Stepwise engineering of a Pichia pastoris D-amino acid oxidase whole cell catalyst
Upload
independentCategory
view
0download
0
doi: 10.1136/gut.2010.210229 2010 59: 1169-1177 originally published online June 4, 2010Gut
Roos E Pouw, Stefan Seewald, Joep J Gondrie, et al. neoplasia in a cohort of 169 patientseradication of Barrett's oesophagus with early Stepwise radical endoscopic resection for
http://gut.bmj.com/content/59/9/1169.full.htmlUpdated information and services can be found at:
These include:
References
http://gut.bmj.com/content/59/9/1169.full.html#related-urlsArticle cited in:
http://gut.bmj.com/content/59/9/1169.full.html#ref-list-1This article cites 28 articles, 2 of which can be accessed free at:
serviceEmail alerting
box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://gut.bmj.com/cgi/reprintformTo order reprints of this article go to:
http://gut.bmj.com/subscriptions go to: GutTo subscribe to
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from

Stepwise radical endoscopic resection for eradicationof Barrett’s oesophagus with early neoplasiain a cohort of 169 patients
Roos E Pouw,1 Stefan Seewald,2 Joep J Gondrie,1 Pierre H Deprez,3 Hubert Piessevaux,3
Heiko Pohl,4,5 Thomas Rosch,4 Nib Soehendra,2 Jacques J Bergman1
ABSTRACTBackground and Aims Endoscopic resection is safe andeffective to remove early neoplasia (ie,high-grade intra-epithelial neoplasia/early cancer) in Barrett’soesophagus. To prevent metachronous lesions duringfollow-up, the remaining Barrett’s oesophagus can beremoved by stepwise radical endoscopic resection(SRER). The aim was to evaluate the combinedexperience in four tertiary referral centres with SRER toeradicate Barrett’s oesophagus with early neoplasia.MethodsDesign: Retrospective cohort study.Setting: Four tertiary referral centres.Participants: 169 patients (151 males, age 64 years(IQR 57e71), Barrett’s oesophagus 3 cm (IQR 2e5))with early neoplasia in Barrett’s oesophagus #5 cm,without deep submucosal infiltration or lymph nodemetastases, treated by SRER between January 2000and September 2006.Intervention: Endoscopic resection every 4e8 weeks,until complete endoscopic and histological eradication ofBarrett’s oesophagus and neoplasia.Results According to intention-to-treat analysiscomplete eradication of all neoplasia and all intestinalmetaplasia by the end of the treatment phase wasreached in 97.6% (165/169) and 85.2% (144/169) ofpatients, respectively. One patient had progression ofneoplasia during treatment and died of metastasisedadenocarcinoma (0.6%). After median follow-up of32 months (IQR 19e49), complete eradication ofneoplasia and intestinal metaplasia was sustained in95.3% (161/169) and 80.5% (136/169) of patients,respectively. Acute, severe complications occurred in1.2% of patients, and 49.7% of patients developedsymptomatic stenosis.Conclusions SRER of Barrett’s oesophagus #5 cmcontaining early neoplasia appears to be an effectivetreatment modality with a low rate of recurrent lesionsduring follow-up. The procedure, however, is technicallydemanding and is associated with oesophageal stenosisin half of the patients.
INTRODUCTIONIn patients with Barrett’s oesophagus containinghigh-grade intraepithelial neoplasia (HGIN) orearly cancer (EC), oesophagectomy used to be thetreatment of choice.1e3 However, since lymphnode involvement occurs rarely with these earlylesions (0% for HGIN and less then 3% for earlycancer),4e7 treatment with less invasive endoscopic
Significance of this study
What is already known about this subject?< Endoscopic therapy for early Barrett’s neoplasia
has been proven a safe and effective alternativeto surgical resection in selected patients.
< Mono-therapy of neoplastic lesions with endo-scopic resection is associated with a significantnumber of recurrences (30%) in the residualBarrett’s mucosa during follow-up.
< Stepwise radical endoscopic resection (SRER) ofthe complete Barrett’s segment, to decrease therisk of metachronous lesions during follow-up,has been proven feasible in a number of small,single centre studies with limited follow-up.
What are the new findings?< This largest series worldwide shows that in
expert hands, SRER is safe and highly effectivefor complete removal of all neoplasia (97.6%)and all Barrett’s mucosa (85.2%).
< Neoplasia recurrence after complete eradicationof the Barrett’s segment was rare duringa follow-up of 32 months, which shows thatall Barrett’s mucosa should be removed fora persistent treatment effect.
< Thorough endoscopic work-up of Barrett’s patientswith early neoplasia accurately identifies the mostinvolved area: all submucosal lesions were resectedduring the first treatment session; and after removalof the most suspicious area, histological evaluationdid not reveal worse tumour characteristicsduring subsequent treatment sessions.
< Almost half of the patients developed an oeso-phageal stenosis. The rate of oesophageal stenosiswas related to the length of the resected Barrett’ssegment (ManteleHaenszel test; p¼0.002).
How might it impact on clinical practice in theforeseeable future?< Complete eradication of Barrett’s oesophagus
with early neoplasia appears to decrease therate of recurrences during follow-up. SRER canbe used for initial staging of the most involvedarea, and for subsequent safe and effectiveremoval of all residual Barrett’s mucosa. Giventhe high rate of oesophageal stenosis; however,future research should be aimed at prevention ofoesophageal stricturing or different techniquesmay be used to eradicate the whole Barrett’ssegment after diagnostic endoscopic resection.
See Commentary, p 11631Department ofGastroenterology andHepatology, Academic MedicalCenter, University ofAmsterdam, Amsterdam, theNetherlands2Department of InterdisciplinaryEndoscopy, University HospitalEppendorf, Hamburg, Germany3Department ofGastroenterology, CliniquesUniversitaires Saint-Luc,Universite Catholique deLouvain, Brussels, Belgium4Department ofGastroenterology, Charite eCampus Virchow, Berlin,Germany5VA White River Junction,Vermont, andDartmoutheHitchcock MedicalCenter, One Medical CenterDrive, Lebanon, NewHampshire, USA
Correspondence toDr Jacques J. Bergman,Department of Gastroenterologyand Hepatology, AcademicMedical Center, Meibergdreef 9,1105 AZ Amsterdam,Netherlands;[email protected]
For author footnote see end ofthe article.
Revised 22 March 2010Accepted 27 March 2010Published Online First4 June 2010
Gut 2010;59:1169e1177. doi:10.1136/gut.2010.210229 1169
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from

techniques has emerged and has been shown to be an effectiveand safe alternative for selected patients.8e11 The cornerstone ofendoscopic treatment is endoscopic resection (ER) of focallesions, which provides a relatively large tissue specimen foraccurate histological assessment. Focal ER, however, is associ-ated with recurrent lesions elsewhere in the Barrett’s oesoph-agus in 25e33% of patients during follow-up if the residualBarrett mucosa is left untreated.9e11 To minimise this risk ofrecurrence, not only the neoplasia but all Barrett mucosa can beremoved by stepwise radical endoscopic resection (SRER). InSRER the whole Barrett’s oesophagus is resected by subsequentER-sessions resulting in complete removal of the Barrett’soesophagus with histological correlation of the whole Barrettsegment. SRER has been shown to effectively eradicateneoplastic Barrett’s oesophagus in relatively small-sizedsingle-centre studies.12e18 The aim of the current multi-centrestudy was to retrospectively evaluate SRER in four Europeantertiary referral centres for early Barrett neoplasia, all usinga prospective treatment protocol. This study aimed atevaluating the safety and efficacy of SRER in a significantlylarger cohort with a longer follow-up period than reportedthus far.
PATIENTS AND METHODSData collectionAll participating centres used a comparable protocol for SRERtreatment. In two centres, data were prospectively entered intoa dedicated database whereas the other two centres documentedtheir findings in endoscopy and pathology reports. For thepurpose of this study, all centres were visited by two researchersexperienced in the field of endoscopic treatment of early Barrettneoplasia. Standardised case record forms were used to extractrelevant data from the prospective databases and/or endoscopyand pathology reports. The collected data were then entered intoa central database for further evaluation. After a first analysis, allcentres were revisited by the same researcher to update follow-up data for included patients, collect missing data, and to reviewcharts of all patients that underwent ER at the participatingcentres again to ensure that no patients were inadvertentlyexcluded.
Selection criteriaFor this retrospective multi-centre cohort study, all patientsthat underwent an ER at the University Hospital Eppendorf(Hamburg), Charité-Campus Virchow (Berlin); CliniquesUniversitaires Saint-Luc (Brussels) and Academic Medical Centre(Amsterdam), from January 2000 until September 2006, werereviewed. Patients were included if they met all of the followingcriteria:1. Maximum estimated Barrett’s oesophagus length of 5 cm,
with intestinal metaplasia (IM) upon biopsy2. A histological diagnosis of HGIN or invasive cancer in
biopsies or ER-specimens3. In the case of a diagnostic ER (always performed during the
first ER session), specimens could not show any of thefollowing criteria: invasion >T1sm1, poorly/undifferentiatedcancer (G3/G4), lymphevascular invasion, irradical deepresection margins (Note: T1sm1 cancer with G1/G2 differen-tiation and no lymphevascular invasion, was considereda relative indication for endoscopic treatment, if patients hadserious contraindications for surgery or refused surgery. Bothendoscopic and surgical options were discussed with thesepatients before treating them with SRER);
4. No signs of lymph node or distant metastasis on endo-sonography or CT
5. Patients were considered eligible for complete eradication oftheir Barrett’s oesophagus by means of SRER.Patients were excluded if, after focal ER of visible lesions, they
were not additionally treated by SRER, but with endoscopicablation (eg, argon plasma coagulation (APC), photodynamictherapy (PDT) or radiofrequency ablation (RFA)), or if residualBarrett’s oesophagus was kept under surveillance.
Treatment protocolIn the case of visible lesions suspicious for submucosal invasion,patients first underwent a diagnostic ER to assess their eligibilityfor further endoscopic treatment by means of SRER. If there wasno suspicion on deep submucosal infiltration on endoscopy orendosonography, 50% of the circumference of the Barrett’soesophagus, including the most suspicious lesion, was removedduring the first SRER session. Subsequent SRER sessions wereperformed with an interval of 4e8 weeks until endoscopiceradication of all Barrett’s oesophagus mucosa and neoplasia wasconsidered complete. Histological eradication of IM andneoplasia was confirmed by biopsies from the neosquamousmucosa and immediately distal to the neo-squamocolumnarjunction (neo-SCJ) (figure 1).Patients were prescribed high-dose proton pump inhibitor
therapy (esomeprazole/omeprazol 40 mg b.i.d.) as maintenancemedication during the entire treatment phase and aftercompletion of the protocol.
Endoscopic resection proceduresSRER procedures were generally performed on an outpatient basisusing propofol sedation, or conscious sedation with midazolamand fentanyl. Therapeutic procedures were performed usingstandard therapeutic video endoscopes (Olympus GIF-1T140/160;Olympus Europe, Hamburg, Germany). ER was performed usingeither the ER-cap technique, with oblique caps (diameter 12.8/14.8/18 mm, MAJ-296/297 or D206-5; Olympus Europe),19 20 thesimple snare technique using a monofilament steel wire(30e50 mm Erlangen-type polypectomy snare; Ch. Grosse,Daldorf, Germany),12 or multi-band mucosectomy (Duette Multi-Band Mucosectomy kit; Cook Endoscopy, Limerick, Ireland).14 20
In all cases, the area to be resected was delineated with coagula-tion markings, followed by ER of the target area using one of theabove-mentioned techniques that have been described in detailelsewhere.12 14 20 All ER specimens were retrieved, pinned on corkor paraffin and fixed in formalin.
Additional ablationAPC was used to ablate small areas of Barrett’s oesophagusmucosa that could not be resected (eg, tissue bridges betweenadjacent resections, areas difficult to reach due to stenosis), orto ablate the neo-SCJ in some patients. A 2.3 mm forwardspraying APC probe (Erbe APC 300; Erbe Elektromedizin,Tubingen, Germany) was used (power 80e99 W, argon flow1.6e2.0 l/min).
Histopathological evaluationFormalin-fixed biopsies and ER specimens were processed tohaematoxylin & eosin stained slides for routine histologicalevaluation by experienced GI pathologists. Biopsies and ERspecimens were evaluated for the presence of (subsquamous)intestinal metaplasia and neoplasia, graded according to theWHO classification.21 Furthermore, tumour infiltration depth,
1170 Gut 2010;59:1169e1177. doi:10.1136/gut.2010.210229
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from

differentiation grade, lymphevascular involvement and radi-cality at the deep resection margins were assessed in ER speci-mens as described elsewhere.22
Follow-upFollow-up started after complete removal of all endoscopicallyvisible columnar epithelium in the oesophagus, confirmedhistologically by biopsies. All patients underwent at least thefirst follow-up endoscopy in the centre where they were treatedand a strict biopsy protocol was applied with random four-quadrant biopsies distal to the neosquamocolumnar junctionand for every 1e2 cm of the neosquamous epithelium. Subse-quent follow-up endoscopies were performed every 3e6months during the first year with six monthly or annualendoscopic follow-up thereafter. Follow-up endoscopy consistedof standard video endoscopy combined with chromoendoscopy
using Lugol staining or narrow-band imaging to detect recur-rent columnar epithelium. Targeted biopsies were obtainedfrom visible columnar-like epithelium in the oesophagus, andrandomly from neosquamous mucosa and immediately distal tothe neo-SCJ.
EndpointsPrimary endpoints were assessed at the end of the treatmentphase and at the end of the follow-up:1. Complete eradication of all HGIN/cancer, defined as absence
of HGIN/cancer in biopsies (complete response of neoplasia,CR-N)
2. Complete eradication of all Barrett’s oesophagus, defined asabsence of IM in biopsies obtained from neosquamousmucosa and immediately distal to the neo-SCJ (completeresponse of IM, CR-IM).
Figure 1 Endoscopic images a Barrett’s oesophagus with early cancer treated by stepwise radical endoscopic resection (SRER). (A) C1M4 Barrett’soesophagus with at the 10 o’clock position a 0eIIaeIIc lesion. (B, C) Acute bleeding during diagnostic endoscopic resection (ER) of the lesion treatedby placement of a clip. (D) Resection specimen pinned down on paraffin. (E) Prior to the second ER session, 6 weeks after the diagnostic ER a scar isobserved at the 9 o’clock position. (F) Resection wound after the SRER session. (G) View on the resection wound with the endoscope in the retrogradeposition. (H) Complete regeneration of squamous mucosa after SRER and four dilatations sessions for symptomatic stenosis. (I) Extensive biopsiesfrom the neo-squamous mucosa during follow-up.
Gut 2010;59:1169e1177. doi:10.1136/gut.2010.210229 1171
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from

Secondary endpoints were:1. Number of treatment sessions and need for additional
treatment during the treatment phase to achieve completeeradication of neoplasia and complete endoscopic removal ofall Barrett’s oesophagus
2. Number of patients that required surgery3. Histological outcome of subsequent ER procedures4. Complications during the treatment phase, defined as ‘acute’
(during procedure), ‘early’ (0e48 h) and ‘late’ (>48 h).Complications were only recorded if they were clinicallysignificant and graded as ‘mild’ (unplanned hospital admis-sion, hospitalisation <3 days, haemoglobin drop <3 g, notransfusion), ‘moderate’ (4e10 days hospitalisation, <4 unitsblood transfusion, need for repeat endoscopic intervention,radiological intervention), ‘severe’ (hospitalisation >10 days,ICU admission, need for surgery, > 4 units blood transfusion,in the case of stenosis: >5 dilatations, stent placement orincision therapy) or ‘fatal’ (death attributable to procedure<30 days or longer with continuous hospitalisation)
5. Need for re-treatment during follow-up.
Statistical analysisFor intention-to-treat analysis the primary endpoints at the endof the treatment phase and at the end of follow-up wereaccounted for in all patients who were included for this study.Patients lost to follow-up were considered a failure for bothprimary endpoints. For patients who discontinued treatment orfollow-up, CR-N and CR-IM were defined at the exit from thestudy and in case these endpoints were unknown, they wereconsidered a failure. The treatment approach used to achieve andsustain CR-N and CR-IM was a secondary endpoint.
For the per-protocol analysis at the end of the treatmentphase, patients who were lost for further treatment or whodiscontinued treatment for unrelated reasons were censored.For per-protocol analysis at the end of the follow-up phase,patients who were lost to follow-up were censored and forpatients who discontinued follow-up CR-N and CR-IM weredefined at the exit from the study. Patients undergoing surgeryduring the treatment or follow-up phase were considereda failure
For descriptive statistics, mean (6SD) was used in case ofa normal distribution of variables and median (25%e75%) wasused for variables with a skewed distribution. Where appro-priate, the Student t test, ManneWhitney U test, orManteleHaenszel test was used.
RESULTSPatientsFrom a total of 341 patients undergoing ER in Barrett’soesophagus at the four centres from January 2000 untilSeptember 2006, 172 patients were excluded. Exclusion reasonswere: Barrett’s oesophagus >5 cm (n¼91); histological evalua-tion of diagnostic ER specimens showing contraindications forendoscopic treatment (n¼27); no signs of HGIN/EC in biopsiesor ER specimens (n¼18); ER monotherapy followed by surveil-lance (n¼15), extensive APC (n¼2), PDT (n¼8) or RFA ofresidual Barrett’s oesophagus (n¼11).
A total of 169 patients (151 males, median age 64 years(57e71), median Barrett’s oesophagus 3 cm (2e5)) wereincluded. Visible lesions were identified in 127 patients (78%)and the worst histological grade prior to ER was HGIN in 88patients and EC in 54 patients. Twenty-seven patients hadno histological diagnosis based on biopsies prior to ER, but
underwent immediate diagnostic ER of focal lesions that wereendoscopically suspicious for neoplasia (all showing HGIN/ECin resected specimens).EUS was performed in 86 patients, of which 12 underwent
EUS-FNA (fine-needle aspiration) without any signs ofmalignancy.
Primary endpointsIntention-to-treat analysis at the end of the treatment phaseA total of 169 patients were included, there were no deathsduring the treatment phase. Five patients discontinued SRERtreatment due to the following non-related reasons: withdrawalof consent (n¼1), poor mental state (n¼1), cardiovascular co-morbidity (n¼1), second primary cancer detected during thetreatment phase (n¼2). Status at time of discontinuation inthese five patients was: CR-N (n¼5) and CR-IM (n¼0). Threepatients were lost for further treatment and were considered asa failure for both endpoints.A total of 161/169 patients (95%) finished the SRER protocol.
Complete eradication of neoplasia (CR-N) was reached in 160/161 patients (99%). Complete eradication of all IM(CR-IM) was reached in 144/161 patients (89%), with small
remnants of endoscopically visible Barrett mucosa in tenpatients (6%) and a once-only histological finding of IM in sevenpatients (4%) during the first follow-up in biopsies immediatelydistal to the neo-SCJ (n¼2, 1%) and underneath neosquamousmucosa (n¼5, 3% ‘buried Barrett’s’).According to an intention-to-treat analysis the overall primary
endpoints after the treatment phase for the whole cohort of 169patients were: CR-N 165/169 (97.6%) and CR-IM 144/169(85.2%) (figure 2).Of the four patients in whom CR-N was not reached, three
were lost to follow-up as described above and one patient,initially treated for HGIN, was a failure of the endoscopictreatment protocol. This patient had a C2M3 Barrett’s oesoph-agus with inconspicuous HGIN in biopsies. After four SRERsessions, with HGIN as the worst histology in ER specimens,a rim of Barrett’s oesophagus mucosa with HGIN persisted atthe gastro-oesophageal junction. The area was treated withAPC, since ER was impeded by scarring after prior ERs.However, a visible lesion developed in this area and repeat-ERshowed a partially removed, poorly differentiated mucosalcarcinoma. Subsequent surgery revealed residual HGIN anda lymph node metastasis at the celiac trunk. Seventeen monthsafter surgery the patient was diagnosed with abdominalmetastasis and died 12 months later.
Per-protocol analysis at the end of the treatment phaseFor the per-protocol analysis patients who were lost for furthertreatment (n¼3) or who discontinued treatment for unrelatedcauses (n¼5) were censored. Patients undergoing surgery (n¼3)were considered a failure for both endpoints. By per-protocolanalysis the primary endpoints at the end of the treatmentphase were: CR-N 158/161 (98.1%) and CR-IM 141/161 (87.6%).
Intention-to-treat analysis at the end of the follow-up phaseA total of 160 patients entered the follow-up phase after eradi-cation of neoplasia. Median follow-up time from the start of thetreatment until the last follow-up endoscopy was 32 (19e49)months, and 27 months (12e42) from the last therapy sessionto the last follow-up endoscopy. Patients underwent a median of4 (2e5) follow-up endoscopies. Follow-up was discontinued in10 patients due to unrelated death (n¼7), advanced age (n¼2), ora second primary cancer detected during the follow-up phase
1172 Gut 2010;59:1169e1177. doi:10.1136/gut.2010.210229
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from

(n¼1). Status at the time of discontinuation of these 10 patientswas: CR-N (n¼10) and CR-IM (n¼7). Four patients were lost tofollow-up and were considered failures for both endpoints. Bythe time of the last data review, 146 patients were alive andunder follow-up, of which nine patients underwent re-treat-ment during the follow-up phase (see below). Complete eradi-cation of neoplasia (CR-N) was sustained in 146/146 patients(100%) whereas sustained eradication of all IM (CR-IM) wasaccomplished in 129/146 patients (88%): seven patients (5%)had a small island (<5 mm) of non-dysplastic Barrett mucosaand in 10 patients (7%) focal IM was found in biopsies obtainedimmediately distal to the neo-SCJ at the last follow-up endos-copy. The overall primary endpoints at the end of the follow-upphase were: CR-N 156/160 (97.5%) and CR-IM 136/160 (85.0%).
The overall primary endpoints at the end of treatment andfollow-up phase according to intention-to-treat analysis were:CR-N: 161/169 (95.3%) and CR-IM: 136/169 (80.5%) (figure 2).
Per-protocol analysis at the end of the follow-up phaseFor per-protocol analysis at the end of the follow-up phase,patients who were lost to follow-up (n¼4) were censored and
for patients who discontinued follow-up (n¼10) CR-N and CR-IM were defined at the exit from the study. Patients undergoingsurgery (n¼2) were considered a failure for both endpoints. Byper-protocol analysis the primary endpoints at the end of thefollow-up phase were: CR-N 152/154 (98.7%) and CR-IM 134/154 (87.0%). The overall primary endpoints at the end oftreatment and follow-up phase according to per-protocol anal-ysis were: CR-N: 152/157 (96.8%) and CR-IM: 134/157 (85.4%).
Secondary endpointsNumber of treatment sessions and the need for additional treatmentduring the treatment phasePatients underwent a median number of two (two to three) ERsessions, with a median number of four (two to six) resectionsper session. The ER-cap technique was used in 46%, multibandmucosectomy in 23%, simple snare technique in 22% anda combination of these techniques in 8% of procedures (table 1).Additional ablation with APC was performed in 103 patients
(61%), either during the ER procedure, or at a separate APCsession (n¼55 patients, median of one additional APC session).In 57 patients APC was used to ablate small islands (<10 mm2),
Figure 2 Flowchart illustrating patientflow as well as primary and secondaryendpoints in 169 patients with Barrett’soesophagus containing high-gradeintraepithelial neoplasia (HGIN)/cancer,treated with stepwise radicalendoscopic resection (SRER).
Gut 2010;59:1169e1177. doi:10.1136/gut.2010.210229 1173
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from

in 20 patients areas between 10e20 mm2 were ablated and in 26patients APC was performed for areas >20 mm2.
Overall, patients underwent a median of three (two to four)endoscopic treatment sessions, including all ER and additionalAPC sessions.
Number of patients who required surgeryA total of five patients underwent surgical oesophagectomy(5/169, 3%). Two patients were referred for surgery to removepersisting neoplasia that could not be removed endoscopically;one of these patients, with intra-abdominal tumour recurrence,has been described above; the other patient had a T1m3 G1cancer in a C0M1 Barrett’s oesophagus removed by ER; however,residual HGIN could not be removed by ER due to pre-existingscarring resulting from reflux ulceration. Two patients weretreated surgically for a perforation caused by ER (n¼1) or bydilatation of a stricture (n¼1). Finally, one patient in whoma C2M4 Barrett’s oesophagus with a T1m2 G1 cancer wascompletely removed during two SRER sessions, had recurrenceof neoplasia during follow-up (see below). Repeat ER showeda radically removed T1sm1 cancer, for which the patient wasreferred for subsequent surgery. However, no tumour rest orpositive lymph nodes were found in the surgical resectionspecimen.
Histological outcomeTable 2 displays the worst histological outcome at the subse-quent ER sessions. The worst overall diagnosis in ER specimensper patient was a radically removed T1sm1 cancer in sevenpatients (4%); mucosal cancer in 69 patients (41%); HGIN in72 patients (43%); LGIN in 10 patients (6%); and no neoplasia in11 patients (7%). The latter 21 patients with LGIN/no dysplasiain their ER specimens, all had confirmed HGIN/cancer in biop-sies obtained during endoscopic work-up.
During subsequent ER sessions, histological evaluation did notreveal worse tumour characteristics as diagnosed during the firstER session (ie, no submucosal invasion, no G3/G4 differentia-tion, no lymphevascular invasion).
Complications during the treatment phaseFour acute complications occurred during 415 ER procedures, allperforations (1.0% of procedures, 2.4% of patients). Two perfo-rations were considered severe: one was treated surgically; theother by placement of a covered stent (Esophageal Choo Stent;Fujinon Medical Holland, Veenendaal, Netherlands) and ICUadmission. Two perforations were graded as moderate: one wasclosed with clips and the patient was hospitalised for 5 days, theother was hospitalised for 7 days with conservative treatment.A moderate, early complication occurred in four patients
(1.0% of procedures, 2.4% of patients), all delayed bleedingstreated by repeat endoscopy and placement of haemoclips(n¼3).Late complications, all symptomatic stenoses, developed in 84
patients (49.7%). The rate of oesophageal stenosis was related tothe length of the resected Barrett’s oesophagus(ManteleHaenszel test; p¼0.002). Using either Savarybougienage or balloon dilatation, all patients were adequatelytreated by a median of 3 (IQR 2e6) dilatation sessions,supplemented by placement of a stent (n¼2) or incision therapy(n¼4). In 56 (67%) patients the stenosis was graded asa moderate complication due to the need for endoscopic dilata-tion, and in 28 (33%) patients the stenosis was graded as severesince >5 endoscopic dilatations, stent placement or incisiontherapy were required, or because a perforation occurred duringdilatation (n¼2, treated conservatively (n¼1) and surgically(n¼1)). None of the patients had persisting complaints ofdysphagia after dilatation therapy.
Need for re-treatment during follow-upThree patients underwent repeat ER for recurrence of HGIN(n¼2) and T1sm1 cancer (n¼1); in all cases located immediatelydistal to the neo-SCJ without a clearly visible Barrett segment intwo patients and with a small columnar-lined tongue in onepatient. Six patients were additionally treated for visiblecolumnar epithelium in the tubular oesophagus with IM uponbiopsy; using APC (n¼2), repeat ER (n¼1) or a biopsy forceps(n¼3). In all cases these were small islands (<5 mm), likelyoverlooked during the treatment phase.
DISCUSSIONUntil recently, oesophagectomy was considered the standardtherapy for patients with HGIN/EC in Barrett’s oesophagus.1
Although modern series in centres of excellence have reporteda mortality of almost 0% for HGIN and <5% for EC,2 3 oeso-phagectomy remains an invasive procedure and less invasiveendoscopic alternatives have therefore been considered. Endo-scopic resection is the cornerstone of endoscopic therapy, since it
Table 1 Overview of the different endoscopic resection (ER)techniques used in the participating centres
Centre ER-cap MBM Snare Combination
Hamburg 0.7% 24.8% 56.4% 18.1%
Amsterdam 67.2% 29.3% 0.6% 2.9%
Brussels 95.3% 4.7% 0% 0%
Berlin 95.8% 4.2% 0% 0%
MBM, multiband mucosectomy.
Table 2 Worst histological diagnosis in work-up biopsies and endoscopic resection (ER) specimens from subsequent ER sessions
Work-upbiopsies(n[142)
Worsthistology1st ER(n[169)
Worsthistology2nd ER(n[121)
Worsthistology3rd ER(n[71)
Worsthistology4th ER(n[18)
Worsthistology5th ER(n[4)
Worsthistology6th ER(n[1)
Worsthistologyoverall(n[169)
Submucosal cancer 0 7 0 0 0 0 0 7
Intramucosalcancer
54 67 7 4 1 1 0 69
High-grade IN 88 70 28 11 5 1 0 71
Low-grade IN 0 13 33 12 0 0 0 10
No neoplasia 0 12 53 44 12 2 1 12
Note: In 27 patients with macroscopic lesions suspicious for cancer, no work-up biopsies were obtained prior to treatment. All 27 patients had high-grade intraepithelial neoplasia (HGIN)/cancerin ER specimens from the first ER session. IN: intraepithelial neoplasia.
1174 Gut 2010;59:1169e1177. doi:10.1136/gut.2010.210229
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from

provides a relatively large tissue specimen for histopathologicalevaluation, enabling proper selection of patients for subsequentendoscopic versus surgical therapy.8e11 22 In the case ofsubmucosal invading lesions (T1sm), the significant risk forlymphatic involvement (15e30%) warrants surgical oesopha-gectomy with resection of surrounding lymph nodes.6 7
However, in selected patients with HGIN or EC limited to themucosal layer (T1m), the risk of lymphatic involvement isminimal, and ER in these patients has been reported to havea 5-year disease specific survival of 98%.4e8 In addition, endo-scopic treatment is associated with few complications, mostpatients are treated in an outpatient setting and the functionalintegrity of the oesophagus is preserved.8e11 After focal ER ofHGIN/EC, the residual Barrett’s oesophagus stills holds thepotential of malignant degeneration, and metachronous lesionsoccur in 30% of patients.10 11 Additional treatment of theresidual Barrett’s oesophagus after focal ER is therefore advo-cated; for example, using stepwise radical endoscopic resection(SRER). In this retrospective multi-centre study we evaluatedthe results of SRER for Barrett’s oesophagus containingHGIN/EC in four tertiary referral centres. The protocol involvedstepwise resection of the whole Barrett’s oesophagus in multipleendoscopic sessions and was limited to patients with a Barrett’soesophagus #5 cm in length.
A total of 169 patients were included in the study andaccording to intention-to-treat analysis complete eradication ofall neoplasia was reached in 97.6% of patients. Three of the fourfailures were due to patients who were lost to follow-up duringthe treatment phase and were considered failures according tothe intention-to-treat analysis. In one patient (0.6%), however,neoplasia progressed under treatment with eventually a fataloutcome.
The SRER protocol proved to be relatively safe: acute, severecomplications occurred in 1.2% of patients and the vast majorityof patients were treated with endoscopic procedures only,generally in an outpatient setting, with oesophagectomy beingperformed in 2.9% of patients.
Complete eradication of all histological IM was reached in85.2% of patients, with only small remnants of visible Barrettmucosa in ten patients and seven patients without any endo-scopic signs of residual Barrett’s oesophagus had ‘hidden’ IM inbiopsies from neosquamous mucosa or immediately distal to theneo-SCJ at the first follow-up endoscopy. Due to our strictcriteria, these patients were considered failures for the CR-IMendpoint although we feel that the extent of residual Barrett’soesophagus might be considered negligible.
A prior study from Amsterdam has demonstrated that theneosquamous mucosa that regenerates after SRER is free ofoncogenic abnormalities as present in the pre-treatmentBarrett’s oesophagus.23 This may be reflected in the low recur-rence rate during follow-up: three patients (1.8%) developedrecurrence of neoplasia that was effectively treated in all cases.After median follow-up of 32 months, intention-to-treat anal-ysis resulted in a sustained complete eradication of neoplasia in95.3% of patients. The recurrence rate for neoplasia after SRERis thus much lower than the 25e33% that can be expected aftermono-therapy with ER.10 11 Also bearing in mind that theseseries have reported their outcomes per-protocol and notaccording to the intention-to-treat principle as in our currentstudy. For comparison, per-protocol analysis of our studyshowed sustained complete eradication of neoplasia in 98.7% ofpatients.
SRER is, however, technically demanding and a number ofissues need to be discussed. First, after SRER it may be difficult
to assess if the distal end of the Barrett’s oesophagus has beencompletely resected, since it is almost impossible to endoscopi-cally distinguish residual Barrett’s from gastric mucosa at thelevel of the gastric folds. It is therefore important that the ERextends deep enough into the cardia since additional resectionsat a later stage may prove difficult due to scarring. Completenessof SRER should ideally be confirmed by biopsies taken imme-diately distal to the neo-SCJ. Despite absence of endoscopicallyvisible Barrett’s oesophagus, focal IM was incidentally found ina small number of patients during follow-up and since all threerecurrences of neoplasia occurred in the neo-SCJ area, this maybe a relevant finding. Other groups have also reported on theissue of neoplasia developing in the cardia months to years aftercomplete removal of the Barrett’s segment.24 25 However, thereason for these undesirable events is still unknown and it istherefore recommendable to focus on the neo-SCJ during follow-up, by detailed endoscopic inspection in the antegrade as well asretrograde position and by obtaining four-quadrant biopsiesfrom this area.Histological IM underneath neosquamous mucosa (buried
Barrett’s) was diagnosed in a small number of patients at a singlefollow-up endoscopy. The clinical relevance of buried Barrett’s isstill unclear. Despite anecdotal reports of subsquamous cancersthat supposedly originated from areas with buried Barrett’s afterAPC and PDT,26 some believe that the risk of malignantdegeneration in buried glands is negligible since they areprotected from the harmful effects of gastro-esophagealrefluxate.27 In this series, the clinical relevance of buried glandsmay also be questioned since they were only diagnosed earlyduring follow-up, without being reproduced at a later stage.In 21 patients no HGIN/EC was found in any of the ER
specimens during SRER treatment, even though all thesepatients had HGIN/EC in pre-treatment biopsies, confirmedafter revision by a second pathologist. There are three possibleexplanations for this discrepancy: first, patients did not haveHGIN/EC and the diagnosis was misinterpreted by multipleexpert pathologists; second, the very small foci of HGIN/ECwere effectively removed by biopsies; and third, residual HGIN/EC removed during SRER was overlooked either due to histo-logical misinterpretation or because the area of the ER specimencontaining neoplasia was not assessed by the pathologist.However, irrespective of the reason for this discrepancy, thedecision to treat the patients with SRER was made according tostandard guidelines. In countries were endoscopic managementof Barrett’s oesophagus neoplasia is less well accepted, thesepatients would likely have been considered for surgery.Symptomatic oesophageal stenosis occurred in almost half of
the patients and in 33% of these patients the stenosis met ourdefinitions of a severe complication because they required >5dilatation sessions, additional incision therapy, stent placementor dilatation resulted in a perforation. The stenosis rate wascorrelated with the length of the resected Barrett’s oesophagusand although we anticipate that SRER may also be successful inpatients with Barrett’s oesophagus >5 cm, we feel that thiscurrently is the upper limit for safe and effective SRER. Todecrease the high stenosis rate after SRER, studies on methodsto prevent stricturing after ER would be helpful; for example,placement of biodegradable stents, injection of steroids,‘prophylactic’ dilatation during the healing phase, or applicationof autologous stem cells.28 29
Recent studies combining focal ER of neoplasia with RFA ofresidual Barrett’s oesophagus have shown high efficacy rates foreradication of Barrett’s oesophagus and associated neoplasia,with absent or low rates of stenosis even when used for
Gut 2010;59:1169e1177. doi:10.1136/gut.2010.210229 1175
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from

long-segment Barrett’s oesophagus.30 Yet, a downside of allablation techniques is the lack of histological correlation. Thismay pose patients at unnecessary risk for lymph node metas-tases if a lesion with submucosal invasion, poor differentiationor lymph-vascular invasion is not diagnosed as such, andablated. In this respect, the total histological correlation of theSRER protocol may be considered an important advantage. Inthe current study, however, the most suspicious area within theBarrett’s oesophagus was identified during endoscopic work-upand removed during the first SRER session. In all patients, thehistological findings of the first SRER procedure correspondedwith the overall worst histopathology of the patient: all T1sm1cancers were identified as a suspicious lesion and removed duringthe first procedure and no G3/G4 cancers or lymphevascularinvasion were diagnosed at subsequent ER sessions. This maysuggest that after thorough endoscopic work-up and ER of themost involved area with histological correlation, the remainingBarrett’s oesophagus can be safely treated with ablation therapywithout significant risk of leaving submucosal lesions undiag-nosed and under-treated. A randomised comparison of SRER andfocal ER supplemented with RFA for residual Barrett’s oesoph-agus is currently under way.31
This study has a number of limitations that need to beaddressed. First, the endoscopists at the four study centres hadextensive experience in endoscopic detection and work-up forearly neoplasia in Barrett’s oesophagus, and in performing safeand effective piecemeal resections in Barrett’s oesophagus.The safety and efficacy results of SRER reported inthis study may, therefore, be different in centres where endo-scopic treatment of early Barrett neoplasia is practised lessfrequently.
Second, this was a retrospective study without a prede-termined mutual protocol and without central histopathologicalassessment. We acknowledge that review by a single pathologistwould have increased the homogeneity of our cohort. However,all four centres have a tertiary referral function for early Barrett’sneoplasia, which ensures a certain level of histopathologicalexpertise.
Lastly, despite prospective registration of SRER data, theretrospective inclusion of patients may have resulted in exclu-sion of patients that were initially considered for SRER treat-ment, but who did not finish treatment because of adverseeffects, for example poor healing, stricturing or otherwise.However, according to the intention-to-treat principle thesecases should be included in the cohort. After the initial dataanalysis it was therefore decided to re-visit all centres to reviewnot only patients treated with SRER, but to review all patientsundergoing an ER between January 2000 and September 2006.By surveying the course of all ER patients at each centre, weaimed at minimising the number of intention-to-treat patientswho were missed during the first data collection.
In summary, focal endoscopic resection for early Barrett’sneoplasia has been proven safe and effective with 5 year survivalrates up to 98%.8 To minimise the 30% risk of recurrentneoplasia in the residual Barrett’s segment during follow-up,9e11
SRER can be used to remove all Barrett mucosa at risk formalignant progression, with histological correlation. The resultsof this study demonstrate that SRER of Barrett’s oesophagus#5 cm containing HGIN/EC is an effective treatment modalityto remove all neoplasia and all Barrett’s mucosa, with a low rateof recurrent lesions during follow-up. However, the high rate ofoesophageal stenosis in almost half of the patients is a signifi-cant drawback of this approach that needs to be overcome bydevelopments to prevent post-ER stricturing.
Author footnote:Details of authors: R.E. Pouw (conception and design, analysis and interpretation ofdata, drafting the article, final approval to be published); S. Seewald (conception anddesign, critical revision of the manuscript for important intellectual content, finalapproval); J.J. Gondrie (conception and design, analysis and interpretation of data,drafting the article, final approval); P.H. Deprez (conception and design, criticalrevision of the manuscript for important intellectual content, final approval);H. Piessevaux (conception and design, critical revision of the manuscript for importantintellectual content, final approval); H. Pohl (conception and design, critical revision ofthe manuscript for important intellectual content, final approval); T. Rosch (conceptionand design, critical revision of the manuscript for important intellectual content, finalapproval); N. Soehendra (conception and design, critical revision of the manuscript forimportant intellectual content, final approval); J.J. Bergman (conception and design,analysis and interpretation of data, critical revision of the manuscript for importantintellectual content, final approval).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed
REFERENCES1. Holscher AH, Bollschweiler E, Schneider PM, et al. Early adenocarcinoma in
Barrett9s oesophagus. Br J Surg 1997;84:1470e3.2. Williams VA, Watson TJ, Herbella FA, et al. Esophagectomy for high grade
dysplasia is safe, curative and results in good alimentary outcome. J GastrointestSurg 2007;11:1589e97.
3. Rice TW. Esophagectomy is the treatment of choice for high-grade dysplasia inBarrett’s esophagus. Am J Gastroenterol 2006;101:2177e84.
4. Vieth M, Rosch T. Endoscopic mucosal resection and the risk of lymph-nodemetastases: indications revisited? Endoscopy 2006;38:175e9.
5. Bergman JJ. Endoscopic treatment of high-grade intraepithelial neoplasia and earlycancer in Barrett’s oesophagus. Best Pract Res Clin Gastroenterol 2005;19:889e907.
6. Westerterp M, Koppert LB, Buskens CJ, et al. Outcome of surgical treatment forearly adenocarcinoma of the esophagus or gastro-esophageal junction. VirchowsArch 2005;446:497e504.
7. Van Sandick JW, Van Lanschot JJ, Ten Kate FJ, et al. Pathology of early invasiveadenocarcinoma of the esophagus or esophagogastric junction: implications fortherapeutic decision making. Cancer 2000;88:2429e37.
8. Ell C, May A, Pech O, et al. Curative endoscopic resection of early esophagealadenocarcinomas (Barrett’s cancer). Gastrointest Endosc 2007;65:3e10.
9. Pech O, Behrens A, May A, et al. Long-term results and risk factor analysis forrecurrence after curative endoscopic therapy in 349 patients with high-gradeintraepithelial neoplasia and mucosal adenocarcinoma in Barrett’s oesophagus. Gut2008;57:1200e6.
10. May A, Gossner L, Pech O, et al. Local endoscopic therapy for intraepithelial high-grade neoplasia and early adenocarcinoma in Barrett’s oesophagus: acute-phase andintermediate results of a new treatment approach. Eur J Gastroenterol Hepatol2002;14:1085e91.
11. Peters FP, Kara MA, Rosmolen WD, et al. Endoscopic treatment of high-gradedysplasia and early stage cancer in Barrett’s esophagus. Gastrointest Endosc2005;61:506e14.
12. Seewald S, Akaraviputh T, Seitz U, et al. Circumferential EMR and completeremoval of Barrett’s epithelium: a new approach to management of Barrett’sesophagus containing high-grade intraepithelial neoplasia and intramucosalcarcinoma. Gastrointest Endosc 2003;57:854e9.
13. Giovannini M, Bories E, Pesenti C, et al. Circumferential endoscopic mucosalresection in Barrett’s esophagus with high-grade intraepithelial neoplasia or mucosalcancer. Preliminary results in 21 patients. Endoscopy 2004;36:782e7.
14. Soehendra N, Seewald S, Groth S, et al. Use of modified multiband ligatorfacilitates circumferential EMR in Barrett’s esophagus. Gastrointest Endosc2006;63:847e52.
15. Peters FP, Kara MA, Rosmolen WD, et al. Stepwise radical endoscopic resection iseffective for complete removal of Barrett’s esophagus with early neoplasia:a prospective study. Am J Gastroenterol 2006;101:1449e57.
16. Larghi A, Lightdale CJ, Ross AS, et al. Long-term follow-up of complete Barrett’seradication endoscopic mucosal resection (CBE-EMR) for the treatment of high gradedysplasia and intramucosal carcinoma. Endoscopy 2007;39:1086e91.
17. Pouw RE, Peters FP, Sempoux C, et al. Stepwise radical endoscopic resection forBarrett’s esophagus with early neoplasia: report on a Brussels’ cohort. Endoscopy2008;40:892e8.
18. Chennat J, Konda VJ, Ross AS, et al. Complete Barrett’s eradication endoscopicmucosal resection: an effective treatment modality for high grade dysplasia andintramucosal carcinomadan American single-center experience. Am J Gastroenterol2009;2684e92.
19. Peters FP, Brakenhoff KP, Curvers WL, et al. Endoscopic cap resection for treatmentof early Barrett’s neoplasia is safe: a prospective analysis of acute and earlycomplications in 216 procedures. Dis Esophagus 2007;20:510e15.
20. Peters FP, Kara MA, Curvers WL, et al. Multiband mucosectomy for endoscopicresection of Barrett’s esophagus: feasibility study with matched historical controls.Eur J Gastroenterol Hepatol 2007;19:311e15.
21. Hamilton SR, Aaltonen LA, eds. WHO classification. Tumours of the digestivesystem. Lyon: IARC Press, 2000:18e24.
1176 Gut 2010;59:1169e1177. doi:10.1136/gut.2010.210229
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from
22. Peters FP, Brakenhoff KP, Curvers WL, et al. Histologic evaluation of resectionspecimens obtained at 293 endoscopic resections in Barrett’s esophagus.Gastrointest Endosc 2008;67:604e9.
23. Peters FP, Krishnadath KK, Rygiel AM, et al. Stepwise radical endoscopic resectionof the complete Barrett’s esophagus with early neoplasia successfully eradicates pre-existing genetic abnormalities. Am J Gastroenterol 2007;102:1853e61.
24. Weston AP, Sharma P, Banerjee S, et al. Visible endoscopic and histologic changesin the cardia, before and after complete Barrett’s esophagus ablation. GastrointestEndosc 2005;61:515e21.
25. Sampliner RE, Camargo E, Prasad AR. Association of ablation of Barrett’sesophagus with high grade dysplasia and adenocarcinoma of the gastric cardia.Dis Esophagus 2006;19:277e9.
26. Van Laethem JL, Peny MO, Salmon I, et al. Intramucosal adenocarcinomaarising under squamous re-epithelialisation of Barrett’s oesophagus. Gut2000;46:574e7.
27. Hornick JL, Blount PL, Sanchez CA, et al. Biologic properties of columnar epitheliumunderneath reepithelialized squamous mucosa in Barrett’s esophagus. Am J SurgPathol 2005;29:372e80.
28. Rajan E, Gostout C, Feitoza A, et al. Widespread endoscopic mucosal resection ofthe esophagus with strategies for stricture prevention: a preclinical study. Endoscopy2005;37:1111e15.
29. Nieponice A,McGrath K, Qureshi I, et al. An extracellular matrix scaffold for esophagealstricture prevention after circumferential EMR. Gastrointest Endosc 2009;69:289e96.
30. Pouw RE,Wirths K, Eisendrath P, et al. Efficacy of radiofrequency ablation combinedwith endoscopic resection for Barrett’s esophagus with early neoplasia. ClinGastroenterol, Published Online First: 2009 August 11.
31. Van Vilsteren FG, Pouw RE, Seewald S, et al. A multi-center randomized trialcomparing stepwise radical endoscopic resection versus radiofrequency ablation forBarrett esophagus containing high-grade dysplasia and/or early cancer. GastrointestEndosc 2009;69:AB133.
Editor’s quiz: GI snapshot
Is indeterminate colitis reallyindeterminate?
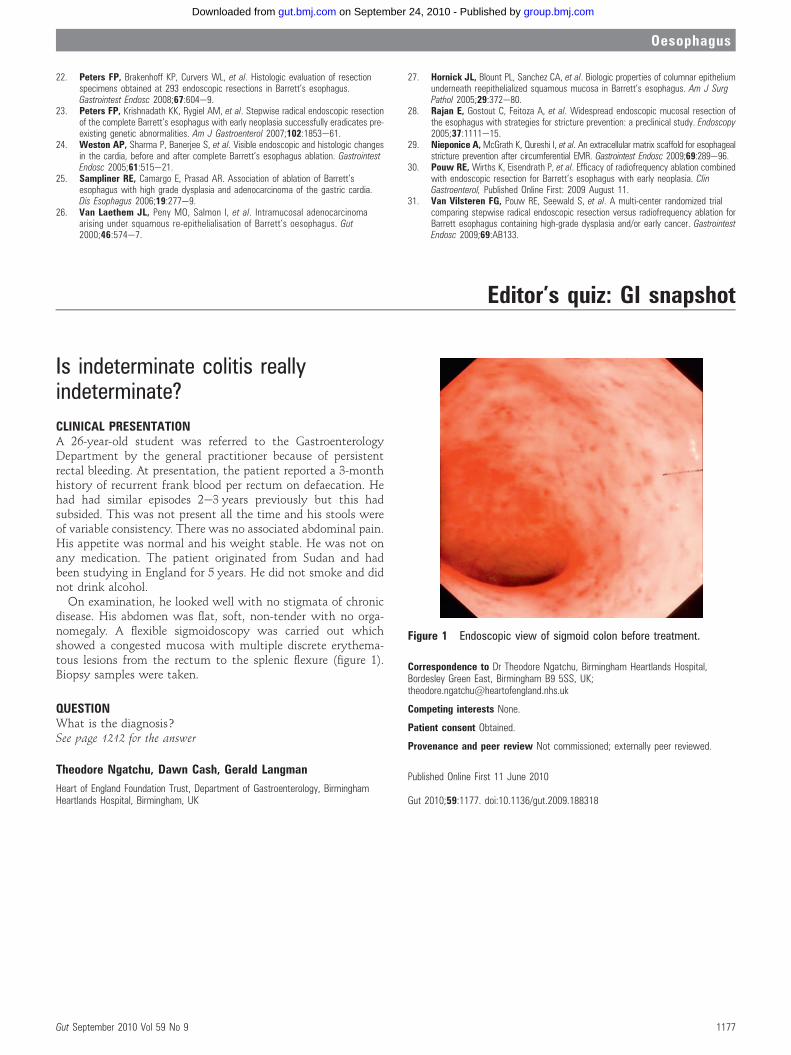
CLINICAL PRESENTATIONA 26-year-old student was referred to the GastroenterologyDepartment by the general practitioner because of persistentrectal bleeding. At presentation, the patient reported a 3-monthhistory of recurrent frank blood per rectum on defaecation. Hehad had similar episodes 2e3 years previously but this hadsubsided. This was not present all the time and his stools wereof variable consistency. There was no associated abdominal pain.His appetite was normal and his weight stable. He was not onany medication. The patient originated from Sudan and hadbeen studying in England for 5 years. He did not smoke and didnot drink alcohol.
On examination, he looked well with no stigmata of chronicdisease. His abdomen was flat, soft, non-tender with no orga-nomegaly. A flexible sigmoidoscopy was carried out whichshowed a congested mucosa with multiple discrete erythema-tous lesions from the rectum to the splenic flexure (figure 1).Biopsy samples were taken.
QUESTIONWhat is the diagnosis?See page 1212 for the answer
Theodore Ngatchu, Dawn Cash, Gerald Langman
Heart of England Foundation Trust, Department of Gastroenterology, BirminghamHeartlands Hospital, Birmingham, UK
Correspondence to Dr Theodore Ngatchu, Birmingham Heartlands Hospital,Bordesley Green East, Birmingham B9 5SS, UK;[email protected]
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Published Online First 11 June 2010
Gut 2010;59:1177. doi:10.1136/gut.2009.188318
Figure 1 Endoscopic view of sigmoid colon before treatment.
Gut September 2010 Vol 59 No 9 1177
Oesophagus
group.bmj.com on September 24, 2010 - Published by gut.bmj.comDownloaded from
Copyright © 2022 FDOKUMEN