
Proizvodnja vitamina B12 pomoću Pseudomonas denitrificans ...
Upload
independentCategory
view
3download
0
Nutrition, Metabolism & Cardiovascular Diseases (2005) 15, 100e108
www.elsevier.com/locate/nmcd
Role of vitamins B6, B12 and folic acid onhyperhomocysteinemia in a Pakistani populationof patients with acute myocardial infarction
M.P. Iqbal a,*, M. Ishaqb, K.A. Kazmi c, F.A. Yousuf a, N. Mehboobali a,S.A. Ali a, A.H. Khana, M.A. Waqar a
a Department of Biological & Biomedical Sciences, The Aga Khan University, Stadium Road,PO Box 3500, Karachi 74800, Pakistanb National Institute of Cardiovascular Diseases, Rafique Shaheed Road, Karachi, Pakistanc Department of Medicine, The Aga Khan University, Stadium Road, PO Box 3500,Karachi 74800, Pakistan
Received 4 December 2003; accepted 27 May 2004
KEYWORDSFolic acid;Vitamin B6;Pyridoxal phosphate;Vitamin B12;Cobalamine;Hyperhomo-cysteinemia;Acute myocardialinfarction;Cardiovascular disease
Summary Background and aim: Pakistani people belong to an ethnic group whichhas the highest rate of coronary artery disease (CAD). We investigated the possiblecorrelation between deficiency of vitamins B6, B12 or folic acid and hyperhomo-cysteinemia in Pakistani patients with acute myocardial infarction (AMI). A case-control study was carried out involving 224 AMI patients (age 30e70 years; 55females and 169 males) and 126 normal healthy subjects (age 31e70 years; 35females and 91 males).Methods and results: Fasting venous blood was obtained from cases and controls.Serum was analyzed for folic acid and B12 using radioassays. Plasma was analyzedfor pyridoxal phosphate (PLP; coenzymic form of B6) using a radioenzymatic assayand for total homocysteine using a fluorescence polarization immunoassay. Meanserum B12 concentration in AMI patients was found to be significantly lower thanthe mean for controls (241G185 pg/ml vs 608G341 pg/ml; p!0.001). Mean serumfolate level in patients was also found to be lower than controls (3.35G3.78 ng/mlvs 4.93G2.93 ng/ml), however, the differences were not statistically significant.Similarly, mean PLP concentration in plasma of cases (19.4G24.4 nmol/l) was lowerthan the concentration in controls (23.2G17.6 nmol/l), but the difference was notstatistically significant. Mean plasma homocysteine level in AMI cases (18G8.36mmol/l) was higher than the mean level in controls (16.4G4.9 mmol/l), but not toa significant extent. However, this mean homocysteine concentration in normal
* Corresponding author. Tel.: C92 21 493 0051x4463; fax: C92 21 493 4294.E-mail address: [email protected] (M.P. Iqbal).
0939-4753/$ - see front matter � 2005 Elsevier Ltd. All rights reserved.doi:10.1016/j.numecd.2004.05.003

B6, B12 and folate deficiency in Pakistani AMI patients 101
healthy subjects was among the highest reported in the literature and wassignificantly more than mean values reported in most Eastern and Western studies.Compared to controls, there was significantly greater deficiency of folate (32.5% vs67.1%), B12 (3.2% vs 63.4%) and PLP (49.2% vs 74.1%) in AMI patients. Deficiencies offolate, B12 and PLP were defined as serum folate levels less than 3.5 ng/ml, serumlevels of B12 less than 200 pg/ml and plasma PLP levels less than 20 nmol/l. Meanplasma homocysteine levels in smokers were found to be significantly higher in bothcases and controls. Similarly, mean serum folate levels in smokers (compared tononsmokers) were significantly lower in both cases and controls.Conclusions: Substantial nutritional deficiencies of these three vitamins along withmild hyperhomocysteinemia, perhaps through an interplay with the classicalcardiovascular risk factors (highly prevalent in this population), could be furtheraggravating the risk of CAD in the Pakistani population.� 2005 Elsevier Ltd. All rights reserved.
Introduction
Cardiovascular disease (CVD) is the leading cause ofdeath in both industrialized and developing coun-tries. Recent reports have indicated that Pakistanipeople belong to an ethnic group which has thehighest rates of coronary artery disease (CAD) [1].Moreover, the relative risk of CAD in South Asianmen is highest at early ages [2,3] suggesting thatboth intrinsic and extrinsic factors contribute to thedevelopment of CAD in this population.
A number of studies during the past few yearshave indicated a protective role of vitamins B6,B12 and folate against the development of CAD[4,5]. More recent reports have shown an associ-ation between deficiency of these B-complexvitamins and hyperhomocysteinemia, a known riskfactor for myocardial infarction [6e8]. This hasfocused attention on these B-complex vitaminsand the important role they might play in pro-tection against the development of CAD [9]. Todate, no studies have been carried out in Pakistanto investigate the role of deficiency of thesevitamins in the development of CAD.
The objective of this study is to investigatewhether or not our patients suffering from acutemyocardial infarction (AMI) have lower levels ofplasma B6, B12 or folate and enhanced homocys-teine compared to healthy subjects who do nothave CAD. If deficiency of B-complex vitamins isfound to exist in this population, then interventionin the form of supplementations might significantlyreduce the incidence of CAD.
Methods
Patients
Two hundred and twenty four consecutive Pakis-tani patients with AMI (age 30e70 years) admitted
to the National Institute of Cardiovascular Diseases(NICVD), Karachi from January 2001 to June 2001,were included in this study. They were enrolledwithin the index admission after confirmation ofdiagnosis based on WHO criteria of clinical historysuggestive of myocardial ischemia, ECG indicationsof myocardial damage, and elevation of biochem-ical markers (creatine kinase and creatine kinase-MB). All patients were assessed as having riskfactors for CVD, such as diabetes mellitus, hyper-tension, obesity, hypercholesterolemia, smokingand a parental history of ischemic heart disease(IHD). Criteria for diabetes were set as an abnor-mal fasting blood glucose level O125 mg/dl atadmission, or having taken hypoglycemic agents.All those with systolic blood pressure greater than140 mmHg and/or diastolic blood pressure of 90mmHg or those on regular antihypertensive med-ications were classified as hypertensive. Thosehaving serum cholesterol level greater than 200mg/dl were considered to have hypercholesterol-emia. A body mass index (BMI) above 30 wasclassified as obese, and a parental history of IHDwas considered positive if any of the parents hadIHD at or below the age of 60 years. Subjects wereconsidered smokers if they had been smokingcigarettes regularly (one or more per day). Thosecases (as well as controls) who were pregnant,using antiepileptics, taking oral contraceptives,having malabsorption syndrome, suffering fromtuberculosis, liver disease, uremia, or cancer orusing vitamin B-complex supplements during thepast 6 months were not included.
Similarly, 126 normal healthy subjects who hadbeen matched for age and sex and belonged to thesame socio-economic class, were selected from thepersonnel of the Aga Khan University and CivilHospital, Karachi, for this study from January2001 to June 2001. They were also assessed forthe above mentioned risk factors. However, morestringent criteria were used for the selection of

102 M.P. Iqbal et al.
normal healthy control subjects. In addition tobeing matched for age, sex and socioeconomicbackground, they had no evidence of CAD, diabetesmellitus, hypertension, obesity or hypercholester-olemia. The objective was to have an assessment ofthe levels of folate, B12, B6 and homocysteine ina ‘‘normal healthy population’’ and compare theirlevels with those obtained from AMI patients.Informed consent was obtained from the partici-pants and the study was approved by the EthicsReview Committee of the Aga Khan University.
Estimation of glucose, total cholesterol,high density lipoprotein (HDL)-cholesterol,triglycerides and low density lipoprotein(LDL)-cholesterol
Fasting serum glucose, total cholesterol, HDL-cholesterol and triglycerides were analyzed usingcolorimetric kit methods (RANDOX, UK) fromvenous blood obtained within 24 h of AMI. Theconcentration of LDL-cholesterol was calculatedusing the Friedewald formula [10].
Estimation of B12, folate, B6 andhomocysteine in serum/plasma
Fasting venous blood was obtained from cases aswell as controls. Serum samples were analyzed forfolate and vitamin B12 using radioassays [11e14].Plasma samples from both cases and controls werescreened for pyridoxal phosphate (PLP; coenzymicform of vitamin B6) and homocysteine. PlasmaPLP concentration was chosen as standard forvitamin B6 status because this measure appearsto reflect tissue stores [15]. For determination ofPLP in plasma, a modification of the method byCamp et al. [16] as described previously was used[17]. Determination of plasma homocysteine wascarried out using a kit based on fluorescencepolarization immunoassay (Abbott Laboratories,Ltd., Pakistan).
Vitamin deficiency
To provide a perspective on blood concentrationsof the vitamins, we compared them to values thatrepresent deficiency states. Thus, vitamin B12deficiency was defined as a plasma concentrationless than 200 pg/ml. Folate deficiency was definedas a serum concentration less than 3.5 ng/ml. PLPdeficiency was defined as a plasma level less than20 nmol/l [18,19].
Statistical analysis
All mean values were expressed as meanGstan-dard deviation (SD). Percentages were comparedby test of proportions using chi-square. Meanvalues of various groups were compared usinganalysis of variance (ANOVA). The analyses wereperformed with the statistical package (Epi Info 6,version 6.04 d, 2001, WHO). Two-way ANOVAwas carried out using the SPSS� (statistical pack-age for social sciences), Software Version 10 forWindows�. A p value less than 0.05 was consideredsignificant.
Results
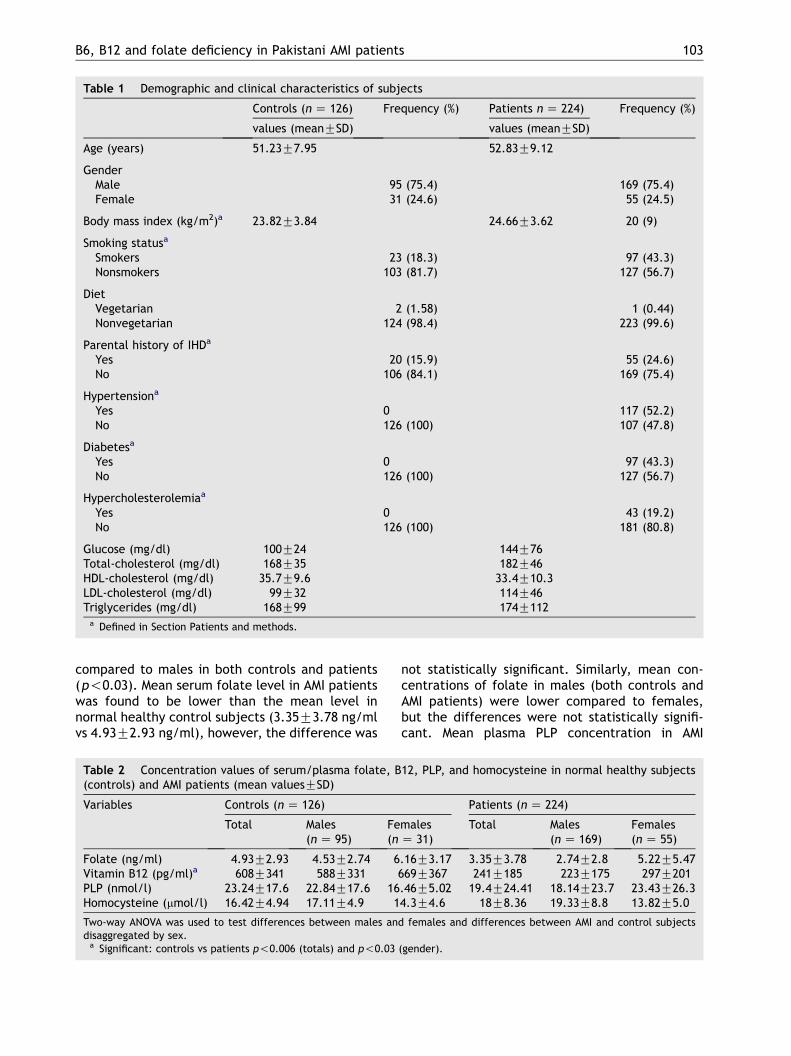
Demographic and clinical characteristics of patientsare listed in Table 1. The patient group comprised 55females and 169 males providing a female to maleratio of 1:3. The mean age was 52.83G9.12 years(range 30e70 years) in this group. Mean BMI was24.66G3.62 kg/m2. Nine percent were obese, 43%were smokers, 52% were hypertensive, 43% werediabetic, while 19% were hypercholesterolemic.Twenty-five percent of the patients had parentalhistory of ischemic heart disease (IHD). Only onepatient was a strict vegetarian. Mean serum levelsof glucose, total cholesterol, HDL-cholesterol, LDL-cholesterol and triglycerides were 144G76 mg/dl,182G46 mg/dl, 33.4G10.3 mg/dl, 114G46 mg/dland 174G112 mg/dl, respectively.
Among the controls, the mean age was51.23G7.95 years (range 31e70 years). Therewere 31 females and 95 males and the mean BMIfor this group was 23.82G3.84 kg/m2, which wasquite close to the mean BMI of cases. Eighteenpercent of the controls were smokers. There wereonly two vegetarians and 16% of the controlsubjects had parental history of IHD.
Concentrations of folate, B12, PLP andhomocysteine
Table 2 shows the mean concentrations of serumfolate, serum B12, plasma PLP and plasma homo-cysteine in normal healthy subjects (controls) andAMI patients. Analysis of the data by two-wayANOVA revealed that the mean serum B12 concen-tration in AMI patients (241G185 pg/ml) wassignificantly less than the mean serum B12 con-centration (608G341 pg/ml) in normal healthysubjects (p!0.006). Mean concentration of B12was also found to be significantly higher in females
B6, B12 and folate deficiency in Pakistani AMI patients 103
Table 1 Demographic and clinical characteristics of subjects
Controls (n Z 126) Frequency (%) Patients n Z 224) Frequency (%)
values (meanGSD) values (meanGSD)
Age (years) 51.23G7.95 52.83G9.12
GenderMale 95 (75.4) 169 (75.4)Female 31 (24.6) 55 (24.5)
Body mass index (kg/m2)a 23.82G3.84 24.66G3.62 20 (9)
Smoking statusa
Smokers 23 (18.3) 97 (43.3)Nonsmokers 103 (81.7) 127 (56.7)
DietVegetarian 2 (1.58) 1 (0.44)Nonvegetarian 124 (98.4) 223 (99.6)
Parental history of IHDa
Yes 20 (15.9) 55 (24.6)No 106 (84.1) 169 (75.4)
Hypertensiona
Yes 0 117 (52.2)No 126 (100) 107 (47.8)
Diabetesa
Yes 0 97 (43.3)No 126 (100) 127 (56.7)
Hypercholesterolemiaa
Yes 0 43 (19.2)No 126 (100) 181 (80.8)
Glucose (mg/dl) 100G24 144G76Total-cholesterol (mg/dl) 168G35 182G46HDL-cholesterol (mg/dl) 35.7G9.6 33.4G10.3LDL-cholesterol (mg/dl) 99G32 114G46Triglycerides (mg/dl) 168G99 174G112a Defined in Section Patients and methods.
compared to males in both controls and patients(p!0.03). Mean serum folate level in AMI patientswas found to be lower than the mean level innormal healthy control subjects (3.35G3.78 ng/mlvs 4.93G2.93 ng/ml), however, the difference was
not statistically significant. Similarly, mean con-centrations of folate in males (both controls andAMI patients) were lower compared to females,but the differences were not statistically signifi-cant. Mean plasma PLP concentration in AMI
Table 2 Concentration values of serum/plasma folate, B12, PLP, and homocysteine in normal healthy subjects(controls) and AMI patients (mean valuesGSD)
Variables Controls (nZ 126) Patients (nZ 224)
Total Males(nZ 95)
Females(n Z 31)
Total Males(n Z 169)
Females(n Z 55)
Folate (ng/ml) 4.93G2.93 4.53G2.74 6.16G3.17 3.35G3.78 2.74G2.8 5.22G5.47Vitamin B12 (pg/ml)a 608G341 588G331 669G367 241G185 223G175 297G201PLP (nmol/l) 23.24G17.6 22.84G17.6 16.46G5.02 19.4G24.41 18.14G23.7 23.43G26.3Homocysteine (mmol/l) 16.42G4.94 17.11G4.9 14.3G4.6 18G8.36 19.33G8.8 13.82G5.0
Two-way ANOVA was used to test differences between males and females and differences between AMI and control subjectsdisaggregated by sex.a Significant: controls vs patients p!0.006 (totals) and p!0.03 (gender).
104 M.P. Iqbal et al.
patients was also found to be lower than thecontrols (19.4G24.4 nmol/l vs 23.24G17.6 nmol/l), however, the values were not significantlydifferent. Mean homocysteine concentration inplasma of AMI patients was higher compared tocontrols (18G8.36 mmol/l vs 16.42G4.94 mmol/l)and males in both controls and AMI patients hadmean homocysteine concentrations higher thanfemales. However, the differences were notstatistically significant. It is important to notethat the mean homocysteine concentration innormal healthy subjects (controls) was well abovethe higher limit of the normal homocysteineconcentration (15 mmol/l) in most Western andEastern populations.
Deficiency of folate, B6 and B12
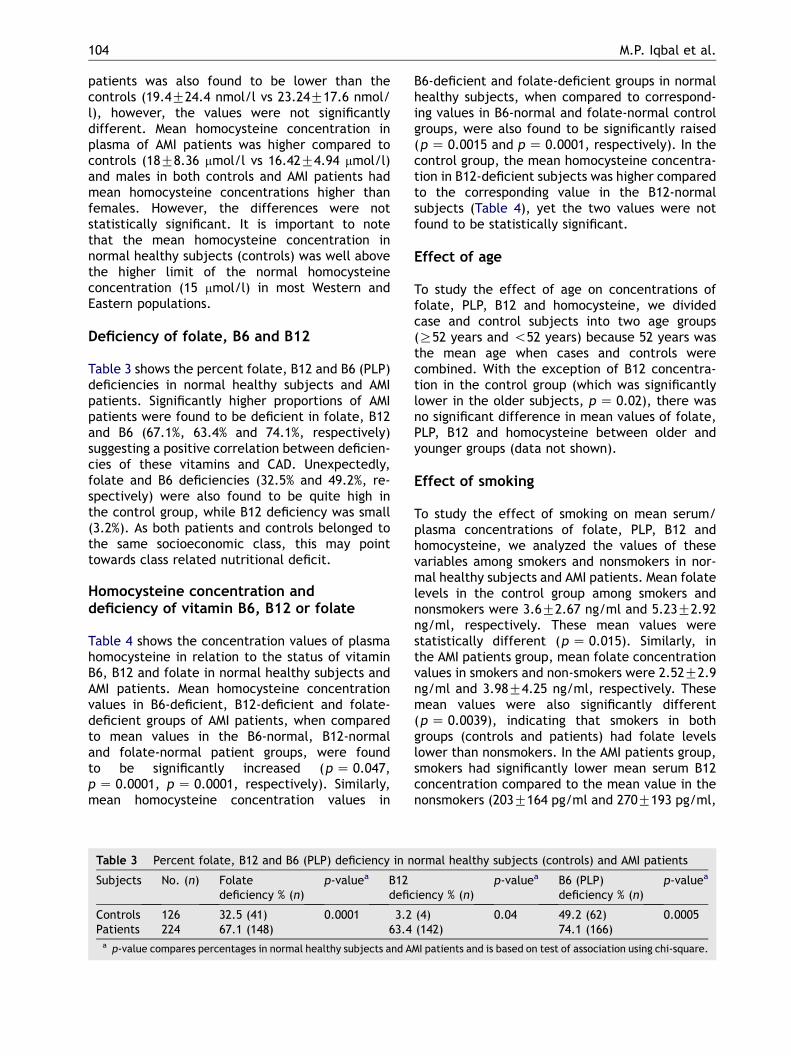
Table 3 shows the percent folate, B12 and B6 (PLP)deficiencies in normal healthy subjects and AMIpatients. Significantly higher proportions of AMIpatients were found to be deficient in folate, B12and B6 (67.1%, 63.4% and 74.1%, respectively)suggesting a positive correlation between deficien-cies of these vitamins and CAD. Unexpectedly,folate and B6 deficiencies (32.5% and 49.2%, re-spectively) were also found to be quite high inthe control group, while B12 deficiency was small(3.2%). As both patients and controls belonged tothe same socioeconomic class, this may pointtowards class related nutritional deficit.
Homocysteine concentration anddeficiency of vitamin B6, B12 or folate
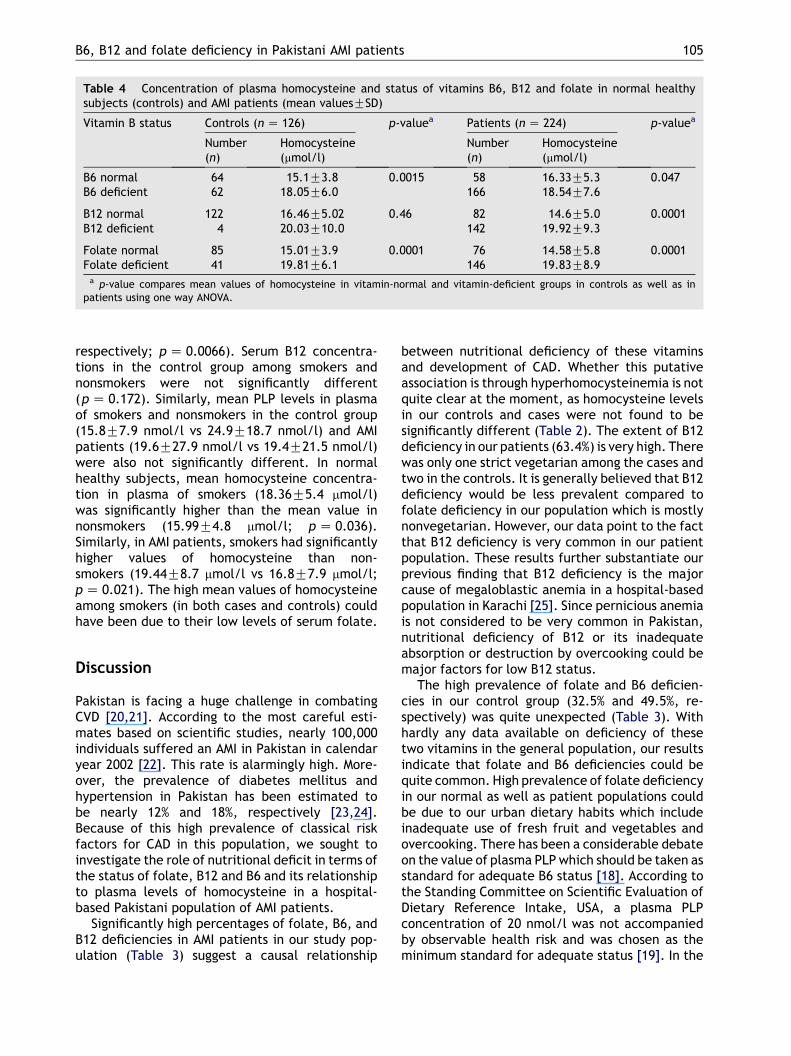
Table 4 shows the concentration values of plasmahomocysteine in relation to the status of vitaminB6, B12 and folate in normal healthy subjects andAMI patients. Mean homocysteine concentrationvalues in B6-deficient, B12-deficient and folate-deficient groups of AMI patients, when comparedto mean values in the B6-normal, B12-normaland folate-normal patient groups, were foundto be significantly increased (p Z 0.047,p Z 0.0001, p Z 0.0001, respectively). Similarly,mean homocysteine concentration values in
B6-deficient and folate-deficient groups in normalhealthy subjects, when compared to correspond-ing values in B6-normal and folate-normal controlgroups, were also found to be significantly raised(p Z 0.0015 and p Z 0.0001, respectively). In thecontrol group, the mean homocysteine concentra-tion in B12-deficient subjects was higher comparedto the corresponding value in the B12-normalsubjects (Table 4), yet the two values were notfound to be statistically significant.
Effect of age
To study the effect of age on concentrations offolate, PLP, B12 and homocysteine, we dividedcase and control subjects into two age groups(R52 years and !52 years) because 52 years wasthe mean age when cases and controls werecombined. With the exception of B12 concentra-tion in the control group (which was significantlylower in the older subjects, p Z 0.02), there wasno significant difference in mean values of folate,PLP, B12 and homocysteine between older andyounger groups (data not shown).
Effect of smoking
To study the effect of smoking on mean serum/plasma concentrations of folate, PLP, B12 andhomocysteine, we analyzed the values of thesevariables among smokers and nonsmokers in nor-mal healthy subjects and AMI patients. Mean folatelevels in the control group among smokers andnonsmokers were 3.6G2.67 ng/ml and 5.23G2.92ng/ml, respectively. These mean values werestatistically different (p Z 0.015). Similarly, inthe AMI patients group, mean folate concentrationvalues in smokers and non-smokers were 2.52G2.9ng/ml and 3.98G4.25 ng/ml, respectively. Thesemean values were also significantly different(p Z 0.0039), indicating that smokers in bothgroups (controls and patients) had folate levelslower than nonsmokers. In the AMI patients group,smokers had significantly lower mean serum B12concentration compared to the mean value in thenonsmokers (203G164 pg/ml and 270G193 pg/ml,
Table 3 Percent folate, B12 and B6 (PLP) deficiency in normal healthy subjects (controls) and AMI patients
Subjects No. (n) Folatedeficiency % (n)
p-valuea B12deficiency % (n)
p-valuea B6 (PLP)deficiency % (n)
p-valuea
Controls 126 32.5 (41) 0.0001 3.2 (4) 0.04 49.2 (62) 0.0005Patients 224 67.1 (148) 63.4 (142) 74.1 (166)a p-value compares percentages in normal healthy subjects and AMI patients and is based on test of association using chi-square.
B6, B12 and folate deficiency in Pakistani AMI patients 105
Table 4 Concentration of plasma homocysteine and status of vitamins B6, B12 and folate in normal healthysubjects (controls) and AMI patients (mean valuesGSD)
Vitamin B status Controls (n Z 126) p-valuea Patients (nZ 224) p-valuea
Number(n)
Homocysteine(mmol/l)
Number(n)
Homocysteine(mmol/l)
B6 normal 64 15.1G3.8 0.0015 58 16.33G5.3 0.047B6 deficient 62 18.05G6.0 166 18.54G7.6
B12 normal 122 16.46G5.02 0.46 82 14.6G5.0 0.0001B12 deficient 4 20.03G10.0 142 19.92G9.3
Folate normal 85 15.01G3.9 0.0001 76 14.58G5.8 0.0001Folate deficient 41 19.81G6.1 146 19.83G8.9a p-value compares mean values of homocysteine in vitamin-normal and vitamin-deficient groups in controls as well as in
patients using one way ANOVA.
respectively; pZ 0.0066). Serum B12 concentra-tions in the control group among smokers andnonsmokers were not significantly different(pZ 0.172). Similarly, mean PLP levels in plasmaof smokers and nonsmokers in the control group(15.8G7.9 nmol/l vs 24.9G18.7 nmol/l) and AMIpatients (19.6G27.9 nmol/l vs 19.4G21.5 nmol/l)were also not significantly different. In normalhealthy subjects, mean homocysteine concentra-tion in plasma of smokers (18.36G5.4 mmol/l)was significantly higher than the mean value innonsmokers (15.99G4.8 mmol/l; pZ 0.036).Similarly, in AMI patients, smokers had significantlyhigher values of homocysteine than non-smokers (19.44G8.7 mmol/l vs 16.8G7.9 mmol/l;pZ 0.021). The high mean values of homocysteineamong smokers (in both cases and controls) couldhave been due to their low levels of serum folate.
Discussion
Pakistan is facing a huge challenge in combatingCVD [20,21]. According to the most careful esti-mates based on scientific studies, nearly 100,000individuals suffered an AMI in Pakistan in calendaryear 2002 [22]. This rate is alarmingly high. More-over, the prevalence of diabetes mellitus andhypertension in Pakistan has been estimated tobe nearly 12% and 18%, respectively [23,24].Because of this high prevalence of classical riskfactors for CAD in this population, we sought toinvestigate the role of nutritional deficit in terms ofthe status of folate, B12 and B6 and its relationshipto plasma levels of homocysteine in a hospital-based Pakistani population of AMI patients.
Significantly high percentages of folate, B6, andB12 deficiencies in AMI patients in our study pop-ulation (Table 3) suggest a causal relationship
between nutritional deficiency of these vitaminsand development of CAD. Whether this putativeassociation is through hyperhomocysteinemia is notquite clear at the moment, as homocysteine levelsin our controls and cases were not found to besignificantly different (Table 2). The extent of B12deficiency in our patients (63.4%) is very high. Therewas only one strict vegetarian among the cases andtwo in the controls. It is generally believed that B12deficiency would be less prevalent compared tofolate deficiency in our population which is mostlynonvegetarian. However, our data point to the factthat B12 deficiency is very common in our patientpopulation. These results further substantiate ourprevious finding that B12 deficiency is the majorcause of megaloblastic anemia in a hospital-basedpopulation in Karachi [25]. Since pernicious anemiais not considered to be very common in Pakistan,nutritional deficiency of B12 or its inadequateabsorption or destruction by overcooking could bemajor factors for low B12 status.
The high prevalence of folate and B6 deficien-cies in our control group (32.5% and 49.5%, re-spectively) was quite unexpected (Table 3). Withhardly any data available on deficiency of thesetwo vitamins in the general population, our resultsindicate that folate and B6 deficiencies could bequite common. High prevalence of folate deficiencyin our normal as well as patient populations couldbe due to our urban dietary habits which includeinadequate use of fresh fruit and vegetables andovercooking. There has been a considerable debateon the value of plasma PLPwhich should be taken asstandard for adequate B6 status [18]. According tothe Standing Committee on Scientific Evaluation ofDietary Reference Intake, USA, a plasma PLPconcentration of 20 nmol/l was not accompaniedby observable health risk and was chosen as theminimum standard for adequate status [19]. In the
106 M.P. Iqbal et al.
absence of any data in this part of the world, thisvalue was taken as theminimum value for adequatestatus of B6. Since nearly 49% of our healthysubjects had values in the deficiency range, it ispossible that for our population, the normalrange might be different from that accepted inthe West.
The folate deficiency of 32.5% in our normalhealthy subjects, mostly from personnel of the AgaKhan University and the Civil Hospital, Karachi,compares well with that of 33% reported for theIndian population [26]. Community based, largescale studies would be required to find out theextent of this nutritional problem in Pakistan.
Although a mild hyperhomocysteinemia hasbeen observed in our patients suffering from AMI(Table 2), it does not appear to be an independentrisk factor for development of CAD. The causes ofhyperhomocysteinemia are multifactorial, but ourpreliminary data indicate that folate deficiencyand B6 deficiency certainly appear to have anassociation with it (Table 4). This could be due tothe fact that most of the subjects in our cases andcontrol populations belonged to the lower middleclass, a group with a relatively modest socio-economic background and perhaps receiving some-what poor and unbalanced nutrition.
It is noteworthy that the mean plasma homocys-teine levels in normal healthy subjects (controls) inour study were well above the range of ‘‘normalhomocysteine concentration’’ (5e15 mmol/l) inmost Eastern and Western populations [27e29].Similar high values of plasma homocysteine innormal healthy subjects have also been reportedin certain populations in South India [30], Thailand[31] and Turkey [32]. High levels of homocysteine inour controls, which fall into the category of ‘‘mildhyperhomocysteinemia’’ (15e30 mmol/l), havebeen observed in our younger age group (!52years). Similar findings have also been reported byRefsum et al. on a population from South India [33].This may explain why rates of CAD are highest in ourpopulation [1] and why South Asian men are atgreater risk of developing CAD at a younger age[2,3]. However, no significant increase in homocys-teine levels was observed in AMI patients. This lackof association between plasma homocysteine levelsand development of CAD in our population shouldnot be viewed as an unusual finding, as strength ofassociation of homocysteine concentration andatherosclerosis may vary between populations.Knekt et al. have shown that the genetic back-ground of the Finnish population differs somewhatfrom that of peoples from other Western countries[34]. Therefore, a lack of association of homocys-teine concentration and risk of CAD in Finland,
contrary to the results of most studies on otherWestern countries, is quite understandable [34].
A number of studies have shown increasedplasma homocysteine levels in aged individuals[35e38]. However, our study, though indicatingincreased homocysteine levels in the age groupR52 years (in both cases and controls), failedto show a significant difference from mean valuesof plasma homocysteine in the age group less than52 years.
Our observation of significantly lower levels ofserum folate in smokers compared to nonsmokers inthe normal control group (p Z 0.015), as well as inthe AMI patients group (p Z 0.0039), is consistentwith the results reported by Mansoor et al. [39] whoshowed a significant decrease in both serum anderythrocyte folate in smokers. Lower intake of fruitand vegetables, free radicals in cigarette smoke,and increased excretion of folate might havecontributed to a decline in body stores of folate[40e43]. With low folate and low B12 concentra-tions in smokers, mean plasma homocysteine con-centrations among smokers (both in controls as wellas AMI patients), as expected, were found to besignificantly higher than in nonsmokers. Nygardet al. [35] in a study involving nearly 16,000subjects from a general community in Norway havealso reported significantly increased levels of totalhomocysteine in smokers compared to nonsmokers.
On the basis of these observations, it canbe suggested that very significant deficiencies offolate, B6 and B12 along with mild hyperhomo-cysteinemia could act synergistically in concertwith other classical risk factors in the Pakistanipopulation, thereby further aggravating the riskof CAD.
Conclusions
Our study reports the prevalence of folate, B6 andB12 deficiency and its relationship with plasmahomocysteine levels in a Pakistani population. Ourdata show substantial nutritional deficiency of allthese three vitamins. Deficiencies of folate, B6 andB12 were even more pronounced in AMI patients,consistent with their important role in preventingthe development of CAD. Any single nutritionalintervention, such as supplementation with folatealone, may not be enough to protect against CAD ina population that has the highest rates of thisdisease compared to any other in the world.However, supplementations with all three vitaminswould, perhaps, offer some protection. Large scale‘‘community-based’’ studies would be required toassess the prevalence of the deficiency of these
B6, B12 and folate deficiency in Pakistani AMI patients 107
three vitamins in Pakistan, since the present studywas only on a hospital-based population in Karachi.The association between B-complex vitamin de-ficiency, hyperhomocysteinemia, other classicalrisk factors and the risk of developing CAD meritsour serious attention.
Acknowledgements
The study was supported by a grant # S-AKU(185)Med by the Pakistan Science Foundation and a URCgrant by the Aga Khan University to Dr M. PerwaizIqbal. Professional help provided by Dr Ayela Bakarin collection of some of the control samplesfrom Civil Hospital, Karachi is also gratefullyacknowledged. We greatly appreciate the supportby Mr Haseeb-ur-Rehman and Mr Akbar Khan(Abbott Laboratories Ltd, Pakistan). We also thankMr Iqbal Azam for his assistance in analysis ofthe data by two-way ANOVA and Professor John D.Connor for editorial corrections in the manuscript.The valuable suggestions by Professor Sheldon P.Rothenberg and Dr Edward V. Quadros (SUNYDownstate Medical Center, New York) regardingoptimization of folate and B12 assays are alsogratefully acknowledged.
References
[1] McKeigue PM, Marmot MG. Mortality from coronary heartdisease in Asian communities in London. Br Med J 1988;297:903.
[2] Balarajan R. Ethnic differences in mortality from ischae-mic heart disease and cerebrovascular disease in Englandand Wales. Br Med J 1991;302:560e4.
[3] McKeigue PM. Coronary heart disease in Indians, Pakistanisand Bangladeshis: etiology and possibilities of prevention.Br Heart J 1992;67:341e2.
[4] Riemersma RA, Wood DA, Macintyre CCH, Elton RA, Gey KF,Oliver MF. Risk of angina pectoris and plasma concen-trations of vitamin A, C, and E and carotene. Lancet 1991;337:1e5.
[5] Losonczy KG, Harris TB, Havlik RJ. Vitamin E and vitamin Csupplement use and risk of all-cause and coronary heartdisease mortality in older persons: the established pop-ulations for epidemiological studies of the elderly. Am JClin Nutr 1996;64:190e6.
[6] Ubbink JB, Vermaak WJH, van der Merwe A, Becker PJ.Vitamin B12, Vitamin B6 and folate nutritional status inmen with hyperhomocysteinemia. Am J Clin Nutr 1993;57:47e53.
[7] Verhoef P, Stampfer MJ, Buring JE, Gaziano JM, Allen RH,Stabler SP, et al. Homocysteine metabolism and risk ofmyocardial infarction: relation with vitamins B6, B12 andfolate. Am J Epidemiol 1996;143:845e59.
[8] Bates CJ, Pentieva KD, Prentice A, Mansoor MA, Finch S.Plasma pyridoxal phosphate and pyridoxic acid and their
relationship to plasma homocysteine in a representativesample of British men and women aged 65 years and over.Br J Nutr 1999;81:191e201.
[9] Nishtar S. The role of vitamins as risk modifying agents incoronary artery disease. Pak J Cardiol 1999;10:5e7.
[10] Friedewald WT, Levy RI, Fredrickson DS. Estimation of theconcentration of low density lipoprotein cholesterol inplasma without use of the preparative ultracentrifuge.Clin Chem 1972;18:499e502.
[11] Rothenberg SP, daCosta M, Rosenberg Z. A radioassay forserum folate: use of a two-phase sequential incubation,ligand-binding system. N Engl J Med 1972;286:1335e9.
[12] Rothenberg SP. Application of competitive ligand bindingfor the radioassay of vitamin B12 and folic acid. Metabo-lism 1973;22:1075e82.
[13] Rothenberg SP. A radioassay for serum vitamin B12 usingunsaturated transcobalamine 1 as the B12 binding protein.Blood 1968;31:44e54.
[14] Rothenberg SP. Radioassay of serum vitamin B12 byquantitating the competition between 57CoB12 andunlabeled B12 for binding sites of intrinsic factor. J ClinInvest 1963;42:1391e8.
[15] Lui A, Lumeng L, Aronoff GR, Li TK. Relationship betweenbody store of vitamin B6 and plasma pyridoxal-P clear-ance: metabolic balance studies in humans. J Lab Clin Med1985;106:491e7.
[16] Camp VM, Chipponi J, Faraj BA. Radioenzymatic assay fordirect measurement of plasma pyridoxal 5#-phosphate.Clin Chem 1983;29:642e4.
[17] Iqbal MP, Khan AH, Yousuf F. A simple and sensitiveradioenzymatic assay for pyridoxal-5#-phosphate in humanplasma. Pak J Zool 2003;35(3):231e5.
[18] Hansen CM, Shultz TD, Kwak HK, Memon HS, Leklem JE.Assessment of vitamin B-6 status in young women consum-ing a controlled diet containing four levels of vitamin B-6provides an estimated average requirement and recom-mended dietary allowance. J Nutr 2001;131:1777e86.
[19] Institute of Medicine. DRI reference intake for thiamin,riboflavin, niacin, vitamin B6, folate, vitamin B12, pan-tothenic acid, biotin and cholin. Washington, DC: NationalAcademy Press; 1998.
[20] Ahmad K. Facing up to Pakistan’s cardiovascular challenge.Lancet 2002;359:859.
[21] Bhopal R. Epidemic of cardiovascular disease in SouthAsians. Br Med J 2002;324:625e6.
[22] Samad A. Coronary artery disease in Pakistan; preventiveaspects. Pak J Cardiol 2003;14(2):59e60.
[23] Khan NR, Mallick IA. Economic situation in Pakistan’sNational Health Survey of Pakistan. Pak J Med Res 1992;31(4):282e8.
[24] Ghaffar A, Reddy KS, Singhi M. Burden of noncommuni-cable diseases in South Asia. Br Med J 2004;328:807e10.
[25] Kakepoto GN, Iqbal MP, Iqbal SP. Megaloblastic anaemia ina hospital-based population. Med Sci Res 2000;28:45e7.
[26] Antony AC. Prevalence of cobalamin (vitamin B-12) andfolate deficiency in India e audi alteram partem. Am J ClinNutr 2001;74:157e9.
[27] de Jong SC, Stehouwer CDA, van den Berg M, Kostense PJ,Alders D, Jakobs C, et al. Determinants of fasting and post-methionine homocysteine levels in families predisposed tohyperhomocysteinemia and premature vascular disease.Arterioscler Thromb Vasc Biol 1999;19:1316e24.
[28] Dalery K, Lussier Cacan S, Selhub J, Davignon J, Latour Y,Genest Jr J. Homocysteine and coronary artery disease inFrench Canadian subjects: relation with vitamins B12, B6,pyridoxal phosphate, and folate. Am J Cardiol 1995;75:1107e11.

108 M.P. Iqbal et al.
[29] Lolin YI, Sanderson JE, Cheng SK, Chan CF, Pang CP, Woo KS,et al. Hyperhomocysteinaemia and premature coronaryartery disease in the Chinese. Heart 1996;76:117e22.
[30] Sastry BK, Indira N, Anand B, Kedarnath Prabha BS,Raju BS. A case-control study of plasma homocysteinelevels in South Indians with and without coronary arterydisease. Indian Heart J 2001;53:749e53.
[31] Leowattana W, Mahanonda N, Bhuripunyo K, Pokum S.Association between serum homocysteine, vitamin B12,folate and Thai coronary artery disease patients. J MedAssoc Thai 2000;83:536e42.
[32] Tokgozoglu SL, Alikasifoglu M, Unsal Atalar E, Aytemir K,Ozer N, Ovunc K, et al. Methylene tetrahydrofolatereductase genotype and the risk and extent of coronaryartery disease in a population with low plasma folate.Heart 1999;81:518e22.
[33] Refsum H, Yajnik CS, Gadkari M, Schneede J, Vollset SE,Orning L, et al. Hyperhomocysteinemia and elevatedmethylmalonic acid indicate a high prevalence of co-balamin deficiency in Asian Indians. Am J Clin Nutr 2001;74:233e41.
[34] Knekt P, Reunanen A, Alfthan G, Heliovaara M, Rissanen H,Marniemi J, et al. Hyperhomocystinemia: a risk factor ora consequence of coronary heart disease? Arch Intern Med2001;161:1589e94.
[35] Nygard O, Vollset SE, Refsum H, Stensvold I, Tverdal A,Nordrehaug JE, et al. Total plasma homocysteine andcardiovascular risk profile. The Hordaland HomocysteineStudy. JAMA 1995;274:1526e33.
[36] Bates CJ, Mansoor MA, van der Pols J, Prentice A, Cole TJ,Finch S. Plasma total homocysteine in a representativesample of 972 British men and women aged 65 and over.Eur J Clin Nutr 1997;51:691e7.
[37] Chou ST, Ko LE, Lim PS, Huang JL, Yang CS. Effect of ageand sex on plasma total homocysteine in Taiwanesesubjects. Chin J Physiol 2000;43:159e64.
[38] Andersson A, Brattstrom L, Israelsson B, Isaksson A,Hamfelt A, Hultberg B. Plasma homocysteine before andafter methionine loading with regard to age, gender, andmenopausal status. Eur J Clin Invest 1992;22:79e87.
[39] MansoorMA,BergmarkC,SvardalAM,LonningPE,UelandPM.Redox status and protein binding of plasma homocysteineandotheraminothiols inpatientswithearly-onset peripheralvascular disease. Homocysteine and peripheral vasculardisease. Arterioscler Thromb Vasc Biol 1995;15:232e40.
[40] Subar AF, Harlan LC, Mattson ME. Food and nutrient intakedifferences between smokers and non-smokers in the US.Am J Public Health 1990;80:1323e9.
[41] Pryor WA, Stone K. Oxidants in cigarette smoke. Radicals,hydrogen peroxide, peroxynitrate, and peroxynitrite. AnnNY Acad Sci 1993;686:12e28.
[42] Gey KF. Prospects for the prevention of free radicaldisease, regarding cancer and cardiovascular disease. BrMed Bull 1993;49:679e99.
[43] Herbert V. Development of human folate deficiency. In:Picciano MF, Stokstad ELR, Gregory JF, editors. Folic acidmetabolism in health and disease. New York: Willey-Liss;1990. p. 195e210.
Copyright © 2022 FDOKUMEN




















