Seroepidemiology of dengue fever in Khyber Pakhtunkhawa, Pakistan
6
Seroepidemiology of dengue fever in Khyber Pakhtunkhawa, Pakistan Amjad Ali a , Habib ur Rehman b , Muhammad Nisar a,c , Shazia Rafique d , Sadia Ali c , Abrar Hussain e , Nausheen a,c , Muhammad Idrees e, *, Sabeen Sabri f , Hakeem Zada g , Shah Hussain a a Department of Biotechnology University of Malakand, Chakdara, Khyber Pakhtunkhawa, Pakistan b District Head Quarter Hospital, Mardan, Khyber Pakhtunkhawa, Pakistan c Department of Botany, University of Malakand, Chakdara, Khyber Pakhtunkhawa, Pakistan d Centre for Applied Molecular Biology, Ministry of Science and Technology, Thokar Niaz Baig, Lahore, Pakistan e Division of Molecular Virology, National Centre of Excellence in Molecular Biology, University of the Punjab, 87 West Canal Bank Road, Thokar Niaz Baig, Lahore 53700, Pakistan f Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore, Pakistan g Department of Microbiology, Abasyn University, Peshawar, Khyber Pakhtunkhawa, Pakistan International Journal of Infectious Diseases 17 (2013) e518–e523 A R T I C L E I N F O Article history: Received 13 July 2012 Received in revised form 27 December 2012 Accepted 9 January 2013 Corresponding Editor: Ziad Memish, Riyadh, Saudi Arabia Keywords: Dengue fever Seroprevalence IgM IgG Clinical signs Travel history Residence Khyber Pakhtunkhawa S U M M A R Y Background: Dengue is the most important vector-borne disease in many different parts of the world and is expanding into other areas of the globe without hindrance. The morbidity and mortality due to dengue complications are increasing globally at an alarming rate. Although transmission of the dengue virus has been documented in well-characterized areas of Pakistan, its incidence in Khyber Pakhtunkhawa has not been characterized. To address this issue we aimed to determine the seroprevalence of dengue (IgM and IgG) antibodies and the disease symptoms in the population of Khyber Pakhtunkhawa, and to investigate the incidence of dengue fever in different seasons and in urban as well as in rural areas. Methods: From August to October 2011, data of suspected dengue patients were collected from different primary, secondary, and tertiary collection centers situated in Khyber Pakhtunkhawa in order to determine the actual seroprevalence of dengue antibodies (IgM and IgG) in Khyber Pakhtunkhawa. Results: A total 612 subjects with a suspected infection were enrolled in our study. Of the 612 suspected cases, 319 were found positive for dengue IgG, IgM, or both IgG and IgM. The overall weighted prevalence of dengue-specific antibodies (IgM and/or IgG) was 52.12%. Overall, of the 52.12%, 31.86% (95% confidence interval (CI) 28.17–35.55) were positive for dengue IgM and 20.26% (95% CI 17.03–23.39) were positive for dengue IgG. Only 23 (3.75%) samples showed both IgG and IgM antibodies. A higher prevalence of IgM (39.35%, 95% CI 32.84–45.86) and IgG (22.42%, 95% CI 16.86–27.98) antibodies was found in the age group 21–30 years as compared to the children age group (10 years) and the oldest age group (51 years). The mean age of the febrile cohort was 53.16 44.22 years, ranging from 4 to 85 years. Age group was not statistically associated with IgM (p = 0.64) or IgG (p = 0.49) positivity. A higher seroprevalence of IgM (37.24%, 95%CI 32.84–45.86) was observed in males as compared to females (IgM 17.88%, 95% CI 11.11–24.65) while higher seroprevalnce of IgG (22.76%, 95% CI 15.35–30.17) was seen in females as compared to males (IgG 17.58%, 95% CI 14.21–20.95). Gender was not significantly associated with IgM (p = 0.06) or IgG (p = 0.53) positivity. Dengue IgM (35.38%, 95% CI 38.61–62.91) and IgG (50.76%, 95% CI 38.61–62.91) were higher in patients who had a history of travel to a dengue endemic area as compared to those who did not (IgM 33%, 95% CI 29.06–36.94, and IgG 15%, 95% CI 12.01–17.99). History of travel to an endemic area was significantly associated with IgM (p = 0.023) and IgG (p = 0.041) positivity. A higher incidence of IgM (41.13%, 95% CI 35.55–46.71) and IgG (27.42%, 95% CI 22.36–32.48) was observed in urban areas than in rural areas (IgM 23%, 95% CI 18.34– 27.66, and IgG 13.41%, 95% CI 9.63–17.19). IgM (p = 0.0005) and IgG (p = 0.0007) positivity was significantly associated with area of residence. Symptoms including fever (p = 0.007), headache (p = 0.001), Skin rash (0.005), joint pain (0.004) and Fatigue were significantly linked to dengue fever. IgM and IgG antibodies were more frequently seen in the post-monsoon season (68.33%) than in the monsoon period (31.68%). The death ratio in the overall weighted prevalence was 2.19%. Conclusion: The results of the present cohort study of febrile subjects show that young people and males are more susceptible to dengue fever. Dengue infection was most prominent in the post-monsoon season, in urban areas, and in patients with a history of travel to an endemic locality. Furthermore seven deaths were found in our cohort study. ß 2013 International Society for Infectious Diseases. Published by Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +92 42 5293141; fax: +92 42 5293149. E-mail address: [email protected] (M. Idrees). Contents lists available at SciVerse ScienceDirect International Journal of Infectious Diseases jou r nal h o mep ag e: w ww .elsevier .co m /loc ate/ijid 1201-9712/$36.00 – see front matter ß 2013 International Society for Infectious Diseases. Published by Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.ijid.2013.01.007
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Seroepidemiology of dengue fever in Khyber Pakhtunkhawa, Pakistan

International Journal of Infectious Diseases 17 (2013) e518–e523
Seroepidemiology of dengue fever in Khyber Pakhtunkhawa, Pakistan
Amjad Ali a, Habib ur Rehman b, Muhammad Nisar a,c, Shazia Rafique d, Sadia Ali c, Abrar Hussain e,Nausheen a,c, Muhammad Idrees e,*, Sabeen Sabri f, Hakeem Zada g, Shah Hussain a
a Department of Biotechnology University of Malakand, Chakdara, Khyber Pakhtunkhawa, Pakistanb District Head Quarter Hospital, Mardan, Khyber Pakhtunkhawa, Pakistanc Department of Botany, University of Malakand, Chakdara, Khyber Pakhtunkhawa, Pakistand Centre for Applied Molecular Biology, Ministry of Science and Technology, Thokar Niaz Baig, Lahore, Pakistane Division of Molecular Virology, National Centre of Excellence in Molecular Biology, University of the Punjab, 87 West Canal Bank Road, Thokar Niaz Baig, Lahore 53700, Pakistanf Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore, Pakistang Department of Microbiology, Abasyn University, Peshawar, Khyber Pakhtunkhawa, Pakistan
A R T I C L E I N F O
Article history:
Received 13 July 2012
Received in revised form 27 December 2012
Accepted 9 January 2013
Corresponding Editor: Ziad Memish,
Riyadh, Saudi Arabia
Keywords:
Dengue fever
Seroprevalence
IgM
IgG
Clinical signs
Travel history
Residence
Khyber Pakhtunkhawa
S U M M A R Y
Background: Dengue is the most important vector-borne disease in many different parts of the world and
is expanding into other areas of the globe without hindrance. The morbidity and mortality due to dengue
complications are increasing globally at an alarming rate. Although transmission of the dengue virus has
been documented in well-characterized areas of Pakistan, its incidence in Khyber Pakhtunkhawa has not
been characterized. To address this issue we aimed to determine the seroprevalence of dengue (IgM and
IgG) antibodies and the disease symptoms in the population of Khyber Pakhtunkhawa, and to investigate
the incidence of dengue fever in different seasons and in urban as well as in rural areas.
Methods: From August to October 2011, data of suspected dengue patients were collected from different
primary, secondary, and tertiary collection centers situated in Khyber Pakhtunkhawa in order to
determine the actual seroprevalence of dengue antibodies (IgM and IgG) in Khyber Pakhtunkhawa.
Results: A total 612 subjects with a suspected infection were enrolled in our study. Of the 612 suspected
cases, 319 were found positive for dengue IgG, IgM, or both IgG and IgM. The overall weighted prevalence
of dengue-specific antibodies (IgM and/or IgG) was 52.12%. Overall, of the 52.12%, 31.86% (95%
confidence interval (CI) 28.17–35.55) were positive for dengue IgM and 20.26% (95% CI 17.03–23.39)
were positive for dengue IgG. Only 23 (3.75%) samples showed both IgG and IgM antibodies. A higher
prevalence of IgM (39.35%, 95% CI 32.84–45.86) and IgG (22.42%, 95% CI 16.86–27.98) antibodies was
found in the age group 21–30 years as compared to the children age group (�10 years) and the oldest age
group (�51 years). The mean age of the febrile cohort was 53.16 � 44.22 years, ranging from 4 to 85 years.
Age group was not statistically associated with IgM (p = 0.64) or IgG (p = 0.49) positivity. A higher
seroprevalence of IgM (37.24%, 95%CI 32.84–45.86) was observed in males as compared to females (IgM
17.88%, 95% CI 11.11–24.65) while higher seroprevalnce of IgG (22.76%, 95% CI 15.35–30.17) was seen in
females as compared to males (IgG 17.58%, 95% CI 14.21–20.95). Gender was not significantly associated with
IgM (p = 0.06) or IgG (p = 0.53) positivity. Dengue IgM (35.38%, 95% CI 38.61–62.91) and IgG (50.76%, 95% CI
38.61–62.91) were higher in patients who had a history of travel to a dengue endemic area as compared to
those who did not (IgM 33%, 95% CI 29.06–36.94, and IgG 15%, 95% CI 12.01–17.99). History of travel to an
endemic area was significantly associated with IgM (p = 0.023) and IgG (p = 0.041) positivity. A higher
incidence of IgM (41.13%, 95% CI 35.55–46.71) and IgG (27.42%, 95% CI 22.36–32.48) was observed in urban
areas than in rural areas (IgM 23%, 95% CI 18.34– 27.66, and IgG 13.41%, 95% CI 9.63–17.19). IgM (p = 0.0005)
and IgG (p = 0.0007) positivity was significantly associated with area of residence. Symptoms including fever
(p = 0.007), headache (p = 0.001), Skin rash (0.005), joint pain (0.004) and Fatigue were significantly linked to
dengue fever. IgM and IgG antibodies were more frequently seen in the post-monsoon season (68.33%) than
in the monsoon period (31.68%). The death ratio in the overall weighted prevalence was 2.19%.
Conclusion: The results of the present cohort study of febrile subjects show that young people and males
are more susceptible to dengue fever. Dengue infection was most prominent in the post-monsoon
season, in urban areas, and in patients with a history of travel to an endemic locality. Furthermore seven
deaths were found in our cohort study.
Contents lists available at SciVerse ScienceDirect
International Journal of Infectious Diseases
jou r nal h o mep ag e: w ww .e lsev ier . co m / loc ate / i j id
ci
� 2013 International So* Corresponding author. Tel.: +92 42 5293141; fax: +92 42 5293149.
E-mail address: [email protected] (M. Idrees).
1201-9712/$36.00 – see front matter � 2013 International Society for Infectious Disea
http://dx.doi.org/10.1016/j.ijid.2013.01.007
ety for Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
ses. Published by Elsevier Ltd. All rights reserved.

A. Ali et al. / International Journal of Infectious Diseases 17 (2013) e518–e523 e519
1. Introduction
Dengue is a most significant febrile illness caused by a singlestranded an enveloped RNA virus belongs to the family Flaviviridae,genus Flavivrus.1 Dengue infection is caused by any one of fourdistinctive antigenically related dengue virus serotypes: DENV-1,DENV-2, DENV-3, and DENV-4.2 Medical manifestations of dengueinfection range from asymptomatic, to mild flu-like symptoms, tosevere life-threatening dengue complications such as dengue shocksyndrome (DSS) and dengue hemorrhagic fever (DHF).3,4 The denguevirus is transmitted to humans through the bite of an infectedmosquito of the genus Aedes (namely Aedes aegypti and Aedes
albopictus) during daylight hours.5 An estimated 50–100 millioncases of dengue fever (DF), 250 000–500 000 of DHF, and 25 000deaths occur each year globally.6 Frequent international/nationaltravel and trade can lead to the movement of viruses and mosquitoesfrom one part of the globe to another, increasing the risk ofepidemics.7 Both viral and host factors are thought to contribute tothe manifestations of the disease in each infected person.8
Since the first isolation of the dengue virus in Japan in 1943, ithas been active sporadically in different parts of the world;however in the last decade, major outbreaks of this highly endemicvirus were seen in many subcontinents.9 The earliest well-knownoutbreak of DHF occurred in the city of Manila, Philippines in1953–1954. It has now been transmitted geographically fromSoutheast Asian states to Asian states including Sri Lanka, India,and Pakistan.10
The first case of DHF in Pakistan was reported in 1994,11 andsince then its prevalence has increased rapidly. It frequently affectsthe older age groups, with the adult to child ratio being 3.3:1.12
Pakistan was considered a non-endemic country until 1993, but isnow considered endemic for dengue.11
In 2005 an outbreak of dengue with DENV-3 serotype wasdocumented in Karachi;13 in the same area, Khan and colleaguesfound co-circulation of serotypes DENV-2 and DENV-3 andconcluded that dengue is now hyperendemic in Pakistan.14 Morerecently, Fatima et al. reported that the most frequent serotypes ofthe dengue virus circulating in the country are DENV-2 and DENV-3. The reported principal genotypes described were subtype IV ofDENV-2 and subtype III of DENV-3.15
Although Pakistan has a history of outbreaks of dengue viralinfection, reported from districts, towns, and cities,11,14–18 not asingle dengue outbreak has been reported from Khyber Pakhtun-khawa Province. To address this issue we aimed to evaluate theseroprevalence of dengue antibodies (IgM and IgG) and the clinicalsymptoms of the disease in the population of Khyber Pakhtun-khawa, and to investigate the incidence of dengue fever in thedifferent seasons and in urban as well as in rural areas. The studydesign and questionnaire were approved by the ethics committeeof the university.
2. Materials and methods
2.1. Study area
Khyber Pakhtunkhawa, formerly known as the North-WestFrontier Province (NWFP), is located in the north-west of Pakistanand is one of the four provinces of the country. It shares boundarieswith Afghanistan to the north-west, Federal Administrative TribalAreas (FATA) to the west and south, Gilgit-Baldistan to the north-east, Azad Jammu and Kashmir to the east, Balochistan to thesouth, and Islamabad Capital Territory and Punjab to the south-east (Figure 1). Khyber Pakhtunkhawa is the third most importantpopulated territory of the country. Pakhtuns form the major part ofthe population, followed by smaller groups such as Hindkowans,Gujjars, Chatralis, and Dards. In this study we evaluated the
seroprevalence of IgM and IgG dengue antibodies specifically in thepopulation of Khyber Pakhtunkhawa.
2.2. Data collection
Data were collected from different primary, secondary, andtertiary collection centers situated in Khyber Pakhtunkhawa,Pakistan. The data were obtained from records and registers/filledforms, and a questionnaire was administered to obtain informationincluding the patient’s gender, clinical manifestations, area ofresidence, admission date, and their history of travel to endemicareas of the country. A total of 612 patients with a suspectedinfection were selected for the study; 489 (79.90%) were males and123 (20.09%) were females. Briefly, 3 ml of venous blood werecollected aseptically then labeled and processed at the differentdiagnostic centers. The blood was centrifuged at 3000 rpm for5 min and the serum was used for the detection of IgG and IgMantibodies against dengue virus using a highly sensitive ELISA kit(Diagnostic Automation, Cortez Diagnostics Inc., CA, USA) inaccordance with the manufacturer’s protocol. The specificity andsensitivity of the IgG ELISA kit are 96% and 100%, respectively, andof the IgM ELISA kit are 100% and 86%, respectively.
2.3. Statistical analysis
The data analysis was done using SPSS v. 16 software. Chi-square analysis was used to determine the relationship betweengender, age group, history of travel to an endemic area, and area ofresidence (urban or rural) and dengue IgM and IgG seroprevalence.Logistic regression analysis was done to investigate various factorsrelated to a positive dengue IgM and IgG. A p-value of <0.05 wasconsidered statistically significant.
3. Results
Sum of 612 dengue suspected subjects were enrolled in thissetup. Of the 612 suspected cases, 319 were seen positive fordengue IgG, IgM, or both IgG and IgM. The entire weightedprevalence of dengue-specific antibodies (IgM and/or IgG) was52.12%. Overall, of the 52.12%, 31.86% (95% confidence interval (CI)28.17–35.55) were positive for dengue IgM and 20.26% (95% CI17.03–23.39) were positive for dengue IgG. Only 23 (3.75%)samples showed both IgG and IgM antibodies.Mean age of febrilecohort was 53.16 � 44.22 years ranging from 4 years to 85 yearsolder.
3.1. Distribution of dengue fever by gender in the different districts of
Khyber Pakhtunkhawa
Serum was collected from 612 suspected dengue patientsfrom the following districts: Peshawar (n = 148), Mansehra(n = 61), Abbottabad (n = 59), Mardan (n = 64), Nowshera(n = 37), Swat (n = 24), Kohat (n = 31), Dir (lower) (n = 22),Haripur (n = 29), Charsadda (n = 24), Shangla (n = 33), Bannu(n = 27), Karak (n = 21), Swabi (n = 15), and Dera Ismail khan(n = 17). A total of 319 (52.12%) samples were found ELISA-positive for dengue antibodies: 195 IgM (31.86%) and 124 IgG(20.26%). The highest seropositivity of IgM and IgG was reportedfrom the district of Peshawar (n = 93, 29.15%), followed byMansehra (n = 40, 12.5%), Abbottabad (n = 39, 12.2%), Mardan(n = 38, 11.9%), Nowshera (n = 17, 5.32%), Swat (n = 14, 4.38%),Kohat (n = 13, 4%), Dir (lower) (n = 13, 4%), Haripur (n = 12,3.76%), Charsadda (n = 10, 13.13%), Shangla (n = 8, 2.50%), Bannu(n = 7, 2.19%), Karak (n = 6,1.88%), Swabi (n = 5,1.56%),and DeraIsmail Khan (n = 4, 1.25%) (Figure 2).
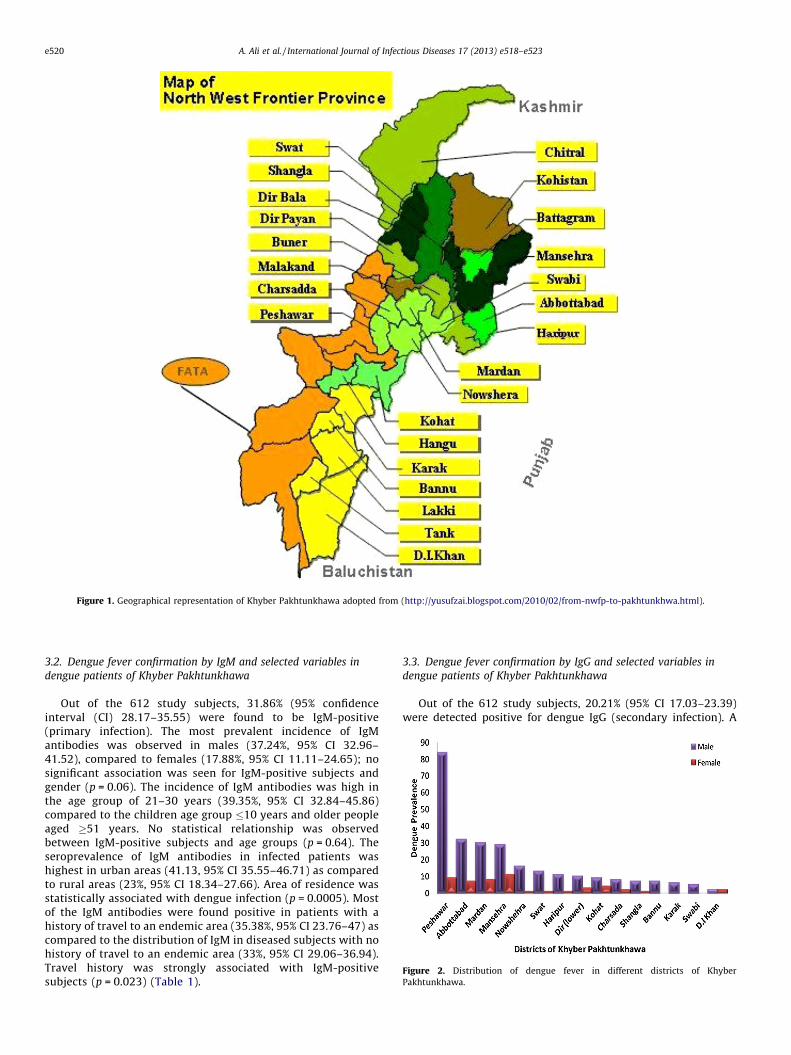
Figure 1. Geographical representation of Khyber Pakhtunkhawa adopted from (http://yusufzai.blogspot.com/2010/02/from-nwfp-to-pakhtunkhwa.html).
Figure 2. Distribution of dengue fever in different districts of Khyber
Pakhtunkhawa.
A. Ali et al. / International Journal of Infectious Diseases 17 (2013) e518–e523e520
3.2. Dengue fever confirmation by IgM and selected variables in
dengue patients of Khyber Pakhtunkhawa
Out of the 612 study subjects, 31.86% (95% confidenceinterval (CI) 28.17–35.55) were found to be IgM-positive(primary infection). The most prevalent incidence of IgMantibodies was observed in males (37.24%, 95% CI 32.96–41.52), compared to females (17.88%, 95% CI 11.11–24.65); nosignificant association was seen for IgM-positive subjects andgender (p = 0.06). The incidence of IgM antibodies was high inthe age group of 21–30 years (39.35%, 95% CI 32.84–45.86)compared to the children age group �10 years and older peopleaged �51 years. No statistical relationship was observedbetween IgM-positive subjects and age groups (p = 0.64). Theseroprevalence of IgM antibodies in infected patients washighest in urban areas (41.13, 95% CI 35.55–46.71) as comparedto rural areas (23%, 95% CI 18.34–27.66). Area of residence wasstatistically associated with dengue infection (p = 0.0005). Mostof the IgM antibodies were found positive in patients with ahistory of travel to an endemic area (35.38%, 95% CI 23.76–47) ascompared to the distribution of IgM in diseased subjects with nohistory of travel to an endemic area (33%, 95% CI 29.06–36.94).Travel history was strongly associated with IgM-positivesubjects (p = 0.023) (Table 1).
3.3. Dengue fever confirmation by IgG and selected variables in
dengue patients of Khyber Pakhtunkhawa
Out of the 612 study subjects, 20.21% (95% CI 17.03–23.39)were detected positive for dengue IgG (secondary infection). A
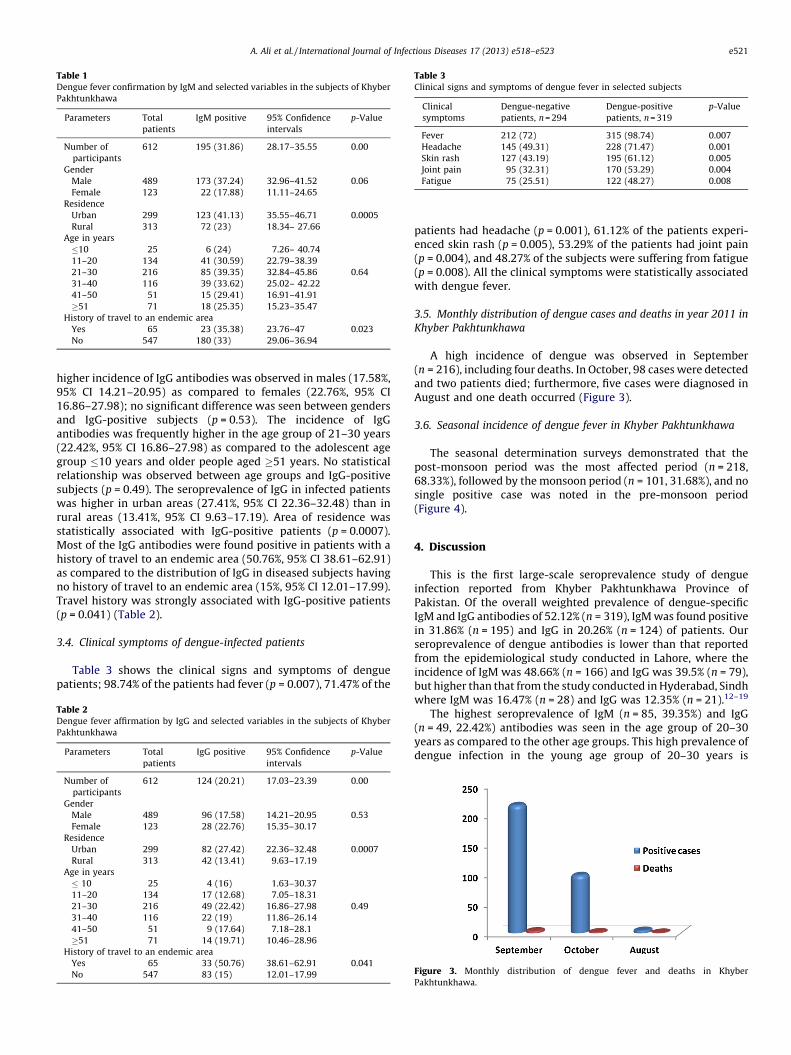
Table 1Dengue fever confirmation by IgM and selected variables in the subjects of Khyber
Pakhtunkhawa
Parameters Total
patients
IgM positive 95% Confidence
intervals
p-Value
Number of
participants
612 195 (31.86) 28.17–35.55 0.00
Gender
Male 489 173 (37.24) 32.96–41.52 0.06
Female 123 22 (17.88) 11.11–24.65
Residence
Urban 299 123 (41.13) 35.55–46.71 0.0005
Rural 313 72 (23) 18.34– 27.66
Age in years
�10 25 6 (24) 7.26– 40.74
11–20 134 41 (30.59) 22.79–38.39
21–30 216 85 (39.35) 32.84–45.86 0.64
31–40 116 39 (33.62) 25.02– 42.22
41–50 51 15 (29.41) 16.91–41.91
�51 71 18 (25.35) 15.23–35.47
History of travel to an endemic area
Yes 65 23 (35.38) 23.76–47 0.023
No 547 180 (33) 29.06–36.94
Table 3Clinical signs and symptoms of dengue fever in selected subjects
Clinical
symptoms
Dengue-negative
patients, n = 294
Dengue-positive
patients, n = 319
p-Value
Fever 212 (72) 315 (98.74) 0.007
Headache 145 (49.31) 228 (71.47) 0.001
Skin rash 127 (43.19) 195 (61.12) 0.005
Joint pain 95 (32.31) 170 (53.29) 0.004
Fatigue 75 (25.51) 122 (48.27) 0.008
A. Ali et al. / International Journal of Infectious Diseases 17 (2013) e518–e523 e521
higher incidence of IgG antibodies was observed in males (17.58%,95% CI 14.21–20.95) as compared to females (22.76%, 95% CI16.86–27.98); no significant difference was seen between gendersand IgG-positive subjects (p = 0.53). The incidence of IgGantibodies was frequently higher in the age group of 21–30 years(22.42%, 95% CI 16.86–27.98) as compared to the adolescent agegroup �10 years and older people aged �51 years. No statisticalrelationship was observed between age groups and IgG-positivesubjects (p = 0.49). The seroprevalence of IgG in infected patientswas higher in urban areas (27.41%, 95% CI 22.36–32.48) than inrural areas (13.41%, 95% CI 9.63–17.19). Area of residence wasstatistically associated with IgG-positive patients (p = 0.0007).Most of the IgG antibodies were found positive in patients with ahistory of travel to an endemic area (50.76%, 95% CI 38.61–62.91)as compared to the distribution of IgG in diseased subjects havingno history of travel to an endemic area (15%, 95% CI 12.01–17.99).Travel history was strongly associated with IgG-positive patients(p = 0.041) (Table 2).
3.4. Clinical symptoms of dengue-infected patients
Table 3 shows the clinical signs and symptoms of denguepatients; 98.74% of the patients had fever (p = 0.007), 71.47% of the
Table 2Dengue fever affirmation by IgG and selected variables in the subjects of Khyber
Pakhtunkhawa
Parameters Total
patients
IgG positive 95% Confidence
intervals
p-Value
Number of
participants
612 124 (20.21) 17.03–23.39 0.00
Gender
Male 489 96 (17.58) 14.21–20.95 0.53
Female 123 28 (22.76) 15.35–30.17
Residence
Urban 299 82 (27.42) 22.36–32.48 0.0007
Rural 313 42 (13.41) 9.63–17.19
Age in years
� 10 25 4 (16) 1.63–30.37
11–20 134 17 (12.68) 7.05–18.31
21–30 216 49 (22.42) 16.86–27.98 0.49
31–40 116 22 (19) 11.86–26.14
41–50 51 9 (17.64) 7.18–28.1
�51 71 14 (19.71) 10.46–28.96
History of travel to an endemic area
Yes 65 33 (50.76) 38.61–62.91 0.041
No 547 83 (15) 12.01–17.99
patients had headache (p = 0.001), 61.12% of the patients experi-enced skin rash (p = 0.005), 53.29% of the patients had joint pain(p = 0.004), and 48.27% of the subjects were suffering from fatigue(p = 0.008). All the clinical symptoms were statistically associatedwith dengue fever.
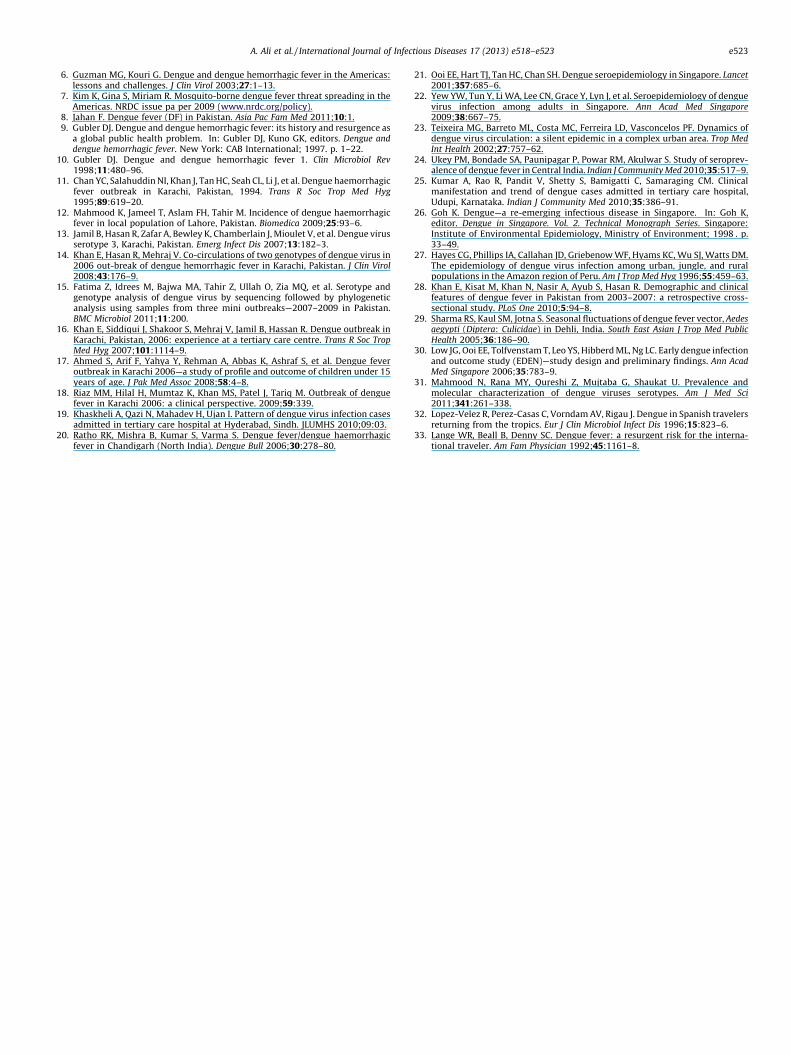
3.5. Monthly distribution of dengue cases and deaths in year 2011 in
Khyber Pakhtunkhawa
A high incidence of dengue was observed in September(n = 216), including four deaths. In October, 98 cases were detectedand two patients died; furthermore, five cases were diagnosed inAugust and one death occurred (Figure 3).
3.6. Seasonal incidence of dengue fever in Khyber Pakhtunkhawa
The seasonal determination surveys demonstrated that thepost-monsoon period was the most affected period (n = 218,68.33%), followed by the monsoon period (n = 101, 31.68%), and nosingle positive case was noted in the pre-monsoon period(Figure 4).
4. Discussion
This is the first large-scale seroprevalence study of dengueinfection reported from Khyber Pakhtunkhawa Province ofPakistan. Of the overall weighted prevalence of dengue-specificIgM and IgG antibodies of 52.12% (n = 319), IgM was found positivein 31.86% (n = 195) and IgG in 20.26% (n = 124) of patients. Ourseroprevalence of dengue antibodies is lower than that reportedfrom the epidemiological study conducted in Lahore, where theincidence of IgM was 48.66% (n = 166) and IgG was 39.5% (n = 79),but higher than that from the study conducted in Hyderabad, Sindhwhere IgM was 16.47% (n = 28) and IgG was 12.35% (n = 21).12–19
The highest seroprevalence of IgM (n = 85, 39.35%) and IgG(n = 49, 22.42%) antibodies was seen in the age group of 20–30years as compared to the other age groups. This high prevalence ofdengue infection in the young age group of 20–30 years is
Figure 3. Monthly distribution of dengue fever and deaths in Khyber
Pakhtunkhawa.

Figure 4. Seasonal occurrence of dengue cases in 2011.
A. Ali et al. / International Journal of Infectious Diseases 17 (2013) e518–e523e522
congruent with previous studies conducted in other epidemiclocalities,20,21 but in contrast with a study conducted in Singaporein which a higher prevalence of IgM and IgG antibodies wereobserved in older aged people.22
A higher incidence of dengue IgM (n = 173, 37.24%) and IgG(n = 96, 17.58%) antibodies was noted among males than females(IgM n = 22, 17.88%; IgG n = 28, 22.76%), which is consistent withother studies conducted in tropical/subtropical countries in whichmales were found to be more susceptible to dengue thanfemales.4,23–26 This difference may be associated with disparitiesin gender-specific contact, according to confined intellectualsettings and daily activities in the outdoors. Disparity by genderwas not statistically significant with IgM (p = 0.06) and IgG(p = 0.53).
Dengue is noticed an urban disease and the deadly diseasepartially attributed to gradually more populated towns in rural areasas well.5 We identified dengue cases during the period of August–October in 2011. Lower percentages of IgM (23%) and IgG (13.41%)dengue antibodies were observed in rural areas compared to urbanareas (IgM 41.13% and IgG 27.42%), in concordance with the study ofHayes et al. who found the dengue antibody seroprevalence to behigher in urban populations as compared to rural populations.27
Residence was significantly associated with IgM (p = 0.0005) and IgG(p = 0.0007) positive subjects. In addition to expanding vectornumbers, improved routes of transportation allow the migration ofviremic humans from one region to another, which might facilitatethe spread of dengue from urban into rural areas.
This outbreak of dengue infection occurred mostly in the post-monsoon period (n = 218, 68.33%) compared to the monsoonperiod (n = 101, 31.68%), which is consistent with previousoutbreaks in Pakistan28 and in the neighboring country of Indiaas well.29 The post-monsoon season is a peak period for dengueinfection due to the high humidity after the rainy season, whichprovides sufficient breeding sites for mosquitoes.
In a study from Singapore, Low et al. reported that fever,headache, joint pain, fatigue, and skin rashes were statisticallyassociated with dengue.30 Similarly, the majority of our entirefebrile cohort were symptomatic and symptoms were statisticallyrelated to dengue infection. Fever, headache, joint pain, andfatigue, as well as skin rashes were statistically linked with dengueinfection. Therefore the detection of a DENV infection should beundertaken for patients who present with a wide variety of signsand symptoms and who inhabit or have passed through a dengueendemic area. Of the 319 patients who had a clinical diagnosis ofDENV infection, seven (2.19%) died and 312 (97.8%) recovered. Allseven of the patients who died presented with fever, fatigue,headache, and skin rash.
One important finding of our study was that the seropreva-lences of IgM (35.38%) and IgG (50.76%) antibodies were higher inpatients who presented a history of travel to an endemic area as
compared to the incidence in patients who presented no suchhistory (IgM 33% and IgG 15%). Moreover travel history wassignificantly associated with IgM (p = 0.023) and IgG (p = 0.041)positive subjects. This observation suggests that the higherprevalence could be because of the heavy load in the floatingpopulation from the dengue epidemic areas of Pakistan wheredengue cases have been diagnosed previously,13–18 and currentlyfrom Punjab where dengue infection hit a large population ofLahore in 2011.31
These results are in agreement with those of several studies onthis topic. Dengue virus is increasingly recognized as the mostprevalent agent of febrile illness in travelers returning from dengueepidemic areas.31–33 Familial outbreaks of dengue viral infectionintroduced through travelers have to be regarded as a potential riskin the non-endemic geographical areas in which competentdengue vectors are already present.
The government and policy makers urgently need to makeextensive efforts towards disease prevention and vector controlthrough biological and/or environmental measures, chemicalmeasures, and education strategies in the community, so thatpatients seek timely medical care, and knowledge of familydispensers/physicians/general practitioners to identify the admis-sion signs and symptoms of dengue viral infection is strengthened.Moreover a strong campaign would be indispensable to increaselocal awareness in the population of this area so that they follow allthe preventive measures against dengue infection to avoid furtherspreading of the virus.
Finally there is an urgent need to conduct further seropreva-lence studies on a large scale to determine the real magnitude ofthe problem. The timely detection and regular management of thiscondition can help to decrease the morbidity and mortality rates tosome extent; without due care, this situation could lead toconsiderable dengue complications in the forms of DHF and DSS infuture episodes.
In conclusion, these results indicate a large earlier exposure ofthe people of Khyber Pakhtunkhawa to dengue infection andhighlight the risks of febrile illness due to the prospect of denguevirus. The present febrile cohort study showed that young peopleand males are more disposed to dengue fever. Dengue infectionwas most frequent in the post-monsoon season, in urban areas, andin patients with a history of travel to an endemic area. Sevenpatients died due to dengue fever in our infected population.Further critical analysis is necessary to characterize the currentdengue virus circulation patterns and to identify the linkedserotypes and genotypes.
Acknowledgements
We are thankful to all the clinicians and paramedical staff ofKhyber Pakhtunkhawa for facilitation and providing data.
Conflict of interest: None of the authors have any conflict ofinterest (financial or personal). No fund was received from anysource for the present study.
References
1. Naeem-Ullah U, Akram W. Dengue knowledge, attitudes and practices inMultan, Pakistan: an urban area at the verge of dengue infestation. PublicHealth 2009;123:452–3.
2. Chakravarti A, Kumaria R, Berry N, Sharma VK. Serodiagnosis of dengue infec-tion by rapid immunochromatography test in a hospital setting in Delhi, 1999–2001. Dengue Bull 2002;26:936–9.
3. Halstead S, Suaya J, Shepard D. The burden of dengue infection. Lancet2007;369:1411–2.
4. Gupta E, Dar L, Kapoor G, Broor S. The changing epidemiology of dengue inDelhi, India. Virol J 2006;3:92.
5. Gubler DJ, Clark GG. Dengue/dengue hemorrhagic fever: the emergence of aglobal health problem. Emerg Infect Dis 1999;52:55–7.
A. Ali et al. / International Journal of Infectious Diseases 17 (2013) e518–e523 e523
6. Guzman MG, Kouri G. Dengue and dengue hemorrhagic fever in the Americas:lessons and challenges. J Clin Virol 2003;27:1–13.
7. Kim K, Gina S, Miriam R. Mosquito-borne dengue fever threat spreading in theAmericas. NRDC issue pa per 2009 (www.nrdc.org/policy).
8. Jahan F. Dengue fever (DF) in Pakistan. Asia Pac Fam Med 2011;10:1.9. Gubler DJ. Dengue and dengue hemorrhagic fever: its history and resurgence as
a global public health problem. In: Gubler DJ, Kuno GK, editors. Dengue anddengue hemorrhagic fever. New York: CAB International; 1997. p. 1–22.
10. Gubler DJ. Dengue and dengue hemorrhagic fever 1. Clin Microbiol Rev1998;11:480–96.
11. Chan YC, Salahuddin NI, Khan J, Tan HC, Seah CL, Li J, et al. Dengue haemorrhagicfever outbreak in Karachi, Pakistan, 1994. Trans R Soc Trop Med Hyg1995;89:619–20.
12. Mahmood K, Jameel T, Aslam FH, Tahir M. Incidence of dengue haemorrhagicfever in local population of Lahore, Pakistan. Biomedica 2009;25:93–6.
13. Jamil B, Hasan R, Zafar A, Bewley K, Chamberlain J, Mioulet V, et al. Dengue virusserotype 3, Karachi, Pakistan. Emerg Infect Dis 2007;13:182–3.
14. Khan E, Hasan R, Mehraj V. Co-circulations of two genotypes of dengue virus in2006 out-break of dengue hemorrhagic fever in Karachi, Pakistan. J Clin Virol2008;43:176–9.
15. Fatima Z, Idrees M, Bajwa MA, Tahir Z, Ullah O, Zia MQ, et al. Serotype andgenotype analysis of dengue virus by sequencing followed by phylogeneticanalysis using samples from three mini outbreaks—2007–2009 in Pakistan.BMC Microbiol 2011;11:200.
16. Khan E, Siddiqui J, Shakoor S, Mehraj V, Jamil B, Hassan R. Dengue outbreak inKarachi, Pakistan, 2006: experience at a tertiary care centre. Trans R Soc TropMed Hyg 2007;101:1114–9.
17. Ahmed S, Arif F, Yahya Y, Rehman A, Abbas K, Ashraf S, et al. Dengue feveroutbreak in Karachi 2006—a study of profile and outcome of children under 15years of age. J Pak Med Assoc 2008;58:4–8.
18. Riaz MM, Hilal H, Mumtaz K, Khan MS, Patel J, Tariq M. Outbreak of denguefever in Karachi 2006: a clinical perspective. 2009;59:339.
19. Khaskheli A, Qazi N, Mahadev H, Ujan I. Pattern of dengue virus infection casesadmitted in tertiary care hospital at Hyderabad, Sindh. JLUMHS 2010;09:03.
20. Ratho RK, Mishra B, Kumar S, Varma S. Dengue fever/dengue haemorrhagicfever in Chandigarh (North India). Dengue Bull 2006;30:278–80.
21. Ooi EE, Hart TJ, Tan HC, Chan SH. Dengue seroepidemiology in Singapore. Lancet2001;357:685–6.
22. Yew YW, Tun Y, Li WA, Lee CN, Grace Y, Lyn J, et al. Seroepidemiology of denguevirus infection among adults in Singapore. Ann Acad Med Singapore2009;38:667–75.
23. Teixeira MG, Barreto ML, Costa MC, Ferreira LD, Vasconcelos PF. Dynamics ofdengue virus circulation: a silent epidemic in a complex urban area. Trop MedInt Health 2002;27:757–62.
24. Ukey PM, Bondade SA, Paunipagar P, Powar RM, Akulwar S. Study of seroprev-alence of dengue fever in Central India. Indian J Community Med 2010;35:517–9.
25. Kumar A, Rao R, Pandit V, Shetty S, Bamigatti C, Samaraging CM. Clinicalmanifestation and trend of dengue cases admitted in tertiary care hospital,Udupi, Karnataka. Indian J Community Med 2010;35:386–91.
26. Goh K. Dengue—a re-emerging infectious disease in Singapore. In: Goh K,editor. Dengue in Singapore. Vol. 2. Technical Monograph Series. Singapore:Institute of Environmental Epidemiology, Ministry of Environment; 1998 . p.33–49.
27. Hayes CG, Phillips IA, Callahan JD, Griebenow WF, Hyams KC, Wu SJ, Watts DM.The epidemiology of dengue virus infection among urban, jungle, and ruralpopulations in the Amazon region of Peru. Am J Trop Med Hyg 1996;55:459–63.
28. Khan E, Kisat M, Khan N, Nasir A, Ayub S, Hasan R. Demographic and clinicalfeatures of dengue fever in Pakistan from 2003–2007: a retrospective cross-sectional study. PLoS One 2010;5:94–8.
29. Sharma RS, Kaul SM, Jotna S. Seasonal fluctuations of dengue fever vector, Aedesaegypti (Diptera: Culicidae) in Dehli, India. South East Asian J Trop Med PublicHealth 2005;36:186–90.
30. Low JG, Ooi EE, Tolfvenstam T, Leo YS, Hibberd ML, Ng LC. Early dengue infectionand outcome study (EDEN)—study design and preliminary findings. Ann AcadMed Singapore 2006;35:783–9.
31. Mahmood N, Rana MY, Qureshi Z, Mujtaba G, Shaukat U. Prevalence andmolecular characterization of dengue viruses serotypes. Am J Med Sci2011;341:261–338.
32. Lopez-Velez R, Perez-Casas C, Vorndam AV, Rigau J. Dengue in Spanish travelersreturning from the tropics. Eur J Clin Microbiol Infect Dis 1996;15:823–6.
33. Lange WR, Beall B, Denny SC. Dengue fever: a resurgent risk for the interna-tional traveler. Am Fam Physician 1992;45:1161–8.