
NMDARs Mediate the Role of Monoamine Oxidase A in Pathological Aggression
Upload
khangminh22Category
view
5download
0
PDF hosted at the Radboud Repository of the Radboud University
Nijmegen
The following full text is a publisher's version.
For additional information about this publication click this link.
https://repository.ubn.ru.nl/handle/2066/240240
Please be advised that this information was generated on 2022-08-21 and may be subject to
change.
Monoamineneurotransmitter
disorders
from biochemical aspectsand clinical observations to
recommendations for management
Tessa Wassenberg
Uitn
od
igin
g
529Tessa W
assenbergM
ON
OA
MIN
E N
EU
RO
TR
AN
SM
ITT
ER
DIS
OR
DE
RS
Tessa_Wassenberg-Omslag-order154547_Dondersversie-rfp-v2.indd 2-6Tessa_Wassenberg-Omslag-order154547_Dondersversie-rfp-v2.indd 2-6 10/13/2021 1:06:00 PM10/13/2021 1:06:00 PM

Uitnodigingvoor het bijwonen van deopenbare verdediging vanmijn proefschrift getiteld
Monoamineneurotransmitter
disorders
from biochemical aspectsand clinical observations to
recommendations formanagement
Op 22 december 2021om 14:30 precies
in Academiezaal Aulavan de Radboud UniversiteitComeniuslaan 2, te Nijmegen
Livestream: https://tinyurl.com/PhD-Tessa
U bent van harte welkombij deze plechtigheid
en de aansluitende receptie
Tessa [email protected]
ParanimfenAnouke van Rumund
Lianne van de [email protected]
Tessa_Wassenberg-Omslag-order154547_Dondersversie-rfp-v2.indd 7-11Tessa_Wassenberg-Omslag-order154547_Dondersversie-rfp-v2.indd 7-11 10/13/2021 1:06:00 PM10/13/2021 1:06:00 PM

Monoamine neurotransmitter disorders
From biochemical aspects and clinical observations to recommendations for management
Tessa Wassenberg
Voorbereid document _Tessa Wassenberg_V03.indd 1Voorbereid document _Tessa Wassenberg_V03.indd 1 25/10/2021 09:3225/10/2021 09:32

Copyright 2021 © Tessa Wassenberg, 2021
ISBN 9789462842618Cover design and illustrations: Ilse Schauwers, isontwerp.nlProvided by thesis specialist Ridderprint, ridderprint.nlPrinting: RidderprintLayout and design: Anke Muijsers, persoonlijkproefschrift.nl
The work presented in this thesis was carried out at the Radboud university medical center (Radboudumc), Department of Neurology, Donders Institute for Brain, Cognition and Behaviour, and the Department of Laboratory Medicine, Translational Metabolic Laboratory, Nijmegen, the Netherlands, with financial support from the AADC Research Trust and Hersenstichting Nederland Benny Vleerlaag fonds (2009(2)-80).
The publication of this thesis was financially supported by the Department of Neurology, Donders Institute for Brain, Cognition and Behaviour and the Department of Pediatrics, Amalia Children’s Hospital Radboudumc.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without permission of the author, or, when appropriate, of the publishers of the publications.
Voorbereid document _Tessa Wassenberg_V03.indd 2Voorbereid document _Tessa Wassenberg_V03.indd 2 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 3Voorbereid document _Tessa Wassenberg_V03.indd 3 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 4Voorbereid document _Tessa Wassenberg_V03.indd 4 25/10/2021 09:3225/10/2021 09:32

Voor mijn ouders
Voorbereid document _Tessa Wassenberg_V03.indd 5Voorbereid document _Tessa Wassenberg_V03.indd 5 25/10/2021 09:3225/10/2021 09:32

Abbreviations (synonym)
3-OMD 3-O-methyldopa (3-MTYR)3-MT 3-Methoxytyramine3-MTYR 3-Methoxytyrosine (3-OMD)5-HIAA 5-Hydroxyindoleacetic acid5-HTP 5-Hydroxytryptophan5-HT 5-Hydroxytryptamine (serotonin)5-MTHF 5-MethyltetrahydrofolateAADC Aromatic L-amino acid decarboxylaseAADCD Aromatic l-amino acid decarboxylase deficiency;AD Autosomal dominantADH Alcohol dehydrogenaseAR Aldose reductaseAR Autosomal recessiveBH4 TetrahydrobiopterinCOMT Catechol-O-methyltransferaseCNS Central nervous systemCSF Cerebrospinal fluidDA DopamineDA Dopamine agonistDAT Dopamine transporterDBH Dopamine beta hydroxylase (DβH)DβH Dopamine beta hydroxylase (DBH)DDC Dopa decarboxylaseDHPG DihydroxyphenylglycolDHPR Dihydropteridine reductaseDRD Dopa responsive dystoniaE Epinephrine (adrenaline)EEG ElectroencephalographyGCH1 GTP-cyclohydrolase IGFR Glomerular filtration rateGPP Good practice pointGRADE Grading of recommendations, assessments, development and
evaluationGTP Guanosine triphosphateHPLC High pressure liquid chromatographyHVA Homovanillic acidIHC ImmunohistochemistryiNTD international working group on neurotransmitter related disordersL-DOPS L-threo- 3,4- dihydroxyphenylserineL-DOPA L-3,4- dihydroxyphenylalanine (Levodopa/ L-dopa)
Voorbereid document _Tessa Wassenberg_V03.indd 6Voorbereid document _Tessa Wassenberg_V03.indd 6 25/10/2021 09:3225/10/2021 09:32

MAO Monoamine oxidaseMET MetanephrineMHPG 3-methoxy 4-hydroxyphenylglycolNE Norepinephrine (noradrenaline)NH2P3 Dihydroneopterin-3-phosphateNMET NormetanephrinePAH Phenylalanine hydroxylaseP4αCD Pterin-4α-carbinolaminePCD Pterin-4-carbinolamine dehydratasePLP Pyridoxal phosphate;PNMT Phenylethanolamine N-methyltransferasePNPO Pyridox(am)ine 5-phosphate;PTE Proximal tubular epitheliumPTP 6-PyrovoyltetrahydrobiopterinPTPS Pyruvoyl-tetrahydrobiopterin synthaseqBH2 Quinonoid dihydrobiopterinSAM s-AdenosylmethionineSERT Serotonin transporterSIGN Scottish Intercollegiate Guideline NetworkSR Sepiapterin reductaseSSRI Selective serotonin reuptake inhibitorTβH Tyramine beta hydroxylaseTDC Tyrosine decarboxylase;TH Tyrosine hydroxylaseTrH Tryptophan hydroxylaseTML Translational Metabolic LaboratoryVLA Vanillactic acidVMA Vanillylmandelic acidVMAT Vesicular monoamine transporterWB Western blot
Voorbereid document _Tessa Wassenberg_V03.indd 7Voorbereid document _Tessa Wassenberg_V03.indd 7 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 8Voorbereid document _Tessa Wassenberg_V03.indd 8 25/10/2021 09:3225/10/2021 09:32
Index
Part I Prologue 11
Chapter 1 General introduction 13Chapter 2 Aims and outline of the thesis 25
Part II Biochemical aspects and the importance of different body compartments
31
Chapter 3 Urinary dopamine in aromatic l-amino acid decarboxylase deficiency: the unsolved paradox
33
Chapter 4 The paradox of hyperdopaminuria in aromatic l-amino acid deficiency explained
55
Chapter 5 Blood, urine and cerebrospinal fluid analysis in TH and AADC deficiency and the effect of medical treatment
69
Part III Beyond the classic phenotype: clinical observations 99Chapter 6 Pyramidal predominant presentation of GCH1 mutations 101Chapter 7 Congenital eyelid ptosis, decreased glomerular filtration
and orthostatic hypotension: questions and answers121
Part IV Reviews and guidelines for management 133Chapter 8 Consensus guideline on the diagnosis and treatment of
AADC deficiency135
Chapter 9 Clinical presentation and long-term follow-up of Dopamine Beta Hydroxylase Deficiency
179
Part V General discussion and summary 213Chapter 10 General discussion and future perspectives 215Chapter 11 Summary 233Chapter 12 Dutch summary (Nederlandse samenvatting) 239
Appendices 247Dankwoord/Acknowledgements 248About the author 252List of publications 253Research data management 256PhD Portfolio 257Donders Graduate School for Cognitive Neuroscience 260
Voorbereid document _Tessa Wassenberg_V03.indd 9Voorbereid document _Tessa Wassenberg_V03.indd 9 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 10Voorbereid document _Tessa Wassenberg_V03.indd 10 25/10/2021 09:3225/10/2021 09:32

PART I
Prologue
Voorbereid document _Tessa Wassenberg_V03.indd 11Voorbereid document _Tessa Wassenberg_V03.indd 11 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 12Voorbereid document _Tessa Wassenberg_V03.indd 12 25/10/2021 09:3225/10/2021 09:32
CHAPTER 1
General introduction
Voorbereid document _Tessa Wassenberg_V03.indd 13Voorbereid document _Tessa Wassenberg_V03.indd 13 25/10/2021 09:3225/10/2021 09:32

14
Chapter 1
Dopamine, norepinephrine, epinephrine, and serotonin are monoamine neurotransmitters with many different actions inside and outside of the human brain. Dopamine is involved in the regulation of movement, endocrine regulation, motivational processes, learning, affective behavior and cognition1, and is needed for blood pressure regulation and natriuresis2. Norepinephrine is important for arousal, attention, and vigilance in the central nervous system, and the functioning of the sympathetic autonomous nervous system1,3. Epinephrine is important in vital functions such as regulation of respiration, is involved in memory consolidation, and is a key player in the fight-or-flight response4. Serotonin is involved in practically every type of behavior, is a modulator of neuroendocrine function and circadian rhythm, and has important functions outside the central nervous system in platelets and the gastrointestinal tract5,6. Figures 1 and 2 show the distribution of monoamine neurotransmitters in the human brain, depicting the areas where dopamine, norepinephrine and epinephrine (the catecholamines), and serotonin are produced and how they are projected.
Figure 1. Distribution of catecholamine neurotransmitters in the human brain
Figure 1. Schematic representation of the distribution of dopamine, norepinephrine and epinephrine in the human brain. Dopamine is formed in the substantia nigra and ventral tegmental area, and follows different projection pathways. Norepinephrine is formed in the locus coeruleus in the mesencephalon and projects widely to the brain and spinal cord. Epinephrine is formed in the medullary epinephrine neurons and projects to the thalamus, brain stem, and spinal cord. Figure created with Biorender.com
Voorbereid document _Tessa Wassenberg_V03.indd 14Voorbereid document _Tessa Wassenberg_V03.indd 14 25/10/2021 09:3225/10/2021 09:32

15
General introduction
Figure 2. Distribution of serotonin in the human brain
Figure 2. Schematic representation of the distribution of serotonin in the human brain. Serotonin is formed in the raphe nuclei in the medulla oblongata and formatio reticularis of the pons and mesencephalon. It projects to the cortex, basal ganglia, cerebellum, brain stem, and spinal cord. Figure created with Biorender.com
The synthesis and breakdown of monoamine neurotransmitters involves several enzymatic steps. Many enzymes involved in monoamine synthesis only function optimally when specific cofactors are present. Tetrahydrobiopterin (BH4) is one of these important cofactors, whose synthesis and recycling also involves multiple enzymatic reactions7. Primary monoamine neurotransmitter disorders are rare genetic disorders in which there is a defect in one of the enzymes that is needed in the synthesis, breakdown, storage or transport of serotonin, dopamine, and/or norepinephrine and epinephrine8. More recently, also disorders in chaperone proteins and electron shuttles that can lead to monoamine deficiency have been described9,10.
In Figures 3-5, the synthesis, breakdown and transport of monoamine neurotransmitters, and the known primary monoamine neurotransmitter disorders including the BH4 disorders are schematically shown. Until now, 14 different monoamine neurotransmitter disorders have been described involving 13 different genes (Table 1).
Clinically, monoamine neurotransmitter disorders can present with a broad spectrum of symptoms and signs, ranging from severe early infantile encephalopathy, to mild adult onset movement disorders, or isolated young-onset orthostatic hypotension8,11. In general, movement disorders (especially dystonia and/or parkinsonism, oculogyric crises) and/or autonomic disorders (e.g. orthostatic hypotension, ocular ptosis) are present. Developmental delay and hypotonia are present in the more severe clinical phenotypes of several monoamine neurotransmitter disorders. All primary monoamine neurotransmitter disorders are rare disorders with unknown precise epidemiology. Autosomal dominant GTP-cyclohydrolase I (GCH1) deficiency (Ib in Figure 3 and Table 1) is the most common
1
Voorbereid document _Tessa Wassenberg_V03.indd 15Voorbereid document _Tessa Wassenberg_V03.indd 15 25/10/2021 09:3225/10/2021 09:32

16
Chapter 1
disorder with an estimated prevalence of 0.5-3:1.000.00012. Dopamine beta hydroxylase (DBH) deficiency (XI in Figure 5 and Table 1) has only been described in 25 patients worldwide13. In general clinical practice, recognition of monoamine neurotransmitter disorders is difficult due to its rarity and potential overlap with more common disorders like cerebral palsy14-16 or epilepsy17. However, correct diagnosis is of utmost importance because some of these disorders are excellently treatable with medication and/or dietary regimens, and for AADC deficiency (VIII in Figure 4) intraparenchymal gene therapy has been developed. Knowledge on the biochemical background of monoamine neurotransmitter disorders is essential to understand the clinical presentation, and the principles of diagnosis and treatment. In Figure 6, the principles of medical treatment are schematically presented. A short summary of all known monoamine neurotransmitter disorders to date can be found in Table 1.
Figure 3. The tetrahydrobiopterin (BH4) cycle and associated monoamine neurotransmitter disorders.
Figure 3. Tetrahydrobiopterin (BH4) is formed in several steps from GTP. The BH4 recycling consists of a hydroxylation reaction where BH4 is converted to the inactive P4αCD, and a two-step conversion to regenerate active BH4. The BH4 hydroxylation reaction is an obligate cofactor reaction for PAH, TH and TrH. Furthermore, BH4 is an important cofactor for nitric oxide synthases and alkylglycerol monooxygenase (not shown). PAH is primarily located in the liver (shown in purple). TH and TrH are present in dopaminergic neurons (shown in blue) and serotonergic neurons (shown in yellow) respectively, but are also expressed in peripheral organs like gut and kidneys. Pterin measurements in cerebrospinal fluid and urine typically quantify total pterin, biopterin, neopterin, sepiapterin and primapterin, and its pattern can help to localize a specific BH4-defect. Hyperphenylalaninemia can be present in all disorders shown in the figure except for Ib and III. A deficiency in PAH is better known as phenylketonuria (PKU), and not considered to be a monoamine neurotransmitter disorder. Pathogenic variants in DNAJC12 hinder the function of PAH, TH and TrH and therefore leads to decreased monoamine neurotransmitters. Abbreviations see p5-6, different disorders (I-VI, XIII) see Table 1.
Voorbereid document _Tessa Wassenberg_V03.indd 16Voorbereid document _Tessa Wassenberg_V03.indd 16 25/10/2021 09:3225/10/2021 09:32

17
General introduction
Figure 4. Dopamine and serotonin formation, breakdown and transport and associated mono-amine neurotransmitter disorders
Figure 4. Simplified representation of neuronal synthesis, transport, uptake and breakdown of dopamine (in blue) and serotonin (in yellow). Dashed arrows: intermediate steps not shown. Dopamine and serotonin receptors are located in the pre- and postsynaptic membrane. There are 5 different dopamine receptors (D1-D5), and 7 different serotonin receptors (5-HT1 – 5-HT7). HVA and 5-HIAA are the main diagnostic breakdown products that can be measured in cerebrospinal fluid. Furthermore, L-DOPA, 5-HTP, 3-O-methyldopa and vanillactic acid (the major breakdown products of L-dopa, not shown), and 3- methoxytyramine (an intermediate breakdown product of dopamine, not shown) can be quantified by some laboratories. Abbreviations see p5-6. Different disorders (VI-X) see Table 1.
1
Voorbereid document _Tessa Wassenberg_V03.indd 17Voorbereid document _Tessa Wassenberg_V03.indd 17 25/10/2021 09:3225/10/2021 09:32

18
Chapter 1
Figure 5. Norepinephrine and epinephrine formation and breakdown, and associated monoamine neurotransmitter disorders
Figure 5. Dopamine is converted to norepinephrine by DBH. CYB561 functions as an electron shuttle for this reaction. Norepinephrine is converted to epinephrine by PNMT. Breakdown of norepinephrine and epinephrine follows several step in which the enzymes MAO and COMT play a major role. Plasma NMET and MET can be used as peripheral markers of norepinephrine and epinephrine breakdown respectively. In CSF, MHPG is the major breakdown product. VMA is the common breakdown product of norepinephrine and epinephrine and can be found in urine. Abbreviations see p5-6, different disorders (X-XII) see Table 1.
Voorbereid document _Tessa Wassenberg_V03.indd 18Voorbereid document _Tessa Wassenberg_V03.indd 18 25/10/2021 09:3225/10/2021 09:32

19
General introduction
Figure 6. The biochemical rationale of the treatment of monoamine neurotransmitter disorders
Figure 6. Schematic presentation of the treatment possibilities in monoamine neurotransmitter disorders. Dopamine and serotonin do not cross the blood-brain barrier (BBB, dashed square). L-dopa and 5-HTP are available as oral supplements that are able cross the blood-brain barrier. This constitutes the hallmark of treatment of all primary monoamine deficiencies where the defect is located upstream of levodopa and 5-HTP conversion, including the BH4-deficiencies. To increase the fraction of L-dopa and 5-HTP that is available to cross the BBB, peripheral decarboxylase inhibitors like carbidopa or benserazide are added. In some BH4 disorders, BH4 can be given in the form of sapropterin (Kuvan©). In AADC-deficiency, vitamin B6 can be used to improve residual activity of the AADC enzyme. A part of the dopamine and serotonin that is released into the synaptic cleft will be directly transported back into the presynaptic neuron by the transporters DAT (dopamine) and SERT (serotonin). SSRI’s inhibit this reuptake of serotonin. Dopamine receptors in the postsynaptic neuron also respond to dopamine agonists, that can be used in the medical treatment of several primary monoamine neurotransmitters disorders. Breakdown of dopamine and serotonin is a multistep process in which MAO and COMT are involved. MAO- and COMT-inhibitors can therefore be used to increase dopamine and serotonin concentrations. L-DOPS can be used to treat DBH deficiency, because it is converted to norepinephrine by AADC. Serotonin is a precursor of melatonin. Therefore, in case of sleep disturbances in patients with monoamine neurotransmitter disorders in which the serotonergic pathway is involved, melatonin should be considered. Abbreviations see page 5-6.
1
Voorbereid document _Tessa Wassenberg_V03.indd 19Voorbereid document _Tessa Wassenberg_V03.indd 19 25/10/2021 09:3225/10/2021 09:32

20
Chapter 1
Table 1. Overview of the monoamine neurotransmitter disorders and main treatment options
Disorder Gene OMIM Synonyms Level of defect
Main treatment
Ia AR GCH1 deficiency GCH1 233910 AR-DRD with or without HPA
BH4 synthesis(cofactor)
L-dopa5-HTP
Ib AD GCH1 deficiency GCH1 128230 DYT5aAD-DRDSegawa syndromeDYT/PARK-GCH1
BH4 synthesis(cofactor)
L-dopa5-HTP
II PTPS deficiency PTS 261640 HPA, BH4 deficient due to PTPS deficiency
BH4 synthesis(cofactor)
SapropterinL-dopa5-HTP
III Sepiapterin reductase deficiency (SRD)
SPR 612716 DRD due to SRD BH4 synthesis(cofactor)
L-dopa5-HTPDA-agonist
IV DHPR-deficiency QDPR 261630 HPA, BH4 deficient, due to DHPR deficiency
BH4 recycling(cofactor)
L-dopa5-HTPDietFolinic acid(sapropterin?)
V PCD-deficiency PCBD1 264070 HPA, BH4 deficient due to PCD deficiency;HPA with Primapterinuria
BH4 recycling(cofactor)
Sapropterin
VI TH-deficiency TH 605407 AR-DRDAR-Segawa syndromeDYT-5b
Synthesis L-dopaDA-agonists
VII AADC-deficiency DDC 608643 Dopa decarboxylase deficiency
Synthesis Vitamin B6DA-agonistsMAO-inhibitors.Gene therapy
VIII VMAT2-deficiency SLC18A2 618049 Parkinsonism-Dystonia Infantile, 2
Transport DA-agonists
IX DAT-deficiency SLC6A3 613135 Parkinsonism-Dystonia Infantile, 1
Transport DA-agonists
X MAO-deficiency MAOA 300615 Brunner syndrome
Breakdown SSRI?
Voorbereid document _Tessa Wassenberg_V03.indd 20Voorbereid document _Tessa Wassenberg_V03.indd 20 25/10/2021 09:3225/10/2021 09:32

21
General introduction
Table 1. [Continued]
Disorder Gene OMIM Synonyms Level of defect
Main treatment
XI DBH-deficiency DBH 223360 Orthostatic hypotension 1
Synthesis LDOPS
XII CYB561 mutations CYB561 618182 Orthostatic hypotension 2
Electron shuttle
LDOPS
XIII DNAJC12 mutations DNAJC12 617384 HPA, mild, non BH4 deficient
Co-chaperone
SapropterinL-dopa5HTP
Table 1. Roman numerals refer to numerals in Figures 3-5 where the location of the defect can be found. All disorders are inherited in an autosomal recessive manner except for autosomal dominant GCH1 deficiency and X-linked MAO-deficiency. OMIM number reflects the phenotype MIM (mendelian inheritance of man) number (https://omim.org). Main treatment gives a short overview of the main treatment options, that are also schematically shown in Figure 6. L-dopa is always given together with an AADC-inhibitor (e.g. benserazide or carbidopa, normally in a 4:1 ratio). Diet is a phenylalanine restricted diet. BH4 can be given in the form of sapropterin (Kuvan ©). It is not always necessary to treat PCD-deficiency because this sometimes lead to transient mild HPA, but early screening for diabetes mellitus should be performed. Abbreviations see page 5-6.
1
Voorbereid document _Tessa Wassenberg_V03.indd 21Voorbereid document _Tessa Wassenberg_V03.indd 21 25/10/2021 09:3225/10/2021 09:32

22
Chapter 1
References
1. Gnegy MT. Catecholamines. In: Brady ST, ed. Basic Neurochemistry. 8 ed. Oxford: Elsevier Academic Press; 2012:283-299.
2. Aperia A. Dopamine action and metabolism in the kidney. Current opinion in nephrology and hypertension. 1994;3(1):39-45.
3. Goldstein DS. Noradrenergic neurotransmission. In: Robertson D, ed. Primer on the autonomous nervous system. 3 ed. Oxford: Elsevier Academic Press; 2012.
4. Tank AW, Lee Wong D. Peripheral and central effects of circulating catecholamines. Compr Physiol. 2015;5(1):1-15.
5. Hensler JG. Serotonin. In: Brady ST, ed. Basic Neurochemistry. 8 ed. Oxford: Elsevier Academic Press; 2012:300-322.
6. Berger M, Gray JA, Roth BL. The expanded biology of serotonin. Annu Rev Med. 2009;60:355-366.7. Werner ER, Blau N, Thony B. Tetrahydrobiopterin: biochemistry and pathophysiology. The
Biochemical journal. 2011;438(3):397-414.8. Ng J, Papandreou A, Heales SJ, Kurian MA. Monoamine neurotransmitter disorders- clinical
advances and future perspectives. Nature reviews Neurology. 015;11(10):567- 584.9. Anikster Y, Haack TB, Vilboux T, et al. Biallelic Mutations in DNAJC12 Cause
Hyperphenylalaninemia, Dystonia, and Intellectual Disability. Am J Hum Genet. 2017;100(2):257-266.
10. van den Berg MP, Almomani R, Biaggioni I, et al. Mutations in CYB561 Causing a Novel Orthostatic Hypotension Syndrome. Circulation research. 2018;122(6):846-854.
11. Brennenstuhl H, Jung-Klawitter S, Assmann B, Opladen T. Inherited Disorders of Neurotransmitters: Classification and Practical Approaches for Diagnosis and Treatment. Neuropediatrics. 2019;50(1):2-14.
12. Dobricic V, Tomic A, Brankovic V, et al. GCH1 mutations are common in Serbian patients with dystonia-parkinsonism: Challenging previously reported prevalence rates of DOPA-responsive dystonia. Parkinsonism & related disorders. 2017;45:81-84.
13. Wassenberg T, Deinum J, van Ittersum FJ, et al. Clinical presentation and long-term follow-up of Dopamine Beta Hydroxylase deficiency. Journal of inherited metabolic disease. 2020.
14. Nygaard TG, Waran SP, Levine RA, Naini AB, Chutorian AM. Dopa-responsive dystonia simulating cerebral palsy. Pediatr Neurol. 1994;11(3):236-240.
15. Fink JK, Filling-Katz MR, Barton NW, Macrae PR, Hallett M, Cohen WE. Treatable dystonia presenting as spastic cerebral palsy. Pediatrics. 1988;82(1):137-138.
16. Neville B. Congenital DOPA-responsive disorders: a diagnostic and therapeutic challenge to the cerebral palsies? Developmental medicine and child neurology. 2007;49(2):85.
17. Wassenberg T, Molero-Luis M, Jeltsch K, et al. Consensus guideline for the diagnosis and treatment of aromatic l-amino acid decarboxylase (AADC) deficiency. Orphanet journal of rare diseases. 2017;12(1):12.
Voorbereid document _Tessa Wassenberg_V03.indd 22Voorbereid document _Tessa Wassenberg_V03.indd 22 25/10/2021 09:3225/10/2021 09:32

23
General introduction
1
Voorbereid document _Tessa Wassenberg_V03.indd 23Voorbereid document _Tessa Wassenberg_V03.indd 23 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 24Voorbereid document _Tessa Wassenberg_V03.indd 24 25/10/2021 09:3225/10/2021 09:32

CHAPTER 2
Aims and outline
of the thesis
Voorbereid document _Tessa Wassenberg_V03.indd 25Voorbereid document _Tessa Wassenberg_V03.indd 25 25/10/2021 09:3225/10/2021 09:32

26
Chapter 2
In this thesis, clinical and biochemical characteristics of several monoamine neurotransmitter disorders are investigated, with emphasis on aromatic l-amino acid decarboxylase (AADC) deficiency and dopamine beta hydroxylase (DBH) deficiency. Furthermore, autosomal dominant GCH1 deficiency and tyrosine hydroxylase (TH) deficiency are discussed. The scientific work reflects a research project that spans over a decade, performed primarily at the Radboud university medical center departments of Neurology, Pediatric Neurology, and the Translational Metabolic Laboratory (TML). It combines several methodologies, including laboratory research, database research, literature review, chart review, case reports, and guideline development. With this thesis, we aim to explain differences found in neurotransmitter metabolites in different body compartments, better delineate clinical characteristics, and improve early diagnosis and clinical care for patients suffering from these rare disorders.
Part I: Prologue
Monoamine neurotransmitter disorders are uncommon and can present in many ways. Therefore, they are hard to recognize in clinical practice and the diagnostic delay can be long. However, identification is crucial because some of these disorders are excellently treatable, and all disorders require a specific approach regarding diagnosis, medical treatment, and surveillance. Whereas the following parts of this thesis focus on specific aspects of these disorders, chapter 1 focuses on the general presentation and overarching principles of monoamine neurotransmitter disorders.
Part II:Biochemical aspects and the importance of different body compartments
Part II focuses on biochemical aspects of two monoamine neurotransmitter disorders: AADC deficiency and TH deficiency. It aims to outline and understand the differences that can be found in different body compartments (reflected by cerebrospinal fluid, blood and urine) when measuring monoamine metabolites. Although it seems attractive and more patient friendly to use blood or urine biomarkers in these disorders instead of cerebrospinal fluid, we identified several caveats that are discussed in this chapter.
In chapter 3 we investigated a puzzling observation made in our laboratory and repeatedly reported in the literature, namely that patients with AADC-deficiency can have normal or even increased levels of dopamine and dopamine metabolites in their urine. This seemingly paradoxical finding – it is expected that patients with AADC-deficiency have an overall lack of dopamine due to the metabolic defect – prompted us to do several laboratory studies to replicate this finding in a larger group of patients, and search for possible explanations by investigating genotype/phenotype correlations and testing possible alternative metabolic routes for the formation of urinary dopamine. In chapter 4, we propose an explanation for normal or increased levels of urinary
Voorbereid document _Tessa Wassenberg_V03.indd 26Voorbereid document _Tessa Wassenberg_V03.indd 26 25/10/2021 09:3225/10/2021 09:32

27
Aims and outline of the thesis
dopamine in AADC-deficiency by calculating residual renal AADC-activity in two patients. To further investigate the neurotransmitter metabolite profiles in different body compartments, we performed a literature study on neurotransmitter metabolites in blood, urine and cerebrospinal fluid in patients with AADC- and TH-deficiency, and combined this with findings from the TML database from 1997-2020. Additionally, serum prolactin levels were recorded. Results are presented in chapter 5.
Part III: Beyond the classical phenotype: clinical observations
Case reports that highlight new or unexpected features of disorders are important for clinical practice and can guide further research. They also have educational value.
During the course of this research project, we identified several adult patients with autosomal dominant GCH1-mutations that had a deviant phenotype that was characterized by pyramidal predominant onset instead of the well-known dystonia phenotype. In chapter 6, the long-term clinical course of these patients is described, illustrated by video fragments, and combined with a literature review on spasticity in GCH1-mutations.
In chapter 7, a patient with dopamine beta hydroxylase (DBH)-deficiency is presented who came to the attention of our pediatric nephrologist many years ago because of decreased renal function. Her symptoms and signs are described, as well as the diagnostic steps that ultimately led to the correct diagnosis. This chapter is structured in a question and answer mode and highlights the previously overlooked renal involvement in DBH-deficiency.
Part IV: Reviews and guidelines for management
Because monoamine neurotransmitter disorders are so rare, management is mainly based on expert opinion and large randomized controlled trials are barely feasible. However, because of the complexity of these disorders, patients will benefit greatly from guidelines in which state of the art approach to diagnosis, treatment, and follow-up is described. Also for rare disorders, evidence based recommendations can be made when SIGN/GRADE methodologies are followed (https://www.sign.ac.uk/assets/sign_grading_system_1999_2012.pdf). In 2014 we decided to develop a consensus guideline for AADC deficiency as part of the iNTD initiative (international working group on neurotransmitter related disorders). For this guideline, an extensive literature review was performed and several international group meetings were held that ultimately led to the publication of the first iNTD guideline in 2017. This consensus guideline on the diagnosis and treatment of AADC deficiency is presented in chapter 8.
2
Voorbereid document _Tessa Wassenberg_V03.indd 27Voorbereid document _Tessa Wassenberg_V03.indd 27 25/10/2021 09:3225/10/2021 09:32

28
Chapter 2
DBH-deficiency is one of the rarest among the uncommon monoamine neurotransmitter disorders. In the literature, information on long-term follow-up of this disorders was lacking. In the Netherlands, we identified a relatively large group of 10 patients with DBH deficiency. In chapter 9, we present the outcome of our research project that combined literature review with chart review of the Dutch patients, and provide an extensive overview on the clinical presentation and long-term follow-up of this disorder with recommendations for clinical practice.
Voorbereid document _Tessa Wassenberg_V03.indd 28Voorbereid document _Tessa Wassenberg_V03.indd 28 25/10/2021 09:3225/10/2021 09:32

29
Aims and outline of the thesis
2
Voorbereid document _Tessa Wassenberg_V03.indd 29Voorbereid document _Tessa Wassenberg_V03.indd 29 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 30Voorbereid document _Tessa Wassenberg_V03.indd 30 25/10/2021 09:3225/10/2021 09:32

PART II
Biochemical aspects
and the importance
of different body
compartments
Voorbereid document _Tessa Wassenberg_V03.indd 31Voorbereid document _Tessa Wassenberg_V03.indd 31 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 32Voorbereid document _Tessa Wassenberg_V03.indd 32 25/10/2021 09:3225/10/2021 09:32

CHAPTER 3
Urinary dopamine in aromatic l-amino acid decarboxylase deficiency: the unsolved paradoxTessa Wassenberg, Michèl A.A.P. Willemsen, Ben P.B.H. Geurtz, Martin Lammens, Kiek Verrijp, Martijn Wilmer, Wang Tso Lee, Ron A. Wevers, Marcel M. Verbeek
Mol Genet Metab. 2010; 101(4) 349-356DOI: 10.1016/j.ymgme.2010.08.003
Voorbereid document _Tessa Wassenberg_V03.indd 33Voorbereid document _Tessa Wassenberg_V03.indd 33 25/10/2021 09:3225/10/2021 09:32

34
Chapter 3
Abstract
Introduction: In aromatic L-amino acid decarboxylase (AADC) deficiency, a neurotransmitter biosynthesis defect, paradoxical normal or increased levels of urinary dopamine have been reported. Genotype/phenotype correlations or alternative metabolic pathways may explain this remarkable finding, but were never studied systematically.
Methods: We studied the mutational spectrum and urinary dopamine levels in 20 patients with AADC-deficiency. Experimental procedures were designed to test for alternative metabolic pathways of dopamine production, which included alternative substrates (tyramine and 3-methoxytyrosine) and alternative enzymes (tyrosinase and CYP2D6).
Results/ discussion: In 85% of the patients the finding of normal or increased urinary levels of dopamine was confirmed, but a relation with AADC genotype could not be identified. Renal microsomes containing CYP2D were able to convert tyramine into dopamine (3.0 nmol/min/g protein) but because of low plasma levels of tyramine this is an unlikely explanation for urinary dopamine excretion in AADC-deficiency. No evidence was found for the production of dopamine from 3-methoxytyrosine. Tyrosinase was not expressed in human kidney.
Conclusion: Normal or increased levels of urinary dopamine are found in the majority of AADC-deficient patients. This finding can neither be explained by genotype/phenotype correlations nor by alternative metabolic pathways, although small amounts of dopamine may be formed via tyramine hydroxylation by renal CYP2D6. CYP2D6-mediated conversion of tyramine into dopamine might be an interesting target for the development of new therapeutic strategies in AADC-deficiency.
Voorbereid document _Tessa Wassenberg_V03.indd 34Voorbereid document _Tessa Wassenberg_V03.indd 34 25/10/2021 09:3225/10/2021 09:32

35
Urinary dopamine in AADC deficiency: the unsolved paradox
Introduction
Aromatic L-amino acid decarboxylase (AADC; EC 4.1.1.28, also known as dopa decarboxylase) is an essential enzyme in the biosynthesis of the monoamine neurotransmitters serotonin and dopamine. AADC converts both 5-hydroxytryptophan (5-HTP) into serotonin and 3,4-dihydroxyphenylalanine (L-dopa) into dopamine, requiring pyridoxal-5-phosphate (activated vitamin B6) as co-factor. Dopamine is further metabolized towards norepinephrine (NE) and epinephrine (E) (Fig. 1). AADC-deficiency is a rare autosomal recessive disorder, characterized by developmental delay, prominent motor abnormalities, oculogyric crises and autonomic features1, 2. Prognosis is poor, and available treatment options like dopamine agonists, vitamin B6 and monoamine oxidase (MAO; EC 1.4.3.4) inhibitors only have marginal therapeutic effect3, 4. Diagnosis of AADC-deficiency is made by analysis of cerebrospinal fluid (CSF), the determination of AADC-enzyme activity in plasma, and mutation analysis 3, 5. In urine, vanillactic acid (VLA), a breakdown product of L-dopa, is increased and may alert clinicians to perform additional investigations5, 6.
In a number of AADC-deficient patients normal or increased levels of urinary dopamine are reported 6-10. This apparently paradoxical finding has not been studied systematically before. Although dopamine is not uniquely synthesized in the nervous system, its biosynthesis is essentially mediated by AADC irrespective of the site of production. The kidneys synthesize dopamine by AADC after uptake of L-dopa in the cortical peripheral tubular epithelium (PTE) cells. The intrarenal autocrine–paracrine dopamine system is critical for sodium homeostasis11-13. However, the finding of normal or increased levels of urinary dopamine remains unexplained10.
We aimed to find a genetic or metabolic explanation for normal or increased levels of urinary dopamine in AADC-deficiency. Identification of alternative metabolic pathways for dopamine synthesis, different from that mediated by AADC, might reveal a potential therapeutic target for patients with AADC-deficiency. Furthermore, better understanding of peripheral dopamine synthesis will shed light on the underlying mechanisms of AADC-deficiency and may contribute to the development of therapeutic strategies in dopamine deficient ailments. Potential alternative metabolic pathways for dopamine production are depicted in Fig. 1, with 3-methoxytyrosine (3-MTYR) and tyramine shown as possible alternative substrates, and cytochrome P450 2D6 (CYP2D6) and tyrosinase shown as possible alternative enzymes involved in dopamine formation.
3
Voorbereid document _Tessa Wassenberg_V03.indd 35Voorbereid document _Tessa Wassenberg_V03.indd 35 25/10/2021 09:3225/10/2021 09:32

36
Chapter 3
Figu
re 1
. Bio
synt
hesis
of c
atec
hola
min
es a
nd m
elan
in; k
now
n an
d pr
opos
ed p
athw
ays o
f dop
amin
e sy
nthe
sis.
Voorbereid document _Tessa Wassenberg_V03.indd 36Voorbereid document _Tessa Wassenberg_V03.indd 36 25/10/2021 09:3225/10/2021 09:32

37
Urinary dopamine in AADC deficiency: the unsolved paradox
Figure 1. Established pathways in humans are shown in straight black arrows. If intermediate products and enzymes are not depicted, straight grey arrows are shown. Human enzymes are shown in black rectangles, with cofactors depicted next to arrows. TDC is shown in a grey ovale because it is only found in invertebrate tyrosine metabolism. Proposed alternative pathways of dopamine formation are shown in interrupted arrows with enzymes in corresponding interrupted rectangles: dopamine formation from tyramine using the alternative enzymes CYP2D6 or tyrosinase; dopamine formation from 3-MTYR using unknown enzymes or non-enzymatic reactions; dopamine formation from L-dopa formed in melanin synthesis, using AADC Abbreviations: PhH, phenylalanine hydroxylase; TH, tyrosine hydroxylase; AADC, aromatic L-amino acid decarboxylase; DβH, dopamine beta hydroxylase; PNMT, phenylethanolamine N-methyltransferase; COMT, catechol-O-methyltransferase; VLA, vanillactic acid; BH4, tetrahydrobiopterin; Vit B6, vitamin B6; Vit C, vitamin C; SAM, s-adenosylmethionine; SAH, s-adenosylhomocysteine; Cu2+, copper; TDC, tyrosine decarboxylase.
3-MTYR has been described in several publications to serve as an alternative substrate for dopamine formation14-16. Hydroxylation of tyramine leads to dopamine production. Tyrosinase is essential in melanin formation (Fig. 1) and tyrosinase deficiency results in albinism. Protein expression is thought to be highly confined to cells containing melanosomes17. Catecholamine synthesis was noted in pigmented tyrosine hydroxylase (TH; EC 1.14.16.2) deficient mice, suggesting a role for tyrosinase in the dopamine production by using tyrosine as substrate18, 19. Although AADC is still required in this alternative metabolic pathway of catecholamine synthesis (Fig. 1), these data support our hypothesis of existing alternative pathways for dopamine production in the absence of one of the key enzymes (in this case, TH). Interestingly, tyrosinase may also use tyramine as substrate for dopamine production. Since mushroom tyrosinase may convert tyramine to dopamine20, 21, we investigated if human tyrosinase could be responsible for renal dopamine biosynthesis in AADC-deficiency by studying its expression in peripheral human tissues including kidney. The other enzyme tested, CYP2D6, is described to hydroxylate tyramine to dopamine in human liver and brain22,23.We investigated if this reaction also occurs in kidneys and therefore could be an explanation for normal or increased levels of urinary dopamine in AADC-deficiency.
Materials and methods
We collected urinary dopamine levels of AADC-deficient patients and searched for a genotype/phenotype correlation in this group. Peripheral dopamine production was investigated in several human and rat tissues and AADC-dependency of dopamine production in human kidney cortex was investigated by applying AADC-inhibitors. Furthermore, alternative metabolic pathways were tested to find possible AADC-independent ways of dopamine formation. The collection and use of laboratory data were in accordance with the regulations of the ethical committee of the Radboud University Nijmegen Medical Centre, Nijmegen, the Netherlands. Use of human tissue was according to the code for proper secondary use of human tissues in the
3
Voorbereid document _Tessa Wassenberg_V03.indd 37Voorbereid document _Tessa Wassenberg_V03.indd 37 25/10/2021 09:3225/10/2021 09:32

38
Chapter 3
Netherlands. Use of rat tissue for this study was approved by the ethical committee of the Radboud University Nijmegen Medical Centre, Nijmegen, the Netherlands.
MaterialsL-dopa, tyramine-HCl and L-3-methoxtyrosine were all purchased from Sigma (St Louis, MO). Carbidopa (peripheral AADC-inhibitor), 3-hydroxylbenzylhydrazine (NSD-1015, a central AADC-inhibitor), pargyline (monoamine oxidase (MAO)-inhibitor) and 3,5-dinitrocatechol (catechol-O-methyltransferase (COMT; EC 2.1.1.6)-inhibitor) were also from Sigma. Recombinant AADC protein was purchased from Abcam, Cambridge, UK. Primary antibodies comprised of polyclonal rabbit anti-AADC (dilution in western blot (WB) 1:1000 and immunohistochemistry (IHC) 1:200, Acris Antibodies, Herford, Germany) and anti-tyrosinase mouse antibody (T311; WB 1:1000, IHC 1:10, Calbiochem, Merck). Secondary antibodies for WB were goat-anti rabbit IgG and goat-anti-mouse IgG (Alexa Fluor 680, Invitrogen, Paisly UK). For IHC of AADC, biotinylated horse-anti-goat (1:200) was used as secondary antibody followed by an avidin–biotin peroxidase complex (1:100, Vector, Burlingame, CA). IHC on tyrosinase was performed using PowerVision peroxidase-labeled polyclonal goat-anti-mouse IgG (Immunologic, Duiven, the Netherlands).
PatientsCharacteristics of AADC-deficient patients were collected by sending out a questionnaire to referring physicians regarding age, ethnicity, clinical presentation, mutation analysis, plasma AADC-activity and urinary dopamine levels with corresponding reference values, and medication at time of analysis. Eleven patients were analyzed for urinary catecholamine levels in our lab using a commercial assay (Bio-Rad, Veenendaal, the Netherlands), as described previously24. Only patients with confirmed mutations in the dopa decarboxylase (DDC)-gene and known urinary levels of dopamine were included for this study. Twelve patients have been reported previously (Table 1).
Literature study on alternative splicingPubmed was searched for alternative splicing events of the human AADC gene with search terms AADC, DDC, dopa decarboxylase [Mesh], aromatic l-amino acid decarboxylase [Mesh], alternative splicing, with or without the limit [humans]. Last search was performed in April 2010.
Tissue preparationThe following tissues were used for the experiments: human kidney cortex (n = 3), adrenal gland (n = 2), jejunum (n = 2), liver (n = 2), cerebral cortex (n = 2) and striatum (n = 2), and rat kidney (n = 2) and liver (n = 2). Furthermore, we used human tumor tissues from pheochromocytoma (n = 2), neuroblastoma (n = 2) and melanoma (n = 1), essentially as positive controls. Human serum was used for control purposes in dopamine production assays. For the dopamine production assays, a total of 50–100 mg
Voorbereid document _Tessa Wassenberg_V03.indd 38Voorbereid document _Tessa Wassenberg_V03.indd 38 25/10/2021 09:3225/10/2021 09:32

39
Urinary dopamine in AADC deficiency: the unsolved paradox
of 10 μm sections of tissue (all except melanoma) were homogenized on ice using a glass potter and sonification (Sonifier-II W250/W450 Classic, Branson) in 0.1 M phosphate buffer pH 7.0, containing 39 mM dithiotreitol (Aldrich, Steinheim, Germany) and 0.167 mM NaEDTA (Baker, Deventer, the Netherlands). Protease inhibitor cocktail was added according to supplier instructions (Roche, Switzerland). Supernatant was obtained after centrifugation for 10 min at 10,000 × g at 4 °C. For the WB, lysates were made of all tissues after homogenization of 10 μm sections in RIPA-buffer (50 mM TRIS pH 7.5, 150 mM NaCl (Merck)), 1% (w/v) Nonidet P40 (Sigma), 0.5% (w/v) 10% SDS (Gibco) with protease inhibitors cocktail, incubated on ice for 20 min and subsequently centrifuged at 10,000 × g at 4 °C for 20 min. IHC expression of AADC was performed in triplicate in all tissues except melanoma. IHC expression of tyrosinase was performed in triplicate in all tissues except pheochromocytoma and neuroblastoma. Four micrometer sections of frozen tissue were prepared and subsequently fixed for 10 min in acetone at −20 °C and dried.
Since fresh human tissue was not available for studying CYP2D6 activity, the liver and the kidney of two female adult Wistar rats were collected after decapitation and immediately frozen in liquid nitrogen. Microsomes (vesicle-like artifacts formed from the endoplasmatic reticulum when eukaryotic cells are broken-up by differential centrifugation) were prepared as described in Bromek et al.23, using a mini-ultracentrifuge (Mini Sorval RCM150GX), and stored at − 80 °C in storage solution containing 20% (v/v) glycerol until use.
Protein determination of tissue lysates was performed by the method of Lowry et al.25
Dopamine production assays modified from AADC-activity assays in plasmaFirstly, dopamine production in human tissue homogenates was measured as described previously 26 and expressed in nmol/min/g protein. Secondly, to mimick renal dopamine production in AADC-deficiency, methods were modified by testing dopamine production in human kidney cortex homogenate in the presence of carbidopa and NSD-1015 at increasing concentrations. Human serum was used as control. Thirdly, to test for alternative metabolic pathways for dopamine production in the kidney, L-dopa was replaced by other substrates (tyramine or 3-MTYR, 2 mM) and dopamine and L-dopa production was tested in human kidney cortex homogenate and serum. In these last experiments, MAO was inhibited by pargyline (100 μM) and COMT by 3,5-dinitrocatechol (1 μM) to prevent metabolism of dopamine to homovanillic acid. Furthermore, incubation time was prolonged to 18 h. To mimic AADC-deficiency, NSD-1015 (500 μM) or carbidopa (1000 μM) was added.
HPLC analysis of dopamine and L-dopaHPLC analysis to detect dopamine production in enzyme activity assays with L-dopa as substrate was performed as described previously26. In the enzyme activity assays
3
Voorbereid document _Tessa Wassenberg_V03.indd 39Voorbereid document _Tessa Wassenberg_V03.indd 39 25/10/2021 09:3225/10/2021 09:32

40
Chapter 3
with alternative substrates, HPLC with fluorometric detection was used to detect both dopamine and L-dopa. A Partisphere C18 5 μm 4.6 × 250 mm column was used (Whatman, Meadstone, UK). Mobile phase consisted of 0.025 M citric acid, 0.025 M Na2HPO4, 0.015 M sodium perchlorate, 0.5 mM sodium octansulfonic acid, 50 mM NaCl, 0.3 mM EDTA, and 4% methanol. Detection was performed by fluorometric detection (excitation: 278 nm; emission: 325 nm, FP1520 Jasko, Japan), at a flow of 1.50 mL/min. A Triathlon autosampler (Spark) was used for injection of samples (volume 250 μL). PC1000 software (Thermo separations, San Jose, CA) was used for automated data collection.
Western blottingFor WB analysis of AADC, equivalent amounts of protein (20 μg total protein) from tissue lysates, and 0.05 μg recombinant AADC protein were diluted in a reduced sample buffer containing 0.5 M Tris–HCl (pH 6.8), 25% glycerol, 20% sodium dodecyl sulfate (SDS), 0.001% bromophenol blue (Pharmacia Biotech AB, Uppsala, Sweden) and 30 mM DL-dithiotreitol (Sigma), heated at 99 °C for 5 min, cooled on ice for 5 min and subsequently centrifuged at 7000 × g for 5 min. If negative results on the blots were obtained, procedures were repeated with 200 μg total protein. For WB of tyrosinase, the same procedure was followed except that of all tissues 200 μg total protein was used, except for melanoma as positive control (50 μg). Precision plus protein (PPP; Bio-Rad) was used as molecular weight marker. Electrophoresis was performed on 12% Tris–HCl sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) gels and proteins were transferred to nitrocellulose membranes (Schleicher and Schuell, Dassel, Germany). For immunodetection, membranes were incubated subsequently (i) overnight at 4 °C in Odyssey blocking buffer (LI-COR; Westburg, Leusden, The Netherlands), (ii) for 2 h in primary antibody and (iii) for 1 h in secondary antibody with washing steps in between. Blots were scanned with the LI-COR Odyssey infrared scanner.
ImmunohistochemistrySections were pre-incubated with 20% normal horse serum in phosphate buffered saline (PBS) for 10 min. Incubation with primary antibody diluted in 1% BSA/PBS was performed for 1 h at room temperature. Incubation with secondary antibodies was performed for 30 min at room temperature, followed by incubation with an avidin–biotin peroxidase complex in case of AADC. Detection was carried out with the use of aminoethylcarbazole as substrate.
CYP2D6 activity assaysThe hydroxylation of tyramine to dopamine by renal microsomes was tested as previously described23, with modifications. Microsomes (mean protein content 1.1 ± 0.3 mg/mL) were incubated with potassium phosphate buffer (0.1 M, pH 7.4), NADPH (Sigma) (1 mM) and pargyline (100 μM). Tyramine was added to the incubation mixture at a concentration of 1 mM. The final incubation volume was 1.0 mL. The mixture was
Voorbereid document _Tessa Wassenberg_V03.indd 40Voorbereid document _Tessa Wassenberg_V03.indd 40 25/10/2021 09:3225/10/2021 09:32

41
Urinary dopamine in AADC deficiency: the unsolved paradox
incubated at 37 °C for 20 min. The reaction was stopped by adding 15 μL of perchloric acid (60%) and cooling the samples on ice. Supernatant was collected by centrifugation for 10 min at 3000 × g.
Results
Phenotype and genotype of 20 AADC-deficient patientsPatient characteristics are shown in Table 1. Urinary dopamine levels were obtained from 20 patients with AADC-deficiency with confirmed mutations. Eight patients were from European descent, one from Arabic descent and 11 from Asian descent. Mean age at time of investigation was five years and six months (range: three months to 26 years). Only one patient used medication (L-dopa) during the time of analysis. Three patients had decreased levels of urinary dopamine (Pt 1–3), seven patients had normal levels (Pt 4–10) and ten patients (Pt 11–20) had increased levels of urinary dopamine. Thus, in 85% of the patients the finding of normal or increased levels of urinary dopamine was confirmed. There was no correlation between the level of urinary dopamine and the clinical phenotype. All patients described in the article gradually showed the complete, characteristic neurological disorder including developmental delay and severe motor abnormalities, ptosis and oculogyric crisis, and autonomic dysfunction. In this group, seventeen different mutations were found throughout the whole gene, residing in exons 2, 3, 4, 7, 8, 11, 12 and 14, and in intron 6 (Fig. 2, lower panel). The most common mutation was found in intron 6 (IVS6 + 4A > T) which occurred exclusively in the Asian population. This mutation was found in homozygous form in patients with either decreased, normal or increased levels of urinary dopamine.
Table 1. Urinary dopamine levels and corresponding mutations in AADC-deficient patientsCharacteristics of 20 AADC-deficient patients. Patient characteristics: age is given in years. Mutation found in allele 1 and allele 2, medication at time of laboratory findings (i.e. urinary dopamine and plasma AADC-activity) are given. Laboratory findings under medication are given only if the untreated values were not available. Reference to first occurrence in literature and corresponding JakeID number (if recorded) from Jake Database (http://www.biopku.org/BioPKU_databaseJAKE.asp; curated by N. Blau) are given. Urinary dopamine levels are defined as decreased, normal and increased. Absolute values are presented between brackets, with local reference values for age and sex. Reference value for plasma AADC-activity: 16-48 mU/L or 36-129 pmol/min/mL (patient 17 and 18) Abbreviations: M= male, F=female NF= not found, ND = not detectable, ref= reference value, med= medication
3
Voorbereid document _Tessa Wassenberg_V03.indd 41Voorbereid document _Tessa Wassenberg_V03.indd 41 25/10/2021 09:3225/10/2021 09:32

42
Chapter 3
#Pa
tient
cha
ract
eris
tics
sex,
age
, orig
in,
(fam
ily re
latio
n)
Mut
ation
:Al
lele
1M
utati
on:
Alle
le 2
Med
Dop
amin
e le
vel i
n ur
ine
Plas
ma
AAD
C ac
tivity
(m
U/L)
Refe
renc
e
1M
, 3/1
2, F
renc
hE2
5KV4
60G
-De
crea
sed
(38
nmol
/mm
ol k
reat
; ref
65-
1700
)0.
5Ve
rbee
k et
al 2
007,
Jake
ID 2
1
2F,
1,Ta
iwan
ese
IVS6
+4A>
TIV
S6+4
A>T
-De
crea
sed
(28
μg/2
4h ;
ref 5
0-45
0)-
-
3F,
2, T
aiw
anes
eIV
S6+4
A>T
NF
-De
crea
sed
(14
μg/2
4h; r
ef 5
0-45
0)-
-
4M
, 2, B
elgi
anA9
1VA2
75T
-N
orm
al (1
90 n
mol
/mm
ol k
reat
; ref
70-
795)
0.7
-
5M
, 1, T
aiw
anes
eIV
S6+4
A>T
Y79C
-N
orm
al (1
00 μ
g/24
h; re
f 50-
450)
--
6F,
2, T
aiw
anes
eIV
S6+4
A>T
IVS6
+4 A
>T-
Nor
mal
(222
μg/
24h;
ref 5
0-45
0 )
--
7M
, 6/1
2, T
aiw
anes
eIV
S6+4
A>T
IVS6
+4 A
>T-
Nor
mal
(314
μg/
24h;
ref 5
0-45
0)-
-
8F,
1, T
aiw
anes
eIV
S6+4
A>T
IVS6
+4 A
>T-
Nor
mal
(113
μg/
24h
; ref
50-
450)
--
9M
, 1, T
aiw
anes
eIV
S6+4
A>
IVS6
+4 A
>T-
Nor
mal
(166
μg/
24h
; ref
50-
450)
--
10M
, 6/1
2, A
rabi
cR4
47H
R447
H-
Nor
mal
(922
nm
ol/m
mol
kre
at; r
ef 6
5-17
00)
1.0
Verb
eek
et a
l 200
7, Ja
keID
50
11F,
26, S
erbi
an (s
iblin
g 12
+13)
G102
SG1
02S
-In
crea
sed
(451
nm
ol/m
mol
kre
at; r
ef 1
5-22
5)N
DBr
autig
am e
t al 2
000,
Jake
ID 1
5
12M
, 24,
Ser
bian
(sib
ling
11+1
3)G1
02S
G102
S-
Incr
ease
d (8
11 n
mol
/mm
ol k
reat
; ref
15-
225)
0.9
Brau
tigam
et a
l 200
0, Ja
keID
14
13M
, 16,
Ser
bian
(sib
ling
11+1
2)G1
02S
G102
SL-
dopa
Incr
ease
d (3
145
nmol
/mm
ol k
reat
; ref
15-
225)
ND
Brau
tigam
, Jak
eID
13
14M
, 8, J
apan
ese
A110
QN
F-
Incr
ease
d (5
369
μg/2
4h; r
ef 3
10-1
140)
-Id
e et
al 2
009,
Jake
ID 3
6
15M
, 3, I
talia
nS2
50F
S250
F-
Incr
ease
d (1
3,73
3 nm
ol/m
mol
kre
at; r
ef 7
0-82
5)-
Fium
ara
et a
l 200
2, Ja
keID
4
16F,
9/12
, Tai
wan
ese
IVS6
+4 A
>TIV
S6+4
A>T
-In
crea
sed
(899
μg/
d; re
f 50-
450)
--
17F,
6, S
inga
pore
(sib
ling
18)
R285
WIV
S6+4
A>T
-In
crea
sed
(161
1 nm
ol/m
mol
kre
at; r
ef 7
0-82
5)<1
pm
ol/m
l/m
inTa
y et
al 2
007,
Jake
ID 2
7
18F,
7, S
inga
pore
(sib
ling
17)
R285
WIV
S6+4
A>T
-In
crea
sed
(182
1 nm
ol/m
mol
kre
at; r
ef 7
0-70
0)<1
pm
ol/m
l/m
inTa
y et
al 2
007,
Jake
ID 2
6
19M
, 7/1
2, F
renc
hR3
47Q
R358
H-
Incr
ease
d (1
974
nmol
/ mm
ol k
reat
; ref
65-
1100
)1.
9Ve
rbee
k et
al 2
007,
Jake
ID 2
3
20M
, 7, P
ortu
gese
R462
PR4
62P
-In
crea
sed
(848
nm
ol/ m
mol
kre
at; r
ef 7
0-82
5)0.
1Ve
rbee
k et
al 2
007,
Jake
ID 2
5
Voorbereid document _Tessa Wassenberg_V03.indd 42Voorbereid document _Tessa Wassenberg_V03.indd 42 25/10/2021 09:3225/10/2021 09:32
43
Urinary dopamine in AADC deficiency: the unsolved paradox
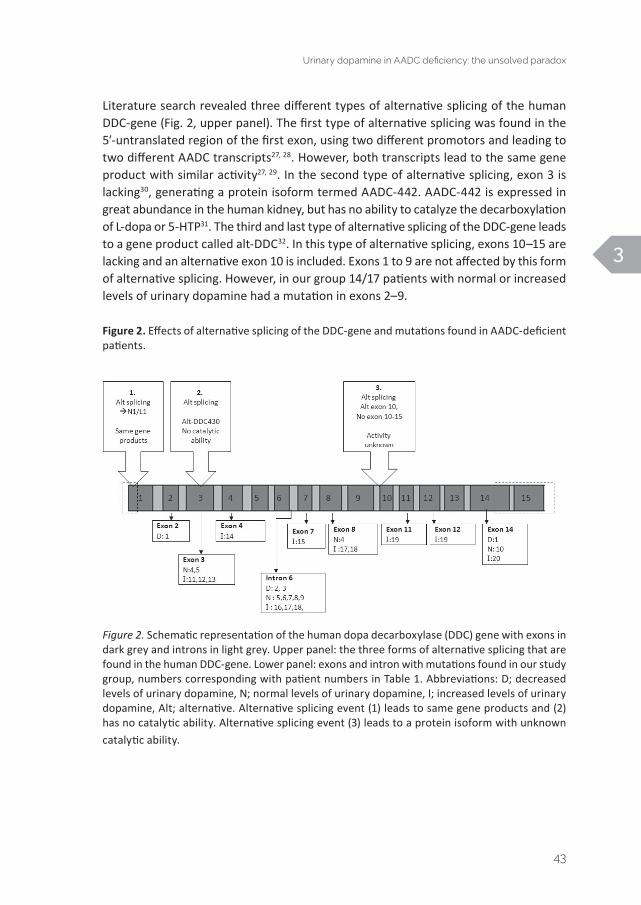
Literature search revealed three different types of alternative splicing of the human DDC-gene (Fig. 2, upper panel). The first type of alternative splicing was found in the 5′-untranslated region of the first exon, using two different promotors and leading to two different AADC transcripts27, 28. However, both transcripts lead to the same gene product with similar activity27, 29. In the second type of alternative splicing, exon 3 is lacking30, generating a protein isoform termed AADC-442. AADC-442 is expressed in great abundance in the human kidney, but has no ability to catalyze the decarboxylation of L-dopa or 5-HTP31. The third and last type of alternative splicing of the DDC-gene leads to a gene product called alt-DDC32. In this type of alternative splicing, exons 10–15 are lacking and an alternative exon 10 is included. Exons 1 to 9 are not affected by this form of alternative splicing. However, in our group 14/17 patients with normal or increased levels of urinary dopamine had a mutation in exons 2–9.
Figure 2. Effects of alternative splicing of the DDC-gene and mutations found in AADC-deficient patients.
Figure 2. Schematic representation of the human dopa decarboxylase (DDC) gene with exons in dark grey and introns in light grey. Upper panel: the three forms of alternative splicing that are found in the human DDC-gene. Lower panel: exons and intron with mutations found in our study group, numbers corresponding with patient numbers in Table 1. Abbreviations: D; decreased levels of urinary dopamine, N; normal levels of urinary dopamine, I; increased levels of urinary dopamine, Alt; alternative. Alternative splicing event (1) leads to same gene products and (2) has no catalytic ability. Alternative splicing event (3) leads to a protein isoform with unknown catalytic ability.
3
Voorbereid document _Tessa Wassenberg_V03.indd 43Voorbereid document _Tessa Wassenberg_V03.indd 43 25/10/2021 09:3225/10/2021 09:32

44
Chapter 3
Peripheral dopamine production and AADC-expression in tissueTable 2 and Figure 3 and 4 show dopamine production and AADC-expression by WB and IHC in the various human tissues. As expected, the kidney cortex shows high dopamine production activity and AADC-expression levels compared with other normal human tissues. Figure 3 shows cell-type specific IHC of AADC-expression in the kidney cortex, jejunum, adrenal gland (cortex and medulla) and liver. Levels of dopamine production activity corresponded well with AADC-expression in the various tissues (Table 2). We were able to achieve 100% inhibition of dopamine production when carbidopa was applied, in serum as well as in the kidney cortex. Compared to serum, high concentrations of carbidopa were needed to achieve complete inhibition of AADC-activity in kidney (1000 μM carbidopa for kidney and 125 μM for serum). At 62.5 μM NSD-1015 a maximum inhibition of 97% was achieved in the kidney cortex. In serum, 100% inhibition of dopamine production was achieved at 6.25 μM NSD-1015.
Table 2. AADC-activity and expression of AADC in various human tissues
Tissue AADC-activity(nmol/min/g protein)
Immunohistochemical expression
Western Blot expression
Pheochromocytoma 7301 +++ ++
Kidney cortex 2996 +++ +++
Liver 354 ++ ++
Jejunum 304 +++ ++
Neuroblastoma 232 ++ +
Adrenal gland 152 +++/ + +
Striatum (n=2) 5 +/- +/-
Table 2. All AADC-activity assays were performed in duplicate, value shown is mean of two separate samples except for kidney cortex (mean of three separate samples). +++: strong positive, ++: intermediate positive, +: positive, +/-: weak positive. IHC of the adrenal gland showed a strong positive signal in the medulla and a weak positive signal in the cortex.
Voorbereid document _Tessa Wassenberg_V03.indd 44Voorbereid document _Tessa Wassenberg_V03.indd 44 25/10/2021 09:3225/10/2021 09:32

45
Urinary dopamine in AADC deficiency: the unsolved paradox
Figure 3. IHC expression of aromatic L-amino acid decarboxylase in several human tissues.
Figure 3. AADC-expression by immunohistochemistry of several human tissues; 10×. A: Kidney cortex, high expression in proximal tubular epithelial cells. B: Jejunum, expression in epithelial cells. C: Adrenal gland; high expression in medulla and weak expression in cortex. D: Liver, weak positive expression in sinusoidal capillaries.
Figure 4. Western blot of AADC and in several human tissues.
Figure 4. Protein precision plus molecular weight marker is shown to the left. 1: recombinant AADC protein (major band at 54 kDa). 2: pheochromocytoma, 3: neuroblastoma, 4: jejunum, 5: kidney cortex, 6: adrenal gland, 7: liver, 8: striatum. 2–7 are results of 20 μg total protein/well, 8 is a result of 200 μg total protein/well because of negative results at 20 μg. Highest AADC protein expression is seen in the kidney cortex (lane 5).
3
Voorbereid document _Tessa Wassenberg_V03.indd 45Voorbereid document _Tessa Wassenberg_V03.indd 45 25/10/2021 09:3225/10/2021 09:32

46
Chapter 3
Dopamine production with alternative substratesThe dopamine production activity assay in the kidney cortex homogenate and plasma was used to test the possibility that substrates other than L-dopa, namely 3-MTYR and tyramine, may be converted into dopamine. However, neither dopamine nor L-dopa production was found, also if AADC-inhibitors were applied (data not shown).
Peripheral expression of tyrosinaseIf the hypothetical pathway shown in Fig. 1 (tyrosinase catalyzing the conversion from tyramine to dopamine) would explain dopaminuria in AADC-deficiency, a substantial amount of tyrosinase should be expressed in peripheral tissues, especially in the kidneys. However, IHC showed the lack of tyrosinase expression in all peripheral human tissues tested (kidney, liver, adrenal gland, and jejunum). Besides melanoma, only striatum showed a weak positive signal for tyrosinase. In line with these findings, only weak bands at the expected molecular weight of 70–80 kDa for tyrosinase were observed in melanoma and cerebral cortex, but not in the other tissues tested, including the kidney cortex by WB (data not shown).
CYP2D dopamine production from tyramineCYP2D isoforms may potentially catalyze the conversion of tyramine to dopamine. We confirmed the presence of this pathway in rat liver and kidney microsomes. Under the experimental conditions described in the CYP2D6 activity assays section, dopamine production of 18 nmol/min/g protein in rat liver, and 3 nmol/min/g protein in rat kidney was found. In comparison, mean dopamine production by AADC was 8348 nmol/min/g protein for rat liver, and 14,084 nmol/min/g protein for rat kidney.
Discussion
We confirmed that the majority of patients with AADC-deficiency (85%) have normal or increased levels of urinary dopamine excretion. In fact, even the patients with hypodopaminuria still excrete substantial amounts of dopamine. Genotype/phenotype correlations do not explain this finding. In our search for alternative metabolic pathways, we found that tyramine can be converted to dopamine by rat renal microsomes, presumably by CYP2D isoforms. Other alternative metabolic pathways for dopamine formation were not found. Tyrosinase, another enzyme that is thought to catalyze the conversion of tyramine to dopamine, is not expressed in human peripheral tissues including the kidney and therefore is not a likely explanation for normal to increased levels of urinary dopamine in AADC-deficiency. The kidney cortex contained the highest dopamine production activity and AADC-expression of human tissues we tested.
None of the mutations (genotypes) found in our population were specifically associated with either normo-, hyper- or hypodopaminuria. Furthermore, described forms of alternative splicing cannot explain this finding. The alternative splicing event in exon 1
Voorbereid document _Tessa Wassenberg_V03.indd 46Voorbereid document _Tessa Wassenberg_V03.indd 46 25/10/2021 09:3225/10/2021 09:32

47
Urinary dopamine in AADC deficiency: the unsolved paradox
leads to the same gene product, and alternative splicing of exon 3 leads to an isoform without catalytic ability. The catalytic ability of alt-DDC, formed in alternative splicing of exon 10, is unknown, but it is unlikely that this isoform explains normal to increased levels of dopamine in AADC-deficiency, since the majority of patients with mutations in exons 1–9 were able to produce normal or increased levels of urinary dopamine (Figure 2). Other forms of alternative splicing events are not described in human DDC. Because many different mutations affecting the whole DDC-gene are associated with normal or increased levels of urinary dopamine in AADC-deficiency, alternative splicing events are very unlikely to be the explanation for normal or increased function of AADC in the kidneys.
CYP2D6 is a human cytochrome P450 isoform and involved in metabolism of approximately 20% of all clinical drugs33. It is expressed in the liver, and to a lesser extent also in extrahepatic organs, e.g. in human kidney34 and brain35. Tyramine has been described as an endogenous substrate for CYP2D6 in human liver22 and in rat brain microsomes and human CYP2D6 expressing bactosomes and supersomes23. CYP2D6 catalysis involves O-demethylation and ring hydroxylation, which may lead to conversion of tyramine into dopamine36. In kidneys, tyramine conversion by CYP2D6 has not been described previously. We have shown that rat kidney microsomes can convert tyramine to dopamine in vitro. Rats express CYP2D isoforms with similar properties as human CYP2D623. However, the amount of dopamine found in urine of AADC-deficient patients can reach very high levels (Table 1), especially compared to the low levels of dopamine formation found in our in vitro experiments. Although we did not formally assess this, it does not seem likely that CYP2D6-mediated conversion of tyramine to dopamine alone can explain this finding. Notably, substrate availability (plasma tyramine) is also low in normal controls37 and AADC-deficient patients (unpublished observations). Two sources of tyramine are available in humans, namely dietary tyramine, that mostly is converted by MAO (especially in the intestines38, and AADC-dependent endogenous synthesis from tyrosine39. Humans do not exhibit the invertebrate enzyme tyrosine decarboxylase (TDC; EC4.1.1.25) and solely rely on AADC for this catalysis40 (Fig. 1). Like dopamine, tyramine is thought not to cross the blood brain barrier. However, tyramine levels are detectable in CSF, specific trace amines receptors exist in the brain, and plasma tyramine is increased in patients with primary headache syndromes41. Despite these drawbacks, the CYP2D6-mediated pathway of dopamine formation from tyramine is an interesting topic for further research because it may be of value in designing therapeutic strategies for AADC-deficiency, especially because this metabolic pathway is also functional in the brain.
We did neither observe protein expression of tyrosinase by IHC nor a protein band on WB in peripheral tissues that do not contain melanosomes. This is in accordance with Chen et al., who obtained negative results in kidney, and several other tissues42. However, tyrosinase mRNA was detected in, amongst others, kidney43, which apparently—
3
Voorbereid document _Tessa Wassenberg_V03.indd 47Voorbereid document _Tessa Wassenberg_V03.indd 47 25/10/2021 09:3225/10/2021 09:32

48
Chapter 3
therefore—is not translated into detectable protein levels. Although tyrosinase is able to use monohydroxy-phenols (e.g. tyrosine and tyramine) as substrate20, only mushroom tyrosinase may convert tyramine to dopamine20, 21. With our negative finding of protein expression of tyrosinase in human peripheral tissues, it is very unlikely that the hydroxylation of tyramine by tyrosinase will contribute to normal or increased levels of urinary dopamine in AADC-deficiency, let alone that available substrate levels of tyramine are low.
We did not find evidence that 3-MTYR may serve as substrate for dopamine formation in AADC-deficiency. In previous reports, the demethylation of 3-MTYR to L-dopa, or direct conversion to dopamine has been proposed14, 44, 45. Also more recently, demethylation of 3-MTYR as a source for urinary dopamine was demonstrated in vivo and in vitro in rats16. However, we neither found L-dopa nor dopamine production with 3-MTYR as substrate. It cannot be excluded that the tested conditions were not optimal for demethylation of 3-MTYR. However, the final step in dopamine formation from demethylated 3-MTYR still requires a decarboxylation step by AADC44.
We found high levels of dopamine production activity in human kidney cortex homogenate. Although the high AADC-activity in PTE-cells is established, to our knowledge, no other studies tested AADC-activity in human kidney cortex homogenate using the same conditions as we did. The only other study on human kidney cortex homogenate found an activity of only 70 nmol/min/g protein, but no vitamin B6 was added as co-factor and incubation time was much shorter46. Studies on rat kidney cortex homogenate showed similar or higher AADC-activities compared to our results47, 48. In our assay, enzyme activity is determined as dopamine production, hence no direct measurement of AADC is made and dopamine production could be dependent on other enzymes. However, we established that this dopamine production is indeed AADC-dependent, because a complete inhibition of dopamine production was reached when the peripheral AADC-inhibitor carbidopa was applied. Therefore, and in combination with our other results, in the human kidney the conversion of L-dopa to dopamine by AADC is probably the only possible pathway. The importance of L-dopa in renal dopamine formation is also illustrated in previous reports that showed an increase of urinary dopamine excretion in AADC-deficient patients with increased levels of plasma L-dopa because of L-dopa medication8, 10.
In conclusion, we found normal to increased levels of urinary dopamine in the majority of AADC-deficient patients. There are no genotype/phenotype correlations, including alternative splicing events, to explain this finding and no alternative metabolic pathways can satisfactorily explain renal dopamine formation in AADC-deficient patients. Although it does not provide an explanation for normal or increased levels of urinary dopamine, CYP2D-mediated conversion of tyramine to dopamine is possible in the
Voorbereid document _Tessa Wassenberg_V03.indd 48Voorbereid document _Tessa Wassenberg_V03.indd 48 25/10/2021 09:3225/10/2021 09:32

49
Urinary dopamine in AADC deficiency: the unsolved paradox
kidney. This finding might lead to the design of new therapeutic strategies for AADC-deficiency, e.g. by stimulating cerebral CYP2D6 activity or substrate availability.
AcknowledgmentsWe thank the referring clinicians for sharing patient material and J.D.A. Olivier, PhD, Donders Institute for Cognition, Brain and Behavior, Department of cognitive neuroscience: Molecular neurobiology, Radboud University Nijmegen Medical Centre, for providing animal material. This work was financially supported by the AADC Research Trust and Hersenstichting Nederland/Benny Vleerlaag Fonds (2009(2)-80). 3
Voorbereid document _Tessa Wassenberg_V03.indd 49Voorbereid document _Tessa Wassenberg_V03.indd 49 25/10/2021 09:3225/10/2021 09:32

50
Chapter 3
References
1. Hyland K, Surtees RA, Rodeck C, Clayton PT. Aromatic L-amino acid decarboxylase deficiency: clinical features, diagnosis, and treatment of a new inborn error of neurotransmitter amine synthesis. Neurology. 1992 10/1992;42(10):1980-8.
2. Swoboda KJ, Saul JP, McKenna CE, Speller NB, Hyland K. Aromatic L-amino acid decarboxylase deficiency: overview of clinical features and outcomes. Annals of neurology. 2003 2003;54 Suppl 6:S49-S55.
3. Brun L, Ngu LH, Keng WT, et al. Clinical and biochemical features of aromatic L-amino acid decarboxylase deficiency. Neurology. 2010 Jul 6;75(1):64-71.
4. Pons R, Ford B, Chiriboga CA, et al. Aromatic L-amino acid decarboxylase deficiency: clinical features, treatment, and prognosis. Neurology. 2004 4/13/2004;62(7):1058-65.
5. Hyland K, Clayton PT. Aromatic L-amino acid decarboxylase deficiency: diagnostic methodology. Clinical chemistry. 1992 12/1992;38(12):2405-10.
6. Abeling NG, van Gennip AH, Barth PG, van CA, Westra M, Wijburg FA. Aromatic L-amino acid decarboxylase deficiency: a new case with a mild clinical presentation and unexpected laboratory findings. Journal of inherited metabolic disease. 1998 6/1998;21(3):240-2.
7. Abdenur JE, Abeling N, Specola N, et al. Aromatic l-aminoacid decarboxylase deficiency: unusual neonatal presentation and additional findings in organic acid analysis. Mol Genet Metab. 2006 Jan;87(1):48-53.
8. Fiumara A, Brautigam C, Hyland K, et al. Aromatic L-amino acid decarboxylase deficiency with hyperdopaminuria. Clinical and laboratory findings in response to different therapies. Neuropediatrics. 2002 8/2002;33(4):203-8.
9. Ito S, Nakayma T, Ide S, et al. Aromatic l-amino acid decarboxylase deficiency associated with epilepsy mimicking non-epileptic involuntary movements. Dev Med Child Neur 2008 2008;50:876-8.
10. Abeling NG, Brautigam C, Hoffmann GF, et al. Pathobiochemical implications of hyperdopaminuria in patients with aromatic L-amino acid decarboxylase deficiency. Journal of inherited metabolic disease. 2000 6/2000;23(4):325-8.
11. Aperia AC. Intrarenal dopamine: a key signal in the interactive regulation of sodium metabolism. Annu Rev Physiol. 2000 2000;62:621-47.
12. Goldstein DS, Eisenhofer G, Kopin IJ. Sources and significance of plasma levels of catechols and their metabolites in humans. The Journal of pharmacology and experimental therapeutics. 2003 6/2003;305(3):800-11.
13. Lee MR. Dopamine and the kidney: ten years on. Clinical science. 1993 4/1993;84(4):357-75.14. Bartholini G, Kuruma I, Pletscher A. 3-O-methyldopa, a new precursor of dopamine. Nature.
1971 4/23/1971;230(5295):533-4.15. Carlsson A, Waldeck B. Formation of dopamine from 3-methoxytyrosine. Fact or artifact?
Naunyn Schmiedebergs 1972 1972;272(4):441-6.16. Ibarra FR, Aguirre J, Nowicki S, Barontini M, Arrizurieta EE, Armando I. Demethylation of
3-O-methyldopa in the kidney: a possible source for dopamine in urine. Am J Physiol. 1996 5/1996;270(5 Pt 2):F862-F8.
Voorbereid document _Tessa Wassenberg_V03.indd 50Voorbereid document _Tessa Wassenberg_V03.indd 50 25/10/2021 09:3225/10/2021 09:32

51
Urinary dopamine in AADC deficiency: the unsolved paradox
17. Fedorow H, Tribl F, Halliday G, Gerlach M, Riederer P, Double KL. Neuromelanin in human dopamine neurons: comparison with peripheral melanins and relevance to Parkinson’s disease. Prog Neurobiol 2005 2/2005;75(2):109-24.
18. Eisenhofer G, Tian H, Holmes C, Matsunaga J, Roffler-Tarlov S, Hearing VJ. Tyrosinase: a developmentally specific major determinant of peripheral dopamine. FASEB journal : official publication of the Federation of American Societies for Experimental Biology. 2003 7/2003;17(10):1248-55.
19. Rios M, Habecker B, Sasaoka T, et al. Catecholamine synthesis is mediated by tyrosinase in the absence of tyrosine hydroxylase. The Journal of neuroscience : the official journal of the Society for Neuroscience. 1999 5/1/1999;19(9):3519-26.
20. Fenoll LG, Rodriguez-Lopez JN, Varon R, Garcia-Ruiz PA, Garcia-Canovas F, Tudela J. Kinetic characterisation of the reaction mechanism of mushroom tyrosinase on tyramine/dopamine and L-tyrosine methyl esther/L-dopa methyl esther. Int J Biochem Cell Biol 2002 12/2002;34(12):1594-607.
21. Gandia-Herrero F, Escribano J, Garcia-Carmona F. Characterization of the monophenolase activity of tyrosinase on betaxanthins: the tyramine-betaxanthin/dopamine-betaxanthin pair. Planta. 2005 10/2005;222(2):307-18.
22. Hiroi T, Imaoka S, Funae Y. Dopamine formation from tyramine by CYP2D6. Biochemical and biophysical research communications. 1998 8/28/1998;249(3):838-43.
23. Bromek E, Haduch A, Daniel WA. The ability of cytochrome P450 2D isoforms to synthesize dopamine in the brain: An in vitro study. Eur J Pharmacol 2009 10/8/2009.
24. Verbeek MM, Willemsen MA, Wevers RA, et al. Two Greek siblings with sepiapterin reductase deficiency. Mol Genet Metab. 2008 8/2008;94(4):403-9.
25. Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with the Folin phenol reagent. The Journal of biological chemistry. 1951 11/1951;193(1):265-75.
26. Verbeek MM, Geurtz PB, Willemsen MA, Wevers RA. Aromatic L-amino acid decarboxylase enzyme activity in deficient patients and heterozygotes. Mol Genet Metab. 2007 4/2007;90(4):363-9.
27. Ichinose H, Sumi-Ichinose C, Ohye T, Hagino Y, Fujita K, Nagatsu T. Tissue-specific alternative splicing of the first exon generates two types of mRNAs in human aromatic L- amino acid decarboxylase. Biochemistry. 1992 11/24/1992;31(46):11546-50.
28. Sumi-Ichinose C, Ichinose H, Takahashi E, Hori T, Nagatsu T. Molecular cloning of genomic DNA and chromosomal assignment of the gene for human aromatic L-amino acid decarboxylase, the enzyme for catecholamine and serotonin biosynthesis. Biochemistry. 1992 3/3/1992;31(8):2229-38.
29. Krieger M, Coge F, Gros F, Thibault J. Different mRNAs code for dopa decarboxylase in tissues of neuronal and nonneuronal origin. Proceedings of the National Academy of Sciences of the United States of America. 1991 3/15/1991;88(6):2161-5.
30. Chang YT, Mues G, Hyland K. Alternative splicing in the coding region of human aromatic L- amino acid decarboxylase mRNA. Neuroscience letters. 1996 1/5/1996;202(3):157-60.
31. O’Malley KL, Harmon S, Moffat M, Uhland-Smith A, Wong S. The human aromatic L-amino acid decarboxylase gene can be alternatively spliced to generate unique protein isoforms. Journal of neurochemistry. 1995 12/1995;65(6):2409-16.
3
Voorbereid document _Tessa Wassenberg_V03.indd 51Voorbereid document _Tessa Wassenberg_V03.indd 51 25/10/2021 09:3225/10/2021 09:32

52
Chapter 3
32. Vassilacopoulou D, Sideris DC, Vassiliou AG, Fragoulis EG. Identification and characterization of a novel form of the human L-dopa decarboxylase mRNA. Neurochemical research. 2004 10/2004;29(10):1817-23.
33. Yu AM, Idle JR, Gonzalez FJ. Polymorphic cytochrome P450 2D6: humanized mouse model and endogenous substrates. Drug Metab Rev 2004 5/2004;36(2):243-77.
34. Nishimura M, Yaguti H, Yoshitsugu H, Naito S, Satoh T. Tissue distribution of mRNA expression of human cytochrome P450 isoforms assessed by high-sensitivity real-time reverse transcription PCR. Yakugaku Zasshi. 2003 5/2003;123(5):369-75.
35. Siegle I, Fritz P, Eckhardt K, Zanger UM, Eichelbaum M. Cellular localization and regional distribution of CYP2D6 mRNA and protein expression in human brain. Pharmacogenetics. 2001 4/2001;11(3):237-45.
36. Miller GP, Hanna IH, Nishimura Y, Guengerich FP. Oxidation of phenethylamine derivatives by cytochrome P450 2D6: the issue of substrate protonation in binding and catalysis. Biochemistry. 2001 Nov 27;40(47):14215-23.
37. Yonekura T, Kamata S, Wasa M, et al. Simultaneous determination of plasma phenethylamine, phenylethanolamine, tyramine and octopamine by high-performance liquid chromatography using derivatization with fluorescamine. Journal of chromatography. 1988 6/3/1988;427(2):320-5.
38. Rapaport MH. Dietary restrictions and drug interactions with monoamine oxidase inhibitors: the state of the art. J Clin Psychiatry. 2007 2007;68 Suppl 8:42-6.
39. Berry MD, Juorio AV, Li XM, Boulton AA. Aromatic L-amino acid decarboxylase: a neglected and misunderstood enzyme. Neurochemical research. 1996 Sep;21(9):1075-87.
40. Lange AB. Tyramine: from octopamine precursor to neuroactive chemical in insects. Gen Comp Endocrinol 2009 5/15/2009;162(1):18-26.
41. D’Andrea G, Terrazzino S, Leon A, et al. Elevated levels of circulating trace amines in primary headaches. Neurology. 2004 May 25;62(10):1701-5.
42. Chen YT, Stockert E, Tsang S, Coplan KA, Old LJ. Immunophenotyping of melanomas for tyrosinase: implications for vaccine development. Proceedings of the National Academy of Sciences of the United States of America. 1995 8/29/1995;92(18):8125-9.
43. Battyani Z, Xerri L, Hassoun J, Bonerandi JJ, Grob JJ. Tyrosinase gene expression in human tissues. Pigment Cell Res 1993 12/1993;6(6):400-5.
44. Bartholini G, Kuruma I, Pletscher A. The metabolic pathways of L-3-O-methyldopa. The Journal of pharmacology and experimental therapeutics. 1972 10/1972;183(1):65-72.
45. Chalmers JP, Davies DS, Draffan GH, Reid JL, Thorgeirsson SS. Demethylation of 3-O- methyldopa. British journal of pharmacology. 1971 10/1971;43(2):455P-6P.
46. Soares-da-Silva P, Fernandes MH, Pestana M. A comparative study on the synthesis of dopamine in the human, dog and rat kidney. Acta physiologica Scandinavica. 1993 7/1993;148(3):347-51.
47. Moreira-Rodrigues M, Sampaio-Maia B, Pestana M. Renal dopaminergic system activity in rat remnant kidney up to twenty-six weeks after surgery. Life sciences. 2009 3/27/2009;84(13- 14):409-14.
Voorbereid document _Tessa Wassenberg_V03.indd 52Voorbereid document _Tessa Wassenberg_V03.indd 52 25/10/2021 09:3225/10/2021 09:32

53
Urinary dopamine in AADC deficiency: the unsolved paradox
48. Sampaio-Maia B, Serrao P, Vieira-Coelho MA, Pestana M. Differences in the renal dopaminergic system activity between Wistar rats from two suppliers. Acta physiologica Scandinavica. 2003 5/2003;178(1):83-9.
3
Voorbereid document _Tessa Wassenberg_V03.indd 53Voorbereid document _Tessa Wassenberg_V03.indd 53 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 54Voorbereid document _Tessa Wassenberg_V03.indd 54 25/10/2021 09:3225/10/2021 09:32

CHAPTER 4
The paradox of hyperdopaminuria in aromatic l-amino acid deficiency explained
Tessa Wassenberg, Leo A.H. Monnens, Ben P.B.H. Geurtz, Ron A. Wevers, Marcel M. Verbeek, Michèl A.A.P. Willemsen
JIMD Reports 2012; 4: 39-45DOI 10.1007/8904_2011_84
Voorbereid document _Tessa Wassenberg_V03.indd 55Voorbereid document _Tessa Wassenberg_V03.indd 55 25/10/2021 09:3225/10/2021 09:32

56
Chapter 4
Abstract
Aromatic L-amino acid decarboxylase (AADC) decarboxylates 3,4-L-dihydroxyl-phenylalanine (L-dopa) to dopamine, and 5-hydroxytryptophan to serotonin. In AADC deficiency, dopamine and serotonin deficiency leads to a severe clinical picture with mental retardation, oculogyric crises, hypotonia, dystonia, and autonomic dysregulation. However, despite dopamine deficiency in the central nervous system, urinary dopamine excretion in AADC-deficient patients is normal to high.
In human, renal AADC-activity is very high compared to other tissues including brain tissue. Plasma L-dopa levels are increased in AADC deficiency. In this study, the hypothesis that in AADC deficiency relatively high-residual renal AADC-activity combined with high substrate availability of L-dopa leads to normal or elevated levels of urinary dopamine is tested and verified using 24-h urine collection of two AADC-deficient patients.
Renal dopamine is a major regulator of natriuresis and plays a crucial role in the maintenance of sodium homeostasis. Therefore, the preservation of sufficient renal AADC-activity in AADC deficiency might be crucial for survival of AADC-deficient patients.
In this study, we underpinned an empirical finding with theory, thereby putting a clinical observation into its physiological context. Our study stresses the difference - not qualitatively but quantitatively - between dopamine production in the central nervous system and peripheral organs. Furthermore, this study clarifies the so far unexplained observation that neurotransmitter profiles in urine should be interpreted with extreme caution in the diagnostic work-up of patients suspected to suffer from neurometabolic disorders.
Voorbereid document _Tessa Wassenberg_V03.indd 56Voorbereid document _Tessa Wassenberg_V03.indd 56 25/10/2021 09:3225/10/2021 09:32

57
The paradox of hyperdopaminuria in AADC deficiency explained
Introduction
Aromatic l-amino acid decarboxylase (AADC; EC 4.1.1.28) decarboxylates 3,4-l-dihydroxylphenylalanine (L-dopa) to dopamine, and 5-hydroxytryptophan to serotonin (Figure 1). AADC deficiency (OMIM 608643) is a rare autosomal recessive neurometabolic disorder characterized by mental retardation, oculogyric crises, hypotonia, dystonia, and autonomic dysregulation1. Unfortunately, no successful therapeutic strategies are available.
Figure 1. Overview of the biosynthesis of serotonin and the catecholamines (dopamine, norepi-nephrine, and epinephrine).
Figure 1. Abbreviations: PhH phenylalanine hydroxylase, BH 4 tetrahydrobiopterine, TH tyrosine hydroxylase, TrH tryptophan hydroxylase, AADC aromatic l-amino acid decarboxylase, l -dopa l-3,4-dihydroxyphenylalanine, Vit B6 vitamin B6, COMT catechol-O-methyl-transferase, DβH dopamine β hydroxylase, PNMT phenyletholamine N-methyltransferase, MAO monoamine oxidase, AD aldehyde dehydrogenase, DOPAC dihydroxyphenylacetic acid, 3-MT 3-methoxytyramine, AR aldehyde reductase, ADH alcohol dehydrogenase, DHPG 3,4-dihydroxyphenylethyleneglycol, MHPG 3-methoxy 4-hydroxyphenylethyleneglycol, 5-HIAA 5-hydroxy indole acetic acid, HVA homovanillic acid, VMA vanilmandelic acid. Dopal, dopegal, and mopegal are intermediate aldehydes.
4
Voorbereid document _Tessa Wassenberg_V03.indd 57Voorbereid document _Tessa Wassenberg_V03.indd 57 25/10/2021 09:3225/10/2021 09:32

58
Chapter 4
Urine is easily accessible for diagnostic purposes and is often used in the diagnostic work-up of neurometabolic disorders. However, its usefulness to diagnose these disorders is limited, e.g., it is not appropriate in the case of tyrosine hydroxylase deficiency2. Urinary vanillactic acid (VLA), a catabolic end-product of L-dopa, is increased in AADC deficiency. However, in some patients urinary VLA is only mildly increased1, and most laboratories do not include VLA in their organic acid analysis3. Furthermore, the neurotransmitter profile in urine shows unexpected findings in AADC deficiency, not at all reflecting the deficiencies in the central nervous system as found in the cerebrospinal fluid (CSF). Most notably, the majority of AADC-deficient patients shows paradoxically normal or even increased levels of free urinary dopamine and homovanillic acid (HVA)4,
5, the metabolic end-product of dopamine breakdown. This is paradoxical because renal dopamine production, taking place in proximal tubular epithelial (PTE)-cells in the renal cortex, is thought to be AADC-dependent6, 7. In a recent study, we confirmed the presence of high AADC-activity in normal human renal cortex and found no alternative metabolic pathways of renal dopamine formation4.
Complete loss of AADC-activity is thought to be incompatible with life, as is complete loss of catalytic activity of tyrosine hydroxylase, the neighboring enzyme in dopamine biosynthesis8. In line with this assumption, in almost all AADC-deficient patients, some residual plasma AADC-activity can be demonstrated3. It is very likely that PTE-cells of AADC-deficient patients will also exhibit residual AADC-activity. In this chapter, we tested the hypothesis that residual renal AADC-activity combined with high levels of substrate availability (L-dopa from plasma) is sufficient to account for urinary dopamine excretion in AADC-deficient patients.
Methods
Data CollectionA 24-h urine collection and a single venous blood sample were obtained from a 6-years-old AADC-deficient male patient (patient 1), first reported in 2007 3 and a 9-months-old male patient (patient 2) not previously described. Patient 1 used selegiline (monoamine oxidase (MAO)-B inhibitor) 6 mg/day and vitamin B6 100 mg/day as medication. Patient 2 did not use any relevant medication at the moment of sampling. Informed parental consent and approval of the Medical Ethical Committee of the Radboud University Nijmegen were obtained for this study. In urine, creatinine, L-dopa, HVA, DOPAC, and dopamine were determined using standard HPLC procedures. In plasma, L-dopa, HVA, and AADC-activity, the latter as described previously3, were determined. Plasma dopamine was determined but was below the detection limit (nM range). Glomerular filtration rate (GFR) was determined by creatinine clearance using the following standard formula: GFR (mL/min) = (urine creatinine (μmol/L)/plasma creatinine (μmol/L)) × urine production (mL/min).
Voorbereid document _Tessa Wassenberg_V03.indd 58Voorbereid document _Tessa Wassenberg_V03.indd 58 25/10/2021 09:3225/10/2021 09:32

59
The paradox of hyperdopaminuria in AADC deficiency explained
Calculation of L-dopa Availability and Dopamine ProductionIf urinary dopamine arises from blood-derived L-dopa, filtered L-dopa should exceed urinary dopamine plus urinary HVA and DOPAC because dopamine is metabolized, ultimately to HVA, inside PTE-cells (Figs. 1 and 2)9. Furthermore, a portion of dopamine formed inside PTE-cells will be taken up into the body by basolateral reabsorption of dopamine. However, this uptake is very small compared to dopamine excretion10, 11 and, therefore, neglected in the following calculation. Once secreted in the tubulus, virtually no reabsorption of dopamine12 and HVA13 takes place. Urinary HVA is partially derived from the blood and partially formed within the kidneys14. The following calculations were used to estimate the amount of substrate availability (L-dopa) and extent of metabolism of dopamine:
Calculations:
(Ia) L-dopa filtered load (nmol/min) = GFR(mL/min) x L-dopa in plasma (nmol/mL)(Ib) L-dopa excretion (nmol/min) = urinary L-dopa (nmol/mL) x urine production
(mL/min)(Ic) Substrate availability (nmol/min) = (Ia) – (Ib)(II) Dopamine excretion (nmol/min) = urinary dopamine (nmol/mL) x urine
production (mL/min)(III) DOPAC excretion (nmol/min) = urinary DOPAC x urine production (mL/min)(IVa) HVA filtered load (nmol/min) = GFR x plasma HVA (nmol/L)(IVb) HVA excretion (nmol/min) = urinary HVA (nmol/ml) x urine production (ml/min)(IVc) Renal metabolism of dopamine to HVA (nmol/min) = (IVb) – (IVa)(V) Renal dopamine production: II+III+Ivc
Equation (A): Substrate availability should be greater than renal dopamine production:
(A) : (Ic)>(V)
4
Voorbereid document _Tessa Wassenberg_V03.indd 59Voorbereid document _Tessa Wassenberg_V03.indd 59 25/10/2021 09:3225/10/2021 09:32

60
Chapter 4
Figure 2. Renal handling of L-dopa
Figure 2. Schematic representation of renal handling of L-dopa and its metabolites. Dopamine filtration and reabsorption, shown in gray, is very small compared to dopamine formation and excretion, and therefore not considered in the calculation of L-dopa availability. L-dopa is decarboxylated to dopamine inside proximal tubular epithelium cells, and metabolism of newly formed dopamine (simplified representation) also takes place inside these cells. Roman numbers indicate formulas that are given in the text. Ia: L-dopa filtered load. Ib: L-dopa excretion. Ic: L-dopa reabsorption. II: dopamine excretion. III: DOPAC excretion. IVa: HVA filtered load. IVb: HVA excretion. IVc: HVA renal production (adapted from Wassenberg T et al, JIMD Reports 2012)
Renal AADC-Activity with In Vivo Range of L-dopa SupplyHuman renal AADC-activity is 100 to 1000 times higher than plasma AADC-activity when tested with micromolar to millimolar L-dopa concentrations4, 15, 16. Although no material was available to actually measure residual renal AADC-activity in kidney homogenate of AADC-deficient patients, it seems inevitable that there will be at least some residual enzyme activity since complete loss of AADC-function is considered incompatible with life8, and because some residual AADC-activity is also found in plasma of (almost all) AADC-deficient patients. Renal dopamine biosynthesis depends on AADC-activity and substrate availability. In vivo, substrate availability to PTE-cells of AADC-deficient patients will be in the nanomolar range. To investigate renal AADC-activity with L-dopa availability as present in vivo, dopamine production in human kidney homogenate was
Voorbereid document _Tessa Wassenberg_V03.indd 60Voorbereid document _Tessa Wassenberg_V03.indd 60 25/10/2021 09:3225/10/2021 09:32

61
The paradox of hyperdopaminuria in AADC deficiency explained
tested under Michaelis–Menten conditions with L-dopa concentrations ranging from 0 to 1,000 μM in AADC-activity assays as previously described4.
Results
Patient characteristics are shown in Table 1, and results of calculations are shown in Table 2. The urinary dopamine level of both AADC-deficient patients was increased compared to age matched controls. Urinary L-dopa excretion (Ib) was found to be less than the filtered L-dopa (Ia) leading to L-dopa substrate availability (Ic) of 20 (patient 1) and 18 (patient 2) nmol/min. Equation (A) was confirmed in both patients with renal dopamine production being three (patient 1) or two (patient 2) times less than L-dopa substrate availability and, therefore, dopamine production could have originated from filtered L-dopa.
The substrate curve of AADC-activity for human kidney cortex homogenate is shown in Fig. 3a (0–1,000 μM) and Fig. 3b (0–100 μM). At L-dopa availability in the nanomolar/ low micromolar range, the relation between AADC-activity and L-dopa availability is linear. In other words, small increase in substrate availability will lead to high increase in dopamine production.
Table 1. Patient Characteristics
Patient 1 Patient 2
Sex, age (years) M, 6 M, 0.8
Medication Vit B6, selegiline none
Length (cm), Weight (kg) 107, 15 70, 9.2
Urine production (ml/min) 0.1 0.5
Plasma creatinine (µmol/l) 27 23
Urine creatinine (µmol/l) 7500 1500
GFR (mL/min) 30 32.4
Plasma L-dopa (nmol/ml) 0.8 0.8
Urine L-dopa (nmol/ml) 35.3 19.1
Plasma HVA (nmol/ml) 0.05 0.003
Urine HVA (nmol/ml) 51 13.1
Urine DOPAC (nmol/ml) 11.3 5.9
Plasma DA (nmol/ml) ND ND
Urine DA (nmol/ml) 10.2 2.4
Serum AADC-activity (nmol/min/l) 0.3 1.7
4
Voorbereid document _Tessa Wassenberg_V03.indd 61Voorbereid document _Tessa Wassenberg_V03.indd 61 25/10/2021 09:3225/10/2021 09:32

62
Chapter 4
Table 2. Results of calculations
Patient 1 Patient 2
Ia L-dopa filtered load (nmol/min) 24 27
Ib L-dopa excretion (nmol/min) 4 10
Ic L-dopa substrate availability (IIa-IIb) (nmol/min) 20 18
II Dopamine excretion (nmol/min) 1.1 1.2
III DOPAC excretion (nmol/min) 1.1 2.9
IVa HVA filtered load (nmol/min) 1.4 0.1
IVb HVA excretion (nmol/min) 5.5 6.5
IVc Renal metabolism of dopamine to HVA (IVb-IVa) (nmol/min) 4.2 6.4
V Renal dopamine production (II+III+IVc) (nmol/min) 6.5 10.5
A Ic > V Yes Yes
Figure 3. Substrate curves for AADC-activity of human renal cortex
Substrate curves for AADC-activity of human renal cortex with an L-dopa concentration of 0-1000 μM (3a) and 0-100 μM (3b). AADC-activity was measured as dopamine production in nmol/min/L. Figure adapted from Wassenberg T, JIMD Reports 2012.
Discussion
In this chapter, we showed that the – seemingly paradoxical – finding of normal or increased levels of urinary dopamine in AADC deficiency can be explained by the combination of three factors. First, AADC deficiency is characterized by profoundly diminished, but not totally absent, enzymatic activity as confirmed by measurement of
Voorbereid document _Tessa Wassenberg_V03.indd 62Voorbereid document _Tessa Wassenberg_V03.indd 62 25/10/2021 09:3225/10/2021 09:32

63
The paradox of hyperdopaminuria in AADC deficiency explained
residual plasma AADC-activity in almost all patients3. Second, human kidneys have an efficient system to synthesize dopamine from blood derived L-dopa as reflected by the very high AADC-activity found in kidney cortex compared to other organs including the brain. Third, as the consequence of the metabolic defect, large amounts of substrate (i.e., L-dopa in plasma) are readily available for the kidneys of AADC-deficient patients. We hypothesized that the combination of these three factors may logically explain urinary dopamine excretion in AADC deficiency. This hypothesis was confirmed in a process where we first defined the most appropriate theoretical calculation of urinary dopamine excretion, and subsequently demonstrated in a clinical setting that this calculation is in line with our empirical observations of normo- or hyperdopaminuria in AADC-deficient patients.
There might be a drug-induced effect of dopamine excretion in patient 1 who used selegiline at the time of investigation. MAO-B inhibitors increase extracellular dopamine content by inhibiting dopamine breakdown, and in an experimental design Ibarra et al. showed increase of proximal tubular dopamine concentration when MAO-B inhibitors were applied17. This means that in patient 1, intratubular concentration of L-dopa – and, therefore, actual substrate availability – was higher than calculated and that use of selegiline does not conflict with the outcome of Equation (A).
Dopamine is a major regulator of the body’s sodium homeostasis. Experimental studies showed that rats with reduced renal mass showed increased dopamine production per gram tissue9. In humans with reduced renal perfusion, dopamine excretion is not decreased18. It is not surprising that the body is capable of increasing dopamine production in certain situations, because renal dopamine is crucial in natriuresis and maintenance of sodium homeostasis19. Therefore, the preservation of sufficient renal AADC-activity in AADC deficiency, although leading to seemingly paradoxical normal or increased levels of urinary dopamine, might be crucial for the survival of AADC-deficient patients.
A methodological consideration might be that we did not use healthy, age-matched controls to prove that L-dopa substrate availability is sufficient to explain the amount of urinary dopamine that is normally excreted. However, it has been clearly shown in the literature that L-dopa is the substrate for renal dopamine biosynthesis7, 20, and in a systematic study, we have not found any alternative metabolic pathways to explain renal dopamine formation in AADC-deficient patients4. Furthermore, a direct relationship between L-dopa availability and renal dopamine excretion is illustrated by the observation that urinary dopamine levels increase upon L-dopa medication, both in normal controls21, and AADC-deficient patients5, 22.
4
Voorbereid document _Tessa Wassenberg_V03.indd 63Voorbereid document _Tessa Wassenberg_V03.indd 63 25/10/2021 09:3225/10/2021 09:32

64
Chapter 4
Another consideration is that we present a theoretical calculation which gives a simplified representation of renal physiology. We think that the most important simplification might be that we have assumed a one to one ratio of L-dopa concentrations in PTE-cells and the intraluminal compartment of the proximal tubule. It could be argued that this ratio is not physiologically correct and that deviations from this ratio would interfere with the accuracy of the model. Indeed, L-dopa uptake in PTE-cells is mediated by active transport23, and under experimental conditions up to 70 times higher L-dopa concentrations are found inside cultured renal epithelial cells than in the culture medium24-26. Reported intracellular concentrations24, 26 are in the linear part of the substrate curve (Fig. 3b), and increasing amounts of available L-dopa inside PTE-cells will, therefore, lead to linear increases of dopamine production. In our model, this means that substrate availability (freely filtered tubular L-dopa) will lead to even higher intracellular dopamine concentrations and, therefore, higher dopamine production than calculated. Altogether, the most critical assumption in our model of renal dopamine handling does not conflict with the main conclusions of this study.
Take-Home Message
The combination of residual renal AADC-activity and pathologic increases of L-dopa substrate availability explains normo- to hyperdopaminuria in AADC-deficient patients.
Voorbereid document _Tessa Wassenberg_V03.indd 64Voorbereid document _Tessa Wassenberg_V03.indd 64 25/10/2021 09:3225/10/2021 09:32

65
The paradox of hyperdopaminuria in AADC deficiency explained
References
1. Brun L, Ngu LH, Keng WT, et al. Clinical and biochemical features of aromatic L-amino acid decarboxylase deficiency. Neurology. 2010 Jul 6;75(1):64-71.
2. Willemsen MA, Verbeek MM, Kamsteeg EJ, et al. Tyrosine hydroxylase deficiency: a treatable disorder of brain catecholamine biosynthesis. Brain : a journal of neurology. 2010 Jun;133(Pt 6):1810-22.
3. Verbeek MM, Geurtz PB, Willemsen MA, Wevers RA. Aromatic L-amino acid decarboxylase enzyme activity in deficient patients and heterozygotes. Mol Genet Metab. 2007;90(4):363-9.
4. Wassenberg T, Willemsen MA, Geurtz PB, et al. Urinary dopamine in aromatic L-amino acid decarboxylase deficiency: the unsolved paradox. Mol Genet Metab. 2010 Dec;101(4):349-56.
5. Abeling NG, Brautigam C, Hoffmann GF, et al. Pathobiochemical implications of hyperdopaminuria in patients with aromatic L-amino acid decarboxylase deficiency. Journal of inherited metabolic disease. 2000;23(4):325-8.
6. Baines AD, Drangova R, Hatcher C. Dopamine production by isolated glomeruli and tubules from rat kidneys. Can J Physiol Pharmacol 1985;63(2):155-8.
7. Soares-da-Silva P, Fernandes MH. Synthesis and metabolism of dopamine in the kidney. Effects of sodium chloride, monoamine oxidase inhibitors and alpha-human atrial natriuretic peptide. American journal of hypertension. 1990;3(6 Pt 2):7S-10S.
8. Chen L, Zhuang X. Transgenic mouse models of dopamine deficiency. Annals of neurology. 2003;54 Suppl 6:S91-102.
9. Sampaio-Maia B, Moreira-Rodrigues M, Pestana M. Role of chronic inhibition of dopamine- metabolizing enzymes in the regulation of renal sodium and phosphate excretion in the rat remnant kidney. Nephron Physiol. 2006;103(1):p14-24.
10. Eisenhofer G, Aneman A, Friberg P, et al. Substantial production of dopamine in the human gastrointestinal tract. The Journal of clinical endocrinology and metabolism. 1997 11/1997;82(11):3864-71.
11. Wang Y, Berndt TJ, Gross JM, Peterson MA, So MJ, Knox FG. Effect of inhibition of MAO and COMT on intrarenal dopamine and serotonin and on renal function. American journal of physiology Regulatory, integrative and comparative physiology. 2001;280(1):R248- R54.
12. Chan YL. Cellular mechanisms of renal tubular transport of I-dopa and its derivatives in the rat: microperfusion studies. The Journal of pharmacology and experimental therapeutics. 1976;199(1):17-24.
13. Pestana M, Jardim H, Correia F, Vieira-Coelho MA, Soares-da-Silva P. Renal dopaminergic mechanisms in renal parenchymal diseases and hypertension. Nephrol Dial Transplant 2001;16 Suppl 1:53-9.
14. Goldstein DS, Eisenhofer G, Kopin IJ. Sources and significance of plasma levels of catechols and their metabolites in humans. The Journal of pharmacology and experimental therapeutics. 2003;305(3):800-11.
15. Moreira-Rodrigues M, Sampaio-Maia B, Pestana M. Renal dopaminergic system activity in rat remnant kidney up to twenty-six weeks after surgery. Life sciences. 2009;84(13- 14):409-14.
4
Voorbereid document _Tessa Wassenberg_V03.indd 65Voorbereid document _Tessa Wassenberg_V03.indd 65 25/10/2021 09:3225/10/2021 09:32

66
Chapter 4
16. Sampaio-Maia B, Serrao P, Vieira-Coelho MA, Pestana M. Differences in the renal dopaminergic system activity between Wistar rats from two suppliers. Acta physiologica Scandinavica. 2003;178(1):83-9.
17. Ibarra FR, Armando I, Nowicki S, et al. Dopamine is metabolised by different enzymes along the rat nephron. Pflugers Arch 2005;450(3):185-91.
18. Soares-da-Silva P, Pestana M, Ferreira A, Damasceno A, Polonia J, Cerqueira-Gomes M. Renal dopaminergic mechanisms in renal parenchymal diseases, hypertension, and heart failure. Clin Exp Hypertens. 2000 (3):251-68.
19. Aperia AC. Intrarenal dopamine: a key signal in the interactive regulation of sodium metabolism. Annu Rev Physiol. 2000;62:621-47.
20. Baines AD, Chan W. Production of urine free dopamine from DOPA; a micropuncture study. Life sciences. 1980;26(4):253-9.
21. Barthelmebs M, Mbou P, Stephan D, Grima M, Imbs JL. Renal dopamine excretion in healthy volunteers after oral ingestion of L-dopa. Fundam Clin Pharmacol. 1993;7(1):11-6.
22. Fiumara A, Brautigam C, Hyland K, et al. Aromatic L-amino acid decarboxylase deficiency with hyperdopaminuria. Clinical and laboratory findings in response to different therapies. Neuropediatrics. 2002;33(4):203-8.
23. Quinones H, Collazo R, Moe OW. The dopamine precursor L-dihydroxyphenylalanine is transported by the amino acid transporters rBAT and LAT2 in renal cortex. American journal of physiology Renal physiology. 2004;287(1):F74-F80.
24. Soares-da-Silva P, Vieira-Coelho MA, Serrao MP. Uptake of L-3,4-dihydroxyphenylalanine and dopamine formation in cultured renal epithelial cells. Biochem Pharmacol 1997;54(9):1037-46.
25. Soares-da-Silva P, Serrao MP, Vieira-Coelho MA. Apical and basolateral uptake and intracellular fate of dopamine precursor L-dopa in LLC-PK1 cells. Am J Physiol. 1998;274(2 Pt 2):F243-F51.
26. Vieira-Coelho MA, Soares-Da-Silva P. Uptake and intracellular fate of L-DOPA in a human intestinal epithelial cell line: Caco-2. Am J Physiol. 1998 Jul;275(1):C104-12.
Voorbereid document _Tessa Wassenberg_V03.indd 66Voorbereid document _Tessa Wassenberg_V03.indd 66 25/10/2021 09:3225/10/2021 09:32

67
The paradox of hyperdopaminuria in AADC deficiency explained
4
Voorbereid document _Tessa Wassenberg_V03.indd 67Voorbereid document _Tessa Wassenberg_V03.indd 67 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 68Voorbereid document _Tessa Wassenberg_V03.indd 68 25/10/2021 09:3225/10/2021 09:32

CHAPTER 5
Blood, urine and cerebrospinal fluid analysis in TH and AADC deficiency and the effect of medical treatment
Tessa Wassenberg, Ben P.B.H. Geurtz, Leo Monnens, Ron A. Wevers RA, Michèl A.A.P. Willemsen, Marcel M. Verbeek.
Molecular Genetics and Metabolism Reports, 2021; 27: 100762.DOI: 10.1016/j.ymgmr.2021.100762.
Voorbereid document _Tessa Wassenberg_V03.indd 69Voorbereid document _Tessa Wassenberg_V03.indd 69 25/10/2021 09:3225/10/2021 09:32

70
Chapter 5
Abstract
Background: Aromatic L-amino acid decarboxylase (AADC) deficiency and tyrosine hydroxylase (TH) deficiency are rare inherited disorders of monoamine neurotransmitter synthesis which are typically diagnosed using cerebrospinal fluid examination of monoamine neurotransmitter metabolites. Until now, it has not been systematically studied whether analysis of monamine neurotransmitter metabolites in blood or urine has diagnostic value as compared to cerebrospinal fluid examination, or whether monoamine neurotransmitter metabolites in these peripheral body fluids is useful to monitor treatment efficacy.
Methods: Assessment, both by literature review and retrospective analysis of our local university hospital database, of monoamine neurotransmitter metabolites in urine, blood and cerebrospinal fluid, and serum prolactin levels, before and during treatment in patients with AADC and TH deficiency.
Results: In AADC deficiency, 3-O-methyldopa in serum or dried blood spots was reported in 34 patients and found to be (strongly) increased in all, serotonin in serum was decreased in 7/7 patients. Serum prolactin was increased in 34/37 and normal in 3 untreated patients. In urine, dopamine was normal or increased in 21/24 patients, 5-hydroxyindoleacetic acid was decreased in 9/10 patients, and vanillactic acid was increased in 19/20 patients. No significant changes were seen in monoamine neurotransmitter metabolites after medical treatment, except for an increase of homovanillic acid in urine and cerebrospinal fluid after levodopa therapy, sometimes even in absence of a clinical response. After gene therapy, cerebrospinal fluid homovanillic acid increased in most patients (8/12), but 5-hydroxyindoleacetic acid remained unchanged in 9/12 patients.In TH deficiency, serum prolactin was increased in 12/14 and normal in the remaining untreated patients. Urinary dopamine was decreased in 2/8 patients and normal in 6. Homovanillic acid concentrations in cerebrospinal fluid increased upon levodopa treatment, even in the absence of a clear treatment response.
Conclusions: This study confirms that cerebrospinal fluid is the most informative body fluid to measure monoamine neurotransmitter metabolites when AADC or TH deficiency is suspected, and that routine follow-up of cerebrospinal fluid measurements to estimate treatment response is not needed. 3-O-methyldopa in dried blood spots and vanillactic acid in urine are promising peripheral biomarkers for diagnosis of AADC deficiency. However, in many patients with TH or AADC deficiency dopamine in urine is normal or increased thereby not reflecting the metabolic block. The value of serum prolactin for follow-up of AADC and TH deficiency should be further studied.
Voorbereid document _Tessa Wassenberg_V03.indd 70Voorbereid document _Tessa Wassenberg_V03.indd 70 25/10/2021 09:3225/10/2021 09:32

71
Blood, urine and CSF in TH and AADC deficiency
Introduction
Monoamine neurotransmitter deficiencies are rare, usually autosomal recessively inherited neurometabolic disorders in which an enzyme deficiency leads to impaired synthesis, metabolism, or transport of catecholamines (dopamine, norepinephrine and epinephrine) and/or serotonin, depending on the specific deficiency1. In aromatic L-amino acid decarboxylase (AADC; EC 4.1.1.28) deficiency synthesis of serotonin and catecholamines2, 3 is affected, which leads to hypotonia, developmental delay, movement disorders (especially oculogyric crises), and autonomic symptoms4. Tyrosine hydroxylase (TH; EC 1.14.16.2) deficiency only affects catecholamine synthesis and clinically leads to dopa-responsive dystonia or a more severe infantile onset complex encephalopathy5. AADC and TH deficiency can be diagnosed by quantification of monoamine neurotransmitter metabolites in cerebrospinal fluid (CSF) and molecular analysis of the DDC or TH gene4, 5. In addition, AADC (but not TH) enzyme activity can be determined in plasma4. Treatment of AADC deficiency is complex and often little successful4, although promising results of gene therapy have been obtained recently6,7. Treatment of TH deficiency is often more straightforward and consists primarily of L-dopa supplementation with a peripheral decarboxylase inhibitor like carbidopa5.
TH and DDC genes are expressed throughout the body8-10, and dopamine and serotonin not only act as neurotransmitters but also as endocrine, autocrine and paracrine substances11-14. However, it is generally accepted that – in contrast to what is seen in CSF – the quantity of monoamine neurotransmitter metabolites in urine do not reflect the metabolic defect in patients with primary monoamine neurotransmitter disorders. In AADC deficiency, monoamine neurotransmitter excretion patterns have been studied quite extensively and it has been shown that urinary dopamine is often paradoxically increased due to the combination of excessive availability of the precursor L-dopa and residual enzymatic capacity of AADC in the kidneys10, 15. For monoamine neurotransmitter metabolites in blood, fewer data are available. Consensus in AADC deficiency is that urine and plasma measurements of monoamine neurotransmitter metabolites are not suitable for diagnostic purposes4, with the exception of vanillactic acid (VLA) and 3-O-methyldopa (3-OMD) in plasma4, 16 and urine17, which may serve as “red flags” that make AADC deficiency highly suspicious. In TH deficiency, urine and plasma are probably not useful for diagnostic purposes at all, but monoamine neurotransmitter metabolite patterns in both blood and urine have not been systematically studied.
Pituitary prolactin release is controlled by dopamine through a negative feedback18. Therefore, in disorders with low dopamine levels like TH and AADC deficiency, serum prolactin levels would be expected to be high. However, the diagnostic value of hyperprolactinemia in AADC deficiency is unclear4, and its significance in TH deficiency has not been systematically studied before. The serum prolactin concentration is
5
Voorbereid document _Tessa Wassenberg_V03.indd 71Voorbereid document _Tessa Wassenberg_V03.indd 71 25/10/2021 09:3225/10/2021 09:32

72
Chapter 5
easily influenced by multiple factors, including stress of a venous puncture and diurnal variation, and references ranges are age- and gender specific18. Therefore, values should always be interpreted with caution. Nonetheless, serum prolactin could be an interesting biomarker to support diagnosis, and potentially also to monitor the efficacy of treatment in patients with a primary monoamine neurotransmitter disorder. The analysis of prolactin is widely available (in contrast to analysis of monoamine neurotransmitter metabolites in body fluids, which is restricted to specialized labs), relatively cheap, and does not require a lumbar puncture. Therefore, in this study we also reviewed available data of prolactin measurements in AADC and TH deficiency before and during treatment.
The value of CSF monoamine neurotransmitter analysis to diagnose AADC and TH deficiency and many other primary monoamine disorders is solid1, 4, 5, and needs no confirmation. Routine follow-up CSF measurements are generally neither used nor needed in the management of stable patients with primary monoamine neurotransmitter deficiencies4, and therefore it is not well known how CSF profiles change due to treatment in these disorders. Therefore, we evaluated available data on CSF monoamine neurotransmitter metabolites before and during treatment.
In this study, we combined a literature review of laboratory measurements in AADC and TH deficiency with a study of the database of the Translational Metabolic Laboratory (TML) of our hospital, to analyze patterns of monoamine neurotransmitter metabolism in urine, blood, and CSF before and during treatment, and prolactin levels in blood before and during treatment. With this, we aim to further expand the knowledge on central and peripheral patterns of dopamine and serotonin metabolites, expose knowledge gaps to guide further research, and provide practical advice concerning body fluid examination in the management of these disorders.
Materials and methods
Data collectionWe searched the PubMed database using the following search terms: dopa responsive dystonia, tyrosine hydroxylase deficiency, TH-deficiency, aromatic L-amino acid decarboxylase deficiency, AADC-deficiency, and dopa decarboxylase. Language filters used were English, French, and Dutch. The last search was performed May 2020. Reference lists of all relevant papers were checked for missing articles. The TML database was searched to include all patients with TH and AADC deficiency diagnosed and/or followed in our laboratory from January 1997 until May 2020. This database contains all records of all neurochemical investigations that were performed in body fluids collected form patients for whom these ancillary laboratory investigations were indicated as part of the diagnostic process. Patients (both from the literature and TML database) were included if (I) any of the monoamine neurotransmitter metabolites
Voorbereid document _Tessa Wassenberg_V03.indd 72Voorbereid document _Tessa Wassenberg_V03.indd 72 25/10/2021 09:3225/10/2021 09:32

73
Blood, urine and CSF in TH and AADC deficiency
(dopamine, norepinephrine, epinephrine, serotonin, homovanillic acid (HVA), 5-hydroxyindole acid (5-HIAA), ratio HVA/5-HIAA, 3-methoxy 4-hydroxyphenylglycol (MHPG), 3-O-methyldopa (3-OMD), L-Dopa, 5-hydroxytryptophan (5-HTP), vanillylmandelic acid (VMA), and vanillactic acid (VLA)) were reported in urine and/or blood, and/or (II) prolactin levels were reported in serum/plasma, and/or (III) monoamine neurotransmitter metabolites in CSF were reported before and during medical treatment.
Data were excluded if it was not described if the samples were taken before or during treatment and/or no information on the method by which the patient was diagnosed (genetic analysis, CSF studies, enzyme activity) was available. For each included patient, it was recorded which core diagnostic characteristics (CSF monoamine neurotransmitter profile and/or molecular analysis in TH and AADC deficiency, and additionally AADC activity in AADC deficiency) were available. Because it was not described in most case reports if samples from different body compartments were taken on the same day – this could only be confirmed for data included in the TML database- no direct comparisons between monoamine neurotransmitter metabolites in different body compartments were made. All patients that were included in the TML database have been reported previously (Supplement A and B).
Laboratory methodologiesThe laboratory methodologies used for monoamine neurotransmitter analysis in TML have previously been described19, 20. In other laboratories, local methodologies may apply. For literature references of included articles, see supplemental material (Supplement A and B).
Data analysisReference values of monoamine neurotransmitter metabolites are age dependent and differ between different laboratories. In order to be able to compare data, we classified values as decreased, normal, or increased according to the reference range in the corresponding laboratory. We defined mildly decreased as 50–99% of lower limit of reference range, moderately decreased as 10–49% of lower limit of reference range, strongly decreased as <10% of lower limit of reference range, mildly increased as 101–199% of upper limit of reference range, moderately increased as 200–499% of upper limit of reference range, and strongly increased as ≥500% of upper limit of reference range. To compare monoamine neurotransmitter metabolites in CSF before and during treatment, 1-tailed dependent t-test was used for all measurements except 3-OMD (1-tailed independent t-test). These basic statistical analyses were performed using Microsoft Windows Excel 2007. For prolactin, measurements were classified as decreased, normal, or increased compared to reported reference value
5
Voorbereid document _Tessa Wassenberg_V03.indd 73Voorbereid document _Tessa Wassenberg_V03.indd 73 25/10/2021 09:3225/10/2021 09:32

74
Chapter 5
Ethical considerationsThis study was in accordance with the International Declaration of Helsinki and consisted of purely retrospective and anonymous use of data. The retrospective use of data from the TML database was approved by the local ethical committee of Radboud university medical center (registration number: 2016-3011).
Results
Supplements A (AADC deficiency) and B (TH deficiency) give an overview of included patients regarding reference (TML and/or literature), core diagnostic tests which were reported to ascertain diagnosis, and which data was available for inclusion to answer our research questions. In TH deficiency, we found no reports of monoamine neurotransmitter metabolites in blood.
AADC deficiency: monoamine neurotransmitter metabolites in plasma en DBS in untreated patientsThe profile of monoamine neurotransmitter metabolites in untreated patients is summarized in Table 1, and resembles the profile found in CSF with high levels of metabolites upstream from the metabolic defect (L-dopa, 3-OMD and 5-HTP), and decreased levels of metabolites downstream from the metabolic defect (HVA, VMA, MHPG, NE, E, 5-HIAA, 5-HTP and serotonin), except that in one patient a normal 5-HIAA level was reported. Measurements in more than five patients were present for serotonin (n = 7) and 3-OMD (n = 34) only. 3-OMD was increased in all patients. When a precise value was reported, 3-OMD was always very strongly increased (766–13.350% of upper limit of reference range, median 2312%).
Table 1. Profile of monoamine neurotransmitter metabolites in plasma in untreated patients with AADC deficiency
L-dopa 3-OMD HVA VMA MHPG NE E 5-HTP 5-HIAA 5-HT
N 5 34 3 3 4 3 2 3 2 1 7
Result ↑↑↑ ↑↑↑* ↓↓ ↓↓ ↓↓ ↓↓ ↓↓↓ ↑↑↑ ↓↓↓ n ↓↓-↓↓↓
Table legend: Description of monoamine neurotransmitter metabolites in plasma in untreated patients with AADC deficiency. ↓: mildly decreased (50-99% of lower limit of reference range) ↓↓: moderately decreased (10-49% of lower limit of reference range ), ↓↓↓: strongly decreased (<10% of lower limit of reference range), ↑: mildly increased (101-199% of upper limit of reference range); ↑↑: moderately increased (200-499% of upper limit of reference range), ↑↑↑: strongly increased (>500% of upper limit of reference range), n = normal.*only in 13 patients a precise value was given, the others were described as ‘increased’. 3-OMD was measured in DBS in 29 patients and in plasma in 5 patients.Abbreviations: 3-OMD: 3-O-methyldopa, DBS: dried blood spot; HVA: homovanillic acid; VMA: vanillylmandelic acid; NE: norepinephrine, E: epinephrine, 5HTP: 5-hydroxytryptophane, 5HIAA: 5-hydroxyindoleacetic acid ; 5HT: serotonin.
Voorbereid document _Tessa Wassenberg_V03.indd 74Voorbereid document _Tessa Wassenberg_V03.indd 74 25/10/2021 09:3225/10/2021 09:32

75
Blood, urine and CSF in TH and AADC deficiency
AADC deficiency: monoamine neurotransmitter metabolites in plasma during treatmentIn three patients, monoamine neurotransmitter metabolites in plasma could be compared before and during two treatment strategies. Under vitamin B6 monotherapy, which gave no clear clinical response in these three patients, 5-HTP, 3-OMD, L-DOPA, 5-HT and NE remained unchanged. Epinephrine was reported in two patients and remained below detection limit21,22. Treatment with vitamin B6 and tranylcypromine (a MAO inhibitor) yielded some positive effects in these patients with improvement in muscle tone and oculogyric crises. Biochemically, MHPG increased from 15% to 86% of lower limit of reference range in one patient, norepinephrine normalized in two patients, epinephrine remained below detection limit in two patients, and serotonin increased from strongly to moderately decreased in two patients, but did not change in another patient. L-DOPA, 3-OMD and 5-HTP remained strongly elevated in all three patients, although 3-OMD levels diminished by about 50%21, 22.
Table 2. Profile of monoamine neurotransmitter metabolites in urine in untreated AADC and TH deficiency
Table 2a. AADC deficiency
AADCD VLA 3-OMD 5HIAA HVA VMA DA NE E
N 1 21 1 5 9 1 1 6 7 3 3 9 12 4 2 5
Result n ↑↑↑* n ↑↑↑ ↓↓↓-↓ n ↓ n ↓↓-↓ n ↓ n ↑↑↑-↑ ↓↓↓-↓↓ n ↓↓↓-↓↓
Table 2b. TH deficiency
THD VLA 3-OMD 5HIAA HVA VMA DA NE E
N - - 7 1 8 3 8 1 2 6 5 3 1 6 1
Result n ↑ ↓↓↓-↓ n ↓↓↓-↓ n ↓↓ n ↓↓-↓ n ↓↓↓ n ↑↑
Table legend: Description of monoamine neurotransmitter metabolites in urine in untreated patients with AADC (2a) and TH deficiency (2b).↓: mildly decreased (50-99% of lower limit of reference range) ↓↓: moderately decreased (10-49% of lower limit of reference range ), ↓↓↓: strongly decreased (<10% of lower limit of reference range), ↑: mildly increased (101-199% of upper limit of reference range); ↑↑: moderately increased (200-499% of upper limit of reference range), ↑↑↑: strongly increased (>500% of upper limit of reference range), n = normal.* in 16/21 patients, no value was given, only a description (increased).Abbreviations: AADCD: AADC deficiency, n: number of patients in which data was recorded. THD: tyrosine hydroxylase deficiencyVLA: vanillactic acid, 3-OMD: 3-O-methyldopa, 5HIAA: 5-hydroxyindoleacetic acid, HVA: homovanillic acid; VMA: vanillylmandelic acid; DA: dopamine; NE: norepinephrine, E: epinephrine
5
Voorbereid document _Tessa Wassenberg_V03.indd 75Voorbereid document _Tessa Wassenberg_V03.indd 75 25/10/2021 09:3225/10/2021 09:32

76
Chapter 5
AADC deficiency: monoamine neurotransmitter metabolites in urineThe profile of monoamine neurotransmitter metabolites in urine of untreated patients is summarized in Table 2a. Although urine measurements were recorded in 49 patients with AADC deficiency (Supplement A), simultaneously reported multiple metabolites were available for only 15 patients, of which for four only measurements during treatment were available.
Urine before treatment did not reflect the typical CSF profile in most patients, with normal HVA in 6/7 patients and normal or increased dopamine in 21/24 patients. Urinary epinephrine was decreased in all patients. 5-HIAA was decreased in most patients (9/10), and normal in one. VLA in urine was reported in 20 patients and was increased in 19 of them. The patient with normal VLA levels in urine had a severe classical phenotype of AADC deficiency complicated by epilepsy and was genetically confirmed (p.R347Q homozygous), but neither CSF analysis nor AADC enzyme activity was available23. 3-OMD in urine was reported in 6 patients, and was normal in one patient and increased in five. There was insufficient data available for other monoamine neurotransmitter metabolites.
Upon treatment with L-dopa there was a strong increase of HVA and dopamine. Epinephrine did not clearly increase in response to different treatment regimens and remained decreased in all patients.
AADC deficiency: serum prolactinSerum prolactin was reported in 37 untreated patients with AADC deficiency. Concentrations were increased in 34 patients and normal in three. In two patients, the treatment effect of rotigotine (a dopamine agonist) and vitamin B6 was reported, with normalization of prolactin levels24. In two patients, only measurements during treatment (vitamin B6 in one, DA-agonist, vitamin B6 and MAO-inhibitor in the other) were given, and also showed normal prolactin levels.
AADC deficiency: CSF monoamine neurotransmitter metabolites before and during medical treatmentCSF HVA and 5-HIAA measurements could be compared in untreated and treated condition in 14 patients.
As expected, HVA and 5-HIAA were decreased in all these untreated patients (mean HVA 25.5% of lower limit of reference range, range 2.3–54.5%; mean 5-HIAA 12.5% of lower limit of reference range, range 0.0–41.6%). The CSF MHPG concentration in untreated patients was decreased in nine patients (mean percentage of lower limit of reference range 19.5%, range 4.1–43.3%) but normal in one.
Voorbereid document _Tessa Wassenberg_V03.indd 76Voorbereid document _Tessa Wassenberg_V03.indd 76 25/10/2021 09:3225/10/2021 09:32

77
Blood, urine and CSF in TH and AADC deficiency
Treatment conditions were variable and consisted of dopamine agonists, MAO-inhibitors, vitamin B6, L-dopa, or selective serotonin reuptake inhibitors in various combinations. HVA levels in CSF could increase, remain stable or decrease upon treatment. Significant HVA increase was only reached when treatments included L-dopa, a drug which is only effective in a small subset of patients with AADC deficiency due to L-dopa responsive mutations. In three of these responsive patients (siblings), normalization of the HVA level was reached upon treatment with L-dopa and vitamin B6. One other, clinically non-responsive, patient also had normalization of HVA level under treatment with L-dopa, vitamin B6 and a MAO-inhibitor. 5-HIAA and MHPG levels did not change significantly upon treatment, regardless of whether L-dopa was used or not.
Table 3. Summary of CSF findings before and during medical treatment in AADC and TH-deficiency
AADC deficiencyUntreated
Mean (range)Number of patients
AADC deficiency Treated(L-dopa excluded)
Mean(range)p-valueNumber of patients
AADC deficiencyTreated(total, L-dopa included
Mean(range)p-value Numberof patients
TH deficiencyUntreated
Mean (range)Number of patients
TH deficiencyTreated
Mean(range)p-value Numberof patients
HVA ↓↓(↓↓↓-↓)n=14
↓↓(↓-↓↓)p=0.14n =9
↓(↓↓-n)p=0.03 n=14
↓↓(↓↓↓-↓)n=16
↓(↓↓↓-↑)p<0.001n=16
5-HIAA ↓↓(↓↓↓-↓↓)n=14
↓↓(↓↓↓-↓)p=0.22n=9
↓↓(↓↓↓-↓)p=0.07n=14
n(↓-↑)n=16
n(↓-↑)p=0.06n=16
MHPG ↓↓(↓↓↓-n)n=10
↓↓↓(↓↓↓- ↓↓)p=0.05 n=6
↓↓(↓↓↓-n)p=0.47n=10
↓↓(↓↓↓-↓)n=9
↓(↓↓↓ - n)p=0.01n=9
3-OMD ↑↑↑(↑↑-↑↑↑)n=9
↑↑↑(↑↑-↑↑↑)p=0.29n=7
↑↑↑(↑↑-↑↑↑)p=0.06n=9
n(↓↓↓ - n)n=14*
↑↑↑(↑↑-↑↑↑)p<0.001n=13*
L-dopa ↑↑↑(↑-↑↑↑)n=10
↑↑(↑↑-↑↑↑)p=0.03n= 7
↑↑↑(↑↑-↑↑↑)p=0.13n=10
No data ↑↑(n - ↑↑↑)n=6
5
Voorbereid document _Tessa Wassenberg_V03.indd 77Voorbereid document _Tessa Wassenberg_V03.indd 77 25/10/2021 09:3225/10/2021 09:32

78
Chapter 5
Table 3. [Continued]
AADC deficiencyUntreated
Mean (range)Number of patients
AADC deficiency Treated(L-dopa excluded)
Mean(range)p-valueNumber of patients
AADC deficiencyTreated(total, L-dopa included
Mean(range)p-value Numberof patients
TH deficiencyUntreated
Mean (range)Number of patients
TH deficiencyTreated
Mean(range)p-value Numberof patients
5-HTP ↑↑↑(↑↑-↑↑↑)n=10
↑↑↑(↑-↑↑↑)p=0.12n=6
↑↑(↑-↑↑↑)p=0.04n=10
Table legend: ↓: mildly decreased (50-99% of lower limit of reference range) ↓↓: moderately decreased (10-49% of lower limit of reference range), ↓↓↓: strongly decreased (<10% of lower limit of reference range), n: normal, ↑: mildly increased (101-199% of upper limit of reference range), ↑↑: moderately increased (200-499% of upper limit of reference range), ↑↑↑: strongly increased (>500% of upper limit of reference range). p-value refers to the significance level of the change in metabolite levels in untreated vs. treated conditions (1-tailed dependent t-test). *no direct comparison of patients, independent t-test performed
AADC deficiency: CSF metabolites before and during gene therapyTo date, intraparenchymal gene therapy has been reported in 16 patients6, 7. In 12 patients, HVA and 5-HIAA in CSF has been reported in treatment naïve condition and after gene therapy. HVA increased in 8 patients, but remained strongly decreased in 5 of these 8 patients. In one patient, who had moderately decreased HVA before gene therapy, normal HVA levels after gene therapy were reached. HVA remained unchanged in four patients (strongly decreased in three, moderately decreased in one). All patients showed a favourable motor response after gene therapy.
5-HIAA remained strongly decreased in 9 patients. In three patients, 5-HIAA increased, to moderately (n = 1) or to mildly (n = 2) decreased levels. 3-OMD was reported in 6 patients before treatment and after gene therapy, but remained moderately to strongly increased without a significant change (p = 0.17).
TH deficiency: monoamine neurotransmitter metabolites in urineThe profile of monoamine neurotransmitter metabolites in urine (HVA, 5-HIAA, VMA, dopamine, norepinephrine and epinephrine) in untreated TH deficiency is summarized in Table 2b. There were insufficient data for the other monoamine neurotransmitter metabolites, or for urinary monoamine neurotransmitter metabolites on medical treatment (reported in one patient only).
Although in most patients before treatment urinary HVA and VMA were decreased and 5-HIAA was normal (in line with the neurometabolic block), this was not found in all
Voorbereid document _Tessa Wassenberg_V03.indd 78Voorbereid document _Tessa Wassenberg_V03.indd 78 25/10/2021 09:3225/10/2021 09:32

79
Blood, urine and CSF in TH and AADC deficiency
patients. Three patients had normal HVA, one patient had normal VMA and one patient had increased 5-HIAA levels.
Urinary dopamine was normal in 6/8 patients and decreased in the other two patients. Norepinephrine was normal in 3/8 patients and decreased in the other five patients. Epinephrine was decreased in only one patient, normal in 6, but increased in one. Normal epinephrine concentrations were found in patients with decreased dopamine (n = 2) and/or decreased norepinephrine (n = 4).
TH deficiency: serum prolactinIn untreated TH deficiency, prolactin was increased in 12 and normal in two patients. In two patients, only measurements under L-dopa treatment were available, which showed normal levels. In two patients under L-dopa and selegiline treatment, prolactin levels did not change. In one male patient, multiple measurements of prolactin were reported from age 1.8 until the age of 15 years under different treatment regimes. He had very high levels at the time of diagnosis and clinically was a very slow responder to medication. On follow-up, prolactin could be normal (n = 1), decreased (n = 3) or increased (n = 6). There was no clear correlation between treatment regime, clinical response, and prolactin levels (see Leuzzi et al. 2017 for a detailed description25).
TH deficiency: CSF monoamine neurotransmitter metabolites before and during treatmentIn 16 patients, CSF measurements before and during treatment were available. The summary of results is shown in Table 3.
In all untreated patients, HVA was decreased (mean percentage of lower limit of reference range 16.8%, range 0.00–63.0%), 5-HIAA was normal in 13/16 patients, mildly increased in two and mildly decreased in one patient. CSF HVA/5-HIAA ratio was decreased in all untreated patients.
Upon treatment, which always included L-dopa/carbidopa, there were no significant changes in 5-HIAA levels. In contrast, there was a clear significant increase in HVA to a mean of 81.3% of lower limit of reference range. Normal levels of HVA were reached in five patients; three on a combination therapy of L-dopa and a MAO-inhibitor, two on an L-dopa monotherapy. However, in two patients with a severe, early onset phenotype that exhibited normal HVA levels, clinical response was described as only partial or minimal26, 27. In one patient, mildly increased HVA levels (133% of upper limit of reference range) occurred on L-dopa monotherapy. The clinical response in this patient was not described.
A comparison of MHPG concentrations before and during treatment could be made in 9 patients. MHPG was decreased in all untreated patients (mean percentage of lower
5
Voorbereid document _Tessa Wassenberg_V03.indd 79Voorbereid document _Tessa Wassenberg_V03.indd 79 25/10/2021 09:3225/10/2021 09:32

80
Chapter 5
limit of reference range 32.8%, range 5.71–85.0%) and increased upon treatment to a mean of 56.1% of lower limit of reference range, with a normal level reached in three patients, all on L-dopa/carbidopa monotherapy. HVA in two of these patients remained decreased, while in one patient it reached mildly increased levels (clinical response not described).
Insufficient data for CSF 3-OMD prohibited a direct intra-individual comparison. 3-OMD in untreated patients was normal in 11 patients, and mildly, moderately, or strongly decreased in one patient each. Levels in treated condition (L-dopa with or without dopamine agonist) were increased in all patients.
Discussion
In this study of patients with TH and AADC deficiency, we retrospectively evaluated the literature and our laboratory database for monoamine neurotransmitter metabolite patterns in blood and urine and prolactin levels in blood, and analyzed the influence of medical treatment on monoamine neurotransmitter metabolites in CSF. This was the first structured study in both TH and AADC deficiency to evaluate this, yielding both expected and unexpected findings which are outlined below.
It is considered good practice to use CSF, but not blood or urine, to diagnose primary monoamine neurotransmitter disorders, and our study supports this habit. Although in patients with AADC deficiency the monoamine neurotransmitter profile in blood seems to reflect the metabolic block and the profile found in CSF, this was only reported in a very limited number of patients and 5-HIAA in blood was normal in one of these patients. In TH deficiency, no reports of monoamine neurotransmitter metabolites in blood were found at all. In urine, we confirm that the monoamine neurotransmitter profile does not reflect the metabolic block in many patients with AADC deficiency, in whom normal to high levels of dopamine metabolites are often found. We show here that also when TH is deficient, normal levels of dopamine and HVA can be found. Overall, we confirm that quantities of monoamine neurotransmitter metabolites in urine in patients with AADC and TH deficiency should be interpreted with extreme caution and are of very limited diagnostic value.
An exception to the rule above regards the metabolites that accumulate in AADC deficiency, namely 3-OMD, L-dopa, and VLA, and possibly 5-HTP. These metabolites are not only highly elevated in CSF, but also in blood and urine, a finding we could confirm here in a relatively large group of patients. The work that is done to develop newborn screening for AADC deficiency measuring 3-OMD in DBS16, 28, 29 is therefore interesting and promising to decrease the long diagnostic delay that is often present in this disorder3. However, some caution regarding these accumulating metabolites is warranted. Firstly, in patients with AADC deficiency normal urinary VLA levels have been
Voorbereid document _Tessa Wassenberg_V03.indd 80Voorbereid document _Tessa Wassenberg_V03.indd 80 25/10/2021 09:3225/10/2021 09:32

81
Blood, urine and CSF in TH and AADC deficiency
reported23, although recently it was shown that this might be overcome by measuring VLA/VMA ratios in patients with AADC deficiency17. Secondly, other conditions in which 3-OMD, L-dopa and VLA accumulate do exist. Besides due to treatment with L-dopa30, 31, accumulation can occur in the case of ‘secondary AADC deficiency’ due to deficiency of its co-factor pyridoxin, e.g. in some of the primary vitamin B6 responsive disorders like pyridoxamine 5′- phosphate oxidase (PNPO) deficiency32, 33, or pyridoxal phosphate binding protein (PLPBP) deficiency34, which in fact can give a monoamine neurotransmitter metabolite profile indistinguishable from AADC deficiency. Clinically, these disorders are usually different from AADC deficiency because of prominent neonatal seizures33. Recently however, one patient with PLPBP deficiency was described who did not suffer from seizures but displayed a movement disorder compatible with AADC deficiency. Also in this patient, increased levels of VLA were found in urine34. This highlights the fact that molecular confirmation of a specific genetic diagnosis is crucial because treatment strategies of vitamin B6 responsive disorders and AADC deficiency are different.
In TH deficiency, neither accumulated metabolites in CSF, urine or blood are known nor identified with our study. At this moment, newborn screening for TH-deficiency using metabolites in blood therefore seems beyond the horizon. However, innovative techniques, e.g. using metabolomics or complexomics, might identify new biomarkers of TH deficiency in the future35, 36.
Although it can be argued that nowadays the use of biomarkers in CSF, blood and urine is losing its relevance since patients with a suspected neurometabolic disorders will first be investigated using a genetic approach37, we believe that it is still important to delineate and understand the profile of monoamine neurotransmitter metabolites in body fluids. Not only can this help to establish or reject a diagnosis in patients in which genetic variants of uncertain significance are found, it is also relevant to the new ‘omics’ techniques mentioned above35.
We found that serum prolactin is often increased in patients with AADC and TH deficiency, but that it can be normal as well. We cannot extrapolate these findings to all patients with TH and AADC deficiency because of the retrospective nature of this study with lack of information on withdrawal conditions which is important for correct interpretation of prolactin levels18. Although increased prolactin might serve as a possible clue towards monoamine neurotransmitter deficiencies, especially in low-resource countries 38, normal prolactin does not exclude TH or AADC deficiency. However, the usefulness of prolactin for diagnosis and treatment monitoring of primary monoamine deficiencies is an interesting topic for further prospective studies.
In patients with TH deficiency and AADC deficiency who are treated rationally (targeting the metabolic defect), CSF metabolite concentrations tend to become less deviant, but
5
Voorbereid document _Tessa Wassenberg_V03.indd 81Voorbereid document _Tessa Wassenberg_V03.indd 81 25/10/2021 09:3225/10/2021 09:32

82
Chapter 5
their characteristic diagnostic profile mostly remains present. Treatment with L-dopa leads to strongly increased 3-OMD levels, not only in patients with AADC deficiency who already have strongly increased levels, but also in patients with TH-deficiency. Interestingly, this is also found in patients with Parkinson’s disease upon L-dopa treatment39, and even in healthy volunteers who receive a single dose of L-dopa30. In our small and retrospective series, there is no clear correlation between alterations in CSF monoamine neurotransmitter metabolites and clinical response to medical treatment in TH or AADC deficiency. Normalization of CSF HVA levels may follow L-dopa supplementation in both disorders, but does not always reflect the clinical response. Remarkably, after intraputaminal gene therapy - a new treatment available for patients with AADC-deficiency - HVA in CSF shows a modest increase in most patients, but can remain strongly decreased even when there is a clear clinical response6, 7. Therefore, we think it wiser and more patient friendly to use clinical parameters rather than biochemical measurements to target treatment response in the follow-up of AADC and TH deficiency.
Some findings we cannot easily explain relate to monoamine neurotransmitter metabolites in urine. Interestingly, epinephrine was consistently found to be decreased in AADC deficiency (5/5 patients), but was mostly normal or even increased in patients with TH deficiency (7/8 patients). In contrast, in both disorders urinary norepinephrine was decreased in most patients. There was no clear intra-individual correlation between the levels of urinary dopamine and epinephrine, and medical treatment did not change the level of urinary epinephrine in patients with AADC deficiency. For TH deficiency, there was insufficient data available to evaluate the treatment effect on urinary monoamine neurotransmitter metabolites. Possibly, urinary epinephrine is decreased in AADC but not TH deficiency due to the highly accumulated levels of L-dopa that are present in AADC deficiency only. L-dopa is metabolized to 3-OMD by COMT in a methylation reaction that uses s-adenosylmethionine as methyl donor40. If s-adenosylmethionine is depleted, the same methylation reaction that is needed to metabolize norepinephrine to epinephrine by phenylethanolamine N-methyltransferase might be hindered.
Another remarkable finding in urine metabolites in patients with AADC-deficiency is that 5-HIAA was most often decreased (9/10 patients). In line with our previous explanation for the often normal or even increased urinary dopamine concentration in patients with this disorder, namely the combination of excessive availability of the precursor L-dopa and sufficient residual capacity of AADC enzyme activity in the kidneys10, 15, one might expect that also 5-HIAA would be normal or increased because of redundant availability of the precursor 5-HTP. A possible explanation why this is not seen is that AADC has a higher affinity for L-dopa than for 5-HTP20. Indeed, it has been shown in rats that chronic L-dopa supplementation leads to increased excretion of dopamine
Voorbereid document _Tessa Wassenberg_V03.indd 82Voorbereid document _Tessa Wassenberg_V03.indd 82 25/10/2021 09:3225/10/2021 09:32

83
Blood, urine and CSF in TH and AADC deficiency
but decreased excretion of serotonin31. However, further research is needed to exclude sampling error and better understand this observation.
We used purely retrospective data mainly derived from case reports with non-uniform sampling methods. Correct sampling is essential, especially for monoamine neurotransmitter metabolites in CSF because of a rostrocaudal gradient that is present for HVA, 5-HIAA and MHPG, but it was not always stated whether this was indeed taken into account. Furthermore, for most observations only a limited number was available. However, we think we can draw some valuable conclusions. Firstly, CSF should be regarded as the main body fluid to test monoamine neurotransmitter metabolites when there is a suspicion of TH or AADC deficiency. Secondly, accumulated metabolites in AADC deficiency (VLA, 3-OMD, L-Dopa) are promising biomarkers for neonatal screening, but some hurdles still need to be overcome before it can be implemented in clinical practice. Thirdly, the applicability of serum prolactin in diagnosis and follow-up of primary monoamine neurotransmitter disorders should be further studied in a standardized and prospective manner, ideally using international collaboration initiatives like the international working group on neurotransmitter related disorders (iNTD)41. Fourthly, regular follow-up of CSF measurements to target treatment response is not needed in these disorders. Furthermore, we show that, just like in AADC deficiency, in TH deficiency monoamine neurotransmitter metabolites in urine do not completely reflect the metabolic block and HVA and dopamine can be normal in both disorders. An interesting observation includes that in TH deficiency normal levels of urinary epinephrine are often reported, whereas these are generally decreased in AADC-deficiency. This finding highlights the complex and incompletely understood physiology of monoamine metabolism outside the central nervous system, and calls for further research on this topic. These rare primary monoamine neurotransmitter disorders may serve as unique models for this.
AcknowledgementsWe thank Claudia S. Wouters for her help in data collection and thank Erik Verbruggen for critical proofreading of the manuscript.
5
Voorbereid document _Tessa Wassenberg_V03.indd 83Voorbereid document _Tessa Wassenberg_V03.indd 83 25/10/2021 09:3225/10/2021 09:32

84
Chapter 5
Reference
1. Ng J, Papandreou A, Heales SJ, Kurian MA. Monoamine neurotransmitter disorders-clinical advances and future perspectives. Nature reviews Neurology. 2015 Oct;11(10):567-84.
2. Hyland K, Clayton PT. Aromatic amino acid decarboxylase deficiency in twins. Journal of inherited metabolic disease. 1990 1990;13(3):301-4.
3. Brun L, Ngu LH, Keng WT, et al. Clinical and biochemical features of aromatic L-amino acid decarboxylase deficiency. Neurology. 2010 Jul 06;75(1):64-71.
4. Wassenberg T, Molero-Luis M, Jeltsch K, et al. Consensus guideline for the diagnosis and treatment of aromatic l-amino acid decarboxylase (AADC) deficiency. Orphanet journal of rare diseases. 2017 Jan 18;12(1):12.
5. Willemsen MA, Verbeek MM, Kamsteeg EJ, et al. Tyrosine hydroxylase deficiency: a treatable disorder of brain catecholamine biosynthesis. Brain : a journal of neurology. 2010 Jun;133(Pt 6):1810-22.
6. Kojima K, Nakajima T, Taga N, et al. Gene therapy improves motor and mental function of aromatic l-amino acid decarboxylase deficiency. Brain : a journal of neurology. 2019 Feb 1;142(2):322-33.
7. Chien YH, Lee NC, Tseng SH, et al. Efficacy and safety of AAV2 gene therapy in children with aromatic L-amino acid decarboxylase deficiency: an open-label, phase 1/2 trial. Lancet Child Adolesc Health. 2017 Dec;1(4):265-73.
8. Nagatsu T. Genes for human catecholamine-synthesizing enzymes. Neuroscience research. 1991 Oct;12(2):315-45.
9. Johnson ME, Salvatore MF, Maiolo SA, Bobrovskaya L. Tyrosine hydroxylase as a sentinel for central and peripheral tissue responses in Parkinson’s progression: Evidence from clinical studies and neurotoxin models. Prog Neurobiol. 2018 Jun - Aug;165-167:1-25.
10. Wassenberg T, Willemsen MA, Geurtz PB, et al. Urinary dopamine in aromatic L-amino acid decarboxylase deficiency: the unsolved paradox. Mol Genet Metab. 2010 Dec;101(4):349-56.
11. Berger M, Gray JA, Roth BL. The expanded biology of serotonin. Annu Rev Med. 2009;60:355-66.12. Martin AM, Young RL, Leong L, et al. The Diverse Metabolic Roles of Peripheral Serotonin.
Endocrinology. 2017 May 1;158(5):1049-63.13. Rubi B, Maechler P. Minireview: new roles for peripheral dopamine on metabolic control
and tumor growth: let’s seek the balance. Endocrinology. 2010 Dec;151(12):5570-81.14. Goldstein DS, Eisenhofer G, Kopin IJ. Sources and significance of plasma levels of catechols
and their metabolites in humans. The Journal of pharmacology and experimental therapeutics. 2003 6/2003;305(3):800-11.
15. Wassenberg T, Monnens LA, Geurtz BP, Wevers RA, Verbeek MM, Willemsen MA. The paradox of hyperdopaminuria in aromatic L-amino Acid deficiency explained. JIMD reports. 2012;4:39-45.
16. Chen PW, Lee NC, Chien YH, Wu JY, Wang PC, Hwu WL. Diagnosis of aromatic l-amino acid decarboxylase deficiency by measuring 3-O-methyldopa concentrations in dried blood spots. Clinica chimica acta; international journal of clinical chemistry. 2014 Feb 7;431C:19- 22.
Voorbereid document _Tessa Wassenberg_V03.indd 84Voorbereid document _Tessa Wassenberg_V03.indd 84 25/10/2021 09:3225/10/2021 09:32

85
Blood, urine and CSF in TH and AADC deficiency
17. Brennenstuhl H, Garbade SF, Okun JG, et al. Semi-quantitative detection of a vanillactic acid/vanillylmandelic acid ratio in urine is a reliable diagnostic marker for aromatic L-amino acid decarboxylase deficiency. Mol Genet Metab. 2020 Jul 7.
18. Saleem M, Martin H, Coates P. Prolactin Biology and Laboratory Measurement: An Update on Physiology and Current Analytical Issues. Clin Biochem Rev. 2018 Feb;39(1):3-16.
19. Brautigam C, Wevers RA, Jansen RJ, et al. Biochemical hallmarks of tyrosine hydroxylase deficiency. Clinical chemistry. 1998 Sep;44(9):1897-904.
20. Verbeek MM, Geurtz PB, Willemsen MA, Wevers RA. Aromatic L-amino acid decarboxylase enzyme activity in deficient patients and heterozygotes. Mol Genet Metab. 2007 4/2007;90(4):363-9.
21. Hyland K, Surtees RA, Rodeck C, Clayton PT. Aromatic L-amino acid decarboxylase deficiency: clinical features, diagnosis, and treatment of a new inborn error of neurotransmitter amine synthesis. Neurology. 1992 10/1992;42(10):1980-8.
22. Maller A, Hyland K, Milstien S, Biaggioni I, Butler IJ. Aromatic L-amino acid decarboxylase deficiency: clinical features, diagnosis, and treatment of a second family. J Child Neurol 1997 9/1997;12(6):349-54.
23. Spitz MA, Nguyen MA, Roche S, et al. Chronic Diarrhea in L-Amino Acid Decarboxylase (AADC) Deficiency: A Prominent Clinical Finding Among a Series of Ten French Patients. JIMD reports. 2017;31:85-93.
24. Leuzzi V, Mastrangelo M, Polizzi A, et al. Report of Two Never Treated Adult Sisters with Aromatic L-Amino Acid Decarboxylase Deficiency: A Portrait of the Natural History of the Disease or an Expanding Phenotype? JIMD reports. 2014 May 1.
25. Leuzzi V, Mastrangelo M, Giannini MT, Carbonetti R, Hoffmann GF. Neuromotor and cognitive outcomes of early treatment in tyrosine hydroxylase deficiency type B. Neurology. 2017 Jan 31;88(5):501-2.
26. Ludecke B, Knappskog PM, Clayton PT, et al. Recessively inherited L-DOPA-responsive parkinsonism in infancy caused by a point mutation (L205P) in the tyrosine hydroxylase gene. Human molecular genetics. 1996 Jul;5(7):1023-8.
27. Yeung WL, Wong VC, Chan KY, et al. Expanding phenotype and clinical analysis of tyrosine hydroxylase deficiency. J Child Neurol. 2011 Feb;26(2):179-87.
28. Chien YH, Chen PW, Lee NC, et al. 3-O-methyldopa levels in newborns: Result of newborn screening for aromatic l-amino-acid decarboxylase deficiency. Mol Genet Metab. 2016 Aug;118(4):259-63.
29. Brennenstuhl H, Kohlmuller D, Gramer G, et al. High throughput newborn screening for aromatic L-amino-acid decarboxylase deficiency by analysis of concentrations of 3-O- methyldopa from dried blood spots. Journal of inherited metabolic disease. 2019 Dec 18.
30. Benetello P, Furlanut M, Fortunato M, Pea F, Baraldo M. Levodopa and 3-O-methyldopa in cerebrospinal fluid after levodopa-carbidopa association. Pharmacol Res. 1997 Apr;35(4):313- 5.
31. Garcia NH, Berndt TJ, Tyce GM, Knox FG. Chronic oral L-DOPA increases dopamine and decreases serotonin excretions. Am J Physiol. 1999 Nov;277(5):R1476-80.
32. Brautigam C, Hyland K, Wevers R, et al. Clinical and laboratory findings in twins with neonatal epileptic encephalopathy mimicking aromatic L-amino acid decarboxylase deficiency. Neuropediatrics. 2002 6/2002;33(3):113-7.
5
Voorbereid document _Tessa Wassenberg_V03.indd 85Voorbereid document _Tessa Wassenberg_V03.indd 85 25/10/2021 09:3225/10/2021 09:32

86
Chapter 5
33. Mills PB, Surtees RA, Champion MP, et al. Neonatal epileptic encephalopathy caused by mutations in the PNPO gene encoding pyridox(am)ine 5’-phosphate oxidase. Human molecular genetics. 2005 Apr 15;14(8):1077-86.
34. Johnstone DL, Al-Shekaili HH, Tarailo-Graovac M, et al. PLPHP deficiency: clinical, genetic, biochemical, and mechanistic insights. Brain : a journal of neurology. 2019 Mar 1;142(3):542- 59.
35. Wevers RA, Blau N. Think big - think omics. Journal of inherited metabolic disease. 2018 May;41(3):281-3.
36. Tristan-Noguero A, Borras E, Molero-Luis M, et al. Novel Protein Biomarkers of Monoamine Metabolism Defects Correlate with Disease Severity. Movement disorders : official journal of the Movement Disorder Society. 2020 Nov 5.
37. Willemsen MA, Harting I, Wevers RA. Neurometabolic disorders: Five new things. Neurol Clin Pract. 2016 Aug;6(4):348-57.
38. Goswami JN, Sankhyan N, Singhi PD. An Indian Family with Tyrosine Hydroxylase Deficiency. Indian Pediatr. 2017 Jun 15;54(6):499-501.
39. Andersen AD, Blaabjerg M, Binzer M, et al. Cerebrospinal fluid levels of catecholamines and its metabolites in Parkinson’s disease: effect of l-DOPA treatment and changes in levodopa- induced dyskinesia. Journal of neurochemistry. 2017 May;141(4):614-25.
40. Brautigam C, Wevers RA, Hyland K, Sharma RK, Knust A, Hoffman GF. The influence of L- dopa on methylation capacity in aromatic L-amino acid decarboxylase deficiency: biochemical findings in two patients. Journal of inherited metabolic disease. 2000 6/2000;23(4):321-4.
41. Opladen T, Cortes-Saladelafont E, Mastrangelo M, et al. The International Working Group on Neurotransmitter related Disorders (iNTD): A worldwide research project focused on primary and secondary neurotransmitter disorders. Molecular genetics and metabolism reports. 2016 Dec;9:61-6.
Voorbereid document _Tessa Wassenberg_V03.indd 86Voorbereid document _Tessa Wassenberg_V03.indd 86 25/10/2021 09:3225/10/2021 09:32

87
Blood, urine and CSF in TH and AADC deficiency
Supplemental material Chapter 5
Supplement A. AADC deficiency: included patients
Pt NR
Level of diagnosis References TML Prolactin Blood NT Urine NT CSF NT CSFGT
1 CSF, AADC [1,2] x**
2 CSF, AADC, DNA [2-4] x x x x** x
3 CSF, DNA [5] x
4 CSF, AADC [6] x
5 CSF, AADC, DNA [7,8] x x
6 CSF, AADC, DNA [8,9] x x x
7 CSF, AADC, DNA [10, 100] x x x
8 CSF, AADC, DNA [2, 12-16] x x** x
9 CSF, AADC, DNA [2,3,12-16] x x** x
10 CSF, AADC, DNA [2,3,12-16] x x** x
11 CSF, AADC, DNA [3,13,15,17] x** x
12 CSF, AADC, DNA [13,17,18] x x x**
13 CSF, AADC, DNA [19] x
14 CSF, AADC, DNA [20-23] x x x
15 CSF, AADC, DNA [20-23] x x x
16 CSF, AADC, DNA [11,24] x x
17 CSF, AADC, DNA [11,24] x x
18 CSF, AADC, DNA [14,25] x x
19 CSF, DNA [26] x x**
20 CSF, DNA [27,28] x**
21 CSF, DNA [29] x**
22 CSF, AADC, DNA [30] x x x
23 CSF, AADC, DNA [30] x x x
24 CSF, AADC [31] x
25 CSF, AADC, DNA [14] x
26 CSF, AADC, DNA [32] x
27 CSF, AADC, DNA [14] x
28 CSF, AADC, DNA [33] x
29 CSF, AADC, DNA [15,33] x
30 CSF, AADC, DNA [2,13,15] x x**
31 CSF, AADC, DNA [2,13,15] x x**
5
Voorbereid document _Tessa Wassenberg_V03.indd 87Voorbereid document _Tessa Wassenberg_V03.indd 87 25/10/2021 09:3225/10/2021 09:32

88
Chapter 5
Supplement A. [Continued]
Pt NR
Level of diagnosis References TML Prolactin Blood NT Urine NT CSF NT CSFGT
32 CSF, AADC, DNA [2,13,15] x x x
33 CSF, AADC, DNA [2,13,15] x x x** x
34 CSF, AADC, DNA [2] x
35 CSF, DNA [2] x x
36 CSF, AADC [2] x
37 CSF, DNA [2] x
38 CSF, AADC [2] x
39 CSF, AADC [2] x
40 CSF, AADC [2] x
41 CSF, DNA [2] x
42 CSF, DNA [2] x
43 CSF, DNA [2] x
44 CSF, DNA [2] x
45 CSF [2] x x
46 CSF [2] X x
47 DNA [15] x
48 DNA [15] x
49 DNA [15] x x x**
50 DNA [15] x
51 DNA [15] x
52 DNA [15] x
53 DNA [15] x
54 DNA [15] x
55 DNA [15] x
56 DNA [34] x**
57 CSF, AADC, DNA [8] x
58 CSF, AADC, DNA [8] x
59 CSF, AADC, DNA [8] x
60 CSF, AADC, DNA [8] x
61 DNA [8] x
62 CSF, DNA [8] x
63 CSF, AADC, DNA [8] x
64 CSF, AADC, DNA [8] x
Voorbereid document _Tessa Wassenberg_V03.indd 88Voorbereid document _Tessa Wassenberg_V03.indd 88 25/10/2021 09:3225/10/2021 09:32

89
Blood, urine and CSF in TH and AADC deficiency
Supplement A. [Continued]
Pt NR
Level of diagnosis References TML Prolactin Blood NT Urine NT CSF NT CSFGT
65 CSF, AADC, DNA [11,35] X x
66 DNA [36] x x*
67 DNA [36] x x*
68 DNA [36] x x*
69 DNA [36] x x*
70 CSF, DNA [37] x*
71 CSF, DNA [38] x*
72 CSF, DNA [38] x* x
73 CSF, DNA [38] x* x
74 CSF, DNA [38] x* x
75 CSF, DNA [38] x* x
76 CSF, DNA [38] x* x
77 CSF, DNA [38] x* x
78 CSF, DNA [38] x* x
79 CSF, DNA [38] x* x
80 CSF, DNA [38] x* x
81 CSF, AADC, DNA [11] x
82 CSF, AADC, DNA [11] x
83 DNA [39] x
84 DNA [39] x x*
85 DNA [39] x*
86 DNA [39] x*
87 DNA [39] x*
88 DNA [40] x* x
89 DNA [40] x* x
90 DNA, AADC, CSF [41] x*
91 DNA, AADC, CSF [41] x*
92 DNA, AADC, CSF [41] x*
93 DNA, AADC, CSF [41] x*
94 DNA, AADC, CSF [41] x*
95 DNA, AADC, CSF [41] x*
97 DNA, AADC, CSF [41] x*
5
Voorbereid document _Tessa Wassenberg_V03.indd 89Voorbereid document _Tessa Wassenberg_V03.indd 89 25/10/2021 09:3225/10/2021 09:32

90
Chapter 5
Supplemental Table 1.• Level of diagnosis: diagnostic tests that were performed to confirm AADC-deficiency. CSF:
typical neurotransmitter profile in cerebrospinal fluid. AADC: low aromatic l-amino acid decarboxylase enzyme activity. DNA: molecular diagnosis confirmed.
• TML: Translational Metabolic Laboratory, data included from TML database that was not previously reported in the literature.
• Prolactin: serum prolactin reported.• Blood NT: measurements of neurotransmitter metabolites in blood. *: only 3-OMD
measurements available (DBS or plasma)• Urine NT: measurements of neurotransmitter metabolites in urine. **:measurements of
multiple metabolites performed. In the patients without asterix, only dopamine or VLA was reported.
• CSF NT: measurement of neurotransmitter metabolites in cerebrospinal fluid before and during medical treatment
• CSF GT: measurement of neurotransmitter metabolites in cerebrospinal fluid before and after gene therapy.
Reference list Supplement A AADC deficiency
1. J.E. Abdenur, N. Abeling, N. Specola, L. Jorge, A.B. Schenone, A.C. van Cruchten, N.A. Chamoles, Aromatic l-aminoacid decarboxylase deficiency: unusual neonatal presentation and additional findings in organic acid analysis Mol Genet Metab 87 (2006) 48-53.
2. L. Brun, L.H. Ngu, W.T. Keng, G.S. Ch’ng, Y.S. Choy, W.L. Hwu, W.T. Lee, M.A. Willemsen, M.M. Verbeek, T. Wassenberg, L. Regal, S. Orcesi, D. Tonduti, P. Accorsi, H. Testard, J.E. Abdenur, S. Tay, G.F. Allen, S. Heales, I. Kern, M. Kato, A. Burlina, C. Manegold, G.F. Hoffmann, N. Blau, Clinical and biochemical features of aromatic L-amino acid decarboxylase deficiency Neurology 75 (2010) 64-71.
3. N.G. Abeling, C. Brautigam, G.F. Hoffmann, P.G. Barth, R.A. Wevers, J. Jaeken, A. Fiumara, A. Knust, A.H. van Gennip, Pathobiochemical implications of hyperdopaminuria in patients with aromatic L-amino acid decarboxylase deficiency Journal of inherited metabolic disease 23 (2000) 325-328.
4. N.G. Abeling, A.H. van Gennip, P.G. Barth, C.A. van, M. Westra, F.A. Wijburg, Aromatic L- amino acid decarboxylase deficiency: a new case with a mild clinical presentation and unexpected laboratory findings Journal of inherited metabolic disease 21 (1998) 240-242.
5. M. Alfadhel, R. Kattan, Aromatic amino Acid decarboxylase deficiency not responding to pyridoxine and bromocriptine therapy: case report and review of response to treatment Journal of central nervous system disease 6 (2014) 1-5.
6. I.A. Anselm, B.T. Darras, Catecholamine toxicity in aromatic L-amino acid decarboxylase deficiency Pediatr Neurol 35 (2006) 142-144.
7. J.B. Arnoux, L. Damaj, S. Napuri, V. Serre, L. Hubert, M. Cadoudal, G. Simard, I. Ceballos, L. Christa, P. de Lonlay, Aromatic L-amino acid decarboxylase deficiency is a cause of long- fasting hypoglycemia The Journal of clinical endocrinology and metabolism 98 (2013) 4279- 4284.
Voorbereid document _Tessa Wassenberg_V03.indd 90Voorbereid document _Tessa Wassenberg_V03.indd 90 25/10/2021 09:3225/10/2021 09:32

91
Blood, urine and CSF in TH and AADC deficiency
8. M.A. Spitz, M.A. Nguyen, S. Roche, B. Heron, M. Milh, P. de Lonlay, L. Lion-Francois, H. Testard, S. Napuri, M. Barth, S. Fournier-Favre, L. Christa, C. Vianey-Saban, C. Corne, A. Roubertie, Chronic Diarrhea in L-Amino Acid Decarboxylase (AADC) Deficiency: A Prominent Clinical Finding Among a Series of Ten French Patients JIMD reports 31 (2017) 85-93.
9. M. Barth, V. Serre, L. Hubert, Y. Chaabouni, N. Bahi-Buisson, M. Cadoudal, D. Rabier, S.N. Tich, M. Ribeiro, D. Ricquier, A. Munnich, D. Bonneau, P. de Lonlay, L. Christa, Kinetic analyses guide the therapeutic decision in a novel form of moderate aromatic Acid decarboxylase deficiency JIMD reports 3 (2012) 25-32.
10. S. Ito, T. Nakayma, S. Ide, Y. Ito, H. Oguni, Y.I. Goto, M. Osawa, Aromatic l-amino acid decarboxylase deficiency associated with epilepsy mimicking non-epileptic involuntary movements Dev Med Child Neur 50 (2008) 876-878.
11. K. Kojima, T. Nakajima, N. Taga, A. Miyauchi, M. Kato, A. Matsumoto, T. Ikeda, K. Nakamura, T. Kubota, H. Mizukami, S. Ono, Y. Onuki, T. Sato, H. Osaka, S.I. Muramatsu, T. Yamagata, Gene therapy improves motor and mental function of aromatic l-amino acid decarboxylase deficiency Brain : a journal of neurology 142 (2019) 322-333.
12. Y.T. Chang, R. Sharma, J.L. Marsh, J.D. McPherson, J.A. Bedell, A. Knust, C. Brautigam, G.F. Hoffmann, K. Hyland, Levodopa-responsive aromatic L-amino acid decarboxylase deficiency Annals of neurology 55 (2004) 435-438.
13. M.M. Verbeek, P.B. Geurtz, M.A. Willemsen, R.A. Wevers, Aromatic L-amino acid decarboxylase enzyme activity in deficient patients and heterozygotes Mol Genet Metab 90 (2007) 363-369.
14. C. Manegold, G.F. Hoffmann, I. Degen, H. Ikonomidou, A. Knust, M.W. Laass, M. Pritsch, E. Wilichowski, F. Horster, Aromatic L-amino acid decarboxylase deficiency: clinical features, drug therapy and follow-up Journal of inherited metabolic disease 32 (2009) 371-380.
15. T. Wassenberg, M.A. Willemsen, P.B. Geurtz, M. Lammens, K. Verrijp, M. Wilmer, W.T. Lee, R.A. Wevers, M.M. Verbeek, Urinary dopamine in aromatic L-amino acid decarboxylase deficiency: the unsolved paradox Mol Genet Metab 101 (2010) 349-356.
16. C. Brautigam, R.A. Wevers, K. Hyland, R.K. Sharma, A. Knust, G.F. Hoffman, The influence of L-dopa on methylation capacity in aromatic L-amino acid decarboxylase deficiency: biochemical findings in two patients Journal of inherited metabolic disease 23 (2000) 321-324.
17. A. Fiumara, C. Brautigam, K. Hyland, R. Sharma, L. Lagae, B. Stoltenborg, G.F. Hoffmann, J. Jaeken, R.A. Wevers, Aromatic L-amino acid decarboxylase deficiency with hyperdopaminuria. Clinical and laboratory findings in response to different therapies Neuropediatrics 33 (2002) 203-208.
18. M. Mastrangelo, C. Caputi, S. Galosi, M.T. Giannini, V. Leuzzi, Transdermal rotigotine in the treatment of aromatic L-amino acid decarboxylase deficiency Movement disorders : official journal of the Movement Disorder Society 28 (2013) 556-557.
19. K. Gucuyener, C.S. Kasapkara, L. Tumer, M.M. Verbeek, Aromatic L-Amino acid decarboxylase deficiency: A new case from Turkey with a novel mutation Annals of Indian Academy of Neurology 17 (2014) 234-236.
20. K. Hyland, P.T. Clayton, Aromatic amino acid decarboxylase deficiency in twins Journal of inherited metabolic disease 13 (1990) 301-304.
5
Voorbereid document _Tessa Wassenberg_V03.indd 91Voorbereid document _Tessa Wassenberg_V03.indd 91 25/10/2021 09:3225/10/2021 09:32

92
Chapter 5
21. K. Hyland, R.A. Surtees, C. Rodeck, P.T. Clayton, Aromatic L-amino acid decarboxylase deficiency: clinical features, diagnosis, and treatment of a new inborn error of neurotransmitter amine synthesis Neurology 42 (1992) 1980-1988.
22. R. Pons, B. Ford, C.A. Chiriboga, P.T. Clayton, V. Hinton, K. Hyland, R. Sharma, V. De, D.C., Aromatic L-amino acid decarboxylase deficiency: clinical features, treatment, and prognosis Neurology 62 (2004) 1058-1065.
23. K.J. Swoboda, J.P. Saul, C.E. McKenna, N.B. Speller, K. Hyland, Aromatic L-amino acid decarboxylase deficiency: overview of clinical features and outcomes Annals of neurology 54 Suppl 6 (2003) S49-S55.
24. S. Ide, M. Sasaki, M. Kato, T. Shiihara, S. Kinoshita, J.Y. Takahashi, Y.I. Goto, Abnormal glucose metabolism in aromatic l-amino acid decarboxylase deficiency Brain Dev (2009).
25. G.C. Korenke, H.J. Christen, K. Hyland, D.H. Hunneman, F. Hanefeld, Aromatic L-amino acid decarboxylase deficiency: an extrapyramidal movement disorder with oculogyric crises Eur J Paediatr Neurol 1 (1997) 67-71.
26. H.C. Lee, C.K. Lai, K.C. Yau, T.S. Siu, C.M. Mak, Y.P. Yuen, K.Y. Chan, S. Tam, C.W. Lam, A.Y. Chan, Non-invasive urinary screening for aromatic L-amino acid decarboxylase deficiency in high-prevalence areas: a pilot study Clinica chimica acta; international journal of clinical chemistry 413 (2012) 126-130.
27. W.T. Lee, J.H. Lin, W.C. Weng, S.S. Peng, Microstructural changes of brain in patients with aromatic L-amino acid decarboxylase deficiency Hum Brain Mapp 38 (2017) 1532-1540.
28. S. Camargos, A.J. Lees, A. Singleton, F. Cardoso, DYT16: the original cases Journal of neurology, neurosurgery, and psychiatry 83 (2012) 1012-1014.
29. L.K. Lee, K.M. Cheung, W.W. Cheng, C.H. Ko, H.H. Lee, C.K. Ching, C. Mak, A rare cause of severe diarrhoea diagnosed by urine metabolic screening: aromatic L-amino acid decarboxylase deficiency Hong Kong medical journal = Xianggang yi xue za zhi / Hong Kong Academy of Medicine 20 (2014) 161-164.
30. C. Dionisi-Vici, G.F. Hoffmann, V. Leuzzi, H. Hoffken, C. Brautigam, C. Rizzo, G.C. Steebergen-Spanjers, J.A. Smeitink, R.A. Wevers, Tyrosine hydroxylase deficiency with severe clinical course: clinical and biochemical investigations and optimization of therapy The Journal of pediatrics 136 (2000) 560-562.
31. A. Maller, K. Hyland, S. Milstien, I. Biaggioni, I.J. Butler, Aromatic L-amino acid decarboxylase deficiency: clinical features, diagnosis, and treatment of a second family J Child Neurol 12 (1997) 349-354.
32. L. Brun, L.H. Ngu, W.T. Keng, G.S. Ch’ng, Y.S. Choy, W.L. Hwu, W.T. Lee, M.A. Willemsen, M.M. Verbeek, T. Wassenberg, L. Regal, S. Orcesi, P. Accorsi, D. Tonduti, H. Testard, J.E. Abdenur, S. Tay, G.F. Allen, S. Heales, I. Kern, K. Kato, A. Burlina, C. Manegold, G. Hoffmann, N. Blau, Laboratory diagnosis, treatment, and follow-up of 78 patients with aromatic l-amino acid decarboxylase deficiency JIMD 33 (2010) S164.
33. S.K. Tay, K.S. Poh, K. Hyland, Y.W. Pang, H.T. Ong, P.S. Low, D.L. Goh, Unusually mild phenotype of AADC deficiency in 2 siblings Mol Genet Metab 91 (2007) 374-378.
34. T. Wassenberg, L.A. Monnens, B.P. Geurtz, R.A. Wevers, M.M. Verbeek, M.A. Willemsen, The paradox of hyperdopaminuria in aromatic L-amino Acid deficiency explained JIMD reports 4 (2012) 39-45.
Voorbereid document _Tessa Wassenberg_V03.indd 92Voorbereid document _Tessa Wassenberg_V03.indd 92 25/10/2021 09:3225/10/2021 09:32

93
Blood, urine and CSF in TH and AADC deficiency
35. K. Kojima, R. Anzai, C. Ohba, T. Goto, A. Miyauchi, B. Thony, H. Saitsu, N. Matsumoto, H. Osaka, T. Yamagata, A female case of aromatic l-amino acid decarboxylase deficiency responsive to MAO-B inhibition Brain Dev 38 (2016) 959-963.
36. Y.H. Chien, P.W. Chen, N.C. Lee, W.S. Hsieh, P.C. Chiu, W.L. Hwu, F.J. Tsai, S.P. Lin, S.Y. Chu, Y.J. Jong, M.C. Chao, 3-O-methyldopa levels in newborns: Result of newborn screening for aromatic l-amino-acid decarboxylase deficiency Mol Genet Metab 118 (2016) 259-263.
37. W.L. Hwu, Y.H. Chien, N.C. Lee, M.H. Li, Natural History of Aromatic L-Amino Acid Decarboxylase Deficiency in Taiwan JIMD reports 40 (2018) 1-6.
38. Y.H. Chien, N.C. Lee, S.H. Tseng, C.H. Tai, S.I. Muramatsu, B.J. Byrne, W.L. Hwu, Efficacy and safety of AAV2 gene therapy in children with aromatic L-amino acid decarboxylase deficiency: an open-label, phase 1/2 trial Lancet Child Adolesc Health 1 (2017) 265-273.
39. W. Dai, D. Lu, X. Gu, Y. Yu, A.R.D. Mainland Chinese League of, Aromatic L-amino acid decarboxylase deficiency in 17 Mainland China patients: Clinical phenotype, molecular spectrum, and therapy overview Mol Genet Genomic Med 8 (2020) e1143.
40. B. Monteleone, K. Hyland, Case report: discovery of 2 gene variants for aromatic L-amino acid decarboxylase deficiency in 2 African American siblings BMC Neurol 20 (2020) 12.
41. H. Brennenstuhl, D. Kohlmuller, G. Gramer, S.F. Garbade, S. Syrbe, P. Feyh, S. Kolker, J.G. Okun, G.F. Hoffmann, T. Opladen, High throughput newborn screening for aromatic L- amino-acid decarboxylase deficiency by analysis of concentrations of 3-O-methyldopa from dried blood spots Journal of inherited metabolic disease (2019).
5
Voorbereid document _Tessa Wassenberg_V03.indd 93Voorbereid document _Tessa Wassenberg_V03.indd 93 25/10/2021 09:3225/10/2021 09:32

94
Chapter 5
Supplement B. Tyrosine Hydroxylase Deficiency: included patients
Pt NR Level of diagnosis Reference TML Prolactin Urine NT CSF NT
1 CSF, DNA [1-4] x x x X
2 CSF, DNA [5-7] x X
3 CSF, DNA [5-8] x x X
4 CSF, DNA [5-8] x X
5 CSF, DNA [5-8] x x X
6 CSF, DNA [9] x
7 CSF, DNA [9] x
8 CSF, DNA [3,10,11] x x X
9 CSF, DNA [3] x
10 CSF, DNA [12] x X
11 CSF, DNA [13,14] x
12 CSF, DNA [13,14] X
13 CSF, DNA [13,14] x
14 CSF, DNA [13-15] x X
15 CSF, DNA [14,15] x X
16 CSF, DNA [16,17] X
17 CSF, DNA [18] x x X
18 DNA [19,20] x
19 DNA [19,20] x
20 CSF, DNA [21] x X
21 CSF, DNA [22] x X
22 CSF, DNA [14] x X
23 CSF, DNA [14] x X
24 CSF, DNA [23] x x x
25 DNA [24] x
26 DNA [24] x
27 DNA [25] x
Supplemental Table B: Level of diagnosis: diagnostic tests that were performed to confirm TH-deficiency. CSF: typical neurotransmitter profile in cerebrospinal fluid. DNA: molecular diagnosis confirmed.
• TML: Translational Metabolic Laboratory, data included from TML database that was not previously reported in the literature.
• Prolactin: serum prolactin• Urine NT: measurements of multiple neurotransmitter metabolites in urine.• CSF NT: measurement of neurotransmitter metabolites in cerebrospinal fluid before and
during medical treatment
Voorbereid document _Tessa Wassenberg_V03.indd 94Voorbereid document _Tessa Wassenberg_V03.indd 94 25/10/2021 09:3225/10/2021 09:32

95
Blood, urine and CSF in TH and AADC deficiency
Reference list supplement B TH deficiency
1. C. Brautigam, G.C. Steenbergen-Spanjers, G.F. Hoffmann, C. Dionisi-Vici, L.P. van den Heuvel, J.A. Smeitink, R.A. Wevers, Biochemical and molecular genetic characteristics of the severe form of tyrosine hydroxylase deficiency Clinical chemistry 45 (1999) 2073-2078.
2. C. Dionisi-Vici, G.F. Hoffmann, V. Leuzzi, H. Hoffken, C. Brautigam, C. Rizzo, G.C. Steebergen-Spanjers, J.A. Smeitink, R.A. Wevers, Tyrosine hydroxylase deficiency with severe clinical course: clinical and biochemical investigations and optimization of therapy The Journal of pediatrics 136 (2000) 560-562.
3. G.F. Hoffmann, B. Assmann, C. Brautigam, C. Dionisi-Vici, M. Haussler, J.B. de Klerk, M. Naumann, G.C. Steenbergen-Spanjers, H.M. Strassburg, R.A. Wevers, Tyrosine hydroxylase deficiency causes progressive encephalopathy and dopa-nonresponsive dystonia Annals of neurology 54 Suppl 6 (2003) S56-65.
4. V. Leuzzi, M. Mastrangelo, M.T. Giannini, R. Carbonetti, G.F. Hoffmann, Neuromotor and cognitive outcomes of early treatment in tyrosine hydroxylase deficiency type B Neurology 88 (2017) 501-502.
5. C. Brautigam, R.A. Wevers, R.J. Jansen, J.A. Smeitink, J.F. de Rijk-van Andel, F.J. Gabreels, G.F. Hoffmann, Biochemical hallmarks of tyrosine hydroxylase deficiency Clinical chemistry 44 (1998) 1897-1904.
6. R.A. Wevers, J.F. de Rijk-van Andel, C. Brautigam, B. Geurtz, L.P. van den Heuvel, G.C. Steenbergen-Spanjers, J.A. Smeitink, G.F. Hoffmann, F.J. Gabreels, A review of biochemical and molecular genetic aspects of tyrosine hydroxylase deficiency including a novel mutation (291delC) Journal of inherited metabolic disease 22 (1999) 364-373.
7. J.F. de Rijk-Van Andel, F.J. Gabreels, B. Geurtz, G.C. Steenbergen-Spanjers, L.P. van Den Heuvel, J.A. Smeitink, R.A. Wevers, L-dopa-responsive infantile hypokinetic rigid parkinsonism due to tyrosine hydroxylase deficiency Neurology 55 (2000) 1926-1928.
8. L.P. van den Heuvel, B. Luiten, J.A. Smeitink, J.F. de Rijk-van Andel, K. Hyland, G.C. Steenbergen-Spanjers, R.J. Janssen, R.A. Wevers, A common point mutation in the tyrosine hydroxylase gene in autosomal recessive L-DOPA-responsive dystonia in the Dutch population Hum Genet 102 (1998) 644-646.
9. T. Giovanniello, D. Claps, C. Carducci, C. Carducci, N. Blau, F. Vigevano, I. Antonozzi, V. Leuzzi, A new tyrosine hydroxylase genotype associated with early-onset severe encephalopathy J Child Neurol 27 (2012) 523-525.
10. R.J. Janssen, R.A. Wevers, M. Haussler, J.A. Luyten, G.C. Steenbergen-Spanjers, G.F. Hoffmann, T. Nagatsu, L.P. Van den Heuvel, A branch site mutation leading to aberrant splicing of the human tyrosine hydroxylase gene in a child with a severe extrapyramidal movement disorder Ann Hum Genet 64 (2000) 375-382.
11. M. Haussler, G.F. Hoffmann, R.A. Wevers, L-dopa and selegiline for tyrosine hydroxylase deficiency The Journal of pediatrics 138 (2001) 451-452.
5
Voorbereid document _Tessa Wassenberg_V03.indd 95Voorbereid document _Tessa Wassenberg_V03.indd 95 25/10/2021 09:3225/10/2021 09:32

96
Chapter 5
12. B. Ludecke, P.M. Knappskog, P.T. Clayton, R.A. Surtees, J.D. Clelland, S.J. Heales, M.P. Brand, K. Bartholome, T. Flatmark, Recessively inherited L-DOPA-responsive parkinsonism in infancy caused by a point mutation (L205P) in the tyrosine hydroxylase gene Human molecular genetics 5 (1996) 1023-1028.
13. C.M. Mak, C.W. Lam, T.S. Siu, K.Y. Chan, W.K. Siu, W.L. Yeung, J. Hui, V.C. Wong, L.C. Low, C.H. Ko, C.W. Fung, S.P. Chen, Y.P. Yuen, H.C. Lee, E. Yau, B. Chan, S.F. Tong, S. Tam, Y.W. Chan, Biochemical and molecular characterization of tyrosine hydroxylase deficiency in Hong Kong Chinese Mol Genet Metab 99 (2010) 431-433.
14. W.L. Yeung, V.C. Wong, K.Y. Chan, J. Hui, C.W. Fung, E. Yau, C.H. Ko, C.W. Lam, C.M. Mak, S. Siu, L. Low, Expanding phenotype and clinical analysis of tyrosine hydroxylase deficiency J Child Neurol 26 (2011) 179-187.
15. W.L. Yeung, C.W. Lam, J. Hui, S.F. Tong, S.P. Wu, Galactorrhea-a strong clinical clue towards the diagnosis of neurotransmitter disease Brain Dev 28 (2006) 389-391.
16. M. Ribases, M. Serrano, E. Fernandez-Alvarez, S. Pahisa, A. Ormazabal, A. Garcia-Cazorla, B. Perez-Duenas, J. Campistol, R. Artuch, B. Cormand, A homozygous tyrosine hydroxylase gene promoter mutation in a patient with dopa-responsive encephalopathy: clinical, biochemical and genetic analysis Mol Genet Metab 92 (2007) 274-277.
17. C. Ortez, S.T. Duarte, A. Ormazabal, M. Serrano, A. Perez, R. Pons, M. Pineda, Z. Yapici, E. Fernandez-Alvarez, R. Domingo-Jimenez, P. De Castro, R. Artuch, A. Garcia-Cazorla, Cerebrospinal fluid synaptic proteins as useful biomarkers in tyrosine hydroxylase deficiency Mol Genet Metab 114 (2015) 34-40.
18. D.E.L. P, M.C. Nassogne, A.H. van Gennip, A.C. van Cruchten, T. Billatte de Villemeur, M. Cretz, C. Stoll, J.M. Launay, G.C. Steenberger-Spante, L.P. van den Heuvel, R.A. Wevers, J.M. Saudubray, N.G. Abeling, Tyrosine hydroxylase deficiency unresponsive to L-dopa treatment with unusual clinical and biochemical presentation Journal of inherited metabolic disease 23 (2000) 819-825.
19. P. Rondot, M. Ziegler, Dystonia--L-dopa responsive or juvenile parkinsonism? Journal of neural transmission. Supplementum 19 (1983) 273-281.
20. R.J. Swaans, P. Rondot, W.O. Renier, L.P. Van Den Heuvel, G.C. Steenbergen-Spanjers, R.A. Wevers, Four novel mutations in the tyrosine hydroxylase gene in patients with infantile parkinsonism Ann Hum Genet 64 (2000) 25-31.
21. K. Szentivanyi, H. Hansikova, J. Krijt, K. Vinsova, M. Tesarova, E. Rozsypalova, P. Klement, J. Zeman, T. Honzik, Novel mutations in the tyrosine hydroxylase gene in the first Czech patient with tyrosine hydroxylase deficiency Prague Med Rep 113 (2012) 136-146.
22. M.M. Verbeek, G.C. Steenbergen-Spanjers, M.A. Willemsen, F.A. Hol, J. Smeitink, J. Seeger, P. Grattan-Smith, M.M. Ryan, G.F. Hoffmann, M.A. Donati, N. Blau, R.A. Wevers, Mutations in the cyclic adenosine monophosphate response element of the tyrosine hydroxylase gene Annals of neurology 62 (2007) 422-426.
23. D.I. Zafeiriou, M.A. Willemsen, M.M. Verbeek, E. Vargiami, A. Ververi, R. Wevers, Tyrosine hydroxylase deficiency with severe clinical course Mol Genet Metab 97 (2009) 18- 20.
24. J.N. Goswami, N. Sankhyan, P.D. Singhi, An Indian Family with Tyrosine Hydroxylase Deficiency Indian Pediatr 54 (2017) 499-501.
Voorbereid document _Tessa Wassenberg_V03.indd 96Voorbereid document _Tessa Wassenberg_V03.indd 96 25/10/2021 09:3225/10/2021 09:32

97
Blood, urine and CSF in TH and AADC deficiency
25. B. Feng, G. Sun, Q. Kong, Q. Li, Compound heterozygous mutations in the TH gene in a Chinese family with autosomal-recessive dopa-responsive dystonia: A case report Medicine (Baltimore) 97 (2018) e12870.
5
Voorbereid document _Tessa Wassenberg_V03.indd 97Voorbereid document _Tessa Wassenberg_V03.indd 97 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 98Voorbereid document _Tessa Wassenberg_V03.indd 98 25/10/2021 09:3225/10/2021 09:32

PART III
Beyond the
classic phenotype:
clinical observations
Voorbereid document _Tessa Wassenberg_V03.indd 99Voorbereid document _Tessa Wassenberg_V03.indd 99 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 100Voorbereid document _Tessa Wassenberg_V03.indd 100 25/10/2021 09:3225/10/2021 09:32

CHAPTER 6
Pyramidal predominant presentation of GCH1 mutations
Tessa Wassenberg, Meyke I. Schouten, Rick C. Helmich, Michèl A.A.P. Willemsen, Erik-Jan Kamsteeg, Bart P.C. van de Warrenburg
Parkinsonism Relat Disord. 2020; 74: 12-15DOI doi: 10.1016/j.parkreldis.2020.03.019
Voorbereid document _Tessa Wassenberg_V03.indd 101Voorbereid document _Tessa Wassenberg_V03.indd 101 25/10/2021 09:3225/10/2021 09:32

102
Chapter 6
Abstract
Background: Autosomal dominant GCH1 mutations are known to cause dopa-responsive dystonia (DRD). In this case series, we confirm a variant phenotype, characterized by predominant spastic paraplegia at disease onset with development of dystonia and/or parkinsonism only decades later.
Methods: Clinical trajectories of four patients from three families with pathogenic variants in GCH1 are described, illustrated by videos of the motor phenotype before and during treatment with levodopa. An extensive literature review was performed on previous reports of spasticity in patients with autosomal dominant GCH1 mutations.
Results: All patients presented during childhood or early adolescence with gait and leg spasticity. Three patients developed basal ganglia signs only in the fifth decade; the youngest patient has not yet developed dystonia, bradykinesia or hypokinesia. All patients responded to levodopa/carbidopa with improvement of gait and of dystonia, hypokinesia and/or rigidity. In all patients, spasticity decreased but did not disappear. Spasticity has been described previously in DRD, but in most cases co-existent basal ganglia signs were identified early in the disease course.
Conclusion: GCH1 mutations may cause a phenotype initially resembling hereditary spastic paraplegia (HSP) rather than DRD, with basal ganglia signs developing only after decades. In order not to miss this treatable condition, GCH1 should be included in HSP gene panels and its testing is pivotal in patients with spastic paraplegia, especially if there are concomitant basal ganglia signs and/or diurnal fluctuation.
Voorbereid document _Tessa Wassenberg_V03.indd 102Voorbereid document _Tessa Wassenberg_V03.indd 102 25/10/2021 09:3225/10/2021 09:32

103
Pyramidal predominant presentation of GCH1 mutations
Introduction
Autosomal dominant GTP Cyclohydrolase I (GCH1) gene mutations cause dopa-responsive dystonia (DRD), typically presenting with childhood-onset lower limb dystonia with diurnal fluctuations and an excellent response to levodopa1. More recently, adult-onset parkinsonism due to nigral degeneration, thus resembling Parkinson’s disease2 has been added to the clinical spectrum of GCH1 mutations.
DRD is part of the differential diagnosis of hereditary spastic paraplegias (HSP), the main reason being that lower limb dystonia can be confused with spastic paraparesis3. Furthermore, patients with GCH1 mutations can be misdiagnosed for having spastic diplegic cerebral palsy4. Interestingly, GCH1 mutations have also been found in patients with phenotypes that are in fact compatible with hereditary spastic paraplegia (HSP)5, 6. This is surprising and warrants confirmation, as it is difficult to link the neurobiological consequence of GCH1 mutations (dopamine and serotonin deficiency) to spasticity.
We here describe a series of patients with GCH1 mutations and initial HSP-like phenotypes, in whom basal ganglia signs developed only after decades. We also provide a literature overview of earlier reports on spasticity in DRD.
Methods
All patients were referred to our tertiary movement disorder expert center for clinical and molecular evaluation because of suspected HSP.
Whole-exome sequencing (WES), read mapping and variant calling were performed by BGI-Europa (Copenhagen, DK). Variant annotation and prioritization was done as described7. Exome data was analyzed using a gene panel for movement disorders (patient A2 version DGD200614, patient B and C version DGD141114) consisting of >150 genes each. The panels can be found online (https://www.radboudumc.nl/en/patientenzorg/onderzoeken/exome-sequencing-diagnostics/exomepanelspreviousversions/movement-disorders). Variants were classified as pathogenic according to the American College of Medical Genetics and Genomics8.
Clinical exome sequencing was approved by the Medical Review Ethics Committee Arnhem-Nijmegen (no. 2011/188). Written informed consent for genetic analysis and publication including video material was obtained from all patients.
An extensive literature search was performed on Pubmed using (dopa responsive dystonia, GCH1, spasticity, cerebral palsy) and [Dystonia, dopa responsive] (Mesh) in various combinations.
6
Voorbereid document _Tessa Wassenberg_V03.indd 103Voorbereid document _Tessa Wassenberg_V03.indd 103 25/10/2021 09:3225/10/2021 09:32

104
Chapter 6
Case descriptions
All patients were born after normal pregnancies and deliveries and had normal early milestone development unless otherwise described. All patients have normal cognitive abilities. Table 1 summarizes molecular and main clinical findings, including diurnal fluctuation. Fig. 1 graphically summarizes the individual clinical trajectories with onset of spasticity and basal ganglia signs, age of clinical examination in our center, and ages at molecular diagnosis and at start of treatment.
Table 1. Main clinical findings before treatment with levodopa/carbidopa.
Case
Sex
Mut
ation
Age
at o
nset
gai
t di
stur
banc
e (y
)
Age
at o
nset
bas
al g
angl
ia
sign
s (y)
Age
at d
iagn
osis
(y)
Firs
t clin
ical
dia
gnos
is
Diu
rnal
fluc
tuati
ons
Blad
der s
ympt
oms
Spas
tic g
ait
Spas
ticity
legs
(L/R
)
Hyp
erre
flexi
a (L
/R)
Plan
tar r
espo
nse(
L/R)
Dys
toni
a
Park
inso
nism
1.1 F c.454-2A>G (r.spl?)
≈ 2 54 56 Cerebral palsy
+ + ++ ++/++ +/+ ↑/↑ + -/+
1.2 F c.454-2A>G (r.spl?)
3 - 25 HSP ++ - + ++/++ +/+ ↑/↓ - -
2 F c.193del (p.Glu65fs)
14 42 49 Cervical stenosis
HSP
+ + ++ ++/++ +/+ ↓/↑ ++ +
3 M c.631_632del (p.Met211fs)
7 49 50 HSP + - ++ ++/+ ++/+ ↑/= - ++
Table 1. summarizes main clinical findings in four patients with an autosomal dominant GCH1 mutation. Disease onset was in childhood or early adolescence in all patients, with spastic gait. Basal ganglia signs developed only in the fifth decade. Diurnal fluctuation was present in all patients. All three genetic variants are considered likely pathogenic by applying ACMG guidelines (criteria PVS1 and PM2) [8]. None of the three variants were detected in gnomAD (https://www.biorxiv.org/content/10.1101/531210v3). Almost 250 different pathogenic variants are described in The Human Gene Mutation Database: hgmd.cf.ac.uk/ac/gene.php?gene = GCH1.Abbreviations: F: female, M: male, y: year, L: left, R: right. HSP: hereditary spastic paraparesis. NA: not applicable. Plantar responses: ↑: extensor, ↓: flexor, = : equivocal.
Voorbereid document _Tessa Wassenberg_V03.indd 104Voorbereid document _Tessa Wassenberg_V03.indd 104 25/10/2021 09:3225/10/2021 09:32

105
Pyramidal predominant presentation of GCH1 mutations
Figure 1. Graphical representation of clinical trajectories
Figure 1. Graphical representation of clinical trajectories in four patients with an autosomal dominant GCH1 mutation, with time in years on the x-axis. All patients had pyramidal-predominant signs (spastic gait, increased reflexes, Babinski sign in some) that preceded basal ganglia signs (dystonia in patient 1.1, dystonia and parkinsonism in patient 2, parkinsonism in patient 3) by many years and have not yet developed in the youngest patient (1.2). Levodopa/carbidopa treatment was started directly after molecular diagnosis in all patients. Furthermore, timing of the first neurological examinations in our clinic and videos are indicated.
Cases 1.1 and 1.2 (Mother and daughter)Case 1-1. This 58-years-old woman was born full term with severe growth restriction (1200 g) and signs of perinatal asphyxia (Apgar scores and umbilical cord pH values are unknown). Still, she had normal early milestone development. She was never able to walk long distances and complained of leg stiffness. She carried a diagnosis of cerebral palsy, but at age 54 years, she deteriorated and was referred to our department with fatigue, balance problems, and urinary urgency with frequent nocturia. Gait worsened over the course of the day. Neurological examination showed a broad based, predominantly spastic gait with constant upward extension of both halluces [VIDEO 1], brisk knee and ankle jerks and bilateral Babinski signs. There was mild cervical dystonia, and no hypokinesia except for reduced arm swing on the right. Imaging of brain and spinal cord was normal. At this time, her daughter (case 1.2) was referred for WES
6
Voorbereid document _Tessa Wassenberg_V03.indd 105Voorbereid document _Tessa Wassenberg_V03.indd 105 25/10/2021 09:3225/10/2021 09:32

106
Chapter 6
because of suspected HSP. Following her daughters’ WES result (see below), GCH1 was sequenced and confirmed to harbour the same mutation. Her gait showed a swift and good response to levodopa/carbidopa. Recent neurological exam showed mildly increased tone in the left leg, increased tendon reflexes without clonus [VIDEO 2], and equivocal plantar responses.
Case 1.2: From age three years, this 28-years-old woman suffered from mildly progressive walking difficulties that increased over the course of the day with associated fatigue. At age 17 years, she first visited a neurologist who diagnosed spastic paraplegia. MRI of the brain and spinal cord were normal. Genetic investigations showed no mutations in spastic paraplegia genes (SPG) 3A, 4, 7, 10 and 31. WES analysis then revealed a GCH1 mutation. Clinical reassessment at our department confirmed a mild bilateral spastic gait and evident spasticity of both legs when tested on the bench. Knee jerks were bilaterally increased with non-sustained clonus on the left, and ankle jerks were increased with non-sustained clonus on the right. She had a left-sided Babinski sign (not shown). Foot tapping was slow, irregular and demanding for the patient from the start onwards, without progressive loss of speed or amplitude or dystonic posturing [VIDEO 3]. Levodopa/carbidopa therapy was started and she responded within two days with a marked improvement of gait and fatigue. Furthermore, speed and fluency of foot tapping improved. Leg tone and knee and ankle jerks remained somewhat increased [VIDEO 4]. Babinski sign was no longer present. There were still no signs of dystonia or parkinsonism on follow-up.
Case 2From age 14 years, this 52-years-old woman manifested progressive walking difficulties with leg stiffness and circumduction (right > left). At age 40, a cervical stenosis without myelopathy was diagnosed and a laminectomy (C4–C7) was performed. Subsequently, her gait transiently improved but deteriorated over the following years with progressive spasticity of the legs and mild urinary urgency, despite a sufficiently wide cervical canal on follow-up MRI. Therefore, HSP was suspected and she was referred to our center. Neurological examination at age 48 years showed mixed pyramidal and basal ganglia signs with spastic gait with upward deviation of both halluces, mild dystonia of the left arm, cervical dystonia, facial hypomimia and bradykinesia of the right hand [VIDEO 5]. There was no ankle clonus; it has to be noted that she previously underwent phenolization of the right tibial nerve. Plantar reflexes showed extension on the right and flexion on the left. At age 49 years, WES showed a GCH1 mutation. Levodopa/carbidopa was started with clear improvement of gait, bradykinesia, and dystonia. Leg tone remained increased [VIDEO 6]. Interestingly, she had evening dyskinesias that restricted levodopa/carbidopa dose to 100/25 mg bid +12.5/6.25 mg an.
Voorbereid document _Tessa Wassenberg_V03.indd 106Voorbereid document _Tessa Wassenberg_V03.indd 106 25/10/2021 09:3225/10/2021 09:32

107
Pyramidal predominant presentation of GCH1 mutations
Case 3From age seven years, this 54-years-old man developed slowly progressive walking difficulties described as a stiff gait. At age 40 years, he was first seen at our tertiary movement disorder clinic, showing a mild bilateral spastic gait, more pronounced on the right, with markedly increased tendon reflexes of the lower limbs, suggestive of HSP. No basal ganglia signs were noted. Unfortunately, video material of this examination is not available. A year later, he suffered a severe traumatic brain injury, with cerebral contusion and right-sided subdural hematoma, which led to a left-sided pyramidal syndrome. At age 50 years, fine motor skills and reaction speed had declined. Neurological reassessment showed a mixed bilateral pyramidal (left > right) and hypokinetic rigid syndrome with hypomimia and mild bradykinesia on finger tapping, but no dystonia. Tendon reflexes were increased, more so on the left, with a Babinski sign on the left. WES was performed, after SPG 3, 4, 7 and 31 mutations had been excluded earlier, and showed a mutation in GCH1. Parkinsonian features and gait clearly improved on low dose levodopa/carbidopa, while spasticity, including tendon and plantar reflexes, did not change.
Literature review
We identified 48 patients with dopa responsive dystonia and spasticity from 20 publications, of which 16 patients were identified on clinical grounds only, four patients on clinical and cerebrospinal fluid characteristics, and the remaining patients on clinical grounds and dominant GCH1 mutations. All references and clinical and molecular details can be found in Supplemental Table 1. In summary, of these 48 patients, 26 had a more progressive course than the patients we present in our series, with severe functional impairment before the age of 20 years and/or additional clear dystonia before the age of 20 years. In four patients with predominant spasticity at disease onset, diagnoses were made before the age of 13 years, possibly before the appearance of basal ganglia signs. In nine patients, there was not enough information available to adequately compare the clinical course to our cases. The remaining nine patients had a clinical course that seems comparable to our patients, with predominant lower limb spasticity at disease onset and basal ganglia signs developing later in life. Only Fan et al. provided photographic material to support their findings5.
Discussion
Our case series provides the confirmation that patients with dominant GCH1 mutations can present with lower limb spasticity5, 6 and shows that it can evolve into a mixed pyramidal-dystonia-parkinsonism phenotype only after long-term follow-up. To our knowledge, we are the first to provide video material of this phenotype. Although lower limb dystonia can easily be mistaken for spasticity in patients with DRD (e.g. upward extension of hallux representing striatal toe rather than Babinski sign), and
6
Voorbereid document _Tessa Wassenberg_V03.indd 107Voorbereid document _Tessa Wassenberg_V03.indd 107 25/10/2021 09:3225/10/2021 09:32

108
Chapter 6
brisk tendon reflexes and ankle clonus are often present in this patient group1, the initial presentation in our patients was that of spastic paraplegia rather than lower limb dystonia. Neurological exam in the youngest patient shows leg spasticity and spastic gait, without clear dystonia or parkinsonism. In the three older patients, clear basal ganglia signs have emerged in addition to lower limb spasticity.
All patients clearly improved on levodopa/carbidopa therapy. We appreciate that the treatment effect in cases 2 and 3 is probably driven most by the effect of levodopa on the basal ganglia features. The evening dyskinesias in case 2, who is clearly parkinsonian at this stage, could possibly be related to nigrostriatal degeneration2, although we did not perform imaging studies to confirm this. However, in case 1.1 and 1.2 the disappearance of Babinski signs and improvement of spastic gait argue for an effect of levodopa on pyramidal signs as well. The etiology of spasticity in patients with a GCH1 mutation is not easily explained. Nonetheless, tetrahydrobiopterin (the end product of the biopterin pathway in which GCH1 is an enzyme) has multiple metabolic functions beside monoamine production9, and spasticity might arise from other deficiencies than dopamine.
We did not perform neurophysiological testing in our case series to further explore the corticospinal tract in GCH1 mutations. As such, we cannot convincingly link the spasticity in our cases neuro-anatomically to actual dysfunction of the pyramidal tract. Still, the clinical constellation and disease course in our patients is highly suggestive of a predominantly pyramidal phenotype at disease onset, and clearly different from the classic disease course in patients with DRD. On the other hand, distinguishing dystonia and spasticity can be notoriously difficult, illustrated by a low interobserver agreement in a study of patients with cerebral palsy10. Although we show in our literature review that in most patients in whom spasticity was described basal ganglia signs already clearly existed early in disease course, HSP-like presentations have been described in the literature before, and this phenotype might be less rare than currently assumed. It is therefore important to appreciate this particular phenotype of GCH1 mutations and to include this gene in the genetic work-up of HSP.
In our case series, 1 splicing and 2 frameshift mutations were found. The splicing mutation in family 1 and two base pair deletion leading to a frameshift in patient 3 have previously been described in patients with a classical DRD phenotype11, 12. The deletion leading to a frameshift in patient 2 is newly reported here. In previously reported patients with predominantly pyramidal presentations of GCH1 mutation, both truncating and missense mutations were found (Supplementary Table 1). Besides variation in expression, the large inter- and intrafamily variability of autosomal dominant GCH1 mutations is not well understood.
Voorbereid document _Tessa Wassenberg_V03.indd 108Voorbereid document _Tessa Wassenberg_V03.indd 108 25/10/2021 09:3225/10/2021 09:32
109
Pyramidal predominant presentation of GCH1 mutations
Identification of a GCH1 mutation is crucial because of the excellent treatment response to levodopa. A clinical clue pointing to the possibility of a GCH1 mutation in a patient with a HSP phenotype is diurnal fluctuation, with deterioration in the course of the day and improvement after sleep and/or daytime naps that was present in all of our patients (Table 1). Diurnal fluctuation is a well-known feature of classic DRD but not always present1. GCH1 should be included in HSP gene panels and its testing is particularly – but not exclusively-warranted in patients with lower limb spasticity with childhood onset, and co-existing basal ganglia signs and/or diurnal fluctuation later in disease course.
AcknowledgementsWe thank all patients for participating. We thank dr. Björn van Geel, MD PhD, neurologist NoordWest Ziekenhuis Alkmaar, the Netherlands for the referral and assistance in obtaining video material. Several authors of this publication are members of the European Reference Network for Rare Neurological Diseases - Project ID No 739510.
6
Voorbereid document _Tessa Wassenberg_V03.indd 109Voorbereid document _Tessa Wassenberg_V03.indd 109 25/10/2021 09:3225/10/2021 09:32

110
Chapter 6
References
1. Furukawa Y. GTP Cyclohydrolase 1-Deficient Dopa-Responsive Dystonia. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, et al., editors. GeneReviews(R). Seattle (WA)1993.
2. Mencacci NE, Isaias IU, Reich MM, et al. Parkinson’s disease in GTP cyclohydrolase 1 mutation carriers. Brain : a journal of neurology. 2014 Sep;137(Pt 9):2480-92.
3. Fink JK. Hereditary spastic paraplegia: clinical principles and genetic advances. Seminars in neurology. 2014 Jul;34(3):293-305.
4. Lee JH, Ki CS, Kim DS, Cho JW, Park KP, Kim S. Dopa-responsive dystonia with a novel initiation codon mutation in the GCH1 gene misdiagnosed as cerebral palsy. J Korean Med Sci. 2011 Sep;26(9):1244-6.
5. Fan Z, Greenwood R, Felix AC, et al. GCH1 heterozygous mutation identified by whole- exome sequencing as a treatable condition in a patient presenting with progressive spastic paraplegia. Journal of neurology. 2014 Mar;261(3):622-4.
6. Tassin J, Durr A, Bonnet AM, et al. Levodopa-responsive dystonia. GTP cyclohydrolase I or parkin mutations? Brain : a journal of neurology. 2000 Jun;123 ( Pt 6):1112-21.
7. Neveling K, Feenstra I, Gilissen C, et al. A post-hoc comparison of the utility of sanger sequencing and exome sequencing for the diagnosis of heterogeneous diseases. Hum Mutat. 2013 Dec;34(12):1721-6.
8. Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015 May;17(5):405-24.
9. Werner ER, Blau N, Thony B. Tetrahydrobiopterin: biochemistry and pathophysiology. The Biochemical journal. 2011 Sep 15;438(3):397-414.
10. Eggink H, Kremer D, Brouwer OF, et al. Spasticity, dyskinesia and ataxia in cerebral palsy: Are we sure we can differentiate them? Eur J Paediatr Neurol. 2017 Sep;21(5):703-6.
11. Weber Y, Steinberger D, Deuschl G, Benecke R, Muller U. Two previously unrecognized splicing mutations of GCH1 in Dopa-responsive dystonia: exon skipping and one base insertion. Neurogenetics. 1997 Sep;1(2):125-7.
12. Bandmann O, Valente EM, Holmans P, et al. Dopa-responsive dystonia: a clinical and molecular genetic study. Annals of neurology. 1998 Oct;44(4):649-56.
Voorbereid document _Tessa Wassenberg_V03.indd 110Voorbereid document _Tessa Wassenberg_V03.indd 110 25/10/2021 09:3225/10/2021 09:32

111
Pyramidal predominant presentation of GCH1 mutations
Supplemental material Chapter 6
Video legends• Video 1: Case 1.1, female, aged 54 years, before start of levodopa/carbidopa
therapy. Gait is broad based and spastic with stiff legs, limited foot dorsiflexion, and circumduction. There is mild increase of toe walking with increasing walking distance. There is spontaneous upward extension of both halluces (R>L). Speed of gait and turning speed is slow. Also, there is reduced arm swing on the right.
• Video 2: Case 1.1, female, aged 58 years, after 2 years of treatment with levodopa/carbidopa 50/12.5 mg three times daily. Overall, gait is more fluent with increased gait speed and reduced step width. Arm swing is still reduced on the right. On the bench, hypertonia of the left leg is demonstrated. Knee jerks are brisk (L>R).
• Video 3: Case 1.2, female, aged 25 years , before start of levodopa/carbidopa therapy. Gait is mildly affected. Gait speed is somewhat slow, gait is slightly broad-based, and there is mild leg stiffness with upward extension of the halluces. On the bench, there is clear spasticity of both legs with increased tone and spastic catch. Knee jerks are increased with unsustained clonus on the left, ankle jerks are increased with unsustained clonus on the right. Toe tapping is slow and irregular from the start onward, without evident bradykinesia. It is a difficult test for the patient to perform.
• Video 4: Case 1.2, female, aged 28 years, during treatment with levodopa/carbidopa 50/12.5 mg three times daily. Her gait is clearly improved: increased speed, less stiffness, normal-based, and more fluent. By testing on the bench, there is still leg hypertonia and increased knee and ankle jerks, without clonus. Toe tapping evidently improved in speed and ease.
• Video 5: Case 2, female, aged 48 years, before start of levodopa/carbidopa therapy. Gait is predominantly spastic with slow speed and slow turning, circumduction and scissoring; there is upward deviation of both halluces. Arm swing is normal. Trunk and head are deviated laterally. By testing on the bench, there is marked hypertonia and pes equinus bilaterally. Facial hypomimia is evident. There is a torticollis to the right with lateroflexion to the left, and mild dystonic posturing of the fingers and arms. Finger tapping is irregular on both sides, with bradykinesia on the right.
• Video 6: Case 2, female, aged 49 years, during treatment with levodopa/carbidopa 100/25 mg twice a day and 12.5/ 3.125 mg at night. Gait has clearly improved, with increased speed and decreased circumduction; there is less axial deviation. On the bench, there is still hypertonia of both legs. Facial hypomimia has improved. Cervical and brachial dystonia have also improved but are still present. Finger tapping is more regular on both side without definite bradykinesia.
Videos can be found online through sciencedirect: https://www.sciencedirect.com/science/article/pii/S1353802020300754?via%3Dihub
6
Voorbereid document _Tessa Wassenberg_V03.indd 111Voorbereid document _Tessa Wassenberg_V03.indd 111 25/10/2021 09:3225/10/2021 09:32

112
Chapter 6
Supp
lem
enta
ry T
able
1. L
itera
ture
rep
orts
of p
yram
idal
sig
ns in
pati
ents
with
aut
osom
al d
omin
ant G
CH1
mut
ation
s/ d
opa
resp
onsi
ve d
ysto
nia
and
com
paris
on w
ith o
ur c
ase
serie
s.
Auth
or, y
ear
Num
ber o
f pa
tient
s, a
geLe
vel o
f dia
gnos
isCl
inic
al d
escr
iptio
nVi
deo/
phot
o m
ater
ial
Com
paris
on w
ith
curr
ent c
ase
serie
s
[1]
Fink
et a
l, 19
885
patie
nts
5-30
yCl
inic
alN
onpr
ogre
ssiv
e sp
astic
par
apar
esis
(spa
stic
cere
bral
pal
sy)
was
pre
viou
sly d
iagn
osed
. All
gait
diffi
culti
es b
egan
in fi
rst
24 m
onth
s.In
add
ition
to
hype
rrefl
exia
of
the
low
er e
xtre
miti
es, a
ll pa
tient
s had
gen
eral
ized
dyst
onia
, par
ticul
arly
affe
cting
the
trun
k an
d lo
wer
ext
rem
ities
. All
had
diur
nal fl
uctu
ation
.
NA
Dyst
onia
ear
lier i
n co
urse
[2]
Boyd
, 198
9Fe
mal
e, 1
8yCl
inic
alO
nset
at a
ge 5
y w
ith ti
ptoe
wal
king
. Pro
gres
sive,
whe
elch
air
boun
d be
fore
18y
ears
. Exa
min
ation
at 1
8y: a
bnor
mal
pos
ture
, dy
ston
ia fi
nger
s, an
kles
and
neck
. On
stan
ding
, tipt
oe p
ositi
on
with
flex
ion
at th
e hi
ps. I
ncre
ased
tone
and
cog
whe
elin
g in
bo
th a
rms
and
legs
. Gen
eral
ized
hype
rrefl
exia
, ext
enso
r pl
anta
r res
pons
e.
NA
Mor
e pr
ogre
ssiv
e co
urse
, mor
e dy
ston
ia e
arly
in th
e co
urse
Fem
ale,
27y
Clin
ical
Ons
et a
t ag
e 5y
with
tipt
oe w
alki
ng. P
rogr
essiv
e sp
astic
pa
rapl
egia
was
dia
gnos
ed. I
n th
e fo
llow
ing
year
s, w
heel
chai
r bo
und
and
appe
aran
ce o
f dys
toni
c sym
ptom
s.
NA
Mor
e pr
ogre
ssiv
e co
urse
, mor
e dy
ston
ia
[3]
Brow
n an
d Br
itton
, 199
0
Fem
ale,
24y
Clin
ical
Ons
et a
t ag
e 1y
with
gai
t di
sord
er. T
rem
or f
rom
age
6y.
Ex
amin
ation
at a
ge 2
9y: h
esita
nt g
ait w
ith lo
ss o
f pos
tura
l re
flexe
s, in
crea
sed
tone
in lo
wer
lim
bs (a
ppar
ently
spa
stic)
, hy
perr
eflex
ia, e
xten
sor p
lant
ar re
spon
ses.
Norm
al se
nsati
on
NA
Com
para
ble,
bes
ides
tr
emor
Voorbereid document _Tessa Wassenberg_V03.indd 112Voorbereid document _Tessa Wassenberg_V03.indd 112 25/10/2021 09:3225/10/2021 09:32

113
Pyramidal predominant presentation of GCH1 mutations
Supp
lem
enta
ry T
able
1. [
Conti
nued
]
Auth
or, y
ear
Num
ber o
f pa
tient
s, a
geLe
vel o
f dia
gnos
isCl
inic
al d
escr
iptio
nVi
deo/
phot
o m
ater
ial
Com
paris
on w
ith
curr
ent c
ase
serie
s
[4]
Nyga
ard
et a
l, 19
94
Girl,
12y
Clin
ical
, CSF
(re
duce
d HV
A,
biop
terin
and
ne
opte
rin)
Dela
yed
wal
king
(22m
) Age
2y:
incr
ease
d to
ne in
add
ucto
r m
uscl
es o
f th
igh
and
Achi
lles
tend
ons,
gen
eral
ized
hy
perr
eflex
ia a
nd b
ilate
ral
exte
nsor
pla
ntar
res
pons
es.
Clin
ical
impr
essio
n of
spas
tic q
uadr
ipar
esis.
In th
e fo
llow
ing
year
s pro
gres
sive
cour
se w
ith m
ore
appa
rent
dys
toni
a ne
xt
to p
yram
idal
sign
s.
NA
Mor
e pr
ogre
ssiv
e co
urse
with
mor
e an
d ea
rly d
ysto
nia
4 ad
ditio
nal
patie
nts
Clin
ical
, CSF
in 3
pa
tient
s (re
duce
d HV
A, b
iopt
erin
, ne
opte
rin)
Less
ext
ensi
vely
des
crib
ed.
All h
ad a
dduc
tor
tight
enin
g,
Achi
lles t
endo
n sh
orte
ning
, ank
le cl
onus
and
ext
enso
r pla
ntar
re
spon
se.
NA
Not e
noug
h in
form
ation
[5]
Harw
ood
et a
l, 19
94
Fem
ale,
54y
Clin
ical
Ons
et a
t ag
e 6y
with
foo
t in
vers
ion.
Age
16y
ope
ratio
n to
len
gthe
n bo
th A
chill
es t
endo
ns,
no b
enefi
t. Ag
e 39
y m
ore
clea
r dys
toni
c ga
it. E
xagg
erat
ed te
ndon
refle
xes
and
appa
rent
ly e
xten
sor p
lant
ar re
spon
ses.
NA
Com
para
ble,
bes
ides
fo
ot in
vers
ion
[6]
Pate
l et a
l, 19
95
Girl,
10y
Clin
ical
Ons
et a
t age
5y
with
pro
gres
sive
gait
diso
rder
dia
gnos
ed a
s he
redi
tary
spa
stic
para
pare
sis. A
t age
10y
spa
stic
gait
with
to
e w
alki
ng, m
aske
d fa
ce, m
arke
dly
incr
ease
d to
ne in
low
er
limbs
with
bris
k re
flexe
s, an
kle
clon
us, a
nd s
pont
aneo
usly
up
-goi
ng p
lant
ars
NA
Com
para
ble,
but
ea
rlier
dia
gnos
is6
Voorbereid document _Tessa Wassenberg_V03.indd 113Voorbereid document _Tessa Wassenberg_V03.indd 113 25/10/2021 09:3225/10/2021 09:32

114
Chapter 6
Supp
lem
enta
ry T
able
1. [
Conti
nued
]
Auth
or, y
ear
Num
ber o
f pa
tient
s, a
geLe
vel o
f dia
gnos
isCl
inic
al d
escr
iptio
nVi
deo/
phot
o m
ater
ial
Com
paris
on w
ith
curr
ent c
ase
serie
s
[7]
Tass
in e
t al,
2000
Fem
ale,
47
y (m
othe
r)Cl
inic
al a
nd
gene
tic(c
.631
-632
delA
T;
p.M
ET21
1Val
(sto
p249
))
Spas
tic ga
it fro
m a
ge 1
2y w
ith b
road
gait,
incr
ease
d re
flexe
s in
the
low
er lim
bs, p
lant
ar fl
exor
resp
onse
s, pe
s cav
us a
nd m
ild
scol
iosis
. Pos
tura
l tre
mor
in u
pper
lim
bs. N
o dy
ston
ia. A
ge
47y:
not
abl
e to
wal
k w
ithou
t can
e, re
st tr
emor
wor
sene
d.
NA
Com
para
ble,
bes
ides
tr
emor
Girl,
19y
(d
augh
ter)
Clin
ical
and
ge
netic
(c.6
31-6
32de
lAT;
p.
MET
211V
al(s
top2
49))
Freq
uent
fal
ls an
d ga
it di
sord
er f
rom
age
8y,
whe
elch
air
boun
d ag
e 13
y. L
ower
lim
b sp
astic
ity w
ith n
orm
al re
flexe
s, de
crea
sed
ankl
e je
rks,
pla
ntar
ext
enso
r re
spon
ses.
Mild
po
stur
al t
rem
or i
n th
e ar
ms,
dys
toni
c w
riting
pos
ture
. Sc
olio
sis
NA
Mor
e pr
ogre
ssiv
e co
urse
, ear
lier
dyst
onia
and
trem
or
3 ad
ditio
nal
patie
nts
Clin
ical
and
ge
netic
al (c
.534
A>T,
p.
Arg1
78Se
r)(c
.539
A>T;
p.
Gln1
80Ar
g)(c
.645
C>T;
p.
Arg2
16St
op)
Gene
raliz
ed d
ysto
nia
with
add
ition
al lo
wer
lim
b sp
astic
ity
desc
ribed
in 2
pati
ents
, and
low
er li
mb
dyst
onia
with
low
er
limb
spas
ticity
in 1
pati
ent.
NA
Mor
e dy
ston
ia e
arly
in
cour
se
[8]
Chen
g an
d Ko
ng, 2
002
Girl,
7y
Clin
ical
Clin
ical
pic
ture
dom
inat
ed b
y th
e pr
esen
ce o
f upp
er m
otor
ne
uron
sign
s in
both
low
er lim
bs, a
nd co
ntra
ctur
es o
f Ach
illes
te
ndon
s. Br
isk re
flexe
s, bi
late
ral B
abin
ski s
igns
, inc
reas
ed le
g to
ne, a
sym
met
ric ti
p to
e w
alki
ng. S
ome
diur
nal fl
uctu
ation
.
NA
Com
para
ble,
but
ea
rlier
dia
gnos
is
Voorbereid document _Tessa Wassenberg_V03.indd 114Voorbereid document _Tessa Wassenberg_V03.indd 114 25/10/2021 09:3225/10/2021 09:32

115
Pyramidal predominant presentation of GCH1 mutations
Supp
lem
enta
ry T
able
1. [
Conti
nued
]
Auth
or, y
ear
Num
ber o
f pa
tient
s, a
geLe
vel o
f dia
gnos
isCl
inic
al d
escr
iptio
nVi
deo/
phot
o m
ater
ial
Com
paris
on w
ith
curr
ent c
ase
serie
s
[9]
Kang
et a
l, 20
04
Girl,
12y
Clin
ical
and
ge
netic
(p
.Met
137A
rg)
Ons
et a
t age
12y
with
gai
t dist
urba
nce:
stiff
gait
with
pla
ntar
fle
xed
feet
, hyp
erre
flexi
a of
legs
with
ext
ensio
n of
gre
at
toe.
Ton
ic fo
ot m
aneu
ver c
orre
cted
the
exte
nsor
resp
onse
. In
itial
ly d
iagn
osed
as h
avin
g sp
astic
par
apar
esis.
NA
Com
para
ble,
but
ea
rlier
dia
gnos
is
[10]
Gara
vagl
ia e
t al
, 200
4
Mal
e, 2
5yCl
inic
al a
nd
gene
tic (c
.614
T>G;
p.
V205
G)
Ons
et a
t age
7y
with
stiff
ness
and
tipt
oe w
alki
ng. A
ge 8
y:
spas
tic p
arap
ares
is le
ft m
ore
than
righ
t. Ag
e 25
y: s
low
ness
of
mov
emen
ts a
nd ri
gidi
ty in
upp
er li
mbs
.
NA
Com
para
ble
[11]
Jan,
200
4Bo
y, 3
yCl
inic
al, g
eneti
cs
not d
escr
ibed
Tip-
toe
wal
king
with
evi
dent
diu
rnal
fluc
tuati
on a
nd e
piso
dic
char
acte
r, aft
er in
itial
nor
mal
ear
ly d
evel
opm
ent.
Refe
rral
di
agno
sis m
ild sp
astic
dip
legi
c cer
ebra
l pal
sy.
NA
Com
para
ble,
but
ea
rlier
dia
gnos
is
Girl,
11y
Clin
ical
, gen
etics
no
t des
crib
edRe
ferr
al
diag
nosi
s pr
ogre
ssiv
e sp
astic
di
pleg
ia.
On
exam
inati
on d
ysto
nia
of lo
wer
lim
bs w
ith h
yper
refle
xia,
cl
onus
, and
nor
mal
pla
ntar
resp
onse
s.
NA
Mor
e dy
ston
ia e
arly
in
cour
se
Girl,
12y
Clin
ical
, gen
etics
no
t des
crib
edGe
nera
l pro
gres
sive
mot
or a
nd sp
eech
det
erio
ratio
n, d
iffus
e hy
pert
onia
, w
alki
ng d
ifficu
lties
. O
n ex
amin
ation
diff
use
limb
and
trun
cal d
ysto
nia,
dys
arth
ria, m
aske
d fa
cies
and
hy
perr
eflex
ia
NA
Mor
e pr
ogre
ssiv
e co
urse
with
mor
e dy
ston
ia e
arly
in
cour
se
Girl,
13y
Clin
ical
, gen
etics
no
t des
crib
edGe
nera
l pro
gres
sive
mot
or a
nd sp
eech
det
erio
ratio
n, d
iffus
e hy
pert
onia
, w
alki
ng d
ifficu
lties
. O
n ex
amin
ation
diff
use
limb
and
trun
cal d
ysto
nia,
dys
arth
ria, m
aske
d fa
ces
and
hype
rrefl
exia
NA
Mor
e pr
ogre
ssiv
e co
urse
with
mor
e dy
ston
ia e
arly
in
cour
se
6
Voorbereid document _Tessa Wassenberg_V03.indd 115Voorbereid document _Tessa Wassenberg_V03.indd 115 25/10/2021 09:3225/10/2021 09:32

116
Chapter 6
Supp
lem
enta
ry T
able
1. [
Conti
nued
]
Auth
or, y
ear
Num
ber o
f pa
tient
s, a
geLe
vel o
f dia
gnos
isCl
inic
al d
escr
iptio
nVi
deo/
phot
o m
ater
ial
Com
paris
on w
ith
curr
ent c
ase
serie
s
[12]
Chai
la e
t al,
2006
4 fe
mal
e sib
sCl
inic
al a
nd
gene
tic (m
utati
on
not d
escr
ibed
)
All h
ad d
ysto
nia
and
pyra
mid
al tr
act s
igns
; mild
spas
ticity
in
uppe
r lim
bs, m
ild-m
oder
ate
pyra
mid
al re
flexe
s. Th
ree
had
exte
nsor
pla
ntar
res
pons
es, a
ll ha
d so
me
dyst
onia
, 2 h
ad
brad
ykin
esia
, 1 h
ad tr
emor
NA
Mor
e dy
ston
ia e
arly
in
cour
se
[13]
Liu
et a
l, 20
102
fem
ale
pts
Clin
ical
and
ge
netic
Pt 4
: p.M
et10
2Leu
Pt 8
: p.G
ly20
3Arg
Both
pati
ent h
ad d
ysto
nia,
but
spas
tic p
arap
legi
a as a
dditi
onal
sy
mpt
om.
NA
Mor
e dy
ston
ia e
arly
in
cour
se
[14]
Cao
et a
l, 20
10Fe
mal
e, 2
2yCl
inic
al a
nd
gene
tic(c
.2T>
C; p
.M1T
)
Wea
knes
s in
left
leg
at a
ge 1
0y, a
ge 1
1y a
lso ri
ght l
eg. M
ild
limb
spas
ticity
and
mild
pyr
amid
al w
eakn
ess i
n lo
wer
lim
bs.
Pes e
quin
ovar
us d
efor
mity
misd
iagn
osed
as fi
xed
for w
hich
op
erati
on w
as p
erfo
rmed
. Bris
k re
flexe
s.
NA
Com
para
ble
Fem
ale,
30y
Clin
ical
and
ge
netic
(c.2
45T>
C; p
.L82
P)
Ons
et 8
y w
ith le
g sti
ffnes
s, eq
uino
varu
s ga
it aft
er e
xerc
ise,
pes e
quin
ovar
us d
efor
mity
misd
iagn
osed
as fi
xed
for w
hich
op
erati
on w
as p
erfo
rmed
. Ag
e 17
y: t
rem
or,
uppe
r lim
b sti
ffnes
s, w
riter
s cr
amp.
Mod
erat
e lim
b sp
astic
ity a
nd
mod
erat
e py
ram
idal
wea
knes
s. Br
isk re
flexe
s.
NA
Com
para
ble,
bes
ides
tr
emor
[15]
Tsao
et a
l, 20
12Gi
rl, 4
yCl
inic
al a
nd
gene
tic(c
.595
C>T;
p.
P199
S)
Ons
et 1
1m w
ith t
oe w
alki
ng, d
iagn
osis
of s
pasti
c di
pleg
ic
cere
bral
pal
sy a
t age
2y.
At a
ge 4
y le
g sp
astic
ity, w
orse
on
the
right
, inc
reas
ed d
eep
tend
on r
eflex
es a
t leg
s. E
xerc
ise
indu
ced
dyst
onia
led
to cl
inic
al su
spic
ion
of D
RD.
NA
Dyst
onia
ear
lier i
n co
urse
[16]
Kark
heira
n et
al
, 201
3
5 pa
tient
s fr
om o
ne
fam
ily
Clin
ical
and
ge
netic
(exo
n 1
dele
tion)
5 pa
tient
s w
ere
initi
ally
dia
gnos
ed a
s ha
ving
her
edita
ry
spas
tic p
arap
legi
a du
e to
‘pse
udop
yram
idal
sig
ns’,
but
no
furt
her i
nfor
mati
on is
giv
en. A
ll of
them
also
had
dys
toni
a an
d/ o
r tre
mor
.
NA
Not e
noug
h in
form
ation
Voorbereid document _Tessa Wassenberg_V03.indd 116Voorbereid document _Tessa Wassenberg_V03.indd 116 25/10/2021 09:3225/10/2021 09:32

117
Pyramidal predominant presentation of GCH1 mutations
Supp
lem
enta
ry T
able
1. [
Conti
nued
]
Auth
or, y
ear
Num
ber o
f pa
tient
s, a
geLe
vel o
f dia
gnos
isCl
inic
al d
escr
iptio
nVi
deo/
phot
o m
ater
ial
Com
paris
on w
ith
curr
ent c
ase
serie
s
[17]
Fan
et a
l, 20
14Fe
mal
e, 3
6yGe
netic
s (W
ES):
(c.6
46C>
T,
p.R2
16X)
Ons
et a
t age
6y
with
tipt
oe w
alki
ng. D
epen
dent
on
crut
ches
at
age
18y
. Leg
stiff
ness
and
pai
n. E
xam
inati
on: s
pasti
c ga
it,
incr
ease
d de
ep t
endo
n re
flexe
s w
ithou
t cl
onus
, big
toe
s ex
tend
ed a
t res
t, re
mai
ning
toes
flex
ed to
nica
lly.
Phot
ogra
phs
Com
para
ble
[18]
Jain
et a
l, 20
162
fem
ale
siblin
gsCl
inic
al, g
eneti
cal.
(p.K
160E
)Tr
emor
s of h
ead
and
legs
in in
fanc
y. W
alke
d at
10m
, fre
quen
t fa
lling
subs
eque
ntly.
Age
3y:
onl
y abl
e to
craw
l and
sit u
prig
ht
for a
shor
t per
iod
of ti
me
in th
e m
orni
ng. T
one
was
incr
ease
d in
bot
h lo
wer
lim
bs, e
spec
ially
ach
illes
, with
bila
tera
lly b
risk
deep
tend
on re
flexe
s and
ext
enso
r pla
ntar
resp
onse
s
NA
Mor
e pr
ogre
ssiv
e co
urse
[19]
Dobr
icic
et a
l, 20
17
3 fe
mal
e pa
tient
sCl
inic
al, g
eneti
cal
(c.4
70T>
C,
P.L1
57P)
in tw
o;(c
.209
delA
, p.
N70T
fs*1
0) in
on
e
Initi
al a
nd o
nly s
ympt
om o
f spa
stic p
arap
ares
is in
two
fam
ily
mem
bers
, with
bris
k refl
exes
and
seve
re sp
astic
ity. T
reat
men
t st
arte
d at
age
28
and
29 y
ears
with
com
plet
e re
solu
tion
of
sym
ptom
s.In
the
othe
r pati
ent fi
rst d
ysto
nia a
nd la
ter s
pasti
c par
apar
esis.
NA
Com
para
ble
in 2
, ot
her p
atien
t mor
e dy
ston
ia e
arly
in
cour
se
[20]
Yang
et a
l, 20
181,
age
?Cl
inic
al, g
eneti
cal
c.67
9A>G
(p
.T22
7A)
Ons
et in
ear
ly c
hild
hood
with
low
er li
mb
dyst
onia
with
w
alki
ng d
ifficu
lties
and
diu
rnal
fluc
tuati
on. A
lso in
crea
sed
mus
cle
tone
with
hyp
erre
flexi
a, e
spec
ially
in lo
wer
lim
bs,
and
bila
tera
l Bab
insk
i sig
n. A
chill
es te
ndon
sep
arati
on a
nd
nerv
e ro
ot rh
izoto
my a
t age
s 3 a
nd 4
year
s, w
ith p
oor r
esul
ts.
NA
Mor
e dy
ston
ia e
arly
in
cour
se
Supp
lem
enta
ry T
able
1. s
umm
ary
of a
ll ca
ses
iden
tified
by
exte
nsiv
e lit
erat
ure
sear
ch in
whi
ch p
atien
ts w
ith p
yram
idal
sig
ns w
ere
repo
rted
. Lev
el o
f di
agno
sis is
giv
en, i
n w
hich
clin
ical
dia
gnos
is m
eans
impr
ovem
ent o
f sym
ptom
s afte
r tre
atm
ent w
ith le
vodo
pa. I
f ava
ilabl
e, re
port
ed p
atho
geni
c var
iant
s ar
e de
scrib
ed. A
bbre
viati
ons:
CSF
= ce
rebr
ospi
nal fl
uid.
NA
= no
t ava
ilabl
e
6
Voorbereid document _Tessa Wassenberg_V03.indd 117Voorbereid document _Tessa Wassenberg_V03.indd 117 25/10/2021 09:3225/10/2021 09:32

118
Chapter 6
References Supplementary Table 1, Chapter 6
1. Fink JK, Filling-Katz MR, Barton NW, Macrae PR, Hallett M, Cohen WE. Treatable dystonia presenting as spastic cerebral palsy. Pediatrics. 1988 Jul;82(1):137-8.
2. Boyd K, Patterson V. Dopa responsive dystonia: a treatable condition misdiagnosed as cerebral palsy. Bmj. 1989 Apr 15;298(6679):1019-20.
3. Brown P, Britton TC. Cortico-motor neurone conduction in dopa responsive dystonia. Movement disorders : official journal of the Movement Disorder Society. 1990;5(4):338.
4. Nygaard TG, Waran SP, Levine RA, Naini AB, Chutorian AM. Dopa-responsive dystonia simulating cerebral palsy. Pediatr Neurol. 1994 Oct;11(3):236-40.
5. Harwood G, Hierons R, Fletcher NA, Marsden CD. Lessons from a remarkable family with dopa-responsive dystonia. Journal of neurology, neurosurgery, and psychiatry. 1994 Apr;57(4):460-3.
6. Patel K, Roskrow T, Davis JS, Heckmatt JZ. Dopa responsive dystonia. Archives of disease in childhood. 1995 Sep;73(3):256-7.
7. Tassin J, Durr A, Bonnet AM, et al. Levodopa-responsive dystonia. GTP cyclohydrolase I or parkin mutations? Brain : a journal of neurology. 2000 Jun;123 ( Pt 6):1112-21.
8. Cheng WW, Kong CK. Girl with dopa-responsive dystonia. J Paediatr Child Health. 2001 Jun;37(3):300-2.
9. Kang JH, Kang SY, Kang HK, Koh YS, Im JH, Lee MC. A novel missense mutation of the GTP cyclohydrolase I gene in a Korean family with hereditary progressive dystonia/dopa- responsive dystonia. Brain Dev. 2004 Aug;26(5):287-91.
10. Garavaglia B, Invernizzi F, Carbone ML, et al. GTP-cyclohydrolase I gene mutations in patients with autosomal dominant and recessive GTP-CH1 deficiency: identification and functional characterization of four novel mutations. Journal of inherited metabolic disease. 2004;27(4):455-63.
11. Jan MM. Misdiagnoses in children with dopa-responsive dystonia. Pediatr Neurol. 2004 Oct;31(4):298-303.
12. Chaila EC, McCabe DJ, Delanty N, Costello DJ, Murphy RP. Broadening the phenotype of childhood-onset dopa-responsive dystonia. Archives of neurology. 2006 Aug;63(8):1185-8.
13. Liu X, Zhang SS, Fang DF, et al. GCH1 mutation and clinical study of Chinese patients with dopa-responsive dystonia. Movement disorders : official journal of the Movement Disorder Society. 2010 Mar 15;25(4):447-51.
14. Cao L, Zheng L, Tang WG, et al. Four novel mutations in the GCH1 gene of Chinese patients with dopa-responsive dystonia. Movement disorders : official journal of the Movement Disorder Society. 2010 Apr 30;25(6):755-60.
15. Tsao CY. Guanine triphosphate-cyclohydrolase 1-deficient dopa-responsive dystonia presenting as frequent falling in 2 children. J Child Neurol. 2012 Mar;27(3):389-91.
16. Karkheiran S, Hubert B, Moghaddam H, Darvish H, Paisan-Ruiz C. Phenotypic heterogeneity and full penetrance in a family with dopa-responsive dystonia. Clinical genetics. 2013 Apr;83(4):392-4.
Voorbereid document _Tessa Wassenberg_V03.indd 118Voorbereid document _Tessa Wassenberg_V03.indd 118 25/10/2021 09:3225/10/2021 09:32

119
Pyramidal predominant presentation of GCH1 mutations
17. Fan Z, Greenwood R, Felix AC, et al. GCH1 heterozygous mutation identified by whole- exome sequencing as a treatable condition in a patient presenting with progressive spastic paraplegia. Journal of neurology. 2014 Mar;261(3):622-4.
18. Jain R, Shukla B, Mittal M. Delayed Diagnosis of Dopa responsive Dystonia in Two Siblings. Indian Pediatr. 2016 May 8;53(5):427-8.
19. Dobricic V, Tomic A, Brankovic V, et al. GCH1 mutations are common in Serbian patients with dystonia-parkinsonism: Challenging previously reported prevalence rates of DOPA- responsive dystonia. Parkinsonism & related disorders. 2017 Dec;45:81-4.
20. Yang K, Yin R, Lan X, et al. Dopa-Responsive Dystonia in Han Chinese Patients: One Novel Heterozygous Mutation in GTP Cyclohydrolase 1 (GCH1) and Three Known Mutations in TH. Med Sci Monit. 2018 Feb 6;24:751-7.
6
Voorbereid document _Tessa Wassenberg_V03.indd 119Voorbereid document _Tessa Wassenberg_V03.indd 119 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 120Voorbereid document _Tessa Wassenberg_V03.indd 120 25/10/2021 09:3225/10/2021 09:32

CHAPTER 7
Congenital eyelid ptosis, decreased glomerular filtration and orthostatic hypotension: questions and answers
Adapted from:Congenital eyelid ptosis, decreased glomerular filtration, and orthostatic hypotension: Questions.Tessa Wassenberg, Michèl A.A.P. Willemsen, Henry Dijkman, Jaap Deinum, Leo Monnens
Pediatr Nephrol. 2017 Jul;32(7):1169-1170.DOI: 10.1007/s00467-016-3494-2
ANDCongenital eyelid ptosis, decreased glomerular filtration, and orthostatic hypotension: Answers.Tessa Wassenberg, Michèl A.A.P. Willemsen, Henry Dijkman, Jaap Deinum, Leo Monnens
Pediatr Nephrol. 2017 Jul;32(7):1171-1174.DOI: 10.1007/s00467-016-3515-1.
Voorbereid document _Tessa Wassenberg_V03.indd 121Voorbereid document _Tessa Wassenberg_V03.indd 121 25/10/2021 09:3225/10/2021 09:32

122
Chapter 7
Case presentation
An 18-year-old girl was referred to our department of pediatric nephrology due to elevated serum creatinine level. She was born premature and dysmature (gestational age 31 weeks + 5 days, birth weight 1210 g) to consanguineous parents. She had a good start but a very low blood glucose level directly after birth (0.2 mmol/L); this was corrected with an intravenous glucose infusion, and there was no further hypoglycemia in the neonatal period. She had mild bilateral eyelid ptosis from birth. Psychomotor development was normal. During childhood, she had a history of recurrent airway infections and bronchitis, mild failure to thrive, and mild anemia for which she visited a general pediatrician regularly.
At age 4 years, routine serum creatinine measurements were 58 μmol/L, with an estimated glomerular filtration rate (eGFR) of 60 ml/min/1.73 m2. The lower than expected eGFR escaped the attention of the local pediatrician, and it was only at age 15 years, during routine testing, that a mildly elevated serum creatinine was noted for the first time (106 μmol/L, eGFR 53 ml/min/1.73 m2). At age 18 years, the serum creatinine level had increased to 139 μmol/L (eGFR 48 ml/min/1.73 m2), and she was referred to our university hospital for further examination. At that time, she reported exercise intolerance and lightheadedness on rising in the morning. Physical examination showed a height of 1.56 m (−2 standard deviations [SD]), a weight of 60 kg (+1SD), and a supine blood pressure of 106/55 mmHg; results were normal for heart, lungs, and abdomen examination, and, with the exception of the eyelid ptosis, for the neurological examination.
Her symptoms and signs, especially the exercise intolerance and eyelid ptosis, raised the suspicion of a mitochondrial disorder. Laboratory investigations showed normal values for serum lactate and electrolytes (Na+ 140 mmol/L, K+ 4.4 mmol/L, Ca2+ 2.2 mmol/L, Mg2+ 0.75 mmol/L, P3− 1.33 mmol/L). There was no proteinuria nor hematuria. Kidney size and structure were normal on the renal ultrasound images. In order to obtain a diagnosis, we performed a renal biopsy. Light microscopic examination revealed a few vascular sclerosed glomeruli with only discrete interstitial fibrosis. Electron microscopic examination revealed notable abnormal, fused mitochondria in the proximal tubules but not in the distal tubules (Fig. 1). This prompted the performance of a muscle biopsy for further evaluation of a mitochondrial defect. However, muscle histology was normal, and extensive biochemical testing of the respiratory chain also did not show any evidence of a mitochondrial disorder1 .Mutation analysis of mitochondrial DNA was performed in leucocytes and muscle tissue, but did not show any abnormalities. At that time, current techniques, such as whole exome sequencing, were not yet available, and so the patient was managed further by our department without a classifying diagnosis. At age 19 years, she fainted while her height was being measured during a routine visit to the outpatient clinic. She reported that she was increasingly suffering from dizziness,
Voorbereid document _Tessa Wassenberg_V03.indd 122Voorbereid document _Tessa Wassenberg_V03.indd 122 25/10/2021 09:3225/10/2021 09:32

123
Ptosis, decreased GFR and orthostatic hypotension: Q&A
especially in the morning. Orthostatic blood pressure measurements were performed, showing severe orthostatic hypotension with preserved heart rate increase. Her blood pressure decreased from supine values of 116/76 mmHg (heart rate 54 bpm) to 56/30 mmHg (heart rate 84 bpm) after standing for 3 min. Upon asking, she reported that sweating was normal.
Questions
1. What diagnosis can be suspected and which tests can be used to confirm this?2. What could be the explanation of the mitochondrial abnormalities in the proximal
tubule (Fig. 1), and the decreased glomerular filtration rate in this patient?3. Is treatment possible?
Figure 1.
Figure 1. Electron microscopic image of kidney biopsy showing notable abnormal mitochondria. Asterisk Basal membrane, BB brush border proximal tubule, arrow fused mitochondria. Inset: Arrowhead swollen mitochondria exhibit electron-lucent areas, arrow fused mitochondria present amorphous matricial densities.
7
Voorbereid document _Tessa Wassenberg_V03.indd 123Voorbereid document _Tessa Wassenberg_V03.indd 123 25/10/2021 09:3225/10/2021 09:32

124
Chapter 7
Answers
What diagnosis can be suspected and which tests can be used to confirm this?
The combination of congenital eyelid ptosis and severe orthostatic hypotension with preserved heart rate acceleration suggests sympathetic failure with intact parasympathetic function. Sweating, sympathetically mediated by acetylcholine, was intact, which implies that there was isolated absence of noradrenergic sympathetic function. Indeed, noradrenaline and adrenaline in plasma at rest and after standing were below detection limits (<0.01 nmol/L, normal values 0.4–3 nmol/L and 0.012–0.2 nmol/L respectively), whereas the dopamine level was greatly increased (1.1 nmol/L, normal values 0.02–0.19 nmol/L). These very low plasma levels of noradrenaline and adrenaline with an increased level of dopamine in this young adult patient are typical of dopamine beta hydroxylase (DBH) deficiency. DBH deficiency in this patient was genetically confirmed, with homozygous known pathogenic variants (IVS1 + 2 T > C) of the DBH gene (chromosome locus 9q34.2)2. As shown in Fig. 1, DBH is the enzyme that converts dopamine to noradrenaline. Noradrenaline can then be further converted to adrenaline. DBH deficiency is an extremely rare metabolic disorder of catecholamine synthesis, described in less than 20 patients worldwide. It leads to a lack of sympathetic noradrenergic function with normal parasympathetic and cholinergic-mediated sympathetic function, as is extensively reviewed by Robertson and Garland3. In DBH deficiency, the autonomic nervous system is structurally intact, but functionally impaired by the lack of noradrenaline, which leads to profound orthostatic hypotension and mild eyelid ptosis, but has no effect on sweating. In most patients, baroreflex afferents to the heart are at least partially intact, as demonstrated by the increase in heart rate on standing4.
In DBH deficiency, it is described that orthostatic hypotension mostly becomes manifest during adolescence. The reason for this relatively late presentation in the context of severe catecholamine deficiency from birth onward is unknown. It may be partly due to tardy recognition, as was probably the case in our patient. In general, orthostatic intolerance is often considered and evaluated in puberty and adulthood, but not in childhood. We are not aware of studies on normal values for blood pressure after orthostatic provocation in young children. Moreover, orthostatic complaints may become more apparent during puberty, because children may be protected from it owing to reduced gravitational force on their limited body height, or because of increased angiotensin II levels in childhood. Angiotensin II is part of the neurohumoral response on standing5.
Voorbereid document _Tessa Wassenberg_V03.indd 124Voorbereid document _Tessa Wassenberg_V03.indd 124 25/10/2021 09:3225/10/2021 09:32

125
Ptosis, decreased GFR and orthostatic hypotension: Q&A
What could be an explanation for the mitochondrial abnormalities in the proximal tubule, and the decreased glomerular filtration rate in this patient?
Electron microscopy of the kidney biopsy (Fig. 1) showed notable mitochondrial abnormalities, with extensive mitochondrial fusion and mitochondria with irregular shape and/or loss of cristae. This indicates mitochondrial dysfunction, especially in the activity of fission and fusion, which is critical for preserving normal cellular physiology6, and can be an indicator of changed environmental conditions. No histological abnormalities were seen at the distal tubules, and mitochondrial function in muscle tissue was normal, suggesting a local damaging factor in the proximal tubule in our patient. A possible damaging factor here is the high L-DOPA concentration in proximal tubules, because of increased filtered load and enhanced transport of L-DOPA in this compartment6. In DBH deficiency, plasma L-DOPA concentration is doubled2,8. L-DOPA is metabolized to dopamine inside the proximal tubular cells and dopamine is transported out of the cell to activate dopamine receptors. In urine, the concentration of dopamine is about 1,000 times the serum concentration and a small increase in L-DOPA concentration can lead to greatly increased dopamine levels9. Goldstein et al. reviewed the inherent cytotoxicity of catecholamines including dopamine in cells in which they are produced10,11. Monoamine oxidase (MAO), one of the enzymes that metabolize dopamine to its inactive metabolite homovanillic acid, yields hydrogen peroxide, resulting in the production of reactive oxygen species (ROS). Increased production of mitochondria-derived ROS was shown in opossum proximal tubular cells treated with dopamine in a concentration-dependent manner12. Mitochondrial DNA is particularly susceptible to modification by ROS13. Furthermore, mitochondrial toxicity can be due to increased levels of quinones, which are intermediates in L-DOPA metabolism14.
Besides mitochondrial dysfunction, the function of the tubuloglomerular system itself may be an explanation for the decreased eGFR in our patient. Dopamine leads to decreased reabsorption of sodium in the proximal tubule and loop of Henle, and this could initiate a vasoconstrictor response in the afferent arteriole via a Na+-K+-2Cl− cotransporter, and a vasodilator response, probably via the Na+ transporter in the connecting tubule. Both transporters, however, are inhibited by dopamine. Dopamine can also directly stimulate renin expression and release15. It is difficult to predict the effect of increased dopamine on glomerulotubular balance. Other factors, caused by defective reabsorption by damaged proximal tubular cells such as succinic acid, can stimulate the system16. However, dopaminergic stimulation of the tubuloglomerular feedback system leading to reduced filtration pressure remains an attractive possibility.
Decreased kidney function was found in 4 out of 9 patients with DBH deficiency3. Garland et al. proposed that a decrease in renal perfusion may lead to renal damage in
7
Voorbereid document _Tessa Wassenberg_V03.indd 125Voorbereid document _Tessa Wassenberg_V03.indd 125 25/10/2021 09:3225/10/2021 09:32

126
Chapter 7
patients with autonomic failure16. However, if hypoperfusion leading to hypoxia would be the main explanation of kidney failure in this patient group, tubulointerstitial fibrosis would be expected18. Fibrosis was only discreetly seen in our patient (Fig. 1).
Is treatment possible?
Dopamine beta hydroxylase deficiency can be treated successfully by using L-threo-3,4-dihydroxyphenylserine (L-DOPS, droxidopa), which is converted directly to noradrenaline by aromatic L-amino acid decarboxylase (AADC), thereby bypassing the metabolic block (Fig. 2)8, 19. With L-DOPS treatment, patients no longer experience the symptoms associated with orthostatic hypotension20, have an increased exercise tolerance, and markedly improved quality of life21. Our patient also achieved an impressive functional improvement after starting on L-DOPS. Furthermore, her eGFR showed a significant improvement, as is shown in Fig. 3. The negative effects of high dopamine levels on the kidney, therefore, whatever their exact mechanism, seemed to be reversible in this patient. The serum magnesium concentration before (0.64–0.77 mmol/L) and during (0.64–0.78 mmol/L) L-DOPS treatment remained in the low normal or subnormal range, with increased fractional urinary magnesium excretion (7.25–9.75 %, normally <4 %) during both states. The renal function study in this patient is a strong impetus for further detailed studies in more patients with DBH deficiency.
Voorbereid document _Tessa Wassenberg_V03.indd 126Voorbereid document _Tessa Wassenberg_V03.indd 126 25/10/2021 09:3225/10/2021 09:32

127
Ptosis, decreased GFR and orthostatic hypotension: Q&A
Figure 2.
Figure 2. Simplified scheme of catecholamine biosynthesis. The diagram shows how catecholamines (dopamine, noradrenaline and adrenaline) are formed from tyrosine and L-DOPA, and how they are metabolized to homovanillic acid (HVA) and vanillylmandelic acid (VMA). The metabolic block in DBH deficiency can by bypassed by supplying the patient with L-DOPS, represented in a capsule. Enzymes, represented in ovals, are abbreviated: TH: tyrosine hydroxylase, AADC: aromatic l-amino acid decarboxylase, DBH: dopamine beta hydroxylase, PNMT: phenylethanolamine N-methyltransferase. Dashed arrows do not show intermediate steps/ enzymes.
7
Voorbereid document _Tessa Wassenberg_V03.indd 127Voorbereid document _Tessa Wassenberg_V03.indd 127 25/10/2021 09:3225/10/2021 09:32

128
Chapter 7
Figure 3.
Figure 3. Repeated measurements of estimated glomerular filtration rate (eGFR; ml/min/1.73m2) in our patient with DBH deficiency, showing decreased eGFR (<60 ml/min/1.73 m2). After she started on L-DOPS, her eGFR increased to between 68 and 78 ml/min/1.73m2.
Voorbereid document _Tessa Wassenberg_V03.indd 128Voorbereid document _Tessa Wassenberg_V03.indd 128 25/10/2021 09:3225/10/2021 09:32

129
Ptosis, decreased GFR and orthostatic hypotension: Q&A
References
1. Rodenburg RJ. Biochemical diagnosis of mitochondrial disorders. Journal of inherited metabolic disease. 2011 Apr;34(2):283-92.
2. Kim CH, Zabetian CP, Cubells JF, et al. Mutations in the dopamine beta-hydroxylase gene are associated with human norepinephrine deficiency. American journal of medical genetics. 2002 Mar 1;108(2):140-7.
3. Robertson D, Garland EM. Dopamine Beta-Hydroxylase Deficiency. In: Pagon RA, Adam MP, Bird TD, Dolan CR, Fong CT, Stephens K, editors. GeneReviews. Seattle (WA)1993.
4. Man in ‘t Veld A, Boomsma F, Lenders J, et al. Patients with congenital dopamine beta- hydroxylase deficiency. A lesson in catecholamine physiology. American journal of hypertension. 1988 Jul;1(3 Pt 1):231-8.
5. Wagoner AL, Shaltout HA, Fortunato JE, Diz DI. Distinct neurohumoral biomarker profiles in children with hemodynamically defined orthostatic intolerance may predict treatment options. American journal of physiology Heart and circulatory physiology. 2016 Feb 1;310(3):H416- 25.
6. Archer SL. Mitochondrial dynamics--mitochondrial fission and fusion in human diseases. The New England journal of medicine. 2013 Dec 5;369(23):2236-51.
7. Pinto V, Pinho MJ, Soares-da-Silva P. Renal amino acid transport systems and essential hypertension. FASEB journal : official publication of the Federation of American Societies for Experimental Biology. 2013 Aug;27(8):2927-38.
8. Man in ‘t Veld AJ, Boomsma F, van den Meiracker AH, Julien C, Lenders J, Schalekamp MA. d,l-threo-3,4-dihydroxyphenylserine restores sympathetic control and cures orthostatic hypotension in dopamine beta-hydroxylase deficiency. Journal of hypertension Supplement : official journal of the International Society of Hypertension. 1988 Dec;6(4):S547-9.
9. Wassenberg T, Monnens LA, Geurtz BP, Wevers RA, Verbeek MM, Willemsen MA. The paradox of hyperdopaminuria in aromatic L-amino Acid deficiency explained. JIMD reports. 2012;4:39-45.
10. Goldstein DS. Catecholamines 101. Clinical autonomic research : official journal of the Clinical Autonomic Research Society. 2010 Dec;20(6):331-52.
11. Goldstein DS, Kopin IJ, Sharabi Y. Catecholamine autotoxicity. Implications for pharmacology and therapeutics of Parkinson disease and related disorders. Pharmacology & therapeutics. 2014 Dec;144(3):268-82.
12. Acquier AB, Mori Sequeiros Garcia M, Gorostizaga AB, Paz C, Mendez CF. Reactive oxygen species mediate dopamine-induced signaling in renal proximal tubule cells. FEBS Lett. 2013 Oct 1;587(19):3254-60.
13. Gutierrez J, Ballinger SW, Darley-Usmar VM, Landar A. Free radicals, mitochondria, and oxidized lipids: the emerging role in signal transduction in vascular cells. Circulation research. 2006 Oct 27;99(9):924-32.
14. Meiser J, Weindl D, Hiller K. Complexity of dopamine metabolism. Cell communication and signaling : CCS. 2013;11(1):34.
7
Voorbereid document _Tessa Wassenberg_V03.indd 129Voorbereid document _Tessa Wassenberg_V03.indd 129 25/10/2021 09:3225/10/2021 09:32

130
Chapter 7
15. Yang S, Yao B, Zhou Y, Yin H, Zhang MZ, Harris RC. Intrarenal dopamine modulates progressive angiotensin II-mediated renal injury. American journal of physiology Renal physiology. 2012 Mar 15;302(6):F742-9.
16. Peti-Peterdi J. Mitochondrial TCA cycle intermediates regulate body fluid and acid-base balance. The Journal of clinical investigation. 2013 Jul;123(7):2788-90.
17. Garland EM, Gamboa A, Okamoto L, et al. Renal impairment of pure autonomic failure. Hypertension. 2009 Nov;54(5):1057-61.
18. Fine LG, Norman JT. Chronic hypoxia as a mechanism of progression of chronic kidney diseases: from hypothesis to novel therapeutics. Kidney international. 2008 Oct;74(7):867-72.
19. Biaggioni I, Robertson D. Endogenous restoration of noradrenaline by precursor therapy in dopamine-beta-hydroxylase deficiency. Lancet. 1987 Nov 21;2(8569):1170-2.
20. Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Autonomic neuroscience : basic & clinical. 2011 Apr 26;161(1-2):46-8.
21. Garland EM, Raj SR, Demartinis N, Robertson D. Case report: Marathon runner with severe autonomic failure. Lancet. 2005 Dec;366 Suppl 1:S13.
Voorbereid document _Tessa Wassenberg_V03.indd 130Voorbereid document _Tessa Wassenberg_V03.indd 130 25/10/2021 09:3225/10/2021 09:32

131
Ptosis, decreased GFR and orthostatic hypotension: Q&A
7
Voorbereid document _Tessa Wassenberg_V03.indd 131Voorbereid document _Tessa Wassenberg_V03.indd 131 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 132Voorbereid document _Tessa Wassenberg_V03.indd 132 25/10/2021 09:3225/10/2021 09:32

PART IV
Reviews
and guidelines
for management
Voorbereid document _Tessa Wassenberg_V03.indd 133Voorbereid document _Tessa Wassenberg_V03.indd 133 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 134Voorbereid document _Tessa Wassenberg_V03.indd 134 25/10/2021 09:3225/10/2021 09:32

CHAPTER 8
Consensus guideline on the diagnosis and treatment of AADC deficiency
Tessa Wassenberg, Marta Molero-Luis, Kathrin Jeltsch, Georg F. Hoffmann, Birgit Assmann, Nenad Blau, Angeles Garcia-Cazorla, Rafael Artuch, Roser Pons, Toni S. Pearson, Vincenco Leuzzi, Mario Mastrangelo, Phillip L. Pearl, Wang Tso Lee, Manju A. Kurian, Simon Heales, Lisa Flint, Marcel Verbeek, Michèl Willemsen and Thomas Opladen
Orphanet J Rare Dis 2017 Jan 18;12(1):12.DOI: 10.1186/s13023-016-0522-z.
Voorbereid document _Tessa Wassenberg_V03.indd 135Voorbereid document _Tessa Wassenberg_V03.indd 135 25/10/2021 09:3225/10/2021 09:32

136
Chapter 8
Abstract
Aromatic L-amino acid decarboxylase deficiency (AADCD) is a rare, autosomal recessive neurometabolic disorder that leads to a severe combined deficiency of serotonin, dopamine, norepinephrine and epinephrine. Onset is early in life, and key clinical symptoms are hypotonia, movement disorders (oculogyric crisis, dystonia, and hypokinesia), developmental delay, and autonomic symptoms.
In this consensus guideline, representatives of the International Working Group on Neurotransmitter Related Disorders (iNTD) and patient representatives evaluated all available evidence for diagnosis and treatment of AADCD and made recommendations using SIGN and GRADE methodology. In the face of limited definitive evidence, we constructed practical recommendations on clinical diagnosis, laboratory diagnosis, imaging and electroencephalograpy, medical treatments and non-medical treatments. Furthermore, we identified topics for further research.
We believe this guideline will improve the care for AADCD patients around the world whilst promoting general awareness of this rare disease.
Voorbereid document _Tessa Wassenberg_V03.indd 136Voorbereid document _Tessa Wassenberg_V03.indd 136 25/10/2021 09:3225/10/2021 09:32

137
Consensus guideline on the diagnosis and treatment of AADC deficiency
Background
Aromatic L-amino acid decarboxylase (AADC; EC 4.1.1.28) is the final enzyme in the biosynthesis of the monoamine neurotransmitters serotonin and dopamine, and dopamine is the precursor for norepinephrine and epinephrine. AADC deficiency (AADCD; OMIM 608643) is a rare, autosomal recessive neurometabolic disorder that leads to a severe combined deficiency of serotonin, dopamine, norepinephrine and epinephrine (Fig. 1)1. About 100 patients have been described in case reports or case series since the initial description of the index family in 19902,3. The global incidence of AADCD is unknown, and there are no newborn screening programs, but it is more prevalent in certain Asian (especially Taiwanese and Japanese) populations, probably due to a founder effect4. Symptom onset typically occurs during the first months of life2. While most patients present a severe phenotype with early onset hypotonia, oculogyric crises, ptosis, dystonia, hypokinesia, impaired development and autonomic dysfunction2, a few patients with a milder disease course are known5.
Due to the rarity of AADCD, there is limited international clinical expertise for evidence-based management. Treatment response is often disappointing and treatment strategies vary between single expert centers6. Some patients are treated with a variety of different drugs, while others only receive one or two different drug classes2. A small subset of patients shows a good response to L-Dopa7 or dopamine agonists5, but often patients show no or poor response2. For most patients, treatment response cannot be predicted.
To improve care for patients with neurotransmitter related disorders, including AADCD, the International Working Group on Neurotransmitter Related Disorders (iNTD) was founded in 20138. Today, iNTD is a growing worldwide network of 38 neurometabolic centers from 24 countries. In addition to keeping a patient registry9, one of its goals is to develop consensus care guidelines for neurotransmitter related disorders by pooling all published evidence and experience of leading expert centers. This guideline on diagnosis and treatment of AADCD is the first guideline developed by iNTD.
In this guideline, developed with the Scottish Intercollegiate Guideline Network (SIGN) methodology, we present the key clinical symptoms and the recommended strategy for diagnosis and management of AADCD based on a systematic review of the literature and consensus meetings of the iNTD guideline working group. The guideline is intended for metabolic specialists, child and adult neurologists, pediatricians, intensive care specialists, nurses, and paramedical specialists involved in the care of patients with AADCD.
8
Voorbereid document _Tessa Wassenberg_V03.indd 137Voorbereid document _Tessa Wassenberg_V03.indd 137 25/10/2021 09:3225/10/2021 09:32

138
Chapter 8
Figure 1. Biosynthesis and breakdown of serotonin and the catecholamines, and the metabolic block in AADC deficiency
Figure 1. Simplified scheme of the biosynthesis and breakdown of serotonin and the catecholamines (dopamine, norepinephrine and epinephrine), and melatonin synthesis. Cofactors (BH4, PLP, Cu) and methyldonor (SAM) are connected to the respective enzyme with dashed lines. Dashed arrows do not show intermediate steps. The metabolic block caused by AADC deficiency is shown as a red bar. Metabolites above the block are increased, metabolites below the block are decreased, indicated by red arrows. The implication of 5-MTHF in L-dopa to 3-OMD metabolism is shown in a simplified manner. Norepinephrine and epinephrine are broken down to NMET and MET only in the periphery. In CSF, the main metabolite of norepinephrine and epinephrine is MHPG. Abbreviations: AADC: aromatic l-amino acid decarboxylase; BH4: tetrahydrobiopterin; COMT: catechol O-methyl transferase; CSF: cerebrospinal fluid; Cu: cupper; DβH: dopamine beta hydroxylase; DOPAC: dihydroxyphenylacetic acid; HCys: homocysteine; 5-HIAA: 5-hydroxyindoleacetic acid; 5-HTP: 5-hydroxytryptophan; HVA: homovanillic acid; L-Dopa: 3,4-dihydroxyphenylalanine; MAO: monoamine oxidase; MET: metanephrine; Met: metionine; MHPG: 3-methoxy 4-hydroxyphenylglycol; 3MT: 3-Metyramine; 5-MTHF: methyltetrahydrofolate; NMET: normetanephrine; 3-OMD: 3-O-methyldopa (=3-methoxytyrosine); Phe: phenylalanine; PhH: phenylalanine hydroxylase; PNMT: phenylethanolamine N-methyltransferase; SAH: S-adenosylhomocysteine; SAM: s-adenosylmethionine; TH: tyrosine hydroxylase; TrH: tryptophan hydroxylase; Tryp: tryptophan; Tyr: tyrosine; VLA: vanillactic acid; VMA: vanillmandelic acid: Vit B6 vitamin B6 (pyridoxine)
Voorbereid document _Tessa Wassenberg_V03.indd 138Voorbereid document _Tessa Wassenberg_V03.indd 138 25/10/2021 09:3225/10/2021 09:32

139
Consensus guideline on the diagnosis and treatment of AADC deficiency
Methods
Composition of the guideline working group and timelineAn executive committee (TO (chairman), TW (secretary), MM and KJ) was appointed to oversee the guideline development process and to function as coordinators for the subgroups focusing on different topics. The guideline working group consisted of 13 child neurologists (TW, GH, BA, AC, MK, WL, RP, TP, VL, MMa, PP, MW, TO), 5 biochemists (MM, NB, RA, SH, MV), and 1 research project manager (KJ) from several European countries, the USA and Taiwan. All group members are affiliated to iNTD and are experienced in the diagnosis and treatment of AADCD. Furthermore, a representative of the European AADCD patient organization (LF, AADC Research Trust) participated in guideline development. Finally, according to SIGN guidelines, two external academic reviewers with expertise in neurometabolic and movement disorders (Ron Wevers, Nijmegen, the Netherlands and Russell Dale, Sydney, Australia), and one additional lay reviewer were asked to comment on the draft before submission. The final version of the guideline was pilot-tested for use in clinical practice by non-specialist neurologists in training. A preliminary guideline working group meeting took place in November 2014 (London, UK) during the AADC Research Trust Conference. The start-up meeting took place in Barcelona, Spain (February 2015). Further face-to-face meetings were held in Heidelberg, Germany (September 2015, executive committee only), in Venice, Italy (November 2015), and a final wrap-up meeting was held during the AADC Research Trust Conference in May 2016 (London, UK).
Developing topics and key questionsDuring the start-up meeting, the initial list of key questions compiled by TW and TO was discussed and refined. The group was divided in subgroups focusing on the following topics: (I) Clinical Presentation; (IIa) Diagnosis: laboratory tests; (IIb) Diagnosis: imaging; (III) Treatment; (IV) Complications and Long-Term Management; (V) Social Issues and Transition; and (VI) Special Situations. The final list of key questions can be found online as additional file 1, Table S1 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5241937/#MOESM1).
Systematic literature searchA systematic literature review on AADCD was performed through December 2015 on Pubmed, Cochrane database, and the Cinahl database, using “aromatic (l) amino acid decarboxylase deficiency” and “AADC deficiency” as search terms. No language or data filters were used. The literature database on the official website of the AADC research trust was searched for applicable articles10. The reference list of the large case series of Brun2 was screened for additional sources. Furthermore, reviews on monoamine neurotransmitter deficiencies were searched using Pubmed, search term “monoamine neurotransmitter disorders’, limits: review, English, from 1990. The WHO registry for clinical trials11 and the NIH registry for clinical trials12 were searched. Finally, reference
8
Voorbereid document _Tessa Wassenberg_V03.indd 139Voorbereid document _Tessa Wassenberg_V03.indd 139 25/10/2021 09:3225/10/2021 09:32

140
Chapter 8
lists from review articles and key case series were screened for additional hits and members of the guideline group were asked to suggest relevant book chapters. Because of the limited number of publications on AADCD, conference abstracts from posters or symposia were included for literature review, but only if they were not followed by a peer reviewed publication from the group. The flow chart with results of the literature search can be found as Additional file 2: Figure S1.
Grading of evidence and recommendationsThe guideline was developed according to SIGN13. For rating the quality of evidence and defining strength of recommendations, SIGN is committed to using the GRADE methodology14-17. Level of evidence of individual studies was rated in a range from 4 (lowest) to 1++ (highest) (Table 1). Specific outcomes (e.g. effect of a specific drug on hypotonia) were described with a certain level of evidence (very low, low, moderate or high) for the total body of evidence. Recommendations were rated as strong (for or against), conditional (for or against), or recommendation for further research (Table 2). Furthermore, Good Practice Points (GPP) were formulated based on the clinical experience of the guideline development group. Relevant papers were evaluated by at least two guideline working group members. Before and during meetings, the guideline group members were trained on standardized literature evaluation using SIGN/ GRADE methodologies. All recommendations were discussed for consensus during guideline group meetings.
Table 1. Levels of evidence according to SIGN
Levels of evidence
1++ High quality meta-analyses, systematic reviews of RCTs or RCTs with a very low risk of bias
1+ Well conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort studiesHigh quality case control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal
2+ Well conducted case control or cohort studies with a low risk of confounding bias and a moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
Voorbereid document _Tessa Wassenberg_V03.indd 140Voorbereid document _Tessa Wassenberg_V03.indd 140 25/10/2021 09:3225/10/2021 09:32

141
Consensus guideline on the diagnosis and treatment of AADC deficiency
Table 2. Forms of recommendations according to GRADE
Judgment Recommendation
Undesirable consequences clearly outweigh desirable consequences
Strong recommendation against
Undesirable consequences probably outweigh desirable consequences
Conditional recommendation against
Balance between desirable and undesirable consequences is closely balanced or uncertain
Recommendation for research and possibly conditional recommendation for use restricted to trials
Desirable consequences probably outweigh undesirable consequences
Conditional recommendation for
Desirable consequences clearly outweigh undesirable consequences
Strong recommendation for
Disclaimer
The purpose of this guideline is to improve care for patients with AADCD and is based on the best available evidence. However, AADCD being a very rare disorder, the body of evidence encompasses mainly non-analytical studies and case reports. Therefore, many recommendations reflect expert opinion. This guideline is meant to give a solid foundation to caregivers who look after AADCD patients, but should never replace sensible, well-informed clinical care.
Part I: Clinical presentation
Number of reports; literature searchIn addition to the 78 patients reported in the large case series of Brun et al in 20102, 39 individual patients were identified in a total of 13 reports3,5,18-28). A further 22 cases, partly described in conference abstracts, could not with certainty be distinguished as individual patients24,29-33. In other words, 117 to 139 AADCD patients have been described so far, and 117 patients were used for calculations of patient characteristics. The comprehensiveness of the clinical information and the amount of biochemical and molecular data available differed substantially between included reports. Six families with multiple affected members were described1,7,34-37. Of the 117 patients clearly identified as individual AADCD cases, 56 were male, 42 were female, and in 19 gender was not reported.
8
Voorbereid document _Tessa Wassenberg_V03.indd 141Voorbereid document _Tessa Wassenberg_V03.indd 141 25/10/2021 09:3225/10/2021 09:32

142
Chapter 8
Ethnic originMany reported patients (50/117) are Asian. It is known that there is an increased prevalence of AADCD in patients from southern Chinese descent, especially from Taiwan and Japan, due to the founder variant IVS6 + 4A > T4. Other reported ethnic origins are: Caucasian (n = 33), Arabic (n = 4), Iranian (n = 1) and Jewish (n = 2). Ethnic origin was not described or remained uncertain in 21 cases.
• R#1 (strong): There should be an increased level of awareness for AADCD in patients of Chinese/Taiwanese/Japanese descent, because of the presence of a founder variant (IVS6 + 4A > T).
Age of onset and age of diagnosisThe age of onset of signs and symptoms, clearly documented in 68 cases only, was within the first year of life (mean: 2.7 months, SD ± 2.7). Eleven patients presented in the neonatal period with hypotonia, or floppiness. Based on available data (mostly level 3, with non-standardized methods of reporting symptoms), it was not possible to describe the precise age of onset and duration of every symptom associated with AADCD. Table 3 summarizes the best available data from published cases regarding the onset of symptoms. Despite the early onset of symptoms, mean age of diagnosis was 3.5 years (median 13 months, range 2 months – 23 years, 26 % missing data).
Key symptoms and signsKey symptoms of AADCD are: hypotonia (present in n = 91 patients, absent in n = 3 patients, not mentioned in n = 23 patients), movement disorders (present n = 99, absent n = 3, not mentioned n = 15), developmental delay (present n = 84, absent in n = 1 only [18], not mentioned n = 32), and autonomic symptoms (present n = 76, absent n = 3, not mentioned n = 38). All key symptoms ranged in severity from mild to very severe. Hypotonia is most often axial, and sometimes accompanied by limb hypertonia. Movement disorders most often described are oculogyric crises (n = 91), dystonia (n = 63), and hypokinesia (n = 40). Most prominent autonomic signs are ptosis, excessive sweating, and nasal congestion. Hypotension or orthostatic hypotension was reported in 15 patients, with onset mostly in late childhood or adolescence. In 14 patients, blood pressure was reported to be normal. A complete list of movement disorders, autonomic symptoms and signs, and other clinical characteristics is given in Table 3.
• R#2(strong): In children with unexplained hypotonia, movement disorders (especially oculogyric crisis), developmental delay, and autonomic symptoms, AADCD should be considered.
Other neurological findingsEpileptic seizures were described in 9 patients2,7,22,38-40. Behavioral problems can be a great burden to patients and caregivers but are not well defined in the literature. They
Voorbereid document _Tessa Wassenberg_V03.indd 142Voorbereid document _Tessa Wassenberg_V03.indd 142 25/10/2021 09:3225/10/2021 09:32

143
Consensus guideline on the diagnosis and treatment of AADC deficiency
were reported to be present in 41 cases, mostly described as irritability, excessive crying, dysphoria2,40,41 and autistic features31. Sleep disturbance (both insomnia and hypersomnia) was described in 34 patients. Some patients may suffer from severe sleep apnea, which may be lethal (personal observation WL). In some patients, diurnal fluctuations and improvement after sleep, a classical finding for many neurotransmitter disorders6, is reported. On neurological examination, deep tendon reflexes can be decreased, normal or increased. Pathological reflexes including Babinski sign are sometimes reported.
• R#3 (research): Behavioral symptoms and sleep disturbances in AADCD should be better defined, to improve patient care.
Additional clinical findingsGastrointestinal problems can be prominent in AADCD. Symptoms can include diarrhea, constipation, gastroesophageal reflux, and feeding difficulties. Many patients receive and benefit from a gastrostomy (expert experience). Failure to thrive and short stature is often reported. In 13 patients, intermittent hypoglycemia was reported, at birth or in the first five years of life. Hypoglycemia can occur during intercurrent illnesses41. In one patient, hypoglycemia with reduced level of consciousness was found after sedation for MRI42. There are no reports of growth hormone deficiency, thyroid deficiency, or other hormone deficiencies in AADCD.
Phenotypic spectrum and clinical courseBased on clinical description, cases were broadly classified as mild (mild delay in developmental milestones, ambulatory without assistance, mild intellectual disability), severe (no or very limited developmental milestones, fully dependent), and moderate (in between). Six cases could be classified as mild (reported in5,18,19,35,43), 15 as moderate (reported in2,5,7,20,22,31,35,40,44,45), and 82 as severe. For 14 cases, insufficient information about the clinical picture was available. Importantly, a mild phenotype can present predominantly with autonomic symptoms (diarrhea, episodic hypoglycemia, nasal congestion) and without evident movement disorders18. Two adult sisters had a very atypical clinical course, with hypotonia at birth, moderate to severe motor developmental delay in infancy, and mild to moderate symptoms in childhood, with improvement during puberty5. The two other patients who were diagnosed as adults did not show transient improvement in puberty, but rather a deteriorating clinical picture7. Deterioration with loss of skills, e.g. regression of language skills20,22, is described in some patients but in the majority of cases, there is no evident progressive clinical course with loss of function described. A decline in motor function can sometimes be due to secondary factors like joint contractures46.
8
Voorbereid document _Tessa Wassenberg_V03.indd 143Voorbereid document _Tessa Wassenberg_V03.indd 143 25/10/2021 09:3225/10/2021 09:32

144
Chapter 8
• R#4 (conditional): The phenotypic spectrum of AADCD is broad and can range from very severe to relatively mild. AADCD should also be considered in patients with autonomic symptoms without obvious movement disorders.
• R#5 (strong): A deteriorating clinical course is not expected in patients with AADCD and should trigger a diagnostic work-up for other diseases.
Phenotype correlations with genotype or biochemical phenotypeThere are >50 different DDC gene disease causing variants described in AADCD but clear genotype/ phenotype correlations could not be established. However, patients with the founder splice variant IVS6 + 4A > T (36 patients in total, 26 with homozygous variants) all had a severe phenotype without reaching clear developmental milestones, except for two sisters with the compound heterozygous variants p.[R285W];[IVS6 + 4A > T] and a mild to moderate clinical picture with response to treatment35. The variant p.[R285W],c.[853C > T] is not reported in other patients. Gender is not associated with phenotype (severe phenotype in 72 % of females and 77 % of males).
There is evidence for a genotype/ treatment response correlation in two families with different L-Dopa binding site variants and a convincing response to L-Dopa. Three siblings, extensively represented in the literature, with a homozygous p.[G102S], c.[304G > A] variant became able to walk independently (n = 1) or with assistance (n = 2) and showed improvement of dystonia, truncal hypotonia and speech after L-Dopa treatment was started7,40/47. More recently, a patient with other variants affecting the L-Dopa binding site p.[R347Q];[R160W], c.[1040G > A];[478C > T], also showed a good response to L-Dopa19. Currently, therapeutic implications of other DDC gene variants in AADCD are being investigated48.
There is overlap in cerebrospinal fluid (CSF) values of biogenic amines in mild, moderate and severe cases without a clear correlation of the biochemical (CSF) and clinical phenotype. Plasma AADC enzyme activity does not correlate with clinical phenotype; in both mild and severe cases it can be below the detection limit of the assay.
• R#6 (conditional): There are no clear genotype/ biochemical or clinical phenotype correlations in AADCD except for the homozygous IVS6 + 4A > T splice variant that is associated with a severe phenotype in all cases reported to date, and rare L-Dopa binding site variants that are associated with L-Dopa responsiveness.
Voorbereid document _Tessa Wassenberg_V03.indd 144Voorbereid document _Tessa Wassenberg_V03.indd 144 25/10/2021 09:3225/10/2021 09:32

145
Consensus guideline on the diagnosis and treatment of AADC deficiency
Table 3. Symptoms and signs described in AADC deficiency
Sym
ptom
/ si
gn
Neo
Nat
al
Infa
ncy
Child
hoo
d
Adol
esce
nce
Adul
thoo
d
CNS Tone regulation Floppy infant + ++
Hypotonia (mainly truncal) + ++ ++ ++ ++
Poor head control + + + + +
Hypertonia (mainly limbs) + + + + +
Movement disorders
Dyskinesia (eg hyperkinesia, chorea, athetosis) + + + + +
Dystonia - ++ ++ ++ ++
Oculogyric crisis + ++ ++ ++ ++
Hypokinesia and/ or bradykinesia + ++ ++ ++ ++
Myoclonus + + + + +
Tremor + + + + +
Developmental Delay
Delayed motor development + ++ ++ ++ ++
Delayed cognitive development + + + +
Delayed speech development + + + +
Behavioural Problems
Irritability ++ ++ + + +
Autistic features + + +
Dysphoria/ Mood problems + + + + +
Excessive crying + ++ + - -
Sleeping Problems Insomnia and or hypersomnia + + + +
Other Epileptic seizures - + + + +
Fatiguability + + + + +
Diurnal fluctuation + + + +
Dysarthria + + +
Poor eye fixation + + + +
Increased startle + + + + +
8
Voorbereid document _Tessa Wassenberg_V03.indd 145Voorbereid document _Tessa Wassenberg_V03.indd 145 25/10/2021 09:3225/10/2021 09:32

146
Chapter 8
Table 3. [Continued]
Sym
ptom
/ si
gn
Neo
Nat
al
Infa
ncy
Child
hoo
d
Adol
esce
nce
Adul
thoo
d
ANS Eyes Ptosis + + + + +
Miosis + + + + +
Upper respiratory tract
Nasal congestion - + + + +
Excessive drooling - + + + +
Stridor + + + + +
Skin Excessive sweating - + + + +
Homeostasis Temperature instability + + + + +
Cardiovascular (Orthostatic) Hypotension - - + + +
Bradycardia + + + + +
Heart rhytm abnormalities + + + +
Gastrointestinal Diarrhea + + + + +
Obstipation + + + + +
Metabolic/ endocrine Hypoglycemia + + + - -
Hyperprolactinemia + + + + +
General Feeding/ Swallowing Problems + + + + +
Gastrointestinal reflux + + + + +
Gastrointestinal problems unspecified + ++ + + +
Failure to thrive + + + +
Contractures - - - + +
Small hand and feet + + + + +
Table 3. Best available evidence for all published clinical symptoms and the age of occurrence (additional literature used: [77]). CNS Central Nervous System. ANS autonomic nervous system. ++ very often (key symptom); + often; ± sometimes; - not expected
Voorbereid document _Tessa Wassenberg_V03.indd 146Voorbereid document _Tessa Wassenberg_V03.indd 146 25/10/2021 09:3225/10/2021 09:32

147
Consensus guideline on the diagnosis and treatment of AADC deficiency
Part IIa: Diagnosis: laboratory tests
Key diagnostic tests: CSF, AADC activity and genetic testing
Lumbar punctureThe typical CSF pattern in AADCD consists of (1) low levels of 5-hydroxyindoleacetic acid (5-HIAA), homovanillic acid (HVA) and 3-methoxy-4-hydroxyphenylglycol (MHPG), (2) normal pterins including neopterin and biopterin, and (3) high concentrations of 3-O-methyldopa (3-OMD), L-Dopa and 5-OH tryptophan (5-HTP). This reflects the metabolic block at the level of AADC (Fig. 1). Low HVA and 5-HIAA was reported in 99 % of patients. Only two sisters with a mild phenotype had normal HVA (124 and 169 nmol/L; ref 98-450 nmol/L), one of them also had normal 5-HIAA (50 nmol/L; ref 45-135 nmol/L). In both patients, 3-OMD and -5-HTP were increased and MHPG was decreased5. In only one patient, normal MHPG was reported, with decreased HVA and 5-HIAA19. Normal CSF pterins (neopterin, dihydrobiopterin and tetrahydrobiopterin) are essential to differentiate AADCD from the tetrahydrobiopterin disorders6.
The CSF profile of AADCD may be similar to the profile found in pyridox(am)ine 5-phosphate (PNPO) deficiency, in which there is a secondary failure of AADC due to a deficiency of its cofactor pyridoxal phosphate (PLP). However, additional findings in this disorder are very low PLP, and increased glycine and threonine in CSF. Furthermore, the clinical picture of PNPO deficiency, namely a severe neonatal epileptic encephalopathy, is different from the clinical presentation of AADCD49,50.
Mildly decreased CSF 5-methyltetrahydrofolate (5-MTHF) was reported in only 1 patient with AADCD47, and 5-MTHF levels decreased during L-Dopa treatment in 3 patients40. It was proposed that this could be due to a depletion of CSF s-adenosylmethionine (SAM) in states with increased L-Dopa concentrations51, but serial CSF measurements for 5-MTHF have not been performed in other patients.
Neurotransmitter metabolite analysis is performed in a limited number of specialized laboratories. For an online list of iNTD affiliated laboratories, see8. Collection and handling of CSF should be performed strictly following standardized procedures to ensure correct interpretation of results. For a review see Hyland52.
• R#7 (strong): AADCD can be diagnosed in CSF. Specific measurements in CSF should include the core metabolites HVA, 5-HIAA, 3-OMD, L-Dopa, and 5-HTP, and pterins. If available, 5-MTHF and PLP should also be measured. Reduced 5-HIAA and HVA, and elevated 3-OMD, L-Dopa and 5-HTP, with normal pterins, point to AADCD.
• R#8 (GPP): CSF measurements should always include standard measurements (cells, protein, glucose, lactate). Collection and handling of CSF should be performed
8
Voorbereid document _Tessa Wassenberg_V03.indd 147Voorbereid document _Tessa Wassenberg_V03.indd 147 25/10/2021 09:3225/10/2021 09:32

148
Chapter 8
strictly following standardized procedures to ensure correct interpretation of results.
AADC activity in plasmaEnzyme assays measuring AADC activity in plasma can be performed using both L-Dopa and 5-HTP as substrate. Since L-Dopa gives a higher analytical yield it is used as the standard method. All 57 papers that reported results of plasma AADC activity assays, described decreased activity in patients with AADCD. In about 30 % of reported cases, AADC activity was below detection limits. The highest reported residual enzyme activity in AADCD was 12 pmol/mL/min (33 % of the lower limit of normal), reported in 1 patient [41]. AADC activity is also decreased in heterozygous carriers (35-40 % of normal)18,34,35,53. For an online list of iNTD affiliated laboratories that perform AADC activity assays, see8.
• R#9 (strong): AADCD can be diagnosed by demonstrating severely decreased AADC activity in plasma. Plasma AADC activity is moderately reduced in heterozygous carriers.
Molecular diagnosisAbout 50 disease causing DDC variants have been described so far: 39 substitution variants, 2 nonsense, 5 deletions, 1 insertion and 4 splice variants. For an up to date list of DDC variants, see online locus-specific database on PNDdb54. In only two AADCD patients with the classical CSF profile and decreased AADC activity in plasma, no variants of the DDC gene were found despite Sanger analysis of the coding region, the exon/intron boundaries and flanking untranslated regions39,41. In two other patients (siblings),with the classical CSF profiles and very low plasma AADC enzyme activity, only one variant was detected36. It is assumed that in these cases a second variant may be intronic, within the promoter region or a heterozygous deletion or duplication, undetectable by current standard diagnostic techniques. Two recent reports detected AADCD patients using whole exome sequencing20,55.
• R#10 (strong): In the great majority of patients, AADCD can be genetically confirmed.
Concluding statements regarding key diagnostic tests• R#11 (strong): There are three core diagnostic keys for identifying AADCD:
• (1) low CSF levels of 5-HIAA, HVA, and MHPG, increased CSF levels of 3-OMD, L-Dopa and 5-HTP, and normal CSF pterins
• (2) compound heterozygous or homozygous pathogenic variants in the DDC gene
• (3) decreased AADC enzyme activity in plasma
Voorbereid document _Tessa Wassenberg_V03.indd 148Voorbereid document _Tessa Wassenberg_V03.indd 148 25/10/2021 09:3225/10/2021 09:32

149
Consensus guideline on the diagnosis and treatment of AADC deficiency
To diagnose AADCD, genetic testing should be performed and at least two out of three core diagnostic tests should be positive.
• R#12 (strong): If genetic diagnosis is performed as the first step (e.g. whole exome sequencing or affected family member), functional confirmation should be completed by measuring AADC enzyme activity in plasma and/or neurotransmitter metabolites in CSF.
• R#13 (conditional): If local resources allow, we recommend performing all three key diagnostic tests in patients with this rare disorder.
• R#14 (GPP): The results of CSF analysis and plasma AADC activity measurement are generally available before results of genetic testing. Genetic confirmation should not be awaited before initiating therapy.
Other diagnostic tests in AADCD
ProlactinProlactin in blood can be increased in dopamine biosynthesis disorders, because dopamine serves as an inhibitor of prolactin secretion6. Prolactin was reported in 13 AADCD patients. Elevated prolactin was found in 6 patients; in the others it was normal. Also, members of the guideline group reported normal prolactin in multiple AADCD patients (non-published observations).
• R#15 (research): Normal prolactin level in blood does not exclude AADCD. To better understand this mechanism we recommend further research on this topic.
Neurotransmitter (metabolites) in bloodWhole blood serotonin was reported in 15 patients and found to be decreased in all of them1,34,39,40,56. Plasma monoamine and monoamine metabolites (L-Dopa, 3-OMD, vanillactic acid (VLA), HVA, vanillylmandelic acid (VMA), MHPG, norepinephrine, epinephrine, and 5-HTP) are reported in a very limited number of patients and it is not possible to draw conclusions about the diagnostic accuracy of these tests. Plasma measurements cannot replace measurements in CSF.
• R#16 (strong): Measurement of catecholamine metabolites in blood are not useful in routine clinical practice, because it neither diagnoses nor excludes AADCD.
8
Voorbereid document _Tessa Wassenberg_V03.indd 149Voorbereid document _Tessa Wassenberg_V03.indd 149 25/10/2021 09:3225/10/2021 09:32

150
Chapter 8
Dried blood spot measurement of 3-OMDOne report studied the use of dried blood spot (DBS) testing of 3-OMD in 15 patients57. All samples showed an at least 15-fold increase of 3-OMD. In 6 patients, newborn values were available, showing very high levels of 3-OMD. However, 3-OMD is also increased in PNPO deficiency. There are no other reports on this subject available. If (newborn) screening can reliably diagnose AADCD, this will greatly improve the diagnostic delay that is often encountered now. A clinical trial on newborn screening of AADCD is currently recruiting patients in Taiwan12.
• R#17 (research): The development, diagnostic accuracy, and cost effectiveness of DBS analysis of 3-OMD for (newborn) screening for AADCD should be further investigated.
Urine measurements of neurotransmitter metabolitesIncreased urine vanillactic acid (VLA) levels, measured by organic acid analysis, are reported in AADCD. However, this elevation is often subtle and easily missed if not specifically looked for in a specialised laboratory2.
Dopamine, HVA and vanilylmandelic acid (VMA) in urine are not reliable as biomarkers in AADCD because they can either be normal, decreased or increased2,26,58. This is due to very high AADC activity within the kidneys, accounting for sufficient residual AADC activity to form dopamine and its metabolites27.
• R#18 (conditional): If urinary VLA is increased, AADCD should be considered. However, normal levels do not exclude the diagnosis.
• R#19 (strong): Measurement of catecholamine metabolites in urine is not useful as a diagnostic test in clinical practice, because it can neither diagnose nor exclude AADCD.
Other diagnostic testsMelatonin is formed from serotonin and would be expected to be decreased in AADCD. Theoretically, it is therefore a possible diagnostic tool for this patient group, but no reports on melatonin measurements are available. One recent report used global metabolomics assisted pathway screening with plasma samples in one AADCD patient, and showed an increased 3-OMD. This finding was also seen in subjects using L-Dopa/ carbidopa medication55.
• R#20 (research): Other diagnostic tests that might increase knowledge on AADCD and/ or serve as possible biomarkers are melatonin and broad metabolomic screening for specific AADCD related markers.
Voorbereid document _Tessa Wassenberg_V03.indd 150Voorbereid document _Tessa Wassenberg_V03.indd 150 25/10/2021 09:3225/10/2021 09:32

151
Consensus guideline on the diagnosis and treatment of AADC deficiency
Part IIb: Diagnosis: imaging and electroencephalography
Magnetic resonance imaging (MRI) of the brainBrain imaging was performed in 38 cases (36 MRI, 2 CT), and was described as normal in 25. In the remaining cases, described abnormalities were heterogeneous, including: diffuse mild cerebral atrophy2,38, cortical atrophy41, reduced prefrontal volume with normal myelination and normal basal ganglia36, focal demyelination changes over bilateral frontal and left parietal area4, leukomalacia4, degenerative changes of white matter, thinning of corpus callosum, prominent ventricular bodies, leukodystrophy-like patterns, and hypomyelination2. Since there is no specific MRI pattern, imaging is not helpful in the diagnosis of AADCD. However, it is usually necessary in the work-up of a patient with neurodevelopmental delay to exclude other conditions in the differential diagnosis. Following standards of good clinical care, neuroimaging is always indicated if there is an unexpected deviation of clinical course in a diagnosed AADCD patient (see also R #5).
• R#21 (conditional): Routine imaging of the brain is not needed to diagnose AADCD.• R#22 (GPP): In the work-up of patients with neurodevelopmental delay, and in
unexpected deviation of clinical course in AADCD patients, brain imaging should be considered.
Electroencephalography (EEG)EEG, reported in 28 cases, was described as normal in 21. In the remaining cases described abnormalities included: epileptiform abnormalities in a patient with clinical seizures38, epileptiform abnormalities (paroxysmal discharges, (multifocal) sharp waves, polyspikes) without evident clinical seizures in three patients2,56,59, unspecific changes41, and rapid activity or slowing2. EEG is not needed to diagnose AADCD. However, if there is a clinical suspicion of epilepsy, to differentiate oculogyric crises from epileptic events7, or in the general work-up of neurodevelopmental delay, EEG can be performed following local standards of good clinical care.
• R#23 (conditional): EEG is not needed to diagnose AADCD.• R#24 (GPP): EEG can be used in the work-up of AADCD if there is a clinical suspicion
of epilepsy, to differentiate oculogyric crises from epileptic events, or in the general work-up of neurodevelopmental delay.
Other imaging modalitiesA brain fluorodeoxyglucose (18F-FDG) PET scan was performed in only 1 patient36, and demonstrated reduced uptake in the prefrontal cortex and bilateral basal ganglia. Striatal uptake of fluorodopa (FDOPA) on PET/CT was reported to be very low at baseline, and increased after gene therapy in 3 patients24. There were no published reports of DAT scans in AADCD.
8
Voorbereid document _Tessa Wassenberg_V03.indd 151Voorbereid document _Tessa Wassenberg_V03.indd 151 25/10/2021 09:3225/10/2021 09:32

152
Chapter 8
• R#25 (research): Other imaging modalities (FDG PET, FDOPA PET, DAT-scan) have no role in routine clinical care but can be useful in research settings, e.g. the assessment of the efficacy of gene therapy.
Part III: Treatment
IIIa: Medical treatment
Available evidenceBased on the literature evaluation, considered judgments leading to recommendations for use in clinical practice could be constructed for dopamine agonists, monoamine oxidase (MAO) inhibitors, pyridoxal phosphate, pyridoxine, anticholinergic agents, folinic acid, L-Dopa with carbidopa, L-Dopa without carbidopa, 5-hydroxytryptophan, benzodiazepines, melatonin, and selective serotonin reuptake inhibitors (SSRIs). For catechol O-methyl transferase (COMT)-inhibitors there was insufficient literature available to come to a recommendation. The quality of the total body of evidence for specific outcomes was rated as low or very low. There are currently no active medical treatment trials in AADCD registered.
First line treatment
Dopamine agonistsDopamine agonists activate postsynaptic dopamine receptors directly. Ergot-derived dopamine agonists with strong serotonergic (5HT2b) agonist action (pergolide and cabergoline) are strongly associated with cardiac valvulopathy and other fibrous complications60, and should not be used in AADCD. Ergot-derived dopamine agonists without 5HT2b agonist action (bromocriptine) have a lower risk, although incidentally, pulmonary, retroperitoneal and (peri)cardial fibrosis have been described, with a dose-effect relation61. Non-ergot derived dopamine agonists are pramipexole, ropinirole, rotigotine (transdermal patches) and apomorphine (subcutaneous). The risk of fibrotic complications with non-ergot derived dopamine agonists is probably very low62.
Use of dopamine agonists in AADCD was described in 58 individual cases, with bromocriptine being used most often (26 patients), followed by pergolide (11 patients). Reports on non-ergot derived dopamine agonists were fewer (4 patients on pramipexole, 4 on rotigotine, and 2 on ropinirole). One patient on cabergoline was described. In 9 patients the dopamine agonist was not specified. There are no reports of the use of subcutaneous apomorphine in AADCD. Positive responses (e.g. improvement of head control, hypotonia, oculogyric crises, voluntary movements and autonomic symptoms) have been reported for bromocriptine, pramipexole, rotigotine patches and pergolide. Also, neutral effects were reported. Reported side effects included irritability, weight loss, worsening of failure to thrive, vomiting, and also mild to severe
Voorbereid document _Tessa Wassenberg_V03.indd 152Voorbereid document _Tessa Wassenberg_V03.indd 152 25/10/2021 09:3225/10/2021 09:32

153
Consensus guideline on the diagnosis and treatment of AADC deficiency
dyskinesia45. Overall, benefits outweighed side effects in most cases. It is important to consider that many patients were treated simultaneously with more than one drug class, therefore assessment of the impact of a single drug is often problematic. For dose recommendations of dopamine agonists, see Table 4.
• R#26 (strong): Dopamine agonists should be tried in the treatment of AADCD. Non-ergot derived dopamine agonists (pramipexole, ropinirole, rotigotine) are preferred.
• R#27 (strong): Cabergoline and pergolide should not be used for the treatment of AADCD because of the high risk of fibrotic complications.
• R#28 (GPP): Cardiac screening (see R#48) before and during treatment with bromocriptine (ergot derived dopamine-agonists) is indicated, because of the potential risk of cardiac fibrosis.
MAO inhibitorsMAO inhibitors prevent breakdown of dopamine and serotonin, thereby increasing monoamine availability. The effect of MAO inhibitors in AADCD was described for 31 cases in 17 studies. All patients had co-treatment with dopamine agonists and/ or pyridoxine. MAO inhibitors used were tranylcypromine (n = 14), selegiline (n = 7), phenelzine (n = 1), or unspecified (n = 9). No studies were found on rasagiline. The majority of studies described an improvement in at least one clinical endpoint (e.g. hypotonia), with no effects on others. Some studies reported no clinical improvement at all, e.g. Anselm et al39, or only temporary improvement40. Side effects were rarely reported, apart from one patient who developed a dystonic crisis on withdrawal of tranylcypromine45, and one patient with increased oculogyric crises40. For dose recommendations, see Table 4.
• R#29 (strong): From the biochemical viewpoint there is strong recommendation for giving patients with AADCD a trial of MAO inhibitors, although there is little evidence of clinical benefit.
Pyridoxine / pyridoxal phosphate (PLP)Pyridoxal phosphate (PLP), the active form of pyridoxine, is a cofactor of AADC (Fig. 1). Therefore, treatment with one of several available forms of vitamin B6 might increase residual activity of the AADC enzyme. Pyridoxine is more readily available and cheaper than PLP, therefore it is the form used most often in AADCD. It has been reported in about 50 individual patients. The use of PLP was described in only one study22. Pyridoxine monotherapy was reported in only 8 patients, of which only one patient (with a mild phenotype) showed a clear favorable response18. In patients with concurrent medications, a favorable effect was sometimes seen. In 19 patients, no clear response was described at all. Reported side effects were gastrointestinal complaints, sleeping problems and extreme motor restlessness in patients with very high doses of pyridoxine and concurrent treatment with L-Dopa. Pyridoxine and PLP can cause
8
Voorbereid document _Tessa Wassenberg_V03.indd 153Voorbereid document _Tessa Wassenberg_V03.indd 153 25/10/2021 09:3225/10/2021 09:32

154
Chapter 8
reversible polyneuropathy when used in high doses for long periods of time. For dose recommendations, see Table 4.
• R#30 (strong): Vitamin B6 is considered a first line treatment from a biochemical standpoint, but dose limits should be respected because of possible side effects.
• R#31 (conditional): Pyridoxine is preferred over PLP because of availability and costs. If it is not tolerated, PLP can be tried instead.
Additional symptomatic treatment
Anticholinergic drugsAnticholinergic drugs (e.g. trihexyphenidyl, benztropine, biperiden) are commonly used to treat certain movement disorders, especially parkinsonism63 and dystonia64. Although their exact mechanism of action is not known, it is thought that they influence the relative imbalance between dopaminergic and cholinergic pathways. In AADCD, they can be used to treat autonomic symptoms, dystonia, and oculogyric crisis. The effect of anticholinergic medication is described in only 11 patients, who all received concurrent medications (dopamine agonist and/ or L-Dopa and/ or pyridoxine and/ or MAO-inhibitors). In the majority of cases there was an improvement of at least one clinical endpoint (e.g. hypotonia, excessive sweating, dystonia). Not all patients were reported to benefit, however. Side effects were reported in two articles, including significant sedation in one patient39 and aggressive behavior in another41. For dose recommendations, see Table 4.
• R#32 (conditional): Anticholinergic agents can be considered in AADCD, especially (additionally) to treat autonomic symptoms, dystonia, and oculogyric crisis.
MelatoninThere is very limited evidence for the use of melatonin in AADCD. It was reported in only 6 cases. An improvement in sleep pattern was described in 2 cases41,45, 1 patient showed no effect21, and in 3 cases the clinical effect was not described45. No side effects have been reported although some members of the guideline working group reported experience with patients who had transient night terrors (unpublished observation). From a pathophysiological perspective, supplementation for disorders of sleep induction is reasonable because melatonin is formed from serotonin and therefore may be decreased in AADCD. Many AADCD patients suffer from sleeping disorders, and unpublished observations of the guideline group support the effect of melatonin in this patient group. For dose recommendations, see Table 4.
• R#33 (conditional): Melatonin should be considered for the treatment of sleep disturbances in AADCD.
Voorbereid document _Tessa Wassenberg_V03.indd 154Voorbereid document _Tessa Wassenberg_V03.indd 154 25/10/2021 09:3225/10/2021 09:32

155
Consensus guideline on the diagnosis and treatment of AADC deficiency
BenzodiazepinesThere is very limited evidence for the use of benzodiazepines in AADCD, since it was reported in only 4 patients38,42,65. In one patient, there was a slight improvement of dystonia on clobazam65. In another patient, rectal diazepam was effective in the treatment of prolonged oculogyric crises42. General dose recommendations can be used.
• R#34 (conditional): Benzodiazepines, especially when used intermittently, can be considered in specific settings, e.g. in sustained oculogyric or dystonic crises.
Other symptomatic treatmentAlthough no reports specifically evaluate the use of alpha-adrenoreceptor nose drops in AADCD, its value is evident in clinical practice to treat nasal congestion. To reduce side effects of long-term application, the lowest possible dose should be used. Application should be accompanied by local care, e.g. with dexpanthenol containing ointments. During long-term treatment an intermittent application of a topical steroid (e.g. fluticasone; one spray in each nostril per day for 6 weeks; maximal twice per year) can restore the nose drops effect and reduce the necessary dose (expert opinion). Clonidine, an imidazoline and alpha-2 agonist, can be used for irritability and sleep disturbance6. For dose recommendations, see Table 4. Botulinum toxin injections can be used in the treatment of dystonia. We have limited clinical experience with its use in AADCD.
Other treatment options
L-Dopa with or without carbidopaPatients with AADCD already have highly elevated levels of L-Dopa, therefore treatment with L-Dopa is counterintuitive, and only reported in 10 cases. However, in 4 patients with variants at the L-Dopa binding site, a sustained effect of L-Dopa was seen (see part I). Reported side effects (diarrhea and restlessness) in these patients were minimal and dose-dependent19. No improvement was reported in 3 cases40,42, and in 3 cases response was not described2. The use of carbidopa, an AADC inhibitor, is potentially dangerous in AADCD from a pathophysiological point of view because it further inhibits an already deficient enzyme. For dose recommendations of L-Dopa, see Table 4. In patients on L-Dopa therapy, extra attention should be given to folinic acid supplementation because of possible depletion.
• R#35 (strong): L-Dopa is first line treatment only for patients with L-Dopa binding-site variants (e.g. p.[G102S], p.[R347Q], p.[R160W]). On theoretical grounds, L-Dopa without carbidopa is preferred.
• R#36 (conditional): In patients without proven L-Dopa binding-site variants,, an L-Dopa trial can be considered if other treatment options fail.
8
Voorbereid document _Tessa Wassenberg_V03.indd 155Voorbereid document _Tessa Wassenberg_V03.indd 155 25/10/2021 09:3225/10/2021 09:32

156
Chapter 8
• R#37 (strong): CSF 5-MTHF levels should be determined before and during L-Dopa therapy.
Folinic acidIn theory, secondary cerebral folate deficiency may develop in AADCD since O-methylation of the excessive amounts of L-Dopa to 3-OMD depletes methyl donors including SAM and 5-MTHF. However, decreased levels of CSF 5-MTHF were only reported in a very limited number of patients (see part IIa). The therapeutic use of folinic acid in AADCD is reported in 4 patients21,24,47. In three patients, some improvement was seen. No side effects were published, but several members of the guideline working group reported gastro-intestinal side effects in AADCD patients (unpublished observations). Costs and insurance covering of folinic acid varies amongst countries. Low CSF 5-MTHF levels must be supplemented with folinic acid, not folic acid. Dose recommendations can be found in Table 4.
• R#38 (conditional): Supplementation with folinic acid can be considered in all patients, and is clearly recommended when 5-MTHF in CSF is low.
• R#39 (research): Further research on 5-MTHF is needed to be able to give strong recommendations on folinic acid supplementation and 5-MTHF follow-up in AADCD. At this moment, we do not recommend regular follow-up lumbar punctures in stable patients. In case of unexpected clinical deterioration, measurements of CSF 5-MTHF should be considered to rule out secondary folate deficiency.
5-Hydroxytryptophan5-HTP is the substrate for AADC to form serotonin, and its use in AADCD is as counterintuitive as the use of L-Dopa. Use of 5-HTP in AADCD was described in 5 patients34,40,47,56. None showed a positive effect. In contrast, 2 patients showed side effects: lethargy, increased axial hypotonia, and abdominal pain.
• R#40 (strong): Based on the current evidence and pathophysiological mechanisms, 5-HTP should not be used in the treatment of AADCD.
Selective serotonin reuptake inhibitors (SSRIs)The use of SSRIs (paroxetine, ergotamine and fluoxetine) was reported in 4 patients with AADCD5,40,45,56. Only one patient showed a possible, unspecified response. The other 3 patients showed no clinical benefit, but experienced side effects including worsening of oculogyric crises and hypotonia, lethargy, and dystonic reactions.
• R#41 (conditional): Based on the current evidence, the use of SSRIs in AADCD is not recommended.
Voorbereid document _Tessa Wassenberg_V03.indd 156Voorbereid document _Tessa Wassenberg_V03.indd 156 25/10/2021 09:3225/10/2021 09:32

157
Consensus guideline on the diagnosis and treatment of AADC deficiency
Treatment schedule AADCD
In Table 4, recommended drugs and doses are summarized. Figure 2 shows a schematic example of how a patient with newly diagnosed AADCD can be treated. In recommendation 42 the most important treatment principles of AADCD are given:
• R#42 (strong): The core recommendations for medical treatment of AADCD are:
1. First line treatment agents are selective dopamine agonists, MAO-inhibitors, and pyridoxine
2. Additional symptomatic treatment agents are anticholinergic agents, melatonin, benzodiazepines, and alpha-adrenoreceptor blockers.
3. In general, therapy with multiple drugs will be needed and doses should be titrated individually and sequentially.
4. General treatment principles to adhere to are: step-wise approach, start low and go slow when increasing the doses, and discontinue/ wean off medication that is not helpful.
• R#43 (research): Since the evidence for medical treatment in AADCD is low to very low, it would be desirable to conduct randomized clinical trials in AADCD to improve the proposed treatment schedule. 8
Voorbereid document _Tessa Wassenberg_V03.indd 157Voorbereid document _Tessa Wassenberg_V03.indd 157 25/10/2021 09:3225/10/2021 09:32

158
Chapter 8
Tabl
e 4.
Rec
omm
ende
d dr
ugs a
nd d
oses
in A
ADC
defic
ienc
y
Clas
sD
rug
Mec
hani
smD
ose
reco
mm
enda
tion
Prec
autio
n/ c
omm
ents
FIRST LINE TREATMENT AGENTS
Vita
min
B6
Pyrid
oxin
e (v
it B6
)Co
fact
or, o
ptim
izes
resi
dual
AAD
C ac
tivity
Star
t: 10
0 m
g/d
in 2
dos
esM
ax 2
00 m
g/d
May
be
pref
erre
d ov
er p
yrid
oxal
5-p
hosp
hate
be
caus
e of
cos
t and
ava
ilabi
lity
Mai
ntai
n fo
r 1
year
, the
n di
scon
tinue
whe
n in
st
able
circ
umst
ance
s. If
no
dete
riora
tion,
leav
e di
scon
tinue
d.Ch
roni
c us
e in
hig
h do
se c
an c
ause
sev
ere
sens
orim
otor
pol
yneu
ropa
thy
Side
effe
cts:
gen
eral
ly w
ell t
oler
ated
, som
etim
es
naus
ea, v
omiti
ng.
Pyrid
oxal
5-
Phos
phat
eCo
fact
or, o
ptim
izes
resi
dual
AAD
C ac
tivity
Star
t:100
mg/
d in
2 d
oses
.M
ax 2
00m
g/d
Cons
ider
tria
l if p
yrid
oxin
e gi
ves
too
man
y si
de
effec
ts o
r is n
ot e
ffecti
ve.
Chro
nic
use
in h
igh
dose
can
cau
se s
ever
e se
nsor
imot
or p
olyn
euro
path
y
Dopa
min
e ag
onis
tsPr
amip
exol
eN
on-e
rgot
der
ived
D2
-ago
nist
with
pr
efer
ence
for D
3 re
cept
or su
btyp
e.
Star
t 0.
005
– 0.
010
mg/
kg/d
of
BAS
E in
1-3
div
ided
dos
es,
incr
ease
eve
ry 3
-7*
days
by
0.00
5mg/
kg/d
, max
0.0
75m
g/kg
or 3
.3m
g/d
of B
ASE
Disti
nctio
n in
salt
and
base
con
tent
.Ta
ke ta
blet
s with
wat
er, o
ption
al w
ith fo
odHi
gh ri
sk o
f dru
g-in
duce
d dy
skin
esia
s
Ropi
niro
leN
on-e
rgot
der
ived
D2
-ago
nist
with
pr
efer
ence
for D
3-re
cept
or su
btyp
e.
Sugg
estio
n: S
tart
0.2
5mg/
d1
daily
2h
befo
re b
edtim
e;
incr
ease
eve
ry 3
-7*
days
to
0.5-
4.0
mg/
d in
3 d
ivid
ed
dose
s, m
ax 0
.3m
g/kg
/d o
r 24
mg/
d
Do n
ot u
se in
seve
re k
idne
y fa
ilure
Take
tabl
ets w
ith fo
odVe
ry l
imite
d ex
peri
ence
in
AAD
C de
ficie
ncy,
ph
ysic
ian
shou
ld e
xtra
pola
te a
nd ti
trat
e ca
refu
lly.
Prob
ably
hig
h ris
k of
dru
g-in
duce
d dy
skin
esia
s as
in o
ther
dop
amin
e ag
onis
ts.
Voorbereid document _Tessa Wassenberg_V03.indd 158Voorbereid document _Tessa Wassenberg_V03.indd 158 25/10/2021 09:3225/10/2021 09:32

159
Consensus guideline on the diagnosis and treatment of AADC deficiency
Tabl
e 4.
[Con
tinue
d]
Clas
sD
rug
Mec
hani
smD
ose
reco
mm
enda
tion
Prec
autio
n/ c
omm
ents
FIRST LINE TREATMENT AGENTS
Dopa
min
e ag
onis
tsRo
tigoti
ne p
atch
Non
-erg
ot d
eriv
ed
D2 a
goni
st w
ith
pref
eren
ce fo
r D3;
al
so e
ffect
on
D2,
D1 a
nd D
5; a
nd α
2B
and
5HT1
A ag
onis
t.
>12y
ears
and
>15
kg:
Star
t 2m
g/d;
wee
kly
incr
ease
by
2m
g, m
ax 8
mg/
d.
No
data
ava
ilabl
e fo
r use
in c
hild
ren
<12y
/ <15
kg.
Do n
ot c
ut p
atch
es.
Dru
g in
duce
d dy
skin
esia
s re
quire
a lo
wer
dos
e an
d/ o
r slo
wer
incr
ease
Skin
reac
tions
occ
ur o
ften
(abo
ut 3
0%).
Sulp
hite
can
lead
to a
llerg
ic re
actio
nsRe
mov
e pa
tch
durin
g M
RI/
elec
troc
ardi
over
sion
(a
lum
iniu
m c
onte
nt)
Brom
ocrip
tine
Ergo
t-de
rived
D2
-ago
nist
with
D1
rece
ptor
ant
agon
ist
effec
t
Star
t 0.
1mg/
kg/d
(m
ax
1.25
mg/
d); i
ncre
ase
wee
kly
by
0.1m
g/kg
/d (m
ax 1
.25m
g/d)
up
to 0
.5m
g/kg
/d (m
ax 3
0mg/
d) in
2-
3 di
vide
d do
ses.
Non
-erg
ot
deri
ved
dopa
min
e ag
onis
ts
are
pref
erre
dTa
ke ta
blet
s with
food
Smal
l ri
sk o
f fib
rotic
com
plic
ation
s, c
onsi
der
card
iac
scre
enin
g be
fore
and
dur
ing
use.
Hig
her
risk
with
hig
her
dose
, dos
e re
stric
ted
to
30m
g/d
in a
dults
. Mai
ntai
n lo
wes
t effe
ctive
dos
e.
Perg
olid
e or
ca
berg
olin
eEr
got-
deriv
edN
one
Do
not
use
beca
use
of h
ighe
r ri
sk o
f fib
rotic
co
mpl
icati
ons
MAO
-inhi
bito
rsSe
legi
line
MAO
-B in
hibi
tor
(non
-sel
ectiv
e in
ve
ry h
igh
dose
s)
Star
t 0.1
mg/
kg/d
in 2
-3 d
ivid
ed
dose
s. In
crea
se e
very
2 w
eeks
by
0.1
mg/
kg/d
up
to 0
.3m
g/kg
/d o
r 10m
g/d
Dos
e at
bre
akfa
st a
nd lu
nch,
avo
id n
ight
-tim
e do
ses i
f ins
omni
a is
expe
rienc
ed.
Dose
subl
ingu
al p
repa
ratio
ns m
uch
low
er
Tran
ylcy
prom
ine
Non
-sel
ectiv
e M
AO-A
and
-B
inhi
bito
r
Star
t 0.
1mg/
kg/d
in 2
dos
es.
Incr
ease
eve
ry 2
wee
ks b
y 0.
1mg/
kg/d
up
to 0
.5m
g/kg
/d
(max
30
mg)
Dos
e at
bre
akfa
st a
nd lu
nch,
avo
id n
ight
-tim
e do
ses i
f ins
omni
a is
expe
rienc
ed.
Occ
urre
nce
of ‘c
hees
e eff
ect’
(hyp
erte
nsiv
e cr
ises
whe
n fo
ods
with
hig
h co
nten
t of
tyr
amin
e ar
e in
gest
ed) i
s ve
ry u
nlik
ely
in p
atien
ts w
ith A
ADC
defic
ienc
y du
e to
the
ir lo
w le
vels
of d
opam
ine,
no
repi
neph
rine
and
epin
ephr
ine.
8
Voorbereid document _Tessa Wassenberg_V03.indd 159Voorbereid document _Tessa Wassenberg_V03.indd 159 25/10/2021 09:3225/10/2021 09:32

160
Chapter 8
Tabl
e 4.
[Con
tinue
d]
Clas
sD
rug
Mec
hani
smD
ose
reco
mm
enda
tion
Prec
autio
n/ c
omm
ents
ADDITIONAL SYMPTOMATIC TREATMENT
Antic
holin
ergi
cs
(dys
toni
a/
auto
nom
ic
sym
ptom
s)
Trih
exyp
heni
dyl
Antic
holin
ergi
c ag
ents
, res
tore
s ne
urot
rans
mitt
er
disb
alan
ce
<15k
g: s
tart
0.5
-1m
g/d
in 1
do
se; i
ncre
ase
ever
y 3-
7* d
ays
by 1
mg/
d in
2-4
dos
es/d
>15k
g: s
tart
2m
g/d
in 2
dos
es;
incr
ease
ev
ery
3-7*
da
ys
by2m
g/d
in 2
-4 d
ivid
ed d
oses
.Eff
ectiv
e do
se h
ighl
y va
riabl
e (6
-60m
g)M
axim
um d
ose:
<10
kg 3
0mg/
d;
>10k
g 60
mg/
d
In g
ener
al,
the
youn
ger,
the
bett
er t
oler
ated
; do
sage
s oft
en e
xcee
d re
com
men
ded
dose
for
ad
ults
(15m
g/d)
.M
axim
um d
ose
is di
ctat
ed b
y sid
e eff
ects
: e.g
. dry
m
outh
, dry
eye
s, b
lurr
ed v
ision
(myd
riasis
), ur
ine
rete
ntion
, con
stipa
tion.
Sed
ation
in h
igh
dose
s.
Benz
trop
ine
Cent
rally
acti
ng
antic
holin
ergi
c ag
ent.
Also
do
pam
iner
gic
effec
t by
inhi
bitin
g pr
esyn
aptic
re
upta
ke
Star
t 1m
g in
2 d
ivid
ed d
oses
, in
crea
se w
eekl
y up
to 4
mg/
dAn
ticho
liner
gic
side
effe
cts:
e.g
. dry
mou
th, d
ry
eyes
, blu
rred
vis
ion
(myd
riasi
s), u
rine
rete
ntion
, ob
stipa
tion.
Sed
ation
in h
igh
dose
s.
Nas
al
cong
estio
nO
xym
etaz
olin
e or
xy
lom
etaz
olin
e no
sedr
ops
α-ad
rene
rgic
ag
onis
t lea
ding
to
loca
l va
soco
nstr
ictio
n
Use
gene
ral d
ose
guid
elin
es fo
r ag
e, tr
y to
use
low
est a
vaila
ble
dose
in c
hron
ic u
se
Try
to i
nclu
de i
nter
mitt
ent
wee
ks w
itho
ut
trea
tmen
t to
prev
ent h
abitu
ation
Hyp
erte
nsiv
e cr
ises
if u
sed
conc
omita
ntly
with
M
AO-in
hibi
tors
is v
ery
unlik
ely
in p
atien
ts w
ith
AADC
defi
cien
cy d
ue to
thei
r lev
els o
f dop
amin
e,
nore
pine
phrin
e an
d ep
inep
hrin
e
Slee
ping
pr
oble
ms
Mel
aton
inRe
gula
tes o
nset
of
slee
p an
d da
y/ni
ght
cycl
ing
Star
t 3m
g/d,
giv
en 4
hou
rs
befo
re o
nset
of
slee
p. M
ax
dose
5-8
mg/
d
Tran
sien
t ni
ght
terr
ors
on in
itial
tre
atm
ent
can
occu
r (pe
rson
al e
xper
ienc
e)Av
aila
bilit
y di
ffers
bet
wee
n co
untr
ies.
Irrita
bilit
y/
slee
p di
stur
banc
e
Clon
idin
eCe
ntra
lly a
cting
an
tihyp
erte
nsiv
e dr
ug; i
mid
azol
ine
(I1-)
and
α2-a
goni
st
Star
t 0.
1mg/
d an
te n
octu
m,
incr
ease
to
max
3m
g/d
ante
no
ctum
Mon
itor b
lood
pre
ssur
e in
hig
her d
ose
Seda
tive,
ther
efor
e gi
ve A
N
Voorbereid document _Tessa Wassenberg_V03.indd 160Voorbereid document _Tessa Wassenberg_V03.indd 160 25/10/2021 09:3225/10/2021 09:32

161
Consensus guideline on the diagnosis and treatment of AADC deficiency
Tabl
e 4.
[Con
tinue
d]
Clas
sD
rug
Mec
hani
smD
ose
reco
mm
enda
tion
Prec
autio
n/ c
omm
ents
SPECIAL CASES ONLY
L-Do
pa b
indi
ng
site
var
iant
L-Do
pa w
ithou
t ca
rbid
opa
Subs
trat
e fo
r AAD
C to
form
dop
amin
e;
effec
tive
in c
erta
in
bind
ing
site
var
iant
s
Star
t 0.5
-1m
g/kg
/d in
3 d
ivid
ed
dose
s, i
ncre
ase
2 w
eekl
y by
1m
g/kg
to
5mg/
kg/d
. O
nly
if cl
inic
al e
ffecti
ve,
furt
her
incr
ease
to m
ax 1
5mg/
kg/d
Star
t as fi
rst l
ine
trea
tmen
t onl
y if
know
n bi
ndin
g si
te v
aria
nt.
Oth
erw
ise,
con
side
r as
thi
rd-li
ne t
reat
men
t tria
l fo
r 2
mon
ths
(or
less
if d
eter
iora
tion)
whe
n in
st
able
clin
ical
situ
ation
.M
onito
r CSF
dur
ing
trea
tmen
t, in
clud
ing
5-M
THF
Low
5-M
THF
in C
SFFo
linic
aci
d (c
alci
um fo
linat
e)M
ethy
latio
n of
ex
cess
ive
amou
nts
of L-
Dopa
in
AADC
D m
ay c
ause
de
pleti
on o
f met
hyl
dono
rs.
1-2m
g/kg
/d, m
ax 2
0mg/
dO
nly
supp
ly if
5-M
THF
is lo
w in
CSF
Mon
itor
5-M
THF
in C
SF d
urin
g tr
eatm
ent
with
L-
Dopa
8
Voorbereid document _Tessa Wassenberg_V03.indd 161Voorbereid document _Tessa Wassenberg_V03.indd 161 25/10/2021 09:3225/10/2021 09:32

162
Chapter 8
Figure 2. Treatment algorithm in AADC deficiency
Figure 2. reflects a possible treatment scheme for a newly diagnosed AADCD patient. Drug dose and escalating schemes are given in Table 4. At the left, first line treatment is depicted in which pyridoxine is started at diagnosis (step (1)), followed after two weeks by step (2): either one of the dopamine agonists in escalating scheme or one of the MAO-inhibitors. After two months of treatment at target dose, step (3) is added: either a dopamine agonist or a MAO-inhibitor. The order of introducing dopamine agonist or MAO-inhibitors is interchangeably. Dose escalation depends on effect and tolerability. If an agent is not effective or has too many side effects, consider replacing it with another agent from the same class before going to the next step. In case of intolerable side effects, treatment should be stopped. After about 1 year in stable treatment regimen, reassessment should take place: consider to discontinue drugs (only 1 at a time) without clear treatment effect. Frequent assessment is then again necessary, and agents should be reinstated in case of deterioration. At the right, additional symptomatic treatment is depicted, with different drug classes that could be added for specific symptoms. Always avoid starting more than 1 agent at the time. Assess tolerability and effect frequently, and discontinue drugs that have no clear effect, or give intolerable side effects. Treatment in special situations (L-Dopa, folinic acid) is not depicted in this figure (see text). Abbreviations: DA-agonist: dopamine agonist; MAOI: MAO-inhibitor; OGC: oculogyric crisis
Drugs to avoid in AADCDCentrally acting dopamine antagonists, used for their antiemetic and antipsychotic properties, should be avoided in AADCD because they have the potential to worsen symptoms of dopamine deficiency. The detrimental effects of haloperidol (antagonist
Voorbereid document _Tessa Wassenberg_V03.indd 162Voorbereid document _Tessa Wassenberg_V03.indd 162 25/10/2021 09:3225/10/2021 09:32

163
Consensus guideline on the diagnosis and treatment of AADC deficiency
at dopamine 2 receptors) are illustrated in one case report39. Metoclopramide should not be used for the treatment of nausea. Levomepromazine, an agent with antagonistic properties to epinephrine, histamine, acetylcholine, dopamine, and serotonin, led to severe side effects in one patient46. Less is known about serotonin antagonists like 5-HT3 receptor blockers that are used as antiemetics (e.g. ondansetron, granisetron). From a pathophysiological standpoint, side effects can be expected and their use should be avoided, but there is no literature or clinical experience available. It is important to realize that many drugs have antagonistic properties for several neurotransmitters, and before introducing any drug to AADCD patients, its potential benefits and harms should be considered carefully.
In case of nausea and vomiting in AADCD patients, supportive care to avoid dehydration and hypoglycemia is most important. If possible, anti-dopaminergic and anti-serotonergic agents should be avoided. If medical therapy is needed, low dose domperidone can be considered. Local guidelines on availability, cardiac concerns and dose recommendations should be followed. Although domperidone is a dopamine antagonist, it does not cross the blood brain barrier and therefore side-effects in AADCD are expected to be limited.
• R#44 (strong): Centrally acting dopamine antagonists should be avoided in AADCD.• R#45 (GPP): Supportive care in nausea and vomiting in AADCD patients should be
optimal. If medical treatment is needed, low-dose domperidone can be considered.
Dystonic crisis (status dystonicus)Dystonic crisis can occur in AADCD patients, but limited data is available about the prevalence of and treatment approach to this rare, potentially life-threatening complication. A dystonic crisis is often triggered by infection or medication adjustments. It is characterized by sustained severe dystonic muscle contractions that can lead to airway compromise and metabolic complications such as rhabdomyolysis leading to acute renal failure66. The approach to dystonic crisis in AADCD should be similar to the general approach, with admission to an intensive care unit, fluid and nutrition supplementation, sedation (usually with benzodiazepines) and respiratory support if needed. Dopamine antagonists and L-Dopa should not be used in AADCD. For a review, see67.
• R#46 (GPP): Dystonic crisis in AADCD is a potentially life-threatening condition and should be treated promptly.
8
Voorbereid document _Tessa Wassenberg_V03.indd 163Voorbereid document _Tessa Wassenberg_V03.indd 163 25/10/2021 09:3225/10/2021 09:32

164
Chapter 8
IIIb: Non-medical treatment
Paramedical treatment in AADCDAlthough there are no studies or reports on the effects of paramedical treatment in AADCD, a multidisciplinary approach with physiotherapy, speech therapy, occupational therapy, feeding and nutritional assessment, and (neuro)psychological treatment and support is essential to prevent secondary complications and promote development. A physiatrist (rehabilitation specialist) is also a valuable member of the team. In this respect, approach to a patient with AADCD is comparable to the approach of other chronic neurological disorders, e.g. cerebral palsy.
• R#47 (GPP): Involvement of a multidisciplinary team that includes a rehabilitation physician (physiatrist) and allied health professionals (paramedical therapy services) is essential in the care for AADCD patients.
Gene therapy and other surgical treatment optionsGene therapy in which a viral vector (adeno-associated virus type 2) encoding cDNA of the human DDC gene is delivered to targeted brain structures was originally developed for patients with Parkinson’s disease68. Gene transfer to the bilateral putamen has been performed in four AADCD patients in Taiwan with modest but promising results24. Further research is ongoing. Clinical trials are presently recruiting patients in Taiwan and Japan11,12, and trials in the USA and Europe, in which gene transfer will target midbrain structures, are anticipated69. There is no experience with deep brain stimulation or other surgical treatment options in AADCD.
• R#48 (research): Gene therapy for AADCD is currently under development in research setting. Clinical trial results will determine whether further implementation of this promising therapy may occur in the future.
Part IV: Complications and long-term management in AADCD
Cardiac decompensationStructural cardiac abnormalities in AADCD are not expected from a pathophysiological perspective. In one case report, electrocardiogram and heart ultrasound were reported as normal34, but in most reports information regarding cardiac status is lacking. There are individual descriptions of one patient with bradycardia on ECG20, and one patient who suffered from a witnessed cardiac arrest at age 9 years, with ensuing permanent neurological damage59. It is possible that cathecholaminergic deficiency and autonomic dysfunction may potentially lead to cardiac complications, which may be more evident during illness or stress (e.g. intercurrent infections, surgical interventions).
Voorbereid document _Tessa Wassenberg_V03.indd 164Voorbereid document _Tessa Wassenberg_V03.indd 164 25/10/2021 09:3225/10/2021 09:32

165
Consensus guideline on the diagnosis and treatment of AADC deficiency
• R#49 (strong): There should be awareness for possible cardiac complications in AADCD patients during potentially stressful situations and cardiac monitoring during these instances is recommended. Regular follow-up cardiac screening is not needed, but recommended before any anesthesia or intervention. If available in local care setting, cardiac screening should consist of a referral to a (pediatric) cardiologist for clinical evaluation, ECG and echocardiogram. For cardiac screening for patients on dopamine agonists, see recommendation #28.
Orthopaedic complicationsOrthopaedic complications are reported in AADCD secondary to severe motor impairment (abnormalities of tone, posture, paucity of movement). Contractures leading to mobilization problems are described in a few patients7,39. A multidisciplinary approach for follow-up and treatment is recommended. Orthopaedic monitoring (e.g. hip and spine X-rays) is recommended, preferably in a local care setting.
• R#50 (GPP): AADCD patients should be monitored for orthopaedic complications following standards of good care for patients with motor impairment.
InfectionsThere is an increased risk of infections in AADCD patients, likely not because of disease-specific mechanisms but secondary to complications including impaired feeding and swallowing, reduced mobility, and recurrent hospitalization. A disease specific aspect of AADCD could be the reduced response to stress of infections, which can be fatal. Treating physicians (specialists and primary care physicians) should be aware of this. Furthermore, hyperthermia in AADCD can be due to autonomic temperature dysregulation and may not always represent a fever due to underlying infection. Vaccinations following local vaccination programs are recommended.
• R #51 (GPP): Because AADCD patients have a reduced response to stress, close monitoring during infections is recommended.
• R#52 (GPP): Vaccinations following local vaccination programs are recommended in AADCD.
Follow-up visits• R#53 (strong): AADCD patients should be seen at least yearly by a (child) neurologist
with experience in movement disorders or neurometabolic disease, ideally in a multidisciplinary setting (see R#46), facilitating a shared-care approach.
Emergency card• R#54 (GPP): It is recommended that all AADCD patients receive an emergency
card including short information on AADCD, possible complications, and drugs to avoid in this disorder. An agreed emergency card can be found as Additional file 3 .
8
Voorbereid document _Tessa Wassenberg_V03.indd 165Voorbereid document _Tessa Wassenberg_V03.indd 165 25/10/2021 09:3225/10/2021 09:32

166
Chapter 8
PART V: Social issues and transition
Psychological support for familiesThere are no reports on the health and well-being of caregivers of children with AADCD available. However, studies in families with children with chronic diseases show that caregivers are at risk of reduced quality of life. Family stress and parental coping are factors that are associated with quality of life70. For more background information and strategies to improve support for parents of chronically ill children, see e.g. Newton and Lemarche71. Quality of life assessment and the evaluation of disease burden in family members of AADCD patients are an essential part of the ongoing iNTD registry study9.
In isolated case reports, an increased prevalence of psychiatric disorders in carriers of AADCD has been described. To date, this has neither been systematically evaluated nor consistently reported35,45.
• R#55 (strong): If available in local care setting, psychological support (e.g. psychologist, social worker) to caregivers, siblings, and patients with AADCD is recommended
• R#56 (research): Further research is needed to clarify whether DDC gene variant carriers have a primary (genetically determined) increased risk of psychiatric symptoms.
Genetic counselingAlthough there is no specific literature on genetic counseling in AADCD available, it can be considered good clinical practice for all parents of children with AADCD to be offered standard genetic counseling, considering the autosomal recessive nature of the disorder. See also R#60.
• R#57 (strong): If available in local care settings, all parents of patients with AADCD should be offered standard genetic counseling.
Parental organizationsThere are two internationally operating non-profit parental organizations for patients with AADCD: the UK based AADC Research Trust (www.aadcresearch.org) and the USA based Pediatric Neurotransmitter Disease Association (www.pndassoc.org). Furthermore, there is the Spanish neurotransmitter diseases association “De neu” (www.deneu.org). The major aim of these organizations is to help and support patients with AADCD by providing information and organizing family meetings, promoting disease awareness and funding scientific research.
• R#58 (strong): It is recommended that caregivers of AADC deficient patients be informed about existing parental organizations for this rare disorder.
Voorbereid document _Tessa Wassenberg_V03.indd 166Voorbereid document _Tessa Wassenberg_V03.indd 166 25/10/2021 09:3225/10/2021 09:32

167
Consensus guideline on the diagnosis and treatment of AADC deficiency
Transition from child to adulthoodNo specific reports are available on the healthcare transition of patients with AADCD from childhood to adolescence to adulthood. Most reports focus on patients in infancy and childhood. There is no information published on puberty. Also fertility concerns or pregnancy has not been described in AADCD. Considering the often severe phenotype, for the majority of patients this will not be an issue. However, relatively mildly affected patients have been described35 and the phenotypic spectrum continues to expand. Based on experience with other disorders that cause neurodevelopmental disability, it is known that there are significant gaps in our knowledge and practice about healthcare transition for young adults72. The transfer from intense, family-oriented pediatric care, to primarily individually focused adult care is often perceived as difficult for both patients and caregivers73. Local differences in health care organization for patients with neurodevelopmental disabilities will be present across countries. Based on the literature, it is not possible to give specific recommendations on transition of care for patients with AADCD. However, the guideline committee clearly states that this process should be adequately prepared. Continuation of the multidisciplinary care setting is recommended.
• R#59 (GPP): Transition of AADCD patients to adult care should be prepared well, and continue to take place in specialized centers. Multidisciplinary care should be continued.
• R#60 (research): Follow-up studies of adult patients with AADCD are strongly recommended to better define prognosis and possible new clinical symptoms and signs in adolescence and adulthood.
Part VI: Special situations
Anesthesia for interventionsIt is not unusual for patients with AADCD to need anesthesia for (minor) interventions such as gastrostomy. Only two reports described anesthesia management in two different AADCD patients39,30. It should be noted that intravenous phenylephrine and dopamine may lead to an exaggerated hemodynamic response in these patients. In case of hypotension during intervention, dopamine should be initiated at low dose (e.g. 1-2 ug/kg/min)29. Monitoring of hemodynamic function, temperature and glucose levels is important, especially in prolonged interventions.
• R#61 (strong): Anesthesia should be well prepared in patients with AADCD because patients have an increased risk of hemodynamic instability and hypoglycemia. In addition to cardiovascular monitoring, monitoring of temperature and glucose levels during procedures is recommended. In general, it is recommended to continue standard treatment (including MAO inhibitors) during interventions.
8
Voorbereid document _Tessa Wassenberg_V03.indd 167Voorbereid document _Tessa Wassenberg_V03.indd 167 25/10/2021 09:3225/10/2021 09:32

168
Chapter 8
Intensive Care managementInformation on ICU management of AADC deficient patients is limited. In a case report of one patient, cardiac complications are described during ICU treatment with exogenous catecholamines39. Another case report described one patient with a 5-h period of hypotension with bradycardia following sedation at age 11 years59. Autonomic testing in two patients showed severe impairment of sympathetic blood pressure modulation in both. In the more severely affected patient, recurrent episodes of cardiorespiratory arrest, preceded by profound bradycardia, were described, evoked by painful stimuli (e.g. blood draw)45.
• R#62 (strong): AADCD leads to sympathetic impairment with possible cardiac complications. This should be anticipated during ICU admissions.
Prenatal diagnosisPrenatal diagnosis of AADCD might be possible by measuring 3-OMD, 5-HTP and L-Dopa in amniotic fluid or fetal plasma74, but if both disease-causing genetic variants are known, the most reliable method of prenatal diagnosis is to perform genetic analysis of chorionic villi or amniotic fluid cells.
In two reports, successful pre-implantation genetic diagnosis has been described. In four of five families, unaffected live births were achieved75. In a report from the same group, Chen et al describe this technique in a diverse group of single gene disorders including AADCD76.
• R#63 (strong): If local resources allow, prenatal genetic diagnosis or preimplantation techniques should be offered to carriers of AADCD.
Conclusions
AADCD is an early onset disorder with a combined deficiency of serotonin, dopamine, norepinephrine and epinephrine. Key clinical symptoms are hypotonia, movement disorders (especially oculogyric crisis, dystonia and hypokinesia), developmental delay, and autonomic symptoms. The phenotypic spectrum is broad and can range from very severe to relatively mild. There are no clear genotype/ phenotype correlations in AADCD except for the homozygous IVS6 + 4A > T splice variant that is associated with a severe phenotype in all cases reported to date, and has an increased incidence in people of Chinese ethnicity.
Voorbereid document _Tessa Wassenberg_V03.indd 168Voorbereid document _Tessa Wassenberg_V03.indd 168 25/10/2021 09:3225/10/2021 09:32

169
Consensus guideline on the diagnosis and treatment of AADC deficiency
There are three core diagnostic tools for identifying AADCD:1. Low CSF levels of 5-HIAA, HVA and MHPG, with normal CSF pterins, and increased
CSF levels of L-Dopa, 3-OMD and 5-HTP2. Genetic diagnosis showing compound heterozygous or homozygous disease
causing variants in the DDC gene3. Decreased AADC enzyme activity in plasma
To diagnose AADCD, genetic testing should be performed and at least two out of three core diagnostic tests should be positive. If local resources allow, we recommend performing all three key diagnostic tests in patients with this rare disorder.
The core recommendations for treatment of AADCD are:1. First line treatment with selective dopamine agonists, MAO-inhibitors, and
pyridoxine2. Additional symptomatic treatment agents with anticholinergic agents, melatonin,
benzodiazepines, and alpha-adrenoreceptor blockers3. In general, multiple drug classes will be needed4. Overall treatment principles to adhere to are: step-wise approach, start low and
go slow when increasing dosages, and discontinue/ gradually withdraw medication that is not helpful.
Involvement of a multidisciplinary team, including physiatrist and paramedical therapy services, is essential in the care for AADCD patients, and psychological support should be offered to caregivers, siblings and patients. Patients and caregivers should be informed about the AADCD parental organizations. AADCD patients should be seen at least yearly by a (child) neurologist with experience in movement disorders or neurometabolic disease, ideally in a multidisciplinary setting, facilitating a shared-care approach.
Although the level of evidence mainly consisted of level 3 and 4 (non-analytical studies and expert opinion), using SIGN and GRADE methodology permitted us to form the strong and conditional recommendations provided in this guideline. We believe that this consensus guideline will improve the care of AADCD patients around the world. Furthermore, we determined several knowledge voids that should be addressed in future research.
8
Voorbereid document _Tessa Wassenberg_V03.indd 169Voorbereid document _Tessa Wassenberg_V03.indd 169 25/10/2021 09:3225/10/2021 09:32

170
Chapter 8
References
1. Hyland K, Clayton PT. Aromatic amino acid decarboxylase deficiency in twins. J Inherit Metab Dis. 1990;13(3):301–4.
2. Brun L, Ngu LH, Keng WT, Ch’ng GS, Choy YS, Hwu WL, et al. Clinical and biochemical features of aromatic L-amino acid decarboxylase deficiency. Neurology. 2010;75(1):64–71. doi:10.1212/WNL.0b013e3181e620ae.
3. Alfadhel M, Kattan R. Aromatic amino Acid decarboxylase deficiency not responding to pyridoxine and bromocriptine therapy: case report and review of response to treatment. J Cent Nerv Syst Dis. 2014;6:1–5. doi:10.4137/JCNSD.S12938.
4. Lee HF, Tsai CR, Chi CS, Chang TM, Lee HJ. Aromatic L-amino acid decarboxylase deficiency in Taiwan. Eur J Paediatr Neurol. 2009;13(2):135–40.
5. Leuzzi V, Mastrangelo M, Polizzi A, Artiola C, van Kuilenburg AB, Carducci C et al. Report of two never treated adult sisters with aromatic L-amino acid decarboxylase deficiency: a portrait of the natural history of the disease or an expanding phenotype? JIMD Rep. 2014. doi:10.1007/8904_2014_295.
6. Ng J, Papandreou A, Heales SJ, Kurian MA. Monoamine neurotransmitter disorders-clinical advances and future perspectives. Nat Rev Neurol. 2015;11(10):567–84. doi:10.1038/nrneurol.2015.172.
7. Chang YT, Sharma R, Marsh JL, McPherson JD, Bedell JA, Knust A, et al. Levodopa- responsive aromatic L-amino acid decarboxylase deficiency. Ann Neurol. 2004;55(3):435–8.
8. INTD. International Working Group on Neurotransmitter Related Disorders. 2013. www.intd- online.org.
9. INTD. International working group on neurotransmitter related disorders Patient Registry. 2013. https://intd-registry.org.
10. AADC research trust. The AADC research trust literature database. 2015. http://www.aadcresearch.org/page/by-leading-author/. Accessed 09 Feb 2016.
11. WHO. International clinical trials registry platform. 2016. http://apps.who.int/trialsearch/. Accessed Feb 2016.
12. NIH. ClinicalTrials.gov, a service of the U.S. National Institutes of Health. 2015. https://clinicaltrials.gov/. Accessed Feb 2016.
14. Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94. doi:10.1016/j.jclinepi.2010.04.026.
15. Guyatt GH, Oxman AD, Kunz R, Atkins D, Brozek J, Vist G, et al. GRADE guidelines: 2. Framing the question and deciding on important outcomes. J Clin Epidemiol. 2011;64(4):395– 400. doi:10.1016/j.jclinepi.2010.09.012.
16. Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–6. Doi:10.1016/j.jclinepi.2010.07.015.
Voorbereid document _Tessa Wassenberg_V03.indd 170Voorbereid document _Tessa Wassenberg_V03.indd 170 25/10/2021 09:3225/10/2021 09:32

171
Consensus guideline on the diagnosis and treatment of AADC deficiency
17. Guyatt GH, Oxman AD, Schunemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. 2011;64(4):380–2. doi:10.1016/j.jclinepi.2010.09.011.
18. Arnoux JB, Damaj L, Napuri S, Serre V, Hubert L, Cadoudal M, et al. Aromatic L-amino acid decarboxylase deficiency is a cause of long-fasting hypoglycemia. J Clin Endocrinol Metab. 2013;98(11):4279–84. doi:10.1210/jc.2013-2740.
19. Barth M, Serre V, Hubert L, Chaabouni Y, Bahi-Buisson N, Cadoudal M, et al. Kinetic analyses guide the therapeutic decision in a novel form of moderate aromatic Acid decarboxylase deficiency. JIMD Rep. 2012;3:25–32. doi:10.1007/8904_2011_43.
20. Graziano C, Wischmeijer A, Pippucci T, Fusco C, Diquigiovanni C, Noukas M, et al. Syndromic intellectual disability: a new phenotype caused by an aromatic amino acid decarboxylase gene (DDC) variant. Gene. 2015;559(2):144–8. doi:10.1016/j.gene.2015.01.026.
21. Gucuyener K, Kasapkara CS, Tumer L, Verbeek MM. Aromatic L-amino acid decarboxylase deficiency: a new case from Turkey with a novel mutation. Ann Indian Acad Neurol. 2014;17(2):234–6. doi:10.4103/0972-2327.132652.
22. Helman G, Pappa MB, Pearl PL. Widening phenotypic spectrum of AADC deficiency, a disorder of dopamine and serotonin synthesis. JIMD Rep. 2014. doi:10.1007/8904_2014_327.
23. Lee HC, Lai CK, Yau KC, Siu TS, Mak CM, Yuen YP, et al. Non-invasive urinary screening for aromatic L-amino acid decarboxylase deficiency in high-prevalence areas: a pilot study. Clin Chim Acta. 2012;413(1-2):126–30. doi:10.1016/j.cca.2011.09.008.
24. Hwu WL, Muramatsu S, Tseng SH, Tzen KY, Lee NC, Chien YH, et al. Gene therapy for aromatic L-amino acid decarboxylase deficiency. Sci Transl Med. 2012;4(134):134ra61. doi:10.1126/scitranslmed.3003640.
25. Molero-Luis M, Serrano M, Ormazabal A, Perez-Duenas B, Garcia-Cazorla A, Pons R, et al. Homovanillic acid in cerebrospinal fluid of 1388 children with neurological disorders. Dev Med Child Neurol. 2013;55(6):559–66. doi:10.1111/dmcn.12116.
26. Wassenberg T, Willemsen MA, Geurtz PB, Lammens M, Verrijp K, Wilmer M, et al. Urinary dopamine in aromatic L-amino acid decarboxylase deficiency: the unsolved paradox. Mol Genet Metab. 2010;101(4):349–56. doi:10.1016/j.ymgme.2010.08.003.
27. Wassenberg T, Monnens LA, Geurtz BP, Wevers RA, Verbeek MM, Willemsen MA. The paradox of hyperdopaminuria in aromatic L-amino Acid deficiency explained. JIMD Rep. 2012;4:39–45. doi:10.1007/8904_2011_84.
28. Haliloglu G, Vezir E, Baydar L, Onol S, Sivri S, Coskun T, et al. When do we need to perform a diagnostic lumbar puncture for neurometabolic diseases? Positive yield and retrospective analysis from a tertiary center. Turk J Pediatr. 2012;54(1):52–8.
29. Vutskits L, Menache C, Manzano S, Haenggeli CA, Habre W. Anesthesia management in a young child with aromatic l-amino acid decarboxylase deficiency. Paediatr Anaesth. 2006;16(1):82–4. doi:10.1111/j.1460-9592.2005.01605.x.
30. Berkowitz DH, Ganesh A. Combined general and regional anesthetic in a child with aromatic L-amino acid decarboxylase deficiency. Anesth Analg. 2006;103(6):1630–1. doi:10.1213/01.ane.0000247197.78421.93.
31. Burlina AB, Burlina AP, Hyland K, Bonafé L, Blau N. Autistic syndrome and aromatic L- amino acid decarboxylase (AADC) deficiency. J Inherit Metab Dis. 2001;24(S1):34.
8
Voorbereid document _Tessa Wassenberg_V03.indd 171Voorbereid document _Tessa Wassenberg_V03.indd 171 25/10/2021 09:3225/10/2021 09:32

172
Chapter 8
32. Choy YS, Ngu LH, Chen BC, Ong LC, Blau N. Variable manifestations and therapeutic response of aromatic l-amino acid decarboxylase deficiency. JIMD. 2006;29(144):15.1.
33. Chang YT, Mues G, McPherson JD, Bedell JA, Marsh JL, Hyland K. Mutations in the human aromatic l-amino acid decarboxylase gene. J Inherit Metab Dis. 1998;21(S2):4.
34. Fiumara A, Brautigam C, Hyland K, Sharma R, Lagae L, Stoltenborg B, et al. Aromatic L- amino acid decarboxylase deficiency with hyperdopaminuria. Clinical and laboratory findings in response to different therapies. Neuropediatrics. 2002;33(4):203–8.
35. Tay SK, Poh KS, Hyland K, Pang YW, Ong HT, Low PS, et al. Unusually mild phenotype of AADC deficiency in 2 siblings. Mol Genet Metab. 2007;91(4):374–8.
36. Ide S, Sasaki M, Kato M, Shiihara T, Kinoshita S, Takahashi JY, et al. Abnormal glucose metabolism in aromatic l-amino acid decarboxylase deficiency. Brain Dev. 2010;32:506–10.
37. Menache C, Manzano S, Cruzado D, Mirabeau M, Haenggeli CA. Aromatic l-amino acid38. Ito S, Nakayma T, Ide S, Ito Y, Oguni H, Goto YI, et al. Aromatic l-amino acid decarboxylase
deficiency associated with epilepsy mimicking non-epileptic involuntary movements. Dev Med Child Neur. 2008;50:876–8.
39. Anselm IA, Darras BT. Catecholamine toxicity in aromatic L-amino acid decarboxylase deficiency. Pediatr Neurol. 2006;35(2):142–4.
40. Manegold C, Hoffmann GF, Degen I, Ikonomidou H, Knust A, Laass MW, et al. Aromatic L- amino acid decarboxylase deficiency: clinical features, drug therapy and follow-up. J Inherit Metab Dis. 2009;32(3):371–80.
41. Pons R, Ford B, Chiriboga CA, Clayton PT, Hinton V, Hyland K, et al. Aromatic L-amino acid decarboxylase deficiency: clinical features, treatment, and prognosis. Neurology. 2004;62(7):1058–65.
42. Korenke GC, Christen HJ, Hyland K, Hunneman DH, Hanefeld F. Aromatic L-amino acid decarboxylase deficiency: an extrapyramidal movement disorder with oculogyric crises. Eur J Paediatr Neurol. 1997;1(2-3):67–71.
43. Abeling NG, Brautigam C, Hoffmann GF, Barth PG, Wevers RA, Jaeken J, et al. Pathobiochemical implications of hyperdopaminuria in patients with aromatic L-amino acid decarboxylase deficiency. J Inherit Metab Dis. 2000;23(4):325–8.
44. Hyland K, Surtees RA, Rodeck C, Clayton PT. Aromatic L-amino acid decarboxylase deficiency: clinical features, diagnosis, and treatment of a new inborn error of neurotransmitter amine synthesis. Neurology. 1992;42(10):1980–8.
45. Swoboda KJ, Saul JP, McKenna CE, Speller NB, Hyland K. Aromatic L-amino acid decarboxylase deficiency: overview of clinical features and outcomes. Ann Neurol. 2003;54 Suppl 6:S49–55.
46. Knust A. Aromatischer L-aminosauredecarboxylasemangel: charakterisierung und therapiestudie einer ‘neuen’ neurometabolischen erkrankung der dopamin- und serotoninbiosynthese [Human Medicine]. Marburg: Phillips-Universitat Marburg; 2002.
47. Brautigam C, Wevers RA, Hyland K, Sharma RK, Knust A, Hoffman GF. The influence of L- dopa on methylation capacity in aromatic L-amino acid decarboxylase deficiency: biochemical findings in two patients. J Inherit Metab Dis. 2000;23(4):321–4.
Voorbereid document _Tessa Wassenberg_V03.indd 172Voorbereid document _Tessa Wassenberg_V03.indd 172 25/10/2021 09:3225/10/2021 09:32

173
Consensus guideline on the diagnosis and treatment of AADC deficiency
48. Montioli R, Dindo M, Giorgetti A, Piccoli S, Cellini B, Voltattorni CB. A comprehensive picture of the mutations associated with aromatic amino acid decarboxylase deficiency: from molecular mechanisms to therapy implications. Hum Mol Genet. 2014;23(20):5429–40. doi:10.1093/hmg/ddu266.
49. Mills PB, Surtees RA, Champion MP, Beesley CE, Dalton N, Scambler PJ, et al. Neonatal epileptic encephalopathy caused by mutations in the PNPO gene encoding pyridox(am)ine 5’- phosphate oxidase. Hum Mol Genet. 2005;14(8):1077–86. doi:10.1093/hmg/ddi120.
50. Brautigam C, Hyland K, Wevers R, Sharma R, Wagner L, Stock GJ, et al. Clinical and laboratory findings in twins with neonatal epileptic encephalopathy mimicking aromatic L- amino acid decarboxylase deficiency. Neuropediatrics. 2002;33(3):113–7.
51. Surtees R, Hyland K. L-3,4-dihydroxyphenylalanine (levodopa) lowers central nervous system S-adenosylmethionine concentrations in humans. J Neurol Neurosurg Psychiatry. 1990;53(7):569–72.
52. Hyland K. Clinical utility of monoamine neurotransmitter metabolite analysis in cerebrospinal fluid. Clin Chem. 2008;54(4):633–41. doi:10.1373/clinchem.2007.099986.
53. Verbeek MM, Geurtz PB, Willemsen MA, Wevers RA. Aromatic L-amino acid decarboxylase enzyme activity in deficient patients and heterozygotes. Mol Genet Metab. 2007;90(4):363–9.
54. Blau N. PNDdb: locus-specific database of gene variants causing BH4 deficiencies and other PND (formerly BIOMDB). 2016. http://www.biopku.org/home/pnddb.asp.
55. Atwal PS, Donti TR, Cardon AL, Bacino CA, Sun Q, Emrick L, et al. Aromatic L-amino acid decarboxylase deficiency diagnosed by clinical metabolomic profiling of plasma. Mol Genet Metab. 2015;115(2-3):91–4. doi:10.1016/j.ymgme.2015.04.008.
56. Swoboda KJ, Hyland K, Goldstein DS, Kuban KC, Arnold LA, Holmes CS, et al. Clinical and therapeutic observations in aromatic L-amino acid decarboxylase deficiency. Neurology. 1999;53(6):1205–11.
57. Chen PW, Lee NC, Chien YH, Wu JY, Wang PC, Hwu WL. Diagnosis of aromatic l-amino acid decarboxylase deficiency by measuring 3-O-methyldopa concentrations in dried blood spots. Clin Chim Acta. 2014;431C:19–22. doi:10.1016/j.cca.2014.01.034.
58. Abeling NG, van Gennip AH, Barth PG, van CA, Westra M, Wijburg FA. Aromatic L-amino acid decarboxylase deficiency: a new case with a mild clinical presentation and unexpected laboratory findings. J Inherit Metab Dis. 1998;21(3):240–2.
59. Lee LK, Cheung KM, Cheng WW, Ko CH, Lee HH, Ching CK, et al. A rare cause of severe diarrhoea diagnosed by urine metabolic screening: aromatic L-amino acid decarboxylase deficiency. Hong Kong Med J. 2014;20(2):161–4. doi:10.12809/hkmj133922.
60. Antonini A, Poewe W. Fibrotic heart-valve reactions to dopamine-agonist treatment in Parkinson’s disease. Lancet Neurol. 2007;6(9):826–9. doi:10.1016/S1474-4422(07)70218-1.
61. (EMA) EMA. Amendments to be included in the relevant sections of the summaryor product characteristics for bromocriptine containing medicinal products..In: Union E, editor. London; 2009. http://www.ema.europa.eu/docs/en_GB/document_library/Referrals_document/Ergot_derived _dopamine_agonists_31/WC500011454.pdf.
62. Andersohn F, Garbe E. Cardiac and noncardiac fibrotic reactions caused by ergot-and nonergot-derived dopamine agonists. Mov Disord. 2009;24(1):129–33. doi:10.1002/mds.22385.
8
Voorbereid document _Tessa Wassenberg_V03.indd 173Voorbereid document _Tessa Wassenberg_V03.indd 173 25/10/2021 09:3225/10/2021 09:32

174
Chapter 8
63. Katzenschlager R, Sampaio C, Costa J, Lees A. Anticholinergics for symptomatic management of Parkinson’s disease. Cochrane Database Syst Rev. 2003;2:CD003735. doi:10.1002/14651858.CD003735.
64. Jankovic J. Medical treatment of dystonia. Mov Disord. 2013;28(7):1001–12. doi:10.1002/mds.25552.
65. Abdenur JE, Abeling N, Specola N, Jorge L, Schenone AB, van Cruchten AC, et al. Aromatic l-aminoacid decarboxylase deficiency: unusual neonatal presentation and additional findings in organic acid analysis. Mol Genet Metab. 2006;87(1):48–53. doi:10.1016/j.ymgme.2005.09.007.
66. Manji H, Howard RS, Miller DH, Hirsch NP, Carr L, Bhatia K, et al. Status dystonicus: the syndrome and its management. Brain. 1998;121(Pt 2):243–52.
67. Allen NM, Lin JP, Lynch T, King MD. Status dystonicus: a practice guide. Dev Med Child Neurol. 2014;56(2):105–12. doi:10.1111/dmcn.12339.
68 Christine CW, Starr PA, Larson PS, Eberling JL, Jagust WJ, Hawkins RA, et al. Safety and tolerability of putaminal AADC gene therapy for Parkinson disease. Neurology. 2009;73(20):1662–9. doi:10.1212/WNL.0b013e3181c29356.
69. San Sebastian W, Kells AP, Bringas J, Samaranch L, Hadaczek P, Ciesielska A et al. Safety and tolerability of MRI-guided infusion of AAV2-hAADC into the mid-brain of non-human primate. Mol Ther Methods Clin Dev. 2014;3. doi:10.1038/mtm.2014.49.
70. Fidika A, Salewski C, Goldbeck L. Quality of life among parents of children with phenylketonuria (PKU). Health Qual Life Outcomes. 2013;11:54. doi:10.1186/1477-7525-11- 54.
71. Newton K, Lamarche K. Take the challenge: strategies to improve support for parents of chronically ill children. Home Healthc Nurse. 2012;30(5):E1–8. doi:10.1097/NHH.0b013e318252c3d5.
72. Racine E, Bell E, Yan A, Andrew G, Bell LE, Clarke M, et al. Ethics challenges of transition from paediatric to adult health care services for young adults with neurodevelopmental disabilities. Paediatr Child Health. 2014;19(2):65–8.
73. Camfield P, Camfield C. Transition to adult care for children with chronic neurological disorders. Ann Neurol. 2011;69(3):437–44. doi:10.1002/ana.22393.
74. Hyland K, Clayton PT. Aromatic L-amino acid decarboxylase deficiency: diagnostic methodology. Clin Chem. 1992;38(12):2405–10.
75. Kuo SJ, Ma GC, Chang SP, Wu HH, Chen CP, Chang TM, et al. Preimplantation and prenatal genetic diagnosis of aromatic L-amino acid decarboxylase deficiency with an amplification refractory mutation system-quantitative polymerase chain reaction. Taiwan J Obstet Gynecol. 2011;50(4):468–73. doi:10.1016/j.tjog.2011.10.012.
76. Chen HF, Chang SP, Wu SH, Lin WH, Lee YC, Ni YH, et al. Validating a rapid, real-time, PCR-based direct mutation detection assay for preimplantation genetic diagnosis. Gene. 2014;548(2):299–305. doi:10.1016/j.gene.2014.07.039.
77. Hoffmann GF, Assmann BE. Aromatic l-amino acid decarboxylase deficiency. In: Hoffmann GF, Blau N, editors. Congenital neurotransmitter disorders: a clinical approach. 1 ed. New York: Nova Science Publishers; 2014. p. 65-80.
Voorbereid document _Tessa Wassenberg_V03.indd 174Voorbereid document _Tessa Wassenberg_V03.indd 174 25/10/2021 09:3225/10/2021 09:32

175
Consensus guideline on the diagnosis and treatment of AADC deficiency
Supplemental material Chapter 8
Additional file 1:List of key questions can be accessed online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5241937/#MOESM1
Additional file 2: Figure S1. Flow chart showing the systematic literature search and number and type of included sources.
8
Voorbereid document _Tessa Wassenberg_V03.indd 175Voorbereid document _Tessa Wassenberg_V03.indd 175 25/10/2021 09:3225/10/2021 09:32

176
Chapter 8
Additional File 3: Emergency Card AADC deficiency
Emergency CardAromatic L-amino acid decarboxylase deficiency
Synonyms AADC deficiency AADCD
Definition AADC deficiency is a rare autosomal recessive neurometabolic disorder that leads to a deficiency of the neurotransmitters serotonin, dopamine, norepinephrine (noradrenaline) and epinephrine (adrenaline).
Key clinical symptoms• Severe hypotonia• Movement disorders
• Oculogyric crisis, dystonia, hypokinesia• Prolonged oculogyric crisis/ status dystonicus possible
• Developmental delay• Autonomic symptoms
• Excessive sweating, drooling, temperature instability, hypotension• Sympathetic impairment with possible cardiac complications
• Impaired stress response• Hypoglycemia possible• Sudden death possible
Emergency treatment Clinical admission and surveillance, including monitoring of glucose levels, during acute illness and/ or any medical intervention
Attention Anesthesia should be well prepared because of increased risk of hemodynamic instability and hypoglycemia. Ensure regular monitoring of temperature and glucose levels. Standard treatment (including MAO inhibitors) should be continued before and during interventions.
Drugs to avoid• DO NOT GIVE any centrally acting antidopaminergic medication (e.g.
metoclopramide, haloperidol and most other neuroleptics)• Avoid phenothiazines because of antidopaminergic, antiadrenergic and
antiserotonergic properties• Caution when using drugs with antiserotonergic properties (e.g. ondansetron)• Low dose of domperidone can be considered if antiemetic treatment is needed.
Voorbereid document _Tessa Wassenberg_V03.indd 176Voorbereid document _Tessa Wassenberg_V03.indd 176 25/10/2021 09:3225/10/2021 09:32

177
Consensus guideline on the diagnosis and treatment of AADC deficiency
8
Voorbereid document _Tessa Wassenberg_V03.indd 177Voorbereid document _Tessa Wassenberg_V03.indd 177 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 178Voorbereid document _Tessa Wassenberg_V03.indd 178 25/10/2021 09:3225/10/2021 09:32

CHAPTER 9
Clinical presentation and long-term follow-up of Dopamine Beta Hydroxylase Deficiency
Tessa Wassenberg, Jaap Deinum, Frans J van Ittersum, Erik-Jan Kamsteeg, Maartje Pennings, Marcel M Verbeek, Ron A Wevers, Mirjam E van Albada, Ido P Kema, Jorie Versmissen, Ton van den Meiracker, Jacques W M Lenders, Leo Monnens, Michèl A Willemsen
J Inherit Metab Dis 2021; 44 (3): 554-565. doi: 10.1002/jimd.12321. Epub 2020 Oct 15.
Voorbereid document _Tessa Wassenberg_V03.indd 179Voorbereid document _Tessa Wassenberg_V03.indd 179 25/10/2021 09:3225/10/2021 09:32

180
Chapter 9
Abstract
Dopamine beta hydroxylase (DBH) deficiency is an extremely rare autosomal recessive disorder with severe orthostatic hypotension, that can be treated with L-threo-3,4-dihydroxyphenylserine (L-DOPS). We aimed to summarize clinical, biochemical, and genetic data of all world-wide reported patients with DBH-deficiency, and to present detailed new data on long-term follow-up of a relatively large Dutch cohort. We retrospectively describe 10 patients from a Dutch cohort and 15 additional patients from the literature. We identified 25 patients (15 females) from 20 families. Ten patients were diagnosed in the Netherlands. Duration of follow-up of Dutch patients ranged from 1 to 21 years (median 13 years). All patients had severe orthostatic hypotension. Severely decreased or absent (nor)epinephrine, and increased dopamine plasma concentrations were found in 24/25 patients. Impaired kidney function and anemia were present in all Dutch patients, hypomagnesaemia in 5 out of 10. Clinically, all patients responded very well to L-DOPS, with marked reduction of orthostatic complaints. However, orthostatic hypotension remained present, and kidney function, anemia, and hypomagnesaemia only partially improved. Plasma norepinephrine increased and became detectable, while epinephrine remained undetectable in most patients. We confirm the core clinical characteristics of DBH-deficiency and the pathognomonic profile of catecholamines in body fluids. Impaired renal function, anemia, and hypomagnesaemia can be part of the clinical presentation. The subjective response to L-DOPS treatment is excellent and sustained, although the neurotransmitter profile in plasma does not normalize completely. Furthermore, orthostatic hypotension as well as renal function, anemia, and hypomagnesaemia improve only partially.
Voorbereid document _Tessa Wassenberg_V03.indd 180Voorbereid document _Tessa Wassenberg_V03.indd 180 25/10/2021 09:3225/10/2021 09:32

181
Clinical presentation and long-term follow-up of DBH deficiency
Introduction
Dopamine beta hydroxylase (DBH) deficiency (MIM#223360) is an autosomal recessive neurometabolic disorder due to pathogenic variants in the DBH gene. A gene transcript is present in (nor)adrenergic neurosecretory vesicles in the central and peripheral nervous system, the retina, and chromaffin cells of the adrenal medulla, where the enzyme DBH (EC 1.14.17.1) converts dopamine to norepinephrine1,2. DBH-deficiency leads to undetectable levels of norepinephrine and epinephrine and increased levels of dopamine in the central and autonomous nervous system and peripheral organs3-5
(Figure 1). Key symptom in DBH-deficiency is profound orthostatic hypotension3, while patients—surprisingly—have no clear central nervous system manifestations, like neurocognitive abnormalities6 or major sleep disturbances7.
DBH-deficiency is an extremely rare disorder. From its first description in the mid-1980s, both in the United States of America4 and the Netherlands5, only about 20 additional patients have been described. Despite its rarity, however, DBH-deficiency offers a unique opportunity to study the role of catecholamines in the human autonomic and central nervous system. DBH-deficiency leads to a selective and functional noradrenergic failure of a structurally normal sympathetic nervous system8,9. This is nicely illustrated by normal sweating patterns in patients with DBH-deficiency4,10, a function of the sympathetic nervous system mediated by acetylcholine instead of norepinephrine11. Of utmost importance, DBH-deficiency is a treatable disorder, in which the metabolic block can be bypassed by oral supplementation with L-threo-3,4-dihydroxyphenylserine (L-DOPS/Droxidopa)12 (Figure 1). This makes DBH-deficiency a diagnosis not to be missed.
Literature on DBH-deficiency consists mainly of case reports, and many patients are presented in multiple publications. In order to summarize the available body of evidence, we performed a literature review on DBH-deficiency with attention to clinical presentation, biochemical, and genetic diagnosis and treatment, and combined this with a retrospective chart review of a relatively large Dutch cohort of patients with DBH-deficiency. The latter includes also data on long-term follow-up during treatment. In this overview, clinical presentation and treatment recommendations are summarized, and several new observations regarding female fertility, anemia, kidney function, and serum electrolytes are described.
9
Voorbereid document _Tessa Wassenberg_V03.indd 181Voorbereid document _Tessa Wassenberg_V03.indd 181 25/10/2021 09:3225/10/2021 09:32

182
Chapter 9
Figure 1. Simplified scheme of catecholamine synthesis and breakdown in DBH-deficiency
Figure 1. depicts the simplified scheme of the biosynthesis and catabolism of catecholamines (dopamine, norepinephrine, and epinephrine), and shows the metabolic block in DBH-deficiency (black bar). The artificial compound L-DOPS can bypass this block because it can be converted to norepinephrine using the enzyme AADC. Breakdown of catecholamines can involve multiple steps (dashed arrow) and differs in different body compartments. HVA is the major stable end-product of dopamine catabolism in cerebrospinal fluid, blood and urine. MHPG is the major end-product of (nor)epinephrine catabolism in cerebrospinal fluid. NMET and MET are breakdown products of norepinephrine and epinephrine in the peripheral circulation and urine, VMA is the major common end-product of (nor)epinephrine catabolism.Abbreviations: AADC, aromatic l-amino acid decarboxylase; ADH, alcohol dehydrogenase; DBH, dopamine beta hydroxylase; DHPG, dihydroxyphenylglycol; COMT: catechol-O-methyltransferase; HVA, homovanillic acid; L-DOPA, L-3,4 dihydroxyphenylalanine; L-DOPS: l-threo-3,4-dihydroxyphenylserine; MAO, monoamine oxidase; MET, metanephrine; MHPG, 3-methoxy-4-hydroxyphenylglycol; NMET, normetanephrine; PNMT, phenylethanolamine N-methyltransferase; VMA, vanillylmandelic acid
Methods
We performed a literature search on DBH-deficiency using Pubmed indexed for Medline, Cochrane library, clinicaltrials.gov, and WHO clinical trial registry through August 2019 with search terms “dopamine beta hydroxylase deficiency,” “DBH deficiency” and
Voorbereid document _Tessa Wassenberg_V03.indd 182Voorbereid document _Tessa Wassenberg_V03.indd 182 25/10/2021 09:3225/10/2021 09:32

183
Clinical presentation and long-term follow-up of DBH deficiency
[dopamine beta hydroxylase deficiency] (MESH). Neither language nor date filters were used in the initial search. Reference lists of key papers were manually screened for additional publications.
Patients from the Dutch cohort were diagnosed and are followed by four university clinics in the Netherlands.
Patients were included in this study if they had a confirmed genetic diagnosis of DBH-deficiency and a plasma catecholamine profile with low/undetectable in levels of norepinephrine and epinephrine and increased levels of dopamine. If only one of the two diagnostic biomarkers was available, patients were included only if clinical description was of a clear purely noradrenergic failure.
We evaluated the published case reports and medical charts of the Dutch patients for clinical symptoms, initial diagnosis, age of onset, age of diagnosis, diagnostic tests, blood pressure values, treatment and treatment response, and long-term follow-up. Orthostatic hypotension was defined as a sustained reduction of systolic blood pressure of at least 20 mm Hg or diastolic blood pressure of at least 10 mm Hg within 3 minutes of standing13.
We classified levels of catecholamines (norepinephrine, epinephrine, and dopamine) and their breakdown products in plasma, urine, and cerebrospinal fluid arbitrarily as low if decreased but >10% of local lower reference value, very low if <10% of local lower reference value, extremely low if <5% of local lower reference value or below detection limit, high if increased but <2 times local upper reference value, very high if >2 times local upper reference value, and extremely high if >5 times local upper reference value.
We recorded all reported routine biochemical measurements including hematological parameters, serum creatinine, and electrolytes. Kidney function was estimated by calculating the estimated glomerular filtration rate (eGFR), using the updated bedside Schwartz formulae (CKiD) for children14, and the CKD-EPI formula for adults15.Estimated GFR (mL/min/1.73 m2) was classified as normal if ≥90, mildly decreased if 60 to 89, moderately decreased if 30 to 59, severely decreased if 15 to 29, and kidney failure if <15 mL/min/1.73 m2 (or dialysis) according to the National Kidney Foundation practice guidelines16.We used Dutch national reference values for blood hemoglobin and magnesium: hemoglobin: 7.5 to 10 mmol/L for females and 8.5 to 11 mmol/L for males, magnesium 0.7 to 1.0 mmol/L. We calculated fractional excretion of magnesium by the following general formula: (magnesium (urine, mmol/L) × creatinine (plasma, μmol/L))/(0.7 × magnesium (plasma, mmol/L) × creatinine (urine, μmol/L)) × 100, with normal values 2% to 4%17.
9
Voorbereid document _Tessa Wassenberg_V03.indd 183Voorbereid document _Tessa Wassenberg_V03.indd 183 25/10/2021 09:3225/10/2021 09:32

184
Chapter 9
Statistical analysis was performed using IBM SPSS statistics 22. Data were explored by descriptive statistics and scatter plots. To compare means, independent samples t-test was used.
This study was retrospective, in accordance with the Declaration of Helsinki, and approved by the research ethics committee of the Radboud University Medical Center (2019-5281). All Dutch patients gave informed consent for retrospective analysis of their medical files, and for anonymized publication of data.
Results
The literature search ultimately revealed 39 publications containing information that could be deduced to individual patients (Figure S1, supplemental material). One patient was excluded because no genetic analysis was reported and he had an atypical clinical presentation (fixed heart rate on tilt table test suggesting concomitant parasympathetic failure)18. In total, we identified 22 unique patients from 18 families reported in the literature. Furthermore, we identified three Dutch patients of whom data had never been published before, including a twin brother of a previously reported patient. Characteristics of all 25 patients (15 females) with DBH-deficiency from 20 families are shown in Table S1 and summarized below. Data represent a combination of literature review and chart review unless specified otherwise.
Clinical presentation
Clinical symptoms and signsAll patients with DBH-deficiency had severe orthostatic hypotension. Orthostatic complaints (mostly described as reduced standing time, lightheadedness, fainting spells, and exercise intolerance) started in early childhood (1-4 years of age) in the majority of patients (n = 18), at school age (4-12 years) in four patients, and in two patients during early adulthood of which one patient had onset of complaints after start of olanzapine. One patient who was diagnosed at age 40 years because of a positive family history did not report complaints, but had severe orthostatic hypotension on measurement and improved in overall functioning with L-DOPS treatment. Orthostatic symptoms became more severe during adolescence in 11 patients.
Blood pressure within 3 minutes of standing fell to a mean of 72 mmHg systolic (range 44-115, SD 15) and 49 mm Hg diastolic (range 20-75, SD 13, with undetectably low diastolic blood pressure in three patients). Overall, the untreated drop in systolic and diastolic blood pressure within 3 minutes of standing was profound: mean systolic difference 58 mm Hg (range 32-115 mm Hg, SD 21), mean diastolic difference 38 mm Hg (range 18-74, SD 18). Supine blood pressure (office measurements) was <135/90 mm Hg in all patients (mean 109/68 mm Hg SD 13/11).
Voorbereid document _Tessa Wassenberg_V03.indd 184Voorbereid document _Tessa Wassenberg_V03.indd 184 25/10/2021 09:3225/10/2021 09:32

185
Clinical presentation and long-term follow-up of DBH deficiency
Eyelid ptosis was present in 18 patients and was absent in two patients who did have a mild miosis. In five patients, ptosis was not described. Ptosis could be unilateral or asymmetric. Other autonomic symptoms and signs were not reported systematically but included intermittent diarrhea and chronic nasal congestion. Nycturia was reported in three patients.
Information on the neonatal period was available for 14 patients and was reported as normal in five. Five patients (including one pair of twins) were born preterm and had low birth weight. Childhood hypoglycemia was reported in four patients.
Dysmorphic features were described non-systematically and included brachydactyly and/or short hands or feet (n = 7), high palate (n = 6), mild hypertelorisme (n = 1), and micrognathia (n = 1). Additional dysmorphic features including coloboma in patient 14 were thought to be due to a concomitant mosaic 11p13 deletion.
Reproductive function in males was described in 5/10 patients and was abnormal in three (difficulty maintaining erections and/or retrograde ejaculation). Menarche and menstrual cycle were described in 7/15 female patients and were normal in all. Primary infertility before diagnosis was described in two female patients, it persisted during L-DOPS treatment in one. The other patient had an early abortion during treatment with L-DOPS. One other patient became pregnant with assisted fertility treatment before diagnosis. Spontaneous pregnancy before diagnosis was described in two patients, they delivered without complications, but lactation did not start.
Cognitive development was described in 18 patients, and found to be normal in 16. One patient had mildly delayed motor and speech milestones with normal mental capacities subsequently. One patient with a complicated neonatal period after premature birth and a severe infection at age 6 months had mild intellectual disability. In five patients extensive neurocognitive testing was performed, with a mean total IQ of 106 (range 98-119)6.
Three patients were initially diagnosed as having epilepsy with generalized seizures and were treated with anti-epileptic drugs. Their interictal EEGs were normal and seizures only occurred on assuming the upright position. One additional patient with epilepsy was reported, with focal onset seizures with rainbow visual aura, without information on triggers for the attacks. Two patients first came under medical attention because of anemia, three patients because of decreased kidney function. Median age of diagnosis of DBH-deficiency was 24 years (range 13-73, SD 13.5).
9
Voorbereid document _Tessa Wassenberg_V03.indd 185Voorbereid document _Tessa Wassenberg_V03.indd 185 25/10/2021 09:3225/10/2021 09:32

186
Chapter 9
Diagnostic tests
Catecholamine measurements in plasma, urine, and CSFIn plasma, norepinephrine and dopamine measurements were reported in 24/25 patients, epinephrine in 22/25 patients (Table S1). Norepinephrine was decreased in all patients: extremely low in 20 and very low in four. Epinephrine was decreased in 21 patients: extremely low in 18, very low in two, and low in one patient. In one patient (pt 23), plasma epinephrine surprisingly was within the normal range. Dopamine was increased in all patients: extremely high in 12 patients, very high in seven, high in one patient. Norepinephrine and epinephrine remained extremely low when changing to standing position (reported in eight patients). Dopamine further increased on standing position in seven patients, and remained extremely high without further increase in one.
Urine measurements of norepinephrine, epinephrine, and dopamine were reported in six, five, and four patients, respectively, with a profile similar to plasma: very low to extremely low levels of norepinephrine and epinephrine, and very high levels of dopamine. The one patient (pt 23) with normal plasma epinephrine also had normal urinary epinephrine levels. Metanephrine (a metabolite of epinephrine, see Figure 1) in plasma was also normal in this patient and urinary dopamine was only slightly elevated. Catecholamines in cerebrospinal fluid were reported in three patients, and showed undetectable levels of norepinephrine and epinephrine, and increased dopamine (3-20-fold increase) in all.
DBH enzyme activityDBH enzyme activity in plasma was reported in 18 patients and absent or severely decreased in all (Table S1). In three patients, DBH enzyme activity was tested in CSF and also absent there.
Molecular diagnosisMolecular diagnosis was reported in 19 patients from 16 families; 10 different pathogenic variants were identified. In 12 patients, compound heterozygous pathogenic variants were found. The most frequently reported pathogenic variant (19 patients total, seven homozygous) is the intronic mutation c.339+2T>C (also reported as IVS1+2T>C) leading to aberrant splicing19.Table 1 shows all reported pathogenic variants. Distribution of pathogenic variants is schematically represented in Figure 2. Due to small sample size and relatively large number of variants, no phenotype/genotype correlations can be made.
Voorbereid document _Tessa Wassenberg_V03.indd 186Voorbereid document _Tessa Wassenberg_V03.indd 186 25/10/2021 09:3225/10/2021 09:32

187
Clinical presentation and long-term follow-up of DBH deficiency
Table 1. Pathogenic DBH variants reported in patients with DBH-deficiency
NR Location DNA(NM_000787.4)
Protein(NP_000778.3)
Reference
1 Intron 1 c.339+2T>C1 None (affects splicing) Kim et al 2002
2 Exon 1 c.301G>A p.(Val101Met)2 Kim et al 2002
3 Exon 2 c.342C>A p.(Asp114Glu) Kim et al 2002
4 Exon 3 c.617del p.(Glu206Glyfs*82) Deinum et al 2004
5 Exon 4 c.806G>T p.(Cys269Phe) Deinum et al 2004
6 Exon 6 c.1033G>A p.(Asp345Asn)2 Kim et al 2002
7 Exon 6 c.1085C>A p.(Ala362Glu) Kim et al 2011
8 Intron 8 c.1374+2_1374+20del None (affects splicing) Deinum et al 2004
9 Exon 9 c.1409_1410delinsTG p.(Thr470Met) Bartoletti-Stella et al 2015
10 Exon 11 c. 1667A>G p.(Tyr556Cys) Deinum et al 2004
Table 1. Pathogenic DBH variants reported in patients with DBH-deficiency. Numbers in column 1 correspond with numbers in column 12 (Molecular diagnosis) of Supplemental Table 1. RefSeq IDs are NM_000787.4 for DNA and NP_000778.3 for protein. Notes: 1 Also reported as IVS1+2T>C. 2Has only been described in trans with c.1033G>A, one of the two may not be pathogenic.
Figure 2. Schematic representation of pathogenic variants in the dopamine beta hydroxylase gene and pathogenic variants in DBH deficiency.
Figure 2. Introns are shown in gray, exons in black and numbered 1 to 12, and UTR’s in dark-gray. Intron lengths are not to scale, while exon sizes are. The coding DNA positions of the first bases of each exon are shown above the schematic. In DBH-deficiency, 2 intronic pathogenic variants and 8 exonic pathogenic variants have been described so far, and are depicted under the schematic. The HGVS nomenclature is done using reference sequence NM_000787.4. The respective protein variants are given in Table 1
Biochemical parameters: kidney function, hemoglobin, and electrolytesKidney function, hemoglobin, and electrolytes have sparsely been reported in the literature and therefore data is mainly derived from chart review of the Dutch patients. Kidney function (eGFR) before treatment was available in all Dutch patients (Table 2) and in two additional patients from the literature. Decreased kidney function before treatment was present in all patients: mildly decreased in seven (of which three patients
9
Voorbereid document _Tessa Wassenberg_V03.indd 187Voorbereid document _Tessa Wassenberg_V03.indd 187 25/10/2021 09:3225/10/2021 09:32

188
Chapter 9
had a range including normal values >90 mL/min/1.73 m2), moderately decreased in four, and moderately to severely decreased in one patient.
Hemoglobin before treatment was recorded in all Dutch patients (Table 2) and in four additional patients from the literature review. Mean hemoglobin level was below lower limit of normal for age and sex in 12/14 patients, while mean corpuscular volume was normal in 10/10 patients. Mild thrombocytopenia (100-149 × 109/L) was reported in four patients before treatment, leukocytes were normal in all patients except for one who had mild leucopenia.
Serum magnesium was not reported in the literature but available from chart review of all Dutch patients (Table 2). Two siblings evidently had hypomagnesaemia, while serum magnesium in the third sibling was normal. In three additional patients, serum magnesium was mildly decreased before treatment. Compared to mean serum magnesium level in a large general adult follow-up cohort (0.86 mmol/L, range 0.34-1.17, SD 0.0622), mean magnesium levels in patients with DBH-deficiency were much lower: untreated mean 0.60 mmol/L, range 0.33-0.87, SD 0.18. Available serum sodium and potassium levels were normal in all patients. Fractional magnesium excretion could be calculated for five patients before treatment and was increased in all (range 5.0-15.1%; Table 2).
Other additional testingCerebral MRI was performed in five patients as part of a research protocol,6 and described in two additional patients21,23, and was structurally normal. EMG and nerve conduction studies were reported as normal in four patients and abnormal in one patient with a concomitant genetically confirmed hereditary neuropathy. Extensive physiologic autonomic function tests were performed in several patients and are excellently summarized in a review3.
Voorbereid document _Tessa Wassenberg_V03.indd 188Voorbereid document _Tessa Wassenberg_V03.indd 188 25/10/2021 09:3225/10/2021 09:32

189
Clinical presentation and long-term follow-up of DBH deficiency
Tabl
e 2.
Cha
ract
eris
tics o
f the
Dut
ch co
hort
with
DBH
-defi
cien
cy a
nd fo
llow
-up
of c
atec
hola
min
es, k
idne
y fu
nctio
n, h
emog
lobi
n, a
nd m
agne
sium
bef
ore
and
durin
g tr
eatm
ent
Patient number
Sex (M/F)
FU before diagnosis (y)
Age at diagnosis (y)
FU after diagnosis (y)
Cate
chol
-am
ines
(p
lasm
a)Ki
dney
func
tion
Anem
iaM
agne
sium
Befo
re
trea
tmen
t N
E/E/
DA
Dur
ing
trea
tmen
t N
E/E/
DA
Befo
re
trea
tmen
tD
urin
g tr
eatm
ent
Befo
re
trea
tmen
tD
urin
g tr
eatm
ent
Seru
m
Mg2
+ be
fore
tr
eatm
ent
Frac
tiona
l M
g2+
excr
etion
be
fore
tr
eatm
ent
(%)
Seru
m
Mg2
+ du
ring
trea
tmen
t
Frac
tiona
l M
g2+
excr
etion
du
ring
trea
tmen
t (%
)
3F
126
21↓
↓↓
↓↓
↓↑
↑↑
↓↓ -
↑↑
↓N
-↓↓
++
N
4F
1520
17↓
↓↓
↓↓
↓↑
↑↑
↓↓
↓↓
↓ -N
-↓↓
N-↓
↓+
+N
-↓
8F
334
18↓
↓↓
↓↓
↓↑
↓↓
↓↓
↑↑
N-↓
N-↓
++
N↑
NN
9 Sib
10,1
1M
145
11↓
↓^
↓^
↑↑
- - -↓
↓-↓
↓↓
↓↓
-↓↓
↓+
+↓
↓↓
↑↑
*
10 Sib
9,11
F4
3611
↓↓
^↓
↓↓
↑↑
- - -↓
↓-↓
↓+
+N
NN
9
Voorbereid document _Tessa Wassenberg_V03.indd 189Voorbereid document _Tessa Wassenberg_V03.indd 189 25/10/2021 09:3225/10/2021 09:32

190
Chapter 9
Tabl
e 2.
[Con
tinue
d]Patient number
Sex (M/F)
FU before diagnosis (y)
Age at diagnosis (y)
FU after diagnosis (y)
Cate
chol
-am
ines
(p
lasm
a)Ki
dney
func
tion
Anem
iaM
agne
sium
Befo
re
trea
tmen
t N
E/E/
DA
Dur
ing
trea
tmen
t N
E/E/
DA
Befo
re
trea
tmen
tD
urin
g tr
eatm
ent
Befo
re
trea
tmen
tD
urin
g tr
eatm
ent
Seru
m
Mg2
+ be
fore
tr
eatm
ent
Frac
tiona
l M
g2+
excr
etion
be
fore
tr
eatm
ent
(%)
Seru
m
Mg2
+ du
ring
trea
tmen
t
Frac
tiona
l M
g2+
excr
etion
du
ring
trea
tmen
t (%
)11 Si
b 9,
10F
940
15↓
↓↓
↓↓
↓↑
↓↓
↓↓ -
↓↓
↓-↓
↓+
+↓
↓↑
↑↓
-↓↓
↑-↑
↑
19 Sib 25
F23
2315
↓↓
↓↓
↓↓
↑↑
↑
↓↓
↓↓
↑↑
↓↓
↓-↓
↓+
+N
-↓↑
N-↓
↑
23F
238
6↓
↓↓
N↑
↑↑
↓↓ N ↑↑
↓-↓
↓↓
-↓↓
++++
↓N
-↓
24M
013
1
urin
e↓
↓↓
↓↓
↓↑
↑↑
-↓
↓-
-N
↑N
↑
Voorbereid document _Tessa Wassenberg_V03.indd 190Voorbereid document _Tessa Wassenberg_V03.indd 190 25/10/2021 09:3225/10/2021 09:32

191
Clinical presentation and long-term follow-up of DBH deficiency
Tabl
e 2.
[Con
tinue
d]
Patient number
Sex (M/F)
FU before diagnosis (y)
Age at diagnosis (y)
FU after diagnosis (y)
Cate
chol
-am
ines
(p
lasm
a)Ki
dney
func
tion
Anem
iaM
agne
sium
Befo
re
trea
tmen
t N
E/E/
DA
Dur
ing
trea
tmen
t N
E/E/
DA
Befo
re
trea
tmen
tD
urin
g tr
eatm
ent
Befo
re
trea
tmen
tD
urin
g tr
eatm
ent
Seru
m
Mg2
+ be
fore
tr
eatm
ent
Frac
tiona
l M
g2+
excr
etion
be
fore
tr
eatm
ent
(%)
Seru
m
Mg2
+ du
ring
trea
tmen
t
Frac
tiona
l M
g2+
excr
etion
du
ring
trea
tmen
t (%
)25 Si
b 19M
035
1↓
↓↓
↓↓
↓↑
↑↑
-↓
↓↓
↑↑
N-↓
N-↓
++
N↑
N↑
Cate
chol
amin
es: N
E: n
orep
inep
hrin
e, E
: epi
neph
rine,
DA:
dop
amin
e. ↓
: low
(bel
ow re
fere
nce
valu
e), ↓
↓: v
ery
low
(< 1
0% o
f loc
al lo
wer
ref
eren
ce
valu
e), ↓
↓↓
: ext
rem
ely
low
(< 5
% o
f loc
al lo
wer
refe
renc
e va
lue
or b
elow
det
ectio
n lim
it), ↑
↑: v
ery
high
(> tw
o tim
es lo
cal u
pper
refe
renc
e va
lue)
, ↑
↑↑
: ext
rem
ely
high
(> fi
ve ti
mes
loca
l upp
er re
fere
nce
limit)
, N: n
orm
al, ^
prob
able
ove
resti
mati
on d
ue to
tech
nica
l rea
sons
(Jep
ma
et a
l, 20
11).
• Ki
dney
func
tion:
N: n
orm
al (e
GFR
>90
ml/m
in/1
.73m
2 ), ↓
: mild
ly d
ecre
ased
(eG
FR 6
0-90
ml/m
in/1
.73m
2 ), ↓
↓: m
oder
atel
y de
crea
sed
(eG
FR 3
0-59
m
l/min
/1.7
3m2 ),
↓↓
↓: s
ever
ely
decr
ease
d (e
GFR
15-
29 m
l/min
/1.7
3m2 ).
• An
emia
: - a
bsen
t, +
pres
ent (
mild
), ++
pre
sent
(mod
erat
e) .
• M
agne
sium
: ↓: m
ildly
dec
reas
ed, ↓
↓: m
oder
atel
y de
crea
sed
↑: i
ncre
ased
, N=n
orm
al. F
racti
onal
mag
nesi
um e
xcre
tion:
nor
mal
val
ue 2
-4%
. n=
norm
al, ↑
= 4-
10%
↑↑
>10%
. * fr
actio
nal m
agne
sium
exc
retio
n ca
lcul
ation
unr
elia
ble
due
to e
GFR
<40
ml/m
in/1
.73m
2 .
Abbr
evia
tions
: M: m
ale,
F: f
emal
e. F
U: fo
llow
-up.
y=y
ears 9
Voorbereid document _Tessa Wassenberg_V03.indd 191Voorbereid document _Tessa Wassenberg_V03.indd 191 25/10/2021 09:3225/10/2021 09:32

192
Chapter 9
Treatment and follow-up
L-DOPS: effect, dose, and tolerabilityAll patients were treated with L-DOPS, and remained on the same dose of L-DOPS over the years. Doses ranged from 400 to 1800 mg/day, given in 2 to 3 doses. For the Dutch cohort, treatment follow-up ranged from 1 to 21 years (median 13 years; Table 2). Treatment response was favorable and sustained in all patients and mostly subjectively described as “orthostatic symptoms disappeared” or “symptoms improved greatly.” Side effects were not reported apart from one patient with possible increase of nightmares on L-DOPS. In the Netherlands, L-DOPS was prescribed for compassionate use and imported from Sumitomo pharmaceuticals, Japan.
Other clinical features during treatmentMild ptosis persisted under L-DOPS treatment (reported in 7 patients). Response of diarrhea and nasal obstruction to L-DOPS treatment was not reported in the literature or medical charts. Quality of life was not objectively recorded by questionnaires, but a great and continuous improvement in overall functioning was reported by all patients, for example, becoming able to work-full time and to do sports. In one patient, fatigue remained present, especially during menstrual periods.
Blood pressure measurements under L-DOPS treatmentOffice orthostatic blood pressure measurements during treatment with L-DOPS were not systematically reported. In some patients, it was stated that orthostatic hypotension disappeared. When exact blood pressure measurements were available for analysis, all patients (n = 7) still fulfilled the criteria for orthostatic hypotension during treatment in the great majority of measurements, with a mean systolic (supine minus standing) difference of 38 mm Hg (range 8-60) and a mean diastolic difference of 21 mm Hg (range 4-40). Overall, this was a less pronounced drop than before treatment was installed. There was no significant increase in supine office blood pressure during L-DOPS treatment. However, in the Dutch patient who was diagnosed during adolescence L-DOPS 100 mg twice daily led to mild hypertension, necessitating to decrease the dose to 75 mg twice daily, with still adequate clinical response. Figure 3 shows representative 24-hours blood pressure measurements in one patient, before and during L-DOPS treatment. Before treatment, there is no nightly dip in blood pressure. During treatment, there is no increase in overall blood pressure, and there is a more physiological dip in blood pressure during the night although still less than expected.
Voorbereid document _Tessa Wassenberg_V03.indd 192Voorbereid document _Tessa Wassenberg_V03.indd 192 25/10/2021 09:3225/10/2021 09:32

193
Clinical presentation and long-term follow-up of DBH deficiency
Figure 3. 24-h bloodpressure measurements in one patient before and during L-DOPS treatment
Figure 3. 24h blood pressure measurements in one patient before (left panel) and during (right panel L-DOPS treatment. The night is shaded in grey. Sys: systolic blood pressure, MAP: mean arterial pressure, Dia: diastolic blood pressure, HF: heart frequency, bpm: beats per minute
Followup of catecholamines during treatmentNorepinephrine and epinephrine levels in plasma before and during treatment were reported in 13 patients. Follow-up for the Dutch cohort is shown in Table 2. With L-DOPS, plasma norepinephrine increased in all patients: it became detectable but still below the lower limit of normal in 11, and reached normal levels in two. Epinephrine in plasma remained undetectable in nine and became detectable but still below lower limit of normal in three patients. Patient 23 had normal levels of epinephrine before and during L-DOPS treatment. Plasma dopamine before and during treatment was reported in 12 patients and decreased with L-DOPS in all, but in 10 patients remained above upper limit of normal.
Kidney function, hematological parameters, and electrolytes during treatmentFor biochemical parameters under L-DOPS treatment, only data from chart review of the Dutch patients was available (Table 2). With L-DOPS treatment, there was an improvement of kidney function in only three patients.
In four patients, there was an increase of hemoglobin during treatment with L-DOPS, with no other associated treatments at the time (eg, erythropoetin, ferrofumarate). There was no change in leucocyte and thrombocyte counts during treatment.
Overall, serum magnesium showed a significant increase under treatment (treated mean 0.67 mmol/L, range 0.37-0.98, SD 0.15, P = .019). Fractional magnesium excretion could be calculated for seven patients during treatment and was normal in two patients who both had normal serum magnesium levels. In one patient (pt 9), calculation of fractional magnesium excretion was unreliable because of eGFR <40 (24 mL/min/1.73 m2; Table 2).
9
Voorbereid document _Tessa Wassenberg_V03.indd 193Voorbereid document _Tessa Wassenberg_V03.indd 193 25/10/2021 09:3225/10/2021 09:32

194
Chapter 9
MortalityOne fatal case is extensively described in the literature (pt 13). This man had a severe phenotype with frequent syncopes from early childhood, and died at age 28 years after maximum 4 years of L-DOPS treatment. Autopsy showed isolated microfoci of cortical gliosis, cardiac arteriolar smooth muscle hypertrophy, dispersed fibrosis in the cardiac conduction system, and sclerotic renal glomeruli. There was absent DBH immunoreactivity in the central nervous system (ventrolateral medulla) and the authors felt that his early death might have resulted from cardiac dysrhythmia. Furthermore, three deceased patients have been reported in a review (age 20; suspected suicide, and age 57 and 63 years; suspected natural cause, not specified)3. One Dutch patient died at age 60 years due to urogenital cancer.
Discussion
We describe the clinical characteristics of 25 patients with DBH-deficiency and detailed follow-up data of the 10 Dutch patients within this group. The study gives a comprehensive overview of clinical presentation, diagnosis, treatment, and long-term follow-up of this extremely rare neurogenic orthostatic hypotension syndrome, and has—for the first time—disclosed the high prevalence of decreased kidney function, hypomagnesaemia, and anemia in DBH-deficiency.
Core clinical characteristics of DBH-deficiency are confirmed3, namely a combination of profound orthostatic hypotension with onset mostly in early childhood, and eyelid ptosis. Patients often present with nonspecific symptoms and long diagnostic delays are common. Nonetheless, the clue to the diagnosis, that is, orthostatic hypotension, can easily be tested, and underscores the value of a complete physical examination in patients with poorly understood complaints.
In patients with a clinical suspicion of DBH-deficiency, measurement of plasma catecholamines is the first ancillary diagnostic test. The pathognomonic metabolite profile shows undetectable levels of norepinephrine and epinephrine, and increased dopamine. This profile was found in all but one patient, who had thus far unexplained normal levels of epinephrine in plasma (and urine), despite previously reported pathogenic DBH variants, absent DBH enzyme activity, and a classical clinical phenotype.
The differential diagnosis of orthostatic hypotension varies from volume depletion and drug effects to primary autonomic failure. The latter includes a wide variety of neurological disorders, varying from pure autonomic failure, neurodegenerative disease (eg, multiple system atrophy), toxic and paraneoplastic neuropathies, amyloidosis, inflammatory disease (eg, Guillain Barré syndrome) and genetical disorders such as Fabry disease and DBH-deficiency24. Other than in late adulthood, in childhood true orthostatic hypotension is rare and a genetic cause should be considered early in the
Voorbereid document _Tessa Wassenberg_V03.indd 194Voorbereid document _Tessa Wassenberg_V03.indd 194 25/10/2021 09:3225/10/2021 09:32

195
Clinical presentation and long-term follow-up of DBH deficiency
diagnostic work-up25,26. Recently, a novel young onset cause of orthostatic hypotension caused by mutations in CYB561 was identified27. Although clinically quite similar to DBH deficiency, this disorder is characterized by normal plasma dopamine in the presence of severely reduced levels of norepinephrine and epinephrine28.
To diagnose DBH-deficiency, a clinical presentation with severe young-onset orthostatic hypotension, undetectable levels of norepinephrine and epinephrine and increased levels of dopamine in plasma, and pathogenic variants in the DBH gene should be present. Although the diagnosis of DBH-deficiency can be supported by demonstration of absent to severely decreased DBH enzyme activity, it should be noted that plasma DBH enzyme activity is absent in 4 % of the healthy population due to a specific variant (−1021C>T) of the DBH gene, leading to pseudodeficiency with normal levels of plasma norepinephrine29. It is not necessary to test catecholamines in urine and cerebrospinal fluid for the diagnosis of DBH-deficiency.
In the Dutch cohort, it is clearly shown that impaired kidney function is part of the clinical presentation of DBH-deficiency. Our initial hypothesis was that this is caused by chronic, intermittent renal hypoperfusion due to severe orthostatic hypotension. However, the results of the kidney biopsy in one patient with DBH-deficiency, which showed only discrete fibrosis, make this a less likely explanation30 because renal hypoxia would cause clear histological abnormalities31,32. Renal failure in peripheral autonomic failure is attributed to supine hypertension33, but this is not found in patients with DBH-deficiency. A potential damaging factor to the kidneys, which is quite unique to patients with DBH-deficiency, is the very high level of dopamine intracellularly in the proximal tubular cells. In high concentrations, dopamine and intermediate dopamine metabolites are thought to be autotoxic34, possibly because of increased radical oxygen species production35. This might also explain why there is only partial improvement of kidney function after treatment is started, because dopamine levels remain evidently increased in most patients.
Anemia is also clearly part of the clinical presentation of DBH-deficiency in most Dutch patients. It is mostly mild, and can improve on treatment with L-DOPS. In general, chronic kidney disease is often associated with anemia due to relative erythropoietin deficiency, especially in moderate to severe kidney failure36. However, we also found anemia in patients with DBH-deficiency who only had mildly decreased kidney function and therefore this is not likely to be the only explanation. Sympathetic innervation of the bone marrow plays an important role in hematopoiesis. Adrenergic signals induce mobilization of hematopoetic stem cells, and continuous trafficking of stem cells between bone marrow and blood compartments likely contributes to the maintenance of normal hematopoiesis37. Also in several other autonomic disorders, anemia with or without reduced kidney function has been described38. The precise mechanism of
9
Voorbereid document _Tessa Wassenberg_V03.indd 195Voorbereid document _Tessa Wassenberg_V03.indd 195 25/10/2021 09:3225/10/2021 09:32

196
Chapter 9
anemia in DBH-deficiency and why it does not resolve completely with treatment in most patients is unknown.
Hypomagnesaemia was present in five Dutch patients with DBH-deficiency before and during treatment. Fractional magnesium excretion was increased in four Dutch patients. Magnesium handling depends on gastro-intestinal uptake and renal excretion, with fine regulation of magnesium transport in the distal tubule39. The precise pathophysiology, clinical significance and optimal treatment strategy of hypomagnesaemia in patients with DBH-deficiency needs further investigation.
While plasma norepinephrine showed the expected—although incomplete—increase on L-DOPS treatment, epinephrine remained below the detection limit in four Dutch patients during follow-up and showed a slight increase in only one patient. This is puzzling because physiologically, it is expected that patients with DBH-deficiency who are treated with L-DOPS can synthesize epinephrine in the adrenal medulla. Lamotte et al showed that in patients with neurogenic orthostatic hypotension treated with L-DOPS, norepinephrine excretion is much higher than expected and hypothesized that this is due to norepinephrine built up in the cytoplasm of proximal tubular cells exiting to the interstitium of the kidney40. Probably, norepinephrine excretion is also increased in patients with DBH-deficiency under L-DOPS treatment, preventing further metabolization to epinephrine.
Healthy pregnancy and delivery is possible in patients with DBH-deficiency before and during L-DOPS treatment, and with the limited data at hand continuing L-DOPS during pregnancy appears safe and desirable. However, in the Dutch cohort three female patients had problems conceiving which might indicate that the rate of female fertility problems is increased before and during treatment with L-DOPS. Oocytes express DBH, can take up dopamine, and convert it to norepinephrine41. Oocyte derived norepinephrine may be necessary to regulate follicular development and oocyte maturation41,42. Higher levels of dopamine might lead to more reactive oxygen species in human follicular cells43. Hypothetically both mechanisms (absence of norepinephrine and presence of high dopamine concentrations in oocytes) could lead to decreased fertility in DBH-deficiency. Another issue concerning reproduction is that successful lactation has not been described in patients with DBH-deficiency, probably due to the increased levels of dopamine that inhibit the secretion of prolactin44.
DBH-deficiency is a treatable disorder: L-DOPS leads to an almost immediate and sustained clinical response. In adults, Federal Drug Administration (FDA) approved dosing schedules can be followed, starting with 100 mg two to three times daily, increasing to a maximum of 1800 mg divided in three doses. Dose should be titrated individually based on clinical response, and last dose should be given more than 4 hours before bedtime to avoid nightly hypertension45. In our experience, more than 1200 mg
Voorbereid document _Tessa Wassenberg_V03.indd 196Voorbereid document _Tessa Wassenberg_V03.indd 196 25/10/2021 09:3225/10/2021 09:32

197
Clinical presentation and long-term follow-up of DBH deficiency
per day is rarely needed. Temporary increase of daily dose during periods with more complaints, for example, illness or hot weather, can be of use (personal observation JD). For children, a starting dose of 2 mg/kg/d divided in 2 to 3 doses seems reasonable, eventually increasing to 5 to 10 mg/kg/d in 2 to 3 doses, with careful monitoring of side effects and blood pressure. L-DOPS is excellently tolerated in patients with DBH-deficiency45. Although the FDA approved L-DOPS for neurogenic orthostatic hypotension in adults, in many countries including the Netherlands L-DOPS is not registered and should be prescribed off-label or for compassionate use.
Treatment of DBH-deficiency with L-DOPS greatly improves quality of life and exercise intolerance. However, catecholamine levels, kidney function, anemia, and hypomagnesaemia do not or only partially respond to treatment. Furthermore, ptosis often does not disappear, and blood pressure does not normalize; many patients still have (less pronounced) orthostatic hypotension on office measurements. The clinical relevance of these observations is unclear. Because of the extreme rarity of this disorder, clinical trials to determine optimum treatment strategy in DBH-deficiency seem hard to effectuate. We think it is important that routine biochemical parameters including kidney function, hematological parameters, and electrolytes are regularly followed, while structured outcome measures like the orthostatic hypotension questionnaire46, could be used to monitor treatment response. Whether 24-hours blood pressure measurements during L-DOPS treatment are useful to improve long-term outcome, for example, by aiming at a more physiological blood pressure course including the nocturnal dip, should be further investigated.
In conclusion, DBH-deficiency is an extremely rare but fascinating cause of neurogenic orthostatic hypotension. It should be suspected in patients with profound, young-onset orthostatic hypotension and ptosis. We have shown that decreased kidney function, hypomagnesaemia, and anemia are part of the clinical picture at presentation. DBH-deficiency is a treatable disorder: L-DOPS strongly improves the clinical symptoms and quality of life, even though orthostatic hypotension does not disappear. Laboratory parameters, including catecholamine profile in plasma, impaired kidney function, anemia, and hypomagnesaemia only partially respond to L-DOPS treatment. The questions whether long-term outcome can be improved by optimizing dosing strategies of L-DOPS, and which parameters should be used to guide this, remain to be answered.
9
Voorbereid document _Tessa Wassenberg_V03.indd 197Voorbereid document _Tessa Wassenberg_V03.indd 197 25/10/2021 09:3225/10/2021 09:32

198
Chapter 9
References
1. Nagatsu T. Genes for human catecholamine-synthesizing enzymes. Neurosci Res. 1991; 12(2): 315- 345.
2. Levin EY, Levenberg B, Kaufman S. The enzymatic conversion of 3,4-dihydroxyphenylethylamine to norepinephrine. J Biol Chem. 1960; 235: 2080- 2086.
3. Robertson D, Garland EM. Dopamine beta-hydroxylase deficiency. In: RA Pagon, MP Adam, TD Bird, CR Dolan, CT Fong, K Stephens, eds. GeneReviews. Seattle, WA: University of Washington; 1993.
4. Robertson D, Goldberg MR, Onrot J, et al. Isolated failure of autonomic noradrenergic neurotransmission. Evidence for impaired beta-hydroxylation of dopamine. N Engl J Med. 1986; 314(23): 1494- 1497.
5. Man in’t Veld AJ, Boomsma F, Moleman P, Schalekamp MA. Congenital dopamine-beta-hydroxylase deficiency. A novel orthostatic syndrome. Lancet. 1987; 1(8526): 183- 188.
6. Jepma M, Deinum J, Asplund CL, et al. Neurocognitive function in dopamine-beta-hydroxylase deficiency. Neuropsychopharmacology. 2011; 36(8): 1608- 1619. 7. Tulen JH, Man in’t Veld AJ, Mechelse K, Boomsma F. Sleep patterns in congenital dopamine beta-hydroxylase deficiency. J Neurol. 1990; 237(2): 98- 102.
8. Donadio V, Liguori R, Incensi A, et al. Skin biopsy and microneurography disclose selective noradrenergic dysfunction due to dopamine-beta-hydroxylase deficiency. Auton Neurosci. 2016; 197: 56- 59.
9. Rea RF, Biaggioni I, Robertson RM, Haile V, Robertson D. Reflex control of sympathetic nerve activity in dopamine beta-hydroxylase deficiency. Hypertension. 1990; 15(1): 107- 112. 10. Magnifico F, Misra VP, Murray NM, Mathias CJ. The sympathetic skin response in peripheral autonomic failure—evaluation in pure failure, pure cholinergic dysautonomia and dopamine-beta-hydroxylase deficiency. Clinical Autonomic Research. 1998; 8(3): 133- 138. 11. Wehrwein EA, Orer HS, Barman SM. Overview of the anatomy, physiology, and pharmacology of the autonomic nervous system. Compr Physiol. 2016; 6(3): 1239- 1278.
12. Biaggioni I, Robertson D. Endogenous restoration of noradrenaline by precursor therapy in dopamine-beta-hydroxylase deficiency. Lancet. 1987; 2(8569): 1170- 1172.
13. Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton Neurosci. 2011; 161(1–2): 46- 48.
14. Mian AN, Schwartz GJ. Measurement and estimation of glomerular filtration rate in children. Adv Chronic Kidney Dis. 2017; 24(6): 348- 356.
15. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009; 150(9): 604- 612.
16. Levey AS, Coresh J, Balk E, et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003; 139(2): 137- 147.
17. Elliott C, Newman N, Madan A. Gentamicin effects on urinary electrolyte excretion in healthy subjects. Clin Pharmacol Ther. 2000; 67(1): 16- 21.
Voorbereid document _Tessa Wassenberg_V03.indd 198Voorbereid document _Tessa Wassenberg_V03.indd 198 25/10/2021 09:3225/10/2021 09:32

199
Clinical presentation and long-term follow-up of DBH deficiency
18. Gentric A, Fouilhoux A, Caroff M, Mottier D, Jouquan J. Dopamine B hydroxylase deficiency responsible for severe dysautonomic orthostatic hypotension in an elderly patient. J Am Geriatr Soc. 1993; 41(5): 550- 551.
19. Kim CH, Zabetian CP, Cubells JF, et al. Mutations in the dopamine beta-hydroxylase gene are associated with human norepinephrine deficiency. Am J Med Genet. 2002; 108(2): 140- 147.
20. Deinum J, Steenbergen-Spanjers GC, Jansen M, et al. DBH gene variants that cause low plasma dopamine beta hydroxylase with or without a severe orthostatic syndrome. Journal of medical genetics. 2004; 41(4):e38.
21. Bartoletti-Stella A, Chiaro G, Calandra-Buonaura G, et al. A patient with PMP22-related hereditary neuropathy and DBH-gene-related dysautonomia. J Neurol. 2015; 262(10): 2373- 2381.
22. Kieboom BCT, Ligthart S, Dehghan A, et al. Serum magnesium and the risk of prediabetes: a population-based cohort study. Diabetologia. 2017; 60(5): 843- 853.
23. Cheshire WP Jr, Dickson DW, Nahm KF, Kaufmann HC, Benarroch EE. Dopamine beta-hydroxylase deficiency involves the central autonomic network. Acta Neuropathol. 2006; 112(2): 227- 229.
24. Brown TP. Pure autonomic failure. Pract Neurol. 2017; 17(5): 341- 348.25. Axelrod FB. Genetic autonomic disorders. Semin Pediatr Neurol. 2013; 20(1): 3- 11.26. Stewart JM, Boris JR, Chelimsky G, et al. Pediatric disorders of orthostatic intolerance.
Pediatrics. 2018; 141(1): e20171673.27. van den Berg MP, Almomani R, Biaggioni I, et al. Mutations in CYB561 causing a novel
orthostatic hypotension syndrome. Circ Res. 2018; 122(6): 846- 854.28. Shibao CA, Garland EM, Black BK, et al. Congenital absence of norepinephrine due to CYB561
mutations. Neurology. 2020; 94(2): e200- e204.29. Zabetian CP, Anderson GM, Buxbaum SG, et al. A quantitative-trait analysis of human
plasma-dopamine beta-hydroxylase activity: evidence for a major functional polymorphism at the DBH locus. Am J Hum Genet. 2001; 68(2): 515- 522.
30. Wassenberg T, Willemsen M, Dijkman H, Deinum J, Monnens L. Congenital eyelid ptosis, decreased glomerular filtration, and orthostatic hypotension: questions. Pediatr Nephrol. 2017; 32(7): 1169- 1170. https://doi.org/10.1007/s00467-016-3494-2.
31. Nangaku M. Hypoxia and tubulointerstitial injury: a final common pathway to end-stage renal failure. Nephron Exp Nephrol. 2004; 98(1): e8- e12.
32. Fine LG, Norman JT. Chronic hypoxia as a mechanism of progression of chronic kidney diseases: from hypothesis to novel therapeutics. Kidney Int. 2008; 74(7): 867- 872.
33. Garland EM, Gamboa A, Okamoto L, et al. Renal impairment of pure autonomic failure. Hypertension. 2009; 54(5): 1057- 1061.
34. Goldstein DS, Kopin IJ, Sharabi Y. Catecholamine autotoxicity. Implications for pharmacology and therapeutics of Parkinson disease and related disorders. Pharmacol Ther. 2014; 144(3): 268- 282.
35. Acquier AB, Mori Sequeiros Garcia M, Gorostizaga AB, Paz C, Mendez CF. Reactive oxygen species mediate dopamine-induced signaling in renal proximal tubule cells. FEBS Lett. 2013; 587(19): 3254- 3260.
36. Fishbane S, Spinowitz B. Update on anemia in ESRD and earlier stages of CKD: Core curriculum 2018. Am J Kidney Dis. 2018; 71(3): 423- 435.
9
Voorbereid document _Tessa Wassenberg_V03.indd 199Voorbereid document _Tessa Wassenberg_V03.indd 199 25/10/2021 09:3225/10/2021 09:32

200
Chapter 9
37. Garcia-Garcia A, Korn C, Garcia-Fernandez M, et al. Dual cholinergic signals regulate daily migration of hematopoietic stem cells and leukocytes. Blood. 2019; 133(3): 224- 236.
38. Biaggioni I, Robertson D, Krantz S, Jones M, Haile V. The anemia of primary autonomic failure and its reversal with recombinant erythropoietin. Ann Intern Med. 1994; 121(3): 181- 186.
39. de Baaij JH, Hoenderop JG, Bindels RJ. Regulation of magnesium balance: lessons learned from human genetic disease. Clin Kidney J. 2012; 5(Suppl 1): i15- i24.
40. Lamotte G, Holmes C, Sullivan P, Goldstein DS. Substantial renal conversion of L-threo-3,4-dihydroxyphenylserine (droxidopa) to norepinephrine in patients with neurogenic orthostatic hypotension. Clin Autonom Res. 2019; 29(1): 113- 117.
41. Mayerhofer A, Smith GD, Danilchik M, et al. Oocytes are a source of catecholamines in the primate ovary: evidence for a cell-cell regulatory loop. Proc Natl Acad Sci U S A. 1998; 95(18): 10990- 10995.
42. Greiner M, Paredes A, Rey-Ares V, Saller S, Mayerhofer A, Lara HE. Catecholamine uptake, storage, and regulated release by ovarian granulosa cells. Endocrinology. 2008; 149(10): 4988- 4996.
43. Saller S, Kunz L, Berg D, et al. Dopamine in human follicular fluid is associated with cellular uptake and metabolism-dependent generation of reactive oxygen species in granulosa cells: implications for physiology and pathology. Hum Reprod. 2014; 29(3): 555- 567.
44. Fitzgerald P, Dinan TG. Prolactin and dopamine: what is the connection? A review article. J Psychopharmacol. 2008; 22(2 Suppl): 12- 19.
45. Strassheim V, Newton JL, Tan MP, Frith J. Droxidopa for orthostatic hypotension: a systematic review and meta-analysis. J Hypertens. 2016; 34(10): 1933- 1941.
46. Kaufmann H, Malamut R, Norcliffe-Kaufmann L, Rosa K, Freeman R. The orthostatic hypotension questionnaire (OHQ): validation of a novel symptom assessment scale. Clin Autonom Res. 2012; 22(2): 79- 90.
Voorbereid document _Tessa Wassenberg_V03.indd 200Voorbereid document _Tessa Wassenberg_V03.indd 200 25/10/2021 09:3225/10/2021 09:32

201
Clinical presentation and long-term follow-up of DBH deficiency
Supplemental material
Table S1. Clinical characteristics of 25 patients with DBH-deficiencyCharacteristics of the 25 patients with DBH-deficiency identified with structured literature review and chart review, including three previously unpublished Dutch patients (patient 23-25). Patients are presented in chronological order from appearance in the literature. All references per patient are given, the reference list can be found in supplementary material. Numbers in the column with molecular diagnosis correspond to numbers of the pathogenic DBH variants in Table 2. Definitions: -: not measured or unknown. Early childhood 1-4 y, School age 4-12 y, Adolescence 12-18y. Legend: *miosis present. ^ reported to be probably overestimated due to technical reasons. ↓: low (below local reference value), ↓↓: very low (< 10% of local lower reference limit), ↓↓↓: extremely low (< 5% of local lower reference limit/ below detection limit), ↑: high (above local reference value), ↑↑: very high (> two times local upper reference limit), ↑↑↑: extremely high (> five times local upper reference limit).Abbrevations: bw: birth weight. Y: yes, N: no, NE: norepinephrine, E: epinephrine, DA: dopamine. DBH: dopamine beta hydroxylase. PAF: pure autonomic failure. HNPP: hereditary neuropathy with liability to pressure palsies, PAN: peripheral autonomic neuropathy. DM1: diabetes mellitus type 1. TIQ: total intelligence quotient. N: normal. ICSI: intracytoplasmic sperm injection.US: United States of America, NL: the Netherlands, UK: United Kingdom, AU: Australia, CA: Canada, FR: France.
9
Voorbereid document _Tessa Wassenberg_V03.indd 201Voorbereid document _Tessa Wassenberg_V03.indd 201 25/10/2021 09:3225/10/2021 09:32

202
Chapter 9
Pt n
umbe
r
Sex
(M/F
)
Neo
nata
l and
in
fanti
le p
rob-
lem
s
Ptos
is
Ons
et o
f or
thos
tatic
co
mpl
aint
s
Initi
al d
iagn
osis
Deve
lopm
ent/
in
telli
genc
e
Oth
er a
uto -
nom
ic fe
atur
es
Addi
tiona
l sig
ns
on p
hysic
al
exam
inati
on
Repr
oduc
tive
func
tion
Age
at d
iagn
osis
(y
ears
)
Cate
chol
amin
e pr
ofile
(pla
sma)
N
E/E/
DA
DBH
enzy
me
ac-
tivity
(pla
sma)
Mol
ecul
ar
diag
nosis
(see
ta
ble
2)
Com
orbi
dity
Coun
try
Year
of fi
rst
publ
icati
on
Firs
t ref
eren
ce
Addi
tiona
l re
fere
nces
1 F - Y Early child-hood
Epilepsy Normal Chronic nasal congestion, occasional diarrhea
- Regular cycle 33 ↓↓↓/ ↓↓↓/ ↑↑ absent (1); (2,6) US 1986 [1] [2-8]
2 M Bilateral ptosis Y Early child-hood
Epilepsy Normal Chronic nasal congestion, occasional diarrhea
Deep tendon reflexes reduced, hypermobile joints
Retrograde ejaculation, diffi-culty maintaining erection
42 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(3) US 1987 [3] [4-7, 9]
3 F At birth: hypoton-ic and cyanotic.4 episodes with vomiting, hypoglyce-mia, hypo-thermia during first year of life
Y Early child-hood
- Normal None record-ed
High palate, brachydac-ty-ly, sluggish deep tendon reflexes, hypermobile joints.
Menarche at 14y, regular cycle, no pregnancies
26 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(1) NL 1987 [10] [6,7,11-19]
4 F AD 37 weeks, dys-mature, failure to thrive
Y Early child-hood
Epilepsy Mildly delayed motor and lan-guage mile-stones, later normal intellectual abilities
None record-ed
Mild hypertelo-rism, high palate, brachydac-tyly, hypotonia, hypermobile joints, sluggish deep tendon reflexes
Menarche at 13y, normal cycle. No children (preg-nancy discour-aged by treating physicians at the time)
20 ↓↓↓/ ↓↓↓/ ↑↑ absent (1);(4) NL 1988 [13] [6,7, 14-19]
5Sib6
M No abnormalities N* School age Cardiac disorder
Normal Nocturnal polyuria
- Normal erections, ejaculation de-layed or absent
29 ↓↓↓/ ↓↓↓/ ↑↑↑ absent - UK 1990 [20] [6,7, 21-24]
6Sib 5
F No abnormalities N* Early child-hood
- Normal Nocturnal polyuria
- Menarche at 12y, regular cycle
23 ↓↓↓/ ↓↓↓/ ↑↑↑ absent - UK 1990 [20] [6,7, 21-24]
7 F Pre- and dys-mature (AD 36 weeks)
Y Early child-hood
- - - - Menarche at 12y, regular cycle. Pregnancy at age 22y (LDOPS+)
14 ↓↓^/ ↓↓↓/ ↑↑↑ absent - AU 1994 [25] [7,26,27]
8 F No abnormalities Y School age Anemia NormalTIQ 112
Intermittend diarrhea
Mild brachydac-tyly, hy-permobile joints, sluggish deep tendon reflexes
Menarche at 12y. Primary infertility, successful preg-nancy with ICSI before diagnosis. No lactation
34 ↓↓↓/ ↓↓↓/ ↑ absent (5);(5) NL 2003 [28] [7,18,19, 29]
9Sib 10,11
M No abnormalities Y No spon-taneous complaints
None Normal None record-ed
Sluggish deep tendon reflexes
No children (no active child wish)
45 ↓↓^/ ↓^/ ↑↑ absent (1);(10) Chronic kidney disease
NL 2004 [18] [7,19]
10Sib 9, 11
F No abnormalities Y Early adulthood after start olanzapine
None Normal None record-ed
Sluggish deep tendon reflexes
No pregnancies (no active child wish)
36 ↓↓^/ ↓↓↓/ ↑↑ absent (1);(10) Mood disorder NL 2004 [18] [7,19]
Voorbereid document _Tessa Wassenberg_V03.indd 202Voorbereid document _Tessa Wassenberg_V03.indd 202 25/10/2021 09:3225/10/2021 09:32

203
Clinical presentation and long-term follow-up of DBH deficiency
Pt n
umbe
r
Sex
(M/F
)
Neo
nata
l and
in
fanti
le p
rob-
lem
s
Ptos
is
Ons
et o
f or
thos
tatic
co
mpl
aint
s
Initi
al d
iagn
osis
Deve
lopm
ent/
in
telli
genc
e
Oth
er a
uto -
nom
ic fe
atur
es
Addi
tiona
l sig
ns
on p
hysic
al
exam
inati
on
Repr
oduc
tive
func
tion
Age
at d
iagn
osis
(y
ears
)
Cate
chol
amin
e pr
ofile
(pla
sma)
N
E/E/
DA
DBH
enzy
me
ac-
tivity
(pla
sma)
Mol
ecul
ar
diag
nosis
(see
ta
ble
2)
Com
orbi
dity
Coun
try
Year
of fi
rst
publ
icati
on
Firs
t ref
eren
ce
Addi
tiona
l re
fere
nces
1 F - Y Early child-hood
Epilepsy Normal Chronic nasal congestion, occasional diarrhea
- Regular cycle 33 ↓↓↓/ ↓↓↓/ ↑↑ absent (1); (2,6) US 1986 [1] [2-8]
2 M Bilateral ptosis Y Early child-hood
Epilepsy Normal Chronic nasal congestion, occasional diarrhea
Deep tendon reflexes reduced, hypermobile joints
Retrograde ejaculation, diffi-culty maintaining erection
42 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(3) US 1987 [3] [4-7, 9]
3 F At birth: hypoton-ic and cyanotic.4 episodes with vomiting, hypoglyce-mia, hypo-thermia during first year of life
Y Early child-hood
- Normal None record-ed
High palate, brachydac-ty-ly, sluggish deep tendon reflexes, hypermobile joints.
Menarche at 14y, regular cycle, no pregnancies
26 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(1) NL 1987 [10] [6,7,11-19]
4 F AD 37 weeks, dys-mature, failure to thrive
Y Early child-hood
Epilepsy Mildly delayed motor and lan-guage mile-stones, later normal intellectual abilities
None record-ed
Mild hypertelo-rism, high palate, brachydac-tyly, hypotonia, hypermobile joints, sluggish deep tendon reflexes
Menarche at 13y, normal cycle. No children (preg-nancy discour-aged by treating physicians at the time)
20 ↓↓↓/ ↓↓↓/ ↑↑ absent (1);(4) NL 1988 [13] [6,7, 14-19]
5Sib6
M No abnormalities N* School age Cardiac disorder
Normal Nocturnal polyuria
- Normal erections, ejaculation de-layed or absent
29 ↓↓↓/ ↓↓↓/ ↑↑↑ absent - UK 1990 [20] [6,7, 21-24]
6Sib 5
F No abnormalities N* Early child-hood
- Normal Nocturnal polyuria
- Menarche at 12y, regular cycle
23 ↓↓↓/ ↓↓↓/ ↑↑↑ absent - UK 1990 [20] [6,7, 21-24]
7 F Pre- and dys-mature (AD 36 weeks)
Y Early child-hood
- - - - Menarche at 12y, regular cycle. Pregnancy at age 22y (LDOPS+)
14 ↓↓^/ ↓↓↓/ ↑↑↑ absent - AU 1994 [25] [7,26,27]
8 F No abnormalities Y School age Anemia NormalTIQ 112
Intermittend diarrhea
Mild brachydac-tyly, hy-permobile joints, sluggish deep tendon reflexes
Menarche at 12y. Primary infertility, successful preg-nancy with ICSI before diagnosis. No lactation
34 ↓↓↓/ ↓↓↓/ ↑ absent (5);(5) NL 2003 [28] [7,18,19, 29]
9Sib 10,11
M No abnormalities Y No spon-taneous complaints
None Normal None record-ed
Sluggish deep tendon reflexes
No children (no active child wish)
45 ↓↓^/ ↓^/ ↑↑ absent (1);(10) Chronic kidney disease
NL 2004 [18] [7,19]
10Sib 9, 11
F No abnormalities Y Early adulthood after start olanzapine
None Normal None record-ed
Sluggish deep tendon reflexes
No pregnancies (no active child wish)
36 ↓↓^/ ↓↓↓/ ↑↑ absent (1);(10) Mood disorder NL 2004 [18] [7,19]
9
Voorbereid document _Tessa Wassenberg_V03.indd 203Voorbereid document _Tessa Wassenberg_V03.indd 203 25/10/2021 09:3225/10/2021 09:32

204
Chapter 9
Pt n
umbe
r
Sex
(M/F
)N
eona
tal a
nd
infa
ntile
pro
b-le
ms
Ptos
is
Ons
et o
f or
thos
tatic
co
mpl
aint
s
Initi
al d
iagn
osis
Deve
lopm
ent/
in
telli
genc
e
Oth
er a
uto-
nom
ic fe
atur
es
Addi
tiona
l sig
ns
on p
hysic
al
exam
inati
on
Repr
oduc
tive
func
tion
Age
at d
iagn
osis
(y
ears
)Ca
tech
olam
ine
profi
le (p
lasm
a)
NE/
E/DA
DBH
enzy
me
ac-
tivity
(pla
sma)
Mol
ecul
ar
diag
nosis
(see
ta
ble
2)
Com
orbi
dity
Coun
try
Year
of fi
rst
publ
icati
on
Firs
t ref
eren
ce
Addi
tiona
l re
fere
nces
11Sib 9, 10
F No abnormalities Y Adulthood Ortho-stat-ic hypo-ten-sion eci
Normal None record-ed
Sluggish deep tendon reflexes
Uncom-plicated pregnancy before diagnosis.No lactation
40 ↓↓↓/ ↓↓↓/ ↑ absent (1);(10) Hy-po-magne-sae-mia
NL 2004 [18] [7,19]
12 F - Y Early child-hood
- - - - - 22 ↓↓↓/ ↓↓↓/ ↑↑↑ - - - US 2005 [30]
13 M Spells of apnea and staring
Y Early child-hood
Ortho-sta-tic hypo-ten-sion, epilepsy
Normal - Micrognathia high palate, brachydac-tyly
No children, died at young age
24 ↓↓↓/ ↓↓↓/ ↑↑ - Not found
US 2006 [31]
14 F - - Early child-hood
DBHD and dys-mor-phic features
NormalTIQ 107
Enuresis nocturna
Iris coloboma, short hands, short high-arched feat
- 16 ↓↓/ ↓↓/ ↑↑ - (2,6); (2,6)
Mosaic deletion 11p13
CA 2010 [32] [29]
15 M No abnormalities - School age PAF Normal No urinary or gastro-intes-tinal complaints
- Sexual function normal, two children
73 ↓↓↓/ ↓↓↓/ ↑ absent - FR 2010 [33]
16 F - - Early child-hood
- - - - - 20 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(7) US 2011 [34]
17Sib 18
M - Y Early child-hood
- Normal TIQ 100
Chronic nasal congestion
- - 15 ↓↓↓/ NR/ ↑↑ - (1);(6) US 2011 [29] [35]
18Sib 17
M Aspeptic menin-gitis, operative correction ptosis
Y Early child-hood
- NormalTIQ 119
- - - 22 ↓↓↓/ NR/ ↑↑↑ - (1);(6) DM1 US 2011 [29] [35]
19Sib25
F Pre- and dysma-ture (AD 31w, bw 1210g), hypogly-cemia at birth, sustained feeding difficulties
Y Early child-hood
Mito-chon-drial disorder
Normal Chronic nasal congestion
High palate, small hands and feet, brachydactyly
Normal menstrual cycle.Problems conceiv-ing, first trimester abortion at age 37 years.
23 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(1) NL 2011 [29] [36]
20 F - Y Early child-hood
Ptosis - - - - 16 - absent (2,6); (2,6)
US 2013 [35]
21 M - - School age PAN - - - - 38 ↓↓↓/ ↓↓/ ↑ absent (8);(9) HNPP (PNP22 del), traumatic brain injury
IT 2015 [37] [38]
22 F - - Early child-hood
- - - - - <15 ↓↓↓/ ↓↓↓/ ↑↑↑ - (1);(1) US 2017 [39
23 F No abnormalities Y Early child-hood
Anemia, mild kidney failure
Normal None High palate, small hands and feet
Normal menstrual cycle. Primary infertility (also under LDOPS)
38 ↓↓↓/ N/ ↑↑↑ absent (1);(9) NL This publi-cation
Voorbereid document _Tessa Wassenberg_V03.indd 204Voorbereid document _Tessa Wassenberg_V03.indd 204 25/10/2021 09:3225/10/2021 09:32

205
Clinical presentation and long-term follow-up of DBH deficiency
Pt n
umbe
r
Sex
(M/F
)N
eona
tal a
nd
infa
ntile
pro
b-le
ms
Ptos
is
Ons
et o
f or
thos
tatic
co
mpl
aint
s
Initi
al d
iagn
osis
Deve
lopm
ent/
in
telli
genc
e
Oth
er a
uto-
nom
ic fe
atur
es
Addi
tiona
l sig
ns
on p
hysic
al
exam
inati
on
Repr
oduc
tive
func
tion
Age
at d
iagn
osis
(y
ears
)Ca
tech
olam
ine
profi
le (p
lasm
a)
NE/
E/DA
DBH
enzy
me
ac-
tivity
(pla
sma)
Mol
ecul
ar
diag
nosis
(see
ta
ble
2)
Com
orbi
dity
Coun
try
Year
of fi
rst
publ
icati
on
Firs
t ref
eren
ce
Addi
tiona
l re
fere
nces
11Sib 9, 10
F No abnormalities Y Adulthood Ortho-stat-ic hypo-ten-sion eci
Normal None record-ed
Sluggish deep tendon reflexes
Uncom-plicated pregnancy before diagnosis.No lactation
40 ↓↓↓/ ↓↓↓/ ↑ absent (1);(10) Hy-po-magne-sae-mia
NL 2004 [18] [7,19]
12 F - Y Early child-hood
- - - - - 22 ↓↓↓/ ↓↓↓/ ↑↑↑ - - - US 2005 [30]
13 M Spells of apnea and staring
Y Early child-hood
Ortho-sta-tic hypo-ten-sion, epilepsy
Normal - Micrognathia high palate, brachydac-tyly
No children, died at young age
24 ↓↓↓/ ↓↓↓/ ↑↑ - Not found
US 2006 [31]
14 F - - Early child-hood
DBHD and dys-mor-phic features
NormalTIQ 107
Enuresis nocturna
Iris coloboma, short hands, short high-arched feat
- 16 ↓↓/ ↓↓/ ↑↑ - (2,6); (2,6)
Mosaic deletion 11p13
CA 2010 [32] [29]
15 M No abnormalities - School age PAF Normal No urinary or gastro-intes-tinal complaints
- Sexual function normal, two children
73 ↓↓↓/ ↓↓↓/ ↑ absent - FR 2010 [33]
16 F - - Early child-hood
- - - - - 20 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(7) US 2011 [34]
17Sib 18
M - Y Early child-hood
- Normal TIQ 100
Chronic nasal congestion
- - 15 ↓↓↓/ NR/ ↑↑ - (1);(6) US 2011 [29] [35]
18Sib 17
M Aspeptic menin-gitis, operative correction ptosis
Y Early child-hood
- NormalTIQ 119
- - - 22 ↓↓↓/ NR/ ↑↑↑ - (1);(6) DM1 US 2011 [29] [35]
19Sib25
F Pre- and dysma-ture (AD 31w, bw 1210g), hypogly-cemia at birth, sustained feeding difficulties
Y Early child-hood
Mito-chon-drial disorder
Normal Chronic nasal congestion
High palate, small hands and feet, brachydactyly
Normal menstrual cycle.Problems conceiv-ing, first trimester abortion at age 37 years.
23 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(1) NL 2011 [29] [36]
20 F - Y Early child-hood
Ptosis - - - - 16 - absent (2,6); (2,6)
US 2013 [35]
21 M - - School age PAN - - - - 38 ↓↓↓/ ↓↓/ ↑ absent (8);(9) HNPP (PNP22 del), traumatic brain injury
IT 2015 [37] [38]
22 F - - Early child-hood
- - - - - <15 ↓↓↓/ ↓↓↓/ ↑↑↑ - (1);(1) US 2017 [39
23 F No abnormalities Y Early child-hood
Anemia, mild kidney failure
Normal None High palate, small hands and feet
Normal menstrual cycle. Primary infertility (also under LDOPS)
38 ↓↓↓/ N/ ↑↑↑ absent (1);(9) NL This publi-cation
9
Voorbereid document _Tessa Wassenberg_V03.indd 205Voorbereid document _Tessa Wassenberg_V03.indd 205 25/10/2021 09:3225/10/2021 09:32

206
Chapter 9
Pt n
umbe
r
Sex
(M/F
)N
eona
tal a
nd
infa
ntile
pro
b-le
ms
Ptos
is
Ons
et o
f or
thos
tatic
co
mpl
aint
s
Initi
al d
iagn
osis
Deve
lopm
ent/
in
telli
genc
e
Oth
er a
uto-
nom
ic fe
atur
es
Addi
tiona
l sig
ns
on p
hysic
al
exam
inati
on
Repr
oduc
tive
func
tion
Age
at d
iagn
osis
(y
ears
)Ca
tech
olam
ine
profi
le (p
lasm
a)
NE/
E/DA
DBH
enzy
me
ac-
tivity
(pla
sma)
Mol
ecul
ar
diag
nosis
(see
ta
ble
2)
Com
orbi
dity
Coun
try
Year
of fi
rst
publ
icati
on
Firs
t ref
eren
ce
Addi
tiona
l re
fere
nces
24 M Pre- and dysma-ture (AD34w,bw 1810g)
Y Early child-hood
Impaired nasal passage
Normal Chronic nasal stuffiness
None Retrograde ejac-ulation
13 ↓↓↓/ ↓↓↓/ ↑ Severely de-crea-sed
(1);(6) NL This publi-cation
25Sib 19twn
M Pre- and dysma-ture (AD31+5w), neonatal convul-sions.Severe sepsis at age 6 months
N Early child-hood
Cerebral palsy
Mild intellecutal disability
None High palate No children, no active child wish
35 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(1) Hearing loss and neurolo-gical sequelae after infantile sepsis
NL This publi-cation
Voorbereid document _Tessa Wassenberg_V03.indd 206Voorbereid document _Tessa Wassenberg_V03.indd 206 25/10/2021 09:3225/10/2021 09:32

207
Clinical presentation and long-term follow-up of DBH deficiency
Pt n
umbe
r
Sex
(M/F
)N
eona
tal a
nd
infa
ntile
pro
b-le
ms
Ptos
is
Ons
et o
f or
thos
tatic
co
mpl
aint
s
Initi
al d
iagn
osis
Deve
lopm
ent/
in
telli
genc
e
Oth
er a
uto-
nom
ic fe
atur
es
Addi
tiona
l sig
ns
on p
hysic
al
exam
inati
on
Repr
oduc
tive
func
tion
Age
at d
iagn
osis
(y
ears
)Ca
tech
olam
ine
profi
le (p
lasm
a)
NE/
E/DA
DBH
enzy
me
ac-
tivity
(pla
sma)
Mol
ecul
ar
diag
nosis
(see
ta
ble
2)
Com
orbi
dity
Coun
try
Year
of fi
rst
publ
icati
on
Firs
t ref
eren
ce
Addi
tiona
l re
fere
nces
24 M Pre- and dysma-ture (AD34w,bw 1810g)
Y Early child-hood
Impaired nasal passage
Normal Chronic nasal stuffiness
None Retrograde ejac-ulation
13 ↓↓↓/ ↓↓↓/ ↑ Severely de-crea-sed
(1);(6) NL This publi-cation
25Sib 19twn
M Pre- and dysma-ture (AD31+5w), neonatal convul-sions.Severe sepsis at age 6 months
N Early child-hood
Cerebral palsy
Mild intellecutal disability
None High palate No children, no active child wish
35 ↓↓↓/ ↓↓↓/ ↑↑↑ absent (1);(1) Hearing loss and neurolo-gical sequelae after infantile sepsis
NL This publi-cation
9
Voorbereid document _Tessa Wassenberg_V03.indd 207Voorbereid document _Tessa Wassenberg_V03.indd 207 25/10/2021 09:3225/10/2021 09:32

208
Chapter 9
Reference list to Table S1 Chapter 9
1. Robertson, D., et al., Isolated failure of autonomic noradrenergic neurotransmission. Evidence for impaired beta-hydroxylation of dopamine. N Engl J Med, 1986. 314(23): p. 1494-7.
2. Biaggioni, I., A.S. Hollister, and D. Robertson, Dopamine in dopamine-beta-hydroxylase deficiency. N Engl J Med, 1987. 317(22): p. 1415-6.
3. Biaggioni, I. and D. Robertson, Endogenous restoration of noradrenaline by precursor therapy in dopamine-beta-hydroxylase deficiency. Lancet, 1987. 2(8569): p. 1170-2.
4. O’Connor, D.T., et al., Dopamine beta-hydroxylase immunoreactivity in human cerebrospinal fluid: properties, relationship to central noradrenergic neuronal activity and variation in Parkinson’s disease and congenital dopamine beta-hydroxylase deficiency. Clin Sci (Lond), 1994. 86(2): p. 149-58.
5. Kim, C.H., et al., Mutations in the dopamine beta-hydroxylase gene are associated with human norepinephrine deficiency. Am J Med Genet, 2002. 108(2): p. 140-7.
6. Senard, J.M. and P. Rouet, Dopamine beta-hydroxylase deficiency. Orphanet J Rare Dis, 2006. 1: p. 7.
7. Timmers, H.J., et al., Congenital dopamine-beta-hydroxylase deficiency in humans. Ann N Y Acad Sci, 2004. 1018: p. 520-3.
8. Biaggioni, I., et al., Dopamine-beta-hydroxylase deficiency in humans. Neurology, 1990. 40(2): p. 370-3.
9. Rea, R.F., et al., Reflex control of sympathetic nerve activity in dopamine beta-hydroxylase deficiency. Hypertension, 1990. 15(1): p. 107-12.
10. Man in ‘t Veld, A.J., et al., Congenital dopamine-beta-hydroxylase deficiency. A novel orthostatic syndrome. Lancet, 1987. 1(8526): p. 183-8.
11. Superti-Furga, A., P.M. Royce, and B. Steinmann, Congenital dopamine beta-hydroxylase deficiency. Lancet, 1987. 1(8534): p. 693.
12. Man in ‘t Veld, A.J., et al., Effect of unnatural noradrenaline precursor on sympathetic control and orthostatic hypotension in dopamine-beta-hydroxylase deficiency. Lancet, 1987. 2(8569): p. 1172-5.
13. Man in ‘t Veld, A., et al., Patients with congenital dopamine beta-hydroxylase deficiency. A lesson in catecholamine physiology. Am J Hypertens, 1988. 1(3 Pt 1): p. 231-8.
14. Man in ‘t Veld, A.J., et al., d,l-threo-3,4-dihydroxyphenylserine restores sympathetic control and cures orthostatic hypotension in dopamine beta-hydroxylase deficiency. J Hypertens Suppl, 1988. 6(4): p. S547-9.
15. Tulen, J.H., et al., Sleep patterns in congenital dopamine beta-hydroxylase deficiency. J Neurol, 1990. 237(2): p. 98-102.
16. Tulen, J.H., et al., D,L-threo-3, 4-DOPS enhances rapid eye movement sleep in patients with congenital dopamine beta-hydroxylase deficiency. J Clin Psychopharmacol, 1990. 10(1): p. 73-4.
17. Tulen, J.H., et al., Sleeping with and without norepinephrine: effects of metoclopramide and D,L-threo-3,4-dihydroxyphenylserine on sleep in dopamine beta-hydroxylase deficiency. Sleep, 1991. 14(1): p. 32-8.
Voorbereid document _Tessa Wassenberg_V03.indd 208Voorbereid document _Tessa Wassenberg_V03.indd 208 25/10/2021 09:3225/10/2021 09:32

209
Clinical presentation and long-term follow-up of DBH deficiency
18. Deinum, J., et al., DBH gene variants that cause low plasma dopamine beta hydroxylase with or without a severe orthostatic syndrome. J Med Genet, 2004. 41(4): p. e38.
19. Deinum, J., et al., [From gene to disease; dopamine-beta-hydroxylase deficiency and orthostatic hypotension]. Ned Tijdschr Geneeskd, 2004. 148(36): p. 1771-5.
20. Mathias, C.J., et al., Clinical, autonomic and therapeutic observations in two siblings with postural hypotension and sympathetic failure due to an inability to synthesize noradrenaline from dopamine because of a deficiency of dopamine beta hydroxylase. Q J Med, 1990. 75(278): p. 617-33.
21. Smith, G.D., et al., Abnormal cardiovascular and catecholamine responses to supine exercise in human subjects with sympathetic dysfunction. J Physiol, 1995. 484 ( Pt 1): p. 255-65.
22. Smith, S.A. and S.E. Smith, Bilateral Horner’s syndrome: detection and occurrence. J Neurol Neurosurg Psychiatry, 1999. 66(1): p. 48-51.
23. Magnifico, F., et al., The sympathetic skin response in peripheral autonomic failure--evaluation in pure failure, pure cholinergic dysautonomia and dopamine-beta-hydroxylase deficiency. Clin Auton Res, 1998. 8(3): p. 133-8.
24. Brooks, D.J., et al., The effect of orthostatic hypotension on cerebral blood flow and middle cerebral artery velocity in autonomic failure, with observations on the action of ephedrine. J Neurol Neurosurg Psychiatry, 1989. 52(8): p. 962-6.
25. Kingwell, B.A., et al., Heart rate spectral analysis, cardiac norepinephrine spillover, and muscle sympathetic nerve activity during human sympathetic nervous activation and failure. Circulation, 1994. 90(1): p. 234-40.
26. Thompson, J.M., et al., Total norepinephrine spillover, muscle sympathetic nerve activity and heart-rate spectral analysis in a patient with dopamine beta-hydroxylase deficiency. J Auton Nerv Syst, 1995. 55(3): p. 198-206.
27. Scurrah, N.J., A.W. Ross, and M. Solly, Peripartum management of a patient with dopamine beta-hydroxylase deficiency, a rare congenital cause of dysautonomia. Anaesth Intensive Care, 2002. 30(4): p. 484-6.
28. Gomes, M.E., et al., Occam’s razor; anaemia and orthostatic hypotension. Lancet, 2003. 362(9392): p. 1282.
29. Jepma, M., et al., Neurocognitive function in dopamine-beta-hydroxylase deficiency. Neuropsychopharmacology, 2011. 36(8): p. 1608-19.
30. Garland, E.M., et al., Case report: Marathon runner with severe autonomic failure. Lancet, 2005. 366 Suppl 1: p. S13.
31. Cheshire, W.P., Jr., et al., Dopamine beta-hydroxylase deficiency involves the central autonomic network. Acta Neuropathol, 2006. 112(2): p. 227-9.
32. Erez, A., et al., Mosaic deletion 11p13 in a child with dopamine beta-hydroxylase deficiency-case report and review of the literature. Am J Med Genet A, 2010. 152A(3): p. 732-6.
33. Despas, F., et al., DBH deficiency in an elderly patient: efficacy and safety of chronic droxidopa. Clin Auton Res, 2010. 20(3): p. 205-7.
34. Kim, C.H., et al., Norepinephrine deficiency is caused by combined abnormal mRNA processing and defective protein trafficking of dopamine beta-hydroxylase. J Biol Chem, 2011. 286(11): p. 9196-204.
9
Voorbereid document _Tessa Wassenberg_V03.indd 209Voorbereid document _Tessa Wassenberg_V03.indd 209 25/10/2021 09:3225/10/2021 09:32

210
Chapter 9
35. Phillips, L., et al., Pediatric Ptosis as a Sign of Treatable Autonomic Dysfunction. Am J Ophthalmol, 2013.
36. Wassenberg, T., et al., Congenital eyelid ptosis, decreased glomerular filtration, and orthostatic hypotension: Questions. Pediatr Nephrol, 2016.
37. Bartoletti-Stella, A., et al., A patient with PMP22-related hereditary neuropathy and DBH-gene-related dysautonomia. J Neurol, 2015. 262(10): p. 2373-81.
38. Donadio, V., et al., Skin biopsy and microneurography disclose selective noradrenergic dysfunction due to dopamine-beta-hydroxylase deficiency. Auton Neurosci, 2016. 197: p. 56-9.
39. Arnold, A.C., et al., Hyperinsulinemia and Insulin Resistance in Dopamine beta-Hydroxylase Deficiency. J Clin Endocrinol Metab, 2017. 102(1): p. 10-14.
Voorbereid document _Tessa Wassenberg_V03.indd 210Voorbereid document _Tessa Wassenberg_V03.indd 210 25/10/2021 09:3225/10/2021 09:32

211
Clinical presentation and long-term follow-up of DBH deficiency
Figure S1. Literature search flowchart
Figure S1. Flow-chart of literature search. Literature search performed on Pubmed, Cochrane database, clinicaltrials.gov, and WHO trial registry. The 39 publications that ultimately where identified containing unique patient information can be found in de reference list of Table S1
9
Voorbereid document _Tessa Wassenberg_V03.indd 211Voorbereid document _Tessa Wassenberg_V03.indd 211 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 212Voorbereid document _Tessa Wassenberg_V03.indd 212 25/10/2021 09:3225/10/2021 09:32

PART V
General discussion and summary
Voorbereid document _Tessa Wassenberg_V03.indd 213Voorbereid document _Tessa Wassenberg_V03.indd 213 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 214Voorbereid document _Tessa Wassenberg_V03.indd 214 25/10/2021 09:3225/10/2021 09:32

CHAPTER 10
General discussion
and future perspectives
Voorbereid document _Tessa Wassenberg_V03.indd 215Voorbereid document _Tessa Wassenberg_V03.indd 215 25/10/2021 09:3225/10/2021 09:32

216
Chapter 10
The general aim of this thesis has been to elucidate clinical and biochemical aspects of several monoamine neurotransmitter disorders, with an emphasis on two disorders of impaired monoamine synthesis: aromatic L-amino acid decarboxylase (AADC) deficiency and dopamine beta hydroxylase (DBH) deficiency. Furthermore, tyrosine hydroxylase (TH) deficiency and autosomal dominant GTP-cyclohydrolase I (GCH) deficiency have been studied. Laboratory work, clinical observations, literature, and chart reviews were scrutinized and synthesized to better understand the pathophysiology of these disorders inside and outside the central nervous system. A recurring problem in the study of extremely rare disorders is a limitation of resource availability, both in the financial as the literal sense where subjects are scarce. Here, we have dealt with this twin problem by taking a multidimensional approach, answering several fundamental questions about monoamine neurotransmitter pathophysiology by carefully examining our patients and the literature.
Furthermore, this thesis aimed to function as a reference work for physicians to guide their diagnostic approach and clinical management of patients with AADC and DBH deficiency. This was achieved by (inter)national collaboration which is essential in the field of ultrarare disorders.
In the next paragraphs of this discussion we will put our findings in context of prior and current research in the field, identify knowledge gaps, consider methodological issues, and discuss future perspectives for research and clinical management of this fascinating group of disorders.
Part I: Biochemical aspects and the importance of different body com-partments
Monoamine neurotransmitter metabolites in the urine of patients with AADC and TH deficiency: dopamine and homovanillic acidThe starting point of the work in this thesis was to try to understand a peculiar observation in the urine of patients with AADC deficiency. These patients have a severe deficiency of dopamine production, which is illustrated clinically by the profound hypotonia/ hypokinesia and impressive oculogyric crises many of them suffer from1, and biochemically by the very low levels of homovanillic acid (HVA) in the cerebrospinal fluid2. However, it was noted in several reports3-7 that HVA and dopamine concentrations in the urine of these patients is normal or even elevated. To better understand this finding we evaluated the urine of 20 patients with AADC deficiency, and found that 17 had normal or increased urinary dopamine while the remaining three patients excreted decreased but still substantial amounts of dopamine (chapter 3). In healthy humans, renal expression of AADC is very high (chapter 3). Mouse studies have shown that complete knockout of the DDC gene is incompatible with life8, as was found in TH knockout models as well9. Indeed, in patients with AADC deficiency, some residual
Voorbereid document _Tessa Wassenberg_V03.indd 216Voorbereid document _Tessa Wassenberg_V03.indd 216 25/10/2021 09:3225/10/2021 09:32

217
Summary
AADC enzyme activity can be detected in plasma10. In patients in whom the AADC activity is reported as non-detectable, it is more likely that it is not quantifiable with the performed enzyme assay rather than completely absent. Furthermore, in AADC deficiency L-dopa accumulates throughout the body, which is reflected by elevated levels of L-dopa in CSF, plasma and urine2.
Taking the facts of very high AADC expression in healthy kidneys, no complete loss of AADC activity in patients with AADC deficiency, and high L-dopa substrate availability in the kidneys together, we postulated that patients with AADC deficiency will have sufficient residual AADC activity in the kidneys to produce substantial amounts of dopamine. In chapter 4, we confirmed that residual AADC activity in the kidneys combined with high L-dopa substrate availability in the proximal tubuli can explain the finding of normal to elevated levels of dopamine in the urine of patients with AADC deficiency. We are aware that chapter 4 should mainly be regarded as a proof-of-concept study because we used data of only two patients, and the calculations we used are a somewhat simplified representation of the complex interplay between catecholamine synthesis, breakdown, reuptake, and excretion in the central nervous system and the periphery. However, in both patients the final equation that substrate availability should be greater than renal dopamine production was met. We believe that this is a reliable and reproducible finding, that shows that normo- or hyperdopaminuria in AADC deficiency should be regarded as an expected rather than a paradoxical finding.
Also in patients with TH deficiency, normal dopamine excretion is common (6/8 patients, chapter 5) which had not been clearly reported in the literature before. However, in TH deficiency, urinary HVA was diminished in 8/11 patients, in contrast to AADC deficiency where it was normal in 6/7 patients and decreased in only one. We hypothesize that the finding of normal urinary dopamine concentrations in patients with TH deficiency is in line with the findings in AADC deficiency, and residual TH activity in the kidneys will be sufficient to deliver substrate (L-dopa) to the abundantly present renal AADC. However, we think that the retrospective and non-standardized data collection that we used in chapter 5 has clear methodological weaknesses that prevents settling this at this stage and more research is needed.
This does not prevent us from having a strong believe that our findings in chapter 3, 4 and 5 have significant clinical implications, the most important of which is that concentrations of dopamine and HVA in urine can neither be used to reliably diagnose nor to exclude AADC or TH deficiency, because they can be normal, increased or decreased. Although it could be argued that this will not change clinical practice – cerebrospinal fluid examination of monoamine neurotransmitter metabolites is the cornerstone for diagnosis in these disorders11, 12 – we think it is important that we not only show that normo- or hyperdopaminuria is very common, but also offer an explanation for this observation. In this explanation, we combined observations from
10
Voorbereid document _Tessa Wassenberg_V03.indd 217Voorbereid document _Tessa Wassenberg_V03.indd 217 25/10/2021 09:3225/10/2021 09:32

218
Chapter 10
the dopaminergic system in the central nervous system, and the renal dopamine system, two entities that are very intensively studied separately from each other, but rarely in combination.
Dopamine and other monoamines inside and outside the central nervous system: worlds apart?The renal dopamine system is extensively studied by physiologists and nephrologists and known for its natriuretic actions, stimulation of renal blood flow, and diuretic effect13, 14. Intravenously administered dopamine became widely used as vasopressor in critical care medicine from the late 1960s onwards15, and although its use has been questioned16, and its indication is limited nowadays17, it is still available in the armamentarium of the intensive care specialist and anesthesiologist, both in adult medicine and pediatrics18, 19. In the central nervous system, dopamine is a virtually inexhaustible source for research in neurology, psychiatry, cognitive behavioral sciences, and neuroscience (see references for recent reviews20-23), and many drugs that are used in neurological and psychiatric disorders modulate dopaminergic function. Interestingly, the blood-brain barrier quite literally separates the peripheral circulation from the central nervous dopaminergic system by preventing dopamine from crossing it24. This leaves the (pediatric) neurologist with L-dopa and dopamine agonists as surrogates to treat patients that suffer from dopamine deficiency. In ‘dopa responsive states’ like autosomal dominant GCH1 deficiency and TH deficiency, this usually poses no major problems since these patients can metabolize L-dopa to dopamine in the brain12, 25. For AADC deficient patients this is different because AADC is needed for this reaction. Only a small subset of patients with AADC deficiency with specific pathogenic variants respond to L-dopa supplementation26, 27.
In this thesis, we highlight one difference between different body compartments, namely the concentration of dopamine in urine vs. that in cerebral spinal fluid (CSF) in patients with AADC and TH deficiency, and alert that it is important to be aware of this difference. However, many questions about dopamine and serotonin as neurotransmitter versus hormone or autocrine/paracrine substance, and the interplay between different body compartments remain. For example, little is known about the stress response – normally partially mediated by norepinephrine and epinephrine28 - in patients with monoamine neurotransmitter disorders. Furthermore, although serotonin stores are much more abundant in the gut than in the brain29, the consequence of serotonin deficiency to the gastro-intestinal system of patients with AADC deficiency and the tetrahydrobiopterin (BH4) disorders has not yet been investigated in detail. Likewise, the observation that patients with DBH deficiency have no apparent clinical consequences of norepinephrine and epinephrine deficiency in the central nervous system30 remains intriguing. Moreover, to our knowledge, extensive standardized sympathetic nervous system testing (for example using tilt tables) has only been performed in DBH deficiency and not in the other monoamine neurotransmitter disorders. Although many patients
Voorbereid document _Tessa Wassenberg_V03.indd 218Voorbereid document _Tessa Wassenberg_V03.indd 218 25/10/2021 09:3225/10/2021 09:32

219
Summary
will be too fragile to perform this kind of tests, knowing the peripheral consequences of monoamine deficiency will likely be of clinical benefit to these patients and deserves further scientific attention. In conclusion, monoamine neurotransmitter disorders provide a unique opportunity to increase our fundamental understanding concerning the consequences of monoamine deficiencies inside and outside of the brain.
Monoamine neurotransmitter metabolites: old-school but not outdatedThe main conclusions in part I of this manuscript are that (I) in AADC and TH deficiency, neurotransmitter metabolite concentrations in urine do not completely mirror concentrations in cerebrospinal fluid, (II) there is insufficient data to draw firm conclusions on the usefulness of monoamine neurotransmitter metabolites in plasma or dried blood spots (DBS) for diagnosing monoamine neurotransmitter disorders, except for 3-O-methyldopa (3-OMD) in AADC deficiency, and (III) routine follow-up measurements of cerebrospinal fluid (CSF) monoamine neurotransmitter metabolites are not needed in these disorders. However, the analysis of body fluids clearly holds its clinical value in monoamine neurotransmitter disorders, even in the present times when ‘genetic-first’ diagnostic approaches are more and more common.
To diagnose AADC deficiency using metabolic testing, it is an advantage that in this disorder typically specific metabolites accumulate in body fluids, i.e. L-dopa, and its derivates 3-OMD and vanillactic acid (VLA). The increase in urinary VLA can be detected by organic acid analysis, which is a routine screening test in metabolic medicine. However, the increase can be subtle and therefore easily overlooked, and does not occur in all patients. A recent study showed that the ratio between VLA and vanillylmandelic acid (VMA) is more informative, because this ratio is clearly increased in all patients with AADC deficiency31. Therefore, urine can alert to the diagnosis of AADC deficiency in routine metabolic testing, but laboratories are not always aware of this possibility and associated pitfalls. Furthermore, urine is an attractive and easily accessible body fluid for new diagnostic techniques like metabolomics, proteomics, lipidomics, and complexomics32. These techniques – applied either to urine, plasma or CSF- can potentially lead to fast and accurate diagnosis in rather unselected patients with unexplained disorders33, and have the advantage over exome or genome sequencing that they give information on functional changes. This complements untargeted molecular genetic techniques that often report variants of unknown significance. Interestingly, the accumulation of 5-hydroxytryptophan (5-HTP), which reflects the accumulation of metabolites in the serotonergic pathway in AADC deficiency, is much less well defined in the literature and would be an interesting subject for further studies. Besides AADC deficiency, dopamine beta hydroxylase (DBH) deficiency may also be detectable by urine-based metabolomics because of the highly increased dopamine levels that are present in all body fluids, which is a specific finding in this disorder. Whether ‘omics’ techniques can be reliably used for diagnostics in the near future will also depend on the choice of the correct body fluid to perform the screening in. Potentially, these
10
Voorbereid document _Tessa Wassenberg_V03.indd 219Voorbereid document _Tessa Wassenberg_V03.indd 219 25/10/2021 09:3225/10/2021 09:32

220
Chapter 10
untargeted screening methodologies may shorten the diagnostic delay, identify new phenotypes, and guide treatment choices.
As discussed in chapter 5, 3-OMD in plasma or dried blood spots (DBS) seems to be a reliable diagnostic marker for AADC deficiency. It has been studied by different research groups around the world (Taiwan34, Germany35, Italy36, and Brazil37), and these studies consistently yielded highly elevated 3-OMD levels in DBS of patients with AADC deficiency compared to normal controls. However, 3-OMD can also be increased due to L-dopa supplementation38, 39, or, in neonates, by maternal L-dopa usage35. Furthermore, 3-OMD in CSF is increased in pyridoxamine 5’- phosphate oxidase (PNPO) deficiency40, 41
and pyridoxal phosphate binding protein (PLPBP) deficiency42, two primary vitamin B6 responsive disorders that lead to secondary AADC deficiency because vitamin B6 is a cofactor for AADC. In general, these disorders are clinically distinguishable from AADC deficiency because of prominent neonatal seizures. Recently however, in a series of 12 patients with PLPBP deficiency, one patient did not suffer from seizures but displayed a movement disorder compatible with AADC deficiency42. Probably, 3-OMD is not only elevated in CSF but also in DBS in these primary vitamin B6 responsive disorders, but to our knowledge this has not been studied yet. In three patients with PNPO deficiency 3-OMD in DBS was not elevated, but these patients were under pyridoxine therapy and clinically well controlled35. The other causes for 3-OMD elevation should be taken into account and necessitate further biochemical testing and molecular confirmation when AADC deficiency is suspected.
The research groups that have been working on 3-OMD measurements in DBS are aiming to implement a neonatal screening for AADC deficiency. In Taiwan, where the prevalence of AADC deficiency is higher than in Europe due to a founder pathogenic variant in intron 6 (IVS6+4 A>T), four patients were identified after more than 2 years of screening 127,987 newborns34. In Italy, no patients were identified in a limited pilot project screening only 21,867 samples36. Although newborn screening is an appealing concept – the recognition of AADC deficiency can be difficult, diagnostic delay is often long, and gene therapy has been developed for this disorder – it is important to note that at this moment disease modifying treatments in infants are not available yet. Although gene therapy using an intraparenchymal injection of the DDC gene is promising with improvement in motor and mental function, the median age of inclusion was 11 years (range 5-19 years, 6 patients) in a Japanese study43, and 4.3 years (range 1.6-8.4 years, 8 patients) in a Taiwanese study44. The results of a National Institute of Health (NIH) trial (clinical trial identifier NCT02852213) that targets the substantia nigra instead of the putamen are pending, but in this study inclusion starts from five years of age. However, in the Taiwanese studies, clinical outcome43 and improvement in white matter tractography45 was more pronounced in younger patients, making it likely that early intervention is preferred (as expected). Furthermore, to our knowledge gene therapy has not yet been performed in patients with a mild phenotype of AADC deficiency, who
Voorbereid document _Tessa Wassenberg_V03.indd 220Voorbereid document _Tessa Wassenberg_V03.indd 220 25/10/2021 09:3225/10/2021 09:32

221
Summary
will probably also be identified with neonatal screening using 3-OMD in DBS. Therefore, we feel that some caution is warranted before newborn screening for AADC deficiency can be implemented. Indeed, early diagnosis has the advantage of sparing patients and their families a long diagnostic journey, and gives parents the opportunity to consider prenatal or preimplantation genetic diagnosis in further family planning. However, this advantage is not unique to AADC deficiency and has historically not been an argument to include disorders in neonatal screening programs that have their focus on disorders that are (only) treatable at very young age.
Part II: Clinical observations: beyond the classic phenotype
Although case reports and case series are positioned low in the traditional pyramid of evidence-based medicine because of their high risk of bias (Figure 1), we included a case series and case report in part II of this thesis. As outlined below, we think these reports can give valuable new insights in monoamine neurotransmitter disorders that have clinical implications, and can also direct further research. Especially, novel insights in natural history and treatment are excellently presented using case reports, as are observations in diseases for which the clinical course, pathophysiology or management is unexplored yet in larger series46.
Autosomal dominant GCH1 mutation can present with spastic paraplegiaIn chapter 6, we describe four patients from three families with autosomal dominant GCH1 mutations that presented with a pyramidal predominant phenotype (lower leg spasticity) instead of the expected basal ganglia signs. This is a deviant phenotype of this disorder, which is historically coined Segawa syndrome after the first description of the disorder in 1976 by Segawa et al47, and frequently referred to as one of the dopa responsive dystonias (DRD). However, at a young age the patients from our case series were not suspected to have a monoamine neurotransmitter disorder but where thought to have (hereditary) spastic paraplegia. Therefore, treatment with levodopa/carbidopa was not considered at symptom onset but started only many years later.
Unfortunately, there were neither videos nor neurophysiological tests available of our patients early in the disease course. The phenotype with pure lower limb spasticity (which was still present in the youngest patient as shown on video) was only derived ad-posteriori from the clinical description in the case files of the three older patients. This is a weakness of our report, and one might argue that these patients had lower limb dystonia all along that was mistaken for spasticity. Dystonia and spasticity can be difficult to distinguish48. However, we are confident that the clinical course in our patients was different from the usual presentation of autosomal dominant GCH1 mutation, and we found that several other patients with the same pyramidal predominant phenotype had been described in the literature previously49-55. In TH deficiency, to our knowledge only one patient with a pyramidal predominant phenotype
10
Voorbereid document _Tessa Wassenberg_V03.indd 221Voorbereid document _Tessa Wassenberg_V03.indd 221 25/10/2021 09:3225/10/2021 09:32

222
Chapter 10
has been described to date56. Although in a publication from our department a patient with pure spastic paraplegia was first thought to have TH deficiency due to homozygous class 4 variants in TH, he was later found to carry the pathogenic variants in CAPN157, 58. The clinical insignificance of the class IV variants in TH in this patient was proven by an absent clinical effect of L-dopa/carbidopa, and normal monoamine neurotransmitter metabolites in CSF. This prompted further genetic testing in this patient, and illustrates how lucky we are in the field of monoaminergic neurotransmitter disorders to have clinical and biochemical biomarkers at hand, as opposed to many genetic disorders for which no functional testing or biomarkers are available to prove causality when new variants are found. We think it is of utmost importance to precisely delineate different phenotypes of monoamine neurotransmitter disorders, especially because of the potential treatment implications. Therefore, case series clearly have their value in these rare disorders. Next steps to further clarify the finding of spasticity in monoamine neurotransmitter disorders are to better outline the prevalence and natural history in a larger cohort, and perform basic research to understand the mechanism of spasticity in hypomonoaminergic states.
Dopa responsive dystonia is a confusing termSince it is evident that we need to look beyond the classic phenotype when considering monoaminergic neurotransmitter disorders, we would like to make a case against the use of the term ‘dopa responsive dystonia/ DRD’. Firstly, it does not accurately describe all patients with monoamine neurotransmitter disorders that respond to L-dopa supplementation, because dystonia can be absent early in the disease course as we show in chapter 6. Secondly, some patients who are considered to suffer from DRDs are not dopa responsive, as is for example true for the more severe phenotypes of TH deficiency12. Thirdly, the – understandable - fear of missing a DRD can lead to the unwise impulse of subjecting all patients with early onset dystonia to treatment with L-dopa/carbidopa, without first seeking biochemical or molecular justification for this treatment59. Other authors have also been struggling with the term DRD and have proposed subdivisions like DRD, DRD-plus, and DRD-look alike60; or classic DRD, DRD with parkinsonism, and early onset atypical DRD61, supplemented with atypical late-onset DRD with Parkinson`s disease62. However, we feel that these subdivisions only complicate matters further and we would suggest that the monoaminergic neurotransmitter disorders are named after their genetic or enzymatic defect, eventually followed by the most defining sign in that particular patient. This follows the recommendations of the international Parkinson and movement disorder task force on nomenclature of genetic movement disorders63. The patients in chapter 6 would then be described as having ‘HSP-GCH1’ which accurately describes the predominant phenotype and the causative gene.
Voorbereid document _Tessa Wassenberg_V03.indd 222Voorbereid document _Tessa Wassenberg_V03.indd 222 25/10/2021 09:3225/10/2021 09:32

223
Summary
Further beyond the classic phenotype?Recently, more and more attention has been given to the non-motor symptoms in ‘movement disorders’, like Parkinson’s disease and dystonia. In Parkinson’s disease, it was found that non-motor symptoms (e.g. impulse control disorders, apathy, pain, sleep disorders, depression, cognitive problems, autonomic disorders) have a greater impact on health-related quality of life than motor symptoms64 and although treatment is still mainly focused on motor symptoms, the management of non-motor symptoms is an important part of guidelines on Parkinson’s disease nowadays. In dystonia, although it is evident that this is not a psychogenic disorder as was thought in the past65, psychiatric symptoms like anxiety and depression are nevertheless common66. This has also been found in patients with autosomal dominant GCH1 mutations67. The prevalence, extensiveness, and impact of non-motor symptoms in monoaminergic neurotransmitter disorders are important topics for further study, ultimately hopefully leading to better treatment strategies. Clinical observations – whether or not published as case reports – can be a starting point for more extensive research on this topic.
Figure 1. the traditional evidence based pyramid
10
Voorbereid document _Tessa Wassenberg_V03.indd 223Voorbereid document _Tessa Wassenberg_V03.indd 223 25/10/2021 09:3225/10/2021 09:32

224
Chapter 10
Part III: Reviews and guidelines for management
In Part III of this thesis, we provided an overview of the clinical presentation, diagnosis, and management of AADC deficiency (chapter 8) and DBH deficiency (chapter 9). For both disorders, an extensive literature review was performed to gather existent evidence. For AADC deficiency, this was done by a joint effort of a subgroup of the international working group on neurotransmitter related disorders (iNTD), following the Scottish Intercollegiate Guideline Network (SIGN)68 and Grading of Recommendations Assessment, Development and Evaluation (GRADE)69 methodology. This ultimately led to an evidence based consensus guideline. For DBH deficiency, being an even rarer disorder than AADC deficiency, this was done by a literature review and chart review of the relatively large population of patients with DBH deficiency in the Netherlands. Whereas the first publication was effectively aimed to serve as a practice guideline and the second more as an overview paper, we believe that both papers can help guide clinicians in the management of these disorders. For AADC deficiency, clear recommendations for the diagnosis and management are given, combined with good practice points and recommendations for further research. Indeed, in the years that passed since the publication of the guideline, several research topics signaled therein have already been further investigated, such as the value of 3-OMD measurements (see above). We plan to make an update of the guideline on AADC deficiency with the iNTD guideline working group in 2021/2022. In our review on DBH deficiency, we clearly showed that anemia, decreased kidney function, and hypomagnesemia can be part of the disorder and should be screened for at diagnosis and be regularly assessed during follow-up. In the discussion section, we give recommendations for the dosage of LDOPS therapy, not only for adults but also for children with DBH deficiency, which has not been reported in the literature before.
However, it should be kept in mind that most literature on the management of AADC and DBH deficiency that we reviewed consisted of non-analytical studies with a high risk of bias and a low sample size, which are therefore placed low in the traditional pyramid of evidence-based medicine (Figure 1). The SIGN/GRADE methodology makes it possible to faithfully formulate strong recommendations even if evidence comes (only) from non-analytical studies, which is why it has been used in guideline development for other rare disorders as well (e.g. phenylketonuria70 and urea cycle disorders71). Recently, iNTD published the consensus guidelines on diagnosis and treatment of BH4 disorders, using the same methodology25. Nonetheless, we would like to repeat the disclaimer we give in chapter 8: “the guideline is meant to give a solid foundation to caregivers who look after patients with AADC deficiency, but should never replace sensible, well-informed clinical care”.
Voorbereid document _Tessa Wassenberg_V03.indd 224Voorbereid document _Tessa Wassenberg_V03.indd 224 25/10/2021 09:3225/10/2021 09:32

225
Summary
The challenges of performing evidence-based medicine in ultrarare disordersIn a narrative review, three fundamental challenges in generating robust evidence for the management of rare diseases were identified. Firstly, because of the (extreme) rarity of the disorders, it is often not feasible to recruit a sufficient number of patients to achieve statistical power. Secondly, natural history of the disorder is often unclear especially when there is a broad clinical spectrum within one disorder. Thirdly, outcome measures are often short-term with unclear clinical relevance72. Indeed, all these factors are at play in the field of monoamine neurotransmitter disorders.
The first challenge regarding sample size is inherent to the field of (ultra)rare disorders. There is only a limited number of patients with monoamine neurotransmitter disorders, dispersed around the globe. Studies that are traditionally placed on top of the traditional evidence-based pyramid like double-blind, placebo-controlled and randomized controlled trials (Figure 1) are therefore very difficult or simply impossible to perform with sufficient sample size. Luckily, other study types are emerging that are aimed to minimize bias and maximize internal validity, also in ultrarare disorder. One possibility is to use factorial trials, in which multiple interventions are tested simultaneously using the same study population, thus reducing the overall number of participants needed72,
73. However, this is only of use when interventions will be used in combination anyway. In the AADC guideline, we discouraged starting different drugs at the same time, as it complicates the assessment of responses to individual drugs, and the informed discontinuation of certain drugs that have no benefit (chapter 8). A study design that we think holds more potential to improve evidence-based medicine in monoamine neurotransmitter disorders is the N-of-1 trial, which is increasingly used in the field of rare neurodevelopmental disorders74. N-of-1 trials are essentially randomized clinical trials in individual patients75, which therefore have great internal validity and can be used in a research setting or directly in clinical care76.
The second challenge, regarding natural history, was addressed in a natural history study of a large group of patients with AADC deficiency1. However, although it gives an important overview of the clinical presentation and evolution of AADC deficiency, also in this study the full clinical spectrum – including mild phenotypes – is not represented in its entirety. The prospective clinical registry database of iNTD (https://intd-registry.org/) is a valuable tool to better outline the natural history of all monoamine neurotransmitter disorders, although assuring accurate data collection is a challenge nonetheless. It is practically impossible for a doctor working in the field of rare disorders to keep an up-to-date registry for each rare disease. Support in the form of allocated time, staff and adequate technology, is essential to ensure reliable and sustained record keeping in registry studies.
The third challenge regards the lack of reliable, clinically relevant outcome measures in rare disorders. Indeed, when we evaluated the literature for the AADC guideline one
10
Voorbereid document _Tessa Wassenberg_V03.indd 225Voorbereid document _Tessa Wassenberg_V03.indd 225 25/10/2021 09:3225/10/2021 09:32

226
Chapter 10
of the difficulties we encountered was that the clinical response to a certain treatment was often not well defined, making it more difficult to give solid recommendations. In the AADC gene therapy trials, outcome is better defined using motor scales like the Peabody Developmental Motor Scale second edition and Alberta Infant Motor Scale43, 44, but this is not practical to implement in daily clinical practice. An outcome measure in the gene therapy trials that was more difficult to objectively assess was the reduction in oculogyric crises43, which was rated as clinically very important to parents. Implementing scales that reflect clinical relevant outcomes is important to select the correct treatment.
Future perspectives in general
As outlined above, much progress has been made in recent years concerning natural history, diagnosis, and management of AADC deficiency. The consensus guidelines on diagnosis and treatment of AADC deficiency and the BH4 disorders are major steps forward in the care for these patients. Our review on DBH deficiency highlighted the importance of screening for anemia, kidney failure, and hypomagnesemia in this disorder. The results of intraparenchymal gene therapy in patients with AADC deficiency are promising. However, for the other monoamine neurotransmitter disorders, developments are less pronounced, and also for AADC deficiency, the BH4 disorders, and DBH deficiency many questions still remain unanswered. Therefore, the monoamine neurotransmitter disorders remain complex and challenging, not only for physicians and researchers, but above all for the patients and their families who will have to cope with them.
The impact on parents of having a child with a rare disorder is immense, and living with a monoamine neurotransmitter disorder has profound consequences on everyday life. In daily clinical practice, it is impressive to experience the great resilience that many parents and children possess when being faced with disease. In present times, in which there is a major focus on the technical advances of medicine, it is humbling to note that parental support and socio-economic status remain key factors in quality of life, neurodevelopmental outcome, and survival of several disorders like Down’s syndrome77, extremely preterm birth78, and childhood-onset leukemia79. We expect this to be no different for the monoamine neurotransmitter disorders. Therefore, attention for the social background is pivotal, and a holistic approach to the needs of the patients and their families indispensable. In the care for patients with monoamine neurotransmitter disorders, multidisciplinary care integrating medical and paramedical disciplines, patient advocacy groups, and networks that connect specialists on rare disorders like European Reference Networks (ERN) and iNTD can help to achieve this.
Voorbereid document _Tessa Wassenberg_V03.indd 226Voorbereid document _Tessa Wassenberg_V03.indd 226 25/10/2021 09:3225/10/2021 09:32

227
Summary
References
1. Pearson TS, Gilbert L, Opladen T, et al. AADC deficiency from infancy to adulthood: Symptoms and developmental outcome in an international cohort of 63 patients. Journal of inherited metabolic disease. 2020 Sep;43(5):1121-30.
2. Hyland K, Clayton PT. Aromatic L-amino acid decarboxylase deficiency: diagnostic methodology. Clinical chemistry. 1992 12/1992;38(12):2405-10.
3. Abeling NG, Brautigam C, Hoffmann GF, et al. Pathobiochemical implications of hyperdopaminuria in patients with aromatic L-amino acid decarboxylase deficiency. Journal of inherited metabolic disease. 2000 6/2000;23(4):325-8.
4. Abeling NG, van Gennip AH, Barth PG, van CA, Westra M, Wijburg FA. Aromatic L-amino acid decarboxylase deficiency: a new case with a mild clinical presentation and unexpected laboratory findings. Journal of inherited metabolic disease. 1998 6/1998;21(3):240-2.
5. Abdenur JE, Abeling N, Specola N, et al. Aromatic l-aminoacid decarboxylase deficiency: unusual neonatal presentation and additional findings in organic acid analysis. Mol Genet Metab. 2006 Jan;87(1):48-53.
6. Fiumara A, Brautigam C, Hyland K, et al. Aromatic L-amino acid decarboxylase deficiency with hyperdopaminuria. Clinical and laboratory findings in response to different therapies. Neuropediatrics. 2002 8/2002;33(4):203-8.
7. Ito S, Nakayma T, Ide S, et al. Aromatic l-amino acid decarboxylase deficiency associated with epilepsy mimicking non-epileptic involuntary movements. Dev Med Child Neur 2008 2008;50:876-8.
8. Lee NC, Shieh YD, Chien YH, et al. Regulation of the dopaminergic system in a murine model of aromatic L-amino acid decarboxylase deficiency. Neurobiology of disease. 2013 Apr;52:177-90.
9. Chen L, Zhuang X. Transgenic mouse models of dopamine deficiency. Annals of neurology. 2003 2003;54 Suppl 6:S91-102.
10. Verbeek MM, Geurtz PB, Willemsen MA, Wevers RA. Aromatic L-amino acid decarboxylase enzyme activity in deficient patients and heterozygotes. Mol Genet Metab. 2007 4/2007;90(4):363-9.
11. Brun L, Ngu LH, Keng WT, et al. Clinical and biochemical features of aromatic L-amino acid decarboxylase deficiency. Neurology. 2010 Jul 6;75(1):64-71.
12. Willemsen MA, Verbeek MM, Kamsteeg EJ, et al. Tyrosine hydroxylase deficiency: a treatable disorder of brain catecholamine biosynthesis. Brain : a journal of neurology. 2010 Jun;133(Pt 6):1810-22.
13. Aperia A. Dopamine action and metabolism in the kidney. Current opinion in nephrology and hypertension. 1994 1/1994;3(1):39-45.
14. Aperia AC. Intrarenal dopamine: a key signal in the interactive regulation of sodium metabolism. Annu Rev Physiol. 2000 2000;62:621-47.
15. Goldberg LI. Dopamine--clinical uses of an endogenous catecholamine. The New England journal of medicine. 1974 Oct 3;291(14):707-10.
10
Voorbereid document _Tessa Wassenberg_V03.indd 227Voorbereid document _Tessa Wassenberg_V03.indd 227 25/10/2021 09:3225/10/2021 09:32

228
Chapter 10
16. Debaveye YA, Van den Berghe GH. Is there still a place for dopamine in the modern intensive care unit? Anesthesia and analgesia. 2004 Feb;98(2):461-8.
17. Russell JA. Vasopressor therapy in critically ill patients with shock. Intensive Care Med. 2019 Nov;45(11):1503-17.
18. Barreto HAG, Sestren B, Boergen-Lacerda R, Soares L. Standard concentration infusions of inotropic and vasoactive drugs in paediatric intensive care: a strategy for patient safety. The Journal of pharmacy and pharmacology. 2019 May;71(5):826-38.
19. Kirupakaran K, de Sousa P, Le Roux C, Redwood L, Rabe H, Patel BA. Evaluation of the causal effects between dopamine infusion changeover and fluctuations in mean arterial pressure in neonates. Archives of disease in childhood. 2020 Apr;105(4):390-4.
20. Berke JD. What does dopamine mean? Nature neuroscience. 2018 Jun;21(6):787-93.21. Kesby JP, Eyles DW, McGrath JJ, Scott JG. Dopamine, psychosis and schizophrenia: the
widening gap between basic and clinical neuroscience. Transl Psychiatry. 2018 Jan 31;8(1):30.22. Lerner TN, Holloway AL, Seiler JL. Dopamine, Updated: Reward Prediction Error and Beyond.
Curr Opin Neurobiol. 2020 Nov 13;67:123-30.23. Kaasinen V, Vahlberg T, Stoessl AJ, Strafella AP, Antonini A. Dopamine Receptors in
Parkinson’s Disease: A Meta-Analysis of Imaging Studies. Movement disorders : official journal of the Movement Disorder Society. 2021 May 6.
24. Bertler A, Falck B, Owman C, Rosengrenn E. The localization of monoaminergic blood-brain barrier mechanisms. Pharmacological reviews. 1966 Mar;18(1):369-85.
25. Opladen T, Lopez-Laso E, Cortes-Saladelafont E, et al. Consensus guideline for the diagnosis and treatment of tetrahydrobiopterin (BH4) deficiencies. Orphanet journal of rare diseases. 2020 May 26;15(1):126.
26. Chang YT, Sharma R, Marsh JL, et al. Levodopa-responsive aromatic L-amino acid decarboxylase deficiency. Annals of neurology. 2004 Mar;55(3):435-8.
27. Barth M, Chaabouni Y, Hubert L, et al. Kinetic analysis guide the therapeutic decision in a novel form of moderate aromatic acid decarboxylase deficiency. JIMD. 2010;33(S1):S165.
28. Charmandari E, Tsigos C, Chrousos G. Endocrinology of the stress response. Annu Rev Physiol. 2005;67:259-84.
29. Gershon MD. 5-Hydroxytryptamine (serotonin) in the gastrointestinal tract. Curr Opin Endocrinol Diabetes Obes. 2013 Feb;20(1):14-21.
30. Jepma M, Deinum J, Asplund CL, et al. Neurocognitive function in dopamine-beta- hydroxylase deficiency. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology. 2011 Jul;36(8):1608-19.
31. Brennenstuhl H, Garbade SF, Okun JG, et al. Semi-quantitative detection of a vanillactic acid/vanillylmandelic acid ratio in urine is a reliable diagnostic marker for aromatic L-amino acid decarboxylase deficiency. Mol Genet Metab. 2020 Jul 7.
32. Wevers RA, Blau N. Think big - think omics. Journal of inherited metabolic disease. 2018 May;41(3):281-3.
33. Kyle JE, Stratton KG, Zink EM, et al. A resource of lipidomics and metabolomics data from individuals with undiagnosed diseases. Sci Data. 2021 Apr 21;8(1):114.
Voorbereid document _Tessa Wassenberg_V03.indd 228Voorbereid document _Tessa Wassenberg_V03.indd 228 25/10/2021 09:3225/10/2021 09:32

229
Summary
34. Chien YH, Chen PW, Lee NC, et al. 3-O-methyldopa levels in newborns: Result of newborn screening for aromatic l-amino-acid decarboxylase deficiency. Mol Genet Metab. 2016 Aug;118(4):259-63.
35. Brennenstuhl H, Kohlmuller D, Gramer G, et al. High throughput newborn screening for aromatic L-amino-acid decarboxylase deficiency by analysis of concentrations of 3-O- methyldopa from dried blood spots. Journal of inherited metabolic disease. 2020 May;43(3):602-10.
36. Burlina A, Giuliani A, Polo G, et al. Detection of 3-O-methyldopa in dried blood spots for neonatal diagnosis of aromatic L-amino-acid decarboxylase deficiency: The northeastern Italian experience. Mol Genet Metab. 2021 May;133(1):56-62.
37. Kubaski F, Herbst ZM, Pereira DAA, et al. Evaluation of 3-O-methyldopa as a biomarker for aromatic L-amino acid decarboxylase deficiency in 7 Brazilian cases. Molecular genetics and metabolism reports. 2021 Jun;27:100744.
38. Benetello P, Furlanut M, Fortunato M, Pea F, Baraldo M. Levodopa and 3-O-methyldopa in cerebrospinal fluid after levodopa-carbidopa association. Pharmacol Res. 1997 Apr;35(4):313- 5.
39. Garcia NH, Berndt TJ, Tyce GM, Knox FG. Chronic oral L-DOPA increases dopamine and decreases serotonin excretions. Am J Physiol. 1999 Nov;277(5):R1476-80.
40. Brautigam C, Hyland K, Wevers R, et al. Clinical and laboratory findings in twins with neonatal epileptic encephalopathy mimicking aromatic L-amino acid decarboxylase deficiency. Neuropediatrics. 2002 6/2002;33(3):113-7.
41. Mills PB, Surtees RA, Champion MP, et al. Neonatal epileptic encephalopathy caused by mutations in the PNPO gene encoding pyridox(am)ine 5’-phosphate oxidase. Human molecular genetics. 2005 Apr 15;14(8):1077-86.
42. Johnstone DL, Al-Shekaili HH, Tarailo-Graovac M, et al. PLPHP deficiency: clinical, genetic, biochemical, and mechanistic insights. Brain : a journal of neurology. 2019 Mar 1;142(3):542- 59.
43. Hwu WL, Muramatsu S, Tseng SH, et al. Gene therapy for aromatic L-amino acid decarboxylase deficiency. Science translational medicine. 2012 May 16;4(134):134ra61.
44. Chien YH, Lee NC, Tseng SH, et al. Efficacy and safety of AAV2 gene therapy in children with aromatic L-amino acid decarboxylase deficiency: an open-label, phase 1/2 trial. Lancet Child Adolesc Health. 2017 Dec;1(4):265-73.
45. Tseng CH, Chien YH, Lee NC, et al. Gene therapy improves brain white matter in aromatic l- amino acid decarboxylase deficiency. Annals of neurology. 2019 May;85(5):644-52.
46. Bhattacharrya S, Miller J, Ropper AH. The case for case reports. Annals of neurology. 2014 Oct;76(4):484-6.
47. Segawa M, Hosaka A, Miyagawa F, Nomura Y, Imai H. Hereditary progressive dystonia with marked diurnal fluctuation. Advances in neurology. 1976;14:215-33.
48. Eggink H, Kremer D, Brouwer OF, et al. Spasticity, dyskinesia and ataxia in cerebral palsy: Are we sure we can differentiate them? Eur J Paediatr Neurol. 2017 Sep;21(5):703-6.
49. Brown P, Britton TC. Cortico-motor neurone conduction in dopa responsive dystonia. Movement disorders : official journal of the Movement Disorder Society. 1990;5(4):338.
50. Harwood G, Hierons R, Fletcher NA, Marsden CD. Lessons from a remarkable family with dopa-responsive dystonia. Journal of neurology, neurosurgery, and psychiatry. 1994 Apr;57(4):460-3.
10
Voorbereid document _Tessa Wassenberg_V03.indd 229Voorbereid document _Tessa Wassenberg_V03.indd 229 25/10/2021 09:3225/10/2021 09:32

230
Chapter 10
51. Tassin J, Durr A, Bonnet AM, et al. Levodopa-responsive dystonia. GTP cyclohydrolase I or parkin mutations? Brain : a journal of neurology. 2000 Jun;123 ( Pt 6):1112-21.
52. Garavaglia B, Invernizzi F, Carbone ML, et al. GTP-cyclohydrolase I gene mutations in patients with autosomal dominant and recessive GTP-CH1 deficiency: identification and functional characterization of four novel mutations. Journal of inherited metabolic disease. 2004;27(4):455-63.
53. Cao L, Zheng L, Tang WG, et al. Four novel mutations in the GCH1 gene of Chinese patients with dopa-responsive dystonia. Movement disorders : official journal of the Movement Disorder Society. 2010 Apr 30;25(6):755-60.
54. Fan Z, Greenwood R, Felix AC, et al. GCH1 heterozygous mutation identified by whole- exome sequencing as a treatable condition in a patient presenting with progressive spastic paraplegia. Journal of neurology. 2014 Mar;261(3):622-4.
55. Dobricic V, Tomic A, Brankovic V, et al. GCH1 mutations are common in Serbian patients with dystonia-parkinsonism: Challenging previously reported prevalence rates of DOPA- responsive dystonia. Parkinsonism & related disorders. 2017 Dec;45:81-4.
56. Furukawa Y, Graf WD, Wong H, Shimadzu M, Kish SJ. Dopa-responsive dystonia simulating spastic paraplegia due to tyrosine hydroxylase (TH) gene mutations. Neurology. 2001 Jan 23;56(2):260-3.
57. van de Warrenburg BP, Schouten MI, de Bot ST, et al. Clinical exome sequencing for cerebellar ataxia and spastic paraplegia uncovers novel gene-disease associations and unanticipated rare disorders. European journal of human genetics : EJHG. 2017 Feb;25(3):393.
58. Shetty A, Gan-Or Z, Ashtiani S, et al. CAPN1 mutations: Expanding the CAPN1-related phenotype: From hereditary spastic paraparesis to spastic ataxia. Eur J Med Genet. 2018 Dec 17.
59. Maas R, Wassenberg T, Lin JP, van de Warrenburg BPC, Willemsen M. l-Dopa in dystonia: A modern perspective. Neurology. 2017 May 9;88(19):1865-71.
60. Lee WW, Jeon B, Kim R. Expanding the Spectrum of Dopa-Responsive Dystonia (DRD) and Proposal for New Definition: DRD, DRD-plus, and DRD Look-alike. J Korean Med Sci. 2018 Jul 9;33(28):e184.
61. Wijemanne S, Jankovic J. Dopa-responsive dystonia--clinical and genetic heterogeneity. Nature reviews Neurology. 2015 Jul;11(7):414-24.
62. Mottet L. Classification of dopa-responsive dystonia - a patient’s perspective. Nature reviews Neurology. 2016 Jul;12(7):427.
63. Marras C, Lang A, van de Warrenburg BP, et al. Nomenclature of genetic movement disorders: Recommendations of the international Parkinson and movement disorder society task force. Movement disorders : official journal of the Movement Disorder Society. 2016 Apr;31(4):436-57.
64. Martinez-Martin P, Rodriguez-Blazquez C, Kurtis MM, Chaudhuri KR, Group NV. The impact of non-motor symptoms on health-related quality of life of patients with Parkinson’s disease. Movement disorders : official journal of the Movement Disorder Society. 2011 Feb 15;26(3):399-406.
65. Munts AG, Koehler PJ. How psychogenic is dystonia? Views from past to present. Brain : a journal of neurology. 2010 May;133(Pt 5):1552-64.
Voorbereid document _Tessa Wassenberg_V03.indd 230Voorbereid document _Tessa Wassenberg_V03.indd 230 25/10/2021 09:3225/10/2021 09:32

231
Summary
66. Stamelou M, Edwards MJ, Hallett M, Bhatia KP. The non-motor syndrome of primary dystonia: clinical and pathophysiological implications. Brain : a journal of neurology. 2012 Jun;135(Pt 6):1668-81.
67. Timmers ER, Kuiper A, Smit M, et al. Non-motor symptoms and quality of life in dopa- responsive dystonia patients. Parkinsonism & related disorders. 2017 Dec;45:57-62.
68. SIGN. Scottish Intercollegiate Guideline Network. 2014; Available from: http://www.sign.ac.uk.69. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles
and summary of findings tables. Journal of clinical epidemiology. 2011 Apr;64(4):383-94.70. van Spronsen FJ, van Wegberg AM, Ahring K, et al. Key European guidelines for the diagnosis
and management of patients with phenylketonuria. Lancet Diabetes Endocrinol. 2017 Sep;5(9):743-56.
71. Haberle J, Burlina A, Chakrapani A, et al. Suggested guidelines for the diagnosis and management of urea cycle disorders: First revision. Journal of inherited metabolic disease. 2019 Nov;42(6):1192-230.
72. Tingley K, Coyle D, Graham ID, et al. Using a meta-narrative literature review and focus groups with key stakeholders to identify perceived challenges and solutions for generating robust evidence on the effectiveness of treatments for rare diseases. Orphanet journal of rare diseases. 2018 Jun 28;13(1):104.
73. Montgomery AA, Peters TJ, Little P. Design, analysis and presentation of factorial randomised controlled trials. BMC Med Res Methodol. 2003 Nov 24;3:26.
74. Muller AR, Brands M, van de Ven PM, et al. Systematic Review of N-of-1 Studies in Rare Genetic Neurodevelopmental Disorders: The Power of 1. Neurology. 2021 Mar 16;96(11):529-40.
75. Guyatt G, Sackett D, Adachi J, et al. A clinician’s guide for conducting randomized trials in individual patients. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne. 1988 Sep 15;139(6):497-503.
76. Stunnenberg BC, Deinum J, Nijenhuis T, et al. N-of-1 Trials: Evidence-Based Clinical Care or Medical Research that Requires IRB Approval? A Practical Flowchart Based on an Ethical Framework. Healthcare (Basel). 2020 Feb 27;8(1).
77. Roizen NJ, Patterson D. Down’s syndrome. Lancet. 2003 Apr 12;361(9365):1281-9.78. Benavente-Fernandez I, Synnes A, Grunau RE, et al. Association of Socioeconomic Status
and Brain Injury With Neurodevelopmental Outcomes of Very Preterm Children. JAMA Netw Open. 2019 May 3;2(5):e192914.
79. Petridou ET, Sergentanis TN, Perlepe C, et al. Socioeconomic disparities in survival from childhood leukemia in the United States and globally: a meta-analysis. Ann Oncol. 2015 Mar;26(3):589-97.
10
Voorbereid document _Tessa Wassenberg_V03.indd 231Voorbereid document _Tessa Wassenberg_V03.indd 231 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 232Voorbereid document _Tessa Wassenberg_V03.indd 232 25/10/2021 09:3225/10/2021 09:32

CHAPTER 11
Summary
Voorbereid document _Tessa Wassenberg_V03.indd 233Voorbereid document _Tessa Wassenberg_V03.indd 233 25/10/2021 09:3225/10/2021 09:32

234
Chapter 11
Monoamine neurotransmitter disorders are rare genetic disorders that are caused by impaired synthesis, breakdown, storage or transport of monoamines, or impaired synthesis or recycling of tetrahydrobiopterin (BH4), which is an important cofactor in dopamine and serotonin synthesis. Many monoamine neurotransmitter disorders are treatable disorders. In this thesis, clinical and biochemical characteristics of several disorders within this group are discussed, with the focus on aromatic l-amino acid decarboxylase (AADC) and dopamine beta hydroxylase (DBH) deficiencies. Furthermore, tyrosine hydroxylase (TH) and autosomal dominant GTP-cyclohydrolase I (GCH1) deficiencies are discussed.
Part I: Prologue
Part I of this thesis consists of an introduction (chapter 1) to the field of monoamine neurotransmitter disorders. The biochemical pathway of monoamine synthesis and breakdown is presented, showing the enzymes and their cofactors that are involved. The main monoamine neurotransmitter metabolites that are used in diagnosis are 5-hydroxyindoleacetic acid (5-HIAA) and homovanillic acid (HVA) as the main breakdown products of serotonin and dopamine, respectively, and vanillylmandelic acid (VMA) and 3-methoxy 4-hydroxyphenylglycol (MHPG) as the main breakdown products of norepinephrine and epinephrine. Key clinical symptoms, diagnostic approach, and treatment options of AADC deficiency, DBH deficiency, TH deficiency and autosomal dominant GCH1 deficiency are briefly discussed. Furthermore, Table 1 in this chapter gives a brief overview of the primary monoamine neurotransmitter disorders that are known to date. Chapter 2 describes the aims and outline of this thesis.
Part II: Biochemical aspects and the importance of different body compartments
Serotonin, dopamine, norepinephrine and epinephrine are not only present in the central nervous system where they act as neurotransmitters, but are also active in the periphery. For example, dopamine is important in the regulation of blood pressure and natriuresis. However, the relationship between central and peripheral dopamine is not well understood. In part II, we performed several studies to better understand this relationship.
In chapter 3, we explored a peculiar finding in the urine of patients with AADC deficiency. It had anecdotally been noted that patients with this disorder had increased levels of dopamine and its metabolite HVA in the urine. This observation was in stark contrast with the low levels of dopamine and HVA in the cerebrospinal fluid, and remained unexplained for many years. We found that 17/20 patients with AADC deficiency indeed had normal or increased levels of dopamine in the urine, and the remaining three patients excreted low, but still substantial, levels of dopamine. We found no
Voorbereid document _Tessa Wassenberg_V03.indd 234Voorbereid document _Tessa Wassenberg_V03.indd 234 25/10/2021 09:3225/10/2021 09:32

235
General discussion
genotype/phenotype correlation to explain this finding. Therefore, we searched for alternative pathways for the formation of dopamine in the kidneys using alternative substrates (tyramine and 3-methoxytyrosine) and alternative enzymes (tyrosinase and CYP2D6). We also performed experiments on peripheral dopamine production and AADC expression in several tissues using an AADC activity assay, immunohistochemical expression, and Western Blot. We found that renal microsomes were indeed able to convert tyramine to dopamine using the CYP2D6 enzyme (3.1 nmol/min/g protein). However, because of low plasma levels of tyramine this is an unlikely explanation for urinary dopamine excretion in AADC deficiency. We found no evidence for the production of dopamine from 3-methoxytyrosine. Tyrosinase was not expressed in human kidney. We found a very high AADC activity (2996 nmol/min/g protein) and AADC expression (by both immunohistochemical and Western Blot analysis) in human kidney cortex. The AADC activity in human striatum was much lower (5 nmol/min/g protein).
Patients with AADC deficiency will have some residual enzyme activity, because a complete loss of AADC is thought to be incompatible with life. The extremely high AADC expression and activity in (healthy) kidney cortex led us to the hypothesis that even minimal amounts of residual AADC activity, in combination with excessive substrate (i.e. L-dopa) availability in patients with AADC deficiency might be sufficient to explain the finding of normal or increased urinary dopamine in these patients. In patients with AADC deficiency, L-dopa is highly increased because AADC is needed to convert L-dopa to dopamine. In chapter 4, we tested our hypothesis by calculating residual renal AADC activity and L-dopa substrate availability in two patients with AADC deficiency. For this, we collected 24-h urine samples and performed blood tests to measure L-dopa. In both patients, who both had increased levels of urinary dopamine, our hypothesis was verified. This study showed that normal or increased levels of urinary dopamine are an expected rather than a paradoxical finding in AADC deficiency, because of the qualitative difference between dopamine production in the central nervous system and the kidneys.
In chapter 5, we further examined the difference between monoamine neurotransmitter metabolites in the central nervous system (reflected by their concentrations in cerebrospinal fluid) and peripheral body fluids, and tried to clarify the diagnostic value of blood and urine in AADC and TH deficiencies. Furthermore, we studied serum prolactin levels, and neurotransmitter metabolites in cerebrospinal fluid before and during treatment. For this, we performed a literature review and a retrospective analysis of our local university hospital database (1997-2020). In AADC deficiency, we found that 3-O-methyldopa (a metabolite of L-dopa) in serum or dried blood spots was strongly increased in 34/34 patients. In urine, dopamine was normal or increased in 21/24 patients, 5-HIAA was decreased in 9/10 patients, and vanillactic acid was increased in 19/20 patients. No significant changes were seen in monoamine neurotransmitter metabolites after medical treatment, except for the (expected) increase of HVA in urine
11
Voorbereid document _Tessa Wassenberg_V03.indd 235Voorbereid document _Tessa Wassenberg_V03.indd 235 25/10/2021 09:3225/10/2021 09:32

236
Chapter 11
and cerebrospinal fluid after L-dopa therapy. After gene therapy, HVA in cerebrospinal fluid increased in 8/12 patients, but 5-HIAA remained very low in 9/12 patients. In TH deficiency, urinary dopamine was normal in 6/8 patients and decreased in two. The HVA concentrations in cerebrospinal fluid increased upon levodopa treatment, even in the absence of a clear treatment response. Prolactin was increased in 34/37 patients with AADC deficiency, and 12/14 patients with TH deficiency. We concluded that 3-O-methyldopa in serum and dried blood spots and urinary vanillactic acid are promising biomarkers in the diagnosis of AADC deficiency, but discussed also some pitfalls especially regarding the potential confusion with the primary vitamin B6 disorders. We showed that also in TH deficiency, urinary dopamine is normal in the majority of patients, which was not clearly stated in the literature before. Furthermore, cerebrospinal fluid examination of neurotransmitter metabolites remains the most informative body fluid when AADC or TH deficiency is suspected, but routine follow-up lumbar punctures are not needed in these disorders, and should only be performed in case of unexpected clinical deterioration. Finally, the value of serum prolactin for screening and follow-up of AADC and TH deficiency seems promising but should be further studied.
Part III: beyond the classic phenotype: clinical observations
In part III, we presented a case series on patients with autosomal dominant GCH1 deficiency, and a case report on DBH deficiency.
In chapter 6, we described four patients from three families with an uncommon clinical presentation of autosomal dominant GCH1 deficiency. Instead of (lower-limb) dystonia, they presented with spastic paraplegia. The youngest patient did not show clear basal ganglia signs at diagnosis, and the other patients developed basal ganglia signs (dystonia and/or parkinsonism) only in their fifth decade. We described the clinical trajectories, and showed videos of the neurological examination before and during treatment with L-dopa. We performed a literature search in which we identified nine patients with a clinical course compatible with the patients in our case series, with predominant lower limb spasticity at disease onset, and basal ganglia signs developing later in life. Because autosomal GCH1 deficiency is a treatable disorder, with an excellent response to L-dopa, we stress that this disorder should be considered in patients that present with spastic paraplegia, especially if there are concomitant basal ganglia signs and/or diurnal fluctuations, and that the GCH1 gene should be included in HSP gene panels.
In chapter 7, we presented a didactic case report on DBH deficiency, structured in a question and answer module. We described a young woman who was ultimately diagnosed with DBH deficiency at the age of 19 years. Her referral diagnosis was kidney failure. She complained of exercise intolerance and showed eyelid ptosis, therefore a mitochondrial disorder was suspected. When profound orthostatic hypotension
Voorbereid document _Tessa Wassenberg_V03.indd 236Voorbereid document _Tessa Wassenberg_V03.indd 236 25/10/2021 09:3225/10/2021 09:32

237
General discussion
was noted, DBH deficiency was suspected and confirmed. In the answer module, we described key clinical signs and symptoms of DBH deficiency, and highlighted the importance of performing office orthostatic blood pressure measurements. It is important to be aware of the extremely rare diagnosis of DBH deficiency, also in children or adolescents who present with reduced kidney function, because it is a treatable disorder. The patient in our report had an excellent clinical response to L-DOPS, and also her kidney function improved.
Part IV: Reviews and guidelines for management
Part IV consists of two overview articles on monoamine neurotransmitter disorders.
In chapter 8, the consensus guideline on diagnosis and treatment of AADC deficiency is presented. This guideline was developed by the AADC guideline group of the international working group on neurotransmitter related disorders (iNTD) using Scottish Intercollegiate Guideline Network (SIGN) and Grading of Recommendations, Assessments, Development and Evaluation (GRADE) methodology. SIGN and GRADE methodology enables to make strong (or conditional) recommendations, even in the field of rare disorders where most evidence consists of case reports, case series and expert opinion. In the guideline, 63 recommendations were formulated regarding clinical presentation, diagnosis, treatment, complications, long-term management, social issues and transition, and special situations (e.g. anesthesia, intensive care management).
In chapter 9, we described the clinical presentation and long-term follow-up of patients with DBH deficiency. It consists of a literature review, combined with a chart review of the relatively large population of patients with DBH deficiency in the Netherlands. In total, we identified 10 patients in the Netherlands, and 15 additional patients from the literature. The duration of follow-up of the Dutch patients ranged from 1 to 21 years (median 13 years). All patients had severe orthostatic hypotension. The pathognomonic metabolite pattern with strongly decreased or absent (nor)epinephrine, and (highly) increased dopamine plasma concentrations was found in 24/25 patients. All Dutch patients had impaired kidney function and anemia, 50% had hypomagnesaemia. The clinical response to L-DOPS treatment was excellent and sustained in all patients, but the neurotransmitter profile in plasma did not normalize completely, and renal function, anemia and hypomagnesemia improved only partially.
Part V: General discussion and summary
In chapter 10, a general discussion is given in which we put our findings in context of prior and current research in the field, identify knowledge gaps, consider methodological issues, and discuss future perspectives for research and clinical management of monoamine neurotransmitter disorders.
11
Voorbereid document _Tessa Wassenberg_V03.indd 237Voorbereid document _Tessa Wassenberg_V03.indd 237 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 238Voorbereid document _Tessa Wassenberg_V03.indd 238 25/10/2021 09:3225/10/2021 09:32

CHAPTER 12
Dutch summary
(Nederlandse samenvatting)
Voorbereid document _Tessa Wassenberg_V03.indd 239Voorbereid document _Tessa Wassenberg_V03.indd 239 25/10/2021 09:3225/10/2021 09:32

240
Chapter 12
Monoamine neurotransmitter stoornissen zijn zeldzame genetische aandoeningen die worden veroorzaakt door een verstoorde synthese, afbraak, opslag of transport van monoamines, of een verstoorde synthese of recycling van tetrahydrobiopterine (BH4), een belangrijke cofactor bij de synthese van dopamine en serotonine. Veel monoamine neurotransmitter stoornissen zijn behandelbare aandoeningen. In dit proefschrift worden de klinische en biochemische kenmerken van verschillende stoornissen binnen deze groep besproken, met de nadruk op aromatische l-aminozuur decarboxylase (AADC) en dopamine beta hydroxylase (DBH) deficiënties. Verder worden tyrosine hydroxylase (TH) en autosomaal dominante GTP-cyclohydrolase I (GCH1) deficiënties besproken.
Deel I: Proloog
Deel I van dit proefschrift bestaat uit een inleiding (hoofdstuk 1) op het gebied van monoamine neurotransmitter stoornissen. De biochemische route van monoamine synthese en afbraak wordt gepresenteerd, waarbij de enzymen en hun cofactoren worden getoond die hierbij betrokken zijn. De belangrijkste monoamine neurotransmitter metabolieten die gebruikt worden in de diagnostiek zijn 5-hydroxyindoleazijnzuur (5-HIAA) en homovanillinezuur (HVA) als de belangrijkste afbraakproducten van respectievelijk serotonine en dopamine, en vanillyl-amandelzuur (VMA) en 3-methoxy 4-hydroxyfenylglycol (MHPG) als de belangrijkste afbraakproducten van noradrenaline en adrenaline. De belangrijkste klinische symptomen, de diagnostische aanpak en de mogelijke behandelingen van AADC-deficiëntie, DBH-deficiëntie, TH-deficiëntie en autosomaal dominante GCH1-deficiëntie worden kort besproken. Verder geeft tabel 1 in dit hoofdstuk een kort overzicht van de monoamine neurotransmitter stoornissen die tot op heden bekend zijn. Hoofdstuk 2 beschrijft de doelstellingen en opzet van dit proefschrift.
Deel II: Biochemische aspecten en het belang van verschillende lichaamscompartimenten
Serotonine, dopamine, noradrenaline en adrenaline zijn niet alleen aanwezig in het centrale zenuwstelsel waar ze als neurotransmitters fungeren, maar zijn ook actief in de periferie. Zo is dopamine bijvoorbeeld belangrijk bij de regulering van de bloeddruk en de natriurese. De relatie tussen centrale en perifere dopamine is echter niet goed bekend. In deel II hebben wij verschillende studies uitgevoerd om deze relatie beter te begrijpen.
In hoofdstuk 3 onderzochten we een eigenaardige bevinding in de urine van patiënten met AADC deficiëntie. Het was eerder reeds anekdotisch opgemerkt dat patiënten met deze aandoening verhoogde niveaus van dopamine en zijn metaboliet HVA in de urine hadden. Deze waarneming stond in schril contrast met de lage niveaus van dopamine
Voorbereid document _Tessa Wassenberg_V03.indd 240Voorbereid document _Tessa Wassenberg_V03.indd 240 25/10/2021 09:3225/10/2021 09:32

241
Dutch summary (Nederlandse samenvatting)
en HVA in de cerebrospinale vloeistof, en bleef gedurende vele jaren onverklaard. Wij stelden vast dat 17/20 patiënten met AADC-deficiëntie inderdaad normale of verhoogde dopaminegehaltes in de urine hadden, en dat de overige drie patiënten lage, maar nog steeds substantiële, dopaminegehaltes uitscheidden. Wij vonden geen genotype/fenotype correlatie om deze bevinding te verklaren. Daarom zochten wij naar alternatieve routes voor de vorming van dopamine in de nieren met behulp van alternatieve substraten (tyramine en 3-methoxytyrosine) en alternatieve enzymen (tyrosinase en CYP2D6). We hebben ook experimenten uitgevoerd naar perifere dopamineproductie en AADC-expressie in verschillende weefsels met behulp van een AADC-activiteitstest, immunohistochemische expressie, en Western Blot. We ontdekten dat renale microsomen inderdaad in staat waren tyramine om te zetten in dopamine met behulp van het CYP2D6-enzym (3,1 nmol/min/g eiwit). Gezien de lage plasmaniveaus van tyramine is dit echter een onwaarschijnlijke verklaring voor de uitscheiding van dopamine in de urine bij AADC-deficiëntie. Wij vonden geen aanwijzingen voor de productie van dopamine uit 3-methoxytyrosine. Tyrosinase werd niet tot expressie gebracht in de menselijke nieren. We vonden een zeer hoge AADC activiteit (2996 nmol/min/g eiwit) en AADC expressie (door zowel immunohistochemische als Western Blot analyse) in menselijke niercortex. De AADC activiteit in het menselijke striatum was veel lager (5 nmol/min/g eiwit).
Patiënten met AADC-deficiëntie zullen nog enige residuele enzymactiviteit hebben, omdat een volledig verlies van AADC onverenigbaar met het leven wordt geacht. Bij patiënten met AADC deficiëntie is L-dopa sterk verhoogd omdat AADC nodig is om L-dopa om te zetten in dopamine. De extreem hoge AADC expressie en activiteit in (gezonde) nier cortex leidde ons tot de hypothese dat zelfs minimale hoeveelheden van restactiviteit van het AADC enzym, in combinatie met een overmatige beschikbaarheid van substraat (d.w.z. L-dopa) in patiënten met AADC deficiëntie voldoende zou kunnen zijn om de bevinding van normale of verhoogde dopamine uitscheiding in de urine te verklaren. In hoofdstuk 4 hebben we onze hypothese getest door de residuele renale AADC activiteit en de beschikbaarheid van L-dopa substraat te berekenen bij twee patiënten met AADC deficiëntie. Hiervoor verzamelden we 24-uurs urinemonsters en voerden bloedtesten uit om L-dopa te meten. Bij beide patiënten, die beide verhoogde niveaus van dopamine in de urine hadden, werd onze hypothese geverifieerd. Deze studie toonde aan dat normale of verhoogde niveaus van dopamine in de urine eerder een verwachte dan een paradoxale bevinding zijn bij AADC deficiëntie, vanwege het kwalitatieve verschil tussen dopamine productie in het centrale zenuwstelsel en de nieren.
In hoofdstuk 5 onderzochten we het verschil tussen monoamine neurotransmitter metabolieten in het centrale zenuwstelsel (weergegeven door hun concentraties in cerebrospinale vloeistof) en perifere lichaamsvloeistoffen, en probeerden we de diagnostische waarde van bloed en urine bij AADC en TH deficiënties te verduidelijken.
12
Voorbereid document _Tessa Wassenberg_V03.indd 241Voorbereid document _Tessa Wassenberg_V03.indd 241 25/10/2021 09:3225/10/2021 09:32

242
Chapter 12
Verder bestudeerden wij serum prolactine spiegels, en neurotransmitter metabolieten in cerebrospinale vloeistof voor en tijdens de behandeling. Hiervoor voerden wij een literatuurstudie uit en een retrospectieve analyse van onze lokale universitaire ziekenhuisdatabase (1997-2020). Bij AADC deficiëntie vonden we dat 3-O-methyldopa (een metaboliet van L-dopa) in serum of dried blood spots sterk verhoogd was bij 34/34 patiënten. In urine was dopamine normaal of verhoogd bij 21/24 patiënten, 5-HIAA was verlaagd bij 9/10 patiënten, en vanillezuur was verhoogd bij 19/20 patiënten. Er werden geen significante veranderingen gezien in monoamine neurotransmitter metabolieten na medische behandeling, met uitzondering van de (verwachte) toename van HVA in urine en cerebrospinale vloeistof na L-dopa therapie. Na gentherapie nam HVA in cerebrospinaal vocht toe bij 8/12 patiënten, maar 5-HIAA bleef zeer laag bij 9/12 patiënten. Bij TH deficiëntie was het dopamine in de urine normaal bij 6/8 patiënten en verlaagd bij twee. De HVA-concentraties in cerebrospinaal vocht stegen bij behandeling met levodopa, zelfs zonder een duidelijke behandelingsrespons. Prolactine was verhoogd bij 34/37 patiënten met AADC deficiëntie, en bij 12/14 patiënten met TH deficiëntie. Wij concludeerden dat 3-O-methyldopa in serum en dried blood spots en urine vanillezuur veelbelovende biomarkers zijn in de diagnose van AADC deficiëntie, maar bespraken ook enkele valkuilen, vooral met betrekking tot de mogelijke verwarring met de primaire vitamine B6 stoornissen. Wij toonden aan dat ook bij TH deficiëntie de dopamine in de urine normaal is bij de meerderheid van de patiënten, hetgeen niet eerder duidelijk was vermeld in de literatuur. Verder blijft onderzoek van cerebrospinaal vocht van neurotransmitter metabolieten de meest informatieve lichaamsvloeistof wanneer AADC of TH deficiëntie wordt vermoed, maar routine follow-up lumbaalpuncties zijn niet nodig bij deze aandoeningen, en moeten alleen worden uitgevoerd in geval van onverwachte klinische verslechtering. Ten slotte lijkt de waarde van serumprolactine voor screening en follow-up van AADC en TH deficiëntie veelbelovend, maar moet dit verder worden onderzocht.
Deel III: het klassieke fenotype voorbij: klinische observaties
In deel III presenteerden wij een case serie over patiënten met autosomaal dominante GCH1 deficiëntie, en een case report over DBH deficiëntie.
In hoofdstuk 6 beschreven we vier patiënten uit drie families met een ongebruikelijke klinische presentatie van autosomaal dominante GCH1 deficiëntie. In plaats van (onderste ledematen) dystonie, presenteerden zij zich met spastische paraplegie. De jongste patiënt vertoonde geen duidelijke basale ganglia symptomen bij diagnose, en de andere patiënten ontwikkelden basale ganglia symptomen (dystonie en/of parkinsonisme) pas in hun vijfde decennium. Wij beschreven de klinische trajecten, en toonden video’s van het neurologisch onderzoek voor en tijdens de behandeling met L-dopa. Wij verrichtten een literatuurstudie waarin wij negen patiënten vonden met een klinisch beloop dat overeenkomt met de patiënten in onze case-serie, met
Voorbereid document _Tessa Wassenberg_V03.indd 242Voorbereid document _Tessa Wassenberg_V03.indd 242 25/10/2021 09:3225/10/2021 09:32

243
Dutch summary (Nederlandse samenvatting)
overheersende spasticiteit van de onderste ledematen bij aanvang van de ziekte, en basale ganglia verschijnselen die zich pas later in het leven ontwikkelden. Omdat autosomale GCH1 deficiëntie een behandelbare aandoening is, met een uitstekende respons op L-dopa, benadrukken wij dat deze aandoening overwogen moet worden bij patiënten die zich presenteren met spastische paraplegie, vooral als er gelijktijdige basale ganglia verschijnselen en/of diurnale fluctuaties zijn, en dat het GCH1 gen opgenomen moet worden in HSP genpanels.
In hoofdstuk 7 presenteerden wij een didactische casusbespreking over DBH deficiëntie, gestructureerd in een vraag-en-antwoord module. We beschreven een jonge vrouw bij wie uiteindelijk DBH deficiëntie werd vastgesteld op de leeftijd van 19 jaar. Haar doorverwijzingsdiagnose was nierfalen. Ze klaagde over inspanningsintolerantie en vertoonde ooglidptosis, waardoor een mitochondriale aandoening werd vermoed. Toen een ernstige orthostatische hypotensie werd vastgesteld, werd DBH deficiëntie vermoed en bevestigd. In de antwoordmodule hebben we de belangrijkste klinische tekenen en symptomen van DBH-deficiëntie beschreven en hebben we het belang benadrukt van het uitvoeren van orthostatische bloeddrukmetingen tijdens routine lichamelijk onderzoek. Het is belangrijk om op de hoogte te zijn van de uiterst zeldzame diagnose van DBHdeficiëntie, ook bij kinderen of adolescenten die zich presenteren met een verminderde nierfunctie, omdat het een behandelbare aandoening is. De patiënte in ons rapport had een uitstekende klinische respons op L-DOPS, en ook haar nierfunctie verbeterde.
Deel IV: Reviews en klinische richtlijnen
Deel IV bestaat uit twee overzichtsartikelen over monoamine neurotransmitter stoornissen.
In hoofdstuk 8 wordt de consensusrichtlijn over de diagnose en behandeling van AADC deficiëntie gepresenteerd. Deze richtlijn is ontwikkeld door de AADC richtlijngroep van de internationale werkgroep voor neurotransmitter gerelateerde aandoeningen (iNTD) met behulp van de Schotse Intercollegiate Guideline Network (SIGN) en Grading of Recommendations, Assessments, Development and Evaluation (GRADE) methodologie. De SIGN en GRADE methodologie maakt het mogelijk om sterke (of voorwaardelijke) aanbevelingen te doen, zelfs op het gebied van zeldzame aandoeningen waar het meeste bewijs bestaat uit case reports, case series en expert opinion. In de richtlijn zijn 63 aanbevelingen geformuleerd met betrekking tot klinische presentatie, diagnose, behandeling, complicaties, langetermijn management, sociale kwesties en transitie, en speciale situaties (bijv. anesthesie, intensive care management).
In hoofdstuk 9 wordt de klinische presentatie en lange termijn follow-up van patiënten met DBH deficiëntie beschreven. Het hoofdstuk bestaat uit een literatuuroverzicht,
12
Voorbereid document _Tessa Wassenberg_V03.indd 243Voorbereid document _Tessa Wassenberg_V03.indd 243 25/10/2021 09:3225/10/2021 09:32

244
Chapter 12
gecombineerd met een statusonderzoek van de relatief grote populatie van patiënten met DBH deficiëntie in Nederland. In totaal identificeerden wij 10 patiënten in Nederland, en 15 aanvullende patiënten uit de literatuur. De follow-up duur van de Nederlandse patiënten varieerde van 1 tot 21 jaar (mediaan 13 jaar). Alle patiënten hadden ernstige orthostatische hypotensie. Het pathognomonische metabolietenpatroon met sterk verlaagde of afwezige (nor)adrenaline, en (sterk) verhoogde dopamine plasmaconcentraties werd gevonden bij 24/25 patiënten. Alle Nederlandse patiënten hadden een verminderde nierfunctie en anemie, 50% had hypomagnesiëmie. De klinische respons op L-DOPS-behandeling was uitstekend en aanhoudend bij alle patiënten, maar het neurotransmitterprofiel in plasma normaliseerde niet volledig, en de nierfunctie, anemie en hypomagnesemie verbeterden slechts gedeeltelijk.
Deel V: Algemene discussie en samenvatting
In hoofdstuk 10 geven we een algemene discussie van de bevindingen in dit proefschrift, en relateren we dat aan ander onderzoek in het veld. Kennishiaten worden besproken evenals methodologische overwegingen. Ook bespreken we toekomstperspectieven voor onderzoek en klinische behandeling van monoamine neurotransmitter stoornissen.
Voorbereid document _Tessa Wassenberg_V03.indd 244Voorbereid document _Tessa Wassenberg_V03.indd 244 25/10/2021 09:3225/10/2021 09:32

245
Dutch summary (Nederlandse samenvatting)
12
Voorbereid document _Tessa Wassenberg_V03.indd 245Voorbereid document _Tessa Wassenberg_V03.indd 245 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 246Voorbereid document _Tessa Wassenberg_V03.indd 246 25/10/2021 09:3225/10/2021 09:32

APPENDICES
Acknowledgements (Dankwoord)
About the author
List of publications
Research data management
PhD Portfolio
Donders Graduate School for Cognitive Neuroscience
Voorbereid document _Tessa Wassenberg_V03.indd 247Voorbereid document _Tessa Wassenberg_V03.indd 247 25/10/2021 09:3225/10/2021 09:32

248
Appendices
Acknowledgements/ Dankwoord
In twaalf jaar tijd zijn er zoveel mensen geweest die mij geholpen, geïnspireerd of gesteund hebben bij de uitvoering van dit onderzoek! Ik ben hen allen enorm dankbaar. Een aantal wil ik graag in het bijzonder noemen.
Ten eerste wil ik graag de patiënten en hun families bedanken die hebben meegewerkt aan dit proefschrift. Wat heb ik bewondering voor jullie veerkracht. Jullie zijn de beste motivatie om de diagnostiek en behandeling van monoamine neurotransmitter stoornissen te blijven proberen te verbeteren.
Beste Michèl, vanaf het allereerste begin mijn promotor en mentor. Wat ben ik blij dat ik zoveel jaar geleden eens mocht komen praten over hoe je eigenlijk kinderneuroloog wordt. Je hebt me altijd gesteund en gestimuleerd om mijn eigen pad te volgen, en me veel vrijheid en kansen gegeven in de uitvoering van dit onderzoek. Bedankt voor alles, bedankt voor het vertrouwen!
Beste Marcel, net uit de schoolbanken in jouw lab terecht komen was een fantastische ervaring, waar ik met veel plezier aan terug denk. Enorm bedankt dat je me altijd bent blijven steunen als betrouwbare, nuchtere promotor en uitstekende wetenschapper, met een groot hart voor de mens achter de patiënt en onderzoeker.
Hartelijk dank aan de manuscriptcommissie, prof. Han Brunner, prof. Nanda Verhoeven-Duif, en prof. Tom de Koning, voor het beoordelen van mijn manuscript.
Professor Leo Monnens, beste prof, u hebt een grote rol gespeeld in het kritisch leren denken over de wisselwerking tussen hersenen en nieren, en u bent een grote stimulans geweest om het DBH stuk af te ronden. Ik bewonder uw intelligentie en vasthoudendheid, en ben blij dat u met zoveel enthousiasme mijn begeleider bent geweest!
Beste Ben, je bent tijdens de start van mijn onderzoeksperiode onmisbaar geweest. Het was vast niet altijd makkelijk om een dokter alles te leren over fosfaatbuffers en HPLC. Gelukkig bezit je een grote dosis geduld en eigenzinnigheid, en een feilloos geheugen voor verschillende catecholamine pathways en afbraakproducten. Ook de andere medewerkers van TML wil ik heel hartelijk bedanken voor hun hulp en gezelligheid tijdens de start van mijn onderzoekscarrière.
Beste Ron, je bent een autoriteit op het gebied van klinische biochemie en neurotransmitterziekten, en ik waardeer jouw enthousiasme over het onderwerp en je feedback enorm. Menig artikel is door jouw kritische commentaar op een hoger plan getild, bedankt daarvoor!
Voorbereid document _Tessa Wassenberg_V03.indd 248Voorbereid document _Tessa Wassenberg_V03.indd 248 25/10/2021 09:3225/10/2021 09:32

249
Acknowledgements/ Dankwoord
Veel coauteurs hebben meegewerkt aan de totstandkoming van de artikelen in dit proefschrift, en ik wil hen allen heel hartelijk bedanken voor hun bijdrage.
Thanks to all co-authors for their valuable contributions!
Dear members of the AADC deficiency guideline group, it was such an honor to develop the first iNTD guideline together with you, me as a young researcher working closely with all those renowned experts in the field.
Dear Thomas, you are the driving force behind iNTD and I greatly admire how you combine clinic and science, and the fantastic neurotransmitter research group you have set up in das wunderschöne Heidelberg. Thank you so much for including me in the AADC deficiency guidelines, and for the great support during the whole process of writing it.
Beste Jaap en Jacques, bedankt dat jullie je expertise over DBH deficiëntie hebben willen delen en mij als neuroloog hebben meegenomen in de wereld van bloeddrukmetingen en orthostatische hypotensie.
Beste Bart, bedankt dat je me de kans hebt gegeven om te werken aan het PREPARE project en de REEB Biobank, en me daarmee ook extra neurotransmittertijd hebt gegund. Er zijn weinig mensen die zo scherp een probleem kunnen analyseren – of het nu om een bewegingsstoornis, een manuscript, of onhandige logistiek gaat. Wat een eer dat je in mijn promotiecommissie zit!
Studenten Anna en Claudia, het is dapper om voor een afstudeerstage te kiezen binnen een extreem zeldzame groep ziektes zoals de neurotransmitterziekten, maar jullie hebben het fantastisch gedaan. Ik vond het heel leuk om jullie begeleider te mogen zijn, bedankt voor al het werk wat jullie hebben verzet!
Beste Monja, ons project om de neuropsychologische effecten van dragerschap van TH deficiëntie in kaart te brengen was heel speciaal en super leerzaam. Ik denk met veel plezier terug aan alle ritjes kriskras door Nederland, waarbij we goede gesprekken hebben kunnen voeren over het leven, de wetenschap, en het verschil in lunchgewoontes tussen Nederlanders en Duitsers. Binnenkort toch nog eens afstemmen over het vervolg?
Een groot deel van dit onderzoek is verricht tijdens mijn opleiding tot neuroloog. Ik wil alle neurologen en kinderneurologen van het Radboudumc bedanken voor de stimulerende omgeving en de uitstekende opleiding. Wat ben ik blij met zo‘n stevige basis! Die is ook te danken aan alle supervisoren die me hebben begeleid tijdens stages op andere afdelingen binnen en buiten het Radboudumc. Een speciaal woord van dank
A
Voorbereid document _Tessa Wassenberg_V03.indd 249Voorbereid document _Tessa Wassenberg_V03.indd 249 25/10/2021 09:3225/10/2021 09:32

250
Appendices
aan de opleiders (prof. Padberg, Arnoud Kappelle, Karin Klijn en Bart Post) voor de mogelijkheid en het vertrouwen om mijn opleiding zo vorm te geven dat ik het steeds heb kunnen combineren met onderzoek, en er echt mijn eigen richting aan heb kunnen geven.
AIOS neurologie van het Radboudumc, bedankt voor de gezelligheid, weekendjes, filmpjes, goede discussies en collegialiteit. Lieve Corinne, Anouke, Rianne, Bas, Lonneke, Jeroen, Mayte en Joery: sommige van ons zijn inmiddels doorgewinterd specialist maar ik hoop dat onze Jonge Klaren app nog lang actief zal blijven. Het was een eer en groot plezier om met jullie de opleiding te delen!
Mijn collega’s kinderneurologie in het UZ Brussel: Luc, Danièle, Nathalie, Viki, Helen, Ine en Berthold, wat ben ik blij om in zo’n fijn team te werken. Bedankt dat jullie altijd geïnteresseerd zijn in mijn onderzoek, en me ondersteunen met een luisterend oor, lezen van EEG’s, of overnemen van patiënten als ik weer eens tegen drie deadlines tegelijk aanzit.
Beste Inge, bedankt dat je het combineren van onderzoek en kliniek van harte ondersteunt als afdelingshoofd pediatrie. Ook dank aan prof. Vandenplas voor de steun bij mijn start in het UZ.
Lieve An, je hebt me de kans gegeven om mijn onderzoek in Nijmegen te blijven combineren met het fellowship kinderneurologie, en me enorm gesteund op alle vlakken. Ik ben blij dat ik destijds voor jou en Linda de grote stap naar Brussel heb gewaagd!
Lieve vrienden, bedankt voor jullie interesse, soms gemengd met ongeloof, voor mijn onderzoek en opleiding die maar voortduurden en voortduurden, maar vooral voor de fijne gesprekken, wandelingen, feestjes en weekendjes weg die me altijd weer duidelijk maken wat echt belangrijk is.
Lieve Lianne, we zijn onze onderzoekscarrière samen begonnen met het profielwerkstuk in 6VWO, en jij hebt België alvast voor me verkend tijdens je studie. Wat ben ik blij met jouw vriendschap, die gelukkig meer over het leven gaat dan over het werk. Ik ben blij dat je vandaag naast me staat!
Lieve Anouke, jouw scherpe geest gecombineerd met sterke sociale antennes maken je tot een geweldige neuroloog en fijne vriendin. We begonnen onze opleiding samen, wat fijn dat je vandaag naast me staat!
Voorbereid document _Tessa Wassenberg_V03.indd 250Voorbereid document _Tessa Wassenberg_V03.indd 250 25/10/2021 09:3225/10/2021 09:32

251
Acknowledgements/ Dankwoord
Lieve schoonfamilie, door mijn onderzoek en werk heb ik helaas wel eens een verjaardag of samenkomst moeten missen… Hopelijk in het vervolg wat minder vaak want ik vind het altijd fijn om elkaar te zien. Jan en Maria, bedankt dat jullie Izaak elke woensdag zo’n heerlijke dag laten beleven!
Lieve zussen, met Rens deel ik de verhalen over het ziekenhuis, met Co de liefde voor ingewikkelde recepten, en met jullie beiden de stevige basis van het Goor. Bedankt voor jullie steun en relativeringsvermogen. Wat is het fijn om elkaar te zien, zeker als Peter, Marc, Siebren, Nienke, Hasse, Senne en Valke er ook bij zijn.
Lieve papa en mama, bedankt voor alles. Van de vele elementen die mij gemaakt hebben tot wie ik nu ben zijn jullie het fundament.
Zonder Otto waren vele uurtjes achter de laptop een stuk kouder en minder gezellig geweest.
Lieve Erik, jij bent mijn thuis. Bedankt dat je er voor me bent!
Lieve Izaak, wat ben ik blij met jou! Je maakt het leven zoveel mooier.
A
Voorbereid document _Tessa Wassenberg_V03.indd 251Voorbereid document _Tessa Wassenberg_V03.indd 251 25/10/2021 09:3225/10/2021 09:32

252
About the Author
About the author
Tessa Wassenberg was born on January 2nd, 1985, in Veghel, Noord-Brabant. She grew up in Boekel and graduated secondary school at Udens College in 2003 (cum laude). She started medical school in 2003 at Maastricht University where she passed her doctoral exam in 2008 (cum laude). During her studies in Maastricht, she combined the regular curriculum with the research track (OTG) from 2005-2008 at the Department of Basal Neuroscience, studying the neuropathology of schizophrenia. For this, she spent an internship abroad in 2006 at Mount Sinai Medical School, New York. She spent her final year of medical school (2008/2009) at Máxima Medisch Centrum Veldhoven at the Department of Pediatrics. Her master thesis was on the brain development of extremely premature infants using amplitude integrated EEG, supervised by dr. Peter Andriessen.
After finishing medical school in 2009, she started as a junior researcher on AADC deficiency at the Radboudumc Nijmegen, under the supervision of prof. dr. Michèl Willemsen en dr. ir. Marcel Verbeek. Here, the foundation of this doctoral thesis was laid. From July 2010, she worked as a junior medical doctor at Medisch Centrum Alkmaar at the Department of Neurology and Neurosurgery. She started her residency in Neurology at the Radboudumc Nijmegen in January 2012 (supervisors prof. dr. George Padberg, dr. Arnoud van Kappelle, dr. Bart Post, prof. dr. Karin Klijn). In 2018, she finished her neurology residency and started a fellowship in child neurology and metabolic disorders at UZ Brussel (supervisors prof. dr. Linda De Meirleir, prof. dr. Anna Jansen, dr. Luc Régal). As of April 2020, she works as a child neurologist at UZ Brussel KidZ Health Castle, with a special interest in neurometabolic disorders and movement disorders.
Tessa lives together with Erik Verbruggen and their son Izaak (2020) in Mortsel, Belgium.
Voorbereid document _Tessa Wassenberg_V03.indd 252Voorbereid document _Tessa Wassenberg_V03.indd 252 25/10/2021 09:3225/10/2021 09:32

253
List of publications
List of publications
This Thesis1. Wassenberg T, Geurtz BPH, Monnens L, Wevers RA, Willemsen MA, Verbeek MM. Blood, urine and cerebrospinal fluid analysis in TH and AADC deficiency and the effect of treatment. Molecular Genetics and Metabolism Reports. 2021; 27: 100762.
2. Wassenberg T, Deinum J, van Ittersum FJ, Kamsteeg EJ, Pennings M, Verbeek MM, Wevers RA, van Albada ME, Kema IP, Versmissen J, van den Meiracker T, Lenders JWM, Monnens L, Willemsen MA. Clinical presentation and long-term follow-up of Dopamine Beta Hydroxylase deficiency. Journal of Inherited Metabolic Disease. 2021; 44(3): 554-565.
3. Wassenberg T, Schouten MI, Helmich RC, Willemsen MA, Kamsteeg EJ, van de Warrenburg BPC. Autosomal dominant GCH1 mutations causing spastic paraplegia at disease onset. Parkinsonism & related disorders. 2020;74:12-5.
4. Wassenberg T, Willemsen MA, Dijkman H, Deinum J, Monnens L. Congenital eyelid ptosis, decreased glomerular filtration, and orthostatic hypotension: Questions. Pediatric Nephrology 2017;32(7):1169-70. AND Wassenberg T, Willemsen M, Dijkman H, Deinum J, Monnens L. Congenital eyelid ptosis, decreased glomerular filtration, and orthostatic hypotension: Answers. Pediatric Nephrology. 2017;32(7):1171-4.
5. Wassenberg T, Molero-Luis M, Jeltsch K, Hoffmann GF, Assmann B, Blau N, Garcia-Cazorla A, Artuch R, Pons R, Pearson TS, Leuzzi V, Mastrangelo M, Pearl PL, Lee WT, Kurian MA, Heales S, Flint L, Verbeek MM, Willemsen MA. Consensus guideline for the diagnosis and treatment of aromatic l-amino acid decarboxylase (AADC) deficiency. Orphanet Journal of Rare Diseases. 2017;12(1):12.
6. Wassenberg T, Monnens LA, Geurtz BP, Wevers RA, Verbeek MM, Willemsen MA. The paradox of hyperdopaminuria in aromatic L-amino Acid deficiency explained. JIMD Reports. 2012;4:39-45.
7. Wassenberg T, Willemsen MA, Geurtz PB, Lammens M, Verrijp K, Wilmer M, Lee WT, Wevers RA, Verbeek MM. Urinary dopamine in aromatic L-amino acid decarboxylase deficiency: the unsolved paradox. Molecular Genetics and Metabolism. 2010;101(4):349-56.
A
Voorbereid document _Tessa Wassenberg_V03.indd 253Voorbereid document _Tessa Wassenberg_V03.indd 253 25/10/2021 09:3225/10/2021 09:32

254
Appendices
Other publications8. Kuseyri Hübschmann O, Horvath G, Cortès-Saladelafont E, Yildiz Y, Mastrangelo M, Pons R, Friedman J, Mercimek-Andrews S, Wong SN, Pearson TS, Zafeiriou DI, Kulhánek J, Kurian MA, López-Laso E, Oppebøen M, Kilavuz S, Wassenberg T, Goez H, Scholl-Bürgi S, Porta F, Honzík T, Santer R, Burlina A, Serap Sivri H, Leuzzi V, Hoffmann GF, Jeltsch K, Hübschmann D, Garbade SF, iNTD Registry Study Group; García-Cazorla A, Opladen T. Insights into the expanding phenotypic spectrum of inherited disorders of biogenic amines. Nature Communications. 2021; 12(1): 5529.
9. Meester K, Wassenberg T, Vanbesien J. Hypocalcemia as a cause of complex febrile seizures in a toddler. Case Reports in Pediatrics. 2021; 1798741.
10. Tristán-Noguero A, Borràs E, Molero-Luis M, Wassenberg T, Peters T, Verbeek MM, Willemsen MA, Opladen T, Jeltsch K, Pons R, Thony B, Horvath G, Yapici Z, Friedman J, Hyland K, Agosta GE, López-Laso E, Artuch R, Eduard Sabidó, Àngels García-Cazorla. Novel protein biomarkers of monoamine metabolism defects correlate with disease severity. Movement Disorders. 2021; 36: 690-703.
11. Opladen T, López-Laso E, Cortès-Saladelafont E, Pearson TS, Sivri HS, Yildiz Y, Assmann B, Kurian MA, Leuzzi V, Heales S, Pope S, Porta F, García-Cazorla A, Honzík T, Pons R, Regal L, Goez H, Artuch R, Hoffmann GF, Horvath G, Thöny B, Scholl-Bürgi S, Burlina A, Verbeek MM, Mastrangelo M, Friedman J, Wassenberg T, Jeltsch K, Kulhánek J, Kuseyri Hübschmann O; International Working Group on Neurotransmitter related disorders (iNTD). Consensus guideline for the diagnosis and treatment of tetrahydrobiopterin (BH4) deficiencies. Orphanet Journal of Rare Diseases. 2020;15(1):126.
12. Shetty A, Gan-Or Z, Ashtiani S, Ruskey JA, van de Warrenburg B, Wassenberg T, Kamsteeg EJ, Rouleau GA, Suchowersky O. CAPN1 mutations: Expanding the CAPN1-related phenotype: From hereditary spastic paraparesis to spastic ataxia. European Journal of Medical Genetics. 2019; 62(12): 103605.
13. Maas R, Wassenberg T, Lin JP, van de Warrenburg BPC, Willemsen M. L-Dopa in dystonia: A modern perspective. Neurology. 2017;88(19):1865-71.
14. Timmers ER, Kuiper A, Smit M, Bartels AL, Kamphuis DJ, Wolf NI, Poll-The BT, Wassenberg T, Peeters EAJ, de Koning TJ, Tijssen MAJ. Non-motor symptoms and quality of life in dopa-responsive dystonia patients. Parkinsonism & Related Disorders. 2017;45:57-62.
15. Opladen T, Cortès-Saladelafont E, Mastrangelo M, Horvath G, Pons R, Lopez-Laso E, Fernández-Ramos JA, Honzik T, Pearson T, Friedman J, Scholl-Burgi S, Wassenberg T, Jung-Klaaitter S, Kuseyri O, Jeltsch K, Kurina MA, Garcia-Cazorla A; International Working
Voorbereid document _Tessa Wassenberg_V03.indd 254Voorbereid document _Tessa Wassenberg_V03.indd 254 25/10/2021 09:3225/10/2021 09:32

255
List of publications
Group on Neurotransmitter related disorders (iNTD). The International Working Group on Neurotransmitter related Disorders (iNTD): A worldwide research project focused on primary and secondary neurotransmitter disorders. Molecular Genetics and Metabolism Reports. 2016;9:61-6.
16. Niemarkt HJ, Jennekens W, Maartens IA, Wassenberg T, van Aken M, Katgert T, Kramer BW, Gavilanes AW, Zimmermann LJ, Bambang Oetomo S, Andreissen P. Multi-channel amplitude-integrated EEG characteristics in preterm infants with a normal neurodevelopment at two years of corrected age. Early human development. 2012;88(4):209-16.
17. Maartens IA, Wassenberg T, Buijs J, Bok L, de Kleine MJ, Katgert T, Andriessen P. Neurodevelopmental outcome in full-term newborns with refractory neonatal seizures. Acta Paediatrica. 2012;101(4):e173-8.
18. Brun L, Ngu LH, Keng WT, Ch’ng GS, Choy YS, Hwu WL, Lee WT, Willemsen MA, Verbeek MM, Wassenberg T, Régal L, Orcesi S, Tonduti D, Accorsi P, Testard H, Abdenur JE, Tay S, Allen GF, Heales S, Kern I, Kato M, Burlina A, Manegold C, Hoffmann GF, Blau N. Clinical and biochemical features of aromatic L-amino acid decarboxylase deficiency. Neurology. 2010;75(1):64-71.
19. Maartens IA, Wassenberg T, Halbertsma FJ, Marres HA, Andriessen P. Neonatal airway obstruction caused by rapidly growing nasopharyngeal teratoma. Acta Paediatrica. 2009;98(11):1852-4.
20. Vermaning S, Jansen A, Vanderhasselt T, Régal L, Wassenberg T. Transient headache and neurological deficits with lymphocytosis (HaNDL-syndrome) with an acute confusional state and papilledema in a 10-years old girl: a case report. Belgian Journal of Paediatrics 2021; 23: 72-75
21. Wassenberg T, Maartens IA, Wagener-Schimmel LJJC, Willemsen MA, Halbertsma FJJ. Acute hoofdpijn bij een meisje van 9 jaar veroorzaakt door een spontaan chronisch subduraal hematoom. Tijdschrift voor Kindergeneeskunde 2010; 4.
Book ChaptersDopamine Beta Hydroxylase. Wassenberg T, Verbeek MM. In: Inherited Disorders of Biogenic Amines: a Practical Guide. Blau N and Hoffmann GF (editors). Uni-Med. 2020
A
Voorbereid document _Tessa Wassenberg_V03.indd 255Voorbereid document _Tessa Wassenberg_V03.indd 255 25/10/2021 09:3225/10/2021 09:32

256
Research data management
Research data management
The data presented in this thesis and collected during this PhD project at the department of Neurology and Laboratory Medicine TML was archived according to Findable, Accessible, Interoperable and Reusable (FAIR) principles.
Ethical considerationsThe studies described in chapter 3,4 and 5 were conducted in accordance with the International Declaration of Helsinki. All procedures performed in studies involving human participants were in accordance with local regulations. Use of human tissue in chapter 3 was according to the code for proper secondary use of human tissue in the Netherlands. Informed consent was obtained from patients and/or parents where applicable (chapter 4,6, 7 and 9). The retrospective use of data from the TML database in chapter 5 was approved by the local research ethical committee of the Radboud university medical center (registration number 2016-3011). Clinical exome sequencing as described in chapter 6 was approved by the Medical Review Ethics Committee Arnhem-Nijmegen (2011/188). The work in chapter 9 was approved by the local research ethics committee of the Radboud university medical center (2019-5281). The research in chapter 3 was funded by the AADC Research Trust and Hersenstichting Nederland/ Benny Vleerlaag fonds.
Findable, accessibleRaw and processed data are stored digitally at a server of the Radboudumc, and are accessible to authorized researchers of child neurology and laboratory medicine. Daily back-ups are made of this server, which is supported by the Radboudumc ICT department. All experiments described in this thesis are logged at a paper labjournal stored at the department of laboratory medicine (TML). Datasets are available from the corresponding author upon reasonable request. Chapter 4,5,7,8 and 9 are published as open access articles.
Interoperable, ReusableThe data are documented in English or Dutch, and are adequately documented to be reusable for further research and analysis.
Voorbereid document _Tessa Wassenberg_V03.indd 256Voorbereid document _Tessa Wassenberg_V03.indd 256 25/10/2021 09:3225/10/2021 09:32

257
PhD Portfolio
PhD Portfolio
International conferences2019 European Federation of Autonomic Societies (EFAS) International Congress, Leiden, The Netherlands Poster presentation: ‘Dopamine Beta Hydroxylase deficiency: clinical presentation and long-term follow-up of a treatable neurogenic orthostatic hypotension syndrome’ 2018 Society for the Study of Inborn Errors of Metabolism (SSIEM), Annual symposium, Athens, Greece Poster presentation: ‘Autosomal dominant GCH-1 mutations causing spastic paraplegia at disease onset’ 2018 EPNS Research meeting 2018, Alicante, Spain Oral presentation: ‘Catecholamine and serotonin biosynthesis defects, from biochemical aspects and important observations to evidence based guidelines’ 2017 International symposium on Paediatric Movement Disorders, Barcelona, Spain Oral presentation: ‘Evidence based guideline for AADC deficiency- the First iNTD guideline’ 2016 International Child Neurology Congress (ICNC), Amsterdam, the Netherlands Poster presentation: ‘Non-motor symptoms in tyrosine hydroxylase deficiency’ 2016 AADC Research Trust meeting, Londen, United Kingdom Oral presentation: ‘Developing the guideline for the diagnosis and treatment of AADC deficiency’
National conferences2021 Romanian Child Neurology Society: annual meeting (online) Oral presentation: ‘AADC-deficiency, an overview’2020 Fifth Brussels Paediatric Day , Meise, Belgium Oral presentation: ‘What a pediatrician needs to know about monoamine neurotransmitter disorders’ 2019 Fourth Brussels Pediatric Day, Meise, Belgium Oral presentation: ‘Rare bewegingen, functioneel of neurologisch?’| 2019 Belgian Society of Pediatric Neurology, Spring Meeting, Brussels, Belgium Oral presentation: ‘Dopamine Beta Hydroxylase deficiency: clinical presentation of a treatable orthostatic hypotension syndrome 2018 Valediction prof. Linda De Meirleir, Brussels, Belgium Oral presentation: ‘Neurotransmitter defects: update and treatment’
A
Voorbereid document _Tessa Wassenberg_V03.indd 257Voorbereid document _Tessa Wassenberg_V03.indd 257 25/10/2021 09:3225/10/2021 09:32

258
Appendices
2016 Nederlandse Vereniging voor Kinderneurologie (NVKN): spring meeting, Oral presentation: ‘Erfelijke neurotransmitterstoornissen – een overzicht’ 2014 Nederlandse Vereniging voor Kinderneurologie (NVKN): spring meeting, Alkmaar Oral presentation: DOBH-deficientie: een aangeboren tekort aan noradrenaline en adrenaline
Webinars speaker2021 EPNS/ young EPNS Journal club: ‘2021 European guideline on the management of narcolepsy in adults and children’ 2021 AADC deficiency, seventh PTC-therapeutics webinar: ‘The key role of a multidisciplinary team approach in clinical practice’ 2020 AADC deficiency, first PTC-therapeutics webinar: ‘The road to diagnosis’
Courses2018 International Course Movement Disorders in Children and Adolescents, UMC Groningen 2016 Academic writing course, Radboudumc Nijmegen 2016 Basic course rules and organization clinical researchers (BROK) 2015 Recordati Neurotransmitter Focus Course, Venice, Italy
Voorbereid document _Tessa Wassenberg_V03.indd 258Voorbereid document _Tessa Wassenberg_V03.indd 258 25/10/2021 09:3225/10/2021 09:32

259
PhD Portfolio
Teaching2017 Supervision of master thesis C.S. Wouters, Radboudumc Nijmegen Neurotransmitter excretion patterns in inborn errors of monoamine neurotransmitter synthesis 2016 Supervision of master thesis A. de Kort, Radboudumc Nijmegen Promising first steps into developing a tyrosine hydroxylase activity assay in cerebral spinal fluid 2014-2017 Teaching fifth year medical students acute neurology and neurological examination, Radboudumc Nijmegen
Other2020 – present Member of the Young EPNS (European Paediatric Neurology Society) committee active in the education and career working group 2020 – present Secretary of the VNZZ-RND (Vlaams Netwerk Zeldzame Ziekten Rare Neurological disorders) 2018-2019 Member of the iNTD BH4 Guideline working group – subgroup Sepiapterin Reductase Deficiency 2017 Preparation of the application for the ‘REEB Biobank’ (Radboud Expertisecentrum voor Erfelijke Bewegingsstoornissen) 2016-2018 Clinical research assistant for PREPARE (Preparing for therapies in Autosomal Recessive ataxias) at Radboudumc Nijmegen 2012 – present Review activities for various journals (Molecular Genetics and Metabolism, Journal of Inherited Metabolic Disease, Belgian Journal of Neurology, Current Medical Research and Opinion)
A
Voorbereid document _Tessa Wassenberg_V03.indd 259Voorbereid document _Tessa Wassenberg_V03.indd 259 25/10/2021 09:3225/10/2021 09:32

260
Donders Graduate School for Cognitive Neuroscience
Donders Graduate School for Cognitive Neuroscience
For a successful research Institute, it is vital to train the next generation of young scientists. To achieve this goal, the Donders Institute for Brain, Cognition and Behaviour established the Donders Graduate School for Cognitive Neuroscience (DGCN), which was officially recognised as a national graduate school in 2009. The Graduate School covers training at both Master’s and PhD level and provides an excellent educational context fully aligned with the research programme of the Donders Institute.
The school successfully attracts highly talented national and international students in biology, physics, psycholinguistics, psychology, behavioral science, medicine and related disciplines. Selective admission and assessment centers guarantee the enrolment of the best and most motivated students.
The DGCN tracks the career of PhD graduates carefully. More than 50% of PhD alumni show a continuation in academia with postdoc positions at top institutes worldwide, e.g. Stanford University, University of Oxford, University of Cambridge, UCL London, MPI Leipzig, Hanyang University in South Korea, NTNU Norway, University of Illinois, North Western University, Northeastern University in Boston, ETH Zürich, University of Vienna etc.. Positions outside academia spread among the following sectors: specialists in a medical environment, mainly in genetics, geriatrics, psychiatry and neurology. Specialists in a psychological environment, e.g. as specialist in neuropsychology, psychological diagnostics or therapy. Positions in higher education as coordinators or lecturers. A smaller percentage enters business as research consultants, analysts or head of research and development. Fewer graduates stay in a research environment as lab coordinators, technical support or policy advisors. Upcoming possibilities are positions in the IT sector and management position in pharmaceutical industry. In general, the PhDs graduates almost invariably continue with high-quality positions that play an important role in our knowledge economy.
For more information on the DGCN as well as past and upcoming defenses please visit: http://www.ru.nl/donders/graduate-school/phd/
Voorbereid document _Tessa Wassenberg_V03.indd 260Voorbereid document _Tessa Wassenberg_V03.indd 260 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 261Voorbereid document _Tessa Wassenberg_V03.indd 261 25/10/2021 09:3225/10/2021 09:32

Voorbereid document _Tessa Wassenberg_V03.indd 262Voorbereid document _Tessa Wassenberg_V03.indd 262 25/10/2021 09:3225/10/2021 09:32

Uitnodigingvoor het bijwonen van deopenbare verdediging vanmijn proefschrift getiteld
Monoamineneurotransmitter
disorders
from biochemical aspectsand clinical observations to
recommendations formanagement
Op 22 december 2021om 14:30 precies
in Academiezaal Aulavan de Radboud UniversiteitComeniuslaan 2, te Nijmegen
Livestream: https://tinyurl.com/PhD-Tessa
U bent van harte welkombij deze plechtigheid
en de aansluitende receptie
Tessa [email protected]
ParanimfenAnouke van Rumund
Lianne van de [email protected]
Tessa_Wassenberg-Omslag-order154547_Dondersversie-rfp-v2.indd 7-11Tessa_Wassenberg-Omslag-order154547_Dondersversie-rfp-v2.indd 7-11 10/13/2021 1:06:00 PM10/13/2021 1:06:00 PM

Monoamineneurotransmitter
disorders
from biochemical aspectsand clinical observations to
recommendations for management
Tessa Wassenberg
Uitn
od
igin
g
529Tessa W
assenbergM
ON
OA
MIN
EN
EU
RO
TR
AN
SM
ITT
ER
DIS
OR
DE
RS
Tessa_Wassenberg-Omslag-order154547_Dondersversie-rfp-v2.indd 2-6Tessa_Wassenberg-Omslag-order154547_Dondersversie-rfp-v2.indd 2-6 10/13/2021 1:06:00 PM10/13/2021 1:06:00 PM
Copyright © 2022 FDOKUMEN




















