
Effects of Hyperhomocysteinemia on Arterial Pressure and Nitric Oxide Production in Pregnant Rats
10
Effects of Hyperhomocysteinemia on Arterial Pressure and Nitric Oxide Production in Pregnant Rats DL Chandler, MT Llinas, JF Reckelhoff, B LaMarca, J Speed, and JP Granger University of Mississippi Medical Center, Department of Physiology and Biophysics and the Center for Excellence in Cardiovascular-Renal Research, 2500 N. State Street, Jackson, Mississippi 39216-4505 Abstract Background—An elevated plasma level of homocysteine (hyperhomocysteinemia) is thought to be an important risk factor for a variety of cardiovascular diseases including preeclampsia. Although clinical studies have reported a 2-3 fold elevation in plasma levels of homocysteine in women who developed preeclampsia, the importance of hyperhomocysteinemia in causing endothelial dysfunction and increases in arterial pressure during pregnancy is unknown. Method—Therefore, the purpose of this study was to determine the effects of a 2-3 fold elevation in plasma homocysteine levels on arterial pressure, chronic pressure natriuresis relationship, and endothelial factors during pregnancy in the rat. Homocysteine treatment for 4 weeks increased plasma homocysteine levels in pregnant rats from 7.1 ± 1.9 to 16.7 ± 2.3 μmol/L. Results—Homocysteine treatment decreased urinary nitrate/nitrite levels from 53 +/- 7 vs. 39 +/- 5 (umol/24 h/kg BW) in pregnant rats while having no effect on urinary excretion of endothelin. Homocysteine treatment had no effect on MAP in pregnant rats (104 +/- 2 vs. 107 +/- 3 mmHg) nor on the chronic pressure natriuresis relationship. Conclusion—These results suggest that while hyperhomocysteinemia decreases nitric oxide production in pregnant rats, hyperhomocysteinemia does not affect MAP, the chronic pressure- natriuresis relationship, or urinary excretion of endothelin in pregnant rats. Moreover, the reported 2-3 fold elevation in plasma level of homocysteine in women with preeclampsia is unlikely to contribute to the hypertension of preeclampsia. Keywords hyperhomocysteinemia; preeclampisa; urinary nitrate/nitrite Introduction Preeclampsia is a multisystemic disorder of pregnancy estimated to affect 5% to 10% of all pregnancies in the United States. 1 Preeclampsia is also one of the leading causes of maternal death and prenatal morbitity. 1,2,3 Although widespread vascular dysfunction and increases in blood pressure occurs during preeclampsia, the mechanisms responsible for this disorder are unclear. 1,2,3 Endothelial dysfunction, decreases in nitric oxide production, and enhanced endothelin production have all been suggested to be important factors in the pathophysiology of hypertension during preeclampsia. 4,5,6,7,8 Please address all correspondence to: Joey P. Granger, Ph.D., Department of Physiology and Biophysics, University of Mississippi Medical Center, 2500 N. State Street, Jackson, MS 39216-4505, Phone: (601) 984-1801, Fax: (601) 984-1817. Disclosures: There are no financial disclosures and no conflict of interest to report from any of the authors. NIH Public Access Author Manuscript Am J Hypertens. Author manuscript; available in PMC 2010 October 1. Published in final edited form as: Am J Hypertens. 2009 October ; 22(10): 1115–1119. doi:10.1038/ajh.2009.130. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Effects of Hyperhomocysteinemia on Arterial Pressure and Nitric Oxide Production in Pregnant Rats
Effects of Hyperhomocysteinemia on Arterial Pressure and NitricOxide Production in Pregnant Rats
DL Chandler, MT Llinas, JF Reckelhoff, B LaMarca, J Speed, and JP GrangerUniversity of Mississippi Medical Center, Department of Physiology and Biophysics and theCenter for Excellence in Cardiovascular-Renal Research, 2500 N. State Street, Jackson,Mississippi 39216-4505
AbstractBackground—An elevated plasma level of homocysteine (hyperhomocysteinemia) is thought tobe an important risk factor for a variety of cardiovascular diseases including preeclampsia.Although clinical studies have reported a 2-3 fold elevation in plasma levels of homocysteine inwomen who developed preeclampsia, the importance of hyperhomocysteinemia in causingendothelial dysfunction and increases in arterial pressure during pregnancy is unknown.
Method—Therefore, the purpose of this study was to determine the effects of a 2-3 fold elevationin plasma homocysteine levels on arterial pressure, chronic pressure natriuresis relationship, andendothelial factors during pregnancy in the rat. Homocysteine treatment for 4 weeks increasedplasma homocysteine levels in pregnant rats from 7.1 ± 1.9 to 16.7 ± 2.3 μmol/L.
Results—Homocysteine treatment decreased urinary nitrate/nitrite levels from 53 +/- 7 vs. 39 +/-5 (umol/24 h/kg BW) in pregnant rats while having no effect on urinary excretion of endothelin.Homocysteine treatment had no effect on MAP in pregnant rats (104 +/- 2 vs. 107 +/- 3 mmHg)nor on the chronic pressure natriuresis relationship.
Conclusion—These results suggest that while hyperhomocysteinemia decreases nitric oxideproduction in pregnant rats, hyperhomocysteinemia does not affect MAP, the chronic pressure-natriuresis relationship, or urinary excretion of endothelin in pregnant rats. Moreover, the reported2-3 fold elevation in plasma level of homocysteine in women with preeclampsia is unlikely tocontribute to the hypertension of preeclampsia.
Keywordshyperhomocysteinemia; preeclampisa; urinary nitrate/nitrite
IntroductionPreeclampsia is a multisystemic disorder of pregnancy estimated to affect 5% to 10% of allpregnancies in the United States.1 Preeclampsia is also one of the leading causes of maternaldeath and prenatal morbitity.1,2,3 Although widespread vascular dysfunction and increasesin blood pressure occurs during preeclampsia, the mechanisms responsible for this disorderare unclear.1,2,3 Endothelial dysfunction, decreases in nitric oxide production, and enhancedendothelin production have all been suggested to be important factors in thepathophysiology of hypertension during preeclampsia.4,5,6,7,8
Please address all correspondence to: Joey P. Granger, Ph.D., Department of Physiology and Biophysics, University of MississippiMedical Center, 2500 N. State Street, Jackson, MS 39216-4505, Phone: (601) 984-1801, Fax: (601) 984-1817.Disclosures: There are no financial disclosures and no conflict of interest to report from any of the authors.
NIH Public AccessAuthor ManuscriptAm J Hypertens. Author manuscript; available in PMC 2010 October 1.
Published in final edited form as:Am J Hypertens. 2009 October ; 22(10): 1115–1119. doi:10.1038/ajh.2009.130.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
A number of clinical studies have shown that women with higher plasma homocysteine(hyperhomocysteinemia) levels early in pregnancy have a higher incidence of preeclampsia,intra-uterine growth restriction (IUGR), as well as first trimester miscarriages. 8,9,10,11,12
Elevated homocysteine levels, a demethylated derivative of methionine, has been suggestedas a risk factor for a variety of cardiovascular diseases including coronary artery disease,stroke, and peripheral arterial disease.13,14 Hyperhomocysteinemia has been reported tocause endothelial dysfunction by scavenging or trapping nitric oxide.15 We and others havereported that nitric oxide (NO) plays an important role in mediating the cardiovascular andhemodynamic changes during pregnancy.5,16,17,18 In addition, a decrease in nitric oxideproduction and/or availability has been shown to increase endothelin production, reduce therenal pressure natriuresis relationship, and cause a salt-sensitive form of hypertension.19
Therefore, it is possible that hyperhomocysteinemia during pregnancy may decrease thenitric oxide levels during pregnancy and lead to hypertension. Although there is a strongcorrelation between hyperhomocysteinemia and preeclampsia there are no studies to ourknowledge that demonstrate a physiological role for elevated homocysteine levels duringpregnancy.20,21 Therefore, the purpose of this study was to assess the effect ofhyperhomocysteinemia; comparable to plasma levels observed in women in preeclampsia,on arterial pressure, renal pressure natriuresis relationship, and nitric oxide and endothelinproduction during pregnancy.
MethodsAll experimental procedures executed in this study were in accordance with NationalInstitutes of Health guidelines for use and care of animals with approval of all protocols bythe Animal Care and Use Committee at the University of Mississippi Medical Center.Female, virgin Sprague Dawley rats purchased from Harlan Sprague Dawley Inc.(Indianapolis, IN) were housed in a temperature-controlled room (23°C) with a 12:12 hourlight/dark cycle with food and water available ad libitum.
Experimental designRats treated with homocysteine were administered DL-homocysteine (Sigma, St. Louis,MO) in the drinking water (0.67 mg/ml) one week prior to breeding and maintained on thistreatment throughout the experiment to create a condition of hyperhomocysteinemia. On day17 and 18 pregnancy, rats on a normal sodium diet were placed in individual metabolismcage for 24 hours for collection of urine. Control (n=7) and homocysteine treated (n=9) ratswere surgically instrumented with femoral catheters on day 18 of pregnancy. Arterialpressure measurements and subsequent harvesting of kidneys were performed on day 19 - 20of pregnancy.
To assess the chronic pressure natriuresis relationship, arterial pressure and sodiumexcretion were measured in four groups of pregnant rats on day 19 of pregnancy: pregnantcontrol rats-normal 1% NaCl diet (n=7), pregnant control rats-high 8% NaCl diet (n=6),pregnant rats treated with homocysteine- normal 1% NaCl diet (n=9), and pregnant ratstreated with homocysteine-high 8% NaCl diet (n=5).
The effects of hyperhomocysteinemia on arterial pressure and the chronic pressurenatriuresis relationship were also examined in virgin rats: virgin control-normal sodium diet(n=12), virgin control-high sodium diet (n=6), virgin treated with homocysteine-normalsodium diet (n=10) and virgin treated with homocysteine-high sodium diet (n=6).
Chandler et al. Page 2
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mean arterial pressure measurements in conscious ratsRats were anesthetized with 5% isoflurane (W.A. Butler Co., Memphis, TN) delivered by ananesthesia apparatus (Vaporizer for Forane Anesthetic, Ohio Medical Products, Madison,WI). During isoflurane anesthesia, rats were surgically instrumented with catheters (PE 50tubing) in the femoral artery for blood sampling and blood pressure monitoring. The arterialcatheter was tunneled to the back of the neck and exteriorized. Arterial pressure wasmonitored with a pressure transducer connected to a recorder for continuous recording.
Analysis of Plasma HomocysteineTotal plasma homocysteine (tHcys) was measured by fluorescence HPLC analysis asdescribed previously by Chen and Zou.22 Briefly, blood samples of 1 mL were collected intoVacutainer tubes containing sodium heparin (Becton Dickinson) and immediatelycentrifuged at 1000g for 10 minutes at 4°C. Plasma samples (100-μL) or solutions mixedwith 10 μL internal standard, (2-mercaptoethylamine (ME) (2.0 mmol/L)), were treated with10 μL of 10% tri-n-butylphosphine (TBP) in dimethylformamide at 4°C for 30 minutes.Subsequently, 100 μL of the supernatant was transferred into a solution containing 20 μL of1.55 mol/L sodium hydroxide, 250 μL of 0.125 mol/L borate buffer (pH 9.5), and 100 μL of1.0 mg/mL ABD-Fsolution. The resulting mixture was incubated at 60°C for 30 minutes toaccomplish derivatization of plasma thiols. HPLC was performed with a Hewlett-PackardModel 1090 Series II system with an autosampler. Separation was carried out at ambienttemperature on an analytical column, Supelco LC-18-DB (150×4.6 mm ID, 5 μm) with aSupelcosil LC-18 guard column (20×4.6 mm ID, 5 μm). Fluorescence intensities weremeasured spectrophotometrically (Hewlett-Packard Model 1046A) at an excitationwavelength of 385 nm and emission wavelength of 515 nm. The peak area of thechromatographs was quantified with a Hewlett-Packard 3392 integrator. The analyticalcolumn was eluted with 0.1 mol/L potassium dihydrogenphosphate buffer (pH 2.1)containing 6% acetonitrile (vol/vol) as mobile phase with a flow rate of 2.0 mL/min.
Urinary nitrite/nitrate excretion24-hour nitrite/nitrate excretion was used to determine whole body NO production. Animalswere fed a low nitrite/nitrate diet (AIN76, ICN Biomedicals, Inc., Aurora, OH) starting 5days prior to placement in the metabolism cages. Nitrite/nitrate excretion determination wasdescribed previously.23 Briefly, E. coli was the source of nitrate reductase for conversion ofnitrate to nitrite and sodium nitrate will be used as the standard to verify that all nitrate isconverted to nitrite. The concentration of nitrite was measured colorimetrically using theGriess reagent. Sodium nitrite was used as the standard with data expressed as μmole nitrate/nitrite excreted/24 h of the rat.
Measurement of endothelinThe urinary excretion of endothelin was measured in 24-hour urine samples. The sampleswere frozen and stored at −80°C until determination of endothelin concentration byradioimmunoassay kit (Amersham Internatal, Amersham, UK) utilizing competitive bindingwith a fixed quantity of 125I-labeled endothelin-1 (synthetic) for an endothelin-1 specificantibody.
Determination of Urinary Protein LevelsUrinary excretion of protein was measured in animals with 24 hour urine collection andstorage of final sample at −20°C. Protein concentration was determined using a SigmaProtein Determination kit (P5656, Sigma Chemical Co.)24
Chandler et al. Page 3
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Statistical AnalysesSigma-STAT version 1.0 was used for all statistical analysis. All data are expressed as mean± SEM. All treated group were compared to their respective controls. When comparisonswere made between groups, an unpaired student t-test was used. A value of P<0.05 wasconsidered statistically significant. A 3 way ANOVA and multiple comparison test (Holm-Sidak method) was utilized to compare the effects of Na diet and homocysteine in bloodpressure between virgin and pregnant groups.
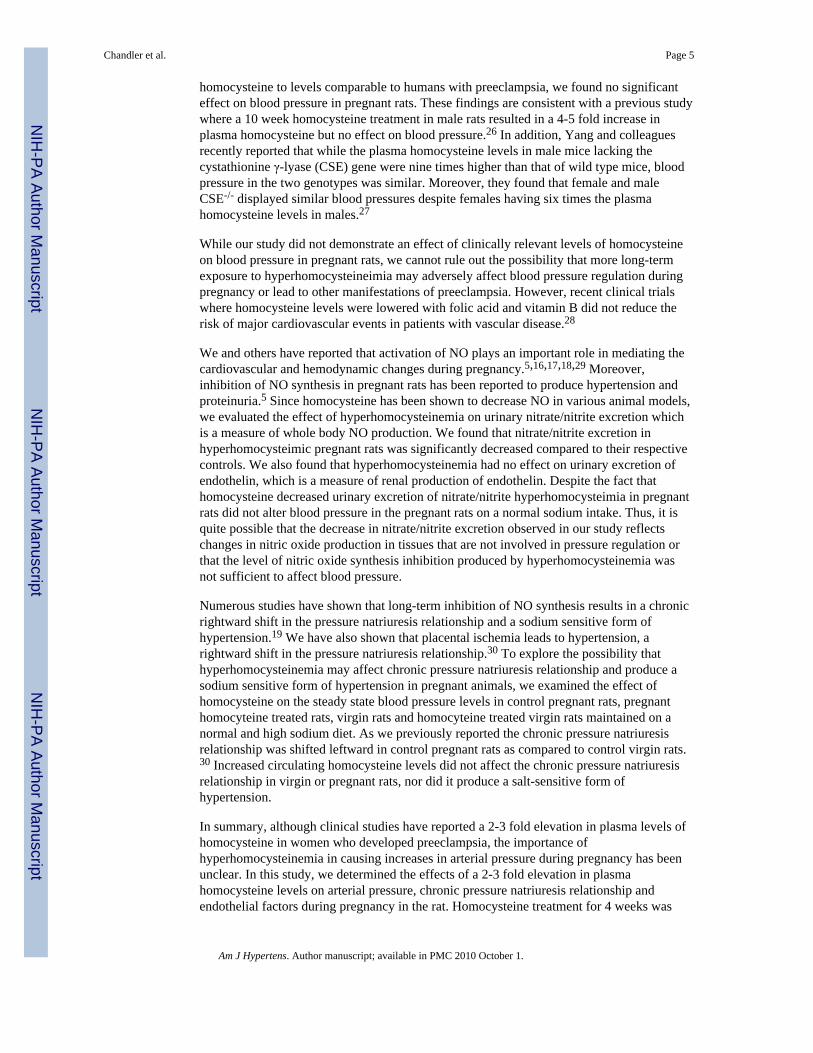
ResultsFigure 1 illustrates the effect of increasing plasma homocysteine levels on mean arterialpressure in pregnant rats on a normal sodium intake. Increasing plasma homocysteine from7.1 ± 1.9 to 16.7 ± 2.3 μmol/ L (p<0.05) did not have an effect on mean arterial pressure inhomocysteine treated pregnant rats (107± 3 mmHg) as compared to control pregnant rats(104± 2 mmHg).
Figure 2 depicts the effect of elevated homocysteine levels on urinary nitrate/nitrite,endothelin and protein excretion. Urinary nitrate/nitrite excretion was significantly reducedfrom 53 ± 7 to 39 ± 5ρg/day (p<0.05) when pregnant rats were treated with homocysteine.Homocysteine treatment did not have an effect on endothelin or protein excretion.Endothelin excretion averaged 1.2± 0.2 pg/day in pregnant rats and 1.3± 0.2 pg/day inhomocysteine treated pregnant rats. Urinary protein excretion averaged 19.1 ± 9 mg/day incontrol pregnant rats and 29.1± 2 mg/day in homocysteine treated pregnant rats.
Figure 3 illustrates the effect of increasing homocysteine levels in virgin and pregnant ratson the slope of the pressure natriuresis relationship. As we previously reported the chronicpressure natriuresis relationship was shifted leftward in control pregnant rats as compared tocontrol virgin rats. Increasing plasma homocysteine levels did not affect the chronic pressurenatriuresis relationship in virgin or pregnant rats.
DiscussionClinical studies have shown that elevated plasma levels of homocysteine in early pregnancyincreases the risk factor for preeclampsia.20,21 For example, Lopez-Quesada and colleaguesreported that pregnant women with hyperhomocysteinemia in the third trimester ofpregnancy have a 8-fold increased risk for developing preeclampsia.21 Normal plasmahomocysteine levels for pregnant women are ∼ 8.4 μmol/L and hyperhomocysteinemia isclassified as a plasma level of homocysteine of ∼ 10.5 μmol/L or higher.20,21 In this studywe elevated the plasma levels of homocysteine one week before breeding and continued thehomocysteine treatment throughout the three weeks of pregnancy in rats. Our pregnant ratshad plasma homocysteine levels of of ∼ 17 μmol/L on day 19 of pregnancy, a 2.5-foldincrease over our control pregnant rats and comparable to the values observed in womenwith preeclampsia.
Experimental and clinical evidence support a correlation between plasma homocysteinelevels and blood pressure.11,12,13,21 Increased homocysteine levels has been proposed tocause hypertension through arterial stiffening.25 Hyperhomocysteinemia has also beensuggested to cause hypertension via an oxidative stress and endothelial dysfunction.11,12,13
However, most of the animal studies that have observed an effect of homocysteine treatmenton blood pressure did not measure plasma homocysteine or utilized doses of homocysteinethat would achieve concentrations far beyond those observed in preeclamptic women. In thepresent study we evaluated the effects of experimentally induced hyperhomocysteinemia onblood pressure in pregnant rats. Although we increased our plasma concentration of
Chandler et al. Page 4
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
homocysteine to levels comparable to humans with preeclampsia, we found no significanteffect on blood pressure in pregnant rats. These findings are consistent with a previous studywhere a 10 week homocysteine treatment in male rats resulted in a 4-5 fold increase inplasma homocysteine but no effect on blood pressure.26 In addition, Yang and colleaguesrecently reported that while the plasma homocysteine levels in male mice lacking thecystathionine γ-lyase (CSE) gene were nine times higher than that of wild type mice, bloodpressure in the two genotypes was similar. Moreover, they found that female and maleCSE-/- displayed similar blood pressures despite females having six times the plasmahomocysteine levels in males.27
While our study did not demonstrate an effect of clinically relevant levels of homocysteineon blood pressure in pregnant rats, we cannot rule out the possibility that more long-termexposure to hyperhomocysteineimia may adversely affect blood pressure regulation duringpregnancy or lead to other manifestations of preeclampsia. However, recent clinical trialswhere homocysteine levels were lowered with folic acid and vitamin B did not reduce therisk of major cardiovascular events in patients with vascular disease.28
We and others have reported that activation of NO plays an important role in mediating thecardiovascular and hemodynamic changes during pregnancy.5,16,17,18,29 Moreover,inhibition of NO synthesis in pregnant rats has been reported to produce hypertension andproteinuria.5 Since homocysteine has been shown to decrease NO in various animal models,we evaluated the effect of hyperhomocysteinemia on urinary nitrate/nitrite excretion whichis a measure of whole body NO production. We found that nitrate/nitrite excretion inhyperhomocysteimic pregnant rats was significantly decreased compared to their respectivecontrols. We also found that hyperhomocysteinemia had no effect on urinary excretion ofendothelin, which is a measure of renal production of endothelin. Despite the fact thathomocysteine decreased urinary excretion of nitrate/nitrite hyperhomocysteimia in pregnantrats did not alter blood pressure in the pregnant rats on a normal sodium intake. Thus, it isquite possible that the decrease in nitrate/nitrite excretion observed in our study reflectschanges in nitric oxide production in tissues that are not involved in pressure regulation orthat the level of nitric oxide synthesis inhibition produced by hyperhomocysteinemia wasnot sufficient to affect blood pressure.
Numerous studies have shown that long-term inhibition of NO synthesis results in a chronicrightward shift in the pressure natriuresis relationship and a sodium sensitive form ofhypertension.19 We have also shown that placental ischemia leads to hypertension, arightward shift in the pressure natriuresis relationship.30 To explore the possibility thathyperhomocysteinemia may affect chronic pressure natriuresis relationship and produce asodium sensitive form of hypertension in pregnant animals, we examined the effect ofhomocysteine on the steady state blood pressure levels in control pregnant rats, pregnanthomocyteine treated rats, virgin rats and homocyteine treated virgin rats maintained on anormal and high sodium diet. As we previously reported the chronic pressure natriuresisrelationship was shifted leftward in control pregnant rats as compared to control virgin rats.30 Increased circulating homocysteine levels did not affect the chronic pressure natriuresisrelationship in virgin or pregnant rats, nor did it produce a salt-sensitive form ofhypertension.
In summary, although clinical studies have reported a 2-3 fold elevation in plasma levels ofhomocysteine in women who developed preeclampsia, the importance ofhyperhomocysteinemia in causing increases in arterial pressure during pregnancy has beenunclear. In this study, we determined the effects of a 2-3 fold elevation in plasmahomocysteine levels on arterial pressure, chronic pressure natriuresis relationship andendothelial factors during pregnancy in the rat. Homocysteine treatment for 4 weeks was
Chandler et al. Page 5
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
associated with a 2-3 fold increase in plasma homocysteine levels in pregnant rats. Whilehomocysteine treatment decreased urinary nitrate/nitrite levels in pregnant rats,hyperhomocysteinemia had no effect on mean arterial pressure nor on the chronic pressurenatriuresis relationship in pregnant rats. These results suggest that while clinical studies havereported elevations in plasma levels of homocysteine in women who developedpreeclampsia, it is unlikely that a 2-3 fold increase in homocysteine contributes to thehypertension observed in preeclamptic women.
AcknowledgmentsThis work was supported by National Institute of Health Grants HL-51971 and HL-07635. We also thank KathyCockrell and Elizabeth Sullivan for their excellent technical assistance.
References1. National High Blood Pressure Education Program working Group Report on High Blood Pressure in
Pregnancy. Am J Obstet Gynecol. 1990; 163:1691–1712. [PubMed: 2104525]2. Granger JP, Alexander BT, Llinas MT, Bennett WA, Khalil RA. Pathophysiology of Hypertension
During Preeclampsia Linking Placental Ischemia With Endothelial Dysfunction. Hypertension.2001; 38(3):718–722. [PubMed: 11566964]
3. Davison JM, Homuth V, Jeyabalan A, Conrad KP, Karumanchi SA, Quaggin S, Dechend R, LuftFC. New Aspects in the Pathophysiology of Preeclampsia. J Am Soc Nephrol. 2004; 15(9):2440–2448. [PubMed: 15339993]
4. de Groot C, Taylor R. New insights in to the etiology of preeclampsia. Ann Med. 1993; 25:243–249.[PubMed: 8333923]
5. Baylis C, Suto T, Conrad K. Importance of nitric oxide in control of systemic and renalhemodynamics during normal pregnancy: studies in the rat and implications for preeclampsia.Hypertens Pregnancy. 1996; 15:147–169.
6. LaMarca BB, Gilbert J, Granger JP. Recent Progress Toward the Understanding of thePathophysiology of Hypertension During Preeclampsia. Hypertension. 2008 Apr; 51(4):982–8.[PubMed: 18259004]
7. Wolf M, Kettyle E, Sandler L, Ecker JL, Roberts J, Thadhani R. Obesity and Preeclampsia: ThePotential Role of Inflammation. Obstet Gynecol. 2001; 98(5):757–762. [PubMed: 11704165]
8. Dekker G, De Vries J, Doelitzsch P. Underlying disorders associated with severe early-onsetpreeclampsia. Am J Obstet Gynecol. 1995; 173:1042–1048. [PubMed: 7485291]
9. Hogg B, Tamura T, Johnston K, Dubard M, Goldendberg R. Second-trimester plasma homocysteinelevels and pregnancy-induced hypertension, preeclampsia, and intrauterine growth restriction. Am JObstet Gynecol. 2000; 183:805–809. [PubMed: 11035317]
10. Mudd SH, Finkelstein JD, Irreverre F, Laster L. Homocystinuria: An Enzymatic Defect. Science.1964; 143(3613):1443–1445. [PubMed: 14107447]
11. Powers R, Evans R, Majors A. Plasma homocysteine concentration is increased preeclampsia andis associated with evidence of endothelial activation. Am J Obstet Gynecol. 1998; 179:1605–1611.[PubMed: 9855605]
12. Rajkovic A, Mahomed K, Malinow MR, Sorenson TK, Woelk GB, Williams MA. PlasmaHomocyst(e)ine Concentrations in Eclamptic and Preeclamptic African Women Postpartum.Obstet Gynecol. 1999; 94(3):355–360. [PubMed: 10472859]
13. McDowell IFW, Lang D. Homocysteine and Endothelial Dysfunction: A Link with CardiovascularDisease. J Nutr. 2000; 130(2):369.
14. Brattstrom L, Wilcken DEL. Homocysteine and cardiovascular disease: cause or effect? Am J ClinNutr. 2000; 72(2):315–323. [PubMed: 10919920]
15. Li N, Yi FX, Rute E, Zhang DX, Slocum GR, Zou AP. Effects of homocysteine on intracellularnitric oxide and superoxide levels in the renal arterial endothelium. Am J Physiol Heart CircPhysiol. 2002; 283(3):H1237–1243. [PubMed: 12181155]
Chandler et al. Page 6
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
16. Abram SR, Alexander BT, Bennett WA, Granger JP. Role of neuronal nitric oxide synthase inmediating renal hemodynamic changes during pregnancy. Am J Physiol Regul Integr CompPhysiol. 2001; 281(5):R1390–1393. [PubMed: 11641107]
17. Alexander BT, Cockrell K, Cline FD, Granger JP. Inducible Nitric Oxide Synthase InhibitionAttenuates Renal Hemodynamics During Pregnancy. Hypertension. 2002; 39(2):586–590.[PubMed: 11882613]
18. Williams DJ, Vallance PJ, Neild GH, Spencer JA, Imms FJ. Nitric oxide-mediated vasodilation inhuman pregnancy. Am J Physiol Heart Circ Physiol. 1997; 272(2):H748–752.
19. Granger JP, Alexander BT. Abnormal pressure natriuresis in hypertension: Role of nitric oxide.Acta Physiologica Scandinavia. 2000; 168(1):161–168.
20. Cotter A, Molloy A, Scott J, Daly S. Elevated plasma homocysteine in early pregnancy: a riskfactor for the development of severe preeclampsia. Am J Obstet Gynecol. 2001; 185(4):781–209.[PubMed: 11641651]
21. Lopez-Quesada E, Vilaseca M, Lailla J. Plasma total homocysteine in uncomplicated pregnancyand in preeclampsia. European Journal of Obstetrics and Gynecology. 2003; 108:45–49.
22. Li N, Chen YF, Zou AP. Implications of Hyperhomocysteinemia in Glomerular Sclerosis inHypertension. Hypertension. 2002; 39(2):443–448. [PubMed: 11882587]
23. Reckelhoff JF, Kellum JA, Blanchard EJ, Bacon EE, Wesley AJ, Kruckeberg WC. Changes innitric oxide precursor, L-arginine, and metabolites, nitrate and nitrite, with aging. Life Sci. 1994;55(24):1895–1902. [PubMed: 7990649]
24. Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurements with the folin phenolreagent. J Biol Chem. 1951; 193:265–275. [PubMed: 14907713]
25. Bartolotto L, Safar M, Blacher J. Plasma homocysteine, aortic, stiffness and renal function inhypertensive patients. Hypertension. 1999; 34(part2):837–842. [PubMed: 10523370]
26. Joseph J, Joseph L, Shekhawat NS, Devi S, Wang J, Melchert RB, Hauer-Jenson M, Kennedy RH.Hyperhomocysteinemia leads to pathological ventricular hypertrophy in normotensive rats. AM JPhysiol Heart Circ Physiol. 2003 Aug; 285(2):H679–86. Epub 2003 May 1. [PubMed: 12730062]
27. Yang G, Wu L, Jiang B, Yang W, Qi J, Cao K, Meng Q, Mustafa AK, Mu W, Zhang S, SnyderSH, Wang R. H2S as a physiologic vasorelaxant: hypertension in mice with deletion ofcystathionine gamma-lyase. Science. 2008 Oct 24; 322(5901):587–90. [PubMed: 18948540]
28. Lonn E, Yusuf S, Arnold MJ, Sheridan P, Pogue J, Micks M, McQueen MJ, Probstfield J, Fodor G,Held C, Genest J Jr. Heart Outcomes Prevention Evaluation (HOPE) 2 Investigators Homocysteinelowering with folic acid and B vitamins in vascular disease. N Engl Med. 2006 Apr 13; 354(15):1567–77.
29. Alexander BT, Kassab SE, Miller MT, Abram SR, Reckelhoff JF, Bennett WA, Granger JP.Reduced Uterine Perfusion Pressure During Pregnancy in the Rat Is Associated With Increases inArterial Pressure and Changes in Renal Nitric Oxide. Hypertension. 2001; 37(4):1191–1195.[PubMed: 11304523]
30. Granger JP, Alexander BT, Abram SR, Reckelhoff JF, Wilson J, Rinewalt AN. Chronic reductionsin uterine perfusion pressure in the pregnant rat produces hypertension and reduces pressure-natriuresis. Hypertension. 2001; 36(4):682. abstract.
Chandler et al. Page 7
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Figure 1.Effect of increasing plasma homocysteine levels (pregnant, n=5, versus homocysteinepregnant, n=6) on mean arterial pressure (pregnant, n=7, versus homocysteine pregnant,n=9) in pregnant rats. All values are expressed as means ± SE. * denotes p < 0.05.
Chandler et al. Page 8
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
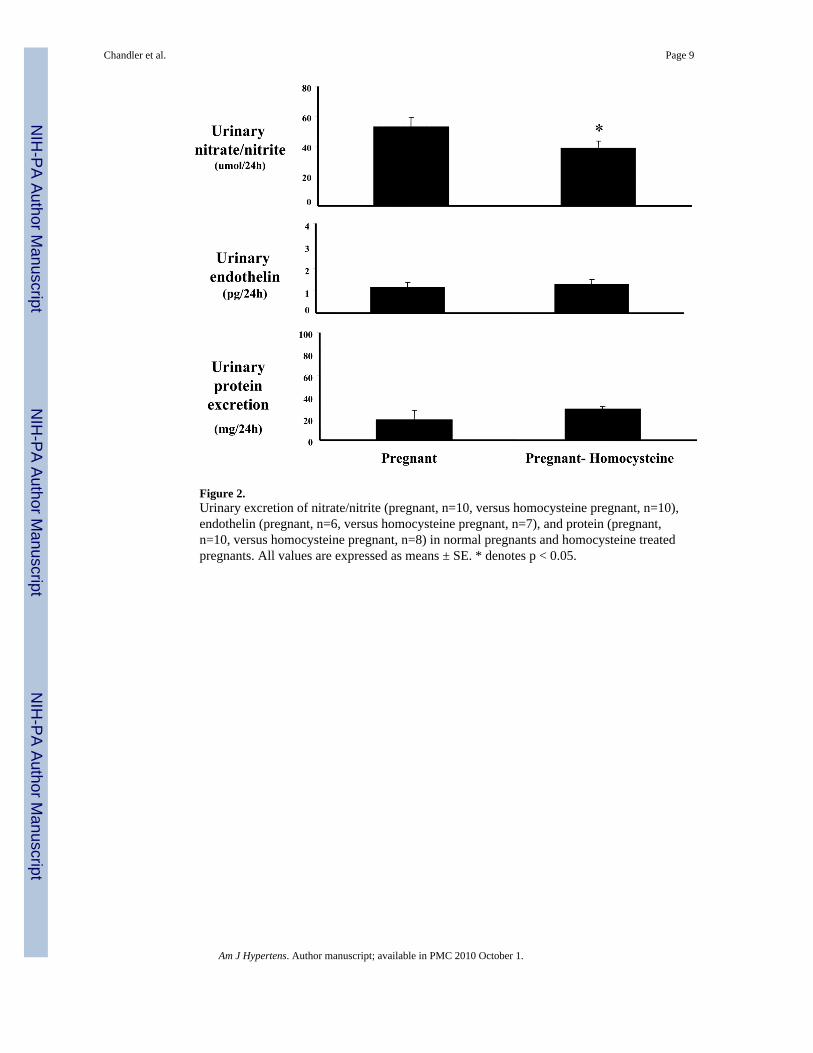
Figure 2.Urinary excretion of nitrate/nitrite (pregnant, n=10, versus homocysteine pregnant, n=10),endothelin (pregnant, n=6, versus homocysteine pregnant, n=7), and protein (pregnant,n=10, versus homocysteine pregnant, n=8) in normal pregnants and homocysteine treatedpregnants. All values are expressed as means ± SE. * denotes p < 0.05.
Chandler et al. Page 9
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
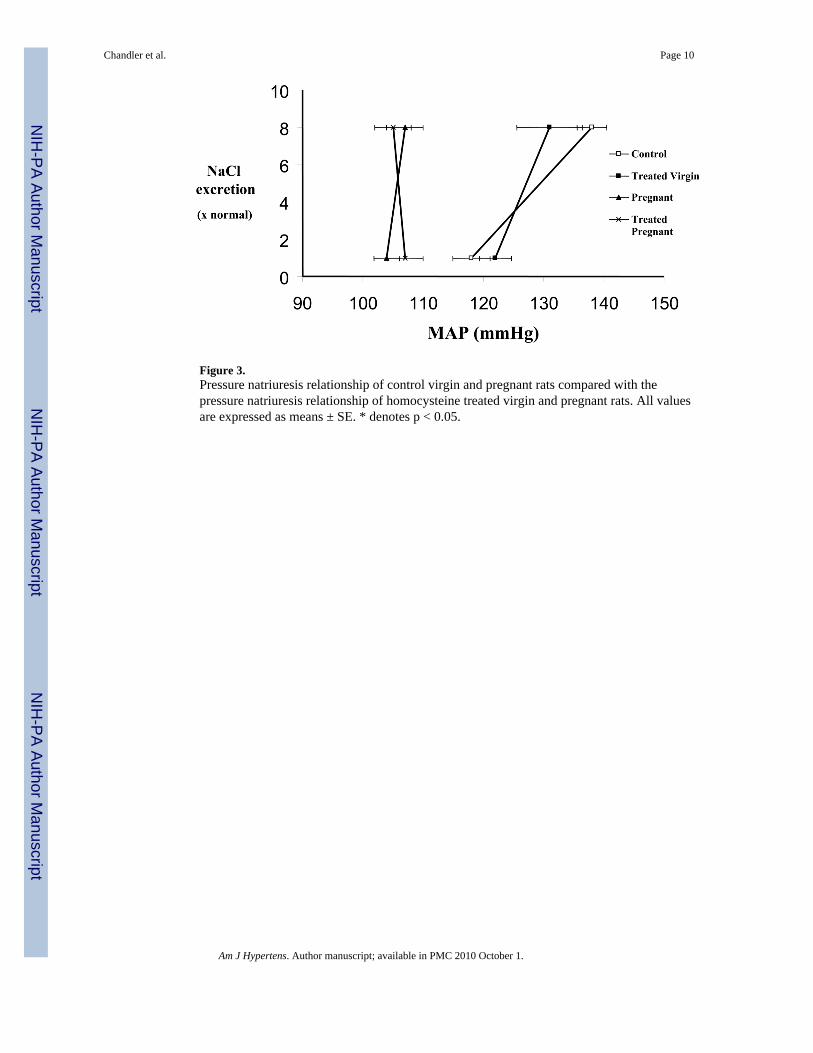
Figure 3.Pressure natriuresis relationship of control virgin and pregnant rats compared with thepressure natriuresis relationship of homocysteine treated virgin and pregnant rats. All valuesare expressed as means ± SE. * denotes p < 0.05.
Chandler et al. Page 10
Am J Hypertens. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript




















