
Research Repository - ePrints Soton
313
Research Repository Copyright © and Moral Rights for this thesis and, where applicable, any accompanying data are retained by the author and/or other copyright owners. A copy can be downloaded for personal non-commercial research or study, without prior permission or charge. This thesis and the accompanying data cannot be reproduced or quoted extensively from without first obtaining permission in writing from the copyright holder/s. The content of the thesis and accompanying research data (where applicable) must not be changed in any way or sold commercially in any format or medium without the formal permission of the copyright holder/s. When referring to this thesis and any accompanying data, full bibliographic details must be given, e.g. Thesis: Kaveri Mayra (2021) "’Women are supposed to endure that!’ A critical feminist exploration of obstetric violence in women’s and midwives’ birth narratives in India", University of Southampton, Faculty of Social Science, PhD Thesis, pp 305.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Research Repository - ePrints Soton

Research Repository
Copyright©andMoralRightsforthisthesisand,whereapplicable,anyaccompanyingdataare
retainedbytheauthorand/orothercopyrightowners.Acopycanbedownloadedforpersonal
non-commercialresearchorstudy,withoutpriorpermissionorcharge.Thisthesisandthe
accompanyingdatacannotbereproducedorquotedextensivelyfromwithoutfirstobtaining
permissioninwritingfromthecopyrightholder/s.Thecontentofthethesisandaccompanying
researchdata(whereapplicable)mustnotbechangedinanywayorsoldcommerciallyinany
formatormediumwithouttheformalpermissionofthecopyrightholder/s.
Whenreferringtothisthesisandanyaccompanyingdata,fullbibliographicdetailsmustbegiven,
e.g.
Thesis:KaveriMayra(2021)"’Womenaresupposedtoendurethat!’Acriticalfeministexploration
ofobstetricviolenceinwomen’sandmidwives’birthnarrativesinIndia",Universityof
Southampton,FacultyofSocialScience,PhDThesis,pp305.


UniversityofSouthampton
FacultyofSocialSciences
DepartmentofSocialStatisticsandDemography
‘Womenaresupposedtoendurethat!’Acriticalfeministexplorationofobstetric
violenceinwomen’sandmidwives’birthnarrativesinIndia
by
KaveriMayra
ORCIDID0000-0001-8395-0738
ThesisforthedegreeofDoctorofPhilosophy
November2021


UniversityofSouthampton
Abstract
FacultyofSocialSciences
ThesisforthedegreeofDoctorofPhilosophy
‘Womenaresupposedtoendurethat!’Acriticalfeministexplorationofobstetricviolencein
women’sandmidwives’birthnarrativesinIndia
by
KaveriMayra
Birthandviolenceagainstwomenaresensitiveareasofresearchsurroundedbyathickculturalsilence.
Womenaroundtheworldexperiencedifferentformsofobstetricviolenceduringchildbirthinavarietyof
settingsbyprovidersandsupportworkerswithinhealthcaresystems.Whilethereisevidenceofobstetric
violenceasaglobalissue,moresystematicexplorationisneededonitscausesfromtheperspectivesof
womenandtheircarers.Obstetricviolenceiscloselylinkedwithissuesofwomen’spositioningatthe
intersectionsofdifferentformsofoppressionandtheirexperiencesandperceptionsofobstetricviolence
canbeinfluencedbysocio-cultural,demographicandeconomiccharacteristics,theirimmediatecontexts,
theirreproductivehistoriesandgeographies.Inthisthesis,Iapplyafeministperspectivetoexplorethe
natureofobstetricviolenceandthefactorsthatmakeswomenvulnerableduringchildbirth,considering
thatwomen’sandnurse-midwives’perspectivesandexperiences.Ifirstconductaquantitativeexamination
ofthedeterminantsofobstetricviolenceinoneoftheeconomicallydeprivedstatesofBiharinIndia,and
findwomen’sexperiencesofobstetricviolenceareoftenpluralandmulti-layered.Age,parityand
educationarefoundstatisticallysignificantattributesthatincreasewomen’svulnerabilitytoobstetric
violenceinBihar.Ifollowthiswithaqualitativeexplorationthroughparticipatoryarts-basedmethodsto
cutacrossthepower-basedandlanguage-basedbarriersandlearnfromandpresentwomen’sembodied
experiencesofchildbirthandobstetricviolence.Iusedfeministmethodssuchasbirthmapping,birthing
story,poeticinquiry,feminist-relationaldiscourseanalysisandvoice-centeredrelationalanalysisfordata
collection,analysis,interpretationandpresentation,tobringforthwomen’sandnurse-midwives’voiceson
thissensitiveembodiedissue.Myresearchindicatesthatthedeterminantsdrivingobstetricviolenceare
relatedtowomenandtheirnurse-midwives,attheindividuallevel,intheirimmediatebirthing
environmentandinthelargersocialandpolicylevel.Gender,power,cultureandstructurearethekey
themesholdingtheindividualandtheinteractionsofthedeterminantsleadingtoobstetricviolence.They
needtobeaddressedateachoftheselevelsthroughmulti-sectoralapproacheswithwomenandtheir
midwivesaskeystakeholdersdrivingthechangetowardsensuringrespectfulmaternitycare.
Keywords:Obstetricviolence,Feministmethods,Respectfulmaternitycare,Bodymapping,Birth,Nurse,Midwife,Healthsystems,Bihar,India

Idedicatemydissertationtowomen
Womeninmylife,mymother,mysister,myniece,mygrandmother,myfriends,mymidwives,
mynurses,mytribe.Womenwhohaveexperiencedrespectfulcareandobstetricviolenceduring
childbirth.
Womenwhohavekindlyandbravelysharedtheirstoriesofbirthandviolence.
LineartofabirthmapbyAditiParischa

TableofContents
i
TableofContents
TableofContents............................................................................................................i
TableofTables.............................................................................................................vii
TableofFigures.............................................................................................................ix
TableofBoxes..............................................................................................................xii
Introduction........................................................................Error!Bookmarknotdefined.
ResearchThesis:DeclarationofAuthorship.................................................................xix
Acknowledgements.....................................................................................................xxi
DefinitionsandAbbreviations....................................................................................xxv
Chapter1 Whystudyobstetricviolence?.....................................................................1
1.1 Introduction...............................................................................................................1
1.2 Researchobjectives...................................................................................................4
1.3 Researchquestions....................................................................................................4
1.4 Thesisorganisation....................................................................................................4
Chapter2 ObstetricViolence:Aliteraturereview&positionality................................7
2.1 Obstetricviolencefromarightsperspective.............................................................8
2.2 ‘Obstetricviolence’:Terminologies,definitions,resistance,movementsandthe
history......................................................................................................................10
2.3 Typesofobstetricviolenceduringchildbirth..........................................................17
Source:Bohrenetal.2015................................................................................................19
2.4 Globalevidenceofobstetricviolenceduringchildbirth..........................................19
2.5 Impactofobstetricviolenceduringchildbirthonhealthandwellbeing.................22
2.6 Determinantsofobstetricviolenceduringchildbirth.............................................23
2.6.1 Individualandhouseholddriversofobstetricviolence...................................24
2.6.2 Systemicdriversofobstetricviolence.............................................................25
2.7 Situating‘obstetricviolence’withingender-basedviolence...................................28
2.8 Positionality:Myassociationwith‘obstetricviolence’...........................................29
2.9 Summary.................................................................................................................32
Chapter3 BirthinginBihar:settingthecontext.........................................................33

TableofContents
ii
3.1 QualityofmaternalcareinIndia.............................................................................33
3.2 EvidenceofobstetricviolenceduringchildbirthinIndia........................................34
3.3 ThestateofmidwiferyeducationinIndia...............................................................36
3.3.1 Pre-serviceeducation......................................................................................36
3.3.2 In-serviceeducation........................................................................................37
3.4 Bihar........................................................................................................................39
3.5 MaternalhealthcareinBihar..................................................................................40
3.6 StatusofwomeninBihar........................................................................................42
3.7 Pleasure,shame,endurance:conversationsaroundbirthing.................................44
3.8 ViolenceagainstwomeninBihar............................................................................45
Chapter4 Shesmileswhenshetalksaboutviolence:Epistemologicalunderpinnings
andmethodologicalapproaches................................................................47
4.1 Epistemologicalunderpinnings...............................................................................47
4.1.1 Feministtheory................................................................................................49
4.1.2 Criticalfeministtheory....................................................................................49
4.1.3 Feministstandpointtheory.............................................................................51
4.1.4 Intersectionality...............................................................................................53
4.2 Conceptualframework............................................................................................54
4.3 Studydesignandanalysis........................................................................................56
4.4 Researchethicalapproval.......................................................................................59
Chapter5 SocialdeterminantsofobstetricviolenceinBihar:evidencefroma
householdsurvey......................................................................................61
5.1 Introduction.............................................................................................................61
5.2 Objective..................................................................................................................63
5.3 Methods..................................................................................................................63
5.3.1 Datacollection.................................................................................................64
5.3.2 Dataanalysis....................................................................................................65
5.4 Results.....................................................................................................................66
5.4.1 Participantprofile............................................................................................66
5.4.2 Experienceofobstetricviolence.....................................................................69

TableofContents
iii
5.4.3 Socialdeterminantsofobstetricviolence.......................................................77
5.5 Discussionandconclusion.......................................................................................89
Chapter6 Whatdoeswomen’sexperienceofrespect,disrespectandabuselooklike?
Breakingthesilencesurroundingobstetricviolence..................................93
6.1 Background..............................................................................................................93
6.2 Researchquestions..................................................................................................96
6.3 Objectives................................................................................................................96
6.4 Methods..................................................................................................................96
6.4.1 Bodymapping..................................................................................................98
6.4.2 Planningthedatacollectionwithbodymapping..........................................100
6.4.3 BirthmappinginBihar...................................................................................102
6.4.4 Methodologicalchallenges............................................................................104
6.4.5 Dataanalysis..................................................................................................105
6.4.6 Positionalityandreflexivity...........................................................................108
6.5 Findings..................................................................................................................109
6.5.1 ‘Good’births,‘Bad’birthsandexpectedbirths.............................................111
6.5.2 Respect,disrespectandabuseduringmedicalinterventions.......................130
6.5.2.1 Painmanagement...............................................................................133
6.5.3 Birthsetting/placerelatedrespect,disrespectandabuse............................134
6.5.4 Respect,disrespectandabuserelatedtobirthingenvironment..................138
6.5.5 Respectful,disrespectfulandabusivecommunicationaroundchildbirth....144
6.5.6 Respectful,disrespectfulandabusivepeoplearoundchildbirth..................150
6.5.7 Respect,disrespectandabuseinpersonalspaceandrelationships:household
andhusband..................................................................................................161
6.5.8 Birthinginformation,birthpreparednessandmythsaroundbirth...............167
6.6 Discussion..............................................................................................................171
6.7 Strengthsandlimitations......................................................................................176
6.8 Conclusion.............................................................................................................176
Chapter7 “Ihavetolistentothemortheymightharmme”:Whydowomenendure
obstetricviolence?..................................................................................178

TableofContents
iv
7.1 Background............................................................................................................178
7.2 Researchquestion.................................................................................................179
7.3 Objective................................................................................................................180
7.4 Findings..................................................................................................................180
7.4.1 Powerinfluencescareduringchildbirth........................................................180
7.4.2 Genderinfluencescareduringchildbirth......................................................185
7.4.3 Structureinfluencescarearoundchildbirth..................................................189
7.4.4 Cultureinfluencescarearoundchildbirth.....................................................194
7.5 Discussionandconclusion.....................................................................................197
Chapter8 “It’seasytoabuseobesewomen!”:Whydosomecareprovidersengagein
obstetricviolence?..................................................................................202
8.1 Background............................................................................................................202
8.2 Researchquestion.................................................................................................204
8.3 Objectives..............................................................................................................205
8.4 Methods................................................................................................................205
8.4.1 Studyinstrument...........................................................................................206
8.4.2 Datacollection...............................................................................................207
8.4.3 Dataanalysis..................................................................................................208
8.4.4 Positionalityandreflexivity...........................................................................208
8.5 Findings..................................................................................................................209
8.5.1 Reactiontothepaintingofawomangivingbirth.........................................210
8.5.2 Factorsbehinddisrespectandabuseofwomenduringchildbirth...............211
8.5.2.1 Woman-relatedfactors.......................................................................211
8.5.2.2 Nurse-midwiferelatedfactors............................................................214
8.5.3 Participant’srecommendationsforrespectfulmaternitycare.....................218
8.5.4 Respectfulmaternitycareeducationforthenextgenerationofcare
providers........................................................................................................222
8.5.5 Domidwiveshaverespectfulbirths?............................................................224
8.6 Discussion..............................................................................................................225
8.7 Limitations.............................................................................................................228

TableofContents
v
8.8 Conclusion.............................................................................................................229
Chapter9 Expectedrespectabilityfromanintersectionallens:discussionand
conclusion...............................................................................................230
9.1 Expectedrespectability.........................................................................................230
9.2 Applyinganintersectionallens..............................................................................233
Chapter10 Summary,policyrecommendationsandwayforward.............................235
10.1 Summaryofresearch............................................................................................235
10.2 Researchcontributions..........................................................................................236
10.3 Policyrecommendations.......................................................................................237
10.4 Limitations.............................................................................................................238
10.5 Futureresearch.....................................................................................................238
Postscript:Thestoryofmybirth.................................................................................241
AppendixATrahi’sbirthingexperience......................................................................245
AppendixBBodymappingaidedin-depthinterviewguide.........................................247
AppendixCNursemidwives’perspectivesonrespect,disrespect&abuseduring
childbirth.................................................................................................251
AppendixDKnowledgetranslation.............................................................................254
ListofReferences.......................................................................................................259


TableofTables
vii
TableofTables
Table2.1 Violationwomen’srightduringchildbirth........................................................9
Table2.2 Definitionsofdisrespectandabuse;andobstetricviolenceduringchildbirth13
Table2.3 Typologyofmistreatmentofwomenduringchildbirth..................................18
Table3.1 IndicatorsofviolenceagainstwomeninBiharandIndia...............................45
Table4.1 Studydesign....................................................................................................56
Table5.1 Participantprofile...........................................................................................67
Table5.2 Participant’sbirthrelatedvariables................................................................69
Table5.3 Typesofmistreatmentduringchildbirthexperiencedbywomen..................72
Table5.4 Percentageofwomenreportingobstetricviolencebywomen’sbackground74
Table5.5 Binarylogisticregression(oddsratio)(95%CI)...............................................79
Table5.6 Factoranalysis.................................................................................................83
Table5.7 Linearregressioncoefficientsofbackgroundcharacteristicsandthenew
obstetricviolencescores.................................................................................88
Table6.1 ParticipantsProfile........................................................................................110
Table6.2 Women’sunderstandingofgood,badandexpectedbirth..........................112
Table6.3 Women’sexperienceagainstBohrenet.al’sadaptedcategoriesofmistreatment
duringchildbirth............................................................................................119
Table8.1 Participantbydomainofleadership.............................................................205
Table8.2 Participantprofile.........................................................................................209


TableofFigures
ix
TableofFigures
Figure1.1 TheWHOqualityofcareframework(Source:WHO,2018,p.12)....................2
Figure2.1 Definitionofdisrespectofabuseduringchildbirth(Source:Freedmanetal.,
2014,p.916)...................................................................................................12
Figure2.2 Terminologicalterritoriesaround‘obstetricviolence’(Author’sown)...........14
Figure2.3 Evidenceofmistreatmentofwomenincountriesaroundtheworld(Author’s
own)................................................................................................................20
Figure2.4 Determinantsofdisrespectandabuseduringchildbirth................................24
Figure2.5 Personalchallengesinmidwifery(Source:Filbyetal.,2016,p.15)...............26
Figure2.6 Structuralandpolicychallengesinmidwiferycare(Source:Bradleyetal.,2019.
p.4).................................................................................................................27
Figure2.7 Meandmyclassmatesinouruniform............................................................31
Figure3.1 MapshowingpercentagesofinstitutionalbirthsinIndiabystate(Source:IIPS,
2015)...............................................................................................................34
Figure5.1 Socialdeterminantsofmaternalhealth(Source:Khanna&Sri,2018.p.194)63
Figure5.2 Women’sexperienceofobstetricviolenceunderBohrenetal.typology(2015)
........................................................................................................................70
Figure5.3 Thenumberoftypesofobstetricviolencesufferedbywomen.....................77
Figure5.4 ScreePlot........................................................................................................81
Figure5.5 Meanscoresofobstetricviolencebyagegroup............................................84
Figure5.6 Meanscoresofobstetricviolencebyeducation............................................85
Figure5.7 Meanofobstetricviolencebysocio-economicstatus....................................86
Figure5.8 Meanscoresofobstetricviolencebycaste....................................................86
Figure5.9 Meanscoresofobstetricviolencebyparity...................................................87
TableofFigures
x
Figure6.1 Themesofexplorationforrespect,disrespectandabuseduringbirth(Author’s
own)................................................................................................................97
Figure6.2 Birthmappingpilot.......................................................................................101
Figure6.3 Birthingmappinginaction............................................................................103
Figure6.4 Feministrelationaldiscourseanalysis...........................................................107
Figure6.5 Thehybridmapoftheworstexperiencefromtheeightbodymaps...........122
Figure6.6 Birthingposturesofwomen(Author’sown).................................................127
Figure6.7 Anju’sbodymapshowingherhomebirths..................................................129
Figure6.8 Birthplaceoptionsandchanges(Author’sown)..........................................135
Figure6.9 Ria’sBodyMap..............................................................................................140
Figure6.10 Levelsofprivacytobeprotectedforthewomeninbirthingroom(Author’sown)
......................................................................................................................141
Figure6.11 Pairo’sBodyMap..........................................................................................143
Figure6.12 Pratima’sbodymap......................................................................................157
Figure6.13 Sujata’sbodymap.........................................................................................158
Figure6.14 Amrita’sbirthmap........................................................................................166
Figure6.15 Rangeofwomen’scontrapuntalvoicesaboutselfdecision-makingandsurrogate
decisionmakingduringchildbirthandinlife(Author’sown).......................172
Figure7.1 Hierarchyofpowerrelations(Author’sown)................................................180
Figure7.2 Urmila’sbirthmap........................................................................................192
Figure7.3 Impactofgender,power,culture&structureonwomen(Author’sown)...198
Figure8.1 FlashcardshowingabirthingenvironmentinIndia.....................................207
Figure8.2 RecommendationsforrespectfulmaternitycareinIndia(Author’sown)....219
Figure8.3 Midwiferyleaders’perceptionsofobstetricviolence(Author’sown)..........226
Figure9.1 ContinuumofRespectfulExperiences(CORE)model(Author’sown)..........231

xi
Figure9.2 Intersectionalitywheelofobstetricviolence(AdaptedfromSimpson,2009,p.3)
......................................................................................................................234
TableofBoxes
xii
TableofBoxes
Box6.1 Pairo’sI-poem-Thisisthefateofwomenandwomenmustendureit!.......132
Box6.2 Pratima’sI-poem-Bornathome...................................................................137
Box6.3 Sita’sIpoemonJananiSurakshaYojana(JSY)..............................................138
Box6.4 Pairo’sI-poem-Doll.......................................................................................147
Box6.5 Urmila’sI-poem-Theladydoctorwasreallynice!........................................152
Box6.6 Ria’sI-poem-Thedeadbaby.........................................................................160
Box6.7 Ria’sI-poem-Ithasstayed............................................................................163
Box6.8 Urmila’sI-poem-Inevermadeadecisionaboutmyself...............................164
Box6.9 Amrita’sIpoem-Becauseofhim,Iaminthissituation!..............................167
Box6.10 Pairo’sIpoemaboutconversationaboutbirthingandpreparedness..........169
Box7.1 Pairo’sbirthingstory.....................................................................................184
Box7.2 Amrita’sI-poem-‘I’.......................................................................................187
Box7.3 Urmila’sbirthingstory...................................................................................193
Box7.4 Ria’sIpoem-HadIbeenfairerandhadbirthedaboy..................................196

Preface
xiii
Preface
‘I’
Iamarestlesssoul
Ilovedancing
IwastwoorthreewhenIfirstperformedonstage
Iamlovedfordancing
Iamstigmatisedfordancing
Ihadanomadicupbringing
ImovedtoanewstateinIndiaevery3-4years,myfatherisaretiredairman
IgetrestlesswhenIliveinastateorcountryformorethan3years
Ifeelrootsgrowingfrommywholebody
Ifindanewdestination,Imove
Iwaseducatedbymymother,shewasmymostpersistentteacher,verystricttoo
Iamadoctoralresearcher
Iamamidwiferyresearcher
Ihaveassistedchildbirths,themostlifechangingexperience
Iamanursingresearcher
Ihavefeltlifeleavingpeople’sbody
Ihavewashedthatbodyforthefamily

Preface
xiv
Igetattached
Iadvocate forgender-equality, for respectfulcare, fororgasmequality, formidwives’&
nurse’sroleinhealthpolicymakingandagainstallformsofgender-basedviolence
Iamafeminist
Iamaglobalhealthleader
Idoabitofsalsa,swing,bachata,folk,classicalandawholelotoffreestyle
Idanceintheshower
IdancewhenIcook
Ilovetravelling
Ihaveledcampaigns
Ilovecooking,Iamnotafoodie,Iamafussyeater,Ilovepostoandchingri
Ilovetherapy
Iwantedtoflyplanes
Idonotlikemaths
Ilovetalkingaboutintersectionality,positionality,inclusivityanddiversity
Ilovepeople
Ilovepeople’sstoriesofbirth
Idobirthmapping
Iampassionate,Iamkind,Iamveryweird
Ihavebeensexuallyharassed,multipletimes,atallages
Ithinkthestigmaaroundfemalemasturbationshouldend
Ithinkwomenexperiencingpleasureissexy
Iamaconfidentpublicspeaker
IamanervouswreckbeforeIfaceanaudience
Iamimpatient,Iamincapableofmeditating

Preface
xv
Iloveresearch,Ihavealwayslovedresearch
Iamawomanofscience
Ihavemadeawesomefriends,99%don’tlivearoundme
Ihaveasister,Keya,sheismylife,wehaveourparent’snamestattooedonourarms,her
tattooisnicer,it’scolourful,sheismyfavouritecompany,she’sanartist
Ifeltliberatedaftermydivorce
Ibondedthestrongestwithmyparentsaftermydivorce,Ilovethemverymuch
Ihavetwotattoos
IgotmyKalpanaSamar’stattooedonmyarminrebellionbeforemymarriage
Ialwayswantedtogetmarried,sinceIwasachild
Ithoughtthekeytofreedomfromoppressionisinfindingthemostequal-mindedhusband
Ilovemyeyes,everyonedoes,IwantedtodonatethemsinceIwasachild
Ihavetokophobia
Ilovebeinginlove
IproposewhenIfallinlove,it’sapattern
Ilikestickynotes,bignotes,whiteboards,postcards,letters,stationery
Iamscaredofpetdogs
Ithinkmusiccanhealeverything
IwriteaboutDocsplanation
IthinkonedayIwilladoptachild,Ialwayswantedto,sinceIwasachild
Ithinkfeministwritingisamazing
Ireadeverymorning
Ican’tdowithoutChikki,Chikklettismyniece,sheisChikktasticandallthingsChikk
Ilovemysurnamemorethanmyfirstname,Iwishitwasmyfirstname
IknitscarveswhenIgothroughanxietyanddepression

Preface
xvi
Ilearntknittingfrommymom
Ilearntembroideryfrommydad,no-oneembroidersbetterthanhim
Ihavetravelledtooverfourteencountries
Ithinkpeoplehaveno-ideahowtobehavearoundadivorcedwoman,theyfeelnowthatherlifeis
ruinedletthepoor-thingdowhatevermakesherhappy,itisfascinating
IamaBengali,fromIndia
Ispeakthreelanguageswell
Iunderstandmanymore
Iamaworkaholic
Ineedtolearntodrive
Ilovecolours,Iwearcolours,Idresstoresist
Iamawesomeinverbalcommunication
Iwritetoresist
Ifeelthatswitchingtoamenstrualcupwasthebestdecision
Ithinkpeoplewhoauthorgoodbooksaresuper-humans,soarevegans
Iwillwriteabooksomeday
Iknowsomereallyamazingwomen
Ipickeduphula-hoopinginthepandemic
Iamboxingthesedays,Ilovepunching
Icarryseverallayersofguilt
IhopeKeya,ChikkiandIlivetogetherfor3yearsinanothercountry,justus
Iwillhavearoomwithacupboardsomewhereintheworld,tocallmyown
Ican’tsettle,Icanneversettle
Iwillfindpatienceandcalm
Ilovewaterfalls,oceans&rivers

Preface
xvii
Iamnamedafterariver

ResearchThesis:DeclarationofAuthorship
xix
ResearchThesis:DeclarationofAuthorship
Printname:KaveriMayra
Titleofthesis:‘Womenaresupposedtoendurethat!’Acriticalfeministexplorationofobstetric
violenceinwomen’sandmidwives’birthnarrativesinIndia
Ideclarethatthisthesisandtheworkpresentedinitaremyownandhasbeengeneratedbyme
astheresultofmyownoriginalresearch.
Iconfirmthat:
1. Thisworkwasdonewhollyormainlywhileincandidatureforaresearchdegreeatthis
University;
2. Whereanypartofthisthesishaspreviouslybeensubmittedforadegreeoranyother
qualificationatthisUniversityoranyotherinstitution,thishasbeenclearlystated;
3. WhereIhaveconsultedthepublishedworkofothers,thisisalwaysclearlyattributed;
4. WhereIhavequotedfromtheworkofothers,thesourceisalwaysgiven.Withtheexception
ofsuchquotations,thisthesisisentirelymyownwork;
5. Ihaveacknowledgedallmainsourcesofhelp;
6. Wherethethesisisbasedonworkdonebymyselfjointlywithothers,Ihavemadeclear
exactlywhatwasdonebyothersandwhatIhavecontributedmyself;
7. Partsofthisworkhavebeenpublishedas:
• MayraK.,MatthewsZ.,PadmadasSS.2021.Whysosomehealthcareprovidersdisrespect
andabusewomenduringchildbirth.WomenandBirth.Inpress.Doi.
https://doi.org/10.1016/j.wombi.2021.02.003
• MayraK.,MatthewsZ.,SandallJ.Thecaseof‘surrogatedecision-making’inIndiafor
womencompetenttoconsentandchooseduringchildbirth.Agenda.Doi.
https://doi.org/10.1080/10130950.2021.1958549
• MayraK.,SandallJ.,MatthewsZ.,PadmadasSS.2021.Breakingthesilenceabout
obstetricviolence:Bodymappingwomen’snarrativesonrespect,disrespectandabuse
duringchildbirthinBihar,India.BMCPregnancyandChildbirth.Accepted.
Signature: ................................................................Date:21/07/2021


Acknowledgements
xxi
Acknowledgements
ThisthesisisbornoutofadreamthatIhavenurturedforoveradecade.Iamoneofmany
Indianwomenwhohavesuchdreams,butveryfewgetanopportunitylikeIdid.Thisthesis
andmydoctoralresearchwouldnothavebeenpossiblewithoutthesupportfrommany
peopleindifferentcountries,whohavekeptmegoing.Theyhelpedmelivemydream.
DeborahGearingwhogavemeahomeawayfromhomeandbecamemyfamilyawayfrom
family,andsupportedmethroughthetoughestoftimesbeitapandemic,ornumerous
personalcrisis.Shehasalsoentertainedmyseveral‘English’relatedquestions,withimmense
knowledge,supportedbymanydictionariesandlanguagestyleguides.
TomNewton-Lewissawnotjustpotential,buta‘rockstar’inmeandhelpedmeinevery
possibleway,tomakethisPhDhappen.RodantevanderWaal,myphilosophyguruand
EuniceMueni,mystatisticscoach,havebothseenthefearsandtearsupclose.Eunicehas
entertainedmylatenightvideoscreensharingcallswheneverIneededher,whichwastoo
manytimes.SudiptaBosesavedmefrompurchasingseveralpanic-laptopsandishelping
withtechnologyevenasIwritetheacknowledgements,thatisrightnow!Thesefriends,
family,havehelpedmethroughwaytoomanyanxieties,tocount.
SmritikanaMani,mymidwiferyprofessorandM.Prakasamma,mymentor,havebeenrole
modelsandhavebroadenedmyunderstandingofthechallengesinmidwifery,nursingand
maternalhealthathomeandIcontinuetobeinspiredbythem.Allmymidwifery,nursing
andglobalhealthfriendsandcolleaguesinIndiaandeverywhereintheworldwhohave
masteredinsocial-mediasupportandmotivation,andhavebeenabigwarmvirtualfamily.
SandyAvrutin,PabloTrucco,BenRoss,Christian,AparnaJohn,JurajMihalik,VictoriaHobbs,
CamillaPickles,RituKumari,SoumiKarmakar,SubarnaGhosh,SudeshnaDey,ManasMurmu,
KarimaKhalilandVanesaRomero-Kutznerhavebeenimportantcheerleadersandhavebeen
essentialformymentalhealth.
Mysupervisors,ZoëMatthewsandSabuPadmadas,withwhommypassionformaternal
healthresearchalignedfromthemomentwemetandIwantedtodomyPhDwithonly
them.IneverappliedforastudentshipanywhereelsebutUniversityofSouthampton,
becauseitisfortunatetohavethemasprofessors.Iamtheluckiesttohavethembothasmy
supervisors.IhaveproudlyshowedoffasthehappiestPhDstudentanditwasallbecauseof
them.IamtemptedtodoasecondPhDrightawayifthey’llhavemeasastudentagain.My
externalsupervisor,JaneSandall,atKingsCollegeLondon,tookmeupasaPhDstudentand
Acknowledgements
xxii
guidedmethroughuniquefeministresearchmethods.Iamverygratefultoherforher
generositywithhertime,effortsandguidance.
FranMcConville,BrigidMcConville,BashiKumar-HazardandmanyotherfriendsattheWHO
HQ,WhiteRibbonAllianceUKandIndia,WHOIndia,OxfordPolicyManagementLtd.,
WomeninGlobalHealthIndia,AcademyforNursingStudiesandWomen’sEmpowerment
ResearchStudies,HumanRightsinChildbirth,InternationalConfederationofMidwives,
All4BirthandSocietyofMidwivesIndiahavesupportedmethroughthickandthinandhave
enrichedmewiththeirwisdom.
IamgratefulforthefundingsupportfromtheViceChancellor’sScholarshipattheUniversity
ofSouthampton;BurdettTrustforNursing,UK;ParkesFoundation,UKandtheRoyal
NorwegianEmbassy,India.
IwillforeverbegratefulforhavingVarunKakdeinmylife,assomeonewhohasbeena
sourceofconstantsupport,loveandhappinesssincebeforeIstartedmyPhDandtheperson
IcausedthemostpainsoIcouldaccomplishmybiggestdream.
Keya,Chikki,Baba(SamarendraNathMayra)andMa(KalpanaMayra),Icanfinallybook
ticketstoseemyfamilybackinIndia.Iamlookingforwardtothebiggestreunionever!Ithas
beenalmosttwoyearsIhavenotseenthemandIfeelthepandemichasbroughtuscloser.
ThisPhDwouldnotbewrittenwithouttheirsupportandsacrificeandthegenesIrecently
foundoutaboutthatturnsallthewomeninourfamilyintobookworms.Iamtoldmy
grandmother,marriedofbeforeshehitpubertylearnttoreadfromherchildren’sschool
booksandthennoonecouldseparateherbooks,newspapers,advertisements,everything,
withatinylampshewouldhidefromeveryone.Iftherewerewordsanywhere,shewould
readthem.Hertwolibrarycardswerehergreatestpossessionandcouldnotsatisfyher
hungertoread.Thispassionforeducationwassharedbymymotherwhopasseditontome
andmysisterandIseeitinmyniecewhoisneverwithoutabook.Weareallvoracious
readers.
PS:Nowthatyouhaveseenyournamesintheacknowledgement,doreadthethesis.J

Acknowledgements
xxiii


DefinitionsandAbbreviations
xxv
DefinitionsandAbbreviations
ANC......................................AntenatalCare
ANM....................................AuxiliaryNurseMidwives
AMANAT..............................ApaatkalinMatritvaevamNavjaatTatparta
ASHA....................................AccreditedSocialHealthActivist
BPHC....................................BlockPrimaryHealthCentre
BEmONC..............................BasicEmergencyObstetricandNeonatalCare
CHC......................................CommunityHealthCentre
CEMONC..............................ComprehensiveEmergencyObstetricandNeonatalCare
CEDAW................................ConventionontheEliminationofDiscriminationAgainstWomen
CS.........................................CesareanSection
CME.....................................ContinuedMedicalEducation
CMS.....................................CentreforMediaStudies
CAMT...................................CentreforAdvancedMedicalTraining
CORE....................................ContinuumofRespectfulExperiences
EAG......................................EmpoweredActionGroup
ERCC....................................EssentialRespectfulCareCourse
FRDA....................................FeministRelationalDiscourseAnalysis
GE........................................GeneralExamination
GOI......................................GovernmentofIndia
GNM....................................GeneralNurseandMidwife
HH........................................Household
IDI........................................In-depthInterview
IUCD....................................IntrapartumUterineContraceptiveDevice
IMR......................................InfantMortalityRate
INC.......................................IndianNursingCouncil
ICM......................................InternationalConfederationofMidwives

DefinitionsandAbbreviations
xxvi
ICN.......................................InternationalCouncilofNurses
IPV.......................................IntimatePartnerViolence
IV.........................................IntraVenous
JSY.......................................JananiSurakshaYojana
NFHS....................................NationalFamilyHealthSurvey
NHM....................................NationalHealthMission
NPM.....................................NursePractitionerinMidwifery
NRHM..................................NationalRuralHealthMission
MDG....................................MillenniumDevelopmentGoals
MMR....................................MaternalMortalityRatio
MNMT.................................MobileNurseMentoringTraining
LMIC....................................LowerMiddleIncomeCountries
OT........................................OperationTheatre
PSE.......................................Pre-ServiceEducation
PTSD....................................PostTraumaticStressDisorder
PMNCH................................<KaveriMayratofill>
QoC......................................QualityofCare
SDG......................................SustainableDevelopmentGoals
SES.......................................Socio-EconomicStatus
SOMI....................................SocietyofMidwivesIndia
SIDA.....................................SwedishInternationalDevelopmentAgency
SNC......................................StateNursingCouncil
SPSS.....................................StatisticalPackageforSocialSciences
SRS.......................................SampleRegistrationSystem
SBA......................................SkilledBirthAttendants
UNFPA.................................UnitedNationsFundsforPopulationActivities
UNHCR.................................UnitedNationsHighCommissionforRefugees
UN.......................................UnitedNational

DefinitionsandAbbreviations
xxvii
VE........................................VaginalExaminations
WHO....................................WorldHealthOrganisation
WRA.....................................WhiteRibbonAlliance


Chapter1
1
Chapter1 Whystudyobstetricviolence?
1.1 Introduction
“DoNoHarm”isthekeyethicalprincipleforhealthcareproviders,yetevidenceismounting
showingwomen’sexperiencesofobstetricviolenceduringchildbirth–arguablythemost
vulnerablephaseoftheirlife(Vogeletal.,2015;Khoslaetal.,2016;Pateletal.,2015).Childbirth
isanaturalprocessandthoughtheeventismarkedbyritedepassageandcelebrations(Nayak&
Nath,2018),evidencefromoverhalfoftheworld’snationsindicatethatobstetricviolenceisa
globalissue.Thisthesismakesanoriginalcontributiontounderstandingtheextentofobstetric
violenceinresourceconstrainedsettingsinIndiawithafocusonexperiencesandperceptionsof
bothwomenandnurse-midwives,astheirprimarycareproviders.
Irefertotheproblemas‘obstetricviolence’throughoutthisthesiswithreasonsexplained
throughmypositionalityinthenextchapter,althoughthereareseveralterminologiesusedby
researchersthatIrefertowhenIquotestudies.Mistreatmentofwomeninlabourisrecognised
asadeterrenttofacility-basedbirthwhichalsothreatensprogresstowardsreductionsin
maternalmortality(Bohrenteal.,2015).Itisaviolationofwomen’srighttothehighestattainable
standardsofhealth(WHO,2015)thatincludesrespectfulanddignifiedcareduringchildbirth.Itis
importanttounderstandwhatitmeanstoreceivequalityofcareandhowrespectfulcareis
situatedinitsrealmwhilebeingmindfulthateverywoman’sexperience,needsandexpectations
ofrespectfulcarecanbeuniqueandneedstobeunderstoodtoprovideperson-centeredcare
(Downe,2019).
TheWorldHealthOrganization(WHO)definesqualityofcareas‘theextenttowhichhealthcare
servicesprovidedtoindividualsandpatientpopulationsimprovedesiredhealthoutcomes’and
furthersays,‘toachievethis,healthcareneedstobesafe,effective,timely,efficient,equitable
andpeoplecentred’(WHO,2016,p.14).Inrecognitionofthis,WHOhasincludedexperienceof
careasamainaspectintheprocess,whichisfurtherdividedinto:1)effectivecommunication;2)
respectandpreservationofdignityand3)emotionalsupportasthethreecomponentsinthe
WHOframeworkforQualityofCare(Figure1.1)(Hulton,Matthews&Stones,2000).The
frameworkisinlinewithDonabedian’sModelofQualityofCare(Donabedian,1988),butthesub-
componentsonrespectanddignityforwomenseekingcaremakesitmoreresponsivetowomen
centredcareandoutcomes.

Chapter1
2
Figure1.1 TheWHOqualityofcareframework(Source:WHO,2018,p.12)
Respectfulnesshasbeenidentifiedasanessentialactionpointwhenitcomestoperson-centred
careprovision(WHO,2015).WHO’sguidelinesforintrapartumcareconsistsoffournew
recommendationsspecificallyon:1)respectfulmaternitycare;2)effectivecommunication;3)
companionshipduringlabourandchildbirthand4)continuityofcare.Otherrecommendations
alsoaimtoensurerespectfulnessanddignityofwomenduringchildbirthbyensuringherchoice
ofpositionandadequatemobility,byavoidingunnecessaryinterventions,andensuringadequate
painrelief.Theserecommendationsintendtomakechildbirthapositiveexperienceandcareto
bewomencentred(WHO,2018).
Thereisagrowingevidencerelatedtoobstetricviolencefromaroundtheworldbuttherehave
beenlimitedeffortstounderstandwhatdrivesthisissueandthedeterminantsofobstetric
violenceduringchildbirth(Bhattacharyaetal.,2013;Murray,2008;Jefferyetal.,2010;Hunter,
2009).Itisalsoimportanttonotethatoftenwhatdrivestheproblemisnotlearntfromthose
whoexperienceitandthoseatthefrontlineofcareprovision,suchasthenurse-midwives.There
isalackofstudiesexploringwomen’sunderstandingoftheissueofobstetricviolencewherethe
issueexists,giventhecultureandcontextdrivensubjectivenatureofperceptionsofrespect,
dignity,disrespect,abuseandviolence.Thisgapneedstobeaddressedtocallforanendto
obstetricviolencebylearningthewaystoaddressthisissuefromwomenandcareproviders(such
asnurse-midwivesinIndia),asthekeystakeholdersinvolvedinthisprocessofexperiencingcare
andprovidingcare.Thedeterminantsofobstetricviolencelieatdifferentlevelssuchasthe
individual,structuralandpolicylevels(Freedmanetal.,2014).Theythereforeneedtobeexplored
atthesethreelevelstobeaddressedintheserespectivelevels.Whilewomencansharetheir

Chapter1
3
experiencefromthecareseekersendatthesethreelevels,nurseandmidwiferyleaderscan
sharethesideofthecareproviders,havingprovidedcareatfrontlinesofprimarycareprovision,
followingbyreachingthehighestlevelofpolicymaking.Therefore,theinclusionofnursingand
midwiferyleadersisessentialtothisthesistounderstandtheentiregamutofdeterminantsof
obstetricviolence.
Indiaishometoover1.3billionpeople(Census,2011)withthesecondhighestnumberof
birthsintheworld.Indianwomenpresentadiverseprofileindifferentstatesbasedon
attributessuchaseducation,occupation,religion,healthstatusandespeciallywhen
comparedwithmen.Forinstance,thecurrentliteracyrateforwomeninIndiais68%when
comparedtomen(86%),whichfurthervariesforwomenbyrural(62%)andurban(81%),as
reportedbytheNationalFamilyHealthSurvey(NFHS-4).Italsofoundthat27%womenaged
between20-24yearsweremarriedbeforeturning18years,whichisthelegalageof
marriageforwomeninIndiaandhave2.2childrenperwoman.Thereportfurtherssuggests
that8%womenagedbetween15-19werealreadymothersorpregnantatthetimeof
survey.Therearedisparitiesinfamilyplanningtoo,wheremorewomenundergosterilisation
(36%)thanmen(0.3%)(NHFS-4).
Indiafacesuniquechallengesinmaternalhealthcareprovision,whicharemorepronounced
inparticularIndianstates,suchasBihar.Indiaalsohasoneofthemostinstitutionalised
systemsforchildbirthintheworld,bothintermsofspeedandscale,withover79%women
givingbirthathealthcareinstitutions,whichiscreditedtohavebroughtIndia’sshareofthe
globalburdenofmaternaldeathsfrom19%(WHO,2015)to12%(WHO,2019).Although,its
impactonthequalityofcarehasoftenbeenquestionedinitsmovetowardsmedicalisation
thatfurthermakesitaninterestingsettingtounderstandobstetricviolenceduringchildbirth,
consideringover-medicalisationasoneofitsenablersinthiscontext.Thehighcaesarean
sectionrates(17%)indicatesthis,whichshowsfurtherdisparitiesbetweenprivate(41%)and
publicsectors(12%)(NFHS-4).Violenceisgenerallyhighinwomen’sliveswith31%married
womenreportedlyexperiencingspousalviolenceand4%whilebeingpregnant(NFHS-4).
Therearenosystematiceffortstocollectevidenceonobstetricviolenceandresearchonthis
sensitivesubjectistheneedofthehour.
Aim:Mythesisinvestigatesobstetricviolenceandrespectfulnessincareprovisionduring
childbirthandhowitcanbeimprovedthroughmidwiferyleadership,learningfromthe
perspectivesandexperiencesofwomenasprimarycare-receiversandnurse-midwifeleaders
fromtheirexperienceasprimarycare-providersinIndia.
Chapter1
4
1.2 Researchobjectives
Thisthesisispresentedinathreepaperformat,withanexceptionofanadditionalpaper,
addressingthefollowinginterrelatedobjectives:
• Paper1usesquantitativesecondarydatatoexaminethesocialdeterminantsofobstetric
violenceduringchildbirthinBihar,India.
• Paper2and3usebodymappingaidedin-depthinterviewstounderstandwomen’s
perceptionandhowtheyattachmeaningtorespect,disrespectandabusefromtheir
experienceofgivingbirthandtheirunderstandingofwhatdrivesrespectful,disrespectfuland
abusivecareduringchildbirthinBihar,India.
• Paper4qualitativelydocumentsandanalysetheexperiencesofmidwiferyleadersonrespect,
disrespectandabuseandrecommendnewevidence-basedpoliciestostrengthenrespectful
careforwomenduringchildbirthinIndia.
1.3 Researchquestions
• Whatarewomen’sexperienceofobstetricviolenceinBihar?(Paper1and2)
• Whatmakesawomanvulnerabletoexperiencerespect,disrespectandabuseduring
childbirthinpublichealthinstitutionsinBihar?(Paper2)
• Howdowomenattachmeaningtotheirexperiencesofrespect,disrespectandabuseduring
childbirthinBihar?(Paper2)
• Whatarewomen’sunderstandingoftheunderlyingfactorsdrivingrespect,disrespectand
abuseduringchildbirthinBihar?(Overarchingquestion-Paper3)
• WhydosomecareprovidersdisrespectandabusewomenduringchildbirthinIndia?(Paper4)
• Whataremidwives’experiencesofrespect,disrespectandabuseduringchildbirthinIndia?
(Overarchingquestion-Paper4)
1.4 Thesisorganisation
Mythesisisorganisedinto10chapters.Chapter1laysouttherationaleandneedforthePhDand
helpstounderstandtheresearchobjectivesandquestions.Chapter2presentsareviewof
literaturetounderstandthetypologyandthefactorsinfluencingrespect,disrespectandabuse
duringchildbirthglobally.Italsonarratesthechallengesinrespectfulmaternitycareprovision
alongwiththeglobalevidenceofobstetricviolenceduringchildbirth.Itincludesmypositionality
fordoingthisresearchwhichisblendedthroughoutmythesis.Chapter3setsthecontextof
maternalhealthcareprovisionduringchildbirthandthestatusofwomeninBiharandIndiato

Chapter1
5
understandtheissueinthegeopoliticallocationofmyresearch.Chapter4presentsthe
methodologyanddifferentmethodsusedtoexploretheresearchobjectiveswithaconceptual
frameworkthatconnectsthefourpapers.
MyPhDisstructuredinthethreepaperformat,whichispresentedinthenextfourchapters,
whichessentiallyareonepapereach.Chapter5investigatesthesocialdeterminantsofobstetric
violencequantitativelythroughthesecondarydatafromalargescalehouseholdsurveydonein
Biharthatincludesself-reportofthewomenwithinamonthoftheirinstitutionalbirth.Chapter6
presentshowwomenexperienceandperceiverespect,disrespectandabuseduringchildbirth.
Thisisconductedqualitativelythroughavisual-artsbasedparticipatoryresearchinBihar,India.
Chapter7discussestheimpactofgender,power,cultureandstructureonwomen’sbirthing
experienceswhichisanextensionoffindingsfromChapter6butpresentedseparatelyto
acknowledgethethematicchangeincontent.Withthefirstthreefindingschapterexploringthe
experienceandperceptionsofwhatconsistsofobstetricviolenceandwhatdrivesin,Ithen
presentthecareprovider’sexperienceandperspectiveofthesame,fromwhoarenursingand
midwiferyleadersinthecontextofIndia.Chapter8examineswhysomecareprovidersabuse
womenduringchildbirthqualitativelyfrommidwiferyandnursingleadersexperienceand
perceptionsinIndia.InChapter9bindsthefindingstogetherfromanintersectionallensand
concludesthethesis.Inchapter10summarisesthethesis,presentsrecommendationsforpolicies,
futureresearchandlimitations.Thestudytools,apublishedmanuscriptanddetailsonknowledge
translationareappended.


Chapter2
7
Chapter2 ObstetricViolence:Aliteraturereview&
positionality
Obstetricviolenceduringchildbirthisanimportantandsensitiveissueforvariousreasons.Firstly,
itisaviolationofwomen’sfundamentalhumanrights.Secondly,careprovidersandhealth
systemspolicymakershaveacknowledgeditasanindicatorofalackofqualitycarewhichcan
leadtopoormaternalandneonatalhealthoutcomes.Asevidenceonobstetricviolenceduring
childbirthevolves,itbecomesincreasinglydifficulttoignorethewidespreadnatureofthisissue
andtheeffortsrequiredtoaddressthischallenge.
Inthischapter,Ipresenthowobstetricviolenceisperceivedindifferentcountrieswithglobal
evidence,typologiesandchoiceofterminologies.Thesubsequentsectionontheimpactof
obstetricviolencehighlightstheimportanceofrespectfulmaternitycareforapositivebirthing
experience.Whilethereisadearthofliteraturediscussingthefactorslinkedwithobstetric
violenceduringchildbirth,therearesomestudiesconnectingwomen’sbackgroundcharacteristics
andcareproviderattributesthatmayinfluencematernitycareprovision.
Obstetricviolenceduringchildbirthcanbeunderstoodfromtwokeyperspectivesguidedbythe
literature:1)feminism,followingtheprinciplesofequality,equity,diversity,inclusivityand
humanrightsand2)healthsystems,guidedbytheprinciplesofethicsandqualityofcare
provision.Thestakeholdersworkinginthisareaaredividedintousergroupsandadvocatesof
women’srightsdemandingfortheirrighttoadignifiedbirthingexperience.Thecareproviders
andpolicymakersontheotherhand,aretryingtoensurerespectfulanddignifiedcarewhile
addressingtheexistinghealthsystemsconstraints.Theexistingliteratureonthedefinitions,
terminologies,typologies,impact,driversandwaystoaddressobstetricviolenceduringchildbirth
fallunderthesetwodomains,feminismandhealthsystems.
ThefeministrightsactivistAdichie(2014),warnsherreadersaboutthedangersoflisteningtoa
singlestorywithoutunderstandingthecontext.Theissueofobstetricviolenceisnoexception,
andshouldbeunderstoodfromthefeministperspectiveandhealthsystemsperspective;from
thecare-seekerandcare-provider,bothpredominantlywomen,sharingtheirsidesofthestory
fromtheirstandpointbasedontheirlivedexperiences.Thisreviewemphasisesandpresentsboth
perspectivesfromfeministideologyandunderthequalityofcareframework,bothofwhich
eventuallyleadtothecommonlydesiredoutcomeofwomen-centredcareandabirthing
experiencethatisrespectfulanddignified.

Chapter2
8
Genderisakeybackgroundfactorthatinfusestheentirenarrativeandisembeddedinallthe
chaptersofthisthesisstartingwiththisliteraturereview.Eventhoughitisreflectedinthe
narrativesaroundfeministperspectivemorepredominantly,thehealthsystemsperspectiveis
alsopresented.Inthefollowingsections,Ipresentthesetwoperspectivesincludingdefinitions,
determinants,impactandthewayforward.
2.1 Obstetricviolencefromarightsperspective
Obstetricviolenceofwomenduringchildbirthisaviolationofhumanrights(Miller&Lalonde,
2015;Allotey-Reidpathetal.,2018;Miltenburgetal.,2018).Humanrightsacknowledgesthat
“…eachindividualisentitledtoenjoyhisorherrightswithoutdistinctionastorace,colour,sex,
language,religion,politicalorotheropinion,nationalorsocialorigin,property,birthorother
status.”(UnitedNations,1948).Thereare32articlesintheUniversalDeclarationofHumanRights
whichhavebeenratifiedby192countries,includingIndia.Anycountrythatissignatorytothe
UniversalDeclarationofHumanRightsislegallymandatedtoensuretheserightstoitscitizens
(UnitedNations,1948;Khoslaetal,2016).Aspermyunderstanding,obstetricviolenceduring
childbirthisaviolationofhumanrightsunderthesesixarticles,shownintable2.1.

Chapter2
9
Table2.1 Violationwomen’srightduringchildbirth
Article
no.
UniversalDeclarationofHuman
Rights
Whatitmeansforchildbirth
1 Allhumanbeingsarebornfree
andequalindignityandrights
Allwomenandbirthingpeoplearebornfreeand
equalindignityandrightsinlife,includingduring
childbirth.
2 Everyoneisentitledtoallthe
rightsandfreedomssetforthin
thisdeclaration,without
distinctionofanykind,suchas
race,colour,sex,language,
religion,politicalorother
opinion,nationalorsocialorigin,
property,birthorotherstatus
Everywomanandbirthingpersonisentitledtoall
therightsandfreedomsincludingherrightto
satisfactorybirthingexperiencefreefrom
unnecessaryinterventions,disrespect,abuseand
withbestpossiblecareduringchildbirth.
3 Nooneshallbesubjectedto
tortureortocruel,inhumanor
degradingtreatmentor
punishment
Nowomanorbirthingpersonshouldbesubjected
toanyformofdisrespect,abuseandviolencewhen
seekingmaternalandreproductivehealthcare.
7 Allareentitledtoequal
protectionagainstany
discriminationinviolationofthis
declarationandagainstany
incitementtosuch
discrimination
Nowomanorbirthingpersonshouldbe
discriminatedonthebasisofcolour,caste,religion,
background,gender,sexuality,physicalandsocio-
economiccharacteristicswhileseekingmaternal
andreproductivehealthcare,whichwouldbea
violationofthisdeclaration.
21 Everyonehastherighttoequal
accesstopublicserviceinhis
country
Everywomanandbirthingpersonhastherightto
betreatedequallyandfairlyintermsofresource
allocationandmaternalandreproductivehealth
caretheyreceive,includingduringchildbirth.
25 1)Everyonehastherighttoa
standardoflivingadequatefor
thehealthandwellbeing
ofhimselfandhis
family.2)Motherhoodand
1)Everywomanandbirthingpersonhasarightto
qualityandrespectfulmaternalhealthcareduring
childbirthforthehealthandwellbeingofherself,
hernew-bornandherfamily.2)Everywomanand
birthingpersonisentitledtospecialcareduring

Chapter2
10
Article
no.
UniversalDeclarationofHuman
Rights
Whatitmeansforchildbirth
childhoodareentitledtospecial
careandassistance
pregnancy,childbirthandpostnatalperiodwhen
seekingmaternalandreproductivehealthcare.
Thedeclarationofhumanrightsisnotgenderneutralorinclusiveinlanguage.Amajordrawback
ofthedeclarationisthatitfailstorecognisewomenandreferstoonlymen.Itreferstopeopleas
‘he’,‘his’,‘him’and‘himself’around22timesinthedocument,ignoringtheglobalpushfor
genderneutralandgenderfluidlanguage.
TheUniversalDeclarationofHumanRightsalsodoesnotrefertowomen’srightsduringchildbirth
directly,butthisgapwasfilledbytheConventionontheEliminationofallformsofDiscrimination
AgainstWomen(CEDAW).Itisoneoftheeightmajorhumanrightstreaties,theonlyonethat
directlyreferstorespectfulhealthcareforwomenundertheprovisionofArticle11(1)(f),12,14
(2)(b)andgeneralrecommendation24onwomenandhealthfornon-discriminationinthefieldof
healthcare.Itspecificallystates,“…thedutyofthestatespartiestoensure,onabasisofequality
betweenmenandwomen,accesstohealthcareservices,informationandeducationimpliesan
obligationtorespect,protectandfulfilwomen’srightstohealthcare.”(WHO,2007,p.3).There
are180signatoriestoCEDAWthatareliabletoratifythisintheircountry,includingIndia
(CEDAW,1980).
Thethirdkeydocumentinthisregardisthecharteronrespectfulmaternitycarewhichtakesit
furtherbypresentingthesevenUniversalRightsofChildbearingWomen(WRA,2015)whichis
updatedin2019toincludetherightsofthenewborn(WRA,2019).Thischarterembedstherights
ofchildbearingwomenwithinthecontextofhumanrights,thoughitisnotlegallybindingasthe
CEDAWandUniversalDeclarationofHumanRightsare.
2.2 ‘Obstetricviolence’:Terminologies,definitions,resistance,
movementsandthehistory
Namingviolenceinpublicdiscourseisessentialtoendingviolenceagainstwomen.Althoughthere
isadisbelief,areluctancetoacceptandnameviolenceagainstwomen,whichisnotnew.I
wantedtofindoutwhenitwasthatthefirstwomansuffereddomesticviolenceand/orintimate
partnerviolence.ThenIwantedtotracehowlongittookfromwhentheseabuseswerenamed,
towhenprogresswasmadeinconsideringittobeakeyformofviolenceagainstwomen,

Chapter2
11
embeddedingender-basedviolence.Itprobablytookcenturies!Similarly,itwouldbedifficultto
tellwhenthefirstwomanexperiencedobstetricviolence.
ThehistoryoftheSim’sspeculumandthenotoriousexperimentsbyDr.JMarionSims,thefather
ofGynaecology(Davis,2019),onblackenslavedwomen’sbodiesisagorydetailinhistory(Davis,
2019).Itprobablyisasfarbackasrecordedhistorygoesregardingobstetricviolenceembedded
inandindicatingobstetricracism(Davis,2019;Cleghorn,2021;Hamad,2021).Almosttwo
centurieslater,Iseeandreadsimilaranecdotesofwomenbeingtraumatisedthroughun-
anesthetisedepisiotomyrepairs.Theexpectationsforsomewomentobearmorepainbasedon
theirraceorclassandothersocialconstructs,alsocalled‘ObstetricHardiness’,persiststwo
centurieslater(Davis,2019).Ihaveapersonalconnectiontothisconcept.Mymothertoldme
thatshewasonher‘best-behaviour’andnotmakingasound,andclenchingherteeththrough
thepainfulcontractions,asitsavedherfromfacinganyhumiliation.Shereportssatisfactionfrom
herbirthingexperienceasshehadmanagedtoavoid‘misbehaviour’(bajebaiboharinBengali).I
thinkmymotherperformedobstetrichardinesstoavoidobstetricviolencewhenIwasbeingborn
inthemid-eightiesatagovernmentmilitaryhospitalinIndia(elaboratedinChapter6).
Whiletheproblemremainedunnamedinthemid-eighties,aconnectioncanbedrawnfromthe
anecdotesofwomen’srightsactivistssuchasbellhooks,AnnOakleyandSheilaKitzingertothe
beginningofrecordedover-medicalisationofbirthintheeighties.Amanifestationofthiscouldbe
seenintheexodusofwomenfromhometohospitalbirthsandtherisingcesareansectionrates
aroundtheworld.Whilethesefeministauthorsdidnotusespecificterminologies,the
characteristicsofdehumanisedbirthingexperienceswereevidentinthecontentandbooktitles
suchas‘Capturedwomb’and‘Confinedwomen’.Espinoza-Reyes(2020)andSolispositionthis
‘colonisationofthewomb’asobstetricviolenceandahumanrightsviolationintheMexican
context.
‘Obstetric’,atermtreatedasholy,sacrosanct,andimplyingconnectiontoobstetricians,makesit
abattlegroundwhen‘violence’isattachedtoit.Thetermisconsideredfeminist,activist,
journalistic,non-academic,alarminganddangerous.Academicsfinditdifficulttopublishand
makepresentationswithobstetricviolenceinthetitle(Levesque&Parayre,2021).Forexample,
inIndia,twoofmyownpaperswereremovedfromthefinalstagesofreviewbecausetheissueis
deemedcontroversialandcouldcauseapoliticalturmoilwhenreportsofobstetricviolenceare
published.Governments,globally,donotappreciatebeingtoldthatwomenareexperiencing
obstetricviolence,it’stoostrong,harshandreal,theycan’tbearit.Theypreferbeinggentlymade
awarethatwomenareexperiencing‘alackofrespect’whentheygivebirth.Brazil’sMinistryof

Chapter2
12
Health’sdecisiontodroptheterminologyfromofficialdocumentsisanexampleofapatternseen
inmanycountriesthatarestillindenial(Ignacio,2019).
Thecompetingterminologiesinclude‘disrespectandabuse’thathavebeendefinedbyFreedman
(2014)categorisingintoindividual,structuralandpolicyfactorsthatdrivethepractice(Figure
2.1);whileSen,ReddyandIyer(2018)focusedonthecontextofIndiaandexplaineddisrespectas
thelessandabusemoreextremeinstanceswhilereferringtomanyunderlyingfactorsfroman
intersectionalperspective.Boththedefinitionsmainlyreferredtotheprocessanddriversofthe
issue.Othernoteworthytermsincludestructuralviolence(Miltenburg,2018),normalised
violence(Chadwick,2017)andsymbolicviolence(Morgan,Thapar-Björkert2006)thatcanbe
usedtoexplainaspectsofobstetricviolencebringinginthehierarchy,power,statusandcontrol
relatedargumentswhicharealsocoveredinsomewayinthepreviouslymentioneddefinitions.
Figure2.1 Definitionofdisrespectofabuseduringchildbirth
(Source:Freedmanetal.,2014,p.916)
Obstetricviolencecanbeconsideredtofallunderthelargerdomainofreproductiveviolencethat
goesbeyondthe‘obstetric’realm.Mistreatmentisthethirdmostcommonoftheterminologies,
althoughithasnotbeendefinedproperlybuthasbeenusedtopresenttypologiesbyBowserand
Hill(2010)andBohrenetal.(2015).Obstetricviolenceisalsothemostcontestedterminology
(Rost,Arnold&Clerq2018;Sadler,2016).Thefollowingtablebringstogetherthedefinitionsofall
theterminologiesdiscussedinthissection.

Chapter2
13
Table2.2 Definitionsofdisrespectandabuse;andobstetricviolenceduringchildbirth
Terminology Definitions
ObstetricViolence
“theappropriationofthebodyandreproductiveprocessesofwomenbyhealthpersonnel,whichisexpressedasdehumanisedtreatment,anabuseofmedication,andtoconvertthenaturalprocessesintopathologicalones,bringingwithitlossofautonomyandtheabilitytodecidefreelyabouttheirbodiesandsexuality,negativelyimpactingthequalityoflifeofwomen.”(PerezD’Georgio,2010,p.201)
“anassemblageofdisciplinary,bodilyandmaterialrelationsthatareshapedbyracialised,medicalisedandclassesnormsaboutgoodpatients,goodwomenandgoodbirthingbodies.”(Chadwick,2017,p.504)
Disrespectandabuseduringchildbirth
“theindividualdisrespectandabuse(i.e.specificproviderbehaviourexperiencedorintendedasdisrespectfulorhumiliatingsuchasslappingorscoldingwomen)andthestructuraldisrespectandabuse(i.e.systemicdeficienciesthatcreateadisrespectfulandabusiveenvironment,suchasovercrowdedandunderstaffedmaternitywardwherewomendeliveronthefloor,alone,inunhygienicconditions).”(Freedman&Kruk,2014,p.915)
“Inthecontextofobstetriccare,wedefinedisrespectastheviolationofawoman’sdignityasapersonandasahumanbeingonthebasisofhereconomicstatus,gender,caste,race,ethnicity,maritalstatus,disability,sexualorientation,orgenderidentity.Disrespectisoftenrevealedinthebiasednormativejudgmentsthathealthworkersmakeaboutwomenandtheresultingactsofomissionorcommission.Abusereferstoactionsthatincreasetheriskofharmtothewomanandarenotinthebestinterestsofherhealthorwell-being.Suchactionsmaybelearnedandreproducedthroughthepracticesofinstitutionalmedicine.Theymayormaynotbeintendedtocauseharmandareoftenjustifiedbyresourceconstraintsthatcanbecomeacoverforprioritisingtheconvenienceofhealthprovidersoverthewell-beingofthewoman.”(Sen,Reddy&Iyer2018,p.8)
Structuralviolence
“socialforcesthatcreateandmaintaininequalitieswithinandbetweensocialgroups,whichmakewayforconditionswhereinterpersonalmaltreatmentandviolencemaybeenacted…theessenceofstructuralviolenceliesintheindirect,systematicandofteninvisibleinflictionofharmonindividualsbysocialforcesthatdisableindividualfromhavingtheirbasicneedsmet.”(Miltenburgetal.,2018,p.2)
ObstetricviolenceisacommonlyusedterminologyintheLatinAmericaandtheCaribbean
(Savage&Castro,2017).Thedefinitionsofobstetricviolencefocusmainlyonwomenasthe
objectofvictimisationanditsimpactonherselfandherbody.Italsodrawsfromthegender
perspectiveasanunderlyingfactorinthedefinitionsthatauthorshavepresentedovertheyears
influencedbyfeministliteratureonwomen’srightsandwomen’sbodiesasmentionedinPerezD’
Giorgio’sdefinition.
Chadwick’sdefinitionshedslightonhowsocietyexpectswomentobe,whichinfluenceshowthey
areexpectedtobehaveduringlabourandbirth.Womenareexpectedtoappearandbehaveina
dignifiedway(Kitzinger,1992)ingeneral.Actionsofscreaming,notbeingabletobearpainand
beingincontroloftheactionsofthephysicalpainduringlabour,areconsideredundignifiedand
Chapter2
14
henceneedtobedisciplined.Studiessuggestthatanyworkattemptingtounderstanddisrespect
andabuseincareduringchildbirthneedstorecognisemanyrelevanttheoriesandprinciples.At
thecoreofthisissueliesthehumanrightsviolationatthewomen’smostvulnerablephaseoflife
whichisinfluencedbytheculturalcontextonhowwomenareregardedinacommunitywhichis
bestexplainedinfeministliteratureonwomen’srights,choicesandbodies(Friedan,1963;
Oakley,1986;Kitzinger,1992;Stones,2004;Menon,2012;Nayak&Nath,2018;Davis,2019;
Criado-Perez,2019;Cleghorn,2021).
ThedefinitionofstructuralviolencebyMiltenburgetal.(2018)takesthemeaningofstructurea
levelhigherfromthebirthingenvironmentandhealthsystemstructuretothelargersocial
constructofthesociety.Themostrecentdefinitionofdisrespectandabuseduringchildbirthisa
blendofthefeministperspective,thehealthsystemsconstraintsandthedeep-rootedcultural
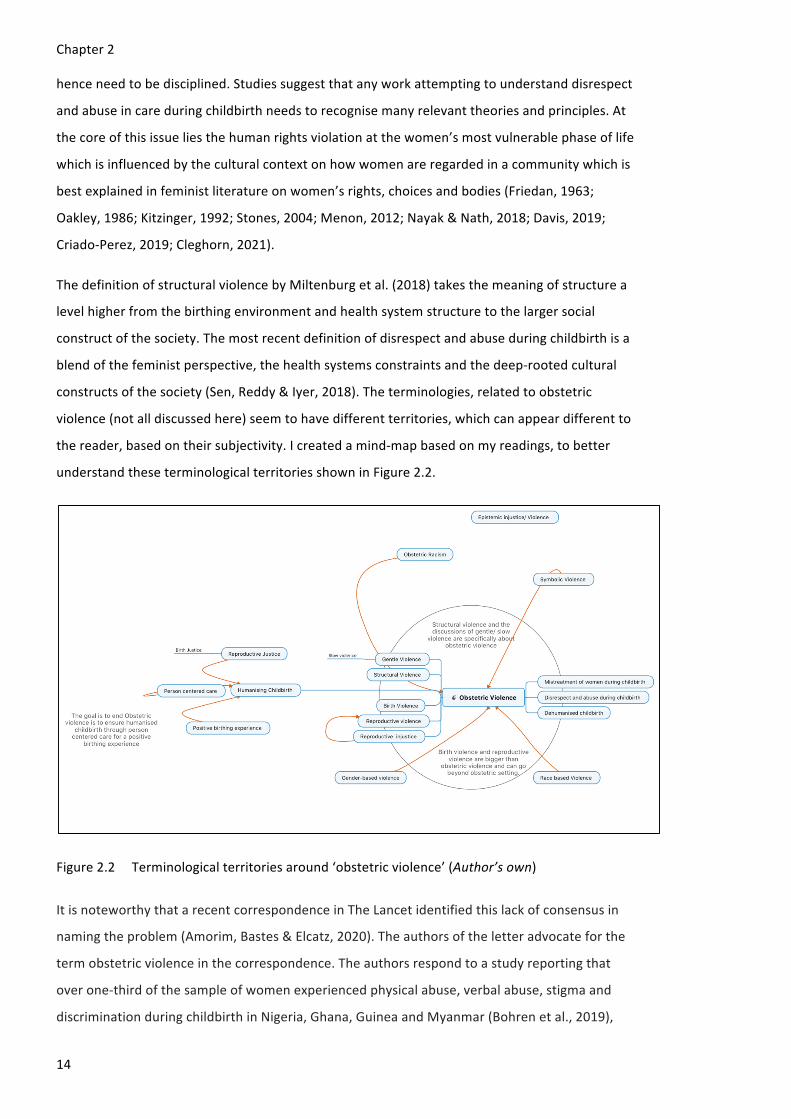
constructsofthesociety(Sen,Reddy&Iyer,2018).Theterminologies,relatedtoobstetric
violence(notalldiscussedhere)seemtohavedifferentterritories,whichcanappeardifferentto
thereader,basedontheirsubjectivity.Icreatedamind-mapbasedonmyreadings,tobetter
understandtheseterminologicalterritoriesshowninFigure2.2.
Figure2.2 Terminologicalterritoriesaround‘obstetricviolence’(Author’sown)
ItisnoteworthythatarecentcorrespondenceinTheLancetidentifiedthislackofconsensusin
namingtheproblem(Amorim,Bastes&Elcatz,2020).Theauthorsoftheletteradvocateforthe
termobstetricviolenceinthecorrespondence.Theauthorsrespondtoastudyreportingthat
overone-thirdofthesampleofwomenexperiencedphysicalabuse,verbalabuse,stigmaand
discriminationduringchildbirthinNigeria,Ghana,GuineaandMyanmar(Bohrenetal.,2019),

Chapter2
15
whilenotnamingtheissueonthetitle.Amorim,BastesandElcatz(2020)arguethatobstetric
violencetranscendsstructuralandlogisticalissuesbyindicatingtheviolationofwomen’shuman
rights,equality,healthandreproductiveeconomy.Bohrenetal.(2020)respondedtoitreferring
totheissueofintentionalitythattheterm‘obstetricviolence’poses,makingitdifficulttoengage
withhealthcareworkersandpolicymakers,hencetheywerekeentocontinueengagingwiththe
issuebyreferringtotheissueas‘mistreatmentduringchildbirth’.Iacknowledgeandunderstand
whyresearchersoftenhavetopickandnavigatebetweenterminologiesforreasonsofreachand
preference,toinfluencepoliciesandpolicymakers,topublishandsecurefunding,aseach
terminologyhasacertainboundary.Ihavedonethattoo,andIamtryingtochangethatby
placing‘obstetricviolence’atthecentreinmywork.Thereasonsbehindtheneedfornavigation
betweenterminologies,theargumentsaround‘obstetricviolence’anditsmisinterpretations,can
bebestexplainedbytworecentexamples,oneeachfromtheglobalnorthandtheglobalsouth.
InItaly,Rivaldietal.(2018)reportedevidenceofobstetricviolencefromanonlinecommunity
survey.ThePresidentsofthreeobstetricianassociationsandonemidwives’associationwrotea
strongcorrespondenceobjectingtotheevidenceproduced,callingit‘presumeddeplorable
behaviour’;‘damaging’and‘alarming’toput‘violence’nextto‘obstetric’.Theystatethatthe
findings‘donottakeintoaccountthepower-dutyoftheprofessionalstoco-decide,guidewomen’s
choices,acturgently,evenwithoutconsent,toavoidseriousdangertotheperson’slifeor
integrity.’(Scambiaetal.,2018).SimilarlanguagehasbeenusedinaGermanarticlewherethe
authorreferredto‘obstetricviolence’asanattemptof‘boilinguptheproblemofviolence’
(DeutschesÄezteblatt,2019).
Rost,Arnold&Clerq(2020)respondedtothediscourseinItalyandGermanyfromanethics
perspective,condoningtheharshlanguageusedintheseresponsearticleswhicharedevoidof
empathy,andsuperciliouslydenyingtheissueratherthanlisteningtowomen’sexperiences.They
alsoraisedthepertinentquestionindicatingthelanguageoffuriousrejectionoftheterminology,
andtheassumptionthatanissueofthisnaturecanbe‘boiledup’.Thisraisesthequestionof
whetherhealthcareprovidersareactuallyunawareofthisproblem,inanyname,whileservingin
thesamesystem,nowthatthereisampleevidenceaboutobstetricviolenceglobally.Isobstetric
violencethenawell-preservedproblemtowhichthereisaseriousresistancetoacknowledge?Is
itawantedphenomenontodisciplinewomen’sbodies,toensurecontinuedoppressionof
womenthroughvariousformsofviolence,includingintheobstetricsettingandtokeepcontrolof
wombandbirth?Thishasbeennotedandexplainedinfeministwritingsasaclassicfeatureof
patriarchalpost-colonialstructurethatbenefitsfromobstetricviolencebycontinuingtheculture
ofdehumanisationofwomeninvarioussettings(Chattopadhyay,2018),alsoamanifestationof
patriarchalviolence(hooks,2000).

Chapter2
16
Intentionalityisatthecentreofthediscourseofnamingandaddressingobstetricviolence,
frequentlyreferredtotheWHO’sdefinitionof‘violence’thatlaysemphasisontheintentof
causingharm.Whilethereissufficientliteratureondriversofobstetricviolencethatacknowledge
careprovider’schallengesandsupportthelackofintent(Barbosa,Jardim&Modena,2018),that
isnotanargumenttodenyobstetricviolenceandthefactthathealthcareprovidersinflict
violenceinbirthsettingswhetherintentionallyorunintentionally.ArecentcasestudyfromSouth
Africaexplainsthisdiscoursebest.ThisstartedwithChadwick’s(2017)bookonobstetricviolence
inSouthAfrica,specificallyreferringto‘gentleviolence’whichhidesinplainsightandis
embeddedinthecultureandisnormalisedbutregardless,isindeedobstetricviolence.Astudyby
LappemanandSchwartzmadeanargumentaboutthelackofintentonthehealthcareproviders
partwhilepresentingfindingsfromastudyconductedintwopublichospitalsinSouthAfrica,
whilestronglycriticisingChadwick’suseoftheterm‘obstetricviolence’inherresearchwitha
diversegroupofwomen’sexperienceofbirth.LappemanandSchwartzexpressconcernsthat
namingthe‘silentwardmilieu’as‘gentleviolence’,whiledrawingtheterm’ssimilaritieswithslow
violence(Nixon,2011),isdemoralisingforhealthcareproviderswhoprovidegoodqualitycare
againstall(systemic)odds.Theyfurtheraddwhetherthetermdisempowersinadvertentlythe
womenitaimstoempower.Theircentralargumentliesinthequestion-‘Howgentlemust
violencebeinorderforittonotbeviolent?’.
Threecommentaries,stronglyrejectingthiscentralargument,arepublishedinresponseinthe
sameissueofjournal‘ViolenceAgainstWomen’,allofwhomadeargumentsinsupportofusing
thetermobstetricviolence.LevesqueandParayre(2021),whilehighlightingWHO’sdefinitionof
intentinviolenceasoutdated,raiseanimportantpointofwhetheranactisviolentonlywhen
perceivedassuch,indicatingitsrootsinsexism,whichisanindicatorofapatriarchalandsexist
system.Burnett(2021),criticisedthenotionofmakingtheissueabouttime(slowvsfast)and
intensity(gentlevsharsh)whilealsodrawingattentiontothecontextofwomenthatguidestheir
perceptionofviolence.Inmyexperience,thisargumentalsoholdsfortheIndiancontext.The
authorsresttheircaseemphasisingontheimportanceoflanguagewhichhastheabilitytodrive
changeorleaveanissueunaddressedwhennotnamedfairly.Inthesamevein,Salter(2021)
arguesthattheactofcallingviolenceoutdoesnotoutweighthechallengesthehealthcare
providersfaceduetothesystemicissues,whichisinherentlydiscriminatory,disempowering,
harmfulandoppressivetowardswomenwhomitpromisestodonoharm.Theycentrethe
terminologyintothereproductivejusticeframeworkwhilereflectingontheintersectionalitythat
couldinfluencewomen’svulnerabilitytoobstetricviolence;finallyrejectingthefocusonthe
argumentfixatedonintentionalityforactsofphysicalabuse,belittling,sexuallyabusingand
humiliatingwomenwhichareevidentlyintentional(Salter,2021).

Chapter2
17
LappemanandSchwartz(2021)acknowledgeallthethreecommentariesagreeingtoseveral
pointsraisedbytheauthorsbutre-statetheiropinionthatthetermisprovokingandundermines
thegoodpracticesbyhealthcareproviderswhoarethemselvesvictimsofsystem’sinternalised
oppression.Shamingthembymakingthemtakeblameandaccepting‘jarringterminologies’,in
theiropinion,iscounterproductivetoensuringrespectfulcare,inlinewithbehaviorchange
literature.Idon’tthinkthatresearcherswhoreportonobstetricviolence,includingmyself,
attempttogeneralisethatallcareworkersareabusers,nordotheyunderminetheeffortsofall
thosehealth-careproviderswhoareprovidingrespectfulanddignifiedcaretowomenandtaking
astandagainstallodds.Referringtomaritalrapeandintimatepartnerviolenceasmarital
dispute;orrapeandsexualabuseas‘offence’isjustasharmfulasisreferringto‘obstetric
violence’as‘mistreatment’,‘misbehavior’or‘alackofrespectfulcare’,makesusallaccomplices
inlettingaseriousissuegounaddressedwhilewellrecognisingitsconsequencesandimpacton
womenandtheirfamilies.AsimpleresponsetoLappemanandSchwartz’squestion(howgentle
shouldobstetricviolencebeforittonotbeviolence?),wouldbethatthereshouldbenoviolence
againstwomeninorderforittonotbeviolent.
2.3 Typesofobstetricviolenceduringchildbirth
ThefirsttypologyofdisrespectandabuseduringchildbirthwaspresentedbyBowserandHill
(2010)fromtheirlandscapeanalysisbasedonacomprehensivereviewofevidencefromtheir
workinTanzania.Theycategoriseddisrespectandabuseduringchildbirthinto:1)physicalabuse,
2)nonconsentedcare,3)nonconfidentialcare,4)nondignifiedcare,5)discriminationbasedon
specificpatientattributes,6)abandonmentofcareand7)detentioninfacilities.
Thesecondtypologyofmistreatmentofwomenduringchildbirthwaspresentedthroughthree
levelsofdomains,subdomainsandspecificindicators.Thedomainsinclude;1)physicalabuse,2)
sexualabuse;3)verbalabuse;4)stigmaanddiscrimination;5)failuretomeetprofessional
standards;6)poorsupportbetweenwomenandproviders;7)healthsystemconditionsand
constraints(Bohrenetal.,2015).Thistypologybreakstheactionsofabusedowntothespecifics
andhenceiseasytoidentifyinhealthcarefacilities(Table2.3).

Chapter2
18
Table2.3 Typologyofmistreatmentofwomenduringchildbirth
Domains Sub-domains Indicators
Physicalabuse Useofforce Womenbeaten,slapped,kickedorpinchedduringchildbirth
Physicalrestraint Womenphysicallyrestrainedtothebedorgaggedduringchildbirth
Sexualabuse Sexualabuse Sexualabuseandrape
Verbalabuse Harshlanguage Harshorrudelanguage
Judgementaloraccusatorycomments
Threatsandblaming Threatsofwithholdingtreatmentorthreatsthatpooroutcomeswillensue
Blamingwomenforpooroutcomes
Stigmaanddiscrimination
Discriminationbasedonsociodemographiccharacteristics
Discriminationbasedonethnicity/race/religion
Discriminationbasedonage
Discriminationbasedonsocio-economicstatus
Discriminationbasedonmedicalconditions
DiscriminationbasedonHIVstatus
Failuretomeetprofessionalstandardsofcare
Lackofinformedconsent
Lackofinformedconsentprocess
Breachesofconfidentiality
Physicalexaminationsandprocedures
Unnecessarilypainfulvaginalexaminations
Refusaltoprovidepainrelief
Performanceofunconsentedsurgicaloperations
Neglectandabandonment
Neglectabandonmentsorlongdelays
Skilledattendantabsentattimeofdelivery
Poorsupportbetweenwomenandproviders
Ineffectivecommunication
Poorcommunication
Dismissalofwomen’sconcerns
Language&interpretationissues
Poorstaffattitudes
Lackofsupportivecare Lackofsupportivecarefromhealthworkers
Denialorlackofhealthcompanions
Lossofautonomy Womentreatedaspassiveparticipantsduringchildbirth
Denialoffood,fluidsormobility
Lackofrespectofwomen’spreferredbirthpositions
Denialofsafetraditionalpractices
Objectificationofwomen
Detainmentinfacilities
Lackofresources Physicalconditionoffacilities

Chapter2
19
Domains Sub-domains Indicators
Healthsystemconditions&constraints
Staffingconstraints
Staffingshortages
Supplyconstraints
Lackofprivacy
Lackofpolicies Lackofredress
Facilityculture Unclearfeestructure
Unreasonablerequestsofwomenbyhealthworkers
Briberyandextortion
Source:Bohrenetal.2015
AthirdtypologyofmistreatmentduringchildbirthisanadaptationoftheBohrenetal.typology
formistreatmentofnewborns(Sacks,2018).Thisisthefirsttypologyfocusingonrespectful
newborncare.Thoughitincludessomeexampleswhichindicatedisrespectandabuseofwomen
too,forinstance“womenblamedforpoorneonataloutcomes,smallinfantandfemalenewborn”.
(Sacks,2018).Noneofthesetypologiesincorporateobstetricviolenceofwomenduringchildbirth
byfamilymembersathomeorhospitalsettings.Thesetypologieshavebeenusedtogenerate
evidenceinmanycountries,asdescribedinthenextsection.
2.4 Globalevidenceofobstetricviolenceduringchildbirth
Evidenceofobstetricviolencehasbeenreportedfromaroundtheworldregardlessoftheincome
andlevelofdevelopmentofthecountry.Whileundertakingtheliteraturereview,Ifound
evidenceofobstetricviolenceinover75countriesglobally,indicatedinredinFigure2.3.

Chapter2
20
Figure2.3 Evidenceofmistreatmentofwomenincountriesaroundtheworld(Author’sown)
Theliteratureisdividedinreportingonobstetricviolenceduringchildbirth.Therearesome
studiesthatusetheBowserandHillandotherwiseBohrenet.al’stypologytoclassifythetypesof
mistreatmentatbirthsystematically(Abuyaetal.,2015;Srivastava&Sivakami,2020).Thereis
someoverlapwhenitcomestoreporting,ifthetypeofobstetricviolenceisunclear.Somestudies
reportonnon-dignifiedcare,verbalandphysicalabuseseparately,othersmaylookatphysical
andverbalabuseastypesofnon-dignifiedcare.Thislackofconsensusisquiteevidentinthe
literature,failingtorecognisethattheperceptionofrespectissubjectiveanddependsonthe
conditioningintowhatisacceptableandwhatisnot.Therefore,studiesemploydifferent
approachesthatincludeaskingwomenabouttheirperceptionsandexperiencesafterbirth,or
sometimesreportingdirectobservationsofthechildbirthprocess(Dey,2018;Mayra&Kumar,
2017;Jhaetal.,2017).
Kitzinger,(1992)referstotheabsenceofgreetingandwelcomingwomenintothebirthingspace
orenvironmentasakindofdisrespectthateverywomanexperienceswhenshevisitsaservice
providerforchildbirth,oftenalongsideotherextremeformsofobstetricviolence(Miltenburget
al.,2018).ThiswasreportedinastudydoneinTanzania,withauthorsindicatingthatallwomen
experienceddisrespectandabuseduringchildbirth.Womenhavesharedreportsofobstetric
violencestartingfromalackofcommunication,tounconsentedcareandsexualabuse(Reedet
al.,2017).InastudyconductedinJordan,women(averageageof28years)reportedneglect
(32.2%)andverbalabuse(37.7%)duringtheirlastchildbirth(Alzyoudetal.,2018).Across
sectionalstudycarriedoutamong173womenthroughanexitinterviewinEthiopiafound39.3%
womenreportingofbeingleftunattendedduringlabour(Asefa&Bekele,2015).Researchers

Chapter2
21
categoriseddisrespectandabuseaspertheBowserandHilltypologyinasurveywith641women
in13Kenyanfacilitiesandreportedonnon-confidentialcare(8.5%),nondignifiedcare(18%),
neglectandabandonment(14.3%),non-consensualcare(4.3%),physicalabuse(4.2%)and
detainmentfornon-paymentoffees(8.1%)(Abuyaetal.,2015).
Studiessuggestpotentialunder-reportingofobstetricviolenceduringchildbirth(Kitzinger,1992).
Thiscanbearesultofwomen’slowexpectationsornotknowingwhattoexpectduringchildbirth;
experiencingdisrespectandabusebutconsideringitapartofcareprovision;beingawareofthe
experienceofdisrespectandabuseduringchildbirthbutconsideringitwomen’sfaultduetothe
fearofconsequencessuchasnottospeakagainsttheonlycareproviderintheareaorfearofnot
beingheardandtakenseriously(Kitzinger,1992).InEthiopia,78.6%womeninastudyhad
reportedlyexperiencedobstetricviolenceduringchildbirth,butonly16.2%reportedaboutit
(Asefa&Bekele,2015).Thischangedwhenthe‘WhatWomenWant’campaignreachedoutto1.2
millionwomenin114countriesaskingtheironedemandforqualityreproductiveandmaternal
healthcare.Womenbroketheirsilenceinsolidaritystatingtheirtopranking‘want’from1,03,584
women(10%)asrespectfulmaternitycare(WRA,2019).
Recognitionofobstetricviolenceisnotlimitedtotheindividualbutdependsonthelarger
systemsofcommunitiesandcountries,aspreviouslydiscussed.Over-medicalisation,forexample,
hasgraduallybeenrecognisedasakeyformofobstetricviolenceinmanycountries,duetothe
underlyingstructuralinequality,thatleadstoobstetricviolencewhennotprescribedfortheright
diagnosis(Sadleretal.,2016).WHOrecommendsanormalrateofcaesareansection(CS)at10-
15%,whichhasbeenincreasingexponentiallyinmanycountries.TherateofCSincreasedfrom
11%to21%inJapan(Behrouzi,2010).Around98%womengivebirthinhealthfacilitiesinBrazil,
wheretherateofCSwasashighas53.5%in2013.ItisparticularlychallengingintheBrazilian
privatesectorwheretherateofCSwas80%in2007(Dinizetal.,2018).TheCSratesinChileare
39%inpublichospitaland72%inprivatehospitals(Sadleretal.,2016).HighratesofCSare
reportedfromtheUSAandCanadaaswell,whereobstetriciansreportedlypreferCStoavoid
lawsuitsresultingfromanadversebirthoutcome,sotheyconvincewomenforanelectiveCS
(Hausman,2005;Nayak&Nath,2018).Therehasbeenanincreaseintokophobiaandcaesarean
sectiononmaternalrequest.Studiestrackingepisiotomyratesfromdifferentcountriesrange
from21%to91%.Eventhoughitisdifficulttodetermineanacceptablerate,WHOdoesnot
recommendroutineorliberaluseofepisiotomyforspontaneousvaginalbirth(WHO,2018).
Studiesreportthepresenceofdifferentformsofobstetricviolenceembeddedinthemedical
education,whichisbecomingapartofcareproviderslearnedbehaviour(Sen,Reddy&Iyer,2018;
Nayak&Nath,2018;Dinizetal.,2018;Mayra2020b;Srivastava&Sivakami,2020).Thisleadsto

Chapter2
22
particularlyextremecasesofdisrespectandabuseinthetertiarylevelteachinghospitals,where
muchattentionisgiventomedicalstudent’spractice,whichsurpassestheimportancethatshould
begiventowomen.Thiscouldbeareasonwhywomenmaybemorevulnerabletoobstetric
violencewhenexperiencingandbeingcaredforcomplications(Srivastava&Sivakami,2020).In
Brazil,astudyreportedacasein2014,whereablackundergraduatestudentwasreportedlygiven
twoepisiotomycuts,ontherightandleft,sothattwomedicalstudentscouldpracticeepisiotomy
andsuturingonthesamewoman(Dinizetal.,2018).Obstetricviolenceduringchildbirthcanlead
tosomesevereconsequences,asarediscussedinthenextsection.
2.5 Impactofobstetricviolenceduringchildbirthonhealthand
wellbeing
Discouragingandaddressingobstetricviolenceduringchildbirthisnotjustaboutsurviving
childbirth,butacknowledgingthatwomendeservemuchmorethanthat.StudiesinIndiahave
foundthatobstetricviolenceduringchildbirthleadstofearofbirth,thatcandiscouragewomen
fromcareseeking(Mayra&Kumar,2017;Jhaetal.,2017),evenwhencomplicationsarise
(Bhattacharyaetal.,2013).Itdiscourageswomenfromfacility-basedbirthduringcomplications
whichthreatensprogresstowardreductionsinmaternalmortality(Bohren,2015;Bohrenetal.,
2014).Neglectandabandonmentinacarefacilityhasnegativeoutcomesforthemotherand
newborn,asreportedintheDominicanRepublic,wheremissingheartbeatsofinfantand
ruptureduterusforthewomanwentunnoticed(Miller,2015).Lackofprivacyisacommonly
reportedfactormakingwomendecideagainstinstitutionalbirth(Afsana&Rashid2001;Oxnevad,
2011;Doctoretal.,2012;Otisetal.,2008;Sorensenetal.,2011;Mrishoetal.,2007;Hadwinger&
Hadwinger,2012;Bhattacharya,Srivastava&Avan,2013).
Obstetricviolencecanhavealastingnegativeimpactonwomenthatmayleadtopostnatal
depression,duetofeelingoutofcontrolandtraumatisedduringchildbirth(Kitzinger,1992;
Larsonetal.,1988;Greenetal.,1988;Scotland,2020).Womensufferingfromposttraumatic
stressdisorder(PTSD),havingexperiencedatraumaticchildbirthmayoftenrelivethetrauma
everyyearontheirchild’sbirthday.Theymaysufferfromguiltofnotenjoyingtheirchild’s
birthdayandhavingtoputupanacttolookhappyontheoutside,whilerecountingthetrauma
bytheminute.Womenhavereportedlychangedthenarrativeoftheirchild’sbirthsotheycan
reduceitsimpactonthem.Womenhavealsochangedtheirchild’sbirthdaytodealwiththe
traumabetter(Beck,Driscoll&Watson,2013).
AstudybyKitzinger(1992)reportsthatvictimsofrapeandviolenceduringchildbirthhave
similaritiesinhowtheyholdbackfromsharingaboutit,intheirfeelingofdepersonalisation
Chapter2
23
leadingtofear,painanddistress;denialandfeelingofisolation,feelinghelplessthinkingnoone
wouldunderstand,self-disgustandself-blame(Kitzinger,1992).Womenfinditdifficultto
describetheirexperienceandoftenusethelanguageoftheiroppressor.Inthiscase,itisthe
medicalterminologiesthatthecareproviderstellthemwerenecessaryforthesurvivalofthe
babyandwoman.Whentheydofindthewordstosharetheirexperiencetheydrawparallelswith
feelingrapedandthelanguageincludesbeing‘strippedoff’,‘tethered’,‘forciblyexposed’,‘sexual
organsputondisplay’,‘disempowered’,‘shocked’,‘numb’,and‘feelinglikebeingaslabofmeat
beingbutchered’.Victimsofbothexperiencesrememberdetailsofthetraumafordecades
(Kitzinger,1992).Ihaveexperiencedandobservedthiscommunicationgapbetweenthe
informationseeker(suchasresearcher)andinformationholder(womenwithbirthingexperience)
foroveradecadeinmyresearchexperiencesoftryingtounderstandwomen’sbirthnarrativesin
differentpartsoftheworldparticularlyinfluencedbypatriarchy,genderandissuesthatare
sensitiveinnature.
Unnecessaryinterventionsduringchildbirthisalsoaformofobstetricviolencethathasbeen
reportedextensivelyaroundtheworld.Thisover-medicalisationgraduallytakesthepowerand
controlofwomen’sbodyawayfromthemandovertothehealthcareproviders,mainlydoctors
andobstetricians,whoareatthetopofthemedicalandsocialhierarchyinmostcommunities,
countriesandcultures(Oakley,1986;Kitzinger,1992;Bohrenetal,2015;Sadleretal,2016;Nayak
&Nath,2018).ThereisevidencefrommanycountriesincludingTanzania(Magomaetal.,2010),
Nigeria(Shifrawetal.,2013;Parkhurstetal.,2007),Ethiopia(Seljeskogetal.,2006),Iran(Ghaziet
al.,2012),Kenya(Mwangomeetal.,2012),Bangladesh(Afsana&Rashid,2001)andMalawi,
(Seljeskogetal.,2006)whereover-medicalisationhasleadtothefearofcutting(episiotomy),that
discourageswomenfromseekingcare(Bohrenetal.,2014).Womenmayevenchooseanelective
caesareansection,justtoavoidthehumiliationaroundover-medicalisedandaviolent
institutionalvaginalbirth,asseeninBrazil(Dinizetal.,2018).
2.6 Determinantsofobstetricviolenceduringchildbirth
Itisessentialtounderstandthedeterminantsofobstetricviolencetofindsustainablesolutions.
Therearesomestudiesthathavefounddeterminantsthatareeitherrelatedtothebackground
characteristicsofwomensuchaslevelofeducationandsocio-economicstatusorothersystemic
factorsrelatedtocare-providers.Thereissomementionofthestructuralandsystemicdriversof
obstetricviolence.Whilethereisadearthofstudiesthatspecificallytrytounderstandthe
reasonsbehindobstetricviolenceduringchildbirth(Sen,Reddy&Iyer,2018)butonecansee
patternsindriversfromtheexistingliterature.Thesedriverscanbecategorisedinto:1)individual,

Chapter2
24
2)structural,and3)socialandsystemiclevelasshowninFigure2.4.Theindividualandstructural
factorshavebeendiscussedinthenextsub-section.
Figure2.4 Determinantsofdisrespectandabuseduringchildbirth
(Author’sownbasedonliteraturereview)
2.6.1 Individualandhouseholddriversofobstetricviolence
Personal,demographicandsocio-economiccharacteristicsmayincreasewomen’svulnerabilityto
obstetricviolenceduringchildbirth.Studiesreportthatsociodemographiccharacteristicscan
makewomenpronetopoorqualityofcare,onthebasisofsocietalinequalities(Gilmore,2017).
Thismayincludeeducationlevel,location,maritalstatus,age,gender,socio-economicstatus,
parityandphysicalappearance(Murray,2008).StudiesinIndiahavereportedpoorqualityofcare
provisiontowomenwhoareilliterateorlesseducated,belongingtolowincomegroups,withtwo
tofourchildren(Bhattacharyaetal.,2013;Jefferyetal.,2010;Sen,Reddy&Iyer,2018),arepoor
andlivinginruralareas(Chattopadhyayetal.,2017).Discriminationshavebeenreportedonthe
basisofthenewborn’ssex(Chawla,2019).Thesereasonshavebeenreportedintermsofintimate
partnerviolence(IPV)againstwomenwhoarepooranduneducated(Dharetal.,2018)inBihar.
Theassociationofobstetricviolencewithwomen’sbackgroundcharacteristicswasnotedinthe
northeastpartsofIndiatoo(Chattopadhyay,2018).
AstudycarriedoutintheUnitedKingdomfoundthatchildhoodexperienceofsexualabusecan
makewomenrelivethoseexperiencesduringchildbirth(Montgomery,2015).Reportsstatethat
oneineveryfivewomenhavebeensexuallyabusedasachild,whichsuggeststhatcareproviders
Individual
Women Related-Literacy
-socio economic status-marital status
-Gender-physical appearance
-Parity-Age
-History of childhoodsexual abuse
Structural
Health systems related-Hierarchy
-Level of care provision-Culture of birthing
-Perception of respect -Care provider challenges
Community related-Position of women in
society-Traditional birthing norms
-Perception of respect
Social and Systemic
-Constructs of society -Gender related barriers
-Political will -Lack of Policies
-Normalization of disrespect and abuse during childbirth
-Patriarchy-Incentive based health policies
-Lack of awareness of human rights
Disrespect and Abuse of women
during childbirth
Feminist perspective
Health Systems perspective

Chapter2
25
needtobesensitiveandeducatedabouttraumainformedcare,evenwhenwomenmaynot
sharesuchexperiences(Montgomery2013;Montgomery,2015;WRA,2019).
2.6.2 Systemicdriversofobstetricviolence
Systemrelatestotheinstitutionalenvironment,includingthecareprovidersandthepolicies.
Careproviders-relateddriversfollowaspectrum,whichchangesfromtheirpre-serviceeducation
toserviceprovision,particularlymidwivesandnurses.Studiesraisetwokeychallengesthatare
cadrerelevanttounderstandinthiscontextandinclude:1)alackofrespectformidwivesand
nurses;and2)medicalhierarchy,thatincludestertiarylevelcareprovisioninteachinghospital
andtheresultingpowerdynamics.Midwives’andnurse’schallengesareimportanttoconsideras
theyareprimarystakeholdersincareprovisionduringchildbirthandtheirproblemsarestemming
fromthesetwofacts.
Alackofsupportiveattendanceduringchildbirthcanbeconsideredasignofdisrespectfulbirthing
environmentthatdiscouragescareseeking(Bohrenetal.,2014;Bohrenetal.,2015).Retaining
trainednursesandmidwiveshasbeenanomnipresenthealthsystemschallenge.Theworld
currentlylacksmorethan900,000midwivesparticularlyinthelowandmiddleincomesettings
(SOWMY,2021).Inthelastfewyears,markedincreasehavebeennoticedintheestablishmentof
trainingandeducationinstitutestoproduceskillednurse-midwives’fortheinternationalmarket
(Kodath,2013).Thishasnotnecessarilyledtoanimprovementincareprovisionbytargetting
workload.
Midwiveshavehistoricallybeencomparedwith‘witches’(Ehrenreich&English,1970)andhave
beenlabelled‘half-taught’,‘totallyignorant’(Oakley,1993)andevenblamedfornegativebirth
outcomes.Midwiferyisconsideredanextensionofawomen’sroleofcaringathome.Thismind-
setisslowlychangingwithmorereportsofmidwifery-ledcarebeingquotedasawaytomost
satisfyingbirthingexperiencesinmanycountries(Oakley,1993)andwithmoreresearchreporting
theimpactofmidwives.ArecentstudyinTheLancetreportedthatwhenenabledtoperformat
theirfullcapacity,midwivescanreducematernaldeaths,neonataldeathsandstillbirths
substantially,whilealsosaving4.3millionlivesannuallyby2035(Noveetal.,2021).Yet,most
countriesdonothaveanindependentmidwiferyprofessionandtheinvestmentinmidwifery
remainsnon-prioritised.
Thecadreofnurse-midwives’faceuniqueprofessional,economic,socialandgender-based
challengesthatleadstoburnoutandstress(Sadleretal.,2016;Sheikhetal.,2012).Studies
suggestthatburnoutandstresscombinedwithpoortreatmentofnursemidwivesascare
providers,reducescompassionincareprovision(Hall,2013;Deery,2009).The‘Midwives’Voices,

Chapter2
26
Midwives’Realities’reporthighlightstheseissuesraisedby2470midwivesfrom93countries
(Figure2.5).Midwivesreportbeingdisrespectedatwork(36%)byseniormedicalstaffandfeltnot
beinglistenedto(32%).Workplaceharassmentsuchasverbalabuse,bullying,physicalandsexual
abusearealsoreportedby37%midwives.Onefifthoftheparticipantsdependonasecondary
sourceofincomeforsurvival(Filbyetal.,2016).
Figure2.5 Personalchallengesinmidwifery(Source:Filbyetal.,2016,p.15)
Thehierarchicalnatureoftheteamprovidingcarealsodeterminestheexperienceofawoman
aroundchildbirth(Deery,2009).Midwivesoftensharethattheirroleincareprovisionis
unrecognisedandissuppressedbythemedicalprofession(Philbyetal.,2016;Mayra,2019;
Mayra2020a).Figure2.6presentschallengesandbarriersthatmidwivesfaceincareprovision,as
aresultofthelargercommunityandsystemtheyareapartof.Thesearecategorisedintomacro,
mesoandmicrochallengesthateventuallyleadtoobstetricviolence.

Chapter2
27
Figure2.6 Structuralandpolicychallengesinmidwiferycare(Source:Bradleyetal.,2019.p.4)
Bradleyetal.(2019)furtherreportthatmidwivesareoftentrappedandlefttostrugglebetween
the‘socialmodelofcare’andthe‘medicalmodelofcare’.Thisrequiresthemtoswitchbetween
theorganisationalsystemofcareandvalues,andthewaymidwiveswouldwanttoprovidecare
(Deery,2009).Caringforwomenduringchildbirthisemotionalwork(notbeconfusedwith
emotionallabour),whichrequirescopingmechanismstoprovidecare.Inotherwords,nothaving
ahealthystateofmindforcareprovisionmayhavenegativeeffectonthecare-seeker.Coping
withone’spersonalstrugglesandthestresstheworkbringswithit,isdoneinmanyways.Some
midwivesjust‘switchoff’andputontheir‘masks’or‘smiles’or‘happyfaces’toappeardignified
whichleadstoemotionalwithdrawingandphysicaldistancing(Hunter,2009).Theyfeeltheneed
to‘donnetheiremotionalarmour’,whichsomerefertoas‘surfaceaction’or‘impression
management’,tobeabletoperformwhatthejobrequires(Deery,2009;Hunter,2009)while
insidetheymightbefeelinglikea‘foodmixer’(Edwards,2009).Thishelpswithcareprovisionbut
itcancostthemidwives,whomaygetoverwhelmedandburnoutinthelongrun.Midwivesare
expectedtobeadvocatesforwomenandtheirhumanrightsdefenders(Gilmore,2017)butthe
challengessurroundingtheirworkneedstobeaddressedforthemtodotheirjobwell.Midwives’
humanrightsneedtobeprotectedalongsidewomen’srights.Itcannotbeside-lined,astheyare
victimsofthesamesystemicissues.
Chapter2
28
2.7 Situating‘obstetricviolence’withingender-basedviolence
Obstetricviolenceisafeministissue,embeddedintheinherentgender-basedinequalitythat
appliestothewomenascare-receiverandmidwives(andnurses)ascareproviders,whoare
predominantlywomen(9outof10globally).Allthesectionsdescribedinthischapterhave
presentedaninterplaywithgender,beittheterminology,definitions,typologies,evidence,
impactanddeterminants.Itisimportanttounderstandandinvestigateobstetricviolenceduring
childbirthfromthegenderlens,toaddresstheinequalitiesitposes(Betron,2018)andthefact
thatitisaresultofgenerationsofhistoricsuppressionofwomen.
Beingawoman,makesonevulnerabletoanykindofviolenceandvictimisation(Jeejebhoy,2018).
Womenareconsideredthe‘secondsex’(Beauvoir,1949)andtheirprioritiesarealsoconsidered
secondary(Betron,2018).Asawoman,oneissupposedtobehaveinafashionguidedbythe
rules,stigmaandnormsofthesociety.Thishasbeennoticedinwomen’snarrativesofpowerand
controlaroundchildbirth,whichresembleshowtheyinteractwiththepatriarchalstructuresand
howsocietycontrolsthem(Bradleyetal.,2016).Therearerulesandregulationstodetermine
whatwomenshoulddowiththeirbodiesandthiscontrolusuallytakesthepowerovertheirown
bodies,awayfromthem.Anyresistancefromwomenisconsidered‘misbehaviour’andmeted
with‘punishment’.Womenareexpectedtoquietlyendurethelabourpainsbecausescreamingor
cryingviolatesthesocialnormsandcallsforpunishmentthroughscoldingandmanyotherforms
ofmistreatmentduringchildbirthtodisciplineherbody(Bradleyetal.,2016;Senetal.,2018).
Thispunishmentforwomenisbasedonthecontextofthecommunity,countryandculture
dependingonprevailingnormsofviolenceagainstwomen.Thediversityintheviolenceagainst
womeninacontext,makesobstetricviolencediverseaswell.
Women’sbodiesandbodily‘purity’isattachedtothehonourofmen,whoownherbodyandthe
body’s‘purity’.Onewaytoensurethis‘purity’inthehospitalenvironmentcanbeseenwhenthe
familyensuresaparticulargenderforthetreatingdoctor(Jeejebhoy,2018;Silanetal.,2012).The
controlofthefemalebodyduringchildbirthinahospitalsettingisareflectionofhowsocietyis
conditionedtotreatwomenathome,inthecommunityandingeneral(Senetal.,2018).Birth,
beinganaturalprocess,hastraditionallybeenanaffairofwomen,tobedealtwithathome,
thoughguidedbypatriarchalnormsofthesociety(Kitzinger,2012).Therehavebeenrituals
aroundbirthandpregnancythathavebroughtwomenofcommunitytogetherthathashelped
theminbonding(Chawla,2019).Thegradualshiftfromthissocialmodelofmaternitycaretothe
medicalmodel,hasledtomedicalisationofthebirthingprocess.Theobjectificationofwomen’s
bodiesduringchildbirthisstemmingfromtheasymmetricgender-basedpowerimbalance
betweenthewomenandthemedicalprofessionmanagingchildbirththatisusuallymasculine

Chapter2
29
(Sadler,2016).Thisgenderinequalityissystemicandnormalisesviolenceduringchildbirthtoan
extent,wherethewomenbeingvictimised,startstoacceptit,considersitapartofthebirthing
processandmanagesherownbehaviourarounditwithanexpectationofbeingabused(Sadler,
2016;Miltenburg,2018).ThisiswhatDavis(2019)referredtoasobstetrichardiness(section2.2).
Ontheotherhand,subjectingmidwiferytohumiliationandprofessionalshamingisdeeply-rooted
ingendertoo.Thishindersthegrowthofmidwifery,graduallytakingmidwivesoutofthepicture,
andgoesagainstthesocialmodelofbirthing,bymakingbirthingariskybusinessthatneedstobe
handledbydoctorsguidedbynumerousmedicalinterventions(Oakley,1984;Davis,2019;
Cleghorn,2021).Thefemale-dominatedmidwiferyprofessionissubjectedtomanystereotypes
andhasoftenbeensubjectedtoalowerstatusinthehealthsystem.Withinthehealthcareteam
environment,midwiveshavebeenbulliedandmadetofeelundervalued.Theunduework
pressurealongwiththelackofrecognitionhasledtoburnoutandalackofcompassion(WHO,
2019;Deery,2009;Hunter,2009;Sadleretal.,2016).Thishasbeenevidentinthelackof
midwives’involvementinpolicymaking,lowersalaries,lesssecurityandlowmarketvalue
becauseitisseenasa‘women’swork’(WHO,2019).ThishasbeenhighlightedinWHO’s
‘DeliveredbyWomen,LedbyMen’report(2019).
Genderactsadoubleedgedswordinthecontextofobstetricviolenceduringchildbirth,that
negativelyinfluencesthecareseekerandthecare-provider.IexplainthisfurtherintheIndian
contextandinthecontextofBihar,astateinIndia,inChapter3.
Finally,Ipresentmypositionality,asanAsianfeministresearcherconductingresearchonAsian
womeninIndia,toknowcertainpositionsIhavetakenandhowithasguidedtheresearch-related
decisionsImadeinmyresearchandhowmybackground,experiencesandcontextmakesme
understandandapproachthecontextinwhichIconductmyresearch.Iamsharingmyassociation
withobstetricviolenceandwhatinspired,encouragedorpushedmetoplantodothisresearch
forovertenyearsofmylifeandthenmakingitpossibleforthelastfouryears.Researcher
positionalityandreflexivityareimportantaspectsofmystudy,especiallybecauseshiftingpower
dynamicneedswerenegotiatedintheprocessofconductingresearchandispresentingthe
findings.Thisisessentialbecauseobstetricviolenceisdeeplyentrenchedinandinfluencedbythe
constructsofpowerwhicharenotfixedbutfluidandisshiftingbasedontheinteractionsand
intersectionsaroundtheindividuals,theircontexts,andbackgrounds(Hamilton,2020).
2.8 Positionality:Myassociationwith‘obstetricviolence’
IamaBengaliAsianwomaninmymid-thirties,bornandraisedinlower-middleincomesettingsin
differentstatesinIndia,courtesyofmyfather’sfrequentlytransferablemilitarydeployment,with

Chapter2
30
himasasoleearnerinthefamily.Whileituprooteduseveryfewyears,italsoopenedmeuptoa
diverseupbringingandculturewherehomogeneityincultureandcontextwasneverthenormand
this diversity is my normality. I received an undergraduate degree in nursing with midwifery
embedded in it, inagovernment college,affiliated to the largest tertiary levelhospital inWest
Bengal, ineastern India (myparent’shomestate), thatpredominantlyservedpeople frompoor
incomebackgrounds.WhileIcallIndiahome,Istruggletoplacemyselfinaparticulargeography,
soIwillnotdothat.
Igotselectedinoneoftheonly15seatsavailabletomillionsofgirlsfromeightstatesintheeastern
partofthecountryandmyfeewasaround250rupeesperyear(approx.2.5pounds),whichwas
affordable for my family and it guaranteed a government job thereafter. In the four years of
'training’,mymidwiferyeducationbeganinthe3rdyearwhenIwas19andhadstartedassisting
birthsinaveryhighcaseloadfacility‘labourroom’.Myfriend(studentnurse-midwife)andIassisted
‘deliveries’sidebysidewithoutrest,althoughnightshiftswerebusierandtheywerelessviolentto
women.Exchangingsmileswastheonlyencouragementforusinabusymaternityunit.Therewas
neveradearthof‘cases’toconductwithfourorfive‘labourtables’placednexttoeachotherand
oneheavymetalricketyscreen,thatscreamedforattentionwhendragged,andwasrarelyused.
Weobservedsomeformof‘mistreatment’and‘abuse’ofwomeneveryday,numeroustimes.
Itwascommontoseedoctors,juniorandsenior,shoutatwomen.Slappingorpinchingontheouter
thighwitharteryforcepswascommonwhenassistingbirths.Slappingontheinnerthighorhitting
on the vulva with an instrument was common during episiotomy repair, when this was done
withoutanesthesiaorwhennotenoughtimewasgivenbetweenanesthesiaandrepair.Seniorstaff
nurses would shout and make derogatory humiliating remarks ‘why did you not think before
spreadingyourlegs’;‘rememberthepainnexttime’;‘yourageisn’trecedingisit,yetyoushowup
everyyear’; ‘this iscommon intheir religion’; ‘youmustgetoperated(tubectomy)oracopper-T
inserted1’.Iregisteredtheminmymindasunnecessaryabusivebehavior,thatthewomendidnot
deserve.Inmycontext,thesepracticeswerenormalised‘misbehavior’ofcareproviders.Istoodat
the centre of the scenewith obstetric violence unfolding aroundme, conditioningme andmy
friendsintoit.
Itwouldbefairtostatethattheseviolentpracticesarepartofamedical,midwiferyandnursing
student’seducation(Madhiwalaetal.,2018;Mayra,2020b).Thecontextofinequityteachesone
totakeadvantageofthepower-basedinequalityinaviciouscycle,subconsciously.Alackofprivacy
andconfidentiality,verbalabuse, repeatedvaginalexaminationswereusualandblended inour
1AlsoknownasIntraUterineContraceptiveDevice(IUCD)

Chapter2
31
practice,thatwentunregisteredinourminds.Observingtheexperiencewomenweresubjectedto
everyday,whilechangingoutofuniform(abrightfluorescentyellowsareeasshowninFigure2.7)
aftershift,somefriendswouldsay‘Iamdefinitelygettinganelectivecesarean,thereisnopointof
thisembarrassmentforahealthcareprofessional!’Somesavedforyearsforanelectivecesareanin
a private hospital. After experiencing sexual abuse and violence myself, during a vaginal
examination,inthehospitalIpracticedin,whileinuniform,Iwaspositivethatmypositionhadno
positiveinfluenceonhowIwillbetreatedintheplacewhereIprovidedcare.Idecidedtonever
givebirth.Mydecision,asavirgin,involvedrefrainingfromsexualintercourse.Icouldnottakea
chanceofcontraceptivefailureoranabortion,exposingmyselfoncemoretosimilarhumiliation
and abuse. Itmademe go on ‘birth strike’ (Brown, 2018). Having experienced sexual violence
numeroustimes(Mayra2020a;Mayra2020b),IwantedtosteerclearofacircumstanceIcouldnot
protectmyselffrom.
Figure2.7 Meandmyclassmatesinouruniform
(Illustrationby:SoumiKarmakarespeciallyforthisresearch,includedwithpermission)
DuringmyundergraduatecourseItriedtofileacomplaintagainstadoctorwhoabusedthe
womanIwascaringforsaying‘howdoesyourhusbandwanttodoanythingwiththejungleyou
havegrownthere’,beforeperforminganunconsentedvaginalexamination.Beingatthebottom
ofthehierarchy,myvoicedidnotreachfar.Frustratedanddetermined,IdecidedtodoaPhDon

Chapter2
32
this,somyvoiceisnotignored,andIamabletoinfluencepoliciesthatchangecarethatviolates
women.Asplanned,Ihavenotgivenbirth,Ihaveneverconceived,andIdonotintendtodoso
either.Obstetricviolenceduringchildbirthremainsmybiggestnightmareandthegreatest
mysteryandIamfinallydoingaPhDaboutit.
2.9 Summary
Thereisagrowingbodyofevidenceofdifferentkindsofobstetricviolenceofwomenduring
childbirth,whichneedstobeaddressedattheindividual,structuralandpolicylevel,asthedrivers
andimpactsareinterconnectedthroughalltheselevels.Thereissomeresearchthathelpsto
understandthedeterminantsofobstetricviolenceduringchildbirth,butmoreeffortsareneeded
tounderstandwhatmakeswomenmorevulnerableinrelationtosocialdeterminantsandwhat
canbedonetoaddressit.
Globalcampaignssuchas‘WhatWomenWant’,‘MeToo’and‘Time’sUp’haveopenedupthe
platformforwomentosharetheirexperiencesagainstabuseandaskforrespectfulmaternity
care.Itisthereforetimelytoaddresstheissueofobstetricviolenceagainstwomeninthelabour
roomstoo,aimingforquickeractionsandsustainablechanges.Obstetricviolenceofwomen
duringchildbirthhasbeencalled‘MeToointheLabourRoom’inpopularculturewitharesulting
outpouringofexperiencesofwomenfrommoreeducatedsectionsofsocietywithspecific
campaignsdedicatedtoobstetricviolencerelatedexperiencesinLatinAmerica,Canadaand
Europe.Storiesofwomenfromruralareasandurbanslumsofpoorsocioeconomicstatusand
lowereducationremainunheard.Understandingrespect,disrespectandabusearoundchildbirth
fromwomen’sperspectivesinaholisticwayisanothergapintheliterature.
Experienceofcareprovisionandofreceivingmaternalhealthcarearethetwokeyaspectswhen
understandingqualityofhealthcarethatIwillstudyunderthelargerframeworkofqualityof
maternalhealthcareprovision.Itisimportanttoexplorewhatrespectmeansfromthe
perspectiveandexperienceofwomenandcareproviderstounderstandtheproblemand
sustainablesolutionslocally.Mythreepaperthesisfillsthisresearchgapbystartingwiththe
explorationofdisrespectandabusefromtheperspectivesofwomenandofcareproviders.

Chapter3
33
Chapter3 BirthinginBihar:settingthecontext
Indiapresentsadiversecontext,influencedbydifferentstates.Inthischapter,Iprovide
informationfromliteraturetounderstandthiscontextaboutIndia,asacountryandBiharasthe
statewheremostofmyresearchisgeographicallylocated.Ipresentinformationaboutmaternal
health,childbirth,women’sstatus,empowermentandviolence,tobetterunderstandthestudy
context.
3.1 QualityofmaternalcareinIndia
Indiamadeconsiderableprogressinthereductionofmaternalmortalitybetween1990to2015,
butcouldnotmeettheMillenniumDevelopmentGoal(MDG)5targets,aimedatimprovingthe
maternalhealthcareprovision(Shah,2016).Indiarepresents12%oftheglobalburdenof
maternalmortality.WHOestimatesitscurrentMaternalMortalityRatio(MMR)at145(WHO,
2017;Shah,2016).Thewiderangeinhealthserviceindicatorsisevidentinthedifference
betweenthestatesinothermaternalhealthindicators.Thenorth-easternstateofAssam,for
instance,hasthehighestMMRof237(SRS,2018)andthesouthernstateofKeralahasthelowest
MMRof46(SRS,2018).Uptakeofmaternitycareelementssuchasantenatalcareand
institutionalbirth,remainslow,incomparisontootherLowandMiddle-IncomeCountries
(LMICs).Evenwithincountry,giventhediversityandsizeofpopulation,thestatusofmaternal
healthcareprovisionvariesbetweenstates.TheinstitutionalbirthsinKerala,forexample,is
99.8%whereasinNagalanditis45.7%(NFHS4).Statewisepercentagesofinstitutionalbirthsin
IndiafromNFHS4areshowninFigure3.1.
Healthbeingastatesubject,individualstateshavetheirownpoliciestomanagehealthcareand
tacklestatebasedchallenges,andhencetherateofprogressvariesbystate.Itis,therefore
importanttounderstandthehealthstatusandservicedeliveryforeverystateinitscontext.The
upcomingsectionsdescribethecontextofmaternalhealthcareduringchildbirthinIndiaand
specificallyinBihar,wheremuchofthisstudyislocated.

Chapter3
34
Figure3.1 MapshowingpercentagesofinstitutionalbirthsinIndiabystate(Source:IIPS,2015)
3.2 EvidenceofobstetricviolenceduringchildbirthinIndia
Thereisagrowingbodyofevidenceonobstetricviolenceduringchildbirthcomingfromdifferent
statesinIndia(Nayak&Nath,2018).Asystematicreviewreportedevidenceofobstetricviolence
inIndiaagainsttheBohrenetal.(2015)typologyunderallthesixkeydomainsexceptsexual
abusewhichisoftenleftoutoftheresearchduetothesensitivityofaskingquestionsofthis
naturetowomen(Srivastava&Sivakami,2020;Bhattacharya&Ravindran,2018).Inmyprevious
qualitativestudy,conductedintheeasternstateofWestBengal,participants(pregnantwomen)
reportedverbal,physical,sexualabuseandunethicalcareprovision(Mayra&Kumar,2017).
VerbalabuseisacommonformofobstetricviolenceseeninIndia.Womenoftenreportthattheir
careprovidersmakederogatoryandjudgementalcommentsparticularlywhentheyareinpain.
Thetimeofbirthhasbeenusedasasiteforhumiliatingwomenwithdifferentversionsofinsults,
inmanycountriesincludingIndia(Senetal.,2018).Inmypreviousresearch,Ihavefoundthat
careproviderswhoclaimthatobstetricviolence(notmentionedwiththatterminologybut
translatedinlocallanguages)isamyththatcanbebrokenbyhavingahusbandasyourbirth

Chapter3
35
companionduringchildbirth.Ahusband’spresenceisconsideredmoreasawitness,thana
supportinlabourandbirth.
AstudycarriedoutinAssam,Indiareportedextremeformsofobstetricviolencethatinclude
routineepisiotomywithoutanaesthesia,hittingwithastickforsoilingthebed,verbalabuseand
neglect(Chattopadhyay,2017).StudiesfromUttarPradeshstatethat90%womenreportillegal
payments,28%verbalandphysicalabuse(Bhattacharya,2015;Rajetal.,2017),80%women
reportedroutinemanualexplorationofuterusand92%werenotallowedabirthingpositionof
choice(Sharmaetal.,2019).Notinformingwomenbeforevaginalexaminationandphysical
violence,arecommonlyseeninpublichospitals,whereasroutineperinealshavingiscommonin
theprivatehospitalsinUttarPradesh(Sharmaetal.,2019).Womenfromthewesternstateof
Gujaratreportunconsentedcare(57%),verbalabuse(55%)andphysicalabuse(40%)(Pateletal.,
2015).ArecentstudyconductedinIndia’snationalcapital,NewDelhi,bringsforthseveralreports
ofunconsentedpost-partumintra-uterinedevice(PPIUCD)insertions,fromthenarrativesof
elevenmuslimwomenwhoareallhomemakersfromlow-incomebackgrounds(Nazdeek,2020).
Theincreasingtrendofunnecessaryinterventionsduringbirth,especiallytherateofepisiotomy
andcaesareansections(CS),isnoticedinIndia.Currently,theaveragerateofCSis17%(nearly9%
in2005-06)rangingbetween6%inNagalandto58%inTelangana(Radhakrishnanetal.,2017).
Therearevariationswithinstatesinthepublicandprivatesectors.Forinstance,thelowestCS
rateinthepublicsectorisnearly3%inBiharandthehighestisinTelengana(40%).ThelowestCS
rateintheprivatesectorisinRajasthan(23%)andthehighestisinJammu&Kashmir(75.5%)
(NFHS4,2015-16).Thelowestdifferencebetweenthepublicandprivatesector’sCSrateis7%in
Keralaandhighestdifferenceis52%inWestBengal(NFHS4,2015-16).Astudyconductedattwo
tertiaryhospitalsinMaharashtrainvestigatedstructuralviolencethroughinterviewswithcare
providersandfoundnormalisationofobstetricviolenceduringchildbirth.Theyalsofoundmedical
studentsengagingincarethatisdisrespectfulandabusivetowomen,similartowhatwas
mentionedintheprevioussectioninBrazil(Madhiwalaetal.,2018).Therearenostudies
specificallyexploringthedeterminantsofobstetricviolenceduringchildbirthinIndia.Thisisa
crucialgapintheliteraturethatisaddressedinthisPhD.
Afrequentlystatedreasonforpoorqualityofmaternalhealthcareisthelackofnurse-midwives
asprimarymaternalhealthcareproviders(Sheikh,Raman&Mayra,2012),atrendobserved
globally(presentedinChapter2).Indiaisyettoestablishanindependentcadreofprofessional
midwives;thishasbeenofbenefittomanyothercountriesincludingAustralia,UKandNew
Zealand,thathavebeenattheforefrontofbestcareprovisionduringchildbirth.TheGOIisnow
makingorganisedeffortstoimplementmidwiferyinIndia.Theoperationalguidelineshavebeen

Chapter3
36
launchedinDecember2018duringthePartnershipofMaternal,NeonatalandChildHealth’s
(PMNCH)Partner’sForum,hostedbyGovernmentofIndia.Iplayedakeyroleindraftingthe
operationalguidelinesasaconsultantwithWHOIndia.
Nursingandmidwiferyistaughtasacombineddegreewithtwoseparateregistrations.Thiscadre
formsthelargestproportionofthehealthworkforceandperformsmajorityofcarerelated
services.Indiarankssecondintermsofnursingandmidwiferyworkforcemigration,thoughwithin
countrythepopulationissupportedbyonly24careprovidersper10,000populations,17outof
thesearenurse-midwives(WHO,2015).Thelackofskillednursemidwivesisaseriousissuein
India.ThiswasconfirmedinWHO’s2010projectionthatIndianeeds2.4millionadditionalnurse-
midwives’toensuregoodqualityuniversalcaretoitscitizens(WHO,2010).Theissuesfacedin
preparinganursingandmidwiferyworkforcethatcouldprovidequalityandrespectfulcare,is
furtherdiscussedinthenextsection.
3.3 ThestateofmidwiferyeducationinIndia
Therearemanyinitiativesinvolvedincapacitybuildingofnurses-midwivesinpre-serviceandin-
serviceeducationaimingtoimprovecareatthefrontline(Fisheretal.,2015;Dasetal.,2016),but
thereislittleevidenceontheirutilitybeyondimmediatesuccess.Idiscussthiswithinthedomains
ofpre-serviceandin-serviceeducationofmidwivesinIndia.
3.3.1 Pre-serviceeducation
Nurse-midwivesinIndiajointhehealthcareworkforceaftercompleting2-4yearsofmandatory
pre-serviceeducation.Althoughthecoursecurriculumiscentrallydesignedandapprovedbythe
IndianNursingCouncil(INC),yetthequalityofeducationvariesacrossstatesandinstitutions.
MidwiferyeducationisimpartedaspartofthethreeyeardiplomacoursecalledGeneralNursing
andMidwifery(GNM)andthefour-yeardegreecoursecalledBScNursing,withanadditionalsix
months’internship.ThereareelementsofmidwiferyskillsintheAuxiliaryNursingandMidwifery
(ANM)education,whichisacertificatecourse.Thecurriculumofthesethreelevelsofmidwifery
educationarenotcomparablewiththeInternationalConfederationofMidwives(ICM)
recommendedskill-setrequiredtoensureknowledgeandskillsonsevencompetenciesof
midwifery(ICM,2013).InIndia,plansfordirectentrymidwiferyeducationhavebeeninthe
pipelineforyears.

Chapter3
37
3.3.2 In-serviceeducation
Withthefast-evolvingnatureofhealthcare,itisessentialthatcareprovidersgetupdated
frequentlywhilein-service,throughContinuedMidwiferyEducation(CME).Overthelasttwo
decades,manyinitiativeshavebeenimplementedinIndia,withanaimtoimprovenursingand
midwiferyeducation,mainlythroughin-serviceeducation(Figure3.2).Someareimplementedin
partnershipwithGovernmentofIndiaandotherswithvariousstategovernmentsincollaboration
withnationalandinternationaldevelopmentorganisations.
Figure3.2 TimelineofmidwiferystrengtheninginitiativesinIndianstates(Author’sown)
TheSkilledBirthAttendant’s(SBA)trainingisthemostcommonamongthese,thatisdeliveredto
ANMs,staffnursesanddoctors,throughoffsitetraining,providedbyateamofdoctorsand
nursesoveraperiodof21days(GOI,2010).
OthertrainingmodelsincludetheUnitedStatedAidforInternationalDevelopment(USAID)
fundedtwodaystrainingcalled‘CareAroundBirth’underalargerinterventioncalledVriddhiin
2016(IPEGlobal,2016).ThethreedaystrainingcalledDAKSHATAhasfour‘pausepoints’based
onWHO’ssafechildbirthchecklist(GOI,2015).TheBillandMelindaGatesFoundation(BMGF)
fundedaninemonthsin-serviceeducationcalledtheMobileNurseMentoringTeam(MNMT)
trainingunderthelargerinterventionsofANANYAandAMANAT2in2014inBihar.Fewother
stateshaveimplementedtheeducationformat(Das,2017).TheMedakmodelprojectprovided
MidwiferySkillsEnhancementTrainingsinMedakdistrict,AndhraPradeshin2007.Allthese
trainingstargetedANMsandstaffnursesforimprovementinmaternalhealthcareprovision
2ApatkalinMatritvaAvamNAvjatTatparta(AMANAT)thatlooselytranslatesintoBasicEmergencyObstetricandNeonatalCare(BEmONC)

Chapter3
38
includingcareduringchildbirth.TheSwedishInitiativeforDevelopmentAssistance(SIDA)
supported(IIPH-G2010)theCentreforAdvancedMidwiferyTraining(CAMT)thatstartedskill
buildingofmidwiferytutorsfromschoolsandcollegesofnursing,whowentontobuildthe
capacityofcareproviders.TheCAMTswerealsousedforprovidingtheninemonthsNurse
Practitioner’sinMidwifery(NPM)courseintwoIndianstateswiththeSocietyofMidwivesIndia
(SOMI)asakeypartner(Prakasamma,2010).FernandezhospitalinHyderabadisimplementing
theProfessionalMidwiferyEducationandTraining(PMET)whichisbasedonUnitedKingdom’s
modelofmidwiferyeducation,foundedonICM’ssevencompetencyskills.Thisisan18months’
course,adaptedtoeducate30nursesfromKarimnagardistrict,withsupportfromTelengana
Governmentthatwaspilotedin2017.
Mostoftheseinitiativesareledbyobstetricians,withminimumtonoinvolvementofnursesand
midwiferyleadershipintheconceptualisationanddesigningphases,exceptfortheMedakModel
ProjectandCAMT.MostoftheseeducationmodelshadoverseasmidwivesvisitingIndiato
implementthem,whichmakesculturalsensitivityoftheseinitiativesquestionable.Itisalso
unclearifthesetrainingmodelsweredesignedwithsupportfromtheINCorthevariousState
NursingCouncils(SNC).In2012,theGOIbroughtoutguidelinesforstrengtheningthePSEnursing
andmidwiferyincollaborationwithINC.Thedifferenceincareprovidereducationandtraining
mayleadtodifferencesinqualityofcareprovision,thatisparticularlypoorinafewstates.The
commonfactoristheabsenceofanycontentonrespectfulmaternitycareinallthesetraining
initiatives.
Intermsofrecentprogress,theGOIisimplementingan18monthsNPMcourse.Thetimeline
(Figure3.2)doesnotincludethis18monthadaptedNPMcoursethatispilotedinthreestatesin
Indiabutit’sprogresshasbeenstalledduetothepandemic.Thiscourse’scurriculumhasbeenco-
designedbyIndianNursingCouncil(INC)andICM.IworkedwithICMasaconsultanttoco-
developthecurriculumandalsoworkedwiththeWHOtodrafttheGOI’soperationalguidelines
formidwiferyimplementationinIndia(GOI,2018).ThedraftNursingandMidwiferyBill,2020is
currentlyintheparliament.Whenpassed,itwillreplacethe75-year-oldINCActof1946.
Although,thereareseveralchallengeswiththeimplementationofthisbill.Itwouldbea
regressivestepthatwouldnotsupportmidwiferyimplementationinIndiaasthebilldoesnot
definethedesignationorthescopeofpracticeandcontinuestounderminetheprofessionby
attachingittonursingascanalsobeseeninthetitleofNPMwhichmaysuggestthatmidwifery
wilcontinuetobedependentonnursing(Mayra,Padmadas&Matthews,2021).

Chapter3
39
3.4 Bihar
Biharhasbeenanareaofinterestforinternationaldonorsanddevelopmentsectorsalikeforover
adecade,givenitscontinuedpoorperformanceofmaternalhealthcareindicators.Obstetric
violenceduringchildbirthremainsunderstudiedinBihartoo,whichcouldbeduetoalackof
politicalwill,thesensitivenatureofthisissueandthefactthatviolenceagainstwomentakestime
toreceiveattention.ThenextsectionsarededicatedtodiscussthereasonsthatmakesBiharan
interestingcasestudytoexploreobstetricviolence.
Geographyanddemography
BiharisintheeastofIndiathatsharesboundarieswiththreeIndianstatesofWestBengal,
Jharkhand,UttarPradeshandaninternationalboundarywithNepal.Thestatecoversanareaof
94,163squarekilometreswhichisfurtherdividedinto9regions,38districts,101subdivisions,
534blocksand44,874revenuevillages.Biharhasthehighestbirthrate(26)inthecountryagainst
thenationalaverageof20(SRS,2020),whichmakesitallthemoreimportanttogetbirthingright
inBihar.ThepopulationofBiharis107million,88%populationresidesinruralareasand48%
comprisesofwomen.Biharconsistsofthesecondhighestruralpopulationinthecountry(GOI,
2011).Thesexratiois916femalesper1000malesandthefemaleliteracyrateis53%againstthe
statetotalof64%andtheInfantMortalityRate(IMR)is29,againstthenationalaverageof32
(SRS,2020).Biharunderperformsinmostotherpopulationandhealthrelatedindicatorsin
comparisontothenationalaverage,asshowninTable3.1.
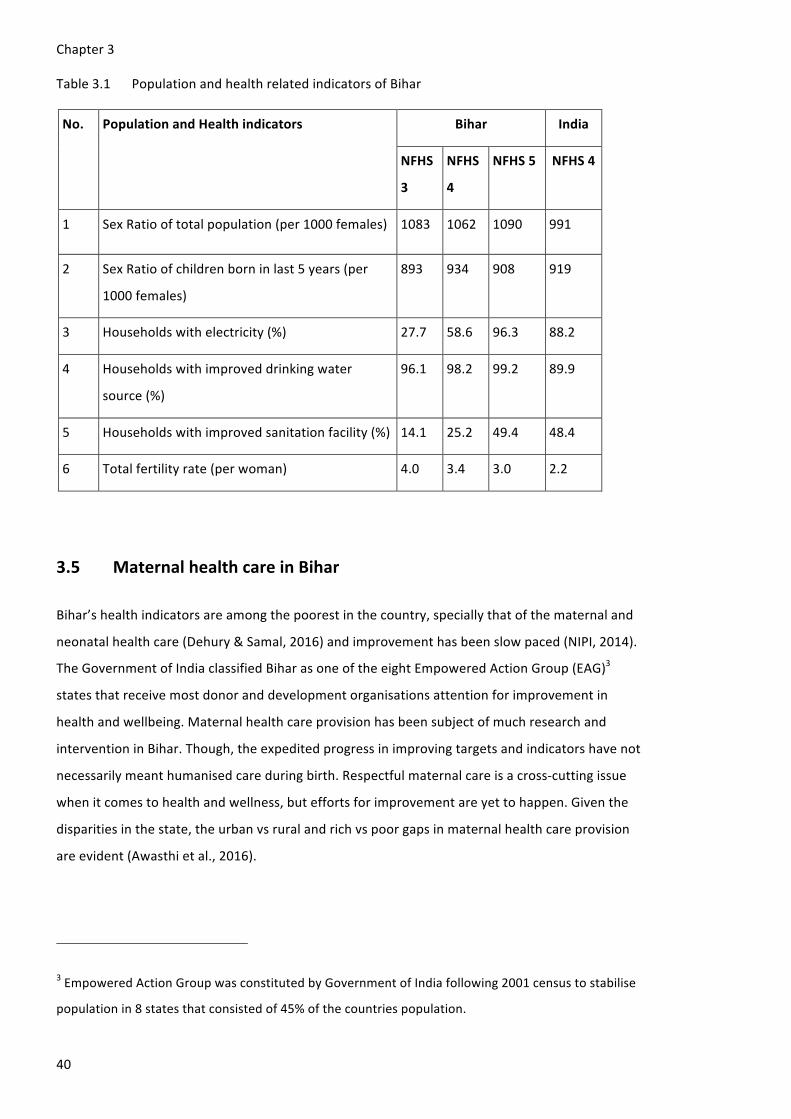
Chapter3
40
Table3.1 PopulationandhealthrelatedindicatorsofBihar
No. PopulationandHealthindicators Bihar India
NFHS
3
NFHS
4
NFHS5 NFHS4
1 SexRatiooftotalpopulation(per1000females) 1083 1062 1090 991
2 SexRatioofchildrenborninlast5years(per
1000females)
893 934 908 919
3 Householdswithelectricity(%) 27.7 58.6 96.3 88.2
4 Householdswithimproveddrinkingwater
source(%)
96.1 98.2 99.2 89.9
5 Householdswithimprovedsanitationfacility(%) 14.1 25.2 49.4 48.4
6 Totalfertilityrate(perwoman) 4.0 3.4 3.0 2.2
3.5 MaternalhealthcareinBihar
Bihar’shealthindicatorsareamongthepoorestinthecountry,speciallythatofthematernaland
neonatalhealthcare(Dehury&Samal,2016)andimprovementhasbeenslowpaced(NIPI,2014).
TheGovernmentofIndiaclassifiedBiharasoneoftheeightEmpoweredActionGroup(EAG)3
statesthatreceivemostdonoranddevelopmentorganisationsattentionforimprovementin
healthandwellbeing.Maternalhealthcareprovisionhasbeensubjectofmuchresearchand
interventioninBihar.Though,theexpeditedprogressinimprovingtargetsandindicatorshavenot
necessarilymeanthumanisedcareduringbirth.Respectfulmaternalcareisacross-cuttingissue
whenitcomestohealthandwellness,buteffortsforimprovementareyettohappen.Giventhe
disparitiesinthestate,theurbanvsruralandrichvspoorgapsinmaternalhealthcareprovision
areevident(Awasthietal.,2016).
3EmpoweredActionGroupwasconstitutedbyGovernmentofIndiafollowing2001censustostabilise
populationin8statesthatconsistedof45%ofthecountriespopulation.

Chapter3
41
ThecurrentMMRinBiharis165(SRS,2018)andtheInfantMortalityRate(IMR)is32(SRS,2020),
bothhigherthanthenationalaverageof130(SRS,2018)and33(SRS,2020)respectively.NFHS5
carriedoutinBiharin2019-20,showsmarkedimprovementsinsomematernalhealthindicators
incomparisonwithNFHS3and4from2005-06and2015-16,asshowninTable3.2.
Table3.2 BirthindicatorsinBihar
No. Birthrelatedindicators Bihar
India
NFHS
3
NFHS
4
NFHS
5
NFHS4
1 WomenwhohavehadfourANCvisits(%) 11.2 14.4 25.2 51.2
2 Womenwhohadinstitutionalbirth(%) 19.9 63.8 76.2 78.9
3 Womenwhowereassistedbyskilledcare
providerduringchildbirth(%)
29.3 70.0 79.0 81.4
4 Institutionalbirthinpublicfacility(%) 3.5 47.6 56.9 52.1
5 BirthsbyCS(%) 3.1 6.2 9.7 17.2
6 BirthsbyCSinpublichospital(%) 7.6 2.6 3.6 40.9
7 BirthsbyCSinprivatehospital(%) 17.2 31.0 39.6 11.9
8 Womenwhowerevisitedbyacareprovider
withintwodaysofbirth(%)
NA 10.8 57.3 62.4
9 Childrenbornathomewhoweretakentoa
healthfacilityforacheckupwithin24hours
ofbirth(%)
NA NA 59.3 NA
NA=Notavailable
Biharlagsbehindthenationalaverageinmanybirthindicators,includinginstitutionalbirths
(Figure3.1),evenaftersubstantialincreasesininstitutionalbirthsowingtothewidely
implementedincentivisationscheme,JananiSurakshaYojana(JSY)(Karvandeetal.,2016;Dehury
&Samal,2016).Thishasnotledtocomparableprogressintermsofantenatal,postnatalcare
(Dharetal.,2018)andneonatalcare(Dasetal.,2016),ashasbeenthetrendinIndia.

Chapter3
42
Evenwithinthestate,therearedisparitiesintermsofinstitutionalbirthsatthedistrictlevel,
rangingfrom37%to87%,asshownintheFigure3.3.
Figure3.3 ProportionofinstitutionalbirthsindistrictsofBihar(AuthorsOwn)
(Source:NFHS4)
3.6 StatusofwomeninBihar
Obstetricviolenceduringchildbirthcannotbetreatedasanisolatedissuewithoutunderstanding
theculturalcontextandthestatusofwomeninBihar.NFHSreportsonseveralgender-based
indicatorswhicharepoorerforwomenwhencomparedtomen.Genderisakeyunderlyingfactor
whichshowsinthefactthatwomen’sliteracyislessthanmenbyalmost23%orsterilisationrate
being35%inastatewhere0.1%mengotsterilisedorthatdoublethewomenareanaemicthan
men(NFHS5)asshowninTable3.3.Inequalityingenderrolesmakewomenmorevulnerable
towardsvictimisationinasocietythattreatstheirwomenlessthanmen(Jejeebhoy&Santhya,
2018).Women’shighlevelofaccesstomobilephonesandbankaccountsisafalseindicatorof
theirlevelofautonomy.ThiscouldhaveincreasedtofacilitatetheJSYincentivethatisdirectly
transferredtotheclient’sbankaccount,soitmaynotsignifymorethanthat.
32.2% -53.5%53.5% - 62.1%62.1% - 71%71% - 78.9%78.9% - 86.6%
Institutional births in Bihar (%)

Chapter3
43
Table3.3 Womenempowermentandgender-basedindicatorsinBihar
No. Womenempowermentandgender-relatedIndicators Bihar India
NFHS
3
NFHS
4
NFHS
5
NFHS
4
1 Womenwhoareliterate(%) 37.0 49.6 57.8 68.4
2 Menwhoareliterate(%) 70.4 77.8 78.5 85.7
3 Womenwith10ormoreyearsschooling(%) 13.2 22.8 28.8 35.7
4 Womenage20-24yearsmarriedbeforeage18years
(%)
69.0 42.5 40.8 26.8
5 Womenage15-19yearswhowerealreadymothersor
pregnantatthetimeofthesurvey(%)
25.0 12.2 11.0 7.9
6 Femalesterilisation(%) 23.8 20.7 34.8 36.0
7 Malesterilisation(%) 0.6 0.0 0.1 0.3
8 Allwomenage15-49whoareanemic(%) 67.4 60.3 63.5 53.1
9 Menage15-49whoareanemic(%) 34.3 32.3 34.8 22.7
10 Womenwhoworkedinthelast12monthswhowere
paidincash(%)
17.2 12.5 12.6 24.6
11 Womenhavingbankorsavingsaccountthatthey
themselvesuse(%)
8.2 26.4 76.7 53.0
12 Womenwhohaveamobilephonethattheythemselves
use(%)
NA 40.9 51.4 45.9
13 Womenage15-24yearswhousehygienicmethodsof
protectionduringtheirmenstrualperiod(%)
NA 31.0 56.0 57.6
NA=Notavailable
Thisgender-basedinequalitypresentsonenarrativeofoppressionofwomeninBiharandIndia.
Asdiscussedinthepreviouschapter,women’sgeographiclocation,theirculturalcontextand
history,forexamplebeinginapostcolonialpatriarchalcontextandtheirpositioningatparticular
intersections,maymakethemmorevulnerabletoanykindofviolence.Thisisfurtherdiscussedin
thenextsection,thoughitisimportanttodrawconnectionstotheirintersectionsinregardsto

Chapter3
44
theirlevelofeducation,financialindependenceandreproductivedecision-makingfromthis
sectionandtheprevioustable.
3.7 Pleasure,shame,endurance:conversationsaroundbirthing
Women’sjourneytothe‘labourroom’,pre-dominantly,isaresultofsexualintercourse.Indian
womenexperienceextremepressuretoachieveapregnancyandgivebirth,preferablytoamale
child,assoonastheygetmarried.Womenneedtoprovetheirfertilityandmentheirmanhood
throughquickprocreation,thesoonerthebetter.Butthatdoesnotmeanthatthereisalotof
franknessintheconversationsaboutsexualityandbirth.Women’ssexualityisahushedtopicand
thereisnoconversationaboutwomen’spleasure.Sexisconsideredshamefulbecausethe‘act’
hasbeenperformedtoreachthelabourroom.Shamingwomenthroughjudgementalcomments
abouttheirsexualityisacommonformofabuseseenduringinstitutionalbirths.Itistherefore
highlylikelythatawomanisviolatedduringchildbirthforbeingthereafterexercisingher
sexuality,whichisoftennotoutofchoice.Thefollowingquoteconnectsthisshame,sexuality,
silenceandviolencewell(Bhasin&Menon,1998,p.58).
‘neitherabsolutenormonolithicthisconsensusis,nevertheless,atoncedeepandwideranging
andencompassesmostformsofviolence…Ithastwocriticalanddistinguishingfeatures:it
sanctionstheviolent“resolution”ofthetroublesomequestionofwomen’ssexualityandsexual
status-chaste,polluted,impure-andsimultaneouslyinsistsonwomen’ssilenceregardingit
throughtheattachmentofshameandstigmatothisveryprofoundviolationofself.Thus,the
womanraped,thewomanwhomayberaped,therapedchild,theyoungwidowwhosesexuality
cannolongerbechannelised,thewiferapedbykinsmanorothers,thewomenwhomustbekilled
sothattheirsexualityisnotmisappropriated,thewives,daughtersandsisterswhomustbe
recoveredsothatsexualtransgressionisreversed-areallcompelledintoacquiescing.’
Thiscontinuumofviolenceandenduranceinwomen’slivespresentedbyBhasinandMenon
(1998)intheSouthAsiancontext,haspreviouslybeenexplainedbyKelly(1988)inherworkon
sexualviolence.Thenarrativeofenduranceoftentranscendsfromthebedroomtothebirthing
room,whereexperiencesthatshouldbepleasurable,endupbecomingtraumatising,anda
sourceofshameforexercisingfemalesexuality.Incaseofobstetricviolenceparticularly,aprivate
experienceofbirthingbecomespublicandtheprivateexperiencesofexercisingsexualityis
draggedoutinpublicdiscoursetoo,touseasadeviceforhumiliationandoppression.

Chapter3
45
3.8 ViolenceagainstwomeninBihar
Biharisknownforitshistoricallyviolentpoliticalclimate(Rodgers&Satija,2012).Studieshave
reportedtheevidenceofviolenceembeddedinthecasteandreligion-basedfeudalsystemin
Bihar(Satija,2013;Stephenson,2013).Biharleadsintermsofviolenceagainstwomentoo.It
rankshighinIntimatePartnerViolence(IPV)duringpregnancyagainstotherstates(NFHS-5)
(Table3.1).
Table3.1 IndicatorsofviolenceagainstwomeninBiharandIndia
No. Indicatorsofviolenceagainstwomen Bihar India
NFHS
3
NFHS
4
NFHS
5
NFHS
4
1 Evermarriedwomenwhohaveeverexperienced
spousalviolence(%)
59 43 40 31
2 Evermarriedwomenwhohaveexperienced
violenceduringpregnancy(%)
NA 5 3 4
3 Youngwomenage18-29yearswhoexperienced
sexualviolencebyage18(%)
NA NA 2 NA
NA=Notavailable
Evidencesuggeststhatviolenceagainstwomenduringpregnancyhasmanynegativeoutcomes
forthewomanandherbaby(Dharetal.,2018).Dharetal,reportongenderbeingakeyfactorfor
violenceagainstwomenathome,where43%marriedwomenarestillexperiencingspousal
violenceand5%whilepregnant.Associationswerefoundwithcasteandreligionaswell(Satija,
2013).
Thereisacriticalthirdangletothecultureofviolenceagainstwomenthatneedstobe
considered,whichhappensintheirchildhood.Astudyconductedin2007found47%offemale
childrenreportbeingsexuallyabusedinIndia.Thisstudywascarriedin13statesincludingBihar,
wherethereportedfigurewas30%(WCD,2007).Childbirthisauniqueexperienceandexposes
onetonewproceduresthatmayresultinwomenrelivingexperiencesofabusefromchildhood
(Montgomery,2013).Researchsuggeststhatcompassionatecareisneededinhandlingwomen
withsuchexperiencesthatshouldbeperformedwithutmostsensitivity(Montgomery,2013).This
isyetanotherchallengethatneedstobeaddressedincareduringchildbirthandmaternalhealth
careprovisioningeneral.

Chapter3
46
Biharreportshighratesofallformsofviolenceagainstwomen,althoughtherearenostudies
aimingtoinvestigatingobstetricviolenceinthestate.Otherstateswithsimilarcontextof
women’sstatusandviolencehavereportedhighratesofdifferentformsofobstetricviolence,
suchasUttarPradesh,WestBengal,AssamandGujarat,aspresentedinthischapter.Allthese
aspectsmakeBiharaparticularlyinterestingstatetostudyregardinghowwomenascare
receiversand;midwivesandnursesascareproviders,perceiverespectanddisrespectduring
childbirthandwhywomenarenotreceivingmaternalcarethatisrespectfulanddignifiedin
nature.

Chapter4
47
Chapter4 Shesmileswhenshetalksaboutviolence:
Epistemologicalunderpinningsand
methodologicalapproaches
Inthischapter,Idescribetheepistemologicalunderpinningsandthekeymethodsadoptedinthis
thesis.Thisresearchisembeddedincriticalfeministtheory.Feministapproachesandmethodsof
inquiryhaveguidedalltheaspectsofmydoctoralresearch,includingthepresentationofthe
thesis.Inthefourpapers,Iexploretheexperiences,expectations,determinantsand
recommendationstoaddressobstetricviolenceduringchildbirthfromtheperspectivesofwomen
ascareseekersandmidwives’ascareproviders.Inchapter5,Ipresenttheexperienceof
obstetricviolencefromahouseholdquantitativesurvey(Paper1)andexplorethesocial
determinantsofobstetricviolencethatmakewomenmorevulnerabletoadehumanisedbirthing
experience.Iinvestigatethedepthandthenatureofwomen’sexperiencesofrespect,disrespect
andabuseduringchildbirthinchapter6(Paper2).Chapter7(Paper3)presentswomen’s
perceptionsofwhytheyhadexperiencedobstetricviolenceand/orrespectfulmaternitycare
whichemergedfromdata.Thisisfollowedbychapter8(Paper4)withnursingandmidwifery
leader’sperceptionofthedriversofobstetricviolenceasaprimarycareprovider,particularlyin
thecontextofIndia.Ihavedescribedthemethodsforeachofthefourchaptersindetailinthe
respectivechapters5,6,7and8.
4.1 Epistemologicalunderpinnings
Violenceagainstwomeninpublicandprivatesphereshavebeenthesubjectofincredulityanda
centralfocusoffeministmovementsthatcanbecreditedforprogressinaddressingviolence
againstwomen(Federici,2018).‘Feminismisamovementtoendsexism,sexistexploitationand
oppression’(hooks,2000,p.8).Feministresearchaimstouncoverandbringforthnarrativesof
silenced,andwomenresisting,asaresultofcenturiesofoppression,owingtopower-based
imbalancethatwomenexperience,asaresultofpatriarchyandcolonialism.Feministscholars
havechampionedresearchwiththemarginalised,oppressedandsecluded,bybreakingthe
‘norms’ofacademicscholarship.FeministscholarssuchasMcKenzie,Chadwick,Montgomeryuse
innovativeparticipatoryfeministmethodssuchasarts-basedresearchtoovercomethe
challengesoftraditionalsciencethatisembeddedinsexism,racism,casteismandsystemic
biases,andthereforetendstoreproduceoppressivestructures(Weisstein,1993;Magnusson&
Marecek,2017;Criado-Perez,2019;Ali,2019).

Chapter4
48
Underepistemology,IunderstandthewayinwhichI,asascientist,produceknowledge.It
concernsfundamentalquestionssuchas‘Whatisknowledge?’,‘Howisknowledge(re)produced?’
and‘Whoownsit?’(McEwan,2001).Feministepistemologyaccountsforthefactthatnot
everybodyisequallyconsideredtobeasubjectcapableofreproducingknowledgeandthatthe
knowledgethatisproducedbytheelitebastionofuniversitiesoftenexcludestheknowledgeand
waysofknowingofthelessprivileged.ThishasbeenapointofdepartureforSouthAsianfeminist
theoristswhoexplainandcritise,fromusingthefeministpost-colonialtheory,thepatternof
researchersandacademics(westernandwhite)consistingresearchinthe‘third-world’countries
presentingahomogenousnarrativeofoppressedthird-worldwomenwithnorecognitiontotheir
resistanceandheterogeneity(TalpadeMohanty,1988).ThisisanessentialinsightIhavedrawn
frommyexperiencesofresearchinginlowincomesettingsoverthelastdecadewithparticipants
whosevoicesareseldomconsideredimportantwhilealsobeingaresearcherwhosevoicehas
beensidelinedforbeingawomanandanurse-midwife.Iamattemptingtochangethatthrough
mydoctoralresearch,becausewomenandnurse-midwives(pre-dominantlywomen)belongto
thegroupexcludedfromknowledge-production,resultinginthesilencingoftheir/our
perspectiveswithinthehegemonicscienceofobstetricsandhealth.Ihaveaimedtoresistthis
traditionalpower-imbalancebetweentheresearcherandtheresearchsubjectbyaddressingthe
womenandnurse-midwiveswhoparticipate,as‘knowers’.Ihavedonethistoensurethatthe
women’snarrativesoftheirembodiedexperienceofbirthandthenurse-midwives’experienceof
providingcareareatthecentreofmyresearch.
Withthisaim,theresearchmethodologiesIchoosetouseallcomeforthoutofcriticalfeminist
theory.Formydatacollection,Ihaveusedparticipatoryresearchandvisualarts-basedmethods
suchas‘birthmapping’,anadaptationofbodymapping.Formydataanalysis,Ihaveused
feministrelationaldiscourseanalysisandvoice-centeredrelationalanalysis.IhaveusedI-poems,
birthingstoriesandthebirthmaps,asresearchoutputs.Hence,thetheoreticalunderpinningsof
mydoctoralresearcharethoseoffeministtheorybecauseIhavebeenmindfuloftheinfluenceof
genderandpoweronmydatacollection,analysis,andontheconstructsandcontextsthatI
explore.Below,Iwillspecifytheepistemologicalunderpinningsofmyresearchasawhole,along
withhowotherspecifictheorieshaveinfluenceddifferentaspectsofresearchandmethodological
decisions,thatincludeintersectionaltheoryandfeministstandpointtheory.Thethreeaspectsof
feminismtoconsiderformyresearchare1)feminismanditsrelationtogenderandpower-based
oppression;2)feminismformedicalhealthcareresearchand3)feminismrelatedtoviolence.This
approachisbestexplainedbythisstatementfromAllen(2013,p.268)‘fromthedirectionofa
feministtheorythatstrivestobegenuinelyinclusiveoftheperspectivesandexperiencesofall

Chapter4
49
women,(includingnurses-midwives’inpredominantlyfemale-ledprofessions)includingthosein
theGlobalSouth,bydevelopinganintersectionalanalysisofthecross-cuttingaxesofracial,
gender,andimperial(medicalandpatriarchal)domination;andfromthedirectionofacritical
theorythatcanonlybetrulycriticalifitcantakeonboardapostcolonialperspective.’
4.1.1 Feministtheory
Feministtheoryprimarilypresentsanexplanationofsexistthinkingandhowitcanbechallenged
andchanged(hooks,2000).Itunderstandsgendertobeanideologicalconstruct,whichmeans
thatwomenareexpectedtodisplayandperformasetroleandfollowthenormsthatarelaidout
forwomeninourparticularcontextandcultures.Thisalsoexplainswomen’sroleinwomen-
dominatedprofessionssuchasmidwiferyandnursing,thatareoftenconsideredanextensionof
women’sdomesticrole.Thisisembeddedingender-basedinequalitywhichcaninfluence
women’sactivities,experiences,choicesandvalueseverydayintheirroutinelives(Butler,1993).
Thiseventuallysubordinateswomen,generationaftergeneration,beingconsideredasthe
inferiorsex.Feministtheoristsbelievethatsexismwasnotnecessarilyconsciouslystructuredto
oppresswomen,butintheprocessithascertainlyresultedintocentralisingpowerwithmenand
establishingpatriarchalconcepts,masculinenormsandmaledominatedconstructsthatbenefit
onlymen(Keeling,2011)suchasthemale-ledmedicalmodel.
Feministresearchisabroadfield.Itconsistsofcriticismsofandrocentricresearch.Globalhealth
policymaking,forinstance,ispredominantlywhitemaledoctorled.DorothySmith(1987)refers
tothisasthecirclesofmen(usuallywhiteandintheglobalnorth)whoconductresearchrelevant
tomen,writtenandreadbymen(McEwan,2001).Formidwiferyandmaternalhealthis
supplementedbywhitewomenpublishingresearch.Thisissueexistsinmaternalhealthcare
deliveryresearchwherenurses,midwivesandwomen’sperspectivesandexperiencesareoften
measuredorexaminedthroughincompetentmethods.Thesewereparticularlyconcerningwith
sensitiveareasofresearchsuchasviolenceagainstwomenandresearchonmaternaland
reproductivehealth,whichledfeministscholarstothinkoutoftheboxanddoresearch
differently(Wigginton&Lafrance,2019).
4.1.2 Criticalfeministtheory
Criticalfeministtheoryprovidestheessentialtheoreticalframeworktounderstandwomen’s
experienceofchildbirthandspecificallytheirexperienceofobstetricviolencegivenchildbirthand
obstetricviolenceisapre-dominantlywomen’sexperience.Italsolocatesobstetricviolenceas

Chapter4
50
gender-basedviolence,rootedinpower-basedimbalanceasaresultofwomen’ssocial
positioning.
Criticalfeministtheoryisacombinationoffeministtheoryandcriticaltheories.Itisimportantto
understandthisamalgamationthatcreatescriticalfeministtheory,asnotallfeministtheoriesare
criticalandnotallcriticaltheoriesarefeminist.CriticalFeministtheoryexplainstheresistanceand
deploymentofpowerandaimsto‘identify,questionandseektoreformpatriarchalideologies
thatgiverisetoasymmetricalrightsandopportunities,rolesandmaterialcircumstances’(Wood,
2015,p.293).GenderandpatriarchyaretwokeyaspectsoffeministtheoryinmyPhD,that
intersectswiththestructuresofpowerandequity-basedoppression.Intermsofobstetric
violence,itrelatestothestructuresthatupholdtheobstetricsystemofmaternalhealthcare
provision,thatallowsthisformofviolencetogoon(McEwan,2001;Ray,2020).Theimbalance
couldbeinformalandinformalpower-basedrelationshipsorinteractions(Wood,2015).Inthe
contextofmydoctoralresearch,themedicalinstitutionshaveformalpoweroverthenurse-
midwivesasaresultofahierarchicalhealthcaregovernancestructure.Thepowerofthemedical
professionalsoverwomenwhoareseekingcare,withthedoctorusuallyheadingthestructure,is
informalpower,becausethewomenarenotobligedtoformallyacceptorobeytheirorders.
Doctors,areinthemostrespectedprofession.Theyholdpowerinthesocietyinformallyoverthe
membersofthecommunityandthepeoplethey‘serve’,thatcomesmainlyfromtheknowledge
theyhold,thepowerofknowledge(McEwan,2001).Womenareconditionedtoobey,be
disciplinedandallowedtoeveryactiontheytakeduringtheirownchildbirth.Inthesamevein,
doctorsandotherhealthcareprovidersarealsoconditionedtoabusethispower,whilewomen
areconditionedtoendureit,whomayoftensharetheirexperiencesofroutineviolenceand
obstetricviolencewithasmileandevenalaughtertoneutralisetheseriousnessoftheissue,and
tonotdrawattentiontothemselves.
Criticalfeministtheoryisinfluencedbypostcolonialscholarship,whichmakesitagoodfitformy
researchinIndia,thathasahistoryofcolonisation,thataddsanotherlayerofoppressionforthe
women.Thisisakeyfeatureofthepatriarchalstructurewhereeveryoneisataparticularposition
basedontheirgender,sexualityandsocialrole,thatguideswhosevoices,perspectivesandvalues
matter,andwillbelistenedto.Thisisacontinuedbattleoftheculturallegitimacyofvoices,also
referredtoasthe‘theatreofstruggle’byStuartHall(1989).Thispower-basedimbalancebetween
doctor-patient(women)anddoctor-nurse-midwife,makestheresearchthroughfeminist
methodologiescrucial,becausethehistoricoppressionmakesitdifficulttoascertainthe
knowledgethroughtraditional,conventionalandman-mademethodsforandrocentricknowledge
(Wigginton&Lafrance,2019;Espinoza-Reyes&Solis,2020).

Chapter4
51
Childbirthisexperiencedpredominantlybywomen,primarilycaredforbymidwives,(couldbe
referredtoasnurse-midwives’inIndia)inaprofessiondominatedbywomen.Bothcategoriesof
womenhaveahistoryofoppression.Thepower-basedimbalanceisacrucialaspectof
researchingwithboththesecategoriesofparticipants,wherewomenareatthebottomofthe
socialhierarchyandnurse-midwivesareatthebottomofthemedicalhierarchy.Bothwomenand
nurse-midwives’facetheconsequentialpowerlessnessthatrequiresforthemtocontinuallyresist
suchstructuresofoppression,henceitisimportanttounderstandhowwomenandnurse-
midwivesinteractwiththesesystemicoppressivestructuresfromtheuniqueperspectivesof
subordination,powerlessnessandresistance(McAra-Couper,Jones&Smythe,2011;Mayra
2020a).
4.1.3 Feministstandpointtheory
Standpointfeminismconsidersthatwomenandmenleadsignificantlydifferentlivesthatare
shapeddifferentlybytheirsocialrolesandexperiences.Standpointtheoryhasbeenusedin
researchaboutreproductionandrelatedexperiencessuchaspregnancy,menstruationandbirth,
becauseonlywomen,predominantly,canhavetheseembodiedexperiences(Woliver2002,Parry,
2008).Standpointtheoryalsoenablesthewomenexperiencingtheoppressivepowerstructures
toconfrontthesave‘oppressivepowerstructures’(Jaggar,1997),itistheobstetriccaresystemin
thiscase.Whilefeministtheoristshavepresentedtheirapproachesandextensionstofeminist
standpointtheory,theconsensusremainsthatfeministstandpointtheorygiveswomenvoiceto
presenttheirnarrativesfromtheirstandpoint(Keeling,2011).Ihaveoftenwonderedaboutthe
actof‘giving’voiceandstronglybelieveditisnotourstogive.Feministresearcherscanfind
feministwaysofresearchtounearthnarrativesthatwerehiddenduetotheinabilityofour
researchmethodstoexamineandourincompetencetolistenandunderstandsuchsensitive
phenomenon.Inmycase,itischildbirthandobstetricviolence,whichIdecidedtolearnfromthe
standpointofwomenascare-seekersandthestandpointofnurse-midwivesasprimarycare
providers,inacontextofcontinuedoppressioninapatriarchalpostcolonialcontext.
Generatingawarenessoftheoppressivestructuresandtheimpactithas,isacrucialstepinmy
study,aswillbepresentedinthefindings.Challengingthesesystemswillbethenextstep,which
somewomenshowintheIndianandBiharicontextintheireffortstocompletelybypasssuch
oppressivesystemsandtakebirthingintheirownhands,byeitherswitchingbirthplaces,
changingcareprovidersorcompletelyrejectingtheobstetricsettingbygivingbirthathome
withoutassistanceofacareproviderorwithatraditionalmidwife.

Chapter4
52
Theknowerknowsbestofwhatisbeingexplored,forbeinginapositionofhavingtheexperience
inacontextthatconstructedtheirperspective,andhencesharesthenarrativefromtheirunique
standpoint(Sprague,2016).AccordingtoDorothySmith(1991)theseknowersare‘theactual
subjectssituatedatparticularsites’thatasresearcherswearetryingtostudy.Inthecontextof
myPhD,theknowerarethewomenwhohavegivenbirthinthepatriarchalculture,ina
postcolonialcontextofBihar,Indiaandareparticularlyfromlow-incomesettings.Iexplorewhat
theycanshareasavirtueoftheirstandpoint,thatotherscannotprovide.Similarly,thenursing
andmidwiferyleaderssharetheirstandpointofprovidingcaretowomeninthesamecontext,as
theirprimarycareprovider,inahealthcaresysteminfluencedbypatriarchalculturewith
remnantsofpostcolonialcontext.Thiscanbeseeninthegovernanceofthelargestprimarycadre
ofcareprovidersofnurses-midwivesinIndia,andthechallengesandstrugglestheyfaceincare
provisionandwhattheyperceiveistheresultoftheirbodilyexistencethatlocatestheir
consciousness(Smith,1991).Smithalsocriticiseshowpastattemptshaveusuallyconsidered
experienceonlywhen‘spoken’bytheparticipantswhilearguingthatitisembeddedinour
feelings,dailypractices,inlocalsettingsandIbelieve,itevenliesinthemundaneandinour
silences.
Womenhaveembodiedtheexperienceofgivingbirthandrespectfulnessand/orobstetric
violencewhilegivingbirth.Nurse-midwiveshaveembodiedgivingbirth,assistingbirths,
experiencingchallengesinensuringqualitycare,participatinginrespectfulcareand/orobstetric
violence,andobservingrespectfulcareandobstetricviolenceunfoldaroundthem.Theselived
experiencesofwomenandnurses-midwivesareatthecenterofmyresearch(Keeling,2011),who
aresharingtheirtruth,basedontheirexperience,relationandinteractionswithpower
(Ramazanoglu&Holland,2006).Itisimportanttounderstandhowtheircontinuedoppression
andresistanceshapestheirexperienceandmakesthemaddmeaningtotheirexperiences.Thisis
the‘concreteexperience’whichIenterintoresearchtoexploreandbringoutfromthe
participant’snarratives.
Howmypositionality,asawoman,fromlower-middleincomebackground,educatedinnursing
andmidwiferyintheworldtheresearchparticipantsandIinhabit,shapesmystandpointand
influencesmyresearchdecisionsandmethodologicalchoices,isdiscussedthroughoutthe
researchpresentationthroughmyreflexivity.Itisimportanttoacknowledgethatthisresearch
couldhavebeendonedifferentlywhendonebyanon-feministand/ormaleand/ornonAsian
and/ornon-healthcareworker’sstandpoint,toconsiderthatmypositionalityinthediscourse
addsvaluetothisresearch(Parry,2008).Insimplewords,itisimportanttotakenoteofwhatis
beingresearched,whoisbeingresearchedandwhoisdoingtheresearchinwhatcontext.

Chapter4
53
4.1.4 Intersectionality
MyPhDisgeographicallylocatedinIndiawithparticipantshailingfromdifferentstates(inthe
studywithnurse-midwives’),andparticularlyfromBihar(inthestudiesaboutwomen’s
experiencesofchildbirth).Thesetwocategoriesofparticipantspresentmanytraitsthatcanbea
breedinggroundforoppression.Genderistheconnectingfactorintheirbackgrounds,
exacerbatedbytheirlevelofeducation,statusofoccupation,geographicallocation,age,caste,
religion,socio-economicstatus,maritalstatusandphysicalappearance,amongmanyothersuch
characteristicsthatmakenurse-midwivesandwomenvulnerabletobeingoppressedand
experienceobstetricviolenceduringchildbirth(Sen&Chattopadhyay,2018;Menon,2012).
FeministAmericanlawyerKimberléCrenshawiscreditedforcoiningthewordandintroducingthe
worldtotheconceptofIntersectionality,tounderstandblackwomen’sdoubledis-advantageat
theintersectionofgenderandrace(Crenshaw,1986).Whilestandpointtheoryhelpsto
understandtheperspectivefromtheparticipant’sstandpointshapedbytheiruniquepositioning,
intersectionalityexplainsthisuniquepositionattheintersectionsofallthecharacteristics
mentionedbeforeandhowthatinfluencestheirexperiences,perceptionsandexpectations.
Intersectionalityprovidesalenstounderstandthesensitiveissuesriddenwithstigmaand
stereotypes,suchasbirth,andmorespecifically,obstetricviolence(Boydelletal.,2020;Hill
Collins,2019).
Theintersectionalframinghelpstofurtherunderstandwomen’sexperiencesfromtheir
standpoint,andhowandwhytheymayexperiencewhattheyexperience,intermsofviolence
duringchildbirthaswellbasedontheirpositioningattheintersectionsofsexuality,gender
identity,racism,sexismandableism(Boydelletal.,2020).Althoughtherearecriticismsthat
intersectionalitydoesnotfocusonsexualidentityandorientation,thatledtothetheoryofsexual
configurations,whichhelpstounderstandthefluidnatureofsexualorientationandpreferences
thatkeepstheperson’sidentityflexibleandopentoconfigurations,astheorisedbyVanAnders
(2016)(Grzanka,2016).Idostronglybelievethatintersectionalityisaboutalltheattributesthat
explainstheinequalitiesandpower,thatarerelevanttoaparticularcontext,andthatsexualityis
oneofthosedeterminingfactorsaswell.Asdescribedintheliteraturereview(chapter2)andin
thecontextofBiharandIndia,(Chapter3),womenandtheirnurse-midwives’positioningat
particularintersectionscouldplayaroleinhowtheyaretreatedandhowtheyresist.Inthe
contextofIndia,birthingandmattersrelatedtowomen’sreproductionareconsideredpolluted
anduncleanrequiringsegregationinmanycommunities(Chawla,2019;Menon,2012).Profession
isakeyattributetoincludeforthenursingandmidwiferywhichhavehistoricallyoppressed
professionsinIndia(Ray,2020;Mayra2020b).Intersectionalityisessentialbecauseitexplains

Chapter4
54
whois‘respectable’inasocialconstructbasedontheirsocialdeterminants(Christensen&
Jensen,2012).
Intersectionalityisthekeyframeworktounderstandmydoctoralresearch,intermsof
understandingtheparticipants,theirexperiences,thedriversoftheviolencetheybearandhow
theyperceiveitandalsotheimpactithasontheirroutinereproductiveandnon-reproductive
livesalongwithmymethodologicalchoices.Itexplainsthestigmaanddiscriminationattachedto
thepainandpleasuresurroundingthereproductiveaspectsoflifeandchoiceswhichisdescribed
indetailintheforthcomingrelevantchapters.Intersectionalityexplainsthepositioningofpeople
fromwheretheyarepresentingtheirstandpoint.
Itisimportantformyresearchtoadoptmultiplelensestounderstandobstetricviolencebecause
themultipleformsofoppressionsandtheircomplexinterrelationshipsthatshapetheexperiences
andperceptionsofwomenandnurse-midwives(McEwan,2001).
4.2 Conceptualframework
Thisconceptualframeworkconnectsallthefourpapers.Overall,Ihaveinvestigatedwomen’sand
midwives’experiencesofrespect,disrespectandabuseduringchildbirth.Ihavealsoexplored
theirperceptionofwhywomenexperienceobstetricviolenceandrespectfulmaternitycare
duringchildbirth.Thedeterminantsaredividedintothreelevels:individual,structuralandpolicy
levels,basedonparticipant’sresponses,inlinewiththedefinitionofdisrespectandabuseduring
childbirthbyFreedmanetal.(2014)aspresentedinchapter2.Theconceptualframeworkshows
thestudycomponents,experiences,determinantsandperceptionsandrecommendationsdivided
atthreedifferentlevels:individual,structuralandpolicy(Figure4.1).

Chapter4
55
Figure4.1 Conceptualframework
(Author’sown,withexclusivepaintingbyS.Karmakarforthisresearch,usedwithpermission)
Paper1:Socialdeterminantsofobstetricviolence-Women’sexperiencesofobstetricviolence
arenotaonetimeoccurrence,butoftenanembodiedexperienceofmultipleexperiencesthat
furtherexplainstheseriousnessofthisissue.Thispaperpresentsthediversityandpluralnature
ofwomen’sexperienceofobstetricviolencealongwithanunderstandingoftheirsocio-
demographicbackground,thatmayincreasetheirvulnerabilitytoobstetricviolence,andmultiple
experiencesofviolenceduringchildbirthinanobstetricsetting.
Paper2and3:Women’sexperiencesandperceptionofrespect,disrespectandabuse-Paper2
discusseswomen’sembodiedexperienceofrespect,disrespectandabuseduringchildbirthto
understandhowtheyattachmeaningtothese,throughparticipatoryvisualarts-basedqualitative
research.Paper3drawsfromthesamedataonexploringwomen’sperceptionofwhythey
experiencerespect,disrespectandabuseduringchildbirthandhowbirthcanbemadewomen-
centeredandsatisfactoryforeachoftheparticipant.
Paper4:Nurses-Midwives’perceptionsofobstetricviolence-Midwiferyandnursingleader’s
experienceandperspectivesofqualityandrespectfulmaternalhealthcareiscrucialforpolicies
andpracticebecausetheyaretheprimarycareprovidersinIndia.Theirperceptionsand
experiencehavebeenexploredqualitativelytopresentthedriversofobstetricviolenceandalso
recommendationsofwhatwillmakecarerespectfulforwomenduringchildbirth.
Women’s experienceof giving
birth
RESPECT DISRESPECT ABUSE
Midwives’ experienceof assisting
birth
EXPERIENCE
Midwives’ experienceof giving
birth
PERCEPTIONS
DETERMINANTS
Midwives’ related
factors that increase women’s
vulnerability to obstetric
violenceduring
childbirth
Women related
factors that increase
vulnerability to obstetric
violence during
childbirth
Midwives’ understand
ing of respect,
disrespect & abuse during
childbirth
INDIVIDUAL STRUCTURAL SYSTEMIC
Women’s perception of respect, disrespect & abuse during
childbirth
Women’s perceived factors of of respect, disrespect & abuse during
childbirth
Midwives’ perceived factors of of respect, disrespect & abuse during
childbirth

Chapter4
56
4.3 Studydesignandanalysis
Thisisamixed-methodsstudythathasqualitativeandquantitativecomponents.Thekey
methodshavebeenmentionedinTable4.1againsteachpaper.
Table4.1 Studydesign
No. Objectives Design Typeofdata
Datacollection
Respondents Analysis
Paper1 Toexaminethesocialdeterminantsofobstetricviolenceduringchildbirth,inBihar.
Quantitative Secondary
StructuredHHsurveyquestionnaire
Newmothers DescriptiveanalysisLogisticregressionFactoranalysisLinearregression
Paper2&3
Toinvestigatetheperceptionsandexperiencesofrespect,disrespectandabuseincareduringchildbirthandthefactorsdrivingit,inBihar.
Qualitative Primary
BodyMappingassistedIDI’s
Womenwithbirthingexperience
FeministRelationalDiscourseAnalysis(FRDA)VoiceCenteredRelationalAnalysis
Paper4 Todocumentandanalysetheexperiencesofnursingandmidwiferyleaderswithrespect,disrespectandabuse,andtorecommendwaystostrengthenrespectfulcareforwomenduringchildbirthinIndia.
Qualitative Primary
Indepthinterview(IDI)
Nursing&midwiferyleaders
Thematicanalysis
Paper1:Socialdeterminantsofobstetricviolence:Thisstudyusessecondarydata.Ihadledan
extensivedatacollectionexerciseinacourseof18months(July2016toDecember2017)before
startingmyPhD.Thisdatacollectionwasdonetounderstandthequalityandrespectfulnessin
careduringchildbirthinallthe38districtsinBihar.Thesurveycoveredallthreelevelsofhealth
careprovision:primary,secondaryandtertiary.Theprocessinvolvedvisitingwomenattheir
householdswithinarecallperiodof30daysofbirthtounderstandthequalityandrespectfulness
ofcareduringchildbirthfromtheirperspectivewiththehelpofastructuredquestionnaire.The
householdinterviewswereconductedbyfemaleenumeratorsexperiencedinconducting
interviewsinthelocallanguagesanddialectsinBihar.Atotalof2194interviewswereconducted

Chapter4
57
withwomenwhohavegivenbirthinanobstetricsettingwithinonemonthprecedingthe
interview.
Myaimistounderstandwhichbackgroundcharacteristicsofwomeninfluencedifferentformsof
obstetricviolenceduringchildbirth.Iconductedadescriptiveanalysisonthehousehold
interviewswithwomen,followedbybinarylogisticregressionanalysistounderstandthesocial
determinantsofobstetricviolence.Iconductedfactoranalysistocreatenewvariablesofobstetric
violencethatexplainthemostvarianceinthestudyfindingsonobstetricviolence.Iconducteda
linearregressiononthenewlycreatedvariablestoexaminetheircorrelationwithwomen’s
backgroundcharacteristics.StatisticalPackageforSocialSciences(SPSS)isusedtoanalysethe
data.
Papers2and3:Women’sexperienceandperceptionofrespectfulmaternitycareinBihar:I
interviewedwomenwhohavegivenbirthinBihar,inurbanslumsandruralvillages,qualitatively
usingavisual-artsbasedparticipatorymethod,bodymapping.Womenfromboththeseareas
belongtothepoorestofstrataandseekmaternalhealthcareatdifferentlevelsofcareprovision.
Womenfromtheruralareasmostlyaccesscareatprimaryandsecondarylevelsofcareprovision
thatmainlyincludetheBlockPrimaryHealthCenters(BPHCs),CommunityHealthCenters(CHCs)
andSubDistrictHospitals(SDHs).Womenintheurbanslumshavequickeraccesstothetertiary
levelsofcareprovisionsuchasatgovernmentsuper-specialtyhospitalsandmedicalcollege
hospitals.
IconductedascopingvisitinBiharinJanuary2019,toidentifythethemestoexplore,the
methodstouseandethicalmeasurestoconsider,toensurethestudyisconductedwithutmost
sensitivity.TheinterviewswereconductedinHindiandotherlocaldialectsconvenienttothe
participant.Havingworkedextensivelyinthesedistrictsandstate,Iamawareofthelanguage
barriersthatmayexist,asaresultofmanydialectsspokeninBiharincludingBhojpuri,Maithili
andMagahi.Audiorecordingwasdoneandpicturesweretakenwhilemaintaininganonymityof
theparticipantwithwomen’sinformedconsent.Participantswererequestedtoselecta
pseudonymtobeusedinthestudythatwillmaketheresultsmorerealisticbyaddingcultural
authenticitytoit(Montgomery,2015).Ianalysedthedatausingfeministrelationaldiscourse
analysis(FRDA),withvoicecenteredrelationalanalysisembeddedinit.IusedNVivo12toaidthe
analysis.
Paper4:Nurse-midwives’experiencesandperspectivesonrespect,disrespectandabuseduring
childbirthinIndia:IconductedthiscomponentofthePhDqualitativelythroughin-depth
interviewswithseniormidwiferyandnursingleaderswhorepresentthedomainsofeducation,
regulation,unionisationorassociation,research,administrationandhealthcareprovision.This

Chapter4
58
datawerecollectedatstateandnationallevelsinIndia,withaglobalperspectivesharedby
expertsengagedinglobalmidwiferyandmaternalhealth-relatedpolicymaking.Thestatelevel
datacollectionwascarriedoutinBihar,Rajasthan,OdishaandMadhyaPradeshthatrepresent
theunderperformingstates,intermsofmaternalhealthcareindicatorsandoutcomes.Giventhe
lackofleadershipinmidwiferyandnursinginIndia,datacollectioninthesefourstateshelpedto
understandthebackgroundandcontextofchallengesforawayforward.WestBengalwas
selectedtorepresentastatewithgoodgovernancestructureinIndiaintermsofnursingand
midwiferyleadershipinpolicymakingforhealthworkforceandhealthserviceprovision(Baggaet
al.,2010;Sharmaetal.,2010;Mayra,Padmadas&Matthews,2021).Dataisalsocollectedatthe
nationallevelinIndia.
Interviewsareconductedwithglobalexpertsforareflectiononhowmidwiferyleadershipcan
helpimproverespectfulnessincareduringchildbirthandwhatdrivesobstetricviolenceduring
childbirth.Iinterviewedparticipantsrepresentinginternationalorganisationsthatinfluence
policiesinIndiaandgloballyincludingWHO,UnitedNations,UnitedNationalsFundforPopulation
Activities(UNFPA),ICM,ICNandtheUnitedNationsHighCommissionforRefugees(UNHCR).I
alsointerviewedmidwiferyexpertsfromUnitedKingdomwhohavesuccessfullyestablisheda
midwiferyledmodelofmaternalhealthcareprovisionandcloselycollaboratewithIndian
counterpartstoaidinmidwiferyimplementationinIndia.Theseinternationalexpertsarealready
playingacrucialroleinimplementingmidwiferyinIndiawiththeGovernmentofIndia.
Interviewsareaudiorecordedalongsidethoroughnotes.Writtenconsentistakenfromthe
participantsforaudiorecording,andfortheirparticipationintheresearch.Theinterviewsare
doneinEnglish,HindiandBengali,basedontheconvenienceofparticipants.Iamfluentinthese
languageswhichensuredthattherewasnolanguagebarrier.Therecordingsaretranslatedand
anonymisedwhilecompletingthenotesbeforestartingdataanalysis.
Iselectedtheparticipantsthroughpurposivesamplingfortheinterviews.Theparticipantshold
keypositionsinthestates,atthenationallevelandinthedevelopmentorganisationsatthe
globalpolicymakinglevel.Thesemi-structuredin-depthinterview(IDI)guide,forthenursingand
midwiferyleaders,isbasedonliteraturereviewofchallengesthatthiscadresexperience
(Appendix3)andmydecadelongexperienceofengagingin,influencingandresearchingnursing
andmidwiferygovernanceandpolicymakinginIndia(Mayra2020a;Mayra,Padmadas&
Matthews,2021).Thecare-seeker’sinterviewsanalysisisguidedbycriticalfeministtheory.The
careprovider’sinterviewsareanalysedusingthematicanalysis.IusedNVivo12toaidthe
qualitativedataanalysis.

Chapter4
59
4.4 Researchethicalapproval
TheethicalapprovalforthePhDwastakenfromtheethicalreviewcommitteeofUniversityof
Southampton.Forpaper1,ethicalapprovalwasalsotakenfromCenterforMedicalStudies(CMS)
ethicalreviewcommitteeinIndia(ReferencenumberIRB00006230),beforeconductingthedata
collection.TheGovernmentofBiharhadalsoapproveddatacollection.Thereferencenumberof
UniversityofSouthampton’sethicsapprovalforthesecondarydataanalysisoffullyanonymised
datais31910.TheethicalreviewcommitteeatUniversityofSouthamptonapproveddata
collectionforthestudyaimingtounderstandwomen’sexperienceandperspectivesofrespect,
disrespectandabuseduringchildbirthinBihar(Referencenumber49734).Duetothesensitive
natureofdatacollectionforpaper2and3,thestudyisassignedcategoryA.Forpaper4,to
understandnursingandmidwiferyleader’sexperiencesandperspectivesofensuring
respectfulnessinthecareduringchildbirth,thereferencenumberforethicsapprovalis41164.

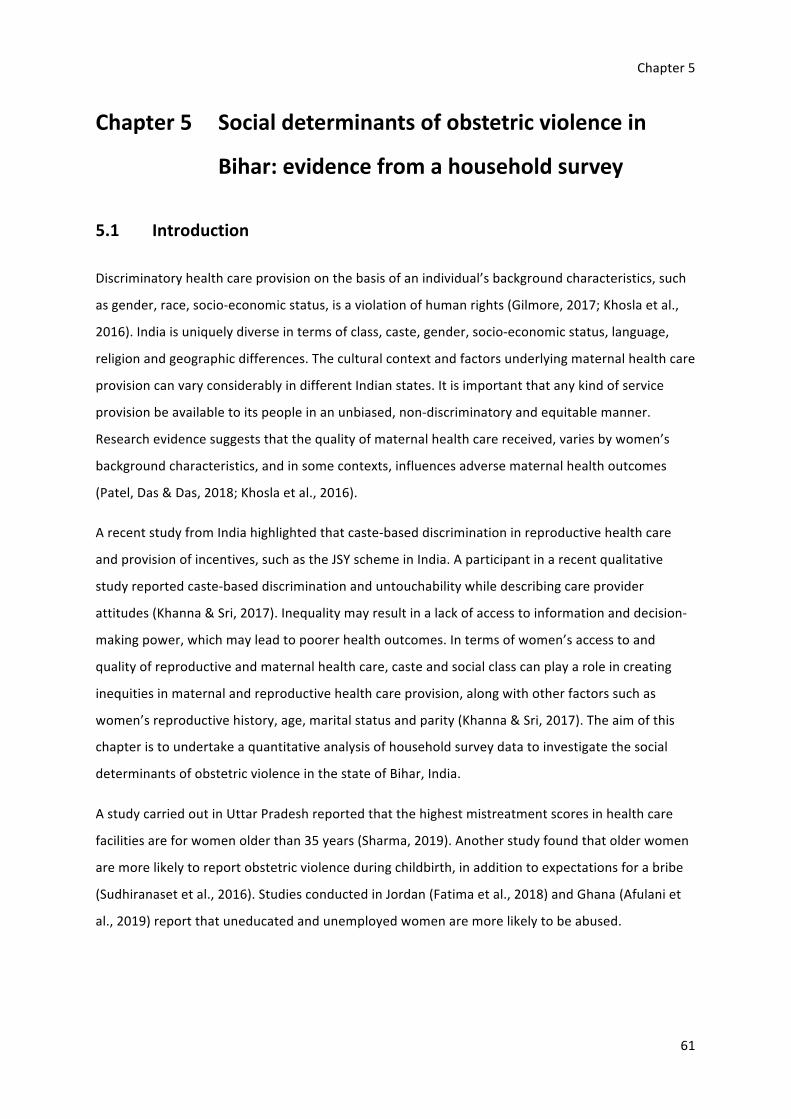
Chapter5
61
Chapter5 Socialdeterminantsofobstetricviolencein
Bihar:evidencefromahouseholdsurvey
5.1 Introduction
Discriminatoryhealthcareprovisiononthebasisofanindividual’sbackgroundcharacteristics,such
asgender,race,socio-economicstatus,isaviolationofhumanrights(Gilmore,2017;Khoslaetal.,
2016).Indiaisuniquelydiverseintermsofclass,caste,gender,socio-economicstatus,language,
religionandgeographicdifferences.Theculturalcontextandfactorsunderlyingmaternalhealthcare
provisioncanvaryconsiderablyindifferentIndianstates.Itisimportantthatanykindofservice
provisionbeavailabletoitspeopleinanunbiased,non-discriminatoryandequitablemanner.
Researchevidencesuggeststhatthequalityofmaternalhealthcarereceived,variesbywomen’s
backgroundcharacteristics,andinsomecontexts,influencesadversematernalhealthoutcomes
(Patel,Das&Das,2018;Khoslaetal.,2016).
ArecentstudyfromIndiahighlightedthatcaste-baseddiscriminationinreproductivehealthcare
andprovisionofincentives,suchastheJSYschemeinIndia.Aparticipantinarecentqualitative
studyreportedcaste-baseddiscriminationanduntouchabilitywhiledescribingcareprovider
attitudes(Khanna&Sri,2017).Inequalitymayresultinalackofaccesstoinformationanddecision-
makingpower,whichmayleadtopoorerhealthoutcomes.Intermsofwomen’saccesstoand
qualityofreproductiveandmaternalhealthcare,casteandsocialclasscanplayaroleincreating
inequitiesinmaternalandreproductivehealthcareprovision,alongwithotherfactorssuchas
women’sreproductivehistory,age,maritalstatusandparity(Khanna&Sri,2017).Theaimofthis
chapteristoundertakeaquantitativeanalysisofhouseholdsurveydatatoinvestigatethesocial
determinantsofobstetricviolenceinthestateofBihar,India.
AstudycarriedoutinUttarPradeshreportedthatthehighestmistreatmentscoresinhealthcare
facilitiesareforwomenolderthan35years(Sharma,2019).Anotherstudyfoundthatolderwomen
aremorelikelytoreportobstetricviolenceduringchildbirth,inadditiontoexpectationsforabribe
(Sudhiranasetetal.,2016).StudiesconductedinJordan(Fatimaetal.,2018)andGhana(Afulaniet
al.,2019)reportthatuneducatedandunemployedwomenaremorelikelytobeabused.

Chapter5
62
Disrespectfulcommentsbycareprovidersoftentargetwomen’sphysicalappearance,socio
economicstatus,parityandage(Sharma,2019).Inthesamevein,treatmentofwomenmayvary
basedon‘favouritism’thatmayresultininequitableuseoflimitedresourcesandrespectfulnessin
careprovisionwhenthelabouringwomanisknowntotheteam,orcomesfromawealthyand
influentialfamily(Freedmanetal,2018).
Freedman(2014)highlightsthatitisimportanttounderstandthedifferentdeterminantsofinequity
incareprovision,thatvariesbydifferentculturesandcountries.Thisistrueforbothdevelopingand
developedcountries,asforinstancecanbelearntfromthepoormaternalhealthoutcomesfor
womenofcolourinAmerica(Shah,2019).EvidencefromBihar,Indiashowsdiscriminatorypractices,
wherebywomenfromuppercastesorsocialclassesaregivenpreferentialcareinhealthfacilities
whilethoseinthelowercastegroupareeitherignoredorforcedtowait(Patel,Das&Das,2018).
AnotherreportsuggeststhatthereisnoASHAinaparticularcommunitybecauseASHA’sarefrom
uppercastefamilieswhooftenignorewomeninthevillagefromthelowercastes.Womenfrom
poorsocioeconomicbackgroundsaremorelikelytoreceivedisrespectfulandabusivecare.Thismay
includeignoringtheirrequestsforattentionorpainrelief,beingphysicallyimmobilised,undergoing
multiplepelvicexaminations,notbeingallowedabirthcompanion,givingbirthlyingdown(supine
position),receivingfundalpressureandhavingtheirculturalandspiritualritualsaroundbirth
ignored(suchasplacentadisposal).Theyarealsomorelikelytobegivenepisiotomiesincomparison
towomenfromaffluentbackgrounds(Sen,Reddy&Iyer,2018).Genderisanunderlyingfactorthat
increaseswomen’svulnerabilityingeneral(Sen,Reddy&Iyer,2018).
Discriminationcanbeseeninhowmedical,nursingandmidwiferystudentsaretaughtandthe
womenthey‘practice’on.Thereislimitedresearchonhospitalandstudentpairingforpracticein
theirpre-serviceeducation(Madhiwalaetal.,2018).Theprivateandpublichospitaldistinctionis
alsoimportanttonotehere.Midwifery,nursingandmedicalstudentsinIndiapracticeinpublic
hospitalsordonotgetenoughpracticeiftheyarestudyinginprivateinstitutionsaffiliatedtoa
privatetertiaryhospital(Mayra,2020b;Mayra,Padmadas&Matthews,2021).Mostprivate
hospitalshaveclientsfromaffluentbackgroundwhomightnotacceptcarefromastudent.Public
hospitalspredominantlyreceiveclientsfrompoorsocio-economicbackgrounds,indicatingmore
power-basedinequitiesbetweencareseekerandcareproviders(Mayra,Padmadas&Matthews,
2021).Studentsandtheirtraininginstitutionsfinditeasiertopracticeskillsonwomenfrompoorer
backgroundseekingcareinthepublichealthfacility.Figure5.1classifiesthesesocialdeterminants
into:1)individualattributes,2)familyandpeerinfluences,3)intermediarydeterminantsofhealth
and4)structuraldeterminantsofhealthinequities.

Chapter5
63
Figure5.1 Socialdeterminantsofmaternalhealth(Source:Khanna&Sri,2018.p.194)
Careprovidersunderstandthataneducatedwomanisoftenawareofthecareshewouldreceive
andhashigherexpectations(Downe,2019).Inlinewiththisargument,astudyfoundthatliterate
womenweremorelikelytohaveinterventionsexplainedtothem(Sudhiranasetetal.,2016).Onthe
otherhand,itisdifficultforwomenfrommarginalisedbackgroundtoreportobstetricviolenceeven
afteridentifyingit.Moststudiesonobstetricviolencefocusondifferentformsofviolence,ascanbe
seenthroughthevarioustypologies,andnotenoughonthepluralityofthesedifferentformsof
obstetricviolenceineachwoman’sexperience,whichIaddressinthisstudyalongwithexamining
thesocialdeterminantsofobstetricviolenceagainstthespecificindicatorsinthesevendomainsof
mistreatmentpresentedbyBohrenetal(2015).
5.2 Objective
• Toinvestigatetheassociationbetweenwomen’sbackgroundcharacteristicssuchasage,
caste,education,occupation,socio-economicstatusandparityandtheirlikelihoodof
experiencingobstetricviolenceduringchildbirthinBihar,India.
• Tounderstandthepluralityandcomplexmultilayerednatureofwomen’sexperienceof
obstetricviolenceinBihar,Indiathatmaybebetterexpressedquantitatively.
5.3 Methods
IanalysedsecondarydatafromahouseholdsurveyconductedinBihar,India.

Chapter5
64
5.3.1 Datacollection
DatawerecollectedbyOxfordPolicyManagementLimitedbetweenJuly2016toDecember2017
coveringallofthe38districtsofBihar,andthehouseholdsurveywascarriedoutasapartofthe
evaluationofqualityofmaternalhealthcareprovisioninthestate.Thehouseholdsurveyincludeda
separatesectiontocapturerespectfulmaternitycare.
Thehouseholdsurveyimplementedastructuredquestionnaire,targetingasampleof2194women
whohadgivenbirthwithinamonthprecedingtheinterviewinhealthcarefacilities(obstetric
settings)inBihar.Thisdatacollectionwasrelatedtoanothersurvey,whichinvolveddirect
observationofchildbirthinpublichospitalsinallthedistrictsofBihar,thataimedtoexplorethe
qualityofcareduringchildbirththroughaquasi-experimentalstudy.Thefindingsofthisstudyare
publishedelsewhere(Ahmedetal.,2019).Consentwastakenfromwomentoobservetheirbirth
andtoalsovisitthemwithin30daysofchildbirthforaninterviewattheirhouse.Theenumerators
visitedthehouseholdofallthewomenwhohadgivenbirthinthelast30dayswhentheyvisitedthe
womanwhosebirthwasobservedinthehealthcarefacilityalongwithcontactingwomenwhose
birthwerenotobservedbutliveinthesamevillageandhavegivenbirthinthelast30days.
Theinformationaboutallthewomenwhohadgivenbirthinthesamevillagecouldbereceivedfrom
theASHA,whichwasfollowedbyinterviewingthewomenafterseekingconsent.Womenwhogave
birthathomewereexcludedfromthesample,asIaimedtoexaminethesocialdeterminantsof
obstetricviolenceinobstetricsettingsonly.
Ofthe2194interviews,964women’sbirthswereobservedbynurse-midwifeenumeratorswith
consent.Theinterviewswerecarriedoutbyfemaleenumeratorswhowerefluentinthelocal
dialectssuchasMaithli,MagahiandBhojpuri.Everyinterviewwasconductedbytwofemale
enumerators,usingComputerAssistedPersonalInterviews(CAPI)systems.Afieldsupervisorwas
deployedwitheachteamtomonitorthesurveyandsupporttheteam.
AstructuredquestionnaireinHindiwasusedtodocumentwomen’sbackgroundcharacteristics,
experienceofcarearoundchildbirth,respect,disrespectandabuse,andsatisfactionwiththecare
received.
AstheNationalQualityofCareEvaluationManageratOxfordPolicyManagement,Iwasclosely
involvedinthedesignandimplementationofthehouseholdsurveyinBiharincludingdatacollection
andprocessing.Iwasalsoresponsibleforcoordinatingthefieldworkwhichincludedhiringand
trainingtheenumeratorsandsupervisoryteamandperformingtheoverallmanagementofthedata

Chapter5
65
collection,datamanagementandqualitycontrol.Ihavealsoparticipatedinreportwritingand
disseminationofthestudyfindings.Mybackgroundinnursingandmidwiferyandinresearchon
sexual,reproductiveandmaternalhealthcareaddedvaluetothedevelopmentandimplementation
offieldwork.
Ethicalapproval:TheethicalclearancefordatacollectionwastakenfromCentreforMediaStudies
institutionalreviewcommitteeinIndiabeforestartingdatacollection(Referencenumber:
IRB00006230).Informedconsentwastakenfromalltheparticipantsfortheinterviewattheir
household.Inaddition,IobtainedethicalapprovalforsecondarydataanalysisfromtheFacultyof
SocialSciencesResearchEthicsandGovernanceCommittee,attheUniversityofSouthampton
(Referencenumber:31910).
5.3.2 Dataanalysis
Forthedescriptiveandmultipleregressionanalyses,Iuseddatafrom2194womenwhogavebirth
inobstetricsettings.Basedontheliterature,Iselectedrelevantbackgroundvariablestounderstand
thesocialcharacteristicsassociatedwithobstetricviolence.Theseinclude:women’sage,education,
caste,occupation,socio-economicstatus,religionandparity.Ihaveconsideredthehousehold’s
socioeconomicstatustobetheparticipant’ssocio-economicstatuswhichwasmeasuredthrough
questionsonthehousehold’slandandcarownershipasanindicatorofwealth.
First,IcreatednewvariablesthatmatchedindicatorsundertheBohrenetal.(2015)typologyof
mistreatmentduringchildbirth,tounderstandtheextentofwomen’sexperienceofobstetric
violence.Thesevariablesareclassifiedunderallthesevenkeydomainsofthetypology:1)physical
abuse;2)sexualabuse;3)verbalabuse;4)stigmaanddiscrimination;5)poorrapportbetween
womenandcareproviders;6)failuretomeetprofessionalstandardsofcare;and7)healthsystems
conditionsandconstraints.Second,Iconductedbinarylogisticregressionanalysistounderstandthe
statisticalassociationbetweenthesespecificformsofobstetricviolenceunderBohren.etal(2015)
typologyandwomen’sdemographicandsocialcharacteristics.
Finally,Iconductedfactoranalysistocreatescorestoquantifyobstetricviolence,therebyreducing
thedifferentdimensionsasidentifiedunderthesevendomainsofBohrenetal.(2015)typology.
BasedontheScreeplot,Iextractedthefirstthreecomponentsthatrepresentedmorethan30%of
thevarianceinmydataset.Iconductedlinearregressiononthethreenewlycreatedobstetric
violencevariableswiththebackgroundcharacteristicstoinvestigatetheirassociationwithwomen’s
vulnerabilitytoexperienceobstetricviolenceduringchildbirth.

Chapter5
66
5.4 Results
5.4.1 Participantprofile
Atotalof2194womenwhoparticipatedinthisstudygavebirthinahealthcarefacilityinBihar.As
showninTable5.1,theparticipant’sagerangedbetween18-25years(72%),only1.5%participants
wereagedabove36years.Halfofthewomeninterviewedhavenotreceivedanyformaleducation
andonly8%hadreceivedahigherordegree(5%)leveleducation.Themajorityofparticipants
belongedtoHindureligion(83%)andweremarried(99.9%).About26%ofsurveyparticipants
belongedtoschedulecaste.Scheduletriberepresentationwasinsignificant(0.5%),whileother
backwardcastesrepresented61%ofallparticipants.Littlemorethan50%ofwomenlivedin
householdswithbettersocio-economicconditionswhichmeanttheirhouseholdsownedeitherland
orcar,orboth.

Chapter5
67
Table5.1 Participantprofile
Backgroundcharacteristics Numberofwomen(N=2194) Percentage
Age
18-25 1587 72.3
26-35 574 26.2
36-45 31 1.4
46+ 2 0.1
Education
Noeducation 1084 49.4
Primaryeducation 226 10.3
Secondaryeducation 594 27.1
Highersecondaryeducation 179 8.2
Degreelevel 111 5.1
Occupation
Homemaker 2179 99.3
Farmer 10 0.5
Employee 1 0.0
Ownbusiness/selfemployed 2 0.1
Student 2 0.1
Religion
Christian 3 0.1
Hindu 1816 82.8
Muslim 375 17.1
Marriage
Married 2191 99.9

Chapter5
68
Backgroundcharacteristics Numberofwomen(N=2194) Percentage
Separated 3 0.1
Caste
General 265 12.1
ScheduleCaste 573 26.1
ScheduleTribe 12 0.5
Otherbackwardcastes 1342 61.2
Socioeconomicstatus
BetterSES 1182 53.9
PoorSES 1012 46.1
Itisessentialtoexaminetheparticipant’sbirthingrelatedprofiles.Almostallwomenreceivedsome
antenatalcare(Table5.2).About4%womenhadabirthwerereferredfromanotherfacility.Most
womenweremultiparous(70%),withamaximumninebirths.Mostofthewomeninterviewed,
reportedsatisfactionwiththeirbirthingexperienceatthehealthcarefacility(96%)andwouldprefer
toseekcareatthesamehealthcarefacilityiftheygavebirthagain(92%).

Chapter5
69
Table5.2 Participant’sbirthrelatedvariables
Birthrelatedindicators Numberofwomen
(N=2194)
Percentage
Receivedanyantenatalcare 2180 99.4
Referredfromanotherfacility 95 4.3
Receivedepisiotomy 123 5.6
Givenanesthesiabeforeepisiotomy 82(N=123)
Prefertobirthinthesamefacilityagain 2009 91.6
Womensatisfiedwiththeirbirth
experience
2106 95.9
Parity
1 652 30.0
2-3 1055 48.0
4+ 487 22.2
Womenratingrespectfulnessincare
Excellent 138 6.3
Verygood 1386 63.2
Good 488 22.2
Fair 130 5.9
Poor 52 2.4
5.4.2 Experienceofobstetricviolence
Noneofthewomenreportedexperiencingsexualabuse,beingrestrainedandbeingdiscriminated
basedoncaste.Thegraphbelow(Figure5.2)showsthepercentageofwomenwhoexperienced
obstetricviolence,classifiedunderBohrenetal.(2015)sevenkeydomains.

Chapter5
70
Figure5.2 Women’sexperienceofobstetricviolenceunderBohrenetal.typology(2015)
Thetablebelow(5.3)showswomen’sexperienceofobstetricviolencebasedonBohrenetal.(2015)
typologyonmistreatmentofwomenduringchildbirthinanobstetricsetting.Thesurveydatashow
that,whileJSYpolicyisthekeydriverforwomentogivebirthinthehealthcareinstitutions,98%of
womendidnotreceivethemoneyfromgovernmentwithin30daysofgivingbirth.Unclearfee
structureisthecommonestformofabusefollowedbybriberyandextortion(84%),whichtogether
suggeststhatallwomenhadachallengingexperiencerelatedtohealthsystemconditionsand
constraints,whichisthe7thdomainofthetypology.Thiswasfollowedbythe6thdomain,‘Failureto
meetprofessionalstandardsofcare’,underwhich,womenweredeniedfoodandfluid(27%),not
allowedtowalkaround(22%)andnotallowedtheirchosenpositiontogivebirth(12%).Theywere
treatedasapassiveparticipantduringtheirchildbirth,andwerenotinformedaboutthefindingsof
theirgeneralexamination(31%)andvaginalexamination(7%),whichindicatespoorstaffattitude.
Womenreportedpoorrapportwiththecareproviders(Domain5).Theyexperiencedalackofclarity
incommunicationintermsofnotexplainingthewardenvironment(13%),theprogress(7%)and
movement(21%)inlabour.Somewomen(5%)feltneglectedorabandonedwhentheyneededa
careprovider.Afewwomenreportedbeingdiscriminatedandstigmatizedbasedontheirage
(0.2%),socioeconomicstatus(0.4%)andHIVstatus(16%).Althoughthenumberdoesnotsuggest
thattheywereHIVpositive,insteadthattheycouldhavefeltdiscriminatedwhentheywereasked
aboutit.Afewwomenreportedbreachofprivacy(4%)andconfidentiality(1%).

Chapter5
71
Womenalsoreportedthatsomeofthemostextremeformsofobstetricviolence:verbal(5%)and
physicalabuse(2%).Womenwerehit,slappedandpinched(2%)andweresubjectedtojudgemental
andaccusatorycomments(5%),rudelanguage(5%)andwerethreatenedtowithholdservices(1%).
Somewomenreceivedanepisiotomycutwithoutanesthesia(2%),thatcanbeconsideredoneofthe
harshestformsofobstetricviolence.

Chapter5
72
Table5.3 Typesofmistreatmentduringchildbirthexperiencedbywomen
Domainof
obstetricviolence
Specificmistreatmentcategory Frequency%
(N=2194)
Physicalabuse Slapping,hitting,pinching 1.6(35)
Restraining 0.0(0)
Sexualabuse Rape 0.0(0)
Verbalabuse Judgementalandaccusatorycomments 5.0(109)
Rudelanguage 5.0(109)
Threatenedwomentowithholdservices 0.6(14)
Stigmaand
discrimination
Discriminationbasedonage 0.1(2)
Discriminationbasedoncaste 0.0(0)
DiscriminationbasedonSES 0.2(4)
DiscriminationbasedonHIVstatus(askedaboutHIV
status)
15.5(341)
Poorrapport
betweenwomen
andproviders
Nopainrelief(episiotomywithoutanesthesia) 1.9(12)
Neglectandabandonment 4.7(103)
Lackofconfidentiality 1.2(27)
Poorcommunication-wardenvironmentnotexplained 13.2(289)
Poorcommunication-progressinlabournotexplained 6.1(134)
Poorcommunication-movementforfoetusinlabour
notexplained
20.7(454)
Nonconsensualsurgery(episiotomy) 0.5(12)
Nonconsensualcare 3.7(81)
Notallowedtowalk 21.9(481)
Womanorbabydetainedatthefacility 2.4(53)

Chapter5
73
Domainof
obstetricviolence
Specificmistreatmentcategory Frequency%
(N=2194)
Failuretomeet
professional
standards
Denialoffoodandfluid 27.3(600)
Birthcompanionnotallowed 1.5(34)
Deniedchoiceofbirthposition 12.1(266)
Treatedasapassiveparticipant(GEnotexplained) 30.8(675)
Poorstaffattitude(VEfindingsnotexplained) 7.2(157)
Healthsystem
conditionand
constraints
Lackofprivacyduringbirth 3.9(85)
Bribeandextortion 84.2(1848)
Reportedgrievance 4.7(104)
Unclearfee(receivedanyfunds/JSYmoneyfromthe
institutionalbirth)
98.0(2150)
Table5.4showsthepercentagesofdifferentformsofobstetricviolencebywomen’sbackground
characteristics,basedonBohrenetal.(2015)classification.Morethan30%ofthewomenaged
between36-45yearsexperiencedstigmaanddiscrimination,whichismuchhigherthanotherage
groupsofparticipants.Thisistwiceashighsuggestingwomenmayexperiencemoreabusewhen
givingbirthatanolderagethanwomenagedbetween18-25and26-35yearsofage.Similarly,
womenwhowerehighlyeducated,withdegreelevelofeducation,didnotreportanyexperiencesof
physicalabuse.However,highlyeducatedwomenreportedcomparativelymorestigmaand
discriminationthanotherwomeninthiscategory.
Religionisalsoanimportantfactor.Hinduwomenreportedexperiences(82%)ofverbalabuseata
higherratethanMuslimwomen(5%).Scheduledtribewomenreportedexperiencingphysical(8%)
andverbalabuse(8%)atahigherratethantheaverage(2%&5%)andwomen’sexperiencefrom
othercastes.Parityisanimportantfactor,asprimiparawomenhavebeenmorelikelytoexperience
physicalabuseandpoorrapportwiththecareprovider.

Chapter5
74
Table5.4 Percentageofwomenreportingobstetricviolencebywomen’sbackground
Variables Physical
abuse
Verbal
abuse
Stigma&
discrimina
tion
Poor
rapport
between
woman&
care
provider
Failureto
maintain
profession
al
standard
ofcare
Health
systems
conditions
and
constraints
TOTAL 1.6 5.0 15.8 3.2 56.6 100.0
Age
18-25years 1.7 5.4 16.4** 4.0** 55.3 99.9
26-35years 1.4 3.8 13.4** 1.0** 60.6 100.0
36-45years 0.0 3.2 32.3** 0.0** 48.4 100.0
46yearsandabove 0.0 0.0 0.0** 0.0** 50.0 100.0
Education
Noeducation 1.6 4.8 15.9 2.2 58.9 100.0***
1-5years(Primary) 0.9 4.4 13.3 3.1 56.2 100.0***
6-10years(Secondary) 2.4 5.9 15.0 3.5 55.4 100.0***
11-12(Higher
secondary)
1.1 4.5 17.9 5.0 51.4 100.0***
13+(Degree) 0.0 3.6 21.6 8.1 50.5 99.1***
Religion
Muslim 1.1 4.5*** 15.5 3.7 59.7 100.0
Christian 0.0 66.7*** 0.0 0.0 100.0 100.0
Hindu 1.7 82.6*** 15.9 3.1 55.9 99.9
Caste
Generalcaste 1.5 4.5 19.9 4.5 58.3 100.0
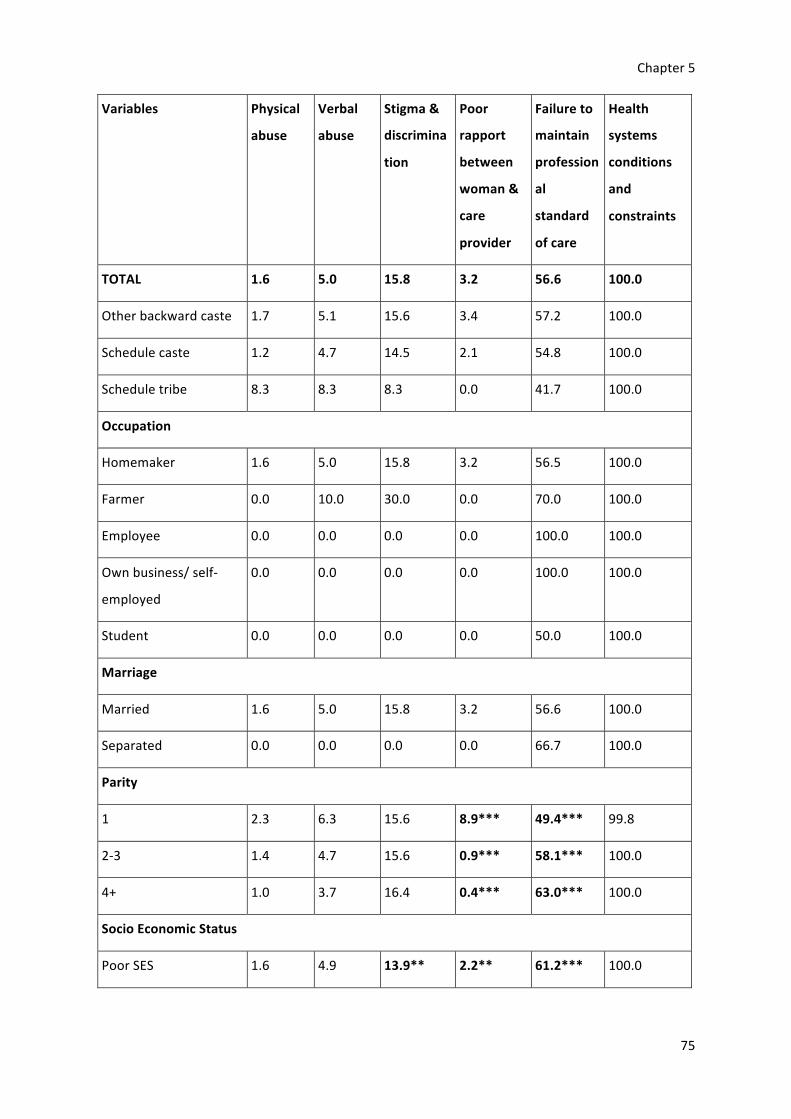
Chapter5
75
Variables Physical
abuse
Verbal
abuse
Stigma&
discrimina
tion
Poor
rapport
between
woman&
care
provider
Failureto
maintain
profession
al
standard
ofcare
Health
systems
conditions
and
constraints
TOTAL 1.6 5.0 15.8 3.2 56.6 100.0
Otherbackwardcaste 1.7 5.1 15.6 3.4 57.2 100.0
Schedulecaste 1.2 4.7 14.5 2.1 54.8 100.0
Scheduletribe 8.3 8.3 8.3 0.0 41.7 100.0
Occupation
Homemaker 1.6 5.0 15.8 3.2 56.5 100.0
Farmer 0.0 10.0 30.0 0.0 70.0 100.0
Employee 0.0 0.0 0.0 0.0 100.0 100.0
Ownbusiness/self-
employed
0.0 0.0 0.0 0.0 100.0 100.0
Student 0.0 0.0 0.0 0.0 50.0 100.0
Marriage
Married 1.6 5.0 15.8 3.2 56.6 100.0
Separated 0.0 0.0 0.0 0.0 66.7 100.0
Parity
1 2.3 6.3 15.6 8.9*** 49.4*** 99.8
2-3 1.4 4.7 15.6 0.9*** 58.1*** 100.0
4+ 1.0 3.7 16.4 0.4*** 63.0*** 100.0
SocioEconomicStatus
PoorSES 1.6 4.9 13.9** 2.2** 61.2*** 100.0
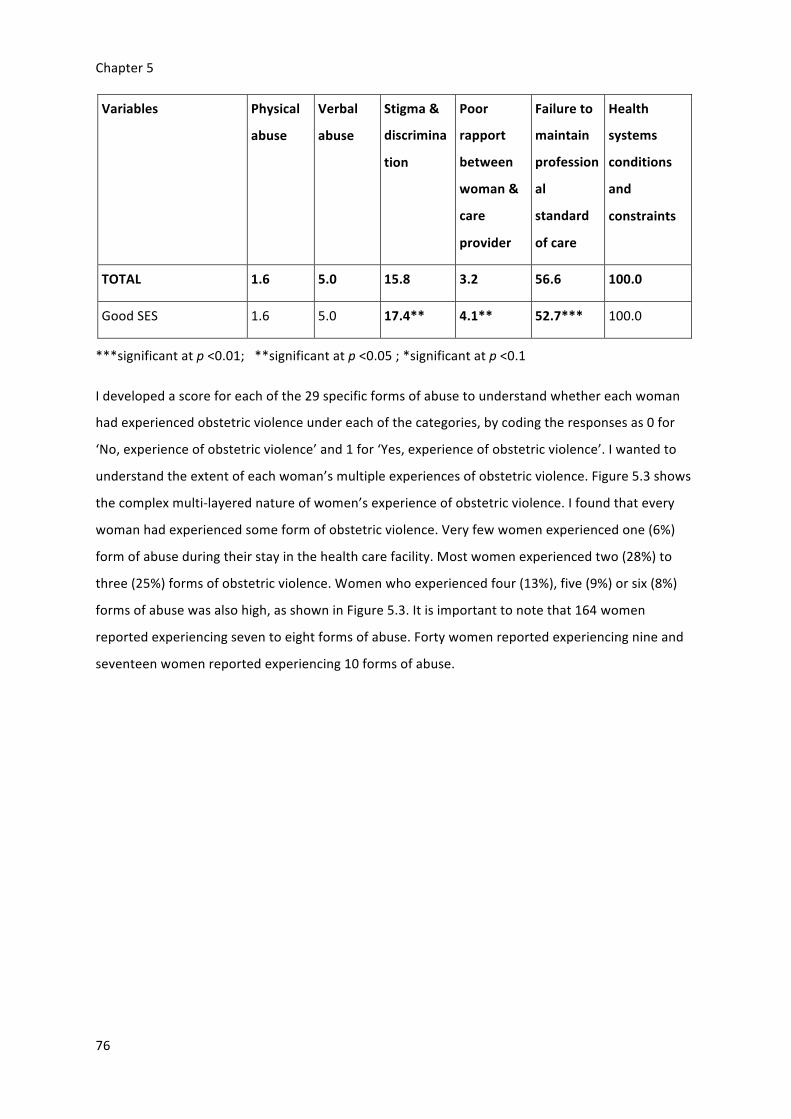
Chapter5
76
Variables Physical
abuse
Verbal
abuse
Stigma&
discrimina
tion
Poor
rapport
between
woman&
care
provider
Failureto
maintain
profession
al
standard
ofcare
Health
systems
conditions
and
constraints
TOTAL 1.6 5.0 15.8 3.2 56.6 100.0
GoodSES 1.6 5.0 17.4** 4.1** 52.7*** 100.0
***significantatp<0.01;**significantatp<0.05;*significantatp<0.1
Idevelopedascoreforeachofthe29specificformsofabusetounderstandwhethereachwoman
hadexperiencedobstetricviolenceundereachofthecategories,bycodingtheresponsesas0for
‘No,experienceofobstetricviolence’and1for‘Yes,experienceofobstetricviolence’.Iwantedto
understandtheextentofeachwoman’smultipleexperiencesofobstetricviolence.Figure5.3shows
thecomplexmulti-layerednatureofwomen’sexperienceofobstetricviolence.Ifoundthatevery
womanhadexperiencedsomeformofobstetricviolence.Veryfewwomenexperiencedone(6%)
formofabuseduringtheirstayinthehealthcarefacility.Mostwomenexperiencedtwo(28%)to
three(25%)formsofobstetricviolence.Womenwhoexperiencedfour(13%),five(9%)orsix(8%)
formsofabusewasalsohigh,asshowninFigure5.3.Itisimportanttonotethat164women
reportedexperiencingseventoeightformsofabuse.Fortywomenreportedexperiencingnineand
seventeenwomenreportedexperiencing10formsofabuse.

Chapter5
77
Figure5.3 Thenumberoftypesofobstetricviolencesufferedbywomen
Tobetterunderstandthegraphaboveintermsoftheseverityofwomen’sexperiences,Ipresenta
casestudyfrommydataset.IpresentTrahi’s(pseudonym)story,astheparticipantwhoexperienced
themaximum(17)formsofobstetricviolence,whichwasthehighestinmydatasetinAppendixA.I
constructedthisstoryfromherdata,forabetterunderstandingofwomen’sexperiencesofobstetric
violencewithmorecontext,andtohighlightthevalueofeverysinglewoman’sexperienceof
obstetricviolence,thatIwillexploreinmoredetailinthenextchapters.
5.4.3 Socialdeterminantsofobstetricviolence
Binarylogisticregressionanalysis
Iconductedlogisticregressionsonfiveoutofthesevenkeydomainsofobstetricviolence
(dependentvariables)fromBohrenetal.(2015)typologytoexaminetheirassociationwithwomen’s
backgroundcharacteristics(Table5.5).Ididnotincludesexualabusebecausenoonereportedit
whilehealthsystemsconditionsandconstraintsreportingwasuniversal.Thebackground
characteristicsdescribingwomen’sreligion,age,education,caste,parityandsocio-economicstatus
aretheindependentvariablesalongwithavariableonwhethertheparticipant’sbirthwasobserved
inthesurveybyresearchersinthehealthcarefacility.Ididnotuseoccupationdatabecause99.9%
womenarehomemakers.Iusethe1stcategoryineachvariableasthereferencecategory.

Chapter5
78
Theresultsshowthatwomenhadhigheroddsofexperiencingphysicalabuse,verbalabuse,and
failuretomeetprofessionalstandardsbycareproviders,whentheirbirthwasnotobserved.Women
weremorelikelytoexperiencestigmaanddiscriminationwhentheirbirthwasobserved.These
resultswerehighlysignificant.Increasingparitydecreasedthelikelihoodofwomenexperiencing
poorrapportwithcareproviderbutincreasedthelikelihoodoffailureonthecareprovider’spartto
provideprofessionalstandardofcare.Womenwithmorechildrenweremorelikelytoexperience
failuretomaintainprofessionalstandardofcare.Inaddition,womenagedbetween25-36years
werelesslikelywhilewomenaged36-45yearsweremorelikelytoexperiencestigmaand
discriminationcomparedtowomengivingbirthatbetween18-25yearsofage.Poorrapportwith
careproviderwasmorelikelyifthewomenareeducated,withthemosteducatedwomen
experiencingthehighestlikelihoodofpoorrapportwithcareprovider.Womenweremorelikelyto
experiencepoorrapportwithcareproviderandlesslikelytoexperienceafailuretomaintain
professionalstandardofcareiftheybelongedtoahouseholdwithagoodsocio-economicstatus.
Womenfromotherbackwardcastesandscheduletribeweresignificantlylesslikelytoexperience
stigmaanddiscriminationincomparisontowomenfromgeneralcaste.
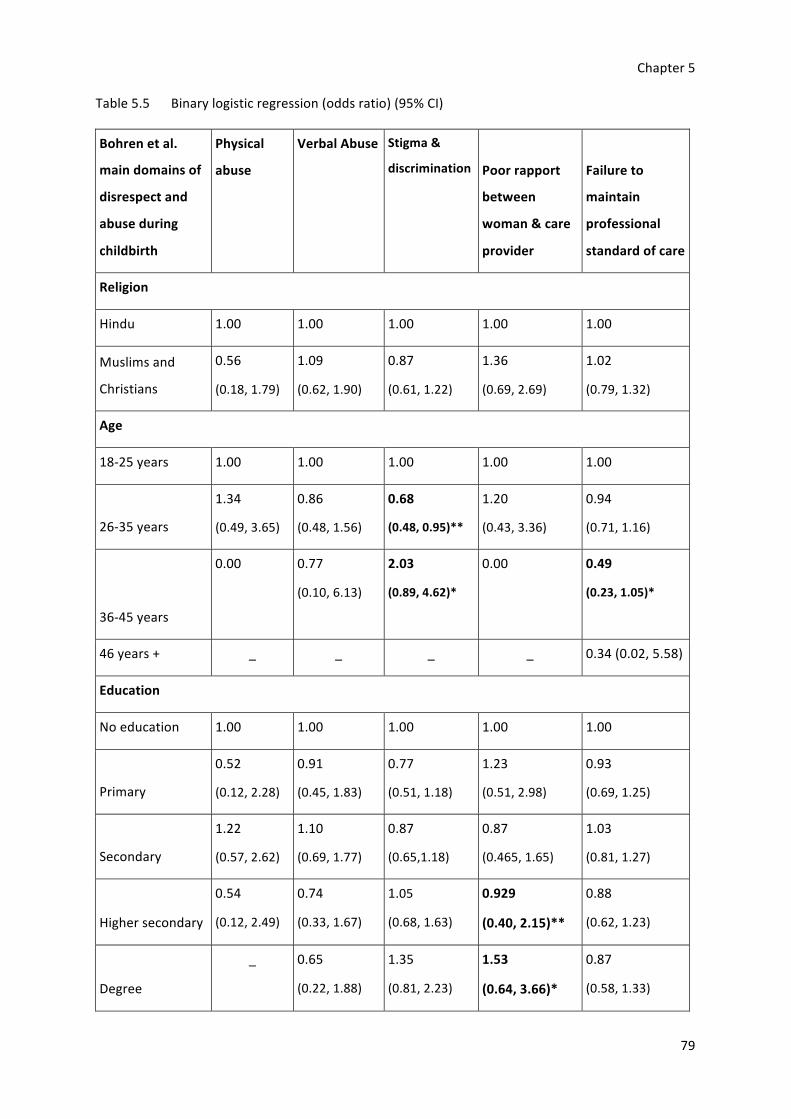
Chapter5
79
Table5.5 Binarylogisticregression(oddsratio)(95%CI)
Bohrenetal.
maindomainsof
disrespectand
abuseduring
childbirth
Physical
abuse
VerbalAbuse Stigma&
discrimination Poorrapport
between
woman&care
provider
Failureto
maintain
professional
standardofcare
Religion
Hindu 1.00 1.00 1.00 1.00 1.00
Muslimsand
Christians
0.56
(0.18,1.79)
1.09
(0.62,1.90)
0.87
(0.61,1.22)
1.36
(0.69,2.69)
1.02
(0.79,1.32)
Age
18-25years 1.00 1.00 1.00 1.00 1.00
26-35years
1.34
(0.49,3.65)
0.86
(0.48,1.56)
0.68
(0.48,0.95)**
1.20
(0.43,3.36)
0.94
(0.71,1.16)
36-45years
0.00 0.77
(0.10,6.13)
2.03
(0.89,4.62)*
0.00 0.49
(0.23,1.05)*
46years+ _ _ _ _ 0.34(0.02,5.58)
Education
Noeducation 1.00 1.00 1.00 1.00 1.00
Primary
0.52
(0.12,2.28)
0.91
(0.45,1.83)
0.77
(0.51,1.18)
1.23
(0.51,2.98)
0.93
(0.69,1.25)
Secondary
1.22
(0.57,2.62)
1.10
(0.69,1.77)
0.87
(0.65,1.18)
0.87
(0.465,1.65)
1.03
(0.81,1.27)
Highersecondary
0.54
(0.12,2.49)
0.74
(0.33,1.67)
1.05
(0.68,1.63)
0.929
(0.40,2.15)**
0.88
(0.62,1.23)
Degree
_ 0.65
(0.22,1.88)
1.35
(0.81,2.23)
1.53
(0.64,3.66)*
0.87
(0.58,1.33)
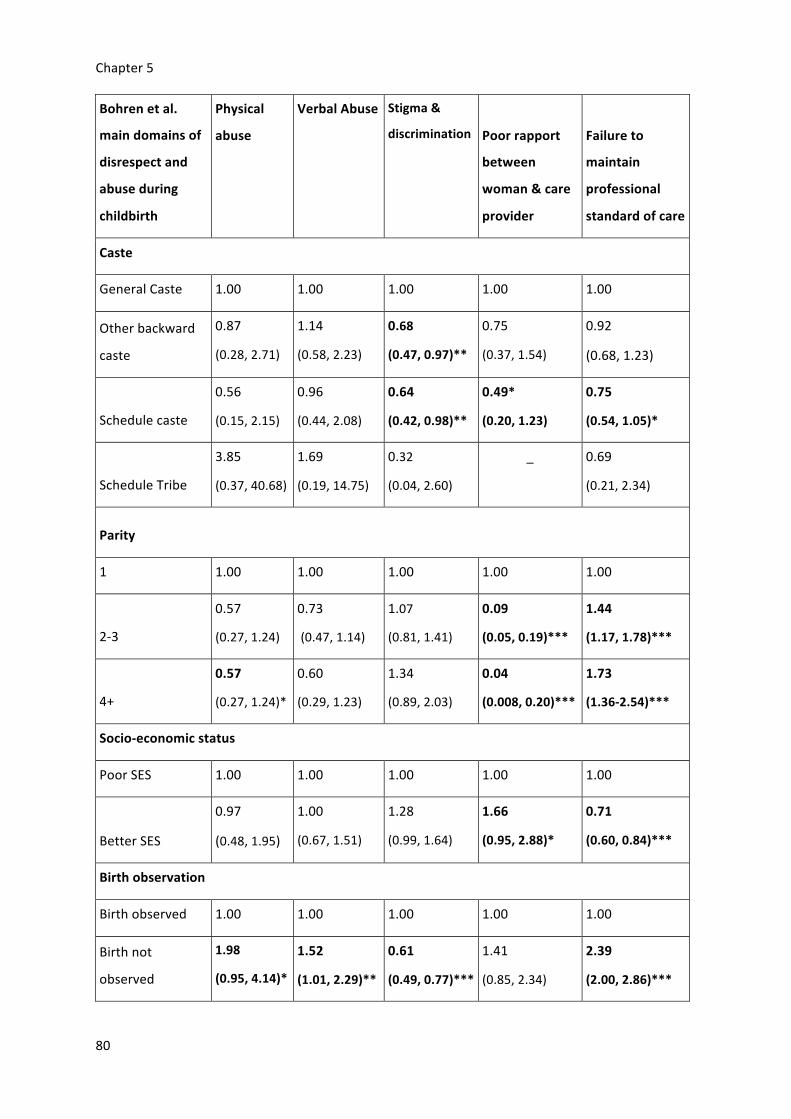
Chapter5
80
Bohrenetal.
maindomainsof
disrespectand
abuseduring
childbirth
Physical
abuse
VerbalAbuse Stigma&
discrimination Poorrapport
between
woman&care
provider
Failureto
maintain
professional
standardofcare
Caste
GeneralCaste 1.00 1.00 1.00 1.00 1.00
Otherbackward
caste
0.87
(0.28,2.71)
1.14
(0.58,2.23)
0.68
(0.47,0.97)**
0.75
(0.37,1.54)
0.92
(0.68,1.23)
Schedulecaste
0.56
(0.15,2.15)
0.96
(0.44,2.08)
0.64
(0.42,0.98)**
0.49*
(0.20,1.23)
0.75
(0.54,1.05)*
ScheduleTribe
3.85
(0.37,40.68)
1.69
(0.19,14.75)
0.32
(0.04,2.60)
_ 0.69
(0.21,2.34)
Parity
1 1.00 1.00 1.00 1.00 1.00
2-3
0.57
(0.27,1.24)
0.73
(0.47,1.14)
1.07
(0.81,1.41)
0.09
(0.05,0.19)***
1.44
(1.17,1.78)***
4+
0.57
(0.27,1.24)*
0.60
(0.29,1.23)
1.34
(0.89,2.03)
0.04
(0.008,0.20)***
1.73
(1.36-2.54)***
Socio-economicstatus
PoorSES 1.00 1.00 1.00 1.00 1.00
BetterSES
0.97
(0.48,1.95)
1.00
(0.67,1.51)
1.28
(0.99,1.64)
1.66
(0.95,2.88)*
0.71
(0.60,0.84)***
Birthobservation
Birthobserved 1.00 1.00 1.00 1.00 1.00
Birthnot
observed
1.98
(0.95,4.14)*
1.52
(1.01,2.29)**
0.61
(0.49,0.77)***
1.41
(0.85,2.34)
2.39
(2.00,2.86)***

Chapter5
81
Factoranalysis
AnalysingeachseparateBohrenetal.,(2015)categorywasonewaytoreducethedimensionalityof
theobstetricviolencedata.However,onlyfiveofthesevendatagroupscouldbeusedandthe
approachdidnotreducethedimensionalityenough.I,therefore,usedfactoranalysiswithprinciple
componentanalysisasthemethodofextraction,tocreatescoresthatcapturedthevariationmore
succinctly.Iselectedthefirstthreecomponentswhichexplainedthemostvarianceinthedata,as
canbeseenintheScreePlot(Figure5.4)whichshowsthatthefactorsstarttailingoffafterthe3rd
componentandthefirstthreecomponentsexplain32%ofthetotalvariance.
Tocarryoutthefactoranalysis,Iselected26ofthe29typesofobstetricviolencebasedonthe
entireBohrenetal.(2015)classificationbecausethreeformsofviolencenamely,sexualviolence,
restrained,anddiscriminationagainstcaste,werenotreportedbyparticipants.Table5.6presents
thethreecomponentsthatrepresentedthemostvarianceinthe25typesofobstetricviolence.I
selectedacutoffvalueforfactorloadingsat0.3(Tabachnich&Fidell,2013)andhighlightedthe
elementsthatloadedpositivelyandstronglyundertheparticularformsofviolence.
Figure5.4 ScreePlot
Component1loadedpositivelyforindicatorsconcerningphysicalandverbalabuse.Thethree
variablesthatloadedstronglyunderthiscomponentforverbalabuseare:1)rudelanguage;2)
judgementalandaccusatorycomments;and3)threatenedwomentowithholdservices.Poor
communicationhasstrongpositivefactorloadingfortwomainobstetricviolencedomainsi.e.poor
rapportbetweenwomanandcareproviderandafailuretoprovideprofessionalcare,for

Chapter5
82
component2.Thereisapatterninthehighpositivefactorloadingforthespecificvariableswhich
weremostlyrelatedtopoorcommunicationandalackofexplanation,thatinclude:1)vaginal
examinationfindingsnotexplained;2)wardenvironmentnotexplained;3)progressinlabournot
explained;4)generalexaminationfindingsnotexplained;and5)movementinlabournotexplained.
Factorsloadingwerepositiveandstrongfordenialoffoodandfluidsandnotallowingwomento
walkwheninlabour.Thisshowsafailuretoprovidecompassionatecareduringchildbirth,andcan
beconsideredrelatedtopoorcommunicationwhenwomenarerestrictedfromwalkingandeating.
Thethirdcomponent,coercion,indicatesalackofconsent,asthefactorloadingwaspositively
correlatedwith1)non-consensualcareand2)non-consensualsurgery.

Chapter5
83
Table5.6 Factoranalysis
IndividualdisrespectandabuseindicatorsfromBohrenetal’sclassification
Components
Physical&verbalabuse
Poorcommunication
Coercion
Womanorbabydetainedatfacility
0.188 0.038 0.122
AskedaboutHIVstatus -0.111 -0.197 -0.009
Nobirthcompanion 0.011 0.108 0.103
Deniedchoiceofbirthposition 0.250 0.235 -0.032
Denialoffood&fluid 0.188 0.547 -0.193
Physicalabuse 0.511 -0.155 -0.057
Leftunattendedwhenneeded 0.437 -0.017 0.202
GEexaminationsnotexplained 0.226 0.370 0.041
VEfindingsnotcommunicated 0.222 0.458 0.322
Lackofprivacyduringbirth 0.156 0.000 0.246
Confidentialitybreach 0.215 -0.085 0.245
Wardenvironmentnotexplained
0.247 0.305 0.052
Progressinlabourunexplained 0.238 0.371 0.476
Non-consensualsurgery 0.244 0.044 0.556
Non-consensualcare 0.372 -0.028 0.487
Rudelanguage 0.906 -0.271 -0.201
Receivedanyfundsfromtheinstitutionalbirth
-0.014 -0.038 -0.115
Judgementalandaccusatorycomments
0.906 -0.271 -0.201
Movementinlabourunexplained
0.223 0.816 -0.256
Threatenedwomentowithholdservices
0.483 -0.140 0.068
Bribeandextortion 0.154 0.107 0.055
Reportedgrievance 0.883 -0.270 -0.204
Notallowedtowalk 0.215 0.809 -0.270
Agebaseddiscrimination 0.185 -0.004 -0.059

Chapter5
84
DiscriminationbasedonSES 0.213 -0.057 -0.125
Extractionmethod-PrincipleComponentAnalysis
Rotationmethod-ObliminwithKaiserNormalisation
Exploringtheobstetricviolencefactorscoresbywomen'sbackgroundcharacteristics
Icreatedscoresagainstthreeobstetricviolencevariablesfromthefirstthreeprinciplecomponents
foralltheparticipants,tounderstandthepatternofobstetricviolencebyselectedbackground
characteristics,asshownthroughthefollowinggraphs.Ahigherscoreofeachofthenewdomain,
meansmoreexperienceofobstetricviolence.Poorcommunicationscoresincreasewithwomen’s
age,whereascoercion,physicalandverbalabusescoresdecreaseswithage(Figure5.5).
Figure5.5 Meanscoresofobstetricviolencebyagegroup
Communicationimprovedandphysicalandverbalabusedecreasedwithincreaseineducation,but
coercionincreased(Figure5.6).Thecommunicationscoresdecreasedformultigravidawomen,while
primigravidawomenweremorephysicallyandverballyabusedandcoerced(Figure5.9).The
increaseinpositivefactorscoresshowanincreaseinpoorcommunicationasthepositiveloadings
indicateincreaseinobstetricviolenceandthenegativeloadingindicateadecreaseintheparticular
-0.30-0.20-0.10
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
18-25 26-35 36-45 46+
Meanfactorsc
ore
Agegroup(inyears)
Physical&verbalabuse Poorcommunication Coercion

Chapter5
85
formofobstetricviolence.Womenfromgeneralcastewerewelltreated,whilewomenfrom
scheduletribewerephysicallyandverballyabused.Coercionscoreswerehighforwomenfrom
otherbackwardcastes(Figure5.8).
Figure5.6 Meanscoresofobstetricviolencebyeducation
-0.15
-0.10
-0.05
0.00
0.05
0.10
0ornone 1-5 6-10 11-12 13+
Meanfactorsc
ore
Educationattainment(inyears)
Physical&verbalabuse Poorcommunication Coercion

Chapter5
86
Figure5.7 Meanofobstetricviolencebysocio-economicstatus
Figure5.8 Meanscoresofobstetricviolencebycaste
-0.08
-0.06
-0.04
-0.02
0.00
0.02
0.04
0.06
0.08
0.10
Poor Rich
Meanfactorsc
ore
SocioeconomicStatus
Physical&verbalabuse PoorCommunication Coercion
-0.10
-0.05
0.00
0.05
0.10
0.15
0.20
0.25
Generalcaste Otherbackwardcaste
Schedulecaste Scheduletribe
Meanfactorsc
ore
Caste
Physical&verbalabuse PoorCommunication Coersion

Chapter5
87
Figure5.9 Meanscoresofobstetricviolencebyparity
Linearregressionwiththenewcomponents
Iconductedlinearregressionwiththethreenewvariables(physicalandverbalabuse;poor
communicationandcoercion)tounderstandtheirrelationshipwithwomen’sbackground
characteristics.Backgroundcharacteristicsselectedincludeage,religion,education,parity,socio-
economicstatusandcaste.Theregressioncoefficientshowsthatparityhadasignificantnegative
effectoncoercionscores,whichimpliesthatmultiparouswomenarelesslikelytoexperience
coercion.Similarsignificantandnegativeeffectwasnotedforpoorcommunication,suggestingthat
communicationtendstoimprovewithnumberofbirths.Womenlivinginbetterlivingconditions
werelesslikelytoreportpoorcommunication,andtherelationshipwasstatisticallysignificant.The
relationshipbetweenobstetricviolencescoresandwomenwhosebirthwasnotobservedwas
positiveandsignificant.Thissuggeststhatwomenwhosebirthwasnotobservedweremorelikelyto
reportcoercion,poorcommunicationandphysicalandverbalabuse.
-0.20
-0.15
-0.10
-0.05
0.00
0.05
0.10
0.15
1 2-3 4+
Meanfactorsc
ore
Parity
Physical&verbalabuse PoorCommunication Coercion

Chapter5
88
Table5.7 Linearregressioncoefficientsofbackgroundcharacteristicsandthenewobstetric
violencescores
Backgroundcharacteristics
Coercion PoorCommunication
Physical&verbalabuse
Age 18-25years 0.000 0.000 0.000
26yearsandabove -0.007(0.060) 0.008(0.06) -0.008(0.06)Education Noeducation 0.000 0.000 0.000Primaryeducation -0.002(0.07) 0.002(0.07) -0.010(0.07)Secondaryeducation -0.002(0.05) 0.038(0.05) 0.012(0.05)H.secondaryeducation
0.001(0.08) -0.009(0.08) -0.019(0.09)
Degreeeducation 0.011(0.10) 0.015(0.10) -0.023(0.10)Religion Hindu 0.000 0.000 0.000Muslim&Christian -0.014(0.06) -0.010(0.06) -0.012(0.63)
Caste SCST 0.000 0.000 0.000Generalcaste 0.012(0.08) -0.033(0.08) 0.012(0.08)
Otherbackwardcaste
0.020(0.05) 0.031(0.05) 0.020(0.05)
Parity 1 0.000 0.000 0.000
2-3 -0.079***(0.05) 0.115***(0.05) -0.036(0.05)4+ -0.081***(0.08) 0.116***(0.07) -0.048(0.08)Socioeconomicstatus
Good 0.000 0.000 0.000Poor -0.008(0.045) -0.073***(0.044) -0.003(0.46)BirthobservationBirthobserved 0.000 0.000 0.000Birthnotobserved 0.044**(0.04) 0.225***(0.042) 0.038*(0.43)Rsquare 0.01 0.07 0.01
Note:StandardErrorinbrackets.

Chapter5
89
5.5 Discussionandconclusion
Theforegoinganalysesshowsthatwomen’sexperienceofobstetricviolenceisnotaone-time
occurrenceduringchildbirth.Theseexperiencesaremultilayered,non-linearandconsistsof
differentformsofviolence.Acrucialfindingisthatallparticipantshaveexperiencedatleastone
formofobstetricviolenceduringchildbirth.Itisalsonoteworthythatnoneofthewomen
experiencedjustoneformofviolenceduringchildbirthbasedontheBohren’sclassification.Ifound
thatwhilenowomanreportedexperiencingsexualviolence(2nddomain),everywomanreported
experiencingdisrespectandabuserelatedtohealthsystemsconditionsandconstraints.Theleast
abusiveexperienceofwomenincluded,undergoingatleasttwoformsofobstetricviolence.Onthe
otherhand,onewomanexperienced17formsofdisrespectandabuseasperBohrenetal.(2015)
sub-classification.Whileitwaspossibletoreportdifferentformsofabuse,thequestionnairedidnot
allowtocapturehowmanyinstancesofabuseanddisrespectoccurredundereachform.Thisisa
limitationthatshouldbeexploredinthefuturetoobtainacompletepictureofthenatureand
extentofwomen’sexperiencesofobstetricviolence.
Iconductedlogisticregressionswiththemainformsofobstetricviolenceandwomen’sbackground
characteristicssuchasage,education,caste,socio-economicstatus,parityandwhethertheir
childbirthwasobservedtounderstandthesocialdeterminantsofobstetricviolence.Ifoundthat
womenwithmorechildrenweremorevulnerabletoexperiencingunprofessionalcare.Womenaged
between18-25yearsweremorelikelytoexperiencestigmaanddiscrimination,whencomparedto
womenaged26-35years.Thisisinlinewiththeassumptionthatwomenatthebeginningandthe
endoftheirreproductiveagemayexperiencemoreobstetricviolenceintheformofstigmaand
discriminationforgivingbirthtooearlyortoolate.Aseducationincreased,womenweremorelikely
toexperiencepoorrapportwithcareproviders.Thiscouldbebecauseeducatedwomenmayask
morequestions,knowtheirrightsandaskaboutprocedures,whichmayleadtopoor
communicationasthecareprovidersmaynotentertainit.Religionhadnosignificantinfluenceon
obstetricviolenceinthesedata.Itisinterestingtonotethatwomenfromschedulecasteand
backwardcastesweremorelikelytoexperiencestigmaanddiscriminationandpoorrapportwhen
comparedwithwomenfromgeneralcaste.Thiscouldbebecauseover88%oftheparticipantswere
fromlowcastesincludingschedulecastes,scheduletribesandotherbackwardcastes.Theopposite
hasbeenreportedinpreviousstudiesinadifferentstateinIndia(Khanna&Sri,2017).Inthatstudy,
womenfrompoorsocio-economicstatusweremorelikelytoexperienceobstetricviolencethan
womenfromaffluentbackgrounds,asisreportedelsewheretoo(Sharma,2019).Icouldnot
examinetheinfluenceofoccupationandmaritalstatusonobstetricviolenceasmorethan99%

Chapter5
90
participantsaremarriedhomemakers.Giventhatasubstantialnumberofwomenwereinterviewed
afterobservationoftheirchildbirthexperience,itisimportanttonotethattheyexperiencemore
obstetricviolencewhentheirbirthisnotobserved.Thiscanbeexplainedbytheimpactof
hawthorneeffectoncareprovider’sbehaviourasaresultofbeingobserved,ashasbeenreportedin
ourpublicationfromthedirectobservationofbirthdata(Ahmedetal.,2019)andreportedbyother
researcherstoo(Goodwinetal.,2018;Choi,Jung&Grantchrov,2019).
Iconductedfactoranalysistoexaminethevariationinthevariablesofobstetricviolencethrough
whichIcreatedthreenewobstetricviolencescoreswhichrepresentalargeproportionofvariance
in(32%)thedataset.Thepatternsinthespecificvariableshelpedtonamethem:1)coercion;2)
poorcommunicationand3)physicalandverbalabuse.Parityisanimportantfactorandsignificant
forallthethreevariables.Whileprimigravidawomenweremorephysicallyandverballyabusedand
coerced.Withmorenumberofbirths,multigravidawomenexperiencedpoorercommunication
fromthecareproviders.Ialsoconductedlinearregressionanalysisagainstselectedvariablesfrom
women’sbackgroundcharacteristicsasdependentvariable.Ifoundthatwomenexperiencedpoor
communicationwithincreaseinparity.Ialsofoundthatgoodsocio-economicstatusresultedin
bettercommunicationwithwomen.Finally,morewomenwhosebirthswerenotobservedwere
coerced,physically,verballyabusedandexperiencedpoorcommunication.Theseresultsareinline
withtheresultsfromlogisticregressiontoo.
Studiesconductedgloballyhavefoundthatwomenfrommarginalisedcommunitiesmaybemore
vulnerabletoexperiencingobstetricviolenceduetotheirage,socio-economicstatus,race,gender
expression,sexualorientation,healthstatusandmigration(Khoslaetal.,2016;Chadwick,2019).
Obstetricviolence,asIdiscussedinChapter2,makeswayfornegativehealthoutcomes,for
maternal,reproductiveandsexualhealth.InthecaseofIndia,women’ssocialanddemographic
characteristicssuchaseducation,parity,obstetrichistory,socialposition,culture,valuesandnorms
playakeyroleindeterminingtheirvulnerabilitytoobstetricviolence(Nambiar&Muralidharan,
2017).Someofthesefactorshavebeenfoundtoinfluenceintimatepartnerviolenceaswell,inthe
contextofBiharandotherstatesinIndia(Dharetal.,2018;Sharmaetal.,2019;Deyetal.,
Sudhiranasetetal.,2016),asIdiscussedinChapter3.Futurestudieswouldbenefitfromexploring
obstetricviolencealongsideallotherformsofviolenceexperiencedbywomenastheprevalenceof
violenceinwomen’slives,increaseswomen’svulnerabilityforviolenceinotherphasesoftheirlives.
ThecultureofviolenceisprevalentinBihar(NFHS,2020;Dharetal.,2018).Women’spositioningat
theintersectionsoftheirbackgroundcharacteristicsincreasestheinequalities,furtherincreasing
Chapter5
91
theirvulnerabilitytoobstetricviolence(Sen,Reddy&Iyer,2018).Obstetricviolenceisanegative
outcomeofcareprovisioninitself.
ThisstudyisthefirstofitskindbasedonarepresentativehouseholdsurveyinBihar,whichcovers
allthedistrictsofthestateandaddressesthesocialfactorsunderlyingobstetricviolenceand
respectfulmaternitycare.Amongstthebackgroundcharacteristics,Ifoundparity,ageand
educationtobesignificantassocialdeterminantsofobstetricviolence.Ifoundthatparitymade
womenmorevulnerabletobeingcoercedwithanincreaseinparityandexperiencepoor
communication,whilewomengivingbirthforthefirsttimeexperiencedmorephysicalandverbal
abuse.
Thereisanevidenceofunder-reportingoftheextremeformsofobstetricviolencesuchasphysical,
verbalandsexualabuse(Afulanietal.,2019).Thiscouldbebecauseofwomen’slackofawareness
aboutgoodqualityandrespectfulcare,theiracceptanceofviolenceandreluctancetoshare
sensitiveanecdotesofviolence(Afulanietal.,2019).Thissuggeststhatnewermethodsarerequired
tounderstandwomen’sembodiedexperiencesthatcutacrossthestigmaandshameofsharingbirth
andobstetricviolencerelatedstories.Iexplorethisinthenexttwochapters.Thisisoneofthefirst
studiestopresentthemultilayeredandcomplexnatureofwomen’sexperienceofobstetricviolence
withadetailedunderstandingoftheirexperiences,whichIfurtherpresentedthroughTrahi’sstory
(AppendixA),thesurveyrespondentswhoreportedexperiencingthemostformsofobstetric
violence.DevelopingTrahi’sstoryismyattempttohelpdrawthereader’sattentiontowomenas
peopleandunderstandtheircontextandthecontextofobstetricviolence(Jeffery&Jeffery,2010).
Women’sstoriesofviolence,birthingandobstetricviolenceareuniqueandimportanttobe
understoodinthewholegamutoftheirsexual,reproductiveandmaternallives,whichIpresentin
theupcomingchapters.
5.6 Limitations
ThesurveydatadoesnotcaptureeverythingaboutthenatureofobstetricviolenceinBihar,India.
Whileitcapturesthedifferentformsofobstetricviolence,itdoesnotreportonhowmanyaccounts
ofviolencewomenexperienceundereachcategory.Surveysaresubjecttosamplingerrorswhich
cannotbeunderestimated.Underreportingcouldbeachallengeinlowresourcesettingssuchas
Bihar,wherewomen’sexpectationsofcarecouldbelow,whichmayleadtoacceptanceofpoor
quality,disrespectfulandabusivecare.Thiscouldalsobedrivenbywomen’slackofawarenessof
whatqualityandrespectfulcarestandardsforthehealthcaredeliverysystemsareorcouldbefrom
theawarenessthattheyarenotimportantenoughinthesocialhierarchytobetreatedrespectfully.

Chapter5
92
Thiscouldlimitthecapacityofthehealthcareprovidersandfacilitiestolearnfromwomen’s
experiences,toaddressthemwellandtoprovidewomen-centeredcaretothecareseeker’s
satisfaction,particularlyforwomenfrompoorandmarginalizedcommunities,giventhediverse
natureofpopulationsinIndia.

Chapter6
93
Chapter6 Whatdoeswomen’sexperienceofrespect,
disrespectandabuselooklike?Breakingthe
silencesurroundingobstetricviolence
6.1 Background
Respectoriginatesfromthelatinwordrespecterewhichmeansto‘treatwithdeferentialregardor
esteem’.The‘WhatWomenWant’campaignreceived350,696responsesinIndia,whereitisalso
called‘HamaraSwasthyaHamariAwaaz4’(WRA,2019).Thereisagrowingbodyofliterature,
indicatingthatrespectfulmaternitycareistheneedofthehour(Jeejebhoy&Santhya2018;Mayra,
2017).Studieshavebroughtoutevidenceofvariousformsofobstetricviolenceduringchildbirth
acrossmanyIndianstates.Insomestates,reportssuggestthatalmosteverywomanexperiences
somekindofobstetricviolence(Bhattacharya,2015;Shreeporna,2015),butthesewomenmaynot
reporttheirexperience.ThisisofparticularconcerninIndia,whichaccountsfor12%oftheglobal
burdenofmaternaldeaths(WHO,2019),andhasapoorlyresourcedhealthsystem.
Respectfulmaternitycareisafairlynewareaofresearchforaneverexistentissue.Contextplaysa
keyroleinunderstandingobstetricviolenceduringchildbirth,becausethemeaningofrespect,
disrespectandabusechangeswithpeopleandacrossculturesandgeographies.TheLancetserieson
maternalhealthbroughtoutthechallengesofwomenwhoreceivedcarethatiseithertoomuchtoo
soonortoolittletoolate.Thisvariationinthequalityofcareisdependentoncultureandcontext.
Researcherscontinuetoexplorethemeaningofrespectfulmaternitycareandhowtoprovide
person-centeredcare(Downe,2019;Afulanietal.,2019).Theresponsibilityofwomen-centered
careisontheteamofcareproviders,toensurethathealthcareprotectswomen’srightsanddignity,
andissatisfactoryforthem.Healthcareprovidersneedtounderstandwomen’sperceptionof
respect,disrespectandabusefromtheirexperienceofchildbirth,tobeabletoproviderespectful
maternitycare(Bhattacharya,2013).Inthepreviouschapter,Ipresentedhowwomen’sexperiences
consistofmultipletypesofobstetricviolencewhichcontinuesthroughouttheirpresenceinthe
obstetricsetting.Women-centeredcarerequiresadeeperunderstandingofwhatwomenwant
duringchildbirth.Thismaynotbesameasthecareproviderorthepolicymaker’sperceptionof
obstetricviolenceandrespectfulcare,whichIexploreinChapter8.
4Translatesto‘Ourhealth,ourvoice’

Chapter6
94
Becketal.(2013)aptlydefinesthatitisnotjustbeautythatliesintheeyeofthebeholder,itisalso
traumaticchildbirth.Previousstudiessuggestafewreasonswhyrespect,disrespectandabusecan
beperceiveddifferentlybywomenandothers,includingcareproviders.Firstly,asKitzinger(2005)
showsinherwork,womenoftenlackthelanguagetonarratetheirbirthexperience.Painisoften
thecommonexplanationoftheirexperienceofchildbirth.Womenmaynotbeaccustomedto
medicallanguageandterms.Theymaybesilencedbythestigmaandshamerelatedto
conversationsthatinvolvereferencetobodypartssuchasreferringtoone’sgenitalsandthefact
thatbirthisaresultofintercourse(Chadwick,2018;Becketal.,2013;Kitzinger,2005).‘Theclinical
languageusedbycareproviderscouldbedifficultforwomentounderstandandincorporateinto
theirnarrative.Allthesefactorsindicatetheneedforamethodofexploringwomen’sembodied
experienceofsuchsensitiveareasofstigmaandshame(Chadwick,2017)particularlyinapatriarchal
postcolonialsetting,suchasIndia.
Studieshavefoundthatwomen’snarrativesoftraumaticbirthexperienceareoftensimilarto
narrativesofrapevictims(Beck,Driscoll&Watson2013;Kitzinger,2005).Thesameistrueofnon-
verbalcommunication,suchastouch.Touchcanbecomfortingaswellasdiscomforting.Giventhe
experienceofthispainusuallyendswiththebirthofachild,thereusuallyisadilemmaforwomen.
Reportingatraumaticbirthingexperiencebecomessecondarywhenawomanisexpectedtobe
gratefulforsurvivingchildbirthandreturninghomewithalivebaby(Kitzinger,2005).Somewomen,
havingexperiencedtraumaticchildbirth,mayrelivethebirthtraumaeveryyearontheirchild’s
birthdayastraumaanniversary.Thisdilemmaleadsthemtofeeldisgustedanddepressedeveryyear
onadaytheyaresupposedtocelebrate(Beck,Driscoll&Watson,2013;Scotland2020).
Secondly,womenmaynotbeawarethatcertainactionsorbehaviourarenotpartofcare(Downe,
2019),eventhoughtheyfelt‘bad’whentheyexperiencedit,ortheymayexpecttobemistreated
(Lambertetal.,2018).Theymaynotobjecttoobstetricviolence,thinkinghealthcaredoesnothave
tobeapleasantexperienceandsometimesneedstobeendured.Theirexpectationsareoftenso
lowthatsatisfactionisnotapriority.AstudyinIndiareportsthatwomenconsideredtheavailability
ofhealthcareprovidersandhealthsupplies,suchasmedicines,astwokeyaspectsofgoodquality
care(Bhattacharya,2013).Theyrecommendthatreducingwaitingtime,provisionofseating
arrangementandgoodlaboratoryserviceswillincreasewomen’ssatisfactionwiththeservices(Das
etal.,2010).
Womenmayrefrainfromreportingtraumaticchildbirth,astheymayfeelthatishowhealthcareis
supposedtobe(D’entremont,2014)andevenblamethemselvesfortheviolencetheyexperience.
Personal,socialandculturalcontextplaysanimportantroleinshapingwomen’sperceptionsof

Chapter6
95
respectanddisrespect;andinfluencestheirintenttoreportit(Sen,Reddy&Iyer,2018).Findings
fromChapter5showthatwhileeverywomanreportedexperiencingsomeformofobstetric
violenceintheobstetricsettingsinBihar,only5%(2194)consideredreportingtheirgrievance
formally.Notopeninguptogivinganaccountofobstetricviolenceduringbirthcanbeduetothe
starkinequalitiesinsocietyleadingtoapower-basedimbalanceandthefearofconsequences(Sen,
Reddy&Iyer,2018;Roberts,1981).
Finally,women’sautonomyanddecision-makingpowercoulddeterminewhatasatisfactory
experienceofchildbirthcanbe.Indeeplypatriarchalcultures,womenhavealimiteddecision
makingrole,especiallyabouttheirsexual,reproductiveandmaternalhealthandneeds(Jeejebhoy&
Santhya2018;Koski,Stephenson&Koenig,2011).Thereareseveralindicatorsthatconfirmalackof
women’sagencyinBihar.TheNFHS-5reportsthatonly29%womenhadcompletededucationupto
10yearsand41%(agedbetween20-24yearsatthetimeofthesurvey)weremarriedbeforethey
turned18.Thishighlightsthatchild-marriageisapersistentissueinthestate.Thehighratesof
gender-basedviolenceandcrimeagainstwomenshowsfurtherdisempowermentandoppressionof
women(Dharetal.,2018;Jejebhoy&Santhya,2018).Intimatepartnerviolenceisanotherkeyissue
inthestate(Dharetal.,2018),with40%womenhavingexperiencedspousalviolenceand3%
experienceditduringpregnancy.Amongstthewomensurveyedbetween18-29years’age,8%
reportedexperiencingsexualviolencebeforetheyturned18.Gender-baseddiscriminationisevident
inotherindicatorsaswell.Forinstance,femalesterilisation(35%)ismuchhigherthanmale
sterilisation(0%)(GOI,2020).
Acultureofviolenceandsubjugationispartofapatriarchalstructure,wherewomenandgirlshave
limitedagencyovertheirbodiesandlives.Thisextendstoobstetricsettingstoo.Lackofconsentand
explanationofobstetricinterventionsarekeyindicatorsinthiscontext,whichisoftenveryhigh
(Bhattacharya,2013;Patel,Das&Das,2018)asseenforBiharinChapter5,whichconfirmsalackof
women’sconsentandchoiceinobstetricbirthenvironments.Thisisacharacteristicofthemedical
modelofcare,asaresultofthegradualtransitionofhomeasthemorecommonandacceptedbirth
setting,todominationbytheobstetricbirthsetting,overlastmanydecadeswhichcontinuedthe
alienationofwomen’sreproductiverights(Oakley,1984;Menon,2012;Hill,2018;Cleghorn,2021).
Allthesereasonsnormaliseobstetricviolence,asanextensionofwomenbeing‘allowed’todo
anythingintheirroutinelives.Itisaresultofgirl’sandwomen’spositioningattheintersectionsof
several‘female’disadvantages,whichincreasewomen’svulnerability(Sen&Iyer,2012:
Chattopadhyay,2018;Chadwick,2018).Itmayfurtherindicatethatwomenfindabusivecare
acceptableorfeelthatwomendeservetobetreatedordisciplinedduringchildbirthandact

Chapter6
96
accordingly(McAra-Cooper,2011).Womenmaychangetheirplaceofbirthandnotgivebirthina
healthcarefacilitybasedontheirpreviousbirthexperience(Silanetal.,2018),ratherthanreporting
theirexperiences.Alltheseexplanationspointtothenormalisationofobstetricviolenceduring
childbirthastheextremeformsofabuse(includingphysicalabuse)becomeincreasinglyacceptable
andpartofcareprovision(Bradley,2016;Freedmanetal.,2018;Senetal.,2018;Lambert,2018).
Thischapter,aimstoexplorehowwomenattachmeaningtorespect,disrespectandabusethrough
theirexperiencesofchildbirthusinguniqueparticipatoryarts-basedresearchmethodsthatenable
understandingoftheirembodiedexperiences.
6.2 Researchquestions
• Howdowomenattachmeaningtotheirexperiencesofrespect,disrespectandabuseduring
childbirthinBihar,India?
• Howcanwomen’sembodiedexperiencebeexploredthroughsensoryinterviewing?
6.3 Objectives
• Tounderstandhowwomenperceiveandattachmeaningtorespect,disrespectandabuse
duringchildbirthinBihar.
• Toundertakefeministparticipatoryarts-basedresearchinexploringsensitiveembodied
experiencesofchildbirth.
• Todocumentwomen’sexpectationsofrespectfulcarenecessarytoensureapositive
birthingexperience.
6.4 Methods
ThisisaqualitativestudyundertakeninBihar,whereIconductedin-depthinterviewsaidedbya
participatoryvisualarts-basedresearchmethodcalledbodymapping.Criticalfeministtheory
informedallaspectsofthisstudy,whichenabledanunderstandingofchildbirthasahuman
experience,whichisembodied,inter-subjective,contingent,andwovenintopersonalandcultural
websofsignification.
WomeninIndiausuallygivebirthinfourtypesofsettings:1)publichospital;2)privatehospital;3)
homeand4)onthewaytohospital(Figure6.1).Thefigureshowstheareasthatwereexploredin
datacollectionineachofthesesettings.Someofthemhaveoverlappingdomains.Thecommon

Chapter6
97
themesofrespect,disrespectandabusewereexploredineachofthesettingwiththehelpofsome
overarchingquestionsoncommunication,touch,information,decision-makingandconsentduring
childbirthtounderstandthenatureofthisineachofthesebirthsettings.Allthesekeyareasof
explorationhavespecificprobesasshowninthein-depthinterviewguide(AppendixB)andmay
indicaterespect,disrespectandabuseduringchildbirth.
Bothprimigravidaandmultigravidawomenwereselectedfortheinterviews,underthecriterion
thatstudyparticipantshadgivenbirthatleastonceinBihar.Iselectedeightwomenpurposively,to
participateinabodymappingassistedin-depthinterview.
Figure6.1 Themesofexplorationforrespect,disrespectandabuseduringbirth(Author’sown)
TheparticipantswereselectedfromanurbanslumfromPatnaandaruralvillagefromMuzaffarpur,
bothinBihar.Patnaisthecapitalofthestateandhasaccesstospecialisedtertiary-levelhealthcare
facilities,whichismoreaccessibletowomenlivinginurbanslumswhicharelocatedindifferent
partsofthecitycapital.TheinstitutionaldeliveryrateinPatnaisamongthehighestinIndia,
between79-87%.Muzaffarpur,ontheotherhand,hasanoverallinstitutionaldeliveryratebetween
62-71%,whichmatchespercentageofinstitutionalbirthsatthestatelevel.Itisalsoadjoinedby
neighbouringdistrictslikeSamastipurwhereinstitutionalbirthrateisbetween53-62%and
Darbhanga,Seohar,Sitamarhi,WestChamparan;whereitisthelowest,between32-53%(NFHS4).

Chapter6
98
6.4.1 Bodymapping
Bodymappingisauniqueparticipatoryapproachthatcombinesvisualartsandtherapeuticpractice
toguideparticipantsintheartfulcommunicationabouttheirembodiedlifeexperiencesinwaysthat
aresafeandsupportive(Orchard,2017).BirthingmapsisatermIcoinedtorefertomyadaptation
oftheestablishedbodymappingmethod,wherebyIuseittoexplorewomen’sexperiencesofgiving
birth.Thiswasanidealmethodfordatacollectionasitreducedliteracy,stigmaandpower-related
barrierstorespondents’abilitytocommunicatetheirexperiencesandtheresearcher’sabilityto
listenandlearn.Collectingnarrativesofbirthinvolvestalkingaboutbodypartsthatareshamefulto
talkaboutinthelocalcontext.Birthmappingisaculturallyappropriatemethodbecauseofits
flexiblenature,whichgivesroomforadaptionandenableswomentobypassstigmaandsharerich
accountsoftheirexperiences.Theexercisestartswiththeinterviewerrequestingtheparticipantto
liedownonthesheetinthepositiontheygavebirthinordertodrawalivesizeoutlinearoundthe
person.Idemonstratethisbylyingdownonthesheet,whichIfoundhelpedtoovercomeany
hesitationthatwomenmayhavefeltaboutlyingdownonthepaper.Talkingaboutbirthissensitive
andbodymappinghelpswomentoopenupoverthecourseofafewinteractionsthatallow
developmentoftrustbetweentheinterviewerandinterviewee.Birthmappinghavethree
components:1)thebirthmap;2)thebirthingstory,and3)thebodykey.
Bodymappingisarelativelynewmethodofdatacollectioninpublichealthresearch.Itwasfirst
developedbyMacCormackandusedinruralJamaicaforastudyonwomen’sunderstandingoftheir
fertility(MacCormack,1985).ItwassubsequentlyusedinZimbabwetoinitiateconversationsabout
sexuality,reproductivehealthandtheanatomyofwomen(Cornwall,1992)andinotherpartsof
AfricainthecontextofHIV/AIDs(CATIE,2006).Thismethodhasprimarilybeenusedinstudies
involvingwomen’sbodieswheretheirunderstandingabouttheirbody,aparticularfunctionofit
(reproduction)orimpactofacondition(e.g.obesity,HIV/AIDS)hasbeenexplored.Researchers
havefoundittobeagoodapproachwhentryingtounderstandsensitiveissues.Theyreportthat
bodymappingisanapproachtobridgethegapsbetweenembodiedexperiencesandtraditional
researchmethodswhilealsoempoweringthepeoplewhoparticipateintheprocess(Cornwall,
1992).Bodymappinghelpstounearthdifficultand‘meaningful,embodiedexperiencesandlife
events’,whichjustifiesusingthisapproachtounderstandwomen’sexperienceofchildbirth
(Orchard,2017).
Thoughotherstudieshaveusedbodymappingtounderstandconstructsofgenderandbody,there
islittleornoattentiongiventobodymappingtounderstandbirthingexperienceasaparticularform
ofparticipatoryvisualarts-basedresearch.Otherformsofarts-basedresearch,suchasI-poems,

Chapter6
99
havebeenusedintheanalysisofbirthingexperiencesbefore(Montgomery,2014;Chadwick,2018;
McKenzie,2021).Studiesthathaveusedbodymappinghavefoundhighsatisfactionfromthe
participantsabouttheapproachtodatacollection.Theyalsoreportthatresearchersgoingbackto
themandfinishingthemappingexerciseoverafewdayshelpsthemtoformulatetheirthoughtsand
experiencesbetter,enablingakeenerengagementintheprocess(Orchard,2017).
Whiletherearegeneralguidelinestoconductthebodymappingmethod,Iadaptedthoseguidelines
forbirthmappinginBihar.Itisessentialtoallowthisflexibilitytoincorporatethecontextand
setting-basedchanges.
Aspectsforbirthmapping
1. Peopleinvolved-Apartfromtheparticipant,theprocessofbirthmappingconsistsoftwo
researchers:afacilitatorandanotetaker.
2. Facilitator-Guidestheprocessofbirthmapping,demonstratesonthesheet,drawsthe
outlineofparticipantwithconsent,answersanyquestions,asksthequestionswhile
facilitatingtheprocessofbirthmapping.
3. Notetaker-Takesthoroughnotesoftheparticipantresponsesandpreparesthebodykey,
assistsintheprocesswiththearts-basedsupplies.
4. Indexbirth-Theparticipantisrequestedtopickanindexbirth,whichwillbethebirththe
mapwillmainlyfocuson.Butthatwillnotrestrictherfromsharingaboutherotherbirths.
Thismayormaynotbehermostrecentbirth.
5. Outline-Theexercisebeginsbytracinganoutlineoftheparticipant’sbodyonalargesheet
ofpaper.Theparticipantisrequestedtoliedownonthepaperinthepositionthatshegave
birthin.Ifshegavebirthinastandingposition,wewillshowitthroughverticalarrows.The
facilitatorliesdowntodemonstrate.
6. Colours-Theparticipantisrequestedtochooseanycolourshewantstoshowthegoodand
badfeelings,skin,clothes,environmentandotheraspectsofthenarrativewhiletryingto
maintainascloseresemblancetothedayofbirthaspossible.
7. Symbols-Theparticipantchoosesanysymbolstosignifytheexperiences(holdinghands),
people(birthcompanion;careproviders)oremotions(pain;shame;fear;disgust;
happiness).Shemaydraworwriteaboutherexperiencesonthemap.Shecanalsowrite
quotesofpeoplearoundher.Thefacilitatorcanparticipateinwritingthequoteswiththe
participant,basedonparticipant’sliteracylevelandrequestforhelp.
8. Bodykey-Thenotetakerkeepsanoteofwhatthecoloursandsymbolssignify,whichguides
thebirthingstorytounderstandthebirthmapwell.
Chapter6
100
9. Birthingbody-Theparticipantisrequestedtoshowherexperienceofgivingbirthby
indicatingtheexperiencewithintheoutlineofthebodythatmayincludeemotionsand
interventions.
10. Birthingenvironment-Theparticipantisrequestedtoshowotheraspectsofthebirthing
environmentoutsidetheoutlineofthebody.Thismayincludethenumberofpeople
around,whotheywereandtheirrole.Thiscanincludeimportantaspectsofthenarrativesin
thesocialenvironment,familialenvironment,community,alongwiththehospital
environment.
11. Birthingstory-Itisaone-pagesummaryoftheconversationsandinteractionsco-created
withtheparticipantandisapprovedbytheparticipantonthelastmeeting.Thisisalsoan
analyticoutcomeoftheprocesswhichbeginsinthefieldwiththeparticipant.
12. Finalmeeting-Theparticipantisrequestedtocheckthebirthmapbeforeendingthelast
interactiontoseeifanythinghasbeenleftoutthattheywouldliketoadd.Sheisasked
abouthersatisfactionwiththeinterviewprocess.Theco-createdbirthingstoryisreadbyor
readouttotheparticipantintheirlanguagetotaketheirapprovaloftheinformation
sought.
13. Pictureofbodymap-Theparticipantisgivenanoptiontotakepicturesofthemapandthe
birthingstory.
6.4.2 Planningthedatacollectionwithbodymapping
IconductedascopingstudyinJanuary2019inanurbanslumandaruralvillageinPatnadistrictof
Bihartounderstandthefeasibilityofbirthmapping.Thescopingstudyalsohelpedtodevelopa
semi-structuredguidewiththeadviceofwomentoaidtheexercise.Thestructureandmethodsof
conductingbodymappinghaveevolvedsince.Istartedwitharoughoutlineofapersonona
notepad,followeditbyabodyoutlineonlytoshowafewthingswithcolouredpens(Figure6.2).
Finally,Iconductedtobodymappingduringthedatacollection,whereIusedmanyotherarts-based
supplies.Expertconsultationswithqualitativeresearchers,midwivesandpeoplewhohavebeen
involvedinarts-basedmethodsandstorytelling,helpedtoshapetheprocess.Thereareveryfew
publishedstudiesonhowtoconductbodymaps,whichincludesacoupleofguidelinesthathave
beenusedtoprepareadetailedguideforthisstudy(Gastaldo,2012).

Chapter6
101
Figure6.2 Birthmappingpilot
Researchethicsapproval-Ethicalclearanceforarts-basedresearchmethodsisimportantand
severalethicaldimensionsneedtobethoughtthroughandplannedfor,whichincludes
understandingthesensitivityofthemethod(Orchard,2017).Itrequiresmanyinteractionsand
seekingtimefromparticipants.Giventhisisaparticipatorymethod,itneedsparticipant’sactive
involvementwheretheywillbespeaking,lyingdownonthepaperforanoutlineandthen
participateinshowingtheirbirthingstoryonthemap.Mystudyinvolvedrecallingsensitiveaspects
ofthebirthingexperience,soIhadinformationofthenearestcounsellorinapublichospital,incase

Chapter6
102
theparticipantsfeltandexpressedtheneedtotalktoacounselororahealthcareproviderabout
theirexperience.TheethicalclearancewasprovidedbytheethicalreviewboardoftheUniversityof
Southampton(Referencenumber49730).Theethicalconsiderationsofconsent,confidentiality,
anonymityhavebeenaddressedintheethicsapplicationwhichisbasedontheintegralprinciplesof
autonomy,beneficenceandnon-maleficence.Participantswererequestedforwrittenorverbal
consentinlinewiththeuniversityethicalclearance.Sevenoftheeightinterviewswereaudio
recordedwithconsent.Ialsorequestedparticipant’sconsenttotakepictureswhilemaintaining
theiranonymity.Everypicturewasshowntotheparticipantbeforekeepingthemforthestudyand
onestheydidnotapproveofweredeletedinfrontoftheparticipant.Participantswererequestedto
selectapseudonamewhichisusedtoaddresstheminthestudy.
6.4.3 BirthmappinginBihar
IconductedthedatacollectioninurbanslumsandruralvillagesinBihartoexploreexperiencesof
birthingindifferentbirthsettingsatdifferentlevelsofcareforwomenwhoweresocio-economically
disadvantaged.TheslumswereselectedinthestatecapitalPatna,whichhasoptionsfortertiary-
levelofcareinbothpublicandprivatehospitals.TheruralvillagesareselectedinMuzaffarpur
district.Iselectedthesedistrictsbasedonthematernalmortalityratio,whichisveryhighinPatna
andmoderatelyhighinMuzaffarpur.Ihiredafemaleresearchassistant(note-taker)fromBiharto
assistmewiththedatacollection.Theresearchassistanthadpreviousexperienceofqualitative
interviewingandisadeptinmanyofthedialectsinBihar.SheworkedwithmeinBiharonadifferent
initiativeforacoupleofyears.
Womenwhohavegivenbirthinthelast5yearsinBiharareincludedinthestudy.Wevisitedurban
slumsinPatnaandruralvillagesinMaraulblockinMuzaffarpurdistricttorecruitparticipants.We
wentfromdoortodoortotalktowomenandseekconsent.Weplannedtointerviewwomen
regardlessofwheretheyhavegivenbirth.Therewerenoexclusioncriteria.Betweentwotofive
interactionswerearrangedwithalltheeightparticipants.Allparticipantsprovidedtheirconsentand
sharedbackgroundinformationinthefirstinteractionandweinitiatedthebirthmappingexercise.
Intwocases,womengaveusanotherappointmenttobeginworkingonthemapwiththem.Thelast
interactioninvolvedclarifyinganyqueriesfromtheinterview,takingwomen’sapprovalofthe
completedbirthmap,makinganyfinalchangesonthemap,andreadingandfinalisingthebirthing
story.Theresearchteamspentonaveragetwotosixhourswitheachparticipant.

Chapter6
103
Wecarriedlargesheetsofthickwhitepaper,7feetlongand3.5feetwide.Wecarriedcoloured
sketchpens,markers,crayons,andcutoutsoffacialexpressions,smallminiaturecutoutsofpeople,
children,fetusandcareproviders,medicalequipment,cut-outsofinjections,intravenousfluids,
weighingmachineandbloodtransfusions.Wecarriedthesheetsinalargepostercarriertube
(Figure6.3).
Figure6.3 Birthingmappinginaction
(Includedwithethicalclearanceandwomen’sconsent)
Wemaintainedtheprivacyofthewomenatalltimes.Weconductedtheexerciseintheirbedroom
onawoodenplank,onthefloorofastoragearea,ontherooftopandinthebackyardofamud
house.Womenfromtheneighbourhoodandfemalefamilymemberswouldoftenvisittoseewhat
wearedoing.Weexplainedourpurposeandrequestedforprivacy.Weoftenengagedindiscussions
notrelevanttothestudy,becausethewomenwantedtotalk.Wetoldparticipantsaboutourrole,
researchandaboutourbackgroundwithpeople.Intwointerviews,themother-in-lawhad
interruptedtheinteractionafewtimes,butwemadesuretonotworkonthemaporaskinterview
questionstotheparticipantwhenwewereinterrupted.Everyparticipantselectedapseudonymfor
herselftoputonthebirthmapandtobeaddressedasinthestudy.Noneofthepicturestaken
showedtheparticipant’sfacesandallwereapprovedbythem.Audiorecordingsweremadein
sevenoftheeightinterviewswithparticipant’sconsent.Detailednotesweretakeninallthe
interviews.
Body Mapping Body Mapping
Pictures taken by : Ritu Kumari
Chapter6
104
6.4.4 Methodologicalchallenges
Weexperiencedmanychallengesoverthecourseofdatacollection.Wefacedahighrefusalrateto
participateinthestudybecausebirthmappingistimeconsuming.Refusaltoparticipatewashigher
intheruralareas.Inonevillageeverywomanweapproachedrefusedtoparticipate.Thiswasa
smallvillagewherewereachedoutto12households.Someofthesewomendidnotrefuseinitially,
gaveconsentandaskedustocomebackanotherday.Inournextvisitwerealisedtheydidnotwant
toparticipatebutcouldnotsaynotous,expectingthatwewillnotreturn.Onoursubsequentvisit
wewouldwaitforthemtotalktousforhourswhentheywoulddotheirhouseholdworkafter
givingusanappointment.Womenoftendidnotsaynotousbutratherignoreduswhilewetriedto
talktothem.Oftentheeldersofthefamilysuchasmother-in-lawwouldtellustogoaway.Often
womenwhowouldwanttotalktousbutcouldnotbecausetheirhusbandoreldersinthefamilydid
notapprove.Thiswasapatternwhichweunderstoodafteraseriesofexperiencesoverafewdays.
Thecooperationofthefamilywasimportant.Beforeinterviewingoneparticipant,wesatoutside
thehousewiththemother-in-lawwhoinvitedustotellhermoreaboutourwork.Womenwe
interviewedhadonetofourchildrenandagedlessthanten-year-old.Innuclearfamilies,itwas
difficultforthemtostaywithusforlongstretchesoftimeandtheywouldoftentendtotheir
children’sneedsmid-interviewwhilewepausedtherecorderandwaited.Wehelpedtomindthe
childrenwhenpossible.Childrenwouldoftenappearintheareaofinterviewbecausewewere
workingwithcoloursandcut-outs,whichmadethemcurious.Wegaveawaycoloursandpaperto
keepthembusy.Onelittleboytriedtotearawaythemapwithanailandtriedtoprickuswiththe
nailtoo,hewastakenawaybyanelderinthefamily.
Mosthouseholdshadpetsandrodents.InRia’shouseholdwehadtoentertheroomcrossingavery
tinyroomwhichwasanurbancowshed,withtwocows.Intwohouses,UrmilaandSita,therewere
ratsthatwouldcomeoutofholesonthegroundorthewallsandtwiceIhadtoliedownonthe
sheettodemonstratewhiletheratwasveryclose.Iamscaredofrats.Thisdatacollectiontested
manyofmyfearsbutithelpedtowintheparticipant’strust.ThereweregoatsinAmrita’s
household,whichweretakenoutsidewhilewedidtheexerciseinthegoat-shedaftercleaningthe
goatfaeces.Pratimahastworabbits,whoappearinherbirthmapaswell.Shetooktherabbitsto
theroofwhentheystartedchewingthemap.Husbandswereinthehouseinafewcases,butthey
usuallydidnotinterrupt,exceptonewhokeptcallinghiswifeandaskinghowlongitwilltakeus,
whileAmritakeptconfirmingthatit’sfineforustotalktoher.Itwasarareexperienceforthe
participanttotalktosomeoneandshewantedtotalktousasshesaid‘nooneevercomestomeet
me’.

Chapter6
105
Findingspacetospreadthesheetandworkarounditwaschallenging.Theparticipantswerevery
helpfulinmakingspace.Itwasdifficulttoencouragethemtoparticipateaswellbecausesevenout
oftheeightparticipantswerenotusedtoholdingapen,andwereconcernedtheywouldnotbe
abletodoagoodjob.Theywerenotusedtowritingordrawing,butoverthecourseofinteractions
theybecamecomfortableandparticipatedactively.Theyalsoopenedupmoreinlatterinteractions
astrustdevelopedandtheyrealisedweourselvesdidnothaveanyartisticabilities,butfoundthe
processeasierandmoreengagingasitunfolded.
Womenfoundverylittletimeforthemselvesawayfromtheirdomesticchoresandoutsidework,
whichstretchedourworkinghours.Weoftenconductedinterviewsintheeveningandlatenight,or
startedbefore6amtogetanhourwiththeparticipantbeforetheirday’sworkbegan.Wemade
suretomakeourselvesavailableatallhourswhenevertheygaveustime.Wehadadayofthorough
disinfectionafterwerealisedoneofourparticipants,whomwecameinclosecontactwithwhile
creatingthebirthmap,complainedofliceinfestation.Theresearchassistant’sroleintheexercise
waschallengingandunpredictable.Sheparticipatedintakingreflexivenotesandnotesoninterview
environment,providedtheresourcestopreparethemapandalsohelpedinmindingthechildren
andattimesengagedinconversationswiththeparticipant’sfamilysothattheywouldnotinterrupt
theparticipantand‘allowher’tocontinuetalkingtous.Thiswasoftenrequestedbytheparticipant
herself.
Workwasdonealsowhenwewerebackinourhotel,whichincludedgettingmorecut-outsthatwe
wouldneedintheongoingexercise.Weaccomplishedsomeofthecolouringworkforthelast
interactionandwithpermissionfromtheparticipantwhenwefilledintheskincolour,orother
parts.Theparticipantsselectedthecoloursthatwestartedfillinginherpresenceatherhome.We
alsoworkedonthebirthingstoryafterlisteningandre-listeningtotheaudiorecordingsofthe
interviews,manyofwhichwereindicatedtobeimportantaspectsofthestorybytheparticipants.
Thebirthmapshavemanycut-outspastedonthemwhichwerefixedwithadhesivetape.Thismade
themapsveryheavy.Themapsarescannedinlivesizeandthenprintedonwhiteclothintheirtrue
sizetomakeiteasiertocarryanddisplay,becausethepaper-basedmapsarepronetowearand
tear.Theseclothmapsareverygoodfordissemination.
6.4.5 Dataanalysis
Phenomenologicalconstructsofdifferenttheoristswereemployedtounderstandandpresenthow
womenattributemeaningtorespect,disrespectandabusefromtheirexperienceofchildbirth.Van
Manen’sworkonexistentialismthatdrawsonlivedtime,livedbody,livedspaceandlived
Chapter6
106
relationshipshelpedtoexplorehowwomenexperiencebirthing.Thishasbeenusedinthecontext
ofchildbirthinpreviousstudies(Thomson,2011).Ifurtherexploredtheconceptsofunpleasant
sight,unpleasantsound,unpleasantfeel,unpleasanttouchandunpleasanttastewhichwerealso
introducedbyVanManen.Theseconceptsareimportanttoexplore,giventhechallengesdiscussed
byotherresearcherswithregardtolanguagebarrierswhenitcomestounderstandingchildbirth
throughwomen’sexperience.
Criticalfeministtheoryincludestheconstructsfromcriticaltheoryandfeministtheory(Keedleetal.,
2009)aselaboratedinChapter4.Feministphenomenologycanbedefinedasacritical
phenomenologysinceitenablesunderstandingofhumanexperiencessuchaschildbirth,whichis
embodied,inter-subjective,andcontingent,andwovenintopersonalandculturalwebsof
significationandareinfluencedbyimbalancesinpower.Experiencesofchildbirthalsovarybasedon
cultureandcontext.Thismethodhelpstointerpretwomen’sexperiencesfromtheperspectiveof
imbalanceofpowerandpositionintheircommunityinacriticalperspective(Simms&Stawarska,
2013).Therearestudiesthatreportthattheissueofdisrespectandabuseduringchildbirthcanbe
attributedtogenderandgender-basedsubordination.ThisisseeninBiharaswell,asdescribedin
Chapter3.Sincechildbirthisinfluencedbypowerimbalancesinthesocietyattributingtoaperson’s
gender,andthelivedexperiencenarratesabout‘women’ssubordinationinthesociety’,feminist
theoryprovidesalensforanalysis.
Ianalysedthedatausingembodiedfeministmethods(Chadwick,2017).Mydataincludeaudio
recordingsoftheinterviews,thetranscriptswithreflexivenotesandthebodymapsalongwiththeir
summaries.Iusedfeministrelationaldiscourseanalysistoanalysethedata,whichisdividedinto
twokeydomainsofpost-structuralistdiscourseanalysis(steps1-6)andemergentvoicesinrelation
todiscourses(steps7-10)(Thomson,Rickett&Day,2018).FRDAguidesanalysisthroughaseven
stepprocess(Figure6.4):1)readingthetranscriptsandlisteningtotheaudiorecordings;2)
‘chunking’thetalkintosections;3)labellingthechunksoftalkwithdescriptivecodes;4)identifying
recurrentcodesorthemes;5)identifyingdiscourses;6)identifyingdiscursivepatterns;5)filtering
outtheI-voice;6)listeningtotherecordingforreflexivity;7)multiplelistening;8)generatingtheI-
poems;9)listeningforcontrapuntalvoices;and10)puttingthepersonalinthepolitical.Icreated
memosandannotationsthroughouttheanalysis.Thisanalysismethoddoesnotguidehowto
analysethebirthmapsandbirthingstories.Ithereforeadaptedthemethodtoaddtwomoresteps
intotheprocess:11)applyingthethemesandcodestothebirthsmaps,12)arrangingtheI-poems
againstthebirthmapsandbirthingstories.Thisisamultilayerednon-linearembodiedanalysisthat
ensuresthattheparticipant’svoicetakesdominanceintheanalysis,overtheresearcher’s
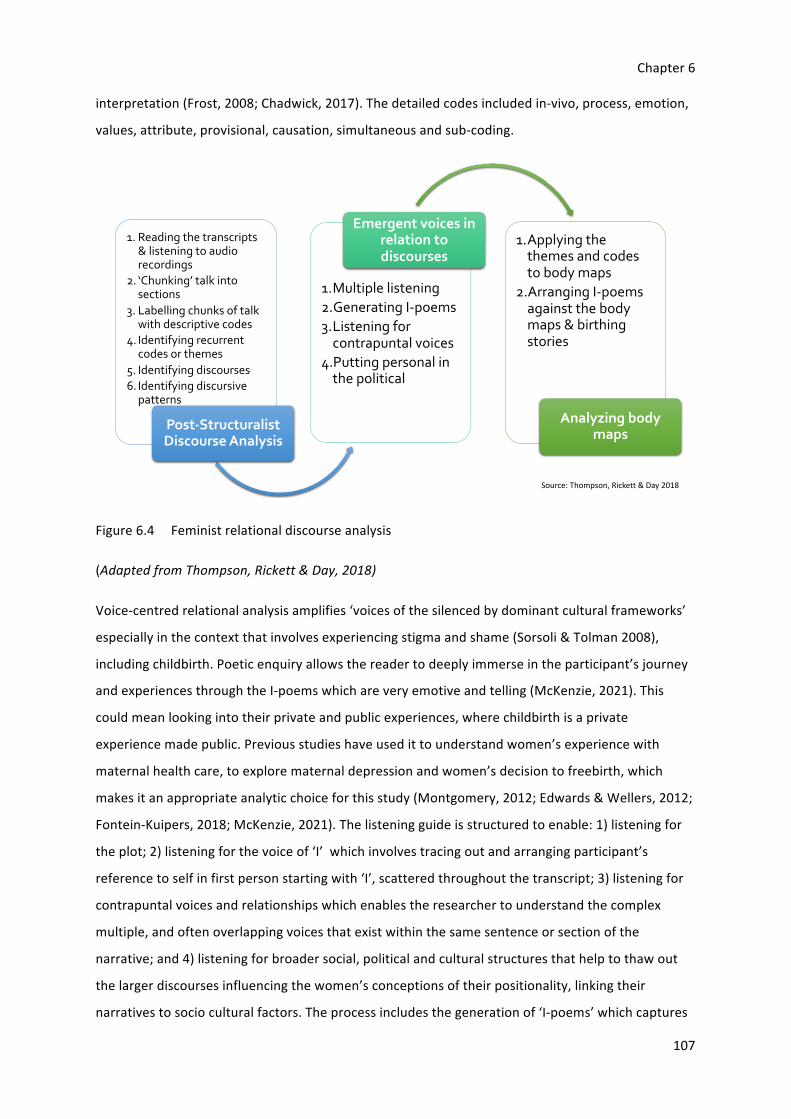
Chapter6
107
interpretation(Frost,2008;Chadwick,2017).Thedetailedcodesincludedin-vivo,process,emotion,
values,attribute,provisional,causation,simultaneousandsub-coding.
Figure6.4 Feministrelationaldiscourseanalysis
(AdaptedfromThompson,Rickett&Day,2018)
Voice-centredrelationalanalysisamplifies‘voicesofthesilencedbydominantculturalframeworks’
especiallyinthecontextthatinvolvesexperiencingstigmaandshame(Sorsoli&Tolman2008),
includingchildbirth.Poeticenquiryallowsthereadertodeeplyimmerseintheparticipant’sjourney
andexperiencesthroughtheI-poemswhichareveryemotiveandtelling(McKenzie,2021).This
couldmeanlookingintotheirprivateandpublicexperiences,wherechildbirthisaprivate
experiencemadepublic.Previousstudieshaveusedittounderstandwomen’sexperiencewith
maternalhealthcare,toexplorematernaldepressionandwomen’sdecisiontofreebirth,which
makesitanappropriateanalyticchoiceforthisstudy(Montgomery,2012;Edwards&Wellers,2012;
Fontein-Kuipers,2018;McKenzie,2021).Thelisteningguideisstructuredtoenable:1)listeningfor
theplot;2)listeningforthevoiceof‘I’whichinvolvestracingoutandarrangingparticipant’s
referencetoselfinfirstpersonstartingwith‘I’,scatteredthroughoutthetranscript;3)listeningfor
contrapuntalvoicesandrelationshipswhichenablestheresearchertounderstandthecomplex
multiple,andoftenoverlappingvoicesthatexistwithinthesamesentenceorsectionofthe
narrative;and4)listeningforbroadersocial,politicalandculturalstructuresthathelptothawout
thelargerdiscoursesinfluencingthewomen’sconceptionsoftheirpositionality,linkingtheir
narrativestosocioculturalfactors.Theprocessincludesthegenerationof‘I-poems’whichcaptures
1. Reading the transcripts & listening to audio recordings
2. ‘Chunking’ talk into sections
3. Labelling chunks of talk with descriptive codes
4. Identifying recurrent codes or themes
5. Identifying discourses
6. Identifying discursive patterns
Post-StructuralistDiscourse Analysis
1.Multiple listening
2.Generating I-poems
3.Listening for contrapuntal voices
4.Putting personal in the political
Emergent voices in relation to discourses
1.Applying the themes and codes to body maps
2.Arranging I-poems against the body maps & birthing stories
Analyzing body maps
Source: Thompson, Rickett & Day 2018

Chapter6
108
theiractualvoices.Inourstudytheparticipant’sreferencesto‘I’weresupplementedbyreferences
to‘my’and‘me’onafewoccasions,toensuremoredetailanddepthinthenarrativeandfora
richerunderstandingofthecontext.Thereareotherpronounpoemsthatresearchershaveusedto
addtopresentadifferentperspectiveandanotherangle(Chadwick2017).Therearedifferentways
ofcreatingandconstructingtheI-poems,Ifocusoncreatingthe‘full’poemstoallowsomecontext
intothepoemsandaddmoredepthtothenarrative.Partsofthetextsarebold,basedonmy
subjectivitytoemphasisecertainaspectsofthepoem.
6.4.6 Positionalityandreflexivity
Itisessentialformeastheresearchertobeina‘reflexiveengagement’withmyownassumptions
andknowledge.IsoughthelpfromProf.GillThomsonatUniversityofCentralLancashiretoconduct
apre-understandinginterviewwithmebeforeIstarteddatacollection.Ithelpedmetounderstand
andidentifymy‘forehaving5’,‘foresight6’and‘foreconception7’.
“Idon’tthinkIwentthroughanabusivebirth.Iknewaboutthedoctorwhowasgoingtodeliveryou.
Ihadheardthathedoesn’tlikewhenwomenscreamduringchildbirth.Iwasinmybestbehavior.
WitheverypainthatIclenchedmyteethanddidn’tmakeasound.Soitallwentverywell.Ididnot
getscoldedatallbecauseIdidnotgiveanyoneachancetoscoldme.”–Mymother
Thisismymother’snarrationofmybirththatIhaveincludedwithherconsent.Iremembersaying
thatsheshouldhavescreamedifshewantedtoscream.Itwasarespectfulbirthfrommymother’s
perspective,becauseshewastreatedwell.Butitwasnotapositivebirthingexperience,inmyview.
Asastudentnurse-midwife,Iwitnessedmanyexamplesofobstetricviolenceduringchildbirth,most
ofwhichwasnormalisedtoanextentthatwentunnoticedbythecareprovidersandwerenot
reportedbythewomenwhowereabused.Inmythirdyearasastudentmidwife,Iprovidedcarefor
awomanwhowassupposedtoundergoavaginalexamination.Therewasanareawithcurtainsand
alabourtable.Iaccompaniedherwherethedoctorwoulddotheexamination.Therewerethree
morepeopleinattendance,includingstaffnursesandapeonwhoevenafterImentionedthereare
toomanypeople.Thedoctorworeagloveinonehand,liftedthewoman’spetticoatandsaree
withoutanyexplanationandsaid,“howdoesyourhusbandwanttodoanythingwithyou,withthe
jungleyouhavegrownthere?”.EveryonestartedlaughingandIfrozenotknowingwhattodo.The
5Forehaving-myfamiliarityandbackgroundtothestudy.6Foresight-myperspectivewhichisinfluencedbymybackground.7Foreconception-whatIfeelIamgoingtofind.

Chapter6
109
womandidnotsayawordbutjustcoveredherfacewiththepallu8ofhersaree.Italmostfeltasif
sheexpectedtobeabused.Thestaffnurselookedatmeandsaid,“thedoctorisjustjoking!”.The
doctorwasjustjoking.Ireportedtheincidenttothenurse-in-chargeinthelabourroomandalsoto
mysupervisor.Theycould,atbest,advisemetoneverpracticewhatIwitnessed.
OverthenextcoupleofyearsIsawwomenbeingslappedontheirface,ontheirthighs,pinchedon
theirthighswitharteryforceps,pulleddownbyherhair,leftnakedonthelabourtableswithout
curtainsorclothes,givenepisiotomywithoutanesthesia,fundalpressure,subjectedtomultiple
vaginalexaminations(asaresultofbirthinginateachinghospital),screamedat,commentedon
(basedontheirageornumberofchildrenorphysicalappearanceorlevelofeducation)bycare
providers.“What’sthepointofscreamingnow,didn’tyouthinkaboutthispainwhenyoulaidwith
yourhusband?”,wasacommoncommentwhichIlaterheardbeingsaidtowomeninmanyother
states.Privacyandconfidentialitywerenotmaintained.Iidentifiedmanyexamplesofwomennot
beingrespectedbyhospitalstaff.Forinstance,notgivingwomenalltheinformation,callingwomen
bytheirbednumberorthecolouroftheirsaree,notintroducingthemselvestowomenandnot
encouragingwomentoaskquestionsoranswerquestionswomenhave.Manyoftheseexamplesof
obstetricviolence,IcontinuetorealiseasIreadmoreliteratureonthesubject.
6.5 Findings
Theeightwomenwhowereinterviewed,focusedonanyonebirthexperienceoftheirchoice,in
detail,topresentontheirbirthmap.Intotal,theyhad20livebirths(10eachfromurbanandrural)
andtwostillbirths,atdifferentlevelsofgovernmenthospital,atprivatehospitalsandathome.
Womensharedtheirexperienceandperceptionsofrespect,disrespectandabuseduringvaginaland
cesareanbirth.MoreinformationabouttheparticipantsisprovidedinTable6.1.
8Palluisapartofsareethathangsfromshoulderwhenworn.
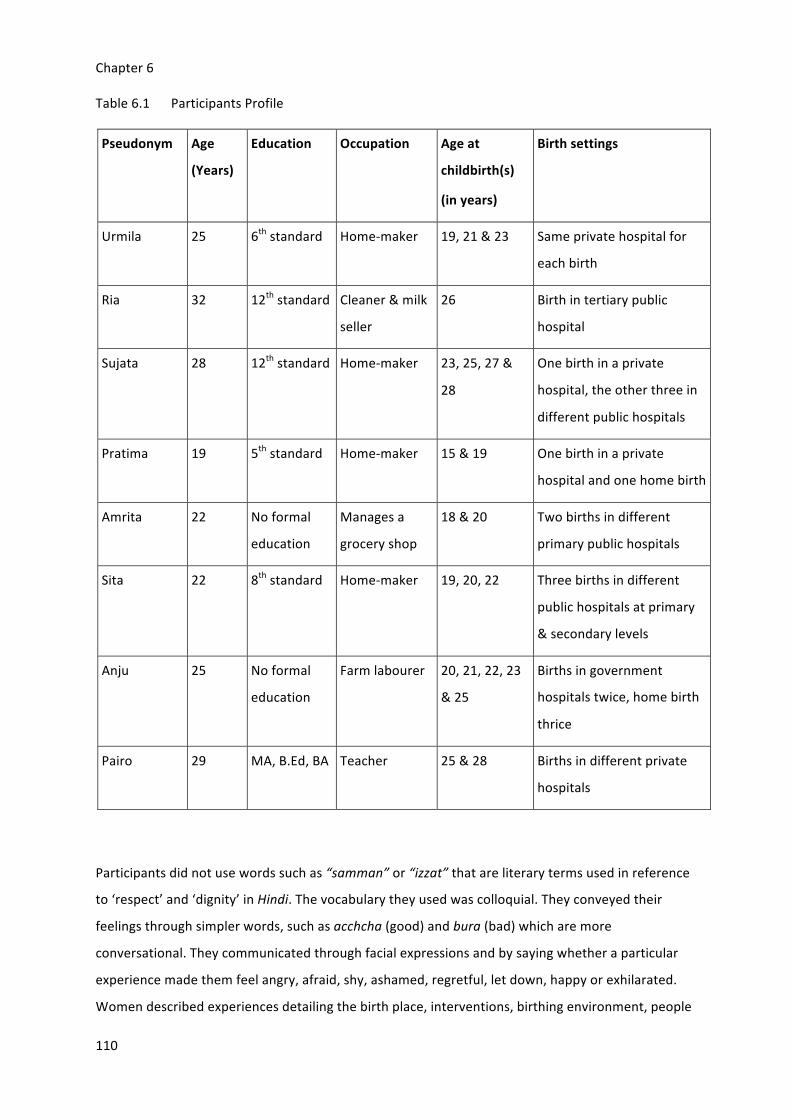
Chapter6
110
Table6.1 ParticipantsProfile
Pseudonym Age
(Years)
Education Occupation Ageat
childbirth(s)
(inyears)
Birthsettings
Urmila 25 6thstandard Home-maker 19,21&23 Sameprivatehospitalfor
eachbirth
Ria 32 12thstandard Cleaner&milk
seller
26 Birthintertiarypublic
hospital
Sujata 28 12thstandard Home-maker 23,25,27&
28
Onebirthinaprivate
hospital,theotherthreein
differentpublichospitals
Pratima 19 5thstandard Home-maker 15&19 Onebirthinaprivate
hospitalandonehomebirth
Amrita 22 Noformal
education
Managesa
groceryshop
18&20 Twobirthsindifferent
primarypublichospitals
Sita 22 8thstandard Home-maker 19,20,22 Threebirthsindifferent
publichospitalsatprimary
&secondarylevels
Anju 25 Noformal
education
Farmlabourer 20,21,22,23
&25
Birthsingovernment
hospitalstwice,homebirth
thrice
Pairo 29 MA,B.Ed,BA Teacher 25&28 Birthsindifferentprivate
hospitals
Participantsdidnotusewordssuchas“samman”or“izzat”thatareliterarytermsusedinreference
to‘respect’and‘dignity’inHindi.Thevocabularytheyusedwascolloquial.Theyconveyedtheir
feelingsthroughsimplerwords,suchasacchcha(good)andbura(bad)whicharemore
conversational.Theycommunicatedthroughfacialexpressionsandbysayingwhetheraparticular
experiencemadethemfeelangry,afraid,shy,ashamed,regretful,letdown,happyorexhilarated.
Womendescribedexperiencesdetailingthebirthplace,interventions,birthingenvironment,people

Chapter6
111
aroundbirth,beingtouchedduringbirthandcommunicationandabouttheirdecision-makinginall
oftheseareas.Theysharedtheirexperiencesofgivingbirth,howtheirbirthingexperiences
influencedtheirsubsequentbirths,andtheimpactonebirthingexperiencehadonanotherinterms
ofperceptionandexpectationofrespect,disrespectandabuse.Theyexplainedwhattheymeantby
a‘goodbirth,’whichalsoinfluenceddecision-makingduringchildbirth,theirexpectationsoffuture
birthsandthebirthingexperiencesandexpectationsofwomenaroundthem.
6.5.1 ‘Good’births,‘Bad’birthsandexpectedbirths
Womenwererequestedtochooseoneoftheirbirthingexperiences(incaseofamultigravida)to
showonthebirthingbodymap.Riawastheonlyprimi-gravidaparticipant.Amrita,Pairo,Sujataand
Urmilachosetonarratetheirmosttraumaticbirthingstoryonthemap.Pratima,SitaandAnjuchose
tonarratetheirgoodbirthingexperiences.Womenweresuggestedtoranktheirbirthing
experiencestohelpthemchoosewhichbirthtocreateonthemap.Thishelpedwomento
understandwhataccordingtothemisa‘goodbirth’ora‘badbirth’.Agoodoutcomeintheir
perceptionwaspartofagoodbirthingexperience.Theyreportedthebirthofasonasagood
outcome.Thisisanindicationofsonpreference,reflectingthepatriarchalsocietalstructure,ascan
beseeninAmrita’sbirthingbodymap(Figure6.14).
“Theboy!IfeltbetterwhenIhadtheboybecauseIhadgoodpainandtookverylesstime.Mygirl’s
birthwasverypainfulforme.Ihadsomuchproblem.Iwouldliketoshowthegirl’sbirthonthe
map.”(Amrita)
Women’sunderstandingofanidealbirthwasexpressedinparts,throughoutthemultiple
interactions,totheextentwherebirthswhichwereconsidered‘better’became‘bad’.Asthetrust
developedovertheinteractions,theyopenedupmore.Theexpectedbirthwasaskedintermsof
respectfulness,apartfromexperiencedbirth,ascompiledinTable6.2.

Chapter6
112
Table6.2 Women’sunderstandingofgood,badandexpectedbirth
Participant
(livebirths)
Experiencedbirth Expectedbirth
Goodbirth Badbirth
Amrita(2) -shortdurationof
labour
-toopainful
-neglectand
abandonment
-verbalabuse
discriminatedagainst
onthebasisofsexof
newborn
-notouching
-propercommunication
-timelyexamination
-nodelayincare
-politecareprovider,servewitha
smile
-abed
-careprovidershouldtreatas
familymember
-nondiscriminatorycare
regardlessofnewbornssex
-availabilityofhospitalsupplies
-nodisrespect
-noextortion
-notmorethantwopeople
aroundherduringchildbirth
-incentiveforinstitutionalbirth
Pairo(2) -betterpreparedfrom
experience
-lowerexpectation
thanpreviousbirth
-toomanyvaginal
examinationsby
differentcareproviders
withoutmaintaining
privacyorseeking
consent
-extortion
-blindfolded
-inhumanetreatment
-manymenaroundin
thebirthingroom(OT)
-vaginal(normal)birth
-comfortingtouch
-novaginalexaminations
-seekconsentbeforetouching
-explanationandconsentbefore
interventions
-birthcompanioninOT

Chapter6
113
Participant
(livebirths)
Experiencedbirth Expectedbirth
Goodbirth Badbirth
Pratima(2) -homebirth
-betterneonatal
outcome
-respectful
communicationin
hospitalbirth
-privatehospitalbirth
-unaffordablecare
-journeytohospitalto
givebirth,travelalong
abumpyroad
-unexplained,
unconsented
augmentation
-homebirth
-novaginalexamination
Sita(3) -cleantoilet
-quickambulance
-swellingoflegsand
arms
-difficultywalking
-unconsentedand
forcedvaginal
examination
-restrained,physical
abuse
-notouching
-verbalabuse(hopeditwon’t
happen)
-nodelayincare
-nocomplications
-respectfulcommunication
-birthcompanionofchoice
-foodtobeprovidedathospital
-cleanbed,birthingroomand
bathroom
-birthinthehospital
-incentiveforinstitutionalbirth
Ria(1) -comfortingtouch
fromanotherbirthing
woman’scompanion
-affordablecare
-verbalabuse
-shoutedat
-uterineprolapserepair
withoutanesthesia
-Babydeclareddeadby
daiswithoutnewborn
assessment
-nophysicalabuse
-comfortingtouch
-birthcompanionofchoice
-extortion,buthopeditwon’t
happen
-1:1care
-onebed,oneroom
-curtainsforprivacy

Chapter6
114
Participant
(livebirths)
Experiencedbirth Expectedbirth
Goodbirth Badbirth
-respectfulbehaviourfromcare
providers
-careprovidersshouldintroduce
themselves
-babyshouldbereceivedwith
careandassessedproperlyafter
birth
-properlight&ventilation
Sujata(4) -presenceof
‘guardian’thoughnot
ofchoice
-careproviders
followedherbeliefs
(norms)afterinsisting
-careprovidersdid
notdovaginal
examinationafter
refusal
-extremepain
-forgottentoremove
gaugepiecebefore
episiotomyrepair
-extortion
-unexplainedand
unconsentedvaginal
examination,
episiotomy,episiotomy
repair,uterine
explorationand
augmentation
-noanesthesiabefore
episiotomyrepair
-husband’spresenceasabirth
companion
-noepisiotomy
-birthingwoman’snormsand
beliefstobefollowed
Urmila(3) -nomedicine
-novaginal
examination
-lesspain
-quickdelivery
-privacyprotected
-shoutedat,verbally
abused
-unconsented,
unexplainedvaginal
examination,
episiotomy,episiotomy
repair,augmentation
-nocut
-littlepain
-nostitchingwithoutanesthesia
-nounnecessarytouching
-seekpermissionbeforetouching
andinterventions

Chapter6
115
Participant
(livebirths)
Experiencedbirth Expectedbirth
Goodbirth Badbirth
-restrained,physically
abused
-detentionofnewborn
-extortion
-respectfulbehaviourfromcare
providers
-comehomealiveafterbirth
-nobirthcompanion
Anju(3) -homebirth
-threelivebirths
-samedagarin
-hospital
-twostillbirths
-homebirths
-continuityofcareacrossall
births
Disrespectfulandabusivebirths
Womenreferredtovariouskindsofdisrespectfulandabusiveencounterswiththehealthandnon-
healthcareprovidersduringtheirstayatthehospital.Theyreportedhearingsimilarexperiences
fromtheirfriends,familymembersandwomenintheneighbourhoodwhooftenmadesimilar
choicesofbirthplace.Storiesofrespect,disrespectandabusewereconsideredwhengivingbirth
again,andthesestoriessymboliseddesiredbehaviours,self-disciplineandwaystoavoidbeing
violated,humiliatedandhaveasclosetoadignifiedbirthingexperienceaspossible.Womenoften
saidthattheydiscussedobstetricviolenceinahushedmanneramongstpeerswhensomeoneisdue
togivebirth.Thesestorieswerenotsharedwithauthoritiesasagrievance,notevenwithsenior
membersofthefamilyincludingtheirhusband,withwhomtheconversationsaboutbirthwererare.
Alltheparticipantshadexperiencedobstetricviolenceduringchildbirth.
Verbalabusewasthemostcommonformofviolenceexperienced.Somecareprovider’scomments
weresodisgustingthatwomenrefusedtorepeattheirwords.
“Twosisters(nurses)wereverybadbecausetheywereabusingmeandshoutingatmelikeanything,
Ican’teventellyouthethingstheysaidtome.”(Urmila)
“ThedoctorinsertedherfingersinsidemeandIscreamedveryloudly.Shesaid,‘Pairohasnopain
threshold,shecanneverhaveanormalbirth!’”(Pairo)
“Shesaid,‘Shutup!Whyareyouscreamingsomuch?’…‘behave!Lookhowyouarescreaming!’”
(Ria)

Chapter6
116
Incidentsofphysicalabusewerementioned.Womendidnotperceiverestrainingasabuse.They
reportedthatitiscommonandtheyconsidereditasabadtouch,butapartofqualitycare.Women
dislikedbeinghelddown,butwerehesitanttosaythatbecauseoftentheirfamilymemberswere
theonesrestrainingthem.Episiotomyrepairwithoutanaesthesiaisacommonkindofphysical
abusethatwomen(Ria,Urmila,Sujata)haveexperienced,buttheyconsideredthatapartofcare
duringchildbirthaswell.Everywomanwastouchedwithoutconsent.Theyreportedfeeling
‘uncomfortable’and‘ashamed’butcouldnotsaythistothepeoplearoundthem.
“Theydohitwomeninthatcondition…Awomanhadcome,shewasscreamingsomuchfromthe
painthatshecouldnotstayinherbed.Thesister(nurse)gavehertwotightslapsacrossherface.”
(Ria)
“Peopledon’tlikebeingtouched,buteveryonehastogothroughit!”(Sita)
Womendidnotspeakaboutexperiencingsexualabuse,butthenarrationandnon-verbal
communicationsconveyedotherwise.Oneoftheparticipantsreferredtocommentswithsexual
connotationas‘colourfulthings’whilealsosharinghowuncomfortableitmadeherfeel,butshe
believedthateveryonehadtoendure.
“Thedoctorsaid‘youarenotscaredofotherthings,ofdoingit,butyouarescaredofinjections!’
Manypeopleabuselikethat.Theysaid‘ifyouaresoafraidthenwhydidyouconceive?Whenthe
babyhadstayed,youshouldhavetakenthepilltogetridofit!What’stheneedofhavingchildren
then?’”(Ria)
Extortionisthecommonestformofabusethatwasmentionedbyeveryparticipant,exceptAnju.It
hasbecomeatraditionforcareproviderstoaskfor‘khushikepaise’(happinessmoney),thatalso
determinesrespectfulnessandqualityofcarebasedonacareseeker’saffordabilitytotipthem.
Moneyissoughtassoonasthebabyisborn.Thecareprovidersdonotmissanopportunityto
demandmoney,astheydonotknowwhenthefamilymightleavethehospital.Participantshave
reportedthatalltypesofhealth(doctors,nurses)andnon-healthcareproviders(ASHA,Mamta,
cleaner,dagarin/dai)askformoneyalthoughhowthemoneyisdividedbetweentheteamcould
notbeascertained.Theydemandmoney,foreveryoneinthehospital,regardlessofhowmany
peoplewereinvolvedincare.
“Happinessmoney!Shesaid‘yourgrand-daughterislikeGoddessLakshmi’theneveryoneaskedfor
money.Myhusbandgave100-150rupeestoeveryone.Therewere11-12peoplethere…Happily!?

Chapter6
117
Somepeoplegiveithappilybuttheyhavemadeahabitoutofit.Peoplewhocan’tafford,theyask
themtoo.Thatisgreed!”(Pairo)
“Myhusbanddoesgarbagework(rag-picker)…helosthisjobandwehave300rupees.Shouldwego
tohospitalortakecareofthehouse!Wehadnomoneytogotohospitalinthesecondbirth…
everyonehadtaken100rupeeslasttimeinthenameofhappiness,therewereninepeople.”
(Pratima)
AparticipantmentionedthatshehadtobribetheNew-bornIntensiveCareUnit(NICU)staffevery
timeortheydidn’tlethervisithernew-borndaughter.Thiswastraumaticforher.Asimilar
experiencewasreportedbyUrmila,whichledtoherbaby’sdetentionintheprivatehospitaluntil
theypaidextra,overthehospitalfees.Thebabywaskeptforhoursuntilthecareprovidersreceived
the‘happinessmoney’.
“Thereweretwobadsisters(nurses).Myfathergavethem1000rupeesbuttheywerenothappy.
Theytoldusthatotherpeoplegivethemgoldearringsandnecklace.Myfatherwasnotgivingthem
moneysotheykeptthebabyfortwohoursandwhenmyfatherfinallygavemoremoneythesisters
(nurses)handedoverourbabytous.”(Urmila)
“Someguardianscannotpayasmuchasthedoctorsaskfor.Thenursesdetainthebabysaying‘we
wantthismuchorwewon’tgivethebaby’.Manypeopledon’thaveenoughmoneytofreethebaby
fromthem.Sometimesitturnsintoconflicts.”(Sujata)
Unconsentedproceduresshowedafailuretomeetprofessionalstandardsandtherearemany
instancesshowingpoorrapportbetweencareprovidersandwomen,whichincludesalackof
explanation,detentionandtreatingwomenaspassiveparticipants(asshowninPairo’sexperience
inFigure6.11).
“Thedoctorsaid,Ionlywenttobedat1amandyoupeoplestartedcallingme.Stopthischaos!Go
away!Iwillcomeinthemorning”(Amrita)
Theaccountsofobstetricviolencebasedonthefindingsreportedbyeightparticipants,areshown
(Table6.3)againstanupdatedtypologyofmistreatmentduringchildbirthbyBohrenetal.(2015).

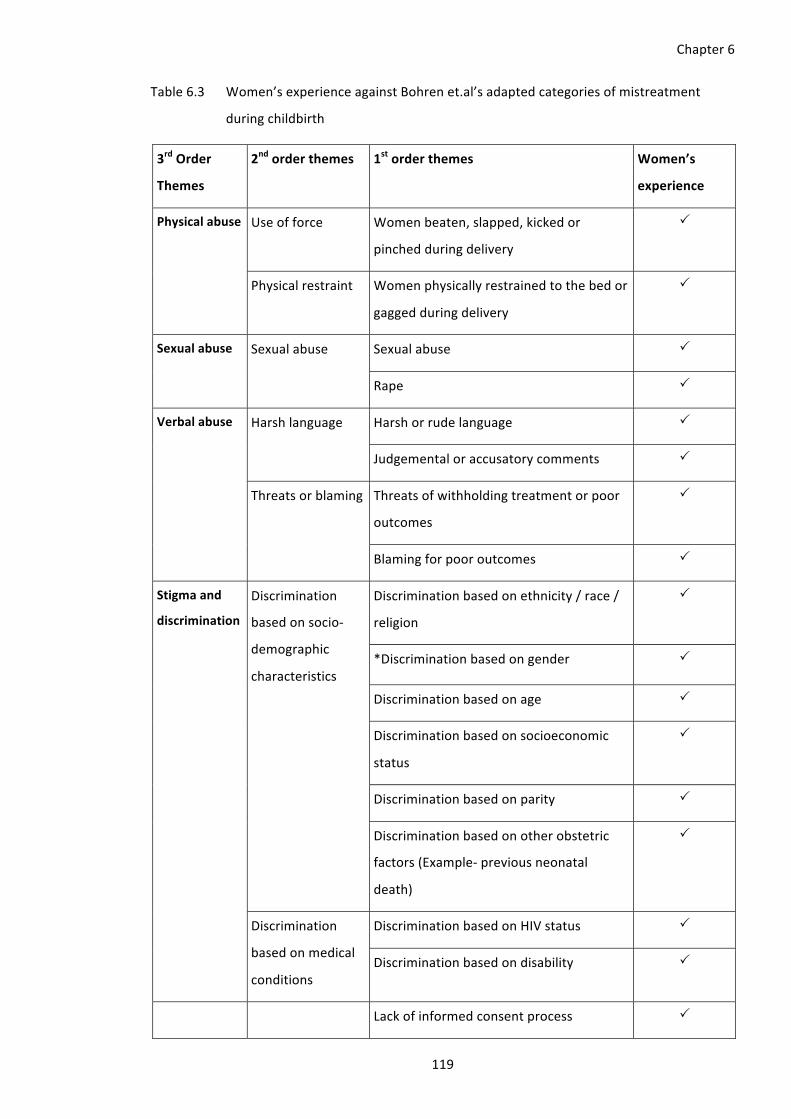
Chapter6
119
Table6.3 Women’sexperienceagainstBohrenet.al’sadaptedcategoriesofmistreatment
duringchildbirth
3rdOrder
Themes
2ndorderthemes 1storderthemes Women’s
experience
Physicalabuse Useofforce Womenbeaten,slapped,kickedor
pinchedduringdelivery
P
Physicalrestraint Womenphysicallyrestrainedtothebedor
gaggedduringdelivery
P
Sexualabuse Sexualabuse Sexualabuse P
Rape P
Verbalabuse Harshlanguage Harshorrudelanguage P
Judgementaloraccusatorycomments P
Threatsorblaming Threatsofwithholdingtreatmentorpoor
outcomes
P
Blamingforpooroutcomes P
Stigmaand
discrimination
Discrimination
basedonsocio-
demographic
characteristics
Discriminationbasedonethnicity/race/
religion
P
*Discriminationbasedongender P
Discriminationbasedonage P
Discriminationbasedonsocioeconomic
status
P
Discriminationbasedonparity P
Discriminationbasedonotherobstetric
factors(Example-previousneonatal
death)
P
Discrimination
basedonmedical
conditions
DiscriminationbasedonHIVstatus P
Discriminationbasedondisability P
Lackofinformedconsentprocess P

Chapter6
120
3rdOrder
Themes
2ndorderthemes 1storderthemes Women’s
experience
Failureto
meet
professional
standardsof
care
Lackofinformed
consent&
confidentiality
Breachesofconfidentiality P
Physical
examinations&
procedures
Painful(and*forced)vaginalexaminations P
Refusaltoprovidepainreliefand
*anaesthesia
P
Performanceofunconsentedsurgical
operations
P
Neglect&
abandonment
Neglect,abandonmentsorlongdelays P
Skilledattendantabsentattimeofdelivery P
Poorrapport
between
womenand
providers
Ineffective
communication
Poorcommunication P
Dismissalofwomen’sconcerns P
Language&interpretationissues P
Poorstaffattitudes P
Lackofsupportive
care
Lackofsupportivecarefromhealth
workers
P
Denialorlackofhealthcompanions P
Lossofautonomy Womentreatedaspassiveparticipants
duringchildbirth
P
Denialoffood,fluidsormobility P
Lackofrespectforwomen’spreferred
birthpositions
P
Denialofsafetraditionalpractices P
Objectificationofwomen P
Detainmentinfacilities P
Lackofresources Physicalconditionoffacilities P
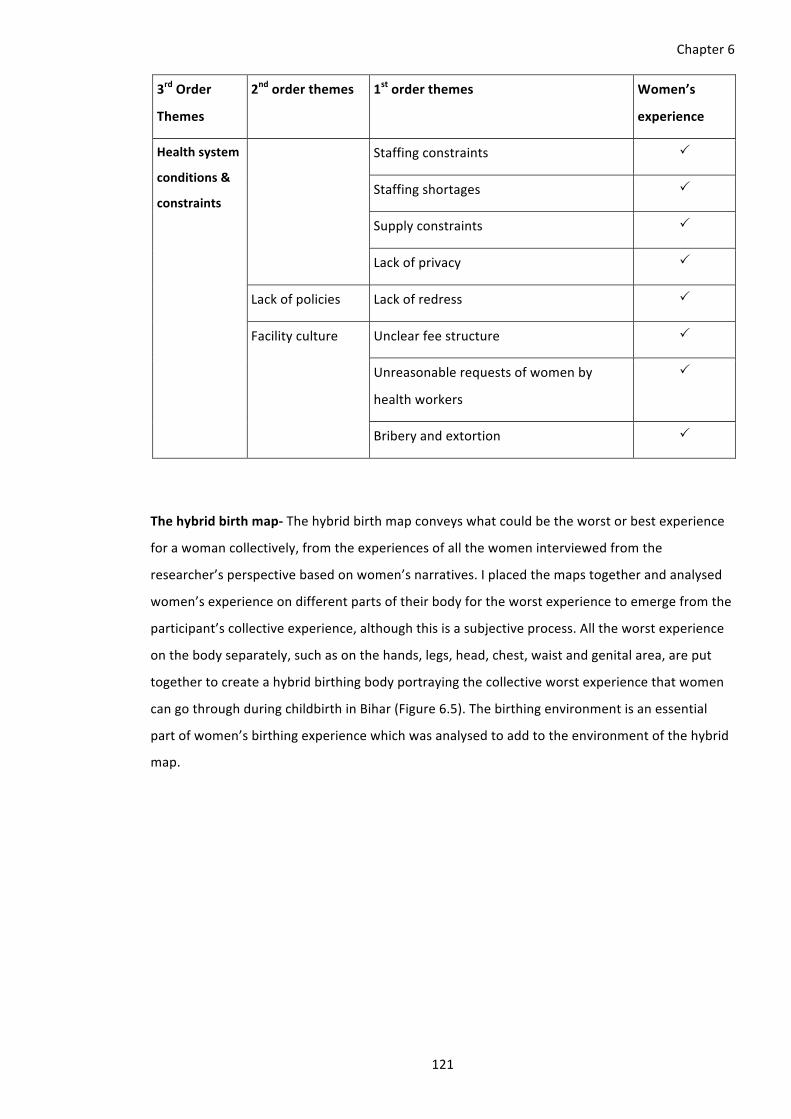
Chapter6
121
3rdOrder
Themes
2ndorderthemes 1storderthemes Women’s
experience
Healthsystem
conditions&
constraints
Staffingconstraints P
Staffingshortages P
Supplyconstraints P
Lackofprivacy P
Lackofpolicies Lackofredress P
Facilityculture Unclearfeestructure P
Unreasonablerequestsofwomenby
healthworkers
P
Briberyandextortion P
Thehybridbirthmap-Thehybridbirthmapconveyswhatcouldbetheworstorbestexperience
forawomancollectively,fromtheexperiencesofallthewomeninterviewedfromthe
researcher’sperspectivebasedonwomen’snarratives.Iplacedthemapstogetherandanalysed
women’sexperienceondifferentpartsoftheirbodyfortheworstexperiencetoemergefromthe
participant’scollectiveexperience,althoughthisisasubjectiveprocess.Alltheworstexperience
onthebodyseparately,suchasonthehands,legs,head,chest,waistandgenitalarea,areput
togethertocreateahybridbirthingbodyportrayingthecollectiveworstexperiencethatwomen
cangothroughduringchildbirthinBihar(Figure6.5).Thebirthingenvironmentisanessential
partofwomen’sbirthingexperiencewhichwasanalysedtoaddtotheenvironmentofthehybrid
map.

Chapter6
122
Figure6.5 Thehybridmapoftheworstexperiencefromtheeightbodymaps

Chapter6
123
RespectfulBirth
Womenoftenjustsaidthey‘feltgood’aboutaspectsofbirthwhentheytalkedaboutrespectful
birth.Butasstatedbefore,betterbirthdidnotalwaysmeanagoodandrespectfulbirth.Women
sharedtheirexpectationsthatcouldmaketheirbirthsrespectful.Amritahadvisitedatertiary
levelhospitalinadifferentstateforafewantenatalvisitsbeforemovingbacktoBihartogive
birth.Shetalkedaboutthecleanlinessandgoodbehaviorofthehospitalstaffthere,comparing
withherbirthingexperiences.Gettingacleanambulancetogotothehospitalontimewasthe
onlypositiveaspectfromherexperience.Sheexpectedcleanlinessintheentirehospital.Shehas
averyclearvisionofwhatrespectfulcaremeanstoher.
“Careshouldbelike,whenItoldthemwhatproblemIhave,theyshouldcomeandcheckme
completelyandtellmeaboutmycondition,thatinhowmuchtimeIwilldeliver.Iwillfeel
respectfulwhentheywilldomydeliveryontimewithoutdelay,whentheywillspeakwithme
politelywithasmile.Whentheywilltakecareofmenicely.Iftheygaveusabed.Thingsshouldgo
well.Theyshouldtreatuslikefamilymembers.NomatterwhetherIambirthingaboyoragirl,I
shouldbetreatedwell.Iftheytalktomenicely,thenonlyIwillcomehere…nomatterwhetheritis
thenurse,doctorordai.Theyshouldgiveimmunization,injection,medicinesandothersupplies
fromhospitalifitisavailable.Ifitisnotavailable,theyshouldbringitfromoutsideandgiveus.
Thenonlywewillshareourgoodexperiencewithotherwomenintheneighbourhoodthatweare
notdisrespectedthereandpeoplearenotgreedy.What’sthepointofgoingthereotherwise!”
(Amrita)
Atouchthatfeltgoodwasmentionedasacalmingandrarelyexperiencedaspectofbirth.Pairo
wasrelievedtohavebeengivenbirthpain-free.Afterhavingatraumaticbirthexperience(Figure
6.11),itwasdifficultforhertogothroughanothercesareaneventhoughshehadchangedthe
hospitalandthedoctor.Memoriesofherfirstbirthexperiencecausedsevereanxietywhenshe
waslyingontheoperationtable,blindfolded,andshegotsupportfromastrangerwhoheldher
handandhelpedhercalmdown.Riahasasimilarstoryofhervaginalbirthinapublictertiary
hospitalwhenshewassurroundedbyfiveotherwomeninlabour,withoutanyprivacy(Figure
6.9).Bothofthemdidnothavethesupportfromfamilywhentheyweregivingbirth,butwere
supportedbyastranger,whichwasthebestaspectoftheirexperience.ForPairo,itwasthe
‘stem-cell-guy’andforRiaitwasthebirthcompanionofanotherwomanbirthingnexttoher.
CordbloodbankingisavailableinmostprivatehospitalsinIndia,whichexplainsthepresenceof
thispersonintheOTwhomPairoreferredtoasthe‘stem-cell-guy’.
“ThereweremanypeopleintheOTandIhadthestemcellguyintheOTwithme.Heheldmy
hand.IknewIwasgoingtobeoperatedsoIwentcompletelynumbinmyheart.Itwashurtinglike

Chapter6
124
aninjectionduetofear.Itoldhimtopresstightlyonmyheart,onmychest.HeofferedwaterbutI
refusedtodrink…‘justpresstightlyhere’andhedidso.(laughs)Noonewilltellanyonelikethis
butIwasblindfoldedandIdidn’tevenknowwhohewas.Ididn’tseehisface.Aftersometimehe
asked‘areyouokay?’,Isaid‘yes’…Ifeltlikeheismyown,someonefamiliar.”(Pairo)
“Iwantedonlytwopeoplearoundme,anurseandadoctor.Thepeoplewhogivemedicineand
injectionshouldremainandtheothersshouldnotbethere.”(Amrita)
Theabsenceofbadbehaviorincludingwhattheyconsiderbadtouch,wasalsoexpected.Pairo
recallednovaginalexaminationsbeingareliefinhersecondbirth.Goodbehaviorcouldbeseen
inusualandunusualforms.
“She(doctor)wasverynicebecauseshealsostartedprayingwithus(forthebaby).Shewasan
innocentnicelady.Shewassogood.Ifeltgoodbecausethoseweregoodpeople,doinggood
thingsandtakingcareofmenicely.Wewerehappy!”(Pratima)
Theplaceofbirthmattersaswell.Pratimafeltthatshewasmostrespectedathomewhen
comparedtoherpreviousbirthinaprivatehospital.Riaperceivedthatwomenareabusedin
governmenthospitalbecausetheyhavenotpaid.Inprivatehospitalonepaysfortheservices,so
canexpecttobetreatedwithrespect.Thisalsowasrelatedtoworkloadinthegovernment
hospital.Havingfamilymembersmayalsoensurerespectfulcareandifnot,oneatleastfelt
supportedwithfamily’spresence.
“Ingovernment,theydoonework,thenleavethatandgotodoanother,thenleavethattoo.They
areconstantlyjugglingbetweenyouandotherpatients.Theyonlycomewhenthebabyiscoming
out.Butintheprivatehospitaltheywillstandnexttoyoufromthebeginninguntiltheend.The
moremoneyyougive,themoreconvenienceyouget.”(Ria)
Participantsoftenchangedbirthplacesafteratraumaticbirthingexperience.Inmanycasesthat
wasnotanoption.Anjugavebirthathomethreetimesaftertwostillbirthsatthehospitaland
sheisconvincedthathomeiswhereherbabiessurvived,whichwouldnothavehappenedina
hospital.Sujata,PairoandSitachangedhospitalsaswell.Pratimahadahospitalbirthwhich
wasn’tverybadinheropinion,butaffordabilitywasachallengeforherandhomebirthwaslight
onthepocket.
“ObviouslyIwillbemostrespectfullytreatedathomeduringbirth!Yougetgoodcareathome.If
yougivebirthathome,thenitishomeonly.Thereisnoneedtogoanywhereelse.Didnothaveto
reserveavehicle.Thereisnoneedtogorunningaround,arrangingthings.Everythinghappensat

Chapter6
125
home.Theroadshavepotholes,itsbumpy,whichisoneofthereasonsofdiscomfortwhile
travellingtothehospital.That’swhyIgotmybirthdoneathome.”(Pratima)
ReceivingtimelyattentionfromthecareproviderswasmentionedbyAmritaandSita.Thiswasa
causeofworryformostparticipantswhogavebirthinahospital,andexperiencedneglectand
abandonment.Apartfromgoodbehavior,thereweremanybirthingenvironment-relatedaspects
thatSitathoughtwouldberespectfultothebirthingwomen.
“Theyshoulddodeliveryquicklywithoutmuchdelay,Imeanontime.Thereshouldnotbeany
problemorcomplication.Theyshouldtalknicelywitheveryone.Mealsshouldbegiveninthe
hospital.Bathroomshouldbeclean,roomshouldbeclean,bedshouldbeclean.Ifyouarealone,
youwillbescared.Nobodyshouldtouch.Idonotwanttobetouchedbyanyone.Thereshouldbe
someonewithyou,it’simportant.”(Sita)
Birthcompanionsareconsideredimportant,althoughthehusbandisnotconsideredabirth
companion.Husbandsareusuallykeptaway,asitisdeemedinappropriateculturallyformento
bearoundbirth.Birthcompanionor‘guardian’couldensuretheygetrespectfulcarebecause
theirpresencewillmeanthecareproviderswillgetmoneyafterthebirth,whichwillensurethey
treatthewomenbetter.Womenfromthefamilyaccompanyabirthingwoman,thoughtheyare
notallowedintheOT,aswasseenforPairo.Thepresenceofhusbandisdebatableandismostly
frownedupon.AsmentionedbyPratimaandSitawhofelttherewasnoneedforherhusbandto
bethere.Box6.19hasAmrita’sI-poemonherfeelingsabouthavingherhusbandaroundwhile
givingbirth,andexpressingthatshefeelsshehadtogothroughpainfulbirthsbecauseofhim.
Anju’shusbandplayedakeyroleinallherbirthsastheonlypersonaround,otherthanthe
dagarin.Hewasalsotheonetocatchthebabyinherfirsthomebirth,thoughhewaitedoutside
inthetwofollowingbirths.Urmila’shusbandwasinprisononetimeandnotaroundherduring
restofherbirthsandRia’shusbandabandonedheraftershegotpregnant.Sujata’shusbandhad
towaitoutsidethebirthingroominallofherfourbirthsandthatisoneaspectofherbirthshe
wantedtochange.
“ThebenefitwouldbethatwhenIwascryingoutofpain,Icouldhaveheldmyhusband’shand.I
couldhavesharedmypainwithhimandthatwouldbegoodforme(laughs).Hemaynothavefelt
anything,butIwouldhavefelteverything.Itwasallaboutme,Iwasinpainsolet’sfocusonhow
thatwouldhavehelpedme(laughs)Iwouldhavebenefitedfrommyhusband’spresenceforsure.
Hewasoutside,waitingtohearaboutthebaby.Iwantedhimintheroomwithme.Ifmyhusband
wouldhavebeenthere,Iwouldhaveaskedhimtocomenearme(laughs)…Justthefeelingthat
someonefromfamilyisthere.Buthavinghusbandnexttoyouissomethingdifferent…holdinghis
handwillbemorethanenough(laughs)Inthisconditionhusbandisneededmore.Hecanalsohug

Chapter6
126
me.Iwillbeinpainbutbecauseofmyhusband’scompany,mypainwillbeless.Iwillfeelrelaxed.
Beingwithhimwillmakemehappier.”(Sujata)
Womenwanttoavoidunnecessaryinterventionsduringchildbirthandgivebirthnaturally.Some
oftheseinterventionsareperceivedasbadtouchtothemandtheywanttogivebirthwhere
thereare‘nocuts,nochecks’becauseepisiotomy,repairandvaginalexaminationsaresomeof
themostdisrespectfulandabusiveaccountsnarratedbyparticipantsincludingunnecessary
exposure,thatisshamefulandtraumaticforthem.Theywanttheirprivacytobemaintainedatall
times.Itisimportanttoensurethattheirnormsandbeliefsarevalued,asSujataexperienced
whenshefeltthebabyisnotcomingoutbecausethefanneedstobeturnedofftoincreaseher
bodyheat.ThenursedidthatforherandSujatareportedthatherbabycameoutquicklyafter
that.Whenwomenhavetoundergointerventions,theywanttobetoldaboutthemandbegiven
enoughinformationtounderstandthepurposeofit.
“Theyshouldhaveexplained(aboutvaginalexamination)tome.ThenIwouldhavethought,okay
theywilldothistomeanditisrequired.SoIwouldhaveconvincedmyselftohavecourage.I
wouldhavepreparedmyself.”(Pairo)
Manyoftherespondentssharedwhattheir‘birthingexperienceofdreams’wouldbelike,ifthey
hadalltheresourcesimaginable,vestedtomaketheirbirthingexperiencemorerespectfuland
satisfactory.ThefollowingquoteshowsRia’shopesforherdaughter’sbirth(Figure6.9),because
shedoesnotplantogivebirthagain.
“Thereshouldbeonlyonebed,surroundedbycurtainsonallsides…hereeveryonewasscreaming,
hereandthere,everywhere.Thereshouldbeasister(nurse)whowilltalknicelyandpolitelywith
love.Theywillguideuswhattodosaying‘dearthisisthisandit’saboyoragirl’…Iwillgivebirth
lyingdownonly,inaseparateroom.Theyshouldbeencouraging.Iwanttobefamiliarwiththem
(doctor,nurse).IwouldthinkthatsomeoneisthereandIwillfeellessafraidandnotpanic.
Encouragingenvironment!Everythingshouldbedonewithloveandcare,thenIwillfeelhappy
andsatisfied…oncethebabyisreceivedwithcare,checkthegeneralconditionofthebaby,assess
thebabythoroughly,identifythepresenceofanyproblem…providecare.Aftercleaningthebaby,
itshouldbeshowntomesoIknowwhetherIbirthedasonordaughter.Theroomshouldbeclean,
nosmells,thefloorshouldbeclean.Thebedshouldbesuchthattheheadrisesup.Thereshould
beproperlight,ventilation,workingairconditionerandrunningfanspeciallyinhotweather.If
televisionistherethatwouldbebetter.Thereshouldbeabedformyfamilytoointhesameroom.
Ishouldnothavetospendsomuchmoney,buteverythinghappensasperincome.Can’tspread

Chapter6
127
thelegssomuchthatitgoesoutofthequilt!9Thepoorandneedyshouldgetallthesefacilitiesin
thegovernmenthospital.”(Ria)
Participantsgavebirthinarestrainedsupinepositioninthehospitalanddidnothaveanopinion
onanidealpositiontogivebirthin,thoughAnjugavebirthsquattinginthreeofherbirthsat
homeasshowninherbirthmap(Figure6.7).Havingthesamedagarin10forallherbirthswas
comforting,assheknewhercarerandhaddevelopedarelationshipoftrust.Urmilawasalso
caredbyateamofhealthcareprovidersknowntoherinallthreeofherbirthsinaprivate
hospital.Thebirthmapsarealsoanalysedinanotherwaythatincreasedunderstandingofthe
differentwayswomenbirthinBihar,inoneimage.Forthis,Itracedalltheeightmapsleavingout
alltheotheraspectsofthemapstofocusonlyontheposturewomentakeoraremadetotake
whentheyaregivingbirthathospitalorhomeandinnaturalorcesareanbirth.Therangeof
birthingpositionsshowshowdiversebirthingcanbe(Figure6.6).
Figure6.6 Birthingposturesofwomen(Author’sown)
Thefinalaspectwasaboutthechoiceofhowtogivebirth,andallwomenwantedtogivebirth
‘normally’.Pairospentdayscryingwhenshecouldnotgivebirthvaginallyeventhesecondtime,
becauseherfirstbirthwascesarean.Eventhosewhodidhaveavaginalbirthreportedhaving,
9ThisisacommonIndiansaying.10Dagarinisdaiortraditionalbirthattendant.

Chapter6
128
whattheycalled,a‘mini-operation’(episiotomy)whichwasthemosttraumaticaspectoftheir
birth,asUrmilaandRianarrated.Theirhappiestexperienceswereinterventionfreevaginal
births,buttheyfelttheydidnothavetherighttomakethatchoiceovertheirownbody.
AhybridbodymapofthebestexperiencescouldbecreatedbutthatwouldequatetoAnju’s
originalbirthmap(Figure6.7)thatmajorlydepictedthebirthingpositionandbirthing
environmentofoneparticipant,Anju,whochosetogivebirthathomethrice,withthesame
traditionalbirthattendanti.e.adaiaftertwostillbirthsathospitals.Anjusquattedtogivebirth
everytime,takingsupportfromthetwobamboopoles,inthepresenceofherdai.Acoupleof
otherparticipants,oneofwhomfeltthatquickaccesstoacleanambulanceandthecleantoilets
inthehospitals,werekeyaspectsofhergoodbirthingexperience.Incontrast,Pratima,whoalso
gavebirthathomewithadai,feltthepresenceofherrabbitsduringherbirthassomethingshe
wouldpreferifshegavebirthagain.

Chapter6
129
Figure6.7 Anju’sbodymapshowingherhomebirths

Chapter6
130
6.5.2 Respect,disrespectandabuseduringmedicalinterventions
Womenexperiencedarangeofmedicalinterventions.Alltheeightparticipantsgavebirthina
hospitalatsomepoint.Theseinterventionsincludegettingintravenousfluids(IV),augmentation,
episiotomy,episiotomyrepair,perinealshavingandvaginalexamination.Theinterventionsalso
includebloodtransfusion,fetalmonitoringanduterineexploration.Cesareansectionhasalso
beenincludedasanintervention.
Augmentationandintravenousfluidtransfusion-Allwomenwereaugmented;exceptone
womanwhogavebirthathome.Mostofthemwereinducedwithoutconsentandsomewere
inducedmultipletimes.Someofthemunderstoodonlyafterrealisingthatsuddenlytheintensity
oftheircontractionshadincreasedafteraninjectionwasaddedtothe‘bottle’,withoutany
communication.Sitawantedtobeinduced,toavoidvaginalexaminations.Womengenerally
reactedtoaugmentationwithannoyance,thoughoneofthemfeltitwasanactofcare.Itis
difficulttosayhowmanyofthesewomenwereinducedonprescription,butitiscertainthat
augmentationinlabourisaroutineprocedurethatwomenarewellawareof.
“My‘dard’(pain)increasedalotafterthetwoinjections.Ididnotnotaskthemtoincreasemy
pain”(Urmila)
“Theygavemedicinetoincreasemypain.Ididnotask,butshegaveitsothatthebabywillbe
bornquicklyasshewaswatchingmeallnight,Iwasrestlessduetopain.Shewasverynice!”
(Pratima)
IVfluidswerecommonlygiventowomenwhentheywereadmitted.InfusingoxytocinintheIV
fluidisacommonpractice.WomenunderstoodthisandoftenacceptedIVinfusedoxytocinas
partofthecareduringchildbirth.
“Shesaidmouth(cervix)isnotopenenoughanditisleakingwater,soitneedstobeinfused.
Otherwisethebabywilldryupinside.Theyranwaterdayandnight.19bottlesin3days!”(Pairo)
“Shehungthebottleofwater,addedtheinjectioninitandwhenitfinished,thenurseaskedme
‘how’syourpain?’,gavemetwoinjectionsandafterthatmyconditionwaspatheticandIstarted
cryingandscreamingloudly.”(Sujata)
Episiotomyandrepair-Womenreportedunpleasantandtraumatisingexperiencesofepisiotomy
andrepair.Noneofthewomenwereaskedfortheirpermissionbeforethecareprovider
subjectedthemtoanepisiotomy.Manywerenotinformedaboutitbeforegiving‘thecut’or
‘chotaoperation’(mini-operation),asitiscommonlyreferredto.Womenoftensaidtheygave
Chapter6
131
birththrough‘chota-operation’andnotnormal/natural/vaginalbirth.Theseexperiencesare
etchedintheirmemorywithgreatdetail,eventhoughyearshavegonebysincetheygavebirth.
“…8stitches!Iknowfromtouchingit.Whenshewasstitchingme,itwashurtingalot.Whenever
theneedlewouldpiercemefromoneend,Iwouldcountwhenitwouldturnaroundandcome
backagain.Icouldfeelallofit!ItoldthemtogivemeaninjectionsoI’llbeunconscious.Somany
timesItoldthem.Butshedidnotgivemetheinjection.Iscreamedalot!Shekeptsaying,‘it’s
done!’.Itwasverypainful!Itwasverypainful!”(Ria)
Riagavebirthinatertiarylevelgovernmenthospitalinthestatecapital.Urmila,23yearsold,
motherofthree,alsohadaverysimilarnarrativeofherepisiotomyandrepair.Shegavebirthina
privatehospital.Sujata,experienced‘thecut’inhertwoinitialbirthsinthegovernmenthospital.
Shewasscared,anticipatingshewouldbecutinherthirdchildbirth,inaprivatehospitalthis
time.Shewaspreparingherselfmentally,butwasrelievedwhenthisdidnothappen.
“…that’swhyIcalleditagoodbirth!”(Sujata)
Pairosharedastoryofherdistantauntwhohadgonethroughpainfulepisiotomyandrepair,
whichtookverylongtoheal,leavingherinpainformonthsandunabletosit.Sheultimately
decidedtoneverhavechildrenagain.
Vaginalexaminationanduterineexploration-Women’saccountsofvaginalexaminationsare
harrowinganditisanexperienceeverywomanhasenduredmultipletimes.Theycalledit‘bauaa
walacheck’.Everyvaginalexaminationisunpleasantandmanyaretraumatic.Aparticipantwould
usuallyknowaboutvaginalexaminationwhenthecareprovidersays‘liftyoursaree’orwould
announce‘Iamgoingtocheck’.TheI-poeminBox6.1isanarrativeofPairo’sexperiencesof
multiplevaginalexaminationsbydifferentcareproviders.OneofSujata’sIpoemstitled‘Iamtoo
important!Ishouldnotbecheckedfrombelow’isanotheraccountofanequallydisturbing
experienceofvaginalexaminations.
“Shesaidliedown,holdyourlegswithbothhands,Iamcheckingyou!...liftyourclothes.”
(Pratima)
“Peoplecomeineachshiftandeveryonechecks.Therewasnodoctor.Everyhourshewas
checkingandsaying‘mouthisnotopen’.(expressionofdiscomfort)Don’tyouthinkitfeelsbad?...
Firstmymothertoldmethatlethercheckonce.Itoldher‘no’Iamalreadyhavingalotofproblem
withmybaby,Idon’twantthesethings.Butmymotherinsisted‘howwillsheknowifshedoesn’t
check.’(Sita)

Chapter6
132
Womendidnotalwaysknowbeforeexperiencingvaginalexamination,thatitisaprocedure.This
isalackofcommunication.Theywonderedwhytheywerebeingtreatedlikethat.Theywerenot
toldwhatwasfoundintheexaminationandwhentherewasanexplanationitwasvague,suchas
‘there’stime!’or‘itwilltaketime’.
“Iwouldneverhaveselectedtheonewheretheyputtheirhandinsideme(ifIhadachoice)”
(Pratima)
Box6.1 Pairo’sI-poem-Thisisthefateofwomenandwomenmustendureit!
“Thisisthefateofwomenandwomenmustendureit!”
Ifeltveryuncomfortable!
Iwasscared!
Ikeptshouting.
Icomplainedtothedoctorlater,“Whyiseveryonecheckingmelikethis?”.
Itoldthedoctorwhyareyourpeoplecheckingmelikethis.
Icomplainedtothedoctor.
Ifounditoutallintheend.
Iwasfindingitverydifficulttoacceptthattheyshoulddolikethat.
Ifeltveryuncomfortable!
Ihavemyownroom,menarearound,thereisacrowdandthereareotherpatients,thentheyshouldnotcheckmeinfrontofeveryone.
Ididnotunderstandwhenthenursediditforthefirsttime.
Ithought,whatwasshedoingandinfrontofeveryone?
Iwaswearinganightie.
Ithoughtwhatisshedoing?
Itoldthistomymotheragainandagain,aftergoinghomethatwhatevershehasdoneinfrontofeveryone,itwasnotright.
Iusedtosayhertheyshouldnothavedonethat.
Ishouldhavebeentold.
Iusedtofeelveryuncomfortable!
Iwouldhavethoughtthatokaytheywilldothistomeandit’srequired.
Iwouldhaveconvincedmyself,tohavecourage.
Iwouldhavepreparedmyself.
Ithoughtwhataretheydoingwithme?
Iwasfeelinguncomfortable.
Iwasnotatallsupportingthattheytouchmelikethis.
Iwouldhaveneverselectedtheonewhentheyputtheirhandinsideme.

Chapter6
133
Uterineexplorationwasalsoreportedbeingcarriedouttoremoveany‘kachra’(dirt)fromthe
uterusafterchildbirthorwasdonetotakethefoetusout.Thedifferencebetweenuterine
explorationfromvaginalexaminationwasunderstoodwhentheyspecificallymentionedthattwo
fingerswereinsertedassomeonealsosaid‘twophinter’buttheymentionedthatthe‘whole
hand’wasputinsideincaseofauterineexploration.Twoparticipantsreportedthisexperience
andnonewereinformedorconsentedbeforeitwasdonebyunqualifiedcareproviders.
“Sheworeagloveandputherwholehandinsideme.Mypainincreasedalotafterthis.”(Sujata)
6.5.2.1 Painmanagement
Painisthecommonaspectthateveryparticipantknewandfearedaboutchildbirth.Theytalked
oftheextentofpainandhowunbearableitwas.Theydescribedthatitwasthekindofpainthat
couldleadtodeath.Contractionswerereferredtoaspain.Womendidnottellthefamily
memberswhentheystartedgettingpain,theywaiteduntilitgotunbearable.Theyhadwaysto
describethedegreeandnatureofpain.Sujatasharedthatthepainbeforeone’swaterbreaksas
‘drypain’,evenafterthepainisnotintenseandisinfrequent,itiscalled‘sweetpain’.Topush,
wasalsoreferredtoas‘givingpain’.Theydiscussedthedurationofpainintermsofdaysand
sometimesjusthoursbutthenatureofbirthwasdependentonthekindofpaintheyhad.Agood
birthmaymeantheshortestdurationandlowestintensityofpaininaparticularbirthoutofall
thebirthingexperiencesawomanmayhavehad.
“WhenIaminpainobviouslyIwillgetveryangry.”(Amrita)
“IwaslaughingandgoingtothehospitalbecauseIhadnopain…IwashappybecauseatleastI
wasbirthingwithoutpain(cesareansection)”(Pairo)
“Iwasinsomuchpain,Ikeptonturningallnight.”(Pratima)
Women’smobilitywasdependentonthepain.Theposturetheytookduringcontractionsand
givingbirthoftendependedonwhatpositionmadeitalittleeasiertobearthepain.Participants
didnotmentionbirthinginapositionofchoiceandoftenbirthedinasupinepositionina
hospital,asshowninmostofthebirthmaps.Theysharedthatitissupposedtobethebest
positiontogivebirthbecausetheyhavebeentoldaboutthatorthatthebabymayfallifbirthed
inadifferentposition.Thiswasoftennotencouragedbythecareproviders,whodidnot‘allow’a
positionofchoiceanddisciplinedwomenwhentheyreactedtopainbycryingorscreaming.
“Iwasinsomuchpain.Iwassittingonthefloor.Iwaslyingdownbeforebutthepainwas
increasingsoIgotdownandmymother-in-lawwasholdingmyhandandIwascrying.”(Amrita)

Chapter6
134
Painwasconsideredinevitableandwomendidnotaskaboutpainrelief.Thelanguageusedto
converseaboutpaininthehospitallacksclarity.Womenwouldoftenaskfortheinjectionfor
pain,orthecareproviderwouldsaytheyhavegivenmedicineorinjectionforpain.Thisoften
meantaugmentationandnotpainrelief.Womenwereoftenshockedwhenthecareproviders
increasedtheirpain,withoutinformationorconsent.Painwasrelatedtomanyother
interventionsthatthewomenhadnotconsentedto.Givinganepisiotomycutwithoutanesthesia
wascommonwiththenotionthatwomenwouldnotfeelitalongsidethepainfulcontractions.
Womenreportedfeelingeverything,includingwhentheywerebeingsuturedwithoutanesthesia.
Thecareproviderscontinuedsuturingthroughthepainregardlessofwomen’spleastostop.
Womencomplainedofpainwhenforcedvaginalexaminationswereconducted,fundalpressure
wasappliedanduterineexplorationwasconducted.Painwasalsooftentheonlyquestioncare
providersaskedwomenandwomenaskedcareproviders.
“Mypainincreasedwhenshegavemetheinjection.”(Sita)
“Afterthenursegavemethesecondpaininjectionmyconditionwaspathetic.Istartedcryingand
screamingloudly.Ihadtoomuchpain.”(Sujata)
“Itoldherdon’tputyourhandinsidebecauseit’shurtingbutstilltheycontinuedtodosoand
didn’tlistentome.”(Urmila)
Twoparticipantssharedtheyhadtoliedowntobearthepainandwalkwhenitwasless.One
participantwaskeentohaveherhusbandholdherhand,eventhoughhewouldnotunderstand
herpain,buthispresencewouldmakeiteasiertobearthepain.
6.5.3 Birthsetting/placerelatedrespect,disrespectandabuse
Theparticipantshave22birthingexperienceswhichincludedgovernmenthospital(10),private
hospital(8)andhomebirths(4),including20livebirthsand2stillbirths.Thegovernmenthospital
birthsincludefouratmedicalcollegehospitalsinthestatecapital,whichareatthetertiarylevel
ofcareprovisionandtheremainingfourareattheprimaryhealthcentres(PHCs),whichareat
theprimarylevelofcareprovision.Thewomenoftenchosebetweenthesethreeoptionsofbirth
placeintheirsubsequentbirthsexceptUrmila,whobirthedallherthreechildreninthesame
privatehospitalclosetohermaternalhouseandRia,whogavebirthonce.Women(Sujata,
Pratima,Sita,Anju)havechangedtheirbirthsettingsintermsofsectoraswell.Pratimagavebirth
ataprivatehospitalthefirsttimeandathomethesecondtime.Somewomen(Pairo,Amrita,
SujataandSita)changedtheplaceofbirthsometimeswithinthesector.Pairogavebirthtwicein

Chapter6
135
twodifferentprivatehospitals.Figure6.8showsmoreaboutbirthsettingchangeswherethe
orderofarrowsshowtheorderofbirth.
Figure6.8 Birthplaceoptionsandchanges(Author’sown)
Theplaceswomenchosetogivebirthwasnotnecessarilytheirnearestaccesstohealthcare,as
seenwithPairo,Sujata,AmritaandSita.Thewomenchangedthesetting:1)togivebirthcloserto
thematernalhome,2)avoidhighfeesatprivatehospitals,3)avoidcesareansection,4)provision
ofahigherfacilityforbetterservicessuchasbloodtransfusionand5)alastminuteshiftto
hospitalafterdaicouldnotmanagethebirthathome.Themostunusualreasonwasbecausea
mobilecompanywentbankruptandtheparticipantcouldnotcontactherhusbandwhowould
havetakenhertothegovernmenthospital,whichledtohergivingbirthatthenearestprivate
hospital.Thisalsosuggeststhattheclosesthospitaltoherwasnotpublic.Manywomenchanged
thevenueofbirthtoavoidobstetricviolenceduringchildbirth.Theirnarrativesshowthatthey
arelookingforrespectfulcareandcontinuityofcare.
Womenpreferredtohavethesamebirthplaceunlesstheyexpectedbettercareorwerelooking
foraffordablecare.Urmilabirthedinthesamehospitaleverytime,atanaddedunaffordable
cost,butherpreferencewassupportedbyhermaternalfamily.Riahadonebabyinthetertiary
governmenthospitalandvowstonevertakeherdaughterthereforherbirthunlesssystems
improve.Hermothergavebirthtoherinthesamehospital.SitachosetogotoaparticularPHC
becauseitwasclosetohermaternalhouseasdidAmrita.Anjucalledthesamedagarintoher
homeallthreetimes,asdidPratima.However,Pratimahadtobetransferredtothenearby
privatehospitalinthelastminute.

Chapter6
136
“Ingovernmenthospitaloneneedstocallthedoctorandnurseeverytime.Theywaitforyour
death.Youhavenorighttosayanything,youhavenotpaid.Inprivatehospital,Iaskformyright
sinceIhavepaid(money).Ihaveheardsomanycasesofexchangingbabiesingovernment
hospitals.Thosewhowantamalebaby,getmalebaby…thereisnoguaranteeyouwillleavethe
hospitalwithyourownbaby…inprivate,eventhoughyoupay20,000rupeesatleastyoucome
homealive.”(Urmila)
“Isawthedoctorcheckingallthewomenqueueingup,downthere(vaginalexamination)wearing
apolytheneglove.IwassoscaredtoseeitIranfromthere!”(Pairo)
“Thereisanadvantageofgovernmenthospitalthattheywillnotoperateonyouimmediately.
Theyletnormalbirthtakeitscourse,aslongaspossible.Privatehospitalslookforeveryexcuseto
cutyouopen,allformoney.Normalbirthisnotprofitabletothem.Ingovernment,Icangivebirth
inthemorningandleaveintheevening.Inprivatetheykeepyouadmittedforminimum2-3days.”
(Ria)
Sita’sstoryisuniquetooanditshowssomeamountofdecisionmakingbyher,inchoosingthe
birthsetting,whichisrare.Hermother-in-lawisadagarinwhoassistsalltheneighbourhood
births,butSitarefusedtoletherassistherbirthandwenttoahospitalallthreetimes.
“Thesedaysnoonegivesbirthathome.Igavebirthtoallmythreebabiesathospital.Hospitalis
betterforme.”(Sita)
“They(hospital)killedtwoofmybabiessoIdidnotgotherethethirdtime.EverytimeIhad
bleedingallthroughmypregnanciesandeverytimeIwenttothehospitalmybabiesdied.Every
timeIgavebirthathome,mybabiessurvived!”(Anju)
HomebirthsweretheprimarychoiceforPratimaandAnju.ThoughPratimacouldonlyhavea
homebirthforhersecondchildbirth,Anjuhadthreehomebirthsassistedbythesamedagarin,
followedbytwostillbirthsatagovernmenthospital.Pratima’shomebirthingexperiencehasbeen
narratedinherI-poeminBox6.2.

Chapter6
137
Box6.2 Pratima’sI-poem-Bornathome
Bornathome
Ilikedthehomebirth!
Ihadmyfirstchild.
Ihaveonemoresister-in-law,shealsohasfourmembersinherfamily.
Ididnotreleasewater11.
IhadcompletedallmyworkintheeveningandmymotherwasinPujarituals.
Iwashavingpainsincethatthemorning.
Ihadameal,Ikepteatingandworking.
Ididallmyworklikecooking,cleaningupanddownworkfromterrace.
Idideverything.
Ididalltheworkevenintheevening.
Iwashedtheclothes.
Imoppedthecorridorandterrace.
Ipreparedthedinner.
Ihadpreparedthemeal.
Iservedthedinnertoeveryone,thenIwentupstairswithamobile.
Iwaswatchingamovie.
IwaswatchingtheBhojpuriMovie.
Idon’trememberthename.
Idon’tknowheroandheroine.
Iusedtohangupthephoneandroamaround.
Iusedtogoupanddownthestairs.
IgotdownfromtheterraceandIinformedmymother-in-lawthatIamhavingpain.
Ihadthesametypeofpain.
Iwaslyingonit.
Ilaydownthisway.
Iwasholdingthemtightly.
Iwasholdingmythightoo.
Iworeasareebuttheyremovedit,petticoatwasthere.
Iwasonajuterag.
Iamshameless!
Ihadpainforanhour.
Iwasaloneinthatroom,thenIcalledmysister-in-lawtoholdmeatthetimeofbirth.
Itookabathintheevening,sothehairremainedopenandsoitremainedopenallnight.
Ifeeltwokidsareenough.
Isay,‘see,asonisbornbygod’sgrace!’
IgotmybirthdoneathomeandIwouldnotliketochangeanything.
11 Amniotic fluid

Chapter6
138
NoneoftheparticipantsmentionedanyaidtheyreceivedoraresupposedtoreceivefromJanani
SurakshnaYojana,oranyothergovernmentincentivepolicies,asareasonforgivingbirthatthe
governmenthospital.Itwasoftenseenthatwomenwouldgetantenatalcarefromprivateor
missionhospitalsandwouldonlygotothegovernmenthospitaltogivebirth,asseeninRiaand
Anju’sstory.
“Ireceived(JSYmoney)formyfirstbirthbutnotforthesecond.ASHAblamedmesaying‘howdoI
know?Youprobablyreceivedthemoneyanddidnottellme’.Ihavearight!...ifgovernmentdoes
notgiveanythingtoyouhowcanyoutrustthem?…Iwillnotgetit,sowhythinkaboutit
unnecessarily!Whygetworried!”(Amrita)
Sita’snarrativeisverysimilartoAmrita’sinthisregard,asshowninherI-poeminBox6.3.There
wereothercomparisonstoowhichweremadebetweengovernmentandprivatethatincluded
participant’slackoftrustintermsofcleanliness.
Box6.3 Sita’sIpoemonJananiSurakshaYojana(JSY)
“JananiSurakshaYojanamoneyisforthemotherandthebaby,Iheard”
Ireceived[themoney].
Ihadmythirdchildalsobutdidnotreceive[themoney].
Iupdatedthepassbookbutitwasnotshowinginthat.
ItoldASHAtotakemyaccountdetailsandcheckitiftheydon’ttrustme,buttheydidnotdoso.
Ididnotknow,butwhenIwenttomymother’shousethenmymothertoldme.
Ididn’tgetit.
Ihavenotchecked.
Idon’tknowwhetherIreceiveditornot.
Idon’trememberexactly,butitwasapproximatelyRs3400/-.
Iusedtotalktomymothereveryday.
Ididnotchecktilldate.
Iheardthatthemoneyisgiventoutiliseforthemotherandthebaby.
6.5.4 Respect,disrespectandabuserelatedtobirthingenvironment
Thebirthingenvironmentincludestheinfrastructureinthatarea,thepeoplegivingcareandthe
toiletaswell.Womennotonlydescribedthebirthingenvironmentintheirbirthmapsbutalsothe
onesthatarenotonit.Thenumberofpeoplearoundbirthwasrelatedtowhethertheygave

Chapter6
139
birthinagovernmenthospital,privatehospitalorhome.Evenwhengivingbirthatagovernment
hospital,birthingatatertiarylevelofcaremeantbirthinginacrowdedhallwithmanyother
women,ascanbeseeninRia’sbirthmap(Figure6.9).
“Birthwashappeningallaroundme!Therewere6beds.Itwasfull!Everyonewasscreaming,
whichwasmakingmemoreanxiousandscared.Everyone’sbirthwashappening!Someonewas
receivingwater(IV).Doctorwasscoldinganotherfornotpushing,‘Push!Push!’.”(Ria)
Theinfrastructureofthebirthingroomoftenmadeitmorechaoticwheremultiple‘labourtables’
werekeptnexttoeachother,asnoticedinthestoriesofRiaandSujata;bothbirthstookplaceat
governmenttertiaryhospitals.Theprivatehospitalsonlyhadtheparticipant(Urmila,Pratima)in
thebirthingroom.Thehomebirthswerealsoconductedprivately,eitherjustwiththedagarin
(Anju)orassistedbythewomeninthefamily(Pratima)alongwiththedagarin.A‘Labourtable’
wascommoningovernmenthospitalbirthingstoriesandinprivatehospital.Therewerewomen
whoalsobirthedonawiderbed.Womenathomegavebirthonthefloor.
“Windowswerecoveredwiththicknetandglasses.Thelabourroomhadairconditionerandfan
butbothwereswitchedoff.Thelabourtablewasquitehigh.Therewasabluecolourmattresson
thebedandstepsnexttoit.Therewasathickrodattheheadendtoholdandbeardown.”
(Urmila)

Chapter6
140
Figure6.9 Ria’sBodyMap

Chapter6
141
Privacyisakeyaspectofthebirthingenvironmentandismentionedinallthewomen’s
narratives.Womenwanttheirprivacytobeprotected,theyalsodemonstratedaforced
acceptanceofthislackofprivacy.Theirprivacyneededtobeprotectedatsixlevelsasseeninthe
narratives,showninFigure6.10.
Level1-iscoveringtheirbodyduringinterventions,notexposingitunnecessarilyandexposing
onlyasmuchasneededwithconsent;
Level2-protectingprivacyfromthebirthcompanionandtheimmediatehealthcareproviders
whoareassistingthebirth;
Level3-protectingprivacybetweenotherbirthingwomenandtheirfamilymembers,ifmultiple
womenarebirthinginthesameroom,byensuringcurtains/screensbetweenthem;
Level4-ensuringthatoutsidersarenotabletopeepinfromanyopenwindowsbyputting
curtainsinthewindowsoraroundthewomen;
Level5-protectingprivacyfromalltheothercareandnonhealthcareproviderssuchascleaners,
whomaybeinthebirthingroom,atthenurse’sstationorweighingstation;
Level6-fromthefamilymembers,outsiders,othersinthewaitingareaoutsidethedoorwhich
usuallyopenstoahallway.
Figure6.10 Levelsofprivacytobeprotectedforthewomeninbirthingroom(Author’sown)

Chapter6
142
Curtainswerementionedwheremultiplewomenwerebirthinginthesameroombuttheywere
toprotecttheprivacyofallthefourtosixwomenbirthingtogetherfromoutsiders.Therewere
nocurtainsbetweenthelabourtablestoprotecttheprivacyofbirthingwomenfromeachother
andtheirbirthcompanions.
“Iwasabletoseewithmyowneyeswhentheladyinthecornerwasgivingbirth.Therewereno
curtains.Therewasonlyahall.Whenyougoinsideyouwillfindeveryonenakedthere.Evenif
attendantswouldcomethentheywillalsosee…Dhat!(Ohgod!)It’ssoembarrassing!Ifeltvery
bad!Youdon’twantanyonetolookatyouinthatstate.”(Ria)
“Myprivacywasmaintained…mybodywasnotexposedmuch.Doctoronlyexposedmylowerleg
toknee.Restofitwascoveredwiththenightie.Theladydoctorwasgood.”(Urmila)
Theissueofprivacyworsenedifmenareallowedaroundbirthingwomen.Thatisconsidered
shameful,ahugeinvasionofprivacyandsomeevenconsiderthisprivacytohavebeenprotected
ifnomenwereallowedinthelabourroom,regardlessofhowmanywomenareinthevicinity.
Thebirthingareaforthecesareansectionisverydifferentfromthelabourroom,asseenin
Pairo’sstory.Thisalsoincludedalotofmenaroundbirthinanoperationtheatreasshownin
Pairo’sbodymapinFigure6.11.
“Theywerenottakingmypermissionforanything…Ifeltsomeoneremovedmypetticoat.Ifeltit.”
(Pairo)
“Notasinglemanwasthere.Menarenotallowed.Ladiesstaytherewithladies!Mendonotgo
therebecausewomenarenaked…Assoonastheyseemen,theystartchasingthemaway.‘Go…
Go…whatareyoudoinghere?’Theydonotletanyonein.”(Sujata)
“Theywereallmen.Therewerenowomen(intheOT).Gentswhodoultrasoundwerealsothere.
Therewerearound8-9men.Thedoctorwasalsomale.Ifeelallthosemenshouldhaveworn
uniform…Theywerethereasiftheyaretourists.”(Pairo)

Chapter6
143
Figure6.11 Pairo’sBodyMap

Chapter6
144
Cleanlinessofthebirthingenvironment,includingthelabourtable,thetoiletsandtheoverall
cleanlinessofthehospital,isofutmostimportance.Thewomenwhogavebirthathomehadno
complainsaboutcleanliness.Mostoftheissueswerereportedamongthosewhohadabirthin
governmenthospitals,excludingoneofSita’sbirthataPHCwhichshereportedtobeveryclean.
Itiscertainthatthisisakeyaspectintermsofrespectfulnessforwomen.
“Mygoodness!Thetoiletwasdirty.Itwasverymuchdirty!Toomuchdirty!Dirtwaseverywhere.
Therewasevenmoredirtbecauseofnowater.Thewaterwasnotdrinkableandtheywereasking
ustodrinkfromthetoilettap.Ithadsuchastench!Dirtypiecesofclothdrenchedinbloodand
fluidseverywhere.”(Sujata)
“Theentirehospital…therewasbloodanddirtyliquideverywhere.Supposeyouhavesomeillness
andIusedyourdirtytoilet,willInotcatchitthen?Bloodyfloorseverywhere!Ididnoturinate
there.That’swhyIdidn’tgothere.Iwenttothejunglebehindthebushes.Thereweresome
abandonedbrokenhousesnearbyandjungle,butitwascleanerthanthehospital.Iwentthereto
urinate.Imightbedarkskinned,butIamverydisgustedbydirtI”(Amrita)
6.5.5 Respectful,disrespectfulandabusivecommunicationaroundchildbirth
Womenbarelyspokeinthebirthingroomanditbeginsfromtheminutetheysteppedintothe
hospitalcompound.Theyusuallycomeincontactwithhealthcareproviderssuchasdoctors,
nurse-midwives’andnonhealthcareprovidersincludingtheMamta,cleaner,daiandASHA.They
rarelyaskanyquestionsorobjecttoanythingthatisdonetothemduringandaroundchildbirth.
Asurrogatedecision-makerfromthewoman’sfamily,whomshemaynothavechosenatthefirst
place,takesontheroleofcommunicatingonthewoman’sbehalfwhowasoftenreferredtoby
thewomenas‘guardian’.Allthesewomenareabovetheageof18atthetimeofgivingbirth,
exceptone.
“Ihavenotaskedanythingtoanyone.Mymother-in-lawaskedeveryonewhateverIhadtoask…I
didnotfeelliketalkingtoanyone.”(Amrita)
“Iwasallalonethere…Icouldnotsayanything.IwasfeelingbadbutIcouldnotsayanything
becausewewereinthehospital.WhoamIsupposedtotell?...ifIsaysomethingtothemtheywill
say‘youarenottheonlyonehavingababyhere.Thereareotherstooandtheydon’thaveany
problem.Youdon’thavesomethingspecialdownthere.”(Ria)

Chapter6
145
“WhywouldIaskthem?Whatisthepointofaskingthemthingsunnecessarilywhentheeldersare
there?They(parents)needtoknowanddecidethings.”(Urmila)
Thelackofcommunicationfromthecareprovider’ssidebeginswhenthewomanisadmitted
undertheircare.Thelackofawelcomeisthefirstinstanceofdisrespecteverywoman
experiences.
“Welcome?!(laughs)…Whotalkswithyouanyway!...loudlyshesaid‘liedown’,Itoosaid,‘where
toliedown?’.‘Findanemptybedandliedown’shesaid.Iwentandlaydown”(Ria)
Thereisnointroductionoranyefforttoknoweachother’snamesbecauseknowingnamesisnot
consideredimportantwherecareprovider’sfirstwordsorinstructionstothewomanistolie
downandpartherlegs.Thatis,ifsheisspokentodirectlybythecareproviders,theusual
scenariowouldbeanurse,doctor,daiorMamtapartingthewoman’slegsforcefullywithout
sayingawordtoher.
“Theydon’tcareaboutthenameofpatient.Theywerenotcallingbyname.Theywerecallingby
whatishappening,ortoknowhowmuchpainoneisin.Therewasnoneedtocallaswewereall
justlyingdown.Therewasnohelloorthankyou!...whatwillIcall?Ishouted-‘listen’,‘Iamin
pain’,‘pleasesomeonecomehere’.”(Sujata)
Therewasalackofcommunicationaboutexaminationsandinterventions.Careprovidersdidnot
tellthewomenaboutthecaretheywerereceiving.Theywouldcomeandstartintravenousfluids
andgiveinjectionswithouttellingthemwhatitisfor.Itisnotjustaboutwhatisbeing
communicatedandhowitisbeingcommunicated;butalsowhoiscommunicating,asseenwith
Sita,whichwassomethingthatshouldsurelyhavebeenconveyedbyamedicalpersonnelandnot
aMamta.
“Theykeptmeinthehospitalforthreedaysandsaid‘wecansaveonlyone,eitherthemotheror
thebaby’Mamtasaid.”(Sita)
“Theycheckedwiththatmachineonmyabdomenandsaidthebabywillnotsurvive!”(Anju)
Thecommunicationaroundvaginalexaminationisespeciallysensitiveanditisanintervention
which,asSujataexplains,‘theworstaspectofgivingbirthinahospital!’.Clearly,itrequiresan
explanationandseekingconsentbeforestartingthevaginalexamination.Thedoctorsandnurses
wouldatbestsaytheyarecheckingifthe‘mouth’isopenornot.Participant’swerehorrifiedat
thelackofsensitivityandcommunicationaroundthisinterventionandwereleftfeelingashamed
andhumiliated.Thislackofcommunicationalsosubjectedthewomentoafearofnotknowing
whatisnextandleftthemexpectingtheworst.

Chapter6
146
“Shestarteddrawingtheinjectionandsettingupwater…Iwasreallyscaredtoseethis…she
askedformyhand.Isaid‘whatareyoudoing?’…howcouldIaskherwhatshewasdoing?We
don’task.Wedon’thavethehabitofasking…IgotscaredthatprobablyIshouldnothaveasked
anything,shouldnothaveinterfered.”(Sujata)
“Shesaid‘liedown,Iwillseeifthemouthisopen’.Sheinsertedherfingers.Shedidnotsay
anything.Iwasscaredandstartedscreamingveryloudly.Thedoctorsaid,‘shehasnopain
threshold,shecannothaveanormalbirth.’”(Pairo)
“Sheinsertedherfingersinsidemewithouttellingme.Theydidn’taskmeorinformme.”(Urmila)
Thelackofcommunicationwasn’tjustlimitedtoexaminationsandinterventions,thatmost
womenwentthrough.ThemostharrowingaccountcamefromPairowhowasdraggedtothe
operationtheatrebyanurseandontheoperatingtableshefiguredoutsheisgoingtobe
operatedaftershewasgivenaninjectionwhichmadeherlegsgonumbwhileshewasalso
blindfolded.HernarrationhasbeencapturedinherI-poemtitled‘Doll’inBox6.4.
Womenfeltlikeanobject,apassiveparticipantintheprocessandisolatedevenwhentheywere
surroundedbypeoplewhoweretheretotakecareofthem.Theyoftenfoundthatpeoplewere
talkingoverthemandnottothem.
“Ineverhadanyconversationwiththecareproviders.Theyweretalkingaboutme,aroundme,
butnottome…Afterdoingmycheckup,theyweretellingmyparents,notme,andIwasalsonot
talkingtothem.”(Urmila)
Someacceptedthislackofcommunicationanddisplayedanunquestioningbehaviornotbecause
thatistheirnature,asseeninsomeoftheearlierquotes.Itwasoftenledbythefearofinviting
obstetricviolenceandthefearofconsequences.Theyarriveatthehealthcarefacilityhaving
discountedonalltheirrightsandgivenuponalltheirchoiceswithanacceptancethatthereis
nothingtheycandoorsay,theyareexpectedtofollowinstructionstoleavethebirthingroom
withtheleastharmdone,evenwithsomeawarenessoftheirrightsinthebirthingroom.
“IfeelangrybutIamadmittedunderyourcare,soIwillhavetodowhatyousay.IfIdonotdoas
peryourorder,thenyouwillagaindosomethingtoharmme.Mymotherwasaskingmenotto
talkback,orargue,becausethesepeoplemightdosomethingulta-pulta(inappropriatetoharm
you)!”(Ria)

Chapter6
147
Box6.4 Pairo’sI-poem-Doll
Doll
Ihadnoguardiansaccompanyingme.
Iwasscreaming,Mummy!Mummy!
Iwastakeninside.
Ifeltliketheygavemeaninjection.
Ifeltmylegsweregettingcoldandnumb.
Icouldnotseewhogaveittome.
Ithinkaspecialisthadcomeforthat.
Iguesshewasananaesthesiadoctor.
Iguesshehasonlygivenmethatinjection.
Itrustthematleastthatmuch,thatanyrandompersonwon’tstickinjectionsinme.
Iwaswearingthesamenightie.
Ihadnotchanged,itwasdirty.
Iwouldhavefeltfreshiftheyhadallowedmetotakeabath.
TheymademeliedownonOTtable.
Iwassitting.
Iwasputtosleep.
Iwasblindfoldedwithcottonballsonmyeyeandthentherewasacloththeytiedontopofthat.
SoIwouldn’tseeanything.
Ifelt,thereweresomanymen.
Iwouldhavefeltuncomfortablebecausethereweremen.
Iaskedhim‘whereismadam(ladydoctor)?’
Iwasblindfolded.
Iheardavoicethatmadamhadarrived.
Ifelttheyremovedmyclothes,mylegshadnosensation.
Theydidnotconsidermeasahuman.
Theyweretreatingmelikeadoll!
Doingwhatevertheywanttodowithme.
Theywerenotaskingformypermission.
Ifeltsomeoneraisedmynightie.
Ifeltthisbecauseofthelossofsensationbelowmywaist.

Chapter6
148
Ifeltlikethis.
Iwaslyingdown.
Iwaslyingonthisadjustablething,theycouldturnitaroundastheywanted,totheir
convenience.
Theycouldjustoperatemelikethat.
Iremember,clotheswereremoved.
Ifeltso!
IfeltmylegsgettingcoldsoIthoughtmypetticoatwasremovedbysomeone.
Theydidnothaveanythingtodowithme.
Alotofmachinesandwireswereconnectedtome,onetomyheartandoneonmyfinger.
Myeyeswerekeptshut.
Idon’tknow.
Icouldnottellwhatwashappeningaroundme,orwhatwasgoingtohappennext.
Iwasconsciousbutnobodywastalkingtome.
Ijustlaythere.
Iwasnotsleeping.
Ikeptmyeyesclosed.
Iwashearingeveryone’svoices.
Icouldfeelthatsomeoneiscuttingmybelly.
Iwashearingthesoundofmachinesandinstruments.
Idid.
Iheardmybellybeingcut.
Icouldhearsomebodycuttingme,likecuttingajuterag.
Theycutme,tookmydaughterout,stitchedmeandsentmebacktomyroomimmediately.
IrememberprayingtoGod,sothateverythinggoeswell.
Idon’tknowwhostitchedmeorcutme.
Ididnotknowanything,nordidIfeelanything.
Myeyeswereclosed.
Ihaveadaughter.
Istartedimagining.

Chapter6
149
Iwillmaketwoponytailsandtakehertoschoolwithme.
Iwashappy.
Ihaveagirl.
IwasfeelinglikeIamadoll.
Ididn’tknowwhatwillbedonetomenext.
Mymothersaid,‘Theyweretreatingyoulikeananimal’.
Idofeelonething,thebadexperienceswerewithmybody.
Ilovemydaughteralotmorethanmyson.
Thosethingsdon’tmattertomeanymore.
Whathappened,happenedtomybody,myspiritisuntouched.
Mybabycameintothisworldthroughthatexperience.
Iamhappyaboutthat.
Ifeelthatthebadexperienceswerewithmybody.
IfeeltheythoughtofmelikeIamacoworabuffalooradoll.
Therewereacoupleofinstanceswherethewomensaidthatthenurseorthedoctorwastalking
tohernicely.Thiswasoftenararepersonamongstallthepeopletheparticipantswouldhave
comeincontactwith,whichmadethemsuspiciousovertheunusualnicety.Aparticipantalso
sharedhowthecareproviderdidnotproceedwiththevaginalexaminationaftersherequested
hernotto.
“ThenursewasthefirstpersonImetthatmorning.Shewascallingmedearone,dearone!She
wastalkingtomeproperly.”(Sujata)
“Mymaternaluncle,anMBBSdoctor,gavemearecommendationletter.She(therecommended
doctor)usedtogivemetimeandtalktomenicely.Iusedtowonderifshetalksnicelyonlywith
meorwitheveryone.”(Pairo)
“Theladydoctorandonesisterweregoodwhowerecaringforme.Thereweretwosisterswho
werealwaysfrowning,shoutingandscreamingatme.Sheabusedmesomanytimes.”(Urmila)

Chapter6
150
6.5.6 Respectful,disrespectfulandabusivepeoplearoundchildbirth
Fourtypesofpeoplehaveplayedarolearoundchildbirthinthehospitalsandhomes:1)qualified
healthcareprovidersinthehospital(nurse-midwife,doctor);2)women’scompanionsfrom
family/neighbourhood(husband,mother,mother-in-lawandothers);3)unqualifiedcare
providers(cleaners,Mamtas,dais)and4)mobilisers(ASHA).
Thequalifiedhealthcareprovidersincludednurse-midwives(mostlyreferredtoasnurseorsister
bywomen)anddoctors.Allthewomenwereexaminedandcaredforbydoctorsandnursesat
somepointduringtheirchildbirth(s)exceptinhomebirths.Theirinteractionswiththedoctorsand
nurseswererespectful,disrespectfulandabusivewhichalsoshapedtheirperceptionsfortheir
prospectivechildbirthandtheirexpectationfromcareingeneral.
Doctor’sroleduringchildbirth
Thedoctor’sroleduringchildbirthislimitedtovaginalexaminationsingovernmenthospitals,
aftertheinitialexamination.Intheprivatehospital,theyarealsoseenconductingcesarean
sectionandalsoperformingepisiotomyrepair.Participantshaduniqueinteractionswiththeir
doctors.Amritacameincontactwithtwodoctorsoverthecourseoftwochildbirths.She
experiencedobstetricviolenceintheformofdisrespectfulcommunicationfrombothofthem.
Thefirstdoctorinherfirstchildbirthrefusedtoassistherbirthbecauseshewasanaemicandthe
doctordidnotwanttotakearisk.Theseconddoctorshoutedatallherfamilymembersbecause
shevisitedthehealthcentreinlabourveryearlyinthemorningandthedoctorwantedtosleep
in.Afterrepeatedrequeststhedoctorarrivedinthelastminutetocatchthebaby.Pairocamein
contactwithfivedoctorsincludingonepaediatrician.Thefifthdoctorshemet,whowastheonly
doctorinhersecondcesareansection,wasrespectfultoher.Threeofthefourdoctorsshecame
incontactwithinherfirstchildbirthweredisrespectfulandabusive.Shewasn’tsureifthethird
doctor(seconddoctor’sson)wasadoctor,heronlycontactwithhimwasintheoperation
theatre,whilebeingblindfolded.Sheassumedhewasadoctorbecausehewasthereandhe
calledPairo’sdoctor,hismother.Shedidnothaveanyinteractionswiththefirstdoctorshesaw
inthegovernmenthospital.Shesawhimperformingvaginalexaminationwearingthesame
‘polythenegloves’,forwomenwhoqueuedoutsidehisclinic,soshelefttheplacedisgusted.
“TheyheldmedownbecauseIwasinpain…Iliftedmywaistandshe(doctor)pusheditdown
sayingthebabywillgetinjured.Then,Ineverlifteditup.”(Amrita)
“Theformerdoctor’sbehaviorwasnotgoodwithme.Ididnotlikeherbecauseshedidnottalkto
menicely.Sheusedtothinkveryhighlyofherselfasifsheisageniusandaknow-it-all!Sheused
tojustprescribewithoutexplainingwhatthemedicinesarefor.ShewasoverconfidentandIdon’t

Chapter6
151
knowwhatshethoughtofherself?ShethoughtverylittleofmeorthatIamworthnothing
comparedtoher.Didn’teventalktomemuch.Iusedtothinkthatitsmewhowillhavethisbaby,
atleasttalktome,saysomething!”(Pairo)
BothPratimaandUrmilacameincontactwithjustonedoctorwhilegivingbirthinaprivate
hospital.Urmilafoundherdoctortobeabusive.Pratimafoundherdoctortoberespectful.Urmila
wascaredforbytwodoctorsandshewenttothesamehospitalforallherbirths.Urmila’s
experiencewithherdoctorissharedthroughherI-poem‘Theladydoctorwasreallynice’,inBox
6.5.Whilethedoctorwasdisrespectfulandabusive,shetookcomfortinthefactthatitwasa
femaledoctor.
“Thenthepoorlady(doctor)searchedformyveinandgavemeaninjection.Shewasinnocentand
nicelady.Thewayshetookcareofme,Ifeltlikeherowndaughter.Ifeltgood.Iwasfeelinggood
becausethosepeopleweregoodpeople.Wewerehappy!”(Pratima)
“Onlyfemaledoctorcheckedmethroughoutmydelivery…IwasfeelingsomanythingswhichI
couldnotsharewithanyoneelse.Idon’tknowwhy.Iwassoangrywiththedoctorbecauseshe
calledmesomanytimesforvaginalcheck-ups…Ididnotlikeit.Thedoctorinthedeliveryroom
wasgood.Sheencouragedmewithherwords,‘Don’tworry,everythingwillbealright!’shesaid.”
(Urmila)

Chapter6
152
Box6.5 Urmila’sI-poem-Theladydoctorwasreallynice!
Theladydoctorwasreallynice!
Itoldhernottodoit,butsheforcedherhandinsideme.
Itoldherdon’tputyourhandin,itwashurting,butshecontinuedtodoso,didn’tlistentome.
Iwassoangrywiththedoctor,shecalledmesomanytimesforvaginalcheck-ups,everytime
shetoldmethepassagedidnotopen.
Ididn’tlikeit.
Iwasshoutingandcryingduetopainbutstilldoctorkeptonsuturing.
Iaskedthemfor‘behoshikidawa’(anesthesia),buttheywerenotlisteningtomeandkeptdoing
it.
Ithoughtmyproblemswereoveraftergivingbirth,buttherealchallengewaspostbirth.
Iwasscreaming,thedoctorandsisterswereholdingmedownfromallsidesandkeptstitching
me.
Ifeltallofit.
Ikeptscreamingandaskingforanesthesia.
Ifeltallofit!
Ididn’thavesuchpaininmyfirstdeliverywhilestitching.
Ilikedthebehaviourofmydoctorandoneofthenurses.
Ididn’tlikethosetwofrowningsisterswhoshoutedatme.
RiaandSujatahadalmostnointeractionwithanydoctorafteradmission,wheretheyhadonly
seenonedoctorlookingatlaboringwomenfromadistance.Bothofthembirthedingovernment
tertiarylevelhospitalsatthestatecapital,inabigroomwithfourtofivewomenbirthing
together.DoctorsappearedinSujata’sstorywhenshetalkedaboutbribes.Thedoctorwasseen
walkingaroundinbothcases,oftenjustatthefoot-endofthelabourtablewhilethewomen
birthedandnevercommunicatingwiththewomeninlabour.
“Therewasadoctor.Shegaveadvicetoeveryoneandwentaway.”(Ria)
“Myhusbandgaverupees1001tothedoctorand500tonurses.”(Sujata)
“Ifshe(doctor)hastoaskanything,thenshecanaskfromthere(foot-end)that‘areyouhaving
painornot?’or‘whatistheproblem?’…theydon’tcomeclose,theydon’tfeeltheneedforthat.
Thereisonlysomuchspacebetweenthelabourtablessothereisnoneedforthataswell.”
(Sujata)

Chapter6
153
Thelackofcommunicationwasacommonthemewithalltheparticipants.Thedoctorsdidnot
explaintheiractionsorproceduresanddidnotseekconsentfromthewomenforanything.When
theydidcommunicate,itwaswiththefamilymembers,ofteninthecareseekingwoman’s
absenceorintheformofinstructionstothenurseoraideforsomethingtheconsciousparticipant
iscapableofdoing.ThesamescenarioplayedoutinacompletelydifferentwayinPratima’scase
whereshefoundthedoctorwastalkingtohernicely.InPairo’scase,shewasnottoldthatshe
wouldundergoacesareansection,herparentsalsodidnotinformher,shefoundoutafterspinal
anesthesiawasgivenintheoperationtheatre.
“She(doctor)askedtothenursetobendmyleg.”(Pairo)
“Shesaid‘liedownandholdyourlegswithbothhandsandIamcheckingyou’.Sheaskedmeto
liftup(mysaree)andIdidthesame.Thenshecheckedme.Noonewasthere.Justmeandher
(doctor).”(Pratima)
“Thedoctorhadalreadyspokenwithmymotheraboutthis(cesareansection).Theydidnottell
meanything.Theyjustkepttalkingamongstthemselves,noinformationhadcometome.”(Pairo)
TwopediatricianswerementionedinPairoandSujata’snarrative.Inprivatehospitalsthey
seemedtohavemoreresponsibilities,whichincludedgivingmedicineandinjectionsandstarting
theintravenousline,alongwiththeirinitialroleinsendingthewomenforadmissionandsigning
fordischarge.
Nurse’sroleduringchildbirth
Womencouldconfidentlyidentifythedoctors,bytitleorbysensingthepowerdynamics.Any
womancaringforthemwasconsideredanurseandeventhoughtheyconfidentlysharedan
interactionaboutthenursetheyweren’tsure.Therewasnointroductionabouteachother’srole
betweencareproviderandcareseekerduringtheirstayatthehospital.
“Yestheywerenursesonly.Shewasgivinginjectionandhelpinginthebirth.”(Pratima)
“Shegavehertwotightslapsonherface.Iguessshewasasister(nurse).Yes,theyweresisters
only.”(Ria)
“Nursemeansdai!”(Sujata)
“Iwasinthewaitingareawhennursesapproachedme…theladieswhodoallthecleaningwork
aroundbirth…theytookmeinsidethelabourroom.”(Urmila)

Chapter6
154
Nursesareusuallyreferredtoas‘sister’.Nursesatthetertiarygovernmenthealthfacilitieswere
seengivinginjections,runningIVfluids,augmentingandperformingepisiotomyrepairs.Atthe
secondaryorprimarylevelofcareprovisiontheywerementionedwithsimilarrolesbutnotfor
episiotomyrepair.
“…nursesdon’tgetinvolvedincleaningworkusually.”(Amrita)
Intheprivatehospitalitwasnotclearwhetherthepeople,participantswerereferringtoasa
nurseorsister,wereactuallylicensednurses.Theywereoftenonlyseeninthebirthingarea.In
bigprivatehospitals,theywereseendoingmultiplevaginalexaminations.Onenursewas
mentionedasperforminganabdominalpalpation.Butmostwereseenfollowingdoctor’s
instructionstoparttheparticipant’slegsortorestrainherforvaginalexaminationorduring
episiotomyrepair.Itseemslikebeinganaideinobstetricviolencebyphysician’sorder.
“Therewasjustoneoldnurse.Sheshiftedmetothatroomforbirth.Shecheckedmefromupon
theabdomen,notbelow.Thentookmeinsidetheroomandgavemeaninjection.”(Sita)
Mostparticipantscameincontactwithnursesandoftenmorethanone.Theysharedhownurses
workedinshiftsintertiaryhospitals,oraboutanurseataPHCwhomtheyhadknownforyears,
whohadpassedaway.Thischangeinrelationshiporinknowingthecareprovider,wasseen
betweenurbanandruralareas.Itdidnotnecessarilyhaveanyeffectontherespectfulnessofcare
thesewomenreceived.Therewerecontrastingopinionsonwhetherthenurseswereinvolvedin
extortion.Sujatafelttheywere,thoughothersfelttheywerenot.Inprivatehospitals,theywere
seenaskingforhappinessmoney.
Communicationwithnurseswaslimited,although,oneconversationwithPairo’smotherstands
out.Theabsenceofanydisrespectfullanguageandactionsoftencountedasbeingrespectfuland
insomecasesitinvolvedspecificactionsthatconveyedrespect.
“Anurse…toldmymotherthattheclothesofpatientareremovedatthetimeofoperationinthe
OT.Butshedidnotlikethatatall…thereareladiesandgentseveryone.Shesaidshetriestokeep
thepatientsascoveredaspossibleinthatsituation.”(Pairo)
“Outofthosethreenursesonewasverygoodbecausesheusedtoholdmyhandinbetween
labourpains.”(Urmila)
“Shewastalkingnicely.Shewassayingnottopanicandthateverythingwillgowell.”(Sita)

Chapter6
155
Dai’sroleduringchildbirth
Daiwasoftenconfusedwithanurse,MamtaandASHA.Daiwasmentionedbywomenwhogave
birthatalllevelsofgovernmenthealthcaredeliverysystemandathome.Withthewomen
interviewedintheruralarea,Sita,AmritaandAnjumentionedthepresenceofadaiaroundtheir
birth.Intheurbanareainterview,Ria,SujataandPratimawereaidedbydaisintheirchildbirthas
well.SitaandAmrita’snarrativeshedslightontheirroleintheprimarycarehospitalwherethey
cleanthebirthingarea,callthedoctorswhenneededandrestrainwomenwhenrequired.Dai
oftenaccompaniedwomenfromtheirhomestothehospital,iftheyarefromthesame
neighbourhoodorvillage.
SujataandRiahadsimilarnarrativesofdai’spresenceinthelabourroomandtheirroleduring
childbirth,eventhoughtheygavebirthindifferenttertiarylevelhospitalsinthestatecapitalof
Bihar.Theycameincontactwithmanydais.Twotothreedaiswereseenassistingtheirbirthsand
thatofthewomenbirthingonthefourtofivelabourtablesnexttothem.Daisreportedlyworked
indifferentshiftsandwereattheforefrontofaskingformoneyateverylevelofpublichospital.
Peoplepaidalottodaisatthetertiarylevel,especiallybecausethereweresomanyofthem.
“Thedaiaskedfor5000rupees,1000rupeeseach…‘areyougivingmealms?AmIabeggar?You
keepit,youaretreatingmelikeabeggar…’Therewerethreedaisinoneshift.Theyusedtocome
forcleaningandmopping.Thedaiswhosweepthefloorarenotthesamedais.”(Ria)
Sita’s50-year-oldmother-in-lawhasbeenadagarin(dai)forover20years,assistingbirthsinher
villageandnearbyvillages,yetSitainsistedongivingbirthatthehospital.Sita’smother-in-law
goestowomen’shousesandputsherhandinsidetoknowhowmuch‘themouth’isopen‘one
phinter,twophinter’.Shegivestheinjectionssothefoetuscancomeoutquickly.Shealsostocks
IVfluidsathome.Herworkisinlessdemandbecausethehospitalsarefunctioningbetter.Sita
sharedthatdagarin/daisfromthevillageareelectedtoworkinthehospitalsometimesbuther
mother-in-lawwasnotselected.
Atthehospital,thedaiswereseendoingeverythingfromgivinginjections,vaginalexaminations,
episiotomy,assistingbirths,weighingbabies,conductinguterineexplorationandcleaningthe
labourtablethereafter.Thedoctorornurse’sroleinthelabourroomwasthebareminimum.
Theywerealsomentionedinrelationtomuchoftheabuse.
“Theyweresaying‘youarescreamingunnecessarilywhilejustproducingonechild.Howmuchwill
youscreamwhenyouproducemore!Wehaveallbirthed15childreneachandneverbehavedlike
you.’Daisweresaying.Onewasstandingnearmyfeet.Shewasanoldlady,keptsayingrubbish
anddisgustingthings.”(Ria)

Chapter6
156
“Mydeliverywasdonebydais.Daigavemeaninjectiontoo…sheworeagloveandcheckedme
byputtingherhandinside…threedaiswerethere…saying‘push,push’…theywereconductingthe
delivery…Iwasnotabletofigureoutwhowasdoingwhat.Whenthebaby’sheadwasout,all
threewerebusyremovingthebaby…oncethebabywasouttheycleanedeverything.Theytorea
clothandwipedthebabyandcutthecordlater.Theyremovedtheplacentabyapplyingpressure
ontheabdomen.Shetookitoutbyputtingherwholehandinsideandcheckedsothereisnodirt
leftinsidetheuterus…sheheldmyhandandgotmyclotheschanged.Askedaboutmypainand
gavememedicine.Theywerenotlettinganyone(fromfamily)goinsideatthetimeofbirth
becausetheywerethere.”(Sujata)
DaiassistedAnju’sthreehomebirths.Pratima’ssecondbirthwasassistedbyadai,asshownin
herbodymap(Figure6.17).Shewantedherfirstbirthathomeaswell,butthedaisentthemto
hospitalaftershethoughtthelabourhadlastedtoolong.Thisissimilartothepatternwithbirths
inpublicsectorhospitals,beittertiarylevelhospitalorathome.Birthsassistedbydaisareseen
withPratima(Figure6.12)andSujata(Figure6.13).
“Shedidallthedeliveries.Dagarincameat12atnight.Shewasmassagingmyhandsandlegs.
Shecutthecordwithblade.Shemassagedthebabywithoil.”(Anju)
“Myfather-in-lawwentandbroughtthedaihome…wheneveryougotocallher,shecomes.Poor
thing!Eveninthemiddleofthenight.Sheisanoldwidow.”(Pratima)

Chapter6
157
Figure6.12 Pratima’sbodymap

Chapter6
158
Figure6.13 Sujata’sbodymap

Chapter6
159
ASHA’sroleduringchildbirth
ASHAswerementionedinAmritaandSita’sstory.Herroleistocalltheambulanceandhelpthe
womanreachthenearbyinstitutionforbirth.ShealsoaidsingettingtheJSYincentive.Butin
bothcasesthewomenhadnotreceivedtheirJSYincentivesfortheirrecentbirths.On
complainingaboutthistotheASHAs,theyblamedthecomplainants,sayingthattheyprobably
receivedthemoneyandspentit.ASHAswerealsoseenhelpingtogetthebirthcertificate,but
theychargedafeesof300rupees.Inthelabourroom,theyweresometimesseenrestraining
womenwhoaregivingbirth.OneparticipanthadanASHAwhowasafamilymember.Participants
oftenfounditdifficulttodifferentiatebetweenwomenaroundbirthandcouldnottellASHAand
mamtaapart.ASHA’srolewasthatofamediatorofservicesandamotivatorforthewomenand
familytoseekhealthcareservices.
“Sheisinmymaternalhousehold.Sheisourfamilymember,soshehaddonealltheproceedings.”
(Sita)
“Igavehermypassbookandtoldherifyoudon’tbelievemethenwhydon’tyoucheckit.Itoldher
‘youthinkIwillgrowricherby1400rupees?’Thenshetookandupdatedthepassbookbutshedid
notfindoutanything.ShesaidnowIwillnotgetthemoney.”(Amrita)
Mothersandmother-in-law’sroleduringchildbirth
Motherandmother-in-lawwerenotmentionedtobetogetheraroundbirth.Amrita,Sitaand
Pratimahadtheirmother-in-law’spresence,whilePairo,Ria,UrmilaandAmritahadtheirmother
besidethem.Sister-in-lawswerepresentatSujataandPratima’sbirths.Theirrolewasthatofa
femalefromfamilywhowasaroundtocallthecareproviderswhentheyfelttheneedand
facilitatecommunicationfromthefamily.Womenwereaskingquestionssuchas,howlongwillit
taketogivebirth.Theydidnotnecessarilyconveytheinformationtothebirthingwomen,asis
seenwithPairowhowasn’tinformedbyhermotherthatshewasgoingtobeoperatedthenext
day.Theycommunicatedtheinformationtorestofthefamilymembers,includingthehusband/
fatherofthechild.Theymadesomedecisionsaroundbirthtoo.Mother,mother-in-lawand
sisters-in-lawswereamongstthefamilymemberswhorestrainedthebirthingwomen.Sita’s
mother-in-lawinterruptedtheinterviewafewtimesandalsotookovertheconversation,untilwe
couldtalkprivatelyagain.
“She(mother)washoldingmyclothesandkeepingmylegsdown.”(Amrita)

Chapter6
160
Womensaidtheypreferredtheirmother’scompany,exceptUrmilawhofeltveryangrywithher
mother’spresence.Riafeelshermothersavedherbaby’slife,aftershemadealotofnoise
becausethedaisannouncedastillbirthand‘threw’thebabyunderthetable.Thisiscapturedin
herIpoem(Box6.6).Pairohasasimilarstorywherehermotherfoundthenewborn’scordstump
bleeding,hoursafterbirthandreportedtothedoctors.
Box6.6 Ria’sI-poem-Thedeadbaby
Thedeadbaby
Mybabywasbornwithgreatdifficulty.
Mybabywasmovinginmywomb,butafterbirtheveryonesaidthatthebabyisdeadandtheythrewmybabyunderthetable.
Mymothershoutedatthem,‘Howcanthebabybedead?’
Mymothertoldmethebabyisdead.
Iwasnotawareofitwhileitwashappening.
Mymotherwentthereandquestionedeveryonebecausethebabygetsexchangedoften.
Ididn’tknowanythingafterthat.
Iwasjustlyingdown.
Iwasinalotofpain.
Iwasdrowsy.
Iwasrestlesstooandmymotherwenttothebaby.
Iaskedmymother,‘howisshe?’
Irepeatedlyaskedmymotherhowthebabywas.
Iwouldhavebecomefamiliarwiththem.
Iwouldthinkthat‘Yes,Ihavesomeonehere’.
Iwillfeellessafraidandnotpanic.
Mymotherwouldhavebeenthere.
Ihadthebaby,afterhalfanhourtheystitchedmeupandIwasalmostunconscious.
Iwasunconsciousandtheyshiftedmetoanotherroom.
Iwouldhavenotknownaboutthebaby.
Mymothersavedmybaby!
Iwasupstairs,mybabywasinNICU.
Ihadtopaytoseemybaby,whomIgavebirth!
IusedtosaythatIamgoingtotellthistohigherauthority.
Iwassaying,‘letusseethebabyonce’.
Irequested,‘showmefromafaratleast.Howismybaby?’
Mybabyfinallycameinmylapafter8days.
Mybabywascoveredinherstoolafter8days.
Iexpressedmilkinaglassandgaveittothem.
Iwasnothappyfortwentydaysatleast.

Chapter6
161
Iusedtobeveryrestless.
Istartedspendingmoretimewithmybaby,Iusedtofeelmuchbetter,satisfied.
Womendidnotchoosetheirbirthcompanion.Womenoftenfelttheyhadnochoiceinmaking
thatdecisionandfoundthathavingtheirmotheroranywomenamongstrelatives,wasthemost
acceptableoption.Sujatawastheonlyparticipantwhofreelyexpressedherwishtohaveher
husbandbyhersideoveranyoneelse,butshedidnotvoicethatchoiceduetosocietalbarriers.
Shealsohadtofollowtraditionalnorms,suchaswearingsignsofmarriage,becauseherin-laws
werepresentduringchildbirth.Theyalsohadaroleinconvincingwomentoacceptinterventions
thattheydidnotagreewithandfelttheyhadnochoicetodeny.
“Iwaswearingbindiandvermillion,becausemyin-lawswerethere.”(Sujata)
“Mymothersaidtolether(nurse)checkonce.”(Sita)
“Ididnotwantanyonetotouchme.EvenwhenmymothercametoholdmeIfeltlikeIwillhit
her…itwasnotcomfortingme…mostofthetimeshewasjustsittinginthelabourroom.WhenI
waswalkingshewastryingtoholdmyhand,Ididnotlikethat.Iwantedtodoitonmyown.
What’sthepointofholdinghand?Itmakesmelookweak!”(Urmila)
6.5.7 Respect,disrespectandabuseinpersonalspaceandrelationships:householdand
husband
Therewerenodirectquestionsaboutwomen’shouseholdenvironmentotherthanhousehold
incomeandsourceofincome.Womensharedabouttheirrelationshipwiththeirhusband,while
talkingaboutthebirthcompanion,theirhusband’soccupation,themainsourceofhousehold
incomeandtheirhusband’sroleduringchildbirth.Womenoftenworkeduntiltheywentinto
labour(pleaseseePratima’spoem‘Bornathome’inBox6.3andAmrita’spoem‘I’inBox7.2).
Thisincludedtheirpaidworkandunpaiddomesticwork.Thisworkwasoftendescribedasa
burdenthatwasrarelyshared.Oftheeightwomeninterviewed,fourdidnotengageinpaidwork.
Anjuisalaboureronothersfarms;Riaworksasacleanerandrearedcowstosellmilk;Amritaran
asmallgroceryshopandPairoisagovernmentschoolteacher.RiaandAnjuarethesoleearners
ofthefamily.AmritaandPairo’sincomewassupplementedbytheirhusband’s,buttheyranthe
household.Anjuhadthelowesthouseholdincome(1000rupeespermonth),forafive-member
familyandPairohadthehighesthouseholdincome(65,000rupeespermonth)forafour-member
family.Womenwhoengagedinpaidwork,managedallthedomesticworkaswell.Womenin
jointfamiliesordomiciledattheirmother’splace,wereabletorestforthefirstfourtosixweeks
aftergivingbirth,thiswasfoundtobeacommonnorm.Thiswasnotpossibleinnuclearfamilies.
Chapter6
162
“Nooneistheretolookaftermykidsandfamily.Ionlygotothemarkettopurchasegroceryfor
theshop.Ileavethechildrenforafewhoursattheanganwadi.Iwas8monthspregnantandhad
tolift25kgjutesacks.”(Amrita)
“Afterthefirst3monthswhenmymotherwenthome,IusedtowashclothesandIusedtositand
feeltiredandthinkhowwillIgobacktoschool,howwillItakecareofmybabyandhowwillIdo
everything?TwomonthslaterIstartedtakingbauua(daughter)toschool…itwasquite
troublesomebutImanaged.”(Pairo)
“AtleastinthefirstmonthandahalfIdidnothavetodoanything.Usedtojustroamaround.
Cookedfoodwasbroughttome…Iwasatmyin-law’shouse.”(Pratima)
Womenfeltshytalkingaboutpregnancyandbirthwiththeirhusband,andthenarrativesdepict
thatthiskindofconversationwasnotnecessarilyencouragedbetweenthem.Box6.7showsRia’s
communicationwithherhusbandwhensheannouncedherpregnancytohim.Hernarrative
showshowherpregnancyledtoherseparationfromhim,whicheventuallyledtoadivorce.She
recountedexperiencingintimate-partnerviolencefromherhusbandandoflivinginaviolent
domesticenvironment.

Chapter6
163
Box6.7 Ria’sI-poem-Ithasstayed
Ithasstayed!
Iusedtoaskwhatthedoctorsaidexactly.
Myfriendsaid,doctorusedtosaythat,‘whenyoudon’thavethestrengthtogivebirthandbearthepain,thenwhydidyoukeepthebaby?’
Myhusbandtoldmethathewantsason.
Itoldhim,‘Myperiodshavestopped,IguessIampregnant.’Hecurledhislipsinangerandsaid,‘Idon’twantababyrightnow’.
Igotpregnant.
Ididnoteatordrinkmuch,IusedtoliftheavyweightandIusedtocarrytwobucketsofwater,atatime.
Ihavebeenmarriedfor6years.
Myhusbanddoesnotstaywithme.
Iamdivorced.
Iwaspregnant,hedidnotgivemeanymoney.
Ialsosaid,‘Don’tgive!’
Iwentforthedelivery;hedidnotgivemoney.
Iwenttohospitalwithmymother.
Icalledhimfrommymother’sphonebuthedidnottakemycall.
Ialsoleftitlikethat.
Iwasscared.
Iwasnothappy.
Itoldhim,evenifIampregnant,Iwillnottakeapill.
Iwillnottakethatpill.
Ialsotoldhim,‘don’tdo,Iwillmanage’.
Isaidtomymotherto‘helpme.Idon’thaveanythingtodayandIdon’tearn,Ihavenoonetospreadmyhandsinfrontofformoney.Yougivemetoeat’.
Ialsosaidthendon’targuewithme,whotoldyoutoarguewithme…abuseme.
Urmiladisclosedaboutherhusbandbeinganalcoholicandabusive,whichledtohercallingthe
police,followedbyhisimprisonment,asseeninherI-poeminBox6.8.Nothavingaproductive,
respectfuldialoguewithhusbandwasacommontheme.ThiswasseenwithSujataaswell,who
wasotherwisequitefrankwithherhusbandabouteverything.Husbandsoftenconveyedtheir
opinionaboutthefamilysize,andtheirwordwasusuallythefinaldecision.
“Myguardian(husband)didnotletme…saysourchild(son)remainsverysick.That’swhyIdid
notgetitdone.They(in-laws)saidyouhaveonlytwochildren.Operation(tubectomy)wasmy
thought.”(Amrita)

Chapter6
164
“Icouldnotaskhim‘howwillitcomeout’.ButhewishedIwoulddelivernormally…hesometimes
says‘doyouwantmorechildrenthatyoudidnotgetfamilyplanningoperationdone?’.Inthe
secondtimehesaidregardlessofboyorgirl,gettheoperationdone…ifthebabyishealthythen
onlyIwillgetitdone.NeitherIhavedonetheoperationnorhehas.Itellhimwhydon’tyougetit
done.Hesays‘Iwillhavetositandworkallday,Iwillgetweak!’.Sonowwheneverweget
intimate,Itellhim‘mylifeisinyourhands!’.Hegetsscared!(laughs)”(Pairo)
“Ifeeltwokidsareenoughbutmyhusbandkeepssayinghewantsonemore.Asin,ason!Isay
see,asonisbornoutofgod’sgrace…howwilloneoperate(Vasectomy)onhusband?!(shocked)
No,no,no…ahowcanamangetoperated!”(Sita)
Box6.8 Urmila’sI-poem-Inevermadeadecisionaboutmyself
Inevermadeadecisionformyself
IleftmyeducationwhenIwas13.
Igotmarriedveryyoung.
Ihavenoideaaboutmoney,myhusbandtakescareofmoney.
Idon’tknowwhatheearns.
WhatdoIhavetodoaskingaboutmoneyanyway!
Iputmyhusbandinjailbecauseofhisaddiction.
Ishouldnothavedonethat.
Idon’tknowwhenmyhusbandwillbereleased.
Iwasbetteroffalone.
Iwouldhavedonesomething,earnedsomemoney.
Ijustdon’tlikewhenhecomeshomedrunk.
Ifeellikelockingmyselfinanotherroom.
Ididnotlikethesmell.
Myhusbandhadmoneytodrinkalcoholbutnomoneyformychildren’seducation.
Ifeel,Ishouldjusttakecareofmychildren.
Iwillfindthemoneytofeedthem,evenifIdivorcedhim.
Hedrinksandhitsme.

Chapter6
165
Iputhiminjail.
Noneofthehusbandswereallowedintothebirthingenvironmentinthehospitalsettings.The
husband’srolewaslimitedtocallingforthedaiorambulance.Inthehospitalsettinghusbands
paidthebills,paidthebribestocareworkers,boughtthesuppliesinstructedfromthehospital
andwaitedoutsidethelabourroomoroperationtheatre,asseeninthecaseofSujataandPairo.
Amrita,SitaandPratima’shusbandscouldnotmakeittothehospital.Amrita’shusbandwas
workinginanotherstate,asheisamigrantworker,andanothertimehedidnotwanttogotothe
hospitalbecausethebabywasgoingtobebroughthomeanyway.Pratima’shusbandisarag
pickerandcouldnotmissaday’sworkashewasearningadailywageof250rupeesthatensured
foodfor22householdmemberseveryday.Pairo’shusbandworksinabankandwasawayduring
thetimeofherpregnancybutarrivedrightbeforechildbirthfromanothercity.
Thehusband’spresencearoundchildbirthwasn’talwaysdesired,asnarratedinAmrita’sIPoem
inBox6.9andshowninherbirthmapinFigure6.14.Sujatawastheonlyparticipantwhowanted
herhusbandtobethereduringherbirthsasmentionedintheprevioussection.Anju’shusband
playedakeyroleinallherbirths,fromcallingtheambulancetoaccompanyherforfirsttwobirths
whichwerestillbirths,followedbycallingthedaiforhomebirthinhernextthreebirths.Heeven
assistedherfirsthomebirthasthedaiarrivedlateandhewaitedoutsidetheroomfortherestof
thetwobirths.
“Nonono…whywillIcallmyhusbandtoholdme!Iwasinsomuchpain!Ididnotthinkof
husbandandall.”(Sita)
“Tofranklytellyou,itwouldhavebeenmostencouragingifmyhusbandwastherewithme,but
mencannotbethere.Theyarenotallowed.So,ifheisn’tthere,itdoesn’tmatterwhois!All
othersaresame!Husband’spresenceissomethingentirelydifferent.Inthisconditiononly
husbandisneededmore.”(Sujata)

Chapter6
166
Figure6.14 Amrita’sbirthmap

Chapter6
167
Box6.9 Amrita’sIpoem-Becauseofhim,Iaminthissituation!
Becauseofhim,Iaminthissituation!
Ifeltgood!
Iaminpain,obviouslyIgetveryangrywhenIwilllookathim.
IalsogetangrywheneverIwasinpain.
Iamthere,justbecauseofhim,Iamhereinthissituation.
Ifeelheshouldbeaway.
Ididn’twanthimtobetherewithme.
Idon’tknowaboutitexactly,guardianspaidthatbutthepeoplewhowerecleaningthere,theyallhaveaskedformoneytoeatsweets.
Idon’tknowhowmuchtheypaid.
Ididn’taskanythingtoanyone.
IwasjustprayingtoGodsoIdon’thaveanymorebabies.
Iwascrying.
Ididnotfeelliketalkingtoanyone.
Iwasthinkingabouttheoperation(tubectomy).
Ithinkthereisnopointofhavingmorethantwochildren.
Iwantedtogivethemagoodlife.
Iwantedtosendthemtoschoolforeducation,whichIhavenotreceived.
I[could]gothereforoperation.
Ididnotgetitdone.
Myguardian(husband)didnotletme.
6.5.8 Birthinginformation,birthpreparednessandmythsaroundbirth
Womendidnottalktoothersaboutpregnancyandchildbirth.Theyoftenhadnoinformation
whengivingbirthforthefirsttime.Noneofthewomenhadanydiscussionaboutpregnancyor
childbirthwiththeirhusbands.Anycommunicationwaslimitedtosomeconversationswithother
womenintheneighbourhood,whichwaslessoften.Oneparticipantdiscusseditwithhergrand-
mothertoo.Theinformationsharedamongstwomenwerenotalwayscorrectandfullofmyths.
Womenwereaskedtoeat,drinkandrestwhiletheyarepregnantandleaveeverythingtoGod.
Nobodytalkedabouthowthebabyisbornorotherdetailsofitforvariousreasonsincluding
shame,asSujatashared.
“Inwinterstheydon’trunwater(IVfluids)becauseitissocold…myneighbourhoodsistertoldme
theyranwaterandthebabycameoutquicklyafterthat.”(Amrita)

Chapter6
168
“It’sasayingthatiftheenvironmentishotter,thebabywillcomeoutquicker.Likeifsomeone
doesnotwanttohavethebabywhensheispregnant,everyoneadvisestoeatanddrinkhot,like
cardamom,whichhasheat.Thatheatsupthebodyandthebabygetsspoiled/wasted.Thesame
waywhengivingbirth,heatwillcausethebabytocomeout.Womenwhoseexpecteddateof
deliveryisupwillhaveasafedeliveryandthosewhoseduedateisfarwillgetitaborted.
Definitelyitwillgetspoiled!”(Sujata)
“Babywaspoisonedinsidethebellyfor3monthsanditstayedinthebellyandmotheralsodied
becauseofthatpoison.(Aladyfromthenearbyvillage)”(Anju)
“Mymotherinlawusedtosayifyouwanttoeatsourthenyouwillhavedaughterandifyouwant
toeatsweetyouwillhaveason.ItoldherIlikeboth.ShesaidthenIwillhaveadaughter.”(Ria)
Womenwereshytotalkaboutbirthwiththewomenaroundthem,withtheirhusbandsandwith
healthcareproviders.ThestigmatotalkaboutbirthcanbeseeninPairo’sI-poemtitled‘Itwas
myinnocence!’inBox6.10.
“Iwasveryanxiousduringmyfirstbirth.Ididnotaskaboutittoanybody.Iwasfeelingvery
ashamedandnotunderstandinganythingsinceIwasveryyoung.Iwasveryashamed.Howwill
theydoit,whattodo,forallthatIwasnervous.”(Sita)
“Ididnotknowbeforehand.IneverwenttohospitalsohowwouldIknow?Idon’ttalktoanyone.
Therewasafairwomaninthenexthouse...Iusedtodiscusswithhersometime.Idon’tgooutof
thehouseatall…whatwillhappenwillbeGod’swill,whenGodwillwantittohappen.It’snotin
ourhands.”(Pratima)
“Youknowhowwomentalkaboutthesethings…theyusedtoshareithappenedlikethisandlike
that.Oneofmyfriendssaidthatdoctorsaid,‘whenyouyoudon’thavethestrengthtobearthe
painandgivebirth,thenwhydidyoukeepthebaby.’Everyonegetstohearthis.Thisisvery
normalconversationaroundchildbirth.”(Ria)

Chapter6
169
Box6.10 Pairo’sIpoemaboutconversationaboutbirthingandpreparedness
‘Itwasmyinnocence!’
Iwasbornin1990.
Iamaschoolteacher.
IampursuingmyMAdegree.
Icallmymothertotakecareofmykidsandfamily.
Ikeepaskinghertocomehere.
Iamtheeldest.
Imusthavebeen10yearsold.
Ihadtomindhim.
Ihadtotakehim.
Iusedtobeathimalot.
Iremember,whenIwasunabletotakecareofhimasachild,sowheneverhecried,Iwouldbeathim.
Ididnotknowwhattodowithhim.
ItoldthistohimthatIusedtobeatyoualotwhenyouweresmall.
ItoldhimthatIusedtodothiswithyou.
Isometimesthinkthatit’snotpossibleforamothertotackletoomanychildren,sosheputsthatburdenofresponsibilityonhereldestchild.
Idothattoo.
Itellmydaughter“youmusttakecareofyourbrother”.
Icompareitwithmychildhoodwhenmymotherdidthesame.
Ithinkthisisagiventhingtodo.
Igotmyjobhere,sowestayedhere.
Ihavealsostudiedfrommymaternalgrandmother’shouse,notevenfrommyownmaternalhouse.
Iusedtolivethere.
Ididnotunderstandsomuchaboutthesethings.
Ihavealwaysjustkeptmyfocusonmyeducation,thensuddenlyIgotmarriedandhadchildrenquitequicklyafterthat.
Igenerallydidnotpayattentiontothesethings.
Ididnottalkaboutthiswithanyonemuch,didnothavemuchinformationaboutthis.
Ihadneverheardaboutit.
Iusedtothinkthatthebabyhasgotteninsidemywomboneway,buthowwillitcomeoutnow(laughs).
Itoothoughtsinceitwalkedlate(inthewomb)thenitwouldbeason.
Iwascarefreeaboutit.
Ithoughtit’sfineandIampregnant.
Ijusthavetokeepeatingandgotowork.
Ikeptgoingtillthelastmonth.

Chapter6
170
IwaswaitinginmyhousethatIwillhavepainanymoment.
Iwasthinking,howwillitcomeout?
IusedtolivealonewhenIhadthesethoughts.
IwasnotsayinganythingtoanyonebecauseIwasthinkingthatthesepeoplewouldthinkaboutmywellbeingonly.
Ibelievethatthesepeopleshouldhavetoldmethis.
Iwasjustapatient.
Ineverdiscussedaboutitwithanyone.
IknewthatIwouldhavenormalbirth.
Iwashappythatmysecondbirthwillbenormal.
Iwantedtoexperiencenormalbirth.
Iwillcometoknowhowwomengivebirthnormally.
IneverevenwatchedavideoonYoutubeabouthowbabycomesoutofthemother’swomb.
Ineveraskedthesethingstomymotheroraunt.
Ineversharedthesethingswithmymotheroraunt.
Ithoughtitwillhappensomehow.
Iwasthinkinghowwillithappen.
IusedtomeetmydoctorforUSG.
Iusedtoaskherpleasetellmewhatisinsideotherwisemyhusbandwillfeelangryeventhoughhewon’ttellmeanything.
IassumedIhaveadaughter,ithadtobeagirlsinceshewasnottellingme.
Iusedtothinkthatitwouldbeason.
Ithinkbecauseofmymindsetwhenwassheborn,shewaslookinglikeaboy.
IthoughtsecondtimeIwillhaveagirlbutitwasaboy.
Ilovehermore.
IusedtotellmybrotherandsisterthatIdon’tlikehimmuch.
Withnoonetotalkto,SujatalookedintoYoutubeforinformationonbirthingandcareduring
pregnancy.Womencarriedmanythingswiththemwhentheywenttotheinstitutiontogive
birth.Wearinganightiewasacommoninstructionthateithercamefromthecareprovidersoras
asuggestionfromwomenintheneighbourhood.Womenoftendidnotwearanyjewellrywhen
theyweregoingtogivebirth.Theycarriedaseparatesetofclothestochangeafterandoldcloths
tobeusedduringbirthinthehospitaltocleanthebaby,thewomanandthelabourtable.
“Wecarriedeverything.Petticoat,nightie,bedsheet.Notpads,theygaveusthere.Theclothes
whichonewearsatthetimeofbirth,theythrowitbecausetheybecomedirtygivingbirth.That’s
whywecarryextraclothes.Theyremovedallmyclothesandaskedmetowearanightie.”(Sita)
“ItshowsonYoutuberight,whatisgoodtoeatandwhatnot.Iusedtowatchit.Myhusbandhas
amobilephone,Iusedtosearchinthat…Iwouldengageinthesemischiefsaftermyhusband
wouldsleepoff.Iusedtolookforallthesesecretly.”(Sujata)

Chapter6
171
Womenfounditdifficulttodeterminewhoisgivingtherightinformationandoftentheywillonly
getthatclarityaftergivingbirthforthefirsttime.Womendidnotfeeltheneedtotalktoanyone
aboutit,asUrmilashared.
“Ihavenevertalkedaboutmybirthswithanyone.Ididnotfeeltheneedtotalkaboutthiswith
anybody.Wedonothavethecultureoftalkingaboutbirth,beforeorafter.Iwasnotabletotalk
aboutthistomymother,husbandanybody.IdidnotknowIneededit,aftertalkingtoyouI
realised,Ilikedtalkingaboutmybirth.”(Urmila)
6.6 Discussion
Breakingthesilencethroughbirthmapping
Womenweresurprisedtofindsomeoneknockattheirdoorwiththepropositionofhearingtheir
birthingstories.Birthisatabooedtopicofconversationamongwomenbecauseitiscommonly
ascribedtoanoutcomeofsexualintercourse(Chawla,2006;Chawla,2019).Womenareoften
verballyabusedwithjudgmentalcommentsusingthisfact,asisseeninRia’snarrative.Thisisnot
justaboutnarrativesoftraumaticbirth,theliteraturesuggeststhatwomensharinggoodbirthing
experiencesareshamedfor‘showingoff’(Hill,2019).Giventheutilityofbodymapsin
understandingwomen’sexperienceofcruciallifeeventssuchaschildbirth,myadaptationcanbe
named‘birthmaps’andtheprocess‘birthmapping’.Birthmappinghelpedtobreakwomen’s
silenceabouttheirbirthingexperiences,wheretheirsisthecrucialvoicedrivingthe
improvementsinsexual,reproductiveandmaternalhealthcare(Oakley,1984;hooks,1989;
Kitzinger2005;Chawla,2006).Birthmappinghasproventobeanexcellentchoiceforamethod
ofdatacollectiontounderstandwomen’sexperienceswhicharesensitiveinnature,suchas
childbirth,andrequiresmoretimeandwillingnessfromparticipantstoshareinatrusting
environment.Itisaneconomicandflexiblemethod(Devine,2008)whichrequiresrelativelylow
costsuppliesfortheartwork(Gubriumetal.,2016).
Theuniqueapplicationofbirthmapshelpedtoaddressthelanguageandpower-basedbarriers
andhelpedwomentobreaktheirsilence,especiallyabouttheirexperiencesofobstetricviolence,
andsharetheirbirthingexperienceindetailwithcomfort.Birthmappingensuredthat
participantswereattentiveandfocusedthroughouttheexercise.Womenhadbetterrecall,more
thantheyexpectedthemselvestoremember.Somewomenwereinterviewedthreetofourtimes
andallthroughtheconversationstheyremainedintriguedandweredeterminedtofindtimeout
oftheirbusyscheduleandcontinuetheirparticipation.Participantsweredeeplyengagedinthe
process.Theirattentivenessreflectsintherichnessofthedatacollectedthroughtheirnarratives
ofbirth(Lysetal.,2018).Thebirthmapsenabledtheconversationtomovefromonepartofthe

Chapter6
172
bodytoanother,fromtheexperiencesthatwomenfeltontheirbodytotheirexperiencesofthe
birthingenvironment.Itwaseasierfortheparticipantstoarticulatetheirfeelingsthroughthe
map.Specificaspectssuchasthecolours,cut-outs,facialexpressionsandpeoplethewomen
chosetoputonthemap,openedthewayforrelevantprobesandgaveoptionsforwomento
choosefromwhattoshareoftheirstory.Thismadeiteasyfortheparticipantstoreflecton
certainprobesandtheirperceptionfromtheirexperience.Thiswasakeyrationaleforusingthis
methodtounderstandwomen’sexperiencesofchildbirth.Birthmappingmadethedata
comprehensiveandrich.
Listeningtothecontrapuntalvoices
Withthechoiceoffeministembodiedmethods,Ihaveensuredthatthewomen’svoiceisprimary
andtheauthor’sinterpretationissecondary.Thishasbeenensuredduringdatacollection,
analysisandinthepresentationofthefindingsthroughthebirthmaps,birthingstoriesandthe
generousinclusionofquotes.Feministmethodsreducethepower-basedimbalancebetweenthe
researcherandparticipant.Feministrelationaldiscourseanalysisandvoice-centeredrelational
analysisarenovelmethodsthatensurewomen’svoicesareprioritisedandareatthecentre.This
multilayeredanalysisisakeystrengthofthisstudywhichguidedmylisteningtothecontrapuntal
voicesthroughoutthedifferentformsofdata.Figure6.15presentsarangeofcontrapuntalvoices
heardinwomen’spoemsinthisstudythroughthelanguageofmusic.
Figure6.15 Rangeofwomen’scontrapuntalvoicesaboutselfdecision-makingandsurrogate
decisionmakingduringchildbirthandinlife(Author’sown)
Chapter6
173
Therangeshows‘discord’ofthenegativeend,wherewomenexperienceextremeformsof
obstetricviolenceanditsconsequences.Ittransitionsthroughthe‘harmonicprogressions’,which
expresswomen’sstruggleandresistance,extendingtotheextremepositiveendof‘concord’fora
satisfyingandpositivebirthingexperience.Women’sexperiencesarenotlinearoronedirectional
butrathercomplexandlayered.Thedominantdiscourseofthecontrapuntalvoicesisofdiscord
andsuspension,ratherthanofconcord.Someofthevoicesprevailmorethanothers.Oneof
thesefigurescanbecreatedforeachparticipant,focusingonjusthercontrapuntalvoices.Even
withinthepoems,themapsandquotes(andthebirthingstoriespresentedinChapter7)show
thatthevoicesdepictingconcordwerelimited,whereasthelengthordurationofthevoicesof
discordwerelongerforallfourwomen’sexperiences.Forinstance,Pairo’spoem‘Doll’hadthe
voiceofdeterminationandhappiness,onceeach,whensheishappythatshehasgivenbirthtoa
girlanddeterminedtotakehertoschoolwithher.Theothervoiceswerethoseofshame,
powerlessness,trauma,fear,silence,isolation,sadness,detachmentandstruggle.Thetwopoems
fromUrmila’sexperiencehaveanalignednarrativeaboutdecision-makinginthebirthing
environmentandaboutherlife.Thesevoicescanbenoticednotjustinthebirth-relatedpoems
butintheirroutinelife-relatedpoemsaswell,allowingthereadertoseeconnectionsemerging
betweenbothaspectsoflives,withbirthingbeinganextensionofhowtheyexperiencelifeand
theoppressionthatcomeswithitinroutinelives.Thevoicesofsilence,powerlessness,isolation,
pain,fear,anger,resistanceandstrugglecanbenoticedinbothdomainsandsimilarlyonthe
positiveside,thelessfrequentvoiceoftriumphcanbeheardwhenshedescribessendingher
husbandtojail.
Complex,richanduniqueexperiencesofrespectfulbirthsandobstetricviolence
Thisstudyhasopeneduptherich,complexandmultilayeredbirthingexperiencesthatarenot
unidirectionalandhaveaspectsofbothrespectfulcareandobstetricviolence,takingitastep
furtherfromthequantitativeanalysisof2194women’sbirthingexperiencesthatIpresentedin
thepreviouschapter.Thischaptershinesalightoneachparticipant’sembodiedexperience,
enablingreflectionbyunderstandingthemasaholisticbeingalongwithadeeperunderstanding
ofthehealthcareinfrastructure,birthingenvironment,policies,normsandmuchmorefromthe
women’sperspectiveandexperience.Thehospitalbirthsettinginaprivatehospitalwasnot
necessarilyverydifferentfromthepublicsettingsatdifferentlevels.Womenreportedthatthe
privatehospitalsdiscussedinthisstudywereadvantageouswhencomparedwiththepublic
hospitalintermsofgettingabedoraseparateroom,andtoreceivequickerattentionfromthe
careproviders.RiaandPairohavebirthedinverycrowdedenvironments,butthisisquitethe
oppositetothecomfortingexperienceofcommunalbirthing,whereeveryonearoundthewoman
isthereforher,supportingherandencouragingher(Chadwick,2018;Shabot,2020).

Chapter6
174
Inhospitalbirths,respectfulcarebeginswiththereceptionofwomen.Anabsenceofbasichuman
interactionisthemostcommonformofdisrespectthatwomenexperience(Vedametal.,2019).
Thereisscopeforcareprovidersandhealthsystemstoembedrespectfulnessateverypointof
interactionwithwomenthroughouttheirsexual,reproductiveandmaternalhealthneeds.
Respectfulcarecouldbeensuredviabetterinterpersonalcommunication,appropriatebirthing
environments,effectiveteamcommunications,avoidingunnecessaryinterventionsand
conductingtheessentialinterventionwithconsentandsensitivity,ensuringcleanbirthingspaces,
accesstocleanwater,hygieneandsanitationandbirthcompanionsofchoice(UnitedNations,
1947;WHO,2018).
Over-medicalisationmakesthebirthworldimpossibleforwomentounderstandanddescribe.
Studiessuggestthatthecultureofsilence,leadingtoacclimatisationtotolerateviolencein
personallives,oftenasaresultofapatriarchalculture,maykeepthemfromreportingtheir
experienceofdisrespectandabuseinthebirthingenvironment,astheymaybeconditionedto
feellessvalued(Chawla,2006;Hill,2019;Oakley,1984;Mayra&Hazard,2020;Jejeebhoy&
Santhya,2018).Thisisconfirmedwhenmedicalinterventionsareprioritisedoverwomen’s
comfort,dignityandchoice(Chawla,2006;Madhiwalaetal.,2018;Dinizetal.,2018;Kapoor,
2006).Womenreportedbeingthelastpriorityinthebirthingenvironment.Thisisasadreality
thatissystemicandapartoftheculturalconditioningofwomenthatmakesthemaccept
unnecessaryunwantedinterventions,includingcesareansections(Dinizetal.,2018),andsothat
birthingbecomesanexperiencethatneedstobeendured.Lambertetal.(2018)arguessaying
‘youbarteryourchoiceinreturnforskilledcare’.
Whileotherstudiessuggestthat“beingpresentwiththewoman”iscrucialforapositivebirthing
experience(Kapoor,2006),inwomen’sopinionthecareproviderswouldrankthefoetus/baby
andtheirownconvenienceastopconcernsintheorderofpreferenceforcare.Thisisreflectedin
careproviderscoercingandcompellingwomenandrestrictingwomen’schoicesabouttheirbody.
Itisimperativetounderstandthedifferencebetweenhavingbirthcompanionschosenbythe
familyandhealthcareproviders,againsthavingasupportivepresenceofsomeonechosenbythe
woman.Acompanionwhoisfocusedonthecareseeker’sneedsandthebirthingprocess
(Chawla,2019).Thecontinuouspresenceofahealth-careproviderwitheverywomanisnot
reportedinthesestoriesfromBihar,apartfromadagarininonecase,whowaswiththewoman
throughoutherhomebirths.Goodtouch,thatissoothing,ishighlightedasessentialinthegood
birthingnarratives(Chadwick,2019)ascouldbeseeninSujata’sexpectations.Thistactilecomfort
isusuallysoughtinanatmosphereandrelationshipthatwomentrust(Shabot,2020;Scotland,
2020).Mystudypredominantlyreportsbadtouch,becausemosttouchwomenreportedduring
childbirthwasuninvited,unconsentedandtraumatising.Thecurrentnarrativesofthebirthworld

Chapter6
175
arehostileandharrowing.Theyincludewomen’sexchangesaboutbirthwiththeirfemalefamily
membersorfriends,whichleadthemtoexpectobstetricviolence.Thatisunlesstheybehaveor
abidebythecareprovidersorletthemdothingsanddonotcomeinthewayofcareandactasa
passiveparticipantinasignificantexperienceoftheirlife.
Fromendurancetoadaptation
WomeninBiharrequest‘dardkidava’(augmentationbyun-prescribeduterotonicstohasten
uterinecontractions).Theyareoftenaugmentedbeforegoingtothehospital,toreducethe
durationoftheirstayinthehospital.Theydonotconsideritasabuse,aswomeninhigher-income
countriesoftendo.Thedifferenceisintheperceptionofbeingabusedandtheextentof
acceptabilityandreporting,whichisdifferentinhigh-incomecountriesbecauseofabetter
understandingbywomenofpoorqualityanddisrespectfulcare.Women’schoicesaremoulded
bytheirpreviousbirthingexperience,andwomenoftenfactorinmemoriesoftherespectfulness
oftheircare,especiallywhentheyhavepreviouslyexperiencedobstetricviolence.Womenoften
recoverfromtheirprevioustraumaticexperienceintheirsubsequentbirthbytryingtodo
everythingpossibletomakeitapositiveexperience,asawaytohealfromtheirprevious
traumaticbirth(Beck,Driscoll&Watson,2013;Kapoor,2006;Shakibazadehetal.,2018;Keedleet
al.,2019).Thiswastrueforwomengivingbirthforthefirsttime,basedonwhattheyhadheard
fromwomenintheirneighbourhood.Womeninlowandmiddle-incomecountriesendureand
oftendonotknowthattheirexperiencecanbebetter,theypreparethemselvesforanalarming
experience.Sometimestheawarenessofchoiceoverwhathappenstotheirbodyandhowthey
willbetreated,comesasarevelation(McAra-Couperetal.,2011).Thiscouldbeattributedto
intersectionalityofthewomen’sbackgroundcharacteristicssuchaseducation,socio-economic
status,gender,maritalstatus,religion,age,gravida,caste,classetc.andthedifferencebetween
hercharacteristicsfromthatofhercareproviderandeveryonewhoplaysaroleduringchildbirth
(Sen,Reddy&Iyer,2018;Chattopadhyay,2018;Sen&Iyer,2012).Intersectionalityisbetter
explainedintermsofraceandgenderbutcouldbeusedtounderstandwhatdrivesobstetric
violenceduringchildbirth(Chadwick,2018).IncountriessuchasIndia,careprovidersneedto
workhardertoensurerespectfulperson-centeredcare,astheyareupagainstwomen’slow
expectationsfromcare(Roder-DeWanetal.,2019).Eventhoughsomeinstancesofabuseare
unintentionaloraparticularcareprovider’sfault,buttheyneedtobeawarethatabusivecare
duringbirthisthedominantdiscourseintheIndianbirthingculture,andonlytheycanchangethis
narrative.Measuresarerequiredtoalsoaddressthestructuralandpolicyrelateddriversthat
makethewomenvulnerabletoobstetricviolencebutthatwillonlybepossiblethroughthe
understandingofwhywomenexperienceobstetricviolence,andarenottreatedinarespectful
anddignifiedmannerduringchildbirth.Idiscussthisinthenextchapterfromthefourimportant

Chapter6
176
constructsofgender,power,cultureandstructurethatemergedfromtheseeightinterviewswith
women.
6.7 Strengthsandlimitations
Thischapterpresentswomen’sexperienceofrespect,disrespectandabuseduringchildbirth
usingthevisualarts-basedparticipatorymethodofbodymapping.Adaptingthismethodtobirth
narrativesbyproducingnovelbirthmapsisakeystrengthofthestudy.Theresultantrich
accountsofwomen’snarrativeshelptoenlightentounderstandtheircontextualsituations
(throughthemapsandtheirbirthingstories)helpthereadertoappreciatetheirperspectives.
Womeninmystudyexperiencedrespect,disrespectandabuseinthehomeenvironmentaswell
asinprivateandpublicfacilities,thoughexploringtheseperspectivesfurtherwasbeyondthe
scopeofthisstudy.Therewereaspectsofdisrespectfulorabusivebehaviourlinkedtofamily
membersorathomethatwomennarratedinregardtobirthingexperiencethathadaninfluence
on,oraddedcontexttotheirperspectives.Childhoodsexualabuseincreaseswomen’s
vulnerabilitytoabuseduringchildbirth,butthiscouldnotbeexploredinthisstudyduetoadded
sensitivitiestothealreadysensitivenatureoftheissuebeingexplored.Women’sexperienceof
respect,disrespectandabusechangeswithcontextandwomen’schangingperspectives
dependingontheirsociodemographicbackground.Itisessentialtounderstandthisthroughthe
intersectionallenstoinvestigatetheroleofdifferentcultures,religionsandsocio-economic
backgrounds,tounderstandhowitinfluencescareduringchildbirth.
6.8 Conclusion
Women’smissingvoicesinresearchaboutdeeplyfeminineissuesconstituteaglobal
phenomenon.Obstetricviolencerelatedresearchisdominatedbysurveysandperspectivesof
everyonebutthewomenwhogivebirth,especiallyinthediverseIndiancontext.Women
rememberthetraumaofanabusivebirththroughouttheirlife,oftenwithoutanopportunityto
shareitwithanyone.Thisresearchmakesanimportantnovelcontributionthroughthecreation
anduseofthebirthingmapsasaparticipatoryandculturally-appropriatevisualarts-based
methodproveusefulforaccuratelyportrayingwomen’srespectful,disrespectfulandabusive
birthsinlowresourcesettings.Ithelpswomentobreaktheirsilenceaboutobstetricviolenceand
expresstheirexperienceofrespectfulmaternitycare.Thisisimportanttounderstand,asevenin
theeightcasestudiesweobserveddiversityinwomen’sexpectationsalongwithsome
similarities.Thisdiversitycanbewellunderstoodthroughbirthingmapsascareneedstoadaptto

Chapter6
177
thesechangingcircumstances,toensurerespectfulperson-centeredcareduringpregnancy,
labourandchildbirth(Afulanietal.,2019).
ThesystemofcareduringchildbirthisverymedicalisedinBihar,asseeninthenarrativesof
womenfromthisstudyandtherampant,oftenunethicaluseofinterventionsperformedsothat
thecareprovidersdonothavetobeatthemercyofthephysiologicalbirthingprocess.They
createsomethingthatcanfittheirscheduleandcalendars.Pairo’sstoryclearlyshowshow
“Docsplanation”hastakenoverthebirthworldbecausethemedicalmodelhaschangedtosuit
theneedsofobstetricians,especiallymale(Mayra,2020a).Remnantsofthiscanbeseenin
hospitalbirthingenvironmentsinIndiawherewomenarerestrainedwhengivingbirth.The
presenceofeightmenintheoperationtheatreforPairo,noneofwhomshehadmetbefore,isa
severeviolationofherprivacy.Insteadofkeepinghercomfortinmind,Pairowasnon-
consensuallyblindfolded,whichperfectlysignifiestheoppressionofwomenintheobstetric
settings.Allwomenhaveauniversalrighttorespectfulmaternitycare,regardlessofthecontext
anddiversebackgrounds.Thismakesitimportanttosystematicallyunderstandwomen’schoices,
experiencesandexpectationsthroughinnovativemethodslikebirthmappingtoinformchanges
inpracticesandpoliciesaroundchildbirth,whicharediverseacrossculturesandcontexts.
Chapter7
178
Chapter7 “Ihavetolistentothemortheymightharm
me”:Whydowomenendureobstetric
violence?
Thepreviouschapterpresentedthenatureofrespect,disrespectandabuseduringchildbirth
fromwomen’snarratives.Thiscouldbeconsideredtheirfirststepinbreakingthesilenceabout
theirexperiencesofobstetricviolenceduringchildbirthandstatetheirexpectationsofrespectful
maternitycare.Women’snarrativesarerichandtheyoftenmentionedtheirperspectiveofwhy
theyexperiencerespect,disrespectandabuseentangledintheirresponsestothenatureoftheir
experience.Iutilisedtheadditionalinformationwomenprovided,byanalysingittounderstand
theunderlyingreasonsbehindrespect,disrespectandabuseduringchildbirth.Thiswas
thematicallydifferentfromtheplannedobjectiveofthepreviouschapter,soIampresentingitin
thisnewchapter.Womenwentastepaheadfromsharingwhattheirexperienceand
expectationsare,byalsostatingwhytheyexpecttobetreatedwithrespect,disrespectandabuse
andwhatdrivesit.Thischapterismorethanbreakingthesilence,itpresentswhatcausedthe
silenceinthefirstplace.
7.1 Background
Silenceisacommonthemewhenexploringwomen’ssexual,reproductiveandmaternalhealth.
Silenceisnoticedathomeandinthehospital,whichpointsatwomen’sunquestioningattitude
whichstartsathomeandextendstotheobstetricsetting.Womenhardlycomplainaboutpain,be
itpainduringintercourseorpainwhengivingbirth(McAra-Couper,2014).
InthepreviouschapterIpresentedevidencethatwomeninBiharraiseconcernsreferringto
aspectsofthecarethattheyconsideredrespectfulordisrespectful.Thelanguagewomenuse
whentheyreferredtobeing‘allowedto’or‘madeto’or‘forcedto’isamanifestationofthe
imbalanceofpowerdeep-rootedingender-baseddiscriminationsandhasbecomepartofthe
structureandculturewhichensuresthisconditioningisperpetuated.Women’snarratives
exemplifyhowpower,gender,cultureandstructureinfluencethecaretheyreceiveandhowthat
isrelatedtowhatshapestheirperceptionofrespect,disrespectandabuseduringchildbirth.
Thesethemeswerenotincludedinthepreviouschapterbecausetheyrelatetothefactorsdriving
respect,disrespectandabusethatemergedfromthedata.Butthisisanimportantpieceofthe
puzzlewhichprovidestheperspectivesofthekeystakeholderofchildbirth,thewomen.Hence
theimpactofgender,power,cultureandstructurearepresentedseparatelyinthischapterI

Chapter7
179
choseadifferentsetofquestionsusingthesamedatafromthebodymappingaidedin-depth
interviewsandfollowingthesamemethodsofanalysisaspresentedinthepreviouschapter.
Thischapterandthenextchapterexploreswhywomenexperienceobstetricviolence.Thishas
thepotentialforpositiveimpactonprovidingrespectfulmaternitycare.Themethodshavebeen
describedinChapter6,butitisimportanttomentionthatIacknowledgethepower-based
inequalityintheinterviewenvironmentbetweenmeandtheparticipant.Iemployedmeasuresin
termsofusingthelanguageofparticipants,dressinglocallyandbeingatthesamelevelinterms
ofpositioningoneselfphysicallytotrytoreducethisinequality.Theseeffortsmaynotgoallthe
wayinbalancingthepowerdynamics,thereforetheresearchteamensuredthatall
communicationandinteractionwiththeparticipantandpeopleinthecommunitiesare
respectful,theinterviewsandthebirthmappingexerciseareconductedwithutmostsensitivity
andtheparticipantsaremadeawarethattheycanrefusetobeapartoftheexerciseoranswer
anyparticularquestions.
Aresearchrelationshipoftenputstheresearcherinapositionofauthorityofpowerascreatorof
knowledgethattheyseektocreate(Sprague,2016).Studieshaveshownthatarts-basedresearch
methods,suchasbodymapping,tendtominimizepower-basedimbalancesbetweenresearcher
andparticipant.Researchmethodsshiftsthepowerdynamicswheretheparticipantistheexpert
knowledgeproducer,andtheresearcherbecomesafacilitatorandco-creatoroftheoutcomeof
thearts-basedresearch(KlienandMilner,2019;Lys2018;Boydell2018;Sweet&Escalante2015;
Boydelletal.,2020).Ifollowedthecourseofdiscussionoftheparticipant,probingonlywhen
required,andnoticedmanyinstancesthatcouldindicateashiftinpowerimbalanceduringthe
courseoftheinteractions,suchasparticipant’scomfortaboutcallingusatoddhours,haltingthe
interviewtoattendtothehouseholdchoreswhenrequiredandwiththeirfrankness,humour,
honestyandopennesswhensharingsensitivedetailsoftheirexperienceofbirthingandother
aspectsoftheirlife.Thistrustwasgrowing,itcouldbeseenmorestronglyinsubsequent
interactionsandinthenatureofthecontentwediscussed,thatoftenwentofftrack,butwomen
sharedwhattheyfoundrelevanttothecontextofmyresearch.Thischapterisaresultofsuch
off-trackconversationsthatprovidedarichunderstandingoftheparticipant’sunique
perspectivesofwhywomenexperiencerespect,disrespectandabuseduringchildbirth.
7.2 Researchquestion
Whatarewomen’sperceptionsoftheunderlyingfactorsdrivingrespect,disrespectandabuse
duringchildbirthinBihar?

Chapter7
180
7.3 Objective
Tounderstandthedriversofrespect,disrespectandabuseduringchildbirth,fromqualitative
participatoryarts-baseddataaboutwomen’sexperienceofgivingbirthinBihar,India.
7.4 Findings
7.4.1 Powerinfluencescareduringchildbirth
Powerwasevidentinthewaywomeninteractedamongstthemselvesandwithothersintheir
homeortheirsocialenvironmentandtheobstetricenvironment.Twokindsofhierarchiescould
benotedfromtheseinteractions;1)socialhierarchyand2)medicalhierarchy(whichisembedded
withinthesocialhierarchy).Powerinrelationshipswithpeopleincreasesasonegoesupwards
andwomenareatthebottomofboththehierarchies,asshowninFigure7.1.Allkindsofpeople
(especiallyasmentionedinsection6.5.6aboutpeopleinthebirthingenvironment)andtheir
relationstowomenmentionedbythemintheirinterviews,areshownhere.Thehierarchyis
createdafteranalysisofwomen’snarrativesabouttheseactorsinthehouseholds,
neighbourhoods,communityandobstetricenvironments.
Figure7.1 Hierarchyofpowerrelations(Author’sown)
Inthehospitalenvironment,thedoctorcouldbeseenatthetopofthehierarchy,asobserved
fromwomen’sresponses.Whenaskedtorankallthepeopleinthebirthingroomintheorderof
theirimportance,Sujatamentionsthatthedoctoristhemostimportantpersoninthebirthing
room,andevenforthecareprovidersaroundherlikethenurseanddai,thedoctorwaspriority.

Chapter7
181
Sujataforgetsherselfwhenrankingeveryoneintheorderofimportanceandpower;andwhen
sheisremindedofherself,shesharesconfidently,withalaugh,thatwhilesheshouldbethemost
importantpersoninthebirthingroomalongsideherbaby,thatisnotthereality.Theinferiority
canbenoticedinthelanguageusedbywomenindescribingthemselvesassomeonewhowill
needtofollowthecareprovider’sordersandthattheyhavenochoiceorrighttoconsentinthe
situation.Thiswasobviousinwomen’snarrativesofbeingtreatedlikeanobject,apassive
participantandoftenbeingatthereceivingendofthecareprovider’sanger.
“‘Ifyouaresoafraidwhydidyouconceive?Whatistheneedofhavingchildren?’Theysaysuch
things,whatcanwesay!Ifeelangry.ButIamadmittedunderyourcare,so,Iwillhavetodowhat
yousay.IfIdonotdoasperyourorder,thenyouwillagaindosomethingtoharmme.SoIhaveto
listentothem….Ortheymightharmmeinsomeway.”(Ria)
“Theydecidedontheirown…Iwasinthedeliveryroom.Weallwanttohaveanormalbirthbutit
dependsonthedoctorwhattheywanttodo.Whatisbest!”(Sujata)
“Thenursewasverysadbecausewewerecreatinginconveniencesforthemearlyinthemorning.”
(Amrita)
Thiswasmanifestedinthewaycommunicationbetweentheseactorsplayedout.Doctorsand
nursesdidnotdirectlycommunicatewiththewomen,nordidtheyexplaintheproceduresto
themorseekconsent.Theytreatedwomenasapassiveparticipant,asanobject.Themost
extremecasewasseeninPairo’sfirstcesareanbirthwhichisalsoshowninherbirthingstory(Box
7.1)12.Pairofeltthatthedoctorwasover-confidentanddidnotcarewhatherpatientsmightbe
thinkingofher,asshewasprescribingmedicineswithoutdescribingwhattheyareforandjust
expectingherprescriptiontobefollowedwithoutanyexplanation.Shealsofeltthatthe
pediatrician,whoscoldedherhusbandafterhavingbeenatfaulthimself,justmadeamistake.
Shefeltshehadnorighttofeelangryorconcernedaboutitbecausehewastreatingherbaby,so
wasonlyexercisingthepowerhehadoverher,andherfamily.Adisplayofphysicaloverpowering
wasalsoseenintermsofrestrainingwomenduringvariousinterventionswherepeoplearound
birthfromhomeandhospitalparticipatedinrestrainingthebirthingwoman.Womendidnotlike
this,butconsidereditnormalandhencedidnotreportgrievance.Powerwasdisplayedby
completelyignoringthebirthingwoman’spresenceintheroom,andnotgivingheranychoiceor
voicebycuttingallcommunicationswithher.ThecommunicationtookplacewithwhatIcallthe
‘surrogatedecisionmakers’whoconverseonbehalfofthebirthingwomanwhoiscapableof
makingherowndecisions.
12For better impact please look at Pairo’s birth map in Figure 6.11 while reading her birthing story in Box 7.1.
Chapter7
182
“Theyweretalkingaboutme,aroundme,butnottome.Theywereonlytalkingtomyparents.
Theywereinformingthemaftercheckingme.Ididnotaskthemanything.Whatisthepointofme
askingthemthingsunnecessarily,theeldersarethereforthat.Theyneedtoknowanddecide
things.”(Urmila)
“Shedidnotneedtoaskmyname.Shewascallingmeyou,you.”(Sujata)
“Iwantedtostraightenmylegforawhilebuteveryonewasholdingmedown,mylegsandhands
fromallfoursidestightly.Icouldnotbearthat,thetouchofanyone.”(Urmila)
Athomewomenfollowthedecisionsoftheirguardianswithoutquestioning.Fatheratmayka
(maternalhome)andhusbandatsasuraal(in-lawsplace)arethepeoplewiththehighest
authority.Inthebirthingenvironmentthefatherandhusbandhavealimitedrolebuttheelderly
womensuchasthemother-in-lawandthemotheroftenmakethedecisionsaboutpregnancyand
childbirthandalsonegotiatedthatwomennotfussabouttheinterventionswiththeclassic
‘womenhavetoendurethisexperience’.Thisisseeninsomeofthequotesingender,cultureand
structureaswell.DaiandASHAshaveadualroletoplayaswell,whichisevidentfromASHA’s
placementinbridgingthegapbetweenhomeandhospital.Daiisoftenseenprovidingcarein
boththeseenvironments.
“She(ASHA)toldme‘youmighthavewithdrawnthemoneyfromyouraccount.’…Igavehermy
passbookandtoldhertocheckifshedoesnotbelieveme”(Amrita)
Participantsoftendidnotquestiontheauthorityofanyoneandfollowedalltheinstructions
withoutresistance.Theywouldgobacktothesamecareproviderwhohaveabusedthem,
avoidinganyconfrontation.Therearenoconsequencesforhealthcareprovidersforviolence
againstwomenandthenewbornintheobstetricenvironment.
“Hewasagooddoctorandweknewthathemadeamistake…hescoldedmyhusband…Ijustfeel
heprobablydidnotdoitintentionally.ItrusthimenoughthatIstillgothereformychild.ButI
neverconfronthim(doctor).Didnotwanttohurthisfeelings.”(Pairo)
“Theyaredoingtheirwork,theyarenotatfault.Theyweredoingastheyshoulddo.Accordingto
mylevelofpain,Iwasalsobehavingacertainway.Atthetimeofbirth,theyusedtoremovethe
clothesandliftitup,butthatisnecessary.”(Sujata)
Thefactthatthe‘surrogatedecisionmakers’donotfeeltheneedtoconveythecommunication
theyhadwiththecareprovidersaboutthecourseoftreatmentordecisionsandchoicesmade
aboutthewoman,isastounding.

Chapter7
183
“Iwasthinkingthesepeoplewouldthinkaboutmywellbeingonly.They’llhavemybestinterestin
heart,mymotherandhusband.Ibelievetheyshouldhavetoldmeaboutitbuttheydidnot.What
shouldIsay,Iwasjustapatient.Butthesethingsshouldhavebeenexplainedtome.”(Pairo)

Chapter7
184
Box7.1 Pairo’sbirthingstory
Pairo’sBirthingStory
Myheartwasbeatingoutofmychest,becauseIknewwhatwasgoingtohappennext.Heheldmyhand
tightly,astranger,butitfeltgood.Asifsomeonemyowniskeepingmecalm.Scared,Iaskedhimtopress
hishandonmychest,onmyheart.Iama29yearsold,governmentschoolteacherandthiswasmy
secondchildbirthayearago.
Memoriesofmy1stbirthhadtraumatizedme.Everythingisstillfreshinmymind.EvennowwhenIthink
aboutit,Ijustknow,neveragain.Iwasn’tinpainbutIwasleakingsomefluid.Soeveryonetookmetothe
governmenthospitalthatmorning.Thereweremanywomenallwaitingfortheirturn,andthenIsawthat
doctorwearingaplasticglovecheckingeveryoneinthatdirtyenvironment.Iranfromthere!Iwastakento
aprivatehospitalnext.Theladydoctorjustmadethenurseliftmypetticoatandnightieup;andforcedher
handinsidemewithoutanyexplanation.Istartedscreamingandcryingoutofpain.“Youcanneverhaveanormalbirth,ifyoucannotbearthispain.”ThenextthreedaysIwasinobservationwhenIwasgivennineteenbottlesoffluids,manyinjectionstoincreasethelabourpainandnumerousvaginalexaminations.
Thenurseswouldjustcomeandinserttheirhand,notevenmindingthecrowdandhowmanypeopleare
aroundme.Iwasfrustratedandcomplainedtothedoctor,“whydoeseveryonehastofirstinsertahandinsideme,withouteventalkingtome.Istherenootherwaytocheck?”.Shesaidnothing.Mymothersays,
“womenhavetoendurethat,tohaveachild”.EvennowsometimesItellmummy,“thatwasn’tright!”
Iwasinthecafeteriawithmyfamilywhenthenursecameandjustdraggedmebymyhandtothe
operationtheatre.Noexplanationgiven!MyfamilystayedoutsidetheOT.Therewere8menintheroom
allinregularclothes,liketheyareonapicnic!Oneofthemsaid,“getup!”.Gavemeaninjectiononmy
backandmademeliedown.Noexplanationgivenagain!That’swhenIrealizedIamgoingtogetoperated,
noonetoldme.Myonlysolacewasthattherewon’tbeanylabourpain.Anothermanblindfoldedme
becausethelessIsee,thelessuncomfortableIwillbe.Ifeltsomeonetalkingmypetticoatoffandlifting
mynightietomychest.Theyweretreatingmelikeadoll…orlikeananimal…doingwhatevertheywant…
notcaringaboutmeatall.LikeIdidnotexist!Iwasfilthyandmyhairtangledwithoutashowerin4days
myclothesgettingdrenchedinmyfluidanddryingonme.Ididnotknowanyoneinthatroom.Iasked
aboutmyladydoctortothisotherguywhowasapparentlyherson.Shearrivedlater.
Theyplayedmusic.Itwascalming.Therewereothersoundstoo,ofinstrumentsandscissorscutting
throughmeliketheyarecuttingajuterag.Everyonewastalkingamongstthemselveswhiletheytookthe
girloutofmybody.It’sagirl,theydiscussedandIthought,“Iwilltieherhairintwopig-tailsandtakehertoschoolwithme.”Istayedinhospitalfor10daysafterthatbecauseIhadfeverandchillsandwasrecoveringfromsurgery.Meanwhilethebaby’sdoctordidnottiemybaby’scordproperlywhichkept
bleeding.Shegotinfectionthesamenightandmyhusbandhadtotakehertoanotherhospital,3
kilometersaway,everydayforinjections.Istruggledtobreastfeedmybabyandevenholdherproperly.
IcriedwhenIcouldnothaveanormalbirththe2ndtimewithmyson,2yearslater.Thedoctorpressedon
theincisionandithurt.“itcangettornandyoumightgetacutdownthereanyways.You’llneedabigoperation.”Shesaid.Thenormalbirth’spainlasts4daysbutthemiseryofCSlastsforyearsandbreaks
yourbody.InthebeginningsometimestheincisionusedtohurtlikesomeonerubbedchillipowderonitforthemedicineIwasprescribedtoapplyonittogetridofpainandrednessinthefirstplace.Thiswasa
quackinourvillagewhoconsidershimselfourarea’sMBBS!
Myhusbandasks,“whydidyounotgetsterilizedifyoudon’twantanotherchild?”.“Yougetsterilized”,Itellhim.Hemakesexcusesthathe’llgetweak.Sowebothdon’tgetitdone.ButIdoteasehimsaying,“mylifeisinyourhands”whenwegetintimate.IfeelIneededtosharethesewithsomeone,itallneededto
comeoutasIcouldnottalkaboutitwithanyone.Thatdaysomehowgotover,butthosehaunting
memorieshavestayedwithme.

Chapter7
185
7.4.2 Genderinfluencescareduringchildbirth
Gendermanifestedinmanywaysandisakeyfactorinfluencingtheimbalanceofpowerbetween
differentactors,asshowninFigure7.1.Sonpreferenceisshownindifferentwaysbypeoplefrom
homeandhospitalinthebirthingenvironment.ThisseemedtobeapartoftheBihariculture,
thatbeginsatbirthandinfluenceseverypartoftheparticipant’slifeincludingtheireducation,
financialstability,occupation,marriageandeveryroletheyplay.Careprovidersdemandmore
moneywhenasonisbornandofferadiscountonthebirthofagirl,tomakeupforthesorrow
thatdescendedonthehousehold.Thefamiliesavailthediscount.
“Nobodywasplayingwithmygirl.Noonewastakingherintheirlap(whenshewasborn).Then
slowlypeoplestartedwarminguptoher…mymother-in-lawwasveryhappywhenitwasaboy.”
(Amrita)
“Ifitisagirlbabytheyaskforlessmoney,it’smoreforaboy.Ifsomeonegivesbirthto2-3girls,
thentheydon’taskforhappinessmoneybecauseit’samatterofgreatsorrowforthefamily.They
(careproviders)understandthesituation,whentoask(formoney)andwhennotto.”(Sujata)
Womenoftenhavenosayinthemajordecisionsoftheirlife,regardlessofeducation.Thisreflects
intheirdecisionsaboutpregnancy,birthandfamilysize.Adoptingfamilyplanningmethodsis
treatedaswomen’sbusinessandwomenacceptitastheyacceptthatdomesticworkiswomen’s
domain.Thiscouldbeseeninthehugedifferenceinthefemaleandmalesterilisationratein
BiharandIndia,indicatingthatifonehastogetsterilisedbetweenthecouple,itwillbethe
woman,andallthefamilymembersweighinonthatdecision.Womendidnotknowmuchabout
money-relatedmatters,theyhadnosayinexpensesandoftendidnotknowhowtomanagea
bankaccount,eventhoughmostwomenhadabankaccountwhichismandatorytoreceivethe
JSYincentive.
“Myworkistojustcookandtakecareofthehouse.SoIdon’tknowmuch.”(Sita)
Womenarenotaccustomedtothesegenderrolesforthemselvesandforothers.Forinstance,
theyassumeawomaninthebirthingareaisanurseandamanisoftenadoctor.Theyalso
assumemenintheOTtobenurses,toensureoneselfthattheirpresencetherewasnecessary.
“WhatwillIcallthem,gentsnurse?Aretheynurse?Imeancompoundermaybe?”(Pairo)

Chapter7
186
“Thedoctorplayedmusiconhismobile…Iaskedwhereismadam?Hesaid‘mummyiscoming!’
ThedoctorwhomIusedtoshowwasaladybuthersoncameintheoperationroom…hehada
degree…Ididnotknow,heisadoctor.”(Pairo)
ThepersonwhoPairoreferredtoasdoctor,mayhavementionedthatthedoctorwashismother
toindicateandexercisethesamelevelofpoweroverPairo.Womencitemanyreasonsforthe
obstetricviolence.Theyfeelthatrespectisfortherichandifonehasthefinancialmeanstopay
the‘happinessmoney’,apartfrombearingthecostofcare,their‘patient’willbecaredforwell.A
‘guardian’accompanyingthemindicatetherearepeoplewhowillpay.Anexperienceofprevious
birthmatters,becausethewomenwouldhavegonethroughthepainbeforeandexperienced
obstetricviolence,andwouldbehaveaccordingly.Povertyandalackofeducationinviteabuse,
accordingtoparticipants.
“Whenpoorcomeforcare,theygetscolded.Wearepoor,uneducated,weakanditisourneed
thatwewent,sowecannotsayanythingandhavetolistentoeverythingtheysay.Aneducated
personknowshowtotalktothem…aneducatedpersonwillbeabletoreasonwellwiththembut
wecan’t.Wehavetobearthebruntoftheiranger.”(Amrita)
“Theonewhoscreamsgetsabused!Theyarenotusingtheirstrengthtopushbuttoscream.
They’llhavetolistentoabusivelanguage.Thosewhohaveahabitofbirthing,donothaveto
listentosuchthings.Newmothersdon’thaveahabitofbirthing,sotheydon’tknowmuch,they
havetolistentosuchthings.So,theywereabusingme.”(Ria)
“IwasblindfoldedbecauseIwouldhavefeltuncomfortablebecausethereweremen.Therewere
noladies.Thedoctorwhowasgoingtoperformtheoperationwasalsoaman.”(Pairo)
Pairoassumesthistobethereasonwhyshewasblindfolded.Therewasnoexplanation.When
womenaskforanexplanationorquestionaboutaprocedureormedicationorthedurationof
labour,itoftenfallsondeafearsandisnotrespondedtobythecareproviders.Treatingwomen
asapassiveparticipantintheirbirthisgender-based.Womenunderstandthis,andthatas
womentheyhavelittlesay.Women’spainisnotaddressedorevenacknowledgedinmost
scenariosasIdiscussinthepreviouschapter.
“Ikeptaskingforanesthesiabuttheywerenotevenlisteningtomeandkeptdoingit(episiotomy
repair)…Ikeptscreamingandeveryonewasholdingandstitchingme.Ididn’thaveasmuchpain
duringdeliveryasIdidwhentheystitchedme.”(Urmila)

Chapter7
187
“Idofeelthatthebadexperienceswerewithmybody.So,thosethingsdon’tmattertome
anymore.Whathappened,happenedwithmybodybutmyspiritisuntouched.”(Pairo)
Themanifestationofgenderindifferentaspectsofawoman’slifecanbeseeninthepoemfrom
Amrita’snarrationtitled‘I’.
Box7.2 Amrita’sI-poem-‘I’
I
Imighthavebeen18or19yearsold.
Ihaveahusband.
Irunmyshop,takecareofmychildrenandmyhouse.
IgotothenearbyPHC.
Igothereformedicinesandall.
Igothere.
Iwenttheretogetchecked.
Ihadmyboythere.
…Ifallsick,mychildfallssick.
Iamfinenow.
Ihavetakenmedicineatnight.
Igetheadachesatnight,Igetfever.
Idon’tknowwhetheritisduetotirednessorsomethingelse.
Iwasveryhealthybefore.
Ihadnofever,nothing.
ItakemedicineandstaywellforaweekandthenagainIfallsick.
Iamallalone.
…Ifallill,thereisnoonetolookafterme.
Ionlylookafterthem.
Igotothemarketforpurchasingthethingsformygroceryshop.
Isellit.
Ileavemychildrenatthenearbycentre.
Ileavemychildrenwiththem.
Igethelp.
Ileavethechildrenwiththewomeninmyneighbourhood.

Chapter7
188
Iwasalone.
Iusedtodoallthehouseholdworkalongwithtakingcareofgroceryshop.
Icarriedbagsofrice,veryheavy.
Iusedtolift25kgjuterags.
Iusedtositatthegroceryshop.
Iwasalmost8monthspregnant.
Iusedtocallmysisterforhouseholdwork…cookingandall.
Itookrestthen.
Ihadatwo-year-olddaughter.
Iusedtotakecareofher,likewashingclothes,cleaningher,bathingher.
Iusedtokeepherwithme.
Iusedtogetalotofrest.
Ijusthadtoeat.
Itook3daystogivebirthtomyfirstchild.
Iwasolder(18years)whengivingbirth.
Iusedtobeverysickwiththesecondchildinmywomb.
Ididnotlikeanyonetalkingtome.
Iusedtoalwaysfeeltired.
Iusedtobelethargic.
Icouldnoteveneatmuchfoodorwater.
Ididn’tlikeanything.
Irelaxed.
Ialsohadnauseaandvomitingduringmyantenatalperiod.
Imeanmylipsandtonguebecameredandblisteredandmouthwasdry.
Iworeasareeforbothmybirths.
Ihadababyboy,theyallweresohappyandtheystartedtalkingwithmepolitely.
Ihadthegirlchild,everyonewashappyatmymothers’side.
Ididn’thavemuchtroubleinmyfirstbaby.
Ibirthedagirl.
Iusedtodoeverythingforher,putakala-tika13onherforeheadandputhertosleep.
13Blackkohldotontheforeheadwithwithculturalsignificanceofprotectionfromevileye.

Chapter7
189
Iwasalsohappy.
Iwashappybothtimes.
Iusedtofeelalotofpainwhilepassingurine.
ImightbedarkskinnedbutIamveryneatandclean.
ItelleveryonehowIgavebirth.
Ihadnormalbirth.
ItoldthemwhatproblemIhad.
Iwillfeelrespectfulwhentheywilldomydeliveryontimewithoutmuchdelay,whentheywill
speaktomepolitely,withasmile.
Iambirthingaboyorgirl,Ishouldbetreatedwell.
Iwantsisters(nurses)tocheckmenicely.
7.4.3 Structureinfluencescarearoundchildbirth
Systemsaroundbirthfollowstructuresthatincludecertainnormsanddeep-rootedcultures,and
areinfluencedbygenderandpower.Women,couples,familiesandcommunitiesareconditioned
tocarryonthesestructureswhichrelatetotheirhome,extendingtothebirthingenvironment
andbeyond.Thisisnoticedintheirnarrativeswheretheywanttofollowaritualbecauseitis
normalized.Thestructureofbirthingmayincludemanygoodandbadaspectswhichmay
encouragewomenandpeopletomakebirthingchoices.Thisstructureencouragespeopleto
strengthenthe‘doctor-knows-best’culturewhichmakesthemfollowcareproviders
unquestioningly.Questioningcanalsobeconsideredoffensivebetweenpeoplewithsuchhuge
hierarchicaldifferences.
“Weallthinkweshouldhaveanormalbirth.That’sthebest!Butaftergoingtothedoctor,it
dependsonherwhatshewillsay.”(Sujata)
“Mymother-in-lawsaidifshedoesn’tcheckyoudowntherehowwillthebabycomeout?’We
don’tunderstandthisbuttheydo.”(Sita)
Sujatafeelswhatthedoctorandothercareprovidersdoinabirthingenvironmentisinthebest
interestofthebirthingwomen.Itmightnotbecomfortable,butthewomenhavetogothroughit
anywaybecausetheydonothaveachoicetodenycare.Participantsbelievethatthecare
providersknowwhatisbestforthemandhopedthattheirrespect,dignityandcomfortwouldbe
consideredwhenmakingchoicesforthem,andthattheyshouldbegivenachoice.Forinstance,

Chapter7
190
Urmilasharedthatbabiesareexchangedatgovernmenthospitalsbasedonsex.Riafeelsherbaby
couldhavebeenexchangedwhenshewasinitiallyinformedaboutastillbirth.Womenhave
assumptionsaboutthequalityofcaretheycanexpectatgovernmentandprivatesectorsandalso
atdifferentlevelsofcareprovisionwhichhelpsthemtodecideandplanaboutchildbirth,starting
withwearingapetticoattoensurealittleprivacybykeepingthelowerhalfofthebodycovered,
inanobstetricstructurethatprovidesbareminimumlogisticsupport,tochoosingwherethey
wanttogivebirth,basedonhowmuchagencytheyhaveinthesematters.
“Ingovernmenthospitaltheydonotcutopenthebellyunnecessarily.”(Amrita)
“Peoplesayaboutgovernmenthospitalthatyougetthefacilitythatyoucanaffordtopayfor.The
moneywegiveascertainstheconvenienceweget.Ifyougotoaprivatehospital,theywillrobyou.
Youhavetobringeverythingyourselfingovernmentbutdon’tneedtopaythedoctor.”(Ria)
“Thosewhoareaccompaniedbytheirguardianaretreatedwell…iftheyfeelthattheywontmake
moneyafterbirthfromguardians,thentheydonottreatwell...theydonotgiveanyattention.”
(Sujata)
CallinganambulanceandASHAwheninlabour,ispartofthestructure,soisexpectingtheJSY
incentiveafterbirthinginagovernmenthospital.
“Weusedit(JSYincentive)uptobuyknickknacksforhome.Forvegetablesandotherimportant
things.Ifyouhavemoneyinyourhands,somanythingscomeup.Weusedupthemoneyfor
householdrelatedthings.”(Sita)
Obstetricviolenceisstructuralandnormalised.Womenexpectsomeextentofdisrespect,abuse
ortheabsenceofrespectfulcare.Theyacceptittoacertainextent,anddonotobjecttowhat
theycanendure,complainingandconfrontingisnotdesirable.Theyseekcare,knowingmany
aspectsofbirthingpracticesthattheydonotnecessarilylike,buttheconsensusisthattheyhave
toendureittogivebirth,everywomanenduresit.Theysharemanyargumentsthatsupportthis
beliefwhichincludestheirlowerstatus,lowlevelofeducationincomparisontothecare
providersandthefactthattheyarecareseekers,sothecareproviderhaspoweroverthemasis
thenatureofthestructure.
“Hesaid,‘getup’andinjectedinmywaist,takingmyclothesoff…theyweretreatingmelikea
doll.Theywerenottakingpermissionfromme…Noexplanation!”(Pairo)
“Iquicklydrankit(soda)asIhadorderedit,butthosepeople(hospitalstaff)wantedittoo.It
happensinthegovernmenthospital,peopleaskyoutofeedthem.”(Sujata)

Chapter7
191
“IleftmyeducationwhenIwas13.Butit’stheir(parents)responsibilitytosendmeforfurther
studieswhichtheydidnotdo.Theyshouldhavebeenstricter.”(Urmila)
Thestructureofsocietyshapespeople’sattitudesandbehaviourabouthowwomenshouldbe
treatedingeneral.Theireducation,mobility,financialindependenceanddecisionmakingright
andchoicesareallpartofthesocietalstructure.Thishasaninfluenceonhowwomenaretreated
inthehospitalandalltheactorsarepartofandactingaccordingtothestructure.Urmila’s
birthingstoryinBox7.3andherbirthmapinFigure7.2,showsthisaboutherlife.

Chapter7
192
Figure7.2 Urmila’sbirthmap
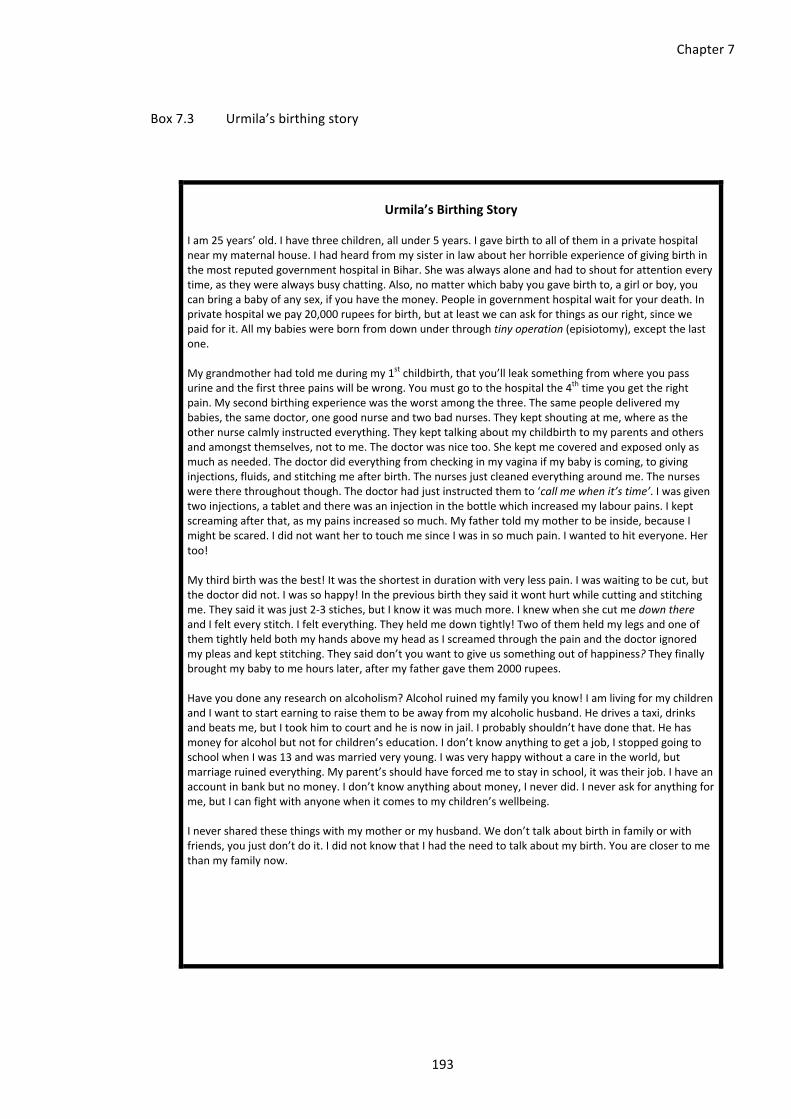
Chapter7
193
Box7.3 Urmila’sbirthingstory
Urmila’sBirthingStory
Iam25years’old.Ihavethreechildren,allunder5years.Igavebirthtoalloftheminaprivatehospital
nearmymaternalhouse.Ihadheardfrommysisterinlawaboutherhorribleexperienceofgivingbirthin
themostreputedgovernmenthospitalinBihar.Shewasalwaysaloneandhadtoshoutforattentionevery
time,astheywerealwaysbusychatting.Also,nomatterwhichbabyyougavebirthto,agirlorboy,you
canbringababyofanysex,ifyouhavethemoney.Peopleingovernmenthospitalwaitforyourdeath.In
privatehospitalwepay20,000rupeesforbirth,butatleastwecanaskforthingsasourright,sincewe
paidforit.Allmybabieswerebornfromdownunderthroughtinyoperation(episiotomy),exceptthelast
one.
Mygrandmotherhadtoldmeduringmy1stchildbirth,thatyou’llleaksomethingfromwhereyoupass
urineandthefirstthreepainswillbewrong.Youmustgotothehospitalthe4thtimeyougettheright
pain.Mysecondbirthingexperiencewastheworstamongthethree.Thesamepeopledeliveredmy
babies,thesamedoctor,onegoodnurseandtwobadnurses.Theykeptshoutingatme,whereasthe
othernursecalmlyinstructedeverything.Theykepttalkingaboutmychildbirthtomyparentsandothers
andamongstthemselves,nottome.Thedoctorwasnicetoo.Shekeptmecoveredandexposedonlyas
muchasneeded.Thedoctordideverythingfromcheckinginmyvaginaifmybabyiscoming,togiving
injections,fluids,andstitchingmeafterbirth.Thenursesjustcleanedeverythingaroundme.Thenurses
weretherethroughoutthough.Thedoctorhadjustinstructedthemto‘callmewhenit’stime’.Iwasgiventwoinjections,atabletandtherewasaninjectioninthebottlewhichincreasedmylabourpains.Ikept
screamingafterthat,asmypainsincreasedsomuch.Myfathertoldmymothertobeinside,becauseI
mightbescared.IdidnotwanthertotouchmesinceIwasinsomuchpain.Iwantedtohiteveryone.Her
too!
Mythirdbirthwasthebest!Itwastheshortestindurationwithverylesspain.Iwaswaitingtobecut,but
thedoctordidnot.Iwassohappy!Inthepreviousbirththeysaiditwonthurtwhilecuttingandstitching
me.Theysaiditwasjust2-3stiches,butIknowitwasmuchmore.IknewwhenshecutmedownthereandIfelteverystitch.Ifelteverything.Theyheldmedowntightly!Twoofthemheldmylegsandoneof
themtightlyheldbothmyhandsabovemyheadasIscreamedthroughthepainandthedoctorignored
mypleasandkeptstitching.Theysaiddon’tyouwanttogiveussomethingoutofhappiness?Theyfinallybroughtmybabytomehourslater,aftermyfathergavethem2000rupees.
Haveyoudoneanyresearchonalcoholism?Alcoholruinedmyfamilyyouknow!Iamlivingformychildren
andIwanttostartearningtoraisethemtobeawayfrommyalcoholichusband.Hedrivesataxi,drinks
andbeatsme,butItookhimtocourtandheisnowinjail.Iprobablyshouldn’thavedonethat.Hehas
moneyforalcoholbutnotforchildren’seducation.Idon’tknowanythingtogetajob,Istoppedgoingto
schoolwhenIwas13andwasmarriedveryyoung.Iwasveryhappywithoutacareintheworld,but
marriageruinedeverything.Myparent’sshouldhaveforcedmetostayinschool,itwastheirjob.Ihavean
accountinbankbutnomoney.Idon’tknowanythingaboutmoney,Ineverdid.Ineveraskforanythingfor
me,butIcanfightwithanyonewhenitcomestomychildren’swellbeing.
Ineversharedthesethingswithmymotherormyhusband.Wedon’ttalkaboutbirthinfamilyorwith
friends,youjustdon’tdoit.IdidnotknowthatIhadtheneedtotalkaboutmybirth.Youareclosertome
thanmyfamilynow.

Chapter7
194
7.4.4 Cultureinfluencescarearoundchildbirth
Cultureguidesmanyactionsduringbirthingthatfunctionatdifferentlevels.Familiesusuallyhave
someculturalnorms,mythsandtraditionswhichcouldbelimitedtothefamilyorsharedbythe
communityoreventhestateorcountry.Thisisbasedontheaspectsthatbindthemtogether
whichcouldbefamilyties,gender,caste,religionetc.Whowillbepresentaroundthewoman
givingbirthisculturalandsoisthepresenceofdai,asnoticedinallthehomebirthsinruralor
urbaninterviewsandeveninthehospitalbirths,althoughthereisnoformalroleforadaiinthe
hospitalbirthingenvironment,andyetsheseemstobeoneofthekeycareproviders.
“Everyonewantedittobenormalbecausenobodyhadgivenbirthbycaesareaninmyfamily
before.Nobodywantedmetohaveacaesarean.That’swhyeveryonewassad,mymotherwas
sadandcryingandsaying‘whathashappenedtomydarlinggirl!’.”(Pairo)
Culturedrivesmanysmallandbigactionsaroundchildbirth.It’sinwomen’sculturetowearsaree
ingeneralandwhentheygivebirth.Wearingasareeand/orpetticoatunderit,helpstoavoid
overexposurewhengivingbirth,beitathomeorhospital.Manycareprovidersrecommend
womentowearanightiewhentheygoinlabour,fortheeaseofwearingandremoving.Notall
theculturesareappropriate,somearequitedamagingforthecommunityandhaveadrastic
impact.SonpreferenceisonesuchdangerousanddominantcultureinBiharthatturnsthebirth
ofagirlintoanatmosphereofsorrow.Eventhoughsexdeterminationinpregnancyisillegalin
India,peopleoftentrytodeterminethesexofthebaby.Ondenial,theymayfeelthattheyare
notbeingtoldbecauseitsnotthe‘preferredsex’.
“For9monthsIassumedIhadadaughterbecauseshe(doctor)won’trevealittome.SoIthought
it’sagirlbecauseshewasn’ttellingme…Thedoctorsaidthatthisisagirl.Peoplewanttheirfirst
childtobeaboy.Theyalsosayifitstartswalkinglateitwillbeaboy.”(Pairo)
“IthoughtIwillhavetwoboysandagirlandthenIwillgetoperated.Butthisisalsoagirl.I
usuallystayunwellsoIdon’twantanymorechildren.”(Sita)
Itisessentialtounderstandhowthecultureofabuseseapsintopeople’sliveswhentheyare
growingupintheirhomeandsurroundings.Thisaidsinnormalisingviolenceagainstwomen,
wherewomenadapttoitaspartoftheircultureanddonotresistviolenceduringpregnancyor
childbirth.Extortionisalsoobstetricviolenceduringchildbirth,whichiscalled‘happinessmoney’
especiallyofferedgenerouslyfollowingbirthofamalebaby.ItisaculturalcharacteristicofBihar.

Chapter7
195
Oppressionofwomen,givingwomenasecondarystatusinsocietyandwomen’soveralllackof
importance,iscultural.Thisisevidentinwomenenduringpain.Womenaresupposedtoendure
painandtheydothataslongastheycan.Theirsilenceaboutanythingthathappensinthe
birthingenvironmentispartcultural.Womenunderstandthattheyarenotsupposedtoconverse
inthebirthingenvironment,theyarenotsupposedtoquestionordoanythingtodrawattention.
“IwasfeelingbadbutIcouldnotsayanythingbecausewewereinthehospital.IfIsayanythingto
themthentheywillsay‘youarenottheonlyonehavingababyhere.Thereareotherpeopletoo
whodon’thaveanyproblem.Youdon’thavesomethingspecialdownthere’.”(Ria)
“EverythingwashappeninginfrontofmebutIcouldnotsayanything.Youarenotsupposedto
talkaboutoperation…youloosealotofbloodandthebodybecomesweak.”(Pairo)
“Ifirsttriedtobearthepainbutwhenitwasunbearableforme,thenItoldmymother.”(Sita)
Birthingisconsideredwomen’sbusiness,butironicallythewomangivingbirthhasnosayinit.
Thewomenaroundthebirthingwomanmanagemostthings.Womenoftengototheirmother’s
housetogivebirth,mainlyexpectingsomerestduringthelatestageofpregnancyand
immediatelyafterbirth.
“Wedon’tdoanyheavyworkjustcookfoodafterbirth.Noliftingheavythings.”(Sita)
“Iwasatmymother’shouse…therewasnoonetotakecareofmeheresoIwenthome.”(Sita)
Womendonottalkaboutbirth,regardlessoftheircuriosity.Theyaresurroundedbywomenwho
havegivenbirthbutdonotsharethegorydetailsofthebirthingprocess,andwomenacceptit
withoutquestioning.Theydonotdiscussitwiththeirhusbandsasitistooshameful.Theculture
istonottalkaboutbirthingandbirthsinBihar,itisstigmatised.
“Atthetimeofbirtheverybodykeepssearchingforallthis(information).Everyoneiscuriousto
knowallthis.”(Sujata)
“HowcouldIaskhim(Husband)‘howwillitcomeout?’”(Pairo)
“WhatwillhappenisGod’swill.WhenGodwillwantittohappen,itwillhappen.”(Pratima)
Thelackofimportanceaccordedtowomenbeginsatbirthandiscultivatedthroughlivingalife
thatisnotvaluedmakingwomenawareofthateveryday.Theirdateofbirthisofless
importance;itwasnotcelebratedorremembered.Decisionsaremadeforthemandtheyare
supposedtofollow.UrmilaandRia’sIpoem(Box7.5)presentthisaspectoftheirupbringing

Chapter7
196
whichmentionshowimportantitistobeafair(lightskinned)girltobemarriageableandtogive
birthtoasonthereafter,assoonaspossible.
“HowoldamI?Idon’tknow.”(Sita)
“Inevertookanydecisionformyselfneitherformychildbirth.”(Urmila)
Box7.4 Ria’sIpoem-HadIbeenfairerandhadbirthedaboy
HadIbeenfairerandhadbirthedaboy…
IwouldhavebeenhappierifIhadason.
Ihavenosonsorbrotheratmyhome.
Ihadonesister,shepassedawayatanearlyage.
Ihaveneverseenmyfather.
Iwas1½yearsold,whenmyfatherpassedaway,hewasmurdered!
Iwasallaloneatmyhome.
MymothertookcareofmeasIgrewup.
IthoughtifIhadason,thenhewouldcarrymyfamily’snameforanothergeneration.
Iwasexpectingason,butIhadadaughter.
Iwassad.
Iswear,Iwassad!
IwonderwhyIdidnothaveason,whyIhaveadaughter.
IliveinthishouseandnooneasksmewhereIwork.
Igotowork,butpeoplesayIamgoingtodowrongthings.
Ifeellikecrying.
Ithink,ifIhadason,hecouldsupportme.
Ishouldhavehadason!
Iwasmarriedwithgreatdifficulty.
Iusedtotellmother,‘Idon’twanttomarryhim.’
Myfamilyruinedmymarriage.

Chapter7
197
MyunclesaidIworkinaboutique,inaparlour.
Iusedtoworkverylate,11amto8or9pm.
Idon’tworkthereanymore.
Myhusbandstarteddoubtingme.
IsaidIwillnotstaywithhim.
IfIhadbeenfair14,Iwouldbebeautiful,mymotherwouldhavemarriedmeofftosomeonenice.
Iwouldhavebeeneducated,Iwouldhavebeenbetteroff.
Myluckwasbad!
7.5 Discussionandconclusion
Gender,power,structureandcultureinfluencethedecisionsmadeforwomenbywomen,by
theirfamilymembersandcareprovidersabouttheirlives,includingpregnancyandchildbirth.
Figure7.4summarisesvariousaspectsofthesefourdomainsthatarecross-cuttingandoverlap
acrossdomains.Forinstance,women’slackofchoiceisgender-based,culturallydeep-rootedand
womenareconditionedintoit,inapatriarchalsocietalstructure.Itmaintainspowerlessnessby
keepingwomeninalowerpositioninthesociety.Similarly,theotheraspectshavebeenputin
onedomaineach,basedontheresearcher’sunderstandingofwhichdomaineachofthese
aspectsrepresentbest.Theircross-cuttingnaturecanbenoticedinthefindingsaswell.Idecided
tokeeptheminaparticulardomainbasedonwhatmademostanalyticsensetome,butthisis
subjectiveandthereadermayfeelthatanaspectbelongstoadifferentdomain.
14Lighterskincolour

Chapter7
198
Figure7.3 Impactofgender,power,culture&structureonwomen(Author’sown)
Womenreportalackofagencyinmakinganydecisionsaboutthemselvesandtheirbody
includingduringpregnancyandchildbirth(McAraCooper,2011).Thisbeginswiththeuncertainty
ofwhetherwomenwillbeallowedtobebornowingtotheunwantednessofafemalechild
(Hawkesetal.,2020).Thisisfollowedbyalifecoursethatincludesnotbeingallowedtomakeany
decisionsabouttheireducation;nothavingfinancialindependence;havingnosayinconception
andcontraception;notbeingabletodecidetheirfamilysize;nosayinageofmarriageorpartner
ofmarriage;notallowedtodecidewheretogivebirth;whomtohaveasabirthcompanion;not
beingaskedtoconsentforthemedicalinterventionsandbeingtreatedlikeanobject;enduring
obstetricviolencewithoutgrievancewhichincludesnotbeingallowedtoscreamduringlabour
painsandnotgettingaresponsetoquestionsandbeinginformed,evenwhenbeingoperated,
andnotgivenasayinthecareoftheirnewborn.Thisoppressionofwomenaroundchildbirthand
alackofagencyindecision-makingisinlinewiththeliteraturefromIndiaandothercountries
(Menon,2012;Chawla2006;Chalwa2019;Senetal.,2018).
Villarmea(2020)explainsthatthereasonbehindalackofwomen’sagency,autonomyandthe
frequentdisregardoftheirrefusaltointerventionsisbecauseofthe‘uterineinfluence’.Women
areconsideredincapableofmakingrationaldecisionsduetopain,andwomen’schoiceand
consentisoftensupersededbecausetheyaremerethe‘container’forthe‘foetus’,whois
consideredthekeystakeholderinchildbirth.Thisisacharacteristicofapatriarchalmedicalmodel
ofcare(Oakley1982;Hill2019)evidentalsointhefailureofthedoctortostoponUrmila’sstrong

Chapter7
199
resistancetounanesthetisedepisiotomyrepair.Urmila’sanxietyoverherdecisiontoputher
husbandinprison,isasignofthepatriarchy-drivenmindsetwhichcomesfromadeep-rooted
conditioningintothatculture.Heranxietyisaboutbreakingthenormsandtherealisationofthe
repercussionsofthisactofresistanceonherandherchildrenfromherhusband’sfamily,society
andfromherhusbandwhenheisreleasedfromprison.Women’snarrativesdisplayapatriarchal
culturewheretheirvoicesandchoiceshavelimitedscope.Whenpatriarchypermeatesthe
birthingenvironment,medicalinterventionsareprioritisedoverwomen’scomfort,dignityand
choice(Villarmea2020;Mayra,Matthews&Padmadas2021).Urmilapraisedherdoctorduring
herinterview,regardlessofthetraumaticexperienceshenarrated.Thisisindicativeofa
structuralissueandapartoftheculturalconditioningofwomen.Wenoticethisinwomen’s
expectations,acceptance,enduranceandtheirreactiontotheviolenceandalackofdecision-
makingroleduringchildbirthinanobstetricenvironmentandintheirroutinelife,intheirsocial
environment.
Women’sresiliencetoendureviolenceinthehospitalenvironmentisinaccordancetotheir
intimatepartnerviolenceanddomesticviolenceintheirhomeenvironmentinBihar(Jeejebhoy,
2018;Koskietal.,2011).Justaswomenoftendonotexpectrepercussionsforviolenceintermsof
intimatepartnerviolenceanddomesticviolenceinthehomeenvironment,theymaynotexpect
anyrepercussionsforobstetricviolenceintheobstetricenvironmentbecauseviolenceagainst
womenisnormalised.Repercussionsareonself,notontheperpetrator.Therearefewexamples
inthisstudyofwomenwhobrokethisnarrativeandshowedresistance,suchasthatofUrmila.
Sitarefusingtoletherdagarinmother-in-lawdoavaginalexaminationanddecidingtogivebirth
atthehospital,inanareawheremostofthebirthsintheneighbourhoodweretraditionally
assistedbyhermother-in-law.InanotherscenarioUrmilawantingtohithermotherwhenshe
washerbirthcompanion,goesagainstthecommoncultureandstructureofbirthinginBihar.In
thepersonallives,bothRiaandUrmilashareaboutintimatepartnerviolenceandbothhavetaken
astandagainstit,Urmilabysendingheralcoholichusbandtojail,andRiabydivorcingher
husbandwithoutalimony,whichisquiteunheardofinIndiawheretherateofdivorceis0.24%of
themarriedpopulation(Thadathil&Sriram,2019).Receivingrespectfulcare,alongwiththebasic
gestureofbeingspokentorespectfully,changesthatpowerdynamicsandindicatesan
equalisationofthepower-basedimbalancewhereinwomenfeeltheyarereceivingwayabove
theirgrade,whichmayleadtoarelationshipoftrustbetweenthecareproviderandcareseeker.
Womenareconstantlynegotiatingpowerathomeandhospitalandeveryotherenvironmentshe
engageswith.Sheknowssheisatthebottomofthehierarchybystructure,moresoinan
obstetricenvironment,soshediscountsthegoodbehaviouranddoeswhatisbeneficialforher
baby,followsorders,enduresobstetricviolenceandshegoeshomewithalivebaby.

Chapter7
200
Thepowerdynamicismoreleveledinhomebirths.Educationorfinancialindependencedidnot
influenceitmuchforPairo,whowantedtobetoldabouttheinterventionsanddenyvaginal
examinations,andatleastrequestforprivacy,butshecouldnotstateanyofthesetoherfamily
membersorthecareproviders.However,theimpactofhereducationandfinancial
independencecouldbeseeninherdecisiontonotgivebirthinagovernmenthospitalandgotoa
privatehospital.Thecultureofsilenceisseeninmostaspectsofwomen’sexperienceswhichthey
acceptandendureintheirusuallivesthatreflectsinthebirthingenvironmentaswell(Shabot,
2020a).Thenormaroundbirthingisthatwomenaresupposedtoendureit,asthatistheusual
courseofinstitutionalbirthanddoesnotfallinthecategoryofviolenceorvictimisationtobe
grieved(Shabot,2020a).
Obstetricviolenceisgender-basedviolence.Theintersectionalityofawoman’sotherbackground
characteristicssuchaseducation,socio-economicstatus,gender,marriage,religion,age,parity,
caste,class,stateandnationmaydeterminehervulnerabilitytoobstetricviolence(Pateletal.,
2018;Jeffery&Jeffery,2010;Senetal.,2018).Thishasalsobeenreportedelsewherewhere
scheduledcastewomenwereseentoreceivetreatmentafterhighercastewomenaretreatedin
Bihar(Pateletal.,2018).Literaturealsosuggeststhataccesstomedicaleducationhas
traditionallybeenlimitedtomostlymenofhighercasteandricherfamilies,whichincreasesthe
socialdistancebetweenthewomanandherdoctor(Prakashetat.,1993).Inmystudywefound
womenbeingabusedduetosomeofthesefactors,whichwerealsoidentifiedbytheparticipants
suchaspoverty,lackofeducation,beingawomanandstateofmarriage.
Structuralintersectionalityexplainswhythewomenareatadisadvantageinapatriarchalculture,
inamale-ledmedicalmodelofcareandthroughthevariousfactorsthatmaintainthedominant
poweroverwomen.Thecurrentstructureofbirthinghaschangedtoinstitutionalbirthsasa
dominantculture,eveninlow-economicsettingswiththeimplementationofJSYaspartofNRHM
(nowNHM).Anjuchallengedthisstatusquowhenshedecidedtofreebirthinherthree
subsequentbirthsfollowedbytwostillbirthsatapublichospital.Freebirthingor‘handsoffbirths’
havebeenontheriseandarebeingincreasinglyreportedincountriessuchasAustralia,
Netherlands,UKandUSforexpressingwomen’sdesiretohaveaninterventionfree,vaginaland
respectfulbirth(Freeze&Tanner,2020;Jackson,2020;Feely&Thomson,2020;Hollander,2020).
Therearemanyaspectsinthestructureofbirthingthatareviolenttowomen,thatviolate
women.Mostwomenstronglyexpressedtheirdisapprovaltowardsvaginalexaminations,when
theywereoftengivennoprivacyandwererestrainedbyothers.Thiscanbeconsideredadisplay
ofphysicaloverpowering.Chawlaconsidersroutineepisiotomyandfemalegenitalmutilationas
violenceagainstwomenassexualbeingstargetedattheirgenitals,women’s‘siteofpower’
(Chawla,2019).Regardlessofthelackofagencyandchoice,thelossofpowerispartofthe

Chapter7
201
culture.Respectfulmaternitycarewasseenwherethefamilyhadsomeinfluence,suchasfor
Pairoinhersecondcesareansectionduetotheinfluenceofherdoctormaternaluncle.The
interplayofthesefourdiscourses,gender,power,cultureandstructure,areessentialto
understandtoensurerespectfulcaretowomen(Figure7.4)(Hutter,1994).
Chapter8
202
Chapter8 “It’seasytoabuseobesewomen!”:Whydo
somecareprovidersengageinobstetric
violence?
Thepreviousfindingschaptersfocussedonwomen’svoiceandembodiedexperiencesof
respectfulmaternitycareandobstetricviolenceduringchildbirthasprimarycare-seeker.Nurse-
midwivesaretheprimarycareproviderstowomen,whentheyseekreproductiveandmaternal
healthcare.Nurse-midwives’standpointaboutobstetricviolenceisessentialtoensurerespectful
maternitycareandtounderstandthebarrierstheyfaceincareprovision,inlowresource
settings.AsisdiscussedintheFreedmanetal.’sdefinition,thedeterminantsofobstetricviolence
needtobeexploredandaddressedatallthreelevels,individual,structuralandpolicylevels.
Nursingandmidwiferyleadershaveservedatthefrontlineofcareprovisionandexperiencedthe
challengesintheircareersspanningdecades.Theyarenowatthehighestdecisionandpolicy
makingpositionsintheirdomain.Theyarebestplacedtosharethedeterminantsofobstetric
violencefromthecareprovidersside,atallthesethreelevels.Thischapterpresentsnurse-
midwives’perspectivefromdifferentpolicy-makingpositions,tounderstandhowtomake
respectfulmaternitycareareality.Somenursingandmidwiferyleadersreflectontheissueand
thesolutionfromtheirownbirthingexperiences.
8.1 Background
Obstetricviolenceisahumanrightsviolationandarecognisedglobalphenomenonthatmayvary
acrossdifferentculturalandsocio-economicsettings.Ihavedescribedthenatureofobstetric
violencefrompreviousstudiesandfromwomen’sownexperiencesandperceptionsinthe
previouschapters.Thisincludesthecommonlyheardabusiveandsexistcommentsthathealth
workersdirectatwomenduringchildbirthandIhavepresentedhowthisisnormalised,endured
andtoleratedresultinginloweringofwomen’sexpectationsfromcareduringchildbirth.Studies
oftenreflectonintentionalityasakeyconstructinthecontextofhealthcareworkersengagingin
obstetricviolence.Intentionalactionstoharmwomen’shealthandwellbeingaredisrespectful
andabusive.Studiesreportevidenceofseveralformsofdisrespectandabuseglobally,which
beginswithanabsenceofgreetingonarrival,acommondisrespectthatmanywomen
experience,toextremeformsofabuseincludingphysicalviolence,reportedfromdevelopingand
developedcountriesalike(Abuyaetal.,2015;Miltenburgetal.,2018).

Chapter8
203
Despitegrowingevidenceontheextentofdisrespectandabuseduringchildbirth,theunderlying
reasonsfromaprovider’sperspectivehavenotbeensystematicallyunderstoodintheIndian
context.Thesecouldbecultural,socialorhealthsystem-relatedfactorsthatmayexplainwhy
womenaredisrespectedandabusedduringchildbirthbytheircareproviders.Between2005and
2016,Indiahasseenanunprecedentedincreaseininstitutionalbirthsfrom39%to79%,yetthere
hasbeenlittleimprovementintheprovisionofqualitymaternalcareservices(NFHS-3;NFHS-4).
Positioningnurse-midwives15inanindependentmidwiferyrolehasbecomemoreimportantin
suchcircumstances,becausetheyaretheclosestcareproviderthatwomencomeincontactwith
duringpregnancyandchildbirth.InIndia,everyyear,approximately27millionbirthsare
reported,andofthese,nurse-midwivesattendoneinfourinruralareasandoneinsixinurban
areas,asprimarycaregivers(Radhakrishnan,Vasanthakumari&Babu,2017).
Studiesshowthat,globally,midwivesfacesignificantprofessionalbarriersbecausetheyarepart
ofaprofessiondominatedbywomen.Midwiveshavehistoricallybeencomparedwith‘witches’
(Ehrenreich&English,1970)andlabelled‘halftaught’,‘totallyignorant’(Oakley,1997)and
blamedfornegativebirthoutcomes.Fromafeministperspective,thisrepresentsadouble
contextofpowerlessnessattributedtosocialhierarchiesforbothwomenintheirsocially
prescribedrolesandnurse-midwivesatalowlevelinthemedicalhierarchy(Sheikh,Raman&
Mayra,2012;Filby,McConville&Portella,2016;Mayra,2020a).Furthermore,alackofleadership
opportunitiesamongnurse-midwivesindecision-makingpreventthemfromadvocating
effectivelyforwomenintheprovisionofquality,respectfulanddignifiedmaternitycare(Maslach
&Leiter,2016;Steege&Rainbow,2016).Midwivesarguethattheirroleincareprovisionis
unrecognisedandtheyareoftendiscriminatedagainstandsuppressedbyphysicians.Such
challengescanleadtoburnout,workplaceharassmentandbullying,causingcareprovidersto
showreducedempathyandcompassion(Maslach&Leiter,2016;Steege&Rainbow,2016)
therebyincreasingthecareseekers’vulnerabilitytodisrespectandabuse.
Theliteraturesuggeststhatpoorworkingconditionsleadingtoburnoutincareprovidersmay
leadtopoormaternalhealthoutcomes(Maslach&Leiter,2016;Steege&Rainbow,2016;Hunter,
2009).Midwives’workhasbeendescribedasemotionalwork(Hunter,2009).Theresulting
depersonalisation,cynicismanddetachmentareusedascopingmechanismstodealwith
workloadandjobstress(Maslach&Leiter,2016;Steege&Rainbow,2016).Thisisevidentin
15IndiadoesnothaveanindependentmidwiferycadreasperthestandardsofInternationalConfederationofMidwives.TheIndiansystemofeducationenablespracticingmidwiferywithnursingthroughadualregistrationofregisteredmidwivesandregisterednurses.Hencetheyarereferredtoasnurse-midwivesinthisstudytoacknowledgetheirdualroleandabsenceofindependentmidwivesinIndia.

Chapter8
204
manyaspectsofcareduringchildbirththatincludesaddressingwomenbythecolouroftheir
attireorbednumber;thatdisplaysalackofempathywhenintentionallymistreatingwomen
duringchildbirth.Midwivesreport‘switchingoff’andputtingontheir‘masks’or‘happyfaces’to
appeardignified,whichleadstoemotionalwithdrawalandphysicaldistancingfromwomenthey
arecaringfor(Hunter,2009).Theyfeeltheneedto‘dontheiremotionalarmour’whichsome
refertoas‘surfaceaction’or‘impressionmanagement’,tobeabletoperformwhatthejob
requires(Hunter,2009;Deery,2009)whileinsidetheymightbefeelinglikea‘foodmixer’
(Edwards,2009).Potentialabuseofthemidwifeandalackofopportunityforthemtoprocessthe
emotionsinajobthatinvolvesdealingwithvitalevents,suchasbirthsanddeathsregularly,may
addtowomen’svulnerabilitytomistreatment.
The‘WhatWomenWant’campaignisveryrelevant,asitaskedwomenandgirlsgloballytheirone
keydemandforimprovementinmaternalandreproductivehealthservicesandthetopranking
demandfrom1.2millionparticipantsin114countrieswasrespectfulmaternitycare(WRA,2019).
Theneedforrespectfulcarecanbebetterunderstoodbyunravellingtheunderlyingcausesof
obstetricviolenceduringchildbirth,whichremainsakeygapintheobstetricviolenceliterature.
Clearly,midwifery,nursingandmedicalstudentsshouldbeprovidedwitheducationfreeof
hierarchy,genderandstatusbaseddifferences,andtheyshouldbesufficientlymentoredto
providecarewithoutanyformofbiasordiscrimination.Theabuseofhierarchyinmedical
educationisasignificantbarriertorespectfulmaternitycare(Madhiwallaetal.,2018;Dinizetal.,
2018).ArecentstudyconductedintwotertiarylevelhospitalsinMaharashtra,Indialooked
specificallyatstructuralviolencethroughinterviewswithcareprovidersandfoundnormalisation
ofdisrespectandabuseduringchildbirthandmedicalstudentsengaginginsuchpractices
(Madhiwallaetal.,2018).Furthermore,respectfuleducation,studentsobservingrespectfulcare
andpracticingitintheirpre-serviceeducationiscrucial,sothattheyarenotconditionedto
providecarethatisdisrespectfulandabusive(Moridietal.,2020;Dzomekuetal.,2020).
Evidently,theseunderlyingcausesmaybeperceiveddifferentlybywomen(ascareseekers)
comparedwiththeperceptionsofmidwives,nurses,doctorsandother(ascareproviders)(Beck,
Driscoll&Watson,2013).Ipresentedwomen’sperceptionofthefactorsbehindobstetric
violenceinthepreviouschapter.Thischapterbridgesthegapbyexploringthenurse-midwives’
perspectiveofthereasonsbehindobstetricviolenceofwomenduringchildbirthinthecontextof
India.
8.2 Researchquestion
Whydosomehealthcareprovidersdisrespectandabusewomenduringchildbirthinindia?

Chapter8
205
8.3 Objectives
1. Toinvestigatemidwiferyandnursingleader’sperceptionsandexperiencesofrespect,
disrespectandabuseduringchildbirthinIndia.
2. Tounderstandthedeterminantsofobstetricviolencefrommidwiferyandnursing
leader’sperspectiveinIndia.
3. Todocumentmidwiferyandnursingleader’srecommendationsforrespectfulmaternity
careprovisionduringchildbirthinIndia.
8.4 Methods
ThestudyparticipantsarethemidwiferyandnursingleadersinIndiaholdingkey,formaland
informalleadershiprolesinthedomainsofeducation,regulation,administration,advocacyand
serviceprovisionaspresentedinTable8.1.Someoftheparticipantsrepresentmorethanone
domain.Itiscrucialtoexplorethestandpointofprimaryhealthcareprovidersandthestudy
participantshavedecadesofexperienceatthefrontline,providingcaretowomenbeforetaking
onvariousleadershippositionstoinfluenceandmakepolicies.Theselectedleadershavereached
alevelofprominenceintermsoftheirofficialposition.Mostofthemhavereportedlimited
decisionandpolicy-makingpowerevenwhentheyareatthehighestattainablepostsfornurse-
midwives’.Theyunderstandthechallengesinherentincareprovisionandhowthesechallenges
maybetackled.Theperceptionsandexperiencesoftheseleadersareusefulindeveloping
practicalsolutionstoensurerespectfulcareduringchildbirthinIndia.
Table8.1 Participantbydomainofleadership
Domains State National Global Total
Administration 3 2 1 6
Advocacy 8 3 4 15
Education 9 4 2 15
Regulation 4 1 2 7
ServiceProvision 6 1 1 8
*someparticipantsrepresentmultipledomains
Chapter8
206
Iusequalitativemethodstoinvestigatethereasonsunderlyingobstetricviolencefromthecare
providers’perceptions.Iselectedparticipantsthroughpurposiveandsnowballsamplinginfive
statesinIndia,namelyBihar(BH),Rajasthan(RJ),Odisha(OD),MadhyaPradesh(MP)andWest
Bengal(WB)andatthenationallevel(NL).Thesestatesrepresentdiversecontextswith
unfavourablematernalhealthindicatorsincludinghighmaternalmortality.Theleadersare
selectedinthreecategoriescomprisingthestatelevelandthenationallevelinIndiaandathird
categoryfromaninternationalperspectivewithparticipantsfromadvancedhealthcaresystems
participatinginglobalpolicymaking.
InIndia,healthisastatesubject,thereforepolicy-makingandgovernanceisdividedbetweenthe
statesandthecentre.Thestatesrepresentawiderangeofhealthcarecontextsthataredifferent
ingeography,cultureandhealthoutcomes,yettheysharethesimilarhealthsystem
infrastructureandfacesimilarchallenges.Theselectionofnurse-midwifeleadersatanational
levelfacilitatestheunderstandingofthelargerpictureofhealthpolicyandgovernancestructure
inIndia.Additionally,IinterviewedmidwiferyleadersintheUnitedKingdombecauseit
representsasuccessfulmodelofmidwiferycarethathasmadecommendableprogressin
respectfulcareprovisionandhascollaborationswithpartnersimplementingmidwiferyinIndia.I
alsointerviewedeightmidwiferyleadersforaglobalperspectivewithprofessionalsfromWHO
Headquarters,ICM,ICNandUNFPA,thatplayakeyroleinmakingandinfluencingpoliciesata
globallevelthathasanimpactoncountriessuchasIndia.
8.4.1 Studyinstrument
Ipreparedasemi-structuredguideforin-depthinterviews.Theinterviewguidehadthree
sections;1)backgroundinformation;2)participant’sroleandresponsibilities;and3)perception
ofrespect,disrespectandabuseincareduringchildbirth.Giventhesensitivityindiscussing
disrespectandabuseofwomenduringchildbirthbycareproviders,Iusedanillustratedpainting
ofawomangivingbirthtoinitiatetheconversation(Figure8.1).Thethemeandcontentsofthe
paintingreflectedtheleadresearcher’sexperienceandobservationsofchildbirthinapublic
hospitalsettinginIndia.
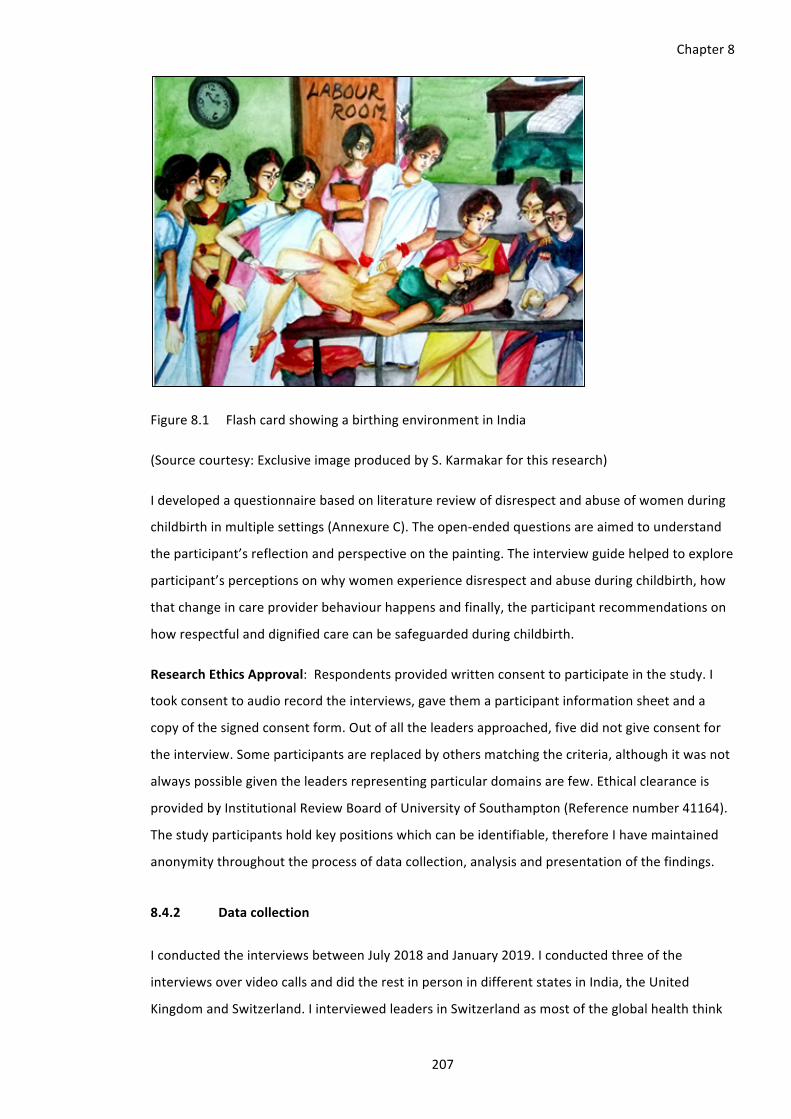
Chapter8
207
Figure8.1 FlashcardshowingabirthingenvironmentinIndia
(Sourcecourtesy:ExclusiveimageproducedbyS.Karmakarforthisresearch)
Idevelopedaquestionnairebasedonliteraturereviewofdisrespectandabuseofwomenduring
childbirthinmultiplesettings(AnnexureC).Theopen-endedquestionsareaimedtounderstand
theparticipant’sreflectionandperspectiveonthepainting.Theinterviewguidehelpedtoexplore
participant’sperceptionsonwhywomenexperiencedisrespectandabuseduringchildbirth,how
thatchangeincareproviderbehaviourhappensandfinally,theparticipantrecommendationson
howrespectfulanddignifiedcarecanbesafeguardedduringchildbirth.
ResearchEthicsApproval:Respondentsprovidedwrittenconsenttoparticipateinthestudy.I
tookconsenttoaudiorecordtheinterviews,gavethemaparticipantinformationsheetanda
copyofthesignedconsentform.Outofalltheleadersapproached,fivedidnotgiveconsentfor
theinterview.Someparticipantsarereplacedbyothersmatchingthecriteria,althoughitwasnot
alwayspossiblegiventheleadersrepresentingparticulardomainsarefew.Ethicalclearanceis
providedbyInstitutionalReviewBoardofUniversityofSouthampton(Referencenumber41164).
Thestudyparticipantsholdkeypositionswhichcanbeidentifiable,thereforeIhavemaintained
anonymitythroughouttheprocessofdatacollection,analysisandpresentationofthefindings.
8.4.2 Datacollection
IconductedtheinterviewsbetweenJuly2018andJanuary2019.Iconductedthreeofthe
interviewsovervideocallsanddidtherestinpersonindifferentstatesinIndia,theUnited
KingdomandSwitzerland.IinterviewedleadersinSwitzerlandasmostoftheglobalhealththink

Chapter8
208
tanksthatinfluenceglobalpoliciesarelocatedthere.LeadersfromUnitedKingdomhave
establishedamidwiferyledmodelandhavecollaboratedwithIndiancounterpartstoimplement
midwiferyinIndia.IcarriedouttheinterviewsinEnglish,afewinHindiandBengali.Iamfluentin
thesethreelanguagesandmynativelanguageisBengali.
Icontactedtheparticipantsbyemailinitially,witharequesttoparticipateinthestudy.I
conductedmostoftheinterviewsintheparticipant’sofficeorresidence.Mostwerefreefrom
anyinterruptions.Iconductedtheinterviewswithparticipantsrepresentingregulatorybodiesin
theiroffices,withquiteabitofinterruption.Mostinterviewslastedbetween30minutesto1.5
hours.Itookreflexivenoteswithdescriptionsoftheinterviewenvironment.Iinformedthe
participantsaboutthestudyobjectivespriortoschedulingtheinterview.Iintroducedmyselfto
theparticipantswithinformationaboutmyqualificationsandprofessionalbackground.Nine
prospectiveparticipantseitherdeclinedtoparticipateordroppedoutfromthestudyduetoalack
oftime.
8.4.3 Dataanalysis
Ianalysedthedatausingthematicanalysis(Green&Thorogood,2014).Theanalysisapproachisin
linewithreflexivethematicanalysiswhichhasthemesdrawnfromtheresearchquestionsandthe
semi-structuredinterviewguide(Braun&Clarke,2019).Thethemesareclustersofcodesthat
haveasharedmeaning(Braun&Clarke,2019).Isupplementeditwithemergingthemeswith
deductivecodingasanalysisprogressed.Idecidedtheinitialcodesbasedonwhatmadethemost
analyticsenseandappearedfrequentlyacrossdata.Furthercodesweregeneratedbasedoneach
code’spropertyandrefinedwithsubcodes.QualitativedataanalysissoftwareNVivo12isusedto
aidinanalysis.Icodedthedata,alongsidedatacollection,toidentifyandexploretheemerging
themesandintheupcominginterviews.
8.4.4 Positionalityandreflexivity
Mybackgroundandinvolvementinresearchingandinfluencingmidwiferyandnursingpoliciesin
Indiaandgloballyplayedakeyroleinparticipant’sagreementtotakepartintheresearch.Ihave
professionalacquaintancewith11outofthe34participants.Mysubjectivity,shapedbymy
experiences,hasbeenapotentialresourcethroughoutmydoctoralresearchandasBraunand
Clarke(2019)state‘itshouldnotbetreatedasathreattoknowledgeproduction’.Myexperience
ofreceivingeducationinnursingandmidwiferyingovernmenthospitalsinWestBengal,along
withoveradecade’sexperienceofresearchingonthechallengesinhealthcareprovision,helped
todesigntheinterviewguide,conducttheinterviews,analyseandinterpretthedata.
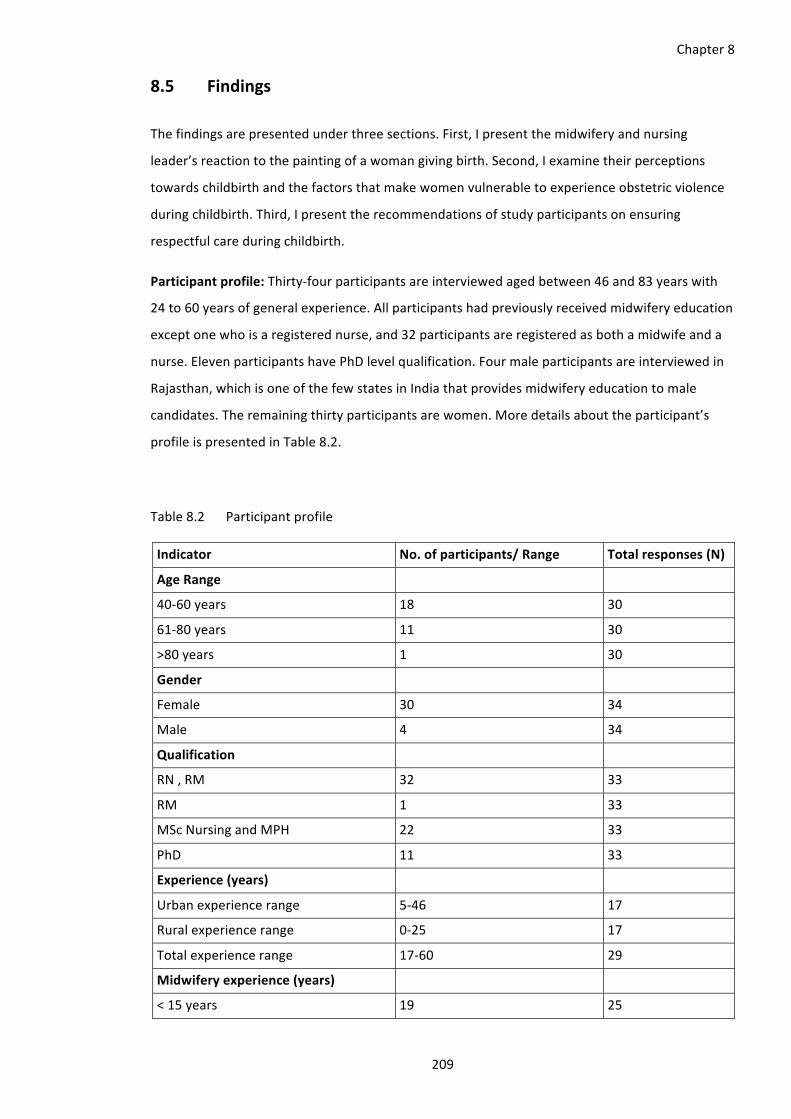
Chapter8
209
8.5 Findings
Thefindingsarepresentedunderthreesections.First,Ipresentthemidwiferyandnursing
leader’sreactiontothepaintingofawomangivingbirth.Second,Iexaminetheirperceptions
towardschildbirthandthefactorsthatmakewomenvulnerabletoexperienceobstetricviolence
duringchildbirth.Third,Ipresenttherecommendationsofstudyparticipantsonensuring
respectfulcareduringchildbirth.
Participantprofile:Thirty-fourparticipantsareinterviewedagedbetween46and83yearswith
24to60yearsofgeneralexperience.Allparticipantshadpreviouslyreceivedmidwiferyeducation
exceptonewhoisaregisterednurse,and32participantsareregisteredasbothamidwifeanda
nurse.ElevenparticipantshavePhDlevelqualification.Fourmaleparticipantsareinterviewedin
Rajasthan,whichisoneofthefewstatesinIndiathatprovidesmidwiferyeducationtomale
candidates.Theremainingthirtyparticipantsarewomen.Moredetailsabouttheparticipant’s
profileispresentedinTable8.2.
Table8.2 Participantprofile
Indicator No.ofparticipants/Range Totalresponses(N)
AgeRange
40-60years 18 30
61-80years 11 30
>80years 1 30
Gender
Female 30 34
Male 4 34
Qualification
RN,RM 32 33
RM 1 33
MScNursingandMPH 22 33
PhD 11 33
Experience(years)
Urbanexperiencerange 5-46 17
Ruralexperiencerange 0-25 17
Totalexperiencerange 17-60 29
Midwiferyexperience(years)
<15years 19 25

Chapter8
210
Indicator No.ofparticipants/Range Totalresponses(N)
15-30years 3 25
31-45years 3 25
Midwiferyexperiencerange 0-41 25
Birthsassistedrange(0-40,000)
<25 4 26
25-100 6 26
101-500 6 26
501-1000 4 26
>1000 6 26
Participant’smidwiferyexperiencerangedfrom0to41years.Theysharedthetotalnumberof
vaginalbirthsassisted,includingduringtheirnursing-midwiferyeducation.Theresponsesrange
from0toapproximately40,000births.Fourofthemassistedlessthan25vaginalbirths,even
thoughitisanessentialcriteriaofpre-servicecurriculumbeforeregisteringasamidwifeinIndia.
Fourrespondentscouldnotciteanumber.
8.5.1 Reactiontothepaintingofawomangivingbirth
TheparticipantsfromIndiausethewords‘terrible’,‘bad’,‘wrong’,‘notright’,‘familiar’,
‘uncomfortable’,‘stressful’,‘notconducive’,‘horrible’,‘extremedisrespectandabuse’and
‘concerning’todescribethepainting(Figure8.1).Oneparticipantsharedherperspectiveofthe
positiveaspectsinthepainting.
“…thepositionsheisin,thewomanisnotcomfortable.Peoplearoundherarestressful…lookat
thestrainedfacesaroundher.Theenvironmentisnotconduciveforher.Thislookslikearural
facility.Inahospitallabourroomsomanypeoplewillnotbearound.Theassistant,doctorand
maximumfourpeoplewillbearound.Studentswillbeallowed.Ascreenislacking,forprivacy.This
lookslikeaprivatefacilityassituationsaredeterioratingintheprivatesector.”(O03)
“She(careprovider)ismassagingtheuterusforcontractionandtoreducethechanceofPPH.This
lookslikePPH.She(labouringwoman)mustbeunconscious,thatiswhythestaffispinchingthe
thighwithforceps.”(R01)
Mostrespondentsacknowledgetheissueandmanyconfidetheyhavenotseenbuthaveheard
fromothersthatdisrespectandabuseduringchildbirthhappens.Afewparticipantsassumethat
thepaintingissetinaprivatehospital,whileothersrefertoapublictertiaryhospital,butdeny
thatnursesengageinsuchbehaviour.

Chapter8
211
“Doctorsengageinthiskindoftreatment”(CL01)
“Staffnurses’don’tdothat,onlyuntraineddais(do).”(O02)
Participantsatthegloballevelreflectonhowsimilarthesituationseemedinmanyotherpartsof
theworldandsayitis‘horrifying’and‘shocking’.Aparticipantalsofoundithardtobelievethat
thelabouringwomanconsentedtohavesomanypeoplearoundherduringchildbirth.
“…thewomenarenotlookingatherbutatthebaby.Thiswomanisstruckwithhorror…blood
pouringfromher.Sheislyingonaflatbedwithnosheet…thefundalpressureisveryhard…Iseea
womanwhoisbeingtortured!Sheisingravepainandisscreaming…thereisonewomanwithher
armaroundherandshehasherhandonherheart.Itindicatessomekindofcompassionforthe
woman.Butbecauseofthesystemofthecareandplace,sheisflatonherback,intheworst
positionpossiblewithoutanycomfortatthetimeofherlife…thisisapictureofextreme
dehumanisation!”.(GL07)
8.5.2 Factorsbehinddisrespectandabuseofwomenduringchildbirth
Factorsaffectingdisrespectandabusethatarerelatedtocharacteristicsofwomen,areorganised
inathreelevelframeworkrangingfromindividualleveltosociallevelcharacteristics.Factors
emergingfromtheresearchthatrelatetonurse-midwives’disrespectfulandabusivetreatmentof
women,asidentifiedbythestudyparticipants,werecategorisedintoindividual,structuralor
policylevels,inlinewithFreedmanetal.(2014)definitionofmistreatmentduringchildbirth.
8.5.2.1 Woman-relatedfactors
Woman-relatedfactorsareorganisedintothreelevelstoo:(i)individual-whichincludespersonal
attributesofthewomanthatincreaseshervulnerability;(ii)communityenvironment-the
woman’simmediatecontextincludinghome,theplaceofbirth,neighbourhoodandcommunity;
and(iii)socialenvironment-includesthestatewomencomefrominIndiaandthecountry.The
differentiationbetweenthelevelsisnotjustgeographicbutalsointermsofimpactthatmaygo
acrosslevels.
Individualattributes
Women’sbackgroundandphysicalappearancecouldmakethemvulnerabletodisrespectand
abuseduringchildbirth.Ageandparityarefrequentlystatedreasonsforpredispositiontopoor
treatmentaswell.Onerespondentmentionedthatwomenwithfourormorechildrenareoften
verballyabused.

Chapter8
212
“Whatdoyouplan,toscoreacentury?”(CL03)
Awomanhadcometogivebirthwithher16-year-olddaughter,whichmayhaveprovokedthe
conversationsuggestingthatthewomanshouldhavestoppedchildbearingafteracertainage.
“Amultigravidashouldnotcometoalabourroomsomanytimes.”(WB03)
Parityisassociatedwithreligiontoo.Onerespondentmentionedthatitiscommontohavemany
childreninsomereligionsandcultures.
“Muslimwomenaremultipara.”(RJ04)
Otherrespondentssaidthatolderwomeninevitablyhearjudgementalcommentsforhavingtoo
manychildrenorhavingthemtoolate.Younggirlshadtohearthemforgettingpregnanttoo
early.
Illiteracyincreaseswomen’svulnerability.Accordingtorespondents,judgementalcommentson
whyuneducatedwomenhavemorechildrenarecommon.Awoman’scooperationduringlabour
oftendependsonhoweducatedsheis.Thishasastronginfluenceonherknowledgeand
expectationsforcareduringchildbirth.Interestingly,manyrespondentsassumethattheonusis
onthewomantobeabletocommunicate,andnotthecareprovideronhowtotalktowomen
fromdifferentbackgrounds.Thedifferenceincareproviderandwomen’sbackgroundcanleadto
obstetricviolence,whichincludestheirlanguage,religionandcultures.
Thewayawomandresses,smells,weighs,maintainsherpersonalhygiene,includinghowher
genitalsarepresented,maydeterminehowshewillbetreatedduringchildbirth.Obesityattracts
judgementalcomments.Physicalappearanceisthefirstthingthatthecareprovidersnotice.
Womenwhopresentwithpoorpersonalhygiene,invisiblydirtyclothesandsmellingbad,are
consideredunpleasanttocarefor.
“Itiseasytoabuseobesewomen.Personalhygieneisafactortoo.Theycomewithskindiseases
attimes.Noonewantstotouchthem.Theyhavetohearalotofbadcommentslyingonthe
labourtable…theydonotbatheandwehavetocleaneverythingasthebabywillbebornthrough
theunhygienicpassage…woodsellers,coalsellers,Bihariwomenareverydirty.Wedonotcareif
onehasshavedornot.Manymotherscomeaftertrimming.Looksliketheyhavecomestraight
fromtheparlour,freshlywaxed.Theygetgoodcare,weliketouchingthem.”(WB03)
Communityattributes
Women’simmediateenvironmentincludesherhome,familyandneighbourhoodandthepeople
shecomesincontactwith,whomaysharethesamevaluesandcultureinthecommunity.

Chapter8
213
Povertyincreaseswomen’svulnerabilitytoobstetricviolence.Itisacross-cuttingfactor,asitis
associatedwithcasteandeconomicstatus.Respondentsopinedthatpoorwomenhavenooption
buttoseekcareinpublichospitals.Manyrespondentscommentedthatstaffmembershavea
tendencytoaskforunofficialpaymentsfromthefamilyafterbirth.
“Shewillhavetolistentoalotofcommentsifsheispoor.Thereisalotofignorancetoo.If
someoneisrichorfrombetterincomebackground,theneverystaffbehavesverypatientlyand
respectfulmaternitycarepoursoutofthem.Theyknowhowtodoit,justdependsonwhetheryou
areworthyofrespect.”(RJ04)
“ThisistheculturalconstructofbirthinginIndiawhichtomeiswheretheissueis.Whenwomen
acceptthatthisisokay,thatiswhattheywillget.WomeninIndiapassonthisculturalconstruct
asbirthpreparedness.Whenwethinkaboutabuseofwomeninhealthcare,weneedtobevery
clearthatinsocietieswhereabuseisnormalit’sgoingtobeverydifficulttochangethatina
healthenvironment.Dothepeoplearoundherfeelthatitisnotokaytopinch,hitwomengiving
birth?”(GL02)
ThestereotypeofMuslimwomenhavingmorechildrenisalsoanormaboutbirthingand
contraceptioninsomecultures,fromthecareproviderspointofview.Thestereotypeabout
Bihariwomenisalsoprevalentandopensdoorstodiscriminationagainsttheminattracting
obstetricviolence.
Socialenvironment
Beingawomanincreasesvulnerabilityespeciallywhenthewomanisuneducated,poor,not
appearingacertainway,oldoryoung,marriedornot.Thewaysheistreatedbycareprovidersin
thelabourroomwhilegivingbirthisanindicationofhowsocietyandherfamilyvaluesher,and
treatsher.Thisshapesherexpectations,assheisconditionedtobetreatedinacertainway,with
acertainlevelofrespectfulness.Whethersheasksquestionsorcommunicateswithcare
providersandtheresponseshereceives,dependsonhowsheisconditionedtobetreated.In
fact,gender-baseddiscriminationbeginsatbirth.Thebirthofaboyoftenmeansmoremoneyfor
careproviders.Thebirthofagirlinvitesverbalabuseanddiscriminationforthenewmother.The
waysheexperiencesbeingvaluedornotingeneral,ishowsheexpectstobevaluedinthelabour
roombycareproviders.Genderisacross-cuttingissuewhichcanbeseenattheindividuallevel,
inthecommunityandinthesocialenvironment.
“Globallywomenareoflowstatus,nottreatedwithrespectorregardedasequalcitizens,not
valued.Littlegirlsgrowupthinkingsheisnotasimportantasherbrother,notlikelytoget
educated,notencouragedtoquestion.Womenaccepttheirlowerplaceinthesociety.Whenthey

Chapter8
214
cometogivebirth,manyofthemdidnotchoosetobepregnant,theydidnothaveaccesstobirth
control,marriedoffveryyoung.Arrangedmarriages,childbrides.Thesealltakeawaytheir
empowerment.Youfinditdifficulttostandupforyourself.Whensheisinlabour,thelastthing
youwantisfightingforyourself.Youaresocaughtupinthepsychologicalprocessthatis
happening.Thatmakesyouvulnerableaswell.”(GL05)
8.5.2.2 Nurse-midwiferelatedfactors
Thenurse-midwiferelatedfactorshavebeenorganisedintothreelevelstoo:(i)individual-
includespersonalandprofessionalattributes;(ii)thebirthingenvironment-includesthebirthing
room(‘labourroom’);and(iii)thepolicyenvironment-thatdeterminesthequalityofcareand
serviceprovisionthroughpoliciesatstate,nationalandgloballevels.
Individualfactors
Participantsfeltthatworkloadoftenmadenurse-midwivesangryandfrustrated,astheyare
overburdened.Atatertiarylevelhealthfacility,forexample,birthshaveincreasedfrom400to
1000permonthoverthelastfewyears,thoughthenumberofstaffremainssame.
“Wehave1nursefor100patients,thatiswhythishappens.Workload!”(OD02)
“Staff’sconfidencebreaksassoonastheyseethecrowd.Theyworryhowtoprovidecaretoso
many.”(RJ06)
“Weusedtogivemorepsychologicalsupportbackthen.”(OD03)
Respondentsfeelthatthelackofpromotionsandstagnantsalaryisdemotivating.Theadded
workloadwithoutincentivesmakesthemfeelunder-appreciatedandunder-valued.
“Nurse-midwives’arenotgettingenoughsalary,recognition.Noonechecksonus.”(CL01)
“...theyarediscriminatedwithotherprofessions.Physiotherapistsandpharmacistsareallgoing
up(intheircareer)andnursing(andmidwifery)isgoingdown.”(O03).
“...sinceromantimes,womenwerenotrespectedandthenChristianitycameinandwomen
startedbeingdisrespected,whichincreasedasthemalemedicalmodelslowlyinstalleditselfinto
theprofession.Atonepoint,nursesandmidwiveswerebeingheldaswitches.Itslikeatrailof
under-representationthatleadstodisrespectandabuseofwomenandmidwives.Thisincreased
inthe80’sand90’sasthemalemedicalmodelmarginalisedmidwives.”(GL06)
Workingconditionsareoftendemotivatinginahierarchicalstructurewheredoctorshavebetter
facilitiesthannurse-midwives.Suchdiscriminationleavesnurse-midwivespowerlessandtaken

Chapter8
215
forgranted.Onerespondentfeltthatthislearnedhelplessnessisanoutcomeofcontinued
oppression,whichmakesmidwives’powerlesstobringanychangesinthesystem.Beingvoiceless
inplanningcareprovisionleadstoassertionofpoweronthewomenwhoarefurtherdowninthe
socialhierarchy.
“Theytakethesewomenforgranted.TheyfeelIamtakingcareofyouandIhavethispowerover
youtoprovidecaretoyou,soyouhavetolistentome.Thisismyterritoryandyouareboundto
listentome.”(WB02)
Manystakeholdersmentionedthatnursesandmidwivesareoftenbulliedbydoctors.Withthe
lackofasupervisor,whoisanurse-midwife,thedoctorastheheadofanyinstitution,overpowers
everyoneleadingtomismanagementofmidwiferyandnursingservices.Nurse-midwivesareill-
treated;andtheirwelfareandworkingenvironmentisnotconsidered.
“Gynaewarddoesnothavetoilet,soifthenursesgotoadifferentwardtousethetoiletandthe
doctorcomesforaroundatthattime…marksherabsentfortheday.Sometimeswequietlyuse
thetoiletinthecabin(meantforwealthypatients)whennooneswatching.Wearenotrespected.
Themedicalsuperintendentdoesnotrespectus.”(BH01)
Stakeholdersexplainthatthenurse-midwives’workinvolvesdealingwithbirthsanddeaths.Due
toanincreasingworkload,theyhavelesstimetocommunicatewiththeirpatients.Thereis
frustrationfrombeingoverburdenedandnotimetoprocessemotionsrelatedtovitaleventslike
birthsanddeaths.
“Theydonotgetattached.Theycallthembybednumberorcolourofsaree.”(RJ04)
Birthingenvironment
Participantsmentionedthelackofinfrastructureasaninterveningfactorinthebirthing
environmentthatisdisrespectfultowomen.Screensareimportanttomaintainprivacyduring
childbirth.Lackofinjectableanaestheticsandanalgesicsaddstoadisrespectfulbirthing
experience.Itleadstowomenenduringmorepainwhentheyundergoanepisiotomyandrepair
withoutanaesthesia.Thecleanlinessofthelabourroomisanissue,resultinginwomenbirthingin
anunhygienicenvironment.
“Thedoctorsaretall,sotheirheightneedstobeconsidered,hencethelabourtableissotall.”
(B02)

Chapter8
216
The‘teamculture’includeshowcareproviderscollectivelyperceiverespectfulcarebasedon
existingwork-placenorms.Thismakescertainpracticesandevenextentsofdisrespectandabuse
duringchildbirthacceptable,thusaddingtonormalisationofdisrespectandabuseduring
childbirth.
“Thereare12labourtablesinthelabourroom,separatedbycurtains.Wedon’tletmenenter,so
theirprivacyisprotected.Thenitisallwomen.”(RJ01)
Extortionisoftenpartofateamculture.Themoneygetsdividedbythewholeteameventhough
thenon-healthcareproviders,suchascleaners,areattheforefrontofaskingforit.Thereare
manyunethicalpracticesthatarepartofteamculture,includingaugmentationoflabour.
“Theywillscream‘push,push’iftheirdutyisendingat1:45pm.Theywillmakesurethewoman
givesbirthwithinone’sdutytimesothatcareprovidergetsthemoney…sotheywillinducewith
oxytocinsometimes.”(RJ04)
Taskshiftingbetweencareprovidersatdifferentlevelsofcareisbasedonthehierarchyofcare
providers,whichstemsfromthecentralisationofpowerandmismanagementoftheincreasing
workload.Respondentsshareexamplesofsystematicshiftingofdutiesfromdoctors,whichisnot
apartofnurse-midwives’role,followedbynurse-midwives’transferringtheirroleinassisting
births,tonon-healthcareworkerssuchasMamta16,ASHAandtraditionaldais.
“He(medicalsuperintendent)isrunningthehospitalinanywayhewants.Nurse-midwives’are
postedinnon-nursingrolesevenwithanexistingshortage.Therearenurse-midwives’postedin
thefireextinguishingdepartment.Sixnursesreadyintheiruniform,twoforeachshift.Theyare
notinvolvedinpatientcareanymore.Tennursesareworkinginpharmacydistributingdrugswhile
thepharmacistschillinaroom.Nursesareworkinginpathologywhiletechniciansareroaming
free.Thetelephonecontrolroomisrunbynursesandsoisthereceptionandhousekeeping.The
nursepatientratiois1:50-75.”(BH01)
Stakeholdersdescribethatwithincreasinglevelofcareprovision,disrespectandabuseofwomen
duringchildbirthincreases.Womenaremorevulnerabletobeabusedatatertiarylevelofcare
provisionthanaprimaryorsecondarylevel.Thisisrelatedtomanyfactors,forinstance,workload
increasesatahigherlevelofcare,reducingpatient-healthworkerinteractiontimeandincreasing
workloadrelatedfrustration.Manystakeholdersfeelthatdoctorsattertiarylevelareengagedin
16MamtaisanonhealthcareproviderwhoworksprovidessomecounselingtowomenonbreastfeedingandtheimportanceofcleanlinessafterwomengivebirthinaninstitutioninBihar.Shealsomaintainscleanlinessinthelabourroomandreceivesincentivesforherwork.

Chapter8
217
moresevereformsofabuse.Beingfurtherupinthelevelofcareprovisionalsomeansthat
womenarenotknowntoanyoneintheteamofcare,whereexperiencesarefurtherover-
medicalisedthanatalowerlevelofcare.Thetertiarylevelincludesteachinghospitals,where
womenbecomesubjectsof‘casediscussion’aspartofthemedicaleducation.
“Everyonelooksatherassomeoneyoucanperformcaseson.Theyseethatthisisacaseinmy
logbook…theywanttogiveanepisiotomysoonecangetanepisiotomyrepairdoneandwrite
aboutitinlogbook.”(CL04)
Disrespectandabuseofwomenduringchildbirthoftenstemsfromalackofcompassionate
leadershipatthecentreofthemanagementsystemorhierarchy,whichalsoinfluencestheteam
culture.
“Itslikearippleinthepond.Youhavegotanabusivepersonatthecentreofthat.Thepersonwho
isabusiveinnature,maybeofpsychopathictendencies.Thepersonatthecentrebecomes
powerfulandinordertomaintainthatpower,buildsrelationships,andslowlypeoplechangetheir
behaviourtofitintothatwayofbeing.Thelongerthatpersonisabletostayinoneplace(centre),
theculture(ofabuse)growsstronger.”(GL06)
AparticipantinIndiacalledthisa‘dominoeffect’whereonecareproviderlearnstoabusefrom
another,establishinganabusiveteamcultureintheprocess,thispeerinfluenceslowlyturns
everyoneintoanabuser.
Policyenvironment
Somenationalpoliciesindirectlycontributetoadisrespectfulbirthingexperience.TheJSYpolicy
incentiviseswomenforgivingbirthinaninstitutionandincentivisesthecommunitybased
motivators,ASHAs.Thispolicyiscriticisedbyparticipantsasinsensitive,asitdoesnotuphold
women’srightsorfacilitatetheirchoicesanddecisionmakingaboutchildbirth.
“Itmakesnosensetohaveagovernmentpolicytomovewomentohospitalswhenthehospitals
treatthemsobadly.Theresponsewillbe‘ohbutyoushouldseehowtheyaretreated(athome)in
India,atleasttheygetfoodinthehospital’.”(GL07)
Participantsalsoidentifiedthatthedehumanisationofwomenbeginsinthepre-serviceeducation
asalearnedbehaviour,wherethemedical,nursingandmidwiferystudentsimbibehowthecare
providersdealwithwomen.Obstetricviolenceduringbirthhasbeenanorm,whichnormalisesit,
thusreducingtheimportanceofthisproblem.

Chapter8
218
“IhaveseentheHeadoftheDepartmentverballyabuseinaround1977-78.Theyarenotproperly
educated.Thegovernmentdidnotcarebackthenaboutrespectfulnessastheyareenforcingit
now.”(WB01)
Birthingisexplainedas‘dirtywork’byaninternationalparticipant(GL03),whosharesthatsince
birthworkstemsfromunpaidwomen’swork,itmayhaveanegativeimpactontheprofession
whichfurtherentrenchesmedicaldominationofmidwifery,nursingandbirthing.
Theprovider-clientrationeedstobemaintainedtoensurerespectfulcare.Under-recruitmentis
anindicatoroflackofthewomen-centricpolicies.Itiscommoninhospitalstorotatenurse-
midwives,respondentsperceivethispracticeasdiscouraginganddeterrenttomaintaining
midwiferyandnursingskills.Theamountofdocumentationworkisanadditionalburdenthat
takesoverdirectcareprovision.
“Weareengagedinmultiplethings,astaffnurseinthelabourroomcannotmaintaincareand
qualityservice,theyjustcannot.Suchahugelogbooktheyhavetofill.Somanyrecordsto
maintain.Howwillsheconductsomanydeliveries?1:1ratioisrequiredforassistingbirths…
tertiarylevelstaffjustdoespaperwork.”(WB05)
8.5.3 Participant’srecommendationsforrespectfulmaternitycare
Participant’srecommendationsarecontext-specificandarebasedonbestpractices.Preventing
disrespectandabuseduringchildbirthandpromotingrespectfulmaternityisadeep-rooted,and
anage-oldproblem,whichrequiresaparadigmshiftinculturetoaddresschallengesatvarious
level.Participantssuggestinvolvingwomenandnurse-midwivesinpolicy-making,astwokey
stakeholdersinmaternalhealthcare.
“It’saboutreallystrongpartnerships.”(GL03)
Participantssuggestedamulti-sectorapproachtoinvolvestakeholdersfromcommunityand
healthsystemsforalastingimpact.Participantsfeeltheneedtodecentralisepower,fromthe
medicalmodelofcare,tomakecareprovisioninclusive.Collaborationswithwomen’srights
organisationsandnursingandmidwiferyassociationswillincreaseaccountability.Global
internationalorganisationshavearoleinadvocacy,settingstandardsandfundinginitiativeswith
asustainableapproach.Theserecommendationsaresummarisedinaframeworkformidwifery
modelforwomencentred-carewithchangessuggestedatdifferentlevels(Figure8.2),similarto
thelevelsdiscussedforthefactorsofdisrespectandabuseduringchildbirth.

Chapter8
219
Figure8.2 RecommendationsforrespectfulmaternitycareinIndia(Author’sown)
Level1-Midwiferymodelforwomencentredcare-Itisimperativetohearwomen’sexpectations
andexperiencesofcaretounderstandwhatisrespectfulandgoodqualitycareforthemand
ensureapersoncentredpositivebirthingexperience.
“Thevoiceofpeopleisoneofthebiggestmotivesbehindchange…youcanregulatethattherehas
tobeawomaninthediscussionbuttheywillfindathousandwaysaroundtonotadheretothat.
Inchangingvaluesandnormsofsocieties,notmuchchanges.Womenneedtostandupandsay‘I
needrespectfulcare!’.Thosearethewaystomakechangehappen.”(GL01)
Participantsfeltthatsharinginformationandcounsellingshouldbeginintheantenatalperiod,to
helppregnantwomenunderstandtheprocessofbirthingandexplainproceduresbeforehand.
Theyalsofeltitisdifficulttocommunicatemanythingswhilethewomanisbearinglabourpain.
Proceduresneedtobeexplainedtogainthewomen’strust.Continuedcommunicationand
psychologicalsupportduringchildbirthisconsideredofutmostimportance.
“…tellthemhowmuchitwillhurt.Thenumberofhoursitwilltake.WeshouldtellthembeforePV
andwhenstartingabottletoincreasepain.”(R01)
Midwiferyandnursingisconsideredemotionalworkandparticipantsfeltitisimportantforcare
providerstotaketimeoutforthemselvesandtakecareoftheirwellbeing.
Chapter8
220
“…takingtimetogetagoodworklifebalance.Doingwhattheyenjoy,switchingofffrom
workplace,gettingsupportfromcolleagues.Gettingaperspectiveandbeingawareofoneself.”
(GL03)
Theroleofnursesandmidwivesisrecommendedtobeenvisionedasadvocatesforwomen’s
rightforqualityandrespectfulcare.Thiswillincludestandingagainstdisrespectandabuseof
womenduringchildbirthintheirfacilityandfindinginnovativewaystopreventit.
Level2-Individualandteamculturefortheidealbirthingenvironmentcareprovider:
Perceptionsaroundqualityandrespectfulnessneedtoalignwithwomen’sperception.
“WelookatIndiaandseewomeninbeautifulsareesinruralareasandfeeleverythingisfine.One
hastolookbeyondthatandseewhattheyfeel,whattheyneed,whattheywantandservethem
well.”(GL02)
Toensureanappropriateteambehaviourtowardswomenundertheircare,itisnecessarythat
stepsbetakentoimprovetheteam’sattitude.Beingrespectfultowardseachotherintheteam
regardlessofgenderandprofessionisrecommended.
“Theteamneedstobetrainedtogether!”(WB04)
“Facilitiesneedtoimprovetheircollectivebehaviour.”(WB03)
Respectfulcommunicationisstronglyrecommended.Respondentsfeltthatcareproviderscould
beeducatedinwhattosay,whatnottosayandhowtocommunicatewithwomen,asthey
acknowledgethat‘theirwordscanhurt’.
Changesareneededattheprimary,secondaryandtertiarylevelofcare,whichcanbedifferent
basedontheissuesthatexistateachlevelofcare.Infrastructuralavailabilityandworkload
distributionneedtobeensuredateachlevelforanidealbirthingenvironment.
Homebirthwassuggestedbymanystakeholders,withscalingupofhome-basedcare.Theyfelt
thereisalesserculturaldifferencebetweenthecareproviderandwomenwhencareishome-
based,wherefamilymembersgetinvolvedasbirthcompanions,makingbirthingmoreculturally
acceptableandsatisfying.
“Let’sjustchangethephysicalenvironment,itsnotthatdifficulttodo.Itwillhaveprivacy.Does
notneedabed.Lotofwomendonotneedabed.Theywanttobirthstandingup,onamat,sitting
down,onalittlechair.Theywantitclean…andwarm…”(GL02)

Chapter8
221
“Idealbirthingenvironmentistheenvironmentforlovemaking.Bothpsychologicalactivities
releaseoxytocinandendorphinonstimulationandobstructedwheninfear,embarrassedorin
doubt.”(WB03)
Level3-Compassionatenursingandmidwiferyleadership:Midwiferyandnursingleadershipis
consideredkeytoensurethatamidwiferymodelofcareisimplementedinIndia.Participants
stronglyfelttheneedforone-to-onemidwiferycareforwomen.Advancedcareisneededif
complicationsarise.Therefore,effortsareneededtoestablishamidwiferymodelofcare.
“Midwiferymodelofcareisinconflictbetweentryingtobalancecarebasedoninstitutional
hierarchies,whereyouareacceptedtointerveneandifyoudonot,thenyouareprofessionallyin
trouble.”(GL03)
Thetertiarylevelofcare,includingteachinghospitals,whichareresponsiblefortheeducationof
careproviders,needstoadoptmeasuresthatcompriserespectfulmaternitycarewhilestudents
canlearnandpractice.Theimportanceofstudentstoimbibevaluesofrespectfulnessintheir
behaviourneedstostartintheirpre-serviceeducation.Thestudentnurse-midwivesoftensuffer
theconsequencesofbeingatthebottomofthemedicalhierarchy.Medicalstudentswereoften
prioritisedintermsofpracticeinteachinghospital,whereasnursingandmidwiferystudentsdo
notgetachance.Thestudentnurse-midwivesareoftentreateddisrespectfully.Respectful
communicationisencouragedforeveryinteractionwiththestudents,evenwhentheymake
mistakes.Thewaytasksaredelegatedtostudentsneedtochange.
“...teachersshouldbecompassionatetothestudents.Iamshockedsometimestoseeintheglobal
workhowthemidwiferystudentsaretreated...thehierarchyisknockon.Everybodyisabusingthe
otherwhoislowerinstatusthanthem...weneeddeepculturalchange.”(GL05)
“Theactualrelationshipbetweentheclinicalinstructorandthestudentshouldberespectful.”
(CL02)
Midwivesandnursesneedtobeempoweredsothattheycantakeupleadershiprolesand
participateindecisionmakingateverylevel.Midwiferyandnursingsupervisorscanrealistically
plancareandmanagemidwivesandnurses.Aparticipantfeltthatcompassionateleadershipat
thecentrecouldpositivelyinfluencetheteamtowardsrespectfulbehaviour,asarippleeffect,but
thisdependsonthekindofleadershipatthecentre.
Level4-Policyreformsandregulation:Withincreasingevidenceofdisrespectandabuse,
midwiferyandnursingleaderssuggestedseveralrecommendationsforpolicychangesinhealth
serviceprovisionthatcanmakebirthingrespectfulanddignified.Theseincludeworkplacepolicies

Chapter8
222
tohavecompassionateleadershipbyinfluencingnormsatworkplacethatcouldfosterrespectful
careandpoliciesthatgoverncareprovisionatthestatesandcountrylevel.Manyparticipants
recommendtoaddresstheincreasingworkloadbyimplementing1:1ratiofornurse-midwifeand
women,whichwilldirectlyinfluencecareprovisionforthebetter.Propermanagementof
workforceanddevelopmentofleadershipinnursingandmidwiferyisessential.
Regulatorybodieshaveakeyroletoplayineducation,practice,maintainingstandardsofcare
andupholdingprofessions.Regulatorybodiesneedtomakechangestodiscouragetheindividual
andinfrastructuraldisrespectandabuseofwomenduringchildbirthbysettingstandards.
“IndianNursingCouncilshouldprovidebestexamples,showcasingwhatitlooksliketohaveasafe
birth.SNCsaremembersofINCandcandoitintheirownstates.”(GL02)
Leadershavedividedopinionsonwhetherthereshouldberegulatoryreformstoaddress
disrespectandabuseduringchildbirth.Theyfeelthatpenalisingcareprovidersisnotasolution,
astheythemselvesaresubjectedtoharshworkingconditions.Theyalsomentiontheneedto
discourageanykindofintentionaldisrespectfulandabusivebehaviourwithinateamandtowards
thebirthingwomen.Thereshouldbezerotoleranceofintentionalabuseofwomenbyallhealth
careproviders,andnon-healthcareprovidersshouldnotbeallowedtoassistbirths.
8.5.4 Respectfulmaternitycareeducationforthenextgenerationofcareproviders
Respectstudent-Nursingandmidwiferyleadersfeelthatthestudentnurse-midwivesoftensuffer
theconsequenceofbeingatthebottomofthemedicalhierarchy.Medicalstudentsareoften
prioritisedtoallowpracticeinteachinghospital,whereas“nursesdonotgetachance”.Respectful
communicationisencouragedforeveryinteractiononehaswiththestudentsevenwhenthe
studentsmakemistakes.Aparticipantfeltthatthewaytasksaredelegatedtostudentsneedto
change.
“…theactualrelationshipbetweentheclinicalinstructorandthestudentshouldberespectful.”
(NL02)
Rolemodelling-Participantsconveytheimportanceofensuringthatthenextgenerationof
nurse-midwives’needtoberespectfulincareprovision.Someofthemfeelthatrespectfulness
cannotbetaughtthroughafewdaystraining.Theyunderstanditasaprocess,thatensurethat
thepersonalitytraitorvaluesystemisembeddedinthestudent,sothattheyarecapableof
respectfulcareandtostandagainstdisrespectandabuseduringchildbirthwhenrequired.Role
modellingismentionedafewtimestoachievethis.Participantsfeelthatteachershaveakeyrole
toplayinthis.Thisroleshouldbeginintheteachinginstitutionforthemtodemonstrate

Chapter8
223
respectfulness,butitisalsoimportanttoshowintheinteractionswithwomenintheteaching
hospital.Theimportanceofgoodcommunication,addressingtheclientbyname,explainingevery
procedureandtakingconsentbeforeengaginginanycareprovisionismentioned.Itisimportant
tostandagainstdisrespectandabusetowardswomenwhenteachersseeanyoneintheteamof
careprovidersengaginginit,asNL03explains.
“…whentheyseedisrespectandabuse,teachersshouldpointoutandcallthestaffoutlaterand
discouragethisbehaviour.Theyshouldhelpthemtoperformbetterandbeanadvocateforthe
mother.”(NL03)
Thefirstchallengeistoletthenursingandmidwiferystudentspractice,whichisakeyhurdle
describedbyparticipants.
“Headofthedepartmentsaysmymedicalstudentswillpracticefirst.Thenursingstudentsobserve
casesandrequestthemtogiveachance.Hundredpercentcasesaredonebymedicalstudentsand
wehavecomplainedaboutthismanytimesbutwhowilllistentous.”(B02)
Thechallengeisgreaterformalestudentspersuingnursingandmidwifery,whotrytogetalittle
practicebyassistingdoctors.Thegapinwhatistaughtintheinstitutionfromthepractice
scenarioinlabourroomcanbereducedbypropersupervisionfromthenursingandmidwifery
supervisors.Participantsfeelitisimportantforcontinuityofcare,startingfromthepreservice
education,asNL06explains.
“Ineverallowedanystudenttopracticewithoutlearningproperly.Theyhadtoidentifythe
woman,giveantenatalcare,providecareduringchildbirthfollowedbyimmediatepostnatalcare
for48hours,ifpossible.Otherwise,Ididnotsigntheircasebook.”(NL06)
Clinicalinstructorsareusuallyassignedinthemorningshifttosupervisestudents,althougha
participantreportsencouragingresultsofassigningteachersinallthethreeshifts,wherestudents
practiced.
Properselection-Participantsfeelthatstudentswhojoinnursingandmidwiferyarenotalways
readyfortherole.Theyfeel,studentsshouldbecounselledonwhattheprofessionalcourse
entails.
“…somepeoplejoinmidwiferywhocannotfunctionindependently.Thereisalotofindependence
inthisareaandoneneedstomakedecisions.Everyonecannotdothat.Somepreferfollowing
orders,theyshouldworkinotherareaslikemedicalsurgicalnursing.Ifyoucannotfunction
independently,don’tworkinmidwifery.”(WB03)
Chapter8
224
Theparticipantalsofeelsthatcandidatesshouldbeselectedbasedonanaptitudetestwhichwill
ensurewillingnessinthestudentsfromthebeginning.
8.5.5 Domidwiveshaverespectfulbirths?
Amongthenursingandmidwiferyleadersinterviewed,twelvehavesharedstoriesoftheirown
childbirth.Participantsnarratebothrespectfulanddisrespectfulbirthingexperiences.Someof
themsharethatbeinganurseandamidwifeisapositionofprivilege,becausetheyknowthe
processandhavetheknowledgeofbirth.Theseparticipantshavetheexperienceofbirthingin
publicandprivatehealthcarefacilitiesandathome.
Powerofmidwiferyknowledge-Manymidwivesfeeltheyhadabetterandrespectfulbirth
becausetheyaremidwives,evenwhentheydidnotgivebirthinthelabourroomtheyworkedin.
AsO03shares,sheguidedherownbirthwithanunderstandingofthecomplicationsinvolved.
“…myhusbandbroughtthemidwifeoncycleandItoldhertobringthecatheter.Herskillsandmy
knowledgeworkedtogether.Itoldhertoboilthecatheterfirst.Iwantedtogivebirthinsitting
position,soIdid…soskillfullyshedeliveredthatIwasveryimpressed.”(O03)
Nursemidwivesoftensharedabouttheirowndesignationthatensuredtheyhaveagoodbirth.
ParticipantB02’sbirthingexperienceisanexampleofthis.
“nursesdidnotbehaveproperly…shewaslisteningtofoetalheartsoundandIrefusedasking‘why
areyoulisteningtoFHSwhenIaminpain,can’tyouwaittillthecontractionisover?’.I
complainedtothenursingsuperintendent.ShesawmynameandrealisedwhoIam…shecalled
thestaffandsaid‘wherehaveyoulearntmidwifery,don’tyouknowsheisateacher?’She
apologisedandtheneveryonecooperated.”(B02)
Beinganurseandamidwifealsomeanstheysometimesknewthestaff,whichprovided
infrastructuralbenefitsandtheadvantageofhavingsomeoneassistingtheirbirthwhomthey
trustedasGL02describesit.
“…itsokaytofeeloutofcontrolbecauseyouarehavingacompletelyoutofbodyexperience,but
youneedtotrustthepeoplebirthingwithyou.”Beingacareprovideroftenhasextendedbenefits
fortheirfamilyandrelativesasWB03putsit,“thisisacommunalfeelingwhichwehave,where
wegetbettercarebecauseweprovidecareallourlivesandwefeelwehaveearnedit.”(GL02)
Birthingintheworkplace-Inonecasetheparticipantgivingbirthinherownplaceofwork
ensuredthateveryonewasveryrespectfultoher.Butshealsotriedtobe“inherbestbehaviour”
asshedidnotwanttobemadefunofthewayshewasscreamingorcryingduringchildbirth.She

Chapter8
225
(NL04)furtheraddsthatherdoctorencouragedherbysaying‘sheisverybraveandwehavenot
seenanywomanwithsomuchpatience’butshehasalsoseenthesamedoctorsexuallyabusing
otherwomeninlaboursaying‘thisisallyoucandoathome,andthenyoucomehere.’Notall
experienceswereasgood,GL06sharedhowshewasbulliedinherworkplace,whichextendedto
herbirthingspace.Shefeelsthatherbirthcouldbemanagednormally,butduetoaugmentation
hercontractionsgrewstrongerandledto‘difficultforceps’withoutanyepiduralorpainrelief.
TheexperienceofbirthinginherownworkplacewastraumaticforGL08tooasshedescribesit.
“Iwasslappedonmybuttocksinmyfirstbirthcausemylabourmeantdelayinher(midwife’s)
leavingforhome.ShealsoforcedmetohaveanenemaevenafterIrefusedtohaveit.…Sheknew
Iamamidwife,weworkedtogether.…Iwaspowerlesstorefuseanything.SincethenIhavebeen
frightenedofmidwivesanddoctors.”(GL08)
Inthesubsequentbirths,theparticipantensuredtohaveamidwifeshetrusted,whoprovided
continuityofcare.Also,sheestablishedherownhomebirthpracticetoensurewomeninherarea
hadrespectfulbirths.
8.6 Discussion
Themidwiferyandnursingleadersperceivedthatthepainting(Figure8.1)depictedthewoman
beingabusedduringchildbirth.Theypointedoutmanyunacceptableactionsfromthepeople
aroundthebirthingwoman,intheobstetricenvironment.Thoughthereisadifferenceinthe
perceptionofparticipantsinIndiaandelsewhere,abouttheseverityofobstetricviolencethe
womaninthepaintingisbeingsubjectedto.Thisdifferenceinperspectivescouldbearesultof
theparticipant’scontext,thecultureofviolencetheyareexposedto,progressinthediscussions
aboutobstetricviolence,thelevelofeffortstoensurerespectfulcareandwomen’svaried
expectationofqualityandrespectfulcareindifferentcontextsandcountries.Participant’sown
contextofsharedoppressionsandpowerlessnessmayhaveanimpactontheirperceptionof
violenceaswell.Indianparticipant’sperspectiveconveysnormalisationofobstetricviolencetoan
extentwhereunlesstheactofabuseisextreme,itisunnoticeableandisside-lined.Aparticipant
fromIndiafeltthatthepictureshowsgoodqualityofcarewhileanotherbelievedthatsome
amountofshoutingatthewomanduringchildbirthiscompletelyjustifiable,aswomenareunable
tohearduetopainandfollowtheinstructionsduringchildbirth.Thiscouldbefuelledalsobythe
lowexpectationsofwomenandtheconditioningaboutbirthing,thatalivebabyandalive
womanareconsideredgoodenoughoutcomesofchildbirth(Shakibazadehetal.,2018).
Participantstouchedupondifferenttypesoffactorsassociatedwithobstetricviolenceand
increasewomen’svulnerability.Thesefactorsarenotlimitedtowomenbutalsothenurse-

Chapter8
226
midwivesastheprimarycareprovider.Womenandnurse-midwivesareattheintersectionsof
differentindividual,structuralandpolicyrelatedattributesinthelargercontextofoppressionof
women(Sen,Reddy&Iyer,2018).Allthefactorsdiscussedinthispapershouldbeaddressedto
ensurethatcareisrespectfulandpersoncentred.Freedmanetal.(2014)discussedindividual,
structuralandpolicylevelsintheirunderstandingofmistreatmentofwomenduringchildbirth.I
createdaframeworkbasedonthepatternsIlearntfromthedifferentfactorsfromthemidwifery
andnursingleader’sstandpointforthecare-seekingwomanandthecareprovidersthemselves.
Someofthesefactors,suchasgender,arecross-cuttingforboththewomenandthenurse-
midwivesthatgoesagainstthemandleadstodisrespectedwomenanddisrespectedcare
provider.
Figure8.3 Midwiferyleaders’perceptionsofobstetricviolence(Author’sown)
Thenursingandmidwiferyworkforcefacesnumerousgender-basedandhierarchicalchallenges
thatimpedetheirleadershipanddecisionmakingpowers(Sheikh2012;Guptaetal.,2003;Langer
etal;2015).Thesocial,economicandprofessionalchallengesleadtomoraldistressandburnout
(Maslach&Leiter,2009;Steege&Rainbow,2009).Nurse-midwives’challengessuchasunsafe
workingconditions,alackofpromotions,pooranddelayedsalaries,longworkinghoursandalack
ofsupervisionarewelldocumented(Filbyetal.,2016;Mayra,2020b;Maslach&Leiter;2016).
However,usingnurse-midwivesforfireextinguishingservices,isadefinitenewlow.Itisclear
fromtheresponsesthatnursingandmidwiferyleadersunderstandthechallenge,andarecapable
ofmakingreformativechangeswithmulti-sectoralcollaborationthroughadministration,
regulation,advocacy,researchandserviceprovision(Ratcliffeetal.,2016).Currently,participants

Chapter8
227
representingtheeducationsectorhavenoflexibilityandlittleinfluencewithoutasupportive
regulatoryframework.Theyalsohavelimitedpowertomakeanychangeinthehospitalswhere
themidwiferyandnursingstudentspractice.Inadifferentstudy,Ihavepublishedthesechanges
requiredineducationandregulationurgentlyinIndiawhichwillbeakeysteptowardsensuring
respectfulmaternitycare,inlinewiththerecommendationsthatparticipantssharedinthisstudy
(Mayra,Padmadas&Matthews,2021).Amidwiferymodelofcareiscrucialtoensuringrespectful
maternitycare,whichwillbeaculturalshiftfromthecurrentmedicalmodelofcare,thatledto
over-medicalisationofbirthandhasnormalisedobstetricviolenceduringchildbirth(Homeretal.,
2014;Renfrew,McFadden&Bastos,2014).Thisnowseemspossible,withIndiamakingstridesto
startmidwiferyinthecountry,whichwillincreaseaccountabilityforrespectfulmaternitycarefor
women(Ratcliffeetal.,2016;GOI,2018;Afulani&Moyer,2019).
Healthsystemmanagementexpectsnurse-midwivestobe‘supernurses’byprovidingthemless
thanidealworkconditionswhiledemandinggoodqualitycare.Policiescomewithanadditional
workloadwithoutincreasingworkforce,whichleadstounmanageablefatigue(Steege&Rainbow,
2016;Lui,Andres&Johnston,2018),asseeninthenarratives(insection3.2.2.3).Thenurse-
midwives’themselvesarevictimsofpoorworkforceandhealthsystempolicies,institutional
mismanagementandhierarchy(Moridietal.,2020).Thisisalsowhyitisveryimportanttolearn
fromthediscoursearoundintentionalityofhealthcareprovidersinobstetricviolencethatIhave
discussedatlengthintheliteraturereview(section2.3).
Thepolicyenvironmentiscrucialtoensurelongtermchanges.Thoughrespectfulmaternitycare
ismentionedintheLAQSHYAguidelinesinIndia,thecontentisnotenoughtoensurerespectful
caretowomen(GOI,2017).Studiessuggestthatexistingpoliciesorinitiativestargetedat
improvingmaternalhealthcaredelivery,suchastheJSY,arenotunderpinnedbytheessential
infrastructure(Randiveetal.,2014)toencouragerespectfulcareandcontinuityofcare.Itis
essentialtocalloutactionsofdisrespectandabuseandstaterespectfulcarespecificallytomake
itanorm(Morton&Simpkin,2019).Recentstudieshavepresentedknowledge,skillsand
behavioursforrespectfulcarewhichcanbecontextualisedandadaptedforIndia(Butleretal.,
2020;Shakibazadehetal.,29)whichcanbeimplementedwithcontinuedin-servicetraining,
birthinginfrastructureandpolicyreforms(Moridietal.,2020;Mselleetal.,2018).
Beingawomanincreasesone’svulnerabilitytoanykindofviolenceandvictimisation(Jejeebhoy
&Santhya,2018)inIndiaandapatriarchalcultureincreasesthisvulnerabilityespeciallyduring
childbirth.Women’sprioritiesareconsideredsecondary,whichensuresthatthelimitedreportsof
obstetricviolencesharedbythem,fallondeafears(Betronetal.,2018).Womenareoften
blamedforpoorbirthoutcomesandinsomeculturesthebirthofagirlchildisconsideredapoor

Chapter8
228
outcome(Sacks,2017).Rulesandregulationsdeterminewhatwomenareallowedtodowith
theirbodiesandthiscontrolusuallytakesthepowerovertheirownbodies,awayfromthen
(Bradleyetal.,2016).Anyresistanceisconsidered‘misbehaviour’andmetwith‘punishment’.
Womenareexpectedtoquietlyendurethelabourpains,screamingorcryingviolatesthesocial
normsandcallsforpunishmentintermsofscoldingandmanyotherformsofobstetricviolence
duringchildbirth,todisciplineherbody(Bradleyetal.,2016;Sen,Reddy&Iyer,2018).Thecontrol
ofthefemalebodyduringchildbirthinahospitalsettingisareflectionofhowsocietyis
conditionedtotreatwomenathome,inthecommunityandingeneral(Sen,Reddy&Iyer,2018).
TheIndianparticipantsdidnotmentiongenderasafactor,thoughtherearesomereferencesto
poorstatusorlackofwomen’sawarenessdeterminingrespectfulcare.Respondentssharedthat
veryfewwomenaskanyquestion.Theyjustwanttoknowhowlongitwilltaketogivebirth,even
thatismetwitharuderesponseifthewomanaskstoomanytimes.
Itisclearfromthisstudythatmidwivesandnurseshaveanin-depthunderstandingofthefactors
underlyingdisrespectandabuseofwomenandcancollaborateinbringingchangesthrough
advocacy,administration,education,regulationandserviceprovision.Thisisthekeystrengthof
thisstudy.Thesefindingscanbestrengthenedbyunderstandingtheexperiencesofmidwifery
caretofurtherunderstandthechallengesthatcareprovidersfaceroutinelyindirectcare
provision,includinginthecurrenttimewherenewerformsofabuseandanincreaseofobstetric
violenceisbeingreportedinmediaasaresultoftheCOVID-19pandemic(Sadleretal.,2020;
Kumarietal.,2020).Thisisanaddeddisadvantagealongwiththeintersectionalityofwomen’s
manyattributesthatgivesrisetogender-basedinequalities,therebyincreasingwomen’s
vulnerabilitiestoabusivebehaviour(Betronetal.,2018).However,collaborativeeffortsare
requiredtoensurethatallthefactorsareaddressedatthethreelevels,forlastingchanges,while
keepingwomenandtheirnurse-midwivesatthecentreoftheeffortsandaskeystakeholders.
8.7 Limitations
Thisstudycouldbenefitfromtheexperiencesofdirectmidwiferycareproviderstofurther
understandthechallengesthatcareprovidersfaceroutinelyindirectcareprovisionatpresent.
Giventhestudyparticipantsareallnursesandmidwives,itmayhavesomebiasedopinions
againstothermembersoftheteamofcareproviders.Indiadoesnothaveaseparatecadreof
midwivesyet,hencetherespondentshavebeenaddressedasnurse-midwivesinthechapter.Asa
result,theresponsesareamixoftherespondentsnursingandmidwiferyroles,butthatisa
challengeinitself.Solongasthesetwostreamsofcarearenotseparated,itwouldbedifficultto
filteroutthemidwiferyrelatedchallengesfromnursingwhenunderstandingandworking
towardsrespectfulmaternitycare.

Chapter8
229
8.8 Conclusion
Obstetricviolenceduringchildbirthisdrivenbyfactorsrelatedtothecareprovider,birthing
environmentandpolicyenvironmentandthewomanasacarereceiver.Itisevidentfromthis
studythatthenursesandmidwiveshavein-depthunderstandingofwhatconsistsofrespect
duringchildbirthandwhatleadstodisrespectandabuseofwomen.Theyfaceseveralchallenges
thatmakeitdifficulttosustainchanges.Implementingmidwiferypracticeandempoweringthe
existingnurse-midwivesinthecurrentworkforce,fromthestudentstotheleadersservinginthe
highestpositionsinthestateandcentre,iskeytoensuregoodqualityandrespectfulcarefor
womeninIndia.
Chapter9
230
Chapter9 Expectedrespectabilityfromanintersectional
lens:discussionandconclusion
IaimtolearnwhatmakeswomenmorevulnerabletoobstetricviolenceinBihar,India.Todothis,
Iexploredthenatureofobstetricviolenceandfactorsthatdriveobstetricviolence.Iwantedto
understandthisfromtheexperiencesandperceptionsofwomenwhoshouldbethekey
stakeholderincareseekingandaspeoplewhoownthisknowledge;andfromtheexperiences
andperceptionsofleaderswhoaremidwives,nurse-midwivesandnurses,asprimary
stakeholdersinmaternalandreproductivehealthcareprovision,whoowntheknowledgefrom
thecareprovider’sposition.Thesetwostandpointsareessentialtoensurerespectfulmaternity
careforwomen.Iusedfeministmethodstohighlightwomen’svoicesandtheirexperiences,
supplementedbyvoicesandnarrativesoftheirnurse-midwives.
Iconcludemythesisbyansweringthequestionof‘what’and‘why’aboutobstetricviolence
throughtwoconstructs:1)expectedrespectability-thatexplainswhysomeoneisconsidered
respectableaccordingtowomen’sexpectationsofbeingrespected,disrespectedandabused
basedonthecomplexnatureoftheirexperiencesduringchildbirth;and2)intersectionality-that
explainswhywomenexperienceobstetricviolence.Parallelscanbedrawnbetweenboththese
constructs,toalsounderstandmidwivesornurse-midwives’experiencesofrespectabilityand
whatdrivestheviolenceanddisrespectagainstthem,throughintersectionality.Forwomenand
midwives(predominantlywomenintheIndiancontext),thesediscoursesinthebirth
environmentareanextensionoftheirlivesintheirsocialenvironment.
9.1 Expectedrespectability
Childbirth,asanarrative,isbeingpassedonthroughgenerationsasanexperiencethatshouldbe
endured.Women’sbirthingexperiencesbringclarityaboutwhyithasbeenanexperiencethat
Indianwomenendure,anditcanbeunderstoodasacontinuum,whichhasaspectsof
respectfulnessandobstetricviolencewhichtogetherdecidewhetherwomen’sbirthing
experiencewillbepositiveortraumatic.Ihaveattemptedtosummariseandshowthisuniquemix
ofrespectful,disrespectfulandabusiveinstancesinwomen’sexperiencesthroughtheContinuum
ofRespectfulExperiences(CORE)Model.IpresentanevolvingprototypedevelopedfromPairo’s
narrative,byplottingherexperiencesontheCOREmodelretrospectivelytoshowaspectsof
respect,disrespectandabuseinherbirthingexperience(Figure9.1).TheCOREmodelenables
visualisationofthecomplex,multi-layerednatureofbirthingexperiences,whicharenot
unidirectionalandarelonglasting.Someoftheseactionsappearonce,othersappearmultiple

Chapter9
231
timesandmanyare‘ongoingbehaviour’(shownvertically)thatwomenexperiencethroughout
thedurationoftheirstayinthehospital.TheconfigurationsofPairo’sidentitiesandbackground
helptounderstandherintersections.Thismodelcanbeusedasatoolforfutureresearch,to
continuemakingprogressandmeasurechangingpatternsofrespectfulnessincareprovision.It
canbeoperationalisedforcareproviderstodevelopcompetenciesandwaystoaddressspecific
formsofobstetricviolence;informedbyparticipant’sexperiencesandperceptionsofrespectful
care,enablingperson-centereddecision-makinginformedbythedifferentneedsofpeople
representingdifferentidentities.Thegoalistomakethecontinuumgreenalltheway,toensurea
humanisingbirthingexperience.
Figure9.1 ContinuumofRespectfulExperiences(CORE)model(Author’sown)
Thefindingsfromchapter5demonstratedevidencethateverywomanexperiencedatleasttwo
tothreeformsofabuseduringchildbirthrangingtoamaximumof17formsofabusesmakingit
anextremelytraumaticchildbirthexperiencefortheparticipant(AppendixA).Nowoman
reportedexperiencingsexualviolenceandbeingrestrainedduringchildbirth,andreportsof
physical(2%)andverbalabuse(5%)areataminimum.Thisisinlinewithseveralstudiesthat
explainreasonsbehindunderreportingofexperiencesofobstetricviolenceinresource
constrainedsettings.Thepaperondeterminantsofobstetricviolenceduringchildbirthidentified
bythequantitativeanalysis,doesnotexplainthenumberofaccountsofviolenceundereachof
theseforms,howmanypeoplethesewomenwereabusedbyandthenatureoftheobstetric
violencewithitsdiversityinthecontextandtheimpactonwomen.I,therefore,godeeperinto
women’sembodiedexperiencesinthefollowingchaptersthroughparticipatoryarts-based
feministmethodsthatputwomen’snarrativesatthecentre,whilecuttingthroughthebarriersof
language,stigmaandpower.

Chapter9
232
Acommonthreadinallthefindingschapters(chapter5,6,7and8),fromthestandpointof
womenandtheirnurse-midwives,isthatgrievancereportingisunusual.Women’sreportingof
violenceisinfluencedbytheirexperienceofreportingviolenceintheirroutinelives,drivenbythe
contextwithinitsdomainsofsensitivityandstigma,thatguideswhetherandwhattotalkabout
birthingexperienceswithinthediscoursesaroundsexual,reproductiveandmaternalhealthand
wellbeing.
Inthequantitativestudy(chapter5),nowomanreportedbeingrestrained.Although,being
restrainedisoneofthemosttraumaticanecdotesinmostwomen’sbirthingstoriesinthe
qualitativestudy(chapter6),becauseofitsconnectednesstounconsentedvaginalexaminations,
toepisiotomy,tounanesthetisedepisiotomyrepairs,uterineexplorationsandfundalpressure.
Womenconsideredmanyoftheseinterventionstobeapartofqualityhealthcareprovision,
whichissupposedtobeendured.Sexualviolence,asanAsianfeministtheoristexplains,is
consideredafateworsethandeath,andhasnegativerepercussionstowardsthewomen,instead
oftheperpetrator,asthecurrentdiscourseinmostpartsofIndiagoes.Womenstandthechance
ofbeingdisbelieved,asisseenintheglobaldiscourseandinIndia,concerningtheincredulity
surroundingdomesticviolence,intimatepartnerviolenceandnowobstetricviolence.Itis
thereforenotsurprisingthatnowomanreportedsexualviolenceinthequantitativestudy,
althoughthatchangedinthebirthmappingexercisewhichcapturedwomen’sexperiencesfrom
theiruniquewaysofverbalandnon-verbalexpressions,suchasRia’sreferencetosexualviolence
as‘colourfulthings’.
Itisobviousfromwomen’snarrativesthattheattempttodisciplinewomenbodiesbyhealthcare
providers,asisinthenatureofobstetricsystems,iswellunderstoodandobeyedbywomenand
acceptedasacultureleadingtoself-disciplineinadisplayofobstetrichardiness,inlinewiththe
genderedexpectationsfromwomeningeneral,moresofromwomenrepresentingparticular
backgroundcharacteristicssuchasbeingmultiparous.Ialsopresentreportsfromwomen’sand
nurse-midwives’narrativesabouthowthisguideswomen’sexpectationofbeingrespected,
disrespectedandabusedduringchildbirth,whichIrefertoas‘expectedrespectability’.Itexplains
whetherandhowwomenexpecttobetreatedbycareproviderstreatthembasedonthesocietal
andculturalnorms,andwomen’spositioning,definingtheirrespectabilityfromanoutsider’s
perspectiveandinthiscase,careprovider’sperspective.Iexplainthisfromanintersectionallens
inthefollowingsection.

Chapter9
233
9.2 Applyinganintersectionallens
Intersectionalitycanhelptounderstandwhywomenexperienceobstetricviolenceandwhysome
careprovidersengageininflictingobstetricviolenceduringchildbirth.Women’snarratives
indicatehowtheyaretreatedinthebirthingenvironment,obstetricandnon-obstetric,andhow
theyexpecttobetreatedduringchildbirth.Womenaretreatedinacertainmannerbecauseof
theirpositioningattheintersectionsofgender,parity,abilities/disabilities,maritalstatus,caste,
financialstatus,physicalappearance,language,religion,nationality,statehood,age,education
andhealthstatus.Ihaveattemptedtopresentthisthroughtheintersectionalitywheel,adapted
forobstetricviolence(Figure9.2).Theseintersectionsaredynamic,basedonpeople’scontext
andbackgroundcharacteristics.Theyareflexibleandcanbefluid,becausetheintersectionsare
constantlyshiftinginrelationtothechangesinwomen’sbackgroundcharacteristicsandcontext,
asisexplainedbythetheoryandconceptofconfigurations.
Inthequantitativeanalysispresentedinchapter5,Ifoundthatage,parityandeducationwere
significantindeterminingwomen’svulnerabilitytoobstetricviolence.This,alongwithother
determinants,weresharedbywomenthroughtheirbirthmaps,althoughIdidnotdirectly
exploretheunderlyingfactorsdrivingobstetricviolenceinthequalitativestudy,butwomen
completedtheirnarrativessharingthereasonsbehindbeingtreatedrespectfully,ingeneraland
inthebirthingenvironment.ThisismorepronouncedinAmrita’scommentthatalthoughsheis
darkskinnedbutshepreferscleanliness,drawingtheconnectiononhowwomen’streatmentin
thesocietyandbirthingenvironmentisdependentonthecolouroftheirskin,whilealso
indicatingtowardsthediscriminationswomenface,basedontheirskincolourandphysical
appearance.Isawapatterninwomen’snarratives,onhowthesedeterminantsinteractand
influenceeachunderthefourkeydomainsofgender,power,cultureandstructurewhile
increasingwomen’svulnerabilitytoobstetricviolenceinpaper3.Someofthesedeterminants
weremissingfromwomen’snarrativebutcouldbelearntfromnurse-midwives’perspectivesin
paper4.OneoftheseaboutvulnerabilityofwomenparticularlyfromBiharcouldbenoticedina
nurse-midwives’judgementriddencommentthatBihariwomendisplaypoorerpersonalhygiene.
Thisreflectedthestereotypesrelatedtowomen’sgeographicalpositioninginastateorcountry
couldalsoleadtoobstetricviolence.

Chapter9
234
Figure9.2 Intersectionalitywheelofobstetricviolence(AdaptedfromSimpson,2009,p.3)
Theclarityonthiscomesfromthenurse-midwives’standpoint,whoreflectonthedeterminants
ofobstetricviolence,asprimarycareprovidersandasapartofthehealthsystem.Theyhave
experiencedthechallengesofworkinginthemedicalmodelofcare.Itisoftenmale-ledandhas
remnantsofpatriarchyembeddedinapostcolonialcontext.Apatterncanbenoticedinthe
importantfactorsthatnurse-midwifeleadersmentioned,andcouldbedividedintofactorsthat
arerelatedtothemandtowomen,inincreasingboundariesofself,immediatesurroundingsand
largerenvironment,thatinteractwitheachotherwhiledeterminingwomen’svulnerabilityto
obstetricviolence.Manyofthesefactorsarecross-cutting,betweenwomenandnurse-midwives,
suchasgender,whichconnectedthemintheirsharedvulnerabilitiesanddrewparallelsonhow
similartheirstoriesare,forwomenbeingatthebottomofthesocialhierarchyandnurse-
midwives’positionedatthebottomofthemedicalhierarchy.Thispositioning,influencedthe
otherfactorswhileconstantlyshiftingthecontextofhowwomen,nurse-midwivesandother
stakeholdersincareprovisionandcareseekinginteractwitheachotherrespectfully,
disrespectfullyandinanabusivemannerwhileconstantlycreatingnewdiscoursesowingtotheir
diversities.

Chapter10
235
Chapter10 Summary,policyrecommendationsandway
forward
Iaimedtoexplorewomenandnurse-midwives’experiencesandperceptionsaboutthenatureof
obstetricviolenceandtheunderlyingfactorsdrivingthisissueinBihar,India.Inthisfinalchapter,
Isummarisethefindingsfromchapter5,6,7and8,andconcludewiththepolicy
recommendationsandsuggestionsforfutureworkalongwithstatingthelimitationsofthethesis.
10.1 Summaryofresearch
Paper1(Chapter5)-
• Women’sexperiencesofobstetricviolencearepluralandmultilayered,whichmaygoon
fortheentiredurationoftheirstayintheobstetricsetting.Mostoftheparticipantsofthe
studyexperiencedatleast2-3formsofobstetricviolenceduringchildbirthinBihar,while
themaximumformsofabusesexperiencedbyawomanwas17.
• Bribery,extortionandunclearfeestructureisthecommonestformofabusethatevery
womanexperienced,regardlessofherbackgroundcharacteristics.
• Parity(numberofbirths),ageandeducationincreasedwomen’svulnerabilityto
experienceobstetricviolenceduringchildbirthinBihar.
• Noparticipantreportedbeingsexuallyabused.
• ThreetypesofobstetricviolenceemergefromthedatainBihar:1)coercion;2)poor
communication;3)physicalandverbalabuse.
• Thesurveydatadoesnotnecessarilyelicitfulldisclosureorabusefromwomen.Butthe
extentwasconsiderableandislikelytobemore.
Paper2(Chapter6)-
• Women’sexperienceofbirthiscomplex,multilayeredanduniquewiththeircontrapuntal
voicesrepresentingthediversityandtheupsanddowns,therespect,disrespectand
abuseintheirbirthingexperienceswhicharenotunidirectional.Theseareablendoftheir
voicesofsilence,knowing,resistance,resilience,depression,sadness,trauma,isolation,
powerlessness,determination,hopelessness,relief,satisfaction,struggle,conditioning,
denial,anger,happinessandmore.
• Obstetricviolenceisexploredinseveraldomainswhichincludes,butisnotlimitedto
communication,touch,obstetricinterventions,peoplearoundchildbirth,birthsettingand
birthingenvironmenttounderstandthenatureofobstetricviolenceinordertoensure
respectfulmaternitycareineachofthesedomains.

Chapter10
236
• Feministmethodsareessentialwhenexploringissuesbornoutofcenturiesofwomen’s
oppression.
• Arts-basedresearchisanappropriatewayoflearningaboutsensitiveissuesaround
women’ssexual,reproductiveandmaternalhealthcareandwellness.
• Birthmappingisafeministvisualarts-basedparticipatorymethodtoenablelearningfrom
women’sembodiedbirthingexperiences.
Paper3(Chapter7)-
• Gender,power,cultureandstructurebasedbarriersdriveobstetricviolenceand
respectfulmaternitycare.Thisisanextensionofthehowthesefactorsdriveotherforms
ofviolencesuchassexualharassment,intimatepartnerviolenceanddomesticviolence,
intheotherroutinephasesofwomen’sliveswhichmayincreasetheirvulnerabilityby
normalisingviolence.Thishasbeencommonlyseeninpatriarchalculturesinpostcolonial
settings.
• Thefactorsunderthesefourdomainscanbeoverlapping,thisisinthefluidnatureof
thesecross-cuttingfactorsthatmakesthemcomplexandarethereforeessentialto
explorethroughuniqueapproachesofresearch.
Paper4(Chapter8)-
• Therearemanyfactorsrelatedtothenurse-midwivesthatfunctionattheindividual,birth
environmentandpolicyenvironmentlevels;similarly,therearefactorsrelatedtowomen
thatfunctionattheindividual,communityandsocialenvironmentlevels.Thesefactors
togetherdeterminewomenandbirthingpeople’svulnerabilitytoobstetricviolence.
Manyofthesefactors,suchasgender,arecross-cutting.
• Midwivesandwomenarebothvictimsofaviolentbirthingenvironmentandan
insensitivepolicyenvironment,asaresultofmidwives’beingatthebottomofthe
medicalhierarchyandwomenpositionedatthebottomofthesocialhierarchy,
experiencingaformofdeep-rootedandcontinuedoppression.
• Midwives’perceptionofrespect,disrespectandabuseisbasedintheircontextand
culture,andhowtheyperceiveitiscrucialtoensurerespectfulmaternitycarethrough
theirrecommendationsaroundmidwiferymodelofcare,shiftingfromthecurrent
medicalmodelofreproductiveandmaternalhealthcare.
10.2 Researchcontributions
• Betterunderstandingofsocialdeterminantsofobstetricviolencefromwomenandnurse-
midwives’experienceandperspectivestoensurerespectfulmaternitycareinIndia.

Chapter10
237
• Adetailedframeworkpresentingthedriversofobstetricviolencewithrecommendations
forrespectfulcareprovisionduringchildbirth.
• WHO’sEssentialRespectfulCareCourse(ERCC)-ThefindingsofthisPhDwillguide
educationofmidwivesgloballyasprimarycareprovidersbetterunderstandingobstetric
violence,itsfactorstoproviderespectfulmaternitycareblendedwithresearchfrom
otherpartsoftheworld,withtheERCC,thatisunder-developmentatWHOAcademy,
WHO,HQ.
• Apolicyframeworkreflectingontheexperienceofmidwiferyleadersandwomento
advocateforimprovedrespectfulnessinmaternalhealthcareprovisionandtothereby
ensurequalityofcare.
• Birthmapping,avisualarts-basedresearchmethodtounderstandsensitiveissuessuchas
respect,disrespectandabuselearntfromwomen’sperspectivesandexperienceofcare
duringchildbirthtoguidecareprovisioninIndia,whichcanbeadoptedtoexplore
sensitiveissueswithsensitivityinothercontexts.
10.3 Policyrecommendations
• ThecentralandstategovernmentsofIndiashouldcollaboratewithpartnerswhoplaya
keyroleinprovidingsexual,reproductiveandmaternalhealthcareanddevelopa
roadmapforawayforwardtoensureperson-centeredcompassionatecare,guidedby
womenandmidwives’.Theyneedtomakesystemicchangesbeginningatthetoplevels
ofpolicymakingwhilestayingengagedforcontinuedlearningfromthegroundrealities
fromwomenandmidwivesasthetwokeystakeholders.
• Birthmapscanbeutilisedinthecurriculumformidwifery,nursingandmedicalstudents
tolearnaboutobstetricviolenceandensurerespectfulmaternitycaretowomenfrom
women’sexperiencesandperspectives.Birthmappingisauniquewaytolearnwomen’s
embodiedexperiencesandbeforestudentspracticehealthcareprovisiononpeople.
• GovernmentofIndiashouldensureimplementationofprofessionalmidwiferycadre,
independentoftheirnursingroletoensurecompassionaterespectfulmaternitycarefor
allwomenandbirthingpeople,regardlessoftheirbackground,inanequitablemanner.
• Governmentsshouldenactlawsatthecentralandstates,againstobstetricviolenceinline
withothercountriessuchasinLatinAmerica,whohavelawsinplaceagainstviolencein
obstetricsettings.
• Largescalesurveysarerequiredtogenerateevidenceforobstetricviolence.Government
canensureinclusionofquestionsexploringnatureandextentofobstetricviolencein
NationalFamilyHealthSurveysjustasitexploresquestionsonintimatepartnerviolence.

Chapter10
238
• Inclusionofnursingandmidwivesandnursingandmidwiferyleadersateverylevelof
decisionmakingandpolicymaking,startingfromthegrassrootsandprimarylevelofcare
provision.Thiswillhaveimplicationsineducationandpractice.
• Empowermenthastobeatalllevelsformidwifery,nursingandmedicinestudentsand
careprovidersandteachingprofessionalsonhowtotakeastandforwomenandpeople
whoserightsarebeingviolated,onhowtopreservetheirdignity,throughrolemodelling.
• Everytimethereisanindicatorfallingbehindinhealthcare,nursesandmidwivesareon
thefiringlineandinterventionsareparticularlydesignedjusttotrainorretrainthem.This
impliesashiftingofblameonthem,forbeingapre-dominantlywomendominated
profession.Thisisagender-basedchallengeandsystemicbiasthatneedstobeaddressed
throughteam-basedinter-professionallearningforrespectfulmaternitycare.Thisneeds
tobeinthecurriculumandeducationalstandardssothattheregulatoryandaccreditation
systemsofIndiacanincorporateit.
10.4 Limitations
• SurveydatadoesnotcaptureeverythingaboutthenatureofobstetricviolenceinBihar,
India.
• Surveysaresubjecttosamplingerrorswhichcannotbeunderestimated.
• UnderreportingcouldbeachallengeinlowresourcesettingssuchasBihar,where
women’sexpectationsofcarecouldlowwhichmayleadtoacceptanceofpoorquality
anddisrespectfulandabusivecare.
• Whilebodymappingcaptureswomen’sembodiedexperiences,culturalunderstandings
andsocialcontextcouldpotentiallyinfluencethecontentsofmappingexercise.
• Althoughmeasureswereinplacetoreduceresponsebiases,thenursingandmidwifery
leaders’interviewscouldhavebeeninfluencedbytheirrolesaskeypolicymakersand
beingapartofhealthcaresystems.
• Practicingmidwives(nurse-midwives’intheIndiancontext)werenotincludedinthe
study.
10.5 Futureresearch
• Researchaimingtocreateanatlasofbirthmapsfromcountriesandcontextsaroundthe
worldtounderstandthediversenatureofwomenandbirthingpeople’sexperiencesof
respectfulmaternitycareandobstetricviolenceduringchildbirth.

Chapter10
239
• Researchshouldexploretheextentofobstetricviolencewithindifferentformsofabuse
whichhavebeenrecognisedandtheonesthatarecontextspecificandremaintobe
identifiedindifferentstatesandinIndia.
• Researchonwomen’sexperiencesofallformsofviolencealongwithobstetricviolence
throughsensitive,feminist,embodiedparticipatorymethodstounderstandtheconstruct
ofallformsofviolenceinwomen’sliveswithoutsegregatingthedifferentformsof
violence.
• Researchandconsultationbasedonlearningsfromsystemicliteraturereviewtodevelop
plansforawayforwardtoaddressthedriveridentifiedatallthelevels,individual,
birthingenvironment,socialandpolicylevels,whichcanenablerespectfulmaternitycare
provision.
• Researchtounderstandobstetricviolenceinuniquecircumstancessuchassurrogacy,
prison,conflictandhumanitariansettings,naturalcalamitiesandpandemictoensure
respectfulcareinthesecontextsforsexual,reproductiveandmaternalhealthcare.
• Researchonoverlappingterritoriesandconstructssuchasreproductiveviolence,
reproductiveinjustice,reproductivepoliticsandgovernanceetc.howtheyoverlapwith
anddifferfromobstetricviolence,tofurtherunderstandthewholegamutofwomen’s
experiencewithinsexual,reproductiveandmaternalhealthandhealthcare.
• Researchonmidwivesandnurse-midwives’experienceofobstetricviolenceand
respectfulmaternitycarewhentheygivebirth,andhowthatinfluenceshealthcare
provision.
• Researchonteamcultureonobstetricviolenceandalsoonrespectfulmaternitycare,and
howteamscanbeaddressedtogetherininitiativestoensurecompassionatecare.
• Largescalequantitativeresearchoncareprovidersrelatedbarrierstoensurerespectful
maternitycareinIndia.
• Researchexploringpainandpleasureinwomen’ssexual,reproductiveandmaternal
healthrelatedembodimentstounderstandhowtheyinfluenceeachother,andtheir
experiencesandexpectationsfromhealthcare.
• Researchonobstetricviolenceandrespectfulmaternitycarefromtheperspectiveof
senseofsight,smell,speech,soundandtouch.
• Researchonbirthingenvironmentinfrastructureandarchitectureforlowresource,high
workloadsettings.
• Understandingthecontrapuntalvoicesquantitativelytoknowthedurationofthese
voicesrepresentingconcordanddiscordinanattempttomakeashifttowardsmore
concord,insensitiveissuesofbirthingwherewomen’smayhesitatetosharetheir
experiencesofobstetricviolence.

Chapter10
240
• ResearchandimplementationoftheContinuumofRespectfulExperiences(CORE)model.

0
241
Postscript:Thestoryofmybirth
My1stfamilypicture:Baba(curlyhair),Ma(wearingasareecutfromtheclothofthecurtain),me
(camouflagingonmymother’slap)andDidi(turtleneck)
IwasborninamilitaryhospitalinthewesternstateofRajasthaninIndia,at10amonathursday,December11th,1986.
Soonafter,mymawasshiftedtoapostnatalcareroomthatshesharedwithaRajasthaniaunty.
Let'scallherBinti.
Bintiauntygavebirthtoher4thsonandwasverysad!
MrsandMrBintialwayswantedagirlandhad4sonswhiletryingforagirl.
Mymahadadaughteralready,ourbelovedKeya.
Iamhersecondgirl,soBintiauntydrooledallovermefromthesecondshesawmeandhadabrilliantidea.
"Let'sexchangeourbabies,Kalpana"shesaidtomymother"thatwaywewillbothcompleteourdreamfamilywithperfectmale:femaleratioandthesecretwillremaininthispostnatalroom".
Let'scallhersonDhinku.
Concerned,IlookedatDhinkuandthoughtthere'snowaymymawillgivemeupforhim.
(PleaserefertomeinthepictureinExhibitA:Myfirstfamilypicture)
Importantdetail-noneofthefathershadseentheirrespectivebabiesyet.
Bintikeptpleading.
Masaidno.
Shesaidplease.
Masaidno.

0
242
DhinkuandImadeeyecontactandcried,undecidedwho'sgoingtogetaBengaliupbringingandwhowillberaisedRajasthani.
Bintibrokeintotears,inconsolable.
Mr.Bintijumpedin,saidplease.
Masaidno.
Everybodystartedcrying!
TheysaidaskMr.Kalpana,he'llsurelywantDhinku(2.5kgs)inexchangeofa2nddaughter(4kgs).
Keya,mydidi,clueless,ifherparentsarebringinghomeasisterorabrother.
Mr.Kalpanaheardaboutthedealofbabyexchangeonthetable(inthecrib)andgotfurious.
Mr.Kalpanaranhishandthroughhiscurlyheadfullofhairandsaidno.
Forwhateverreason,together,MrsandMrKalpanadecidedtokeeptheirdaughter(4kgs)andtheylivedhappilyeverafter.
****************************

0
243


AppendixA
245
AppendixA Trahi’sbirthingexperience
Trahi(pseudonym)isa21-year-oldhomemaker.Shehastwochildren,andherlastchildwasborn
18daysago.SheisaHindubyreligionandbelongstoschedulecaste.Shehasreceived4yearsof
formaleducation,belongstoahouseholdfrompoorsocio-economicbackground,whoareall
casuallabourersinothersfarms.Thehouseholddoesnothaveaccesstoelectricity.
Trahitravelledwithhermother-in-lawandarelativetothehealthcarecentre.Shemadetwo
visitsforantenatalcareatapublichealthcarefacilityduringherpregnancyandfeltthatsheis
treatedveryrespectfullyduringherante-natalvisits.Goingtothisfacilitywasherfamily
member’sdecision.Itwasthesamefacilitywhereshewentforherantenatalcareandfeltthe
providerstreattheirclientswell.Sheexpectedawellequippedfacility,cleanenvironment,good,
affordableandspecialisedservices.Whenshevisitedthehealthcarecentretogivebirththe
healthcareproviderscheckedherbloodpressure,thefetalheartrateandconductedan
ultrasonography.Herbirthwasassistedbyadoctor,nurse,mamtaandASHA.Hermother-in-law
accompaniedasherbirthcompanion.
Trahiexperiencedmanyinstancesofobstetricviolenceduringherstayatthehealthcarefacility
duringchildbirth.Sheexperiencedphysicalabuse,verbalabuse,stigma,discrimination,therewas
poorrapportwithhealthcareproviders,afailuretomeetprofessionalstandardsofcareand
healthsystemconstraints.Thehealthcareprovidersusedrudelanguagewithherandmade
judgementalandaccusatorycomments.Shewasthreatenedtobehitbecauseshewasscreaming
fromthepainfulcontractions.Theyphysicallyabusedherbypullingherbyherleg,shewasalso
slappedorhitorpinched.Therewaspoorcommunicationandshefeltlikeapassiveparticipant
becauseshewasnotinformedthefindingsofhergeneralandvaginalexaminations.Shewasnot
communicatedaboutthewardenvironmentandtheprogressinherlabour.Shefeltneglected
andabandoned.Herprivacywasnotmaintainedandconfidentialitywasbreached.Herconsent
wasnotsoughtwhenconductinginterventionsonher.
Trahi,orthebabyweredetainedatthehealthcarefacilityfortheinabilitytomakepayment.Her
familypaid500rupeesinbribeand3500rupeesformedicationatthegovernmenthealthcare
facility.ShehadnotreceivedtheJSYmoneyinthe18dayssincebirth,whichsheissupposedto
receiveimmediatelyinherbankaccount.Shefeltthatthestaffattitudetowardsherwasvery
poor.Shewasnotallowedanyfoodorfluidduringlabourandbirth,andwasnotallowedtowalk
around.Shewasnotallowedtogivebirthinapositionofherchoiceandhadtogivebirth
standing.Herbabywasputonherchestrightafterbirth.Shetooknoactionabouttheobstetric

AppendixA
246
violencesheexperienced.Shesharesthatshewillnotrecommendthishealthcarefacilityto
otherstogivebirth.Trahiratedtherespectfulnessshowntoherduringchildbirthandstayinthe
facilityaspoor.

AppendixB
247
AppendixB Bodymappingaidedin-depthinterview
guide
Background
No. Question Response
A1 Participantcode
A2 Participantchosenpseudonym
A3 Age
A4 Numberofchildren
A5 Education(no.ofyears)
A6 Occupation
Householdinformation
No. Question Response
B1 Istherewatersupplyinthehousehold?
B2 Isthereelectricityinthehousehold?
B3 Doestheparticipanthaveabankaccounttohername?
B4 Distance(kms)tothenearesthealthcarefacility?(PHC/CHC/DH/Tertiaryhospital)
B5 Urban/Rural
B6 Durationofstayatcurrentaddress
Birthhistory
No. Mother’sageatbirth
Placeofbirth(Hospital,Home,CSother)
Sexofnewbornatbirth
Birthcompanion Anycomplications/comments/remarks
C1
C2
C3
C4
C5

AppendixB
248
Experience,expectationsandperceptionsaboutchildbirth
No. Questionsandprobes ReflexiveNotes
Experienceofchildbirth
D1 Howwasyourbirthexperience?Probes:Shemaytalkaboutanybirthexperienceofherchoiceandevenmentionexperiencesfromdifferentbirthsshehashad.
D2 Howwereyoureceivedatthehealthfacilitywhenyouarrivedandhowwastheexperience?Probes:Whoreceivedyou,howmanypeoplewerethere,whosaidwhat,whodidwhat,waitingtimefromarrivaltolabourroomorward
D3 Whathappenedafteradmission?Wereyoutakentothelabourroomorawardtowait?Whathappenedintheantenatalroom?Probes:Wereyouallowedtomovearound?Wassomeonewithyoufromfamily?Wasthereanythingthatyoulikedordidnotlike?Didyoufeelanythingdisrespectfulorabusive?
D4 *Howwouldyoudescribethebirthingenvironment/roomwhereyougavebirth?Probes:whatwasaroundyou?Curtains,airconditioning,otherlabourtables,cleanliness,monitor
D5 *Howwasyourprivacymaintainedduringlabourandwhilegivingbirth?Probes:Whatwerepeopledoingaroundyou?Canyoushowonthemapwherearoundyoutheywerestanding?Didyoufeelyouwereproperlycovered?Howdidyoufeelaboutit?
D6 *Whatpositiondidyougivebirthinandhowdidyoufeelaboutit?Probes:lyingdown,restraints,peopleholdingdown,howwasbirthingonalabourtable
D7 *Whatinterventionswereperformedonyouinthehospitalfromadmissiontodischarge?Howdidyoufeelaboutit?Probes:consent,information,communication
D8 Didthesamecareprovidergivecaretoyoufromantenatalperiodtochildbirth?Probes:Yes,no?why?Whatwouldyouhaveliked?Howwouldithavehelped?
D9 *Howdidtheperson/peoplefromfamilyaroundyouhelpwhileyouwereinthehealthcarefacility(orhome)andwhenyouweregivingbirth?
D10 *Howdidyoudecideaboutyourbirthcompanionandwhy?
D11 Howwasthebehaviorofthecareprovideraroundyouduringchildbirth?
D12 Whatconversationsdidyouhavewiththecareprovider?Probes:Didanyonesayanythingtoyouthatyoudidnotlike?Anythingthatyouliked?

AppendixB
249
D13 Howdidyoufeelaboutaskingquestionstothecareprovidersduringchildbirth?Probe:Couldyoutalkfreelytoyourcareprovider?
D14 *Whatkindoftouchisokayduringchildbirth?Probes:Howmanypeopletouchedyouinanyway?Careprovidersandfamily?Whotouchedyouwhereandhowmanytimes?Howdidyoufeelaboutit?
D15 *Whatcomfortedyouduringlabourpains?Who(family,careproviders)helpedyou?How?Probes:Walkaround,drinkingwater,takingsomefood,usingwashroom,backmassages;Whatwasthemostdiscomforting?
D16 *Whatarethethingsthatyoulikedduringchildbirth?Whatarethethingsthatyoudidnotlike?Probes:wasinformationaboutyousharedwithothersthatyoudidnotwant?Didyouhavetopayforanyservice?
D17 *Howdidyoudecidewheretogivebirthandwhy?Howdidyoufeelaboutthatdecision?
Hopes
E1 *Whatdidyoualreadyknowaboutgivingbirth?Whatisthelanguageyouusetotalkaboutbirth?Whodoyoutalktoaboutbirth,questions,fears,doubts?
E2 *Whatdidyouhopewouldhappenwhenyougivebirth?Probes:Listallthethingsshesaysandkeepaskingspecificquestionsbasedonherresponse,couldbeunrealistic
E3 *Whatservicesshouldbethereinthehospitalthatwillmakeyourexperienceofchildbirthsatisfactoryandrespectful?Probes:birthenvironment,privacy,cleanliness,behaviorofcareproviders,wayoftalking
E4 Multipara-whatisthedifferenceinyourexperienceofbirthingintwosettings?Goodandbad?Whichwasmorerespectful&disrespectful?Why?
F Concludingquestion-Howdoyoufeelaboutthisexercise?Isthisasatisfyingexercise?Why?Probes:likes,dislikesabouttheprocessofbodymapping
Note-*Tobeaskedforhomebirthsaswell.

AppendixB
250
BodyMapKey
RespondentID/Pseudonym-
Symbolorcolour Meaningorinterpretation
Postinterviewdebrief
Debrief
Reflexivenotes
Interviewenvironment

AppendixC
251
AppendixC Nursemidwives’perspectivesonrespect,
disrespect&abuseduringchildbirthA. Backgroundinformation(Tobefilledbyparticipantifpossible)
A1 Participantcode
A2 Age
A3 Sex
A4 Designation
A5 Organisation/department
A6 State
A7 Category(selectallthatapplies) • MOHFW• INC/SNC• Hospital• TeachingInstitution• CivilSocietyOrganization• Private• Others______________________
A8 Numberofyearsofserviceinurbanandruralarea
Urban____________Rural_____________
A9 Educationalbackground(selectallthatapplies)
• ANM• GNM• BScNursing• PBBScNursing• MScNursingin_______________• PhDin______________________• Other_______________________
A10 Allthedesignationsworkedonwithpromotions(mentionpositionandnumberofyearsworkedonthesame,Eg.StaffNurses-10years)
Designation Yearsofservice
A11 Totalyearsofexperience
A12 Haveyoueverdonemidwiferyprofessionally?
Professionally-Yes/No
A13 Ifyes,forhowmanyyearsormonths?
A14 Howmanybirthshaveyouconductedintotal?(anyinthelastoneyear?Public/Private)
B. CurrentRoleandresponsibilities
B1 Howwouldyoudescribeyournursingand/ormidwiferycareer?
B2 Whatisyourcurrentroleandresponsibilities?

AppendixC
252
B3 Whatsupervisoryroledoyoucurrentlyplay?(Probes:Visitstohospitals,teachinginstitutions,meetingswithpeopleetc.)
B4 Howarevariousnursingandmidwiferypoliciesmade?Howarethosedecisionsmade?(Probes:regulation,deployment,transfer,etc.)
B5 Whatroledoyouplayinnursing&midwiferyworkforcegovernance?Probe:recruitment,salary,posting&transfer,continuededucation,careerprogression,promotionCollect:policydocuments,acts,etc.Whatpercentageofthemarewithnursingandmidwiferybackground?Whoarethestakeholdersinvolvedinthesedecisionmaking?
B6 Doyoufeelnurse-midwivesareplayinganequalroleatpolicymaking?Doyoufeeltheycancontributeinanyotherwayinimprovingnursing-midwiferyworkforcegovernance?
C. Perceptionofquality&respectfulnessincarearoundbirth
Information:Hereisapaintingdrawnbyamidwifebasedonherandmyexperienceofadeliverywehadobservedtogether.(Refertoimage)
C1 Whatisyourreactiontothepainting?Probe:familiarornot,realisticornot,typeoffacility,urban/rural,home,private,public
C2 Whatdoyoufeelaretheessentialcomponentsofgoodqualityofcarearoundchildbirth?
C3 Whatdoesrespectmeantoyou?
C4 Howwouldyoudefinerespectfulmaternitycare?
Information:ThereissomeevidencecomingupfromstateslikeBihar,UttarPradesh,Jharkhand,WestBengaletc.thatwomenhavebeenphysicallyabused(hit,slapped,pinched)orverballyabused(commentsonsexlife,discriminatorycommentsbasedongender,religionorsocioeconomicstatus,physicalappearance)ortherewaslackofprivacyduringchildbirth&confidentialityduringorafter.
C5 Haveyouheardofchildbearingwomenundergoingdisrespectandabuseduringchildbirth?Whatkindofdisrespectandabusedoyouthinkwomenface?Couldyousharesomeexamplesfromwhatyoumayhaveseenorheard?
C6 Whydoyouthinksomecareprovidersabusewomenduringchildbirth?Probe:workenvironment,workpressure
C7 Howdoesthisstart?Why?Probe:Whiletheyarestudents,laterinprofession
C8 Howdoyouthinkthechildbearingwoman’sbackgroundcharacteristicplaysanyroleinwhyshegetsabusedduringchildbirth,ifany?Probe:Gender,Socioeconomicstatus,educationlevel,class,caste,religion,HIVstatus,numberofchildren,age
C9 Howdoyouthinkawoman’sphysicalappearanceplaysaroleinwhysheget’sabused?Probe:Height,weight,age,colorofskin,attire/clothing,personalhygienelevel,genitals
C10 Howdoyoufeelthetransformationhappensfromastudentwhoislearningtogivecarearoundbirthtoaprofessionalsomeyearslaterwhoabuseswomenaroundchildbirth?Probe:Medicine,midwifery,otherstaff
C11 Howcanyouensurethatrespectfulmaternitycareisprovided?Probe:Disrespectandabuseduringchildbirthisviolationofhumanrights.Howcanitberegulated?Disincentive,punishment
C12 Givenyouarenursingand/ormidwiferyleader(inIndia)howdoyouthinknursingand/ormidwiferyleadershipcanhelpimproverespectfulnessofcarearoundchildbirth?

0
253
C13 Howcanournursing&midwiferystudentsbeshowntoprovideRMCintheirPreserviceeducation?
C14 Canyoulistthreethings/actionsyoucantakefromyourleveltoseethatcareprovisionaroundchildbirthisrespectful?Andwhatbarriersandfacilitatorsdoyouforeseeforthesame?
C15 Doyouhaveanychildren?Wouldyoumindsharinghowyourchildbirthexperiencewas?(Probe:Respectful,disrespect&abuse,incontrol,choice,whatdidyoulikeordislike)

AppendixD
254
AppendixD Knowledgetranslation
ThisPhDenablesunderstandingofobstetricviolenceduringchildbirth.Thefindingshighlight
needforfutureresearchtopromoteandimplementrespectfulmaternitycareandfindshortterm
andlongtermsolutionstoaddressobstetricviolenceduringchildbirth.MyPhDbeganinJanuary
2018andthefollowingactivitieshelpedinknowledgetranslationofmyPhDresearchoverthelast
fouryears.
TableD:Knowledgetranslationactivities
Month,year Event Activity
2018
August-September2018
SeminaratWHOHeadQuarters,Geneva,Switzerland
RespectfulMaternityCare:Definitions,typologies,evidenceandpoliciesPresentedtohealthandpolicyexpertsatanopentoallseminarattheWHOHQ.
August-September2018
Globalguidelinesfortrainingmidwivesonrespectfulmaternitycare,WHOToolkit(upcoming)
InternedonMidwiferyLeadershipatWHOHQPreparedacrosscuttingmoduleonRMCforaglobaltoolkitonmidwiferyeducationasadeliverableoftheinternship.Thistoolkitwillbepublishedwhenothermoduleswillbeready.
December2018
PartnershipofMaternalNeonatalChildHealth,Partner’sForum,NewDelhi,India
MidwivesVoices,Women’sChoicesOrganisedasideeventtothepartners’forumthatbroughtmidwives,womenandadolescentgirlsfrom13statesinIndiawheretheysharedtheirexperiences,needsandchallenges.Theaudienceofthiseventincludedinternationaldevelopmentorganisers,policymakers,academiciansandresearchersfrommanycountries.TheNormalBirthCampaigninIndiawasalsolaunchedinthisevent.https://www.change.org/p/government-of-india-promote-normal-birth-in-india-be-a-normal-birth-ambassador
2019
March2019 DepartmentofSocialSciencesSeminar,UniversityofSouthampton,UK
Whydocareprovidersabusewomenduringchildbirth?Presentedfindingsfromthefirstanalysisbasedonmidwiferyleadersinterviews
March2019 WhatWomenWantCampaign,UK
LeadtheglobalWhatWomenWantcampaigninUKtocollectwomenandgirl’swantsforreproductiveandmaternalhealthcare.

AppendixD
255
April2019 3MinuteThesisUniversityofSouthampton
Wonthefacultylevel3MTRepresentedFacultyofSocialSciencesattheUniversitylevelcompetition.https://www.youtube.com/watch?v=LNA6cAfzDAE
May2019 AllWalesStudentNursesConference,Cardiff,Wales
Howcanstudentmidwivesensurerespectfulmaternitycare?Invitedtospeakontherolestudentmidwiveshaveinprovidingrespectfulcareandhowrespectfulcommunicationintheteachingenvironmentinfluencesthat.
May2019 72ndWorldHealthAssembly,Geneva,Switzerland
WASHinHCFandMidwiferyStrengtheningRepresentedICMasayoungmidwiferyleaderandinvitedtospeakattwopanelsalongsideDirectorGeneralDr.TedrosAGhebreyesus.
June2019 WhatWomenWantReport,WhiteRibbonAlliance
Gotfeaturedinthereportasoneofthe5keyinfluencersforthecampaignthatranin114countriesandfoundrespectfulmaternitycareasthe1strankingdemandfromatotal1.2millionwants.https://www.whiteribbonalliance.org/wp-content/uploads/2019/06/What-Women-Want_Global-Results.pdf
June2019 14thNormalLabourandBirthResearchConference,Lancashire,UK
EmpowermidwivesforrespectfulmaternitycarePresentedfindingsfromfirstanalysischapterondriversofdisrespectandabuseduringchildbirthfrommidwiferyleader’sperspective.
July2019 ParlayParlour;WhiteRibbonAlliance,GlastonburyFestival2019,UK
Women’sbodies,Women’srightsSpokeonapanelfocusingonchoicesinbirthandfertilityrevolvingaroundpainandpleasure;alongsideJessePhillips,MPBirminghamYardley.https://www.theguardian.com/music/2019/jun/30/glastonbury-gender-balance-performers-headline-acts-men
August2019 RespectfulMaternityandNewbornCareGuidelines,GovernmentofIndia
ReviewedandgaveinputstothenationalguidelinesonRespectfulmaternityandneonatalcarebyGovernmentofIndia.
September2019
Resolutiontorevolution:WASHinhealthcarefacilities,Livingston,Zambia
Howdoeswater,hygieneandsanitationservicesinhealthcarefacilitieseffectcareprovider’ssafety&dignity?Presentedatathree-daymeetingorganisedbyWHOHQ,UNICEFandGovernmentofZambiabasedonpersonalexperiencesandaquicksurveyofnursesandandmidwivesonsocialmediafromotherlowermiddleincomecountries.https://www.youtube.com/watch?v=Su53NTLFkdA&feature=youtu.be
September2019
14thAnnualSocietyofMidwivesIndiaConference,Raipur,India
Domidwiveshaverespectfulbirths?InvitedtospeakonapanelonRespectfulMaternityCare(RMC)inIndiaorganisedbyWhiteRibbonAllianceIndiaatthe14thSOMIconference.

AppendixD
256
September2019
InternationalConfederationofMidwives’(ICM)
Midwiferyeducator’scurriculum;andNursePractitionerinMidwiferyCurriculum;GovernmentofIndiaConsultedwithICMonafive-memberteamofmidwiferyexpertsledbyProf.LesleyPagetopreparetwocurriculumsformidwiferyeducatorsandnursepractitionersinmidwifery(NPM)inIndia.AnewcadreofmidwivesisfinallybeingtrainedinIndiatoenablemidwiferyledcarethatisgoodqualityandrespectful.
2020
February2020
Birthingoutsidethesystem:TheCanaryintheCoalmine,Routledge
WhySouthAsianwomenmakeextremebirthchoices(BookChapter)Co-writtenwithBashiKumarHazard,fromHumanRightsinChildbirthwhoiseditingthisbookwithHannahDahlenandVirginiaSchmiedfromWesternSydneyUniversity,Australia.https://www.routledge.com/Birthing-Outside-the-System-The-Canary-in-the-Coal-Mine-1st-Edition/Dahlen-Kumar-Hazard-Schmied/p/book/9781138592704
March2020 EconomicandPoliticalWeekly(EPW)
Docsplanation!It’sanopinionpiecetohighlightthedominationandinfluenceofmedicalprofessiononmidwiferyandnursinginIndia.https://www.epw.in/journal/2020/10/postscript/docsplanation.html
April2020 WashingtonUniversityofSt.Louis
Gaveaguestlecturetoundergraduatestudentson‘Birth,genderandmidwifery’
May2020 73rdWHA,Geneva
WASHfornursesandmidwives’inCOVID-19
June2020 ThePracticingMidwifeJournal
Astarchedcottonfluorescentyellowsaree,khopa,bellybuttonandsafetypins:decodingthe‘dignifiedIndiannurse-midwife’https://www.all4maternity.com/a-starched-cotton-fluorescent-yellow-saree-khopa-belly-button-and-safety-pins-decoding-the-dignified-indian-nurse-midwife/
July2020 CollegeofObstetrics,Argentina
ParteríaInterculturalGotfeaturedinaSouthAmericanmidwiferymagazinebytheCollegeofMidwives’sinArgentinaintheirglobalinterculturalmidwiferysection.
September2020
GLOWConference
Presentedapostertitledwhysomecareprovidersdisrespectandabusewomenduringchildbirth.
December2020
15thNormalLabourandBirthResearchConference
2021

AppendixD
257
February2021
UniversityofSouthampton,UK
June2021 InternationalConfederationofMidwivesCongress,Bali,Indonesia
Abstractselectedfor3MinuteThesis:1. DisrespectandabuseofwomenduringchildbirthinIndia
(3minutethesisentry)
2021-22 Publicationsunderrevieworin-print
ThefollowingpapersareplannedfromthePhD:1. MayraK.,MatthewsZ.,SandallJ.Thecaseofsurrogate
decisionmakersforwomencompetenttoconsentduringchildbirthinBihar,India.Agenda.Inprint
2. MayraK.,MatthewsZ.,SandallJ.,PadmadasSS.Women’sexperienceofrespect,disrespectandabuseinBihar,India:abodymappingaidedcriticalfeministstudy(underreviewwithBMCPregnancyandChildbirth)
3. MayraK.BodyMapping:aparticipatorymethodtounderstandwomen’sbirthingexperience(UnderreviewwithQualitativeHealthResearch)
4. VanderwaalR.,MayraK.Obstetricviolenceasgenderbasedviolence(BookChapter,Underreview)
5. VanderwaalR.,MayraK,ObstetricViolence:It’sabolition(UnderreviewwithFeministAnthropology)

ListofReferences
259
ListofReferences
1. Abuya,T.,Warren,EC.,Miller,N.,etal.,(2015).Exploringtheprevalenceofdisrespect
andabuseduringchildbirthinKenya.PlosOne.10(4).
2. Adichie,CN.2014.Weshouldallbefeminists.FourthEstate.
3. Afsana,K.,RashidSF.(2001).ThechallengesofmeetingruralBangladeshiwomen’sneeds
indeliverycare.ReproductiveHealthMatters.9(18).Pp.79-89.
4. Afulani,PA.,PhillipsB.,Aborigo,RA.,Moyer,CA.(2019).Person-centeredmaternitycare
inlow-incomeandmiddleincomecountries:analysisofdatafromKenya,Ghanaand
India.LancetGlobalHealth.(7).pp.96-109.
5. Afulani,PA.,Moyer,CA.(2019).Accountabilityforrespectfulmaternitycare.TheLancet.
394.
6. Ahmed,S.,etal.(2019).Theimpactofanursementoringprogramonthequalityof
labouranddeliverycareatprimaryhealthcareatprimaryhealthcarefacilitiesinBihar,
India.BMJGlobalHealth.4:e001767.Doi.doi:10.1136/bmjgh-2019-001767
7. Ali,N.(2019).Whatwearetoldnottotalkaboutbutwearegoingtoanyway!Penguin
Viking.
8. Allen,A.(2013).Feminism,modernityandcriticaltheory.Internationalcriticalthought.
3(3).pp.268-281.Doi:10.1080/21598282.2013.817986
9. Allotey-Reidpath,KD.,Allotey,P.,Reidpath,DD.(2018).Ninemonthsaslave:when
pregnancyisinvoluntaryservitudetoafoetus.ReproductiveHealthMatters.26(52).Doi.
10.1080/09688080.2018.1451173
10. Alzyoud,F.,Khoshnood,K.,Alnatour,A.,etal.,(2018).Exposuretoverbalabuseand
neglectduringchildbirthamongJordanianwomen.Midwifery.58.pp.71-76.Doi.
10.1016/j.midw.2017.12.008
11. Amorim,MM.,Bastos,MHS.,Katz,L.(2020).Mistreatmentduringchildbirth.TheLancet.
12. ANSWERS.2009.NursingServicesinBihar:currentsituation,requirementsandmeasures
toaddressshortages.NationalHealthSystemsResourceCentre.
13. Asefa,A.,Bekele,D.(2015).Statusofrespectfulandnonabusivecareduringfacilitybased
childbirthinahospitalandhealthcentersinAddisAbaba,Ethiopia.ReproductiveHealth.
12(33).Doi.10.1186/s12978-015-0024-9
14. Bagga,R.etal.(2010).MidwiferyandmotherhoodinIndia.
15. Baxter,J.(2008).FeministPost-StructuralistDiscourseAnalysis-Anewtheoreticaland
methodologicalapproach?

ListofReferences
260
16. Beard,M.(2017).WomenandPower.AManifesto.
17. Behruzi,R.,Hatem,M.,Fraser,W.,etal.,(2010).Facilitatorsandbarriersinhumanization
ofchildbirthpracticeinJapan.BMCPregnancyandChildbirth.10(25).
18. Betron,ML.,McClairm,TL.,Currie,S.,etal.,(2018).Expandingtheagendaforaddressing
mistreatmentinmaternitycare:amappingreviewandgenderanalysis.Reproductive
Health.15(143).Doi.10.1186/s12978-018-0584-6
19. Bender,PTH.,MacDonagh,S.,Liljestrand,J.,(2006).Humanresourcesandaccessto
maternalhealthcare.InternationalJournalofGynaecologyandObstetrics.94.pp.226-
233.
20. Bhattacharya,S.,Srivastava,A.,Avan,B.I.,(2013).Deliveryshouldhappensoonandmy
painwillbereduced:understandingwomen’sperceptionofgooddeliverycareinIndia.
GlobalHealthAction.6.doi.10.3402/gha.v6i0.22635
21. Bhasin,K.,Menon,R.1(998).Bordersandboundaries:WomeninIndia’spartition.Kalifor
women.pp.58.
22. Bohren,MA.,etal.,(2014).Facilitatorsandbarrierstofacilitybaseddeliveryinlowand
middleincomecountries:aqualitativeevidencesynthesis.ReproductiveHealth.11(71).
23. Bohren,MA.,etal.(2015).Themistreatmentofwomenduringchildbirthinhealth
facilitiesglobally:Amixed-methodssystematicreview.PLOSOne.12(6).Doi.
10.1371/journal.pmed.1001847
24. Bohren,MA.,Adu-Bonsaffoh,K.,Irinyenikan,TA.,Maung,TM.,Balde,MD.,Tuncalp,O.
(2020).Authorsreply.TheLancet.
25. Bowser,D.,HillK.,(2010).Exploringevidencefordisrespectandabuseinfacilitybased
childbirth.USAIDTRActionProject.
26. Boylan,J.,Dacre,J.,Gordon,H.(2019).Addressingwomen’sunder-representationin
medicalleadership.TheLancet.393.
27. Boydell,KM.,etal.(2020).Womenandstigma:Aprotocolforunderstandingthe
intersectionsofexperiencethroughbodymapping.InternationalJournalofEnvironmental
ResearchandPublicHealth.17(5432).
28. Bradley,S.,McCourt,C.,RaymentJ.,ParmerD.(2016).Disrespectfulintrapartumcare
duringfacilitybaseddeliveryinsub-saharanAfrica:Aqualitativesystematicreviewand
thematicsynthesisofwomen’sperceptionsandexperiences.SocialScienceandMedicine.
169.pp.157-170.Doi.10.1016/j.socscimed.2016.09.039
29. Braun,V.,Clarke,V.(2019).Reflectingonreflecxivethematicanalysis.Qualitative
Research.11(4).pp.589-597.Doi.https://doi.org/10.1080/2159676X.2019.1628806
30. Brown,J.(2019).Isitabirthstrike?WomenTestify.BirthStrike:TheHiddenfightover
women’swork.pp.42-59.

ListofReferences
261
31. Burnett,C.(2021).CommentaryontheArticle“Howgentlemustviolenceagainstwomen
beinordertonotbeviolent?Rethinkingtheword‘violence’inobstetricsettings,”
Reframedwithinacriticaldiscourseorientation.ViolenceAgainstWomen.
32. Butler,J.(1990).Gendertrouble.RoutledgePublishers.
33. Butler,MM.,Fullerton,J.,Aman,C.(2020).Competenciesforrespectfulmaternitycare:
Identifyingthosemostimportanttomidwivesworldwide.Birth:Issuesinperinatalcare.
00.pp.1-11.
34. Chadwick,R.(2017).Ambiguoussubjects:Obstetricviolence,assemblageandSouth
Africanbirthnarratives.FeminismandPsychology.27(4).pp.489-509.
35. Chadwick,R.(2019).Goodbirthnarratives:DiverseSouthAfricanwomen’sperspectives.
Midwifery.77.pp.1-9.
36. Charmaz,K.(2006).Constructinggroundedtheory:apracticalguidethroughqualitative
analysis.Sagepublications.
37. Chattopadhyay,S.,Mishra,A.,Jacob,S.,(2017).‘Safe’,yetviolent?Women’sexperiences
withobstetricviolenceduringhospitalbirthsinruralnortheastIndia.Culture,Healthand
Sexuality.
38. Chattopadhyay,S.(2018).Theshiftingaxesofmarginalities:thepoliticsofidentities
shapingwomen’sexperiencesduringchildbirthinNortheastIndia.Sexualand
ReproductiveHealthMatters.26(53).
39. Chawla,J.(2019).Towardsafemaleshastra.
40. Choi,WJ.,Jung,JJ.,Crantcharov,TP.(2019).Impactofhawthorneeffectonhealthcare
professionals:asystematicreview.RuralHealth.96(2)/
41. Choudhury,UK.(1997).TraditionalpracticesofwomenfromIndia:Pregnancy,childbirth
andnewborncare.JournalofObstetric,GynaecologicandNeonatalNursing.26.pp.533-
539
42. Christensen,A.,Jensen,SQ.(2012).Doingintersentionalanalysis:methodological
implicationsforqualitativeresearch.NordicJournalofFeministandGenderResearch.
20(2).pp.109-125.Doi.https://doi.org/10.1080/08038740.2012.673505
43. Cleghorn,E.(2021).Unwellwomen:ajourneythroughmedicineandmythinaman-made
world.Weidenfeld&Nicolson.
44. Coetzee,B.Roomaney,R.Willis,N.Kagee,A.(2019).BodyMappinginresearch.Hand
bookofresearchmethodsinHealthSocialSciences.Springer.pp.1237-1253.
45. Cornwall,A.(1992).BodymappinginRPA/PRA.RPANotes.16:pp.69-76.
46. Crawford,A.(2010).If‘Thebodykeepsthescore’:Mappingthedissociatedbodyin
TraumaNarrative,InterventionandTheory.UniversityofTorontoQuarterly.79(2).

ListofReferences
262
47. Criado-Perez,C.(2019).Invisiblewomen:exposingdatabiasinaworlddesignedformen.
PenguinRandomHouse.
48. Das,P.,Basu,M.,Tikadar,T.,Biswas,GC.,Mridha,P.,PalR.(2010).Clientsatisfactionon
maternalandchildhealthservicesinruralBengal.IndianJournalofCommunityMedicine.
35(4);pp.478-81.
49. Das,A.,etal.(2016).Impactofanursingskillimprovementinterventiononnewborn
specificdeliverypractices:AnexperiencefromBihar,India.Birth.
50. Davis,D.(2019).ReproductiveInjustice:Racism,PregnancyandPrematurebirth.New
YorkUniversityPress.
51. Deery,R.,(2009).Communitymidwifery‘performances’andthepresentationofself.
Emotionsinmidwiferyandreproduction.pp.73-89.
52. Dehury,RK.,Samal,J.(2016).MaternalhealthsituationinBiharandMadhyaPradesh:A
comparativeanalysisofstatefactsheetsofNationalFamilyHealthSurvey(NFHS)3and4.
JournalofClinicalandDiagnosticResearch.10(9).Doi.10.7860/JCDR/2016/19079.8404
53. Devsenapathy,N.,etal.(2014).Whywomenchoosetogivebirthathome:asituational
analysisfromurbanslumsofDelhi.BMJOpen.4.
54. Devine,C.(2008).Themoon,thestartsandascar:bodymappingstoriesofwomenliving
withHIV/AIDS.Bordercrossings.
55. DeutschesÄrzteblatt,(2019)PrävalenzzurGewaltinderGeburtshilfeweiterhinunklar.
Availableat:https://www.aerzteblatt.de/nachrichten/107793/Praevalenz-zur-Gewalt-in-
der-Geburtshilfe-weiterhin-unklar
56. D’Gregorio,P.(2010).ObstetricViolence:AnewlegaltermintroducedinVenezuela.
InternationalJournalofGynaecologyandObstetrics.111.pp.201-202.
57. Dhar,D.,etal.,(2018).Associationsbetweenintimatepartnerviolenceandreproductive
andmaternalhealthoutcomesinBihar,India:acrosssectionalstudy.Reproductive
Health.15(109).Doi.10.1186/s12978-018-0551-2
58. Diamond-Smith,N.etal,.(2016).Therelationshipbetweenwomen’sexperiencesof
mistreatmentatfacilitiesduringchildbirth,typesofsupportreceivedandperson
providingthesupportinLucknow,India.Midwifery.40.pp114-123.
59. Diniz,CSG.,etal.,(2018).DisrespectandAbuseinchildbirthinBrazil:socialactivism,
publicpoliciesandproviderstraining.ReproductiveHealthMatters.Doi.
10.1080/09688080.2018.1502019
60. Doctor,HV.,etal.,(2012).Usingcommunitybasedresearchtoshapethedesignand
deliveryofmaternalhealthservicesinNorthernNigeria.ReproductiveHealthMatters.
20(39).pp.104-112.

ListofReferences
263
61. Donabedian,A.,(1988).Thequalityofcare.Howitcanbeassessed?.Journalofthe
AmericanMedicalAssociation.260(12).Pp.1743-1748.
62. Downe,S.,Finlayson,K.,Oladapo,O.,Bonet,M.,Gülmezoglu,AM.(2018).Whatmatters
towomenduringchildbirth:Asystematicqualitativereview.PLOSONE.13(4).
63. Downe,S.(2019).Focusingonwhatworksforpersoncenteredmaternitycare.The
Lancet.7.
64. Dzomeku,VM,Mensah,ABB,Nakua,E,Agbadi,P,Lori,JR,Donkor,P.(2020).“Iwouldn’t
havehityou,butyouwouldhavekilledyourbaby”:exploringmidwives’perspectiveson
disrespectandabusivecareinGhana.BMCPregnancyandChildbirth.20(15).
65. Edwards,PN.(2009).Women’semotionworkinthecontextofcurrentmaternityservices.
Emotionsinmidwiferyandreproduction.pp.36-55.
66. Edwards,R.,Weller,S.(2012).Shiftinganalyticontology:usingI-poemsinqualitative
longitudinalresearch.QualitativeResearch.12(2).pp.202-217.Doi.
10.1177/1468794111422040
67. Ehrenreich,B.,English,D.(1970).Witchesmidwivesandnurses:Ahistoryofwomen
healers.GlassMountainPamphlets.
68. Espinoza-ReyesE.,SolisM.2020.Decolonizingthewomb:agencyagainstobstetric
violenceinTijuana,Mexico.JournalofInternationalWomen’sStudies.21(14).pp.189-
206.
69. Fatima,A.,Khoshnood,K.,Alnatour,A.,Oweis,A.(2018).Exposuretoverbalabuseand
neglectduringchildbirthamongJordanianwomen.Midwifery.58.pp.71-76.
70. Federici,S.(2018).Witches,witch-huntingandwomen.PMPress.
71. Feely,C.,Thomson,G.(2020)Understandingwomen’smotivationstoandexpriencesof,
freebirthingintheUK.In:Birthingoutsidethesystem.Thecanaryinthecoalmine.Ed.
DahlenH.,Kumar-HazardB.,SchmiedV.RoutledgePublishers.
72. Filby,A.,McConville,F.,Portella,A.(2016).Whatpreventsqualitymidwiferycare?A
systematicmappingorbarriersinLowandMiddleIncomeCountriesfromtheprovider
perspective.PloSOne.11(5).
73. Fisher,EA.(2015).Nursementorstoadvancequalityimprovementinprimaryhealth
centres:lessonsfromapilotprograminnorthernKarnataka,India.GlobalHealth:Science
andPractice.3(4).
74. Fontein-Kuipers,Y.,Boele,A.,StuiJ.(2016).Midwives’perceptionsofinfluencesontheir
behaviourofwoman-centeredcare:aqualitativestudy.FrontiersinWomen’sHealth.
1(2).pp.20-26.Doi.10.15761/FWH.1000107
ListofReferences
264
75. Freedman,LP.(2003).Humanrights,constructiveaccountabilityandmaternalmortalityin
theDominicanRepublic:acommentary.InternationalJournalofGynaecologyand
Obstetrics.82.pp.111-114.
76. Freedman,LP.,etal.,(2014).Definingdisrespectandabuseofwomeninchildbirth:a
research,policyandrightsagenda.BulletinofWorldHealthOrganization.92.pp.915-
917.Doi.10.2471/BLT.14.137869
77. Freedman,LP.,Kruk,ME.(2014).Disrespectandabuseofwomeninchildbirth:
challengingtheglobalqualityandaccountabilityagendas.TheLancet.384.pp.42-44.
78. FreedmanP.,KujawskiSA.,MbuyitaS.,etal.,2018.Eyeofthebeholder?Observation
versusselfreportinthemeasurementofdisrespectandabuseduringfacilitybased
childbirth.ReproductiveHealthMatters.26(53).Pp.107-122.Doi.
10.1080/09688080.2018.1502024
79. Freeze,R.,Tanner,L.(2020)FreebirthintheUnitedStates.In:Birthingoutsidethesystem.
Thecanaryinthecoalmine.Ed.DahlenH.,Kumar-HazardB.,SchmiedV.Routledge.2020.
80. Friedan,B.,1963.Thefemininemystique.
81. Ghazi,TM.,Moudi,Z.,Vedadhir,A.(2012).Homebirthandbarrierstoreferringwomen
withobstetriccomplicationstohospitals:amixedmethodsstudyinZahedan,Southeast
Iran.ReproductiveHealth.9(18).pp.79-89.
82. Gilmore,K.(2017).Midwives:Makingadifferencethroughsupportingwomen’sandgirls
rights.Thesignificanceofmidwivesasgeneratorsoffemaleempowermentinhealthand
humanrightscontexts.31stInternationalConfederationofMidwivesTriennialCongress.
83. Gilligan,C.(1982).Inadifferentvoice:Psychologicaltheoryandwomen’sdevelopment.
Cambridge,MA:HarvardUniversityPress.
84. Goberna-Tricas,J.,Bańus-Giménez,M.,Palacio-Tauste,A.,Linares-Sancho,S.(2011).
Satisfactionwithpregnancyandbirthservices:Thequalityofmaternitycareservicesas
experiencedbywomen.Midwifery.27.
85. GOI.2005-2006.NationalFamilyHealthSurvey-3.StatefactsheetBihar.International
InstituteforPopulationSciences.
86. GOI.2015-16.NationalFamilyHealthSurvey-4.StateFactsheetBihar.International
InstituteforPopulationSciences.
87. GOI.2015-16.NationalFamilyHealthSurvey-4.IndiasheetBihar.InternationalInstitute
forPopulationSciences.
88. GOI.2019-2020.NationalFamilyHealthSurvey-5.StatefactsheetBihar.International
InstituteforPopulationSciences.
89. GOI.2007.StudyonchildabuseinIndia.MinistryofWomenandChildDevelopment.

ListofReferences
265
90. GOI.(2010).GuidelinesforantenatalcareandskilledattendanceatbirthbyANMs/LHVs/
SNs.MaternalHealthDivision.MinistryofHealthandFamilyWelfare.
91. GOI.(2011).CensusofIndia.
92. GOI.(2015).DAKSHATA:EmpoweringprovidersforimprovedMNHcareduring
institutionaldeliveries.
93. GOI.(2017).LAQSHYA.Labourroomqualityimprovementinitiative.NationalHealth
Mission.
94. GOI.(2018).GuidelinesonMidwiferyServicesinIndia.
95. GOI.(2020).SRSBulletin.SampleRegistrationSystem.53(1).Availableat:
https://censusindia.gov.in/vital_statistics/SRS_Bulletins/SRS%20Bulletin_2018.pdf
96. Goodwin,MA.,Stange,KC.,Zyzanski,SJ.,Crabtree,BF.,Borawski,EA.,Flocke,SA.(2017).
Thehawthorneeffectindirectobservationresearchwithphysiciansandpatients.JEval
ClinPract.23(6):pp.1322-1328.Doi.10.1111/jep.12781
97. Greer,G.(1984).Achildisborn.Sexanddestiny:thepoliticsofhumanfertility.
98. Grzanka,P.(2016).Intersectionsandconfigurations.ArchivesofSexualBehaviour.45(3).
Doi.10.1007/s10508-015-0624-z
99. Gubrium,AC.,etal.(2016).Realizingreproductivehealthequityneedsmorethanlong-
actingreversiblecontraception(LARC).AmericanJournalofPublicHealth.106(1).Doi.
https://doi.org/10.2105/ajph.2015.302900
100. Gupta,N.,Diallo,K.,Zurn,P.,DalPoz,MR.(2003).Assessinghumanresourcesfor
health:whatcanbelearnedfromlabourforcesurveys?.HumanResourcesforHealth.
1(1).
101. Hadwinger,MC.,Hadwinger,SC.(2012).Filipinamothers’perceptionsabout
childbirthathome.IntNursRev.59(1).pp.125-131.
102. Hamilton,P.(2020).‘NowthatIknowwhatyou’reabout’:blackfeministreflections
onpowerintheresearchrelationship.QualitativeResearch.20(5).519-533.Doi.
10.1177/1468794119891583
103. HamadR.(2020).Whitetears/brownscars:Howwhitefeminismbetrayswomenof
colour.TrapezePublishers.
104. Hall,J.,(2013).Developingacultureofcompassionatecare-Themidwives’voice?.
Midwifery.29.pp.269-271.
105. Hausman,LB.(2005).Riskybusiness:Framingchildbirthinhospitalsettings.Journal
of26(1).pp.23-38.
106. Hawkes,S.,Allotey,P.,Elhadj,AS.,Clark.J.,Horton,R.(2020).TheLancetCommission
onGenderandGlobalHealth.
107. HooksB.(1989).Feminismisforeverybody.

ListofReferences
266
108. Hollander,M.(2020).Birthing‘outsidethesystem’inNetherlands.In:Birthing
outsidethesystem.Thecanaryinthecoalmine.Ed.DahlenH.,Kumar-HazardB.,Schmied
V.RoutledgePublishers.
109. Homer,CSE.,etal.,(2014).Theprojectedeffectofscalingupmidwifery.TheLancet.
384.pp-1146-57.
110. Hulton,LA.,Matthews,Z.,Stones,RW.,(2007).Applyingaframeworkforassessing
thequalityofmaternalhealthservicesinUrbanIndia.SocialScienceandMedicine.64.pp.
2083-2095.Doi.10.1016/j.socscimed.2007.01.019
111. Hunter,B.,(2009).‘Mixedmessages’:midwives’experiencesofmanagingemotion.
Emotionsinmidwiferyandreproduction.pp.173-191.
112. Hutter,I.(1994).BeingpresentinruralSouthIndia:nutritionofwomenandwell-
beingofchildren.
113. ICM.(2013).Essentialcompetenciesforbasicmidwiferypractice.
114. Ignacio,A.(2019).Brazil’sdebateover‘ObstetricViolence’shineslightonabuse
duringchildbirth.HuffpostBrazil.Availableat:
https://www.huffpost.com/entry/obstetric-violence-brazil-
childbirth_n_5d4c4c29e4b09e72974304c2
115. IIPH-G.(2010).RapidevaluationofMedakModelProject.
116. IPEGlobal.(2016).Trainingtostrengthencarearoundbirth.
117. Jackson,M.(2020).GivingbirthoutsidethesysteminAustralia:freebirthandhigh
riskhomebirth.In:Birthingoutsidethesystem.Thecanaryinthecoalmine.Ed.DahlenH.,
Kumar-HazardB.,SchmiedV.RoutledgePublishers.
118. Jaggar,A.(1997).Loveandknowledge:Emotioninfeministepistemology.InFeminist
socialthought:Areader.Eds.MeyersD.London:Routledge.pp.385-405.
119. Janet,C.(2019).Towardsafemaleshastra.Self-published.
120. Jeffery,P.,Jeffery,R.,(2010).Onlywhentheboathasstartedsinking.Amaternal
deathinruralnorthIndia.SocialScienceandMedicine.71.Pp.1711-1718.Doi.
10.1016/j.socscimed.2010.05.002
121. Jejeebhoy,SJ.,Santhya,K.G.,(2018).Preventingviolenceagainstwomenandgirlsin
Bihar:challengesforimplementationandevaluation.ReproductiveHealthMatters.
26(52).Doi.10.1080/09688080.2018.1470430
122. Jha,P.,etal.,(2017).Satisfactionwithchildbirthservicesprovidedinpublichealth
facilities:resultsfromacrosssectionalsurveyamongpostnatalwomeninChattisgarh,
India.GlobalHealthAction.10(1).Doi.10.1080/16549716.2017.1386932

ListofReferences
267
123. Karvande,S.,etal.,(2016).Whatdoesqualityofcaremeanformaternalhealth
providersfromtwovulnerablestatesofIndia?CasestudyofBiharandJharkhand.Journal
ofHealth,PopulationandNutrition.35(6).Doi.10.1186/s41043-016-0043-3
124. Kaur,J.(2012).Theroleofensuringwomen’sreproductiverights:ananalysisofthe
ShantiDevijudgmentinIndia.ReproductiveHealthMatters.20(39).Pp21-30.
125. Keedle,H.,Schmied,V.,Burns,E.,Dahlen,HG.(2019).Anarrativeanalysisof
women’sexperiencesofplanningavaginalbirthaftercesarean(VBAC)inAustraliausing
criticalfeministtheory.BMCPregnancyandChildbirth.19(142).
https://doi.org/10.1186/s12884-019-2297-4
126. Keeling,JJ.(2011).Usingafeministstandpointtoexplorewomen’sdisclosureof
domesticviolenceandtheirinteractionwithstatutoryagencies.DoctoralDissertation.
UniversityofChester,UnitedKingdom.
127. Kelly,L.(1988).Survivingsexualviolence.PolityPress.
128. Khaliq,AA.,Broyles,RW.,Mwachofi,AK.(2008).Globalnursemigration:Itsimpact
ondevelopingcountriesandprospectsforfuture.WorldHealthandPopulation.10(3).
pp.5-23.
129. Khanna,R.,Sri,S.(2017).Socialdeterminantsofmaternalhealth”:Deadwomen
talking.TheSocialDeterminantsofHealthinIndia:ConceptsProcessesandIndicators.pp.
189-208.
130. Khosla,R.,etal.,(2016).Internationalhumanrightsandthemistreatmentofwomen
duringchildbirth.HealthandHumanRightsJournal.18(2).pp.131-143
131. Kilaru,A.,etal.(2004).Shehasatenderbody:postpartummorbidityandcareduring
BananthanainruralSouthIndia.
132. Kitzinger,S.(1992).Birthandviolenceagainstwomen:generatinghypothesesfrom
women’saccountsofunhappinessafterchildbirth.Women’sHealthMatters.Routledge.
133. Kitzinger,S.(2005).ThePoliticsofbirth.
134. Kitzinger,S.(2012).Rediscoveringthesocialmodelofchildbirth.Birth:Issuesin
perinatalcare.39(4).
135. Klein,M.,Milner,RJ.(2019).Theuseofbodymappingininterpretative
phenomenologicalanalysis:amethodologicaldiscussion.InternationalJournalofSocial
ResearchMethodology.22(5).
136. Kodoth,P.(2013).InternationalmobilityofnursesfromKerala(India)totheEU:
ProspectsandChallengeswithspecialreferencetoNetherlandsandDenmark.Indian
InstituteofManagementBangalore.

ListofReferences
268
137. Koski,AD.,Stephenson,R.,Koenig,MR.(2011).Physicalviolencebypartnerduring
pregnancyanduseofprenatalcareinRuralIndia.JournalofHealth,Populationand
Nutrition.29(3).pp.245-254.
138. Kruk,EM.,Kujawski,S.,Mbarku,G.(2014).Disrespectfulandabusivetreatment
duringfacilitydeliveryinTanzania:afacilityandcommunitysurvey.HealthPolicyand
Planning.pp.1-8.Doi.10.1093/heapol/czu079
139. Kumari,V.,Mehta,K.,Choudhary,R.(2020).COVID-19outbreakanddecreased
hospitalizationofpregnantwomeninlabour.TheLancetGlobalHealth.
140. Lambert,J.,Etsane,E.,Bergh,AM.,Pattison,R.,BroekN.,(2018)‘Ithoughttheywere
goingtohandlemelikequeenbuttheydidn’t’:Aqualitativestudyexploringthequalityof
careprovidedtowomenatthetimeofbirth.Midwifery.(62).pp.256-263.
141. Langer,A.,Meleis,A.,Knaul,FM.,Atun,R.,Aran,M.,(2015)Womenandhealth:the
keyforsustainabledevelopment.TheLancet.386(9999).pp.1165-1210.
142. Lappeman,M.,Swartz,L.(2019).Rethinkingobstetricviolenceandthe“neglectof
neglect”:thesilenceofalabourwardmilieuinaSouthAfricadistricthospital.BMCHealth
andHumanRights.pp.19:30.
143. Lappeman,M.,Swartz,L.(2021).Howgentlemustviolenceagainstbeinordertonot
beviolent?Rethinkingtheword“violence”inobstetricsettings.ViolenceAgainstWomen.
144. Levesque,S.,Ferron-Parayre.(2021).Touseornottousetheterm“Obstetric
Violence”:CommentaryontheArticlebySwartzandLappeman.ViolenceAgainst
Women.
145. Lokot,M.,Avakyan,Y.(2020).IntersectionalityasalenstotheCOVID-19pandemic:
implicationsforsexualandreproductivehealthindevelopmentandhumanitarian
contexts.SexualandReproductiveHealthMatters.28(1).
146. Lui,J.NM.,Andres,EB.,Johnston,JM.(2018).Presenteeismexposuresandamongst
hospitaldoctorsandnurses:systematicreview.BMCHealthServicesResearch.18(985).
147. Lys,C.Gesink,D.Strike,C.Larkin,J.2018.Bodymappingasayouthsexualhealth
interventionanddatacollectiontool.QualitativeHealthResearch.28(7).
148. Madhiwala,N.,etal.,(2018).Identifyingdisrespectandabuseinorganizational
culture:astudyoftwohospitalsinMumbai,India.ReproductiveHealthMatters.DOI:
10.1080/09688080.2018.1502021
149. Magnusson,E.,Marecek,J.(2017).Feminisms,psychologiesandthestudyofsocial
life.InB.Gough(Ed.)ThePalgravehandbookofcriticalsocialpsychology.London,UK:
SpringerNature.

ListofReferences
269
150. Magoma,M.,etal.,(2010).HighANCcoverageandlowskilledattendanceinarural
Tanzaniandistrict:acaseforimplementingabirthplanintervention.BMCPregnancyand
Childbirth.10(13).pp.1-12.
151. Maslach,C.,Leiter,MP.(2016).Understandingtheburnoutexperience:recent
researchanditsimplications.WorldPsychiatry.15(2).pp.103-111.
152. Matthews,Z.,etal.,(2005).BirthrightsandritualsinruralSouthIndia:Careseeking
intheintrapartumperiod.JournalofBiosocialScience.37(4).pp.385-411.Doi.
10.1017/S0021932004006911
153. Matsuno,A.,NurseMigration:theAsianperspective.
154. Maung,TM.,etal.,(2020).Aqualitativestudyonacceptabilityofthemistreatmentof
womenduringchildbirthinMyanmar.ReproductiveHealth.17(56).
155. Maya,TE.,.,etal.,(2018).Women’sperspectiveofmistreatmentduringchildbirthat
healthfacilitiesinGhana:findingsfromaqualitativestudy.ReproductiveHealthMatters.
Doi.10.1080/09688080.2018.1502020
156. Mayra,K.,Kumar,AIK.(2017).Perceptionsofantenatalwomen,husbandsandhealth
careprovidersonhusbandbeingbirthcompanionduringchildbirth:Aqualitativestudy.
PublicHealthOpenAccess.1(1).
157. Mayra,K.(2020a).Docsplanation:amaladyofthehealthcareprofession.Economic
andPoliticalWeekly;55(10).
158. Mayra,K.(2020b).Astarchedcottonfluorescent-yellowsaree,khopa,bellybutton
andsafetypins:decodingthe‘dignifiedIndiannurse-midwife’ThePracticingMidwife
Journal.23(6).
159. Mayra,K.,Padmadas,SS.,Matthews,Z.(2021).Challengesandneededreformsin
midwifeandnursingregulatorysystemsinIndia:Implicationsforeducationandpractice.
PLOSONE.16(5).Doi:https://doi.org/10.1371/journal.pone.0251331
160. McAra-Couper,J.,Jones,M.,Smythe,L.(2011).Cesarean-section,mybody,my
choice:Theconstructionof‘informedchoice’inrelationtointerventioninchildbirth.
FeminismandPsychology.0(0).pp.1-18.
161. McEwan,C.(2001).Postcolonialism,feminismanddevelopment:intersectionsand
dilemmas.ProgressinDevelopmentStudies.1(2).pp.93-111.
162. McKenzie,E.(2021).FreebirthingintheUnitedKingdom:TheVoiceCentered
RelationalMethodandthe(de)constructionoftheI-poem.InternationalJournalof
QualitativeMethods.20.pp.1-13.Doi.10.1177/1609406921993285
163. McMahon,SA.,George,AS.,Chebet,JJ.,Mosha,IH.,Mpembeni,RNM.Winch,PJ.
(2014).Experiencesofandresponsestodisrespectfulmaternitycareandabuseduring

ListofReferences
270
childbirth;aqualitativestudywithwomenandmeninMorogoroRegion,Tanzania.BMC
PregnancyandChildbirth.14(268).
164. Miller,S.,Lalonde,A.(2015).Theglobalepidemicofabuseanddisrespectduring
childbirth:History,evidence,interventionsandFIGO’smother-babyfriendlybirthing
facilitiesinitiative.InternationalJournalofGynecologyandObstetrics.131.Pp.549-552.
165. Miltenburg,AS.,etal.(2018).Disrespectandabuseinmaternitycare:individual
consequencesofstructuralviolence.ReproductiveHealthMatters.Doi.
10.1080/09688080.2018.1502023
166. Montgomery,E.(2013).Feelingsafe:Ameta-synthesisofthematernitycareneedsof
womenwhoweresexuallyabusedinchildhood.Birth.40(2).pp.88-95.
167. Montgomery,E.,PopeC.,RogersJ.(2015).Afeministnarrativestudyofthe
maternitycareexperiencesofwomenwhoweresexuallyabusedinchildhood.Midwifery.
Pp.54-60.
168. Montgomery,E.,Pope,C.,Rogers,J.,(2015).There-enactmentofchildhoodsexual
abuseinmaternitycare:aqualitativestudy.BMCPregnancyandChildbirth.15(194).Doi.
10.1186/s12884-015-0626-9
169. Morgan,K.,Thapar-Bjorkert,S.(2006).“I’dratheryou’dlaymeonthefloorandstart
kickingme”:Understandingsymbolicviolenceineverydaylife.Women’sStudies
InternationalForum.29(5).489-498.
170. Moridi,M.,Pazandeh,F.,Hajian,S.,Potrata,B.(2020).Midwives’perspectivesof
respectfulmaternitycareduringchildbirth:Aqualitativestudy.PLOSONE.15(3).
171. Morton,CH.,Simpkin,P.(2019).Canrespectfulmaternitycaresaveandimprove
lives?Birth:Issuesinperinatalcare.46.pp.391-395.
172. Mrisho,M.,etal.,(2007).FactorsaffectinghomedeliveryinruralTanzania.TropMed
IntHealth.12(7).pp.862-872.
173. Murray,AF.(2008).Women’shealth,povertyandrights.FromOutragetoCourage.
174. Mselle,LT,Kohi,TW,Dol,J.(2018).Barriersandfacilitatorstohumanizingbirthcare
inTanzania:findingsfromsemi-structuredinterviewswithmidwivesandobstetricians.
ReproductiveHealth.15:137.
175. Mwangome,FK.,etal.,(2012).BarrierstohospitaldeliveryinaruralsettinginCoast
Province,Kenya:communityattitudeandbehaviours.RuralRemoteHealth.12.
176. Nayak,AK.,Nath,A.(2018).ThereisanurgentneedtohumanizechildbirthinIndia.
EconomicandPoliticalWeekly.53(2).
177. Narayan,T.(2002)Genderandpowerissuesinmedicaleducation.In:Genderand
medicaleducation.

ListofReferences
271
178. NAZDEEK.(2020).Hiddentraumas:uncoveringexperiencesofobstetricviolence.
Availableat:https://indd.adobe.com/view/2e6edb7d-050c-474a-a380-ca09c9ebb326
179. Nixon,R.(2011).Slowviolenceandtheenvironmentalismofthepoor.Cambridge.
HarvardUniversityPress.
180. NorwayIndiaPartnershipInitiative.(2014).AssessmentofQualityofHealthCarefor
childreninDistrictHospitals.
181. Nove,A.,etal.,(2021).Potentialimpactofmidwivesinpreventingandreducing
maternalandneonatalmortalityandstillbirths:aLivesSavedToolmodellingstudy.The
LancetGlobalHealth.9(1).Doi:https://doi.org/10.1016/S2214-109X(20)30397-1
182. Oakley,A.(1981).Interviewingwomen:acontradictioninterms.Doingfeminist
research.1981.pp.30-61.
183. Oakley,A.,(1984).Thecapturedwomb.Ahistoryofthemedicalcareofpregnant
women.OxfordpublishingServices.Oxford.
184. Oakley,A.(1993).EssaysonWomen,MedicineandHealth.EdinburghUniversity
Press.
185. Orchard,T.(2017).RememberingtheBody:Ethicalissuesinbodymappingresearch.
Springer.
186. Otis,KE.,Brett,JA.(2008).Barrierstohospitalbirths:whydoBolivianwomengive
birthathome?RevPamanSaludPublica.24(1).pp.46-53.
187. OxnevadM.,2011.Perceptionsandpracticesrelatedtohomebasedandfacility
basedbirth.AqualitativestudyfromAgemssa,Ethiopia.
188. Pankhurst,JO.,Rahman,SA.(2007).Lifesavingormoneywasting?Perceptionsof
caesareansectionsamongusersofservicesinruralBangladesh.HealthPolicy.80(3).
pp.392-401.
189. Parry,DC.(2008).“Wewantedabirthexperience,notamedicalexperience”:
exploringCanadianwomen’suseofmidwifery.Healthcareforwomeninternational.29.
Pp784-806.Doi:10.1080/07399330802269451
190. Patel,P.,Makadia,K.,Kedia,G.(2015).Studytoassesstheextentofdisrespectand
abuseinfacilitybasedchildbirthamongwomenresidinginurbanslumareaof
Ahmedabad.InternationalJournalofMultidisciplinaryResearchandDevelopment.2(8),
pp.25-27.
191. Patel,P.,Das,M.,Das,U.(2018).Theperceptions,healthseekingbehavioursand
accessofScheduledCastewomentomaternalhealthservicesinBihar,India.
ReproductiveHealthMatters.pp1-12.

ListofReferences
272
192. Perera,D.,etal.(2018).‘Whenhelpershurt’:women’sandmidwives’storiesof
obstetricviolenceinstatehealthinstitutions,Colombodistrict,SriLanka.BMCPregnancy
andChildbirth.18(211).Doi.10.1186/s12884-018-1869-z
193. Perez,CC.(2019).Invisiblewomen:exposingdatabiasinaworlddesignedformen.
194. Perkins,J.,etal.(2019).Humanizedchildbirth:thestatusofemotionalsupportof
womeninruralBangladesh.SexualandReproductiveHealthMatters.27(1).
195. Prakasamma,M.(2010).MaternalmortalityreductionprograminAndhraPradesh.
MidwiferyandmaternalhealthinIndia:SituationAnalysisandlessonsfromthefield.
196. Prakash,P.,George,A.,Panalal,R.(1993).Sexisminmedicineandwomen’srights.
IndianJournalofSocialWork.54(2).
197. Radhakrishnan,T.,Vasanthakumari,KP.,Babu,PK.(2017).Increasingtrendof
caesareanratesinIndia:EvidencefromNFHS-4.JournalofMedicalScienceandClinical
Research.5(8).
198. Raj,A.etal.,(2017).Associationsbetweenmistreatmentbyaproviderduring
childbirthandmaternalhealthcomplicationsinUttarPradesh,India.MaternalChild
HealthJournal.21.Pp.1821-1823.Doi.10.1007/s10995-017-2298-8
199. Raman,PS.,etal.,(2010).Historicalperspectivesofnursingandmidwifery:training,
educationandpracticeinIndia.MidwiferyandmaternalhealthinIndia:Situationanalysis
andlessonsfromthefield.pp.3-13.
200. Ramazanoglu,C.,Holland,J.(2002).Feministmethodologies:Challengesandchoices.
SagePublications.
201. Randive,B.,etal.,(2014).Inequalitiesininstitutionaldeliveryuptakeandmaternal
mortalityreductioninthecontextofcashincentiveprohram,JananiSurakshaYojana:
ResultsfromninestatesinIndia.SocialScienceandMedicine.123.Doi.
10.1016/j.socscimed.2014.10.042
202. Ratcliffe,HL.,Sando,D.,Mwanyika-Sando,M.,Chalamilla,G.,Langer,A.,McDonald,
KP.(2016).Applyingaparticipatoryapproachtothepromotionofacultureofrespect
duringchildbirth.ReproductiveHealth.13(80).
203. Rivaldi,C.,Skoko,E.,Cericco,M.,Vannacci,A.(2018).Abuseanddisrespectin
childbirthassistanceinItaly:Acommunity-basedsurvey.EuropeanJournalofObstetric
andGynaecologyandReproductiveBiology.
204. Rawat,LK.,Prasad,JB.,Kumar,P.(2015).Maternalhealthcareservicesandits
utilizationinBihar,India.InternationalJournalofHumanitiesandSocialScienceInvention.
4(1).pp.73-86.
205. Ray,P.(2016).Care(un)skilled:fragmentedmarketsandnursinglabour,
contemporaryKolkata.Land,labourandlivelihoods:Indianwomen’sperspectives.
ListofReferences
273
206. Ray,P.(2019).Caringorwhoring?Nursesandthepoliticsofrepresentation.Colonial
tocontemporaryCalcutta.
207. Reed,R.,Sharman,R.,Inglis,C.(2017).Women’sdescriptionofchildbirthtrauma
relatingtocareprovideractionsandinteractions.BMCPregnancyandChildbirth.17(21).
208. Renfrew,M.,McFadden,A.,Bastos,HM.,(2014).Midwiferyandqualitycarefroma
newevidenceinformedframeworkformaternalandnewborncare.TheLancet.384.
209. Roberts,H.(1981).Womenandtheirdoctors:powerandpowerlessnessinthe
researchprocess.DoingFeministResearch.pp.7-29.
210. Rodgers,D.,Satija,S.(2012).Violence,crimeandpovertyinPatna,Bihar.13.
Availableat:
https://assets.publishing.service.gov.uk/media/57a08a7fe5274a27b200061b/60712_Rod
gers_violence.pdf
211. Roder-DeWan,S.,Gage,AD.,Hirschhorn,LR.etal.(2019).Expectationsofhealthcare
quality:Across-sectionalstudyofinternetusersin12low-andmiddleincomecountries.
PLOSMedicine.16(8).Doi.https://doi.org/10.1371/journal.pmed.1002879
212. Rost,M.,Arnold,L.,DEClerq,E.(2020).“Boilinguptheproblemofviolence”in
childbirth?-anethicalviewpointonmedicalprofessionalresponsestowomen’sreportsof
mistreatmentinchildbirth.OfficialJournaloftheGermanAcademyofEthicsinMedicine.
213. Rubashkin,N.,Ateva,E.(2019).Fromdisrespectandabusetorespectfuland
compassionatecare:aglobalperspective.Squaringthecircle.pp.289-296.
214. Sacks,E.(2017).Definingdisrespectandabuseofnewborns:areviewoftheevidence
andanexpandedtypologyofrespectfulmaternitycare.ReproductiveHealth.14(66).Doi.
10.1186/s12978-017-0326-1
215. Sadler,M.,Ruiz-Berdun,D.,Rojas,GL.(2016).Movingbeyonddisrespectandabuse:
addressingthestructuraldimensionsofobstetricviolence.ReproductiveHealthMatters.
24(47).pp.47-55.Doi.10.1016/j.rhm.2016.04.002
216. Sadler,M,Leiva,G,Olza,L.(2020).COVID-19asariskfactorforobstetricviolence.
SexualandReproductiveHealthMatters.
217. Salter,CL.,Olaniyan,A.,Mendez,DD.,Chang,JC.(2021).Namingsilenceand
inadequateobstetriccareasobstetricviolenceisanecessarystepforchange.Violence
AgainstWomen.
218. Satija,S.(2013).ViolenceagainstwomeninRuralBihar:Acaseoffourvillages.
Workingpapers7621.eSocialSciences.PublishedbyInstituteofHumanDevelopment.
219. Savage,V.,Castro,A.(2017).Measuringmistreatmentofwomenduringchildbirth:a
reviewofterminologyandmethodologicalapproaches.ReproductiveHealth.14(138).Doi.
10.1186/s12978-017-0403-5

ListofReferences
274
220. Scambia,G.,Viora,E.,Colacurci,N.,Vicario,M.(2018).“ObstetricViolence”:Between
misunderstandingandmystification.EuropeanJ0urnalofObstetricsandGynaecologyand
ReproductiveBiology.
221. Scotland,M.(2020).BirthShock.PinterandMartin.
222. Seljeskog,L.,Sundby,J.,Chimango,J.(2006).Factorsinfluencingwomen’schoiceof
placeofdeliveryinruralMalawi-anexploratorystudy.AfricanJournalofReproductive
Health.10(3).pp.66-75.
223. Shabot,SC.(2020a).Why‘normal’feelssobad:violenceandvaginalexaminations
duringlabour–a(feminist)phenomenology.Feministtheory.0(0).
224. Shabot,SC.(2020b).Webirthwithothers:TowardsaBeauvoirianunderstandingof
obstetricviolence.EuropeanJournalofWomen’sStudies.1(16).
225. Shakibazadeh,E,etal.(2018).Respectfulcareduringchildbirthinhealthfacilities
globally:aqualitativeevidencesynthesis.BritishJournalofObstetricsandGynaecology.
125:pp.932-942.
226. Shah,P.,(2016).MDGstoSDGs:Reproductive,Maternal,NeonatalandChildHealth
inIndia.ObserverResearchFoundation.
227. Sharma,B.,etal.,(2010).Roleofnursingcouncilsinregulatingnursingandmidwifery
education,trainingandpracticeinIndia.MidwiferyandmaternalhealthinIndia:Situation
analysisandlessonsfromthefield.pp.14-30.
228. Sharma,G.,Penn-Kekana,L.,Halder,K.,Filippi,V.(2019).Aninvestigationinto
mistreatmentofwomenduringlabourandchildbirthinmaternitycarefacilitiesinUttar
Pradesh,India:amixedmethodsstudy.ReproductiveHealth.16(7).
229. Sheikh,K.,Raman,VR.,Mayra,K.(2012).NursinggovernanceinLowandMiddle
IncomeCountries(LMICs):LiteratureReview.PublicHealthFoundationofIndia.
230. Shiferaw,S.,etal.(2013).WhydowomenpreferhomebirthsinEthiopia?BMC
PregnancyandChildbirth.13(1).
231. Simms,EM.,Stawarska,B.(2013).Introduction.Conceptsandmethodsin
InterdisciplinaryFeministPhenomenology.JanusHead.
232. Silan,V.,Kant,S.,Archana,S.,Misra,P.,Rizwan,SA.(2014).Determinantsof
underutilizationoffreedeliveryservicesinanareawithhighinstitutionaldeliveryrate:a
qualitativestudy.NorthAmericanJournalofMedicalSciences.6(7).pp.315-320.
233. Simpson,J.(2009).EveryoneBelongs:Atoolkitforapplyingintersectionality.Ottawa,
Ontario.
234. Skop,M.(2016).Theartofbodymapping:amethodologicalguideforsocialwork
researchers.AotearoaNewZealandSocialWork.28(4).

ListofReferences
275
235. Smith,D.(1987).Theeverydayworldasproblematic:Afeministsociology.Toronto,
Canada:UniversityofTorontoPress.
236. Smith,D.(1991).Writingwomen’sexperiencesintosocialscience.Feminism&
Psychology.1(1).
237. Spraque,J.(2016).Feministmethodologiesforcriticalresearchers.Bridging
difference.Rowman&LittlefieldPublishers.
238. Sorensen,BL.,et.al.,(2011).Userandproviderperspectivesonemergencyobstetric
careinaTanzanianruralsetting:Aqualitativeanalysisofthethreedelaysmodelinafield
study.AfricanJournalofReproductiveHealth.15(2).
239. Sorsoli,L.,Tolman,DL.(2008).Hearingvoices:listeningformultiplicityand
movementininterviewdata.InS.N.Hesse-Biber&P.Leavy(Eds.),Handbookofemergent
methods.TheGuildfordPress.
240. Swartz,L.,Lappeman,M.(2021).Makingcarebetterinthecontextofviolence:The
limitsofblame.ViolenceAgainstWomen.
241. Sweet,E.Escalante,SR.(2015).Bringingbodiesintoplanning:visceralmethods,fear
andgenderviolence.UrbanStudies.52(10).
242. Srivastava,A.,etal.(2015).Determinantsofwomen’ssatisfactionwithmaternal
healthcare:areviewofliteraturefromdevelopingcountries.BMCPregnancyand
Childbirth.15(97).
243. Srivastava,S.,Sivakami,M.(2019).Evidenceof‘obstetricviolence’inIndia:an
integrativereview.JournalofBiosocialScience.52(4).pp610-628.Doi:
https://doi.org/10.1017/S0021932019000695
244. Sen,G.,Reddy,B.,Iyer,A.(2018).Beyondmeasurement:thedriversofdisrespect
andabuseinobstetriccare.ReproductiveHealthMatters.26(53),pp.6-18.
245. Steege,LM.,Rainbow,JG.(2016).Fatigueinhospitalnurses-‘Supernurse’cultureisa
barriertoaddressingproblems:Aqualitativeinterviewstudy.InternationalJournalof
NursingStudies.67.pp-20-28.
246. StephensonR.,WinterA.,HindinM.,2013.Frequencyofintimatepartnerviolence
andruralwomen’smentalhealthinfourIndianstates.ViolenceAgainstWomen.19(9).
pp.1133-1150.Doi.10.1177/1077801213501898
247. Stones,W.(2004).Women,DoctorsandPain.Reproductiveagency,medicineand
state:CulturaltransformationsinChildbearing.
248. Sudhiranaset,M.,etal.(2016).Women’sstatusandexperiencesofmistreatment
duringchildbirthinUttarPradesh:amixedmethodsstudyusingculturalhealthcapital
theory.BMCPregnancyandChildbirth.16(332).Doi.10.1186/s12884-016-1124-4
ListofReferences
276
249. Talpade-Mohanty,C.(1988).Underwesterneyes:feministscholarshipandcolonial
discourses:Thirdworldwomenandthepoliticsoffeminism.Feministliterarytheory.Ed
by.EagletonM.WileyPublishers.
250. Thadathil,A.,Sriram,S.(2019).Divorce,familiesandadolescentsinIndia:areviewof
research.JournalofDivorceandRemarriage.
251. Thompson,L.,Rickett,B.,Day,K.(2018).Feministrelationaldiscourseanalysis:
puttingthepersonalinthepoliticalinfeministresearch.QualitativeResearchin
Psychology.15(1).pp.93-115.Doi.https://doi.org/10.1080/14780887.2017.1393586
252. Thomson,G.,Feeley,C.(2019).The‘trustingcommunion’ofapositivebirth:an
existentialperspective.Squaringthecircle.47-53.
253. Thomson,G.(2011).‘Abandonmentofbeing’inchildbirth.Qualitativeresearchin
midwiferyandchildbirth:Phenomenologicalapproaches.133-152.
254. Tavris,C.(1993).Themis-measureofwoman.Feminism&Psychology.3(2).149-168.
255. TuncalpO.,etal.,(2015).Qualityofcareforpregnantwomenandnewborns–the
WHOvision.BritishJournalofObstetricsandGynaecology.
256. UnitedNations.(1947).UniversalDeclarationofHumanRights.DignityandJustice
forallofus.
257. UnitedNations.(2019).Ahumanrights-basedapproachtomistreatmentand
violenceagainstwomeninreproductivehealthserviceswithafocusonchildbirthand
obstetricviolence.Item26(a):Advancementofwomen:advancementofwomen.
258. UNFPA,ICM,WHO.(2014).Thestateofworldsmidwifery:universalpathway,a
woman’srighttohealth.Availableat:https://www.unfpa.org/sowmy-2014
259. UNFPA,WHO,ICM.(2021).Thestateofworldsmidwifery.Availableat:
https://www.unfpa.org/publications/sowmy-2021
260. VanAnders,SM.(2015).Beyondsexualorientation:Integratinggender/sexand
diversesexualitiesviaSexualConfigurationsTheory.ArchivesofSexualBehaviour.44.pp.
1177-1213.Doi.https://doi.org/10.1007/s10508-015-0490-8
261. VanManen,M.(1997).Researchingthelivedexperience:Humanscienceforanaction
sensitivepedagogy.TheAlthousePress.
262. Varkey,LC.(2010).Qualityofcaregiventodeliveringwomenandthepivotalroleof
nurse-midwivesintheprocess.MidwiferyandmaternalhealthinIndia:Situationanalysis
andlessonsfromthefield.Pp.89-111.
263. Vogel,JP.,etal.,(2015).Howwomenaretreatedduringfacilitybasedchildbirth:
developmentandvalidationofmeasurementtoolsinfourcountries-phase1formative
researchstudyprotocol.ReproductiveHealth.12(60).Doi.10.1186/s12978-015-0047-2

ListofReferences
277
264. Vora,K.,etal.(2010).MaternalhealthsituationinIndia.MidwiferyandMaternal
HealthinIndia:SituationAnalysisandlessonsfromthefield.pp.165-192.
265. Weisstein,N.(1993).Psychologyconstructsthefemale:orthefantasylifeofthe
malepsychologist(withsomeattentiontothefantasiesofhisfriends,themalebiologist
andthemaleanthropologist).FeminismandPsychology.3(2).pp.195-210.Doi.
https://doi.org/10.1177/0959353593032005
266. Wigginton,B.,Lafrance,MN.(2019).Learningcriticalfeministresearch:Abrief
introductiontofeministepistemologiesandmethodologies.FeminismandPsychology.
DOI:10.1177/0959353519866058
267. WHO.(2007).Women’shealthandhumanrights:Monitoringtheimplementationof
CEDAW.WorldHealthOrganization.
268. WHO.(2010).Wanted:2.4millionnursesandthat’sjustinIndia.Pp.327-328.
269. WHO.(2015).WorldHealthStatistics.WorldHealthOrganization.
270. WHO.(2015).Thepreventionandeliminationofdisrespectandabuseduringfacility-
basedchildbirth.
271. WHO,UNICEF,UNFPA,WorldBank,UnitedNations.(2015).Trendsinmaternal
mortality1990-2015.WorldHealthOrganization.
272. WHO.(2018).Intrapartumcareforapositivechildbirthexperience.WorldHealth
Organization.
273. WHO,GHWN,WGH.(2019.Deliveredbywomen,Ledbymen:agender&equity
analysisoftheglobalhealthandsocialworkforce.HumanResourcesforHealthObserver
SeriesNo.24.
274. Woliver,L.(2002).Ethicaldilemmasinpersonalinterviewing.Politicalscienceand
politics.35(4).pp.677-678.Doi.10.1017/S1049096502001154
275. Wood,J.(2015).Criticalfeministtheories:givingvoiceandvisibilitytowomen’s
experiencesininterpersonalrelations.Engagingtheoriesininterpersonalcommunication.
Ed.BraithwaiteDO.,SchrodtP.Sagepublishers.
276. WhiteRibbonAlliance.(2015).RespectfulMaternityCareCharter:universalrighstof
childbearingwomen.Availableat:https://www.whiteribbonalliance.org/wp-
content/uploads/2017/12/RMC-Impact-Brief.pdf
277. WhiteRibbonAlliance.(2019).WhatWomenWantsreport.Availableat:
https://www.whiteribbonalliance.org/wp-content/uploads/2019/06/What-Women-
Want_Global-Results.pdf
278. WhiteRibbonAlliance.(2019).RespectfulMaternityCareCharter:universalrightspof
motherandnewborns.Availableat:https://www.whiteribbonalliance.org/respectful-
maternity-care-charter/

ListofReferences
278
279. Yuval-DavisN.(2011).Power,Intersectionalityandthepoliticsofbelonging.FREIA
WorkingpaperseriesNo.75.

279

![arXiv:1912.05704v1 [astro-ph.HE] 12 Dec 2019 - ePrints Soton](https://static.fdokumen.com/doc/165x107/631962ea1a1adcf65a0ea184/arxiv191205704v1-astro-phhe-12-dec-2019-eprints-soton.jpg)

















