Squamous Cell Cancer of the Head and Neck
137
Doctoral Thesis Squamous Cell Cancer of the Head and Neck – a 10 year follow up Prospective factors and treatment options for patients suffering a squamous cell cancer of the head and neck submitted by Martin Christoph Lanzer Date of birth: 18.04.1984 to obtain the medical degree Doctor of medical science (Dr. sci. med.) conducted at the Department of otorhinolaryngolgoy, division of general othorhinolaryngology, head and neck surgery Medical University Graz under supervision of OA Dr. Sabine Reinisch and Prof. Dr. Heinz Stammberger
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Squamous Cell Cancer of the Head and Neck

Doctoral Thesis
Squamous Cell Cancer of the Head and Neck – a 10 year
follow up
Prospective factors and treatment options for patients suffering a
squamous cell cancer of the head and neck
submitted by
Martin Christoph Lanzer
Date of birth: 18.04.1984
to obtain the medical degree
Doctor of medical science (Dr. sci. med.)
conducted at the
Department of otorhinolaryngolgoy, division of general
othorhinolaryngology, head and neck surgery
Medical University Graz
under supervision of
OA Dr. Sabine Reinisch and Prof. Dr. Heinz Stammberger

i
Sworn Declaration
I declare by word of honor, that I’ve written and conducted the present doctoral thesis unaided
and autonomously; there were no other quotes and citations used than the marked and fully
reproduced quotes and citations
Eidesstattliche Erklärung
Ich erkläre ehrenwörtlich, dass ich die vorliegende Arbeit selbstständig und ohne fremde Hilfe
verfasst habe, andere als die angegebenen Quellen nicht verwendet habe und die den benutzten
Quellen wörtlich oder inhaltlich entnommenen Stellen als solche kenntlich gemacht habe.
Place, Date Signature

ii
Dedicated to my parents for their lifelong support, that finally brought me to this point.
A very special and cordially thank to Sabine Reinisch, MD as well as Prof. Heinz Stammberger, MD
for their guidance throughout this doctoral thesis.

iii
Zusammenfassung
Trotz leicht rückläufiger Zahlen in der Krebsstatistik, stellen Tumore im Bereich des Kopfes und
des Halses nach wie vor ein wachsendes Problem in der Bevölkerung dar. Die steigende Zahl an
neu auftretenden Tumoren bei zum Teil immer jünger werdenden Patienten und das Aufkommen
von neuen – zum Teil – aggressiven Therapieoptionen führt zu mehreren herausfordernden
Entscheidungen. Bei der Frage, welche Therapie für den Patienten die beste Lösung darstellt
fließen viele Einflussfaktoren gleichzeitig ein. Auch ist zu berücksichtigen dass der Patient
Therapieangebote nicht akzeptiert oder andere Einflussfaktoren wie zum Beispiel der allgemeine
Zustand des Patienten die gewählte Therapie nicht zulässt. Wie kommt man zur richtigen
Therapiewahl? Was sind die Faktoren die den Medizinern die Anhaltspunkte geben, welcher
Tumor aggressiver therapiert werden soll und bei welchem Tumor die adjuvante Therapie dem
Patienten einen entscheidenden Vorteil – oder doch nur eine zusätzlich Belastung - bringen kann.
Der initiale Gedanke, der die Forschung vorantreibt, ist im Endeffekt immer die Optimierung von
bestehenden Systemen und Therapien. Dies war auch in erster Linie unsere Fragestellung: durch
die Aufarbeitung unserer Therapieentscheidungen bei Patienten mit Kopf-, Halstumoren wollten
wir einerseits unsere Ergebnisse darstellen und überprüfen, und uns – insbesondere - mit der
angloamerikanischen Literatur vergleichen, um konsequenterweise Therapieschemata zu
optimieren und Überlebensraten bei gleichzeitiger Senkung der Morbidität des Menschen zu
steigern. Bei allem Enthusiasmus und Engagement, die zur Bekämpfung des Tumorleidens
aufgebracht werden, sollte nicht außer Acht gelassen werden, was der Patient für eine
Lebensqualität unter der Therapie hat: können wir dem Patienten wirklich helfen - und ist es nicht
nur der Stolz der behandelnden Ärzte - alles zu versuchen um schlussendlich die dem Patienten
noch verbliebenen Tage so ertragbar als möglich zu gestalten.
Zusammenfassend konnten wir mehrere entscheidende Faktoren des Überlebens erkennen:
1)Einerseits sind es vor allem die chirurgisch Fertigkeiten, die überlebensnotwendig sind.
Prognosen von Tumoren, die nicht in sano reseziert werden konnten, sind deutlich schlechter.
Dies kann auch durch eine adjuvante Therapie (in erster Linie Strahlentherapie) nicht kompensiert
werden. 2)Weiters zeigte sich, dass das Verhältnis der exzidierten Lymphknoten zu den
metastatisch befallenen Lymphknoten in Zukunft eine entscheidende Rolle spielen kann. Je mehr
Lymphknoten in den abfließenden Lymphbahnen nicht befallen sind, umso eher die
Wahrscheinlichkeit dass diese Lymphknoten – im Sinne von Wächterlymphknoten – die Aussaat
von Tumorzellen verhindern konnten.

iv
3)Wir konnten demonstrieren, dass bei Tumoren der Mundhöhle sowie des Oropharynx bei
bekannt hoher Wahrscheinlichkeit von kreuzenden, mittellinienübergreifenden
Lymphabflusswegen eine bilaterale Hals-Dissektion nicht zwingend indiziert ist. Mit Ausnahme
von Tumoren größer als 4cm, Infiltration von mehr als 4mm, mittellinienüberschreitende
Tumoren, Lymphgefäßeinbrüche sowie mehrfacher ipsilateraler Lymphknotenbefall stellen
bilaterale Hals-Dissektionen ein „Over Treatment“ dar. 4)Radikale Hals-Dissektionen führen - bei
deutlicher Zunahme der Patientenmorbidität – nicht zu höheren Überlebensraten. Vielmehr zeigt
sich die Kombination von selektiven Dissektionen mit adjuvanter Strahlen(-Chemo)therapie als
effektive und zugleich patientenschonende Therapie zur lokoregionären Tumorfreiheit. 5)Wir
konnten die schon in der Literatur beschriebenen negativen Prognosefaktoren bestätigen:
Hypopharynxtumoren, Größe des Tumors sowie Lymphknotenbefall – insbesondere mehrerer
Lymphknotenlevel. Auch die histologischen Faktoren wie perineurale Invasion,
Lymphgefäßeinbrüche, Blutgefäßeinbruch, Lymphknotenkonglomerate sowie - sehr bedeutend -
Kapseldurchbruch der Lymphknoten konnten wir als prädiktive Faktoren demaskieren.

v
Abstract
Head and neck cancer is a serious and still growing problem around the world. The increasing
incidence of newly diagnosed cancer with the decreasing age of the patients diagnosed, in
combination with newly – partly aggressive – therapeutic options, leads to many challenging and
unsolved problems. Especially the decision regarding the treatment plan is of outstanding
importance. Factors of influence, such as ambition or rejection of the patient as far as for example
surgical procedures or radiotherapy are concerned, common physical state of the patient –
thinking of the kidney malfunction or blood count, and possibilities as well as limits of
chemotherapeutical agents must be considered. What is the pathway for the best treatment
plan? What are the factors building the evidence on which more aggressive treatment options
are chosen, and how to weigh, whether adjuvant therapy might be a benefit or just an additional
burden for the patient?
Initially, scientific research in medicine is based either upon the striving for optimization or
progress to develop new treatment options, or to improve existing treatment modalities. By
analyzing our own treatment decisions we have made for the last 10 years in patients with
squamous cell carcinoma of the head and neck, we wanted to evaluate our results and outcomes
of our patients and particularly compare the disease free and overall survival of our patients with
the outcome of patients described in the Anglo-American literature. The aim of this study was to
optimize our treatment modalities, prolong patients survival and - probably most important –
reduce patients morbidity.
In our results, we were able to conclude various determining variables for survival:
1)It is of outstanding importance, that surgical skills are at highest level to assure negative
resection margin whenever possible. Patients not being operated in sano have by far a worse
prognosis – even if adjuvant therapies (radiotherapy, chemotherapy or both) are applied.
2)Relationship between excised positive lymph nodes and total number of excised lymph nodes
during a neck dissection might play a very important role in future decisions whether adjuvant
therapy should be applied or not. The more lymph nodes are not affected with metastatic tumor
cells, the better it is for the prognosis. This might be similar to sentinel lymph nodes in other
tumor entities. 3)In tumors of the oropharyngeal region and the oral cavity, a bilateral neck
dissection is not mandatory in every case, despite the high probability of crossing lymph drainage
to the other side. With the exception of tumors bigger than 4cm, infiltration deeper than 4mm,
tumor crossing the midline and multiple ipsilateral metastatic lymph nodes, a bilateral neck
dissection is not indicated. 4) Radical neck dissection, including excision of the
sternocleidomastoid muscle, the jugular vein and the submandibular gland do not lead to better

vi
prognosis, despite the high patient morbidity related to this procedure. Instead, combination of
selective neck procedures with adjuvant radiotherapy or radio-chemotherapy are effective and
tolerated treatment options. Although side effects are known, quality of life is not diminished
dramatically.
5) Analog to the literature, we could confirm the negative prognostic factors for overall survival
and disease free survival: localization of the tumor in the hypopharyngeal region, size of the
tumor and lymph node status – especially if more than one lymph node level is affected.
Furthermore the histological factors such as perineural invasion, lymph vessel invasion, blood
vessel invasion, conglomerate lymph node and capsule penetration could be unmasked as
predictive factors for survival.

7
1 Introduction ................................................................................................................................... 11
1.1 Definition ............................................................................................................................. 11
1.2 Epidemiology ........................................................................................................................ 11
1.2.1 Global incidence .............................................................................................................. 11
1.2.2 Global mortality ............................................................................................................... 13
1.3 Classification of squamous cell carcinoma .......................................................................... 15
1.3.1 Primary tumor ................................................................................................................. 15
1.3.2 Lymph node ..................................................................................................................... 18
1.3.3 TNM-Staging .................................................................................................................... 19
1.4 Classification of neck lymph nodes ...................................................................................... 21
1.5 Classification of neck dissection .......................................................................................... 22
1.6 Risk factors for squamous cell carcinoma ............................................................................ 24
1.6.1 Alcohol ............................................................................................................................. 24
1.6.2 Tobacco ............................................................................................................................ 25
1.6.3 Human Papilloma Virus (HPV) ......................................................................................... 25
1.6.4 Diet and Nutrition ............................................................................................................ 26
1.6.5 Proteomics and genomics................................................................................................ 26
2 Material and Methods ................................................................................................................... 27
2.1 Methods ............................................................................................................................... 27
2.2 Measured endpoints ............................................................................................................ 27
2.2.1 Recurrence free survival .................................................................................................. 27
2.2.2 Disease free survival ........................................................................................................ 27
2.2.3 Overall survival ................................................................................................................ 28
2.3 Database .............................................................................................................................. 28
2.4 Statistical analyses ............................................................................................................... 33
2.5 Neck Dissection .................................................................................................................... 34
2.6 Treatment plan .................................................................................................................... 34

8
2.6.1 Radiotherapy ................................................................................................................... 34
2.6.2 Chemotherapy ................................................................................................................. 35
3 Results ........................................................................................................................................... 38
3.1 Patients ................................................................................................................................ 38
3.2 Distribution of localizations and sub-localizations .............................................................. 38
3.3 Distribution of gender, classification, lymph node status and grading ............................... 40
3.4 Time of follow-up ................................................................................................................. 40
3.5 Overall survival ..................................................................................................................... 42
3.6 Tumor localization ............................................................................................................... 44
3.6.1 Disease free survival depending on tumor localization................................................... 44
3.6.2 Overall survival depending on tumor localization ........................................................... 44
3.6.3 Does the tongue carcinoma represent a special entity within the oral cavity? .............. 45
3.6.4 Tumor localization and further outcome ........................................................................ 46
3.7 Tumor classification ............................................................................................................. 47
3.7.1 Disease free survival considering tumor classification .................................................... 47
3.7.2 Overall survival considering tumor classification ............................................................ 48
3.8 Lymph nodes ........................................................................................................................ 50
3.8.1 Lymph node status .......................................................................................................... 50
3.8.2 Number of positive lymph nodes .................................................................................... 53
3.8.3 Number of positive and overall lymph nodes excised .................................................... 55
3.8.4 Lymph node ratio as a predictive factor for disease free and overall survival ................ 57
3.9 Tumor stage ......................................................................................................................... 60
3.10 Tumor grade ......................................................................................................................... 60
3.11 Histological aspects: ............................................................................................................. 62
3.11.1 Association of histological aspect and localization of recurrence: ............................. 64
3.12 Neck dissection: ................................................................................................................... 65
3.12.1 Correlation between extent of neck dissection and outcome: ................................... 66
3.12.2 Impact of radical neck dissection: ............................................................................... 69

9
3.12.3 Does type of neck dissection effect locoregional recurrence free survival? .............. 72
3.12.4 Benefit of elective bilateral neck dissection in patients with a clinical negative
contralateral neck: ........................................................................................................................ 75
3.13 Effect of excision of non-lymphatic structures on disease free and overall survival: ......... 77
3.14 Resection margin: ................................................................................................................ 77
3.14.1 Disease free survival considering resection margin: ................................................... 77
3.14.2 Overall Survival considering Resection Margin: .......................................................... 79
3.14.3 Influence of postoperative therapy in patients with resection margins R0, R1 or R2 on
disease free survival: ..................................................................................................................... 80
3.14.4 Influence of postoperative therapy in patients with resection margin R0, R1, or R2 on
overall survival: .............................................................................................................................. 83
3.15 Adjuvant therapy: ................................................................................................................ 86
3.15.1 Radiotherapy: .............................................................................................................. 86
3.15.2 Chemotherapy: ............................................................................................................ 87
3.16 Impact and importance of adjuvant therapy: ...................................................................... 88
3.16.1 Impact of adjuvant therapy considering tumor classification: ................................... 88
3.16.2 Impact of adjuvant therapy considering Lymph Node Status: .................................... 92
3.17 Adjuvant therapy in early stage tumors (stage I and stage II) ............................................. 96
3.18 Adjuvant therapy in advanced tumors (stage III and stage IV): ........................................... 97
3.19 Multivariate data analysis: ................................................................................................. 100
3.19.1 Recurrence free survival:........................................................................................... 100
3.19.2 Disease free survival: ................................................................................................. 101
3.19.3 Overall survival: ......................................................................................................... 102
3.20 Recurrence: ........................................................................................................................ 103
3.21 Cause of death: .................................................................................................................. 107
4 Discussion: ................................................................................................................................... 109
4.1 Tumor Stage: ...................................................................................................................... 109
4.2 Tumor Grade: ..................................................................................................................... 109
4.3 Histological aspects: ........................................................................................................... 110

10
4.4 Tumor Localization: ............................................................................................................ 111
4.4.1 Hypopharynx: ................................................................................................................ 111
4.4.2 Tongue Cancer: .............................................................................................................. 112
4.5 Lymph Node Status: ........................................................................................................... 112
4.6 Lymph Node Ratio: ............................................................................................................. 112
4.7 Resection Margin: .............................................................................................................. 113
4.8 Neck Dissection: ................................................................................................................. 114
4.8.1 Preserving non lymphatic tissue: ................................................................................... 114
4.8.2 Preserving lymphatic tissue: .......................................................................................... 114
4.8.3 Clinical Node Negative Neck – is there a need of elective contralateral Neck Dissection?
....................................................................................................................................... 116
4.9 Adjuvant therapy in advanced disease: ............................................................................. 117
References ........................................................................................................................................... 120
Tables .................................................................................................................................................. 130
Figures ................................................................................................................................................. 133

11
1 Introduction:
1.1 Definition(1): Head and neck squamousa cell carcinomab arises from the oral, pharyngeal, or laryngeal mucosa and
resembles the squamous cells that comprise most of the upper layers. Squamous cells are found in
the tissue that forms the surface of the skin, the lining of hollow organs of the body, and the
passages of the respiratory and digestive tracts.
According to the 9th volume of the World Health Organization Classification of Tumors(2), squamous
cell carcinoma can histologically be divided into six (for hypopharynx, larynx and trachea) and seven
(for oropharynx and oral cavity) subgroups: verrucous carcinoma, basaloid squamous cell carcinoma,
papillary squamous cell carcinoma, spindle cell carcinoma, acantholitic squamous cell carcinoma,
adenosquamous carcinoma, and for oral cavity and oropharyngeal cancer also carcinoma
cuniculatum.
1.2 Epidemiology: Head and neck cancer is a serious and still growing problem around the world. Oral and pharyngeal
cancer, grouped together, is the sixth most common cancer worldwide(3). More than 90 % of cancer
in this tumor sites are squamous cell carcinomas.
1.2.1 Global incidence(4):
According to the International Agency for Research on Cancer, there is a wide geographical variation
in the incidence of this cancer. Countries with high incidence rates are found in parts of both eastern
and western Europe (e.g. Spain, France, Luxembourg, Hungary, Slovakia, and Romania), parts of
south America (e.g. Brazil and Uruguay) as well as the Caribbean region, parts of South and Southeast
Asia, especially India, Chinese Taipei, Bhutan, Taiwan, Sri Lanka, and in the Pacific region (e.g. Papua
New Guinea).
a Squamous (from Latin squamosus, from squama a scale): consisting of one or more layers of flat platelike cells
b Carcinoma, pl. carcinomas or carcinomata: an invasive malignant tumor derived from epithelial tissue that
tends to metastasize to other areas of the body

12
Figure 1) Worldwide incidence for lip, oral cavity, pharyngeal and laryngeal cancer according to GLOBOCAN (2008)
In 2008, age-standardized incidence ratio for Europe was led by Hungary 27,1 deaths per 100,000,
followed by Luxembourg and Slovakia with 15,8 and 15,4 deaths per 100,000, respectively.
Table 1) Ranking of age-standardized incidence rate of lip, oral cavity, oropharyngeal and laryngeal cancer in Europe according to GLOBOCAN (2008)
HEAD AND NECK CANCER: BOTH SEXES – INCIDENCE, ALL AGES

13
1.2.2 Global mortality(4):
Similar to world-wide incidence of head and neck cancer, the same countries have to be named in
highest mortality rates: Papua New Guinea, Bhutan, Hungary, Bangladesh, Sri Lanka, Chinese Taipei,
and India with age-standardized mortality rates of 16.58, 15.32, 14.53, 13.51, 12.77, 11.52 and 11.39,
respectively.
Table 2) Ranking of age-standardized mortality rate for lip, oral cavity, pharyngeal and laryngeal cancer worldwide according to GLOBOCAN (2008)
Figure 2) Worldwide incidence for lip, oral cavity, pharyngeal and laryngeal cancer according to GLOBOCAN (2008)

14
Countries with the highest age-standardized mortality rate (ASR) in Europe are Hungary, Slovakia,
Romania and Republic of Moldova, with ASR 14,5, 10,1, 9,3 and 8,9, respectively per 100,000 people.
Luxembourg, suffering a high ASR in incidence (15,8 per 100,000) is not in the front line in age-
standardized mortality rate with only 4,0 per 100,000 people.
Austria has an age-standardized incidence rate of 8,9 per 100,000 and an age-standardized mortality
rate of 4,1 per 100,000.
Table 3) Ranking of age-standardized mortality rate of lip, oral cavity, oropharyngeal and laryngeal cancer in Europe according to GLOBOCAN (2008)
According to the World Health Organization (WHO), the number of patients dying because of lip, oral
cavity or pharyngeal tumor is rising in Austria and Germany, while it is declining in countries like
Australia, Canada, United Kingdom and United States of America.
In Austria, crude rate of death because of a tumor in this region is 8,69 per 100,000 for male and 2,85
per 100,000 for female(5). In 2008, 483 males and 150 females died because of lip, oral cavity,
pharyngeal or laryngeal tumor.
Of outstanding importance is the fact that German speaking countries (Austria, Germany, and
Switzerland) with an age standardized incidence rate of 8,5 – 10,4 per 100,000 people have a lower
incidence rate than the United States of America. Nevertheless, in age standardized mortality rate,
German speaking countries with 3,2 - 4,1 per 100,000 people had a significant higher mortality rate
compared to America with only 2,2 per 100,000 people.

15
Figure 3) Mortality crude rate from lip, oral cavity and pharynx in Australia, Austria, Canada, Germany, United Kingdom and United States of America(5)
1.3 Classification of squamous cell carcinoma:
1.3.1 Primary tumor:
Formerly, the classification of tumors into T stages has always been more arbitrary than defined.
There has always been a close inverse relationship between classifications of tumors into T stages
and overall survival; the bigger the tumor, the higher the T stage and the worse the prognosis.
In the sixth edition of the TNM-Staging System of the International Union against Cancer (UICC) and
the American Joint committee on Cancer (AJCC) a uniform descriptor for size for the above head and
neck sites was introduced. Furthermore category T4 was further subcategorized into T4a and T4b;
subcategory a, for tumors being resectable, subcategory b for tumors infiltrating or involving vital
structures and thus not being suitable for surgical resection.
The latest edition of the TNM-Staging System subdivides the localization into 3 groups: oral cavity
and lip, pharyngeal region and larynx.

16
1.3.1.1 Primary tumor of the oral cavity and lip(6):
In classification of primary tumor, it is customary to use the variables “X” if primary tumor is
unknown, “0” if there is no evidence of primary tumor, and “is” in case of a carcinoma in situ. This
classification is used in any site of head and neck carcinoma.
In oral cavity and lip carcinomas, T1 is a tumor smaller than 2cm in diameter. Between 2cm and 4cm
in greatest dimension it is considered T2, and if tumor mass is bigger than 4cm, it is classified as T3. If
tumor invades structures like cortical bone, muscles or nerves but is still resectable, it is considered
T4a, if primary tumor is not resectable, patient is classified with a T4b tumor.
Table 4) Staging system of the oral cavity and lip cancers, according to the sixth-edition of the TNM-Staging System of the International Union Against Cancer (UICC) and the American Joint Committee on Cancer (AJCC)
1.3.1.2 Primary tumor of the pharyngeal region:
Compared to oral cavity and lip cancer, classification of pharyngeal regions is similar, except
nasopharyngeal cancer. In nasopharyngeal cancer, tumors confined to the nasopharynx are classified
as T1. If extend of primary tumor includes soft tissue, it is upstaged to T2 - T2a if parapharyngeal
structures are not involved, T2b if parapharyngeal structures are involved.
In case of bone structure involvement and/or paranasal sinus involvement staging of primary tumor
is T3. A T4 stage is a tumor with intracranial extension, involvement to the infratemporal fossa or
hypopharynx, as well as masticator space, orbit or involvement of cranial nerves. In nasopharyngeal
cancer there is no subdivision of T4.
In oropharyngeal and hypopharyngeal cancer, tumor classification until T3 is comparable with cancer
of oral cavity as described above. In oropharynx, T4a equals invasion of larynx, hard palate or
mandible as well as invasion of muscle of tongue or medial pterygoid. In T4b, lateral pterygoid
muscle or pterygoid plate are involved. Further involvement of lateral nasopharynx, skull base or
tumor encasing carotid artery puts patient into a T4b classification.
T4a in hypopharyngeal cancer is classified in case of invasion of thyroid/cricoid cartilage, hyoid bone,
thyroid gland, esophagus or central compartment of soft tissue. If tumor invades prevertebral fascia,
encases carotid artery, or involves mediastinal structures it is classified as T4b.

17
According to the sixth-edition of TNM staging system of the UICC and AJCC T4b tumors are tumors
that are not resectable.
Table 5) Staging system of pharyngeal cancers, according to the sixth-edition of the TNM-Staging System of the UICC and AJCC, *parapharyngeal extension denotes posterolateral infiltration beyond the pharyngobasilar fascia
1.3.1.3 Primary tumor of the larynx:
For classification of the larynx, the region is subdivided into supraglottis, glottis, and subglottis. For
all laryngeal regions T1 conforms a tumor limited to one subsite, with normal vocal cord mobility. To
simplify T2 and T3 for the different sub-regions, T2 tumors show impaired vocal cord mobility,
whereas T3 tumors are tumors with vocal cord fixation (detailed classification see table below). T4a
equals invasion of cricoid or thyroid cartilage and/or invasion of tissues beyond the larynx and T4b
equals invasion of prevertebral space, encased carotid artery, or invasion of mediastinal structures.

18
Table 6) Staging system of laryngeal cancers, according to the sixth-edition of the TNM-Staging System of the UICC and AJCC
1.3.2 Lymph node:
The sixth-edition of TNM-Staging System of the UICC and the AJCC defines the classification of lymph
node staging similarly to that of the T-stage. The N stage is also subdivided into two subgroups: all
head and neck sites except nasopharynx and the nasopharyngeal cancer.
1.3.2.1 Lymph node staging for all head and neck sites except nasopharynx:
Points of interest in lymph node classification are size (i.e. 3cm and 6cm) and bilateral lymph node
metastasis. If there is no pathological lymph node, patients are classified as N0. If only one lymph
node is positive, classification is either N1 for lymph nodes smaller than 3cm in diameter, N2 if lymph
node is between 3 – 6cm, and N3 if lymph node is bigger than 6cm.
Within N2 classification, there are three subgroups: N2a, N2b and N2c. If only one lymph node (3-
6cm in diameter) is positive, it is considered N2a, if there are more ipsilateral positive lymph nodes of
any size smaller than 6cm, it is considered N2b. Contralateral or bilateral lymph node metastasis is
considered to be N2c.

19
Table 7) Staging system for lymph nodes of all head and neck sites except nasopharynx, according to the sixth-edition of the TNM-Staging System of the UICC and AJCC
1.3.2.2 Lymph node staging for nasopharyngeal tumors:
Different to lymph node status of other regions, margin between N1 and N3 for nasopharyngeal
tumors is 6cm in diameter. Extension to the supraclavicular fossa automatically puts the patient into
a N3 status. Bilateral lymph node metastasis is considered a N2 status.
Table 8) Staging system for lymph nodes of nasopharyngeal tumor, according to the sixth-edition of the TNM-Staging System of the UICC and AJCC, *midline nodes are considered to be ipsilateral nodes
1.3.3 TNM-Staging(7)
With three variables (TNM) offering a high possibility of different variation, a stage grouping was
necessary. Stage grouping, currently proposed by the American Head and Neck Society is as follows:

20
Table 9) Tumor staging of squamous cell carcinomas in oral cavity, oropharynx, hypopharynx and larynx
Table 10) Tumor staging of nasopharyngeal tumors

21
1.4 Classification of neck lymph nodes: Classification of neck regions was made according to the American Head and Neck society(8,9):
Level I includes the submental and submandibular nodes. It is divided into Level IA - the submental
nodes - between the medial margins of the anterior bellies of the digastric muscles, and Level IB –
the submandibular nodes – which are lateral to level IA and anterior to the vertical plane, defined by
the posterior edge of the submandibular gland. Previously, the stylohyoid muscle was defined as the
posterior border of level IB. The dissection plane typically used to separate Level IB and Level IIA is
along the fascia overlying the posterior aspect of the submandibular gland.
Level II holds the upper internal jugular nodes. Level II is from the posterior aspect of the
submandibulary gland to the posterior border of the sternocleidomastoid muscle and above the level
of the bottom of the body of the hyoid bone. The middle jugular nodes are in level III, between the
two anatomical landmarks - the body of the hyoid bone superiorly and the bottom of the cricoid arch
inferiorly. Lower to level III is level IV – the lower jugular nodes – between the level of the bottom of
the cricoid arch and the level of the clavicle. The boundaries of Level III and Level IV anteriorly was
previously the lateral aspect of the sternohyoid muscle, and changed now to the medial border of
the common carotid artery, so that positive lymph nodes can be allocated by radiologist, since
sternohyoid muscle is not a landmark easily to discern. Nevertheless, intraoperative, surgeons can
choose the lateral aspect of the sternohyoid muscle as the anterior border.
Table 11) Borders of neck lymph node regions(10)
Posteriorly, the posterior edge of the sternocleidomastoid muscle is the borderline of Level II-IV to
Level V, the so called posterior triangle nodes. Level V is divided into Level VA and Level VB by the

22
bottom level of the cricoid arch. Lymph nodes above this level are considered Level VA, lymph nodes
below are considered Level VB. Level V is limited posteriorly by the medial aspect of the trapezius
muscle.
The upper visceral nodes – Level VI – lies between the carotid arteries, from the level of the bottom
of the body of the hyoid bone to the level of the top of the manubrium.
Level VII is below the level of the top of the manubrium but above the innominate vein – the superior
mediastinal nodes. Lateral margins of Level VII are the carotid arteries.
Retropharyngeal nodes are medial to the carotid arteries and behind the pharyngeal tube, from the
skull base to the level of the hyoid bone, and supraclavicular nodes are at or caudal to the level of the
clavicle and lateral to the carotid arteries.
Figure 4) Anatomical subsites of the head and neck region(11)
1.5 Classification of neck dissection: In 1991 the American Academy of Otolaryngology-Head and Neck Surgery in conjunction with the
Education committee of the American Society for Head and Neck Surgery, developed a classification
system of neck dissection. The concept based on the radical neck dissection as the fundamental
procedure with which every other neck dissection has to be compared. In the modified radical neck
dissection, at least one or more non-lymphatic structures have to be spared. In the selective neck
dissection, at least one or more lymphatic levels are spared:
They concluded the radical neck dissection and the modified radical neck dissection together, as
comprehensive neck dissection, since no lymphatic tissue is spared. Both include the complete

23
removal of all the lymph node levels I-V. In the radical neck dissection additional resection of the
spinal accessory nerve, the internal jugular vein and the sternocleidomastoid muscle is conducted.
The Academy divides the modified radical neck dissection into 3 groups: Type 1 is a radical neck
dissection, only the spinal accessory nerve is preserved; in Type 2 next to the spinal accessory nerve,
also the internal jugular vein is preserved. Type 3 is a radical neck dissection with preservation of all
non-lymphatic structures (spinal accessory nerve, internal jugular vein and sternocleidomastoid
muscle).
As explained, the selective neck dissection equates any type of lymphadenectomy that spares at least
one or more lymphatic levels. The Academy sub-classifies the selective neck dissection into 4 groups:
supraomohyoid neck dissection, posterolateral neck dissection, lateral neck dissection and anterior
neck dissection.
Supraomohyoid neck dissection refers to the removal of lymph neck node levels I-III. Inferior
boundary of this procedure is the omohyoid muscle. In the posterolateral neck dissection, lymph
neck node levels II-V and the suboccipital and retroauricular nodes are removed. In the lateral neck
dissection the lymph nodes along the jugular vein are removed – levels II-IV. The anterior neck
dissection refers to the removal of the anterior compartment of the neck in lymph node level VI.
Even more aggressive than the radical neck dissection is the extended neck dissection: this operation
includes not only the radical neck dissection with the removal of lymph neck node levels I-V with all
the non-lymphatic structures spinal accessory nerve, internal jugular vein and sternocleidomastoid
muscle but in addition removal of other lymph node groups and/or non-lymphatic structures for
example such as the carotid artery, the hypoglossal or vagal nerve or the anterior lymph neck nodes.
In 2000 Ferlito et al confounded neck dissections and came up with a modified terminology of
classification similar to the terminology offered by the American Association of Head and Neck
Surgery. In addition to the former terminology, he added suprahyoid neck dissection as dissection of
levels I and II, extended supraomohyoid neck dissection as the removal of levels I-IV, and the
anterolateral neck dissection in which neck lymph node levels II-IV and VI are removed:

24
Table 12) Classification and terminology of neck dissection(12)
In 2008, the Acadamy made once again changes in the terminology(9). Their latest recommendation
is to specifically address every level excised in a selective neck dissection as the level excised plus the
non-lymphatic tissue removed, for example: selective neck dissection (II,III,IV,IJV,SCM) as the
removal of levels II to IV with the additional removal of the internal jugular vein and the
sternocleidomastoid muscle.
1.6 Risk factors for squamous cell carcinoma: Risk factors for development of squamous cell carcinoma are multiple - especially alcohol and
tobacco, as well as betel quid, fruits, certain diets, and lately, HPV are considered as etiologic factors.
1.6.1 Alcohol:
It is well accepted throughout the literature that alcohol, aside from smoking, is an independent risk
factor for head and neck cancers(3). Hashibe et al(13) demonstrated that the odds ratio to develop a
squamous cell carcinoma in the head and neck region was 2,04 if someone drank more than three
drinks per day versus no alcohol consumption. It seems that it is not the type of alcohol used, but
more important the total amount of alcohol consumption throughout the lifetime(14).

25
1.6.2 Tobacco:
All forms of tobacco are carcinogenic, and recently, evidence for smokeless tobacco causing oral and
pharyngeal cancer has been evaluated and confirmed(15). Gandini et al(16) conducted a systematic
meta-analysis of observational studies on cigarette smoking and cancer from 1961 until 2003. The
relative risk (RR) in this meta-analysis was 6,98 (95% CI: 3,14-5,52) for current smokers. RR for
smokers to develop a larynx or oral cavity cancer was 3,43 (95% CI 2,37 – 4,94) times higher.
Cigarette smokers who were never drinkers had an increased risk of pharyngeal and laryngeal cancer
(13)
1.6.3 Human Papilloma Virus (HPV):
HPV are a very heterogeneous group of viruses. Less than 100 variants of any HPV type have been
detected by DNA sequence analysis, with each type defined as having more than 10% dissimilarity in
the combined nucleotide sequences of E6 and E7 genes(17,18). Most (>90%) HPV-associated head
and neck squamous cell cancers are caused by one virus type, HPV 16, the same type that leads to
HPV-associated anogenital cancers(19).
1.6.3.1 Epidemiology of HPV:
In a Danish study by Lajer et al(20) investigating and reviewing on the role of human papilloma virus
in head and neck cancer, he demonstrated that the incidence and prevalence of HPV associated
cancer is difficult to evaluate. Range of patients with a positive HPV status was from 0% up to 93%
(33 studies included). In the USA, about 40-80% of oropharyngeal cancers are caused by HPV,
whereas in Europe the proportion varies from around 90% in Sweden to less than 20% in
communities with the highest rates of tobacco use(19). However, while tobacco abusus as an
etiologic factor for head and neck cancer is declining, the role of HPV in oral and oropharyngeal
cancer is increasing, especially in younger ages(19,21).
1.6.3.2 Biology of HPV:
HPV-associated head and neck cancer arises most commonly in the oropharyngeal region, especially
in the lingual and palatinal tonsils(22). Target points of virus DNA are the oncoproteins E6 and E7
leading to a dysregulated expression. Protein E6 induces degradation of p53 through ubiquitin-
mediated proteolysis, leading to substantial loss of p53 activity. E7 protein binds and inactivates the
retinoblastoma tumor suppressor gene product pRB, leading to cell-cycle disruption, proliferation,
and malignant transformation(23,24).
1.6.3.3 Unsolved importance of HPV:
Despite the recognized importance of HPV in oropharyngeal cancer, the epidemiology of oral HPV
infection is not well understood. Shanti Marur et al(19) disclosed the unknown aspects of oral HPV
infection:
Does HPV infection cause cancer at other head and neck subsites than the oropharyngeal
region?

26
How common is prevalent and persistent oral HPV infection in general population
What is the natural history of oral HPV cancer? Which factors affect oral HPV persistence and
progression, and what is the median time from oral HPV infection to cancer?
Why are men more likely to be affected by oral HPV infection, and why is the incidence in
oral HPV infection increasing in men, while this is not seen in women?
Is there an association of P16 immunohistochemistry and HPV 16 status?
Why do we see a better overall survival in HPV-positive cancer; should there be a different
treatment for those being HPV-negative?
Do precancerous oropharyngeal lesions exist, and would testing for persistent oral HPV
infection be a useful screening method?
What impact do HPV vaccines have on oral HPV infection?
1.6.4 Diet and Nutrition:
Diet and nutrition are also risk factors for head and neck squamous cell carcinoma. Although the
individually micronutrients that might be responsible for the development of malignant cells have
not been formally identified, vegetables and fruits that protect against oral cancer and precancer are
rich in ß-carotene, vitamin C, and vitamin E, with antioxidant properties(25). Furthermore,
epidemiologic studies from northern China, parts of Africa and Iran could demonstrate the
association of nutritional zinc deficiency, associated with restricted diet and exposure to carcinogenic
N-nitrosamines and the etiology of esophageal cancer(26).
1.6.5 Proteomics and genomics:
Aside known etiologic factors, such as alcohol, tobacco et cetera, investigation on circumstances,
leading more easily to the development of head and neck cancer are debated throughout the
literature. Especially proteomics and genomics will play a more important role in the future,
especially for diagnostic reasons(27).

27
2 Material and Methods:
2.1 Methods: We analyzed in a retrospective study all neck dissections of patients being operated during the years
1999 until 2009.
Selection Criteria: Histologically confirmed squamous cell carcinoma of the oral cavity, nasopharynx,
oropharynx, hypopharynx and larynx. All patients were operated during the years 1999 until 2009. All
patients were treated with surgical resection of the primary tumor and neck dissection of the neck
lymphatics. Furthermore, patients were consequently observed or treated with radiotherapy,
chemotherapy, or combined radiochemotherapy.
Exclusion Criteria: Other histological diagnosis than squamous cell carcinoma. Localization of a
squamous cell carcinoma other than oral cavity, nasopharynx, oropharynx, hypopharynx or larynx.
Patients undergoing therapy after metastasis from a former squamous cell carcinoma. Patients
having metastasis before undergoing neck dissection. Patients not being operated at the
otorhinolaryngological department of the Medical University Hospital Graz. Patients receiving
palliative treatment initially.
A total of 293 patients, with a histological proven squamous cell carcinoma of the oral cavity,
oropharnyx, nasopharynx, hypopharnyx or larynx were included into the study for further statistical
evaluation.
Patient data were obtained by searching patient records, pathological findings, operation protocols
as well as data extraction out of the datasystem medocs, which was installed in our facility in 2001.
Furthermore CT scans were looked at, as well as patients that were lost to follow up were contacted,
or if contact failed, tumor register and death register were looked at to check whether patient was
still alive.
2.2 Measured endpoints:
2.2.1 Recurrence free survival:
Recurrence free survival was the period of time between date of operation of the primary tumor and
date of occurrence of first recurrence at any location (local recurrence, locoregional neck recurrence,
distant metastis). If the patient died prior to the end of the study, or prior to getting a recurrence
he/she was censored from further follow-up. If the patient died due to on behalf of tumor relapse,
presenting himself at final stage, he therefore was considered as patient with recurrence and later on
as patient dying of disease.
2.2.2 Disease free survival:
Disease free survival was the period of time between date of operation of the primary tumor and
date of occurrence of first recurrence at any location (local recurrence, locoregional neck recurrence,

28
distant metastis), occurrence of second primary, or death. If patient was lost to follow up prior to
death or end of study he therefore was excluded at last time of appearance at our hospital.
2.2.3 Overall survival:
Overall survival was the period of time between date of operation of the primary tumor and date of
death for any reason. If patient was lost to follow up prior to death or end of study he therefore was
excluded at last time of appearance at our hospital.
2.3 Database: For collection of patient data, a database using MS Access as platform was created.
First layer consisted of basic patient information: name, age, gender, and further notes if
necessary:
Figure 5) First layer of database with basic information

29
Second layer was intended for preoperative information of the cancer: localization,
classification, lymph node status, distant metastasis, grading, and histological additional
information, such as perineural invasion. Furthermore, information on preoperative therapy
was filled out on this layer:
Figure 6) Second layer of database with tumor specific information

30
Third layer held information of the surgical treatment of the primary tumor: time of
operation, type of operation, resection margin, and whether neck dissection was conducted
within 30 days of primary surgery:
Figure 7) Third layer of database with information on tumor excision

31
Fourth layer contained all information on the conducted neck dissection: time and type of
neck dissection, side of neck dissection, number of excised lymph nodes, number of positive
lymph nodes, surgeon who made the neck dissection. Furthermore precise information on
lymph node levels excised, as well as information on non-lymphatic tissue such as accessoric
nerve, jugular vein, submandibular gland, sternocleidomastoidal, and omohyoidal muscle.
Figure 8) Fourth layer of database, holding information on neck dissection

32
Fifth layer held information of postoperative chemotherapy and radiotherapy, type of
chemotherapy used, information on recurrence (time of recurrence as well as localization of
recurrence), information on death (time and cause of death), as well as information on the
last patient data entry for follow-up time.
Figure 9) Fifth layer of database holding information of adjuvant therapy, recurrence and death

33
The sixth layer contained information on possible second primary tumors: was there a pre- or
postoperative second malignancy.
Figure 10) Sixth layer of database holding additional information
2.4 Statistical analyses: For statistical analyses SPSS 17 software was used. Initially, patient data was analyzed descriptively,
looking for frequency of occurrences and distribution of occurrences. Based on this distribution,
diverse groups were formed and analyzed for comparability using the chi-square test. Adjacent
groups were compared for outcome.
Points of interest were overall survival (OS), disease free survival (DFS) and recurrence free survival
(RFS). Factors influencing those points of interest were compared using log-rank test and Kaplan-
Meier survival curve, as well as chi-square test to evaluate difference between two groups.
34
2.5 Neck Dissection: Nomenclature of neck dissections used for our patients(9):
Radical neck dissection: Regio I-V, no preservation of non-lymphatic tissue (jugular vein,
m.sternocleidomastoideus, accessoric nerve)
Modified radical neck dissection: Regio I-V, preservation of at least one non-lymphatic tissue
Posterolateral neck dissection: Regio II-V, regardless of non-lymphatic tissue
Lateral selective neck dissection: Regio II-IV, regardless of non-lymphatic tissue
Supraomohyoidal neck dissection: Regio I-III, regardless of non-lymphatic tissue
Suprahyoidal neck dissection: Regio I-II, regardless of non-lymphatic tissue
2.6 Treatment plan: Patients were diagnosed by clinical examination, ultrasound, CT or MRI scan, and histological
evaluation (HE-Stain). In specific situations (i.e. carcinoma of unknown primary, uncertain metastatic
disease) Positron Emission Tomography was conducted for aggregation of further information.
Treatment plan was drawn by an interdisciplinary team including oncologists, radiooncologists,
pathologists and otorhinolaryngologists. Radiotherapy applied was 60Gy for R0 and 66Gy – 70Gy for
R1 and R2, daily dose depending on the patients physical condition between 1,8Gy and 2,0Gy.
Concomitant adjuvant chemotherapy used was either cisplatin or carboplatin/5FU. One patient
received concomitant adjuvant immunotherapy with Erbitux.
2.6.1 Radiotherapy:
Radiotherapy plays a very important role in the treatment of head and neck malignancies. In head
and neck tumors, radiooncologists are confronted with the tumor on the one side, but with a lot of
normal tissue that is of vital importance in near proximity: spinal cord, auditory and optic apparatus,
salivary glands, mandible and vocal cords. Therefore exact targeting of the tumor mass, while at the
same time sparing normal tissue, is a main factor for treatment outcome and quality of life.
For this reason, conventional radiotherapy, although offering a homogenous dose distribution by
lateral beams to encompass the known primary and the lymphatic structures, becomes more and
more inadequate since normal structures in the proximity receive high dose of radiation(28). In head
and neck cancer, especially salivary gland function is at risk during radiotherapy, causing chronic
xerostomia with associated adverse impact on taste, swallowing, dentition, speech and therefore
quality of life; hence, this is one of the most common rationales for intensity modulated radiation
therapy (IMRT). Furthermore, the capacity of IMRT to limit dose to normal tissue structures may also
allow dose escalation and differential dose painting, thereby accomplishing “in field tumor
boosting”(29).

35
2.6.1.1 What is IMRT?
In intensity-modulated radiation therapy, a specific technique of linear accelerator-based radiation
therapy is used, whereby beams are modulated in such a manner to produce highly conformal dose
distributions:
IMRT delivery techniques with linear accelerator can be divided into two classes: techniques with
fixed gantry, “step and shoot” and “sliding window”, and rotational techniques, called “intensity
modulated arc therapy” and “volumetric modulated arc therapy”. In contrast, in conventional head
and neck radiotherapy, static fields are shaped by blocks and modulated by simple beam wedges or
tissue compensators(30). In IMRT variable dose intensities can be delivered through the segment of
each treatment field, thereby maximizing conformality of the ultimate dose distribution(28).
2.6.1.2 Advantage of IMRT:
Advantages of IMRT are most obvious if critical structures are invaginated or completely surrounded
by the tumor mass, building a concavity in its surface. In this type of geometric situation, IMRT can be
used to shape the isodose lines around the critical structures – which was not possible with normal
three dimensional techniques. A target that has regions on its surface that are concave should be a
common condition for the usage of IMRT(31). Staffurth et al reviewed that inverse-planned IMRT
maintains parotid saliva production and reduces acute and late xerostomia during radiotherapy for
locally advanced head and neck cancers(32).
Inverse planning is another advantage of IMRT over traditional 3D conformal radiotherapy. Instead of
the planner, trying a variety of configurations of beams, wedges and beamweights until a suitable
match is found to the dose prescription (forward planning) the reverse is attempted and dose-
volume constraints and/or dose limits are specified. For both, planned target volumes and avoidance
structures dose limitations can be set, for example: “not more than x% of the y structure may receive
dose zGy or more”. Adjacent, the specification drives the optimization and the computer code will do
the best to satisfy the constraint(33).
Nevertheless, improvements of the dose distribution with IMRT are often accomplished at the
expense of dose homogeneity within the target, and high-dose regions sometimes spill over to
surrounding critical structures(31).
2.6.2 Chemotherapy:
Chemotherapeutics used in our patients were cisplatin, carboplatin in combination with 5-
fluorouracil and the epidermal growth factor inhibitor cetuximab. Since cetuximab was not
commonly used at our facility by the end of the study in 2009, only one patient received cetuximab.
Knowing the high potency of platinum-based chemotherapeutics in head and neck cancer compared
to other chemotherapeutic agents(34), either cisplatin or carboplatin represented the treatment of
choice at our department. Introducing carboplatin in clinical daily routine in 1992 as a platinum-
based analogue with a distinctly different toxicity profile favorable to toxicity profile of cisplatin,
carboplatin has become a commonly preferred agent over cisplatin in different solid tumors. In head
and neck cancer, however, cisplatin appears to be superior to carboplatin as far as therapeutic

36
effectiveness is concerned(35). Therefore, if patient’s health condition admitted the usage of
cisplatin, it was our treatment of choice. Likewise, Go et al(36) reviewed the effectiveness of
Cisplatin/5FU versus Carboplatin/5FU, once again demonstrating the high effectiveness of Cisplatin
along with the strong neurotoxic and especially nephrotoxic effects. Chemotherapeutic dose applied
in the literature are most often 3 circles of 100mg/m2 cisplatin or 3 circles of 400mg/m2
carboplatin(37) together with 5FU. For cisplatin as monochemotherapy, either low-dose weekly at 30
to 40 mg/m2 or every 3 weeks at doses of 75 to 100mg/m2 are described in the literature(38).
In our department, cisplatin was used as concurrent radiochemotherapy after resection of the
primary tumor. Dose of cisplatin applied was 100mg/m2 on the 1st, 22nd and 43rd day of radiotherapy.
This traditional cyclical approach of delivery of concurrent cisplatin has not been compared directly
with schedules that utilize smaller doses more frequently. Although studies exist on the effect of
“non-standard” schedules, comparisons between those two treatment options are missing(39).
Therefore we applied 3 circles of 100mg/m2 cisplatin.
2.6.2.1 Cisplatin(40):
Cisplatin is the first introduced platinum-based chemotherapeutic drug. Like all platinum-based
drugs, it interacts in vivo with the DNA, causing crosslinking within the DNA-strand and hence
triggers apoptosis.
Most common side effects(41) are: nephrotoxicity, neurotoxicity, nausea and vomiting, ototoxicity,
and electrolyte disturbance.
2.6.2.2 Carboplatin(42):
Carboplatin is also a platinum-based chemotherapeutic. Introduced in the 1980’s it has gained
popularity in clinical treatment since side-effects, compared to cisplatin, are reduced.
Especially the elimination of nephrotoxic side effects, and more easily controlled nausea and
vomiting is a main advantage over cisplatin. Disadvantages are the myelosuppressive effect(43) on
the one side, and the, less potency compared to cisplatin. Therefore, carboplatin is used together
with 5-Fluorouracil.
2.6.2.3 5-Fluorouracil(44):
5-Fluorouracil (5FU) is a pyrimidine analogue, which operates by a noncompetitive inhibition of
thymidylate synthase.
Main side effects include myelosuppression, mucositis, dermatitis, diarrhea and cardiac toxicity.
Furthermore it also causes both acute central nervous system (CNS) damages and progressively
worsening delayed degeneration of the CNS.

37
2.6.2.4 Cetuximab(45):
Cetuximab (marketed under the name Erbitux®), is a chimeric (mouse/human) monoclonal antibody,
an epidermal growth factor inhibitor.
Cetuximab is indicated for the treatment of patients with squamous cell carcinoma of the head and
neck in combination with platinum-based chemotherapy for first line treatment of recurrent and/or
metastatic disease and in combination with radiation therapy for locally advanced disease.
Known side effects are severe infusion reactions that can even lead to anaphylactic shock and cardiac
arrest. Other common side effects include especially acne-like rash, photosensitivity,
hypomagnesemia due to magnesium wasting, and less commonly, pulmonary and cardiac toxicity.

38
3 Results:
3.1 Patients: In the years 1999 until 2009 a total of 502 neck dissections on 475 patients were conducted:
475 patients underwent any form of neck dissection at the department of otorhinolaryngology of the
Medical University of Graz. 360 patients had a histological proven squamous cell carcinoma. Most
other findings than squamous cell carcinoma was adenocarcinoma, lymphadenitis and sarcoma. 15
patients were diagnosed with malignant melanoma and 20 patients had a carcinoma of the parotid
gland.
Out of the remaining 360 patients, 17 patients had a primary in a different location than the oral
cavity, oropharynx, nasopharynx, laryngopharynx or larynx. 18 patients suffered a distant metastasis
before undergoing neck dissection.
Furthermore, 32 patients were excluded because diagnosis of cancer was either before 1999,
treatment plan was palliative initially, patient underwent neck dissection twice or patient was not
operated at the department of otorhinolaryngology department of the Medical University of Graz.
A total of 293 patients met all inclusion/exclusion criteria.
Figure 11) Distribution of patients who were neck dissected and included into the study during the years 1999-2009
3.2 Distribution of localizations and sub-localizations: Most patients had a squamous cell carcinoma of the oropharynx (94 patients) followed by oral cavity
(74), laryngopharynx (49) and larynx (44). There were 26 patients with an carcinoma of unknown
primary (CUP) and 6 patients had a nasopharyngeal squamous cell carcinoma. In oral cavity cancer,

39
most primaries were in the tongue and floor of the mouth, 40 and 26 respectively. If primary was in
the oropharyngeal region, most patients suffered a tumor of the tonsils (67 patients).
Figure 12) Distribution of sublocalizations: floor of the mouth 26, tongue 40, cheek mucosa 2, lip 6, soft palate 6, root of tongue 19, lateral pharyngeal wall 2, tonsils 67, nasopharynx 6, sinus piriformis 38, postcricoidal region 1, epiglottis 7, lateral laryngopharyngeal wall 1, supraglottic 15, glottis 27, transglottic 2, unknown primary 26

40
3.3 Distribution of gender, classification, lymph node status and grading: Mean age of patients at diagnosis was 64 years. Distribution of gender was 243 male versus 50
female patients. Most patients had a tumor classification of pT2 (86 patients), followed by 68 pT3
and 65 pT1 tumors. 48 patients had a pT4 and as mentioned, 26 had a CUP. As far as lymph node
status is concerned, most patients had a pN2 status (135 patients), followed by pN0 (109) and 38
patients with a pN1 status. 11 patients suffered a pN3 disease.
Most tumors were poorly (151 patients) and moderately (127) differentiated. Only 10 patients were
well differentiated and 5 patients had an anaplastic cancer. Therefore tumor grade was grouped into
high differentiated (well-differentiated and moderately-differentiated) and low differentiated
(poorly-differentiated and undifferentiated) for statistical analysis.
Table 13) Distribution of cancer staging in patients
3.4 Time of follow-up: Median time of follow-up was 34 months. Range of observation was 0 – 128 months (5% - 95%
percentiles; range of observation was 5 - 104 months). As expected, there is no normal dispersion,
therefore median is used in statistical analysis.

41
Figure 13) Time of follow up in months
Figure 14) Test of normality

42
Table 14) Test of normality proving there is no normal dispersion
3.5 Overall survival: Median survival of 293 patients was 108 months. Overall median survival in men was 101 months;
overall median survival in women was 108 months. There was no statistical significance between
overall survival between men and women.
Table 15) Statistic for survival of male, female and overall survival

43
Figure 15) 5 year overall survival
Figure 16) 5 year overall survival considering gender

44
3.6 Tumor localization
3.6.1 Disease free survival depending on tumor localization
Considering tumor localization for disease free survival, there was no statistical significance showing
a particular tumor region as being more likely to undergo a recurrence. Although the nasopharynx
seems to have a better disease free survival, considering the low number of patients (6 patients with
a nasopharyngeal cancer) the result was not statistically significant (Log Rank = 0,342)
3.6.2 Overall survival depending on tumor localization
Tumor localization did not have a statistical significant impact on overall survival according to the
Log-Rank test (Log-Rank = 0,095).
Table 16) Log-Rank test for the impact of tumor localization on overall survival
Figure 17) Kaplan-Meier curve illustrating the overall survival considering tumor localization

45
Nevertheless 25 of 49 patients with a hypopharyngeal cancer died of the disease. Considering other
tumor localizations this was a considerably high number. Therefore, hypopharyngeal cancer was
compared with all other tumor localizations, with the result that hypopharyngeal cancer compared
to other tumor localizations had a significant difference in overall survival (Log Rank = 0.003). This
significant difference in survival remained looking at small tumors separately: pT1 and pT2 tumors of
the hypopharyngeal region compared to other tumor sites remained significant (Log Rank = 0,011)
Figure 18) Small hypopharyngeal cancer compared to small cancer of all other tumor localizations combined showing a significant difference in outcome (Log Rank = 0.011)
Table 17) Test of equality of distribution depending on hypopharyngeal cancer or cancer of other localization
3.6.3 Does the tongue carcinoma represent a special entity within the oral cavity?
Comparing patients suffering a carcinoma of the tongue with other localizations of the oral cavity, we
did not find a statistically significant difference in either disease free survival or overall survival.
Although percentage of overall survival was the lowest in patients with a tongue carcinoma (67,5%)
versus other localizations, Log-Rank test was not significant (Log-Rank = 0,280)

46
Table 18) Overall survival depending on localization of oral cavity carcinoma
3.6.4 Tumor localization and further outcome:
Chi-Square test did not show any significant difference in tumor localization and recurrence or
localization of recurrence. There was no tumor localization more likely to develop a local- or lymph
node recurrence or distant metastasis.
Table 19) Distribution of recurrence, localization of recurrence and number of death according to localization
As mentioned, hypopharyngeal cancer had the worst prognosis for overall survival showing a crude
overall survival rate of 51% dying (25 of 49 patients). Compared with other tumor localizations,
hypopharyngeal cancer had a statistically significant higher percentage of people dying (Chi-Square
test = 0,002).

47
Table 20) Comparison of hypopharyngeal cancer and cancer of other tumor sites in recurrence, localization of recurrence and number of deaths
Looking at the distribution of hypopharyngeal cancer and tumor classification compared to other
cancer sites, there was no statistical significance. Hypopharyngeal cancer did not have a worse tumor
classification.
3.7 Tumor classification:
3.7.1 Disease free survival considering tumor classification:
There was a significant difference in disease free survival considering tumor classification. As
expected, pT1 and pT2 had the best outcome for disease free survival. Nearly the same run of the
curves showed pT3 tumors and tumors with an unknown primary. Tumors classified as pT4 had by far
the worst prognosis (50% have a five year disease free survival). Log-Rank test was significant, Log
Rank = 0,001

48
Figure 19) Kaplan Meier curve illustrating disease free survival considering tumor classification
Table 21) Percentage of patients suffering a recurrence considering tumor classification
3.7.2 Overall survival considering tumor classification:
Similar to disease free survival, overall survival depended strongly on tumor classification. Log-Rank
test showed a statistical significance (Log Rank = 0,020). Likewise to disease free survival, 24 of 48
patients with a pT4 classification died. With same percentage of disease free survival and overall
survival of patients with a pT4 classification, this would imply that those patients who suffered a
recurrence, eventually died.

49
Table 22) Percentag of patients dying considering tumor classification
Figure 20) Kaplan Meier curve illustrating overall survival considering tumor classification

50
3.8 Lymph nodes:
3.8.1 Lymph node status:
3.8.1.1 Disease free survival considering lymph node status:
Although 109 patients presented themselves initially with a pathological negative neck after neck
dissection, only 82 (75%) were disease free after follow up. 21 of 38 patients (55%) with pN1, 85 of
135 (63%) with pN2 and 6 of 11 patients (54%) with pN3 remained disease free. Especially pN1 and
pN2 status presented a very similar run of the curve. Median disease free survival for pN1 was 75
month, for pN2 82 month. pN3 had a median disease free survival of 32 month.
Table 23) Statistical analysis of disease free survival depending on lymph node status

51
Figure 21) Kaplan Meier curve illustrating disease free survival considering lymph node status
3.8.1.2 Overall survival considering lymph node status:
Positive lymph node status was always seen as a bad prognostic factor for outcome and overall
survival, reducing survival up to 50%(46). In our patients, positive lymph node status was also a
strong statistically significant factor for poor outcome (Log Rank = 0,001). 25 of 109 (77%) patients
with a negative lymph node status died, while 69 of 184 patients (62%) died with a positive lymph
node status.
Table 24) Percentage of patients being alive at the end of follow up considering positive or negative lymph node status

52
Figure 22) Kaplan-Meier curve demonstrating the high impact of positive lymph node status on overall survival
Looking at the curves for every lymph node status, pN1 and pN2 had – similar to disease free survival
– once again the same run of the curves. Median survival for pN1 was 78 months versus 88 months in
patients with pN2.
Table 25) Statistical analysis of median overall survival considering lymph node status

53
Figure 23) Kaplan Meier curve illustrating overall survival considering lymph node status (Log-Rank = 0,001)
3.8.2 Number of positive lymph nodes:
Similar to lymph node status, number of positive lymph nodes can also be used for prognosis on
disease free survival and overall survival. Considering the difference of staging within the pN2 stage
(pN2a equates to a single positive lymph node smaller than 6 cm on the ipsilateral side and pN2c
equates to one or more positive lymph nodes on the contralateral side) number of positive lymph
nodes might even deliver a more accurate prognosis.
3.8.2.1 Disease free survival considering number of positive lymph nodes:
Percentage of disease free survival for patients with a negative neck was 75%. By chance, the
number of patients with 1 or 2-5 positive lymph nodes and the number of patients suffering a
recurrence, was the same: 28 of 77 suffered a recurrence, and 49 (64%) remained disease free.
Disease free survival of patients with more than 5 lymph nodes was 47%.
Table 26) Percentage of disease free survival depending on number of positive lymph nodes.

54
Run of the Kaplan-Meier curves of disease free survival depending on number of positive lymph
nodes was similar to the curves of lymph node stage. Kaplan-Meier was statistical significant (Log-
Rank = 0,001).
Figure 24) Kaplan-Meier curve illustrating disease free survival considering number of positive lymph nodes
3.8.2.2 Overall survival considering number of positive lymph nodes:
We did not experience such a high impact on overall survival if one lymph node was positive,
compared to a negative neck. Overall survival was 77% vs. 71% for negative neck and one positive
lymph node, respectively. Also median survival of patients with one positive lymph node offered,
with 108 months a very good prognosis.
In patients with 2 – 5 positive lymph nodes, overall survival was 60%, and in those patients with more
than 5 positive lymph nodes, overall survival went down to 47%. Disease free survival and overall
survival in patients with more than 5 positive lymph nodes at presentation was the same, implicating
that every person with a recurrence died on behalf of the disease.
Median survival for 2-5 positive lymph nodes and more than 5 positive lymph nodes was 52 and 47
months, respectively.

55
Table 27) Statistic of overall survival depending on number of positive lymph nodes (Event = death)
Figure 25) Kaplan-Meier curve illustrating overall survival considering number of positive lymph nodes
3.8.3 Number of positive and overall lymph nodes excised:
Range of positive lymph nodes excised was 0 to 40 lymph nodes. In about one third of patients
(37,2%), lymph node status was negative. 77 patients had one positive lymph node; the same

56
number of patients had 2-5 positive lymph nodes. Only 10% of patients suffered a multiple lymph
node metastasis with more than 5 positive lymph nodes at the neck region.
Figure 26) Number of positive lymph nodes excised
Looking at the relationship between lymph node status and number of lymph nodes excised,
bivariate data analysis (Spearman = 0,000) was statistically significant. The lower the lymph node
status was, the fewer lymph nodes were excised.
Looking at the scatter plot, results of Spearman test is graphically illustrated.

57
Figure 27) Scatter plot of lymph node status and number of lymph nodes excised
3.8.4 Lymph node ratio as a predictive factor for disease free and overall survival:
Looking at our data, both, disease free survival and overall survival was statistically significant
depending on lymph node ratio. As suggested cutoff points(47), we used three groups: <7%, 7-13%,
and >13% ratio.
Percentage of disease free survival for groups of <7%, 7-13%, and >13% was 71,0%, 62,8% and 52,6%,
respectively. Median disease free survival was 108, 48, and 47 months.

58
Table 28) Statistical analysis for disease free survival depending on lymph node ratio
Median overall survival in patients with a lymph node ratio below 7% was 109 months. 76,2% were
still alive after follow-up. In patients with a lymph node ratio between 7-13%, median overall survival
was 48 months, and percentage of survival 58,1%. Worst prognosis was seen in patients with a lymph
node ratio higher than 13%. Median overall survival was 39 months; only 47,4% of patients were still
alive at end of follow-up.
Table 29) Statistical analysis for overall survival depending on lymph node ratio

59
Figure 28) Disease free survival and overall survival considering lymph node ratio (Log-Rank = 0,000 for both disease free and overall survival)
However, comparing lymph node ratio 7-13% with lymph node ratio higher than 13%, there was no
statistical difference found. Log-Rank for disease free survival was Log-Rank = 0,200, and for overall
survival Log-Rank = 0,180.

60
3.9 Tumor stage Tumor stage was highly significantly correlated with overall survival (Log-Rank = 0,001). Looking at
the 5-year overall survival rate, probability of survival at 5 years was 94%, 83%, 61%, and 56% for
stage I, stage II, stage III, and stage IV, respectively.
Figure 29) Kaplan-Meier curve illustrating 5 year overall survival depending on stage
3.10 Tumor grade: Considering tumor grade for disease free survival and overall survival, differentiation did not have a
statistically significant impact on either of them. On the contrary, run of the curves for disease free
survival and overall survival were nearly the same. Log Rank test for disease free survival and for
overall survival were 0,616 and 0,426, respectively.

61
Figure 30) Kaplan Meier curve illustrating no impact of tumor grade on disease free survival
Figure 31) Kaplan Meier curve illustrating no impact of tumor grade on overall survival (well-differentiated and undifferentiated tumor grades were excluded out of the graphic on behalf of small patient number)

62
3.11 Histological aspects: Five histological aspects were of special interest: lymphangiosis carcinomatosa, haemangiosis
carcinomatosa, capsule penetration, conglomerate tumor, and perineural invasion. All of them were
strong prognostic factors for reduction of disease free survival, and all of them – except
haemangiosis carcinomatosa – were strong prognostic factors for poor overall survival (reason for
border significance of haemangiosis carcinomatosa can be explained by the small number of patients
n=5).
Reduction of median disease free survival was between 2-3 times as fast. In overall survival,
reduction of survival time was reduced up to factor 10. Representative for all 5 histological aspects,
results of conglomerate lymph nodes are demonstrated in the following figures.
Figure 32) Impact of conglomerate lymph nodes on disease free survival

63
Figure 33) Impact of conglomerate lymph nodes on 5 year overall survival
Table 30) Statistical analysis of conglomerate lymph nodes as prognostic factor for overall survival; median disease free survival was reduced from 108 months to 29 months

64
3.11.1 Association of histological aspect and localization of recurrence:
Table 31) Statistical analysis of histological aspects and occurrence and localization of recurrence

65
All five histological factors were significant for poor outcome, disease free survival, and overall
survival. Perineural invasion was a strong prognostic factor for contralateral lymph node recurrence
(Log-Rank = 0,002) and ipsilateral lymph node recurrence (Log-Rank = 0,001). Haemangiosis
carcinomatosa and conglomerate lymph nodes were strong prognostic factors for distant metastasis
(Log-rank = 0,011 and 0,001, respectively). Lymphangiosis carcinomatosa was a statistically
significant factor for ipsilateral lymph node recurrence (Log-Rank = 0,048) and capsule penetration
was a significant factor for distant metastasis (Log-Rank = 0,048). None of those factors had an
impact on local recurrences.
3.12 Neck dissection: According to the classification of neck dissection proposed by the American Head and Neck Society
and the American Academy of Otolaryngology–Head and Neck Surgery in 2001(48)(9,48), 41 patients
were operated with a radical neck dissection, 85 patients received a modified radical neck dissection,
76 a posterolateral neck dissection, 26 patients a supraomohyoidale neck dissection, 24 patients had
an expanded supraomohyoidal neck dissection (additional resection of region 5a or region 4), 14
patients a lateral selective neck dissection; in two patients lateral selective neck dissection was
expanded to region 5a, 3 patients underwent a suprahyoidale neck dissection, and the remaining 24
neck dissection were selective neck dissections. In 66 patients, neck dissection was performed
bilaterally.
In total, 293 patients received 359 neck dissections
Figure 34) Distribution of types of neck dissections performed (according to the recommendations of the American Head and Neck Society 2008)
Considering lymph node status, the higher the lymph node status was, the more aggressive was neck
dissection. In patients with pN2 or pN3, nearly every patient was treated with either radical neck
dissection, modified radical neck dissection, or posterolateral neck dissection.

66
3.12.1 Correlation between extent of neck dissection and outcome:
3.12.1.1 Excision of number of lymph node levels and disease free survival:
Disease free survival in patients with a negative lymph neck node status (pN0) was 77,4%, 73,7% and
72,2% for patients treated with excision of 1-3 levels, 4-5 levels and more than 5 levels, respectively.
In patients with a positive lymph node status, disease free survival was 72.7%, 59.2% and 64,5%,
respectively. Median survival for pN0 patients could not be calculated (more than 50% of patients
survived), in pN+ patients, median survival for excision of 1-3 levels, 4-5 levels and more than 5 levels
was 85 months, 69 months and 85 months. There was no statistical significance between percentage
of disease free survival and median disease free survival time.
3.12.1.2 Excision of number of lymph node levels and overall survival:
Percentage of overall survival in patients with a negative neck node status (pN0) was 84,9%, 68,4%,
and 72,2% for resection of 1-3 levels, 4-5 levels, or more than 5 levels, respectively. In patients with a
positive neck status (pN+) overall survival for those three groups was: 63,6%, 61,3%, and 67,7%.

67
Statistical analysis did not show any significant difference between those groups. The poor median
overall survival time in patients with a pN+ and resection of 1-3 levels might evolve out of a small
number of patients (n =11)
3.12.1.3 Correlation between extent of neck dissection and outcome in patients with a N0
lymph node status:
Kaplan-Meier curve did not show any differences in run of curve as far as disease free survival in pN0
patients was concerned. However, Kaplan-Meier analysis demonstrated a border significance in
patients with a pN0 status treated only with excision of 1-3 lymph node levels (Log-Rank = 0,088)

68
Figure 35) Kaplan-Meier curve, showing no statistically significant difference in disease free or overall survival depending on number of excised lymph node levels in patients with a pN0 status.
3.12.1.4 Correlation between extent of neck dissection and outcome in patients with a
positive lymph node status:
Patients with a positive lymph node status pN+ did not have a significantly different outcome
depending on amount of lymph node levels excised during neck dissection.

69
Figure 36) Kaplan-Meier curve, showing no statistically significant difference in disease free or overall survival depending on number of excised lymph node levels in patients with a pN+ status.
3.12.2 Impact of radical neck dissection:
3.12.2.1 Impact of radical neck dissection on disease free survival and overall survival in
patients with positive neck lymph node status:
Patients with a positive lymph neck node status treated with a radical neck dissection did not benefit
from this procedure. On the contrary, run of curves of patients treated with radical neck dissection,
even though lacking statistical significance, was below run of curves of patients not treated in a
radical manner (Log-Rank = 0,074).

70
Separating the group of patients with a positive lymph node status into groups of patients with one,
2-5, or more than 5 positive lymph nodes, radical neck dissection did not offer a benefit in overall
survival in any of these groups.
Figure 37) Impact of radical neck dissection on overall survival in patients with a positive lymph node status (Log-Rank = 0,74)
Table 32) Log-Rank test on effect of radical neck dissection considering number of positive lymph nodes
3.12.2.2 Impact of radical neck dissection on disease free survival and overall survival in
stage IV disease:
Altogether, in 41 patients a radical neck dissection was performed. Most patients (38 patients) had a
stage IV disease; two patients had a stage III disease and one patient a stage I.

71
There was no statistically significant difference in disease free survival for patients considering type
of neck dissection (radical vs. non radical neck dissection) in stage I and stage III disease – numbers of
patients were very small. Comparing patients in stage IV being operated either with a radical neck
dissection vs. non radical neck dissection, there was a statistically significant difference in disease
free survival (Log-Rank = 0,002). Surprisingly, patients treated with radical neck dissection suffered
more often from a recurrence.
Figure 38) Kaplan-Meier curve illustrating the negative effect of radical neck dissection on disease free survival (Log-Rank = 0,002)
This is even more remarkable looking at the distribution of tumor classification and lymph node
status. Within stage IV patients, distribution of surgical therapy (radical neck dissection vs. other neck
dissection) was even.
Table 33) Distribution of tumor classification and lymph node status within stage IV disease treated with or without radical neck dissection
In overall survival, run of Kaplan-Meier curve in patients receiving radical neck dissection was still
below the curve of patients not undergoing radical therapy, but statistical significance was missing.

72
Nevertheless, striving for radical neck dissection to prevent patients from recurrence is not indicated.
Figure 39) Overall survival of patients with stage IV disease depending on type of neck dissection (Log-Rank = 0,115)
3.12.3 Does type of neck dissection effect locoregional recurrence free survival?
Both, in patients with a negative lymph node status (pN0), and in patients with a positive lymph node
status (pN+), there was no significant difference of the impact of type of neck dissection on
locoregional neck lymph node recurrence free survival. Only 7 patients of 109 patients (6,4%) with a
negative neck at diagnosis developed a locoregional lymph node recurrence during follow up.
Patients developing a recurrence were treated with modified radical neck dissection (1),
posterolateral neck dissection (2), supraomohyoidal neck dissection (2), expanded supraomohyoidal
neck dissection (1) and selective neck dissection (1).
In patients with a pN+ neck, 19 of 184 (10,3%) developed a locoregional neck lymph node metastasis.
Likewise, there was no statistically significant difference between different types of neck dissections
performed.

73
Table 34) Percentage of locoregional recurrence free survival depending on type of neck dissection
3.12.3.1 Effect of extensive neck dissection versus selective neck dissection procedures on
locoregional recurrence (LRR) free survival:
Comparing extensive neck dissection (radical neck dissection, modified radical neck dissection and
posterolateral neck dissection) versus selective elective procedures (supraomohyoidal neck
dissection, suprahyoidal neck dissection, lateral neck dissection and selective neck dissection), there
was no statistically significant difference in LRR free survival. Even considering adjuvant therapy, no
statistically significant difference between treatment groups could be found in the Log-Rank test.

74
Figure 40) Kaplan-Meier curve illustrating similar run of curves between different types of neck dissection, considering adjuvant therapy
Further, comparing radical neck dissection versus modified radical neck dissection, run of curves
were hardly different from each other (Log-Rank = 0,884) implying that locoregional control can be
achieved without dissecting all non-lymphatic structures at risk in the neck.

75
Figure 41) Locoregional recurrence free survival considering type of neck dissection
3.12.4 Benefit of elective bilateral neck dissection in patients with a clinical negative
contralateral neck:
Number of patients presenting with a clinical negative contralateral neck were 284. 57 patients were
treated with bilateral neck dissection, 227 patients with unilateral neck dissection. Both disease free
survival and overall survival did not show any significant difference between those two groups in run
of Kaplan-Meier curves (Log-Rank = 0,709 and 0,973), percentage of recurrence (66% vs. 68%),
percentage of death (68% vs. 72%) or median disease free survival (91 months vs. 85 months).
Distribution of adjuvant therapy in patients with unilateral neck dissection and patients with bilateral
neck dissection was not significantly different.
Table 35) Percentage of adjuvant therapy in patients receiving unilateral or bilateral neck dissection

76
Figure 42) Overall survival of patients with clinical contralateral negative neck depending on unilateral or bilateral neck treatment (Log-Rank = 0,973)

77
3.13 Effect of excision of non-lymphatic structures on disease free and
overall survival: Effect of excision of jugular vein, accessoric nerve and sternocleidomastoid muscle could not be
evaluated because distribution of patients to different groups was not even.
Table 36) Chi-Square test did show a significant difference in distribution between patients and excision of non-lymphatic structures, and therefore could not be analyzed
3.14 Resection margin:
3.14.1 Disease free survival considering resection margin:
Postoperative, 230 patients had a negative resection margin (R0). At the end of follow-up, 69% of
patients were still disease free. Out of the other 63 patients, 58 had a histological positive resection
margin (R1) and 5 patients had a macroscopic positive resection margin (R2). 59% of R1 patients still
lived without a recurrence of disease at the end of follow-up, but only 1 of 5 patients with R2 (20%)
was disease free.
Median disease free survival time was 49 months and 20 months for R1 and R2, respectively. Patients
with a negative resection margin had a median disease free survival time of 93 month. Log-Rank test
showed the strong statistic impact of positive resection margin on disease free survival (Log-Rank =
0,002)

78
Table 37) Statistical analysis of disease free survival considering resection margin
Figure 43) Kaplan-Meier curve of disease free survival considering resection margin

79
3.14.2 Overall Survival considering Resection Margin:
At the end of follow-up of 250 patients with a negative resection margin, 72% were still alive. 32 0f
58 (55%) of R1 patients were still alive at the end of follow up, but only 1 of 5 patients with R2 (20%)
survived.
The Kaplan-Meier curve illustrated the strong prognostic factor of resection margin, and the Log-
Rank test demonstrated a strong statistical significance of resection margin for survival (Log-Rank =
0,000). Median survival for R1 was 49 months, for macroscopic positive resection margin only 20
months, the same amount of time that we experienced for disease free survival, implying the close
relationship between recurrence and death.
Table 38) Statistical analysis of overall survival considering resection margin

80
Figure 44) Kaplan-Meier curve of overall survival considering resection margin
3.14.3 Influence of postoperative therapy in patients with resection margins R0, R1 or R2
on disease free survival:
Out of 293 patients, 114 did not receive adjuvant therapy: out of those 114 patients, 108 patients
were diagnosed with a negative resection margin, 6 patients had a R1 postoperative result. 36 of 108
patients (67%) with a negative resection margin did not experience a recurrence, while only 1 of 6
patients (17%) was disease free after follow up in the R1 group. Patients receiving postoperative
adjuvant therapy were 122 patients with a R0, 52 with a R1 and 5 with a R2 situation. Disease free
survival rate in those three groups were 86 of 122 (70%), 33 of 52 (63%), and 1 of 5 (20%),
respectively for R0, R1, and R2.

81
Table 39) Number of patients being treated with or without postoperative adjuvant therapy and percentage of disease free survival (Event = recurrence)
Negative resection margin versus positive resection margin in patients not being treated with
adjuvant therapy was a strong prognostic factor (Log-Rank = 0,000) for disease free survival. R0 and
R1 patients receiving adjuvant therapy did not differ significantly in disease free survival. Patients
with a macroscopic positive resection margin (R2) had an unpromising prognosis (Log-Rank = 0,025
compared to R0 and 0,050 compared to R1).
Although there was no statistically significant difference in R0 and R1 patients receiving adjuvant
therapy, median disease free survival was reduced by 44 month; 105 month vs. 61 month in R0 and
R1 respectively.
Table 40) Statistical analysis for disease free survival considering resection margin and postoperative adjuvant therapy

82
Figure 45) Kaplan-Meier curve illustrating the bad prognosis on disease free survival of patients with a R1 resection margin and no additional treatment compared to patients with negative resection margins (Log-Rank = 0,000)
Figure 46) Kaplan-Meier curve illustrating the effect of adjuvant therapy in positive resection margin (Log-Rank = 0.313 for R0 vs. R1)

83
Table 41) Patients at risk depending on adjuvant therapy and resection margin, after 1, 3 and 5 years
If administered adjuvant therapy was solely radiotherapy, Kaplan-Meier curve showed a similar run
of curve. Difference between disease free survival of R0 or R1 was not significant, whereas R2
remained prudent.
3.14.4 Influence of postoperative therapy in patients with resection margin R0, R1, or R2
on overall survival:
Among 114 patients receiving no adjuvant therapy, 108 had a negative resection margin, and 6
patients had a R1 resection margin. 80 of 108 patients with R0 were still alive at the end of follow-up
(74%) while 2 of 6 patients with R1 survived (33%)
Distribution of resection margin in the group receiving postoperative adjuvant therapy was 122
patients with R0, 52 with R1 and 5 with R2 resection margins. Overall survival in those three groups
was 70%, 58% and 20% for R0, R1 and R2, respectively.
Table 42) Number of patients being treated with or without postoperative adjuvant therapy and percentage of overall survival (Event = death)
Negative resection margin versus positive resection margin in patients not being treated with
adjuvant therapy was a strong prognostic factor (Log-Rank = 0,000) for overall survival. R0 and R1
patients receiving adjuvant therapy did not differ statistical significant in disease free survival;
nevertheless a border significance could be identified (Log-Rank = 0,088).

84
Patients with a R2 resection margin had the same unpromising prognosis in overall survival like they
had in disease free survival (Log-Rank = 0,25 compared to R0 and 0,50 compared to R1).
Figure 47) Kaplan-Meier curve illustrating the bad prognosis on overall survival of patients with a R1 resection margin and no additional treatment compared to patients with negative resection margins (Log-Rank = 0,000)

85
Figure 48) With adjuvant therapy, R1 and R0 did not show a statistical significant difference (Log-Rank = 0,088) in overall survival, while R2 remained a strong prognostic impact on overall survival (Log-Rank = 0,002 compared to R0 and 0,015 compared to R1)
Interestingly enough, looking at patients treated only with postoperative radiotherapy, there was a
significant difference in overall survival between patients with a R0 and R1 resection (Log-Rank =
0,045) compared to patients receiving postoperative radiochemotherapy in which difference
between R0 and R1 in overall survival was not statistical significant (Log-Rank = 0,088)

86
3.15 Adjuvant therapy:
3.15.1 Radiotherapy:
Most patients, 140 of 293 (47,7%), were treated with adjuvant radiotherapy. 114 patients did not
receive any additional therapy, 38 (12,9%) received radiochemotherapy, and only one patient (0,3%)
was additionally treated with cisplatin only.
Figure 49) Number of patients treated with postoperative adjuvant therapy

87
3.15.2 Chemotherapy:
Only 39 patients were treated with postoperative adjuvant chemotherapy. Most of those patients
received radiochemotherapy; only one patient received cisplatin solely (patient refused
radiotherapy).
Distribution between chemotherapeutics used was dominated by cisplatin with 33 patients, followed
by carboplatin/5FU with 5 patients, and one patient was treated with the epidermal growth factor
inhibitor Erbitux.
Figure 50) Number of patients treated with carboplatin/5FU, Cisplatin or Erbitux

88
3.16 Impact and importance of adjuvant therapy:
Figure 51) Overall effect of adjuvant therapy
3.16.1 Impact of adjuvant therapy considering tumor classification:
3.16.1.1 Disease free survival:
Overall disease free survival in patients receiving adjuvant therapy was 67% versus 64% in patients
who did not receive postoperative treatment. Although percentage of disease free survival was
generally higher in patients receiving adjuvant therapy, only patients with a carcinoma of unknown
primary had a statistically significant benefit (Log-Rank = 0,000).
Run of the curves of disease free survival in patients without adjuvant therapy was statistical ly
significant depending on tumor classification. In patients with adjuvant therapy, only T4 tumors had a
statistically significant different run of the curves compared to T1 (Log-Rank = 0,040). There was a
borderline significance in run of the curves between T3 tumors and T2 tumors (Log-Rank = 0,053)
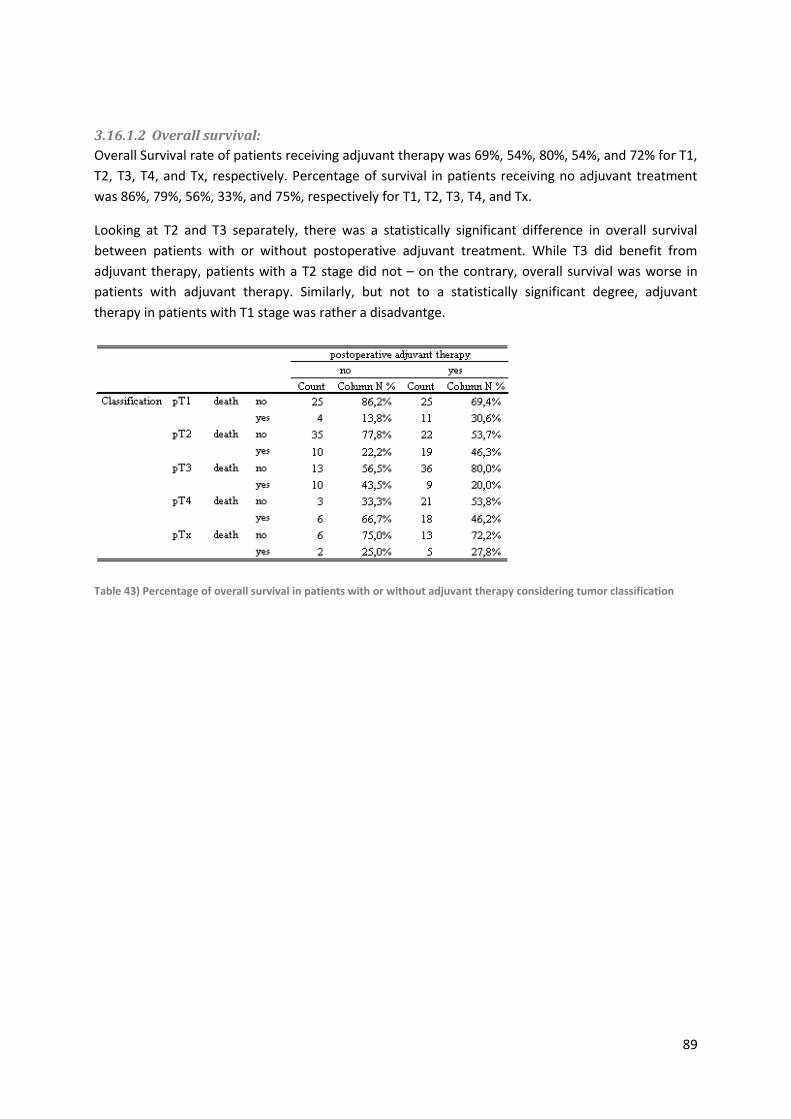
89
3.16.1.2 Overall survival:
Overall Survival rate of patients receiving adjuvant therapy was 69%, 54%, 80%, 54%, and 72% for T1,
T2, T3, T4, and Tx, respectively. Percentage of survival in patients receiving no adjuvant treatment
was 86%, 79%, 56%, 33%, and 75%, respectively for T1, T2, T3, T4, and Tx.
Looking at T2 and T3 separately, there was a statistically significant difference in overall survival
between patients with or without postoperative adjuvant treatment. While T3 did benefit from
adjuvant therapy, patients with a T2 stage did not – on the contrary, overall survival was worse in
patients with adjuvant therapy. Similarly, but not to a statistically significant degree, adjuvant
therapy in patients with T1 stage was rather a disadvantge.
Table 43) Percentage of overall survival in patients with or without adjuvant therapy considering tumor classification

90
Figure 52) Effect of postoperative adjuvant therapy in pT1 tumor patients (Log-Rank = 0,151)
Figure 53) Effect of postoperative adjuvant therapy in pT2 tumor patients (Log-Rank = 0,016)

91
Similar to disease free survival, run of curves for overall survival differed depending on tumor
classification and whether adjuvant postoperative therapy was applied or not. Patients with a T1, T2,
or Tx tumor stage not receiving adjuvant therapy showed a very similar run of curve. Curves of T3
and T4 patients differed significantly compared to T1,T2, and Tx.
Run of curves in patients receiving postoperative adjuvant therapy did not differ to a statistical ly
significant degree.
Table 44) Pairwise comparison of overall survival depending on postoperative adjuvant therapy and tumor classification
Figure 54) Kaplan-Meier curve illustrating overall survival depending on tumor classification of patients receiving no additional postoperative treatment

92
Figure 55) Kaplan-Meier curve illustrating overall survival depending on tumor classification of patients receiving no additional postoperative treatment
3.16.2 Impact of adjuvant therapy considering Lymph Node Status:
3.16.2.1 Disease Free Survival:
In patients with a negative neck, disease free survival for patients with or without postoperative
adjuvant therapy was 76% and 75%, respectively. Only 10 of 30 patients (33%) with a pN+ stage
remained disease free if adjuvant therapy was not applied. Patients with a pN+ stage who did receive
adjuvant therapy had a percentage of disease free survival of 66%. Kaplan-Meier curve demonstrated
the statistical significant benefit of postoperative adjuvant therapy in patients with a pathological
lymph neck node status (Log-Rank = 0,004).
Difference in median disease free survival between patients receiving postoperative treatment
compared to those not receiving postoperative treatment was 85 months vs. 54 months.
Considering run of the curves of patients without adjuvant therapy, pN0 had a significantly better
disease free survival (Log-Rank = 0,000). But if patients were treated with postoperative adjuvant
therapy, run of the curves were not statistically significant (Log-Rank = 0,317).

93
Table 45) Statistical analysis of disease free survival in patients with or without postoperative adjuvant therapy
Figure 56) Kaplan-Meier curve illustrating disease free survival without postoperative adjuvant therapy considering positive or negative lymph node status (Log-Rank = 0,000)

94
Figure 57) Kaplan-Meier curve illustrating disease free survival in patients receiving postoperative adjuvant therapy considering positive or negative lymph node status (Log-Rank = 0,317)
Figure 58) Kaplan-Meier curve illustrating the statistically significant impact on postoperative adjuvant therapy in patients with a positive lymph node status (Log-Rank = 0,004)

95
3.16.2.2 Overall survival:
Kaplan-Meier survival analysis in patients without adjuvant therapy demonstrated a statistically
significant difference in overall survival depending on lymph node status (negative vs. positive lymph
neck node), while patients receiving adjuvant therapy did not differ significantly (Log-Rank = 0,006 vs.
0.228, respectively).
Overall survival was 17 of 30 patients (57%) with pN+ stage, and 65 of 84 patients (77%) with a pN0
stage, if no adjuvant therapy was administered. In comparison to patients receiving additional
postoperative treatment, percentage in patients with a negative neck was similar, 19 of 25 patients
(76%), while 98 of 154 patients (64%) with a positive neck were still alive at the end of follow-up.
Median survival for patients with a positive neck was 66 months without adjuvant therapy versus 85
months in those receiving adjuvant treatment options. Median survival of pN0 patients could not be
calculated.
Table 46) Statistical analysis of overall survival depending on postoperative adjuvant therapy and lymph node status
Although patients with a pN+ neck did benefit significantly from postoperative adjuvant therapy as
far as disease free survival was concerned, this benefit could not be found in overall survival.
Prognosis for overall survival in both patients with a negative and patients with a positive lymph
node stage did not alter in any direction if adjuvant therapy was applied.
The difference of impact on disease free survival and overall survival might be explained by the high
toxicity coming along with adjuvant therapy, regardless of whether chemotherapy, radiotherapy, or
both was administered. Although recurrence was obviated, overall survival did not benefit.

96
Figure 59) Difference in run of curves depending on postoperative adjuvant therapy in patients with a pathological positive neck (Log-Rank = 0,420)
3.17 Adjuvant therapy in early stage tumors (stage I and stage II) Most patients with early stage carcinoma had solely operative treatment. Only 7 of 70 patients
underwent adjuvant therapy in early stage tumors. Adjuvant therapy in all those cases was adjuvant
radiotherapy.
Table 47) Adjuvant therapy applied in early stage carcinoma
Percentage of overall survival was similar. Looking at the Kaplan-Meier curve, patients receiving
adjuvant therapy did not have an event within 5 years. However, Log-Rank test was not significant at
Log-Rank = 0,771

97
Figure 60) Kaplan-Meier curve illustrating impact of adjuvant therapy in early stage cancer on overall survival
3.18 Adjuvant therapy in advanced tumors (stage III and stage IV): A total of 222 patients were staged with a stage III or stage IV tumor. One patient declined
radiotherapy and received postoperative chemotherapy only. Because of this small number, patient
was not included in statistical analysis.
Disease free survival in this group of patients was 62%; 84 patients suffered a recurrence. 133
patients were treated with a postoperative radiotherapy. 50 of those 133 patients experienced a
recurrence (62,4%). Recurrence rate of patients without adjuvant therapy and with combined
postoperative radiochemotherapy was 44% and 84% respectively. Chi square test was highly
significant (Chi-square = 0,001). Log-Rank test could demonstrate a significance (Log-Rank = 0,004).
Table 48) Number of recurrence in patients with a stage III or stage IV disease

98
Figure 61) Disease free survival of patients with stage III or stage IV disease considering adjuvant therapy (Log-Rank = 0,004)
Impact of adjuvant therapy on overall survival showed a similar effect. 22 patients without
postoperative adjuvant treatment died (44%). Overall survival in patients with postoperative
radiotherapy was 57,9%, and 86,8% in patients with postoperative adjuvant radio-, and
chemotherapy. Chi-Square test was significant at p = 0,003. Likewise to disease free survival, Kaplan-
Meier curve demonstrated different run of curves depending on adjuvant therapy, however, Log-
Rank test was not significant at Log-Rank = 0,245.

99
Table 49) Statistical analysis of disease free and overall survival in stage III/IV patients considering adjuvant therapy
Figure 62) Kaplan-Meier curve illustrating different run of curves considering adjuvant therapy in stage III and stage IV disease, however, Log-Rank test did not reach statistical significance (Log-Rank = 0,245)

100
3.19 Multivariate data analysis: After univariate data analysis, multivariate data analysis was performed, using every covariable with
a significance level below p-value of 0,2. Size of tumor, conglomerate lymph nodes, and perineural
invasion remained as the leading covariables for recurrence free survival. In disease free survival,
most powerful effect for an event were tumor size, conglomerate lymph nodes and lymph node ratio
(using threshold at 7%). Stage, lymph node ratio, conglomerate lymph nodes, resection margin, and
adjuvant therapy are most important covariables for overall survival.
3.19.1 Recurrence free survival:
Number of stderr of
observations estimate
Gender 265 1,163 0,286 (0.664, 1.039) 0,5974
Localization (hypopharynx vs. other tumor
sites)265 1,294 0,273 (0.758, 2.209) 0,3455
Staging (1,2 vs. 3,4) 265 2,203 0,303 (1.216, 3.994) 0,0092
pT1/2 vs. 3/4 265 2,07 0,225 (1.331, 3.219) 0,0012
pN0 vs. pN+ 265 1,758 0,241 (1.096, 2.820) 0,0192
Positive Lymph Nodes (1 vs. 0) 265 1,408 0,3 (0.782, 2.536) 0,2538
Positive Lymph Nodes (2-5 vs. 0) 265 1,777 0,29 (1.007, 3.137) 0,0473
Positive Lymph Nodes (>5 vs. 0) 265 2,586 0,343 (1.322, 5.061) 0,0055
Lymph Node Ratio (<7 vs. >7) 265 1,855 0,225 (1.193, 2.886) 0,0061
Grade (high vs. low) 265 1,205 0,224 (0.777, 1.871) 0,405
Perineural Invasion 265 2,274 0,325 (1.201, 4.303) 0,0116
Lymphangiosis 265 1,952 0,354 (0.975, 3.908) 0,0588
Haemangiosis 265 3,573 0,464 (1.438, 8.876) 0,0061
Capsule Penetration 265 2,357 0,244 (1.461, 3.804) 0,0004
Conglomerat Lymph Nodes 265 2,961 0,287 (1.687, 5.195) 0,0002
R0 vs. R+ 265 1,8 0,239 (1.128, 2.873) 0,0138
Radical Neck Dissection 265 2,21 0,28 (1.276, 3.827) 0,0047
Neck Dissection (functional vs.
comprehensive)265 1,395 0,247 (0.860, 2.261) 0,1776
Levels (Level 1-3 vs. 4-5) 265 1,663 0,31 (0.906, 3.051) 0,1005
Levels (Level 1-3 vs. >5) 265 1,625 0,379 (0.773, 3.418) 0,2005
Excision of M. Sternocleidomastoideus 265 1,279 0,229 (0.817, 2.003) 0,2816
Excision of Jugular Vein 265 1,69 0,234 (1.068, 2.676) 0,0251
Excision of Accessoric Nerve 265 1,499 0,223 (0.968, 2.322) 0,0697
Adjuvant Therapy 265 0,917 0,226 (0.589, 1.429) 0,7025
Recurrence Free Survival
p-valuehazard ratio CI
Table 50) Multivariate data analysis for recurrence free survival

101
Number of stderr of
observations estimate
pT1/2 vs. 3/4 265 1,886 0,229 (1.204, 2.953) 0,0056
Perineural Invasion 265 2,28 0,336 (1.179, 4.407) 0,0143
Conglomerat Lymph Nodes 265 3,165 0,293 (1.782, 5.621) < 0.0001
p-valueCIhazard ratio
Multivariate Model with Univariate Significant Covariables (p-Wert < 0.2)
Table 51) Multivariate model for recurrence free survival including univariate significant covariables
3.19.2 Disease free survival:
Number of stderr of
observations estimate
Gender 265 1,086 0,253 (0.662, 1.783) 0,7428
Localization (hypopharynx vs. other
tumor sites)265 1,446 0,228 (0.925, 2.261) 0,1057
Staging (1,2 vs. 3,4) 265 2,306 0,265 (1.372, 3.874) 0,0016
pT1/2 vs. 3/4 265 1,942 0,194 (1.329, 2.838) 0,0006
pN0 vs. pN+ 265 1,669 0,206 (1.115, 2.497) 0,0128
Positive Lymph Nodes (1 vs. 0) 265 1,215 0,265 (0.723, 2.043) 0,4624
Positive Lymph Nodes (2-5 vs. 0) 265 1,892 0,242 (1.178, 3.039) 0,0084
Positive Lymph Nodes (>5 vs. 0) 265 2,289 0,302 (1.266, 4.140) 0,0062
Lymph Node Ratio (<7 vs. >7) 265 2,08 0,193 (1.424, 3.038) 0,0002
Grade (high vs. low) 265 1,126 0,193 (0.772, 1.642) 0,5386
Perineural Invasion 265 1,788 0,307 (0.980, 3.264) 0,0583
Lymphangiosis 265 1,935 0,307 (1.061, 3.529) 0,0312
Haemangiosis 265 2,64 0,46 (1.072, 6.502) 0,0348
Capsule Penetration 265 2,239 0,213 (1.474, 3.401) 0,0002
Conglomerat Lymph Nodes 265 2,754 0,253 (1.676, 4.524) < 0.0001
R0 vs. R+ 265 1,958 0,202 (1.316, 2.914) 0,0009
Radical Neck Dissection 265 1,776 0,259 (1.069, 2.951) 0,0265
Neck Dissection (functional vs.
comprehensive)265 1,399 0,213 (0.922, 2.122) 0,1141
Levels (Level 1-3 vs. 4-5) 265 1,516 0,259 (0.913, 2.518) 0,1081
Levels (Level 1-3 vs. >5) 265 1,5 0,321 (0.800, 2.813) 0,2061
Excision of M. Sternocleidomastoideus 265 1,224 0,196 (0.833, 1.798) 0,3029
Excision of Jugular Vein 265 1,587 0,204 (1.063, 2.369) 0,0238
Excision of Accessoric Nerve 265 1,465 0,193 (1.004, 2.137) 0,0477
Adjuvant Therapy 265 0,904 0,195 (0.617, 1.324) 0,6036
Disease Free Survival
hazard ratio CI p-value
Table 52) Covariables used for multivariate data analysis for overall survival

102
Number of stderr of
observations estimate
pT1/2 vs. 3/4 265 1,838 0,194 (1.256, 2.689) 0,0017
Lymph Node Ratio (<7 vs. >7) 265 1,649 0,214 (1.083, 2.510) 0,0196
Conglomerat Lymph Nodes 265 1,981 0,28 (1.144, 3.431) 0,0147
hazard ratio CI p-value
Multivariate Model with Univariate Significant Covariables (p-Wert < 0.2)
Table 53) Multivariate model for disease free survival including univariat significant covariables
3.19.3 Overall survival:
Number of hazard ratio stderr of CI p-value
observations estimate
Gender 265 0,795 0,34 (0.408, 1.548) 0,4995
Localization (hypoharynx vs. other tumor
sites)265 1,888 0,258 (1.138, 3.130) 0,0138
Staging (1,2 vs. 3,4) 265 5,154 0,427 (2.233, 11.893) 0,0001
pT1/2 vs. 3/4 265 2,02 0,235 (1.274, 3.201) 0,0028
pN0 vs. pN+ 265 2,396 0,267 (1.420, 4.042) 0,0011
Positive Lymph Nodes (1 vs. 0) 265 1,563 0,34 (0.804, 3.041) 0,1883
Positive Lymph Nodes (2-5 vs. 0) 265 2,819 0,303 (1.556, 5.111) 0,0006
Positive Lymph Nodes (>5 vs. 0) 265 3,602 0,361 (1.776, 7.305) 0,0004
Lymph Node Ratio (<7 vs. >7) 265 3,001 0,235 (1.893, 4.756) < 0.0001
Grade (high vs. low) 265 1,392 0,237 (0.875, 2.215) 0,1623
Perineural Invasion 265 1,918 0,357 (0.952, 3.863) 0,0684
Lymphangiosis 265 2,165 0,356 (1.077, 4.352) 0,0302
Haemangiosis 265 2,657 0,594 (0.829, 8.515) 0,1001
Capsule Penetration 265 2,744 0,25 (1.682, 4.475) < 0.0001
Conglomerat Lymph Nodes 265 4,025 0,278 (2.334, 6.941) < 0.0001
R0 vs. R+ 265 2,464 0,241 (1.537, 3.951) 0,0002
Radical Neck Dissection 265 2,204 0,298 (1.228, 3.955) 0,0081
Neck Dissection (functional vs.
comprehensive)265 2,523 0,297 (1.409, 4.517) 0,0018
Levels (Level 1-3 vs. 4-5) 265 2,458 0,361 (1.211, 4.992) 0,0128
Levels (Level 1-3 vs. >5) 265 2,209 0,434 (0.944, 5.174) 0,0678
Excision of M. Sternocleidomastoideus 265 1,726 0,249 (1.060, 2.810) 0,0283
Excision of Jugular Vein 265 2,187 0,24 (1.367, 3.498) 0,0011
Excision of Accessoric Nerve 265 2,275 0,234 (1.439, 3.597) 0,0004
Adjuvant Therapy 265 1,408 0,246 (0.869, 2.282) 0,1649
Overall Survival
Table 54) Covariables used for multivariate data analysis for overall survival

103
Number of stderr of
observations estimate
Staging (1,2 vs. 3,4) 265 5,305 0,47 (2.111, 13.332) 0,0004
Lymph Node Ratio (<7 vs. >7) 265 1,861 0,281 (1.073, 3.229) 0,0271
Conglomerat Lymph Nodes 265 2,442 0,315 (1.317, 4.527) 0,0046
R0 vs. R+ 265 2,069 0,272 (1.215, 3.522) 0,0074
Adjuvant Therapy 265 0,358 0,301 (0.198, 0.646) 0,0007
hazard ratio CI p-value
Multivariate Model with Univariate Significant Covariables (p-Wert < 0.2)
Table 55) Multivariate model for overall survival including univariat significant covariables
3.20 Recurrence: One-third of the patients, 99 of 293 (34%) suffered a recurrence. Highest percentage of recurrence
rate was carcinoma of unknown primary (42%); in 5 out of 11 patients with recurrence in this group
of carcinomas, recurrence equaled the finding of the primary tumor. Lowest percentage of
recurrence rate was found in patients with a laryngeal cancer (29%). No tumor localization was
statistically more at risk to develop a recurrence.
If a recurrence occurred, most patients suffered a local recurrence (13% of patients), followed by
distant metastasis (9%) and lymph node recurrence (12%). Patients with laryngeal cancer had a very
low percentage of local recurrence (4,5%). All other tumor regions aside from nasopharyngeal cancer
had a local recurrence rate of about 15%. Lymph node recurrence happened most often in
nasopharyngeal cancer and cancer of unknown primary, 17% and 15%, respectively. In every 5th
patient with a hypopharyngeal cancer, distant metastasis occurred.
Contralateral recurrence only occurred in 4 of 293 patients (1%):
• 2 patients with a tumor of the oral cavity:
• One patient with a tumor of the tongue, pT1N2b, experienced a local recurrence as
well as a bilateral recurrence after modified radical neck dissection and
postoperative adjuvant radiotherapy.
• Another patient with a tumor of the floor of the mouth, pT2N2c, developed a
submental lymph node recurrence on the contralateral side after extended (Va)
supraomohyoidale neck dissection and selective neck dissection (II and III) on the
contralateral side and postoperative adjuvant radiotherapy.
• One patient with a hypopharyngeal tumor of the sinus piriformis, pT4N2b, developed after
lateral neck dissection a lymph node recurrence at level II on the contralateral side.
• One patient with a laryngeal tumor, pT4, and a pathological negative neck developed a
contralateral lymph node recurrence at level III.

104
Table 56) Percentage of recurrence depending on tumor localization
Percentage of overall survival in patients that remained disease free was 79,9% (155 of 194 patients).
Every second patient with a local recurrence died (19 of 38 patients) and 57,7% of patients with
lymph node recurrence did not survive (15 of 26 patients).
As expected, the worst outcome was experienced by patients with distant metastasis. 28,6% (10 of
25 patients) died during follow-up; the remaining 10 patients received palliative treatment onwards.
Since at some point they did not show up for follow up any more, they are supposed to have died of
the disease as well. Therefore, all patients experiencing distant metastasis died of the disease.
If loco-regional lymph neck node recurrence occurred, in most cases, it happened in the region of the
former neck dissection. In 20 of 26 patients with a lymph node recurrence, recurrence was in the
field of neck dissection (76,9%); in 2 of 26 patients it was in the region of neck dissection and in
another not dissected region; and 4 patients suffered a lymph node recurrence outside the region of
dissection.
According to the statistical analysis, distant metastasis has the worst outcome, with a median overall
survival of 29 months (only patients receiving palliative treatment at our department). Median
overall survival for lymph node recurrence was 84 months and for local recurrence 47 months. One
must keep in mind that those numbers of months are considered from the point of first diagnosis.

105
Table 57) Statistical analysis of overall survival depending on type of recurrence
Kaplan-Meier curves showed the same result: the bad overall survival of patients suffering distant
metastasis, local recurrence and lymph node recurrence showing a better prognosis but still not
comparable if patient remained disease free. Log-Rank test was highly significant at Log-Rank =
0,000.

106
Figure 63) Kaplan-Meier curve illustrating overall survival depending on type of recurrence (Log-Rank = 0,000)
Figure 64) Number of patients dying after recurrence depending on type of recurrence

107
3.21 Cause of death: A total of 94 patients (32%) died during follow-up. In 60 of 94 patients (64%), cause of death was
tumor associated. 6 patients (6%) died therapy associated, and 28 patients (30%) died due to other
reasons.
Reason for therapy associated death was as follows:
One Patient with oropharyngeal cancer: major bleeding in operation field, one week after
operation
One patient with hypopharyngeal cancer died due to infection of the port-a-cath
Three patients with laryngeal cancer died therapy associated: one patient suffered a cardial
decompensation after operation, one died due to an ulcus bleeding in the hypopharyngeal
anastomosis region, and one patient suffered a postoperative ileus, leading to a necrosis of
the gut and furtheron died because of sepsis
One patient with a carcinoma of unknown primary died because of a postoperative ileus
leading to a lethal sepsis.
Table 58) Number and cause of death depending on tumor localization
Table 59) Number and cause of death depending on tumor classification

108
Table 60) Number and cause of death depending on lymph node status

109
4 Discussion:
4.1 Tumor Stage: Yeole et al(49) investigated on the 5 year overall survival of more than 5000 patients in Mumbai,
India. He classified tumor stages of patients as localized, if no neck involvement was found, regionally
spread, if neck lymph nodes were positive, and distant metastasis. 5 year overall survivals of those
patients were 63%, 22%, and 9%, respectively.
In carcinoma of the oral cancer, Shah et al experienced a cause specific survival of 94%, 80%, 66% ,
and 58% for Stage I, II, III and IV, respectively. Overall Survival for Stage III and IV cancer was 68%(50).
Compared to a retrospective study in Taiwan conducted on 703 patients by Chen et al(51), a much
better prognosis. In our patients, overall survival depending on stage, was comparable with the result
of the Memorial Sloan Kettering Center described by Shah. Especially stage I and stage II tumors offer
a very good prognosis(52). The good prognosis in early stage cancer was also described by
Mendenhall et al(53). He could demonstrate the high cause specific 5 year survival rate of early stage
laryngeal cancer: 98% in T1a and 90% in T2b patients and a 5 year overall survival between 82% for
T1a cancer and 77% for T2b.
Other study groups could not obtain such high survival rates(54). Hinerman et al(55) experienced a
stage III and stage IV overall survival of less than 50 percent.
4.2 Tumor Grade: In our patients we only had a very small number of patients with grade I or grade IV disease. Those
with undifferentiated carcinoma included into this study (5 patients), were described as squamous
cell carcinoma by more differentiated parts of the tumor mass. Due to the small numbers of GI and
GIV tumors, tumor grade was confounded into two groups: high differentiated (GI,GII) and low
differentiated (GIII,GIV)
Between those two groups we could not demonstrate a statistically significant difference in
recurrence free and overall survival depending on differentiation of primary tumor. In our tumor
board, decision for adjuvant therapy was not based upon tumor grade. However, lower
differentiation grade correlated with higher pN-status and therefore also with higher tumor stage.
Hence assessment of the impact of tumor grade on disease free and overall survival is difficult to
make, since low differentiated tumors were treated statistically more often with adjuvant therapy
compared to highly differentiated tumors.
In the literature, subjectivity of evaluation(56) into different grading groups is mentioned. In our
patients, pathological reports were made by one experienced examiner, therefore inter-examiner
variability was not an issue. This might be a very important factor considering the inconclusive
literature of the impact of grading on overall survival. Since differentiation of tumor is based on
microscopically conducted pathological evaluation, in which borderlines between well differentiated,

110
moderately differentiated and poorly differentiated tumors are set by the pathologist individually,
comparison and effect of tumor grade on outcome might be difficult if more than one pathologist
was responsible for evaluation.
As mentioned, literature on tumor grade is inconclusive. Janot et al(56) described the risk of early
and more frequently metastases in poorly differentiated tumors, concluding that patients with
poorly differentiated tumors and clinical nodal involvements are at high risk for recurrence and
therefore have a poorer overall survival. Likewise, Jerjes et al(57) could demonstrate in a recent
study the same effect of tumor differentiation in early stage oral squamous cell carcinoma on loco-
regional neck lymph node metastasis and overall survival. Even the relationship between histological
differentiation and perineural invasion is debated in the literature(58).
On the other side, other authors support the thesis of less important effects of tumor differentiation
on outcome. Li et al(59) investigated retrospectively on 391 patients with head and neck squamous
cell carcinoma; similar to our study setting, he investigated on patients primarily treated with surgical
tumor therapy and optional adjuvant therapy. In his patients, tumor grade did not have an impact on
distant metastasis and therefore survival. Kane et al(60), investigating prospectively on patients with
early stage oral carcinoma, could also find no impact of tumor grade on survival.
Trying to merge those two different views, our results to some extent support both theses at the
same time: we also experienced the correlation of tumor grade with lymph node metastases, as
described by Janot and Jerjes. Nevertheless, looking at the outcome, both overall and disease free
survival were not altered just as described by Kane and Li. The unchanged outcome might be
explained due to the adjuvant therapy administered. Looking at our patients treated solely with
surgical therapy, low grade and high grade tumors differed, although statistical significance was
missing. On the other side, run of curves of patients receiving adjuvant therapy did not differ at all.
We did not see the correlation of differentiation of tumor and perineural invasion as proposed by
Rahima. Although expecting the lower differentiated tumors to be more aggressive or more invasive,
we could not see a correlation of tumor grade not only on perineural invasion but also on capsule
penetration, haemangiosis, lymphangiosis, and congolemerate tumors.
4.3 Histological aspects: In our patients, perineural invasion, extracapsular spread, lymphangiosis carcinomatosa,
haemangiosis carcinomatosa and conglomerate tumors played an important role for disease free and
overall survival.
Perineural invasion is a strong predictor for local and locoregional recurrence and has to be looked
for and is requested to be reported in pathological examination(61) and treated with adjuvant
therapy(55). Also in cutaneous cancer of head and neck, perineural invasion is known as a predictive
factor for survival, nevertheless importance of adjuvant radiotherapy is still under debate in this
entity(62) - on a wide basis of discussion. Liao et al(63) did not see a statistically significant difference
in disease free survival and overall survival if patients with perineural invasion received adjuvant
radiotherapy or not. He therefore concluded that surgical resection alone is a sufficient treatment
even for patients with perineural invasion. This is in complete contrast to our patient data, showing
the importance of adjuvant therapy in patients with perineural invasion. Le Tourneau et al(64)

111
supports the importance of adjuvant therapy while he did not find a poorer survival in patients with
perineural invasion after primary surgical treatment and adjuvant radiotherapy. Nevertheless,
prospective trials for impact of adjuvant radiotherapy on patients with perineural invasion should be
realized.
The impact of extracapsular spread on locoregional and overall survival is well documented
throughout the literature(65,66). Even in patients with clinical negative neck, occult metastases with
capsule penetration occur(67), putting the patient at high risk of undertreatment. This disproves the
former thought of extracapsular spread being associated with larger lymph node metastasis and
fixed lymph nodes(68).
Investigating on 266 patients with squamous cell carcinoma of the oral tongue, Myers et al(69)
experienced a 5 year overall survival rate for patients with pathological node-negative neck, node-
positive neck without extracapsular spread, and node-positive neck with extracapsular spread, of
75%, 50%, and 30%, respectively. With 89% of postoperative radiotherapy in patients with
extracapsular spread in this study, nevertheless regional failure rate was 29%, therefore he
concluded that further adjuvant therapy is needed to affect regional and distant control and improve
survival. Our data suggests the significant importance of extracapsular spread on disease free and
overall survival. 6 out of 7 (85,7%) patients with extracapsular spread receiving no adjuvant therapy
died during follow-up. With adjuvant therapy, overall survival was significantly higher in patients with
extracapsular spread. Overall survival in all patients with extracapsular spread was 48% (29 of 56
patients died during follow-up).
Aside from capsule penetration and perineural invasion, further important tumor factors associated
with prognosis are local invasion, angioinvasion, lymphogenic dissemination and soft tissue
extension(57,70). In our patients, conglomerate tumors and haemangiosis carcinomatosa was a
strong predictive factor for distant metastasis. Patients with lymphangiosis carcinomatosa suffered
significantly more often ipsilateral and contralateral recurrence. All of these factors were strong
predictive factors for poor outcome. Both, disease free survival and overall survival were reduced
significantly if angioinvasion, lymphogenic dissemination, or conglomerate tumors were present.
In the literature, reports of haemangiosis carcinomatosa is rare as far as head and neck squamous
cell carcinoma is concerned, but the impact of haemangiosis on survival is documented in other
topics such as breast cancer(71). Likewise, impact of conglomerate lymph nodes – so called bulky
lymph nodes – is not documented in the literature for head and neck surgery. However, bulky
disease plays an important role for overall survival for example in penile cancer(72).
Similar to our results McMahon et al demonstrated in a prospective audit of patients in 1999 until
2001 with oral and oropharyngeal cancer, the bad prognostic impact of perineural invasion,
extracapsular spread, and vascular invasion(54).
4.4 Tumor Localization:
4.4.1 Hypopharynx:
In our data, patients with a hypopharyngeal tumor had a significantly lower recurrence free and
overall survival compared to other tumor localizations. Overall survival was 49% in patients with a

112
hypopharyngeal cancer compared to 71,7% of patients with cancer in other localizations. The poor
outcome in hypopharyngeal tumors is also described in the literature(73,74). In a study by Johansen
et al(75), an overall survival of 21% in hypopharyngeal cancer was described. Hypopharyngeal cancer
tends to present with advanced primary disease, and nodal metastasis is highly likely(76). Although
advanced stage of disease at time of diagnosis seems to be mainly responsible for poor outcome, and
T1 and T2 hypopharyngeal tumors have satisfying disease free survival and local control according to
Karatzanis et al(77), we have to contradict this statement, since results of our patient data showed
the bad prognosis of T1 and T2 hypopharyngeal tumors compared to other tumor localizations.
4.4.2 Tongue Cancer:
Looking at the literature, it seems as if within the oral cavity tumors, tongue cancer plays a
substantially different role(78). Looking at the outcome of our patients, we did not see a significant
difference in disease free and overall survival compared to other localizations of the oral cavity, but
similar to Yao et al(79), tongue cancer was always the one behind. Of course, statistic always faces
the problem of small numbers as seen in oral cavity cancer. However, Rusthoven et al(80) could
demonstrate in a study on more than 6700 patients, the bad prognostic factor of tongue cancer.
4.5 Lymph Node Status: Importance of lymph node status for disease free and overall survival is well documented throughout
the literature. Hahn et al(81) described the statistical significance between N0 or N1 versus N2 and
N3 status, finding no difference between N0 and N1. Li et al(59) demonstrated the statistically
significant impact of N-stage and numbers of positive lymph node levels on distant metastasis and
therefore overall survival. In our patients, we experienced the importance of negative lymph node
versus positive lymph node status. As soon as neck lymph node was involved, overall survival was
diminished by 15%. The effect of lymph node status on overall survival remains significant even in
patients with locally advanced (T4) disease(82). In a large retrospective publication by Layland et
al(83) on 3887 patients, he could demonstrate the negative prognostic factor of positive lymph node
status for each tumor site: oral cavity, oropharynx, hypopharynx and larynx, separately.
4.6 Lymph Node Ratio: In certain tumor entities such as gastric cancer(84-86), endometrial cancer(87), colorectal cancer(88-
90) and pancreatic cancer(91,92), lymph node ratio is a very important diagnostic tool.
Based upon those findings in other cancer entities, Shrime et al(47,93) postulated that lymph node
ratio between number of excised lymph nodes and number of positive lymph nodes is a predictive
factor for outcome. Investigating on 386 patients with an oral squamous cell carcinoma, Gil et al(94)
came to the same conclusion. While Shrime et al used two cut off points (6% and 13%) Gil only
compared the lymph node ratio below and above 6%. In both studies, results were similar showing a
statistically significant difference in disease free and overall survival depending on the lymph node
ratio. Süslü et al(95) also came to the conclusion of the importance of lymph node ratio; however,
this group used 4% as the cutoff point for different outcomes.

113
Comparing our data with the literature, we had a very similar result compared to the study
conducted by Gil. As suggested by Shrime, we also used two cutoff points, finding out that there was
no significant difference between patients with a lymph node ratio between 7-13% and patients with
a lymph node ratio higher than 13%. But patients with a lymph node ratio of 6% or lower had a
better disease free and overall survival.
4.7 Resection Margin: As expected, resection margin played a very important role in disease free and overall survival in our
patients. While macroscopic positive resection margin offered a crucial prognosis, microscopic
positive resection margins had a significant better prognosis. However, if microscopic positive
resection margin was not treated with adjuvant therapy (radiotherapy or radiochemotherapy),
prognosis was bleak.
If adjuvant therapy was administered in case of microscopic positive resection margin, Kaplan-Meier
curve could be converged to run of curve of negative resection margin. Still, median overall survival
differed by many months, indicating the importance of tumor free resection margins.
The importance of resection margin on disease free and overall survival is well documented
throughout the literature. Patel et al(96) concluded that, aside fromT-stage, N-stage, extracapsular
spread and tumor thickness, resection margin is a very important predictive factor for disease free
survival. Karatzanis et al(77) emphasized the importance of negative resection margin. Similar to
Patel, McMahon et al filtered resection margin, among other predictive factors, as a very important
statistically significant factor for outcome(54).

114
4.8 Neck Dissection:
4.8.1 Preserving non lymphatic tissue:
In the mid-20th century, it became evident that radical neck dissection was too aggressive in a large
number of situations. The group of surgeons aiming for preservation of non-lymphatic tissue was led
by Osvaldo Suarez and his pupils Ettore Bocca and Cesar Gavilan(97). Kokemueller et al(98) however
disagreed with the idea of preserving non-lymphatics. At least as far as advanced stages were
concerned, because curves for actuarial neck control demonstrated a remarkable divergence.
Nevertheless, he could not find a statistically significant influence on prognosis for different types of
comprehensive neck dissections, but explained the missing significance by the usually more extensive
disease when radical procedure was performed.
In our patients, we did not see a difference in disease free survival or overall survival comparing
whether non-lymphatic tissues were excised or not. For all three (sternocleidomastoid muscle,
accessoric nerve and jugular vein), Kaplan-Meier curves had a similar run. However, likewise with
Kokemueller, groups were not eligible for comparison, because distribution of disease stage was not
even, and therefore validity of evidence was missing.
4.8.2 Preserving lymphatic tissue:
With the discussion on preserving non-lymphatic tissue at debate at the end of the 20th century, also
discussion about whether selective neck dissection could be a sufficient treatment option for some
patients or whether the need of radical neck dissection remained, was coming up and was
investigated by some study groups(99-102). All of those investigations are based on distribution of
neck lymph node metastases described by earlier studies of Lindberg(103) and Shah(104). In oral
cancer, most commonly, lymph nodes at levels I-III are involved while positive lymph nodes in level IV
are rare. In oropharyngeal and hypopharyngeal cancer, Candela et al(105) described the likelihood of
level II to level IV metastasis, while involvement of level I and level V was seen very randomly (less
than 1 percent). It appears that the pattern of metastasis in laryngeal cancer is very similar to
hypopharyngeal cancer(106,107).
In 1998, Clayman et al(108) reviewed existing literature, confounding lymph node levels at highest
risk for lymph node metastasis and set recommendations of selective procedures for every tumor
site:
Oral cavity: lymph node levels I-III, in case of tongue carcinoma also IV are at risk for lymph
node metastasis and therefore, the recommended neck procedure is a supraomohyoidal
neck dissection, in case of tongue carcinomas recommendation includes extension to region
IV.
Oropharynx: regions at risk are the lymph node levels I-III, also lymph nodes in the
retropharyngeal and parapharyngeal regions should be looked for in a supraomohyoidal neck
dissection.

115
Hypopharynx: levels at risk are especially levels II-IV, but also retropharyngeal and
parapharyngeal lymph nodes. Recommended neck procedure in hypopharyngeal cancer is a
lateral neck dissection with inclusion of retro-, and parapharyngeal basins.
Larynx: most common lymph node metastasis in laryngeal tumors are levels II-IV, in case of
advanced carcinomas also regio VI. Lateral neck dissection or in case of advanced disease,
anterolateral neck dissection should be performed.
In our patient data, we could not find a statistical significant benefit in patients receiving a more
extensive type of neck dissection compared to patients receiving only selective procedures. Looking
at the number of lymph node levels excised, we could demonstrate that with an increasing number
of lymph nodes resected, disease free and overall survival did not increase in the same way but
rather showed a very similar outcome; regardless the benefit of morbidity in patients with neck
dissections of only I-III lymph node levels (especially prevention of shoulder dysfunction(109,110))
Nevertheless, overall survival in patients with neck dissection of 1-3 lymph node levels in patients
with a positive neck did have a very low median overall survival compared to patients being dissected
with more than 3 nodes. But looking at the Kaplan-Meier curve together with the Log-Rank test,
small number of median overall survival (34 months) can be explained by the small number of
patients in this group (11 patients).
As far as radical neck dissection is concerned, we could demonstrate that radical neck dissection does
not provide a better outcome in patients with a stage IV disease, patients with a positive neck, and
also patients with different number of positive neck lymph nodes affected. In every setting, radical
neck dissection did not offer an advantage compared to other types of neck dissections. Kohler et
al(111), comparing radical neck dissection versus modified radical neck dissection, came to the same
conclusion: radical neck dissection, with all its sequels, did not show a better outcome.
Looking at the locoregional recurrence free survival, comparing extensive neck dissection (radical
neck dissection, modified radical neck dissection, and posterolateral neck dissection) with the more
or less elective selective procedures of selective neck dissections (supraomohyoidal neck dissection,
suprahyoidal neck dissection and lateral neck dissection), lymph node recurrence was even. Even if
adjuvant therapy was considered, there was not benefit in any neck procedure on locoregional
recurrence free survival. In our patients, we experienced a locoregional recurrence (LRR) free survival
of 91 percent. Patel et al(99) experienced a LRR free survival of 87 percent, Shepard et al(112) a LRR
free survival of 90 percent. Both could not find a statistically significant benefit of comprehensive
neck dissection versus selective neck dissection for LRR free survival. This is even more remarkable
considering the fact that patients receiving comprehensive neck dissection usually have a higher
disease stage.
Therefore, with the great support of the literature, we would vote for a selective neck procedure,
especially in elective neck dissections, rather than a comprehensive radical, or modified radical neck
dissection.

116
4.8.3 Clinical Node Negative Neck – is there a need of elective contralateral Neck
Dissection?
Knowing the good prognosis of patients with a negative lymph neck node status, and the bad effect
of lymph node metastasis on overall survival, especially in patients receiving no adjuvant therapy,
physicians are faced with the problem of patients with clinical negative lymph nodes but occult neck
metastasis. Is there a need of elective procedure and what is the indication for elective neck
dissection? Today there are at least 4 prospective studies available questioning whether elective
neck dissection or observation and therapeutically treating the clinically negative neck is the best
decision. But still, the issue remains unresolved since answers are inconclusive:
Fakih et al(113,114) showed in 70 patients with a squamous cell carcinoma (SCC) of the oral tongue
that there is no significant difference in disease free survival between patients treated with elective
ipsilateral radical neck dissection versus observation. Similar to Fakih, Vandenbrouck et al(115)
investigated in 75 patients on T1-T3 SCC of mixed oral tongue and floor of mouth carcinomas
showing that there is no benefit if elective radical neck dissection was performed.
Based on their earlier conducted retrospective study(116), showing a significant reduction of node
related mortality from 23% of observation to 3% after selective neck dissection Yuen et al(117)
investigated prospectively on the same issue in 71 patients, trying to confirm their retrospective
study. The 5 year disease-specific survival rate was 87% for the observation arm and 89% for the
elective neck dissection arm showing once again no significant difference. These 3 studies indicate
that if close follow-up is assured, both observation as well as elective neck dissection offers similar
treatment results.
On the other hand, Kligerman et al(118) prospectively analyzed T1-T2 SCC of the oral cavity in 67
patients finding recurrences in 42% of patients of the observation group and 24% of the elective
omohyoidale neck dissection group. The disease-free survival rates at 3,5 years were 49%, and 72%,
respectively, leading to the conclusion that neck dissection remains mandatory.
In 1997 Pillsbury and Clark concluded that considering the high percentage of occult metastases in
oral cavity SCC, observation of the n0 neck with oral cavity primary is ill advised(119). Other
retrospective studies and reviews demonstrated the high incidence of occult metastases in the oral
cavity(46,120-122). In case of oropharyngeal and hypopharyngeal primary tumor, bilateral elective
treatment should be strived for, since probability of occult metastases is – depending on
literature(105,123-125) – between 17% and 55% But even though the rich lymphatic network in this
region puts the patient at higher risk of occult metastases bilaterally, the discussion whether bilateral
neck dissection should be performed in every case is questioned(126)(126).
Therefore it is essential to filter out those patients who might benefit of a bilateral treatment and
those who would not.
Interestingly enough, facing a high number of occult lymph node metastastis in the ipsilateral and
contralateral neck in oral cavity and oropharyngeal cancer, locoregional recurrence rate seems to be
much lower. Moncrieff et al(52) experienced a locoregional lymph node recurrence in 8 % and only
2% in the contralateral neck in T1/T2 tumors of the oropharynx – any N was included. Considering
that only 1 patient was treated bilaterally and 22 out of 92 did not receive lymphadenectomy, a very
small number. 10 out of 155 patients experienced a lymph node recurrence in a recent study by
Sklenicka et al(127) similar to a Korean study(128), finding 25 out of 230 patients with a recurrence in

117
the neck. Unfortunately number and type of lymphadenectomy in those patients with lymph node
recurrence was not described in those studies. Garcia et al(129) investigated in a retrospective study
on 315 patients with oral cavity cancer: 9% developed ipsilateral and only 5% contralateral neck
relapse. 101 patients did not receive any lymphadenectomy, only 2 of them experienced
contralateral lymph node relapse.
Weiss et al(130) calculated a treatment threshold for elective neck dissection if the probability of
occult metastases being higher than 20%. Okura et al(131) calculated the threshold point being at
44%, suggesting an elective treatment of the neck if the probability of occult metastases being above
this threshold percentage.
The literature available exposes two main arguments: 1) how high is the risk of occult metastases to
the neck in different tumor types considering grading and other histopathological subgroups, and 2)
if the risk of occult metastases is known, at what point is prophylactic treatment indicated?
However, we could not find a statistical significant benefit of elective treatment of the contralateral
neck, but rather a very similar result in both groups. Considering the high morbidity of bilateral neck
dissection, we would not suggest such a therapy approach in clinical negative contralateral necks,
except when the tumor is crossing the midline.
4.9 Adjuvant therapy in advanced disease: Throughout the literature, debate about best treatment strategies in head and neck cancer are going
on. Carvalho et al(132) came to the conclusion that surgery should be the first option for initial
clinical stage oral and oropharyngeal cancers. For advanced cases, independently of the site of the
tumor, surgery and postoperative radiotherapy should be the standard of care because it is
associated with the lowest rates of locoregional recurrence. Further discussion on advantage or
disadvantage of surgical procedure (i.e. organ preservation(133)) will not be conducted, since our
patients were included into this study, if primary treatment plan consisted of surgical resection of
primary tumor with additional neck dissection and, if administered, adjuvant therapy. Patients
receiving induction chemotherapy, definitive radiotherapy, et cetera, were not included and
therefore any advantage of those treatment options will not be included into discussion.
Adjuvant therapy is an integral part of treating locally advanced head and neck cancer. In a
comparative analysis of the EORTC 22931(134) and the RTOG 9501(135) studies, Bernier et al(136)
confounded the importance of postoperative adjuvant radiochemotherapy especially in patients with
microscopically positive resection margins and extracaspular rupture outside lymph nodes. Although
detectable, the contribution of adjuvant chemoradiation in the group of patients who have stage III-
IV disease, perineural infiltration, vascular embolisms, and/or level IV-V lymph nodes secondary to
tumors of the oral cavitiy or oropharynx seems to be less important in this combined analysis.
Comparing combined radiochemotherapy with single modality treatment options in advanced
oropharyngeal cancer, Kader et al(137) could demonstrate the superiority of combined
radiochemotherapy in disease free and overall survival.
Reviewing more than 25 papers on the effect of additional adjuvant chemotherapy versus
radiotherapy solely after primary surgery, Furness et al(138) calculated a 16% increase in overall

118
survival if postoperative radiochemotherapy was administered. Oliver et al(139) came to the same
conclusion finding a statistically significant difference in patients being treated with surgery plus
radiochemotherapy compared to patients undergoing surgery plus radiotherapy solely; large
European(134) as well as American(135) studies were included. However, it has to be said, that
overall survival did not differ statistically significant in the American study by Cooper. Comparing the
literature with our results, we could see the benefit of combined postoperative radiochemotherapy
compared to surgery and surgery with postoperative radiotherapy. Percentage of overall and disease
free survival was significantly higher in patients treated with postoperative radiochemotherapy.
However, Log-Rank test in the Kaplan-Meier analysis did not show up to be significant.
Furthermore, in our results, overall survival of patients with stage III and stage IV disease was very
high compared to literature. Bernier et al(134) experienced in 334 patients with stage III and stage IV
disease an overall survival of 40% and 52% respectively for patients with adjuvant radiotherapy and
adjuvant radiochemotherapy. In our patient cohort, with 221 patients, overall survival for the same
group was 58% and 87%. Investigating on the high percentage of overall survival in our patients, we
found out that long time follow-up in patients with radiotherapy could be achieved: after 3 years we
still had 58 patients at risk, 34 patients after 5 years. In patients treated with postoperative adjuvant
radiochemotherapy, only 6 of 37 patients were still at risk after three years, and only 1 patient was
followed up for more than 5 years. This could be responsible for the very high number of percentage
of overall survival in this specific group.
However, one has to keep in mind that with increasing aggressiveness of treatment modalities, side
effects as well as morbidity rises as well. The Radiation Therapy Oncology Group investigated
together with the Eastern Cooperative Oncology Group and the Southwest Oncology Group in 459
patients with high risk squamous cell carcinoma of head and neck (positive mucosal resection
margin, more than 2 positive lymph nodes and extracapsular spread) the effect of postoperative
adjuvant radiotherapy versus postoperative adjuvant chemoradiation. Although local and regional
control was increased significantly in the combined adjuvant therapy group, overall survival did not
benefit of combined postoperative chemoradiation. Adverse side effects of grade 3 or higher were
seen in 34 percent of radiotherapy patients, but 77 percent in patients with chemoradiation(135).
Especially in older age and high T-status, as well as tumors of the hypopharynx and larynx are
associated with severe late toxicity after concurrent chemoradiation(140).
In a meta-analysis by Pignon et al(34), investigating on 17354 patients with advanced disease and
impact of chemotherapy together with locoregional therapy, he could not find a higher percentage of
patients dying of other causes than the cancer between patients receiving chemotherapy to those
patients without chemotherapy. Furthermore, he confounded the positive impact of chemotherapy
especially if applied concomitant with radiotherapy. Considering the different chemotherapeutics, he
identified platin based chemotherapeutics as being the most effective agents considering overall
survival – especially if chemotherapy was a mono-chemotherapy.
In a recent study by Tobias et al(141), investigating on the effect of timing of chemotherapy in a large
cohort of patients with advanced head and neck cancer (966 patients) he agreed with Pignon that
concurrent chemoradiotherapy has the best effect on disease free and overall survival. However,
since he also included patients with inoperable cancer, this conclusion was not right for patients who
were operable and had undergone surgery. Looking at those patients separately, additional
concurrent chemoradiation did not offer a better recurrence free survival or overall survival

119
compared to patients with postoperative radiotherapy. In addition, late toxicity was doubled and
therefore not suggested. Nevertheless, he used non-platinum chemotherapeutics in his study design.
This might explain the missing effect of chemotherapeutics in patients undergoing surgery and
postoperative radiotherapy.
Nevertheless, one has to keep in mind the high toxicity of platinum based chemotherapeutics. Newer
agents, such as taxanes and targeted therapies might improve on the longer established cisplatin. In
this context, a large study on 424 patients with advanced head and neck cancer by Bonner et al(142)
investigating on effect of adjuvant radioimmunotherapy with cetuximab as immunotherapeutic, has
to be mentioned. Bonner came to the conclusion that patients treated with postoperative
radiotherapy and additional cetuximab experienced a significantly better overall survival. However,
validity of this study is doubted, since he did not compare cetuximab with the gold-standard in
advanced carcinomas but with radiotherapy solely. Discussion is on-going, whether all patients would
benefit of concurrent radiotherapy and cetuximab(143), and explanation of the connection between
cetuximab induced rash and overall survival is demanded(144).
Two phase III randomized trials (RTOG 0522 and GORTEC 2007-01) might resolve the question
whether combining cetuximab with chemoradiotherapy is better than chemoradiotherapy alone or
cetuximab and radiotherapy in locally advanced head and neck cancers(145).
Looking at the literature, the issue of treatment associated morbidity and mortality is getting more
into focus of therapists. With all the effective treatment choices available, and with the rise of
combined therapy modalities, one has to weigh the aggressive treatment for cancer control on the
one side with the high therapy associated morbidity on the other side. To oversimplify a bit, cancer
might be controlled by today’s treatment options, but does the patient survive our treatment? And
that should be the most important factor: what is best for the patient, not what is best to treat the
cancer.

120
References
(1) Houghton Mifflin Company. The Free Dictionary. 2010; Available at: http://www.thefreedictionary.com. Accessed 08/20, 2010.
(2) Barnes L, Eveson JW, Reichart P, Sidransky D editors. WHO Classification of Tumours. Pathology and genetics of head and neck tumours. Fifth Edition ed. Lyon: IARC Press; 2005.
(3) Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol 2009 5;45(4-5):309-316.
(4) Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN 2008, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10. 2008; Available at: http://globocan.iarc.fr. Accessed 08/16, 2010.
(5) World Health Organization. Mortality database. 2010; Available at: http://www.who.int/whosis/whosis. Accessed 08/16, 2010.
(6) Patel SG, Shah JP. TNM staging of cancers of the head and neck: striving for uniformity among diversity. CA Cancer J Clin 2005 Jul-Aug;55(4):242-58; quiz 261-2, 264.
(7) Deschler DG editor. TNM Staging of Head and Neck Cancer and Neck Dissection Classification. Alexandria: American Academy of Otolaryngology–Head and Neck Surgery Foundation, Inc.; 2008.
(8) Robbins KT, Medina JE, Wolfe GT, Levine PA, Sessions RB, Pruet CW. Standardizing neck dissection terminology. Official report of the Academy's Committee for Head and Neck Surgery and Oncology. Arch Otolaryngol Head Neck Surg 1991 Jun;117(6):601-605.
(9) Robbins KT, Shaha AR, Medina JE, Califano JA, Wolf GT, Ferlito A, et al. Consensus statement on the classification and terminology of neck dissection. Arch Otolaryngol Head Neck Surg 2008 May;134(5):536-538.
(10) Seethala RR. Current state of neck dissection in the United States. Head Neck Pathol 2009 Sep;3(3):238-245.
(11) SNM. Advancing Molecular Imaging Therapy. Available at: http://tech.snmjournals.org/content/vol35/issue1/images/large/10fig2.jpeg. Accessed 09/19, 2010.
(12) Ferlito A. Classification and terminology of neck dissection. Arch Otolaryngol Head Neck Surg 2002 Jul;128(7):747-748.
(13) Hashibe M, Brennan P, Benhamou S, Castellsague X, Chen C, Curado MP, et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J Natl Cancer Inst 2007 May 16;99(10):777-789.
(14) Curado MP, Hashibe M. Recent changes in the epidemiology of head and neck cancer. Curr Opin Oncol 2009 May;21(3):194-200.

121
(15) International Agency for Research on Cancer editor. Smokeless Tobacco and Some Tobacco-specific N-Nitrosamines. Lyon, France: World Health Organization International Agency for Research on Cancer; 2007.
(16) Gandini S, Botteri E, Iodice S, Boniol M, Lowenfels AB, Maisonneuve P, et al. Tobacco smoking and cancer: a meta-analysis. Int J Cancer 2008 Jan 1;122(1):155-164.
(17) Mannarini L, Kratochvil V, Calabrese L, Gomes Silva L, Morbini P, Betka J, et al. Human Papilloma Virus (HPV) in head and neck region: review of literature. Acta Otorhinolaryngol Ital 2009 Jun;29(3):119-126.
(18) Paz IB, Cook N, Odom-Maryon T, Xie Y, Wilczynski SP. Human papillomavirus (HPV) in head and neck cancer. An association of HPV 16 with squamous cell carcinoma of Waldeyer's tonsillar ring. Cancer 1997 Feb 1;79(3):595-604.
(19) Marur S, D'Souza G, Westra WH, Forastiere AA. HPV-associated head and neck cancer: a virus-related cancer epidemic. The Lancet Oncology ;In Press, Corrected Proof.
(20) Lajer CB, von Buchwald C. The role of human papillomavirus in head and neck cancer. APMIS 2010 Jun;118(6-7):510-519.
(21) Sturgis EM, Cinciripini PM. Trends in head and neck cancer incidence in relation to smoking prevalence: an emerging epidemic of human papillomavirus-associated cancers? Cancer 2007 Oct 1;110(7):1429-1435.
(22) Klussmann JP, Weissenborn SJ, Wieland U, Dries V, Kolligs J, Jungehuelsing M, et al. Prevalence, distribution, and viral load of human papillomavirus 16 DNA in tonsillar carcinomas. Cancer 2001 Dec 1;92(11):2875-2884.
(23) Klussmann JP, Weissenborn SJ, Wieland U, Dries V, Eckel HE, Pfister HJ, et al. Human papillomavirus-positive tonsillar carcinomas: a different tumor entity? Med Microbiol Immunol 2003 Aug;192(3):129-132.
(24) Wiest T, Schwarz E, Enders C, Flechtenmacher C, Bosch FX. Involvement of intact HPV16 E6/E7 gene expression in head and neck cancers with unaltered p53 status and perturbed pRb cell cycle control. Oncogene 2002 Feb 28;21(10):1510-1517.
(25) Negri E, Franceschi S, Bosetti C, Levi F, Conti E, Parpinel M, et al. Selected micronutrients and oral and pharyngeal cancer. Int J Cancer 2000 Apr 1;86(1):122-127.
(26) Yang CS. Research on esophageal cancer in China: a review. Cancer Res 1980 Aug;40(8 Pt 1):2633-2644.
(27) Rezende TMB, Freire MdS, Franco OL. Head and neck cancer. Cancer 2010:n/a-n/a.
(28) Hong TS, Ritter MA, Tome WA, Harari PM. Intensity-modulated radiation therapy: emerging cancer treatment technology. Br J Cancer 2005 May 23;92(10):1819-1824.
(29) Butler EB, Teh BS, Grant WH,3rd, Uhl BM, Kuppersmith RB, Chiu JK, et al. Smart (simultaneous modulated accelerated radiation therapy) boost: a new accelerated fractionation schedule for the treatment of head and neck cancer with intensity modulated radiotherapy. Int J Radiat Oncol Biol Phys 1999 Aug 1;45(1):21-32.

122
(30) Harari PM, Sharda NN, Brock LK, Paliwal BR. Improving dose homogeneity in routine head and neck radiotherapy with custom 3-D compensation. Radiotherapy and Oncology 1998 10;49(1):67-71.
(31) Galvin JM, Ezzell G, Eisbrauch A, Yu C, Butler B, Xiao Y, et al. Implementing IMRT in clinical practice: a joint document of the American Society for Therapeutic Radiology and Oncology and the American Association of Physicists in Medicine. Int J Radiat Oncol Biol Phys 2004 Apr 1;58(5):1616-1634.
(32) Staffurth J. A Review of the Clinical Evidence for Intensity-modulated Radiotherapy. Clin Oncol ;In Press, Corrected Proof.
(33) Webb S. The physical basis of IMRT and inverse planning. Br J Radiol 2003 Oct;76(910):678-689.
(34) Pignon J, Maître Al, Maillard E, Bourhis J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiotherapy and Oncology 2009 7;92(1):4-14.
(35) Lokich J, Anderson N. Carboplatin versus cisplatin in solid tumors: an analysis of the literature. Ann Oncol 1998 Jan;9(1):13-21.
(36) Go RS, Adjei AA. Review of the comparative pharmacology and clinical activity of cisplatin and carboplatin. J Clin Oncol 1999 Jan;17(1):409-422.
(37) Ebeling O, Eckel HE, Volling P, Heitmann K, Vossing M. Cisplatin/5-FU versus carboplatin/5-FU. 5 year follow-up. HNO 1994 Oct;42(10):629-635.
(38) Harari PM, Ritter MA, Petereit DG, Mehta MP. Chemoradiation for upper aerodigestive tract cancer: balancing evidence from clinical trials with individual patient recommendations. Curr Probl Cancer 2004 Jan-Feb;28(1):7-40.
(39) Brizel DM, Esclamado R. Concurrent chemoradiotherapy for locally advanced, nonmetastatic, squamous carcinoma of the head and neck: consensus, controversy, and conundrum. J Clin Oncol 2006 Jun 10;24(17):2612-2617.
(40) Hao D, Ritter MA, Oliver T, Browman GP. Platinum-based concurrent chemoradiotherapy for tumors of the head and neck and the esophagus. Semin Radiat Oncol 2006 Jan;16(1):10-19.
(41) McWhinney SR, Goldberg RM, McLeod HL. Platinum neurotoxicity pharmacogenetics. Mol Cancer Ther 2009 Jan;8(1):10-16.
(42) Wagstaff AJ, Ward A, Benfield P, Heel RC. Carboplatin. A preliminary review of its pharmacodynamic and pharmacokinetic properties and therapeutic efficacy in the treatment of cancer. Drugs 1989 Feb;37(2):162-190.
(43) Schmitt A, Gladieff L, Laffont CM, Evrard A, Boyer JC, Lansiaux A, et al. Factors for Hematopoietic Toxicity of Carboplatin: Refining the Targeting of Carboplatin Systemic Exposure. J Clin Oncol 2010 Sep 20.
(44) Malet-Martino M, Jolimaitre P, Martino R. The prodrugs of 5-fluorouracil. Curr Med Chem Anticancer Agents 2002 Mar;2(2):267-310.

123
(45) Cripps C, Winquist E, Devries MC, Stys-Norman D, Gilbert R. Epidermal growth factor receptor targeted therapy in stages III and IV head and neck cancer. Curr Oncol 2010 Jun;17(3):37-48.
(46) Capote A, Escorial V, Munoz-Guerra MF, Rodriguez-Campo FJ, Gamallo C, Naval L. Elective neck dissection in early-stage oral squamous cell carcinoma--does it influence recurrence and survival? Head Neck 2007 Jan;29(1):3-11.
(47) Shrime MG, Bachar G, Lea J, Volling C, Ma C, Gullane PJ, et al. Nodal ratio as an independent predictor of survival in squamous cell carcinoma of the oral cavity. Head Neck 2009 Nov;31(11):1482-1488.
(48) Robbins KT, Clayman G, Levine PA, Medina J, Sessions R, Shaha A, et al. Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg 2002 Jul;128(7):751-758.
(49) Yeole BB, Sankaranarayanan R, Sunny L, Swaminathan R, Parkin DM. Survival from head and neck cancer in Mumbai (Bombay), India. Cancer 2000;89(2):437-444.
(50) Shah JP, Gil Z. Current concepts in management of oral cancer – Surgery. Oral Oncol 2009 5;45(4-5):394-401.
(51) Chen YK, Huang HC, Lin LM, Lin CC. Primary oral squamous cell carcinoma: an analysis of 703 cases in southern Taiwan. Oral Oncol 1999 3;35(2):173-179.
(52) Moncrieff M, Sandilla J, Clark J, Clifford A, Shannon K, Gao K, et al. Outcomes of primary surgical treatment of T1 and T2 carcinomas of the oropharynx. Laryngoscope 2009 Feb;119(2):307-311.
(53) Mendenhall WM, Werning JW, Hinerman RW, Amdur RJ, Villaret DB. Management of T1?T2 glottic carcinomas. Cancer 2004;100(9):1786-1792.
(54) McMahon JD, Robertson GAJ, Liew C, McManners J, Mackenzie FR, Hislop WS, et al. Oral and oropharyngeal cancer in the West of Scotland—long-term outcome data of a prospective audit 1999–2001. British Journal of Oral and Maxillofacial Surgery ;In Press, Corrected Proof.
(55) Hinerman RW, Mendenhall WM, Morris CG, Amdur RJ, Werning JW, Villaret DB. Postoperative irradiation for squamous cell carcinoma of the oral cavity: 35-year experience. Head Neck 2004;26(11):984-994.
(56) Janot F, Klijanienko J, Russo A, Mamet JP, de Braud F, El-Naggar AK, et al. Prognostic value of clinicopathological parameters in head and neck squamous cell carcinoma: a prospective analysis. Br J Cancer 1996 Feb;73(4):531-538.
(57) Jerjes W, Upile T, Petrie A, Riskalla A, Hamdoon Z, Vourvachis M, et al. Clinicopathological parameters, recurrence, locoregional and distant metastasis in 115 T1-T2 oral squamous cell carcinoma patients. Head Neck Oncol 2010 Apr 20;2:9.
(58) Rahima B, Shingaki S, Nagata M, Saito C. Prognostic significance of perineural invasion in oral and oropharyngeal carcinoma. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology & Endodontics 2004 4;97(4):423-431.

124
(59) Li X, Di B, Shang Y, Zhou Y, Cheng J, He Z. Clinicopathologic risk factors for distant metastases from head and neck squamous cell carcinomas. European Journal of Surgical Oncology (EJSO) 2009 12;35(12):1348-1353.
(60) Kane SV, Gupta M, Kakade AC, D'Cruz A. Depth of invasion is the most significant histological predictor of subclinical cervical lymph node metastasis in early squamous carcinomas of the oral cavity. European Journal of Surgical Oncology 2006 9;32(7):795-803.
(61) Fagan JJ, Collins B, Barnes L, D'Amico F, Myers EN, Johnson JT. Perineural invasion in squamous cell carcinoma of the head and neck. Arch Otolaryngol Head Neck Surg 1998 Jun;124(6):637-640.
(62) Han A, Ratner D. What is the role of adjuvant radiotherapy in the treatment of cutaneous squamous cell carcinoma with perineural invasion? Cancer 2007;109(6):1053-1059.
(63) Liao C, Chang JT, Wang H, Ng S, Hsueh C, Lee L, et al. Does Adjuvant Radiation Therapy Improve Outcomes In pT1-3N0 Oral Cavity Cancer With Tumor-Free Margins and Perineural Invasion? International Journal of Radiation Oncology*Biology*Physics 2008 6/1;71(2):371-376.
(64) Le Tourneau >, Jung G, Borel C, Bronner G, Flesch H, Velten M. Prognostic factors of survival in head and neck cancer patients treated with surgery and postoperative radiation therapy. Acta Otolaryngol 2008 01/01;128(6):706-712.
(65) Shimizu K, Inoue H, Saitoh M, Ohtsuki N, Ishida H, Makino K, et al. Distribution and impact of lymph node metastases in oropharyngeal cancer. Acta Otolaryngol 2006 01/01;126(8):872-877.
(66) Puri SK, Fan CY, Hanna E. Significance of extracapsular lymph node metastases in patients with head and neck squamous cell carcinoma. Curr Opin Otolaryngol Head Neck Surg 2003 Apr;11(2):119-123.
(67) Coatesworth AP, MacLennan K. Squamous cell carcinoma of the upper aerodigestive tract: The prevalence of microscopic extracapsular spread and soft tissue deposits in the clinically N0 neck. Head Neck 2002;24(3):258-261.
(68) Johnson JT, Barnes EL, Myers EN, Schramm VL,Jr, Borochovitz D, Sigler BA. The extracapsular spread of tumors in cervical node metastasis. Arch Otolaryngol 1981 Dec;107(12):725-729.
(69) Myers JN, Greenberg JS, Mo V, Roberts D. Extracapsular spread. Cancer 2001;92(12):3030-3036.
(70) Gil Z, Fliss DM. Contemporary management of head and neck cancers. Isr Med Assoc J 2009 May;11(5):296-300.
(71) Rack B, Janni W, Gerber B, Strobl B, Schindlbeck C, Klanner E, et al. Patients with recurrent breast cancer: does the primary axillary lymph node status predict more aggressive tumor progression? Breast Cancer Res Treat 2003 Nov;82(2):83-92.
(72) Margulis V, Sagalowsky AI. Penile Cancer: Management of Regional Lymphatic Drainage. Urol Clin North Am 2010 8;37(3):411-419.
(73) Martin A, Jackel MC, Christiansen H, Mahmoodzada M, Kron M, Steiner W. Organ preserving transoral laser microsurgery for cancer of the hypopharynx. Laryngoscope 2008 Mar;118(3):398-402.

125
(74) Edward BK. National Cancer Institute - Surveillance Epidemiology and End Results. 2010; Available at: http://seer.cancer.gov/csr/1975_2007/index.html. Accessed 08/16, 2010.
(75) Johansen LV, Grau C, Overgaard J. Hypopharyngeal squamous cell carcinoma--treatment results in 138 consecutively admitted patients. Acta Oncol 2000;39(4):529-536.
(76) Wycliffe ND, Grover RS, Kim PD, Simental A,Jr. Hypopharyngeal cancer. Top Magn Reson Imaging 2007 Aug;18(4):243-258.
(77) Karatzanis AD, Psychogios G, Waldfahrer F, Zenk J, Hornung J, Velegrakis GA, et al. T1 and T2 hypopharyngeal cancer treatment with laser microsurgery. J Surg Oncol 2010 Jul 1;102(1):27-33.
(78) Bello IO, Soini Y, Salo T. Prognostic evaluation of oral tongue cancer: Means, markers and perspectives (II). Oral Oncol ;In Press, Corrected Proof.
(79) Yao M, Chang K, Funk GF, Lu H, Tan H, Wacha J, et al. The failure patterns of oral cavity squamous cell carcinoma after intensity-modulated radiotherapy-the university of iowa experience. Int J Radiat Oncol Biol Phys 2007 Apr 1;67(5):1332-1341.
(80) Rusthoven K, Ballonoff A, Raben D, Chen C. Poor prognosis in patients with stage I and II oral tongue squamous cell carcinoma. Cancer 2008;112(2):345-351.
(81) Hahn SS, Spaulding CA, Kim JA, Constable WC. The prognostic significance of lymph node involvement in pyriform sinus and supraglottic cancers. Int J Radiat Oncol Biol Phys 1987 Aug;13(8):1143-1147.
(82) Tankéré F, Camproux A, Barry B, Guedon C, Depondt J, Gehanno P. Prognostic Value of Lymph Node Involvement in Oral Cancers: A Study of 137 Cases. Laryngoscope 2000;110(12):2061-2065.
(83) Layland MK, Sessions DG, Lenox J. The influence of lymph node metastasis in the treatment of squamous cell carcinoma of the oral cavity, oropharynx, larynx, and hypopharynx: N0 versus N+. Laryngoscope 2005 Apr;115(4):629-639.
(84) Bando E, Yonemura Y, Taniguchi K, Fushida S, Fujimura T, Miwa K. Outcome of ratio of lymph node metastasis in gastric carcinoma. Ann Surg Oncol 2002 Oct;9(8):775-784.
(85) Persiani R, Rausei S, Biondi A, Boccia S, Cananzi F, D'Ugo D. Ratio of metastatic lymph nodes: impact on staging and survival of gastric cancer. Eur J Surg Oncol 2008 May;34(5):519-524.
(86) Sianesi M, Bezer L, Del Rio P, Dell'Abate P, Iapichino G, Soliani P, et al. The node ratio as prognostic factor after curative resection for gastric cancer. J Gastrointest Surg 2010 Apr;14(4):614-619.
(87) Chan JK, Kapp DS, Cheung MK, Osann K, Shin JY, Cohn D, et al. The impact of the absolute number and ratio of positive lymph nodes on survival of endometrioid uterine cancer patients. Br J Cancer 2007 Sep 3;97(5):605-611.
(88) Ceelen W, Van Nieuwenhove Y, Pattyn P. Prognostic value of the lymph node ratio in stage III colorectal cancer: a systematic review. Ann Surg Oncol 2010 Nov;17(11):2847-2855.

126
(89) Galizia G, Orditura M, Ferraraccio F, Castellano P, Pinto M, Zamboli A, et al. The lymph node ratio is a powerful prognostic factor of node-positive colon cancers undergoing potentially curative surgery. World J Surg 2009 Dec;33(12):2704-2713.
(90) Vaccaro CA, Im V, Rossi GL, Quintana GO, Benati ML, Perez de Arenaza D, et al. Lymph node ratio as prognosis factor for colon cancer treated by colorectal surgeons. Dis Colon Rectum 2009 Jul;52(7):1244-1250.
(91) Showalter TN, Winter KA, Berger AC, Regine WF, Abrams RA, Safran H, et al. The Influence of Total Nodes Examined, Number of Positive Nodes, and Lymph Node Ratio on Survival after Surgical Resection and Adjuvant Chemoradiation for Pancreatic Cancer: A Secondary Analysis of RTOG 9704. Int J Radiat Oncol Biol Phys 2010 Oct 7.
(92) Murakami Y, Uemura K, Sudo T, Hayashidani Y, Hashimoto Y, Nakashima A, et al. Number of metastatic lymph nodes, but not lymph node ratio, is an independent prognostic factor after resection of pancreatic carcinoma. J Am Coll Surg 2010 Aug;211(2):196-204.
(93) Shrime MG, Ma C, Gullane PJ, Gilbert RW, Irish JC, Brown DH, et al. Impact of nodal ratio on survival in squamous cell carcinoma of the oral cavity. Head Neck 2009 Sep;31(9):1129-1136.
(94) Gil Z, Carlson DL, Boyle JO, Kraus DH, Shah JP, Shaha AR, et al. Lymph node density is a significant predictor of outcome in patients with oral cancer. Cancer 2009;115(24):5700-5710.
(95) Suslu N, Hosal AS, Sozeri B. Prognostic value of metastatic lymph node ratio in node-positive head and neck carcinomas. Am J Otolaryngol 2009 Apr 16.
(96) Patel RS, Clark JR, Dirven R, Wyten R, Gao K, O?Brien CJ. Prognostic factors in the surgical treatment of patients with oral carcinoma. ANZ J Surg 2009;79(1-2):19-22.
(97) Gavilan J, Herranz J, DeSanto LW, Gavilan C editors. Functional and Selective Neck Dissection. New York, Stuttgart: Thieme; 2002.
(98) Kokemueller H, Brachvogel P, Eckardt A, Hausamen J-. Neck dissection in oral cancer—clinical review and analysis of prognostic factors. Int J Oral Maxillofac Surg 2002 12;31(6):608-614.
(99) Patel RS, Clark JR, Gao K, O'Brien CJ. Effectiveness of selective neck dissection in the treatment of the clinically positive neck. Head Neck 2008 Sep;30(9):1231-1236.
(100) Byers RM. Modified neck dissection: A study of 967 cases from 1970 to 1980. The American Journal of Surgery 1985 10;150(4):414-421.
(101) Spiro RH, Morgan GJ, Strong EW, Shah JP. Supraomohyoid neck dissection. The American Journal of Surgery 1996 12;172(6):650-653.
(102) Andersen PE, Warren F, Spiro J, Burningham A, Wong R, Wax MK, et al. Results of selective neck dissection in management of the node-positive neck. Arch Otolaryngol Head Neck Surg 2002 Oct;128(10):1180-1184.
(103) Lindberg R. Distribution of cervical lymph node metastases from squamous cell carcinoma of the upper respiratory and digestive tracts. Cancer 1972 Jun;29(6):1446-1449.

127
(104) Shah JP. Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg 1990 Oct;160(4):405-409.
(105) Candela FC, Kothari K, Shah JP. Patterns of cervical node metastases from squamous carcinoma of the oropharynx and hypopharynx. Head Neck 1990 May-Jun;12(3):197-203.
(106) Shah JP, Candela FC, Poddar AK. The patterns of cervical lymph node metastases from squamous carcinoma of the oral cavity. Cancer 1990;66(1):109-113.
(107) Shah JP. Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg 1990 Oct;160(4):405-409.
(108) Clayman GL, Frank DK. Selective neck dissection of anatomically appropriate levels is as efficacious as modified radical neck dissection for elective treatment of the clinically negatice neck in patients with squamous cell carcinoma of the upper respiratory and digestive tracts. Arch Otolaryngol Head Neck Surg 1998 Mar;124(3):348-352.
(109) Cappiello J, Piazza C, Nicolai P. The spinal accessory nerve in head and neck surgery. Curr Opin Otolaryngol Head Neck Surg 2007 Apr;15(2):107-111.
(110) Kowalski LP, Sanabria A. Elective neck dissection in oral carcinoma: a critical review of the evidence. Acta Otorhinolaryngol Ital 2007 Jun;27(3):113-117.
(111) Kohler HF, Cunha IW, Kowalski LP. Impact of modified radical neck dissections on the number of retrieved nodes, recurrence and survival. Braz J Otorhinolaryngol 2010 Jun;76(3):374-377.
(112) Shepard PM, Olson J, Harari PM, Leverson G, Hartig GK. Therapeutic selective neck dissection outcomes. Otolaryngol Head Neck Surg 2010 May;142(5):741-746.
(113) Fakih AR, Rao RS, Patel AR. Prophylactic neck dissection in squamous cell carcinoma of oral tongue: a prospective randomized study. Semin Surg Oncol 1989;5(5):327-330.
(114) Fakih AR, Rao RS, Borges AM, Patel AR. Elective versus therapeutic neck dissection in early carcinoma of the oral tongue. Am J Surg 1989 Oct;158(4):309-313.
(115) Vandenbrouck C, Sancho-Garnier H, Chassagne D, Saravane D, Cachin Y, Micheau C. Elective versus therapeutic radical neck dissection in epidermoid carcinoma of the oral cavity: results of a randomized clinical trial. Cancer 1980 Jul 15;46(2):386-390.
(116) Yuen AP, Wei WI, Wong YM, Tang KC. Elective neck dissection versus observation in the treatment of early oral tongue carcinoma. Head Neck 1997 Oct;19(7):583-588.
(117) Yuen AP, Ho CM, Chow TL, Tang LC, Cheung WY, Ng RW, et al. Prospective randomized study of selective neck dissection versus observation for N0 neck of early tongue carcinoma. Head Neck 2009 Jun;31(6):765-772.
(118) Kligerman J, Lima RA, Soares JR, Prado L, Dias FL, Freitas EQ, et al. Supraomohyoid neck dissection in the treatment of T1/T2 squamous cell carcinoma of oral cavity. Am J Surg 1994 Nov;168(5):391-394.
(119) Pillsbury HC,3rd, Clark M. A rationale for therapy of the N0 neck. Laryngoscope 1997 Oct;107(10):1294-1315.

128
(120) Cheng A, Schmidt BL. Management of the N0 neck in oral squamous cell carcinoma. Oral Maxillofac Surg Clin North Am 2008 Aug;20(3):477-497.
(121) Kowalski LP, Sanabria A. Elective neck dissection in oral carcinoma: a critical review of the evidence. Acta Otorhinolaryngol Ital 2007 Jun;27(3):113-117.
(122) Greenberg JS, El Naggar AK, Mo V, Roberts D, Myers JN. Disparity in pathologic and clinical lymph node staging in oral tongue carcinoma. Implication for therapeutic decision making. Cancer 2003 Aug 1;98(3):508-515.
(123) Barrs DM, DeSanto LW, O'Fallon WM. Squamous cell carcinoma of the tonsil and tongue-base region. Arch Otolaryngol 1979 Aug;105(8):479-485.
(124) Byers RM, Wolf PF, Ballantyne AJ. Rationale for elective modified neck dissection. Head Neck Surg 1988 Jan-Feb;10(3):160-167.
(125) Ogura JH, Biller HF, Wette R. Elective neck dissection for pharyngeal and laryngeal cancers. An evaluation. Ann Otol Rhinol Laryngol 1971 Oct;80(5):646-650.
(126) Cagli S, Yuce I, Yigitbasi OG, Guney E. Is routine bilateral neck dissection absolutely necessary in the management of N0 neck in patients with supraglottic carcinoma? Eur Arch Otorhinolaryngol 2007 Dec;264(12):1453-1457.
(127) Sklenicka S, Gardiner S, Dierks EJ, Potter BE, Bell RB. Survival Analysis and Risk Factors for Recurrence in Oral Squamous Cell Carcinoma: Does Surgical Salvage Affect Outcome? Journal of Oral and Maxillofacial Surgery 2010 6;68(6):1270-1275.
(128) Lim YC, Koo BS, Choi EC. Bilateral neck node metastasis: a predictor of isolated distant metastasis in patients with oral and oropharyngeal squamous cell carcinoma after primary curative surgery. Laryngoscope 2007 Sep;117(9):1576-1580.
(129) Gonzalez-Garcia R, Naval-Gias L, Rodriguez-Campo FJ, Sastre-Perez J, Munoz-Guerra MF, Gil-Diez Usandizaga JL. Contralateral lymph neck node metastasis of squamous cell carcinoma of the oral cavity: a retrospective analytic study in 315 patients. J Oral Maxillofac Surg 2008 Jul;66(7):1390-1398.
(130) Weiss MH, Harrison LB, Isaacs RS. Use of decision analysis in planning a management strategy for the stage N0 neck. Arch Otolaryngol Head Neck Surg 1994 Jul;120(7):699-702.
(131) Okura M, Aikawa T, Sawai NY, Iida S, Kogo M. Decision analysis and treatment threshold in a management for the N0 neck of the oral cavity carcinoma. Oral Oncol 2009 Oct;45(10):908-911.
(132) Carvalho A, Magrin J, Kowalski L. Sites of recurrence in oral and oropharyngeal cancers according to the treatment approach. Oral Dis 2003;9(3):112-118.
(133) Pointreau Y, Garaud P, Chapet S, Sire C, Tuchais C, Tortochaux J, et al. Randomized trial of induction chemotherapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx preservation. J Natl Cancer Inst 2009 Apr 1;101(7):498-506.
(134) Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefèbvre J, Greiner RH, et al. Postoperative Irradiation with or without Concomitant Chemotherapy for Locally Advanced Head and Neck Cancer. N Engl J Med 2004 05/06;350(19):1945-1952.

129
(135) Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, et al. Postoperative Concurrent Radiotherapy and Chemotherapy for High-Risk Squamous-Cell Carcinoma of the Head and Neck. N Engl J Med 2004 05/06;350(19):1937-1944.
(136) Bernier J, Cooper JS, Pajak TF, van Glabbeke M, Bourhis J, Forastiere A, et al. Defining risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 2005;27(10):843-850.
(137) Kader HA, Mydin AR, Wilson M, Alexander C, Shahi J, Pathak I, et al. Treatment Outcomes of Locally Advanced Oropharyngeal Cancer: A Comparison Between Combined Modality Radio-Chemotherapy and Two Variants of Single Modality Altered Fractionation Radiotherapy. International Journal of Radiation Oncology*Biology*Physics ;In Press, Corrected Proof.
(138) Furness S, Glenny AM, Worthington HV, Pavitt S, Oliver R, Clarkson JE, et al. Interventions for the treatment of oral cavity and oropharyngeal cancer: chemotherapy. Cochrane Database Syst Rev 2010 Sep 8;9:CD006386.
(139) Oliver RJ, Clarkson JE, Conway DI, Glenny A, Macluskey M, Pavitt S, et al. Interventions for the treatment of oral and oropharyngeal cancers: surgical treatment. Cochrane Database Syst Rev 2007 Oct 17;(4)(4):CD006205.
(140) Machtay M, Moughan J, Trotti A, Garden AS, Weber RS, Cooper JS, et al. Factors associated with severe late toxicity after concurrent chemoradiation for locally advanced head and neck cancer: an RTOG analysis. J Clin Oncol 2008 Jul 20;26(21):3582-3589.
(141) Tobias JS, Monson K, Gupta N, MacDougall H, Glaholm J, Hutchison I, et al. Chemoradiotherapy for locally advanced head and neck cancer: 10-year follow-up of the UK Head and Neck (UKHAN1) trial. The Lancet Oncology 2010 1;11(1):66-74.
(142) Bonner JA, Harari PM, Giralt J, Cohen RB, Jones CU, Sur RK, et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. The Lancet Oncology 2010 1;11(1):21-28.
(143) Eriksen JG, Lassen P, Overgaard J. Do all patients with head and neck cancer benefit from radiotherapy and concurrent cetuximab? The Lancet Oncology 2010 4;11(4):312-313.
(144) Harrington KJ. Rash conclusions from a phase 3 study of cetuximab? The Lancet Oncology 2010 1;11(1):2-3.
(145) Tao Y, Daly-Schveitzer N, Lusinchi A, Bourhis J. Advances in radiotherapy of head and neck cancers. Curr Opin Oncol 2010 May;22(3):194-199.

130
Tables
Table 1) Ranking of age-standardized incidence rate of lip, oral cavity, oropharyngeal and laryngeal
cancer in Europe according to GLOBOCAN (2008) ................................................................................ 12
Table 2) Ranking of age-standardized mortality rate for lip, oral cavity, pharyngeal and laryngeal
cancer worldwide according to GLOBOCAN (2008) .............................................................................. 13
Table 3) Ranking of age-standardized mortality rate of lip, oral cavity, oropharyngeal and laryngeal
cancer in Europe according to GLOBOCAN (2008) ................................................................................ 14
Table 4) Staging system of the oral cavity and lip cancers, according to the sixth-edition of the TNM-
Staging System of the International Union Against Cancer (UICC) and the American Joint Committee
on Cancer (AJCC) ................................................................................................................................... 16
Table 5) Staging system of pharyngeal cancers, according to the sixth-edition of the TNM-Staging
System of the UICC and AJCC, *parapharyngeal extension denotes posterolateral infiltration
beyond the pharyngobasilar fascia .................................................................................................. 17
Table 6) Staging system of laryngeal cancers, according to the sixth-edition of the TNM-Staging
System of the UICC and AJCC ................................................................................................................ 18
Table 7) Staging system for lymph nodes of all head and neck sites except nasopharynx, according to
the sixth-edition of the TNM-Staging System of the UICC and AJCC .................................................... 19
Table 8) Staging system for lymph nodes of nasopharyngeal tumor, according to the sixth-edition of
the TNM-Staging System of the UICC and AJCC, *midline nodes are considered to be ipsilateral nodes
............................................................................................................................................................... 19
Table 9) Tumor staging of squamous cell carcinomas in oral cavity, oropharynx, hypopharynx and
larynx ..................................................................................................................................................... 20
Table 10) Tumor staging of nasopharyngeal tumors ............................................................................ 20
Table 11) Borders of neck lymph node regions(10) .............................................................................. 21
Table 12) Classification and terminology of neck dissection(12) .......................................................... 24
Table 13) Distribution of cancer staging in patients ............................................................................. 40
Table 14) Test of normality proving there is no normal dispersion ...................................................... 42
Table 15) Statistic for survival of male, female and overall survival ..................................................... 42
Table 16) Log-Rank test for the impact of tumor localization on overall survival ................................ 44
Table 17) Test of equality of distribution depending on hypopharyngeal cancer or cancer of other
localization ............................................................................................................................................ 45
Table 18) Overall survival depending on localization of oral cavity carcinoma .................................... 46

131
Table 19) Distribution of recurrence, localization of recurrence and number of death according to
localization ............................................................................................................................................ 46
Table 20) Comparison of hypopharyngeal cancer and cancer of other tumor sites in recurrence,
localization of recurrence and number of deaths ................................................................................. 47
Table 21) Percentage of patients suffering a recurrence considering tumor classification ................. 48
Table 22) Percentag of patients dying considering tumor classification .............................................. 49
Table 23) Statistical analysis of disease free survival depending on lymph node status ...................... 50
Table 24) Percentage of patients being alive at the end of follow up considering positive or negative
lymph node status ................................................................................................................................. 51
Table 25) Statistical analysis of median overall survival considering lymph node status ..................... 52
Table 26) Percentage of disease free survival depending on number of positive lymph nodes. ......... 53
Table 27) Statistic of overall survival depending on number of positive lymph nodes (Event = death)
............................................................................................................................................................... 55
Table 28) Statistical analysis for disease free survival depending on lymph node ratio....................... 58
Table 29) Statistical analysis for overall survival depending on lymph node ratio ............................... 58
Table 30) Statistical analysis of conglomerate lymph nodes as prognostic factor for overall survival;
median disease free survival was reduced from 108 months to 29 months ........................................ 63
Table 31) Statistical analysis of histological aspects and occurrence and localization of recurrence .. 64
Table 32) Log-Rank test on effect of radical neck dissection considering number of positive lymph
nodes ..................................................................................................................................................... 70
Table 33) Distribution of tumor classification and lymph node status within stage IV disease treated
with or without radical neck dissection ................................................................................................ 71
Table 34) Percentage of locoregional recurrence free survival depending on type of neck dissection 73
Table 35) Percentage of adjuvant therapy in patients receiving unilateral or bilateral neck dissection
............................................................................................................................................................... 75
Table 36) Chi-Square test did show a significant difference in distribution between patients and
excision of non-lymphatic structures, and therefore could not be analyzed ....................................... 77
Table 37) Statistical analysis of disease free survival considering resection margin ............................ 78
Table 38) Statistical analysis of overall survival considering resection margin..................................... 79
Table 39) Number of patients being treated with or without postoperative adjuvant therapy and
percentage of disease free survival (Event = recurrence) ..................................................................... 81

132
Table 40) Statistical analysis for disease free survival considering resection margin and postoperative
adjuvant therapy ................................................................................................................................... 81
Table 41) Patients at risk depending on adjuvant therapy and resection margin, after 1, 3 and 5 years
............................................................................................................................................................... 83
Table 42) Number of patients being treated with or without postoperative adjuvant therapy and
percentage of overall survival (Event = death) ..................................................................................... 83
Table 43) Percentage of overall survival in patients with or without adjuvant therapy considering
tumor classification ............................................................................................................................... 89
Table 44) Pairwise comparison of overall survival depending on postoperative adjuvant therapy and
tumor classification ............................................................................................................................... 91
Table 45) Statistical analysis of disease free survival in patients with or without postoperative
adjuvant therapy ................................................................................................................................... 93
Table 46) Statistical analysis of overall survival depending on postoperative adjuvant therapy and
lymph node status ................................................................................................................................. 95
Table 47) Adjuvant therapy applied in early stage carcinoma .............................................................. 96
Table 48) Number of recurrence in patients with a stage III or stage IV disease ................................. 97
Table 49) Statistical analysis of disease free and overall survival in stage III/IV patients considering
adjuvant therapy ................................................................................................................................... 99
Table 50) Multivariate data analysis for recurrence free survival ...................................................... 100
Table 51) Multivariate model for recurrence free survival including univariate significant covariables
............................................................................................................................................................. 101
Table 52) Covariables used for multivariate data analysis for overall survival ................................... 101
Table 53) Multivariate model for disease free survival including univariat significant covariables ... 102
Table 54) Covariables used for multivariate data analysis for overall survival ................................... 102
Table 55) Multivariate model for overall survival including univariat significant covariables ............ 103
Table 56) Percentage of recurrence depending on tumor localization ............................................. 104
Table 57) Statistical analysis of overall survival depending on type of recurrence ............................ 105
Table 58) Number and cause of death depending on tumor localization .......................................... 107
Table 59) Number and cause of death depending on tumor classification ........................................ 107
Table 60) Number and cause of death depending on lymph node status .......................................... 108

133
Figures
Figure 1) Worldwide incidence for lip, oral cavity, pharyngeal and laryngeal cancer according to
GLOBOCAN (2008) ................................................................................................................................. 12
Figure 2) Worldwide incidence for lip, oral cavity, pharyngeal and laryngeal cancer according to
GLOBOCAN (2008) ................................................................................................................................. 13
Figure 3) Mortality crude rate from lip, oral cavity and pharynx in Australia, Austria, Canada,
Germany, United Kingdom and United States of America(5) ............................................................... 15
Figure 4) Anatomical subsites of the head and neck region(11) ........................................................... 22
Figure 5) First layer of database with basic information ....................................................................... 28
Figure 6) Second layer of database with tumor specific information ................................................... 29
Figure 7) Third layer of database with information on tumor excision ................................................ 30
Figure 8) Fourth layer of database, holding information on neck dissection ....................................... 31
Figure 9) Fifth layer of database holding information of adjuvant therapy, recurrence and death ..... 32
Figure 10) Sixth layer of database holding additional information ....................................................... 33
Figure 11) Distribution of patients who were neck dissected and included into the study during the
years 1999-2009 .................................................................................................................................... 38
Figure 12) Distribution of sublocalizations: floor of the mouth 26, tongue 40, cheek mucosa 2, lip 6,
soft palate 6, root of tongue 19, lateral pharyngeal wall 2, tonsils 67, nasopharynx 6, sinus piriformis
38, postcricoidal region 1, epiglottis 7, lateral laryngopharyngeal wall 1, supraglottic 15, glottis 27,
transglottic 2, unknown primary 26 ...................................................................................................... 39
Figure 13) Time of follow up in months ................................................................................................ 41
Figure 14) Test of normality .................................................................................................................. 41
Figure 15) 5 year overall survival........................................................................................................... 43
Figure 16) 5 year overall survival considering gender ........................................................................... 43
Figure 17) Kaplan-Meier curve illustrating the overall survival considering tumor localization .......... 44
Figure 18) Small hypopharyngeal cancer compared to small cancer of all other tumor localizations
combined showing a significant difference in outcome (Log Rank = 0.011) ......................................... 45
Figure 19) Kaplan Meier curve illustrating disease free survival considering tumor classification ...... 48
Figure 20) Kaplan Meier curve illustrating overall survival considering tumor classification ............... 49
Figure 21) Kaplan Meier curve illustrating disease free survival considering lymph node status ........ 51

134
Figure 22) Kaplan-Meier curve demonstrating the high impact of positive lymph node status on
overall survival ....................................................................................................................................... 52
Figure 23) Kaplan Meier curve illustrating overall survival considering lymph node status (Log-Rank =
0,001) ..................................................................................................................................................... 53
Figure 24) Kaplan-Meier curve illustrating disease free survival considering number of positive lymph
nodes ..................................................................................................................................................... 54
Figure 25) Kaplan-Meier curve illustrating overall survival considering number of positive lymph
nodes ..................................................................................................................................................... 55
Figure 26) Number of positive lymph nodes excised ............................................................................ 56
Figure 27) Scatter plot of lymph node status and number of lymph nodes excised ............................ 57
Figure 28) Disease free survival and overall survival considering lymph node ratio (Log-Rank = 0,000
for both disease free and overall survival) ............................................................................................ 59
Figure 29) Kaplan-Meier curve illustrating 5 year overall survival depending on stage ....................... 60
Figure 30) Kaplan Meier curve illustrating no impact of tumor grade on disease free survival ........... 61
Figure 31) Kaplan Meier curve illustrating no impact of tumor grade on overall survival (well-
differentiated and undifferentiated tumor grades were excluded out of the graphic on behalf of small
patient number) .................................................................................................................................... 61
Figure 32) Impact of conglomerate lymph nodes on disease free survival .......................................... 62
Figure 33) Impact of conglomerate lymph nodes on 5 year overall survival ........................................ 63
Figure 34) Distribution of types of neck dissections performed (according to the recommendations of
the American Head and Neck Society 2008) ......................................................................................... 65
Figure 35) Kaplan-Meier curve, showing no statistically significant difference in disease free or overall
survival depending on number of excised lymph node levels in patients with a pN0 status. .............. 68
Figure 36) Kaplan-Meier curve, showing no statistically significant difference in disease free or overall
survival depending on number of excised lymph node levels in patients with a pN+ status. .............. 69
Figure 37) Impact of radical neck dissection on overall survival in patients with a positive lymph node
status (Log-Rank = 0,74) ........................................................................................................................ 70
Figure 38) Kaplan-Meier curve illustrating the negative effect of radical neck dissection on disease
free survival (Log-Rank = 0,002) ............................................................................................................ 71
Figure 39) Overall survival of patients with stage IV disease depending on type of neck dissection
(Log-Rank = 0,115) ................................................................................................................................. 72
Figure 40) Kaplan-Meier curve illustrating similar run of curves between different types of neck
dissection, considering adjuvant therapy ............................................................................................. 74

135
Figure 41) Locoregional recurrence free survival considering type of neck dissection ........................ 75
Figure 42) Overall survival of patients with clinical contralateral negative neck depending on
unilateral or bilateral neck treatment (Log-Rank = 0,973) .................................................................... 76
Figure 43) Kaplan-Meier curve of disease free survival considering resection margin ........................ 78
Figure 44) Kaplan-Meier curve of overall survival considering resection margin ................................. 80
Figure 45) Kaplan-Meier curve illustrating the bad prognosis on disease free survival of patients with
a R1 resection margin and no additional treatment compared to patients with negative resection
margins (Log-Rank = 0,000) ................................................................................................................... 82
Figure 46) Kaplan-Meier curve illustrating the effect of adjuvant therapy in positive resection margin
(Log-Rank = 0.313 for R0 vs. R1) ............................................................................................................ 82
Figure 47) Kaplan-Meier curve illustrating the bad prognosis on overall survival of patients with a R1
resection margin and no additional treatment compared to patients with negative resection margins
(Log-Rank = 0,000) ................................................................................................................................. 84
Figure 48) With adjuvant therapy, R1 and R0 did not show a statistical significant difference (Log-
Rank = 0,088) in overall survival, while R2 remained a strong prognostic impact on overall survival
(Log-Rank = 0,002 compared to R0 and 0,015 compared to R1) .......................................................... 85
Figure 49) Number of patients treated with postoperative adjuvant therapy ..................................... 86
Figure 50) Number of patients treated with carboplatin/5FU, Cisplatin or Erbitux ............................. 87
Figure 51) Overall effect of adjuvant therapy ....................................................................................... 88
Figure 52) Effect of postoperative adjuvant therapy in pT1 tumor patients (Log-Rank = 0,151) ......... 90
Figure 53) Effect of postoperative adjuvant therapy in pT2 tumor patients (Log-Rank = 0,016) ......... 90
Figure 54) Kaplan-Meier curve illustrating overall survival depending on tumor classification of
patients receiving no additional postoperative treatment ................................................................... 91
Figure 55) Kaplan-Meier curve illustrating overall survival depending on tumor classification of
patients receiving no additional postoperative treatment ................................................................... 92
Figure 56) Kaplan-Meier curve illustrating disease free survival without postoperative adjuvant
therapy considering positive or negative lymph node status (Log-Rank = 0,000) ................................ 93
Figure 57) Kaplan-Meier curve illustrating disease free survival in patients receiving postoperative
adjuvant therapy considering positive or negative lymph node status (Log-Rank = 0,317) ................. 94
Figure 58) Kaplan-Meier curve illustrating the statistically significant impact on postoperative
adjuvant therapy in patients with a positive lymph node status (Log-Rank = 0,004) ........................... 94
Figure 59) Difference in run of curves depending on postoperative adjuvant therapy in patients with a
pathological positive neck (Log-Rank = 0,420) ...................................................................................... 96

136
Figure 60) Kaplan-Meier curve illustrating impact of adjuvant therapy in early stage cancer on overall
survival .................................................................................................................................................. 97
Figure 61) Disease free survival of patients with stage III or stage IV disease considering adjuvant
therapy (Log-Rank = 0,004) ................................................................................................................... 98
Figure 62) Kaplan-Meier curve illustrating different run of curves considering adjuvant therapy in
stage III and stage IV disease, however, Log-Rank test did not reach statistical significance (Log-Rank
= 0,245) .................................................................................................................................................. 99
Figure 63) Kaplan-Meier curve illustrating overall survival depending on type of recurrence (Log-Rank
= 0,000) ................................................................................................................................................ 106
Figure 64) Number of patients dying after recurrence depending on type of recurrence ................. 106