Characterization of the glycoproteins of Crimean-Congo hemorrhagic fever virus
Upload
khangminh22Category
view
1download
0
PDF hosted at the Radboud Repository of the Radboud University
Nijmegen
The following full text is a publisher's version.
For additional information about this publication click this link.
http://hdl.handle.net/2066/146791
Please be advised that this information was generated on 2022-07-08 and may be subject to
change.

Dengue Hemorrhagic Fever in Indonesia
the role of cytokines in plasma leakage, coagulation and fibrinolysis


Dengue Hemorrhagic Fever in Indonesia:
the role of cytokines in plasma leakage, coagulation and
fibrinolysis

Copyright Catharina Suharti. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the author.
ISBN 90 373 0584 9 Publisher: Nijmegen University Press

Dengue Hemorrhagic Fever in Indonesia:
the role of cytokines in plasma leakage, coagulation and fibrinolysis
Een wetenschappelijke proeve op het gebied van de Medische Wetenschappen
Proefschrift
ter verkrijging van de graad van doctor aan de Katholieke Universiteit Nijmegen, volgens besluit van het College van Decanen in het openbaar te verdedigen op
Dinsdag 11 september 2001 des namiddags om 1.30 uur precies
door
Catharina Suharti
geboren op 25 November 1947 te Muntilan, Central Java, Indonesia

Promotores: Prof. Dr. J.W.M, van der Meer Prof. Dr. R.J. Djokomoeljanto (Diponegoro University)
Co-promotores:
Manuscriptcommissie:
Dr. W.M.V. Dolmans Dr. D.P.M. Brandjes (Universiteit van Amsterdam)
Prof. Dr. R. Holdrinet Prof. Dr. L. G. Thijs Prof. Dr. P.M. Hoogerbrugge
The study was supported by a grant from The Royal Netherlands Academy of Arts and Sciences
The studies presented in this thesis were performed at the Departments of Medicine and Paediatrics, Dr. Kariadi Hospital, Diponegoro University, Semarang, Indonesia; the Department of General Internal Medicine, University Medical Centre St. Radboud, Nijmegen, The Netherlands; Department of Internal Medicine, Slotervaart Hospital, Amsterdam, The Netherlands and at the Institute of Virology, Erasmus Medical Centre, Rotterdam, The Netherlands.

To my parents, husband
and all relatives,
and
my institutions
Dr Kanadi Hospital and
Diponegoro University

Contents
Dengue hemorrhagic fever in Indonesia, the role ot cytokines in plasma leakage, coagulation and fibrinolysis.
Chapter 1 Introduction dengue hemorrhagic fever in 8 Indonesia and outline of thesis
Chapter 2 Differential diagnosis of adult dengue 24
infections in Indonesia
Chapter 3 Human hantavirus infections in Indonesia 35
Chapter 4 Clinical picture and risk factors for 38 mortality in dengue shock syndrome
Chapter 5 Cytokine patterns during dengue shock 50 syndrome
Chapter 6 Plasma interleukin-1 receptor antagonist 64 (IL-IRa) concentration is associated with plasma leakage in dengue shock syndrome
Chapter 7 Infectious diseases and coagulation 75 disorders
Chapter 8 Activation ot coagulation factor XI, 97 without detectable contact activation in dengue hemorrhagic fever
Chapter 9 The role of cytokines in activation of 108 coagulation and fibrinolysis in dengue shock syndrome
Chapter 10 Summary and directions for future research Ringkasan Samenvatting
Acknowledgements Curriculum vitae List of publications
120
124 128
132 135 136
Chapter 1
Introduction: dengue hemorrhagic fever in Indonesia and outline of thesis

Introduction: dengue hemorrhagic fever in Indonesia
Illustrative case
Marni, a smart six year old Javanese child m Semarang did not want to go to school because she had fever and headache since 3 days. Her mother decided to bring her to the nearest Puskesmas (Health Centre) The doctor gave her some tablets for fever and asked her to come hack if there was no improvement. Two days later she still had fever and at that lime she looked very ill Her mother brought her hack to the Puskesmas. On examination she had cold extremities and a decreased consciousness. The doctor told the mother to bring her straight to Dr Kanadi Hospital In the outpatient clime Marni was in shock and she was admitted to the Pediatric Intensive Care Unit immediately The blood pressure was 50/30 mmHg Plasma expanders were given, blood for laboratory tests taken and a chest x-ray done Six hours later she had severe hematemesis and melena. Pulse and blood pressure were undetectable The chest x-ray showed bilateral pleural effusion She was given a blood transfusion, but died that same day
The case of Marni reflects the tragedy of severe dengue virus infection (in this case dengue shock syndrome) in children in Indonesia This case is not a rare one, per year in Indonesia 400 to 1200 people die due to this severe virus infection and 34 to 60% of cases are children between 5 and 14 years
Geographical and historical background
Indonesia is an archipelago stretching from latitudes 6° north to 11° south. All areas have a tropical climate. By 1998 census the total population was 204 millions The country is divided into 27 provinces, 306 distncs, 3 911 sub distncs and 67.008 villages (1)
The first major epidemic compatible with and thought possibly to be dengue occurred in Batavia (Jakarta) in 1779 and was reported by David Beylon (2) The disease is characterized by fever, headache, retro-orbital pain, back pain, joint pain and muscular pain, therefore, the disease was designated "knokkelkoorts" (Dutch for knuckle fever) or "break-bone fever" The first outbreaks of Dengue Hemorrhagic Fever (DHF) occurred in Jakarta and Surabaya in 1968, with 54 cases and 24 deaths (3) Since then, the number of reported cases has increased sharply. Outbreaks of the disease occurred in major urban areas, as well as in some rural areas In 1994, the disease had spread to all (27) provinces in Indonesia At present, the disease is endemic in many large cities and small towns (1,4).
Epidemiology of dengue fever and dengue hemorrhagic fever
DHF is now widespread in South-East Asia, the Western Pacific and the Caribbean Indonesia ranks third, based on the number of DHF cases reported to the World Health Organization (WHO) Regional Offices, 1991-1995, ranks first

9
for the number of death, and ranks fourth for the case fatality rate (5) (Table 1 ) Even though the case fatality rate of DHF showed a decreasing trend, during 1968-1988 DHF incidence tended to increase However, following the epidemic of 1988, DHF incidence decreased until 1996, when it increased again, with the highest peak in 1998 (4). (Table 2)
During the early epidemic years, the disease mostly affected children During 1968-1973 about 95 percent of cases were children under 15 years During 1991-1998 most of DHF cases were children of 5-14 years but the proportion of adult cases (> 15 years) showed an increasing trend (4) (Table 3) Epidemics occurred in general during the rainy seasons, beginning after September and reaching its peak in January However, in densely populated urbans areas such as Jakarta and Surabaya, the peak is already reached in June or July, the beginning of the dry season ( 1 )
Four serotypes of dengue virus are found in Indonesia, Den-1, Den-2, Den-3, and Den-4 (1, 4, 6-10) A study of dengue virus conducted in several cities in Indonesia showed that Den-3 was the predominant virus in suspected dengue hemorrhagic fever cases (11, Suharyono W, unpublished data) A study in Jakarta from 1975-1978 showed that 73 of 154 (47 4%) DHF cases and 21 of 30 (70 0%) fatal DHF cases were caused by Den-3 (11) From 680 DHF cases diagnosed on four islands of Indonesia and confirmed by hemagglutination inhibition (HI) test, dengue virus was isolated in 212 The distribution of Den-1, Den-2, Den-3 and Den-4 was 32, 44, 112 and 24 cases, respectively (Suharyono W, unpublished data).
Tablel. DHF cases reported to WHO Regional Offices, 1991-1995 *)
Country
Philippines Vietnam Thailand Laos Kampuchea Myanmar Malaysia Singapore Indonesia India Sn Lanka Americas Pacific Islands
Number of cases
7580 329429 263512 624 15528 25283 13460 9249 110043 35440 3170 18428 948
Number of death
77 1093 801 9 691 901 125 12 2861 65 105 253 6
Case fatality rate (%)
1 0 0 3 0 3 1 4 4 4 36 09 0 1 26 02 3 3 1.4 0.6
*) ReflS

10
Table 2. Number of dengue hemorrhagic fever cases, death and incidence rates in Indonesia, 1968-1999*)
Year
1968 1969 1970 1971 1972
1973 1974 1975 1976 1977
1978 1979 1980 1981 1982
1983 1984 1985 1986 1987
1988 1989 1990 1991 1992
1993 1994 1995 1996 1997 1998 1999
Number of DHF cases
58 167 477 267 1400
10189 4586 4563 4548 7826
6989 3422 5007 5978 5451
13668 12710 13588 16529 23864
47573 10362 22807 21120 17620
17418 18783 35102 45548 31784 72133 21134
Number of death
24 40 90 40 135
470 180 368 214 320
384 165 243 231 255
491 382 460 608 1105
1527 464 821 578 509
418 471 885 1234 705 1414 422
CFR (%)
41.3 23.9 18.8 14.9 9.6
4.6 3.9 8.1 4.7 4.1
5.5 4.8 4.8 3.9 4.7
3.6 3 3.4 3.7 4.6
32 4.5 3.6 2.7 2.9
2.4 2.5 2.5 2.7 2.2 2.0 2.0
Incidence rate/ 100.000 population
0.05 0.14 0.40 0.22 1.14
8.14 3.57 3.47 3.38 5.69
4.96 2.37 3.39 3.96 3.53
8.65 7.86 8.14 9.79 13.50
27.09 6.09 12.70 11.56 9.45
9.17 9.72 18.50 23.22 15.28 35.19 10.17
*) Ref.4
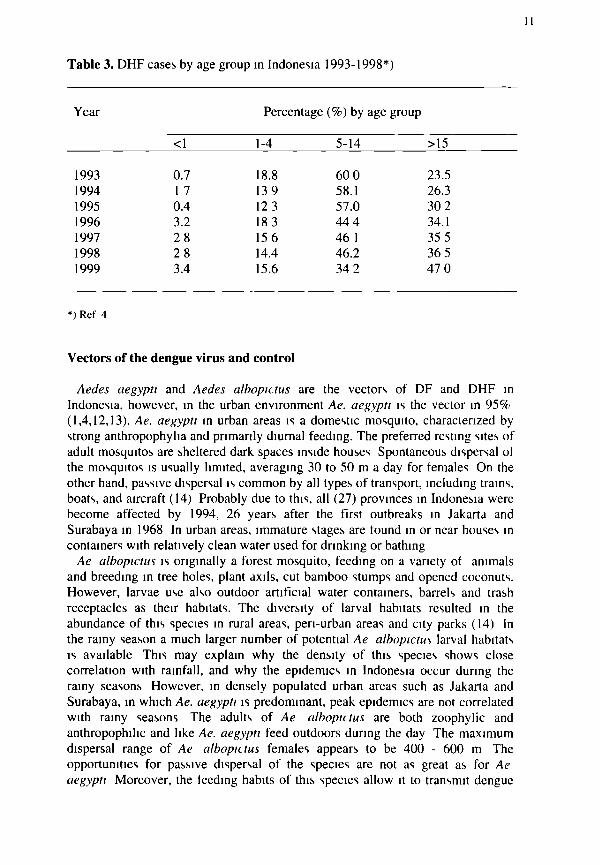
Table 3. DHF cases by age group in Indonesia 1993-1998*)
Year
1993 1994 1995 1996 1997 1998 1999
<1
0.7 1 7 0.4 3.2 28 28 3.4
Percentage
1-4
18.8 139 12 3 183 15 6 14.4 15.6
(%) by
5-14
60 0 58.1 57.0 444 46 1 46.2 34 2
age group
>15
23.5 26.3 30 2 34.1 35 5 36 5 47 0
*) Ref 4
Vectors of the dengue virus and control
Aedes aegypti and Aedes albopittus are the vectors of DF and DHF in Indonesia, however, in the urban environment Ae. aegypti is the vector in 95% (1,4,12,13). Ae. aegypti in urban areas is a domestic mosquito, characterized by strong anthropophylia and primarily diurnal feeding. The preferred resting sites of adult mosquitos are sheltered dark spaces inside houses Spontaneous dispersal ol the mosquitos is usually limited, averaging 30 to 50 m a day for females On the other hand, passive dispersal is common by all types of transport, including trains, boats, and aircraft (14) Probably due to this, all (27) provinces in Indonesia were become affected by 1994, 26 years after the first outbreaks in Jakarta and Surabaya in 1968 In urban areas, immature stages are found in or near houses in containers with relatively clean water used for drinking or bathing
Ae albopictus is originally a forest mosquito, feeding on a variety of animals and breeding in tree holes, plant axils, cut bamboo stumps and opened coconuts. However, larvae use also outdoor artificial water containers, barrels and trash receptacles as their habitats. The diversity of larval habitats resulted in the abundance of this species in rural areas, pen-urban areas and city parks (14) In the rainy season a much larger number of potential Ae albopictus larval habitats is available This may explain why the density of this species shows close correlation with rainfall, and why the epidemics in Indonesia occur during the rainy seasons However, in densely populated urban areas such as Jakarta and Surabaya, in which Ae. aegypti is predominant, peak epidemics are not correlated with rainy seasons The adults of Ae albopictus are both zoophylic and anthropophihc and like Ae. aegypti feed outdoors during the day The maximum dispersal range of Ae albopictus females appears to be 400 - 600 m The opportunities for passive dispersal of the species are not as great as for Ae aegypti Moreover, the feeding habits of this species allow it to transmit dengue

12
viruses from monkey to man, or vice versa (14) The eggs of Ae albopictus can resist desiccation for several months
During a DHF epidemic in Bantul, a densely populated rural area on Central Java in December 1976, both Ae aegypti and Ae albopictus were prevalent, the latter species being more abundant There was considerable overlap in the breeding habitats of the two species in Bantul Preliminary results indicate that in Yogyakarta wells serve as important permanent habitats for Ae Aegypti, especially during the dry season (15).
Dengue control programs centre around vector control through community participation at village level and supervised by Health Center personnel In addition, an early warning system to prevent dengue outbreaks has been established, based on case surveillance and focal control using insecticide fogging in areas within 100 m from the residence of DHF cases Also, health education of the community at village level and of elementary school children has been performed by distribution of teaching materials and posters, as well as through television and radio broadcasting The strategy of dengue prevention and control consist of. (i) to empty and to refill water containers, (n) to cover water containers, (ni) to burry unused articles and all water recepticles which could be possible vector breeding sites such as bottles and tins (I). Vector control programs have not been highly eftective however due to the irregularity of control and limited coverage due to lack of supplies, equipments and budget ( 1, 16, 17)
Surveillance of DHF cases is mostly based on clinically diagnosed cases because only in few patients the diagnosis is confirmed serologically During 1994-1996, a total of 7707 HI tests and 11612 of dengue blot tests were done in Indonesia representing less than 20 percent of suspected DHF cases (4) By clinical picture alone it is difficult to differentiate dengue infections from other hemorrhagic fevers, because signs and symptoms overlap a great deal Thus a simple, rapid, and cheap diagnostic assay is greatly needed tor surveillance
The first generation of on attenuated dengue virus vaccine has been developed at the vaccine center of Mahidol University, Bangkok, Thailand The industrially produced vaccine is undergoing phase II trials in Thai adults for safety, immunogemcity, dose and formula adjustment and will go into phase I trials in children (18, 19) Second generation attenuated dengue virus vaccines are being developed by genetic engineering, and are undergoing preclinical studies (20)
Clinical presentation and case definition
Dengue fever (DF) and DHF are caused by the dengue virus, which belongs to the genus Flavivirus, family Flavivmdae and has tour serotypes- DEN-1, DEN-2, DEN-3 and DEN-4 Dengue virus infections cause a spectrum of illness: asymptomatic infection, mild undifferentiated fever, DF, DHF and dengue shock syndrome (DSS) Dengue fever is charactenzed by fever, headache, joint and muscle pain, and skin rash A positive Tourniquet test and / or petechiae may be present (21, 22) Typical cases of DHF are characterized by tour major clinical manifestations high fever, bleeding, thrombocytopenia (100 000 cells/ mm3 or less) and evidence

of plasma leakage (21, 22) The severity of DHF has been classified into four grades according to two pathophysiological hallmarks, shock and bleeding Grade I cases are characterized by fever accompanied by non-specific constitutional symptoms The only hemorrhagic manifestation is a positive tourniquet test and/or easy bruising Grade II cases are patients with spontaneous bleeding (usually in the skin and / or other hemorrhages) in addition to manifestations as in grade I. Grade III is characterized by circulatory failure, manifested by rapid and weak pulse, narrowing of pulse pressure (20 mmHg or less) or hypotension with the presence of cold clammy skin and restlessness Grade IV cases are characterized by profound shock with undetectable blood pressure and pulse (21,22) DHF I and DHF II during the acute phase of illness are difficult to distinguish from dengue fever or other illnesses found in tropical areas caused by Chikungunya virus, Rickettsia typhi, influenza virus, mild Hantavirus, leptospira infection or Salmonella typhi or paratyphi (typhoid fever) (21,23- 29)
Laboratory diagnosis
The diagnosis of dengue virus infection may be complicated by serological cross reaction with other members of the family Flaviviridae such as Japanese encephalitis (JE) virus JE virus has been isolated from mosquitos in 1974 and anti-JE-antibodies were found among human and pig populations The first two confirmed human JE cases were reported from Bah in 1999 (30) Appropriately timed specimens are needed for virus isolation as well as for serological assays The reliability of laboratory diagnosis depends on the quality of the specimens received, viraemia and antibody responses in dengue infections, as well as optimal procedures for handling of specimens (31) Several tests are used to diagnose dengue infection
Hemagglutination inhibition test (HI) The HI test was developed by Clarke and Casals in 1958 (32) This test detects
IgG antibody, and has become the WHO standard test for the serological confirmation and classification of dengue infections (21) The endpoint of the titration is the highest dilution of serum that inhibits agglutination of a standard amount of antigen Interpretation of the HI test is based on titers and time after onset of disease Fourfold or greater changes in HI titer between paired specimens are considered recent infections In primary infections, detectable HI antibodies generally appear on day six or more after onset of symptoms In secondary or tertiary infections, an anamnestic IgG response may occur, which results in a rapid elevation of the titer within a few days of onset, resulting m a positive HI test in acute phase samples Titers equal to or greater than 1 2560 in a specimen are classified as presumed secondary infections (21) Disadvantages of the HI test are that it is time consuming, that other flaviviruses may cross react and that for a definitive diagnosis acute and convalescent paired specimens of at least 7 days apart are needed (33-37)

14
Enzyme-linked immunosorbent assay (ELISA) The ELISA for IgM antibodies is the most useful serological procedure
available for determining a recent infection with dengue virus. IgM antibody titres to dengue viruses can also be measured by the antibody-capture assay (MAC-ELISA). In this test, IgM antibody is non-specifically captured in the wells of a microliter plate by anti-human IgM antibody. The captured antibody is then exposed to the four dengue antigens, either separately or as a cocktail of four antigens. If anti-dengue IgM antibody is present in the test serum, the antigen is bound and the signal-generating system gives a positive reaction. The latter system usually consists of an anti-dengue or anti-flavivirus antibody conjugated to an enzyme, which produces a colored product (31). This test is rapid and sensitive and as opposed to the HI test, in case IgM is detected, only a single specimen is needed (31, 34-41). The crucial point is the use of appropriately timed specimens, since six days or more after onset of disease are needed to produce detectable antibodies (31, 34, 38, 42, 43). The ELISA for IgG antibodies is sensitive and convenient since many sera may be tested in a single day. No serum processing is required and a few microliters of serum are sufficient for a test (31 ).
Plaque reduction neutralization test (PRNT) The PRNT is a type specific test to diagnose dengue, but the test is technically
complicated. In this test, a diluted heat-inactivated serum is incubated with defined amounts of virus. The non-neutralized viral fraction is subsequently absorbed onto a monolayer of susceptible cells and the resultant plaques are counted. The endpoint of titration is the highest dilution of serum that reduces the number of plaques by 50 to 90 percent (31). Even though the PRNT test is dengue virus type specific, cross-reactivity with other flaviviruses has been observed (44).
Dot blot test and dipstick ELISA These tests are simple and rapid, do not require the equipment needed for
conventional serology and can be performed in a small laboratory or field station. Dot blot tests may detect IgG, while a dipstick ELISA may detect IgM and IgG antibodies. These tests are not practical for testing large series of samples, since individual strips of paper or dip sticks must be used for each serum. In addition, these tests are expensive (31). Compared with IgG/IgM ELISA as a standard, the IgG blot had a sensitivity of 48.8% and specificity of 88,7%. However, in primary dengue infection, the IgG blot had a sensitivity of only 1.7% but of 93.5% in secondary dengue. Therefore, this test is especially useful in secondary dengue infections which are the most common infections in hospitalized cases in Asia (33). With IgG/IgM dipstick ELISA, the sensitivity as well as the specificity appeared to be better. A study on samples collected from 125 individuals living in an area endemic for dengue, the IgG dipstick ELISA showed a sensitivity of 95.2% and a specificity of 100% compared with an IgG microplate ELISA, while an IgM dipstick ELISA showed a sensitivity of 97.9% and specificity of 100% when compared with IgM antibody capture microplate ELISA. Therefore, the

15
IgM/IgG dipstick ELISA is a sensitive and specific test for the detection of dengue IgM and IgG in human serum (45)
Virus isolation Isolation and identification of virus is time consuming, it requires acute phase
specimens, is technically complicated, and only laboratories with insectary facilities or able to provide cell lines can perform the test (7, 31, 42, 43, 46). Three methods are used for dengue virus isolation, namely suckling mouse inoculation, inoculation of cell cultures of either mammalian or insect origin and inoculation of adult or larval mosquitoes The use of Toxorhynchites splendens larvae as the host for inoculation, is considered a rapid and sensitive method for isolation of dengue viruses. Dengue specific monoclonal antibodies are used for identification of the isolated dengue virus
Pathogenesis of dengue hemorrhagic fever and dengue shock syndrome
The pathogenesis of DHF and DSS is still debated. The most commonly accepted hypothesis is immune enhancement or antibody-dependent enhancement (47), implying that patients experiencing a second infection with heterologous dengue virus serotype have a significantly higher risk of developing DHF/DSS Preexisting heterologous dengue antibody recognizes the infecting virus and forms an antigen-antibody complex, which is then bound to and internalized by immunoglobulin Fc receptors on the cell membrane of leukocytes, especially monocytes or macrophages Because the antibody is heterologous, the virus is not neutralized and is free to replicate in the monocytes or macrophages (48) Epidemiologal studies in Thailand and Cuba (48-51) and in-vitro studies (52) supported this theory
Monocytes or macrophages infected by dengue virus produce and secrete cytokines and other mediators in response to dengue virus infection (53-56), which may trigger vascular permeability and activation of coagulation and fibrinolysis leading to plasma leakage and bleeding disorders Cytokines are small, nonstructural proteins with molecular weights ranging from 8 to 40 000 D, and are important in the acute inflammatory response initiated by infection or trauma Some cytokines clearly promote inflammation and are called proinflammatory cytokines, whereas other cytokines suppress the activity of proinflammatory cytokines and are called anti-inflammatory cytokines (57) TNF-α and IL-Iß are proinflammatory cytokines with a plethora of overlapping biological effects they cause fever and regulate the acute phase response, which includes leukocytosis and the increased synthesis of acute phase proteins by hepatocytes (58) Cytokines also have a series of effects on endothelial cells. IL-1 and TNF induce endothelial adhesion molecules, which are essential for the adhesion of leukocytes to the endothelial surface before they migrate into the tissues, they are also inducers of endothelial cell permeability and in addition, they stimulate endothelial procoagulant activity and plasminogen activator inhibitor synthesis (57,58,59,60)

16
Some cytokines that possibly contribute to the pathogenesis of DHF have been studied within the context of DHF In patients with DHF compared with patients with DF and healthy children, elevated levels of TNF-a have been reported (53,61,62) The levels of TNF-a were higher in hospitalized dengue patients than in out-patients with dengue and elevated IL-6 levels were positively associated with the seventy of dengue infection, while the levels of IL-Iß were negatively associated with disease seventy (63) Levels of IL-2 and IFN-γ were strongly elevated in serum specimens of patients with DHF or DF, however the difference was not significant (64) Increased levels of IL-1 have not been detected in the sera of patients with DHF (53) Other cytokines which have been studied in dengue infection are IL-8 (65,66), IL-10 (67,68 ), IL-12 (69), transforming growth factor beta-1 (TGF-ß) (70,71) and human cytotoxic factor (hCF) (72-74)
Apart from the immune enhancement hypothesis, it may also be that the complications of DHF/DSS are due to infection with one or more specific virus-subtypes Dengue virus type 2 and 3 appear to be more pathogenic than Den-1 and Den-4, but all four types can cause severe DHF (9, 75-79) Molecular studies have demonstrated that dengue viruses vary genetically in nature Study on dengue virus genome differences may give a better understanding of the true composition of viral RNA populations in the natural host and permit their association with pathogenesis (80)
Thus, the pathogenesis of DHF/DSS is still largely unknown and constitutes a wide area for further study

17
Outline of the thesis
In DHF/DSS two major pathological changes occur plasma leakage and bleeding.
The leading hypothesis for this thesis is that there is an intimate interplay between cytokines (released by dengue virus infected monocytes and activated-T cells), coagulation disorders and plasma leakage
Chapter 1 describes the epidemiology of dengue in Indonesia, and addresses the problems of dengue control, laboratory diagnosis and pathogenesis of DHF
Signs and symptoms of dengue virus infections are not specific and overlap with febrile illnesses caused by bacteria or other viruses In chapter 2 we report which diagnoses can be made in patients presenting with dengue-like symptoms, of whom in many recent dengue virus infection could not be confirmed with dengue IgM/IgG ELISA; and in chapter 3 we describe the evidence for hantavirus in Indonesia
Chapter 4 addresses the question, which factor involved in the pathological changes of DHF/DSS is related to mortality plasma leakage or bleeding We study the association of mortality with severe bleeding manifestations, activation markers of coagulation and fibrinolysis, as well as markers of plasma leakage
In chapter 5, we investigate the patterns of cytokines released in the course of DHF/DSS- tumor necrosis factor-α, interleukin-lß, interleukin-6, interferon-γ and interleukin-1 receptor antagonist, to answer the questions- what are the concentrations of these cytokines in the blood during the course of disease9, are there differences in the concentrations of cytokines between survivors and non-survivors during the acute phase of disease9, what is the ex-vivo production capacity of blood cells with and without LPS stimulation, and which of these cytokines is associated with mortality9
In chapter 6, we investigate the hypothesis that cytokines play a pivotal role in the endothelial permeability changes, the major pathology in DHF/DSS We ask the question which cytokines are associated with markers of plasma leakage
Chapter 7 gives an overview of bleeding disorders in systemic infections, since viral and bacterial infections may influence hemostasis and can lead to thrombohemorrhagic complications
In chapter 8, we investigate the role of the intrinsic pathway of coagulation, notably of thrombin-activatable fibrinolysis inhibitor (TAFI), in the onset of coagulation in DSS

In chapter 9, we investigate the hypothesis that in DSS cytokines may activate coagulation and fibnnolysis, as was shown already in experimental endotoxaemia and sepsis
In chapter 10 we summarize our findings and give directions for future dengue research.
References
1. Suroso Τ Epidemiological situation of dengue hemorrhagic fever and its control in Indonesia. In Proceedings International Seminar on Dengue Fever/Dengue Hemorrhagic Fever (Surabaya). Indonesia. 1999 11.
2. Kouwenaar W, Van Steenis PB, Winckel CH WF. Leerboek der tropische geneeskunde Tweede druk. Amsterdam Scheltema & Holkema, 1956; 223
3 Setyorogo D The review and control of DHF in Indonesia Dengue Newsletter 1981;7:41-42
4. Suroso T. A review of dengue hemorrhagic fever and its control in Indonesia In Proceeding International Seminar Recent Advances in Molecular Diagnostics Yogyakarta, Indonesia, 1997:4.
5 Halstead SB Epidemiology of dengue and dengue hemorrhagic fever. In-
Gubler DJ, Kuno G. Dengue and dengue hemorrhagic fever Walhngford, UK-Cab International, 1997, 23-44
6. Gubler DJ, Suharyono W, Lubis I, Eram S, Gunarso S Epidemic Dengue 3 in Central Java, associated with low viraemia in man Am J Trop Med Hyg 1981,30· 1094-99
7. Samsi TK, Wulur H, Sugianto D, Bartz CR, Tan R, Sie A. Some clinical and epidemiological observations on virologically confirmed dengue hemorrhagic fever Paediatr Indones 1990; 30. 293-303
8 Richards AL, Bagus R, Baso SM, Follows GA, Tan R, Graham RR, Sandjaja B, Corwin AL, Punyabi Ν The first reported outbreak of dengue hemorrhagic fever in Irian Jay a, Indonesia Am J Trop Med Hyg 1997; 57 49-55.
9. Graham RR, Juffne M, Tan R, Hayes CG, Laksono I, Ma'roef C, Erhn, Sutaryo, Porter KR, Halstead SB A prospective seroepidemiologic study on dengue in children four to nine years of age in Yogyakarta, Indonesia I. Studies in 1995-1996 Am J Trop Med Hyg 1999; 61 · 412-19
10 Hills S, Pnspanen J, Foley P, Smith G, Humphreys J, Simpson J, McDonald G Public health implications of dengue in personnel returning from East Timor. Commun Dis Intell 2000, 24 365-68
11 Sumarmo, Wulur H, Jahja E, Gubler DJ, Suharyono W, Sorensen K. Clinical observations on virologically confirmed fatal dengue infections in Jakarta, Indonesia Bull World Health Organ 1983; 61. 693-701.
12. Jumali, Sunarto, Gubler DJ, Nahm S, Eram S, Sulianti Saroso J Epidemic dengue hemorrhagic fever in rural Indonesia III Entomological studies. Am J Trop Med Hyg 1979, 28· 717-24

19
13 Ishak H, Miyagi I, Toma Τ, Kamimura Κ Breeding habitats of Aedes aegypty and Aedes albopictus in villages of Barru, South Sulawesi, Indonesia Southeast Asian J Trop Med Public Health 1997, 28 844-50
14 Rhodain F, Rosen L Mosquito vectors and dengue virus-vector relationships In Gubler DJ, Kuno G Dengue and dengue hemorrhagic fever Wallingford, UK Cab Intrnational, 1997,45-60
15 Gionar YR, Rusmiarto S, Susapto D, Bangs MJ Use of funnel trap for collecting immature Aedes aegypti and copepods from deep wells in Yogyakarta, Indonesia J Am Mosq Control Assoc 1999, 15 576-80
16 Anms B, Knsnowardojo S, Atmosoedjono S, Supardi Ρ Suppression of larval Aedes aegypty populations in household water storage containers in Jakarta, Indonesia, through release of first-instar Toxorhynchites splendens larvae J Am Mosq Control Assoc 1989, 5 235-38
17 Anms B, Nalim S, Hadisuwasono, Widiarti, Boewono DT Toxorynchites amboinensis larvae released in domestic containers fail to control dengue vectors in a rural village in central Java J Am Mosq Control Assoc 1990, 6 75-78
18 Bhamarapravati Ν Dengue vaccine development Monograph on Dengue/Dengue Haemorrhagic Fever World Health Organization New Dehh 1993,161-163
19 Bhamarapravati N, Yoksan S Live attenuated tetravalent dengue vaccine In Gubler DJ, Kuno G (eds) Dengue and dengue hemorrhagic fever Wallingford, UK Cab International, 1997,367-377
20 Trent DW, Kinney RM, Huang Y-Η C Recombinant dengue virus vaccines In Gubler DJ, Kuno G (eds) Dengue and dengue hemorrhagic fever Wallingford, UK Cab International, 1997, 379-403
21 World Health Organization Dengue hemorrhagic fever diagnosis, treatment, prevention and control 2d ed Geneva WHO 1997, 12-47
22 Pan American Health Organization Dengue and dengue hemorrhagic fever in the Americas guidelines for prevention and control Washington DC, USA 1994,8-21
23 Gubler DJ Dengue and dengue hemorrhagic fever Clin Microbiol Rev 1998, 11 480-496
24 Nur YA, Groen J, Heuvelmans H, Tuynman W, Copra C, Osterhaus AD An outbreak of West Nile Fever among migrants in Kisangani, Democratic Republic of Congo Am J Trop Med Hyg 1999, 61 885-88
25 Silarug N, Foy HM, Kupradinon S, Nisalak A, Pongsuwant Y Epidemic ot fever of unknown origin in rural Thailand, caused by influenza A (HINI) and dengue fever Southeast Asian J Trop Med Pub Hlth 1990, 21 61-67
26 Levett PN, Branch SL, Edwards CN Detection of dengue in patients investigated for leptospirosis in Barbados Am J Trop Med Hyg 2000, 62 112-14
27 KO AI, Galvao Reis M, RibeiroDourado CM, Johnson WD Jr, Riley LW Urban epidemic of severe leptospirosis in Brazil, Salvador Leptospirosis Study Group Lancet 1999, 354 820-25

20
28 Clement J, Neild G, Hinnchsen SL, Crescente JA, Van Ranst M Urban leptospirosis versus urban hantavirus infection in Brazil Lancet 1999, 354 2003-04.
29. Sudjana P, Yusuf H Concurrent dengue hemorrhagic fever and typhoid fever infection in adult case port Southeast Asian J Trop Med Public Health 1998, 29. 370-2
30 Yoshida M, Igarashi A, Suwendra P, Inada K, Maha MS, Kan K, Suda H, Antonio MT, Arhana BN, Takikawa Y, Maesawa S, Yoshida H, Chiba M. The first report on human cases serologically diagnosed as Japanese encephalitis in Indonesia. Southeast Asian J Trop Med Public Health 1999, 30: 698-706
31 Vomdam V, Kuno G Laboratory diagnosis of dengue virus infections. In. Gubler DJ, Kuno G (eds) Dengue and dengue hemorrhagic fever Wallingford, UK. Cab International, 1997, 313-333
32 Clarke DH, Casals J Techniques for hemagglutination and hemagglutination inhibition test with arthropod-borne viruses. Am J Trop Med Hyg 1958,7: 561-577
33 Tan R, Kumiawan H, Hartati S, Widjaya S, Jenning GB. Comparative sensitivity of laboratory methods to diagnose dengue virus infection at Husada Hospital, Jakarta Southeast Asian J Trop Med & Pub Hlth 1994, 25. 262-5.
34. Inms BL, Nisalak A, Nimmannitya S, Kusalerdcharya S, Chongswasdi V, Suntayakorn S, Puttisn P, Hoke CH An enzyme-linked immunosorbent assay to characterize dengue infections where dengue and Japanese Encephalitis co-circulate Am J Trop Med Hyg 1989, 40. 418-427
35 Lam S Κ Rapid dengue diagnosis and interpretation Malayasia J Pathol 1993; 15-9-12
36 Lam SK, Devi S, Pang Τ Detection of specific IgM in dengue infection Southeast Asian J Trop Med Pub Hlth 1987, 18: 533-8
37 Chungue E, Marché G, Phchart R, Boutin JP, Roux J Comparison of immunoglobulin G enzyme-linked immunosorbent assay (IgG-ELISA) and hemagglutination inhibition (HI) test tor the detection of dengue antibodies Prevalence of IgG-ELISA antibodies in Tahiti Transactions of the Royal Society ot Tropical Medicine and Hygiene 1989; 83 708-711
38 Rurchusatsawat K, Monta K, Tanaka M, Vongcheree S, Rojanasuphot S, Warachit Ρ, Kanal K, Thongtradol Ρ, Nimnakom M, Kanungkid S, Igarashi A Daily observation of antibody levels among dengue patients detected by enzyme-linked immunosorbent assay (ELISA) Jpn J Trop Med Hyg 1994; 22 9-12
39. Kuno G, Gomez I, Gubler DJ Detecting artificial anti-dengue IgM immune complexes using an en/yme-hnked immunosorbent assay Am J Trop Med Hyg 1987, 36 153-9
40 Kuno G, Gomez I, Gubler DJ An ELISA procedure for the diagnosis of dengue infections. J Virol Methods 1991; 33 101-13.
41 Bundo K, Igarashi A. Antibody-capture ELISA for detection of immunoglobulin M antibodies in sera from Japanese encephalitis and dengue hemorrhagic fever patients J Virol Methods 1985, 11 15-22.

42 Perez-R JG, Clark GG, Gubler DJ, Reiter Ρ, Sanders EJ, Vorndam AV Dengue and dengue hemorrhagic fever The Lancet 1998, 352 971-77
43 Sharp TW, Wallace MR, Hayes CG, Sanches JL, DeFraites RF, Arthur RR, Thornton SA, Batchelor RA, Ro/majzl PJ, Hanson RK, Wu SJ, Inye C, Burans JP Dengue fever in U S troops during operation restore hope, Somalia, 1992-1993 Am J Trop Med Hyg 1995, 53 89-94
44 Makino Y, Tadano M, Saito M, et al Studies on cross-reaction in sequential flavivirus infections Microbiol Immunol 1994, 38 951-5
45 Wu SJL, Hanson B, Paxton H, et al Evaluation ot a dipstick en/yme-linked immunosorbent assay for detection of antibodies to dengue virus Clinical and Diagnostic Laboratory Immunology 1997, 4 452-7
46 Gubler DJ, Suharyono W, Tan R, Abidin M, Sie A Viraemia in patients with naturally acquired dengue infection Bulletin of World Health Organization 1981,59 623-630
47 Halstead SB Pathogenesis of dengue challenges to molecular biology Science 1992,45 292-98
48 Vaughn DW Dengue lessons from Cuba Am J Epidemiol 2000, 152 800-3 49 Sangkawibha N, Rojansuphot S, Ahandnk S, Vinyapongse S, Jatanasen S,
Sahtul V, Phanthumachinda B, Halstead SB Risk factors in dengue shock syndrome a prospective epidemiologic study in Rayong, Thailand Am J Epidemiol 1984,20 653-69
50 Guzman MG, Kouri GP, Bravo J, Soler M, Vasquez S, Morier L Dengue hemorrhagic fever in Cuba, 1981 a retrospective seroepidemiologic study Am J Trop Med Hyg 1990, 42 179-84
51 Burke DS, Nisalak A, Johnson DE, Scott RM A prospective study of dengue infections in Bangkok Am J Trop Med Hyg 1988, 38 172-180
52 Anderson R, Wang S, Osiowy C, Issekutz AC Activation of endothelial cells via antibody-enhanced dengue virus infection of peripheral blood monocytes J Virol 1997,71 4226-4232
53 Hober D, Poh L, Roblin B, Gestas P, Chungue E, Grame G, Imbert Ρ, Pecarere JL, Vergez-Pascal R, Wattre Ρ Serum levels of tumor necrosis factor-alpha (TNF-alpha), interleukin-6 (IL-6), and interleukin-lß (IL-1 beta) in dengue-infected patients Am J Trop Med Hyg 1993, 48 324-31
54 Pinto LMO, Oliveira SA, Braga ELA, Nogueira RMR, Kubclka CF Increased Pro-inflammatory Cytokines (TNF-a and IL-6) and Ann-inflammatory Compounds (sTNFRp55 and sTNFRp75) in Brazilian Patients during exanthematic Dengue Fever Mem Inst Oswaldo Cruz 1999, 94 387-394
55 Chaturvedi UC, Elbishbishi EA, Agarwal R, Raghupathy R, Nagar R, Tandon R, Pacsa AS, Younis OI, Azizieh F Sequential production of cytokines by dengue virus-infected human peripheral blood leukocytes cultures J Med Virol 1999,59 335-40
56 lyngkaran N, Yadav M, Sinniah M Augmented intlammatory cytokines in primary dengue infection progressing to shock Singapore Med J 1995, 36 218-21
57 Dinarello CA Proinflammatory cytokines Chest 2000, 118 503-08

22
58 Hamblin AS Cytokines and cytokine receptors New York Oxford University Press, 1993 55-64
59 Bonner SM, O'Sullivan MA Endothelial cell monolayers as a model system to investigate dengue shock syndrome J Virol Methods 1998, 71 159-67
60 Nawroth PP, Stern DM Modulation of endothelial cell hemostatic properties by tumor necrosis factor J Exp Med 1986, 163, 740-745
61 Vitarana T, de Silva H, Withana Ν, Gunasekera C Elevated tumor necrosis factor in dengue fever and dengue hemorrhagic fever, Ceylon Med J 1991, 36 63-65
62 Yadav M Kamath KR, lyngkaran N, Sinniah M Dengue hemorrhagic fever and dengue shock syndrome are they tumor necrosis factor-mediated disorders' FEMS Microbiol Immunol 1991, 4 45-49
63 Kuno G, Bailey RE Cytokine responses to dengue infection among Puerto Rican patients Mem Inst Oswaldo Cruz 1994, 89 179-182
64 Kurane I, Innis BL, Nimmannitya S, Nisalak A, Meager A, Janus J, Enms FA Activation of Τ lymphocytes in dengue virus infections high levels ot soluble interleukin-2 receptor, soluble CD4, soluble CD8, interleukin 2 and interferon gamma in sera of children with dengue J Clin Invest 1991, 88 1473-80
65 Raghupathy R, Chaturvedi UC, Al-Sayer H, Elbishbishi EA, Agarwal R, Nagar R, Kapoor S, Misra A, Mathur A, Nusrat H, Azmeh F, Khan MA, Mustafa AS Elevated ot levels IL-8 in dengue hemorrhagic tever J Med Virol 1998,56 280-85
66 Juffne M, van der Meer GM, Hack CE, Haasnoot Κ, Sutaryo, Veerman AJP, Thijs LG Inflammatory mediators in dengue virus infection in children interleukin-8 and its relationship to neutrophil degranulation Infect Immun 2000,68 702-707
67 Chaturvedi UC, Raghupathy R, Pacsa AS, Elbishbishi EA, Agarwal R, Nagar R, Misra A, Kapoor S, Mathur A, Khan MAY, Azizieh F Shift from a Thl-type response to Th2-type in dengue hemorrhagic fever Curr Sci 1999, 76 63-69
68 Green S, Vaughn DW, Kalayanarooj S, Nimmannitya S, Suntayakorn S, Nisalak A, Rothman AL, Enms FA Elevated plasma interleukin levels in acute dengue correlate with disease severity J Med Virol 1999,59 329-34
69 Pacsa AS, Agarwal R, Elbishbishi EA, Chaturvedi UC, Nagar R, Mustafa AS Interleukin-12 in patients with dengue hemorrhagic fever FEMS Immunol Med Microbiol 2000, 27
70 Laur F, Murgue B, Depans X, Roche C, Cassar O, Chungue E Plasma levels of tumor necrosis factor alpha and transforming growth factor beta-1 in children with dengue 2 virus infection in French Polynesia Trans R Soc Trop MedHyg 1998,92 654-56
71 Agarwal R, Elbishbishi EA, Chaturvedi UC, Nagar R, Mustafa AS Profile of transforming growth factor-beta 1 in patients with dengue hemorrhagic fever Int J Exp Pathol 1999, 80 143-49
72 Shaio MF Cheng SN, Yuh YS, Yang KD Cytotoxic factors released by dengue virus-infected human blood monocytes J Med Virol 1995,46 216-23

2λ
73 Agarwal R, Chaturvedi UC, Misra A, Mukerjee R, Kapoor S, Nagar R, Tandon R, Mathur A Production of cytotoxic factor by penpheral blood mononuclear cells (PBMC) in patients with dengue hemorrhagic fever. Clin Exp Immunol 1998, 112. 477-81.
74. Chaturvedi UC, Elbishbishi EA, Agarwal R, Mustafa AS. Cytotoxic factor-autoantibodies possible role in the pathogenesis of dengue hemorrhagic fever FEMS Immunol Med Microbiol 2001; 30 181-86
75 Vaughn DW, Green S, Kalayanarooj S, Innis BL, Nimmannitya S, Suntayakom S, Endy TP, Raengsakulrach B, Rothman AL, Enms FA, Nisalak A Dengue viremia titer, antibody respons pattern, and virus serotype correlate with disease seventy J Infect Dis 2000, 181 2-9
76. Pandey BD, Igarashi A. Seventy-related molecular differences among nineteen strains of dengue type 2 viruses. Microbiol Immunol 2000; 44 179-88
77. Guzman MG, Koun G, Valdes L, Bravo J, Alvarez M, Vazques S, Delgado I, Halstead SB. Epidemiologic studies on dengue in Santiago de Cuba, 1997 Am J Epidemiol 2000; 152. 793-9.
78 Kobayashi N, Thayan R, Sugimoto C, Oda Κ, Saat Ζ, Vijayamalar Β, Sinniah M, Igarashi A Type-3 dengue virusesresponsible for the dengue epidemic in Malayasia during 1993-1994. Am J Trop Med Hyg 1999; 60 904-9
79 Pandey BD, Monta Κ, Hasebe F, Parquet MC, Igarashi A Molecular evolution, distnbution and genetic relationship among the dengue 2 viruses isolated from different clinical severity Southeast Asian J Trop Med Public Health 2000; 31 266-72.
80 Leitmeyer KC, Vaughn DW, Watts DM, Salas R, Villalobos I, de Chachon, Ramos C, Hesse RR. Dengue virus structural differences that correlate with pathogenesis J Virol 1999,73-4738-4747

24
Chapter 2
Differential diagnosis of adult dengue virus infections in Indonesia
Catharma Suhdrti,(l) Eric C M van Gorp,<2) Wil M V Dolmans,0' Jan Groen,(4, Suharyo Hadisaputro,"1 Robert J Djokomoeljanto,1" Osterhaus Ab D M E ,<4) Jos W M van der Meer0)
Department of Internal Medicine, School of Medicine, Diponegoro University and Dr Kanadi Hospital, Semarang, Indonesia,'" Department of Internal Medicine, Slotervaart Hospital, Amsterdam,'"' Department oi Medicine, University Medical Centre St Radboud, Nijmegen, The Netherlands,' ' Institute of Virology, WHO Collaborating Center for Arboviruses and Hemorrhagic Fevers, Erasmus University Hospital, Rotterdam, The Netherlands <4,
Submitted for publication

25
Abstract
The clinical spectrum of dengue virus infection may vary from asymptomatic illness, undifferentiated fever, dengue fever (DF) to dengue hemorrhagic fever (DHF) Signs and symptoms are non-specific and overlap with febrile illnesses caused by other viruses or bacteria During a dengue epidemic in Indonesia, we investigated 118 adult patients fulfilling the WHO criteria tor dengue (91 DF, 8 DHF I, 13 DHF II, 5 DHF III and 1 DHF IV) In all but 4 patients, IgG antibodies against dengue virus was found, but only in 58 patients recent dengue virus infection was confirmed by the presence of dengue specific IgM antibodies or a significant rise in IgG titer To determine which infection was the cause of disease in the remaining 60 patients, we performed additional serological tests In 20 sera (33.3%) serological evidence of a recent infection with another agent was demonstrated hantavirus (5), Chikungunya virus (2), influenza A virus (1), rubella virus (3), Rickettsia typhi (5), R. tsutsugamushi (2) and leptospira (2) Clinical and laboratory characteristics of these patients and the 58 with dengue overlapped In addition, evidence for infection with Chikungunya virus or hantavirus in the past (IgG antibodies but no rising titer) was found in 12 and two patients, respectively We conclude that based on clinical criteria alone, it is not easy to diagnose dengue. Specific laboratory assays are needed to differentiate dengue from other febrile illnesses Among these, in Indonesia hantavirus infection should be considered as well.

26
Introduction
Indonesia has a tropical climate and humidity which is conducive to perpetuation of Aedes aegypti, the main vector of dengue. Dengue virus belongs to the genus Flavivirus, family Flaviviridae and may cause a wide spectrum of illness: asymptomatic infection, undifferentiated febrile illness, dengue fever (DF) and dengue hemorrhagic fever (DHF).1" Clinical signs and symptoms of dengue fever are not specific and include sudden onset of fever, weakness, headache, joint pain, muscle pain, retro-orbital pain, nausea, vomiting, rash and bleeding. The less severe grades of DHF (grade I and II) manifest similar to DF with signs of plasma leakage, and are difficult to distinguish from other viral illnesses such as Chikungunya virus infection (which is also transmitted by Ae. Aegypti), influenza, mild hantavirus infection and rubella, as well as bacterial infections such as mild leptospirosis and rickettsiosis."" '
Epidemiological studies have demonstrated that during outbreaks of dengue 10.5 to 42.7% of cases can be detected by virus isolation,(8·9,46.3% by IgM/IgG ELISA,<9) 41.8% by hemagglutination inhibition (HI) tests,<l0) 41.4 to 66% by IgM ELISA and/or virus isolation, ' " '2) and 73% by HI and/or virus isolation."3' Thus, the rest of these patients may actually suffer from another febrile illnesses. Alternatively, the sensitivity of assays used may have been low, or a wrong sampling time-point for the analysis was used.
We studied a group of patients > 13 years clinically suspected of recent dengue virus infection, according 1997 WHO definition, and performed serological assays to confirm the diagnosis. In case dengue was not confirmed, we performed additional serological tests to determine which other infectious agent could be the cause of their present illness. Since infections with Chikungunya virus, hantavirus, Rickettsia typhi, R. tsutsugamushi, leptospira, rubella virus and influenza virus may present with similar clinical characteristics as dengue and may be encountered in Indonesia, the specimens were examined for serological evidence of these infections. We also investigated whether clinical symptoms and signs may help to differentiate between these infections.
Materials and methods
Study setting The prospective study was performed in Dr. Kariadi Hospital, the university hospital of
Diponegoro University, Semarang, Indonesia. The research protocol was approved by the Review Board of the Dr. Kariadi Hospital. Written informed consent was obtained from patients or legal guardians.
Patients and data collection Between May 1995 and May 1996, during an outbreak of dengue in Indonesia, 118
consecutive adults (>13 years), clinically suspected by the WHO 1997 case definition <')
of DF or DHF, were examined prospectively. Of each patient, data were collected on a clinical record form, listing for each patient
during hospital slay: name, age, sex, history of illness (date of onset of disease and date of admission), symptoms, physical findings and laboratory findings, including blood tests
27
for: cell counts, prothrombin time (PT), activated partial thromboplastin time (aPTT), liver function (bilirubin, ASAT, ALAT), renal function (creatinine). Chest x-ray, ECG and ultrasonography were not done routinely.
For serological assays, 4 ml of blood was collected in vacutainer tubes (Becton Dickinson, Rutherford, NJ 07417) on day of admission, on day of discharge, and 1 week after discharge. The third specimen was omitted if the second specimen was two weeks
or more after the first. Specimens were kept at minus SO^C before testing and shipped on dry ice to the Virology Laboratory of the Erasmus University Hospital Rotterdam, The Netherlands for serological analysis.
Serological assays Samples were tested for the presence of specific antibodies against dengue virus by
IgM capture/IgG enzyme linked immunosorbent assay (ELISA)."4' A recent dengue infection was diagnosed if IgM antibodies were demonstrated or if a significant rise of IgG antibodies in paired serum samples was demonstrated.
All samples in which no recent dengue virus infection was found, were tested for antibodies against Chikungunya virus, hantavirus, influenza A virus, leptospira, and Rickettsia typhi. For the detection of antibodies against Chikungunya virus (IgG), Hantavirus (IgM and IgG) and influenza A (IgA), different ELISA-based systems were used, as described previously.13'15"18' In the ELISA for hantavirus antibodies, microplates coated with a mixture of Seoul and Sin Nombre virus recombinant nucleoproteins (MRL Diagnostics, Cypress, USA) were used."6' A greater than two times rise of IgG antibody titer against Chikungunya virus in paired-samples was considered to represent a recent infection. If IgM antibodies against hantavirus were detected in ELISA, those were confirmed by immunofluorescence (IFA); the presence of IgM antibodies, if confirmed by IFA, was considered to represent a recent infection. Presence of IgA antibodies against influenza A in any of the three serum samples was considered to represent a recent infection with influenza A virus.17 For the diagnosis of leptospirosis a haemagglutination inhibition (HI) test was performed."'" Only seroconversion in paired samples was considered to represent recent infection. IgM antibodies against R. typhi were measured by immunofluorescence (INDX, Baltimore, USA); an IgM antibody titer > 1:32 was considered to represent recent infection.
The sera in which no evidence for a recent infection with dengue virus, nor with any of the above mentioned other agents was demonstrated, were tested for presence of IgM antibodies against rubella virus, using a IgM capture assay (Organon Technika, Boxtel, The Netherlands) and for presence of IgM antibodies against R. tsutsugamushi by immunofluorescence (INDX, Baltimore, USA; positive titer >1:32).
Statistical analysis Continuous data were described as median (range) and nominal data were described in number (%). All statistical analyses were performed with SPSS for Windows version 9.0.
Results
Patients with confirmed recent dengue virus infection (n-58) In 58 patients, recent dengue virus infection was serologically confirmed. According

28
the 1997 WHO criteria, the classification of these 58 patients were· DF (42), DHF I (4), DHF II (7). DHF III (4), DHF IV (1) Their median age (range) in years was 19 (14-53) and sex ratio (M/F) 28/30
Patients without serological evidence of recent dengue virus infection (n=60) On clinical grounds, the remaining 60 patients had been classified as follows DF (49),
DHF I (4), DHF II (6), and DHF III (1). In all but 4 patients, dengue virus specific IgG was found, but there was no rise ot titer, indicating dengue virus infection in the past In 20 of the 60 patients, we found serological evidence of another recent infection hantavirus (5), Chikungunya virus (2), R. typhi (5), R tsutsugamushi (2), rubella virus (3), influenza A virus in (1), and leptospira (2). No evidence for recent infection with any of the mentioned agents was detected in the remaining 40 specimens Evidence for infection with Chikungunya virus in the past was found in 12 patients (IgG antibodies, but no rising titer) Three of these 12 patients had recent infections with dengue virus (1), hantavirus (1) and R. typhi (1) Also, evidence for hantavirus infection in the past was found in two patients.
Clinical characteristics Table 1 shows the distribution of clinical variables of 58 patients with confirmed recent
dengue and 20 with evidence of recent infection with Chikungunya virus, hantavirus, R typhi, R tsutsugamushi, rubella virus, influenza A virus or leptospira Headache, weakness, joint and/or muscle pain, epigastric pain, nausea, vomiting, were the most commonly presented symptoms/signs in all patients regardless their final diagnosis Bleeding manifestations were usually mild consisting of petechiae, gum bleeding and epistaxis Hematemesis and/or melena were found in some patients with dengue and one with hantavirus infection classified on admission as DHF III One patient with confirmed recent dengue virus infection (DHF IV) died, the remaining 117 patients recovered fully after a hospital stay of 2 to 18 days (median 6 days)
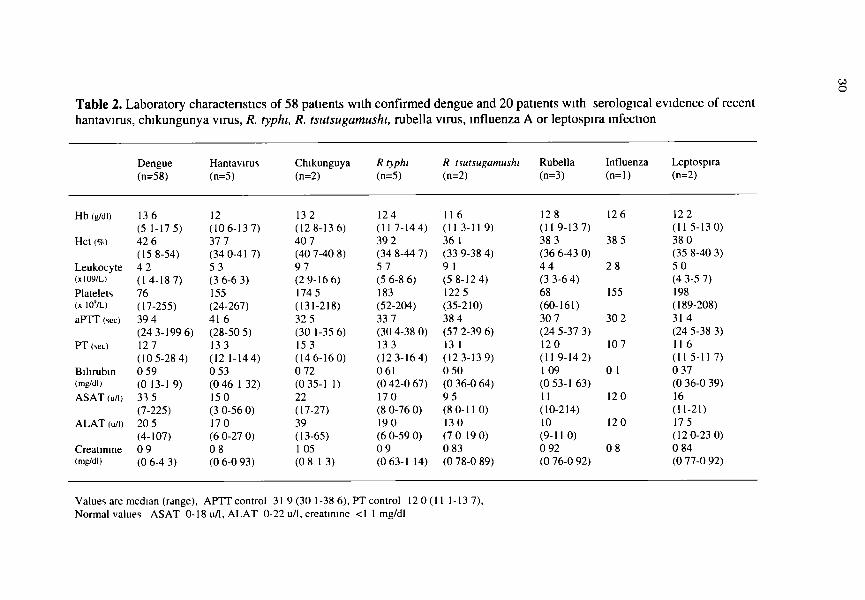
Laboratory results As shown in table 2 the median levels of hemoglobin, hematocrit and leukocytes were
normal in all cases Marked thrombocytopenia was found in patients with dengue and in some patients with hantavirus and R tsutsugamushi infection A prolongation of coagulation parameters was seen in some patients with dengue (aPTT, PT), Chikungunya (PT), hantavirus infection (aPTT) and R typhi infection (PT) A mild to moderate elevation of ASAT and ALAT were found in dengue virus infection and in some patients with rubella virus, hantavirus, Chikungunya virus and R. typhi infection A moderate increase of creatinine (up to 4 3 mg/dl) was found in some patients with dengue virus infection. Three of five patients with hantavirus infection had proteinuria and microscopic hematuria, but in all of them serum creatinine was normal

Table 1. Clinical characteristics of 58 patients with confirmed dengue and 20 patients with serological evidence of recent
hantavirus, Chikungunya virus, R. typhi, R. tsutsugamushi, rubella virus, influenza A or leptospira infection
Characteristics Dengue Hantavirus Chikungunya R typhi* R tsutsugamushi* Rubella Influenza A Leptospira (n=2) (n=58) (n=5) (n=2) (n=5) (n=2) (n=3) (n=l)
19 0/3
2/3 3/3 3/3 2/3 3/3 3/3
2/3 1/3 2/3 1/3 3/3 3/3 0/3
46 0/1
1/1 1/1 0/1 1/1 0/1 0/1
0/1 0/1 0/1 0/1 1/1 0/1 0/1
19 0/2
2/2 2/2 1/2 1/2 1/2 0/2
0/2 0/2 0/2 0/2 0/2 0/2 0/2
Median age (years) Male/Female ratio Symptoms Headache Weakness Joint/muscle pain Nausea/vomiting Epigastric pain Retro-orbital pain Signs Exanthema (rash) Pharyngitis Lymphadenopathy Hepatomegaly Petechiae Epistaxis/gum bleeding Hematemesis / melena
19 28/30
57/58 51/58 40/58 49/58 45/58 10/58
13/58 7/58 7/58 8/58 37/58 21/58 8/58
15 1/4
5/5 4/5 4/5 4/5 4/5 1/5
2/5 0/5 1/5 2/5 4/5 1/5 1/5
26 5 1/1
0/2 2/2 1/2 2/2 1/2 0/2
0/2 1/2 0/2 0/2 1/2 1/2 0/2
16 2/3
5/5 5/5 1/5 5/5 3/5 0/5
0/5 0/5 0/5 1/5 4/5 3/5 0/5
27 5 0/2
2/2 2/2 2/2 2/2 1/2 0/2
0/2 0/2 0/2 0/2 2/2 0/2 0/2
*Nonc of these patients had an eschar
to CD
03 O
Table 2. Laboratory characteristics of 58 patients with confirmed dengue and 20 patients with serological evidence of recent hantavirus, Chikungunya virus, R. typhi, R. tsutsugamusht, rubella virus, influenza A or leptospira infection
Dengue Hantavirus Chikunguya R typhi R tsutsugamushi Rubella Influenza Leptospira (n=58) (n=5) (n=2) (n=5) (n=2) (n=3) (n=l) (n=2)
Hb (g/dl)
Hct (%)
Leukocyte (X109/L)
Platelets (x lO'/L)
aPTT (sec)
PT (sec)
Bilirubin (mg/dl)
ASAT (u/1)
ALAT (u/i)
Creatinine (mg/dl)
136 (5 1-175) 42 6 (15 8-54) 4 2 (14-187) 76 (17-255) 39 4 (24 3-199 6) 127 (10 5-28 4) 0 59 (0 13-1 9) 33 5 (7-225) 20 5 (4-107) 0 9 (0 6-4 3)
12 (106-137) 37 7 (34 0-417) 5 3 (3 6-6 3) 155 (24-267) 416 (28-50 5) 133 (12 1-144) 0 53 (0 46 1 32) 150 (3 0-56 0) 170 (6 0-27 0) 0 8 (0 6-0 93)
132 (128-136) 40 7 (40 7-40 8) 9 7 (2 9-16 6) 174 5 (131-218) 32 5 (30 1-35 6) 153 (146-160) 0 72 (0 35-1 1) 22 (17-27) 39 (13-65) 105 (0 8 13)
124 (11 7-144) 39 2 (34 8-44 7) 5 7 (5 6-8 6) 183 (52-204) 33 7 (30 4-38 0) 133 (123-164) 061 (0 42-0 67) 17 0 (8 0-76 0) 19 0 (6 0-59 0) 0 9 (0 63-1 14)
II 6 (11 3-11 9) 36 1 (33 9-38 4) 9 1 (5 8-12 4) 122 5 (35-210) 38 4 (57 2-39 6) 13 1 (12 3-13 9) 0 50 (0 36-0 64) 9 5 (8 0-11 0) 130 (7 0 19 0) 0 83 (0 78-0 89)
12 8 (11 9-137) 38 3 (36 6-43 0) 4 4 (3 3-6 4) 68 (60-161) 30 7 (24 5-37 3) 120 (11 9-14 2) 109 (0 53-1 63) 11 (10-214) 10 (9-11 0) 0 92 (0 76-0 92)
126
38 5
2 8
155
30 2
107
0 1
120
120
0 8
122 (11 5-130) 38 0 (35 8-40 3) 5 0 (4 3-5 7) 198 (189-208) 314 (24 5-38 3) 11 6 (11 5-117) 0 37 (0 36-0 39) 16 (11-21) 17 5 (12 0-23 0) 0 84 (0 77-0 92)
Values are median (range), APTT control 31 9 (30 1-38 6), PT control 120(11 1-137), Normal values ASAT 0-18 u/1, ALAT 0-22 u/1, creatinine <1 1 mg/dl

31
Discussion
In 114 of 118 (97%) adult patients clinically suspected of dengue virus infection by the 1997 WHO criteria, antibodies to dengue virus were found This shows the high endemicity of dengue in the area of study. However, in only 58 patients, the clinical suspicion of dengue virus infections could be confirmed serologically In 20 ot the remaining 60 patients who presented dengue-like illness, a recent infection with hantavirus, Chikungunya virus, R typhi, R tsutsugamushi, rubella virus, influenza A virus, or leptospira was demonstrated The clinical symptoms and signs of these 20 patients (table 1) were very similar to those of the 58 patients whose present illness was due to dengue Most of these patients had mild dengue virus infection (DF or DHF I or II). Our findings in adult patients with suspected dengue contrast with those in 50 children with dengue shock syndrome (DHF III or DHF IV), in whom the diagnosis dengue virus infection was confirmed in all cases ' 'The explanation probably is that the clinical picture of severe dengue virus infection (DSS) is more specific.
IgM antibodies against hantavirus were detected in 5 patients indicating recent infection, and in 2 patients with IgG with no rising titer indicating infection in the past On admission, 4 of these 5 patients with recent hantavirus infection were clinically diagnosed as DF, whereas one patient had a more severe clinical presentation, and was originally diagnosed as DHF III. None of these patients had traveled outside Indonesia These are the first reported hantavirus infections in humans from Indonesia Hantavirus infection may manifest as mild or severe disease The different hantavirus types are associated with different types of disease manifestations, both in terms of target organs and disease severity (21) Severe disease may manifest itself as Hantavirus Pulmonary Syndrome (HPS) or Hemorrhagic Fever with Renal Syndrome (HFRS) HPS may present as a non-specific illness with fever, myalgia, headache, and gastrointestinal symptoms, followed by a non-productive cough, culminating rapidly in respiratory insufficiency Severe HFRS is characten/ed by extreme albuminuria and impaired renal function l22 "S)
Three of five patients with hantavirus infection had proteinuria and microscopic hematuria tor several days, but no impaired renal function
We demonstrated antibodies against Chikungunya in 14 patients but only in two patients the antibody profile indicated recent infection On admission, these two patients were clinically diagnosed as DF and DHF I. Chikungunya is difficult to differentiate from DF or mild DHF due to the overlap in clinical symptoms and signs (table 2) as also was described previously (13 261
We detected IgM antibodies against R. typhi in 5 patients This disease is known to occur in Indonesia ( l ) Our five patients had mild nckettsiosis and had clinically been suspected of DF Antibodies against R. isutsugamushi were found in 2 patients The clinical characteristics and laboratory finding of R tsutsugamushi were similar to those of R. typhi infection.
We detected antibodies against rubella virus in 3 patients These patients were originally diagnosed as DF in one and DHF II in two patients. A similar finding has been reported previously .<1Ü,
Antibodies against influenza A virus were found in one patient, clinically diagnosed as DF on admission Also previous studies demonstrated that influenza can mimic mild

32
dengue infection We found antibodies against leptospira in two patients Manifestations of leptospirosis
may vary from a mild flu-like illness to an acute life-threatening condition with renal failure (Weil's disease). Our two patients had mild leptospirosis and were mistaken for DF on admission Both dengue and leptospirosis are endemic in Indonesia. During a large outbreak of leptospirosis in Salvador, Brazil, 42 percent of cases were misdiagnosed as dengue fever in the outpatient clinic <6) Also, substantial misdiagnosis of dengue and leptospirosis occurred in Barbados During 1995, 48 of 108 sera during 1996, 21 of 64 sera from leptospirosis-negative patients were found to have IgM antibodies to dengue virus <5) On the other hand, after hurricane-generated floods in Puerto Rico, leptospirosis was diagnosed in patients suspected clinically of dengue, but testing dengue-seronegative 02)
In 40 of the patients, we failed to demonstrate the presence of another recent infection This may be due to the presence of yet another disease, not tested for For instance, in patients clinically suspected of dengue, typhoid fever with a positive culture for Salmonella typhi (Hadinegoro SR, unpublished), and measles ( 3 3 ) have been diagnosed.
We did not test for Japanese encephalitis which manifests with neurologic illness and is often fatal. The other flavivirus, causing Yellow Fever, does not occur in Indonesia
In conclusion, it is difficult to distinguish clinically dengue from other febrile illnesses. This applies particularly to dengue fever and mild in adults. Which specific laboratory tests are to be used, depends on the geographical area Differentiating other infectious agents not only is of epidemiological but also clinical interest, because adequate antibiotic treatment can be instituted in some of these infections, reducing morbidity and mortality. Hantavirus infection should be added to the differential diagnosis of dengue virus infection in Indonesia
Acknowledgements
Participants in this project, besides the authors, were dr Budi Riyanto, dr M H Gasem and dr L.Widiono from the Department of Internal Medicine, Dr Kanadi Hospital, Diponegoro University, Semarang, Indonesia. We thank Υ Τ van der Heide from the Clinical Chemistry and Hematology Laboratory, Slotervaart Hospital, Amsterdam, The Netherlands, for managing the blood samples Ms P.Koraka and C. Copra of the Virological laboratory, Erasmus University Hospital Rotterdam, The Netherlands for exellent technical assistence
References
1 World Health Organization Dengue hemorrhagic fever diagnosis, treatment, prevention and control 2d ed. Geneva WHO 1997 12-47
2 Gubler DJ Dengue and dengue hemorrhagic fever. Clin Microbiol Rev 1998; 11 480-96
3. Nur YA, Groen J, Heuvelmans H, Tuynman W, Copra C, Osterhaus AD An outbreak of West Nile Fever among migrants in Kisangani, Democratic Republic of Congo Am J Trop Med Hyg 1999, 61 · 885-88
4. Silarug N, Foy HM, Kupradinon S, Nisalak A, Pongsuwant Y Epidemic of fever

33
of unknown origin in rural Thailand, caused by influenza A (HINI) and dengue fever Southeast Asian J Trop Med Pub Hlth 1990; 21 61-67
5 Levett PN, Branch SL, Edwards CN Detection of dengue in patients investigated for leptospirosis in Barbados. Am J Trop Med Hyg 2000, 62. 112-14
6 KO AI, Galvao Reis M, RibeiroDourado CM, Johnson WD Jr, Riley LW. Urban epidemic of severe leptospirosis in Brazil, Salvador Leptospirosis Study Group Lancet 1999, 354. 820-25.
7 Clement J, Neild G, Hinrichsen SL, Crescente JA, Van Ranst M Urban leptospirosis versus urban hantavirus infection in Brazil Lancet 1999, 354· 2003-4.
8 Sharp TW, Wallace MR, Hayes CG, Sanchez JL, DeFraites RF, Arthur RR, Thornton SA, Batchelor RA, Rozmajzl PJ, Hanson RK, Wu SJ, Inye C, Burans JP Dengue fever in U.S troops during operation restore hope, Somalia, 1992-1993 Am J Trop Med Hyg 1995, 53 89-94
9 Inms BL, Nisalak A, Nimmanmtya S, Kusalerdcharya S, Chongswasdi V, Suntayakorn S, Puttisn P, Hoke CH. An enzyme -linked immunosorbent assay to characterize dengue infections where dengue and Japanese Encephalitis co-circulate. Am J Trop Med Hyg 1989, 40 418-27
10. Chairulfatah A, Setiabudi D, Ridad A, Colebunders R Clinical manifestations ot dengue hemorrhagic fever in children in Bandung, Indonesia Ann Soc Belg Med Trop 1995,75-291-95
11. Depans X, Murgue B, Roche C, Cassar O, Chungue E Changing clinical and biological manifestations of dengue during the dengue-2 epidemic in French Polynesia in 1996/1997-description and analysis in a prospective study Trop Med Int Health 1998,3:859-65
12 Richards AL, Bagus R, Baso SM, Follows GA, Tan R, Graham RR, Sandjaja B, Corwin AL, Punjabi Ν The first reported outbreak of dengue hemorrhagic fever in Irian Jaya, Indonesia Am J Trop Med Hyg 1997,57 49-55
13 Kuberski T, Rosen L, Reed D Mataika J Clinical and laboratory observations on patients with primary and secondary dengue type 1 infections with hemorrhagic manifestations in Fiji Am J Trop Med Hyg 1977, 26 775-83
14. Velzing J, Groen J, Drouet MT, van Amerongen G, Copra C, Osterhaus AD, Deubel V Induction of protrective immunity against Dengue virus type 2 companson of candidate live attenuated and recombinant vaccines. Vaccine 1999, 17 1312-20
15 Groen J, Gerding M, Jordans JG, Clement JP, Osterhaus AD Class and subclass distribution of Hantavirus-specific serum antibodies at different times after the onset of nephropathia epidemica. J Med Virol 1994, 43 39-43
16 Koraka P, Avsic-Zupanc T, Osterhaus AD, Groen J Evaluation of two commercially available immunoassays for the detection of hantavirus antibodies in serum samples J clin Virol 2000, 17. 189-196
17 Rothbarth PH, Groen J, Bohnen AM, de Groot R, Osterhaus AD Influenza virus serology a comparative study. J Virol Methods 1999; 78 163-69.
18 Moll van Charante AW, Groen J, Mulder PGH, Rijpkema SG, Osterhaus ADME Occupational risks of zoonotic infections in Dutch forestry workers and muskrat catchers Eur J Epidemiol 1998, 14 109-16

34
19 Levett PN, Whittington CU Evaluation of the indirect hemagglutination assay for diagnosis of acute leptospirosis J Clin Microbiol 1998, 36 11-14
20 Suharti C, Tatty E Senati, van Gorp ECM, Djokomoeljanto RJ, Trastotenoyo MS, van der Meer JWM, Dolmans WMV Clinical picture and risk factors for mortality in dengue shock syndrome, submitted for publication
21 Mc Caughey C, Hart CA Hantaviruses J Med Microbiol 2000, 49 587-99 22 Khan AS, Ksiazek TG, Peters CJ Hantavirus pulmonary syndrome Lancet 1996,
347 739-41 23 Bonn D Hantaviruses an emerging threat to human health9 Lancet 1998, 352
86 24 Aker S, Ivens Κ, Pilaski J, Grabensee Β, Heering Ρ Acute renal failure in
hantavirus infections Med Klin 2000, 95 213-17 25 Ferreira MS, Nishioka SD, Santos TL, Santos RP, Santos PS, Rocha A
Hantavirus pulmonary syndrome in Brazil clinical aspects of three new cases Rev Inst Med Trop Sao Paulo 2000, 42 41-46
26 Thaikruea L, Charearnsook O, Reanphumkamkit S, Dissomboon P, Phonjan R, Ratchbud S, Kounsang Y, Buranapiyawong D Chikungunya in Thailand a re-emerging disease9 Southeast Asian J Trop Med Public Health 1997, 28 359-64
27 Richards AL, Soeatmadji DW, Widodo MA, Sardjono TW, Yanuwiadi B, Hemowati TE, Baskoro AD, Roebiyoso, Hakim AL, Soendoro M, Rahardjo E, Putrì MP, Saragih JM, Stnckman D, Kelly DJ, Dasch GA, Olson JG, Church CJ, Corwin AL Seroepidemiologic evidence for murine and scrub typhus in Malang, Indonesia Am J Trop Med Hyg 1997, 57 91-95
28 Corwin AL, Soeprapto W, Widodo PS, Rahardjo E, Kelly DJ, Dash GA, Olson JG, Sie A, Larasati RP, Richards AL Short report surveillance of rickettsial infections in Indonesian military personnel during peace keeping operations in Cambodia Am J Trop Med Hyg 1997,57 569-70
29 Parola Ρ, Vogelaers D, Roure C, Janbon F, Raoult D Murine typhus in travelers returning from Indonesia Emerg Infect Dis 1998, 4 677-80
30 Tan DSK, Chew V, Nuruddin NM Rubella cases mistaken for dengue fever Singapore Med J 1980, 21 769-70
31 Thaung U, Ming CK, Thein M Dengue hemorrhagic lever in Burma Southeast Asian J Trop Med Public Health 1975, 6 580-91
32 Sanders EJ, Rigau-Perez JG, Smits HL, Deseda CC, Vomdam VA, Aye Τ, Spiegel RA, Weyant RS, Bragg SL Increase of leptospirosis in dengue-negative patients after a hurricane in Puerto Rico In 1996 Am J Trop Med Hyg 1999, 61 399-404
33 Dietz VJ, Nieburg P, Gubler DJ, Gomez I Diagnosis ol measles by clinical case definition in dengue endemic areas implications for measles surveillance and control Bull World Health Organ 1992, 70 745-50

35
Chapter 3
Human hantavirus infections in Indonesia
J. Groen PhD*, C. Suharti M.D.1, P. Koraka BSc*, E.C.M. van Gorp Y M.D., PhD, J. Sutaryo M.D, PhD*, A.D.M.E. Osterhaus D.V.M, PhD*
* Laboratory for Exotic Viral Infections University Hospital Rotterdam, The Netherlands. 1 Department of Internal Medicine, Dr. Kariadi Hospital, Diponcgoro University, Semarang, Indonesia. ' Department of Internal Medicine, Slotervaart Hospital, Amsterdam, The Netherlands. Department of Paediatrics, Faculty of Medicine, Gadjah Mada University,
Yogyakarta, Indonesia.
Submitted for publication

36
To the Editor: Here we describe the first evidence of Hantavirus (HV) infection in humans in Indonesia. Hantaviruses belong to the family Bunyavmdae Several serotypes have been described to cause disease in man Hantaan-, Seoul-, - Dobrava-and Puumala-hke viruses cause mild to severe haemorrhagic fever with renal syndrome (HFRS) (1). New World hantavirus serotypes (e g Sin Nombre, Andes) are associated with pulmonary syndrome (hantavirus with pulmonary syndrome [HPSJ) (1) In South East Asia, evidence of HV has been reported from Korea, the Philippines, Singapore and Thailand (2,3,4,5). In Indonesia, a serological study indicated the presence of Seoul-like virus in wild rats (6) So far no human cases of HV infection have been reported from this country
Serum samples from 94 febrile patients suspected of a dengue virus infection were investigated for the presence of HV specific antibodies All patients were residents of Yogyakarta or Semarang and had presented as outpatients or had been admitted to hospital with symptoms of febrile illness between May 1995 and January 1996 during a dengue epidemic Patients were divided into two age groups, the first group included 69 patients in the age ranging between 2-20 years (mean 13.9 years), the second group included 25 patients in the age ranging between 21-47 years (mean 27 2 years) Dengue virus specific serology in serum samples of these patients was not indicative for recent infection with this virus Therefore the aetiology of their illness remained elusive. Serial serum samples of each patient were tested for the presence of HV specific IgM and/or IgG antibodies with a commercially available enzyme immunoassay (EIA) (MRL Diagnostics, Cypress, USA), using microplates coated with a mixture of Seoul and Sin Nombre virus recombinant nucleoproteins (7) Positive EIA results were confirmed by immunofluorescence assay (8)
In ten (11%) of the 94 patients, HV specific serology indicated a recent HV infection Five had HV specific IgM and IgG serum antibodies and five had HV specific IgM but no HV specific IgG serum antibodies In two patients only HV specific IgG serum antibodies were demonstrated, indicating a past HV infection Nine of the ten, recently infected patients were under 20 years of age (mean 17 6 years), the youngest being 13 years old This finding is in agreement with previous observations, showing that the majority of HV patients is older than 15 years (9) Previous epidemiological studies have demonstrated that the distribution of HV infection in Europe is skewed towards the male population, whereas in South East Asia the distribution of HV infections is almost equal among the sexes, which may be related to outdoor occupational activities (3, 9) In our study, eight of the HV positive patients proved to be women All ten patients had suffered from fever and headache, whereas the majority of the patients displayed other symptoms including weakness, nausea, vomiting, joint-, muscular- and retro-orbital pain, lymphadenopahty, hepatomegaly and petechiae These clinical symptoms are consistent with those of HV infection causing HFRS ( 1 )
This first demonstration of HV infection in Indonesia is important for differential diagnosis ot acute febrile illness, which may present with haemorrhagic complications.

37
References
1 Schmaljohn C , Hjelle Β Hantaviruses a global disease problem Emerg Infect Dis 1997,3 95-104
2 Lee HW, Lee PW, Johnson KM Isolation of the enologie agent of Korean Hemorrhagic fever J Infect Dis 1978,137 298-308
3 Quelapio ID, Villa L, Clarin SM, Bacosa M, Tupasi TE Seroepidemiology of Hantavirus in the Philippines Ini J Infect Dis 2000,4 104-107
4 Wong TW, Chan YC, Joo YG, Lee HW, Lee PW, Yanagihara R Hantavirus infections in humans and commensal rodents in Singapore Trans R Soc Trop MedHyg 1989,83 248-251
5 Elwell MR, Ward GS, Tingpalapong M, LeDuc JW Serologic evidence of Hantaan-like virus in rodents and man in Thailand Southeast Asian J Trop Med Public Health 1985,16 349-354
6 Ibrahim IN, Sudomo M, Monta C, Uemura S, Muramalsu Y, Ueno H el al Seroepidemiological survey of wild rats for Seoul virus in Indonesia Jpn J Med Sci Biol 1996,49 69-74
7 Koraka P, Avsic-Zupanc T, Osterhaus AD, Groen J Evaluation of two commercially available immunoassays for the detection of hantavirus antibodies in serum samples J Clin Virol 2000,17 189 196
8 Groen J, Osterhaus AD, Avsic-Zupanc T, van der GG, Clement JP, Letevre A et al Different hantavirus serotypes in western Europe Lancet 1991,337 621-622

38
Chapter 4
Clinical picture and risk factors for mortality in dengue shock syndrome
Catharina Suharti', Tatty E. Setiati2, Eric CM. Van Gorp1, Robert J. Djokomoeljanto', Moeljono S. Trastotenojo2, Jos W. M. van der Meer4, Wil M.V. Dolmans4
Departments of Internal Medicine1 and Paediatrics2, School of Medicine, Diponegoro University and Dr. Kariadi Hospital, Semarang, Indonesia; Department of Internal Medicine Slotervaart Hospital, Amsterdam", The Netherlands; Department of General Internal Medicine, University Medical Center St. Radboud, Nijmegen4, The Netherlands
Submitted for publication

39
Abstract
Dengue shock syndrome (DSS) is the most severe form of dengue hemorrhagic fever (DHF) and has a high mortality In 50 children with DSS, of whom Π (26%) died, we investigated which clinical signs and laboratory findings are related to mortality We found that gastrointestinal bleeding and bilateral pleural effusion were significantly more frequent in non-survivors than in survivors (p<0 02 and p-0 0006, respectively) Also, mean admission levels of thrombin-antithrombin complexes (TATc) and plasminogen activator inhibitor type 1 (PAI-1), activation markers of coagulation and fibrinolysis, respectively, were significantly higher in non-survivors (p=0 004 and p-0 0006, respectively) In regression analysis, bilateral pleural effusion and admission levels of TATc were significantly associated with mortality (p=0 007 and p=0 048, respectively) Our data provide evidence for a relationship of mortality with pleural effusion, a marker of plasma leakage, and coagulation activation, both characteristic pathological changes in dengue shock syndrome

40
Introduction
Dengue virus infection is an arthropod-borne disease, caused by any of four closely related serotypes of dengue virus, belonging to the genus Flavivirus, family Flavivindae. DEN-1, DEN-2, DEN-3 and DEN-4. Infection confers life-long homotypic, but not heterotypic, immunity Clinical manifestation can be asymptomatic infection, dengue fever (DF) and dengue hemorrhagic fever (DHF) The severity of DHF can vary from DHF I to DHF IV The severe forms (DHF III and IV) are also referred to as dengue shock syndrome (DSS), characterized by shock due to leakage of plasma from blood vessels (1).
The pathogenesis of DSS is controversial Epidemiological studies indicate that preexisting dengue virus antibodies may predispose an individual to DHF on subsequent infection with another dengue virus serotype (2-4) Other studies have demonstrated that DEN-2 and DEN-3 are more virulent than DEN-1 and DEN-4, but all four serotypes can cause severe or fatal disease (5-9). Epidemiological observations have provided evidence that age and race may be risk factors tor DHF DSS has been almost confined to children (10) and the age group most severely affected was 5-9 years (11). Blacks are less susceptible to dengue shock syndrome than whites and Asians (3).
There are two major pathological changes in DHF determining the severity of disease, plasma leakage and bleeding The mechanism responsible for the increased permeability of vascular endothelial cells and bleeding in DHF has not been elucidated, although cytokines released during the immune response to dengue virus have been thought to be mediators of the process (12-14) The mortality rate ot DHF is high, ranging from 2 to 10 9% (15-19), reaching 47% in patients with profound shock (20).
We conducted a prospective clinical study, to investigate which clinical signs and laboratory parameters are associated with mortality in DSS.
Patients and Methods
Study setting This prospective study was performed in Dr. Kanadi Hospital, the university hospital of
Diponegoro University, Semarang, Indonesia The research protocol was approved by the Review Board of the Dr Kanadi Hospital. Written informed consent was obtained trom children's parents or legal guardians
Patients Between June and November 1996, during an outbreak of dengue in Indonesia, 50
consecutive children with the clinical diagnosis of DSS, who were admitted to the Paediatnc Intensive Care Unit were enrolled in the study Only children with age > 3 years were included.
Case definition The clinical diagnosis of DSS (DHF grade III and grade IV) was finally based on the
1997 WHO criteria (1) Patients presenting all criteria for DHF (i) fever or history of acute fever 2-7 days, (n) bleeding (mild to severe), (m) thrombocytopenia 100.000/mm1
or less (iv) evidence of plasma leakage plus evidence of circulatory lailure manifested by

41
(a) rapid and weak pulse; (b) narrow pulse pressure (20 mmHg); (c) hypotension and (d) cold, clammy skin and restlessness, were classified DHF III. If profound shock with undetectable blood pressure and pulse was present, patients were classified as DHF IV. Decreased consciousness was based on the Glasgow Coma Scale (21).
Patient monitoring Thorough clinical assessment was performed daily during hospitalization, using a
medical record form. Laboratory tests to support clinical management included blood cell counts, tests for hemostasis (prothrombin time and activated partial thromboplastin time) as well as biochemical tests for kidney and liver functions and electrolyte status. Thrombin-antithrombin complexes (TATc) and plasminogen activator inhibitor type 1 (PAI-1), activation markers for coagulation and fibrinolysis, respectively, were also assayed. Chest x-ray and ECG were done routinely.
Specimen collection and methods of assay Blood specimens were collected in vacutainer tubes (Becton Dickinson, Rutherford, NJ
07417). Two ml of blood for serological assays was collected on day of admission and at discharge. Blood was centrifuged 1000-1500 rpm for 10 minutes, after which serum was
transferred to screw cap Eppendorf tubes and stored at -80^C, until assayed. Full blood counts were measured with QBC, Becton Dickinson, NJ 07417. For measurement of aPTT, PT and TATc, venous blood (9 vol.) was drawn into vacutainer tubes containing 0.105 M sodium citrate (1 vol.). aPTT and PT were measured by a coagulometer, KG Behnk Elektronik, and TATc levels were determined by means of a commercially available ELISA kit, according to the manufacturer's instructions (Enzygnost TAT micro, Dade Behring, Marburg Germany); normal value < 4.1mg/l. For measurement of PAI-1, blood was collected in siliconized vacutainer tubes containing Polybrene (Janssen Chimica, Belgium) and EDTA (0.05%, w/v, and 10 mM, respectively, final concentrations), to prevent in vitro complex formation. PAI-1 was measured with sandwich ELISA kits using specific monoclonal antibodies as described (22). All blood samples for analysis of coagulation and fibrinolysis were immediately immersed in melting ice and subsequently centrifuged at 40C for 20 min, at 1600 χ g. Plasma samples were stored at -80 C, until assayed. Normal value for PAI-1 is 30-60 ng/ml. Biochemical tests, including liver as well as renal function tests and electrolytes, were measured with Auto Analyzer, Hitachi, 7050. Normal value for serum protein were 5.9-8.6 g/dl, and for serum albumin were 3.5-5.6 g/dl. TATc and PAI-1 measurements were done at the Slotervaart Hospital, Amsterdam, The Netherlands. For the transport from Indonesia to The Netherlands (which last longer than 15 hours) the samples for coagulation, fibrinolysis, and serological assays were kept on dry ice.
Serological assays The diagnosis of dengue virus infection was confirmed by serological assays. A capture
and indirect enzyme-linked immunosorbent assay (ELISA) detected dengue specific IgM and IgG antibodies in serum samples, according to a previously described procedure (23).
Statistical analysis Continuous data were described in mean (SD) and nominal data in number (%).

42
Nominal variables between survivors and non-survivors were compared using x" Test Fisher's Exact test was performed if the number of cells with expected frequency less than 5 were more than 20% Independent t-tests were done to compare numeric variables between survivors and non-survivors The assumption of normality of the data was checked before the t-test Mann-Whitney U tests were done when the data were not normally distributed The cut-of-point of significance was p=0 05 with 95 % confidence interval Regression analysis was done to determine factors associated with mortality Survival time was calculated with Kaplan-Meier curves Log-rank test was used for curve comparison All statistical analyses were pertormed with SPSS for Windows version 9 0
Results
Between June and November 1996, 50 children with a clinical diagnosis ot DSS, were enrolled in the study Thirteen patients (26%) died during follow up in the Intensive Care Unit The clinical diagnosis of DSS was confirmed by serological assays in all patients, either by an IgM response or a fourfold rise in IgG titers All antibody profiles were typical for secondary dengue infection
Table 1. Clinical characteristics of survivors and non-survivors in 50 patients with dengue shock syndrome
Survivors Non-Survivors ρ value (n=37) (n=13)
Clinical characteristics Age (years) Sex ratio (M/F) DHF III/DHF IV Days since onset ol disease Bleeding manifestations Positive Tourniquet test Skin bleeding Epistaxis Gum bleeding Gastrointestinal bleeding Hematuna Signs of disease seventy Cold extremities Clammy skin Delirium Decreased consciousness Convulsions Bilateral pleural effusion Lowest systolic blood pressure Lowest diastolic blood pressure
6 8+2 8 20/17 34/1 4 2±0 9
16 14 7 0 17 1
35 3 13 16 2 2 92±11 59+24
6 0±2 8 4 / 9 9/4 40±1 3
7 7 3 3 11 1
13 6 11 11 3 6 83+11 45±31
051 031 0 74 <0 003 <0 02 0 43
0 39 0 002 0 002 001 0 07 0 0006
Values indicated are mean±SD and number

43
Clinical characteristics of survivors and non-survivors As shown in table 1, most patients were young children who presented after
about 4 days of illness. Relatively more female patients died than males. Of the non-survivors 4 of 13 (30.7%) were classified as DHF IV, as compared with 3 of 37 (8.1%) survivors. The proportion of patients with gastrointestinal and gum bleeding was significantly higher in non-survivors than in survivors. A clammy skin, delirium, decrease of consciousness and bilateral pleural effusion were significantly more frequent in non-survivors than in survivors.
Table 2. Laboratory tests for hemostasis and markers of plasma leakage on day of admission in survivors and non-survivors in 50 patients with dengue shock syndrome
Survivors Non-Survivors ρ value *) (n=37) (n=13)
Tests for hemostasis APTT (sec) PT (sec) PAI-1 (ng/ml) TATc (ng/ml) Plalelets(xl09/1)
Markers of plasma leakage Serum protein (g/l) Serum albumin (g/l) Albumin/protein ratio Plasma sodium (mmol/1) Hematocrit (%)
56.6±24.1 15.3+4.7 285.11491.8 32.7+77.3 63.8±35.7
5.2±1.0 3.5±0.7 0.67+0.08 134.9+6.2 38.3±6.4
107.01102.2 24.2+12.0 1126.4+1314.6 67.5+43.3 48.6112.9
ρ value (95% CI)
4.5+0.9 3.2+0.6 0.71+0.07 133.8+8.0 36.417.4
0.06 0.001 0.0006 0.004 0.15
0.035 (0.052 to 1.335) 0.22 (-0.164 to 0.682) 0.10 (-0.103 to 0.010) 0.63 (-3.639 to 5.872) 0.39 (-2.519 to 6.227)
Mann-Whitney U test for differences of APTT, PT, PAI-1, TATc, and platelets; Independent t-lest for serum protein, serum albumin, albumin/protein ratio, plasma sodium and hematocrit: APTT: activated partial thromboplastin time (control value: 31.911.7 sec); PT: prothrombin time (control value: 12+0.6 sec); PAI-1: plasminogen activator inhibitor-type 1 (normal value 30-60 ng/ml); TATc: thrombin-antithrombin complex (normal value <4.1 ng/ml).
Laboratory tests for hemostasis and markers of plasma leakage Table 2 shows that the prothrombin time (a measure for both the extrinsic and
the common coagulant pathway) was significantly longer in non-survivors than in survivors. Also the levels of thrombin-antithrombin complexes (TATc) and plasminogen activator inhibitor type 1 (PAI-1), activation markers of coagulation

44
and fibrinolysis, respectively, were significantly higher in non-survivors than in
survivors
The levels of serum protein were significantly lower in non-survivors than in
survivors
Association of markers of coagulation and fibrinolysis and of plasma leakage
with mortality In the logistic regression analysis lor mortality of day of admission levels ol TATc and
PAI 1 activation markers of coagulation and fibrinolysis, respectively, wc found a significant association of TATc with mortality (p=0 048, regression coefficient 0 023) Such association was not found for PAI 1 (table 3)
In the logistic regression analysis of albumin/protein ratio on day of admission and bilateral pleural etlusion tor mortality, a significant association was found tor bilateral pleural effusion but not for albumin/protein ratio The odds ratio lor bilateral pleural effusion was 12 2 and p-value 0 007, implying that patients with bilateral pleural effusion had a 12 2 times increased nsk of death (table 3) This effect is also shown in the cumulative survival curve ot patients with and without bilateral pleural effusion (Figure)
Table 3. Association ot markers of coagulation and fibrinolysis and of plasma
leakage with mortality in 50 patients with dengue shock syndrome
Ρ value Exp (ß)/OR
Activation markers of coagulation and fibrinolysis
TATc (ng/ml) PAI-1 (100 ng/ml) Constant
0 02 0 08 2 79
0 048 0 12 0 0002
102 1 08
Markers of plasma leakage
Bilateral pleural etlusion 2 5 0 007 12 2 Albumin protein ratio*) 3 7 0 39 40 7 Constant -4 109 0 172
β regression coefficienl Exp β exponent β OR odds ratio TATc thrombin antithrombin complex PAI 1 plasminogen activator inhibitor type 1 *) day of admission levels

45
•̂ 4-
I
No bilateral pleural effusion
1 I I
+ Bilateral pleural effusion
2 Ò 2 4 6 8 10 12 14 16
Days since admission
Kaplan Meier survival curves of patients with bilateral pleural effusion compared with those without bilateral pleural effusion (p=0 002) The median survival time of patients with bilateral pleural effusion was 4 days (95% CI, 1 32 to 6 68)
Discussion
In this prospective study of 50 children with DSS, we found that bilateral pleural effusion and elevated TATc concentrations were significantly associated with mortality in logistic regression analysis Bilateral pleural effusion indicates severe vascular leakage whereas high TATc concentrations reflect markedly activated coagulation
Our finding that bilateral pleural effusion is associated with poor prognosis corroborates the data of a study from Jakarta of 30 fatal cases ot virologically confirmed dengue virus infection In that study plasma leakage appeared to be the main cause of death, because 19 of the 30 cases (63.3%) had profound shock with hemoconcentration (24) In an autopsy study from Thailand of 100 children with latal DSS plasma leakage was also likely the main cause of death, as evidenced by > 4g/dl protein content of serous effusions in the pleural, abdominal and pericardial cavities Also, the mucosa, submucosa and serosa of the gastrointestinal tract of these children showed oedema and hemorrhage, especially in children with prolonged shock (25,26).
The admission level of TATc appeared to be a strong predictor of mortality, indicating the pathophysiological implication of coagulation activation This finding is in line with the result from an earlier study, in which we found that high PAI-1 levels and hence activation of coagulation were most pronounced in non-survivors, indicating an ongoing procoagulant state (27). Studies on fatal cases demonstrated evidence ot severe bleeding
100c
80
60
40
20
0

46
followed by shock (24), foci of hemorrhage in the brain (28), histological evidence of intravascular coagulation (26, 29), sero-hemorrhagic effusions (29) and renal impairment (30)
We also tound that prothrombin time was significantly longer in non-survivors than in survivors This suggests that the extrinsic (tissue lactor/tactor Vila) pathway may be the main route in the activation of coagulation in DSS.
A number of clinical signs were more frequently seen in non-survivors than in survivors although these signs did not qualify in the logistic regression analysis, because these are not specific for DSS Clammy skin was significantly more frequent (p=0.0002) and the systolic and diastolic blood pressures were lower in non-survivors (table 1) In addition, we found that delirium and decreased consciousness were significantly more frequent in non-survivors than in survivors (p=0 002 and p=0.0l0, respectively). Dengue virus subtypes 2 and 3 have been isolated from cerebrospinal fluid and have known to be neurovirulent (31) Histological studies from fatal DHF cases with signs of encephalopathy have provided evidence that the brain cell is also a target cell for dengue virus (32-36) In addition, loss of integrity of the cerebral vascular endothelium leading to cerebral oedema and cerebral bleeding has been observed (28, 37)
In conclusion, our data provide evidence for a relationship of mortality with both, plasma leakage and coagulation activation in dengue shock syndrome In the absence of interventions to stop vascular leakage, close monitoring and the use of plasma expanders to increase intravascular oncotic pressure is mandatory, especially in children with pleural effusion. In addition strategies to control coagulation activation would be an important area of development
Acknowledgements
Participants in this project, besides the authors, were dr. Herawati Juslam from the Department of Paediatrics, Diponegoro University and Dr Kanadi Hospital, Semarang, Indonesia. We thank dr. Hardian and dr Henry Setiawan from Clinical Epidemiology Unit, Diponegoro University, Semarang, for statistical support, Y T. van der Heide from Clinical Chemistry and Hematology Laboratory Slotervaart Hospital, Amsterdam for managing the blood samples We thank also Dr J Groen and Prof A Osterhaus trom Institute of Virology Erasmus Medical Center Rotterdam for performing the diagnostic assays

47
References
1. World Health Organization. Dengue haemorrhagic fever: diagnosis, treatment, prevention and control. 2nd ed. Geneva 1997; 12-47.
2. Sangkawibha N, Rojansuphot S, Ahandrik S, Viriyapongse S, Jatanasen S, Salitul V, Phanthumachinda B, Halstead SB. Risk factors in dengue shock syndrome: a prospective epidemiologic study in Rayong, Thailand. Am J Epidemiol 1984; 20: 653-69.
3. Guzman MG, Kouri GP, Bravo J, Soler M, Vasquez S, Morier L. Dengue hemorrhagic fever in Cuba, 1981: a retrospective seroepidemiologic study. Am J Trop Med Hyg 1990; 42: 179-84.
4. Burke DS, Nisalak A, Johnson DE, Scott RM. A prospective study of dengue infections in Bangkok. Am J Trop Med Hyg 1988; 38: 172-80.
5. Rosen L. Comments on the epidemiology , pathogenesis and control of dengue. Med Trop 1999;59:495-98.
6. Guzman MG, Kouri G, Valdes L, Bravo J, Alvarez M, Vazques S, Delgado I, Halstead SB. Epidemiologic studies on dengue in Santiago de Cuba, 1997. Am J Epidemiol 2000; 152: 793-99.
7. Graham RR, Juffrie M, Tan R, Hayes CG, Laksono I, Ma'roef C, Erlin, Sutaryo, Porter KR, Halstead SB. A prospective seroepidemiologic study on dengue in children four to nine years of age in Yogyakarta, Indonesia I. Studies in 1995-1996. Am J Trop Med Hyg 1999;61:412-19.
8. Kobayashi N, Thayan R, Sugimoto C, Oda Κ, Saat Ζ, Vijayamalar Β, Sinniah M, Igarashi A. Type-3 dengue viruses responsible for the dengue epidemic in Malayasia during 1993-1994. Am J Trop Med Hyg 1999; 60: 904-9.
9. Pandey BD, Morita K, Hasebe F, Parquet MC, Igarashi A. Molecular evolution, distribution and genetic relationship among the dengue 2 viruses isolated from different clinical severity. Southeast Asian J Trop Med Public Health 2000; 31: 266-72.
10. Kouri GP, Guzman MG, Bravo JR, Triana C. Dengue haemorrhagic fever/dengue shock syndrome lessons from the Cuban Epidemic. Bull. W.H.O 1989; 67: 375-380.
11. Chareonsook O, Foy HM, Teeraratkul A, Silarug N. Changing Epidemiology of dengue hemorrhagic fever in Thailand. Epidemiol Infect 1999; 122: 161-66.
12. Kurane I, Ennis FA. Immunopathogenesis of dengue virus infections. In: Dengue and dengue hemorrhagic fever. Gubler DJ, Kuno G, eds. Wallingford, UK: Cab International 1997; 273-90.
13. lyngkaran N, Yadav M, Sinniah M. Augmented inflammatory cytokines in primary dengue infection progressing to shock. Singapore Med J 1995; 36: 218-21.
14. Anderson R, Wang S, Osiowy C, Issekutz AC. Activation of endothelial cells via antibody-enhanced dengue virus infection of peripheral blood monocytes. J Virol 1997;71:4226-32.
IS.Tripathi BK, Gupta B, Sinsha RS, Prasad S, Sharma DK. Experience in adult population in dengue outbreak in Dehli. J Assoc Physicians India 1988; 46: 273-76.
16. Aggarwal A, Chandra J, Aneja S, Patwari AK, Dutta AK. An epidemic of dengue hemorrhagic fever and dengue shock syndrome in children in Dehli. Indian Pediatr 1998; 35: 727-32.

48
17 Anuradha S, Singh NP, Rizvi SN, Agarwal SK, Gur R, Mathur MD The 1996 outbreak of dengue hemorrhagic fever in Delhi, India Southeast Asian J Trop Med Public Health 1998, 29· 503-06.
18. Kabra SK, Jain Y, Pandey RM, Madhulika, Singhal T, Tnpathi P, Broor S, Seth P, Seth V. Dengue hemorrhagic fever in children in the 1996 Delhi epidemic Trans R Soc Trop Med Hyg 1999, 93· 294-98.
19. Wall JP, Biswas A, Handa R, Aggarwal P, Wig N, Dwivedi SN. Dengue hemorrhagic fever in adults a prospective study of 110 cases Trop Doet 1999, 29 27-30.
20 Agarwal R, Kapoor S, Nagar R, Misra A, Tandon R, Mathur A, Misra AK, Srivastava KL, Chaturvedi UC A clinical study of the patients with dengue hemorrhagic fever during the epidemic of 1996 at Lucknow, India Southeast Asian J Trop Med Public Health 1999; 30· 735-40
21 Jams C, 1993 Physical examination and health assessment, ρ 199 WB Saunders, Philadelphia
22. De Boer JP, Creasy AA, Chang A, Roem D, Brouwer MC, Herenberg AJ, Hack CE, Taylor FB Jr. Activation patterns of coagulation and fibrinolysis in baboons following infusion with lethal or sublethal dose ot Escherichia coli Cire Shock 1993 39 59-67.
23. Velzing J, Groen J, Drouet MT, van Amerongen G, Copra C, Osterhaus AD, Deubel V. Induction of protrective immunity against Dengue virus type 2 comparison of candidate live attenuated and recombinant vaccines Vaccine 1999, 17 1312-20
24. Sumarmo, Wulur H, Jahja E, Gubler DJ, Suharyono W, Sorensen K. Clinical observations on virologically confirmed fatal dengue infections in Jakarta, Indonesia Bull World Health Organ 1983; 61 693-701.
25. Bhamarapravati N, Tuchinda P, Boonyapaknavik V Pathology of Thailand haemorrhagic fever: a study of 100 autopsy cases Ann Trop Med Parasitol 1967, 61' 500-10.
26. Bhamarapravati Ν Pathology of dengue infections In Gubler DJ, Kuno G eds Dengue and dengue hemorrhagic lever Cab Inteernational 1997 Wallingford, UK 115-132
27. van Gorp ECM, Suharti C, Tatty E Setiati, Mairuhu ATA, ten Cate H, Dolmans WMV, van der Meer JWM, Hack EC, Brandjes DPM Impaired fibrinolysis in the pathogenesis of lethal dengue hemorrhagic fever (DHF). Submitted for publication
28 Chimelh L, Hahn MD, Netto MB, Ramos RG, Dias M, Gray F Dengue neuropathological findings in 5 fatal cases from Brazil. Clin Neuropathol 1990; 9 157-62.
29 Strobel M, Jattiot F, Boulard F, Lamaury I, Salin J, Jarnge B, Mazille V, Vachon F, Goursaud R Emergence of dengue hemorrhagic fever in French Antilles. Three initial fatal cases in Guadeloupe Presse Med 1998, 27 1376-78
30 George R, Liam CK, Chua CT, Lam SK, Pang T, Geethan R, Foo LS Unusual clinical manifestations of dengue virus infection Southeast Asian J Trop Med Public Health 1988, 19 585-90
31. Lum C, Lam SK, Choy YS, George R, Harun F Dengue encephalitis a true entity9
Am J Trop Med Hyg 1996· 54 256-59 32 Miagostovich MP, Ramos RG, Nicol AF, Nogueira RM, Cuzzi-Maya Τ, Oliveira AV,
Marchevsky RS, Mesquita RP, Schatzmayr HG. Retrospective study on dengue fatal

49
cases Clin Neuropathol 1997, 16 204-08 33 Desprès Ρ, Frenkiel MP, Ceccaldi ΡΕ, Dos Santos CD, Deubel V Apoptosis in the
mouse central nervous system in response to infection with mouse-neurovirulent dengue viruses J Virol 1998,72 823-29
34 Ramos C, Sanchez G, Pando RH, Baquera J, Hernandez D, Mota J, Ramos J, Flores A, Llausas E Dengue virus in the brain of fatal case of hemorrhagic dengue fever J Neurovirol 1998, 4 465-68
35 Hommel D, Talarmin A, Deubel V, Reynes JM, Drouet MT, Sarthou JL, Huhn A Dengue encephalitis in French Guiana Res Virol 1998, 149 235-38
36 Guzman MG, Alvarez M, Rodnquez R, Rosario D, Vazquez S, Vald SL, Cabrera MV, Koun G Fatal dengue haemorrhagic fever in Cuba, 1997 Int J Infect Dis 1999, 3 130-35
37 Janssen HL, Bienfait HP, Jansen CL, van Duinen SG, Vriesendorp R, Schimsheimer RJ, Groen J, Osterhaus AD Fatal cerebral oedema associated with primary dengue infection J Infect 1998, 36 344-46

so
Chapter 5
Cytokine patterns during Dengue Shock Syndrome
CatharinaSuharti'.EncC M van Gorp2, Wil M V Dolmans1, Tatty E Setiati4, C Enk Hdck\ Robert J Djokomoeljanto', Jos W M van der Meer1
Departmens of Medicine and Paediatrics, School ot Medicine, Diponegoro University and Dr Kanadi Hospital, Semarang, Indonesia, Department of Medicine, Slotervaart Hospital, Amsterdam2, Department of Medicine, University Medical Center St Radboud, Nijmegen , Central Laboratory of The Netherlands Red Cross Blood Transfusion Service, and Department Clinical Chemistry, Academic Hospital Vrije Universiteit, Amsterdam,5 The Netherlands
Submitted for publication

SI
Abstract
Dengue shock syndrome (DSS) is the most severe form of dengue Cytokines released during the immune response to dengue virus are thought to play a pivotal role in the pathogenesis of the disease We performed a prospective clinical study in 50 patients with DSS, to investigate the patterns of TNF-a, IL-Iß, IL-6, IFN-yand IL-lRa dunng the course of the disease During the acute phase, the plasma concentrations and the ex-vivo production without LPS of IL-lRa were considerably elevated and returned to normal on recovery However, the ex-vivo LPS stimulated production of the proinflammatory cytokines TNF-a and IL-Iß were considerably depressed Also these concentrations returned towards normal on recovery In non-survivors, the plasma concentrations of IL-6 and IL-lRa were significantly higher than in survivors (p<0 00001 and ^=0 0005, respectively) Also the ex-vivo production of IL-lRa in non-survivors was significantly higher than in survivors, both without LPS stimulation (p=0 0008) and with LPS (p<0 004) Since IL-lRa was significantly associated with mortality (/7=0 007), this measurement may be used as an index of disease seventy

Ï2
Introduction
Dengue virus infections are caused by any of four serotypes of the virus (DEN-1, DEN-2, DEN-3, and DEN-4). The disease may manifest itself as a dengue fever (DF), characterized by sudden onset of fever and a variety of nonspecific signs and symptoms, including headache, joint and muscle pains, retro-orbital pain, rash and bleeding manifestations (1,2), or as dengue hemorrhagic fever (DHF), the severe form of disease Patients with DHF develop thrombocytopenia, increased capillary permeability, resulting in plasma leakage, hemoconccntration, and sometimes hemorrhage DHF may develop into dengue shock syndrome (DSS), the most severe form of DHF, with signs of circulatory failure, including narrow pulse pressure (20 mm Hg), hypotension, or frank shock (1) Plasma leakage and bleeding are the two major pathophysiological changes in DHF/DSS that determine the seventy of the disease The pathogenetic mechanisms responsible for the increased permeability of vascular endothelial cells in DHF has not been elucidated, however, it has been suggested that cytokines and other mediators which are released during the immune response to dengue virus infection may form the underlying mechanism (3). It is hypothesized that in secondary infections with a virus of a different of serotype from that causing the primary infection, cross-reactive antibodies enhance the infection and replication of dengue virus in mononuclear phagocytic cells (4, 5). In addition, these cells produce and secrete pro-inflammatory cytokines, including tumor necrosis factor-α (TNF-a), interleukin-lß (IL-Iß), and IL-6 (6-8), as well as antiinflammatory mediators, the soluble TNF-Receptor p55 (sTNFRp55), sTNFRp75 and IL-1 receptor antagonist (sIL-IRa) (9) CD4+T lymphocytes are activated and produce a number of cytokines including gamma interferon (IFN-γ), IL-2, IL-4, IL-5, IL-10 (ΙΟΙ 2) Previous studies have observed a relationship between high levels of TNF-a, IL-6 and disease severity (6-8) In addition, the role of TNF-a in plasma leakage has been demonstrated indirectly by the correlation of soluble tumor necrosis factor receptors (sTNFRs) with the degree of subsequent pleural effusion (13), and, the role of cytokine in the initiation of coagulation and fibrinolysis has been studied intensively in Gram negative-sepsis and endotoxacmia (14)
We performed a prospective clinical study to investigate the patterns of TNF-a, IL-Iß, IL-6, IFN-γ and IL-IRa during the course of the disease and to identity which of these cytokines were related to mortality
Patients and methods
Study setting This prospective study was performed in Dr Kanadi Hospital, the university hospital of
Diponegoro University, Semarang, Indonesia The research protocol in this study was reviewed and approved by the institutional Review Board of Dr Kanadi Hospital/Diponegoro University Written informed consent was obtained from children's parents or legal guardians
Patients Between June and November 1996, during an outbreak of dengue in Indonesia, 50
consecutive children with the clinical diagnosis of DSS and admitted to the Paediatnc

53
Intensive Care Unit were enrolled in the study. The diagnosis of DSS (DHF grade III and grade IV) was finally based on WHO criteria (1997) (1). Only children with age > 3 years old were included
Patient monitoring Thorough clinical assesment using a medical record form was performed daily from
day of admission to the Intensive Care Unit until discharge from that Unit or death Laboratory tests to support clinical management included blood cell counts, tests for hemostasis (prothrombin time and activated partial thromboplastin time) as well as biochemical tests for kidney and liver functions and electrolytes status Also, chest x-ray and ECG were done routinely
Specimen collection Blood specimens were collected in vaculainer tubes (Becton Dickinson, Rutherford, NJ
07417) Specimen for cytokine assays were collected in the acute phase of the disease (on day of admission day 0, on day 1 and 2), and on day 7 or the day of discharge if the patient was hospitalized less than 7 days Two tubes of 4 ml of blood were collected into sterile tubes containing EDTA from each patient. To each tube 125 μ ι aprotinin (Trasylol, Bayer, Leverkusen, Germany, final concentration 625 kallikreine inactivating umts/mL) was added through the stopper by a tuberculin needle and syringe One tube was centnfuged directly at 1250 g for 10 minutes, and thereafter at 15000 g tor 1 minute to remove platelets The plasma was stored in aliquots at -800C until assayed for cytokines. To one of the remaining tube, 50 μL· LPS (E coli serotype 055 B5, Sigma, St Louis, USA; final concentration 10 μg/mL) was added to stimulate cytokine production The tube was incubated at 37()C for 24 hours, and afterwards stored in - 80()C, until assayed for cytokines
To collect appropriately timed specimens for serological assay (> day 6 after onset of fever) (15-18), 2 ml of blood was collected on day of admission and at discharge Blood was centnfuged at 1000-1500 rpm for 10 minutes, then, serum was transferred to screw cap Eppendorf tubes and stored at -800C until assayed. For the transport from Indonesia to The Netherlands, the samples for cytokines and serological assays were kept on dry ice
Cytokine assays TNF-a, IL-Iß and IL-IRa were measured in duplicate by nonequihbnum
radioimmunoassay (RIA) (19) Recombinant human TNF-a, IL-Iß and IL-IRa were calibrated against standards provided the National Institute of Biological Standards and Control (Potters Bar, UK), with the sensitivity of the assay with 100 μΐ sample of 40 pg/ml, 40 pg/ml, and 80 pg/ml, respectively TNF: normal median value 90 pg/ml (range 50-170) IL-Iß. normal median value 50 pg/ml (range <40-l 15) IL-IRa normal median value 139 pg/ml (range <80-502) IFN-γ and IL6 were measured with ELIS As obtained from the Central Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands, according to manufacturer's instruction Levels of IFN-γ exceeding 40 pg/ml and levels of IL6 exceeding 10 pg/ml were considered to be elevated

54
Serological assays The diagnosis of dengue infection was confirmed by serological assays. A capture and
indirect enzime-linked immunosorbent assay (ELISA) detected dengue specific IgM and IgG antibodies in serum samples, according to a previously described procedure (20).
Statistical analysis Continuous data were described in mean (SD), and median; whereas nominal data were
described in number. Independent Independent i-tests were done to compare numeric variables between survivors and non-survivors. The assumption of normality of the data was checked before the f-test. Mann-Whitney U tests were done when the data were not normally distributed. The cut-of-point of significance was p=0.05 with 95 % confidence interval. Logistic regression analysis was done to calculate association between cytokines and mortality. All statistical analyses were performed using SPSS for Windows version 9.0.
Results
Between June and November 1996, 50 children with a clinical diagnosis of DSS were enrolled in the study. Baseline characteristics of the patients are listed in the table 1. All children were admitted during the acute phase of the disease. Symptoms had started 2-7 days (mean 4.2±1) before admission to the Intensive Care Unit. Thirteen patients (26%) died during follow up. The clinical diagnosis was confirmed by serological assay in all patients, either by an IgM response or a fourfold rise in IgG titres. Antibody profiles were typical for secondary dengue infection.
Table 1. Characteristics in 50 patients with dengue shock syndrome
Age in years 6.6±2.8 (3-13) Days since onset of disease 4.2±1 (2-7) Male 24 (48%) Female 26 (52%) Clinical diagnosis (WHO criteria) DHF III 43 (86%) DHFIV 7(14%) Positive serology result 50 ( 100%) Number of deaths 13 (26%)
Age and days since onset of disease are mean ±SD (range)
Plasma concentrations of cytokines in the course of the disease We found (figure la,b) that the plasma concentrations of proinflammatory
cytokines TNF-a and IL-Iß were only mildly elevated during the course of the disease. Median values (range) in pg/ml for TNF-a: 155 (95 - 2500) on admission

55
(day 0), 140 (85 - 315), 150 (95 - 305) and 135 (90 - 1100), on day 1, day 2 and day 7 / discharge, respectively; for IL-Iß: 72.5 (<40 - 320) on admission, 80 (<40-140), 80 (<40 - 145) and 70 (<40 - 155), on day 1, day 2 and day 7 / discharge, respectively. However, (figure l,c) the plasma concentrations of the anti-inflammatory cytokine IL-IRa were considerably elevated during the acute phase to decrease during recovery: 795 (220-2500) on admission, 555 (180 -2400), 590 (225 - 2050) and 395 (240 - 2900), on day 1, day 2 and day 7/discharge, respectively. Median plasma concentrations of IFN-γ and IL-6 were not elevated. IL-6: <2 (<2 - 199000) on admission, 2.1 (<2 - 1058), 3.5 (<2 - 155) and <2 (<2 -48), on day 1, day 2 and day 7 / discharge, respectively. IFN-γ: 20 (20 - 54) on admission, 20 (20 - 86), 20 (20 - 582) and 20 (20 - 53), on day 1, day 2 and day 7/discharge, respectively.

56
2ϋΟ -
200 -
=1 t
7/(* schare*
-r-J f-,H E~
Figure la,b,c. Plasma concentrations of TNF-α, IL-Iß and IL-lRa on day of admission (D 0), the following two days (DI, D2) and on day 7 or day of discharge if earlier (D7 / discharge) in 50 patients with DSS. Normal median value of TNF-a 90 pg/ml (range 50-170), IL-Iß 50 pg/ml (range <40-l 15), IL-lRa 139 pg/ml (range <80-502).

s?
Ex-vivo production of TNF-OL, IL-1 β and IL-1 Ra As shown in table 2, the ex-vivo production of IL-IRa after incubation for 24 hours
without LPS was elevated m the acute phase of the disease, and nearly normalized on recovery, while the ex-vivo production of TNF-a and IL-Iß were very little elevated However, after stimulation with LPS, the median ex-vivo production of TNF-a and IL-1 β were considerably depressed dunng the acute phase of the disease These levels returned towards normal on recovery
Table 2. Median ex-vivo production of TNF-a, IL-Iß, and IL-IRa after 24 hr incubation without LPS and with LPS on day of admission (DO), the following two days (D1,D2), and on day 7 or day of discharge if earlier (D7/discharge) in 50 children with dengue shock syndrome
Cytokine
Without LPS
TNF-a (pg/ml) IL-lß(pg/ml) IL-IRd (pg/ml)
With LPS
TNF a (pg/ml) IL-Iß (pg/ml) IL-IRa (pg/ml)
DO
345 0 65 0 2400 0
520 0 660 0 6975 0
Dl
365 0 80 0 2700 0
5100 755 0 8750 0
D2
330 0 80 0 3100 0
590 0 1320 0 9850 0
D7/dischdrgc
330 72 5 1400 0
3850 0 9450 10500 0
Normal value
275 0 40 0 1030 0
4930 0 6460 0 10500 0
Plasma concentrations of cytokines on day of admission in survivors and non-survivors The plasma concentrations of TNF-a, ILI-β and IFN-γ on day of admission of
survivors and non-survivors were not significantly different (mean values ± SD in pg/ml, and ρ value) TNF-a 154 7 ± 540 vs 556 6 ± 909 3, p=0 254, IL-lß 7 3 2 ± 2 1 5 v s 115 7 ± 91 6, p=0 089, IFN-γ 22 2 ± 7 8 vs 25 0 ± 11 8, p=0 376 However (figure 2), compared to survivors, the plasma concentrations IL-IRa were significantly higher in non-survivors 802 2 ± 566 4 vs 1566 9 ± 675 6, p=0QQ05 Also for IL-6 the plasma concentrations were higher in non-survivors compared to survivors (219 50 ± 58 262 0 vs 172 1 ± 956 8, p=<0 00001), but the median values of IL-6 in both groups were 9 5 and 1 0 pg/ml, respectively (normal level up to 10 pg/ml)

58
Figure 2 Plasma concentrations of IL-lRa on day of admission (D 0) in survivors and non survivors of 50 patients with DSS. The difference is significant (p<0.0005). Normal value 139 pg/ml (range <80-502).
Ex-vivo production of TNF-OC, IL!-β and IL-lRa on day of admission in survivors and non-survivors
Table 3 shows the patterns of the proinflammatory cytokines TNF-a and ILI-β and of the anti-inflammatory cytokine IL-lRa. The ex-vivo production of IL-lRa was significantly higher in non-survivors than in survivors, both without LPS stimulation (p=0.0008) and with LPS (p<0.004). The LPS stimulated production of IL-Iß was lower in non-survivors than in survivors (516.1 ± 270.0 vs 2252.2 ± 4152.9 pg/ml) but the difference did not reach statistical significance.
Association of plasma concentrations of cytokines on day of admission with mortality We calculated the association of plasma concentrations of TNF-a, IL-Iß, IL-6, IFN-γ
and IL-lRa on day of admission with mortality. IL-lRa was significantly associated with mortality in these 50 children with DSS (Table 4).

59
Table 3. Ex-vivo production of TNF-α, IL-Iß and IL-lRa after 24 hr incubation without LPS and with LPS on day of admission in survivors and non survivors
Cytokine
Without LPS TNF-α (pg/ml) IL-lß(pg/ml) IL-lRa (pg/ml)
With LPS TNF-α (pg/ml) IL-Iß (pg/ml) IL-lRa (pg/ml)
Survivors (n=37)
362 51219 2 76 8±38 9 2506 912388 9
714 21791 7 2252 214152 9 7141 413436 5
Non-survivors (n=13)
1748 013356 1 86 9149 3 6823 015435 5
1622 312946 7 516 11270 0 11750 015473 9
ρ value*)
0 107 0 584 0 0008
0719 0 084 <0 004
Values are mean+SD, *) Mann-Whitney U-Wiltoxon Rank Sum W Test, Normal value cytokines without LPS in mean+SD, pg/ml TNF-α 286187, IL-ß 46±12,IL-lRd 1144 + 423, with LPS TNFa 51601 1910, IL-Iß 7080 +3430, IL-lRa 10790 + 2460
Table 4. Association of plasma concentrations of TNF-α, IL-1 β, IL-6, IFN-γ and
IL-lRa on day of admission with mortality in 50 children with dengue shock
syndrome
Variable p-value
TNF-α (per 10pg/ml) IL-Iß (per 10pg/ml) IL-6 (per 1000pg/ml) IFN-γ (pg/ml) IL-lRa (100pg/ml) Constant
-0 125 0 203 0 203
-0 290 0 266 2 403
0 275 0 377 0 734 0 887 0 007 0 953
β regression coefficient

60
Discussion
In 50 children with DSS we found that plasma concentrations ot IL-IRa were considerably elevated and that high concentrations of this antiinflammatory cytokine correlated with mortality
It is generally assumed that high concentrations ot antiinflammatory cytokines in the circulation reflect proinflammatory cytokine production in the tissues Also, compared to an antiinflammatory cytokine like IL-IRa, the proinflammatory cytokine responses are relatively short lived in serious infections, and elevated concentrations in plasma are only found shortly after onset (21) Since our patients with DSS were admitted a mean ot 4 2 days since onset of disease (table 1), this may explain why we have found only slightly elevated median plasma concentrations ot TNF-a and IL-6, although strongly elevated TNF-a concentrations (both 2500 pg/ml) and IL-6 (86 000 and 199000 pg/ml) were found in two patients, both of whom died Other investigators have reported high concentrations of circulating proinflammatory cytokines in dengue, correlating with disease activity We could not however confirm the data of Hober et al, who found high TNF concentrations in children with dengue of all severity grades (the highest values in the sera of DHF HI and DHF IV were 300 and 400 pg/ml, respectively, and in DHF I and DHF II patients, 180 and 250 pg/ml, respectively) (6) One reason for this discrepancy may be the timing of blood sampling In our study, the earliest samples in which cytokines were measured, were collected 4 (median) days (range 2-7) after onset of disease Therefore, we may have missed a possible high released of IL-6 and IFN-γ during the first days of infection. An additional explanation may be the use of a different TNF assay There is still a rather poor standardization between the assays and it is known that validated RIA's such as used by us generally have a higher read out than many of the commercial ELISA's (Johanna van der Ven-Jongeknjg, et al, manuscript in preparation)
However, the tact that we also found low median IL-6 concentrations gives support to our TNF data In addition, we noted that the patterns of IL-6 correlated with TNF-a (data not shown) In general, IL-6 which is induced mainly by TNF and persists in plasma, is a very sensitive marker for activation of the cytokine network Apparently IL-6 concentrations normalize relatively soon in dengue even when patients are (still) critically ill
In the acute phase of the disease, the ex-vivo production of TNF-a and IL-Iß after incubation with LPS was considerably depressed but returned to normal on recovery Such low production capacity of proinflammatory cytokines has been found in severe bacterial infections such as sepsis (22, 23), typhoid fever (24), and acute meningococcal disease (25) and apparently also occurs in this severe viral infection The degree ot down regulation ot proinflammatory cytokine production has been shown to correlate with disease severity in the bacterial infections mentioned and seems to mirror the magnitude ot the initial systemic cytokine response In our patients, the degree ot down regulation of IL-Iß in non-survivors was less than in survivors Conversely, the upregulation of the anti-inflammatory cytokine IL-IRa was significantly more pronounced in non-survivors (figure 2) This provides evidence that the regulation of pro- and anti-inflammatory cytokines in this severe viral infection (DSS) is similar to that in severe bacterial infections

61
We did not find evidence for production of the type I cytokine IFN-γ in DSS Other investigators observed that IFN-γ levels were increased and decreased abruptly 1 day after defervescence (13), coinciding with the disappearance of viraemia (26) Therefore, like for TNF-a and IL-6, we may have missed the IFN-γ peak due to relatively late sampling
We conclude that in hospitalized children with DSS (DHF III and DHF IV), IL-IRa is a valid prognostic marker, since it is associated with mortality and because of its relatively long half life it can be reliably measured. Its presence provides indirect evidence tor preceding proinflammatory cytokine activity, such as of IL-Iß. The transient proinflammatory cytokine patterns in the blood with the pronounced anti-intlammatory response observed lend little support for anti-cytokine strategies in DSS when patients are already ill for 3-4 days.
Acknowledgements
Participants in this project, besides the authors, were Prof Moeljono S Trastotenojo, dr Herawati Yuslam from the Department of Paediatrics and Prof Soenarto from the Department of Internal Medicine, Dr Kanadi Hospital, Diponegoro University, Semarang, Indonesia. We thank dr Hardian and dr Henry Setyawan from the Clinical Epidemiology Unit of Diponegoro University for statistical support, Υ Τ van der Heide from the Clinical Chemistry and Hematology Laboratory, Slotervaarl Hospital, Amsterdam, The Netherlands, for managing the blood samples, and Dr J Groen and Prof A Osterhaus from the Institute of Virology, Erasmus Medical Centre, Rotterdam, tor performing the diagnostic assays We thank also Johanna van der Ven-Jongeknjg from the laboratory of the Department ot General Internal Medicine, University Medical Centre St Radboud, Nijmegen, The Netherlands and GJ van Mierloo and AJM Eerenberg from the Central Laboratory of The Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands, for performing the cytokine assays.

I World Health Organization Dengue hemorrhagic fever diagnosis, treatment, prevention and control 2nü ed, 1997, Geneva, 12-47
2. Gubler DJ Dengue and Dengue Hemorrhagic Fever. Clin Microbiol Rev 1998, 11.480-96
3. Kurane I, Ennis FA. Immunopathogenesis of dengue virus infections In' Dengue and dengue hemorrhagic fever Gubler DJ, Kuno G, eds Wallingford, UK Cab International 1997; 273-290
4 Halstead SB Pathogenesis of dengue challenges to molecular biology Science 1988; 239.476-81.
5 Halstead SB, Venkateshan CN, Gentry MK, Larsen LK. Heterogeneity of infection enhancement of dengue 2 strains by monoclonal antibodies. J Immunol 1984; 132: 1529-32
6. Hober D, Poli L, Roblin B, Gestas P, Chungue E, Grame G, Imbert Ρ, Pecarere JL, Vergez-Pascal R, Wattre Ρ Serum levels of tumor necrosis factor-alpha (TNF-alpha), interleukin-6 (IL-6), and interleukin-lß (IL-1 beta) in dengue-infected patients. Am J Trop Med Hyg 1993; 48: 324-31
7. Kuno G, Bailey RE. Cytokine responses to dengue infection among Puerto Rican patients. Mem Inst Oswaldo Cruz 1994; 89. 179-82.
8 lyngkaran N, Yadav M, Sinniah M. Augmented inflammatory cytokines in primary dengue infection progressing to shock. Singapore Med J 1995, 36. 218-21.
9. Pinto LMO, Oliveira SA, Braga ELA, Nogueira RMR, Kubelka CF. Increased Pro-inflammatory Cytokines (TNF-a and IL-6) and Anti-inflammatory Compounds (sTNFRp55 and sTNFRp75) in Brazilian Patients during exanthematic Dengue Fever Mem Inst Oswaldo Cruz 1999; 94 387-394.
10 Chaturvedi UC, Elbishbishi EA, Agarwal R, Raghupathy R, Nagar R, Tandon R, Pacsa AS, Younis 01, Azizieh F Sequential production of cytokines by dengue virus-infected human peripheral blood leukocytes cultures J Med Virol 1999, 59: 335-40
II Kurane I, Meager A, Ennis FA Dengue virus-specific human Τ cell clones Serotype crossreactive proliferation, interferon gamma production, and cytotoxic activity. J Exp Med 1989; 170 763-75
12. Kurane I, Innis BL, Nimmannitya S, Nisalak A, Meager A, Janus J, Ennis FA Activation of Τ lymphocytes in dengue virus infections High levels of soluble interleukin 2 receptor, soluble CD4, soluble CD8, interleukin 2, and interferon-gamma in sera of children with dengue. J Clin Invest 1991; 88 1473-80
13 Green S, Vaughn DW, Kalayanarooj S, Nimmannitya S, Suntayakom S, Nisalak A, Lew R, Innis BL, Kurane I, Rothman AL, Ennis FA. Early immune activation in acute dengue illness is related to development of plasma leakage and disease seventy. J Infect Dis 1999; 179· 755-62
14 Van Gorp ECM, Suharti C, ten Gate H, Dolmans WMV, van der Meer J WM, ten Cate JW, Brandjes DPM Infectious Diseases and Coagulation Disorders J Infect Dis 1999; 180· 176-186

61
15 Rigau-Perez JG, Clark GG, Gubler DJ, Reiter Ρ, Sanders EJ, Vorndam AV. Dengue and dengue hemorrhagic fever Lancet 1998; 352: 971-7
16 Sharp TW, Wallace MR, Hayes CG, Sanche/ JL, DeFraites RE, Arthur RR, Thornton SA, Batchelor RA, Rozmajzl PJ, Hanson RK, Wu SJ, Inye C, Burans JP. Dengue fever in U.S. troops during operation restore hope, Somalia, 1992-1993 Am J Trop Med Hyg 1995, 53. 89-94
17 Innis BL, Nisalak A, Nimmannitya S, Kusalerdcharya S, Chongswasdi V, Suntayakom S, Puttisn P, Hoke CH An enzyme-linked immunosorbent assay to characterize dengue infections where dengue and Japanese Encephalitis co-circulate Am J Trop Med Hyg 1989, 40: 418-427
18. Ruechusatsawat K, Monta Κ, Tanaka M, Vongcheree S, Rojanasuphot S, Warachit Ρ, Kanal Κ, Thongtradol Ρ, Nimnakom M, Kanungkid S, Igarashi A Daily observation of antibody levels among dengue patients detected by enzyme-linked immunosorbent assay (ELISA) Jpn J Trop Med Hyg 1984; 22 9-12
19. Drenth JP, van Uum SH, van Deuren M, Pesman GJ, van der Ven-Jongeknjg J, van der Meer J WM. Endurance run increases circulating IL-6 and IL-IRa but downregulates ex-vivo TNF-alpha and IL-1 beta production J Appi Physiol 1995, 79 1497-03
20. Velzing J, Groen J, Drouet MT, van Amerongen G, Copra C, Osterhaus AD, Deubel V. Induction of protective immunity against dengue virus type 2 companson of candidate live attenuated and recombinant vaccine Vaccine 1999; 17· 1312-1320
21 Van Deuren M, van der Ven-Jongeknjg J, Bartelink AKM, Sauerwein RW, van der Meer JWM Correlation between proinflammatory cytokines and antiinflammatory mediators and the severity of disease in meningococcal infections J Infect Dis 1995, 172 433-39
22. Munoz C, Carlet J, Fitting C, Misset Β, Bleriot JP, Cavaillon JM. Dysregulation of in vitro cytokine production by monocytes during sepsis J Clin Investig 1991, 88. 1747-1754.
23. Ertel W, Kremer JP, Kenney J, Steckhol/er U, Jarrar D, Trentz O, Schildberg FW. Downregulation of proinflammatory cytokine release in whole blood from septic patients Blood 1995, 85 1341-1347
24. Keuter M, Edi Dharmana, Gasem MH, Van der Ven-Jongeknjg J, Djokomoeljanto R, Dolmans WMV, Demacker PNM, Sauerwein RW, Gallati Η, Van der Meer JWM. Patterns of proinflammatory cytokines and inhibitors during typhoid fever J Infect Dis 1994, 169:1306-1311.
25. Van Deuren M, Van der Ven-Jongeknjg J, Demacker PNM, Bartelink AKM, Van Dalen R, Sauerwein RW, Gallati H, Vannice JL, Van der Meer JWM Differential expression of proinflammatory cytokines and their inhibitors during the course of meningococcal infections. J Infect Dis 1994, 169· 157-161
26. Vaughn DW, Green S, Kalayanarooj S, Innis BL, Nimmannitya S, Suntayakorn S, Rothman AL, Ennis FA, Nisalak A. Dengue in the early febrile phase: viremia and antibody responses J Infect Dis 1997, 176: 322-30.

64
Chapter 6
Plasma Interleukin-1 receptor antagonist (IL-IRa) concentration is associated with plasma leakage in Dengue Shock Syndrome
Cathanna Suharti', Eric C M van Gorp2, Tatty E Setiati1, Wil M V Dolmans4, Robert J Djokomoeljanto', C Erik Hack'', Hugo ten Gate26, Jos W M van der Meer4
Departments of Internal Medicine' and Paediatrics1, School of Medicine, Diponegoro University and Dr Kanadi Hospital, Semarang, Indonesia, Department of Internal Medicine, Slotervaart Hospital, Amsterdam, The Netherlands , Department of Internal Medicine, University Medical Centre St Radboud, Nijmegen, The Netherlands4, Central Laboratory of The Netherlands Red Cross Blood Transfusion Service and Department Clinical Chemistry, Academic Hospital Vrije Universiteit, Amsterdam, The Netherlands5, Laboratory for Experimental Internal Medicine, Academic Medical Center, Amsterdam, The Netherlands6
Submitted for publication

65
Abstract
Plasma leakage is the most characteristic pathological change in dengue hemorrhagic fever (DHF), of which dengue shock syndrome (DSS) is the severest form Cytokines are thought to be involved in the endothelial cell permeability changes leading to the leakage We investigated the association of tumor necrosis factor-α, interleukin-lß, interleukin-1 receptor antagonist (IL-IRa), interleukin-6 and interferon-γ with plasma leakage, manifested by the concentrations of serum protein, serum albumin and the presence of pleural effusion in 50 children with DSS IL-IRa was significantly associated with both, bilateral pleural effusion (p=0.03; regression coefficient. 0 186) and the albumin/protein ratio (p=0 018, 95% CI 0 001-0 01). We conclude that IL-IRa contributes to the capillary permeability changes in DSS

66
Introduction
Dengue hemorrhagic fever (DHF) is the severe form of dengue viral infection and is characterized by an acute onset ot fever, bleeding, and plasma leakage, the evidence of which is hemoconcentration, pleural and other effusions, hypoalbuminaemia, hypoproteinaemia, and hyponatremia. Dengue Shock Syndrome (DSS) is defined as DHF with signs of shock (1,2) The pathological mechanisms which increase permeability of vascular endothelial cells in DHF/DSS have not been clarified.
Since in-vitro studies have demonstrated that endothelial cells can be infected with dengue virus (3-6), it has been postulated that these cells play a key role in the pathogenesis of DHF/DSS Histological studies have shown swelling of vascular endothelial cells and perivascular tissues without structural damage to endothelial cells (7) and electron microscopy of the microvasculature has demonstrated non-specific changes, consistent with increased transport activities of the endothelial cell (8); no apparent morphological changes in these cells were observed in patients who recovered (7) In addition to direct viral effects on endothelium, it has been hypothesized that cytokines released from dengue virus-infected monocytes trigger plasma leakage in DHF/DSS (9) Observations in other critical illnessess have demonstrated that cytokines and other mediators may induce increased capillary permeability, plasma leakage and shock. These cytokines include tumor necrosis factor-α (TNF-a), interleukin-1 β (IL-Iß), interleukin-6 (IL-6) and interferon-γ (IFN-γ) (10-12). Moreover, a synergistic effect has been shown among these cytokines. For example, TNF-a and IFN-γ increase permeability of human vascular endothelial cell monolayers (HUVEC) more than each cytokine alone in vitro (11). IL-1 and TNF-a act synergistically m the induction of shock in animal models in vivo (13) Limited data suggest that dengue virus indeed may modulate endothelial cell function by releasing TNF-a from virus infected-monocytes in vitro (14) In a clinical study, the elevation of plasma concentrations of soluble tumor necrosis factor receptors (sTNFRs), correlated with the degree of plasma leakage in DHF which argues in favor of cytokine involvement in the pathogenesis of capillary leakage in DHF (15) In the present study we have further investigated the role of cytokines in plasma leakage in patients with dengue shock syndrome.
Patients and methods
Study setting The study was performed in Dr Kanadi Hospital, the University Hospital of
Diponegoro University, Semarang, Indonesia Dengue is endemic in Indonesia
Patients Between June and November 1996, during an outbreak of dengue in Indonesia, 50
consecutive children with the clinical diagnosis of DSS and admitted to the Paediatnc Intensive Care Unit, were enrolled in the study Only children aged > 3 years old were included

67
Case definition The clinical diagnosis of DSS (DHF grade III and grade IV) was finally based on the
1997 WHO criteria (1). Patients presenting all criteria for DHF: (i) fever or history of acute fever 2-7 days; (ii) bleeding (mild to severe); (iii) thrombocytopenia 100.000/mm or less (iv) evidence of plasma leakage plus evidence of circulatory failure manifested by (a) rapid and weak pulse; (b) narrow pulse pressure (20 mmHg); (c) hypotension and (d) cold, clammy skin and restlessness, were classified DHF III. If profound shock with undetectable blood pressure and pulse was present, patients were classified as DHF IV. Decreased consciousness was based on the Glasgow Coma Scale (16).
Patient monitoring A detailed clinical record form was kept for each patient on which findings of physical
examination were entered daily during hospitalization. Daily laboratory tests included blood cell counts and tests for hemostasis. Renal and liver function tests, and electrolytes were measured with Auto Analyser, Hitachi, 7050, on day of admission (day 0), on day 1, and on day 2. Chest x-rays were done routinely to confirm pleural effusion.
Specimens collection Blood specimens were collected in vacutainer tubes (Beclon Dickinson, Rutherford, NJ
07417). To collect appropriately timed specimens for virus isolation (< day 5 after onset of fever) (17-21) and for serological assays (> day 6 after onset of fever) (17, 21, 22, 23), 2 ml of blood was collected on day of admission (for virus isolation), and on day of admission and discharge (for serological assays). Blood was centrifuged at 1000-1500 rpm for 10 minutes, whereafter serum was transferred to screw cap Eppendorf tubes and stored at -80^C, until assayed. Specimens for cytokine assays were collected three times: on the day of admission (day 0), on day 1 and on day 2. Four ml of blood was collected into sterile tubes containing EDTA in each patient. To this tube 125 μL· of aprotinin (Trasylol, Bayer, Leverkusen, Germany; final concentration 625 kallikreine inactivating units/mL) was added through the stopper by a tuberculin needle and syringe. The tube was centrifuged directly at 1250 g for 10 minutes, and thereafter at 15000 g for 1 minute) to remove platelets. The plasma was stored in aliquols at -80^C until assayed for cytokines. During transport of the samples from Semarang to The Netherlands, samples were kept on dry ice.
Cytokine assays
TNF-a, IL-Iß and IL-IRa were measured in duplicate by nonequilibrium radioimmunoassay (RIA) (24). Recombinant human TNF-a, IL-Iß and IL-IRa were calibrated against standards provided the National Institute of Biological Standards and Control (Potters Bar, UK), with the sensitivity of the assay with 100 μΙ sample of 40 pg/ml,40 pg/ml,and 80 pg/ml, respectively. TNF-a: normal median value 90 pg/ml (range 50-170). IL-Iß normal median value 50 pg/ml (range <40-l 15). IL-IRa: normal median value 139 pg/ml (range <80-502). IFN-γ and IL6 were measured with ELIS As obtained from the Central Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands, according to manufacturer's instruction. Levels of IFN-γ exceeding 40 pg/ml and levels of IL6 exceeding 10 pg/ml were considered to be elevated.

68
Serological assays The diagnosis of dengue infection was confirmed by serological assays. A capture and
indirect enzyme-linked immunosorbent assay (ELISA) detected dengue specific IgM and IgG antibodies in serum samples, according to a previously described procedure (25).
Statistical analysis Continuous data were described as mean (SD) or median with range, while nominal
data were described as percentage (%). Linear and logistic regression analysis were done to determine association of cytokines (TNF-a, IL-Iß, IL-IRA, IL-6 and IFN-γ) with the concentrations of protein, albumin in serum, and with pleural effusion. A p-value (2-sided) < 0.05 was considered to represent a significant difference or association. All statistical analyses were performed using SPSS for Windows version 9.0.
Results
Between June and November 1996, 50 children with the clinical diagnosis of DSS, were enrolled in the study. Baseline characteristics are listed in Table 1. Thirteen patients died (26%) 1 to 9 days (median 4 days) after hospitalization. Pleural effusion (right-sided or bilateral) was present in 25 (50%) patients, of whom 8 (16%) had a bilateral pleural effusion. Virus isolation was done in the first 28 of 50 patients with specimens collected on day of admission. No virus was isolated, even though 26 of 28 specimens were collected within the first 5 days after onset of fever. The clinical diagnosis of DHF/DSS was confirmed by serological assay in all patients, either by an IgM response or by a fourfold rise in IgG titres. Antibody profiles were typical for secondary infection.
Table 1. Patient characteristics in 50 children with dengue shock syndrom
Age (year) 6.6 ± 2.8 (3-13) Days since onset of disease 4.2 ± 1 (2-7) Male / Female 24 (48) / 26 (52) Positive dengue serology result 50 (100) Clinical diagnosis *: DHF III 43 (86)
DHFIV 7(14) Number of death 13 (26) Pleural effusion 25 (50) Bilateral pleural effusion 8(16) Hematocrit (%)** 37.8 ± 6.7 (22-58.9) Sodium (mmol/1)** 135(121-148)
* WHO criteria ** on day of admission The values indicated are mean ± SD (range) and number (7c)

69
Plasma concentrations of cytokines, protein and albumin The cytokine concentrations in this study are also presented in a parallel paper dealing
with cytokine measurements in dengue (26) (chapter 5) We found that the plasma concentrations of IL-lRa were markedly elevated, while the plasma concentrations of TNF-a and IL-Iß were only mildly elevated (table 2) Although, the median plasma concentrations of IFN-γ and IL-6 were not elevated, in occasional patients strongly elevated values were found.
We observed a decrease of the median levels of protein and albumin on the day of admission, which returned to normal on day 2 (table 2)
Table 2. The median plasma concentrations of cytokines, protein and albumin during the study period
Day 0 Day 1 Day 2 Normal value
Cytokine
TNF-a (pg/ml)
IL-lß(pg/ml)
IL-IRA (pg/ml)
IL-6 (pg/ml)
IFN-γ (pg/ml)
155 (95-2500) 72 5 «40 320) 795 (220 2500)
<2 (<2-199000) 20
(20-54)
140 (85 315) 80 (<40 140) 555 (180 2400) 2 100 « 2 1058) 20 (20 86)
150 (95 305) 80 (<40-145) 590 (225-2050)
3 5 « 2 155) 20 (20 582)
90 (50-170) 50 «40 115) 139 «80 502)
<10
<40
Markers oj pia sma leakage Protein (g/dl) 5 1 5 5 5 9 5 9-8 6
(18-6 9) (3 17 5) (3 9-9 1) Albumin (g/dl) 3 5 3 6 3 8 3 5-5 6
(10-5 2) (15 4 7) (2 0-5 4)
The values indicated are median (range)
Association of plasma concentrations of cytokines with albumin/protein ratio
In a multiple linear regression model, the association of TNF-a, IL-Iß, IL-lRa, IL-6 and IFN-γ with albumin/protein ratio on day of admission was calculated Table 3 shows that IL-lRa was significantly associated with albumin/protein ratio (p-Q 018)
Association of plasma concentration', of cytokines with pleural effusion In a multiple logistic regression model, the association of TNF-a, IL-lß, IL-lRa, IL-6
and IFN-γ on admission with bilateral pleural effusion was calculated Table 4 shows that IL-lRa was significantly associated with bilateral pleural effusion with />=0 03 The
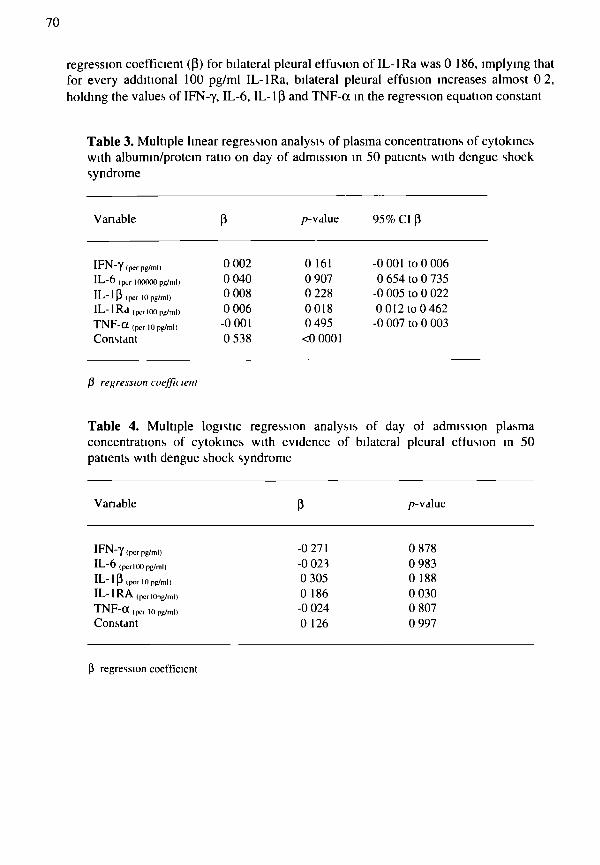
70
regression coefficient (β) for bilateral pleural effusion of IL-lRa was 0 186, implying that for every additional 100 pg/ml IL-lRa, bilateral pleural effusion increases almost 0 2, holding the values of IFN-γ, IL-6, IL-lß and TNF-a in the regression equation constant
Table 3. Multiple linear regression analysis of plasma concentrations of cytokines with albumin/protein ratio on day of admission in 50 patients with dengue shock syndrome
Vanable β p-value 95% CI β
I F N - γ (per pg/ml)
I L - 6 (ρ,,Γ 100000 pg/ml)
I L - l ß (per 10 pg/ml)
I L - I R d (pcrlOO pg/ml)
T N F - a (per 10 pg/ml)
Constant
0 002 0 040 0 008 0 006 -0 001 0 538
0 161 0 907 0 228 0018 0 495 <0 0001
-0 001 to 0 006 0 654 to 0 735
-0 005 to 0 022 0 012 to 0 462 -0 007 to 0 003
β regression coeffu lent
Table 4. Multiple logistic regression analysis of day of admission plasma concentrations of cytokines with evidence of bilateral pleural effusion in 50 patients with dengue shock syndrome
Variable β p-value
I F N - γ (per pg/m|)
I L - 6 (pcrlOO pg/ml)
I L - l ß (per 10 pg/ml)
I L - I R A (pcrlOpg/ml)
T N F - 0 t (per 10 pg/ml)
Constant
-0 271 -0 023 0 305 0 186 -0 024 0 126
0 878 0 983 0 188 0 030 0 807 0 997
β regression coefficicnl

71
Discussion
In 50 children with DSS we found that plasma concentrations of IL-IRa were considerably elevated and that the concentration of this anti-inflammatory cytokine correlated with markers of plasma leakage, ι e with albumin/protein ratio and pleural effusion
It is generally assumed that high concentrations of antiinflammatory cytokines in the circulation reflect proinflammatory cytokine production in the tissues Also, compared to an antiinflammatory cytokine like IL-IRa, the proinflammatory cytokine responses are relatively short lived in serious infections, and elevated concentrations in plasma are only found shortly after onset (27) In addition, the short half live may also be due to the induced leakage This explains probably why we have found only slightly elevated median plasma concentrations of the proinflammatory cytokines TNF Nevertheless, strongly elevated ot TNF-oc concentrations (up to 2500 pg/ml) were found in some patients, leading to the unanswered question whether this reflects heterogeneity in the cytokine response ot patients. It is also possible that high concentrations in the other patients have been present at earlier time points.
We found an association of IL-IRa with bilateral pleural effusion and with albumin/protein ratio. This finding suggest involvement of IL-Iß in vascular permeability. The role of IL-Iß in inducing capillary leakage has been demonstrated m experimental animals (13, 28) as well as in vitro studies (29,30) The way in which IL-lß and other proinflammatory cytokines induce endothelial permeability is not fully understood, but eicosanoids (prostaglandins, leucotnenes and platelet-activating factor) and induced nitric oxyde appear to play a role (13,29, 31-35) IFN-γ, IL-lß and TNF-a are potent inducers of inducible nitric oxide synthetase (iNOS), an cn/yme which is responsible for NO biosynthesis, and hyperpermeabihty to hydrophihc solutes in cultured enterocytic monolayers The cytopathic effects ot NO may be mediated by peroxynitnte, which is produced by the reaction of NO with superoxide radical anion (35) F actin cytoskeleton has a crucial role in endothelial tight junction barrier regulation In-vitro, TNF-a and IFN-γ are able to cause a 50% decrease in the electrical resistances across endothelial cells, and a striking fragmentation of the basal, continuous interendothelial cell zonula occludens-1 protein distribution (36). The finding of others that the concentrations of soluble tumor necrosis factor receptors (sTNFRs) correlate with the degree of plasma leakage should also be seen as evidence for a role of TNF, since this cytokine is the major stimulus for solubilization of the TNF receptors (15) The sTNFRs have a longer half life than TNF itself and are present in a relatively high concentrations Therefore they act as a marker which is relatively easy to measure, with the problem, however, of a clear dependence on renal function
If we take all data together it's very likely that endothelial permeability changes in DSS and the subsequent plasma leakage is driven by proinflammatory cytokines such as IL-lß and TNF Further studies are needed to determine whether intervention with anticytokines is able to prevent plasma leakage and improve prognosis

72
Acknowledgements
Participants in this project, besides the authors, were Prof. Moeljono S Trastotenojo and dr Herawati Yuslam from the Department of Paediatrics, Diponegoro University and Dr. Kanadi Hospital, Semarang, Indonesia We thank dr Hardian and dr. Henry Setiawan from the Clinical Epidemiology Unit, Diponegoro University, Semarang, for statistical support, Y.T. van der Heide from the Clinical Chemistry and Hematology Laboratory, Slotervaart Hospital, Amsterdam for managing the blood samples, and Dr. J. Groen and Prof. A Osterhaus from the Institute of Virology, Erasmus Medical Centre, Rotterdam for performing the serological assays We thank also Johanna van der Ven-Jongekrijg from the Department of Internal Medicine, University Medical Centre St Radboud, Nijmegen, The Netherlands and GJ van Mierloo and AIM Eerenberg from the Central Laboratory of The Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands for performing the cytokine assays
References
1. World Health Organization Dengue haemorrhagic fever, diagnosis, treatment, prevention and control 2nd ed Geneva 1997, 12-47
2 Pan American Health Organization Dengue and dengue hemorrhagic fever in the Amencas guidhnes for prevention and control.Washington, DC PAHO Sci Pubi 1994; 3-38
3. Friedman H, Macarak E, MacGregor R, Wolfe J, Kefahdes Ν. Virus infection in endothelial cells J Int Dis 1981, 143 266-73
4. Friedman H, Wolfe J, Kefahdes Ν, Macarak E. Susceptibility of endothelial cells derived from different blood vessels to commom viruses In Vitro Cell Dev Biol 1986,22 397-401.
5 Friedman Η Infection of endothelial cells by common human viruses. Rev Infect Dis 1989, 11 S700-S704.
6 Butthep P, Bunyaratvej A, Bhamarapravati Ν Dengue virus and endothelial cell: a related phenomenon to thrombocytopenia and granulocytopenia in dengue hemorrhagic fever. Southeast J Trop Med Pubi Health 1993, 24 246-49
7 Bhamarapravati Ν Pathology of dengue infections In Gubler DJ and Kuno G eds Dengue and dengue hemorrhagic fever Walhngford UK Cab International 1997·! 15-132
8 Sahaphong S, Rienggrojpita S, Bhamarapravati N, and Chirachanyavej T. Electron microscopic study of the vascular endothelial cell in dengue hemorrhagic fever Southeast Asian Journal of Tropical Medicine and Public Health 1980, 11 194-204
9 Kurane I, Rothman AL, Livingston PG, et al Immunopathologic mechanisms of dengue hemorrhagic fever and dengue shock syndrome Arch Virol 1994, (Suppl) 9 59-64
10 Minghim A, Bntt LD, Hill MA. Interleukin-1 and interleukin-6 mediated skeletal muscle arteriolar vasodelatation- in vitro versus in vivo studies Shock 1998, 9.210-5

73
11. Stolpen AH, Guinan EC, Fiers W, Pober JS. Recombinant tumor necrosis factor and immune interferon act singly or in combination to reorganize human vascular endothelial cell monolayers. Am J Pathol 1986, 123 16-24.
12 Yi ES, Ulich TR Endotoxin, interleukin-1, and tumor necrosis factor cause netrophil-dependent microvascular leakage in postcapillary venules. Am J Pathol 1992, 140:659-63
13 Dinarello CA, Okusawa S, Gelfand JA Interleukin-1 induces a shock-like state in rabbits, synergism with tumor necrosis factor and the effect of cyclooxygenase inhibition Prog Clin Biol Res 1989, 286 243-63
14 Anderson R, Wang S, Osiowy C, Issekutz AC Activation of endothelial cells via antibody-enhanced dengue virus infection of peripheral blood monocytes J Virol 1997,71:4226-4232
15 Green S, Vaughn DW, Kalayanarooj S, et al. Early immune activation in acute dengue illness is related to development ot plasma leakage and disease severity J Infect Dis 1999; 179 755-62.
16 Jarvis C. Physical examination and health assessment Philadelphia WB Saunders, 1993 178
17 Perez-Rigau JG, Clark GG, Gubler DJ, Reiter Ρ, Sanders EJ, Vomdam AV Dengue and dengue hemorrhagic fever. Lancet 1998; 352 971-77
18 Samsi TK, Wulur H, Sugianto D, Bart/ CR, Tan R, Sie A Some clinical and epidemiological observations on virologically confirmed dengue hemorrhagic fever Paediatr Indones 1990, 30· 293-303
19 Sharp TW, Wallace MR, Hayes CG, et al Dengue fever in U S troops during operation restore hope, Somalia, 1992-1993 Am J Trop Med Hyg 1995; 53 89-94.
20 Vomdam V, Kuno G. Laboratory diagnosis of dengue virus infections In Gubler DJ, Kuno G eds Dengue and dengue hemorrhagic fever Wallingford. Cab International, 1997 313-333
21. Gubler DJ, Suharyono W, Tan R, Abidin M, Sie A. Viraemia in patients with naturally acquired dengue infection Bull. W.H.O 1981; 59· 623-630
22 Innis BL, Nisalak A, Nimmannitya S, et al An enzyme -linked immunosorbent assay to charactenze dengue infections where dengue and Japanese Encephalitis co-circulate Am J Trop Med Hyg 1989, 40. 418-427
23. Ruechusatsawat K, Monta Κ, Tanaka M el al Daily observation of antibody levels among dengue patients detected by enzyme-linked immunosorbent assay (ELISA) Jpn J Trop Med Hyg 1984; 22 9-12
24 Drenth JP, van Uum SH, van Deuren M, Pesman GJ, van der Ven-Jongeknjg J, van der Meer JWM Endurance run increases circulating IL-6 and IL-IRa but downregulates ex-vivo TNF-alpha and IL-lbeta production J Appi Physiol 1995, 79· 1497-503
25 Velzing J, Groen J, Drouet MT, van Amerongen G, Copra C, Osterhaus AD, Deubel V Induction ot protrective immunity against Dengue virus type 2. comparison of candidate live attenuated and recombinant vaccines Vaccine 1999; 17: 1312-20
74
26 Suharti C, van Gorp ECM, Dolmans WMV, Tatty E. Senati, Hack CE, Djokomoeljanto RJ, van der Meer JWM. Cytokine patterns during dengue shock syndrome (submitted for publication)
27 van Deuren M, van der Ven-Jongekrijg J, Bartelmk AKM, van Dalen R, Suaerwein RW, van der Meer JWM Correlation between proinflammatory cytokines and anti-inflammatory mediators and the severity of disease in meningococcal infections. J Infect Dis 1995, 172. 433-39
28 Luna JD, Chan CC, Derevjanik NL, Mahlow J, Chiu C, Peng B, To Campochiaro PA, Vinores SA. Blood-retinal barrier (BRB) breakdown in experimental autoimmune uveoretimtis· comparison with vascular endothelial growth factor, tumor necrosis factor alpha, and interleukin-1 beta-mediated BRB breakdown J Neurosci Res 1997, 49· 268-80
29. Chen DB, Yang ZM, Hilsenrath R, Le SP, Harper MJ Stimulation of prostaglandin (PG) F2 alpha and PGE2 release by tumor necrosis factor-alpha and interleukin-1 alpha in cultured humen luteal phase endometrial cells
30 Dentener MA, Francot GJ, Hiemstra PS, Tool AT, Verhoeven AJ, Vandenabeele P, Buurman WA Bactencidal/permeability-increasing protein release in whole blood ex vivo strong induction by lipopolysacchande and tumor necrosis factor-alpha J Infect Dis 1997, 175 108-17
31 de Vries HE, Blom-Roosemalen MC, van Osten M, de Boer AG, van Berkel TJ, Breimer DD, Kuiper J The influence of cytokines on the integrity of the blood-brain barrier in vitro. J Neuroimmunol 1996, 64 37-43
32 Zemel D, Krediet RT Cytokine patterns in the effluent of continuous ambulatory peritoneal dialysis- relationship to peritoneal permeability Blood Punf 1996, 14 198-216.
33. Sirois MG, Plante GE, Braquet Ρ, Sirois P. Tumor necrosis factor pnmes the effects of platelet-activating factor on rat vascular permeability J Lipid Médiat 1990, 2Suppl:S109-17
34. Gad MZ, Khattab M Modulation of nitric oxide synthesis in inflammation Relationship to oxygen-derived free radicals and prostaglandin synthesis Arzneimittelforschung 2000, 50 449-55
35. Chavez AM, Menconi MJ, Hodin RA, Fink MP. Cytokine-induced intestinal epithelial hyperpermeability role of nitric oxide Cnt Care Med 1999, 27: 2246-51
36. Blum MS, Tonmelh E, Anderson JM, Balda MS, Zhou J, O'Donnel L, Pardi R, Blender JR Cytoskeletal rearrangement mediates human microvascular endothelial tight junction modulated by cytokines Am J Physiol 1997, 273 H286-94

75
Chapter 7
Review: Infectious Diseases and Coagulation Disorders
van Gorp ECM (1), Suharti C (2), ten Gate H (1)(3), Dolmans WMV (4), van der Meer JWM (4), ten Gate JW (3), Brandjes DPM (1)(3).
(1) Dept of Internal Medicine Slotervaart Hospital, Amsterdam, the Netherlands; (2) Dept of Internal Medicine Dr. Kariadi Hospital, Semarang, Indonesia; (3) Center for Hemostasis, Thrombosis, Atherosclerosis and Inflammation research, Academic Medical Center, Amsterdam, the Netherlands; (4) Dept of Internal Medicine University Hospital Nijmegen, Nijmegen, the Netherlands.
The Journal of Infectious Diseases 1999; 180: 176-86

76
Abstract.
Infection, both bacterial and non-bacterial, may be associated with coagulation disorders, resulting in disseminated intravascular coagulation (DIC) and multiorgan failure (MOF). In the last few decades a series of both in-vivo and in-vitro studies has provided more insight into the pathogenetic mechanisms and the role of cytokines in these processes. Because of the growing interest in this field, the complexity of the subject and the fact that many physicians have to deal with a variety of infections, we will review current data on the association between infectious diseases and the coagulation system. In the conclusions we will speculate about novel therapeutic intervention strategies that probably will become available in the near future and are of special interest for those infectious disorders for which only supportive care can be given.

Introduction
Systemic infections may be complicated by activation of the coagulation cascade, varying from subclinical activation, indicated by a rise in laboratory markers for thrombin and fibrin generation, to fulminant disseminated intravascular coagulation (DIC), with the formation of microvascular thrombi in various organs [1]. Bleeding, thrombosis, or both may be the presenting clinical features. DIC may contribute to multiorgan failure (MOF) and is associated with a high mortality in both bacterial and non-bacterial disease. [2,3J As we have learned from studies of Gram negative sepsis in man and experimental animals, cytokines play a pivotal role in the activation and regulation of the coagulation cascade, although the interactions are complicated and the effects are time-dependent and transient [41. Activation of the coagulation system has also been documented for non-bacterial pathogens, i.e. viruses (causing hemorrhagic fevers) [5,6], protozoa (Malaria) [7,8] and fungi [9]. Since a specific effective treatment of DIC is not available at present, therapy focuses on treatment of the underlying disorder, e.g. antibiotics for bacterial infection. For many infectious diseases, such as viral hemorrhagic fever, causal therapy is not available and only supportive care can be provided. To improve therapy and supportive care, a better understanding of the pathogenesis of bleeding and thrombotic complications is needed. Novel therapeutic agents which intervene in the coagulation and cytokine cascades will become available in the near future and may have a positive clinical effect, especially for those infections for which only supportive care can be given. Because of the growing interest in this field, the complexity of the subject and the fact that many physicians have to deal with a variety of infections, we will review current data on the association between infectious diseases and the coagulation system.
Clinical aspects of hemostasis in bacterial and viral infections.
Viral and bacterial infections may influence hemostasis and this can lead to thrombohemorrhagic complications. Infection may result in thrombohemorrhagic syndromes such as DIC, hemolytic uremic syndrome (HUS), thrombotic thrombocytopenic purpura (TTP)or vasculitis. Symptoms and signs may be dominated by bleeding, thrombosis, or both. DIC is an acquired disorder in which the hemostatic system is activated, resulting in activation of platelets and the conversion of fibrinogen to fibrin. [31[10] This may lead to generalized microvascular thrombosis and MOF as well as life threatening hemorrhage due to consumption of coagulation factors and activation of the fibrinolytic system. DIC as a consumptive coagulopathy, with consumption of both platelets and clotting factors, has to be distinguished from the non-consumptive coagulopathies such as HUS and TTP, characterized by the consumption of platelets but not clotting factors. HUS and TTP are regarded as variants of a single syndrome characterized by thrombocytopenia, hemolytic anemia, fever, renal abnormalities and neurologic disturbances. Endothelial injury is considered the primary event which, as demonstrated in recent studies, may lead to excessive release of extremely large polymers of von Willebrand factor that cannot be processed to smaller forms due to deficiency of von Willebrand factor-cleaving protease. [11-14]

78
Vasculitis, which may be triggered by infection, is characterized by local or more generalized vascular changes, resulting from infarction secondary to occlusion by thrombi of the lumen of small blood vessels in the upper part of the dermis. Vascular occlusion may lead to ischemic tissue injury due to local vascular occlusion or bleeding due to local tissue damage [15,16] None of these syndromes (DIC, MOF, HUS, TTP or vasculitis) are specific for a certain pathogen and their occurrence depends on factors such as virulence of the pathogen, the prior condition of the patient, source and si/e of the innoculum and availability of antimicrobial treatment For example these coagulopathic syndromes are encountered more frequently in Gram negative infection in comparison with Gram positive and other non bacterial infections Vasculitis, ι e. Cytomegalovirus vasculitis is a known entity in immuno-compromised HIV patients, whereas it is a rarity in patients who are not immuno-depressed, underlining the role of the host status. There is a relation between the si/e of innoculum and the occurrence of the sepsis syndrome as has been demonstrated in an experimental Gram negative sepsis model in baboons [17]
In some cases of MOF bleeding and (microvascular) thrombosis may be co-existing features, which makes it impossible to determine the principal defect (thrombosis or bleeding). Taking these considerations into account the classification of clinical entities according to bleeding and/or thrombosis will be the basis for discussion, although the complexity and overlap in clinical presentation must be kept in mind.
Hemorrhage Hemorrhage may occur as a single clinical phenomenon or may be part of a more complex derangement of the coagulation cascade due to DIC or septic vasculitis, as in Gram negative bacterial sepsis, i e meningococcemia [1,3,16] Seventy may vary from local defects in hemostasis with oozing from arterial or venous puncture sites to more general complications such as petechiae, purpura, ecchymosis, gut bleeding, hemoptysis or even MOF due to adrenal bleeding (as in the Waterhouse Fndenchsen syndrome). The clinical signs are not pathogen specific and in general depend on the seventy of infection
In specific infections, such as viral hemorrhagic fever, bleeding complications are prominent. [18-20] Among the viral hemorrhagic fevers. Dengue hemorrhagic fever [18-20], Marburg hemorrhagic fever [21,22], and Ebola hemorrhagic fever [23,24] are the most important, Dengue being the most prevalent
Bacterial and viral infections may result in a vascuhtis-like syndrome with either bleeding manifestations or ischemic injury [15,16,25] Vasculitis is a well-documented phenomenon in CMV infection [26,27], occurring predominantly in the vasculature of the gastrointestinal tract where it causes colitis [28,29], the central nervous system where it causes cerebral infarction [30,31] and the skin where it results in petechiae, purpura papules, localized ulcers or a diffuse maculopapular eruption. [32] HIV (human immunodeficiency virus) infection may be accompanied by vasculitis syndromes, e g. Polyarteriitis nodosa, Henoch Schonlein purpura and leukocytoclastic vasculitis [33-36] Hepatitis Β and C infection may cause polyartentis-like vasculitis [37-39] Parvovirus Β19 has been suggested to be associated with vascuhtis-like syndromes including Kawasaki disease, polyarteritis nodosa and Wegener's granulomatosis [40-42]

79
Table 1. Viral Infections hallmarked by hemorrhage; Viral hemorrhagic fevers (VHF).
Virus Geographic distribution Source of infection
Dengue HF
Chikungunya Ebola Marburg HF Lassa Fever Yellow fever Omsk HF Hantaan
Southeast Asia, Carribean, Middle/South America, China Southeast Asia Zaire, Sudan Zimbabwe, Kenya, Uganda West Africa South America, Africa Former Soviet Union Central Europe, former Soviet Union, Korea, Japan, eastern China
Mosquito
Mosquito Unknown Unknown Rodent Mosquito Tick Rodent
Leptospirosis, especially Weil's syndrome, may present with hemoptysis, epistaxis, intestinal bleeding, adrenal bleeding, hematuria and even subarachnoid hemorrhage. [43] The pathogenesis may be either primary activation of coagulation or diffuse vasculitis, resulting in bleeding or ischemia of the vascularized tissue. TTP, with bleeding as the presenting symptom, may also occur in the course of Weil's syndrome.[44] In other viral and bacterial infections associated with TTP or HUS, bleeding also is often the prominent and presenting symptom. [45-47]
Thrombosis and hemorrhage; Disseminated intravascular coagulation (D/C) Viral and bacterial infections may theoretically result in local thromboembolic disease, i.e. deep venous thrombosis (DVT) or pulmonary embolism (PE). In a recently published thrombo-embolic prevention study of low-dose subcutaneous standard heparin for hospitalized patients with infectious diseases, morbidity due to thromboembolic disease was significantly reduced in the heparin group compared to the group receiving no prophylaxis. There was however no beneficial effect of prophylaxis on mortality due to thromboembolic complications. [481 In chronic viral diseases, such as CMV or HIV infection, the risk of thromboembolic complications is relatively low. [49,50] MOF is a clinical entity characterized by generalized microvascular thrombosis that may develop as part of the DIC syndrome, especially in bacterial Gram negative sepsis but also in severe viral infections. Viral hemorrhagic fever (table 1) is complicated by DIC in the most severe cases. [ 18-24] DIC is not frequently encountered in other viral infections [51,52], but has been reported in cases of infection with Rotavirus [53,54], Varicella, Rubella, Rubeola and Influenza. [55-61] TTP and HUS, triggered by a viral or bacterial infection, [45-47] frequently lead to bleeding symptoms, as has been discussed, but also platelet and fibrin thrombi may be generated in various organs, leading to prominent symptoms with organ dysfunction.

80
The variety and complexity of the clinical presentation of the coagulopathy syndromes
confront the clinician with the difficult question of whether, when and how to provide
optimal supportive care, to combat the coagulation disorders in addition to giving
antimicrobial therapy. In making this decision he will probably be guided by the
clinically most pronounced presenting symptom.
Principles of hemostasis, coagulation and fibrinolysis; general aspects
Contact system
XII PK HK
Γ/ssue factor system
TFPI-Θ.. TF-Vlla
Prothrombin
T A p . Fibrinolysis
Figure 1 Coagulation cascade
Model of the hypothetical coagulation cascade Products of coagulation activation are shown in squares. IXp= factor IX activation peptide, Xp= factor X activation peptide, Fl+2= prothrombin fragment 1+2, FPA = fibrinopeptide A , D-dimer= fibrin split product, TAT= thrombin - antithrombin complex The following natural inhibitors are shown TFP 1= tissue factor pathway inhibitor, AT= antithrombin, Pca= activated protein C (which cleaves activated factors V and VIII) Coagulation proteins are given in roman numbers, PK = prekallikrein, HK= high molecular weight kminogen TAFI= the recently identified "thrombin activatable fibrinolytic inhibitor"
The hemostatic mechanism consists of primary hemostasis, coagulation and
fibrinolysis. Primary hemostasis is maintained by the adhesion and aggregation of
81
platelets to form a hemostatic plug which is stabilized by fibrin strands [62,63] Coagulation, the second hemostatic defense mechanism, is generated by a series of linked coagulation protease-zymogen reactions, ultimately resulting in the formation of fibrin. In the current concept of coagulation, thrombin generation is induced by the assembly of tissue factor (TF)-factor Vila complex, the so-called extrinsic route of coagulation.
Coagulation is counteracted by different inhibitory mechanisms A first mechanism is made up of the circulating inhibitors of blood coagulation, ι e antithrombin, protein C and S and tissue factor pathway inhibitor (TFPI) A second inhibitory mechanism consists of the endothehum-bound modulators heparan sulfate and thrombomodulin, which facilitate the inhibitory activity of antithrombin and protein C, respectively The third, the fibrinolytic system, is activated by tissue plasminogen activator (tPA) and urokinase, following their synthesis and release from the endothelial cell system These activators initiate the conversion of plasminogen to plasmin, which hydrolyzes polymen/ed fibrin strands into soluble fibrin degradation products. Infection may lead to an imbalance between platelet I unction and the regulatory mechanisms of the coagulation cascade and fibrinolysis, resulting in bleeding, thrombosis or both.
Pathophysiological mechanisms of hemostasis in bacterial and viral infection
On the basis of data from experimental studies which have revealed the complexity ol the interactions between infectious pathogens, cytokines, effector cells and the coagulation system, we will discuss current insights into the pathogenesis of abnormal hemostasis in infectious diseases Cytokines are thought to play an essential role in activation of the coagulation system during viral and bacterial infections [64,65)
Coagulation activation
Tissue fat tor pathway The tissue factor pathway (extrinsic route) is the main route for activation of the coagulation cascade in sepsis Endotoxins , lipopolysacchande constituents of the outer membrane of Gram negative microorganisms, play a pivotal role in the development of the Gram negative sepsis syndrome [66] Levels of circulating endotoxin are prognostic markers for the clinical outcome of the septic syndrome [67,68] Injection of endotoxin or TNF alpha into healthy volunteers results in activation of the coagulation system via activation of the tissue factor pathway [64,69-71] TNF alpha injected into volunteers initiates the release of interleukin 6 and interleukin 8, which is followed by an increase in the levels of circulating markers of thrombin and fibrin generation (Prothrombin fragments (Fl+2), thrombin-antithrombin complexes (TAT), fibnnopeptide A) [17,64,72] This activation is preceded by a primary but transient activation of fibrinolysis, in contrast after activation of the coagulation cascade, activation of fibrinolysis is secondary [52] The net effect of an injection of endotoxin or TNF alpha is a procoagulant state In this experimental model coagulation and fibrinolysis seem to be activated independently, which may lead to an imbalance between activation of coagulation and regulation (activation/inhibition) of fibrinolysis [73] The same imbalance has been observed in baboons after injection of interleukin-1 [74] Administration of IL-6 into patients with renal cell carcinoma also results in activation of coagulation, as reflected by a rise in

82
the concentration of F1+2 and TAT complexes, but here fibrinolysis is not affected [75] TNF alpha induces the expression of tissue factor on monocytes [76] and endothelial cells [77-79] In chimpanzees and baboons, antibodies directed against tissue factor or Factor Vila or treatment with tissue factor pathway inhibitor (TFPI) prevents activation of the common pathway [71,80-84], whereas antibodies directed against Factor XII do not prevent activation [85,86], emphasizing the role of the tissue factor pathway IL-10 can inhibit the coagulant response during systemic infection by influencing the expression of TF on monocytes [87,88] As mentioned above, TNF is not an essential factor in the mediation of activation of coagulation in sepsis This has become evident from studies of volunteers treated with anti-TNF in which endotoxin-induced activation of coagulation did not change [89,90] Surprisingly, administration of IL-Ira, a major natural inhibitor of IL-1, results in inhibition of both the coagulation cascade and fibrinolysis in baboons with lethal bacteremia and patients with the sepsis syndrome [74,91] Treatment of patients with ILl-ra is associated with decreases in the concentrations of thrombin-anti thrombin complexes (TAT) and plasmin-alfa 2 antiplasmin complexes (PAP) complexes and tissue plasminogen activator (tPA) and plasminogen activator inhibitor (PAI-1) [91] Treating chimpanzees with anti-IL-6 after the administration of low-dose endotoxin prevents activation of the coagulation cascade but does not affect fibrinolysis [92]
In conclusion, activation of the tissue factor pathway after endotoxin release is largely, although not exclusively, mediated and regulated by cytokines
Contact activation Although the factor XII pathway does not seem to play an essential role in activation of the coagulation cascade in experimental sepsis in baboons [85,86], blocking of the contact activation system by the administration of monoclonal antibodies against Factor Xlla could prevent lethal hypotension This effect is most probably mediated by the generation of kinins, such as bradykmin [85] Moreover the contact system seems to play an independent role in the activation of the fibrinolytic system [93] However the importance of this route in sepsis has not yet been completely tlanfied
Table 2. Viruses infecting endothelial cells
Viruses
Dengue virus Herpes simplex virus Ebola virus Polio virus Marburg virus Adenovirus Hantaan virus Parainfluenza virus Cytomegalovirus Echovirus Measles Human Immunodeffiuency virus (HIV) HTLV-1 Mumps

83
Endothelial cell and Tissue Factor expression
The role of endothelial cells seems to be crucial in the development of shock and activation of coagulation. [94-96] Endothelial cell injury is a common feature of viral infection and can alter hemostasis in a direct or indirect manner. The endothelial cell can be directly infected by different viruses [97-99], e.g. HSV, Adenovirus, Parainfluenzavirus, Poliovirus, Echovirus, Measles virus, Mumps virus [100), Cytomegalovirus [101], HTLV-1 [102] and HIV. [103] The ability to infect endothelial cells has also been demonstrated in hemorrhagic fevers due to Dengue virus, Marburg virus, Ebola virus, Hantaan virus, Lassa virus. [104] Such infections may result in a procoagulant state, mainly by inducing tissue factor expression on the endothelial surface [105-107], probably mediated by cytokines such as IL-1 [105-112], TNF alpha and IL-6. [113-115] An additional cause of enhanced coagulability may be prothrombinase complex assembly on the CMV surface. [116] This observation suggests that the CMV surface contains the necessary procoagulant phospholipids for assembly of the coagulation enzyme complex leading to thrombin generation. A similar observation has been made for HIV. [117] However not all viral infections affecting endothelial cells result in activation of coagulation, which may indicate that activation of endothelium is one factor in a multifactorial process.
tmcro-organem and/or
mediators (cytokines)
molecule·
leukocyte rolling and adhesion Î
local mflammalion
increased permeability
\ plasma leakage
Figure 2 The endothelial cell in infection. During infection the endothelial cell may change to a procoagulant state, by expressing tissue factor on the membrane. Tissue factor is the main inducer of the extrinsic pathway of blood coagulation Increased endothelial permeability resulting in plasma leakage may be the consequence of a local or more generalized inflammatory response, with increased leukocyte adherence to the endothelial cell. This mechanism is triggered by the upregulation of endothelial cell adhesion molecules, i.e. Intercellular adhesion molecule I (ICAM 1), Vascular cell adhesion molecule 1 (VCAM I), E -selectin, P- selectin.

84
Fibrinolysis
General aspects The process of fibrinolysis involves the enzymatic cascade which helps to breakdown crosslmked fibrin molecules Fibrinolysis may be activated primarily and thus independently of activation of the coagulation cascade or secondarily in response to fibrin formation. If fibrinolysis is not balanced in time and scope, either bleeding or thrombosis may ensue After the injection of TNF into healthy volunteers activation of the coagulation cascade is preceded by a transient activation of fibrinolysis, which is reflected by increased circulating levels of tissue plasminogen activator (tPA) and urokinase plasminogen activator (UPA), followed by an increase in plasminogen activator inhibitor (PAI I), suppressing fibrinolysis [64,72,118,119] Coagulation activation triggers a secondary activation of fibrinolysis [52], which is rapidly shut-off by the release of relatively large amounts of PAI-I, such that the net effect of the injection of a bolus of endotoxin is a procoagulant state
Infusion of IL-1 alpha into baboons also elicits an early and transient activation of fibrinolysis [74], followed by the production of PAI-1 leading to a balance. Fibrinolytic activation is followed by activation of coagulation, thus showing the same imbalance between coagulation and fibrinolysis observed after the administration of TNF alpha This procoagulant imbalance is also present in DIC, where the net effect will be a tendency toward diffuse bleeding and microvascular thrombosis Treatment with anti-TNF in the human and chimpanzees sepsis model inhibits the fibrinolytic system, as reflected by the absence of a rise in tPA, PAI-l and PAP complexes [89,90,120], whereas coagulation is not affected, showing that TNF plays an important role in regulation of the fibrinolytic response Administration of IL-Ira into baboons with lethal bacteremia or patients with sepsis inhibits both coagulation and fibrinolysis [74,91], as indicated by decreased concentrations of TAT and PAP complexes and tPA and PAI-1 [91] Treating chimpanzees with anli-IL-6 after the administration of low-dose endotoxin prevents activation of the coagulation cascade and does not affect fibrinolysis [91 ]
Protein C/S sy stem During sepsis the protein C/S system is downregulated. [121] After the release of TNF alpha thrombomodulin is also downregulated, resulting in a further decrease in protein C activity, thereby enhancing the procoagulant stale Some viruses have the ability to induce specific changes in the coagulation inhibitory system During the course of HIV infection the protein CI S system may be impaired as a result of an acquired protein S deficiency, the pathogenesis of which is not yet clarified [122-125] In children protein S deficiency seems to correlate with the duration of HIV infection [122] , but such a relationship has not been demonstrated in adults [123] Increased plasma concentrations of the C4b-binding protein, an acute phase protein which binds protein S, may result in decreased levels of free protein S. Antiphosphohpid antibodies, which may be present in HIV patients, might interfere with the protein C/protein S complex and diminish its activity [123,126-129] In patients with Dengue hemorrhagic fever we also found decreased levels of both protein C and protein S activity (unpublished data) As in Dengue, HIV can affect the endothelial cell, hypothetically this could lead to decreased production of protein S

85
Thrombocytopenia
Thrombocytopenia is seen in the course of many viral infections but is only occasionally serious enough to lead to hemostatic impairment and bleeding complications [130] It is assumed that thrombocytopenia is mainly immune-mediated. [131] The mechanism is decreased thrombopoiesis [132,133], increased platelet consumption [134], or a combination of both Direct interaction of the virus with platelets [5,135,136] may lead to thrombocytopenia and/or thrombocytopathy Endothelial injury by the virus 1137] may lead to increased adherence and consumption of platelets [138].
Viral infections that have been associated with thrombocytopenia are Mumps [139,140], Rubella [141-143], Rubeola [144], Varicella [145-147], disseminated Herpes simplex [148|, CMV [149,150], infectious mononucleosis [151-155], Hantaan virus infection [156,157], Dengue HF [5,135,158], Crimean-congo HF [159] and Marburg HF [160] Dengue fever is associated with thrombocytopenia even in mild and uncomplicated cases [5] and therefore thrombocytopenia cannot be the only explanation for the occurrence of bleeding
Soluble adhesion molecules
The change of the endothelial cell from a resting to a procoagulant state may be associated with expression of endothelial surface adhesion molecules [112,161,162] These molecules, ι e. ICAM, VCAM, E Seleclin and von Willebrand factor (vWF), play an essential role in the binding of leukocytes, resulting in a local inflammatory response, endothelial cell damage and subsequent plasma leakage and shock [163-166] Vasculitis also occur, as has been documented in association with such viruses, as CMV and HIV [26,167,168] The finding of increased plasma concentrations of these endothelial surface adhesion molecules is thought to be a reflection of the level of activation and perhaps damage of the endothelial cell Measuring circulating endothelial cells by immunofluorescence or immunomagnetic separation may provide additional information about the activation of vascular endothelium [169-171]
Conclusions.
Infectious diseases are often accompanied by activation of coagulation. Although direct interactions between the infectious agent and the coagulation system occur, cytokines are beleived to be important mediators in this process During systemic Gram negative and Gram positive bacterial infections, activation ol coagulation is mediated via the extrinsic tissue factor pathway Experimental studies suggest that as a rule coagulation and fibrinolysis occur independently of one another and the overall result is usually a procoagulant tendency The latter situation may result in DIC with microvascular thrombosis and organ failure Bleeding may result from consumption of platelets and clotting proteins in traumatized tissues Although this scenario has been derived largely Irom studies with purified endotoxin or Gram negative bacteria, we expect similar alterations to occur in Gram positive as well as specific viral infections, due to the fact that some ol the key intermediate cytokines (TNF, IL-1, IL-6) are involved. It should be noted however, that the mechanisms by which viruses presumably induce coagulation in vivo are still speculative, since only in vitro data are available The critical cellular elements

86
involved in these reactions may not be the same for bacterial and viral infections, but we speculate that the vascular endothelium is one of the main targets Endothelial cells may turn into a procoagulant state either by stimulation of cytokines in concert with circulating blood cells, such as lymphocytes or platelets, or by direct infection (viruses) of endothelial cells.
Bleeding in infectious disease is most likely a multifactorial process, resulting from a combination of thrombocytopenia, consumption of clotting factors, (local) hyperfibnnolysis, and vascular damage or leakage. In addition immunologically mediated vasculitis may contribute to bleeding in specific infections The clinical consequences of chronic viral infections (such as CMV and HIV), for the development of thrombotic complications, vasculitis and atherosclerosis are of great interest One could hypothesize that due to the fact that CMV infection may lead to transformation of the endothelial cell to a procoagulant state but may also induce vasculitis and atherosclerosis [172], it could well be that there is a common pathway in the pathophysiological mechanism of these physiological and anatomical entities The role ot other pathogens, e g Chlamydia pneumoniae, which have the potency to affect the endothelium and contribute to the pathogenesis of atherosclerosis is of interest [173-175]
Knowledge of the underlying mechanisms leading to thrombosis and/or bleeding is fundamental for the development of therapeutic strategies In Gram negative infections the insight into the important roles of endotoxin and specific cytokines has already led to clinical therapeutic trials with selective inhibitors of the TF pathway (monoclonal antibodies, Fab fragments, modified Factor Vila, NAPc2 (nematode anticoagulant protein), TFPI) [176,177]
Studies with anti-TF antibodies and TFPI in primates have indicated that, in addition to inhibition of coagulation activity, these agents may have significant antiinflammatory properties and may markedly reduce mortality in otherwise lethal infections. [178,179]
Given the potential role that endothelial TF may play in some of the thrombo-hemorrhagic complications of viral disease, we expect that therapeutic intervention at the TF level or aimed at one ot the critical cytokines that mediates its cellular expression may potentially alter the clinical course of these infections favorably Many issues remain to be answered and therefore there is an urgent need for more clinical and experimental studies, particularly with respect to the relationship between viral infections and the mechanisms leading to bleeding/DIC Needless to say treatment of the causal infectious agent remains the cornerstone of therapy
Acknowledgments
E C M van Gorp and C Suharti are supported by a KNAW (Royal Netherlands Academy of Art and Science) grant and working on a collaborative project between Indonesia and the Netherlands on the pathogenesis of Dengue hemorrhagic fever. H ten Cate is a Clinical Established Investigator of the Netherlands Heart Foundation Participants in this project, besides the authors, are R. Djokomoeljanto (1), L W Statius van Eps (2,3), C E Hack (4),
J. Sutaryo (5), M Juffrey (5), L G. Thijs (3) and A J Ρ Veerman (3) (l)University of Diponegoro, Semarang, Indonesia, (2)Dept of Internal Medicine Slotervaart hospital Amsterdam, (3) Free University, Amsterdam, Netherlands, (4) Central Laboratory of the Bloodtransfusion Service, Amsterdam, Netherlands, (5) Gadjah Mada University, Yogyakarta, Indonesia.

87
References
01 Levi M, ten Gate H, van der Poll Τ, van Deventer SJH Pathogenesis of disseminated intravascular coagulation in sepsis JAM, 1993,270 975-979
02 Bauer Κ A and Weitz J I (1994) Laboratory markers ot coagulation and fibrinolysis pp 1197-1210 In Hemostasis and Thrombosis Basic Principles and Clinical Practice, Third edition (ed R W Colman, J Hirsh, V J Marder and E W Salzman) J Β Lippincott Company, Philadelphia
03 ten Gate H, Brandjes D P M , Wolters Η J , van Deventer S J H (1993) Disseminated intravascular coagulation Pathophysiology, diagnosis and treatment New Hori/ons, 1, 312-23
04 ten Cate JW, van der Poll T, Levi M, ten Cale Η, van Deventer SJH Cytokines, Triggers of clinical thrombotic disease Thromb Haemost, 1997,78(1) 415-419
05 Bhamarapravati Ν Hemostatic defects in Dengue hemorrhagic fever Rev Inf Dis, 1989, Il Suppl S826-829
06 Heller MV, Marta RF, Sturk A et al Early markers of blood coagulation and fibrinolysis activation in Argentine hemorrhagic fever Thromb Haemost, 1995, 73(3) 368-73
07 Clemens R, Pramoolsinsap C, Loren/ R et al Activation of the coagulation cascade in severe falciparum malaria through the intrinsic pathway Br J Haemat, 1994,87 100-105
08 Mohanty D, Ghosh K, Nandwam SK et al Fibrinolysis, inhibitors of blood coagulation and monocyte derived coagulant activity in acute Malaria Am J Hemat, 1997,54 23-29
09 Fera G, Semararo Ν, De Mitrio V, Schiraldi Ο Disseminated intravascular coagulation associated with disseminated cryptococcosis in a patient with acquired immunodeficiency syndrome Infection, 1993, 21(3) 171-3
10 Ten Cate H, Levi M, Biemond BJ, van Deventer SJH, van der Poll T, Buller HR, ten Cate JW Markers of hemostatic activation in experimental endotoxemia implications for therapy In DIG Pathogenesis, diagnosis and therapy of disseminated intravascular fibrin formation Muller-Berghaus G, Madlcner K, Blomback M, ten Cate JW (Eds) Excerpta Medica, 1993, Pg 81-89
11 Furlan M, Robles R, Galbusera M, et al Von Willebrand factor cleaving protease in thrombotic thrombocytopenic purpura and the hemolytic uremic syndrome Ν Engl J Med 1998,339 1578-84
12 Tsai HM, Chun-Yet Lian E Antibodies to von Willebrand factor cleaving protease in acute thrombotic thrombocytopenic purpura Ν Engl J med 1998, 339 1585-94
13 Moake JL Moschcowitz, muitimers, and metalloprotease Editorial Ν Engl J Med 1998,339 1629-31
14 Moake JL, Eisenstaedt RS Thrombotic thhrombocytopenic purpura and the hemolytic uremic syndrome In Colman RW, Hirsh J, Marder VJ, Salzman EW, eds Hemostasis and thrombosis basic principles and clinical practice 3rd ed Philadelphia JB Lippincott 1994 1064-75
15 Lie JT Vasculitis associated with infectious agents 1996, Current Opinion Rheumatol 1996, 8 26-29
16 Ackerman AB, Chongchitnant N, Sanchez J, Guo Y et al Inflammatory diseases In Histologic diagnosis of inflammatory skin diseases 2nd ed Williams and Wilkins 1997 170-786

88
17 De Boer JP, Creasy AA, Chang A, et al Activation patterns of coagulation and fibrinolysis in baboons following infusion with lethal or sublethal dose of Escherichia coli Cire Shock 1993, 39. 59-67
18 Hayes EB, Gubler DJ Dengue and dengue hemorrhagic fever Pediatr Inf Dis J 1992, 11 311-17.
19. Sumarmo, Wulur H, Jahja E, Gubler DJ, Suharyono W, Sorensen Κ Clinical observations on virologically confirmed fatal dengue infections in Jakarta, Indonesia Bull WHO, 1983, 61(4)· 693-701
20. Kuberski T, Rosen L, Reed D, Mataika J. Clinical and laboratory observations on patients with primary and secondary dengue type I infections with hemorrhagic manifestations in Fiji Am J Trop Med Hyg, 1977, 26(4) 775-83
21 Egbnng R, Slenczka W, Baltzer G Clinical manifestations and mechanism of the haemorrhagic diathesis in Marburg viral disease In- Martini GA, Siegert R, eds Marburg virus disease New York- Springer Verlag, 1971· 41-8
22 Gear JSS, Cassel GA, Gear AJ, et all. Outbreak ot Marburg virus disease in Johannesburg Br Med J 1975; 4 489-93
23. Report of a WHO international study team Ebola haemorrhagic fever in Sudan, 1976 Bull WHO 1978; 56. 247-70
24 Report ot an international commission Ebola haemorrhagic fever in Zaire, 1976. Bull WHO 1978; 56271-93
25. Guillevin L, Lhote F, Ghérardi R The spectrum and treatment of virus associated vasculitides. Curr Opinion Rheumatol 1997 9 31-36
26 Golden MP, Hammer SM, Wanke CA, Albrecht MA Cytomegalovirus vasculitis Case reports and review of the literature Medicine, 1994, 73(5) 246-255
27 Ho DD, Rota TR, Andrews CA, Hirsch MS. Replication of human cytomegalovirus in endothelial cells J Infect Dis 1984, 150 956-57
28. Goodman MD, Porter DD Cytomegalovirus vasculitis with fatal colonic hemorrhage Arch Pathol 1973,96 281-84
29. Foucar E, Mukai K, Foucar K, Sutherland DER, van Buren CT Colon ulceration in lethal cytomegalovirus infection Am J Clin Pathol 1981,76 788-801
30. Booss J, Dann PR, Winkler SR, Griffith BP, Kim JH Mechanisms of injury to the central nervous system following experimental cytomegalovirus infection Am J Otolaryngol 1990; 11 313-17.
31. Koeppen AH, Lansing LS, Peng SK, Smith RS Central nervous system vasculitis in cytomegalovirus infection J Neurol Sci 1981, 51 395-410
32 Lin CS, Penha PD, Knshman MN, Zak FG Cytomegalic inclusion disease of the skin. Arch Dermatol 1981, 117 282-84.
33 Libman BS, Quinsmorio FP, Stimmler MM Polyarteritis nodosa like vasculitis in human immunodeficiency virus infection J Rheumatol 1995, 22. 3511-55.
34 Calabrese LH Vasculitis and infection with the human immunodeficiency virus Rheum Dis Clin North Am 1991, 17 131-147
35 Gherardi R, Belec L, Mhin C et al The spectrum of vasculitis in human immunodeficiency virus infected patients Arthritis Rheum 1993, 36. 1164-74
36. Oehler R. Vaskulitis bei HIV infizierten patiënten Med Klin 1993,5 327-329 37 Sergent JS, Lockshin MD, Christian CL, Gocke DJ Vasculitis with hepatitis Β
antigenemia Medicine (baltimore) 1976, 55 1-18 38. Carson CW, Conn DL, Czaja AJ, Wright TL, Brecher ME Freqeuncy and
significance of antibodies to hepatitis C virus in polyarteritis nodosa J Rheumatol 1993,20 304-309

89
39 Quint L, Deny Ρ, Guillevin L et al Hepatitis C virus in patients with polyarteritis nodosa, prevalence in 38 patients Clin Exp Rheumatol 1991,9 253-257
40 Leruez-Ville M, Laugé A, Morinet F, Guillevin L, Deny Ρ Polyarteritis nodosa and parvovirus Β19 Lancet 1994, 344. 263-64.
41 Nikkari S, Mertsola J, Korvenranta H, Vainionpaa R, Toivanen Ρ Wegener's granulomatosis and parvovirus Β19 infection Arthritis Rheum 1994, 37' 1707-08
42 Yoto Y, Kudoh T, Haseyama K, Suzuki N, Chiba S, Matsunaga Y Human parvovirus Β19 infection in Kawasaki disease. Lancet 1994; 344 58-59
43 Lecour H, Miranda M, Magro C et al Human Leptospirosis- a review of 50 cases Infection 1989, 17(1) 8-12.
44 Laing RW, Teh C, Toh CH Thrombotic thrombocytopenic purpura (TTP) complicating Leptospirosis, a previously undescnbcd association J Clin Pathol 1990,43(11) 961-2.
45 Badesha PS, Saklayen MG. Hemolytic uremic syndrome as a presenting form of HIV infection Nephron 1996,72(3) 472-5
46 Chu QD, Medeiros LJ, Fisher AE, Chaquette RF, Crowley JP Thrombotic thrombocytopenic purpura and HIV infection South Med J 1995,(88)1 82-6
47 Qadn SM, Kayali S Enterohemorrhagic Escherichia coli A dangerous food borne pathogen Postgrad Med 1998, 103(2)· 179-80
48 Gardlund Β Randomised controlled trial ot low dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The heparin prophylaxis study group. Lancet, 1996, 347· 1357-61
49 Laing RBS, Brettle RP, Leen CLS Venous thrombosis in HIV infection. Int J STD AIDS 1996,7 82-85
50 Jenkins RE, Peters BS, Pinchin AJ. Thromboembolic disease in AIDS is associated with cytomegalovirus disease AIDS 1991,5 1540-2
51 Marder VJ Consumptive thrombohemorrhagic disorders In Williams WJ, Beutler E, Erslev AJ, Lichtman MA, eds Hematology 3rd ed New York McGraw-Hill, 1983 1433-61
52 Marder VJ, Feinstein DI, Francis CW, Coiman RW Consumptive thrombohemorrhagic disorders In Coiman RW, Hirsh J, Marder VJ, Sal/man EW, eds Hemostasis and thrombosis- basic principles and clinical practice 3rd ed Philadelphia· JB Lippmcott 1994 1023-1063
53 Limbos MA, Lieberman JM Disseminated intravascular coagulation associated with Rotavirus gastroenteritis- Report of two cases Clin Inf Dis 1996, 22 834-6.
54 WHO scientific working group Rotavirus and other viral diarrheas Bull World Health Organ 1980,58. 183-98
55 McKay DG, Margaretten W Disseminated intravascular coagulation in virus diseases Arch Intern Med 1967, 120 129-52
56 Gagel C, Linder M, Muller-Berghaus G, Lasch HG Virus infection and blood coagulation Thromb Diath Haemorrh 1970, 23 1-11.
57 Talley NA, Assumpcao CAR Disseminated intravascular clotting complicating viral pneumonia due to influenza Med J Aust 1971, 2 763-6
58 Davison AM, Thomson D, Robson JS Intravascular coagulation complicating Influenza A virus infection Br Med J 1973; l· 654-5
59 Whitaker AN, Bunce I, Graeme ER Disseminated intravascular coagulation and acute renal failure in Influenza A2 infection Med J Aust 1974, 2 196-201.
60. Settle H, Glueck HI Disseminated intravascular coagulation associated with influenza. Ohio State Med J 1975,71 541-3

90
61 Anderson DR, Schwartz J, Hunter NJ, Cottnll C, Bisaccia E, Klainer AS. Varicella hepatitis A fatal case in a previously healthy, immunocompetent adult. Arch Intern med 1994; 154 2101-5
62 Davie EW., Fujikawa K. and Kisiel W (1991). The coagulation cascade-initiation, maintenance and regulation Biochemistry, 30, 10363-10370
63 Van Gorp ECM, ten Gate H Coagulation monitoring In Oxford textbook ol critical care medicine Webb AR, Shapiro MJ, Singer M, Suter PM editors. Oxford university press 1999 1170-1173.
64 Van Deventer SJH, Buller HR, ten Gate JW, Aarden LA, Hack CE, Sturk A Experimental endotoxinaemia in humans, analysis of cytokine release and coagulation, fibrinolytic, and complement pathways Blood 1990; 76. 2520- 2526
65. Michie HR, Manogue KR, Spnggs DR, et al Detection of circulating tumor necrosis factor after endotoxin administration Ν Engl J Med 1988, 318 1481-1486.
66 Morrison DC, Ryan JC Endotoxin and disease mechanisms Annu Rev Med, 1987;38:417-432
67. Brandtzaeg P, Kieruit P, Gaustad Ρ et al. Plasma endotoxin as a predictor of multiple organ failure and death in systemic meningococcal disease. J Infect Dis 1989; 159. 195-204
68. Van Deventer SJH, Buller HR, ten Gate JW, Sturk A, Pauw W. Endotoxinaemia an early predictor of septicemia in febrile patients. Lancet 1988,1 605-609
69 Bauer KA, ten Gate H, Barzegar S, Spriggs DR, Sherman ML, Rosenberg RD. Tumor necrosis factor infusions have a procoagulant effect on the hemostatic mechanism of humans Blood 1989,74:165-172.
70. Van der Poll T, Buller HR, ten Cate H, et al. Activation ot coagulation after administration ot tumor necrosis factor to normal subjects Ν Engl J Med 1990, 322 1622-27
71 Levi M, ten Gate Η, Bauer ΚΑ, Buller HR, te Cate JW, Rosenberg RD. Dose dependent endotoxin induced cytokine release and cpagulation activation in chimpanzees Thromb Haemost 1991,65.793
72. Suttredini AF, Harpel PC, Panilo JE Promotion and subsequent inhibition of plasminogen activator after administration of intravenous endotoxin to normal subjects. Ν Engl J Med 1989, 320. 1165-72
73 Van der Poll T, Levi M, van Deventer SJH TNF and the dysbdlance between coagulant and anticoagulant mechanisms in septicemia Update Intensive Care Emerg. Med. 1990, 14:21-25.
74. Jansen PM, Boermeester MA, Fischer E, de Jong IW, van der Poll T, Moldawer LL, Hack CE, Lowry SF Contribution of interleukin-1 to activation of coagulation and fibrinolysis, to neutrophil degranulation and the release of sPLA2 in sepsis Studies in non-human pnmates following interleukin 1 alfa administration and during lethal bacteremia Blood 1995,86 1027-34
75. Stouthard JML, Levi M, Hack CE, Veenhof CHN, Romijn JA, Sauerwein HP, van der Poll Τ Interleukin-6 stimulates coagulation, not fibrinolysis, in humans. Thromb Haemost 1996, 76 738-42.
76 Conkling PR, Greenberg CS, Weinberg JB. Tumor necrosis factor induces tissue factor like activity in human leukemia cell line U937 and penpheral blood monocytes Blood 1988,72 128-133
77. Conway EM, Bach R, Rosenberg RD, Königsberg WH Tumor necrosis factor enhances expression of tissue factor mRNA in endothelial cells Thromb Res 1989,53 231-241

91
78 Bevilacqua MP, Pober SS, Majeau GR, Fiers W, Cotran RS, Gimbrone MA Recombinant tumor necrosis factor produces pro-coagulant activity in cultured human vascular endothelium Proc Natl Acad Sci USA 1986,83 4533-4537
79 Osterud B, Flaegstad Τ Increased tissue thromboplastin activity in monocytes ot patients with meningococcal infections related to unfavourable prognosis. Thromb Haemost 1983; 49 5-7
80. Levi M, ten Gate H, Bauer KA, van der Poll T, Edgington TS, Buller HR, van Deventer SJH, Hack CE, ten Gate JW, Rosenberg RD Inhibition of endotoxin induced activation of coagulation and fibrinolysis by pentoxifylline or by a monoclonal anti-tissue factor antibody in chimpanzees J Clin Invest 1994, 93 114-20
81 Taylor jr FB, Chang A, Ruf W, Momssey JH, Hinshaw L, Cdtlett R, Blick Κ, Edgington TS. Lethal E Coli septic shock is prevented by blocking tissue factor with monoclonal antibody Circ Shock 1991; 33 127-34
82 Creasy AA, Chang ACK, Feigen L, Wun TC, Taylor jr FB, Hinshaw LB. Tissue factor pathway inhibitor reduces mortality from Escherichia Coli septic shock J Clin Invest 1993; 91· 2850-60
83. Biemond BJ, ten Gate H, Levi M, Soule HR, Moms LD, Foster DL, Bogowitz CA, vander Poll Τ, Buller HR, ten cale JW Complete inhibition of endotoxin-induced coagulation activation in chimpanzees with a monoclonal Fab fragment against factor Vll/VIIa. Thromb Haemost 1995, 73 223-30
84 Biemond BJ, ten Gate H, Levi M, et al Complete inhibition ot endotoxin induced coagulation activation in chimpanzees with a monoclonal antibody to factor Vn/VIIa Circulation 1992; 86· 679
85 Pixley RA, De La Cadena R, Page JD, Kaufman N, Wyshock EG, Chang A, Taylor jr FB, Colman RW The contact system contributes to hypotension but not to disseminated intravascular coagulation in lethal bacteremia J Clin Invest 1993 91 61-8
86 Pixley RA, De La Cadena, Page JD, et al Activation of the contact system in lethal hypotensive bacteremia in a baboon model Am J Pathol 1992, 140 897-906
87 Pajkrt D, van der Poll T, Levi M et al Intcrlcukin 10 inhibits activation of coagulation and fibrinolysis during human endotoxemia Blood 1997, 89(8) 2701-05
88 Pradier O, Gerard C, Delvaux A, Lybin M, Abramowic/ D, Capei Ρ, Velu Τ, Goldman M. Interleukin-10 inhibits the induction ot monocyte procoagulant activity by bacterial hpopolysacchande Eur J Immunol 1993, 23 2700-4
89. Van der Poll T, Levi M, van Deventer SJH, ten Gale H, Haagmans BL, Biemond BJ, Buller HR, Hack CE, ten Cate JW Differential effects ot anti-tumor necrosis factor monoclonal antibodies on systemic inflammatory responses in experimental endotoxemia in chimpanzees Blood 1994,83 446-51
90 Van der Poll T, Coyle SM, Levi M, Jansen PM, Dentener M, Barbosa Κ, Buurman WA, Hack CE, ten Cate JW, Agost JM, Lowry SF Effect of recombinant dimeric tumor necrosis factor receptor on inflammatory responses to intravenous endotoxin in normal humans Blood 1997, 89 3727-34
91 Boermeester MA, van Leeuwen PAM, Coyle SM, Houdijk AJP, Eerenberg AM, Wolbink GJ, Pnbble JP, Stiles DM, Wesdorp RIG, Hack CE, Lowry SF. Interleukin-1 receptor blockade in patients with sepsis syndrome evidence that interleukin-l contributes to the release of interleukin-6, elastase and

92
phospholipase A2, and to the activation of the complement, coagulation and fibrinolytic systems Arch Surg 1995, HO 739-48
92 Van der Poll T, Levi M, Hack CE, ten Gate H, van Deventer SJH, Eerenberg AJM, de Groot ER, Jansen J, Gallati H, Buller HR, ten Gate JW, Aarden LA Elimination of interleukin 6 attenuates coagulation activation in experimental endotoxcmia in chimpanzees J Exp Med 1994, 179 1253-9
93 Levi M, Hack CE, de Boer JP, Brandjes DPM, Buller HR, ten Gate JW Reduction of contact activation related fibrinolytic activity in factor XII deficient patients further evidence for the role of the contact system m fibrinolysis in vivo J Clin Invest 1991,88 1155-1160
94 Cotran RS The endothelium and inflammation new insights Monogr Pathol 1982,23 18-37
95 Stemerman MB, Colton C, Morell E Perturbations of the endothelium Progr HemostThromb 1984, 7 289-324
96 Kaiser L, Sparks HV jr Endothelial cells not just a celophane wrapper Arch Intern Med 1987, 147 569-73
97 Friedman H, Macarak E, MacGregor R, Wolfe J, Kefahdes Ν Virus infection in endothelial cells J Inf Dis 1981, 143 266-73
98 Friedman H, Wolfe J, Kefahdes Ν, Macarak E Susceptibility of endothelial cells denved from different blood vessels to common viruses In Vitro Cell Dev Biol 1986,22 397-401
99 Friedman Η Infection ol endothelial cells by common human viruses Rev Infect Dis 1989, 11 S700-S704
100 Friedman HM, Macarak EJ, MacGregor RR, Wolfe J, Kefahdes NA Virus infection of endothelial cells J Infect Dis 1981, 143 266-73
101 Ho DD, Rota TR, Andrews CA, Hirsch MS Replication of human cytomegalovirus in endothelial cells J Infect Dis 1984, 150 956-7
102 Hoxie JA, Matthews DM, Cines DB Infection of human endothelial cells by human T-cell leukemia virus type I Proc Natl Acad Sci USA 1984, 81 7591-5
103 Wiley CA, Schner RD, Nelson JA, Lampert PW, Oldstone MBA Cellular localization of human immunodeficiency virus infection within the brains of acquired immune deficiency syndrome patients Proc Natl Acad Sci USA 1986, 83 7089-93
104 Butthep P, Bunyaratvcj A, Bhamarapravati Ν Dengue virus and endothelial cell a related phenomenon to thrombocytopenia and granulocytopenia in Dengue hemorrhagic fever Southeast J Trop Med Pubi Health 1993, 24 246-49
105 Bevilacqua M, Pober J, Wheeler M, Cotran R, Gimbrone M Interleukine-1 activation of vascular endothelium effects on procoagulant activity and leucocyte adhesion Am J Pathol 1985, 121 393-403
106 Adams DH, Wyner LR, Kamovsky MJ Experimental graft arteriosclerosis, 2 immunocytochemical analysis of lesion development Transplantation 1993, 56 794-99
107 Schorer A, Kaplan M, Rao G, Moldow C Interleukin-1 stimulates endothelial cell tissue factor production and expression by a prostaglandin-independent mechanism Thromb Haemost 1986, 56 256-59
108 Van Dam Mieras MCE, Muller AD, van Hinsbergh VWM, Mullers WJHA, Bomans PHH, Bruggeman CA The procoagulant response ol cytomegalovirus infected endothelial cells Thromb Haemost 1992, 68 364

9")
109 Van Dam-Mieras MCE, Bruggeman CA, Muller AD Debie WHM, Zwaai RFA Induction of endothelial cell procoagulant activity by cytomegalovirus infection ThrombRes 1987,47 69
HOEtingin OR, Silverstein RL, Friedman HM, Hajjar DP Viral activation of the coagulation cascade Molecular interaction at the surface of infected endothelial cells Cell 1990,61 657
111 Visser MR, Tracy PB, Vercelotti CM, Goodman JL, White JG, Jacob HS Enhanced thrombin generation and platelet binding on herpes simplex virus-infected endothelium Proc Natl Acad Sci USA 1988, S1) 8227
112 Etingin OR, Silverstein RL, Hajjar DP Identification of a monocyte receptor on herpes virus-infected cells Proc Natl Acad Sci USA 1991, 88 7200
113 Dudding L, Haskel S, Clark BD, Auron PE, Sporn S, Huang ES Cytomegalovirus infection stimulates expression ot monocyte associated mediator genes J Immunol 1989, 143 3343-52
114 Smith PD, Saini SS, Raffeid M, Manischewitz JF, Wahl SM Cytomegalovirus induction of tumor necrosis factor-alpha by human monocytes and mucosal macrophages J Clin Invest 1992, 90 1642-48
115 Almeida GD, Porada CD, St Jeor S, Ascensao J Human cytomegalovirus alters interleukin 6 production by endothelial cells Blood 1994, 83 370 76
116Pryzdial ELG, Wright JF Prothrombinase assembly on an enveloped virus evidence that the cytomegalovirus surface contains procoagulant phopholipid Blood 1994,84 3749-3757
117 Aloia RC, Tian H, Jensen FC Lipid composition and fluidity of the human immunodeficiency virus envelope and host cell plasma membranes Proc Natl Acad Sci USA 1993, 90 5181
118 Voss R, Matthias FR, Borkowski G, Reit/ D Activation and inhibition of fibrinolysis in septic patients in an intensive care unit Br J Haematol 1990, 75 99-102
119 Van der Poll T, Levi M, Buller HR, et al Fibrinolytic response to tumor necrosis lactor in healthy subjects J Exp Med 1991,174 729 73
120 Biemond BJ, Levi M, ten Gate H, van der Poll T, Buller HR, Hack CE, ten Gate JW Plasminogen activator and PAI-I release during experimental endotoxemia in chimpanzees eifects of various interventions in the cytokine and coagulation cascades Clin Sci 1995, 88 587-94
121 Esmon CT The regulation of natural anticoagulant pathways Science 1987,235 1348-52
122 Sugerman RW, Church JA, Goldsmith JC, Ens GE Acquired protein S deficiency in children infected with human immunodeficiency virus Pediatr Infect Dis J 1996, 15 106-11
123 Stahl CP, Wideman CS, Spira TJ, Haff EC, Hixon GJ, Evatt BL Protein S deficiency in men with long term human immunodeficiency virus infection Blood 1993, 81 1801-07
124 Lafeuillade A, Alessi MC, Poi/ol-Martin I et al Endothelial cell dysfunction in HIV infection J Acquir Immune Defic Syndr 1992, 5 127-31
125 Bissuel F, Verruyer M, Causse X, Dechavane M, Trepo C Acquired protein S deficiency correlation with advanced disease in HIV-infected patients J Acquir Immune Defic Syndr 1992, 5 484-9
126 Malia RG, Kitchen S, Greaves M, Preston FE Inhibition of activated protein C and its co-factor protein S by antiphospholipid antibodies Β J Haematol 76, 101 1990

94
127.Lo SCL, Salem HH, Howard MA, Oldmeadow MJ, Firkin BG Studies of natural anticoagulant proteins and anticardiohpin antibodies in patients with the lupus anticoagulant Β J Haematol 76, 380 1990
128 Hassell KL, Kressin DC, Neumann A, Ellison R, Marlar RA Correlation of antiphosphohpid antibodies and protein S deficiency with thrombosis in HIV infected men. Blood Coagulation Fibnnol 1994; 5(4) 455-62
129 Llorente MR, Carton JA, Carcaba V, Rodriguez-Pinto C, Maradona JA, Asensi V, Femandez-Urgelles M Antiphosphohpid antibodies in human immunodeficiency virus infection Medicina Clinica 1994, 103. 10-13
130.Levin J. Bleeding with infectious diseases In Disorders of hemostasis, 1984 367-378. Ratnoff OD, Forbes CD editors. Grune and Strattonane
131.Kelton J, Neame Ρ Hemorrhagic complications of infection in Hemostasis and thrombosis. Philadelphia, Pa JB Lippincott, 1987: 965-74.
132.Bierman HR, Nelson ER. Hematodepressive virus diseases of Thailand Ann Intern Med 1965; 62 867-84
133.Nakao S, Lai CJ, Young NS. Dengue virus, a flavi virus, propagates in human bone marrow progenitors and hematopoietic cell lines Blood 1989, 74 1235-40
134 Na-Nakom S, Suingdumrong A, Pootrakul S, Bhamarapravati Ν Bone marrow studies in Thai hemorrhagic fever. Bull WHO 1966, 35 54-5
135 Halstead SB Antibody, Macrophages, Dengue virus infection, shock and hemorrhage a pathogenetic cascade Rev Inf Dis 1989, 11 S830-S839
136.Terada H, Baldini M, Ebbe S, Madoff MA. Interaction of Influenza virus with blood platelets Blood 1966,28 213-28.
137.Stemerman MB Vascular intimai componenets. precursors of thrombosis Progr HemostThromb 1974, 2 1-47
138.Curwen KD, Gimbrone Majr, Handln RI In vitro studies of thromboresistance the role of prostacyclin (PGI2) in platelet adhesion to cultured normal and virally transformed human vascular endothelial cells. Lab Invest 1980, 42 366-74
139 Kolars CP, Spink WW Thrombopemc purpura as a complication of mumps JAMA 1958, 168 2213-15
140.Graham DY, Brown CH III, Benrey J, Butel JS. Thrombocytopenia a complication of mumps JAMA 1974, 227 1162-4.
141.Myllyla G, Vahen A, Vesikan T, Penttinen Κ Interaction between human blood platelets, viruses and antibodies Post Rubella thrombocytopenic purpura and platelet aggregation by Rubella antigen-antibody interaction Clin Exp Immunol 1969, 4· 323-32
142. Hirsch EO, Gardner FH. The transfusion of human blood platelets, with a note on the transfusion of granulocytes. J Lab Clin Med 1952; 39 556-69
143.Morse EE, Zinkham WH, Jackson DP Thrombocytopenic purpura following Rubella infection in children and adults. Arch Intem Med 1966, 117 573-9.
144 Hudson JB, Weinstein L, Chang TW Thrombocytopenic purpura in measles. J Pediatr 1956;48:48-56
145 Charkes ND Purpuric chickenpox report ot a case, review of the literature, and classification by clinical features Ann Intern Med 1961, 54 745-59
146.Tobin JD jr, ten Bensei RW Varicella with thrombocytopenia causing fatal intracerebral hemorrhage Am J Dis Child 1972, 124· 577-8
147 Brook I Disseminated Varicella with pneumonia, memngoencefalitis, thrombocytopenia,, and fatal intrcramal hemorrhage South Med J 1979, 72 756-7

9S
148 Whitaker JA, Hardison JE Severe thrombocytopenia after generalized herpes simplex virus-2 (HSV-2) infection 1978,71 864-5
149Chanarin I, Walford DM Thrombocytopenic purpura in Cytomegalovirus mononucleosis Lancet 1973, 2 238-9
150 Sahud MA, Bachelor MM Cytomegalovirus-induced thrombocytopenia an unusual case report Arch Intern Med 1978, 138 1573-5
151 Carter RL Platelet levels in infectious mononucleosis Blood 1965, 25 817-21 152 Sharp AA Platelets, bleeding and haemostasis in infectious mononucleosis In
Carter RL, Penman HG, eds Infectious mononucleosis 1st ed Oxford Blackwell Scientific Publications 1969 99-110
153 Casey TP, Matthews JRD Thrombocytopenic purpura in infectious mononucleosis NZMed J 1973, 77 318-20
154 Ellman L, Carvalho A, Jacobson BM, Colman RW Platelet autoantibody in acase of infectious mononucleosis presenting as thrombocytopenic purpura Am J Med 1973,55 723-6
155 Mazza J, Magnin GE Severe thrombocytopenia in infectious mononucleosis report of two cases and review of the literature Wis Med J 1975, 74 S124-7
156 Lee M Korean hemorrhagic fever (hemorrhagic fever with renal syndrome) 2nd edition Seoul Seoul National University press, 1986 83-106
157 Lo TT, Wang SH, Hwang HF, Pan NC, Qing WO, Wei WY Mechanisms of bleeding and the search for treatment in epidemic hemorrhagic fever Chinese Journal of Infectious Diseases 1986,4 716-9
158 Suvatte V Dengue hemorrhagic fever hematologic abnormalities and pathogenesis J med Assoc Thai 1978,61 (Suppl) 53-8
159 Swanepoel R, Shepherd AJ, Leman PA, Shepherd SP, McGillivray GM, Erasmus MJ, Searle LA, Gill DE Epidemiologic and clinical features of Crimean-Congo hemorrhagic fever in Southern Africa Am J Trop Med Hyg 1987, 36 120-32
160 Martini GA Marburg virus disease clinical syndrome In Martini GA, S legert R eds Marburg virus disease New York Springer Verlag, 1971 1-9
161 Mc Ever R GMP-140 a receptor for neutrophils and monocytes on activated platelets and endothelium J Cell Biochem 1991, 45 156-61
162Etingin O, Silverstein R, Hajjar D Von Willebrand factor mediates platelet adhesion to virally infected endothelial cells Proc Natl Acad Sci USA 1993, 90 5153-56
163 Van Gorp ECM, Suharti C, ten Cate H et al Endothelial cell activation in (Dengue) hemorrhagic fever Abstract 38th ICAAC 1998
164 Anderson R, Wang S, Osiowy C, Issekutz AC Activation of endothelial cells via antibody-enhanced dengue virus infection of peripheral blood monocytes J Virol 1997,71(6)4226-4232
165 Takahashi M, Ikeda U, Masuyama J et al Monocyte-endothelial cell interaction induces expression of adhesion molecules on human umbilical cord endothelial cells Cardiovasc Res 1996, 32(2) 422-29
166 Seigneur M, Constans J, Blann A et al Soluble adhesion molecules and endothelial cell damage in HIV infected patiënten Thromb Haemost 1997, 77(4), 646-649
167 Calabrese LH Vasculitis and infection with the human immunodeficiency virus Rheum Dis Clin North Am 1991, 17 131 -47
168 Gherardi R, Belec L, Mhin C, Gray F, Lescs MC, Sobel A, Guillevin L, Wechsler J The spectrum of vasculitis in human immunodeficiency virus infected patients Arthritis Rheum 1993, 36 1164-1174

96
169 Drancourt M, George F, Brouqui Ρ, Sampol J, Raoult D Diagnosis of mediterranean spotted fever by indirect immunofluorescence of Rickettsia conorn in circulating endothelial cells isolated with monoclonal antibody coated immunomagnetic beads J Inf Dis 1992, 166 660-3
170 George F, Brouqui Ρ, Boffa MC, Mutin M, Drancourt M, Bnsson C, Raoult D, Sampol J Demonstration of Rickettsia conorii-induced endothelial injury in vivo by measuring circulating endothelial cells, thrombomodulin, and von Willebran factor in patients with Mediterranean spotted fever Blood 1993, 82 2109-2116
171 Solovey A, Lin Y, Browne P, Choong S, Wayner E, Hebbel RP Circulating activated endothelial cells in sickle cell anemia Ν Engl J Med 1997, 337(22) 1584-90
172 Nicholson AC, Hajjar DP Herpesviruses in atherosclerosis and thrombosis Enologie agents or ubiquitous bystanders 9 Arteriosclerosis thromb vase biol 1998, 18 339-48
173 Danesh J, Collins R, Peto R Chronic infections and coronary heart disease is there a link Review Lancet 1997, 350 430-36
174 Gurfmkel E, Bozovich G, Daroca A et al Randomised trial of roxithromycin in non Q wave coronary syndromes Roxis pilot study Lancet 1997, 350 404-7
175 Gupta S, Leatham EW, Carnngton D el al Elevated Chlamydia pneumoniae antibodies, cardiovascular events, and a/ithromycine in male survivors of myocardial infarction Circulation 1997, 96 404-7
176 Cappello M, Vlasuk GP, Bergum PW et al Ancylostoma caninum anticoagulant peptide A hookworm-derived inhibitor of human coagulation factor Xa Proceedings of the National Academy of Sciences (USA) 1995, 92 6152-6156
177 Stanssens P, Bergum PW, Gansemans Y et al Anticoagulant repertoire of the hookworm Ancylostoma caninum Proceedings of the National Academy of Sciences (USA) 1996, 93 2149-2154
178 Taylor Jr FB, Chang A, Rut W et al Lethal E coli septic shock is prevented by blocking tissue factor with monoclonal antibodies Circ Shock 1991,33 127-37
179 Creasey A A, Chang ACK, Feigen L, Wun TC, Taylor Jr FB, Hinshaw LB Tissue factor pathway inhibitor reduces mortality from Escherichia coli septic shock J Clin Invest 1993,91 2850

Chapter 8
Activation of coagulation Factor XI, without detectable contact activation in dengue haemorrhagic fever.
Eric CM van Gorp (1), Monique C Minnema (2,3), Cathanna Suharti (4), Albert TA Mairuhu(l), Dees Ρ M Brandjes ( 1,2), Hugo ten Gate ( 1,5), C Erik Hack (3), Joost C M. Meyers (2).
Department ot Internal Medicine Slotervaart Hospital, Amsterdam, Netherlands (1), Department of Vascular Medicine, Academic Medical Centre, Amsterdam, Netherlands (2); Central Laboratory of the Netherlands Red Cross Blood Transfusion Service and Department Clinical Chemistry, Academic Hospital Vrije Universiteit, Amsterdam, Netherlands (3), Department of Internal Medicine and Paediatnc Department University of Diponegoro, Semarang, Indonesia (4); Laboratory for Experimental Internal Medicine, Academic Medical Centre, Amsterdam, Netherlands (5),.
The British Journal of Haematolology 2001; 113- 94-99.

98
Summary
A prospective cohort study was performed in 50 patients with dengue haemorrhagic fever (DHF) to determine the potential role of the contact activation system and factor XI activation (intrinsic pathway) in the coagulation disorders in DHF. To establish whether TAFI (thrombin-activatable fibrinolysis inhibitor) was involved in the severity of the coagulation disorders, the TAFI antigen and activity levels were also determined. Markers of contact activation (kalhkrein-Cl-inhibitor complexes), the intrinsic pathway of coagulation (factor XIa-Cl-inhibitor complexes) and TAFI were measured and correlated to thrombin generation markers (Thrombin-antithrombin complexes (TAT), prothrombin fragment 1+2 (Fl+2)) and a marker for fibrinolysis (plasmin-a2-antiplasmin complexes (PAP)) Activation of the intrinsic pathway of coagulation was clearly demonstrated by elevated levels of factor XIa-Cl-inhibitor complexes, without evidence of contact activation, reflected by undetectable kallikrein-Cl-inhibitor complexes. TAFI levels, both antigen and activity, were decreased in all patients which may contribute to the severity of bleeding complications in DHF because of the impaired capacity of the coagulation system to protect the fibrin clot from fibrinolysis. These findings in a human viral infection model, are in accordance with earlier findings in bacterial sepsis.

99
Introduction
The viral haemorrhagic fevers (VHF), i.e dengue haemorrhagic fever (DHF), are hallmarked by bleeding complications which may be life threatening Dengue fever (DF) is the most prevalent VHF world-wide, with over half of the world's population living in areas at risk of infection (Perez-Rigau et al, 1998) Annually, millions of people are infected and an estimated 250,000 to 500,000 patients develop severe DHF, which is associated with a mortality rate of 1-10%.
The pathogenesis of bleeding in DHF is poorly understood Thrombocytopenia may enhance the risk, but it is unknown what is the primary cause of bleeding Limited data suggest that activation of coagulation and fibrinolysis play a role in the pathogenesis of DHF (Bhamarapravati, 1989, Snchaikul et al, 1977) An imbalance in the regulation of coagulation and fibrinolysis, as in the disseminated intravascular coagulation syndrome (DIC), in conjunction with the characteristic thrombocytopenia may contribute to the bleeding tendency in DHF and other VHP's (van der Poll et al, 1990, van Gorp et al, 1997)
The main route for activation of the coagulation cascade in sepsis and probably also DHF is the tissue factor (TF) pathway (extrinsic pathway) (van Gorp et al, 1999) The factor XII pathway, or contact system, does not seem to play an essential role in the activation of coagulation in experimental sepsis in baboons (Pixlcy et al, 1993) Blocking of the contact activation system by administration of monoclonal antibodies against factor XII did not affect activation of coagulation, whereas it prevented lethal hypotension Rather, the contact system contributes to the activation and regulation of the fibrinolytic system in sepsis (Jansen et al, 1996). After thrombin formation via the TF pathway, factor XI may become involved in the coagulation process via positive feed back activation by thrombin (Naito and Fujikawa, 1991, Bro/e et al, 1992) Factor XIa generates additional thrombin via activation of factors IX and X (von dem Borne et al, 1995, ten Gate et al, 1996)
High concentrations of thrombin are needed for the activation of TAFI (thrombin-activatable fibrinolysis inhibitor) (von dem Bome et al 1995, von dem Borne et al 1997) Activated TAFI, also known as carboxypeptidase Β, carboxypeptidase U and carboxypeptidase R, down regulates fibrinolysis by removing C-terminal lysine residues that are essential for binding and activation of plasminogen (Baj/ar et al 1995, Wang et al 1998) Activation of TAFI by the coagulation system results in the protection of the fibrin clot from fibrinolysis TAFI was found to be responsible for the factor XI dependent down regulation of the fibrinolytic system (von dem Borne et al, 1997, Minnema et al, 1998a) In fact, any disturbance in the intrinsic pathway resulted in an increased clot lysis because of a reduced thrombin formation (Broze and Higuchi, 1996) These regulatory roles of both factor XI and TAFI may explain the bleeding tendency that occasionally accompanies deficiency states of these proteins (Minnema et al, 1999)
In this study we investigated the possible role of the contact activation pathway and activation of the intrinsic pathway in relation to thrombin generation and TAFI. We hypothesised that an inadequate factor XI/thrombin/TAFI feed back loop, resulting in an imbalance between coagulation and fibrinolysis, may contribute to the bleeding tendency in DHF

100
Methods
Study setting The study was executed in Semarang, Central Java, Indonesia, in the Dr Kanadi
University Hospital of the University of Diponegoro in Semarang Dengue is endemic in Java, with yearly outbreaks
Patients and monitoring Consecutive patients (children) who were admitted to the paediatnc intensive care
unit of the University Hospital of Diponegoro, Semarang, Indonesia, with a clinical diagnosis of severe DHF (grade III to IV) according to WHO criteria (World Health Organization, 1997) were included The study protocol received approval from the Institutional Review Board of this hospital and informed consent was obtained from the children's parents or guardians pnor to study inclusion
Activation markers of the intrinsic pathway of coagulation, ie factor XIa-Cl inhibitor complexes (activation marker of XI), Kallikrein-Cl inhibitor complexes (activation marker of the contact pathway) and TAFI were studied in samples obtained on the day of admission in the hospital and correlated to markers of thrombin generation (thrombin-anti-thrombin complexes (TAT) and prothrombin fragment 1+2 (Fl+2)) and plasmin formation (plasmin-a2-anti-plasmin complexes (PAP)
Diagnosis The presence of dengue was objectively confirmed by serological assays A capture
and indirect enzyme-linked immunosorbent assay (ELISA) detected dengue specific IgM and IgG antibodies in serum samples, according to a previously described procedure (Groen et al, 1999) Blood cultures were obtained in all patients to exclude bacterial infections
Blood collection Blood samples for analysis were collected on the day of admission Venous blood
was drawn into siliconized vacutainer tubes (Becton Dickinson, Great Britain) containing Polybrene (Janssen Chimica, Belgium) and EDTA (0 05%, w/v, and 10 mM, respectively, final concentrations) to prevent in vitro complex formation
All blood samples were immediately immersed in melting ice and subsequently centnfuged at 4°C for 20 mm at 1600 χ g Plasma samples were stored at -70°C until assayed Routine laboratory tests (haematology and chemistry) were done in Indonesia Research assays were carried out on samples transported to the Netherlands on dry ice
Coagulation assays TAT and Fl+2 levels were determined by means of commercially available ELISA
kits, according to the manufacturer's instructions (Enzygnost TAT micro and Fl+2 micro, Dade Behring, Marburg Germany) PAP complexes were measured with a radioimmuno-assay, as described previously (Levi et al, 1992) Upon activation in plasma, factor XI forms complexes with several protease inhibitors, the dominant inhibitor being CI-inhibitor (Wuillemin et al, 1995) Hence, to assess activation of factor XI in the patients, levels of factor XIa-Cl-inhibitor complexes were measured according to a method described previously (Wuillemin et al, 1995) In plasma of normal volunteers levels of these complexes are below the detection limit of 10 pmol/1 of this assay

101
Complexes between kallikrein with CI-inhibitor were measured with ELISA's modified from radioimmunoassays (Minnema et al, 1998b) Normal values were < 350 pmol/l for kalhkrein-Cl -inhibitor complexes
TAFI antigen and activity levels were measured according to a previously described procedure (Mosnier et al, 1998) A pool of plasma of 150 healthy adult hospital workers was used as a reference for the TAFI assays
Statistical analysis The plasma levels of the analytes measured were presented as median values with
their corresponding interquartile range (IQR) The Mann-Whitney-U test was used to compare the respective plasma levels of patients who died during the study (non-survivors) with those without a lethal clinical course (survivors) Two-tailed p-values of less than 0 05 were considered to indicate statistical significance Spearman rank correlation coefficients were calculated Analyses were performed using statistical software (SPSS 9 0)
Results
Patients From July 1996 through October 1996, a total of 50 consecutive children with a
clinical diagnosis of DHF were enrolled in the study Thirteen patients died during follow up on the intensive care unit (26%) due to DIC and multi-organ failure related complications The base-line characteristics of the subgroups, ι e survivors and non-survivors, were similar (Table 1)
The clinical diagnosis of DHF was confirmed by serological assay in all patients, either by an IgM response or a fourfold nse in IgG titres Antibody profiles were typical for secondary DF infection All patients were of Javanese origin, excluding racial differences
In all patients, blood cultures revealed no bacterial growth
Table 1. Baseline characteristics of the patients
Age (yr) Female sex (%) Admission day Clinical diagnosis DHF III DHF IV Thrombocytes (x lO'/L) White blood cell count (x IO'VL)
CRP (μδ/πιΙ)
Survivors (n=37)
6 8 + 2 8 46% 4 3 ± 0 9
34 3 63 9 ±35 7 7 5 ± 4 3
22 6 ± 33 5
Non-survivors (n=13)
6 0 ±2 8 69% 4 1± 1 4
9 4 4 8 7 1 1 2 9 10 2 ±5 1
1 3 6 ± 1 8 8
Values are means ± SD Clinical diagnosis according WHO criteria (WHO 1997)

102
Coagulation and fibrinolysis Thrombin generation was increased in all patients, as reflected by a marked
elevation of plasma levels of TAT and Fl+2 We also performed a sub-analysis in the survivors (n=37) and the non-survivor group (n=13), which demonstrated that thrombin generation was significantly more pronounced in the non-survivor group. (Table 2) Likewise, activation ot the fibrinolytic system, reflected by a rise in PAP complexes, occurred in nearly all patients, but was most pronounced in the survivor group (Table 2)
Table 2. Markers ot coagulation and fibrinolysis
TAT N<4 lmg/1 Fl+2 N<1 InMol/l PAP N<7nMol/l
All patients
(n=50)
27 2 (13 3 65 7) 3 2 (2 0-5 0) 8 6 (6 3-12 0)
Survivors
(n=37)
2 1 0 (10 9-52 0) 2 8 (19-4 0) 10 0 (7 1-13 0)
Non-survivors (n=13)
50 9
(28 5 117 5) 4 9 (2 7-7 2) 6 4 (4 1-8 5)
Ρ value*
0 004
0 008
0 03
Values ot markers of coagulation and fibrinolysis at day of ddmittance, all patients (n=50), Survivors (n=37) and Non survivors (n=13) Median values with 25% and 75% interquartile ranges (1QR) * Ρ value for comparison between survivors and non-survivors (Mann-Whitney U test) Ν is reference value
Activation of the intrinsic pathway of coagulation and the contact system The intrinsic pathway of coagulation was activated, as demonstrated by an increase
in factorXIa-Cl-inhibitor complexes Median values ot factor XI activation complexes were elevated In the sub analyses between survivors (n=37) and non-survivors (n=13) no significant differences were demonstrated (Table 3)
Although the intrinsic pathway was clearly activated we didn't demonstrate contact activation in our patients Kallikrein-Cl-inhibitor complexes, as a marker for contact activation, were only slightly elevated, but remained within the normal range The subgroup analyses between survivors and non-survivors also revealed no significant differences (Table 3)
TAFI ( thrombin -activatable fibrinolysis inhibitor) TAFI antigen and activity levels, were markedly decreased in all patients (Table 3)
In the subgroup analyses between survivors and non-survivors we demonstrated that this decrease was significantly more pronounced in the non-survivor group (Table 3) Spearman rank correlation coefficients between TAFI levels and the markers of thrombin generation were calculated. We lound a negative correlation between TAFI antigen and activity levels and TAT and Fl+2 levels (correlation coefficients between -0 2 and -0 6)

103
Table 3. Activation markers of the intrinsic pathway of coagulation and TAFI
Factor Xla-Cl inhibitor complexes N<10pmol/1
Kallikrein-Cl inhibitor complexes N<350pmol/1
TAFI activity Ν 100%
TAFI antigen Ν 100%
All patients (n=50)
13.5 (0-31.8)
13.2 (5.9-47.8)
31.8 (21.0-39.9)
46.0 (33.4-61.8)
Survivors
(n=37)
15.0 (12.0-20.5)
9.5 (5.8-38.8)
34.0 (25.7-41.1)
48.7 (39.4-68.4)
Non-survivors
(η=Ι3)
15 0 (0-48.0)
24.4 (7.6-69.6)
20.1 (12.7-31.8)
33.5 (24.7-45.8)
Ρ value*
0.7
0.3
0.004
0.006
Values of factor XIa-C I -inhibitor complexes and kallikrein C1 -inhibitor complexes and of thrombin aclivatable fibrinolysis inhibitor (TAFI) antigen and activity for all patients (n=50) and for the subgroups; survivors (n=37) and non-survivors (n=13). Median values with 25% and 75% interquartile ranges (IQR). * Ρ value for comparison between survivors and non-survivors (Mann-Whitney-U-tesl) Ν is reference value.
Discussion
In the present study we demonstrated that the intrinsic pathway of coagulation, i.e. factor XI pathway, is involved in the pathogenesis of coagulation disorders in DHF. Factor XI activation was demonstrated and at the same time thrombin generation was present reflected by elevated levels of TAT and F 1+2. In contrast we did not find evidence for contact activation, since kallikrein-Cl-inhibitor remained in the normal range. This observation is in line with the observations and results from studies in bacterial infection, but it is the first time that this mechanism is demonstrated in a viral infection.
The results from earlier studies in sepsis, recently resulted in a new comprehensive model of coagulation. In this model it is thought that the TF pathway is the main route of activation of the coagulation cascade. In 1991 two publications demonstrated the capacity of thrombin to activate factor XI, providing an alternative route for activation of factor XI (Naito and Fulikawa, 1991; Gailani and Broze, 1991). A new comprehensive model of coagulation was presented based on the following concept: Coagulation is initiated by the extrinsic, TF pathway, leading to the generation of thrombin and the formation of fibrin. After the formation of small amounts of factor Xa, the extrinsic pathway is rapidly inhibited by the tissue factor pathway inhibitor (TFPI) (Broze, 1992; Broze 1995). Continued thrombin formation now depends on the intrinsic pathway, activated by positive feedback (amplification) pathways consisting of thrombin-induced activation of factors V, VIII and XI (Davie et al, 1991 ; Broze and Gailani, 1993). The contact system does not play a role in physiological blood coagulation in this model. The absence of detectable contact activation, but detectable

HM
factor XI activation, in conjunction with enhanced thrombin generation suggests that coagulation activation in DHF follows this revised model
The coagulation system not only results in the formation of the fibrin clot, but also protects the fibrin clot by activation of TAFI Activated TAFI protects the fibnn clot by removing c-terminal lysine residues that are involved in binding and activation of plasminogen (Bajzar et al, 1995, Wang et al, 1998) TAFI levels, both antigen and activity, were markedly decreased in all patients In acute promyelocytic leukemia, often characterised by severe bleeding complications, only TAFI activity was decreased, whereas antigen levels remained unchanged (Meijers et al, 2000) It was demonstrated that, as a result of hyperfibnnolysis elevated plasmin levels may reduce TAFI activity, only slightly reducing the antigen level (Meijers et al, 2000) It is very likely that the decrease of both TAFI activity and antigen levels in the present study, is a manifestation of excessive thrombin generation, resulting in a disturbed factor XI-thrombin-TAFI feed back loop. This phenomenon is also demonstrated by the negative correlation between TAFI antigen and activity levels and markers of thrombin generation
The low TAFI levels, found in our patients, may also contribute to the impaired capacity of the coagulation system to stabilise clot formation and thereby lead to a dysbalance between coagulation and fibrinolysis, resulting in haemorrhage Yet, no data are available about TAFI levels in other infectious diseases and especially infections characterised by a bleeding tendency
Several issues of the present study merit further comment Firstly we have not determined TAFI levels in a control population with the same ethnic background. Recently it has been published that TAFI antigen levels may vary in populations with different ethnic background (Chetaille et al, 2000) Nevertheless, the lowest values measured in that study, in a black afncan population were above 80 % (mean value), whereas antigen levels in our study group varied between 33 5 and 48 7 % (median) (Table 3). In a group healthy Caucasian children (n=l 1 ), in the same age group (mean age 7 5 years), we measured mean TAFI antigen levels of 82% Taking these results together the TAFI levels measured in our study are extremely low Secondly we investigated only patients with the severest form of DHF Hence, our findings are only applicable to patients with this spectrum of disease and further studies are required to establish the role of the intrinsic pathway of coagulation and TAFI in patients with milder DF On the third place, it was rather surprising for us that all the enrolled patients who were clinically classified as having DHF on the basis of widely accepted clinical criteria, indeed had the disease, objectively confirmed by serological assays. This occurred despite the inclusion of consecutive patients in order to avoid selection bias and explains the lack of a non-dengue control group in this study. Taking these restrictions into account we believe that the possibility to study such a clinical cohort is rather unique
In conclusion it is clearly demonstrated that factor XI, i.e. the intrinsic pathway of coagulation, is involved in the activation of coagulation in DHF, whereas there is no contact activation This means that in viral infection (DHF) the similar route of activation occurs, that has recently been postulated and demonstrated in sepsis The low TAFI levels may be an attributable factor leading to the dysbalance in coagulation, resulting in bleeding complications These observations may indicate new molecular interactions for therapeutic intervention

105
Appendix
Besides the authors, the following investigators participated in this study J.W.M. van der Meer and W M.V. Dolmans (Department of Internal Medicine University Medical Centre St Radboud, Nijmegen, The Netherlands); L W Statius van Eps (Slotervaart Hospital, Amsterdam, The Netherlands); J Sutaryo (Gadjah Mada University, Yogyakarta, Indonesia); L G Thijs, A.J.P Veerman (University Hospital Vrije Universiteit, Amsterdam, The Netherlands), Υ Τ van der Heide (Clinical Chemistry and Haematology Laboratory, Slotervaart Hospital, Amsterdam); A.J.M Herenberg, G J van Mierloo (Central Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam); A Osterhaus, J Groen (Institute of Virology, Erasmus Medical Center, Rotterdam), M R Mac Gillavry, J.G Lijmer, (Department of Clinical Epidemiology and Biostatistics, Academic Medical Center, Amsterdam).
References
I Bajzar L, Manuel R, Nesheim ME (1995) Purification and characterization ot TAFI, a thrombin-activatable fibrinolysis inhibitor Journal of Biological Chemistry, 271, 14477-14484.
2. Bhamarapravati Ν Hemostatic defects in Dengue Hemorrhagic fever (1989) Review of Infectious Diseases, 11, S826-29
3. Broze GJ. The role of tissue factor pathway inhibitor in a revised coagulation cascade. (1992) Seminars in Hematology, 29, 159-169
4. Broze GJ, Gailani D. The role of factor XI in coagulation (1993) Thrombosis and Haemostasis, 70, 72-74
5. Broze GJ. Tissue factor pathway inhibitor (1995) Thrombois and Haemostasis, 74, 90-93
6 Broze GJ, Higuchi DA. (1996) Coagulation dependent inhibition of fibrinolysis, role of carboxypeptidase-U and the premature lysis of clots from hemophilic plasma. Blood, 88, 3815-3823
7. Chetaille P, Alessi MC, Kouassi D, Morange PE, Juhan-Vague I. (2000) Plasma TAFI antigen variations in healthy subjects Thrombois and Haemostasis, 83, 902-5
8 Davie EW, Fujikawa K, Kisiel K. (1991) The coagulation cascade Initiation, maintenance, and regulation Biochemistry, 30, 10363-10370
9. Gailani D, Bro/e GJ (1991) Factor XI activation in a revised model ot blood coagulation Science, 253, 909-12.
10. Groen J, Velzing J, Copra C, Balentien E, Deubel V, Vorndam V, Osterhaus ADME (1999) Diagnostic value of dengue virus-specific IgA and IgM serum antibody detection. Microbes and infection, 1,1-6
II Jansen PM, Pixley RA, Brouwer M, de Jong IW, Chang AC, Hack CE, Taylor FB, Coiman RW (1996) Inhibition of factor XII in septic baboons attenuates the activation of complement and fibrinolytic systems and reduces the release of interleukin-6 and neutrophil elastase. Blood, 87, 2337-44.
12 Levi M, de Boer JP, Roem D, ten Gate JW, Hack CE (1992) Plasminogen activation in vivo upon intravenous infusion of DDAVP Quantitative

106
assessment of plasmin-alpha-2-antiplasmin complex with a novel monoclonal antibody based radioimmunoassay Thrombosis and Haemoslasis, 67, 111-6
13 Meijers JCM, Oudijk EJ, Mosmer LO, Bos R, Bouma BN, Nieuwenhuis HK, Fijnheer R (2000) Reduced activity of TAFI (thrombin-activatable fibrinolysis inhibitor) in acute promyelocytic leukaemia British Journal of Haematology, 108,518-23
14. Minnema MC, Friederich PW, Levi M, von dem Borne PA, Mosmer LO, Meijers JCM, Biemond BJ, Hack CE, Bouma BN, ten Gate H. (1998) Enhancement of rabbit jugular vein thrombolysis by neutrali/ation of factor XI in vivo evidence for a role of factor XI as an anti-fibnnolytic factor Journal of Clinical Investigation, 101, 10-14
15 Minnema MC, Pajkrt D, Wuillemin WA, Roem D, Bleeker WK, Levi M, van Deventer SJH, Hack CE, ten Gate H (1998) Activation of clotting factor XI, without detectable contact activation in experimental human endotoxemia Blood, 92, 3294-3301
16. Minnema MC, ten Gate H, Hack CE (1999) The role of factor XI in coagulation: a matter of revision Seminars in Thrombosis and Hemostasis, 25,419-28
17 Mosmer LO, von dem Bome PA, Meyers JCM, Bouma BN (1998) Plasma TAFI levels influence the clot lysis time in healthy individuals in the presence of an intact intrinsic pathway of coagulation. Thrombosis and Haemostasis, 80, 829-35.
18 Naito K, Fujikawa Κ (1991) Activation of human blood coagulation factor XI independent of factor XII. Journal of Biological Chemistry, 266, 7353-7358
19. Perez-Rigau JG, Clark GC, Gubler DJ, Reiter Ρ, Sanders EJ, Vomdam AV. (1998) Dengue and dengue haemorrhagic fever Lancet, 352, 971-77
20. Pixley RA, de la Cadena R, Page JD, Kaufman N, Wyshock EG, Chang A, Taylor FB Jr,Colman RW (1993) The contact system contributes to hypotension but not disseminated intravascular coagulation in lethal bacteremia In vivo use of a monoclonal anti-factor XII antibody to block contact activation in baboons Journal of Clinical Investigation, 91, 61-68
21 Schatteman KA, Goossens FJ, Schärpe SS, Neels HM, Hendriks DF. (1999) Assay of procarboxypeptidase U, a novel determinant of the fibrinolytic cascade, in human plasma Clinical Chemistry, 45, 807-13
22 Snchaikul T, Nimmamtaya S, Artcharant N, Sinasawakul T, Sungpeuk Ρ (1977) Fibrinogen metabolism and disseminated intravascular coagulation in dengue hemorrhagic fever American Journal of Tropical Medicine and Hygiene, 26, 525-532
23 Ten Gate H, Biemond BJ, Levi M, Wuillemin WA, Bauer KA, Barzegar S, Buller HR, Hack CE, ten Gate JW, Rosenberg RD (1996) Factor XIa induced activation ol the intrinsic cascade in vivo Thromb Haemost, 75, 445-9
24 Van der Poll T, Levi M, van Deventer SJH (1990) TNF and the dysbalance between coagulant and anticoagulant mechanisms in septicemia Update Intensive Care Emerging Medicine, 14, 269-73
25 Van Gorp ECM, Suharti C, Setidti TE, Trastotenojo MS, ten Gate H, Keuter M, Dolmans WMV, Van den Ende A, Brandjes DPM (1997) Coagulation disorders in children with viral haemorrhagic fever Clinical Microbiology and Infection, 3, Suppl 2, 356

107
26 Van Gorp ECM, Suharti C, ten Gate H, Dolmans WMV, van der Meer JWM, ten Gate JW, Brandjes DPM (1999) Review Infectious diseases and coagulation disorders Journal of Infectious Diseases, 180, 176-86
27 Von dem Borne PA, Meijers JCM, Bouma BN (1995) Feedback activation ot factor XI by thrombin in plasma results in additional formation of thrombin that protects fibnn clots from fibrinolysis Blood, 86, 3035-42
28 Von dem Borne PA, Bajzar L, Meijers JCM, Nesheim ME, Bouma BN (1997) Thrombin-mediated activation of factor XI results in a thrombin-activatable fibrinolysis inhibitor-dependent inhibition of fibrinolysis Journal of Clinical Investigation, 99, 2323-27
29 WangW, BoffaMB, Bajzar L, Walker J B, Nesheim ME (1998) A study of the mechanism of inhibition of fibrinolysis byactivated thrombin-activable fibrinolysis inhibitor Journal of Biological Chemistry, 273, 27176-27181
30 World Health Organization (1997) Dengue haemorrhagic tever diagnosis, treatment, prevention and control 2d ed Geneva 12-47
31 Wuillemin WA, Minnema MC, Meijers JCM, Roem D, Eerenberg AJM, Nuijens JH, ten cate H, Hack CE (1995) Inactivation of factor XIa in human plasma assessed by measuring factor Xia-protease inhibitors major role tor Cl-inhibitor Blood, 85, 1517-26

108
Chapter 9
The Role of Cytokines in Activation of Coagulation and Fibrinolysis in Dengue Shock Syndrome
Cathanna Suharti', Eric C M van Gorp2, Tatty E Setiati1, Wil M V Dolmans4, Robert J Djokomoeljanto', C Erik Hack 5, Hugo ten Cate6 , D Ρ M Brandjes2, Jos W M van der Meer4
Departments of 'Medicine and 3Paediatrics, Faculty of Medicine, Diponegoro University and Dr Kariadi Hospital, Semarang, Indonesia, "Department of Medicine, Slotervaart Hospital, Amsterdam, 4Department of Medicine, University Medical Centre St Radboud, Nijmegen, Central Laboratory of The Netherlands Red Cross Blood Transfusion Service and Department Clinical Chemistry, Academic Hospital Vrije Universiteit, Amsterdam, laboratory for Experimental Internal Medicine, Academic Medical Center, Amsterdam, The Netherlands
Submitted for publication

109
Summary
In a prospective clinical study of 50 patients with Dengue Shock Syndrome (DSS), we investigated the association of tumor necrosis factor-α (TNF-a), interleukin-lß (IL-Iß), IL-1 receptor antagonist (IL-lRa), and IL-6 with activation markers of coagulation (Fl+2 and TATc) and fibrinolysis (t-PA, PAPc, and D-dimer). We found that TNF-a, IL-1 β and Il-lRa, but not IL-6, concentrations in the circulation were elevated during the early stage of infection and at discharge from hospital TNF-a was significantly associated with D-dimer, an activation marker of fibrinolysis ( p<0.003), but not with activation markers of coagulation. IL-Iß was significantly associated with t-PA (p<0 03) IL-lRa was significantly associated with F1+2, TATc (p<0.04 and p<0.02, respectively), whereas IL-6 was significantly associated with both, activation markers of coagulation (Fl+2, p<0.03) and fibrinolysis (PAPc; p=0.002) Our data are in line with studies in bacterial sepsis. In severe dengue virus infection the same cytokines are involved in the onset and regulation of hemostasis.

110
Introduction
The association between infection and activation of coagulation and fibrinolysis has been studied extensively in Gram negative-sepsis and endotoxemia (1) Activation of coagulation, as reflected by increasing plasma levels of prothrombin fragment 1 and fragment 2 (Fl+2) and thrombin-antithrombin complexes (TATc), and activation of fibrinolysis, as reflected by increasing plasma levels of tissue plasminogen activator (t-PA) and plasminogen activator inhibitor type 1 (PAI-1), have been detected in sepsis (2-4) and in experimental endotoxemia in humans (5, 6) Cytokines appear to play a crucial role in the initiation of coagulation and fibrinolysis under these circumstances (1). Tumor necrosis factor α (TNF-cc), interleukin-lß (IL-Iß), and interleukin-6 (IL-6) seem to be the most prominent mediators in this respect (1,6-10)
Dengue hemorrhagic fever (DHF) is a severe form of the infection caused by any of four serotypes of the dengue virus It is characterized by fever, thrombocytopenia, bleeding manifestations ranging from mild to severe, and evidence of plasma leakage According to the 1997 WHO criteria, dengue shock syndrome (DSS) is defined as DHF with signs of circulatory failure, including narrow pulse pressure (20 mm Hg) and hypotension (DHF grade III) or trank shock (DHF grade IV) (11, 12). Plasma leakage and bleeding are the two major pathophysiological changes in DHF/DSS, determining the seventy of disease (11-14) Little is known about the pathogenesis of bleeding in DHF/DSS and in analogy to sepsis it is attractive to speculate that cytokines are key mediators Preexisting heterotypic dengue antibodies augment dengue virus infection of monocytes or macrophages (15). An increased number of dengue virus-infected monocytes may result in T-lymphocyte activation, the activation of both types of cell may result in the production of elevated levels of the aforementioned cytokines (16)
We designed a prospective clinical study to investigate the association ot cytokines with activation markers of coagulation and fibrinolysis in DSS. We investigated those cytokines which are known to play a role in the activation ot coagulation and fibrinolysis in bacterial sepsis
Patients and methods
Study setting The study was executed in Dr Kanadi Hospital, Semarang, Indonesia, the university
hospital of Diponegoro University The research protocol was reviewed and approved by the institutional Review Board of the Dr Kanadi Hospital Written informed consent was obtained from children's parents or legal guardians
Patients Between June and November 1996, during an outbreak of dengue in Indonesia, 50
consecutive children with the clinical diagnosis of DSS and admitted to the Paediatnc Intensive Care Unit, were enrolled in the study The diagnosis of DSS (DHF grade III and grade IV) was based on WHO criteria (1997) (11) The assessment of decreased consciousness was based on the Glasgow coma scale (17) Only children aged > 3 years were included

I l l
Patient monitoring Thorough clinical assessment was performed daily during hospitalization, using a
medical record form Laboratory tests to support clinical management included blood cell counts, tests tor hemostasis (prothrombin time and activated partial thromboplastin time) as well as biochemical tests for kidney and liver functions and electrolyte status
Specimen collection Blood specimens were collected in vacutainer tubes (Becton Dickinson, Rutherford, NJ
07417) Specimens for cytokine assays were collected in the acute phase of disease (on day of admission· day 0, on day 1 and 2), and on day 7 or the day ot discharge if the patient was hospitalized less than 7 days Four ml of blood were collected into sterile tubes containing EDTA in each patient To this tube 125 μ ι of aprotmin (Trasylol, Bayer, Leverkusen, Germany; final concentration 625 kallikreine inactivating units/mL) was added through the stopper by a tuberculin needle and syringe The tube was centnfuged directly at 1250 g for 10 minutes, and thereafter at 15000 g for 1 minute to remove platelets. The plasma was stored in ahquots at -80^C until assayed tor cytokines
Blood samples for analysis of coagulation and fibrinolysis were collected on the same days as the samples for cytokines Venous blood (9 vol ) for measurement ot F1+2, TATc and D-dimers was drawn into vacutainer tubes containing 0 105 M sodium citrate (1 vol ) For measurement of PAPc, t-PA, blood was collected in siliconized vacutainer tubes containing Polybrene (Janssen Chimica, Belgium) and EDTA (0.05% w/v, and 10 mM, respectively, final concentrations) to prevent in-vitro complex formation All blood samples were immediately immersed in melting ice and subsequently centnfuged at 4()C for 20 mm at 1600 χ g Plasma samples were stored at -800C until assayed
To collect appropriately timed specimens for serological assays (> day 6 after onset of fever) (18-21), 2 ml of blood was collected on day of admission and at discharge Blood was centnfuged 1000-1500 rpm tor 10 minutes, afterwards, serum was transferred to screw cap Eppendorf tubes and stored at -80^C, until assayed For the transport from Indonesia to The Netherlands (which lasts longer than 15 hours) the samples for cytokines, coagulation, fibrinolysis, and serological assays were kept on dry ice
Cytokine assays
TNF-a, IL-ß and IL-IRa were measured in duplicate by nonequilibnum radioimmunoassay (RIA) (22) Recombinant human TNF-a, IL-Iß and IL-IRa were calibrated against standards provided the National Institute of Biological Standards and Control (Potters Bar, UK), with the sensitivity of the assay with 100 μΐ sample of 40 pg/ml, 40 pg/ml, and 80 pg/ml, respectively IL-6 was measured with ELISA obtained from the Central Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands, according to manufacturer's instruction, circulating concentrations exceeding 10 pg/ml were considered to be elevated
Coagulation and fibrinolysis assays Fl+2 and TATc levels were determined with the use ot commercially available ELISA
kits, according to the manufacturer's instructions (Enzygnost F1+2 micro and TAT micro, Dade Behring, Marburg, Germany) For the measurement of D-dimer levels, the TintElize D dimer ELISA from Biopool (Sweden) was used, according to the

112
manufacturer's instructions t-PA was measured with sandwich ELISA kits using specific monoclonal antibodies as described before (23) PAPc was measured with radioimmunoassay as described previously (24)
Serological assays The diagnosis of dengue infection was confirmed by serological assays A capture and
indirect enzyme-linked immunosorbent assay (ELISA) detected dengue specific IgM and IgG antibodies in serum samples, according to a previously described procedure (25)
Statistical analysis Continuous data were described as mean with SD or median with range Nominal data
were described as percentage (%) Multiple linear regression analysis was done to determine the association between cytokines and activation markers of coagulation and fibrinolysis on the day of admission Ρ values of less than 0 05 were considered to indicate statistical significance All statistical analyses were performed with SPSS for Windows, version 9 0
Results
Between June and November 1996, 50 children with a clinical diagnosis of DSS, were enrolled in the study Baseline charactenstics of the patients are listed in table 1 Thirteen patients (26%) died during follow up on the intensive care unit The clinical diagnosis was confirmed by serological assay in all patients, either by an IgM response or a fourfold rise in IgG titres Antibody profiles were typical for secondary dengue infection
Plasma concentrations of cytokines in the course of DSS The circulating plasma concentrations of TNF-a, IL-ß, IL-1 Ra, and IL-6 were assayed
on the day of admission (day 0), on day 1 and 2 after admission, and on day 7 after admission or at discharge it this was earlier than day 7 As shown in Table 2, concentrations of TNF-a and IL-Iß were mildly elevated and concentrations of IL-IRa were moderately elevated during the early stage of infection and at discharge The median plasma concentrations of IL-6 were low during the observation penod, although three patients had extremely high plasma concentrations

113
Table 1. Characteristics in 50 patients with dengue shock syndrome
Age in years * Days since onset of disease* Male Female Clinical diagnosi·, (WHO criteria)
DHF III DHFIV Positive serology result Number of death Bleeding manifestations
Positive Tourniquet test Skin bleeding (petechiae,purpura,hematoma) Epistaxis Gum bleeding Hematemesis and / or melena Hematuria
6.6±2.8(3-13) 4.2±1 (2-7) 24 (48) 26 (52)
43 (86) 7(14) 50(100) 13(26)
23(46) 21(42)
10(20) 3(6) 28(56) 2(4)
* Age and Days since onset of disease are mean ±SD (range), all other characteristics are numbers (%)
Activation of coagulation and fibrinolysis As shown in Table 3, Fl+2 and TATc were persistently high from admission to
discharge, reflecting activation of coagulation. Also, persistently elevated levels of t-PA, PAPc, and D-dimer were found during the study period, reflecting activation of the fibrinolytic system.

114
Table 2. Median circulating plasma concentrations (range) of TNF-a, IL-Iß, IL-1 Ra and IL-6 on day of admission (DO), the following two days (Dl, D2) and on day 7 or at discharge if earlier (D7 / discharge) in 50 patients with dengue shock syndrome
TNF-a (pg/n,,,
IL-1 β (pg/ml)
IL-1 Ra (pg/mi)
IL-6 (pg/mi)
DO
155 (95-2500) 72.5 (<40-320) 795 (220-2500) < 2 (<2-199000)
D 1
140 (85-315) 80 (<40-140) 555 (180-2400) 2.1 (<2-1058)
D 2
150 (95-305) 80 (<40-145) 590 (225-2050) 3.5 (<2-155)
D 7 (discharge)
135 (90-1100) 70 (<40-155) 395 (240-2900) <2 «2-48)
Normal value
90 (50-170) 50 (<40-115) 139 (<80-502) <10
Table 3. Median plasma concentrations (range) of activation markers of coagulation and
fibrinolysis on day of admission (DO), the following two days (Dl, D2) and on day 7 or
at discharge if earlier (D7 / discharge) in 50 patients with dengue shock syndrome
DO
Markers of coagulation
F1+2 (nMol/l)
TATc (mg/i)
3.2 (1.2-14.2) 27.1 (3.8- 120)
Markers ofjibrmolysh
t-PA (ng/ml)
PAPC („Mol)
D-dimer (ng,ml)
52.5 (5.5 - 143) 8.6 (2.3-25) 241 (85-2000)
D l
2.6 (0.9-40.8) 15 (1.9-120)
56 (7.6-112) 7.4 2.1-14 312 (69-1600)
D 2
2.7 (0.8-21.4) 15.5 (3.3-120)
41.5 (9 - 86) 10 (3.3-32 481 (53-1778)
U /[discharge)
2.2 (0.8 - 7.6) 6.6 (1.7- 101.5)
16.5 (5.7 - 89) 12 (3.4-60) 265 (59-1600)
Normal value
<1.1
<4.1
<10
<7
<39

115
Association of plasma concentrations of cytokines with activation markers of coagulation and fibrinolysis As shown in Table 4, TNF-a was significantly associated with D-dimer, an activation marker of fibrinolysis, but not with activation markers of coagulation. IL-Iß was significantly associated with activation marker of fibrinolysis l-PA; the regression coefficient (β) for t-PA of IL-1 β was 4.05, meaning that for every additional 10 pg IL-1 β, t-PA increases 4.05 ng/ml. IL-lRa was significantly associated with activation markers of coagulation Fl+2 as well as TATc. The regression coeffisien (β) for Fl+2 of IL-lRa was 0.11, meaning that for every additional 100 pg/ml of IL-lRa, Fl+2 increases 0.11 nMol. IL-6 was significantly associated with F 1+2, an activation marker of coagulation and with PAPc, an activation marker of fibrinolysis. The regression coefficient (β) for Fl+2 of IL-6 was 0.05, implying that for every additional 1000 pg/ml of IL-6, Fl+2 increases 0.05 nMol. Similarly, β for PAPc of IL-6 was 0.17, and for D-dimer of TNF-a was 13.77; this means that for every additional 1000 pg of IL-6, PAPc increases 0.17 nMol, and for every additional 10 pg of TNF-a, D-dimer increases 13.77 ng/ml.
Table 4. Results of multiple linear regression analysis showing significant associations of cytokines with activation markers of coagulation and fibinolysis on day of admission in 50 patients with dengue shock syndrome
Markers of coagulation
F l + 2 („Mol/l)
TATC (mg/i)
Markers of fibrinolysis
t-"A (ng/ml)
P A P c (nMo|>
D-dimer ( „ ^ D
Cytokine
IL-6 (per llXXIpf.)
I L - l R a (ptr loopg)
I L - l R a (per 100 pg)
IL-lßipcHOpg)
IL-6 (per 1000 pg)
T N F - a (per io pg)
/7-value
0.0260 0.0348 0.0108
0.0265 0.0020 0.0023
ß
0.05 0.11 2.09
4.05 0.17 13.77
β: regression coefficient

116
Discussion
The present study in severe dengue virus infection demonstrates, that cytokines are associated with activation markers of coagulation and fibrinolysis
TNF-a was significantly associated with D-dimer, a marker of fibrinolysis, but not with activation markers of coagulation. Studies in bacterial infection have clearly indicated the role of TNF-a in the activation of the fibrinolytic system, but the role of TNF-a in the activation ot the coagulation system seems to be less direct. A single intravenous injection of recombinant TNF into human volunteers induced activation of the common pathway of the coagulation cascade, resulting in thrombin formation, as reflected by elevated plasma levels ot Fl+2 (3), and activation of the fibrinolytic system characterized by increased levels ot urokinase-type PA (u-ΡΑ) and t-PA, followed by PAI-1 (4) An injection of E. coli endotoxin induced increased levels of TNF-a and IL-6, and resulted in activation of fibrinolysis as reflected by increased levels of t-PA, PAPc, which was subsequently otfset by release of PAI-1, and a long-lasting onset of coagulation activation characterized by increase of prothrombin F1+2 and TATc (9) However, further studies have demonstrated that anti-TNF treatment did not affect endotoxin-induced coagulation activation (26-28), but did inhibit the activation of the fibrinolytic system in animal and human models with low-grade endotoxaemia (26,27,29) Thus our findings in DHF are in line with these findings in endotoxemia
We demonstrated that IL-Iß was significantly associated with tPA, a marker for activation of fibrinolysis. The role of IL-Iß in the activation of coagulation as well as fibrinolysis has been demonstrated by injection ot IL-lß, or, indirectly by injection of IL-IRa (5,6) Infusion of IL-1 into baboons induced activation of the fibrinolytic system, reflected by increased levels of t-PA, and subsequently offset of fibrinolysis by PAI-1, followed by the activation ot coagulation, characterized by increased levels of TATc (5) Administration of ILl-Ra in baboons with lethal bacteremia, and in patients with sepsis have significantly attenuated the activation of coagulation and fibrinolysis (6).
We also found that IL-IRa was significantly associated with the activation markers ot coagulation F1+2 and TATc, leading to the conclusion that the regulation of coagulation and fibrinolysis by IL-lß and IL-IRa in this severe viral infection is similar to that in sepsis
We demonstrated that IL-6 is significantly associated with activation markers of both coagulation and fibrinolysis The role of this cytokine in the activation of coagulation has been demonstrated by injection ot recombinant IL-6, as well as by administration of anti-IL-6 antibody Infusion of recombinant IL-6 into patients with renal cell carcinoma resulted in increased levels of Fl+2 and TATc, while fibrinolysis was not clearly affected (30)
In the present study we found that the median levels ot IL-6 were normal, but with extremely high values in 3 patients (5823, 86000 and 199000 pg/ml) Two of these 3 patients died and in these two patients, very high levels of TNF-a (2500 and 2500 pg/ml), IL-IRa (2500 and 2500 pg/ml), and Fl+2 (7.51 and 14 2 nMol/1, normal <1 InMol/l) were found The very high levels of Fl+2 reflect the degree of coagulation activation, which may result in a considerable fibrin formation, leading to multiorgan failure and ultimately to death

117
We conclude that in dengue shock syndrome the same cytokines are involved in the onset and regulation of coagulation and Fibrinolysis as in bacterial infections.
Acknowledgements
Participants in this project, besides the authors, were Prof. Moeljono S. Trastotenojo, dr. Herawati Juslam, from the Deparment of Paediatrics and Prof. Soenarto, from the Department of Internal Medicine, Dr. Kariadi Hospital, Diponegoro University, Semarang, Indonesia. We thank Y.T. van der Heide from the Clinical Chemistry and Hematology Laboratory, Slotervaart Hospital, Amsterdam, The Netherlands, for managing the blood samples, and Dr. J. Groen and Prof. A. Osterhaus from the Institute of Virology, Erasmus Medical Centre, Rotterdam, for performing the diagnostic assays. We thank also Johanna van der Ven-Jongekrijg from the laboratory of the Department of General Internal Medicine, University Medical Centre St Radboud, Nijmegen, The Netherlands and GJ van Mierloo and AJM Herenberg from the Central Laboratory of The Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands, for performing the cytokine assays.
References
1. Van Gorp ECM, Suharti C, ten Gate H, Dolmans WMV, van der Meer JWM, ten Cate JW, Brandjes DPM. Infectious Diseases and Coagulation Disorders. J Infect Dis 1999; 180: 176-86.
2. Osterud B, Flaegstad T. Increased tissue thromboplastin activity in monocytes of patients with meningococcal infections related to unfavourable prognosis. Thromb Haemostats 1983; 49: 5-7.
3. Voss R, Matthias FR, Borkowski G, Reitz D. Activation and inhibition of fibrinolysis in septic patients in an internal intensive care unit. Β J Haematol 1990;75:99-105.
4. Brandtzaeg P, Joo GB, Brusletto B, Kierulf P, Plasminogen activator inhibitor 1 and 2, and a2-antipla.smin, and endotoxin levels in systemic meningococcal disease. Thromb Res 1990; 57: 271-78.
5. Van Deventer SJH, Büller HR, Ten Cate JW, Aarden LA, Hack CE, Sturk A. Experimental endotoxaemia in humans: analysis of cytokine release and coagulation, fibrinolytic and complement pathways. Blood 1990; 76: 2520-26.
6. Suffredini AF, Harpel PC, Parrillo JE. Promotion and subsequent inhibition of plasminogen activator after administration of intravenous endotoxin to normal subjects. Ν Engl J Med 1989; 320: 1165-72.
7. Van der Poll T, Büller HR, Ten Cate H, Wortel CH, Bauer KA, van Deventer SJH, Hack CE, Sauerwein HP, Rosenberg RD, ten Cate JW. Activation of coagulation after administration of tumor necrosis factor in healthy subjects. Ν Engl J Med 1990; 322: 1622-27.
8. Van der Poll T, Levi M, Büller HR, van Deventer SJH, de Boer JP, Hack CE, ten Cate JW. Fibrinolytic response to tumor necrosis factor in healthy subjects. J Exp Med 1991; 174:729-32.

118
9 Jansen PM, Boermeester MA, Fischer E, de Jong IW, van der Poll T, Moldawer LL, Hack CE, Lowry SF Contribution of interleukin-1 to activation of coagulation and fibrinolysis, to neutrophil degranulation and the release of sPLA2 in sepsis. Studies in non-human primates following interleukin-lcc administration and during lethal bacteremia Blood 1995, 86 1027-34
10 Boermeester MA, van Leeuwen PAM, Coy le SM, Houdijk AJP, Herenberg AM, Wolbink GJ, Pnbble JP, Stiles DM, Wesdorp RIC, Hack CE, Lowry SF Interleukin-1 receptor blockade in patients with sepsis syndrome evidence that interleukin-1 contributes to the release of interleukin-6, elastase and phospholipase A2, and to the activation of the complement, coagulation and fibrinolytic system Arch Surg 1995, 130 739-48.
11. Dengue haemorrhagic fever- diagnosis, treatment, prevention and control 2d ed. Geneva World Health Organization 1997, 12-47
12. Dengue and dengue hemorrhagic fever in the Americas guidlines for prevention and control Washington, DC Pan Amencan Health Organization Sci Pubi 1994, 3-21
13 Bhamarapravati Ν. Pathology of dengue infections. In Dengue and dengue hemorrhagic fever Gubler DJ, Kuno G, eds. Wallingford, UK. Cab International 1997, 115-32
14 Nimmannitya S Dengue hemorrhagic fever diagnosis and management. In-
Dengue and dengue hemorrhagic fever Gubler DJ, Kuno G, eds. Wallingford, UK: Cab International 1997, 133-45
15. Halstead SB, O'Rourke EJ Dengue viruses and mononuclear phagocytes I Infection enhancement by non-neutralizing antibody J Exp Med 1977; 146 201-17
16 Kurane I, Rothman AL, Livingstone PG, Green S, Gagnon SJ, Janus J, Innis BL, Nimmannitya S, Nisalak A, Ennis FA Immunopathologic mechanisms ot dengue hemorrhagic fever and dengue shock syndrome. Arch Virol (Suppl) 1994; 9: 59-64
17. Jarvis C Physical examination and health assessment. Philadelphia WB Saunders 1993, 178.
18 Rigau-Pere/ JG, Clark GG, Gubler DJ, Reiter Ρ, Sanders EJ, Vorndam AV Dengue and dengue hemorrhagic fever Lancet 1998, 352 971-77
19. Sharp TW, Wallace MR, Hayes CG, Sanche/ JL, DeFraites RF, Arthur RR, Thornton SA, Batchelor RA, Rozmaj/l PJ, Hanson RK, Wu SJ, Inye C, Burans JP Dengue fever in U.S troops during operation restore hope, Somalia, 1992-1993 Am J Trop Med Hyg 1995; 53 89-94
20 Innis BL, Nisalak A, Nimmannitya S, Kusalerdcharya S, Chongswasdi V, Suntayakorn S, Puttisn P, Hoke CH An enzyme-linked immunosorbent assay to characterize dengue infections where dengue and Japanese Encephalitis co-circulate. Am J Trop Med Hyg 1989, 40 418-427.
21 Ruechusatsawat K, Monta Κ, Tanaka M, Vongcheree S, Rojanasuphot S, Warachit Ρ, Kanai Κ, Thongtradol Ρ, Nimnakom M, Kanungkid S, Igarashi A Daily observation of antibody levels among dengue patients detected by enzyme-linked immunosorbent assay (ELISA) Jpn J Trop Med Hyg 1984, 22 9-12
22 Drenth JP, van Uum SH, van Deuren M, Pesman GJ, van der Ven-Jongeknjg J,

119
van der Meer JWM Endurance run increases circulating IL-6 and IL IRa but downregulates ex-vivo TNF-alpha and IL-1 beta production J Appi Physiol 1995, 79 1497-03
23 De Boer JP, Creasy AA, Chang A, Roem D, Brouwer MC, Eerenberg AJ, Hack CE, Taylor FB Jr Activation patterns of coagulation and fibrinolysis in baboons following infusion with lethal or sublethal dose of Escherichia coli Cire Shock 1993, 39 59-67
24 Levi M, de Boer JP, Roem D, ten Cate JW, Hack CE Plasminogen activation in vivo upon intravenous infusion of DDAVP Quantitative assessment of plasmin-alpha-2 antiplasmin complex with a novel monoclonal antibody based radioimmunoassay Thromb Haemost 1992, 67 111-16
25 Velzing J, Groen J, Drouet MT, van Amerongen G, Copra C, Osterhaus AD, Deubel V Induction of protective immunity against Dengue virus type 2 comparison of candidate live attenuated and recombinant vaccines Vaccine 1999, 17 1312-20
26 Van der Poll T, Levi M, Van Deventer SJH, Ten Cate H, Haagmans BL, Biemond BJ, Buller HR, Hack CE, Ten Cate JW Differential effects of anti-tumor necrosis factor monoclonal antibodies on systemic inflammatory responses in experimental endotoxaemia in chimpanzees Blood 1994, 83 446-51
27 Van der Poll T, Coyle SM, Levi M, Jansen PM, Dentener M, Barbosa Κ, Buurman WA, Hack CE, ten Cate JW, Agosti JM, Lowry SF Effect of recombinant dimeric tumor necrosis factor receptor on inflammatory responses to intravenous endotoxin in normal humans Blood 1997, 89 3727-34
28 Hinshaw LB, Tekamp-Olson P, Chang ACK, Lee PA, Taylor Jr FB, Murray CK, Peer GT, Emerson Jr TE, Passey B, Kuo GC Survival of primates in LD100 septic shock following therapy with antibody to tumor necrosis factor (TNF) Cire Shock 1990,30 279-92
29 Biemond BJ, Levi M, ten Cate H, van der Poll T, Buller HR, Hack CE, ten Cate JW Plasminogen activator and PAI-1 release during experimental endotoxaemia in chimpanzees, effects of various intervention in the cytokine and coagulation cascades Clin Sci 1995, 88 587-94
30 Stoudhardt JML, Levi M, Hack CE, Veenhof CHN, Romijn JA, Sauerwein HP, van der Poll Τ Interleukin-6 stimulates coaagulalion, not fibrinolysis, in humans Thromb Haemostas 1996, 76 738-42

120
Chapter 10
Summary and directions for future research Ringkasan Samenvatting

121
Summary and directions for future research
Dengue and its complicated form, dengue hemorrhagic fever (DHF) is one of the emerging diseases in the world. In chapter 1 the epidemiology and possibilities for vector control of dengue in Indonesia, the clinical presentation of dengue fever and DHF and how to diagnose dengue virus infection is reviewed Also insights into the pathogenesis of the disordered coagulation and fibrinolysis and the role of cytokines in this process are presented. Next, an outline of the thesis is given In chapters 2 and 3 the differential diagnosis of mild dengue virus infection in adults and in chapter 4 the clinical presentation and mortality in severe DHF is studied In chapters 5 and 6 studies on the pathogenesis of dengue shock syndrome (DSS) in a cohort of children are presented, with emphasis on the role of cytokines in the process of plasma leakage. After a review of coagulation disorders in chapter 7, in chapters 8 and 9 the outcome of studies on activation of coagulation and fibrinolysis in DSS in the same cohort of children is presented.
In chapter 2 a study is reported on 118 adult patients suspected clinically of dengue virus infection. Only in 58 patients recent dengue virus infections could be confirmed although in 114 of the 118 patients (97%) antibodies to dengue virus were found In 20 of the remaining 60 patients whose present clinical symptoms were not due to a recent dengue virus infection, serological evidence was found of a recent infection with hantavirus (5), Rickettsia t\phi (5), R tsutsugamushi (2), rubella virus (3), Chikungunya virus (2), influenza A virus (1) and leptospira (2) This the first report of human hantavirus infection in Indonesia In chapter 3, the evidence for the presence of hantavirus in Indonesia is presented in a larger sample of patients.
In chapter 4 we report a study in 50 children with dengue shock syndrome (DSS), of whom 13 (26%) died, in which we investigated which clinical signs and laboratory findings are related to mortality Gastrointestinal bleeding, bilateral pleural effusion and blood levels on admission of thrombin-antithrombin complexes (TATc) and plasminogen activator inhibitor type 1 (PAI-1) were significantly higher in non-survivors than survivors In the regression analysis, only bilateral pleural effusion and admission blood levels of TATc were significantly associated with mortality This shows that mortality in DSS is related to plasma leakage and coagulation activation, which are characteristic changes in this disease
In chapter 5 the results are presented of a prospective clinical study in the same cohort of 50 children with DSS, to investigate the patterns of tumor necrosis factor-α (TNF-a), interleukm-lß (IL-Iß), IL-6, interferon-γ (IFN-γ) and interleukin-l receptor antagonist (IL-IRa) During the acute phase, the plasma concentrations and the ex-vivo production without lipopolysaccharide (LPS) of IL-IRa were elevated, however, the ex-vivo LPS stimulated production of the proinflammatory cytokines TNF-a and IL-Iß were depressed Concentrations returned towards normal on recovery In non-survivors, the plasma concentrations

122
and the ex-vivo production of IL-IRa were significantly higher than in survivors Since we found that IL-IRa was significantly associated with mortality, this measurement may be used as an index of disease severity
In chapter 6 we report a study on the association of TNF-a, IL-Iß, IL-IRa, IL-6 and IFN-γ with concentrations of protein and albumin in the serum and the presence of pleural effusion in 50 children with DSS. Since IL-IRa was significantly associated with both, bilateral pleural effusion and the albumin/protein ratio, we conclude that IL-IRa contributes to the capillary permeability changes in DSS
In chapter 7 a review is presented of bacterial and non-bacterial infections associated with coagulation disorders, resulting in disseminated intravascular coagulation (DIC) and multiorgan failure (MOF). This review puts the disorders of coagulation and fibrinolysis as they occur in dengue in perspective and serves as an introduction to the studies presented in chapters 8 and 9
In chapter 8 we report on a study in the same cohort of 50 children with DSS to determine the potential role of contact activation and factor XI activation (intrinsic pathway) in the coagulation disorders in DHF Markers of contact activation (kallikrein-Cl-inhibitor complexes), the intrinsic pathway of coagulation (factor XIa-Cl-inhibitor complexes) and thrombin activatable fibrinolysis inhibitor (TAFI) were measured and correlated to thrombin generation markers TATc, prothrombin fragment 1+2 (Fl+2) and plasmin-a2-antiplasmin complexes (PAPc) a marker for fibrinolysis. Activation of the intrinsic pathway of coagulation was demonstrated by elevated levels of factor XIa-Cl-inhibitor complexes, without evidence of contact activation, reflected by undetectable kallikrein-Cl-inhibitor complexes TAFI levels were decreased in all patients which may contribute to the severity of bleeding complications in DHF because of the impaired capacity of the coagulation system lo protect the fibrin clot from fibrinolysis Our finding in DSS are in accordance with those in bacterial sepsis
In chapter 9 we report on the association of TNF-a, IL-Iß, IL-IRa, and IL-6 with activation markers of coagulation (Fl+2 and TATc) and fibrinolysis (t-PA, PAPc, and D-dimer) in the same cohort of 50 children with DSS We found that median plasma concentrations of TNF-a, IL-Iß and IL-IRa, but not ot IL-6 were elevated during the early stage of infection and at discharge from hospital TNF-a was significantly associated with D-dimer, an activation marker of fibrinolysis, but not with activation markers of coagulation IL-Iß was significantly associated with t-PA. IL-IRa was significantly associated with Fl+2, TATc, whereas IL-6 was significantly associated with both, activation markers of coagulation (Fl+2), and fibrinolysis (PAPc) In severe dengue virus infection the same cytokines are involved in the onset and regulation of hemostasis as in bacterial sepsis.

123
Directions for future research
Given the results obtained in the studies reported in this thesis, we have asked ourselves the question which directions future research on dengue in Indonesia should take Five major areas can be distinguished
A It is clear that the diagnostic procedures for dengue can be improved especially in adults In Indonesia, a wide spectrum of febrile illnesses should be investigated in suspected dengue Particularly, the index of suspicion for hantavirus needs to be raised and surveillance for the disease in different parts of the country is warranted A rapid assay for diagnosis of dengue, for instance a dipstick test, capable of detecting infection in the first two days, should be developed
Β The prognosis ot patients with complicated dengue can be improved if those at risk of developing dengue shock syndrome could be identified early It facilities would allow, rapid and on-site determination of levels of thrombin-antithrombin complexes and interleukin-1 receptor antagonist and otherwise of the albumin/protein ratio is helpful
C Future research should be directed at possibilities to effectively combat plasma leakage by interfering with the endothelial permeability changes In addition restoration ot the balance between coagulation and fibrinolysis is another important area for future studies. Whether anticytokine strategies may be of use is questionable, in view ot the poor results of such therapies in sepsis syndrome. In addition, these kind of therapies are far beyond the budgets available for the Indonesian patients. The serine protease inhibitors, which affect intrinsic coagulation and fibrinolysis, as well as CI esterase inhibitor could have a place Activated protein C cannot be applied because it is much too expensive Meanwhile, cheaper solutions should be contemplated like the use of colloid or fresh plasma followed by crystalloids
D Prevention would be an important issue One way would be an effective vector control program So tar, vector control programs have not been very successful in Indonesia; in fact, the incidence of dengue is increasing. Through operational research ways should be found to improve health education of the community and vector control
E Another prevention measure would be vaccination Research towards the development of a safe and immunogenic vaccine against all four serotypes ol the dengue virus should be strengthened. This would be facilitated of (part ot) the genome of the dengue virus could be identified

124
Ringkasan dan arah penelitian untuk masa yang akan datang
Dengue fever (DF) dan dengue hemorrhagic fever (DHF) merupakan salah satu penyakit yang sedang berkembang pesat di dunia Bab 1 dan buku tesis im mengulas tentang epidemiologi, cara pemberantasan vektor virus dengue di Indonesia, gambaran klinik dan DF dan DHF, serta bagaimana menegakkan diagnosis infeksi virus dengue Juga disajikan pengertian tentang patogenesis, khususnya tentang gangguan koagulasi dan fibnnolisis serta peran sitokin dalam proses im Penelitian tentang diagnosis banding infeksi virus dengue derajad nngan pada orang dewasa disajikan pada bab2 dan 3, sedangkan pada bab 4 bensì penelitian tentang gambaran klinik dan faktor nsiko untuk kematian pada DHF derajad berat Bab 5 dan 6 bensì penelitian kohort tentang patogenesis dengue shock syndrome (DSS), dengan penekanan peran sitokin pada proses kebocoran plasma Bab 7 bensì ulasan tentang gangguan koagulasi, sedangkan pada bab 8 dan 9 disajikan hasil penelitian tentang pengaktifan sistem koagulasi dan fibnnolisis pada DSS dan studi kohort pada pasien yang sama.
Bab 2 bensì laporan hasil penelitian pada 118 penderita dewasa yang secara klinik diduga mendenta infeksi virus dengue Ternyata hanya pada 58 penderita dapat dibuktikan secara serologik adanya infeksi baru virus dengue, meskipun 114 dan 118 penderita (97%) didapatkan antibodi terhadap virus dengue Pada 20 dan 60 penderita yang tersisa, dimana gejala klinik yang ada bukan disebabkan karena infeksi baru virus dengue, ditemukan bukti serologik adanya infeksi baru dengan virus hanta pada 5 penderita, Rickettsia typhi (5), R tsutsugamushi (2), rubella virus (3), Chikungunya virus (2), influenza A virus (1) dan leptospira (2) Infeksi terhadap virus hanta ini merupakan laporan pertama infeksi virus hanta pada manusia di Indonesia. Bab 3 menampilkan adanya infeksi virus hanta di Indonesia dalam sampel yang lebih besar
Pada bab 4 kami melaporkan penelitian pada 50 penderita DSS anak, dimana 13 diantaranya (26%) memnggal Dalam penelitian ini kami mencan temuan klinik maupun laboratonk yang berasosiasi dengan kematian. Frekuensi perdarahan gastrointestinal dan efusi pleura bilateral lebih sering terjadi pada pendenta yang memnggal dibanding penderita yang hidup Selain itu kadar kompleks trombin-antitrombin (TAT) serta inhibitor aktivator plasminogen tipe 1 pada han pertama perawatan lebih tinggi pada pendenta yang memnggal dibandingkan dengan pendenta yang hidup Pada anahsis regresi, efusi pleura bilateral dan kadar kompleks TAT pada han pertama perawatan mempunyai asosiasi yang bermakna dengan kematian. Hal ini menunjukkan bahwa kematian pada DSS berhubungan dengan kebocoran plasma dan pengaktifan sistem koagulasi, dimana keduanya merupakan kelainan patologik yang khas pada penyakit ini
Pada bab 5 ditampilkan hasil penelitian klinik prospektif secara kohort pada 50 pendenta DSS yang sama, dimana diteliti pola dan sitokin tumor necrosis factor-α (TNF-α), interleukin-lß (IL-lß), IL-6, interferon-γ (IFN-γ) dan antagoms

125
reseptor interleukin-1 (IL-lRa) Pada fase akut, kadar plasma serta produksi ex-vivo dan IL-lRa tanpa stimulasi lipopolisakanda (LPS) meningkat, tetapi produksi ex-vivo dengan stimulasi LPS dan sitokin proinflamasi TNF-a and IL-lß rendah Kadar sitokin ini kembali kearah normal pada fase penyembuhan Pada pendenta yang meninggal, konsentrasi plasma serta produksi ex-vivo dan IL-lRa lebih tinggi secara bermakna dibanding pendenta yang hidup Selain Uu IL-lRa juga terbukti mempunyai asosiasi yang bermakna dengan kematian, sehingga pengukuran kadar IL-lRa mungkin bisa digunakan sebagai indeks beratnya penyakit
Pada bab 6 kami melaporkan suatu penehtian tentang hubungan antara TNF-a, IL-Iß, IL-lRa, IL-6 and IFN-γ dengan kadar protein dan albumin dalam serum serta efusi pleura pada 50 pendenta DSS Oleh karena IL-lRa mempunyai hubungan yang bermakna baik dengan efusi pleura bilateral maupun rasio albumin protein, kami menyimpulkan bahwa IL-lRa ikut berperan pada perubahan permeabilitas kapiler pada DSS.
Bab 7 bensì ulasan tentang hubungan antara infeksi yang disebabkan oleh bakten maupun non-bakten dengan gangguan koagulasi hingga terjadi koagulasi intravakuler diseminata (DIC) serta kegagalan multiorgan Ulasan mi menempatkan gangguan koagulasi dan fibrinolisis dalam perspcktif yang juga terjadi pada infeksi virus dengue dan menyajikan sebagai penddhuluan pada penelitian dalam bab 8 dan 9.
Pada bab 8 kami melaporkan suatu penelitian kohort pada 50 pendenta DSS yang sama untuk mengetahui peran pengaktifan kontak dan pengaktifan faktor XI (jalur intnnsik) pada gangguan koagulasi pendenta DHF. Dalam penelitian mi dilakukan pemenksaan terhadap petanda pengaktifan kontak (kompleks kalhkrein-inhibitor CI), jalur intnnsik sistem koagulasi dan trombin yang mengaktifkan inhibitor fibrinolisis (TAFI), temyata hasilnya mempunyai korelasi dengan petanda pembentukan trombin (TATc, F1+2) dan petanda fibrinolisis, kompleks plasmin-a2-antiplasmin (PAPc) Pengaktifan sistem koagulasi jalur intnnsik dibuktikan dengan pemngkatan kadar kompleks taktor XIa-inhibitor CI, tanpa adanya bukti pengaktifan kontak, yang dicerminkan oleh tidak terdeteksinya kompleks kalhkrein-inhibitor CI. Kadar TAFI menurun pada semua pasien dan hai im mungkin berperan pada beratnya komplikasi perdarahan pada DHF karena adanya kegagalan dan kapasitas sistem koagulasi dalam mempertahankan bekuan fibrin dan fibrinolisis Temuan kami pada pendenta DSS sesuai dengan apa yang ditemukan pada sepsis yang disebabkan oleh bakten
Pada bab 9 kami melaporkan hubungan sitokin TNF-a, IL-Iß, IL-lRa, and IL-6 dengan petanda koagulasi (Fl+2 and TATc) dan fibrinolisis (t-PA, PAPc, and D-dimer) pada studi kohort dengan 50 pendenta DSS yang sama Kami menemukan bahwa median kadar plasma TNF-a, IL-Iß and IL-lRa (kecuali kadar IL-6), meningkat pada stadium awal infeksi dan pada saat keluar dan rumah sakit TNF-α mempunyai asosiasi yang bermakna dengan D-dimer, petanda pengaktifan

126
fibrinolisis, tetapi tidak dengan petanda pengaktifan koagulasi. IL-lß berasosiasi secara bermakna dengan t-PA. IL-IRa berasosiasi secara bermakna dengan Fl+2, TATc, sedangkan IL-6 berasosiasi secara bermakna dengan petanda koagulasi (Fl+2), maupun dengan petanda fibrinolisis (PAPc). Pada infeksi virus dengue derajad berat, sitokin yang sama ikut berperan pada awal dan pengaturan hemostasis seperti yang terjadi pada sepsis karena bakteri.

127
Arah penelitian untuk masa yang akan datang
Dan hasil penelitian yang kami dapat dan kami laporkan ddldm buku tesis ini, timbul pertdnyddn ddldm dm kami, ke arah mana penelitian dengue di Indonesia untuk masa yang akan datang Ada 5 bidang utama yang berbeda A Kiranya jelas bahwa prosedur diagnostik untuk dengue perlu ditingkatkan,
terutamd untuk dewasa Di Indonesia, kasus-kasus yang dicungdi dengue harus dipenksa untuk suatu spektrum yang luas dan penyakit yang disertai demam Khususnya indeks kecungaan untuk inveksi virus hanta perlu ditingkatkan, serta surveilens penyakit ini di berbdgdi dderah perlu ditekankan Perlu dikembangkan uji diagnostik dengue yang cepat, misalnya seperti metoda dipstik, yang mampu mendeteksi penyakit ini dalam 2 han pertama
Β Prognosis penderita dengue yang berat bisa ditingkatkan bila perubahan kearah DSS bisa diidentifikasi secara awal Apabila fasihtas memungkinkan, pemenksaan secara cepat kadar kompleks trombin anti trombin serta kadar antagonis reseptor interleukin-1 dan, kalau tidak rasio albumin/protein bisa membantu
C Penelitian yang akan datang harus diarahkan untuk kemungkindn mcngdtdsi kebocoran plasma, dengan cara intervensi perubahan permeabihtas endotel Disamping itu pemulihan keseimbdngan koagulasi dan fibnnolisis merupakan bidang penehti yang penting untuk masa yang dkan ddtdng
D Manfaat penggunaan antisitokin dalam hal mi masih merupakan tanda tanya mengingat hasil ydng kurdng menggembirakan dan penggunaan terapi mi pada penderita dengan sindroma sepsis Lagi puld, jenis terdpi tersebut sulit dijangkau bagi penderita infeksi dengue di Indonesia Inhibitor protease serine, yang ddpdt mempengdruhi sistem intnnsik jalur koagulasi dan fibnnolisis, maupun inhibitor CI esterase mungkin bisa dipertimbdngkdn Penggunaan protein C yang diaktifkan sulit diterapkan karena harganya yang terlalu mahal Sementara itu, manfaat penggunaan cairan yang lebih murah seperti keloid, plasma segar dnkuti dengan knstaloid perlu direnungkan lebih lanjut
E Pencegahan merupakan suatu masalah yang penting Salah satu cara adalah program pemberantasan vektor Hingga saat ini program pemberantasdn vektor di Indonesia belum berhasil, terbukti dengan insidens yang meningkat Perlu diteliti untuk mendapatkan cara guna memngkatkdn pendidikan kesehatan pada masyarakat dan pemberantasan vektor
F Cara pencegahan lain adalah vaksinasi Penelitian kearah pengembangan vaksin yang aman dan bersifat imunogenik yang ddpdt meldwdn ke empat jenis virus dengue harus ditingkatkan, diantaranya dengan dapat dndentifikasinya genome virus dengue

128
Samenvatting en aandachtsvelden voor toekomstig onderzoek
Dengue en de gecompliceerde vorm, dengue hemorrhagic fever (DHF) is een van de opkomende ziekten in de wereld In hoofdstuk 1 wordt een overzicht gegeven van de epidemiologie, de mogelijkheden voor vector bestrijding van dengue in Indonesie, de klinische presentatie van dengue fever (DF) en DHF en van de diagnostiek van dengue virus infectie Ook worden de huidige inzichten in de Pathogenese van de ontregelde stolling en fibrinolysis en de rol van cytokines in dit proces besproken Hierna wordt de opzet van het proefschrift uiteengezet In de hoofdstukken 2 en 3 wordt de differentiaal diagnose van lichte dengue virus infecties bij volwassenen en in hoofdstuk 4 de klinische presentatie en sterfte bij ernstige DHF bestudeerd In de hoofdstukken 5 en 6 worden studies over de Pathogenese van dengue shock syndrome (DSS) in een cohort van 50 kinderen gepresenteerd, met nadruk op de rol van cytokines bij plasma lekkage Na een overzicht van de stoornissen in de stolling bij infectieziekten in hoofdstuk 7, wordt m de hoofdstukken 8 en 9 het resultaat gespresenteerd van studies over activatie van stolling en fibnnolyse bn DSS in hetzelfde cohort kinderen
Hoofdstuk 2 gaat over een studie bij 118 volwassen patiënten met de klinische diagnose dengue virus infectie Slechts bij 58 patiënten kon een recente dengue virus infectie serologisch worden bevestigd, ofschoon bij 114 van de 118 patiënten (97%) antihchamen tegen dengue virus werden gevonden Bij 20 van de overige 60 patiënten van wie de klinische symptomen niet op een recente dengue virus infectie berustten, werden serologische aanwijzingen gevonden voor recente infectie met hantavirus (5), Rickettsia typhi (5), R tsutsugamushi (2), rubella virus (3), Chikungunya virus (2), influenza A virus (1) resp leptospira (2) Dit is de eerste keer dat humane hantavirus infectie in Indonesie wordt aangetoond In hoofdstuk 3, worden de aanwijzingen voor het voorkomen van hantavirus bij patiënten in Indonesie verder uitgewerkt bij een grotere groep patiënten
In hoofdstuk 4 wordt een studie besproken bij 50 kinderen met dengue shock syndrome (DSS), van wie er 13 (26%) stierven Onderzocht werd welke klinische symptomen en laboratorium uitslagen zijn gerelateerd aan sterfte Het bleek dat gastrointestinaal bloedverlies, bilateraal pleuravocht en de concentraties in het bloed bij opname van thrombine-antithrombine complexen (TATc) en van plasminogeen activator inhibitor type 1 (PAI-1) significant hoger waren bij de overleden kinderen vergeleken met degenen die herstelden In de regressie analyse waren alleen bilateraal pleuravocht en de concentraties van TATc bij opname significant geassocieerd met sterfte Dit toont aan dat de sterfte bij DSS is gerelateerd aan plasma lekkage and stollingsactivatie, welke beide karakteristieke veranderingen zijn bij deze ziekte
In hoofdstuk 5 worden de resultaten gepresenteerd van een prospectieve klinische studie in hetzelfde cohort van 50 kinderen met DSS, waarbij het patroon van tumor necrosis factor-α (TNF-α), interleukin-1 β (IL-Iß), IL-6, interferon-γ (IFN-γ) en interleukin-l receptor antagonist (IL-IRa) werd bestudeerd In de

129
acute fase van de ziekte waren de plasma concentraties en de ex-vivo productie zonder LPS van IL-lRa verhoogd, echter de door LPS gestimuleerde ex-vivo productie van de proinflammatoire cytokines TNF-α en IL-Iß was verlaagd De concentraties normaliseerden vrijwel geheel in de herstelfase van de ziekte Bij kinderen die overleden was de plasma concentratie en de ex-vivo productie van IL-lRa significant hoger dan bij degenen die herstelden. Omdat wij vaststelden dat IL-lRa significant was geassocieerd met sterfte, kan meting van IL-lRa gebruikt worden als een indicator voor de ernst van de ziekte
In hoofdstuk 6 wordt een studie gerapporteerd waarbij de associatie werd onderzocht van een aantal cytokines (TNF-α, IL-Iß, IL-lRa, IL-6 en IFN-γ) met serumeiwit, serumalbumine en aanwezigheid van pleuravocht bij 50 kinderen met DSS Omdat IL-lRa significant geassocieerd was met zowel bilateraal pleuravocht als met de albumine/eiwit ratio, concludeerden wij dat IL-lRa bijdraagt aan de toegenomen capillaire permeabiliteit bij DSS
In hoofdstuk 7 wordt een overzicht gepresenteerd van bactenele and niet-bactenele infecties waarbij afwijkingen in de stolling leiden tot gedisscmineerde intravasale slolling (DIC) en multi-orgaan falen (MOF) Door dit overzicht worden de afwijkingen in de stolling en fibrmolyse, zoals deze bij dengue voorkomen, in perspectief geplaatst Het hoofdstuk dient tevens als introductie op de studies die worden gepresenteerd in de eropvolgende hoofdstukken 8 en 9
Hoofdstuk 8 gaat over een studie, gedaan in hetzelfde cohort van 50 kinderen met DSS, naar de mogelijke betekenis van contactactivatie en van factor XI activatie (de intrinsieke stollmgsroute) bij het optreden van slollingsstoormssen Gemeten werden als maatstaf voor contactactivatie kallikreine-Cl-inhibitor complexen, als maatstaf voor de intrinsieke stolling factor XIa-Cl-inhibitor complexen, alsook thrombin activatable fibrinolysis inhibitor (TAFI) Deze werden gecorreleerd met TATc en prothrombine fragment 1+2 (Fl+2) als maatstaf voor thrombinegeneratie, alsook met plasmine-a2-antiplasmine complexen (PAPc), welke een maatstaf zijn voor fibrmolyse Wij vonden dat de intrinsieke stolling geactiveerd was, immers er waren verhoogde concentraties van factor XIa-Cl-inhibitor complexen Er was echter geen contactactivatie, hetgeen bleek uit ondetecteerbare concentraties van kallikrein-Cl-inhibitor complexen. De concentraties van TAFI waren verlaagd bij alle patiënten, hetgeen kan bijdragen aan de ernst van de bloedingscomplicalies bij DHF doordat lysis van het fibrincstolsel niet wordt tegengegaan Onze bevindingen bij DSS komen overeen met die bij sepsis
In hoofdstuk 9 rapporteren wij een onderzoek naar de associatie van TNF-α, IL-lß, IL-lRa, en IL-6 met activatie van stolling (Fl+2 and TATc) en fibrmolyse (t-PA, PAPc, and D-dimer) in hetzelfde cohort van 50 kinderen met DSS We vonden dat de mediane plasmaconcentraties van TNF-α, IL-lß and IL-lRa, maar niet die van IL-6 verhoogd waren in de vroege fase van de infectie en bij ontslag uit het ziekenhuis. TNF-α was significant geassocieerd met D-dimer, een maatstaf

130
voor activatie van de fibnnolyse, maar niet met stolling IL-Iß was significant geassocieerd met t-PA en IL-lRa met Fl+2 en TATc, terwijl IL-6 significant geassocieerd was met zowel stollingsactivatie (Fl+2) als fibnnolyse (PAPc) Bij patiënten met ernstige dengue virus infectie zijn dezelfde cytokines betrokken bij de regulatie van de hémostase als bij sepsis

131
Aandachtsvelden voor toekomstig onderzoek
Gezien de resultaten van de verschillende studies die in dit proefschrift worden gerapporteerd, stelden wij ons de vraag op welke gebieden het dengue onderzoek in Indonesie zich in de toekomst zou moeten concentreren Wij willen vijf belangrijke gebieden noemen A. Het is duidelijk dat de diagnostiek van dengue verbeterd kan worden, met
name bij volwassenen In Indonesie moet een veelheid van koortsende ziekten in de differentiaal diagnose worden overwogen bij patiënten met klinische verdenking op dengue. Met name moet ook aan hantavirus gedacht worden en onderzoek naar het voorkomen van deze ziekte in verschillende delen van het land is aangewezen Ook moeten snelle tests voor de diagnose van dengue worden ontwikkeld die de infectie kunnen vaststellen in de eerste paar dagen van de ziekte.
Β De prognose van patiënten met gecompliceerde dengue kan worden verbeterd als patiënten die risico lopen om dengue shock syndroom te ontwikkelen vroegtijdig kunnen worden geïdentificeerd. Als de faciliteiten het zouden toelaten, zou snelle bepaling van de concentratie van thrombine-antithrombine-complexen en van interleukine-1 receptor antagonist ter plaatse nuttig zijn. Is dit niet mogelijk, dan is bepaling van de albumine/eiwit ratio zinvol.
C Toekomstig onderzoek moet gericht worden op het effectief bestrijden van plasma lekkage door beïnvloeding van de veranderingen op het niveau van de endotheelcel Bovendien is onderzoek naar mogelijkheden om het evenwicht te herstellen tussen stolling en fibnnolyse een belangrijk aandachtsveld Of behandeling met anticytokines van nut is, is nogal de vraag gezien de slechte resultaten van deze therapie bij sepsis syndroom. Bovendien zijn degelijke middelen veel te duur voor de meeste patiënten in Indonesie. Toepassing van geactiveerd Proteïne C stuit eveneens op financiële bezwaren. Misschien is er een plaats voor serine protease inhibitors die de intrinsieke stolling en fibnnolyse beïnvloeden Ook zou de werking van Cl esterase inhibitor kunnen worden onderzocht Inmiddels moeten alternatieve en goedkopere mogelijkheden onderzocht worden, zoals toepassing van vers plasma en colloïden, gevolgd door electrolytoplossingen
D Preventieve maatregelen moeten verbeterd worden, bijvoorbeeld door een meer effectief vector bestrijdingsprogramma Tot nu toe zijn dergelijke programmas in Indonesie niet erg suksesvol geweest, jazelfs, de incidentie van dengue is stijgende Door operationeel onderzoek dienen manieren gevonden te worden om de gezondheidsvoorlichting van de bevolking en de vectorbestnjding te verbeteren
E Vaccinatie zou een andere preventiestrategie zijn Onderzoek bedoeld om een veilig en immunogeen vaccin tegen alle vier serotypen van het dengue virus te ontwikkelen moet bevorderd worden Dit zou worden vergemakkelijkt als (een deel van) het genoom van het dengue virus zou worden geïdentificeerd

132
Acknowledgements
I am sincerely grateful to all who guided and supported me during my study period
Firstly, I like to thank my promotor Professor Djokomoeljanto Professor Djoko, I had so many questions when you asked me to be the sparring partner in the collaborative dengue research between Diponegoro University/Dr. Kanadi Hospital and The Nijmegen University, The Netherlands However, the questions remained unanswered and I just did what I had to do Now, the findings reported in this booklet are the results of taking up my responsibility. I am sincerely grateful for your confidence and guidance in this dissertation
My co-promotor Dr Wil M.V Dolmans Dr Dolmans, I always remember how you pushed me to do all my best and how you have worked hard on my drafts to read them, to give comments and ideas Also, in between of a hard time you gave me an episode of cooling time in your "rumah-kaca" to drink a cup of coffee and eat pieces of cake made by Mechy I am sincerely grateful for this I also would like to thank Mechy, your beloved wife, tor what she has done for me during my stay in Nijmegen
I am greatly indebted to Professor Jos M W van der Meer, my other promotor. Professor van der Meer, even in the weekend you worked hard on my drafts to read, to make comments and give many ideas especially on aspects of cytokines, rather a new field lor me I never would imagine that you as my promotor, when it was raining, cycled to Dr Dolmans' house to give me back part of my manuscripts with your comments. My deepest gratitude for all that you have done forme
My co-promotor Dr Dees Ρ M Brandjes Dees, your attention tor me did not only concern my manuscript, but also other things. You gave your support and tried to lessen my burden during my hard time I am sincerely grateful for this
I like to thank Dr Eric van Gorp, my PhD partner Eric, since we worked together, we have been family In the early period of our study, I was busy with patients and collecting samples, while you were busy managing different laboratory assays. Thanks to E-mail, while being busy writing each our manuscript far away from each other, we seemed to be working at the same place. Also, I would like to thank Alice, Vallery, Steven and Oma for a nice stay at your house
I am sincerely grateful to Professor Erik C. Hack, Dr Hugo ten Gate, and Dr J Groen for your contributions to my manuscript
I would like to thank Koninklijke Nederlandse Akademie van Wetenschappen (KNAW)/ Royal Netherlands Academy of Arts and Sciences for the financial support for this study
I would like to thank Dr Pierre Demacker and Johanna van der Ven- Jongeknjg from the Laboratory of the Department of General Internal Medicine, University Medical Centre St Radboud, Nijmegen, for performing the cytokine assays, and Yvonne van der Heide from the Laboratory of Hemostasis, Slotervaarl Hospital, Amsterdam, for the coagulation and fibrinolysis assays I also would like to thank

133
all the colleagues from the Department of General Internal Medicine, University Medical Centre St Radboud, Nijmegen, for their help, especially Dr. Monique Keuter, Dr. Marcel van Deuren, Drs. P. Vrylandt and also the secretaries for their help during my work in Nijmegen.
I am also thankful to the present and past Directors of Dr. Kariadi Hospital and to the Dean of the Medical Faculty, Diponegoro University, including dr. Gatot Suharto, dr. Anityo Mochtar, dr. M. Sulaiman, dr Anggoro B. Sachro and Professor Subowo for the opportunity to do my PhD.
I am also thankful to the present and past Heads of the Department of Internal Medicine, the Head of the Hematology/Medical Oncology Subdivision, the Heads of Infection and Tropical Diseases Subdivision, Diponegoro University and Dr.Kariadi Hospital, including Professor Djokomoeljanto, dr. Priyanto Poerjoto, Dr. Darmono, Professor Soenarto, Professor Suharyo and dr. Budi Rijanto for giving me the opportunity in doing my PhD research program. I also would like to thank the present and past Heads of the Department of Pediatrics, including Professor I. Sudigbia, Dr. Harsoyo, dr. Kamilah B. Also, my deepest gratitude to Professor Moeljono S. Trastotenojo, the late dr. Sutono, dr. Herawati Juslam and dr. Tatty E. Setiati for the opportunity in doing research in the Department of Paediatrics. I hope dr. Tatty will be successful in continuing the dengue research and be the next to get a PhD.
I would like to thank all the staff members of the Department of Internal Medicine, especially dr. Mika L. Tobing and dr. Suyono from Hematology /Medical Oncology Subdivision, who have taken up most of my tasks during my study period. I also would like to thank dr. Lukas Widiono, who participated in this research during his Internal Residency; dr. Lukas, you have done a lot for this study. I am also grateful to drg. Henry Setiawan, dr. Hardian and dr. Wahyu Rochadi for their support and teaching me statistical analysis.
I am also thankful to all patients and nurses from the Departments of Internal Medicine, Paediatrics and Paediatric Intensive Care Unit, and all laboratory analysts especially Jujuk, Agus, Wiwiek and others, who participated in this study.
My gratitude goes also to dr. Edi Dharmana, dr. M. Hussein Gasem for their support in this research. Before the dengue research started, you have had a lot of experience in the typhoid fever study, especially in specimen processing for cytokine assays. Through your experience the progress of dengue research could be faster.
I am also thankful to the present and past Directors and laboratory staff of Telogorejo and St. Elisabeth Hospital, Semarang including dr. A. Gambiro, dr. Ag Suwito, Maya and colleagues as well as Sr. Ignace Marie, for the support in storing the samples. Also my gratitude goes to the present and past Heads of Laboratory of Biotechnology including Drs. Damin, dr. Tjahjati, Professor Djokomoeljanto, Dr. Hendrowahjono, for the support in storing samples and performing some laboratory assays.
I am also indebted to dr. Thomas Suroso, from the Division of Communicable Disease Control, Ministry of Health, Jakarta, who gave me the dengue data in Indonesia and dr. W. Suharyono for his advice in samples processing for virus

134
isolation. Also, my gratitude to Dr. Sutaryo, from the Pediatric Department, dr. Sardjito Hospital, Gajahmada University, Yogyakarta, for his advice in the dengue research.
Finally, I am most grateful to my dear parents, beloved husband, mas Wiet, and all relatives for their support, understanding and keeping up my spirit during my PhD program and lifelong study in medicine.

135
Curriculum vitae
The writer of this thesis was bom in Muntilan, Central Java, Indonesia on 25 November 1947. She received the degree in Medicine in 1972 from the School of Medicine at Diponegoro University, Semarang, Indonesia. From 1972 to 1983 she served as Head of the Blood Transfusion Unit at Dr. Kariadi Hospital in Semarang. From 1975 to 1981 she studied Internal Medicine at the Department of Medicine, Diponegoro University. In 1981, she joined in the Division of Hematology/Medical Oncology, Department of Medicine as Lecturer. In 1988, she went to Sydney, Australia, to study cytohematology at The Prince of Wales Hospital and in 1990 she completed her postgraduate studies in Hematology/Medical Oncology. On May 1995 she started the study of dengue hemorrhagic fever, which led to this PhD. She is married to P. Prawito.

136
List of publications:
1 Van Gorp ECM, Suharti C, ten Gate H, Dolmans WMV, van der Meer JWM, ten Gate JW, Brandjes DPM Infectious Diseases and Coagulation Disorders J Infect Dis 1999, 180 176-86
2 Van Gorp ECM, Minnema MC, Suharti C, Mairuhu ATA, Brandjes DPM, ten Cate H, Hack CE, Meijers JCM Activation of coagulation factor XI, without detectable contact activation in dengue haemorrhagic fever Β J Haematol 2001, 113 94-99
3 Van Gorp ECM, Suharti C, Setiati TE, Trastotenojo MS, ten Gate H, Keuter M, Dolmans WMV, Van den Ende A, Brandjes DPM (1997) Coagulation disorders in children with viral haemorrhagic fever Clinical Microbiology and Infection, 3, Suppl 2, 356
4 Suharti C, van Gorp ECM, Dolmans WMV, Groen J, Hadisaputro S, Djokomoeljanto RJ, Osterhaus AbDME, van der Meer JMW Differential diagnosis of adult dengue virus infections in Indonesia Submitted tor publication
5 Groen J, Suharti C, Koraka P, van Gorp ECM, Sutaryo J, Osterhaus ADME Human hantavirus infections in Indonesia Submitted for publication
6 Suharti C, Tatty E Setiati, van Gorp ECM, Djokomoeljanto RJ, Trastotenojo MS, van der Meer JMW, Dolmans WMV Clinical picture and risk factors tor mortality in dengue shock syndrome Submitted tor publication
7 Suharti C, van Gorp ECM, Dolmans WMV, Tatty E Sellati, Hack CE, Djokomoeljanto RJ, van der Meer JWM Cytokine patterns during dengue shock syndrome Submitted for publication
8 Suharti C, van Gorp ECM, Tatty E Setiati, Dolmans WMV, Djokomoeljanto RJ, Hack CE, ten Cate H, van der Meer JWM Plasma Interleukin-1 receptor antagonist (IL-IRa) concentration is associated with plasma leakage in Dengue Shock Syndrome Submitted for publication
9 Suharti C. van Gorp ECM, Tatty E Setiati, Dolmans WMV Djokomoeljanto RJ, Hack CE, ten Cate H, van der Meer JWM The role of cytokines in activation of coagulation and fibrinolysis in dengue shock syndrome Submitted tor publication

Π7
10 Koraka Ρ, Suharti C, T E Setiati, Mairuhu A T A , Van Gorp E C M, Hack C.E , Juffrie M, Sutaryo J, Van der Meer G.M , Groen J, Osterhaus A D Μ E Kinetics of dengue virus specific serum immunoglobulin classes and subclasses and correlation with clinical outcome of infection Accepted in J Microbiol
11 van der Meer G M., van Gorp E C M., Juffrie M, Groen J, Suharti C. Tatty E Setiati, Veerman A J P., Thijs LG, Hack C E Extracellular granzyme A and Β are released in children with dengue virus infection Submitted for publication
12. van Gorp E C.M , Suharti C, ten Gate H, Dolmans W M V , Brandjes DPM, van der Ven J, Demacker Ρ Ν M , van der Meer J W M Changes in the plasma lipid profile in dengue haemorrhagic fever Submitted for publication.
13. van Gorp E.C M , Suharti C, Mairuhu AT.A , Tatty E Setiati, van den Ende A, ten Gate H, Mac Gillavan MR, van der Meer J.W M , Brandjes D.P M. The role of endothelial cells in dengue hemorrhagic fever (DHE) and dengue shock syndrome (DSS) Submitted for publication
14. van Gorp E C M , Suharti C, Tatty E setiati, Mairuhu A Τ A , ten Gate H, Dolmans W.M V , van der Meer J W M , Hack C E, Brandjes D P M Impaired fibrinolysis in the pathogenesis of lethal dengue hemorrhagic fever (DHF) Submitted for publication
15 F J Giles, Κ A Salim, B.L Rapoporl, V Poovalingam, I Supandiman, V.Kuchopillai, Ρ Tan, R. Torres, M Gonzaga, Y.C. Chen, C H Ho, G.Y Tee, L.L. Heng, C Suharti, M Patel, D Tian, R Sumantri, Ρ M Shah, L X.Wang, S.N Lee, Β S. Ho, S Chen, Ν Ona, Κ Y Kim S.W Lim, M.M Franco, M.P. Fuerst, G Ν Lawrence, D A Kusuanco and F Guilhot. Presenting Features of PH+ Chronic-Phase CML (CP CML) A Comparison between Asian and French Patients on the International Oncology Study (ISOG) CML 1 Study and the French CML 88 Study Published in the British Journal of Haematology (Abstract)
16. Giles FJ, Lim SW, Chaimongkol B, Bapsy PP, Villalon A, Jootar S, Harryanto RA, Sagar TG, Thamprasit T, Kim SW, Suh C, Song HS, Suharti C, Schwarer AP, Kim SY, Roslan M, Lekhakula A, Kumar R, Kannan T, Rapoport BL, Wickham NR, Sotamaphan N, Intragumtornchai T, Cheong SK, Raafat J, Esfaham FS, Coccia-Portugal MA, Chuncharunee S, Prayoonwiwat W, Doyeun O, Smruti BK, Voges CW, Shah PM, Fuerst MP, Lawrence GN, Kusuanco DA Oncology Study Group (ISOG) NHLI Study American Society of Clinical Oncology (ASCO) Annual Meeting, Philadelphia, PA, USA, May 18-21, 1996 Published in the Journal of Clinical Oncology (Abstract)

138
17 Giles FJ, Kantarjian HM, Lim SW, Salim KA, Rapoport BL, Poovalingam V, Supandiman I, Kochupillai P, Tan P, Torres R, Gonzaga M, Chen JC, Tee GY, Heng LL, Suharti C, Patel M, Sumantri R, Shah PM, Wang LX, Ho BS, Shanshan C, Ona N, Kim KY, Fuerst MP, Lawrence GN, Kusuanco DA Presenting Features of Chronic-Phase CML (CP CML)· A Comparison Between Asian and U S Patients An International Oncology Study Group (ISOG) Study. 1996 American Society of Clinical Oncology (ASCO) Annual Meeting, Philadelphia, PA, USA, May 18-21, 1996 Published in the Journal of Clinical Oncology (Abstract)
18 Look RM, Salim KA, Rapoport BL, Suharti C, Sumantri R, Supandiman I, Torres R, Tee GY, Ho BS, Lim SW,Kusuanco DA, Giles FJ Treatment ot Early Chronic Phase Chronic Myeloid Leukemia (CML) Patients with Recombinant Alpha b Interferon (Intron) and Hydroxyurea (H) versus Intron and Low-Dose Ara-C (C): An International Oncology Study Group (ISOG) Protocol Acta Hematologica 1995, 93 180.
19 Look RM, Chaimongkol B, Jootar S, Villalon A, Sagar TG, Suh C, Harryanto RA, Thamprasit T, Song HS, Muthalib A, Bapsy PP, Suharti C, Lekhakula A, Lim SW, Kusuanco DA, Giles FJ Treatment of Intermediate-Grade (IG) and High-Grade (HG) NHL with CHOP plus Alpha 2b Interferon Followed by Intron Maintenance versus CHOP Induction Alone Versus CHOP followed by COP Maintenance. An International Oncology Study Group (ISOG) Protocol Acta Hematologica 1995; 93 189.
20. Look RM, Supandiman I, Suh C, Muthalib A, Suharti C, Rapoport BL, Tan P, Chen YC, Salim KAHarryanto RA, Radheshyam D, Suwansela M, Ruff GP, Lim SW, Kusuanco DA, Giles FJ Treatment of Multiple Myeloma (MM) Patients after an Objective Response to Induction Melphalan/Predmson with Maintenance Recombinant Alpha 2b Interferon (Intron) Alone from Response to Relapse vs. Intron Alone for 1 Year from Response to Relapse vs Intron combined with Monthly Pulse Dexamethasone from Response to Relapse- An International Oncology Study Group (ISOG) Protocol Acta Hematologica 1995, 93· 196


BN 90 373 0584 9
Copyright © 2022 FDOKUMEN