic ab−normalities in Barrett’s esophagus after photodynamic therapy. Gas−troenterology 2000; 119: 624± 630
21 Ragunath K, Krasner N, Raman VS et al. Endoscopic ablation of dysplas−tic Barrett’s oesophagus comparing argon plasma coagulation andphotodynamic therapy: a randomized prospective trial assessing effi−cacy and cost−effectiveness. Scand J Gastroenterol 2005; 40: 750±758
22 Sharma VK, Wang KK, Overholt BF et al. Balloon−based, circumferen−tial, endoscopic radiofrequency ablation of Barrett’s esophagus: 1−year follow−up of 100 patients. Gastrointest Endosc 2007; 65: 185 ±195
23 Bergman JJ, Fockens P. Ablating Barrett’s metaplastic epithelium: arethe techniques ready for clinical use? Gut 2006; 55: 1222 ± 1223
24 Sharma P, Dent J, Armstrong D et al. The development and validation ofan endoscopic grading system for Barrett’s esophagus: the Prague C &M criteria. Gastroenterology 2006; 131: 1392 ± 1399
25 Aiko T, Sasako M. The new Japanese Classification of Gastric Carcino−ma: Points to be revised. Gastric Cancer 1998; 1: 25 ± 30
26 Peters FP, Kara MA, Curvers WL et al. Multiband mucosectomy for en−doscopic resection of Barrett’s esophagus: feasibility study with mat−ched historical controls. Eur J Gastroenterol Hepatol 2007; 19: 311±315
27 Dunkin BJ, Martinez J, Bejarano PA et al. Thin−layer ablation of humanesophageal epithelium using a bipolar radiofrequency balloon device.Surg Endosc 2006; 20: 125± 130
28 Ganz RA, Utley DS, Stern RA et al. Complete ablation of esophageal epi−thelium with a balloon−based bipolar electrode: a phased evaluationin the porcine and in the human esophagus. Gastrointest Endosc2004; 60: 1002± 1010
29 Morales TG, Camargo E, Bhattacharyya A et al. Long−term follow−up ofintestinal metaplasia of the gastric cardia. Am J Gastroenterol 2000;95: 1677± 1680
Original article 369
Gondrie JJ et al. Stepwise circumferential and focal ablation of Barrett’s esophagus with HGD ¼ Endoscopy 2008; 40: 359 ± 369
Copyright © 2022 FDOKUMEN