
Increasing incidence of Barrett’s oesophagus: a population-based study
7
GASTRO-INTESTINAL EPIDEMIOLOGY Increasing incidence of Barrett’s oesophagus: a population-based study Helen G. Coleman • Shivaram Bhat • Liam J. Murray • Damian McManus • Anna T. Gavin • Brian T. Johnston Received: 7 April 2011 / Accepted: 1 June 2011 / Published online: 14 June 2011 Ó Springer Science+Business Media B.V. 2011 Abstract Oesophageal adenocarcinoma, a highly fatal cancer, has risen in incidence in Western societies, but it is unclear whether this is due to increasing incidence of its pre- cursor condition, Barrett’s oesophagus (BO) or whether the proportion of BO patients undergoing malignant progression has increased in the face of unchanged BO incidence. Data from population-based studies of BO incidence is limited, with equivocal results to date difficult to distinguish from changes in endoscopic practices. The aim of this study was to assess population trends in Barrett’s oesophagus (BO) diag- noses in relation to endoscopy and biopsy rates over a 13 year period. The Northern Ireland Barrett’s oesophagus Register (NIBR) is a population-based register of all 9,329 adults diagnosed with columnar epithelium of the oesophagus in Northern Ireland between 1993 and 2005, of whom 58.3% were male. European age-standardised annual BO incidence rates were calculated per 100,000 of the population, per 100 endoscopies and per 100 endoscopies including an oesopha- geal biopsy. Average annual BO incidence rates rose by 159% during the study period, increasing from 23.9/100,000 during 1993–1997 to 62.0/100,000 during 2002–2005. This elevation far exceeded corresponding increases in rates of endoscopies and oesophageal biopsies being conducted. BO incidence increased most markedly in individuals aged \ 60 years, and most notably amongst males aged \ 40 years. This study points towards a true increase in the incidence of BO which would appear to be most marked in young males. These findings have significant implications for future rates of oesophageal adenocarcinoma and surveillance programmes. Keywords Barrett’s oesophagus Á Epidemiology Á Population-based Á Trends Abbreviations BO Barrett’s oesophagus NIBR Northern Ireland Barrett’s oesophagus Register UK United Kingdom US United States Introduction Oesophageal adenocarcinoma is relatively rare in the UK [1], but is recognised as a growing public health problem. H. G. Coleman (&) Cancer Epidemiology & Health Services Research Group, Centre for Public Health, Queen’s University Belfast, Room 02:031 ICS-B Building, RVH Site, Grosvenor Road, Belfast BT12 6BA, Northern Ireland, UK e-mail: [email protected] S. Bhat Cancer Epidemiology & Health Services Research Group, Centre for Public Health, Queen’s University Belfast, Room 1:49 Mulhouse Building, RVH Site, Grosvenor Road, Belfast BT12 6BJ, Northern Ireland, UK L. J. Murray Cancer Epidemiology & Health Services Research Group, Centre for Public Health, Queen’s University Belfast, ICS-B Building, RVH Site, Grosvenor Road, Belfast BT12 6BA, Northern Ireland, UK D. McManus Belfast Health & Social Care Trust, BCH Site, Belfast BT9 7AB, Northern Ireland, UK A. T. Gavin Northern Ireland Cancer Registry, Mulhouse Building, RVH Site, Grosvenor Road, Belfast BT12 6BJ, Northern Ireland, UK B. T. Johnston Belfast Health & Social Care Trust, RVH Site, Grosvenor Road, Belfast BT12 6BJ, Northern Ireland, UK 123 Eur J Epidemiol (2011) 26:739–745 DOI 10.1007/s10654-011-9596-z
Transcript of Increasing incidence of Barrett’s oesophagus: a population-based study
GASTRO-INTESTINAL EPIDEMIOLOGY
Increasing incidence of Barrett’s oesophagus:a population-based study
Helen G. Coleman • Shivaram Bhat •
Liam J. Murray • Damian McManus •
Anna T. Gavin • Brian T. Johnston
Received: 7 April 2011 / Accepted: 1 June 2011 / Published online: 14 June 2011
� Springer Science+Business Media B.V. 2011
Abstract Oesophageal adenocarcinoma, a highly fatal
cancer, has risen in incidence in Western societies, but it is
unclear whether this is due to increasing incidence of its pre-
cursor condition, Barrett’s oesophagus (BO) or whether the
proportion of BO patients undergoing malignant progression
has increased in the face of unchanged BO incidence. Data
from population-based studies of BO incidence is limited,
with equivocal results to date difficult to distinguish from
changes in endoscopic practices. The aim of this study was to
assess population trends in Barrett’s oesophagus (BO) diag-
noses in relation to endoscopy and biopsy rates over a 13 year
period. The Northern Ireland Barrett’s oesophagus Register
(NIBR) is a population-based register of all 9,329 adults
diagnosed with columnar epithelium of the oesophagus in
Northern Ireland between 1993 and 2005, of whom 58.3%
were male. European age-standardised annual BO incidence
rates were calculated per 100,000 of the population, per 100
endoscopies and per 100 endoscopies including an oesopha-
geal biopsy. Average annual BO incidence rates rose by 159%
during the study period, increasing from 23.9/100,000 during
1993–1997 to 62.0/100,000 during 2002–2005. This elevation
far exceeded corresponding increases in rates of endoscopies
and oesophageal biopsies being conducted. BO incidence
increased most markedly in individuals aged\60 years, and
most notably amongst males aged \40 years. This study
points towards a true increase in the incidence of BO which
would appear to be most marked in young males. These
findings have significant implications for future rates of
oesophageal adenocarcinoma and surveillance programmes.
Keywords Barrett’s oesophagus � Epidemiology �Population-based � Trends
Abbreviations
BO Barrett’s oesophagus
NIBR Northern Ireland Barrett’s oesophagus Register
UK United Kingdom
US United States
Introduction
Oesophageal adenocarcinoma is relatively rare in the UK
[1], but is recognised as a growing public health problem.
H. G. Coleman (&)
Cancer Epidemiology & Health Services Research Group,
Centre for Public Health, Queen’s University Belfast,
Room 02:031 ICS-B Building, RVH Site, Grosvenor Road,
Belfast BT12 6BA, Northern Ireland, UK
e-mail: [email protected]
S. Bhat
Cancer Epidemiology & Health Services Research Group,
Centre for Public Health, Queen’s University Belfast,
Room 1:49 Mulhouse Building, RVH Site, Grosvenor Road,
Belfast BT12 6BJ, Northern Ireland, UK
L. J. Murray
Cancer Epidemiology & Health Services Research Group,
Centre for Public Health, Queen’s University Belfast,
ICS-B Building, RVH Site, Grosvenor Road,
Belfast BT12 6BA, Northern Ireland, UK
D. McManus
Belfast Health & Social Care Trust, BCH Site, Belfast BT9 7AB,
Northern Ireland, UK
A. T. Gavin
Northern Ireland Cancer Registry, Mulhouse Building, RVH
Site, Grosvenor Road, Belfast BT12 6BJ, Northern Ireland, UK
B. T. Johnston
Belfast Health & Social Care Trust, RVH Site, Grosvenor Road,
Belfast BT12 6BJ, Northern Ireland, UK
123
Eur J Epidemiol (2011) 26:739–745
DOI 10.1007/s10654-011-9596-z

Oesophageal adenocarcinoma incidence approximately
quadrupled in England and Wales between 1971 and 1998
[2] and rates have continued to rise in the past decade [3].
Similar striking increases in oesophageal adenocarcinoma
incidence have been observed across many Western soci-
eties [1, 4–7]. Such increases in incidence cannot be
entirely attributed to detection bias from improved diag-
nostic procedures [8], misclassification bias from reclassi-
fication of adjacent gastric cancers [8, 9], nor over-
diagnosis since mortality rates from this cancer have also
increased [9].
It is possible that a rise in Barrett’s oesophagus (BO)
incidence, the pre-cursor for oesophageal adenocarcinoma,
could be accounting for the observed escalating oesopha-
geal adenocarcinoma rates. There is considerable debate
over whether there is a true rise in BO incidence in the UK
population, or if such an occurrence simply reflects chan-
ges in endoscopy practices and improvements in recogni-
tion of the disease [10]. One of the major difficulties in
accurately assessing BO incidence is a lack of robust
population-based data. Many of the studies published to
date that have identified increases in clinical BO diagnoses
exceeding those of concurrent increased rates of endoscopy
and biopsy included only relatively small numbers of BO
patients [10–13]. Nevertheless, a recent national study of
BO incidence originating from The Netherlands does
suggest an increased incidence of BO over an eleven year
period, particularly in younger males who are at a height-
ened risk of developing oesophageal adenocarcinoma [14].
By contrast two US studies have suggested that the
increase they found was largely accounted for by data
recording issues [15, 16]. The study conducted in The
Netherlands did not have available data on the numbers of
endoscopies performed [14]. Therefore, controversy
remains as to whether true changes in population BO trends
have occurred.
The aim of this investigation was to assess trends in BO
incidence in relation to endoscopy and biopsy rates over a
thirteen year period using data from the population-based
Northern Ireland Barrett’s oesophagus register.
Materials and methods
Data collection
The Northern Ireland Barrett’s oesophagus register (NIBR)
includes all patients diagnosed with BO (defined as
columnar-lined oesophagus) in Northern Ireland from
January 1993 until December 2005. The NIBR was con-
structed by performing a standardised review of pathology
reports from all oesophageal biopsies conducted in
Northern Ireland between 1993 and 2005 (corresponding to
SNOMED2 codes T62* and SNOMED3 codes T56*). Any
reports diagnosing histologically confirmed columnar epi-
thelium of the oesophagus, or synonymous terms, were
deemed to be BO and were eligible for inclusion. Reports
relating to the oesophagogastric junction or carcinoma of
either the oesophagus or oesophagogastric junction were
excluded, as were patients aged \16 years of age. Trained
staff extracted information on age, sex, date of BO diag-
nosis and, where possible, Barrett’s segment length from
the pathology reports. Data on Barrett’s segment length
were supplemented by a case note review of medical notes
conducted by three trained Tumour Verification Officers
from the Northern Ireland Cancer Registry. This case note
review was conducted for approximately one-third of
NIBR patients who were reported as having specialised
intestinal metaplasia. Finally, duplicate biopsies and
patients were removed so that only the index BO diagnosis
biopsy was retained in the NIBR.
Data on all upper gastrointestinal endoscopies and
oesophageal biopsies conducted in Northern Ireland within
the same time period were obtained from all public
healthcare providers. The largest private healthcare pro-
vider contributed endoscopy records from 1998 to 2005,
which amounted to only 2% of all endoscopies performed.
All electronic data from endoscopy to biopsy reports were
received to the Northern Ireland Cancer Registry. Infor-
mation on other conditions diagnosed at endoscopy,
including oesophagitis, gastritis, duodenitis and hiatus
hernia, were also recorded. Repeat endoscopies and
endoscopies including a biopsy that were performed after a
diagnosis of BO were removed from the endoscopy and
biopsy datasets. After rigorous electronic and manual res-
olution, 594 patients in the NIBR could not be matched to
any endoscopy records, probably due to name changes or
data entry differences, and these patients were added to the
endoscopy dataset for completion since they had to have
undergone an endoscopy to receive a BO diagnosis.
Ethical approval for the Northern Ireland Barrett’s reg-
ister and related research has been granted by the regional
ethics committee of Northern Ireland.
Statistical analysis
Annual European age-standardised incidence rates of BO
were calculated per 100,000 of the Northern Ireland pop-
ulation using mid-year population estimates (Northern
Ireland Statistics and Research Agency). European age-
standardisation was conducted using standard methods as
outlined by the International Agency for Research on
Cancer [17]. For comparison purposes, incidence rates of
oesophagitis, gastritis, duodenitis and hiatus hernia per
100,000 of the population were also calculated. To deter-
mine BO incidence in relation to endoscopy rates, firstly
740 H. G. Coleman et al.
123
the annual number of endoscopies (excluding repeat
endoscopies after a BO diagnosis) in Northern Ireland were
calculated per 100,000 of the population and age-stand-
ardised according to European rates. Annual BO incidence
was then divided by endoscopy rates and multiplied by 100
to give BO incidence per 100 endoscopies performed. BO
incidence per 100 endoscopies that included oesophageal
biopsies (hereafter referred to as BO incidence per 100
biopsies) was calculated in a similar way. Incidence rates
are also presented in three time bands to maximise com-
parability with other published population-based estimates
of BO incidence [14]. Stratified analyses were conducted
according to gender, age groupings, deprivation quintiles
and BO segment length although results are not presented
for the latter as segment length was unknown for two-thirds
of patients. Comparisons between characteristics in BO
patients were performed using independent t-tests or chi-
squared tests, as appropriate. Poisson regression was
applied to assess trends in BO incidence over time. All data
cleaning and statistical analyses were conducted using
Microsoft Office Excel 2007 and Intercooled Stata version
11.0 (College Station, Texas, USA).
Results
Over the 13 year time period in Northern Ireland, 261,725
endoscopies of the upper gastrointestinal tract were con-
ducted and 24,876 of these included oesophageal biopsies
(excluding repeat endoscopies and biopsies performed after
a BO diagnosis). This corresponded to 197,635 unique
patients who underwent an endoscopy, and resulted in
9,329 individuals aged C16 years being diagnosed with
BO.
Males accounted for 58.3% of BO patients, and were
significantly younger than females at the time of BO
diagnosis (Table 1). Overall mean age of BO diagnosis
declined from 61.9 years in 1993–1997 to 60.4 years in
2002–2005. As shown in Table 1, BO segment length was
unknown for the majority of patients.
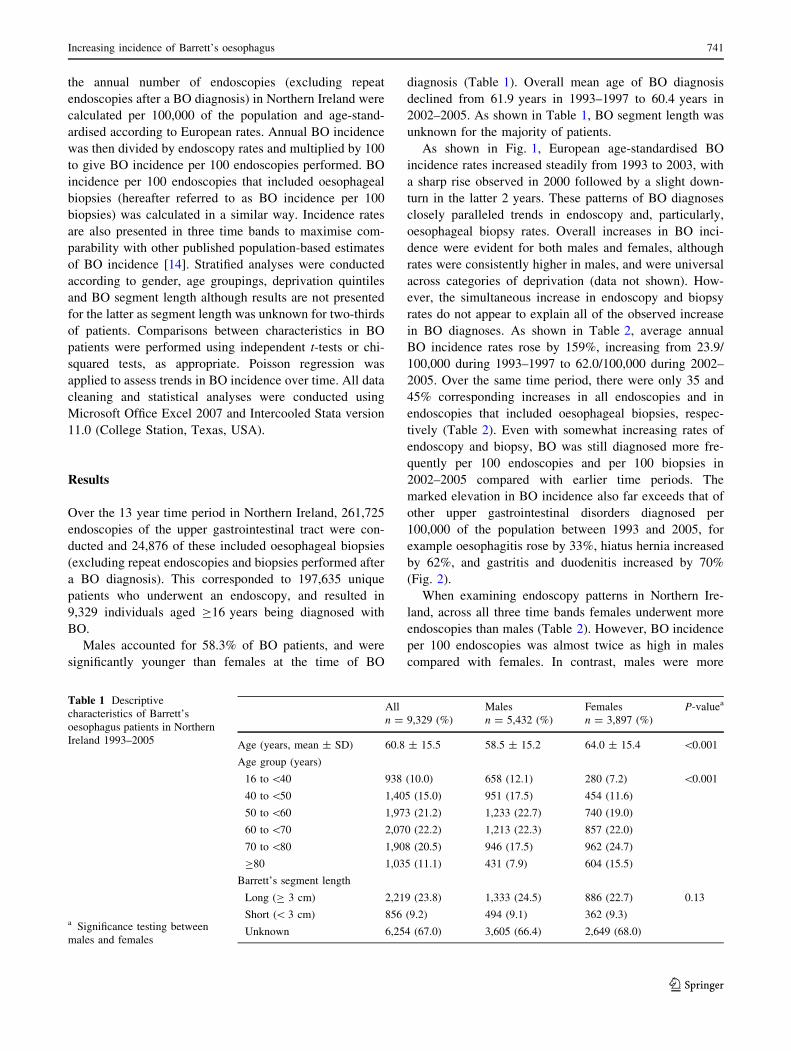
As shown in Fig. 1, European age-standardised BO
incidence rates increased steadily from 1993 to 2003, with
a sharp rise observed in 2000 followed by a slight down-
turn in the latter 2 years. These patterns of BO diagnoses
closely paralleled trends in endoscopy and, particularly,
oesophageal biopsy rates. Overall increases in BO inci-
dence were evident for both males and females, although
rates were consistently higher in males, and were universal
across categories of deprivation (data not shown). How-
ever, the simultaneous increase in endoscopy and biopsy
rates do not appear to explain all of the observed increase
in BO diagnoses. As shown in Table 2, average annual
BO incidence rates rose by 159%, increasing from 23.9/
100,000 during 1993–1997 to 62.0/100,000 during 2002–
2005. Over the same time period, there were only 35 and
45% corresponding increases in all endoscopies and in
endoscopies that included oesophageal biopsies, respec-
tively (Table 2). Even with somewhat increasing rates of
endoscopy and biopsy, BO was still diagnosed more fre-
quently per 100 endoscopies and per 100 biopsies in
2002–2005 compared with earlier time periods. The
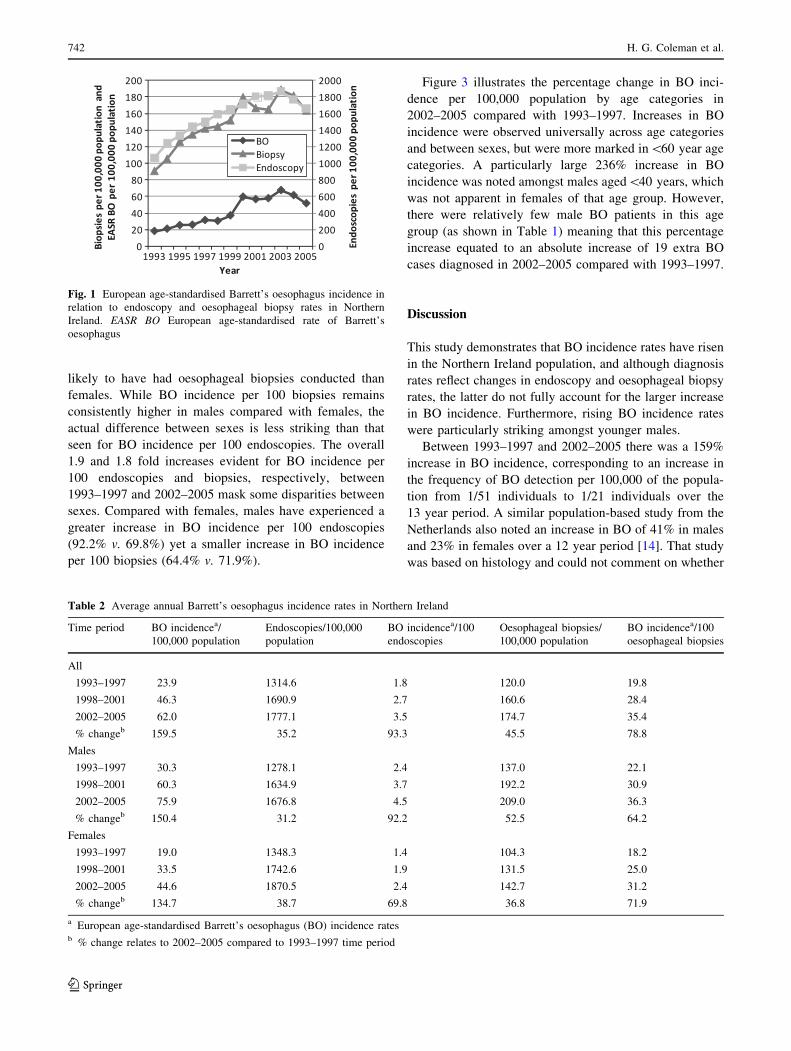
marked elevation in BO incidence also far exceeds that of
other upper gastrointestinal disorders diagnosed per
100,000 of the population between 1993 and 2005, for
example oesophagitis rose by 33%, hiatus hernia increased
by 62%, and gastritis and duodenitis increased by 70%
(Fig. 2).
When examining endoscopy patterns in Northern Ire-
land, across all three time bands females underwent more
endoscopies than males (Table 2). However, BO incidence
per 100 endoscopies was almost twice as high in males
compared with females. In contrast, males were more
Table 1 Descriptive
characteristics of Barrett’s
oesophagus patients in Northern
Ireland 1993–2005
a Significance testing between
males and females
All Males Females P-valuea
n = 9,329 (%) n = 5,432 (%) n = 3,897 (%)
Age (years, mean ± SD) 60.8 ± 15.5 58.5 ± 15.2 64.0 ± 15.4 \0.001
Age group (years)
16 to \40 938 (10.0) 658 (12.1) 280 (7.2) \0.001
40 to \50 1,405 (15.0) 951 (17.5) 454 (11.6)
50 to \60 1,973 (21.2) 1,233 (22.7) 740 (19.0)
60 to \70 2,070 (22.2) 1,213 (22.3) 857 (22.0)
70 to \80 1,908 (20.5) 946 (17.5) 962 (24.7)
C80 1,035 (11.1) 431 (7.9) 604 (15.5)
Barrett’s segment length
Long (C 3 cm) 2,219 (23.8) 1,333 (24.5) 886 (22.7) 0.13
Short (\ 3 cm) 856 (9.2) 494 (9.1) 362 (9.3)
Unknown 6,254 (67.0) 3,605 (66.4) 2,649 (68.0)
Increasing incidence of Barrett’s oesophagus 741
123
likely to have had oesophageal biopsies conducted than
females. While BO incidence per 100 biopsies remains
consistently higher in males compared with females, the
actual difference between sexes is less striking than that
seen for BO incidence per 100 endoscopies. The overall
1.9 and 1.8 fold increases evident for BO incidence per
100 endoscopies and biopsies, respectively, between
1993–1997 and 2002–2005 mask some disparities between
sexes. Compared with females, males have experienced a
greater increase in BO incidence per 100 endoscopies
(92.2% v. 69.8%) yet a smaller increase in BO incidence
per 100 biopsies (64.4% v. 71.9%).
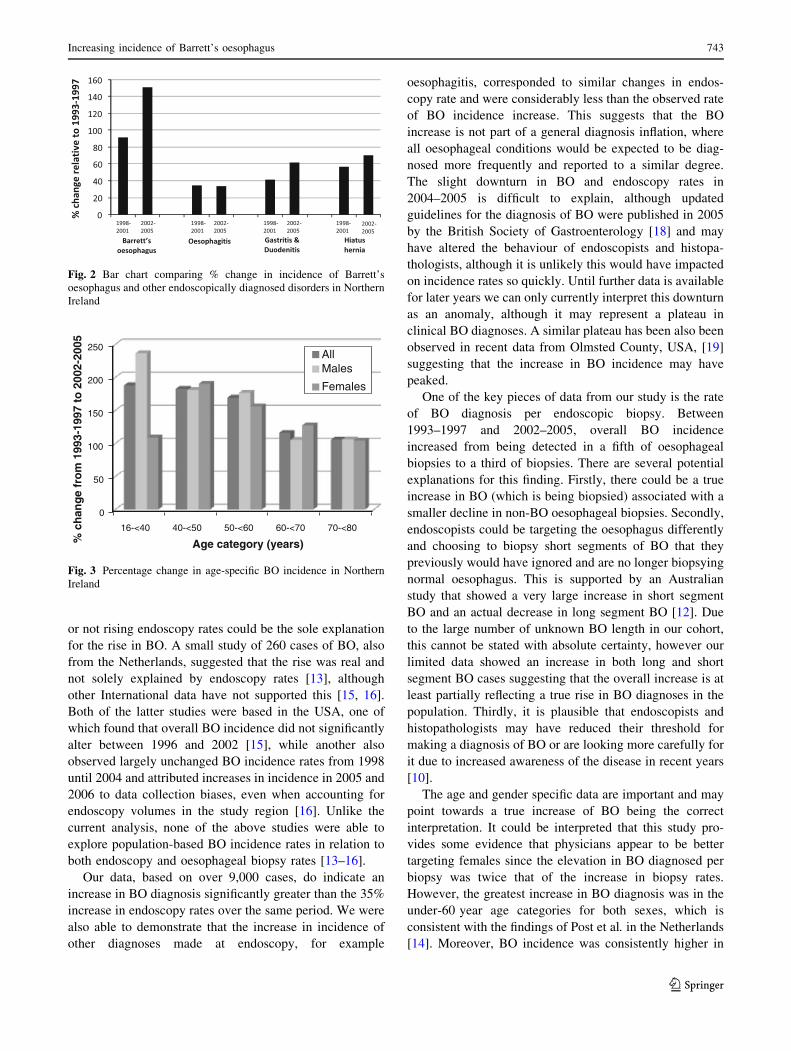
Figure 3 illustrates the percentage change in BO inci-
dence per 100,000 population by age categories in
2002–2005 compared with 1993–1997. Increases in BO
incidence were observed universally across age categories
and between sexes, but were more marked in\60 year age
categories. A particularly large 236% increase in BO
incidence was noted amongst males aged\40 years, which
was not apparent in females of that age group. However,
there were relatively few male BO patients in this age
group (as shown in Table 1) meaning that this percentage
increase equated to an absolute increase of 19 extra BO
cases diagnosed in 2002–2005 compared with 1993–1997.
Discussion
This study demonstrates that BO incidence rates have risen
in the Northern Ireland population, and although diagnosis
rates reflect changes in endoscopy and oesophageal biopsy
rates, the latter do not fully account for the larger increase
in BO incidence. Furthermore, rising BO incidence rates
were particularly striking amongst younger males.
Between 1993–1997 and 2002–2005 there was a 159%
increase in BO incidence, corresponding to an increase in
the frequency of BO detection per 100,000 of the popula-
tion from 1/51 individuals to 1/21 individuals over the
13 year period. A similar population-based study from the
Netherlands also noted an increase in BO of 41% in males
and 23% in females over a 12 year period [14]. That study
was based on histology and could not comment on whether
Fig. 1 European age-standardised Barrett’s oesophagus incidence in
relation to endoscopy and oesophageal biopsy rates in Northern
Ireland. EASR BO European age-standardised rate of Barrett’s
oesophagus
Table 2 Average annual Barrett’s oesophagus incidence rates in Northern Ireland
Time period BO incidencea/
100,000 population
Endoscopies/100,000
population
BO incidencea/100
endoscopies
Oesophageal biopsies/
100,000 population
BO incidencea/100
oesophageal biopsies
All
1993–1997 23.9 1314.6 1.8 120.0 19.8
1998–2001 46.3 1690.9 2.7 160.6 28.4
2002–2005 62.0 1777.1 3.5 174.7 35.4
% changeb 159.5 35.2 93.3 45.5 78.8
Males
1993–1997 30.3 1278.1 2.4 137.0 22.1
1998–2001 60.3 1634.9 3.7 192.2 30.9
2002–2005 75.9 1676.8 4.5 209.0 36.3
% changeb 150.4 31.2 92.2 52.5 64.2
Females
1993–1997 19.0 1348.3 1.4 104.3 18.2
1998–2001 33.5 1742.6 1.9 131.5 25.0
2002–2005 44.6 1870.5 2.4 142.7 31.2
% changeb 134.7 38.7 69.8 36.8 71.9
a European age-standardised Barrett’s oesophagus (BO) incidence ratesb % change relates to 2002–2005 compared to 1993–1997 time period
742 H. G. Coleman et al.
123
or not rising endoscopy rates could be the sole explanation
for the rise in BO. A small study of 260 cases of BO, also
from the Netherlands, suggested that the rise was real and
not solely explained by endoscopy rates [13], although
other International data have not supported this [15, 16].
Both of the latter studies were based in the USA, one of
which found that overall BO incidence did not significantly
alter between 1996 and 2002 [15], while another also
observed largely unchanged BO incidence rates from 1998
until 2004 and attributed increases in incidence in 2005 and
2006 to data collection biases, even when accounting for
endoscopy volumes in the study region [16]. Unlike the
current analysis, none of the above studies were able to
explore population-based BO incidence rates in relation to
both endoscopy and oesophageal biopsy rates [13–16].
Our data, based on over 9,000 cases, do indicate an
increase in BO diagnosis significantly greater than the 35%
increase in endoscopy rates over the same period. We were
also able to demonstrate that the increase in incidence of
other diagnoses made at endoscopy, for example
oesophagitis, corresponded to similar changes in endos-
copy rate and were considerably less than the observed rate
of BO incidence increase. This suggests that the BO
increase is not part of a general diagnosis inflation, where
all oesophageal conditions would be expected to be diag-
nosed more frequently and reported to a similar degree.
The slight downturn in BO and endoscopy rates in
2004–2005 is difficult to explain, although updated
guidelines for the diagnosis of BO were published in 2005
by the British Society of Gastroenterology [18] and may
have altered the behaviour of endoscopists and histopa-
thologists, although it is unlikely this would have impacted
on incidence rates so quickly. Until further data is available
for later years we can only currently interpret this downturn
as an anomaly, although it may represent a plateau in
clinical BO diagnoses. A similar plateau has been also been
observed in recent data from Olmsted County, USA, [19]
suggesting that the increase in BO incidence may have
peaked.
One of the key pieces of data from our study is the rate
of BO diagnosis per endoscopic biopsy. Between
1993–1997 and 2002–2005, overall BO incidence
increased from being detected in a fifth of oesophageal
biopsies to a third of biopsies. There are several potential
explanations for this finding. Firstly, there could be a true
increase in BO (which is being biopsied) associated with a
smaller decline in non-BO oesophageal biopsies. Secondly,
endoscopists could be targeting the oesophagus differently
and choosing to biopsy short segments of BO that they
previously would have ignored and are no longer biopsying
normal oesophagus. This is supported by an Australian
study that showed a very large increase in short segment
BO and an actual decrease in long segment BO [12]. Due
to the large number of unknown BO length in our cohort,
this cannot be stated with absolute certainty, however our
limited data showed an increase in both long and short
segment BO cases suggesting that the overall increase is at
least partially reflecting a true rise in BO diagnoses in the
population. Thirdly, it is plausible that endoscopists and
histopathologists may have reduced their threshold for
making a diagnosis of BO or are looking more carefully for
it due to increased awareness of the disease in recent years
[10].
The age and gender specific data are important and may
point towards a true increase of BO being the correct
interpretation. It could be interpreted that this study pro-
vides some evidence that physicians appear to be better
targeting females since the elevation in BO diagnosed per
biopsy was twice that of the increase in biopsy rates.
However, the greatest increase in BO diagnosis was in the
under-60 year age categories for both sexes, which is
consistent with the findings of Post et al. in the Netherlands
[14]. Moreover, BO incidence was consistently higher in
Fig. 2 Bar chart comparing % change in incidence of Barrett’s
oesophagus and other endoscopically diagnosed disorders in Northern
Ireland
0
50
100
150
200
250
16-<40 40-<50 50-<60 60-<70 70-<80
% c
han
ge
fro
m 1
993-
1997
to
200
2-20
05
Age category (years)
AllMales
Females
Fig. 3 Percentage change in age-specific BO incidence in Northern
Ireland
Increasing incidence of Barrett’s oesophagus 743
123

males, which could possibly be attributed to patterns of
obesity and central adiposity in the population [20, 21].
Indeed, there is a gender discrepancy in the under-40 year
age group with a large increase in BO diagnosis among
males and less so among females. This would be consistent
with the known older presentation of BO in females that is
demonstrated in both the current study and other smaller
published studies [13, 22]. These age and gender differ-
ences make altered endoscopic behaviour or altered histo-
pathology reporting less likely explanations for the
increase, as neither of these would be expected to apply
differentially across age groups or gender. If our data do
represent a true increase, this has implications for a
potentially increasing pool of individuals at risk of OAC in
the coming decades especially as the largest percentage
increase in BO diagnosis was in the youngest group of
males. Moreover, results from this study also indicate that
mean age of BO diagnosis is declining, which is consistent
with other reports from the UK [23], fuelling concerns over
possible future rises in oesophageal adenocarcinoma inci-
dence in a younger population.
Two important strengths of this study are its size and the
fact that it is a comprehensive, population-based analysis of
a relatively stable community. Through the NIBR we have
been able to capture all diagnoses of BO within a single
geographic location, allowing accurate comments to be
made regarding the emerging pattern of BO incidence.
Another major strength of this study is the accountability of
both endoscopy and oesophageal biopsy rates in our cal-
culations of BO incidence. One issue which needs to be
taken into account when comparing BO incidence in our
study with others is that Northern Ireland has a higher rate
of endoscopy compared with the rest of the UK (12.5 v.
8/1,000 population per year) (R. Hulatt, personal commu-
nication). Therefore, the generalisability of our findings
with BO incidence in other populations may be limited. We
were also unable to match 594 BO patients to their initial
endoscopy records, and so added them into the endoscopy
dataset, which may have artificially inflated the number of
endoscopies performed over this time period slightly,
however these patients only accounted for 6% of all BO
patients, and therefore any potential dilution effect on BO
rates per endoscopy is minimal. In addition, despite the
thorough analysis of endoscopy and biopsy data we are
unable to account for any changes in BO detection due to
increased awareness of the condition amongst practitioners.
We were also unable to obtain information on BO segment
length for a substantial proportion of patients therefore
analysis into increases in short v. long segment BO was
limited.
In conclusion, this large population-based study pro-
vides evidence pointing towards a true increase in the
incidence of BO which would appear to be most marked in
young males. These findings have significant implications
for future rates of oesophageal adenocarcinoma and
increased demand on surveillance programmes. Future
research should be directed towards identifying factors that
may reduce BO incidence in the population and minimise
the proportion of these patients that will undergo malignant
progression.
Acknowledgments We would like to acknowledge the contribution
of the tumour verification officers in the Northern Ireland Cancer
Registry and all staff in the Centre for Public Health who contributed
to the development of the Northern Ireland Barrett’s register. This
work was supported by funding from the Ulster Cancer Foundation
and the Health and Social Care Research and Development Office,
Northern Ireland. The Northern Ireland Cancer Registry is funded by
the Public Health Agency for Northern Ireland. The funding bodies
had no role in the study design and all researchers involved in this
study are independent of the funding bodies. All authors had full
access to all of the data (including statistical reports and tables) in the
study and can take full responsibility for the integrity of the data and
the accuracy of the data analysis.
References
1. Bosetti C, Levi F, Ferlay J, Garavello W, Lucchini F, Bertuccio
P, et al. Trends in oesophageal cancer incidence and mortality in
Europe. Int J Cancer. 2008;122:1118–29.
2. Newnham A, Quinn MJ, Babb P, Kang JY, Majeed A. Trends in
the subsite and morphology of oesophageal and gastric cancer in
England and Wales 1971–1998. Aliment Pharmacol Ther.
2003;17:665–76.
3. Lepage C, Rachet B, Jooste V, Faivre J, Coleman MP. Contin-
uing rapid increase in esophageal adenocarcinoma in England
and Wales. Am J Gastroenterol. 2008;103:2694–9.
4. Botterweck AA, Schouten LJ, Volovics A, Dorant E, van Den
Brandt PA. Trends in incidence of adenocarcinoma of the
oesophagus and gastric cardia in ten European countries. Int J
Epidemiol. 2000;29:645–54.
5. Devesa SS, Blot WJ, Fraumeni JF Jr. Changing patterns in the
incidence of esophageal and gastric carcinoma in the United
States. Cancer. 1998;83:2049–53.
6. Pera M, Manterola C, Vidal O, Grande L. Epidemiology of
esophageal adenocarcinoma. J Surg Oncol. 2005;92:151–9.
7. Crane SJ, Richard Locke G III, Harmsen WS, Diehl NN, Zins-
meister AR, Joseph Melton L III, et al. The changing incidence of
oesophageal and gastric adenocarcinoma by anatomic sub-site.
Aliment Pharmacol Ther. 2007;25:447–53.
8. Wei JT, Shaheen N. The changing epidemiology of esophageal
adenocarcinoma. Semin Gastrointest Dis. 2003;14:112–27.
9. Pohl H, Welch HG. The role of overdiagnosis and reclassification
in the marked increase of esophageal adenocarcinoma incidence.
J Natl Cancer Inst. 2005;97:142–6.
10. Prach AT, MacDonald TA, Hopwood DA, Johnston DA.
Increasing incidence of Barrett’s oesophagus: education, enthu-
siasm, or epidemiology? Lancet. 1997;350:933.
11. Conio M, Cameron AJ, Romero Y, Branch CD, Schleck CD,
Burgart LJ, et al. Secular trends in the epidemiology and outcome
of Barrett’s oesophagus in Olmsted County, Minnesota. Gut.
2001;48:304–9.
12. Kendall BJ, Whiteman DC. Temporal changes in the endoscopic
frequency of new cases of Barrett’s esophagus in an Australian
health region. Am J Gastroenterol. 2006;101:1178–82.
744 H. G. Coleman et al.
123

13. van Soest EM, Dieleman JP, Siersema PD, Sturkenboom MC,
Kuipers EJ. Increasing incidence of Barrett’s oesophagus in the
general population. Gut. 2005;54:1062–6.
14. Post PN, Siersema PD, Van Dekken H. Rising incidence of
clinically evident Barrett’s oesophagus in The Netherlands: a
nation-wide registry of pathology reports. Scand J Gastroenterol.
2007;42:17–22.
15. Musana AK, Resnick JM, Torbey CF, Mukesh BN, Greenlee RT.
Barrett’s esophagus: incidence and prevalence estimates in a rural
Mid-Western population. Am J Gastroenterol. 2008;103:516–24.
16. Corley DA, Kubo A, Levin TR, Block G, Habel L, Rumore G,
et al. Race, ethnicity, sex and temporal differences in Barrett’s
oesophagus diagnosis: a large community-based study, 1994–
2006. Gut. 2009;58:182–8.
17. Boyle P, Parkin DM. Chapter 11. Statistical methods for regis-
tries. In: Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet
RG, editors. Cancer registration: principles and methods. Lyon,
France: International Agency for Research on Cancer Scientific
Publication No. 95; 1991. p. 126–158.
18. British Society of Gastroenterology. Guidelines for the diagnosis
and management of Barrett’s columnar-lined oesophagus. 2005;
28:1–42.
19. Jung KW, Talley NJ, Romero Y, Katzka DA, Schleck CD,
Zinsmeister AR, et al. Epidemiology and natural history of
intestinal metaplasia of the gastroesophageal junction and Bar-
rett’s esophagus: a population-based study. Am J Gastroenterol.
Epub 12 Apr 2011.
20. Kamat P, Wen S, Morris J, Anandasabapathy S. Exploring the
association between elevated body mass index and Barrett’s
esophagus: a systematic review and meta-analysis. Ann Thorac
Surg. 2009;87:655–62.
21. Edelstein ZR, Farrow DC, Bronner MP, Rosen SN, Vaughan TL.
Central adiposity and risk of Barrett’s esophagus. Gastroenter-
ology. 2007;133:403–11.
22. van Blankenstein M, Looman CW, Johnston BJ, Caygill CP. Age
and sex distribution of the prevalence of Barrett’s esophagus
found in a primary referral endoscopy center. Am J Gastroenterol.
2005;100:568–76.
23. Wall CM, Charlett A, Caygill CP, Gatenby PA, Ramus JR,
Winslet MC, et al. Are newly diagnosed columnar-lined
oesophagus patients getting younger? Eur J Gastroenterol Hepa-
tol. 2009;21:1127–31.
Increasing incidence of Barrett’s oesophagus 745
123




















