
Periodontal Disease, Dental Caries and Hypersensitivity : A millennial view
19
Transcript of Periodontal Disease, Dental Caries and Hypersensitivity : A millennial view


1
Periodontal Disease, Dental Caries and Hypersensitivity
An Update for NEW GEN
Editor-in-chief: Lakshman P. Samaranayake
Supported by
Editorial development by Sharon O’ Brien MIMS. The opinions expressed in this publication are not necessarily those of the editor, publisher or sponsor. Any liability or obligation for loss or damage however so arising is hereby disclaimed. © 2013 MIMS. All rights reserved. No part of this publication may be reproduced by any process in any language without the written permission of the publisher.
Acknowledgements
Johnson and Johnson would like to thank Lakshman P. Samaranayake, Sukumaran Anil, Prathip Phantumvanit, Domenick T. Zero, C.H. Chu Chun Hung, and Christine Charles for kindly agreeing to become authours for this textbook.
First Edition 2013
Published by: MIMS Pte Ltd6 Shenton Way #15-08 Tower 2 Singapore 068809Tel: +65 6290 7400 Fax: +65 62907401Email: [email protected] Website: www.mims.com

2
ContentsChapter I Biofilm as Root Cause of Oral Disease L.P. Samaranayake
What is biofilm ........................................................................................................................... 1
Oral Biofilm ................................................................................................................................... 1
Plaque biofilm formation as a multistage process ...................................................... 2
Biofilm maturation ................................................................................................................... 3
Biofilm architecture and functionality ............................................................................ 4
Molecular biology of biofilms .............................................................................................. 5
Metagenomics and plaque biofilms ..................................................................... 5
The role of biofilms in oral infections ............................................................................. 5
Bofilm and periodontal disease ........................................................................... 5
Biofilm and dental caries ......................................................................................... 7
The role of biofilms in systemic infections ................................................................... 9
Conclusion .................................................................................................................................. 10
Chapter II Periodontal Disease S. Anil
Prevalence and Epidemiology ........................................................................................... 12
Etiology ....................................................................................................................................... 14
Pathogenesis ............................................................................................................................. 15
Microbial species ........................................................................................................ 16
Impact on general health: systemic perio interrelations ........................................ 18
Management of periodontal disease .............................................................................. 20
Non-surgical periodontal therapy ....................................................................... 20
Surgical methods ..................................................................................................... 21
Prevention of periodontal diseases ................................................................................ 22
Self-care .......................................................................................................................... 22
Dentifrice ..................................................................................................................... 22
Tooth brushing ............................................................................................................ 22
Interdental cleaning .................................................................................................. 22
Mouthrinses ................................................................................................................... 23
Oral irrigation ............................................................................................................... 23
Future risk .................................................................................................................... 23

3
Modifiable risk factors ......................................................................................................... 24
Tobacco ........................................................................................................................... 24
Diabetes mellitus and other systemic risk factors ...................................... 24
Nutrition .......................................................................................................................... 24
Conclusion ................................................................................................................................. 24
Chapter III Dental Caries P. Phantumvanit & D. Zero
Prevalence and epidemiology ........................................................................................... 26
Etiology and pathogenesis .................................................................................................. 29
Fermentable carbohydrates ................................................................................. 30
Cariogenic pathogens ............................................................................................... 30
Impact on health and quality of life ............................................................................... 32
Caries prevention strategies for a new generation .................................................. 34
Fluoride ........................................................................................................................... 34
Xylitol .............................................................................................................................. 35
Antimicrobial agents ................................................................................................. 36
Conclusion .................................................................................................................................. 36
Chapter IV Hypersensitivity C.H. Chu
Prevalence and epidemiology ........................................................................................... 38
Etiology and pathogenesis ................................................................................................. 39
Mechanism of dentine hypersensitivity ....................................................................... 41
Impact on health and quality of life ................................................................................ 42
Managing hypersensitivity ................................................................................................. 43
Home management desensitisation ............................................................................... 44
Professional management desensitisation .................................................................. 46
Conclusion .................................................................................................................................. 48

4
Chapter IV 130 year Listerine; Efficacy and Safety for Life The Essential Formulation
The efficacy from in vitro to clinical
C. Charles
Antimicrobial Mouthrinse Ingredients ......................................................................... 50
Chlorhexidine .............................................................................................................. 51
Cetylpyridinium chloride ........................................................................................ 51
Fixed combination of four Essential Oils ......................................................... 52
In Vitro Antimicrobial Efficacy ......................................................................................... 54
Clinical Efficacy ........................................................................................................................ 55
Short term ..................................................................................................................... 56
Long term .................................................................................................................... 56
Professional uses .................................................................................................................... 57
Implants ....................................................................................................................... 57
In office pre-procedural rinsing ....................................................................... 58
Orthodontics .............................................................................................................. 58
Cariology ...................................................................................................................... 58
Recurrent aphthous ulceration ......................................................................... 59
Oral malodour ........................................................................................................... 59
Daily use safety ........................................................................................................................ 60
FDA ................................................................................................................................ 60
ADA ................................................................................................................................ 61
Safety of alcohol-containing mouthrinses .................................................... 62
Safety in individuals with xerostomia ........................................................... 65
pH effect ...................................................................................................................... 65
Conclusion ................................................................................................................................. 66
12
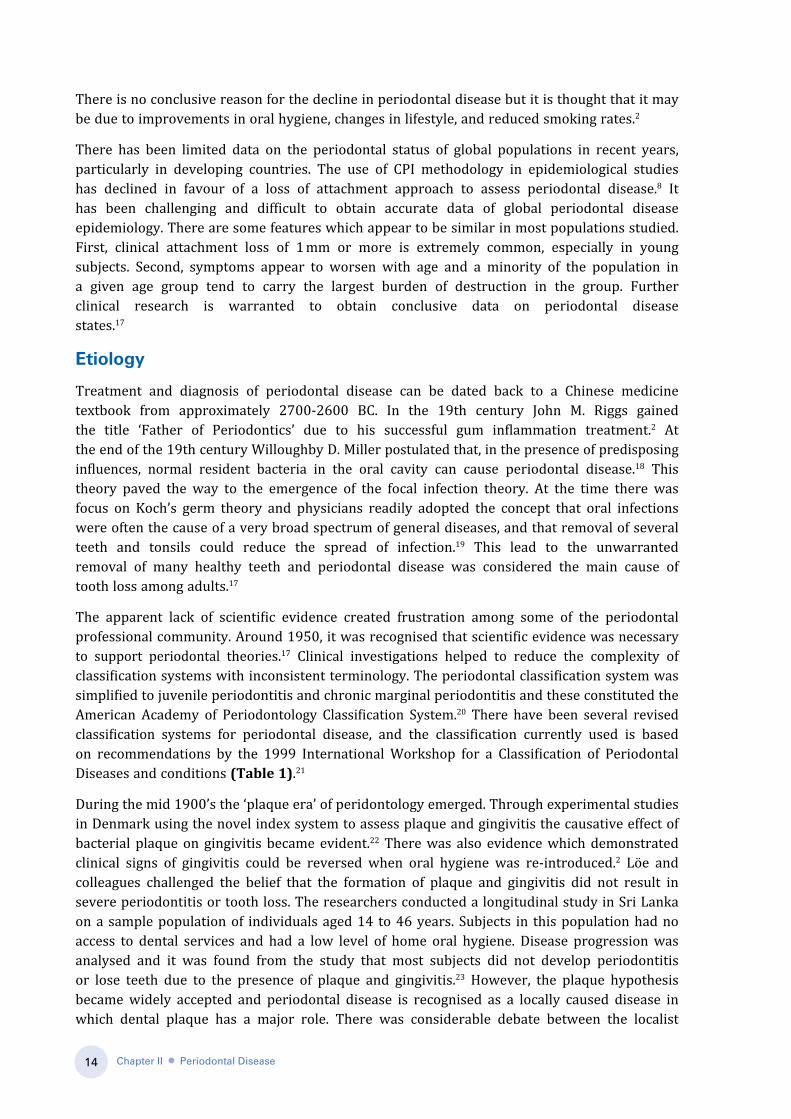
B. A case of chronic Periodontitis note the gingival recession, attachment loss and spacing of the teeth
CHAPtER II.
Periodontal DiseaseS. Anil
Prevalence and epidemiology
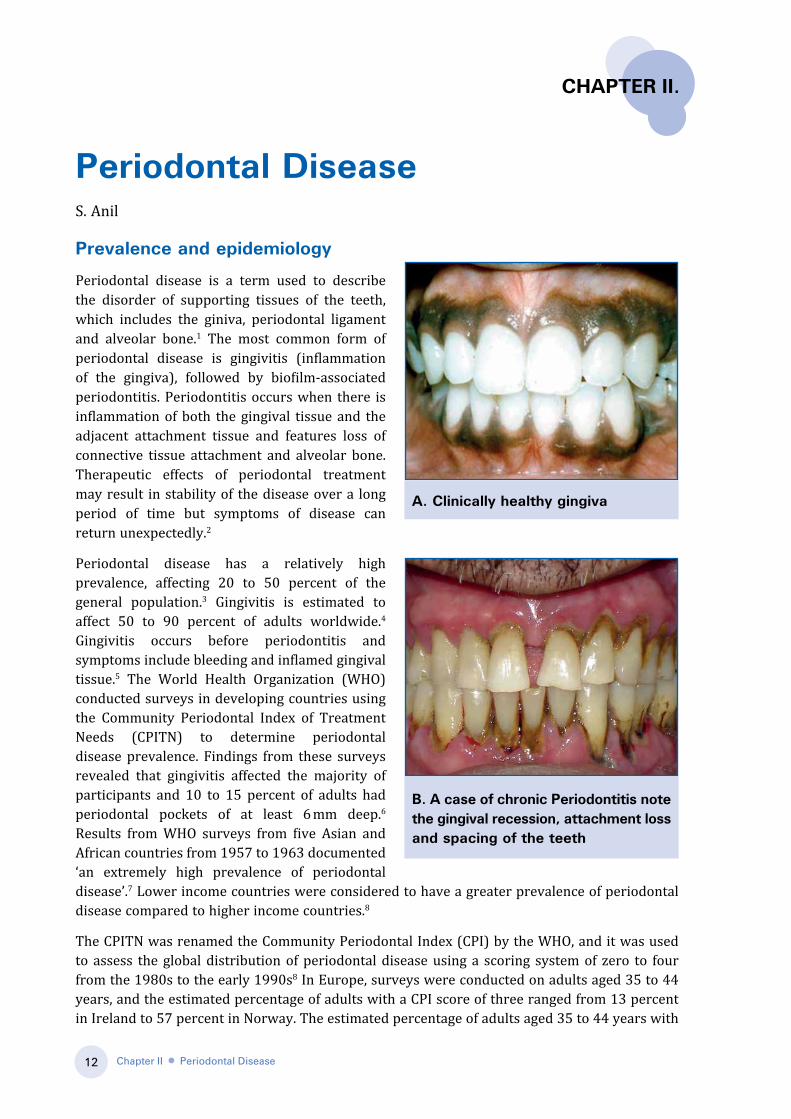
Periodontal disease is a term used to describe the disorder of supporting tissues of the teeth, which includes the giniva, periodontal ligament and alveolar bone.1 The most common form of periodontal disease is gingivitis (inflammation of the gingiva), followed by biofilm-associated periodontitis. Periodontitis occurs when there is inflammation of both the gingival tissue and the adjacent attachment tissue and features loss of connective tissue attachment and alveolar bone. Therapeutic effects of periodontal treatment may result in stability of the disease over a long period of time but symptoms of disease can return unexpectedly.2
Periodontal disease has a relatively high prevalence, affecting 20 to 50 percent of the general population.3 Gingivitis is estimated to affect 50 to 90 percent of adults worldwide.4 Gingivitis occurs before periodontitis and symptoms include bleeding and inflamed gingival tissue.5 The World Health Organization (WHO) conducted surveys in developing countries using the Community Periodontal Index of Treatment Needs (CPITN) to determine periodontal disease prevalence. Findings from these surveys revealed that gingivitis affected the majority of participants and 10 to 15 percent of adults had periodontal pockets of at least 6 mm deep.6 Results from WHO surveys from five Asian and African countries from 1957 to 1963 documented ‘an extremely high prevalence of periodontal disease’.7 Lower income countries were considered to have a greater prevalence of periodontal disease compared to higher income countries.8
The CPITN was renamed the Community Periodontal Index (CPI) by the WHO, and it was used to assess the global distribution of periodontal disease using a scoring system of zero to four from the 1980s to the early 1990s8 In Europe, surveys were conducted on adults aged 35 to 44 years, and the estimated percentage of adults with a CPI score of three ranged from 13 percent in Ireland to 57 percent in Norway. The estimated percentage of adults aged 35 to 44 years with
A. Clinically healthy gingiva
Chapter II ● Periodontal Disease

13
a CPI score of four ranged from three percent in Malta to 40 percent in Turkmenistan. It was estimated that 14 percent of Europeans from the sample populations had a CPI score of four.9
Other surveys focused on Asia and Oceania. The percentage of 35 to 44 year old adults with a CPI score of three ranged from 57 percent in Hong Kong to 8 percent in Saudi Arabia.10 The proportion of adults aged 35 to 44 years with a CPI score of four ranged from 28 percent in Nepal to 5 percent or less in Sri Lanka, Syria and New Zealand. Similar CPI scores were recorded in Africa for both a CPI of three and four.11 Data on CPI scores for the United States showed a 20 percent CPI score of four for adults aged 35 to 44 years.12 The use of CPI scores in epidemiological studies gradually decreased and instead pocket depth and attachment loss became a more common method to assess periodontal disease in populations.8 An Australian that study used clinical attachment of teeth and pocket dept as measurements for periodontal disease found that a quarter of adults aged 35 to 54 years had moderate or severe periodontal attachment loss.13,14
Data from the United States National Health and Nutrition Examinations Surveys (NHANES) from 1988 to 1994 indicated that 7.3 percent of adults had moderate to severe signs of periodontitis. It was calculated that one in every 14 adults suffered from periodontitis with approximately one in five adults having slight periodontitis, one in ten having moderate periodontitis, and one in 30 with signs of severe periodontitis. It was also noted from these surveys that prevalence of periodontitis increased with age. However, the prevalence of the most severe forms were highest at 70 years and did not increase any further.3 Data from the NHANES conducted between 1999 to 2000 found a lower prevalence (4.2 percent) of moderate to severe periodontitis compared to the previous NHANES from 1988 to 1994. This may indicate a decline in periodontal disease over the last decade.15 Hugoson et al examined trends in prevalence and severity of periodontal disease in a Swedish population over 30 years. The researchers found that there were large improvements in alveolar bone index scores in adults aged 20 to 60 years (Figure 1).16 Improvements in periodontal health ranged from 8 to 44 percent, however, severe periodontal disease prevalence remained unchanged over time.16
1973
200370
Bo
ne
Leve
l In
dex
(%
) 60
50
40
30
20
10
020 30 40 50 60
Age group (years)
Figure 1. An improvement in alveolar bone index over a 30-year time period in Scandinavians (Modified from Dentino et al, 2013 and Hugoson et al, 2008).
Chapter II ● Periodontal Disease
14
There is no conclusive reason for the decline in periodontal disease but it is thought that it may be due to improvements in oral hygiene, changes in lifestyle, and reduced smoking rates.2
There has been limited data on the periodontal status of global populations in recent years, particularly in developing countries. The use of CPI methodology in epidemiological studies has declined in favour of a loss of attachment approach to assess periodontal disease.8 It has been challenging and difficult to obtain accurate data of global periodontal disease epidemiology. There are some features which appear to be similar in most populations studied. First, clinical attachment loss of 1 mm or more is extremely common, especially in young subjects. Second, symptoms appear to worsen with age and a minority of the population in a given age group tend to carry the largest burden of destruction in the group. Further clinical research is warranted to obtain conclusive data on periodontal disease states.17
Etiology
Treatment and diagnosis of periodontal disease can be dated back to a Chinese medicine textbook from approximately 2700-2600 BC. In the 19th century John M. Riggs gained the title ‘Father of Periodontics’ due to his successful gum inflammation treatment.2 At the end of the 19th century Willoughby D. Miller postulated that, in the presence of predisposing influences, normal resident bacteria in the oral cavity can cause periodontal disease.18 This theory paved the way to the emergence of the focal infection theory. At the time there was focus on Koch’s germ theory and physicians readily adopted the concept that oral infections were often the cause of a very broad spectrum of general diseases, and that removal of several teeth and tonsils could reduce the spread of infection.19 This lead to the unwarranted removal of many healthy teeth and periodontal disease was considered the main cause of tooth loss among adults.17
The apparent lack of scientific evidence created frustration among some of the periodontal professional community. Around 1950, it was recognised that scientific evidence was necessary to support periodontal theories.17 Clinical investigations helped to reduce the complexity of classification systems with inconsistent terminology. The periodontal classification system was simplified to juvenile periodontitis and chronic marginal periodontitis and these constituted the American Academy of Periodontology Classification System.20 There have been several revised classification systems for periodontal disease, and the classification currently used is based on recommendations by the 1999 International Workshop for a Classification of Periodontal Diseases and conditions (Table 1).21
During the mid 1900’s the ‘plaque era’ of peridontology emerged. Through experimental studies in Denmark using the novel index system to assess plaque and gingivitis the causative effect of bacterial plaque on gingivitis became evident.22 There was also evidence which demonstrated clinical signs of gingivitis could be reversed when oral hygiene was re-introduced.2 Löe and colleagues challenged the belief that the formation of plaque and gingivitis did not result in severe periodontitis or tooth loss. The researchers conducted a longitudinal study in Sri Lanka on a sample population of individuals aged 14 to 46 years. Subjects in this population had no access to dental services and had a low level of home oral hygiene. Disease progression was analysed and it was found from the study that most subjects did not develop periodontitis or lose teeth due to the presence of plaque and gingivitis.23 However, the plaque hypothesis became widely accepted and periodontal disease is recognised as a locally caused disease in which dental plaque has a major role. There was considerable debate between the localist
Chapter II ● Periodontal Disease
15
theory and the generalists theory which postulated that remote causes such as nutrition and tobacco use can weaken periodontal tissues and make tissues vulnerable to infection. However, the generalist theory of periodontal disease remains largely unaccepted and even tobacco use is often only considered a modifying factor and not a primary causal factor of disease.24
Pathogenesis
Periodontal disease develops through opportunistic infection. This usually occurs when there is an imbalance between the oral biofilm and host defences. It is initiated by plaque formation but it is the periodontal tissue’s response to bacterial biofilm which determines the severity and progression of the disease.2
Gingival and periodontal lesions are caused by biofilm-induced inflammatory cascades that involve both the innate and adaptive immune response systems.2 The host response to bacterial biofilm initiates an immuno-inflammatory response with the release of destructive cytokines and enzymes, which can trigger periodontal tissue breakdown. The host response to the bacterial biofilm is influenced by genetic, systemic, and environmental factors such as stress, diabetes and smoking. This genetic link may help to explain why aggressive periodontitis usually has a familial aggregation.25 Inflammation that is localised to the gingiva is the result of a well-balanced symbiosis between biofilms and the host tissues, and periodontitis occurs when there is breakdown of this symbiosis.2
Signalling pattern recognition receptors (PPRs) located on the surface of immune cells interact with pathogen-associated molecular patterns (PAMPs) to initiate a cascade of events.2
Toll-like receptors are triggered which initiates transition from the innate to the adaptive response. In conjunction with other transcriptional activations, formation of reactive oxygen species, reactive nitrogen species, cytokines (interleukin (IL)-1, IL-12, and tumor necrosis factor-α [TNF-α]) and chemokines (IL-8 and monocyte chemoattractant protein-1) occurs. These compounds trigger an inflammatory response and allow migration of additional leukocytes from the blood circulatory system to the site of inflammation. A complex of CD14,
Chapter II ● Periodontal Disease
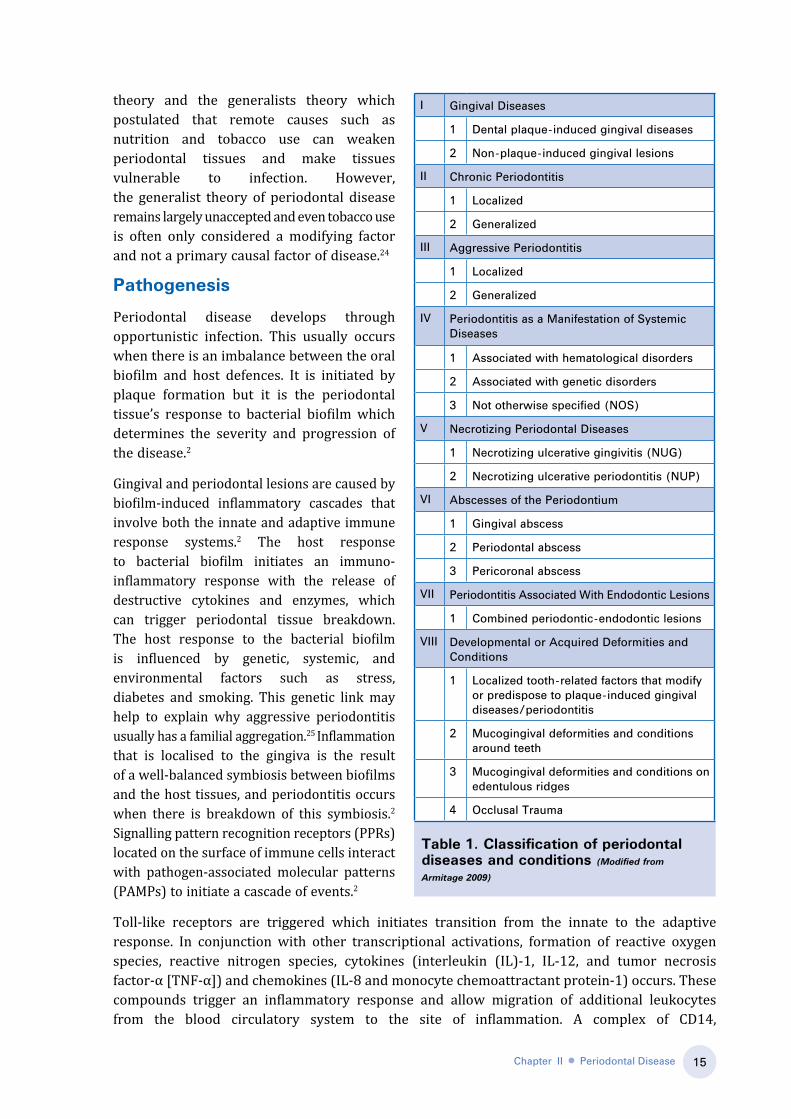
table 1. Classification of periodontal diseases and conditions (Modified from
Armitage 2009)
I Gingival Diseases
1 Dental plaque-induced gingival diseases
2 Non-plaque-induced gingival lesions
II Chronic Periodontitis
1 Localized
2 Generalized
III Aggressive Periodontitis
1 Localized
2 Generalized
IV Periodontitis as a Manifestation of Systemic Diseases
1 Associated with hematological disorders
2 Associated with genetic disorders
3 Not otherwise specified (NOS)
V Necrotizing Periodontal Diseases
1 Necrotizing ulcerative gingivitis (NUG)
2 Necrotizing ulcerative periodontitis (NUP)
VI Abscesses of the Periodontium
1 Gingival abscess
2 Periodontal abscess
3 Pericoronal abscess
VII Periodontitis Associated With Endodontic Lesions
1 Combined periodontic-endodontic lesions
VIII Developmental or Acquired Deformities and Conditions
1 Localized tooth-related factors that modify or predispose to plaque-induced gingival diseases/periodontitis
2 Mucogingival deformities and conditions around teeth
3 Mucogingival deformities and conditions on edentulous ridges
4 Occlusal Trauma
16
lipopolysaccharide (LPS) and toll like receptor 4 further enhances the production of cytokines and chemokines. This triggers the complement cascade, the coagulation pathway and leads to further inflammation.2
A normal inflammatory response will eradicate the unwanted pathogen and stimulate tissue repair. However, if inflammation and infection persists then T-cells and B cells begin to accumulate and dominate the lesion. Toll-like receptors trigger dendritic cells to initiate a specific T-cell response.2 This involves activation of antigen-presenting cells, which interact with T and B cells, triggering an expansion of antibody-secreting plasma B cells, and formation of the chronic lesion.26
Inflammatory pathways can trigger bone destruction. Pro-inflammatory cytokines such as IL-1β, IL-6, IL-17 and TNF-α can trigger periodontal osteoblasts to express membrane bound receptor activator of nuclear factor-kappa B ligand (RANKL). Activation of RANKL in periodontal tissues triggers the differentiation of monocyte-macrophage precursor cells into osteoclasts. Maturation of osteoclasts results in alveolar bone loss.26
CD4+ T lymphocytes are major players in the adaptive immune response, and are the main cell type located in periodontitis gingival tissue. CD4+ T cells proliferate and based on cytokine production, differentiate into T helper (Th) 1, Th2 cells, Th17, and the regulatory T (Treg) cell subset. Th1 cells secrete interferon (IFN)-γ, IL-2, IL-12, TNF-α, and TNF-β, and aid the elimination of intracellular pathogens. Th2 secrete IL-4, IL-5, IL-6, IL-9 and IL-13 that strongly activate B cells and facilitate the eradication of extracellular microorganisms. Th17 has only recently been characterised, and is thought to have a destructive role by inducing bone resorption through secretion of IL-17 and RANKL.26
Matrix metalloproteinases (MMPs) are a family of enzymes that can degrade extracellular matrix (ECM) proteins that are intrinsically linked to periodontal tissue homeostasis. MMP-8, MMP-9, and MMP-13 are able to degrade collagen, and are considered the most important proteases that contribute to periodontal tissue destruction. An imbalance of ECM degradation will disrupt periodontal tissue homeostasis, and impact on a chronic periodontitis state.26
Microbial species
Inflammation of the periodontal tissue occurs in response to Gram-negative pathogenic bacteria such as Porphyromonas gingivalis and spirochetes in the dental plaque biofilm. It has been considered that even a small rise in pH provides a suitable environment for P. gingivalis to overgrow and override other microorganisms in the biofilm. However, P. gingivalis appears to be disrupted by cleaning and it can take many days to re-establish.27 Periodontal disease develops from a pre-existing gingivitis. However, some individuals with severe plaque and calculus formation will develop gingivitis and not periodontitis. On the other hand, some individuals may have good oral hygiene but develop periodontitis, with early tooth loss.28 Typically, poor oral hygiene changes the environment so more periodontal pathogens can survive and multiply.
Chapter II ● Periodontal Disease
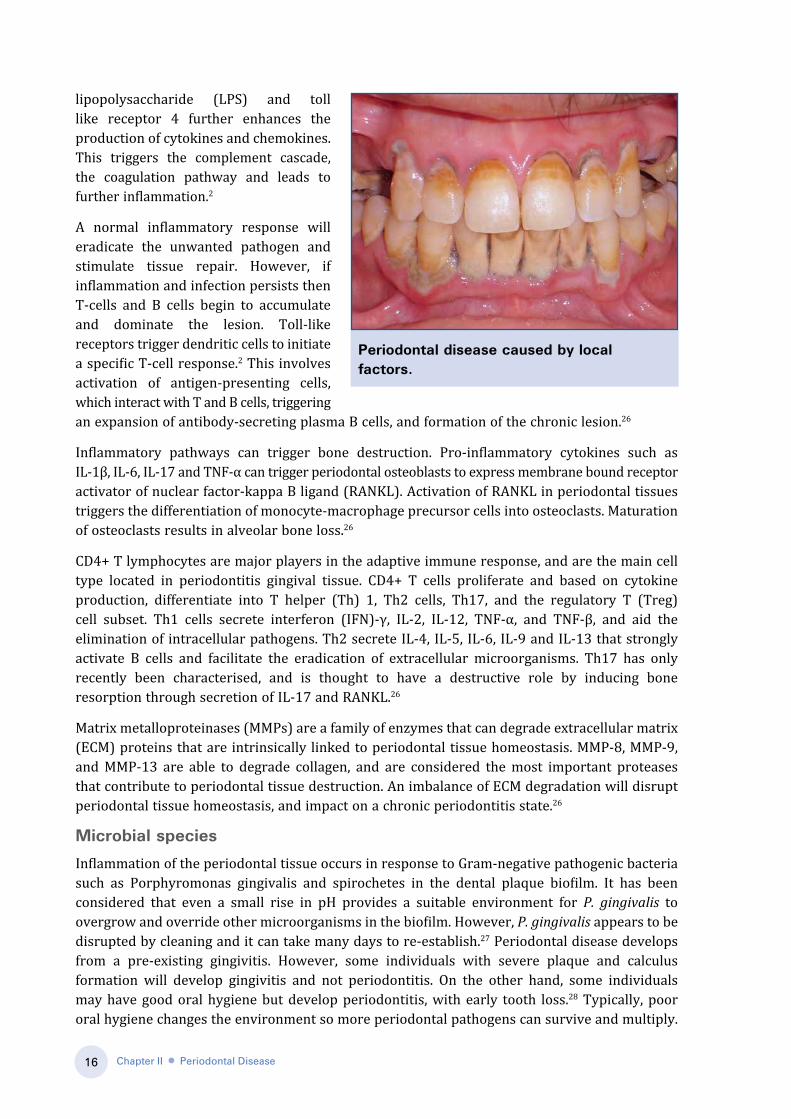
Periodontal disease caused by local factors.

17
There is a direct association between biofilm build-up and the development of gingivitis in humans. The removal of biofilm through brushing and flossing may reverse oral disease states.29
Development of rinse treatments that prevent biofilm colonisation of gum tissues will help to prevent periodontal disease states.
There appears to be a defined order of microbial succession in early supragingival and subgingibal biofilm re-establishment after professional cleaning. Streptococcus mitis and Neisseria mucosa have been shown to significantly increase in supragingival biofilms by day one. These early colonisers either attach themselves to hydroxyapatite or to the salivary glycoproteins covering periodontal tissue. Capnocytophaga gingivalis and Eikenella corrodens were shown to significantly increase by day 2 to 4 post-cleaning. An increased proportion of Veillonella Parvula and streptococcus oralis have been observed between days 1 to 4. Campylobacter rectus, Campylobacter showae, Prevotella melaninogenica and Prevotella nigrescens have been shown to significantly increased between days 4 to 7 post-cleaning in both healthy and diseases supragingival biofilms. It has been proposed that Veillonella may be a critical genus which can guide multispecies development and may be an integral part of a metabolic food chain. Subgingival biofilms have been shown to redevelop at a slower rate and do not follow supragingival biofilm formation after professional cleaning. An elevated number of S. mitis, followed by V. Parvula and C. gingivalis have been observed at the early stages of redevelopment. An increased proportion of Campylobacter Sputigena and P. nigrescens were recorded at day 7.27
The presence of anaerobic bacteria in the biofilm is the main initiating factor associated with periodontal disease development. A healthy gingival sulcus will have an equal ratio of gram- positive cocci. As the biofilm develops and matures, a greater proportion of gram-negative flora colonises. An increased proportion of anaerobic, Gram-negative and motile organisms are associated with progressive periodontal disease. Periodontopathogens are considered to misguide host defense and stimulate tissue-destructive inflammatory pathways.29
Biofilm in the form of supra-gingival and sub-gingival plaque is the etiological agent in periodontal disease. The sub-gingival microbial flora varies from one person to another. The most important Gram-negative bacteria in relation to periodontal disease include P. gingivalis, Aggregatibacter actinomycetemcomitans, Prevotella intermedia, Bactereroides forsythus, Fusobacterium nucleatum, Capnocyophaga species, and C. rectus. It is considered that bacterial colonies can produce disease by tissue invasion, or through the release of enzymes and toxins.1
The following criteria is necessary for a microorganism to be considered a periodontal pathogen● There must be greater numbers of organisms in disease-active sites as compared to non-
disease sites.● Removal of the organism should stop disease progression.● The microorganism needs to have virulent factors relevant to the disease process.● The organism should activate a humoral or cellular immune response.
Porphyromonas gingivalis: P gingivalis, is a Gram-negative rod. It has a protective carbohydrate covering on its outer surface which inhibits opsonisation by complement and also inhibits phagocytosis by neutrophils. This bacterium is an important periodontopathogen which expresses many virulence factors. The main virulence factors it possesses are fimbriae, gingvipains, and lipopolysaccharides. It has the ability to adhere and to invade oral epithelia in vitro. There has been considerable research in developing a vaccine against this bacterium.1
Chapter II ● Periodontal Disease

18
Aggregatibacter actinomycetemcomitans: A. actinomycetemcomitans is a Gram-negative facultative non-motile coccoid bacillus. Colonisation in the periodontal pocket is associated with pre-adolescent, localised juvenile, and advanced adult aggressive periodontal disease. Endotoxin production can modulate host responses and promote tissue destruction. A. actinomycetemcomitans has several virulence factors, with leukotoxin as the most significant.1
Prevotella intermedia: P.intermedia is a black pigmented Gram-negative bacterium. It is thought that it is resistant to phagocytosis through its enclosing capsule.1
Fusobacterium nucleatum: F. nucleatum is an important bacterium at the initial stage of periodontal disease. It forms lipopoysaccharide and butyric acid as metabolic end products.1
Capnocyophaga species: Capnocytophaga are Gram-negative rods. There are three species: C. ochracea, C. sputigena, and C. gingivalis. C. ochracea appears to be most prevalent at the start of a juvenile periodontal disease and in adult periodontal disease.1
Spirochaetes: These are flagellated, motile spiral-shaped microorganisms. Treponema denticola and Treponema vincentii are associated with periodontal disease. These species produce lipopolysaccharide, and other metabolic end products, such as indole, hydrogen sulphide, and ammonia, which can be harmful to host cells.1
A study by Socransky and Haffajee identified spirochetes and P. gingivalis as being more prevalent in diseased sites of diseased patients than in healthy sites of diseased patients. The researchers also identified more of these microorganisms in healthy sites of diseased patients than in healthy sites of healthy patients.30
Although it has been thought that patients with chromosomal abnormalities such as trisomy 21 (Down Syndrome) are predisposed to periodontal disease, there is no firm data to support this theory. Rather, the often lack of dental care services for patients with Down syndrome and mental disability per se may hinder effective control of dental plaque as they may have difficulty in learning an effective brushing technique, and may also lack the concentration required. Poor oral hygiene, poor nutrition and local irritants can exacerbate the problem. Therefore, it is important to adopt effective measures to control biofilm particularly in these cohorts, and thereby reduce the risk of periodontal disease.29
Impact on general health: systemic perio interrelations
Periodontal disease is thought to have a serious impact on systemic health. Evidence is mounting for the potential association between periodontitis and cardiovascular disease (CVD), diabetes mellitus, low birth weight and pulmonary diseases.31,32 The most common reasoning is that circulating periodontal bacterial components may be transported to other tissues, and trigger various host responses which may lead to disease.33
In 1998, Page proposed three different mechanisms by which periodontitis may influence the development of other systemic diseases. He proposed that shared risk factors may be the underlying cause of both periodontal disease and other systemic diseases that may develop. Factors such as tobacco use, stress, aging, race, ethnicity and gender are risk factors for CVD but these are also periodontal disease risk factors. Another proposed mechanism involved subgingival biofilms that harbours lipopolysaccharides and Gram-negative bacteria which can induce vascular responses. Page also proposed that the periodontium may act as a cytokine reservoir as pro-inflammatory cytokines such as TNF-α, IL-1β, gamma interferon and prostaglandin E2 (PGE2) are present in high proportions in periodontitis.34
Chapter II ● Periodontal Disease

19
Figure 2. Schematic overview of potential inflammatory mechanisms linking periodontitis to systemic diseases - Periodontal infection and systemic conditions -(CRP-C-reactive protein, LPS - lipopolysaccharide, IL-1- interleukin-1,IL-6 - interleukin-6, IL-8 - interleukin-8, SSA- Sjogrens’s antibodies , INF-γ-Interferon-gamma, TNF-α Tumor necrosis factor-alpha) [Modified from Anil et al, 2012)
Periodontitis appears to have its strongest association with atherosclerotic cardiovascular disease (ACVD). A consensus report concluded that there is “consistent and strong epidemiological evidence that periodontitis imparts increased risk for future cardiovascular disease” but further intervention trials are necessary before any further conclusions can be made.35 Periodontitis has been shown to be a greater independent risk factor for cerebrovascular disease than with coronary heart disease, and the risk is also greater in males and younger adults. The most plausible biological mechanism by which periodontal disease exerts it effects on cardiovascular disease (CVD) was determined to be via transportation of oral bacteria in the blood stream and eliciting an inflammatory response. It was also documented that periodontal treatment often triggers an increase in systemic inflammatory or pro-thrombotic mediators, and reduces endothelial function within 24 to 48 hours. Periodontal treatment can also reduce C-reactive protein, a marker of inflammation and a CVD risk factor.35 The host response to bacteria circulating in the blood is thought to vary between individuals due to variation in genetic influence on inflammatory pathways (Figure 2).33
Blood StreamSystemic inflammatory process
Acute Phase ProteinsCRP, SSA, IL-6, TNF-α, IL-1
AtherosclerosisCVS disease
DiabetesPre term
Low birth weight
Heart & Blood VesselsEndothelial injury, Lipid deposition, Monocyte
migration, Smooth muscle proliteration
Placenta/UterusContraction of uterine
smooth muscle, Preterm rupture of membrances
Liver & PancreasInsulin resistenceGlucose tolerence
BacteriaBacteria Products
LPSInflammatory
mediators
Periodontal infection
Chapter II ● Periodontal Disease
20
A review of periodontal systemic associations found weak associations between periodontitis and chronic obstructive pulmonary disease (COPD), rheumatoid arthritis, chronic kidney disease, obesity and cancer. A possible association between periodontitis and chronic obstructive pulmonary disease (COPD) was considered from analysis of NHANES data and also from the Veterans Administration Dental Longitudinal Study (VADLS). Further analysis of NHANES III revealed a near threefold increase in COPD in smokers with severe periodontitis. This was the only significant association found and accounted for 1.3 percent of the subjects. It was considered that smoking should be treated only as an effect modifier in any association between periodontitis and COPD. Although there are studies which have showed an association between periodontitis and a number of systemic diseases, the authors of this review concluded that there needs to be further studies to gain evidence which can support associations both in smoking and non-smoking individuals with COPD.36 Once associations are support by stronger evidence there will then need to be more extensive research before periodontal disease is implicated as a causative factor for any of these systemic diseases.
Management of periodontal disease
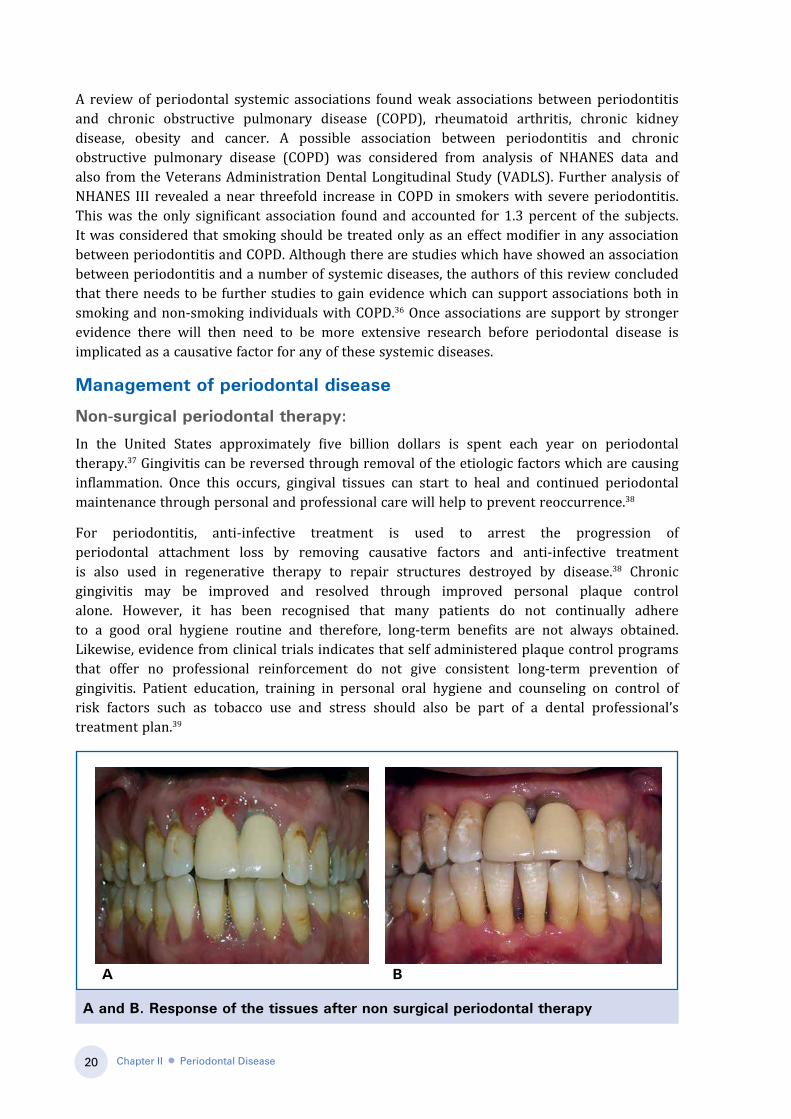
Non-surgical periodontal therapy:
In the United States approximately five billion dollars is spent each year on periodontal therapy.37 Gingivitis can be reversed through removal of the etiologic factors which are causing inflammation. Once this occurs, gingival tissues can start to heal and continued periodontal maintenance through personal and professional care will help to prevent reoccurrence.38
For periodontitis, anti-infective treatment is used to arrest the progression of periodontal attachment loss by removing causative factors and anti-infective treatment is also used in regenerative therapy to repair structures destroyed by disease.38 Chronic gingivitis may be improved and resolved through improved personal plaque control alone. However, it has been recognised that many patients do not continually adhere to a good oral hygiene routine and therefore, long-term benefits are not always obtained. Likewise, evidence from clinical trials indicates that self administered plaque control programs that offer no professional reinforcement do not give consistent long-term prevention of gingivitis. Patient education, training in personal oral hygiene and counseling on control of risk factors such as tobacco use and stress should also be part of a dental professional’s treatment plan.39
A and B. Response of the tissues after non surgical periodontal therapy
Chapter II ● Periodontal Disease
A B
21
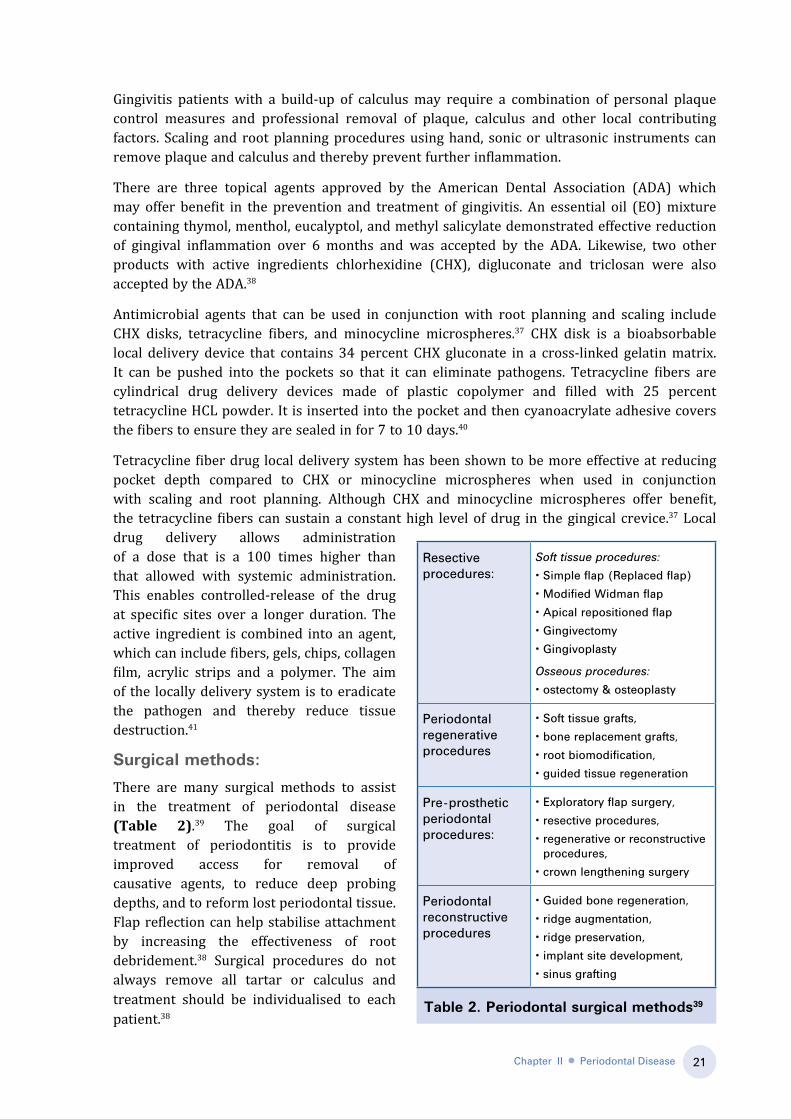
table 2. Periodontal surgical methods39
Gingivitis patients with a build-up of calculus may require a combination of personal plaque control measures and professional removal of plaque, calculus and other local contributing factors. Scaling and root planning procedures using hand, sonic or ultrasonic instruments can remove plaque and calculus and thereby prevent further inflammation.
There are three topical agents approved by the American Dental Association (ADA) which may offer benefit in the prevention and treatment of gingivitis. An essential oil (EO) mixture containing thymol, menthol, eucalyptol, and methyl salicylate demonstrated effective reduction of gingival inflammation over 6 months and was accepted by the ADA. Likewise, two other products with active ingredients chlorhexidine (CHX), digluconate and triclosan were also accepted by the ADA.38
Antimicrobial agents that can be used in conjunction with root planning and scaling include CHX disks, tetracycline fibers, and minocycline microspheres.37 CHX disk is a bioabsorbable local delivery device that contains 34 percent CHX gluconate in a cross-linked gelatin matrix. It can be pushed into the pockets so that it can eliminate pathogens. Tetracycline fibers are cylindrical drug delivery devices made of plastic copolymer and filled with 25 percent tetracycline HCL powder. It is inserted into the pocket and then cyanoacrylate adhesive covers the fibers to ensure they are sealed in for 7 to 10 days.40
Tetracycline fiber drug local delivery system has been shown to be more effective at reducing pocket depth compared to CHX or minocycline microspheres when used in conjunction with scaling and root planning. Although CHX and minocycline microspheres offer benefit, the tetracycline fibers can sustain a constant high level of drug in the gingical crevice.37 Local drug delivery allows administration of a dose that is a 100 times higher than that allowed with systemic administration. This enables controlled-release of the drug at specific sites over a longer duration. The active ingredient is combined into an agent, which can include fibers, gels, chips, collagen film, acrylic strips and a polymer. The aim of the locally delivery system is to eradicate the pathogen and thereby reduce tissue destruction.41
Surgical methods:
There are many surgical methods to assist in the treatment of periodontal disease (Table 2).39 The goal of surgical treatment of periodontitis is to provide improved access for removal of causative agents, to reduce deep probing depths, and to reform lost periodontal tissue. Flap reflection can help stabilise attachment by increasing the effectiveness of root debridement.38 Surgical procedures do not always remove all tartar or calculus and treatment should be individualised to each patient.38
Resective procedures:
Soft tissue procedures:
• Simple flap (Replaced flap)
• Modified Widman flap
• Apical repositioned flap
• Gingivectomy
• Gingivoplasty
Osseous procedures:
• ostectomy & osteoplasty
Periodontal regenerative procedures
• Soft tissue grafts,
• bone replacement grafts,
• root biomodification,
• guided tissue regeneration
Pre-prosthetic periodontal procedures:
• Exploratory flap surgery,
• resective procedures,
• regenerative or reconstructive procedures,
• crown lengthening surgery
Periodontal reconstructive procedures
• Guided bone regeneration,
• ridge augmentation,
• ridge preservation,
• implant site development,
• sinus grafting
Chapter II ● Periodontal Disease

22
When there is a large amount of periodontal attachment loss, then regeneration of lost tissue can be extremely beneficial. Bone grafting, and guided tissue regeneration techniques may help to restore lost tissue when there has been advanced attachment loss.
Prevention of periodontal diseases
Self-care
Periodontal self-care is the greatest factor which can help improve gingival health and prevent further attachment loss. The most common ways to perform self-care include tooth brushing with a dentifrice. Adjunction aids such as dental floss, inter dental cleaning devices, mouth rinses, irrigation devices and other less common approaches can be incorporated into a daily oral self-care regimen. Although whether this is the most effective way to prevent and treat periodontal disease compliance is questionable.42
Dentifrice
Brushing teeth once to twice a day with fluoride-containing toothpaste has become a commonly practiced daily routine of people in developed countries. Review of epidemiological evidence found that a stannous fluoride dentifrice had greater reduction in gingivitis compared to sodium fluoride dentifrice.43 A triclosan/copolymer dentifrice was shown to be a more effective antiplaque and antigingivitis agent compared to a stannous fluoride dentifrice.44 However, safety of triclosan/copolymer has become questionable.42
tooth brushingConsistent tooth brushing greater than once a day can reduce the risk of tooth loss by nearly half compared to those who do not consistently brush their teeth daily.45 Surfaces that are 80 percent plaque-free are more likely to maintain long-term periodontal health.46 Therefore, the best approach is to keep plaque formation consistently to less than 20 percent.42 This can be difficult to achieve and is improved with regular professional mechanical plaque removal. Frequent professional mechanical plaque removal using scaling, and/or polishing can positively influence dental plaque, bleeding, inflammation, probing depth and attachment levels.42
However, professional mechanical plaque removal in the absence of oral-hygiene instructions provides little benefit.47
In the 1960s, powered toothbrushes were introduced. There has been little evidence to show that these toothbrushes have a proven benefit over manual toothbrushes. Most evidence points to an equivocal benefit with either a manual or powered toothbrush. There is some evidence to support tooth brushes with rotational oscillation are superior to side-to-side brushes. Professionals can recommend powered toothbrushes but future studies are necessary to determine the influence they have on dental health.42
Interdental cleaning
Regular interdental cleaning is necessary to maintain periodontal health because no toothbrush effectively disrupts true interproximal plaque, particularly in the posterior dentition. Interdental area is more prone to the initiation and progression of periodontal diseases.48
Flossing was introduced in 1819, as an adjunct to tooth brushing to prevent periodontal disease and caries disease. Flossing is considered beneficial to periodontal health as periodontitis and gingivitis mainly occur in the interproximal sites. Biofilm located in the interproximal sites are not easily reached by normal tooth brushing, and can therefore even accumulate when there is regular toothbrushing been performed. Compliance with flossing is often low and the
Chapter II ● Periodontal Disease
23
time taken to perform this activity has a negative impact on routine performance.42 Although benefits of flossing have been widely accepted, a systematic review in 2011 found that there was only a weak statistically benefit associated with flossing in conjunction with tooth brushing compared with toothbrushing alone, in reducing gingivitis. The consensus from research to date is that there is a weak association between flossing and plaque reduction.49 However, there is still strong support for daily flossing to aid plaque removal and gingivitis reduction.42
Interdental brushes as an adjunct to toothbrushing removes greater amounts of plaque than tooth brushing alone. Interdental brushing has also been shown to remove more plaque than dental floss and wood sticks. However, interdental brushing did not shown any additional benefit on gingival inflammation when compared to flossing.50 The superior effects on plaque removal support interdental brushes as a likely first choice for interdental cleaning.42
Mouthrinses
Mouthrinses offer additional beneficial effects on plaque reduction and gingivitis. A review of mouthrinse efficacy found 21 studies that supported an EO mouthrinse and 7 studies that supported 0.12 percent CHX mouthrinse. The active agents in these two mouthrinses have been shown to statistically improve plaque and gingivitis.44 An EO-containing mouthrinse has been proven to be just as effective as floss in reducing interproximal plaque and gingivitis.51 CHX mouthrinses have greater utility when short-term plaque control is critical.52 This situation includes the postoperative phase following periodontal surgery, when mechanical oral hygiene is difficult.
Oral irrigation
Subgingival irrigation can be performed at home or in-office by a dental professional. It has some positive influence on inflammation and may be beneficial when used in conjunction with routine oral hygiene.42 Oral irrigation with water as part of a regular oral hygiene program can decrease the concentration of pro-inflammatory cytokines in gingival fluids.53
Future risk
Maintaining a daily oral hygiene routine that includes tooth brushing in conjunction with flossing or other interdental cleaning methods and mouthrinsing will help to prevent future risk
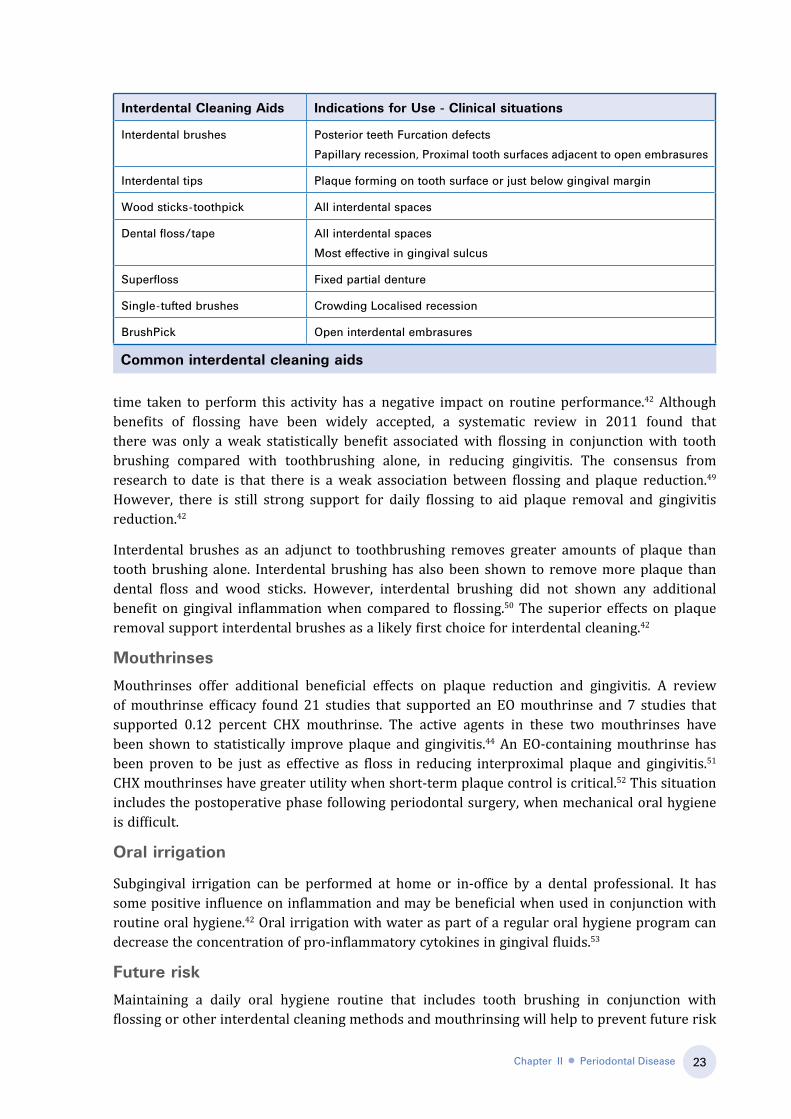
Common interdental cleaning aids
Chapter II ● Periodontal Disease
Interdental Cleaning Aids Indications for Use - Clinical situations
Interdental brushes Posterior teeth Furcation defects
Papillary recession, Proximal tooth surfaces adjacent to open embrasures
Interdental tips Plaque forming on tooth surface or just below gingival margin
Wood sticks-toothpick All interdental spaces
Dental floss/tape All interdental spaces
Most effective in gingival sulcus
Superfloss Fixed partial denture
Single-tufted brushes Crowding Localised recession
BrushPick Open interdental embrasures

24
of periodontal disease. Supportive periodontal care (SPC) can help reduce clinical attachment loss, and overall improve outcomes for patients. SPC is delivered by dental professionals and supports patients own efforts to control periodontal infections and to reduce the risk of future infections.54
Modifiable risk factors
tobacco
Tobacco use is a significant modifiable risk factor for periodontal disease. Approximately half of all periodontal disease cases in the United States between 1988 and 1994 were attributed to current or former tobacco use.55 Smokers have a four times greater risk of periodontitis than non-smokers. There also appears to be an association with the number of cigarettes smoked per day and the risk of developing periodontal disease.56 It can be reasoned that eliminating cigarette use will help prevent periodontal disease.
Diabetes mellitus and other systemic risk factors
Patients with diabetes mellitus are at a greater risk for periodontal disease. Diabetics with poor glycemic control have a faster recurrence of periodontal pockets after periodontal treatment than non-diabetics.57 Good diabetes control can help maintain healthy periodontal tissue. Other possible systemic risk factors for periodontal disease are CVD, hypertension, and obesity. These diseases feature underlying systemic inflammation which could influence gingivitis and periodontitis.
Nutrition
Deficiency of vitamin C can lead to generalised alveolar changes. Analysis from NHANES III surveys found that intake of less than 30 mg per day of vitamin C was associated with a slightly increased occurrence of periodontitis compared to those who consumed greater than 180 mg of vitamin C per day. There is also evidence to show a reduced likelihood of periodontal disease with higher intakes of whole grains. Greater antioxidant intake may also reduce the risk of periodontitis.55
Conclusion
It is evident that modifiable factors and non-modifiable factors such as ethnicity, age and genetics can influence the likelihood of periodontal disease development. However, the most important consideration is to maintain good oral health by establishing a regular daily oral hygiene routine. Regular dental visits and professional mechanical tooth cleaning also help prevent periodontal disease. Dental professionals can advise on an effective oral hygiene routine which may also help increase compliance.
Chapter II ● Periodontal Disease

25
References1. Kesic L, Milasin J, Igic M, Obrodovic R. Microbial etiology of periodontal disease-mini review. Medical Biology 2008;15:1-6.2. Dentino A, Lee S, Mailhot J, Hefti AF. Principles of periodontology. Periodontology 2000 2013;61(1):16-53.3. Albandar JM, Rams TE. Global epidemiology of periodontal diseases: an overview. Periodontol 2000 2002;29:7-10.4. Heaton B, Dietrich T. Analytic epidemiology and periodontal diseases. Periodontology 2000 2012;58(1):112-20.5. Rouabhia M, Chmielewski W. Diseases Associated with Oral Polymicrobial Biofilms. Open Mycology Journal 2012;6:27-32.6. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bulletin of the World Health Organization
2005;83(9):661-9.7. Ramfjord SP, Emslie RD, Greene JC, Held AJ, Waerhaug J. Epidemiological studies of periodontal diseases. American Journal of Public Health and the Nations
Health 1968;58(9):1713-22.8. Dye BA. Global periodontal disease epidemiology. Periodontology 2000 2012;58(1):10-25.9. Sheiham A, Netuveli GS. Periodontal diseases in Europe. Periodontology 2000 2002;29:104-21.10. Corbet EF, Zee KY, Lo EC. Periodontal diseases in Asia and Oceania. Periodontology 2000 2002;29:122-52.11. Baelum V, Scheutz F. Periodontal diseases in Africa. Periodontology 2000 2002;29:79-103.12. Petersen PE, Ogawa H. Strengthening the prevention of periodontal disease: the WHO approach. Journal of Periodontology 2005;76(12):2187-93.13. Thomson WM, Slade GD, Beck JD, et al. Incidence of periodontal attachment loss over 5 years among older South Australians. Journal of Clinical Periodontology
2004;31(2):119-25.14. Brennan DS, Spencer AJ, Roberts-Thomson KF. Periodontal disease among 45-54 year olds in Adelaide, South Australia. Australian Dental Journal 2007;52(1):55-
60.15. Borrell LN, Burt BA, Taylor GW. Prevalence and trends in periodontitis in the USA: the [corrected] NHANES, 1988 to 2000. Journal of Dental Research 2005;84(10):924-
30.16. Hugoson A, Sjodin B, Norderyd O. Trends over 30 years, 1973-2003, in the prevalence and severity of periodontal disease. Journal of Clinical Periodontology
2008;35(5):405-14.17. Baelum V, Lopez R. Periodontal disease epidemiology - learned and unlearned? Periodontology 2000 2013;62(1):37-58.18. Miller WD. The micro-organisms of the human mouth: the local and general diseases which are caused by them. The Micro-organisms of the Human Mouth: White
Dental Mfg. Company; 1890.19. Grob GN. The rise and decline of tonsillectomy in twentieth-century America. Journal of the History of Medicine and Allied Sciences 2007;62(4):383-421.20. Wiebe CB, Putnins EE. The periodontal disease classification system of the American Academy of Periodontology--an update. Journal of the Canadian Dental
Association. Journal de L’Association Dentaire Canadienne 2000;66(11):594-7.21. Armitage GC. Development of a classification system for periodontal diseases and conditions. Annals of Periodontology 1999;4(1):1-6.22. Loe H, Silness J. Periodontal Disease in Pregnancy. I. Prevalence and Severity. Acta Odontologica Scandinavica 1963;21:533-51.23. Loe H, Anerud A, Boysen H, Morrison E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46
years of age. Journal of Clinical Periodontology 1986;13(5):431-45.24. Hujoel P, Zina LG, Cunha-Cruz J, Lopez R. Historical perspectives on theories of periodontal disease etiology. Periodontology 2000 2012;58(1):153-60.25. Gu Y, Ryan ME. Overview of Periodontal Disease: Causes, Pathogenesis, and Characteristics. Periodontal Disease and Overall Health: A Clinician’s Guide 2010:5.26. Hernández M, Vernal R, Sorsa T, et al. The Role of Immuno-Inflammatory Response in the Pathogenesis of Chronic Periodontitis and Development of Chair-Side
Point of Care Diagnostics. In: Buduneli, editor. Pathogenesis and Treatment of Periodontitis; 2012.27. Teles FR, Teles RP, Uzel NG, et al. Early microbial succession in redeveloping dental biofilms in periodontal health and disease. Journal of Periodontal Research
2012;47(1):95-104.28. Ryan ME. Nonsurgical approaches for the treatment of periodontal diseases. Dental Clinics of North America 2005;49(3):611-36.29. Teitelbaum AP, Czlusniak GD. Control of Dental Biofilm and Oral Health Maintenance in Patients with Down Syndrome. In: Dey SK, editor. Down Syndrome; 2013.30. Socransky SS, Haffajee AD. Periodontal microbial ecology. Periodontology 2000 2005;38:135-87.31. Cullinan MP, Ford PJ, Seymour GJ. Periodontal disease and systemic health: current status. Australian Dental Journal 2009;54 Suppl 1:S62-9.32. Scannapieco FA, Dasanayake AP, Chhun N. “Does periodontal therapy reduce the risk for systemic diseases?”. Dental Clinics of North America 2010;54(1):163-81.33. Anil S, Varma S, Preethanath R, Anand P. The Emerging Concepts on the Impact of Periodontitis on Systemic Health. Periodontal Diseases - A Clinician’s Guide:
Available at: http://www.intechopen.com. Accessed 25 May, 2013.34. Page RC. The pathobiology of periodontal diseases may affect systemic diseases: inversion of a paradigm. Annals of Periodontology 1998;3(1):108-20.35. Tonetti MS, Van Dyke TE, Working group 1 of the joint EFPAAPw. Periodontitis and atherosclerotic cardiovascular disease: consensus report of the Joint EFP/AAP
Workshop on Periodontitis and Systemic Diseases. Journal of Clinical Periodontology 2013;40 Suppl 14:S24-9.36. Linden GJ, Lyons A, Scannapieco FA. Periodontal systemic associations: review of the evidence. Journal of Clinical Periodontology 2013;40(s14):S8-S19.37. Niederman R, Abdelshehid G, Goodson JM. Periodontal therapy using local delivery of antimicrobial agents. Dental Clinics of North America 2002;46(4):665-77.38. Denstistry. TAAoP. Treatment of plaque-induced gingivitis, chronic periodontitis, and other clinical conditions. Reference Manual. The American Academy of
Pediatric Denstistry 2004;34(6):317-26.39. AAP-2003. Guideline for Periodontal therapy. Reference Manual. The American Academy of Peridontology 2003;34(6):312-16.40. Verma E, Belludi SA, Banthia R. Local drug delivery with chlorhexidine chip and tetracycline fibers as an adjunct to mechanical therapy in isolated periodontal
pockets-a case report. International Journal of Clinical Dentistry 2011;4(4):383-90.41. Perno M. Pharmactotherapy in periodontal Therapy. Access 2001:1-11.42. Drisko CL. Periodontal self-care: evidence-based support. Periodontology 2000 2013;62(1):243-55.43. Paraskevas S, van der Weijden GA. A review of the effects of stannous fluoride on gingivitis. Journal of Clinical Periodontology 2006;33(1):1-13.44. Gunsolley JC. A meta-analysis of six-month studies of antiplaque and antigingivitis agents. Journal of the American Dental Association 2006;137(12):1649-57.45. Kressin NR, Boehmer U, Nunn ME, Spiro A, 3rd. Increased preventive practices lead to greater tooth retention. Journal of Dental Research 2003;82(3):223-7.46. Axelsson P, Nystrom B, Lindhe J. The long-term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. Results after 30
years of maintenance. Journal of Clinical Periodontology 2004;31(9):749-57.47. Needleman I, Suvan J, Moles DR, Pimlott J. A systematic review of professional mechanical plaque removal for prevention of periodontal diseases. Journal of
Clinical Periodontology 2005;32 Suppl 6:229-82.48. Ryder MI, Pons B, Adams D, et al. Effects of smoking on local delivery of controlled-release doxycycline as compared to scaling and root planing. Journal of Clinical
Periodontology 1999;26(10):683-91.49. Sambunjak D, Nickerson JW, Poklepovic T, et al. Flossing for the management of periodontal diseases and dental caries in adults. Cochrane Database Syst Rev
2011(12):CD008829. 50. Slot DE, Dorfer CE, Van der Weijden GA. The efficacy of interdental brushes on plaque and parameters of periodontal inflammation: a systematic review. International
Journal of Dental Hygiene 2008;6(4):253-64.51. Stoeken JE, Paraskevas S, van der Weijden GA. The long-term effect of a mouthrinse containing essential oils on dental plaque and gingivitis: a systematic review.
Journal of Periodontology 2007;78(7):1218-28.52. Charles CH, Mostler KM, Bartels LL, Mankodi SM. Comparative antiplaque and antigingivitis effectiveness of a chlorhexidine and an essential oil mouthrinse: 6-month
clinical trial. Journal of Clinical Periodontology 2004;31(10):878-84.53. Payne JB, Reinhardt RA. Potential application of low-dose doxycycline to treat periodontitis in post-menopausal women. Advances in Dental Research 1998;12(2):166-9.54. Pennington M, Heasman P, Gaunt F, et al. The cost-effectiveness of supportive periodontal care: a global perspective. Journal of Clinical Periodontology 2011;38(6):553-
61.55. Tomar SL, Asma S. Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey. Journal
of Periodontology 2000;71(5):743-51.56. Albandar JM, Streckfus CF, Adesanya MR, Winn DM. Cigar, pipe, and cigarette smoking as risk factors for periodontal disease and tooth loss. Journal of Periodontology
2000;71(12):1874-81.57. Tervonen T, Karjalainen K. Periodontal disease related to diabetic status. A pilot study of the response to periodontal therapy in type 1 diabetes. Journal of Clinical
Periodontology 1997;24(7):505-10.
Chapter II ● Periodontal Disease




















