Surgical Complications Do Not Affect Longterm Survival after Esophagectomy for Carcinoma of the...
9
Surgical Complications Do Not Affect Longterm Survival after Esophagectomy for Carcinoma of the Thoracic Esophagus and Cardia Ermanno Ancona, MD, FACS, Matteo Cagol, MD, Magdalena Epifani, PhD, Francesco Cavallin, PhD, Giovanni Zaninotto, MD, FACS, Carlo Castoro, MD, Rita Alfieri, MD, Alberto Ruol, MD, FACS BACKGROUND: Surgical resection is the only real chance of cure for carcinoma of the esophagus and esophago- gastric junction, although it carries considerable postoperative morbidity and mortality. The longterm prognosis for patients undergoing operation depends largely on the pathologic stage of the disease. The real impact of postoperative complications on survival is still under evaluation. STUDY DESIGN: A retrospective analysis was performed on patients with squamous cell carcinoma and adeno- carcinoma of the thoracic esophagus and esophagogastric junction, undergoing surgical resec- tion between January 1992 and December 2002. For the 522 patients considered for esopha- gogastroplasty, we analyzed comorbidities, preoperative staging, neoadjuvant treatments, surgical data, histopathology, postoperative surgical or medical complications, and survival. RESULTS: Surgical complications occurred in 85 of 522 patients (16.3%); their survival rate was entirely similar to that of the group of patients without surgical complications (p 0.9). The survival rate was worse for patients with concurrent surgical and medical complications. Analysis of the 99 patients (19%) who had only medical complications postoperatively revealed a survival rate comparable (p 0.9) with that of the 338 patients (63.7%) with an uneventful postoperative course. The median postoperative hospital stay was 14 days for all 522 patients, and 18 days for patients with medical or surgical postoperative complications. Multivariate analysis of the predictive factors showed that surgical complications do not affect longterm prognosis. CONCLUSIONS: Surgical complications have no negative impact on survival rates, which seem to depend exclu- sively on the pathologic stage of the tumor. (J Am Coll Surg 2006;203:661–669. © 2006 by the American College of Surgeons) Esophageal carcinoma is still one of the solid tumors with the most dismal prognosis. Radical surgery with lymphadenectomy is the only real chance for cure, but it carries considerable postoperative morbidity and mortality. 1-4 Most patients present with locally advanced tumors, and neoadjuvant chemoradiotherapy has been used more frequently in recent years; in responders, it in- creases the R0 resection rate, improving the prognosis and quality of life. 5,6 The chemoradiotherapeutic regimen also has a far-from-negligible toxicity rate, however, and it in- creases the postoperative morbidity and mortality. Recent studies have emphasized a notable improve- ment in morbidity and mortality rates at high-volume referral centers, 7-10 recommending that this type of op- eration be performed only at specialized centers. Hospi- tal mortality rates are known to depend on postoperative morbidity rates; the longterm prognosis for patients un- dergoing surgery depends on the pathologic stage of their disease, and particularly, on lymph node positivity and visceral metastases. 11 The real impact of postopera- tive complications on survival is a matter of debate. A recent retrospective analysis on 510 patients who underwent surgery for carcinoma of the esophagus or cardia at Memorial Sloan-Kettering Cancer Center 12 showed that postoperative surgical complications have a severly negative impact on longterm survival. We com- Competing Interests Declared: None. Received February 15, 2006; Revised May 26, 2006; Accepted July 17, 2006. From the Instituto Oncologico Veneto (Ancona, Cagol, Epifani); and the Department of Surgery, Clinica Chirurgica III (Cavallin, Zaninotto, Castoro, Alfieri, Ruol), University of Padova, Padova, Italy. Correspondence address: Ermanno Ancona, MD, FACS, Department of Sur- gery, Clinical Chirurgica III, Via Giustinani 2, Padova, Italy. 661 © 2006 by the American College of Surgeons ISSN 1072-7515/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jamcollsurg.2006.07.017
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Surgical Complications Do Not Affect Longterm Survival after Esophagectomy for Carcinoma of the...
SSo
EG
Ewlbmtucq
C
RFDACg
©P
urgical Complications Do Not Affect Longtermurvival after Esophagectomy for Carcinomaf the Thoracic Esophagus and Cardia
rmanno Ancona, MD, FACS, Matteo Cagol, MD, Magdalena Epifani, PhD, Francesco Cavallin, PhD,iovanni Zaninotto, MD, FACS, Carlo Castoro, MD, Rita Alfieri, MD, Alberto Ruol, MD, FACS
BACKGROUND: Surgical resection is the only real chance of cure for carcinoma of the esophagus and esophago-gastric junction, although it carries considerable postoperative morbidity and mortality. Thelongterm prognosis for patients undergoing operation depends largely on the pathologic stageof the disease. The real impact of postoperative complications on survival is still underevaluation.
STUDY DESIGN: A retrospective analysis was performed on patients with squamous cell carcinoma and adeno-carcinoma of the thoracic esophagus and esophagogastric junction, undergoing surgical resec-tion between January 1992 and December 2002. For the 522 patients considered for esopha-gogastroplasty, we analyzed comorbidities, preoperative staging, neoadjuvant treatments,surgical data, histopathology, postoperative surgical or medical complications, and survival.
RESULTS: Surgical complications occurred in 85 of 522 patients (16.3%); their survival rate was entirelysimilar to that of the group of patients without surgical complications (p � 0.9). The survivalrate was worse for patients with concurrent surgical and medical complications. Analysis of the99 patients (19%) who had only medical complications postoperatively revealed a survival ratecomparable (p � 0.9) with that of the 338 patients (63.7%) with an uneventful postoperativecourse. The median postoperative hospital stay was 14 days for all 522 patients, and 18 days forpatients with medical or surgical postoperative complications. Multivariate analysis of thepredictive factors showed that surgical complications do not affect longterm prognosis.
CONCLUSIONS: Surgical complications have no negative impact on survival rates, which seem to depend exclu-sively on the pathologic stage of the tumor. (J Am Coll Surg 2006;203:661–669. © 2006 by the
American College of Surgeons)hc
mretmdtat
ucs
sophageal carcinoma is still one of the solid tumorsith the most dismal prognosis. Radical surgery with
ymphadenectomy is the only real chance for cure,ut it carries considerable postoperative morbidity andortality.1-4 Most patients present with locally advanced
umors, and neoadjuvant chemoradiotherapy has beensed more frequently in recent years; in responders, it in-reases the R0 resection rate, improving the prognosis anduality of life.5,6 The chemoradiotherapeutic regimen also
ompeting Interests Declared: None.
eceived February 15, 2006; Revised May 26, 2006; Accepted July 17, 2006.rom the Instituto Oncologico Veneto (Ancona, Cagol, Epifani); and theepartment of Surgery, Clinica Chirurgica III (Cavallin, Zaninotto, Castoro,lfieri, Ruol), University of Padova, Padova, Italy.orrespondence address: Ermanno Ancona, MD, FACS, Department of Sur-
sery, Clinical Chirurgica III, Via Giustinani 2, Padova, Italy.
6612006 by the American College of Surgeons
ublished by Elsevier Inc.
as a far-from-negligible toxicity rate, however, and it in-reases the postoperative morbidity and mortality.
Recent studies have emphasized a notable improve-ent in morbidity and mortality rates at high-volume
eferral centers,7-10 recommending that this type of op-ration be performed only at specialized centers. Hospi-al mortality rates are known to depend on postoperativeorbidity rates; the longterm prognosis for patients un-
ergoing surgery depends on the pathologic stage ofheir disease, and particularly, on lymph node positivitynd visceral metastases.11 The real impact of postopera-ive complications on survival is a matter of debate.
A recent retrospective analysis on 510 patients whonderwent surgery for carcinoma of the esophagus orardia at Memorial Sloan-Kettering Cancer Center12
howed that postoperative surgical complications have a
everly negative impact on longterm survival. We com-ISSN 1072-7515/06/$32.00doi:10.1016/j.jamcollsurg.2006.07.017

popecti
MAVbnarTrtttgp
PAtCseseeatuwd
SPrtcgTrr
ce
pcntcwrboaaudaa
CIlrdhCti
tmems
ldtwgfsatics
662 Ancona et al Longterm Survival after Esophagectomy J Am Coll Surg
ared the results of this study with results obtained atur own center, based on a retrospective analysis on 522atients who underwent surgery for carcinoma of thesophagus or cardia, evaluated the impact of surgicalomplications on postoperative mortality and survival inhe long and short term, and identified factors influenc-ng the prognosis.
ETHODSretrospective analysis was conducted on the data in theeneto Region’s Center for Esophageal Diseases data-ase, considering all patients with squamous cell carci-oma and adenocarcinoma of the thoracic esophagusnd esophagogastric junction who underwent surgicalesection between January 1992 and December 2002.here were 522 eligible patients who had undergone
esection and esophagogastroplasty for reconstruction ofhe digestive tract. Variables considered were clinical his-ory, comorbidities, preoperative staging, neoadjuvantreatments, surgical data, histologic findings on the sur-ical specimen, postoperative surgical or medical com-lications, and survival.
reoperative stagingll patients were staged preoperatively by endoscopy of
he upper digestive tract with biopsy, barium swallow,T scan, otolaryngology examination, tracheobroncho-
copy for patients with upper and median thoracicsophageal tumor, plus hepatic ultrasonography or bonecan, when necessary. From 2000 onward, esophagealco-endoscopic ultrasonography was also used. Thesophageal tumors of patients given neoadjuvant ther-py (45 to 50 Gy radiotherapy and three cycles chemo-herapy) were staged before and after treatment to eval-ate their response. An accurate anesthesiologic workupas performed, examining the patient’s respiratory, car-iovascular, hepatic, and renal functions.
urgeryatients with a neoplasm in the infracarinal thoracicegion and cardia underwent a transthoracic esophagec-omy through laparotomy and right thoracotomy ac-ording to Ivor Lewis, with an intrathoracic esophago-astric anastomosis, routinely performed with a stapler.he chosen approach for patients with supracarinal tho-
acic neoplasms was a transthoracic esophagectomy by
ight thoracotomy, laparotomy, and cervicotomy, ac-ording to McKeown.The cervical anastomosis was gen-rally fashioned manually.
In all patients, an en-bloc lymph node dissection waserformed, which included the periesophageal, infra-arinal, posterior mediastinal, and paracardial lymphodes and those located along the lesser gastric curva-ure, the origin of the left gastric artery, celiac trunk,ommon hepatic artery, and splenic artery. In patientsith upper thoracic tumor, paratracheal, cervical, and
ecurrent lymph nodes were removed.The median num-er of lymph nodes harvested was 17. Where thoracot-my was contraindicated, patients underwent a transhi-tal esophagectomy by laparotomy and cervicotomy,nd cervical anastomosis. All patients had postoperativepper gastrointestinal study with gastrografin on the 7th
ay for intrathoracic and on the 10th day for cervicalnastomoses. All patients received epidural analgesia toccomplish better postoperative pain control.
omplicationsntraoperative complications included tracheobronchialesions, including recurrent nerve injury from oncologicadicality, and splenectomies prompted by accidentalamage. Cases of diaphragmatic hernia, postoperativeemorrhage, and chylothorax were also considered.omplications related to reconstruction of the digestive
ract included anastomotic leakages (radiologic and clin-cal), necrosis, and esophageal transit impairments.
Tracheobronchial lesions were diagnosed intraopera-ively and immediately sutured and reinforced withuscle flaps. Recurrent nerve lesions were identified by
ndoscopic otolaryngologic examination. Diaphrag-atic hernias were diagnosed by barium swallow or CT
can, and then confirmed intraoperatively.Chylothorax was defined as an excessive (� 1,000 mL/d)
eakage from the thoracic drainage tube, lasting at least 2ays, and confirmed by a physical-chemical analysis ofhe fluid. Radiologically identified anastomotic leakagesere asymptomatic and were found at followup gastro-rafin swallow; clinically symptomatic fistulas were con-irmed by gastrografin swallow and endoscopy. Diagno-is of necrosis was clinical, radiologic, and endoscopic,nd treatment involved take-down of the esophagogas-roplasty and cervical esophagostomy. Digestive transitmpairments were defined as pathologic, symptomatichanges in the transit and were diagnosed by bariumwallow and endoscopy.
Medical complications that correlated with the oper-
adtrolknr
aciabetpi
p3d
HAcTawsrmgs
FAlfwcw
SD(w
mmWttupaatwf
RTtcpav
TC
TMGCRHDNN
P
H
P
663Vol. 203, No. 5, November 2006 Ancona et al Longterm Survival after Esophagectomy
tion, but were not strictly caused by the surgical proce-ure, were also considered. The most frequent complica-ions were respiratory, including respiratory insufficiencyequiring orotracheal intubation for more than 48 hoursr transient postoperative tracheostomy, ARDS, radio-ogically demonstrated pneumonia with fever and leu-ocytosis requiring specific antibiotic treatment, pulmo-ary atelectasis, and tracheobronchial obstructionequiring multiple selective bronchial aspirations.
Pulmonary thromboembolism was investigated byngio-CT scan, perfusion-ventilatory lung scintigraphyombined with vascular color echo-Doppler, or both, todentify any deep venous thrombosis. Cardiac alter-tions, such as arrhythmia or ischemia, were investigatedy electrocardiography or echocardiography and cardiacnzyme monitoring. Other minor medical complica-ions included diabetic decompensation, renal or he-atic insufficiency, acute pancreatitis, and others requir-ng specialist examination and treatment.
Perioperative mortality was considered in terms ofostoperative 30-day mortality (deaths occurring within0 days of surgery) and overall in-hospital mortality (alleaths occurring at the hospital).
istologyll patients had squamous cell carcinoma or adenocar-inoma of the esophagus or esophagogastric junction.he surgeon separately submitted the lymph node tissue
nd surgical specimen for histologic analysis. Stagingas done according to the pTNM classification.13 Re-
ection was defined as curative, or R0, when there was noesidual macro- or microscopic disease; R1 in cases oficroscopic residual disease or positive resection mar-
ins; R2 in cases of incomplete resection with macro-copic residual tumor.
ollowup and survivalll patients had accurate clinical and instrumental fol-
owups and outpatient visits at least twice a year for theirst 5 years, and once a year thereafter. Survival ratesere calculated from the date of operation. Survival
urves include postoperative deaths. All followup dataere stored in a database updated as of December 2004.
tatistical analysisata were analyzed using SAS Stat and SAS Graf, rel. 8.2
SAS Institute). Categorical variables were compared
ith the chi-square and Fisher’s exact tests, and the teans were compared with Student’s t-test. Nonpara-etric analysis was conducted according to Kruskal-allis. Survival analysis was done with the Life Test, and
he survival curves were compared using the Log-Rankest. Multivariate analysis on the survival times was donesing Cox’s logistic regression. Univariate analysis waserformed to correlate single variables, complicationsnd survival. Age, respiratory, cardiovascular, hepaticnd neurologic comorbidities, diabetes, neoadjuvantreatments, histotype, tumor site, and pathologic stageere entered in the multivariate analysis to evaluate the
actors predicting survival.
ESULTSable 1 summarizes the characteristics of the 522 pa-ients with adenocarcinoma (38.3%) or squamous cellarcinoma (61.7%). All 522 patients were followed upostoperatively for at least 2 years. Patients had a meange of 62 years, and the majority were men (79.7%ersus 20.3%, M/F 4:1). The most frequent comorbidi-
able 1. Patient Characteristicsharacteristics n %
otal 522ean age, y 62ender, male 416 79.7ardiovascular comorbidities 203 38.9espiratory comorbidities 93 17.8epatic comorbidities 72 13.8iabetes 44 8.4ephropathies 12 2.3eoadjuvant therapiesChemotherapy (3 cycles) 53 10.1Radiotherapy (45–50 Gy) 3 0.6Chemoradiotherapy 92 17.6
rocedureIvor-Lewis: thoracic anastomosis 382 73.2McKeown: cervical anastomosis 102 19.4Transhiatal 38 7.4istologyAdenocarcinoma 200 38.3Squamous cell carcinoma 322 61.7
athologic stage0 60 11.51 79 15.22 139 26.73 190 36.34 54 10.3
ies were cardiovascular (38.9%), followed by respira-

t(
tc1egw7
PTpwanthhrttmhm
sh
laiarp
(a
sinws
awrpspw
RmPe
T
V
I
pT
pA
p
* re on
664 Ancona et al Longterm Survival after Esophagectomy J Am Coll Surg
ory (17.8%) and hepatic disorders (13.8%), diabetes8.4%) and nephropathies (2.3%).
In 28% of the sample, patients received neoadjuvantreatment for locally advanced tumors; this involvedhemoradiotherapy in 17.6%, chemotherapy alone in0.1% and radiotherapy alone in 0.6%. The infracarinalsophagus was the most common tumor site, so the sur-ical procedure was usually esophagogastric resectionith esophagogastroplasty according to Ivor-Lewis (in3.2% of patients).
ostoperative complicationshere were 94 surgical complications (16.3%) in 85atients: 30 patients (5.7%) had an anastomotic leakage,hich was radiologically detectable in 12 patients (40%)
nd clinically detectable in 18 (60%); 8 patients hadecrosis (1.5%); 2 had impaired transit through theransposed viscera (1 suffered from colonic transhiatalernia requiring surgical reduction and closure of theiatus and 1 had stenosis at the diaphragmatic hiatus,equiring enlargement by means of a right pillar sec-ion); 5 patients had postoperative hemorrhage (1 fromhe transposed gastric viscera, requiring surgery and he-ostasis; 3 cases of surgically treated hemothorax and
emostasis; and 1 hemothorax with concurrent massiveyocardial infarction and subsequent death).Lesions to contiguous anatomic structures during re-
ective surgery occurred in 47 patients (9%): 32 (6.1%)
able 2. Surgical Complications and Patient Characteristics
ariableAnastomotic leak
n %
nduction therapyChemotherapy 2 3Chemoradiotherapy 3 3None 25 6Value 0.1umor locationProximal 11 10Middle 11 7Distal 3 3Gastroesophageal junction 5 2Value 0.47nastomotic locationChest 15 3Neck 15 10Value 0.002
The recurrent nerve lesions also include those performed deliberately to assu
ad unilateral recurrent nerve lesions, 7 (1.3%) had chy- w
othorax, treated conservatively in 1 and by en-bloc lig-ture of the thoracic duct in 6; 1 patient (0.2%) had anntraoperative tracheobronchial injury that was suturednd reinforced with a muscle flap; and 7 patients (1.3%)equired splenectomy. Table 2 shows the surgical com-lications according to the characteristics considered.Medical complications were seen in 148 patients
28%); 110 of them had medical complications alone,nd 38 also had surgical complications.
By analyzing 100 randomly chosen patients and con-idering the median duration of the operation and thentraoperative blood loss, there was no statistically sig-ificant difference between patients with and thoseithout complications. The number of blood transfu-
ion in the two groups was not markedly different.To establish whether preoperative chemoradiother-
py affects the rate of surgical complications, patientsere divided acccording to whether or not they had
eceived neoadjuvant treatment: 26 (17.6%) of the 148atients who had received neoadjuvant treatment hadurgical complications versus 59 (15.8%) of the 374atients who had not, so the surgical complication rateas comparable in the two groups (p � 0.6).
elationships between complications, postoperativeortality, and survivalostoperative mortality and survival (including postop-rative deaths) were compared for the groups of patients
ChylothoraxRecurrent nerve
injury*n % n %
0 5 9.41 1.0 10 10.86 1.0 17 4.5
3 2.8 20 18.72 1.4 6 4.21 1.2 2 2.41 0.5 4 2.1
2 1.4 27 19.15 1.3 5 1.3
cologic radicality.
.8
.2
.7
.2
.7
.6
.6
.9
.7
ith and without surgical complications. There were 7
pcwcTp
pm1c
ttFe(mFp(gs
Mswd
DIfhde
hrncagcl
ikplrhc(sots
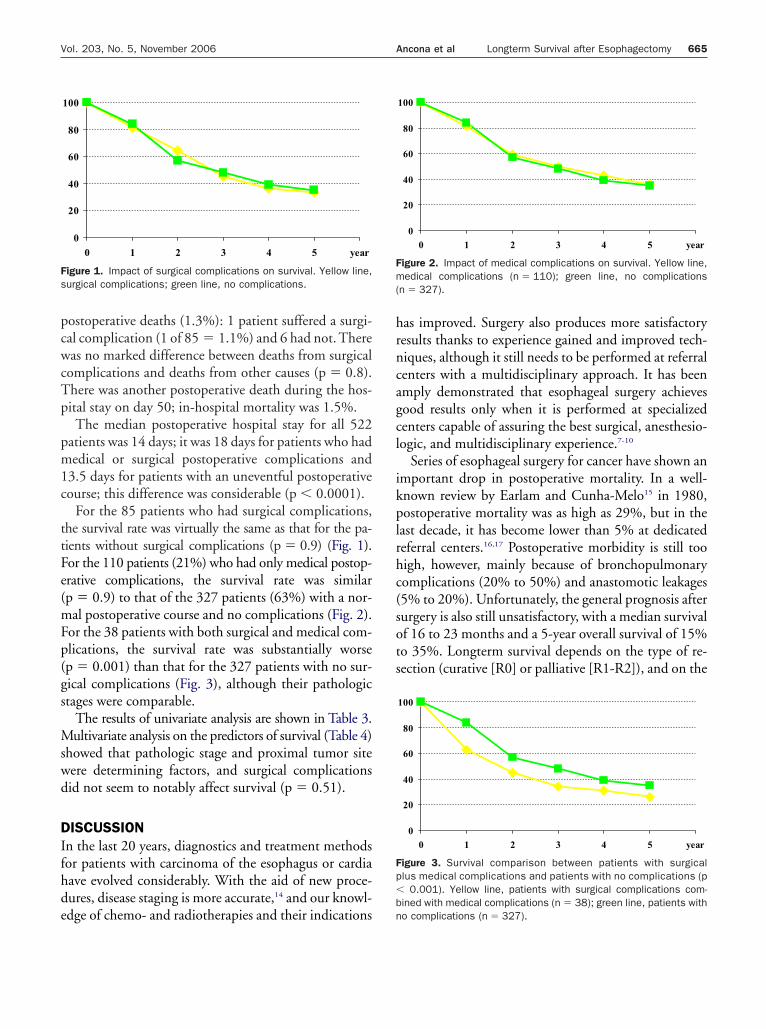
Fs
Fm(
Fp�b
665Vol. 203, No. 5, November 2006 Ancona et al Longterm Survival after Esophagectomy
ostoperative deaths (1.3%): 1 patient suffered a surgi-al complication (1 of 85 � 1.1%) and 6 had not. Thereas no marked difference between deaths from surgical
omplications and deaths from other causes (p � 0.8).here was another postoperative death during the hos-ital stay on day 50; in-hospital mortality was 1.5%.The median postoperative hospital stay for all 522
atients was 14 days; it was 18 days for patients who hadedical or surgical postoperative complications and
3.5 days for patients with an uneventful postoperativeourse; this difference was considerable (p � 0.0001).
For the 85 patients who had surgical complications,he survival rate was virtually the same as that for the pa-ients without surgical complications (p � 0.9) (Fig. 1).or the 110 patients (21%) who had only medical postop-rative complications, the survival rate was similarp � 0.9) to that of the 327 patients (63%) with a nor-al postoperative course and no complications (Fig. 2).
or the 38 patients with both surgical and medical com-lications, the survival rate was substantially worsep � 0.001) than that for the 327 patients with no sur-ical complications (Fig. 3), although their pathologictages were comparable.
The results of univariate analysis are shown in Table 3.ultivariate analysis on the predictors of survival (Table 4)
howed that pathologic stage and proximal tumor siteere determining factors, and surgical complicationsid not seem to notably affect survival (p � 0.51).
ISCUSSIONn the last 20 years, diagnostics and treatment methodsor patients with carcinoma of the esophagus or cardiaave evolved considerably. With the aid of new proce-ures, disease staging is more accurate,14 and our knowl-
0
20
40
60
80
100
0 1 2 3 4 5 year
igure 1. Impact of surgical complications on survival. Yellow line,urgical complications; green line, no complications.
dge of chemo- and radiotherapies and their indications n
as improved. Surgery also produces more satisfactoryesults thanks to experience gained and improved tech-iques, although it still needs to be performed at referralenters with a multidisciplinary approach. It has beenmply demonstrated that esophageal surgery achievesood results only when it is performed at specializedenters capable of assuring the best surgical, anesthesio-ogic, and multidisciplinary experience.7-10
Series of esophageal surgery for cancer have shown anmportant drop in postoperative mortality. In a well-nown review by Earlam and Cunha-Melo15 in 1980,ostoperative mortality was as high as 29%, but in the
ast decade, it has become lower than 5% at dedicatedeferral centers.16,17 Postoperative morbidity is still tooigh, however, mainly because of bronchopulmonaryomplications (20% to 50%) and anastomotic leakages5% to 20%). Unfortunately, the general prognosis afterurgery is also still unsatisfactory, with a median survivalf 16 to 23 months and a 5-year overall survival of 15%o 35%. Longterm survival depends on the type of re-ection (curative [R0] or palliative [R1-R2]), and on the
0
20
40
60
80
100
0 1 2 3 4 5 year
igure 2. Impact of medical complications on survival. Yellow line,edical complications (n � 110); green line, no complications
n � 327).
0
20
40
60
80
100
0 1 2 3 4 5 year
igure 3. Survival comparison between patients with surgicallus medical complications and patients with no complications (p
0.001). Yellow line, patients with surgical complications com-ined with medical complications (n � 38); green line, patients with
o complications (n � 327).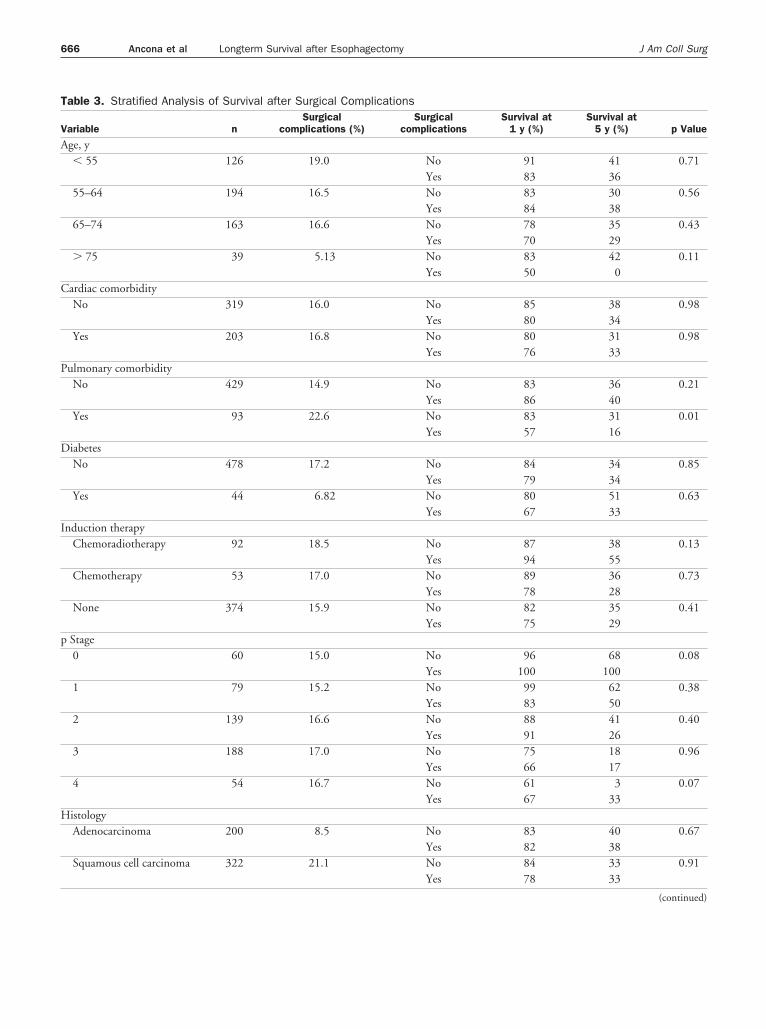
T
V
A
C
P
D
I
p
H
666 Ancona et al Longterm Survival after Esophagectomy J Am Coll Surg
able 3. Stratified Analysis of Survival after Surgical Complications
ariable nSurgical
complications (%)Surgical
complicationsSurvival at
1 y (%)Survival at
5 y (%) p Value
ge, y� 55 126 19.0 No 91 41 0.71
Yes 83 3655–64 194 16.5 No 83 30 0.56
Yes 84 3865–74 163 16.6 No 78 35 0.43
Yes 70 29� 75 39 5.13 No 83 42 0.11
Yes 50 0ardiac comorbidityNo 319 16.0 No 85 38 0.98
Yes 80 34Yes 203 16.8 No 80 31 0.98
Yes 76 33ulmonary comorbidityNo 429 14.9 No 83 36 0.21
Yes 86 40Yes 93 22.6 No 83 31 0.01
Yes 57 16iabetesNo 478 17.2 No 84 34 0.85
Yes 79 34Yes 44 6.82 No 80 51 0.63
Yes 67 33nduction therapy
Chemoradiotherapy 92 18.5 No 87 38 0.13Yes 94 55
Chemotherapy 53 17.0 No 89 36 0.73Yes 78 28
None 374 15.9 No 82 35 0.41Yes 75 29
Stage0 60 15.0 No 96 68 0.08
Yes 100 1001 79 15.2 No 99 62 0.38
Yes 83 502 139 16.6 No 88 41 0.40
Yes 91 263 188 17.0 No 75 18 0.96
Yes 66 174 54 16.7 No 61 3 0.07
Yes 67 33istologyAdenocarcinoma 200 8.5 No 83 40 0.67
Yes 82 38Squamous cell carcinoma 322 21.1 No 84 33 0.91
Yes 78 33
(continued)

pc
oSseotvc
awwatwpmsicnAwnj
4cws1sm
lest
g(qto
T
V
L
TV
SA
GC
IHT
p
G
667Vol. 203, No. 5, November 2006 Ancona et al Longterm Survival after Esophagectomy
athologic stage.18,19 The real impact of postoperativeomplications on survival is still under debate.
Our retrospective analysis can be compared with thene conducted by Rizk and colleagues12 at Memorialloan-Kettering Cancer Center. This study investigatedurgical complications in 510 patients who underwentsophagogastroplasty for carcinoma of the esophagusr cardia between 1996 and 2001, showing that pa-ients with an uneventful postoperative course sur-ived considerably longer than those who had surgicalomplications.
When the two studies were compared, the postoper-tive mortality was lower at our center: 1.6% of patientsithout surgical complications and 1.2% of patientsith surgical complications died (p � NS). Rizk and
ssociates’ study reported a 12% mortality rate for pa-ients who had surgical complications and 4% for thoseho did not (p � 0.001); it is remarkable that 28% ofatients in our study underwent neoadjuvant treat-ents, compared with 50% in Rizk and coworkers’
tudy. So the overall incidence of surgical complicationss different: 16.2% in our series versus 27% in Rizk andolleagues’, and the incidence of leakages and cases ofecrosis vary even more (7.3% in our series versus 21%).lso in this case, the different incidences of leakage,hich is the worst complication, may be the effect ofotably different numbers of patients receiving neoad-
uvant treatment.It is worth noting that, in our study population,
3% of the leakages were detectable only radiologi-ally (found at followup gastrografin swallow) andere clinically silent. These patients were treated con-
ervatively, and they recovered completely within 7 to5 days. At our department, intrathoracic anastomo-es are performed with a stapler, and cervical anasto-
able 3. (continued)
ariable nSurgical
complications (%)
ocationProximal 107 33.7
Middle 142 16.9
Distal 83 10.9
Cardia 190 8.4
oses are done by hand. Fistulas are generally more
ikely to develop in manually fashioned anastomoses,specially in the cervical region (as confirmed in oureries, with 10.7% cervical fistulas versus 3.9% in-rathoracic leakages).
A second complication observed was recurrent laryn-eal nerve injury, which occurred in 32 of our patients6.1%) and was unilateral in all cases. It was more fre-uent during esophagectomy for upper-median thoracicumors, and it was often a necessary sacrifice to achievencologic radicality.20
The impact of postoperative chylothorax varies in dif-
Surgicalcomplications
Survival at1 y (%)
Survival at5 y (%) p Value
No 79 29 0.13Yes 81 44No 91 33 0.14Yes 71 25No 77 33 0.38Yes 89 11No 82 41 0.63Yes 81 40
able 4. Multivariable Predictors of Death after Esophagectomyariable p Value Risk ratio 95% CI
urgical complication 0.78ge, y� 55 0.2855–64 0.4865–74 0.24� 75 0.07
ender 0.22omorbidityCardiac 0.14Pulmonary 0.66Diabetes 0.50
nduction therapy 0.49istology 0.99umor locationProximal 0.03 1.40 1.03–1.91Middle 0.93Distal 0.58Cardia 0.10StagepTNM �0.0001 1.54 1.34–1.78
radingG1 0.24G2 0.66
G3 0.09
fipcnepocdoar
mtsl
amaccwt(r
stfplrtaprma
ottds
ASAA
DCSS
R
1
1
1
1
1
668 Ancona et al Longterm Survival after Esophagectomy J Am Coll Surg
erent reports and some investigators describe a very lowncidence when en-bloc ligature of the thoracic duct iserformed during operation.21-23 The incidence of thisomplication in our series was 1.3%, and we have seeno cases of chylothorax since 2000, when intraoperativen-bloc ligature of the thoracic duct became routineractice. Rizk and colleagues12 found a higher incidencef chylothorax in patients treated preoperatively withhemoradiotherapy (4% versus 1%), but this differenceid not emerge in our series. So we recommend intra-perative ligature to all patients undergoing esoph-gocardial resection because it guarantees excellentesults.
One of our patients had a postoperative diaphrag-atic hernia requiring colonic reduction and closure of
he hiatus and another had severe dysphagia caused bytenosis at the diaphragmatic hiatus, requiring right pil-ar section.
The overall incidence of medical complications wascceptable and there is no evidence that they have aajor impact on prognosis. Improved anesthesiologic
nd reanimation techniques and postoperative careould probably notably reduce the severity of medicalomplications. The most dismal prognosis coincidedith the combination of surgical and medical complica-
ions (Fig. 3). It is remarkable that 27 of these patients71%) suffered from serious sepsis, which might cause aeduction in immunologic defenses.
In our series, the surgical complication rates were theame between patients with and without neoadjuvantreatment, although several reports in the literatureound postoperative mortality and morbidity higher inatients who had received first-line therapies, particu-
arly if this involved regimens combining chemo- andadiotherapy. Candidates for surgery after neoadjuvantreatment should have a more accurate selection andnesthesiologic workup to help minimize the risk ofostoperative complications. Interesting to note, as al-eady reported by others and also in our study, in theultivariable analysis, neoadjuvant treatments did not
ffect survival.In conclusion, when performed at referral centers,
ncologic surgery on the esophagus has acceptable mor-ality and morbidity rates, and the surgical complica-ions do not affect longterm prognosis, which seems toepend exclusively on the pathologic stage and proximal
ite of the tumor.uthor Contributionstudy conception and design: Ancona, Cagol, Ruolcquisition of data: Cagol, Alfierinalysis and interpretation of data: Ancona, Zaninotto,Castoro, Ruolrafting of manuscript: Ancona, Cagol, Ruolritical revision: Ancona, Ruoltatistical expertise: Epifani, Cavallinupervision: Ancona
EFERENCES
1. Atkins BZ, Shah AS, Hutchenson KA, et al. Reducing hospitalmorbidity and mortality following esophagectomy. Ann ThoracSurg 2004;78:1170–1176.
2. Law S, Wong KH, Kwok KF, et al. Predictive factors for postop-erative pulmonary complications and mortality after esophagec-tomy for cancer. Ann Surg 2004;240:791–800.
3. McCulloch P, Ward J, Tekkis PP, ASCOT group of surgeons;British Oesophago-Gastric Cancer Group. Mortality and mor-bidity in gastro-esophageal cancer surgery: initial results ofASCOT multicentre prospective cohort study. BMJ 2003;327:1192–1197.
4. Cariati A, Casano A, Campagna A, et al. Prognostic factorsinfluencing morbidity and mortality in esophageal carcinoma.Rev Hosp Clin Fac Med Sao Paolo 2002;57:201–204.
5. Stahl M, Wilke H, Fink U, et al. Combined preoperative che-motherapy and radiotherapy in patients with locally advancedesophageal cancer. Interim analysis of a phase II trial. J ClinOncol 1996;14:829–837.
6. Yano M, Tsujinaka T, Shiozaki H, et al. Concurrent chemother-apy (5-fluorouracil and cisplatin) and radiation therapy fol-lowed by surgery for T4 squamous cell carcinoma of the esoph-agus. J Surg Oncol 1999;70:25–32.
7. Casson AG, Van Lanschot JJ. Improving outcomes after esoph-agectomy: the impact of operative volume. J Surg Oncol 2005;92:262–266.
8. Dimick JB, Wainess RM, Upchurch GR Jr, et al. National trendsin outcomes for esophageal resection. Ann Thorac Surg 2005;79:212–216.
9. Finlayson EV, Goodney PP, Birkmeyer JD. Hospital volume andoperative mortality in cancer surgery: a national study. ArchSurg 2003;138:721–725.
0. Metzger R, Bollschweiler E, Vallbohmer D, et al. High volumecenters for esophagectomy: what is the number needed toachieve low postoperative mortality? Dis Esophagus 2004;17:310–314.
1. Hermanek P. pTNM and residual tumor classifications. Prob-lems of assessment and prognostic significance. World J Surg1995;19:184–190.
2. Rizk NP, Bach PB, Schrag D, et al. The impact of complicationson outcomes after resection for esophageal and gastroesophagealjunction carcinoma. J Am Coll Surg 2004;198:42–50.
3. Sobin LH, Wittekind C, eds. UICC TNM classification of ma-lignant tumors. 5th ed. New York: Wiley-Liss; 1997.
4. Moreto M. Diagnosis of esophago-gastric tumors. Endoscopy
2005;37:26–32.
1
1
1
1
1
2
2
2
2
669Vol. 203, No. 5, November 2006 Ancona et al Longterm Survival after Esophagectomy
5. Earlam R, Cunha-Melo JR. Oesophageal squamous cell carcinoma:I. A critical review of surgery. Br J Surg 1980;67:381–390.
6. AbunasraH,LewisS,BeggsL,etal.Predictors of operative death afteroesophagectomy for carcinoma. Br J Surg 2005;92:1029–1033.
7. Lerut T, Coosemans W, Decker G, et al. Surgical techniques.J Surg Oncol 2005;92:218–229.
8. Collard JM, Giuli R. Surgical and multimodal approaches tocancer of the esophagus: state of the art. Acta Gastroenterol Belg1999;62:272–282.
9. Wu PC, Posner CM. The role of surgery in the management of
esophageal cancer. Lancet Oncol 2003;4:481–488.0. Gockel I, Kneist W, Keilmann A, Junginger T. Recurrent laryn-geal nerve paralysis (RLNP) following esophagectomy for carci-noma. Eur J Surg Oncol 2005;31:277–281.
1. Lagarde SM, Omloo JM, de Jong K, et al. Incidence and man-agement of chyle leakage after esophagectomy. Ann Thorac Surg2005;80:449–454.
2. Bolger C, Walsh TN, Tanner WA, et al. Chylothorax afteresophagectomy. Br J Surg 1991;78:587–588.
3. Merigliano S, Molena D, Ruol A, et al. Chylothorax complicat-ing esophagectomy for cancer: a plea for early thoracic duct
ligation. J Thorac Cardiovasc Surg 2000;119:453–457.JACS CME-1 PROGRAMAs of October 2006, 1.0 credit will be given for completingboth questions for each article (.50 for each completed question).Completion of all four articles (8 questions) earns a CME-1 credit of4.0 each month.




















