
Optimal Exposure Time for Diagnosis of Approximal Caries ...

SCiENTIFIC ARTICLE
Oral Conditions in Children withCerebral Palsy
Maria Teresa Botti ROdrigues dos Santos DDSe PhDDanilo Masiero MD PhD
Neil Ferreira Novo DDSe PhDMaria Regina Lorenzetti Simionato DDSe PhD
ABSTRACTPurpose Cerebral palsy (CP) is a major severechildhood disability and its prevalence is increasingparticularly among premature low-weight newborns The oral conditions observed demonstratethe need for home and professional care for these individuals This study aimed to investigatedental caries plaque index time of eruption malocclusion bruxism and motor oral skills in agroup of 62 CP children (study group)Methods The results were compared to those obtained for a control group with 67 normal chil-dren Nonparametric statistical tests including the Mann-Whitney test FishersExact test (P) Chi-square test (Xl) and Cochrans Q test were used according to the nature of the variables studiedwith the level of significance set at Plt05Results The results showed a significantly higher DMFS index for CP children with permanentdentition of both sexeswhen compared to normal children A significantly higher plaque index wasalso observed in the study group A high tendency to delayed eruption of permanent molars andsignificantly higher percentages of malocclusion and bruxism were observed in the study groupwith permanent dentition Residual food and mouth breathing have been frequently found in CPchildrenConclusions Earlier preventive measures for CP patients are required because they are a high-riskgroup for dental caries (J Dent Child 20037040-46)
KEYwORDS CEREBRAL PALSY DENTAL CARIES ORAL HYGIENE PLAQUE INDEX
Cerebral palsy (CP) belongs to the group of the mostcommon and severe disabilities of childhood char-acterized by a set of non-progressive motor disor-
ders of posture and movement due to a lesion in the devel-oping brain 1 The rate of CP has risen in spite of fallingperinatal and neonatal mortality rates a rise that is evenmore pronounced when the mildest and least reliably ascer-tained cases were excluded The effect of modern care seemsto be that many babies lt2500 g who would have died dur-ing the perinatal period now survive with severe Cp2Thusthese children need special or intensive care requiring theinterest of investigators not only in the prevention of the
Dr Rodrigues dos Santos Is full professor Division of Dentistryfor Persons with Disabilities University Cruzeiro Do Sui SaoPaulo BrazilDr Maslero Isassociate professor Department of Orthopaedicsand Traumatology Federal University of Sao Paulo BrazilDr Novo is professor Department of Preventltlve MedicineFederal University of Sao Paulo BrazilDr Smonato Is professor Department of MicrobiologyInstitute of Biomedical Sciences University of Sao Paulo BrazilCorrespond with Dr Simlonato at mrslmlonlcbuspbr
disease but also in the prevention of the problems relatedto it such as dental caries
The pathogenesis of CP seemsto involvefactorsoperating dur-ing pregnancy and the neonatal period The most important pre-natal factor appears to be intrauterine infection3 The prevalenceof the disease has been reported to range from 1 to 2 per 1000livebornsl being significantlyhigher in males and black people4-5
The problems due to the diseaseare definitely becoming worseThe most common disorders associated with CP are mental
retardation sensory limitations epilepsy learning difficultiesspeech disorders and hearing loss6There is contradictory infor-mation in the literature regarding the incidence of oral diseasesin patients with Cp According to Brown these controversiesare due to failure of the criteria used to choose the population tobe studied absence of control groups and use of non-standard-ized criteria for diagnosis inexperienced investigators and lackof statistical analysis of the results
The purpose of this study was to investigate the prevalenceofthe main oral disorders such asdental cariesplaque index time oferuption of permanent teeth malocclusionand bruxism in agroupof children with Cp and compare these results with those ob-tained for a control group of normal children Oral motor skills
40 dos Santos et al Oral Conditions in Children with CP Journal ofDentistry for Children
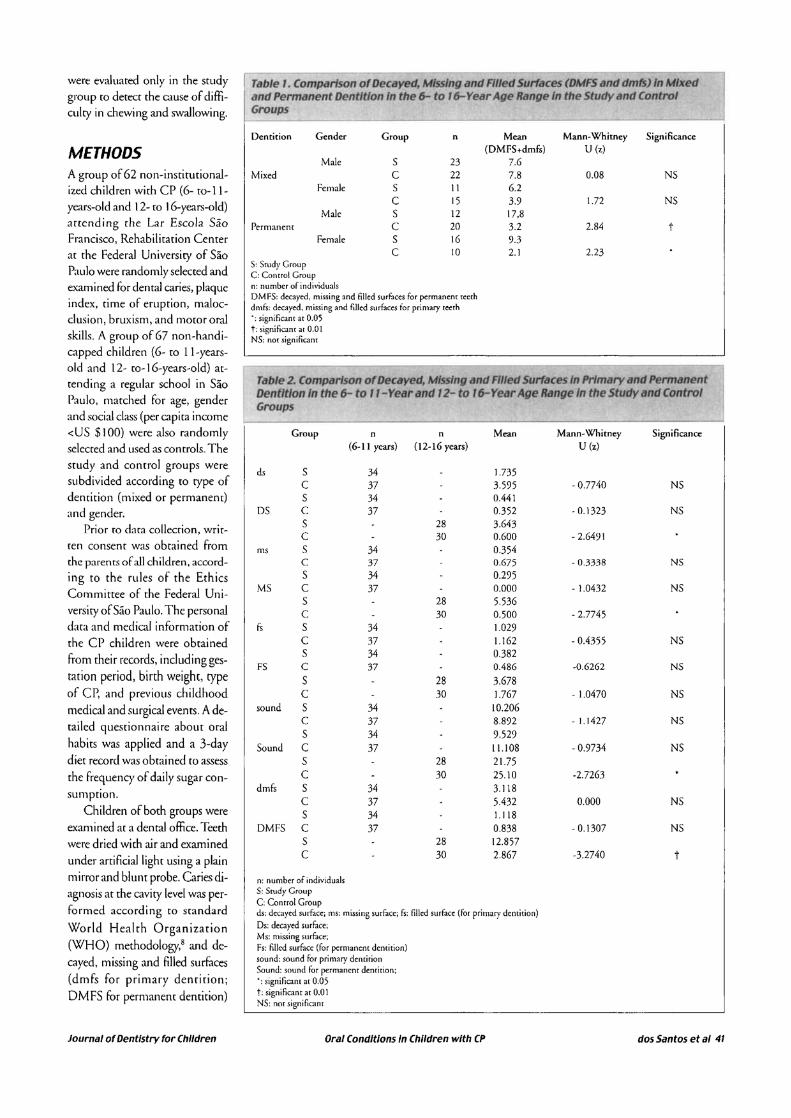
were evaluated only in the studygroup to detect the cause of diffi-culry in chewing and swallowing
Table Comparison of Decayed Ml5slng and Riled Surfaces (DMFS and dmfs) In Mixedand Permanent Dentition In the 6- to 6- Year Age Range In the Study and ControlGroups
S Study GroupC Control Groupn number of individualsDMFS decayed missing and filled surfaces for permanent teethdmfs decayed missing and filled surfaces for primary retrh significant at 005t signifIcant at 00 INS not significant
Table 2 Comparison of Decayed Missing and Filled Surfaces In Primary and PermanentDentition In the 6- to - Year and 11- to 6- Year Age Range In the Study and ControlGroups
Group n n Mean Mann-Whitney Significance(6-11 years) (12-16 years) U(z)
ds S 34 1735C 37 3595 - 07740 NSS 34 0441
DS C 37 0352 - 01323 NSS 28 3643C 30 0600 - 26491
ms S 34 0354C 37 0675 - 03338 NSS 34 0295
MS C 37 0000 - 10432 NSS 28 5536C 30 0500 - 27745
fs S 34 1029C 37 1]62 - 04355 NSS 34 0382
FS C 37 0486 -06262 NSS 28 3678C 30 1767 - 10470 NS
sound S 34 10206c 37 8892 -11427 NSS 34 9529
Sound C 37 11108 - 09734 NSS 28 2175C 30 2510 -27263
dmfs S 34 3ll8C 37 5432 0000 NSS 34 1118
DMFS C 37 0838 - 01307 NSS 28 12857C 30 2867 -32740 t
n number of individualsS Study GroupC Control Groupds decayed surface ms missing surface fs tilled surface (fot primary dentition)Os decayed sutfaceMs missing surbceFs filled surFace(for petmanent dentition)sound sound for primary delUirionSound sound for permanent dentition
significant at 005t significant at 00 INS nor significant
Oral Conditions In Children with CP dos Santos et al 41
METHODSA group of 62 non-institutional-ized children with CP (6- to-I 1-years-old and 12- to 16-years-old)anending the Lar Escola SaoFrancisco Rehabilitation Centerat the Federal Universiry of SaoPaulo were randomly selecced andexamined for dental caries plaqueindex time of eruption maloc-clusion brLLxismand mo(Or oralskills A group of 67 non-handi-capped children (G- to II-years-old and 12- (0- IG-years-old) at-tending a regular school in SaoPaulo matched for age genderand social class (per capita incomeltUS $100) were also randomlyselected and used as controls Thestudy and control groups weresubdivided according to rype ofdemition (mixed or permanent)and gender
Prior to dara collecrion wrir-ten consent was obtained fromthe parents of all children accord-ing to the rules of the EthicsCommittee of the Federal Uni-versiry of Sao Paulo The personaldata and medical information ofthe CP children were obtainedfrom their records including ges-tation period birth weight typeof cr and previous childhoodmedical and surgical events A de-railed questionnaire about oralhabits was applied and a 3-daydiet record was obrained (0 assessthe frequency of daily sugar con-sumption
Children of both groups wereexanlined at a dental office Teethwere dried with air and examinedunder arrificiallight using a plainmirror and blunt probe Caries di-agnosis at rhe caviry level was per-formed according (0 standard
World Health Organizarion(WHO) methodologyS and de-cayed missing and filled surfaces(dmfs for primary dentirionDMFS for permanent dentirion)
Journal of Dentistry for Children
Dentition
Mixed
Permanent
Gender Group n Mean Mann-Whitney Significance(DMFS+dmfs) U(z)
Male S 23 76C 22 78 008 NS
Female S II 62C 15 39 172 NS
Male S 12 178C 20 32 284 t
Female S 16 93C 10 21 223
RESULTS
Tlfble 4 ComplJrlson of the Results of the Exlfmlnlftlon fOr Pllfque Index In the Study IfndControl Groups
t
t
NS
NS
Significance
P=05
P=05
The study group consisted of 62CP children Of these 34 chil-dren had mixed dentition Theywere ages 6- to-II-years 23males (37 mean age 86years) 11 females (18 meanage 87 years) The remaining 28children had permanent denti-tion They were ages 12- to-16-years 12 males (19 mean age146 years) 16 females (26mean age 142 years)
The control group consistedof67 normal children Of these37 children had mixed denti-tion They were ages 6- [0-] ]-years-old 22 males (33 meanage 82 years) and 15 females(22 mean age being 76years) The remaining 30 chil-dren had permanent dentitionThey were ages] 2- ro-16-years-
old 20 males (30 mean age125 years) 10 females (15mean age 149 years)
In the study group 68 ofthe children had spastic quad-riplegia or spastic diplegia 13had spasticity plus athetosis and13 had athetosis plus ataxia(mixed cases) and 6 of the chil-
dren had other mixed conditionsThe results of the study are presented in Tables 1 to 8 The
results for dental caries in the 6- to 16-year-old age group aresummarized in Table 1 CP children had statistically more DMFS(Plt05)
The results for the 6- to II-year-old and 12- to 16-year-oldage groups are summarized in Table 2 There was no statisticaldifference between the study group and the control group forthe first age group Nevertheless significantly more decayed andmissing surfaces and higher DMFS were seen in the study groupfor the 12- to 16-year-old age group More sound permanentteeth were seen in the control group
The results for caries-free children are presented in Table3 The frequency of caries-free children with mixed dentitionwas 21 in the study group and 43 in the control groupand the frequency of caries-free children with permanent den-tition was 18 in the study group and 43 in the controlgroup The results for affected children with mixed and per-manent dentition are also presented in this table Fishers ex-act test shows a significantly higher percentage of affectedteeth for both dentition
Data concerning dental plaque are presented in Table 4 andclearly show that the plaque index was significantly higher in bothfemales and males with permanent teeth in the study group (Plt05)
P=006
Fishers Exacr Tesr Significance
169
203
340
0147
Mann-WhitneyVIz)
Gender Group n Mean
Male S 23 383C 22 368
Female S II 427C 15 342
Male S 12 424C 20 272
Female S 16 388C 10 313
To 3lercetrtage ofChIldren WJtIJ ntI MWhout CM1e51ntile 0- to -ltIId r to 6-rAIle llitnges In the Study ~ Control Groups
Dentition Group n AfFecred Caries free
Mixed S 34 79 21C 37 57 43
Permanent S 28 82 18C 30 57 43
Mixed + Permanent S 62 81 19C 67 57 43
n number of individualsS scudy groupC control group signifiC3ntat 005t signiflcam a[ 00 1
Mixed
Permanent
Dentition
n number of individualsS srudy groupC control group significant at 005t significant at 001NS noc significant
were recorded For children with mixed dentition dmfS and DMFSwere summed A single examiner who was trained and calibratedin detecting caries malocclusion and bruxism carried out all pro-cedures The intra-examiner reliability was established by re-ex-aminarion of20 children in 2 different visits (kappa=O 93) Plaque
index was assessed using the oral hygiene index proposed byPodshadley and Haley9 For the presence of permanent teeth thecriterion of counting the first permanent molars at ages 5- to-7-years and second permanent molars at ages 12- to-13 years wasapplied Code 0 was used for non-erupted teeth and code 1 wasused when at least 13 of the crown had erupted WH08 criteriawere used to determine the prevalence of malocclusion which wasclassified according to Angles classification Bruxism was recordedwhen there was abnormal grinding of the primary or permanentteeth resulting in clinically detectable facets To evaluate oral skillsthe CP group was assessed by a rehabilitation center speech thera-pist who visually determined how children performed suckingbitingbreathing functions as well as the presence of residual foodafter eating Children were observed at lunchsnack time seated intheir custom-fitted wheelchairs
Nonparametric statistical tests including the Mann-Whitneytest Fishers exact test (P) Chi-square test (X2) and Cochrans Gtest were used according to the nature of the variables studied 10
with the level of significance set at Plt05
42 dos Santos et al Oral Conditions In Children with CP Journal of Dentistry for Children
Table 6 Comparison of the Presence of Malocclusion (Class II Division type) In Mixedand Permanent Dentition In the Study and Control Groups
Table S Comparison of the Results of the Examination for the Presence ofthe flrstPermanent Molar In Mixed Dentition and of the second Permanent Molar In PermanentDentitIon In the Study and Control Groups
Gender Group n of presence Fishers Exact Test Significance
Presence Male S 8 381st perm C 7 71 P=2 NSmolar Female S 5 60
C 7 100 P=2 NSPresence Male S 3 672nd perm C II 91 P=4 NSmolar Female S 6 83
C 2 100 P=8 NS
n number of individualsS srudy groupC conrrol groupNS nOl significant
A tendency to a delayed time ofemption of permanent molars wasobserved for both males and femalesin the smdy group (Table 5)
Table 6 shows a significantlylower percentage of malocclu-sion in females with mixed teethin the control group and a sig-nificantly higher percentage ofmalocclusion in males with pet-manent teeth in the study group(PltO 5) The malocclusionfound in the study group withanterior open bite was Class fIdivision 1 type according toAngles classification
The statistical analysis of thedata in Table 7 shows a signifi-cantly higher percentage ofbrux-ism in males of the study groupthan the control group with per-manent dentition (Plt05)
Evaluation of oral motor skillsshowed significant characteristicssuch as the presence of residualfood and mouth breathing in thestudy group (Table 8)
Dentition
Mixed
Permanent
Gender Group n of Presenceof Malocclusion
Male S 23 65C 22 77
Female S 11 82C 15 47
Male S 12 83C 20 55
Female S 16 81C 10 60
Chi-square test Significance
X =095 NS
X=668
X=764
X=180 NS
Table 7 Comparison of the Presence of Bruxl m In Mixed and Permanent Dentition In theStudy snd Control Groups
NS
NS
NS
Significance
1=1
1=7
1=004
X =179
Fishers Exact Test
groups since [here were no significant differences between agesAuthors also compared the groups mixed and permanent denti-tion No significant differences were observed between femalesand males in both groups but significantly higher values wereobserved for the study group with permanent teeth which coin-cides with the literature 16middot20 The higher occurrence of caries inpermanent dentition verified in [his study was probably due tothe higher presence of residual food
Group n of Presenceof Bruxism
S 23 61
C 22 415 II 27
C 15 27
S 12 42
C 20 0
S 16 25
C 10 0
Male
Male
Female
Female
Gender
Permanent
Dentition
Mixed
n number of individualsS study groupC conrrol group significant at 005NS not significant
0 number of individualsS srudy groupC conrrol group significant at 005NS nor significanr
DISCUSSIONMany studies reporr that livingconditions the presence offluo-ride in water diet oral hygieneand social factors are imporrantfor the prevalence of oral diseasesin handicapped patientsII14
These studies show differencesbetween institutionalized andnon-institutionalized individu-als In general institutionalizedpatients presented a lower preva-lence of dental caries when com-pared to non-institutionalizedpatients probably due to dietarycontrol7IS Handicap severityshould also be taken into ac-count since it is a determinantfactor not only for oral hygienestatus but also for dental
therapy which is hampered bythe inability of CP children to communicate and cooperatebecause of their oral pathologic reflexes These facts reinforcethe need to study the factors related to the etiology of the dis-ease in these patients
To record dental caries clinicians used only clinical criteriaNo radiographs were obtained to aid the diagnosis of caries dueto the lack of sufficient patient cooperation To determine cariesprevalence authors chose to compare the DMFS between the 2
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 43
Table B Orill Motor Sldlls In the Study Group
Dentition Gender n Suction capacicy Bite capacicy Nasal breathing Residual food Coch ranG test Significance
Male 23 70 30 44 74 3389 +Mixed
Female II 64 46 46 73 1733 +
Male 12 50 25 8 75 1970 +Permanent
Female 16 63 31 50 88 1929 +
n number of individualy+ significant at 00 I
When dmfs and DMFS were examined in the 6- to 11-year-old group no differences were found between the studyand control groups Magnusson and Devall7 found no signifi-cant difference in dmfs in subjects with mixed dentitionShmarak and Bernstein21 summed dmfs and DMFS and theyfound higher decay experience levels in CP children Swallowl2
found lower dmfs and DMFS values in this age group in CPchildren but these subjects had a much lower number of filledsurfaces Fishman et al23 described very similar DMF valuesand components of DMFS in CP children and siblings butslightly higher dmf (not statistically significant) in CP chil-dren The conflicting results verified in different studies wereprobably due to different characteristics of the studied popula-tions and different control groups
There were significantly higher values of DMFS for the 12-to 16-year-old children in the study group Swallow22 andMagnusson and Devall7 reported a similar DMF but Swallowl2
found far fewer fillings in the CP children Pope and Curzonl3
found more decayed and extracted teeth in mentally handicappedCP children However Nielsen20 in a study of 14- and 15-year-old CP children detected lower mean DMFS scores and morecaries-free mouths in CP children than in controls Nielsen20
found that moror alterations in handicapped persons were thebest caries predictors The evidence of the present study showedthe opposite situation for this age and group
Plaque index values were significantly higher in both sexeswith permanent dentition in the study group However thefrequency of rooth-brushing in the CP group was consideredcomparable ro that of the general pediatric population No childreported the use of fluoride supplements
According ro many parents there was an association betweenthose who had difficulty in maintaining satisfactory oral hygieneand those who had difficulty in properly brushing their teethMoror and mental alterations as well as dyskinetic movementsmay have hanlpered dental hygiene Position of the child at thetime or oral hygiene the presence of pathological oral reflexessuch as biting and vomiting and alterations in intraoral sensitiv-ity were also very important factors for the mechanical removalof plaque Most of the studies in the literature reported unsatis-factory oral hygiene in individuals with CP7 11-1317-2124-28
Increasing discrepancy in oral hygiene with age between handi-capped and non-handicapped children was seen in the presentstudy and has also been described by Brown and Schodel IIMaclaurin et al12and Murray and McLeod 26
Dietary habits were difficult to assess due to incomplete datafor me CP group In many of me diets soft loosely textured andsemisolid foods were consumed thereby increasing the risk offermentable carbohydrate retention and subsequent decay
Lower percentages for the expected time of eruption of perma-nent molars were observed in the experimental group Pope andCurzon13 Morales18 Nielsen2deg and Album et al29 also reporteddelay in the time of eruption Molina et al2Srelated the degree ofmental involvement to the delay in time of eruption HoweverWesselsl6 reported that the pattern of eruption of primary andpermanent teeth and the time of eruption in CP children did notsignificantly differ from those of normal children
The results showed significantly higher percentages of malocclu-sion in males wim permanent dentition in the srudy group Whenpresent the malocclusion found was only Class II division 1 typeaccording to Angles classification The simple orthodontic assess-ment indicated that CP children most of whom were affected byspasticity had a higher prevalence of increased overjet and lowerprevalence of crowding than controls Brown and Schodel II Popeand Curzon13 Wessels16 Miller and Taylor19 Shamarak andBernstein21 and Album et al29also obtained similar results Strodel28
suggested that CP children tended to develop increased overjet due
to buccal breathing and tongue thrusting which was rdated to poorswallowing reflex This clinician considered that this may have pre-disposed the upper incisor teeth of CP children to rrawna
Wesselsl6 considered the prevalence and severity of malocclu-sion to increase with age in CP children and the fact that theoverjet was significantly higher in the older population of thisstudy but nor in the 6- to ll-year-old group It has been sug-gested that CP children have significantly different skull and jawdimensions compared with controls When combined with ab-normal muscular activity this would result in severe malocclu-sion11 Foster et al30 demonstrated variable differences in skulldimensions in CP children when compared with controls andthey found that the most severe CP children had the most ab-normal and reduced skull dimensions Strodel28 stated that themotor disorders in individual children accentuated tendenciesroward malocclusion and the spastic CP children had a greatertendency roward a Class II dental and skeletal formation
Bruxism was present in a significantly higher percentage of maleswith permanent dentition in the study group Bruxism was gener-ally accepted as a frequent finding in CP children 17and the presentstudy agreed with the literature Albwn et al29reported that theathetoid group exhibited the highest percentage of bruxism In
44 dos Santos et al Oral Conditions In Children with CP Journal of Dentistry for Children
the present smdy the presence of bruxism was not cypicll of onlychildren with athetosis
Eating efficiency represented the final outcome of the oral skillsused to prepare food for swallowing In this study the authors in-tended to determine which aspects of oral skills were impaired Thepresence of residual food was the result of the inability of the tonguelips and cheeks to perform normal deglutition Nowakll also pointedout that the difficulty in mastication and deglutition of CP subjectsmighr have lead them to eat pasty foods rich in carbohydrates witha reduced duration of the masticatory cycle Poor lip closure tonguethrust and lip retraction leading to mouth breathing were frequentcharacteristics observed in the smdy group The authors would liketo emphasize that accumulation of food deposits associated withthe increased plaque index observed in the smdy group were highrisk factors for the increase in caries prevalence in these patients
At present much attention has focused on the rehabilitationof CP patients so that they can integrate into society throughproper health care education and employment Neverthelessoral conditions in CP patients were not satisfactory accordingto the variables studied On this basis it is important to empha-size that to rehabilitate these patients dental therapy must beincluded The energy needed to maintain their vital processeswill be provided by a balanced diet which will be greatly influ-enced by their healthy oral caviry Based on these results earlierpreventive measures for CP patients are required because theyare a high-risk group for dental caries
CONCLUSIONSCP children presented significantly higher DMFS indexesfor permanenr teeth than normal children The plaque indexfound in the group of CP children was significantly higherfor permanenr teeth than normal children CP children hada rendency to a delay in the rime of eruption of permanentmolars compared to normal children CP children with per-manent denrition presenred significantly higher percentagesof malocclusion and bruxism rhan normal children In thestudy group oral breathing and the presence of food depos-its were freq uenr characteristics
ACKNOWLEDGEMENTSWe thank Fundarao de Amparo a Pesquisa do Estado de SaoPaulo (FAPESP) for financial support (9612474-0) (FAPESPis an institution of the state of Sao Paulo that provides grantsfor research)
REFERENCESI Stanley F The etiology of cerebral palsyEarry Hum Dev
19943681-88
2 Colver AF Gibson M Hey EN et aI Increasing rates of cerebralpalsy across the severity spectrum in northeast England Collabora-rive cerebral palsy survey Arch Dis Child Fetal Neonatal Ed200083 F7-F 12
3 OShea TM Dammann O Anrecedents of cerebral palsy in verylow-birth weighr infants Clin Perinatol 200027285-302
4 Murphy C Yeargin-AJlsopM Decoufle Pet al Prevalence of cere-bral palsyamong ten-year-old children in metropolitan Atlanta 1985through 1987 Pediatr 1993123513-20
5 Cummis S Nelson K Grether J et al Cerebral palsy in four north-ern California counties births 1983 through 1985 Pediatr1993123 230-237
6 Schwartzman S Paralisia cerebral Temassobre 0 desenvolvimento19933 4-21
7 Brown J The efficacy and economy of comprehensive dental carefor handicapped children Int Dent 198030 14-27
8 World Health Organization Oral health surveysbasic methods 3rded Geneva World Health Organization 1987
9 Podshadley A Haley T A method for evaluating oral hygiene per-formance Public Health Rep 196883 259-264
1OSiegelS Castellan JR Nonparametric statistics2ed New York NYMcGraw-Hili 1988399
11Brown J Schodel BA reviewof controlled surveysof dental disease inhandicapped persons Dent Child 197643313-320
12MacLaurin E Shaw L Foster T Dental study of handicapped chil-dren attending special schools in Birmingham Part I Dental cariesexperience of children living in a fluoridated area Community DentHealth 19852259-265
13Pope J Curzon M The dental status of cerebral palsied childrenPediatr Dent 199113156-162
14Bhavsar JP Damle SG Dental caries and oral hygiene amongst 12-14-year-old handicapped children of Bombay India Indian SocPedodPrevDent1995131-3
15Novak AJThe effect of dietary and brushing habits on dental cariesin noninstitutionalized handicapped children Dem Handicap]977315-19
16Wessels K Oral conditions in cerebral palsy Dent Clin North Am1960455-468
17Magnusson B Deval R Oral conditions in a group of children withcerebral palsy Odontol Revy 1963 14385-402
I8Morales C Paralisiscerebral sus efectos sobre la erupci6n del primermolar permanenre y las condiciones de salud-enfermedad ActaOdontolVenez 198725 13-33
19Miller J Taylor PA survey of the oral health of a group of orthope-dically handicapped children Dent Child 197037 331-343
20Nielsen 1 Caries among children with cerebral palsy Relation roCP-diagnosis mental and moror handicap Dent Child199057267 -273
21Shmarak K Bernstein J Caries incidence among cerebral palsiedchildren A preliminary study Dent Child 1961 28 154- 156
22Swallow J The dental problems of handicapped children J R SocHealth 196885152-157
23Fishman 5 Young W Haley J et al The status of oral health incerebral palsy children and their siblings Dent Child196734219-227
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 45
24Melville M Pool D Jaffe E er aI A denral service for handicapped
children Br Dent 1981 151 259-261
25Molina I Vinas L Garcia F Erupci6n clfnica de los dienres
permanenres en nifios can impedimenros menrales de Sanro
Domingo Acta Odonto Pedjatr 1982369-73
26Murray J McLeod J The denral condirion of severely subnormal
children in rhree London boroughs Br Dent 1973 134380-385
27Nunn J Murray J The denral healrh of handicapped children in
Newcasrle and Northumberland Br Dent 1987] 629-14
28Srrodel B The effecrs of spasric cerebral pals) on occlusion j DentChild ]98754255-260
29Album M Krogman W Baker D er al An evaluarion of denral
profile of neuromuscular deficir parienrs A pilor Srudy Dent Child196431 204-227
30Fosrer TD Griffirh MI Gordon PH The effecrs of cerebral palsy
on rhe size and form of rhe skull Am j Orthod 19746640-49
31 Nowak AJ Denral disease in handicapped persons Spec Care Den-tist 1984466-69
46 dos Santos et al Oral Conditions in Children with CP Journal of Dentistry for Children
were evaluated only in the studygroup to detect the cause of diffi-culry in chewing and swallowing
Table Comparison of Decayed Ml5slng and Riled Surfaces (DMFS and dmfs) In Mixedand Permanent Dentition In the 6- to 6- Year Age Range In the Study and ControlGroups
S Study GroupC Control Groupn number of individualsDMFS decayed missing and filled surfaces for permanent teethdmfs decayed missing and filled surfaces for primary retrh significant at 005t signifIcant at 00 INS not significant
Table 2 Comparison of Decayed Missing and Filled Surfaces In Primary and PermanentDentition In the 6- to - Year and 11- to 6- Year Age Range In the Study and ControlGroups
Group n n Mean Mann-Whitney Significance(6-11 years) (12-16 years) U(z)
ds S 34 1735C 37 3595 - 07740 NSS 34 0441
DS C 37 0352 - 01323 NSS 28 3643C 30 0600 - 26491
ms S 34 0354C 37 0675 - 03338 NSS 34 0295
MS C 37 0000 - 10432 NSS 28 5536C 30 0500 - 27745
fs S 34 1029C 37 1]62 - 04355 NSS 34 0382
FS C 37 0486 -06262 NSS 28 3678C 30 1767 - 10470 NS
sound S 34 10206c 37 8892 -11427 NSS 34 9529
Sound C 37 11108 - 09734 NSS 28 2175C 30 2510 -27263
dmfs S 34 3ll8C 37 5432 0000 NSS 34 1118
DMFS C 37 0838 - 01307 NSS 28 12857C 30 2867 -32740 t
n number of individualsS Study GroupC Control Groupds decayed surface ms missing surface fs tilled surface (fot primary dentition)Os decayed sutfaceMs missing surbceFs filled surFace(for petmanent dentition)sound sound for primary delUirionSound sound for permanent dentition
significant at 005t significant at 00 INS nor significant
Oral Conditions In Children with CP dos Santos et al 41
METHODSA group of 62 non-institutional-ized children with CP (6- to-I 1-years-old and 12- to 16-years-old)anending the Lar Escola SaoFrancisco Rehabilitation Centerat the Federal Universiry of SaoPaulo were randomly selecced andexamined for dental caries plaqueindex time of eruption maloc-clusion brLLxismand mo(Or oralskills A group of 67 non-handi-capped children (G- to II-years-old and 12- (0- IG-years-old) at-tending a regular school in SaoPaulo matched for age genderand social class (per capita incomeltUS $100) were also randomlyselected and used as controls Thestudy and control groups weresubdivided according to rype ofdemition (mixed or permanent)and gender
Prior to dara collecrion wrir-ten consent was obtained fromthe parents of all children accord-ing to the rules of the EthicsCommittee of the Federal Uni-versiry of Sao Paulo The personaldata and medical information ofthe CP children were obtainedfrom their records including ges-tation period birth weight typeof cr and previous childhoodmedical and surgical events A de-railed questionnaire about oralhabits was applied and a 3-daydiet record was obrained (0 assessthe frequency of daily sugar con-sumption
Children of both groups wereexanlined at a dental office Teethwere dried with air and examinedunder arrificiallight using a plainmirror and blunt probe Caries di-agnosis at rhe caviry level was per-formed according (0 standard
World Health Organizarion(WHO) methodologyS and de-cayed missing and filled surfaces(dmfs for primary dentirionDMFS for permanent dentirion)
Journal of Dentistry for Children
Dentition
Mixed
Permanent
Gender Group n Mean Mann-Whitney Significance(DMFS+dmfs) U(z)
Male S 23 76C 22 78 008 NS
Female S II 62C 15 39 172 NS
Male S 12 178C 20 32 284 t
Female S 16 93C 10 21 223
RESULTS
Tlfble 4 ComplJrlson of the Results of the Exlfmlnlftlon fOr Pllfque Index In the Study IfndControl Groups
t
t
NS
NS
Significance
P=05
P=05
The study group consisted of 62CP children Of these 34 chil-dren had mixed dentition Theywere ages 6- to-II-years 23males (37 mean age 86years) 11 females (18 meanage 87 years) The remaining 28children had permanent denti-tion They were ages 12- to-16-years 12 males (19 mean age146 years) 16 females (26mean age 142 years)
The control group consistedof67 normal children Of these37 children had mixed denti-tion They were ages 6- [0-] ]-years-old 22 males (33 meanage 82 years) and 15 females(22 mean age being 76years) The remaining 30 chil-dren had permanent dentitionThey were ages] 2- ro-16-years-
old 20 males (30 mean age125 years) 10 females (15mean age 149 years)
In the study group 68 ofthe children had spastic quad-riplegia or spastic diplegia 13had spasticity plus athetosis and13 had athetosis plus ataxia(mixed cases) and 6 of the chil-
dren had other mixed conditionsThe results of the study are presented in Tables 1 to 8 The
results for dental caries in the 6- to 16-year-old age group aresummarized in Table 1 CP children had statistically more DMFS(Plt05)
The results for the 6- to II-year-old and 12- to 16-year-oldage groups are summarized in Table 2 There was no statisticaldifference between the study group and the control group forthe first age group Nevertheless significantly more decayed andmissing surfaces and higher DMFS were seen in the study groupfor the 12- to 16-year-old age group More sound permanentteeth were seen in the control group
The results for caries-free children are presented in Table3 The frequency of caries-free children with mixed dentitionwas 21 in the study group and 43 in the control groupand the frequency of caries-free children with permanent den-tition was 18 in the study group and 43 in the controlgroup The results for affected children with mixed and per-manent dentition are also presented in this table Fishers ex-act test shows a significantly higher percentage of affectedteeth for both dentition
Data concerning dental plaque are presented in Table 4 andclearly show that the plaque index was significantly higher in bothfemales and males with permanent teeth in the study group (Plt05)
P=006
Fishers Exacr Tesr Significance
169
203
340
0147
Mann-WhitneyVIz)
Gender Group n Mean
Male S 23 383C 22 368
Female S II 427C 15 342
Male S 12 424C 20 272
Female S 16 388C 10 313
To 3lercetrtage ofChIldren WJtIJ ntI MWhout CM1e51ntile 0- to -ltIId r to 6-rAIle llitnges In the Study ~ Control Groups
Dentition Group n AfFecred Caries free
Mixed S 34 79 21C 37 57 43
Permanent S 28 82 18C 30 57 43
Mixed + Permanent S 62 81 19C 67 57 43
n number of individualsS scudy groupC control group signifiC3ntat 005t signiflcam a[ 00 1
Mixed
Permanent
Dentition
n number of individualsS srudy groupC control group significant at 005t significant at 001NS noc significant
were recorded For children with mixed dentition dmfS and DMFSwere summed A single examiner who was trained and calibratedin detecting caries malocclusion and bruxism carried out all pro-cedures The intra-examiner reliability was established by re-ex-aminarion of20 children in 2 different visits (kappa=O 93) Plaque
index was assessed using the oral hygiene index proposed byPodshadley and Haley9 For the presence of permanent teeth thecriterion of counting the first permanent molars at ages 5- to-7-years and second permanent molars at ages 12- to-13 years wasapplied Code 0 was used for non-erupted teeth and code 1 wasused when at least 13 of the crown had erupted WH08 criteriawere used to determine the prevalence of malocclusion which wasclassified according to Angles classification Bruxism was recordedwhen there was abnormal grinding of the primary or permanentteeth resulting in clinically detectable facets To evaluate oral skillsthe CP group was assessed by a rehabilitation center speech thera-pist who visually determined how children performed suckingbitingbreathing functions as well as the presence of residual foodafter eating Children were observed at lunchsnack time seated intheir custom-fitted wheelchairs
Nonparametric statistical tests including the Mann-Whitneytest Fishers exact test (P) Chi-square test (X2) and Cochrans Gtest were used according to the nature of the variables studied 10
with the level of significance set at Plt05
42 dos Santos et al Oral Conditions In Children with CP Journal of Dentistry for Children
Table 6 Comparison of the Presence of Malocclusion (Class II Division type) In Mixedand Permanent Dentition In the Study and Control Groups
Table S Comparison of the Results of the Examination for the Presence ofthe flrstPermanent Molar In Mixed Dentition and of the second Permanent Molar In PermanentDentitIon In the Study and Control Groups
Gender Group n of presence Fishers Exact Test Significance
Presence Male S 8 381st perm C 7 71 P=2 NSmolar Female S 5 60
C 7 100 P=2 NSPresence Male S 3 672nd perm C II 91 P=4 NSmolar Female S 6 83
C 2 100 P=8 NS
n number of individualsS srudy groupC conrrol groupNS nOl significant
A tendency to a delayed time ofemption of permanent molars wasobserved for both males and femalesin the smdy group (Table 5)
Table 6 shows a significantlylower percentage of malocclu-sion in females with mixed teethin the control group and a sig-nificantly higher percentage ofmalocclusion in males with pet-manent teeth in the study group(PltO 5) The malocclusionfound in the study group withanterior open bite was Class fIdivision 1 type according toAngles classification
The statistical analysis of thedata in Table 7 shows a signifi-cantly higher percentage ofbrux-ism in males of the study groupthan the control group with per-manent dentition (Plt05)
Evaluation of oral motor skillsshowed significant characteristicssuch as the presence of residualfood and mouth breathing in thestudy group (Table 8)
Dentition
Mixed
Permanent
Gender Group n of Presenceof Malocclusion
Male S 23 65C 22 77
Female S 11 82C 15 47
Male S 12 83C 20 55
Female S 16 81C 10 60
Chi-square test Significance
X =095 NS
X=668
X=764
X=180 NS
Table 7 Comparison of the Presence of Bruxl m In Mixed and Permanent Dentition In theStudy snd Control Groups
NS
NS
NS
Significance
1=1
1=7
1=004
X =179
Fishers Exact Test
groups since [here were no significant differences between agesAuthors also compared the groups mixed and permanent denti-tion No significant differences were observed between femalesand males in both groups but significantly higher values wereobserved for the study group with permanent teeth which coin-cides with the literature 16middot20 The higher occurrence of caries inpermanent dentition verified in [his study was probably due tothe higher presence of residual food
Group n of Presenceof Bruxism
S 23 61
C 22 415 II 27
C 15 27
S 12 42
C 20 0
S 16 25
C 10 0
Male
Male
Female
Female
Gender
Permanent
Dentition
Mixed
n number of individualsS study groupC conrrol group significant at 005NS not significant
0 number of individualsS srudy groupC conrrol group significant at 005NS nor significanr
DISCUSSIONMany studies reporr that livingconditions the presence offluo-ride in water diet oral hygieneand social factors are imporrantfor the prevalence of oral diseasesin handicapped patientsII14
These studies show differencesbetween institutionalized andnon-institutionalized individu-als In general institutionalizedpatients presented a lower preva-lence of dental caries when com-pared to non-institutionalizedpatients probably due to dietarycontrol7IS Handicap severityshould also be taken into ac-count since it is a determinantfactor not only for oral hygienestatus but also for dental
therapy which is hampered bythe inability of CP children to communicate and cooperatebecause of their oral pathologic reflexes These facts reinforcethe need to study the factors related to the etiology of the dis-ease in these patients
To record dental caries clinicians used only clinical criteriaNo radiographs were obtained to aid the diagnosis of caries dueto the lack of sufficient patient cooperation To determine cariesprevalence authors chose to compare the DMFS between the 2
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 43
Table B Orill Motor Sldlls In the Study Group
Dentition Gender n Suction capacicy Bite capacicy Nasal breathing Residual food Coch ranG test Significance
Male 23 70 30 44 74 3389 +Mixed
Female II 64 46 46 73 1733 +
Male 12 50 25 8 75 1970 +Permanent
Female 16 63 31 50 88 1929 +
n number of individualy+ significant at 00 I
When dmfs and DMFS were examined in the 6- to 11-year-old group no differences were found between the studyand control groups Magnusson and Devall7 found no signifi-cant difference in dmfs in subjects with mixed dentitionShmarak and Bernstein21 summed dmfs and DMFS and theyfound higher decay experience levels in CP children Swallowl2
found lower dmfs and DMFS values in this age group in CPchildren but these subjects had a much lower number of filledsurfaces Fishman et al23 described very similar DMF valuesand components of DMFS in CP children and siblings butslightly higher dmf (not statistically significant) in CP chil-dren The conflicting results verified in different studies wereprobably due to different characteristics of the studied popula-tions and different control groups
There were significantly higher values of DMFS for the 12-to 16-year-old children in the study group Swallow22 andMagnusson and Devall7 reported a similar DMF but Swallowl2
found far fewer fillings in the CP children Pope and Curzonl3
found more decayed and extracted teeth in mentally handicappedCP children However Nielsen20 in a study of 14- and 15-year-old CP children detected lower mean DMFS scores and morecaries-free mouths in CP children than in controls Nielsen20
found that moror alterations in handicapped persons were thebest caries predictors The evidence of the present study showedthe opposite situation for this age and group
Plaque index values were significantly higher in both sexeswith permanent dentition in the study group However thefrequency of rooth-brushing in the CP group was consideredcomparable ro that of the general pediatric population No childreported the use of fluoride supplements
According ro many parents there was an association betweenthose who had difficulty in maintaining satisfactory oral hygieneand those who had difficulty in properly brushing their teethMoror and mental alterations as well as dyskinetic movementsmay have hanlpered dental hygiene Position of the child at thetime or oral hygiene the presence of pathological oral reflexessuch as biting and vomiting and alterations in intraoral sensitiv-ity were also very important factors for the mechanical removalof plaque Most of the studies in the literature reported unsatis-factory oral hygiene in individuals with CP7 11-1317-2124-28
Increasing discrepancy in oral hygiene with age between handi-capped and non-handicapped children was seen in the presentstudy and has also been described by Brown and Schodel IIMaclaurin et al12and Murray and McLeod 26
Dietary habits were difficult to assess due to incomplete datafor me CP group In many of me diets soft loosely textured andsemisolid foods were consumed thereby increasing the risk offermentable carbohydrate retention and subsequent decay
Lower percentages for the expected time of eruption of perma-nent molars were observed in the experimental group Pope andCurzon13 Morales18 Nielsen2deg and Album et al29 also reporteddelay in the time of eruption Molina et al2Srelated the degree ofmental involvement to the delay in time of eruption HoweverWesselsl6 reported that the pattern of eruption of primary andpermanent teeth and the time of eruption in CP children did notsignificantly differ from those of normal children
The results showed significantly higher percentages of malocclu-sion in males wim permanent dentition in the srudy group Whenpresent the malocclusion found was only Class II division 1 typeaccording to Angles classification The simple orthodontic assess-ment indicated that CP children most of whom were affected byspasticity had a higher prevalence of increased overjet and lowerprevalence of crowding than controls Brown and Schodel II Popeand Curzon13 Wessels16 Miller and Taylor19 Shamarak andBernstein21 and Album et al29also obtained similar results Strodel28
suggested that CP children tended to develop increased overjet due
to buccal breathing and tongue thrusting which was rdated to poorswallowing reflex This clinician considered that this may have pre-disposed the upper incisor teeth of CP children to rrawna
Wesselsl6 considered the prevalence and severity of malocclu-sion to increase with age in CP children and the fact that theoverjet was significantly higher in the older population of thisstudy but nor in the 6- to ll-year-old group It has been sug-gested that CP children have significantly different skull and jawdimensions compared with controls When combined with ab-normal muscular activity this would result in severe malocclu-sion11 Foster et al30 demonstrated variable differences in skulldimensions in CP children when compared with controls andthey found that the most severe CP children had the most ab-normal and reduced skull dimensions Strodel28 stated that themotor disorders in individual children accentuated tendenciesroward malocclusion and the spastic CP children had a greatertendency roward a Class II dental and skeletal formation
Bruxism was present in a significantly higher percentage of maleswith permanent dentition in the study group Bruxism was gener-ally accepted as a frequent finding in CP children 17and the presentstudy agreed with the literature Albwn et al29reported that theathetoid group exhibited the highest percentage of bruxism In
44 dos Santos et al Oral Conditions In Children with CP Journal of Dentistry for Children
the present smdy the presence of bruxism was not cypicll of onlychildren with athetosis
Eating efficiency represented the final outcome of the oral skillsused to prepare food for swallowing In this study the authors in-tended to determine which aspects of oral skills were impaired Thepresence of residual food was the result of the inability of the tonguelips and cheeks to perform normal deglutition Nowakll also pointedout that the difficulty in mastication and deglutition of CP subjectsmighr have lead them to eat pasty foods rich in carbohydrates witha reduced duration of the masticatory cycle Poor lip closure tonguethrust and lip retraction leading to mouth breathing were frequentcharacteristics observed in the smdy group The authors would liketo emphasize that accumulation of food deposits associated withthe increased plaque index observed in the smdy group were highrisk factors for the increase in caries prevalence in these patients
At present much attention has focused on the rehabilitationof CP patients so that they can integrate into society throughproper health care education and employment Neverthelessoral conditions in CP patients were not satisfactory accordingto the variables studied On this basis it is important to empha-size that to rehabilitate these patients dental therapy must beincluded The energy needed to maintain their vital processeswill be provided by a balanced diet which will be greatly influ-enced by their healthy oral caviry Based on these results earlierpreventive measures for CP patients are required because theyare a high-risk group for dental caries
CONCLUSIONSCP children presented significantly higher DMFS indexesfor permanenr teeth than normal children The plaque indexfound in the group of CP children was significantly higherfor permanenr teeth than normal children CP children hada rendency to a delay in the rime of eruption of permanentmolars compared to normal children CP children with per-manent denrition presenred significantly higher percentagesof malocclusion and bruxism rhan normal children In thestudy group oral breathing and the presence of food depos-its were freq uenr characteristics
ACKNOWLEDGEMENTSWe thank Fundarao de Amparo a Pesquisa do Estado de SaoPaulo (FAPESP) for financial support (9612474-0) (FAPESPis an institution of the state of Sao Paulo that provides grantsfor research)
REFERENCESI Stanley F The etiology of cerebral palsyEarry Hum Dev
19943681-88
2 Colver AF Gibson M Hey EN et aI Increasing rates of cerebralpalsy across the severity spectrum in northeast England Collabora-rive cerebral palsy survey Arch Dis Child Fetal Neonatal Ed200083 F7-F 12
3 OShea TM Dammann O Anrecedents of cerebral palsy in verylow-birth weighr infants Clin Perinatol 200027285-302
4 Murphy C Yeargin-AJlsopM Decoufle Pet al Prevalence of cere-bral palsyamong ten-year-old children in metropolitan Atlanta 1985through 1987 Pediatr 1993123513-20
5 Cummis S Nelson K Grether J et al Cerebral palsy in four north-ern California counties births 1983 through 1985 Pediatr1993123 230-237
6 Schwartzman S Paralisia cerebral Temassobre 0 desenvolvimento19933 4-21
7 Brown J The efficacy and economy of comprehensive dental carefor handicapped children Int Dent 198030 14-27
8 World Health Organization Oral health surveysbasic methods 3rded Geneva World Health Organization 1987
9 Podshadley A Haley T A method for evaluating oral hygiene per-formance Public Health Rep 196883 259-264
1OSiegelS Castellan JR Nonparametric statistics2ed New York NYMcGraw-Hili 1988399
11Brown J Schodel BA reviewof controlled surveysof dental disease inhandicapped persons Dent Child 197643313-320
12MacLaurin E Shaw L Foster T Dental study of handicapped chil-dren attending special schools in Birmingham Part I Dental cariesexperience of children living in a fluoridated area Community DentHealth 19852259-265
13Pope J Curzon M The dental status of cerebral palsied childrenPediatr Dent 199113156-162
14Bhavsar JP Damle SG Dental caries and oral hygiene amongst 12-14-year-old handicapped children of Bombay India Indian SocPedodPrevDent1995131-3
15Novak AJThe effect of dietary and brushing habits on dental cariesin noninstitutionalized handicapped children Dem Handicap]977315-19
16Wessels K Oral conditions in cerebral palsy Dent Clin North Am1960455-468
17Magnusson B Deval R Oral conditions in a group of children withcerebral palsy Odontol Revy 1963 14385-402
I8Morales C Paralisiscerebral sus efectos sobre la erupci6n del primermolar permanenre y las condiciones de salud-enfermedad ActaOdontolVenez 198725 13-33
19Miller J Taylor PA survey of the oral health of a group of orthope-dically handicapped children Dent Child 197037 331-343
20Nielsen 1 Caries among children with cerebral palsy Relation roCP-diagnosis mental and moror handicap Dent Child199057267 -273
21Shmarak K Bernstein J Caries incidence among cerebral palsiedchildren A preliminary study Dent Child 1961 28 154- 156
22Swallow J The dental problems of handicapped children J R SocHealth 196885152-157
23Fishman 5 Young W Haley J et al The status of oral health incerebral palsy children and their siblings Dent Child196734219-227
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 45
24Melville M Pool D Jaffe E er aI A denral service for handicapped
children Br Dent 1981 151 259-261
25Molina I Vinas L Garcia F Erupci6n clfnica de los dienres
permanenres en nifios can impedimenros menrales de Sanro
Domingo Acta Odonto Pedjatr 1982369-73
26Murray J McLeod J The denral condirion of severely subnormal
children in rhree London boroughs Br Dent 1973 134380-385
27Nunn J Murray J The denral healrh of handicapped children in
Newcasrle and Northumberland Br Dent 1987] 629-14
28Srrodel B The effecrs of spasric cerebral pals) on occlusion j DentChild ]98754255-260
29Album M Krogman W Baker D er al An evaluarion of denral
profile of neuromuscular deficir parienrs A pilor Srudy Dent Child196431 204-227
30Fosrer TD Griffirh MI Gordon PH The effecrs of cerebral palsy
on rhe size and form of rhe skull Am j Orthod 19746640-49
31 Nowak AJ Denral disease in handicapped persons Spec Care Den-tist 1984466-69
46 dos Santos et al Oral Conditions in Children with CP Journal of Dentistry for Children

RESULTS
Tlfble 4 ComplJrlson of the Results of the Exlfmlnlftlon fOr Pllfque Index In the Study IfndControl Groups
t
t
NS
NS
Significance
P=05
P=05
The study group consisted of 62CP children Of these 34 chil-dren had mixed dentition Theywere ages 6- to-II-years 23males (37 mean age 86years) 11 females (18 meanage 87 years) The remaining 28children had permanent denti-tion They were ages 12- to-16-years 12 males (19 mean age146 years) 16 females (26mean age 142 years)
The control group consistedof67 normal children Of these37 children had mixed denti-tion They were ages 6- [0-] ]-years-old 22 males (33 meanage 82 years) and 15 females(22 mean age being 76years) The remaining 30 chil-dren had permanent dentitionThey were ages] 2- ro-16-years-
old 20 males (30 mean age125 years) 10 females (15mean age 149 years)
In the study group 68 ofthe children had spastic quad-riplegia or spastic diplegia 13had spasticity plus athetosis and13 had athetosis plus ataxia(mixed cases) and 6 of the chil-
dren had other mixed conditionsThe results of the study are presented in Tables 1 to 8 The
results for dental caries in the 6- to 16-year-old age group aresummarized in Table 1 CP children had statistically more DMFS(Plt05)
The results for the 6- to II-year-old and 12- to 16-year-oldage groups are summarized in Table 2 There was no statisticaldifference between the study group and the control group forthe first age group Nevertheless significantly more decayed andmissing surfaces and higher DMFS were seen in the study groupfor the 12- to 16-year-old age group More sound permanentteeth were seen in the control group
The results for caries-free children are presented in Table3 The frequency of caries-free children with mixed dentitionwas 21 in the study group and 43 in the control groupand the frequency of caries-free children with permanent den-tition was 18 in the study group and 43 in the controlgroup The results for affected children with mixed and per-manent dentition are also presented in this table Fishers ex-act test shows a significantly higher percentage of affectedteeth for both dentition
Data concerning dental plaque are presented in Table 4 andclearly show that the plaque index was significantly higher in bothfemales and males with permanent teeth in the study group (Plt05)
P=006
Fishers Exacr Tesr Significance
169
203
340
0147
Mann-WhitneyVIz)
Gender Group n Mean
Male S 23 383C 22 368
Female S II 427C 15 342
Male S 12 424C 20 272
Female S 16 388C 10 313
To 3lercetrtage ofChIldren WJtIJ ntI MWhout CM1e51ntile 0- to -ltIId r to 6-rAIle llitnges In the Study ~ Control Groups
Dentition Group n AfFecred Caries free
Mixed S 34 79 21C 37 57 43
Permanent S 28 82 18C 30 57 43
Mixed + Permanent S 62 81 19C 67 57 43
n number of individualsS scudy groupC control group signifiC3ntat 005t signiflcam a[ 00 1
Mixed
Permanent
Dentition
n number of individualsS srudy groupC control group significant at 005t significant at 001NS noc significant
were recorded For children with mixed dentition dmfS and DMFSwere summed A single examiner who was trained and calibratedin detecting caries malocclusion and bruxism carried out all pro-cedures The intra-examiner reliability was established by re-ex-aminarion of20 children in 2 different visits (kappa=O 93) Plaque
index was assessed using the oral hygiene index proposed byPodshadley and Haley9 For the presence of permanent teeth thecriterion of counting the first permanent molars at ages 5- to-7-years and second permanent molars at ages 12- to-13 years wasapplied Code 0 was used for non-erupted teeth and code 1 wasused when at least 13 of the crown had erupted WH08 criteriawere used to determine the prevalence of malocclusion which wasclassified according to Angles classification Bruxism was recordedwhen there was abnormal grinding of the primary or permanentteeth resulting in clinically detectable facets To evaluate oral skillsthe CP group was assessed by a rehabilitation center speech thera-pist who visually determined how children performed suckingbitingbreathing functions as well as the presence of residual foodafter eating Children were observed at lunchsnack time seated intheir custom-fitted wheelchairs
Nonparametric statistical tests including the Mann-Whitneytest Fishers exact test (P) Chi-square test (X2) and Cochrans Gtest were used according to the nature of the variables studied 10
with the level of significance set at Plt05
42 dos Santos et al Oral Conditions In Children with CP Journal of Dentistry for Children
Table 6 Comparison of the Presence of Malocclusion (Class II Division type) In Mixedand Permanent Dentition In the Study and Control Groups
Table S Comparison of the Results of the Examination for the Presence ofthe flrstPermanent Molar In Mixed Dentition and of the second Permanent Molar In PermanentDentitIon In the Study and Control Groups
Gender Group n of presence Fishers Exact Test Significance
Presence Male S 8 381st perm C 7 71 P=2 NSmolar Female S 5 60
C 7 100 P=2 NSPresence Male S 3 672nd perm C II 91 P=4 NSmolar Female S 6 83
C 2 100 P=8 NS
n number of individualsS srudy groupC conrrol groupNS nOl significant
A tendency to a delayed time ofemption of permanent molars wasobserved for both males and femalesin the smdy group (Table 5)
Table 6 shows a significantlylower percentage of malocclu-sion in females with mixed teethin the control group and a sig-nificantly higher percentage ofmalocclusion in males with pet-manent teeth in the study group(PltO 5) The malocclusionfound in the study group withanterior open bite was Class fIdivision 1 type according toAngles classification
The statistical analysis of thedata in Table 7 shows a signifi-cantly higher percentage ofbrux-ism in males of the study groupthan the control group with per-manent dentition (Plt05)
Evaluation of oral motor skillsshowed significant characteristicssuch as the presence of residualfood and mouth breathing in thestudy group (Table 8)
Dentition
Mixed
Permanent
Gender Group n of Presenceof Malocclusion
Male S 23 65C 22 77
Female S 11 82C 15 47
Male S 12 83C 20 55
Female S 16 81C 10 60
Chi-square test Significance
X =095 NS
X=668
X=764
X=180 NS
Table 7 Comparison of the Presence of Bruxl m In Mixed and Permanent Dentition In theStudy snd Control Groups
NS
NS
NS
Significance
1=1
1=7
1=004
X =179
Fishers Exact Test
groups since [here were no significant differences between agesAuthors also compared the groups mixed and permanent denti-tion No significant differences were observed between femalesand males in both groups but significantly higher values wereobserved for the study group with permanent teeth which coin-cides with the literature 16middot20 The higher occurrence of caries inpermanent dentition verified in [his study was probably due tothe higher presence of residual food
Group n of Presenceof Bruxism
S 23 61
C 22 415 II 27
C 15 27
S 12 42
C 20 0
S 16 25
C 10 0
Male
Male
Female
Female
Gender
Permanent
Dentition
Mixed
n number of individualsS study groupC conrrol group significant at 005NS not significant
0 number of individualsS srudy groupC conrrol group significant at 005NS nor significanr
DISCUSSIONMany studies reporr that livingconditions the presence offluo-ride in water diet oral hygieneand social factors are imporrantfor the prevalence of oral diseasesin handicapped patientsII14
These studies show differencesbetween institutionalized andnon-institutionalized individu-als In general institutionalizedpatients presented a lower preva-lence of dental caries when com-pared to non-institutionalizedpatients probably due to dietarycontrol7IS Handicap severityshould also be taken into ac-count since it is a determinantfactor not only for oral hygienestatus but also for dental
therapy which is hampered bythe inability of CP children to communicate and cooperatebecause of their oral pathologic reflexes These facts reinforcethe need to study the factors related to the etiology of the dis-ease in these patients
To record dental caries clinicians used only clinical criteriaNo radiographs were obtained to aid the diagnosis of caries dueto the lack of sufficient patient cooperation To determine cariesprevalence authors chose to compare the DMFS between the 2
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 43
Table B Orill Motor Sldlls In the Study Group
Dentition Gender n Suction capacicy Bite capacicy Nasal breathing Residual food Coch ranG test Significance
Male 23 70 30 44 74 3389 +Mixed
Female II 64 46 46 73 1733 +
Male 12 50 25 8 75 1970 +Permanent
Female 16 63 31 50 88 1929 +
n number of individualy+ significant at 00 I
When dmfs and DMFS were examined in the 6- to 11-year-old group no differences were found between the studyand control groups Magnusson and Devall7 found no signifi-cant difference in dmfs in subjects with mixed dentitionShmarak and Bernstein21 summed dmfs and DMFS and theyfound higher decay experience levels in CP children Swallowl2
found lower dmfs and DMFS values in this age group in CPchildren but these subjects had a much lower number of filledsurfaces Fishman et al23 described very similar DMF valuesand components of DMFS in CP children and siblings butslightly higher dmf (not statistically significant) in CP chil-dren The conflicting results verified in different studies wereprobably due to different characteristics of the studied popula-tions and different control groups
There were significantly higher values of DMFS for the 12-to 16-year-old children in the study group Swallow22 andMagnusson and Devall7 reported a similar DMF but Swallowl2
found far fewer fillings in the CP children Pope and Curzonl3
found more decayed and extracted teeth in mentally handicappedCP children However Nielsen20 in a study of 14- and 15-year-old CP children detected lower mean DMFS scores and morecaries-free mouths in CP children than in controls Nielsen20
found that moror alterations in handicapped persons were thebest caries predictors The evidence of the present study showedthe opposite situation for this age and group
Plaque index values were significantly higher in both sexeswith permanent dentition in the study group However thefrequency of rooth-brushing in the CP group was consideredcomparable ro that of the general pediatric population No childreported the use of fluoride supplements
According ro many parents there was an association betweenthose who had difficulty in maintaining satisfactory oral hygieneand those who had difficulty in properly brushing their teethMoror and mental alterations as well as dyskinetic movementsmay have hanlpered dental hygiene Position of the child at thetime or oral hygiene the presence of pathological oral reflexessuch as biting and vomiting and alterations in intraoral sensitiv-ity were also very important factors for the mechanical removalof plaque Most of the studies in the literature reported unsatis-factory oral hygiene in individuals with CP7 11-1317-2124-28
Increasing discrepancy in oral hygiene with age between handi-capped and non-handicapped children was seen in the presentstudy and has also been described by Brown and Schodel IIMaclaurin et al12and Murray and McLeod 26
Dietary habits were difficult to assess due to incomplete datafor me CP group In many of me diets soft loosely textured andsemisolid foods were consumed thereby increasing the risk offermentable carbohydrate retention and subsequent decay
Lower percentages for the expected time of eruption of perma-nent molars were observed in the experimental group Pope andCurzon13 Morales18 Nielsen2deg and Album et al29 also reporteddelay in the time of eruption Molina et al2Srelated the degree ofmental involvement to the delay in time of eruption HoweverWesselsl6 reported that the pattern of eruption of primary andpermanent teeth and the time of eruption in CP children did notsignificantly differ from those of normal children
The results showed significantly higher percentages of malocclu-sion in males wim permanent dentition in the srudy group Whenpresent the malocclusion found was only Class II division 1 typeaccording to Angles classification The simple orthodontic assess-ment indicated that CP children most of whom were affected byspasticity had a higher prevalence of increased overjet and lowerprevalence of crowding than controls Brown and Schodel II Popeand Curzon13 Wessels16 Miller and Taylor19 Shamarak andBernstein21 and Album et al29also obtained similar results Strodel28
suggested that CP children tended to develop increased overjet due
to buccal breathing and tongue thrusting which was rdated to poorswallowing reflex This clinician considered that this may have pre-disposed the upper incisor teeth of CP children to rrawna
Wesselsl6 considered the prevalence and severity of malocclu-sion to increase with age in CP children and the fact that theoverjet was significantly higher in the older population of thisstudy but nor in the 6- to ll-year-old group It has been sug-gested that CP children have significantly different skull and jawdimensions compared with controls When combined with ab-normal muscular activity this would result in severe malocclu-sion11 Foster et al30 demonstrated variable differences in skulldimensions in CP children when compared with controls andthey found that the most severe CP children had the most ab-normal and reduced skull dimensions Strodel28 stated that themotor disorders in individual children accentuated tendenciesroward malocclusion and the spastic CP children had a greatertendency roward a Class II dental and skeletal formation
Bruxism was present in a significantly higher percentage of maleswith permanent dentition in the study group Bruxism was gener-ally accepted as a frequent finding in CP children 17and the presentstudy agreed with the literature Albwn et al29reported that theathetoid group exhibited the highest percentage of bruxism In
44 dos Santos et al Oral Conditions In Children with CP Journal of Dentistry for Children
the present smdy the presence of bruxism was not cypicll of onlychildren with athetosis
Eating efficiency represented the final outcome of the oral skillsused to prepare food for swallowing In this study the authors in-tended to determine which aspects of oral skills were impaired Thepresence of residual food was the result of the inability of the tonguelips and cheeks to perform normal deglutition Nowakll also pointedout that the difficulty in mastication and deglutition of CP subjectsmighr have lead them to eat pasty foods rich in carbohydrates witha reduced duration of the masticatory cycle Poor lip closure tonguethrust and lip retraction leading to mouth breathing were frequentcharacteristics observed in the smdy group The authors would liketo emphasize that accumulation of food deposits associated withthe increased plaque index observed in the smdy group were highrisk factors for the increase in caries prevalence in these patients
At present much attention has focused on the rehabilitationof CP patients so that they can integrate into society throughproper health care education and employment Neverthelessoral conditions in CP patients were not satisfactory accordingto the variables studied On this basis it is important to empha-size that to rehabilitate these patients dental therapy must beincluded The energy needed to maintain their vital processeswill be provided by a balanced diet which will be greatly influ-enced by their healthy oral caviry Based on these results earlierpreventive measures for CP patients are required because theyare a high-risk group for dental caries
CONCLUSIONSCP children presented significantly higher DMFS indexesfor permanenr teeth than normal children The plaque indexfound in the group of CP children was significantly higherfor permanenr teeth than normal children CP children hada rendency to a delay in the rime of eruption of permanentmolars compared to normal children CP children with per-manent denrition presenred significantly higher percentagesof malocclusion and bruxism rhan normal children In thestudy group oral breathing and the presence of food depos-its were freq uenr characteristics
ACKNOWLEDGEMENTSWe thank Fundarao de Amparo a Pesquisa do Estado de SaoPaulo (FAPESP) for financial support (9612474-0) (FAPESPis an institution of the state of Sao Paulo that provides grantsfor research)
REFERENCESI Stanley F The etiology of cerebral palsyEarry Hum Dev
19943681-88
2 Colver AF Gibson M Hey EN et aI Increasing rates of cerebralpalsy across the severity spectrum in northeast England Collabora-rive cerebral palsy survey Arch Dis Child Fetal Neonatal Ed200083 F7-F 12
3 OShea TM Dammann O Anrecedents of cerebral palsy in verylow-birth weighr infants Clin Perinatol 200027285-302
4 Murphy C Yeargin-AJlsopM Decoufle Pet al Prevalence of cere-bral palsyamong ten-year-old children in metropolitan Atlanta 1985through 1987 Pediatr 1993123513-20
5 Cummis S Nelson K Grether J et al Cerebral palsy in four north-ern California counties births 1983 through 1985 Pediatr1993123 230-237
6 Schwartzman S Paralisia cerebral Temassobre 0 desenvolvimento19933 4-21
7 Brown J The efficacy and economy of comprehensive dental carefor handicapped children Int Dent 198030 14-27
8 World Health Organization Oral health surveysbasic methods 3rded Geneva World Health Organization 1987
9 Podshadley A Haley T A method for evaluating oral hygiene per-formance Public Health Rep 196883 259-264
1OSiegelS Castellan JR Nonparametric statistics2ed New York NYMcGraw-Hili 1988399
11Brown J Schodel BA reviewof controlled surveysof dental disease inhandicapped persons Dent Child 197643313-320
12MacLaurin E Shaw L Foster T Dental study of handicapped chil-dren attending special schools in Birmingham Part I Dental cariesexperience of children living in a fluoridated area Community DentHealth 19852259-265
13Pope J Curzon M The dental status of cerebral palsied childrenPediatr Dent 199113156-162
14Bhavsar JP Damle SG Dental caries and oral hygiene amongst 12-14-year-old handicapped children of Bombay India Indian SocPedodPrevDent1995131-3
15Novak AJThe effect of dietary and brushing habits on dental cariesin noninstitutionalized handicapped children Dem Handicap]977315-19
16Wessels K Oral conditions in cerebral palsy Dent Clin North Am1960455-468
17Magnusson B Deval R Oral conditions in a group of children withcerebral palsy Odontol Revy 1963 14385-402
I8Morales C Paralisiscerebral sus efectos sobre la erupci6n del primermolar permanenre y las condiciones de salud-enfermedad ActaOdontolVenez 198725 13-33
19Miller J Taylor PA survey of the oral health of a group of orthope-dically handicapped children Dent Child 197037 331-343
20Nielsen 1 Caries among children with cerebral palsy Relation roCP-diagnosis mental and moror handicap Dent Child199057267 -273
21Shmarak K Bernstein J Caries incidence among cerebral palsiedchildren A preliminary study Dent Child 1961 28 154- 156
22Swallow J The dental problems of handicapped children J R SocHealth 196885152-157
23Fishman 5 Young W Haley J et al The status of oral health incerebral palsy children and their siblings Dent Child196734219-227
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 45
24Melville M Pool D Jaffe E er aI A denral service for handicapped
children Br Dent 1981 151 259-261
25Molina I Vinas L Garcia F Erupci6n clfnica de los dienres
permanenres en nifios can impedimenros menrales de Sanro
Domingo Acta Odonto Pedjatr 1982369-73
26Murray J McLeod J The denral condirion of severely subnormal
children in rhree London boroughs Br Dent 1973 134380-385
27Nunn J Murray J The denral healrh of handicapped children in
Newcasrle and Northumberland Br Dent 1987] 629-14
28Srrodel B The effecrs of spasric cerebral pals) on occlusion j DentChild ]98754255-260
29Album M Krogman W Baker D er al An evaluarion of denral
profile of neuromuscular deficir parienrs A pilor Srudy Dent Child196431 204-227
30Fosrer TD Griffirh MI Gordon PH The effecrs of cerebral palsy
on rhe size and form of rhe skull Am j Orthod 19746640-49
31 Nowak AJ Denral disease in handicapped persons Spec Care Den-tist 1984466-69
46 dos Santos et al Oral Conditions in Children with CP Journal of Dentistry for Children

Table 6 Comparison of the Presence of Malocclusion (Class II Division type) In Mixedand Permanent Dentition In the Study and Control Groups
Table S Comparison of the Results of the Examination for the Presence ofthe flrstPermanent Molar In Mixed Dentition and of the second Permanent Molar In PermanentDentitIon In the Study and Control Groups
Gender Group n of presence Fishers Exact Test Significance
Presence Male S 8 381st perm C 7 71 P=2 NSmolar Female S 5 60
C 7 100 P=2 NSPresence Male S 3 672nd perm C II 91 P=4 NSmolar Female S 6 83
C 2 100 P=8 NS
n number of individualsS srudy groupC conrrol groupNS nOl significant
A tendency to a delayed time ofemption of permanent molars wasobserved for both males and femalesin the smdy group (Table 5)
Table 6 shows a significantlylower percentage of malocclu-sion in females with mixed teethin the control group and a sig-nificantly higher percentage ofmalocclusion in males with pet-manent teeth in the study group(PltO 5) The malocclusionfound in the study group withanterior open bite was Class fIdivision 1 type according toAngles classification
The statistical analysis of thedata in Table 7 shows a signifi-cantly higher percentage ofbrux-ism in males of the study groupthan the control group with per-manent dentition (Plt05)
Evaluation of oral motor skillsshowed significant characteristicssuch as the presence of residualfood and mouth breathing in thestudy group (Table 8)
Dentition
Mixed
Permanent
Gender Group n of Presenceof Malocclusion
Male S 23 65C 22 77
Female S 11 82C 15 47
Male S 12 83C 20 55
Female S 16 81C 10 60
Chi-square test Significance
X =095 NS
X=668
X=764
X=180 NS
Table 7 Comparison of the Presence of Bruxl m In Mixed and Permanent Dentition In theStudy snd Control Groups
NS
NS
NS
Significance
1=1
1=7
1=004
X =179
Fishers Exact Test
groups since [here were no significant differences between agesAuthors also compared the groups mixed and permanent denti-tion No significant differences were observed between femalesand males in both groups but significantly higher values wereobserved for the study group with permanent teeth which coin-cides with the literature 16middot20 The higher occurrence of caries inpermanent dentition verified in [his study was probably due tothe higher presence of residual food
Group n of Presenceof Bruxism
S 23 61
C 22 415 II 27
C 15 27
S 12 42
C 20 0
S 16 25
C 10 0
Male
Male
Female
Female
Gender
Permanent
Dentition
Mixed
n number of individualsS study groupC conrrol group significant at 005NS not significant
0 number of individualsS srudy groupC conrrol group significant at 005NS nor significanr
DISCUSSIONMany studies reporr that livingconditions the presence offluo-ride in water diet oral hygieneand social factors are imporrantfor the prevalence of oral diseasesin handicapped patientsII14
These studies show differencesbetween institutionalized andnon-institutionalized individu-als In general institutionalizedpatients presented a lower preva-lence of dental caries when com-pared to non-institutionalizedpatients probably due to dietarycontrol7IS Handicap severityshould also be taken into ac-count since it is a determinantfactor not only for oral hygienestatus but also for dental
therapy which is hampered bythe inability of CP children to communicate and cooperatebecause of their oral pathologic reflexes These facts reinforcethe need to study the factors related to the etiology of the dis-ease in these patients
To record dental caries clinicians used only clinical criteriaNo radiographs were obtained to aid the diagnosis of caries dueto the lack of sufficient patient cooperation To determine cariesprevalence authors chose to compare the DMFS between the 2
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 43
Table B Orill Motor Sldlls In the Study Group
Dentition Gender n Suction capacicy Bite capacicy Nasal breathing Residual food Coch ranG test Significance
Male 23 70 30 44 74 3389 +Mixed
Female II 64 46 46 73 1733 +
Male 12 50 25 8 75 1970 +Permanent
Female 16 63 31 50 88 1929 +
n number of individualy+ significant at 00 I
When dmfs and DMFS were examined in the 6- to 11-year-old group no differences were found between the studyand control groups Magnusson and Devall7 found no signifi-cant difference in dmfs in subjects with mixed dentitionShmarak and Bernstein21 summed dmfs and DMFS and theyfound higher decay experience levels in CP children Swallowl2
found lower dmfs and DMFS values in this age group in CPchildren but these subjects had a much lower number of filledsurfaces Fishman et al23 described very similar DMF valuesand components of DMFS in CP children and siblings butslightly higher dmf (not statistically significant) in CP chil-dren The conflicting results verified in different studies wereprobably due to different characteristics of the studied popula-tions and different control groups
There were significantly higher values of DMFS for the 12-to 16-year-old children in the study group Swallow22 andMagnusson and Devall7 reported a similar DMF but Swallowl2
found far fewer fillings in the CP children Pope and Curzonl3
found more decayed and extracted teeth in mentally handicappedCP children However Nielsen20 in a study of 14- and 15-year-old CP children detected lower mean DMFS scores and morecaries-free mouths in CP children than in controls Nielsen20
found that moror alterations in handicapped persons were thebest caries predictors The evidence of the present study showedthe opposite situation for this age and group
Plaque index values were significantly higher in both sexeswith permanent dentition in the study group However thefrequency of rooth-brushing in the CP group was consideredcomparable ro that of the general pediatric population No childreported the use of fluoride supplements
According ro many parents there was an association betweenthose who had difficulty in maintaining satisfactory oral hygieneand those who had difficulty in properly brushing their teethMoror and mental alterations as well as dyskinetic movementsmay have hanlpered dental hygiene Position of the child at thetime or oral hygiene the presence of pathological oral reflexessuch as biting and vomiting and alterations in intraoral sensitiv-ity were also very important factors for the mechanical removalof plaque Most of the studies in the literature reported unsatis-factory oral hygiene in individuals with CP7 11-1317-2124-28
Increasing discrepancy in oral hygiene with age between handi-capped and non-handicapped children was seen in the presentstudy and has also been described by Brown and Schodel IIMaclaurin et al12and Murray and McLeod 26
Dietary habits were difficult to assess due to incomplete datafor me CP group In many of me diets soft loosely textured andsemisolid foods were consumed thereby increasing the risk offermentable carbohydrate retention and subsequent decay
Lower percentages for the expected time of eruption of perma-nent molars were observed in the experimental group Pope andCurzon13 Morales18 Nielsen2deg and Album et al29 also reporteddelay in the time of eruption Molina et al2Srelated the degree ofmental involvement to the delay in time of eruption HoweverWesselsl6 reported that the pattern of eruption of primary andpermanent teeth and the time of eruption in CP children did notsignificantly differ from those of normal children
The results showed significantly higher percentages of malocclu-sion in males wim permanent dentition in the srudy group Whenpresent the malocclusion found was only Class II division 1 typeaccording to Angles classification The simple orthodontic assess-ment indicated that CP children most of whom were affected byspasticity had a higher prevalence of increased overjet and lowerprevalence of crowding than controls Brown and Schodel II Popeand Curzon13 Wessels16 Miller and Taylor19 Shamarak andBernstein21 and Album et al29also obtained similar results Strodel28
suggested that CP children tended to develop increased overjet due
to buccal breathing and tongue thrusting which was rdated to poorswallowing reflex This clinician considered that this may have pre-disposed the upper incisor teeth of CP children to rrawna
Wesselsl6 considered the prevalence and severity of malocclu-sion to increase with age in CP children and the fact that theoverjet was significantly higher in the older population of thisstudy but nor in the 6- to ll-year-old group It has been sug-gested that CP children have significantly different skull and jawdimensions compared with controls When combined with ab-normal muscular activity this would result in severe malocclu-sion11 Foster et al30 demonstrated variable differences in skulldimensions in CP children when compared with controls andthey found that the most severe CP children had the most ab-normal and reduced skull dimensions Strodel28 stated that themotor disorders in individual children accentuated tendenciesroward malocclusion and the spastic CP children had a greatertendency roward a Class II dental and skeletal formation
Bruxism was present in a significantly higher percentage of maleswith permanent dentition in the study group Bruxism was gener-ally accepted as a frequent finding in CP children 17and the presentstudy agreed with the literature Albwn et al29reported that theathetoid group exhibited the highest percentage of bruxism In
44 dos Santos et al Oral Conditions In Children with CP Journal of Dentistry for Children
the present smdy the presence of bruxism was not cypicll of onlychildren with athetosis
Eating efficiency represented the final outcome of the oral skillsused to prepare food for swallowing In this study the authors in-tended to determine which aspects of oral skills were impaired Thepresence of residual food was the result of the inability of the tonguelips and cheeks to perform normal deglutition Nowakll also pointedout that the difficulty in mastication and deglutition of CP subjectsmighr have lead them to eat pasty foods rich in carbohydrates witha reduced duration of the masticatory cycle Poor lip closure tonguethrust and lip retraction leading to mouth breathing were frequentcharacteristics observed in the smdy group The authors would liketo emphasize that accumulation of food deposits associated withthe increased plaque index observed in the smdy group were highrisk factors for the increase in caries prevalence in these patients
At present much attention has focused on the rehabilitationof CP patients so that they can integrate into society throughproper health care education and employment Neverthelessoral conditions in CP patients were not satisfactory accordingto the variables studied On this basis it is important to empha-size that to rehabilitate these patients dental therapy must beincluded The energy needed to maintain their vital processeswill be provided by a balanced diet which will be greatly influ-enced by their healthy oral caviry Based on these results earlierpreventive measures for CP patients are required because theyare a high-risk group for dental caries
CONCLUSIONSCP children presented significantly higher DMFS indexesfor permanenr teeth than normal children The plaque indexfound in the group of CP children was significantly higherfor permanenr teeth than normal children CP children hada rendency to a delay in the rime of eruption of permanentmolars compared to normal children CP children with per-manent denrition presenred significantly higher percentagesof malocclusion and bruxism rhan normal children In thestudy group oral breathing and the presence of food depos-its were freq uenr characteristics
ACKNOWLEDGEMENTSWe thank Fundarao de Amparo a Pesquisa do Estado de SaoPaulo (FAPESP) for financial support (9612474-0) (FAPESPis an institution of the state of Sao Paulo that provides grantsfor research)
REFERENCESI Stanley F The etiology of cerebral palsyEarry Hum Dev
19943681-88
2 Colver AF Gibson M Hey EN et aI Increasing rates of cerebralpalsy across the severity spectrum in northeast England Collabora-rive cerebral palsy survey Arch Dis Child Fetal Neonatal Ed200083 F7-F 12
3 OShea TM Dammann O Anrecedents of cerebral palsy in verylow-birth weighr infants Clin Perinatol 200027285-302
4 Murphy C Yeargin-AJlsopM Decoufle Pet al Prevalence of cere-bral palsyamong ten-year-old children in metropolitan Atlanta 1985through 1987 Pediatr 1993123513-20
5 Cummis S Nelson K Grether J et al Cerebral palsy in four north-ern California counties births 1983 through 1985 Pediatr1993123 230-237
6 Schwartzman S Paralisia cerebral Temassobre 0 desenvolvimento19933 4-21
7 Brown J The efficacy and economy of comprehensive dental carefor handicapped children Int Dent 198030 14-27
8 World Health Organization Oral health surveysbasic methods 3rded Geneva World Health Organization 1987
9 Podshadley A Haley T A method for evaluating oral hygiene per-formance Public Health Rep 196883 259-264
1OSiegelS Castellan JR Nonparametric statistics2ed New York NYMcGraw-Hili 1988399
11Brown J Schodel BA reviewof controlled surveysof dental disease inhandicapped persons Dent Child 197643313-320
12MacLaurin E Shaw L Foster T Dental study of handicapped chil-dren attending special schools in Birmingham Part I Dental cariesexperience of children living in a fluoridated area Community DentHealth 19852259-265
13Pope J Curzon M The dental status of cerebral palsied childrenPediatr Dent 199113156-162
14Bhavsar JP Damle SG Dental caries and oral hygiene amongst 12-14-year-old handicapped children of Bombay India Indian SocPedodPrevDent1995131-3
15Novak AJThe effect of dietary and brushing habits on dental cariesin noninstitutionalized handicapped children Dem Handicap]977315-19
16Wessels K Oral conditions in cerebral palsy Dent Clin North Am1960455-468
17Magnusson B Deval R Oral conditions in a group of children withcerebral palsy Odontol Revy 1963 14385-402
I8Morales C Paralisiscerebral sus efectos sobre la erupci6n del primermolar permanenre y las condiciones de salud-enfermedad ActaOdontolVenez 198725 13-33
19Miller J Taylor PA survey of the oral health of a group of orthope-dically handicapped children Dent Child 197037 331-343
20Nielsen 1 Caries among children with cerebral palsy Relation roCP-diagnosis mental and moror handicap Dent Child199057267 -273
21Shmarak K Bernstein J Caries incidence among cerebral palsiedchildren A preliminary study Dent Child 1961 28 154- 156
22Swallow J The dental problems of handicapped children J R SocHealth 196885152-157
23Fishman 5 Young W Haley J et al The status of oral health incerebral palsy children and their siblings Dent Child196734219-227
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 45
24Melville M Pool D Jaffe E er aI A denral service for handicapped
children Br Dent 1981 151 259-261
25Molina I Vinas L Garcia F Erupci6n clfnica de los dienres
permanenres en nifios can impedimenros menrales de Sanro
Domingo Acta Odonto Pedjatr 1982369-73
26Murray J McLeod J The denral condirion of severely subnormal
children in rhree London boroughs Br Dent 1973 134380-385
27Nunn J Murray J The denral healrh of handicapped children in
Newcasrle and Northumberland Br Dent 1987] 629-14
28Srrodel B The effecrs of spasric cerebral pals) on occlusion j DentChild ]98754255-260
29Album M Krogman W Baker D er al An evaluarion of denral
profile of neuromuscular deficir parienrs A pilor Srudy Dent Child196431 204-227
30Fosrer TD Griffirh MI Gordon PH The effecrs of cerebral palsy
on rhe size and form of rhe skull Am j Orthod 19746640-49
31 Nowak AJ Denral disease in handicapped persons Spec Care Den-tist 1984466-69
46 dos Santos et al Oral Conditions in Children with CP Journal of Dentistry for Children

Table B Orill Motor Sldlls In the Study Group
Dentition Gender n Suction capacicy Bite capacicy Nasal breathing Residual food Coch ranG test Significance
Male 23 70 30 44 74 3389 +Mixed
Female II 64 46 46 73 1733 +
Male 12 50 25 8 75 1970 +Permanent
Female 16 63 31 50 88 1929 +
n number of individualy+ significant at 00 I
When dmfs and DMFS were examined in the 6- to 11-year-old group no differences were found between the studyand control groups Magnusson and Devall7 found no signifi-cant difference in dmfs in subjects with mixed dentitionShmarak and Bernstein21 summed dmfs and DMFS and theyfound higher decay experience levels in CP children Swallowl2
found lower dmfs and DMFS values in this age group in CPchildren but these subjects had a much lower number of filledsurfaces Fishman et al23 described very similar DMF valuesand components of DMFS in CP children and siblings butslightly higher dmf (not statistically significant) in CP chil-dren The conflicting results verified in different studies wereprobably due to different characteristics of the studied popula-tions and different control groups
There were significantly higher values of DMFS for the 12-to 16-year-old children in the study group Swallow22 andMagnusson and Devall7 reported a similar DMF but Swallowl2
found far fewer fillings in the CP children Pope and Curzonl3
found more decayed and extracted teeth in mentally handicappedCP children However Nielsen20 in a study of 14- and 15-year-old CP children detected lower mean DMFS scores and morecaries-free mouths in CP children than in controls Nielsen20
found that moror alterations in handicapped persons were thebest caries predictors The evidence of the present study showedthe opposite situation for this age and group
Plaque index values were significantly higher in both sexeswith permanent dentition in the study group However thefrequency of rooth-brushing in the CP group was consideredcomparable ro that of the general pediatric population No childreported the use of fluoride supplements
According ro many parents there was an association betweenthose who had difficulty in maintaining satisfactory oral hygieneand those who had difficulty in properly brushing their teethMoror and mental alterations as well as dyskinetic movementsmay have hanlpered dental hygiene Position of the child at thetime or oral hygiene the presence of pathological oral reflexessuch as biting and vomiting and alterations in intraoral sensitiv-ity were also very important factors for the mechanical removalof plaque Most of the studies in the literature reported unsatis-factory oral hygiene in individuals with CP7 11-1317-2124-28
Increasing discrepancy in oral hygiene with age between handi-capped and non-handicapped children was seen in the presentstudy and has also been described by Brown and Schodel IIMaclaurin et al12and Murray and McLeod 26
Dietary habits were difficult to assess due to incomplete datafor me CP group In many of me diets soft loosely textured andsemisolid foods were consumed thereby increasing the risk offermentable carbohydrate retention and subsequent decay
Lower percentages for the expected time of eruption of perma-nent molars were observed in the experimental group Pope andCurzon13 Morales18 Nielsen2deg and Album et al29 also reporteddelay in the time of eruption Molina et al2Srelated the degree ofmental involvement to the delay in time of eruption HoweverWesselsl6 reported that the pattern of eruption of primary andpermanent teeth and the time of eruption in CP children did notsignificantly differ from those of normal children
The results showed significantly higher percentages of malocclu-sion in males wim permanent dentition in the srudy group Whenpresent the malocclusion found was only Class II division 1 typeaccording to Angles classification The simple orthodontic assess-ment indicated that CP children most of whom were affected byspasticity had a higher prevalence of increased overjet and lowerprevalence of crowding than controls Brown and Schodel II Popeand Curzon13 Wessels16 Miller and Taylor19 Shamarak andBernstein21 and Album et al29also obtained similar results Strodel28
suggested that CP children tended to develop increased overjet due
to buccal breathing and tongue thrusting which was rdated to poorswallowing reflex This clinician considered that this may have pre-disposed the upper incisor teeth of CP children to rrawna
Wesselsl6 considered the prevalence and severity of malocclu-sion to increase with age in CP children and the fact that theoverjet was significantly higher in the older population of thisstudy but nor in the 6- to ll-year-old group It has been sug-gested that CP children have significantly different skull and jawdimensions compared with controls When combined with ab-normal muscular activity this would result in severe malocclu-sion11 Foster et al30 demonstrated variable differences in skulldimensions in CP children when compared with controls andthey found that the most severe CP children had the most ab-normal and reduced skull dimensions Strodel28 stated that themotor disorders in individual children accentuated tendenciesroward malocclusion and the spastic CP children had a greatertendency roward a Class II dental and skeletal formation
Bruxism was present in a significantly higher percentage of maleswith permanent dentition in the study group Bruxism was gener-ally accepted as a frequent finding in CP children 17and the presentstudy agreed with the literature Albwn et al29reported that theathetoid group exhibited the highest percentage of bruxism In
44 dos Santos et al Oral Conditions In Children with CP Journal of Dentistry for Children
the present smdy the presence of bruxism was not cypicll of onlychildren with athetosis
Eating efficiency represented the final outcome of the oral skillsused to prepare food for swallowing In this study the authors in-tended to determine which aspects of oral skills were impaired Thepresence of residual food was the result of the inability of the tonguelips and cheeks to perform normal deglutition Nowakll also pointedout that the difficulty in mastication and deglutition of CP subjectsmighr have lead them to eat pasty foods rich in carbohydrates witha reduced duration of the masticatory cycle Poor lip closure tonguethrust and lip retraction leading to mouth breathing were frequentcharacteristics observed in the smdy group The authors would liketo emphasize that accumulation of food deposits associated withthe increased plaque index observed in the smdy group were highrisk factors for the increase in caries prevalence in these patients
At present much attention has focused on the rehabilitationof CP patients so that they can integrate into society throughproper health care education and employment Neverthelessoral conditions in CP patients were not satisfactory accordingto the variables studied On this basis it is important to empha-size that to rehabilitate these patients dental therapy must beincluded The energy needed to maintain their vital processeswill be provided by a balanced diet which will be greatly influ-enced by their healthy oral caviry Based on these results earlierpreventive measures for CP patients are required because theyare a high-risk group for dental caries
CONCLUSIONSCP children presented significantly higher DMFS indexesfor permanenr teeth than normal children The plaque indexfound in the group of CP children was significantly higherfor permanenr teeth than normal children CP children hada rendency to a delay in the rime of eruption of permanentmolars compared to normal children CP children with per-manent denrition presenred significantly higher percentagesof malocclusion and bruxism rhan normal children In thestudy group oral breathing and the presence of food depos-its were freq uenr characteristics
ACKNOWLEDGEMENTSWe thank Fundarao de Amparo a Pesquisa do Estado de SaoPaulo (FAPESP) for financial support (9612474-0) (FAPESPis an institution of the state of Sao Paulo that provides grantsfor research)
REFERENCESI Stanley F The etiology of cerebral palsyEarry Hum Dev
19943681-88
2 Colver AF Gibson M Hey EN et aI Increasing rates of cerebralpalsy across the severity spectrum in northeast England Collabora-rive cerebral palsy survey Arch Dis Child Fetal Neonatal Ed200083 F7-F 12
3 OShea TM Dammann O Anrecedents of cerebral palsy in verylow-birth weighr infants Clin Perinatol 200027285-302
4 Murphy C Yeargin-AJlsopM Decoufle Pet al Prevalence of cere-bral palsyamong ten-year-old children in metropolitan Atlanta 1985through 1987 Pediatr 1993123513-20
5 Cummis S Nelson K Grether J et al Cerebral palsy in four north-ern California counties births 1983 through 1985 Pediatr1993123 230-237
6 Schwartzman S Paralisia cerebral Temassobre 0 desenvolvimento19933 4-21
7 Brown J The efficacy and economy of comprehensive dental carefor handicapped children Int Dent 198030 14-27
8 World Health Organization Oral health surveysbasic methods 3rded Geneva World Health Organization 1987
9 Podshadley A Haley T A method for evaluating oral hygiene per-formance Public Health Rep 196883 259-264
1OSiegelS Castellan JR Nonparametric statistics2ed New York NYMcGraw-Hili 1988399
11Brown J Schodel BA reviewof controlled surveysof dental disease inhandicapped persons Dent Child 197643313-320
12MacLaurin E Shaw L Foster T Dental study of handicapped chil-dren attending special schools in Birmingham Part I Dental cariesexperience of children living in a fluoridated area Community DentHealth 19852259-265
13Pope J Curzon M The dental status of cerebral palsied childrenPediatr Dent 199113156-162
14Bhavsar JP Damle SG Dental caries and oral hygiene amongst 12-14-year-old handicapped children of Bombay India Indian SocPedodPrevDent1995131-3
15Novak AJThe effect of dietary and brushing habits on dental cariesin noninstitutionalized handicapped children Dem Handicap]977315-19
16Wessels K Oral conditions in cerebral palsy Dent Clin North Am1960455-468
17Magnusson B Deval R Oral conditions in a group of children withcerebral palsy Odontol Revy 1963 14385-402
I8Morales C Paralisiscerebral sus efectos sobre la erupci6n del primermolar permanenre y las condiciones de salud-enfermedad ActaOdontolVenez 198725 13-33
19Miller J Taylor PA survey of the oral health of a group of orthope-dically handicapped children Dent Child 197037 331-343
20Nielsen 1 Caries among children with cerebral palsy Relation roCP-diagnosis mental and moror handicap Dent Child199057267 -273
21Shmarak K Bernstein J Caries incidence among cerebral palsiedchildren A preliminary study Dent Child 1961 28 154- 156
22Swallow J The dental problems of handicapped children J R SocHealth 196885152-157
23Fishman 5 Young W Haley J et al The status of oral health incerebral palsy children and their siblings Dent Child196734219-227
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 45
24Melville M Pool D Jaffe E er aI A denral service for handicapped
children Br Dent 1981 151 259-261
25Molina I Vinas L Garcia F Erupci6n clfnica de los dienres
permanenres en nifios can impedimenros menrales de Sanro
Domingo Acta Odonto Pedjatr 1982369-73
26Murray J McLeod J The denral condirion of severely subnormal
children in rhree London boroughs Br Dent 1973 134380-385
27Nunn J Murray J The denral healrh of handicapped children in
Newcasrle and Northumberland Br Dent 1987] 629-14
28Srrodel B The effecrs of spasric cerebral pals) on occlusion j DentChild ]98754255-260
29Album M Krogman W Baker D er al An evaluarion of denral
profile of neuromuscular deficir parienrs A pilor Srudy Dent Child196431 204-227
30Fosrer TD Griffirh MI Gordon PH The effecrs of cerebral palsy
on rhe size and form of rhe skull Am j Orthod 19746640-49
31 Nowak AJ Denral disease in handicapped persons Spec Care Den-tist 1984466-69
46 dos Santos et al Oral Conditions in Children with CP Journal of Dentistry for Children

the present smdy the presence of bruxism was not cypicll of onlychildren with athetosis
Eating efficiency represented the final outcome of the oral skillsused to prepare food for swallowing In this study the authors in-tended to determine which aspects of oral skills were impaired Thepresence of residual food was the result of the inability of the tonguelips and cheeks to perform normal deglutition Nowakll also pointedout that the difficulty in mastication and deglutition of CP subjectsmighr have lead them to eat pasty foods rich in carbohydrates witha reduced duration of the masticatory cycle Poor lip closure tonguethrust and lip retraction leading to mouth breathing were frequentcharacteristics observed in the smdy group The authors would liketo emphasize that accumulation of food deposits associated withthe increased plaque index observed in the smdy group were highrisk factors for the increase in caries prevalence in these patients
At present much attention has focused on the rehabilitationof CP patients so that they can integrate into society throughproper health care education and employment Neverthelessoral conditions in CP patients were not satisfactory accordingto the variables studied On this basis it is important to empha-size that to rehabilitate these patients dental therapy must beincluded The energy needed to maintain their vital processeswill be provided by a balanced diet which will be greatly influ-enced by their healthy oral caviry Based on these results earlierpreventive measures for CP patients are required because theyare a high-risk group for dental caries
CONCLUSIONSCP children presented significantly higher DMFS indexesfor permanenr teeth than normal children The plaque indexfound in the group of CP children was significantly higherfor permanenr teeth than normal children CP children hada rendency to a delay in the rime of eruption of permanentmolars compared to normal children CP children with per-manent denrition presenred significantly higher percentagesof malocclusion and bruxism rhan normal children In thestudy group oral breathing and the presence of food depos-its were freq uenr characteristics
ACKNOWLEDGEMENTSWe thank Fundarao de Amparo a Pesquisa do Estado de SaoPaulo (FAPESP) for financial support (9612474-0) (FAPESPis an institution of the state of Sao Paulo that provides grantsfor research)
REFERENCESI Stanley F The etiology of cerebral palsyEarry Hum Dev
19943681-88
2 Colver AF Gibson M Hey EN et aI Increasing rates of cerebralpalsy across the severity spectrum in northeast England Collabora-rive cerebral palsy survey Arch Dis Child Fetal Neonatal Ed200083 F7-F 12
3 OShea TM Dammann O Anrecedents of cerebral palsy in verylow-birth weighr infants Clin Perinatol 200027285-302
4 Murphy C Yeargin-AJlsopM Decoufle Pet al Prevalence of cere-bral palsyamong ten-year-old children in metropolitan Atlanta 1985through 1987 Pediatr 1993123513-20
5 Cummis S Nelson K Grether J et al Cerebral palsy in four north-ern California counties births 1983 through 1985 Pediatr1993123 230-237
6 Schwartzman S Paralisia cerebral Temassobre 0 desenvolvimento19933 4-21
7 Brown J The efficacy and economy of comprehensive dental carefor handicapped children Int Dent 198030 14-27
8 World Health Organization Oral health surveysbasic methods 3rded Geneva World Health Organization 1987
9 Podshadley A Haley T A method for evaluating oral hygiene per-formance Public Health Rep 196883 259-264
1OSiegelS Castellan JR Nonparametric statistics2ed New York NYMcGraw-Hili 1988399
11Brown J Schodel BA reviewof controlled surveysof dental disease inhandicapped persons Dent Child 197643313-320
12MacLaurin E Shaw L Foster T Dental study of handicapped chil-dren attending special schools in Birmingham Part I Dental cariesexperience of children living in a fluoridated area Community DentHealth 19852259-265
13Pope J Curzon M The dental status of cerebral palsied childrenPediatr Dent 199113156-162
14Bhavsar JP Damle SG Dental caries and oral hygiene amongst 12-14-year-old handicapped children of Bombay India Indian SocPedodPrevDent1995131-3
15Novak AJThe effect of dietary and brushing habits on dental cariesin noninstitutionalized handicapped children Dem Handicap]977315-19
16Wessels K Oral conditions in cerebral palsy Dent Clin North Am1960455-468
17Magnusson B Deval R Oral conditions in a group of children withcerebral palsy Odontol Revy 1963 14385-402
I8Morales C Paralisiscerebral sus efectos sobre la erupci6n del primermolar permanenre y las condiciones de salud-enfermedad ActaOdontolVenez 198725 13-33
19Miller J Taylor PA survey of the oral health of a group of orthope-dically handicapped children Dent Child 197037 331-343
20Nielsen 1 Caries among children with cerebral palsy Relation roCP-diagnosis mental and moror handicap Dent Child199057267 -273
21Shmarak K Bernstein J Caries incidence among cerebral palsiedchildren A preliminary study Dent Child 1961 28 154- 156
22Swallow J The dental problems of handicapped children J R SocHealth 196885152-157
23Fishman 5 Young W Haley J et al The status of oral health incerebral palsy children and their siblings Dent Child196734219-227
Journal of Dentistry for Children Oral Conditions In Children with CP dos Santos et al 45
24Melville M Pool D Jaffe E er aI A denral service for handicapped
children Br Dent 1981 151 259-261
25Molina I Vinas L Garcia F Erupci6n clfnica de los dienres
permanenres en nifios can impedimenros menrales de Sanro
Domingo Acta Odonto Pedjatr 1982369-73
26Murray J McLeod J The denral condirion of severely subnormal
children in rhree London boroughs Br Dent 1973 134380-385
27Nunn J Murray J The denral healrh of handicapped children in
Newcasrle and Northumberland Br Dent 1987] 629-14
28Srrodel B The effecrs of spasric cerebral pals) on occlusion j DentChild ]98754255-260
29Album M Krogman W Baker D er al An evaluarion of denral
profile of neuromuscular deficir parienrs A pilor Srudy Dent Child196431 204-227
30Fosrer TD Griffirh MI Gordon PH The effecrs of cerebral palsy
on rhe size and form of rhe skull Am j Orthod 19746640-49
31 Nowak AJ Denral disease in handicapped persons Spec Care Den-tist 1984466-69
46 dos Santos et al Oral Conditions in Children with CP Journal of Dentistry for Children

24Melville M Pool D Jaffe E er aI A denral service for handicapped
children Br Dent 1981 151 259-261
25Molina I Vinas L Garcia F Erupci6n clfnica de los dienres
permanenres en nifios can impedimenros menrales de Sanro
Domingo Acta Odonto Pedjatr 1982369-73
26Murray J McLeod J The denral condirion of severely subnormal
children in rhree London boroughs Br Dent 1973 134380-385
27Nunn J Murray J The denral healrh of handicapped children in
Newcasrle and Northumberland Br Dent 1987] 629-14
28Srrodel B The effecrs of spasric cerebral pals) on occlusion j DentChild ]98754255-260
29Album M Krogman W Baker D er al An evaluarion of denral
profile of neuromuscular deficir parienrs A pilor Srudy Dent Child196431 204-227
30Fosrer TD Griffirh MI Gordon PH The effecrs of cerebral palsy
on rhe size and form of rhe skull Am j Orthod 19746640-49
31 Nowak AJ Denral disease in handicapped persons Spec Care Den-tist 1984466-69
46 dos Santos et al Oral Conditions in Children with CP Journal of Dentistry for Children
Copyright © 2022 FDOKUMEN




















