
Semi-Quantitative Evaluation of Access and Coverage (SQUEAC) of Kalgo LGA’s CMAM programme. Kebbi...
52
i Semi-Quantitative Evaluation of Access and Coverage (SQUEAC) of Kalgo LGA’ s CMAM programme. Kebbi State, Northern Nigeria April - May 2014 Adamu Abubakar Yerima, Ayobami Oyedeji, Salisu Sharif Jikamshi and Ode Okponya Ode Save the Children International
Transcript of Semi-Quantitative Evaluation of Access and Coverage (SQUEAC) of Kalgo LGA’s CMAM programme. Kebbi...

i
Semi-Quantitative Evaluation of Access and Coverage (SQUEAC) of Kalgo LGA’s CMAM programme. Kebbi State, Northern Nigeria
April - May 2014
Adamu Abubakar Yerima, Ayobami Oyedeji, Salisu Sharif Jikamshi and Ode Okponya Ode
Save the Children International

ii
Acknowledgement
This SQUEAC assessment in Kalgo LGA was accomplished through the generous support of Children Investment Fund Foundation (CIFF). Special thanks goes to the Federal Ministry of Health (FMOH), Kebbi State Ministry of
Health (SMOH), Kalgo Local Government Area (LGA) and Kalgo LGA Health Facilities’ Staff. Of prominent note are
Director Public Health & State Nutrition Officer of Kebbi State (SMOH), the Chairman and Director PHC of Kalgo LGA for their collaboration in the implementation of the SQUEAC1 assessment in the state.
Our profound gratitude goes to the care givers and various community leaders for sparing their precious time and opening their doors to the SQUEAC team without which this investigation would not have been a reality. Finally and most importantly, we wish to appreciate the technical inputs of Lindsey Pexton (Senior Nutrition Adviser, Save the Children International), Joseph Njau of ACF International and Coverage Monitoring Network (CMN) in analyzing the data and compilation of this report.
1 Semi Quantitative Evaluation of Access and Coverage

iii
Table of contents
Acknowledgement ................................................................................................................................................ ii
Table of contents ................................................................................................................................................. iii
Abbreviations ........................................................................................................................................................ v
Executive summary .............................................................................................................................................. vi
1. Introduction .................................................................................................................................................. 1
2. Objectives ..................................................................................................................................................... 2
3. Methodology ................................................................................................................................................ 2
3.1. Stages of SQUEAC of Kalgo LGA CMAM program....................................................................................... 3
4. Results and Findings ..................................................................................................................................... 6
4.1. Stage 1 : Identification of barriers and boosters and of potential areas of high or low coverage .......... 6
4.1.1. Routine monitoring data and individual OTP cards ........................................................................ 7
4.1.1.1. Admission data........................................................................................................................... 7
4.1.1.2. Exit Data (Discharge Outcomes) ............................................................................................... 11
4.1.2. Qualitative data ........................................................................................................................... 16
4.1.3. Boosters and Barriers ................................................................................................................... 18
4.1.4. Concept Map ................................................................................................................................ 20
4.2. Stage 2: Confirmation areas of high and low coverage ........................................................................ 20
4.2.1. Small area survey ......................................................................................................................... 20
4.2.2. Barriers of the small area survey .................................................................................................. 21
4.2.3. Defaulter Study ............................................................................................................................ 22
4.3. Stage 3: The coverage estimate (application of Bayesian Theory) ....................................................... 23
4.3.1. Development of Prior ................................................................................................................... 23
4.3.2. Likelihood .................................................................................................................................... 28
4.3.3. Posterior ...................................................................................................................................... 31
5. Discussion ................................................................................................................................................... 31
6. Conclusion .................................................................................................................................................. 32
7. Recommendations ...................................................................................................................................... 33
8. Annexure .................................................................................................................................................... 35
Annex I: List of Participants ................................................................................................................................. 35
Annex II: Local Terms to describe Malnutrition................................................................................................... 36
Annex III: Concept Maps ..................................................................................................................................... 37
Annex IV: Itinerary of Survey .............................................................................................................................. 39
Annex V: Seasonal Calendar ................................................................................................................................ 40
Annex VI: Questionnaires ................................................................................................................................... 41

iv
List of figures
FIGURE 1: MAP OF KALGO LGA SHOWING THE WARDS WITH OTP SITE AND THOSE WITHOUT THE OTP ...................................................... 1 FIGURE 2: STAGES OF SQUEAC ........................................................................................................................................ 3 FIGURE 3: PROCESS OF COLLATION ENTRY AND ANALYSIS OF THE ROUTINE AND OTHER PROGRAM DATA ....................................................... 3 FIGURE 4: SHOWS THE NUMBER OF ADMISSION FOR EACH HF FOR THE 15 MONTHS PERIOD. ................................................................... 7 FIGURE 5: PROPORTION OF CASES ADMITTED BY LGA ................................................................................................................ 8 FIGURE 6: THE DIAGRAM DEPICTS THE ADMISSION TREND FOR TOTAL ADMISSION WITH RAW DATA = CASES AND M3A3 -SMOOTHED TO REFLECT
SEASONALITY AND TREND ........................................................................................................................................ 8 FIGURE 7: ADMISSION TREND AND SEASONAL CALENDAR ............................................................................................................ 9 FIGURE 8: ADMISSION TREND FOR EACH HF COMPARED WITH THE TOTAL ADMISSION TREND. .................................................................. 9 FIGURE 9: THE FIGURE ABOVE PLOTS ADMISSION MUACS SHOWING THE MEDIAN ADMISSION MUAC ..................................................... 10 FIGURE 10: A HISTOGRAM REPRESENTATION OF THE LOS WITH MEDIAN LOS SHOWN BY ARROW IN BLACK ................................................ 10 FIGURE 11: A BAR CHART REPRESENTATION OF EXIT MUAC ................................................................................................... 11 FIGURE 12: PIE CHART REPRESENTATION OF EXIT PROPORTIONS FOR THE PERIOD JAN 2013 TO MAR 2014 ............................................... 11 FIGURE 13: TREND OF PERFORMANCE INDICATORS ................................................................................................................. 12 FIGURE 14: BAR CHART REPRESENTATION OF RECOVERY RATE BY HF............................................................................................. 13 FIGURE 15: A BAR CHART REPRESENTATION OF NON-RECOVERED RATE DISAGGREGATED BY HF .............................................................. 13 FIGURE 16: A PIE-CHART REPRESENTATION OF THE PROPORTION REFLECTING PERFORMANCE INDICATORS (WITH DISAGGREGATED TO NORMAL
DEFAULTER AND ‘HIDDEN DEFAULTER’ RATES. ............................................................................................................... 14 FIGURE 17: A GRAPHIC REPRESENTATION OF DEFAULT RATE BY HF ............................................................................................... 14 FIGURE 18: PROPORTION OF NUMBER OF VISITS AT DEFAULT FOR DEFAULTED CASES FOR THE PERIOD JANUARY 2014 TO MARCH, 2014 ............. 15 FIGURE 20: A BAR CHART PRESENTATION OF MUAC AT DEFAULT ................................................................................................ 15 FIGURE 21: SHOWS DISTRIBUTION OF DEFAULTERS BY LGA ....................................................................................................... 16 FIGURE 22: PLOT OF OBSERVED TIME TO TRAVEL PLOT FROM THE CMAM SITE ................................................................................ 16 FIGURE 23: BARRIERS TO ACCESS FOUND IN SMALL AREA SURVEY................................................................................................. 22 FIGURE 24: A GRAPHIC REPRESENTATIONS OF THE REASONS FOR DEFAULTING PUT FORWARD BY THE DEFAULTED CASES DURING DEFAULTER STUDY .. 23 FIGURE 25: GRAPHICAL REPRESENTATION OF BELIEF HISTOGRAM ................................................................................................. 24 FIGURE 26: A GRAPHICAL REPRESENTATION OF THE TRIANGULATION OF THE PRIOR MODE .................................................................... 27 FIGURE 27: THE PLOT OF THE PRIOR MODE IN BAYES SQUEAC CALCULATOR SHOWING SUGGESTED SAMPLE SIZE CIRCLED IN RED ...................... 28 FIGURE 28: BARRIERS TO PROGRAM ACCESS AND UPTAKE DURING WAS ........................................................................................ 30 FIGURE 29: FINAL RESULT OF THE COVERAGE-BINOMIAL CONJUGATE ANALYSIS ................................................................................ 31 FIGURE 30 CONCEPT MAP 1 .......................................................................................................................................... 37 FIGURE 31 CONCEPT MAP 2 .......................................................................................................................................... 37 FIGURE 32 CONCEPT MAP 3 .......................................................................................................................................... 38
List of tables
TABLE 1: SHOWS THE DISTRIBUTION OF HEALTH FACILITIES BY WARD AND THE PROPORTION OF HF HAVING OTP SERVICES ................................ 2 TABLE 2 BARRIERS AND BOOSTERS FOUND DURING THE QUALITATIVE DATA COLLECTION WITH THE SOURCE AND METHODS. .............................. 19 TABLE 3 RESULT OF SMALL AREA SURVEY ........................................................................................................................... 21 TABLE 4 BARRIERS TO ACCESS FOUND DURING SMALL AREA SURVEY .............................................................................................. 22 TABLE 5: TABULAR REPRESENTATION OF WEIGHED BARRIERS AND BOOSTERS OBTAINED IN STAGE 1 BY THE 3 GROUPS .................................... 25 TABLE 6: TABULAR REPRESENTATION OF UN-WEIGHTED BARRIERS AND BOOSTERS ............................................................................. 26 TABLE 7: GROUP REPRESENTATION OF POTENTIAL COVERAGE USING CONCEPT MAP ............................................................................ 26 TABLE 8: THE TABLE SHOWING THE RESULTS OF THE WIDE IS SURVEY ............................................................................................. 29 TABLE 9: RESULTS OF THE WIDE AREA SURVEY-KALGO LGA ....................................................................................................... 29 TABLE 10 BARRIERS TO ACCESS AND UPTAKE FOUND AT WAS .................................................................................................... 30
v
Abbreviations
CIFF Children Investment Fund Foundation
CMAM Community-based Management of Acute Malnutrition
CMN Coverage Monitoring Network
CV Community Volunteers
FMOH Federal Ministry of Health
HF Health Facility
HW Health Worker
LGA Local Government Area
MUAC Mid-Upper Arm Circumference
NBS National Bureau of Statistics
NGO Non-Governmental Organization
NFP Nutrition Focal Person
OTP Outpatient Therapeutic Programme
RC Recovering Case
RUTF Ready to Use Therapeutic Food
SAM Severe Acute Malnutrition
SC Stabilization Centre
SCI Save the Children International
SLEAC Simplified Lot Quality Assurance Sampling Evaluation of Access and Coverage
SMART Standardized Monitoring Assessment of Relief and Transitions
SMOH State Ministry of Health
SNO State Nutrition Officer
SPHCDA State Primary Health care Development Agency
SQUEAC Semi-Quantitative Evaluation of Access and Coverage
UNICEF United Nations Children's Fund
VI Valid International

vi
Executive summary
Kalgo Local Government Area (LGA) is one of the Local Government Areas supported by UNICEF in the implementation of the Community Management of Acute Malnutrition program (CMAM) program since 2009.The result of the Simplified Lot Quality Assurance Sampling Evaluation of Access and Coverage (SLEAC) survey in Kalgo (LGA) revealed a low classification of coverage2 for the CMAM program. The SQUEAC investigation was carried out as a follow-up to the SLEAC assessment conducted between October – November, 2013 3 by Valid International (VI) in collaboration with National Bureau of Statistics (NBS) and the Federal Ministry of Health (FMOH). The coverage assessments are funded by Children Investment Fund Foundation (CIFF).
In order to investigate the CMAM program in the LGA, quantitative data were extracted from the individual beneficiary/OTP cards from the 5 health facilities (HFs) with CMAM services or Outpatient Therapeutic Program (OTP) sites4 while the qualitative information were collected from the communities which form the catchment population of these HFs. The information obtained from this investigation was continuously analyzed to yield the barriers and boosters5 that affect the CMAM coverage. Qualitative information was collected from various sources6 using various methods7. The information gathered was triangulated for consistency and were used as evidence of the findings in this SQUEAC assessment.
The CMAM program performance indicators revealed that the recovery and the defaulter rates did not meet the minimum SPHERE standards8 particularly in year 2013. The trend of the recovery rate was consistently below 75% while, defaulter rate was above 15% in year 2013 except death rate which was within the SPHERE minimum standard (see figure 13 in main report). However, the 2014 data (January – March) shows recovery rate that meets the SPHERE standards and a reducing defaulter rate (below 20% in March). The upward trend of the recovery rate may be attributed to improvement in quality of service delivery when the health workers (HWs) were trained in September 2013 and also, to increased supervision by UNICEF and SMOH beginning the same period. The analysis of the routine program data reveals that the proportion of the recovered cases was 64% while that of defaulting cases was 31% which when compared SPHERE standards are low and high respectively. It is important to note that only 22% of the defaulters had been identified as defaulter exits in the beneficiary/OTP cards with the remaining 9% being “Hidden Defaulters” that had not been identified as normal defaulter exits and had been kept in the program for treatment despite them being eligible defaulter exits.
The analysis of the Mid-Upper Arm Circumference (MUAC) measurement at admission9 yielded a median MUAC at admission of 102mm which is indicative of late treatment seeking behavior. Further still, the histogram representation of the data reveals a long right tail indicative of late admissions (admission when the condition is critical).
The SQUEAC investigation identified the following factors affecting coverage; Boosters: self-referrals and peer-to-peer referral; referral by Community Volunteers(CVs) /Traditional Birth Attendances (TBA) & passive referral by HWs, good beneficiary-to-HW relationship, good awareness of the program, HWs from non-CMAM HFs site were trained on CMAM and are involved in delivering CMAM services in CMAM HFs, financial support to CVs to carry out their activities, Ready to Use Therapeutic Food (RUTF) is well accepted and there is a formed good opinion about the program. Barriers: lack of awareness about malnutrition, far distance to CMAM HFs, poor health
2 Less than 20% 3 Chrissy B., Bina S., Safari B., Ernest G., Lio F. & Moussa S.; Simplified Lot Quality Assurance Sampling Evaluation of Access and Coverage (SLEAC) Survey of Community-based Management of Acute Malnutrition program; Northern States of Nigeria-(Sokoto, Kebbi, Zamfara, Kano, Katsina, Gombe, Jigawa, Bauchi, Adamawa, Yobe, Borno). Valid International. February 2014 4 Dangoma, Kalgo, Keta, Diggi and Kuka PHCs 5 Barriers refers to the negative factors while boosters refer to the positive factors that affect the CMAM program and coverage. 6 caregivers (in the program and not in the program), community leaders, community members, health workers, and the State and LGA nutrition officers 7 Semi-structured interview, informal group discussion and in-depth interview 8 SPHERE standards define the minimum performance of a Therapeutic Feeding Program (TFP) in emergency setting. Thus recovery rate of >75%, death rate of <10% and defaulter rate of <15% 9 Measurement of the MUAC at admission is a strong indicator of late/early detection as well as treatment seeking behavior and the effectiveness of community mobilization activities.

vii
seeking behavior, long waiting time at the CMAM/OTP HFs, poor outreach activities, absence of CVs in non OTP wards (wards without HF offering CMAM services), husband refusal to attend CMAM services, RUTF consumption and sharing, RUTF shortage/stock-out, routine drugs stock-out, wrong admission/discharge criteria, Lack of motivation to HWs, Refusal by caregivers to attend SC, lack of collaboration between CVs and HWs, ineffective supply chain structure for RUTF, high defaulters/non-defaulter tracing, no Stabilization Centre in the LGA, Poor program monitoring and Poor referral system between OTP and SC, OTP to OTP and Community and OTP. The findings from the SQUEAC investigation reveal a coverage estimate of 30.5% (21.7 – 41% CI; 95%) and z-test p-value of 0.5765 which implies that there is no Prior-Likelihood conflict.
The following actions were recommended for the program improvement: o Improving community mobilization & sensitization o Improve program monitoring and capacity building for Health workers o Follow-up SQUEAC assessment in the state/LGA. o Creation of basket fund for the support of CMAM activities in Kebbi State. o Improvement in health education to emphasize on display of information, education and communication
(IEC) materials at the CMAM HFs.

1
1. Introduction Kebbi state located in the North Western Nigeria was created from old Sokoto state on 27th August, 1991. It is located on latitude 11° 30′ 0″ N and longitude 4° 0′ 0″ E, bordered by Sokoto state to the North, Zamfara state to the Northeast, and Niger state to the south. Internationally, it is bordered by Niger Republic to the Northwest and Benin Republic to the Southwest. It is subdivided into 21 administrative units called the Local Government Areas (LGAs)10. It has an estimated population of 3,137,989 people (est. 1991 census) and covers a total area of 36,800 km².
Kalgo LGA is one of the UNICEF supported LGAs and is bordered by Birnin Kebbi LGA to the East, Jega Southeast, Maiyama to the South, Suru to the South west, Bunza to the West and Arewa Dandi to the North. It has an estimated population of 85,403 and a total of area of 1,173 km². It is subdivided into 10 distinct administrative areas or wards namely; Dangoma, Diggi, Etene, Hirishi, Kalgo, Kuka, Mutubare, Nayelwa, Wuro-Gauri and Zuguru11.
Figure 1: Map of Kalgo LGA showing the wards with OTP site and those without the OTP
Kebbi State Ministry of Health (SMoH) with support from UNICEF started implementing CMAM in 10 LGAs in 2009; these LGAs are Argungu, Augie, Arewa Dandi, Bagudo, Birnin Kebbi, Kalgo, Koko/Besse, Sakaba, Shanga and Suru. There are seven stabilization centres (SC) feeding the OTP centers which are Sir Yahaya Memorial Hospital in Birnin Kebbi, Federal Medical Center in Birnin Kebbi, General Hospital Dirin Daji, General Hospital Koko, General Hospital Argungu, General Hospital Yauri and General Hospital Jega. SCI had begun the implementation of CMAM services in 3 additional LGAs of Maiyama, Gwandu and Dandi. The CMAM geographical coverage is 61.90% with 13 out of the 21 LGAs offering CMAM services. The SMART survey in 2013 puts the prevalence of SAM using MUAC at 1.2% (0.7-2.2% CI; 95%) in the state12. Kalgo LGA has 5 wards with Health Facilities (HF) which has CMAM services integrated (as shown in Figure 1 above) and the remaining 24 as non-OTP HFs thereby giving a Geographical Coverage of 17.24% based on the proportion of HF (see table 1) 10 The LGAs are: Aleiro, Arewa Dandi, Argungu, Augie, Bagudo, Birnin Kebbi, Bunza, Dandi, Fakai, Gwandu, Jega, Kalgo, Koko/Besse, Maiyama, Ngaski, Sakaba, Shanga, Suru, Wasagu/Danko, Yauri and Zuru. 11 Map drawn from map of Zamfara obtained through google search and features inserted from google maps 12 SMART Survey, (September, 2013); the prevalence estimate using Weight for Height Z-score (WHZ) is 1.8%( 0.9-3.3% CI)

2
Table 1: Shows the distribution of Health Facilities by ward and the proportion of HF having OTP services
S/No Wards CMAM Services HF with OTP HF without OTP Total Proportion
1. Diggi yes 1 0 1 100.00%
2. Kalgo yes 1 3 4 25.00%
3. Hirishi no 0 4 4 0.00%
4. Etene Yes 1 2 3 33.33%
5. Zuguru no 0 1 1 0.00%
6. Kuka Yes 1 5 6 16.67%
7. Wuro-Gauri no 0 1 1 0.00%
8. Nayelwa no 0 3 3 0.00%
9. Mutubare no 0 2 2 0.00%
10. Dangoma Yes 1 3 4 25.00%
Total 5 5 24 29 17.24%
The SQUEAC investigation was carried out as a follow-up to a SLEAC assessment conducted in period Octobers and November, 201313. This SQUEAC investigation was implemented in the period 22nd April and 20th May 2014.
2. Objectives The objectives of the SQUEAC investigation were to:
• Investigate the barriers and boosters of the CMAM program in Kalgo LGA • Evaluate the spatial pattern of coverage. • Estimate the overall program coverage of the LGA • Issue action oriented-recommendations in order to reform and to improve activities of the CMAM
program and • Build the capacity of SMoH, LGA staff and NBS in Kebbi state on SQUEAC methodology (learning by
doing).
3. Methodology SQUEAC comprise a set of tools that are used to investigate coverage as well as positive and negative factors that affect the coverage of CMAM program. SQUEAC uses Bayesian approach14 to estimate overall program coverage. In SQUEAC investigation collection and collation of information to generate more information is based on the generated level of evidence during the process of investigation15. SQUEAC investigation, while using the principles
13 Chrissy B., Bina S., Safari B., Ernest G., Lio F. & Moussa S.; Simplified Lot Quality Assurance Sampling Evaluation of Access and Coverage (SLEAC) Survey of Community-based Management of Acute Malnutrition program; Northern States of Nigeria-(Sokoto, Kebbi, Zamfara, Kano, Katsina, Gombe, Jigawa, Bauchi, Adamawa, Yobe, Borno). Valid International. February 2014. 14 Refer to Myatt, Mark et al. 2012. Semi-Quantitative Evaluation of Access and Coverage (SQUEAC)/Simplified Lot Quality Assurance Sampling Evaluation of Access and Coverage (SLEAC) Technical Reference. Washington, DC: FHI 360/FANTA for details. 15 Investigative. Involves a technique for investigating coverage and factors influencing coverage. A SQUEAC investigation will, if needed, include surveys, but is not limited to undertaking surveys. •Iterative. The process of a SQUEAC investigation is not fixed, but is modified as knowledge is acquired. This can be thought of as a process of ‘learning as you go’. New information is used to decide the next steps of the investigation. •Innovative. Different tools may be used and new tools may be developed as required. •Interactive. The method collects information through intelligent interaction with program staff, program beneficiaries, and community members using semi-structured interviews, case histories, and informal group discussions. •Informal. The method uses informal but guided interview techniques as well as

3
of triangulation and sampling to redundancy ensures that the body of evidence generated in the process gradually builds up a picture of the “truth” about program coverage whilst simultaneously indicating what practical measures can be undertaken to improve access and coverage. It is semi-quantitative in nature and uses a mixture of quantitative data collected from routine program monitoring, anecdotal program information, small studies, small-area surveys and wide area surveys, as well as qualitative data collected using informal group discussions (IGDs), semi structured interviews and case histories with a variety of respondents (involving but not limited to community leaders, caregivers, community gatherings, religious leaders, traditional birth attendants, traditional healers and other leaders in the community).
3.1. Stages of SQUEAC of Kalgo LGA CMAM program
SQUEAC investigation was conducted in 3-stages as illustrated in the Figure 2 below;
Figure 2: Stages of SQUEAC
Stage 1 The objective at this stage was to identify possible areas of low and high coverage as well as reasons for coverage failure. This involved analysis of quantitative and qualitative data. Quantitative data was extracted from the existing routine program data in individual OTP cards, while qualitative data was obtained from IGD and semi structured interviews with care-givers, village leaders, health workers, community volunteers, lay people (majalis16 and tea-shop gathering), religious leaders, key influential people and traditional healers. The Routine programme data were collected from the 5 OTP centers (that is, Dangoma, Kalgo, Keta, Diggi and Kuka) in the LGA. The analysis yielded various plots that would enable the SQUEAC team to establish whether the coverage could be homogenous or patchy. The process of collation of the OTP cards is illustrated in the figure below:
Figure 3: Process of collation entry and analysis of the routine and other program data
formal survey instruments to collect information about coverage and factors influencing coverage. •In the community. Much of the information used in SQUEAC investigations is collected in the community through interaction with community members. SQUEAC lets you see your program as it is seen by the community. •Intelligent. Triangulation is a purposeful and intelligent process. Data from different sources and methods are compared with each other. Discrepancies in the data are used to inform decisions about whether to collect further data. 16 Majalis; is a gathering of peers in a specific location (be it under a tree, or a shed or simply by the roadside) and at a specified time (depending on seasonality but mostly at the close of work)
4
Qualitative data was collected at the qualitative data phase of SQUEAC investigation and lasted for 3 days. Data was collected from:
• Health workers working within the CMAM health facilities and in the community.
• Caregivers of the beneficiaries in the program
• Various members of the community from 20 villages across the LGA
Qualitative data collection was done from sampled communities (villages) close to the CMAM HF and also from village(s) that were far from the CMAM HF within the same Ward (see the hypothesis below for relative distance comparison). In another way qualitative data were collected in a community within the ward having a CMAM HF and also, in a community that was not within the Ward and far from the CMAM HF. This was done with an aim of
development of the hypotheses in an advanced study. It is important to note that the “thinking” of forming a
hypothesis which would be done in further study began during the analysis of routine programme data.
Qualitative data provided vital information concerning the causes of low or high coverage with an objective of identifying principal barriers to programme access and coverage. It was essential to triangulate the information gathered by source and method until not new information was forthcoming. The main methods of qualitative data collection used during the SQUEAC investigations included; IGD, in-depth interview, semi-structured interview, IGDs, simple-structured interview and observations.
The results yielded in this process are described in the sections below.
Stage 2 In this stage the following processes were carried out:
• Formulation of the hypothesis that would be tested in the LGA to establish spatial coverage.
• Small area survey to gather data which when analyzed will prove the hypothesis formulated and also barriers to access and coverage. This stage was meant to confirm the location of areas of low and high coverage and establish the homogeneity or heterogeneity of the program geographical coverage. It is worth noting that the results confirming the hypothesis would determine the next course of action in the SQUEAC investigation. That is, if the hypotheses were rejected in the sense that the areas that we believed were of low coverage turned out to be areas of high coverage, more data would need to be gathered until the “certainty” of the spatial coverage was established. This would be important at a later
stage when the ‘prior’ of the program coverage would be determined. This process outlines the iterative nature of SQUEAC investigation. The hypothesis that was formulated (as described in the below section of the report) was tested using the small area survey.
The small area survey aimed at verifying our beliefs about the program and confirmed our belief about program coverage on whether it was patchy or not. In a nutshell the steps involved in analysis of the small area survey data and then testing the formulated hypothesis were done as follows:
1. Setting a standard (p): It is often reasonable to set ‘p’ in line with the SPHERE minimum standards17 for therapeutic feeding programme. Considering that the SLEAC18 assessment that was done in October 2013
17 Minimum standards for nutrition are a practical expression of the shared beliefs and commitments of humanitarian agencies and the common principles, rights and duties governing humanitarian action set out in the Humanitarian Charter. For CMAM programme, the minimum standard for coverage is 90% for camp setting, 70% for urban area and 50% for rural areas. 18 Simplified lot quality assurance sampling Evaluation of Access and Coverage
5
in Kalgo LGA (and that unveiled results of program classification of coverage) a 20% threshold19 was used to classify coverage as either low or high.
2. Undertaking of the small area survey
3. Use of the total number of cases found (n) and the standard (p) to calculate the decision rule (d) using the formula for 20% coverage.
4. Application of the decision rule: if the number of cases in the program is > d then the coverage is classified as good and if < d then it is classified as low.
5. Determination of the areas that have low and those that have high coverage. If the results do not agree with the hypothesis formulated then more information would need to be collected.
The Process of field data collection in Kalgo
Identification of villages to be visited
Eight villages were selected; 4 from a ward that has OTP (2 host/near villages and 2 far villages >1hour walk) and 4 villages (2 from OTP ward; 1 host & 1 far village and 2 villages from non-OTP wards). The zones selected are distributed between the survey teams.
Active and adaptive case finding
Each team used an exhaustive active & adaptive case-finding method to search for SAM cases. The process involved:
a) Case definition of malnutrition using local terms recognized in the community;
b) Identification of key informants who were given the description of the children that are being searched. The key informant would then direct the SQUEAC team to the households perceived by the informant to have the described children;
c) Use the caregiver of the SAM case that has been identified to lead the team to another dwelling that could have similar case
d) Repeat the process until the SQUEAC team is led to the dwellings they have previously visited. A simple structured questionnaire was administered to the beneficiaries of non-covered cases identified during the process. In some cases house to house search was done in settlements close to the urban areas to search for SAM cases.
Stage 3 At this stage it was considered that adequate information about the program had been collected and analyzed. The following processes were carried out:
Building of the ‘Prior’ (statistical representation of our belief about the program coverage).
The barriers, boosters and questions were re-analyzed based on the available sources and methods to confirm that information has been exhaustively gathered. The data gathered from the small area survey was also
19 The coverage threshold used to define classes of coverage in hypothesis was adopted from the two-standard three class classification used in SLEAC survey that is: < 20; >=20 to <50; and >=50 for low, moderate and high coverage classification respectively. In Kalgo SQUEAC stage two, results <= 20% was classified as low while that >20% was classified as high.

6
considered at this stage. Concept map was completed to show relationship of all the factors affecting the
program coverage and whether they interlink to reflect the ‘true picture’ of the program.
Belief histogram was drawn. This was done by the team whereby the team determined the minimum and maximum probable coverage (i.e. the coverage limits that the team believes the coverage will not go below or beyond) based on the evidence generated in stage 1 & 2 first. Then each of the team members gave his/her own estimate of the coverage based on a preselected interval of 5% (10%, 15%, 20%...X%) and the result is tallied
according to preselected interval (5% interval), the interval with the highest tally is selected as the ‘prior mode’ and the tallied data is presented in the form of histogram.
Using the built ‘prior’, the lowest and the highest possible values of the program coverage, the Bayes SQUEAC
Calculator was used to present the prior distribution and the relevant shaping parameters. The calculator helped to give a sample size of SAM cases required to estimate our coverage in the wide area survey (likelihood survey).
The number of villages to be visited was determined. The (MUAC) SAM prevalence of the SMART Nutrition survey20, the median village population and estimated percentage of under 5 children were used in the following formula to calculate the number of the villages to be visited.
The actual villages to be visited were selected from a complete list of villages21 which were stratified by Wards and the CMAM facility. The sampling interval was calculated as:
Field data collection
Twenty four villages were selected from the village list based on SAM sample size stratified by ward. The villages selected were distributed between the survey teams. Each team used an exhaustive active & adaptive case-finding methodology where a key informant was identified and house to house search in the absence of key informants or in places with settings close to urban to identify cases (children between 6-59months, MUAC <11.5, presence of edema and the child that is in the program) that are either covered or not by the programme in the selected villages.
4. Results and Findings
4.1. Stage 1 : Identification of barriers and boosters and of potential areas of high or low coverage
In stage 1, the quantitative data extracted from the individual beneficiary/OTP cards and the qualitative data collected from the community were analyzed and the results presented below; 20 SMART nutrition survey done in Kebbi state in 2013 21 Provided by the National Bureau of Statistics, Kebbi State

7
4.1.1. Routine monitoring data and individual OTP cards
The routine data was extracted from the individual beneficiary/OTP cards of all the 5 HFs offering CMAM service in the LGA. The data was extracted from a total of 1770 OTP cards for the period of January 2013 to March 2014 (15 months period). The results were presented as follows:
4.1.1.1. Admission data
The admission data analyzed include admission trend, admission MUAC and HF’s admissions.
HF admissions
The number of admissions varies from HF to HF with Kalgo and Diggi HFs having the highest number of admission followed by Kuka HF with >300 cases. Keta HF showed the least number of admissions with less than 200 admissions per year.
Figure 4: Shows the number of admission for each HF for the 15 months period.
A further analysis of the admission by LGA where the cases are coming from reveals that only 51.84% of the cases are from Kalgo LGA with the remaining coming from other LGAs of Aliero, Birnin Kebbi, Bunza, Dandi, Jega and Mayamma LGAs respectively. The proportion of cases by LGA is as presented in the figure 5 below.

8
Figure 5: Proportion of cases admitted by LGA
Admission Trend
The number of admissions was compiled for the period analysed (January, 2013 - March, 2014) from the 5 HFs offering CMAM services. A total of 1,770 admissions were recorded for the period. The trend of admission provides a good picture about the evolution of admission over time. The admission trend is depicted in the figure 6 below.
Figure 6: The diagram depicts the admission trend for total admission with raw data = cases and M3A3 -smoothed to reflect seasonality and trend
The smoothing was applied to the data using a moving average of a span of 3 months (that is median of 3 and average of 3 months-that is, M3 and A3 respectively) so as to hide the random ‘noise’ component and reveal the seasonality and trend component of the data (Figure 6). A comparison of trend of admission and seasonal calendar is presented in the figure 7 below.

9
Figure 7: Admission trend and seasonal calendar
There is an increase in the number of admission corresponding to the hunger gap, the admission increases gradually up to June 2013 but there is a downward trend in July-August corresponding to shortage of RUTF and HWs strike. Further analysis of the admission trends disaggregated by individual HFs reveals fluctuations in the trend (Figure 8).
Figure 8: Admission trend for each HF compared with the total admission trend.
The downward trend of admission in August 2013 was as a result of RUTF shortage and most importantly health workers strike which led to closure of the facilities during the strike. The fall in admission between January and March 2014 was due to the fact that not all the beneficiary/OTP cards were analyzed in the period when routine

10
data analysis was done. For this period only Kalgo OTP presented the cards completely with Keta CMAM site presenting only 2 cards from January admission and none for the months of February and March. Therefore, the trend during this period would not be analyzed reliably.
Admission MUAC
The measurement of the MUAC at admission is a strong indicator of late/early detection as well as treatment seeking behaviour and the effectiveness of community mobilization activities. The median MUAC at admission was 102mm which is indicative of late treatment seeking behaviour. Further still, the histogram representation of the data reveals a long right tail indicative of late admission (admission when the condition is critical), see Figure 9 below.
Figure 9: The figure above plots admission MUACs showing the median admission MUAC
Length of Stay (LOS) The median LOS observed is 5 weeks which means that half of the cured cases are discharged from OTP in under 5 weeks (Figure 10). When interpreted, this indicates that the programme admission and discharge is good. However, this is not consistent with the plot of admission MUAC data which shows that there is late health seeking behaviour and that a good percentage of the cases were admitted late when their condition is critical. This necessitates the need to further investigate the exit data to ascertain why the LOS is short.
Figure 10: A histogram representation of the LOS with median LOS shown by arrow in black

11
Further investigation into the LOS results was done by looking at exit MUAC for all cured or recovered cases. And the result reveals that only 18% of the exits have a MUAC measurement of above 125mm with 41% being discharge at exactly 125mm, the remaining 42% were discharge with a MUAC measurement of less than 125mm which is below the minimum discharge MUAC (Figure 11). This explains why median LOS looks acceptable when the admission data suggest that the LOS could be longer. Hence, the LOS results should be treated with caution.
Figure 11: A bar chart representation of exit MUAC
4.1.1.2. Exit Data (Discharge Outcomes)
The discharge outcomes (referred as the program performance indicators) are generally classified into four; recovery, death, defaulter and non-recovered rates. The analysis of the routine program data was done in proportions to reflect a picture of the performance rates that could be expected from such a program as shown in figure 12 below;
Figure 12: Pie chart representation of exit proportions for the period Jan 2013 to Mar 2014

12
Performance Indicator Trends
The trend of the indicators revealed that throughout 2013, all the indicators except the death rate were below SPHERE minimum standard with the defaulter rate consistently above 20% (Figure 13). However, the 2014 data (January – March) shows a remarkable improvement with the recovery rate meeting the SPHERE standards and the default rate reducing to below 20% in March. This upward trend started in September and may be attributed to the improved monitoring of data by health workers (when they received refresher training) as well as increased supportive supervision by UNICEF and SMOH.
Figure 13: Trend of performance indicators
Recovery Rate
The analysis of the routine programme data reveals that the recovery rate for the entire duration is below the SPHERE minimum standard of 75% except for January – March, 2014 (see figure 13). However, further analysis disaggregated by HF reveals that none of the 5 CMAM HF has reached the SPHERE standard of >=75% (see figure 14 below for details).

13
Figure 14: Bar chart representation of recovery rate by HF
Non-recovered rate
The overall non-recovered rate for the period in question is 4% and the breakdown of the non-recovered rate by
HF is shown in figure 15 below. All the HFs have non-recovered rate of below 5% with the exception of Keta PHC
which returns a rate of 20.18%.
Death rate
The overall death rate stands at 1% which is below the SPHERE minimum standard of 10%. However, since this program is a high default program, the death rate might have been greatly under reported as a good number of defaulters might have ended up dying without being reported. This has been investigated and was reported in the defaulter Study in Stage 2.
Figure 15: A bar chart representation of non-recovered rate disaggregated by HF

14
Defaulter rate
The routine data analysis reveals an overall defaulter proportion of 31% (figure 16) which doubles the maximum recommended rate by the SPHERE standards (<15%). In the analysis, however, only 22% of the defaulters were captured in the OTP card with the remaining 9% as “Hidden Defaulters” see Figure 16.
Figure 16: A pie-chart representation of the proportion reflecting performance Indicators (with disaggregated to
normal defaulter and ‘hidden defaulter’ rates.
This high defaulter rates implies potential coverage is low since default cases are non-covered cases. The analysis of the number of defaulters over time reveals a defaulter trend as shown in the figure 13 above. The trend shows that the default rate is consistently above the SPHERE minimum standard throughout the 15 months period. A further analysis of the default rate by health facility reveals that all the HFs has a default rate of above 15%. Only Kuka CMAM HF has a default rate of 16% which is slightly above maximum recommended by the SPHERE minimum standards, with the remaining 4 OTPs having a default rate of between 28-40% (Figure 17).
Figure 17: A graphic representation of default rate by HF

15
Analysis of numbers of visit at default reveals that majority (over 70%) default early which implies that they are likely to be current SAM cases. About 26% default after 4 weeks and are likely to be recovering cases. (See figure 18 below for details). Disaggregation of the defaulters by number of visit at default shows that only 26.4% defaulted after the 4th visit with the remaining 73% early defaulters (defaulted before the 5th visit).
Figure 18: Proportion of number of visits at default for defaulted cases for the period January 2014 to March, 2014
Analysis of defaulters by MUAC at default reveals that only 25% of the defaulters defaulted with a MUAC of above 115mm (outside the admission MUAC) with 75% having a MUAC of below or within the admission criteria (defaulted while still being current SAM cases). See figure 19 below.
Figure 19: A bar chart presentation of MUAC at default
Disaggregation of defaulters by LGA reveals that 38.70% of the default cases are from Kalgo LGA with the remaining 61.30% from neighboring LGAs of Aliero, Birnin Kebbi, Bunza, Dandi, Jega and Mayamma. The breakdown of the default cases by LGA is presented in the figure 20 below;

16
Figure 20: Shows distribution of defaulters by LGA
Time to Travel to CMAM site
The observed time to travel plot shows that greater than 50% of the cases came to the OTP from within <1hour travel from the OTP; no cases were observed from beyond 2 hours travel time from the HF as shown in figure 21 below. Not much information of distances of the beneficiaries coming from far was available and the reason why this was not captured on the plot of time to travel to site. Nonetheless, available qualitative information (as discussed in the qualitative results section) indicate that far distance to the CMAM site is a major impediment that affect attendance.
Previous plot (as shown in figure 5 above) has shown that there is close to 50% of the admissions that comes from other LGAs other than Kalgo. 51.84% of the total admissions are from Kalgo LGA.
Figure 21: Plot of observed time to travel plot from the CMAM site
4.1.2. Qualitative data During the qualitative data collection phase which lasted for 3 days, a total of 20 villages were visited in the LGA. The qualitative data collection was organized in the following visits:

17
• 2 villages per ward (one hosting or near the HF and one far away from the HF within the wards with OTP services)
• Villages in OTP ward22 and villages in non-OTP wards.
The results are explained below;
Understanding of Malnutrition
Informal group discussions were conducted in Majalis, semi structured interviews with care-givers (in the program and not in the program), community leaders, religious leaders and CVs from across 20 villages, 2 each from the HF’s catchment area; 1st village (hosting the HF) and the 2nd village is chosen based on the distance from HF. For the other 10 villages 2 were chosen each from non-OTP wards. The result reveals that the community does not have a complete understanding of malnutrition as only cases resulting from sicknesses such as diarrhea, malaria etc. are recognized as SAM. Cases resulting in wasting such as those from lack of sufficient breast feeding or breast feeding while pregnant shanciki23, marasmic kwashiorkor and Oedema were not recognized as SAM. In general, SAM is refer to with various local names with Tamowa being the most common and simply means wasting. Oedema is refer to in many different ways such as Ciwon Kaba24, Ciwon iska25, Ciwon Sanyi26 etc and all are not associated with community’s understanding of SAM cases hence not recognized as such, see Annex II for details of local terms used in describing SAM in the community.
Treatment Seeking Behaviour
The communities visited all have a late treatment seeking behavior as they visit a chemist, traditional healer and or use herbal remedies before visiting a CMAM site as a last resort. Some of the traditional healers interviewed revealed that they have some special herbs which they give to children with SAM (wasting) in which they drink and bath with, while others said that they have a special remedy mixed with rabbit’s ear that is given to child to get well and the mother to make her breast milk good as SAM results from the mother having bad breast milk. Further still, the care-givers most of the time decline to attend SC. This may be attributed to the fact there is no SC in the LGA and the community felt disconnected with the 2 SCs in Birnin Kebbi and the one at General Hospital, Jega.
Awareness about the Program
Generally, all the community members interviewed were fully aware about the program. They know the HF which offers CMAM services, the OTP day and duration of treatment. However, there is huge gap as there are no CVs in wards that do not have a CMAM HF while the existing CVs in wards with CMAM HFs are not active. It was evident that most of the respondents within the community had never seen a MUAC tape. Furthermore, except for the community leaders who were sensitized at the LGA level, no sensitization were done in the community, the only sensitization going on in the communities are announcement by town criers.
Perception about program
The community’s perception about the program is very good mainly due to the evident physical response observed as a result of SAM treatment. The people in the community all like the program. Generally, the community members witnessed that that almost all SAM cases that received treatment recovered which is good for the program. Furthermore, majority of the referrals are community referrals especially peer-to-peer referral.
22 This is a political Ward which has HF offering CMAM services 23 A local term used to describe breastfeeding while pregnant 24 A local term for diseases manifesting in the form of tumour or a generalized tumour 25 A local term for disease resulting from evil spirits 26 A local term for diseases associated with too much exposure to cold temperatures

18
Although there is little or no mobilization activity in the community with the exception of announcement by town criers about the program, the community had fully accepted the program and are expressed positive comments about the “miracle of RUTF” in SAM treatment.
Skills of OTP staff
During the investigation, the SQUEAC teams had the opportunity to observe the process of admission of SAM cases into the CMAM program in 3 out of 5 OTP sites in the LGA. The main challenge at the CMAM HF is lack of enough HWs trained in CMAM. as such, the SMOH had come up with a brilliant idea in which one HW each from neighboring non-CMAM HFs were trained in CMAM and they come to the CMAM site to help out on OTP days. Besides the skills of the HWs being low the SMOH had set a rule to limit the number of SAM cases that are admitted at any one time due to regularly shortage at the state level. This is by limiting admission for only those SAM cases that had MUAC of less than 100mm. In the same way, those that reached the discharge criteria of 120mm were discharge from the program. Thus, the admission and discharge criteria were generally not adhered to according to the national guidelines. However, this rule had been revised recently so that admission and discharges should be according to the national CMAM guideline. But most of the HWs interviewed were still not aware of this and continued to follow the rule. There were few and critical cases admitted and discharged at 120mm of MUAC. The qualitative information was analyzed into boosters and barriers and presented in the sections below.
4.1.3. Boosters and Barriers The result of the qualitative data collected from the community was analyzed using the BBQ tool and presented in the table below;
19
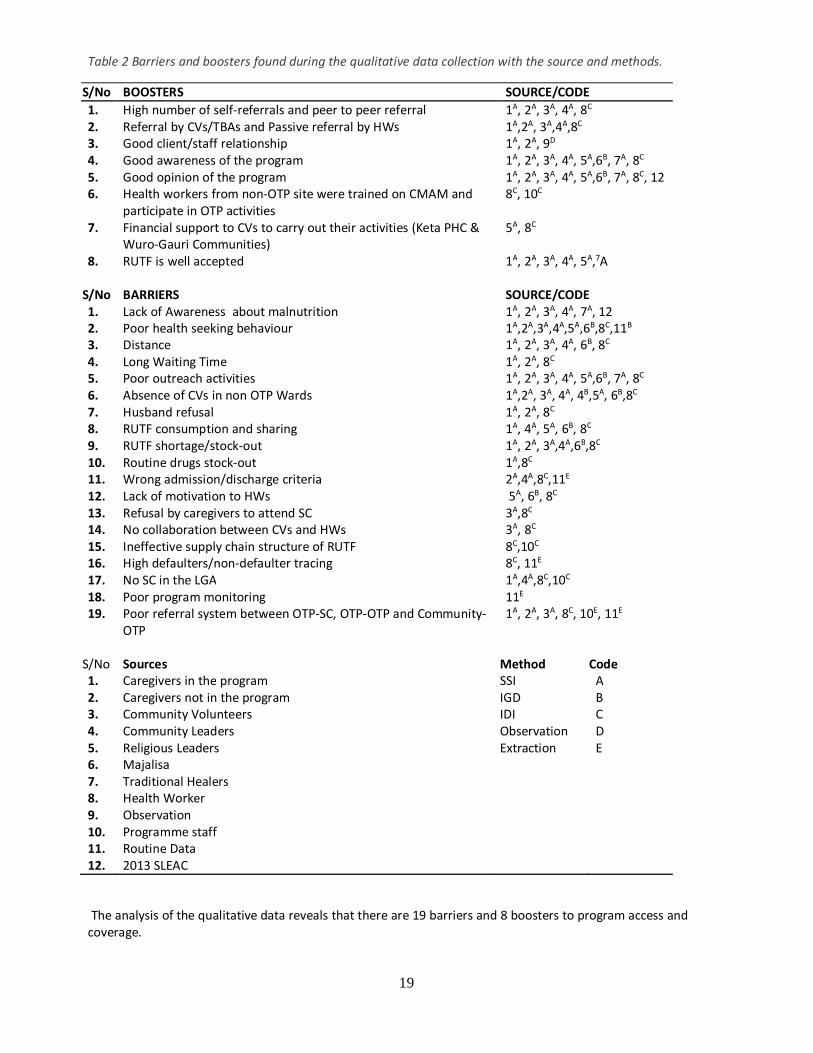
Table 2 Barriers and boosters found during the qualitative data collection with the source and methods.
S/No BOOSTERS SOURCE/CODE 1. High number of self-referrals and peer to peer referral 1A, 2A, 3A, 4A, 8C 2. Referral by CVs/TBAs and Passive referral by HWs 1A,2A, 3A,4A,8C 3. Good client/staff relationship 1A, 2A, 9D 4. Good awareness of the program 1A, 2A, 3A, 4A, 5A,6B, 7A, 8C 5. Good opinion of the program 1A, 2A, 3A, 4A, 5A,6B, 7A, 8C, 12 6. Health workers from non-OTP site were trained on CMAM and
participate in OTP activities 8C, 10C
7. Financial support to CVs to carry out their activities (Keta PHC & Wuro-Gauri Communities)
5A, 8C
8. RUTF is well accepted
1A, 2A, 3A, 4A, 5A,7A
S/No BARRIERS SOURCE/CODE 1. Lack of Awareness about malnutrition 1A, 2A, 3A, 4A, 7A, 12 2. Poor health seeking behaviour 1A,2A,3A,4A,5A,6B,8C,11B 3. Distance 1A, 2A, 3A, 4A, 6B, 8C 4. Long Waiting Time 1A, 2A, 8C 5. Poor outreach activities 1A, 2A, 3A, 4A, 5A,6B, 7A, 8C 6. Absence of CVs in non OTP Wards 1A,2A, 3A, 4A, 4B,5A, 6B,8C 7. Husband refusal 1A, 2A, 8C 8. RUTF consumption and sharing 1A, 4A, 5A, 6B, 8C 9. RUTF shortage/stock-out 1A, 2A, 3A,4A,6B,8C 10. Routine drugs stock-out 1A,8C 11. Wrong admission/discharge criteria 2A,4A,8C,11E 12. Lack of motivation to HWs 5A, 6B, 8C 13. Refusal by caregivers to attend SC 3A,8C 14. No collaboration between CVs and HWs 3A, 8C 15. Ineffective supply chain structure of RUTF 8C,10C 16. High defaulters/non-defaulter tracing 8C, 11E 17. No SC in the LGA 1A,4A,8C,10C 18. Poor program monitoring 11E 19. Poor referral system between OTP-SC, OTP-OTP and Community-
OTP
1A, 2A, 3A, 8C, 10E, 11E
S/No Sources Method Code 1. Caregivers in the program SSI A 2. Caregivers not in the program IGD B 3. Community Volunteers IDI C 4. Community Leaders Observation D 5. Religious Leaders Extraction E 6. Majalisa 7. Traditional Healers 8. Health Worker 9. Observation 10. Programme staff 11. Routine Data 12. 2013 SLEAC
The analysis of the qualitative data reveals that there are 19 barriers and 8 boosters to program access and coverage.

20
4.1.4. Concept Map After completing the analysis of barriers, and boosters, the SQUEAC investigators were divided into three teams. Each team drew their own concept map in which they presented how different barriers and boosters interact with each other and how they affect the program coverage. The key findings of all the 3 groups is that lack of knowledge about malnutrition, poor outreach activities, high defaulters/absence of defaulter tracing and far distance to CMAM site have a direct negative effect on coverage. While ineffective supply chain structure leads to RUTF shortage/stock-out which in turn leads to defaulting and subsequently affects coverage. Others such as long waiting time, poor health seeking behaviors, absence of SC in the LGA/refusal to attend SC by care-givers, routine drug stock-out, poor referral system, poor program monitoring, absence of CVs in non-OTP wards, lack of collaboration between CVs and HWs all contribute indirectly to low coverage. On the other hand, good opinion and awareness about program, community referrals by peer/self, passive referral by HWs and acceptability of RUTF all contributed positively to the coverage. The concept maps for the 3 groups are presented in Annex III.
4.2. Stage 2: Confirmation areas of high and low coverage
4.2.1. Small area survey At the end of Stage 1 and 2, the location of areas of high and low coverage and the reasons for coverage failure identified were tested in a small-area survey. In this stage, active and adaptive case finding methodology was used in the search of SAM cases in the community. It was hypothesized that;
Hypothesis
I). Coverage will be higher (in villages which are near the CMAM HF/OTP centres (within <1hour walk) than in villages which are far from the CMAM HF (>1hour walk).
II). Coverage will be different between wards hosting the OTP centre and the wards without OTP
Based on the results of SLEAC survey conducted in November, 2013 a threshold of 20% was chosen for Kalgo LGA because of its low coverage classification of <20%.
The result was presented in the table below which confirms our hypothesis of areas of low and high coverage;

21
Table 3 Result of Small Area Survey
Hypothesis Village Total SAM = n
SAM Covered
( C )
SAM not Covered
(NC)
Recovering (RC)
Decision rule
d=n/5
Coverage classification Threshold =
20%
OTP
War
d
Near villages
Kuka 11 5 6 0 2 Ok Gulari Sani 6 0 6 0 1 Total 17 5 12 0 3
Far villages
Kokani 9 1 8 0 1 Ok Nasarawa 1 0 1 0 0 Total 10 1 9 0 2
War
d
With OTP Diggi 20 10 10 5 4 Ok Ung/Arawa 2 0 2 0 9 Total 22 10 12 5 4
Without OTP
Wuro Gauri 7 1 6 3 1 Ok Shadadi 0 0 0 0 0 Total 7 1 6 3 1
Grand Total 56 17 39 8
Hypothesis I: The table above show that a total number of 17 SAM cases were found in the settlements that are near the OTP sites (Health facilities with CMAM services) in which out of these 5 cases are covered while the remaining 12 were not covered. This measures to proportion of 29% of the coverage which is classified above 20% threshold. Also 10 SAM cases were found in the settlements that are far away from the OTP Wards out of which 1 case is covered and the remaining 9 cases found were not covered. This represent a proportion of 10% coverage which is classified below the 20% threshold. This implies that, our hypothesis of having a high coverage in villages hosting/near OTP site than villages far from the OTP holds true.
Hypothesis II: A total number of 22 SAM cases were found in the OTP ward27 out of which 10 current cases were covered while 12 were not covered with 5 of the cases found as recovering cases. Thus, 45% of the cases were covered and this is above the 20% threshold. A total number of 7 SAM cases were found in the Non-OTP ward out of which 1 is covered and 6 are not covered. This measures to 14% of the current cases that are covered and is below the 20% threshold. This also reaffirms our hypothesis of having a higher coverage in wards hosting OTP than those not hosting an OTP.
In conclusion, a total number of 56 SAM cases were found in the OTP ward out of which 17 SAM cases were covered and 39 cases were not covered while the remaining 8 cases found were recovering cases. These results reflects the potential patchy spatial coverage in the LGA as either hypothesis (or conjectures) testing potential spatial coverage holds true.
4.2.2. Barriers of the small area survey
Barriers to coverage brought forth by caregivers during this small area survey were presented in the table below;
27 Wards with HF with CMAM services
22
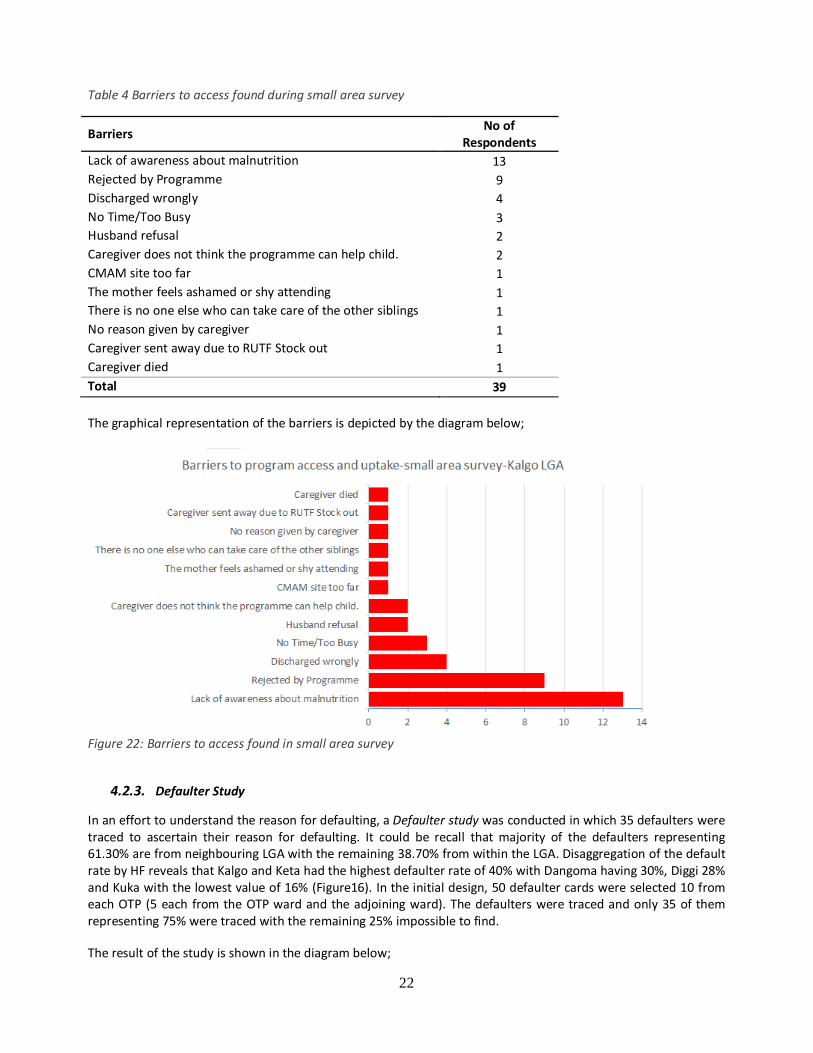
Table 4 Barriers to access found during small area survey
Barriers No of Respondents
Lack of awareness about malnutrition 13 Rejected by Programme 9 Discharged wrongly 4 No Time/Too Busy 3 Husband refusal 2 Caregiver does not think the programme can help child. 2 CMAM site too far 1 The mother feels ashamed or shy attending 1 There is no one else who can take care of the other siblings 1 No reason given by caregiver 1 Caregiver sent away due to RUTF Stock out 1 Caregiver died 1 Total 39 The graphical representation of the barriers is depicted by the diagram below;
Figure 22: Barriers to access found in small area survey
4.2.3. Defaulter Study
In an effort to understand the reason for defaulting, a Defaulter study was conducted in which 35 defaulters were traced to ascertain their reason for defaulting. It could be recall that majority of the defaulters representing 61.30% are from neighbouring LGA with the remaining 38.70% from within the LGA. Disaggregation of the default rate by HF reveals that Kalgo and Keta had the highest defaulter rate of 40% with Dangoma having 30%, Diggi 28% and Kuka with the lowest value of 16% (Figure16). In the initial design, 50 defaulter cards were selected 10 from each OTP (5 each from the OTP ward and the adjoining ward). The defaulters were traced and only 35 of them representing 75% were traced with the remaining 25% impossible to find.
The result of the study is shown in the diagram below;

23
Figure 23: A graphic representations of the reasons for defaulting put forward by the defaulted cases during defaulter study
Further analysis of the reasons of defaulting reveals that 12 of the defaulters representing 34.29% defaulted because the mother was busy or unavailable, closely followed by migration at 8 (22.86%). Distance and death came a third with 4 (11.43%) responses each; child rejects RUTF and child recovered has 3 (8.57%) responses each and only 1 (2.86%) case reported being unable to afford transport to site as reason for defaulting. In as much as there is low death rate as reflected in performance indicators, there are chances of ‘hidden deaths’ who are not able to be known in situation of low defaulter tracing.
4.3. Stage 3: The coverage estimate (application of Bayesian Theory)
4.3.1. Development of Prior SQUEAC methodology utilizes Bayesian technique in which existing information such as routine monitoring data were extracted, additional qualitative information collected and the result of small area survey analyzed to give us a fair idea about the program coverage in the LGA. This fair idea or our belief about the program is known as the ‘Prior’ which is aimed at giving us a fair estimate of the program coverage. Relevant information collected from the routine data i.e. qualitative information, the quantitative data and small area survey were used to inform and develop the prior. Informed guess was done in the process of investigation of what the coverage value is most likely to be, that is the mode of probability density. The factors affecting the coverage positively are the booster and those affecting the coverage negatively are the barriers. Information collected was separated into the boosters and the barriers of CMAM coverage. A procedure was employed to weigh the barriers and booster in four ways; weighted barriers and boosters, Un-weighted barriers and boosters, concept map and belief histogram. The result of the various prior modes for belief histogram, weighted and un-weighted BBQ prior modes and the prior mode from the concept map are presented below; The belief histogram

24
Prior 1: Histogram of belief = 17%
Figure 24: Graphical representation of belief histogram
The belief histogram was based on probability of occurrence of a certain coverage percentage by individual team members of the coverage assessment. The agreement was based on their knowledge about the coverage gotten from the result of routine data analysis and qualitative information from the first stage and the small area survey of the SQUEAC investigation.. The value of the belief histogram coverage varied between 15% and 45% for each participant and minimum values of 5% with a maximum value of 50% were agreed. Five of the participants gave a potential coverage of between 14 – 18 % which was averaged to give a prior mode of 17% whereas all the other participants gave a potential coverage of 20, 25, 30, 35 and 45% respectively. The result is as presented in figure 24 above. Prior from the weighted barriers and boosters Estimation of prior mode from the BBQ was calculated based on the data in the table below as;

25
Table 5: Tabular representation of weighed barriers and boosters obtained in Stage 1 by the 3 groups
S/No Barriers Boosters
GP1 GP2 GP3 Average GP1 GP2 GP3 Average
1 Lack of Awareness about malnutrition 4 4 3 3.7 High number of self-referrals and peer to peer referral 5 5 4 4.7
2 Poor Health Seeking Behaviour 4 5 3 4.0 Referral by CVs/TBAs and Passive referral by HWs 2 5 2 3
3 Distance 5 3 4 4.0 Good client/staff relationship 4 3 4 3.7 4 Long Waiting Time 3 1 3 2.3 Good awareness of the program 5 5 5 5 5 Poor outreach activities 5 5 4 4.7 Good opinion of the program 5 5 5 5
6 Absence of CVs in non OTP Wards
4 4 4 4.0 Health workers from non-OTP site were trained on CMAM and participate in OTP activities
2 3 3 2.7
7 Husband refusal 2 1 1 1.3 Financial support to CVs to carry out their activities 1 2 2 1.7
8 RUTF consumption and sharing 1 3 3 2.3 RUTF is well accepted 5 5 5 5 9 RUTF shortage/stock-out 2 2 2 2.0
10 Routine drugs stock-out 1 1 1 1.0 11 Wrong admission/discharge criteria 2 2 2 2.0 12 Lack of motivation among HWs 1 1 1 1.0 13 Refusal by caregivers to attend SC 3 2 4 3.0 14 No collaboration between CVs and HWs 2 2 4 2.7 15 Ineffective supply chain structure of RUTF 3 2 2 2.3 16 High defaulters/lack of defaulter tracing 5 4 3 4.0 17 No SC in the LGA 2 1 2 1.7 18 Poor program monitoring 4 2 3 3.0
19 Poor referral system between OTP-SC, OTP-OTP and Community-OTP 2 2 1 1.7
Total 55 47 50 50.7 29 33 30 30.7

26
Prior from the un-weighted barriers and boosters
The barriers and booster in the Barriers and Boosters table were given equal score of 5 to assume that each of the barriers and booster affects the coverage in the same manner. The result is presented in the table below Table 6: Tabular representation of un-weighted barriers and boosters
S/N Barriers Value Boosters Value 1 Lack of Awareness about malnutrition 5 High number of self-referrals and peer to
peer referral 5
2 Poor Health Seeking Behavior 5 Referral by CVs/TBAs and Passive referral by HWs
5
3 Distance 5 Good client/staff relationship 5 4 Long Waiting Time 5 Good awareness of the program 5 5 Poor outreach activities 5 Health workers from non-OTP site were
trained on CMAM and participate in OTP activities
5
Absence of CVs in non OTP Wards 5 Financial support to CVs to carry out their activities (Keta PHC & Wuro-Gauri Communities)
5
7 Husband refusal 5 Rutf is well accepted 5 8 RUTF consumption and sharing 5 Good opinion of the program 5 9 RUTF shortage/stock-out 5 10 Routine drugs stock-out 5 11 Wrong admission/discharge criteria 5 12 Lack of motivation to HWs 5 13 Refusal by caregivers to attend SC 5 14 No collaboration between CVs and HWs 5 15 Ineffective supply chain structure of RUTF 5 16 High defaulters/non-defaulter tracing 5 17 No SC in the LGA 5 18 Poor program monitoring 5 19 Poor referral system between OTP-SC, OTP-
OTP and Community-OTP 5
TOTAL 95% 40%
Prior with Concept map Table 7: group representation of potential coverage using concept map
Group Boosters Barriers Prior Mode Arrows # Weight Total Arrows # Weight Total
Group 1 10 3.5 35 27 3.5 94.5 20.25 Group 2 10 5 50 18 5 90 30 Group 3 9 5 45 18 5 90 27.5
Prior Mode (Concept Map) = Average 25.9
1

27
2
3
4
5
6
7
8
9
Triangulating the Prior Mode The different prior mode estimations were used to give a final Prior mode of 26.4% as depicted by the equation and figure 25 below;
���������� =17% + 25.9% + 40% + 22.5%
4 = �26.35%�= 26
Figure 25: A Graphical representation of the triangulation of the prior mode
Therefore, the Prior Mode is 26% which was plotted using the Bayes SQUEAC Calculator and presented in the figure 26 below;

28
Figure 26: The plot of the Prior Mode in Bayes SQUEAC calculator showing suggested sample size circled in red
4.3.2. Likelihood
After plotting the prior, the suggested sample size for SAM cases was obtained from the Bayes SQUEAC calculator, the number of villages to be visited was calculated to get the required number of SAM cases for the likelihood survey. The number of villages was then calculated from the number of SAM cases, median village population, percentage of children 6-59 months and the prevalence of SAM in the state. Therefore:
This meant that to obtain 47 SAM cases a minimum of 24 villages needed to be sampled and find the cases using active and adaptive case finding methodology. Stratified spatial systematic sampling
Since there was no reliable map for LGA Kalgo, systematic stratified spatial sampling of villages was done. A total of 24 villages were selected for the wide area survey.
Therefore, an active and adaptive case finding method was carried out in these 24 villages. The case definition was a child who:
• Had MUAC less than 11.5 cm • Had bilateral pitting oedema and • Was aged 6-59 month

29
Results of the wide are survey The results of the active case finding of the wide are survey (stage 3) are shown in the table 7 below. The complete result of the WAS is presented in Table 8 below; Table 8: The table showing the results of the wide is survey
Total SAM = n SAM Covered ( C ) SAM not Covered (NC) Recovering (RC) 59 19 40 6
Point coverage estimate was used. This considered the proportion of current SAM cases found who are in the program among total SAM cases found. The likelihood was then calculated using the following standard formula for point coverage:
Therefore:
Point coverage = 32.2%
Table 9: Results of the wide area survey-Kalgo LGA
Ward Village Population Total SAM = N SAM Covered (C)
SAM not Covered
(NC)
Recovering (RC)
Dangoma/Gayi Asarara Babba 695 3 3 0 0 Dangoma/Gayi Dangoma 6320 4 4 0 1 Dangoma/Gayi Gayi 5850 6 3 3 2 Dangoma/Gayi Ruggar Bakoshi 100 1 0 1 0 Dangoma/Gayi Tsola 655 0 0 0 0 Diggi Ung. Illo 955 3 3 0 1 Etene S/Taru 945 3 0 3 0 Etene Shiyar Umaru Sarki 1292 6 4 2 2 Hirishi/Magarza Hirishi 1305 1 0 1 0 Hirishi/Magarza Badariya 1970 2 0 2 0 Kalgo Kwartagi 615 1 0 1 0 Kalgo S/Kabawa 675 1 0 1 0 Kalgo Shiyar Kasuwa 825 1 0 1 0 Kalgo U/Saini 575 0 0 0 0 Kukah illela 480 0 0 0 0 Kukah Unguwar Abdu Goni 150 1 0 1 0 Kukah Unguwar Mai shinkafa 305 2 0 2 0 Mutubare kwaidowo 130 1 0 1 0 Mutubare illela 825 2 0 2 0 Nayelwa Kokire 665 0 0 0 0 Nayelwa Nayelwa Fulani 590 6 0 6 0 Nayelwa Sandare 1170 5 0 5 0 Nayelwa UNG.Mai Kudi 530 0 0 0 0 Zuguru Zuguru 2965 10 2 8 0
Total 59 19 40 6
30
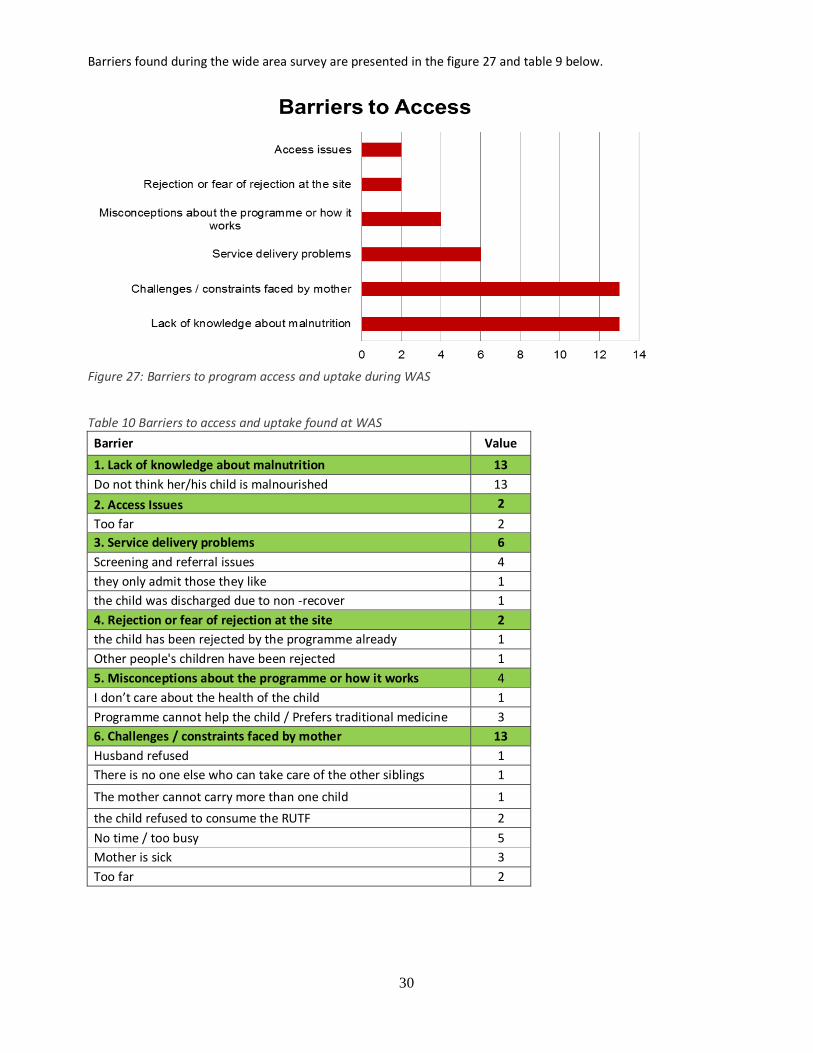
Barriers found during the wide area survey are presented in the figure 27 and table 9 below.
Figure 27: Barriers to program access and uptake during WAS
Table 10 Barriers to access and uptake found at WAS Barrier Value 1. Lack of knowledge about malnutrition 13 Do not think her/his child is malnourished 13 2. Access Issues 2 Too far 2 3. Service delivery problems 6 Screening and referral issues 4 they only admit those they like 1 the child was discharged due to non -recover 1 4. Rejection or fear of rejection at the site 2 the child has been rejected by the programme already 1 Other people's children have been rejected 1 5. Misconceptions about the programme or how it works 4 I don’t care about the health of the child 1 Programme cannot help the child / Prefers traditional medicine 3 6. Challenges / constraints faced by mother 13 Husband refused 1 There is no one else who can take care of the other siblings 1
The mother cannot carry more than one child 1 the child refused to consume the RUTF 2 No time / too busy 5 Mother is sick 3 Too far 2

31
4.3.3. Posterior
Using the Binomial conjugate analysis, the result of stage 1 (Prior) and the stage 3 (Likelihood) were combined to give us the final coverage estimate in the Bayes SQUEAC Calculator (Figure 28)
Figure 28: Final result of the coverage-Binomial conjugate analysis
The final coverage was estimated as 30.5% (21.7 – 41% CI28: 95%). The satisfactory overlap of the prior and the likelihood distributions coupled with z-test p-value of 0.5765 which is greater than 0.05 implies that there is no Prior-Likelihood conflict and the results are valid.
5. Discussion The total coverage of CMAM program in Kalgo LGA was estimated to be 30.5% (21.7-41.0%; 95% CI). This is below the SPHERE standard of a minimum coverage of 50 % for rural area. Although the coverage is below the SPHERE minimum standard, there is a significant improvement as the 2013 SLEAC survey classified it as low (below 20% or with a coarse estimate of 10.19%). This increase could be attributed to the availability of RUTF at the time of the SQUEAC investigations that ensured new admissions and children continued stay in the program. Also the SMOH nutrition unit had just began relaxing the restricted admissions to only 15 cases per day and or admission of severe cases with MUAC below 100mm and discharges at 120mm MUAC measurement. This may be attributed to the improved coverage. Kebbi state has the largest stock of RUTF in the country, aside of stock supplied by UNICEF to the state the state government had a procured a large stock of RUTF for treatment of SAM cases in the state. However, despite the availability of RUTF in the state, RUTF stock pipeline breaks at HF remain one of the major challenges of CMAM in the LGA. There is no formal and consistent supply chain structure for transporting RUTF from the state to LGA and then to HFs. The LGA only provide the sum of Nigerian Naira 3,000 for the transportation which is often delayed thereby putting the whole burden of the transportation on the NFP. Shortage of trained health workers on CMAM is by far the biggest impediment to CMAM activities in the LGA. It is pertinent to note that the SMOH had developed a model of dealing with health workers shortage; they put 2 adjacent wards to share an OTP and HWs from non-OTP HFs were trained on CMAM and were mandated to come
28 Credible interval

32
to the OTP on OTP day to help in service delivery to the clients. Aside from performing duties on OTP day, they also serve as a means of referring SAM cases (verbal referral) to the OTP. An important barrier to coverage was rejection by care-givers to bring SAM cases with complications the SC. This is mainly due to long distance to the SC (General Hospitals and Federal Medical Centre in neighboring LGAs of Birnin-Kebbi and Jega). The community outreach activity is virtually non-existent in the LGA. Except for the village leaders who were sensitized at the LGA level, none of the community members ever reported being mobilized and or sensitized about the CMAM program in the communities. The only sensitizations going on were done by town criers on the behest of the village leaders. Furthermore, there are no CVs in the 5 wards that do not have OTP sites and even in the OTP wards the CVs are no more active and there is no home visit, follow-up, defaulter tracing by CVs with zero collaboration with the health workers. These have totally paralyzed the community outreach part of the CMAM program in the LGA. Key booster of the program was provision of transportation to health volunteers (non CMAM CVs) to help in referring cases from far settlements to the OTP by the religious leader of Wuro-Gauri. This was happening because the religious leader was sensitized in the LGA and understood the importance of seeking treatment for SAM cases. Also, the HW in charge of Keta PHC occasionally provided food and travel facilitation to CVs that came from neighboring villages to come to the CMAM site on the OTP service days. The admission data in the LGA reveals that only 51.84% of cases are from Kalgo LGA with the remaining coming from neighboring LGAs. Smoothing of the admission data over time using the median and averages of 3 months period (M3A3)29 reveals that the admission trend is in tandem with seasonal trends as more cases are enrolled in the period corresponding to hunger peaks and increase disease burdens (June-September) except for an unusual down ward trend in August which was attributed to RUTF stock-out and HWs strike. In general, the communities have a very poor understanding of what constitute a SAM case as only cases showing manifestation of malnutrition when it has deteriorated (such as thinness (marasmus) and from other diseases are considered as SAM. Other cases that results from other causes other than illness such as breast-feeding difficulties or other conditions that leads to outcomes such as Oedema (kwashiorkor) and marasmic kwashiorkor were not considered as SAM and attributed to superstitious causes hence they resort to wrong treatment seeking pathways thereby leading to late treatment seeking. This was further confirmed by traditional healers in the community who reported treating SAM cases. It is also important to note that those traditional healers were not factored during community mobilization at all. This is a huge lost opportunity as they are still being patronized by the care-givers. Overall, the barriers obtained in stage 1 were reaffirmed by the barriers found during the small area survey and likelihood surveys.
6. Conclusion
In conclusion, the program was designed by UNICEF in such a way that it will cater for at least 50% of SAM cases in the LGA (meaning the CMAM program expected target is 50% of SAM cases in the LGA). Thus if the program was able to have a Met Need of 50%, then it must have reached its intended target. In our effort to investigate this, the Met Need of the LGA was calculated using parameters for cases that are from the LGA only.
The calculation was as follows;
Thus the Met Need of the program is 21.08% which is far below the intended target of 50% set in the initial set up of the program in the LGA. This implies that there is much that is needed to be done in order to reach the minimum of target of 50% target.
29 Done to remove noise and enhanced seasonal trends and comparing it to the seasonal calendar

33 竹
7. Recommendations According to the barriers found by SQUEAC investigation, key recommendations perceived to strengthen the CMAM program were identified and presented for further deliberations in a meeting with SNO, director of primary health and other key officials in the state and LGA. These are tabulated below:
SHORT TERM MEASURES TARGET ISSUE PROCESS OF IMPLEMENTATION RESPONSIBLE PARTY EXPECTED OUTPUT TIME LINE IMPROVING COMMUNITY MOBILIZATION & SENSITIZATION
Community advocacy and re-orientation of husbands about the need for their wives to seek treatment from health facilities
Community leaders, NFP • Drop in defaulter rate • Increase in admission • Exit interview with mothers
June – July 2014
Sensitization on the Majalis and religious gatherings (Juma’at prayers) on the importance of CMAM
Community leaders, NFP As above Routine Data
June – July 2014
Display of social mobilization posters in the communities about the availability of service.
NFP, Health Facilities I/C CMAM posters displayed in the communities to improve knowledge on SAM and Malnutrition
June, 2014
HEALTH EDUCATION
Health talks on nutrition to new cases during OTPs days for the caregivers
NFP, Health Facilities I/C Improvement in Cure Rate in routine data
June, 2014
Frequent home visit and follow up by community volunteers NFP, Health Facilities I/C Reduction in Defaulter and Non-recovered Rates
June-August, 2014
Provision and display of posters and other IEC materials in the health facility
UNICEF, Partners, SNO,NFP, Health Facilities I/C
Improvement in admission and discharges based on National guideline
July-August, 2014
PROGRAM MONITORING AND CAPACITY BUILDING
Provision of referral slips to the health workers for passive referral from non-OTP health facilities
NFP Documentation of passive referrals and DNA cases
June, 2014
Conduct regular supportive supervision to health facilities by DPH & DPHC to provide support to CMAM
DPH, DPHC Provision of top level support to Health workers
July, 2014
Health facilities visits for on the job coaching and mentoring by SNO, DSNO, NFP, DNFP
SNO, NFP Capacity building of Health Workers
June – July, 2014
Development of tracking system of referral between OTP-SC and OTP-OTP.
SNO, NFP Improve collaboration/ coordination between HFs
July, 2014
Development and printing of Coloured Cards for CVs to track their referral and active case finding
SNO, NFP Records of CVs activities and DNA cases
July-August, 2014

34
LONG TERM MEASURES TARGET ISSUE
PROCESS OF IMPLEMENTATION RESPONSIBLE PARTY
EXPECTED OUTPUT TIME LINE
IMPROVING COMMUNITY MOBILIZATION & SENSITIZATION
Advocate for printing and distribution of posters translated in local languages, in Arabic text (Ajami)
DPH,SNO, UNICEF, SCI Posters using Arabic text in local languages produced & displayed in communities
September – December, 2014
Incorporating CMAM awareness into existing Radio Health Programs
Director Public Health, SNO
Nutrition/CMAM talks conducted on Radio
July – December, 2014
Production and airing of Drama and documentary on CMAM Director Public Health, SNO, UNICEF
Drama to be performed in communities
November, 2014
PROGRAM MONITORING AND CAPACITY BUILDING
Re-training of HWs Director Public Health, SNO, UNICEF
Health workers in low performing LGAs update their knowledge of CMAM
July-August, 2014
Training of new CVs and refresher training of existing CVs Director Public Health, SNO, NFP, Community Leaders, UNICEF
CVs recruited and trained where absent and existing CVs retrained
August – September, 2014
Routine data quality assessment(DQA) to be conducted in all OTP site to bring the data up to date
SNO, UNICEF CMAM Database updated and gaps identified for targeted training to HWs on data management
September – October, 2014
Trained health workers should only be transferred between OTPs offering Health Facilities
NFP, Director PHC Kalgo LGA, LGA Secretary
All trained HWs transferred only from an OTP to OTP
June – December, 2014
FINANCIAL SUPPORT
Advocacy visit to ALGON Chairman to request the setting aside of a certain amount of money deducted from source to support nutrition activities in the LGAs
UNICEF, Director Public Health and SNO
A dedicated amount of money set aside for nutrition activity to each LGA and deducted from source
June – December, 2014
Full SQUEAC assessment
Advocate for allocation of funding for a low scale follow-up SQUEAC study
Director Public Health, SNO, UNICEF
SQUEAC report November/December 2014

35
8. Annexure Annex I: List of Participants S/No. Name Position Organization
1 Beatrice U. Kwere DSNO State 2 AbdulMalik Muhammad State State 3 Abbas Abdullahi NFP LGA 4 Suwaiba Garba ANFP LGA 5 Aliyu Abubakar Enumerator NBS 6 Naomi Bello Sale Enumerator NBS 7 Usman Alkali Enumerator State 8 Hadiza Dange Enumerator State 9 Fati Zagi Enumerator State
10 Amina Ibrahim Enumerator State 11 Aishatu Abubakar Dogo Enumerator State 12 Suwaiba Usman Enumerator State 13 AbdurRahman Zubairu Yerima Enumerator SCI 14 Hauwa Adamu Sakaba Enumerator SCI 15 Anna Garba Enumerator SCI 16 Dada Ahmad Manga Enumerator SCI 17 Adamu Abubakar Yerima Coverage Coordinator SCI 18 Ode Okponya Ode Coverage Officer SCI 19 Salisu Sharif Jikamshi Coverage Officer SCI 20 Ayobami Oyedeji Coverage Officer SCI 21 Dominic Abi Log Assistant/Driver SCI 21 Yusuf Abel Log Assistant/Driver SCI

36
Annex II: Local Terms to describe Malnutrition S/No Description Local Terms 1. Wasting Tamowa 2. Sunken Fontanel Ciwon Madiga 3. Oedema Ciwon Kaba 4. Wasting Shan Ciki 5. Oedema Ciwon Iska 6. Oedema Uffu (Fulfulde) 7. Oedema Kwakwabo 8. Oedema Ciwon Sanyi 9. Oedema Ciwon Zafi 10. Wasting Onogo Fulfulde) 11. Tonsilitis Hakin Wuya 12. Weaned child Dan Yaye 13. Wasting Bamduti 14. Wasting Tsotsewar Jiki 15. Oedema Mai Gudima 16. Wasting Tamakari 17. Wasting Marainiya 18. Wasting Garjen Giwa 19. Wasting Kenane 20. Wasting Ciwon da Mai-Goyo ba ta fadi
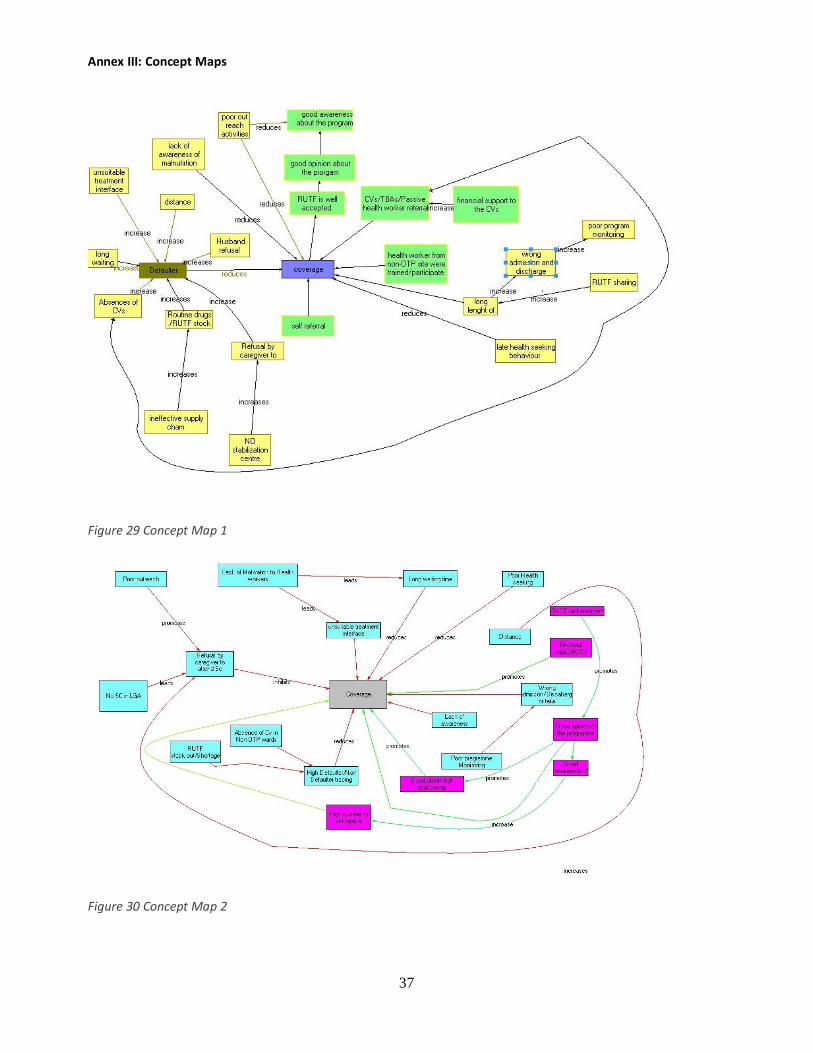
37
Annex III: Concept Maps
Figure 29 Concept Map 1
Figure 30 Concept Map 2

38
Figure 31 Concept Map 3

39
Annex IV: Itinerary of Survey Days Date Activity Tuesday – Friday 22nd - 24th April Meeting with SCI Kebbi field office, SMOH, LGA and
Routine Data extraction Saturday 25th April Routine Data extraction Sunday 26th April Monday 27th April Training of Enumerators and Government counterparts Tuesday 28th April Training continues Wednesday 29th April Training finalized, field testing and MUAC standardization Thursday 30th April Data Extraction Friday 1st May Data Extraction Saturday 2nd May Sunday 3rd May Monday 4th May Routine Data Analysis Tuesday 5th May Qualitative data gathering; visit Hirishi, Badariya Wuro
Gauri, Shadadi and Unguwar Wa Wednesday 6th May Qualitative data gathering; visit Ruga Dan Bagga, Diggi,
Etene, Keta Thursday 7th May Qualitative data gathering; visits Zuguru, Kwimi, Nayelwa Friday 8th May Qualitative data analysis, Development of BBQ and Mind
Mapping Saturday 9th May Qualitative data analysis, Development of BBQ and Mind
Mapping finalized Sunday 10th May Hypothesis setting, Concept map and Mind mapping
finalized Monday 11th May Small Area Survey Tuesday 12th May Small Area Survey Wednesday 13th May Development of Prior and Sample size for likelihood survey Thursday 14th May Wide Area Survey Friday 15th May Wide Area Survey Saturday 16th May Wide Area Survey Sunday 17th May Wide Area Survey Monday 18th May Binomial conjugate analysis; Posterior Tuesday 19th May Debriefing of Stakeholders/Dissemination Meeting
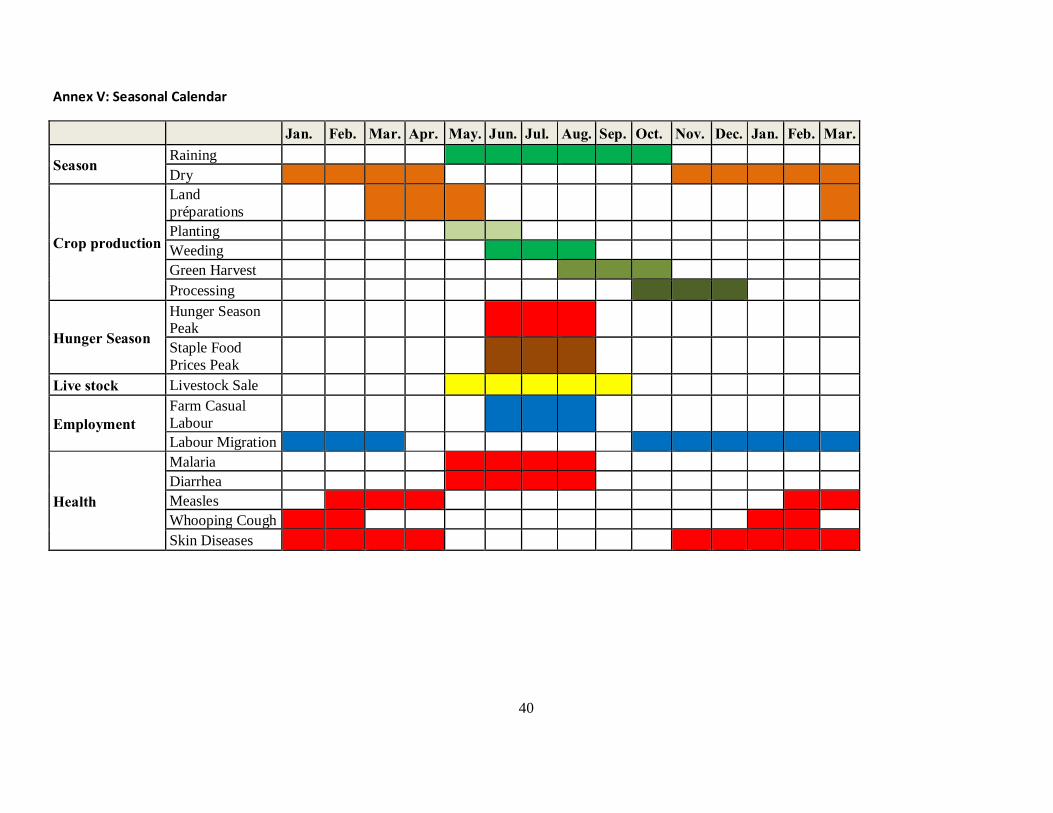
40
Annex V: Seasonal Calendar
Jan. Feb. Mar. Apr. May. Jun. Jul. Aug. Sep. Oct. Nov. Dec. Jan. Feb. Mar.
Season Raining Dry
Crop production
Land préparations Planting Weeding Green Harvest Processing
Hunger Season
Hunger Season Peak Staple Food Prices Peak
Live stock Livestock Sale
Employment Farm Casual Labour Labour Migration
Health
Malaria Diarrhea Measles Whooping Cough Skin Diseases

41
Annex VI: Questionnaires
Carer Interview Form
Name of Health facility/CMAM Site: __________________________ LGA:________________________ Ward Name: __________________________Interviewer Name/ Team#: __________________ State: _____________________________ Date: ______/______/ 2014 Village name: _______________________ Description of Questions: BOLD fonts define questions while ITALIC fonts declare guidance notes. Question# 1: How did this child get to be in this program? Guidance notes: Take history Explore local terms used for SAM children ________________________________________________________________________________________________________ Where did you take the child the first time you noticed he/she was malnourished? Find out its treatment seeking behavior ________________________________________________________________________________________________________ Who told/referred you to visit the CMAM site? Program case findings and referrals methods ________________________________________________________________________________________________________ Question#2 Do you know of any children in your village that are like your child and are not attending this program? Yes No Guidance Notes: (Then ask about index child specific history from above, common SAM etiologies(with specific local names for severe malnutrition) like e.g description of illness with specific signs e.g thin arms, swollen feet, kwashiorkor signs etc, Treatment seeking behavior/pathways to care). if YES please follow Part-A if NO please follow Part-B Part-A why do you think child is not attending this program? (How do you know this, any other reasons, any other children, record name and home location of the informant for follow up). ________________________________________________________________________________________________________ Part-B: if there were children like your child that are not attending this program why do you think they would not attend the program? (Explore of any other reason that stops peoples coming to health facility?) ________________________________________________________________________________________________________ Question#3 if I wanted to find children like your child and the children we have spoken about, how would I best describe them to other people? (discover local terms used to describe SAM in in local language, any other names used to describe sever malnourished children’s, are these the same things as malnutrition). ________________________________________________________________________________________________________ Question# 4 if I wanted to find a children like your child and the children we have spoken about who would best be able to help me to find them? (Ask directly about midwives, traditional birth attendants, traditional healer’s, LHW, Community volunteer’s, the people mentioned in history when exploring treatment seeking behaviors and the peoples use by the programs for case findings/ referrals, Ask “why” and “why not” ________________________________________________________________________________________________________ Q#5 where do you come from, how do you reach here? Guidance Notes: Is CMAM sites nearby/ Far/or very far from your home, walk by feet, time to travel to site, if there is an need for transport how much does it cost? ________________________________________________________________________________________________________ Q#6 What are some challenges you face accessing this programme? Guidance Notes: Is the queue unusually long? Do you usually wait for a long time before being attended to? Are you asked to pay for some services? Are the health workers friendly to you? ________________________________________________________________________________________________________ Q#7 What do you think we can do to improve this programme? ________________________________________________________________________________________________________ Q#8 Is there any other place you/other carers can get/buy RUTF in your village or nearby community? Chemist shop, tea shop, market, other mothers/carers, Okada. Q#9. Is RUTF being tasted, eaten or shared by adult or siblings in your village or nearby community? Guidance Note; probe further if sharing/consumption of RUTF is being done by non-SAM children & adults. ________________________________________________________________________________________________________ Q#10. How do you give RUTF to your child and how many sachets per day? (Guidance Note; probe further on number of sachet given to the mother at the OTP site).

42
Community Questionnaire Community elders opinion leaders, religious leaders Tea shop gatherings/majalisa, (Age- range) Gender
Name of Health facility/CMAM Site: __________________________ State:________________________ LGA:__________________________ Ward:_____________________________ Village:__________________________________ Distance from the CMAM Site:________________ Date:______/______/ 2014 Interviewer Name/ Team#: __________________ Instruction: ask all the question and probe where necessary. 1. What does the community refer “malnutrition” (probe for local terms used in describing malnutrition and
explain the local meanings e.g. ‘Tamowa’ means wasted while ‘Kumburi’ means swollen body) 2. How are the cases who have the condition mentioned above treated/where are the sick cases currently
treated in the community? 3. Have you heard about the CMAM program/program treating malnutrition?
4. If there is a program/health facility treating malnutrition (use local term for malnutrition), what is the name of the facility giving treatment?
5. Do you see malnourished children going to this program/facility that treats malnutrition (CMAM programme)?
6. Do you know of any carer/mother taking their child for treatment? Give the name of the Child and the parent and the village where they come from?
7. Has anyone come to the community to talk to you about the malnutrition (use local terms) and how it is treated?
8. Have you seen a MUAC tape (show the MUAC strip to the interviewees)? 9. Have you seen RUTF (Show sachets of RUTF in use in the program e.g plumpy nut)? 10. Have you ever seen adults eating RUTF (Plumpy nut)? 11. Apart from the CMAM site, is there any other place in this community where I can obtain/buy RUTF? 12. What is your involvement/contribution to the programme? 13. What do you think about the program and how can we improve it?(keep on probing)
43
For the carers of children (Severe cases) who are NOT in the programme
Name of Health facility/CMAM Site: __________________________ LGA:________________________ Ward Name: __________________________Interviewer Name/ Team#: __________________ State: _____________________________ Date: ______/______/ 2014 Village name: ________________________
********************************************************************* 1. DO YOU THINK YOUR CHILD IS MALNOURISHED? * YES * NO
2. ARE YOU AWARE OF THE EXISTENCE OF A PROGRAMME WHICH CAN HELP MALNOURISHED CHILDREN? * YES * NO (→ stop!) If yes, what is the programme’s name? ______________________________________
3. WHY IS YOUR CHILD CURRENTLY NOT ENROLLED IN THE PROGRAMME?
* Too far (How long does it take to walk….…hours) * No time / too busy. What is the parent doing instead?________________________ * Mother is sick * The mother cannot carry more than one child * The mother feels ashamed or shy about coming * Security problems * There is no one else who can take care of the other siblings * The amount of RUTF was too little to justify the journey * The child has been rejected by the programme already. When? ______ (approx.) * Other parents’ children have been rejected * My husband refused * I thought it was necessary to be enrolled at the hospital first * I do not think the programme can help my child (prefer traditional healer, etc.) * Other reasons (specify): ___________________________________________________
4. WAS YOUR CHILD PREVIOUSLY ADMITTED TO THE PROGRAMME? * YES * NO (→ stop!) If yes, why is he/she not enrolled anymore? * Defaulted (when?........ why?.....) * Condition improved and discharged by the programme (when?........) * Discharged because he/she was not recovering (when?........) * Other:___________________________________________ (Thank the carer)

44
Health Facility Staff (clinic staff) Interview Form
Name of Health facility/CMAM Site: __________________________ LGA:________________________ Ward Name:__________________________Interviewer Name/ Team#: __________________ State:_____________________________ Date:______/______/ 2014 ********************************************************************* Question# 1 a. Have you being trained on CMAM? If yes, how many times and when did you receive the last training? b. How many beneficiaries do you see on daily basis (average flow of admission)?
a)OTP ___________________________________________________________________________________ b) Other Patients________________________________________________
Question#2: How do you get new OTP beneficiaries who come here (SAM- children)? Question#3: From where do your OTP beneficiaries (SAM- children) come from? Nearest villages
a) What is/are the name(s) of the nearest village(s)_______________________________ b) What do the carers mostly use to come to facility _______________________ eg: motor cycle, walking,
bus etc c) If walking how long (in estimated minutes/hours) does it take carer to walk to facility________________
Furthest villages a) What is/are the name(s) of the farthest village(s)________________________________ b) What do the carers mostly use to come to facility _______________________ eg: motor cycle, walking,
bus etc c) If walking how long (in estimated minutes/hours) does it take carer to walk to facility________________
Question#4 what is community impression about OTP program (that is part of this CMAM program)? Question# 5 What are the main challenges that you think are related to OTP program here? Question# 6 How do you deal with OTP defaulters? Question# 7 what are major diseases children suffer from in this Locality? Question# 8 Do you get malnourished children referred from another facility? Question#9: How do you routinely assess malnutrition? Question#10: Is there stock out of supplies in OTP within the last 1 year? (e.g RUTF, Amoxicillin etc.). If yes then how does this affects program services? Question#11 Are there communities/certain persons in the community which are not able to access CMAM services? Guidance Notes: Specifically ask about high class/nomads/minority ethnic group or any other specific population group who are not able to come to CMAM site due to stigma or any other reason. please explain? Question#12 What is your collaboration with CV? Guidance Notes: Specifically ask about referral, follow-up, home visit and DNA cases. please explain?

45
Community Volunteers Questionnaire
LGA: ___________________Ward:____________ Health Facility:______________Date: _____________ Name of the interviewer/Team No._______________________________________ Villages/settlements covered: ___________________________________________ Distances from the CMAM Site: __________________________________________
1. How long have you been working as a CV for CMAM programme? 2. Give brief history of your work as a CV (activities; what do you do?)
……………………………………………………………………………………………………………………………………………………
3. How Many Times have you been trained on CMAM and when did you receive the last training?
4. How do you identify malnourished child (probe for signs and symptoms)? ……………………………………………………………………………………………………………………………………………………
5. Do you have MUAC tape? Yes (if yes, show me) No
6. How do you use MUAC tape? Make notes on whether it is done correctly
7. What are the names given to malnutrition in the local community (use local terms)? Probe for names of different types of malnutrition: e.g Oedema (Swollen arms, legs and stomach), Sagging Buttocks, wasting etc)
8. Where do the carers (Mothers) seek help first when their child is sick? Probe to determine health seeking behavior, if mothers visit chemists, community volunteer, traditional healers/native doctors etc first before visiting the health facility
9. Have you ever referred malnourished child to CMAM site? 10. After you refer children to the CMAM site, how do you know they attended the program? 11. What do you think about the CMAM program (aikin kwamazo)? 12. What do you think Plumpy nut (RUTF) is and how do you describe it to the mothers (do they think it is
chocolate or food)? 13. Is Plumpy nut (RUTF) food/Chocolate shared in the family/community? 14. Is Plumpy nut (RUTF) a medicine for malnourished children in the community? 15. How do you follow-up on defaulters in the CMAM program 16. How often do you meet with the health worker to discuss on CMAM programme? 17. What is the community perception of the program? Probe 18. Are there certain communities who do not have access to CMAM Program? 19. If there are such communities what could be the reasons preventing them access? 20. What are the challenges you are facing in performing your duties? 21. What do you think we can do to improve this programme?



















