
Immunological Approach in the Evaluation of Regional Lymph Nodes of Patients with Squamous Cell...
11
Immunological Approach in the Evaluation of Regional Lymph Nodes of Patients with Squamous Cell Carcinoma of the Head and Neck Emma Verastegui,* ,1 Rocio Morales,* Jose ´ Luis Barrera,² Anja Mu ¨ eller,‡ John Hadden, 2 Beatriz Guzman,* Abelardo Meneses,§ and Guillermo Alfaro ¶ *Department of Immunology, ²Division of Surgery, and §Division of Pathology, Instituto Nacional de Cancerologia, Avenida San Fernando 22, Tlalpan, 14000 Me ´xico City, D.F., Me ´xico; ‡Department of Radiation Oncology, Heinrich-Heine University, Moorenstrasse 5, D40225 Du ¨ sseldorf, Germany; and ¶ Department of Immunology, Instituto de Investigaciones Biomedicas, Avenida San Fernandozz, Universidad Nacional Autonoma de Mexico, Mexico City 014000, Mexico In cancer, regional lymph node (LN) cells are one of the first components of the immune system to have contact with tumor cells or their products. Therefore, the phenotype and functional properties of hemato- poietic cells present within the tumor-draining LN are important to understanding their role in the control of malignant cells. Based on the locoregional metastatic behavior of squamous cell carcinoma of the head and neck (SCCH&N) region, we analyzed tumor-draining lymph nodes from SCCH&N patients to obtain insights into regional tumor immunity. Using a three-color flu- orescent labeling technique, surface antigen expres- sion was visualized in mononuclear cells of lymph nodes that were obtained from head and neck cancer patients and compared to mononuclear cells of normal lymph nodes. Cell cycle analyses were performed us- ing propidium iodide. Proliferation after phytohemag- glutinin stimulation was measured by a sodium tetra- zolium-based assay. LN histology was correlated with flow cytometric findings. Regional lymph nodes of head and neck cancer patients undergo morphologic and functional changes. Flow cytometry revealed a decrease in CD8 1 T cells and in some lymph nodes the presence of second or third populations of larger cells with distinct size and granularity that expressed both T(gd/ab) and different natural killer cell markers. Moreover, cell cycle analyses and proliferation assays showed a diminished response to mitogenic stimuli. These changes were found in both metastatic and hy- perplastic lymph nodes from head and neck cancer patients; however, no alterations were found in con- trol lymph nodes or peripheral blood mononuclear cells from noncancer patients. The immune alter- ations detected in lymphocytes present within the draining lymph nodes of head and neck cancer pa- tients may improve our understanding of how tumor cells escape host immunosurveillance. However, this dysfunction in local draining lymph nodes may not be detected systemically. © 2001 Elsevier Science Key Words: head and neck; cancer; lymph nodes; flow cytometry; T-cell subsets. INTRODUCTION The highly specialized cellular and anatomical orga- nization of lymph nodes (LN) facilitates the interaction of antigens and/or antigen-presenting cells with lym- phocytes. Since T and B lymphocytes express specific and clonally distributed antigen receptors, stimulation with foreign or self-modified molecules may induce lo- cal immune responses. Activated lymphoid cells are characterized by the initiation of several rounds of proliferation, the synthesis and secretion of soluble molecules, and the generation of memory cells (1, 2). The migration of hematopoietic cells into and out of the lymph nodes is determined by the interaction of specialized molecules expressed on the cell surface with their corresponding ligands expressed by antigen- presenting or endothelial cells (3). While some of these molecules are constitutively expressed, others are in- duced upon antigen recognition and may contribute to the differential expression of cell surface proteins by down-regulating preexisting molecules (4 –7). There- fore, it is conceivable that characterization of the res- idential LN lymphocytes may help in understanding the role of the immune system in preventing the dis- semination of malignant cells. Although morphological changes within the draining lymph nodes are a common finding in a variety of diseases, they are particularly relevant in cancer. Lo- cal or widespread lymphadenopathy is a hallmark of metastatic activity and has been used as a prognostic factor for the establishment of new therapeutic strat- egies (8, 9). Notably, in cancer patients, changes lead- ing to lymph node hyperplasia are not necessarily ac- companied by the presence of tumor cells (9, 10). These changes may be induced by the interaction of immune cells in response to products secreted by different cel- lular types (10 –14). 1 To whom correspondence should be addressed. Fax: 011 525 513-1623. E-mail: [email protected]. 2 Consultant for the Clinical Immunology Department, Instituto Nacional de Cancerologia. Clinical Immunology Vol. 102, No. 1, January, pp. 37– 47, 2002 doi:10.1006/clim.2001.5130, available online at http://www.idealibrary.com on 1521-6616/01 $35.00 © 2001 Elsevier Science All rights reserved. 37
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Immunological Approach in the Evaluation of Regional Lymph Nodes of Patients with Squamous Cell...

Immunological Approach in the Evaluation of Regional Lymph Nodes
Clinical ImmunologyVol. 102, No. 1, January, pp. 37–47, 2002doi:10.1006/clim.2001.5130, available online at http://www.idealibrary.com on
of Patients with Squamous Cell Carcinoma of the Head and Neck
Emma Verastegui,*,1 Rocio Morales,* Jose Luis Barrera,† Anja Mueller,‡ John Hadden,2 Beatriz Guzman,*Abelardo Meneses,§ and Guillermo Alfaro¶
*Department of Immunology, †Division of Surgery, and §Division of Pathology, Instituto Nacional de Cancerologia, Avenida SanFernando 22, Tlalpan, 14000 Mexico City, D.F., Mexico; ‡Department of Radiation Oncology, Heinrich-Heine University, Moorenstrasse 5,
D40225 Dusseldorf, Germany; and ¶Department of Immunology, Instituto de Investigaciones Biomedicas,Avenida San Fernandozz, Universidad Nacional Autonoma de Mexico, Mexico City 014000, Mexico
In cancer, regional lymph node (LN) cells are one ofdysfunction in local draining lymph nodes may not be
the first components of the immune system to havecontact with tumor cells or their products. Therefore,the phenotype and functional properties of hemato-poietic cells present within the tumor-draining LN areimportant to understanding their role in the control ofmalignant cells. Based on the locoregional metastaticbehavior of squamous cell carcinoma of the head andneck (SCCH&N) region, we analyzed tumor-draininglymph nodes from SCCH&N patients to obtain insightsinto regional tumor immunity. Using a three-color flu-orescent labeling technique, surface antigen expres-sion was visualized in mononuclear cells of lymphnodes that were obtained from head and neck cancerpatients and compared to mononuclear cells of normallymph nodes. Cell cycle analyses were performed us-ing propidium iodide. Proliferation after phytohemag-glutinin stimulation was measured by a sodium tetra-zolium-based assay. LN histology was correlated withflow cytometric findings. Regional lymph nodes ofhead and neck cancer patients undergo morphologicand functional changes. Flow cytometry revealed adecrease in CD81 T cells and in some lymph nodes thepresence of second or third populations of larger cellswith distinct size and granularity that expressed bothT (gd/ab) and different natural killer cell markers.Moreover, cell cycle analyses and proliferation assaysshowed a diminished response to mitogenic stimuli.These changes were found in both metastatic and hy-perplastic lymph nodes from head and neck cancerpatients; however, no alterations were found in con-trol lymph nodes or peripheral blood mononuclearcells from noncancer patients. The immune alter-ations detected in lymphocytes present within thedraining lymph nodes of head and neck cancer pa-tients may improve our understanding of how tumorcells escape host immunosurveillance. However, this
1 To whom correspondence should be addressed. Fax: 011 525513-1623. E-mail: [email protected].
2 Consultant for the Clinical Immunology Department, InstitutoNacional de Cancerologia.
37
detected systemically. © 2001 Elsevier Science
Key Words: head and neck; cancer; lymph nodes; flowcytometry; T-cell subsets.
INTRODUCTION
The highly specialized cellular and anatomical orga-nization of lymph nodes (LN) facilitates the interactionof antigens and/or antigen-presenting cells with lym-phocytes. Since T and B lymphocytes express specificand clonally distributed antigen receptors, stimulationwith foreign or self-modified molecules may induce lo-cal immune responses. Activated lymphoid cells arecharacterized by the initiation of several rounds ofproliferation, the synthesis and secretion of solublemolecules, and the generation of memory cells (1, 2).
The migration of hematopoietic cells into and out ofthe lymph nodes is determined by the interaction ofspecialized molecules expressed on the cell surfacewith their corresponding ligands expressed by antigen-presenting or endothelial cells (3). While some of thesemolecules are constitutively expressed, others are in-duced upon antigen recognition and may contribute tothe differential expression of cell surface proteins bydown-regulating preexisting molecules (4–7). There-fore, it is conceivable that characterization of the res-idential LN lymphocytes may help in understandingthe role of the immune system in preventing the dis-semination of malignant cells.
Although morphological changes within the draininglymph nodes are a common finding in a variety ofdiseases, they are particularly relevant in cancer. Lo-cal or widespread lymphadenopathy is a hallmark ofmetastatic activity and has been used as a prognosticfactor for the establishment of new therapeutic strat-egies (8, 9). Notably, in cancer patients, changes lead-ing to lymph node hyperplasia are not necessarily ac-companied by the presence of tumor cells (9, 10). Thesechanges may be induced by the interaction of immunecells in response to products secreted by different cel-lular types (10–14).
1521-6616/01 $35.00© 2001 Elsevier Science
All rights reserved.

In head and neck cancer, the majority of tumors are TABLE 1
38 VERASTEGUI ET AL.
squamous cell carcinomas that readily metastasizeinto the local draining lymphoid chain (15). The pres-ence of LN metastasis is indicative of poor prognosis,despite the use of combined therapeutic modalities,including radical neck node dissection (16–20).
The purpose of this study was to characterize lym-phocyte populations isolated from regional lymphnodes involved in cellular immunity against tumorcells in patients with squamous cell carcinoma of thehead and neck (SCCH&N). The evaluations were madeby cytometric analyses of T and NK cell surface anti-gens and the proliferative capacity of T cells. The re-sults of these analyses revealed that lymph nodes ofSCCH&N patients contain lower numbers ofCD31CD81 T lymphocytes than normal controls. Fur-thermore, we detected that mononuclear cells in somelymph nodes (13) cluster in a second or a third popu-lation of larger cells with differing granularity. Thosecells expressed both T cells and a higher percentageand heterogeneity of NK surface markers. Thesechanges in cellular populations may have been inducedby an enhanced rate of apoptosis of CD31CD81 T cellsinduced by tumor-released factors or cytokines pro-duced by T helper (TH)2 or natural killer (NK) T cells(21). In addition, cell cycle analyses and proliferationassays showed a diminished response of lymph nodecells to mitogenic stimuli in both metastatic and hy-perplastic lymph nodes from SCCH&N patients,whereas no alterations were found in control lymphnodes or peripheral blood mononuclear cells from non-cancer patients.
MATERIAL AND METHODS
Patients
Thirty patients were selected at random from thosescheduled for surgical treatment for SCCH&N at theInstituto Nacional de Cancerologia. The local EthicsCommittee approved the research protocol, and appro-priate consent from each patient was obtained. A sum-mary of the main clinical characteristics of the patientsand their tumors is presented in Table 1. Control nodeswere obtained from noncancer patients (5) undergoingsurgical procedures of the neck area.
Monoclonal Antibodies
The following monoclonal antibodies were used tocharacterize T cell subsets: CD2, CD3, CD4, and CD8,labeled with FITC, RPE, or RPE-Cy5 (DAKO, Carpen-teria, CA). T cell antigen receptors (TCR) were detectedwith monoclonal antibodies directed against a/b (anti-TCR-a/b-1, recognizes a conformational epitope formedby the TCR and the CD3 e-chain) and g/d (anti-g/d-1,reacts with a framework epitope) (Beckton Dickinson,
San Jose, CA). Anti-CD45RO-RPE and -CD45RA-FITC(Beckton Dickinson, San Jose CA) were used to deter-mine the proportions of memory and naive mononu-clear cell populations present in preparations. Thepresence of NK cells was demonstrated with anti-CD16(DAKO), CD56 (Coulter, Hialeah, FL) (FITC or RPE),and CD57-FITC (Serotec, Kidlington, Oxford, England)to evaluate NK T cells. B cells were detected withanti-CD19-RPE (DAKO). The isotype control used in-cluded IgG1-FITC, IgG1-RPE, and IgG1-RPE/CY(DAKO). These antibodies were used in different com-binations to analyze the lymphocyte populations ineach LN.
Clinical Summary
Patient characteristics Patients Controls
Number 30 5Gender
Male 25 3Female 5 2
AgeMean (range) 61 (25–86) 48 (35–65)
DiagnosisSquamous cell carcinoma 30 0Nontoxic bocio 0 2Lymph node hyperplasia 0 3
Tumor location
Site Number
Larynx 9Oral cavity 20
Tongue 7Retromolar trygone 3Gum 10
Oropharynx 1Tonsil
Clinical stage
T2/N1-N2 T3/N1-N2 T4/N1
Larynx 3 4 2Oral cavity 9 6 5Oropharynx 0 0 1
Lymph node characteristics
Cancer nodes analyzed 38Metastasic 20Sinusoidal hyperplasia 18
Control (noncancer patients)Follicular hyperplasia 5
Note. Principal clinical characteristics of patients from whomlymph nodes were studied. All samples had a histological correlation.None of the lymph nodes obtained as controls was from a patientwith previous malignancy or infectious diseases (bacterial or viral,including HIV).

Samples Studied (red). Electronic compensation was used among the
39EVALUATION OF LN OF SCCH&N
One (22 patients) and in some cases (8 patients) twolymph nodes were collected aseptically. One half of thenode was placed in RPMI 1640 media for further anal-ysis and the other half was fixed and processed forhistological analysis. Also, from each patient 20 ml ofblood was obtained before surgery and stored at roomtemperature in sterile tubes treated with heparin be-fore being used for evaluation of T cell subsets andproliferation assays.
Control lymph nodes were obtained from noncancerpatients attending the General Hospital and undergo-ing surgery of the neck area. The histologic analyses ofthese samples showed follicular hyperplasia; “normal,”unstimulated LNs were never obtained.
Lymphocyte Preparation
Cell suspensions were obtained by disruption of thelymph nodes in tissue culture media, the debris wasremoved by filtration through a stainless steel mesh,and cells were diluted in RPMI. Mononuclear cellswere isolated by centrifugation of cell suspensions lay-ered on Ficoll/Hypaque (Pharmacia, Uppsala, Sweden)(22). Cells were washed (with phosphate-buffered sa-line), and the concentration was adjusted as requiredfor the different assays.
Cell Culture
Cells were cultured in RPMI 1640 supplementedwith sodium pyruvate, nonessential aminoacids, and10% fetal calf serum (all from GIBCO BRL, GrandIsland, NY). Cells were incubated at 37°C in a humid-ified atmosphere with 5% CO2.
Flow Cytometry Analysis
Aliquots of mononuclear cells (MC) (5 3 105) wereincubated with appropriate dilutions of monoclonal an-tibodies for 30 min at 4°C. Subsequently, the cells werewashed, resuspended in 500 ml of PBS/2% formalde-hyde, and stored on ice (23). Flow cytometric analyseswere performed with a FACSort equipped with a15-mW air-cooled 488-nm argon-ion laser. Calibrationsetup was performed using CaliBRITE beads and Au-toCOMP software (all from Becton Dickinson). Sizeand granularity (forward and right-angle scatter char-acteristics) were the parameters used to identify lym-phocyte populations. Care was taken to reset the in-strument before each analysis. If more than one cellpopulation was detected, the corresponding regionswere marked and analyzed separately. Discriminationbetween fluorochromes was made using the followingfilters: 518 nm (green), 560 nm (orange), and 650 nm
fluorescence channels to remove residual spectral over-lap. Fluorescence data (10,000 events) was displayedon four-decade log scales using a Beckton DickinsonFACSort interfaced with a Hewlett–Packard (PaloAlto, CA) 340 computer. Multiparameter data analysiswas performed with LYSYS II software (Becton Dick-inson) (24). For LN cells, pooled data are expressed asmean percentage 6 standard deviation (SD). Periph-eral blood mononuclear cells (PBMC) values are re-ported in absolute numbers of cells/mm3.
Proliferation Assay
Half a million cells were incubated for 72 h in dupli-cates in 96-well flat-bottom microtiter plates containing100 ml of RPMI supplemented with one of the followingconcentrations of phytohemagglutinin (PHA): 0.01, 0.1,1.0, or 10 mg/ml (Murex Biotech Ltd., Dratford, England).Subsequently, 50 ml of XTT (sodium 39-[1-(phenylamino-carbonyl)-3,4-tetrazolium]-bis(4-methoxy-nitro-6) ben-zenesulfonic acid hydrate) (Roche Diagnostics GmbH,Mannheim, Germany) labeling mixture was added andthe reaction mixture was incubated for 4 h. Finally, theincorporation of the dye was measured at 450 nm usingan ELISA reader (Tecan Spectra Classic, Austria). Theresults were expressed as mean percentage 6 SD (25).
Cell Cycle Analysis
The distribution of cells in different phases of the cellcycle was investigated by cytofluometric analysis of theDNA content, using a detergent and proteolytic en-zyme-based technique. Briefly, cell suspensions (1 3106) were incubated in RPMI without or with PHA (1mg/ml) for 48 h, fixed in 70% ethanol, washed, andsuspended in 1 ml of a solution containing appropriateconcentrations of propidiumiodide (PI) and RNase A.After the dye had been incorporated into the DNA, thesamples were analyzed in a Beckton Dickinson FACS-can using a CELL FITT program. Statistical analyseswere conducted using RFIT software (26).
Statistics
Statistical analyses were carried out using InStatGraphPad software. The mean values for each popula-tion were compared with control values using aKruskal–Wallis test.
RESULTS
Histology
The histological analyses of lymph nodes showedsome changes in the architecture and in the types ofcells present. Most LNs without the histologic evidence

40 VERASTEGUI ET AL.
of neoplasm showed sinusoidal hyperplasia (47%) (Fig.1A); the presence of hypoplastic follicles (Figs. 1B and1C) was observed in both tumor-free and metastaticregional nodes. The presence of squamous cell carci-noma metastasis in the lymph node was documented in53% of the nodes studied (Figs. 1D and 1E). In thosecases in which nodal neoplasic involvement waspresent, at least 75% of the lymph node was tumor free.
FIG. 1. Histologic evaluation of representative lymph nodes obtainode with sinusoidal hyperplasia; (B) hypoplasic follicle and sinushypoplasic follicle in a metastatic lymph node (tumor cells not shownI) (2503, H&E); (E) tumor cell contact with lymphoid cells (3003, H
Control nodes (5) were reported with follicular hyper-plasia (data not shown); normal unstimulated LNswere never obtained.
Cell Size and Immunophenotype
Mononuclear cells (MNC) of lymph nodes from non-cancer patients (Fig. 2A) and from the majority of
from SCCH&N patients showing: (A) hyperplasic tumor-free lymphl hyperplasia (Level I) (2503, hematoxylin and eosin (H&E)); (C)
D) subcapsular metastasis of SCC and sinusoidal hyperplasia (Level).
nedoida); (&E

patients with SCCH&N (Fig. 2B) clustered as a homo- These changes did not correlate with the anatomical
41EVALUATION OF LN OF SCCH&N
geneous population located between 200 and 600 FSC-HFSC-height linear scale. In 13 lymph nodes (43%) ofSCCH&N patients, two or three distinct cell clusterswere detected and will be referred to hereafter as P1,P2, and P3 (Figs. 2C and 2D).
The average number of gated events was similar innoncancer LNs (5462.14 gated events) and in LNs ob-tained from cancer patients (5963.52 gated events).The nodes with more than one population had a highernumber of gated events (;7378) that were distributedbetween the different clusters: P1 (3106), P2 (2507),and P3 (1765).
The cell surface phenotype analyses of MNC fromhyperplastic lymph nodes obtained from patients withdiseases other than cancer were distributed as follows:CD31 (76%), CD41 (58%), and CD81 (19%), with aCD4/CD8 ratio of 3:1 (Table 2). Lymph nodes fromindividuals with SCCH&N showed a nonsignificant de-crease in CD31 and CD41 T cells (56 and 45%, respec-tively); however, the number of CD81 lymphocytes wassignificantly lower than in control lymph nodes (5%,P , 0.001), and the CD4/CD8 ratio was of 9:1 (Table 2).
FIG. 2. Cytofluorometric evaluation by size and granularity of LNLN cells from control noncancer patients (A) and tumor-bearing patiobtained from SCCH&N patients showed two (C) (P1 and P2) or thgranularity. The figure shows representative data of four different p
locations of the tumors. Notably, when two lymphnodes were obtained from the same patient (n 5 8), theLNs marked as proximal to the tumors (Level I)showed a more pronounced decrease in CD81 cell sub-sets than did lymph nodes in Level III (Table 2) (moredistal from the tumors).
Lymph nodes with more than one cell populationwere different; cells within P1 were smallerCD31CD41 lymphocytes (Fig. 3A), with varying butconsistently low numbers of cells expressingCD31CD81 (Figs. 3B and 3C), having similar charac-teristics to those found in lymph nodes with a singlecell population. The cells in P2 and P3 were larger andmore heterogeneous, as determined by the pattern ofexpression of T cell surface markers and the differ-ences in the intensity of fluorescence. The total numberof CD31 cells exceeded (;17%) the sum of CD31CD41
and CD31CD81 lymphocytes (Figs. 3D, 3E, and 3F). Itis possible that these CD31 cells may correspond todouble-negative T cells and/or to a subset of nonclassi-cal NK cells.
NC showing single or multiple cell populations in lymph nodes. Mosts (B) clustered in a single homogeneous population. Some LN MNC
(D) populations of cells (P1 , P2, and P3), as defined by size andents.
Mentreeati
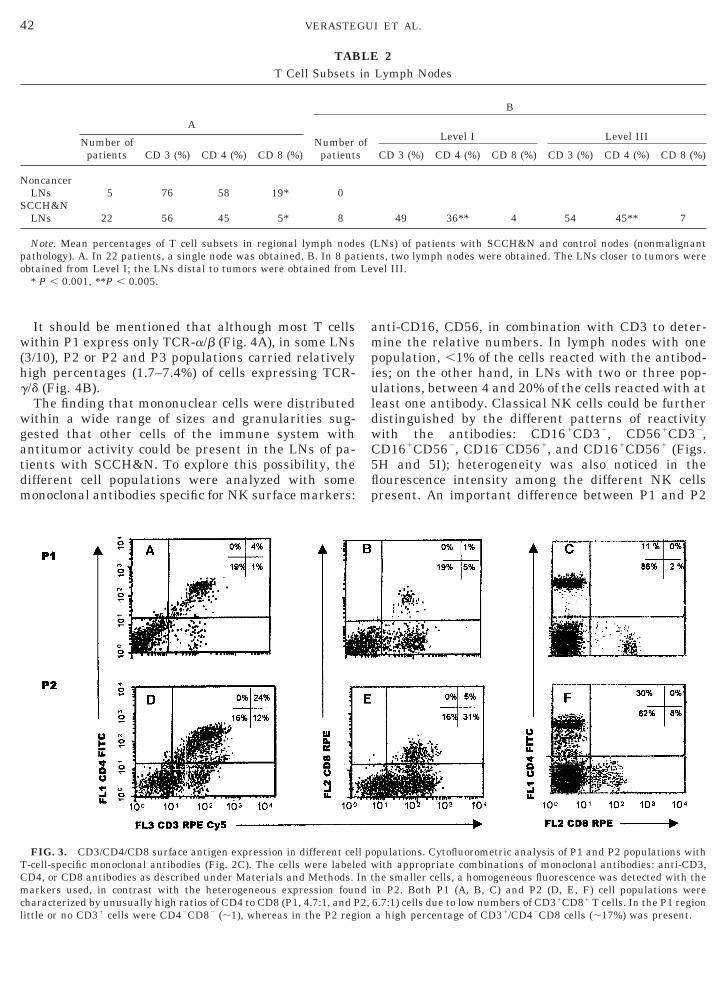
TABLE 2
42 VERASTEGUI ET AL.
It should be mentioned that although most T cellswithin P1 express only TCR-a/b (Fig. 4A), in some LNs(3/10), P2 or P2 and P3 populations carried relativelyhigh percentages (1.7–7.4%) of cells expressing TCR-g/d (Fig. 4B).
The finding that mononuclear cells were distributedwithin a wide range of sizes and granularities sug-gested that other cells of the immune system withantitumor activity could be present in the LNs of pa-tients with SCCH&N. To explore this possibility, thedifferent cell populations were analyzed with somemonoclonal antibodies specific for NK surface markers:
FIG. 3. CD3/CD4/CD8 surface antigen expression in different ceT-cell-specific monoclonal antibodies (Fig. 2C). The cells were labelCD4, or CD8 antibodies as described under Materials and Methods.markers used, in contrast with the heterogeneous expression founcharacterized by unusually high ratios of CD4 to CD8 (P1, 4.7:1, and Plittle or no CD31 cells were CD42CD82 (;1), whereas in the P2 reg
T Cell Subsets
A
Number ofpatients CD 3 (%) CD 4 (%) CD 8 (%)
Numberpatient
NoncancerLNs 5 76 58 19* 0
SCCH&NLNs 22 56 45 5* 8
Note. Mean percentages of T cell subsets in regional lymph nodpathology). A. In 22 patients, a single node was obtained. B. In 8 paobtained from Level I; the LNs distal to tumors were obtained from
* P , 0.001, **P , 0.005.
anti-CD16, CD56, in combination with CD3 to deter-mine the relative numbers. In lymph nodes with onepopulation, ,1% of the cells reacted with the antibod-ies; on the other hand, in LNs with two or three pop-ulations, between 4 and 20% of the cells reacted with atleast one antibody. Classical NK cells could be furtherdistinguished by the different patterns of reactivitywith the antibodies: CD161CD32, CD561CD32,CD161CD562, CD162CD561, and CD161CD561 (Figs.5H and 5I); heterogeneity was also noticed in theflourescence intensity among the different NK cellspresent. An important difference between P1 and P2
opulations. Cytofluorometric analysis of P1 and P2 populations withith appropriate combinations of monoclonal antibodies: anti-CD3,
he smaller cells, a homogeneous fluorescence was detected with thein P2. Both P1 (A, B, C) and P2 (D, E, F) cell populations were6.7:1) cells due to low numbers of CD31CD81 T cells. In the P1 regiona high percentage of CD31/CD42CD8 cells (;17%) was present.
Lymph Nodes
B
Level I Level III
CD 3 (%) CD 4 (%) CD 8 (%) CD 3 (%) CD 4 (%) CD 8 (%)
49 36** 4 54 45** 7
LNs) of patients with SCCH&N and control nodes (nonmalignantts, two lymph nodes were obtained. The LNs closer to tumors werevel III.
ll ped wIn td2,
ion
in
ofs
es (tienLe

present time, the analysis of lymph nodes in cancer is
43EVALUATION OF LN OF SCCH&N
and P3 was that the latter two carried onlyCD561CD162 NK cells (Fig. 5J). Differences in func-tion among these subtypes were not analyzed.
An interesting find in some lymph nodes (5/38) wasthe presence of CD571 cells; these cells were CD571/CD31 (data not shown), CD571CD41 (Figs. 6B and 6C),or CD571CD81 (Fig. 6E). Most CD41CD571 were abun-dant small mononuclear cells located in the P1 region(Fig. 6B), in contrast to CD571CD81, which were largercells gated in the P3 region.
Cell Cycle Analyses and Proliferation Assays
Under basal conditions, both lymph nodes and bloodsamples obtained from SCCH&N patients and patientswith nonmalignant disease contained similar numbersof cells in one of the following phases of the cell cycle:G1, S, G2–M. However, after stimulation with PHA,only PBMC from cancer patients and normal donorsinitiated a new round of proliferation, as determinedby the increase of cells in the S and G2–M phases, whileMNC obtained from cancer patient lymph nodes didnot show any changes when compared to basal condi-tions (Table 3). These findings were confirmed in pro-liferation assays using XTT: LN cells obtained fromSCCH&N patients proliferated poorly or showed noresponse to PHA (data not shown). Conversely, normalproliferative responses were observed in PBMC fromboth cancer and noncancer patients, with no differ-ences among the two groups (data not shown).
DISCUSSION
The importance of the regional lymph nodes in pa-tients with cancer is well established; the presence oftumor cells in the regional LNs is a frequent findingthat is usually seen as a poor prognostic factor andcorrelates with decreased survival (16–20). At the
FIG. 4. TCR expression by lymphocytes isolated from lymphnodes from patients with SCCH&N. Most T cells expressed ab-subunits (90%) (A); however, a small but easily detectable subgroupof cells [;5–10%] carried TCR-gd (B).
a routine histologic procedure that focuses on the de-tection of tumor cells, with constant innovation in tech-niques to improve accuracy (27).
Although the lymph nodes are essential for the ini-tiation of immune responses, their role in tumor con-trol is not fully understood. The events taking place inthe LNs in order to mount an efficient immune re-sponse are dynamic and require certain local environ-mental conditions (28). The lymphocytes may reach,transit, and leave the LN under the influence of signalsprovided by cytokines, chemokines, extracellular ma-trix proteins, and receptors expressed by endothelialcells (29–34).
It has been shown recently that by taking advantageof the same or similar mechanisms that direct thetrafficking of lymphoid cells into the LNs, tumor cellsmay gain access to them (35). The cellular events tak-ing place once the cancer cell reaches the LN are illdefined, and, although the possibility of sensitization ofspecific lymphoid cells by tumor antigens has beenpointed out recently (36), the presence of lymph nodemetastasis is seen as a failure of the body’s immunesurvillance. Furthermore, the role that uninvolved yetstimulated lymph nodes play in the control or progres-sion of malignant diseases is even less understood.Thus, a dynamic view of the LN microenvironmentmay help to understand regional immune responsesand LN pathology.
In this study, microscopic examination of lymphnodes showed patterns suggestive of a regional im-mune response induced by tumor cells and/or unknownantigens in both metastatic and hyperplastic lymphnodes of head and neck cancer patients. However, thehistologic observations in the tumor-free cancer nodes(hypoplastic follicles, sinusoidal hyperplasia) com-pared with those found in LNs form noncancer patients(follicular hyperplasia) suggest that the immune re-sponse in draining cervical lymph nodes may be influ-enced by tumor-related factors contributing to func-tional abnormalities and to cell distribution.
Furthermore, cytofluorometric analyses of lymphnodes from head and neck cancer patients revealed adecreased percentage of CD81 T cells compared to con-trol lymph nodes from noncancer patients. The mech-anism(s) involved in this response may be complex andin vitro correlation may not be precise; suppression bytumor-related factors, signal transduction alterations,or the immunosuppressive effect mediated by cyto-kines is important to consider (21, 37–39). Severalauthors have reported a selective depletion of CD81 Tcells as a consequence of chronic antigenic stimulationand the induction of cell death signals (40). The possi-bility that tumor antigens may be the source of thisstimulation in the cervical nodes of patients withSCCH&N, inducing the death of antigen-specific CD81
cells, requires further exploration.

44 VERASTEGUI ET AL.
FIG. 5. Heterogeneity of NK cells. In those LN with multiple clusters (A), a higher percentages of NK cells was found (5–20%). These NKcells were a heterogeneous population detected with appropriate combinations of CD16 and CD56 monoclonal antibodies (classical NK) (B–J).Some cells showed, additionally, T cell markers (CD3) (B–G). Heterogeneity was also due to differences in the intensity of expression of thedifferent antigenic determinants (B–J).
FIG. 6. Three cell populations of LN (A), showing the presence of NK T CD41 cells (B, C), and CD81CD571 cells (E).

analyzed in all the lymph nodes, the five lymph nodesTABLE 3
45EVALUATION OF LN OF SCCH&N
Key to understanding the mechanism of immunesurveillance is the identification of regulatory cyto-kines and their sources. The low number of CD81 Tcells may be the result of a CD41 T-cell-mediatedmechanism/dysfunction. In head and neck cancer pa-tients the decreased ability of the lymph node cells toproliferate suggests functional abnormalities of thepredominant T cell population (CD31/CD41 cells) (41–43).
The dynamic processes that contribute to the popu-lation of lymph nodes (28) may be influenced by thepresence of the tumor or tumor-related factors andfavor the homing of the heterogeneous cell populationsdetected in the present work; their role in tumor-drain-ing lymph nodes needs to be further evaluated. The g/dT cells may have been driven to the lymph nodes by“stress” signaling under conditions of CD3/CD8 deple-tion and may represent a compensatory immune mech-anism directed against tumor metastasis (44). Al-though NK cells are not frequently present in lymphnodes, this work shows the presence of a higher per-centage of NK cells, mostly in those nodes with two orthree cell populations. The LNs analyzed showed het-erogeneous classical NK populations as defined by dif-ferent combinations of surface markers. Several mech-anisms may have contributed to their presence in theregional LNs, and the cell surface markers expressedcould represent different functional types that inhibitor stimulate the cytotoxic effect against tumor cells(45–47).
The simultaneous expression of specific T cell (CD3)and NK (CD16, CD56) surface molecules suggest thepresence of NK T cells; their presence may contributeto a novel immune surveillance mechanism, but theymay be responsible for some of the alterations detected.Recent evidence from experimental animal studiessuggest that CD41 NK T cells may suppress T-cyto-toxic, mediated antitumor immunity in an IL-13-de-pendent manner (48). Although in this work the pres-ence of CD41/CD571 cells (NK T cells) was not
Cell Cycle Analyses of Regional Lymph Nodes and PBMC
Number ofpatients
Cell cycle phases
G1 G2-M S
LN 8Basal 89% 3% 5%Post-PHA 90% 5% 8%
PBMC 32Basal 82% 11% 7%Post-PHA 69% 21% 10%
Note. Cell cycle distribution of peripheral blood mononuclear cells(PBMC) and mononuclear cells of regional lymph nodes, before andafter PHA stimulation.
from cancer patients analyzed for these surface mark-ers showed increased percentages of CD571 cells. Mostof them were CD571/CD31/CD41/CD82 cells.
Our results, together with the findings in the litera-ture, suggest that this NK T cell population may havealtered the function of other hematopoietic cells withinthe LNs, and, as a consequence, facilitated the estab-lishment of metastases (49–51). Whether thesechanges in lymph node T cells reflect a state of anergyor simply different metabolic conditions characteristicof the LNs remains to be determined.
In peripheral blood mononuclear cells, no alterationswere detected regarding the numbers or functions ofthe different lymphocyte populations. Although we didnot analyze distant lymph nodes, the findings pre-sented here and those reported by others suggest thatthe functional alterations of immune cells may not besystemic, but rather local or zonal within the lym-phatic drainage of the tumor (52).
Conclusions
The differences observed in lymph node T cells fromhead and neck cancer patients suggest that the capac-ity to respond to antigenic stimulation may be dimin-ished and may therefore facilitate metastasis.
ACKNOWLEDGMENT
This work was funded by the Clinical Research Division, InstitutoNacional de Cancerologia, Instituto de Investigaciones Biomedicas,UNAM.
REFERENCES
1. Vitetta, E. S., Berton, M. T., Burger, C., Kepron, M., et al.,Memory B and T cells. Annu. Rev. Immunol. 9, 193–217, 1991.
2. Kelsoe, G., Life and death in germinal certer (redux). Immunity4, 107–111, 1996.
3. Young, A. J., The physisiology of lymphocyte migrationthrough the single lymph node in vivo. Semin. Immunol. 11,73– 83, 1999.
4. McHeyzer-William, M. G., and Davis, M. M., Antigen specificdevelopment of primary and memory T cells in vivo. Science 268,106–111, 1995.
5. Chaplin, D. D., and Yanf-xi, F., Cytokine regulation of secundarylymphoid organ development. Curr. Opin. Immunol. 10, 289–297, 1998.
6. Mac Lennan, I. C. M., Germinal centers. Annu. Rev. Immunol.12, 117–139, 1994.
7. Liu, Y. J., Grouuarrd, G., de Boutellier, O., and Banchereau, J.,Follicular dendritic cells and germinal centers. Int. Rev. Cytol.166, 139–179, 1996.
8. Jess, R. H., and Fletcher, G. H., Treatment of the neck in pa-tients with squamous cell carcinoma of the head and neck. Can-cer 39, 868–872, 1977.
9. Pohris, E., Eichhorn, T., Glanz, H., and Kleinsasser, O., Immu-nohistological reaction patterns of cervical lymph nodes in pa-

tients with laryngeal carcinomas. Arch. Otorhinolaryngol. 244,278–283, 1987.
transcriptase–polymerase chain rection. Cancer Res. 15, 3417–3420, 1995.
46 VERASTEGUI ET AL.
10. Patt, B. S., Close, L. G., and Vuitch, F., Prognostic significance ofsinus histiocytosis in metastatic laryngeal cancer. Laryngoscope103, 498–502, 1993.
11. Eremin, O., Roberts, P., Plumb, D., and Sthephens, P., Humanregional tumor lymph nodes: Alterations of microarchitectureand lymphocyte subpopulations. Br. J. Cancer 40, 62–72,1980.
12. Lores, B., Garcia-Estebez, J. M., and Arias, C., Lymph nodes inhuman tumors. Int. J. Mol. Med. 1, 729–733, 1998.
13. O’Sullivan, G., Corbett, A. R., Sdhanahan, F., and Colins, K.,Regional immune suppression in esophageal squamous cancer:Evidence from functional studies with matched lymph nodes.J. Immunol. 157, 4717–4720, 1996.
14. Hadden, J. W., The immunopharmacology of head and neckcancer: An update. Int. J. Immunopharmacol. 19, 629–644,1997.
15. Shantz, S., Harrison, L. B., and Forastiere, A. A., Tumors of thenasal cavity and paranasal sinuses, nasopharynx, oral cavityand oropharynx. In “Cancer Principles and Practice of Oncology”(V. T. De Vita, S. Hellman, and S. A. Rosenberg, Eds.), 5th ed.,pp. 741–801, Lippincott, Philadelphia, 1997.
16. Gluckman, J. L., Crissman, J. D., and Donegan, J. O., Thesurgical management of early oral cavity cancers. In “Head andNeck Cancer” (J. T. Johnson, and M. S. Didolkar, Eds.), Vol. 3,pp. 329–331, Elsevier, Amsterdam, 1999.
17. Gluckman, J. L., Management of advanced cancer of head andneck. In “Current Therapy in Otolaryngology—Head and NeckSurgery” (G. Gates, Ed.), Vol. 3, pp. 99–102, Decker, Trenton,NJ, 1986.
18. O’Brien, C. J., Smith, J. W., and Soong, S. J., et al., Neckdissection with or without radiotherapy-prognostic factors, pat-tern of recurrence and survival. Am. J. Surg. 152, 456–463,1986.
19. Shah, J. P., Strong, E., Spiro, R. H., and Vikram, B., Neckdissection: Current status and future possibilities. Clin. Bull. 11,25–33, 1981.
20. Barrera Franco, J. L., Granados Garcıa, M., Herrera Gomez, A.,et al., Tratamiento neoadyuvante en el carcinoma epidermoidede cabeza y cuello: Experiencia del Instituto Nacional de Can-cerologia. Rev. Inst. Nal. Cancerol. 44, 9–14, 1998.
21. Terabe, M., Matsui, S., Noben-Trauth, N., and Chen, H., et al.,NKT cell-mediated repression of tumor immunosurviallance byIL-13 and the IL-4R-STAT6 pathway. Nat. Immunol. 1, 515–520,2000.
22. Boyum, A., Separation of lymphocytes from blood and bone mar-row. Scand. J. Clin. Lab. Invest. Suppl. 97, 51–76, 1968.
23. Holmes, K., and Fowlkes, B. J., Preparation of cells and reagentsfor flow cytometry. In “Current Protocols in Immunology,” (J. E.Coligan, A. M. Kruisbeek, D. H. Margulles, E. M. Shevac, and W.Strober, Eds.), pp. 5.3.1–5.3.7, Wiley, New York, 1991.
24. Yokoyama, W. M., Flow cytometry analysis using Beckton Dick-inson FACScan. In “Current Protocols in Immunology” (J. E.Coligan, A. M. Kruisbeek, D. H. Margulles, E. M. Shevac, and W.Strober, Eds.), pp. 5.4.1–5.4.9, Wiley, New York, 1991.
25. Nogushi, P. D., Use of flow cytometry for DNA analysis. In“Current Protocols in Immunology” (J. E. Coligan, A. M. Kruis-beek, D. H. Margulles, E. M. Shevac, and W. Strober, Eds.), pp.5.7.1–5.7.5, Wiley, New York, 1991.
26. Shankey, T. V., Rabinovich, P. S., Bagwell, B., and Bauer, K. D.,et al., Guidelines for implementation of clinical DNA cytometry.Cytometry 12, 472–477, 1993.
27. Mori, M., Mimori, K., Inoue, H., and Barnard, G. F., et al.,Detection of cancer micrometastases in lymph nodes by reverse
28. Fu, Y.-X., and Chaplin, D. D., Development and maturation ofsecondary lymphoid tissues. Annu. Rev. Immunol. 17, 399–433,1999.
29. Stamper, H. B., and Woodruff, J. J., Lymphocyte homing intolymph nodes: In vitro demonstartion of selectivity affinity ofrecirculating lymphocytes for high endotehlial venules. J. Exp.Med. 144, 828–833, 1976.
30. Tangemann, K., Tam, C., Cyster, J. G., Rosen, S. D., and Wil-liam, L. T., A chemokine expressed in lymphoid high endothelialvenules promotes the adhesion and chemotaxis of naive T lym-phocytes. Proc. Natl. Acad. Sci. USA 95, 258–263, 1998.
31. Zlotnik, A., and Yoshie, O., Chemokines: A new classificationand their role in immunity. Immunity 12, 121–127, 2000.
32. Young, A. J., The physiology of lymphocyte migration throughthe single lymph node in vivo. Semin. Immunol. 11, 73– 83,1999.
33. Costanos-Velz, E., Biberfeld, P., and Patarroyo, M., Extracellu-lar matrix proteins and integrin receptors in reactive and non-reactive lymph nodes. Immunology 86, 270–278, 1995.
34. Jeltsch, M., Kaipainen, A., Joukov, V., and Meng, X., et al.,Hyperplasia of lymphatic vessels in VEGF-C transgenic mice.Science 276, 1423–1425, 1997.
35. Muller, A., Homey, B., Soto, H., and Ge, N., et al., Involvement ofchemokine receptors in breast cancer metastasis. Nature 410,50–56, 2001.
36. Santin, A. D., Lymph node metastases: The importance of themicroenviroment. Cancer 88, 175–179, 2000.
37. Lapointe, H., Lampe, H., and Banerjee, D., Head and neck squa-mous cell carcinoma cell line-induced suppression of in vitrolymphocyte proliferative response. Otolaryngol. Head NeckSurg. 106, 149–158, 1992.
38. Whiteside, T. L., Immune cells in the tumor microenviroment:Mechanism responsible for functional and signal defects. Adv.Exp. Med. Biol. 451, 167–171, 1998.
39. Sloan-Lancaster, J., Evavold, B. D., and Allen, P. M., Inductionof T cell anergy by altered T cell receptor ligand on live antigenpresenting cells. Nature 363, 156, 1993.
40. Akbar, A. N., Borthwick, N., Salmon, M., and Gombert, W., et al.,The significance of low bcl-2 expression by CD45RO T cells innormal individuals and patientes with acute viral infectionas.The role of apoptosis in T cell memory. J. Exp. Med. 178, 427,1993.
41. Altfeld, M., and Rosemberg, E. S., The role of CD41 T helper cellsin the cytotoxcic T lymphocyte responses to HIV. Curr. Opin.Immunol. 12, 375–380, 2000.
42. Matloubian, M., Concepcion, R. J., and Ahmed, R., CD41 T cellsare required to sustain cytotoxic T cell responses during chronicviral infection. J. Virol. 68, 8056–8063, 1994.
43. Tatake, R. J., Krishnan, N., Rao, R. S., and Fakih, A. R., et al.,Lymphokine activated killer cell function of lymphocytesfrom peripheral blood, regional lymph nodes and tumor tissuesof patients with oral cancer. Int. J. Cancer 43, 560–566, 1989.
44. Laad, A. D., Thomas, M. L., Fakih, A. R., and Chiplunkar, S. V.,Human gamma delta cells recognize heat shock protein-60 onoral tumor cells. Int. J. Cancer 80, 709–714, 1999.
45. Thrinchieri, G., Biology of natural killer cells. Adv. Immunol. 47,187–376, 1989.
46. Raulet, D. H., Vance, R. E., and McMahon, C. W., Regulation ofthe natural killer cell repertoire. Annu. Rev. Immunol. 19, 291–330, 2001.

47. Moretta, A., Biassoni, R., Bottino, C., and Moretta, L., Surfacereceptors delivering opposite signals regulate the function of
50. Moodycliffe, A. M., Nghiem, D., Clydesdale, G., and Ulrich, S. E.,Immune suppression and skin cancer development: Regulation
47EVALUATION OF LN OF SCCH&N
human NK cells. Semin. Immunol. 12, 129–138, 2000.48. Terabe, M., Matsui, S., Noben-Traith, N., and Chen, H., et al.,
NK T cell mediated repression of tumor immunosurveillance byIL-13 and the IL-4R-STAT6 pathway. Nat. Immunol. 1, 515–520,2000.
49. Vicari, A. P., and Zlotnik, A., Mouse NK1.1-T-cells: A new familyof T cells. Immunol. Today 17, 71–76, 1996.
Received June 1, 2001; accepted with revision September 25, 2001; pub
by NKT cells. Nat. Immunol. 1, 521–525, 2000.51. Yoshimoto, T., Bendelac, A., Watson, C., Hu-Li, J., and Paul,
W. E., Role of NK1.1 T cells in a Th2 response and in immuno-globulin IgE production. Science 270, 1845–1847, 1995.
52. Schuller, D. E., Koolemans-Beynen, A. R., Libby, D. H., et al.,Impact of metastases on nodal immunoreactivity in head andneck cancer. Laryngoscope 96, 1189–1192, 1986.
lished online December 5, 2001




















