
Revista Mexicana de - Neurociencia
38
Editorial We are at war 79 Ildefonso Rodríguez-Leyva Original Article Frequency of hypertension, age and gender in cerebrovascular disease in Paraguay 80 Luis Díaz-Escobar, Alan Flores, Laia Seró-Ballesteros, Christian Otto, Ricardo Mernes, Fátima Pedrozo, Fabiola Riquelme, and Romina Gonzalez Electro-clinical relationship and source analysis of absence seizures in childhood 86 Liane Aguilar-Fabré, René F. Rodríguez-Valdés, Lídice Galán-García, Jorge F. Bosch-Bayard, Hebert L. Hernández-Montiel, and Ramiro J. García-García Are different degrees of lymphopenia for FTY720 associated with serious infectious-type events? No 92 Catalina Márquez-Martín, Ricardo J. García-Bermúdez, and Brenda Bertado-Cortés Review Articles The legacy of polio: 2 cases of post-polio syndrome and review 97 Katherine A. Mafla-Ayub, Luisa F. Guzmán-Molano, Gabriel A. Centanaro-Meza, and Jairo A. Mejia-Mójica Systematic review and effect of conscious breathing on adult attention and learning task 105 Viviana Chavez, Lenin Ochoa-de-la-Paz, and Jorge Parodi Mechanical thrombectomy in children: A little known and scarcely utilized resource 111 Yolanda Aburto-Murrieta, Beatriz Méndez, and Juan M. Marquez-Romero PERMANYER www.permanyer.com VOLUME 23 - NUMBER 3 / May-June 2022 – ISSN: 2604-6180 www.revmexneurociencia.com Revista Mexicana de Neurociencia Publicación oficial de la Academia Mexicana de Neurología A.C.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Revista Mexicana de - Neurociencia

Editorial We are at war 79Ildefonso Rodríguez-Leyva
Original Article Frequency of hypertension, age and gender in cerebrovascular disease in Paraguay 80Luis Díaz-Escobar, Alan Flores, Laia Seró-Ballesteros, Christian Otto, Ricardo Mernes, Fátima Pedrozo, Fabiola Riquelme, and Romina Gonzalez
Electro-clinical relationship and source analysis of absence seizures in childhood 86Liane Aguilar-Fabré, René F. Rodríguez-Valdés, Lídice Galán-García, Jorge F. Bosch-Bayard, Hebert L. Hernández-Montiel, and Ramiro J. García-García
Are different degrees of lymphopenia for FTY720 associated with serious infectious-type events? No 92Catalina Márquez-Martín, Ricardo J. García-Bermúdez, and Brenda Bertado-Cortés
Review ArticlesThe legacy of polio: 2 cases of post-polio syndrome and review 97Katherine A. Mafla-Ayub, Luisa F. Guzmán-Molano, Gabriel A. Centanaro-Meza, and Jairo A. Mejia-Mójica
Systematic review and effect of conscious breathing on adult attention and learning task 105Viviana Chavez, Lenin Ochoa-de-la-Paz, and Jorge Parodi
Mechanical thrombectomy in children: A little known and scarcely utilized resource 111Yolanda Aburto-Murrieta, Beatriz Méndez, and Juan M. Marquez-Romero
PERMANYERwww.permanyer.com
VOLUME 23 - NUMBER 3 / May-June 2022 – ISSN: 2604-6180
www.revmexneurociencia.com
Revista Mexicana de
NeurocienciaPublicación oficial de la Academia Mexicana de Neurología A.C.

79
We are at warIldefonso Rodríguez-Leyva*Department of Neurology, Faculty of Medicine, Hospital Central Dr. Ignacio Morones Prieto, Universidad Autónoma de San Luis Potosí, SLP, Mexico
Revista Mexicana de Neurociencia
Editorial
Correspondence: *Ildefonso Rodríguez-Leyva
E-mail: [email protected]
Available online: 02-05-2022
Rev Mex Neuroci. 2022;23(3):79
www.revmexneurociencia.com
Date of reception: 04-03-2022
Date of acceptance: 04-03-2022
DOI: 10.24875/RMN.M22000086
The difficult situation that humanity faces when one part of it confronts another could be compared to a social disease. Without having yet emerged from a pandemic, we are now facing another conflict that will have an impact on mortality and the global economy. War is a social conflict that goes with the same history of humanity and it is usually experienced not only be-tween nations but also within each country, each small society, and even within families. Neurologists often find it necessary to certify that the patriarch or the mother of a family is unable to make decisions due to a fixed or progressive cognitive deterioration, while the children break their ties out of economic ambition or simply for the sake of power. The same happens in social groups, organizations, and societies. The quest to have more, the envy, the desire to transcend or to feel powerful makes people’s and nations’ leaders to be both admired and hated at the same time.
The followers will applaud the aggressions, while the opponents will mark distance and will try to convince others about the unfairness of the warlike maneuver that the leader is exercising. The same happens with organizations: the representative tends to forget those who supported him and exercises their power by re-warding those close to them, their friends, and corner-ing those who dare to raise their voices demanding justice or at least space. Are these social struggles a reflection of the illness of a leader who tries to exercise his will? The answer is not simple, justice has its edges and what is valid in one society may be punished in another, what is logical and adequate for one group may be crushing and impoverishing for another. What I
believe is always terrible, no matter which perspective it belongs to, is the loss of lives that were not even participating or had minimal interest in the conflict gen-erated, as well as the fact that people have to leave their homes, their homeland, and their family, for the interest of others. It is unfortunate to have to leave a whole history, belongings, and memories behind or to have them destroyed by someone who feels superior because they carry a weapon. In what area of our brain does the war process initiate? There is no doubt that this is the organ that creates good and bad actions, the one generates envy, ambition, destruction, and war.
Countries like ours are living their own war, as incredible as it may seem, as many people die because of social conflicts as the lives that are being lost in Ukraine and the most unfortunate thing seems to be the indifference in which many of us seem to carry the situation, “as long as, it does not affect me, my family, my friends, and my inter-ests, it does not matter.” However, every social change ends up affecting us and that is why we must insist that the search for truth is the only answer to every social in-justice we face. Education is the best way to understand the importance of respect for others, tolerance, coexis-tence, and having other ways of looking at reality. It is seeing the perspective of the other that allows us to un-derstand that my idea may be wrong that I may be wrong.
In this publication, we extend our solidarity to those who are suffering the loss of a loved one, of their home, of their homeland, and of their past, and we hope that our society will be more educated, more equitable, productive, healthy, and just. We wish peace for the world and especially for those who are at war.
2604-6180 / © 2022 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

80
Frequency of hypertension, age and gender in cerebrovascular disease in ParaguayLuis Díaz-Escobar, Alan Flores*, Laia Seró-Ballesteros, Christian Otto, Ricardo Mernes, Fátima Pedrozo, Fabiola Riquelme, and Romina GonzalezUnidad de Ictus, Hospital de Clínicas, Servicio de Urgencias, Facultad de Ciencias Médicas, Universidad Nacional de Asunción, San Lorenzo, Paraguay
Revista Mexicana de Neurociencia
oriGiNal artiClE
abstract
Background: Hypertension, age, and gender are relevant factors associated to cerebrovascular disease. In Paraguay, cerebrovascular disease is the fourth cause of mortality; however, information about demographics and baseline character-istics is not widely knowledge. Our aim was determinate the prevalence of hypertension, age, and gender in the setting of acute-phase stroke in our population. Methods: This is a descriptive, single-center study. Data were collected from a pro-spective registry of stroke patients admitted in the stroke unit of our center, from April 2015 to December 2016. results: From 996 stroke patients, 252 (25.3%) presented intracerebral hemorrhage (ICH). Three hundred ninety (39.1%) were female. The hypertension rate was 74% and 78% in ischemic stroke and ICH, respectively, being hypertensive hemorrhagic etiology 79.5% of the ICH and lacunar infarct 11.6% of ischemic strokes. In ICH patients, mean age differences between genders were re-markable (mean years 55.41 [SD ± 14.8] vs. 62.48 [SD ± 15.2] p ≤ 0.001). In the multivariant analysis, lower age than 60 years old (OR: 4.893; CI 95%: 1.772-13.509 p = 0.029) and higher systolic blood pressure at admission (OR: 1.098; CI 95% 1.044-1.155, p = 0.009) were independent factors associated to ICH. Conclusion: In our population, ICH rates are similar to region-al findings, occurring at an early age than other series, being remarkable in males. Hypertension rates in ischemic stroke and ICH are higher than other series, and the variability of presumed hypertensive microangiopathy phenotype could be in rela-tion to age (hypertensive hemorrhage vs. lacunar). These findings would be related to ethnics, social, environment, and ge-ographies factors.
Keywords: Stroke epidemiology. Hypertensive hemorrhage. Female stroke. Vascular risk factors. Intracerebral hemorrhage.
Frecuencia de la hipertensión arterial, la edad y el género en la enfermedad cerebrovascular en Paraguay
resumen
Background: La hipertensión, la edad y el género son factores relevantes asociados a enfermedad cerebrovascular (ECV). En Paraguay, la ECV es la cuarta causa de mortalidad, sin embargo, la información sobre sus características no es de amplio conocimiento. Nuestro objetivo fue determinar la frecuencia de la hipertensión, la edad y el género en la ECV en fase agu-da en nuestra población. Métodos: Se trata de un estudio observacional descriptivo monocéntrico. Se recogieron datos de
Correspondence: *Alan Flores
E-mail: [email protected]
Available online: 02-05-2022
Rev Mex Neuroci. 2022;23(3):80-85
www.revmexneurociencia.com
Date of reception: 24-04-2019
Date of acceptance: 29-05-2019
DOI: 10.24875/RMN.19000078
2604-6180 / © 2019 Academia Mexicana de Neurología A.C. Published by Permanyer México. This is an open access article under the terms of the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

81
L. Díaz-Escobar et al.: Frecuencia de los FR en el ictus en Paraguay
introduction
Stroke is one of the diseases with the greatest impact on public health, being the third cause of mortality and the leading cause of disability in the Western world since most patients suffer sequels, which is 30% of cases disable them to perform daily activities1,2.
The proportion and frequency between the ischemic types and intracerebral hemorrhage (ICH) are variables according to a determined region; while in Spain, the rates of ICH are around to 12%3, in regions of South America such as Ecuador and Chile the ICH reach rates between 37 and 46%4. In Paraguay, cerebrovas-cular disease is the fourth cause of death5. However, another data about the baseline characteristics in our population are not widely known.
Among the cardiovascular risk factors related to stroke, hypertension is the most frequent and important risk factor. The prevalence is around 70% in both isch-emic and hemorrhagic patients, and its optimal control is possibly one of the most important interventions in secondary prevention for both types of stroke3,6. In Par-aguay, the prevalence of hypertension is high, with rates of 53% in men and 40% in women between 35 and 45 years, reaching up to 81% in the general population between 65 and 74 years7.
Another known and controversial stroke risk factor is gender, and their disparities in baseline and clinical outcomes. Several descriptive studies have shown an association of older age, frequency of hypertension, obesity, and atrial fibrillation in women than in men8,9.
Objective
The objective of the study was to determine the rates of hypertension, age, gender, and other known risk
factors in patients with stroke in the acute phase in our environment.
Methodology
This is a descriptive, observational study in a single center. Data were collected from a prospective of stroke patients admitted in the Stroke Unit of our center from April 2015 to March 2019.
The known modifiable and non-modifiable risk fac-tors have been recorded. In patients with hemorrhagic stroke, the etiology of hypertensive ICH has been de-termined according to the history of hypertension, the topography of the parenchymal lesion, and the vascular study10. The diagnosis of ischemic stroke was made according to the criteria of the Oxfordshire Community Stroke Project and the Trial of ORG 10172 in Acute Stroke Treatment11.
The descriptive statistical analysis was performed for all the parameters, which included measurements of the central tendency and dispersion for the quantitative variables, as well as absolute and relative frequencies for the qualitative variables, with their 95% CI in both cases. If the data did not meet the assumptions of nor-mality for the analysis, non-parametric statistical meth-ods were used (Student’s t-test or Mann–Whitney test, respectively). The Chi-square test was applied for the comparison between the proportions. To determine the weight of each of the risk factors between ischemic and hemorrhagic stroke, multiple logistic regression models were established, with a 95% CI. The statistical tests were performed with a significance level of 5%. The statistical program SPSS v. 23.0 was used to perform the analysis.
un registro prospectivo de pacientes con ictus ingresados en la Unidad de Ictus de nuestro centro, desde abril de 2015 a marzo de 2019. resultados: De 996 pacientes con ictus, 252 (25,3%) presentaron hemorragia intracerebral (HIC). Trescien-tos noventa (39.1%) fueron mujeres. La tasa de hipertensión arterial fue elevada tanto en isquémicos (74%) como en hemo-rrágicos (78%), siendo la hemorragia hipertensiva el 79.5% de las HIC y los lacunares, el 11.6% de ictus isquémicos. En pacientes con HIC, la diferencia de edad entre géneros fue significativa (media/años 55.41 (SD ± 14.8) vs. 62.48 (SD ± 15.2) p ≤ 0.001). En el análisis multivariante, fueron factores independientes asociados a HIC: la edad menor a 60 años (OR: 4.893; IC 95%: 1.772-13.509 p = 0.029) y una elevada presión arterial sistólica al ingreso (OR: 1.098; IC 95% 1.044-1.155, p = 0.009). Conclusión: En nuestra población, la frecuencia de HIC es similar a lo descrito en la región, observándose una edad más temprana que en otras series y siendo remarcable en el género masculino. La tasa de hipertensión en HIC e ictus isquémi-co es mayor que en otras series y la variación de distintos fenotipos por presunta microangiopatía hipertensiva estaría re-lacionado en parte a la edad (hemorragia hipertensiva vs. lacunares). Estos resultados podrían explicarse por razones étni-cas, socioambientales y geográficas.
Palabras clave: Ictus epidemiologia. Hemorragia cerebral hipertensiva. Ictus en la mujer. Factores de riesgo. Hemorragia intracerebral.

82
Rev Mex Neuroci. 2022;23(3)
results
From 996 patients with stroke, 744 (74.7%) were isch-emic, and 252 (25.3%) were ICH, and 390 (39.1%) were women. The mean age was 62.8 years (SD ± 15.3). Overall, 75.4% had known antecedent of hypertension, 27% DM, and 6.4% dyslipidemia. The median baseline NIHSS was 8 (IQR: 4-12). The baseline characteristics in general and of the ischemic and hemorrhagic groups are shown in table 1.
In ischemic stroke patients, the mean age was 64.3 (SD ± 15.2) years, the median of NIHSS was 8 (IQR 4-12), and 39.8% were women. Patients with isch-emic stroke were significantly older (mean years 64.3 SD ± 15.2 vs. 58.1 SD ± 14.8), had higher glycemia at admission (mean mgr./dl 168.6 SD ± 97.7 vs. 155.9 SD ± 120.3 p = 0.513), frequency of diabetes mellitus (23.5% vs. 3.4% p = 0.001), atrial fibrillation (13.6% vs. 1.3% p = 0.001), prior history of stroke (15.4% vs. 2.5% p = 0.001), prior antiplatelet treatment (8.1% vs. 1.0% p = 0.001), and lower systolic blood pressure on arrival than patients with ICH (mean mmHg, 169.8 SD ± 38.3 vs. 189.9 SD ± 43.2).
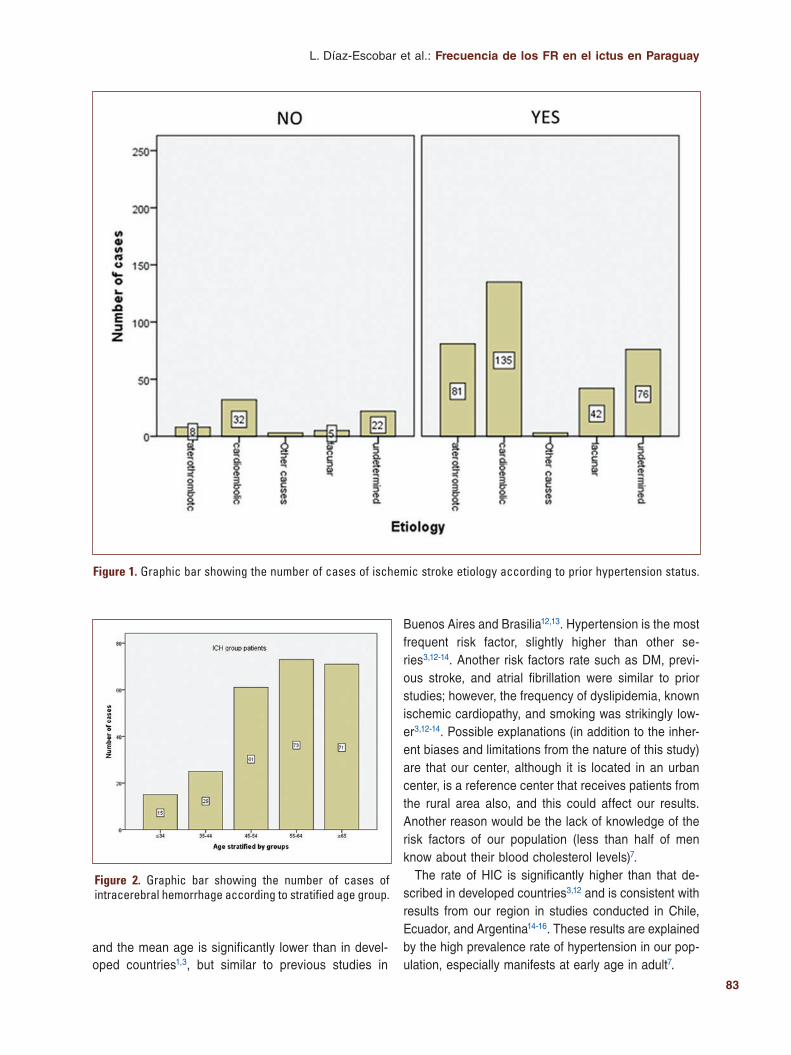
The most frequent etiology was (422 cases work-up performed) cardioembolic 41.2%, indeterminate in 24.1%, lacunar infarcts in 11.6%, and atherothrombotic in 21.5%. Hypertension was present in 91% of athero-thrombotic strokes, 89.6% of lacunary strokes, 80.8% of cardioembolic, and 77.6% of indeterminate strokes (Fig. 1).
ICH patients had a mean age of 58.1 (SD ± 14.8) years, the median of NIHSS was 9 (IQR 5-13), and 36.9% were women. From 142 cases with etiological workup, 79.5% were due to hypertensive hemorrhage. The factors significantly related to hypertensive hemorrhage (113 cases evaluated) were hypertension (p ≤ 0.001) and the lower age stratified by groups (p = 0.006) (Fig. 2).
In the multivariate analysis adjusted for sex, hyper-tension, diabetes mellitus, previous stroke, and atrial fibrillation, age < 60 years old (OR: 4.893, 95% CI: 1.772-13.509, p = 0.029) and a higher systolic blood pressure at admission (OR: 1.098, 95% CI 1.044-1.155, p = 0.009) were independent factors associated with ICH.
In relation to gender, hypertension was present in 79.3% in men and 83.5% in women. In men, smoking habit was significantly more frequent (23.9% vs. 3.4% p < 0.001) and they presented more ischemic heart disease (7.9% vs. 2.3% p = 0.001) than women. Men were younger (61.75 SD ± 13.6 vs. 64.16 SD ± 17.4 p = 0.003), being in the ICH group, even more remark-able the difference (mean years 55.41 [SD ± 14.8 vs. 62.48 [SD ± 15.2 p ≤ 0.001) (Fig. 3).
discussion
This is a descriptive study, with data from a prospec-tive cohort over a period of 41 months. In general, there is a higher proportion of men than women with stroke,
Table 1. Baseline characteristics of all patients with stroke and subgroups; ischemic and hemorrhagic with their significance in the univariate analysis
All(n = 996)
Ischemic(n = 744)
ICH(n = 252)
p-value
Age, year 62.8DS ± 15.3 64.3DS ± 15.2 58.1 ± 14.8 < 0.001
Glicemia at admission mgr/dl. (n:169) 165.4DS ± 120.3 168.6DS ± 97.7 155.9DS ± 120.3 0.513
Female gender n (%) 390 (39.1) 295 (39.6) 93 (36.9) 0.585
Hypertension n (%) 749 (75.2) 553 (74.3) 195 (77.3) 0.102
Diabetes mellitus n (%) 237 (23.6) 206 (23.5) 30 (3.4) < 0.001
Dyslipidemia n (%) 56 (5.6) 47 (5.4) 9 (1) 0.144
Atrial fibrillation 128 (12.7) 117 (13.6) 11 (1.3) < 0.001
Prior antiplatelet treatment 996 (99.1) 81 (8.1) 10 (1.0) 0.003
Prior stroke 150 (14.9) 129 (15.4) 21 (2.5) 0.001
Baseline NIHSS median (interquartile range) 8 (4) 8 (4) 9 (4) 0.796
Systolic blood pressure at admission 169.8 ± 38.3 161.4 ± 32.5 189.9 ± 43.2 < 0.001
83
L. Díaz-Escobar et al.: Frecuencia de los FR en el ictus en Paraguay
Figure 1. Graphic bar showing the number of cases of ischemic stroke etiology according to prior hypertension status.
Buenos Aires and Brasilia12,13. Hypertension is the most frequent risk factor, slightly higher than other se-ries3,12-14. Another risk factors rate such as DM, previ-ous stroke, and atrial fibrillation were similar to prior studies; however, the frequency of dyslipidemia, known ischemic cardiopathy, and smoking was strikingly low-er3,12-14. Possible explanations (in addition to the inher-ent biases and limitations from the nature of this study) are that our center, although it is located in an urban center, is a reference center that receives patients from the rural area also, and this could affect our results. Another reason would be the lack of knowledge of the risk factors of our population (less than half of men know about their blood cholesterol levels)7.
The rate of HIC is significantly higher than that de-scribed in developed countries3,12 and is consistent with results from our region in studies conducted in Chile, Ecuador, and Argentina14-16. These results are explained by the high prevalence rate of hypertension in our pop-ulation, especially manifests at early age in adult7.
Figure 2. Graphic bar showing the number of cases of intracerebral hemorrhage according to stratified age group.
and the mean age is significantly lower than in devel-oped countries1,3, but similar to previous studies in

84
Rev Mex Neuroci. 2022;23(3)
In relation to ischemic stroke, the etiology by TOAST (in 422 cases) showed a high rate of cardioembolic (41.2%), however a lower frequency of atheromatous disease (21.5%) and lacunar (11.6%). These results are more sim-ilar to those found in Santiago14 than in those shown in Brasilia, Guayaquil, and Buenos Aires13,15,16. It should be noted that in South America the frequency in relation to the etiology of stroke is very heterogeneous and diverse, mainly due to ethnic, geographical, and sociocultural dif-ferences4. Finally, the relatively high rate of indeterminate etiology would be related in many cases to an incomplete study and is a clear limitation in the present study.
Interestingly, while hypertension rates are high (79.3%) in ischemic patients, the percentage of lacunar strokes for presumed hypertensive microangiopathy as a cause is lower than expected (11.6%). In contrast, hypertensive hemorrhage represents the cause of up to 79.5% of ICH. Previous studies in relation to this possible common sub-strate have shown that the cerebral vascular phenotype (ICH vs. lacunar infarcts) due to hypertensive microangi-opathy would be related in part to age and cholesterol levels17,18. Therefore, a possible explanation to our find-ings could be related to age (remarkably younger patients) and the lower frequency of dyslipidemia (5.6%) known in our population. Another possible explanation would be in relation to the less severe clinical deficit associated with lacunar stroke19, which may affect the arrival or referral of these patients. These results are consistent in the region with previous studies in Santiago de Chile and Bogotá13,20. Unfortunately, the body mass index, which has been shown to be a prognostic factor for the development of ICH or lacunar infarctions in hypertensive microangiopa-thy18, has not been evaluated in the present study. Future prospective and comparative studies should be taken into account to confirm these findings.
Regarding gender, women presented a stroke less frequently, with greater age (according to the
literature)8,21,22, and significantly less known cardiovas-cular risk factors than men, which is also consistent with previous studies. Factors such as hypertension and atri-al fibrillation, which in other series showed a significantly higher frequency in women, have not been seen in our study8,9. The age difference in HIC is remarkable among genders, being the higher hypertension prevalence in early age7 and the hypothetical hormonal preventive ef-fect in women20,21 probable reasons for this finding.
As a relevant limitation at the present study; it is a monocentric study, involving patients from urban and rural areas that may not represent a specific geographic area.
Conclusion
In this prospective study in our country, hypertension is a risk factor highly related to stroke with a higher frequency of hypertensive hemorrhages in younger pa-tients than other series, especially in men. The frequen-cy of different stroke subtypes would be related to environmental, sociocultural, and biological factors. Multicenter and comparative studies are warranted to confirm these findings. The intensification of public health programs focused on the control of risk factors, especially hypertension, is necessary to prevent cere-brovascular disease in our environment.
Funding
There was no particular funding source for this sci-entific report.
Conflicts of interest
The authors declare that in this study, there are no relevant conflicts of interest.
Figure 3. Bars showing the mean age according to gender in overall A: ischemic; B: intracerebral; and C: stroke patients.
A B C

85
L. Díaz-Escobar et al.: Frecuencia de los FR en el ictus en Paraguay
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
right to privacy and informed consent. The authors declare that no patient data appear in this article.
references 1. Bonita R. Epidemiology of stroke. Lancet. 1992;339:342-4. 2. Truelsen T, Piechowski-Jóźwiak B, Bonita R, Mathers C, Bogousslavsky J,
Boysen G, et al. Stroke incidence and prevalence in Europe: a review of available data. Eur J Neurol. 2006;13:581-98.
3. Arias-Rivas S, Vivancos-Mora J, Castillo J, En Nombre de Los Investi-gadores Del Registro Epices. Epidemiology of the subtypes of stroke in hospitalised patients attended by neurologists: results of the EPICES registry (I). Rev Neurol. 2012;54:385-93.
4. Saposnik G, Del Brutto OH, Iberoamerican Society of Cerebrovascular Diseases. Stroke in South America: a systematic review of incidence, prevalence, and stroke subtypes. Stroke. 2003;34:2103-7.
5. Boletín de Vigilancia. Enfermedades No Transmisibles Y Factores De RIESGO 2015. Ministerio de Salud Pública y Bienestar Social. Available from: http://www.mspbs.gov.py.
6. Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare pro-fessionals from the American heart association/American stroke associa-tion. Stroke. 2014;45:2160-236.
7. Primera Encuesta Nacional de Factores de Riesgo de Enfermedades No Transmisibles. Primera Edición. Asunción. 2012 Ministerio de Salud Pú-blica y Bienestar Social. Available from: http://www.mspbs.gov.py.
8. Andersen KK, Andersen ZJ, Olsen TS. Age-and gender-specific prevalen-ce of cardiovascular risk factors in 40,102 patients with first-ever ischemic stroke: a nationwide Danish study. Stroke. 2010;41:2768-74.
9. Reeves MJ, Bushnell CD, Howard G, Gargano JW, Duncan PW, Lynch G, et al. Sex differences in stroke: epidemiology, clinical presentation, me-dical care, and outcomes. Lancet Neurol. 2008;7:915-26.
10. Lang EW, Ren Ya Z, Preul C, Hugo HH, Hempelmann RG, Buhl R, et al. Stroke pattern interpretation: the variability of hypertensive versus amyloid angiopathy hemorrhage. Cerebrovasc Dis. 2001; 12:121-30.
11. Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet. 1991;337:1521-6.
12. Saposnik G, Caplan LR, Gonzalez LA, Baird A, Dashe J, Luraschi A, et al. Differences in stroke subtypes among natives and Caucasians in Boston and Buenos Aires. Stroke. 2000;31:2385-9.
13. Carod-Artal FJ, Casanova Lanchipa JO, Cruz Ramírez LM, Pérez NS, Siacara Aguayo FM, Moreno IG, et al. Stroke subtypes and comorbidity among ischemic stroke patients in Brasilia and Cuenca: a Brazilian-spa-nish cross-cultural study. J Stroke Cerebrovasc Dis. 2014;23:140-7.
14. Nogales-Gaete J, Núñez L, Arriagada C, Sáez D, Figueroa T, Fernán-dez R, et al. Caracterización clínica de 450 pacientes con enfermedad cerebrovascular ingresados a un hospital público durante 1997. Rev Med Chil. 2000;128:1227-36.
15. Del Brutto OH, Mosquera A, Sánchez X, Santos J, Noboa CA. Stroke subtypes among hispanics living in Guayaquil, Ecuador. Results from the luis vernaza hospital stroke registry. Stroke. 1993;24:1833-6.
16. Saposnik G, Gonzalez L, Lepera S, Luraschi A, Sica RE, Caplan LR, et al. Southern Buenos Aires stroke project. Acta Neurol Scand. 2001;104:130-5.
17. Labovitz DL, Boden-Albala B, Hauser WA, Sacco RL. Lacunar infarct or deep intracerebral hemorrhage: who gets which? The Northern Manhat-tan study. Neurology. 2007;68:606-8.
18. Lioutas VA, Beiser A, Himali J, Aparicio H, Romero JR, DeCarli C, et al. Lacunar infarcts and intracerebral hemorrhage differences: a nested case-control analysis in the FHS (Framingham heart study). Stroke. 2017;48:486-9.
19. Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010;9:689-701.
20. Peña I, Ruiz C, Morillo LE, Pedraza OL, Sánchez E, Santín LC, et al. Clasificación del TOAST en la práctica clínica de un hospital universita-rio. Acta Neurol Colomb. 2001;17:304-8.
21. Alonso de Leciñana M, Egido JA, Fernández C, Martínez-Vila E, Santos S, Morales A, et al. Risk of ischemic stroke and lifetime estrogen exposure. Neurology. 2007;68:33-8.
22. Murphy SJ, McCullough LD, Smith JM. Stroke in the female: role of biological sex and estrogen. ILAR J. 2004;45:147-59.

86
Electro-clinical relationship and source analysis of absence seizures in childhoodLiane Aguilar-Fabré1*, René F. Rodríguez-Valdés1, Lídice Galán-García2, Jorge F. Bosch-Bayard3, Hebert L. Hernández-Montiel1, and Ramiro J. García-García4
1Neurobiology and Cell Bioengineering Laboratory, School of Medicine, Universidad Autónoma de Querétaro, Querétaro, Mexico; 2Department of Neurostatistics, Centro de Neurociencias de Cuba, Havana, Cuba; 3McGill Centre for Integrative Neurosciences, Montreal Neurological Institute-Hospitall, McGill University, Montreal, Canada; 4Neuropediatric Service, Hospital Pediátrico Juan Manuel Márquez, Havana, Cuba
Revista Mexicana de Neurociencia
oriGiNal artiClE
abstract
Purpose: This study was to deepen into the electro-clinical relationship and source analysis of absence seizures in childhood. Methods: Thirty-three subjects were studied with clinical and electrophysiological diagnosis of absence seizures without antiepileptic medication, video-electroencephalogram was applied. We obtained clinical behavior and electrophysiological variables during seizures and General Linear Model was applied, with p < 0.05. Source analysis was carried out with VARE-TA method. results: 174 seizures were evaluated. 75.75% showed interictal epileptiform discharges (IED) and 12.12% showed posterior delta activity. There was an unequal behavior in relation with total electro-clinical seizures and presence or no of IED (p = 0.02), namely between subjects without IED in EEG and multifocal EEG (p = 0.008). Quantity of seizures recorded during HPV had a different behavior between subjects without IED in EEG and multifocal EEG (p = 0.03) and between focal and multifocal EEG (p = 0.04). Source analysis (VARETA) evidence the onset frontal of seizures in 57.47%, mesial and dor-solateral regions in 43% and 57%, respectively. Conclusion: These data suggest that absence seizures are not “generalized” if we considered global cortical activation but rather involve localized discharges from specific cortical regions, mainly fron-tal lobe.
Keywords: Absence seizures. VARETA. Source analysis.
Relación electro-clínica y análisis de fuentes de las crisis de ausencia en la infancia
resumen
objetivo: Profundizar en las relaciones electro- clínica y el análisis de fuentes de las crisis de ausencia en la infancia. Métodos: Se estudiaron 33 sujestos con el diagnóstico clínico y electrofisiológico de crisis de ausencia sin medicación antiepiléptica, se realizó Video-EEG. Se recogieron los comportamientos clínicos y variables electrofisiológicas durante las crisis y se aplicó un Modelo General Lineal, con p < 0.05. El análisis de las fuentes se realizó con el método VARETA. resultados: Se evaluaron 174 crisis El 75,75% mostró descargas epileptiformes interictales (DEI) y el 12,12% mostró acti-vidad delta posterior. Existió un comportamiento desigual en relación con el total de crisis electroclínicas y la presencia o no de DEI (p = 0.02) y entre los sujetos sin DEI y DEI multifocales (p = 0.008). El número de crisis registradas durante la HPV tuvo un comportamiento diferente entre sujetos sin DEI y EEG con DEI multifocales (p = 0.03) y entre EEG focal y
Correspondence: *Liane Aguilar-Fabré
E-mail: [email protected]
Available online: 02-05-2022
Rev Mex Neuroci. 2022;23(3):86-91
www.revmexneurociencia.com
Date of reception: 26-05-2021
Date of acceptance: 13-09-2021
DOI: 10.24875/RMN.21000049
2604-6180 / © 2021 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

87
L. Aguilar-Fabré et al.: Absences epilepsy and source analysis
introduction
Childhood absence epilepsy (AE) represents the prototype of idiopathic generalized epilepsies (IGEs). AE is a specific type of brief, generalized nonconvulsive epileptic seizure disorder. The seizures are characterized by a transitory alteration in consciousness associated with electroencephalograms (EEGs) indicating bilateral 3-4 Hz spike-wave discharges (SWDs) of variable duration1-3.
Typical SWD in absence seizures is dependent on long range corticothalamic and corticocortical network interactions1,4,5. Today, however, the neural networks involved in the generation and propagation of these seizures remain under debate. Despite advances in knowledge about the etiology of IGE and evidence of the involvement of thalamus-cortical networks at the onset of generalized tip-wave discharges, there is no consensus about a common cortical source for gener-alized spike-wave6-11.
Quantitative electroencephalography provides the opportunity to study measurements of brain electrical activity using non-invasive means, such as mathemat-ical algorithms, for the solution of the inverse problem in electroencephalography, which consists in estimat-ing the location of the generators of the electrical ac-tivity of the brain from voltage measurements on the scalp. Modern techniques for locating sources of brain activity allow mapping brain sources in physiological and physiopathology processes in a non-invasive way12-15.
The purpose of this study was to deepen the electro-physiological and clinical characteristics of the absence seizures in childhood.
Methods
Subjects
The study were included those patients with the clinical diagnosis of childhood absence crisis and nor-mal neurological examination. The electro-clinical sei-zures were confirmed through the evaluation by vid-eo-electroencephalogram (V-EEG) performed at the
time of diagnosis. Patients who had a history of other types of seizures or were under antiepileptic treatment were excluded from the study. Demographic variables and related to AE were collected.
EEG-video
The records were acquired using a digital vid-eo-electroencephalograph of 32 channels, Medicid 5 (Neuronic SA). The electrodes of AgCl surface were placed according to the international system of place-ment of electrodes 10-20 and the ears circuited as reference. The bandwidth was 0.5-30 Hz, the digitiza-tion of the electroencephalographic signal was carried out with a sampling period of 5 ms, and the gain of the amplifiers was 10,000. The impedance of the elec-trodes considered acceptable was <5 000 Ω. V-EEG evaluations were performed awake for a minimum du-ration of 30 minutes, with opening activation manoeu-vres, and hyperventilation (HPV) for 3 min, recovery and intermittent light stimulation between 1 and 33 Hz.
Sources analysis
Variable Resolution Electric and Magnetic Tomogra-phy (VARETA) is a type of Distributed Inverse Solution (IS)16. This mathematical algorithm poses a smooth solution discrete distributed to the inverse problem. The sources of currents are restricted to the estimates of probability of existence of gray matter derived from the probabilistic cerebral atlas (PCA) developed at the Neu-rological Institute of Montreal17. Three-dimensional to-mographic images generated with a color code show the IS on the trans axial, coronal, and sagittal cuts of the PCA. In each case, the site of maximum energy was taken as the main IS, considering the large number of measurements and their correlation.
The method of locating distributed sources VARETA was used in the time domain to confirm the ictal start zone, defined by spectral analysis (amplitude maps). For the analysis of the ictal current generators, the point of maximum energy of the tip component of the
multifocal (p = 0.04). El análisis de las fuentes evidenció el inicio frontal de las crisis en el 57,47%, con la participación de las regiones mesial y dorsolateral en el 43% y 57% respectivamente. Conclusiones: Los datos sugieren que las crisis de ausencia no son ¨generalizadas¨ si se considera la activación cortical global, sino que involucran descargas localizadas en regiones corticales específicas, principalmente del lóbulo frontal.
Palabras clave: Crisis de ausencia. VARETA. Análisis de fuentes.

88
Rev Mex Neuroci. 2022;23(3)
spike-wave complexes contained in the first second of each of the electro-clinical seizures was measured.
Statistical analysis
To know if there were different behaviors for the elec-tro-clinical variables: time of evolution of the disease, total electro-clinical seizures, duration of the seizures, topography of the interictal epileptiform discharges (IED), presence of the IED, focal and multifocal IED, a general linear model was applied, with a 95% confi-dence in the hypothesis tests (p < 0.05). The frequency distribution of the variables as well as their average and standard deviation is described. IS percent are described.
Ethical considerations
For the inclusion of the children in this investigation, the informed consent of the parents was requested, the individual data were not divulged, and the established ethical norms were fulfilled. The investigation was ap-proved by the Ethics Committee of the investigations of the Pediatric Hospital “Juan Manuel Márquez” fulfill-ing with the ethical norms of the declaration of Helsinki.
results
We studied 33 patients (16 of the female sex). The age range of the patients was between 5.62 and 10.92, (7.63 ± 1.79 SD) (SD, standard deviation), the time of evolution of the disease varied between 10 and 365 days (112 ± 95 SD). The electro-clinical seizures were recorded in 100% of the subjects. A total of 174 seizures (5.27 ± 3.4 DS) were recorded and majority percent occurred at HPV (Table 1).
The average duration of the seizures was 10.57 s ± 6.79 SD. Other clinics features of the AE showed in Table 2.
The totality of the patients showed a normal back-ground activity with the presence of IEDs in a 75.75% (25/33) and the presence of posterior delta activity in a 12.12% (4/33). Focal IED were present in 72% (18/25) and multifocal IED in 28% (7/25) of subjects.
The statistical analysis by a Linear General Model revealed that there was no different behavior in relation to the time of evolution of the disease, the duration of the seizures and the localization of the IED p = 0.55 and p = 0.26, respectively.
However, there is an unequal behavior in the total of electro-clinical seizures and the presence or not of IED (p = 0.02), particularly among subjects without IED and IED with multifocal presentation (p = 0.008). The number of seizures recorded during HPV be-haves in a different way between subjects with nor-mal interictal EEG and with multifocal IED p = 0.03 and between the EEG with focal and multifocal IED p = 0.04.
The topographic analysis in the time domain using the VARETA method was applied to ictal discharges to the 174 electro-clinical seizures, it showed that the ictal onset area was in the frontal lobes in 57.47% (100/174), mesial and dorsolateral regions in 43% and 57%, re-spectively (Fig. 1).
At the same, the frontal structures most involved in the ISs were the supplementary motor area, middle and superior frontal gyrus and the cingulum. Generators of the ictal epileptiform activity were also found in parietal 25.86% (45/174), temporal 9.77% (17/174), and occipital 6.89% (12/174) regions.
Table 2. Clinics features of the absence seizures
n %
Arrest or Detention of the activity 120 68.96
Opening eyes 75 43.10
Oral Automatism 47 27.01
Others automatism 26 14.94
Clonic component 22 12.64
Atonic component 11 6.32
Between 4 and 20 s 118 67.81
Less than 4 s 40 22.99
More than 20 s 16 9.19
Table 1. Distribution of the absence seizures
Maneuvers n %
Closed eyes 39 22.41
Open eyes 8 4.60
HPV 90 51.72
Recovery 30 17.24
Intermittent light stimulation 7 4.02

89
L. Aguilar-Fabré et al.: Absences epilepsy and source analysis
discussion
There is little research that addresses the study of the electro-clinical characteristics of absence seizures despite representing approximately a quarter of epilep-sy in childhood18,19.
In this research, the average seizures per capita reg-istered was 5.5, and the highest percentage of the seizures was obtained during HPV 51.72% very similar to the values of 5.8 and 47% reported by Saldier20. The same author reported the average duration (9.4 s), du-ration <4 s (26%) and more than 20 s (8%) similar val-ues were found in this study.
One result of this investigation was that exist a dif-ferent behave in relation to the total of seizures, in those patients whose had or no IED, especially those presenting with independent presentation of IED in var-ious regions of the cortex brain. These results are ex-pected if we consider that the interictal epileptiform activity constitutes a good marker of epileptogenicity and the extension of the epileptogenic focus.
Approximately, 76% of the patients assessed showed IED. The high percentage of patients with IED in their
EEG could be related to the high frequency of absence seizures that characterizes this epileptic syndrome21. It is also reported that there is an increase in the inci-dence of IED in those patients who have presented seizures between 2 and 7 days before the EEG and describes a strong association between a high frequen-cy of clinical seizures and a greater likelihood of detect-ing IED22,23.
In the pathophysiology of IGEs, there are two pillars they are: pathological thalamus-cortical interaction and the so-called light diffuse epileptogenic state of the cor-tex11,24-26. The existence of areas of the cerebral cortex with icthyogenic properties have been demonstrated by numerous investigations carried out with neuroimaging that reveal significant morphological and functional dis-turbances restricted to various regions of the cerebral cortex in patients with IGE, more notable toward the frontal regions. By definition, there should be no struc-tural anomalies in patients with IGE. However, the report of diffuse cortical abnormalities and focal cortical micro-dysgenesis in subjects with IGEreaffirms the possible focal cortical origin of this epilepsy27-33.
Figure 1. EEG with generalized spike-wave discharge at 3.1 Hz in patient with absence seizure. Inverse solution in the supplementary motor area by applying the VARETA method.

90
Rev Mex Neuroci. 2022;23(3)
The results of this study indicate the selective in-volvement of cortical networks including lateral dorsum and mesial frontal regions in the generation of ictal discharges, which coincides with that reported by oth-ers investigator6,7,9,34. From the pathophysiologic point of view, the cortical areas where the generators of the ictal discharges are found suggest having ichthyogenic properties possibly as a result of an increase in syn-chronized neural activity6.
A study using magnetoencephalography to deter-mine the cortical and subcortical contribution to the formation of ictal SWDs showed the location of the generators in the frontal cortex and thalamus in more than 70% of the seizures9. The quantitative analysis of the generalized interictal discharges in patients with IGE also reveals the frontal lobe as the main generator, highlighting in this lobe structures such as the middle frontal gyrus and the anterior cingulum cortex10. The results of both works coincide with the findings of this research.
More recently, a paper with Magnetoencephalogra-phy data from 14 patients with AE were recorded during and between seizures at a sampling rate of 6000 Hz and analyzed in seven frequency bands. Neuromagnetic sources were volumetrically scanned with accumulated source imaging. Effective connec-tivity networks of the entire brain, including the corti-co-thalamo-cortical network. It showed that the low-frequency (1-80 Hz) activities showed significant frontal cortical and parieto-occipito-temporal junction source localization around seizures. The high-fre-quency (80-250 Hz) oscillations showed predominant activities consistently localized in deep brain areas and medial frontal cortex34.
Conclusions
The results of this research suggest that in the gener-ation of childhood absence seizures there is no homo-geneous activation of the cerebral cortex. The genera-tion of these seizures mainly involves cortical networks circumscribed mostly to the frontal regions, which pres-ent abundant connections with structures as the thala-mus and the ascending reticular activator systems.
Funding
This research has not received any specific grant from public, commercial, or non-profit sector agencies.
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animal for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
right to privacy and informed consent. The authors declare that no patient data appears in this article.
references 1. Blumenfeld H. Cellular and network mechanisms of spike-wave seizures.
Epilepsia. 2005;46:21-33. 2. Hughes JR. Absence seizures: a review of recent reports with new con-
cepts. Epilepsy Behav. 2009;15:404-12. 3. Panayiotopoulos CP, Michael M, Sanders S, Valeta T, Koutroumanidis M.
Benign childhood focal epilepsies: assessment of established and newly recognized syndromes. Brain. 2008;131:2264-86.
4. Avoli M, Gloor P. Interaction of cortex and thalamus in spike and wave discharges of feline generalized penicillin epilepsy. Exp Neurol. 1982;76: 196-217.
5. Meeren H, van Luijtelaar G, da Silva FL, Coenen A. Evolving concepts on the pathophysiology of absence seizures: the cortical focus theory. Arch Neurol. 2005;62:371-6.
6. Holmes MD, Brown M, Tucker DM. Are generalized seisures truly gene-ralized? Evidence of localized mesial frontal and frontopolar discharges in absence. Epilepsia. 2004;45:1568-79.
7. Craiu D, Magureanu S, van Emde Boas W. Are absence truly generalized seizures or partial seizures originating from or predominantly involving the pre-motor areas? Some clinical and theoretical observations and their implications for seizures classification. Epilepsy Res. 2006,70:141-55.
8. Clemens B, Bessenyer M, Piros P, Tóth M, Seress L, Kondákor I. Cha-racteristic distribution of interictal brain electrical activity in idiopathic generalized epilepsy. Epilepsia. 2007;48:941-9.
9. Tenney JR, Fujiwara H, Horn PS, Jacobson SE, Glauser TA, Rose DF. Focal corticothalamic sources during generalized absence seizures: a MEG study. Epilepsy Res. 2013;106:113-22.
10. Bragas MA, Fujisao EK, Betting LE. Analysis of generalized interictal discharges using quantitative EEG. Epilepsy Res. 2014;108:1740-7.
11. Amor F, Baillet S, Navarro V, Adam C, Martinerie J, Le van Quyen M. Cortical local and long-range synchronization interplay in human absen-ce seizure initiation. Neuroimage. 2009;45:950-62.
12. Urretarazu E, Iriarte J. Análisis matemáticos en el estudio de señales electroencefalográficos. Rev Neurol. 2005;41:423-34.
13. Cho JH, Hong SB, Jung YJ, Kang HC, Kim HD, Suh M, et al. Evaluation of algorithms for intracranial EEG (iEEG) source imaging of extended sources: feasibility of using iEEG source imaging for localizing epileptoge-nic zones in secondary generalized epilepsy. Brain Topogr. 2011;24:91-104.
14. Cosandier-Rimélé D, Merlet I, Badier JM, Chauvel P, Wendling F. The neuronal sources of EEG: modeling of simultaneous scalp and intrace-rebral recordings in epilepsy. Neuroimage. 2008;42:135-46.
15. Grech R, Cassar T, Muscat J, Camilleri KP, Fabri SG, Zervakis M, et al. Review on solving the inverse problem in EEG source analysis. J Neu-roeng Rehabil 2008;5:25.
16. Valdes-Sosa P, Marti F, García F, Casanova R. Variable resolution electric-magnetic tomography. In: Aine CJ, Stroink G, Wood CC, Okada Y, Swithenby SJ, editors. Biomag 96. New York: Springer; 2000.
17. Evans AC, Collins DL, Neelin P, MacDonald D, Kamber M, Marrett TS. Three-dimensional correlative imaging: applications in human brain ma-pping. In: Thatcher R, Hallet M, Zeffiro T, John ER, Huerta M, editors. Functional Neuroimaging: Technical Foundations. San Diego, CA: Aca-demic Press; 1994. p. 145-62.
18. Poblano A, Ibarra J, Muniz A, Garza S. Absence seizures effects on reading revealed by video-electroencephalography. Rev Invest Clin. 2001;53:136-40.

91
L. Aguilar-Fabré et al.: Absences epilepsy and source analysis
19. Capovilla G, Rubboli G, Beccaria F, Lorenzetti ME, Montagnini A, Resi C, et al. A clinical spectrum of the myoclonic manifestations associated with typical absences in childhood absence epilepsy. A video-polygraphic study. Epileptic Disord. 2001;3:57-61.
20. Sadleir LG, Farrel K, Smith S, Connolly MB, Scheffer IE. Electroclinical features of absence seizures in childhood absence epilepsy. Neurology. 2006;67:413-8.
21. Sundaram M, Hogan T, Hiscock M, Pillay N. Factors affecting interictal spike discharges in adults with epilepsy. Electroencephalogr Clin Neuro-physiol. 1990;75:358-60.
22. Janszky J, Hoppe M, Clemens Z, Janszky I, Gyimesi C, Schulz R, et al. Spike frequency is dependent on epilepsy duration and seizure frequen-cy in temporal lobe epilepsy. Epileptic Disord. 2005;7:355-9.
23. Krendel R, Lurger S, Baumgartner C. Absolute spikes frequency predicts surgical outcomes in TLE with unilateral hippocampal atrophy. Neurology. 2008;71:4138.
24. Gloor P, Avoli M, Kostopoulos G. Thalamo-cortical relationships in gene-ralized epilepsy with bilaterally synchronous spike-and-wave discharge. In: Avoli M, Gloor P, Kostopoulos G, Naquet R, editors. Generalized Epilepsy. Neurobiological Approaches. Boston: Birkhauser; 1990. p. 190-212.
25. Salek-Haddadi A, Lemieux L, Merschhemke M, Friston KJ, Duncan JS, Fisch DR. Functional magnetic resonance imaging of human absence seizures. Ann Neurol. 2003;53:663-7.
26. Szaflarski JP, DiFrancesco M, Hirschauer T, Banks C, Privitera MD, Gotman J, et al. Cortical and subcortical contributions to absence seizu-re onset examined with EEG/fMRI. Epilepsy Behav. 2010;18:404-13.
27. Duncan JS. Paper by invitation: imaging idiopathic generalized epilepsy. Clin EEG Neurosci. 2004;35:168-72.
28. Betting LE, Mory SB, Lopes-Cendes I, Li ML, Guerreiro MM, Cam G, et al. MRI volumetry shows increased anterior thalamic volumes in pa-tients with absence seizure. Epilepsy Behav. 2006;8:575-80.
29. Savic RJ, Seitz RJ, Pauli S. Brain distortions in patients with primarily generalized tonic-clonic seizures. Epilepsia. 1998,39:364-70.
30. Woermann SM, Free MJ, Koepp SM, \ Duncan JS. Abnormal cerebral structure in juvenile myoclonic epilepsy demonstrated with voxel-based analysis of MRI. Brain. 1999,122:2101-8.
31. Meencke HJ, Janz D. Neuropathological findings in primary generalized epilepsy: a study of eight cases. Epilepsia. 1984,25:8-21.
32. Meencke H, Janz D. The significance of microdysgenesia in primary generalized epilepsy: an answer to the considerations of Lyon and Gas-taut. Epilepsia. 1985,26:368-71.
33. Liang JS, Lee SP, Pulli B, Chen JW, Kao SC, Tsang YM, et al. Micros-tructural changes in absence seizure children: a diffusion tensor magne-tic resonance imaging study. Pediatr Neonatol. 2016;57:318-25.
34. Caiyun W, Jing X, Jintao S, Shuyang H, Lu T, Ailiang M, et al. Quantify neuromagnetic network changes from pre-ictal to ictal activities in absen-ce seizures. Neuroscience. 2017;357:134-44.
92
are different degrees of lymphopenia for FtY720 associated with serious infectious-type events? NoCatalina Márquez-Martín, Ricardo J. García-Bermúdez, and Brenda Bertado-Cortés*Neurology Department, Specialty Hospital, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social, Mexico City, Mexico
Revista Mexicana de Neurociencia
oriGiNal artiClE
abstract
objective: Describing the occurrence of infections in patients with relapsing-remitting multiple sclerosis (RRMS) treated with fingolimod and with different degrees of lymphopenia in our unit. Patients and Methods: Observational, descriptive, longi-tudinal, and retrospective study in the Hospital Centro Médico Nacional Siglo XXI. Patients with RRMS and treatment with fingolimod were grouped based on lymphocyte count and infections. Quantitative variables were expressed as mean, standard deviation, and interquartile range; qualitative variables were expressed as frequencies and percentages. results: 110 patients, 76 (69.1%) female, 34 (30.9%) male, mean age 38.3 years (17-63, SD 9.85). Mean of initial expanded disability status scale 1.59 (0-5.5, SD 1.15) with a mean diagnosis time of 63.6 months (3-252, SD 50.96). Prior to starting fingolimod, 90.09% of patients had lymphocyte count >1,000. At six months of treatment, 35.64% had lymphocyte >1,000. At twelve months 32.95% had lymphocyte from 501 to 700. At 24 months, 34.21% had lymphocyte from 701 to 1,000. Of the 110 patients, 31.8% had mild infections, of which pharyngitis was reported in 10%, gastroenteritis 2.7%, urinary tract infection 10.9%, HPV infection 0.9%, SARS-CoV-2 infection 3.6%, ophthalmic herpes 0.9%, molluscum contagiosum 0.9%, oral candidiasis 0.9%. 68.18% did not present infections of any kind, no serious infections were reported even with lymphocyte levels below 200. Conclu-sions: Selective lymphopenia caused by fingolimod was not associated with infections of any kind in this population even at levels of 200-500 cells/mm3.
Keywords: Fingolimod. Lymphopenia. Relapsing-remitting multiple sclerosis. Sphingosine 1-phosphate.
¿Los diferentes grados de linfopenia por FTY720 se asociaron a eventos graves de tipo infeccioso? No
resumen
objetivo: Describir la ocurrencia de infecciones severas en pacientes con EMRR tratados con fingolimod y con diferentes grados de linfopenia en nuestra unidad Métodos: Estudio observacional, descriptivo, longitudinal y retrospectivo realizado en el Hospital Centro Médico Nacional Siglo XXI. Pacientes con EMRR tratados con fingolimod, se agruparon por grados de linfopenia e infecciones. Las variables cuantitativas se expresaron como media, desviación estándar y rango intercuartil; las variables cualitativas se expresaron en frecuencias y porcentajes. resultados: 110 pacientes, 76 mujeres (69.1%), 34 hombres (30.9%), media de edad 38.39 (17-63 DE 9.85). Media EDSS inicial 1.59 (0-5.5, DE 1.15), tiempo diagnóstico medio 63.67 meses (3-252, DE 50.96). Previo al inicio de fingolimod, 90.09% de los pacientes tenía linfocitos absolutos >1,000. A los 6 meses de tratamiento, 35.64% tenía >1,000 linfocitos. A los 12 meses el 32.95% tenía 501-700 linfocitos, a los
Correspondence: *Brenda Bertado-Cortés
E-mail: [email protected]
Available online: 02-05-2022
Rev Mex Neuroci. 2022;23(3):92-96
www.revmexneurociencia.com
Date of reception: 25-05-2021
Date of acceptance: 17-09-2021
DOI: 10.24875/RMN.21000048
2604-6180 / © 2021 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

93
C. Márquez-Martínn et al.: Lymphopenia-FTY270. Severe infections?
introduction
The correlation between lymphopenia and the incidence of severe infections in patients with relaps-ing-remitting multiple sclerosis (RRMS) treated with fin-golimod have been a topic of interest and debate for a long time.
Multiple sclerosis (MS) is a chronic, inflammatory, and demyelinating central nervous system disease as-sociated with a wide range of axonal and neuronal damage1-4 the immune response is mainly given by T-cells, with a contribution of B cells and plasmatic cells, as well as activation of macrophages and microglia5-9.
Fingolimod-1-phosphate, the active form of fingoli-mod, is an agonist of S1PR1,3,4 and 5 receptors; Its anti-inflammatory activity is through S1P lymphocyte receptors, with a joint that produces the receptor inter-nalization and functional antagonism concludes in the decrease of lymphocyte count in blood, with a variable grade of lymphopenia (redistributive lymphopenia)10,11.
With a daily dose, lymphocyte count decreased along two weeks, with a minimum value of 30% from initial lymphocyte count. Furthermore, selective lymphopenia keeps memory lymphocytes in blood circulation, which reduces the risk of opportunistic infections12-14
.
In the pivotal phase III study FREEDOMS the overall incidence of serious infections occurred in 1.6-2.6% of patients. Bronchitis and pneumonia were more common with fingolimod than with placebo (occurring in 41 patients [9.6%] receiving 0.5 mg of fingolimod and 49 patients [11.4%] receiving 1.25 mg of fingolimod vs. Twenty-five patients [6.0%] receiving placebo)15-17.
Infection is defined as a process caused by the inva-sion of normally sterile tissues, fluids, or cavities of the body by pathogenic or potentially pathogenic microorganisms.
Mild infection: the presence of systemic inflammatory response that does not require hospital admission: na-sopharyngitis, bronchitis, influenza, gastroenteritis, and urinary tract infection.
Severe infection is a systemic inflammatory response that requires hospital admission due to its high degree of mortality and sequelae: herpes virus encephalitis, dis-seminated herpes zoster, pulmonary tuberculosis, Pneu-mocystis jirovecii pneumonia, toxoplasma gondii infec-tions, and progressive multifocal leukoencephalopathy.
In our country, there are no studies about Fingolimod effects on lymphocyte count, as well as the incidence of serious infectious events with the different grades of lymphopenia.
The aim of our study was to describe the occurrence of infections in patients with RRMS treated with fingo-limod and with different degrees of lymphopenia in our unit. Finding different results to those reported in the pivotal studies.
Patients and methods
We implemented an observational, descriptive, lon-gitudinal and retrospective study at the Clínica de Enfermedades Desmielinizantes, Hospital de Espe-cialidades Centro Médico Nacional Siglo XXI, Insti-tuto Mexicano del Seguro Social. Patients with RRMS and treatment with fingolimod 0.5 mg orally daily dose for at least 6 months, from January 2015 to July 2021 were included. We gathered the information from medical records (age, gender, expanded disabil-ity status scale [EDSS], time from diagnosis, lympho-cyte count at 6, 12, 18, and 24 months). Patients were grouped based on lymphocyte count: 0-200, 201-500, 501-700, 701-1000, and >1000, infections were also grouped into two groups; mild or severe/oppor-tunistic. Getting the percentage of each group during the follow-up. Our population has a parametric dis-tribution so that the quantitative variables were ex-pressed as mean and standard deviation and inter-quartile range; qualitative variables were expressed as frequencies and percentages. The statistical package of social sciences (SPSS) version 24 for Windows was used.
24 meses el 34.21% tenía 701-1,000 linfocitos. De los 110 pacientes, el 31.8% presentó infecciones leves, de las cuales se informó faringitis en 10%, gastroenteritis 2.7%, infección del tracto urinario 10.9%, infección por VPH 0.9%, infección por SARS-CoV-2 3.6%, herpes oftálmico 0.9%, molusco contagioso 0.9%, candidiasis oral 0.9%. El 68.18% no presentó infeccio-nes de ningún tipo, no se reportó infecciones graves incluso con niveles de linfocitos inferiores a 200. Conclusiones: La linfopenia selectiva causada por fingolimod no se asoció a infecciones severas en esta población incluso en niveles de 200 a 500 células/mm3.
Palabras clave: Esclerosis múltiple remitente recurrente. Esfingosina 1-fosfato. Fingolimod. Linfopenia.

94
Rev Mex Neuroci. 2022;23(3)
results
110 patients were included; 101 completed 6 months, 88 completed 12 months, 61 completed 18 months, and 38 completed 24 months of follow-up. 76 (69.1%) pa-tients were female and 34 (30.0%) were male, with a mean age of 38.39 years (17,63, SD 9.85). Mean initial EDSS was 1.59 (0-5.5, SD 1.15), with a mean time from diagnosis of 63.67 months (3-252, SD 50.96). In Ta-ble 1 are shown all patients characteristics.
From all 110 patients, 25 (22.7%) were naive, and prior to fingolimod treatment, 90.09% had lymphocyte count greater than 1000 cells/mcL. At 24 months, 34.21% had 701-1000 lymphocytes/mcL, and 31.57% had 201-500 cells/mcL. Figure 1 shows the proportion of patients in each lymphocyte group during the follow-up.
Of the 110 patients, 68.18% did not present infections of any kind, 31.8% presented mild infections, of which pharyngitis was reported in 10%, gastroenteritis 2.7%, urinary tract infection 10.9%, HPV infection 0.9%, SARS-CoV-2 infection 3.6%, ophthalmic herpes 0.9%, molluscum contagiosum 0.9%, and oral candidiasis 0.9%. There were no severe infections 0%; such as herpes encephalitis, progressive multifocal leukoen-cephalopathy, pulmonary tuberculosis, pneumocystis pneumonia, or toxoplasmosis during follow-up even with lymphocyte levels less than 200.
discussion
MS affects young adults between 20 and 40 years, with a greater prevalence in females18. In our study, the
mean age was 38.39 years and females were more prevalent than males (69.1% vs 30.9% respectively), which agree with the references.
Table 1. Patients characteristics
Characteristics Results (%)
Male n (%) 34 (30.9)
Female n (%) 76 (69.1)
Age *(SD) 38.39 (17-63, SD 9.85)
EDSS *(SD) 1.59 (0-5.5, SD 1.15)
Time from diagnosis * (SD) 63.67 (3-252, SD 50.96)
Previous treatments n (%)
Naïve 25 (22.7)
6 millions interferon 23 (20.9)
8 millions interferon 18 (16.36)
12 millions interferon 8 (7.27)
Glatiramer acetate 25 (22.72)
Dimethyl fumarate 1 (0.9)
Teriflunamide 1 (0.9)
Rituximab 1 (0.9)
Mitoxantrone 1 (0.9)
Natalizumab 3 (2.72)
Ocrelizumab 1 (0.9)
Azathioprine 2 (1.80)
Immunoglobulin 1 (0.9)
*Mean. SD: standard deviation.
Figure 1. Lymphocyte count for 24 months.

95
C. Márquez-Martínn et al.: Lymphopenia-FTY270. Severe infections?
The indications of fingolimod are RRMS with EDSS between 0 and 5.5, naive patients with an aggressive disease or treatment failure19. All patients included in our study had these characteristics.
Fingolimod works as a functional antagonist of sphin-gosine phosphate receptor, which produces a selective lymphocytic redistribution concluding in lymphopenia20-22.
In our study, 0.9% of patients had treatments that re-duce lymphocyte count; whence, these patients had lym-phocyte count between 201 and 500 previous fingolimod started. This group of patients completed 24 months of treatment without infections or lower lymphopenia. At 18 months, 1.63% of patients had lymphocyte count lower than 200 cells/mcL, in whom fingolimod administration was modified from daily dose to every other day, complet-ing 48 months (maintaining this dose for 6 months) with-out opportunistic infections or other complications. The patients had a mean baseline EDSS of 1.59 (0-5.5, SD 1.15), after treatment with fingolimod, showed a statistical-ly significant decrease in EDSS at 6 months with a mean EDSS of 1.2 (0-5, SD 1.13, p = 0.001). In our study, no difference was observed in the efficacy of treatment with fingolimod at alternate doses and daily doses.
The lack of severe infections/opportunistic is because of the selective lymphopenia, which prevents the migra-tion of naive lymphocytes from lymph nodes and the retention of memory T-cells in secondary lymph tissue. Therefore, in blood circulation, there are more memory T-cells, which reduce the infection risk. We prevent se-vere herpesvirus infections by performing serology against varicella-zoster virus prior to the start of treat-ment and vaccination in seronegative subjects23.
Conclusions
During the follow-up, the lymphocyte count was not linearly downward as it is described in references; at 24 months of treatment, 34.21% of patients had lym-phocyte count between 701 and 1,000 cells/mcL, which make us conclude that lymphopenia induced by fingo-limod is not duration of treatment dependent and se-lective lymphopenia caused by fingolimod was not as-sociated with severe infections in this population even at levels of 200-500 cells/mm3.
Funding
This research has not received any specific grant from public, commercial, or non-profit sector agencies.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
right to privacy and informed consent. The au-thors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
references 1. Nourbakhsh B, Mowry E. Multiple sclerosis risk factors and pathogenesis.
Continuum (Minneap Minn). 2019;25:596-610. 2. Reich D, Lucchinetti C, Calabresi P. Multiple sclerosis. N Engl J Med.
2018;378:169-80. 3. Loma I, Heyman R. Multiple sclerosis: pathogenesis and treatment. Curr
Neuropharmacol. 2011;9:409-16. 4. Mallada-Frechín J, Meca-Lallana V, Barrero F, Martínez-Ginés M, Mar-
zo-Sola M, Ricart J, et al. Efectividad y seguridad del fingolimod en la práctica clínica habitual en pacientes con esclerosis múltiple remitente recurrente en España: análisis intermedio del estudio MS NEXT. Rev Neurol. 2018;67:157-67.
5. Porras-Betancourt M, Núñez-Orozco L, Plascencia-Álvarez NI, Quiño-nes-Aguilar S, Sauri-Suárez S. Esclerosis múltiple. Rev Mex Neuroci. 2007;8:57-66.
6. Dendrou C, Fugger L, Friese M. Immunopathology of multiple sclerosis. Nat Rev Immunol. 2015;15:545-58.
7. Ciccarelli O, Barkhof F, Bodini B, de Stefano N, Golay X, Nicolay K, et al. Pathogenesis of multiple sclerosis: insights from molecular and metabo-lic imaging. Lancet Neurol. 2014;13:807-22.
8. Popescu B, Pirko I, Lucchinetti C. Pathology of multiple sclerosis: where do we stand? Continuum (Minneap Minn). 2013;19:901-21.
9. Rose J, Carlson N. Pathogenesis of multiple sclerosis. Continuum Life-long Learn Neurol. 2007;13:35-62.
10. Mazdeh M, Monhaser SK, Taheri M, Ghafouri-Fard S. A non-randomized clinical trial to evaluate the effect of fingolimod on expanded disability status scale score and number of relapses in relapsing-remitting multiple sclerosis patients. Clin Transl Med. 2019;8:11.
11. Cohen JA, Chun J. Mechanisms of fingolimod’s efficacy and adverse effects in multiple sclerosis. Ann Neurol. 2011;69:759-77.
12. Fox E, Buckle J, Singer B, Singh V, Boster A. Lymphopenia and DMTs for relapsing forms of MS considerations for the treating neurologist. Neurol Clin Pract. 2019;9:53-63.
13. Johnson T, Shames I, Keezer M, Lapierre Y, Haegert D, Bar-Or A, et al. Reconstitution of circulating lymphocyte counts in FTY720-treated MS patients. Clin Immunol. 2010;137:15-20.
14. Fragoso YD, Spelman T, Boz C, Alroughani R, Lugaresi A, Vucic S, et al. Lymphocyte count in peripheral blood is not associated with the level of clinical response to treatment with fingolimod. Mult Scler Relat Disord. 2018;19:105-8.
15. Devonshire V, Havrdova E, Radue EW, O’Connor P, Zhang-Auberson L, Agoropoulou C, et al. Relapse and disability outcomes in patients with multiple sclerosis treated with fingolimod: subgroup analyses of the dou-ble-blind, randomised, placebo-controlled FREEDOMS study. Lancet Neurol. 2012;11:420-8.
16. Khatri BO, Pelletier J, Kappos L, Hartung HP, Comi G, Barkhof F, et al. Effect of prior treatment status and reasons for discontinuation on the efficacy and safety of fingolimod vs. interferon β 1a intramuscular: sub-group analyses of the trial assessing injectable interferon vs. fingolimod oral in relapsing-remitting multiple sclerosis (TRANSFORMS). Mult Scler Relat Disord. 2014;3:355-63.

96
Rev Mex Neuroci. 2022;23(3)
17. Derfuss T, Ontaneda D, Nicholas J, Meng X, Hawker K. Relapse rates in patients with multiple sclerosis treated with fingolimod: subgroup analy-ses of pooled data from three phase 3 trials. Mult Scler Relat Disord. 2016;8:124-30.
18. Cardenas R, Otero R, Montalban X, Tintoré M. Prevalencia e impacto de las comorbilidades en pacientes con esclerosis múltiple. Rev Neurol. 2020;71:151-8.
19. Sanford M. Fingolimod: a review of its use in relapsing-remitting multiple sclerosis. Drugs. 2014;74:1411-33.
20. Brinkmann V, Billich A, Baumruker T, Heining P, Schmouder R, Gordon F, et al. Fingolimod (FTY720): discovery and development of an oral drug to treat multiple sclerosis. Nat Rev Drug Discov. 2010;9:883-97.
21. Alcalá-Vicente C, Pérez-Miralles F, Gascón-Giménez F, Boscá-Blasco I, Navarré-Gimeno A, Coret Ferrer F. Tratamiento de la esclerosis múltiple remitente recurrente con fingolimod en la práctica clínica habitual. Rev Neurol. 2017;64:445-53.
22. Tedim Cruz V, Fonseca J. Efectos del fingolimod en el sistema nervioso central. Rev Neurol. 2014;59:121-8.
23. Cervera C. Infecciones y fingolimod. Rev Neurol. 2012;55:227-37.

97
the legacy of polio: 2 cases of post-polio syndrome and reviewKatherine A. Mafla-Ayub1,2*, Luisa F. Guzmán-Molano2, Gabriel A. Centanaro-Meza2, and Jairo A. Mejia-Mójica1,2
1Department of Neurology, Hospital Militar Central; 2Universidad Militar Nueva Granada. Bogotá, Colombia
Revista Mexicana de Neurociencia
rEViEW artiClE
abstract
Post-polio syndrome (PPS) is a rare neurological disorder that affects 20-40% of paralytic and non-paralytic polio survivors. It is estimated that about 15 million people worldwide are survivors of the polio infection that occurred during the 1940s and 1950s, until the vaccine was first introduced. Its main characteristic is the appearance of de novo muscle weakness or its increase and atrophy, accompanied by other symptoms such as fatigue, joint, bone or muscle pain, intolerance to cold, and bulbar symptoms (involvement of swallowing, speech and breathing). PPS usually affects performance in daily activities with a negative effect on patients’ quality of life. We present two cases with a diagnosis of PPS, with a current review of the lit-erature.
Keywords: Post-polio syndrome. New neuromuscular symptoms. Poliomyelitis. Polio. Electromyography.
El legado del polio: 2 casos de síndrome postpolio y revisión
resumen
El síndrome post-polio (SPP) es un trastorno neurológico raro que afecta del 20 al 40% de los sobrevivientes del polio paralítico y no paralítico. Se estima que alrededor de 15 millones de personas en todo el mundo son sobrevivientes de la infección por poliomielitis que ocurrió durante las décadas de 1940 y 1950, hasta que se introdujo por primera vez la vacu-na. Su característica principal es la aparición de debilidad muscular de novo o su aumento y atrofia, acompañado de otros síntomas como fatiga, dolor articular, óseo o muscular, intolerancia al frío y síntomas bulbares (compromiso de la deglución, el habla y la respiración). El SPP generalmente afecta el rendimiento en las actividades diarias con un efecto negativo en la calidad de vida de los pacientes. Presentamos dos casos con diagnóstico de síndrome postopolio, con una revisión actual de la literatura.
Palabras clave: Síndrome post-polio. Nuevos síntomas neuromusculares. Poliomielitis. Polio. Electromiografía.
Correspondence: *Katherine A. Mafla-Ayub
E-mail: [email protected]
Available online: 02-05-2022
Rev Mex Neuroci. 2022;23(3):97-104
www.revmexneurociencia.com
Date of reception: 06-11-2019
Date of acceptance: 03-03-2020
DOI: 10.24875/RMN.20000147
2604-6180 / © 2020 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

98
Rev Mex Neuroci. 2022;23(3)
introduction
Post-polio syndrome (PPS) is a neurological disorder affecting 20-40% of paralytic and nonparalytic polio survivors, characterized by a range of neuromuscular manifestations that occur years after initial infection with poliovirus1-3. The interval between acute infection and PPS is approximately 35 years, with a range vary-ing from 20 to 70 years4,5.
Its main characteristic is the appearance of de novo muscle weakness or its increase and atrophy, accom-panied by other symptoms such as fatigue, joint, bone or muscle pain, intolerance to cold, and bulbar symp-toms (involvement of swallowing, speech, and breath-ing). PPS usually affects performance in daily activities with a negative effect on patients’ quality of life3-5.
In this paper, we report two cases of PPS with differ-ent clinical manifestations and fatal outcomes. We con-sider of interest to our continent due to the large num-ber of patients with a history of paralytic and non-paralytic polio, in addition to the wide spectrum of differential diagnoses.
Case report 1
A 69-year-old female, natural from Nocaima (COL), housewife, was referred with a 5 years of progressive, asymmetric weakness that begins in the right foot, and then progresses to compromise the entire limb with lim-itation for walking until prostration in a wheelchair within 3 years, associated with joint and muscle pain in general management with non-steroidal anti-inflammatory drugs. She had history of paralytic poliomyelitis at age 2 years with shrinking of lower left limb as sequelae and con-trolled arterial hypertension. During school she had par-ticipated in all activities without difficulty. Neurological examination shows normal mental status, loss of cephal-ic support, bilateral interosseous atrophy in both hands, predominantly in the right and both quadriceps, quadri-paresis with distal predominance, and hypoactive reflex-es in lower limbs. Sensory examination was normal.
Additional studies were carried out considering alter-native diagnoses; immunological, infectious, and/or paraneoplastic etiologies were ruled out. Spinal mag-netic resonance imaging (MRI) showed degenerative changes without medullary lesions. The neuro-conduc-tion and electromyography (EMG) show signs of acute denervation with very large, long-duration, and polypha-sic motor unit action potentials (MUAPs) (Figs. 1 and 2). She received 1 cycle of human Immunoglobulin G ac-companied by a rehabilitation plan, with stabilization of symptoms for 1 year. Subsequently, she presented
increased weakness with greater axial, cephalic, and upper limb involvement. During the past 6 months de-pendent on supplemental oxygen per nasal cannula. Finally, she presented acute ventilatory deterioration and died of ventilatory failure.
Case report 2
A 54-year-old male patient, from Bogota (COL), me-chanical engineer, currently retired, was referred with
Figure 1. Neuropathic PUM in right lateral vastus.
Figure 2. Positive wave in right L4 Paraspinalis.

99
K.A. Mafla-Ayub et al.: The legacy of polio
5 years of evolution of progressive asymmetric weakness that begins in upper limbs, of distal predom-inance, and then progresses to lower limbs of ascend-ing characteristics, until limited for standing and walk-ing, with subsequent appearance of hypophonia and solids dysphagia. He had history of paralytic polio at 1 year old with shrinking of the lower right limb and foot drop as a sequel with surgical correction during child-hood (Fig. 3), moderate sleep apnea/hypopnea syn-drome, heart failure (Fev1 50%), atrial fibrillation, pul-monary hypertension with public-safety answering point 50 mmHg, recurrent deep vein thrombosis, and heavy ex-smoker. Physical examination with evidence of central obesity, grade II edema in lower limbs, and skin changes secondary to heart failure (Fig. 3). Neu-rological examination showed hypomimia, nasal voice, hypotrophy, and generalized hypotonia, quadriparesis of distal predominance, reflexes were absent and steppe gait. Studies were performed in search of alter-native diagnoses ruling out immunological, infectious, and/or paraneoplastic etiologies. Additional screening for negative Pompe was done. Biopsy of gastrocnemius muscle was normal and neurophysiological studies with acute denervation signs, with very large, long-duration, polyphasic MUAPs, and the presence of pseudomyo-tonic discharges (Figs. 4 and 5). He received 5 cycles of human immunoglobulin G as a treatment, accompa-nied by a rehabilitation plan with clinical stabilization of symptoms. One year ago, he began with multifactorial respiratory insufficiency and subglottic stenosis with two tracheal dilation attempts plus stent placement, post-resuscitation state, and requirement of prolonged stay in intensive care unit for more than 4 months, with the need for tracheostomy and gastrostomy placement. Now, he remains hospitalized.
discussion
Both patients meet the criteria for PPS. The patients present a chronic weakness of asymmetric onset that progresses to compromise mobility until prostration in a wheelchair and in case 2 associated with hypophonia and dysphagia for solids. Immunological, infectious, and/or paraneoplastic etiologies were ruled out with additional Pompe negative screening, and also normal muscle biopsy. EMG shows signs of acute denervation with neurogenic MUAPs and the presence of pseudo-myotonic discharges. Despite the immunomodulatory therapy received, the weakness progressed to compro-mise respiratory function, and in the first case it ended with a fatal outcome.
Figure 3. Shrinking and atrophy of the lower right limb and foot drop as a sequel with surgical correction during childhood in patient with PPS and heart failure.
Natural history of disease in the world
It is estimated that about 15 million people worldwide are survivors of the Polio infection that occurred during the 1940s and 1950s, until the vaccine was first intro-duced6,7. Since then, the number of people affected has dropped by nearly 99%8. However, polio remains en-demic in two countries (Afghanistan and Pakistan) with 74 cases reported in 2015 and according to global polio surveillance data as of March 2016, five wild poliovirus cases were reported in Pakistan and one in Afghanistan8,9.
The exact incidence and prevalence of PPS are un-known, for 2004 were estimated 250,000 patients with PPS in Europe and 20 million worldwide. Ragonese showed a prevalence of PPS of 31% in 2005 with pre-dominance in women10,11.

100
Rev Mex Neuroci. 2022;23(3)
More than 80% of people who contracted polio as children develop new or increased disability decades after initial infection, considered late effects of polio12.
Physiopathology
The etiology and pathogenesis of PPS is unknown. It has been hypothesized that the new weakness appears to be related to degeneration of individual nerve termi-nals in motor units. The overuse of these motor units for years generates an overload that eventually leads them to lose their ability to respond, producing a slow
deterioration which leads to a reduction in muscle strength13,14.
It is probably an effect of motor neuron damage during acute poliovirus infection that leads to overload-ing and degeneration of the remaining motor neurons in the frontal horns of the spinal column15,16.
More than 50% death must occur in the anterior horn neuron population before weakness can be detected clinically. EMG studies suggest that many of the clini-cally unaffected muscles were sub-clinically involved during the acute episode of the disease7. This hypoth-esis explains why PPS occurs after so many years and has a slow progressive course17.
Sharief et al. demonstrated the presence of immuno-globulin M antibodies against poliovirus and cells sen-sitized to poliovirus in the cerebrospinal fluid (CSF) of patients with PPS. However, no conclusive evidence of CSF poliovirus has been found in such patients18.
In addition, histopathological damage to the reticular activation system has been demonstrated in patients with PPS, which is probably related to cognitive perfor-mance impairment and chronic fatigue syndrome19.
Risk factors
No strong associations have been found between risk factors and PPS; however, some risk factors have been described such as age, genetics, time since acute polio, stress, and inactive lifestyle20. Among those that stand out are the female gender and the severe course of the initial infection15.
Klingman et al. noted that patients who developed PPS had a history of greater generalized paralysis during acute illness or greater lower extremity involvement, but also those who had greater functional recovery. This indicated that the degree of functional recovery could be a predictor for skin perfusion pressure (SPP)7,21.
Several viruses are known to cause chromosomal abnormalities in circulating lymphocytes during infec-tions in humans (such as measles, chickenpox, mumps, and hepatitis viruses), such as chromosomal breakage. However, these chromosomal abnormalities due to di-rect or indirect effects as well as the immediate or delayed effects of the poliovirus have not been fully understood22. Bhattacharya et al. reported a significant increase in chromosomal aberrations in patients with PPS than in controls, showing a delayed effect of the poliovirus in humans22.
The poliovirus has a common receptor known as a poliovirus receptor (PVR) that belongs to the CD155
Figure 5. Pseudomyotonic discharge into right rectus femoris muscle.
Figure 4. Pseudomyotonic discharge into right rectus femoris muscle.

101
K.A. Mafla-Ayub et al.: The legacy of polio
immunoglobulin superfamily, a poliovirus cell surface receptor found on chromosome 19q1323.
Polymorphism of the PVR gene in patients with pro-gressive muscle atrophy was reported by Saunderson et al. in 200424. Later, it was reported that Ala67Thr polymorphism in the PVR gene was a possible risk factor for the etiology of polio25. Single nucleotide het-erozygous polymorphism (Ala67Thr) in the CD155 gene has been reported in healthy populations (6.8-8.5%) and the incidence has been shown to be significantly higher in patients with polio paresis (13.3%) and pro-gressive muscle atrophy (20%)24,25.
Clinical course
PPS was described 15 years after the first polio out-break, when new neuromuscular symptoms were re-ported. Affecting 20-75% of survivors of acute infection, 15 years or more after acute illness15,26-28.
The new symptoms are characterized by muscle weakness, generalized atrophy and fatigue, pain at rest or during activities and intolerance to cold, and bulbar symptoms (compromised swallowing, speech, and breathing)3-5,29.
Joint and muscle pain is present in 70% of patients with PPS. Muscle atrophy and intolerance to cold tem-peratures are rarer and about 50% are seen30. Apnea and dysphagia are observed in 30% of patients31.
Symptoms may be seen in clinically affected and unaffected muscles during primary polio infection. Post-polio progressive muscle atrophy is the term des-ignated to describe the clinical picture, and muscle weakness progression is usually slow and lasts for many years. About 90% of patients with PPS also com-plain of general fatigue, concentration problems, and mood swings32,33.
There are two aspects of fatigue related to PPS, a central fatigue involving central nervous system in-volvement due to SRA involvement leading to mental fatigue related to difficulties in cognitive functions, such as planning and inhibition tasks, concentration prob-lems, and mental sustainability. Moreover, the periph-eral fatigue that mainly derives from the peripheral sys-tem, that is, the compromise of the motor units34.
The new symptomatology may further limit the ability to perform daily activities, especially those related to standing, walking, and climbing stairs, which increases the risk of falls35. This, in turn, can negatively impact the quality of life of patients with PPS36. In addition, psychological factors such as feelings of shame or dis-comfort, fear of injury, lack of motivation, and energy,
along with environmental factors are perceived as bar-riers to physical activity and participation12,37,38.
Respiratory involvement
The leading cause of death during acute polio is respi-ratory disorder. Although respiratory failure is often caused by weak breathing muscles or bulbar dysfunction, it is also related to the high incidence of secondary com-plications such as scoliosis, obesity, and sleep breathing disorders (sleep apnea) in individuals with PPS39-41.
According to pathophysiology, polio survivors suffer mainly from restrictive respiratory deterioration. At present, approximately 27-36% of patients with PPS suffer from respiratory failure42. The main respiratory conditions have been described as dyspnea, fatigue, or sleep-related respiratory disorders, increasing the risk of morbidity and mortality43.
The restrictive defect in ventilatory function is second-ary to the weakness of the respiratory muscles, which are unable to generate the intrathoracic vacuum neces-sary for complete inspiration or the positive pressure necessary for complete exhalation. Generating reduc-tions in Total Lung Capacity below the 5th percentile of predicted value, vital capacity, and maximum voluntary ventilation44. In an 11-year prospective study of 31 pa-tients with PPS, more than half of patients with cardio-vascular < 50% developed the need for ventilation or suffered a death related to respiratory failure45.
Halstead and Rossi46 observed that in patients with PPS, altered lung function was associated with age of onset (progression of 10 years or more), need for mechanical ventilation during the acute phase of the disease, quadriparesis, and time of exposure to the dis-ease. In another study, Lane et al.47 described an asso-ciation between respiratory dysfunction and the pres-ence of kyphoscoliosis or diaphragmatic paralysis.
Sleep disturbances
Sleep disorders are common in patients with PPS48. Their insidious nature can make it difficult for patients, family members, and caregivers to recognize these disorders49-51.
Among the sleep disorders associated with PPS, peri-odic leg movements (PLM), hypopnea, and especially obstructive sleep apnea (OSA) are the most common52.
A prospective study of 60 patients with PPS showed a prevalence of sleep disturbance of 78.3%, with sleep efficiency decreasing from 67.4% (patients with OSA, using non-invasive ventilation) to 69.5% (patients not

102
Rev Mex Neuroci. 2022;23(3)
using non-invasive ventilation). This inefficiency was related to more than 10 awakenings per hour, disor-dered breathing, PLM, changes in the different stages of sleep and muscle and/or joint pain51,53.
Diagnostic
Electrodiagnostic studies play an important role in the diagnostic process of PPS. Although they cannot differ-entiate patients with PPS from those with asymptomatic post-polio, they are important for excluding other neu-romuscular diseases such as amyotrophic lateral scle-rosis, radiculopathy, polyneuropathy, myasthenia gravis, radiculopathies, neuropathies, and myopathies54,55.
Blood test results are generally normal, except for elevated serum creatine kinase (CPK) levels in some patients, which may suggest overuse and damage to muscle fibers56,57.
Imaging studies (e.g., computed tomography scan and MRI) may be needed to exclude spinal conditions such as spondylosis, spinal stenosis, and neoplasms7.
Diagnostic criteria
The current diagnostic criteria for PPS were first de-scribed by Mulder et al. in 197258. These criteria are:1. Previous episode of polio with residual loss of motor
neurons.2. A period of at least 15 years of neurological and
functional stability after recovery from acute illness.3. The gradual or, rarely, abrupt onset of new weakness
or abnormal muscle fatigue and generalized fatigue.
4. The exclusion of other conditions that could cause similar manifestations.In the differential diagnosis, it is important to exclude
orthopedic and neurological diseases similar to PPS such as amyotrophic lateral sclerosis, cervical spondy-losis, tumors of the cervical and thoracic spine, and other causes of chronic fatigue syndrome, myasthenia gravis, myopathies and cardiac diseases, hematologi-cal, endocrine, cancer, chronic systemic infections, among others59,60.
Electromyography findings
Symptoms of PPS should be evaluated by EMG, Single Fiber EMG (SFEMG), and macro-EMG. Muscle fatigue can be caused by neuromuscular junction trans-mission defects58. Muscle weakness and atrophy may be associated with distal degeneration of motor units,
resulting in irreversible denervation of muscle fiber58. The most characteristic finding of EMG in SPP is the presence of potential giants; these units are greater than 8 mV and occur as a result of chronic denervation and reinnervation by shoots of the same motor unit, generating motor units of great amplitude and area61.
In Chang’s study, 31 patients with PPS were diag-nosed with the use of EMG. In 41 (78.8%) of the 52 muscles, the duration of the motor unit increased. Am-plitudes of larger motor units were observed in 43 (82.7%) of the 52 muscles. Polyphasia of more than 20% of the affected muscles was found and sponta-neous activities such as fibrillation and positive acute waves were observed in approximately 30% of the muscles examined in this study. Fasciculations oc-curred in 26.9% of patients with PPS62.
At present, surface EMG is considered as a potential alternative to needle EMG or nerve conduction studies when neuromuscular disorders are investigated63. It has an advantage in the detection of large non-invasive signals, it provides additional information in the study of fatigue in patients with PPS64.
SFEMG has become the most sensitive method for di-agnosing neuromuscular transmission disorders, even subclinical alterations in transmission can be detected with the use of this method65. The SFEMG can provide infor-mation on the reorganization of the motor unit with fiber density, and increased instability is related to mild to se-vere disturbances recognized by impulse blockages64,65.
These findings in the SFEMG confirm the theory that PPS is the result of degradation of nerve endings that influence the condition of neuromuscular unions61.
Neuroconduction findings
Electroneurography is usually normal in patients with PPS. Hachisuka studied 43 polio survivors and 20 healthy controls with studies of motor nerve conduction of the median and tibial nerves. They found a signifi-cant increase in abnormally stereotyped F-waves and a reduction in F-wave persistence in both nerves in polio patients compared to the control group. They conclude that the F wave reveals the electrophysiolog-ical characteristics of the anterior horn cells in polio survivors and reflects the loss of their motor units58.
Treatment
There is no cure for PPS. The main objective of treat-ment is to improve the quality of life of patients through rehabilitation and intervention by the orthopedic group

103
K.A. Mafla-Ayub et al.: The legacy of polio
of the affected limb. Attempts have been made to treat with pyridostigmine and amantadine, but their efficacy in this disease has not been demonstrated66-68.
Attempts are also made with intravenous immunoglobu-lins to achieve stabilization of symptoms, with no studies reporting confirmatory results yet. Assisted ventilation may be necessary in patients with respiratory symptoms32.
Finally, L-citrulline is known to modify the synthesis of muscle metabolism by increasing nitric oxide levels and increasing protein synthesis. Schmidt et al. are conducting a randomized, placebo-controlled, and dou-ble-blind trial aimed at demonstrating that L-citrulline positively influences muscle function and increases muscle energy production in patients with SPP69.
Conclusion
PPS is a rare and disabling chronic neurological con-dition that affects millions of people around the world with unknown pathophysiology and no evidence of spe-cific treatment to date. Controversial treatments such as immunomodulatory therapy are described, where the main objective is to improve patients’ quality of life. Weakness associated with history of paralytic and no paralytic polio now is seen most often in the EMG lab-oratory. The neuro-conduction and EMG test are man-datory to exclude a superimposed process, related to entrapment neuropathy, radiculopathy, myopathy, and or motor neuron disease.
Funding
None of the authors report a source of funding for this work.
Conflicts of interest
None of the authors has any conflicts of interest to disclose.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
right to privacy and informed consent. The au-thors have obtained the written informed consent of the
patients or subjects mentioned in the article. The cor-responding author is in possession of this document.
references 1. Garip Y, Eser F, Bodur H. Health related quality of life in Turkish polio
survivors: impact of post-polio on the health related quality of life in terms of functional status, severity of pain, fatigue, and social, and emotional functioning. Rev Bras Reumatol Engl Ed. 2017;57:1-7.
2. Radha S. The genetics of post-polio syndrome-much to be unraveled? Indian J Med Res. 2016;144:9-10.
3. Silver JK, Aiello DD. What internists need to know about postpolio syn-drome. Cleve Clin J Med. 2002;69:704-6, 709-12.
4. Khan F. Rehabilitation for postpolio sequelae. Aust Fam Physician. 2004;33:621-4.
5. Pascuzzi RM. Poliomyelitis and the post-polio syndrome. Semin Neurol. 1992;12:193-9.
6. Pastuszak Ż, Stępień A, Tomczykiewicz K. Post-polio syndrome. Cases report and review of literatura. Neurol Neurochir Pol. 2017;51:140-5.
7. Lin KH, Lim YW. Post-poliomyelitis syndrome: case report and review of the literature. Ann Acad Med Singapore. 2005;34:447-9.
8. Snider CJ, Diop OM, Burns CC. Surveillance systems to track progress toward polio eradication-worldwide, 2014-2015. MMWR Morb Mortal Wkly Rep. 2016;65:346-51.
9. WHO. Poliomyelitis. WHO. Available from: http://www.who.int/csr/don/13-June-2017-polio-drc/en. [Last accessed on 2017 Apr 24].
10. Bosch X. Post-polio syndrome recognised by European parliament. Lan-cet Neurol. 2004;3:4-5.
11. Ragonese P, Fierro B, Salemi G, Randisi G, Buffa D, D’Amelio M, et al. Prevalence and risk factors of post-polio syndrome in a cohort of polio survivors. J Neurol Sci. 2005;236:31-5.
12. Hammarlund CS, Lexell J, Brogårdh C. Perceived consequences of ageing with late effects of polio and strategies for managing daily life: a qualitative study. BMC Geriatrics. 2017;17:179.
13. Dalakas MC. Pathogenetic mechanisms of post-polio syndrome: morpho-logical, electrophysiological, virological, and immunological correlations. Ann N Y Acad Sci. 1995;753:167-85.
14. Sandberg A, Stålberg E. Changes in macro electromyography over time in patients with a history of polio: a comparison of 2 muscles. Arch Phys Med Rehabil. 2004;85:1174-82.
15. Ramlow J, Alexander M, LaPorte R. Epidemiology of the post-polio syn-drome. Am J Epidemiol. 1992;136:769-86.
16. Halstead L. Assessment and differential diagnosis for post-polio syndro-me. Orthopedics. 1991;14:1209-17.
17. Koopman FS, Beelen A, Gilhus NE. Treatment for postpolio syndrome. Cochrane Database Syst Rev. 2015;5:CD007818.
18. Sharief MK, Hentges R, Ciardi M. Intrathecal immune response in pa-tients with the post-polio syndrome. N Engl J Med. 1991;325:749-55.
19. Bodian D. Poliomyelitis: neuropathologic observations in relation to motor symptoms. J Am Med Assoc. 1947;134:1148-54.
20. Gonzalez H, Olsson T, Borg K. Management of postpolio syndrome. Lancet Neurol. 2010;96:634-42.
21. Klingman J, Chui H, Corgiat M, Perry J. Functional recovery. A major risk factor for the development of postpoliomyelitis muscular atrophy. Arch Neurol. 1988;45:645-7.
22. Bhattacharya SK, Saraswathy R, Sivakumar E. Genotoxic assessment in peripheral blood lymphocytes of post-polio individuals using sister chro-matid exchange analysis and micronucleus assay. Hum Exp Toxicol. 2011;30:636-48.
23. Koike S, Horie H, Ise I, Okitsu A, Yoshida M, Iizuka N, et al. The polio virus receptor protein is produced both as membrane-bound and secreted forms. EMBO J. 1990;10:3217-24.
24. Saunderson R, Yu B, Trent RJ. A polymorphism in the poliovirus recep-tor gene differs in motor neuron disease. Neuroreport. 2004;15:3836.
25. Kindberg E, Ax C, Fiore L. Ala67Thr mutation in the poliovirus receptor CD155 is a potential risk factor for vaccine and wild-type paralytic po-liomyelitis. J Med Virol. 2009;81:933-6.
26. Baj A, Colombo M, Headley JL, McFarlane JR, Liethof MA, Toniolo A. Post-poliomyelitis syndrome as a possible viral disease. Int J Infect Dis. 2015;35:107-16.
27. Dalakas MC. The post-polio syndrome as an evolved clinical entity. Definition and clinical description. Ann N Y Acad Sci. 1995;753:68-80.
28. Rekand T, Korv J, Farbu E, Roose M, Gilhus NE, Langeland N, et al. Long term outcome after poliomyelitis in different health and social con-ditions. J Epidemiol Community Health. 2003;575:368-72.
29. McNalley TE, Yorkston KM, Jensen MP, Truitt AR, Schomer KG, Baylor C, et al. Review of secondary health conditions on postpolio syn-drome. Am J Phys Med Rehabil. 2015;94:139-45.
30. Jubelt B, Lipton H. Enterovirus Infections. Vol. 56. Netherlands: Elsevier Science; 1989. p. 307-47.

104
Rev Mex Neuroci. 2022;23(3)
31. Jubelt B, Cashman N. Neurological manifestations of the post-polio syn-drome. Crit Rev Neurobiol. 1987;3:199-20.
32. Kalpakjian C, Quint E, Toussaint L. Menopause and post-polio symptoms as predictors of subjective sleep disturbance in poliomyelitis survivors. Climacteric. 2007;10:51-62.
33. Jubelt B, Drucket J. Poliomyelitis and the post-polio syndrome in motor disorders. Motor Disord. 1999;34:381-95.
34. Östlund G, Wahlin Å, Sunnerhagen KS. Post polio syndrome: fatigued patients a specific subgroup? J Rehabil Med. 2011;43:39-45.
35. Brogårdh C, Lexell J. Falls, fear of falling, self-reported impairments, and walking limitations in persons with late effects of polio. PM R. 2014;6:900-7.
36. Lexell J, Brogårdh C. Life satisfaction and self-reported impairments in persons with late effects of polio. Ann Phys Rehabil Med. 2012;55:577-89.
37. Buffart LM, Westendorp T, van den Berg-Emons RJ, Stam HJ, Roebroeck ME. Perceived barriers to and facilitators of physical activity in young adults with childhood-onset physical disabilities. J Rehabil Med. 2009;41:881-5.
38. Thorén-Jönsson AL, Willén C, Sunnerhagen KS. Changes in ability and use of assistive devices in everyday life: a 4-year follow-up study in people with late effects of polio. Acta Neurol Scand. 2009;120:324-30.
39. Han SJ, Lim JY, Suh JH. Obesity and pulmonary function in polio survi-vors. Ann Rehabil Med. 2015;396:888-96.
40. Bach JR, Tilton M. Pulmonary dysfunction and its management in post-polio patients. Neurorehabilitation. 1997;82:139-53.
41. Shoseyov D, Cohen-Kaufman T, Schwartz I, Portnoy S. Comparison of activity and fatigue of the respiratory muscles and pulmonary characte-ristics between post-polio patients and controls: a pilot study. PLoS One. 2017;12:e0182036.
42. Berlly MH, Strauser WW, Hall KM. Fatigue in postpolio syndrome. Arch Phys Med Rehabil. 1991;722:115-8.
43. Morales IJ, Gay PC. Respiratory complications of poliomyelitis and mul-tiple sclerosis. Semin Respir Crit Care Med. 2002;233:267-74.
44. Lira CA, Minozzo FC, Sousa BS, Vancini RL, Andrade MS, Quadros AA, et al. Lung function in post-poliomyelitis syndrome: a cross-sectional study. J Bras Pneumol. 2013;39:455-60.
45. Midgren B. Lung function and clinical outcome in postpolio patients: a prospective cohort study during 11 years. Eur Respir J. 1997;101:146-9.
46. Halstead LS, Rossi CD. New problems in old polio patients: results of a survey of 539 polio survivors. Orthopedics. 1985;8:845-50.
47. Lane DJ, Hazleman B, Nichols PJ. Late onset respiratory failure in pa-tients with previous poliomyelitis. Q J Med. 1974;43:551-68.
48. Trojan DA, Arnold DL, Shapiro S, Bar-Or A, Robinson A, Le Cruguel JP, et al. Fatigue in post-poliomyelitis syndrome: association with disease-re-lated, behavioral, and psychosocial factors. PM R. 2009;1:442-9.
49. Fischer JR, Headley J. Post-polio breathing and sleep problems revisited. Post-Polio Health. 2004;20:5-7.
50. Garip Y, Eser F, Bodur H, Baskan B, Sivas F, Yilmaz O. Health related quality of life in Turkish polio survivors: impact of post-polio on the health related quality of life in terms of functional status, severity of pain, fatigue, and social, and emotional functioning. Rev Bras Reumatol. 2015;57(1):1-7.
51. Orsini M, Lopes AJ, Guimarães FS, Freitas MR, Nascimento OJ, de Sant’ Anna M Jr., et al. Currents issues in cardiorespiratory care of patients with post-polio syndrome. Arq Neuropsiquiatria. 2016;74:574-9.
52. Silva TM, Moreira GA, Quadros AA, Pradella-Hallinan M, Tufik S, Olivei-ra AS. Analysis of sleep characteristics in post-polio syndrome patients. Arq Neuropsiquiatr. 2010;68:535-40.
53. Siegel H, McCutchen C, Dalakas MC, Freeman A, Graham B, Alling D, et al. Physiologic events initiating REM sleep in patients with the postpo-lio syndrome. Neurology. 1999;52:516-22.
54. Mulder DW, Rosenbaum RA, Layton DD Jr. Late progression of poliomyelitis or forme fruste amyotrophic lateral sclerosis? Mayo Clin Proc. 1972;47:756-61.
55. Rowland L, Shneider N. Amyotrophic lateral sclerosis. N Engl J Med. 2001;344:1688-700.
56. Stark R, Kennard C, Swash M. Hand wasting in spondylotic high cord compression: an electromyographic study. Ann Neurol. 1981;9:58-62.
57. Cashman NR, Maselli R, Wollmann RL, Roos R, Simon R, Antel JP. Late denervation in patients with antecedent paralytic poliomyelitis. N Engl J Med. 1987;317:7-12.
58. Trojan D, Gendron D, Cashman N. Electrophysiology and electrodiagno-sis of the post-polio motor unit. Orthopedics. 1991;14:1353-61.
59. Jones DA, Newham DJ, Round JM, Tolfree SE. Experimental human muscle damage: morphological changes in relation to other indices of damage. J Physiol. 1986;375:435-48.
60. Newham DJ, Jones DA, Edwards RH. Plasma creatine kinase changes after eccentric and concentric contractions. Muscle Nerve. 1986;9:59-63.
61. Feinberg J. EMG: myths and facts. HSS J. 2006;2:19-21. 62. Chang C, Huangpinal S. Varied clinical patterns, physical activities, mus-
cle enzymes, electromyographic and histologic findings in patients with post-polio syndrome in Taiwan. Spinal Cord. 2001;39:526-31.
63. Meekins GD, So Y, Quan D. American association of neuromuscular and electrodiagnostic medicine evidenced-based review: use of surface elec-tromyography in the diagnosis and study of neuromuscular disorders. Muscle Nerve. 2008;384:1219-24.
64. Drost G, Stegeman DF, Schillings ML, Horemans HL, Janssen HM, Massa M, et al. Motor unit characteristics in healthy subjects and those with postpoliomyelitis syndrome: a high-density surface EMG study. Mus-cle Nerve. 2004;303:269-76.
65. Nandedkar S, Stalberg E. Quantitative measurements and analysis in electrodiagnostic studies: present and future. Future Neurol. 2008; 3:745-64.
66. Horemans HL, Nollet F, Beelen A, Drost G, Stegeman DF, Zwarts MJ, et al. Pyridostigmine in postpolio syndrome: no decline in fatigue and limited functional improvement. J Neurol Neurosurg Psychiatry. 2003; 74:1655-61.
67. Farbu E. Update on current and emerging treatment options for post-po-lio syndrome. Ther Clin Risk Manage. 2010;21:307-13.
68. Stanghelle J, Festvag L. Postpolio syndrome: a 5 year follow-up. Spinal Cord. 1997;35:5038.
69. Schmidt S, Gocheva V, Zumbrunn T, Rubino-Nacht D, Bonati U, Fischer D, et al. Treatment with L-citrulline in patients with post-polio syndrome: study protocol for a single-center, randomised, placebo-con-trolled, double-blind trial. Trials. 2017;18:116.

105
Systematic review and effect of conscious breathing on adult attention and learning taskViviana Chavez1, Lenin Ochoa-de-la-Paz2, and Jorge Parodi1*1Laboratorio Biosocial Tonalli ltda, Tiburcio Saavedra, Temuco, Chile; 2Department of Biochemistry, Faculty of Medicine, Universidad Nacional Autónoma de México, Mexico City, Mexico
Revista Mexicana de Neurociencia
rEViEW artiClE
abstract
In recent years, the control of physiological processes has been strengthened, which show metabolic changes that can generate effects at a neuronal level. Our objective is to review what has been described as conscious breathing theory and how this can affect cognitive tasks, which have been described as very affected in adults and which reduce with age. How-ever, we have begun to understand a new phenomenon of andragogic learning, which indicates that the task of learning must be understood differently, and that attention is something that must be understood as something that does not decrease with age but changes. It also seems that conscious breathing tasks can improve this type of task and that it can be bene-ficial. What has been published suggests that breathing, or at least conscious breathing exercise, improves certain cellular and neuronal capacities and that this can lead to real changes in cognitive tasks in adults.
Keywords: Meditation. Learning. Breathing. Aging.
Revisión sistemática, efecto de la respiración consciente en la atención de los adultos y tarea de aprendizaje
resumen
En los últimos años se ha potenciado el control de los procesos fisiológicos, que muestran cambios metabólicos que pueden generar efectos a nivel neuronal. Nuestro objetivo es revisar lo que se ha descrito como teoría de la respiración consciente y cómo ésta puede afectar a las tareas cognitivas, que se han descrito como muy afectadas en los adultos y que se redu-cen con la edad. Sin embargo, hemos empezado a comprender un nuevo fenómeno de aprendizaje andragógico, que indi-ca que la tarea de aprendizaje debe entenderse de forma diferente, y que la atención es algo que debe entenderse como algo que no disminuye con la edad, sino que cambia. También parece que las tareas de respiración consciente pueden mejorar este tipo de tareas y que pueden ser beneficiosas. Lo que se ha publicado sugiere que la respiración, o al menos el ejercicio de respiración consciente, mejora ciertas capacidades celulares y neuronales y que esto puede llevar a cambios reales en las tareas cognitivas en los adultos.
Palabras clave: Meditación. Aprendizaje. Respiración. Envejecimiento.
Correspondence: *Jorge Parodi
E-mail: [email protected]
Available online: 02-05-2022
Rev Mex Neuroci. 2022;23(3):105-110
www.revmexneurociencia.com
Date of reception: 02-04-2021
Date of acceptance: 03-05-2021
DOI: 10.24875/RMN.21000029
2604-6180 / © 2021 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

106
Rev Mex Neuroci. 2022;23(3)
General ideas
For several years, attempts have been made to rec-oncile meditation tasks and cognitive function. However, it has been difficult to reconcile esoteric definitions with the real scientific background; we can observe in this type of exercise 1. Luckily, and driven by various re-searchers, more pragmatic study methods have recently been applied to this type of activity and we can indicate a relation between physiological balance states, second-ary to conscious breathing activities, and beneficial ef-fects with cognitive tasks2. This review aims to present psychological, physiological, and neurophysiological ev-idence of the advantage of conscious breathing practice on cognitive tasks, particularly learning in the adults.
the task of learning and the andragogy
Defining this activity is complex, with various view-points according to the professional area which studies it. These are all variables to respect, but I must agree on one to define it. A decision, we would like to con-struct, is that learning will be any stimulus generating a behavioral change which leads to survival3. These ideas have also been reinforced by the introduction of the concept of synaptic plasticity4 and have been re-viewed as an important and fundamental phenomenon for the task of learning5. Thus, this neurophysiological phenomenon will be a focus for observing adults when we consider the task of conscious breathing.
The history of definitions of education is long. Within it, pedagogy or teaching has been installed as educa-tion for children perpetuated in various models6. How-ever, the concept of andragogy arose with strength in the 1960s, as a new identity for who was to be taught7. This model was taken as teaching adults, but neurobi-ological concepts let us redefine it as the process of educating a mature, full, and conscious brain, some-thing which arises once this organ is already mature, and the ego emerges8. Learning in adults, andragogy recognizes the importance of tutor participation as an extrinsic motivator7, which concurs with support in guid-ed information searches9. It defines learning in context, which suggests that continuous learning exists, where in any moment; we can acquire new skills10.
attention as a complex task, description on adults
Within the task of learning, attention is a phenome-non to be studied11 as we can define this concept in
neurosciences. We can use the concept that attention is a form of feedback, of self-stimulating learning pro-cesses12. Thus, we can think of it as a part of learning and deem it important to develop to achieve better learning task performance13.
Attention is a fundamental axis of the teaching-learn-ing process, and in this way, we will consider it to be selective14. Furthermore, implicit learning modulates the assignation of attention in the first stages of the perceptive processing of learning and will become im-plicit only when attending to the relevant predictive in-formation15. The information is redundant because its subjects can, in principle, select the right answer based on only one of these signs and ignore the others, so that consequently this signal is learned and the others are not14. This could basically be solved in adult indi-viduals and is achieved in the selection of tasks which are known and to a lesser degree with new tasks. Sub-jects can also learn about stimuli which do not reach consciousness, particularly when they are near the perception threshold and are combined with a reward16, a topic which becomes relevant in earlier stages of life. Attention, environment, and reward jointly determine how we learn and are some of the factors determining neuronal plasticity17, which makes it even more import-ant to investigate new learning environments and their determining factors, such as attentive breathing.
imaging changes in learning tasks
There is apparently an idea that learning new tasks become harder with aging, especially those tasks de-pending on the hippocampus and structures related to the medial temporal lobe to form episodic or declarative memories. It has even been suggested that age-related cognitive deficits begin at age 2018. Various studies suggest that not only are there changes in cerebral microstructure and volume manifesting in cognitive function shifts19 but also metabolic changes20. De-creased cerebral mass and diminished cognitive func-tion are often seen with advanced age20. Therefore, it is important to distinguish between metabolic changes in the brain caused by healthy aging and pathological states21.
Conscious breathing, physiology and molecular changes
The term meditation covers a wide range of mental training practices varying between cultures and tradi-tions. They go from techniques for promoting physical

107
V. Chavez et al.: Breathing and learning task
health, relaxation, or improved concentration, develop-ing an improved sensation of well-being and cultivating altruistic behavior22. Meditation is generally associated with a concurrent state of greater waking conscious-ness and lower metabolic activity, leading to better physical health, psychological balance, and emotional stability23. Mindfulness meditation is a promising basis for interventions, with particular potential relevance for psychiatric comorbidity. The successes and challenges of researching mindfulness meditation are based on the interactions between contemplative traditions and clin-ical psychological science24. The conclusions of these studies determined that attention is the fundamental process strengthened in these interventions25. To un-derstand this, we can investigate that evidence exists supporting mindfulness-based cognitive therapy for treating depression26 and obsessive-compulsive disor-der. At present, there are studies about its efficacy on chronic and terminal diseases. This marks it as effec-tive technique which can help cultivate positive mental health in normal individuals27 and be an effective in-strument regarding preventive medicine and public health.
Studies suggest that long-term meditation practice can reduce stress reactions, a fall in reduction-oxida-tion metabolic conditions and could be therapeutically beneficial in chronic inflammatory conditions character-ized by neurogenic inflammation28. The cumulative ef-fects of regular mediation practice may, in the long run, help improve the physiochemical conditions where syn-apses occur and could represent a useful preventive strategy for age-related chronic diseases29. Even so, there is still much to study given the technical limita-tions and molecular changes which mindfulness prac-tice and conscious breathing could induce, but we may directly infer that metabolic changes improve synaptic tasks and that this improves the task of learning. Med-itation and conscious breathing measurements suggest that this metabolic change occurs and that we can infer cognitive improvement.
Conscious breathing and cognitive effects
Studies suggest that mental training, meditation, and other similar tasks may be used as tools in neurosci-entific studies of the brain and cognitive plasticity30. The brain changes as a function of experience or learn-ing, dependent on stimuli, creating changes in neuronal pathways,31 and deeper molecular remodeling giving evidence of the phenomenon of metaplasticity32. There-fore, some authors mention in their publications that
some cognitive processes and executive functions can be improved with meditation, secondary to synaptic changes. A study was done on adolescents where the participants (N = 198 adolescents) were randomly as-signed to mindfulness meditation, hatha yoga, or a control group. The mindfulness meditation group par-ticipants showed significant improvements in their working memory, unlike the control and hatha yoga groups33. Other short-term meditation studies show that meditation improves executive functions, including attention and working memory processes. However, they argue that it is unclear how much contextual ef-fects contribute to these improvements34, although we can suggest metabolic changes related to improved synaptic function.
Consequently, meditation training improves perfor-mance on tasks evaluating attention, control, and mem-ory function35. To explain these effects, current theo-retical models emphasize attention as the central component influenced by meditation36. However, can it impact adult learning enough to be used within teach-ing-learning processes? Apparently, studies confirm that these individuals improve performance related to sequence repetition, allowing for the implementation of response-based planning, and generating benefits from learning them37.
There is evidence suggesting positive physical and psychological clinical results from meditation. These studies show relief for clinical disorders, including anx-iety and depression38, eating disorders, addictions and disorders caused by psychoactive drug use39, stress normalization, arterial pressure and cholesterol levels, and cardiovascular disease prevention40, of how it could improve metabolic states, diminishing reduc-tion-oxidation balance, which has been suggested to modulate synaptic function, with effects on what we consider the base of learning, metaplasticity41. It has also been suggested that its effect is achieved by low-ering the intensity of emotional excitement; therefore, the task of meditation not only allows us to infer an improved physicochemical environment where synaps-es occur, but also to achieve better balance in the au-tonomous system, allowing us to indicate an improved learning environment. For this reason, since 1996, Va-rela has spoken about neurophenomenology, regarding consciousness studies where subjective experience and brain dynamics are integrated, allowing for simul-taneous measurement of subjective experience (expe-riential correlations), phenomenological correlations, and neurophysiological correlations for the same time period or event42. In this, the state produces a change

108
Rev Mex Neuroci. 2022;23(3)
in brain activity together with a phenomenological change according to the qualitative research done with people in hypnosis or meditation43.
Electrophysiological and imaging evidence
In 2011, Hölzel, et al. analyzed magnetic resonance images and compared cortical density, before and after meditation training, and found structural changes which are secondary to increased synaptic connections in med-itators. These changes are represented by an increased amount of grey matter in the left hippocampus, the pos-terior cingulate cortex, the temporoparietal union and the cerebellum, all areas involved in learning, memory pro-cessing, and emotional regulation44. The increased hip-pocampal structure may be secondary to the activation of the hippocampus. This change in function could be related to the consolidation of declarative memory long-term memory, such as the recovery of spatial information coding and autobiographical memory45. Researchers have also documented the effects of meditation on spa-tio-visual memory spatial memory recovery and recogni-tion of objects and codification of distances between reference points46 and the visualization of interior or ex-terior scenes representing a spatial design47 including the
imagination and representation of complex scenes48, also activating the parahippocampal area, this latter ef-fect being mainly due to structural changes, but which as mentioned are secondary to functional modulations.49
Conclusions
Figure 1 shows a summary of our idea, present now, in this review. We suggested some of the cellular efects of conscious breathing. Synaptic activity is modulable at the molecular level, due to a phenomenon known as metaplasticity. Recent evidence indicates that this is an ongoing phenomenon in the brain and accounts for learn-ing in various models. This phenomenon also does not disappear, but rather changes its form of stimulation sug-gesting that it does not decline in age, but rather adapts to new conditions, Molecular changes occur in appropri-ate physiochemical conditions and with the right level of attention, especially regulating the autonomous system. The tasks of meditation and breathing have been de-scribed as affecting this type of process, improving met-abolic parameters and regulating the autonomous sys-tem, thereby reducing stress. This could allow us to infer a mechanism carrying out structural changes in relevant brain areas for cognitive task development. These points could suggest that conscious breathing activities improve
Figure 1. The figure is a summary model of our review, where we indicate that the use and development of conscious breathing improves cognitive tasks, enabling better behavior in adults. This can be explained by changes in the physiological conditions in which metaplastic phenomena occur and we can suggest that learning can be enhanced by this type of simple and easy to introduce activity.

109
V. Chavez et al.: Breathing and learning task
metabolic processes, allowing for improved synaptic function modulating remodeling culminating in changes in critical brain areas and improved cognitive function. This, in the framework of andragogic learning, could be a new paradigm for working on adult learning, where teaching conscious breathing may be helpful in adults for cognitive tasks in a context of new learning.
Funding
This research received the support of Proyecto Inter-no Universidad Mayor, and Tonalli ltda.
Conflicts of interest
The authors declare that they have no conflict of interests.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
right to privacy and informed consent. The au-thors declare that no patient data appear in this article.
references 1. Thompson E, Varela FJ. Radical embodiment: neural dynamics and
consciousness. Trends Cogn Sci. 2001;5:418-25. 2. Mosini AC, Saad M, Braghetta CC, Medeiros R, Peres MF, Leao FC.
Neurophysiological, cognitive-behavioral and neurochemical effects in practitioners of transcendental meditation - A literature review. Rev Assoc Med Bras (1992). 2019;65:706-13.
3. Voss P, Thomas ME, Cisneros-Franco JM, de Villers-Sidani É. Dynamic brains and the changing rules of neuroplasticity: implications for learning and recovery. Front psychol. 2017;8:1657.
4. Cooke SF, Bliss TV. Plasticity in the human central nervous system. Brain. 2006;129:1659-73.
5. Chavez-Mancilla V, Parodi J. Neurobiological bases of learning and their role for the paradigm shift in education. Psychology. 2015;6:9.
6. Sadaf S, Ali SK, Zuberi RW. Educational models and strategies in heal-th education. Introduction. Educ Health (Abingdon). 2009;22:96.
7. Youde A. Andragogy in blended learning contexts: effective tutoring of adult learners studying part-time, vocationally relevant degrees at a dis-tance. Int J Lifelong Educ. 2018;37:255-72.
8. Wang VC, Storey VA. Andragogy and teaching english as a foreign language in China. Ref Libr. 2015;56:295-314.
9. Watts KA. Tools and principles for effective online library instruction: andragogy and undergraduates. J Libr Inform Serv Distance Learn. 2018;12:49-55.
10. Bergman EM, de Bruin AB, Vorstenbosch MA, Kooloos JG, Puts GC, Leppink J, et al. Effects of learning content in context on knowledge acquisition and recall: a pretest-posttest control group design. BMC Med Educ. 2015;15:133.
11. Hopfinger JB. Introduction to special issue: attention and plasticity. Cogn Neurosci. 2017;8:69-71.
12. Rombouts JO, Bohte SM, Roelfsema PR. How attention can create sy-naptic tags for the learning of working memories in sequential tasks. PLoS Comput Biol. 2015;11:e1004060.
13. Swingler MM, Perry NB, Calkins SD. Neural plasticity and the develop-ment of attention: intrinsic and extrinsic influences. Dev Psychopathol. 2015;27:443-57.
14. Ahissar M, Hochstein S. Attentional control of early perceptual learning. Proc Natl Acad Sci USA. 1993;90:5718-22.
15. Couperus JW. Implicit learning modulates selective attention at sensory levels of perceptual processing. Atten Percept Psychophys. 2009;71:342-51.
16. Sasaki Y, Nanez JE, Watanabe T. Advances in visual perceptual learning and plasticity. Nat Rev Neurosci. 2010;11:53-60.
17. Vartak D, Jeurissen D, Self MW, Roelfsema PR. The influence of atten-tion and reward on the learning of stimulus-response associations. Sci Rep. 2017;7:9036.
18. Salthouse TA. When does age-related cognitive decline begin? Neurobiol Aging. 2009;30:507-14.
19. Raz N, Rodriguez KM. Differential aging of the brain: patterns, cognitive correlates and modifiers. Neurosci Biobehav Rev. 2006;30:730-48.
20. Ding XQ, Maudsley AA, Sabati M, Sheriff S, Schmitz B, Schutze M. Physiological neuronal decline in healthy aging human brain-an in vivo study with MRI and short echo-time whole-brain (1)H MR spectroscopic imaging. Neuroimage. 2016;137:45-51.
21. Holmes MJ, Robertson FC, Little F, Randall SR, Cotton MF, van der Kouwe AJ, et al. Longitudinal increases of brain metabolite levels in 5-10 year old children. PLoS One. 2017;12:e0180973.
22. Slagter HA, Davidson RJ, Lutz A. Mental training as a tool in the neuros-cientific study of brain and cognitive plasticity. Front Hum Neurosci. 2011;5:17.
23. Lutz A, Brefczynski-Lewis J, Johnstone T, Davidson RJ. Regulation of the neural circuitry of emotion by compassion meditation: effects of meditative expertise. PLoS One. 2008;3:e1897.
24. Wielgosz J, Goldberg SB, Kral TR, Dunne JD, Davidson RJ. Mindful-ness meditation and psychopathology. Annu Rev Clin Psychol. 2019;15:285-316.
25. Dahl CJ, Davidson RJ. Mindfulness and the contemplative life: pathways to connection, insight, and purpose. Curr Opin Psychol. 2019;28:60-4.
26. MacKenzie MB, Abbott KA, Kocovski NL. Mindfulness-based cognitive therapy in patients with depression: current perspectives. Neuropsychia-tr Dis Treat. 2018;14:1599-605.
27. Sanivarapu S. Free your mind: mindfulness practice of Buddhist philoso-phy. Indian J Psychiatry. 2016;58:345.
28. Rosenkranz MA, Lutz A, Perlman DM, Bachhuber DR, Schuyler BS, MacCoon DG, et al. Reduced stress and inflammatory responsiveness in experienced meditators compared to a matched healthy control group. Psychoneuroendocrinology. 2016;68:117-25.
29. Chaix R, Alvarez-Lopez MJ, Fagny M, Lemee L, Regnault B, Davidson RJ, et al. Epigenetic clock analysis in long-term meditators. Psychoneuroen-docrinology. 2017;85:210-4.
30. Slagter HA, Lutz A, Greischar LL, Francis AD, Nieuwenhuis S, Davis JM, et al. Mental training affects distribution of limited brain resources. PLoS Biol. 2007;5:e138.
31. Lazar SW, Kerr CE, Wasserman RH, Gray JR, Greve DN, Treadway MT, et al. Meditation experience is associated with increased cortical thick-ness. Neuroreport. 2005;16:1893-7.
32. Yee AX, Hsu YT, Chen L. A metaplasticity view of the interaction between homeostatic and Hebbian plasticity. Philos Trans R Soc Lond B Biol Sci. 2017;372:20160155.
33. Quach D, Jastrowski Mano KE, Alexander K. A randomized controlled trial examining the effect of mindfulness meditation on working memory capacity in adolescents. J Adolesc Health. 2016;58:489-96.
34. Pratzlich M, Kossowsky J, Gaab J, Krummenacher P. Impact of short-term meditation and expectation on executive brain functions. Behav Brain Res. 2016;297:268-76.
35. Gallant SN. Mindfulness meditation practice and executive functioning: breaking down the benefit. Conscious Cogn. 2016;40:116-30.
36. Moore A, Gruber T, Derose J, Malinowski P. Regular, brief mindfulness meditation practice improves electrophysiological markers of attentional control. Front Hum Neurosci. 2012;6:18.
37. Chan RW, Immink MA, Lushington K. The influence of focused-attention meditation states on the cognitive control of sequence learning. Cons-cious Cogn. 2017;55:11-25.
38. Manuello J, Vercelli U, Nani A, Costa T, Cauda F. Mindfulness meditation and consciousness: an integrative neuroscientific perspective. Conscious Cogn. 2016;40:67-78.
39. Khanna S, Greeson JM. A narrative review of yoga and mindfulness as complementary therapies for addiction. Complement Ther Med. 2013;21:244-52.
40. Anderson JW, Liu C, Kryscio RJ. Blood pressure response to transcen-dental meditation: a meta-analysis. Am J Hypertens. 2008;21:310-6.
41. Crestani AP, Krueger JN, Barragan EV, Nakazawa Y, Nemes SE, Quill-feldt JA, et al. Metaplasticity contributes to memory formation in the hi-ppocampus. Neuropsychopharmacology. 2019;44:408-14.
42. Varela F. Neurophenomenology. A methodological remedy to the hard problem. J Conscious Stud. 1996;3:330-49.

110
Rev Mex Neuroci. 2022;23(3)
43. Cardena E. The phenomenology of deep hypnosis: quiescent and phy-sically active. Int J Clin Exp Hypn. 2005;53:37-59.
44. Holzel BK, Carmody J, Vangel M, Congleton C, Yerramsetti SM, Gard T, et al. Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Res. 2011;191:36-43.
45. Cipolotti L, Moscovitch M. The hippocampus and remote autobiographical memory. Lancet Neurol. 2005;4:792-3.
46. Tsukiura T, Fujii T, Okuda J, Ohtake H, Kawashima R, Itoh M, et al. Time-dependent contribution of the hippocampal complex when remem-bering the past: a PET study. Neuroreport. 2002;13:2319-23.
47. O’Craven KM, Kanwisher N. Mental imagery of faces and places activa-tes corresponding stiimulus-specific brain regions. J Cogn Neurosci. 2000;12:1013-23.
48. Hassabis D, Kumaran D, Maguire EA. Using imagination to unders-tand the neural basis of episodic memory. J Neurosci. 2007;27:14365-74.
49. Lv J, Feng H, Chen L, Wang WY, Yue XL, Jin QH. Activation of beta-adre-noceptor facilitates active avoidance learning through enhancement of glutamate levels in the hippocampal dentate gyrus. Neuroreport. 2017;28:973-9.

111
Mechanical thrombectomy in children: a little known and scarcely utilized resourceYolanda Aburto-Murrieta1, Beatriz Méndez1, and Juan M. Marquez-Romero2*1Department of Endovascular Neurological Therapy, Instituto Nacional de Neurología y Neurocirugía “MVS,” Mexico City; 2Department of Neurology, Hospital General de Zona 2, Instituto Mexicano del Seguro Social (IMSS), Aguascalientes. Mexico
Revista Mexicana de Neurociencia
rEViEW artiClE
abstract
Mechanical thrombectomy (MT) in children with acute ischemic stroke (AIS) and large vessel occlusion is a feasible treatment modality. However, the published experience is limited to case reports and small case series that yield a low grade of evi-dence. In this narrative review, we summarize the published literature regarding the topic of MT in pediatric patients with AIS. We conclude that MT is a powerful tool that all clinicians need to keep in mind when treating pediatric patients under sus-picion of AIS. We hope that the present manuscript aids in increasing awareness about this critical topic.
Keywords: Stroke. Mechanical thrombectomy. Pediatric. Review.
Trombectomía mecánica en niños: un recurso poco conocido y raramente utilizado
resumen
La trombectomía mecánica (TM) es una modalidad de tratamiento factible en niños con infarto cerebral agudo (ICA) y oclusión de gran vaso. Sin embargo, la experiencia publicada se limita a reportes de caso y pequeñas series de casos que proveen un bajo grado de evidencia. En esta revisión narrativa, resumimos la literatura publicada en el tema de la TM en pacientes pediátricos con ICA. Concluimos que la TM es una herramienta ponderosa que todos los clínicos necesitan tener en mente cuando tratan pacientes con sospecha de ICA. Deseamos que el presente manuscrito ayude a incrementar la conciencia acerca de este importante tema.
Palabras clave: Enfermedad vascular cerebral. Trombectomía mecánica. Pediatría. Revisión.
Correspondence: *Juan M. Marquez-Romero
E-mail: [email protected]
Available online: 02-05-2022
Rev Mex Neuroci. 2022;23(3):111-115
www.revmexneurociencia.com
Date of reception: 23-04-2021
Date of acceptance: 20-07-2021
DOI: 10.24875/RMN.21000033
introduction
Acute ischemic stroke (AIS) constitutes a rare entity in the pediatric population. Nevertheless, it carries a significant diagnostic delay due to a low index of clinical suspicion when it occurs. In adults, acute recanalization therapies, whether be with intravenous (IV)/intra-arterial (IA) thrombolysis with recombinant tissue plasminogen
activator (rTPA) or with mechanical thrombectomy (MT), are the current standards of treatment. In those present-ing within the 4.5 h, time windows IV rTPA is still the angular stone for treatment. Nevertheless, patients with occlusions affecting the internal carotid artery or the proximal segments of the major cerebral arteries within 6 h from onset of symptoms are candidates to MT1. Since 2018 and mainly due to the results of the DAWN
2604-6180 / © 2021 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

112
Rev Mex Neuroci. 2022;23(3)
and DEFUSE 3 trials, patients with up to 24 h from symptom onset are also candidates to MT in what is currently known as extended time window MT2.
However, trials that provide evidence for the current treatment guidelines selectively excluded patients younger than 18 years. However, MT in children with AIS and large vessel occlusion (LVO) is a feasible treat-ment modality3. Still, the published experience of MT in pediatric AIS is limited to case reports and small case series that yield a Grade IV level of evidence4.
In this narrative review, we summarize the published literature regarding the topic of MT in pediatric patients with AIS, a matter of great interest for all pediatric and adult neurologists.
Epidemiology
AIS during the pediatric ages (0-16 years) has an incidence of 2-8 per 100,000 children. It is a rare event that carries a devastating prognosis due to its long-term economic and social impacts. Reported mortality was 5% in the Canadian Pediatric Ischemic Stroke Registry. Among survivors, 67% exhibit some degree of neuro-logical disability (52% moderate to severe)5.
Clinical presentation
The clinical presentation differs from that in adults, and it varies depending on the patient’s age, clinical context, and etiology of the infarct. One of its main manifestations is irritability, but seizures, conscience impairment, and hemiplegia can all be present. The symptoms above can thus be erroneously attributed to migraine, focal sei-zures, post-ictal hemiparesis (Todd’s paralysis), central nervous system demyelination, or brain tumors. AIS is initially suspected only in about 38% of all cases, leading to a substantial delay in the diagnosis6.
Etiology
Data from multicentric hospital registries have con-firmed that the disorders leading to AIS are different in children than in adults. The most common cause is non-atherosclerotic vasculopathy in up to 49% of the cases, congenital cardiac disease (30%), and thrombo-philias (30%)5.
Focal cerebral arteriopathy characterizes by an irreg-ularity in the arterial inner wall in the absence of acute inflammation of autoimmune or infectious origin7. The arterial occlusion without visible abnormalities of the arterial wall is associated with embolic sources, mainly
cardiac8. Focal cerebral arteriopathy has a reversible course in 68% of the patients and is progressive in 20%. The self-limited inflammatory process present in focal cerebral arteriopathy has a reversible course in 68% of the patients lasting 1-3 months, but can have a progressive course in 20% of the patients9.
diagnosis
Due to its low sensitivity in children, the utilization of computed tomography (CT) scans as the initial diag-nostic approach for pediatric AIS constitutes one of the causes for diagnostic delay6. Only 10% of the patients receive a confirmatory diagnosis of AIS during their first 3 h hospitalized; this figure reaches 20% at 6 h from symptoms onset. When the initial neuroimaging modal-ity does not identify the diagnosis of AIS, the mean time to diagnosis is 44 h. Magnetic resonance imaging (MRI) is conclusive in 100% of the cases and must be the first choice in the pediatric population10.
treatment
Up to this date, there are no randomized controlled trials to sustain the recommendations for the treatment of AIS in pediatric patients. The current guidelines are loosely derived from the evidence obtained from adults and based mainly on expert consensus11. Acute reper-fusion interventions such as IV rTPA and MT are rec-ommended only as a rescue maneuver in selected patients2. Recanalization of LVO is pursued to improve neurological outcomes. Despite the lack of data regard-ing safety and efficacy in children, rTPA employment in the USA is ≤ 2%12. The consensus group for the Throm-bolysis in Pediatric Stroke (TIPS) suggests applying the standard dose (0.9 mg/kg) when rTPA is considered for the treatment of pediatric stroke.
Regarding MT, the Guidelines from the American Heart Association published in 2015 state that benefits from this procedure have not been established for pa-tients younger than 18 years; therefore, MT with stent retriever might be reasonable in selected patients un-der 18 years with AIS due to LVO in whom treatment can be initiated within 6 h from symptom onset1. In 2018, after the publication of the DAWN and DEFUSE 3 trials, a revision of the same guideline extended the therapeutic window for MT up to 16-24 h from symptom onset. Nevertheless, the modification did not address the possibility of extrapolating the extension in the ther-apeutic window to pediatric patients2.

113
Y. Aburto-Murrieta et al.: Mechanical thrombectomy in children
Notwithstanding the facts mentioned earlier, MT ap-pears as a feasible and attractive option for the treat-ment of pediatric AIS3. This is because the low rate of early diagnosis excludes most patients from receiving other acute reperfusion interventions such as IV rTPA. According to current diagnostic delays, even a 6 h time window MT is challenging to perform, leaving the only treatment option the extended window time MT. Still, it is worth noting that this therapeutic conduct is support-ed by Class IV evidence4.
The published evidence suggests that the safety pro-file of MT in children does not differ from that in adults. Most of the children that receive MT achieve favorable neurological outcomes. Special cautions are warranted in those younger than 5 years and those weighing <15 kg because the narrower arteries predispose them to complications from the use of endovascular devic-es13. Another concern is the execution of MT in patients with focal cerebral arteriopathy, Moya-Moya disease, and arterial dissections in whom the contact of foreign materials with the damaged arterial wall has the poten-tial to aggravate the primary injury. In this regard, data from the Save ChildS Study did not show a higher complication rate in the 14 patients treated with MT3.
Standard window time Mt
The Save Childs Study is a cohort that registered data from 27 European and American centers; it recruit-ed 73 pediatric patients that underwent MT within the 6 h time window. The results showed 87% of successful recanalization and neurologic outcome improvement, a median PedNIHSS score of 10 points. The complication rate was 1.37, with only one event of post-interventional bleeding3. There are other published case series that describe 100% rates of at least partial endovascular recanalization and a favorable clinical outcome in 91%14. In an analysis of 12 patients that underwent MT with stent retrievers, 50% were treated within 6 h from symptom onset; there were no procedure-related com-plications, and the clinical outcome at 3 months was 1 point in the modified Rankin scale15.
A sub-analysis of the Multicenter Randomized Clini-cal Trial of Endovascular Treatment for AIS in the Neth-erlands attempted to show efficacy and safety data by prospectively following nine children with AIS second-ary to LVO treated with 6 h time window MT. Outcomes demonstrated functional independence at 6-month fol-low-up in all the patients without cardiac disease. In four patients with ventricular assist devices, the clinical
outcome was not optimal due to the base cardiac pa-thology complications16.
Extended window time Mt
The extended window time MT in pediatric stroke does not count with evidence from prospective studies, and due to its rare nature and low incidence, the prospects of ever acquiring such data are limited16. After considering this fact, it is crucial to generate practical strategies that allow clinicians to adequately identify those children prone to benefit from MT after the standard window for treatment. Image-guided protocols that include some form of perfu-sion neuroimaging can determine the existence of penum-bral tissue potentially salvageable regardless of the time from onset of symptoms. Such protocols have been tested with good results in adults and allow the treatment of pa-tients well beyond the standard window of treatment17.
In a retrospective review of data from 68 patients younger than 18, the mean time to treatment was 13.7 h, with patients receiving MT up to 72 h after onset of symptoms. Nineteen out of the total received extend-ed time window MT and 79.5% achieved an excellent clinical prognosis; this proportion increased to 87.5% when only considering the patient who underwent MT with FDA approved devices such as the Solitaire and Trevo stents and the Penumbra aspiration system18.
In a retrospective cohort of 12 pediatric patients with < 18 years of age, eight received MT and five were treated with extended window time MT. Successful re-canalization was accomplished in 87.5% and an excel-lent clinical outcome in 78%. Criteria for MT were image guided; other inclusion criteria included NIHSS > 6 and evidence for LVO19.
Although MRI is the preferred neuroimaging modality for AIS in children, there might be some situations where it can be contraindicated or unavailable. In these cases, perfusion CT with a Tmax >6 s can be used to determine core/penumbra mismatch20. It is important to stress that without some form of perfusion imaging, the estimation of the ischemic core is not possible, and the lack of this data precludes MT. Thus, some children will be excluded from receiving a potentially beneficial procedure.
Conclusions
AIS constitutes a major neurologic emergency. Due to its low incidence and unusual clinical presentation, AIS is a diagnostic entity scarcely recognized in the pediatric population. The 1st h after the onset of symp-toms is fundamental for an early diagnosis and better

114
Rev Mex Neuroci. 2022;23(3)
clinical outcome. Whenever there exists a suspicion of AIS, the clinician should promptly order an MRI. In the current absence of evidence-based guidelines for treat-ment, it is up to the experts in vascular neurology to guide on a case by case basis, table 1 depicts a sum-mary of the published MT cases performed in the pe-diatric age group. Both the risks of acute recanalization techniques and the potential benefits are to be pon-dered. Still, MT is a powerful tool that all clinicians need to keep in mind when treating pediatric patients under suspicion of AIS. We hope that the present manuscript aids in increasing awareness about this critical topic.
Funding
This work did not receive any funding.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical disclosures
Protection of human and animal subjects: The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data: The authors declare that no patient data appear in this article.
right to privacy and informed consent: The au-thors declare that no patient data appear in this article.
references 1. Powers WJ, Derdeyn CP, Biller J, Coffey CS, Hoh BL, Jauch EC, et al.
2015 American heart association/American stroke association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. 2015;46:3020-35.
2. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare profes-sionals from the American heart association/American stroke association. Stroke. 2019;50:e344-418.
3. Sporns PB, Strater R, Minnerup J, Wiendl H, Hanning U, Chapot R, et al. Feasibility, safety, and outcome of endovascular recanalization in child-hood stroke: the save childs study. JAMA Neurol. 2020;77:25-34.
Table 1. Summary of the published mechanical thrombectomy case reports performed in the pediatric age group
Authors,year
Age Sex NIHSS TTT Treatment technique TICI Clinical outcome
Felker et al.21, 2010 14 M NR 9 Merci 0 NR
Taneja et al.22, 2011 14 F NR 24 SR 3 NR
Xavier et al.23, 2012 16 M 11 ˃72 A + Stent 2A mRs 1
Stidd et al.24, 2014 2 M NR 7 SR 2B mRs 1
Garnés Sánchez et al.25, 2016 9 M 35 36 SR 3 NIHSS 3PSOM 0
Ladner et al.26, 2014 5 M 22 9 SR 2b PSOM 0
Rhee et al.27, 2014 99
MM
610
77
SRSR
33
NIHSS 3NIHSS 3
Sainz de la Maza et al.28, 2014 12 F 18 8 SR 2B NIHSS 1
Savastano et al.29, 2015 22 months F NR 16 SR 3 NR
Huded et al.30, 2015 6 M 15 26 SR 3 NIHSS 0
Weiner et al.31, 2016 15 M 9 8 SR 2B NIHSS 0
Lena et al.32, 2017 NR NR NR ˃17 A 2B mRs 1
Nicosia et al.33, 2017 23 months NR NR 18 SR 3 NR
Wilkinson et al.34, 2017 17 months F NR 50 SR 2B NR
Ghannam et al.35, 2021 7 F 4 11 SR 2B NIHSS 1
NIHSS: National Institutes of Health Stroke Scale; TTT: time to treatment; TICI: thrombolysis in cerebral infarction; EVT: endovascular thrombectomy; NR: not reported; SR: stent retriever (Solitaire: Solitaire FR revascularization device by Medtronic, Minneapolis, MN, USA, or Trevo: Trevo Provue Retriever by Stryker, Kalamazoo, MI, USA); A: aspiration (Penumbra reperfusion catheter system, Penumbra Inc., Alameda, CA, USA); RD: Revive: Revive SE clot retrieval device (Codman & Shurtleff Inc., Raynham, MA); mRs: modified Rankin scale; PSOM: pediatric stroke outcome measure; WS: wake-up stroke.

115
Y. Aburto-Murrieta et al.: Mechanical thrombectomy in children
4. Sporns PB, Psychogios MN, Straeter R, Hanning U, Minnerup J, Chapot R, et al. Clinical diffusion mismatch to select pediatric patients for embolectomy 6 to 24 hours after stroke: an analysis of the save childs study. Neurology. 2021;96:e343-51.
5. deVeber GA, Kirton A, Booth FA, Yager JY, Wirrell EC, Wood E, et al. Epidemiology and outcomes of arterial ischemic stroke in children: the canadian pediatric ischemic stroke registry. Pediatr Neurol. 2017;69:58-70.
6. Rafay MF, Pontigon AM, Chiang J, Adams M, Jarvis DA, Silver F, et al. Delay to diagnosis in acute pediatric arterial ischemic stroke. Stroke. 2009;40:58-64.
7. Marquez-Romero JM, Capristo F, Arauz A. Ischaemic stroke secondary to unilateral focal cerebral arteriopathy. An Pediatr (Barc). 2015;82: 370-1.
8. Goyal P, Malhotra A, Almast J, Sapire J, Gupta S, Mangla M, et al. Neuroimaging of pediatric arteriopathies. J Neuroimaging. 2019;29: 287-308.
9. Yeon JY, Shin HJ, Seol HJ, Kim JS, Hong SC. Unilateral intracranial arteriopathy in pediatric stroke: course, outcome, and prediction of rever-sible arteriopathy. Stroke. 2014;45:1173-6.
10. Mallick AA, Ganesan V, Kirkham FJ, Fallon P, Hedderly T, McShane T, et al. Diagnostic delays in paediatric stroke. J Neurol Neurosurg Psychia-try. 2015;86:917-21.
11. Ferriero DM, Fullerton HJ, Bernard TJ, Billinghurst L, Daniels SR, De-Baun MR, et al. Management of stroke in neonates and children: a scientific statement from the American heart association/American stroke association. Stroke. 2019;50:e51-96.
12. Rivkin MJ, deVeber G, Ichord RN, Kirton A, Chan AK, Hovinga CA, et al. Thrombolysis in pediatric stroke study. Stroke. 2015;46:880-5.
13. Hoffman CE, Santillan A, Rotman L, Gobin YP, Souweidane MM. Com-plications of cerebral angiography in children younger than 3 years of age. J Neurosurg Pediatr. 2014;13:414-9.
14. Madaelil TP, Kansagra AP, Cross DT, Moran CJ, Derdeyn CP. Mecha-nical thrombectomy in pediatric acute ischemic stroke: clinical outcomes and literature review. Interv Neuroradiol. 2016;22:426-31.
15. Sporns PB, Kemmling A, Hanning U, Minnerup J, Strater R, Niederstadt T, et al. Thrombectomy in childhood stroke. J Am Heart Assoc. 2019; 8:e011335.
16. Adriaan CG, Hunfeld MA, van den Wijngaard I, Kraemer U, Engelen M, van Hasselt B, et al. Endovascular treatment for acute ischemic stroke in children: experience from the MR CLEAN registry. Stroke. 2021; 52:781-8.
17. Lee S, Felling RJ. Moving toward a new horizon of pediatric stroke inter-vention. Stroke. 2021;52:789-91.
18. Cobb MI, Laarakker AS, Gonzalez LF, Smith TP, Hauck EF, Zomorodi AR. Endovascular therapies for acute ischemic stroke in children. Stroke. 2017;48:2026-30.
19. Lee S, Heit JJ, Albers GW, Wintermark M, Jiang B, Bernier E, et al. Neuroimaging selection for thrombectomy in pediatric stroke: a sin-gle-center experience. J Neurointerv Surg. 2019;11:940-6.
20. Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, Ortega-Gutie-rrez S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018;378:708-18.
21. Felker MV, Zimmer JA, Golomb MR. Failure of a clot retrieval device in an adolescent stroke patient. Pediatr Neurol. 2010;43:435-8.
22. Taneja SR, Hanna I, Holdgate A, Wenderoth J, Cordato DJ. Basilar artery occlusion in a 14-year old female successfully treated with acute intra-vascular intervention: case report and review of the literature. J Paedia-tr Child Health. 2011;47:408-14.
23. Xavier A, Kansara A, Majjhoo AQ, Norris G. CT perfusion guided delayed recanalization with favorable outcome in pediatric stroke. J Neurointerv Surg. 2012;4:e33.
24. Stidd DA, Lopes DK. Successful mechanical thrombectomy in a 2-year-old male through a 4-French guide catheter. Neurointervention. 2014;9:94-100.
25. Sanchez CM, Parrilla G, Villalba BG, Martinez HA, Salcedo EM, Domin-guez SR. A paediatric case of basilar occlusion treated with mechanical thrombectomy using stent retrievers. Neurologia. 2016;31:347-50.
26. Ladner TR, He L, Jordan LC, Cooper C, Froehler MT, Mocco J. Mecha-nical thrombectomy for acute stroke in childhood: how much does res-tricted diffusion matter? BMJ Case Rep. 2014;2014:bcr2014011465.
27. Rhee E, Hurst R, Pukenas B, Ichord R, Cahill AM, Rossano J, et al. Mechanical embolectomy for ischemic stroke in a pediatric ventricular assist device patient. Pediatr Transplant. 2014;18:E88-92.
28. de la Maza SS, de Felipe A, Matute MC, Fandino E, Mendez JC, Morillo P, et al. Acute ischemic stroke in a 12-year-old successfully treated with mechanical thrombectomy. J Child Neurol. 2014;29:269-73.
29. Savastano L, Gemmete JJ, Pandey AS, Roark C, Chaudhary N. Acute ischemic stroke in a child due to basilar artery occlusion treated success-fully with a stent retriever. J Neurointerv Surg. 2016;8:e33.
30. Huded V, Kamath V, Chauhan B, de Souza R, Nair R, Sapare A, et al. Mechanical thrombectomy using solitaire in a 6-year-old child. J Vasc Interv Neurol. 2015;8:13-6.
31. Weiner GM, Feroze RA, Agarwal N, Panczykowski DM, Ares WJ, Koos-hkabadi A, et al. Successful manual aspiration thrombectomy in a pedia-tric patient. Pediatr Neurol. 2016;61:107-13.
32. Lena J, Eskandari R, Infinger L, Fargen KM, Spiotta A, Turk A, et al. Basilar artery occlusion in a child treated successfully with mechanical thrombectomy using ADAPT. J Neurointerv Surg. 2017;9:e2.
33. Nicosia G, Cicala D, Mirone G, Spennato P, Trischitta V, Ruggiero C, et al. Childhood acute basilar artery thrombosis successfully treated with mechanical thrombectomy using stent retrievers: case report and review of the literature. Childs Nerv Syst. 2017;33:349-55.
34. Wilkinson DA, Pandey AS, Garton HJ, Savastano L, Griauzde J, Chaud-hary N, et al. Late recanalization of basilar artery occlusion in a previous-ly healthy 17-month-old child. BMJ Case Rep. 2017;2017:bcr2017013277.
35. Ghannam M, Zakarna L, Alawneh I, Al-Chalabi M, Kenney-Jung D. En-dovascular therapy for childhood ischemic stroke. Am J Case Rep. 2021; 22:e926529.




















