Plasmid/liposome transfer of the human manganese superoxide dismutase transgene prevents ionizing...
10
Plasmid/Liposome Transfer of the Human Manganese Superoxide Dismutase Transgene Prevents Ionizing Irradiation-Induced Apoptosis in Human Esophagus Organ Explant Culture Michael W. Epperly, Ph.D., 1 Christine Sikora, B.S., 1 Stacy Defilippi, B.S., 1 Jenifer Bray, B.S., 1 Gary Koe, Ph.D., 2 Denny Liggitt, D.V.M., Ph.D., 2 James D. Luketich, M.D., 3 and Joel S. Greenberger, M.D. 1 * 1 Department of Radiation Oncology, University of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania 2 Valentis Corporation, Burlingame, California 3 Department of Cardiothoracic Surgery, University of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania SUMMARY Esophagitis is a major limiting factor in the treatment of lung cancer by radiation alone or in combination with chemotherapy. We have previously demonstrated that intraesophageal injection of manganese superoxide dismutase–plasmid/liposome (MnSOD–PL) complex into C3H/HeNsd mice blocks irradiation-induced esophagitis. To determine whether the human esophagus can be similarly transfected, normal human esophageal sections obtained from the margins of esophagectomy specimens from esoph- ageal cancer patients were transfected in vitro with alkaline phosphatase (AlkP)–PL com- plex and stained for AlkP activity, and the percent of cells expressing AlkP was calculated. At 24 hr after transfection with 20 or 200 μg of AlkP–PL complex, 55.0% and 85.8% of esophageal epithelial cells expressed detectable AlkP, respectively. Other sections trans- fected with MnSOD–PL complex showed transgene mRNA by nested reverse transcrip- tase-polymerase chain reaction (RT-PCR) assay and increased MnSOD biochemical ac- tivity for at least 96 hr after transfection. Irradiated MnSOD–PL complex–transfected sections demonstrated a significantly decreased percentage of apoptotic cells when com- pared to irradiated control sections. Following 1,000 cGy, MnSOD–PL-treated samples showed 7.5 ± 2.8% and 33.3 ± 7.3% apoptotic cells at 24 and 48 hr compared to 53.6 ± 6.9% and 59.0 ± 13.8% for nontransfected controls (P < 0.0001 and P < 0.1175). After 2,000 cGy, results at 24 and 48 hr were 25.0 ± 7.6% and 66.9 ± 4.9% for MnSOD-transfected sections compared to 65.6 ± 4.3% and 90.0 ± 4.1% for control sections (P < 0.0001 and P = 0.0353), respectively. Thus, human esophageal sections can be transfected with MnSOD–PL com- plex in vitro and thereby protected against ionizing irradiation-induced apoptosis. Int. J. Cancer (Radiat. Oncol. Invest.) 90, 128–137 (2000). © 2000 Wiley-Liss, Inc. Key words: manganese superoxide dismutase; plasmid/liposome; radiation esophagi- tis; radioprotective gene therapy Contract grant sponsor: National Institutes of Health (RO1 ? HL60132). *Correspondence to: Joel S. Greenberger, M.D., Department of Radiation Oncology, University of Pittsburgh Cancer Institute, 200 Lothrop Street, B346-PUH, Pittsburgh, PA 15213. Phone: (412) 647-3607; Fax: (412) 647-6029; E-mail: [email protected] Received 2 November 1999; Revised 20 March 2000; Accepted 31 March 2000 Int. J. Cancer (Radiat. Oncol. Invest): 90, 128–137 (2000) © 2000 Wiley-Liss, Inc. Publication of the International Union Against Cancer
-
Upload
washington -
Category
Documents
-
view
3 -
download
0
Transcript of Plasmid/liposome transfer of the human manganese superoxide dismutase transgene prevents ionizing...

Plasmid/Liposome Transfer of the HumanManganese Superoxide Dismutase Transgene
Prevents Ionizing Irradiation-Induced Apoptosisin Human Esophagus Organ Explant Culture
Michael W. Epperly, Ph.D.,1 Christine Sikora, B.S.,1 Stacy Defilippi, B.S.,1Jenifer Bray, B.S.,1 Gary Koe, Ph.D.,2 Denny Liggitt, D.V.M., Ph.D.,2
James D. Luketich, M.D.,3 and Joel S. Greenberger, M.D.1*1Department of Radiation Oncology, University of Pittsburgh Cancer Institute,
Pittsburgh, Pennsylvania2Valentis Corporation, Burlingame, California
3Department of Cardiothoracic Surgery, University of Pittsburgh Cancer Institute,Pittsburgh, Pennsylvania
SUMMARY Esophagitis is a major limiting factor in the treatment of lung cancer byradiation alone or in combination with chemotherapy. We have previously demonstratedthat intraesophageal injection of manganese superoxide dismutase–plasmid/liposome(MnSOD–PL) complex into C3H/HeNsd mice blocks irradiation-induced esophagitis. Todetermine whether the human esophagus can be similarly transfected, normal humanesophageal sections obtained from the margins of esophagectomy specimens from esoph-ageal cancer patients were transfected in vitro with alkaline phosphatase (AlkP)–PL com-plex and stained for AlkP activity, and the percent of cells expressing AlkP was calculated.At 24 hr after transfection with 20 or 200 µg of AlkP–PL complex, 55.0% and 85.8% ofesophageal epithelial cells expressed detectable AlkP, respectively. Other sections trans-fected with MnSOD–PL complex showed transgene mRNA by nested reverse transcrip-tase-polymerase chain reaction (RT-PCR) assay and increased MnSOD biochemical ac-tivity for at least 96 hr after transfection. Irradiated MnSOD–PL complex–transfectedsections demonstrated a significantly decreased percentage of apoptotic cells when com-pared to irradiated control sections. Following 1,000 cGy, MnSOD–PL-treated samplesshowed 7.5 ± 2.8% and 33.3 ± 7.3% apoptotic cells at 24 and 48 hr compared to 53.6 ± 6.9%and 59.0 ± 13.8% for nontransfected controls (P < 0.0001 and P < 0.1175). After 2,000 cGy,results at 24 and 48 hr were 25.0 ± 7.6% and 66.9 ± 4.9% for MnSOD-transfected sectionscompared to 65.6 ± 4.3% and 90.0 ± 4.1% for control sections (P < 0.0001 and P = 0.0353),respectively. Thus, human esophageal sections can be transfected with MnSOD–PL com-plex in vitro and thereby protected against ionizing irradiation-induced apoptosis. Int. J.Cancer (Radiat. Oncol. Invest.) 90, 128–137 (2000). © 2000 Wiley-Liss, Inc.
Key words: manganese superoxide dismutase; plasmid/liposome; radiation esophagi-tis; radioprotective gene therapy
Contract grant sponsor: National Institutes of Health (RO1? HL60132).*Correspondence to: Joel S. Greenberger, M.D., Department of Radiation Oncology, University of Pittsburgh Cancer
Institute, 200 Lothrop Street, B346-PUH, Pittsburgh, PA 15213. Phone: (412) 647-3607; Fax: (412) 647-6029;E-mail: [email protected]
Received 2 November 1999; Revised 20 March 2000; Accepted 31 March 2000
Int. J. Cancer (Radiat. Oncol. Invest):90, 128–137 (2000)© 2000 Wiley-Liss, Inc. Publication of the International Union Against Cancer

INTRODUCTION
Despite the use of modern megavoltage linear ac-celerators and multileaf collimated radiotherapytreatment beams, the clinical radiotherapy of neo-plasms of the thoracic cavity remains limited bynormal tissue toxicity [1–4]. Prominent in earlyclinical toxicity of radiotherapy for lung cancer inother mediastinal tumors is irradiation-inducedesophagitis [5]. Clinical irradiation esophagitis isdose- and volume-dependent, with the time of onsetand severity of symptoms dependent on the dosedelivered per daily fraction, total dose deliveredover the usual 4- to 6-week treatment course of5 days per week, and perhaps most importantly,total volume of the esophagus in the treatment field[1,5,6].
The problem of irradiation esophagitis hasbeen exacerbated by use of the clinically effectivechemotherapeutic drugs carboplatin and paclitaxel(Taxol) (CT) [4,7,8]. These drugs, which havegreatly increased the likelihood of local controlwith radiotherapy of non-small-cell lung cancer(NSCLC), have been associated with an increasedseverity of irradiation esophagitis. The successfuluse of carboplatin and paclitaxel, in addition toradiotherapy, has resulted in long-term local con-trol and disease-free survival in up to 30% of pa-tients with unresectable NSCLC. Furthermore,there is an emerging consensus that escalation ofradiotherapy doses to above 65 Gy may furtherimprove clinical outcomes. These facts point to theneed to develop new strategies for reducing che-moradiotherapy toxicity to the esophagus as well asother normal tissues [1,4].
Currently, clinical esophagitis is scored byseveral criteria, with grades 3 and 4 esophagitisbeing the most debilitating [1]. Patients with grade3 esophagitis may require hospitalization for intra-venous hyperalimentation since swallowing is verypainful and there is a significant risk of dehydrationand/or starvation. Patients with grade 4 esophagitismay suffer esophageal tears or perforation.
The pathology of irradiation esophagitis hasbeen well correlated between experimental rodentmodels and clinical histopathology [9–11]. Thesquamous lining cells of the esophagus demon-strate vacuolization at around 15 days after single-fraction, whole-thorax irradiation in mice [12]. Un-der higher magnification, these vacuoles areidentified as apoptotic cells [12]. Between 15 and30 days, clusters of cells with vacuoles are replacedby areas of ulceration, sloughing of sections ofsquamous lining cells, and infiltration of inflamma-tory cells. After completion of irradiation, reepithe-
lialization of ulcerated areas is detectable over thesubsequent 30 days [9,10]. A late lesion of esoph-ageal stricture has been detected in both experi-mental animal models and patients in the clinicalsetting, involving fibrosis, a lack of esophageal mo-tility, and narrowing of the esophageal lumen.Pharmacological approaches to radiation protectionof the esophagus have met with limited success.The use of sulfhydryl compounds, which scavengeirradiation-induced free radicals; pilocarpine; atro-pine; corticosteroids; nonsteroidal antiinflamma-tory drugs; and other agents known to decreaseproduction of irradiation-induced cytokines hasdemonstrated limited effectiveness at reducing ir-radiation esophagitis [13–15].
We have developed a technique of irradiationprotection of the esophagus through gene therapyusing topically delivered manganese superoxidedismutase–plasmid/liposome (MnSOD–PL) com-plex [12]. MnSOD protection has been shown todecrease apoptotic damage induced by tumor ne-crosis factor-a (TNF-a) or irradiation [16–19]. In amouse model, delivery of pRK5-manganese super-oxide dismutase plasmid (pRK5-MnSOD) and li-pofectin liposomes 1 day prior to irradiation re-sulted in a significant decrease in irradiation-induced vacuolization of the C3H/HeJ mouseesophagus at 15 days, decreased ulceration, de-creased irradiation-induced weight loss, and im-proved survival [12]. In other studies, the molecu-lar mechanism of MnSOD-mediated irradiationprotection has been partially elucidated [20]. At theorgan level, MnSOD transgene expression de-creases cytokine gene transcription [16–19]. Mn-SOD-overexpressing permanent cell lines demon-strated an increased shoulder on the irradiationsurvival curve, decreased irradiation-induced DNAstrand breaks, and decreased irradiation-inducedapoptosis [20].
To translate the effectiveness of MnSOD–PL-mediated irradiation protection from experi-mental animal to human esophageal tissue, using aclinical grade plasmid with a clinical grade lipo-some preparation, we first tested sections of normalhuman esophageal tissue explanted to tissue cul-ture. The results demonstrated efficient uptake oftransgene by human esophageal squamous epithe-lial cells in vitro, using both a histochemicallydetectable alkaline phosphatase (AlkP) markergene as well as the human MnSOD transgene. In-creased MnSOD biochemical activity was detectedin MnSOD transgene–transfected esophageal cellsin vitro and correlated to a significant decrease inirradiation-induced cell death.
Epperly et al.: Esophageal Radioprotective Gene Therapy 129

MATERIALS AND METHODS
Human Esophageal Tissue Sections
Sections of normal human esophagus (1.0 to 2.0 cmcylindrical sections) were dissected from the proxi-mal and distal margins of esophagectomy speci-mens from two esophageal cancer patients andstudied separately. Sections were directly placed inDulbecco’s modified Eagle medium (DMEM) con-taining 10% fetal calf serum (FCS) at room tem-perature and taken to a tissue culture laboratory,where longitudinal sections of 1.0 × 0.3 × 0.3 cmwere sliced in a sterile tissue culture hood. Sectionswere placed in Petri dishes in DMEM plus 10%FCS. The procedure was approved by the Institu-tional Review Board of the University of PittsburghMedical Center.
pNGVL3-MnSOD andAlkP Plasmids
A pNGVL3 (plasmid obtained from the NationalGene Vector Laboratory)-MnSOD plasmid wasconstructed by excising the human MnSOD trans-gene from the pRK5-MnSOD plasmid [16], cuttingthe 38 end of the transgene with PvuI endonucleaseand blunt-ending the 38 end by incubating with T4DNA polymerase for 5 min at 37°C. The 58 end ofthe MnSOD transgene was cut with EcoRI and theMnSOD transgene (750 bp fragment) isolated byelectrophoresis on a 1% agarose gel. The plasmidwas cut with Bam HI restriction endonuclease andblunt-ended with T4 DNA polymerase as describedabove. The pNGVL3 plasmid was cut with EcoRIand isolated by electrophoresis on a 1% agarosegel. The MnSOD transgene was ligated into thepNGVL3 plasmid using the Boehringer-Mannheim(Mannheim, Germany) Rapid DNA Ligation Kit.DH5a Escherichia colicells were transformed by
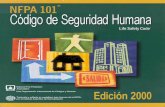
mixing 5 ml of ligation mixture with 50 ml ofDH5a E. coli-competent cells on ice for 5 min,heat-shocking the cells for 30 sec at 37°C, incubat-ing on ice for 2 min, and plating on L-agar platescontaining 10 mg/ml kanamycin. Clones were iso-lated and expanded, and plasmids were isolated.The MnSOD transgene was isolated by cutting theplasmids with EcoRI and Bgl II, electrophoresingon a 1% agarose gel, isolating the 750 bp DNAfragment, and sequencing the isolated fragment.Comparisons of the DNA sequence from the iso-lated fragments and published sequence [21] iden-tified one of the clones as containing MnSOD inthe correct orientation. A map of the pNGVL3-MnSOD plasmid is shown in Figure 1. AlkP plas-mids were provided by Valentis (Burlingame,Calif).
PL TransfectionsPL complexes were prepared at a concentration of2 mg of pNGVL3-MnSOD DNA/ml using endo-toxin-free, clinical grade VC192-208 cationic lipo-somes (Valentis). Esophageal sections werewashed in phosphate-buffered saline (PBS), and ei-ther 200 or 20mg of pNGVL3–MnSOD–PL com-plex (100 ml) were applied for 10 min at roomtemperature; then a second application of the samevolume and weight was immediately applied. Con-trol sections received liposomes only with no DNAinserts. Ten minutes later, sections were coveredwith tissue culture medium consisting of a 50:50mixture of DMEM and F12 medium containing10% FBS, and cultures were incubated at 37°C in ahumidified CO2 incubator.
Detection of AlkP ExpressionMultiple parallel sections from each esophagec-tomy specimen were transfected with a plasmidcontaining the AlkP transgene, as described above.
Fig. 1. Restriction map of the pNGVL3 plasmid (plasmid obtained from the National Gene Vector Laboratory). The humanmanganese superoxide dismutase (MnSOD) transgene was excised from the pRK5 MnSOD plasmid (pRK5-MnSOD) andinserted into the pNGVL3 plasmid as described in Materials and Methods. The plasmid restriction maps for pNGVL3 andpNGVL3-MnSOD are shown.
130 Epperly et al.: Esophageal Radioprotective Gene Therapy

At 24, 48, and 72 hr after transfection, sectionswere removed from the incubator and frozen inOptimum Cutting Temperature (OCT) compound(Sakura Fine Tek, Torrance, Calif.), sectioned, andstained for AlkP expression using the UniTect Rab-bit Immunohistochemistry System (Oncogene Re-search, Cambridge, Mass.). Sections were fixed inmethanol for 5 min at 4°C, then washed three timesin Tris-buffered saline (TBS), covered with 3%goat serum for 30 min at room temperature, andwashed three times in TBS. Sections were coveredwith a 1:500 dilution of a rabbit anti-AlkP anti-body, incubated at room temperature for 2 hr,washed three times in TBS, and covered in a 1:200dilution of a biotinylated goat anti-rabbit antibody.Slides were then incubated for 1 hr at room tem-perature, washed three times in TBS, and coveredwith a 0.5% H2O2 solution for 30 min at roomtemperature to block endogenous peroxidase activ-ity. Slides were washed in TBS and placed in di-aminobenzidine (DAB) solution [5 mg DAB, 40ml30% H2O2, 40 ml 0.1 M Tris (pH 7.6)] for 10 minat room temperature. Sections were next stainedwith propidium iodide by dipping the slides in asolution containing 50mg propidium iodide/ml and0.4 mg/ml RNase in 0.1% glucose [19] for 10 minat room temperature. Slides were mounted usingImmun-Mount (Shandon Lipshaw, Pittsburgh, Pa).Sections were then examined microscopically, andthe percentage of cells expressing AlkP was calcu-lated by scoring at least 100 randomly selectedhigh-power fields containing at least 100 cells perhigh-power field per section studied.
Nested RT-PCR AssayNested RT-PCR was used to demonstrate humanMnSOD transgene activity [17,18] using primersspecific for the pNGVL3-MnSOD transgene. Sincethe human transgene was expressed in a back-ground of endogenous human MnSOD mRNA, wechose the 58 primers located in the cytomegalovirus(CMV) promoter of the pNGVL3-MnSOD plas-mid, while the 38 primers were located in theMnSOD transgene. RNA was extracted from con-trol esophageal sections treated with liposomesonly (no DNA inserts) or transfected with 200mgof MnSOD–PL complex. Sections were homog-enized in 3 ml of Triazol (GIBCO-BRL, Gaithers-burg, Md) using a Polytron PT2000 homogenizer(Brinkmann Instruments, Westbury, NY). Sampleswere then incubated for 5 min at room temperature,followed by addition of 0.6 ml of chloroform, thenvortexing, and incubation for 3 min at room tem-perature. Samples were centrifuged at 12,000g for15 min at 4°C, followed by transfer of the aqueous
phase to a new centrifuge tube and addition of 1.5ml of isopropyl alcohol. Samples were then incu-bated at room temperature for 10 min and centri-fuged at 12,000g for 10 min at 4°C. Next, pelletswere washed with 70% ethanol, centrifuged at7,500g for 5 min at 4°C, air-dried, and resuspendedin 500 ml of water treated with diethylpyrocarbon-ate (DEPC) (Sigma, St. Louis, Mo). Two micro-grams of each RNA sample were mixed with 1.0mlof poly-dT (20 pmol/ml) and incubated for 10 minat 70°C, then placed on ice for 10 min. Each tubereceived 200 U of Superscript II RT (GIBCO-BRL)and 10 mM of the mixture of dCTP, dATP, dGTP,and dTTP and was incubated for 10 min at roomtemperature, 42°C for 50 min, 95°C for 10 min, and4°C for 10 min.
From each RT reaction, 1ml of a 1:100 dilu-tion of the RT reaction was mixed with the first setof 58 and 38 oligonucleotide primers; 10 mM of themixture of dATP, dCTP, dGTP, and dTTP; and0.4 U TAQ DNA polymerase (Boehringer Mann-heim, Indianapolis, Ind.). The mixture was sub-jected to 20 cycles of 94°C (30 sec), 60°C (50 sec),and 72°C (90 sec) in a Gene Amp PCR system(model 9600; Perkin-Elmer, Foster City, Calif.).For the second reaction, 1ml of the first reactionwas diluted 1:1,000 in DEPC-treated water with 1ml mixed with 24 ml of PCR mixture, describedabove, in the presence of the inner oligonucleotideprimers. The second set of primers was chosen tobe internal of the first set of primers and did notoverlap in sequence. Thermocycling was identicalto that of the first PCR, except the reaction was for35 cycles. PCR products were electrophoresed on a1% agarose gel and stained with ethidium bromide.The first set of oligonucleotide sequences consistedof a 58 primer of GGCAGTACATCAATGGGCGT(nucleotides 470–489) and a 38 primer ofTGAGCCTTGGACACCAACAGATGCA (nu-cleotides 1607–1631). The second set of primersconsisted of a 58 primer of CGGTTTGACTCAC-GGGGATT (nucleotides 496–515) and a 38 primerof GCTGAGCTTTGTCCAGAAAATGCTC(nucleotides 1450–1474). The expected size of thePCR product is 978 bp.
Measurement of MnSODBiochemical ActivityEsophageal sections, which were transfected witheither 20 or 200mg of pNGVL3-MnSOD–PL com-plex as described above, were compared to non-transfected sections treated with liposomes onlyand containing no DNA inserts. At 24, 72, or 96 hrafter transfection, control and transfected sectionswere removed and MnSOD biochemical activity
Epperly et al.: Esophageal Radioprotective Gene Therapy 131

was determined [17,18]. Sections were placed in20 mM PBS and homogenized using a PolytronPT2000 homogenizer followed by sonication. Ali-quots of 0, 100, 150, or 200mg protein were incu-bated in 20 mM PBS, 1 mM diethylenetriaminepentaacetic acid (DEPATAC), 1 U catalase, 5.6 ×10–8 M nitroblue tetrazolium (NBT), 0.1 mM xan-thine, 0.05 mM bathocuproinedisulfonic acid(BCS), 0.13 mg/ml defatted bovine serum albumin(BSA), and 5 mM sodium cyanide for 45 min atroom temperature [17,18]. Xanthine oxidase (10–2
M) was added, and the change in absorbance at 560nm as a function of time was measured. In thisreaction, superoxides produced by the reaction ofxanthine with xanthine oxidase reduced NBT, re-sulting in an increased absorbance at 550 nm. In thepresence of MnSOD, superoxides are converted toH2O2, thus preventing the reduction of NBT andinhibiting the increase in absorbance. Samplescontaining higher levels of MnSOD will result inincreased inhibition of the colorimetric assay.Esophageal sections treated with MnSOD–PL com-plex had increased MnSOD activity as seen by theincrease in percent inhibition of NBT reduction bysuperoxides at 24, 72, and 96 hr after application ofthe MnSOD–PL compared to the untreated control.
Quantitation of Cell Death inExplanted EsophagusTissue Sections
Esophageal sections were transfected with eachpNGVL3-MnSOD or control PL preparation as de-scribed above. Control or transfected sections wereirradiated to 1,000 or 2,000 cGy at 24 hr after trans-fection. Following an additional 24 or 48 hr, sec-tions were frozen in OCT and cut by a cryotome(AS620E, Shandon Lipshaw), and slides werestained for DNA strand breaks using the Promega(Madison, Wis.) Apoptosis Detection Kit. Slideswere examined microscopically, and the percentageof dead cells was determined for at least 1,000 cellscounted in at least 10 randomly selected micro-scopic fields for each sample.
RESULTS
Expression of AlkP Transgene inPL-Transfected Human EsophagealTissue Sections In Vitro
The AlkP cationic PLs (Valentis) were added at200 or 20mg in volumes of 100ml to each frag-ment of esophageal tissue in a high-humidity CO2
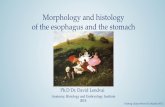
incubator. Complexes were coated on the squa-mous lining surface following washing in low-saltbuffer conditions. Complexes were added directlyto the tissue luminal surface for 10 min, followedby a second addition for 10 min. Sections were thencovered by tissue culture media. Fragments wereharvested at 24, 48, or 72 hr; and the percentage ofAlkP+ cells was calculated using propidium iodideand AlkP staining. As shown in Table 1, at 24 hrafter transfection, esophageal tissue fragments re-ceiving 200mg of PL showed 85.8% of cells con-taining the marker gene. This number decreased to72.1 ± 3.2% of cells at 48 hr and was still 28.4 ±2.9% of cells at 72 hr. With a lower concentrationof 20 mg of PLs at 24 hr after transfection, 55 ±2.9% of cells contained detectable AlkP, with per-sistent detection after 72 hr. Thus, there was strongpositivity at 24 hr with both concentrations of AlkPplasmid. A decreased but still clearly detectablenumber of cells expressing AlkP was scored at 48and 72 hr in sections receiving 200mg of AlkP–PLcomplex. In the esophageal sections receiving20 mg of AlkP–PL complex, there was a gradualchange in the percentage of cells expressing AlkPat 24 and 48 hr; and at 72 hr, there was a furtherdecreased but still detectable percentage of cellsexpressing AlkP. A photograph of representativesections at 24 hr is shown in Figure 2. These resultsestablish the effectiveness of PL transfer of theAlkP marker gene to human esophageal tissue frag-ments in vitro.
Table 1. Percent of Normal HumanEsophageal Cells in Explanted SectionsExpressing the Alkaline Phosphatase(AlkP) Transgene
AlkP–PLcomplex(mg)
Percent of cells at each hourafter transfection
24 hr 48 hr 72 hr
0 0.0 0.0 0.0200 85.8 ± 4.5 72.1 ± 3.2 28.4 ± 2.9
(P 4 0.0207) (P < 0.0001)
20 55.0 ± 2.970.2 ± 3.1
(P 4 0.0769)42.3 ± 2.3
(P 4 0.0130)
Normal human esophageal sections were obtained from the margins ofesophagectomy specimens (as described in Materials and Methods) andwashed in phosphate-buffered saline. Alkaline phosphatase–plasmid/liposome (AlkP–PL) complex (20 or 200mg) was applied to the esophagealsections in a 100ml volume, followed 10 min later with a second application,and covered 10 min later with tissue culture consisting of a 50:50 mixture ofDulbecco’s modified Eagle medium and F12 medium supplemented with10% fetal calf serum. At 24, 48, and 72 hr, a portion of each esophagealsection was removed, frozen in optimum cutting temperature compound,sectioned, and stained for AlkP expression. Sections were examined, and thepercentage of cells expressing AlkP was calculated. Student’st-test wasperformed to compare the percentage of cells expressing AlkP at 48 and 72 hrwith expression at 24 hr, demonstrating little change in gene expression in thefirst 48 hr after transfection.
132 Epperly et al.: Esophageal Radioprotective Gene Therapy

Successful Transfer of HumanMnSOD Transgene by PL toHuman Esophageal SectionsIn Vitro
The pNGVL3-MnSOD–PL preparation was nextadded to human esophageal sections that had beenwashed in PBS, as for the AlkP transgene experi-ments. Two hundred micrograms of pNGVL3-MnSOD–PL complex in 100ml were added for10 min at room temperature, followed by a secondapplication of 200mg of MnSOD–PL. Esophagealsections were covered 10 min later with a 50:50mixture of DMEM and F12 tissue culture mediumand incubated at 37°C. At various time points, sec-tions were removed and placed in liquid nitro-gen. The biochemical assay for detection ofMnSOD activity was carried out (as described inMaterials and Methods). As shown in Figure 3,
biochemical activity was clearly increased inesophageal sections transfected with MnSOD–PLcomplex compared to nontransfected tissuesamples at 24, 72, and 96 hr. At 24 and 72 hr,esophageal sections treated with MnSOD–PL com-plex had 6.7 U MnSOD activity/mg protein, whileat 96 hr the MnSOD activity had decreased to5.0 U compared to 4.3 for normal esophageal sec-tions (P 4 0.0014 and 0.007, respectively). NestedRT-PCR demonstrated that sections transfectedwith pNGVL3-MnSOD–PL showed detectabletransgene, while those treated with liposomes andno insert showed no detectable transgene (Fig. 4).These results establish that the human MnSODtransgene was effectively transferred by PL andexpressed in human esophageal sections in vitro.The results further indicate that the biochem-ical activity of transgene protein produced was
Fig. 2. Positive alkaline phosphatase (AlkP) staining following transfection of esophageal sections with plasmid/liposome(PL) containing the AlkP transgene. Esophageal sections were transfected with AlkP–PL complex (200mg) or liposomes only,as described in Materials and Methods. At 24 hr, sections were stained for AlkP activity. Positive staining (purple) was seenin an esophageal section transfected 24 hr previously with AlkP–PL complex (200mg) (A), while no AlkP staining was seenin sections transfected with liposomes only(B).
Epperly et al.: Esophageal Radioprotective Gene Therapy 133

detectable over the background level of endog-enous MnSOD following varying time periods ofincubation up to 96 hr.
MnSOD–PL Transfection of HumanEsophageal Sections DecreasesIrradiation-Induced Cell DeathIn Vitro
Sections of human esophagus were next transfectedwith 200 mg of MnSOD–PL in two procedures,as described in Materials and Methods. Sectionswere incubated for 24 hr, then irradiated using aVarian 6 MeV linear accelerator to either 1,000 or2,000 cGy. This dose is much greater than thatclinically used, which is fractionated over 5 to7 weeks. However, this dose was required to inducecell death as a single fraction. A group of unirra-diated control cultures was carried to the linear ac-celerator but not treated.
As shown in Table 2, sections treated withliposomes only and containing no DNA insertsdemonstrated 53.6 ± 6.9% of squamous lining cells
with increased DNA strand breaks indicative of in-creased cell death. This number had increased to 59± 13.8% by 48 hr following 1,000 cGy. Followinga higher dose of 2,000 cGy, 65.6 ± 4.3% of cells inthe squamous lining layer of control sections re-vealed increased cell death following transfectionwith naked liposomes containing no DNA inserts.This number increased to 90 ± 4.1% by 48 hr.
In striking contrast, sections receiving Mn-SOD–PL treatment with two transfections using200 mg of plasmid showed a significant reductionin cells with DNA strand breaks at both irradiationdose levels and at both time points. Esophagealsections treated with MnSOD–PL complex had sig-nificantly fewer dead cells than controls at 24 and48 hr after 1,000 cGy (7.5 ± 2.8% and 37.3 ±7.3%). Esophageal sections receiving MnSOD–PLcomplexes plus 2,000 cGy also had significantlyfewer cells with increased DNA strand breaks atboth 24 and 48 hr (25.0 ± 7.0% and 66.9 ± 4.9%,respectively). These results demonstrate that over-expression of the human MnSOD transgene can
Fig. 2. Continued.
134 Epperly et al.: Esophageal Radioprotective Gene Therapy

protect human esophageal sections in vitro againstirradiation-induced cell death.
DISCUSSION
The effectiveness of transmission of the humanMnSOD transgene to human esophageal sections invitro was demonstrated by taking sections of nor-mal human esophagus removed from the resectionmargins of specimens from esophagectomy pa-tients and treating them in vitro with MnSOD–PL.The use of low-salt concentrations in the washingbuffer facilitated increased uptake of cationic lipo-somes. We demonstrated a high efficiency of up-take in esophageal sections of either the AlkPmarker gene or the MnSOD transgene by use ofcationic PL. MnSOD transgene mRNA expressionwas detectable by nested RT-PCR, and MnSODprotein increase was biochemically detected by anassay for NBT dye reduction. Function of the Mn-SOD transgene product in preventing irradiation-induced cell death was demonstrated by in situ
measurement of the percentage of cells having in-creased DNA strand breaks at 24 and 48 hr afterirradiation. This decrease in cell death may nottranslate into a decrease in acute effects if it is theresult of increased cytokine effects following irra-diation. We did not directly measure the percentageof apoptotic cells in explanted, nonirradiatedesophageal sections or the levels of production ofendogenous MnSOD mRNA.
Induction of MnSOD mRNA and protein incells and tissues is known to occur after ionizingirradiation, although this is thought to be a responseto DNA strand breaks induced by irradiation. Thus,radiation induction occurs too late to be protective[17].
The present studies suggest that application ofMnSOD–PL gene therapy technology to clinicalesophageal radioprotection may be feasible. Sincepatients in clinical radiotherapy protocols receivefractionated radiotherapy, usually 180 to 200 cGyto a tumor target volume daily over a treatment
Fig. 3. Manganese superoxide dismutase (MnSOD) bio-chemical activity in human esophageal sections followingadministration of 200mg of MnSOD-plasmid/liposome(MnSOD–PL) complex. Human esophageal sections werewashed in phosphate-buffered saline followed by applica-tion of 200 mg of pNGVL3 (plasmid obtained from theNational Gene Vector Laboratory)–MnSOD–PL complex orliposomes only with no DNA inserts (100ml) for 10 min atroom temperature, followed by a second application. Sec-tions were covered 10 min later with a 50:50 mixture ofDulbecco’s modified Eagle medium and F12 tissue culturemedium and incubated at 37°C. At times ranging from 0 to96 hr, a portion of the esophageal sections were removed,frozen in liquid nitrogen, and assayed (as described in Ma-terial and Methods). The assay was a colorimetric assaybased on the reduction of nitroblue tetrazolium (NBT) bysuperoxides produced by the reaction of xanthine and xan-thine oxidase. Increased MnSOD expression in the esoph-ageal sections reduced the superoxides produced by xan-thine and xanthine oxidase, resulting in increased inhibitionof NBT reduction.
Fig. 4. Nested reverse transcriptase-polymerase chain re-action (RT-PCR) for the manganese superoxide dismutase(MnSOD) transgene in the pNGVL3 (plasmid obtainedfrom the National Gene Vector Laboratory)-MnSOD plas-mid. Esophageal sections were transfected with 200mgpNGVL3–MnSOD–plasmid/liposome (PL) complex orwith liposomes with no DNA inserts as described in Mate-rials and Methods. Duplicate samples were frozen in liquidnitrogen 24 hr later. RNA was extracted and nested RT-PCRwas performed using primers specific for the MnSOD trans-gene only. Positive MnSOD transgene expression wasfound only in sections transfected with the pNGVL3–MnSOD–PL complex.
Epperly et al.: Esophageal Radioprotective Gene Therapy 135

course of 5 to 7 weeks, it is encouraging to note thatthe duration of expression of MnSOD transgene upto 96 hr in vitro suggests that clinical trials mayrequire application of swallowed PL only everyfourth day. Further in vivo animal model studieswill be required to determine the effectiveness ofprotection of esophageal tissue irradiated at timepoints beyond 24 hr after application of PL. In vitrostudies to address this timing question were notpossible in the current in vitro model because of theknown spontaneous background level of apoptoticcells in tissue sections explanted to tissue culture.The available model of explanted human tissue fa-cilitated our studies only over a short duration of 24to 48 hr because the level of spontaneous apoptosisfrom explanted tissue, having lost its blood supplyand tissue integrity, could not be maintained be-yond this time point.
Also supporting a clinical trial of esophagealirradiation protection by MnSOD–PL gene therapyare the results of mouse studies using the samepNGVL3-MnSOD–PL preparation. In other stud-ies, C3H/HeJ mouse esophageal tissue was pro-tected using the same preparation of PL, and a com-plete dose-response curve has been carried outshowing an encouraging protective effect of dosesas low as 2mg plasmid in 500ml liposomes (datanot shown). At the present time, we do not knowhow MnSOD transgene expression in the epitheliallining cells of the mouse esophagus translates toprotection from irradiation-induced apoptosis andulceration of the squamous layer [12]. Direct irra-diation induction of apoptosis in some cells maylead to TNF-a release and secondary induction ofapoptosis in adjacent cells. Since MnSOD protects
against TNF-a, as well as irradiation-induced ap-optosis [16, 19], the positive bystander protectionafforded to nontransfected cells by MnSOD trans-gene-expressing cells may be quite effective at ra-dioprotection of the organ.
Further studies will be required to facilitatetranslation of this potentially important method ofesophageal irradiation protection to the care ofclinical radiotherapy patients.
REFERENCES1. Bahri S, Flickinger JC, Kalend A, Deutsch M, Belani C,
Sciurba F, Luketich J, Greenberger JS. Results of mul-tifield conformal radiation therapy of non-small celllung carcinoma using multileaf collimation beams. Ra-diat Oncol Invest 1999;7:297–308.
2. Byhardt RW, Scott C, Sause WT, Emami B, Komaki R,Fisher B, Lee JS, Lawton C. Response, toxicity, failurepatterns, and survival in five Radiation Therapy Oncol-ogy Group (RTOG) trials of sequential and/or concur-rent chemotherapy and radiotherapy for locally ad-vanced non-small cell carcinoma of the lung. Int JRadiat Oncol Biol Phys 1998;42:469–478.
3. Choi NC, Herndon JE, Rosenman J, Carey RW, ChungCT, Bernard S, Leone L, Seagren S, Green M. Phase Istudy to determine the maximum-tolerated dose of ra-diation in standard daily and hyperfractionated-accelerated twice-daily radiation schedules with con-current chemotherapy for limited-state small-cell lungcancer. J Clin Oncol 1998;16:3528–3536.
4. Choy H, Safran H, Graziano S, Chung C, Williams T,Cole B, Kennedy T. Multi-institutional phase II trial ofpaclitaxel, carboplatin, and concurrent radiationtherapy for locally advanced non-small cell lung can-cer. J Clin Oncol 1998;16:3316–3322.
5. Byhardt RW, Martin L, Pajak TF, Shin KH, Emami B,Cox JD. The influence of field size and other treatment
Table 2. Percent of Cells Having Increased DNA Strand Breaks in HumanEsophageal Sections Following 1,000 or 2,000 cGy Irradiation Is Decreasedby Prior Manganese Superoxide Dismutase–Plasmid/Liposome (MnSOD–PL)Complex Treatment
MnSOD–PLcomplex (mg)
Hours after irradiation (% cells with increased DNA strand breaks)
1,000 cGy 2,000 cGy
24 hr 48 hr 24 hr 48 hr
0 53.6 ± 6.9 59.0 ± 13.8 65.6 ± 4.3 90.0 ± 4.1200 7.5 ± 2.8 33.3 ± 7.3 25.0 ± 7.6 66.9 ± 4.9
(P < 0.0001) (P 4 0.1175) (P < 0.0001) (P 4 0.0353)
Normal esophageal sections were washed in PBS, followed by application to some sections of 200mg of MnSOD–PL complexand incubated at room temperature for 10 min, at which time a second application of 200mg of MnSOD–PL complex wasadministered to the same fraction. Controls received two (100ml) treatments with liposomes only containing no DNA plasmid.Esophageal sections were covered 10 min later with a 50:50 mixture of Dulbecco’s modified Eagle medium and F12 tissue cultuemedium and incubated at 37°C. Samples were irradiated to either 1,000 or 2,000 cGy 24 hr later. At 24 and 48 hr after irradiation,half of each sample was frozen in optimum cutting temperature compound, sectioned, and stained for cells having increasedDNA strand breaks using The Promega Apoptosis Detection Kit. Sections were examined, and the percentage of cells positivefor DNA strand breaks was determined. Student’st-test was used to compare the esophageal sections treated with MnSOD–PLcomplex with the control irradiated sections.
136 Epperly et al.: Esophageal Radioprotective Gene Therapy

factors on pulmonary toxicity following hyperfraction-ated irradiation for inoperable non-small cell lung can-cer (NSCLC)—analysis of a Radiation Therapy Oncol-ogy Group (RTOG) protocol. Int J Radiat Oncol BiolPhys 1993;27:537–544.
6. Greenberger JS, Kalend A, Sciurba F, Jett J, Landre-neau R, Belani C. Development of multifield three-dimensional conformal radiotherapy of lung cancer us-ing a total lung dose/volume histogram. Radiat OncolInvest 1996;3:243–255.
7. Kelly K, Hazuka M, Pan Z, Murphy J, Caskey J, Leo-nard C, Bunn PA. A phase I study of daily carboplatinand simultaneous accelerated, hyperfractionated chestirradiation in patients with regionally inoperable non-small cell lung cancer. Int J Radiat Oncol Biol Phys1998;40:559–567.
8. Langer CJ, Movsas B, Hudes R, Schol J, Keenan E,Kilpatrick D, Yeung C, Curran W. Induction of pacli-taxel and carboplatin followed by concurrent chemora-diotherapy in patients with unresectable, locally ad-vanced non-small cell lung carcinoma: report of FoxChase Cancer Center study 94-001. Semin Oncol 1997;24:S12-89–S12-95.
9. Phillips TL, Margolis L. Radiation pathology and theclinical response of lung and esophagus. Front RadiatTher Oncol 1972;6:254–273.
10. Sherman DM, Carabell SC, Belli JA, Hellman S. Theeffect of dose-rate and Adriamycin on the tolerance ofthoracic radiation in mice. Int J Radiat Oncol Biol Phys1992;8:45–51.
11. Sur M, Sur R, Cooper K, Levin V, Bizos D, DubazanaN. Morphologic alterations in esophageal squamouscell carcinoma after preoperative high-dose-rate intra-luminal brachytherapy. Cancer 1996;77:2200–2205.
12. Stickle RL, Epperly MW, Klein E, Bray JA, Green-berger JS. Prevention of irradiation-induced esophagitisby intraesophageal plasmid/liposome delivery of thehuman manganese superoxide dismutase (MnSOD)transgene. Radiat Oncol Invest 1999;7:204–217.
13. Phillips TL, Kane L, Utley JF. Radioprotection of tu-mor and normal tissues by thiophosphate compounds.Cancer 1973;32:528–525.
14. Nagler RM, Laufer D. Protection against irradiation-induced damage to salivary glands by adrenergic ago-nist administration. Int J Radiat Oncol Biol Phys 1998;40:477–481.
15. Grdina DJ, Carnes BA, Grahn D, Sigdestad CP. Pro-tection against late effects of radiation by S-2-(3-aminopropylamin)-ethylphosphorothioic acid. CancerRes 1991;51:4125–4130.
16. Wong GHW, Elwell JH, Oberley LW, Goeddel DV.Manganese superoxide dismutase is essential for cellu-lar resistance to cytotoxicity of tumor necrosis factor.Cell 1989;58:923–931.
17. Epperly MW, Bray JA, Kraeger S, Zwacka R, Engel-hardt J, Travis E, Greenberger JS. Prevention of lateeffects of irradiation lung damage by manganese super-oxide dismutase (MnSOD) gene therapy. Gene Ther1998;5:196–208.
18. Epperly MW, Bray JA, Krager S, Berry LA, GoodingW, Engelhardt JF, Zwacka R, Travis EL, GreenbergerJS. Intratracheal injection of adenovirus containing thehuman MnSOD transgene protects athymic nude micefrom irradiation-induced organizing alveolitis. Int J Ra-diat Oncol Biol Phys 1999;45:171–182.
19. Epperly MW, Travis EL, Sikora C, Greenberger JS.Magnesium superoxide dismutase (MnSOD) plasmid/liposome pulmonary radioprotective gene therapy:modulation of irradiation-induced mRNA for IL-1,TNF-a, and TGF-b correlates with delay of organizingalveolitis/fibrosis. Biol Blood Bone Marrow Transplant1999;5:204–214.
20. Epperly MW, Bray JA, Esocobar P, Bigbee WL, Wat-kins S, Greenberger JS. Overexpression of the humanMnSOD transgene in subclones of murine hematopoi-etic progenitor cell line 32D cl 3 decreases irradiation-induced apoptosis but does not alter G2/M or G1/Sphase cell cycle arrest. Radiat Oncol Invest 1999;7:331–342.
21. Heckl K. Isolation of cDNAs encoding human manga-nese superoxide dismutase. Nucleic Acids Res 1988;16:6224.
Epperly et al.: Esophageal Radioprotective Gene Therapy 137