
Certificate of Credible coverage - Lockheed Martin
173
This document is a Lockheed Martin Summary Plan Description (SPD). Since SPDs change from time to time, it is important that you always review any updates before reading the document. The updates are located at the front of the SPD. Finding what you want within this SPD is quick and easy. To navigate through the document, click on the Bookmarks tab at the left-hand side to display the document index. All applicable updates appear at the top of the index. After reviewing the updates, scroll down through the document or use the index and go directly to a section of specific interest. If you have any questions about the benefits outlined in this SPD, please call the Lockheed Martin Employee Service Center: 866-562-2363 - Toll-free calls in the U.S. 201-242-4397 - International callers 800-833-8334 - Hearing impaired
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Certificate of Credible coverage - Lockheed Martin
This document is a Lockheed Martin Summary Plan Description (SPD). Since SPDs change from time to time, it is important that you always review any updates before reading the document. The updates are located at the front of the SPD. Finding what you want within this SPD is quick and easy. To navigate through the document, click on the Bookmarks tab at the left-hand side to display the document index. All applicable updates appear at the top of the index. After reviewing the updates, scroll down through the document or use the index and go directly to a section of specific interest.
If you have any questions about the benefits outlined in this SPD, please call the Lockheed Martin Employee Service Center:
866-562-2363 - Toll-free calls in the U.S. 201-242-4397 - International callers 800-833-8334 - Hearing impaired

LMC-ZQB 104SMMB19
April 26, 2019 Summary of Material Modifications Important Information Regarding the Employee Assistance Program This notice is being sent to you to update information in the Summary Plan Descriptions (SPDs) listed in the Attachment. This notice is now part of the official plan documents and is legally referred to as a Summary of Material Modifications (SMM) to this SPD. Employee Assistance Program Information Location Effective Jan. 1, 2018, Employee Assistance Program (EAP) information that appears in your Medical, Dental and/or Vision SPD is removed. Also effective Jan. 1, 2018, the EAP will be described in its own SPD titled “Lockheed Martin Group Benefits Plan – Employee assistance program for eligible employees of Lockheed Martin Corporation” (ZQA – 108SPDB19, effective Jan. 1, 2018). When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Benefits. From LMESC Online, click Library and then Summary Plan Descriptions. https://www.lmpeople.com – on the Internet You will need your User ID (NT ID) and Password to access the website from the Internet. Click on LM Employee Service Center under Benefits. From LMESC Online, click Library and then Summary Plan Descriptions. lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the Claims Administrator.
Please keep this notice with your other important benefits information.

LMC-ZNN 120SMMB18
Aug. 17, 2018 Summary of Material Modifications Important Information Regarding Changes to the Lockheed Martin Health Plan This notice is being sent to you to update information in the Summary Plan Descriptions (SPDs) listed in the Attachment. This notice is now part of the official plan documents and is legally referred to as a Summary of Material Modifications (SMM) to this SPD. Nondiscrimination Notice The Lockheed Martin Health Plan complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. The Lockheed Martin Health Plan does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex. The Lockheed Martin Health Plan:
• Provides free aids and services to people with disabilities to communicate effectively with us, such as: − Qualified sign language interpreters − Written information in other formats (large print, audio, accessible electronic formats, other
formats) • Provides free language services to people whose primary language is not English, such as:
− Qualified interpreters − Information written in other languages
If you need these services, contact the Senior Manager, Compliance through the Lockheed Martin Plan Administration Helpline at 301-548-2320. If you believe that The Lockheed Martin Health Plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with: the Senior Manager, Compliance through the Lockheed Martin Plan Administration Helpline, 6801 Rockledge Drive, CCT-115, Bethesda, MD, 20817, 301-548-2320. You can file a grievance in person or by mail. If you need help filing a grievance, the Senior Manager, Compliance is available to help you. You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 509F, HHH Building Washington, D.C. 20201 1-800-368-1019, 800-537-7697 (TDD) Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html. The effective date of this notice is Oct. 17, 2016.

LMC-ZNN 2 120SMMB18
ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística.
Llame al 866-562-2363.
注意:如果您使用繁體中文,您可以免費獲得語言援助服務。請致電866-562-2363。
CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn. Gọi số 866-
562-2363.
주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 866-562-
2363번으로 전화해 주십시오.
PAUNAWA: Kung nagsasalita ka ng Tagalog, maaari kang gumamit ng mga serbisyo ng tulong sa
wika nang walang bayad. Tumawag sa 866-562-2363.
ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные услуги
перевода. Звоните 866-562-2363.
ATANSYON: Si w pale Kreyòl Ayisyen, gen sèvis èd pou lang ki disponib gratis pou ou. Rele 866-
562-2363.
ATTENTION: Si vous parlez français, des services d'aide linguistique vous sont proposés
gratuitement. Appelez le 866-562-2363.
UWAGA: Jeżeli mówisz po polsku, możesz skorzystać z bezpłatnej pomocy językowej. Zadzwoń
pod numer 866-562-2363.
ATENÇÃO: Se fala português, encontram-se disponíveis serviços linguísticos, grátis. Ligue para
866-562-2363.
ATTENZIONE: In caso la lingua parlata sia l'italiano, sono disponibili servizi di assistenza linguistica
gratuiti. Chiamare il numero 866-562-2363.

LMC-ZNN 3 120SMMB18
ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos sprachliche Hilfsdienstleistungen
zur Verfügung. Rufnummer: 866-562-2363.
.2363-562-866لحوظة: إذا كنت تتحدث اذكر اللغة، فإن خدمات المساعدة اللغویة تتوافر لك بالمجان. اتصل برقم م
注意事項:日本語を話される場合、無料の言語支援をご利用いただけます。866-562-2363
まで、お電話にてご連絡ください。
تماس بگیرید. 2363-562-866اشد. با گفتگو می کنید، تسھیالت زبانی بصورت رایگان برای شما فراھم می ب فارسی: اگر بھ زبان توجھ When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at: Current Employees:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Benefits. From LMESC Online, click Library and then Summary Plan Descriptions. https://www.lmpeople.com – on the Internet You will need your User ID (NT ID) and Password to access the website from the Internet. Click on LM Employee Service Center under Benefits. From LMESC Online, click Library and then Summary Plan Descriptions. lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions.
Retirees:
lmc.lifeatworkportal.com – You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions. http://lockheedmartin.com – Click Employees from the top right corner of the page, then click Retirees. From the Benefits information section, click Lockheed Martin Service Center. You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions.

LMC-ZNN 4 120SMMB18
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the Claims Administrator.
Please keep this notice with your other important benefits information.

LMC-ZNF 101SMMB18
Jan. 1, 2018 Summary of Material Modifications Important Information Regarding a Change Effective Immediately
This notice is being sent to you to update contact information in the Summary Plan Descriptions (SPDs) listed in the Attachment. This notice, describing changes that are effective immediately, is now part of the official plan document and is legally referred to as a Summary of Material Modifications (SMM) to the SPD.
COBRA Administrator Change The name and web site address for the administrator of Lockheed Martin’s COBRA benefits has changed. Following is information about your COBRA administrator: WageWorks Benefit Administrators P.O. Box 226985 Dallas, TX 75222-6985 800-482-4105 877-822-9089 (fax) mybenefits.wageworks.com
When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at:
Current Employees:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Benefits. From the Lockheed Martin Employee Service Center (LMESC) Online, click Library and then Summary Plan Descriptions. https://www.lmpeople.com – on the Internet You will need your User ID (NT ID) and Password to access the website from the Internet. Click on LM Employee Service Center under Benefits. From the Lockheed Martin Employee Service Center (LMESC) Online, click Library and then Summary Plan Descriptions. lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions.

LMC-ZNF 2 101SMMB18
Retirees: lmc.lifeatworkportal.com – You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions. http://lockheedmartin.com – Click Employees from the top right corner of the page, then click Retirees. From the Benefits information section, click Lockheed Martin Service Center. You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the claims administrator.
Please keep this notice with your other important benefits information.

LMC-ZNF 9 101SMMB18
NONDISCRIMINATION NOTICE The Lockheed Martin Health Plan complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. The Lockheed Martin Health Plan does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex. The Lockheed Martin Health Plan:
• Provides free aids and services to people with disabilities to communicate effectively with us, such as:
o Qualified sign language interpreters o Written information in other formats (large print, audio, accessible electronic formats,
other formats) • Provides free language services to people whose primary language is not English, such as:
o Qualified interpreters o Information written in other languages
If you need these services, contact the Senior Manager, Compliance through the Lockheed Martin Plan Administration Helpline at 301-548-2320. If you believe that The Lockheed Martin Health Plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with: the Senior Manager, Compliance through the Lockheed Martin Plan Administration Helpline, 6801 Rockledge Drive, CCT-115, Bethesda, MD, 20817, 301-548-2320. You can file a grievance in person or by mail. If you need help filing a grievance, the Senior Manager, Compliance is available to help you. You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 509F, HHH Building Washington, D.C. 20201 1-800-368-1019, 800-537-7697 (TDD) Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html. ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística. Llame al 866-562-2363. 注意:如果您使用繁體中文,您可以免費獲得語言援助服務。請致電866-562-2363。
CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn. Gọi số 866-562-2363. 주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 866-562-2363번으로 전화해 주십시오. PAUNAWA: Kung nagsasalita ka ng Tagalog, maaari kang gumamit ng mga serbisyo ng tulong sa wika nang walang bayad. Tumawag sa 866-562-2363.

LMC-ZNF 10 101SMMB18
ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные услуги перевода. Звоните 866-562-2363. ATANSYON: Si w pale Kreyòl Ayisyen, gen sèvis èd pou lang ki disponib gratis pou ou. Rele 866-562-2363. ATTENTION: Si vous parlez français, des services d'aide linguistique vous sont proposés gratuitement. Appelez le 866-562-2363. UWAGA: Jeżeli mówisz po polsku, możesz skorzystać z bezpłatnej pomocy językowej. Zadzwoń pod numer 866-562-2363. ATENÇÃO: Se fala português, encontram-se disponíveis serviços linguísticos, grátis. Ligue para 866-562-2363. ATTENZIONE: In caso la lingua parlata sia l'italiano, sono disponibili servizi di assistenza linguistica gratuiti. Chiamare il numero 866-562-2363. ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos sprachliche Hilfsdienstleistungen zur Verfügung. Rufnummer: 866-562-2363.
.2363-562-866ملحوظة: إذا كنت تتحدث اذكر اللغة، فإن خدمات المساعدة اللغویة تتوافر لك بالمجان. اتصل برقم 注意事項:日本語を話される場合、無料の言語支援をご利用いただけます。866-562-2363 まで、お電話にてご連絡ください。
: اگر بھ زبان فارسی گفتگو می کنید، تسھیالت زبانی بصورت رایگان برای شما فراھم می توجھ تماس بگیرید. 2363-562-866باشد. با

LMC-ZPG 122SMMB18
July 17, 2018 Summary of Material Modifications Important Information Regarding Changes Effective April 14, 2017 Effective April 14, 2017, you are eligible to participate in the benefits described in the Summary Plan Descriptions (SPDs) listed below if you are represented by Lowcountry Contract Instructor Pilot Association (LCIPA) F35, MCAS, Beaufort, SC. This notice is now part of the official plan documents and is legally referred to as a Summary of Material Modifications (SMM) to the following SPDs:
• Health Care and Dependent Care Spending Accounts ─ For certain non-represented and represented employees of Lockheed Martin Corporation (ZZE – H10SPD183, effective Jan. 1, 2011)
• LM HealthWorks Plan ─ Health benefits for certain non-represented and certain represented employees (ZAH – 207SPDB11, effective Jan. 1, 2011)
• LM HealthWorks Quit for Life™ Program ─ Tobacco cessation program for eligible employees of Lockheed Martin Corporation (ZN5 – G07SPD154, effective Sept. 25, 2006)
• LM HealthWorks Wellness Center (111SPDB13, effective Jan. 1, 2014) • Lockheed Martin Business Travel Accident Plan ─ For certain non-represented and certain
represented employees (ZZV – 213SPDB11, effective Jan. 1, 2011) • Lockheed Martin Corporation Dental Plans ─ Comprehensive Dental, Comprehensive Plus
Dental and Managed Dental for nonrepresented and certain represented employees of Lockheed Martin Corporation (ZBK – 113SPDB12, effective Jan. 1, 2012)
• Lockheed Martin Corporation International Indemnity Plan (IIP) ─ Health benefits for certain employees of Lockheed Martin Corporation (ZCE – 107SPDB12, effective Jan. 1, 2012)
• Lockheed Martin Corporation Managed Care (HMO and PPO) Medical Plans ─ Medical Plans for non-represented and certain represented employees of Lockheed Martin Corporation (ZBJ – 112SPDB12, effective Jan. 1, 2012)
• Lockheed Martin Corporation Vision Plan ─ Vision Plan for non-represented and certain represented employees of Lockheed Martin Corporation (ZBL –114SPDB12, effective Jan. 1, 2012)
• Lockheed Martin Group Benefits Plan ─ Life and accident insurance for non-represented salaried and certain represented employees of Lockheed Martin Corporation (ZBC – 214SPDB11, effective Jan. 1, 2012)
• Long-Term Disability Insurance Benefits ─ Under the Lockheed Martin Group Benefits Plan and the Lockheed Martin Operations Support, Inc. Benefit Plan (ZBR – 107SPDB14, effective Jan. 1, 2014)
• Short-Term Disability (STD) Insurance ─ For certain non-represented and certain represented employees of Lockheed Martin Corporation (ZEM – 115SPDB15, effective Jan. 1, 2014)

LMC-ZPG 2 122SMMB18
When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Benefits. From the Lockheed Martin Employee Service Center Online, click Library and then Summary Plan Descriptions. https://www.lmpeople.com – on the Internet You will need your User ID (NT ID) and Password to access the website from the Internet. Click on LM Employee Service Center under Benefits. From the Lockheed Martin Employee Service Center Online, click Library and then Summary Plan Descriptions. lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the claims administrator.
Please keep this notice with your other important benefits information.

LMC-ZMW 151SMMB17
Dec. 29, 2017 Summary of Material Modifications Important Information Regarding Changes Effective Jan. 1, 2017 and Jan. 1, 2018 This notice is being sent to you to update information related to dependent eligibility in the Summary Plan Descriptions (SPDs) listed in the Attachment. This notice, describing changes that are effective Jan. 1, 2017 and Jan. 1, 2018, is now part of the official plan document and is legally referred to as a Summary of Material Modifications (SMM) to the SPD. Note: This SMM only applies to eligible Lockheed Martin employees participating in the plans listed in the Attachment to this SMM. The changes outlined in this SMM do not apply to employees who have transitioned to Leidos. Changes to the Dependent Eligibility Definition Effective Jan. 1, 2017, same-sex domestic partners will no longer be eligible to be covered as dependents on Lockheed Martin’s insurance plans. In addition, children of a same-sex domestic partner will no longer be eligible to be covered. Dependents that are removed from coverage as a result of this change will be eligible for COBRA continuation coverage. Effective Jan. 1, 2018, any child(ren), up to age 26, for whom you are a court-appointed legal guardian, will be covered under the Plan. As a result, the following modification will be made: Current language:
You may be able to cover your grandchildren up to age 26, but only if you have court-appointed legal guardianship. Acceptable proof of court appointed legal guardianship will be required before you can enroll a grandchild for the first time and from time to time on request.
Modified language:
Any children (including but not limited to grandchildren) for whom you are a court-appointed legal guardian. Acceptable proof of court-appointed legal guardianship will be required before you can enroll such a child for the first time and from time to time on request.
Dependent Eligibility The following replaces the “Dependent Eligibility” section of the SPD: If you enroll in coverage, you may also enroll your eligible dependents under the Plan.

LMC-ZMW 2 151SMMB17
Your eligible dependents under the Plan include:
Your spouse*; Your children up to age 26 (with no student, marital or financial requirements), if they are:
- Your natural children; - Your legally adopted children; - Children placed with you for legal adoption; - Your stepchildren (natural or legally adopted children of your legal spouse); or - Children (including but not limited to grandchildren) for whom you are a court-appointed
legal guardian. Acceptable proof of court appointed legal guardianship will be required before you can enroll such a child for the first time and from time to time on request.
Your disabled children age 26 and older who, when they first became disabled, would have met the definition of an eligible dependent and who are incapable of self-sustaining employment because of an intellectual disability, serious mental illness, physical sickness or injury. Coverage may continue to age 65 as long as your child remains incapacitated and is otherwise eligible for coverage. To extend this coverage, you must show proof of your child’s incapacity within 30 days after regular coverage ends or within 30 days of your child’s initial eligibility date, if later. Extended coverage ends when: - Your child age 26 and older marries; - Your child age 26 and older becomes capable of self-support; - Your child fails to report for a scheduled physical exam; - Proof of incapacity is requested and not presented; or - Coverage terminates for reasons other than reaching the age limits described earlier.
* NOTE: For purposes of the Plan, the term “spouse” means the person to whom the participant is
legally married under applicable state law, regardless of the sex of the person. This means, for example, that if a participant and his/her same sex partner have a valid state-issued marriage certificate, then the participant’s partner qualifies as his or her spouse. For this purpose, “state” includes the District of Columbia, a U.S. territory or a foreign country having the legal authority to sanction marriages.
Note that the term marriage does not include registered domestic partnerships, civil unions, or similar formal relationships recognized under state law that are not denominated as marriage. Persons in these types of unions do not qualify as spouses for purposes of the Plan, and are not eligible to be covered under the Plan. In certain very limited circumstances, the term spouse may include a common law spouse (where common law marriage is recognized by your state of residence and you have met all requirements of a common law marriage). If requested, you must demonstrate to the satisfaction of the Plan Administrator that you meet the requirements of a common law marriage. Additional Information Other information contained in the SPD, that is specific to the change described above, is impacted by this document. Keep this document with your SPD so that you have the most current information about your benefits and any changes that have occurred since the SPD was published.

LMC-ZMW 3 151SMMB17
When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at: Current Employees:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Benefits. From the Lockheed Martin Employee Service Center Online, click Library and then Summary Plan Descriptions. https://www.lmpeople.com – on the Internet You will need your User ID (NT ID) and Password to access the website from the Internet. Click on LM Employee Service Center under Benefits. From the Lockheed Martin Employee Service Center Online, click Library and then Summary Plan Descriptions. lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions.
Retirees:
lmc.lifeatworkportal.com – You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions. http://lockheedmartin.com – Click Employees from the top right corner of the page, then click Retirees. From the Benefits information section, click Lockheed Martin Service Center. You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, click Library and then Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the claims administrator.
Please keep this notice with your other important benefits information.

LMC-ZMW 4 151SMMB17
NONDISCRIMINATION NOTICE The Lockheed Martin Health Plan complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. The Lockheed Martin Health Plan does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex. The Lockheed Martin Health Plan:
Provides free aids and services to people with disabilities to communicate effectively with us, such as:
o Qualified sign language interpreters o Written information in other formats (large print, audio, accessible electronic formats,
other formats) Provides free language services to people whose primary language is not English, such as:
o Qualified interpreters o Information written in other languages
If you need these services, contact the Senior Manager, Compliance through the Lockheed Martin Plan Administration Helpline at 301-548-2320. If you believe that The Lockheed Martin Health Plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with: the Senior Manager, Compliance through the Lockheed Martin Plan Administration Helpline, 6801 Rockledge Drive, CCT-115, Bethesda, MD, 20817, 301-548-2320. You can file a grievance in person or by mail. If you need help filing a grievance, the Senior Manager, Compliance is available to help you. You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 509F, HHH Building Washington, D.C. 20201 1-800-368-1019, 800-537-7697 (TDD) Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html. ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística. Llame al 866-562-2363. 注意:如果您使用繁體中文,您可以免費獲得語言援助服務。請致電866-562-2363。
CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn. Gọi số 866-562-2363. 주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 866-562-2363번으로 전화해 주십시오.
LMC-ZMW 5 151SMMB17
PAUNAWA: Kung nagsasalita ka ng Tagalog, maaari kang gumamit ng mga serbisyo ng tulong sa wika nang walang bayad. Tumawag sa 866-562-2363. ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные услуги перевода. Звоните 866-562-2363. ATANSYON: Si w pale Kreyòl Ayisyen, gen sèvis èd pou lang ki disponib gratis pou ou. Rele 866-562-2363. ATTENTION: Si vous parlez français, des services d'aide linguistique vous sont proposés gratuitement. Appelez le 866-562-2363. UWAGA: Jeżeli mówisz po polsku, możesz skorzystać z bezpłatnej pomocy językowej. Zadzwoń pod numer 866-562-2363. ATENÇÃO: Se fala português, encontram-se disponíveis serviços linguísticos, grátis. Ligue para 866-562-2363. ATTENZIONE: In caso la lingua parlata sia l'italiano, sono disponibili servizi di assistenza linguistica gratuiti. Chiamare il numero 866-562-2363. ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos sprachliche Hilfsdienstleistungen zur Verfügung. Rufnummer: 866-562-2363.
.2363‐562‐866ملحوظة: إذا كنت تتحدث اذكر اللغة، فإن خدمات المساعدة اللغوية تتوافر لك بالمجان. اتصل برقم 注意事項:日本語を話される場合、無料の言語支援をご利用いただけます。866-562-2363 まで、お電話にてご連絡ください。
: اگر به زبان فارسی گفتگو می کنيد، تسھيالت زبانی بصورت رايگان برای شما فراھم می توجه تماس بگيريد. 2363-562-866باشد. با

LMC-ZMA 100SMMB17
July 5, 2017 Summary of Material Modifications
Important Information Regarding a Change Effective Immediately This notice is being sent to you to update contact information in the Summary Plan Descriptions (SPDs) listed in the Attachment. This notice, describing changes that are effective immediately, is now part of the official plan document and is legally referred to as a Summary of Material Modifications (SMM) to the SPD. COBRA Administrator Contact Information The contact information for CONEXIS Benefit Administrators, the administrator of Lockheed Martin’s COBRA benefits, is: CONEXIS PO Box 226985 Dallas, TX 75222-6985 Phone: 800-482-4105 Fax: 877-822-9089 www.conexis.com When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at: Current Employees:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. https://www.lmpeople.com – on the Internet You will need your User ID (NT ID) and Password to access the website from the Internet. Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.

LMC-ZMA 2 100SMMB17
Retirees: lmc.lifeatworkportal.com – You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. http://lockheedmartin.com – Click Employees from the top right corner of the page, then click Retirees. From the Benefits Information section, click Lockheed Martin Service Center. You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the claims administrator.
Please keep this notice with your other important benefits information.

LMC-ZKW 142SMMB16
Jan. 3, 2017 Summary of Material Modifications Important Information Regarding Changes Effective Jan. 1, 2016 This notice is being sent to you to update information related to Aetna medical plans in the Summary Plan Descriptions (SPDs) listed in the Attachment. This notice, describing changes that are effective Jan. 1, 2016, is now part of the official plan document and is legally referred to as a Summary of Material Modifications (SMM) to the SPD. Precertification Process for Inpatient and Outpatient Hospice Care Effective Jan. 1, 2016, precertification will no longer be required for inpatient and outpatient hospice care or home health care. Enhanced Clinical Review Program Effective Jan. 1, 2016, the Aetna Enhanced Clinical Review Program will replace the High-Technology Imaging Pre-Authorization Program. The following section will replace the “High-Technology Imaging Pre-Authorization Program” section of your SPD: Enhanced Clinical Review (formerly High Technology Imaging Pre-Authorization) Program The program previously called the High-Technology Imaging Pre-Authorization Program is now known as the Enhanced Clinical Review Program. This pre-authorization program requires your provider to obtain authorization BEFORE requesting high-tech imaging services in an outpatient setting and applies to MRIs, CT (CAT) scans, PET scans, nuclear medicine, cardiac imaging, facility-based sleep studies, cardiac implantable devices, interventional pain management and large joint procedures (hip and knee). Prior to your procedure, please confirm that your doctor has pre-certified your test, and is sending you to an approved facility. Because the radiology facilities know that precertification is required, your test could be delayed or you could be denied service if your doctor has not taken this step. If you are seeing an out-of-network provider, it is your responsibility to precertify your procedure. Preauthorization decisions will be made within two business days for standard requests after submitting all required documents. Decisions for urgent requests will be made within four hours. Innovation Health Network for Certain LM HealthWorks Plan Participants Effective Jan. 1, 2016, LM HealthWorks Plan members who live in the Washington D.C. Metropolitan area will have access to the Innovation Health network. As a result, the following content will be added to the “Provider Directory” subsection of the “LM HealthWorks Plan” section of your SPD: LM HealthWorks Plan members who live in the Washington D.C. Metropolitan area now have access to the Innovation Health network of doctors and facilities. Innovation Health is the product of a partnership between Aetna and INOVA, a system of doctors and hospitals based in the D.C. area. Members who utilize the Innovation Health network will save money and receive quality, coordinated care while maintaining access to Aetna’s network of doctors and Aexcel-designated providers.

LMC-ZKW 2 142SMMB16
Behavioral Health Condition Management Effective Jan. 1, 2016, this Behavioral Health Condition Management program replaces the Behavioral Health Disease Management/Case Management programs section of your SPD: Behavioral Health Condition Management Behavioral Health Condition Management is designed to assist you and your covered dependents to understand and better manage behavioral health conditions. This program can assist you with finding behavioral health care counseling resources, provide information to your doctor and counselor to help coordinate treatment, provide you with educational information and assist you with setting realistic goals for improvement of your overall mental health. When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at: Current Employees:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. https://www.lmpeople.com – on the Internet You will need your User ID (NT ID) and Password to access the website from the Internet. Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.
Retirees:
lmc.lifeatworkportal.com – You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. http://lockheedmartin.com – Click Employees from the top right corner of the page, then click Retirees. From the Benefits Information section, click Lockheed Martin Service Center. You will need your Login ID and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the claims administrator.
Please keep this notice with your other important benefits information.

LMC-ZJJ 100SMMB16
June 24, 2016 Summary of Material Modifications
Important Information Regarding Changes Effective Jan. 1, 2015 Effective Jan. 1, 2015, you are eligible to participate in the benefits described in the Summary Plan Descriptions (SPDs) listed below if you are employed by Lockheed Martin MST Services and a member of the Davis-Monthan Flight Simulator Association (DMFSA). This notice, effective Jan. 1, 2015, is now part of the official plan documents and is legally referred to as a Summary of Material Modifications (SMM) to the below-listed SPDs:
LM Essentials Plan, Health benefits for certain non-represented and certain represented employees of Lockheed Martin Corporation (ZBQ – 108SPDB12, effective Jan.1, 2012)
LM HealthWorks Plan, Health benefits for certain non-represented and certain represented employees (ZAH – 207SPDB11, effective Jan. 1, 2011)
Lockheed Martin Corporation Managed Care (HMO and PPO) Medical Plans, Medical Plans for non-represented and certain represented employees of Lockheed Martin Corporation (ZBJ – 112SPDB12, effective Jan. 1, 2012)
Lockheed Martin Corporation Dental Plans, Comprehensive Dental, Comprehensive Plus Dental and Managed Dental for nonrepresented and certain represented employees of Lockheed Martin Corporation (ZBK – 113SPDB12, effective Jan. 1, 2012)
Lockheed Martin Corporation Vision Plan, Vision Plan for non-represented and certain represented employees of Lockheed Martin Corporation (ZBL – 114SPDB12, effective Jan.1, 2012)
Health Care and Dependent Care Spending Accounts, For certain non-represented and represented employees of Lockheed Martin Corporation (ZZE – H10SPD183, effective Jan. 1, 2011)
Short-Term Disability (STD) Insurance, For non-represented and certain represented employees of Lockheed Martin Corporation (ZEM – 115SPDB15, effective Jan. 1, 2014)
Long-Term Disability Insurance Benefits, Under the Lockheed Martin Group Benefits Plan and the Lockheed Martin Operations Support, Inc. Benefit Plan (ZBR – 107SPDB14, effective Jan. 1, 2014)
Lockheed Martin Group Benefits Plan, Life and accident insurance for non-represented salaried and certain represented employees of Lockheed Martin Corporation (ZBC – 214SPDB11, effective Jan. 1, 2012)
Lockheed Martin Business Travel Accident Plan, For certain non-represented and certain represented employees (ZZV – 213SPDB11, effective Jan. 1, 2011)
Lockheed Martin Corporation International Indemnity Plan (IIP), Health benefits for certain employees of Lockheed Martin Corporation (ZCE – 107SPDB12, effective Jan. 1, 2012)
LM HealthWorks Quit for Life™ Program, Tobacco cessation program for eligible employees of Lockheed Martin Corporation (ZN5 – G07SPD154, effective Sept. 25, 2006)
LM HealthWorks Wellness Center (111SPDB13, effective Jan. 1, 2014)

LMC-ZJJ 2 100SMMB16
When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. https://www.lmpeople.com – on the Internet lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the claims administrator.
Please keep this notice with your other important benefits information.

LMC-ZGQ 132SMMB15
July 8, 2015 Summary of Material Modifications Important Information Regarding Changes Effective Jan. 1, 2015 This notice is a Summary of Material Modifications (SMM), a legal document that describes changes to an official plan document called a Summary Plan Description (SPD), effective Jan. 1, 2015. See the Attachment for affected SPDs. LM HealthWorks Facility Charge Review Effective Jan. 1, 2015, an out-of-network facility may bill you for charges—in addition to deductible and coinsurance, as applicable—which exceed the Plan’s reimbursement for a covered service. You may be responsible for these charges and receive an invoice from the facility after your claim has been processed. The following will replace the “Out-of-Network Care” section of your SPD: Out-of-Network Care If you receive care from an out-of-network provider or facility, the LM HealthWorks Plan works a little differently. When your medical service is provided out-of-network, the level of reimbursement from the Plan for covered expenses will usually be lower. This means your out-of-pocket expenses will generally be higher. Depending on the provider or facility, you may need to pay in full at the time of your visit. You must then submit a claim to the LM HealthWorks Plan claims administrator. You can call the LM HealthWorks Plan at 877-458-4975 to request a claim form, or you can download one via the Aetna Navigator Web site. Follow the instructions on the form and remember to include the provider’s or facility’s original bill for services. If there is a balance in your HealthFund, the appropriate amount will be withdrawn automatically to pay the expense. If your HealthFund has been used up before you submit a claim for the expense, you will need to pay for your care out of your pocket. Once you have met the calendar year deductible, the LM HealthWorks Plan pays its share of the expense. If you paid the entire expense when you received care, the LM HealthWorks Plan will reimburse you for the portion of the claim the LM HealthWorks Plan would have paid. You will receive an Explanation of Benefits (EOB) statement that shows the total charge for care and the amount the LM HealthWorks Plan reimbursed you and/or your provider/facility. It also shows you how much of the deductible you have met and how much remains to be met. If you are a registered member with the Aetna Navigator Web site, you will receive an email notification that an EOB is available; otherwise, you will receive the EOB statement by mail. If you would rather receive EOBs online and have not yet registered with Aetna Navigator, you can “turn off” paper EOBs by visiting Aetna Navigator through the LM HealthWorks Plan Web site at www.lmhwplan.com. The EOB is not a bill—your provider or facility will bill you for your share of the cost of the service if you did not pay the entire expense when you received care.

LMC-ZGQ 2 132SMMB15
Please keep in mind that all covered expenses are paid according to what the LM HealthWorks Plan considers the recognized charge. For out-of-network providers or facilities, this is the charge most often made for a service. If your out-of-network provider or facility charges more than the recognized charge, you pay the difference between the provider’s or facility’s charge and the recognized charge. Note: If you are in an active course of treatment with an out-of-network provider when you become a member of the LM HealthWorks Plan, the LM HealthWorks Plan’s Transition of Care provision may be able to help. For certain health conditions, the LM HealthWorks Plan may approve transition coverage to allow you to continue an active course of treatment with an out-of-network provider for a certain period of time while receiving benefits at the in-network level. Prescription Drug Out-of-Pocket Maximum Effective Jan. 1, 2015, the maximum amount you will spend on prescription medications (administered by Express Scripts) in a plan year will be capped at $2,000 per person or $4,000 per family (in-network)*. The up-to-$25 Retail Refill Allowance (RRA) you pay for getting maintenance medications at a retail pharmacy rather than through mail order does not apply to the out-of-pocket maximum. *Note: If you take any prescription medications that are not covered by the Plan, you will continue to pay out-of-pocket for those drugs, regardless of whether you have reached the cap. There is no maximum out-of-network. Effective Jan. 1, 2015, the following row of the “LM HealthWorks Covered Services – Benefit Highlights” chart is being updated to include the prescription drug out-of-pocket maximum and modified to read as follows: LM HealthWorks Covered Services – Benefit Highlights
In-Network Out-of-Network
Calendar Year Deductibles, Out-of-Pocket Maximums, Lifetime Maximum Benefits Calendar Year Out-of-Pocket Maximum
Network: Medical: $2,500 per person up to a $6,000 maximum (includes $1,000/$3,000 deductible); Pharmacy: $2,000 per person up to a $4,000 maximum
Non-Network: Medical: $7,250 per person, up to a $16,750 maximum (includes $2,250/$6,750 deductible); Out-of-Area (OOA): same as Network benefit (combined Network and Non-network)
In addition to the change to the “LM HealthWorks Covered Services – Benefit Highlights” chart shown above, the following replaces the “How the Prescription Benefit Works” section of your SPD: How the Prescription Benefit Works You will receive a prescription benefit packet, including your pharmacy drug ID card, directly from Express Scripts. Use your ID card to fill short-term prescriptions (this generally means up to a 30-day supply), such as those for antibiotics, filled at in-network or out-of-network retail pharmacies. Use the Express Scripts Pharmacy™ to fill prescriptions for medications you use on a continuing basis, such as those used to treat high blood pressure or high cholesterol. You can typically order up to a 90-day supply and have it delivered right to your home.

LMC-ZGQ 3 132SMMB15
There is no deductible to meet before the Plan pays benefits for prescription drugs. When you fill a prescription, either through a retail pharmacy or the Express Scripts Pharmacy™, you will pay either a copayment or a percentage of the cost—called coinsurance. There are three levels of copayment/coinsurance, which depend on whether your doctor prescribes a generic drug, a preferred brand-name drug (one listed on the Plan’s formulary), or a non-preferred brand-name drug (one that is not on the Plan’s formulary). When you purchase prescription medications at network pharmacies, the Plan limits the amount you spend annually out of pocket on covered prescription drugs. (See the “Benefit Highlights” section for more information.) If your physician writes “dispense as written,” you pay the preferred or non-preferred brand-name copayment/coinsurance (depending on the specific prescription drug)—even if a generic equivalent is available. If you request a brand-name drug when a generic is available and the doctor has not requested your medication be dispensed as written, you may pay more. See the “Benefit Highlights” section for more information. Fertility Drug Benefit Maximum and the Prescription Drug Out-of-Pocket Maximum The LM HealthWorks Plan covers up to $5,000 in fertility drugs per lifetime. Copays for fertility drugs purchased at a network pharmacy will apply to the out-of-pocket maximum and will be handled as follows:
• Before the fertility cap is met (if before the out-of-pocket maximum is met), your regular copay will apply to the out-of-pocket maximum.
• Once the fertility cap is met (if before the out-of-pocket maximum is met), you will pay 100% of the fertility drug cost and it will apply to the out-of-pocket maximum.
• If the out-of-pocket maximum is met before the fertility cap is met, the cost for fertility drugs will be $0. Once the fertility cap is met, your cost will be 100%.
Formulary Drugs The formulary is a list of preferred brand-name drugs chosen for their safety, effectiveness and cost. You can review the formulary by registering at www.express-scripts.com or by requesting a formulary guide from Express Scripts. If your medication is not on the list, you will be given alternative options to discuss with your doctor. And, in addition to the change to the “LM HealthWorks Covered Services – Benefit Highlights” chart and the “How the Prescription Benefit Works” section shown above, the following replaces the “Retail Refill Allowance” section of your SPD: Retail Refill Allowance You may pay more for your long-term drugs (such as those used to treat high cholesterol, high blood pressure, depression, or diabetes,) unless you order your prescriptions by mail from the Express Scripts Pharmacy™. After your third purchase of a long-term medication at a participating retail pharmacy, you will pay your regular coinsurance plus up to an additional $25, if you continue to fill at the retail pharmacy. Please note that you will never pay more than the actual cost of the medication. Your mail-order coinsurance will remain the same. This applies to any generic, preferred and non-preferred brand name medication (up to 30-day supply) that is filled more than three times at a retail pharmacy. The amounts you pay for getting maintenance medications at a retail pharmacy rather than through mail order do not apply to the prescription drug out-of-pocket maximum, and you will continue to be responsible for these amounts after the out-of-pocket maximum is met.

LMC-ZGQ 4 132SMMB15
To convert a prescription to the Express Scripts Pharmacy™ or obtain more information, access the Express Scripts Web site at www.express-scripts.com or call Express Scripts at 877-458-4975. Note: The retail refill allowance is not applicable to compound medications. LM HealthWorks HealthFund Credits Effective Jan. 1, 2015, the amount of HealthFund Credits LM HealthWorks Plan participants can earn for completion of certain Healthy Actions are changing. The following chart will replace the current “HealthFund Highlights” chart in “The HealthFund” section of your SPD: HealthFund Highlights The Healthy Actions and the amount of credits that can be earned are subject to change from year to year and will be communicated during annual enrollment. Healthy Actions Complete the Well-Being Assessment* Employee Spouse/Same-sex Domestic Partner
$100 once during the calendar year $100 once during the calendar year
Participate in the Virgin Pulse Physical Activity Tracking Tool Program Level 2: Employee Level 2: Spouse/Same-sex Domestic Partner
$100 once during the calendar year $100 once during the calendar year (must advance from Level 1 to Level 2 during the calendar year)
Level 3: Employee Level 3: Spouse/Same-sex Domestic Partner
$200 once during the calendar year $100 once during the calendar year (must advance from Level 2 to Level 3 during the calendar year)
Level 4: Employee only $300 once during the calendar year (must advance from Level 3 to Level 4 during the calendar year)
Preventive Care – Routine physical exam, routine gynecological/well woman exam, routine mammogram, or colorectal cancer screening (age 50 and older) during the calendar year Employee Spouse/Same-Sex Domestic Partner
$200 once per calendar year $200 once per calendar year
Maximum Credits Earned for the above Healthy Actions Employee Spouse/Same-sex Domestic Partner
$900 maximum per calendar year $500 maximum per calendar year
Registration with Beginning Right® Maternity Management Program (pregnant Employee or pregnant Spouse/Same-sex Domestic Partner registers in first or second trimester during the calendar year)
Over and above the Healthy Actions $150 upon registration, once during the calendar year

LMC-ZGQ 5 132SMMB15
HealthFund Highlights Credits Earned by Health Coaching or ITC/Condition Management Program Participation** (must complete either assessment session and 3 Coaching Sessions or 1 goal (as determined by member and his/her ITC Care Manager, during the calendar year) Employee Spouse/Same-sex Domestic Partner
Over and above the Healthy Actions** $100 once per calendar year $100 once per calendar year
Maximum HealthFund Balance Unlimited HealthFund Exclusions HealthFund does not apply to:
• Prescription drug expenses; and • Any amounts not covered or limited by the
LM HealthWorks Plan such as: - Amounts over the recognized charge; - Amounts you pay because you do not
follow the precertification approval process; or
- Services not covered by the Plan including services above visit limits.
HealthFund Participation Ends Participation ends when you are no longer enrolled in the LM HealthWorks Plan for active employees (or when COBRA or insurance continuation coverage ends). The fund is not a cash account—it is not subject to investment earnings or interest. Any remaining balance in the HealthFund is not payable when enrollment in the LM HealthWorks Plan ends.
* If you are hired or newly eligible for coverage after December 1, you (and your enrolled spouse/same-sex domestic partner) will not be eligible to complete the Well-Being Assessment and earn the related incentive until January 1 of the following Plan Year, provided you continue enrollment.
** Employee and/or Spouse/Same-sex Domestic Partner are eligible for either Condition Management or Health Coaching credits, not both, in a calendar year.
LM HealthWorks Condition Management Effective Jan. 1, 2015, the existing LM HealthWorks condition management program is being modified to include assistance for members experiencing acute medical events, in addition to those managing serious chronic conditions. The program, called Aetna In Touch Care (ITC), offers on-call support, which will allow members to connect by phone with an assigned registered nurse who can provide one-on-one assistance with high-risk health situations, and will extend to your LM HealthWorks-covered family members if applicable. Members will be identified based on claims data or the results of Well-Being Assessments (WBA), and, if eligible, will receive a phone call from Aetna to join this program.

LMC-ZGQ 6 132SMMB15
The following replaces the “Condition Management” section of your SPD, effective Jan. 1, 2015: Aetna In Touch CareSM (ITC) Enhanced Condition Management If you are facing a major medical event (such as surgery) or are living with a chronic health condition, you can receive one-on-one support to help you address your health challenges and avoid more serious health issues in the long term. If your medical records show you have an upcoming surgery or that you have a chronic condition, such as diabetes or high blood pressure, an Aetna In Touch Care (ITC) Care Manager will call you to offer support. You will have an assigned registered nurse who will help you develop and personalize a health action plan based on your needs and health goals. Your Care Manager will work with you one-on-one each time you need help:
• Providing education and information about all your health issues. • Guiding you to the most appropriate health care and helping you coordinate that care.
This program is voluntary, confidential and free. LM HealthWorks Teladoc Service Effective Jan. 1, 2015, Lockheed Martin will offer Teladoc to LM HealthWorks Plan members. The following provision will be added to the “What Is Covered” section of your SPD. Alternatives to Physician Office Visits
• Walk-In Clinic Visits - Charges made by walk-in clinics for unscheduled visits for treatment of non-emergency
illnesses and injuries. - Administration of certain immunizations administered within the scope of the clinic’s license
but not if solely for your employment. • E-Visits
- Charges made by an in-network provider for a routine, non-emergency, online internet medical consultation. You must make your E-visit through an Aetna authorized internet service vendor. You may have to register with that internet service vendor. Information about providers who are signed up with an authorized vendor may be found in the provider directory or online in DocFind on the LM HealthWorks Plan Web site at www.lmhwplan.com or by calling 877-458-4975. Charges made by an out-of-network provider are not covered.
• Telephone and Web Consultations - Teladoc offers access to physicians 24 hours a day, 7 days a week, 365 days a year, via
phone or video consultation (in most states). Teladoc allows you to receive care from a doctor, including diagnosis, recommended treatment and medical prescriptions (when appropriate) for medical issues such as ear infections, coughs or sinus problems. For more information or to register for the program, go to www.teladoc.com/Aetna. Please note there is a $40 copayment per consultation.
Note: Teladoc is not intended to replace the care provided by your PCP, but rather to supplement it. If you are experiencing a life-threatening medical emergency, proceed immediately to the nearest Emergency Room.

LMC-ZGQ 7 132SMMB15
When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. https://www.lmpeople.com – on the Internet lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the claims administrator.
Please keep this notice with your other important benefits information.

LMC-ZFS 146SMMB14
Jan. 26, 2015 Summary of Material Modifications Important Information Regarding a Change Effective Aug. 26, 2014 This notice is a Summary of Material Modifications (SMM), a legal document that describes changes to an official plan document called a Summary Plan Description (SPD). The change described below affects medical, dental and vision plans only, and is effective Aug. 26, 2014. See the Attachment for affected SPDs. When Coverage Ends Currently, when employment terminates, medical, dental and/or vision coverage ends immediately. Effective Aug. 26, 2014, when employment terminates, coverage will end the last day of the pay week. When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. https://www.lmpeople.com – on the Internet lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at: 866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired For specific questions regarding benefits and claim information, please contact the claims administrator.
Please keep this notice with your other important benefits information.

LMC-ZEQ 111SMMB14
Dec. 16, 2014 Summary of Material Modifications Important Information Regarding Changes Effective Jan. 1, 2014 This notice is a Summary of Material Modifications (SMM), a legal document that describes changes to the medical, dental, and vision benefits for eligible employees of the LM HealthWorks Plan included as part of the Lockheed Martin Group Benefits Plan (the “LMC Plan”) and the Lockheed Martin Operations Support, Inc. Benefit Plan (the “LMOS Plan”) (LMC-ZAH – 207SPDB11, effective Jan. 1, 2011). Out-of-Pocket Maximum Effective Jan. 1, 2014, the calendar year deductible will apply towards your out-of-pocket maximum. Therefore, the following list of items that do not count towards your out-of-pocket maximum is modified to read as follows: Certain expenses do not count towards your out-of-pocket maximum. These include, but are not limited to:
• Preventive services that are covered by the plan at 100% of the recognized charge; • Any prescription drug charges that are covered through retail pharmacies (in-network and out-
of-network) and the mail-order service including your share of the cost; • Any amounts you pay because the precertification requirements were not met; • Any expense covered at 50% (for example, non-emergency use of the emergency room); • Any amounts over the recognized charge; and • Any charges not considered covered medical expenses or otherwise excluded or limited by the
Plan. LM HealthWorks Covered Services – Benefit Highlights Effective Jan. 1, 2014, the following LM HealthWorks Covered Services – Benefit Highlights chart will replace the chart in your current SPD. Note: Changes to your benefit have been made. Pay close attention to coinsurance amounts, the deductible and the out-of-pocket maximum. As well, the format of the Benefits Highlights chart now shows the amount you pay, instead of the amount the LM HealthWorks Plan pays. In-Network Out-of-Network Calendar Year Deductibles, Out-of-Pocket Maximums, Lifetime Maximum Benefits Calendar Year Deductible $1,000 per person, up to a $3,000
maximum (no more than $1,000 per person); in-network and out-of-network are not combined
$2,250 per person, up to a $6,750 maximum (no more than $2,250 per person)
Services Excluded From Deductible Calculation
Preventive care, prescription drugs, precertification penalties, recognized charges overages and services not covered under the LM HealthWorks Plan
Preventive care, prescription drugs, precertification penalties, recognized charges overages and services not covered under the LM HealthWorks Plan

LMC-ZEQ 2 111SMMB14
In-Network Out-of-Network Out of Pocket Maximum Network: $2,500 per person, up to
a $6,000 maximum (includes $1,000/$3,000 deductible)
Non-Network: $7,250 per person, up to a $16,750 maximum (includes $2,250/$6,750 deductible); Out-of-Area (OOA): same as Network benefit (combined Network and Non-network)
Services Excluded From OOP Maximum Calculation
Preventive Care, Prescription Drugs, Recognized Charges overages and services not covered under the Plan.
Preventive Care, Prescription Drugs, Recognized Charges overages and services not covered under the Plan.
Lifetime Maximum Per Individual No maximum No maximum Physician Office Visits Primary Care Office Visit 20% after deductible 40% (20% OOA) after deductible Specialist Office Visit Aexcel Designated Provider: 10%
after deductible; Non-Aexcel Designated Provider: 20% after deductible
40% (20% OOA) after deductible
Walk-in Clinic 20% after deductible 40% (20% OOA) after deductible Prescription Drug Coverage Retail: Generic Up to a 30-day supply you pay:
10% up to $25/prescription max. After the 3rd purchase of a long term medication you pay an additional copay of up to $25 for additional fill of that medication at retail.
Up to a 30-day supply you pay: 50%. After the 3rd purchase of a long term medication you pay an additional copay of up to $25 for additional fill of that medication at retail.
Retail: Preferred brand name listed on formulary
Up to a 30-day supply you pay: 30% up to $75/prescription max. After the 3rd purchase of a long term medication you pay an additional copay of up to $25 for additional fill of that medication at retail.
Up to a 30-day supply you pay: 50%. After the 3rd purchase of a long term medication you pay an additional copay of up to $25 for additional fill of that medication at retail.
Retail: Non-Preferred brand name not listed on formulary
Up to a 30-day supply you pay: 50% up to $175/prescription max. After the 3rd purchase of a long term medication you pay an additional copay of up to $25 for additional fill of that medication at retail.
Up to a 30-day supply you pay: 50%. After the 3rd purchase of a long term medication you pay an additional copay of up to $25 for additional fill of that medication at retail.
Mail Order: Generic Up to a 90-day supply you pay: 10% up to $50/prescription maximum, for each prescription or refill.
Not covered
Mail Order: Preferred brand name listed on formulary
Up to a 90-day supply you pay: 30% up to $150/prescription maximum, for each prescription or refill.
Not covered
Mail Order: Non-Preferred brand name not listed on formulary
Up to a 90-day supply you pay: 50% up to $350/prescription maximum, for each prescription or refill.
Not covered

LMC-ZEQ 3 111SMMB14
In-Network Out-of-Network Generic Drug Substitution Rule If you request a brand-name drug
when your physician permits a generic substitution, you will pay the generic drug coinsurance plus the difference between the generic drug cost and the brand-name cost
If you request a brand-name drug when your physician permits a generic substitution, you will pay the generic drug coinsurance plus the difference between the generic drug cost and the brand-name cost
Preventive Care Routine Physicals, Immunizations, and Related Lab Fees Adult Physical Exams No charge, deductible waived (age
and frequency limitations apply) No charge, deductible waived (age and frequency limitations apply)
Colorectal Cancer Screening No charge, deductible waived (age and frequency limitations apply)
No charge, deductible waived (age and frequency limitations apply)
Gynecological No charge, deductible waived (age and frequency limitations apply)
No charge, deductible waived (age and frequency limitations apply)
Mammograms No charge, deductible waived (age and frequency limitations apply)
No charge, deductible waived (age and frequency limitations apply)
Prostate Specific Antigen (PSA) Test and Digital Rectal Exam (DRE)
No charge, deductible waived (age and frequency limitations apply)
No charge, deductible waived (age and frequency limitations apply)
Well Child Care No charge, deductible waived (age and frequency limitations apply)
No charge, deductible waived (age and frequency limitations apply)
Outpatient Services Allergy Injections 20% after deductible 40% (20% OOA) after deductible Allergy Testing and Treatment 20% after deductible 40% (20% OOA) after deductible Ambulance 20% after deductible 20% after deductible Chiropractic 20% after deductible; Up to 20
visits/calendar year (combined in-network and out-of-network limits)
40% (20% OOA) after deductible; Up to 20 visits/calendar year (combined in-network and out-of-network limits)
Colonoscopy 20% after deductible (if not included as part of preventive screening)
40% (20% OOA) after deductible (if not included as part of preventive screening)
Complex Imaging Services (MRA/MRS, MRI, CT Scan, PET Scan)
20% after deductible; precertification required
40% (20% OOA) after deductible; precertification required
Contraceptive Devices, Implants and Injections
No charge, deductible waived 40% (20% OOA) after deductible
Diagnostic Testing: Routine Laboratory
20% after deductible 40% (20% OOA) after deductible
Diagnostic Testing: X-rays 20% after deductible 40% (20% OOA) after deductible Durable Medical Equipment 20% after deductible;
precertification required for recognized charges in excess of $5,000
40% (20% OOA) after deductible; precertification required for recognized charges in excess of $5,000
Emergency Room Care 20% after deductible 20% after deductible Non-emergency use of an Emergency Room
50% after deductible 50% after deductible
Hearing Exams 20% after deductible 40% (20% OOA) after deductible Hearing Aids 20% after deductible; limited to
$1,000 per ear every 3 calendar years (combined in-network and out-of-network limit)
40% (20% OOA) after deductible; limited to $1,000 per ear every 3 calendar years (combined in-network and out-of-network limit)
Maternity: Pre/Postnatal Aexcel Designated Provider: 10% after deductible; Non-Aexcel Designated Provider: 20% after deductible
40% (20% OOA) after deductible

LMC-ZEQ 4 111SMMB14
In-Network Out-of-Network Outpatient Short-Term Rehabilitation
20% after deductible; Limited to 60 visits/calendar year; combined for habilitative, speech, physical and occupational therapies. Office and outpatient treatment combined.
40% (20% OOA) after deductible; Limited to 60 visits/calendar year; combined for habilitative, speech, physical and occupational therapies. Office and outpatient treatment combined.
Outpatient Surgery - Ambulatory Surgical Facility Setting
20% after deductible; precertification required for certain procedures.
40% (20% OOA) after deductible; precertification required for certain procedures.
Outpatient Surgery - Hospital Setting
20% after deductible; precertification required for certain procedures.
40% (20% OOA) after deductible; precertification required for certain procedures.
Outpatient Surgery Performed in Office Setting
20% after deductible; precertification required for certain procedures.
40% (20% OOA) after deductible; precertification required for certain procedures.
Sigmoidoscopy 20% after deductible (if not included as part of preventive screening)
40% (20% OOA) after deductible (if not included as part of preventive screening)
Tubal Ligation 20% after deductible 40% (20% OOA) after deductible Urgent Care Facility 20% after deductible 40% (20% OOA) after deductible Inpatient Hospital Services Inpatient 20% after deductible; Transplant:
Institute of Excellence (IOE) Facility: 10% after deductible, other facilities: 20% after deductible; Bariatric, Cardiac, and Orthopedic Surgery: Institute of Quality (IOQ) Facility: 10% after deductible, other facilities: 20% after deductible; precertification required
40% (20% OOA) after deductible; precertification required
Inpatient Physician and Surgeon Services
20% after deductible 40% (20% OOA) after deductible
Mental Health and Substance Abuse Services Mental Health: Inpatient Services 20% after deductible;
precertification required 40% (20% OOA) after deductible; precertification required
Mental Health: Outpatient Services 20% after deductible; precertification required for certain procedures
40% (20% OOA) after deductible; precertification required for certain procedures
Substance Abuse: Inpatient Services
20% after deductible; precertification required
40% (20% OOA) after deductible; precertification required
Substance Abuse: Outpatient Services
20% after deductible; precertification required for certain procedures
40% (20% OOA) after deductible; precertification required for certain procedures
Other Services Home Health Care 20% after deductible; up to 120
visits/calendar year (Home Health Care and Private Duty Nursing visits combined); precertification required (combined in-network and out-of-network limit).
40% (20% OOA) after deductible; up to 120 visits/calendar year (Home Health Care and Private Duty Nursing visits combined); precertification required (combined in-network and out-of-network limit).
Hospice Care 20% after deductible; precertification required
40% (20% OOA) after deductible; precertification required

LMC-ZEQ 5 111SMMB14
In-Network Out-of-Network Mouth, Jaws, Teeth 20% after deductible; covers
accident related to injury to teeth, and medical in nature oral and jaw surgery; precertification required
40% (20% OOA) after deductible; covers accident related to injury to teeth, and medical in nature oral and jaw surgery; precertification required
Private Duty Nursing (PDN) 20% after deductible; up to 120 visits per calendar year (Home Health Care and Private Duty Nursing visits combined); precertification required (combined in-network and out-of-network limit)
40% (20% OOA) after deductible; up to 120 visits per calendar year (Home Health Care and Private Duty Nursing visits combined); precertification required (combined in-network and out-of-network limit)
Prosthetic Devices 20% after deductible; precertification required for recognized charges in excess of $5,000
40% (20% OOA) after deductible; precertification required for recognized charges in excess of $5,000
Convalescent Facility/Skilled Nursing Facility
20% after deductible; up to 120 days/calendar year; precertification required (combined in-network and out-of-network limits)
40% (20% OOA) after deductible; up to 120 days/calendar year; precertification required (combined in-network and out-of-network limits)
Vision: Screenings Covered only as part of routine physical exam
Covered only as part of routine physical exam
Personal Health Assessment (PHA) to Well Being Assessment (WBA) Effective Sept. 3, 2013, the LM HealthWorks Personal Health Assessment (PHA) has been replaced by the Well-Being Assessment (WBA). There will be no change to the benefit provided to you through the wellness assessment. Note: You will receive Healthy Action incentive credits if you submit either a PHA or WBA during the Plan Year. Address and Phone Change for the Lockheed Martin Qualified Order Department Effective Jan. 1, 2014, the contact information for the Lockheed Martin Qualified Order Department has changed. The Lockheed Martin Qualified Order Department handles questions related to Qualified Medical Child Support Order (QMSCO) and Qualified Domestic Relations Order (QDRO) inquiries. The following is the contact information in effect as of the date mentioned above: Lockheed Martin Qualified Domestic Relations Order (QDRO) Department P.O. Box 3199 Ponte Vedra Beach, FL 32004-3199 877-708-7748 855-775-QDRO (7376) - fax Federal Express and UPS Overnight Mail: Lockheed Martin Qualified Domestic Relations Order (QDRO) Department 130 Corridor Road, Unit #3199 Ponte Vedra Beach, FL 32082-9998

LMC-ZEQ 6 111SMMB14
Lockheed Martin Employee Service Center (LMESC) Address Effective Jan. 1, 2014, the contact information for the Lockheed Martin Employee Service Center has changed. The following is the address in effect as of the date mentioned above: Lockheed Martin Employee Service Center (LMESC) P.O. Box 199731 Dallas, TX 75219-9731 Summary Plan Description Location on Lockheed Martin Intranet Effective Jan. 1, 2014, the location of the SPDs on the Lockheed Martin Intranet has changed. You can access your Summary Plan Descriptions using the path below:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.
Change to Definition of Spouse The definition of “spouse,” as it relates to various Company employee benefit plans, has been updated in light of recent changes in federal law. For purposes of this plan, the term “spouse” means the person to whom the participant is legally married under applicable law, regardless of the sex of the person. This impacts the “Dependent Eligibility” section of the SPD, as well as any sections where the term “spouse” is used. As well, any sections where same-sex spouse is recognized as receiving the same treatment as a same-sex domestic partner no longer apply to same-sex spouse. In certain very limited circumstances, the term spouse may include a common law spouse (where common law marriage is recognized by your state of residence and you have met all requirements of a common law marriage). If requested, you must demonstrate, to the satisfaction of the Plan Administrator, that you meet the requirements of a common law marriage. LM HealthWorks What Is Covered: Preventive Services Effective Jan. 1, 2014, “Immunizations for travel are not covered” is modified from the following bullet in the LM HealthWorks “Preventive Services” section:
• Immunizations for adults who are considered “at risk” for certain medical conditions such as influenza, pneumonia, meningitis, hepatitis and Lyme disease. The Claims Administrator determines “at risk” based on generally accepted medical guidelines. Immunizations for travel may not be covered. Check with your Plan Administrator.
Effective Jan. 1, 2014, the “Prostate-Specific Antigen (PSA) Test and Digital Rectal Exam (DRE) bullet is modified as follows:
• Prostate-Specific Antigen (PSA) Test and Digital Rectal Exam (DRE) – One annual (PSA and DRE) exam for males ages 40 and above. Limitations may apply after age 75.

LMC-ZEQ 7 111SMMB14
LM HealthWorks What Is Covered: Institutes of Quality® (IOQ) (Bariatric, Orthopedic and Cardiac) The following information will replace the “Obesity Surgical Expenses” section of your LM HealthWorks Plan SPD, effective Jan. 1, 2014. The Institutes of Quality network is Aetna's national network of health care facilities that are designated based on measures of clinical performance and efficiency for specific procedures in the areas of Bariatric Surgery, Cardiac Care and Orthopedic care. Hospitals that have been selected to participate in our IOQ network have met enhanced quality thresholds for volumes and outcomes. Bariatric Surgical IOQ facilities provide services to treat people living with morbid (also known as extreme) obesity. Bariatric Surgery IOQ procedures include:
• Gastric bypass • Adjustable gastric band • Sleeve method
Cardiac Care IOQ facilities provide many services, including:
• Rhythm (Pacemakers, Defibrillator) • Interventional (Heart Catheterization, PTCA - balloon opening artery of heart, Stent) • Surgery (CABG, Valve with CABG, Valve without CABG)
Orthopedic IOQs provide a full range of orthopedic care services, including:
• Spine (Primary Fusion, Fusion Revision, Discectomy (without decompression), decompression (without fusion))
• Total Joint Replacement (Knee/Hip) LM HealthWorks What Is Covered: Nutritional Counseling The following section is added as a Covered Service for the LM HealthWorks Plan effective Jan. 1, 2014. Nutritional counseling may be considered medically necessary for chronic diseases in which dietary adjustment has a therapeutic role, when it is prescribed by a physician and furnished by a provider (e.g., licensed nutritionist, registered dietician, or other qualified licensed health professionals such as nurses who are trained in nutrition) recognized under the plan. Medical nutrition therapy has been integrated into the treatment guidelines for a number of chronic diseases, including:
• Cardiovascular disease • Diabetes mellitus • Hypertension • Kidney disease • Eating disorders • Gastrointestinal disorders • Seizures (i.e., ketogenic diet) • Other conditions (e.g., chronic obstructive pulmonary disease) based on the efficacy of diet
and lifestyle on the treatment of these diseased states

LMC-ZEQ 8 111SMMB14
LM HealthWorks What Is Not Covered: Exclusions Effective Jan. 1, 2014, nutritional counseling is considered a covered service, as stated above. Therefore, the current exclusion in the “Exclusions” subsection of the “LM HealthWorks Plan” benefit section will be updated as follows:
• Weight: Any treatment or supply intended to decrease or increase body weight, control weight or treat obesity, including morbid obesity, regardless of the existence of comorbid conditions; except as described in the “What Is Covered” and “Health Management Resources” sections, including but not limited to: - Liposuction, weight control/loss programs and other services and supplies that are
primarily intended to treat, or are related to the treatment of obesity, including morbid obesity;
- Preparations, foods or diet supplements, dietary regimens and supplements, food or food supplements;
- Coaching, training, hypnosis or other forms of therapy; and - Exercise programs, exercise equipment, membership to health or fitness clubs,
recreational therapy or other forms of activity or activity enhancement. Prescription Drugs The following changes impact the “Prescription Drug” section of your SPD effective Jan. 1, 2014. Medco Pharmacy to Express Scripts Pharmacy Effective Jan. 1, 2014, Medco Pharmacy has changed its name to Express Scripts Pharmacy. There will be no change to the benefit provided to you through the prescription drug program. Health Care Reform and Pharmacy (Regarding Preventive Benefits) The Plan continues to comply with Health Care Reform legislation. Over-the-counter legislation recommended products and services are covered without cost-sharing only when prescribed by a health care provider at an in-network pharmacy. Prescription Drugs and Changes to the Formulary The Plan includes a list of preferred drugs that are either more effective at treating a particular condition than other drugs in the same class of drugs, or as effective as and less costly than similar medications. Non-preferred drugs may also be covered under the prescription drug program, but at a higher cost-sharing tier. Collectively, these lists of drugs make up the Plan’s Formulary. The Plan’s Formulary is updated periodically and subject to change. To get the most up-to-date list go online to www.express-scripts.com. Drugs that are excluded from the Plan’s Formulary are not covered under the Plan, unless approved in advance through a Formulary exception process managed by Express Scripts. The process of determining if approved is based on if the drug requested is medically necessary and essential to your health and safety and/or you have tried all Formulary drugs comparable to the excluded drug. If approved through the Formulary exception process, the applicable Formulary copay will apply based on the Plan’s cost share structure. If approval is not provided, you will be required to pay the full cost of the drug without any reimbursement under the Plan. If your Physician believes that an excluded drug meets the requirements described above, the Physician should take the necessary steps to initiate a Formulary exception review.

LMC-ZEQ 9 111SMMB14
The Formulary will continue to change from time to time. For example: • A drug may be moved to a higher or lower cost-sharing Formulary tier. • Additional drugs may be excluded from the Formulary. • A restriction may be added on coverage for a Formulary-covered drug (e.g. prior
authorization). • A Formulary-covered brand name drug may be replaced with a Formulary-covered generic
drug. Because you may not receive notice that a drug has been removed from the Formulary, be sure to check that a drug is covered before the drug is purchased. Certain drugs, even if covered on the Formulary, will require prior authorization in advance of you receiving the drug. Other Formulary-covered drugs may not be covered under the Plan unless an established protocol, known as Step Therapy, is first followed. As with all aspects of the Formulary, these requirements also may change from time to time. Change to Compound Medications Effective Jan. 1, 2014, the following apply to compound medications:
• Compound medication prescriptions will no longer be filled through home delivery. This applies to new prescriptions and existing prescriptions with refills remaining.
• You will continue to have coverage to purchase compound medications at participating retail pharmacies. If a compound medication is purchased at retail pharmacy using your ID card, the retail pharmacy will submit the claim electronically and charge you the applicable copay and/or coinsurance amount. If a compound medication is purchased at a nonparticipating retail pharmacy or if the ID card isn’t used, you must submit a claim form for reimbursement.
• Retail Refill Allowance is not applicable to compound medications. Aetna Navigator® and Claims Appeals (for Aetna plan participants only) The following pertains to participants in an Aetna plan. If you are unsure of the Claims Administrator for your plan, refer to your Medical Benefits Card or see the “Claims Administration” section of your SPD. Through Aetna Navigator®, you can monitor the activity of your claims and appeals. You also now have the option of appealing claims online. To locate specific claims, follow the directions below:
• If you are registered in Aetna Navigator® at www.aetna.com, you will see a menu of options, including “View Claims.”
• If you would like to see claims made on your benefits, click on “View Claims” and your claims will appear. You will then be able to filter by selecting by claimant (self, family member), claim type (medical) and the timeframe of claims (last 365 days, last 90 days).
• Click on the specific claim you want to appeal. • You will then have the option of contacting Member Services. When you click on “Contact
Member Services,” you will have the option to write your appeal in the comment box provided. Note: Content is based on your benefit and subject to change.

LMC-ZEQ 10 111SMMB14
Correction to Dental Plan Summary of Material Modifications (SMM) The Dental Plan SMM (104SMMB14-ZEU) dated Sept. 2, 2014, for dental changes effective in 2014 does not impact the LM HealthWorks Plan. The following is removed from the Attachment list of the Dental Plan SMM:
• Medical, dental, and vision benefits for eligible employees of the LM HealthWorks Plan included as part of the Lockheed Martin Group Benefits Plan (the “LMC Plan”) and the Lockheed Martin Operations Support, Inc. Benefit Plan (the “LMOS Plan”) (LMC-ZAH – 207SPDB11, effective Jan. 1, 2011)
When You Have Questions If you have questions about this document or want to obtain a copy of the SPD, please access Lockheed Martin Employee Service Center Online (LMESC Online) at:
https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on LM Employee Service Center under Pay and Benefits, then My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions. https://www.lmpeople.com – on the Internet lmc.lifeatworkportal.com – on the Internet You will need your Login ID (not your NT ID) and Password to access the website from the Internet. Refer to Login Help on the login screen for guidance. Once logged in, choose My Benefits>Health and Welfare. From the Health and Welfare page, click the drop down menu in the Resources section and click Find Summary Plan Descriptions.
Or, you can call the Lockheed Martin Employee Service Center (LMESC) at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the Claims Administrator.
Please keep this notice with your other important benefits information.

LMC-ZDJ 133SMMB12
April 9, 2013
Summary of Material Modifications Notice of Changes to the LM HealthWorks Plan Effective Jan. 1, 2013
This notice is a Summary of Material Modifications (SMM), a legal document that describes changes to an official plan document called a Summary Plan Description (SPD), effective Jan. 1, 2013. See the attachment for the affected SPDs.
The HealthFund 2013 HealthFund Credits Effective Jan. 1, 2013, the amount of HealthFund Credits that LM HealthWorks Plan participants can earn for completion of certain Healthy Actions are as follows. The following chart will replace the current “HealthFund Highlights” chart in “The HealthFund” section of your SPD.
HealthFund Highlights The Healthy Actions and the amount of credits that can be earned are subject to change from year to year and will be communicated during annual enrollment. Healthy Actions Complete the Personal Health Assessment
Employee Spouse/Same-sex Domestic Partner
$100 once during the calendar year $100 once during the calendar year
Participate in the Virgin HealthMiles Physical Activity Tracking Tool Program*
Level 2: Employee Level 2: Spouse/Same-sex Domestic Partner
$100 once during the calendar year
$100 once during the calendar year (must advance from Level 1 to Level 2 during the calendar year)
Level 3: Employee Level 3: Spouse/Same-sex Domestic Partner
$200 once during the calendar year $100 once during the calendar year (must advance from Level 2 to Level 3 during the calendar year)
Level 4: Employee only $300 once during the calendar year (must advance from Level 3 to Level 4 during the calendar year)

LMC-ZDJ 2 133SMMB12
HealthFund Highlights Preventive Care – Routine physical exam, routine gynecological/well woman exam, routine mammogram, or colorectal cancer screening (age 50 and older) during 2013
Employee Spouse/Same-Sex Domestic Partner
$200 once per calendar year $200 once per calendar year
Maximum Credits Earned for the above Healthy Actions
Employee Spouse/Same-sex Domestic Partner
$900 maximum per calendar year $500 maximum per calendar year
Registration with Beginning Right® Maternity Management Program (pregnant Employee or pregnant Spouse/Same-sex Domestic Partner registers in first or second trimester during 2013)
Over and above the Healthy Actions $150 upon registration, once during the calendar year
Credits Earned by Condition Management Program or Health Coaching Participation (must complete assessment session and 5 Coaching Sessions, during the calendar year)
Employee Spouse/Same-sex Domestic Partner
Over and above the Healthy Actions** $100 once per calendar year $100 once per calendar year
Maximum HealthFund Balance Unlimited
HealthFund Exclusions HealthFund does not apply to:
Prescription drug expenses; and Any amounts not covered or limited by the
LM HealthWorks Plan such as: • Amounts over the recognized charge; • Amounts you pay because you do not
follow the precertification approval process; or
• Services not covered by the plan including services above visit limits.
HealthFund Participation Ends Participation ends when you are no longer enrolled in the LM HealthWorks Plan for active employees (or when COBRA or insurance continuation coverage ends). The fund is not a cash account—it is not subject to investment earnings or interest. Any remaining balance in the HealthFund is not payable when enrollment in the LM HealthWorks Plan ends.
* Must complete the Personal Health Assessment in order to earn these additional incentives. ** Employee and/or Spouse/Same-sex Domestic Partner are eligible for either Condition Management or
Health Coaching credits, not both, in a calendar year.

LMC-ZDJ 3 133SMMB12
Preventive Services Recent changes to preventive services coverage and women’s preventive health coverage under the Federal Affordable Care Act (ACA) impact the preventive care services currently listed in your SPD. Effective Jan. 1, 2013, the following content will replace what is currently stated in the “Preventive Services” sections of your SPD. The Plan is administering medical and outpatient prescription drug coverage in compliance with the applicable components of the ACA. Preventive services, as required by ACA, will be paid without cost-sharing such as coinsurance, copayments or deductibles. The visit maximums at the age intervals are combined for both in-network and out-of-network. Well-child care. Routine adult physical examinations. A routine physical examination includes a complete history
and physical with associated x-ray and laboratory services according to generally accepted medical guidelines.
Immunizations for children covered in accordance with generally accepted medical guidelines. Immunizations for adults who are considered “at risk” for certain medical conditions such as
influenza, pneumonia, meningitis, hepatitis and Lyme disease. The Claims Administrator determines “at risk” based on generally accepted medical guidelines. Immunizations for travel are not covered.
Gynecological – one routine well woman preventive exam office visit, including Pap smears and related laboratory fees, in accordance with the recommendations by the Health Resources and Services Administration.
Routine mammogram – one baseline mammogram age 35 to 39; one per calendar year age 40 and over.
One Prostate Specific Antigen (PSA) test per calendar year for males age 40 and over. Colorectal cancer screening (age 50 and older) – including occult blood stool test (once per year);
sigmoidoscopy (one every five years); double contrast barium enema (one every five years) and colonoscopy (one every 10 years).
For covered females: • Screening and counseling services as provided for in the comprehensive guidelines
recommended by the Health Resources and Services Administration. These services may include but are not limited to:
• Screening and counseling services, such as: — Interpersonal and domestic violence; — Sexually transmitted diseases; and — Human Immunodeficiency Virus (HIV) infections.
• Screening for gestational diabetes. • High-risk Human Papillomavirus (HPV) DNA testing for women age 30 and older and limited to
once every three years. • Screening and counseling services to aid in weight reduction due to obesity. Coverage
includes: — Preventive counseling visits and/or risk factor reduction intervention; — Medical nutrition therapy; — Nutritional counseling; and — Healthy diet counseling visits provided in connection with hyperlipidemia (high
cholesterol) and other known risk factors for cardiovascular and diet-related chronic disease.

LMC-ZDJ 4 133SMMB12
Comprehensive lactation support (assistance and training in breast feeding) and counseling services provided by a certified lactation support provider, in a group or individual setting, to females during pregnancy and in the post-partum period.
The rental or purchase of breast feeding durable medical equipment for the purpose of lactation support (pumping and storage of breast milk), and the purchase of the accessories and supplies needed to operate the item. The Claims Administrator reserves the right to limit the payment of charges up to the most cost efficient and least restrictive level of service or item which can be safely and effectively provided. The decision to rent or purchase is at the discretion of your Claims Administrator. Benefits may be subject to maximums.
For females with reproductive capacity, coverage includes: • FDA-approved contraceptive methods including certain FDA-approved generic drugs,
implantable devices, sterilization procedures and patient education and counseling for women with reproductive capacity.
• Counseling services provided by a physician in either a group or individual setting on contraceptive methods. Benefits may be subject to visit maximums.
• Female voluntary sterilization procedures and related services and supplies including tubal ligation and sterilization implants. Coverage does not include charges for a voluntary sterilization procedure to the extent that the procedure was not billed separately by the provider or because it was not the primary purpose of a confinement.
FDA-approved female generic emergency contraceptive methods that are prescribed by your physician.
Prescription Drugs The following changes will impact the “Prescription Drug” section of your SPD effective Jan. 1, 2013. Medco Moving to Express Scripts Name Earlier in 2012, Express Scripts merged with Medco Health Solutions, Inc. There are no changes to your pharmacy benefit; however, you will see changes to the naming conventions used in your SPD.
The following will not change: You can continue to use the same retail pharmacy. You can continue to refill your prescriptions as you normally would. The toll-free Member Services telephone number on your pharmacy ID card is still correct.
The following reference changes will be effective Jan. 1, 2013 unless otherwise noted below: Medco Health Solutions, Inc. changed to Express Scripts earlier in 2012. Express Scripts and
Medco are now one company and will operate under the Express Scripts name. Medco’s Web site at www.medco.com changed to the Express Scripts Web site at
www.express-scripts.com on Oct.1, 2012. Medco Member Services will change to Express Scripts Member Services; however, the phone
number will remain (877) 458-4975 for those enrolled in the LM HealthWorks plan. Medco’s Health, Allergy & Medication Questionnaire will change to Express Scripts’ Health,
Allergy & Medication Questionnaire. Medco’s Coverage Review unit will change to Express Scripts’ Coverage Review unit; however,
the phone number will remain (800) 753-2851.

LMC-ZDJ 5 133SMMB12
Generics Rx Advantage The Generics Rx Advantage program will be discontinued, effective Jan. 1, 2013, although a description of the program is outlined in the 2012 LM HealthWorks Plan Summary of Materials Modifications (SMM). This program eliminated your first payment on any new 90-day supply of a generic prescription that you filled through the Medco Pharmacy mail-order service. Health Care Reform and Pharmacy (Regarding Preventive Benefits) Health Care Reform provides that some preventive care medications must be covered at 100%. Effective Jan. 1, 2013, in accordance with this legislation, the LM HealthWorks Plan will cover in-network generic prescription contraceptive medications for females through the age of 50 in full (Plan pays: 100%, You Pay: $0). The Retail Refill Allowance outlined in your 2012 Summary of Materials Modifications (SMM) will continue to apply to these medications. This means that after your third purchase (at no cost) of a generic contraceptive medication at a participating retail pharmacy, you will pay up to $25, if you continue to fill at the retail pharmacy. All brand medications will be covered according to the applicable copayment or coinsurance. Over-the- counter contraceptives will continue to be excluded from coverage. Pervasive Development Delays Effective Jan. 1, 2013, the following content will replace the information currently provided in the “Pervasive Development Delays” section of your SPD. Charges for the diagnosis of pervasive, developmental delays, including autism. All other services and treatment of pervasive developmental delays are not covered under the LM HealthWorks Plan except for outpatient short-term rehabilitation. Coverage is limited to 60 visits per year, combined for speech, physical and occupational therapies. Short-term rehabilitation at an outpatient hospital setting is included in the 60-visit maximum. Outpatient Physical Therapy, Occupational Therapy and Speech Therapy Effective Jan. 1, 2013, the following content will replace the information currently provided in the “Outpatient Physical Therapy, Occupational Therapy and Speech Therapy” subsection of the “LM HealthWorks Plan” benefit section. Coverage is subject to the limits shown in the “Benefit Highlights” section. Inpatient rehabilitation benefits for the services listed will be paid as part of the Inpatient Hospital and Skilled Nursing Facility benefits. Rehabilitation services received in the home will also count toward the benefit maximum for Home Health Care. Instead of hospitalization, the LM HealthWorks Plan allows for extension of certain outpatient benefits beyond the LM HealthWorks Plan limits. Care must be medically necessary and be precertified. Physical therapy is covered for non-chronic conditions and acute illnesses and injuries, as long
as the therapy expects to significantly improve, develop or restore physical functions lost or impaired as a result of an acute illness, injury or surgical procedure. Physical therapy does not include educational training or services designed to develop physical function (except as provided for the treatment of Pervasive Developmental Disorders/Autism Spectrum Disorders). Coverage for physical therapy is available for the treatment of Pervasive Developmental Disorders/Autism Spectrum Disorders (as an exception to the above non-chronic condition coverage criteria).

LMC-ZDJ 6 133SMMB12
Occupational therapy (except for vocational rehabilitation or employment counseling) is covered for non-chronic conditions and acute illnesses and injuries, as long as the therapy expects to significantly improve, develop or restore physical functions lost or impaired as a result of an acute illness, injury or surgical procedure, or to relearn skills to significantly improve independence in the activities of daily living. Occupational therapy does not include educational training or services designed to develop physical function (except as provided for the treatment of Pervasive Developmental Disorders/Autism Spectrum Disorders). Coverage for occupational therapy is available for the treatment of Pervasive Developmental Disorders/Autism Spectrum Disorders (as an exception to the above non-chronic condition coverage criteria).
Speech therapy is covered for non-chronic conditions and acute illnesses and injuries as long as the therapy is expected to restore the speech function or correct a speech impairment resulting from that illness or injury; or for delays in speech function development as a result of disease, injury or gross anatomical defect present at birth. Speech function is the ability to express thoughts, speak words and form sentences. Speech impairment is defined as difficulty with expressing one’s thoughts with spoken words. Coverage for speech therapy is available for the treatment of Pervasive Developmental Disorders/Autism Spectrum Disorders (as an exception to the above non-chronic condition coverage criteria).
A “visit” consists of no more than one hour of therapy. Refer to the “Benefit Highlights” section for the visit maximum that applies to the LM HealthWorks Plan. Covered expenses include charges for two therapy visits of no more than one hour in a 24-hour period. The therapy should follow a specific treatment plan that: Details the treatment, and specifies frequency and duration; and Provides for ongoing reviews and is renewed only if continued therapy is appropriate. What Is Not Covered: Exclusions Effective Jan. 1, 2013, the examples of non-covered diagnoses, provided to explain the therapies for the treatment of delays in development or congenital defects amenable to surgical repair that are not covered, will be modified to exclude Pervasive Developmental Disorders (including Autism). The current exclusion in the “Exclusions” subsection of the “LM HealthWorks Plan” benefit section will be updated as follows:
Therapies for the treatment of delays in development, unless resulting from acute illness or injury,
or congenital defects amenable to surgical repair (such as cleft lip/palate), are not covered. • Examples of excluded therapies include but are not limited to Applied Behavioral Analysis, and
the LEAP, TEACCH, Denver and Rutgers programs. • Examples of non-covered diagnoses include Down Syndrome and Cerebral Palsy, as they are
considered both developmental and/or chronic in nature.
Please keep this notice with your other important benefits information.

LMC-ZCS 1 126SMMB12
Dec. 17, 2012 Summary of Material Modifications Important Information Regarding Changes Effective Jan. 1, 2013 This notice is a Summary of Material Modifications (SMM), a legal document that describes changes to an official plan document called a Summary Plan Description (SPD), effective Jan. 1, 2013. See the attachment for the affected SPDs. Coverage Categories Change The “Coverage Categories” section of this SPD currently states that you have the opportunity to choose between three coverage category options. Effective Jan. 1, 2013, you will have the opportunity to choose between four coverage categories depending on the dependents you enroll. Due to this change, the following content will replace what is currently stated in the “Coverage Categories” section as the coverage level options. Coverage Categories
When you enroll, you select your coverage level based on the dependents you enroll, as follows: Employee Only; Employee + Spouse/Same-sex Domestic Partner; Employee + Child(ren); or Employee + Family.
Please keep this notice with your other important benefits information.

LMC–ZAY 106SMMB12
March 1, 2012 Summary of Material Modifications Important Information Regarding Changes Effective January 1, 2012: Eligibility Requirements for a Same-Sex Domestic Partner This notice is a Summary of Material Modifications (SMM). It is a legal document that describes changes to official plan documents called Summary Plan Descriptions (SPDs). See appendix for list of affected SPDs. This SMM describes changes for same-sex domestic partners/spouses effective January 1, 2012 regarding:
• Eligibility requirements, • Enrollment processes, and • Imputed income if the same-sex domestic partner/spouse and/or the child(ren) of a
same-sex domestic partner/spouse qualify as tax dependents for federal income tax purposes.
These changes apply to medical, dental, vision, life insurance and/or special accident insurance plans that accept same-sex domestic partners/spouses as eligible dependents*. Eligibility requirements for a same-sex domestic partner A same-sex domestic partner must meet the requirements outlined in the Company’s Same-sex Domestic Partner Affidavit and other materials as noted below. To be eligible for coverage, neither you nor your same-sex domestic partner may be married to someone else. A same-sex domestic partner also must:
• Be the same sex as you; • Share financial resources and dependencies with you; • Have resided with you continuously for at least six months in a sole-partner relationship
that is intended to be permanent; and • Be at least 18 years of age and not related to you by blood.
You may also be eligible for same-sex spouse coverage if you and your dependent have a valid marriage certificate from a state that recognizes same-sex marriages. However, under current federal law your coverage will be as a same-sex domestic partner and not as a spouse, even if you have enrolled your partner as a same-sex spouse. * Please refer to the Same-sex Domestic Partner Affidavit or the Same-sex Domestic Partner/Spouse Fact Sheet or call the Lockheed Martin Employee Service Center for a list of the medical plans that do not accept same-sex domestic partners/spouses as eligible dependents.

LMC–ZAY 106SMMB12
Eligibility requirements for children of a same-sex domestic partner/spouse If you enroll your same-sex domestic partner’s/spouse’s child(ren), the dependent(s) must meet the following requirements, as noted in the “Dependent Eligibility” section of your SPD. Child(ren) of your qualified same-sex domestic partner/spouse are eligible for dependent coverage if they are:
• The natural or legally adopted child(ren) of your same-sex domestic partner/spouse; and • Under age 26.
Important Note: You may elect to cover eligible child(ren) of your qualified same-sex domestic partner/spouse even if you do not elect coverage for your partner/spouse. If you elect to cover eligible child(ren) of your qualified same-sex domestic partner, you will need to complete a Same-sex Domestic Partner Affidavit. Coverage of your natural born or legally adopted child(ren), or eligible children of your same-sex spouse, is accomplished through the standard enrollment process and no Affidavit is required. Same-sex Domestic Partner Affidavit If you are enrolling a same-sex domestic partner, you will need to complete the Same-sex Domestic Partner Affidavit form at the time of enrollment. You must complete the required form(s) acknowledging that your same-sex domestic partner and/or his or her enrolled child(ren) meet certain criteria, and return the form along with the required documentation to the Lockheed Martin Employee Service Center within the 30 days following the event. If you are enrolling a same-sex spouse, you are not required to submit the Same-sex Domestic Partner Affidavit. Change in same-sex domestic partnership or spouse eligibility You may change your coverage only during the Annual Enrollment period, unless you experience a qualified life event as defined by the plan. • If your same-sex domestic partnership ends during the plan year, you will need to
complete a Drop Same-sex Domestic Partner event within 30 days following your dependent’s loss of eligibility in order to drop your same-sex domestic partner’s coverage.
• If your same-sex marriage ends during the plan year, you will need to complete a Divorce event within 30 days following your dependent’s loss of eligibility.
Visit the Lockheed Martin Employee Service Center Online or call the Lockheed Martin Employee Service Center to report your event and make coverage changes. Note that if your same-sex domestic partnership/marriage ends, you can no longer cover your same-sex domestic partner’s/spouse’s child(ren) not legally adopted by you. Imputed Income: What You Need to Know Adding a same-sex domestic partner/spouse and/or his or her eligible child(ren) not legally adopted by you to your coverage may have an effect on your federal and state income taxes. You should consult your legal and tax advisors to determine how this may affect you. States vary in the degree to which they recognize same-sex relationships (civil unions, same-sex marriages, registered domestic partners). However, under current federal law same-sex couples are not considered as “married” individuals or “spouses” for purposes of the Internal

LMC–ZAY 106SMMB12
Revenue Code (IRC). Consequently, unless your same-sex domestic partner/spouse qualifies as your dependent under the IRC on some basis other than as your “spouse,” the cost of health plan coverage provided to your same-sex domestic partner/spouse is considered taxable income to you. Similarly, unless the child(ren) of your same-sex domestic partner/spouse qualify as your dependent(s), the cost of health plan coverage provided to them is considered taxable income to you. Lockheed Martin must appropriately report and withhold taxes on the cost of the coverage. You will be taxed on the company-paid portions of that individual’s coverage. In addition, you will also be taxed on the portion of that individual’s coverage paid for by you (and deducted from your paycheck on a pre-tax basis). The company- and employee-paid portions of that individual’s coverage together will be treated as “imputed income,” and the imputed amounts will be added to your taxable income. The imputed amounts are also subject to federal income and employment tax withholding. State income tax treatment of that coverage will depend on the laws of your particular state. For example, you could also be subject to state income tax on the imputed amounts. There may be limited circumstances where your same-sex partner (or his or her child) may qualify as your dependent for federal income tax purposes on some basis other than as your spouse. To qualify as your tax dependent, an individual must meet strict requirements set forth in the Internal Revenue Code. For more detail on the dependent test, you should refer to IRS Publication 17 (http://www.irs.gov/pub/irs-pdf/p17.pdf) and/or IRS Publication 501 (http://www.irs.gov/pub/irs-pdf/p501.pdf). You should also contact your legal and tax advisors to determine how this and/or dependent status under state income tax laws may apply to you. Tax Dependent Certification You may also complete the Tax Dependent Certification form when you enroll your same-sex domestic partner/spouse. By taking this optional step, you are certifying that the individual(s) in question qualify as your tax dependent under the Internal Revenue Code. Certification can be made at any time during the year. Any change in imputed income will be effective after the Lockheed Martin Employee Service Center receives the Tax Dependent Certification. Note that you must certify that the applicable individuals qualify as your eligible tax dependents for the entire year. If you do not complete a Tax Dependent Certification, imputed income will continue to apply. If you certify to Lockheed Martin that your enrolled same-sex domestic partner/spouse and/or his or her enrolled child(ren) who have not been legally adopted by you qualify as dependents for federal income tax purposes for the entire year, Lockheed Martin will not report and withhold amounts as imputed income for federal income tax purposes. You will also be able to pay for the applicable coverage on a pre-tax basis under the health plans. You may certify the tax dependent status of the enrolled child(ren) of your same-sex domestic partner/spouse who have not been legally adopted by you even if your partner/spouse does not qualify as your tax dependent. Claims of the tax dependent status for other dependents may be accomplished through the standard enrollment process. Important note: While Lockheed Martin will accept your certification that your enrolled same-sex domestic partner/spouse and/or his or her child(ren) not legally adopted by you are your tax

LMC–ZAY 106SMMB12
dependents, the IRS will have the final say in determining whether someone qualifies as a dependent for federal income tax purposes. It is your responsibility to make sure that your same-sex domestic partner/spouse and/or his or her enrolled child(ren) not legally adopted by you are eligible based on IRS guidance, as eligibility turns on facts solely within your knowledge; Lockheed Martin cannot make this determination for you. If the IRS or applicable state tax agency determines that any are not eligible as dependents, you may be subject to additional taxes and penalties. You should make this determination in consultation with your legal and tax advisors. To certify tax dependent status of your current same-sex domestic partner/spouse and/or his or her enrolled child(ren) who have not been legally adopted by you in the future, or to request a Tax Dependent Certification form, visit the Employee Service Center Online or call the Lockheed Martin Employee Service Center at 866-562-2363.
Please keep this notice with your other important benefits information.

LMC-ZAV 101SMMB12
April 30, 2012 Summary of Material Modifications Notice of Changes to LM HealthWorks Plan Effective Jan. 1, 2012 This notice is a Summary of Material Modifications (SMM), a legal document that describes changes to an official plan document called a Summary Plan Description (SPD), effective Jan. 1, 2012. See the appendix for the affected SPDs. The HealthFund 2012 HealthFund Credits Effective Jan. 1, 2012, the amount of HealthFund Credits that LM HealthWorks Plan participants can earn for completion of certain Healthy Actions are as follows. The following chart will replace the current “HealthFund Highlights” chart in “The HealthFund” section of your SPD.
HealthFund Highlights The Healthy Actions and the amount of credits that can be earned are subject to change from year to year and will be communicated during enrollment. Healthy Actions Complete the Personal Health Assessment Employee Spouse/Same-sex Domestic Partner
$200 once during the calendar year $200 once during the calendar year
Participate in the Virgin HealthMiles Physical Activity Tracking Tool program* Level 2: Employee only
$100 once during the calendar year (must advance from Level 1 to Level 2 during the calendar year)
Level 3: Employee only $100 once during the calendar year (must advance from Level 2 to Level 3 during the calendar year)
Level 4: Employee only $100 once during the calendar year (must advance from Level 3 to Level 4 during the calendar year)

LMC-ZAV 2 101SMMB12
HealthFund Highlights Complete the Tobacco Non-User Certification (or participate in the Quit for Life® program, if a tobacco user).* Employee Spouse/Same-sex Domestic Partner Tobacco users must enroll in the Quit for Life program and either complete 4 coaching calls or complete the Quit for Life program, during the plan year.
$50 once during the calendar year $50 once during the calendar year
Maximum Credits Earned for the above Healthy Actions
Employee $550 maximum per calendar year Spouse/Same-sex Domestic Partner $250 maximum per calendar year Registration with Beginning Right® Maternity Management Program (in first or second trimester)
Over and above the Healthy Actions $150 upon registration, once during the calendar year
Credits Earned by Condition Management Program or Health Coaching Participation (must complete assessment session and 5 Coaching Sessions, during the calendar year)
Over and above the Healthy Actions**
Employee Spouse/Same-sex Domestic Partner
$150 maximum per calendar year $150 maximum per calendar year
* Must complete the Personal Health Assessment in order to earn these additional incentives. ** Employee and/or Spouse/Same-sex Domestic Partner are eligible for either Condition Management or Health Coaching credits, not both, in a calendar year. If You Leave the LM HealthWorks Plan and Enroll in a Different Plan Year The following provides clarification on what happens to your HealthFund balance if you leave the LM HealthWorks Plan and re-enroll. This content will replace what is currently stated in the “If You Leave the LM HealthWorks Plan and Enroll in a Different Plan Year” subsection of “The HealthFund” section in your SPD. Once your coverage ends, the HealthFund also ends. If you subsequently re-enroll in the LM HealthWorks Plan, any HealthFund balance (regardless of how it was earned) will be reinstated provided you re-enroll within three plan years of termination, including the plan year in which you were previously enrolled. Claims incurred after your coverage begins are eligible for reimbursement from the HealthFund—any claims incurred during the period you were not covered are not eligible for reimbursement.

LMC-ZAV 3 101SMMB12
Prescription Drug Effective Jan. 1, 2012, the following provisions will apply to your prescription drug benefit administered by Medco and will modify the “How the Prescription Benefit Works” section of your SPD. Prescription Drug Mail Order Change: Retail Refill Allowance You may pay more for your long-term drugs (such as those used to treat high cholesterol, high blood pressure, depression, or diabetes) unless you order your prescriptions by mail from the Medco Pharmacy™. After your third purchase of a long-term medication at a participating retail pharmacy, you will pay your regular coinsurance plus up to an additional $25, if you continue to fill at the retail pharmacy. Please note that you will never pay more than the actual cost of the medication. Your mail-order coinsurance will remain the same. This applies to any generic, preferred and non-preferred brand name medication (up to 30-day supply) that is refilled more than three times at a retail pharmacy. To convert a prescription to the Medco Pharmacy™ or obtain more information, access the Medco Web site through the Prescription Drug Benefits page at www.lmhwplan.com or call the LM HealthWorks Plan at 877-458-4975. Preferred Drug Step Therapy Your plan uses a coverage tool called step therapy, which requires you first to try one or more specified drugs to treat a particular condition before the plan will cover another (usually more expensive) drug that your doctor may have prescribed. Step therapy is intended to reduce costs for you and your plan by encouraging the use of medications that are less expensive but can treat your condition effectively. If you’re taking a medication that is newly identified as requiring step therapy, you’ll receive a letter explaining that your plan will not cover it unless you try the alternative first. The letter will also have information on starting a coverage review if your doctor believes that you should take the original medication. The following five drug categories are affected by step therapy:
• Proton pump inhibitors • SSRI- anti depressants (members new to therapy only) • Biphosphonates • Intranasal Steroids • Angiotensin II Receptor Blockers
If you need more detailed information, please call Medco Member Services (the phone number is shown on the back of your member ID card). Or, you can log on to www.medco.com and click on either “My Rx Choices” or “Price a Medication,” and then type in the name of the medication to see if coverage rules apply.
LMC-ZAV 4 101SMMB12
If you fill a prescription for one of the above medications without getting approval, you will be responsible for its entire cost. Ask your doctor to consider changing your prescription to one that doesn’t require a review. If your doctor believes that there are special reasons you should continue this medication, your doctor can request a coverage review by calling 800-417-1764, 8:00 a.m. to 9:00 p.m., Eastern time, Monday through Friday. If coverage is approved, you will pay the plan’s appropriate coinsurance for the medication, which may be higher than what you would pay for a preferred alternative drug that does not require a coverage review. If you obtain approval after filling your prescription, you may not be reimbursed for any amount paid. Preferred Drug Step Therapy program (“the Program”) guidelines are subject to periodic review and change. For more information, access the Medco Web site through the Prescription Drug Benefits page at www.lmhwplan.com or call the LM HealthWorks Plan at 877-458-4975. Generics Rx Advantage The Generics Rx Advantage Program saves you money on generic medications by:
• Eliminating your first payment on any new 90-day supply of a generic prescription you fill through the Medco Pharmacy® mail-order service.
• Providing a one-time discount of $25 off your out-of-pocket costs the first time you order a brand-name drug, that will soon become available as a generic drug, through the Medco Pharmacy.
• Offering free standard delivery of your medications to your home or office. • Providing 24/7 access to pharmacists who can answer your questions.
To participate in the Medco Generics Rx Advantage Program, just visit www.medco.com/generics or call 877-909-4367 from 9:00 a.m. to 9:00 p.m., Monday through Friday, and 9:00 a.m. to 6:00 p.m., Saturday, Eastern time. If you haven’t already registered with Medco, you can complete a simple registration process when you visit the site to get access to Generics Rx Advantage. All you need is a recent Medco prescription number and your member ID card.
Medco will contact your doctor to have your prescriptions sent to you by mail, when possible.
What Prescriptions Are Covered Effective Jan. 1, 2012, the following provision will be added to the list of covered prescriptions that by federal law require a physician’s prescription. This addition is for clarification to a benefit that already exists as a Covered Benefit and is in addition to the information currently noted in the “What Prescriptions are Covered” section of your SPD. The prescription drug benefit covers those medications that by federal law require a physician’s prescription, are prescribed according to approved indications, are not considered experimental or investigational and are not otherwise limited or excluded by the LM HealthWorks Plan. Covered prescriptions include such things as:
• Compounded medications containing at least one federal legend drug (unless drugs contained are excluded from coverage by the Plan.).

LMC-ZAV 5 101SMMB12
What Is Covered Effective Jan. 1, 2012, the following provision will be covered under the LM HealthWorks Plan. This will be in addition to the information currently noted in the “What Is Covered” section of your SPD. The LM HealthWorks Plan covers certain preventive services and a wide range of medically necessary services recommended by a physician for the treatment of an illness, injury or pregnancy including:
• Sex reassignment services. Exclusions Effective Jan. 1, 2012, the following provision will be removed from the “What Is Not Covered: Exclusions” section of your LM HealthWorks Plan.
• Sex change: Any treatment, drug, service or supply related to changing sex or sexual characteristics, except as provided in the “What Is Covered” section, including: – Surgical procedures to alter the appearance or function of the body; – Hormones and hormone therapy; – Prosthetic devices; and – Medical or psychological counseling.
High-Technology Imaging Pre-Authorization Program Effective Jan. 1, 2012, the LM HealthWorks Plan is implementing a high-technology imaging pre-authorization program, known as Radiology Benefit Management, in addition to your current complex imaging services benefit. This pre-authorization program requires your provider to obtain authorization BEFORE requesting high-tech imaging services in an outpatient setting and applies to MRIs, CT (CAT) scans, PET scans, nuclear medicine and cardiac imaging. Prior to your high-tech radiology procedure, please confirm that your doctor has pre-certified your test, and is sending you to an approved facility. Because the radiology facilities know that precertification is required, your test could be delayed or you could be denied service if your doctor has not taken this step. If you are seeing an out-of-network provider, it is your responsibility to pre-certify your procedure.
Please keep this notice with your other important benefits information.

Summary Plan Description LM HealthWorks Plan Health benefits for certain non-represented and certain represented employees
Effective January 1, 2011
LMC-ZAH

Important The Lockheed Martin Group Benefits Plan (the “LMC Plan”) provides medical and other benefits to certain employees of Lockheed Martin Corporation. The Lockheed Martin Operations Support, Inc. Benefit Plan (the “LMOS Plan”) provides medical and other benefits to certain employees of Lockheed Martin Operations Support, Inc. and its affiliates. The LMC Plan and the LMOS Plan will be referred to together in this booklet as the “Plans” or simply the “Plan.” This booklet (referred to as a Summary Plan Description or “SPD”) summarizes the medical, prescription drug and employee assistance benefit components of the Plan. If there is any conflict between this SPD and the official plan document(s), the official plan document(s) will govern. The Company (Lockheed Martin Corporation or Lockheed Martin Operations Support, Inc., as applicable) expects to continue the Plan indefinitely. However, the Company reserves the right to amend, suspend or terminate the Plan, in whole or in part, at any time. A collective bargaining agreement may restrict the Company’s right to amend or terminate the Plan during the term of the agreement. Written or oral statements to you from human resources (HR) business partners or other personnel cannot modify the Plan’s terms. Where conflicts exist, the terms as set forth in the plan documents will govern. Participation in the Plan is not a contract of employment and does not constitute a contract for, nor guarantee of, continued or future employment with the Company. The Plan provisions also do not prohibit changes in the terms of your employment. Please keep this information for future reference.
i

About this Booklet This booklet (referred to as a Summary Plan Description or “SPD”) describes the health and the employee assistance benefit component of the Lockheed Martin Group Benefits Plan (the “LMC Plan”) and the Lockheed Martin Operations Support, Inc. Benefit Plan (the “LMOS Plan”). For purposes of simplicity, the health benefits component of the Plans will be referred to herein as the LM HealthWorks Plan. This SPD summarizes the LM HealthWorks Plan and the Employee Assistance Program available to certain non-represented and certain represented employees of the Company or affiliates (see Appendices A and B). The Plans also cover other employees whose benefits are described in separate SPDs. The Plans also provide other, non-medical benefits (for example, life insurance) which are described in separate SPDs. Your health and quality of life are important to you and to the Company. Lockheed Martin has a strong commitment to your health and well-being, and with the LM HealthWorks Plan, this commitment has been put into action. To help you get healthy and stay healthy, the LM HealthWorks Plan gives you access to a world of tools, resources, programs and one-on-one support from trusted partners that Lockheed Martin has selected. These include Aetna, our medical claims administrator; Healthways, our wellness and condition management partner; and Medco® Health Solutions, Inc, our prescription drug claims administrator. It’s a good idea to take time to learn about all the LM HealthWorks Plan has to offer. You should read through this SPD and share it with your family. Also available is the LM HealthWorks Plan Web site at www.lmhwplan.com, which offers many online tools and resources. You can visit this site as often as you like, use the tutorials, check out links and sample the online resources available to you. Regardless of your health needs or personal situation, the LM HealthWorks Plan has something for you. In this SPD, you will find:
Information about eligibility for coverage, enrolling for coverage, when coverage begins and when coverage ends.
A description of the LM HealthWorks Plan and the Employee Assistance Program. Important administrative information about the Plan and your rights under the Employee Retirement
Income Security Act (ERISA). A glossary of terms.
The benefits described in this booklet are effective January 1, 2011.
ii

Table of Contents Eligibility ...................................................................................................................................................... 1 The LM HealthWorks Plan............................................................................................................................ 4 Prescription Drug ........................................................................................................................................ 56 Employee Assistance Program (EAP) ........................................................................................................ 60 Enrolling for Coverage ............................................................................................................................... 61 When Coverage Begins............................................................................................................................... 67 How Claims Are Handled ........................................................................................................................... 68 When Coverage Ends.................................................................................................................................. 73 Situations Affecting Your Coverage........................................................................................................... 74 Continuing Coverage .................................................................................................................................. 77 Certificate of Creditable Coverage ............................................................................................................. 82 Plan Administration .................................................................................................................................... 83 Claims and Appeals Procedures.................................................................................................................. 87 Your Rights Under ERISA ......................................................................................................................... 94 Glossary of Terms....................................................................................................................................... 97 Appendix A – Participating Business Units*............................................................................................ 109 Appendix B – Participating Unions* ........................................................................................................ 110
iii

Eligibility
Employee Eligibility You are eligible to participate in the LM HealthWorks Plan on your first day of work (or on the day you first become eligible) if you are an employee of the Company at a participating business unit (see Appendix A), and you are:
A regular full-time non-represented employee; or A regular part-time non-represented employee; or An employee represented by one of the bargaining units that have adopted the LM HealthWorks Plan
as listed in Appendix B. You are not eligible to participate unless you are scheduled to work at least 1,000 hours in a year. You are also not eligible to participate if you are:
An intern/co-op student; A consultant; A leased employee; Paid by a third-party employer; or Otherwise not classified as an employee by the Company on its payroll records.
Dependent Eligibility If you enroll for coverage, you may also enroll your eligible dependents under the LM HealthWorks Plan. Your eligible dependents under the LM HealthWorks Plan include:
Your spouse (the lawful female wife of an eligible male employee or the lawful male husband of an eligible female employee) or common-law spouse (the common-law female wife of an eligible male employee or the common-law male husband of an eligible female employee, where legally recognized in the state of residence and all requirements have been met); or
Your same-sex domestic partner, as described under the “Same-sex Domestic Partners” section. Your children up to age 26 (with no student, marital or financial requirements), if they are: • Your natural children; • Your legally adopted children; • Children placed with you for legal adoption; • Your stepchildren (natural or legally adopted children of your legal spouse); or • Natural or legally adopted children of your same-sex domestic partner.
You may also be able to cover your grandchildren, but only if you have court-appointed legal guardianship. Acceptable proof of court appointed legal guardianship will be required before you can enroll a grandchild for the first time and from time to time on request.
Your disabled children age 26 and older who, when they first became disabled, would have met the definition of an eligible dependent and who are incapable of self-sustaining employment because of mental retardation, serious mental illness, physical sickness or injury. Coverage may continue to age 65 as long as your child remains incapacitated and is otherwise eligible for coverage. To extend this coverage, you must show proof of your child’s incapacity within 30 days after regular coverage ends or within 30 days of your child’s initial eligibility date, if later.
1

Extended coverage ends when: • Your child age 26 and older marries; • Your child age 26 and older becomes capable of self-support; • Your child fails to report for a scheduled physical exam; • Proof of incapacity is requested and not presented; or • Coverage terminates for reasons other than reaching the age limits described earlier.
Dependent Exclusions Dependents do not include any individual who is also covered as an employee, former employee or retiree under any other Company-sponsored medical plan or a medical plan where the Company is a participating employer. For example, if you are an LMC employee married to another LMC employee or retiree, you and your spouse cannot be covered as both an employee or retiree and a dependent. One of you may elect to waive coverage and be enrolled under your spouse’s coverage or you may both elect single coverage. In addition, any dependents can only be covered by one of you. NOTE: For purposes of this Plan, dependents do not include any person (including but not limited to nieces or nephews) for whom you are the court-appointed legal guardian, unless that person is your child (as defined in the “Dependent Eligibility” section) or your grandchild. Proof of Dependent Eligibility You must provide reasonable proof of dependent status upon request. Failure to provide proof upon request will result in the cancellation of that dependent’s coverage, and may result in the cancellation of coverage for you and your other dependents as well. Once coverage has been cancelled, coverage can only be reinstated (if at all) on a prospective basis from the date the required information is received by the Lockheed Martin Employee Service Center, and only if reinstatement is permitted under the terms of the LM HealthWorks Plan (for example, during Annual Enrollment or where there has been a qualifying event). You are responsible for maintaining accurate and up-to-date information on the eligibility status of your enrolled dependents. You must notify the Lockheed Martin Employee Service Center within 30 days of a change in a dependent’s status. Intentionally falsifying information is also a violation of Company policy. Domestic Relations Cases An order or administrative notice (including approval of a settlement agreement) issued by a court, state agency or other appropriate state process, often referred to as a Qualified Medical Child Support Order (QMCSO), could require that you enroll your child under a health care plan, even if you do not have custody. The Company will comply with any QMCSO presented if it satisfies all legal requirements. You can obtain a copy of the QMCSO procedures without charge by contacting the Lockheed Martin Employee Service Center, or by calling the Lockheed Martin Qualified Domestic Relations Order office at 732-537-7025.
2

Same-sex Domestic Partners You may cover a “same-sex domestic partner” as an eligible dependent if you are not currently covering a spouse. A same-sex domestic partner must meet the requirements outlined in the Company’s Same-sex Domestic Partner Affidavit and other materials that certify that he or she:
Is the same gender as you; Shares significant financial resources with you; Is at least 18 years of age; and Has lived with you for six months or more in a sole-partner relationship that is meant to be
permanent. Neither you nor your same-sex domestic partner may be married to someone else. You may also be eligible for same-sex domestic partner coverage if you and your same-sex partner have a valid marriage certificate from a state that recognizes same-sex marriages performed in the state. Note that in accordance with federal income tax regulations, coverage will be as a same-sex domestic partner and not as a spouse. The Company’s Same-sex Domestic Partner Affidavit and other materials are available through the online benefits enrollment site, or by calling the Lockheed Martin Employee Service Center. In addition, if you elect to cover your same-sex domestic partner you can also enroll your same-sex domestic partner’s children under the same option you choose, as long as they otherwise meet the eligibility requirements as described under the “Dependent Eligibility” section.
3

The LM HealthWorks Plan The LM HealthWorks Plan combines comprehensive coverage with a HealthFund that helps with medical expenses, subject to limitations and exclusions as described within this SPD. The LM HealthWorks Plan gives you the freedom to receive care from in-network and/or out-of-network providers and the opportunity to save money when you use the LM HealthWorks Plan’s in-network providers. The LM HealthWorks Plan also provides coverage for prescription drugs, at both participating retail pharmacies and through a convenient mail-order service. There are a host of resources available to you as well, from health coaching to help with chronic conditions, to online health references, and a 24-hour nurse advice line to help with your health interests and concerns.
Key Features of the LM HealthWorks Plan 100% coverage for covered preventive care. You typically pay nothing for routine exams, well-
child care, immunizations, routine cancer screenings and other services that protect your health and identify potential problems early.
Freedom to choose, opportunity to save. You can receive care from in-network or out-of-network providers and the Plan will pay benefits. The Plan pays a higher percentage and you pay a lower percentage of the recognized charge for most covered services when you choose in-network providers. You pay an even lower percentage when you choose Aexcel-designated providers for certain specialty care. Aexcel providers are higher performers, in terms of clinical performance and efficiency, in their specialty areas.
No referrals to specialists required. When you need specialty care, simply choose a provider and make an appointment. You may directly access specialists and other providers for covered services. To locate in-network specialists, providers and hospitals in your area, you can use the DocFind® tool on the LM HealthWorks Plan Web site at www.lmhwplan.com.
The HealthFund. This is an account set up for you when you enroll in the LM HealthWorks Plan. You can build your fund by completing certain Healthy Actions. As you incur expenses during the year, any covered expenses that apply to your deductible and coinsurance can be paid from the HealthFund. Any money left in your HealthFund at year-end is rolled over to the following year’s account balance.
Prescription drug benefits. You can save on prescriptions filled at participating retail pharmacies (for up to a 30-day supply) and through the convenient mail-order service (for up to a 90-day supply).
Health and information resources. The LM HealthWorks Plan provides and coordinates tools, resources, programs and coaching from leading health and wellness organizations to help you manage your health and your health care.
Network. You have a nationwide network of doctors, specialists and hospitals available to you. To locate an in-network provider, you can use the DocFind® tool on the LM HealthWorks Plan Web site at www.lmhwplan.com.
Condition and lifestyle management. Coaching support is available to help you manage a chronic medical condition and live a healthier life.
4

How the LM HealthWorks Plan Works
In-Network Care Preventive care is covered at 100% with no deductible. For other services, once you meet the deductible, the LM HealthWorks Plan begins to pay benefits. The LM HealthWorks Plan pays a share of your expense and you pay the rest, called coinsurance. The “Benefit Highlights” section shows how you and the LM HealthWorks Plan share expenses. In most cases, when you see an in-network provider, you do not have to pay anything at the time of your visit. If you have not yet met your deductible, some in-network providers may ask for payment at the time of your visit. (Office staff can check this by calling the plan’s customer service line during your visit.) The in-network provider will submit a claim to request payment from the LM HealthWorks Plan. There is no paperwork for you to complete. If there is a balance in your HealthFund, the appropriate amount will be withdrawn automatically to pay the expense. The amount of the claim will also be applied to your calendar year deductible. If your HealthFund has been used up before the full amount of the deductible is met, you will need to pay for your care out of your pocket. After the in-network provider files a claim, you will receive an Explanation of Benefits (EOB) statement that shows the total charge for care and the amount the LM HealthWorks Plan paid. It also shows you how much of the deductible you’ve met and how much remains to be met. If you are a registered member with the Aetna Navigator® Web site, you will receive an email notification that an EOB is available; otherwise, you will receive the EOB statement by mail. If you would rather receive EOBs online and have not yet registered with Aetna Navigator, you can “turn off” paper EOBs by visiting Aetna Navigator® through the LM HealthWorks Plan Web site at www.lmhwplan.com. The EOB is not a bill—your provider will bill you for your share of the cost of the service. NOTE: If you need a service that is covered under the LM HealthWorks Plan but is not available from an in-network provider or hospital in your area, please contact the LM HealthWorks Plan at 877-458-4975 for assistance. Accessing In-network Providers and Benefits You and your covered dependents have the option to select an in-network provider as your primary care physician (PCP) who can help you manage your care—the decision is yours. A primary care physician can include any primary care provider, a pediatrician as a child’s PCP or an OB/GYN as the PCP for a female participant. The LM HealthWorks Plan does not require you to select a PCP and referrals are not required. You can find in-network providers in your area by using DocFind®, the online provider directory. If you wish to receive a copy of a provider directory or information about in-network providers, contact the LM HealthWorks Plan claims administrator at 877-458-4975. Certain health care services such as hospitalization, outpatient surgery and certain other outpatient services require precertification. Refer to the “Precertification” section for more information on the precertification process and what to do if your request for precertification is denied.
5
Out-of-Network Care If you receive care from an out-of-network provider, the LM HealthWorks Plan works a little differently. When your medical service is provided out-of-network, the level of reimbursement from the plan for covered expenses will usually be lower. This means your out-of-pocket expenses will generally be higher. Depending on the provider, you may need to pay in full at the time of your visit. You must then submit a claim to the LM HealthWorks Plan claims administrator. You can call the LM HealthWorks Plan at 877-458-4975 to request a claim form, or you can download one via the Aetna Navigator Web site. Follow the instructions on the form and remember to include the provider’s original bill for services. If there is a balance in your HealthFund, the appropriate amount will be withdrawn automatically to pay the expense. If your HealthFund has been used up before you submit a claim for the expense, you will need to pay for your care out of your pocket. Once you have met the calendar year deductible, the LM HealthWorks Plan pays its share of the expense. If you paid the entire expense when you received care, the LM HealthWorks Plan will reimburse you for the portion of the claim the LM HealthWorks Plan would have paid. You will receive an Explanation of Benefits (EOB) statement that shows the total charge for care and the amount the LM HealthWorks Plan reimbursed you and/or your provider. It also shows you how much of the deductible you’ve met and how much remains to be met. If you are a registered member with the Aetna Navigator Web site, you will receive an email notification that an EOB is available; otherwise you will receive the EOB statement by mail. If you would rather receive EOBs online and have not yet registered with Aetna Navigator, you can “turn off” paper EOBs by visiting Aetna Navigator through the LM HealthWorks Plan Web site at www.lmhwplan.com.The EOB is not a bill—your provider will bill you for your share of the cost of the service if you did not pay the entire expense when you received care. Please keep in mind that all covered expenses are paid according to what the LM HealthWorks Plan considers the recognized charge. For out-of-network providers, this is the charge most often made for a service. If your out-of-network provider charges more than the recognized charge, you pay the difference between the provider’s charge and the recognized charge. NOTE: If you are in an active course of treatment with an out-of-network provider when you become a member of the LM HealthWorks Plan, the LM HealthWorks Plan’s Transition of Care provision may be able to help. For certain health conditions, the LM HealthWorks Plan may approve transition coverage to allow you to continue an active course of treatment with an out-of-network provider for a certain period of time while receiving benefits at the in-network level.
6

Out-of-Area (OOA) Care In some locations in the United States, you may have limited or no access to in-network providers. If the LM HealthWorks Plan claims administrator determines you live in one of these locations, you are eligible for Out-of-Area (OOA) medical benefits, and it will be noted on your LM HealthWorks Plan ID card. If you are eligible for OOA medical benefits, you may see in-network and/or out-of-network providers. Once you meet the deductible, the LM HealthWorks Plan begins to pay benefits based on recognized charges. Your deductible and out-of-pocket maximums are the same as in-network benefits. See the “Benefit Highlights” section for details. NOTE: If you have questions regarding your eligibility for OOA medical benefits, please contact the LM HealthWorks Plan at 877-458-4975.
How Benefits Are Paid
Your Calendar Year Deductible You must meet a calendar year deductible before most covered medical expenses are reimbursed. For your deductible amounts, see the “Benefit Highlights” section. If two family members are enrolled in the LM HealthWorks Plan, each family member must satisfy the individual deductible. When three or more family members are enrolled, a combination of deductible amounts can be used to satisfy the family deductible limit, subject to the per person limit. When the family deductible limit is met, it is satisfied for all other enrolled family members for the rest of the calendar year. NOTE: There are separate in-network and out-of-network deductibles unless you are eligible for Out-of-Area medical benefits. Out-of-network expenses apply only towards the out-of-network deductible, and in-network expenses apply only to the in-network deductible. Therefore, if you have met your in-network deductible and then see an out-of-network provider, you will need to meet your out-of-network deductible before the LM HealthWorks Plan will begin to share in the cost for out-of-network benefits. The HealthFund may help offset a portion of the deductible. For more information, see the “HealthFund” section. Certain expenses do not count toward meeting your deductible. These include:
Preventive services that are covered by the LM HealthWorks Plan at 100% of the recognized charge; Any prescription drug expenses that are covered through retail pharmacies (in-network and out-of-
network) and the mail-order service including your share of the cost; Any amounts over the recognized charge; Any amounts you pay because the precertification requirements were not met; Any expense covered at 50% (for example, non-emergency use of the emergency room); and Any charges not considered covered medical expenses or otherwise excluded or limited by the
LM HealthWorks Plan.
7

Coinsurance Once you meet the deductible, the LM HealthWorks Plan will pay a percentage of the recognized charge for most covered medical expenses. This percentage is known as coinsurance. The percentage the LM HealthWorks Plan will pay depends on the type of covered service and whether you visit an in-network provider, an Aexcel network physician or an out-of-network provider—and if you are eligible for Out-of-Area medical benefits. For most covered medical expenses, after the LM HealthWorks Plan pays its share of the expenses, you are responsible for any remaining costs. This includes any amounts not covered by the plan or limited by the plan. For out-of-network or Out-of-Area medical benefits, this also includes any amounts in excess of the recognized charges. For specific coinsurance amounts, see the “Benefit Highlights” section. Out-of-Pocket Maximum The out-of-pocket maximum limits the amount you pay for covered medical expenses in a calendar year. For your out-of-pocket maximum amounts, see the “Benefit Highlights” section. If you reach your out-of-pocket maximum, most covered medical expenses will be reimbursed at 100% of the recognized charges until the end of the calendar year. If you elect employee + 1 dependent coverage, each of you must satisfy the applicable in-network or out-of-network individual out-of-pocket maximum. If three or more family members are enrolled, a combination of out-of-pocket maximum amounts may be used to satisfy the applicable family out-of-pocket maximum, subject to the per person limit. When the family out-of-pocket maximum is met, it is satisfied for all other enrolled family members for the rest of the calendar year. As with the deductible, there are separate in-network and out-of-network out-of-pocket maximums. Expenses that count towards your in-network out-of-pocket maximum do not count towards your out-of-network out-of-pocket maximum, and vice versa. As with the deductible, certain expenses do not count towards your out-of-pocket maximum. These include:
Preventive services that are covered by the plan at 100% of the recognized charge; The calendar year deductible; Any prescription drug charges that are covered through retail pharmacies (in-network and out-of-
network) and the mail-order service including your share of the cost; Any amounts you pay because the precertification requirements were not met; Any expense covered at 50% (for example, non-emergency use of the emergency room); Any amounts over the recognized charge; and Any charges not considered covered medical expenses or otherwise excluded or limited by the
LM HealthWorks Plan.
8

Lifetime Maximum Benefit The LM HealthWorks Plan does not include a lifetime maximum amount for covered medical expenses or prescription drugs, except as noted in the “What Is Covered” section of this SPD. Precertification When you are receiving care for inpatient stays, certain tests and procedures and outpatient surgeries, precertification is required by the LM HealthWorks Plan claims administrator. Precertification lets you and your physician know whether the recommended services are covered under the LM HealthWorks Plan, ensures you receive care in the most appropriate setting and facilitates your enrollment in case management or any specialized programs that may apply. When you receive care from an in-network provider, you do not need to precertify—your provider will obtain any necessary precertification for you. However, if you receive care from an out-of-network provider, you are responsible for obtaining precertification from the LM HealthWorks Plan claims administrator for any services and supplies on the following list. If you do not precertify, your benefits may be reduced or the plan may not pay any benefits at all. The Precertification Process Services and Supplies Requiring Precertification Precertification is required for the following types of medical expenses:
Stays in a hospital. Stays in a skilled nursing facility. Stays in a rehabilitation facility. Stays in a hospice facility. Outpatient hospice care. Stays in a residential treatment facility for treatment of mental disorders, alcoholism or drug abuse. Family Support at Home Service for mental health and substance abuse. Home health care. All durable medical equipment in excess of $5,000. Private duty nursing care. Bariatric surgery. Certain outpatient services for mental disorders, alcoholism and drug abuse.
If you are admitted to a hospital or are scheduled to receive certain medical services, you or a member of your family, a hospital staff member or the attending physician must contact the LM HealthWorks Plan claims administrator to precertify your care. To request precertification or determine if precertification is required for certain tests and procedures, you, your physician or the facility need to call the LM HealthWorks Plan claims administrator at 877-458-4975 within the time frames below:
9

For non-emergency admissions: At least 14 days before the date you are scheduled
to be admitted. For an emergency outpatient medical condition: You or your physician should call prior to the
outpatient care, treatment or procedure if possible; or as soon as reasonably possible.
For an urgent admission: An urgent admission is a hospital admission by a physician due to the onset of or change in an illness, the diagnosis of an illness or an injury.
Before you are scheduled to be admitted.
For an emergency admission: You, your physician or the facility must call within 48 hours or as soon as reasonably possible after you have been admitted.
For outpatient non-emergency medical services requiring precertification:
At least 14 days before the outpatient care is provided, or the treatment or procedure is scheduled.
The LM HealthWorks Plan claims administrator will notify you and your physician in writing of the precertification decision. If your precertified expenses are approved, the approval is good for 60 days as long as you remain enrolled in the LM HealthWorks Plan. If you are admitted to the hospital, the LM HealthWorks Plan claims administrator will notify you, your physician and the facility about your precertified length of stay. If your physician recommends that your stay be extended, additional days will need to be certified. You, your physician or the facility will need to call the LM HealthWorks Plan claims administrator at 877-458-4975 as soon as reasonably possible but no later than the final authorized day. The LM HealthWorks Plan claims administrator will review the request and let you and your physician know whether the extension has been approved or denied. If precertification determines that the stay or services and supplies are not covered expenses, the notification will explain why and how you or your provider can appeal the LM HealthWorks Plan claims administrator’s decision. What Happens If You Do Not Precertify Covered expenses will be reduced if you do not obtain a required precertification before incurring non-emergency medical expenses. This means the LM HealthWorks Plan claims administrator will reduce the covered expense, or your expenses may not be covered. You will be responsible for the unpaid balance of the bills. If you receive care from an out-of-network provider (with the exception of emergency services), you are responsible for requesting precertification of your care with the LM HealthWorks Plan claims administrator before receiving services. Your provider may also request precertification for your treatment on your behalf. However, you should verify with the LM HealthWorks Plan claims administrator before the procedure that the provider has obtained precertification from the LM HealthWorks Plan claims administrator. If you or your provider’s request for precertification treatment is not approved, the benefit payable may be significantly reduced or your expenses may not be covered.
10

How Your Benefits Are Affected The chart below illustrates the effect on your benefits if you do not obtain the necessary precertification. Note: Precertification is not required for emergency services.
If Precertification Is: Then the Expenses Are: Requested and approved Covered. Requested and denied Not covered, but may be appealed. For more
information, please refer to the “Appeals Process” section.
Not requested, but would have been covered if requested
Covered after a reduction is applied. The covered expenses are reduced by $500 for a hospital admission or $300 for all other medical services or supplies requiring precertification.
Not requested, and would not have been covered if requested
Not covered, but may be appealed. For more information, please refer to the “Appeals Process” section.
It is important to remember that any additional out-of-pocket expenses incurred because you did not precertify will not count toward your deductible, coinsurance or out-of-pocket maximum. In addition, these amounts are not eligible for reimbursement from the HealthFund. If You Are Pregnant If you are pregnant, you do not need to precertify the hospitalization for the birth of your child, but you should notify the LM HealthWorks Plan claims administrator of your pregnancy within the first trimester and enroll in the Beginning Right® Maternity Program. If you are hospitalized for any condition during your pregnancy, you must precertify that admission. For more information about the maternity benefit, please refer to the “Benefit Highlights” and “Pregnancy-Related Expenses” sections.
11

LM HealthWorks Covered Services - Benefit Highlights The LM HealthWorks Plan includes a HealthFund that helps with medical expenses. For more information about the HealthFund, Healthy Actions and other credits, please refer to the “HealthFund” section. The “Benefit Highlights” chart below is an outline of what the Plan covers and how costs are shared for covered services. All amounts payable are based on the recognized charge for that benefit.
In-Network Out-of-Network Calendar Year Deductibles, Out-of-Pocket Maximums, Lifetime Maximum Benefits
Calendar Year Deductible Employee Only: $650 Employee +1: $1,300 ($650 per person) Employee +2 or more: $2,000 (with no more than $650 per person) In-network and out-of-network are not combined
Employee Only: $1,500 Employee +1: $3,000 ($1,500 per person Employee +2 or more: $4,500 (with no more than $1,500 per person) In-network and out-of-network are not combined Out-of-Area (OOA) same as in-network benefit (combined in-network and out-of-network)
Services Excluded From Deductible Calculation
Preventive care, prescription drugs, precertification penalties, recognized charges, overages and services not covered under the LM HealthWorks Plan
Preventive care, prescription drugs, precertification penalties, recognized charges, overages and services not covered under the LM HealthWorks Plan
Out-of-Pocket Maximum Employee Only: $1,500 Employee +1: $3,000 ($1,500 per person) Employee +2 or more: $3,000 (with no more than $1,500 per person) In-network and out-of-network are not combined
Employee Only: $5,000 Employee +1: $10,000 ($5,000 per person) Employee +2 or more: $10,000 (with no more than $5,000 per person) In-network and out-of-network are not combined Out-of-Area (OOA) same as in-network benefit and cross applies with out-of-network
Services Excluded From OOP Maximum Calculation
Preventive care, deductible, prescription drugs, precertification penalties, recognized charges, overages and services not covered under the LM HealthWorks Plan
Preventive care, deductible, prescription drugs, precertification penalties, recognized charges, overages and services not covered under the LM HealthWorks Plan
Lifetime Maximum Per Individual
No maximum
No maximum
12
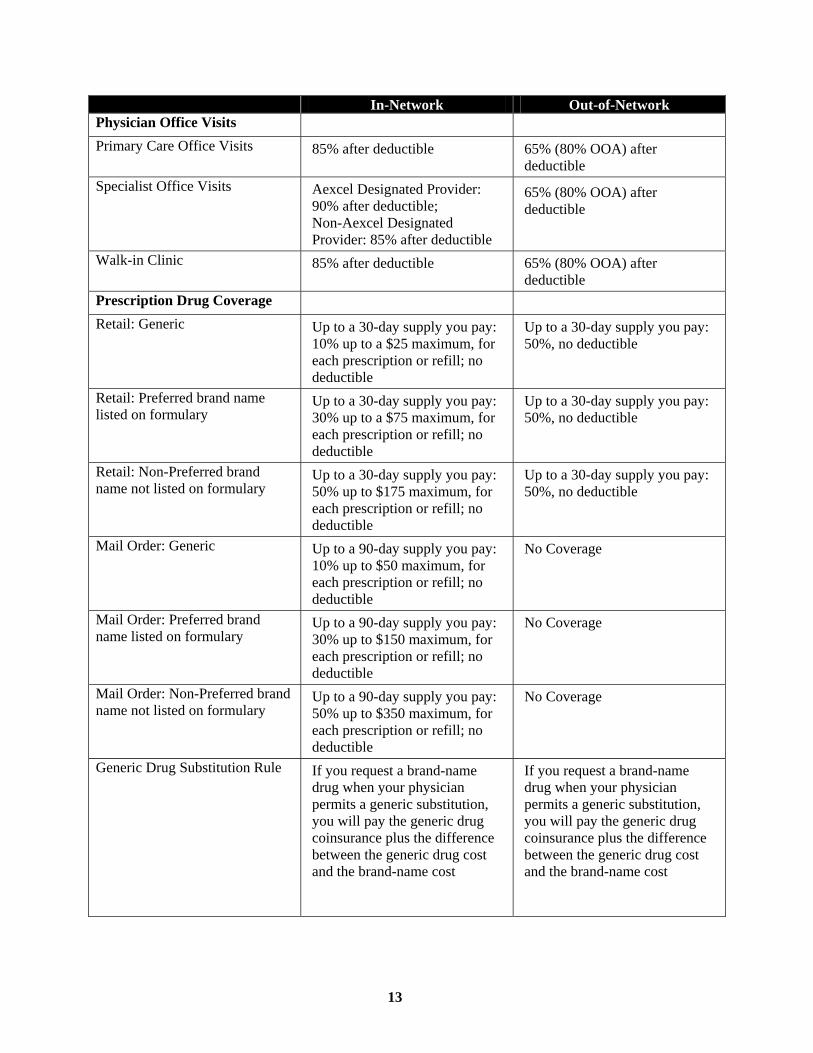
In-Network Out-of-Network Physician Office Visits Primary Care Office Visits 85% after deductible 65% (80% OOA) after
deductible Specialist Office Visits Aexcel Designated Provider:
90% after deductible; Non-Aexcel Designated Provider: 85% after deductible
65% (80% OOA) after deductible
Walk-in Clinic 85% after deductible 65% (80% OOA) after deductible
Prescription Drug Coverage Retail: Generic Up to a 30-day supply you pay:
10% up to a $25 maximum, for each prescription or refill; no deductible
Up to a 30-day supply you pay: 50%, no deductible
Retail: Preferred brand name listed on formulary
Up to a 30-day supply you pay: 30% up to a $75 maximum, for each prescription or refill; no deductible
Up to a 30-day supply you pay: 50%, no deductible
Retail: Non-Preferred brand name not listed on formulary
Up to a 30-day supply you pay: 50% up to $175 maximum, for each prescription or refill; no deductible
Up to a 30-day supply you pay: 50%, no deductible
Mail Order: Generic Up to a 90-day supply you pay: 10% up to $50 maximum, for each prescription or refill; no deductible
No Coverage
Mail Order: Preferred brand name listed on formulary
Up to a 90-day supply you pay: 30% up to $150 maximum, for each prescription or refill; no deductible
No Coverage
Mail Order: Non-Preferred brand name not listed on formulary
Up to a 90-day supply you pay: 50% up to $350 maximum, for each prescription or refill; no deductible
No Coverage
Generic Drug Substitution Rule If you request a brand-name drug when your physician permits a generic substitution, you will pay the generic drug coinsurance plus the difference between the generic drug cost and the brand-name cost
If you request a brand-name drug when your physician permits a generic substitution, you will pay the generic drug coinsurance plus the difference between the generic drug cost and the brand-name cost
13

In-Network Out-of-Network Preventive Care Routine physicals, immunizations, and related lab fees
Adult Physical Exams 100%, deductible waived (age and frequency limitations apply)
100%, deductible waived (age and frequency limitations apply)
Colorectal Cancer Screening 100%, deductible waived (age and frequency limitations apply)
100%, deductible waived (age and frequency limitations apply)
Gynecological 100%, deductible waived (age and frequency limitations apply)
100%, deductible waived (age and frequency limitations apply)
Mammograms 100%, deductible waived (age and frequency limitations apply)
100%, deductible waived (age and frequency limitations apply)
Prostate Specific Antigen (PSA) Test and Digital Rectal Exam (DRE)
100%, deductible waived (age and frequency limitations apply)
100%, deductible waived (age and frequency limitations apply)
Well Child Care 100%, deductible waived (age and frequency limitations apply)
100%, deductible waived (age and frequency limitations apply)
Outpatient Services Allergy Injections 85% after deductible 65% (80% OOA) after
deductible Allergy Testing and Treatment 85% after deductible 65% (80% OOA) after
deductible Ambulance 85% after deductible 85% after deductible Chiropractic 85% after deductible; up to 20
visits per calendar year (combined in-network and out-of-network limit)
65% (80% OOA) after deductible; up to 20 visits per calendar year (combined in-network and out-of-network limit)
Colonoscopy 85% after deductible (if not included as part of preventive screening)
65% (80% OOA) after deductible (if not included as part of preventive screening)
Complex Imaging Services (MRA/MRS, MRI, CT Scan, PET Scan)
85% after deductible 65% (80% OOA) after deductible
Contraceptive Devices, Implants and Injections
85% after deductible 65% (80% OOA) after deductible
Diagnostic Testing: Laboratory 85% after deductible 65% (80% OOA) after deductible
Diagnostic Testing: X-rays 85% after deductible 65% (80% OOA) after deductible
14

In-Network Out-of-Network Durable Medical Equipment 85% after deductible;
precertification required for recognized charges in excess of $5,000
65% (80% OOA) after deductible; precertification required for recognized charges in excess of $5,000
Emergency Room 85% after deductible 85% after deductible Non-emergency use of an Emergency Room
50% after deductible 50% after deductible
Hearing Exams 85% after deductible 65% (80% OOA) after deductible
Hearing Aids 85% after deductible; limited to $1,000 per ear every 3 calendar years (combined in-network and out-of-network limit)
65% (80% OOA) after deductible; limited to $1,000 per ear every 3 calendar years (combined in-network and out-of-network limit)
Maternity OB Visits 85% after deductible 65% (80% OOA) after deductible
Outpatient Short-Term Rehabilitation
85% after deductible; Limited to 60 visits per calendar year combined for speech, physical and occupational therapies. Short-term rehabilitation, combination of office and outpatient treatment in a facility, is included in the 60-visit maximum (combined in-network and out-of-network limit)
65% (80% OOA) after deductible; Limited to 60 visits per calendar year combined for speech, physical and occupational therapies. Short-term rehabilitation, combination of office and outpatient treatment in a facility, is included in the 60-visit maximum (combined in-network and out-of-network limit)
Outpatient Surgery - Ambulatory Surgical Facility Setting
85% after deductible; precertification required for certain procedures
65% (80% OOA) after deductible; precertification required for certain procedures
Outpatient Surgery - Hospital Setting
85% after deductible; precertification required for certain procedures
65% (80% OOA) after deductible; precertification required for certain procedures
Outpatient Surgery Performed in Office Setting
85% after deductible; precertification required for certain procedures
65% (80% OOA) after deductible; precertification required for certain procedures
Sigmoidoscopy 85% after deductible (if not included as part of preventive screening)
65% (80% OOA) after deductible (if not included as part of preventive screening)
Urgent Care Facility (for non-emergency services)
85% after deductible 65% (80% OOA) after deductible
15

In-Network Out-of-Network Inpatient Hospital Services Inpatient 85% after deductible;
precertification required 65% (80% OOA) after deductible; precertification required
Organ and Tissue Transplants Institute of Excellence (IOE) Facility: 90% after deductible; Other Facilities: 85% after deductible; requires preauthorization by National Medical Excellence
65% (80% OOA) after deductible; requires preauthorization by National Medical Excellence
Physician Services 85% after deductible 65% (80% OOA) after deductible
Bariatric Surgery Institute of Quality (IOQ) Facility: 90% after deductible; Other In-Network Facilities: 85% after deductible; precertification required
65% (80% OOA) after deductible; precertification required
Mental Health and Substance Abuse Services
Mental Health: Inpatient Services 85% after deductible; precertification required
65% (80% OOA) after deductible; precertification required
Mental Health: Outpatient Services
85% after deductible; precertification required for certain procedures
65% (80% OOA) after deductible; precertification required for certain procedures
Substance Abuse: Inpatient Services
85% after deductible; precertification required
65% (80% OOA) after deductible; precertification required
Substance Abuse: Outpatient Services
85% after deductible; precertification required for certain procedures
65% (80% OOA) after deductible; precertification required for certain procedures
Other Services Home Health Care 85% after deductible; up to 120
visits per calendar year (Home Health Care and Private Duty Nursing visits combined); precertification required (combined in-network and out-of-network limit)
65% (80% OOA) after deductible; up to 120 visits per calendar year (Home Health Care and Private Duty Nursing visits combined); precertification required (combined in-network and out-of-network limit)
Hospice Care 85% after deductible; precertification required
65% (80% OOA) after deductible; precertification required
16

In-Network Out-of-Network Mouth, Jaws, Teeth 85% after deductible; covers
accident related to injury to teeth, and medical in nature oral and jaw surgery; precertification required
65% (80% OOA) after deductible; covers accident related to injury to teeth, and medical in nature oral and jaw surgery; precertification required
Private Duty Nursing (PDN) 85% after deductible; up to 120 visits per calendar year (Home Health Care and Private Duty Nursing visits combined); precertification required (combined in-network and out-of-network limit)
65% (80% OOA) after deductible; up to 120 visits per calendar year (Home Health Care and Private Duty Nursing visits combined); precertification required (combined in-network and out-of-network limit)
Prosthetic Devices 85% after deductible; precertification required for recognized charges in excess of $5,000
65% (80% OOA) after deductible; precertification required for recognized charges in excess of $5,000
Convalescent Facility/Skilled Nursing Facility
85% after deductible; up to 120 days per calendar year; precertification required (combined in-network and out-of-network limits)
65% (80% OOA) after deductible; up to 120 days per calendar year; precertification required (combined in-network and out-of-network limits)
Vision Screenings Covered only as part of routine physical exam
Covered only as part of routine physical exam
Recognized (Reasonable and Customary) Charges You will be reimbursed based on the recognized charge (formerly known as the “reasonable and customary charge”) for a covered medical expense. The recognized charge is determined by the LM HealthWorks Plan claims administrator based on the fee most commonly charged for a service in a geographic area, or for an in-network provider, a negotiated or discounted fee. (For Medicare eligible participants, when applicable, the recognized charge is the Medicare allowable charge.) Recognized charges are subject to periodic review and change. For in-network providers, you are not responsible for charges in excess of the recognized charge. If you receive care from an out-of-network provider, you must pay any amount above the recognized charge. Charges that are above the recognized fee limit or that are not for covered medical services, do not apply to your deductible, out-of-pocket maximum, or HealthFund maximum.
17

The HealthFund To help offset a portion of covered medical expenses, such as your deductible, the LM HealthWorks Plan offers a HealthFund. The HealthFund is a credit that provides a benefit to offset certain covered medical expenses. The HealthFund is not a cash account, does not vest to employees and does not grow with investment earnings or interest. You and your covered spouse or same-sex domestic partner (if applicable) will be able to add to your HealthFund balance by completing certain Healthy Actions. Generally, eligible expenses that can be reimbursed through the HealthFund are the same as those covered by the LM HealthWorks Plan. Prescription drugs and certain other expenses are not eligible for reimbursement through the HealthFund. The employee + 1 dependent or employee + 2 or more dependents HealthFund balance may be used by one individual or by a combination of covered family members. When coverage ends, any remaining balance in your HealthFund is not payable to you or your dependent(s).
HealthFund Highlights The Healthy Actions and the amount of credits that can be earned are subject to change from year to year and will be communicated during enrollment. Healthy Actions Complete the Personal Health Assessment Employee Spouse/Same-sex Domestic Partner
$250 once during the calendar year $300 once during the calendar year
Participate in the Virgin HealthMiles Physical Activity Tracking Tool program* (must advance from Level I to Level II during the plan year) Employee only
$50 once during the calendar year
Complete the Tobacco Non-User Certification (or participate in the Quit for Life® program, if a tobacco user).* Employee Spouse/Same-sex Domestic Partner Tobacco users must enroll in the Quit for Life program and either complete 4 coaching calls or complete the Quit for Life program, during the plan year.
$50 once during the calendar year $50 once during the calendar year
Maximum Credits Earned for the above Healthy Actions
Employee $350 maximum per calendar year Spouse/Same-sex Domestic Partner $350 maximum per calendar year Credits Earned by Condition Management Program Participation
Over and above the Healthy Actions**
Employee Spouse/Same-sex Domestic Partner
$150 maximum per calendar year $150 maximum per calendar year
18

Credits Earned by Health Coaching Program Participation
Over and above the Healthy Actions**
Employee Spouse/Same-sex Domestic Partner
$150 maximum per calendar year $150 maximum per calendar year
*Must complete the Personal Health Assessment in order to earn these additional incentives. **Employee and/or Spouse/Same-sex Domestic Partner are eligible for either Condition Management or Health
Coaching credits, not both, in a calendar year. Maximum HealthFund Balance Unlimited HealthFund Exclusions HealthFund does not apply to:
Prescription drug expenses; and Any amounts not covered or limited by the LM
HealthWorks Plan such as: • Amounts over the recognized charge; • Amounts you pay because you do not
follow the precertification approval process; or
• Services not covered by the plan including services above visit limits.
HealthFund Participation Ends Participation ends when you are no longer enrolled in the LM HealthWorks Plan for active employees (or when COBRA or insurance continuation coverage ends). The fund is not a cash account—it is not subject to investment earnings or interest. Any remaining balance in the HealthFund is not payable when enrollment in the LM HealthWorks Plan ends.
HealthFund Roll-Overs Any HealthFund credit that is not used in a given year is rolled over to the next calendar year if you continue enrollment in the LM HealthWorks Plan as a subscriber. There is no limit to the amount of HealthFund credits that can be rolled over from one year to the next. Although you may carry over your HealthFund credits from year to year, when you submit a claim for reimbursement, you can only be reimbursed for the amount that was available in the year the expense was incurred. Here is an example to illustrate how a HealthFund credit is carried over and what HealthFund credits are available to pay claims incurred in different calendar years:
If you elected employee only coverage in 2010 (year one) and have $100 remaining at the end of the year, the $100 balance is carried forward to 2011 (year two). You will have to earn HealthFund credits through completing Healthy Actions to increase your HealthFund balance. You complete a Healthy Action worth $50 in year two, which increases your HealthFund balance to $150.
Claims incurred in the second year may be paid up to the $150 credit balance. However, claims incurred in year one and submitted in year two may only be paid up to $100 (which was the credit remaining at the end of year one that was rolled over to year two).
19

You can contact the LM HealthWorks Plan claims administrator at 877-458-4975 if you have questions about the maximum HealthFund limit or what HealthFund credits are available to pay claims incurred in different calendar years. Earning HealthFund Credits Healthy Actions If you are enrolled in the LM HealthWorks Plan, you can build your HealthFund balance by completing certain Healthy Actions. When you complete these actions, a credit is added to the HealthFund in the same calendar year. Descriptions of Healthy Actions are included in the HealthFund Highlights. Healthy Actions and the amount of credits that can be earned are subject to change from year to year and will be communicated during enrollment. Additional Credits Additional credits can be earned over and above those earned through Healthy Actions. The credits that can be earned are subject to change from year to year and will be communicated during enrollment. You and/or your spouse/same-sex domestic partner can earn additional credits for your HealthFund by participating in one of the following programs:
Condition Management Program Participation: If you and/or your spouse/same-sex domestic partner participate in a condition management program, you can earn additional credits for your HealthFund by completing the Condition Management Program, or a one-time initial assessment and participating in a minimum of four coaching calls, during the calendar year.
Health Coaching Program Participation: If you and/or your spouse/same-sex domestic partner participate in the LM6 ( 6-month) or LM12 (12-month) health coaching program, you can earn additional credits for your HealthFund by completing the Health Coaching program, or, a one-time initial assessment and participating in a minimum of four coaching calls, during the calendar year.
Important! You may earn additional credits for only one, not both, of the above programs in a calendar year. If You Leave the LM HealthWorks Plan and Re-Enroll in the Same Plan Year If you re-enroll in the LM HealthWorks Plan in the same calendar year, any remaining balance in the HealthFund is reinstated. When you re-enroll in the same calendar year, only claims incurred while you are covered are eligible for reimbursement from the HealthFund—any claims incurred during the period you were not covered are not eligible for reimbursement from the HealthFund. If You Leave the LM HealthWorks Plan and Enroll in a Different Plan Year Once your coverage ends, the HealthFund also ends. If you subsequently re-enroll in the LM HealthWorks Plan, any HealthFund balance (regardless of how it was earned) will be reinstated if you re-enroll within three years of termination. Claims incurred after your coverage begins are eligible for reimbursement from the HealthFund—any claims incurred during the period you were not covered are not eligible for reimbursement.
20

How the HealthFund Works The LM HealthWorks Plan claims administrator will process eligible HealthFund expenses as part of the claim paying process—there are no separate claim forms to file. Generally, the HealthFund will first be used to satisfy the calendar year deductible for you and/or your covered dependents. If there is a remaining balance, the HealthFund credits can be used to reimburse you and/or your covered dependents’ share of covered in-network and out-of-network expenses. (Remember, prescription drugs and certain other expenses are not eligible for reimbursement through the HealthFund.) Here are two examples to show you how the HealthFund helps offset the cost of health care: Example 1 Assume you elect employee only coverage in 2010 and will be enrolled in the LM HealthWorks Plan for the next two years. You have a carry-over balance of $50 from plan year 2010. In 2011, you complete a Personal Health Assessment ($250), you certify that you don’t use tobacco products ($50) and you reach Level 2 on the physical activity tracking tool ($50) earning $350 in Healthy Actions credits—bringing your total credits to $400—and have no medical expenses. In 2012, you will need outpatient surgery. Here’s what happens to the HealthFund over the three-year period. 1. The HealthFund credit in calendar year 2011 is $400.
($50 carry-over from 2010 + $350 credits for Healthy Actions in 2011) 2. The 2012 HealthFund balance is $400.
($400 carryover from 2011 + $0 HealthFund credit for 2012—no Healthy Actions completed) In calendar year 2012, you need outpatient surgery and the cost is $1,650 for illustrative purposes. You receive care from an in-network provider. Here is how your reimbursement would be calculated:
HealthFund
Pays You Pay Out-
of- Pocket
LM HealthWorks
Plan Pays Covered medical expense $1,650 Individual calendar year deductible - $650 $400 $250
Covered expense after deductible $1,000 Coinsurance percentage x 85% LM HealthWorks Plan pays $850 $850You pay (after deductible) $150 $150 TOTALS $400 $400 $850
21

You are responsible for $800 ($650 for your calendar year deductible + $150 for your share of the cost). Because you have a $400 credit in the HealthFund, $400 of that $800 will be paid from the HealthFund. You will pay $400 for this $1,650 surgery. There will be $0 balance in the HealthFund for the remainder of 2012 unless you complete an available Healthy Action. Example 2 Now let’s assume you elect coverage for employee + 2 or more dependents. You have no carry-over balance from 2010. In 2011, you and your covered spouse both complete Personal Health Assessments ($250 for you and $300 for your spouse) and certify that neither of you use tobacco ($50 for each of you), and you reach Level 2 on the physical activity tracking tool ($50), for $700 in Healthy Action credits. Your covered child incurs the first medical expense. For illustrative purposes, the total expense is $3,150 and your child receives care from an in-network provider. Here’s the reimbursement calculation:
HealthFund
Pays You Pay Out-
of- Pocket
LM HealthWorks
Plan Pays Covered medical expense $3,150 Individual calendar year deductible for your child - $650 $650
Covered expense after deductible $2,500 Coinsurance percentage x 85% LM HealthWorks Plan pays $2,125 $2,125You pay (after deductible) $375 $50 $325 TOTALS $700 $325 $2,125 Your responsibility for your child is $1,025 ($650 for the calendar year deductible + $375 for your share of your child’s cost). Because there is $700 in the HealthFund, $700 of the $1,025 you are responsible for will be paid from the HealthFund, which means you will pay $325 out of your pocket for this surgery and there will be a $0 balance in the HealthFund for the remainder of the year. Remember the following about the HealthFund:
Your HealthFund balance may be used by one individual or a combination of you and/or your covered dependents.
You can use the HealthFund to pay for covered out-of-pocket costs like the deductible and your share of covered expenses.
You cannot use the HealthFund for reimbursement of prescription drugs and certain other expenses, including: • Any amounts not covered or limited by the medical plan such as amounts over the recognized
charge and the amounts you pay because you did not follow the precertification approval process; or
• Services not covered by the LM HealthWorks Plan including services above visit limits.
22

LM HealthWorks Plan Resources An important component of the LM HealthWorks Plan is the many health and wellness resources available to help you better manage your health care needs and to become an informed consumer of health care services. While you are ultimately responsible for your own health and health care decisions, these resources are available to help you and your physician. Health Management Resources The health management resources listed below are available to help you live a healthy lifestyle and in making informed decisions about your health care. The Care Navigator: Single Point of Contact When you have health-related questions and don’t know where to turn, calling the Care Navigator provides you with a single point of contact for referrals to other plan resources. The Care Navigator knows the LM HealthWorks Plan and all that it offers, and can connect you to the resource, service or program that matches your particular health care need or question. The Care Advocate: Care Coordination and Support When you’re facing a health challenge, it can be hard to make important decisions and get the necessary care and support. Your Care Advocate can:
Help you find the right doctors and health care facilities. Arrange diagnostic tests. Help you understand recommended tests, treatments and medications. Facilitate the transfer of medical records, x-rays and lab results to a new doctor.
Your Care Advocate helps you untangle the web of health care options and information. He or she can connect you to the tools and services you need most. Most important, your Care Advocate will stay in the loop every step of the way. The Nurse Advice Line: Guidance and Advice When You Need It If you need help and guidance with a health concern or symptom, or an important health care decision, your Care Navigator will direct you to the Nurse Advice Line. Available 24 hours a day/7 days a week, the Nurse Advice Line is staffed by experienced registered nurses who can answer questions about a particular medical issue, treatment or condition and provide comfort and reassurance to help you find the right care. If you have an immediate, non-emergency health problem or concern and would like to talk with a registered nurse, the Nurse Advice Line’s resources can work with you to determine the best care for your condition, answer questions and provide suggestions for self-care. He or she can also provide information about medications, help you understand a specific diagnosis or condition and help you find convenient access to quality care. If you need to make a major medical decision, the Nurse Advice Line can help you make sense of treatment options, explain medical terms and tell you about the latest developments in health care. He or she can also help you work better with your doctor by giving you the right questions to ask and information to provide during your next office visit.
23

Condition Management If you are living with a chronic health condition, you have an opportunity to lead a healthy life while minimizing the impact that your condition may have on your daily well-being. Through the LM HealthWorks Plan, you can receive one-on-one support and information to help you manage your condition and enjoy better overall health. If you have one or more of the conditions listed below, Condition Management will provide you with access to a team of coaches that are highly trained professionals to help you understand your condition and provider’s recommendations, review your medications and treatment plans and set goals to help manage your health. In addition to the one-on-one support from your team of coaches, you will also have access to educational resources and tools to help manage your condition. Of course, any information you share with your Condition Management team of coaches will always be kept private and confidential.
Cancer — Those who are undergoing cancer treatment, who survived cancer but haven’t hit the five-year cancer-free benchmark or who have advanced cancer and need to plan for end of life, can receive personalized and confidential tools and support.
Diabetes — Highly trained healthcare professionals provide personalized support and health information by telephone and mail. They also help you to better control your blood glucose levels, and keep your doctor involved and informed to ensure that you receive the highest quality care possible.
Congestive Heart Failure — Those who are living with a heart failure diagnosis can get specialized care and support that can increase awareness of what is needed to maintain good health and avoid complications. The Condition Management team of coaches will help you watch your diet, monitor your blood pressure and weight, regularly visit a doctor and complete the necessary laboratory work.
Coronary Artery Disease — Those diagnosed with coronary artery disease, coronary artery intervention or a heart attack or who have had bypass surgery can take advantage of tailored support from the Condition Management team of coaches. You receive support and encouragement that stresses the importance of medication review and education while demonstrating the effectiveness of setting goals.
Chronic Obstructive Pulmonary Disease (COPD) — The Condition Management team of coaches helps those living with COPD to prevent or lessen the severity of COPD exacerbations. You receive education and outreach on how to be aware of your triggers so you can learn how to avoid them, and encouragement to properly use medications along with your doctor’s recommendations.
Chronic Kidney Disease (CKD) and End-Stage Renal Disease (ESRD) — With early detection and therapeutic lifestyle changes such as proper nutrition, blood sugar control and healthy blood pressure, it’s possible to enjoy a high quality of life, delay expensive treatments and avoid unwanted hospitalizations. The Condition Management team of coaches focuses on supporting those on dialysis to ensure appropriate access management, adequate dialysis follow-through, medication and nutrition management. Your Condition Management coach will also help to ensure timely screening and evaluation of kidney function so that you can better manage your condition and enjoy a healthy lifestyle.
Comprehensive Back Pain — The Condition Management program provides you with the support you need to reduce or eliminate recurrent episodes of back pain. It connects you with a qualified team of coaches who can help you learn about specific procedures and treatment options as well as pain management techniques.
Asthma — The Condition Management program provides knowledge and understanding of the causes and consequences of the disease along with help and advice for how you can modify behaviors and environmental exposures that may trigger or aggravate the disease. A highly trained Condition Management coach will help you to learn self-evaluation and self-management techniques and apply them in your everyday life.
24

The program also addresses other conditions that include acid-related stomach disorders, atrial fibrillation, fibromyalgia, inflammatory bowel disease, irritable bowel syndrome and osteoarthritis (in people 18 years of age or older). How the Program Works
Eligible members will be identified by a LM HealthWorks Plan administrator as a result of recent medical care (for example, results and/or data from clinical testing or other filed health care claims).
If you have a chronic condition that is covered by the program, you will receive a welcome packet in the mail as well as a call from a Condition Management coach to get started. The program is voluntary, confidential and free.
Over the course of the program, you will be contacted by a highly trained Condition Management coach who can answer general health questions, advise you on diet and exercise, educate you on your chronic condition(s), help you set and achieve health goals, ensure you are taking medication, counsel you on getting appropriate tests and follow your physician’s plan of care for you.
The frequency of your interaction with the program will depend on the overall status of your health. Your Condition Management coach will increase or decrease the level of coaching needed to provide you with appropriate support.
Educational materials related to your chronic condition(s) will also be provided throughout the program.
The program is designed to address your complete health, not just your chronic condition(s). As such, your Condition Management coach will help you develop a personalized plan for improving your overall health.
You may also call the LM HealthWorks Plan at 877-458-4975 to ask for a Condition Management coach to contact you. Health Coaching If you need to take action on a particular health risk, Health Coaching may be recommended for you. Health Coaching can help you:
Better understand your health risks and how they affect your life; Get answers to pressing health concerns and issues; Find support in your journey to better health; Gain more control over your health and the day-to-day decisions and choices that affect it; and Set goals to reach your personal best health.
You may be offered Health Coaching if your responses to the Personal Health Assessment indicate that you may be at risk for developing a serious and/or chronic medical condition. The Care Navigator, Care Advocate, or the Nurse Advice Line clinician may recommend Health Coaching to you. Or, you may decide to take advantage of this important service on your own. To request a health coach, call the LM HealthWorks Plan at 877-458-4975 and ask the Care Navigator to connect you with a health coach.
25

Your health coach can help with health issues and conditions such as:
High cholesterol. Stress. Weight management. Poor diet. High blood pressure. Physical inactivity.
If you choose to participate, you will be paired with a personal health coach who is a health educator, dietician, nurse or other trained professional, depending on your particular needs. Your health coach will work with you by telephone to review your health status, discuss your risks and suggest possible lifestyle changes. Together, you will set goals that consist of a series of small, manageable changes that you can commit to over time. As part of your personal action plan, your coach may direct you to the Member Wellness Portal for helpful facts and tips on eating healthy, starting an exercise program and other actions you can take to live healthier. Your coach may also provide necessary educational materials by mail. Depression Management Depression Management is designed to assist you and your covered dependents to understand and better manage depression. This program can assist you with finding behavioral health care counseling resources, provide information to your doctor and counselor to help coordinate treatment, provide you with educational information and assist you with setting realistic goals for improvement of your depression and overall mental health. Online services and decision support tools are available to you through Aetna Behavioral Health and the Reawakening Center. You can gain access to these resources through the LM HealthWorks Plan Web site at www. lmhwplan.com. For more information, please see the “Mental Health and Substance Abuse Resources” section. End of Life/Compassionate Care Program The Compassionate Care program is a comprehensive program that offers service and support to members and their families who are facing difficult decisions about advanced illnesses. The program is comprised of nurse support, information and tools and enhanced hospice benefits to help remove barriers for needed care, promote choice and autonomy, and ensure that patients and their families receive comfort and support when dealing with an advanced illness. This program requires a physician to certify that the patient is not likely to live longer than 12 months. Maternity Management If you are expecting or planning a family, the Beginning Right® Maternity Program can provide the information and support you need for a healthier pregnancy. Trained OB/GYN nurses are available via a toll-free phone line to provide:
Answers to questions about pregnancy and delivery. Special attention for at-risk pregnancies. Educational materials on pregnancy-related issues such as breastfeeding and postpartum depression. Information about healthy eating and exercise during pregnancy.
You may call the LM HealthWorks Plan at 877-458-4975 to enroll in the Beginning Right Maternity Program.
26

Medical Services Team The LM HealthWorks Plan Medical Services Team provides members with Case Managers, who are nurses that help you understand the options available to you. Case Managers can also help you understand your illness and the care your doctor and others have ordered. When you and your provider have clear information about your benefit plan, you are in a better position to use your available benefits. The care you receive is still a decision made by you and your provider. Working with a Case Manager does not change your health care coverage in any way. A Case Manager may contact you in the following circumstances:
Your recent medical care indicates you may have a complex medical condition(s); You recently had or scheduled hospital admission or surgery; You have a diagnosis that alerts a Case Manager that you may need some help; and/or You or your family request special assistance managing your care.
If a Case Manager calls or sends you a letter, please return their call and learn how you might benefit from their assistance. You never have an obligation to accept any assistance if you feel it is not necessary. Personal Health Assessment To help you know more about the state of your health and your personal risks, issues and needs, the LM HealthWorks Plan offers the Personal Health Assessment (PHA), a secure online questionnaire. The PHA covers areas such as personal medical history, your current lifestyle and habits, recent biometrics (such as cholesterol measurements) and other health-related factors. The benefit of taking the PHA is early detection of health issues. Because most of the risk factors identified through the PHA have no symptoms, participating in the PHA can help you proactively identify life-threatening risk factors which can lead to chronic illness. Obtaining this in-depth information will allow you to make lifestyle changes or seek treatment in time to avoid serious illness. In addition, when you and your spouse/same-sex domestic partner take the PHA for the first time, you will earn credits towards your HealthFund. The PHA is available to you and your spouse or same-sex domestic partner at no cost and can be taken once per calendar year. In addition, you can go back whenever you like and update self-reported biometric information, such as your most recent cholesterol or other test results. Once you complete the PHA, you will get access to a confidential, personal report that contains:
An easy-to-understand explanation of your health status; A description of health risk factors you may have; and Access to a personalized well-being plan and resources focused to your health risk factors and
wellness needs. Lockheed Martin has partnered with Healthways to administer the PHA. Individual PHA responses and data will not be shared with Lockheed Martin. Only de-identified, collective results are provided to the Company to help understand overall trends and needs. Depending on your personal PHA results, you may be contacted by an LM HealthWorks Plan resource and invited to participate in a Health Coaching Program. If you decide to participate, you will be assigned a health coach who will work with you one-on-one to set goals and create an action plan to achieve them. Your coach will also be available to answer questions, provide support and direct you to other plan resources and programs that can help.
27

Childhood Obesity Childhood Obesity Pilot – GetNHealthy(SM) is designed for children who have a Body Mass Index (BMI) that is too high for their age and gender. Obesity and Nutritional Counseling If your child is between the ages of three and 18 and has a Body Mass Index (BMI) equal to or greater than the 85th percentile for his or her age and gender, he or she may qualify for this program. A child who has already had bariatric surgery is not eligible. Covered services include:
Obesity and nutritional counseling sessions covered at the applicable coinsurance with no deductible. Obesity and nutritional counseling coverage is limited to four obesity and four nutritional counseling
sessions annually. This benefit does not alter or change other obesity or nutritional counseling benefits available under the LM HealthWorks Plan.
Obesity counseling is covered when provided by an in-network pediatrician or other licensed staff within the pediatrician’s office.
Nutritional counseling is covered when provided by an in-network pediatrician or a registered dietician on staff at the pediatrician’s office or an in-network hospital-based registered dietician.
Nutritional counseling addresses the quality of nutrition in an individual’s diet. Registered dieticians offer education in nutritional facts, eating habits, nutrients and weight loss to help individuals develop dietary patterns that suit their lifestyle and health needs. Obesity counseling may include information and advice on dietary intake but also considers others factors on weight management such as an individual’s lifestyle and exercise routines, his or her knowledge and attitude about weight and behavior change stages. There is no out-of-network coverage for obesity and nutritional counseling. Comprehensive Clinically-Based Childhood Obesity Program If your child is between the ages of three and 18, he or she may qualify for this program if he or she meets the following requirements:
Completes the obesity and nutritional counseling sessions; and Has a BMI that remains at or above the 95th percentile (obese and morbidly obese) for his or her age
and gender. The Comprehensive Clinically-Based Childhood Obesity Program uses a multidisciplinary team approach for medical oversight and treatment in the areas of nutrition, behavior therapy and personal training. The program covers one course of treatment per lifetime at the in-network benefit levels for those services, with no deductible. To access the program, you must be referred by an in-network provider. Comprehensive Clinically-Based Childhood Obesity Programs may not be available in all geographic locations and entry requirements may differ from program to program. There is no out-of-network coverage for the Clinically-Based Childhood Obesity Program.
28

Online Tools The LM HealthWorks Plan Web site at www.lmhwplan.com is your portal to plan design information and online resources. In addition to the resources explained below, you can also access the prescription drug administrator’s Web site information. Aetna Navigator® Through Aetna Navigator, you can take care of personal benefit needs and access the site’s tools and information. Using the Aetna Navigator Web site, you will be able to:
Check the status of a claim. Look at the results of claims that were processed and find out when payments were made. This way, you will know your share of the cost.
Request a medical ID card. Print a temporary ID card or request a replacement. Estimate the cost of care. With Navigator’s Cost of Care tools, you can get estimated average costs
for medical treatments and procedures, tests and other services in your area. Use this information to have a discussion with your doctor about care alternatives.
Hospital Comparison Tool. Use Navigator’s Hospital Comparison Tool to compare hospitals in your area on the measures and qualities that mean the most to you.
Health History Report. This report puts all of your claims-based information in one place. Aetna SmartSourcesm. This online tool scans Aetna’s vast online resources to put together health
information specific to you and your needs. Enter a condition or symptom and you will get information about doctors, medications, treatment options, costs and special programs related to your needs.
Contact Member Services. You can email Member Services right from your Navigator home page. Member Services can help with claim and benefits questions, replacement medical ID cards and other needs.
Provider Directory Because in-network providers have agreed to charge special rates for LM HealthWorks Plan members, the LM HealthWorks Plan pays a higher percentage and you pay a lower percentage for most covered services when you use doctors and other health care providers who belong to the Plan’s network. You can find in-network providers in your area by using DocFind®, the online provider directory. If you wish to receive a copy of a provider directory or information about in-network providers, contact the LM HealthWorks Plan claims administrator at 877-458-4975. The directory will be provided free of charge. There are several different ways to search the online provider directory:
You can search by name to find out if a specific doctor belongs to the network. You can enter your ZIP code, city or county to find all in-network providers in your area. You can search by specialty.
DocFind also lets you refine your search with categories such as gender, languages spoken and handicapped accessibility. A blue star ( ) next to a provider’s name in the online provider directory means that he or she belongs to the Aexcel network. The Aexcel network is a group of specialists who are considered higher performers, in terms of clinical performance and efficiency, in their specialty areas. Aexcel specialties include:
Cardiology – heart and circulatory health. Cardiothoracic Surgery – heart surgery, including coronary artery bypass and valve procedures.
29

Gastroenterology – diseases of the digestive system and liver, including ulcers, colitis, intestinal irritation and inflammation, Crohn’s disease and colorectal cancer.
General Surgery – procedures such as appendectomies, hernia repairs, breast surgeries and colorectal surgeries.
Neurology – disorders of the nervous system such as pain syndromes, movement disorders, multiple sclerosis and seizures.
Neurosurgery – surgery performed on the brain, spinal cord and nerves. Obstetrics and Gynecology – childbirth and women’s health. Orthopedics – disorders of muscles, bones and joints. Otolaryngology/ENT – ailments related to ears, nose and throat. Plastic Surgery – surgery to restore form and function to injured or diseased body parts. Urology – health of the male and female urinary tract and the male reproductive organs. Vascular Surgery – surgery to correct problems in arteries and veins.
How are doctors chosen for the Aexcel designation? Aetna considers factors such as 30-day hospital readmission rates, rates of health complications and other specialty-specific treatment measures shown to improve outcomes. Specialists who meet these qualifications are then rated on cost efficiency. The doctors performing highest overall for these measures are chosen for the Aexcel designation. While the provider directory information is believed to be accurate and is updated periodically, it is subject to change without notice. For example, an in-network provider may no longer accept new patients because his or her practice is full. Depending on the timing and notification requirements, this information may not always be included in the directory. For the most current information, you can contact the physician’s office directly or you can call the LM HealthWorks Plan claims administrator at 877-458-4975. Doctor Rates With the LM HealthWorks Plan, you can log onto the Aetna Navigator Web site and learn the actual rates doctors have negotiated with the LM HealthWorks Plan claims administrator for up to 30 widely used services. You can find rates for office visits, vaccinations, routine tests and more. Because you are responsible for paying a share of your health care expenses, knowing rates up front is especially important. It can also help you know how much may be deducted from your HealthFund to pay for certain services. Member Wellness Portal The Member Wellness Portal is an Internet-based health management tool that provides you with:
A personalized, actionable well-being plan that is tailored to focus on relevant health and wellness areas.
Communication tools that allow you to exchange private information with nurses and health coaches over the Web.
A resource center with a variety of recipes and health information. A variety of tools and trackers that allow you to monitor daily progress against goals in areas like
exercise, weight management and healthy eating. A dashboard that allows for a common view of messages, reminders and primary tracker tools.
The Member Wellness Portal is administered by Healthways, our wellness and condition management partner.
30

Mental Health and Substance Abuse Resources To supplement the benefits described under the “What Is Covered” section, online tools are available to help you make more informed decisions about care related to mental health and substance abuse issues. Through the LM HealthWorks Plan Web site at www.lmhwplan.com, you can access the Aetna Behavioral Health Web site where you will find:
Interactive self-assessments. Information about mental health disorders. Guidance and advice for caregivers.
Learn about mental health, take a self-assessment or find a behavioral provider at www.aetnabehavioralhealth.com. The Reawakening Center The Reawakening Center is an online resource that can help you cope with depression and stress. The site offers information, quizzes, interactive tools and other features to help you better understand your feelings and find new, effective ways to cope. Visit www.reawake.com to:
Take a depression self-test. Search an online library for information on depression-related topics that include medications,
therapies, case studies and support groups. Get helpful advice about finding the right treatment. Use the online coaching feature.
What Is Covered The LM HealthWorks Plan covers certain preventive services and a wide range of medically necessary services recommended by a physician for the treatment of an illness, injury or pregnancy including: Preventive Services
Well-child care at the following age intervals: • During the first 12 months of life – seven exams. • Between 13th and 24th months – three exams. • Between 25th and 36th months – three exams. • One exam per calendar year thereafter.
Routine physical examinations, age 18 or older – one exam per calendar year. • A routine physical examination includes a complete history and physical with associated x-ray
and laboratory services according to generally accepted medical guidelines. Immunizations for children– for infectious diseases and the materials for administration of
immunizations as recommended by the Advisory Committee on Immunization Practices of the Department of Health and Human Services, Centers for Disease Control and Prevention.
Immunizations for adults who are considered “at risk” for certain medical conditions such as influenza, pneumonia, meningitis, hepatitis and Lyme disease or for travel. The LM HealthWorks Plan claims administrator determines “at risk” based on generally accepted medical guidelines.
Gynecological – one routine exam and Pap smear per calendar year including the related lab fees. Routine mammogram – one baseline mammogram age 35 to 40; one per calendar year age 40 and
over.
31

One Prostate Specific Antigen (PSA) test per calendar year for males over age 40 to age 75; not covered for ages 76 or older.
Colorectal cancer screening (age 50 and older) – including occult blood stool test (once per year); sigmoidoscopy (one every five years); double contrast barium enema (one every five years) and colonoscopy (one every 10 years).
Vision screenings – covered only as part of routine physical exam. Hearing screenings – covered only as part of routine physical exam in the absence of suspected
hearing impairment. The deductible does not apply to preventive care services and any visit limits or maximums are combined for in-network and out-of-network care for the preventive services listed above. Physician Services Important Reminder The LM HealthWorks Plan’s coinsurance is the highest when you receive specialty care from an Aexcel-designated provider. You can locate Aexcel-designated providers in your area by referring to the provider directory or online in DocFind on the LM HealthWorks Plan Web site at www.lmhwplan.com or by calling 877-458-4975. Physician Visits
Charges made by a physician during a visit to treat an illness or injury. The visit may be at the physician’s office, in your home, in a hospital or other facility during your stay or in an outpatient facility. Covered expenses also include: • Allergy testing and allergy injections; • Supplies, radiological services, x-rays and tests provided by the physician; and • Immunizations for infectious disease, but not if solely for your employment.
Surgery
Charges made by a physician for: • Performing your surgical procedure; • Acting in the capacity of an assistant surgeon or co-surgeon during a surgical procedure where
the services of a second physician are medically necessary; • Pre-operative and post-operative visits; and • Consultation with another physician to obtain a second opinion before the surgery.
Note: The surgical fee includes normal post-operative care. The LM HealthWorks Plan may combine the reimbursement when more than one surgery is performed during the same operative session. Contact the LM HealthWorks Plan claims administrator 877-458-4975 for more information. Anesthetics
Charges for the administration of anesthetics and oxygen by a physician, other than the operating physician, or Certified Registered Nurse Anesthetist (C.R.N.A.) in connection with a covered procedure.
32

Alternatives to Physician Office Visits Walk-In Clinic Visits • Charges made by walk-in clinics for unscheduled visits for treatment of non-emergency illnesses
and injuries. • Administration of certain immunizations administered within the scope of the clinic’s license but
not if solely for your employment. E-Visits • Charges made by a network provider for a routine, non-emergency, online internet medical
consultation. You must make your E-visit through an Aetna authorized internet service vendor. You may have to register with that internet service vendor. Information about providers who are signed up with an authorized vendor may be found in the provider directory or online in DocFind on the LM HealthWorks Plan Web site at www.lmhwplan.com or by calling 877-458-4975. Charges made by a non-network provider are not covered.
Inpatient Hospital Care
Charges for services and supplies provided by a hospital or licensed birthing center while admitted as an inpatient, including: • Room and board charges for a room with two or more beds. Private room and private duty
nursing are not covered unless the LM HealthWorks Plan claims administrator determines that they are medically necessary.
• Ancillary services such as operating room, diagnostic services, therapy services, prescribed drugs and supplies.
• Well-baby care – routine nursery care for a newborn child before the mother’s discharge from the hospital.
NOTE: All inpatient care must be precertified. Please refer to the “Precertification” section for more information. Outpatient Care at a Hospital or Other Facility
Charges for services and supplies provided by a hospital, urgent care facility or other facility on an outpatient basis, including but not limited to: • Outpatient surgery in a surgery center or the outpatient department of a hospital. • Charges made by an urgent care provider, including:
– Use of urgent care facilities; – Physicians services; – Nursing staff services; and – Radiologists and pathologists services.
• Emergency care, including: – Use of emergency room facilities; – Emergency room physician services; – Hospital nursing staff services; and – Radiologist and pathologist services.
If you need emergency care, please follow the guidelines below: • Go to the nearest emergency room, or dial 911 or your local emergency response service for
medical and ambulatory assistance. If possible, call your physician unless it would cause a delay that would be detrimental to your health.
• After assessing and stabilizing your condition, the emergency room should contact your physician to obtain your medical history to assist the emergency physician in your treatment.
33

• If you are admitted to an inpatient facility, you should notify your physician as soon as reasonably possible.
• If you seek care in an emergency room for a non-emergency condition, one that does not meet the criteria for an emergency medical condition, your benefits will be reduced.
Covered expenses include charges made by a hospital or a physician for services provided in an emergency room to evaluate and treat an emergency medical condition. Please contact your physician after receiving treatment for an emergency medical condition.
NOTE: Some outpatient care may require precertification. Please refer to the “Precertification” section for more information. Prescription Drugs For information about prescription drug coverage, refer to the “Prescription Drug” section. Other Covered Health Care Expenses Acupuncture
Acupuncture therapy, only when administered by a health care provider who is a legally qualified physician practicing within the scope of his/her license, to treat or when used for the following: • Post-operative and chemotherapy-induced nausea and vomiting. • Nausea from pregnancy. • Post-operative dental pain. • Post-operative dental care. • Temporomandibular disorders (TMD). • Migraine. • Pain from osteoarthritis of the knee or hip (adjunctive therapy). • Chronic lower back pain (maintenance treatment where symptoms are neither regressing nor
improving is considered not medically necessary). • Anesthesia in connection with a covered surgical expense.
34
Alcoholism and Substance Abuse Charges made for the treatment of alcoholism and substance abuse by behavioral health
providers. In addition to meeting all other conditions for coverage, the treatment must meet the following criteria: • There is a program of therapy prescribed and supervised by a behavioral health provider. • The program of therapy includes either:
– A follow up program directed by a behavioral health provider on at least a monthly basis; or – Meetings at least twice a month with an organization devoted to the treatment of alcoholism
or substance abuse.
Inpatient Treatment for Alcoholism and Substance Abuse • Room and board at the semi-private room rate and other services and supplies provided during
your stay in a psychiatric hospital or residential treatment facility, appropriately licensed by the State Department of Health or its equivalent.
• Coverage includes: – Treatment in a hospital for the medical complications of alcoholism or substance abuse
(“medical complications” include detoxification, electrolyte imbalances, malnutrition, cirrhosis of the liver, delirium tremens and hepatitis); and
– Treatment in a hospital, when the hospital does not have a separate alcoholism and substance abuse treatment facility section.
Outpatient Treatment for Alcoholism and Substance Abuse • Outpatient treatment including partial hospitalization services (more than four hours, but less than
24 hours per day) provided in a facility or program for the intermediate short-term or medically-directed intensive treatment of alcoholism or substance abuse. The partial hospitalization will only be covered if you would need inpatient treatment if you were not admitted to this type of facility.
Partial Confinement Treatment for Alcoholism and Substance Abuse • Charges made for partial confinement treatment provided in a facility or program for the
intermediate short-term or medically-directed intensive treatment of alcoholism or substance abuse.
• The partial confinement treatment will be covered only if you would need a hospital stay if you were not admitted to this type of facility.
Important Reminder Inpatient care and certain outpatient services must be precertified by LM HealthWorks Plan claims administrator. Refer to the “Precertification” section for more information. Ambulance Service
Charges for ground ambulance transportation: • To the first hospital where treatment is given in a medical emergency. • From one hospital to another hospital in a medical emergency when the first hospital does not
have the required services or facilities to treat your condition, and you are transported to the nearest hospital equipped to treat your condition.
• From hospital to home or to another facility when other means of transportation would be considered unsafe due to your medical condition.
35

• From home to hospital for covered inpatient or outpatient treatment when other means of transportation would be considered unsafe due to your medical condition. Transport is limited to 100 miles.
• When during a covered inpatient stay at a hospital, skilled nursing facility or acute rehabilitation hospital, an ambulance is required to safely and adequately transport you to or from inpatient or outpatient medically necessary treatment.
Charges for transportation by air or water ambulance to the nearest hospital equipped to treat your condition when: • Ground ambulance transportation is not available; • Your condition is unstable, and requires medical supervision and rapid transport; and • In a medical emergency, transportation from one hospital to another hospital, when the first
hospital does not have the required services or facilities to treat your condition and you need to be transported to another hospital and the two conditions above are met.
Cardiac and Pulmonary Rehabilitation Benefits
Cardiac rehabilitation benefits are available as part of an inpatient hospital stay. A limited course of outpatient Phase I or Phase II cardiac rehabilitation is covered when following angioplasty, cardiovascular surgery, congestive heart failure or myocardial infarction. The LM HealthWorks Plan will cover charges in accordance with a treatment plan as determined by your risk level when recommended by a physician. This course of treatment is limited to a maximum of 36 sessions in a 12-week period.
Pulmonary rehabilitation benefits are available as part of an inpatient hospital stay. A limited course of outpatient pulmonary rehabilitation is covered for the treatment of reversible pulmonary disease states. This course of treatment is limited to a maximum of 36 sessions in a12-week period
. Chiropractic Treatment
Charges made by a chiropractor on an outpatient basis for manipulative (adjustive) treatment or other physical treatment for conditions caused by (or related to) biomechanical or nerve conduction disorders of the spine. Benefits are subject to the maximum shown in the “Benefit Highlights” section.
Cognitive Therapy
Cognitive therapy associated with physical rehabilitation is covered when the cognitive deficits have been acquired as a result of neurologic impairment due to trauma, stroke or encephalopathy, and when the therapy is part of a treatment plan intended to restore previous cognitive function. Benefits are subject to the Outpatient Short-Term Rehabilitation benefit maximums as shown in the “Benefit Highlights” section.
Contraceptive Services
Charges for contraceptive services and supplies provided on an outpatient basis, including: • Contraceptive drugs and contraceptive devices prescribed by a physician provided they have been
approved by the U.S. Food and Drug Administration; • Related outpatient services such as:
– Consultations; – Exams; – Procedures; and – Other medical services and supplies.
Charges for sterilization.
36

Dental Treatment Dental work, surgery and orthodontic treatment needed to remove, repair, restore or reposition (due to
an injury): • Natural teeth damaged, lost or removed; or • Other body tissues of the mouth fractured or cut. Any such teeth must have been free from decay or in good repair and firmly attached to the jaw bone at the time of the injury.
The dental treatment must be completed in the year of the accident or in the next year. If crowns, dentures, bridges or in-mouth appliances are installed due to injury, covered expenses only include charges for: • The first denture or fixed bridgework to replace lost teeth; • The first crown needed to repair each damaged tooth; and • An in-mouth appliance used in the first course of orthodontic treatment after the injury.
Diabetic Equipment, Supplies and Education
Charges for the following services, supplies, equipment and training for the treatment of insulin and non-insulin dependent diabetes and for elevated blood glucose levels during pregnancy: • External insulin pumps; • Blood glucose monitors without special features unless required due to blindness; • Alcohol swabs; • Glucagon emergency kits; • Self-management training provided by a licensed health care provider certified in diabetes self-
management training; or • Foot care to minimize the risk of infection.
Diagnostic and Preoperative Testing Diagnostic Complex Imaging Expenses
Charges made on an outpatient basis by a physician, hospital or a licensed imaging or radiological facility for complex imaging services to diagnose an illness or injury, including: • Computed Tomography (CAT or CT) Scans; • Magnetic Resonance Imaging (MRI); • Positron Emission Tomography (PET) Scans; and • For any other outpatient diagnostic imaging service costing over $500.
Complex imaging expenses for preoperative testing will be payable under this benefit. Outpatient Lab Work and Radiological Services
Charges for radiological services, lab services and pathology and other tests provided to diagnose an illness or injury. Definite symptoms must be present that start, maintain or change a plan of treatment prescribed by a physician. The charges must be made by a physician, hospital or licensed radiological facility or lab.
37

Outpatient Preoperative Testing Charges made for tests performed by a hospital, surgery center, physician or licensed diagnostic
laboratory before a scheduled surgery, if the charges for the surgery are covered expenses and the tests are: • Related to your surgery, and the surgery takes place in a hospital or surgery center; • Completed within 14 days before your surgery; • Performed on an outpatient basis; • Covered if you were an inpatient in a hospital; and • Not repeated in or by the hospital or surgery center where the surgery will be performed. Test results should appear in your medical record kept by the hospital or surgery center where the surgery is performed, in case you need to access them.
Durable Medical Equipment (DME)
Charges by a DME supplier for the rental of equipment or, in lieu of rental, the initial purchase of DME if: • Long term care is planned; and • The equipment cannot be rented or is likely to cost less to purchase than to rent.
Repair of purchased equipment. Maintenance and repairs needed due to misuse or abuse are not covered.
Replacement of purchased equipment if: • The replacement is needed because of a change in your physical condition; and • It is likely to cost less to replace the item than to repair the existing item or rent a similar item.
The LM HealthWorks Plan limits coverage to one item of equipment for the same or similar purpose and the accessories needed to operate the item. You are responsible for the entire cost of any additional pieces of the same or similar equipment you purchase or rent for personal convenience or mobility. Covered DME includes those items covered by Medicare unless excluded in the “What Is Not Covered” section of this Summary Plan Description. The LM HealthWorks Plan reserves the right to limit the payment of charges up to the most cost efficient and least restrictive level of service or item that can be safely and effectively provided. The decision to rent or purchase is at the discretion of the LM HealthWorks Plan claims administrator. NOTE: To ensure coverage, all DME rentals or purchases of $5,000 or more need to be precertified by the LM HealthWorks Plan claims administrator. Refer to the “Precertification” section for details about precertification. Hearing Aids
Charges for hearing aids to improve or restore hearing, up to the maximum shown in the “Benefit Highlights” section. This includes covered charges for the fitting, adjustments and testing of the appliance up to the maximum benefit allowed.
Hearing Exams
Charges for a hearing screening as part of a routine physical exam are covered as shown in the “Benefit Highlights” section. Other medically necessary hearing exams are a covered expense under the LM HealthWorks Plan.
38
Home Health Care Charges for home health care services when ordered by a physician as part of a home health plan and
provided you are: • Transitioning from a hospital or other inpatient facility, and the services are in lieu of a continued
inpatient stay; or • Homebound.
Covered expenses include only the following: • Skilled nursing services that require medical training of, and are provided by, a licensed nursing
professional within the scope of his or her license. These services need to be provided during intermittent visits of four hours or less, with a daily maximum of three visits. Intermittent visits are considered periodic and recurring visits that skilled nurses make to ensure your proper care, which means they are not on site for more than four hours at a time.
• Home health aide services, when provided in conjunction with skilled nursing care, that directly support the care. These services need to be provided during intermittent visits of four hours or less, with a daily maximum of three visits.
Benefits for home health care visits are payable up to the maximum shown in the “Benefit Highlights” section. Each visit by a nurse or therapist is one visit. In figuring the calendar year maximum visits, each visit of up to four hours is one visit for care given by an R.N. or L.P.N. or home health care aide for skilled nursing services when billed by a home health care agency. Coverage for home health care services is not determined by the availability of caregivers to perform them. The absence of a person to perform a non-skilled or custodial care service does not cause the service to become covered. NOTE: The LM HealthWorks Plan does not cover custodial care, even if care is provided by a nursing professional when a family member or other caretakers cannot provide the necessary care. Home health care must be precertified. Refer to the “Precertification” section for more information. Refer to the “Benefit Highlights” section for details about any applicable home health care visit maximums. Hospice Care
Hospice care provided under the Compassionate Care Program is available if you are terminally ill and receiving care by or under arrangements with a hospice care agency, and have a medical prognosis for which it is substantially likely you will die within 12 months. Covered services include: • Certain facility expenses, respite care expenses and other expenses including grief counseling. • Pain management, in addition to palliative (relief of physical symptoms) and curative care, while
enrolled in the program. • Respite care may include both inpatient and outpatient services, but shall be limited to 15 days to
provide primary care givers temporary relief. • Grief counseling (also called bereavement counseling) is provided for unlimited telephonic
counseling and up to five visits with a provider, within a 12-month period.
39

NOTE: Hospice care must be precertified. Refer to the “Precertification” section for more information. Infertility
Charges made by a physician to diagnose and to surgically treat the underlying medical cause of infertility.
Infertility medications as approved to treat the underlying medical cause of infertility; subject to coverage management by the prescription drug claims administrator and a lifetime benefit maximum of $5,000.
Mental Disorders
Charges made for the treatment of mental disorders by behavioral health providers. In addition to meeting all other conditions for coverage, the treatment must meet the following criteria: • There is a written treatment plan prescribed and supervised by a behavioral health provider; • The plan includes follow-up treatment; and • The plan is for a condition that can favorably be changed.
Benefits are payable for charges incurred in a hospital, psychiatric hospital, residential treatment facility or behavioral health provider’s office as follows:
Inpatient Treatment Charges for room and board at the semi-private room rate, and other services and supplies provided during your stay in a hospital, psychiatric hospital or residential treatment facility. Inpatient benefits are payable only if your condition requires services that are only available in an inpatient setting.
Partial Confinement Treatment Charges made for partial confinement treatment provided in a facility or program for the intermediate short-term or medically-directed intensive treatment of a mental disorder. Such benefits are payable if your condition requires services that are only available in a partial confinement treatment setting.
Outpatient Treatment • Charges for treatment received while not confined as a full-time inpatient in a hospital,
psychiatric hospital or residential treatment facility. • Partial hospitalization services (more than four hours, but less than 24 hours per day) provided in
a facility or program for the intermediate short-term or medically-directed intensive treatment. The partial hospitalization will only be covered if you would need inpatient care if you were not admitted to this type of facility.
Family Support at Home Services • These services are available to your ambulatory (not home bound) covered dependent children
who are less than 18 years of age, have a diagnosed mental health condition and are supported by their immediate family in the home.
• Your outpatient mental health benefit provides for an in-network therapist to provide in home treatment if the services are medically necessary, the home location is determined to be the most effective treatment setting and services at the home location would help prevent an inpatient admission.
• These services are for therapy treatment and not for custodial care. NOTE: Inpatient care, certain outpatient services and Family Support at Home Services must be precertified by the LM HealthWorks Plan claims administrator. Refer to the “Precertification” section for more information.
40

Obesity Surgical Expenses Covered medical expenses include charges made on an inpatient or outpatient basis by a hospital or a physician for the surgical treatment of morbid obesity of a covered person. If the expenses are not incurred at an Institutes of Quality® Bariatric Surgery facility, payment will be made at the lower coinsurance level (see the “Benefit Highlights” section for details). You can search for Institutes of Quality® Bariatric Surgery Facilities using DocFind. Coverage includes the following expenses as long as they are incurred within a two-year period:
One morbid obesity surgical procedure including complications directly related to the surgery; Pre-surgical visits; Related outpatient services; and One follow-up visit.
This two-year period begins with the date of the first morbid obesity surgical procedure, unless a multi-stage procedure is planned. Complications, other than those directly related to the surgery, will be covered under the medical plan’s covered medical expenses, subject to plan limitations and maximums. Organ and Tissue Transplants and Evaluations Under the LM HealthWorks Plan there is a special transplant network. You can call 877-458-4975 for network transplant facilities that are approved for the type of transplant that you need. You can also obtain the list of network transplant facilities from the LM HealthWorks Plan claims administrator’s Web site at www.lmhwplan.com. To receive the highest reimbursement for in-network benefits, you must receive your care from one of the Institute of Excellence facilities designated for the type of transplant you need. You can search for Institutes of Excellence by using DocFind. If you decide to have your transplant at an in-network facility other than one of the designated transplant facilities, you will be reimbursed at the normal in-network rate. If you have your transplant at an out-of-network facility, you will receive out-of-network benefits. (See the “Benefit Highlights” section for details.) You, your representative or your physician must contact the LM HealthWorks Plan claims administrator to receive precertification approval for all inpatient admissions for transplants. Under the transplant program, travel expenses to and from the designated transplant site and reasonable expenses for lodging for the patient and one member of his or her immediate family (up to $10,000 per transplant procedure) may be covered. Precertification approval is required.
41

The following transplants are covered under the transplant program:
Heart; Lung; Heart/lung; Simultaneous Pancreas Kidney (SPK); Pancreas; Kidney; Liver; Intestine; Bone marrow/stem cell; Multiple organs replaced during one transplant surgery; Tandem transplants (stem cell); Sequential transplants; Re-transplant of same organ type within 180 days of the first transplant; and Any other single organ transplant, unless otherwise excluded under the LM HealthWorks Plan.
The following will be considered to be more than one Transplant Occurrence:
Autologous blood/bone marrow transplant followed by allogenic blood/bone marrow transplant (when not part of a tandem transplant);
Allogenic blood/bone marrow transplant followed by an autologous blood/bone marrow transplant (when not part of a tandem transplant);
Re-transplant after 180 days of the first transplant; Pancreas transplant following a kidney transplant; A transplant required by an additional organ failure during the original transplant surgery/process;
and More than one transplant when not performed as part of a planned tandem or sequential transplant
(e.g., a liver transplant with subsequent heart transplant). Transplants or evaluations that the LM HealthWorks Plan claims administrator determines are not medically necessary will not be covered. NOTE: All organ and tissue transplants and evaluations require precertification. Please refer to the “Precertification” section for more information. Transplant Services
Charges made by a physician or transplant team. Charges made by a hospital, outpatient facility or physician for the medical and surgical expenses of a
live donor, but only to the extent not covered by another plan or program, and only when the organ recipient is covered under this LM HealthWorks Plan.
Related supplies and services provided by the facility during the transplant process. These services and supplies may include: physical, speech and occupational therapy; bio-medicals and immunosuppressants; home health care expenses and home infusion services.
Charges for activating the donor search process with national registries. Compatibility testing of prospective organ donors who are immediate family members. For the
purpose of this coverage, an “immediate” family member is defined as a first-degree biological relative. These are your biological parents, siblings or children.
Inpatient and outpatient expenses directly related to a transplant.
42
NOTE: You receive the highest benefit when you receive specialty care from an Institute of Excellence provider. You can locate Institutes of Excellence by referring to the provider directory or online in DocFind on the LM HealthWorks Plan Web site at www.lmhwplan.com or by calling 877-458-4975. Pervasive Developmental Delays
Charges for the diagnosis of pervasive developmental delays, including autism. All other services and treatment of pervasive developmental delays are not covered under the LM HealthWorks Plan.
Pregnancy-Related Expenses
Charges made by a physician for pregnancy and childbirth services and supplies at the same level as any illness or injury. This includes prenatal visits, delivery and postnatal visits.
Charges made by a hospital for inpatient maternity and pediatric care of the mother and newborn child, for a minimum of: • 48 hours after a vaginal delivery; • 96 hours after a cesarean section; and • A shorter stay, if the attending physician, with the consent of the mother, discharges the mother
or newborn earlier. Charges made by a birthing center. Services and supplies provided for circumcision of the newborn during the stay.
Private Duty Nursing
Charges for private duty nursing provided by a R.N. or L.P.N. if the person’s condition requires skilled nursing care and visiting nursing care is not adequate. Each period of private duty nursing of up to eight hours will be deemed to be one private duty nursing visit. Please refer to the “Benefit Highlights” section for LM HealthWorks Plan maximums.
NOTE: Private duty nursing requires precertification. Please refer to the “Precertification” section for more information. Prosthetic Devices
Charges made for internal and external prosthetic devices and special appliances, if the device or appliance improves or restores a body part function that has been lost or damaged by illness, injury or congenital defect. Covered expenses also include instruction and incidental supplies needed to use a covered prosthetic device.
The LM HealthWorks Plan covers the first prosthesis you need that temporarily or permanently replaces all or part of a body part lost or impaired as a result of disease, injury or congenital defects as described in the list of covered devices below for an: • Internal body part or organ; or • External body part.
Replacement of a prosthetic device if: • The replacement is needed because of a change in your physical condition or normal growth or
wear and tear; or • It is likely to cost less to buy a new one than to repair the existing one; or • The existing one cannot be made serviceable.
43

The list of covered devices includes but is not limited to: • An artificial arm, leg, hip, knee or eye; • Eye lens; • An external breast prosthesis and the first bra made solely for use with it after a mastectomy; • A breast implant after a mastectomy; • Ostomy supplies, urinary catheters and external urinary collection devices; • Speech generating devices; • A cardiac pacemaker and pacemaker defibrillators; and • A durable brace that is custom made for and fitted for you.
NOTE: To ensure coverage, all prosthetic devices of $5,000 or more need to be precertified by the LM HealthWorks Plan claims administrator. Refer to the “Precertification” section for more information. Reconstructive or Cosmetic Surgery and Supplies
Charges made by a physician, hospital or surgery center for reconstructive services and supplies, including: • Surgery needed to improve a significant functional impairment of a body part. • Surgery to correct the result of an accidental injury, including subsequent related or staged
surgery, provided that the surgery occurs no more than 24 months after the original injury. For a covered child, the time period for coverage may be extended through age 18.
• Surgery to correct the result of an injury that occurred during a covered surgical procedure provided that the reconstructive surgery occurs no more than 24 months after the original injury.
Note: Injuries that occur as a result of a medical (i.e., non surgical) treatment are not considered accidental injuries, even if unplanned or unexpected.
Surgery to correct a gross anatomical defect present at birth or appearing after birth (but not the result of an illness or injury) when the defect results in: • Severe facial disfigurement; or • Significant functional impairment and the surgery are needed to improve function.
Charges for reconstruction of the breast on which a mastectomy was performed, including an implant and areolar reconstruction. Also included is surgery on a healthy breast to make it symmetrical with the reconstructed breast and physical therapy to treat complications of mastectomy, including lymphedema.
Sexual Disorders
Charges for therapy, supplies or counseling that have a physiological or organic basis. Short-Term Rehabilitation Therapy Services Covered expenses include charges for short-term therapy services when prescribed by a physician as described below up to the benefit maximums listed in the “Benefit Highlights” section. The services have to be performed by:
A licensed or certified physical, occupational or speech therapist; A hospital, skilled nursing facility or hospice facility; or A physician other than a chiropractor.
44

Outpatient Physical Therapy, Occupational Therapy and Speech Therapy Benefits Coverage is subject to the limits shown in the “Benefit Highlights” section. Inpatient rehabilitation benefits for the services listed will be paid as part of the Inpatient Hospital and Skilled Nursing Facility benefits. Rehabilitation services received in the home will also count towards the benefit maximum for Home Health Care. Instead of hospitalization, the LM HealthWorks Plan allows for extension of certain outpatient benefits beyond their LM HealthWorks Plan limits. Care must be medically necessary and be precertified.
Physical therapy is covered for non-chronic conditions and acute illnesses and injuries, as long as the therapy expects to significantly improve, develop or restore physical functions lost or impaired as a result of an acute illness, injury or surgical procedure. Physical therapy does not include educational training or services designed to develop physical function.
Occupational therapy (except for vocational rehabilitation or employment counseling) is covered for non-chronic conditions and acute illnesses and injuries, as long as the therapy expects to significantly improve, develop or restore physical functions lost or impaired as a result of an acute illness, injury or surgical procedure, or to relearn skills to significantly improve independence in the activities of daily living. Occupational therapy does not include educational training or services designed to develop physical function.
Speech therapy is covered for non-chronic conditions and acute illnesses and injuries as long as the therapy is expected to restore the speech function or correct a speech impairment resulting from that illness or injury; or for delays in speech function development as a result of disease, injury or gross anatomical defect present at birth. Speech function is the ability to express thoughts, speak words and form sentences. Speech impairment is difficulty with expressing one’s thoughts with spoken words.
A “visit” consists of no more than one hour of therapy. Refer to the “Benefit Highlights” section for the visit maximum that applies to the LM HealthWorks Plan. Covered expenses include charges for two therapy visits of no more than one hour in a 24-hour period. The therapy should follow a specific treatment plan that:
Details the treatment, and specifies frequency and duration; and Provides for ongoing reviews and is renewed only if continued therapy is appropriate.
Skilled Nursing Facility
Charges made by a skilled nursing facility while admitted as an inpatient for the following services and supplies, up to the maximums shown in the “Benefit Highlights” section, including: • Room and board, up to the semi-private room rate. The LM HealthWorks Plan will cover up to
the private room rate if it is needed due to an infectious illness or a weak or compromised immune system;
• Use of special treatment rooms; • Radiological services and lab work; • Physical, occupational or speech therapy; • Oxygen and other gas therapy; • Other medical services and general nursing services usually given by a skilled nursing facility
(this does not include charges made for private or special nursing, or physician’s services); and • Medical supplies.
45

NOTE: Stays at a skilled nursing facility require precertification. Please refer to the “Precertification” section for more information. Specialized Care Chemotherapy
Charges for chemotherapy treatment. In most cases, chemotherapy is covered as outpatient care. Inpatient hospitalization for chemotherapy is limited to the initial dose while hospitalized for the diagnosis of cancer and when a hospital stay is otherwise medically necessary based on your health status.
Radiation Therapy
Charges for the treatment of illness by x-ray, gamma ray, accelerated particles, mesons, neutrons, radium or radioactive isotopes.
Outpatient Infusion Therapy
Infusion therapy is the intravenous or continuous administration of medications or solutions that are a part of your course of treatment. Coverage is provided for charges made on an outpatient basis for infusion therapy by: • A free-standing facility; • The outpatient department of a hospital; or • A physician in his/her office or in your home.
Charges for the following outpatient infusion therapy services and supplies are covered expenses: • The pharmaceutical when administered in connection with infusion therapy and any medical
supplies, equipment and nursing services required to support the infusion therapy; • Professional services; • Total parenteral nutrition (TPN); • Chemotherapy; • Drug therapy (includes antibiotic and antivirals); • Pain management (narcotics); and • Hydration therapy (includes fluids, electrolytes and other additives).
Benefits payable for infusion therapy will not count toward any Home Health Care maximums that apply. Temporomandibular Joint (TMJ) Disorders
Charges in connection with diagnostic and surgical and non-surgical treatment of conditions affecting the temporomandibular joint when provided by or under the direction of a physician. Coverage includes treatment required as a result of accident, trauma, a congenital anomaly, developmental defect or pathology. Covered treatments include: • Examination. • Radiographs and applicable imaging studies and consultation. • Non-surgical treatment including physical therapy, arthrocentesis and trigger-point injections. • Surgical treatment if:
– There is clearly demonstrated radiographic evidence of significant joint abnormality; – Non-surgical treatment has failed to adequately resolve the symptoms; – Pain or dysfunction is moderate or severe; and – The surgical procedure has been approved as medically necessary by the LM HealthWorks
Plan claims administrator. Oral appliances (orthotic splints) and services that are dental in nature are not covered under the LM HealthWorks Plan.
46

NOTE: Not every service, supply or prescription drug that fits the definition for medical necessity is covered by the LM HealthWorks Plan. Exclusions and limitations apply to certain medical services, supplies and expenses. For example, some benefits are limited to a certain number of days, visits or a dollar maximum. Refer to the “What Is Covered” section and the “Benefit Highlights” section for the Plan limits and maximums. See the “What Is Not Covered” section for more information.
What Is Not Covered
What Health Care Services and Supplies Are Not Covered The LM HealthWorks Plan covers a wide range of expenses. However, benefits are limited under certain circumstances. You will find details of medical benefit limits and exclusions listed below. Please take the time to read them carefully. Not every medical service or supply is covered by the LM HealthWorks Plan, even if prescribed, recommended or approved by your physician or dentist. The LM HealthWorks Plan covers only those services and supplies that are medically necessary and included in the “What Is Covered” section. Charges made for the following are not covered except to the extent listed under the “What Is Covered” section. NOTE: The LM HealthWorks Plan offers medical and prescription drug coverage. The exclusions listed below apply to all coverages under the LM HealthWorks Plan. Additional exclusions apply to specific prescription drug coverage (see the “Prescription Drug” section.). Exclusions The following services will not be covered:
Acupuncture, acupressure and acupuncture therapy, except as provided in the “What Is Covered” section.
Allergy: Specific non-standard allergy services and supplies, including but not limited to skin titration (wrinkle method), cytotoxicity testing (Bryan’s Test), treatment of non-specific candida sensitivity and urine autoinjections.
Ambulance: • If an ambulance service is not medically necessary for your physical condition; • If the type of ambulance service provided is not medically necessary for your physical condition;
or • When received by any form of transportation other than a professional ambulance service.
Amniocentesis, ultrasound or any other procedure requested solely for the sex determination of a fetus.
Any care that is reimbursable in any way through any public program other than Medicare and Medicaid, (i.e., state run programs that provide additional benefits).
47

Any non-emergency prescription drug charges incurred outside of the United States when: • You travel to such location specifically to obtain prescription drugs or supplies, even if otherwise
covered under this plan; • Such drugs or supplies are unavailable or illegal in the United States; or • The purchase of such prescription drugs or supplies outside the United States is considered
illegal. Behavioral health services: • Alcoholism or substance abuse rehabilitation treatment on an inpatient or outpatient basis, except
to the extent coverage for detoxification or treatment of alcoholism or substance abuse is specifically provided in the “What Is Covered” section.
• Treatment of a covered health care provider who specializes in the mental health care field and who receives treatment as a part of their training in that field.
• Treatment of impulse control disorders such as pathological gambling, kleptomania, pedophilia, caffeine or nicotine use.
• Treatment of antisocial personality disorder. • Treatment in wilderness programs or other similar programs. • Treatment of mental retardation, defects and deficiencies. This exclusion does not apply to mental
health services or for the medical treatment of mentally retarded members in accordance with the benefits provided in the “What Is Covered” section.
• Psychological testing for educational purposes. • Psychological testing unless performed to diagnose a psychiatric condition.
Cardiac pulmonary rehabilitation, Phases III and IV. Contraception, except as specifically described in the “What Is Covered” section: • Over the counter contraceptive supplies including but not limited to: condoms, contraceptive
foams, jellies and ointments. Cosmetic services and plastic surgery except when required for an accidental injury received while
covered, or for breast reconstruction following a radical mastectomy, or to treat congenital abnormalities in a child. Any other treatment, surgery (cosmetic or plastic), service or supply to alter, improve or enhance the shape or appearance of the body is not covered, whether or not for psychological or emotional reasons.
Counseling: Services and treatment for marriage, religious, family, career, social adjustment, pastoral or financial counseling.
Custodial care, education or training, except for the hospice care benefit as shown in the “Benefit Highlights” section.
Dental Services: Except as provided in the “What Is Covered” section, any treatment, services or supplies related to the care, filling, removal or replacement of teeth and the treatment of injuries and diseases of the teeth, gums and other structures supporting the teeth. This includes but is not limited to: • Services of dentists, oral surgeons, dental hygienists and orthodontists including apicoectomy
(dental root resection), root canal treatment, soft tissue or bony impactions, treatment of periodontal disease, alveolectomy, augmentation and vestibuloplasty and fluoride and other substances to protect, clean or alter the appearance of teeth;
• Dental implants, false teeth, prosthetic restoration of dental implants, plates, dentures, braces, mouth guards and other devices to protect, replace or reposition teeth; and
• Non-surgical treatments to alter bite or the alignment or operation of the jaw, including treatment of malocclusion or devices to alter bite or alignment.
This exclusion does not include bone fractures, removal of tumors and orthodontogenic cysts.
48

Drugs, medications and supplies: • Over-the-counter drugs, biological or chemical preparations and supplies that may be obtained
without a prescription including vitamins; • Any prescription drug purchased illegally outside the United States, even if otherwise covered
under this plan within the United States; • Immunizations related to work; • Needles, syringes and other injectable aids, except as covered for diabetic supplies; • Drugs related to the treatment of non-covered expenses; and • Androgens and anabolic steroids when prescribed for performance enhancement.
Educational services: • Any services or supplies related to education, training or retraining services or testing, including
special education, remedial education, job training and job hardening programs; • Evaluation or treatment of learning disabilities; minimal brain dysfunction; developmental,
learning and communication disorders; behavioral disorders (including pervasive developmental disorders) or training, regardless of the underlying cause;
• Services, treatment and educational testing and training related to behavioral (conduct) problems, learning disabilities and delays in developing skills; and
• Special education to instruct a person whose speech has been lost or impaired, to function without that ability. This includes lessons in sign language.
Examinations: Any health examinations: • Required by a third party, including examinations and treatments required to obtain or maintain
employment, or which an employer is required to provide under a labor agreement; • Required by any law of a government, securing insurance or school admissions, or professional or
other licenses; • Required to travel, attend a school, camp or sporting event or participate in a sport or other
recreational activity; • Any special medical reports not directly related to treatment except when provided as part of a
covered service; and • Court-ordered forensic or custodial evaluations.
Facility charges, for care services or supplies provided in: • A doctor’s office for surgery; • Rest homes; • Assisted living facilities; • Similar institutions serving as an individual’s primary residence or providing primarily custodial
or rest care; • Health resorts; • Spas, sanitariums; or • Infirmaries at schools, colleges or camps.
Food items: Any food item, including infant formulas, nutritional supplements, medical foods and other nutritional items, even if it is the sole source of nutrition, except as provided in the “What Is Covered” section.
Foot care: Unless required for the treatment of or to prevent complications of diabetes: • Routine foot care, including trimming of toenails and paring of corns or calluses; • Shoes (including orthopedic shoes), therapeutic shoes, foot orthotics or other devices to support
the feet, except for an orthopedic shoe that is an integral part of a covered leg brace; and • Arch supports, shoe inserts, ankle braces, guards, protectors, creams, ointments and other
equipment, devices and supplies, even if required following a covered treatment of an illness or injury.
49
Growth/Height: Any treatment, device, drug, service or supply (including surgical procedures, devices to stimulate growth and growth hormones), solely to increase or decrease height or alter the rate of growth, except as determined by the LM HealthWorks Plan claims administrator to be medically necessary.
Hearing: • Any hearing service or supply that does not meet professionally accepted standards; and • Any tests, appliances and devices to enhance other forms of communication to compensate for
hearing loss or devices that stimulate speech, except as provided in the “What Is Covered” section.
Home and mobility: Any addition or alteration to a home, workplace or other environment or vehicle and any related equipment or device, such as: • Purchase or rental of exercise equipment, air purifiers, central or unit air conditioners, water
purifiers, waterbeds and swimming pools; • Exercise and training devices, whirlpools, portable whirlpool pumps, sauna baths or massage
devices; • Equipment or supplies to aid sleeping or sitting, including non-hospital electric and air beds,
waterbeds, pillows, sheets, blankets, warming or cooling devices, bed tables and reclining chairs; • Equipment installed in your home, workplace or other environment, including stair-glides,
elevators, wheelchair ramps, or equipment to alter air quality, humidity or temperature; • Other additions or alterations to your home, workplace or other environment, including room
additions, changes in cabinets, countertops, doorways, lighting, wiring, furniture, communication aids, wireless alert systems or home monitoring;
• Services and supplies furnished mainly to provide a surrounding free from exposure that can worsen your illness or injury;
• Removal from your home, worksite or other environment of carpeting, hypo-allergenic pillows, mattresses, paint, mold, asbestos, fiberglass, dust, pet dander, pests or other potential sources of allergies or illness; and
• Transportation devices, including stair-climbing wheelchairs, personal transporters, bicycles, automobiles, vans or trucks, or alterations to any vehicle or transportation device.
Home births: Any services and supplies related to births occurring in the home or in a place not licensed to perform deliveries.
Home uterine activity monitoring, except as determined by the LM HealthWorks Plan claims administrator to be medically necessary.
Infertility: Except as specifically described in the “What Is Covered” section, any services, treatments, procedures or supplies that are designed to enhance fertility or the likelihood of conception, including but not limited to: • Drugs related to non-covered treatments; • Infertility medications not approved under the LM HealthWorks Plan or above the lifetime benefit
maximum of $5,000; • Artificial insemination; • Any advanced reproductive technology (“ART”) procedures or services related to such
procedures, including but not limited to in vitro fertilization (“IVF”), gamete intra-fallopian transfer (“GIFT”), zygote intra-fallopian transfer (“ZIFT”), and intra-cytoplasmic sperm injection (“ICSI”)
• Infertility services for couples in which one of the partners has had a previous sterilization procedure, with or without surgical reversal;
• Procedures, services and supplies to reverse voluntary sterilization • Infertility services for females with FSH levels 19 or greater mIU/ml on day three of the
menstrual cycle;
50

• The purchase of donor sperm and any charges for the storage of sperm; the purchase of donor eggs and any charges associated with care of the donor required for donor egg retrievals or transfers or gestational carriers or surrogacy; donor egg retrieval or fees associated with donor egg programs, including but not limited to fees for laboratory tests;
• Charges associated with cryopreservation or storage of cryopreserved eggs and embryos (e.g., office, hospital, ultrasounds, laboratory tests, etc.); any charges associated with a frozen embryo or egg transfer, including but not limited to thawing charges;
• Home ovulation prediction kits or home pregnancy tests; • Any charges associated with care required to obtain ART Services (e.g., office, hospital,
ultrasounds, laboratory tests); and any charges associated with obtaining sperm for any ART procedures; and
• Ovulation induction and intrauterine insemination services if you are not fertile. Maintenance care: Care made up of services and supplies that: • Maintain, rather than to improve, a level of physical or mental function; and • Provide a surrounding free from exposures that can worsen the person’s physical or mental
condition. Medical consumable supplies when they do not require a prescription and can be purchased over the
counter, or when they are given to the patient as take-home supplies. However, diabetic supplies, such as syringes, insulin and strips; self-administered catheters; and ostomy supplies are covered.
Miscellaneous charges for services or supplies including: • Annual or other charges to be in a physician’s practice; • Charges to have preferred access to a physician’s services such as boutique or concierge
physician practices; • Cancelled or missed appointment charges or charges to complete claim forms; • Charges the recipient has no legal obligation to pay; or the charges would not be made if the
recipient did not have coverage (to the extent exclusion is permitted by law) including: – Care in charitable institutions; – Care for conditions related to current or previous military service; – Care while in the custody of a governmental authority; – Any care in a public hospital or other facility is required to provide; or – Any care in a hospital or other facility owned or operated by any federal, state or other
governmental entity, except to the extent coverage is required by applicable laws. Nursing and home health aide services provided outside of the home (such as in conjunction with
school, vacation, work or recreational activities). Non-medically necessary services, including but not limited to those treatments, services, prescription
drugs and supplies which are not medically necessary, as determined by the LM HealthWorks Plan claims administrator, for the diagnosis and treatment of illness, injury, restoration of physiological functions or covered preventive services. This applies even if they are prescribed, recommended or approved by your physician or dentist.
Private duty nursing during your stay in a hospital, and outpatient private duty nursing services, except as specifically described in the Private Duty Nursing provision in the “What Is Covered” section. Charges for the following services are not covered: • Nursing care that does not require the education, training and technical skills of a R.N. or L.P.N. • Nursing care assistance for daily life activities, such as:
– Transportation; – Meal preparation; – Vital sign charting; – Companionship activities; – Bathing; – Feeding;
51

– Personal grooming; – Dressing; – Toileting; and – Getting in/out of bed or a chair.
• Nursing care provided while you are an inpatient in a hospital or health care facility, if the care can adequately be provided by the facility’s general nursing staff, if it were fully staffed.
• A service provided solely to administer oral medicine, except where law requires a R.N. or L.P.N. to administer medicines.
Sex change: Any treatment, drug, service or supply related to changing sex or sexual characteristics, except as provided in the “What Is Covered” section, including: • Surgical procedures to alter the appearance or function of the body; • Hormones and hormone therapy; • Prosthetic devices; and • Medical or psychological counseling.
Services provided where there is no evidence of pathology, dysfunction or disease; except as specifically provided in connection with covered routine care and cancer screenings.
Sexual dysfunction/enhancement: Any treatment, drug, service or supply to treat sexual dysfunction, enhance sexual performance or increase sexual desire, except as provided in the “What Is Covered” section, including: • Surgery, drugs, implants, devices or preparations to correct erectile dysfunction when not caused
by a diagnosable disease or injury; or • Enhance erectile function, enhance sensitivity or alter the shape or appearance of a sex organ and • Sex therapy, sex counseling, marriage counseling or other counseling or advisory services.
Smoking/Tobacco: Any treatment, drug, service or supply to stop or reduce smoking or the use of other tobacco products, or to treat or reduce nicotine addiction, dependence or cravings, including counseling, hypnosis and other therapies, medications, nicotine patches and gum.
Services rendered before the effective date or after the termination of coverage, unless coverage is continued under the “Continuing Coverage” section of the LM HealthWorks Plan. However, if you or an enrolled dependent is confined in a hospital at the time coverage ends, coverage will be continued until the date of discharge, subject to all applicable provisions and limitations of the LM HealthWorks Plan.
Speech therapy for treatment of delays in speech development, except as specifically provided in the “What Is Covered” section. For example, the LM HealthWorks Plan does not cover therapy when it is used to improve speech skills that have not fully developed.
Spinal disorder, including care in connection with the detection and correction by manual or mechanical means of structural imbalance, distortion or dislocation in the human body or other physical treatment of any condition caused by or related to biomechanical or nerve conduction disorders of the spine including manipulation of the spine treatment, except as specifically provided in the “What Is Covered” section.
Strength and performance: Services, devices and supplies to enhance strength, physical condition, endurance or physical performance, including: • Exercise equipment, memberships in health or fitness clubs, training, advice or coaching; • Drugs or preparations to enhance strength, performance or endurance; and • Treatments, services and supplies to treat illnesses, injuries or disabilities related to the use of
performance-enhancing drugs or preparations. Temporomandibular Joint (TMJ) treatment except as described in the “What Is Covered” section.
Appliance therapy and tooth reconstruction for treatment of TMJ are not covered.
52

Therapies for the treatment of delays in development, unless resulting from acute illness or injury, or congenital defects amenable to surgical repair (such as cleft lip/palate), are not covered. • Examples of excluded therapies include but not limited to Applied Behavioral Analysis, and the
LEAP, TEACCH, Denver and Rutgers programs. • Examples of non-covered diagnoses include Pervasive Developmental Disorders (including
Autism), Down Syndrome and Cerebral Palsy, as they are considered both developmental and/or chronic in nature.
Therapies and tests: Any of the following treatments or procedures: • Aromatherapy; • Bio-feedback and bioenergetic therapy; • Carbon dioxide therapy; • Chelation therapy (except for heavy metal poisoning); • Computer-aided tomography (CAT) scanning of the entire body; • Educational therapy; • Gastric irrigation; • Hair analysis; • Hyperbaric therapy, except for the treatment of decompression or to promote healing of wounds; • Hypnosis, and hypnotherapy, except when performed by a physician as a form of anesthesia in
connection with covered surgery; • Lovaas therapy; • Massage therapy; • Megavitamin therapy; • Primal therapy; • Psychodrama; • Purging; • Recreational therapy; • Rolfing; • Sensory or auditory integration therapy; • Sleep therapy; and • Thermograms and thermography.
Transplant – The transplant coverage does not include charges for: • Services and supplies furnished to a donor when the organ recipient is not a covered person; • Home infusion therapy after the transplant occurrence; • Harvesting and/or storage of organs, without the expectation of immediate transplantation for an
existing illness; • Harvesting and/or storage of bone marrow, tissue or stem cells without the expectation of
transplantation within 12 months for an existing illness; and • Cornea (corneal graft with amniotic membrane) or cartilage (autologous chondrocyte or
autologous osteochondral mosaicplasty) transplants, unless otherwise precertified by the LM HealthWorks Plan claims administrator.
Transportation costs, including ambulance services for routine transportation to receive outpatient or inpatient services except as provided in the “What Is Covered” section.
Vision-related services and supplies, except as described in the “What Is Covered” section. The LM HealthWorks Plan does not cover: • Special supplies such as non-prescription sunglasses and subnormal vision aids; • Vision service or supply which does not meet professionally accepted standards; • Special vision procedures, such as orthoptics, vision therapy or vision training; • Eye exams for eyeglasses or contact lenses or their fitting; • Eyeglasses, contact lenses or duplicate or spare eyeglasses or lenses or frames;
53

• Replacement of lenses or frames that are lost or stolen or broken; • Acuity tests; • Eye surgery for the correction of vision, including radial keratotomy, LASIK and similar
procedures; and • Services to treat errors of refraction.
Weight: Any treatment or supply intended to decrease or increase body weight, control weight or treat obesity, including morbid obesity, regardless of the existence of comorbid conditions; except as described in the “What Is Covered” and “Health Management Resources” sections, including but not limited to: • Liposuction, weight control/loss programs and other services and supplies that are primarily
intended to treat, or are related to the treatment of obesity, including morbid obesity; • Preparations, foods or diet supplements, dietary regimens and supplements, food or food
supplements; • Counseling, coaching, training, hypnosis or other forms of therapy; and • Exercise programs, exercise equipment, membership to health or fitness clubs, recreational
therapy or other forms of activity or activity enhancement. General Exclusions The following are not covered:
Any charges in excess of the benefit, dollar, day, visit or supply limits stated in this plan. Charges covered under another Company plan. Charges for a service or supply furnished by an in-network provider in excess of the negotiated
charge, or an out-of-network provider in excess of the recognized charge. Charges submitted for services that are not rendered, or rendered to a person not eligible for coverage
under the Plan. Charges submitted for services by an unlicensed hospital, physician or other provider or not within
the scope of the provider’s license. Charges that are reimbursable through no-fault automobile insurance or uninsured motorist insurance
law. Court ordered services, including those required as a condition of parole or release. Experimental or investigational drugs, devices, treatments or procedures. Injury or loss sustained as a result of war or any act of war in the U.S., declared or undeclared. Payments prohibited by any law you or your covered dependents are subject to at the time services
are rendered. Personal comfort and convenience items: Any service or supply primarily for your convenience and
personal comfort or that of a third party, including: telephone, television, Internet, barber or beauty service or other guest services; housekeeping, cooking, cleaning, shopping, monitoring, security or other home services; and travel, transportation, or living expenses, rest cures, recreational or diversional therapy.
Services provided by a spouse, same-sex domestic partner, parent, child, step-child, brother, sister, in-law or any household member.
Services of a resident physician or intern rendered in that capacity. Services and supplies provided in connection with treatment or care that is not covered under the LM
HealthWorks Plan. Treatment for which you or your dependents are not legally required to pay.
54

Work related: Any illness or injury related to employment or self-employment including any illness or injury that arises out of (or in the course of) any work for pay or profit, unless no other source of coverage or reimbursement is available to you for the services or supplies. Sources of coverage or reimbursement may include your employer, workers’ compensation (except for the hospice care benefit as shown in the “Benefit Highlights” section), or an occupational illness or similar program under local, state or federal law. A source of coverage or reimbursement will be considered available to you even if you waived your right to payment from that source. If you are also covered under a workers’ compensation law or similar law, and submit proof that you are not covered for a particular illness or injury under such law, that illness or injury will be considered “non-occupational” regardless of cause.
55

Prescription Drug Prescription drug coverage is provided as part of your LM HealthWorks Plan and is administered by Medco Health Solutions, Inc. For pharmacy information and services, you can access the Medco Web site through the Prescription Drug Benefits page at www.lmhwplan.com click on the Prescription Drug Benefits page or call the LM HealthWorks Plan at 877-458-4975 to:
Find participating retail pharmacies. Determine the cost of your medications. Look for lower-cost alternatives to your prescription drugs. Look up medications on the formulary. Review the highlights of your prescription drug benefits. Request replacement prescription ID cards.
How the Prescription Benefit Works You will receive a prescription benefit packet, including your prescription drug ID card, directly from Medco. Use your prescription drug ID card to fill short-term prescriptions (this generally means up to a 30-day supply), such as those for antibiotics, filled at in-network or out-of-network retail pharmacies. Use the Medco Pharmacy™ to fill prescriptions for medications you use on a continuing basis, such as those used to treat high blood pressure or high cholesterol. You can typically order up to a 90-day supply and have it delivered right to your home. There is no deductible to meet before the plan pays benefits for prescription drugs. When you fill a prescription either through a retail pharmacy or the Medco Pharmacy,, you will pay either a copay or a percentage of the cost—called coinsurance. There are three levels of copays/coinsurance, which depend on whether your doctor prescribes a generic drug, a preferred brand-name drug (one listed on the plan’s formulary) or a non-preferred brand-name drug (one that is not on the plan’s formulary). (See the “Benefit Highlights” section for more information.) If your physician writes “dispense as written,” you pay the preferred or non-preferred brand-name copay/coinsurance (depending on the specific prescription drug)—even if a generic equivalent is available. If you request a brand-name drug when your physician permits a generic substitution, you will pay the generic coinsurance, plus the difference between the generic drug and the brand-name drug cost. Formulary Drugs The formulary is a list of preferred brand-name drugs chosen for their safety, effectiveness and cost. You can find out if your brand-name medication is on the list by going to Preferred Prescriptions® Drug List and entering the name of your medication. If it is not on the list, you will be given the option of seeing alternatives that you can discuss with your doctor. You can review the formulary at www.lmhwplan.com under Prescription Drug Benefits or by requesting a formulary guide from Medco Member Services.
56

What Prescriptions Are Covered The prescription drug benefit covers those medications that by federal law require a physician’s prescription, are prescribed according to approved indications, are not considered experimental or investigational and are not otherwise limited or excluded by the LM HealthWorks Plan. Covered prescriptions include such things as:
Federal legend drugs (those that require a physician’s prescription). State-restricted drugs. Impotence drugs (with quantity limits). Infertility medications as approved under the prescription drug benefit; subject to coverage
management and a lifetime benefit maximum of $5,000. Insulin. Insulin needles and syringes. Inhaler – assisting devices. Over-the-counter diabetes supplies, including lancets, test strips and blood glucose monitors. Oral contraceptives. Self injected prescription drugs and medications. Anti-obesity medications (subject to coverage management).
Qualification by History (Step Therapy) Some medications are covered only for certain uses and/or require that certain criteria are met, such as age, gender, condition (determined by previous claims history) or use of a first-line therapy. In addition, some categories of drugs may require that you first try a preferred formulary agent before a non-preferred formulary agent is dispensed. In these cases, a coverage review will be required. The step therapy program guidelines are subject to periodic review and change. To find out whether a drug requires step therapy, access the Medco Web site through the Prescription Drug Benefits page at www.lmhwplan.com or call the LM HealthWorks Plan at 877-458-4975. Your physician can request coverage for a step therapy drug by calling Medco’s Coverage Review unit at 800-753-2851. Quantity Management To ensure safe and effective drug therapy, certain covered medications may have quantity restrictions. These quantity restrictions are based on manufacturer and/or clinically approved guidelines and are subject to periodic review and change. Some examples include anti-migraine drugs, rheumatoid arthritis and osteoarthritis drugs, impotence drugs and pain management drugs. If you have any questions, please contact the LM HealthWorks Plan at 877-458-4975. If your physician has any questions, they can call Medco’s Coverage Review unit at 800-753-2851. Coverage Management for Certain Medications Some medications require that you obtain approval through a coverage review before the medication can be covered under your plan. The coverage review process will allow the prescription drug claims administrator to obtain information not available on your original prescription to determine whether a given medication qualifies for coverage under the LM HealthWorks Plan. Medications are periodically added to these programs when new FDA-approved drugs become available.
57

If you are getting the prescription filled through a retail pharmacy, your pharmacist will be notified that the drug cannot be filled without prior approval and that your physician must call Medco’s Coverage Review unit at 800-753-2851 to get approval for the prescription. If you are getting the prescription filled through the mail-order service, the Medco Pharmacy will initiate a call to your provider to get you the approval required.
Mail-Order Service If you use medication on a continuing basis, you will be able to use the mail-order service to make filling long-term prescriptions easier and save on the cost of your drugs. With the Medco Pharmacy mail-order service, you typically can order up to a 90-day supply of medication for the cost of a 60-day supply purchased at a retail pharmacy, with the added convenience of having it delivered right to you. To order medication through the Medco Pharmacy, you can choose from any of the following options:
Online – you first need to register as a new member and set up a personal account. To register, visit www.lmhwplan.com and click on the Prescription Drug Benefit page to access the Medco Web site (www.medco.com) and follow the instructions. Be sure to have the number from your ID card and a recent prescription number handy. You can then click on “Forms & cards” to download a form for your first mail-order.
Phone – have your doctor call in your prescription directly to the Medco Pharmacy. Fax – your doctor can fax your prescription directly to the Medco Pharmacy at the number on the
back of the mail-order form. Remember, only your doctor can fax prescriptions. Mail – mail your original prescription or refill slip, along a completed mail-order form to the Medco
Pharmacy. Medco offers two safe, convenient automatic payment options for prescription orders. You can use e-check to have payments automatically deducted from your checking account. Or you can have payments automatically charged to the credit card of your choice. You can also pay for individual orders by money order, personal check or credit card. For more information, you can access the Medco Web site through the Prescription Drug Benefits page at www.lmhwplan.com or call the LM HealthWorks Plan at 877-458-4975.
Placing your first order. At Medco’s Web site (www.medco.com), download the mail-order form and Medco’s Health, Allergy & Medication Questionnaire (HMQ) for your first order. Just complete both forms and indicate your choice of payment. You can register a credit card with the program or ask to be billed for your order. Remember to include your doctor’s original written prescription with this first order.
Receiving your medication. You can expect to receive your medication within eight days after Medco receives your order. You can request express delivery for an additional charge.
Requesting refills. When it is time for a refill, you can: • Order online at the Medco Web site; • Call the toll-free number shown on your prescription drug ID card; or • Complete and mail the refill form sent with your medication.
58
What Prescription Drugs Are Not Covered The following items are not covered under the prescription drug plan:
Any medication that can be purchased without a prescription. Non-federal legend drugs. Allergy shot serum. Cosmetic agents. Contraceptive jellies, creams, foams, devices, implants. Implantable medications. Nutritional supplements and infant formulas. Smoking cessation agents. Therapeutic devices and appliances. Topical dental fluoride products. Immunizing agents, biologics, blood or blood plasma products (except for hemophilia factors). Any prescription if refilled in excess of the number of refills specified by the physician, or any refill
dispensed after one year from the physician’s original order.
59
Employee Assistance Program (EAP) The Employee Assistance Program (EAP) and work/life service benefits are provided through LifeMatters. The EAP is available to you and anyone living in your immediate household. You do not need to be enrolled in the LM HealthWorks Plan in order to access the EAP or work/life benefits. The EAP offers free confidential and professional behavioral or mental health counseling services to assist with personal problems. You can access up to six face-to-face counseling sessions per case or unlimited telephonic counseling. LifeMatters also offers work/life services, healthy living services and other reliable professional care and guidance in the following areas:
Personal and family problem assessment. Crisis assistance. Referrals for treatment and community resources. Provider searches for child and elder-care needs. Legal and financial consultation. Wellness information and guidance. Education seminars. Assistance with personal or work/life balance concerns. Online information, assessments and interactive tools.
Assistance from the EAP professionals is available 24 hours a day, seven days a week. Face-to-face counseling is available through the EAP on a local basis. If counseling services beyond the EAP are recommended, the counselor will coordinate with your health plan to ensure a smooth transition. To Contact LifeMatters You can access LifeMatters online at: https://www.mylifematters.com To sign in, enter the Company Code—LMC1. You can call LifeMatters at: 888-562-2243 – Toll-free calls in the U.S. and for the hearing impaired 262-574-2500 – International callers
60

Enrolling for Coverage The enrollment materials you will receive from the Lockheed Martin Employee Service Center include the information you need to properly enroll. Please be sure to follow the instructions provided and enroll within the time frame specified.
Coverage Options You can choose your medical coverage from the following options:
LM HealthWorks Plan; or No Coverage.
Coverage Categories When you enroll in the LM HealthWorks Plan, you select your coverage level based on the dependents you enroll, as follows:
Employee only; Employee + 1 dependent; or Employee + 2 or more dependents.
When making your decision, keep the following in mind:
Your eligible dependents can only be covered if you elect coverage. You and your eligible dependents can only be enrolled in one Company-sponsored medical plan. If you enroll your dependents, they will have the same plan you elect. If both you and your eligible dependent work for the Company, your coverage options are: • You may cover your dependent and your dependent may elect no coverage under his or her plan; • You may elect no coverage under your plan and be covered under your dependent’s plan; • You may both separately elect employee only coverage; or • You may both elect no coverage.
If both you and your spouse work or worked for the Company, have eligible dependent children and are covered under a Company-sponsored medical plan, each eligible dependent child can only be covered under the plan of one parent, not both. If you have more than one child, each of you may cover one or more of the children as your dependent, as long as your child does not have duplicate coverage.
Cost of Coverage You and Lockheed Martin Corporation share in the cost of coverage. The amount you pay for coverage is deducted each pay period on a before-tax basis, which reduces your federal and most state and local taxes. If before-tax benefits are prohibited by local law, your cost will be deducted on an after-tax basis. The cost for coverage is included in your enrollment materials each year. Employee contributions are subject to review and periodic change by the Company.
61

Cost for Same-sex Domestic Partner Coverage Same-sex domestic partners, and the children of same-sex domestic partners who you have not legally adopted, may not qualify as spouses or dependents for federal income tax purposes under Sections 105 and 152 of the Internal Revenue Code. Consequently, you will be taxed on the value of the Company-paid portions of the same-sex domestic partner coverage. This is known as “imputed income.” In addition, since the employee-paid portion of a non-tax qualified dependent’s coverage is deducted on a pre-tax basis, that portion attributable to same-sex domestic partner or their dependents’ coverage will be treated as taxable income. These imputed amounts will be added to your taxable income and are also subject to FICA (Social Security), FUTA (federal unemployment) and federal income tax withholding. State income tax treatment of same-sex domestic partner coverage will depend on the law of your particular state. There may be circumstances where you may treat your same-sex domestic partner (and his or her children) as dependents for federal or state income tax purpose on your tax return. You should contact your legal and tax advisors to determine if those circumstances apply to you.
How to Enroll If You: What You Need to Do to Enroll:
Are an eligible employee During the Annual Enrollment period, you can make your elections through the Service Center Online or by calling the Lockheed Martin Employee Service Center. Shortly before each enrollment period, you will receive instructions on how to enroll, as well as information about the choices available to you and their costs. Please review the information carefully and follow the instructions. Once you make your election, you will not be able to change your election until the next Annual Enrollment period unless a qualified status change or special enrollment rule applies. Please see the “Qualified Change in Status” and “Special Enrollment Rules” sections for more information.
Are a newly hired employee or a rehired former employee
If you are enrolling for the first time, or are a rehire in a different plan year, you will receive enrollment materials from the Lockheed Martin Employee Service Center. You will need to make your choices through the Service Center Online or by calling the Service Center within 30 days of your date of hire or rehire. If you are rehired in the same plan year or within 30 days of termination in a different plan year, you will automatically be re-enrolled in the benefits (if available) that you had before your termination. Once you make your election, you will not be able to change your election until the next Annual Enrollment period unless a qualified status change
62

If You: What You Need to Do to Enroll: or special enrollment rule applies. Please see the “Qualified Change in Status,” “Special Enrollment Rules” and “If Your Employment Status Changes” sections for more information.
Have a qualified change in status If you are enrolling during the year because you are a newly eligible employee or you have a qualified change in status, you will have 30 days from the date of the change in status to elect your new choices through the Service Center Online or by calling the Lockheed Martin Employee Service Center. Please note that in most cases coverage can only be effective prospectively from the date you notify the Service Center of the change. Please see the “Qualified Change in Status” and “Special Enrollment Rules” sections for more information, including when coverage will begin.
If You Do Not Enroll
If You: What Happens If You Do Not Enroll: Are an eligible employee If you are already participating in the LM
HealthWorks Plan and do not change your elections or cancel coverage during the Annual Enrollment period, you will continue the same or equivalent coverage for the following plan year. However, you will be subject to any changes in the LM HealthWorks Plan and costs of coverage.
Are a newly hired, newly eligible or rehired former employee
If you are a new hire, rehire in a different plan year or newly eligible employee and do not enroll within 30 days, you will default into no coverage and have to wait until the next Annual Enrollment period to elect medical benefits for the following plan year. Please see the “Qualified Change in Status,” “Special Enrollment Rules” and “If Your Employment Status Changes” sections for more information.
Have a qualified change in status If you have a qualified change in status that allows you to enroll or change coverage levels in the medical plan mid-year and you do not enroll within the designated 30-day period, you will not be able to enroll in coverage until the next Annual Enrollment period. Please see the “Qualified Change in Status” section for more information.
Are enrolled in an option that will no longer be available
If your current medical plan is no longer available, and you are eligible for the LM HealthWorks Plan, you will default into the LM HealthWorks Plan at your current level of coverage (Employee only or Employee + 1 dependent or Employee + 2 or more dependents) as of January 1 of the new plan year.
63

Qualified Change in Status The elections you make during the Annual Enrollment period will stay in effect through the following plan year (or the current plan year if you enroll during the year as a newly eligible employee). However, you may be able to change your elections before the next Annual Enrollment period if you have a qualified change in status (also known as a “life event”) or a special enrollment rule applies. You must make your elections within 30 days of the qualifying event for your election to become effective. (See the “When Coverage Begins” section for more information on effective dates.) If you miss the 30-day deadline, your current elections will remain in effect and you will not be able to change your coverage until the next Annual Enrollment period or until you experience another qualifying event. You need to enroll through the Service Center Online or by calling the Lockheed Martin Employee Service Center. Any change you make must be consistent with your qualified change in status. A qualified status change does not occur when your physician or provider leaves the network. Qualified changes in status under the LM HealthWorks Plan are listed in the following table.
Qualifying Life Event* LM HealthWorks Plan Changes** Marriage Add coverage for you and your eligible
dependents; or Cancel coverage for yourself (for example, if
you will be covered under your spouse’s plan). Birth, legal adoption, or placement for legal adoption of a child
Add coverage for you and your eligible dependents.
Becoming eligible for same-sex domestic partner status after completing the six-month residency requirement
Add coverage for you, your same-sex domestic partner and your same-sex domestic partner’s eligible dependent children.
Changes in employment status that affect coverage (you or your covered dependents)
Cancel coverage for you and/or your covered dependents; or
Add coverage for you and/or your eligible dependents.
Changes in your or your eligible dependent’s coverage (including coverage changes under another employer’s plan) due to an Annual Enrollment change, significant change in cost of coverage or significant change in level of benefits. (Special limitations may apply when the life event is a change in cost or coverage.)
Cancel coverage for you and/or your covered dependents; or
Add coverage for you and/or your eligible dependents.
Change in your place of residence that results in a change in your plan options and/or contributions
Change medical plan option for you and your covered dependents, if another plan is available.
Divorce, legal separation or annulment of a marriage. (Please see the “If Your Dependent Is No Longer Eligible for Coverage” section.)
Cancel coverage for your former spouse and/or dependent children who are no longer eligible. You may be required to continue coverage for your dependent children under the terms of a Qualified Medical Child Support Order (QMCSO).
64

Qualifying Life Event* LM HealthWorks Plan Changes** Death of an eligible dependent Cancel coverage for your deceased dependent and
any dependent children who are no longer eligible. If your spouse dies and he or she was covering your children under his or her plan, you may add coverage for those children if they are otherwise eligible.
Loss of your dependent’s eligibility (i.e., a dependent child who no longer meets the age limitations under the Plan). (Please see the “If Your Dependent Is No Longer Eligible for Coverage” section.)
Cancel coverage for your dependent child.
End of a same-sex domestic partner relationship. (Please see the “If Your Dependent Is No Longer Eligible for Coverage” section.)
Cancel coverage for your same-sex domestic partner, and your same-sex domestic partner’s dependent children.
Change in eligibility for Medicare or Medicaid coverage
Cancel coverage for you and/or your covered dependents; or
Add coverage for you and/or your eligible dependents.
*All changes must be made within 30 days of the qualifying event unless otherwise noted in the “When Coverage Begins” section. **In general, a Social Security number is not required to enroll a dependent in coverage. To request a change in coverage, you must contact the Lockheed Martin Employee Service Center, not the LM HealthWorks Plan claims administrator, in order for coverage to become effective. If Your Employment Status Changes In certain instances an employment status change may affect your benefit options. If your employment status changes (i.e., changing from part-time to full-time, starting or ending an international assignment or transferring jobs or union status), please contact the Lockheed Martin Employee Service Center Online to determine if you need to make new elections. If Your Dependent Is No Longer Eligible for Coverage Some of the preceding events will result in the former dependent ceasing to be eligible for coverage under the LM HealthWorks Plan, whether or not you actually cancel coverage for that dependent. For example, in the event of a divorce, annulment or legal separation, the employee’s former spouse will no longer qualify as a dependent eligible to be covered under the LM HealthWorks Plan. Similarly, if a former dependent child ceases to meet the LM HealthWorks Plan definition of eligible dependent (for example, he or she ceases to satisfy the age requirements), he or she will cease to be covered under the LM HealthWorks Plan.
65

If a dependent loses eligibility under the LM HealthWorks Plan (for example, no longer qualifies as a spouse or other dependent), you must notify the Lockheed Martin Employee Service Center within 30 days of the date he or she loses eligibility. If you do not remove your dependent from coverage within this 30-day period:
Your dependent’s coverage will be terminated retroactively to the date he or she last met the eligibility requirements (which in some circumstances may be the date you fail to provide the requested proof of eligibility); and
Payroll deductions for your current coverage level will be adjusted prospectively from the date your dependent is removed.
See the “Continuing Coverage” section for COBRA or insurance continuation information. Special Enrollment Rules If you decline to enroll yourself or your dependents because of other medical coverage, you may be able to enroll yourself or your dependents later if you request enrollment within 30 days after your other coverage ends (known as HIPAA special enrollment). In addition, if you have a new dependent as a result of marriage, birth, legal adoption or placement for legal adoption, you may be able to enroll yourself and/or your dependents provided you request enrollment within 30 days of the life event. If you qualify for a HIPAA special enrollment, you must contact the Lockheed Martin Employee Service Center within 30 days of the event. The Company will also allow a special enrollment opportunity if you or your eligible dependents either:
Lose Medicaid or Children’s Health Insurance Program (CHIP) coverage because you are no longer eligible; or
Become eligible for a state’s premium assistance program under Medicaid or CHIP. For either of these two enrollment opportunities, you will have 60 days—instead of 30—from the date of the Medicaid/CHIP eligibility change to request enrollment in the health plan, effective on the date you make your election. This 60-day enrollment period only applies to Medicaid/CHIP eligibility changes.
66

When Coverage Begins Following proper enrollment, coverage for you and your dependents will take effect as follows:
Enrollment Time Frames Coverage for You and Your Dependents Takes Effect
If you are a new hire or newly eligible employee who enrolls within 30 days of your initial eligibility date
On your first day of work or the date you meet the eligibility requirements
If you are rehired in the same plan year, your prior coverage is reinstated
On the first day you return to work
If you are rehired within 30 days after termination in a different plan year, your prior coverage is reinstated, if available
On the first day you return to work
If you are rehired in a different plan year (more than 30 days after termination), and enroll within 30 days of your first day of work
On the first day you return to work
If you enroll during an Annual Enrollment period On the first day of the following plan year or as otherwise stated in your enrollment materials
If you enroll your child within 30 days of his or her birth, legal adoption or placement for legal adoption
On the day of the qualifying event
If you enroll within 30 days of an address change that results in a change in your plan options and/or contributions
On the day of the qualifying event only to change your option, not your coverage level
If you enroll within 30 days of any other qualified status change
On the day you make the election
If you enroll within 60 days after losing coverage under Medicaid or the CHIP Plan or becoming eligible for the premium assistance subsidy
On the day you make the election
Generally, if you (or a covered dependent) are in the hospital on the date coverage would normally begin, and your hospitalization is covered under another health plan, benefits under the LM HealthWorks Plan may begin after you are discharged from the hospital. You should contact your claims administrator if this situation applies to you or a dependent. If you are on an approved leave and a qualified status change occurs, call the Lockheed Martin Employee Service Center within 30 days of the change to discuss your options.
Medical and Prescription Drug Identification (ID) Cards If you elect coverage under the LM HealthWorks Plan, medical benefits are administered by Aetna and prescription drug benefits are administered by Medco. You will receive two separate ID cards (one for medical services and one for prescription drug benefits).
67

How Claims Are Handled The following explains when and how to file claims for medical expenses under the LM HealthWorks Plan.
Claim Form Requirements Rules regarding claims depend on where you receive your care, as follows:
In-Network Benefits – you generally do not have to file a claim form. Out-of-Network Benefits – you or your provider must file a claim form. Once the LM HealthWorks
Plan claims administrator has reviewed and approved your completed claim form, you will be reimbursed for the appropriate portion of the cost.
Out-of-Area Benefits – you or your medical provider must file a claim form. Once the LM HealthWorks Plan claims administrator has reviewed and approved your completed claim form, you will be reimbursed for the appropriate portion of the cost.
How to File Claims You must file your claim within 18 months of the date of service or the claim will not be considered for reimbursement. It is your responsibility to ensure the submission of the claim, even if the provider submits the claim for you. You must complete the claim form and sign and date it. If you are attaching an itemized bill, be sure that the bill has the patient’s name, date of service, diagnosis and an itemized list of charges. Records of Expenses It is important you to keep complete records of the itemized expenses of each covered person. Important records include:
Names of physicians and other health care providers. Dates expenses are incurred. Copies of all bills and receipts.
68

Where to Submit Claims The LM HealthWorks Plan claims administrator contact information is listed below. Medical Claims Administrator Aetna
P.O. Box 981106 El Paso, TX 79998-1106
Prescription Drug Claims Administrator Medco Health Solutions, Inc. P.O. Box 14711 Lexington, KY 40512
You may also contact the LM HealthWorks Plan toll-free at 877-458-4975 or visit the LM HealthWorks Plan’s Web site at www.lmhwplan.com for more information.
Appealing Claims If a claim for reimbursement under the Plan is denied, either in whole or in part, you can appeal the denial by following the procedures described in the “Claims and Appeals Procedures” section.
If You Are Covered by More than One Medical Plan The plan has a provision to ensure that payments from all of your group plans do not exceed the amount the plan would pay if it were your only option. This provision is called Coordination of Benefits (COB). If you are enrolled in a managed care plan offered by the Company, the COB provisions (as applicable) are described in the written materials provided by the managed care plan. When you or your enrolled dependents are covered under both this plan and another health care plan, the COB provision applies. For coordination of benefits purposes, other group health plans include:
Group health care plans. State no-fault auto insurance. Pre-payment coverage for hospital or medical care provided by a HMO or other type of health care
facility. Coverage under labor-management trusteed plans, union welfare plans, employer organization plans
or employee benefits plans. Medicare and Medicaid.
How Coordination of Benefits (COB) Works Under COB, one plan is considered primary and the other secondary. The primary plan pays the benefits first, and then the secondary plan pays, depending on its COB policy. Generally, the rules to determine the order of benefit determination are:
The plan without a COB provision is the primary plan and will pay benefits before a plan with a COB provision.
The plan that covers you as an employee will be your primary plan. For example, this plan will be primary for employees of the Company, but will be secondary for employees’ spouses who are also covered by their employers’ plans.
69

When dependent children are covered under both parents’ plans, the primary plan is usually the plan of the parent whose birthday occurs first in the year. The year of birth does not matter. However, if your spouse’s employer uses a different method of determining COB, and that method results in your spouse’s plan paying primary coverage for the dependent children, that method will apply.
If a court decree places financial responsibility for the dependent child’s health care on one parent, that parent’s plan always pays first. Otherwise, the plan of the parent with custody usually pays first. If the person with custody remarries, the stepparent’s plan pays second and the plan of the parent without custody pays third.
The plan that covers the person as an active employee (one who is not laid off or retired) or that employee’s dependent pays before the plan that covers a laid-off or retired employee or that employee’s dependent. If neither plan has this rule, and, if as a result, the plans do not agree on the order of benefits, this rule is ignored.
If a person is covered under the continuation of coverage provisions of COBRA, the plan of the person who is covered as an employee (or as the employee’s dependent) pays first.
If none of these rules establish which plan is primary, the plan that has covered the person for the longest period of time becomes primary.
The claims administrators reserve the right to obtain and exchange benefit information with other organizations, claims administrators, carriers and individuals to determine what other coverage you have. It may also recover overpayments made to you or your dependents as a result of other group coverage.
Non-Duplication of Benefits The medical and dental plans provide non-duplication of benefits COB. This means that if the Company’s plan is secondary, it will pay whatever it would have paid if it were primary, minus whatever the primary plan paid. For example, assume you have covered your spouse under the plan and he or she has met the deductible under the plan. He or she then incurs an in-network charge of $1,000. The plan would pay 85% of that, or $850, if it was the only plan that covered your spouse. But let’s also assume that your spouse is covered under his or her own employer’s plan, and that plan covers the expense at 80%, or $800. The plan will pay $50—or the difference between what it would have paid if it were primary, and what the other plan paid.
COB with Medicare Generally, you become eligible for Medicare when you reach age 65. If you continue working for the Company as an eligible employee beyond age 65, your medical coverage under the plan will continue in the same manner as for any other active employee until you retire. If you are an active employee and enrolled in Medicare, under most circumstances, the plan will be primary and will pay benefits before Medicare.
COB with Medicare If You or a Dependent Is Disabled If you (or an enrolled dependent) are eligible for Medicare because of a disability, Medicare is primary, and the plan is secondary when permitted by law. When Medicare is primary, the plan will pay benefits assuming that you are enrolled in both Medicare Parts A and B—regardless of your actual Medicare enrollment. You are responsible for enrolling in and paying required Medicare Parts A and B premiums. You should contact the claims administrator if you have any questions.
70

COB with Medicaid If you or your covered dependents are covered under a state’s Medicaid program, your plan will be primary and will pay benefits before Medicaid. The plan will not reduce or deny benefits for you or your enrolled dependents to reflect eligibility to receive medical assistance under a state Medicaid program. In addition, the plan will reimburse any state Medicaid program for the cost of any items and services provided under the state program that should have been paid for by the plan and will honor any state’s right of recovery for such mistaken payments.
Recovery of Overpayment If it is determined that the plan has paid benefits in excess of what should have been paid, the plan has the right to recover the overpayment. The Company’s agents may make the collection or the plan claims administrator may choose to offset the amount of overpayment by withholding an amount from a future benefit payment.
Payments from a Third Party As used throughout this section, the term “third party” means any party actually, possibly or potentially responsible for making any payment to you due to your injury, illness or condition, including the liability insurer of such party, or any insurance carrier providing medical expense or liability coverage including, but not limited to, uninsured motorist coverage, underinsured motorist coverage, personal umbrella coverage, medical payments coverage, Workers’ Compensation coverage, no-fault automobile insurance coverage or any first party insurance coverage. For purposes of this section, “you” includes anyone on whose behalf the plan pays or provides any benefit including, but not limited to, you, your spouse or your dependent children who are entitled to receive any benefits from the plan. Immediately upon paying or providing any benefit under this plan, the plan shall be subrogated to all rights of recovery you have against any third party with respect to any payment by a third party to you due to your injury, illness or condition. In addition, if you receive any payment from a third party as a result of an injury, illness or condition, the plan has the right to recover from and be reimbursed by you all amounts this plan has paid and will pay as a result of that injury, illness or condition, up to and including the full amount you receive from all third parties. By accepting benefits (whether the payment of such benefits is made to you or on behalf of you to any provider) from the plan, you agree that if you receive any payment from any third party as a result of any illness, injury or condition, you will serve as constructive trustee over the funds that constitute such payment. Further, the plan will automatically have a lien, to the extent of benefits paid by the plan for the treatment of the illness, injury or condition for which the third party is liable. The lien shall be imposed upon any recovery whether by settlement, judgment or otherwise, related to the treatment for any injury, illness or condition for which the plan paid benefits. The lien may be enforced against any party or other source which possesses funds or proceeds representing the amount of benefits paid by the plan.
71

By accepting benefits (whether the payment of such benefits is made to you or made on behalf of you to any provider) from the plan, you acknowledge that the plan’s recovery rights are a first priority claim against all third parties and are to be paid to the plan before any other claim for damages. The plan shall be entitled to full reimbursement on a first-dollar basis from any third party payments, even if such payment to the plan will result in a recovery to you that is insufficient to make you whole or to compensate you in part or in whole for the damages sustained. The terms of this entire subrogation and right of recovery provision shall apply and the plan is entitled to full recovery regardless of:
Whether any liability for payment is admitted by any third party; or Whether the settlement or judgment received by you identifies the medical benefits the plan provided;
or Whether any portion of the settlement or judgment is allocated for payment of expenses other than
medical expenses. The plan is entitled to recover from any and all settlements or judgments, even those designated as pain and suffering or non-economic damages only. You must fully cooperate with the plan’s efforts to recover its benefits paid. It is your duty to notify the plan within 30 days of the date when any notice is given to any party, including an attorney, of your intention to pursue or investigate a claim to recover damages or obtain compensation due to injuries or illness sustained by you. You shall provide all information requested by the plan, the claims administrator or its representative, including, but not limited to, completing and submitting any applications or other forms or statements as the plan may reasonably request. Failure to provide this information may result in the termination of your health benefits or the institution of court proceedings against you. You shall do nothing to prejudice the plan’s subrogation or recovery interest or to prejudice the plan’s ability to enforce the terms of this provision. This includes, but is not limited to, refraining from making any settlement or recovery that attempts to reduce or exclude the full cost of all benefits provided by the plan.
72

When Coverage Ends Your coverage will end immediately when any of the following occur:
You are no longer an eligible employee; You stop making required contributions; You decline coverage; Your employment terminates; You are disabled and have reached the end of your short-term disability leave (you may qualify for
disability medical coverage – see the “Situations Affecting Your Coverage” section for additional information);
You retire (you may qualify for retiree medical coverage – see the “Situations Affecting Your Coverage” section for additional information);
You die; or The LM HealthWorks Plan is terminated, or is amended such that you do not meet the requirements
for coverage under the LM HealthWorks Plan. Coverage for your dependents will end immediately when any of the following occur:
Your coverage ends; Your spouse or other dependent(s) no longer meet the dependent eligibility requirements under the
LM HealthWorks Plan; You decline coverage for your dependents; You stop making the required contributions for your dependents; You die (see the “Situations Affecting Your Coverage” section for additional information regarding
coverage for your dependents if you die); or The LM HealthWorks Plan is terminated, or is amended such that you or your dependents do not meet
the requirements for coverage under the LM HealthWorks Plan. Your coverage may also be terminated if you fail a health plan dependent audit, fail to comply with a reasonable LM HealthWorks Plan rule, intentionally provide false information or for other LM HealthWorks Plan related misconduct.
73

Situations Affecting Your Coverage The following chart summarizes how your Plan coverage may be affected in certain situations. If you have any questions about the information in the chart, please contact the Lockheed Martin Employee Service Center.
Situation Impact If your work status changes
Your Plan coverage will end as of the date your status changes and you are reclassified as an employee who is no longer eligible for the Plan. If you are not eligible for any other Lockheed Martin coverage as an active employee, you will receive a COBRA or insurance continuation notice when your active medical coverage ends. Please see the “COBRA or Insurance Continuation” section for more information.
If you are on Family Medical Leave If you are on unpaid family medical leave, you have the option to continue participating or to stop participating in the Plan. Please see the “Family Medical Leave” section, and contact the Lockheed Martin Employee Service Center for more information. If you are on an approved unpaid family medical leave and a qualified status change occurs, call the Lockheed Martin Employee Service Center within 30 days of the status change to discuss your options.
If you are a non-represented disabled former employee
If you are eligible for disability medical coverage, you will receive information before the end of your short-term disability leave. Disabled employees whose employment is terminated may be eligible to continue coverage under COBRA or insurance continuation (as applicable). You will receive a COBRA or insurance continuation notice when your active medical coverage ends. Please see the “COBRA or Insurance Continuation” section for more information. The length of time coverage is continued at the end of your short-term disability leave will be included as part of the total amount of coverage allowed under COBRA. Same-sex domestic partners and children of same-sex domestic partners are not eligible for disability medical coverage but may be eligible for insurance continuation. Please see the “COBRA or Insurance Continuation” section for more information.
74

Situation Impact If you are a represented disabled employee If you are a represented employee, continuation of
coverage when you are disabled is based on the terms of your collective bargaining agreement.
If you are on personal leave Your Plan coverage continues for up to 31 days after your last day worked. Your cost will be the same as the active employee cost for coverage, subject to any applicable changes. If you do not return to active service at the end of your personal leave, you and your covered dependents may be eligible to continue coverage under COBRA or insurance continuation by paying the applicable cost. Please see the “COBRA or Insurance Continuation” section for more information.
If you are on a military leave Your Plan coverage continues for up to 31 days after your last day worked. Your cost will be the same as the active employee cost for coverage, subject to any applicable changes. If your military leave extends beyond 31 days, you and your covered dependents may be eligible to continue coverage under COBRA or insurance continuation by paying the applicable cost. Please see the “COBRA or Insurance Continuation” section for more information. Note: In certain extraordinary circumstances, the Company may extend active coverage beyond 31 days. If this occurs, you will be notified in writing.
If you leave the Company If your employment with the Company terminates, coverage for you and your covered dependents ends on the day on which you end active employment. You will receive a COBRA or insurance continuation notice when your active medical coverage ends. Please see the “COBRA or Insurance Continuation” section for more information. Expenses incurred after you leave the Company cannot be reimbursed by the plan unless you choose to continue your participation under COBRA.
75

Situation Impact If you retire Retiree medical coverage may be available to you
and your eligible dependents if you retire from the Company. If you are eligible for retiree medical benefits, you will receive information when you retire. Same-sex domestic partners and children of same-sex domestic partners are not eligible for retiree medical coverage unless required by state law, but may be eligible for insurance continuation coverage. Please see the “COBRA or Insurance Continuation” section for more information.
If you divorce or become legally separated If your spouse and/or dependent children lose coverage as a result of divorce/separation, they may have a right to elect COBRA for up to 36 months. Please see the “COBRA or Insurance Continuation” section for more information. If you divorce or become legally separated, certain court orders could require you to provide medical benefits to covered dependent children. Lockheed Martin Corporation is legally required to recognize qualified medical child support orders within the limits of the plan. If you are a party in a divorce settlement that involves coverage for dependent children under the plan, you should have your attorney contact Lockheed Martin Corporation to make sure the appropriate documents are filed and that the court order in question is actually a Qualified Medical Child Support Order that complies with governing legislation. See the “Domestic Relations Cases” section for more information.
If you die If you die while covered under the plan, coverage for your dependents may continue for six months at no cost. This six month no cost coverage will count toward the total time permitted for continuing coverage under COBRA or insurance continuation (as applicable). Please see the “COBRA or Insurance Continuation” section for more information.
If you are laid off You may be eligible to continue coverage under COBRA or insurance continuation (as applicable). Please see the “COBRA or Insurance Continuation” section for more information.
76

Continuing Coverage
Family Medical Leave If you have been employed at least one year and you have worked at least 1,250 hours within the previous 12 months, you may be able to take an approved family medical leave for up to 12 weeks. During your family medical leave you may continue health benefits coverage for yourself and your covered dependents. Leaves that are taken for the following reasons may qualify as family medical leave:
The birth of your own child. The placement of a child with you for the purpose of adoption or foster care. To care for a spouse, child or parent with a serious health condition. Your own serious health condition rendering you unable to perform your job. A qualifying exigency.
In addition, an employee who is a spouse, child, parent or nearest blood relative of a service member may take up to 26 weeks of family medical leave to care for that service member if he or she has a serious illness or injury. If you take an approved family medical leave, you may continue health benefits coverage for yourself and your covered dependents. Coverage will terminate at the end of your family medical leave period if you do not return from leave. You will then be eligible for COBRA continuation coverage (as described in the next section). To discontinue plan coverage during unpaid family medical leave, you should contact the Lockheed Martin Employee Service Center. If you do not continue your plan coverage during unpaid family medical leave and you return in the same year, your coverage will be reinstated when you return from your leave if your plans are available. If you return in the following year, you will need to make an active election. If you choose to continue coverage during the leave, you will be given the same health care benefit offerings that would have been provided if you were working, at the same cost. Your contributions will be collected in arrears when you return to work. If your coverage under the plan is discontinued during your family medical leave for any reason, your coverage will be restored when you return to work to the same level of benefits as those you would have had if you had not gone on leave and the premium payment(s) had not been missed. This includes coverage for eligible dependents. You will not be required to meet any qualification requirements, such as new or additional waiting periods, waiting for an open enrollment period or passing a medical exam, to reinstate coverage. For additional information about plan coverage during your family medical leave, contact the Lockheed Martin Employee Service Center. Family medical leave will be administered in compliance with the Family Medical Leave Act and applicable state laws.
77

COBRA or Insurance Continuation A federal law known as COBRA permits a person who loses coverage due to a “qualifying event” to continue medical coverage under the plan for a certain period of time by paying the full cost of coverage. Your same-sex domestic partner and/or his or her children may extend coverage under insurance continuation for a period that does not exceed COBRA coverage. In this section, “you” is defined as the person or persons who lost coverage due to a COBRA or insurance continuation qualifying event. If health care coverage for you or your covered dependents ends due to one of the events noted in the following chart, you may be able to continue coverage by making the required contributions under COBRA or insurance continuation. You can contact the COBRA and insurance continuation administrator at: CONEXIS Benefit Administrators P.O. Box 226985 Dallas, TX 75222-6985 Phone: 877-822-0032 Fax: 877-822-0989
COBRA Events Event Length of Coverage
If you leave the Company (for reasons other than gross misconduct)
Coverage for you and your dependents may last for up to 18 months*
If coverage stops because you no longer meet the eligibility requirements
Coverage for you and your dependents may last for up to 18 months*
If coverage stops because you are on a military leave
Coverage for you and your dependents may last for up to 24 months
If you die Coverage for your dependents may last for up to 36 months
If you and your spouse divorce or become legally separated or same-sex domestic partnership requirements are no longer met
Coverage for your spouse, same-sex domestic partner and/or eligible dependent children may last for up to 36 months**
If a child loses dependent status Coverage for that dependent child may last for up to 36 months**
If you are laid off Coverage for you and your dependents may last for up to 18 months*
If you fail to return to work at the end of your family medical leave
Coverage for you and your dependents may last for up to 18 months*
*An 18-month continuation period may be extended to 29 months if you or a dependent is considered disabled under Social Security rules within 60 days of the date you qualify for continuation of coverage due to one of the events noted above. Coverage may continue for up to 29 months as long as the disability continues throughout the continuation period and you notify the COBRA or insurance continuation administrator of the disability within 60 days after the date of the disability determination and before the end of the initial 18-month period. This 11-month extension applies to you and your dependents, not just to the disabled individual. You may be charged up to 150% of the applicable cost during the 11-month extension. **If you do not call or provide written notice to the Lockheed Martin Employee Service Center within 60 days after the event, COBRA or insurance continuation rights will be lost for that event.
78

While COBRA coverage is not available for a same-sex domestic partner and/or children of a same-sex domestic partner, insurance continuation may be available. Except as specifically noted below, insurance continuation is similar to COBRA. COBRA coverage or insurance continuation coverage runs concurrently with other employer provided coverage if a continuation provision applies. Notifying the COBRA or Insurance Continuation Administrator You or your dependent must call or provide written notice to the Lockheed Martin Employee Service Center within 60 days of a divorce, legal separation, loss of same-sex domestic partner eligibility or if a dependent child becomes ineligible for coverage. If you properly notify the Lockheed Martin Employee Service Center within the specified time frame, the Service Center will notify the COBRA administrator or insurance continuation administrator of the change and you will be issued COBRA or insurance continuation rights. Failure to notify the Lockheed Martin Employee Service Center within the required time period will result in the loss of the right to elect COBRA or insurance continuation on account of that event. The Company will notify the COBRA or insurance continuation administrator if coverage stops because you leave the Company for reasons other than gross misconduct, you no longer meet the eligibility requirements for coverage or you die. Electing COBRA or Insurance Continuation Coverage In order to elect COBRA or insurance continuation coverage (if you are entitled to do so), you and/or your covered dependents must complete and return the election form within 60 days after the later of:
The date you and/or your dependents lose coverage; or The date you and/or your covered dependents are notified of your right to continue coverage.
If you elect coverage, the effective date of the coverage is the date of the qualifying event. Premium Due Dates If you elect to continue coverage under COBRA, you must pay the initial premium (including all premiums due but not paid) within 45 days after your election. Thereafter, COBRA premiums must be paid on the first calendar day of the month, but no later than 45 days of each due date. If you elect to continue your coverage under COBRA but do not make timely payments, your coverage will be terminated retroactively to your last payment and will not be reinstated.
79

COBRA Coverage Costs You must pay 100% of the full monthly cost for coverage plus a 2% administrative charge for coverage under COBRA or insurance continuation. If you are disabled, you may be charged up to 150% of the applicable cost after the end of the initial 18-month COBRA or insurance continuation period. The cost of group health coverage is reviewed yearly and is subject to change. If you elect COBRA coverage, you will be notified by the COBRA administrator of any cost changes. COBRA coverage is not effective until you elect it and make the required payment. You have an initial grace period (45 days from the date of your initial election) to make your first premium payment. Claims for reimbursement will not be processed and paid until you have elected COBRA and made the first payment for it. If you do not make your first payment for COBRA coverage within the 45 days after the date of your timely election, you will lose all COBRA rights under the Plan. Your first payment must cover the cost of COBRA coverage from the time your coverage under the Plan would have otherwise terminated up through the end of the month before the month in which you make your first payment. You are responsible for making sure that the amount of your first payment is correct. You may contact the COBRA administrator to confirm the correct amount of your first payment. Thereafter, payments are due by the first day of each month to which the payments apply (payments must be postmarked on or before the end of the 45-day grace period). If you pay part (but not all) of the premium, and the amount you paid is not significantly less than the full amount due, you will have 30 days from the end of the initial 45-day grace period to pay the outstanding amount due. If you do not make timely payments, your COBRA coverage will be terminated as of the last day of the month for which you made timely payment. Continued Coverage Under COBRA You can continue the coverage up to the limit in the “COBRA Events” chart, as long as:
You pay the required cost for continued coverage within 30 days of the due date or within the 45-day grace period;
You do not become covered under another group health plan, or you become covered but have not satisfied any pre-existing condition limitation in that plan;
You do not become entitled to Medicare benefits; and The Company is still offering coverage to its employees.
Continuation of coverage under COBRA (or insurance continuation) will not affect your right to a converted policy—if offered by the claims administrator. You may be able to convert to an individual policy when COBRA or insurance continuation coverage ends. Adding a New Dependent While on COBRA The following provision does not apply to those on insurance continuation—it only applies to those electing coverage under COBRA.
80

If you elect COBRA coverage and you have a new child during your continuation period, your new child is entitled to receive coverage upon his or her birth, legal adoption or placement for legal adoption. You will not have to wait until the next enrollment period to enroll your child. To enroll your new child under COBRA, you must notify the COBRA administrator within 30 days of the child’s date of birth, legal adoption or placement for legal adoption. If you enroll your new child under COBRA, the child is considered a new qualified beneficiary. The child may have limited COBRA rights if a second COBRA qualifying event occurs causing the child to lose coverage under the Plan, as long as the child is otherwise eligible for coverage. For example, if you are on COBRA and later divorce, your child would be able to elect COBRA.
81

Certificate of Creditable Coverage If you lose group health coverage, you will receive a Certificate of Creditable Coverage showing how long you were covered under the Plan. You will receive this certificate from the Lockheed Martin Employee Service Center when you lose coverage or become entitled to COBRA or insurance continuation coverage, and from the COBRA administrator when your COBRA coverage ceases. You may also request a certificate either before you lose group health coverage or within 24 months of losing coverage by calling the Lockheed Martin Employee Service Center, COBRA administrator or insurance continuation administrator. The certificate may be used to reduce or eliminate a waiting period for a pre-existing condition if you become covered under a new group health plan within 63 days of the date your coverage ends under this plan.
Prescription Drug Medicare Notice of Creditable Coverage Lockheed Martin Corporation will send a Notice of Creditable Coverage to all participants stating if the plan provides prescription drug benefits that are, on average, equivalent to the standard Medicare prescription drug plan benefits. The notice is important because it can help you avoid late enrollment penalties associated with Medicare prescription drug plans that may apply given that Lockheed Martin benefits-eligible employees would generally wait until retirement to enroll in Medicare Part B and Part D. If you have a dependent that is eligible for Medicare benefits and you do not receive a Notice of Creditable Coverage, you can contact the Lockheed Martin Employee Service Center to request one.
Converting Medical Coverage You may be able to convert medical coverage to an individual policy when your group coverage ends. You may do so:
Within 31 days after your medical coverage terminates; or During the final 180 days of COBRA or insurance continuation coverage.
You will not have to provide Proof of Insurability (POI). Your converted medical insurance will be one of the insurance company’s current offerings when you pay the first premium, based on its rules for converted policies. The policy will comply with the laws of jurisdiction where the group policy was issued, or where you live if that is different. The converted policy will take effect on the day after your group coverage ends. The premium will be based on your class of risk and age and the level of benefits. For further details, contact the plan’s claims administrator.
82

Plan Administration This section provides you with important information about the Plan as required by the Employee Retirement Income Security Act of 1974, as amended (ERISA). While ERISA doesn’t require the Company to provide you with benefits, it does mandate that the Company clearly communicate to you how the plans subject to the provisions of ERISA operate and what rights you have under the law regarding plan benefits.
General Information The following summarizes important administrative information about the LMC Plan and the LMOS Plan. Please Note: Each plan can be identified by a specific plan number, which is on file with the U.S. Department of Labor.
Plan Information Overview Plan Names and Numbers Lockheed Martin Corporation Group Benefits Plan,
which is identified by the number 594. Lockheed Martin Operations Support, Inc. Benefits Plan, which is identified by the number 504. The Company assigns the plan numbers. Please use these numbers whenever you correspond with anyone about the plan.
Employer Identification Numbers Lockheed Martin Corporation: 52-1893632 Lockheed Martin Operations Support, Inc.: 22-1937239
Plan Sponsor and Plan Administrator For Lockheed Martin Corporation Group Benefits Plan: Lockheed Martin Corporation 6801 Rockledge Drive Bethesda, MD 20817 301-548-2301 For the Lockheed Martin Operations Support, Inc. Benefit Plan: Lockheed Martin Operations Support, Inc 6801 Rockledge Drive Bethesda, MD 20817 301-548-2301
Plan Year January 1 — December 31 Claims Administrator The contact information for claims administrators
for the various benefit plans can be found under “Claims Administrators.”
83

COBRA Administrator CONEXIS Benefit Administrators P.O. Box 226985 Dallas, TX 75222-6985 877-822-0032 www.conexis.com
QMCSO Administrator Lockheed Martin QDRO Department 270 Davidson Avenue, 7th Floor Somerset, NJ 08873 732-537-7025 732-537-4050 (fax)
Employee Assistance Program (EAP) Empathia, Inc. N17 W24100 Riverwood Drive Suite 300 Waukesha, WI 53188 888-562-2243 262-523-0093 (fax)
Agent for Service of Legal Process You can serve legal process on the Plan Administrator at the address listed under Plan Sponsor and Plan Administrator.
Claims Administrators This section provides specific contact information for the Plan described in this SPD.
For Issues on: Contact: At: General Information General plan administration and eligibility to participate in the Plan
Lockheed Martin Employee Service Center
Lockheed Martin Employee Service Center P.O. Box 462 Little Falls, NJ 07424 866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
Employee Service Center Online https://www.lmpeople.com – on the Internet https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on “Health and Wellness” under “Pay & Benefits,” then “Review or Change My Coverage.”
84

For Issues on: Contact: At:
LM HealthWorks Plan Filing an initial claim, benefit provisions under the LM HealthWorks Plan, payment of benefits, denial of LM HealthWorks Plan benefits
Aetna Aetna P.O. Box 981106 El Paso, TX 79998-1106 877-458-4975
Prescription Drugs Under the LM HealthWorks Plan
Filing an initial claim, benefit provisions under the LM HealthWorks Plan, payment of benefits, denial of LM HealthWorks Plan benefits If you have any questions regarding reviews and appeals, contact the LM HealthWorks Plan at 877-458-4975 and select the prescription drug prompt for further assistance.
Medco Medco Health Solutions, Inc. Direct Claims Address (paper claims) P.O. Box 14711 Lexington, KY 40512 877-458-4975 Administrative Determination Reviews & Appeals 8111 Royal Ridge Pkwy Irving, TX 75063 ATTN: Admin Reviews Urgent Administrative Appeals Phone Number: 800-946-3979 Clinical Determination Reviews & Appeals 8111 Royal Ridge Pkwy Irving, TX 75063 ATTN: Coverage Appeals Urgent Clinical Appeals Phone Number: 800-864-1135
Plan Funding The plan is self-insured—claims are paid out of the Company’s general assets.
Future of the Plan The Company expects to continue the plan as described in this booklet. However, the Company reserves to right to amend, suspend or terminate the plan in whole or part at any time. If the plan is terminated, coverage under the plan for you and your covered dependents will end, and payments under the plan will generally be limited to covered expenses incurred before the termination.
85

HIPAA Privacy Rights and Protected Health Information A federal law known as the Health Insurance Portability and Accountability Act of 1996 (HIPAA) requires group health plans to protect the confidentiality of private health information. Plan will not use or further disclose information that is protected by HIPAA (“protected health information”) except as necessary for treatment, payment, health plan operations and plan administration, or as otherwise permitted or required by applicable law. By law, the plan requires all of their business associates to also observe HIPAA’s privacy rules. Under HIPAA, you have certain rights with respect to your protected health information, including certain rights to see and copy the information, receive an accounting of certain disclosures of the information and, under certain circumstances, amend the information. You also have the right to file a complaint with the plan or with the Secretary of the U.S. Department of Health and Human Services if you believe your rights under HIPAA have been violated. To the extent required by applicable law, the plan will maintain a privacy notice, which provides a complete description of your rights under HIPAA’s privacy rules. For a copy of the HIPAA Notice of Privacy Practices, please contact the Lockheed Martin Employee Service Center. If you have questions about the privacy of your health information, or if you wish to file a complaint under HIPAA, you should contact the applicable claims administrator or the Plan’s Privacy Officer.
Protection Against the Use of Genetic Information The Plan will not:
Deny, limit or cancel health care coverage for you or your dependents based on genetic information; Adjust premiums or contributions on the basis of genetic information; or Request, require or purchase genetic information for underwriting purposes or with respect to any
individual in advance of or in connection with such individual’s enrollment.
86

Claims and Appeals Procedures This section includes the general claims and appeals procedures for the Plan. You or your authorized representative may file a claim for eligibility and/or a claim for benefits. An authorized representative is any person (such as a spouse, parent, medical provider, or executor of your estate or attorney) whom you authorize in writing to act on your behalf. The Plan will also recognize representatives authorized through a court order giving a person authority to submit claims on your behalf. Additionally, in the case of a claim involving Urgent Care, a provider with knowledge of your condition may always act as your authorized representative. Please note: If your or your dependent’s coverage is terminated retroactively (often referred to as a rescission of coverage), you may file a claim using the following procedures even if there has not been a specific benefit claim denial associated with that termination.
Claims for Eligibility The Plan Administrator is generally responsible for determining whether someone is eligible for the Plan and for deciding appeals of denied claims involving questions of eligibility to participate in the Plan or changes in coverage elections such as the addition or deletion of dependents (these will be referred to as Eligibility Claims). In carrying out these functions, the Plan Administrator has full discretionary authority to interpret and construe the terms of the Plan, to decide questions regarding eligibility for the Plan and to make any related findings of fact. The Plan Administrator can act through its delegate. The decision of the Plan Administrator shall be final and binding, to the full extent permitted by law. Where the claim involves eligibility to participate, or addition or deletion of dependents, you should contact the Lockheed Martin Employee Service Center at: Lockheed Martin Employee Service Center P.O. Box 462 Little Falls, NJ 07424 866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
Claims for Benefits The applicable claims administrator for the particular benefit (see the “Claims Administrators” section) is responsible for determining whether benefits are payable under the Plan, determining the amount of benefits payable, if any, and deciding appeals of denied claims for benefits (these will be referred to as Benefit Claims). In carrying out these functions, including conducting a full and fair review of denied claims, the claims administrator has the full discretionary authority to interpret and construe the terms of the Plan and to decide questions related to the payment of benefits. The decision of the claims administrator shall be final and binding to the full extent permitted by law.
87

You or your authorized representative should file a written claim for benefits with the claims administrator. To ensure timely processing of your claim, you should contact the claims administrator to confirm the claim filing address. Time Frame for Claim Reviews Regardless of the type of claim (Eligibility Claim or Benefits Claim), the review period varies based on whether the claim is Urgent Care, Pre-Service, Post-Service or ongoing (Concurrent). The review periods for each of these are outlined below. “Urgent Care” Claims An “Urgent Care” claim is one that generally means services received for a sudden illness, injury or condition that is not an emergency but requires immediate outpatient medical care that cannot be put off. An urgent situation is one that is severe enough to need prompt medical attention to avoid serious deterioration of your health; this includes a condition that would subject you to severe pain that could not be adequately managed without proper treatment. If you submit an “Urgent Care” claim, you or your physician will be notified of the claim determination within 72 hours after the claim is received (after January 1, 2012, 24 hours). If additional information is required, the claims administrator will notify you or your physician as soon as possible, but no later than 72 hours after receipt of the claim (after January 1, 2012, 24 hours). You or your physician will be given a reasonable additional amount of time (but no less than 48 hours) to provide the information, and will be notified of the decision no later than 48 hours after the end of that additional time period or after receipt of the information, if earlier. “Pre-Service” Claims and “Post-Service” Claims In some other cases where care is not considered urgent, the Plan may require you to obtain advance approval of a service, supply or procedure before a benefit will be payable. The request for advance approval is considered a “Pre-Service” claim. The claims administrator (or in the case of Eligibility Claim, the Plan Administrator) will notify you of the decision no later than 15 calendar days after receipt of the Pre-Service claim. For claims after the service has taken place, or “Post-Service” claims, you will normally be notified of the decision within 30 calendar days after receipt of the claim. For either a Pre-Service or a Post-Service claim, these time periods may be extended up to an additional 15 calendar days due to circumstances outside the Plan’s control. If an extension is required, you will be notified of the need for the extension before the end of the initial 15- or 30-day period. The notice will set forth the circumstances requiring the extension of time and the date by which the claims administrator expects to make a decision. For example, the 15- or 30-day time period may be extended because you have not submitted sufficient information, in which case, you will be notified of the specific information necessary and given an additional period of at least 45 calendar days after receiving the notice to furnish that information.
88

“Concurrent” Claims If you are receiving an ongoing course of treatment (a “Concurrent” claim), you and your physician will be notified in advance if the Plan intends to terminate or reduce benefits for the course of treatment, so that you or your physician will have an opportunity to appeal the decision before the termination or reduction takes effect. If the course of treatment involves “Urgent Care,” you or your physician may request an extension of the course of treatment at least 24 hours before its expiration. The claims administrator will notify you or your physician of the decision within 24 hours after receipt of the request. Claim Denials If your claim is denied in whole or in part, you will be notified in writing within the time periods outlined above for the applicable type of claim. The notice will state the following:
Specific reasons for the denial. Plan provisions that support the denial. A description of any additional information needed to review your claim request. If an internal rule, guideline, protocol or other similar criterion was relied on in making the benefit
claim denial on your appeal, a copy of the specific rule, guideline, protocol or other similar criterion, or a statement that was relied on in making the benefit claim denial on review will be provided free of charge upon request.
If the denial is based on a medical necessity or experimental treatment or similar exclusion or limit, either an explanation of the scientific or clinical judgment for the determination, applying the terms of the Plan to the claimant’s medical circumstances, or a statement that such explanation will be provided free of charge upon request.
Instructions for requesting a review of your claim denial and the applicable time limits, including information regarding your right to bring a civil lawsuit under Section 502(a) of ERISA following a benefit claim denial on review.
If applicable, a description of the appeal process for claims involving Urgent Care. Internal Appeals Process If your claim is denied in whole or in part, you or your authorized representative can request an internal review of (or appeal) the denied claim within the time limits set forth in this section for the applicable type of claim. The review will take into account all comments, documents, records and other information you submit relating to the claim, without regard to whether such information was submitted or considered in the initial benefit determination. If you wish, you or your authorized representative may review the appropriate Plan documents and submit written information supporting your claim to the claims administrator or Plan Administrator. If you are receiving an ongoing course of treatment, the Plan will not terminate or reduce benefits for the ongoing course of treatment without giving advance notice and the opportunity for review. If you have received pre-authorization for an ongoing course of treatment, you will continue to be covered, pending the outcome of the internal appeal. This means that the Plan cannot terminate or reduce any ongoing course of treatment without providing advance notice and the opportunity for review. If the Plan fails to meet the requirements of the internal claims and appeals process for your claim, you are deemed to have exhausted the internal process, and you may begin an external review request immediately.
89

You will be provided, upon request and free of charge, reasonable access to and copies of all documents, records or other information relevant to your claim for benefits. You will be able to review your file and present information as part of the review. Additional rules apply if the appeal relates to a Benefit Claim, or to an Eligibility Claim which either has a direct adverse effect on a specific benefit claim or involves a retroactive termination of coverage (other than for failure to pay premiums). In that case, before making a benefit determination on review, the Claims Administrator or Plan Administrator, as applicable, will provide you with any new or additional evidence considered or generated by the Plan, as well as any new or additional rationale to be used in reaching the decision. You will be given this information in advance of the date on which the notice of final appeal decision is made to give you a reasonable opportunity to respond. Your internal appeal will be reviewed and decided independently to the original claim process. The appeal decision will not be made by someone who was involved in the original decision or by someone who reports to the initial decision maker. The Claims Administrator or Plan Administrator, as applicable, will ensure that all claims and appeals are handled impartially. The person involved in making the decision will not receive compensation, promotion, continued employment or other similar items based upon the likelihood he or she will support a denial of Plan benefits. In deciding an internal appeal of a claim that was denied based on a medical judgment, a provider with appropriate training and experience in the field of medicine involved will be consulted (such provider will not be someone who was consulted in connection with the original claim denial nor someone who reports to the original consultant). You may request the identity of any medical or vocational experts consulted in making a determination of your appeal. Time Limits You or your authorized representative have 180 calendar days from the date of the claims denial to make a written request for an internal review or appeal to the claims administrator (for benefit claims) or Plan Administrator (where the claim involves an Eligibility Claim). Generally, there may be two levels of internal appeal for appeals relating to benefit claims. Level One Internal Appeal The claims administrator will respond in writing with a decision within 15 calendar days after it receives an appeal for a required Pre-Service or Concurrent claim determination and within 30 calendar days after it receives an appeal for a Post-Service claim determination. If more time or information is needed to make the determination, the claims administrator will notify you in writing of the need for an extension of up to 15 calendar days and to specify any additional information needed to complete the review. Level Two Internal Appeal If you are dissatisfied with the claims administrator’s level one internal appeal decision, you may request a second review. The second level follows the same process as the first level of appeal. Other Rules Regarding Timing For Pre-Service and Concurrent claim determinations, the claims administrator will review the internal appeal within 15 calendar days and for Post-Service claims, the claims administrator will review the claim within 30 calendar days. If more time or information is needed to make the determination, the claims administrator will notify you in writing of the need for an extension of up to 15 calendar days and to specify any additional information needed to complete the review. You will be notified in writing of the appeal decision within the applicable timeframe.
90

Expedited Internal Appeal In the case of a claim involving Urgent Care (generally, where you need to have this process expedited to prevent serious risk to your health, life or ability to regain maximum functionality, or in the opinion of your physician to prevent severe pain that cannot be managed without the requested services), a request for an expedited internal appeal may be submitted orally or in writing. The claims administrator’s medical reviewer, in consultation with your physician, will decide if an expedited appeal is necessary. All necessary information, including the Plan’s benefit determination on review, shall be transmitted between the claims administrator and the claimant by telephone, facsimile or other available similarly expeditious method. The decision on expedited appeals will be communicated orally within 72 hours and will be followed up in writing. Note: In certain situations, you can request an expedited external review at the time you receive the claim denial. You may do this if the Benefit Claim denial involves a medical condition for which the timeframe for completion of an expedited internal appeal would seriously jeopardize the life or health of the claimant or would jeopardize the claimant’s ability to regain maximum function and you have filed a request for an expedited internal appeal. (See “External Review of Claims” section). Eligibility Claims For appeals regarding eligibility to participate or changes in coverage elections such as the addition or deletion of dependents, there is one level of internal appeal. The Plan Administrator or delegate will give you a written decision regarding the review of your claim within 30 calendar days for Urgent Care or Pre-Service claims (or 60 calendar days for Post-Service claims) of receipt of your request for review. Decision on Internal Appeal If your claim is approved, you will receive the appropriate benefit from the Plan. If your claim is denied on internal appeal, in whole or in part, you will receive a written notice from the claims administrator or Plan Administrator within the review period outlined above for the applicable type of claim. The notice will include the following:
The specific reasons for the decision. A reference to the specific Plan provisions upon which the decision is based. A statement that you are entitled to receive, upon request and free of charge, reasonable access to and
copies of all documents, records and other information relevant to your claim for benefits. A statement describing any voluntary appeal procedures offered by the Plan and your right to obtain
these procedures. If an internal rule, guideline, protocol or other similar criterion was relied on in making the benefit
claim denial on your appeal, a copy of the specific rule, guideline, protocol or other similar criterion, or a statement that was relied on in making the benefit claim denial on review will be provided free of charge upon request.
If the adverse decision is based on a medical necessity or experimental treatment or similar exclusion or limit, either an explanation of the scientific or clinical judgment for the determination, applying the terms of the Plan to the claimant’s medical circumstances, or a statement that such explanation will be provided free of charge.
Where required, a statement that there may be other voluntary alternative dispute resolution options. The written denial on appeal will include a statement regarding your right to bring a timely civil lawsuit under Section 502(a) of ERISA following a benefit claim denial on appeal.
91

Claims and Internal Appeals Time Limits – At a Glance The time limits applicable to claims and appeals are summarized in the chart below.
Event Urgent Health Claims
Concurrent Health Claims
Pre-Service Health Claims
Post-Service Health Claims
How long does the Plan have to make an initial claim decision?
ASAP, but no later than 72 hours after receipt of the claim (after January 1, 2012, 24 hours)
ASAP, at least 24 hours before the end of the treatment
No later than 15 days after receipt of the claim
No later than 30 days after receipt of the claim
How long does a participant have to appeal the decision?
180 days after receipt of the adverse decision
180 days after receipt of the adverse decision
180 days after receipt of the adverse decision
180 days after receipt of the adverse decision
How long does the Plan have to determine the appeal?
ASAP, but no later than 72 hours after receipt of the request
Follows the Urgent, Pre-Service or Post-Service time frame appropriate to the service
30 days after receipt of the appeal (15 days if two levels of appeal)
60 days after receipt of the appeal (30 days if two levels of appeal)
External Review of a Claim If your internal appeal is denied, you may request an external review of your claim within four months after being notified of a denied claim. External review is not automatic; you must request it. You will be informed, in writing, of the procedures for requesting an external review. The external review is conducted by an independent review organization (IRO) accredited as required under federal law, and its decision is binding on you and the Plan, except to the extent other remedies are available under federal law. Please note that the external review process does not apply to claims or appeals involving Eligibility Claims or issues (see “Claims for Eligibility” section), even where the Eligibility Claim has a direct adverse effect on a particular benefit claim. Standard External Review Within five days of receiving your request, the Plan will conduct a “preliminary review” to ensure the request can be sent for external review (for example, to ensure the denied claim or appeal does not relate to Plan eligibility and that the request is complete). The Plan will notify you in writing once the preliminary review is complete; you will be informed then if you need to submit additional information and the deadline for doing so. Alternatively, where the decision relates to an Eligibility Claim or issue, the Plan may notify you at the time of the appeal decision that the claim is not subject to eternal review. Such notice will include the reason why the claim is not eligible for external review. The IRO assigned to conduct your external review will notify you of its acceptance of the assignment and you will have 10 business days to submit any additional written information for the IRO to consider. (Within one business day of receiving your additional information, the IRO must share the new material with the Plan. After considering the new information, the Plan may reconsider and reverse its claim or appeal denial, stopping the external review procedure.)
92

The IRO must conduct its external review without giving any weight to the Plan’s earlier conclusions or decision. The IRO may consider information beyond the denied claim’s records, such as the claimant’s medical history, appropriate practice guidelines and Plan terms. The IRO must complete its external review and send notice of its decision to you and the Plan within 45 days. If the IRO reverses the Plan’s earlier decision to deny a claim or appeal, the Plan will immediately provide coverage or payment for the claim. Expedited External Review You may request an expedited external review if the claimant has a medical condition where the timeframe for completion of a standard External Review would seriously jeopardize the life or health of the claimant or would jeopardize the claimant’s ability to regain maximum function, or if the final internal appeal denial concerns an admission, availability of care, continued stay, or health care item or service for which the claimant received emergency services, but has not been discharged from a facility. (As noted in the “Internal Appeals Process” section, in certain circumstances you may also initiate a request for expedited External Review at the time of the initial claims denial). Immediately upon receipt of a request for expedited External Review, the Plan will determine whether the request meets the reviewability requirements set forth above for a standard External Review. The Plan must immediately send you a notice of its eligibility determination. The IRO will render a decision as expeditiously as your medical condition or circumstances require, but in no event more than 72 hours after the IRO receives the request for an expedited External Review. If the notice is not in writing, within 48 hours after the date of providing the notice, the IRO must provide written confirmation of the decision to you and the Plan.
Collective Bargaining Agreements The Plan is maintained pursuant to collective bargaining agreements. Copies of the agreements are available to covered employees and may be requested from your Human Resources office. If you wish to obtain your own copy, submit a written request to your Human Resources office.
93

Your Rights Under ERISA As a participant in the Plan, you are entitled to certain rights and protection under the Employee Retirement Income Security Act of 1974 (ERISA). ERISA provides that all Plan participants shall be entitled to: Receive Information About Your Plan and Benefits
You are entitled to examine without charge, at the Plan Administrator’s office and at other specified locations, such as work sites and union halls, all documents governing the Plan, including insurance contracts and collective bargaining agreements.
You can obtain a copy of the latest annual report (Form 5500 Series) filed by the Plan with the U.S. Department of Labor, which is available at the Public Disclosure Room of the Employee Benefits Security Administration.
You can obtain, upon written request to the Plan Administrator, copies of documents governing the operation of the Plan, including insurance contracts and collective bargaining agreements, copies of the latest annual report (Form 5500 Series) and an updated Summary Plan Description. The Plan Administrator may make a reasonable charge for the copies.
You are entitled to receive a summary of the Plan’s annual financial report. The Plan Administrator is required by law to furnish each participant with a copy of this summary annual report.
You can receive a copy of the Qualified Medical Child Support Order procedures without charge. You can receive a listing of in-network providers without charge.
Continue Group Health Plan Coverage You also have the right to:
Continue health care coverage for yourself, spouse or dependents (if eligible) if you lose coverage as a result of a qualifying event. You or your dependents may have to pay for such coverage.
Reduce or eliminate exclusionary periods of coverage for pre-existing conditions under your group health plan if you have creditable coverage from another plan. The Plan does not limit coverage on account of a pre-existing condition.
Prudent Actions by Plan Fiduciaries In addition to creating rights for Plan participants, ERISA imposes duties upon the people who are responsible for the operation of the employee benefit plan. The people who operate your Plan, called “fiduciaries” of the Plan, have a duty to do so responsibly and in the interest of you and other Plan participants and beneficiaries. No one, including your employer, your union or any other person, may terminate your employment or otherwise discriminate against you in any way to prevent you from obtaining a benefit or exercising your rights under ERISA.
94

Enforce Your Rights If your claim for a benefit is denied or ignored, in whole or in part, you have a right to know why this was done, to obtain copies of documents relating to the decision without charge and to appeal any denial, all within certain time schedules. Under ERISA, there are steps you can take to enforce the above rights. For instance, if you make a written request for a copy of Plan documents or the latest annual report from the Plan and do not receive them within 30 days, you may file suit in a federal court. In such a case, the court may require the Plan Administrator to provide the materials and pay you up to $110 a day until you receive the materials, unless the materials were not sent because of reasons beyond the control of the Plan Administrator. If you have a claim for benefits that is denied or ignored, in whole or in part, you may file suit in a state or federal court. In addition, if you disagree with the Plan’s decision or lack thereof concerning the qualified status of a medical child support order, you may file suit in federal court. If it should happen that the Plan fiduciaries misuse the Plan’s money, or if you are discriminated against for asserting your rights, you may seek assistance from the U.S. Department of Labor, or you may file suit in a federal court. The court will decide who should pay court costs and legal fees. If you are successful, the court may order the person you have sued to pay these costs and fees. If you lose, the court may order you to pay these costs and fees, for example, if it finds your claim is frivolous. Assistance with Your Questions If you have questions about your Plan, you should contact the Plan Administrator. If you have questions about this statement or about your rights under ERISA, or if you need assistance in obtaining documents from the Plan Administrator, you should contact the nearest office of the Employee Benefits Security Administration, U.S. Department of Labor (listed in your local telephone directory), or the Division of Technical Assistance and Inquiries, Employee Benefits Security Administration, U.S. Department of Labor, 200 Constitution Avenue, NW, Washington, DC 20210. You may also obtain certain publications about your rights and responsibilities under ERISA by calling the publications hotline of the Employee Benefits Security Administration. To obtain the addresses and telephone numbers of the District offices, you may access the Department of Labor Employee Benefits Security Administration Web site at http://www.dol.gov/ebsa.
Your Rights Under the Newborns’ and Mothers’ Health Protection Act Group health plans and health insurance issuers offering group insurance coverage generally may not, under federal law, restrict benefits for any otherwise covered hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a normal vaginal delivery, or less than 96 hours following a caesarean section. However, federal law generally does not prohibit the mother’s or newborn’s attending providers, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours, or 96 hours, as applicable. In any case, plans and issuers may not, under federal law, require that a provider obtain authorization from the Plan or issuer for prescribing a length of stay not in excess of 48 hours, or 96 hours, as applicable.
95

Your Rights Under the Women’s Health and Cancer Rights Act Federal law requires a group health plan to provide coverage for the following services to an individual receiving Plan benefits in connection with a mastectomy:
Reconstruction of the breast on which the mastectomy has been performed. Surgery and reconstruction of the other breast to produce a symmetrical appearance. Prostheses and physical complications for all stages of a mastectomy, including lymphedemas
(swelling associated with the removal of lymph nodes). These services shall be provided in a manner determined in consultation with the attending physician and the patient. Coverage for breast reconstruction and related services will be subject to deductibles and coinsurance amounts that are consistent with those that apply to other benefits under the Plan.
96

Glossary of Terms Active course of treatment – a program of planned health care services. It starts on the first day your doctor provided treatment for your condition and covers a certain number of services or treatment period. Aetna Navigator® – an online tool that provides access to information about your benefits and how you are using them. Aexcel® – a network of specialists—called Aexcel-designated providers—who are higher performers, in terms of clinical performance and efficiency, in their specialty areas. Aexcel-designated providers are noted with a blue star in DocFind®, the online provider directory. When you use an Aexcel-designated provider, the plan pays a higher level of in-network benefits. Behavioral health provider/practitioner – a licensed organization or professional providing diagnostic, therapeutic or psychological services for behavioral health conditions. Body Mass Index (BMI) – a practical marker that is used to assess the degree of obesity and is calculated by dividing the weight in kilograms by the height in meters squared. Brand-name drug; brand drug – a medicine made by the pharmaceutical company that developed and patented it (see “Preferred brand-name drug” and “Non-preferred brand-name drug”). Calendar year – the period of time starting January 1 and ending December 31. Chiropractic care – services rendered by a Doctor of Chiropractic (D.C.) and spinal manipulations and related services performed by a doctor of chiropractic care. Chronic condition; chronic disease – a medical condition or disease that is ongoing or lasts for a long time is referred to as “chronic.” Examples of chronic conditions are diabetes, asthma, chronic obstructive pulmonary disease and chronic kidney disease. Claims administrator – the responsible party for managing claims for services received under the LM HealthWorks Plan. Coinsurance – your share of a covered expense, expressed as a percentage. Company – Lockheed Martin Corporation. With respect to the LMOS Plan, “Company” also means Lockheed Martin Operations Support, Inc. Compassionate Care Program – a coordinated, interdisciplinary program designed to meet the physical, psychological, spiritual and social needs of terminally ill persons and their families. Services are provided by hospice care offering palliative, curative, supportive and other health services through home or inpatient care during the terminal illness. Hospice care may be provided by a hospital, skilled nursing facility, home health care agency or hospice facility. Condition Management Program – a program of one-on-one support, information and guidance to help participants manage a specific chronic medical condition or disease and enjoy better overall health.
97

Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA), as Amended – a federal law that allows you and/or your covered dependents to continue health care coverage on an after-tax basis (under certain circumstances) when coverage would otherwise have ended. Cost of Care Tools – online tools, available at Aetna Navigator, you can use to arrive at the average estimated costs of medical procedures, treatments and tests in your area. You may also use the Price-a-Medication Tool at Medco’s prescription drug Web site to receive cost estimate information on the medication(s) you take, as well as lower cost alternatives, if available. Covered active duty – active military duty in connection with a national emergency, or a military action, operation or hostilities outside the U.S. Covered expense – the charge for a health care service or supply allowable under the LM HealthWorks Plan. Covered military member – your spouse, parent or son/daughter of any age on covered active duty in the regular armed forces, reserves or National Guard. Covered person – a Company employee or eligible dependent that is enrolled in the LM HealthWorks Plan. Custodial care – care that provides a level of routine maintenance for the purpose of meeting personal needs or helping with the functions or activities of daily living. This is care that can be provided by a layperson who does not have professional qualifications, skills or training. Deductible – the amount of covered medical expenses you pay each calendar year (January 1 through December 31) before the LM HealthWorks Plan will begin to pay for benefits. The HealthFund helps offset your deductible by paying covered medical expenses as they are incurred during the year, until the HealthFund is depleted. The amount of the deductible depends on the coverage level you select at enrollment (i.e., Employee only, Employee + 1 dependent, Employee + 2 or more dependents) and whether care is provided in-network or out-of-network. The deductible does not apply to prescription drug or preventive care expenses. Detoxification – the process by which an alcohol- or drug-intoxicated or dependent person is medically managed while he or she eliminates from his or her system:
Intoxicating alcohol or drug; Alcohol or drug-dependent factors; or Alcohol in combination with drugs.
The process must minimize the physiological risk to the patient, and take place in a facility that meets any applicable licensing standards established by the jurisdiction in which it is located. DocFind® – the online provider directory that lists doctors, hospitals and other health care providers who belong to the LM HealthWorks Plan’s network (including Aexcel-designated providers). You can use this tool to search for a particular provider or find all in-network providers within a certain geographical area. Durable medical equipment – any equipment that can withstand repeated use, is not disposable, is medically necessary to treat an injury or illness and is generally not useful to a person who is not injured or sick.
98

Eligible expense – cost of services covered under the LM HealthWorks Plan. Emergency; medical emergency – a serious and usually sudden threat to a person’s health or life resulting from illness or injury that requires immediate attention at a hospital or trauma center. Emergency admission – any hospital admission for an inpatient stay for a condition that:
Has a sudden and unexpected onset; and Requires prompt care to protect life, relieve severe pain, or diagnose and treat symptoms that, with
delay, could result in serious injury. Emergency care – treatment given in a hospital’s emergency room to evaluate and treat an emergency medical condition. Emergency medical condition – a recent and severe medical condition, including (but not limited to) severe pain, which would lead a prudent layperson possessing an average knowledge of medicine and health, to believe that his or her condition, illness or injury is of such a nature that failure to get immediate medical care could result in:
Placing your health in serious jeopardy; or Serious impairment to bodily function; or Serious dysfunction of a body part or organ; or In the case of a pregnant woman, serious jeopardy to the health of the fetus.
Experimental or investigational procedures – services or supplies as determined by the claims administrator to be experimental or investigational because:
There are insufficient outcomes data available from controlled clinical trials published in peer reviewed literature to substantiate its safety and effectiveness for the treatment of the disease or injury involved; or
If required by the FDA, approval has not been granted for marketing; or A recognized national medical or dental society or regulatory agency has determined, in writing, that
it is experimental, investigational or for research purposes; or The written protocols or written informed consent used by the treating facility or any other facility
studying substantially the same drug, device, procedure or treatment states that it is experimental, investigational or for research purposes.
However, this exclusion will not apply with respect to services or supplies (other than drugs) received in connection with a disease if the claims administrator determines that:
The disease can be expected to cause death within one year in the absence of effective treatment; and The care or treatment is effective for that disease or shows promise of being effective as demonstrated
by scientific data. In making this determination, the claims administrator will take into account the result of a review by a panel of independent medical professionals (selected by the claims administrator) who treat the type of disease involved.
Also, this exclusion will not apply with respect to drugs that:
Have been granted treatment investigation new drug (IND) or Group C/Treatment IND status; or Are being studied at the Phase III level in a national clinical trial sponsored by the National Cancer
Institute.
99

Explanation of Benefits (EOB) – a brief report that explains what medical services were billed and paid under the LM HealthWorks Plan. Formulary or preferred drug list – list of brand-name and generic drugs that are preferred by your prescription benefit program. This formulary contains a broad list of medications for most medical conditions that are treated on an outpatient basis. Because they are preferred medications, you will usually pay a lower copayment than you would for non-preferred drugs. Generic drug; generic medication – medication that is no longer sold exclusively under the patent of the pharmaceutical company that developed it. According to the U.S. Food and Drug Administration (FDA), generic equivalents are identical to their brand-name counterparts in dosage form, safety, strength, route of administration, quality and performance. The FDA ensures that generic equivalents are as safe and effective as the original brand-name drugs. Generic drugs are generally the most cost effective option under the LM HealthWorks Plan. Health History Report – an online, claims-based report that shows health care services you received (under the LM HealthWorks Plan), when you received them and who provided them. Your Health History Report appears on your Aetna Navigator Web site home page. Hospice care – a coordinated, interdisciplinary program designed to meet the physical, psychological, spiritual and social needs of terminally ill persons and their families. A hospice care program may also provide palliative and supportive medical, nursing and other health services through home or inpatient care during the terminal illness. Hospice care services – any services provided by a hospital, skilled nursing facility or similar institution, home health care agency, hospice facility or any other licensed facility or agency under a hospice care program. Hospital – an institution constituted, licensed and operated in accordance with the laws pertaining to hospitals, which maintains on its premises all the facilities needed to diagnose and treat injury and sickness. It is an institution that qualifies as a hospital and a provider of services under Medicare and is accredited as a hospital by the Joint Commission on the Accreditation of Hospitals. A hospital can specialize in the treatment of mental illness, alcoholism, drug addiction or other related illness. It can also provide residential treatment programs, but only if it is constituted, licensed and operated in accordance with laws of legally authorized agencies responsible for medical institutions. It provides all treatment for a fee, by or under the supervision of physicians on an inpatient basis with continuous 24 hour nursing service by qualified nurses. An institution, which is, other than incidentally, a place for rest, a place for the aged, or a nursing home will not be considered a hospital.
100

Hospitals also include the following:
Ambulatory surgical facility – a facility approved by the claims administrator as meeting established criteria for handling surgical cases on a same-day basis. This may also include a birthing center and surgery performed in a hospital on an outpatient basis.
Skilled nursing facility – an institution that is primarily engaged in providing inpatient skilled nursing care and related services for patients who require medical or nursing care. A skilled nursing facility may also provide physical rehabilitation services for injured or sick persons. To do so, it must be constituted, licensed and operated in accordance with the laws of legally authorized agencies and must maintain on its premises all the facilities needed to provide medical treatment of injury or sickness. It must not be, other than incidentally, a place for rest or domiciliary care; for the aged, blind, deaf, mentally deficient or those suffering from tuberculosis; or a hotel or motel. All skilled nursing care must be provided for a fee by or under the supervision of physicians with nursing service by nurses.
Hospital Comparison Tool – an online tool within the Aetna Navigator Web site under the LM HealthWorks Plan that allows you to compare hospitals in your area according to measures you select. Some of the comparison measures include average inpatient stays, readmission rates and competencies in certain specialized or complex care. In-network or network provider – a health care professional or facility that has contracted with Aetna to provide LM HealthWorks Plan members with services based on pre-agreed fee structures and other criteria. In order to join the network, providers must undergo a credentialing process that considers factors such as education and training, licensure, certification and/or registration to practice in a health care field. Care provided by an in-network provider is called in-network care. Likewise, benefits paid for services given by an in-network provider are called in-network benefits. Injury – an accidental bodily injury that is the sole and direct result of:
An unexpected or reasonably unforeseen occurrence or event; or The reasonable unforeseeable consequences of a voluntary act by the person.
An act or event must be definite as to time and place. Institute of Excellence (IOE) – a hospital or other facility that has contracted with Aetna to furnish services or supplies to an IOE patient in connection with specific transplants at a negotiated charge. A facility is an IOE facility only for those types of transplants for which it has signed a contract. Institute of Quality (IOQ) – a hospital or other facility that has contracted with Aetna to furnish services or supplies to an IOQ patient in for bariatric surgery at a negotiated charge. The hospital or facility must meet Aetna’s designation requirements for clinical quality, value and access for bariatric surgery to be selected for the Institutes of Quality (IOQ) Bariatric Surgery network. Insurance continuation – a provision that allows a same-sex domestic partner and his or her children to continue medical plan coverage on an after-tax basis (under certain circumstances) when coverage would otherwise have ended. Such coverage is similar to that of COBRA. LM6 health coaching program – a six-month Health Coaching program that targets medium-risk individuals. The program involves an average of three to four sessions over a six-month period.
101

LM12 health coaching program – a 12-month Health Coaching program that targets high-risk individuals. The program involves an average of six to eight sessions over a 12-month period. Mail-order service (Medco Pharmacy) – a service that delivers your prescriptions directly to your home. Medicaid – a state program of medical aid for needy persons, established under Title XIX of the Social Security Act of 1965, as amended. Medically necessary – services or supplies to the extent that they are needed for the diagnosis of a sickness, injury or for pregnancy or for the medical care of a diagnosed sickness, injury or pregnancy. To be considered “medically necessary” a service or supply must be determined by the claims administrator to meet all of these tests:
It is ordered by a physician. It is recognized throughout the physician’s profession as safe and effective, is required for the
diagnosis or treatment of a sickness or injury, or pregnancy, and is employed appropriately in a manner and setting consistent with generally accepted United States medical standards.
It is not educational in nature (that is, the primary purpose of the service or supply must not be to provide the patient with any of the following: training in the activities of daily living, instruction in scholastic skills such as reading and writing, preparation for an occupation or treatment for learning disabilities).
It is not experimental or investigational. For purposes of the LM HealthWorks Plan, services or supplies that are provided only because an unnecessary service or supply is being provided will also be considered not medically necessary. In the case of an inpatient hospital stay, in addition to meeting the above tests, the length of the stay and hospital services and supplies will be considered medically necessary only to the extent that the claims administrator determines them to be not allocable to the scholastic education or vocational training of the patient. Medicare – is the Health Insurance for the Aged and Disabled provisions of Title XVIII of the Social Security Act of the United States, as enacted or later amended. Coverage is available to most U.S. residents age 65 and older, those with a disability for at least 29 months, and those with end-stage renal disease (ESRD). Generally, Medicare is the primary coverage for those individuals who are age 65 and older, unless these individuals are actively working.
102

Mental Disorder – an illness commonly understood to be a mental disorder, whether or not it has a physiological basis, and for which treatment is generally provided by or under the direction of a behavioral health provider such as a psychiatric physician, a psychologist or a psychiatric social worker. A mental disorder includes, but is not limited to:
Anorexia/Bulimia Nervosa. Bipolar disorder. Major depressive disorder. Obsessive compulsive disorder. Panic disorder. Pervasive Mental Developmental Disorder (including Autism). Psychotic Disorders/Delusional Disorder. Schizo-affective Disorder. Schizophrenia.
Morbid obesity – a Body Mass Index that is: greater than 40 kilograms per meter squared or equal to or greater than 35 kilograms per meter squared with a comorbid medical condition, such as hypertension, a cardiopulmonary condition, sleep apnea or diabetes. National Medical Excellence® Program – is one of the LM HealthWorks Plan’s Condition Management programs. It consists of the following program components:
National Transplant Program – coordinates care and provides access to covered treatment through the Institutes of ExcellenceTM network.
National Special Case Program – assists members with rare or complex conditions requiring specialized treatment in evaluating treatment options and obtaining appropriate care.
Out-of-Country Care Program – supports members who need emergency medical care while temporarily traveling outside the continental United States.
Patient Management – The National Medical Excellence (NME) program continues to provide the clinical management for transplant cases and special case situations. The Transplant Manager coordinates care from evaluation through post transplant services and assists with access to the Institutes of Excellence network.
Customer Service – The Special Case Customer Service Unit (SCSU) handles claim payment and member/provider services for transplants, transplant-related services and special case situations as well as payment for travel and lodging allowances.
Travel & Lodging – The NME program provides travel and lodging allowances for members in the transplant or special case programs. If the IOE facility needed is more than 100 miles from the patient’s residence, certain travel and lodging expenses for the patient and one companion may be reimbursed if pre-authorized by Aetna. (Note: travel and lodging is NOT offered for out of country care.)
Non-duplication of benefits – the plan does not allow for duplication of benefits. If you and your eligible dependents are covered under more than one group plan, the primary plan (the one responsible for paying benefits first) needs to be determined. You are entitled to receive benefits up to what you would have received under the plan if it were your only source of coverage, but not in excess of that amount. If you have other coverage that is primary to the plan, the claims administrator will reduce the amount of coverage that you would otherwise receive under this plan by any amount you receive from your primary coverage.
103

Non-occupational illness – is an illness that does not:
Arise out of (or in the course of) any work for pay or profit; or Result in any way from an illness that does.
An illness will be considered non-occupational regardless of cause if proof is provided that you are:
Covered under any type of workers’ compensation law; and Not covered for that illness under such law.
Non-occupational injury – is an accidental bodily injury that does not:
Arise out of (or in the course of) any work for pay or profit; or Result in any way from an injury that does.
Non-preferred brand-name drug – a drug that is not included on the LM HealthWorks Plan’s formulary or list of preferred drugs. Online provider directory (DocFind®) – lists doctors, hospitals and other health care providers who belong to the LM HealthWorks Plan’s network (including Aexcel-designated providers). You can use this tool to search for a particular provider or find all in-network providers within a certain geographical area. Out-of-network or non-network provider – a provider that has not contracted with the LM HealthWorks Plan to provide members with services based on pre-agreed fee structures and other criteria. Out-of-network providers can apply to become in-network providers. Out-of-Area – some locations in the United States that have limited or no access to a provider network. Out-of-pocket maximum – the LM HealthWorks Plan’s limit on what you must pay in coinsurance each calendar year. Partial confinement treatment – a plan of medical, psychiatric, nursing, counseling or therapeutic services to treat alcoholism, substance abuse or mental disorders. The plan must:
Be carried out in a hospital, psychiatric hospital or residential treatment facility on less than a full-time inpatient basis.
Be in accord with accepted medical practice for the condition of the person. Not require full-time confinement. Be supervised by a psychiatric physician who review and evaluates the plan’s effectiveness on a
weekly basis. Day care and night care treatment are considered partial confinement treatment. Participating retail pharmacy – a pharmacy that has contracted with LM HealthWorks Plan’s prescription drug claims administrator to provide prescription drug services. Personal Health Assessment (PHA) – a secure online questionnaire that helps you understand your health status and risks. The PHA’s questions cover areas such as personal medical history, lifestyle, habits and recent results of health screenings, such as cholesterol levels.
104

Physician – a licensed medical practitioner who is practicing within the scope of his/her license and who is licensed to prescribe and administer drugs or to perform surgery. Licensed medical practitioners include the following:
Doctor of medicine (M.D.) or doctor of osteopathy (D.O.). Certified registered nurse anesthetist (C.R.N.A.). Chiropractor (D.C.). Dentist (D.D.S. or D.M.D.). Certified or licensed midwife. Optometrist (O.D.). Podiatrist or chiropodist (D.P.M., D.S.C. or D.S.P.). Acupuncturist. Christian Science Practitioner who is authorized by the Mother Church, the First Church of Christ
Scientist in Boston, Massachusetts, and is listed in the Christian Science Journal at the time a service is rendered.
Psychologist (Ph.D., Ed.D. or Psy.D.). Clinical social worker (C.S.W. or L.C.S.W.).
The following are considered covered medical professionals when they are referred by a physician, licensed to practice where the care is given, rendering a service within the scope of that license and providing a service for which benefits are specified in the plan:
Nurse – a nurse is a registered graduate nurse, a licensed practical nurse or a license vocational nurse. A nurse is a professional who has the right to use the respective title and the respective abbreviation R.N., L.P.N. or L.V.N.
Audiologist. Occupational therapist (O.T.). Physical therapist (P.T. or R.P.T.). Speech pathologist or therapist. Marriage, family and child counselor (M.F.C.C. or L.M.F.T.). Home health aide – a person who provides medical or therapeutic care and who reports to and is
under the direct supervision of a home health care agency. Plan year – the 12-month period beginning on January 1 each year and ending on December 31. Precertification or precertify – the process of obtaining approval (certification or authorization) from the claims administrator. Preferred brand-name drug – a drug that is listed on the LM HealthWorks Plan’s formulary or preferred list of prescription drugs. It is not a guarantee that benefits will be payable. Preferred drug list or formulary – is a list of brand-name and generic medications that are preferred by your prescription program. The preferred drug list contains a very broad list of medications for most medical conditions that are treated on an outpatient basis. Because the medications on the list are preferred, you will usually pay a lower copayment than you would for non-preferred drugs. Prescription drug – a drug that you can get only with an order form (prescription) from your doctor or health care professional. Preventive care – health care services that help you stay healthy or help detect early signs of disease.
105

Prescription savings program – My Rx Choices® is available through Medco’s Web site. This online prescription savings program lets you search online for lower-cost alternatives to your medications that are available under the LM HealthWorks Plan. Print out your search results and discuss them with your doctor to see if a lower-cost alternative may be right for you. Price-a-Medication Tool – an online tool available at Medco’s prescription drug Web site. This tool lets you look up your medication and its cost, and search for lower-cost alternatives that may be available and appropriate for you under the LM HealthWorks Plan. Primary care physician (PCP) – a doctor who provides routine and basic care. The LM HealthWorks Plan does not require you to choose a PCP and does not require referrals from a PCP for specialty care. However, you may want to consider using a PCP for the care coordination and continuity that he or she can provide. Qualified Change in Status – (also known as a life event), is a change in your personal circumstances that permits you to change your coverage under the LM HealthWorks Plan during the year. Qualified Medical Child Support Order (QMCSO) – an order from a state domestic relations court, or through an appropriate state administrative process, as defined in Section 609 of ERISA. Qualifying Exigency – a situation arising from a covered military member’s covered active duty that qualifies for family medical leave. Examples of situations that may be qualifying exigencies are:
A covered military member is notified of an impending call or order to covered active duty seven or fewer calendar days before the date of deployment, and during that pre-deployment period needs to arrange for alternative childcare, address financial and legal arrangements or attend certain military event or counseling sessions.
Attendance at post-deployment reintegration briefings and counseling sessions. Spending time with a covered military member who is on short-term, temporary or rest and
recuperation leave during a period of deployment. Recognized charge (formerly reasonable and customary) – the charge most often made for a given health care service or supply in a geographical area. The recognized charge is determined by the claims administrator based on the fee most commonly charged for a service in a geographic area or a negotiated or discounted fee established for an in-network provider. (For Medicare eligible participants, when applicable, the recognized charge is the Medicare allowable charge.) Recognized charges/expenses are subject to review and periodic change. Residential treatment facility (alcoholism and substance abuse) – an institution that meets all of the following requirements:
Maintains an on-site licensed behavioral health provider 24 hours per day/7 days a week. Provides a comprehensive patient assessment (preferably before admission, but at least upon
admission). Requires admission by a physician. Has access to necessary medical services 24 hours per day/7 days a week. Provides 24/7 access to onsite medical treatment, actively supervised by an attending physician, for
patients who need detoxification services. Offers group therapy sessions run by at least an RN or Masters-Level Health Professional. Involves family/support systems in therapy (required for children and adolescents; encouraged for
adults).
106

Provides access to at least weekly sessions with a psychiatrist or psychologist for individual psychotherapy.
Services are managed by a licensed behavioral health provider who meets the claims administrators’ credentialing criteria for individual practitioners and functions under the direction/supervision of a licensed psychiatrist (Medical Director).
Provides an individualized active treatment plan. Provides a level of skilled intervention consistent with patient risk. Meets any and all applicable licensing standards established by the jurisdiction in which it is located. Is not a Wilderness Treatment Program or any such related or similar program, school and/or
education service. Can assess and recognize withdrawal complications that threaten life or bodily functions and to obtain
needed services either on site or externally. Offers 24/7 supervision by a physician with evidence of close and frequent observation.
Residential treatment facility (mental disorders) – an institution that meets all of the following requirements:
Maintains an on-site licensed behavioral health provider 24 hours per day/7 days a week. Provides a comprehensive patient assessment (preferably before admission, but at least upon
admission). Requires admission by a physician. Provides access to necessary medical services 24 hours per day/7 days a week. Provides living arrangements that foster community living and peer interaction consistent with
developmental needs. Offers group therapy sessions run by at least an RN or Masters-Level Health Professional. Involves family/support systems in therapy (required for children and adolescents; encouraged for
adults). Provides access to at least weekly sessions with a psychiatrist or psychologist for individual
psychotherapy. Services are managed by a licensed behavioral health provider who meets the claims administrators’
credentialing criteria for individual practitioners and functions under the direction/supervision of a licensed psychiatrist (Medical Director).
Provides an individualized active treatment plan. Provides a level of skilled intervention consistent with patient risk. Meets any and all applicable licensing standards established by the jurisdiction in which it is located. Is not a Wilderness Treatment Program or any such related or similar program, school and/or
education service. Room and board – all charges commonly made by a hospital on its own behalf for room and meals, and all general services and activities needed for the care of registered bed patients. Serious mental illness – the following psychiatric illnesses, as defined by the American Psychiatric Association in the Diagnostic and Statistical Manual (DSM) IV:
Schizophrenia. Paranoia and other psychotic disorders. Bipolar disorder. Major depressive disorders (chronic or recurrent). Schizo-affective disorder (bipolar or depressive).
107

Specialist – a doctor who provides medical care in a specific area, such as dermatology, cardiology and oncology. Substance Abuse – a physical and/or psychological dependency on a controlled substance or alcohol agent. (These are defined on Axis I in the Diagnostic and Statistical Manual of Mental Disorders (DSM) published by the American Psychiatric Association which is current when you or your insured dependents receive services.) This term does not include conditions not attributable to a mental disorder that are a focus of attention or treatment (the V codes on Axis I of DSM); an addiction to nicotine products or food, or caffeine intoxication. Transition of Care – an LM HealthWorks Plan provision under which you may continue in an active course of treatment with an out-of-network provider and receive benefits at the in-network level for a limited period of time. Urgent care – medical care provided for a sudden illness or injury that is not life-threatening but does require immediate care to avoid severe pain or complications.
108

Appendix A – Participating Business Units* For Lockheed Martin Corporation Group Benefits Plan (Plan 594): All domestic businesses of Lockheed Martin Corporation are eligible effective January 1, 2011, except those listed below: Groups participating in the Lockheed Martin Operations Support, Inc. Benefits Plan as listed below:
LM Canada PAE Sandia National Laboratory Savi Employees permanently residing in Puerto Rico or Hawaii
If you have any questions concerning your eligibility, please contact the Lockheed Martin Employee Service Center. For Lockheed Martin Operations Support, Inc. Benefits Plan (Plan 504): All domestic businesses of the following are eligible effective January 1, 2011:
Lockheed Martin Operations Support, Inc. (except employees working in Puerto Rico or Hawaii) Lockheed Martin Engineering & Sciences, Co. (except employees working in Puerto Rico or Hawaii) LM Global, Inc. (OS) LM Global, Inc. (ES) LM Information Technology Commercial Corporation LM Desktop Solutions, Inc. Sytex, Inc. LM AspenMed Services, Inc. Employees working on the Crossbow contract Employees working on the NASA Facilities Development and Operations contract in LM Services
Inc. LM Logistic Services, Inc. (Field Teams) LM Kelly Aviation Center L P LM Aircraft Center (Greenville) LM Logistics Management, Inc. (Greenville) LM Aeronautics Services, Intl.
If you have any questions concerning your eligibility, please contact the Lockheed Martin Employee Service Center . *This list is current as of the time of publication; participating businesses are subject to change.
109

Appendix B – Participating Unions* The benefits described in this booklet are available to eligible employees of Lockheed Martin Corporation who are represented by the: International Brotherhood of Electrical Workers, AFL – CIO and its Local 949, Eagan, MN. International Union of Electronic, Electrical, Salaried, Machine and Furniture Workers, AFL – CIO
and Engineer Union Local 444, Mitchel Field, NY. If you have any questions concerning your eligibility, please contact the Lockheed Martin Employee Service Center. All unions of Lockheed Martin Operations Support, Inc. and Lockheed Martin Training Solutions, Inc. and their participating affiliates are eligible. *This list is current as of the time of publication; participating unions may change from time to time
110

When you have questions For general enrollment and eligibility questions, please contact the Lockheed Martin Employee Service Center. Visit the Employee Service Center Online at:
https://www.lmpeople.com – on the Internet https://lmpeople.lmco.com – on the Lockheed Martin intranet Click on “Health and Wellness” under “Pay and Benefits,” then “Review or Change My
Coverage.” Call the Lockheed Martin Employee Service Center at:
866-562-2363 – Toll-free calls in the U.S. 201-242-4397 – International callers 800-833-8334 – Hearing impaired
For specific questions regarding benefits and claim information, please contact the claims administrator.
111

207SPDB11




















