Effect of increased intra-abdominal pressure on peristalsis in feline esophagus
9
Effect of increased intra-abdominal pressure on peristalsis in feline esophagus JUNLONG REN, WYLIE J. DODD& CHRISTOPHER J. MARTIN, ROBERTO 0. DANTAS, RAVINDER K. MITTAL, SANDRA S. HARRINGTON, MARK K. KERN, AND JAMES G. BRASSEUR Department of Radiology, Medical College of Wisconsin, Milwaukee, Wisconsin 53226; Department of Surgery, University of Melbourne, Fitzroy, Victoria 3065, Australia; Department of Medicine, University of Virginia Health Sciences Center, Charlottesville, Virginia 22908; and Department of Mechanical Engineering, Pennsylvania State University, University Park, Pennsylvania 16802 REN, JUNLONG, WYLIE J. DODDS, CHRISTOPHER J. MARTIN, ROBERTO 0. DANTAS, RAVINDER K. MITTAL, SANDRA S. HAR- RINGTON, MARK K. KERN, AND JAMES G. BRASSEUR. Effect of increased intra-abdominal pressure on peristalsis in feline esoph- agus. Am. J. Physiol. 261 (Gastrointest. Liver Physiol. 24): G417-G425,1991.-Our aim in this study was to determine the effect of variations in intrabolus pressure on esophageal peri- stalsis. In five cats, intrabolus pressure was altered by increas- ing intragastric pressure to 20-45 mmHg by use of a pressure cuff to compress the abdomen. In each cat, increases in intra- gastric pressure were associated with comparable increases in pressure of the esophageal bolus while the bolus was in the distal esophagus during esophageal peristalsis. Secondary per- istalsis induced by a 5-ml injection of barium into the proximal esophagus was recorded by synchronized videofluoroscopy and esophageal manometry. Graded increases in intrabolus pressure caused an increased prevalence of ineffective, incomplete peri- staltic sequences that did not completely clear barium from the esophagus. At intragastric pressures ~45 mmHg, 63% of the peristaltic sequences were incomplete. Increases in intrabolus pressure elicited by increased intragastric pressure also caused 1) slowing of the peristaltic wave in the distal esophagus, 2) increased pressure wave duration in the distal esophagus, 3) increased esophageal diameter, and 4) increased duration of lower esophageal sphincter opening. The incidence of retro- grade bolus escape was inversely related to the difference be- tween peristaltic wave amplitude and intrabolus pressure. A pressure difference of ~20 mmHg prevented retrograde barium escape at all esophageal levels, whereas a difference of ~20 mmHg was generally associated with retrograde escape of bar- ium in the distal esophagus. We conclude that an increase in intrabolus pressure causes an increase in esophageal distension that is transduced into alterations of esophageal peristalsis by either a myogenic or neural mechanism. esophageal peristalsis; abdominal compression; esophageal ob- struction; cat esophagus IN--PREVIOUS STUDIES, the presence of an esophageal bolus, increased bolus viscosity, increased intra-abdom- inal pressure, and esophageal outflow obstruction have been shown to decrease the velocity of peristalsis in the distal esophagus and increase the duration and in some instances the amplitude of esophageal peristaltic pres- sure waves (6, 7, 12, 14, 16). These previous studies have focused largely on alterations in peristaltic pressure wave variables while giving scant attention to alterations in intrabolus pressure that might have occurred secondary to the test manipulations. Recent publications, however, that focus on esophageal bolus transport emphasize the important spatial distinction between esophageal peri- staltic wave pressure in the esophageal closure segment and that within an intraluminal bolus (3, 4). Thus, for wet swallows, an important distinction exists between the segregated pressure domains of the peristaltic closure segment and that of the swallowed intraluminal bolus (3, 4). The aim of this investigation was to evaluate the effect of increases in intra-abdominal pressure on intra- luminal bolus pressure as well as on peristaltic pressure phenomena within the esophageal closure segment of the feline esophagus. METHODS We did concurrent esophageal manometric and video- fluoroscopic studies in five adult cats of either sex weigh- ing 3.1 to 5.0 kg. For esophageal manometry, we used an eight-lumen manometric catheter with an outer diameter of 4.7 mm. Each recording lumen was 0.8 mm in diame- ter. Side-hole recording orifices were cut in the recording assembly so that site 1 was located 1 cm proximal to the end of the manometric catheter. Site 2 was positioned 4 cm proximal to site 1 and six additional recording sites, numbered site 3 to site 8, respectively, were spaced at Z- cm intervals proximal to site 2. The catheter lumen immediately distal to each recording orifice was plugged with a metal marker, 5 mm in length. On videofluoros- copy, the metal markers served to locate the axial posi- tion of each recording orifice. During recording sessions, each recording lumen was infused with bubble-free water at 0.4 ml/min by a minimally compliant hydraulic infu- sion pump (1). Each manometric recording lumen was connected to an external strain gauge linked in series with a 1%channel polygraph recorder (Grass model D, Grass Instruments, Quincy, MA), run at a paper speed of 10 mm/s. For recording sessions, each animal was fasted 12 h and secured supine on an animal board after ketamine anesthesia. The manometric catheter was passedthrough 0193-1857/91 $1.50 Copyright 0 1991 the American Physiological Society G417
Transcript of Effect of increased intra-abdominal pressure on peristalsis in feline esophagus

Effect of increased intra-abdominal pressure on peristalsis in feline esophagus
JUNLONG REN, WYLIE J. DODD& CHRISTOPHER J. MARTIN, ROBERTO 0. DANTAS, RAVINDER K. MITTAL, SANDRA S. HARRINGTON, MARK K. KERN, AND JAMES G. BRASSEUR Department of Radiology, Medical College of Wisconsin, Milwaukee, Wisconsin 53226; Department of Surgery, University of Melbourne, Fitzroy, Victoria 3065, Australia; Department of Medicine, University of Virginia Health Sciences Center, Charlottesville, Virginia 22908; and Department of Mechanical Engineering, Pennsylvania State University, University Park, Pennsylvania 16802
REN, JUNLONG, WYLIE J. DODDS, CHRISTOPHER J. MARTIN, ROBERTO 0. DANTAS, RAVINDER K. MITTAL, SANDRA S. HAR- RINGTON, MARK K. KERN, AND JAMES G. BRASSEUR. Effect of increased intra-abdominal pressure on peristalsis in feline esoph- agus. Am. J. Physiol. 261 (Gastrointest. Liver Physiol. 24): G417-G425,1991.-Our aim in this study was to determine the effect of variations in intrabolus pressure on esophageal peri- stalsis. In five cats, intrabolus pressure was altered by increas- ing intragastric pressure to 20-45 mmHg by use of a pressure cuff to compress the abdomen. In each cat, increases in intra- gastric pressure were associated with comparable increases in pressure of the esophageal bolus while the bolus was in the distal esophagus during esophageal peristalsis. Secondary per- istalsis induced by a 5-ml injection of barium into the proximal esophagus was recorded by synchronized videofluoroscopy and esophageal manometry. Graded increases in intrabolus pressure caused an increased prevalence of ineffective, incomplete peri- staltic sequences that did not completely clear barium from the esophagus. At intragastric pressures ~45 mmHg, 63% of the peristaltic sequences were incomplete. Increases in intrabolus pressure elicited by increased intragastric pressure also caused 1) slowing of the peristaltic wave in the distal esophagus, 2) increased pressure wave duration in the distal esophagus, 3) increased esophageal diameter, and 4) increased duration of lower esophageal sphincter opening. The incidence of retro- grade bolus escape was inversely related to the difference be- tween peristaltic wave amplitude and intrabolus pressure. A pressure difference of ~20 mmHg prevented retrograde barium escape at all esophageal levels, whereas a difference of ~20 mmHg was generally associated with retrograde escape of bar- ium in the distal esophagus. We conclude that an increase in intrabolus pressure causes an increase in esophageal distension that is transduced into alterations of esophageal peristalsis by either a myogenic or neural mechanism.
esophageal peristalsis; abdominal compression; esophageal ob- struction; cat esophagus
IN--PREVIOUS STUDIES, the presence of an esophageal bolus, increased bolus viscosity, increased intra-abdom- inal pressure, and esophageal outflow obstruction have been shown to decrease the velocity of peristalsis in the distal esophagus and increase the duration and in some instances the amplitude of esophageal peristaltic pres- sure waves (6, 7, 12, 14, 16). These previous studies have
focused largely on alterations in peristaltic pressure wave variables while giving scant attention to alterations in intrabolus pressure that might have occurred secondary to the test manipulations. Recent publications, however, that focus on esophageal bolus transport emphasize the important spatial distinction between esophageal peri- staltic wave pressure in the esophageal closure segment and that within an intraluminal bolus (3, 4). Thus, for wet swallows, an important distinction exists between the segregated pressure domains of the peristaltic closure segment and that of the swallowed intraluminal bolus (3, 4). The aim of this investigation was to evaluate the effect of increases in intra-abdominal pressure on intra- luminal bolus pressure as well as on peristaltic pressure phenomena within the esophageal closure segment of the feline esophagus.
METHODS
We did concurrent esophageal manometric and video- fluoroscopic studies in five adult cats of either sex weigh- ing 3.1 to 5.0 kg. For esophageal manometry, we used an eight-lumen manometric catheter with an outer diameter of 4.7 mm. Each recording lumen was 0.8 mm in diame- ter. Side-hole recording orifices were cut in the recording assembly so that site 1 was located 1 cm proximal to the end of the manometric catheter. Site 2 was positioned 4 cm proximal to site 1 and six additional recording sites, numbered site 3 to site 8, respectively, were spaced at Z- cm intervals proximal to site 2. The catheter lumen immediately distal to each recording orifice was plugged with a metal marker, 5 mm in length. On videofluoros- copy, the metal markers served to locate the axial posi- tion of each recording orifice. During recording sessions, each recording lumen was infused with bubble-free water at 0.4 ml/min by a minimally compliant hydraulic infu- sion pump (1). Each manometric recording lumen was connected to an external strain gauge linked in series with a 1%channel polygraph recorder (Grass model D, Grass Instruments, Quincy, MA), run at a paper speed of 10 mm/s.
For recording sessions, each animal was fasted 12 h and secured supine on an animal board after ketamine anesthesia. The manometric catheter was passed through
0193-1857/91 $1.50 Copyright 0 1991 the American Physiological Society G417
G418 FELINE ESOPHAGUS
a central hole in a hard rubber bite block and positioned so that recording site 1 was located within the stomach and site 2 was positioned 1 cm above the lower esophageal sphincter (LES). With the catheter so positioned, man- ometric recording sites spanned the entire esophageal body at 2-cm intervals. The feline esophageal body av- erages -12-14 cm between the upper margin of the lower and upper esophageal sphincter (2, 11). The tip of a 12. Fr catheter was positioned in the proximal esophagus; secondary peristalsis was induced by an injection of 5- ml barium bolus (Liquid E-Z, E-Z-EM, Westbury, NY) diluted to 40% wt/vol (gravity 1.4 g/cm”). We selected secondary peristalsis for this study because it was more reliable than swallowing for eliciting a reproducible per- istaltic sequence that transported a barium bolus through the esophagus (9, 10).
For videofluoroscopy, the animal was positioned under a g-in. image intensifier locked in position 30 cm above the top of the X-ray table. Videofluoroscopic sequences were obtained at 80 keV and recorded on one-half-inch videotape with a Betamax video recorder (Sony model SLHF 900) run at 30 frames/s. A specially designed modified clock timer (Thalner Electronics, Ann Arbor, MI) synchronized the video and manometric recordings by encoding time in hundredths of a second on each video frame and made an event mark at l-s intervals on one channel of the polygraph tracing.
During each study, we recorded 21-28 esophageal re- sponses in each animal, elicited by injection of 5 ml barium into the proximal esophagus. A total of 118 responses was recorded. Barium-induced peristaltic se- quences were recorded at resting levels of intragastric pressure (5-15 mmHg) and also while intragastric pres- sure was increased by abdominal compression to 20-45
L , Manometry UES
&e mmHg
LES
mmHg using a blood pressure cuff wrapped around the abdomen and secured by a binder. The order of recording sequences at different intragastric pressures was ran- domized.
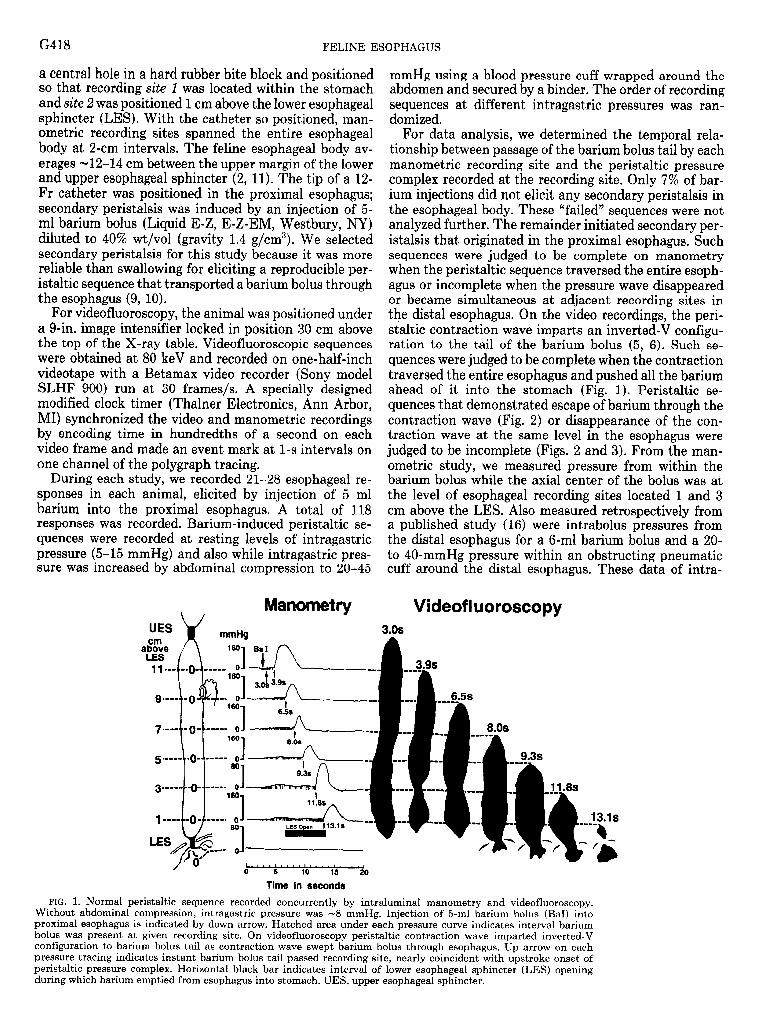
For data analysis, we determined the temporal rela- tionship between passage of the barium bolus tail by each manometric recording site and the peristaltic pressure complex recorded at the recording site. Only 7% of bar- ium injections did not elicit any secondary peristalsis in the esophageal body. These “failed” sequences were not analyzed further. The remainder initiated secondary per- istalsis that originated in the proximal esophagus. Such sequences were judged to be complete on manometry when the peristaltic sequence traversed the entire esoph- agus or incomplete when the pressure wave disappeared or became simultaneous at adjacent recording sites in the distal esophagus. On the video recordings, the peri- staltic contraction wave imparts an inverted-V configu- ration to the tail of the barium bolus (5, 6). Such se- quences were judged to be complete when the contraction traversed the entire esophagus and pushed all the barium ahead of it into the stomach (Fig. 1). Peristaltic se- quences that demonstrated escape of barium through the contraction wave (Fig. 2) or disappearance of the con- traction wave at the same level in the esophagus were judged to be incomplete (Figs. 2 and 3). From the man- ometric study, we measured pressure from within the barium bolus while the axial center of the bolus was at the level of esophageal recording sites located 1 and 3 cm above the LES. Also measured retrospectively from a published study (16) were intrabolus pressures from the distal esophagus for a 6-ml barium bolus and a 20- to 40-mmHg pressure within an obstructing pneumatic cuff around the distal esophagus. These data of intra-
Videofl uoroscopy 3.0s
FELINE ESOPHAGUS G419
UES -- t/ Manometry
3.0s Videofluoroscopy
ImHg
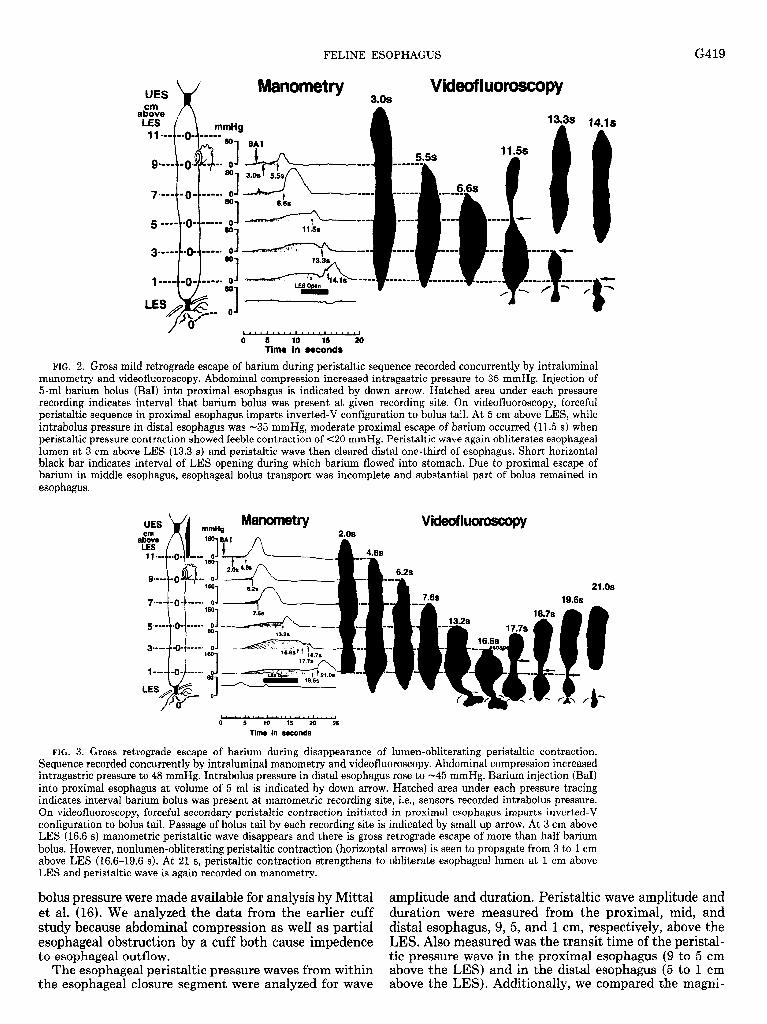
FIG. 2. Gross mild retrograde escape of barium during peristaltic sequence recorded concurrently by intraluminal manometry and videofluoroscopy. Abdominal compression increased intragastric pressure to 35 mmHg. Injection of 5-ml barium bolus (BaI) into proximal esophagus is indicated by down arrow. Hatched area under each pressure recording indicates interval that barium bolus was present at given recording site. On videofluoroscopy, forceful peristaltic sequence in proximal esophagus imparts inverted-V configuration to bolus tail. At 5 cm above LES, while intrabolus pressure in distal esophagus was -35 mmHg, moderate proximal escape of barium occurred (11.5 s) when peristaltic pressure contraction showed feeble contraction of ~20 mmHg. Peristaltic wave again obliterates esophageal lumen at 3 cm above LES (13.3 s) and peristaltic wave then cleared distal one-third of esophagus. Short horizontal black bar indicates interval of LES opening during which barium flowed into stomach. Due to proximal escape of barium in middle esophagus, esophageal bolus transport was incomplete and substantial part of bolus remained in esophagus.
Manometrv *Ee
mm+4 1
LES “1
2.0s BAI 1
Videofl~
3
6.2s
21 .os
L.“““““““ ‘ . ,“ . . . * I
0 5 10 15 20 25
Time in seconds
FIG. 3. Gross retrograde escape of barium during disappearance of lumen-obliterating peristaltic contraction. Sequence recorded concurrently by intraluminal manometry and videofluoroscopy. Abdominal compression increased intragastric pressure to 48 mmHg. Intrabolus pressure in distal esophagus rose to -45 mmHg. Barium injection (Bar) into proximal esophagus at volume of 5 ml is indicated by down arrow. Hatched area under each pressure tracing indicates interval barium bolus was present at manometric recording site, i.e., sensors recorded intrabolus pressure. On videofluoroscopy, forceful secondary peristaltic contraction initiated in proximal esophagus imparts inverted-V configuration to bolus tail. Passage of bolus tail by each recording site is indicated by small up arrow. At 3 cm above LES (16.6 s) manometric peristaltic wave disappears and there is gross retrograde escape of more than half barium bolus. However, nonlumen-obliterating peristaltic contraction (horizontal arrows) is seen to propagate from 3 to 1 cm above LES (16.6-19.6 s). At 21 s, peristaltic contraction strengthens to obliterate esophageal lumen at 1 cm above LES and peristaltic wave is again recorded on manometry.
bolus pressure were made available for analysis by Mittal amplitude and duration. Peristaltic wave amplitude and et al. (16). We analyzed the data from the earlier cuff duration were measured from the proximal, mid, and study because abdominal compression as well as partial distal esophagus, 9, 5, and I cm, respectively, above the esophageal obstruction by a cuff both cause impedence LES. Also measured was the transit time of the peristal- to esophageal outflow. tic pressure wave in the proximal esophagus (9 to 5 cm
The esophageal peristaltic pressure waves from within above the LES) and in the distal esophagus (5 to 1 cm the esophageal closure segment were analyzed for wave above the LES). Additionally, we compared the magni-
G420 FELINE ESOPHAGUS
tude of esophageal pressure wave amplitude above intra- bolus pressure at each recording site and whether inef- fective transport of barium (i.e., barium escape) occurred at the given recording site, as observed on videofluoros- copy by a blinded observer. Lastly, for each intragastric pressure tested, we determined the duration of LES opening during each intact peristaltic sequence and the diameter of the lower esophageal body during peristalsis. From the videofluoroscopy we observed the interval the barium bolus covered each recording site and thereby determined the precise time each recording site recorded pressures from within the barium bolus. The maximal diameter of the distal esophagus was measured 4 cm above the LES while the barium bolus was in the distal esophagus.
For statistical analysis, comparisons between data were done by analysis of variance, Student’s t test, and regression analysis, where appropriate. Averaged values in the text are given as means t SE unless specified otherwise.
RESULTS
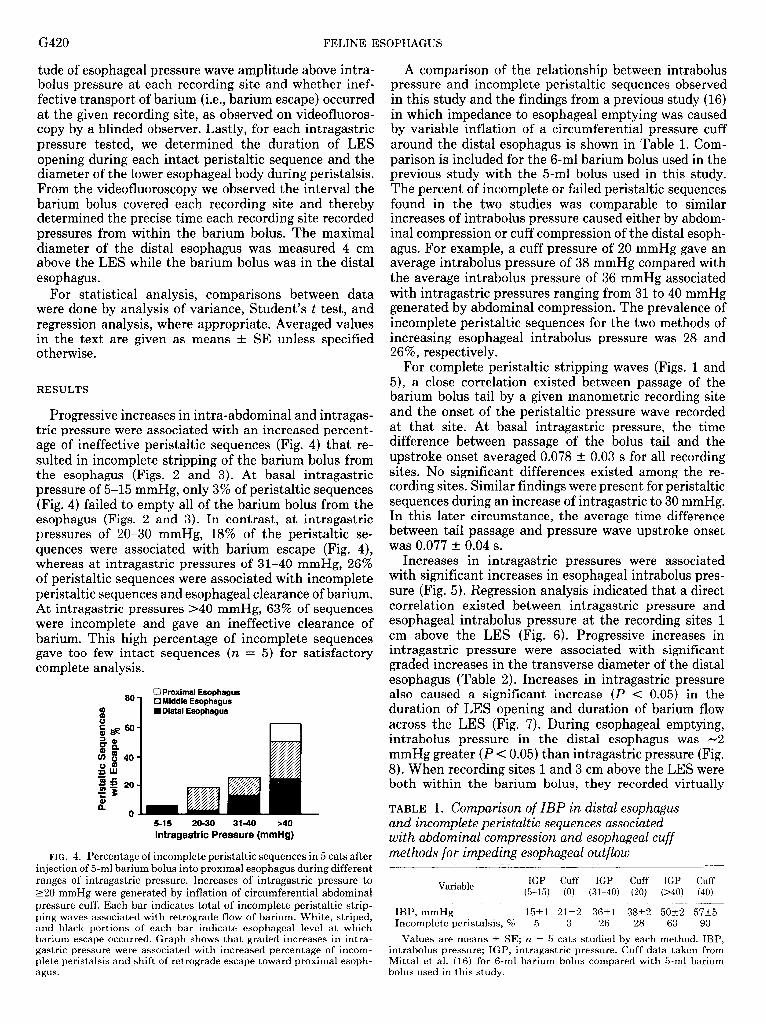
Progressive increases in intra-abdominal and intragas- tric pressure were associated with an increased percent- age of ineffective peristaltic sequences (Fig. 4) that re- sulted in incomplete stripping of the barium bolus from the esophagus (Figs. 2 and 3). At basal intragastric pressure of 5-15 mmHg, only 3% of peristaltic sequences (Fig. 4) failed to empty all of the barium bolus from the esophagus (Figs. 2 and 3). In contrast, at intragastric pressures of 20-30 mmHg, 18% of the peristaltic se- quences were associated with barium escape (Fig. 4), whereas at intragastric pressures of 31-40 mmHg, 26% of peristaltic sequences were associated with incomplete peristaltic sequences and esophageal clearance of barium. At intragastric pressures ~40 mmHg, 63% of sequences were incomplete and gave an ineffective clearance of barium. This high percentage of incomplete sequences gave too few intact sequences (n = 5) for satisfactory complete analysis.
0 Proximal Esophagus fZ Middle Esophagus I Distal Esophagus
lntragastric Pressure (mmHg)
FIG. 4. Percentage of incomplete peristaltic sequences in 5 Cats after injection of 5ml barium bolus into proximal esophagus during different ranges of intragastric pressure. Increases of intragastric pressure to ~20 mmHg were generated by inflation of circumferential abdominal pressure cuff. Each bar indicates total of incomplete peristaltic strip- ping waves associated with retrograde flow of barium. White, striped, and black portions of each bar indicate esophageal level at which barium escape occurred. Graph shows that graded increases in intra- gastric pressure were associated with increased percentage of incom- plete peristalsis and shift of retrograde escape toward proximal esoph- agus.
A comparison of the relationship between intrabolus pressure and incomplete peristaltic sequences observed in this study and the findings from a previous study (16) in which impedance to esophageal emptying was caused by variable inflation of a circumferential pressure cuff around the distal esophagus is shown in Table 1. Com- parison is included for the 6-ml barium bolus used in the previous study with the 5-ml bolus used in this study. The percent of incomplete or failed peristaltic sequences found in the two studies was comparable to similar increases of intrabolus pressure caused either by abdom- inal compression or cuff compression of the distal esoph- agus. For example, a cuff pressure of 20 mmHg gave an average intrabolus pressure of 38 mmHg compared with the average intrabolus pressure of 36 mmHg associated with intragastric pressures ranging from 31 to 40 mmHg generated by abdominal compression. The prevalence of incomplete peristaltic sequences for the two methods of increasing esophageal intrabolus pressure was 28 and 26%, respectively.
For complete peristaltic stripping waves (Figs. 1 and 5), a close correlation existed between passage of the barium bolus tail by a given manometric recording site and the onset of the peristaltic pressure wave recorded at that site. At basal intragastric pressure, the time difference between passage of the bolus tail and the upstroke onset averaged 0.078 t 0.03 s for all recording sites. No significant differences existed among the re- cording sites. Similar findings were present for peristaltic sequences during an increase of intragastric to 30 mmHg. In this later circumstance, the average time difference between tail passage and pressure wave upstroke onset was 0.077 t 0.04 s.
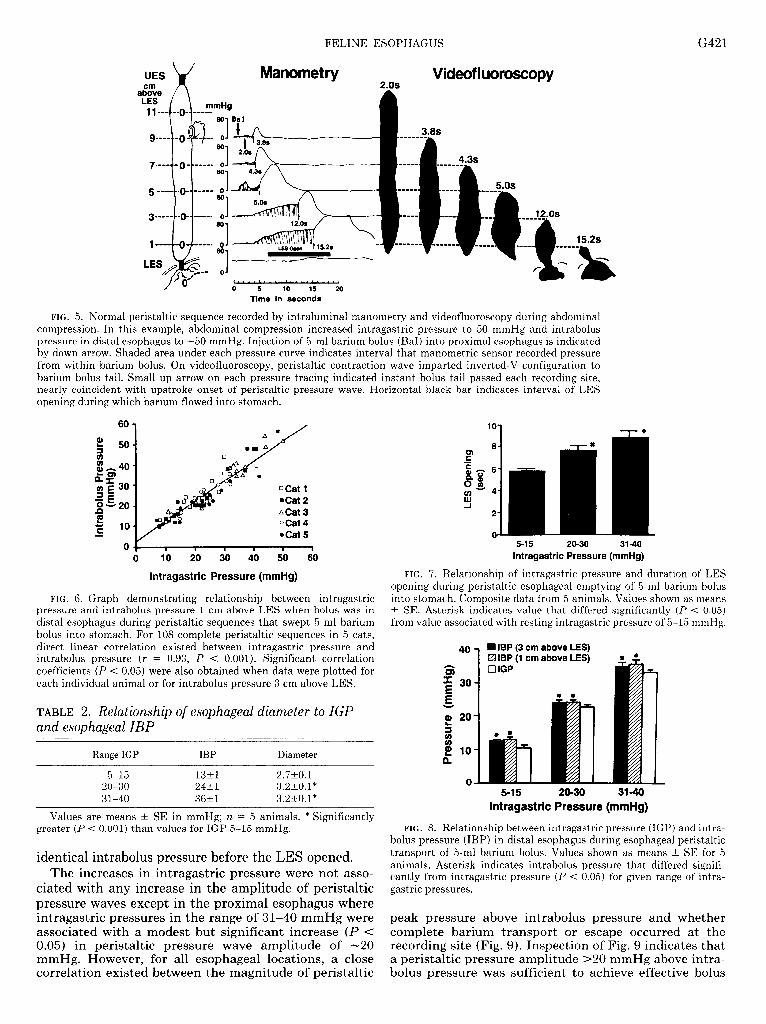
Increases in intragastric pressures were associated with significant increases in esophageal intrabolus pres- sure (Fig. 5). Regression analysis indicated that a direct correlation existed between intragastric pressure and esophageal intrabolus pressure at the recording sites 1 cm above the LES (Fig. 6). Progressive increases in intragastric pressure were associated with significant graded increases in the transverse diameter of the distal esophagus (Table 2). Increases in intragastric pressure also caused a significant increase (P < 0.05) in the duration of LES opening and duration of barium flow across the LES (Fig. 7). During esophageal emptying, intrabolus pressure in the distal esophagus was -2 mmHg greater (P < 0.05) than intragastric pressure (Fig. 8). When recording sites 1 and 3 cm above the LES were both within the barium bolus, they recorded virtually
TABLE 1. Comparison of IBP in distal esophagus and incomplete peristaltic sequences associated with abdominal compression and esophageal cuff methods for impeding esophageal outflow
Variable IGP Cuff IGP Cuff IGP Cuff
(5-15) (0) (31-40) (20) (>40) (40)
IBP, mmHg l&l 211r2 36tl 38&2 50t2 57&5 Incomplete peristalsis, % 5 3 26 28 63 93
Values are means of: SE; n = 5 cats studied by each method. IBP, intrabolus pressure; IGP, intragastric pressure. Cuff data taken from Mittal et al. (16) for 6-ml barium bolus compared with 5-ml barium bolus used in this study.
FELINE ESOPHAGUS G421
UES
aEve LES x
Manometry Videof luoroscopy
3.8s
i.2S
wlx- 0 1. ‘ . . ‘ . . . “ “ “ ‘ . . . .1
0 5 10 15 20
Time in seconds
15.2s
FIG. 5. Normal peristaltic sequence recorded by intraluminal manometry and videofluoroscopy during abdominal compression. In this example, abdominal compression increased intragastric pressure to 50 mmHg and intrabolus pressure in distal esophagus to -50 mmHg. Injection of 5ml barium bolus (BaI) into proximal esophagus is indicated by down arrow. Shaded area under each pressure curve indicates interval that manometric sensor recorded pressure from within barium bolus. On videofluoroscopy, peristaltic contraction wave imparted inverted-V configuration to barium bolus tail. Small up arrow on each pressure tracing indicated instant bolus tail passed each recording site, nearly coincident with upstroke onset of peristaltic pressure wave. Horizontal black bar indicates interval of LES opening during which barium flowed into stomach.
0+ 0
q Cat 1 n Cat 2 Acat 3 0Cat 4 l Cat 5
1 1 I I I 1 lo 20 30 40 50 60
lntragastric Pressure (mmHg)
FIG. 6. Graph demonstrating relationship between intragastric pressure and intrabolus pressure 1 cm above LES when bolus was in distal esophagus during peristaltic sequences that swept 5-ml barium bolus into stomach. For 108 complete peristaltic sequences in 5 cats, direct linear correlation existed between intragastric pressure and intrabolus pressure (r = 0.93, P < 0.001). Significant correlation coefficients (P < 0.05) were also obtained when data were plotted for each individual animal or for intrabolus pressure 3 cm above LES.
TABLE 2. Relationship of esophageal diameter to IGP and esophageal IBP
Range IGP IBP Diameter
5-15 13tl 2.720.1 20-30 24tl 3.2&0.1* 31-40 36tl 3.2tO.l"
Values are means & SE in mmHg; n = 5 animals. * Significantly greater (P < 0.001) than values for IGP 5-15 mmHg.
identical intrabolus pressure before the LES opened. The increases in intragastric pressure were not asso-
ciated with any increase in the amplitude of peristaltic pressure waves except in the proximal esophagus where intragastric pressures in the range of 31-40 mmHg were associated with a modest but significant increase (P c 0.05) in peristaltic pressure wave amplitude of -20 mmHg. However, for all esophageal locations, a close correlation existed between the magnitude of peristaltic
5-l 5 20-30 31-40 lntragastric Pressure (mmHg)
FIG. 7. Relationship of intragastric pressure and duration of LES opening during peristaltic esophageal emptying of 5-ml barium bolus into stomach. Composite data from 5 animals. Values shown as means t SE. Asterisk indicates value that differed significantly (P < 0.05) from value associated with resting intragastric pressure of 5-15 mmHg.
40 n IBP (3 cm above LES) IZA IBP (1 cm above LES)
G x E 30
g
Q) 20 5 2 g 10
e
0 5-15 20-30 314
lntragastric Pressure (mmHg)
FIG. 8. Relationship between intragastric pressure (IGP) and intra- bolus pressure (IBP) in distal esophagus during esophageal peristaltic transport of 5-ml barium bolus. Values shown as means & SE for 5 animals. Asterisk indicates intrabolus pressure that differed signifi- cantly from intragastric pressure (P < 0.05) for given range of intra- gastric pressures.
peak pressure above intrabolus pressure and whether complete barium transport or escape occurred at the recording site (Fig. 9). Inspection of Fig. 9 indicates that a peristaltic pressure amplitude ~20 mmHg above intra- bolus pressure was sufficient to achieve effective bolus
G422 FELINE ESOPHAGUS
mm&l >50-
41-so-
Peristaltic Amplitude 314-
> IBP 21-30-
l&20-
0-10-
qqq n 1138 n -68 n -l!io --------+-------*-------q
Locaum: Proxhnai Middle Distal cm > LES: 9& 7cm 5cm 3&lcm
Esophageal Regions
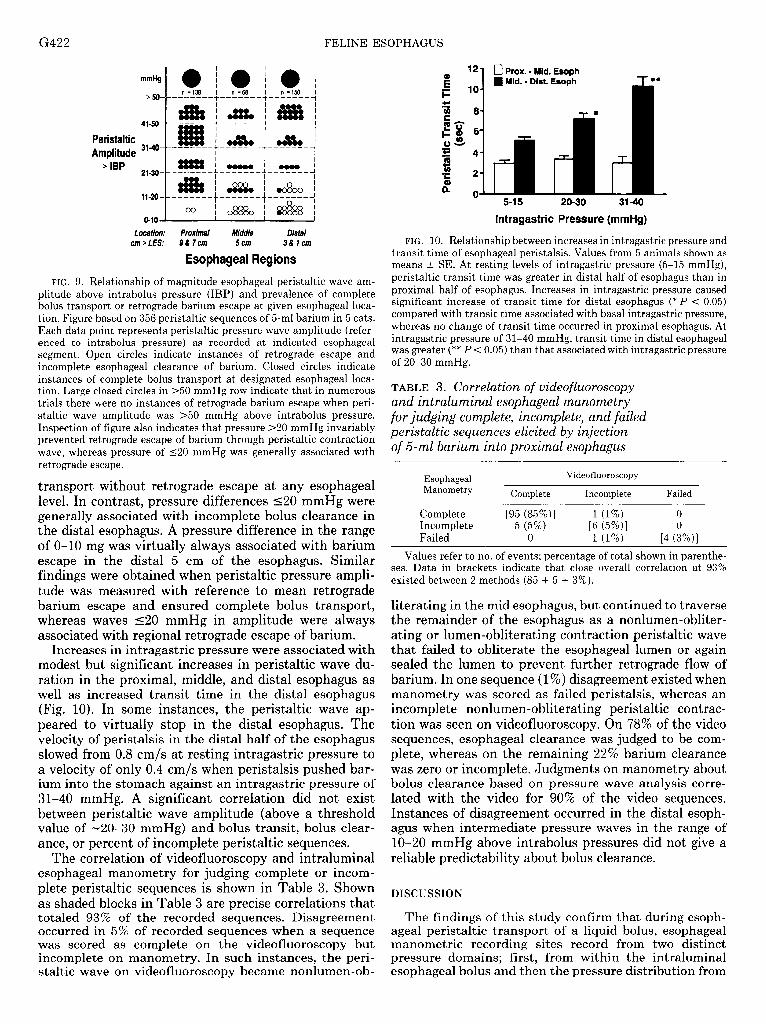
FIG. 9. Relationship of magnitude esophageal peristaltic wave am- plitude above intrabolus pressure (IBP) and prevalence of complete bolus transport or retrograde barium escape at given esophageal loca- tion. Figure based on 356 peristaltic sequences of 5-ml barium in 5 cats. Each data point represents peristaltic pressure wave amplitude (refer- enced to intrabolus pressure) as recorded at indicated esophageal segment. Open circles indicate instances of retrograde escape and incomplete esophageal clearance of barium. Closed circles indicate instances of complete bolus transport at designated esophageal loca- tion. Large closed circles in >50 mmHg row indicate that in numerous trials there were no instances of retrograde barium escape when peri- staltic wave amplitude was ~50 mmHg above intrabolus pressure. Inspection of figure also indicates that pressure >20 mmHg invariably prevented retrograde escape of barium through peristaltic contraction wave, whereas pressure of 520 mmHg was generally associated with retrograde escape.
transport without retrograde escape at any esophageal level. In contrast, pressure differences 520 mmHg were generally associated with incomplete bolus clearance in the distal esophagus. A pressure difference in the range of O-10 mg was virtually always associated with barium escape in the distal 5 cm of the esophagus. Similar findings were obtained when peristaltic pressure ampli- tude was measured with reference to mean retrograde barium escape and ensured complete bolus transport, whereas waves 520 mmHg in amplitude were always associated with regional retrograde escape of barium.
Increases in intragastric pressure were associated with modest but significant increases in peristaltic wave du- ration in the proximal, middle, and distal esophagus as well as increased transit time in the distal esophagus (Fig. 10). In some instances, the peristaltic wave ap- peared to virtually stop in the distal esophagus. The velocity of peristalsis in the distal half of the esophagus slowed from 0.8 cm/s at resting intragastric pressure to a velocity of only 0.4 cm/s when peristalsis pushed bar- ium into the stomach against an intragastric pressure of 31-40 mmHg. A significant correlation did not exist between peristaltic wave amplitude (above a threshold value of -20-30 mmHg) and bolus transit, bolus clear- ance, or percent of incomplete peristaltic sequences.
The correlation of videofluoroscopy and intraluminal esophageal manometry for judging complete or incom- plete peristaltic sequences is shown in Table 3. Shown as shaded blocks in Table 3 are precise correlations that totaled 93% of the recorded sequences. Disagreement occurred in 5% of recorded sequences when a sequence was scored as complete on the videofluoroscopy but incomplete on manometry. In such instances, the peri- staltic wave on videofluoroscopy became nonlumen-ob-
12. 0 Prox. - Mid. Esoph m Mid. - Dist. Esoph
”
5-15 20-30 31-40
lntragastric Pressure (mmHg)
FIG. 10. Relationship between increases in intragastric pressure and transit time of esophageal peristalsis. Values from 5 animals shown as means & SE. At resting levels of intragastric pressure (5-15 mmHg), peristaltic transit time was greater in distal half of esophagus than in proximal half of esophagus. Increases in intragastric pressure caused significant increase of transit time for distal esophagus (* P < 0.05) compared with transit time associated with basal intragastric pressure, whereas no change of transit time occurred in proximal esophagus. At intragastric pressure of 31-40 mmHg, transit time in distal esophageal was greater (** P < 0.05) than that associated with intragastric pressure of 20-30 mmHg.
TABLE 3. Correlation of videofluoroscopy and intraluminal esophageal manometry for judging complete, incomplete, and failed peristaltic sequences elicited by injection of 5-ml barium into proximal esophagus
Esophageal Manometry Complete
Videofluoroscopy
Incomplete Failed
Complete [95 (85%)] 1 (1%) 0 Incomplete 5 (5%) 16 (5%)1 0 Failed 0 1 (1%) [4 (3%)1
Values refer to no. of events; percentage of total shown in parenthe- ses. Data in brackets indicate that close overall correlation at 93% existed between 2 methods (85 + 5 + 3%).
literating in the mid esophagus, but continued to traverse the remainder of the esophagus as a nonlumen-obliter- ating or lumen-obliterating contraction peristaltic wave that failed to obliterate the esophageal lumen or again sealed the lumen to prevent further retrograde flow of barium. In one sequence (1%) disagreement existed when manometry was scored as failed peristalsis, whereas an incomplete nonlumen-obliterating peristaltic contrac- tion was seen on videofluoroscopy. On 78% of the video sequences, esophageal clearance was judged to be com- plete, whereas on the remaining 22% barium clearance was zero or incomplete. Judgments on manometry about bolus clearance based on pressure wave analysis corre- lated with the video for 90% of the video sequences. Instances of disagreement occurred in the distal esoph- agus when intermediate pressure waves in the range of lo-20 mmHg above intrabolus pressures did not give a reliable predictability about bolus clearance.
DISCUSSION
The findings of this study confirm that during esoph- ageal peristaltic transport of a liquid bolus, esophageal manometric recording sites record from two distinct pressure domains; first, from within the intraluminal esophageal bolus and then the pressure distribution from
FELINE ESOPHAGUS G423
within the segment of esophageal closure caused by the circular peristaltic contraction wave that seals the esoph- ageal lumen proximal to the bolus and pushes the bolus aborally toward the stomach. Alterations in intrabolus pressure do not alter pressures within the peristaltic closure segment and, conversely, the pressure wave within the closure segment is not reflected into the esophageal bolus. In this study, we focused mainly on intrabolus pressure as distinct from the variables of the peristaltic pressure wave that is located within the do- main of esophageal closure.
In this investigation, we used concurrent videofluoros- copy and esophageal manometry to determine when manometric pressure sensors recorded from within the bolus and closed segment domains while intrabolus pres- sure was varied by graded increases in intragastric pres- sure. Increases in intra-abdominal pressure elicited by generalized abdominal compression led to graded in- creases in intragastric pressure. Such changes in intra- gastric pressure were associated with corresponding in- creases in pressure within the domain of the esophageal bolus during peristalsis and the duration of LES opening.
The study finding showed that intrabolus pressure within the distal esophagus was slightly greater than the pressure within the stomach. Physical principles of flow would predict a small but significant positive pressure gradient across the LES during fluid flow from the esoph- agus into the stomach. A slight difference between esoph- ageal bolus and intragastric pressure, however, suggests that a truly common cavity phenomenon did not exist between the stomach and esophagus in which case the intraluminal pressure should be isobaric.
The findings in this study confirm the observations made previously in cats and humans that a close tem- poral relationship exists between the passage of the barium bolus tail past a manometric recording site and the onset of the peristaltic pressure wave at the recording site (5, 9, 15, 16, 18). It should be noted, however, that some measurement errors may exist due to imperfect imaging of the barium bolus tail. For all recording sites the mean temporal difference between passage of the bolus tail and pressure wave onset was -0.08 s regardless of whether intrabolus pressure was normal or increased secondary to abdominal compression. The use of a denser barium, a smaller manometric catheter, or video with better resolution, however, might demonstrate an even closer approximation of bolus tail passage and pressure wave onset than shown here, or tail passage might even occur during the early part of the pressure wave upstroke instead of at the pressure onset of the upstroke. The latter relationship is predicted by a theoretical analysis of biomechanical principles (3, 4). Notwithstanding, for practical purposes bolus tail passage and peristaltic wave onset are virtually coincident. This important relation- ship serves as a useful cross index between the radiolog- ical and manometric recordings of esophageal peristalsis. For example, peristaltic transit time or peristaltic wave velocity is comparable when measured by either method.
Increased intragastric and esophageal intrabolus pres- sures were accompanied by a modest increase in peri- staltic wave duration, increased transit time in the distal half of the esophagus, and an increased duration of LES
opening and transsphincteric flow of barium. Unexpect- edly, except in the proximal esophagus, peristaltic pres- sure wave amplitude did not increase during intervals of abdominal compression.
With respect to the variables of esophageal peristalsis, the findings of the present study are similar to an earlier study that determined the effect of abdominal compres- sion on esophageal peristalsis in humans (7). For wet swallows, increases in intragastric pressure up to 25 mmHg were associated with slowing of peristaltic transit in the distal esophagus, increased duration of LES relax- ation, and also increased duration and amplitude of the peristaltic pressure complexes occurring in the distal esophagus. These changes did not occur for dry swallows. In this earlier study, intrabolus pressure was not meas- ured.
In a recent videofluoromanometric study, Mittal et al. (16) evaluated the effect of graded esophageal obstruction elicited by a pneumatic cuff placed around the distal esophagus, on peristalsis elicited by injection of 3, 6, or 9 ml of barium into the esophagus. High cuff pressures and large volumes invariably lead to failed or incomplete peristalsis. For low cuff pressures and bolus volumes of 3 or 6 ml, the partial obstruction caused an increased duration and transit of peristaltic pressure waves in the distal esophagus. The amplitude of the peristaltic pres- sure waves increased only after the 3-ml bolus. Although a different method was used in the study of Mittal et al. (16) to impede esophageal emptying compared with the abdominal compression method used in our study, the findings for a similar-sized bolus (6 vs. 5 ml) were com- parable (Table 1). In the report by Mittal et al. (16) intrabolus pressures were not reported. These intrabolus pressures, however, are reported here. Our analysis (Table 1) indicates that the intrabolus pressure for a 6- ml bolus at a cuff pressure of 40 mmHg was comparable with that elicited by an intragastric pressure of 31-40 mmHg. We suggest that intrabolus pressure is the com- mon denominator for the two studies and accounts for the fact that the study findings were similar.
Some consideration of the mechanism(s) responsible for alteration of esophageal peristalsis during abdominal compression or partial esophageal occlusion warrants discussion. Both methods impede esophageal outflow that leads to slowed transit in the distal esophagus. Slowed transit may explain in part why the increase in pressure wave duration increases the duration of LES opening because the LES remains relaxed until the per- istaltic wave reaches it (6, 7). An increase in peristaltic wave amplitude such as that observed in humans was not verified in our study. What mechanisms might ex- plain the slowing of the peristaltic wave or an increase in its pressure amplitude ? Two types of mechanisms have been proposed, myogenic and neurogenic. As shown in this study, impeded esophageal emptying leads to an increase in intrabolus pressure and distension of the distal esophagus. Such distension may increase the pre- load as well as afterload on circular muscle, thereby slowing its rate of contraction while increasing its force of contraction due to a shift on the circular muscle length tension curve. Another potential explanation is that esophageal stretch elicits a feedback reflex modulation

G424 FELINE ESOPHAGUS
of esophageal peristalsis via extrinsic or intrinsic neural reflexes (14). In our opinion, both explanations have merit and are not mutually exclusive.
In the present study, an increased prevalence of inef- fective peristaltic sequences with incomplete bolus trans- port was associated with 1) increases of intrabolus pres- sure secondary to increases in intra-abdominal pressure and 2) a small difference between peristaltic wave am- plitude and intrabolus pressure. In the cat, these two phenomena are related because increases in intra-ab- dominal pressure were not associated with an increase in peristaltic wave amplitude. Thus, when peristaltic amplitude is constant, the difference between peristaltic wave amplitude and intrabolus pressure decreases with increases in intrabolus pressure. During esophageal transport of a liquid bolus, the circular peristaltic con- traction wave has two functions. First, it seals off the esophageal lumen at the bolus tail and, second, it pushes the bolus through the esophagus. If the force of esopha- geal peristalsis is insufficient to sustain luminal closure, part or all of the bolus passes retrograde through the contracting segment, thereby impairing esophageal clear- ance. In this study, a wave pressure of 20 mmHg above intrabolus pressure invariably prevented retrograde es- cape at any location within the esophagus, whereas a pressure difference of 11-20 mmHg was generally asso- ciated with escape in the distal esophagus. In the distal esophagus, pressure differences between O-l 1 mmHg were nearly always associated with retrograde escape of the bolus. Comparable results were observed by Kahrilas et al. (15) in humans, although the subjects in that study were evaluated only at basal intra-abdominal pressure and pressure wave amplitude was referenced to atmos- pheric pressure as zero and not to intrabolus pressure, which is -10 mmHg in the distal esophagus.
Overall, a 93% correlation existed between the radio- logical and manometric methods for determining whether injection of a barium bolus into the esophagus elicited a peristaltic sequence that traversed the entire esophagus. A comparable correlation has been observed for primary peristalsis in three human studies (5, 13, 17). In some instances, a discrepancy existed between the two methods when a nonlumen-obliterating peristaltic contraction seen on videofluoroscopy was not detected by manometry. In one instance, a low-amplitude pressure wave within the barium bolus was misinterpreted as a peristaltic contraction wave. The radiological method evaluates not only peristalsis but gives a direct observa- tion of esophageal bolus transport and clearance. The manometric method quantitated intrabolus pressure and the magnitude and duration of peristaltic pressure waves. The manometric method also gives good prediction of esophageal bolus transport when peristaltic wave ampli- tude exceeds intrabolus pressure by ~20 mmHg or was in a low range of ~20 mmHg.
In summary, the results of this study suggest that alterations of esophageal motor function elicited by in- creases in intragastric pressure or partial distal esopha- geal obstruction are transduced to the esophagus by increases in intrabolus pressure that distend the esoph- agus and slow peristaltic transit time by either a my-
ogenic or neurogenic mechanism. During peristaltic transport of a fluid bolus the function of the peristaltic contraction wave is to generate a sufficient closure force to seal the esophageal lumen from the fluid bolus that is propelled down from the esophagus and into the stomach. Insufficient circular contraction force fails to maintain esophageal closure and thereby permits retrograde escape of a bolus through the peristaltic contraction segment and an accompanying impairment of esophageal bolus clearance. An appreciation of these biomechanical prin- ciples is essential for an understanding of the mecha- nisms of normal and abnormal esophageal transport of a fluid bolus.
This work was supported in part by National Institute of Diabetes and Digestive and Kidney Diseases Grants DK-25731 and DK-30024.
Address for reprint requests: W. J. Dodds, Medical College of Wis- consin, Dept. of Radiology, Froedtert Memorial Lutheran Hospital, 9200 West Wisconsin Ave., Milwaukee, WI 53226.
Received 30 November 1990; accepted in final form 14 March 1991.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
ARNDORFER, R. C., J. J. STEF, W. J. DODDS, J. H. LINEHAN, AND W. J. HOGAN. Improved infusion system for intraluminal esopha- geal manometry. Gastroenterology 73: 23-27, 1977. BLANK, E. L., B. GREENWOOD, AND W. J. DODDS. Cholinergic control of smooth muscle peristalsis in the cat esophagus. Am. J. Physiol. 257 (Gastrointest. Liver Physiol. 20): G517-G523, 1989. BRASSEUR, J. G. A fluid mechanical perspective on esophageal bolus transport. Dysphagia 2: 32-39, 1987. BRASSEUR, J. G., W. J. DODDS, B. T. MASSEY, M. K. KERN, J. F. HELM, AND P. J. KAHRILAS. Esophageal pressure during peristaltic transport of a fluid bolus: distinction between intrabolus and contractile-segment pressure domains (Abstract). Gastroenterology 96: 56, 1989. DODDS, W. J. Cannon lecture. Current concepts of esophageal motor function. Clinical implications for radiology. Am. J. Radiol. 128: 549-561, 1977. DODDS, W. J., W. J. HOGAN, D. P. REID, E. T. STEWART, AND R. C. ARNDORFER. A comparison between primary esophageal peri- stalsis following wet and dry swallows. J. Appl. Physiol. 35: 851- 857, 1973. DODDS, W. J., W. J. HOGAN, E. T. STEWART, J. J. STEF, AND R. C. ARNDORFER. Effects of increased intra-abdominal pressure on esophageal peristalsis. J. Appl. Physiol. 37: 378-383, 1974. DODDS, W. J., J. J. STEF, E. T. STEWART, W. J. HOGAN, R. C. ARNDORFER, AND E. B. COHEN. Responses of the feline esophagus to cervical vagal stimulation. Am. J. Physiol. 235 (Endocrinol. Metab. Gastrointest. Physiol. 4): E63-E73, 1978. DODDS, W. J., E. T. STEWARD, D. HODGES, AND F. F. ZBORAI,SKE.
Movement of the feline esophagus associated with respiration and peristalsis. An evaluation using tantalum markers. J. Clin. Invest. 52: 1-13, 1973. DODDS, W. J., E. T. STEWART, W. J. HOGAN, J. J. STEF, AND R. C. ARNDORFER. Effect of esophageal movement on intraluminal esophageal pressure recording. Gastroenterology 67: 592-600, 1974. DODDS, W. J., E. T. STEWART, L. J. MCCARTHY, AND F. F. ZBORALSKE. Esophageal labeling with small tantalum wires. Ef- fects on motility and histology. Invest. Radiol. 6: 191-198, 1971. DOOLEY, C. P., B. SCHLOSSMACHER, AND J. E. VALENZEULA. Effects of alterations in bolus viscosity on esophageal peristalsis in humans. Am. J. Physiol. 254 (Gastrointest. Liver Physiol. 17): G8-Gll, 1988. HEWSON, E. G., D. J. OTT, C. B. DAI~TON, Y. M. CHEN, W. C. WV, AND J. E. RICHTER. Manometry and radiology. Complemen- tary studies in the assessment of esophageal motility disorders. Gastroenterology 98: 626-632, 1990. HOLLIS, J. B., AND D. 0. CASTELL. Effect of dry swallows and wet swallows of different volume on esophageal peristalsis. J. Appl.
FELINE ESOPHAGUS G425
Physiol. 38: 1161-l 164, 1975. 15. KAHRILAS, P. J., W. J. DODDS, AND W. J. HOGAN. Effect of
peristalstic dysfunction on esophageal volume clearance. Gastro- enterology 94: 73-80, 1988.
16. MITTAL, R. K., J. REN, R. W. MCCALLUM, H. A. SHAFFER, JR., AND J. SLUSS. Modulation of feline esophageal contractions by bolus volume and outflow obstruction. Am. J. Physiol. 258 (Gas- trointest. Liver Physiol. 21): G208-G215, 1990.
17. OTT, D. J., Y. M. CHEN, E. G. HEWSON, J. E. RICHTER, C. B. DALTON, D. W. GELFAND, AND W. C. WV. Esophageal motility: assessment with synchronous video tape fluoroscopy and manom- etry. Radiology 173: 419-422, 1989.
18. REN, J., W. J. DODDS, C. H. MARTIN, R. 0. DANTAS, M. K. KERN, AND J. G. BRASSEUR. Effect of increased intraabdominal pressure on peristalsis in the feline esophagus (Abstract). Gas troenterology 99: 1228, 1990.