Report of the Committee on Health Care Facilities - NFPA
101
Report of the Committee on Health Care Facilities Technical Correlating Committee (HEA-AAC) Marvin J. Fischer, Chair Brookdale Hospital Medical Ctr., NY Constance Bobik, B&E Fire Safety Equipment Inc., FL Jay Crowley, U.S. Dept. of Health/Human Services, MD Douglas S. Erlckson, American Hospital Assn., IL Ref3. American Hospital Assn. Thomas W. Gardner, Gage-Babcock & Assoc., VA Rep. American Health Care Assn. William T. Guy, The Elizabeth General Medical Ctr, NJ Rep. NFPA Health Care Section Harlan C. Ihlenfeldt, Kemper Nat'l Insurance Companies, IL Stanley D. Kahn, Heckler Electric Co., Inc., NY Rep. Nat'l Electrical Contractors Assn. Ode Richard KeiI,Joint Commission on Accreditation of Healthcare Orgs, IL WiRiam E. Koffel, Koffel Assoc. Inc., MD Nlls A. Maurice, Nils A. Manrice, P.E., CSP, Inc., AZ Rep. American Society of Safety Engr Dasad A. McWhinnle, Mechanical Dynamics Inc., IL * Robert T. Shipley, Fisher Berkeley Corp., CA Rep. Nat'l Electrical Mfrs. Assn. Steven Werner, M&M Protection Consultants, WI Mfl~yer D. Zimmerman, U.S. Dept. of Health and Human Services, Alternates Clement H. Kiffmeyer, Picker Int'l. Inc., OH (Alt. to R. T. Shipley) Kenneth Knight, Bethesda Hospital, OH (AlL to W. T. Guy) Nonvoting Leo G. Foxwell, ITT Hartford, CT FROm. American Insurance Services Group, Inc. e N. Minardl, CIGNA Property & Casualty Companies, CA (Alt. to L. Foxwell) Staff Liaison: Burton IL Klein This list represents the membership at the time the Committee was balloted on the text o_f this edition. Since that time, changes in the membership may have occurred. Committee Scope: This Committee shall have primary responsibil- ity for documents which contain criteria for safe~,marding patients " and health care personnel in the delivery of health care services within health care facilities: a) from fire, explosion, electrical and related hazards resulting either from the use of anesthetic agents, medical gas equipment, electrical apparatus and high frequency electricity, orffom internal or external incidents that disrupt normal patient care; b) from fire and explosion hazards associatedwith Iaboratorypractices; c) in connection with the use of hyperbaric and hypobaric facilities for medical pu(poses; d) through perfor- mance, maintenance and testing criteria for elecu-ical systems, both normal and essential; and e) through performance, maintenance and testing and installation criteria: 1)for vacuum systems for medical or surgical purposes, and 2) for medical gas systems. Technical Committee on Anesthesia Services (HEA-ANE) (5-4.1~ 5-4.2, 5-6.1, 6-2.3, 12-4.1, and 13-4.1) John P. Swope, Chair Derwooc[, MD Pep. NFPA Health Care Section JamesJ. Claffey, McPherson Hospital, MI Rep. American Assn. of Nurse Anethetists Jay Crowle~, U.S. Dept. of Health/Human Services, MD Yadin Dawd, Texas Childrens Hospital, TX RayJ. Nichols, Shriners Burn Inst., TX Rep. American Society of Anethesiologists Gary D. Slack, Healthcare Engr Consultants, OH Rep. American Hospital Assn. Jay IL Sommers, Kim]aerly-Clark Corp., GA Clevis T. Svetlik,Johnso.n & Higgins of Ohio Inc., OH Gregory L. Welyczko, Ohmeda, WI H. Robert Yeager, Caritas Christi, MA Alternates Douglas S. Erickson, American Hospital Assn., IL (Alt. to G. D. Slack) James A. Meyer, Pettis Memorial VA Hospital, CA (Alt. to R.J. Nichols) Staff Liaison: Burton R. Klein This list represents the membership at the time the Committee was balloted on the text of tills edition. Since that time, changes in the membership may have occurred. Technical Committee on Disaster Planning (HEA-DIS) (Annex 1) James W. Kerr, Chair M R Inc., AL DavidJ. Kltchin, Kaiser Permanente Medical Center, CA Pauline N. Minardi, CIGNA Property & Casualty Companies, CA Rep. American Insurance Servfces Group, Inc. Jack-L. Nichols, Truman Medical Center, MO Rep. NFPA Health Care Section Russell Phillips, Russell Phillips & Assoc., Inc., NY W. Thomas S-chipper, Kaiser Foundation Hospitals, CA Rep. American-Hospital Assn. Cleqls T. Svetlik,Johiason & Higgins of Ohio Inc., OH David E. Wacker, Princeton Insurance Co., NJ Altema.te Douglas S. grickson, American Hospital Assn., IL (Alt. to W. T. Schipper) Staff Liaison: Burton IL Klein This list represents the membership at the time the Committee was balloted on the text of tfiis edition. Since that time, changes in the membership may have occurred. Technical Committee on Electrical Equipment (HEA-ELE) (Chapter 7, 9-2.1, X-3.7 in Chapters 12 to 18 and Annex 2) Bryan Parker, Chair Montefiore Medical Ctr, NY Saul Aronow, Waban, MA Jack. Berge.r, Berg er Scientific . Instruments,. MA Yadin Dawdg Texas Chfldrens Hospital, TX Floyd J. DeVore, General Electric Medical Sys Ca~p,WI Albert G. Garlatti, ETL Testing Laboratories, NY Clement H. Kiffmeyer, Pickerlnt'l Inc., OH Rep. Nat'i Electrical Mffs Assn. Alan Lipschultz, The Medical Center of Delaware, DE Rep./gssn. for the Advancement of Medical Instrumentation M. I'. Mere, Underwriters Laboratories Inc., NY James A. Meyer, Pettis Memorial VA Hospital, CA Pep. American Society of Anesthesiologists Timothy Pcglow, La Porte Hospital, IN Rep. American Hospital Assn. Lawi~nce S. Sandier, U.S. Dept. of Veterans Affairs (001T), MD Alternates Britton E. Berek, American Hospital Assn., IL (/kit. to T. Pegiow) Todd L Relyeg, ETL Testing Labortories, NY (AlL toA. G. Garlatfi) Staff Liaison: Burton IL Klein This list represents the membership at the time the Committee was balloted on the text of this edition. Since that time, changes in the membership may have OCCUrr~ 10
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Report of the Committee on Health Care Facilities - NFPA

Report of the Committee on
Health Care Facilities
Technical Correlating Committee (HEA-AAC)
Marvin J. Fischer, Chair Brookdale Hospital Medical Ctr., NY
Constance Bobik, B&E Fire Safety Equipment Inc., FL Jay Crowley, U.S. Dept. of Health/Human Services, MD Douglas S. Erlckson, American Hospital Assn., IL
Ref3. American Hospital Assn. Thomas W. Gardner, Gage-Babcock & Assoc., VA
Rep. American Health Care Assn. William T. Guy, The Elizabeth General Medical Ctr, NJ
Rep. NFPA Health Care Section Harlan C. Ihlenfeldt, Kemper Nat'l Insurance Companies, IL Stanley D. Kahn, Heckler Electric Co., Inc., NY
Rep. Nat'l Electrical Contractors Assn. Ode Richard KeiI,Joint Commission on Accreditation of Healthcare Orgs, IL WiRiam E. Koffel, Koffel Assoc. Inc., MD Nlls A. Maurice, Nils A. Manrice, P.E., CSP, Inc., AZ
Rep. American Society of Safety Engr Dasad A. McWhinnle, Mechanical Dynamics Inc., IL * Robert T. Shipley, Fisher Berkeley Corp., CA Rep. Nat'l Electrical Mfrs. Assn.
Steven Werner, M&M Protection Consultants, WI Mfl~yer D. Zimmerman, U.S. Dept. of Health and Human Services,
Alternates
Clement H. Kiffmeyer, Picker Int'l. Inc., OH (Alt. to R. T. Shipley)
Kenneth Knight, Bethesda Hospital, OH (AlL to W. T. Guy)
Nonvoting
Leo G. Foxwell, ITT Hartford, CT FROm. American Insurance Services Group, Inc.
e N. Minardl, CIGNA Property & Casualty Companies, CA (Alt. to L. Foxwell)
Staff Liaison: Burton IL Klein
This list represents the membership at the time the Committee was balloted on the text o_f this edition. Since that time, changes in the membership may have occurred.
Committee Scope: This Committee shall have primary responsibil- ity for documents which contain criteria for safe~,marding patients
" and health care personnel in the delivery of health care services within health care facilities: a) from fire, explosion, electrical and related hazards resulting either from the use of anesthetic agents, medical gas equipment, electrical apparatus and high frequency electricity, orffom internal or external incidents that disrupt normal patient care; b) from fire and explosion hazards associatedwith Iaboratorypractices; c) in connection with the use of hyperbaric and hypobaric facilities for medical pu(poses; d) through perfor- mance, maintenance and testing criteria for elecu-ical systems, both normal and essential; and e) through performance, maintenance and testing and installation criteria: 1)for vacuum systems for medical or surgical purposes, and 2) for medical gas systems.
Technical Committee on
Anesthesia Services (HEA-ANE)
(5-4.1~ 5-4.2, 5-6.1, 6-2.3, 12-4.1, and 13-4.1)
John P. Swope, Chair Derwooc[, MD
Pep. NFPA Health Care Section
JamesJ. Claffey, McPherson Hospital, MI Rep. American Assn. of Nurse Anethetists
Jay Crowle~, U.S. Dept. of Health/Human Services, MD Yadin Dawd, Texas Childrens Hospital, TX RayJ. Nichols, Shriners Burn Inst., TX
Rep. American Society of Anethesiologists Gary D. Slack, Healthcare Engr Consultants, OH Rep. American Hospital Assn.
Jay IL Sommers, Kim]aerly-Clark Corp., GA
Clevis T. Svetlik,Johnso.n & Higgins of Ohio Inc., OH Gregory L. Welyczko, Ohmeda, WI H. Robert Yeager, Caritas Christi, MA
Alternates
Douglas S. Erickson, American Hospital Assn., IL (Alt. to G. D. Slack)
James A. Meyer, Pettis Memorial VA Hospital, CA (Alt. to R.J. Nichols)
Staff Liaison: Burton R. Klein
This list represents the membership at the time the Committee was balloted on the text of tills edition. Since that time, changes in the membership may have occurred.
Technical Committee on
Disaster Planning (HEA-DIS)
(Annex 1)
James W. Kerr, Chair M R Inc., AL
DavidJ. Kltchin, Kaiser Permanente Medical Center, CA Pauline N. Minardi, CIGNA Property & Casualty Companies, CA
Rep. American Insurance Servfces Group, Inc. Jack-L. Nichols, Truman Medical Center, MO
Rep. NFPA Health Care Section Russell Phillips, Russell Phillips & Assoc., Inc., NY W. Thomas S-chipper, Kaiser Foundation Hospitals, CA
Rep. American-Hospital Assn. Cleqls T. Svetlik, Johiason & Higgins of Ohio Inc., OH David E. Wacker, Princeton Insurance Co., NJ
Altema.te
Douglas S. grickson, American Hospital Assn., IL (Alt. to W. T. Schipper)
Staff Liaison: Burton IL Klein
This list represents the membership at the time the Committee was balloted on the text of tfiis edition. Since that time, changes in the membership may have occurred.
Technical Committee on
Electrical Equipment (HEA-ELE)
(Chapter 7, 9-2.1, X-3.7 in Chapters 12 to 18 and Annex 2)
Bryan Parker, Chair Montefiore Medical Ctr, NY
Saul Aronow, Waban, MA Jack. Be rge.r , Ber g er Scientific . Instruments,. MA Yadin Dawdg Texas Chfldrens Hospital, TX Floyd J. DeVore, General Electric Medical Sys Ca~p, WI Albert G. Garlatti, ETL Testing Laboratories, NY Clement H. Kiffmeyer, Pickerlnt'l Inc., OH Rep. Nat'i Electrical Mffs Assn.
Alan Lipschultz, The Medical Center of Delaware, DE Rep./gssn. for the Advancement of Medical Instrumentation
M. I'. M e r e , Underwriters Laboratories Inc., NY James A. Meyer, Pettis Memorial VA Hospital, CA
Pep. American Society of Anesthesiologists Timothy Pcglow, La Porte Hospital, IN
Rep. American Hospital Assn. Lawi~nce S. Sandier, U.S. Dept. of Veterans Affairs (001T), MD
Alternates
Britton E. Berek, American Hospital Assn., IL (/kit. to T. Pegiow)
Todd L Relyeg, ETL Testing Labortories, NY (AlL toA. G. Garlatfi)
Staff Liaison: Burton IL Klein
This list represents the membership at the time the Committee was balloted on the text of this edition. Since that time, changes in the membership may have O C C U r r ~
10
Technical Committee on
Electrical Systems (HEA-ESE)
(Chapter 3, X-3.3 in Chapters 12 to 18)
Hugh O. Nash, Chair Smith Seckman Reid Inc., TN
Rep. Inst. of Electrical and Electronics Engr, Inc.
Stephen Benesh, Square D Co., WI Rel~. Nat'l Electrical Mfrs Assn.
Jack Berger, Berger Scientific Instruments, MA ] a m e s L . C, rawfoi-d, U.S. Dept. of Health & Human Service, WA Albert G. Garlatti, ETL Testing Laboratories, NY William IL Houser, U.S. ArmyEnvironmental Hygiene Agency, MD
Rep. NFPA Health Care Section .Iambs R. Iverson, Onan Corp., MN Edward A, Lobnitz, Tilden Lobnitz & Cooper Inc., FL Alfrod J. Longhitano, Gage-Babcock & Assoc. Inc., NY
Rep. American Health Care Assn. Terry G. Mclntyre, IRM Insurance, NC M. T. Merrlgan, Underwriters Laboratories Inc., NY David IL Norton, U.S. Dept. of Veterans Affairs, DC Ronald M. Smldt, New Hanover Regional Medical Center, NC Rep. American Hospital Assn.
Howard Stlckley, U.S. Army Corps of Engr, DC Ra_ ymondJ. Swisher, Naval Healthcare Support Office, VA Walter N.'Vernon, Mazzetti & Assoc. Inc., CA Herbert V, Whittall, Caterpillar, Inc., IN
Rep. Electrical Generating Systems Assn.
Alternates
Lawrence A. Bey, Onan Corp., MN (Alt. toJ. R. Iverson)
Do~uglas S. Erickson, American Hospital Assn., IL (Aft. to 1L M. Smidt)
StaffLiaison: Burton 1L Klein
This list represents the membership at the time the Committee was balloted on the text of this edition. Since that time, changes in the membership may have occurred.
Technical Committee on
Gas Equipment (HEA-GAS)
(Chapter 8, X-3.8 in Chapters 12 to 18)
RayJ. Nichols, Chair Shriners Burn Inst., TX
Rep. American Society of Anesthesiologists
M. Lee Bancroft, Beth Israel Hospital, MA Alan Lipschultz, The Medical Center of Delaware, DE
Rep./~ssn. for the Advancement of Medical Instrumentation T. K. Raman, Valley Pulmonary & Medical Assoc., MA
Rep. American College of Chest Physicians Gary D. Slack, Healthcare Engineering Consultants, OH Rep. American Hospital Assn.
Alternate
Britton E. Berek, American Hospital Assn., IL (Air. to G. D. Slack)
Staff Liaison: Burton IL Klein
This llst represents the membership at the time the Committee was balloted on the text of this edition. Since that time, changes in the membership may have O¢curreo~
Technical Committee on
Hyperbaric and Hypobaric Facilities (HEA-HYP)
(Chapter 19)
William H. L. Dornette, Chair Kensington, MD
Grant A. Brown, U.S. Air Force, "IX Dave DeAngelis, U.S. Ocean Engr & Construction Pro Office, DC Robert W. Hamilton, Hamilton Research Ltd, IVY Terry H. Hays , Naval Facilities Engineering Command, DC Eric P. Klndwali, Medical College oTWisconsin, W1 Valerie Messina, Long Beach Memorial Medical Ctr., CA
Rep. Baromedical Nurses Assn. DennisJ. Murray, KMS-Medical Gas System Consultants Ltd, MI Pep. American Hospital Assn.
Stephen D. Reimers, Reimers Engr Inc., VA ]. Ronald Sechrlst, Sechrist Industries, CA PanlJ. Sheffield, Int'l ATMO, Inc., TX Clews T. Svetlik, Johnson& Higgins of Ohio Inc., OH Rep. NFPA Health Care Section
Williur T. Workman, U.S. Air Force, CA
Alternates
Carolyn Jacobs, Scottsdale Memorial Hospital, AZ (Ait. to3/. Messina)
Christopher G. Wallace, Sechrist Industries Inc., CA (/kit. to J. IL Sechrist)
KennethH. Willis, Presbyterian Hospital of Dallas, TX (Alt to D.J. Murray)
Larry L. Wischhoefer, Reimers Engr Inc., VA (Ait. to S. D. Reimers)
Staff Liaison: Burton IL Klein
This list represents the membership at the time the Committee was balloted on the text of this edition. Since that time, changes in the membership may have odctggTea.
Technical Committee on
Laboratories (HEA-LAB)
(Chapter 10, 5-3.1, 5-4.3, 5-4.4, 5-6.2, and associated laboratory requirements in Chapters 12 to 18.)
Gerald A. Hoeltge, Chair Cleveland Clinic Foundation, OH
Pep. College of American Pathologists
John Francis C.apron, The Cleveland Clinic Foundation, OH Arden W. Forrey, Seattle, WA
Rep. American Assn. for Clinical Chemislry George D. Harlow, Tufts New England Medical Ctr, MA Rep. American Hospital Assn.
Harlan C. llalenfeldt, Kemper Nat'l. Insurance Companies, IL Ulrich M. Linder, Earl Walls Assoc., CA }ohn P. McCabe, Nat'l Inst. of Health/Fire Prevention Section, MD auiine N. Minarcli, CIGNA Property & Casualty Companies, CA Rep. American Insurance Sem'ces Group, Inc.
Susan Y. Niekasch, U.S. Dept- of Labor, ID Rep. American Society for Clinical Laboratory Science
Jami~ O. Wear, u.s. Dept. of Veterans Admin. Medical Ctr., AR Rep. NFPA Health Care Section
Alternatres
Britton E. Berek, American Hospital Assn., IL (Alt. to G. D. Harlow)
Robert A. Guy, Earl Walls Associates, CA (Alt. to U. M. Linder)
Staff Liaison: Burton IL Klein
This list represents the membership at the time the Committee was balloted on the text of this edition. Since that time; changes in the membership may have occurred.
Technical Committee on
Piping Systems (HEA-PIP)
(Chapter 4, X-3.4 in Chapters 12 to 18 (Gas), X-3.4 in Chapters 12 to 18 (Vacuum)
Leo G. Foxwell, Chair • 1TT Hartford, CT
Rep. American Insurance Services Group, Inc.
Mark W. Allen, Ohmeda Medical Eng, GA M. Lee Bancroft, Beth Israel Hospital, MA David L. Brittain, PROVAC, OH TerryA. Brouwer, CT Dept of Public Safety, CT + James Coppedge, Littells Oxygen Inc., CA Danlelle S.Y.arhart, U.S. Dept. of Health & Human Services, WA Peter Esherick, Patient Instrumentation Corp., PA P. L. Fan, American Dental Assn., IL Hemy IL Kaht, Squire-Cogswell Go., IL David Eric Lees, Georgetown University Medical Ctr., DC Pep. American Society of Anesthesiologists
Antonio A. Mesa, Nash Engr Co., CT David B. MohUe, Medical Engr Services, Inc., VA DennisJ. Murray, KMS-Medical Gas System Consultants Ltd, MI
Rep. Amercian Hospital Assn.
11

E. Daniel Shoemaker, Matrx Medical Inc., AZ William J. Uhner, Deltech, DE J. Richard Wagner, Poole & Kent CO., MD
Rep. Mechanical Contractos Assn. of America, Inc. F. Davld Wyrick, Cambiare Ltd, NC
Rep. Int'l Analgesia Society
Alternates
Sharon Day, Duke University Medical Center, N.C (AIt. to M. L Bancroft)
Douglas S. Erickson, American Hospital Assn., IL (Alt. to D.J. Murray)
David Eshe/'ick, Patient Instrumentation Corp., PA (Alt. to P. Esherick)
MichaelJ. Lynam, Porter lnsttument Company, Inc., PA (Alt. to D. Wyrick)
James A. Meyer, Pettis Memorial VA Hospital, CA (Alt. to D. E. Lees)
Sharon Stanford, American Dental Association, IL l~arAlt, to P. L. Fan)
kus Yakren, Syska and Hennessy Inc, NY (Vot. Alt. to ASSERep.)
Staff Liaison: Burton IL Klein
This list r_@resents the membership at the time the Committee was balloted o n
the text o f thls edition. Since that time, changes in the membership ma 3 have O c ~ f r ~ T l . " "
The Report of the Committee on Health Care Facilities is pre- sented for adoption in two parts.
Part I of this Report was prepared by the Health Care Facilities Committee andproposes for adoption amendments to NFPA 99- 1993, Standard for Health Care Facilitie~ NFPA 99-1993 is published in Volume 5 of the 1994 National Fire Codes and in separate pamphlet form.
Part I of this Report has been submitted to letter ballot of the individual Technical Committees. The results of the balloting can be found in the i'eport.
Part I of this Report has also been submitted to letter ballot of the Technical Correlating Committee on Health Care Facilities, which consists of 15 voting members; of whom 13 voted affirmative, 1 negative (Mr. McWhinnie) and one ballot was not returned (Mr. Manrice). The reasons for voting negatively or abstaining are as follows:
Mr. McWhinnie voted negatively stating Proposal 99-329 (Log #378) addresses two issues: A. Text Error. B. Performance.
The T/C STATEMENT ignores the technical substantiations of both issues.
1. "other technologies" is irrelevant. Codes are written all the time where practices of all kinds have existed.
2. "... preclude ... use(s) ... in place today" - Incredible (in the • light of Code 99, 1-2 which applies to this circumstance).
3. This applies to "design", "new construction", "inspection" - 99, 1-3.
Issue A. CORRECTION OF TEXT LANGUAGE: "Scavenging apparatus" does not "exhaust the waste anesthetic
gases to the outside of the facility ..." The Waste Anesthetic Gas Disposal System (~vVAGD") does this. The "scavenging apparatus" (confusing, and misleadingly referred
to as an "interface" m the T /C Log #CP4 draft - still under "review- further study") is neither "installed" in, attached to, or in any way connected to the building - (any more than a table lamp is a part of the building's electrical s~stem - or a duct system and fah are-parts of a laboratory test instrument, centrifuge or Bunsen burner).
Nor is the scavenger a part of a WAGD system - any more than is an anesthesia gas machine, ventilator, extra corporeal oxygenator, or any other breathing machine - ALL of which are connected by a hospital supply item (a hose) to an "installed" (permanently) system.
By this rationale a patient oxygen therapy flowmeter, humidifier, vacuum collection bottle, trap, suction regulator, and connecting hoses to a central system would all be parts- of "Piping Systems". -
Leaving 99, 5-4.1.6 as is also leaves open the logic that all hospital secondary equipment is part of any "installed" central system to which they are connected by a hose.
The "Scavenger" breathing machine reservoir) would discharge into the O.R. :except for the hospital provided secondary equi~o- ment (hose), which the staff connects from the breathing m~tchine outlet to a point of "disposal" - the WAGD system permanently "installed" On the building) inlet, which exhausts the waste gases "outside of the facility"..
12
In confirming the T/C ACTION, the T/CC leaves text which is confusing, misleading, wrong - and certainly not "user friendly•'. This ACTION disregards all above - although still under T / C
"review-further study" along with Log #CP4 and 377 - as directed by the T/CC.
Issue B. PERFORMANCE Per Code 99 1-1: NFPA Committee Leadership Conferences: and
(for those unaware) "We intend to be pro-active ... We must (underscore added) make (Codes) easily understandable and adoptable .... growing interest and importance (of) performance based codes and standards ..." (NFPAPresident, George MilDer, May 16, 1994) -" a Positive President's Report (to the entire Association) as to ... how and where NFPA is going." (BRK transmittal June 10, 1994). "Minimum (or maximum) requirements" forpublic safety, the
essence of NFPA Codes/Standffrds, are needed], and foundin almost all NFPA mandatory documents -which took me 25 years to accomplish in Piping Systems - (although performance, criteria were in the MSVS document's first printing (56K, 1980). Where does the astute, and conscientious, designer, contractor,
and user (among others) get authoritative/documented, and safest criteria? - which is available only to those who must make an involved effor~ The most important criteria has been rejected by the T/C, and confirmed by the T/CC.
The most important criteria (quoted below) is the micro-negative pressure (as opposed to a vacuum -just as ventilation exhaust system is never called a vacuum) or -0.5 cm H20. This critical performance criteria in the Proposal has not been addressed by the T / C in its STATEMENT re its ACTION - nor is it in the T /C draft Proposal, Log # CP4. This maximum degree of negative pressure for the anesthetized patient recognizes ANSI/ASA published limit - and ANSI Z79, SC.4 caution to 'avoid exposing the breathing circuit to any pressure less than atmospheric ..." (underscores added).
The T/C on Health Care F~tcilities' mandate was announced as "if we are to err it must be on the safe side".
We are aware of many (yes, many) recommendations for WAGD ranging from atmospheric to over four air expansions (-25"Hg) in theWg-GD system (-top prietary/calculated~).. Anyvacuum lev-el above several inches Hg requires a pump.
Industry should not h~ve fo bear this responsibility. The T/C STATEMENT is untrue per Co-de 99, 1-2. The T/C reject ACTION, based upon its invalid STATEMENT,
warrants reversal as an action not consistent with Regulations Governing Committee Projects 3-3.5.1 and 3-3.6.1. This issue deserves at least Regulation 3-3.6.1. This topic is under T/C "review-further study" as directed by the T /
CC - an t i s interrelated with Log #CP4 and Log #377.
Part I of this report pertaining to gas system requirements has also been submitted for concurrent letter balloting of the T/C on Industrial Medical and Gases, which consists 6f 12 voting members, of whom 7 voted affirmatively, 2 voted negatively (MessrS. Nelson and Pavlovski), and 3 ballots were not returned (Messrs. Caves, Murray and Simon).
Mr. Nelson voted negatively stating: Proposal 99-105 (Log #192) "The restriction of nonflammable gas storage to at least 25 feet
from any "window" in building wall does not appear to be compat- ible with other NFPA codes covering gasses in -6/linders, specifically, NFPA 55." Proposal 99-197 (Log #111) " "It is inappropriate to require components for nonflammable
medicalgas systems to be suitable for use with oxygen. Oxygen compatible components may in fact be incompatiSle with s tme nonflammable medical gases. Also, cleaningmethods and materials may be incompatible with some nonflammable medical gases."
Mr. Pavlovski voted negatively stating: Proposal 99-105 (Log #192) . . . . "Unreasonably restrictive. NFPA 50 requires omy 10 feet trom wait
o~ening for oxygen storage systems!" ropo~al 99-197 (Log #111)
"There is no reason for oxygen-compatible materials to be required for inert gas systems."
Part II of this Report was prepared by the Technical Commi/tee on Hypberbaric & H obaric Facilities, and roposes for ado . . . . tion amendments to ~I~A 99B-1993, Stmad~x~ on Hypobanc FPacdiues. NFPA 99B-1993 is published in Volume 5 of the 1~994 National Fire Codes and in separate pamphlet form.
Part II of this Report has been submitted to letter ballot of the Technical Committee on Hyperbaric & Hypobaric Facilities, which consists of 13 voting members. The results of the balloting can be found in the report.
Part II of this Report has also been submitted to letter ballot of the Technical Correlffting Committee on Health Care Facilities which consists of 15 voting members; of whom 14 voted affirmatively, one ballot was not returned (Mr. Maurice).

NFPA 99--F95 ROP
PART I
99-1 -Unused.
(Log #195) Committee: HEA-P IP
99- 2 - (Entire Standard): Correlating Committee Note: Because of the Technical Correlat-
ing Committee Action of proposal 99-19 (Log#CP81) [i.e., veterinary facilities would be outside the scope of NFPA 99], this proposal is rejected. SUBMITTER: Leo G. Foxweil, ITT Hartford RECOMMENDATION: 1. Develop and publish a standard on the requirements for veterinary hospitals and clinics similar to that in NFPA-99, or
2. Include within NFPA-99 an application chapter similar to chapter 15 for veterinary hospitals and clinics. SUBSTANTIATION: There is an increasing need to have a document to define the requirements for non-flammable medical gases and suction for animal hospitals and clinics. A document is needed to make sure the veterinary medicine doctors and the enforcing authority has appropriate guide lines for a safe installation and not one that is burdened by misinterpretation by lack of a standard. There are approximately 51,000 DVM in USA and presumably 20,000+ installations. The requirements are primarily oxygen and nitrous oxide, vacuum and waste gas systems. This'can readily be developed by T/C on Piping and issued as NFPA-99 V or another number. The Technical Committee on Piping has the knowledge and experience to develop this material. COMMITTEE ACTION: Accept in Principle. See Committee Action on Proposal 99-92 (Log #98).
COMMITPEE STATEMENT: Proposal is similar to Proposal 99-92 (Log #98). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #204) Committee: HEA-PIP
99- 3- (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #CP58). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T/C on Piping Systems is directed to reconsider the action on this proposal. SUBMITTER: PhiUipJ. Long, PA Dept of Health RECOMMENDATION: 1) Change format 2 ways: a. Combined vacuum into medical gas section. b. Arrange all type 1 med. gas sections together, same for type 9,
etc. 2) Arrange format in a logical user friendly readable order: Identify requirements for each area.
SUBSTANTIATION: 1) Present standard material is too confusing for enforcement purposes.
The standard is not user friendly. COMMITYEE ACTION: Accept in Principle. See Committee Action on Proposal 99-99 (Log #CP58).
COMMITrEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITYEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #209) Committee: HEA-PIP
99- 4 - (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #CP5B). The TCC has directed the T /C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T/C on Piping Systems is directed to reconsider the action on this proposal. SUBMITI'ER: Jeffrey L. McManus, Michigan Dept. Public Health RECOMMENBATION: Arrange format of the standard in this order:
1. Identify applications; 2. Define types and areas; 3. Group all typel materials together, all type 2 materials together,
all lab material together. SUBSTANTIATION: The standard is confusing to various users. Difficult to find which provision apply (requirements at back of text) for a given facility type or project. COMMITTEE ACTION: Accept in Principle. See Committee Action on Proposal 99-99 (Log #CP58).
COMMITTEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #210) Committee: HEA-PIP
99-5 - (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #CP58). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T/C on Piping Systems is directed to reconsider the action on this proposal. SUBMITTER: Dennis Ehrlacher, Whitehall, PA RECOMMENDATION: 1) Change format 2 ways:
a) Place medical vacuum into medical gas section. b) Place all type 1 material in one section, type 2 in another
section, etc. 2) Make the text easier to read.
SUBSTANTIATION: 1. a) Vacuum needs to be placed in the same section as other standard pressure gases. To many times vacuum lines are run with substandard materials and poor quality installa- tion, due to the false assumption that vacuum is no ta medical gas. I believe that if all these are combined, vacuum will be treated by inspectors and installers as the critical and important part of the medical gas family that it is.
b) When reading NFPA 99 it is often hard to figure out which code fits which facility. And when you figure that out then you must read the entire book because the information is so scattered.
2. The text should be more direct. There is too much that can be misunderstood due to the wording. COMMITI'EE ACTION: Accept in Principle. See Committee Action on Proposal 99-99 (Log #CP58).
COMMI'FrEE STATI~ENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITYEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
15

N F P A 9 9 - - F 9 5 R O P
(Log #223) Committee: HEA-PIP
99-6- (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #CP58). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T/C on Piping Systems is directed to reconsider the action on this proposal. S U B ~ Franklin L. Gebo, Gebo Architects RECOMMENDATIONi 1) Overall format and setup of these chapter should be rearranged to all of the one type of material together for easier reference. Vacuum and medical gases sections should be combined.
2) Information should be presented in a more user-friendly manner. SUBSTANTIATION: 1) Medical gasses and vacuum should be combined into one section due to the fact that they are concerned together throughout the entire design process.
2) Infong, ation is also confusing and unclear to all parties involved. It is difficult to determine which equipment is required for
different types of facilities. This should be rearrangedin a more user-friendly manner. COMMITTEE ACTION: Accept in Principle. " See Committee Action on Proposal 99-99 (Log #CP58).
COMMITTEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE.TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #300) Committee: HEA-PIP
99- 7 - (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #CP58). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T/C on Piping Systems is directed to reconsider the action on this proposal. SUBMITTER: David A. Brown, Wallace & Watson-Associates, P.C. RECOMMENDATION: Revise text as follows:
1. Combine the vacuum and medical gas sections. 2. Arrange material according to facility/space type (laboratoryvs.
critical care vs. general patient areas, etc.) 3. Arrange the material so that applications, areas, etc. are
identified first with specific requirements for each application, area, etc. to follow. SUBSTANTIATION: 1. Most engineers, contractors and owners consider medical vacuum as a medical gas. In most cases, materials, installation, etc. for vacuum systems are identical to pressure gas systems, therefore, the two should be combined.
2. There is no logical order as to where to find requirements for a particular facility.
3. It is difficult to use the standard with information scattered throughout. The standard should first discuss the types of facilities followed by the requirements.of each type. CO MITIT~ ACTION: Accept in Principle. See Committee Action on Proposal 99-99 (LOg #CP58).
COMMITrEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #305) Committee: HEA-PIP
99- 8- (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log CP58). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T/C on Piping Systems is directed to reconsider the action on this proposal. SUBMITrER: Charlie B. Parker, Sr., Hess Mechanical RECOMMENDATION: Revised text as follows:
1. Need change in 2 ways. A. Integrate vacuum into the medical gas section. B. Arrange all material Type 1 together and all Type 2 together.
All laboratory material together to make easier to understand. 2. Arrange standards in a logical way to make easier to understand.
Identify application area, etc., first and then what is required for each type. SUBSTANTIATION: 1,~. Vacuum and medical gas piping are planned drawn bid constructed and received together. The standards should be together.
1.B. It is too confusing for people piping hospital engineers consulting engineers. It is hard to find what applies to facility it applies to.
2. The standards are not friendly. Application requirements are lost in the back of the standards. First define type of facility then the required .for each. COMMITTEE ACTION: Accept in Principle. See Committee Action on Proposal 99-99 (Log #CP58).
COMMITIT~ STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submltters recommendation. NUMBER OF COMMITTEEMEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMM~WEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #306) Committee: HEA-PIP
99-9 - (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #GP58). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T/G on Piping Systems is directed to reconsider the action on this proposal. SUBMI'I'I~R: Larry Pardoe, Geisinger System Services RECOMMENDATION: Revise text as follows:
1) Arrange format of the standard in a more user friendly order;, identify applications areas, etc. first, then what is required for each type area, eta
2) Change format as follows: a. Arrange all Type 1 material together, all Type 2 material
together and all laboratory material together, etc. b. Integrate vacuum into medical gas section.
SU1K~TANTIATION: 1) At present, the standard, is not user friendly, application requirements are lost in the back of the standard. First define types of facilities, then state what is required for each type.
2) a. It is too confusing for the user to find what applies to the particular facility they are working on. 2) b. Med gases and vacuum are designed and constructed as a
system. Hence, the standards should be together. COMMrITEEACTION: Acceptin Principle. See Committee Action on Proposal 99-99 (Log #GP58).
COMMITTEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
14

NFPA 99-- F95 ROP
(Log #321) "Committee: HEA-PIP
99-10 - (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Lol~ #CP58 ). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T /C on Piping Systems is directed to reconsider the action on this proposal. SUBMITTER: David Esherick, Patient Instrumentation Corp. RECOMMENDATION: 1. Need to have vacuum requirements integrated into the medical gas Section.
2. Put all requirements for Type I together. . . . . . . . Type II together . . . . . . Laboratories together, etc.
SUBSTANTIATION: 1. Hospitals use the medical gases and vacuum together, as well as the new systems being installed, designed and hid for construction together.
2. With health care rapidly changing, we have to define hospital, dental office, and nursing homes, etc. and place all rules in one Pclace so everyone can find out what is required.
OMMITI'EE ACTION: Accept in Principle. See Committee Action on Proposal 9%99 (Log #CP58).
COMMITTEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. • NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #375) Committee: HEA-PIP
99-11 - (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 9%99 (Log #CP58). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T/C on Piping Systems is directed to reconsider the action on this proposal. SUBMrlq'ER: Otto H. Gessner, Medifac RECOMMENDATION: Change format:
1) Better define types 1 & 2 materials. 2) Arrange all type 1 & 2 materials independent according to type. 3) Vacuum should be part of medical gas section. 4) Format of the standard should be more user friendly in
identifying applications, area, etc. first then what requirements apply to that area. SUBSTANTIATION: 1) As a design professional working with the health care facilities, it is confusing to Find what applies to our projects.
2) Medical gases and vacuum systems when designs are planned, drawn, bid and constructed as a complete package. Therefore the standards should be together.
3) Designing the standards I feel that data later described in application, which are in the back of the book, is lost. By first defining types of facilities, provide what is required for this
lication. TrEE ACTION: Accept in Principle.
See Committee Action on Proposal 9%99 (Log #CP58). COMMITTEE STATEMENT: Conlmittee believes Proposal 9999 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #376) Committee: HEA-PIP
99- 12 - (Chapters 1, 2, 4, 10 through 19 and Appendices): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 ( L o g #CP58). The TCC has directed the T /C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the ~r/c on Piping Systems is directed to reconsider the action on this proposal. S U B ~ Steven G. Nann, St.Joseph's Hospital Health'Center RECOMMENDATION: 1) Meld together the requirements for medical gas systems and medical vacuum systems.
2) Separate Type I and Type II systems. Keep all information for Type I together and all information for Type Iltogether.
3) Provide definitions of terms at beginning of each chapter•
SUBSTANTIATION: 1) These systems are installed and tested in the same fashion. This would make code easier to read and comprehend•
2) I f all the requirements for a Type I or Type II system were together, it would be easier to comprehend.
3) Definition of terms (even Type I system vs. Type II system) is not readily available. COMMITTEE ACTION: Accept in Principle in Part. Reject item 3.
COMMITTEE STATEMENT: Committee believes definitions belong only Chapter 2 for use throughout the document as opposed to use specific to a chapter.
For recommendations of other portions, see Proposal 99-99 (Log #CP58). NUMBER OF COMMITI'EE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #311) Committee: HEA-PIP
99- 13 - (1, 2, 4 & 10 thru 19): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #CP58). The TCC has directed the T/C on Piping Systems to resubmit, the proposed chang~es in pro p.er format. Because of the actaon on that proposal, the T /C on Piping Systems is directed to reconsider the action on this proposal. SUBMITTER: Kenneth G. Schultz, George A. Schultz & Son, Inc. RECOMMENDATION: Revise text as follows: A) Include vacuum in the medical gas sections. B) Arrange and define the types of facilities first, then the
requirements for each type of facility. SUBSTANTIATION: A) Medical gas installations including vacuum are designed and installed together.
B): The present standard is difficult to use. The types of facilities should be defined and then the requirements shown for each facility. COMMITTEE ACTION: Accept in Principle. See Committee Action on Proposal 9%99 (Log #CP58).
COMMrI"rEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF CO MITTEE MEMBE1RS ELIGIBLE TO VOTE: 18 VOTE ON COMMITIT~ ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #196) Committee: HEA-PIP
99-14- (Chapter 1, 2, 4, and Appendices, Chapter 10 thru 19): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #CP58). The TCC has directed the T/C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T /C on Piping Systems is directed to reconsider the action on this proposal. SUBMITTER: Clifford E. Case,Jr., Kimble, Inc. RECOMMENDATION: Three revisions:
1. Medical gas and vacuum combine section. 2. Combine material types 1 - together, type 2 - together and lab
material together. 3. Each application should be listed sepmatelywith requirements
included for thatparticular area. SUBSTANTIATION: 1. All medical gas is grouped together for planning and installation. 2. Eliminate confusion in the trenches; help eliminate user
mistakes. 3. Make standards easy to define a hospital a hospital, a nursing
home a nursing home, a doctors office a doctors office, etc., etc. COMMITrEE ACTION: Accept in Principle. See Action on Proposal 99-99 (Log #CP58).
COMMITTEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITFEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
15

N F P A 9 9 - - F 9 5 R O P
(Log#50) Committee: HEA-PIP
99-15 - (Chapters 1, 2, 4 & Appendices and Chapters 10 through 19):
Correlating Committee Note: The Technical Correlating Commit- tee notes the reference in Committee Statement to proposal 99-99 (Log #CP58). The TCC has directed the T /C on Piping Systems to resubmit the proposed changes in proper formal Because of the action on that proposal, the T / C on Piping Systems is directed to reconsider the action on this proposal. SUBMITTER: John Callanan, Coney Island Hospital RECOMMENDATION: Add:
1) Change format 2 ways: a, Integrate vacuum into medical gas section. b. Arrange all type 1 matedal together, all type 2 material together,
all laboratory matedal together, et~ 2) Arrange format of the standard in a logical user fr|endiy or.de F
identify applications, areas, etc. First, then what is required for each type area etc. SUBSTANTIATION: 1) a, Med gases and vacuum are planned, drawn, bid, constructed and received together. Hence, the standards should be together.
b. It is too confusing for the user (Hospital engineer, consulting engineer, contractor, etc.) to find what applies to the particular facility they are working on.
2) At present, the standard is not user friendly. Application requirements are lost in the back of the standard. We should first define types of facility, then state what is required for each type. COMMITTEE ACTION: Accept in Principle.
See Committee Action on Proposal 99-99 (Log #CP58). COMMITrEE STATEMENT: Committee believes Proposal 99-99 (LOg #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrI'rEE ACTION:
AFFIRMATIVE: 16 * NOT RETURNED: Fan, Shoemaker
(Log #92) Committee: HEA-PIP
99- 16 - (Chapter 1, 2, & 4, Appendices Chapter 10 through 19): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #CP58). The TCC has directed the T / C on Piping Systems to resubmit the proposed changes in proper format. Because-of the action on that proposal, the T/C on Piping Systems is directed to. reconsider the action on this proposal. SIJBMITTER: Peter Eshedck, Patient Instrumentation Corporation RECOMMENDATION: Revise text:
1) Change format 2 ways: a. Integrate vacuum into medical gas section. b. Arrange all type 1 matedal together, all type 2 material together,
all laboratory material together etc. 2) Arrange format of the standard in a logical user friendly order:
identify applications, areas etc. First, then what is required for each type area etc. SUBSTANTIATION: 1) a, Med gases and vacuum are planned, drawn, bid, constructed and received together. Hence, the standards should be together.
b. It is too confusing for the user (Hospital engineer, consulting engineer, contractor etc.) to find what appli~t to the particular facility they are working on.
2) At present, the standard is not user friendly. Application requirements are lost in the back of the standard. We should first define types of facility, then state what is required for each type. COMMITTEE ACTION: Accept in Principle. See Committee Action on Proposal 99-99 (Log #CP58).
COMMITTEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #47) Committee: HEA-PIP
99-17 - (Chapter 1, 2, 4, Appendices Chapters 10 through 19): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (LOg #CP58). The TCC has directed the T /C on Piping Systems to resubmit the proposed changes in proper format. Because of the action on that proposal, the T /C on Piping Systems is directed to reconsider the action on this proposal. SUBMITI"ER: DonaldJ. Hetherington, Anne Arundel Medical Center RECOMMENDATION: Revise text:
1. Include Vacuum System piping into Medical Gas Section. Place all sections together i.e. Type 1, Type 2 Laboratory Material etc.
2. Change format of standards by areas, with requirement under, within that area. SUBSTANTIATION: 1. All piping systems are designed together at once. Makes sense that all requirements be grouped together.
2. The way the standard is written now, some requirements are never found until after the fact. Fadlities must be defined first, then requirements. COMMITrEE ACTION: Accept in Principle. See Committee Action on Proposal 99-99 (Log #CP58).
COMMITTEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrrTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(LOg#54) Committee: HEA-PIP
99-18 - (Chapters 1, 2, 4 &Appendices Chapters 10 through 19): Correlating Committee Note: The Technical Correlating Commit-
tee notes the reference in Committee Statement to proposal 99-99 (Log #.CP58). The TCC has directed the T /C on Piping Systems to resubmit the proposed changes in proper formal Because of the action on that proposal, the T / C on Piping Systems is directed to reconsider the action on this proposal SUBMITIXR: Victor H. Wong, Bah Consulting Engineers RECOMMENDATION: Revise: A) Reorganize Format in Chapter Four 1. Vacuum Section should be integrated with the Medical Gas
Section. 2. All Type I Material should be together as well as Type 2, and
laboratory materials. B) Identify areas and applications first and their requirements
after. Reorganize standard in a logical easier to use format. SUBSTANTIATION: Medical gases and vacuum systems are designed, drawn and constructed together, the standards should reflect this. Standards should be easier to use and less confusing. COMMITFEE ACTION: Accept in Principle. See Committee Action on Proposal 99-99 (Log #CP58).
COMMITI'EE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITIT_~ ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP81) Committee: HF_A-AAC
99-19 - (1-1): Accept SUBMIT'I~R: Technical Correlating Committee on Health Care Facilities RECOMMENDATION: Add at end ofsentenc~ one: "providing services to human beings." SUBSTANTIATION: Clarify the scope of document. It is not the intent of NFPA 99 to apply to facilities not treating human beings. COMMITI'EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 15 VOTE ON COMMITI'EE ACTION:
AFFIRMATIVE: 15
16

N F P A 9 9 - - F 9 5 R O P
(Log #25) Committee: HEA-PIP
99- 20 - (Chapter 2): Accept SUBMITTER: Albert L. deRichemond, ECRI RECOMMENDATION: Change "D" to "M" after "Grade" and before "in CGA" in the definitio n of Nitrogen, oil-free, dry in Chapter 2, page 23. SUBSTANTIATION: Grade D nitrogen is not def ined in CGA pamphle t G10.1-1991, Table 1, and has no t been since at least 1985. To ensure minimal oxygen, water, hydrocarbons and particulates, I suggest grade M be specified.
NOTE: Support ing material is available for review at NFPA Headquarters. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #303) Committee: HEA-PIP
99- 21 - (Chapter 2): Accept in Principle SUBMITTER: William G Frank, Win. G. Frank Medical Services, Inc. RECOMMENDATION: Revise text as follows:
Nitrogen, oil-free, dry. Revise SUBSTANTIATION: Referenced paragraph calls for use of Grade D ni trogen per CGA pamphlet G-10-1-1991.
Tiffs pamphle t does not list a grade D nitrogen. COMMITITEE ACTION: Accept in Principl6. See Committee Action on Proposal 99-20 (Log #25).
COMMI'I'rEE STATEMENT: Action on Proposal 99-20 (Log #25) recommends a specific type of nitrogen. NUMBER OF COMMIITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log#320) Committee: HEA-ESE
99- 22 - (Chapter 2 Patient Care Area): Reject SUBMITTER: David Esherick, Padent Instrumentation Corp. RECOMMENDATION: Add "LDR room" to the list of critical care a r e a s .
SUBSTANTIATION: Being born is "very critical" for the baby. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Committee considers an LDR to be a general care area because no inwasive procedures are in tended to be performed. If complications do occur, the patient is moved to a delivery room. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #364) Committee: HEA-PIP
99- 23 - (Chapter 2): Accept in Principle SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: Definition of Medical Compressed Air - Delete Note #2 SUBSTANTIATION: Information presented is of questionable value and may not be of any technological value and at most is editorial. COMMITrEE ACTION: Accept in Principle.
1. Delete Note 2. 2. Insert following new par. 4 in 4-3.1.9.7 to read as follows: "System design shall preclude formation of liquid water in the air
line." COMMITEEE STATEMENT: Committee agrees with deleting the NOTE, but issue of condensat ion in the airline is important for safe
~l~ on. Thus, addit ion of news par. in 4-3.1.9.7. ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP79) Committee: HEA-PIP
99- 24 - (Chapters 2,12,13,15,16,17 (definitions)): Correlating Committee Note: The Technical Correlating Commit-
tee rejects this proposal because of its action on proposal 99-97 (Log #CPS). SUBMITTER: Technical Committee on Piping Systems RECOMMENDATION: NFPA 99 TCC is asked to approve as a minimum the following definition revisions.
(a) Revise the definition of "Hospital Facility" as follows: (The new words are underl ined.)
Hospital Facility. A building or part thereof eauiDoed.to oerform surgical and exoloratorv procedures and used for the medical, psychiatric, obstetrical, "o~ surgical care, on a 2q-hour basis. Treatment and or Drocedures mav render the patient incanable of takin~ action of self oreservation finder emergency care co~nditions. Anesthesia and ventilation suooort are orovid'ed. Hospital F_.a_fj].i~ wherever used in this standar~l. ~ general and specialty hospitals, mental hospitals, tuberculosis hospitals, children's hospitals, and any such facilities providing inpat ient care. (ES, PS)
(b) Retide and revise the definition of "Ambulatory Health C~are Center" as follows: (The new words are underl ined.)
Ambulatory Health Care Facility-Maj.0_r.. A building or part thereof used to provide services or t reatment to four or more patients at the same time and meet ing either (1) or (2) below. Such facilities are not designed to nrovide overnight stays for patients,
1. Those facilities that provide, on an outpatient basis, t reamlent and orocedures for patients that would render them incapable of taking action for serf-preservation under emergency conditions without assistance from others. Examples include but are not restricted to hemodialysis units or freestanding emergency medical units.
2. Those facilities that provide, on an outpatient basis, surgical t rea tment and nrocedures for patients that would render them incapable of tafdng action for self-preservation under emergency conditions without assistance from others. This includes all facilities in which a oatient is subjected to deeo sedation or anesthesia Examples ihclude, but are not restlicied, to Ur~i-care centers. Day surgic~al centers, orthopedic practice and Plastic surgery offices Whe're oatients are sedated w~th ~as. (EE, [~S)
(c) P.~etifle and revise the definition of "nursing home: as follows. (The new words are underlined.)
Nursing Care FaciUtv. A building or part thereof used to rp_.t_Q_~_.~_ housing and acute and sub-acute nursing care, on a 24-hour basis, of four or more persons who, because of mental or physical incapacity, may be unable to provide for their own needs and safety without the assistance of another person. This includes ventilator dependen t Datients and those orovidin~ lon~term personal medical care. No ireatments or was ahalgesia or anesthes~'a are provided. Nursing care
wherever used in this document , includes rehabilitation nursing and convalescent homes, skilled nursing facilities.
intermediate care facilities, and infirmaries in homes for the aged that orovide lon~ term ventilator support. (EE,PS)
(d)" Revise in i~ entirety the definition of "Clinic" to read as follows:
Clinic. A building or part thereof used to provide multiple medical services or t~eatment to four or more patients at the same time where patients are seen on an ambulatory basis. Such facilities are no t designed to provide overnight stays for patients. The facility provides t reatment and procedures for patients that would not render them incapable of taking action for serf-preservation under emergency conditions. Patients are treated for chronic and not acute medical care. (TC, PS)
(e) Revise the definition of "Limited Care Facility" as follows: (The new words are underlined.)
Assisted Livin~ Facility. A building or part thereof used on a 24- hour basis for tlae housing of four or more persons who are incapable of serf-preservation because of age, physical limitation due to accident or illness, or mental limitations such as mental retarda- t ion/developmental disability, mental illness, or chemical depen- dency. Such facilities do not perform invasive procedures or use anesthesia or analgesia. Resoiratorv suot~ort is limited to nasal canual assistance for breathing. (TC, PS)"
(f) Add a new definition for "Ambulatory Care Facility-Minor" to read as follows: Ambulatory Care Facility-Minor. A facility that performs examina-
tions and minor t rea tments /procedures under the continuous supervision of a medical /denta l professional. Procedures involve only conscious sedation or local anesthesia and treatments a n d / o r procedures do not render the patient incapable of taking action for serf-preservation under emergency conditions. Such facilities do no t provide overnight stays for patients nor provide 24 h r /day opera- tion. Examples include: Dental Care Facility, Medical Care Facility, immediate care facility and podiatry office. Veterinary facilities also are included in dais category.
17

NFPA 99-- F95 ROP
(g) Revise the tides of chapters 12,13,15,16,17, as follows: Chapter 12 Hospital Facility Requirements. Chapter 13 Ambulatory Heath Care Facility- Major, Requirements. Chapter 15 Ambulatory Care Facility-Minor, Requirements. Chapter 16 Nursing Care Fadlity, Requirements. Chapter 17 Assisted Living Facility, Requirements.
SUBSTANTIATION: NFPA 99 TCC should explore in cooperation with NFPA 101 revising key definitions used in both standards to:
- Make them current with the terms actively used in health care, and
- Make them more definitive with regard to risk level of the patients, and - Provide examples in the definitions. The current definitions for Hospital, Ambulatory Health Care
Center, Clinic, Nursing Homes, and Medical/Dental office are not adequate. The T / C on Piping Systems is aware that Authorities Having Jurisdiction are having problems in interpretation of the appropriate applications because of this. Revised definitions include greater definition based upon a level of risk. • In addition there presendy is no definition (clarification) of what are the requirements of a dental or medical office to qualify for recognition in Chapter 15, or excluded from chapter 15.
Examples are provided for further clarification. The current nomenclature used in the health care industry is to
incorporate the words "Care Facility" in the tide. The words are addedto be compliant with the industry. Also the term nursing home is appropriately identified as nursing care facility. Limited care facility is also not used in the healthcare industry. The appropriate word is assisted care facility.
The word "shall" should no t be in a definit ion per the style manual and has been deleted. (See existing "hospital definition.") COMMITrEE ACTION: Accept NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #'274) Committee: HEA-ANE
99- 25 - (2-2): Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise text:
1) Revise the definition of Anesthetizing Location to read: L Any area of a facility...the administration of,~,y 7~o~.,a~:c ,,, ,,,,,,-
,q~,,.;.ablc inhalation anesthetic agents... 2) Delete the following definitions: a) Antistatic. b) Conductive. c) Flammable Anesthetizing Location. d) Hazardous Area in a Flammable Anesthetizing Location. e) Hazardous Location. f) Mixed Facility. g) Storage Location for Flammable Inhalation Anesthetics. 3) Revise the definition of Nonflammable Anesthetizing Location
to read: Noc~o~-,,;;,ablc Anesthetizing Location. Any anesthetizing location
designed... SUBSTANTIATION: Over thepast two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologist (ASA), DeparUnent of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITrEEACTION: Acceptin Principle. For submitter's recommendations: 1) Revise definition of "Anesthetizing location" to read as follows:
"Any area of a facility.., the administration of nonflammable inhalation anesthetic agents. . ." Add following NOTE under term: "For guidance on flammable
anesthetizing locations, see Annex 3." 2) Move terms to a new Annex 3. 3) Delete" term "Nonflammable Anesthetizing Location."
COMMITrEE STATEMENT: 1) Since the committee believes that all new construction U.S. is intended for nonflammable inhalation anesthetics, use of term "anesthetizing location" in NFPA 99 is restricted to nonflammable anesthetics.
2) Committee does not want to lose the guidance on 'flammable anesthetics, and is moving all material assodated with this practice to a separate section in NFPA 99.
3) Term no longer needed.
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITFEE ACTION:
AFFIRMATIVE: 10
(Log #CP65) Committee: HEA-PIP
99- 26 - (2-2): Accept SUBMITTER= Technical Committee on Piping Systems RECOMMENDATION: 1. Add the following new definitions:
Alarm System, Type III. An area alarm system for patient nonflammable medical gases system (typically) oxygen, nitrous oxide, and medical compressed air in Dental Care Facilities, and Medical Care Facilities.
Utility Center (J box). The control enclosure for all services used. NOTE: Typically includes electrical receptacle(s), compressed air,
nitrogen, vacuum, and water. Service Outlet. The pneumatic terminus of a piped gas system that
does not serve critical, continuous duty nonflammable medical life support type gasses such as Oxygen, Nitrous Oxide, or Medical Compressed Air. Service Inlet. The pneumatic terminus of a piped vacuum system
that does not serve a critical Type I Medical-Surgical Vacuum System. 2. Revise the existing definition of "Station Inlet" to read: Station Inlet. An inlet point in a Type I medical-surgical piped
vacuum distribution system at which the user makes connections and disconnection's. SUBSTANTIATION: 1. There are a number of new definitions that are needed. At present there is no appropriate definition of an alarm systems for Type Ill systems. At present there is no definition of the term Utility Control Center (J Box) which is used extensively in type III installations. At the present time, the only outlet defined is a "Station Outlet and Station Inlet" that requires a DISS configuration, dual check valves and is intended for continuous duty service at a nominal pressure of 50psig or MSVS. Type III compressed air, and nitrogen systems, andothers, such as Type III vacuum'are intermittent operating, and operate at pressures that .are adjusted by the operator. They also do not need the gas specific features. Most dental & medical facility compressed air or nitrogen piping systems terminate in a shutoff valve with a pipe fitting. It is not appropriate to require a station outlet or a station inlet with DISS requirements.
2. The existing definition of"Station Inlet" needs to be clarified as Type I. COMMITTEE ACTION: Accept. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
c (Log OcPT0) ommittee: HEA-PIP
99- 27- (2-2): Accept $UBMITTER: Technical Committee on Piping Systems RECOMMENDATION: 1. Delete the present definition of Dental Compressed Air.
2. Delete the definition of"Dental compressed air" and add a new definition for "Type III Compressed Air System" to read as follows:
Type III Compressed Air System. A system of component parts, including, but not limited to, air compressor, motor, receiver, controls, filters, dryers, valves and piping, and delivering compressed air < 160 psig to power devices (handpieces, syringe, cleaning devices, etc.) as a power source. NOTE: The system does not produce air to meet the medical
requirements of medical air and is not intended to be used for air life support devices. SUBSTANTIATION: The existing definition of Dental Compressed Air is often being interpreted by the local authorities having jurisdiction to mean that only oil-free compressors can be used. Th~ is not the T/C's intent. In addition the requirement to not ~ ld odor and contaminants is a carry over from the medical compressed air language for breathing type air. The definition of dental compressed air should be revised or deleted. The definition of dental air should not contain a performance specification. The pcefformance requirements belong in Chapter 4.
OMMITrEE ACTION: Accept- NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
18

NFPA 99- - F95 ROP
(Log #268) Committee: HEA-ESE
99- 28 - (2-2 (New)): Accept in Principle SUBMITrER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: New text:
New Construction. The renovation, alteration or modification of any system or individual component. For the purpose of this Standard, only the altered portion of a system or individual component would be required to be upgraded to meet the installation and equipment requirements. SUBSTANTIATION: As NFPA 99 is being referenced by more and more authorities having jurisdiction, there is a need to provide guidance on what portions of NFPA 99 apply to new versus existing installations of systems and equipment. As no definition is included in the 1993 edition, this derision is left up to the enforcing AHJ, who in many instances, does not have the insight of the Technical Committee which wrote the standard. By adding a definition pinning down the TC's intent we will hopefully eliminate the overzealous application of this standard. COMMITrEEACTION: Acceptin Principle. Add at the end of paragraph 1 of 1-2: "Only the altered, renovated or modernized portion of an existing
system or individual component shall be required to meet the installation and equipment requirements stated in this standard. If the alteration, renovation or modernization impacts existing performance requirements of a systems or component, additional upgrading shallbe required." CO]~iITlrEE STATEMENT: Proper section in document for addressing the issue of new construction is considered to be 1-2. Wording by committee is considered to meet the intent of submitter's recommendation. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 17. VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log#CP51) Committee: HEA-ESE
99- 29 - (2-2 Emergency System): Accept SUBMITTER: Technical Committee on Electrical Systems RECOMMENDATION: Revise definition of Emergency System by deleting %vith automatic restoration of elecllical power within 10 seconds." SUBSTANTIATION: Text deleted is performance criteria, and does not belong in a definition. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #CP37) Committee: HEA-LAB
99- 30 - (2-2 Hazardous Area in Laboratories): Accept SUBMITrER: Technical Committee on Laboratories RECOMMENDATION: Delete this term and definition. SUBSTANTIATION: Term not used in text as referenced. CO MM~[' r I~ ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #572) Committee: HEA-PIP
99-31- (2-2 Note 1): Accept SUBMITTER: Mark Allen, Ohmeda Medical Engineering RECOMMENDATION: Alter Note 1 to read: Note 1: Air supplied from on-site compressor and assodated air
treamaent systems (as opposed to Medical Air USP supplied in cylinders) must comply with the above limtts to be considered Medical Compressed Air.
Hydrocarbon carryover from the ~:ompressor into the pipeline distribution system could be detrimental to the safety of the end user and to the integrity of the piping system. Mixing of air and oxygen is a common clinical practice, and the hazards of fire are increased if the air is thus contaminated.
Compliance with these limits is thus considered important to fire and patient safety. The quality of local ambient air should be determined prior to selection for compressors and air treatment equipment. SUBSTANTIATION: The note has been criticized as difficult to understand. This rewrite is an attempt to simplify. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP21) Committee: HEA-ELE
99- 32 - (2-2 Patient Care Area; General Care Area; Critical Care Area): Accept SUBMITTER: Technical Committee on Electrical Equipment RECOMMENDATION: Revise words "electromedical devices" to read:
"patient care related electrical appliances." SUBSTANTIATION: For consistency with a defined term in the document. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #334) Committee: HEA-PIP
99- 33 - (2-2 Medical Compressed Air): Accept in Part SUBMITTER: Saul Axonow, Technology in Medicine lnc RECOMMENDATION: (a) Change title from "Medical Com- pressed Air" to "Medical Air". Also change name in text.
(b) Under "4. Permanent Particulates...", Delete this section of the definition. SUBSTANTIATION: (a) To conform to the terminology of USP XXII and parts of the NFPA-99 text.
(b) A limit on particulates does not appear in USP XXII, nor does a requirement to test appear in Chap. 4. In any case, the number, 5 rag/m3 , is inapprop~ate. It comes from an OSHA requirement for factories. A more reasonable requirement would be the EPA standard for ambient air, 0.15 mg/m 3 , but even this is not needed in the definition. COMMITrEE ACTION: Accept in Part.
1. Accept item 1. 2. Rejectitem 2.
COMMITrEE STATEMENT: 2. Reference to USP, OSHA and EPA requirements are not appropriate for medical piped airpurposes. Committee believes more stringent criteria is necessary tor patient safety. NUMBER OF COMMIT1T, E MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
Committee: HEA-PIP 99-34- (2-2 Station Outlet): Reject S U B ~ Saul Aronow, Technology in Medicine Inc RECOMMENDATION: Add a NOTE or an Appendix item.
The station oudet is the point at which the user makes connection, i.e., connects the operational apparatus. The tests for pressure drop are to be made at this point (4-5.1.3.8, 4-5.1.3.3). This can present a problem when ceiling drops or similar extensions are used. SUBSTANTIATION: Testers are tempted to perform pressure drop tests at the last hard piped position and not at the flexible extension. This should be warned against. COMMITrEE ACTION: Reject. COMMITTEE STATEMENT: 1. Sentence I is covered in Proposal 99-98 (Log #CP6).
2. Sentences 2 and 3 are not in accordance with NFPA style manual of not havin~ requirements in definitions. NUMBER O~F C~)MMITTEE MEMB~EP.S ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
19

NFPA 99-- F95 ROP
(Log #CP80) Committee: HEA-AAC
99- 35 - (Chapter 3): Accept SUBMITTER: Technical Correlating Gommittee on Health Care Facilities RECOMMENDATION: Restructure Chapter 3 as follows:
3-1 Scope [current 3-1] 3-2 Nature of Hazards [current 3-2] 3-3 Normal Electrical System requirements 3-3.1 Sources [current 3-3.1] 3-3.2 Distribution 3-3.2.1 General [current 3-3.1] 3-3.2.2 Isolated power systems [current 3-4.3] 3-3.3 Performance Criteria & testing 3.3.3.1 Source [current 3-5.1.1] 3-3.3.2 Distribution 3-3.3.2.1 Grounding system in p.c.a_ [current 3-5.2.1] 3-3.3.2.2 Receptacles in p.c~a. [current 3-5.2.2] 3-3.3.2.3 GFCIs in p.c.a~ [current 3-5.2.3] 3-3.3.2.4 IPSs [current 3-5.2.4] 3-3.4 Administration 3-3.4.1 Source [current 3-5.2.4] 3-3.4.2 Distribution 3-3.4.2.1 Respon. ofgov, body [current 3-6.2.1] 3.3.4.2.2 Policies [current 3-6.2.2] 3-3.4.2.3 Malnt. & testing [current 3-6.2.3] 3-3.4.3 Record keeping 3-3.4.3.1 General [current 3-6.2.5.1] 3-3.4.3.2 IPS, where installed [current 3-6.2.5.3] 3-3.4.4 Info & warning signs [current 3-6.2.6]
3-4 Essential Electrical System requirements - TYPE 1 3-4.1 Sources 3-4.1.1 On-site generator set [current 3-3.2.1 ] 3-4.1.2 Battery [ cu r r en t 3-3.2.2] 3-4.1.3 Separate utility [current 3-3.2.3] 3-4.2 Distribution 3-4.2.1 General, in¢l. ATS [current 34.2.1] 3-4.2.2 Specific requirements [current 3-4.2.2] 3-4.3 Performance criteria & testing 3-4.3.1 Source [current 3-5.1.2.1(a)] 3-4.3.2 Transfer switches [current 3-5.1.2.2(a)] 3-4.4 Administration 3-4.4.1 Malnt. & testing [current 3-6.2.4] 34.4.2 Record keeping [current 3-6.2.5.2]
3-5 Essential Electrical System requirements - TYPE 2 3-5.1 Sources [same as 34.1 above] 3-5,2 Distribution 3-5,2.1 General, incl. ATS [same as 3-4.2.1 above] 3-5,2.2 Specific requirements [current 34.2.3] 3-5.3 Performance criteria & testing
• 3-5.3.1 Source [current3-5.1.2.1(b)] 3-5.3.2 Transfer switch [current 3-5,1.2.2(b)] 3-5.4 Administration [same as 3-4.4 above]
3-6 Essential Electrical System requirements-TYPE 3 3-6.1 Sources [same as 3-4.1 above] 3-6.2 Distribution 3-6.2.1 General, incl• ATS [same as 3-4.2.1 above] 3-6.2.2 Specific requirements [current 3-4.2.4] 3-6.3 Performance criteria & testing 3-6.3.1 Source [current 3-5.1.2.1(c)] 3-6.3.2 Transfer switches w/eng, gen. sets [current 3-5,1.2.2(c)] 3-6.3.3 Transfer switches w/battery system [current 3-5.1.2.2(d) ] 3-6.4 Administration [same as 3-4.4 above]
SUBSTANTIATION: To make the document more user friendly by placing all requirements for a particular type of system in one section of the document. COMMITI'EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 15 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15
(Log #GP52) Committee: HEA-ESE
99- 36 - (3-3.2.1.5): Accept SUBMITTER: Technical Committee on Electrical Systems RECOMMENDATION: 1. Renumber existing text of 3-3.2.1.5 to 3-3.2.1.5 (a).
2. Add the following new subparagraph (b): (b) Any loads served by the generating equipment not required to
be on the essential electrical system shall be served by their own transfer switch(es) such that these loads:
1. shall not be automatically tTansferred to the generating equipment,
2. shall not be o'ansferred onto the generating equipment if the transfer will overload the generating equipment; and
3. shall be shed upon generating equipment overload, This shall not constitute an 'other use' as described in 3-3.2.1.5(a).
SUBSTANTIATION: Address the problem of users and designers wanting to place non-essential loads on the essential electrical system. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMI'I~EE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #221) Committee: HEA-ESE
99- 37 - (3-3.2.1.5): Accept in Principle SUBMITTER: Hugh O. Nash,Jr., Smith Seckman Reid, Inc~ RECOMMENDATION: Change the second sentence to read - If normally used for other purposes, two or more sets shall be installed, such that the demand and all other performance requirements of the emergency system and medical air compressors, medical/ surgical vacuum pumps, and other life support equipment of the equipment system shall be met with the largest singlegenerator set out of service. (Note that the changed wording is bold.)
Change the Exception to Exception No. 1 and add (4) cogenera- tion to the list included in the exception. Add Exception No. 2 which shall read: Ambulatory health care
centers, clinics, medical and dental offices, nursing homes, and limited care facilities that are contiguous with a hospital shall be permitted to have their essential electrical systems supplied by that of the hospital. Add the following after the exception: Loads not listed specifically in 3-4.2 (Essential System) shall not be
permitted to be connected to the generating equipment. Exception: Selected equipment, task illumination, receptacles, and
power circuits as permitted by 3-4.2.2.2 (C) (9) and 3-4.2.2.3 (D) (8). SUBSTANTIATION: The present wording is more restrictive for multiple generator installations than for single generator installa- tions. As written, the code now penalizes those who would add additional generators in order to provide greater reliability. The present language will also result in grossly oversized generators which is not consistent with the committees recent action on 3-5.1.2.3 (B) (1) which requires testing with a minimum of 50% load. Adding "medical air compressors, medical/surgical vacuum pumps and other life support equipment" answers the concerns of those who feel like load shed systems of multiple generator systems would actually decrease the reliability of service "to these pieces of equipment.
"Cogeneration'.is added to the Exception (No. 1) because cogeneration is the most common "other use" encountered in hospitals.
Exception No. 2 makes legal a practice that is already fairly common in the industry. In fact NFPA 70 (NEG) 517-40(C) already permits contiguous nursing homes to be served by.the hospital generators.
The additional text clarifies a common misconception in the industry - that "other loads" can be indiscriminately added and connected to the generator equipment by means of manual or automatic transfer switches. The new text also points out that the code makes provisions for "selected other loads" in the existing text on Essential Systems. COMMITrEE ACTION: Accept in Principle.
1. Change the second sentence of 3-3.2.1.5 to read: "If normally used for other purposes, two or more sets shall be
installed, such that the maximum actual demand likely to be produced by the connected load of the emergency system as well as medical air compressors, medical/surgical vacuum pumps, electrically operated fire pumps,jockey pumps, fuel pumps and generator accessories shall be met with the largest single generator set out of service."
2. Chan~e the Exception by adding: "(4) cogeneration" to the list included m the exception.
3. Add the following NOTE after paragraph 1 in 3-3.2.1.5 and before the Exception to read:
"NOTE: It is the intent qf this section that load shed circuits, if provided, not shed the above equipment upon loss of the largest singlegenerator."
4. Add to 12-3.3.2: "Hospitals shall be permitted to serve the essential electrical system
needs of contiguous or same-site facilities with the generating equipment of the hospital." - -
2O

N F P A 9 9 - - F 9 5 R O P
COMMITTEE STATEMENT: 1. Since "essential system" was changed to "emergency system," then to avoid decreasing reliability to certain items on the equipment systems, the committee has added them to the list recommended by the submitter.
Change to "maximum actual demand" is for consistency with Committee Proposal 99-43 (Log #CP49).
2. Same recommendation assubmitter. 3. Clarify committee intent that these items not be shed if load
shedding is used. 4. Reworded to darify that it is the generating equipment that is
involved, not the essential system. Current structure of NFPA 99 requires placement of facilitysspecific requirements in facility chapters. Committee expanded concept to allow the essential electrical systems of other buildings to be connected to the generating equipment of the hospital that were both contiguous and on the same site.
Last two items of submitter's recommendation are addressed by Proposal 99-36 (Log #CP52). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACYION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, lverson, Norton, Swisher
(Log #393) Committee: HEA-ESE
99- 38 - (3-3.2.1.5): Accept in Principle StaffNote: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-30(d),FPN (New). It is being acted oia here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITrER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the following fine print note to 517-30(d):
(FPN) Where the essential electrical system power source is comprised of two or more generators, it is recommended that with one generator out of service the remaining generator(s) should have the capacity to operate the life safety branch, critical branch, fire pump, and any loads on the equipment system required for fire
g rotection. UBSTANTIATION: Although two or more generators are not
required by code, it is a common practice and some design guidance is needed for the situation where one generator fails. None of the present NFPA codes address which loads should be shed in the event of a failure of one generator. We have seen much confusion by AHJ's on this matter and many interpretations. Usually NFPA 99 paragraph 3-3.2.1.5 and NFPA 110 paragraph 5-1.6 which address the system when it is "normally used for other purposes" or serves loads "other than Level 1 and Level 2" are incorrectly interpreted. Consistent desig~n guidance is needed throughout the United States. COMMITYEE ACTION: Accept in Principle. COMMITI'EE STATEMENT: See Committee Action on Proposal 99-41 (Log #391) because it addressed this issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #317) Committee: HEA-ESE
99-40- (3-3.2.1.7): Accept in Principle SUBMITTER: A. Dan Chisholm, Motor and Generator Institute RECOMMENDATION: Modify text of 3-3.2.1.7 with wording taken from NFPA 110, 3-4.1. SUBSTANTIATION: To add meaning to current text by stating
"how maximum demand is actually met. COMMITYEE ACTION: Accept in Principle. Delete extract reference from 3-3.2.1.7. Add this extract reference
to 3-3.2.1.8. COMMITrEE STATEMENT: Committee corrects error in extract reference. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #391) Committee: HEA-ES E
99- 41 - (3-3.2.1.7): Accept in Principle Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-30(d). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMI'IqT.R: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the following paragraph to 517-30(d):
(1) It shall be permissible to shed part or all of the equipment system loads not required for fire protection in order to start and/or run the fire pump. Critical and Life Safety Branch loads shall not be shed in order to start or run the fire pump. SUBSTANTIATION: The purpose of the text is to clarify which loads within hospitals are allowed to be shed as allowed by NFPA 20 paragraph fi-7.2 which states, "Automatic shedding of loads not required for fire protection is permitted prior to starting of the fire pump(s)." NFPA 20 appears to allow shedding of the critical and equipment branch. Shedding of the critical system could put lives in danger that are not even close to the fire and this should not be allowed. COMMITTEE ACTION: Accept in Principle. Add a new paragraph to 3-3.2.1.1 to read: "Generator load shed circuits designed for the purpose of load
reduction or for load priority systems shall not shed emergency system loads, medical air compressors, medical/surgical vacuum PcUmps, fuel pumps, jockey pumps or other generator accessories."
OMMITI'EE STATEMENT: 1. It is not common design practice to design an essential electrical system for load shedding if only one generator is used.
2. Committee Action on Proposal 99-37 (Log #221) addressed the issue of load shedding when multiple generator sets are installed.
3. Requirements for fire pumps are covered in NFPA 20. 4. Committee agrees with the intent of submitter with regard to
not shedding critical and life safety branch loads. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #M2) Committee: HEA-ESE
99- 39 - 43-3.9.1.6 (New)): Accept in Principle SUBMITTER: A. Dan Chisholm, Motor and Generator Institute RECOMMENDATION: Replace complete text with NFPA 110:5-2.1 in it's entirety as an extract. SUBSTANTIATION: 3-3.2.1.6 does not cover the subjects of two hour fire rated walls or weather proof outside housings. Addition- ally, NFPA 110:5-2.1 covers all other equipment not just transform- ers which are not allowed to be in the same room. COMMITTEE ACTION: Accept in Principle.
In parentheses at end of paragraph, add "5-2.4." COMMITTEE STATEMENT: Committee notes that extracted text shouM have included reference to NFPA 110, paragraph 5-2.4. Committee has extracted only portions of the two paragraphs referenced from NFPA 110. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMIq[q'EE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #392) Committee: HF~A-ES E
99- 42 - (3-3.2.1.7): Accept in Principle Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-304d ) etal. It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITI~R: Walt Vernon, California Society of Hospital Engineers RECOMMENDATION: Add (b) (5) as follows:
"Any loads served by the standby generators not required to be on the essential system shall be served by their own transfer switch(es), such that these loads shall be shed upon standby generator overloading, and such that standby generators may be sized based upon essential system loads."
Revise 30(d) as follo~'s (changes underlined): ~(d) Capadty of Systems. The essential electrical system shall have
adequate capacity to meet the actual demand likely to be oroduced by the connected load of all functions and equipment to 15e served by each e~enfial system and branch." SUBSTANTIATION: for 517-304b ) 45):
1. Many facilities would like to provide all loads on the generators, and eliminate the various branches of the essential system. This item would clarify this issue.
21

N F P A 9 9 - - F 9 5 R O P
2. Many facilities want to place loads onto the standby generators that are not required. The addition of this item will allow that only- when these loads are isolated from the required essentialsystem loads. 3. This addition will make it clear that the generator need only be
sized to serve the essential system loads.
SUBSTANTIATION for 517-30 (d): 1. Many facilities want to place loads onto the standby generators
that are not required. The addition of this item will allow that only when these loads are isolated from the required essential system loads.
2. To match language in recently updated NFPA 99 (3- 6.2.4.1 (b) (1)NOTE).
3. To make it dear that the intent of this section is to ensure that generators are adequately sized to meet actual demand load, not necessarily demandload as calculated under the other sections of this document. Many local authorities interpret this section as meaning that generators shall be sized based on calculated connected load, as modified by Article 220. COMMYITEE ACTION: Accept in Principle. COMMITrEE STATEMENT: See Committee Action on Proposals 99-37 (Log #'221) and 99-43 (Log #CP49), which address the issues raised here. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #CP49) Committee: HEA-ESE
99- 43 - (5-3.2.1.7): Accept S U B - - R : Technical Cornmittee on Electrical Systems RECOMMENDATION: Revise $-3.2.1.7 to read:
3-3.2.1.7 Capacity and Rating. The generator set(s) shall have sufficient capacity and proper rating to meet the maximum actu~ demand likely to be nroduced by the connected load of the essential electrical ~ at any one time.
IqOTl~; It is the intent of this section to mandate ~enerator s|zin~ based uPOn actual demand likely to be nroduced by the connected load of t~he essential electrical s'~temts)-at any one time. It is not the intent of this section that ~enerator sizin~ bebased uoon connected load or feeder calculation~Drocedures described in N'FPA 70. Na~onal Electrical Code. Demand calculations should be base~l uoon vrudent demand factors and historical data. [changes & new text underlined] SUBSTANTIATION: Clarify the intent of the capadty and rating of ~denerator sets, and address reported misinterpretations of the term
emand" with respect to generator sizing. Committee also addresses multiple essential electrical systems. COMM1TrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITI'EE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger,Iverson, Norton, Swisher
(Log #313) Committee: HEA-ESE
99- 44 - (5-5.2.1.9 (New)): Accept in Pfindple SUBMITrER: A. Dan Chisholm, Motor and Generator Institute RECOMMENDATION: New text as follows: Replace complete text with NFPA 110:5-7.6 and NFPA 110:3-3.1
in their entirety as an extract. SUBSTANTIATION: Present reference of temperature minimums does not agree with the minimums set forth in NFPA 110:5-7.6 nor 5-$.1. The reference to NFPA 110: 5-5.5.2(d) has no validity. COMMITTEE ACTION: Accept in Principle.
I. In 3-$.2.1.9, change "70°F (21.I°C)" to "g&F (32°C)." 2 . Change references for NFPA 110 to "3-3.1 and 5-7.6."
COMMITrEE STATEMENT: 1. To comply with policy on extracts. 2. Correct references.
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #316) Committee: HEA-ESE
99- 45 - (3-3.2.1.10 (New)): Reject SUBMITTER: A~ Dan Chisholm, Motor and Generator Institute RECOMMENDATION: Replace entire text of 5-3.2.1.10 with NFPA 110 5-7.2, 5-7.3, 5-7.4 SUBSTANTIATION: To add meaning to standard. COMMITI'EE ACTION: Reiect. cOMMITI'EE STATEMENT: References currently listed are sufficient. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #$15) Committee: HEA-ESE
99-46- (3-3.2.1.11): Accept in Principle SLrBMITrER: A. Dan Chisholm, Motor and Generator Institute RECOMMENDATION: Replace complete text of 5-3-2.1.11 with NFPA 110:
5-5.4.$ and 5-5.4.4. Appendix item A-3.2.1.11 to be incorporated as part of the revised standard. SUBSTANTIATION: To provide additional wording for full meaning. COMMITrEE ACTION: Accept in Principle.
1. Revise 5-$.2.1.11 to read: "Internal combustion engine cranking batteries shall meet the
cranking requirements of NFPA 1].0." 2. Delete A-5-3.2.1.11.
COMMITTEE STATEMENT: Committee meets intent of recom- mendation by referencing NFPA 110 for requirements for cranking. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #314) Committee: HEA-ESE
99- 47 - (5-$.2.1.13 (New)): Accept in Principle SUBMITTER: A. Dan Chisholm, Motor and Generator Institute RECOMMENDATION: Replace complete texiincluding exception with NFPA 110, section 3-4.2 in it's entirety as an extract. SUBSTANTIATION: Present referenced extract material (NFPA 110 - 1995, 3-1) is the wrong extract reference and the present NFPA 99 text is not extracted from NFPA 110. The wording (text) in NFPA 99, 3-1 is totally different from the referenced extract text. COMMITrEE ACTION: Accept in Principle. Revise 5-3.2.1.15 to read: "Fuel Supply. The fuel supply for the generator set shall comply
with paragraph 5-1.1 and 5-4.2 of NFPA 110." COMMITTEE STATEMENT: Meets the intent ofsubmitter by referencing NFPA 110 instead of extracting text. NUMBER OF COMMITTEE M ] ~ B E R S ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger,.Iverson, Norton, Swisher
(Log #384) Committee: HEA-ESE
99-48- ( M A d ) : Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517.12, Exception 2(New). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITTER: L. Bruce McClung, Union Carbide Corporation RECOMMENDATION: New text as follows:
Exception No. 2: Any temporary elecU'ical power and lighting wiring shall be made only with hard usage or extra-hard usage cords or cables of a type that is specifically marked with an/I_SILC designation and listed for the use. This listing requirement shall become effective January 1, 1997. SUBSTANTIATION: The 1990 Code recognized "/LS" and the 1993 Code recognized "/LC" insulations and outer coverings for conductors for general wiring, for flexible cords and cables and for fmture wires. Any exposed wiring in enclosed spaces where products of combustion would be confined and people (particularly infirm or immobilized people) and /or sensitive electronic equipment that are
22

N F P A 9 9 - - F 9 5 R O P
present should have improved fire safety features. See copy of technical paper tiffed "Improvement in Fire Safety Features of Electrical Conductors and Cables" by L.B. McClung and S. Ramchandran that was presented at IEEE-IAS-PCIC 1993 at St. Louis, Missouri. UL now has available a test by which to measure limited smoke (UL1685). UL is actively pursuing development of a standard test by which to measure low or limited corrosivity of conductors and cables. COMMITrEE ACTION: Reject. COMMITrEE STATEMENT: Temporary wiring is no t within the scope of the Health Care Facilities Project. Requirements are located in NFPA 70, Article 305. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #269) Committee: HEA-ESE
99- 49 - (3-4A.2.1): Reject SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Add to the title after: Wiring, Regular Voltage. (For new construction only.)
SUBSTANTIATION: Many health care organizations are being required to retroactively meet this set o f requirements. With the proposed definition of new construction, this statement for new construction only, after the tide will help Authorities Having Jurisdiction or users in determining when this section will apply. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: See Committee Action on Proposal 9928 (Log #268) which addresses this issue of new construction. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMIIqT.E ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #386) Committee: HEA-ESE
99-50- (3-4.1.2.1(a)): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 5 1 7 , p a r a ~ p h 517-19(a), Exception (New). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. S U B ~ Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the following exception:
Exception: Anesthetizing locations shall be permit ted to be supplied by power from only the critical branch provided that at least two branch circuits are used. SUBSTANTIATION: Most of the clients we have feel it is better to have all emergency power in the OR.'s and Delivery Rooms even if it is f rom a single transfer switch. They are afraid that someone will have life s u p p c ~ equipment plugged into a normal receptacle when the utility power goes off. The probability of a utility power outage is so much greater than the probability of a transfer switch failure that this should be allowed. COMMYVrEE ACTION: Reject. COMMITrEE STATEMENT: Committee believes that transfer switch and circuit failures are likely to occur. NFPA 99 already permits to use critical branch circuit, provided either a "normal" circuit or a second critical branch circuit f rom a separate critical branch transfer switch is provided. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #23) Committee: HEA-ESE
99- 51 - (3-4.1.2.1 (d) (1)): Accept SUBMYITER: Hugh O. Nash,Jr. , Smith Seckman Reid, Inc. RECOMMENDATION: Change 3-4.1.2.1(d) (1) to read as follows:
The main and downstream ground-faultprotective devices (where required) shall be coordinated as r equ i r ed in 3-4.1.5.
FPN: Within the constraints of the equipment provided, consider- ation should be given to coordinating circuit breakers, fuses, and other overcurrent protective devices so that power interruption in that part of the circuit that precedes the interrupting device closest to a fault is no t likely to occur.
SUBSTANTIATION: The cost of provid ingl00% coordinated electrical system is pL'ohibitive. It is impossible to coordinate circuit breakers with instantaneous trip features. It is also difficult (and sometimes impossible) to coordinate current limiting fuses with downstream molded case circuit breakers. In order to satisfy this requirement for 100% coordinated systems, the designer would have to use a 100% fused system with 2:1 or 3:1 ratios (in the sizes of successive fuses) or expensive low voltage power circuit breakers or solid state circuit breakers that utilize a short time trip instead of an instantaneous trip. Such designs are expensive, impractical, and can sometimes compromise equipment protection. Coordination is an art and not a science. It is a trade-off between selectivity and equipment protection, and should be left up to the j udgmen t of the design engineer. Few, if any, hospitals in the United States presently have 100%coordinated electrical systems. COMMITI"EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #218) Committee: HEA-ESE
99- 52 - (3-4.1.2.1 (d) (1)): Accept SUBMITTER: Hugh O. Nash,Jr., Smith Seckman Reid, Inc. RECOMMENDATION: Change 3-4.1.2.1 (d) (1) to read as follows:
The main and downstream ground-fanltprotective devices (where required) shall be coordinated as r equ i red in 3-4.1.5.
FPN: Within the constraints of the equipment provided, consider- ation should be given to coordinating circuit breakers, fuses, and other overcurrent protective devices so that power interruption in that part o f the circuit that precedes the interrupting device closest to a fault is no t likely( to occur. SUBSTANTIATION: The cost of provid ingl 00% coordinated electrical system is prohibitive. It is impossible to coordinate circuit breakers with instantaneous trip features. It is also difficult (and sometimes impossible) to coordinate current limiting fuses with downstream molded case circuit breakers. In order to satisfy this requirement for 100% coordinated systems, the designer would have to use a 100% fused system with 2:1 or 3:1 ratios (in the sizes of successive fuses) or expensive low voltage power circuit breakers or solid state circuit breakers that utilize a short time trip instead of an instantaneous trip. Such designs are expensive, impractical, and can sometimes compromise equipment protection. Coordination is an art and not a science. It is a t rade-offbetween selectivity and equipment protection, and should be left up to the j udgmen t of the design engineer. Few, if any, hospitals in the United States presently have 100%coordinated electrical systems. COMMITFEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #275) Committee: HEA-ESE, HEA-ANE
99- 53 - (3-4.1.2.1 (e)): Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise and delete text:
Modify section as follows: For subpara. (e) (1): ~d~Anesthefizing Locations For suhpara~ (e) (2): Delete in its entirety
SUBSTANTIATION: Over t h e p a s t two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Deparunent o f Veterans Affairs, Depar lment of Defense and major teaching institutions, all of them indicated they have no t used flammable anesthetics for over ten years and have ~ intent ion of permitt ing the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMI'I'I 'EE ACTION: Accept in Principle.
I For subpara. (1): Accept. For subpara. (2): Move to n e w A n n e x 3.
COMMITTEE STATEMENT: 2) Same reason as given in Proposal 99-25 (Log #274). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 (ESE), 10 (ANE)
23

NFPA 99- - F95 ROP
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 12 (ESE), 10 (ANE) NEGATIVE: Longhitano (ESE) NOT RETURNED: Berger (ESE), Iverson (ESE), Norton (ESE),
Swisher (ESE) EXPLANATION OF NEGATIVE: LONGHITANO: If the committee believes that protective features
are needed to make a flammable anesthetizing location safe, we should say so. Keeping the requirement may be one of the factors which makes the use of flammable anesthetics undesirable or uneconomical.
"(b) Wirin~ for low-voltage control systems and non-emergency communications and signaling systems shall be installed in metal raceways unless located outside or above the hazardous area in the flammable anesthetizing location." COMMITTEE STATEMENT: Correlate with Action on Proposal 99.25 (Log #274). NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 17 (ESE), 10 (ANE) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 (ESE), 10 (ANE) NOT RETURNED: Berger (ESE), Iverson (ESE), Norton (ESE),
Swisher (ESE)
" (Log #s88) Committee: HEA-ESE
99- 54 - (3-4.1.2.1 (e) (v)): Accept in Prindple Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-19(h) (New). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITFER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the following paragraph to Section 51%19:
(h) Battery-Powered Lighting Units. Battery-powered lighting units or uninterruptible power systems as described in Section 700-12 shall be provided for selected light fixtures in critical care areas where closure or ending of a procedure would be required in order to sustain human life during failure of the normal and emergency power system.
2. Delete Section 51%63(a) SUBSTANTIATION: 1. It is not uncommon for generators to fail to start. This can provide a substantial risk to hospitals with only one generator. Small rural hospitals are particularly at risL High risk occurs if there is an operation or delivery in progress at the time of power failure. In our experience provision of battery-powered lighting units in these areas is always desired by the Owner and is simply considered good engineering practice. From a liability standpoint for all parties involved, this should be a code require- menu
2. Section 517-65(a) has similar requirements as listed above but as currendy written it only applies to operating rooms. This should be broadened to include other anesthetizifig locations such as deliverf and non-anesthetizing locations such as Labor/Delivery/Recovery Rooms. COMMITTEE ACTION: Accept in Prindple. Revise 34.1.2.I (e) (1) (v) includin~ Exception to read: "Battery-powered emergency ligh~ng units. One or more battery-
powered emergency lighting units shall be provided in accordance with NFPA 70, Section 700-12(0." COMMITYEE STATEMENT: Committee believes that battery- powered units are necessary in anesthetizing locations only.
Committee can not delete sections from other NFPA documents. However, committee has deleted equivalent text in NFPA 99. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TOVOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #'277) Committee: HEA-ESE, HEA-ANE
99- 55 - (3-4.1.2.2(b)): Accept in Principle SUBM/T~R: Douglas S. Erickson, American Hospital Assodation RECOMMENDATION: Revise paragraph to read: Wiring for low-voltage...in metal raceways in u,,,,.'b..,..,,~L;..
anesthetizing locations. ~. ,,,L,-.~ ,,,.Z,;d .... SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITFEE ACTION: Accept in Principle.
1. Revise 3-4.1.2.2(b) to read as follows: "(b) W'uing for low-voltage...installed in metal raceways in
anesthetizing locations." 2. For newAnnex 3, use following wording:
(Log #276) Committee: HEA-ESE, HEA-ANE
99- 56 - (3-4.1.2.3.2): Accept in Principle S U B ~ Douglas S. Erickson, American Hospital Association RECOMMENDATION: Delete subparagraph (2) in its entirety:. SUBSTANTIATION: Over thepast two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupandes. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no inteation of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMM1TIT_,E ACTION: Accept in Prindple. Move to new,annex 3.
COMMITTEE STATEMENT: Correlate with Action on Proposal ~ - ~ (Log #274). NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 17 (mE), 10 (ANE) VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 12 (ESE), 10 (ANE) NEGATIVE: Longhitano (ESE) NOT RETURNED: Berger (ESE), Iverson (ESE), Norton (ESE),
Swisher (ESE) EXPLANATION OF NEGATIVE:
LONGHITANO: If the committee believes that protective features are needed to make a flammable anesthetizing location safe, we should say so. Keeping the requirement may be one of the factors which makes the use of flammable anesthetics undesirable or uneconomical.
(Log #278) Committee: HEA-ESE, HEA-ANE
99-57- (3-4.1.2.4(d),(e),(g)): Accept in Principle SUBMITrER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise as follows:
(d) Anesthetizing Location Receptacles. Receptacles for use in • ~o,..q - . ~ ;.~,Llc anesthetizing locations ,~d . . v . ' . L ~ . , , ~ i C v , ~ , ,,.., " ,'I~- . . . . . L'.,. ~,~a.~G,~,~ : V , ~ G ~ shall be listed for me use.
In . . . . ..q--.n;~,~Ll~ anesthetizing... (e) Receptacles and Amperage. Receptacles for...designed for use
o ;,;,,. . '2. . . . . . aLIc anesthetizing locations... (g) Delete (g) in its entirety.
SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMI'ITEE ACTION: Accept in Prindple.
1. Revise subpara. (d) and (e) as recommended. 2. Move subpara. (g) to new Annex 3.
COMMITI'EESTATEMENT: Correlate with Action on Proposal 99.25 (Log #274). NUMBER OF COMMI'Iq'EE MEMBERS ELIGIBLE TO VOTE: 17 (ESE), 10 (ANE) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 12 (ESE), 10'(ANE) NEGATIVE: Longhitano (ESE) NOT RETURNED: Berger (ESE), Ivecson (ESE), Norton (ESE),
Swisher (ESE)
24

N F P A 9 9 - - F 9 5 R O P
EXPLANATION OF NEGATIVE: LONGHITANO: If the commit tee believes tha t protective features
are needed to make a f lammable anesthet iz ing location safe, we should say so. Keeping the r equ i r emen t may be one of the factors which makes the use of f lammable anesthet ics undesirable or uneconomical .
(Log #CP50) Committee: HEA-ESE
99- 58 - (3-4.1.2.4(h)): Accept SUBMrITER: Technical Commit tee on Electrical Systems RECOMMENDATION: Delete 3-4.1.2.4(b). SUBSTANTIATION: This r equ i r emen t is covered unde r NFPA 70. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #53) Committee: HEA-ESE
99 -59 - (3-4.1.2.6(a) Exception No. 1): Reject SUBMITTER: Peter A. Larrimer, Dept. o f Veterans Affairs, Eastern Region RECOMMENDATION: Delete "toilets, bidets and wash basins" and rewrite as follows:
Exception No. 1: Pat ient beds shall no t be required to be considered wet locations. SUBSTANTIATION: The personnel protect ion requ i rements appear in NFPA 99 to conflict with NFPA 70, National Electrical Code, 1993 Edition, Article 210-8 (b) which identifies ba th rooms with a toilet, tub or shower to require the use of ground-faul t circuit in ter rupt ion protef t ion. Thei r definit ion of a ba th room is an area conta in ing a basin. These s tandards are both referenced by NFPA 101 for Heal th Care Facilities. COMMITI'EE ACTION: Reject. COMMITTEE STATEMENT: Commit tee is unaware of any problems in hea l th care facilities with regard to toilets, bidets and wash basins, and no t requir ing personal protective devices in the area in which they are located. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NEGATIVE: Longhi tano, Merrigan N O T RETURNED: Berger, Iverson, Norton, Swisher
EXPLANATION OF NEGATIVE: LONGHITANO: The submi t te r ' s proposal would change the
s tandard so that a pat ient in a hospital would have electrical protect ion at least comparable to that which be is requi red to provide for h imsel f in his home. Ordinary electrical receptacles are n o t permi t ted in a ba th room of a one-family house. This exception allows electrocution of a pat ient who drops a plugged-in electric shaver into the toilet or sink of the ba th room in his room.
MERRIGAN: Receptacles provided in pat ient ba th rooms should have ground-faul t circuit-interrupter protect ion for personnel per Section 210-8(b) (1) of the National Electrical Code. The most likely use of these receptacles is for personal g rooming or hygiene
~ urposes, as is the case in residential occupancies, and the same azards shou ld be addressed a n d similar protection provided. The
submit ter ' s proposal may no t be the best way to accomplish this but the concept should be supported.
(Log #279) Committee: HEA-ESE, HEA-ANE
99- 60 - (3-4.1.2.7): Accept in Principle Correlat ing Commit tee Note: Secretary Note: Sentence one of
cur ren t text includes word "not" and is thereby included in Commit tee Action since there was no in tent by Commit tee to change requirement- SI .~MITTER: Douglas S. Erickson, Amer ican Hospital Association RECOMMENDATION: Revise paragraph as follows:
An isolated power system is no t requi red to be installed in any pat ient care area_ ~xc,.pz o~ ~pcc~cd ;,J 124.1, "A~,~od,~5,~;,,g L,,cad,,uz." The system shall... SUBSTANTIATION: As the only reference to a r equ i r emen t for isolated power is in section 12-4.1.3.2 unde r requ i rements for a f lammable anesthet iz ing Location this reference needs to be deleted.
COMMrTrEE ACTION: Accept in Principle. Revise sentence 1 to read: "An isolated power system shall no t be required to be installed in
any pat ient care area excez_ep~t as specified in 3-4.. 1.2.6." COMMITrEE STATEMENT: With changes tn 12-4.1, reference to that chapter is no longer appropriate. Commit tee adds correct reference. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 (ESE), 10 (ANE) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 (ESE), 10 (ANE) NOT RETURNED: Berger (ESE), Iverson (ESE), Nor ton (ESE),
Swisher (ESE) COMMENT ON AFFIRMATIVE: YADIN: The sentence proposed by the Commit tee Action suggests
tha t "isolated power system shall be required . . . " ra ther than "shall no t be required. . ." It may be a type error only.
(Log #387) Committee: HEA-ESE
99- 61 - (3-4.1.2.7): Reject Staff Note: This proposal was originally submi t ted on NFPA 70,
Article 517, paragraph 51%19(e) (1) (New). It is being acted on here b y t h e Health Care Commit tee because Panel 17 referred it to NFPA 99. SUBMITTER: Thomas L. Curry, Scalfo Electric, Inc. RECOMMENDATION: Add new text as follows:
517-19(e) (1) In critical care areas used for invasive procedures isolated power systems shall be used. These isolated power systems shall be so des igned and installed as to mee t requ i rements of Section 51%160. SUBSTANTIATION: Due to the p reponde rance of electrical/ electric devices now used in the various invasive procedures . Considerat ion mus t be given as the total leakage currents available t h rough the mult iple parallel paths can exceed a dangerous level. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: ff a rea meets defini t ion of a wet location, t hen IPS may be required. Otherwise, commit tee is unaware of problems with cur ren t requirements . NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O V O T E : 17 VOTE ON C O M M I T r E E ACTION:
AFFIRMATIVE: 13 N O T RETURNED: Berger, Iverson, Norton, Swisher
(Log #390) Committee: HEA-ESE
99- 62 - (3-4.2.2.1): Reject Staff Note: This proposal was originally submi t ted on NFPA 70,
Article 517, paragraph 51%30(b) (4). It is being acted on here by the Health Care Commit tee because Panel 17 referred it to NFPA 99. SUBMITTER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the following sentences to the en d of t h ~ a r a g r a p h :
ere a fire p u m p is provided it shall be provided with a separate transfer switch dedicated solely for the fire pump. Jockey p u m p s and fire p u m p auxiliaries shall be permi t ted to be connec ted to the life safety branch transfer switch." SUBSTANTIATION: The purpose of this proposal is to hel t ) clarify the very confusing issue of how to electrically connect a fire p u m p . The first sentence is to clarify that separate transfer switches are to be provided for fire pumps. These transfer switches are typically suppl ied with the fire p u m p controller. The second sentence is to clarify which b ranch the fire p u m p auxiliaries such as the jockey p u m p shou ld be on. Since it is par t of the fire protect ion system it is my opin ion the jockey p u m p and auxiliaries should be allowed on the life safety branch. Most manufac ture rs do no t allow the auxiliaries to be connec ted to the same transfer switch as the fire p u m p and claim the fire p u m p will operate proper lywi thout the auxiliaries. In any event the p roper electrical b ranch for the fire p u m p auxiliaries to be connec ted to should be clarified. COMMI'[TEE ACTION: Reject. C O M M I T r E E STATEMENT: Jockey p u m p s are no t considered a critical piece of life safety equ ipmen t because its failure does no t compromise the water supply to the fire protect ion systems. Requi rements for fire p u m p s are covered by NFPA 20. NUMBER OF COMMITYEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 N O T RETURNED: Berger, Iverson, Norton, Swisher
25

N F P A 99 m F95 R O P
(Log #29) Committee: HEA-ESE
99- 63 - (3-4.2.2.2): Reject SUBMITTER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Revise 3-4.2.2.2(b) (4) to read "Hospital Communication Systems, where used for issuing instruction during emergency conditions. This shall include nurse call systems and telephone equipment".
Delete nurse call systems and telephone equipment from para-
~ rL~T3-4.2.2-2 (c)- ANTIATION: The purpose is to move nurse call systems and
telephone equipment from the critical branch to the life safety branch. These systems are avery small load on the electrical system and are almost always used for issuing instructions during emer-
ncy conditions. MMITI'EE ACTION: Reject.
COMMITYEE STATEMENT: Committee believes that the nurse call system and telephone equipment are primarily related to patient care and normal facility operation, and not to life safety. These systems can be included under subparagraph (b) (4) if they meet the criteria of being used for issuing instructions during emergency conditions. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO V()TE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #394) Committee: HEA-ESE
99- 64- (3-4.2.2.2(a)): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-31 (New). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99.
• SUBMI'FFER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the following paragraph: "
"517-31 Excepdon: Where fire pumps are provided, the fire pump(s) shalLbe connected with a dedicated transfer switch to the emergency electrical system." SUBSTANTIATION: Neither Article 517, Article 700, NFPA 20, NFPA 99, NFPA 101, or NFPA llO requires the f i repump to be on the essential electrical system. When provided the fire pump is essential to life safety and in the case of hospitals, should be required to have connections to normal and essential electrlcal power. COMMII'I'EE ACTION: Reject. COMMITTEE STATEMENT: It is not within the scope of the Health Care Facilities Project to state how a fire pump is to be connected. This is covered by NFPA 20. NUMBER OF COMMITI'EE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 12 NEGATIVE: Longhitano NOT RETURNED: Berger, Iverson, Norton, Swisher
EXPLANATION OF NEGATIVE: LONGHITANO: The submitter is correct. NFPA 20 specifies
HOW power transfer is accomplished but does not require THAT standby power is required. His proposal would require the fire pump to have standby power.
(Log #395) Committee: HEA-ESE
99- 65 - (3-4.2.2.2(b) (4), 3-4.2.2.2(c) (5),3-4.2.2.2(c) (7)): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-32(d). It is being acted on here by the Health Care Commtttee because Panel 17 referred it to NFPA 99. SUBMITI~R: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Revise text to read "(d) Communication Systems. Hospital communication systems, where used for issuing instructions during emergency conditions; this shall include nurse call systems and telephone equipment."
Delete nurse call systems and telephone equipment from 517- 33(a). SUBSTANTIATION: The purpose is to move nurse call systems and telephone equipment from the critical branch to the life safety branch. These systems are avery small load on the electrical system and are almost always used for issuing instructions during emer-
ncy conditions. MMITI'EE ACTION: Reject.
COMMITTEE STATEMENT: Thisproposal is the same as Proposal 99-63 (Log #29), and is thus rejectedfor the same reasons.
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #396) Committee: HEA-ESE
99. 66 - (3-4.2.2.2(b)): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-32(g) (New), et al. It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITrEITa Robert E. Snider, Sherlock, ~mith and Adams, Inc. RECOMMENDATION: Add the following paragraph to 517-32:
"(g) Automatically operated doors which might be used when evacuating the hospital." And delete 517-34(b) (6) which reads: "(6) Automatically operated doors."
SUBSTANTIATION: Most people are not familiar with how to exit through automatic doors when the power is off. This situation has the potential to induce panic and produce an effective block in the exit caused by non-moving people. The panic can also lead to shoving and pushing and injuries could result. The patient staff trying ~o evacuate the hospital with patients on stretchers could have similar problems. Thisproposal is intended to include automatic doors not in the path of egress such as in O.R. Suites but to exclude automatic roll-up doors such as in Warehouse area. COMMrlTEE ACTION: Reject. COMMITTEE STATEMENT: Thisproposal is the same as Proposal 99-67 (Log #30), and is thus rejectedfor the same reasons. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #30) Committee: HEA-ESE
99. 67- (3-4.2.2.2(b), 3-4.2.2.3(d)): Reject SUBMrrTER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the following paragraph to 3-4.2.2.2(b): "(7) Automatically operated doors which might be used when evacuating the hospital".
and delete 3-4.2.2.3(d) (6) which reads: "(6) Automatically operated doors". SUBSTANTIATION: Most people are not familiar with how to exit through automatic doors when the power is off. This situation has the potential to induce panic and produce an effective block in the exit caused by non-moving people. This can also lead to shoving and pushing and injuries could result. The patient staff trying to evacuate the hospital with stretchers could have similar problems. This is intended to include automatic doors not in the path of egress such as in O.R. Suites but to exclude automatic roll-up doors such in Warehouse area. COMMITTEE ACTION: Reject. COMMITrEE STATEMENT: A~ltomatic doors are required to be
~ le manually per NFPA 101, Life Safety Code. ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
26
(Log #397) Committee: HEA-ESE
99- 68 - (3-4.2.2.2 (b) (7) (new)): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-32(g) (New). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITTER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the following paragraph to the list of items to be on the Life Safety Branch:
517-32(g) Fire Pump Auxiliaries. The associated jockey pump(s) and auxiliaries for the fire pump. SUBSTANTIATION: Neither Article 517, Ardde 700, NFPA 20, NFPA 99, NFPA I01, or NFPA 110 requires the f i repump to be on the essential electrical system. When provided the fire pump is essential to life safety and in the case of hospitals, should be required to have connections to normal and essentialelectrical power. Since the jockey pump(s) and auxiliaries are a part of a proper sprinkler system, they should be allowed on the life ~afety branch.

NFPA 99-- F95 ROP
COMMITYEE ACTION: Reject. COMMITIT.E STATEMENT: See Committee Statement on Proposals 99-02 (Log #390) and 99-64 (Log #394), which address the same issues raised here. NUMBER OF C O ~ E MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMIT'FEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #398) Committee: HF_~-ES E
99- 69 - (3-4.2.`2.2(c)(9)): Accept Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-33(a) (9). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMD1"ER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Revise second sentence to read as follows:
"Single-phase fractional horsepower motors shall be permitted to be connected to the critical branch." SUBSTANTIATION: There are often small exhaust fans and similar equipment in labs and clinics that must be on essential power that are not interlocked with 3-phase motors. Presently the code would require these small motors to be on the equipment branch. Often these may he the only loads required on the equipment branch in that area. This requires establishing equipment branch power in the area for a very small amount of load. These equipment panels, transformers, etc., take up waluable floor space in a hospkal and cause the Owner undue expense in both floor space and electrical equipment. COMMITITAS ACTION: Accept. COMMITrEE STATEMENT: See Proposal 99-71 (Log #27). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #`26) Committee: HEA-ESE
99- 70 - (3-4.`2.`2.2(c)(8)): Reject SUBMIq['rER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Add the foilowing~
(x) Multi-purpose rooms used for Labor and Delivery. SUIK~TANTIATION: In the last few years there has been an increasing popularity in a single room used for Labor, Delivery, Recovery and Post-Recovery. These rooms are not listed in any of the above categories but should re uire critical power. COMMITI~E ACTION: Reject. q COMMITTEE STATEMENT: See Committee Action on Proposal 99-'22 (Log #3`20) which addressed this same issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #`27) Committee: HEA-ESE
99- 71 - (~-4.2.`2.2(c)(9)): Accept SUBMITTER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Revise second sentence to read as follows: "Single phase ffactionai horsepower motors shall be permitted to be connected to the critical branch". SUBSTANTIATION: There are often small exhaust fans and similar equipment in labs and clinics that must be on essential power that are not interlocked with 3-phase motors. Presently, the code would require these small motors to be on the equipment branch. Often, these may be the only loads required on the equipment branch in that area. This requires establishing equipment branch power in the area for a very small amount of load. These equipment panels, transformers, etc~, take up valuable floor space in a hospital and cause the owner undue expense in both floor space andelectrical equipmenL COMMI'ITEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMM/TTEE ACTION: AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #399) Committee: HEA-ESE
99- 72 - (3-4.2.2.2(c)(9)): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-33(a) (9). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITTER: John H. Schwab, Jr., Southeastern Wisconsin Electrical Inspectors Associaton RECOMMENDATION: Change subsection 9 to read as follows: "additional task illumination, receptacles and selected power circuits needed for critical patient care" (the remaining language and second sentence to be deleted). SUBSTANTIATION: Article 517-30(2) defines the critical branch of the emergency system of the essential electrical system of a hospital as "circuits limited to ~ patient care". Article 517-30 (3) defines the equipment system of the essential
electrical system as "supply major electrical equipment necessary for basic hospital operation .
This proposal would help to eliminate confusion as to what should be on "critical" and what should be on the "equipment" branches of hospital power.
Let's stop allowing more changes of faults occurring on the branch which would take out the rnmn critical distribution panel breaker, thus removing the remaining circuits from their power source. A single phase fractional horsepower exhaust fan motor does not
have any reason to be on critical, but should be on the equipment branch similar to a laboratory fume hood. COMMITrEE ACTION: Reject. COMMrITEE STATEMENT: 1. Committee believes certain exhaust fan motors are critical for effective facility operation and patient care, and wants them to be allowed to be connected to the critical branch.
2. Existing wording provides greater latitude for users in determin- ing what items are placed on the critical branch. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #400) Committee: HEA-ESE
99- 73 - (~4.2.2.2(c) (9)): Accept in Principle Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-33(c)(New). It is being acted on here by the Health Gate Committee because Panel 17 referred it to NFPA 99. SUBMITTER: John H. Schwab, Jr., Southeastern "¢VLsconsin Electrical Inspectors Assodaton RECOMMENDATION: Add the following language: "No heating, ventilating, air conditioning equipment or controls for them shall be connected to the critical branch of the emergency system." SUBSTANTIATION: Some contractors, englneers/designers, are trying to use the language in Article 517-]3(a) (9) to have air handling equipment and/or their controls be a part of the "needed for effective hospital operation." Equipment must remain ~ in the emergency equipment branch so that any motor and/or controls having a fault would not take out a critical surgery procedure. COMM1TIq~ACTION: Acceptin Principle. Add to 3-4.2.2.3(d) a new subparagraph (8) to read: "Controls for equipment listed in $-4.2.2.3."
Renumber existing subpara. (8) to subpara. (9). c o m m r l ' r F ~ STATEMENT: Committee believes that the controls. for such equipment belong on the Equipment System and should be so stated, as opposed to a prohibition under 3-4.2.2.2(c). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #GP54) Committee: HEA-ESE
99- 74 - (3-4.2.2.3(c) Note): Accept SUBMITTER: Technical Committee on Electrical Systems
[ RECOMMENDATION: Change "action" to "connection." SUBSTANTIATION: Editorial. Correlate with text of 3-4.2.2.3(c). COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17
27

NFPA 99-- F95 ROP
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #CP53) Committee: HEA-ESE
99- 75 - (3-4.2.2.3(c)(3)): Accept SUBMITTER: Technical Committee on Electrical Systems RECOMMENDATION: Add to existing wording the following:
"It shall be permitted to place such air systems on the critical branch." SUBSTANTIATION: To correlate with committee action on Proposal 99-37 (Log #221 ). COMMITTEE ACTION: A c c e p t NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #402) Committee: HEA-ESE
99- 76 - (3-4.2.4.1): Reject StaffNote: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517-50(b) (3), FPN (New). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITTER: Paul E. Devine, Advisory Committee on the Massafhusetts Electrical Code RECOMMENDATION: Add the following Fine Print Note:
(FPN): For the purposes of this section, the term "electrical life support equipment" includes electric hemodialysis and other equipment that, if inadvertently disconnected, could endanger the patients life. SUBSTANTIATION: The growing use of dialysis clinics which do not have backup emergency power has beefi the subject of concern in two distinct areas. (1) In the event of a power failure, attendants must have proper lighting to attend the manual hand-cranking of the hemodialysis equipment and (2) in the event that too few attendants are present to care for the operating equipment, then a real danger exists in terms of patients receiving care. The former is addressed in Section 517-50(b) (1) and needs no further examina- tion, the latter however, must be addressed since the possibility of loss of life ispresent. The issue of life support is addressed in Section 517-50(a) (2) quite properly but the issue of connection to essential system power must be addressed as proposed to ascertain compliance and uniform enforcement. COMMrI'rEE ACTION: Reject. COMMITTEE STATEMENT: It is not within the scope of the committee to determine whether a specific piece of electrical equipment is-or is not an "electrical life support equipment." f fa device meets the definition of "electrical life support equipment" (as defined in Chapter 2), the type of essential electrical system required is as listed in 13-3.3.2, 14-3.3.2, etc_ NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, lverson, Norton, Swisher
(Log #297) Committee: HEA-ESE
99- 77 - (3-5.2.1.3): Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revised as follows:
...under no-fault conditions between a reference point and exposed conductive surfaces that are likely to become energized ('..clad;;.ts ts.-G~..,I" cG.~;..ct~ .A', cc~vto~l,~ ) i'n a patient care vicinity. SUBSTANTIATION: The testing of all metal surfaces in a patient care vicinity is not cost effective or is it going to enhance the level of safety. This section has been interpreted to required the verification of cubicle curtain tracks, plumbing drains, window frames etc. Adding large surfaces likely to become energized should help provide further guidance to AHJ's and testing organizations. COMMITrEEACTION: Accept in Principle. Revised 3-5.2.1.3 to read as follows: " . . . under no-fault conditions between a reference point and
exposed fixed electrical equipment with conductive surfaces in a patient care vicinity."
Exception: Face plates of wiring devices."
COMMITFEE STATEMENT: Electrical equipment is considered the only equipment with surfaces that are likely to become ener-
~ zed. UMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #298) Committee: HEA-ESE
99- 78 - (3-5.2.1.4(a) & (b)): Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise 3-5.2.1.4 (a) to read:
(a) New Construction: ...the reference point and the grounding contact of eaeh-J~.f,r_C,g~ of all receptade~in th~ patient care vicinities. The...
(b) Delete in its entirety. SUBSTANTIATION: The need to check every receptacle is an excessive requirement. An overall sampling of grounding quality will indicate poor workmanship or inferior system design. With the NEC requirements for multiple pathways to ground, newly installed systems have significandy reduced the probability of an ineffective gtl~thOundingsystem. Deletion of subparagraph (b) is due to the fact
at all testing frequency requirements on existing system was removed from previous editions of NFPA 99. COMMITrEE ACTION: Accept in Principle. Add the following NOTE to submitter's recommendation: "NOTE: It is not the intent that each receptacle be tested. It is
intended that compliance be demonstrated through random testing." COMMITTEE STATEMENT: Clarify that random testing is intended. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 12 NEGATIVE: Longhitano NOT RETURNED: Berger, Iverson, Norton, Swisher
EXPLANATION OF NEGATIVE: LONGHITANO: This change places too much confidence in the
competence of the installer. At least once, when the new work is accepted by the owner, each and every device should be required to be tested and verified.
(Log #219) Committee: HEA-ESE
99- 79 - (3-5.2.1.6 (New)): Reject SUBMITTER: Hugh O. Nash,Jr., Smith Seckman Reid, Inc. RECOMMENDATION: Add FPN after the Exception:
It is not the intent of this section to require installation testing of each device and circuit Random testing of selected devices and circuits will likely reveal any system problems that might create harmful potential differences. System impedance can be deter- mined by observation and by testing selected circuits and devices. SUBSTANTIATION: None. COMMITTEE ACTION: Reject COMMITI'EE STATEMENT: Committee believes that reference to 3-5.2.1.6 is not correct. Committee has added a similar NOTE in 3-5.2.1.4 on the issue of random testing. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log#299) Committee: HEA-ESE
99- 80 - (3-5.2.3, 3-6.2.3.3): Accept SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: 3-5.2.3. delete entire section
3-5.2.3.3 delete entire paragraph SUBSTANTIATION: Newly manufactured GFCIs are very reliable and the need for testing has become unnecessary to assure the devices reliability. As the product reliability has improved drastically, a 12 month testing frequency is not cost effective. COMMITFEE ACTION: Accept NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17
28

NFPA 99-- F95 ROP
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 12 NEGATIVE: Longhitano NOT RETURNED: Berger, Iverson, Norton, Swisher
EXPLANATION OF NEGATIVE: LONGHITANO: f l i t is important to provide the protection
afforded by buying and installing a dewce like a GFCI, it is important to test that the manufacturer 's QC program d idn ' t let a defective device get out of the factory. Zero-defects manufacturing is not yet a reality.
(Log #197) Committee: HEA-ESE
99- 81 - ($-5.2.4.2(b)): Accept SUBMITrER: S tephen Benesh, Square D Company RECOMMENDATION: Add the followin.~ sentence: For a LIM circuit with automated serf-test and self-calibration capabilities. This test shall be per formed at intervals of not more than 12 months. SUBSTANTIATION: Microprocessor-conlxolled LIM's are now available with automated serf-test and self-calibration. These units will activate their visual and audible alarms if self-test and self- calibration are no t accomplished. For preventive maintenance purposes, a one year actuation of the test switch to verify LIM operation is acceptable.
NOTE: Supporting material is available for review at NFPA Headquarters. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #CP55) Committee: HEA-ESE
99- 82 - (3-5.2.4.2(c)): Accept SUBMITTER: Technical Committee on Electrical Systems RECOMMENDATION: Add the following sentence:
"For a LIM circuit with automated serf-test and self-calibration capabilities, this test shall be per formed at intervals of not more than 12 months." SUBSTANTIATION: Correlate with committee action on Proposal 99-81 (Log #197). COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #272) Committee: HEA-ESE
99- 85 - ($-6.2.3.1): Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise text:
Testing shall be per formed after initial installation, replacement, a n d / o r servicing of the device. Additional testing shall be per- formed at intervals def ined by documented performance data. Delete:
& l . ~ a | t v t l ~ t ~
C,:d,~l ~ ~ a-, , , , ,d,z
Delete:
SUBSJ~ANTIATION: Since other NFPA Codes require the use of "hospital grade" receptacles in pat ient care areas, the need to perform receptacle testing as prescribed in the 1993 edition is overkill. While many authorities having jurisdiction permit the use of the current exception others are continuing to mandate the 6 and 12 month frequencies. With the higher grade receptacle in place, we are no t f inding problems with ground pin continuity or blade tension, and of course we have never seen a receptacle switch its polari tywithout work being done to the system. It is time to permit the health care organizations to de termine the frequency of testing versus allowing them to use an exception to the rule. COMMITTEE ACTION: Accept in Principle.
1. Make sentence one ofsubmit te r ' s recommendat ion subpara- graph (a).
2. Make sentence two of submitter 's recommendat ion subpara- ~ a p h (b), and add the following Exception:
Exception'. Receptacles. no t listed as hospital-grade shall be tested at intervals no t exceeding 12 months." COMMITTEE STATEMENT: 2. Take into consideration older, non-listed receptacles that may still be in use. NUMBER OF COMMITIT.E MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NEGATIVE: Housser, Longhitano NOT RETURNED: Berger, Iverson, Norton, Swisher
EXPLANATION OF NEGATIVE: HOUSEP~ I agree with A.J. Longhitano. Second sentence of
proposal is not meaningful with the revised wording of the first sentence and the exception added by committee action 10/11 August 1994.
The original exception was written to increase the interval between testing if documentat ion supported such a decision.
LONGHITANO: I don ' t know what the requi rement means and nei ther will any enforcer. Who will collect the "documented performance data" and how will it be documented? Will it be based on performance data for ALL hospital grade receptacles that are in service, or for ALL receptacles of one manufacturer, or for receptacles of one manufacturer in one hospital in one particular environment in one hospital, etc.? How often will a given receptacle get checked?
(Log #275) Committee: HEA-ESE
99- 84 - (3-6.2.5.2): Accept SUBMITI~R: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Delete entire Section 3-6.2.5.2. SUBSTANTIATION: The need for this section is questionable as there is no requi rement for conducting a test on an existing system. As renovations and alterations are performed, the newly constructed area or systems will need to mee t Section 3-5.2.1.6 for the initial acceptance test, but beyond that, no o ther tests are required. COMMITIT~ ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITIT~ ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #220) Committee: HEA-ELE, HEA-ESE
99- 85 - (3-6.2.3.2, %5.1.3.4): Accept in Principle in Part SUBMrFI~R: Hugh O. Nash,Jr., Smith Seckman Reid, Inc~ RECOMMENDATION: Delete entire text of 3-6.2.3.2 from chapter 3 andp l ace this material in chapter 7. SUBSTANTIATION: The requirements for test ingexist ing systems was deleted f rom Chapter 3 in the 1995 edition. Therefore, the test criteria is no longer needed. However, 7-5.1.3.4 references 3-6.2.5.2. Therefore, this material must be added to Chapter 7. This assumes that the committee responsible for Chapter 7 still feels like this type of equipment testing is required. COMMITrEE ACTION: Accept in Principle in Part.
Delete last sentence of 7-5.1.5.4 ("After installat ion. . .") , and make it new Exception No. 4 under 7-6.2.1.2.
Reword text to read: "Exception No. 4: After installation of fixed equipment, it shall be
tested periodically in accordance with 3-5.2.1.3, and meet the following criteria:
(1) 500 m v f o r general care areas. NOTE: The 500 mV limit is based on physiological values. Since
the actual voltages normally measured in m o d e m consu'uction are usually less than 10 mV with nominal construction, voltages exceeding 20 mV may indicate a deteriorating condition and should be investigated.
(2) ,lO tay lor critical care areas. NOTE: The 40 mV limit is based on physiological values. Since the
actual voltages normally measured in m o d e m construction are usually less than 10 mV with nominal construction, voltages exceeding 20 mV may indicate a deteriorating condition and should be investigated."
Delete 3-6.2.5.2. COMMITrEE STATEMENT: Committee desires to retain the testing of fixed equipment using me thod outl ined in Chapter 3.
Accept submitter 's recommendat ion for $-6.2.3.2 NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 (ELE), 17 (ESE)
29

NFPA 99-- F95 ROP
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 11 (ELE), 13 (ESE) NOT RETURNED: Berger (ELE, ESE), Iverson (ESE), Norton
(ESE), Swisher (ESE)
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, ~lorton, Swisher
(Log #335) Committee: HEA-ESE
99- 86 - (3-6.2.3.2(c) (New)): Reject SUBMITrER: Saul Aronow, Technology in Medicine Inc RECOMMENDATION: Add a new subsection (c):
(c) The acceptability of existing grounding systems shall be tested
~ eriodically. UBSTANTIATION: 3-6.2.3.2 (a) and (b) l?rovide criteria for the
acceptability of existing grounding systems, lout nowhere does it say what to do with the criteria. Periodically is a vague term but it means that over some period, perhaps 5 years, it is reasonable to verify that nothing has ha ppened to the grounding system. This correlates with %5.1.3.4 which discusses fixed equipment but also leaves the time unstated. C O M M r r r E E ACTION: Reject. C O M M I T ~ E STATEMENT: It was, and still is, committee opinion that periodic testing of the grounding system is no t necessary because committee has observed that ,grounding integrity does no t decrease unless the wiring system is modified. See Committee Action on Proposal 99-85 (LOg #220). NUMBER OF COMMITI'EE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON C O M M r I T ~ ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #270) Committee: HEA-ESE
99- 87 - (3-6.2.4.1): Reject SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Delete existing paragraphs (a) & (b) and replace with text extracted f rom NFPA 110 Section 6-4.
6-4 Operational Inspection and Testing.. 6-4.1"_ Level 1 EPSS, including all appur tenant components , shall
be inspected weekly and shall be exercised under load at intervals o f no t more than 30 days.
Exception: If the generator set is used for standby power of for peak load shaving, these uses shall be en tered in written record and may be substituted for scheduled operations and testing of the generator set if the appropriate data are recorded.
6-4.2 Generator sets in Level 1 service shall be exercised under operating temperature conditions and at a capacity no t less than fifty percent of the total connec ted EPSS load (not less than thirty percent of EPS nameplate rating and preferably at least fifty percent of EPS nameplate rating) at least once monthly for a minimfim of thirty minutes. Consideration shall be given to more stringent conditions as r ecommended by the individual energy converter manufacturer.
6-4.2.1 Equivalent loads used for testing shall be automatically replaced with the emergency loads in case of failure of the primary source.
6-4.$ Load tests o f generator sets shall include complete cold starts. 6-4.4 Time delays shall be set as follows: (a) Time delay on start: Minimum 1 second. Exception: Gas turbine cycle: 0.5 second minimum. (b) Time delay on transfer to emergency: no min imum required. (c) Time delay on restoration to normal: 5 minutes minimum.
(See A-4-2.4.7.) (d) Time delay on shutdown: 5 minutes minimum. 6-4.5 The monthly test of a transfer switch shall consist of
electrically operating the transfer switch from normal position to alternate position and return.
6-4.6* EPSS circuit breakers for Level 1 usage, including main and feed breakers between EPS and the transfer switch load terminals, shall be exercised annually.
Exception: Medium and high voltage circuit breakers for Level I usage shall be exercised every six months and tested under simulated overload conditions every two years.
6-4.7 The routine maintenance and operational testing program shall be overseen by a properly instructed individual. SUBSTANTIATION: The installation, testing and maintenance of the alternate power source and transfer switches is the jurisdiction of NFPA 110. NFPA 99 should therefore be exacting this material and no t be in cordlict as is currently the situation. COMMITTEE ACTION: Reject. COMMITTEE STATEMF_2qT: Committee believes that current requirements in NFPA 99 are necessary to insure adequate perfor- mance of the generator in an emergency.
(Log #271) Committee: HEA-ESE
99- 88 - (3-6.2.4.2(a)): Accept in Principle SUBMITTEPa Douglas S. Erickson, American Hospital Associ_ation
I RECOMMENDATION: Revised text: (a) Circuit Breakers. Main and Feeder circuit breakers shall be
visually inspected ~ annually and a program for periodically exercising the components shall be established. SUBSTANTIATION: The requirement for exercising main and feeder circuit breakers has presented hospitals with many problems. Many of our main service breakers are of an ampadty requiring the manufacturer or testing agency to remove them and conduct a bench test at a remote testing facility. To merely require the exercising of these breakers annually may put an organization at extreme risk if the breaker fails to re-energize and adequate contingency plans are no t in place for its immediate replacement. We agree that an annual inspection of these breakers is in order so proper cleaning and evaluation of set points is performed, but disagree with an annual requi rement for exercising. Let the health care organization work out an exercise program with the breaker manufacturei- or local service company to determine the exercise per iod and maintenance requirements. COMMITrEE ACTION: Accept in Principle.
I In submitter 's recommendat ion, delete "visually." Retain existing NOTE. COMMITrEE STATEMENT: Committee believes that more than 'Msual inspection" is necessary. "Inspection" can include touching, smelling, etc. in addit ion to visual. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETIJRNED: Berger, Iverson, Norton, Swisher
(Log #46) Committee: HEA-PIP
99- 89 - (Chapter 4): Accept in Principle SUBMITTER: Thomas A. Pilch, Wassaic Developmental Disabilities Services Office RECOMMENDATION: Revise text:
A. Reformat Text. 1. Include vacuum in medical gas section. 2. Place all similar materials in appropriate groups. B. Rewrite format so it is more easily used and understood.
Current working makes it hard to follow and very confusing. SUBSTANTIATION: A. 1) In almost all cases, vacuum and medical gases are installed or p lanned at the same time they're designed. It would be much easier to use if the two standards were together in text.
2) From a contractor 's and installers' standpoint, it is very confusing to thumb back and forth through the text to determine what standard applies.
B. The standards differ for each type of facility so the types of facilities should be clearly def ined first and then the specific requirements be def ined for each facility. COMMIT1T, E ACTION: Accept in Principle. • Se.e Committee Action on Proposal 99-99 (Log #CP58). COMMITTEE STATEMENT: Committee believes Proposal 99-99 (Log #CP58) meets the intent of the submitters recommendat ion. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON C O M M I T r ~ ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #49) Committee: HEA-PIP
99- 90 - (Chapter 4): Accept in Principle SUBMITTER: Barry Green, Newark, DE RECOMMENDATION: Revise text:
1. Arrange format so that medical vacuum is included in gas section.
2. Put all Type I Facility information together;, Type 2 together; Lab.
30

N F P A 9 9 m F 9 5 R O P
[ 3. Set standards for stand alone ambulatory surgery centers. SUBSTANTIATION: 1. All Bidding for Medical Gases, as well as specs and drawings are done at the same time.
2. Present information is in random order and not very easy to use. Grouping together would be much easier to f ind information.
3. Arab. care or Surgery centers do no t require all the same standard as hospitals - especially master alarm system. COMMITrEEACTION: Accept in Principle.
1. & 2. Accept in Principle. See Committee Action on Proposal 99- 99 (Log #CP58).
[ 3. Accept. COMMITYEE STATEMENT: 1. & 2. Proposal 99-99 (Log #CP58) addresses issue.
3. See Committee Action on Proposal 99-97 (Log #CP5). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #52) Committee: HEA-PIP
99- 91 - (Chapter 4 and Related Chapters): Accept in Principle SUBMrITER: Peter Winders, NewYork, NY RECOMMENDATION: Revise text:
Change format to eliminate need for cross-referencing between chapters. Include all requirements by health care facility type, under their own headings. SUBSTANTIATION: 1. Fmdin~ relevant material for a given application requires more time man is necessary. COMMITYEEACTION: Accept in Principle.
See Action on Proposal 99-99 (Log #CP58). COMMITTEE STATEMENT: Committee Action on Proposal 99-99 (Log #CP58) addresses the issue of cross referencing within Chapter 4, and makes document more user f r iendly . NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #98) Committee: HEA-PIP
99- 92 - (Chapter 4): Correlating Committee Note: Because of the Technical Correlat-
ing Committee action of proposal 99-19 (Log#CP81) [i.e., veterinary facilities would be ou~ide the scope of NFPA 99, this
~ roposal is rejected. UBMITTER: David B. Mobile, Medical Engineering Services, Inc.
RECOMMENDATION: Add new text • Propose that we include veterinary facilities under either (old) type I or (old) Type IL SUBSTANTIATION: Most of the requirements in 99 are for fire safety when constructing and using medical gases. Just because the patient has hair all over his body is no reason no t to protect the staff members that will be using the gases on the patient.
Many research facilities use very expensive animals and they would not like to loose those animals due to problems with the medical gases.
Any veterinary facility that pipes medical gas into rooms for use by human on animals should follow the requirements for use of these
es on humans as currently set up. MMITrEEACTION: Accept in Principle.
1. Revise 1-1 to include reference to veterinary facilities. 2. Revise 4-1 to include reference to veterinary facilities. 3. Create new Chapter 18, Veterinary Facilities, using the current
style of NFPA 99 for text (re, 15-3.4). COMMITTEE STATEMENT: Veterinary facilities present similar fire and related hazards to that of other health care facilities covered by NFPA 99. Thus, they should be included in the document . NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log#211) Committee: HEA-PIP
99-93- (Chapter 4): Reject' SUBMITrER: Dennis Ehrlacher, Whitehall , PA RECOMMENDATION: 1. a) Medical Gas contractors should be required to pull a permit when doing work.
b) Installers should be l icensed before being able to work on a medical gas system. SUBSTANTIATION: 1. a) Contractors should be required to get a ptPhermit to perform work on Medical Gas systems. This would insure
at all work is inspected. Too much work is being pu t in a no t being inspected. This permit could be set up similar to a plumbing permit. AFire Marshall or designated inspector could then oversee all work.
b) Installers should have to be tested and certified to do Med. Gas work. This is one of the most critical piping areas and there is no procedure to insure the qualified people are installing the system. I have seen work being done by people who did no t know that a purge was needed to braze. COMMITTEE ACTION: Reject. COMMITI~E STATEMENT: Recommendat ion is outside the scope of a voluntary standards organization to require permits to conduct business. NUMBER OF COMMITTEE MEMB~.~5 ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #366) Committee: HEA-PIP
99- 94 - (Chap te r 4): Accept in Principle SUBMITrER= Dennis Murray, American Hospital ~$ssociation RECOMMENDATION: Relocate all NOTES to related appendix sections. $ ~ A N T I A T I O N : Notes contain questionable supportive information. Enforcing bodies exwact notes and utilize as minimum requirements. Notes are not user friendly and create confusion. COMMrITEE ACTION: Accept in Principle.
Move all NOTES in text to Appendix. (NOTE: Notes in Figures and tables are not to be moved.) COMMITrEE STATEMENT: Notes in Figures and Tables are necessary for understanding, and are not par t of requirements NUMBER OF COMMrrTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: lfi NOT RETURNED: Fan, Shoemaker
(Log #377) Committee: HEA-PIP
99- 95 - (Chapter 4): Reject S U B - - R : D.A. McWhinnie, Jr., Mechanical Dynamics, Inc. RECOMMENDATION: Delete:
All present references to Waste Anesthetic Gas Disposal - WAGD; and "suggested" 4-9.
New: Add under Chapter 4 heading: Note 4: For Waste Anesthetic Gas Disposal Systems (WAGD) see
Chapter 5 Environmental Systems. SUBSTANTIATION: Not withstanding the error in Chapter 5, 5- 4.1.6 it is dea r that Waste Anesthetic Gas Disposal (WAGD) systems were properly included in the requirements ' text of Chapter 5 Environmental Systems - which was duly approved by the appropri- ate committees; circulated for public comment; approved by the Association; and by the Standards Council for publication - without minority reports. WAGD systems are in the proper Chapter (5) for an Environmental System - which is no t a "piping" system, nor does it carry a "gas" (in NFPA context /defini t ion, and intent in its action above).
To remove WAGD from i t sp roper Chapter 5 requires valid substantiation - andrefu ta t ion of the many valid substantia-
tions for WAGD location in Chapter 5 - as published in NFPA Code 99 Handbook (some of which are listed below).
The present circumstance of many references to WAGD in Chapter 4, without any criteria, requirements, performance guidelines, warnings/cautious as to hazards, etc. has resulted in an industry field-day (voluminously documented) with heavy expense to facilities - with no alternatives to facilities.
31

N F P A 9 9 - - F95 R O P
As Code 99 contains no clear warnings, or cautions (which are "hidden" in the little read Handbook), many facilities are unin- formed - as they also are regarding safer, effective and often less costly alternative methods. The above is largely a result of Code 99, Chapter 4 misleading
PAlermlssive/encou raging/inducing language. I quotations below are from Code 99 requirements and/or
Handbook substantions: AWAGD system is no more a "Gas System" than the Chapter 5
ducted exhaust systems from laboratories, paint spray booths, areas with toxic fumes, building "5-4.1 Ventilation- ", and other environ- mental ducted systems.
If WAGD environmental s~tems "for the protection of Operating Room staff..." (not for patients, who are administered anesthetics intentionally) are included in Chapter 4, then the systems listed in the paragraph last above should also be in Chapter 4. By that same logic WAGD belongs in (;hapter 5, as NFPA published
documentation states: '~AGD is an environmental control system..." (Exact title of
Chapter 5.) '~NAGD is a ventilation function..." ~WAGD ...will appear in Chapter 5." (It has been in Code 99 since
1982.) "WAGD does not fall within the scope (of Chapter 4)." "WAGD is not a function of a medical-surgical vacuum system
(MSVS) ." "WAGD is for protection of operating room staff," "MSVS (medical-surgical vacuum system) is not to be used for
nonmedical or nomurgical applications." Chapter 5 Scope covers all "environmental systems used within
health care facilities." Code 99, Section 12-4.1.2 "Requirements for ALL Anesthetizing
Locations." while its next paragraph "19-4.1.2.1 Ventilation" - "shall conform to (Chapter 5)". The NFPA Technical Committee on Medical-Surgical Vacuum
Systems in Hospitals had voted overwhelmingly twice (once a single vote short of unanimous) to delete the very misleading references to WAGD in Chapter 4. These votes foliowedthe only NFPA research done (within the Vac. T/C) - after uncovering voluminous documen- tation (in NFPA files) of potential patient hazard in the use of MSVS for WAGD.
Present Chapter 4, and "suggested" 4-8.1.2, 4-8.1.2.2 and 4-9.1.2 continue to induce the use of vacuum pumps, and the MSVS system for WAGD. The following is a partial list of documentation concerning the use of MSVS for WAGD. Hazards. "...the maximum safe negative pressure for the patient
(0.5 cm H20 is 0.0012 percent of the minimum degree of vacuum (required) in the MSWS (-12Hg)" or "829.3 times the maximum safe degree of negative pressure...for the anesthetized patient" WAGD applied to MSVS affects "anesthesia and patient safety." "...risks to patients." "Mixing the two creates avery onerous safety problems." (MSVS
and WAGD) "The negative .pressure differential is vast..." "...pressure swings can seriously affect patients." "There is a great disparity in requirements between the two uses." At least three involved Anesthesiologists (NFPA and ANSI
Committee Chairmen) agree to the documented hazards in the use of MSVS for WAGD. MSVS is not to be used for WAGD"...particularly because of the
risks to patients." Exposure of a patient's breathing circuit to the MSVS degree of
vacuum "would not enable patient to breathe and thus kill patient." (Reported to NFPA HCFr/C, June 19,1989). Users are exhorted "to avoid exposing the breathing circuit to any
pressure less than atmospheric." (under score added.) - (NFPA 99, A.5-4.1 and 2 Wentilation of Anestheflzing Locations."/ANSI Z79, SC,-4 - WAGD Scavenging and Disposal.)
"Each scavenger (a device intended to reduce the degree of NFPA Code 99, Chapter 4 required degree of vacuum) tested failed to function safely when wall suction (MSVS) was applied to the exhaust port." (NFPA HCF Handbook, Pg. 288, Ref. 1.) (This reference cites four potential traumas if "wall friction" (MSVS) transverses a failed scavenger.)
"...in normal use some scavenging apparatus, even when operating properly, can alter the normal characteristics of an anesthetic breathing machine..." (ANSI N45.2). Although the Code 99 Vacuum committee has conscientiously....? A major "Problem" (Item 4 on this Proposal Form) is confusion
and/or misinterpretation in the field, resulting from the insertion in Chapter 4 of many permissive and persuasive references to WAGD throughout the MSVS document This enhances the proprietary advantage, and leaves no incentive to com/plicate the process by mentioning the alternates which are effective, safer and less costly (but not mentioned in Code 99). The preferred methods are:
1. Passive/ambient differential (through wall, window, ceiling or floor).
2. Non-return portion ofvenfllaflon exhaust duct. 3. Fan/blower, dampened plenum, duct system.
A current action within NFPA illustrates perfectly the problem of confusion that results from the combining of disparate technologies. A Code 99, Chapter 4 proposal has been filed recently combining
(in the proposal) "Piped Vacuum System" with ~WAGD'. A breathing machine discharge (negative or positive pressure) to a
WAGD system could neither collapse nor burst a paper tube. The maximum allowable breathing machine pressure range is -0.5
cm H20 to +10 cm H20 (+15 H20 ) @ fault condition). This would subject the WAGD negative pressure distribution system
to -0.01446847"Hg. This figure applies to any breathing machine in any facility
anywhere in the world. For NFPA HCF purposes this condition of a fluid is not a "vacuum". Any WAGD system that requires a "Piped System" is improperly
designed. Restudy Reference 1, Pg. 288, NFPA HGF Handbook, 1993 for
hazards in venting anesthesia gases to vacuum. I believe the function of any enforceable document should be
reflected in its rifle. In this case of Waste Anesthetic Gas Disposal I see it as the perfect fit - for the function of "Disposal" of '%gaste".
As important, if not more so, I feel that from the perspective of Administration Chapter 5 responsibility for the facility environment is almost always in the Department of Facility Management, The WAGD function is not a medical one - as is Ghapter 4 - and
WAGD being in Ghapter 5 is consistent with NFPA's published commitments over several years (listed on the previous page). The only reason anyWAGD System would need "piping" would be
because of a high degree of vacuum - and that implies a vacuum pump. With aWAGD system which operates efficiently, and safely, @ -0.5
cm H20 -as any of the three above would - a pump and piping is unnecessary, adds a hazard, reduces the kitty, increases operating and maintenance costs, takes up space, and is noisier. COMMIIq'EE ACTION: Reject. COMMITTEE STATEMF2qT: 1. Over half the WAGD systems in use in this country are connected in some fashion to the MSVS in anesthetizing locations, or are dedicated systems that involve the use of vacuum systems.
2. The use of piped vacuum systems for WAGD is an acceptable method, and thus falls within the scope of Chapter 4.
3. The T/CC on Health Care Facilities has been charged this committee to review this issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrlTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP4) Committee: HEA-PIP
99- 96 - (4): Accept SUBMITIXR: Technical Committee on Piping Systems RECOMMENDATION: Add the following new material on Waste Anesthetic Gas Disposal:
1. Add following new terms and definitions in 2-2: Evacuation -Waste Gas. See definition of ~raste Anesthetic Gas
Disposal." Scavenging - Waste Gas. See definition of "Waste Anesthetic Gas
D~pasosal." te Anesthetic Gas Disposal (WAGD). The process of capturing
and carrying away gases vented from the patientbreathing circuit during the normal operation of gas anesthetic equipment. WAGD Interface. A device provided on the anesthesia gas machine
that connects the WAGD network to the patient breathing circuit NOTE: Interfaces are provided with overpressure, underpressure,
overflow and undertow compensation to ensure the breathing circuit is isolated from the WAGD system.
2. Revise 4-8.1.2 to read as follows: 4-8.1.2 Waste Anesthetic Gas Disposal. (WAGD) 4-8.1.2.1 General. WAGD systems shall be designed and imple-
mented after consultation with the medical staff having knowledge of the requirements to determine the type of system, number and placement of terminals, and other required safety and operating devices.
NOTE 1: A functioning WAGD System will permit the facility to comply with occupational safety requirements by preventing the accumulation of waste anesthetic in the work environment
32

NFPA 99- - F95 ROP
NOTE 2: WAGD using the HVAC (heating, ventilation and air condit ioning) are no t within the scope of this chapter.
4-8.1.2.2 Dedicated WAGD Vacuum Producers (a) The WAGD Source shall consist of a mult iple producers
(vacuum pumps , blowers, fans, etc.) tha t alternately or simulta- neously on d e m a n d serve the WAGD system.
(b) WAGD Source. Producers used exdnsively for WAGD use shall be des igned of materials, and shall use lubricants where needed , tha t are inert in the presence of oxygen, ni t rous oxide, and ha logena ted anesthetics.
(c) WAGD plants shall comply with 4-8.1.1 (a) t h r o u g h (e). (d) The WAGD vacuum producer shall be located to comply with
4-8.1.1 (h). (e) The exhaus t for the WAGD system shall comply with 4-8.1.1 (i). 4-8.1.2.3 Medical-Surgical Vacuum Source used for WAGD (a) A Medical-Surgical Vacuum Source complying with this
s tandard shall be permi t ted to be used for WAGD. (b) Explosion Hazard. Flammable anesthet ic or o ther f lammable
vapors shall be di luted below the lower f lammable limit pr ior to disposal into the medical-surgical vacuum system.
NOTE 1: For fur ther informat ion, see Appendix A-5-4.2 on ANSI Z79.11, and Appendix C-12.1.3.1 on f lammable anesthet ic agents.
NOTE 2: Flammable and nonf lammable gases are known to be incompat ible with some seals and piping used in medical-surgical vacuum systems. If waste anesthet ic gas disposal is to be included as par t of the medical-surgical vacuum system, it should be recognized tha t dais activity may cause deter iorat ion of the vacuum system. The station inlet pe r fo rmance tests out l ined in 4-11.2.1.4 are extremely impor tan t in main ta in ing the integrity of the medical-surgical vacuum system, and they should be made at more f r equen t intervals if waste anesthet ic gas disposal is included in the vacuum system.
4-8.1.2.4 Venturi Driven WAGD (a) Where a venturi within the station inlet is used to produce
WAGD vacuum, the ventori shall no t be user adjustable (ie. shall require the use of special tools).
(b) Venturi WAGD shall be p roduced us ing air or an iner t drive gas.
(c) Drive air for Venturi WAGD shall no t come f rom the medical air system.
3. Revise 4-9.1.2 to read as follows: 4-9.1.2 WAGD System Distribution Network. 4-9.1.2.1 WAGD Distribution Network (a) WAGD Networks shall provide a WAGD inlet at each anesthe-
tizing location. (b) WAGD Distribution Networks shall be const ructed of corrosion
resistant materials appropriate for use with oxygen, ni trous oxide, and ha logena ted anesthet ics in the concentrat ions encoun te red in the anesthet ic brea th ing circuit.
(c) Distribution Network Support . WAGD Distribution Networks shall be suppor ted directly f rom the bui lding structure by pipe hooks, straps, bands or hangers suitable for the size a n d weight of the network material. Supports shall be placed to ensure that suppor t is provided at the joints , and placed at intervals which ensure adequate suppor t for the for the size and weight of the network material.
(d) The Distribution Network shall be provided with balancing valves, dampers , etc. appropria te to balance the flows and pressures th rough the network to those requi red by the WAGD Interfaces in use with. the facility's gas anesthet ic machines .
4-9.1.2.2 WAGD Valves and Dampers . (a) Where valves are provided, they shall be labeled by means of
durable tags, nameplates, or labels: CAUTION
WASTE ANESTHETIC GAS DISPOSAL VALVE DO NOT CLOSE EXCEPT FOR SERVICE
THIS VALVE CONTROLS WAGD TO... (b) Dampers. 4-9.1.2.3 WAGD Inlets. (a) Each station inlet for WAGD shall be of a type appropriate for
the flow and vacuum level required b y t h e WAGD Interfaces in use with the facility's gas aesthetic machines . They shall be located to avoid physical damage to the inlet, ff the inlet can be disassembled for service, each c o m p o n e n t shall be legibly marked "WAGD" or similar. WAGD Inlets shall be no t in terchangeable with o ther systems, including medical-surgical vacuum.
4-9.1.2.4 WAGD Alarms. (a) Alarms or o ther automat ic mechan i sms shall be provided to
inform the user t h a t the WAGD system is operational. 4-9.1.2.5 WAGD System Distribution Network Installation. (a) Assembly. The WAGD Network-shall be assembled us ing such
materials and me thods as will assure the network is free of leaks unde r operat ing vacuum levels.
(b) Labeling. The WAGD Network shall be identified by appropri- ate labeling such as WASTE AESTHETIC GAS DISPOSAL. Such labeling shall be by means of metal tags, stenciling, s tamping or
33
adhesive markers in a m a n n e r that is no t readily removable. Label ing shall appear on the network at intervals of not less than 20 ft (O.1 m) a n d at least once in or above each room and each story traversed by the piping. Arrows (when used) shall po in t f rom the terminal to the vacuum producer .
4. Inset new 4-10.2, and r e n u m b e r existing 4-10.2 and 4-10.3 to 4- 10.3 and 4-10.4:
4-10.2 WAGD System Per formance Criteria and Test ing 4-10.2.1 WAGD DisUdbution Networks shall be sized to deliver
vacuum at a pressure and flow appropr ia te to the WAGD interfaces in use with the facility's gas anesthet ic machines .
4-10.2.2 Include WAGD systems in all cross-connection test ing per 4-10.1.2.4.
4-10.2.3 Vacuum and flow at each terminal inlet shall be as required by the WAGD Interfaces in use with the facility's gas aesthetic machines . The network shall be sized, and the vacu u m producer selected, to provide this level of vacuum and flow simultaneously at all terminal inlets when all inlets are in use.
4-10.2.4 Where required, the network shall be adjusted or balanced prior to c o m m e n c i n g test ing or as part of the testing process.
4-10.2.5 Test ing shall be pe r fo rmed as appropriate to ensure that each inlet is capable of providing vacuum and flow as requi red by the WAGD Interface. At a m i n i m u m , the following tests shall be performed:
(a) Start the vacuum producer and assure it is operat ing correctly. (b) O p e n one inlet per r oom or all inlets to allow a flow equal to
that required by the interface. (c) W h e n all inlets are flowing, test each inlet in succession for
flow and vacuum level. If the inlet is within the requi red limits for the interface, it may be considered ready for use.
4-10.2.6 Venturi drive systems shall follow the requi rements of 4- 5.1 except 4-5.1.3.6 and 4-5.1.3.9 t h rough 10.
5. Insert new 4-11.2.3 to read as follows: 4-11.2.3 WAGD system. 4-11.2.3.1 Maintenance. The facility shall establish rout ine
preventative ma in tenance p rograms applicable to the WAGD system. 4-11.2.3.2 Performance Tests. The facility shall establish rout ine
testing programs to assure the WAGD system performs as required in 4-10.2. SUBSTANTIATION: The 1993 revision cycle left WAGD for fur ther study. The proposal a t tempts to resolve the outs tanding issues in the subject. C O M M r r r E E ACTION: Accept. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP5) Committee: HEA-PIP
99- 97 - (Chapters 2,4,12,13,14,15,16 (restructure)) : Correlating Commit tee Note: The Technical Correlat ing Commit-
tee (TCC) directs the T / C on Piping Systems to reconsider the definit ion por t ion of the proposal not ing that the proposed definit ions are beyond the scope of the T / C on Piping Systems, and involve the entire document . The TCC fur ther notes that the T / C on Piping Systems can define characteristics of care for Chapter 4, and its applicability to Chapters 12 to 17. The TCC supports the concept of establishing needs for e q u i p m e n t based on the character- istics of the pat ient populat ion and the care rendered. SUBMITTER: Technical Commit tee on Piping Systems RECOMMENDATION: (In Chapter 2)
(1) Revise the definit ion of "Hospital Facility" by insert ing the following new sentence between the first and second sentences as follows. "Trea tment a n d o r p r o c e d u r e s may render the pat ient incapable of taking action of self preservation u n d e r emergency care conditions. Anesthesia and ventilation suppor t are provided."
(2) Remove the word "shall" in the s e c o n d s e n t e n c e of the definit ion of "Hospital" and revise the word to include to be "includes" The definit ion would t hen read as follows: (The new words appear
under l ined. ) Hospital Facility. A building or part the reof used for the medical,
psychiatric, obsteu-ical, or surgical care, on a 24-hour basis. T r ea tmen t and or nrocedures mav render the nat ient incanable of taking action of sefforeservat ion unde r emergency care conditions. Anesthesia and venti lat ion suvvo r t are provided. Hospital, wherever used in this standard, ~ ' g e n e r a l and specialty hospitals, menta l hospitals, tuberculosis hospitals, chi ldren 's hospitals, an d any such facilities providing inpat ient care. (ES, PS)

NFPA 99--- F95 ROP
(3) Revise the definition of "ambulatory health care center" as follows: (The new words are underl ined.) Ambulatory Heath Care Center. A building or part thereof used to provide services or t reaunent to four or more patients at the same time and meet ing either (1) or (2) below. Such facilities are not designed to orovide overnight stays for p~tients.
1. ~l'hose facility that prowYde, on an outpat ient basis, t rea tment and procedures for patients that would render them incapable of taking action for serf-preservation under emergency conditions without assistance f rom others. Examples include but are not restricted to hemodialysis units or freestanding emergency medical units.
2. Those facilities that provide, on an outpat ient basis, surgical t rea tment ~ for patients that would render them incapable of taldng action for serf-preservation under emergency conditions without assistance from others. This. includes all facilities in which a nat ient is subiected to deen sedation or anesthesia Examnles include but a~e not restricted to Urcd-care centers. Day sur~ic'ai centers. Ort,/lonedic nractice, and Plastic surgery offices where natients are sedated with was. (EE, PS) ~
(4) Revise the definition of "nursing home" as follows, (The new words are underl ined.)
Nursing Home. A building or part thereof used to ~ housing and acute and sub-acute nursing care, on a 24-hour basis, o f four or more persons who, because of mental or physical incapacity, may be unable to provide for their own needs and safety without the assistance of another person. This includes ventilator d e o e n d e n t oatients and tho~¢ providing longterm personal medical ~:ar¢, NQ ireatments or ~as analgesia or anesthesia are orovided. Nursing Home, wherever u s e d i n this document , inclddes nursing and convalescent homes, skilled nursing facilities, intermediate care facilities, and infirmaries and homes for the aged il2~LIKga~[e, J a I ~ term ventilation suoDort. (EE, PS)
(5) Add a sen tence at the end of the present definition of"Clinic" as follows:
"Such facilities are not des igned to provide overnight stays for patients. The facility provides t reatment and procedures for patients that would not render them incapable of taking action for self- preservation under emergency conditions. Patients are treated for chronic and no t acute medical case. . "(TC, PS)
(6) Revise the definition of "Limited Care Facility" as follows. (The new words are underl ined.) Limited Care Facility. A building or part the reof used on a 24-hour
basis for the housing of four or more persons who are incapable of serf-preservation because of age, physical limitation due to accident or illness, or mental limitations such as mental re tardat ion/ developmental disability, mental illness, or chemical dependency. Such facilities do not nerform invasive procedures or use anesthesia or analgesia. Resoira~orvsunnort is lirr~ited to nasal cmanuai assistance for breathing." (TE, PS)
(7) Add a new definit ion for "Office Practice- Medical or Dental" as follows: Office Practice, Medical - Dental. A facility that performs examina-
tions and minor t rea tments /procedures under the continuous supervision of a medica l /denta l professional. Procedures involve only conscious sedation or local anesthesia and treatments and or procedures do no t render the patient incapable of taking action for serf-preservation under emergency conditions. Such facilities do no t
~ rovide overnight stays for patients or provide 24 h r / d a y operation. xamples include: Dental o f f i ce /d in ic , medical office/clinic,
immediate care facility and podiatry office. Veterinary facilities also are included in this category.
(In Chapter 4) (8) Where ever "Type 1" appears in chapter 4, replace with ~Level
1" (9) Relocate and retitie existing 4-3.4 as new "4-3.5 Level 5 - Other
Gasses (Reserved)" (10) Revise existing 4-3.3 Laboratory Gas Supply Reserved, tO read
"4-3.4 Level 4-Laboratory Gas Supply, (Reserved)" (11 ) Insert new 4-3.3 Gas System, Level 3, and move text f rom
existing 4-3.2 to 4.3.3, and renumber accordingly. (12) Retitle existing 4-3.2 and add new text as follows: 4-3.2 Level 2 - Patient Gas Supply- 4-3.2.1 Cylinder Storage Requirements 4-3.2.1.1 The requirements of 4-3.1.1 through 4-3.1.8 shall apply. 4-3.2.2 Medical Air Compressor Requirements 4-3.2.2.1 The requirements of 2-3.1.9 shall apply except a sde f ined
in 4-3.2.2.2 and 4-3.2.2.3 below. 4-3.2.2.2 One or more compressors shall be permit ted as defined
in 4-3.1.9.3. 4-3.2.2.3 The dryers, aftercoolers, filters and regulators of 4-3.1.9.7
shall be permit ted to be simplexed. (13) Insert new 4-3.3 and 4-3.3.1 as follows:
4-3.3 Level 3 -Gas Supply- 4-3.3.1 Cylinder Storage Requirements (14) Relocate existing 4-3.2.1 and 4-3.2.2 as new 4-3.3.1.1 and
4-3.3.1.2. (15) Retifle and renumber existing "4-3.2.$ Dental /Medical Air
Compressor Requirements" as new "4-3. 3.2 Level'3 Air Compressor Supply Systems. (See figure 4-3.3.2), and change figure number accordingly.
(16) Relocate text under existing 4-3.2.3 to 4-3.3.2 and renumber accordingly.
(17) Retitle existing 4-4.1 as "4-4.1 Level 1 Patient Gas Distribu- tion" ( remainder is the same)
(18) Renumber and retitie, respectfully, existing 4-4.3 and 4-4.4 as "4-4.4 Level 4 Laboratory Gas Distribution," ( remainder is the same) and "4-4.5 Level 5 Other Gases," ( remainder is the same).
(19) Retitle existing 4-4.2 as "4-4.3 Level 3 Patient Gas Distribu- tion" and renumber the text under existing 44.2 accordingly.
(20) Insert new 4-4.2 as follows: 4-4.2 Level 2 Patient Gas Distribution System. 4-4.2.1 "The gas distribution system shall comply with 4-4.1. except
as follows: 4-4.2.1.1. Alarms. (a) Only one alarm panel shall be required for the facility, and it
shall complywith the requirements of 4-4.1.1.2(b), (c), (d),(e), and 4-4.1.1.3(a), (c), and (e). A single alarm panel as def ined in 4-4.1.1.2(a) shall be moun ted in an area of continuous surveillance while the facility is in operation. (Pressure switches shall be moun ted on the main lines and no t down stream of any zone valve.
(b) The required alarm panel shall be permit ted to combine the characteristics of the master and area type alarms into a single panel.
4-4.2.1.2 Valves. (a) Valves identified in 4-4.1.2.2(d) and (e) shall be required to
have a corridor wall intervening between the outlets and the valves. (b) Level 2 facilities shall be required to have a shut offvalve
controlling each gas for each floor in the facility. The valve controlling a given floor shall be on the floor being controlled. The valve shal lbe readily accessible from a standing position !n the event of an emergency.
(21) Retitle 4-5.1 as 4-5.1 Level 1 Patient Gas System (22) Renumber and retide existing 4-5.2 as follows:
4-5.3 Level 3 Patient Gas Testing. (23) Move and renumber existing text under 4-5.2 to under new
4-5.3. (24) Insert new "4-5.2 Level 2 Patient Gas Testhig (Reserved)" (25) Retitle existing 4-6.2.3 as "4-6.2.3 Level 1 Patient Gas Systems." (26) Retide existing 4-6.2.4 as ~4-6.2.5 Level 3 Patient Gas Systems." (27) Insert new "4-6.2.3 Level 2 Patient Gas Systems (Reserved)" (28) Retitie existing 4-8.1.1 as ~Levei 1 Medical Surgical Vacuum
Pumps" (29 )Renumber and retitle existing 4-8.1.3 as 4-8.1.4 Level 3
Vacuum Source (30) Insert new 4-8.1:3 as follows; 4-8.1.3 Level 2 Vacuum Source 4-8.1.3.1 The vacuum system shall comply with 4-8.1 except that
one or more pumps shall be permit ted in 4-8.1.1. (31) Retitle existing 4-8.2 as "Level 4 Vacuum Systems."
(In (a~apter 12) (32) Change "Type" to "Level" where ever it appears in chapter.
(In Chapter 13) (33) Revise 13-3.4.1 as follows: 13-3.4.1.1 Patient gas supply, and gas distribution shall complywith
4-4.1.2.2 as p roposed in this CP 5 (actions 17-20). 13-3.4.1.2 Patient gas testing and administration shall comply with
chapter 4, sections 4-5 and 4-6 level 1.
(34) Revise 13-3.4.2 as follows: 13-3.4.2 Laboratory gas supl31y , distribution systems, testing, and
administration shall comply with Chapter 4 sections 4-3 thru 4-6 Level 4.
(35) Revise 13-3.4.3 as follows: 13-3.4.3 Medical Surgical Vacuum system shall comply with
Chapter 4, sections 4-7 thru 4-11 Level 1.
(In Chapter 14) (36) Revise 14-3.4.1 as follows: 1 4-3.4.1.1 Patient gas supply, and gas distribution shall comply with
Chapter 4, sections 4-3 and 4 4 - level 2., except that the alarms shall comply with 44.2.9. 14-3.4.1.2 Patient gas testing and administration shall comply with
Chapter 4, sections 4-5 and 4-6 Level 1.
34

NFPA 9 9 - - F95 ROP
(37) Revise 14-3.4.2 as follows: 14-3.4.2 Laboratory gas supply, distribution systems, testing, and
administration shall comply with Chapter 4 sections 4-3 thru 4-6 Level 4.
(38) Revise 14-3.4.3 as follows: 14-3.4.3 Medical Surgical Vacuum system shall complywith
Chapter 4, sections 4-7 thru 4-11 Level 1.
(In Chapter 15) (39) In Proposals 99-443 (Log #CP63) to 99-431 (Log #CP77)
change the word "Type" to "Level."
(In Chapter 16) (40) Revise 16-3.4.1 as follows: 16-3.4.1 Patient gas supply, distribution systems, testing and
administration shall comply with chapter 4, sections 4-3 thru 4-6 Level 1.
(41) Revise 16-3.4.2 as follows: 16-3.4.2 Laboratory gas supply, distribution systems, testing, and
administration shall comply with Chapter 4, sections 4-3 thru 4-6 Level 4.
(42) Revise 16-3.4.3 as follows: 16-3.4.3 Medical Surgical Vacuum system shall complywidl
Chapter, 4 sections 4-7 thru 4-11 Level 2. SUBSTANTIATION: For Actions 1 thru 7:
The current definitions for Hospital, Ambulatory Health Care Center, Clinic, Nursing Homes, are insuffident to adequately define and differentiate levels of risk from anesthesia, analgesia, ventilation support crucial to proper system requirements for patient safety. The T/C on PS is aware that owners and authorities having
• jurisdiction are having problems in interpretation of the appropriate applications because of this lack of definition. Some installations are more complex and Overly expensive because of this improper interpretation. Like wise other installations are inadequately equipped for the level of patient risk involved. The proposed definition revisions are intended to minimize
confusion and the prolonged delay thru interpretation. It provides greater differentiation based upon a level of risk to thepatients as worked out with practitioners, installers, AHA, ADA a n d a fire marshall representing AHJ... The definition revisions are intended to be supplemental to the
existing basic definitions used in NFPA 99, and not in conflict with similar major definitions used in NFPA 101.
The word "shall" should not be in a definition per the NFPA style manual and has been deleted. (See existing hospital definition)
In addition there presently is rto definition (clarification) of what are the requirements of a dental or medical office to qualify for recognition in Chapter 15, or to be excluded from chapter 15.
Examples are provided for further clarification.
For committee actions #8 thru #16: To restructure the Gas supply by level of risk designation.
For committee actions #17 thru #20: To restructure the piping distribution system by level of risk
designation.
For committee actions #21 thru #23: To restructure the testing by level of risk designation.
For committee actions #24 thru #26: To restructure the administrative requirements by level of risk
designation.
For committee actions #27 thru #31: To restructure the vacuum by level of risk designation..
For committee actions #31 and up: To restructure the application chapters 12, 13, 14, 15, 16, 17, by
level of gas system riskdesignation as defined in the risk level table below.
FACILI'P/RELATED EQUIPMENT LEVEL REQUIREMENTS
Hospital Nursing Ambulatory Clinics Limited Medical/Dental Home Care Care Office
Manif. or Bulk Supply Level 1 Level l Level I Level I Level I Level 3
Air Plants Level 1 Level 1 Level 2 Level 2 Level 2 Level S
Vacuum
Plants Level 1 Level 2 Level 2 Level 2 Level 2 Level 3
Alarms Level 1 Level 1 Level 2 Level 2 Level S Level 5
Valving Level 1 Level I Level 1 Level t Level 2 Level S
Testing&
Cert. Level I Level 1 Level 1 Level 1 Level I Level 3
COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP5) Committee: HEA-PIP
99- 98 - (4): Accept SUBMITTER: Technical Committee on Piping Systems RECOMMENDATION: Manufactured Assemblies
1. Add the following new definitions in Chapter 2: D.I.S.S. Connector. A threaded medical gas connector complying
with the CGA Pamphlet V-5, Diameter Index Safety System Non Interchangeable Low Pressure Connections for Medical Gas APMPan lications.
ufactured Assembly. A factory assembled product designed for aesthetics or convenience which contains medical gas or vacuum outlets, piping and/or other devices related to medical gases. NOTE: Examples are headwalls, columns, ceiling columns, ceiling
hung pendants, movable track systems, etc. Semi Permanent connection. A non interchangeable gas connec-
tion, usually a D.I.S.S. Connector, which is intended to be detached only for service and is not the point at which the user makes connections or disconnections. Terminal. The end of a flexible hose or tubing used in a Manufac-
tured Assembly where the user is intended to make connection and disconnection.
NOTE: Terminals are constructed to comply with 4-4.1.2.4. 2. Add the following in 4-1A: (4) and Manufactured Assemblies which are intended for connec-
tion to the medical gas or vacuum systems. 3. Add the following new paragraph 4-2.3: 4-2.3 Manufactured Assemblies. Specific hazards associated with
Manufactured Assembliesare the same as those listed in 4.2.2 as well as additional hazards resulting from improper assembly, separation, and leakage resulting from hidden semi-permanent connections, improper connection resulting in cross-connection, and blockage and flow problems resulting from damage to hoses, etc.
4. Add the following new paragraph 4-3.1.3..3: 4-3.1.3.3 Manufactured'Assemblies in which are intended to be
~iped Nitrous oxide or Oxygen shall be a) constructed of metal, or ) tested to pass a minimum flame spread rating of xxxx or if
constructed of polymers (plastic, fiberglass, etc.), a rating of 94 VO or better.
5. Insert the following as new 4-4.1.2.3(b). Renumber existing subparagraph (b) through (f) as (c) through (g):
(b) Medical gas rails shall be permitted only where entirely visible in the room. Medical gas rails shall not pass into or through walls, partitions, etc.
6. Add the following new paragraph 4-4.1.2.4(g): 4-4.1.2.4(g) Outlets (inlets) intended for the connection of
Manufactured Assemblies shall be D.I.S.S. Connectors.
35

- - N F P A 99 m F 9 5 R O P
7. Add the following new paragraph 4-4.1.2.5: 44.1.2.5 Manufactured Assemblies. (a) Manufactured Assemblies employing flexible hoses or tubing
shall: 1. be attached to the medical gas pipelines using semi-permanent
connections to station outlets (inlets). Where the station outlets (inlets) are not fully and immediately accessible (i.e., may be manipulated without necessitating removal of panels, doors, etc.) the station outlets (inlets) shall additionally comply with 4-4.1.2.4(g) and may consist of only a primary check, omitting the secondary check required in 44.1.2.4(a). The station outlet (inlet) shall be permanendy attached to the pipeline.
2. use hoses and flexible connectors complying with 44.1.2.1 (q) except that these may be concealed inside the Manufactured Assembly provided the hoses and connectors can be accessed for replacement or repair.
3. be provided with a terminal complying with 44.1.2.4(a), (c), (d) and (e) at the point where the user makes connections and disconnections.
4. be internally cleaned and provided to the installation site in compliance with 4-4.1.4.1.
5. removal, replacement or addition of the flexible hoses and tubing shall require testing of 4-5.1.3.1 and 4-5.1.3.5.
(b) Manufactured Assemblies employing copper tubing and intended for direct brazed connection to the pipeline shall:
1. complywith 4-4.1.2.1(a), (b), (c), (d), (e), (h) and (j). 2. be provided with a station outlet (inlet) at the point where the
user makes connections and disconnections. 3. be assembled and provided to the installation site in compli-
ance with 4-4.1.4. 8. Add the following new paragraph 4-5.1.1.1: 4-5.1.1.1 Manufactured Assemblies shall, prior to arrival at the
installation site, be pretested to comply with 4-5.1.2.1 through 4-5.1.2.5, except that 4-5.1.2.3 may be performed by any leak testing method which will assure a pressure decay of less than i percent in 24 hours. The manufacturer shall provide documentation attesting to the performance and successful completion of these tests.
9. Add the following paragraph to existing 4-5.1.2: Where Manufactured Assemblies are to be installed, tests required
under section 4-5.1.2 shall be performed at all station outlets (inlets) after completion of the pipeline and after installation of any Manufactured Assemblies employing copper tubing butprior to installation of any Manufactured Assemblies employing flexible hoses or tubing.
10. Add the following paragraph to existing 4-5.1.3: All tests required under section 4-5.1.3 shall be performed after
installation of any Manufactured Assemblies employing flexible hoses or tubing, where there are multiple possible connection points for terminals, each possible position shall he tested indepen- dently.
1 1. Add the following to the beginning of 4-5.1.3.3. Also, delete subparagraph (a), and renumber subparagraph (h) and (c) to (a) and(b). General. These flow tests shall be performed at the station outlet (inlet) or terminal where the user makes connections and discon- nections and may be performed with the use of oil free dry Nitrogen or with the gas of systems designation.
12. Add the following to the beginning of 4-5.1.3.8: General. These flow tests shall be performed at the station outlet
(inlet) or terminal where the user makes connections and discon- nections. SUBSTANTIATION: The present standard contains little guidance to the manufacturer, installer or user of prefabricated or factory fabricated assemblies. The proposal attempts to provide such guidance, recognizing the unique capabilities attainable in a factory setting. COMMITYEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP58) Committee: HEA-PIP
99- 99 - (Chapter 4): Correlating Committee Note: Technical Correlating Committee
notes that the proposal is an improper one according to NFPA Regulations Governing Committee Projects, and directs the T /C on Piping Systems to prepare a committee comment with the details of what it wants to accomplish. SUBMITrER: Technical Committee on Piping Systems RECOMMENDATION: Restructure and integrate gas and vacuum by Type such that gas and vacuum appear sequentially in Chapter 4.
SUBSTANTIATION: Committee believes that vacuum system requirements should be contained immediately following the gas system requirements. Committee wishes to make the document more user friendly by making all Type 1 system requirements together, all Type 2 system requirements together, etc. COMMIT]FEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrI~EE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #1 02) Committee: HEA-PIP
99-100 - (Chapter 4 (New)): Accept in Principle SUBMITrER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Add the following text: x-x.x.x Pressure Gauges. The scale range of pressure gauges shall
be such that the normal reading falls within the middle 1'/3 of the scale. The rated accuracy of pressure gauges used for testing shall be 1% full scale [or better] at the point of reading. SUBSTANTIATION: There is nothing in the standard that prevents
[ gauges from having scale ranges that are too high or too w for reasonable and accurate reading. There is no minimum
accuracy required for test gauges. This proposal establishes a minimum required accuracy of 1% full scale. Better quality gauges having accuracies of 1/2% and 1/4% are available. Lesser quality gauges have 2% accuracy of higher. COMMITTEE ACTION: Accept in Principle.
Insert the following text immediately following the title of 44.1.1.4, and before subpara. (a).
"The scale range of positive pressure analog gauges shall be such that the normal reading falls within the middle fifty percent of the scale. The scale range of digital gauges shall be not more than two times the workingpressure. The rated accuracy of pressure gauges used for testing shall be one percent (full scale) or better at the point of reading." COMMITI3~ STATEMENT: Committee has included both analog and digital gauges for completeness. Committee has also changed recommendation to be in concert with ASME standard on gauges. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #51) Committee: HEA-PIP
99- 101 - (4 & 15): Correlating Committee Note: For item 1, the Technical Correlat-
ing Committee rejects the concept of changing the order. The TCC believes the current order of chapters is most user friendly. For items 2, 3 and 4, recommendations are not in the form of a
~ roper proposal per NFPA Regulations Governing Committee rojects, and are thus rejected.
SUBMITYEI~ Leo G. Foxwell, ITT Hartford RECOMMENDATION: Revise text: There are several potential approaches that could be considered. 1. Rearrange the standard so that the annlications appear in the
first chapters of NFPA-99. i.e., Reposition'the existing chapters 10- 19 in the front as chapters 3 to 12. Have the present chapters 3-9 repositioned as chapters 13 thru 19. This would easily allow anyone to see the applicable sections of the standard and then to proceed to those sections. And,
2. Rearrange the document so that all of the requirements of Type I, Type II and Type 11I are in one location. 3. Print in italics (for example) the paragraphs of Type I, that are
required as they are referenced in Type II & III. Or include them as required as part of Type I and Type II.
4. Consider printing an NFPA 99-D Systems requirements for the Dental and Medical care Facility applications. All the applicable requirements could be printed as they apply. It could be a source of income to the NFPA (25,000 documents/year) and would allow the industry to have a very user friendly document. SUBSTANTIATION: NFPA-99 is not user friendly when used in non-hospital applications, for instance, it is difficult to trace back and forth through the document for all the applicable Type II requirements. And for that matter for all the applicable Type I references that apply in Type II situations. The application of Type II appears at the end of the document and not up front where it can be easily seen and understood. NFPA-99 is not user friendly in the nresent format
36

NFPA 99- - F95 ROP
As a point of reference there are only about 6000+/- hospitals in the Uni ted States where Type I is the mandate . However, there are over 130,000 dental care facilities. It h a s been est imated that, at any given t ime 2 5 p e r c e n t of these installations are u n d e r revision and upgrading. (The n u m b e r of medical care facilities has no t been ascertained.) There is a vasdy greater clientele of Type II applica- tions to which we are trying to reach with the NFPA-99 standard. Yet the s tandard is the least user friendly to this very same group. COMMITTEE ACTION: Accept. COMMITFEE STATEMENT: 4. Commi t tee will consider idea for a new document . NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
(Log #CP75) Committee: HEA-PIP
99-102 - (4-1.4, 2-2, 4-8.1.3): Accept SUBMITTER: Technical Commit tee on Piping Systems RECOMMENDATION: 1. Delete existing 4-1.4.
2. Revise the title of the definit ion of "Medical Surgical Vacuum System" in Chapter 2 to read: "vacuum System-Type I, Medical Surgical Vacuum System." (The text of the definit ion remains the salne.)
3. Change "Medical Surgical Vacuum System" to "Type I Vacuum System" where ever it appears in Chapter 4, and Chapters 10-19.
4. Add a new definit ion for "Vacuum System-Type Ill" in Chapter 2 as follows:
V a c u u m System-Type III. A v a c u u m system, ei ther a wet or dry piping system, des igned to remove liquid, a i r /gas , and solids f rom the treated area.
NOTE 1: The system is not in tended for Type I medical /surgical vacuum applications.
NOTE 2: A wet piping system is des igned to accommoda te liquid, a ir /gas, and solids t h rough the service inlet.
NOTE 3: A dry piping system is des igned to accommodate a i r /gas only t h rough the service inlet. (liquid(s), a n d solid(s) are t r a p p e d before en te r ing the service inlet.)
5. Revise existing 4-8.1.3 in its entirety to read as follows: 4-8.1.3 Vacuum Systems-Type IlL NOTE 1: Type III vacuum systems may be used for dental, podiatry
, and medical care facilities. NOTE 2: See defini t ion of "Vacuum Systems - Type III" in Chapter
2. 4-8.1.3.1 Vacuum General. (a) Service inlets shall be e i ther a shut-offvalve with a th readed
female pipe connector , or a quick-connect fitting with a single check valve.
(b) Type III vacuum p u m p s shall be suitable for the in t ended purpose. Wet vacuum piping system shall have a l i q u i d / a i r separator in the system. (See Figures 4-8.1.3.1(b).)
Equ ipmen t shall be obta ined f rom and be installed unde r the supervision of a manufac turer (s ) or supplier(s) familiar with proper practices for its construct ion and use. Main tenance programs, in accordance with the r ecommenda t ions of manufac turer (s ) , shall be established for the dental air compressor supply system as connec ted in each individual installation.
(c) Liquids f rom a Type III vacuum system, per 4-8.1.3.2, shall be connec ted to the sanitary dra inage system th rough an appropriately
7c~)p ed drain. (See Figures 4-8.1.3.1 (c).) The gas discharge f rom a Type III vacuum system shall be
p iped to the outside. The gas shall be discharged outdoors in a m a n n e r tha t will min imize the hazards o f noise, and contaminat ion to the facility and to the envi ronment .
NOTE: Improper design will permi t gas pressure to build up in the ventilation system and may blow the trap liquid seals.
(e) The exhaus t shall be located remote f rom any door, window, air intake, or o ther openings in the bui lding with particular a t tent ion given to separate levels of intake or discharge.
Care shall also be exercised to avoid discharge locations contraindicated by prevailing winds, adjacent buildings, topography, and o ther influences.
(f) Exhaust to the outdoors shall be protected against the entry of insects, vermin, debris, and precipitation. Exhaus t lines shall be sized to minimize back pressure.
(g) Discharge of the vacuum systems utilizing c o m m o n exhaus t pipes shall be fitted with a check valve, a manua l valve, or a r ranged to permi t capping of the active pipe when removing and servicing a vacuum p u m p or components .
• (h) Vacuum exhaus t f rom separate p u m p s shall follow the manufac ture rs r ecommenda t ions .
NOTE: Care should be taken to insure the dual exhaus t systems do no t develop excessive back pressure when us ing a c o m m o n exhaus t line.
4-8.1.3.2 Piping Distribution. (a) Nonf lammable waste gasses shall be permi t ted to be disposed
of t h rough a Type II vacuum system provided that its inclusion in the system does no t affect the overall pe r fo rmance of the o ther parts of the vacuum system.
(b) Piping materials shall be PVC schedule 40, copper or o ther corrosion-resistant material. Piping shall be sized in accordance with the manufac tu re r ' s r ecommenda t ions . All p ip ing shall be provided with adequate and accessible "clean outs" per the manufac tu re r ' s or des ign engineers ' specifications.
(c) All p iping shall have smoo th interior walls to avoid debris build-up.
(d) Piping shall be s loped a m i n i m u m of one quar te r inch per ten feet toward the vacuum p u m p or a single location before the vacuum pump . Systems shall be free o f local low sections that can collect liquids or debris. Pipe hangers shall be used per manufactur- ers recommenda t ions .
(e) Where any other vacuum systems or p ip ing systems are used, pipe shall be labeled as to type and g a s / v a c u u m being used.
4-8.1.3.3 Alarm. (a) Type III vacuum systems shall no t be requi red to have an a larm
system. 4-8.1.3.4 Testing. (a) The piping system shall be pressurized to 15 psig. (b) The system shall main ta in the static pressure for a m i n i m u m of
24 hours . The pressure drop shall no t exceed 5 psig. (c) The test shall be pe r fo rmed before the vacuum p u m p is
installed. (d) All recorded test informat ion shall be re ta ined at the facility.
(See Hgures following.) SUBSTANTIATION: The presen t scope of chapter 4 is l imited in 4- 1.4 to vacuum systems for medical-surgical systems. The scope needs to be revised to include type III vacuum and o ther vacuum systems used in heal thcare institutions. C O M M H ' r E E ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 18 VOTE ON COMMIT1"EE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Brittain NOT RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: BRITTAIN: "Piping materials shall be PVC..." PVC c a n give off
toxic fumes when burned, and shou ld no t be used. Should sa)n "Piping materials shall be metallic. . ." or some th ing similar.
( Log #17) Committee: HEA-PIP '
99-103 - (4-1.5 (New)): Reject SUBMITTER: David Mohile, Medical Engineer ing Services RECOMMENDATION: Add new text:
"An existing system which is no t in strict compliance with the provisions of this s tandard may be con t inued in use as long as the authori ty havingjur lsdic t ion has de t e rmined that such use does no t consti tute a distinct hazard to life." SUBSTANTIATION: Similar wording existing in NFPA 56F for many years, bu t was removed in the transi t ion to 99 in 1987.
The re are many profiteers in the medical marketplace that are telling facilities that they mus t upgrade to the latest edit ion of the code or be in violation of the code. Many facilities are spend ing h u n d r e d s of thousands of dollars do ing these unnecessary upgrades.
The re int roduct ion o f these words would hopeful ly stop this unnecessary work. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: 1-9 addresses the issue of new verses existing construction. NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Mohile NOT RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: MOHILE: I do no t agree with the Commit tee ' s Action to reject this
proposal. While Paragraph 1-2 does address this problem, 1-2 was no t pr in ted in 99C. Further, many unsc rupu lous privateers are forcing hospitals to spend large a m o u n t s of money to upgrade their medical gas p ipe l ine systems by manipu la t ing the word~ of the document . We need to go back to the wording tha t was in 56F which is very plain and easy to unders tand .
37

NFPA 99- - F95 ROP
, . ~ . . . . -~ . . . . . . . t . . . . . . + . . . t . . , ,....,:'~'~
,,I J Collector ,1 ~ __PJI , , ,151 1 ~ , t " t H Z U ~
k ..~.2 on~. . . . . . . . . . . . . '.,
~..1~.= ,~.., . . J
i SS
Vacuum
I f ° o m ~
! Air/ • Liquid
i Separat°r i • e • w -
To Drain • -= -=% a p ~ = = .
~l~'~l~ =Vacuum Relief Valve (optional Locations)
- ~ =inlet Station
r ~ =Service Inlet
~ =Shut-Off Valve
=Check Valve
=Pipe Isolators
( • =Vacuum Gauge
t ~S~ =Solids Separator (OPTIONAL LOCATIONS)
H2.~I~ Ware r Supply
~ =Utility Center
P Vent to Outside
F'~n'e 4-8.1.3.1(b)(1) Typical Type III wet or dry piping system with single vacuum pump source.
99-102 (Log #CP75)
3 8

NFPA 99- - F95 ROP
P
,----, ~ . 9 . L ~ ' I ) . . . . . . . . . .,. . . . . ' . L~,u,d .,.---~ . . . . . . . -1~ L SS~ ~ ; . . . . . _IL . . . . . . . | . . . . . . Jl_...|..• .~...., "!71 l --J~, ;Separator; |
i .T t r - i -:~ r I ~ ..-<a n ,.@.,, -'.. . j n : ! I ~ / / ! , ~ s s ! / ~.ss.!_ "---,--. / :1 ,i,:,u~d I l U.C. I ~ ,-A--,, . . V 4 ' . ~ ~ I : ICollector I ~ M I~1 : " , , ~ • : ~ • I
/ / : L . L ~ j ~ ;..L~.:~ I i . . ~ . . ~ : i ° n : . . . . . . . . . . . . . i H29--~lVa~uumJ "Z-Q-~lV"cuuml I
. - - - -%
k ~Z]* =Vacuum Relief Y alve (optional Locations)
~ =Inlet Station
[~ ] =Service Inlet
~ =Shut-Off Valve
=Check Valve
S =Pipe Isolators
i • =Vacuum Gauge
~SS ~ =So lids Separator (OPTIONAL LOCATIONS)
H2~Water Supply
r ~ =Utility Center
I
F'tgure 4-8.1.3.1 (b)(2) Typical Type lit wet or dry piping system with duplex vacuum source.
99-102 (Log#CP75)
39
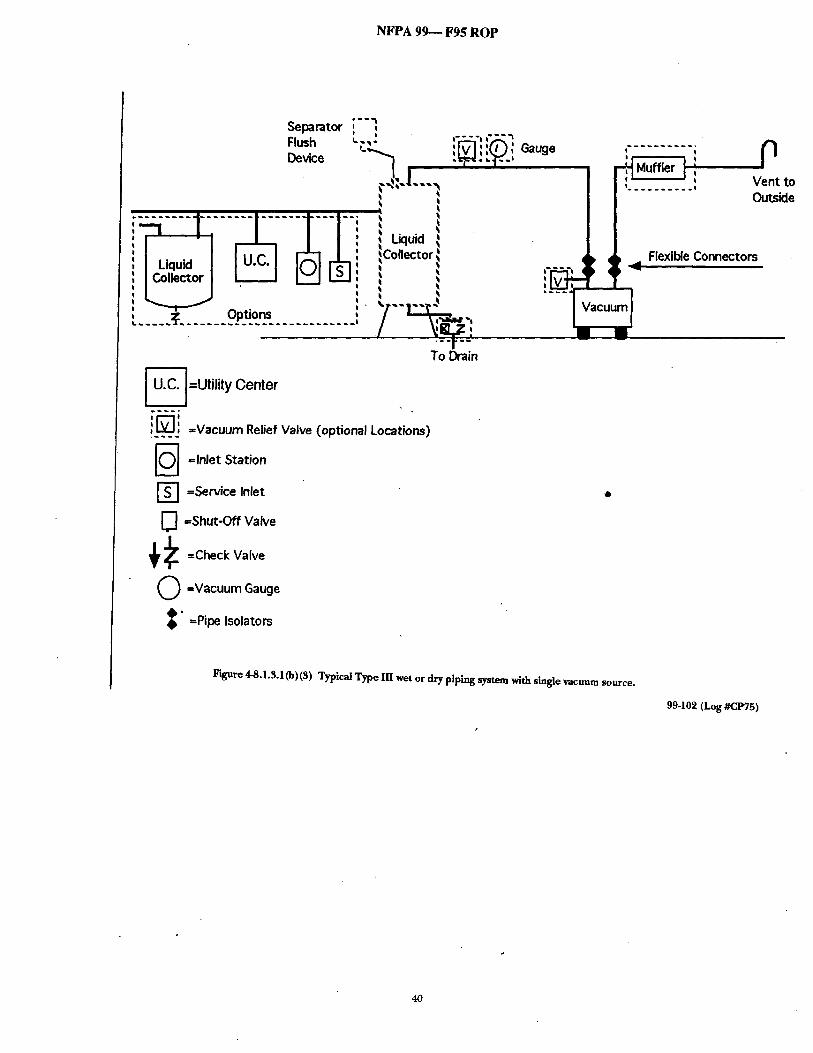
NFPA 99-- F95 ROP
Separator Flush Devk:e
" ; ~ - . . . . I " : . . . . . . . . . . . . . . " - "
L___ j L : j ~L~ J
~, Options
" ' ' ' t I
~~: I ..~
i Liquid Collector
/ y~,.' To Drain
~ =Utility Center
!_~ =Vacoum,e,e, Va,ve ~op,io.al Locatioos~
' ~ =Inlet Station
r ~ =Service Inlet
] =Shut-Off Valve
Q =Vacuum Gauge
, , Gauge t t I
r '~ Muffler l : I t . . . . . . . . . . i
Flexible Connectors
P Vent to Outside
0
~" =Pipe Isolators
Figure 4-8.1.3.1 (b)(3) Typical Type IH wet or dry piping system with single vacuum source.
99-102 (Log#CP75)
40

N F P A 9 9 - - F95 R O P
Separator Flush Device , ' ' : ' " ~ I ; I Muffler O L - - I
.cw ~-:'.L : i ~ , : ~ i ~ . . . . . . I ~ . . . . . . . . . .
. . . . . . . . . . . tO
• Outside
- - - - . . . . . i, . . . . . . . . . . . . . . . . . . . , : Liquid ', I J~ / , ,Collector , • • ~1 b i k Flexible Connectors
Liquid , ' ' . . . . . . . . , 41~ iP ' ' ''-',[~J~ T '
I ¢ I
: . . . . . . V a c u u m V a c u u m :~1 ~ Opti°ns / ~ ' , Isolators
To Drain
[ ~ = U t i l i t y Center
i i E]!..._ =Vacuum Relief Valve <optio.~l Locatio.s)
' ~ =Inlet Station
r ~ l =Service Inlet
==Shut-Off Valve
~ , ~ =Check Valve
Q =Vacuum Gauge
t =Pipe Isolators
F'~ure 4-8.1.3.10))(4) Typical Type III wet or dry piping system with duplex vacuum source.
99-102 (Log #CP75)
41

NFPA 99- - F95 ROP
To the Vacuum Pump{s) r~k A
~ t ~r~g / . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Vent to the PlumbiNg 8ystefll •1" ]
J
• Waste Holding Tank
! | ! | i ! t
i ! ! i Z | | . | | ! ! 1
' : 0
Figure 4-~.1.~.1(c)(1) Drainage from a gravlty-drained, liquid collector tank.
99-102 (Log#CP75)
1 - - E x h a u s t to Outside
AL Vent to the Plumbing System.
~lt illtlll~stmttt Jtltlmmlmmmll~lmlalmmlll;llml| m m j | j |l |l,
!
! o
e
) Drainage System
Figure 4-8.1,3,1(c)(2) Drainage from positive discharge vacuum pump through an Mr/l iquid separator.
99-102 (Log #CP75)
(Log #339) Committee: HEA-PIP
99- 104- (4-3.1.2.1(3)): Accept SUBMITTER: David Wyrick, Sr., Cambiare Ltd. RECOMMENDATION: Revise text as follows: Air Compressors and vacuum pumps shall be located separately
from cylinder patient gas systems or cylinder storage enclosures. SUBSTANTIATION: Statement does not take into consideration dental air or vacuum systems by use of the word Medical. It should state Patient Gas Systems as nitrogen or other non-respirable gases have no effect on air compressor or vacuum pump location. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #192) Committee: HEA-PIP
99-105 - (4-5.1.2.1 (j) (2) (New)): Accept • SIYBMITTI~R: Leo G. FoxweU, I3q" Hartford RECOMMENDATION: 1. Add a new 4-3.1.2.1 (j) (2) as follows:
4-3.1.2.1 (~) (2) Storage facilities that are outside, but adjacent to a building wall, shall be located such that the distance to any window of the adjacent building is greater than 25 feet.
2. Renumber the paragraph that follows. SUBSTANTIATION: The present standard does not address the safety issue of an outdoor cylinder storage location potentially being placed on a wall of a building and under a window of that wall. The 25 feet is in compliance with NFPA 101. COMMITTEE ACTION: AcCept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #370) Committee: HEA-PIP
99- 106 - (4-3.1.2.3): Accept in Prindple in Part SUBMITTER: Peter Ferraro,Jr, Phoenix, AZ RECOMMENDATION: Revise 4-3.1.2.3 as follows:
4-3.1.2.3 Additional Storage Requirements for Nonflammable Gases Less than 3000 cuft (85 m~3). Provide continuous ventingby mechanical means or natural means with at least 72 sq in (0.05m2) free area.
• Note: Louvered openings may not be used when the opening is in a means of egress, nor otherwise located so products of combustion flowing through the opening could jeopardize the use of exits prior to fire damper operation. SUBSTANTIATION: Second sentence of present 4-3.1.2.3, addressing the condition "where the location of the supply system " door opens onto an exit access corridor, provides two alternative (b) and (c) which call for a ventilation opening "with fire damper(s) of appropriate rating." This conflicts with three other NFPA standards. NFPA 101-1991,The Life Safety Code, 12-$.6.4 and 13-$.6.4
prohibit "transfer ~.'lles, whether o rno t protected by fusible link operated dampers in corridor walls or doors of both new and existing Health Care occupancies. NFPA 90-A1993, Standard for Installation of Air Conditioning and
Ventilating Systems, 2-3.11.1, states "air transfer openings(s) are not permitted in walls or in doors separating egress corridors from adjoining areas" in health care, detention and correctional, and residential occupancies.
NFPA 80-1992, Standard for Fire Doors and Windows, 1-3.2 permits fire dampers in fire doors only "wh'ere the opening is not in a means of egress or otherwise located so that products of combustion flowing through, the opening, could jeopardize the use of exits prior to operauon of the louver. This proposal eliminates the conflicts and simplifies the venting
requirement by specifying only venting performance, not how venting is accomplished. The note calls attention to key consider- ations related to means of egress based on other NFPA standards. COMMITI~EE ACTION: Accept in Principle in Part.
Revise submitter's recommendation to read as follows: "4-3.1.2.3 Additional Storage Requirements for Nonflammable
Gases Less than 3000 cu ft (85 m3). Doors to such locations shall be provided with. louvered openings having a minimum of 72 sq. in. (0.05 sq. m.) m total free area. Where the location of the supply system door opens onto an exit access corridor, louvered openings
42
N F P A 9 9 m F 9 5 R O P
shall not be used, and the requirements of 4-3.1.9.2 (c) and 4-3.1.2.2(d) shall be complied with." COMMITrEE STATEMENT: Changes are to comply with require- ments of NFPA 101, Life Safety Code. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #280) Committee: HEA-ANE, HEA-PIP
99-107 - (4-3.1.2.4): Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Delete paragraph in its entirety. SUBSTANTIATION: Over thepast two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Deparmaent of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove anyand all references to flammable anesthetics and " flammable anesthetizing locations. COMMITrEEACTION: Acceptin Principle. Move this text to new Annex 3.
COMIMITrEE STATEMENT: Correlate with action on Proposal 99-25 (Log #274). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 (ANE), 18 (PIP) VOTE ON COMMrlq'EE ACTION:
AFFIRMATIVE: 10 (ANE), 16 (PIP) NOT RETURNED: Fan (PIP), Shoemaker (PIP)
(Log #88) Committee: HEA-ANE, HEA-PIP
99-108 - (4-3.1.2.4(a)): Reject SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise sentence 1 to read:
Enclosures in which tlammable inhalation anesthetic agents are stored shall be individually and continually ventilated by mechanical means at a rate of not less than eight air changes an hour. SUBSTANTIATION: If the gas storage enclosure is located on the ground floor or basement, it is impossible to discharge exhaust air 12' above ground by a gravity system, since many of the i~ases are heavier than air. The only way to do this is by a mechanical means. COMMITTEE ACTION: Reject. See Committee Action on Proposal 99-107 (Log #280).
COMMITFEE STATEMENT: Proposal would delete an acceptable tion for ventilation.
ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 (ANE), 18 (PIP) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 (ANE), 16 (PIP) NOT RETURNED: Fan (PIP), Shoemaker (PIP)
(Log #103) Committee: HEA-PIP
99-109 - (4-3.1.3.1 (New)): Acceptin Principle SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Add the following under 4-3.1.3.1:
NOTE: The following publications may be used for technical reference: ASTM G65, Guide for Evaluating Nonmetallic Materials for Oxygen
Service. ASTM C,88, Guide for Designing Systems for Oxygen Service. ASTM G93, Practice for Gleaning Methods for Material and
Equipment Used in Oxygen-Enriched Environments. ASTM G94, Guide for Evaluating Metals for Oxygen Service. Add the following in Apgendix B under B-1.2.3: ASTM G63-87, Guide for Evaluating Nonmetallic Materials for
Oxygen Service. ASTM G88-90, Guide for Designing Systems for Oxygen Service. ASTM G93-88, Practice for Gleaning Methods for Material and
Equipment Used in Oxygen-Enriched Environments. ASTM G94-90, Guide for Evaluating Metals for Oxygen Service.
SUBSTANTIATION: NFPA 99 presently does not reference any technical sources for evaluating the suitability of materials for use in oxygen systems. COMMI'VI'EE ACTION: Accept in Principle.
Insert submitter's recommendation of list of documents as new endix C~.7, Oxygen Service Related Documents.
FAg STATEMENT: Standards listed are not directly related to medical gas systems, but are general documents of related interest. Placement in Appendix C is considered more appropriate location. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #84) Committee: HEA-PIP
99- 110 - (4-3.1.8.5): Accept SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise sentence 4 to read:
Pressure relief valves set at 50 percent above normal line pressure shall be vented to the outside if the total capacity of the supply system is in excess of 3000 cuft of gas. (Changes are underlined). SUBSTANTIATION: In 1993, NFPA changedthe requirements from 2000 cu ft to 3000 cuft for cylinder and cylinders in storage. The change in 1993 did not include the change requirements for the venting of the relief discharge from 2000 cu. ft. to 3000 cu ft. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #86) Committee: HEA-PIP
99- 111 - (4-3.1.8.5): Reject SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Throughout the text, all references to "pressure relief valve" should be changed to "pressure safety valve". SUBSTANTIATION: Pressure relief valves are used to relieve liquid pressure and pressure safety valves are designed to relieve gas pcressure.
OMMITTEE ACTION: Reject. COMMITrEESTATEMENT: Committee desires to standardize on the use of the term 'pressure relief valve.' See Committee action on Proposal 99-137 (Log #4). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #77) Committee: HEA-PIP
99-112 - (4-3.1.8.7): Accept in Principle SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Delete text: All final line regulators shall be duplexed with isolating valves.
SUBSTANTIATION: The only mechanism in the industry that will maintain a reduced pressure downstream as well as upstream of the piping system is a pressure regulator. Without flow anyvalve on the market will equalize the pressure on both sides of the bypass. COMMITTEE ACTION: Accept in Principle.
1. Revise 4-3.1.8.7 to read: "All final line regulators shall be multiplexed with isolating ~lves to permit service to the regulator without completely shutting down the gas piping system. Each of the regulators shall be sized for 100 percent of the system peak calculated demand at design condition."
2. Revise Figures 4-3.1.5, 4-3.1.6, 4-B.1.7, 4-3.1.9 to reflect change of item 1.
3. Revise 4-3.1.9.7, last paragraph "All final regulators..." to read as follows: "All final line regulators shall be multiplexed with isolating valves to permit service to the regulator without completely shutting down the gas piping system. Each of the regulators shall be sized for 100 percent of the system peak calculated demand at design condition." COMMITI'EE STATEMENT: Committee believes intent of submitter was the deletion of the allowance of three-valve bypass. Committee action addresses additional paragraph and figures for correlation.
43

N F P A 9 9 - - F 9 5 R O P
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #101) Committee: HEA-PIP
99-113- (4-3.1.8.7): Accept in Principle SUBMITTER: David B. Mohile, Medical Engineering Services, Inc. RECOMMENDATION: Delete 4-3.1.8.7, an~l the last sentence of the last paragraph under 4-3.1.9.7. SUBSTANTIATION: We currently permit installing a manifold with a simplex final regulator with a three-valve bypass. This is a very dangerous practice. If the bypass is opened to allow for service of the regulator, high pressure gas will be allowed to enter the hospital pipelines. In the case of tank oxygen, medical air or nitrogen, this pressure could be as high as 300 psig. In the case of nitrofis oxide this pressure could be as high as 185 psig. Regarding medical air compressors, we need to remove the choice
of either simplex regulators with bypass or duplex regulators, and mandate the duplex regulators in all cases. Current installation practice is dual regulators and we should concur. COMMITTEE ACTION: Accept in Prindple. See committee action or~ Proposal 99-112 (Log #77).
COMMITTEE STATEMENT: Committee acdon on Proposal 99-112 (Log #77) addresses the issue raised here. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #193) Committee: HEA-PIP
99-114- (4-3.1.8.7): Reject SUBMITTER: Leo G. Foxweil, ITT Hartford RECOMMENDATION: Revise existing 4-3.1.8.7 in.the second line to add after the words "with isolating valves" or check valves, and then continue.. SUBSTANTIATION: This revision is made to be compatible with 4- 3.1.8.4. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Check valves would not provide the level of safety considered necessary for servicing regulators. NUMBER OF COMMrI'YEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrI'rEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
CLog #3) Committee: HEA-PIP
99-115 - (4-3.1.8.8(c), 4-3.1.8.8, Figure 44.1): Accept in Principle in Part SUBMITTER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Revise text: 4-3.1.8.8(c) "The inlet shall be female NTP sized to carry the
anticipated volume." 4-3.1.8.8 " . . . It shall be labeled "EMERGENCY LOW PRESSURE
GASEOUS OXYGEN INLET" (Low pressure being less than 100 psig)"
Figure 4-4.1 Change reference to paragraph 4-3.1.10 to paragraph 4-3.1.8.8. SUBSTANTIATION: CGA 540 is a high pressure oxygen connec- tion (3,000 ~sig or higher). "The Emergency Oxygen Supply Connection' referredto in paragraph 4-3.1.8.8 is connected to the hospital's oxygen pipeline which operates at a nominal 50 psig. All bulk o en su liars in the ast have had an eme enckcy ~xyg,o en xyg pp p rg supply connection located in the bulk unit installation which is a female NTP. In addition, CGA 540 would not have suiticient flow capacity at 50 jasig and i t is the customary inlet fitting to a high pressure regulator, not the outlet fitting of any regulator.
Low pressure to be added to the label to alert personnel NOT to attach a higher pressure (above 75 psig) source. See Figure 4-4.1 which shows "Emergency Low Pressure Oxygen
Connection (see 4-3.1.10)." Note: This reference was to paragraph in 1990 edition. Correct paragraph in 1993 edition is 4-3.1.8.8. COMMITrEE ACTION: Accept-in Principle in Part.
1. Revise submitter's recommendation for 4-3.1.8.8(c) to read: "The inlet shall be female NTP, sized for 100 percent of the system demand at the emergency source gas pressure."
2. In submitter's recommendation for 4-3.1.8.8, delete "(Low pressure being less than 100 psig.)".
Other recommendations are accepted as submitted. COMMITTEE STATEMENT: 1. The 540 has a defined orifice, and is too small for the purpose intended.
2. Pressures delivered can be over 100 psig. Recommendation is unnecessarily restrictive. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #40) Committee: HEA-PIP
99- 116 - (4-3.1.8.9 (New)): Reject SUBM1TTER: David B. Mohile, Medical Engineering Services RECOMMENDATION: Add a new section which reads
"The oxygen, nitrous oxide, medical air, nitrogen and other medical gas systems shall be connected only to medical gas piping distribution systems used for direct patient application and shall not be used for any other purpose such as laboratory, soiled or clean central sterilizing, dental prosthetics, housekeeping, morgue (other than breathing purposes), or other equipment needs." SUBSTANTIATION: We state some of the above in 4-3.1.9.1 for the medical air. However, we have inadvertently left off the same warning for oxygen and other medical gases in the hospital. As a result, many times medical oxygen and other gases are used for laboratory and other usages. In one facility the medical oxygen was run to a dental lab to he connected with a propane gas line for use as an oxyacetylene torch. This wording wouldprevent any designer from interpreting the code to allow this usage in the future. In another facility medical air was used in the soiled sterile processing area to blow down contaminated instruments prior to cleaning and sterilizing. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: The proposal limits the ability of health care facilities to usepiping systems. If piping systems can be used for multi-purposes with appropriate safeguards, that should be done. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #{_20) Committee: HEA-PIP
99- 117- (4-3.1.8.9 (New)): Reject SUBMITTER: David B. Mohile, Medical Engineering Services, Inc. RECOMMENDATION: Add a new section which reads, "The oxygen, nitrous oxide, medical air, nitrogen and other medical gas systems shall be connected only to medical gas piping distribution systems used for direct patient application and shall not be used for any other purpose such as laboratory, soiled or clean central sterilizing, dental prosthetics, housekeeping, morgue (other than breathing purposes), or other equipment needs." SUBSTANTIATION: We state some of the above in 4-3.1.9.1 for the medical air. However, we have inadvertently left off the same warning for oxygen and other medical gases in the hospital. As a result, many times medical oxygen and other gases are used for iaboratoryand other usages. In one facility the medical oxygen was run to a dental lab to be connected with a propane gas line for use as an oxy-acetylene torch. This wording would prevent any designer from interpreting the code to allow this usage in the future. In another facility medical air was used in the soiled sterile processing area to blow down contaminated instruments prior to cleaning and sterilizing. COMMITTEE ACTION: Reject.
See Committee Action on Proposal 99-116 (Log #40). COMMITTEE STATEMENT: This proposal is a duplicate of Committee Action on Proposal 99-116 (Log #40). NUMBER OF COMMITTEE MEMBERS I~IGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
44

N F P A 9 9 - - F 9 5 R O P
(Log #267) Committee: HEA-PIP
99-118 - (4-3.1.9): Accept in Principle SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Show one condensate trap per aftercooler for conformance to text (4-3.1.9.7, last paragraph, "...individual condensate traps"). SUBSTANTIATION: Figure and text contradict. COMMITTEE ACTION: Accept in Principle. See committee action on Proposal 99-119 (Log #78).
COMMITTEE STATEMENT: Proposal is similar. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrVrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #78) Committee: HEA-PIP
99- 119 - (Figure 4-3.1.9): Accept in Principle in Part SUBMITTER= Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise drawing to reflect a separate condensate trap for each aftercooler and a separate condensate trap for the air receiver. SUBSTANTIATION: Drawing shows two after coolers with a single condensate trap for aftercoolers and air receiver, the air receiver should have its own condensate trap. COMMITI"EE ACTION: Accept in Principle in Part. Add to Fig. 4-5.1.9 a condensate trap for each after-cooler. Remove
the common trapshown. COMMITTEE STATEMENT: Committee believes the automatic drain, in combination with the receiver, serves the same purpose of a condensate trap. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #212) Committee: HEA-PIP
99-120 - (Figure 4.3.1.9): Accept in Principle SUBMITTEPa CorkyJ. Bishop, Medical G ~ Management, Inc. RECOMMENDATION: Show dewpoint and carbon monoxide monitors between the sample connection valve and the source shutoff valve. SUBSTANTIATION: Bring the diagram up to current standards. COMMITrEE ACTION: Accept in Principle. Add arrow between sample connection valve and source shutoff
valve and following text "Connection point for dewpoint monitor, carbon monoxide monitor." COMMITIT~ STATEMENT: Adding arrow is considered to meet the intent of the submitter's recommendation, and reflect text in document. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #263) Committee: HEA-PIP
99- 122 - (4-3.i.9.1 (b)): Accept in Principle in Part SUBMITrEI~ Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Add the underlined: Separation of the oil-containing section from the compression
chamber by ~t least two seals which create and area open to atmosphere which allows direct and unobstructed visual inspection of the interconnecting shaft fQr daily confirmation bv the facilitv ooerators ofnrooer seal ooeration without disassembly of the comore~or. "The vent and insoection onenin~(s) shall each be no smaller than 1.5 shaft d iameter in size." - SUBSTANTIATION: The intent of the original proposal was two fold: 1) to provide double fault failure protection from migration of oil or hydrocarbon into the compressor and into the facilities' medical gas system, and; 2) to allow a means for the facility to detect a seal failure of the oil retaining seal before it could be drawn into the compressor. This proposal adds darity to the intent and insures the facility of
proper venting and inspection capability. Original proposal had no rejection criteria to protect facility operators. COMMITTEE ACTION: Accept in Principle in Part.
In submitter's recommendation, delete the word "daily." COMMITI'EE STATEMENT: Interval for inspection can vary widely, and should be determined by manufac&urer and user based on usage, etc. NUMBER OF COMMI'ITEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITIT.E ACTION: AFFIRMATIVE: 15 NEGATIVE: Brittain NOT RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: BRITTAIN: "1.5 shaft diameters" This is ambiguous. Which
diameter? Shafts usually have multiple diameters. The reference should be ~ as to a diameter (i.e., 2 in. diameter).
(Log #57) Committee: HEA-PIP
99- 123 - (4-3.1.9.2): Accept in Part SUBMITIT~ David Esherick, Patient Instrumentation Corp. RECOMMENDATION: Add:
The medical air intake may be soft soldered. (After 20 ft. (6m) above the ground.) SUBSTANTIATION: The medical air intake is not a pressure line so therefore our reasoning for brazing this line does not apply. Since we deal with construction we should clarify what is necessary here. COMMrUI'EE ACTION: Accept in Part. Add the following paragraph (c) to 4.3.1.9.2: "(c) The medical air
intake shall be permitted to be soft soldered. COMMITTEE STATEMENT: 20 foot distance criteria is not
eUMBrmain to the issue. ER OF COMMITIT..E MEMBERS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP78) Committee: HEA-PIP
99-121 - (4-3.1.9.1; 4-3.1.9.5): Accept SUBMITTER: Technical Committee on Piping Systems RECOMMENDATION: 1. Delete sentence 1 in 4-3.1.9.1.
2. Move sentence 4 of 4.3.1.9.1, including NOTES 1 and 2, and make it new paragraph 1 of 4-3.1.9.5.
3. Delete p ~ a g ~ p h 1 of existing NOTE 3 in 4-3.1.9.1. SUBSTANTIATION: Present wording in 4.3.1.9.1 implies that the definition in Chapter 2 is the requirement for medical air compres- sops. Readers must now proceedto 4-3.1.5 to complete a full understanding of the requirement.
The new order recommended would end the fragmentation, and concentrate requirements to improve user friendliness and enforcement. COMMITI~E ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #66) Committee: HEA-PIP
99-124- (4-3.1.9.2): Accept SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise sentence I to read:
Except as provided in 4-3.1.9.2(a), the intake to medical air compressors shall be located outdoors above roof level, a minimum distance of 10 ft. (3m) from any door, window, e x h a ~ other intake, or opening in the building. (Changes are underlined). SUBSTANTIATION: Added the word "exhaust" to the restrictions of the medical air compressor intake. Although it is good engineer- ing practice, we felt it should be included in the standard. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMM1TI?EE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
45

N F P A 9 9 u F 9 5 R O P
(Log #3!8 ) Committee: HEA-PIP
99-125 - (4-3.1.9.2(a)); Accept SUBMITrER: Milton P. Smith, Nash Engineering RECOMMENDATION: Revise text as follows: Add to end ofpara (a): "Ventilating systems with internally mounted motors and drive
systems, i.e.,belts, couplings and bearings, cannot be used as a source of medical air supply." SUBSTANTIATION: 1. Operation and/or failure of these devices will input hazardous/toxicgas fumes into the medical air supply.
2. HVAC filtration is not designed to stop gas fumes, therefore, will not prevent patient exposure. COMMITFEE ACTION: Accept. Insubmitter's recommendation, change "can noC to %hall not."
COMMITTEE STATEMENT: Conform to NFPA Style Manual. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #225) Committee: HEA-PIP
99-120- (4-3.1.9.3, 4-~1.9.4): Accept SUBMrITER: Antonio A~ Mesa, Nash Engineering Co RECOMMENDATION: Re-arrange organization of requirements so they will read consistently with the new order being proposed for both gas and vacuum source sections.
Topic
Multi Plexlng
Back-Up Operat,on
Alteration
Disconnects & Controls
Power Source
Gas From: To: From:
4-8.1.1 (a)
4-8.1.1(c)
4-8.1.1(b)
4-8.1.1(e)
,t-8.1.1 (d)
4-3.1.92. 4-3.1.9.$
4-3.1.9A 2nd 4-3.1.9.4 (a) Sent 4-3.1.9.4 (b) 4-3.1.9A (a) 4-3.1.9.4(b)
4-$.1.9.4 1st 4-$.1.9A(c) Sent. 4-3.1.9.4(c) 4-$.1.9.4(d) 4-3.1.9A (d)
Vacultm To:
4-8.i.1 (a)
4-&l.l(b)
4-8.1.1(c)
4-8.1.1(d)
d-8.1.1(e)
SUBSTANTIATION: User friendliness. COMMITI'EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 ' VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
( Log #227) Committee: HEA-PW
99- 127- (4-3.1.9.3, 4-3.1.9.4): Accept SUBMITTF.a~ Antonio A. Mesa, Nash Engineering Co
RECOMMENDATION: Delete 4-3.1.9.3 and 4-3.1.9.4 and substitute the attached. Please coordinate committee action with vacuum proposal. 4-3.1.9.3 Multiple Pumps. Two or more compressors shall be
installed that serve this system alternately or simultaneously on demand. The compressor(s) shall be sized to serve peak demand with the largest compressor out of service. Each compressor shall have an automatic means to prevent backflow through off-cycle units and a slmt-offvalve to isolate it from the centrally piped system and other compressors for maintenance or repair without loss of pressure in the system. 4-3.1.9.4(a) Backup Operation. A device shall be provided to
automatically activate the additional compressor(s) if the unit in operation is incapable of adequately maintaining pressure. A local audible and visual alarm and a master alarm signalshall be provided to indicate when the reserve or off-duty compressor is in operation.
4-3.1.9.4(b) Ahemation. Compressors shall be provided with automatic or manual alternation to allow division of operating time. If antomatic alternation of compressors is not provi~led, the facility shall arrange a proper schedule for manual alternation.
4-3.1.9.4(c) Motor Controls. Each compressor shall be provided with a dedicated disconnect switch, motor starting device and overload protection. The disconnect switcl'~es shall be installed in the electrical circuit ahead of each motor starter, circuitry shall be arranged so that control and alarm functions remain energized while any compressor in the system remains electrically on line.
4-3.1.9.4(d) Electrical Power. Electrical equipment and wiring shall conform to the requirements of NFPA 70, National Electrical Code. Emergency electrical service for the compressors shall conform to the requirements of the essential electrical system as described in Chapter 3 of this document. SUBSTANTIATION: User friendiiness and correlation of require- ments with vacuum section. COMMrITEE ACTION: Accept. NUMBER OF COMMITIXE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Fan, Shoemaker
(Log #201) Committee: HEA-PIP
99-128 - (4-3.1.9.4): Accept in Principle SUBMITTER: Henry R. Kaht, Gurnee, IL RECOMMENDATION: Change first paragraph to read: Each compressor shall be provided with a disconnect switch, motor starting device with overload protection and a control circuit transformer. Each compressor system etc. SUBSTANTIATION: When one control circuit transformer is used for two or more compressors and a fault occurs within the circuit, causing the control circuit fuse to be blown, all of the compressors will stop. A control circuit transformer for each compressor will prevent this. COMMrrrEEACTION: Accept in Principle. After sentence one in par. 1 of 4-3.1.9.4, insert the following,: "Each compressor system that utilizes a voltage reducing device
(i.e., transformer) shall have at least two such devices arranged in such a manner that the failure of one device shall not cause an interruption in the operation of the compressor system." COMMITTEE STATEMENT: Allow designer to deride how control circuit is to be constructed. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TOVOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: lfi NOT RETURNED: Fan, Shoemaker
(Log #258) Committee: HEA-PIP
99-129 - (4-3.1.9.4(b)): Accept SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Substitute the following: A signal indicating that the reserve compressor Is running shall
operate a local audio and visual alarm and serve to activate remote master alarms.
Coordinate with vacuum proposal on 48.1.1 (c). SUi~TANTIA.TION: Clarify difference between the requirement for "signal" and "alarm". COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #199) Committee: HEA-PIP
99-130 - (4-3.1.9.5): Reject SUBMITTER: Henry R. Kaht, Gurnee, IL RECOMMENDATION: Revise Paragraph 3:
"type (b), shall monitor air temperature at the immediate discharge of each compressor, before any after cooler, with a "high temperature" switch et~ ~ S ~ A N T I A T I O N : There is confusion by the compressor package manufactures and certifiers as to the intent of the present require- ment. The practical solution seems to be to locate the high temperature switch as close to the discharge of the compressor as possible but before the after cooler. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Proposal would reduce safety by having only one temperature sensor per compressor rather than the current one per cylinder. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Alien NOT RETURNED: Fan, Shoemaker
46

NFPA 99--- F95 ROP
EXPLANATION OF NEGATIVE: ALLEN: The desired result of this provision in the standard is to
protect the user against the supposed hazard caused by overheating of these compressors. The submitter is correct in that the objective can be achieved by alternate arrangements of these temperature sensors. As written, the standard is merely technology restrictive.
(Log #244) Committee: HEA-PIP
99-131 - (4-3.1.9.5): Accept SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Individually identify the requirements for each type compressor within 4-3.1.9.5 as (a), (b) and (c). Make the last sentence pertaining to all compressors as (d). . SUBSTANTIATION: The section is long arid appropriate sections are difficult to reference. COMMITFEE ACTION: Accept. Move par. 4 to beginning of 4-3.1.9.5.
Identify par. beginning "The use of liquid r ing. . ." as "(a)." Identify par. beginning ~The use of permanendy lubricated..." as "(b)'. Identify par. beginning "The use of a medical air compressor.. ." as "(c).~ COMMITI'EESTATEMENT: Editorial. Met intentofrecommen- dation. NUMBER OF COMMITYEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITYEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #245) Committee: HEA-PIP
99-132 - (4-3.1.9.5): Reject S U B ~ Antonio A. Mesa, Nash Engineering Go RECOMMENDATION: 1) Add alarms at 290°F as follows for type A and B compressors:...which shuts down the compressor and activates both master and local alarms at 2~°F.
2) Change last sentence in 4-3.1.9.5 to rea& The cooling water or ambient temperature requirements for any compressor type shall be recommended by the manufacturer. SUBSTANTIATION: High temperatures may effect air quality. Alarms must have criteria for setting, testing and certification. The manufacturer can stipulate cooling requirements necessary to ensure safe operation. I believe 290°F has been used by Squires Cogswell successfully for years. COMMITrEE ACTION: Reject. COMMITI'EE STATEMENT: Recommendation is technology restrictive. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #260) Committee: HEA-PIp
09-133 - (4-3.1.9.5): Accept SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Add as first paragraph: Air compressors shall meet the criteria in 4-3.1.9.1 to be used for
medical air service and shall be alarmed appropriately for conditions which may effect air quality during use or in the event of failure, including: a) water carryover, b) material wear or decomposition, and/or, oil or hydrocarbon carryover. SUBSTANTIATION: 1) To eliminate notion that if the code does not address a compressor type directly, then none of the require* ments apply.
2) To clarify concerns and reasoning for alarms in case "other technology' is applied. COMMITYEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITIq~ ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #213) Committee: HEA-PIP
99- 134- (4-3.1.9.6): Accept SUBMITTER: CorkyJ. Bishop, Medical Gas Management, Inc. RECOMMENDATION: Delete the reference to paragraph (a) of 4- 4.1.2.1 for piping. SUBST.MffI'[AT[ON: Manufacturers continue to use black iron which will rust for the piping in Medical air compressor systems. Paragraph (a) only requires cleaning for oxygen service. COMMITI~E ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 ~" NOT RETURNED: Fan, Shoemaker
(Log #246) Committee: HEA-PIP
99-135 - (4-3.1.9.6): Accept in Principle SUBMITFER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Add the underlined as follows:
of the ASME Boiler and Pressure Vessel Code, and shall be ~alvanized, gUBSTANTIATION: Steel tanks corrode, resulting in rust flakes which may plug drain traps or migrate downstream. Also, galvaniz- ing adds to the longevity of the vessel. COMMITYEE ACTION: Accept in Principle.
In submitter's recommendation, change "galvanized" to "corrosion resistant." COMMITrEE STATEMENT: There are other forms of corrosion resistant receivers other than galvanized. NUMBER O¥ COMI~rlTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #371) Committee: HEA-PIP
99-136 - (43.1.9.6): Accept in Principle SUBMITTER: Mark Allen, Ohmeda Medical Engineering RECOMMENDATION: Replace last sentence 4-3.1.9.6 with:
"Piping within compressor systems upstream of the source shutoff valve shall comply with 4-4.1.2.1 and 4-4.1.4 except that stainless steel shall be permitted to be used as a piping material. Components such as compressors, air receivers, aftercoolers and dryers are permitted to be made of materials suitable for the service." SUBSTANTIATION: The subject of materials within the compres- sor system has been confusing and has led to occasional abuse of the standard. This is particularly true of the various components which are not commercially available in materials compliant with 4-4.1.2.1. The proposal attempts to clarify and allow for the current practice.
COMMITI'EEACTION: Accept in Principle. 1. In submitter's recommendation, in sentence 1, delete "except
that stainless...material." 2. In submitter's recommendation, in sentence 2, delete "air
receivers." 4. Make new last sentence new 4-3.1.9.11.
COMMITI'EE STATEMENT: 1. and 2. Stainless steel is already permitted.
B. Editorial. Make text easier to find in document. NUMBER OF C O M M I ~ MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #4) Committee: HEA-PIP
99-137 - (4-3.1.9.6, Figure 4-3.1.9): Accept SUBMITTER: Peter Esherick, Patient Instrumentation Corporation
I RECOMMENDATION: Revise text: "The receiver shall be equipped with a uressure relief valve . . . "
instead of a SUBSTANTIATION: To be consistent.
Also: Should we state that the pressure reducing valve should be set at 50 percent higher pressure than the highest pressure in the receiver? COMMITTEE ACTION: Accept.
47

NFPA 9 9 - - F95 ROP
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #87) Committee: HEA-PIP
99-138 - (4-3.1.9.7): Accept SUBMITTER: D~e Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text by adding wording underlined:
Final line filters, located upstream of the final line regulators shall be duplexed with appropriate valves to permit service to these devices without shutting down the medical air system. (Changes are underlined). SUBSTANTIATION: Drawing shows change in filter location upstream of regulator, not reflected in written text. C O I ~ E ACTION: Accept. Add text underlined to text in paragraph 6.
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #5) Committee: HEA-PIP
99- 159 - (4-5.1.9.7.1 (New)): Accept SUBMITTER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Add, after "pressure regulators": "and a , pressure relief valve set at 50 percent above nominal line pressure. SUBSTANTIATION: It is shown in Figure 4-3.1.9 but there is no reference in the text. COMMITrF~ ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #247) Committee: HEA-PIP
99-140 - (4-3.1.9.8): Accept SUBMITrEPe Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Change "dryers" to "regulators" as follows:
The monitoring of air quality downstream of the ~ and upstream . . . . SUBSTAWrIATION: Sampling is implied to be done at the sample connection, which is after the dryers, final filters and pressure regulating valves. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #370) Committee: HEA-PIP
99- 141 - (4-3.1.9.8): Accept in Principle SUBMITTER: Mark Alien, Ohmeda Medical En[gineering RECOMMENDATION: Rewrite 4-3.1.9.8 to read:
"The monitoring of air quality and the monitoring system response shall be in accordance with Table 4-3.1.9.8 (exception: existing piping systems provided such piping systems do not constitute a distinct hazard to life.)
Monitoring devices or samples shall be placed or taken at a point immediately downstream of the line regulators and filters."
(Table unchanged) SUBSTANTIATION: The proposal attempts to clarify appropriate practice for these tests. COMMITTEE ACTION: Accept in Principle.
See committee action on Proposal 99-140 (Log #247). COMMITTEE STATEMENT: Action in Proposal 99-140 (Log #247) addresses the issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
(Log #248) Committee: HEA-PIP
99-142 - (Table 4-3.1.9.8): Accept in Principle S L I B ~ Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: 1. Increase table size.
2. Spell out each gas to be monitored, not just dew point, and delete abbreviations.
3. Add frequency and alarm columns to each criteria. 4. Use letters LAand MA to indicate local and master alarms where
applicable. SUBSTANTIATION: 1. Table carries many requirements now carried as small subscript, easily unnoticed.
2. Clarity. 3, Consistency. 4. Clarity.
COMMITTEE ACTION: Accept in Principle. For item 4, use "Local alarm" and "Master alarm" instead of "LA
and "MA." COMMITrEE STATEMENT: Editorial. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
CLog #25~) Committee: HEA-PIP
99-143 - (Table 4-3.1.9.8): Accept S U B ~ Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Change first note under table to read:
Reference Table 4-5.1.3.10 for alarm criteria. SUBSTANTIATION: Effective way m reference all alarm criteria, no t jns t dew point. COMMITTEE ACTION: Accept.
Change reference in NOTE from 4-4.1.1.2(g) to 4-5.1.3.10. NUMBER OF COMMITTEE MEMBERS ELIGIBLETO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #94) Committee: HEA-PIP
99-144 - (4-3.1.9.8.1 (New)): Accept in Principle SUBMITrgR: David B. Mohile, Medical Engineering Services, Inc. RECOMMENDATION: Add a new paragraph to read as follows:
"A valved sample port shall be provided downstream of the final line pressure regulators and upstream oft.he source shut off valve in order to allow for sampling of the medical air produced on a regular basis. This port shall be valved and terminate in a 1 /4 in. female threaded port which shall be plugged with a removable br'4ss plug." SUBSTANTIATION: Figure 4-3.1.9 shows a sample connection valve, but we do not spedfy or mention it in the written text of the code. By defining its location and makeup this clarified the requirement. COMMITrEEACTION: Acceptin Principle. Revise submitter s recommendation by ending paragraph after
"medical air." Paragraph would read as follows: "A valved sample port shall be provided downstream of the final
line pressure regulators and upstream of the source shut off valve to allow for sampling of the medical air." COMMITrEE STATEMENT: To allow facilitate the testing reqtiired in other paragraph. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
48

N F P A 9 9 - - F 9 5 R O P
G (Log #CV66)
ommittee: HEA-PIP 99- 145 - (4-3.2.1 and 4-3.2.2): Accept $UBMITTER: Technical Committee on Piping Systems RECOMMENDATION: 1. Revise the existing text in 4-3.2.2 by deleting reference to only 4-3.1.2.1 (j) and (k), and instead reference 4-3.1.2.1(a) thrn (k). Section 4-3.2.2 would thus read as follows:
4-3.2.2 Supply system and storage locations shall comply with 4-3.1.2.1 (a) through (k) [except 4-3.1.2.1 (k) (3)], and 4-3.1.2.3.
2. Revise 4-3.1.2.10) (3) by deleting the word medical. SUBSTANTIATION: There are several areas in the non-flammable medical gas type II section that have inaccuracies and revisions are required to improve and clarify the intent of the standard.
In 4-3.2.2, reference to 4-3.1.2.2 is deleted as it references a storage system that is >3000 cu ft and is no t compatible with type II systems.
In 4-3.1.2.1, no compressor system should be in a type I or type II cylinder room. It should not just be restrictive to medical air compressor systems. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP72) Committee: HEA-PIP
99-146 - (4-3.2.3): Accept SUBMITTER: Technical Committee on Piping Systems RECOMMENDATION: Revise 4-3.2.3 as indicated below.
1. Re-title existing 4-3.2.3 to read as follows: "4-3.2.3 Compressed Gas (Air/N2) Supply Systems for Power
Devices." 2• Delete existing 4-3.2.3.1, except NOTE. 3. Modify existing NOTE in 4-3.2.$.1 to read as follows, and transfer
to 4-3.2.3: NOTE: Type Ill compressed air and Nitrogen gas systems are
primarily used to drive gas-powered power devices. Similar applica- tions are in podiatry and plastic surgery. Examples of these are air to drive turbine-powered drills and air to dry teeth and gums. Some dental hand pieces have an internal self contained air return system, while other hand pieces may discharge air in the atmosphere. Some may discharge a mixture of air and water. Nitrogen is often piped as an alternate or reserve supply to the compressor system
4. Add new 4-3.2.3.1 to rea&as follows: 4-3.2.3.1 Type Ill Compressed Air Supply Systems. (See new Figure
4-3.2.3.1) Compressed air shall be provided bya Type 1II com- PSressed air system as defined in Chapter 2.
• Renumber existing 4-3.2.3.2 as new 4-3.2.3.1 (a) and replace the first word "Dental" with the words "Type III" so as to read:
Ca) ~ compressed air shall be permit ted to be used to power air-powered devices for evacuation only if the exhaust of the evacuation device is a closed vent to the outside of the building. (change is underl ined) 6. Renumber existing 4-3.2.3.3 as new 4-3.2.3.2.1 (b) 7. Renumber existing 4-3.2.3.4* as new 4-3•2.3.2.1 (c)*. 8. Revise existing 4-3.2.3.5 and renumber as new 4-3.2.3.1(d) as
follows: (d) Each system installation shall include appropriate disconnect
switch(es), motor-starting device(s) and motor overload protection device(s). For single, duplex, or multicompressor systems, a means for activation/deactivation each individual compressor shall be provided by the supplier or contractor. When multiple compressors are used, alternation of units, and a means to activate the additional unit(s) should the in-service unit(s) be incapable of maintaining adequate pressure, shall be provided Manual or automatic switchover shall be permitted.
9. Revise existing 4-3.2.3.6* and renumber as 4-3.2.3.1 (e)* as follows:
. (e) Type III Compressed Air Systems shall be equipped with intake filter-muffler(s) of the dry type; receiver(s); shutoffvalves; air dryer(s); in-line final particulate filters rated at 5 microns, 98 percent efficiency, with filter status indicator; and downstream pressure regulator(s) to ensure the delivery of compressed air with a maximum allowable 0.05 ppm liquid oil and 40% relative humidity at operating pressure and temperature The air intake shall be from outside the building when practical or shall be located within a room where no chemical-based material is stored or used.
The compressor air intake shall be located where no contamina- tion from vacuum system discharges or particulate matter is anticipated. The compressor air intake shall be taken from a space other than an opera toryand other than the room or space in which there is an open or semi-open discharge from aType 1I vacuum system. (See new Figure 4-3.2.3.1.)
10. Revise existing 4-3.2.B.7 and renumber as4-3.2.3.1(f)-as follows:
(0 The system shall be equip~,ed with a pressure relief valve, pressure gauge, and receiver wtth drain plug or a manual drain or an automatic drain. Receiver(s) shall have the capacity to ensure practical o n / o f f operation of the compressor(s). Receiver(s) shall comply with Section VIII ("Unfired Pressure Vessels") of the ASME Boiler and Pressure Vessel Code.
11. Revise existing 4-3.2.3.8 and renumber as 4-3.2.3.1 (g)* as follows:
(g)* An appropriate moisture indicator shall be provided. The moisture indicator shall be located in the active air stream prior to or after the receiver but upstream of any system pressure regulators•
The moisture indicator shall indicate if the relative humidity of the compressed air exceeds 40 percent at line pressure and temperature.
12. Add new 4-3.2.3.1 (h) to read as follows: (h) An oil indicator sensor per 4-3.2.3.1 (e) shall be located
downstream of the receiver as shown in figures 4-3.2.3.1 & 4-3.2.3.2. The oil indication device shall be capable of measuring an oil concentration of 0.05 ppm with an accuracy of+ 0.03 ppm in compressed air at 80 to 100 psig.
13. Revise existing 4-3.2.3.9and renumber as 4-3.2.3.1 (i) as follows:
(i) Any service outlet of a ~ compressed air system that allows for a temporary quick-attach connect ion shall be labeled with the pressure identified as dental compressed air and a warning against using the air for medical air purposes. (changes underl ined)
NOTE: An example of a label:
TYPE III COMPRESSED AIR DO NOT USE FOR MEDICAL AIR PURPOSES
The service outlet shall no t be interchangeable with the medical air station outleL
14. Renumber existing 4-3.2.3.10 as n e w 4-3.2.3.1 (j). 15. Add a new 4-3.2.3.2 to read as follows: 4-3.2.3.2 Nitrogen Gas Supply Systems. (See Proposal 99-147 (Log
#CP73).) REFER to Figure 4-3.2.3.6 in Proposal 99-148 (Log #CP71)
SUBSTANTIATION: The existing dental compressed air definition defines a requi rement as follows: Grade D cylinder air or locally compressed air with:
Maximum humidity of 40% at l inepressure and temperature. Filtered to 5 microns or less with 98% efficiency or better. There is no oil contamination specified. No contaminants in the form of particulate matter, odor, oil
vapor, or other gasses have been added by the system The reference to cylinder air is not realistic. Cylinders of air are
no t used. Locally compressed air or cylinder ni trogen is used. Grade D can have a liquid oil content of 5 milligrams / cu. meter• The requirement of Grade D is no t sufficient for "bonding" purposes in dental procedures•
The ADA task force has def'med the quality of dental air. Their work in part is derived from specifications by USAF. Parameters considered appropriate are:
Relative humidity of 40% at operating pressure. Oil Contamination of 0.05 ppm w/w, at an accuracy of 20%. Particulate matter limit < 5 microns at an accuracy of 20%, no
milligrams per cu. meter are defined. Input from various manufacturers and also f rom the ADA indicates
that the 0.05 ppm is a reasonably attainable oil level• ( Coalescing filters can usually attain 0.01 ppm)
There is agreement on a particulate level of<5 microns with a 98% efficiency with an inlet condition of 20 to 50 ppm.
The manufacturers prefer a 40% RH at line pressure and temperature as that can be easily moni tored by a disk indicator. It is calculated that the 40% RH at line pressure would provide a pressure dew point slightly below or at 4IF.
Testing. A dreager tube measurement can be obtained with either a 1 to 10 milligram, or 2.5 to 10 milligram standard measurement tubes and would not be the test of choice. Johnson Controls makes a Model A4000 disposable instrument ($30-$40) that provides periodic one time testing by flow through a color die indicator over a 4 hour interval. It reportedly can read 0.05 ppm.
The agreed upon parameters to define the quality of air produced by the dental compressed air system is as follows:
Locally compressed air with: Maximum Relative Humidity of 40% at line pressure and
temperature. Fil tered to 5 microns or less with 98% efficiency or better. Maximum allowable Oil Contamination of 0.05 ppm w/w,
COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
49

N F P A 9 9 - - F 9 5 R O P
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP73) Committee: HEA-PIP
99-147 - (4-3.2.3): Accept S U B ~ Technical Committee on Pipinl~ Systems RECOMMENDATION: After renumbering exrsting 4-3.2.3 in accordance with proposal 99-200 (Log #72), add the following new text:
4-3.2.3.2 Type III Nitrogen Gas Supply Systems (See new Hgure 4-3.2.3.2).
(a) The nitrogen operating pressure shall be designed for operating pressures below 160 psig for consideration as type III.
NOTE: If Nitrogen is used as a backup supply to a compressed gas system, the Nitrogen operating pressure should be regulated so not to exceed the operating pressure of the Type III compressed air system.
(b) Supply Systems providing Nitrogen Gas to power devices shall use Nitrogen Oil-Free, Dry as defined in Chapter 2.
(c) Type III Nitrogen systems shall either have regulator(s) mounted on the individual cylinder(s) or the cylinder(s) can be connected to a manifold via pigtail and pressure regulated at the manifold. The cylinder(s) shall be individually secured to prevent fall ing. .
(d) T h e nitrogen cylinder gas supply shall be permitted to be independent of the 3000 cu ft consideration for Type II Pa t i en t Nonflammable Medical Gases classification. Nitrogen gas cylinder storage in compressor rooms and also in the same storage area with nonflammable medical gases shall be permitted.
NOTE: The ol ft of stored Nitrogen gas is not restricted. (e) Cylinder storage shall avoid direct heating from steam, hot
water or other indirect means, cylinder temperatures shall not exceed 130F (54C).
(f) The nitrogen gas supply system shall be asystem of cylinders and necessary supply equipment assembled with that will permit alternately supplying the required supply gas. When the content of one primary cylinder ins unable to supply the normal operating pressures, the secondary cylinder(s) shall be activated manually. Automatic switch over shall be permitted.
(g) Where nitrogen gas is used as a backup for a type 11I com- pressed air system, a check valve and shut offvalve shall be located in each supply line prior to the "T" connection to the main line. (See Figure 4-3.2.3.2 following.) SUBSTANTIATION: Industry practice is to use nitrogen to power dental dynamic devices as an alternated to dental compressedair. In some applications, the nitrogen system is used as a reserve for the dental compressed air when repairs are required. The.standard does not address this application at the present time. A new section 4-3.2.3.2, Nitrogen Gas Systems for Dynamic Devices, is proposed to address the issue. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(LOg #CP71) Committee: HEA-PIP
99-148 - (Figure 4-3.2.3.6): Accept S U B M I T I T ~ Technical Committee on Piping Systems RECOMMENDATION: Revise existing Fig. 4-3.2.3.6 as follows and as shown in the attached:
1. Change the title to Type 11I Air Compressor System 2. Remove the individual regulators and show that the piping
system terminates in a service outlet, 3. Indicate the inclusion of a source isolation valve and source
shutoff valves in the main piping system. 4. Indicate an optional filter location before the dryer in addition
to the existing location. 5. Indicate optional pressure relief valve location 6. Indicate receiver manual or optional automatic drain locations. 7. Indicate moisture indicator location(s).
8. Indicate oll indicator location. (See Figure 4-3.2.3.6 following.) SUBSTANTIATION: The present drawing of a dental air compres- sor system as shown in Figure 4-3.2.3.6 needs revision to correct several errors. The individual regulators as shown in the upper right side of the drawing are not part of the piping system. The dental compressed air system terminates in individual shut-offvalves prior to the regulators. Secondly, this figure excludes filtration before the filter. COMMITIT._£ ACTION: Accept. NUMBER OF COMMIT1T.E MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #74) Committee: HEA-PIP
99-149 - (Figure 4-4.1): Reject SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Include in Figure 4-4.1, the regulator required for the emergency oxygen fill. SUBSTANTIATION: Drawing Figure 4-4.1, does not include new requirements for regulator in the emergency oxygen fill. COMMITI'EE ACTION: Reject.
See committee action Proposal 99-115 (Log #3). COMMITITAg STATEMENT: Regulator does not exist based on Committee Action on Proposal 99-115 (Log #3). NUMBER OF COMMIT1T~ MEMBERS I~LIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #89) Committee: HEA-PIP
99- 150- (Figure 4-4.1): Reject SUBMITTF~ Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Redraw Figure 4-4.1, toshowthe correct installation of zone valve boxes. SUBSTANTIATION: Zone valves are piped from left (inlet) to right (outlet). By looking at this drawing it appears to make no difference how zone valves are piped. It is very dangerous if the line is mistakenly cut on the pressure side of the valve to do future work, because someone piped the zone valve box backwards. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Schematic is representative only, and is not intended to replace text as to what is required. NUMBER OF CoMMrITEE MEMBERS ELIgIBLE TO VOTE: 18 VOTE ON C O ~ ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #'214) Committee: HEA-PIP
99-151 - (Figure 4-4.1): Reject " SUBMITrgR: CorkyJ. Bishop, Medical Gas Management, Inc. RECOMMENDATION: Change label to Emergency oxygen supply connection (see 4-3.1.8.8).
Note $: see 4-4.1.1.2 (f) SUBSTANTIATION: Delete reference to low pressure since a regulator |s now required. Reference paragraph (f) about the actuator in the main line. COMMITIT, E ACTION: Reject.
See committee action on Proposal 99-115 (Log #3). COMMITrF~ STATEMENT: Committee action of Proposal 99-115 (Log #$) addresses issue. Reference in NOTE 5 has been corrected editorially. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemakei"
50
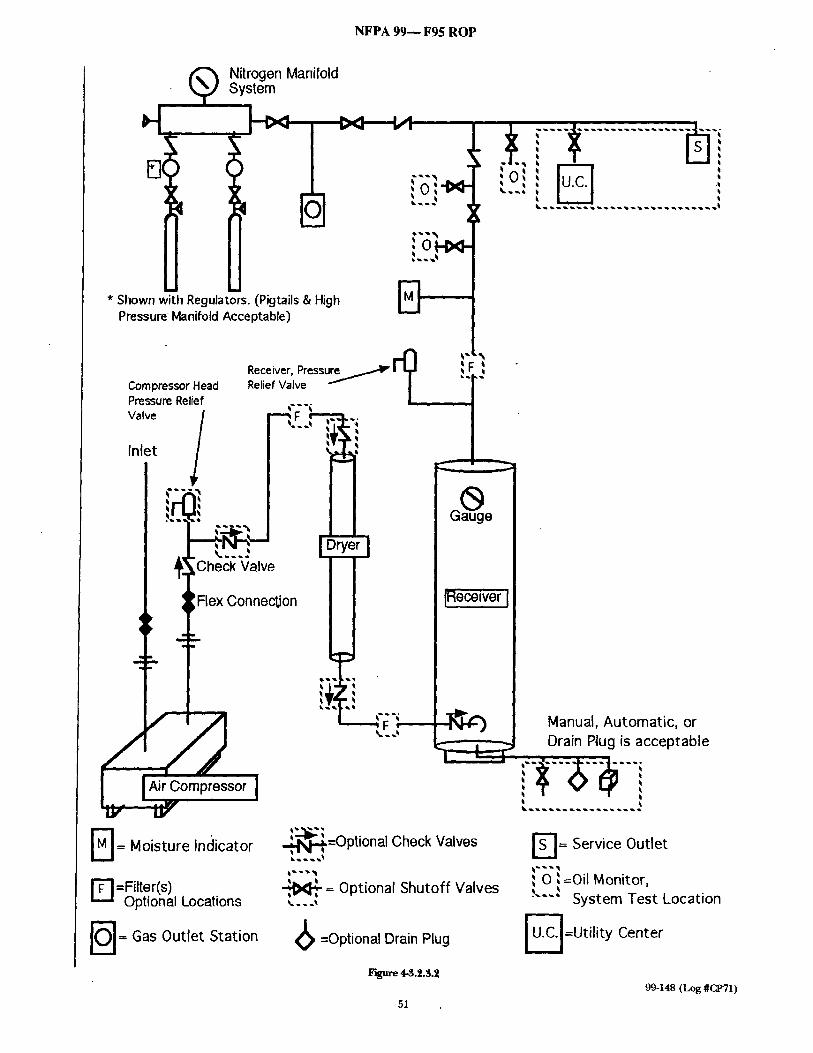
NFPA 99-- F95 ROP
Nitrogen Manifold System
-i
* Shown with Regulators. (Pigtails & High Pressure Manifold Acceptable)
Compressor Head Pressure Relief Valve /
Inlet
F ] = Moisture Indicator
S
Pressure Receiver, Relief Valve
'Y I - GaUge
I_ ~r..~ ~" I DrY er I ~Check Valve
IFlex Connection I Receiver
! i
E3 =Filter(s) Optional Locations
'l--" Gas Outlet Station
Manual, Automatic, or Drain Rug is acceptable
i - - r
d.N.~.=Optional Check Valves
~ = Optional Shutoff Valves
(~ =Optional Drain Plug
F']~tre 4.~.2.3.2
51
'~1 = Service Outlet
I 0 l=Oil Monitor, .~...I System Test Location
~ =Utility Center
99-148 (Log#CP71)

NFPA 99-- F95 ROP
, - - , i iOM: ' ' ' ~ 1 U . C . I
,OM
Receiver, Pressure Relief Valve ~ ,,, '~
Compressor H e a d ~ l _ r l ~'1 "~ Pressure Relief . m m,,,,m / Valve I ...~'~ h....,,.~ I
/ '---' ,,,;~- ~ ,
,o
n ~1~
•
Air Compressor i ~ ~,~ I ~ ! ~ . . . . . . . . . . .~
Manual, Automatic, or Drain Plug is acceptable
= Utility Center (Junction Box, "J-Box")
= Oil Monitor, System Test Location (Optional Locations)
FiKure 4-3.2.&6
= Optional Shutoff Valves ... =Optional Check Valves
I - N I = Moisture Indicator; (optional locations)
[ ~ ] = Filter kocation:(Before or after Dryer or Before or af ter Receiver) t . . . . i
I S 1 = Service Outlet ,b •
u.c.l
IOM I
52
=Optional Drain Plug
99-148{Log#CPfl)

N F P A 99--- F95 R O P
• (Log #341) Committee: HEA-PIP
99- 152 - (4-4.1.1): Reject SUBMYVFER: Mark Allen, Ohmeda Medical Engineering RECOMMENDATION: Rewrite 4-4.1.1 to read:
4-4.1.1 Gas Warning Systems 4-4.1.1.1 General (See Appendix G4.2) (a) All local, master and area alarm panels used for medical gas
systems shall provide: (i) separate visual indicators for each condition monitored. (ii) cancelable audible indication of an alarm condition. The
audible indicator shall p roduce 80 dB measured at 3 feet (1 meter). A second indicated condition occurring while the alarm is silenced shall reinitiate the audible signal.
(iii) visual indication that the audible alarm has been silenced. (iv) indicator lamps in parallel, such that should a single lamp fall,
there continues to be visual indication of the condition, and indication due to change of brightness that the lamp has failed.
(b) Local, master a n d a r e a alarms shall indicate i£ (i) the moni tored condit ion occurs. (ii) the wiring to the sensor or switch is disconnected. (iii) the wiring to the sensor or switch is short circuited. (c) Each local, master and area alarm panel shall be labeled for it's
area of surveillance. Each indicator shall be separately labeled indicating the condit ion monitored.
(d) Where multiple panels are in tended to indicate the same condition, one panel shall be connected directly to the sensor or switch. Other panels may be connected through indirect means such as data trammission lines provided that such indirect means are fully supervised and failure of such indirect transmissions is indicated at all panels so connected.
(e) Local, master and area alarms shall be powered from the life safety branch of the emergency system as described in Chapter 3, "Electrical Systems" or shall include internal power sources (e.g. batteries) to permi t 24 hours of normal operation during power outage. Such internal power sources shall indicate when they are unable to supply the alarm for the necessary 24 hours.
(f) The connect ion of medical gas alarms to a centralized computer (e.g. a building management system) is permitted. The computer shall no t replace any required panel but may be used to supplement any or all panels.
4-4.1.1.9 Master Alarms (a) A master alarm system shall be provided to Monitor the
operation and condit ion of the source of supply, the reserve (ff any) and the pressure of the main line of the medical gas system.
(b) The master alarm system shall consist of two or more alarm panels located in two separate locations. One panel shall be located in the principal working area of the individual responsible for the maintenance of the medical gas system and one or more panels shall be located to assure continuous surveillance during the working hours of the facility (e.g. the te lephone switchboard, security office, or other continuously staffed location).
(e) Each master alarm panel shall include visual indicators for each of the conditions described in 4-4.1.1.2 (b) through (g).
In existing (b) and (d) delete the wording "An audible and noncancellable visual signal shall". Leave "Indicate".
In existing (c) delete the wording "audible and noncancellable visual signal shall". Leave "Indicate".
In existing (e) delete the wording "separate audible and noncancellable visual signals shall indicate". Replace with "Indicate separately".
In existing (f) delete the wording "All medical gas piping systems shall be ~rovided with audible and noncancellable visual signals to indicate . Re~,lace with "Indicate separately for each medical gas piping system '.
In existing (g) reword first paragraph to read: "Indicate separately each of the individual alarms required in 4-3.1.9." Move remainder to new 4-4.1.1.4.
Renumber a m e nded (b) through (g) to become (d) through (i) respectively,
4-4.1.1.3 Area Alarms (a) Area alarms shall be provided in each critical care and
anesthetizing location. (b) Area alarm panels shall be located at or near the nurses station
or other location near the point of use which will provide for responsible surveillance.
(c) Area alarms shall indicate if the pressure in the local line increases or decreases 20% from normal line pressure.
(d) Activating switches or sensors shall be placed in the individual line supplying each such specific area. No valve, other than service , valves located in areas accessible only to authorized personnel, shall intervene between the sensor or switch and the outlets in tended to be moni tored by the alarm. Add new 4-4.1.1.4 Local Alarms
(a) Provide an indicator for each of the individual alarms required in 4-3.1.9 at the air compressor site.
(b) Dew point for medical compressed air shall be moni tored and alarmed per 4-3.1.9.8 to indicate a line pressure d e w p o i n t above 39°F (3.9°C). Move "from the nominal design of 35°F(1.7 °C)" to 4- 3.1.9.7. SUBSTANTIATION: 4-4.1.1.1 General
This section has been reworded for ease of use, consolidating requirements spread all throughout the alarms section.
(a) (iii) visual indication is a new requirement. Panels manufac- tured today have no indication that the alarm has been silenced other than an inference f rom the lamp is being lit and no sound. This is a particular problem with alarms which have been allowed to sound continuously for long periods (e.g. on a construction site) - the sounder wears out. An indication is simple to implement and will guard against this occurrence.
The 80 dB is to ensure that the alarm can be hearcL Canada required 90 dB, which has produced complaints. A reinitiated audible signal upon a second indicated condition is
normal, but should be clearly required to prevent alarms being ignored.
(iv) indicator lamps in parallel guards against a light bulb burning out, or an LED shorting. At present, o ther than the daily "push to test" of C,-4, there is no way to guard against this.
(b) (ii) & (iii) The requirements added here are a guard against damage to a sensor or it 's wiring. Most alarms today already use normally closed circuitry to guard against disconnection, but are no t protected against short circuits in the wiring.
(d) This paragraph brings the 99 into more substantial compliance with the NFPA 72 and standard alarm practice. The present wording uses the term "parallel" which has a distinct electrical definition, which in meaning differs f rom the intent of the NFPA 99 to require only one switch wired as needed to multiple panels. The proposed wording is also less technologically restrictive but equally requires appropriate safeguards.
(e) The use of batteries to power an alarm in the event of a power failure has been suggested for small facilities with limited generation capadty. Appropriately implemented, there is no reason known no t t o p e r m i t such use.
(f) Minor rewording for clarity. 4-4.1.1.2 Master Alartns (b) rewording for clarity and to recognize fxequent limitation of
hours of operation. General rewording of ( b ) t h r o u g h (g) is to reduce redundant wording.
4-4.1.1.3 Area Alarms (d) Location of activating switches brings this section into
harmony with the vacuum section. 4-4.1.1.4 Local Alarms Attempt is to bring the local alarms into the document in a clear
m a n n e r .
(b) Reference to 4-4.1.1.2 (f) is unnecessary. The reference here to the design dew point is inappropriate. This
design requirement should be moved to 4-3.1.9 where other design criteria are place. Allowance for °C or °F is unnecessary. COMMrFrEE ACTION: Reject. , COMMITTEE STATEMENT: Committee finds that new require- ments have been included, which it believes are not necessary. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Kaht NOT RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: KAHT: Section 4-4.1.1 This was originally rejected by the
Committee at the August meeting, then revised by Mark Allen and presented to the Committee again at the September meeting where it was accepted.
I voted no at that time because it is questionable if it is possible to design the 1.e.d. lights for a change in brightness as suggested. Further, the proposal is based on a particular manufacturers design not necessarily superior to other designs available to the market today.
(Log #CP59) Committee: HE/k-PIP
99-153 - (4-4.1.1, 4-3.1.9.7): Accept S U B - - R : Technical Committee on Piping Systems RECOMMENDATION: 1. Revise 4-4.1.1 to read as follows:
4-4.1.1 Gas Warning Systems. 4-4.1.1.1 General (See Appendix G-4.2). (a) All local, master and area alarm panels used for medical gas
systems shall provide:
53
NFPA 9 9 - - F95 RO P
. separate visual indicators for each condition monitored. • cancelable audible indication of an alarm condition.' The
audible indicator shall produce 80 dB measured at 3 ft (1 m). A second indicated condition occurring while the alarm is silenced shall reinitiate the audible signal.
3. the panel shall indicate visually lamp or LED failures (e.g. by change in brightness or a separate indicator).
(b) Local, master and area alarms shall indicate visually and audibly if:
1. the monitoredcondition occurs. 2.. the wiring to the sensor or switch is disconnected. (c) Each local, master and area alarm panel shall be labeled for it's
area of surveillance. Each indicator shall be separately labeled indicating the condition monitored.
(d) Where multiple panels are intended to indicate the same condition(s):
1. at least one panel shall be connected directly to the sensor(s) or switch(es).
2. both Master Alarms required by 4-4.1.1.2(b) shall be connected by dedicated wiring directly to the sensor(s) or switch(es).
3. other panels may be connected through indirect means such as data transmission lines provided that such redirect means are fully supervised and failure of such indirect transmissions is indicated at all panels so connected.
(e) Local, master and area alarms shall be powered from the Life Safety branch of the emergency system as described in Chapter 3, Electrical Systems.
(f) all wiring from switch or sensors shall be protected from physical damage by racewa, ys or conduit in accordance with NFPA 70.
(g) a centralized computer (e.g. a building management system) shall not substitute for any required medical gas alarm panel, but may be used to supplement the medical gas alarm system.
4-4.1.1.2 Master Alarms. (a) A master alarm system shall be provided to monitor the
operation and condition of the source of supply, the reserve (if any) and the pressure of the main lines of all medical gas piping systems.
(b) The master alarm system shall consist of two or more alarm panels located in two separate locations. One panel shall be located m the principal working area of the individual responsible for the maintenance of the medical gas piping systems and one or more panels shall be located to assure continuous surveillance during the working hours of the fadlity (e.g. the telephone switchboard, security office, or other continuously staffed location).
(c) Each master alarm panel shall include visual indicators for each of the following conditions:
1. a separate indicator shall be provided for all systems supplied by a manifold or an alternating type bulk system that has as part of it's normal operation a changeover from one portion of the operating supply to another portion. Indicate when, or just before, this changeover occurs. (See Appendix G-4.1 and C-4.2)
2. when a manifold or bulk supply consists of one or more units that continuously supply the piping system while another unit remains as the reserve supply and operates only in case of an emergency, indicate separately for each system when, or just before, this changeover occurs. (See Appendix C-4.1 and C.4.2)
3. when check valves are not provided for each cylinder lead of the reserve supply for a manifold or bulk supply system, indicate separately for each system when the reserve supply is reduced to one average day's supply. If check valves are provided in each cylinder lead, this signal is not required• (See Appendix G-4.1 and C_~.2.)
4. when a cryogenic liquid storage unit is used as a reserve for a bulk supply system, indicate separately for each system when the contents of the reserve is reduced to one average day's supply and when the gas pressure available in the reserve unit is reducedbelow the pressure required to function properly.
5. indicate separately for each medical gas piping system when the pressure in the main line increases 20 percent or decreases 20 percent from the normal operating pressure. The actuating switch for these signals shall be installed in the main line immediately downstream (on the piping distribution side) of the main line shutoffvalve. (See Appendix C-4.1)
6. indicate each of the individual alarms required in 4-4.1.1.4(a). This shall be either by a separate indicator for each condition monitored or with a single indicator labeled "Medical Air System Fault" or similar wording and which indicates when any of the conditions monitored occurs.
7. provide a separate indicator for each Dew Point and Carbon Monoxide per 4.4.1.1.4 (b) and (c).
4-4.1.1.3 Area Alarms. (a) Area alarms shall be provided for each medical gas piping
system supplying anesthetizing locations and other vital llfe SUl~port and criticai care areas such as postanaesthesia recovery, intensrce care units, coronary care units, etc.
(b) Area alarm panels shall be located at the nurses station or other location which will provide for responsible surveillance.
(c) Area alarms shall indicate if the pressure in the local line increases 20 percent or decreases 20 percent from normal line pressure. (See Appendix G-4.1.)
(d) Activating switches or sensors for critical care areas shall be placed in the individual line supplying each such specific area~ No valve, other than service valves locatedin areas accessible only to authorizedpersonnel, shall intervene between the sensor or switch • and the outlets intended to be monitored by the alarm.
(e) Activating switches or sensors for anesthetizing areas shall be placed in the individual line supplying each such specific area with the individual room shutoffvalve being the only one between the actuating switch and the outlets.
4-4.1.1.4 Local Alarms (a) Provide an indicator for each of the individual alarms required
in 4-3.1.9 at the air compressor site. These indicators shall comply with 4--4•1.1 •1 Ca), (b) and (c) and be grouped together in a single location (e.g. in an alarm panel or with the system controls).
(b) Dew point for medical compressed air shall be monitored and alarmed per 4-3.1.9.8 to indicate a line pressure dew point above 39°F (3.9°C).
(c) Carbon Monoxide for medical compressed air shall be monitored.and alarmed per 4-3.1.9.8 to indicate a level above 10
v~4".'1.1.5. Pressure Gauges for Cases. [Use existing 4-4.1.1.4.]
2. In 4-3.1.9.7, par. 3, revise last sentence to read as follows: "Each dryer system shall be designed toprovide air at a maximum
dew point of 350F (1.7°C) at the peak calculated demand of the system. [See 4-4.1.1.2(c) (vi).]" SUBSTANTIATION: 4-4.1.1.1 General.
This section has been reworded for ease of use, consolidating requirements spread all throughout the alarms section. The General section combines requirements common to all types
of alarms. (a)2. 80 dB is to ensure that the alarm can be heard. Canada
requires 90 dB, which has produced complaints. A reinitiated audible signal upon a second indicated condition is
normal on all manufacturer's panels, but should be clearly required to prevent alarms being ignored.
4. this requirement guards against a light bulb burning Out, or an LED shorting. At present, other than h e daily "push to test" of C-4, there is no way to guard against this.
(b)£. The requirements added here are a guard against damage to a sensor or it's wiring. Most alarms today already use normally dosed circuitry to guard against disconnection.
(d) This paragraph brings the 99 into more substantial compliance with the NFPA 72 and standard alarm practice. The present wording uses the term "parallel" which has a distinct electrical definition, which in meaning differs from the intent of the NFPA 99 to require only one switch wired as needed to multiple panels. The proposed wording is also less technologically restrictive but equally requires appropriate safeguards:
(f) requires the alarms wiring be appropriately safeguarded against damage.
(g) Minor rewording for clarity. 4-4.1.1.2 Master Alarms. (b) rewording for clarity and to recognize frequent limitation of
hours of operation. General rewording of present (b) through (g) is to reduce
redundant wording. Addition of (c)5. is for clarification. Addition of (c)fi. is to address a concern reflected in questions to
the NFPA. 4-4.1.1.3 Area Alarms. Requirements are reworded, but not substantively changed. 4-4.1.1.4 Local Alarms. Attempt is to bring the local alarms into the document in a clear
manner. The reference here to the design dew point is inappropriate. This design requirement should be moved to 4-3.1.9 where other design criteria are placed. Allowance for °C or °F is unnecessary. Dew point and CO Alarlm are clearly spelled out for ease of
understanding. COMMrITEE ACTION: Accept. NUMBER OF COMMITTEE MEMBER$ ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
54

NFPA 99-- F95 ROP
(Log #119) Committee: HEA-PIP
99- 154- (4-4.1.1.1): Accept SUBMITTER: David B. Mohile, Medical Engineering Services, Inc. RECOMMENDATION: Delete items (a), (b), and (c). Re letter (d) and (e). SUBSTANTIATION: Item (a) is covered in 4-4.1.1.2 (a).
Item (b) is covered in 4.4.1.1.2 (b) and (c). Item (c) is covered in 4-4.1.1.3 (a). We need to clean up this section of the code and remove some of
the redundancies. COMMITrEE ACTION: Accept. NLrMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #41) Committee: HEA-PIP
99- 155 - (4-4.1.1.1 (a) (b) and (c)): Accept SUBMITTER: David B. Mohile, Medical Engineering Services RECOMMENDATION: Delete items (a), (b), and (c). Re letter (d) and (e). SUBSTANTIATION: Item (a) is covered in 4-4.1.1.2 (a).
Item (b) is covered in 44.1.1.2 (b) and (c). Item (c) is covered in 4-4.1.1.3 (a). We need to clean up this section of the code and remove some of
the redundancies. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #323) Committee: HEA-PIP
99- 156 - (4-4.1.1.1.1(a)): Reject SUBMITTER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Add: See #4-4.1.1.2(a) and 4-4.1.1.3(e). SUBSTANTIATION: #4-4.1.1.1 (a) states that: "Alarm signals and pressure gauges shall be located to ensure continuous responsible surveillance." It does not say where. The added text says where. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Committee Action on Proposal 99- 154 (Log #119) deleted 4-4.1.1.1(a). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #0) Committee: HEA-PIP
99-157 - (4-4.1.1.2, 4-3.1.9.4(b)): Accept in Principle SUBMITrER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Revise text:
(g) and (a) confusing. Please supply formal interpretation.
SUBSTANTIATION: 4-3.1.9(b) calls for a local signal, yet 4- 4.1.1.2(g) calls for signals in accordance with 4-4.1.1.2(a) which calls for: " . . . master alarm signals in o separate locations...".
nst what is required? ote: The same problem exists with the dew point monitor.
COMMITrEE ACTION: Accept in PrinCiple. See Proposal 99-153 (Log #CP59 ).
COMMITrEE STATEMENT: Proposal 99-153 (Log #CP59), sections 4-4.1.1.2(c)(vi) and (vii), and 44.1.1.4(a) to (c) address the issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #302) Committee: HEA-PIP
99-158- (4-4.1.1.2(0, 4-4.1.1.4(a), 4-9.1.1.7(b), 4-9.1.1.8(a)): Accept in Principle SUBMITrER: William G Frank, Win. G. Frank Medical Services, Inc. RECOMMENDATION: All gauges, pressure switches and pressure sensing devices shall be providedwith a "quick connect" fitting or isolation valve to facilitate replacement. SUBSTANTIATION: Good engineering practice dictates that entire systems should not have to be shut down to replace defective gauges and /o r pressure switches. COMMITI'EE ACTION: Accept in Principle. Add new 4-4.1.1.1 (f) to read: "Allpressure switches and pressure sensing devices shall be
provided with a demand check fitting to facilitate service, testing or replacement." COMMIq[q'EE STATEMENT: The committee agrees in principle that a convenient disconnect for maintenance is desirable. However, it does not wish to permit shutoffvalves in these sensor lines. Also quick disconnect fittings may not have a check valve. The require- naent of a "demand check fitting" accomplishes the submitter~s intent. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18. VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #90) Committee: HEA-PIP
99-159 - (4-4.1.1.2(g)): Accept in Principle SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text: All of the individual alarms as required in 4-3.1.9 shall be provided
with ~ audible and noncancellable visual signals in accordance with 4-4.1.1.2(a). SUBSTANTIATION: In 1993, 4-4.1.1.2 (g) is in error which reads: All of the individual alarms as required in 4-3.1.9 shall be provided with audible and manually resettable visual signal in accordance with ¢4.2.2.2(a). COMMIT17EE ACTION: Accept in Principle.
See Proposal 99-153 (Log #CP59). COMMITI'EE STATEMENT: Proposal 99-153 (Log #CP59), section 4-4.1.1.4(a) to (c) addresses the issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #200) Committee: HEA-PIP
99-1fi0 - (4-4.1.1.2(g)): Reject $UBMITYE~ Henry R. Kaht, Gurnee, IL RECOMMENDATION: Change dew point rise from 39°F (3.9°C) to 45°F (7.2°C). SUBSTANTIATION: During periods of low compressed air demand the 39°F pressure dew point requirement is difficult to maintain with refrigerated type dryers. This can be attributed to dryer inefficiency when flows fall below 60% of the dryers rated capacity. Even with a 45°F pressure dew point problems maystill be incurred during long durations of extreme low flow conditions and perhaps a note should be included that it is normal for dew point low flow alarms to occur under these conditions. COMMITYEE ACTION: Reject. COMMITTEE STATEMENT: Committee is aware that properly designed systems can meet current requirements. NUMBER OF C O ~ E MEMBERS ELIGIBLE TO VOTF~ 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Kaht NOT RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: KAHT: Section 4-4.1.1 (g) A 39°F dew point temperature with a
refrigerated air dryer is not possible when the compressed air demand falls below 90 percent to 95 percent of the dryers capacity.
55

N F P A 9 9 - - F 9 5 R O P
(Log #249) Committee: HEA-PIP
99- 161 - (4-4.1.1.2(g)): Acceptin Principle SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: (g) All of the alarms (delete "individual") required (delete "as") by 4-3.1.9 shall be provided with audible and manually resettable visual signals in accordance with 44.1.1.2 (a). Delete next sentence. The reserve alarm signal in 4-3.1.9.4 (b) and the appropriate signals in 4-3.1.9.5 may be combined into one master alarm signal indicative of equipment malfunction. SUBSTANTIATION: To reduce the number of individual alarms. A master alarm will initiate an inquiry which will conclude with inspection of the individual local alarms at the compressor installa- tion site, COMMITrEE ACTION: Accept in Principle.
See Proposal 99-153 (Log #C259). COMMITrEE STATEMENT: See committee action on Proposal 99-153 (LOg #CP59), section 4-4.1.1.2(c) (vi) and (vii), which address the issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #58) Committee: HEA-PIP
99-165 - (4-4.1.1.3(e)): Accept SUBMITTER: David Esherick, Patient Instrumentation Corp. RECOMMENDATION: Add:
(i.e., 0 2 , Vacuum, Medical Air, etc. service and the room(s) served) after "The appropriately labeled..." SUBSTANTIATION: We need to define and clarify what we feel is the minimum acceptable labeling for alarm panels. COMMITIT_,E ACTION: Accept. COMMITTEE STATEMENT: Change will beincorporated into
I Proposal 99-153 (Log#CP59). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrrTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #250) Committee: HEA-PIP
99-162 - (4-4.1.1.2(g)): Accept in Principle SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Delete the last sentence referendng the local alarms. SUBSTANTIATION: To maintain focus on master alarm require- ments deleting reference to local alarms which have already been covered. COMMITrEE ACTION: Accept in Principle.
See Proposal 99-153 (Log #CP39). COMMITTEE STATEMENT: In Proposal 99-15:5 (Log #CP59), text has been reworded to maintain the focus as requested. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITIT.E ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #251) Committee: HEA-PIP
99.1fi3 - (4-4.1.1.2(g)): Accept in Principle SUBMITrER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Delete last paragraph a n d a d d 4-4.1.1.2 (h):
(h) All of the monitored contaminants requiring master alarming in Table 4-3.1.9.8 shall be provided with individual audible and manually resettable visual signals in accordance with 4-4.1.1.2 (a). SUBSTANTIATION: Proposal changes section to address other contaminants, streamlines presentation ofinformadon and adds to user friendliness. COMMITI3gE ACTION: Accept in Principle.
See Proposal 99..153 (Log #CP59). COMMITTEE STATEMENT: Issue of local alarrm on parameters listed in 4-3.1.9 are included in Proposal 99-153 (Log #CP59). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #45) Committee: HEA-PIP
99-164- (4-4.1.1.3(c), 4-4.1.1.3(d)): Reject SUBMITrER: Roger D. Williams, Patient Instrumentation Corp. RECOMMENDATION:
4-4.1.1.3 (c) "General AreaAlarm" 44.1.1.3 (d) "Local Area Alarm"
SUBSTANTIATION: Need to distinguish between area alarms with sensors before the valve and alarms with sensors after the valve. Current wording leads the confusion, delay and unnecessary cost. c o M M r r r E E ACTION: Reject. COMMITI'EE STATEMENT: Committee does not believe that the addition of new term would improve the usability of the document. Distinction between sensor location is preserved by occupancy of an area (i.e., anesthetizing location vs. critical care area).
(Log #56) Committee: HEA-PIP
99-166 - (4-4.1.1.3(0 (New)): Accept in Principle SUBMITTER: David Esherick, Patient Instrumentation Corp. RECOMMENDATION: Add:
Specify that hospital shall label the area alarm panel with the "as used" room numbers, and not the contractor with the blue print numbers. SUBSTANTIATION: If the contractor labeled the alarm with blue print room numbers, these designations usually become obsolete as soon as the hospital takes over the newly constructed area. This way we eliminate the alarms being labeled incorrecdy. COMMITI3gE ACTION: Accept in Prindple. Add new 4-4.1.1.1 (0 to read as follo~cs: "The responsible authority of the fadlity shall assure that all
labeling of alarms, where room numbers or designations are used, is accurate and up-to-date." COMMITYEESTATilMENT: 1. Respond to submitter's requestfor spedfying labeling of alarms.
2. More appropriate to place requirement in 4-4.1.1.1 NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log 070) Committee: HEA-PIP
99-167 - (4-4.1.1.4(b)): Reject SLIBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise sentence 1:
(b) An appropriately identified pressure gauge, connected to the line being monitored shall be installed at each r n ~ r ~ d area alarm panel location. (Changes are underlined). SUBSTANTIATION: 4-4.1.1.1 General, (a) Alarm signals and pressure gauges shall be located to ensure continuous responsible surveillance. The importance of having gauges at the master alarms is knowing how critical the situation is when the alarm and light signal a problem. COMMITTEE ACTION: Reject. C O ~ STATEMENT: The indicator requirements presendy included in the standard for the master alarm panel were considered
ommittee to be adequate for system monitoring purposes. OF COMMITIXR MEMBERS ELIGIBLE TOwCOTE: 18
VOTE ON COMMITTI/~E ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
56

N F P A 9 9 - - F 9 5 R O P
(Log #308) Committee: HEA-PIP
99-168 - (4--4.1.2.1(c)): Reject SUBMITTER: Gary B. Trinker, Victaulic Company of America RECOMMENDATION: (c) Piping shall be hard-drawn seamless medical gas tube, Type K or L (ASTM B819), and bear one of the following markings: OXY, MED, OXY/MED, ACR/oxry, or ACR/ MED or piping shall be Schedule 5, Type 316 stainless steel approved for use with mechanical pressfitting pipe joining system. Mains and branches... ...Exception: For systems operated at pressures between 200 and 300 psig (1380 and 2070 kPa, respectively), Schedule 5 stainless steel
e with mechanical pressfitting pipe joining system or ASTM B819, K Copper shall be used. TANTIATION: Properly cleaned Type 316 stainless steel
Schedule 5 pipe and the mechanical pressfitting pipe joining system will provide equivalent or superior service to that of the currently
eCifi ed material. MMITTEE ACTION: Reject.
COMMITTEE STATEMENT: Committee is unable to determine from proposal that it will meet the performance criteria currently in Chapter 4 since no data was submitted. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #104) Committee: HEA-PIP
99-169 - (4-4.1.2.1 (d)): Accept in Principle SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Revise 4-4.1.2.1 (d) as follows:
(d) Except as provided under 4-4.1.2.1 (h) and (i),joints in copper. tubes shall be brazed using capillary fittings complying with ANSI B16.22, Wrought Copper and Copper Alloy Solder-Joint Pressure Fittings, except that for joints 1-1/2 in. nominal size and larger, socket depths shall be reduced for brazing in accordance with MSS SP-73, Brazing Joints for Wrought and Cast Copper Alloy Solder Joint Pressure Fittings. Fittings having MSS SP-73 sockets depths for brazing shall be permitted in sizes 1-1/4 in. and smaller. Cast fittings shall n o t b e used for brazed joints.
In Chapter 20, add the following under 20-1.2.10 MSS Publications: SP-73 (1986) Brazing Joints for Wrought and Cast Copper Alloy
Solder Joint Pressure Fittings. Add the following in Appendix A:
A-4-4.1.2.1 (d) A distinction is made between deep-socket solder- jo int fittings (ANSI B16.22) and those having shallow sockets for brazing (MSS SP-73). The use of shallow-socket brazing fittings improves the quality of the brazement with.out decreasing its strength, particularly in larger sizes which are difficult to heat. See Table 4-4.1.2.1 (d) for socket depths conforming to MSS SP-73. The installer may use MSS SP-73 fittings (if available) or have the sockees on ANSI B16.22 fittings cut down to MSS depths. Where shallow- socket fittings are used for the medical gas piping, care shall be taken to avoid their use in other piping system where joints may be soldered instead of brazed.
Table 4-4.1.2.1(d) Socket Depths For MSS SP - 73 Brazing Fittings
Tube Size Socket Depth
1/4" (3/8" OD) 0.17" (3/16") 3/8" (1/2" OD) 0.20" (13/64") 1/2" (5/8" OD) 0.22" (7/32") 3/4" (7/8" OD) 0.25" (1/4") I" (1-1/8" OD) 0.28" (9/32") 1-1/4" (1-3/8" OD) 0.31" (5/16") 1-1/2" (1-5/8" OD) 0.34" .(11/32") 2" (2-1/8" OD) 0.40" (13/32") 2-1/2" (2-5/8" OD) 0.47" (15/32") 3" (3-1/8" OD) 0.53" (17/32") 4" (4-1/8" OD) 0.64" (41/64") 5" (5-1/8" OD) 0.73" (47/64") 6" (6-1/8" OD) 0.83" (53/64")
SUBSTANTIATION: NFPA 99 presendy requires that brazed joints be made using deep-socket fittings designed for solder joints (ANSI B16.22). In larger sizes (starting at 1-1/2" and up), brazers begin to experience problems with applying sufficient heat to the jo int to get a sound braze, even in the shop under near-ideal conditions.
MSS SP-73 fittings with shallow sockets specifig.ally designed for brazing are presently not manufactured. MSS SP-75 fittings comply with ANSI B16.22 in all respects except for decreased socket depth and increased pressure/temperature ratings. Under this proposal, until a market develops for manufactured MSS fittings (potentially both for medical gas and refrigeration), it will be necessary for ANSI B16.22 fittings tobe cut-down to MSS dimensions. It is expected that this will be done by specialty firms who will also clean the fittings for oxygen and package them for medical gas use.
In sizes 1-1/2" and up, the depth of ANSI B16.22 solder fittings is three times that required for brazing under MSS SP-73.
(NOTE: See Table from ANSI B16.22 printed below.)
Tube Size MSS Socket Depth B16,22 Depth for brazing for solder
1/4" (3/8" OD) 0.17" 0.31" 3/8" (1/2" OD) 0.20" 0.38" 1/2" (5/8" OD) 0.22" 0.50" 3/4" (7/8" OD) 0.25" 0.75" 1" (1-1/8" OD) 0.28" 0.91" 1-1/4"(1-3/8" OD) 0.31" 0.97" 1-1/2"(1-5/8" OD) 0.34" 1.09" 2" (2-1/8" OD) 0.40" 1.34" 2-1/2" (2-5/8" OD) 0.47" 1.47" 3" (3-1/8" OD) 0.53" 1.66" 4" (4-1/8" OD) 0.64" 2.16" 5" (5-1/8" OD) 0.73" 2.77" 6" (6-1/8" OD) 0.83" 3.09" 8" (8-1/8" OD) 1.17" 3.97"
This proposal will resolve several issues: 1) First and most important, it will result in a higher percentage of
sound brazed joints in the field where work is frequendy performed in poor light, from awkward positions, with limited access, and under aggressive time schedules. Even i fa brazer passed the qbualification test with full penetration, it is doubtful that he would
e able to achieve the same results in every field joint, or, with larger sizes (1-1/2" and up), would take the time to adequately beat and work each joint. In the case of a 1-1/2"joint, he now has to heat and fill a socket that is 1.09" deep whereas only a 0.34" deep socket is necessary to exceed the full strength of the tube being joined.
2) It will permit the brazer qualification tests to be made using reduced overlap whereby thebrazer will not be faced with the difficult task of trying to get at least 80% penetration into a jo int that is three times deeper than it need be.
3) It will permit near-100% penetration to be made in all size joints, thereby eliminating the concern by some parties that open crevices at the bottom of the socket will promote the growth of bacteria within the gas piping system. COMMITFEE ACTION: Accept in Principle.
1. In sentence one ofsubmitter 's recommendation for (d) after ANSI B 16.22, Wrought Cop per... Fittings, insert the following: "or brazing fittings complying with MSS SP-73 . . . . " Delete remainder of sentence one. Delete sentence 2. Retain sentence 3. Subpar (d) would read as follows: (d) Except as provided under 4-4.1.2.1 (h) and (i),joints in copper
tubes shall be brazed using capillary fittings complying with ANSI B16.22, Wrought Copper and Copper Alloy Solder-Joint Pressure Fittings, or brazing fittings complying with MSS SP-73, BrazingJoints for Wrought and Cast Copper Alloy Solder Joint Pressure Fittings. Cast fittings shall not be used for brazed joints.
2. In submitter's recommendation for Appendix A, last sentence, change "shall" to "should." COMMITTEE STATEMENT: 1. Change permits use of short socket fittings without making it mandatory. , .
2. Conform to NFPAStyle Manual with regard to appendix text. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #105) Committee: HEA-PIP
99- 170- (4-4.1.2.1(e)): Accept SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: (e) Valves, fittings, and other piping components shall be cleaned for oxygen service by the manufacturer in accordance with CGA Pamphlet G-4.1, Cleaning Equipment for Oxygen Service, except that fittings shall be permitted to be cleaned by a supplier or agency other than the manufacturer.
57

N F P A 9 9 - - F 9 5 R O P
SUBSTANTIATION: (Re: proposed change t6 4-4.1.2.1 (d) regarding MSS SP-73 fittings) IfMSS SP-73 brazing fittings are not manufactured and ANSI B16.92 solder fittings must be modified to MSS SP-73 socket depths, this change will permit the firm that cuts the sockets to clean and package the fittings for medical gas use. Valves, stations outlets, alarm switches, pressure gauges, etc. which need to be cleaned prior to or during factory assembly, should continue to be cleaned only by the manufacturer so that he is solely responsible for the performance of his product. Another consideration is that cleaning tube fittings for oxygen
service does not involve assembly of parts or compatibility of materials and thus, need not be limited to the manufacturer. Other firms may be able to perform this function in a more cost-effective or expeditious manner. COMMITTEE ACTION: Accept NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #106) Committee: HEA-PIP
.99-171 - (4-4.1.2.1(g)): Accept in Principle in Part SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Under Gas Piping, change 4-4.1.2.1 (g) to read according:
(g) Piping shall be supported from the bull#rig structure in accordance with MSS Standard Practice SP-69, Piping Hangers and Supports - Selection and Application." Hangers and supports shall comply with MSS standard practice SP-58, "Pipe Hangers and Supports - Materials, Design and Manufacture". Hangers for copper tube shall have a copper finish. In potentially damp locations, copper tube hangers or supports shall be plastic-coated or otherwise insulated from the tube. Maximum support spacing shall be as follows:
1 /4 in. nominal 5 feet 3 /8 in. nominal. 6 feet 1 /2 in. nominal 6 feet 3 /4 in. nominal 7 feet 1 in. nominal 8 feet 1-1/4 in. nominal 9 feet 1-1/2 in. nominal and larger 10 feet
vertical risers every floor
SUBSTANTIATION: The present text does not indude support requirements for 1/4" pipe size and for vertical risers. Also, pipe hanger manufacturers have recently indicated that the copper finish on hangers for copper tube is for identification only and is not sufficiently thick to protect against galvanic corrosion of the hanger. Plastic-coated hangers are available for locations where corrosion may be a problem. COMMITYEE ACTION: Accept in Principle in Part. Revise 44.1.2.1(g), next to last sentence to read: "Portions of
hangers in contact with copper tube shall be protected against galvanic action." COMMITTEE STATEMENT: 1. There is a potential hazard between dissimilar metals tha t could cause corrosion and failure of hangers. Current wording does not address. 2. There are currently restrictions on the use of 1 / 4 in. tubing. NUMBER OF COMMITIYE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #107) Committee: HEA-PIP
99-172 - (4-4.1.2.1 (h)): Accept in Part SUBMITrER: J. Richard Wagner, Baltimord, MD RECOMMENDATION: Revise text:
(h) Joints in medical gas tube shall be brazed except that memory- metal couplings having temperature and pressure ratings not less than that of a brazed joint shall be permitted. Flared and compres- sion-type connections shall be prohibited throughout the piping system, including connections to station outlets, alarm devices, and other components. Threaded connections shall be limited to air compressor sets and devices such as pressure regulators, relief valves, pressure switches, and pressure gauges. Threaded unions and running straight pipe threads are prohibited.
SUBSTANTIATION: The existing language regarding flared and compression joints seems redundant. There are presently no limitations on threaded pipe connections. 4-4.1.2.1(h) could be read to apply only to joining sections of copper tube. COMMITTEE ACTION: Accept in ParL Delete last sentence of proposal ("Threaded unions.., prohib-
ited.") COMMITTEE STATEMENT: The use of threaded unions are an accepted industry practice, and are acceptable for medical gas s o u r c e s
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #309) Committee: HEA-PIP
99-173- (4-4.1.2.1(h), 4-4.1.20)): Reject SUBMITrER: Gary B. Trinker, Victaulic Company of America RECOMMENDATION: New text as follows:
Mechanical pressfittin~ pipe joining system constructed from Type 316 stainless steel couplings and fittings shall be used to join approved Schedule 5,Type 316 stainless steel pipe. Couplings and fittings shall be prepared in accordance with paragraph 4-4.1.2.1 (e) and form joints wi tha maximum rated working pressure of at least 300 psi. SUBSTANTIATION: Properly cleaned Type 316 stainless steel Schedule 5 pipe and the mechanical pressfitting pipe joining system will provide equivalent or superior service to that o f the current specified material. The mechanical presstitting pipe joining system provides perma-
nent mechanical connections for Type 316 stainless steel pipe without requiring heat or open flame (eliminates fire hazards) and provide permanent joints having the mechanical, thermal and sealing integrity of brazed joints for the intended services. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: This is new technology. There has been insufficient data presented to make a decision on whether this method of joining pipes would be equivalent in mechanical, thermal and sealing integrity that is currendy required of brazedioints. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON C O ~ ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #307) Committee: HEA-PIP
99- 174- (4-4.1.2.10)): Reject SUBMITTER: Daniel T. Krebsbach, Advance Mechanical Systems, Inc. RECOMMENDATION: Revise text as follows:
(j) Turns, offsets, and other changes in direction in piping shall be made by bending the pipe or with fittings complying with 4-4.1.2.1 (c). When bending pipe, care shall be taken to use a large enough radius to avoid crimping . . . . SUBSTANTIATION: The use of proper bending procedures and equipment reduces the number of potential leaks and sources of contamination without compromising the integrity of the piping system. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Directional changes using bends can compromise integrity of system. Bends can also decrease flow. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TOVOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: lfi NOT RETURNED: Fan, Shoemaker
(Log #108) Gommittee: HEA-PIP
99- 175 - (4-4.1.2.1(o)): Accept in Principle SUBMITTER: j. Richard Wagner, Baltimore, MD RECOMMENDATION: Change 4-4.1.2.1 (o) to read as follows:
(o) Penetrations. Wherepiping penetrates fire barriers such as walls, partitions, or ceiling/floor assemblies having require0"fire- resistance ratings, the penetration shall be protected in accordance with the requirements of NFPA 101, Life Safety Code, and any applicable building codes.
58

N F P A 99- - - F 9 5 R O P
SUBSTANTIATION: NFPA 101 and mos t bui lding codes now have numerous , specific requ i rements for t reat ing penet ra t ions in fire barriers. Fire-stopping is no t the p roper t e rm to be used for p r o t e c t i n ~ e n e t r a t i o n s . . . . COMMIT]tEE ACTION: Accept m Prmople .
Revise 4-4.1.2.1(o) to read: "Penetrations. Pipe penet ra t ions shall be in accordance with NFPA 101, Life Safety Code." COMMITTEE STATEMENT: There are more t h a n one type of
netrat ion o f barriers that are addressed by NFPA 101. ER OF COMMrVEEE MEMBERS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 N O T RETiJRNED: Fan, Shoemaker
COMMITrEE ACTION: Accept in Principle in Part. Revise submit ter ' s r e c o m m e n d a t i o n to read as an Exception to 4-
4.1.2..2(a): "Exception: Shutoffvalves for use in certain areas, such as
psychiatric or pediatric, shall be permi t ted to be secured to prevent inappropr ia te access." COMMITTEE STATEMENT: The Commit tee believes the submit ters in tent is more appropriately worded t h r o u g h the use of an Exception. The last phrase is deleted so n o t to stifle design or m e t h o d of secur ing access. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TOVOTE: 18 VOTE ON COMMrUrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #15) Committee: HEA-PIP
99- 176 - (4-4.1.2.2 (New)): Accept in Principle SUBMITrER: David Mohile, Medical Engineer ing Services RECOMMENDATION: Add new text:
"Service shu t offvalves shall be placed where the lateral branches off of the r i se rpr io r to any zone valve box assembly on that branch. Only one set o f valves shall be used for each branch off o f a riser regardless of how many zone valve boxes are installed on that lateral. These valves shall be installed to allow a facility to make changes in piping in individual areas without shut t ing down an entire riser or facility.
These valves shall be in a locked chase or shall have their handles locked out or removed, and tagged to prevent accidental closing." SUBSTANTIATION: W h e n a facility wants to change the piping a r r a n g e m e n t in one of its wings, the cur ren t practice is to plan a shu t down of ei ther the riser involved or the entire facility if riser valves were no t originally installed. This is a major under tak ing involving the rental and use of as many as 100 or more large tanks of oxygen, stands, regulators, etc. It also involves many extra personnel and is typically p l anned late at night.
ff a set of valves are installed at the origin of the lateral branch, even if that lateral branch leads to four or five separate zone valve sets, it is easier to plan the temporary s h u t d o w n of those four or five zones ra ther than an entire fadlity.
The cost o f the valves in very small compared to the cost of a shu t down. A 1 in. valve c leaned for medical gas service typically costs less t han $145. COMMITTEE ACTION: Accept in Principle.
1. Add text as new 4-4.1.2.20) 2. In sen tence 2 o f the submit ter ' s r ecommenda t ion , change "Only
one set of valves shall be used for each b r a n c h . . . " to '"Only one valve shall be required for each b r a n c h . . . "
3. In last sentence of the submit ter ' s r ecommenda t ion , change "locked out or removed" to "secured." COMMITrEE STATEMENT: 2. & 3. The proposed intent of wording by submit ter clearly indicates tha t "one valve" is required and is more appropriate than the submit ter choice of the expression "one set o f valves" which could infer tha t more than one valve is required. Also the te rm "secured" is more appropria te as it allows several alternative me ans of secur ing the valve and thus be as effective as tha t p roposed by the submitter . NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #96) Committee: HEA-PIP
99-177 - (4-4.1.2.2(a) (New)): Accept in Principle in Part SUBMITTER: David B. Mobile, Medical Engineer ing Services, Inc. RECOMMENDATION: Add the following wording:
Shutoff~alves for use in psychiatric, pediatric and certain other areas shall be allowed to be secured in some m a n n e r as to prevent inappropriate access such as in a locked valve box with the key accessible only to staff. SUBSTANTIATION: Certain types of patients mus t be prevented f rom unau thor ized operatioff of emergency shut offvalves. However, con f inemen t of these patients to their rooms may not be appropriate. In these instances, it may be necessary for the shu t off valves to be locked up for staff access only. By allowing a locked access pane l to shu t offvalves, or possibly r e m o v i n g t h e handles f rom shut offvalves, we would allow these areas t o h a v e the medical gases that they need but still prevent their unau thor ized usage.
(Log #7) Committee: HEA-PIP
99- 178 - (4-4.1.2.2(c)): Accept in Principle SUBMITYEI~ Peter Esherick, Pat ient Ins t rumenta t ion Corpo .ration RECOMMENDATION: Please clarify'.
Is a shut offvalve required at the immedia te outlet of the source of supply AND a main line shu t offvaive for manifold and air compres- sor installations within a n d / o r immediate ly outside the building? SUBSTANTIATION: Tha t would pu t the source shu t offvalve and main line shu t offvalve almost nex t to each o ther with the m a x i m u m distance be ing one wall thickness in between. COMMITI 'EEACTION: Accept in Principle.
See Commit tee Acdon on Proposal 99-179 (Log #235). COMMITTEE STATEMENT: Proposal 99-179 (Log #235) is considered to clarify issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
(Log #235) Committee: HEA-PIP
99- 179 - (4-4.1.2.2(c)): Accept SUBMITrER: Anton io A. Mesa, Nash Engineer ing Co RECOMMENDATION: Add to end of 4-4.1.2.2 (c)
A main line valve is no t requi red where the source shu t off valve is accessible f rom within the building. SUBSTANTIATION: None. COMMITrEE ACTION: Accept. Accept r ecommenda t ion , except change "is no t required" to "shall
no t be required." COMMITI 'EE STATEMENT: Conform to NFPA Style Manual. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrFTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
(Log #342) Committee: HEA-PIP
99-180 - (4-4.1.2.2(c)): Accept SUBMITTER: Mark Allen, O h m e d a Medical Engineer ing RECOMMENDATION: Rewrite 4-4.1.2.2 (c) to read:
The main supply line shall be provided with a shutoff valve. The valve shall be located to permi t access by author ized personnel only (e.g. by locating in a ceiling or beh ind a locked access door) . Remainder unchanged . SUBSTANTIATION: The present requirement , when combined with figure 4-4.1, is confusing. It is no t desirable that the main line shutoff be used as an emergency shutoff, as it is too remote f rom the users. Locating it to permi t quick access place it in areas which are uncontrol led and therefore subject to vandalism. The valve serves an impor tan t purpose but should no t be accessible to the public. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
59

N F P A 99 - - F 9 5 R O P
(Log #93) Committee: HEA-PIP
99- 181 - (44.1.2.2(c) (New)): Accept in P r indp le SUBMITI'ER: Peter Esherick, Pat ient Ins t rumenta t ion Corporat ion RECOMMENDATION: Add, at the beg inn ing of sub par. (c): W h e n the main supply is r emote (farther t h e n 50 ft. f rom where the main supply line enters the building).. . SUBSTANTIATION: The need for a ma in supply line shu t offvalve is only where the ma in supply is some distance f rom where tha t line enters the building. COMMITTEE ACTION: Accept in Principle.
See Commi t tee act ion on Proposal 99-179 (Log #235). COMMITrEE STATEMENT: Commit tee action on Proposal 99-179 (Log #235) addresses the issue of x;alves. NUMBER OF COMMrITEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #95) Committee: HEA-PIP
99- 182 - (4-4.1.2.2(d) (New)): Accept in P r indp le in Part SUBMITTER= David B. Mohile, Medical Eng inee r ing Services, Inc. RECOMMENDATION: Add the following word i ng t o the above paragraph: Riser valves shall be accessible a n d n o t b l o c k e d by presen t or fu ture installation of duc t work, o ther piping or wiring. SUBSTANTIATION: Frequent ly the riser valves are blocked by o ther service ducts or piping. Since the riser valves are no t ju s t a construct ion valve, bu t allow a facility more flexibility with fu ture work on the medical gas pipeline systems, these valves shou ld always be accessible by service personnel . COMMITrEE ACTION: Accept in Principle in Part.
Revise submit ter ' s r e c o m m e n d a t i o n as follows: "Riser valves shall r emain accessible a n d no t be blocked." COMMITrEE STATEMENT; Commit tee desires such valves to be accessible at all times. List of i tems is restrictive as there are o ther i tems that could be listed. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
(Log #194) Commit tee: HEA-PIP
99-183 - (4-4.1.2.2(e)): Accept SUBMITTER: Leo G. Foxwell, ITT Hartford RECOMMENDATION: Revise existing 4-4.1.2.2 (e) by removing the word "corridor". SUBSTANTIATION: T he phrase "corridor wall" is causing confusion. Requ i rements for sprinklers in a n e w h e a l t h care occupancies, plus change in wall allowed, makes this r e q u i r e m e n t in NFPA 99 out of step with NFPA 1 01 on the te rm "corridor wall". The in tent in 44.1.1.1 (e) is place an in tervening wall between the fire and the shu t offvalve. It does no t have to be an exit corridor barrier. COMMIT'FEE ACTION: Accept. NUMBER OF COMMITIXE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
(Log #24) Committee: HEA-PIP
99-184 - (44.1.2.2(t)): Reject SUBMITTER: Albert L. deRichemond , ECRI ]~ECOMMENDATION: Add "or sensor" after "piping" and before "main tenance" in first sen tence of 4-4.1.2.2(0 SUBSTANTIATION: Pressure a n d con taminan t sensors need periodic calibration or replacement . Main tenance values in l ine with these sensors would greatly ease main ta in ing the sensors while minimally d is rupt ing the system operat ion. COMMITFEE ACTION: Reject. COMMrlTEE STATEMENT: Some sensors can be removed without the need o f a shutoffvalves. Manually opera ted valves for sensors are no t safe as they can be left in the offposi t ion.
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
(Log #222) Committee: HEA-PIP
99-185 - (4-4.1.2.2(1)): Reject SUBMI'iq 'ER: Frederick W. Wiese, Valve Security Systems, Inc. RECOMMENDATION: In general , I wish to address any port ion of this d o c u m e n t which requires valves to be locked either open or closed. Specifically, I would like to address paragraph 44.1.2.2 (F).
"(f) In-line shutoffvalves in tended for use to isolate existing systems for p ip ing ma in tenance or to ex tend to new pip ing systems shall be permit ted. These valves shall be located in a secure area or locked open a n d labeled in accordance with 4-6.4.1.2."
I r e c o m m e n d tha t the last sen tence of this paragraph be changed: "... These valves shall be located in a secure area or locked open or
cont inuously moni to red with active valve sensors and fabe led in accordance with 4-6.4.1.2..." SUBSTANTIATION: "Active valve sensors" m e a n i n g tha t they are no t passive seals, where any t amper ing with the valve for any reason would genera te an electronic sigrral.
It is my view tha t the installation of an active and con t inuous moni to r ing system, t h r o u g h the a t t achmen t of sensors on each valve requi red to be locked open or closed, would satisfy this r eq u i r em en t and, in fact, would make the system far more safe. Th e sensor would signal a . . . . . moni to r by audio and visual a larm when the valve was be ing tu rned m either threctaon. The alarms can be installed at one or more locations, such as a nurses ' station, a n d / o r some central mon i to r ing station already established for o ther systems.
The use of sensors a n d moni tors instead of locks would enhance the safe operat ion o f the gas systems in several ways. First, it would alert s o m e o n e shou ld a lock be inadvertently or intentionally removed and the valve turned. Second, it would el iminate the f requent ly encoun te red d i l emma in hospitals of having to ei ther cut a lock f rom a valve (with tools that are typically no t available) or search frantically, in an emergency, for s o m e o n e with a key.
I do no t suggest that such a moni to r ing system would el iminate the need to cont inue tagging shutoffvalves with the warning requi red in 4-0.4.1.2. Rather, I am suggest ing that any location requi r ing this warning is a candidate for moni tor ing. There is no cur ren t r e q u i r e m e n t to identify the exact location of a mis-posit ioned valve in a critical medical gas application. The master gas pressure a larm system required u n d e r 4-4.1.1.2 will signal when the pressure changes f rom a valve being turned, bu t no t the source o f the problem. In a critical gas system, the t ime n e e d e d to identify the mis-posit ioned valve may be unacceptable.
The benefi t derived f rom a valve moni to r ing system is the rap id identification of the source of p rob lems when an alert is given by the master a larm system. It is no t u n c o n u n o n for hospital personnel to spend hour s trying to identify the source o f a d rop in gas line pressure. Additionally, i f a low use line has an ups t r eam valve closed, the master a larm system may no t alert until a sudden, critical need arises for the gas in tha t line. A valve mon i to r ing system would prevent this si tuation by providing an a larm immediate ly u p o n a change in the posit ion of the valve.
Obviously, our company is in the business of providing valve sensors a n d mon i to r ing systems. We have been very successful at this and we believe our sensors have fit perfectly with the systems requi red by NFPA a n d could well have been responsible for the prevent ion of the loss of life at the facilities where they are installed. We are . . . . no t asking that NFPA change the s tandard or impose a restr ictmn on any gas hne installation that would require the use of our equ ipmen t and no other. We expect tha t there are alternative valve moni to r ing systems available. COMMITTEE ACTION: Reject. COMMITITEE STATEMENT: 1.. S tandard already requires a la rming for pressure to indicate if a valve is closed.
2. NFPA 99 is a m i n i m u m safety s tandard, a n d the system r e c o m m e n d e d by submi t te r can be used. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker "
60

N F P A 99 - - F 9 5 R O P
(Log #81) Committee: HEA-PIP
99- 186 - (4-4.1.2.2(g)): Accept in Principle SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text to read:
New or replacement valves shall be fallLp_oax~ quarter-turn shutoff type with an indicating handle (i.e., bali or butterflyvalve.) This shutoff valve shall be metallic and ofa tvoe that willcreate no ~reater flow restriction than the vining to which they are connected. (Changes are underlined). _ . v SUBSTANTIATION: The importance of having valves full ported is a flow problem in designing systems. A standard ball valve may restrict flow as much as 10 percent of the effective opening. A full ported ball valve has no restriction to the effective opening, causing no flow loss or problems in design. The inside dlam~eter ofa 2 in. full ported valve is 2 in., the inside diameter ofa 2 in. standard ball valve is I 1/2 in. COMMITTEE ACTION: Accept in Principle. See committee action on Proposal 99-189 (Log #232).
COMMITrEE STATEMENT: Proposal 99-189 (Log #232) includes the issue of full-port. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #82) Committee: HEA-PIP
99- 187 - (4-4.1.2.2(g)): Accept in Principle SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text to read as follows:
New or replacement valves shall be of a quarter turn, three niece shu tof ball valve or butterfly valve with indicating handle. (Changes are underlined). SUBSTANTIATION: The words three piece is important because this allows the maintenance of the valve without having to cut the system, purge and braze a new valve in its place. COMMITTEE ACTION: Accept in Principle. See committee action on Proposal 99-189 (Log #232).
COMMITrEE STATEMENT: Committee action on Proposal 99.189 (Log #232) includes the issue of three piece construction.. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #109) Committee: HEA-PIP
• 99-188 - (4-4.1.2.2(g)): Accept in Principle SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Change 4-4.1.2.2(g) to read as follows:
(g) New or replacement shutoffvalves shall be the quarter-turn ball or plug type with indicating handle. Valves in mains and branches shall be full-ported. Seals and packings shall be suitable for oxygen service. SUBSTANTIATION: Plug valves are presently excluded from medical gas piping systems-. There are presently no restrictions on the size of the valve ports, which are related to pressure drop. The present text lists butterflyvalves as an example of a quarter-turn valve. Yet, butterfly valves typically have resilient liners which form gasketed, flanged connections. A resilientgasketed flanged connection does not have the integrity of a brazed joint. COMMITTEE ACTION: Accept in Principle. See Committee Action on Proposal 99.189 (Log #'232).
COMMITrEE STATEMENT: Committee Action on Proposal 99. 189 (Log #232) addresses the issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #232) Committee: HE/k-PIP
99-189 - (4-4.1.2.2(g)): Accept in Principle SUBMI'F~3~ Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: New or replacement shut-offvalves shall be of a quarter-turn type (i.e. ball valve or butterfly valve) with an indicating handle and shall be of metallic conswuction. Bali valves
shall be full port type to prevent excessive restriction to flow. Butterfly valves shall no tbe used in line sizes 2 inches or smaller.
Please coordinate committee action with vacuum proposal. SUBSTANTIATION: 1. Unifyvalverequirementsbetweengasand vacuum sections.
2. Modify pressure drop requirement because btuterflyvalves normally used in larger sizes (3 inches and larger) have minimal, but recognized, pressure drop. COMMITTEE ACTION: Accept in Principle. Revise submitter's recommendation to read as follows: "New or replacement pipeline shut-offvalves shall be of a quarter-
turn ball valve type manufactured with extensions for brazing, and with an indicating handle and shall be of metallic construction. Valves shall be full port to prevent excessive restriction to flow, and three-piece construction to allow for maintenance and brazing." COMMITTEE STATEMENT: 1. Butterfly valves are not suitable for medical gas service.
2. Three-piece construction added for maintenance and brazing
ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #203) Committee: HEA-PIP
99-190 - (4-4.1.2.2(h)): Accept in Principle SUBMITTER: Henry IL Kaht, Gurnee, IL RECOMMENDATION: In patient areas that serve incarcerated persons, psychopathics, children or other similar patients, where valve tampering, intentional or otherwise, is a possibility, then these valves shall be provided with padlocks. A system of rapid access for the valve padlock keys shall be developed by the hospital medical and maintenance staff. SUBSTANTIATION: The possibility of an unauthorized person closing a ~as valve in areas that s~rvice incarcerated persons, psychopams, children, or other similar patients, is a distinct possibility and should be taken into account during the design of health care facilities. COMMITTEE ACTION: Accept in Principle. See Committee Action on Proposal 99-17'7 (Log #96).
COMM1TrEE STATEMENT: Similar recommendation to Proposal 99-177 (Log~96). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITIT, E ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #122) Committee: HEA-PIP
99- 191 - (4-4.1.2.20) (New)): Accept in Principle SUBMITFER: David B. Mobile, Medical Engineering Services, Inc. RECOMMENDATION: Add: Medical gases shall not be installed in the same zone valve box
assembly as natural or propane gas or other flammable gases. SUBSTANTIATION: Dental, laboratory and other uses in hospitals Trequenfly have valve boxes for piped natural gas or other flammable gases. It is not prudent to have oxygen, nitrous oxide, or other medical gases in these boxes since leaks can occur and this could pose a fire hazard when the flammable gas is combined with nonflammable but fire-supporting medical gases. COMMITI'EE ACTION: Accept in Principle. Revise proposal to reac~ "Medical i~ses shall not be installed in the same zone valve box
assembly with flammable gases." COMMI'ITEE STATEMENT: Committee does not want to restrict requirement to just those flammable gases listed in submitter's recommendation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
61

N F P A 99 - - F 9 5 R O P
(Log #338) Committee: HEA-PIP
99-199 - (4-4.1.2.4(d)): Accept SUBMITTER: David Wyrick, Sr., Cambiare Ltd. RECOMMENDATION: Revise text as follows: Station outlets in patient (ADD) or treatment rooms. Add last
sentence: "Floor mounts for Type II shall not be recessed and may be
mounted in or on the dental junction box, when mounted to the f~oor." SUBSTANTIATION: Statement does not take into consideration that outlets are used in other than patient rooms. It reads as ff outlets are ~ e d in hosnitai natient rooms only, The last sentence solves the debate by inspectors and suppliers." The (Dental Junction Box) Utility Center is submitted under revisions for Chapter 2. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #253) Committee: HEA-PIP
99- 193 - (4.4.1.3): Accept in Principle in Part SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Relocate sections of 4-4.1.3 to appropriately and delete 44.1.3.
i.e.: SECTION CHANGE TO: I 4-4.1.3.1 add to 4-4.1.2.2 (d)
4--4.1.3.2 4-4.1.2.2 (e) Renumber existing 44.1.3.3 4-4.1.2.2 (f) Renumber existing 4-4.1.3.4 4-6.2.1.3 (d) 4-4.1.3.5 4-15.9.1.3 (e) 4-4.1.3.6 4-6.2.1.3 (f)
SUBSTANTIATION: Collection of information and requirements in appropriate sections to streamline reading and aid user friendli- ness. COMMITTEE ACTION: Accept in Principle in Part.
1. Accept first three recommendations. 2. Delete sections 4-4.1.3.4, 4-4.1.3.5, 4-4.1.3.6. COMMITrEE STATEMENT: Text to be deleted does not relate to
i~j~l~system requirements. ER OF COMMITTEE MEMBERS ELIGIBLE TO.VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #110) Committee: HEA-PIP
99-194- (4-4.1.3 (New)): Reject SUBMITIXR: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Add the following under 4-4.1.3
4-4.1.3.7 Where medical gas piping penetrates RF shielded rooms or enclosures, connections to brass pipe waveguides through the shielding and to dielectric couplings used to isolate electrical ground paths shall be made by brazing in accordance with 4-4.1.9.1 or by tapered pipe threads in accordance with 4-4.1.4.4. Unions and other straight-threaded connections shall be prohibited. SUBSTANTIATION: Plumbing-type dielectric unions and straight running threads are being used where medical gas tubing penetrates shielded rooms, as in MRIs. These joints do not have the integrity of either a brazed joint or a jo in t having a tapered pipe thread. Unions and straight pipe threads are subject to loosening through normal vibration, thereby creating a fire hazard. COMMITTEE ACTION: Reject. COMMYI'EER STATEMENT: Practice of threaded and other non- brazed connections are already prohibited in document. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATWE: 16 NOT RETURNED: Fan, Shoemaker
(Log #16) Committee: HEA-PIP
99-195 - (4-4.1.3.4, 4-4.1.3.5, 4-4.1.3.6, 4-6.9.1.2): Reject SUBMrrTER: David Mohile, Medical Engineering Services RECOMMENDATION: Delete Sections 4-4.1.3.4, 44.1.3.5, 4-4.1.3.6, 4-6.9.1.2(e), (0, (g), (h), (i), (j), (1), (q), (y), (bb), [cc-whicb is a duplicate of (c).] Remaining sections shall be relettered.
Also delete 4-6-2.1.3, 4-6.9.1.4, 4.6.2.1.5, 4-6.2.1.6. Also delete A-4-4.1.3.4 and Figure A-4-4.1.3.5.
SUBSTANTIATION: All of the above sections deal with the use and administration of cylinders of oxygen and other medical gases in a hospital. They have no place in a construction specification which is primarilyfor the use of construction and design personnel. The removed sections may have to be transferred to another section of the NFPA and the Technical Correlating Committee might have to address this issue.
The appendix information deals solely with small cylinders of oxygen which again, are not used during construction project.
These changes are submitted to assist in making Chapter 4 more user friendly and less cluttered. COMbflTrEE ACTION: Reject. COMMITTEE STATEMENT: 1. Material is necessary safe practices for piped gas systems.
2. Sections 4-4.1.3.4, 5, 6 were deleted by Proposal 99-193 (Log #253). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #75) Committee: HEA-PIP
99-196 - (4-4.1".4.1): Reject SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text:
Reaming of tubingin necessary. SUBSTANTIATION: In the handbook it states that reamingis not recommended. Reaming is very important and is necessarybecause mechanical engineers design systems for flow by full bore of tubing. The elimination of reaming copper tubing will cause system designers to increase systems by one tube size. COMMrITEE ACTION: Reject. COMMITTEE STATEMENT: NFPA 99 is currently silent on the subject of reaming. There is no restriction on the use of reaming per current text. Wording in Handbook is not part of the require- ments of the standard. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COI~IMrrrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #111) Committee: HEA-PIP
99-197 - (4-4.1.4.1): Accept SUBMITTER: j . Richard Wagner, Baltimore, MD RECOMMENDATION: Change 4-4.1.4.1 to read as follows:
4-4.1.4.1 General. (~OmDQnent~ in nonflammBble medical ~as swstems shall be of materials that are suitable for oxwen se r~e . (See 4-3.1.3 Materials - Oxwen ComDatibiliw). Pioe-(tubeL fittings, valves, and other comoonents shall l/ave been thoroughly Cleaned~
od. grease, and other readily oxi~zable iIlternallv to remove " materials, as if for oxv~er~ service. Such materialshall be nlu~ged. q~poed, or otherwise's~ealed until installe~l, Particular care sffall be ta~dn in the storage and handling of such material to maintain its dean condition. Immediately before installation, such material shall be visually examined internally for contamination. Material that has become contaminated and is no longer suitable for oxygen service shall not be installed.
(a) Pipe ~ v a l v e s , and other components shall be ........ (remainder same as existing)
(b) On-site Cleaning (same as existing) [changes are underlined]
SUBSTANTIATION: The important provisions of 4-3.1.3, particu- larly regarding valve sots , seals, and lubricants, are located in a general section of Chapter 4 and are not referenced anywhere under the pipin6 sections. Within 4-4.1.4.1, the proposed change makes several rmnor changes to improve the language. "Assemble" is changed to "install". "Assemble" implies something that is done by the manufacturer rather than the installer.
62

N F P A 9 9 - - F 9 5 R O P
COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #22) Committee: HEA-PIP
99-198 - (4-4.1.4.2): Reject SUBMIT ' rE~ wal te rJ . Sperko, Sperko Engineering Services RECOMMENDATION: Revise text to read:
Procedures and Brazers shall be qualified by tension ~ .t_e_Et~g.~ test coupons in addition to the testing specified by ASME Seiztion IX or AWS B2.2. SUBSTANTIATION: Present words do not indicate whether "modification" means in addit ion to or in place of the requirements of ASME Section IX or AWS B2.2. COMMITrEE ACTION: Reject. COMMITI'EE STATEMENT: Recommendat ion is not consistent with intent of committee. See Committee Action on Proposal 99-201 t ' l ~ z ~ ] l ¢ p i
co E.EMB ELIGIBLE T o VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #48) Committee: HEA-PIP
99-199 - (4-4.1.4.2(4)(ii)): Accept SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Change 4-4.1.4.2(4) (ii) to read as follows:
(ii) The employer shall obtain a copy of both the Brazing Procedure Specification and the support ing qualification records from the group or agency and shall sign and date these records, thereby accepting responsibility for the qualifications that were per formed by the group or agency. SUBSTANTIATION: To make it clear that qualified brazing procedures are permit ted to be exchanged only from a technically competent group or agency to an employer, and not from one employer to another. COMMITrEE ACTION: Accept. NUMBER OF COMMIq['rEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #72) Committee: HEA-PIP
99- 200 - (4-4.1.4.2(a)(1)): Reject SUBMITTER: Dale Dumbleton, American Medical Gas lnstihate RECOMMENDATION: Revise text to read:
Procedures shall be qualified by tension test. SUBSTANTIATION: Procedures should be qualified by tension test to demonstrate the procedure is obtainable. Procedure Qualifica- tion record as per A.S.M.E. section IX and AWS B2.2 does no t required the joints to be tension tested. In our experience in over 1600 brazing coupons, we have found many jo in t penetrat ion failures, but have not found a tension test fai'lure in the same joints. COMMITrEE ACTION: Reject. COMMITTEE STATEMENT: Recommendat ion is no t consistent with intent of committee. See committee action on Proposal 99-201 (Log #112). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
SUBSTANTIATION: The present text has been in terpre ted as requiring tension tests in addition to sectioning or macroetching, which are required tests by ASME Section IX and AWS B2.2 respect ively .The result has been added costs for an unnecessary test. Sectioning or macroetching are superior to the tension test for de termining the ability of the brazer to achieve an acceptable degree of penetrat ion in the test joint . NFPA 99 in tended the tension test to be a minimum level o f performance that was no t based on penetration. If sectioning or macroetching is performed, the tension test serves no purpose. COMMITTEE ACTION: Accept in Principle. Revise 4-4.1.4.2(a) (1) to read as follows: "Brazers shall be qualified by visual examination of the test coupon
followed by sectioning (ASME Section IX) or macroetching (per AWS B2.2), except that a tension test shall be permit ted to be substituted for sectioning or macroetching. Where tension tests are used for brazer qualification, they shall be performed in accordance with ASME IX or AWS B2.2." COMMITrEE STATEMENT: Change adds specific requirements for the tension test, which is acceptable. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #44) Committee: HEA-PIP
99-202- (4-4.1.4.2(a)(1), 4-4.1.4.3(0): Reject SUBMITrER: J. Richard Wagner, The Poole & Kent Company RECOMMENDATION: 1. Change 4-4.1.4.2(a) (1) to read as follows:
(1) For brazer oualification, a visual insnection and tension test may be substituted for sectioning or mactZoetchin~.
2." Change 4-4.1.4.3 (f) as follows: (0 Tube ends shall be inserted fully into the socket of the fitting,
excent that insertion or overlay for the nurnoses of aualification under 4-4,1.4.2 shall be a¢cord[in~ to AS'ME-or AW$ t:eouirements. Where flux is permitted, thejoin~ shall be heated .... SUBSTANTIATION: Reason for Changes:
Change #1: The intent of 4-4.1.4.2 in permitt ing tension testing was to simplify the testing procedure, using a technique that did no t require qualitative j udgmen t on the part of the brazing inspector. The present language in" 4-4.1.4.2(a) (1) is being in terpreted to mean that tension tests are required in addit ion to sectioning or macroetching, which are considered to be required tests by ASME and AWS. Sectioning (per ASME) or macroetching (per AWS) are industry standards which are far superior to tension testing in evaluating the ability of a brazer to make sound, leak-tight joints, ff sectioning or macroetching is used for brazer qualification, a tension test serves no purpose. NFPA 99 has made the qualification process more complicated, more costly, and less effective than normal ASME and AWS procedures.
Change #2: Full penetrat ion of the braze filler metal is not possible when large diameter tube (1" and larger) is inserted fully into the socket of the fitting. An alternative would be that if full insertion is done for qualification testing, then only the first half of the depth of the socket should be considered for penetrat ion of the brazer filler metal. Lack of full penetrat ion into a fully inserted jo in t does no t weaken the jo in t since 50% penetrat ion still provides twice the overlap required to develop the maximum strength of the joint. The overlap required by ASME and AWS is only 4-5 times the wall thickness of the th inner member . COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Proposal does not comply with ASME or AWS procedures. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TOVOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #112) Committee: HEA-PIP
99- 201 - (4-4.1.4.2(a)(1)): Accept in Principle SUBMITI'ER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Changi~ paragraph 4-4.1.4.2(a) (1) to read as follows:
(1) Brazers shall be qualified by visual examination of the test coupon followed by sectioning (ASME Section IX) or macroetching (AWS B2.2). A tension test shall be permit ted as a substitute for sectioning or macroetching.
(Log #60) Committee: HEA-PIP
99- 203 - (4-4.1.4.3(g)): Reject SUBMITTER: Jacob H. Granger, Certified Medical Testing RECOMMENDATION: Delete text.
Exception: Purging of a connect ion to an existing system. SUBSTANTIATION: The intent of the "Exception" is to allow the brazer to tie in one joint, which would be the final jo in t o f a remodel to the piping system without purging that final joint . The language
63
N F P A 9 9 - - F 9 5 R O P
of the "Exception" statement does not specify one joint or final connection, therefore the interpretation of this "Exception" would widely vary throughout the industry. On certain remodel job sites there can be as many as 15-20 connections to an existing system, this would allow for the same amount of opportunities to contaminate the piping system. This "Exception" is also in direct conflict with the following Section/Paragraphs of the same Document: 4-4.1.4.1, 4-4.1.4.30), 4-5.1.3.5, 4-5.1.3.6. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: See Committee Action on Proposal 99-267 (Log #128). Substantiation of this proposal is the same as that one. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #73) Committee: HEA-PIP
99- 2 0 4 - (4-4.1.4.3(g)): Reject SUBMI'ITER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Delete text:
Exception: Purging of a connection to an existing system. SUBSTANTIATION: ff the purge to the connection of the existing system is not performed,, copper oxides will form and. the piping purge test required m 4-5.1.3.5 can not be accomphshed. COMMITI~EE ACTION: Reject. CO MITrEE STATEMENT: Committee believes current requirement of not purging the final connection is appropriate. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrrTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #128) Committee: HEA-PIP
99- 205- (4-4.1.4.3(g) Exception): Reject SUBMITTER: Dan Lehmann, Torrance Nell Burch, Rancho Palo Verdes, CA, (Log #129) Otis Alexander, Riverside, OH, (Log #130) Leo Bisson, Los Angeles, CA, (Log #131) Dave Seiersen, Buena Park, CA, (Log #132) Robert H.Johnson, SantaAna, CA, (Log#133) William C. Corcoran, Los Angeles, CA, (#134) Robert T. Sievert, San Clemente, CA, (Log #135) Chris Rydgren, Santa Monica, CA, (LOg #136) Thomas Welch, Bellflower, CA, (Log #137) Henry Hillebrecht, Orange, CA, (Log#138) George Henry, AnaheimHills, CA, (Log#139) Donald Kimpton, Newport Beach, CA, (Log #140) Joseph Gallegos, Midway City, CA, (Log #141) Louis Cusimaro, Cypress, CA, (Log #142) Javier Ortiz, Los Angeles, CA, (Log #143) Janet E. Sense, Orange, CA, (Log #144) Cesar Escamilla, Los Angeles, CA, (Log #145) Joan Spinosa, Anaheim, CA, (Log #146) Mike Horna, Anaheim, CA, (Log#147) Larry E.Jones, Norco, CA, (Log #148) Earl IL Choate, Fountain Valley, CA, (Log #149) Michael C. Gline, Garden Grove, CA, (Log#150)
A. Wall, Midway City, CA, (Log#151) chard Mantor, Orange, CA, (Log #152)
Richard D. Kennedy, Yorba Linda, CA, (Log #153) Richard Noack, Costa Mesa, CA, (Log#154) Don Boland, Santa Aria, CA, (Log #155) Garland H. Rhodes, Anaheim, CA, (Log #156) Theodore H. Mendoza, Anaheim, CA, (Log #157) Earl IL Choatedr. Moreno Valley, CA, (Log #158) WilliamJ. Wether, Fountain Valley, CA, (Log #159) Shawn Choate, RSM, CA~ (Log#160) Jim Choate, Corona, CA, (Log #161) Michael Housek, Costa Mesa, GA, (Log #162) james vigil, Whittier, CA, (Log #163) Edward W. McGee, Huntington Beach, CA, (Log #164)
~l an Martinez, Torrance, CA, (Log #165) ichaei Lewis, Yorba Linda, CA, (Log #166)
Gheorghe Nicolae, Los Angeles, CA, (Log#167) Brian T. Milone, Canoga Park, CA, (Log #168) James MacBeath, Garden Grove, CA, (Log #169)
oe Cecchini, SantaAna, CA, (Log#170) aul Or$iz, Whittier, CA, (Log #171)
Robert Lamb, Cypress, CA, (Log#172) Janet Sense, Orange, CA, (Log#173) Kurt Sense, CostaMesa, CA, (Log #174) Lee Froehlich, Anaheim, CA, (Log #175) Rudy Celaya, Cypress, CA, (Log #176) Hendk Petersen, San Clemente, (Log #177) Robert R. Modica, Placentia, CA, (Log #178) Gene Genovese, Fountain Valley, CA, (Log #179) Michael A. Cangi, Garden Grove, CA, (Log #180) Chesley M.Johnson, Escondido, CA, (Log #181) Vince Marchetti, Cypress, CA, (Log #182) Paul C.Mathieson, Cypress, CA, (Log #183) Michael D. Robbins, LaVerne, CA, (Log #184) Thomas 1L Lindsey, Dana Point, CA, (Log #.1'85) Thomas Lentine, Burbank, C~ (Log #186) Shawn B. Begin, Aznsa, CA, (Log #187) Panya Surnmaphetrat, Burbank, CA, (Log #188) Robert Roberts, Long Beach, CA, (Log #189) Eddie IL Estiada, Riverside, CA, (Log #190) Dennis Weyer, Lawndale, CA, (Log #191) RECOMMENDATION: Delete the following:
"Exception: Purging of a connection to an existing system". SUBSTANTIATION: The intent of the "Exception" is to allow the brazer to tie in one joint, which would be the final joint of a remodel to the ~iping system without purging that final joint. Thedanguage of the Exception" statement does not specify one joint or final connection, therefore the interpretation of this "Exception" would widely vary throughout the indnstry. On certain remodel job sltes there can be as many as 15-20 connections to an existing system, this would allow for the same amount of opportunities to contaminate the piping system. This "Exception" is also in direct conflict with the following Section/Paragraphs of the same Document: 4-4.1.4.1, 4-4.1.4.$ (j), 4-5.1.3.5, 4-5.1.3.6. COMMITrEE ACTION: Reject. Revise existingException [See Proposal 99-206 (Log #CP7)].
COMMITrEESTATEMENT: Committee could not act on the proposal based on the substantiation provided. Problem is complicated in that tie-ins can vary, from one major connection to many connections.
Committee has developed a proposal in an attempt to address the issue. See Committee Proposal 99-206 (Log#CP7). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP7) Committee: HEA-PIP
99- 206 - (4-4.1.4.3(g) Exception): Accept SUBMITrER: Technical Committee on Piping Systems RECOMMENDATION: Revise Exception to read as follows: "A final connection to an existing pipeline shall be permitted to be made without the use of a nitrogen perge. After final connection, the affected downstream portions of the pipeline shall be tested in accordance with 4-5.1.3.5 and 4-5.1.3.9 with the source gas." SUBSTANTIATION: Clarifying the issue of the final connection of new pipelines to existing systems. COMMITFEE ACTION: Accept. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #70) Committee: HEA-PIP
99- 207 - (4-4.1.4.4(b)): Accept in Principle SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text to read:
(b) Threaded joints in piping systems shall be made up with polytetrafluoroethylene (such as.Teflon) tape or other thread sealant suitable for oxygen service. (Changes are underlined). SUBSTANTIATION: Eliminate tinned, this practice is obsolete in the industry. A problem develops with finning of threads, due to the fact that pieces of the tinning solder fall into the tubing causing contaminates to be added into the medical gas systems.
64

N F P A 9 9 - - F 9 5 R O P
COMMIITEE ACTION: Accept in Principle. Accept submitter's recommendation, but retain last sentence of
current text: "Sealants shall be applied to the male threads only." COMMITTEE STATEMENT: Sentence is necessary because sealant on the female thread would mean sealant would leak into the inside of the pipe and contaminate it. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #83) Committee: HEA-PIP
99- 208 - (4-4.1.4.5(b)): Reject SUBMI'rI~R: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text:
(b) The installation shall be made by qualified, competent technician experienced in making such installations. The qu~ifica- tJon of a comnetent technician shall be by nroof of tralnin~ in m~dical ~as it:lstallations. (Changes are unclerlined). SUBSTAi~ITIATION: Without a definition of a competent technician, this decision if left to anyone to make. In our experi- ence, we have found numerous qualified agencies qualified to educate installers. Further investigation has shown that there are over 3000 people throughout the United States, educated to install medical gas piping. COMMITrEE ACTION: Reject. COMMITrEE STATEMENT: Committee wishes to leave the qualification for a competent technician to the authority having
~ risdiction. UMBER OF CO MITTEE MEMBEKS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #113) Committee: HEA-PIP
99- 209 - (4-4.1.5): Accept SUBMrITER: j. Richard Wagner, Baltimore, MD RECOMMENDATION: Change 4-4.1.5, 4-4.1.5.1 and 4-4.1.5.3 to read according to the followi, ng:
4-4.1.5 Systems Having Nonstandard Operating Pressures. The following requirements apply to gas piping systems having operating pressure other than the standard 50 to 55 psig (345 to 380 kPa) [or 160 psig (1103 kPa) for nitrogen], and are in addition to the minimum requirements listed in 4-4.1.2.
4-4.1.5.1 Pipelines, shutoffvalves, and station outlets in systems having nonstandard operating pressures shall be labeled for gas name and operating pressure. 4-4.1.5.2 (no change). 4-4.1.5.3 Station outlets in systems having nonstandard operating
pressure shall meet the following additional requirements: (a) through (b) same as existing.
SUBSTANTIATION: The existing text gives standard pressures as examples of nonstandard pressures. The proposed change will simplify the text by not repeating the same references to specific pressures. COMMITTEE ACTION: Accept. N MBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #80) Committee: HEA-PIP
99- 211 - (4-4.1.5.3(c)): Reject SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text to read:
If operated at a pressure above 80 psig (550 kPa), but below 200 psig (1380 kPa) shall be DI~S stvle complying with 4-4.1.2.4. (Changes are underlined). SUBSTANTIATION: The existing standard states that (be either DISS style or comply with 4-4.1.2.4.) In paragraph 4-4.1.2.4 states both quick connect and DISS can be used. We feel that NFPA's intent is to limit quick-connect adapters to pressures below 80 psig. COMMITrEE ACTION: Reject. COMMITITEE STATEMENT: There are fittings other than DISS style that are acceptable for the pressures involved. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #79) Committee: HEA-PIP
99- 212 - (4-4.1.5.3(d)): Reject $UBMITI~R: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text:
If operated at a pressure between 200 and 300 psig (1380 to 2068 kPa), the station shall be DISS so designed as to prevent the removal of the adapter until the pressure has been relieved, to prevent the adapter injuring the uses or others when removed from the oudet. (Changes are underlined). SUBSTANTIATION: The word "DISS", in our opinion, has been left out of this paragraph. It's important not to rely on a worn pin in a pin index safety system to hold back 200 to 300 Ibs. of pressure. COMMITrEE ACTION: Reject. COMMITrEE STATEMENT: DISS fittings have been approved for
~ ressures only up to 200 psig by the Compressed Gas Assn (CGA V- ,1989,9ar. 2-1.)
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP67) Committee: HEA-PIP
99- 213 - (4-4.2.2): Accept SUBMITTER: Technical Committee on Piping Systems
[ RECOMMENDATION: Delete 4-4.2.2. SUBSTANTIATION: A revision is required in section 4-4.2. on gas piping. It erroneously references in 4-4.2.2 that indicates 4-3.1.8.3 applies. (Type II systems do not have this type application and it should be deleted.) All other portions of 4-4.2 are adequate. COMMITrEE ACTION: Accept. NUMBER OF COMMITI~E MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #310) Committee: HEA-PIP
99- 210 - (4-4.1.5.2(a)): Reject SUBMITTER= Gary B. Trinker, Victaulic Company of America RECOMMENDATION: Revise text as follows:
(a) Only Schedule 5, Type 316 stainless steel pipe with mechanical pressfitting pipe joining system, or Type KASTM B819 (copper tube) shall be used. SUIK~TANTIATION: Type 316 mechanical pressfitting pipe joints are rated to a maximum working pressure of at least 300 psi and as such are suitable for operating pressures between 200 and 300 psi. COMMITI~E ACTION: Reject. COMMITrEE STATEMENT: Insufficient data presented to committee to demonstrate equivalency to a brazed joint.
(Log #CP76) Committee: H ~ - P I P
99- 214- (4-4.2.12): Accept SUBMITI~R: Technical Committee on Piping Systems RECOMMENDATION: 1. lnsert a new 4-4.2.12.1 to read as follows: 4-4.2.12.1 Non-Emergency Shut-offValves Systems operating at varying op erating~prressures, from 0-200 psig, and not operating at a constant regulated 50 psig, shall have a manual shut off valve between the source and all service outlets. It shall be close to the service outlet.
2. Insert a new 4-4,2.12.2, tided "Emergency ShutoffValves', and renumber existing 4-4.2.12.1 through 4-4.2.12.4 as new (a) through (d) under new 4.4.2.12.2.
65

N F P A 99 - - F 9 5 R O P
3. Renumber affected appendix A material. SUBSTANTIATION: The existing paragraph is tided "Gas Shut off valves". The text that it contains only relates to "emergency shut off valves". There is a need to describe manual type II shutoffvaives. COMMYITEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #59) Committee: HEA-PIP
99-215- (44.2.13.2, 4-9.1.1.6 (New)): Reject SUBMITTER: Paul Rumbos, Major Medical Hospital Services, Inc. RECOMMENDATION: Add:
To install new O-rings in outletsand inlets on a 3 year cycle. SUBSTANTIATION: O-rings tend to go on this cycle due to wear mad tear of in ~ind out use also oxygen is such a dry gas that the rubber goods in outlets usually crystallizes in this time frame. COMMITrEE ACTION: Reject. COMMITTEE STATEMENT: Does not reflect usage pattern. Some O-rings require changing more often than 3-years; others can be changed less often than 3-years. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #'208) Committee: HEA-PIP
99- 216 - (4-4.3): Accept SUBMITTER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Move the following paragraphs in 4-4.3 to 4- 3.3 (Lab Gas Supply): 44.3.1, 44.3.3, 4-4.3.4, 44.3.10,44.3.11, 4- 4.3.2. SUBSTANTIATION: To confirm to structure of NFPA 99, which separates source requirements from distribution requirements. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrYrEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP74) Committee! HEA-PIP
99- 217 - (4-4.3): Accept SUBMITrER: Technical Committee on Piping Systems RECOMMENDATION: Add a new 4-4.3 as follows, renumbering existing 4-4.3 and 4-4.4 to new 44.4 and 4-4.5. 4-4.3. Type III Gas Distribution System 4-4.3.1 The provisions of this section apply to field installed piping
for the distribution of gasses to power devices. (a) Piping shall be Type K or L copper hard drawn or annealed or
brass schedule 40 or 80. If type III dynamic gas piping is installed simultaneously with other pa ten t gas piping systems, either the type IH piping shall be labeled or otherwise identified prior to installa- tion in order to preclude inadvertent inclusion in a non-flammable medical gas piping system, or the type Ill piping shall be cleaned and degreased in accordance with 44.1.4.
(b) Fittings shall be manufactured from corrosion resistant materials suitable for she system pressures (not to exceed 160 psig).
NOTE: Acceptable materials are wrought copper, brass, or bronze. (c) Connectors and joints shall be soldered with 95-5 Tin
Antimony, silver brazed, or threaded NPT. (d) The provisions of 44.1.2.1 (g) piping support, (k) buried
~ iping, (n) trenching, (o) fire stopping, (p) misc. damage, (q) oses, shall apply. 44.3.2 Gas Shutoff Valves. 4-4.3.2.1 Emergency gas shutoffvalves shall not be required.
Shutoffvalves for isolation of a duplex system operation components shall be required per the manufacturers requirements.
4-4.3.2.2 Where nitrogen gas is used as a backup for a type III compressed air system, a check valve and shutoff valve shall be located in each supplyline prior to the "T" connection in the main line. (See new Figure 4-3 .2 .3 .2 . )
44.3.3 Service Outlets.
4-4.3.3.1 Outlets from Type III piping systems shall be either a shut offvalve with a threaded female pipe connect, or quick connect fitting with a single check valve.
44.3.3.2 Service outlets shall be located to avoid physical damage. 4-4.3.4 Alarms. 44.3.4.1 Gasses used to power<tevices such as compressed air, and
nitrogen system, as well as Type III vacuum systems shall not be required to have an alarm system.
44.3.5 Testing. 4-4.3.5.1 Type Ill piping systems shall be static pressure tested to
150 psig or 150 percent of maximum pressur.e, which ever is greater, for 24 hours. The pressure loss shall not exceed a 5 psig loss of pressure. This test shall be conducted after all service outlets are installed and before the compressor system is connected.
44.3.5.2 After a system has been installed, other performance testing shall be conducted per manufactures' requirements.
4-4.3.5.3 Records of all tests shall be maintained in the facility. SUBSTANTIATION: There are currently no requirements for a Type III piping distribution system. The committee believes a Type Ill system category is required, and thus has included requirements for the distribution portion of it. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 1 8 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #206) Committee: HE/k-PIP
99- 218 - (44.3.7): Reject SUBMITTER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: 1. Delete reference to type 1 systems.
2. Add: what is required for non-flammable laboratory gas systems: a. Cleanliness b. Permissible contaminants c. Flow capability d. Purity
SUBSTANTIATION: 1. Type 1 standard do not necessarily apply to laboratory systems.
2. The laboratory personnel should be able to supply the listed min/max limits for parameters a through d. COMMrYrEE ACTION: Reject. COMMrrrEE STATEMENT: Committee believes Type I system requirements are necessary for adequate firesafety for laboratory piped gas systems in health care facilities. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: lfi NOT RETURNED: Fan, Shoemaker
(Log #322) Committee: HF_A-PIP
99-219- (44.3.7): Reject SUBMIT~R: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Delete: ".,..Type I gas systems..." Replace " with: "par. 4-4.2.11 Gas Piping." SUBSTANTIATION: Type I piping specs too restrictive. #4-2.11 refers to type II systems and is less restrictive. COMMrl~EE ACTION: Reject. COMMIT[EE STATEMENT: Reference to 4-4.2.11 is incomplete as it would imply that piping in laboratories meet all Type II piped system requirements. , NUMBEROF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #91) Committee: HEA-PIP
99- 2 2 0 - (44.3.11): Accept in Principle SUBMITrER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Delete text:
If a system is to be connected for use with a gas other than that for which it was originally installed, it shall be inspected for suitability for the proposed gas, purged with an inert gas; (such as nitrogen): cleaned when oil, grease, or other readily oxidizable materials are
66

N F P A 99 - - F95 R O P
present; and pressure tested in accordance with the appropriate piping s tandard. Each outlet of such system shall be identified by chemical n a m e and specifically converted for use with the successor
~"°Ui3STANTIATION: Contradictory statement: 4-4.3.11 states that Piping systems can be used for gases o ther than those for which they are des igned and identified. 4-4.3.10, states tha t Piping systems can no t be used for gases o ther than those for which they are des igned and identified. COMMITTEE ACTION: Accept in Principle.
1. Change section 4-4.3.11 to an Exception to 4-4.3.10. 2. In c.urrent 4.4.3.11, sentence 1, change "connected" to
"converted." COMMITTEE STATEMENT: 1. Laboratory requi rements can change, and Gommit tee wants to allow for the change in use of pip edgasses in laboratories. .
2. To address the issue of systems that are converted to use of o ther
~ I ~ E R OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
(Log #GP60) Committee: HEA-PIP
99- 221 - (4-5.1): Accept SUBMITTER: Technical Commit tee on Piping Systems RECOMMENDATION: 1. Revise paragraph 2 of 4.5.1.1 to read as follows:
"This inspect ion and testing shall inc lude all componen t s o f the system or port ions the reof including, bu t no t l imited to, gas bulk source(s) , manifolds , compressed air source systems (e.g.- compres- sors, dryers, filters, regulators), vacuum source s.vstems, source alarms and mon i to r ing safeguards, master alarms, pipelines, isolation valves, a rea alarms zone valves, station inlets (vacuum) and outlets (pressure ~ases~." (changes under l ined)
2. RevJ~e pa ragraph $ of 4-5.1.1 to read as follows: "All systems that are b reached and componen t s that are subject to
additions, renovations, or rep lacement (e.g., new gas source-bulk, manifolds, compressors, v~cuum pumvs , dryers, alarms) shall be inspected and appropriately tested." (~hanges under l ined)
3. Revise pa ragraph 4 of 4-5.1.1 to read as follows: "Systems shall be d e e m e d breached at the point of pipel ine
intrusion by physical separat ion or by system c o m p o n e n t removal, replacement , or addition. T h e b reached port ions of the systems, subject to inspection and testing, shall be all tile new and existing componen t s in the immedia te zone or area that is located for vacuum systems and downst ream for oressure gases at the point or area of in l rus ion . (changes underline'd) v
4. Revise par. 5 of 4-5.1.1 to read as follows: "The inspect ion and testing reports shall be certified and submit ted
directly to the responsible facility authority, and the installer. These reports shall contain detailed listings of all f indings and results, and any corrective actions tha t may have been performed." (change consists of phrase "authority having jurisdict ion" deleted)
5. Revise par. 7 o f 4.5.1.1 to read as follows: "Before piping systems are initially pu t into use, the hea l th care
facility authori ty shall be responsible for ascer taining that the gas delivered at the outlet is that shown on the outlet label and tha t the
~ roper connec t ing fittings are checked against their labels. This can e accomnl i shed bv accent ing the results of 4-5.1.3 System Verifica-
tion." (cliange under l ined) - 6. Revise the title of 4.5.1.2.2 by delet ing the word "Test." Tide
would thus read: "4-5.1.2.2 Blow Down." 7. Revise the title of 4-5.1.2.4 by adding the word "Test." Title
would thus read: "4.5.1.2.4 Piping Purge Test." 8. Revise par. 2 o f 4.5.1.3 to read as follows: "This testing shall be conduc ted by a party technically c o m p e t e m
and exper ienced in the field of medical ,~s pipeline testing, i rKlenendent of the eQuinment installer . '
9. "Revise 4-5.1.3.1, C~ross-Gonnection Test, as follows: a. Revise and move sentence 1 of 4-5.1.3.1 (a) directly unde r 4-
5.1.5.1 to read as follows: "After closing of walls and comple t ion of requi rements of 4-5.1.2, it shall be de t e rmined that no cross connect ion of p ip ing systems exists by ei ther of the following methods."
b. R e n u m b e r existing 4-5.1.3.1 (a) (3) as new 4.5.1.3.1(b). c. R e n u m b e r existing 4-5.1.3.1 (b) as new 4-5.1.3.11, and tide it:
"Labeling." 10. Revise 4-5.1.3.3(a) byde le t ing "as described in CGA P-9, Inert
Gases: Argon, Ni t rogen and Helium," and moving pa ragraph directly unde r 4-5.1.3.3 so that it reads:
"4-5.1.3.5 Flow Test. All outlets shall be tested for flow. Tests shall be pe r fo rmed with the use of oil-free, dry ni trogen."
R e n u m b e r sub pa ragraph (b) and (c) as subparagraph (a) and (b). 11. Revise 4.5.1.3.4(b) to read as follows: (b) Warn ing Systems. Tests of warning systems for new installations
(initial tests) shall be pe r fo rmed after the cross-connection testing (4.5.1.3.1). Initial tests of warning systems that may be inc luded in an addit ion or extension to an existing piping system shall be comple ted before connec t ion of the addi t ion to the existing system. Test gases for the initial tests shall be oil-free, dry n i t rogen system desLmaation." (changes under l ined)
12. Revise paragraph 2 of 4-5.1.3.5, Piping Purge Test, to read as follows:
"For each positive-pressure gas system, cleanliness o f piping system shall be verified. Filter a m i n i m u m of 35 cu ft (1000 L) of gas th rough a clean, white 0.45-micron filter at a m i n i m u m flow of 3.5 SCFM (100 Lpm) ." Filter shall accrue no more than 0.1 mg of matter. Each zone shall be tested. This test shall be oe r fo rmed at the outlet most remote f rom the source. Test shall be [~erformed with the use ofoi l free, dry ni trogen. (changes under l ined)
13. In last sen tence of 4-5.1.3.6, Piping Purity Test, delete "as described in CGA P-9.
14. Revise 4-5.1.3.10, Medical Air Purity Test (Compressor) , to read as follows:
"Analyze medical air source for concent ra t ion of contaminants , by volume. Take samples for air system test at a sample point. The test results shall n o t exceed the following narameters : (rest the same) (change under l ined) v .
15. Revise 4-5.1.4.1 (b) to read as follows: "(c) f f t h e system has an actuat ing switch and signal to moni to r the
contents of the reserve, its func t ion shall be tested before the system is pu t into service, f f a system uses a liouid source for the reserve. the "Reserve Pressure Low" shall be tested." (change under l ined) SUBSTANTIATION: 1., 2 , 3. Reference to 'Vacuum" added since m a n y gas systems are installed s imultaneously with a vacuum system(s).
4. Reference to AHJ in 4-5.1.1 was deleted since it is beyond the scope o f t h e d o c u m e n t to state who shou ld receive reports o ther than the facility itself.
5. Editorial, for clarification. 6. "Test" was deleted since "blown down" is no t a test. 7. "Test" was added since piping purge includes a test. 8. Independence of tester f rom installer was added to eliminate
the issue of conflict of interest. 0. Editorial, clarifying tha t either test is acceptable. Labeling
criteria moved since it is no t part of cross-connect test. 10. Reference to CGA P-9 deleted since it no t the correct refer-
ence. 11. For change in sentence 1, it is necessary to test warning system,
but it can be done anytime after cross-connection testing; thus delet ion of "before purging". For change in last sentence, gas of system designat ion is acceptable for testing warning systems.
12. Removal of reference to "discoloration" in sen tence 3 was made because it is no t quantifiable. Change in location for test ing of outlets was made as the remotes t outlet is the worst case test. Reference to CGA P-9 in last sentence was deleted since it n o t the correct reference.
13. Reference to GGA P-9 in last sen tence was dele ted since it n o t the correct reference.
14. Editorial change only for clarity. 15. Existing text does not consider a system that used a liquid
source. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Mohile N O T RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: MOHILE: I do no t agree with the Commit tee ' s Action to cont inue
to require testing on a zone by zone basis for cleanliness of the
~ iping system in paragraph 2 of 4-5.1.3.5. According to Doug rickson, Director of Design and Construct ion for the Amer ican
Hospital Association, the AHA wanted to delete this por t ion of the code. However, their representative at the Commit tee mee t ing incorrectly represented the wishes of the AHA. This is a very costly and t ime consuming m e t h o d and entirely no t necessary. It is sufficient to manda te testing at the mos t remote outlet in the system and also allow the certifying agency to do as m u c h additional testing as is necessary to provide a clean system to the authori ty having jurisdiction.
67

N F P A 99 - - F 9 5 R O P .
(Log #365) Committee: HEA-PIP
99- 222 - (4-5.1.1): Accept in Principle SUBMITI~R: Dennis Murray, American Hospital Association RECOMMENDATION: Paragraph 4 Delete. SUBSTANTIATION: Existing text is confusing. Description of breached seems difficult to qualify. COMMr[TEE ACTION: Accept in Principle.
See Committee Proposal 99-221 (Log #CP60). COMMITTEE STATEMENT: Proposal 99-221 (Log #CP60) addressed issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #42) Committee: HEA-PIP
99- 223 - (4-5.1.1.1): Accept in Principle S U B M I ~ David B. Mohile, Medical Engineering Services RECOMMENDATION: The 5th paragraph should be changed to read:
"The inspection and testing reports shall be submitted to the installer, with a copy being sent directly to the responsible facility authority. These reports shall contain detailed listings of all findings and results." SUBSTANTIATION: The first sentence of the existing paragraph . requires the reports to be, "cerafied: This is inconstant since who would 'certify' the report?
The last sentence also indicates that any corrective actions that were done be reported. This is not necessary. I fa problem was found and fixed, why is it necessary to make a big deal about it? We frequently find cross connections on large jobs. As long as the problem is fixed, the installer will have already embarrassed enough. Why make it part of the permanent records? COMMITI'EE ACTION: Accept in Principle. See Committee Proposal 99-221 (Log #CP60).
COMMITI'EE STATEMENT: Proposal 99-221 (Log #CPt0) addressed issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #19) Committee: HEA-PIP
99- 225 - (4-5.1.2): Accept SUBMY[TER: David Mohile, Medical Engineering Services RECOMMENDATION: Change the paragraphs and number to reflect an appropriate testing sequence as follows:
4-5.1.2.1 Blowdown Test (presently 4-5.1.2.2) 4-5.1.2.2 Pressure Test (Initial) (presently 4-5.1.2.1) 4-5.1.2.3 Pressure Test (presently 4-5.1.2.3) 4-5.1.2.4 Piping Purge to remain as currently numbered 4-5.1.2.5 Cross-Connection Test to remain as currently numbered.
SUBSTANTIATION: The purpose of these changes is to more correctly state the normal sequence of events in the installatioh and preliminary testing of a medical gas pipeline. Previously, 4-5.1.2.1 required pressure testing after the installation of the outlet rough in assemblies, and the next paragraph, 4-5.1.2.2, required a blowdown before installation of the oudets and other components.
This merely puts items in the correct sequence. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOTRETURNED: Fan, Shoemaker
(Log #329) Committee: HEA-PIP
99- 226 - (4-5.1.2.4): Reject SUBMITTER: Saul Aronow, Technology in Medicine Inc RECOMMENDATION: Rearrange the order of the sections 4-5.1.2.4, the PIPING PURGE, should be the first thing done. 4-5.1.2.2, BLOWDON TEST should come next because it says it is to be done"., before installation of station outiets..."4-5.1.2.1 PRES- SURE TEST, should come third because it says", after installation of station outlets..." SUBSTANTIATION: Self explanatory. COMMITrEE ACTION: Reject. COMMY[TEE STATEMENT: Blown down needs to be done first to remove larger particles that could be in system. NUMBEROF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #121) Committee: HEA-PIP
99- 224 - (4-5.1.1.1): Accept in Principle SUBMITTER: David B. Mohile, Medical Engineering Services, Inc. RECOMMENDATION: The 5th paragraph should be changed to read:
The inspection and testing reports shall be submitted to the installer, with a copy being sent directly to the responsible facility authority. These reports shall contain detailed listings of all findings and results. SUBSTANTIATION: The first sentence of the existing paragraph requires-the reports to be, "certified". This is inconsistent since who would "certify" the report?
The last sentence also indicates that any corrective actions that were done be reported. This is not necessary. I fa problem was found and fixed, why is it necessary to make a big deal about it? We frequently find cross connections on large jobs. As long as the problem is fixed, the installer will have already been embarrassed enough. Whymake it part of the permanent records? COMMITrEE ACTION: Accept in Principle.
See Proposal 99-221 (Log #GP60). COMMITrEE STATEMENT: Proposal 99-221 (Log #CP60) addressed issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #8) Committee: HEA-PIP
99- 227 - (4.5.1.2.5(a)): Reject SUBMITrER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Delete:
"Prior to closing of walls..." SUBSTANTIATION: It is felt that NFPA should not require that finish cover plates be installed before closing the walls to carry out the initial cross connection test. The installer would have to install the cover plates, test for.~oss connection then remove the cover plates so the walls could be completed. An expensive and time consuming operation.
If the walls are completed and the installer finds a cross connec- tion, they merely cut a hole in the wall, fix the problem and patch the wall - a far less costly solution. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Committee wants testing before walls are closed to minimize delays if cross-connects are found. Open walls facilitates finding and repairing cross-connects. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON GOMMI'Iq'EE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log#9) Committee: HEA-PIP
99- 228 - (4-5.1.$.1 (New)): Reject SUBMITTER= Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Add a new paragraph:
(4) A second alternate method of testing to ensure that no cross connection exists is as follows:
(i) Purge each pressure gas system with the gas of system designa- tion, then perform the following (vacuum should be included with the vacuum source in operation):
68
N F P A 9 9 - - F 9 5 R O P
Test each medical gas outlet with an oxygen analyzer to determine the correct volume percentage of oxygen for that system; i.e., 99 percent oxygen in the oxygen system, 20 percent oxygen in the medical air system and 0 percent oxygen in the nitrous oxide and nitrogen systems. Then use the differential pressure method to verify those systems patency. SUBSTANTIATION: In keeping with NFPA policy of NOT telling how to do something, yet there are two methods of cross connection testing stated, why not add a third method which is equally effective and safe. COMMITrEE ACTION: Reject. COMI~TrEE STATEMENT: Recommendation as worded does not address all potential hazards. NUMBER OF COMMI'Iq'I~ MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #$BB) Committee: HEA-PIP
99- 229 - (4-5.1.3.3): Reject SUBMITTE~ Saul Aronow, Technology in Medicine Inc RECOMMENDATION: Delete this section. SUBSTANTIATION: Under many circumstances this test can not be effectively performe& For example, in an addition to an existing system it may not be practical to connect a nitrogen tank to the system because of the size of the connectors available, to get the required flow without excessive pressure drop in the ~;Qnnectors. This defeats the purpose of the test. In any case, flow and pressure drop will be tested in 4-5.1.5.8, and this preliminary test is not very productive. COMMITrEE ACTION: Reject. COMMITrE£ STATEMENT: How tests can be performed, and allow for early detection of problems that are often difficult to correct later, e.g., piping plugs left in pipe.. Test of 5 psig pressure drop is across the outlet, and this test can be
performed. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP61) Committee: HEA-PIP
99- 250 - (4-5.1.3.5): Accept SUBMITrER: Technical Committee on Piping Systems RECOMMENDATION: 1. Change title to "Outlet flow test."
2. Delete "(a)" from beginning of subparagraph (a). 3. Change "(b)" to "(a) . 4. Change"(c)" to ~(b)'. - •
SUBSTANTIATION: Editorial. Clarify intent that section is an outlet test for flow, not a system test. COMMITIT.E ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #97) Committee: HEA-PIP
99-231- (4-5.1.31B (New)): ReJect SUBMITTER: David B. Mobile, Medical Engineering Services, Inc. RECOMMENDATION: Add new wording to above section to read as follows: Vacuum outlets shall be tested for the ability to flow at a minimum of 3 SCFM with the adjacent outlet also flowing at 3 SCFM. SUBSTANTIATION: The previous vacuum section did not give a minimum performance criteria for testing for newvacuum outlets. This is an attempt to correct this problem by using a generally accepted standard of flow and performance which is mentioned elsewhere in the code (4-10.1.1.3). By locating this testing requirement for vacuum in 4-5.1.1.3 it
groups all oudet testing in one section further making the code more user-friendly.
COMMITrEE ACTION: Reject. COMMITTEE STATEMENT: 1. Vacuum system criteria is located in section 4-10.
2. Test would impact pipe sizing unnecessarily (i.e., dramatically increasing size), and no reasons were included as to why this should be done. NUMBER OF COMMITTEE Ml~MBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #10) Committee: HEA-PIP
99- 252 - (4-5.1.3.3(a) (New)): Reject SUBMITrER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Add after " . . . Helium." the following: "Tests may be performed using gas of the system designation. SUBSTANTIATION: The intended system gas will work equally as well as nitrogen. The test an be carried out with other tests at the same time at reduced cost to the owner without any increase in hazard. COMMIT'I'EE ACTION: R~ect. COMMITTEE STATEMENT: For new construction, use of other m~ceS can contaminate system components. Recommendation could
lude result in gases being brought into workplace during constructionphase, and creating hazards. NUMBER OFCOMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #11 ) Committee: HEA-PIP
99-233- (4-5.1.3.3(b)): Reject SUBMITTER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Delete paragraph 4-5.1.3.3(b) and (c). SUBSTANTIATION: These subparagraphs already covered in paragraph 4-5.1.3.8(d) and (e). COMMI'ITEE ACTION: Reject. COMMITTEE STATEMENT: Par. 4-5.1.3.B is a flow test prior to final tie-in. Subpar. (b) and (c) are the criteria for these tests; using nitrogen as the test gas.
Tests in 4-5.1.3.8 is an operational test using system gas. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #65) Committee: HEA-PIP
99- 234 - (4-5.1.3.3(b)): ReJect SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text to read as follows:
(b) Oxygen, nitrous oxide, and air outlets shall deliver 3.5 SCFM with a pressure drop of no more than 5 psig(35 kpa) and maintain a
pressure of 50 psig (350 kpa) at the source of eouioment. (Changes are underlined). " " SUBSTANTIATION: The terminology of static pressure is in reference to the pressure at "no flow". The words "at the source equipment" are used because placing the gauge downstream of the zone valve, only a small percentage of pipe is being tested for flow and may pass the test, because very little friction is encountere~l. Testing from the source equipment, the filet.ion loss from the entire network of pipe, being much greater, may not pass the test described in the standard. COMMYIq'E~ ACTION: Reject. COMMITTEE STATEMENT: Test in this section is an individual outlet, not a system test. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 1O N O T RETURNED: Ean, Shoemaker
69

N F P A 99 - - F 9 5 R O P
(Log #68) Committee: HEA-PIP
99- 235 - (4-5.1.3.3(c)): Reject SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text:
(c) Nitrogen outlets shall deliver 5~0 SCFM with a pressure drop of no more than 5 psig (35 kpa) and maintain a min imum pressure of 160 psig (1118 kpa) at the source of equipment . (Changes are underl ined). SUBSTANTIATION: The terminology of static pressure is in reference to the pressure at "no flow". The words (at the source equipment) are used because placing the gauge downstream of the zone valve, only a small percentage of pipe is being tested for flow and may pass the test, because very little friction is encountered. Testing from the source equipment, the friction loss from the entire network of pipe, being much greater, may no t pass the test described in the standard. COMMITTEE ACTION: Reject.
See Proposal 99-230 (Log #CP t l ) . COMMrrFEE STATEMENT: Issue is addressed in Proposal 99-230 (Log #GPt l ) . NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #326) Committee: HEA-PIP
99-236- (4-5.1.3.5): Reject SUBMITTER: Saul Aronow, Technology in Medicine lnc RECOMMENDATION: Revise text as follows:
a) Increase the limit for particulate from 0.1 milligrams per cubic meter to 0.5 m gm /m3 .
b) Add a note or an appendix item: It is the intent of this test to require a quantitative measurement , no t a qualitative test such as the clean d o t h test of Section 4-5.1.3.5. SURSTANTIATION: a) It is extremely difficult, and therefore expensive, to make a valid measurement to the limit of 100 u g m / m 3 of particulate. It is a laboratory test requiring well controlled conditions and no t an on-site measurement. But more important, it is no t a direct measure of a property of immediate concern to safety, but an indirect verification of the adequacy of the cleaning of the Pliping
t is bet ter to have a test that is reasonable to perform and that will probably be done, than one that is difficult to do and that therefore invites circumvention.
b) The note is to fur ther advise that the test must be done. COMMITI~E ACTION: Reject. COMMITrEE STATEMENT: Committee member experience has shown that existing test is achievable and can be accomplished with existing technology. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #328) Committee: HEA-PIP
99:237 - (4-5.1.3.5): Reject SUBMIq[TER: Saul Aronow, Technology in Medicine Inc RECOMMENDATION: Revise text as follows:
a) Move the first paragraph to be 4-5.1.3.1 b) Move the second paragraph t o / b e part of 4-5.1.3.6
SUBSTANTIATION: a) The piping purge should be done before any of the system verification tests. At this point it is a check that purgifig had been properly done at an earlier stage of the installa- tion. It may be desirable to add a cautionary note or an appendix item to warn that if the earlier purging had no t been properly done, it may be necessary to open the walls or disassemble the piping system to disclose the source of contamination.
b) This paragraph is no t a purge but is a test to verify the deanli- hess of the p ip ing system. It belongs with the other cleanliness tests. COMMITTEE ACTION: Reject. See committee action on Proposal 99-225 (Log #19).
COMMITTEE STATEMENT: Committee believes the order of tests in Proposal 99-225 (Log #19) is a more appropriate order. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #327) Committee: HEA-PIP
99- 238 - (4-5.1.3.6): Accept in Part SUBMITTER: Saul Aronow, Technology in Medicine Inc RECOMMENDATION: (a) Change the section title to "Piping Cleanliness Test" and move it ahead of 4-5.12k2.
(b) 2nd sentence: change "test each zone" to "Each zone shall be tested..".
(c) 4th sentence: delete "..as described in CGA P-if'. (d) Table: delete +/-sign. (e) Add a note: "The in tent o f these tests is not to check the
qadUality of the ni t rogen but to verify that no contaminants have been ded in the installation.
SUBSTANTIATION: (a) Piping may or may not be clean, but "purity" is no t an attribute of pipeR. Changing the word in the title and the test clarifies the intent.
(b) Code language. (c) Nitrogen is already defined in 2-2, and no t as CGA P-9. (d) The - sign has no meaning. (e) Self explanatory.
COMMI'ITEE ACTION: Accept in Part. a) Reject. b) Accept. ~1~ ccept.
Reject.
C ~ O ~ E E STATEMENT: a) Committee believes order in Proposal 99-225 (Log #19) more appropriate order. Use of te rm "purity" is in concert with industry use of the term.
d) Equipment being used in this test has a tolerance, which must be accounted for.
e) Committee believes existing text is suffidenfly clear as written. Test is a comparative one. NUMBER OF COMMIT1T, E MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMI'ITEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #330) Committee: HEA-PIP
99- 239 - (4-5.1.3.8): Reject SUBMITTEII: Saul Aronow, Technology in Medicine Inc RECOMMENDATION: a) In paragraph (a) add the word "static" in the phrase "shall maintain static pressure..." Delete the last phrase, "..at the maximum flow rate..4-1.3.8 (d) and (e)."
b) In paragraph (b) change to read: "A ni trogen system shall maintain static pressure at 160 psig +5, -0 (l lO0 kPag +35 - 0) at all station outlets. SUBSTANTIATION: a) Present paragraphs (a) and (b) give different numbers than (d) and (e) because of the redundan t wording in (a) and (b). There is no change in intent in this proposal. COMMITI~E ACTION: Reject. COMMITI'EE STATEMENT: For a), test of 4-5.1.3.8 is a dynamic test for outlets. For b), inclusion o f + / - in recommendat ion implies the 160 psig requi rement is a minimum; this is not committee 's intent. Actual
OUMBerational pressure is a user decision. ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #254). Committee: HEA-PIP
99- 240 - (4-5.1.3.8(a)): Accept SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Remove reference to 160 psig
Nitrogen by deleting....7~q~J_(_e.L~ SUBSTANTIATION: "and e" is reference to 160 psig to Nitrogen flow rate which is not applicable to 50 psig systems. COMMITFEE ACTION: Accept.
70

N F P A 9 9 - - F 9 5 R O P
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #71) Committee: HEA-PIP
99- 241 - (4-5.1.3.8(d)): Reject SUBMITrER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text to read:
(d) Oxygen, nitrous oxide, and air outlets shall deliver 3.5 SCFM with a pressure drop of no more than 5 psig (35 kpa) and
pressure of 50 psig (350 kpa). This test shall be ~on- ducted with the desima calculated load on the system. (Changes are underlined). SUBSTANTIATION: The test described above is fine for testing existing functioning facilities. On new hospitals or total new added
tems, we feel that systems can be grossly undersized and still pass tests that are required in the NFPA standard.
COMMITFEE ACTION: Reject. COMMITTEE STATEMENT: The tests in question are meant to be for individual outlets, not system. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #85) Committee: HEA-PIP
99- 242 - (4-5.1.5.8(e)): Reject SUBMrI'I~R: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text to read:
(e) Nitrogen outlets shall deliver 5.0 SCFM with a pr _essure drop of no more than 5 psig. (55 kPa) and static pressure of 1613 psig (1118 kPa). This test shall be conducted with the design calculated load 9n the .system. (Changes are underlined). SUBSTANTIATION: The tests described in the current standard, is fine for testing existing functioning facilities, on new hospitals or totally new added systems, we feel that systems can be grossly undersized and still pass the tests that are required in the NFPA standards. COMMITrEE ACTION: Reject. COMMIT4"EE STATEMENT: The tests in question are meant to be for individual outlets, not system. NUMBER OF COMMIIWEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #100) Committee: HEA-PIP
99- 243 - (4-5.1.3.10): Accept SUBMITTER: David B. Mohile, Medical Engineering Services, In~ RECOMMENDATION: Change the third sentence in this para- graph to read as follows:
The test results shall not exceed the followingparameters: SUBSTANTIATION: When this section was redone for the 1995 code an error was made in referencing the maximum allowable variation table as shown under 4-5.1.3.6. That table (4-5.1.3.6) references the comparison of the test gas parameters taken at the source with the samples taken at the terminus of the pipeline; in other words, a test of the cleanliness of the pipeline. Section 4-5.1.5.10 is an analysis of the air actually produced by the
compressor system and is taken at the test port at the compressor site and not at the terminus of the pipeline. COMMITFEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #255) Committee: HEA-PIP
99- 244 - (4-5.1.3.10): Accept in Principle in Part SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: 1) Change the following: Analyze medical air at sample point for concentration of contami-
nants. The air shall not be acceptable if in excess of the limiting criteria found in Table 4-5.1.3.11. 2) Number table accordingly and label: "MEDICAL AIR LIMITING CRITERIA" 3) Adjust references in alarm sections 4-4.1.1.9 (g) last paragraph
and Table 4-5.1.9.8. (addressed in other proposals). SUBSTANTIATION: Section flawed, deceiwng, and difficult to reference, COMMITFEEACTION: Accept in Principle in Part.
1) Accept in Principle. 2) Reject. 5) Accept in Principle.
COMMITYEE STATEMENT: 1) Similar to Proposal 99-245 (Log #100).
2) Current wording is considered clear. 5) Issue addressed in Proposal 99-155 (Log #CP59). •
NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #256) Committee: HEA-PIP
99- 245 - (4-5.1.3.10): Acceptin Part S U B ~ Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: 1) Change symbol for carbon dioxide -Air to less than or eaual to 500 PPM.
2) Add under Table: NOTE: PPM noted as V/V. SUBSTANTIATION: Editorial:
< (less than or equal to) is a limiting criteria. + implies a tolerance.
COMMITrEE ACTION: Accept in Part. 1) Accept.
2) Reject. C O M M I T ~ STATEMENT: 2) Issue is covered in text of 4- 5.1.3.10. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #331) Committee: HEA-PIP
99- 246 - (4-5.1.3.10): Accept in Part SUBMITTER: Saul Aronow, Technology in Medicine Inc RECOMMENDATION: a) Change title ~rom "Compressor" to "Compressor System". b) Second sentence: change "a sample point" to "the sample point
specified in 4-3.1.9.8" c) Delete the third sentence. d) Fourth sentence: Add "maximum" "Maximum allowable..." e) Table: Delete the signs +/-,_<.
SUBSTANTIATION: a) It is the entire compressor system, not just the compressor, that is being checked.
b) 4-3.1.9.8 specifies a particular place for sampling the system output.
c) This makes no sense. Nothing says what the sample is being to.
d) It is assumed that the intent is to give maximum limits for the output. e) +/- is a typo. _< is not necessary.
COMMYITEE ACTION: Accept in Part. a) Accept. b) Accept. c) Reject. d) Reject. e) Accept.
COMMITrEE STATEMENT: c) Wording changed to clarify, per Proposal 99-243 (Log #100).
d) Wordingchanl~ed to darify, per Proposal 99-221(Log #CP60). NUMBER OF COMMrI'YEE MEMBERS-ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
71

N F P A 9 9 - - F 9 5 R O P
(Log #CP2) Commit tee: HEA-PIP
99- 247- (4-5.1.3.10): Accept SUBMITTER: Technical Commi t tee on Piping Systems RECOMMENDATION: Revise sentences 1 and 2 to read:
"The medical air source shall be analyzed for concent ra t ion of con taminants byvolume. Sample(s) shall be taken for the air system test at a sample point. (See 4-3.1.9.)" SUBSTANTIATION: Editorial to conform to NFPA Style Manual. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemake r
(Log #324) Commit tee: HEA-PIP
99- 248 - (4-5.1.4): Reject SUBMITIT.,R: Dennis Murray, Amer ican Hospital Association RECOMMENDATION: Add new paragraph:
"Source e q u i p m e n t leakage verification shall be pe r fo rmed following the installation o f the in te rconnec t ing pipelines, accesso- ries, and source equipment . This pressure text shall be pe r fo rmed at 50% above the system opera t ing pressure of the system compo- nents. SUBSTANTIATION: T he existing test does no t address the source after total system assembly. This.lack of detail provides for confusion in the field for enforcers. COMMITTEE A~TION: Reject. C O M M I T r E E STATEMENT: Pressurizing systems to 50 pe rcen t above opera t ing pressure is hazardous to some system components . Also, no data was inc luded to indicate what leakage would be acceptable were 50 pe rcen t value used. NUMBER OF COMMITTEE MI~4BERS ELIGIBLE T O VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemaker
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Allen N O T RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: ALLEN: Table as p resen ted in not accurate. Prior to inclusion, it
needs to be corrected.
(Log #12) Committee: I-IF.A-PIP
99- 250 - (4-5.1.4.1(d) (New)): Accept SUBMIIWER: Peter Esherick, Pat ient Ins t rumenta t ion Corporat ion RRCOMMENDATION: Add a new sub pa ragraph after paragraph 4-5.1.4.1 (c):
4-5.1.4.1 (d) If the system has an actuat ing switch and signal to moni to r the pressure of the reserve unit, its func t ion shall be tested before the system is pu t into service.
Relabel paragraphs 4-5.1.4.1 (d) a n d (e) to paragraphs 4-5.1.4.1 (e) and (f). SUBSTANTIATION: It should be m a n d a t e d tha t the a larm signal f r om the pressure o f the reserve uni t be tested for correct func t ion before the uni t is placed in service. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 18 VOTE ON C O M M r r T E E ACTION:
AFFIRMATIVE: 16 N O T RETURNED: Fan, Shoemake r
(Log #34O) Commit tee: HEA-PIP
99- 249 - (Table 4-5.1.4): Accept SUBMIIq 'ER: Mark Allen, O h m e d a Medical Engineer ing RECOMMENDATION:
Cry~enic Bulk Manifold w/cryogenic
Manifold w/reserve reserve Souxce Alarms Changeover Yes Yes Yes
Reserve in Use Yes Yes
Reserve Failure No No Yes
Reserve Low (a) (a) Yes
Dew Point High No No No
Carbon Monoxide High No No No Lag Compressor Running No No No Separator Flooded
No No No Receiver Flooded
No No No High Temperature
No No No
Line Alarms Pressure Gases Vacuum WAGD
High Line Pressure Yes
Low Line Pressure Yes
Low Vacuum Yes No
Cryogenm Bulk Air ~ a Air ~ a Air ~ a w/cyUnder ~3.1.9.1 ~3.1.9.1 Liquid Vacuum WAGD
reserve Para (a) Para. (b) Ring Pump Pump
Yes No No No No No
Yes No No No No No
No No No No No No
(~ No No No No No
No Yes Yes Yes No No
No Yes Yes Yes No No
No Yes Yes Yes Yes No
No No No Yes No No
No (b) (b) Yes No No
No Yes Yes No No No
(a) This signal is required only where cylinder reserves have no check valves for each cylinder lead. (b) This signal is required where the air compressor is water cooled or uses water cooled aftercoolers.
SUBSTANTIATION: T he proposal reconciles the table with changes in the s tandard. C ~ M M I T r E E ACTION: Accept.
72

N F P A 99 - - F 9 5 R O P
(Log #13) Committee: HEA-PIP
99- 251 - (4-5.1.4.1 (e) (3)): Accept in Principle SUBMITTER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Add to paragraph 4-5.1.4.1 (e):
4-5.1.4.1(e) (3) Check all alarm functions of the bulk unit; i.e.: Reserve In Use, Low Reserve Supply, Low Reserve Pressure, etc., to ascertain that the proper signal is indicated and is properly labeled. SUBSTANTIATION: All alarms of the bulk unit must be checked for proper operation and labeling. COMMITrEE~ACTION: Accept in Principle. Revise submi~er 's recommendat ion to read: "Check required alarmed functions of the supply and reserve to
ascertain that the proper signal is indicated and properly labeled." COMMITI'EE STATEMENT: Committee agrees with submitter 's intent. Changes made tb make sure all types of gas systems are included, a n d n o functions are left unchecked. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #257) Committee: HEA-PIP
99- 252 - (4-5.1.4.2): Reject SUBMITrER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Add as 4-5.1.4.2 (a)
(a) After 1 hour of continuous operation for each compressor at or near the compressor 's maximum rating, confirm:
(1) Proper maintenance of liquid levels as alarmed in 4-3.1.9.5. (2) Proper operating temperature as alarmed in 4-3.1.9.5.
SUBSTANTIATION: Proposed test is more representative of compressor conformance under potentially loaded conditions. COMMITI'EE ACTION: Reject. COMMITI'EE STATEMENT: Committee believes that these tests are the responsibility of the manufacturer. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #18) Committee: HEA-PIP
99- 253 - (4-5.1.4.2(b) (2)): Accept in Principle SUBMITI'ER: David Mohile, Medical Engineering Services RECOMMENDATION: Revise text:
"The quality of medical air as delivered by the compressor air supply shall be verified after installation of new components prior to us.e by patients. The test shall be per formed after installation, a m m lm um 24 hours after continuous running of the machinery, at a sample por t downstream of the pressure regulator and upstream of the piping system as defined in Figure 4-3.1.9. To make sure that the machinery is operational, sufficient air shall be bled, f rom the system to cause the compressors to cycle on and off continuously and the dryers to operate for the 24 hour period." SUBSTANTIATION: The previous wording for this section made it seem that testing had to be per formed twice: upon installation and 24 hours afterwards. This change in wording is an at tempt to clarify the wording. It is important to note that the machinery must be in operation with a bleed on the system to allow for any faults in the machinery to appear. It is also important to verify operation of the dryers and filters since some drying equipment needs to operate for a day or more to reach true efficiency. COMMITI'EE ACTION: Accept in Principle. Accept submitter 's recommendat ion with the following change: Revise last sentence ("To make sure . . . " ) to read as follows: "The
system shall operate at 25 percent of its rated capacity to cause the compressors to cycle on and off continuously and the dryers to
erate for the 24 hour period." MMITrEE STATEMENT: Clarify the duty cycle for the
compressor by establishing a min imum criteria for the test. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP68) Committee: HEA-PIP
99- 254 - (4-5.2): Accept SUBMITTER: Technical Committee on Piping Systems RECOMMENDATION: Retitle and revise existing 45.2. in its entirety to read as follows:
4-5.2 Type III Patient Gas Testing. 4-5.2.1 General . Inspection and testing shall be per formed on all
new piped gas systems (including oxygen, nitrous oxide, nitrogen, type HIcompressed air and type III vacuum ), additions, renovations or repaired systems to assure the facility, that all applicable provisions of this document have been adhered to and all system integrity has been achieved or maintained.
This inspection and testing shall include all components of the system or portions thereof including but not limited to , cylinder room equipment, compressed air source systems, vacuum system, alarms, pipelines, shutoffvalves, station outlets and terminal service outlets/inlets. All systems that are breached and components that are subject to
additions, renovations, or replacement shall be appropriately tested. The responsible facility authority shall review all inspection and
testing prior to the use of all systems covered by this document . The responsible authority shall ensure that all findings and results of the inspection and testing have been completed and all documentat ion pertaining thereto shall be maintainedon-si te , within the facility.
4-5.2.2 Piping Integrity Test. The following test shall be conducted by the installer, representative of the supplier, or representative of the manufacturer. The test gas shall be oil-free dry nitrogen.
4-5.2.2.1 Pressure Test Initial. Before at tachment of system components (e.g.), pressure activating switches for alarms, mani- folds, pressure gauges, or pressure relief valves), but after installation of the station outlets, with test caps (if supplied) in place (e.g., rough-in assembly), and before closing of the walls, each section of the piping system shall be subjected to a test pressure of 1.5 times the working pressure [minimum 150 psig (1 MPa gauge)] with oil- free dry nitrogen.
(a) The test pressure shall be maintained until each jo in t has been examined for leakage by means of soapy water or other equally effective means of leak detection safe for use with oxygen. Leaks, if any shall be located, repaired and retested in an accordance with this paragraph.
(b) The source shut-offvalve shall then be closed. The test shall remain static for a per iod of 24 hrs with a maximum allowable pressure loss of 5 psig. Leaks, if any shall be located, repaired and retested in an accordance with this paragraph.
4-5.2.2.2 Blowdown. After installation of the piping, the terminal outlets or station outlets, and after all brazing of joints has been completed, but before other components (Include the balance of 4- 5.1.2.2)
4-5.2.2.3 Piping Purge. (Include here the text of existing 4- 5.1.2.4.) Add the following at the end of the sentence: "Piping shall be capped after testing."
4-5.2.2.4 No fur therbraz ing to the piping system shall be permit- ted after completing the tests in this section. Additional assembly shall be limited to installing the manifold and operating compo- nents of the system.
4-5.2.3 System Verification and Final Testing. The following test shall be performed after those listed in section 4-5.2.2. This testing shall be conducted by a party technically competent and experi- enced in the field of type Ill medical gas, type Ill compressed air, and type III vacuum systems testing and systems.
4-5.2.3.1 All systems will be activated with the in tended "use gas" (i.e. oxygen, nitrous oxide , etc.) at the normal operating pressure (50 psig). The source shut-offvalve shall then be closed. The test shall remain static for a period of 24 hrs with a maximum allowable pressure loss of 5 psig. Leaks, if anyshall be located, repaired and retested in an accordance with this paragraph.
4-5.2.3.2 After walls have been closed in, and all brazing fabrication coml~leted , completion of the system shall be made. Manifolds, regulators., hoses, alarms, compressors, vacuum pumps and all accessones to the system shall be assembled before final testing.
4-5.2.3.3 Static Pressure Test. The pressure test of 4-5.1.2.3 shall be conducted at normal operating pressure. The test gas shall be the in tended service gas. The test shall remain static for a period of 24 hrs with a maximum allowable pressure loss of 5 psig. Leaks, if any shall be located, repaired and retested in an accordance wi.th this paragraph.
4-5.2.3.4 Pressure Relief Test. Test each gas pressure relief valve in the piping system to insure the pressure relief valves actuate at <50% over pressure from their maximum operating pressure. The pressure relief valve specified in 4-4.2.6 shall close automatically when the excess pressure has been released.
4-5.2.3.5 Cross Connection Test Activate the 0 2 system only and all o ther gasses shall be at zero (0) psig. Using appropriate s e c o n d ~ connectors, test all service outlet including vacuum. Only
73

N F P A 9 9 - - F 9 5 R O P
02 shall flow from the 02 station outlet and all other oudets shall have no gas flow. Purge the 02 outlet until a white cloth shows not show any particulate of discoloration.
(a) Repeat section 4-5.2.3.7 for each gas and vacuum piping system.
4-5.2.3.6 Alarm Testing for Gas Systems. Relocate 4-5.2.4 to this paragraph and add to existing text of 4-5.2.4: "Test all functions".
4-5.2.3.7 Additional Test Of Secondary Equipment. Testing shall also be conducted on the piping system with the intended secondary equipment to make sure the safety alarms and provisions of the secondary equipment are verified. The instructions of the manufac- turer or supplier of secondary equipment shall be followed for any additional recommended tests of the piping and or secondary equipment.
NOTE: This will insure required pressure and flow meet the secondary equipment manufacturer's requirements. SUBSTANTIATION: The Type II testing requirements in the '93 edition of NFPA 99 did not properly address the needs of the industry in terms of industry practice while maintaining safety equivalent to Type I systems. The revised testing protocol corrects that problem. COMMITI'EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #198) Committee: HEA-PIP
99- 955 - (4-5.3.10): Reject SUBMITTER: Henry IL Kaht, Gurnee, IL RECOMMENDATION: Change dew point to: +45°F (7.2°C) at 50 PSlG. SUBSTANTIATION: Consistent with 4-4.1.1.2 (g) proposal. COMMITTEE ACTION: Reject. COMMITFEI/I STATEMENT: Since Proposal 99-160 (Log #200) was ~ d , recommended change here can not be made.
ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Kaht NOT RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: KAHT: Section 4-5.3.10 A 39°F dewpoint temperature with a
refrigerated air dryer is not possible when the compressed air demand falls below 90 percent to 95 percent of the dryers capacity.
(Log #14) Committee: HEA-GAS
99- 256 - (4-6.9.1.2 (New)): Reject SUBMITTER: Mayer D. Zimmerman, US DHHS; HCFA RECOMMENDATION: Add a new section:
4-6.2.1.2(0: Cylinders shall be permitted to be dressed with a fabric dress subject to the following:
i - Fabric shall be rendered and maintained flame retardant ii - Dressing shall not cover or obscure markings, fittings, gauges,
regulators or valves. iii - Dressing shall be maintained free from dust, dirt, oil, grease or
flammable substances. SUBSTANTIATION: Marry elderly residents of nursing homes should have their room decorated in such a manner as to promote a home-like environment. A 20-1b oxygen cylinder lacks a degree of esthetics often commensurate with a home-like environment. So long as the precautions listed in the current section 4-6.2.1.2 are observed, there is no compelling technical reason or justification as to why dressing of cylinder should be prohibited. The current text is silent on this issue. The standard should be amended to permit this practice within the limits of the caveats expressed therein. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Committee is of the oplnion that a cover placed over a cylinder would jeopardize patient safety, e.g., maintaining cleanliness of cover, maintaining cut-outs, recognition of cylinder by fire fighters in an emergency. NUMBER OF COMMITI'EE MEMBERS ELIGIBLE TO VOTE: 5 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 4 NOT RETURNIED: Raman
(Log #325) Committee: HEA-GAS, HEA-PIP
99- 257- (4-6.2.1.6): Accept SUBMITrER: Dennis Murray, American Hospital Association RECOMMENDATION: First sentence -Delete as-"if permitted...of the facility," * Add after care areas, complying with 4-3.1.9.1.
SUBSTANTIATION: Existing text does not adequately provide the safety of the environment for which may be compromised during this procedure. Field enforcers find existing text inadequate. COMMITIT, E ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 5 (GAS), 18 (PIP) VOTE ON COMMrlTEE ACTION:
AFFIRMATIVE: 4 (GAS), 16 (PIP) NOT RETURNED: Fan (PIP), Raman (GAS), Shoemaker (PIP)
(Log #CP3) Committee: HEA-PIP
99- 258- (4-6.2.1.6): Accept SUBMlq['rER: Tecfinical Committee on Piping Systems RECOMMENDATION: Revise 4-6.2.1.6 to read:
"Transferring of Liquid Oxygen. Transferring of liquid oxygen from one container to another shall be accomplished at a location specifically designated for the transferring that:
(a) Is separated from any portion of a facility wherein patients are housed, examined or treated by a separation of a fire barrier of one- hour fire resistive construction; and
(b) The area is mechanicallyventilated, sprinklered, and has ceramic or concrete flooring; and
(c) Is posted with signs indicating transferring is occurring, and smoking in the immediate area is not permitted. Tramferring shall be accomplished utilizing equipment designed
to comply with the performance requirements and procedures of CGA Pamphlet P-2.6, Transfilllng of Low Pressure Liquid Oxygen to be Used for Respiration, and adhering to those procedures. SUBSTANTIATION: Clarffyintent of requiring transferring to be "remote from patient care areas." COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #283) Committee: HEA-ANE, HEA-PIP
99- 259 - (4-6.2.2.3): Accept in Principle SUBMITI'ER: Douglas S. Erickson, American H~spital Assodation RECOMMENDATION: Delete paragraph in its entirety. SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupandes. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans AJlalrs, Department of Defense and major te~. ching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITTEE ACTION: Accept in Principle.
Revise 4-6.2.2.3 by deleting "flammable anesthetic" and "(See 4- 3.1.2.4)" in sentence 1; and adding "(See NFPA 45 and NFPA 30 for storage cabinet requirements.)" Move 4-6.2.2.3 to Chapter 6, and designate it 6-2.9.1. COMMITITEE STATEMENT: Material is more appropriate in Chapter 6. Reference to other NFPA documents are added because a l ~ v e r the subject of storage cabinets.
ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 (ANE), 18 (PIP) VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 10 (ANE), 16 (PIP) NOT RETURNED: Fan (PIP), Shoemaker (PIP)
74

N F P A 99 - - F95 R O P
( Log #304) Committee: HEA-PIP
99- 260 - (4-6.2.3.7, 4-6.2.3.9, 4-11.2.1.1): Reject SUBMITTER: William G Frank, Wm. G. Frank Medical Services; Inc. RECOMMENDATION: Revise text as follows:
Prepare a separate section of mandatory and optional maintenance required for medical gas and vacuum systems. SUBSTANTIATION: Medical facilities are in a quandary about requirements for routine maintenance. Private companies are convincing facilities that the procedures in paragraph 4-5 and 4-10 must be per formed annually in order to mee t JCAHO requirements.
Unnecessary monies are being spent for unnecessary testing and routine maintenance is not being performed.
Maintenance statements are scattered through various sections and appendices - they should be expanded in scope and consolidated into a specific section.
Example: Outlet terminal leakage and flow tests shall b e p e r f o r m e d
annually in all critical areas and bi-annually in all o ther areas. Leakage tests must include testing zone valves for internal and
external leakage. Internal leakage is inhe ren t in older zone valves render ing them
useless in the event of fire. Outlet and terminal seal rings deteriorate in 5 to 7 years, resulting
in system leakage. Mechanical parts may fail at any time. These conditions can be detected only by measuring flows and leakage (flow measurement requires use of the correct adaptor, thus the outlet latching mechanism is also tested).
Similar basic information should be published for all system components to clarify all the misinformation being presented to health care facilities. COMMITYEE ACTION: Reject. COMMITTEE STATEMENT: Submitter did no t include any r ecommended text in proposal, in accordance with NFPA regula- tions on submitting proposals. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 15 NEGATIVE: Allen NOT RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: ALLEN: Submitters proposal has meri t and should be submitted to
a task force to develop necessary guidelines.
(Log #GP69) Committee: HEA-PIP
99- 261 - (4-6.2.4.1, 4-6.2.4.5): Accept SLIBMITTER: Technical Committee on Piping Systems RECOMMENDATION: 1. Revise the text of 4-6.2.4.1 (a) by the addit ion of the words as shown in italics and underlined. (a) Have no t more than 3000 cu. ft.(56m3) total capacity of all
gasses (excluding nitrogen and air for powered devices) connected and in storage at one time, except that the total capacity of all grasses shall be permit ted to be increased to 5000 cu. ft. (143 m3) (exclud- ing ni trogen and air for powered devices) if oxygen is ~ . [the rest the same]
2. In 4-6.2.4.5, add the following before the existing text: "An independendy functioning type III system shall be permit ted
within a type I facility. However . . . . (rest the same). SUBSTANTIATION: The criteria for the establishment of Type II nonflammable medical system installations is restricted to <3000 cu. ft. of gas being used in that system. The s torage/use of ni trogen a n d / o r cylinder air for powered devices is i ndependen t of the Type II determinat ion of nonflammable medical gas systems criteria and should no t be a limiting factor to that criteria.
Also clarification is desired to allow an independen t type II system within a facility that is type I. COMM1TrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrFrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #356) Committee: HEA-PIP
99- 262 - (4-6.2.4.5): Accept SUBMITTER: David Wyrick, .Sr., Cambiare Ltd. RECOMMENDATION: Add a last sentence: A stand alone clinic, a part of a larger facility (i.e., hospital), but
complies with 4-6.2.4.1 shall be permit ted to be Type II.
SUBSTANTIATION: This was the intent for the 1993 Edition to allow the Type II facility within larger buildings like, large office buildings, dental or medical schools and self contained dental offices within the hospital. COMMITrEE ACTION: Accept.
Editorial changes. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 1 8 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #99) Committee: HEA-PIP
99- 263 - (4-6.2.4.6): Reject SUBMITTER: David B. Mohile, Medical Engineering Services, Inc, RECOMMENDATION: Delete 4-6.2.4.6 entirely. SUBSTANTIATION: This paragraph is an anachronism. There are many manufacturers and packagers of equipment in the medical and dental marketplace, and they frequently follow the require- ments of design engineers.
It is not p ruden t for this documen t to require a manufacturer t.o be familiar with certain codes and provide on-site personnel to supeiwise installation. This should be a function of the design engineer or authority having jurisdiction. COMMITI'EE ACTION: Reject. COMMITTEE STATEMENT: This section applies to Type II systems, no t Type I systems. Submitter has acknowledged this oversite. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #55) Committee: HE.A-PIP
99- 264 - (4-6.4.1.2 (New)): Accept in Principle S U B ~ David Esherick, Patient Instrumentat ion Corp. RECOMMENDATION: Add:
Specify that hospital shall label the valve box with the "as used" room numbers, not the contractor with blue print numbers. SUBSTANTIATION: If the contractor labeled the valve box with blue p r in t room numbers, these designations usually become obsolete as soon as the hospital takes over the newly constructed area. This way we eliminate the valve box being labeled incorrectly. COMMITrEEACTION: Accept in Principle.
Revise existing 4-6.4.1.2 to read: "The shutoff valves described in 4-4.1.2.2(a), 4-4.1.5.2 and 44.1.3.3
shall be labeled to reflect the rooms that are controlled by such valves. Labeling shall be kept current from initial c6nstruction through acceptance. Valves shall be labeled in substance as follows:" COMMITrEE STATEMENT: The committee believes its wording is preferable, and meets the in tent of the submitter. Committee 's wording also requires the labeling of the valves to be kept current, which the Committee believes the submitter in tended but did not stipulate. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #337) Committee: HEA-PIP
99- 265 - (4-6.5.2.2): Reject SUBMITrER: David Wyrick, Sr., Cambiare Ltd. RECOMMENDATION: Revise text as follows:
8-5.2 should be added to 99-C. SUBSTANTIATION: This is another example of a reference to a paragraph not found in 99-C. Any reference to a section outside of Chapter 4, should be included in 99-C. COMMITrEE ACTION: Reject. COMIMITrEE STATEMENT: Text is f rom Chapter 8 and is not part of piped gas and vacuum system requirements. The request for NFPA 99C asked for medical gas and vacuum systems only. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
75
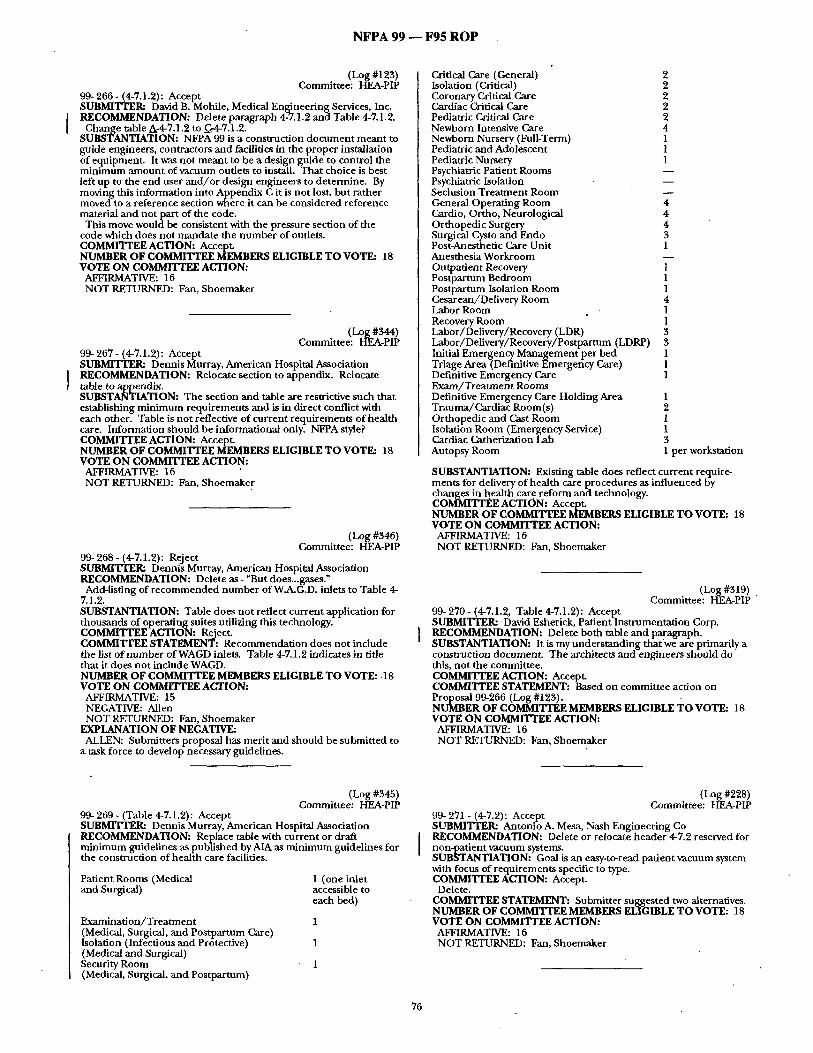
N F P A 99 - - F 9 5 R O P
(Log #123) Committee: HEA-PIP
99- 266 - (4-7.1.2): Accept SUBMITTEI*a David B. MohUe, Medical Engineering Services, Inc. RECOMMENDATION: Delete paragraph 4-7.1.2 and Table 4-7.1.2.
Change table A-4.7.1.2 to _G-4-7.1.2. SUBSTANTIATION: NFPA 99 is a construction document meant to guide engineers, contractors and facilities in the proper installation of equipment. It was not meant to be a design guide to control the minimum amount of vacuum outlets to install. That choice is best left up to the end user and/or design engineers to determine. By moving this information into Appendix C it is not lost, but rather moved to a reference section where it can be considered reference material and not part of the code. This move would be consistent with the pressure section of the
code which does not mandate the number of outlets. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #344) Committee: HEA-PIP
99- 267 - (4-7.1.2): Accept SUBMIITER: Dennis Murray, American Hospital Association RECOMMENDATION: Relocate section to appendix. Relocate table to appendix. SUBSTANTIATION: The section and table are restrictive such that establishing minimum requirements and is in direct conflict with each other. Table is not reflective of current requirements of health care. Information should be informational only. NFPA style? COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #346) Committee: HEA-PIP
99- 268 - (4-7.1.2): Reject SUBMITI'ER: Dennis Murray, American Hospital Association RECOMMENDATION: Delete as - "But does...gases." Add-listing of recommended number of W.A.G.D. inlets to Table 4-
7.1.2. SUBSTANTIATION: Table does not reflect current application for thousands of operating suites utilizing this technology. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Recommendation does not include the list of number of WAGD inlets. Table 4-7.1.2 indicates in title that it does not include WAGD. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 15 NEGATIVE: Allen NOT RETURNED: Fan, Shoemaker
EXPLANATION OF NEGATIVE: ALLEN: Submitters proposal has merit and should be submitted to
a task force to develop necessary guidelines.
Critical Care (General) 2 Isolation (Critical) 2 Coronary Critical Care 2 Cardiac Critical Care 2 Pediatric Critical Care 2 Newborn Intensive Care 4 Newborn Nursery (Full-Term) 1 Pediatric and Adolescent 1 Pediatric Nursery 1 Psychiatric Patient Rooms Psychiatric Isolation Seclusion Treatment Room General Operating Room 4 Cardio, Ortho, Neurological 4 Orthopedic Surgery 4 Surgical Cysto and Endo 3 Post-Anesthetic Care Unit 1 Anesthesia Workroom Outpatient Recovery 1 Postpartum Bedroom 1 Postpartum Isolation Room 1 Cesarean/Delivery Room 4 Labor Room 1 Recovery Room 1 Labor/Delivery/Recovery (LDR) 3 Labor/Delivery/Recovery/Postpartum (LDRP) 3 Initial Emergency Management per bed 1 Triage Area (Definitive Emergency Care) 1 Definitive Emergency Care 1 Exam/Treatment Rooms Definitive Emergency Care Holding Area 1 Trauma/Cardiac Room(s) 2 Orthopedic and Cast Room 1 Isolation Room (Emergency Service) 1 Cardiac Catherization Lab 3 Autopsy Room 1 per workstation
SUBSTANTIATION: Existing table does reflect current require° ments for delivery of health care procedures as influenced by changes in health care reform and technology. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #319) Committee: HEA-PIP
99- 270 - (4-7.1.2, Table 4-7.1.2): Accept SUBMITTER: David Esherick, Patient Instrumentation Corp. RECOMMENDATION: Delete both table and paragraph. SUBSTANTIATION: It is my understanding that we are primarily a construction document. The architects and engineers should do this, not the committee. COMMI'ITEE ACTION: Accept. COMMITTEE STATEMENT: Based on committee action on Proposal 99-266 (Log #123). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TOVOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #345) Committee: HEA-PIP
99- 269 - (Table 4-7.1.2): Accept SUBMITTER: Dennis Murray, American Hospital Assodation RECOMMENDATION: Replace table with current or draft minimum guidelines as published by AIA as minimum guidelines for the construction of health care facilities.
Patient Rooms (Medical 1 (one inlet and Surgical) accessible to
each bed)
Examination/Treatment 1 (Medical, Surgical, and Postpartum Care) Isolation (Infectious and Protective) 1 (Medical and Surgical) Security Room 1 (Medical, Surgical, and Postpartum)
(Log #228) Committee: HEA-PIP
99- 271 - (4-7.2): Accept SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Delete or relocate header 4-7.2 reserved for non-patient vacuum systems. SUBSTANTIATION: Goal is an easy-to-read patient vacuum system with focus of requirements specific to type. COMMITTEE ACTION: Accept. Delete.
COMMITI'EE STATEMENT: Submitter suggested two alternatives. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
76

NFPA 99 -- F95 ROP
(Log #202) Committee: HEA-PIP
99- 272 - (4-8.1.1): Accept in Pr indple SUBMITTEI~ Henry R. Kaht, Gurnee, IL RECOMMENDATION: Change paragraph (e) to read: Each vacuum p u m p shall be provided with a disconnect switch, motor starting device with overload protection and a control circuit transformer, each vacuum pump system, etc. SUBSTANTIATION: When one control circuit t ransformer is used for two or more vacuum pumps and a fault occurs within the circuit, causing the control circuit fuse to be blown, all of the vacuum pumps will stop. A control circuit t ransformer for each vacuum pump will prevent this. COMMITTEE ACTION: Accept in Principle. After sentence two in par. 4-8.1.1 (e), insert the following: "Each vacuum system that utilizes a voltage reducing dewce (i.e.,
transformer) shall have at least two such devices arranged in such a manner that the failure of one device shall no cause an interrupt ion in the operation of the vacuum system." COMMITTEE STATEMENT: Allow designer to decide how control circuit is to be constructed. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
electrical circuit ahead of each motor starter. Circuitry shall be arranged so that control and alarm functions remain energized while any pump in the system remains electrically on line.
4-8.1.1 (e ) Electrical Power. Electrical equipment and wiring shall conform to the requirements of NFPA 70, National Electrical Code. Emergency electrical service for the pumps shall conform to the requirements of the essential electrical system as described in Chapter $ of this document . SUBSTANTIATION: User friendliness and correlation of require- ments with gas section. COMMITrEEACTION: Accept in Principle.
1. In submitter 's recommendat ion for subpara. (b), delete "and a master alarm signal" in sentence 1
2. In submitter 's recommendat ion for subparm (d), delete sentence 3 ("Circuitry shall b e . . . on line.") and replace with the following: "Each vacuum system that utilizes a voltage reducing device (i.e., transformer) shall have at least two such devices arranged in such a manner that the failure of one device shall no t cause an interruption in the operation of the vacuum system." COMMrITEE STATEMENT: 1. Master alarm signal is no t needed because it was never required.
2. To correlate with committee action on Proposal 99-128 (Log #201). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #114) Committee: HEA-PIP
99- 273- (4-8.1.1 (New)): Reject SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Add the following paragraph under 4-8.1.1:
(k) Fluid waste from central vacuum receivers a n d / o r separators shall be directly connected to the sanitary drainage system and discharge through an appropriately-vented, deep-seal trap.
In Figure 4-8.1.1 (j), at the receiver, do no t show an indirect connect ion to the drain. Is a check valve required in the receiver drain line? SUBSTANTIATION: The a tmosphere in a health care facility should no t be exposed to the waste from medical vacuum systems by discharging it to an open drain. Deep-seal traps should be provided in the plumbing system. Appropriate plumbing vents should be installed for the trap, the arrangement of which will vary depending on whether the trap is subject to positive or negative pressures from the vacuum system. COMMITrEE ACTION: Reject. COMMITTEE STATEMENT: Medical-surgical vacuum systems are no t in tended to be operated as wet system, and do no t require a deep-sealed trap. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITI'EE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #226) Committee: HEA-PIP
99- 274 - (4-8.1.1 (a)): Accept in Principle SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Delete 4-8.1.1 (a)-(e) and substitute attached.
Please coordinate committee action with gas proposal. 4-8.1.1 (a) Multiple Pumps. Two or more pumps shall be installed
that serve this system alternately or simultaneously on demand. The pump(s) shall be sized to serve peak demand with the largest pump out of service. Each pump shall have an automatic means to prevent backflow through off-cycle units and a shut-offvalve to isolate it f rom the centrally p iped system and other pumps for maintenance or repair without loss of vacuum in the system.
(Existing notes may be left f rom vacuum section 4-8.1.1 (a)). 4-8.1.1 (b) Backup Operation. A device shall be provided to
automatically activate the additional pump(s) f f the uni t in operation is incapable of adequately maintaining vacuum. A local audible and visu,~l alarm and a master alarm signal shall be provided to indicate when the reserve or off-duty pump is in operation.
4-8.1.1 (c) Alternation. Pumps shall be provided with automatic or manual alternation to allow division of operating time. f fautomatic alternation of pumps is not provided, the facility shall arrange a proper schedule for manua l alternation.
4-8.1.1(d) Motor Controls. Each pump shall be provided with a dedicate disconnect switch, motor starting device and overload protection. The disconnect switches sha l /be installed in the
(Log #224) Committee: HEA-PIP
99- 275 - (4-8.1.1(a) through (e)): Accept in Pr indple SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Re-arrange organization of requirements so they will read consistently with the new order being proposed for both gas and vacuum source sections.
Topic
Multi Plexing
Back-Up Operauon
Alteration
Disconnects & Controls
Power Source
From: To:
4-3.1.9.3
4-3.1.9.42nd Sent 4-3.1.9. 4 (b) 4-3.1.9.4 a)
4-3.1.9.3
4-3.1.9.4(a)
4-S.l.O.4(b)
4-3.1.9.4(c)
4-$.l.g.4(d)
4-8.1.1 (a)
4-8.1.1 (c)
I 4-8,1.1(b)
4-8,1.1 (e)
4-8.1.1(d)
4-3.1.9.4 1st Sent. 4-s.1.9.41¢ /
, 4-$.1.9.4(d)
V~uum From: To:
4-8.1.1 (a)
4-8.1.1(b)
4-8.1.1 (c)
48.1.1 (d)
4-8.1.t (e)
SUBSTANTIATION: User friendliness. COMMITTEE ACTION: Accept in Principle.
See committee action on Proposal 99-274 (Log #226). COMMITTEE STATEMENT: Proposal 99-274 (Log #226) rearranged subparagraphs (a) to (e) in the same order. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #259) Committee: HEA-PIP
99- 276 - (4-8.1.1(c)): Reject SUBMITI'ER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Substitute following for second sentence: A signal indicating that the reserve pump is running shall operate a
local audio and visual alarm and serve to activate remote master alarms.
Coordinate with gas proposal on 4-3.1.9.4 (b). SUBSTANTIATION: Clarify difference between the requirement for "signal" and "alarm". COMMITrEE ACTION: Reject. COMMITrEE STATEMENT: Committee action on Proposals 99-274 (Log #226) and 99-153 (Log #CP59) addressed the issue raised here. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
77

N F P A 9 9 - - F 9 5 R O P
(Log #69) Committee: HEA-PIP
99- 277- (4-8A.l(f)): Reject SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise sentence 3 to read: A manway shall be provided for drainage so that substances that
might accumulate can be cleaned from the receiver(s) tank(s). SUBSTANTIATION: Current wording states, "a suitable method shall be provided", this isnot being done. When questioned they state, by disconnecting the inlet pipe that you can clean and service. COMMITI'EE ACTION: Reject. COMMITTEE STATEMENT: Committee believes it not necessary to have a person go inside a receiver tank to clean it. Current word allows the user to decide how best to clean receiver tank. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
• (Log #125) Committee: HEA-PIP
99- 278 - (4-8.1.1 (f)): Accept in Principle SUBMITTER: David B. Mohile, Medical Engineering Services, Inc. RECOMMENDATION: Change the last two sentences to make a bypass around the vacuum receiver mandatory by adding the following wording: The medical vacuum pump shall be provided with a three valve bypass to permit service to this device without shutting down the vacuum system.
Also, change figure 4-8.1.1 (j) so that the bypass is shown in solid lines as mandatory and not dotted lines as optional. SUBSTANTIATION: The wording in 4-8.1.1 (f) requires a method of draining the vacuum receiver. The proposed wording mandates a bypass to allow for this draining to happen. It also makes it easier to change or service the receiver tank. The addition of the above wording also makes the rules for vacuum
receivers identical to the wording in 4-3.1.9.7 which is for medical air compressor receiver oaks. COMMITI'EE ACTION: Accept in Principle.
1. Revise last sentence of4-8.L1 (t) to read: "The method shall Pthrovide means to drain and service the receiver without interrupting
e vacuum system." 2. Revise diagram 4-8.1.1 (j) as follows: Replace valves and piping
to receiver tank with the two configurations as shown below.
Configurat ion 1 "" -,, ~ . . " Configuration 2
I
• II ]i Receiver
shutoff valve
] vac. switch
C ) gauge
COMMI'ITEE STATEMENT: Submitter's proposal is too restrictive. There are other methods of accomplishing servicing or drainage of receivers. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TOVOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #240) Committee: HEA-PIP
99-.279 - (4-8.1.1 (f)): Accept in Principle SUBMITTERa AntonioA. Mesa, Nash Engineering Co RECOMMENDATION: Change
"...and full vacuum" to "...and full vacuum of 29.92 inches of
~ T I A T I O N : "Full vacuum" not adequately clear to reader. COMMITrEE ACTION: Accept in Principle.
I Revise text to read: "and full vacuum calculated as 14.7 psi of external pressure." COMMITTEE STATEMENT: Clarifies minimum conslruction requirements for receiver tanks. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #368) Committee: HEA-PIP
99- 280 - (4-8.1.1 (f)): Accept in Principle SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: First sentence - Delete as - %vhere the...of the pumps."
Third sentence - Delete as - "suitable method "Replace with "piping/valved by-pass"
(h) Second sentence - Delete as - '~qaere...isolators, "Flexible... SUBSTANTIATION: Exisdng text does not reflect good engineer- ing and manufacturing practices for this technology and does not reflect current field practices. COMM1TIT, E ACTION: Accept in Principle.
1. Accept submitter's first recommendation. 2. See committee action on Proposal 99-278 (Log #125). 3. Accept submitter's recommendation, plus delete "If used," from
sentence three. COMMYITEE STATEMENT: 2. Committee action on item 2 is addressed by Proposal 99-278 (Log #125).
3. Editorial. If accept submitter's recommendation, then sentence three has to be revised to correlate. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log ~61) Committee: HEA-PIP
99- 281 - (4-8.1.1 (g)): Accept in Principle SUBMITTER= AntonioA. Mesa, Nash Engineering Co RECOMMENDATION: Add to end of sentence as Underlined:
...in accordance with 4-9.1.1.1 (a). Schedule 40 welded steel oiDe in nominal sizes $.inches and lar~er shall be permitted in thes~ " are~. SUBSTANTIATION: A~ All this piping.is exposed and accessible.
B. Wall thickness of schedule 40 pipe approaches thickness of many small receiver tanks which require no galvanizing.
C. Galvanizing will bum offwhen welding flanged connections typical for these sizes. COMMITIT~ ACTION: Accept in Principle. Revise submitter's recommendation by adding after "Schedule 40
welded steel pipe" add the following: ", black or galvanized,". COMMI'IT]~ STATEMENT: To make clear that black or galva- nized steel pipe is acceptable. NUMBILR OFCOMM/TFEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrlTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
78

N F P A 99 - - F 9 5 R O P
(Log #262) Committee: HEA-PIP
99- 282 - (4-8.1.1(g)): Accept SUBMITTER: Antonio A. Mesa, Nash Engineering Co
[ RECOMMENDATION: Change main line valve to source-calve. SUBSTANTIATION: a) A main line valve may not exist and may not be required.
b) Piping between source valve and the main line valve should be tested and treated aspart of the distribution system, not source. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITFEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #64) Committee: HEA-PIP
99- 283 - (4-8.1.1 (i)): Reject SUBMITTEI~ Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise sentences 1 and 2:
(i) The exhaust from vacuum pumps shall discharge outdoors above the roof level a minimum distance of 10 fL (3m) from any door, window, other intake, or opening in the building, and a minimum distance of 30' (9m) above the ground. SUBSTANTIATION: Presendy the standard just states to minimize the hazard of noise and contamination to the hospital and its environment. With the problems that can be encountered with vacuum exhaust, we feel that it is necessary to put some minimum restrictions on height and location of vacuum exhaust discharge. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Committee believes recommendation is excessive, and too design restrictive. Quantifying distances varies with each installation. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #241) Committee: HEA-PIP
99- 284- (4-8.1.1(j)): Accept SUBMITrER: Antonio A. Mesa, Nash Engineering Co " RECOMMENDATION: 1. Dash drip legin figure 4-8.1.1 (j).
2. Insert the following between the fifth and sixth sentences (... back pressure. Discharge of...): Discharge piping must be free of dips or loops which may trap condensate or oil. ffsuch discharge piping is unavoidable, a trapped drip leg shall be installed to keep the piping free of fluid build-up. SUBSTAWFIATION: 1. To clarify when drip legs are appropriate.
2. To eliminate implication by figure that drip legs are mandatory. COMMITTEE ACTION: Accept. NUMBER OF COMMI~IXE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #307) Committee: HEA-PIP
99- 285 - (Table 4-8.1.1 (j)): Accept SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: Revise, delete, add and correlate all changes in text to reflect "typical sources" as detailed in section requirements~ SUBSTANTIATION: Table is widely utilized by enforcement bodies. Correlation to changes made to text must be reflected by
dating table to reflect text changes. MMFI'rEE ACTION: Accept.
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #62) Committee: HEA-PIP
99- 286 - (Figure 4-8.1.1 (j)): Accept in Principle SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise text:
Need to change the bypass valving from dotted (optional) to solid line (mandatory). SUBSTANTIATION: Without having the bypass valving mandatory, it is impossible to service and clean the receiver without shutting the vacuum system down. COMI~TrEEACTION: Accept in Principle. See Committee Action on Proposal 99-278 (Log #125).
COMMITITEE STATEMENT: Issue of service of receivers is addressed by Proposal 99-278 (Log #125). NUMBEROF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #350) Committee: HEA-PIP
99- 287 - (4-8.1.2): Accept in Principle SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: Add section and correlate for WA.G.D. under this section." 4-8.1.2.2 requirements 4-8.1 source 4-9 distribution 4-10 perf. criteria testing 4-11 administration
SUBSTANTIATION: Existing sections due not adequately address this technology and enforcement is very difficult due to lack of standard requirements. Not user friendly. COMMITrEE ACTION: Accept in Principle. See Proposal 99-96 (Log #CP4).
COMMITrEE STATEMENT: Issue is addressed by Committee Proposal 99-96 (Log #GP4). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #281) Committee: HEA-ANE, HEA-PIP
99- 288 - (4-8.1.2.1 ) : Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Delete paragraph in its entirety. SUI~TANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITI'EEACTION: Accept in Principle.
Move text to new Annex 3. COMMITI'EE STATEMENT: Correlate with Action on Proposal 99-25 (Log #274). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 (ANE), 18 (PIP) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 (ANE), 16 (PIP) NOT RETURNED: Fan (PIP), Shoemaker (PIP)
(Log #115) Committee: HEA-PIP
09- 280 - (4-8.1.3.2): Reject SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Change 4-8.1.3.2 to read as follows:
4-8.1.3.9 Fluid waste from central receivers and/or separators in dental vacuum systems shall be directly connected to the sanitary drainage system and discharge through an appropriately-vented, deep-seal trap.
79

N F P A 99 - - F95 R O P
SUBSTANTIATION: The existing text does not make it clear that the connection to the sanitary drainage system should be a direct- connection. The atmosphere in a health care facility should not be exposed to the waste from medical vacuum systems by discharging it to an open drain. Deep-seal traps should be provided in the plumbing system. Appropriate plumbing vents should be installed for the trap, the arrangement of which will vary depending on whether the trap is subject to positive or negative pressures form the vacuum system. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Hazard is more appropriately addressed by the plumbing codes. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #116) Committee: HEA-PIP
99- 290 - (4-9.1.1.1): Accept in Principle SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Change all subparagraphs of 4-9.1.1.1 Vacuum Piping System Network to read as follows:
Change the subparagraphs under 4-9.1.1.1 to read as follows: (a) Vacuum Network Piping. Piping shall be corrosion-resistant
metal such as seamless copper water tube (ASTM B88, types K,L,M), copper ACR tube (ASTM B280), copper medical gas tube (ASTM B819), stainless steel tube, or galvanized steel pipe [ 1-1/2 in. minimum size] (ASTM A53). Pipe threads shall comply with ANSI B1.20.1, Pipe Threads, General Purpose. Copper tube shall be hard drawn temper except that annealed tube shall be permitted in concealed locations and underground. Joints in copper tube shall be soldered or brazed. Joints in stainless steel tube shall be brazed or welded. Joints in galvanized steel pipe shall be threaded or flanged. Soldering shall be performed in accordance with ASTM B828, "Making Capillary Joints by Soldering of copper and Copper AlloyTube and Fittings.' Solder metal (ASTM B32) shall contain less than 0.2.% lead. Brazing shall be in accordance with 4-4.1.4.3 except that flux may be used for copper-to-copper joints and nitrogen purgingwhile brazing shall not be required.
(b) Marking. If copper vacuum piping is installedalong with any medical gas piping, either the vacuum piping or the medical gas piping shall, prior to installation, be prominently labeled or otherwise identified to preclude using materials or installation procedures in the medical gas system that are not suitable for oxygen service. If medical gas tube (ASTM B819) with brazed joints is used for the vacuum piping, such special marking shall not be required, provided that the vacuum piping installation meets all requirements for medical gas piping, including the prohibition of flux on copper-to-copper joints and the use of a nitrogen purge while brazing.
(c) Minimum Sizes. Mains and branches shall be not less than 1/2 in. nominal size. Drops to individual vacuum inlets shall be not less then 1/4 in. ID (inside diameter). Connections to gauges and alarm switches and runouts to alarm panels shall be permit tedto be 1/4 in. nominal size.
(d) Support. Piping shall be supported from the building structure in accordance with MSS Standard Practice SP-69, Piping Hangers and Supports - Selection and Application. Hangers and supports shall comply with MSS Standard Practice SP-58, Pipe Hangers and Supports - Materials, Design, and Manufacture. . Hangers for copper tube shall have a copper finish. In potentially damp locations, copper tube hangers or supports shall be plastic- coated or otherwise insulated from the tube. Maximum support spacing shall be as follows:
1 /4 in. nominal 5 feet 3 /8 in. nominal 6 feet 1 /2 in. nominal 6 feet 3 /4 in. nominal 7 feet 1 in. nominal 8 feet 1-1/4 in. nominal 9 feet 1-1/2 in. nominal and larger 10 feet vertical risers every floor
(e) Copper Tube Fittings. Fittings for joining copper tube shall be pressure-rated copper, brass, or bronze, made especially for brazing or soldering, except as provided in 4-9.1.1.1 (O and (g). Fittings shall be wrought or cast, except that cast fittings shal lnot be brazed.
(f) Mechanically-Formed Bi'hnch Connections. The use of drilled and extruded tee-branch connections to copper mains and branches shall be permitted. Such connections shal lbe made in accordance
with the tool manufacturer's instructions and the jo int shall be brazed.
(g) Shape-Memory Couplings. Memory-metal couplings providing joints equivalent to a soldered or brazed joint shall be permitted.
(h) Unions. Unions, flare nuts, and similar straight-threaded connections shall be permitted only in exposed locations and shall not be concealed in walls or ceilings.
(i) Protection. Piping exposed in corridors and other areas where subject to physical damage from the movement of carts, stretchers, portable equipment, or vehicles shall be suitable protected. Buried piping shall be protected from frost, corrosion, and physiaal damage. Piping under roadways, driveways, parking areas, and other locations subject to surface loads shall be installed in a protective sleeve or casing. Piping embedded in concrete floors or walls shall be installed in a continuous conduit.
1 Penetrations. Where piping penetrates fire barriers such as Is, partitions, or ceiling/floor assemblies having required fire-
resistance ratings, the penetration shall be protected in accordance with the requirements of NFPA 101, Life Safety Code, and the applicable building codes.
(k) Conversion. Vacuum piping systems shall not be converted for use as a pressurized gas system. SURSTANTIATION: The existing text on piping requirements for vacuum systems is worded differently from similar requirements for medical gas systems. Certain portions of the existing text include terms that are not commonly used in the piping trades. The proposed change includes specific requirements for the various acceptable pipingmaterials. COMMITrEE ACTION: Accept in Principle. Accept submitter's recommendations with the following changes: 1. Revise subpar. (c) to read: "(c) Minimum Sizes. Mains and branches shall be not less than 3 /
4 in. nominal size. Drops to.individual vacuum inlets shall be not less than 1/2 in. ID (inside diameter), except for the tube attached immediately to the station inlet and not extending more than 8 inches from the station inlet. Connections to gauges and alarm switches and runouts to alarm panels shall be permitted to be 1/4 in. nominal size."
2. In table in subpar. (d): delete "1/4 in. nominal" and "3/8 in. nominal" change "every floor" to "every floor, but not to exceed 15 ft"
3. Delete subpar. (f), and renumber. 4. Delete subpar. (h), and renumber. 5. In subpar. (e), delete ref. to subpar. (f). 6. In subpar. (a), sentence three, delete "or concealed locations."
COMMITTEE STATEMENT: 1. Tube sizes recommended were too restrictive for the design requirements of vacuum systems.
2. Changes to reflect changes in tube sizes. 3. and 4. Because vacuum tubing is installed many times along with
gas tubing, committee ~ t s to avoid the problem of mechanical formed fittings from being inadvertently being made for gas (pressured) systems. 5. To correlate with changes 3 and 4. 6. Correlate action on Proposal 99-291 (Log #61), and allow the
use of annealed tube only in underground applications. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #61) Committee: HEA-PIP
99- 291 - (4-9.1.1.1 (a)): Accept in Part SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Delete:
Copper tube shall be hard tempered for above ground and soft tempered for underground. SUBSTANTIATION." In the text it states that soft tempered copper tubing be used for underground or concealed locatiom. Tubing running above ceilings and in walls are considered to be concealed. We don ' t think it was the subcommittee's intent to have soft tempered copper tubing in walls and ceilings since this poses problems with trapped lines which creates flow problems. COMMITTEE ACTION: Accept in Par t Revise last sentence of 4-9.1.1.1 (a) to read: "Copper tube shall be hard tempered for above ground. Soft
temper tube shall be permitted for underground.-- COMMITrEE STATEMENT: Committee agrees that soft temper should not be allowed in concealed locations above ground. Proposal is too restrictive for tubing underground, and thus makes changes as noted.
80

N F P A 9 9 - - F 9 5 R O P
(Proposal 9%290 (Log #116) incorporates the committee intent of this proposal.) NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #229) Committee: HEA-PIP
99-292 - (4-9.1.1.1(a)): Accept in Principle in Part SUBMITrER: Antonio A~ Mesa, Nash Engineering Co RECOMMENDATION: Change the first sentence as follows (changes are underlined):
(a) Vacuum Piping. All piping shall be constructed of seamless Type L, M, or ACR (ASTM ~ copper tube, or other corrosion- resistant metallic tube such as stainless steel or galvanized steel. If vacuum tube is installed simultaneously with other medical gas tube, either it shall be labeled or otherwise identified prior to installation in order to preclude inadvertent inclusion into a medical gas system, or it shall be ~ in accordance with 4-4.1.2.1 (b) and (c). Copper tube shall be hard temper for exposed locations and soft temper for underground or concealed locations. SUBSTANTIATION: Changes in NFPA 99-1993 discouraged on-site cleaning of tubing and required purchase of pre-deaned tube for gas systems. 4-9.1.1.1 needs to be brought up to date with this change. COMMITrEE ACTION: Accept in Principle in Part.
1. Reject change to sentence 1. 2. For changes to sentences 2, see committee action on Proposal
99-290 (Log #116). COMMITFEE STATEMENT: 1. 17,88 is not the correct reference for ACR tube.
2. Proposal 99-290 (LOg #116) addressed the issue of on-sight cleaning. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker-
(Log #347) Committee: HEA-PIP
9% 293 - (4-9.1.1.1 (a)): Accept in Principle U~cMITTER: Dennis Murray, American Hospital Association
OMMENDATION: Second Sentence - Delete as- "Cleaned and Degreased"
S~l~ace with- "Provided" TANTIATION: Current text is not correlated with existing
requirements of 4-4.1.4. COMMITTEE ACTION: Accept in Principle. See committee action on Proposal 99-290 CLog #116).
COMMITrEE STATEMENT: Proposal 9%290 (Log #116) deleted these terms. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrlTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #$48) Committee: HEA-PIP
99-294- (4-9.1.1.1(a)): Acceptin Principle SUBMITTEI~ Dennis Murray, American Hospital Associadon RECOMMENDATION: First Sentence-Delete as-" or other...such as" SUBSTANTIATION: Existing text confusing, clarification required, not user-friendly. COMMITrEE ACTION: Accept in Principle. See committee action on Proposal 9%290 (Log #116).
COMMITrEE STATEMENT: Issue was addressed in Proposal 9%290 CLog #116). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #349) Committee: HEA-PIP
99- 295 - (4-9.1.1.1 (a)): Accept in Principle SUBM]TrER: Dennis Murray, American Hospital Association RECOMMENDATION: First Sentence-Add-All piping" system, source and exhaust" shall be .... SUBSTANTIATION: Existing text confusing, requires clarification, not user friendly.' COMMIT~E ACTION: Accept in Principle. Add a NOTE 2 under 4-9.1.1.1 (a) to read:
"NOTE 2: For requirements for pi~ing within the source portion of the vacuum system, see 4-8.1.1 (g). COMMITTEE STATEMENT: Section 4-9 covers distribution portion of vacuum system. Addition of NOTE is to remind readers of the' structu re of NFPA 99 NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #351) Committee: HEA-PIP
9% 296 - C4-9.1.1.1(a), Cb)): l~eject SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: (a) last sentence delete as - "copper tube...locations."
(b) first sentence - delete as - "drops...inlets and" (c) Second sentence - delete as "Tube size...diameter (ID)."
SUBSTANTIATION: Existing requirement is inadequate as field installations are not able to achieve adequate performance due to the lack of good engineering practices. COMMITFEE ACTION: Reject. See committee action on Proposal 9%290 (Log #116).
COMMITrEE STATEMENT: 1. Proposed changes per Proposal 99-290 (Log #116) address a portion of the issues raised here.
2. Deletion of text as recommended does not solve problems; it would leave document silent on some piping criteria. Committee believes criteria needs to be included because they are acceptable practices. Proposal 9%290 (Log #116) clarifies these criteria and
mactices ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #230) • Committee: HEA-PIP
99- 297 - (4-9.1.1.1(c)): Accept in Principle SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Substitute requirement and table from gas section 4-4.1.2.1 (g). SUBSTANTIATION: Consistency in wording or requirements with same intent between vacuum and gas sections. COMMITrEE ACTION: Accept in Principle. See committee action on Proposal 99-290 (Log #116).
COMMITTEE STATEMENT: Issue of vacuum tube support intervals was addressed in Proposal 9%290 (Log #116). NUMBER OF COMMITI'EE MEMBERS ELIGIBLE TOVOTE: 18 VOTE ON COMMrlWEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #67) Committee: HEA-PIP
99- 298 - (Table 4-9.1.1.1 (c)): Accept in Principle SUBMITTER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Revise table:
3/8 in. nominal 6 ft. 1/2 in. nominal 6 ft. 3/4 in. nominal 7 ft.
1 in. nominal 8 ft. 1 1/4 in. nominal 9 ft. 1 1/2 in. nominal and larger 10 ft.
SUBSTANTIATION: The spacing of hangers for medical gas and vacuum are different. In most cases the medical gas and vacuum piping is run together on a trapeze hanger system, we thinl/, the
81

N F P A 99 - - F 9 5 R O P
spacing of hangers for both systems should agree. Since the spacing of medical gasis the more strict, we feel this table should apply for both medical gas and vacuum hanger spacing. COMMITrEEACTION: Acceptin Principle.
See committee action on Proposal 99-290 (Log #116). COMMITTEE STATEMENT: Issue of vacuum tube support intervals was addressed in Proposal 99-290 (Log #116). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #352) Committee: HEA-PIP
99- 299 - (4-9.1.1.1 (g)): Accept in Principle SUBMITTER: Dennis Murray, American Hospital Association RECOMME2qDATION: Reference to 4-9.1.1.9(a)? SUBSTANTIATION: Correlation to reference not related to section. Editorial? COMMITrEE ACTION: Accept in Principle.
Change reference to 4-9.1.1.10(a). COMMITrEE STATEMENT: Correct reference. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #243) Committee: HEA-PIP
99- 300 - (4-9.1.1.5): Accept in Principle SUBMITI~R: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Substitute the following as 4-9.1.1.5 (e)
(e) Zone valve. A shut offvalve shall be located immediately outside of each vital life-support, critical care or anesthetizing location in each vacuum line, and located as to be readily accessible in an emergency or for maintenance of the terminals or piping within the individual zone served. Renumber remaining sections, and delete note from existing (e). SUBSTANTIATION: Maintenance and repair of upstream components and piping without requiring a scheduled or emer- gency shutdown of a critical care area. Augments Mr. Allan Currier Proposal 99-315 (Log #20). COMM/TrEE A~I'ION: Accept in Principle. Add recommendation as new 4-9.1.1.5(e), and renumber.
COMMIITEE STATEMENT: Editorial to clarify intent ofsubmitter to add recommendation as a new 4-9.1.1.5 (e). NUMBER OF COMMrITEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: lfi NOT RETURNED: Fan, Shoemaker
(Log #369) Committee: HEA-PIP
99- 301 - (4-9.1.1.5 (f) (New)): Accept in Principle SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: Add (f) main shut offvalve - Revise text using 4-4.1.2.2 (b) correlate to related sections. SUBSTANTIATION: Existing text confusing and not specific regarding requirement for main shutoffvalve. Existing text not user friendly. COMMI'ITEE ACTION: Accept in Principle. See committee action on proposals 99-304 (Log #233) and 99-305
(Log #254). COMMI'I*rEE STATEMENT: With action on proposals 99-304 (Log #233) and 99-$05 (Log #234), a shut valve recommended by submitter is mandated. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #353) Committee: HEA-PIP
99- 302 - (4-9.1.1.5(a), (b)): Accept in Principle SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: (a) Add existing text of 4-4.1.2.2 (c) and correlate for NFPA existing style.
(b) Add existing text of 4-4.1.2.2 (g) and correlate for NFPA existing style.
(c) Delete NOTE at end of 4-9.1.1.5(e). SUBSTANTIATION: Existing text not adequate in detail for enforcement. Correlated 4-4 sections extremely detailed for user friendly applications. COMMITrEE ACTION: Accept in Principle. Accept recommendation (b).
COMMITTEE STATEMENT: Committee action on Proposal 99-300 (Log #243) covered the recommendations (a) and (c). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #'231) Committee: HEA-PIP
99- 303 - (4-9.1.1.5(b)): Accept in Principle SUBM/TTE~ Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: New or replacement shut-offvalves shall be of a quarter-turn type (i.e. bali valve or butterfly valve) with an indicating handle and shall be of metallic construction. Ball valves shall be full port type to prevent excessive restriction to flow. Butterfly valves shall n o t b e used in line sizes 2 inches or smaller.
Please coordinate committee action with gas proposal. SUBSTANTIATION: 1. Unifyvalve requirements between gas and vacuum sections.
2. Modify pressure drop requirement becanse butterilyvalves normally used in larger sizes (3 inches and larger) have minimal, but recogaaized, pressure drop. COI~[MITI~E ACTIOlq: Accept in Prindple.
See committee action on Proposal 99-302 (Log #353). COMMrITEE STATEMENT: Issues are addressed in Proposal 99-302 (Log #355). NUMBER OF COMMIT1T.E MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #233) Committee: I-IFA-P IP
:99- 304- (4-9.1.1.5(c) and Figure 4-8.1.10)): Accept SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: 1) Insert the following as 4-9.1.1.5(c) and re-number accordingly:.
Source shut offvalve. A shut off valve shall be installed immediately upstream (on the terminal or inlet side) of the receiver tank in the vicinity of the source equipment.
2) Revise Figure 4-8.1.10) to showvalve. . SUBSTANTIATION: The valve is presendy defined and the requirement is implied in the master alarm passage, section 4-9.1.1.7. COMMITrEE ACTION: Accept. NUMBER OF COMMIT~E MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #234) Committee:- HEA-PIP
99- 305 - (4-9.1.1.5(d)): Accept in Principle SUBMITTEPa Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Insert the following as 4-9.1.1.5(d) a n d renumber accordingly:.
Main line valve. The main supplyline shall be provided with a shut off valve where the main llne first enters the building. A main line valve is not required if the source valve is accessible from within the building. SUBSTANTIATION: To allow isolation of inaccessible piping for testing or maintenance.
82

N F P A 9 9 - - F 9 5 R O P
COMMI'ITEE ACTION: Accept in Principle. In submitter 's recommendat ion, sentence 2, change "is not
required" to read "shall no t be required." COMMITTEE STATEMENT: Conform to NFPA Style Manual. NUMBER OF COMMITTEE MEMBERS ELIGIBLETO VOTE: 18 VOTE ON COMMNTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #124) Committee: HEA-PIP
99- 306 - (4-9.1.1.5(e)): Accept SUBMITTER: David B. Mohile, Medical Engineering Services, Inc. RECOMMENDATION: Delete the note following 4-9.1.1.5 (e) which states:
Shutoffvalves are not required for each anesthetizing room. SUBSTANTIATION: Common engineer ing practice is to provide a va/ve for vacuum at every location referenced. This valve allows for work to be completed in the vacuum piping within an individual O.R. without shutting down the entire O.1~ suite. When the vacuum section is assimilated into the code as a whole,
this will bring the vacuum section into consistency with the pressure section. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #242) Committee: HEA-PIP
99- 307- (4-9.1.1.5(e)): Accept SUBMITTER: Antonio A. Mesa, Nash Engineering Co
I ECOMMENDATION: Substitute t ex t f rom 4-4.1.2.2 (a) i.e.; (e) Valve boxes. Shut off valves...
SUBSTANTIATION: Correlation of text with gas section. COMMIq[q'EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #354) Committee: HEA-PIP
99- 308- (4-9.1.1.6(a), 4-9.1.2): Accept SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: 1. In 4-9.1.1.6(a), delete NOTE. 2. In 4-9.1.2, delete ", whose vacuum...vacuum source, ".
SUBSTANTIATION: Requirements do not reflect existing established technology utilized in health care.
Not user friendly or correlated with related sections. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #239) Committee: HEA-PIP
• 99- ~09 - (4-9.1.1.7): Reject SUBMrrTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Add the following as 4-9.1.1.7(c)
(c) Reserve Pump. A "reserve p u m p in use" master alarm as described in 4-9.1.1.7 (a) shall be activated by the signal provided in 4-8.1.1 (c).
Renumber the remaining section accordingly. SUBSTANTIATION: To provide a master alarm signal when the reserve pump is activated.
Please coordinate with proposal to amend 4-9.1.1.7(a). COMMITrEE ACTION: Reject. COMMI'['FEE STATEMENT: Proposals 99-276 (Log #259) and 99- 153 (Log#CP59) address the issues raise in this proposal (i.e., the issue of a reserve pump in use is not considered a. master alarm condition).
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #236) Committee: HEA-PIP
99- 310 - (4-9.1.1.7(a)): Accept in Principle SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Substitute the first two sentences of 4-4.1.1.2 (a). SUBSTANTrATION: Unify master alarm requirements between gas and vacuum sections. COMMIIWEE ACTION: Accept in Principle. Accept submitter 's recommendat ion, but revise wording from
4-4.1.1.2(a.) as follows: "To ensure continuous responsible observation, the master alarm signal panels shall be located in two separate warning locations, wired in parallel to. a single sensor to indicate when the vacuum in the main line drops below the level required in 4-10.1.2.6. Audible and noncancellable visual signals shall be installed in the office or principal working area of the individual responsible for the maintenance of the vacuum system and, to ensure continuous surveillance, at the te lephone switchboard, the security office, or at another suitable location." COMMIT]FEE STATEMENT: Changes for correlation purposes, and retain the reference to what is moni tored at the master alarm
el for vacuum systems (as is currently included in 4-9.1.1.7(a). ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #355) Committee: HEA-PIP
99- 311 - (4-9.1.1.7(a), (e), (g)): Accept in Principle in Part SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: (a) Revise text with 4-4.1.1.2 (a) except last sentence. Correlate sections.
(e) Note #1 delete (g) Delete
SUBSTANTIATION: Existing text not correlated or consistent with related sections. Requirements contradlctoryand confusing. Not user friendly. COMMITI]EE ACTION: Accept in Principle in Part.
For (a), accept in principle. See committee action on Proposal 99-310 (Log #236).
For (b), move NOTE 1 under 4-9.1.1.7(e) to Appendix A. For (c), Reject. (See also Proposal 99-314 (Log #237).
COMMITTEE STATEMENT: For (a), proposal 99-310 (Log #'236) correlates gas and vacuum system requirements for master alarms as r ecommended by submitter.
For (b), information is useful, and can be included in the appendix for information purposes, per NFPA Style Manual.
For (c), Committee believes the use of centralized computers for secondary moni tor ing purposes for vacuum systems is an acceptable
ruMBactices, and does not jeopardize patient safety. ER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #215) Committee: HEA-PIP
99- 312 - (4-9.1.1.7(b)): Accept in Principle SUBMITTER: CorkyJ. Bishop, Medical Gas Management, Inc. RECOMMENDATION: Revise text:
b. Actuator Switch. The actuator (vacuum switch) for the master alarm shall be connected to the main line immediately upstream (on the terminal or inlet side) of the source valve [i.e., the source valve is between the receiver (tank) and the master alarm vacuum switch]. SUBSTANTIATION: Use the term source valve to be consistent with the terminology for pressure gas systems. This valve is located in the mechanical room with the equipment it serves. There is no need for a main line shutoff outside the room for a vacuum system from a fire protect ion point of view.
83

N F P A 99 - - F95 R O P
COMMrlTEE ACTION: Accept in Principle. Revise 4-9.1.1.7(b) to read: (b) Actuator Switch. The actuator (vacuum switch) for the master
alarm shall be connected to the main line immediately upstream (on the terminal or inlet side) of the source valve (the main-line valve, if so e;qmppecui ed). COMMITrEE STATEMENT: Action on Proposal 99-305 (Log #234) added the requirement for a main-line valve. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #238) Committee: HEA-PIP
99- 313- (4-9.1.1.7(b)): Reject SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Change to:
(b) Vacuum level. The vacuum level in the main line shall be continuously monitored to indicate when the vacuum drops below the level required in 4-10.1.2.1. The actuator (vacuum switch)... cont. as per existing text. SUBSTANTIATION: To make: 4-9.1.1.7 (a) general (achieved through other proposal),
4-9.1.1.7 (b) specific to vacuum level, so that: 4-9.1.1.7 (c) can address "reserve pump" alarm (achieved through
other proposal.) COMI~TrEE ACTION: Reject. COMMITTEE STATEMENT: Proposal 99-310 (Log#236) included criteria of 4-10.1.2.6 in 4-9.1.1.7(a). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
c (Log #237)
ommittee: HEA-PIP 99- 314- (429.1.1.7(g)): Accept SUBMITTER= Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Substitute the fol lo~ng wording: The connection of the master alarm system to a centralized
computer (e.g., a building management system) is permitted. The computer shall not constitute one of the two master alarm panels required. SUBSTANTIATION: Unify master alarm requirements with gas section.
Section references in existing 4-9.1.1.7 (g) are erroneous and superfluous. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #20) Committee: HEA-PIP
99- 315 - (4.9.1.1.8 (New)): Accept in Principle SUBMITTER: Allan Currier, Madison, WI~ RECOMMENDATION: Insert the following new paragraph in section 4-9.1.1.8:
(e) The actuating switch for anesthetizing locations shall be in the specific line supplying the operating or delivery room suites, with the individual room shutoff valve being the only one between the actuating switch and the room inlets. SUBSTANTIATION: Section 4-9.1.1.5 (a) requires a shutoff valve be provided, "to isolate appropriate sections or portions of the piping system for maintenance, repair, or planned future expansion, andto facilitate periodic testing", (emphasis added). I submit that an operating room is an appropriate section. Inclusion of these valves would allow periodic testing and maintenance of individual rooms without compromising the use of the remainder of the operating suite.
It does not create risk to occupants of the room if installed in accordance with section 4-9.1.1.5(e). A catastrophic failure in one room could compromise the ability of the system to maintain vacuum requirements in adjoining rooms.
The current code would require addition of area alarm actuating switches between these roomshut off valves and the room inlets. This is not consistent with the requirements for compressed gasses [Section 4-4.1.1.3(c) ]. Inclusion of this recommendation would allow installation of room shutoff valves in anesthetizing locations without the additional expense of multiple alarm sensors.
I submit this proposal for inclusion in the 1996 edition. COMMITrEEACTION: Acceptin Prindple. .See Committee Action on Proposal 99-316 (Log #356).
COMMITrEE STATEMENT: Issue was addressed in this proposal. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #356) Committee: HEA-PIP
99- 316 - (4.9.1.1.8(a), (d)): Accept SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: For subpara. (a), revise text using existing 4-4.1.1.3 (a) and correlate with related sections.
Dor subpara. (d), revise text using existing 4-4.1.1.3 (c) and 4- 4.1.1.3(d), and correlate with related sections. SUBSTANTIATION: Existing text 44 provides the necessary detail for adequate enforcement. Current 4-9 section not user friendly and inadequate. COMMITFEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #207) Committee: HEA-PIP
99- 317 - (4.9.1.1.8(d)): Accept in Principle SUBMITTER: Peter Esherick, Patient Instrumentation Corporation RECOMMENDATION: Add underlined:
1. Line 2: "each area except anesthetizing locations..." v
2. Add a new par.: The actuator (vacuum switch) for anesthetizing locations shall be
in the spedfic line supplying the operating or delivery room suites, with the individual room shut off valve being the only one between the actuating switch and the room outlets.
3. Standardize actuator/actuating switch. SUBSTANTIATION: 1. & 2. Existing text does not take into consideration that most operating rooms have individual valves outside each OR.
3. Terminology differs from medical gas to vacuum section of chapter 4. COMMITTEE ACTION: Accept in Prindple. See committee action on Proposal 99-316 (Log #356).
COMMITTEE STATEMENT: Issue was addressed in this pro oosal. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #'216) Committee: HEA-PIP
99- 318 - (4-9.1.1.8(d) (1)): Accept in Principle SUBMITIT.,R: C6rkyJ. Bishop, Medical Gas Management, Inc. RECOMMENDATION: The actuator (vacuum switch) for anesthe- tizing locations shall connect to the vacuum line for that area on the source side (downstream) of the individual room shutoff valve if the O.R,'s and delivery rooms are supplied with their own zone valves. SUBSTANTIATION: Although not required, many hospitals have vacuum included in the zone valve box for each O.R, Under the current requirements, a 12 O.R, suite would have I alarm for each Palressure gas and 12 vacuum alarms. It is very confusing for the
arm signals to be sensed on opposite sides of the zone waives between pressure gases and vacuum in anesthetizing locations. Th~ PCroposal would make them consistent.
OMMITrEE ACTION: Accept in Principle. See committee action on Proposal 99-316 (Log #356).
COMMrITEE STATEMENT: Issue was addressed in this proposal. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18
84

N F P A 99 - - F 9 5 R O P
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #260) Committee: HEA-P!P
99-319- (4-9.1.1.8(e)): Accept in Prindple SUBMrI~'ER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Change as follows: Actuator switch settings. ... respective warning signals a to r below 12 in. Hg of vacuum.
SUBSTANTIATION: Actuation at 8 in. Hg V. being interpreted as beinw lX. COMMITTEE ACTION: Accept in Prindple. Revise submitter's recommendation to read: "...respective at and
below 12 in. Hg of vacuum." COMMrITEEaA'TATEMENT: Committee desires a continuous alarm that starts when system drops to 12 in Fig. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #117) Committee: HF~-PIP
99- 320 - (4-9.1.1.10): Accept in Principle SUBMITTER: J. Richard Wagner, Baltimore, MD RECOMMENDATION: Change 49.1.1.10 to read as follows:
4-9.1.1.10 Installation of Vacuum System Piping (a) Materials and Joints. Piping materials and joining methods
shall be in accordance 4-9.1.L1. (b) Open Ends. Care shall be taken to maintain the interior of the iping system free of debris or other foreign matter. Pipe, tube, and ttings shall be inspected visually prior to installation. During
installation, open ends of piping shall be temporarily sealed. (c) Flux. Where flux.is used for soldered or brazed joints, it shall
be used sparingly to avoid excess flux inside of the finished joint. (d) Cleaning. After soldering or brazing, the outside of all joints
shall be cleaned by washing with water and a stainless steel brush to remove any residue and permit clear visual inspection of thejoinL If flux has been used, joints shall be washed with hot water.
(e) Biowdown. After installation of the piping network, but before installation of vacuum inlets and other vacuum system components, all lines shall be blown clear using compressed air or nitrogen.
(f) Piping Identification. Vacuum piping shall be readily identified by appropriate labeling, such as MEDIC_AI~URGICAL VACUUM, or MED/SURG VAC. Labeling shall be by means of stamped metal tags, stenciling, or printed adhesive markers, and shall not be readily removable. Labels shall be spaced at intervals of not more than 20 ft (6.1 m), except that at least one label shall be visible in or above each room or area. Flow arrows (if used) shall point from the station inlets toward the receiver or pump. SUBSTANTIATION: The existing text is not consistent with similar re uirements for medical gas pi in P . g ' . . C~MMrITEEA~rlON: Accept m Prmaple. Revise submitter's recommendation to read as follows: 4-9.1.1.10 Installation of Vacuum System Piping. (a) General. The provisions of this section shall applyto field-
installed piping for vacuum systems. (b) Materials and Joints. Piping materials and joining methods
shall be in accordance with 4-9.1.1.1. !c! Open Ends. Care shall be taken to maintain the interior of the
piping system free of debris or other foreign matter. Pipe, tube, and fittings shall be inspected visually prior to installation. During installation, open ends of piping shall be temporarily sealed.
(d) Flux. Where flux is used for soldered or brazed joints, it shall be used sparingly to avoid excess flux inside of the fimshedjoint.
(e) Cleaning. After soldering or brazing, the outside of all joints shall be cleaned by washing with water and a stainless steel brush to remove any residue and permit clear visual inspection of the joint. If flux has been used, joints shall be washed with hot water.
(f) Visual Inspection. Each soldered or brazed joint shall be visually examined after deaning of the outside of the joint. The following conditions shall be considered unacceptable:
1. Flux or flux residue. 2. Excessive oxidation of the joint. 3. Presence of unmelted solder or braze filler metal. 4. Failure of the solder or braze filler metal to be clearly visible all
the way around the joint at the interface between the socket and the tube.
5. Cracks in the tube or component.
6. Cracks in the solder or braze filler metal. • 7. Failure of the joint to hold the test pressure under 4-10.1.2.2.2. (g) Repairs. Soldered or brazed joints that are found to be
defective under 4-9.1.1.10(t 0 (1), (3), (4), (6) or (7) shall be permitted to be repaired, except that no joint shall be repaired more than twice. Joints that are found to be defective under 4- 9.1.1.10(f) (2) or (5) shall be replaced•
(h) Piping Identification. Vacuum piping shall be readily identified by appropriate labeling, such as MEDICAE~URGICAL VACUUM, or MED/SURGVAC. Labeling shall be by means of stamped metal tags, stenciling, or printed adhesive markers, and shall not be readily removable. Labels shall be spaced at intervals of not more than 20 ft (6.1 m), except that at least one label shall be visible in or above each room or area. Flow arrows (if used) shall
int from the station inlets toward the receiver or pump. MMITIT_.E STATEMENT: Correlate with actions of Proposal 99.
324 (Lo ~ #CP62). B O V NUMBr..~ OF COMMITTEE MEMBERS ELIGI LET OTE: 18 VOTE ON COMMrrTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #357) Committee: HEA-PIP
99- 321 - (4-9.1.1.10(a), (c), (d)): Accept in Principle SUBMIT~R: Dennis Murray, American Hospital Association RECOMMENDATION: Add "General" - existing text 4-4.1.2.1 first sentence only. Correlate with sections.
(a) First Sentence - Delete as "in copper..Ahread connections," Add last sentence- "Source equipment connections and joints..." (c) Revise with 4-4.1.4.3 (i) (d) Delete as- "or air"
SUBSTANTIATION: Existing text is not detailed adequately to provide enforcement with necessary direction. Text is not user friendly. COMMITTEE ACTION: Accept in Principle. See committee action on Proposal 99-324 (Log #CP62).
COMMITrEE STATEMENT: Proposal 99.324 (Log #CP62) addresses issue raised here. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
. (Log#118) Committee: HEA-PIP
99- 322- (4-9.1.1.11): Accept SUBMITIXR: J. Richard Wagner, Baltimore, MD
[ RECOMMENDATION: Delete Paragraph 4-9.1.1.11 Labeling. SUBSTANTIATION: This paragraph is redundant and serves no clear purpose. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMHTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #358) Committee: HEA-PIP
99- 323 - (4-10.1.2): Accept in Principle SUBMITrER: Dennis Murray, American Hospital Association RECOMMENDATION: Revise text with existing 4-5.1.1 General - and correlate with related sections. SUBSTANTIATION: Existing text inadequate and lacks specific detail for determination of requirements for this section. Not user friendly. Inadequate for enforcement. COMMrFrEE ACTION: Accept in Principle. See committee action on Proposal 99-324 (Log #CP62).
C O M M I ~ STATEMENT: Proposal 99-324 (Log #CP62) addresses issue raised here. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
85

N F P A 99 - - F 9 5 R O P
(Log #CP62) Committee: HEA-PIP
99- 524- (4-10.L2): Accept SUBMrFrER: TechnicafCommittee on Piping Systems
• RECOMMENDATION: Revise 4-10.1.2 in ~ts entirety as follows: 4-10.1.2 Testing. 4-10.1.2.1 General. luspecfion and testing of medical vacuum
systems shall be in accordance with 4-5.1.1. 4-10.1.2.2 Installer Performance Testing. The following tests shall
be conducted by the installer or his representative prior to those tests listed in section 4-10.1.2.3, System Verification. The test gas shall be oil-free dry nitrogen.
4-10.1.2.2.1 Blowdown. After installation of the piping network, but before installation of vacuum inlets and other vacuum system components, all lines shall be blown clear using oil-free dry nitrogen. 4-10.1.2.2.2 Pressure Test (Initial). Before attaching the vacuum
lines to the vacuum pumps, receiver(s) [tank(s) ], and alarm si.gn.aling system(s) switches and gauges, each section of the vacuum ptpmg system shall be subjected to a test pressure not less than 150 psig (1034 kPa gauge) by means of oil-free, dry nitrogen. This test
reSsure shall be maintained until each joint has been examined for akage by use of soapy water or other suitable means. All leaks shall
be repaired and the section retested. 4-10.1.2.2.:5 Standing Pressure Test. After installing a vacuum
system, including station inlets, but before attaching the vacuum lines to the vacuum pumps, receiver(s) [tank(s) ], and alarm system(s) switches and gauges, the entire system or sections of the system shall be subjected to a test pressure of not less than 60 psig (413 kPa gauge) by means of oil-free, dry nitrogen. After allowance for temperature variation, the pressure at ~he end of 24 hours shall be within 5 psig (345 kPa gauge) of the initial pressure. Corrective action shall be taken if this performance is not verified. After completion of the test, corrections, and reverification if necessary, the system shall be connected to the vacuum pumps, receiver(s) [tanks(s) ], alarm actuators (vacuum switches), and gauges. NOTE: For information on how to correct pressure for tempera-
ture changes, see Sections 4-3 through 4-5. 4-10.1.2.2.4 Cross~onnection Test (Initial). Prior to closing walls,
it shall be determined that no cross-connections exist between the vacuum system and any medical gas system. Vacuum systems shall be tested at the same time as medical gas systems, as described in 4- 5.1.2.5.
4-10.1.2.3 System Verification. The following tests shall be performed after those listed in 4-10.1.2.2, "Installer Performance Testing." The test gas shall be oil-free, dry nitrogen.
This testing shall be conducted by a party technically competent and experienced in the field of medical vacuum pipeline testing, and independent of the installer. . . .
4-10.1.2.3.1 Cross-connection Test (Final). After closing Walls and completing the requirements of 4-10.1.2.2, it shall be determined that no cross-connections exist between the vacuum system and any medical gas system, using one of the methods described in 4-5.1.5.1. 4-10.1.2.3.2 Vacuum Test. After connecting the vacuum piping to
the vacuum pumps, receifer(s) [tank(s) ], vacuum gauges, and vacuum alarm switches, a vacuum test shall be performed on the entire system.
NOTE: An acceptable method of testing is by means of shutting downportions of the system using the shutoffvalves described in 4- 9.1.1.5 to determine the capability of that portion to maintain a vacuum. An acceptable condition is a vacuum level loss of less than 1.5 in. Hg in 1 hour with the vacuum system piping initially at a vacuum in excess of 12 in. Hg.
4-10.1.2.3.5 Valve Test. Valves installed invacuum systems shall be tested to verify proper operation and rooms or areas of control. Records shall be made listing the rooms or areas controlled by each valve. The information shall be utilized to assist and verify the P4roper labeling of the valves.
10.1.2.3.4 Alarm TesL (a) General. Alarms for vacuum systems shall be tested to ensure
that all components function properly prior to placing the piping system into service. Permanent records of these tests shall be maintained. Alarms that are part of an addition to an existing vacuum system shall be tested prior to connection of the new piping to the existing system.
(b) Unless otherwise indicated, vacuum system alarms shall indicate if the vacuum in the piping system drops to 12 in. Hg and below." SUBSTANTIATION: Correlation of recommendations in Proposals 99-321 (Log #357), 9%323 (Log #358), 99-325 (Log #359), 9%326 (Log #560) and 99-327 (Log #561). COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16- NOT RETURNED: Fan, Shoemaker
(Log #B59) Committee: HEA-PIP
99- 325 - (4-10.I.ZI): Accept in Principle SUBMITTER: Dennis Murray, American Hospital Association RF.COMMENDATION: Revise text with existing 4-5.1.2 and correlate with related sections and revise text with existing 4-5.1.2.1 and correlate with related sections. Delete reference to C.G.A. SUBSTANTIATION: Existing text inadequate and not detailed to provide the necessary requirements for enforcement. Not user friendly. COMMITTEE ACTION: Accept in Principle. See committee action on Proposal 99-324 (Log #GP62).
COMMITTEE STAT]~[F2qT: Proposal 99-324 (Log#CP62) addresses issue raised here. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 1 6 NOT RETURNED: Far/, Shoemaker
(Log #560) Committee: HEA-PIP
99- 526 - (4-10.1.2.4): Accept in Principle SUBMITrER: Dennis Murray, American Hospital Association RECOMMENDATION: Revise text with existing and correlate with related sections: 4-5.1.3
4-5.1.3.4 4-5.1.3.1 4-5;1.5.7 4-5.1.3.2 4-5.1.3.8 4-5.1.3.3
SUBSTANTIATION: Existing text does not adequately address the requirements for system quality control in detail. The text is not adequate for enforcement and is not user friendly. COMM!TrEEACTION: Accept in Principle. See committee action on Proposal 99-324 (Log #C, P52).
COMMITrEE STATEMENT: Proposal 9%524 (Log #CP62) addresses issue raised here. NUMBER OF COMMITIT, E MEMBERS ELIGIBLE TO VOTE: 1 8 VOTE ON COMMFFFEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #3fil) Committee: HEA-PIP
99- 327 - (4-10.1.2.6): Accept in Principle SUBMIITER: Dennis Murray, American Hospital Association RECOMMENDATION: Revise text with existing 4-5.1.3.4 and correlate with related sections. SUBSTANTIATION: Existing text is inadequate in detail and does not provide the necessary detail for adequate quality control review. Text is inadequate for enforcement and is not user friendly. COMMITTEE ACTION: Accept in Principle. See committee action on Proposal 99-324 (Log #CP62).
COMMITTEE STATEMENT: Proposal 9%324 (Log #CP62) addresses issue raised here. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITFEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #282) Committee: HEA-ANE
9% 328 - (5-4.1, 54.1.1 & 5-4.2): Accept in Principle SUBMYI'Ilgl~ Douglas S. Erickson, American Hospital Association RECOMMENDATION: 5-4.1Ventilation-N,,,=q . . . . . ~LIc Anesthe- tizing Locations.
54.1.1 The mechanicalventilation system supplying a, , ,~,~u,, ,bl~ anesthetizing locations...
54.2 through 5-4.2.5 delete in its entirety. SUBSTANTIATION: Over thepast two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans Affairs, Deparunent of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations.
86

N F P A 99 - - F 9 5 R O P
COMMITTEE ACTION: Accept in Principle. 1. Accept changes to 5-4.1 and 5-4.1.1. 2. Move 5-4.2 to new Annex 3.
COMMITTEE STATEMENT: Correlate with action on Proposal 99-25 (Log #274). NUMBER OF COMMI'FrEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #378) Committee: HEA-ANE, HEA-PIP
99- 329 - (5-4.1.6): Reject SUBMITTER: D.A. McWhinnie, Jr., Mechanical Dynamics, Inc. RECOMMENDATION: Delete: Existing sentence.
New: Waste anesthetic gases from patient breathing machine collecting assembly (scavenger) shaRbe exhausted from the Operating Room through a '~¢AGD" (waste anesthetic gas disposal) inlet.
The WAGD exhaust system shall not exceed a (negative) ]pressure of-0.5 cm H20; and shall vent to the outside of the facility m a manner which will preclude re-entry of vent gasses into the facility.
NOTE: Proven patient-safe WAGD disposal systems: Passive/ ambient differential ( through wall, window, ceiling or floor; Non- return port ion of ventilation exhaust duct; Fan/blower, dampened plenum, duct system. SUBSTANTIATION: A "Scavenging apparatus..." is no t a disposal system, or even a part of one. Without an architecturally built-in disposal system, breathing machine collecting apparatus (Scavenger) would exhaust into the Operating Room. To prevent this, a facility supplied hose is connected to the built-in WAGD terminal (inlet). COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: There are other WAGD technologies than high volume/ low pressure. Proposal would preclude the use of most WAGD in place to day, and op~cating satisfactorily. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 (ANE), 18 (PIP) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 (ANE), 16 (PIP) NOT RETURNED: Fan (PIP), Shoemaker (PIP)
(Log #CP36) Committee: HEA-I_AB
99- 332 - (5-4.3.4): Accept SUBMITTE~ Technical Committee on Laboratories RECOMMENDATION: Delete 5-4,3.4. SUBgTANTIATION: Subject of infectious material and its health hazard is outside scope of committee. COMMITYEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #CP39) Committee: HEA-LAB
99- 333 - (5-4.4.1): Accept SUBMITTER: Technical Committee on Laboratories RECOMMENDATION: 1. Insert "and Biological safety cabinet". after "Fume hoods."
2. In title of 5-4.4, change "Fume Hoods" to "Hood." 3. Add new Appendix A-5.4.4.1 to read: A-5.4.4.1 Biological safety cabinets (BSC) that are vented to the
outside share some characteristics with chemical fume hoods. The interiors of each are at negadve pressure with respect to the ambient environment. BSC are not in tended to be used for protection from exothermic or potentially explosive chemical reactions. (See HHS Publication No. (CDC) 938395, Biosafety in Microbiological and Miomedical Laboratories, for a description of BSG and their ventilating requirements.) SUBSTANTIATION: 1. Biological safety cabinets are not addressed in NFPA 99. Committee believes they present some hazards, and should thus be addressed.
2. Reflect change made in i tem 1. 3. Appendix material is added to explain hazards with BSCa.
COMMrITEE ACTION: Accept. NUMBER OF COMMITFEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #CP8) Committee: HEA-ANE
99- 330- (5-4.1.6): Accept SUBMITTER: Technical Committee on Anesthesia Services RECOMMENDATION: Revise 5-4.1.6 to read:
"Systems that capture or dispose of waste anesthetic gases, if installed, shall prevent their reentry into the facility." SUI~TANTIATION: Recommendat ion widens the methodology of disposing of waste anesthetic gases. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #CP40) Committee: HEA-LAB
99- ~34 - (5-4.4.$ and 5-4.4.4): Accept SUBMITTER: Technical Committee on Laboratories RECOMMENDATION: Delete. SUBSTANTIATION: Subjects are covered in NFPA 45, and 5-4.4.1 references requirements covered in 5-4.4.$ and 5-4.4.4 COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #296) Committee: HEA-LAB
99- 331 - (5-4.3.4): Reject SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise paragraph to read: Air exhausted from areas in which higl'fly infectious oz ,,~'oac~,-.-c
materials are processed or used shall pass through high-efficiency (99-.~ 99.97 percent) filters before discharging to the atmosphere. SUBSTANTIATION: The use of HEPA filters is no t common for radioactive materials. Also I question the need for the entire paragraph as the standard should refer the reader to CDC Contain- ment Level 4 guidelines ff the infectious material is extremely hazardous. It should also refer the reader to NRC standards for fume hoods being used for radioactive material. COMMITTEE ACTION: Reject~ COMMrITEE STATEMENT: See Proposal 99-332 (Log #CP36) which dele ted this paragraph entirely. NUMBER OF COMMITYEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #'217) Committee: HEA-ELE
99- 335 - (Chapter 7): Reject SUBMITTER: Richard P. Kernell, Magic Valley Regional Medical Center, ID RECOMMENDATION: The Standards Council needs to create standards for the use of non-patient equipment being used in a critical care area. There needs to be specific statements on the circumstances where non-UL 544 can be used in critical care areas. SUBSTANTIATION: We are seeing more and more equipment being proposed for use in surgery suites in conjunction with Laparthroscopy carts that are originally in tended for home use. E.G. Video mixer for home enter ta inment to be used to mix with C-arm and lap camera signals to monitor. COMMYITEE ACTION: Reject. COMMITI'EE STATEMENT: 1. No specific recommendat ion was included in proposal.
2. Committee extensively reviewed this subject, and notes the following:
(a) electrical safety requirements for patient care related electrical appliances are covered by 7-5.1.
(b) i ra facility elects to use a 'non-medical ' device in the patient care area, it is the facility's responsibility to assure that the device meets 'medical device' requirements, per 7-6.2.1.1.
87

,I
N F P A 99 - - F95 R O P
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 11 NOT RETURNED: Berger
• (Log #CP18) Committee: HEA-ELE
99- 336 - (%5.1.1): Accept SUBMITTER: Technical Committee on Electrical Equipment RECOMMENDATION: Move 7-5.1.1.2, 7-5.1.1.3, 7-5.1.1.4, and 7-5.1.1.5 to newAnnex 3. SUBSTANTIATION: Correlate with Committee Action on Proposal 99-337 (Log #284). COMMITrEE ACTION= Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMrlTEE ACTION: AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #284) Committee: HEA-ANE, HEA-ELE
99- 337 - (%5.1.2.5, %5.1.2.6, %5.1.2.7, %5.1.2.8): Accept in Prindple SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise text:
%5.1.2.5 Line Voltage Equipment -~dt Anesthetizing Locations 7-5.1.2.5 (b) ...intended for use in a~t anesthetizing... Exception No. 1...in an approved manner. ,,; ~:,,;.,T,;,A , :d , ~,~
• " n ; , 1 L~ : , ~ , L ' Foot-treadle-operateacontrollers a n ~ e i r connector shall be splash proof.
Exception No. 4 ...pedestal-mounted ;.. :- . . . . qa. ...... LI~ --~cg4.~dz- k~ b ,,,.~;~,~. provided...
Exception No. 5 Overhead power receptacles, ;,,, ia . . . . tveatim~, are permitted...
%5.1.2.6 Low Voltage Equipment and Instruments - ~ Anesthetiz- ing Locations
7-5.1.2.7 Delete in its entirety. 7-5.1.2.8 Delete in its entirety.
SUBSTANTIATION: Over thepas t two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), DeparUnent of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over tefi years and have no intention of permltting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITTEE ACTION: Accept in Principle.
1. Revise 7-5.1.2.5 as recommended bysubmitter. 2. Revise 7-5.1.2.6 as recommended by submitter. 3. For newAnnex 3, repeat %5.1.2.5 as currentlyworded in the
document, and move 7-5.1.2.7 and 7-5.1.2.8 into this Annex. COMMITrEESTATEMENT: Correlate with Committee Action Proposal 99-25 (Log #274). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 (ANE), 12 (ELE) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 (ANE), 11 (ELE) NOT RETURNED: Berger (ELE)
COMMITTEE STATEMENT: 2. Correlation. Committee agrees with submitter's recommendation A in that the charging voltage for 9 volt battery systems may require more than 10 volts. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #373) Committee: HEA-ANE, HEA-ELE
99- 339 - (7-5.1.2.7, 7-5.1.2.8): Accept in Prindple SOBMITI'ER: Timothy M. Peglow, La Porte Hospital, Inc. RECOMMENDATION: Delete sections in entirety. SUBSTANTIATION: Flammable anesthetics are not in use in hospitals so this section should be deleted. COMMITI'F_~ ACTION: Accept in Principle.
See Action on Proposal 99-337(Log #284). COMMrlTEE STATEMENT: Committee believes moving text to separate part of document meets intent of submitter. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 (AN'E), 12 (ELE) VOTE ON COMMrrTEE ACTION:
AFFIRMATIVE: 10 (ANE), 11 (ELE) NOT RETURNED: Berger (ELE)
(Log #$9) Committee: HEA-ELE
99- 340 - (7-5.1.3.6): Accept SUBMITTER: MartinJ. Kutik, Chappaqua, NY RECOMMENDATION: Revise text as follows:
(c) Isolation Test (Isolated Inl~Ut ) Change "20 microamperes" to 50 microamperes"
SUBSTANTIATION: I believe this to be a typo error. 20 microam- peres was the old value. The 50 micoramperes is consistent'with paragraphs (b) and (e) and in agreement with ANSI/AAMI ESI- 1993 and proposed UL 544 revisions. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #382) Committee: HEA-ELE
99- 341 - (7-5.1.3.6(c); 9-2.1.13.5(c)): Accept SUBMITTER: Alan Lipschultz, Newark, DE RECOMMENDATION: Change the leakage current limits specified to 50 microamperes. SUBSTANTIATION: Consistency with AAMI Safe Current Limit standard and with IEC-601. The test itself is the single fault condition specified by lEG. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
( Log #21 ) Committee: HEA-ELE
99- 338 - (7-5.1.2.6): Accept in Principle S U B ~ Alan Lipschultz, Newark, DE RECOMMENDATION: A. Change "persons" to "patient."
Change 10 volts to 12 volts Change (c) to "battery-powered... while in operation unless they
meet the requirements of section %5.1.2.5." or B. Delete the whole section. SUBSTANTIATION: The section should be deleted because this equipment is no different in an anesthetizing location than the rest of a health care facility. The section is a remnant of 56A. If the committee does not want to delete it, Option A makes provisions for modifying, so as to make it more in line with actual practice. COMMITrEE ACTION: Accept in Principle.
~ . Accept suhmitter's recommendation B (i.e, delete 7-5.1.2.6). . In %5.1.2.5(b), change "10 volts" to "12 volts."
(Log #294) Committee: HEA-ELE
99- 342 - (7-6.2.1.5): Accept S U B ~ Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise paragraph to read: With the exception of three-to-two-prong adapters, adapters and
extension cords shall be permitted, z,, bc ~,,.~...i-,,,,c, ; ~ v ~ , : ' c ~ . The wiring...thereafter. Adapters and extension cords shall meet the reauirements of 7-5.1.2.9. $LflKSTANTIATION: The current language is overly restrictive and only permits extension cords where distinctive plugs are used. Health care organizations use extension cords daily for. housekeep- ing equipment; maintenance and engineering needs; use in emergency situations, i.e: power outages and other internal disasters; and, for use on medical emergency crash carts. The proposed language will permit the continued use of these cords but will also mandate the cords be of a high quality construction.
88

N F P A 99 - - F 9 5 R O P
COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 11 NOT RETURNED: Berger
EXPLANATION OF NEGATIVE: DAVID: Recent reports indicate that R.F. energy emitted from
electrical equipment interfere with patient-care devices in close proximity. Therefore, the exercise of administrative vigilance in as far as controlling the operation of portable electric drills near anesthesia equipment in the operating theater is a good practice.
(Log #CP20) Committee: HEA-ELE
99- 343 - (7-6.2.1.5): Accept SUBMITTER: Technical Committee on Electrical Equipment RECOMMENDATION: 1. In sentence 1, delete '%Vith the exception of three-to-two prong adapters." Adda new Exception to read: "Exception: Three-to-two prong adapters shall not be permitted." 2. In sentence 2, delete "of the adapter."
SUBSTANTIATION: 1. Clarifies intent of current wording. 2. Testing applies to adapters and extension cords.
COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: II NOT RETURNED: Berger
(Log #285) Committee: HEA-ANE, HEA-ELE
99- 344 - (7-6.2.2.5): Accept SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Dele.te paragraph in its entirety. SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupandes. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans Affairs, Deparmaent of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMI'I~rEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 (EI,E), 10 (AN-E) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 (ELE), 10 (AblE) NEGATIVE: Aronow (ELE), David (ELE) NOT RETURNED: Berger (ELE)
EXPLANATION OF NEGATIVE: ARONOW: I think the vote should be APR and the Action: Move
to newAnnex 3. The material should be retained in the Annex as was done with Proposals 99-337 (Log #284) and 99-336 (Log #CP18).
DAVID: Recent reports indicate that R.F. energy emitted from electrical equipment interfere with patient-care devices in close proximity. Therefore, the exercise of administrative vigilance in as far as controlling the operation of portable electric drills near anesthesia equipment in the operating theater is a good practice.
• (Log #CP9) Committee: HEA-ANE
99- 345 - (7-6.2.2.5): Correlating Committee Note: See Committee Action on Proposal
99-344 (Log #285). The T/C on Electrical Equipment recom- fnended accepting proposal 99.344 (Log #285) which deleted this paragraph. Therefore, recommendation of this proposal is null and void. SUBMITTER: Technical Committee on Anesthesia Services RECOMMENDATION: Revise 7-6.2.2.5 as a NOTE under 7-6.2.2.4 to read:
"Administrative vigilance is required to monitor the use of portable electric equipment and.appliances, such as electri c drills, of a type J unsuitable for use in anesthetizing locations." SUBSTANTIATION: Current text is not enforceable as written. Howe~,er, guidance on the equipment being brought into the anesthetizing location is necessary for patient and staff safety. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NEGATIVE: David
(Log #343) Committee: HEA-ELE
99-346-(7-6.2.4.2 FPN): Accept in Principle SUBMrrTER: Britton Berek, American Hospital Association RECOMMENDATION: Revise 7-6.2.4.2 fine print note to include:
Electrical equipment used within oxygen delivery equipment shall be listed for use in oxygen enriched atmospheres, or sold with the intent to be used in oxygen-enriched atmospheres. FPN: Lowvolta~e nurse call controls which are not used within
oxwen deliverv e-uuinment do not reouire a special listing. For fuhre r informatidn ~onceming the criteria fdr equipmer~t used in oxygen delivery equipment see 9-2.1. SUI~TANTIATION: To avoid special listing for use in oxygen- enriched atmospheres, low voltage equipment - such as nurse call pillow speakers often may carry generic warnings against use with oxygen therapy equipment. Patients and statfhave misinterpreted this labeling and have concluded that these devices are unsafe for use during the administration of any respiratory therapy including routine administration of oxygen. The suggested fine print note clarifies the requirements and obviates the need for spedal warnings to be placed on nurse call pillow speakers. Devices of lowvoltage design have not been implicated in any contemporary fire incidents and presents negligible risk to patients and staff. COMMITIT, E ACTION: Accept in Principle.
1. Revise NOTE in 7-6.2.4.1 to read: "For further information, see manufacturer requirements for
equipment used within the site of intentional expulsion in 9-2.1.9.3." 2. Revise NOTE in 7-6.2.4.2. to read: "For further information, see manufacturer requirements for
equipment used in oxygen delivery equipment in 9-2.1." 3. See committee action on Proposal 99.361 (Log#301).
COMMITI'EE STATEMENT: 1. and 2. NOTES revised to clarify intent that requirements in Chapter 9 are for manufacturers.
3. Committee believes that the action on Proposal 99.361 (Log #301) addresses the concern raised here, and thus recommendation is not necessary NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #CP41) Committee: IqEA-LAB
99- 347 - (745.2.5.1): Accept SUBMI'I~'ER: Technical Committee on Laboratories RECOMMENDATION: 1. Replace existing text of 7-6.2.5.1 with the following:
"The laboratory shall establish policies and protocols for the type of test and intervals of testing for each appliance."
2. Insert new 7-6.2.5.2 to read as follows: [renumber current 7-6.2.5.2 as new 7-6.2.5.$]
"The physical integrity of the power cord and attachment plug and cord strain-relief shall be confirmed at least annually by visual inspection and other appropriate tests."
3. Add new Appendix text to item 2 two read as follows: A-7-6.2.5.2 Most laboratory fires involve biomedical or other
electronic equipment failures. The most cotmnon ignition factors are short circuits or ground faults. Electrical wire or cable insulation is the material most likely to first ignite in a clinical laboratory fire. (Reference: Hoeltge GA, Miller A, Klein BR, Hamlin WB, Accidental Fires in Clinical Laboratories, Arch Pathol Lab Med 17:1200-1204, 1993. SUBSTANTIATION: 1. & 2. Existing text places judgment on AHJ. Committee wants to be more specific in the testing of equipment at least annually.
3. Appendix describes reason for adding new text. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
89

N F P A 9 9 - - F 9 5 R O P
(Log #CP38) Committee: HEA-LAB
99- 348 - (7-6.2.5.2): Accept SUBMITTER: Technical Committee on Laboratories RECOMMENDATION: Revise current 7-6.2.5.2 to read:
"Electrical equipment intetided for use in laboratories shall meet the requirements of NFPA 45, Standard for Laboratories Using Chemicals." Move this text and number as new 7-5.2.2.2(d).
SUBSTANTIATION: Reference to hazardous areas is deleted because all electrical equipment in laboratories need to meet the requirements of NFPA 45.
Movement to section 7-5 is to clarify ~ a t this requirements to new equipment only. COMMITFEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 9 NOT RETURNED: Linder
- (Log #380) Committee: HEA-GAS
99-349- (8-3.1.11): Accept in Principle in Part SUBMITTER: Peter Ferraro,Jr., Phoenix, AZ RECOMMENDATION: Revise 8-3.1.11 in total as follows:
8-3.1.11 Storage Requirements. 8-3.1.11 Storage for Nonflammable Gases Greater than 3000 cuft
(85 m3). Comply with 4-3.1.2 and 4-6.2.2. 8-3.1.11.2 Storage for Nonflammable Gases Less than 3000 cuft (85
m3). (a) Storage locations shall be outdoors in an enclosure or within
an enclosed interior space of non-combustible or limited-combus- tible construction, with doors (or gates outdoors) that can be secured against unauthorized entry.
(b) Oxidizing gases such as oxygen and nitrous oxide shall be separated from combustibles or incompatible materials by either:
(1) A minimum distance of 20 feet (6.1 m); or (2) A minimum distance of 5 ft (1.5 m) if the entire storage
location is protected by an automatic sprinkler system designed in accordance with NFPA 13, Standard for the Installation of Sprinkler Systems; or
(3) A barrier of noncombustible material at least -5 ft (1.5 m) high having a minimum fire resistance rating of one half hour, or
(4) An enclosed cabinet of noncombustible construction having a minimum fire protection rating of one half hour. Note: An approved flammable liquid storage cabinet may be used,
vented to the space. (c) Liquefied gas containers shall be stored outdoors, or in a
location vented by mechanical means or natural means with.at least 72 sq in (0.05 m2) free area. Note: Liquefied gas containers continuallyvent a small amount of
gas to the atmosphere. (d) Cylinders and containers shall be protected so temperatures
do not exceed 125°F (38°C), and protected from the ground and standing water to prevent rusting.
(e) Where cylinders and containers are placed, ordinary electrical wall fixtures shall be installed in fixed locations not less than 5 ft (1.5 m) above the floor to avoid physical damage.
(t) Cylinders and containers shall be protected from abnormal mechanical shock and not placed where heavy moving objects could strike or fall on them.
(g) Cylinders and containers shall be restrained n a rack, stand or cart, to prevent falling or being knocked over.
(h) Flammables shall be prohibited within storage locations for oxidizing gases.
(i) Smoking, open flames, electric heating elements and other sources of ignition shall be prohibited within storage locations and within 20 ft (6.1 m) of outside storage locations.
(j) When provided, cylinder valve protection caps shall be kept in place and hand tightened. $LrI~TANTIATION: Medical gases storage requirements were brought together under 4-3.1.2 and text restructured in 1984 and 1989 editions. In that process, the previously recognized lower hazard traditionally identified as 2000 cu ft or less total capacity for nonflammable medical gas supply systems, as well as the lower hazard associated with storage of cylinders for individual patient respiratory therapy use, were subsumed. The 4-3.1.2 requirements derived from NFPA 56F and were developed and intended only for supply piping systems installations, as clearly stated in the scope provisions of 111 and 113 of NFPA 56F-1977. Further, under 232, even NFPA 56F recognized a lower hazard for 2000 cuft or less total capacity connected or in storage for nonflammable medical gas
supply systems by not requiring rated enclosures or outside venting. (Extract copy of NFPA 56F-1977 provisions attracted.) Supply system requirements of 4-3.1.2 are presently invoked by 8-
3.1.11; and NFPA101-1991, 12-3.2.4 and 13-3.2.4 require medical gases storage protection per NFPA 99 for both new and existing health care occupancies.
Other NFPA standards recognize lesser hazards with smaller quantities of oxidizing gases storage, and establish lesser protection requirements for oxygen storage in occupancies where risk of exposures to flammables, combustibles or ignition sources is far greater than in health care facilities. - NFPA 51-1992, 2-2.1 requires 20 ft separation from flammable and
combustible liquids and easily ignited forms of materials; and, under 2-4.3, requires separation from fuel gas or combustible materials by 20 ft minimum distance, or a noncombustible barrier at least 5 ft high having at least 1/2 hour fire resistance.
- Compressed Gas Association Pamphlets P-1-1984, 4.2.2 required the same, and P-2-1978, 4-3 requiredonly enclosure or separation, but not rated construction. - NFPA 55-1993, 2-1.3 requires separation from flammable,
pyrophoric, and toxic gases; and, under 2-1.6.3, requires separation from incompatible or combustible storage by 20 ft minimum distance, or a noncombustible barrier at least 5 ft high having at lease 1/2 hour fire resistance.
Healthcare facilities must utilize oxygen cylinders when patients move by wheelchair or stretcher, as well as during emergencies should piped uutlets be inoperative or fail. At least some small E-size cylinders are almost always stored on nursing units or floors. It is not unusual to find E-size and occasionally small numbers of larger' oxygen cylinders for respiratory therapy stored in utility rooms or with other storage, including combustible boxed supplies. Even where a separate cylinder storage room exists on the floor, it often does not meet the stringent rated construction or ventilation requirements of 4-3.1.2.
It is reasonable, and in accordance with pgecedent, to provide protection proportional to the lower risk of storage of lesser quantities of individual cylinders and containers, not associated with piped supply systems. Oxygen in larger cylinders may be in use simultaneously at multiple bedsides in a multi-bed room, in proximity to combustible furnishings, bedding and linens, care and comfort items, etc. The 244 cu ft total discharge from a single large cylinder or 23 cuf t total discharge from a single small E-size cylinder pose significantly less risk than a supply system manifold location, where a leak could be expected to discharge many times more than one cylinder's volume over a sustained time. NFPA 99-1993, 4-1.1 clearly states Chapter 4 covers "medical gas .
systems". In response to rejected proposal 99-71 (Log #80), publishes in the 1992 Fall Meeting TCR (pp 251-2), a Committee Statement also indicated "Storage requirements for non-piped gases...are outside the scope of Chapter 4; they need to be addressed in Chapter 8."
This proposal is based on: - Consistency with other NFPA standards protection requirements
for like hazards. - Appropriate separation requirements, proportional to risks, using
the traditional quantity breakpoint of 2000 cu ft to talk capacity based on four oxygen and two nitrous oxide cylinders of G-size (increased in NFPA 99-1993 to 3000 cuf t due to common use of larger size cylinders "to reflect current practices with appropriate safety" per the Health Care Facilities Handbook). Lessened distance separation is provided for spaces having automatic sprinkler protection to recognize the significantly enhanced fire protection provided.
-Ventilation requirements where liquefied containers are stored due to their continuous small venting to the atmosphere.
NOTE: Supporting material is available for review at NFPA headquarters. COMMITI'EE ACTION: Accept in Principle in Part. Accept submitter's recommendations with the following revisions: I. Insert new 8-3.1.11.1 (b) to read: "Oxidizing gases, such as
oxygen and nitrous oxide, shall not be stored with any flammable gas, liquid or vapor." Renumber the remainder of 8-3.1.11 (b) accordingly.
2. In submitter's recommendation, delete 8-3.1.11 (b) (3). 3. In submitter's recommendation, revise 8-3.1.11 (b) (4) to read: (4) An enclosed cabinet of noncombustible construction having a
minimum fire protection rating of one half hour for cylinder storage.. An a proved flammable, liquid storage cabinet shall be permitted to ~e used for cylinder storage.
4. In submitter's recommendation: Replace subpar (c) with following: "(c) Liquified gas container
storage shall comply with 4-3.1.2.2(d)." Replace subpar (d) with the following: "(d) Cylinder and
container storage locations shall meet 4-3.1.2.1 (k) (5) with respect to temperature limitations.
90

N F P A 99 - - F 9 5 R O P
Replace subpar(e) with the following: "(e) Electrical fixtures in storage locations shall meet 4-3.1.2.1 (k) (4)."
Replace subpar (f) with the following: "(f) Cylinder protection from mechanical shock shall mee t 4-6.2.1.2 (m)."
Replace subpar (g) with the following: "(g) Cylinder or container restraint shall meet 4-6.2.1.2(a)."
Delete subpar. (h). Retain subpar (i). Replace subpar (D with the following: "(j) Cylinder valve
protection caps shall meet 4-6.2.1.2(n)." COMMITTEE STATEMENT: 1. Mixing flammable and nonflam- mable gasses, liquids or vapors in the same room is a serious fire hazard. The committee believes that this condition needs to be prevented.
2. Proposed separation is not enforceable. There are many ways that separation could be compromised, and still fall within recom- mendation. Also, submitter failed to provide for adequate horizon- tal separation of the cylinder storage and combustibles, the width of the partition is not specified, which may allow both cylinder and combustible storage to be directly adjacent to each other.
3. To clarify what cabinets can be used for. Venting is deleted since cabinets could placed next to combustible materials.
4. Reference to other paragraphs in document are made to eliminate duplication. Subpar (h) was addressed by committee action number 1. NUMBER OF COMMYVrEE MEMBERS ELIGIBLE TO VOTE: 5 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 4 NOT RETURNED: Raman
(Log #CP17) Committee: HEA-GAS
99- 350 - (8-5.1.2.1(e)): Accept SUBMITTER: Technical Committee on Gas Equil~ment RECOMMENDATION: In last paragraph, delete paramagnetic or polarographic." SUBSTANTIATION: Other technologies are available and are acceptable. COMMITI'EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 5 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 4 NOT RETURNED: Raman
(Log #CP15 ) Committee: HEA-GAS
99- 351 - (8-6.1.2.3): Accept SUBMITrER: Technical Committee on Gas Equipment RECOMMENDATION: In sentence 1, delete "higqa-pressure." SUBSTANTIATION: Hazard exists at any pressure. COMMITFEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 5 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 4 NOT RETURNED: Raman
(Log #CP16) Committee: HEA-GAS
99- 352 - (8-6.1.2.4(e)): Accept SUBMITrER: Technical Committee on Gas Equipment RECOMMENDATION: Delete "ether, cydopropane." SUBSTANTIATION: Agents are no longer in use in the U.S. COMMITTEE ACTION].. Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 5 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 4 NOT RETURNED: Raman
(Log #286) Committee: HEA-ANE, HEA-GAS
99- 353- (8-6.2.2.3): Accept SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise textz
..,combustible liquids , ~ d ~q,~.~Ll, . ~ . . . , s,,cL ~ ,-d,,.,, shall not... *,; ,"-,~, ,q~.,,,,,~,L 1 .... SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Deparunent
of Veterans Affairs, Deparmaent of Defense and major teaching institutions, all of them indicated they have no t used flammable anesthetics for over ten years and have no intention of permitt ing the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMrIWEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 (ANE), 5 (GAS) VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 (ANE), 4 (GAS) NOT RETURNED: Raman
(Log #CPI0) Committee: HEA-ANE
99- 354- (8-6.2.2.4): Accept SUBMITTER: Technical Committee on Anesthesia Services RECOMMENDATION: Delete 8-6.2.2.4. SUBSTANTIATION: Current technology conflicts with this text. Methods used preclude problems; COMMITFEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #CP11) Committee: HEA-ANE
99- 355 - (8-6.2.3.1): Accept SUBMITTER: Technical Committee on Anesthesia Services RECOMMENDATION: 1. Move 8-6.2.3.1 to n e w A n n e x 3.
2. Revise 8-6.2.3 to read "(Reserved)" SUBSTANTIATION: Text covers problems associated with flammable anesthetizing locations. Committee is moving all text on this subject to a n e w A n n e x 3. COMMITI'EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #295) Committee: HEA-G/~
99- 356 - (8-6.4.1.4, 8-6.4.2): Accept in Part SUBMITI'ER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: In both paragraphs add to the proposed sign text the international symbol for no smoking.
In both paragraphs add an exception that reads: Exception: In health care facilities where smoking is prohibi ted
and signs are prominently (strategically) placed at all major entrances, the need for secondary signs with no smoking language is not required. The non-smoking polici" "es shall be strictly enforced. SUBSTANTIATION: The international symbol for no smoking is highly recognizable and will assist in enforcing the smoking regulations. Most if no t all hospitals are non-smoking facilities and therefore a requi rement for secondary signs is r e d u n d a n t COMMITI~E ACTION: Accept in Part. Accept addit ion of symbol for no t smoking.
COMMITTEE STATEMENT: Committee is aware of instances in facilities that prohibi t smoking where persons have used other sources of ignition in areas where oxygen was in use. It therefore believes signs are necessary whenever oxygen is in use. NUMBER OF COMMI'IWEE MEMBERS ELIGIBLE TO VOTE: 5 VOTE ON COMMrrTEE ACTION:
AFFIRMATIVE: 3 NEGATIVE: Lipschultz NOT RETURNED: Raman
EXPLANATION OF NEGATIVE: LIPSCHULTZ: I vote negative on Public Proposal 99-356 (Log
#295) on Section 8-6.4.1.4 and 8-6.4.2. In my opinion, the commit- tee action should have been to accept the comment entirely. While the committee is correct that other sources of ignition are possible, the issue is really if these signs would have prevented any resulting fires; or if discontinuing these signs will result in additional fires. In my opinion, the answer is no. Keeping up with the signage is difficult, and the real benefit s m a l l
The main ignition source continues to be smoking. The proposers recommendat ion addresses this issue adequately.
91

N F P A 99 - - F95 R O P
(Log #383) Committee: HEA-ELE
99-357- (9-2.1.2.1, 9-2.1.2.2): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, paragraph 517.11. It is beingacted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITTER: Frahk Martucci, Fort Lee, NJ RECOMMENDATION: After existing material add: (a) Cord Sets. Cord Sets used for patient care shall be redundantly grounded with two insulated copper conductors. The groundingconductors shall be installed in line and extension cords with thebranch circuit conductors supplying the unfixed equipment.
(1) Grounding poles. Cord connectors and attachment plugs shall be provided with two separate wiring sites at the grounding pole. The cord connectors and attachment plugs shall be designed so that only the grounding pole can be wired with two conductors. SUBSTANTIATION: The extensive assured equipment grounding Pdirogram for construction sites in Section 305-5 (b), substantiates the
re need for an electrocution-proof extension cord for all patient care. The program requires written descriptions, competent persons to implement, daily" inspections and tests, and a written record of the tests. Continuity, and proper terminal connection, tests are made before first use, after repair, before use after suspected damage, and thereafter, every three months. Read the instructions on Wrappers of extension cords for further
substantiation. For example, a few of the instructions given by the Carol Cable company. DANGER: Electric cords can be hazardous, misuse can result in fire, death, or electric shock. Do not use when wet, do not plug one extension cord into another, never drive, drag, or place objects over cord, do not walk on cord, grasp plug to remove from outlet, never unplug by pulling cord, keep away from water, do not splice, adapt, repair, or modify, do not use if cut, worn, or frayed, inspect periodically for damage, etc., etc. How could the Consumer Product Protection Agency permit such a hazardous product?
Compounding the hazards are extension cords with equipment grounding conductors sized less than branch circuit conductors and ground fault circuit interrupters. At a time when proposals are being submitted, AND ACCEPTED, for permitting an increase in the minimum ground path requirements of table 250-95, extension cords are still permitted with equipment grounding conductors sized substantially lower. This increases the chances of loss of grounding from use and abuse, or grounding burnout when unable to conduct any ground fault likely to be imposed on it.
The undersized equipment grounding conductor in lengthy extension cords also violates the adjustment for voltage drop requirements of Section 250-95 of the NEC. This means, extension cord equipment grounding conductors should be increased to sizes even larger than the #12 AWG requirements of Table 25/)-95. Yet exception #1 permits use of equipment grounding conductors as low as #18AWG. This could dangerously energize exposed metal parts of appliances when ground faults occur.
Last, but not least, is the fact that inadvertent wiring errors by even t h e m o s t qualified personnel can also energize the exposed metal parts of appliances. Qualified personnel were responsible for energizing the metal grounding plate that electrocuted a patient March 15,1956 in my hospital. The patient died because an explosion-proof outlet was wired with reversed polarity by an EXPERIENCED electrician and OK'd for service by a QUALIFIED electrical inspector. The patient died because a QUALIFIED factory employee wired an attachment plug to a medical device with reversed green and white conductors. A patient died because a QUALIFIED person, myself, did not u n c o v e r the "Russian Roulette" type of electrocutions built into our grounding system prior to the death of a patient.
Use of an improperly wired extension cord could also energize the exposed metal parts of an appliance in the presence of explosive gases. An energized device contacting adjacent grounded objects will provide the ignition required to cause an explosion. The Sept. 2, 1993 issue of the N.Y. Times reported the death of three patients caused by an energized ventilator that contacted a grounded object in the presence of oxygen gas. The device was actually worked on for giving shocks just two hours before the accident occurred.
The electrocution proof system I propose will prevent both electrocutions and fires by simply eliminatingany chance for the ex osed . . . . metal parts of appliances from everbecoming energu'zed. ~Pest vonng m accordance vath the attached wiring survey will prove
that each and every time wiring errors caused the exposed metal parts of the appliance to become energized, the charge was eliminated when the second grounding conductor was attached.
CONCLUSION: Adoption of the proposal will ameliorate the many hazards
assodated with the use of extension cords. COMMITrEE ACTION: Reject.
COMMITTEE STATEMENT: Subject of grounding conductor.is considered to be adequately addressed in 9-2.1.2.1 and 9-2.1.2.2. Submitter's recommendation would not improve level of safety because the use of two grounding conductors in one cord does not provide the type of redundancy necessary to improve safety level as they are subject to the same failures. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMrITEE ACTION: AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #385) Committee: HEA-ELE
99- 358 - (9-2.1.2.1, 9-2.1.2.2): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517,paragraph 517.12, Exception $(New). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITI'ER: L. Bruce McClung, Union Carbide Corporation RECOMMENDATION: New text as follows:
Exception No. 3: Any other cables: connecting cables, flexible cords with attachment plug cap or cord set assemblies shall be spedfically marked with an/I. .S/LC designation and listed for the use. This listing requirement shall become effective January 1, 1997. SUBSTANTIATION: The 1990 Code recognized "/LS" and the 1993 Code recognized "/LC" instllations and outer coverings for conductors for general wiring, for flexible cords and cables and for fixture wires. Any exposed wiring in enclosed spaces where products of combustion would be confined and people (particularly infirm or immobilized people) and/or sensitive electronic equipment that are present should have improved fire safetyfeatures. See technical paper rifled "Improvement in Fire Safety Features of Electrical Conductors and Cables" by L.B. McClung and S. Ramchandran that was presented at IEEE-IAS-PCIC 1993 at St. Louis, Missouri. UL now has available a test by which to measure limited smoke (UL1685). UL is actively pursuing development of a standard test by which to measure low or limited corrosivity of conductors and cables.
NOTE: Supporting material is available for review at NFPA Headquarters. COMMI'ITEE ACTION: Reject. COMMITTEE STATEMENT: Committee agrees with NEC/Panel 17 in that proposal places unreasonable limits on choices of cables and cords without presenting evidence of a problem that justifies the restriction. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #2) Committee: HEA-ELE
99- 359 - (9-2.1.4.$ (New)): Accept in Principle Note: This proposal appeared as comment 99-166 which was held
for further study from the Fall 92 TCD, which was on proposal 99-185 that appeared in the Fall 92 TCIL SUBMITI~R: Saul Aronow, Technology in Medicine, Inc. RECOMMENDATION: Add a new section 9-2.1.4.3, Patient Lead Connections:
(a) Lead Termination. The connector on a patient lead shall be constructed so that the connector can not be inserted to make contact with the live parts of a power receptacle or to engage any part of the appliance that can introduce a risk of electric shock, fire or personal m'ury l J . . . .
(b) Isolated Patient Lead. The apphance connector of an isolated patient lead shall be constructed so that when not inserted properly in the appliance, the end of the conductor of the lead cannot contact a surface that may be grounded. SUBSTANTIATION: The proposer raised several issues. This comment concerns the proposed "Exception." The intent appears to be to remove the hazard of a lead touching a device or surface that could convey excessive leakage current to the patient. The concern has some validity but the wrong end of the problem is attacked. Many years ago this Committee decided to protect the patient by requiring "isolated leads." However, it did not look at the case of a lead connected to the patient, but with the other end hanging loose, which is what the proposer is concerned with. His PadrOposed Exception is in the wron~ place. It should be in 9-2.1.4,
dressed to the manufacturer, which is why the comment recom- mends that it be placed there. The comment also rephrases the proposed intent to put the solution of the problem at the better place.
92

N F P A 99 - - F95 R O P
COMMITTEE ACTION: Accept in Prindple. In submitter's recommendation a), revise beginning to reach "Lead
Termination. The connector, distal to the natienh on a patient lead . . . " [change underlined] [rest the same] " COMMITrEE STATEMENT: Clarifies which end of the lead is of concern. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #CP23) Committee: HEA-ELE
99. 360 - (9-2.1.7.2): Accept SUBMITrER: Technical Committee on Electrical Equipment RECOMMENDATION: Delete "and NFPA 99B, Standard for Hypobaric Facilities." SUBSTANTIATION: Reference is no longer appropriate. COMMITTEE ACTION: Accept NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #301) Committee: HEA-ELE
99- 361 - (9-2.1.9.3): Accept in Principle SUBMITTER: Joseph P. McClain, Walter Reed Army Medical Center RECOMMENDATION: Revise text as follows:
9-2.1.9.3 Electrical Equipment in Oxygen-EnrichedAtmospheres. Electrically powered equipment intended to be used within oxygen
delivery equipment shall comply with ( a )o r (b) or (c) or (d) ~L-eA as listed below. When only a remote control or signal leads of a device are to be used in the site ofintefitional expulsion, only the control or signal leads shall be required to comply with this section. Low voltage aooliance such as oillow sneakers of 50v or less are not subject to these reouirements ~nless ~ e v are located within the barr iersof the oxygen deliverveouinment. [Chan~esunderlined] SUBSTANTIATION: Based on the 'current definition of oxygen- enriched atmospheres, any control or signal leads such as pillow speakers, intercom, EKG leads can not he used diJring oxygen- merapeutic sessions. The only alternative is to convert all existing electrical devices to manual, non-electrical and pneumatic opera- tion. The definition of oxygen-enriched atmosphere should-be modified to address specific oxygen-therapeutic practices rather than general overall use of oxygen.therapy. The most typical way of delivering oxvgen in health care today is through the use of nasal cannula and mask. It should be noted that oxygen diffuses rapidly and it is difficult to obtain concentration readings greater than 23.5 percent in the proximity of a patient using nasal cannula or mask. Therefore, a boundary shouldbe established for the use of electrical equipment during oxygen therapeutic sessions. I ra boundary can not be established, then all existing structures, such as outlets and all electrically operated medical equipment cannot be used during oxygen therapy sessions without risk to the pat ient A simpler alternative is to modify paragraph 9.2.1.9.3.
NOTE: Supporting material is available for review at NFPA hdadquarters. COMMITrEEACTION: Accept in Principle. Replace sentence 2 of 9-2.1.9.3to read as follows: "Appliances, or part(s) of an appliance or system (e.g., pillow
speaker, remote control, pulse oxymeter probe) to be used in the site of intentional expulsion shall comply with the requirements of this section. Those parts of an appliance or system not within oxygen delivery eqmpment, or not in the site of intentional expulsion, shall not be required to comply with this section." COMMITTEE STATEMENT: Committee recognizes that existing wording is unclear. Revised wording addresses the issue of devices or parts of devices to be used within the site of intentional expulsion. Submitter's new last sentence is already addressed in 9-2.1.9.3(d).
In addition, boundaries On oxygen delivery equipment and on the site of intentional expulsion are already defined in Chapter 2. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TOVOTE: 12 VOTE ON COMMITFEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #381) Committee: HEA-ELE
99- 362 - (9-2.1.13.5(a)): Accept SUBMITTER= Alan Lipschultz, Newark, DE RECOMMENDATION: Change the leakage current limits specified from 50 microamperes to 100 microamperes. SuBKrANTIATION: Consistency with section 7-5.1.3.6(a) and with AAMI gale Current Limit standard and with IEC-601. For non- isolated devices, this test for the reference lead is essentially measuring the chassis leakage current COMMITTEE ACTION: Accept NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON. COMMITTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #CP19) Committee: HEA-ELE
99-363- (9-2.1.13.5(c)): Accept S U B ~ Technical Committee on Electrical Equipment RECOMMENDATION: In sentence 4, change "at the apparatus terminals 10 microamperes" to read "at the apparatus terminals 25 microamperes." SUBSTANTIATION: Correlate with Committee Action on Proposal 99-M1 (Log #382). COMMITIT~ ACTION: Accept. NUMBER OF COMMITIT~ MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMrrTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
• (Log #CP46) Committee: HEA-LAB
99w364- (10-3.1.1 Exception No. 1): Accept SUBMITTER: Technical Committee on Laboratories RECOMMENDATION: Revise Exception 1 by adding the following:
"by the authority having jurisdiction (AHJ)" between "that are not classified" and "as a severe hazard." Add at end of Exception: "(See Appendix A-10-5.1 for one method of calculating the hazard
fire severity.)" SUBSTANTIATION: Assign responsibility for determining fire hazard classification level of a laboratory. COMM1TrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #43) Committee: HEA-LAB
99- 365 - (10-5.1 (b) Note): Accept in Principle SUBMITTER: Harian Ihlenfeldt, Kemper National Insurance RECOMMENDATION: Within the Note following paragraph (b), replace the words "Halon 130I with the words "an approved gaseous agent ' . SUBSTANTIATION: This change is needed to reflect recent chang.es in both technolo, gy and federal., law. Because of its ozone depleuon potential, Halon 1301 is no longer beitlg manufactured. Other gaseous agents have been developed, are being approved, and are covered in NFPA #~2001. Although recycled Halon 1301 remains available, this note in the standard should be made less specific, referring to the various agenm available. This wording is also consistent with NFPA #45. COMMITrEE ACTION: Accept in Principle.
Revise NOTE to read: "Where there is a need to reduce equipment damage and facilitate
return to service, consideration should be given to an approved - a ~ o e ~ n t total-flooding system in laboratories."
EE STATI~ENT: Committee agrees with the intent of submitter with regard to deleting reference to Halon 1501, but also wants to emphasize applicability of this type of extinguishnient to all areas of laboratories ~¢here sensitive equipment is in use. NUMBER OF COMMITTEE MEMBERS-ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
93

N F P A 99 - - F95 R O P
Committee: 99- $66 - (10-5.1(b) Note): Reject. SUBMrITER: Mayer D. Zimmerrnan, US DHHS; HCFA RECOMMENDATION: The first sentence of the note should be deleted. The committee may also wish to check with NFPA 75 for
g ossible substitute language. UBSTANTIATION: Reader should not be advised to consider a
Halon 1501 total flooding system. The use of Halon 1501 has been determined to be an environmen-
tal hazard. COMMITTEE ACTION: Reject COMMITTEE STATEMENT: See Committee Action on Proposal 99-~65 (Log #43). Committee deleted reference to halon 1 $01 via Proposal 99-365 (Log #45). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #CP42) Committee: HEA-LAB
99- $67 - (10-5.$): Accept Correlating Committee Note: The Technical Correlating Commit-
tee notes a problem in the use of the term "ordinary hazard" since other NFPA documents also use this term. The TCC directs the TC on Laboratories to review the use of this term in relation to its me in NFPA 101, Life Safety Code, and NFPA 10, Portable EXtinguisher. S U B ~ Technical Committee on Laboratories RECOMMENDATION: 1. At beginning of paragraph, add -Portable.~
• 2. Add the following new sentence: "For purposes of extinguisher placement, clinical laboratories shall
be gradedas units of ordinary hazard." SUBSTANTIATION: 1. Clarify type of extinguishers being addressed.
2. New sentence is added to designate the number and placement of portable fire extinguishers. COMMITrgR ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMrFtEE ACTION:
AFFIRMATIVE: 10
2. In Chapter 13: " Revise 155.4.3 to read "Vacuum systems for medical/surgical
~, urDoses shall conform to the requirements of Vacuum System-Type Nfedical Surgical as listed in Chapter 4, section 4-7 to 4-11ff
Revise 15-3.4.5 to read "Vacuum s~tems for non-medical/surgical urposes shall conform to the requirements of Vacuum System-Type I, as listed in Chapter 4, section 4-7 to 4-11." 3. In Chapter 14: Retitie existing 14-3.4.3 as "Vacuum Systems." Add new 14-3.4.3.1 to read "vacuum systems for medical surgical
purposes shall conform to the requirements of Vacuum System-Type I, Medical Surgical as listed in Chapter 4, section 4-7 to 4-11." • Add new 14-3.4.3.2 to read "Vacuum systems for non medical
surgical purposes shall conform to the requirements of Vacuum System-Type III, as listed in Chapter 4, section 4-7 to 4-11." Add new 14-3.4.3.3 to read "Laboratory vacuum piping systems shall
conform to the requirements of Section 4-7 through 4-11. 4. In Chapter 16: Retitle existing 16-3.4.3 as "vacuum Systems." Add new 16-3.4.3.1 to read: "Vacuum systems for medical surgical
shall conform to the requirements of Vacuum System-Type Medical Surgical as listed in Chapter 4, section 4-7 to 4-11."
Add new 16-3.4.3.2 to read: "vacuum systems for non medical surgical purposes shall conform to the requirements of Vacuum System-Type Ill, as listed in Chapter 4, Section 4-7 to 4-I 1." Add new 16-$.4.3.3 to read: "Laboratoryvacuum pipingsystems
shall conform to the requirements of Section 4-7 through 4-11. 5. In Chal~ter 17: Retitle existing 17-3.4.3 as Vacuum Systems Add new 17-$.43bl to read: "Vacuum systems for medical/surgical
purposes shall conform to the requirements of Vacuum System-Type ], Medical Surgical as listed in Chapter 4, section 4-7 to 4-11." Add new 17-3.4.3.2 to read: "Vacuum systems for non-medical/
surgical purposes shall conform to the requirements of Vacuum System-Type III, as listed in Chapter 4, section 4-7 to 4-11." Add new 17-3.4.3.3 to read: "Laboratoryvacuum pipingsystems
shall conform to the requirements of Section 4-7 through 4-11. SUBSTANTIATION: Proposal 99-1"02 (Log #CP75) changed the
• vacuum requirements in chal~ter 4. This committee proposal correlates those changes in other application chapters. COMMITTEE ACTION: Accept NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 16 NOT RETURNED: Fan;Shoemaker
(Log #CP47) Committee: HE-LAB
99- 368 - (10-8.1.3): Accept S U B ~ Technical Committee on Laboratories
I RECOMMENDATION: Delete 10-8.1.3. S ~ A N T I A T I O N : Subject of surveiliance for unat tended laboratory operation is covered in 10-2.1.1.3. Committee is unaware of problems of laboratories when not in operafionF.
• COMMrFIT_.EACTION: Accept NUMBER OF COMMITTEE MEMBERS ELIGIBLE TOVOT]~ 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 8 NEGATIVE: ndenfeldt NOT RETURNED: Linder
EXPLANATION OF NEGATIVE: IHLENFELDT: I vote negatively on the proposal to delete this
article. While article 10-2.1.1.3 covers pertodic human supervision of planned unattended operating equipment, it provides no safeguard for equipment which may be inadvertently left on. I would recommend that provision for at least one security tour afte.r departure of the staff remain in the document.
Committee: HF_~-PIP 99-369- (Chapters 12,13,14,16,17): Accept SUBMITIT~ Technical Committee on Piping Systems RECOMMENDATION: 1. In Chapter 12:
Revise 12-3.4.$ to read "Vacuum systems for medical/surgical
~, urposes shall conform to the requirements of Vacuum System-Type Medical Surgical as listed in Chapter 4, section 4-7 to 4-11.
Revise 12-~.4.5 to read "Vacuum systems for non medical/surgical PcUrposes shall conform to Vacuum System-Type III, as listed in
hapter 4, section 4-7 to 4-11."
CLog ~87} Committee: HEA-ANE
99-$70- (12-4.1.1.1, 12-4.1.1.2): Accept in Principle • SUBMITIXR: Douglas S. Erickson, American Hospital Association RECOMMENDATION: 12-4.1.1.1 ,...The increasing use of these agents has cu..'~:l~d, --...i k. ;;,,.~;.
• "..~..=:....0 completely eliminated,... ...human diligence in the maintenance of safe practices l~.~.~.- e.f
. i • t , ~ . * * ~ . _ L t . I " " • = • a n d
electrical shock hazards .... x.compressed gases and their cylinders, ~.c cxvl.;.i;~ .~a~;c ~: . . . . . . . . . . .~,cu:o, and the hazards...
12-4.1.1.2 ...with the administration of L,,tL ~--,,anLl~ -.~,1 ,~,,~,,m,,,,~L:~
inhalation anesthetics. ...facilities that are part of a hospital. ,~, ~;~:: ~,...~ c ...L..'..£~.;.. ".X...This section does not...care facilities.
. . . . . . . . . . . . (see 13-4.1). delete entire sentence - TI,.L. ~c=..u d~c~ ,~,.;...,~,c~ ~--......L:~
SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Sodety of Anesthesiologists (ASA), Department of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no i~tention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMrlTEE ACTION: Accept in Prindple.
1. Move 12-4.1.1.1 to newAnnex 3, and renumber existing 12- 4.1.1.2 to 12-4.1.1.5.
2. For submitter's recommendation on 12-4.1.1.2, revise per items 1 and 2. For item $, retain par. 5 ("This sect ion. . . ) , but delete "and uses flammable anesthetics."
94

N F P A 99 - - F 9 5 R O P
COMMITTEE STATEMENT: 1. Correlate with committee action on Proposal 99-25 (Log #274).
2. Application of the safety requirements in Chapter 12 to animal operative facilities IN hospitals is considered necessary because of the proximity to these areas, as well as for the preservation of systems that mutually support the animal facility and patient care service. NUMBER O~ COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #288) Committee: HVA-ANE
99- 371 - (12-4.1.1.5(b), (c)): Accept in Principle SUBMITTERa Douglas S. Erickson, American Hospital Association RECOMMENDATION: Delete entire subparagraphs ( b ) and (c). SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Depar tment of Veterans Affairs, Depar tment of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intent ion of permitt ing the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITI'EEACTION: Accept in Principle.
1. Move 12.4.1.1.5(b), (c), and (e) to n e w A n n e x 3. 2. For 12-4.1.15(e), change "anesthetizing locations" to "flammable
anesthetizing locations." COMMITTEE STATEMENT: Correlate with committee action on Proposal 99-25(Log #274). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: l0
(Log #CP12) Committee: HEA-ANE
99- 372 - (12-4.1.1.5(f)): Accept SUBMITTER: Technical Committee on Anesthesia Services RECOMMENDATION: Delete 12.4.1.1.5(f) and associated appendix. SUBSTANTIATION: With current equipment, this is no longer a current practice. COMMrlTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #289) Committee: HEA-ANE
99-373- (12-4.1.2.1, 12-4.1.2.4(d), 12-4.1.2.6(a)): Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Association RECOMMENDATION: Revise paragraphs to reack
12.4.1.2.1 Ventilation of anesthetizing locations shall conform to 5-6.1 and to 5-4.1. f ~ . v . ~ . . . . ;~vlc ~.~;k.cG~L.~ "v..+Gv . . . . d
4 g t C . , . t l I I , I + - • I , ,
12-4.1.2.4 Maintenance employees shall be properly acquainted with the importance of the work they are excepted to d o i n lv,.,+GG.~ .%; ~ . . . . . . L:c ~ ,~ .d . cdc .~6c.~; :-.~d anesthetizing locations.
124.1.2.6 (a) A grounded electrical distribution system shall be p.e..,,r~, .itt.e.d to .b e i ns.t~.!.ed !n mle sthetizing !oc~tion~. d.?~ I.,+,, ~.~_ 72: . . . . . v~"yz r . . . . . . . . . . t~ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Note: If a . o , ~ . . . a L l c an anesthetizing location is a wet location,... SUISSTANTIATION: Over t h e p a s t two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban f rom use in health care occupandes. In checking with the American Society of Anesthesiologists (ASA), Deparmaent of Veterans Affairs, Depar tment of Defeuse and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have n o intention of permitt ing the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITrEE ACTION: Accept in Principle.
1. Revise 12.4.1.2.1 and 124.1.2.6(a) as recommended . 2. Revise 12-4.1.2.4(d) to read as follows: "Personnel working in
anesthetizing locations shall be instructed in these electrical safeguards."
95
COMMITI'EE STATEMENT: 2. Current text is restrictive. There are other persons working in anesthetizing locations that need to be aware of these electrical safeguards. NUMBER OF COMMITI~EMEMBF_.RS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log#GP13) Committee: HEA-ANE
99- 374- (12-4.1.2.2(c) Note): Accept SUBMITTER: Technical Committee on Anesthesia Services RECOMMENDATION: 1. Delete sentence 1.
2. Revise seotence 2 to read: "Tinctures and solutions of disinfecting agents maybe flammable,
and can be used improperly during surgical procedures." SUBSTANTIATION: The referenced chemicals are no longer used for the purposes cited. COMMITTEE ACTION: Accept. NUMBER OF C O ~ E MI~BF.RS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #CP14) Committee: HEA-ANE
99- 375 - (12.4.1.2.10(d)(i)): Accept SUBMITI'ER: Technical Committee on Anesthesia Services RECOMMENDATION: Revise to read:
"New operating room/surgical suite personnel, nhvsiciar~_s and sur~eous, shall be t augh t . . . " (rest the same)
cfiange underline] SUBSTANTIATION: Experience of some members of the committee, and reports to the committee, indicate that surgeons and physicians resist in-service education. Committee believes that it needs to apply emphasis to the responsibility of surgeons and Pchysicians.
OMMITI'EE ACTION: Accept. NUMBER OF COMMITTEE MI~MBEI~ ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #290) Committee: HEA-ANE
99- 376 - (12-4.1.3): Accept in Principle SUBMITTERa Douglas S. Erickson, American Hospital Association RECOMMENDATION: Delete entire 12-4.1.3 Requirements for Flammable Anesthetizing Locations. SUI~TANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban f rom use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Depar tment of Veterans Affairs, Depar tment of Defense and major teaching institutions, all of them indicated they have no t used flammable anesthetics for over ten years and have no intent ion of permitt ing the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flamq~able anesthetizing locations. COMMITTEE ACTION: Accept in Principle.
Move 12.4.1.3 to new Annex 3. C O ~ STATEMENT: Correlate with committee action on Proposal 99-25 (Log #274). NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #291) Committee: HEA-ANE
99-377- (12-4.1.4, 12-4.1.4.1, 12-4.1.4.2, 12-4.1.4.3, 12-4.1.4.4, 12- 4.1.4.5): Accept in Pr indple S U B M I T 1 T ~ Douglas S. Erickson, American Hospital Associat ion RECOMMENDATION: Revise text:
12.4.1.4 Delete. 12-4.1.4.1 Delete. 12-4.1.4.2 Delete. 12-4.1.4.3 Delete. 12-4.1.4.4 Flooring in . , , , . 2 ~ , , L ; c anesthetizing locations shall... Move 12.4.1.4.4 to new paragraph number 12-4.1.2.7 and renumber
subsequent paragraphs accordingly.

N F P A 99 - - F 9 5 R O P
12-4.1.4.5 Delete. SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone fi'om an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Sodety of Anesthesiologists (ASA), Department of Veterans Affairs, Departmem of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITITEE ACTION: Accept in Principle.
I Delete all of 12-4.1.4. COMMITI'EE STATEMENT: Tests for flooring is not considered realistic since any floor becomes conductive with routine cleaning. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #292) Committee: HEA-ANE
99- 378 - (124.1.5): Accept in Principle SUBMITTER: Douglas S. Erickson, American Hospital Assodation RECOMMENDATION: Delete entire section 12-4.1.5 Requirements for Mixed Facilities. SUBSTANTIATION: Over the past two decades, the use of flammable anesthetic has gone from an occasional use for research, to a complete ban from use in health care occupandes. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reality and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITI'EE ACTION: Accept in Principle. Move 12-4.1.5 to newAnnex 3.
COMMITI'EE STATEMENT: Correlate with committee action on Proposal 99-25 (Log #274). NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10
(Log #293) Committee: HEA-ANE
99-379- (13-4.1.3, 13-4.1.4, 13-4.1.4.1, 13-4.1.4.2): Accept in Principle SUBMITTER: Douglas S. Erickson, Amedcan Hospital Association RECOMMENDATION: 13-4.1.3 Delete in its entirety.
15-4.1.4 Delete section heading. 13-4.1.4.1 Renumber to 15-4.1.2.11 13-4.1.4.2 Editorial - delete the subparagraph heading of (a) and
renumber to 13-4.1.2.12.
SUBSTANTIATION: Over thepast two'decades, the use of flammable anesthetic has gone fi'om an occasional use for research, to a complete ban from use in health care occupancies. In checking with the American Society of Anesthesiologists (ASA), Department of Veterans Affairs, Department of Defense and major teaching institutions, all of them indicated they have not used flammable anesthetics for over ten years and have no intention of permitting the use of these agents. The time has come to face reallty and remove any and all references to flammable anesthetics and flammable anesthetizing locations. COMMITrEE ACTION: Accept in Principle. Revise 13-4.1 to read: "15-4.1 Anesthetizing Locations. Anesthetizing locations in
ambulatory health care centers shall comply with the requirements in 12-4.1." COMMITTEE STATEMENT: With changes made as a result o f committee action on Proposal 99-25 (Log #274), the requirements for anesthetizing locations in AHO3 are considered the same as those in hospitals. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITFEE ACTION: AFFIRMATIVE: I0
Committee: ( I ~ 3 7 A ~ 4) 99- 380 - (Chapter 15): Accept in Principle SLIBMITI'ER: Timothy M. Peglow, La Porte Hospital, Inc. RECOMMENDATION: Applicability - This chapter does not apply to fadllties wherein general anesthesia or relative analgesia are administered to ambulatory patient. SUBSTANTIATION: Environments where analgesia or anesthesia are administered should have similar code requirements to protect the patients. When patients reflexes are compromised. CO .MMITrEE ACTION: Accept in Principle. Revise 15-1 to read as follows:
15-1 General. 15-1.1 Scope. [same wording as current 15-1.] 15-1.2 Applicability. This chapter applies to facilities wherein
inhalation anesthesia are not administered to ambulatory patients. For facilities that administer inhalation anesthesia, the requirements of Chapter 1 $ shall apply. COMMITTEE STATEMENT: Reference to relative analgesia was deleted became the hazards of relative analgesia as defined in 2-2 do not pertain to patients under these conditions. Committee believes that medical and dental offices that use inhalation anesthesia need to comply with the requirements of Chapter 13. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 10
(Log #CP63) Committee: HEA-PIP
99- 381 - (Chapter 15 and Chapter 2): Correlating Committee Note: The Technical Correlating Commit-
tee (TCC) directs the T /C on Piping Systems to reconsider the placement of proposed terms in Chapter 15 since the terms are
~(~ [icable only to Chapter 15. The TCC questions the use of TF_B that try to further define a term.
SUBMITTER: Technical Committee on Piping Systems RECOMMENDATION: 1. Revise the scope of Chapter 15 to read as follows:
15-1 Scope. This chapter addresses safety requirements for Medical and Dental Care Facilities that comply with the definitions of Medical Care Facility and Dental Care Facility as found in Chapter 2.
2. Add the following definitions in Chapter 2: Dental Care Facility. For purpose of this document, a health care
facility where patients are seen on an ambulatory basis and treated for dental procedures, and retain patients for < than 12 hr post procedure and not over night.
NOTE: Procedures may involve relative analgesia or conscious sedation. Medical Care Facility. For purposes of this document, a health care
facility where patients are seen on an ambulatory basis and treated for minor medical and surgical procedures, and retain patients < than 12 hr postprocedure and not over night.
NOTE: Procedures may involve relative analgesia or conscious sedation. Conscious Sedation. The use of oxygen and nitrous oxide and the
equipment to relieve anxiety and fear of medical and dental procedures.
NOTE: The patient is not rendered unconsdous and does not require an overnight stay in the facility. SUBSTANTIATION: Dental equipment manufacturers and installers report that they are encountering problems by enforcers who are confused, and feel that Type.II systems ~to not apply to situations where the patient is rendered unconscious, such as oral surgetTy. They feel it should be a type I medical facility because of lack of further definition. This is not the committees intent; however confusion in the interpretation is occurring. Conscious sedation is the proper term and the definition is provided by the American Dental Association.
The new definitions and revision are intended to remove the misunderstanding. COMMIlq'EE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMIT17EE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP64) Committee: I-IEA-PIP
99- 382 - (I 5-3.4 and Chapter 4): Accept " S U B ~ Technical Committee on Piping Systems RECOMMENDATION: 1. Revise Chapter 15-3.4 by adding a new note as follows.
96

N F P A 9 9 - - F 9 5 R O P
NOTE: Each of the various piped gas systems has sub classifications of Type I ,II, Ill, or IV. Therefore , it necessary to review each sub- system c o m p o n e n t [Nonf lammable medical gas, compresses g'asses for dynamic devices (air and ni t rogen) , vacuum, a n d WGD] independent ly to see if the requ i rements of a Type I, II, III or Type IV are appropriate.
2. Replace existing 15-3.4.1 with the following: 15-3.4.1 Pa t ien t Nonf lammable Medical Gas Systems 15-3.4.1.1 For purposes of this chapter , pat ient gas p ip ing systems
for nonf l ammable medical gas systems suppl ied f rom cylinders and providing regula ted 50 psig gas shall be classified as Type II if they conform to 4-6.2.4.1; otherwise they shall conform to Type I.
3. Replace existing 15-3.4.3 with the following: 15-3.4.3 Compressed Gas (Air /Nitrogen) Systems For Powered
Devices. 15-3.4.3.1 Air Compressor Supply. For purposes of this chapter , piped compressed air systems used to
power devices shall comply with the definit ion of a Type III Compressed Air System in Chapter 2 and shall conform to Chapter 4, Type III as def ined in 4-3.2.3, 4-4.2, and 4-5.2.
For purposes o f this chapter , p iped compressed air systems used to provide life-supporting air ( e.g., to operate a respirator, or . anes thes ia equ ipment ) shall be considered Type I and shall comply with 4-3.1.9, Type I .
15-3.4.3.2 Ni t logen Systems for Powered Devices. For purposes of this chapter, p iped n i t rogen systems used to power
devices operat ing at design pressures below 160 psig shall be considered Type III and shall conform to Chapter 4, Type III as def ined in 4-3.2.3, 4-4.2, and 4-5.2.
For purposes o f this chapter , any application o f a n i t rogen gas system above a des ign pressure of 160 psig shall be considered a Type I system and conform to Chapter 4 ,Type I.
15-3.4.4 Vacuum Systems. 15-3.4.4.1 For purposes of this chapter, Medical Surgical Vacuum
System applications as def ined in Chapter 2 shall be considered Type I and shall comply with the requi rements of 4-7 to 4-11.
15-3.4.4.2 For purposes of this chapter , vacuum systems complying with the defini t ion of a Type II Vacuum system as def ined in Chapter 2, shall comply with the requ i rements o f 4-7 to 4-11.
15-3.4.4.3 Vacuum systems complying with the definit ion of a laboratory vacuum system, as def ined in Chapter 2, shall comply with the requi rements of a type IV vacuum system as def ined in 4-7 to 4- 11.
15-3.4.5 Waste Gas Disposal. (Reserved.) 4. Retitle 4-6.2.4 to read: "4-6.2.4 Type II Piped Gas Systems." 5. Revise 4-6.2.4.1 to read: "Type II non f lammable medical gas
systems cover installations t h a t : . . . " (Subparagraphs a, b, c, and d remain unchanged . )
6. Delete existing paragraph 4-3.2.3.10. 7. Add a new 4-8.3 to read: "Laboratory Vacuum Systems.
(Reserved)" SUBSTANTIATION: At present, Chapter 15 treats all gas systems as Type II if the application meets the cylinder r equ i rements of 4-6.2.4.1. Tha t defini t ion is appropria te onlv for medical uas suoDiv
employing gas cylinders etc., d ispensing regulated '50 ps~ . " medical gases. It is no t appropriate for dental air supply systems which could be in located in ei ther a medical gas Type I or Type II system. The same s ta tement holds true for n i t rogen systems to power dynamic devices and for dental vacuum. The present T w e II definit ion is only ~errnane to medical ~as sunolv systems Drovid|ne regulated 50 osiiz~as t h rough a station~outldL" "
The T / C off PYpTng Systeffas has reviewed the 1993 edition of NFPA 99. In addit ion 12 type II manufacturers , the American Dental Association, and a m e m b e r of the USAF have been consulted. As issues were deliberated, the classification of gas systems by type came unde r review. The proposed changes are made with the following type classifications.
ype I Pat ient medical gas systems are those usually f ound in a hospital setting. The Type II pat ient medical gas systems are small systems normally found in dental and medical office applications.
Medical Compressed Air is similarly a type I system. However air classified as type II was no t really a small size medical air compressor system. It did no t p roduce medical quality air. It was a compressor system to power dynamic devices with a small a m o u n t of oil permissible, but o f a lower quality of air. It was more appropriate to consider it (dental air) as a type III compressed air system. The char t below resulted f rom tha t t hough t process and is the basis of the Facts that are p resen ted for consideration.
Proposed NFPA-99 Gas and Vacuum SYSTEM TYPES
Piping Systems Type 1 Type 2 Type 3
Medical Gasses Large Life Small Systems, Reserved oF~erating @ 50 Supporting with tank psg. mounted Pegs.
Laboratory Gasses Includes Flammable
Compressed Large Medical Small Medical Air Air @ 50 psig Air Reserved @
50 psig
Nitrogen 0-300 l~ig Reserved Systems srstems to drive
(tynamlC devices
Vacuum Med-Surgical Small norvlife ~tems Vacuum support Vac
sysL
WAGD (Both Large Systems Small systems gas & vacuum typical of typical of powered) Hospitals dental/medical
applications
Powered Device Air, @ 0-160 psig
0-160 p*tg to drive powered devices
Reserved
Type4
Laboratory
Laboratory
Laboratory
Laboratory
C O M M I T r E E ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 18 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP56) Committee: HEA-ELE
99- 383 - (18 (New)): Correlating Commit tee Note:. The Technical Correlating Commit-
tee (TGC) notes that the utle of the proposed chapter gives impression that NFPA 99 would cover "homes." The TCC directs the T / C on Electrical Equ ipmen t to prepare comments , and tide proposed Ch@te r 18 as "Electrical and Gas Equ ipmen t for H o m e Care," and that the scope be a m e n d e d to read as follows: "This chapter addresses the requ i rements for the safe use o f electrical an d gas equ ipmen t used for medical t r ea tment by patients outside heal th care facilities." In section 18-1 of proposal, paragraph one is to be made a Note unde r the above scope s tatement . SUBMITTER: Technical Commit tee on Electrical Eq u ip m en t RECOMMENDATION: Add a new Chapter 18 as follows:
Chapter 18 - H o m e Health Care Requi rements 18-1 Int roduct ion and Scope As part of the current .decentral izat ion of heal th care modalit ies
traditionally the province of hospitals, patients are being treated at h o m e using electrical and gas appliances which, if used in ano the r heal th care facility, would come unde r the purview of this s tandard.
This chapter addresses requ i rements to mitigate the possible hazards in the h o m e use of such equipment .
18-2 Reserved 18-3 Equ ipment 18-3.1 Reserved 18-3.2 Reserved 18-3.3 Reserved 18-3.4 Reserved 18-3.5 Reserved 18-3.6 Reserved 18-3.7 Electrical Equipment . Electrical Equ ipmen t used in the h o m e for hea l th care shall
conform to such requ i rements of Chapter 7 as applicable. 18-3.8 Gas Equ ipmen t Gas equ ipmen t used in the h o m e for heal th care shall conform to
such requ i rements of Chapter 8 as applicable. 18-4 Administrat ion. 18-4.1 Responsibility. It shall be the responsibility of the e q u i p m e n t supplier, which may
be a hospital, an equ ipmen t rental company or an equ ipmen t sales company, to:
(a) Appropriately instruct the equ ipmen t user to operate the equ ipmen t safely. This shall include written instructions, demonst ra- tions, and periodic review of the use.
(b) Provide instruct ion on user ma in tenance of the equipment , provide supervision of the main tenance , and provide such h ighe r level ma in tenance as is appropriate .
97

N F P A 99 - - F 9 5 R O P
SUBSTANTIATION: Recent FDA notification of electrocution from home use of prescribed medical equipment , particularly infant apnea monitors, has raised the committee 's concern regarding standards for medical equipment used outside health care facilities. The committee is r ecommending that a section be created in NFPA 99 to address the issue. COMMITFEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NEGATIVE: Lipschultz, Merrigan NOT RETURNED: Berger
EXPLANATION OF NEGATIVE: LIPSCHULTZ: I vote negative on this proposal because the scope
of the proposal is far too broad. The proposal is also extremely vague when it says "such requirements of Chapter 7 as are appli- cable."
MERRIGAN: My comments are as before: "The creation of a Chapter 18 for Home Health Care Requirements is completely outside the scope of the T/C, and probably the Health Care Facilities Project, as well. However, I would support a committee proposal for an addit ion to Chapter 7 (in Secddn 7-6, Administra- tion) containing the essence of what is in the proposed Section 18-4.1, hut limited to eouioment suPPlied by the health care facility. It could be argued that'th~s is also d~tside the scope of the T/G, but at least it involves requirements directed to health care facilities."
Committee: 99- 384- (19-1): Accept SUBMITTER: Eric P. Kindwall, Milwaukee, WI RECOMMENDATION: Substitute the following for the first sentence:
NOTE: During the past 20 years there has been a widespread interest in the use of oxygen at elevated environmental pressure to increase the partial pressure of oxygen in a patient 's tissues in order to treat certain medical conditions or to prepare a pat ient for surgery. " SUBSTANTIATION: The word drench, which was included in the first sentence previously is no t a medical term and is a translation of the term used by the original Dutch investigator. Using the term "partial pressure of oxygen" is more accurate. Additionally, ~0 io~ranhic theraDv is inaccurate. Radiography is for diagnostic purpJse~, and radiSiherapy is the use of ionizing radiation to kill tumor cells. The adjunctive use of HBO in radiotherapy is today little used. COMMITFEE ACTION: Accept. NUMBER OF COMMITIT~ MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svedik
(Log #CP57) Committee: HEA-HYP
99- 385 - (19-2.1.1): Accept SUBMITTER: Technical Committee on Hyperbaric al~d Hypobaric Facilities RECOMMENDATION: 1. Revise 19-2.1.1 to read as follows:
19-2.1.1 For Class A chambers located inside a building, the chamber(s) and all ancillary service equipment shall be protected by 2-hour fire resistive rated construction.
*Exception No. 1: Free-standing, dedicated buildings containing only a Class A chamber(s) and ancillary service equipment. (See Appendix A-19-2.1.1.)
Exception No. 2: Mobile, vehicle-mounted hyperbaric facilities not contiguous to a health care facility or not permanent ly affixed to a foundation."
2. Add the following new appendix material: A-19-2.1.1 Exception No.-l: For guidance on min imum constrUi>
tion requirements, depend ing on occupancy classification, see NFPA 101, Life Safety Code. SUBSTANTIATION: To clarify intent of requirements with respect housing for Class A chambers, as well as consider new configurations used for housing such chambers. COMI~flTrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 ABSTENTION: Hamilton NOT RETURNED: Hayes, Murray, Svedik
EXPLANATION OF ABSTENTION: HAMILTON: At the 1993 meet ing in Halifax this T / C v o t e d to
remove the requirement for a fire wall for Class A chambers, but this change was lost due to a technicality. It seems inappropriate to modify this section which should instead be eliminated.
(Log #CP28) Committee: HEA.HYP
99- 386 - (19-2.1.1.2): Accept SUBMITTER: Technical Committee on Hypberbaric & Hypobaric
• Facilities RECOMMENDATION: Add at the beginning of 19-2.1.1.2 to following:
"When used for hyperbaric procedures," SUBSTANTIATION: To allow m.ore flexible use a rogm(s) when such room(s) are no t being used for hyperbaric operations. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMrITEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #33) Committee: HEA-HYP
99- 387 - ( 1 9 - 2 . 2 . 2 . 3 Note 1): Accept in Principle SUBMITTER: Eric P. Kindwall, Milwaukee, WI RECOMMENDATION: Delete Note 1 entirely. SUBSTANTIATION: It is impossible to build a chamber without ;~ bilge, unless it is made of concrete. In Gratz, Austria, a large surgical chamber was built, and the bilge was filled with concrete. The concrete separated f rom the chamber wall when the chamber was
~ ressurized, however, and water and other contaminants ran down etween the concrete and the steel. Corrosion and bad smells
developed, and the concrete had to be removed with pneumatic hammer. C O i ~ I I T r E E ACTION: Accept in Principle.
Delete Notes 1 and 2. CoMMrITEE STATEMENT: Given the design of multiplace chambers, it is no t possible to construct a chamber without a bildge. NOTE 2 states the obvious, and is unnecessary. NUMBER OF COMMITTEE.MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #CP34) Committee: HEA-HYP
99- 388- (19-2.4.1.5): Accept SUBMITTERa Technical Committee on Hyperbaric & Hypobaric Facilities RECOMMENDATION: Revise beginning to read: "An alternative source for breathing air shall be available. . . " Rest the same. SUBSTANTIATION: There are other means of providing breathing sources other than SCBA. C O I ~ I I T r E E ACTION: Accept.
• NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #362) Committee: HEA-HYP
99- 389 - (19-2.4.2): Reject" SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: Add sentence as- "The compressor shall meet the requirements as def ined in Chapter 2 for medical air." SUBSTANTIATION: The existing text does no t address the quality of the compressor and air for which is produced regardless of technology. The existing text presents hazards and warnings but does not provide requirements for safety. Chapter 2 addresses these issues. COMMITrEE ACTION: Reject. COMMITTEE STATEMENT: Par. 19-2.4.2 addresses compressor intake. Issue of air quality and its monitoring is addressed in 19-2.8.7.1. NUMBER OF COIVlMITTEE MEMBERS ELIGIBLE TO VOTE: 13
98

N F P A 9 9 - - F 9 5 R O P
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svedik
(Log #1 ) Committee: HEA-HYP
99- 390 - (19-2.4.2.1): Reject Note: This proposal appeared as comment 99-181 which was held
for further study from the Fall 92 TCD, which was on proposal 99- 279 that appeared in Fall 92 TCR. SUBMITTER: John Howard Kimzey, Eagle Engineering RECOMMENDATION: Revise paragraph 19-2.4.2.1 to read:
19-2.4.2.1 Air purity shall be validated for Class A chambers by periodic gas analysis. As a minimum the TLV values of ACGIH, or OSHA's Chapter XVII - 29 CFR 1910.1000, shall be met except for the following:
Carbon dioxide - 500 ppm, byvolume, maximum Carbon monoxide - 10 ppm, by volume, maximum Halogenated compounds - 0.2 ppm, byvolume, maximum Total hydrocarbons (as methane - 25 ppm, byvolume, maximum.
SUBSTANTIATION: Ambient air qualityvaries considerably. Therapy may require exposures longer than 8 hours.
Safe TLV limits for 760 mm Hg may be unsafe for persons at hyperbaric pressures. COMMITrEE ACTION: Reject. COMMITTEE STATEMENT: The record of chamber operation and safety has been salutory using present requirements, e.g., 19- 2.8.7.1 requirements. NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #CPS0) Committee: HEA-HYP
99- 391 - (19-2.6.1): Accept SUBMY[q'ER: Technical Committee on Hypberaric & Hypobaric Facilities RECOMMENDATION: Revise to read:
"The room or rooms housing Class B chambers shall be afforded tection in accordance with 19-2.1.2."
ON: The hazards posed to the room in which Class B chambers are used are comparable to those created by Class A chambers. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 8 NEGATIVE: Messina, Workman NOT RETURNED: Hayes, Murray, Svetlik
EXPLANATION OF NEGATIVE: ME&SINA: Negative vote on Committee Action to accept - should
read to add as 2-6.3, not to replace or change 2-6.1. WORKMAN: Concur with Messina's rationale.
(Log #CP35) Committee: HEA-HYP
99- 392 - (19-2.7.1.6): Accept SUBMII~I'ER: Technical Committee on Hyperbaric & Hypobaric Facilities RECOMMENDATION: Revise "safely terminate a dive" to read "safely decompress the chamber." SUBSTANTIATION: Avoid use of slang terminology. COMMITTEE ACTION: Accept NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svedik
C o mmitte e :( ~-~2~1]-~ 99- 395 - (19-2.7.3): Accept in Principle in Part SUBMITTER: Maurice Brooks, Sechrist Industries, Inc. RECOMMENDATION: Revise the following:
19-2.7.3 Wiring and Equipment inside CI~sA Chambers. Wording added.
SUBSTANTIATION: The requirements of 19-2.7.3.11 are too restrictive for speakers and microphones used in Class B Chambers for communications. Adequate safety precautions for Class B Chambers are already required bySection 19-2.7.6, in which the types of equipment are limited to communications or patient physiological monitoring leads, the power is limited to 28v and 1/2w and flammable liquids, gases, or v'4pors are prohibited inside the chamber. This does not change the requirements for wiring inside the chamber. COMMITTEE ACTION: Accept in Principle in Part.
1. Add a new subpar. (d) in 19-2.7.3.11 to read as follows: "(d) For communication equipment such as speakers and
microphones, the allowable energy (voltage andpower) shall meet the requirements of 19-2.7.6.1." 2. Revise title of 19-2.7.6 to read as follows: "Additional Wiring and Equipment Requirements inside Class B Chambers." 3. Delete 19-2.7.6.2., and renumber accordingly. COMMITTEE STATEMENT: 1. Adding this paragraph addresses submitter's concerns by expanding the scope of 19-2.7.3.11 to allow continuation of speakers and microphones currently in Class A and B chambers that have proven effective for many years, but do not meet the strict criteria in 19-2.7.3.11 (a) to (c). 2. Clarify intent that 19-2.7.5 and 19-2.7.6 applies to Class B chambers. 3. Editorial in light of action of item 2. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svedik
(Log #CP25) Committee: HEA-HYP
99- 394 - (19-2.7.6.4): Accept SUBMITIXR: Technical Committee on Hyperbaric & Hypobaric Facilities RECOMMENDATION: Move 19-2.7.6.4, and make it new 19-3.5.1.2(b). Make existing text of 19-3.1.5.2 as 19-5.1.5.2(a). For existing Exception, add at the beginning "For Class A chambers, f lammable. . ." remainder the same. SUBSTANTIATION: Editorial as current 19-2.7.6.4 is not in an appropriate location. COMMITTEE ACTION: Accept. NUMBER OF COMMITIT_~ MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 7 NEGATIVE: Messina, Sheffield, Workman NOT RETURNED: Hayes, Murray, Svedik
EXPLANATION OF NEGATIVE: ME&SINA: Negative vote on Committee Action - error in Recom-
mendation: should be "make it new 19-3.1.5.2(b)." SHEFFIELD: Recommendation: Should read "Move 19-2.7.6.4 and
make it new 19-5.1.5.2(b)..." WORKMAN: Concur with rationale of both Sheffield/Messing.
(Log #127) Committee: HEA-HYP
99- 395 - (19-2.8.1 (New)): Accept in Principle SUBMITTER: Manrice Brooks, Sechrist Industries, Inc RECOMMENDATION: Add:
Exception: communications and monitoring equipment located inside Class B Chambers shall meet the requirements of 19-2.7.6.1. SUBSTANTIATION: The requirements of 19-2.7.3~11 are too restrictive for speakers and microphones used in class B Chambers for communications. Adequate safety precautions for Class B Chambers are already required by Section 19-2.7.6, in which the
• types of equipment are limited to communications or patient physiological monitoring leads, the power is limited to 28v and 1/2w and flammable liquids, gases, or vapors are prohibited insid, e the chamber. COMM/"/TEE ACTION: Accept in Principle. See committee action on Proposal 99-393 (Log #126).
COMMI'VI'EE STATEMENT: Issue is addressed by committee action on Proposal 99-395 (Log #126). NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 1B VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svedik
99

N F P A 99 - - F95 R O P
(Log #264) Committee: HEA-HYP
99- 396 - (19-2.8.7.1): Reject SUBMITTER: Antonio A~ Mesa, Nash Engineering Co RECOMMENDATION: Change fom~h sentence to read: Air compressors shall be as defined in Chapter 2-2, Medical Air Compres- sor, and meet the criteria of 4-3.1.9.1 and 4-3.1.9.5. SUBSTANTIATION: Hydrocarbon vapor in oil lubricated compressors cannot be filtered effectively and may pose a fire and air quality hazard. Carbon monoxide may also be generated form hydrocarbons during compression. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: With proper maintenance and current purification techniques, the use ofoil lubricated compres- sors have been found to meet air quality criteria for hyperbaric chambers. Alarms, monitors and shutdown capabilities are currently included in compressors used for chambers. Text is being clarified to further reflect this [See Committee
Proposal 99-399 (Log #CP26).] NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
Committee: " 99- 397- (19-2.8.7.1): Reject
SUBMITTER: Antonio A. Mesa, Nash Engineering Co RECOMMENDATION: Change the last sentence as underlined:
...shall meet the requirements of Chapter 2-2, Medical Compressed Air. SUBSTANTIATION: 1. Consistency.
2. Grade D allows higher levels of carbon monoxide and carbon dioxide than is allowed inUSP.
3. USP reference considered more appropriate for medical air. 4. CGA grade D allows "condensed hydrocarbon", which is oil.
COMMITrEE ACTION: Reject. COMMITTEE STATEMENT: Same reason as given in Proposal 99-390 (Log#l) since issue is the same. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #363) Committee: HEA-HYP
99-398- (19-2.8.7.1): Reject SUBMITTER: Dennis Murray, American Hospital Association RECOMMENDATION: Add to the last sentence - as Grade D "and medical compressed air as defined in Chapter 2." SUBSTANTIATION: The existing text does not address the quality of air produced beyond the CGA reference. Chapter 2 addresses these issues. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Same reason as given in Proposal 99-390 (Log#l) as issue is the same. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #CP26) Committee: HEA-HYP
99- 399 - (19-2.8.7.1): Accept SUBIVl]TTER: Technical Committee on Hyperbaric & Hypobar~c Facilities RECOMMENDATION: Revise sentence 4 to read:
"Air supplied from oil-lubricated compressors, capable of contami- natin~ the comnressor outout due to wear or failure, shall be continuously.. '." (rest the same) [change underlined] SUBSTANTIATION: Clarifying that there are oil-lubricated compressors that will not contaminate compressor output with oil under any failure condition (e.g. rotary or screw drive compressors). COMMITI'EE ACTION: Accept. NIYMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #CP31) Committee: HEA-HYP
99- 400 - (19-2.8.7.1): Accept SUBMITTEI~a Technical Committee on Hyperbaric & Hypobaric RECOMMENDATION: 1. Make sen tence2a NOTE.
2. Delete "sometimes" in sentence 2. SUBSTANTIATION: 1. Conform to NFPA style manual.
2. Redundant. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 8 NEGATIVE: Sheffield, Workman NOT RETURNED: Hayes, Murray, Svetlik
EXPLANATION OF NEGATIVE: SHEFFIELD: Recommendation: Does not make sense unless it is
referring to sentence 3, not 2. WORKMAN: Concur with Sheffield's rationale.
(Log #CP32) Committee: HEA-HYP
99- 401 - (19-3.1.3.1): Accept SUBMITTE~ Technical Committee on Hyperbaric & Hypobaric Facilities RECOMMENDATION: Revise 19-3.1.3.1 to read:
"Personnel having, res.ponsibility . . . . . . . for the hyperbaric facility, and those responsible for hcensmg, accrediung, or approwng msutuuons or other facilities in which hyperbaric installations are employed shall establish and enforce appropriate programs to fulfill the
g rovisions of this chapter." UBSTANTIATION: Current text does not conform to NFPA Style
Manual. Change establishes clarity of responsibility. COMMITrEE ACTION: Accept. NLVMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #CP27) Committee: HEA-HYP
99- 402 - (19-5.1.5.3(c)): Accept SUBMITTER: Technical Committee on Hyperbaric Hypobaric Facilities RECOMMENDATION: Revise 19-3.1.5.3(c) "conductive strap" to read "conductive pathway" SUBSTANTIATION: Present wording is too restrictive, Patients . can be adequately grounded using other modalities, such as conductive mattress covers. COMMITrEE ACTION: Accept. NUMBER OF COMMI'VrEE MEMBERS ELIGIBEE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #205) • Committee: HEA-HYP
99-403- (19-3.1.5.4(c)): Accept in Principle SUBMITTER: John S. Selby, S.O.S. Limited RECOMMENDATION: In Class A and Class B chambers with oxygen-enriched atmospheres, electrical grounding of the
g atient... (as before) UBSTANTIATION: SOS Limited have developed a non-metaUic
folding portable hyperbaric chamber as per the enclosed brochure. We have used NFPA 99 in the development of the chamber. However the 'Hyperlite' chamber differs from normal Class B chambers in that the chamber is pressurized with air and the patient breathes oxygen through a BIBS system. In our view neither the "Hyperlite" chamber or its patient needs earthing. COMMITrEE ACTION: Accept in Principle. Wording in 19-3.1.5.3(c) in the 1994 edition of NFPA 99 [formerly
19-3.1.5.4(c) in the 1990 edition] was revised. COMMITrEE STATEMENT: Par. referenced is from 1990 edition. Wording was revised meeting submitter's concern. NUMBER OF COMMITTEEMEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
100 4

N F P A 99 - - F 9 5 R O P
(Log #CP33) Committee: HEA-HYP
99- 404- (19-3.1.5.7): Accept SUBMrVrER: Technical Committee on Hyperbaric & Hypobaric Facilities RECOMMENDATION: Delete sentence 2. SUBSTANTIATION: Provision is not enforceable. COMMITTEE ACTION: Accept. NUMBER OF COMMITrEE MEM]~ERS ELIGIBLE TO VOTI~: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svetlik
(Log #63) Committee: HEA-PIP
09- 405 - (A-4-4.2.11): Reject SUBMITrER: Dale Dumbleton, American Medical Gas Institute RECOMMENDATION: Delete following text:
One of the major concerns is the cross-connection of piping systems of diite(ent gases. The problem of cross-connection of oxygen and other gases such as nitrous oxide, air and nitrogen can readily be recognized/prevented by the use of different sizes of tubing. It is recommended that piping and manifolds for oxygen servicb be of a different size than-the l~ping intended for other gas services. The piping for other than oxygen may be of smaller size. Generally, oxyktn is installed in 1/2-in. O.D. tube size and other gases with 3/8-]n. O.D. tube size. SUBSTANTIATION: The design criteria for systems of medical gases are predicated on flow, pressure, and friction loss due to pipe runs and quantity of fittings. In normal design each piping system will have a variety of pipehne sizes making it virtnally'ln~possible to distinguish oxygen piping from other gas systerus by line size. COMMITTEE ACTION:- Reject. COMMrlTEE STATEMENT: Text is applicable to Type II medical
i ed tems, and is informato only_. ~ ' a R S ~ F COMMITTEE M ~ I ~ ELIGIBLE TO VOTE: 18 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 16 NOT RETURNED: Fan, Shoemaker
(Log #CP22) Committee: HEA-ELE
99- 406 - CA-7.5.1.3.$ and A-9-2.1.13.3): Accept SUBMITrER: Technical Committee on Electrical Equipment RECOMMENDATION: 1. Revise value for capacitor in diagram from "0.015 microfarad" to "0.05 microfarad."
2. Add at end of current text: "For maximum chassis leakage current allowed (i.e., 300 microam-
peres) below 1 KHz, this network will yield the limiting current of 10 ma above 30 KHz." SUBSTANTIATION: To reflect the increase in the value of chassis leakage current allowed (from 100 to 300 microamperes). COMMITrF..E ACTION: Accept. N MBER OF COMMYI'rEE MEMBERS ELIGIBLE TO VOTE: 12 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 11 NOT RETURNED: Berger
VOTE ON COMMITTEE ACTION: AFFIRMATIVE: 11 NOT RETURNED: Berger
(Log #CP43) Committee: HEA-LAB
99- 408 - (A-10-1.1): Accept SUBMITrE_Ik Technical Committee on Laboratories RECOMMENDATION: Delete reference to NFPA SPP-51 docu- ment. SUBSTANTIATION: Out of print. COMMITTEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #CP44) Committee: HEA-LAB
99- 409 - (A-10-8): Accept Sl . IBMrrrE~ Technic~al Committee on Laboratories RECOMMENDATION: I. Replace current text of A-10-8 with the following:
"Comprehensive discussions of the goals and procedures to provide safe working conditions in clinical laboratories are available from the National Ctmmittee for Clinical Laboratory S/andards. (See A~.pendix B-1.2.6.)"
Replace existing reference in Appendix B-1.2.6 with the following new references:
GP17-T" Guidelines for Laboratory Safety GP5-A Clinical Laboratory Waste Management M~3-T2 Protection of Laboratory Workers from Infectious Disease
Transmitted by Blood, Body Fluids, and Tissue. SUBSTANTIATION: NC, CI_.S AS-1 is no longer available, and there are other more relevant documents now published by NCCLS. COMMITrEEACTION: Accept. " NUMBER OF COMMI'VrEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log #CP45) Committee: HEA-I_AB
99- 410 - (B-1.2.5 and B-3): Accept SUBMITTER= Technical Comrm'ttee on Laboratories RECOMMENDATION: 1. For B-1.2.5, change address of JCAHO to:
One Renaissance Blvd., Oakbrook Terrace, IL 60181 2. For B-3, change address of College of American Pathologists to: 325 Wankegan Road, Northfield, IL 60093
SUBSTANTIATION: Organizations have moved. COMMITrEE ACTION: Accept. NUMBER OF COMMI'VI'EE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 9 NOT RETURNED: Linder
(Log#CP24) Committee: HEA-ELE
99- 407 - (A-9-2.1.13.4(c)): Accept SUBMITTER: Technical Committee on Electrical Equipment RECOMMENDATION: 1. Revise paragraph 3 ("For equipment in t he . . . ' ) to read as follows:
"For equipment in the patient care vidnity, it seems reasonable to reduce thig- limit ~ because of . . . " [change underlined]
2. In paragraph 3, subparagraph (f), change "100" to "300." 3. In paragraph 4: , a) Delete sentence 1 (' For the above reasons . . . . "). b) Revise sentence 2 to read: "It should be emphasized that the
reduced leakage current limit is no t . . . " c) In sentence 3, change "100" to "300." 4. In paragraph 5, next to last sentence, change "10 microam-
peres" t-o '10 ..micr°amperes with the ground inLact (i..e under normal conditions)."
5. In paragraph 5, subparagraph (c), change "10 micro amperes" to "10 microamperes with the ground intact (i.e. under normal conditions)." SUBSTANTIATION: Correlate with changes made in requirements
rtion of document. MMITTF~ ACTION: Accept.
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 12
(Log #28) Committee: HEA-ESE
99- 411 - (G-3-1): Reject SUBMIT1T, R: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Revise Figure C-3.1 to indude fire pump and add new Figures C-3.2 and C-3.3 such that there are Typical Hospital Wirinl~Arrangements for small and large hospital~. SUI~TANTIATION: The intent is to resolve the confusion and provide some guidance on how fire pumps are to be connected in the complicated electrical systems found]n hospitals.
Most major hospitals have fire pumps and the issue needs to be addressed. COMM/TrEE ACTION: Reject. COMMITTEE STATEMENT: Committee believes NFPA 20 adequately describes fire pump installation for emergency power syste'ms. Drawings are mis-leading because there are multA'ple ways of making the utifity connection. NUMBF~ OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
101

N F P A 99 - - F95 R O P
Small electric system-hospitals (single transfer switch)
Normal sources
M o i ~
Nonessential loads
Fire Pump
Alternot,
M J v
Essential electrical system (150 kVA or less)
17 Overcurrent protection -
[ - ~ Automatic switching equipment
Transformer
(~) Generator
source ;)
Main
Fm~u'e C-3.1 99-411 (Log #28)
lyp*col large electrical system - hospitals Normo~ Normo~ sources sources
~ ~ Normal;y open secondary tie ~'~fcvercurrent d e v i c e (outcm~otic
Nonessenh¢31 loads Fire Equipment L CnticoI ;)ump system . br~n~h
• Life safely branch
Y Essentio~ electrlcal system
/dlecnate sources
T,ronsformer [ ] Automatic switching equipment
Generator [ ] Delay outomot,c switching means O~erc~rtent I=ro~ect~oo [ ] Ma~UQI switching meons
Figure C-~-3 Typical hospital wiring arrangemenL - - 99-411 (Log #28)
(Log #389) Committee: HEA-ESE
99- 412 - (Figure C-5-1): Reject Staff Note: This proposal was originally submitted on NFPA 70,
Article 517, Diagram 517-30(1),(2),(3). It is being acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SUBMITTER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Revise the diagrams as shown on the attached sketches to include automatic transfer switches for fire pumps.
Smotl electrical system - hospitals
Small electrical system - hospitals
Main
Nonessential loads
Normal sources
Life safety Critical branch branch
v Essential electrical system
Alternate source
Main
!,.! Normal sources
Main
Nonessential loads
Alternate source
Main
Life safety Critical branch branch
V Essential electrical system
I-I Overeurrent protection --~ Automotic switching
equipment
[ " ~ Delay automatic switching equipment
Transformer"
(~) Generator
Figure C-3.2 99-411 (Log #28) '
C] Overcurrent protection ~ ] Automatic switching
equipment
" ~ Delay automatic switching equipment
Transformer
(~ Generator
F~ure C-$.1 99-412 (Log #389)
102
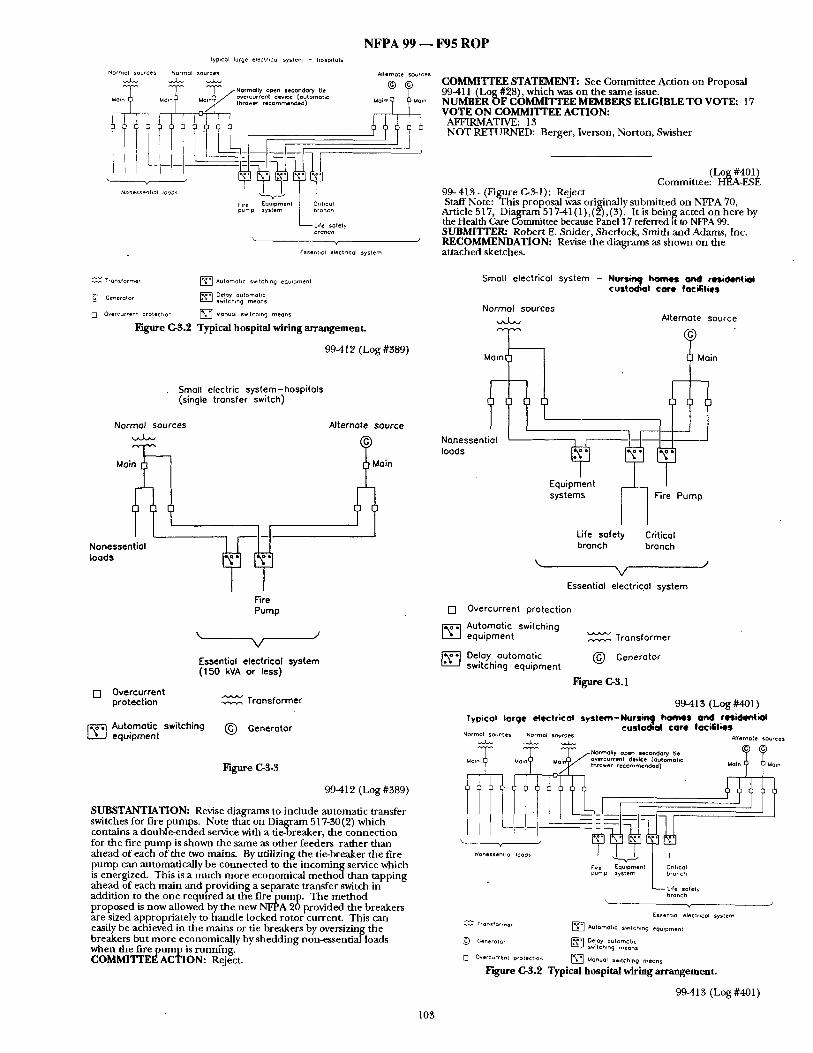
N F P A 9 9 - - F 9 5 R O P lyp,cal laroe electrlcol syslem - hospdoIs
Norrno~ sources Normal sources
T T T / N .. . . ,,yD.. . . . . . . o ° ~ , , . .. overcurrent device {outomotlc
Fire Equ*pmennt L Cr't Ical pump system branch
Life sofety b r o a c h
\ v
Essent,ol electrical system
A*ternot e sources i~n COMMI'VrEE STATEMENT: See Commit tee Action on Proposal 99-411 (Log #28), which was on the same issue. NUMBER OF COMMITTEE MEMBERS ELIGIBLE T O VOTE: 17 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #401) Committee: HEA-ESE
99- 413 - (Figure Cr3-1): Reject Staff Note: T h i s proposal was originally submit ted on NFPA 70,
Article 517, Diagram 517-41(1),(2),(3). It is bein~g acted on here by the Health Care Committee because Panel 17 referred it to NFPA 99. SLrBMITTER: Robert E. Snider, Sherlock, Smith and Adams, Inc. RECOMMENDATION: Revise the diagrams as shown on the at tached sketches.
Transformer [ ] Autamot,c switch,n O eQu,pment
C~ Generotor [ ] Deloy outomoh¢ switch,no meons
00ve rcu r ren t protect,on [ ] MonuQI swdchmg means
F~b~me C-S.2 Typical hospital wiring arramgemeat.
99-412 (Log #389)
Small electric system-hospitals (single transfer switch)
Normal sources Alternate source
Nonessential loads
Fire Pump
I°in \ J
V
Essential electrical system (150 kVA or less)
F'I Overcurrent protection ~ Transformer
-----;] Automatic switching equipment
(~) Generator
Figure C-S-3
99.412 (Log #389)
SUBSTANTIATION: Revise d iagrams to include automat ic transfer switches for f i r epumps . Note that on Diagram 517-30(2) which contains a double -ended service with a tie-breaker, the connect ion for the fire p u m p is shown the same as o ther feeders ra ther than ahead of each o f the two mains. By utilizing the tie-breaker the fire p u m p can automatically be connec ted to the incoming service which is energized. This is a m u c h more economical m e t h o d than tapping ahead of each main and providing a separate transfer switch in addit ion to the one required at the fire pump. T he m e t h o d proposed is now allowed by the new NFPA 20 provided the breakers are sized appropriately to handle locked rotor current . This can easily be achieved in the mains or tie breakers by oversizing the breakers but more economically by shedd ing non-essential loads when the fire p u m p is runn ing . COMMITTEE ACTION: Reject.
Small electrical system - Nuts.. homel Or~ll resident~l custodial core focilitiel
Normal sources
Mainl
Nonessential loads
Alternate source
Main -) 1
Pump
Life safety Critical branch branch
\ J V
Essential electrical system
[] Overcurrent protection
[ ~ utomatlc switching equipment Transformer
[ ] Delay automatic ( ~ Generator switching equipment
F ~ u r e C-S.1
9941 $ (Log #401 ) Iypleat large electrical s y s t e m - N u r $ ~ , homes ond relfidentiol
custodial core focifities Normal sources NormoJ sources ~Uternote sources
.. ~ / o v e r c u t r e n t device (automohc
Nonessenhot IDeaS
Flre Equ'pment L Cnbcol pump SyStem branch
Life safety bra~c~
y--. /
Essent,ol electrical system Transformer [ ] Automobc swdch,n o eoulpmen t
Generator [ ] Delay automc[*c swat ch,n O means
[ ] Overcurr~nt protechon [ ~ M(~nuol s~,tchlng means
Figure C-3.2 Typical hospital wiring ar rangement .
99.4413 (Log #401)
105

N F P A 9 9 - - F 9 5 R O P
Small electric system-Nurstn9 homes anO resiOentiol custodial core f ocilitie$ (single transfer switch)
Normal sources
M o i ~
Nonessentiol Ioods
F~re Pump
Alternote source
i oin
V
Essential electrical system (150 kVA or less) [ ] Overcurrent protection Transformer
~--~ Automatic switching equipment (~) Generot0r
F'~gure C-$-$
99-413 (Log #401)
SUBSTANTIATION: Revise diagrams to include automatic transfer switches for fire pumps. COMMITYF_.E ACTION: Reject. COMMITTEE STATEMENT: This proposal is the same as Proposal 99411 (Log #28), and is reiected for the same reasons. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 17 VOTE ON COMMITITEE ACTION:
AFFIRMATIVE: 13 NOT RETURNED: Berger, Iverson, Norton, Swisher
(Log #CP48) Committee: HEA-LAB
99- 414- (C-10-1): Accep t SUBMITTER: Technic~d Committee on Laboratories RECOMMENDATION: 1. Delete the following incidents from the current list o f fire incidents: Walking motor fire, Incinerator explosion, Perchloric acid
explosion, Cellulose nitrate centrifuge tubes, Explosion hazard of scintillation counter, Pressure filter fire, Ampuls Explode, Chroma- tography fire hazard, Cyclopropane explosion, Centrifuge fire, Sp-m " n-ing gas cylinder, Stea/n b~th flasfi, Fume hood ape-ration. [Retain following incidents: Tissue processor fire, Hot plate fires, Refrigerator explosion, Water bath fire, Peroxide explos-ion]
2. Add the following incidents to the list of fire incidents:
Iowa October 1980 A hospital fire, originating in a second-floor pathology laboratory,
occurre-d when electri- ca l w~res arced and ignited clotli-towels placed under beakers. The beakers contained tissue samples, alcohoI and formaldehyde. The contents of the beakers causei!l the fire to spread to other larger containers of chemicals in the lab. There was2120 to 30 minute delay in detect ion of this fire because
there was no automatic smoke detection equipment in the labora- tory. Smoke detectors in the air ducts Ioc~tedin the hallways did operate when the smoke filtered out of the lab. There was no automatic sprinkler system.
No other specifics were repor ted as to the cause of the electrical arcing.
Direct property damage was estimated at $20,000. Pennsylvafiia December 1980 A small fire, of electrical nature, broke out in a hospital laboratory.
The fire involved a condensate drip tray which was used to dissipate
104
water from a refri~:emtor unit. The probable fire scenario was that a short circuit re'surfed from the aging rubber insulation of the cord. The unit is always left "on."
No direct property damage was repor ted for this fire. There were no automatic sprinklers in the lab area of the hospital. There were heat detectors in the area, but no smoke detectors. The fire generated large amounts of smoke.
Rhode Island October 1981 A fire occurred in a blood b a n k / d o n o r lab in a hospital. A pat ient
was lying on one of three contour couches in the donor room giving blood. The technician pushed a button to raise the couch, then heard a pop, and saw flames and smoke coming from the couch. The technician tried unsuccessfully to extinguish the fire with a PAortable fire extingt~)sher.
supervisor pulled the manual pull station and the fire depart- m e n t arrived within 3 minutes. -
One civilian and one fire fighter were injured in the fire. There was extensive smoke and soot dafiaage in the area. Direct
property damage was estimated at $12,000. The fire occurred in an unsprinklered building.
The cause of the fire was de te rmined to be a short circuit in the wiring in the motor of the couch.
New Jersey April 1982 A small hospl'tal fire occurred in a processing laboratory where
tissue samplts are cut and moun t ed in metal or polypropytene cassettes and then run through a processor. In the processor, the moun t ed samples are d i p p e d i n a-series of baths. The cassettes were stored in polystyrene cabinets.
The cause of the fire was undetermined. Damage was confined to a six square foot area in the c o m e r of the tissue lafi. The fronts of the cassette cabinets suffered partial meltinl~ and some cassettes had the p a r ~ m melted. It was esumated that 81)% of the specimencasset tes were intact and salvageable.
Total direct property damage was estimated at $70,000 and business interrupt ion at $4,000. A single sprinkler head operated and extinguished the fire. The
waterffow ~larm was received by the hospital switchboard an.d the municipal dispatching service.
Massa-chnse(ts April 1982 A tissue laboratory in a hospital was the scene of a fire which
resulted in $50,000 in direct property damage. An additional $50,000 was lost due to tmsiness interruption.
The tissue lab was located in the pathology area of the lab building and housed 11 tissue processing machines. Eight o f the machines were used to dehydrate tissue samples in a xylene concentrated solution or an alcohol solution.
When a technician left the room at 5:15 p.m., all the machines were functioning properly. Twenty minutes later, a waterflow and smoke detection alarm was received at the command center with direct transmission to the fire depar tment . Two sprinkler heads he lped control the fire. The fire was extinguished by the fire depar tment ruing a 1 1/2" hand line f rom an interior standpipe. The fire was atWibuted to the j amming of one of the baskets at a p r o c e s s i n g machine as itwas being moved from one carriage to a n o t h e r . T h e motor failed to shut down as it should have, overheated, and eventually ignited the flammable xylene and alcohol solutions. Tennessee May 1984 The overheating of xylene inside a distiller located in the hospital
lab resulted in a/ ire. Apparendy, the escaping flammable vapors were ignited by ordinary electrical equipment~m the room. Prompt and effective automatic sprinkler activaiion he lped minimize fire damage.
The fire occurred in a fourth floor histology lab. Among the contents of the lab were small xylene stills f t r reclaiming used solvent, and also tissue processing equipment. A techniC:Jan had filled the distiller with xylene. Some time later, another person working in the area of the distiller noticed that an odor x~as coming f rom die uni t and that the solution had a brown color to it. This employee left to f ind someone to inspect the distiller. This employee re turned with another worker to f ind a grayish haze a r o u n d t h e console. Just after leaving the room, the employees saw smoke coming f rom under the door. A "Code Red" was-sounded and the lab was evacuated. The technician who originally was running the machine re turned at the sound of the alarm and tried to turn off the ins t rument by crawling on the floor, but was unable to do so because of the smoke and smell of xylene.
Property loss was estimated at $150,000, and business interrupt ion resulted in an additional $15,000.
Florida December 1985 A fire broke out in a hospital pathology lab and resulted in
$100,000 in property damage, and an additional $2,000 in business interruption. The pathology lab analyzes tissue samples f rom patients. These samples a represe rved in an embedding center using paraffin as the preservfng agent.
• The cause of the fire was de te rmined to be the failure of a thermostat which controls the temperature of the heating e lement that melts the paraffin in the tissue-embedding center. -
The fire damaged two tissue embedding cen(ers, an ultrasonic cleaner, two light fixtures., a wood wall cabinet, as well as damaging
N F P A 99 - - F 9 5 R O P
the wall and ceiling. Microscopes, computer terminals, measuring equipment, and tissue slides and samples were among the items ddmaged by smoke and soot. The fire dainage was confine~! to the lab.
An employee smelled smoke coming from the lab and noticed that the lab door was hot. A security guard was called immediately and pulled the alarm at a manual stauon in the hallway. The fire depar tment extinguished the fire with dry chemicals and an inside hose stream located in the hallway. There were no heat or smoke detectors inside the pathology lab. The building was unsprinklered.
New York April 1988 A hospital laboratory was the scene of $250,000 fire. The fire
started when a professor was sterilizing a pair of scissors using the "flaming" procedure. The "flaming" method involves dipping an item into filcohol and then burning off that alcohol with a Bunsen burner. Theprofessor carried out ihe procedure once, then tried to do it a second time because he thought he had contaminated the scissors. D u r i n g the second attempt, the alcohol he dipped the scissors into ignited because the sossors were still h o t The container of alcohol was d ropped and the fire spread to nearby combustibles, including other flammable liquids. A security guard not iced the fire and immediately pulled the alarm
signaling the fire depar tment and hospital fire brigade. The fire d tpar t rdent responded promptly and extinguished the fire.
There were n t a u t o m a t i c sprinklers in the fire area. Three civilians were injured in the fire.
California April 1989 The thermostat of a low temperature lab oven (incubator)
malfunctioned, causing the oven to overheat. The unit heated to approximately 200 ° overnight, causing a smoldering fire. An employee discovered the fire in the sixth-floor laboratory in the medical center when he arrived early to work. His first action was to shut o f f the incubator, after which he called the fire depar tment .
Fire destroyed the contents of the incubator, and the incubator itself neededrepa i r s due to exposure to dry powder agent. Smoke damage also occurred in the lab and hallway. Property damage was estimated at $1,000. An alarm sounded after the fire depar tment had used an extin-
guisher on the fire. The type of alarm was not reported. California November 1989 Four fire fighters were injured at a fire in a pathology lab at a multi-
story hospita] medical center when they were exposed to toxic chemical debris and human tissue. The fire originated in a stainless steel cabinet which had two glass windowed doors. There were two pieces of equipment in the cabinet which were used to process tissue by dipping ixays of tissues into a series of containers. The machines were about 20 years old.
The official cause of the fire was listed as a malfunctioning piece of electrically powered lab equipment igniting volatile f lammable liquid. The exact point offal'lure could not be determined. Automatic de tecuon equipment was present and operated. There
was no automati'c sprinkler system present in the lab. Direct property loss was estimated at $32~,000. No estimates were given for business interruption. .
Michigan March 1981 A buiRiing which housed various analytical research and develop-
men t laboratories was the scene of a $60,000 fire. The' laboratory involved in the fire was used essentially for liquid and gas chroma- tography.
The fire occurred when solvent leakage inside, or adjacent to, a liquid chromatograph ignited f rom an electrical source. Apparendy, a small amount of solvent was spilled for up to 25 minutes and subsequently ignited. The fire bu rned through a plastic tube feeding a waste solvent container on a shelf. T h e spilled waste solvent intensified the fire. Liquid chromatography uses solvents of methanol and iso-octane.
An employee first heard a crackling and then saw flames at the base of the liquid chromatography instrument. Employees immediately attacked the fire with a dr~ chemical fire extinguisher. Also, two sprinkler heads operated, limiting the spread of fire within the la-boratory. The fire depar tment received a watertlow alarm, a manual fire alarm box, and several phone calls. Fire fighters found the fire nearly out on arrival because of sprinkler activation ancl consumption of the spilled liquid.
Virginia June 1981 A small fire occurred in a laboratory which manufactures inter-
feron. During this process, red and white blood cells are separated, and the white cells are placed in beakers with nutrients. A~nrus is in t roduced to the white cell cultures which then produce the interferon. A centrifuge is used to separate the interferon from the white cells. The process is carried out in a small refrigerated room isolated from other areas by insulated metal panel wails and ceiling.
In the early afternoon, an employee stabilized a magnetic stirring rod which had been banging the side of one of the glass beakers. Minutes later, personnel no~ced smoke and fire within the refrigerated room and immediately extinguished the fires with extinguishers. The fire depar tment also was notified. Alcohol spilling onto the-electrical parts of the magnetic stirrer
caused the-fire. ~l'he spilling was caused by inadequate supervision of the magnetic stirrer.
The fire resulted in $235,000 in direct property damage and an additional $40,000 in business interrupUon. Metal walls and ceiling panels, some laboratory equipment, and an unknown quantity ot mterferon were destroyed or damaged in the fire.
There were no automatic detection or suppression systems in the building. There were manual pull stations and portable extinguish- e r s .
SUBSTANTIATION: Laboratory practices have changed. As an aid to users of document , Committee wants to have a list of incidents that are relevant or typical to current laboratory practice. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 10 VOTE ON COMMITTEE ACTION: • AFFIRMATIVE: 9
NOT RETURNED: Linder
Committee: ~-~fi~#I-~ 99- 415 - (G-19-1.2.5.1): Accept in Principle SUBMITFER: Eric P. Kindw:all, Milwaul(ee, WI RECOMMENDATION: Delete paragraph C-19.1.2.5.1 SUBSTANTIATION: All of the vcords contained in the above-names paragraph were contained in C-19.1.2.5, namely illuminating lamps, vacuum tubes, and overloaded fans, as sources of ignition. COMMITrEE ACTION: Accept in Principle.
Revise C-19-1.2.5.1 to a NOTE-under C-19.1.2.5. COMMITTEE STATEMENT: Information is relevant, but only as a clarification, and thus made a NOTE. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 ' NOT RETURNED: Hayes, Murray, Svetlik
(Log #CP29) Committee: HEA-HYP
99- 416 - (C-19-1.3.1): Accept Correlating Committee Note: The Technical Correlating Commit-
tee desires the TC to review the applicability of this recommendat ion to any occupant or occupants of c~iamber. SUBMITTER: Technic.ill Committee on Hyperbaric & Hypobaric Facilities RECOMMENDATION: 1. Change title of C-19-1.3 to: "Pathophysi- olo~cal, Medical, and other related hazards.
2. Insert new C-19.1.3.1 to read: "Exposure of p r egnan t chamber attendants to hyperbaric atmospheres may result in fetal risk." Renumber accordingly. SUBSTANTIATION: Research suggests t ha tp reg~an t woman, exposed to hypbaric air, maybe have increased lethal risk. COMMITTEE ACTION: Accep t NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITFEE ACTION:
AFFIRMATIVE: 13
Committee: ~°Fa~?I~ 99- 417 - (C-19-1.3.1.2): Accept $ U B M I T r E ~ Eric P. Kindwfill, Milwaukee, WI RECOMMENDATION: Delete the words, "...and, u[) to a certain point, the durat ion of pressurization," which appear m the second sentence in the section. SUBSTANTIATION: In terms of the ni trogen narcosis to be experienced by physicians or patient attenffants inside a hyperbaric chamber, the dura t ion of pressurization does no t affect the degree of ni trogen narcosis.
"The l~ngth of time spent at pressure does no t significantly affect the degree of narcosis", A.R. Behnke in Shilling et al The Phvsidan's Guide to Divinu Medidne . Phenum Press, 1984, pg. 131. " COMMITrEE~CTION: Accept. NUMBER OF COMMITrEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 NOT RETURNED: Hayes, Murray, Svedik
(Log #37) Committee: HEA-HYP
99- 418 - (C-19.1.3.1.3): Accept S U B ~ Eric P. Kindwall, Milwaukee, WI RECOMMENDATION: Revise first sentence to read: "Oxygen toxicity may develop from breathing of o x ~ e n at partial pressures above 0.50 atmospheres absolute for a significant length of t ime' . SUBSTANTIATION. The present wording uses 0.21 atmospheres absolute. Breathing oxygen at pressures less than 0.5 atmospheres for indefinite periods does no t produce oxygen toxicity of the lung, which is measurable, or CNS toxicity.
105

N F P A 99 - - F95 R O P
COMMITITEE ACTION: Accept. NUMBER OF COMMFITEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 N O T RETURNED: Hayes, Murray, Svedik
Committee: (HL°F~-#I-~ 99- 419 - (C-19-1.3.3.1): Accept SUBMITTER: Eric P. Kindwall, Milwaukee, WI RECOMMENDATION: Revise text as follows:
Second sentence: "Such a level can be hazardous because it is distractive, interferes with communica t ion , and may produce
~ e r m a n e n t sensory-neural deafness". UBSTANTIATION: T he p resen t sen tence states that, instead of
sensory neura l deafiaess, h igh noise levels can produce "headaches or o ther problems in susceptible individuals". I doub t that one can substantiate the diagnosis o f headache based on h igh noise levels. Sensory neura l deafness is the actual problem, which is quite real and has been d o c u m e n t e d at noise le~¢els over 85 db. - COMMIq['I'EE ACTION: Accept. NUMBER OF COMMITI'EE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 10 N O T RETURNED: Hayes, Murray, Svetlik
Commit tee: ( ~ - # I - ~ 99- 420 - (C-19-4): Accept SUBMITTER: Eric P. Kindwall, Milwaukee, WI RECOMMENDATION: Revise text as follows:
Correct Equivalent Dep th in Meters Seawater shown below:.
ATA Eouivalent Deo th in Meters Seawater 1 0 1.5 4.90 2.0 9.93 2.5 14.89 3.0 19.85 3.5 24.82 4.O 29.78 5.0 39. 71
SUIKSTANTIATION: Equivalent dep th in meters seawater is e r roneous at all dep ths shown, (Undersen Biomedical Research. Mar. 1974, vol 1, No 1 , p g IV, P/essure Conversion Table) COMMITTEE ACTION: Accept.
1. Correct me te r co lumn only as r e c o m m e n d e d . 2. Correct Depth in feet seawater as follows: 33 to 33.1; 82.9 to
82.7; 132.4 to 1~2.3. COMMIITEE STATEMENT: 1 a n d 2. Editorial. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITrEE ACTION:
AFFIRMATIVE: 8 NEGATIVE: Hamil ton, W o r k m a n N O T RETURNED: Hayes, Murray, Svetlik
EXPLANATION OF NEGATIVE: HAMILTON: There is still a serious p rob lem with the last i tem, ,
and I have had to vote against the commit tee on this as it now stands. The last i tem, Log #38, which a t tempts to revise the units conversion chart, is still w~rong. ' I sen t an explanat ion about this on [uly 11, 1994, which I hope you will refer to. T he p rob lem here ~eems to come f rom the briginal 1974 reference, v~hich was wrong in its defini t ion o f a met re of sea water~(later corrected). Perhaps this was jus t sk immed over at the meet ing. The re is no a r g u m e n t abou t msw (nowadays), bu t the re are still small differences in def in ing the foot of sea water tha t are more or less irreconcilable. T he best defini t ion is 1 /33 a t m = 1 fsw, bu t some use 1/33.08 a tm = 1 fsw. Se t t i ng this one is no t our j o b and is well outside our capability;, j u s t pick one of t he fsw definit ions a n d go with it. - B u t there is no ambiguity about msw. Look at it this way. The defini t ion of a met re of sea water is 0.1 bar. A bar is smaller t han at a tmosphere (1.01325 bars = 1 arm). Therefore it has to take slightly more ~han 10 msw to make an a tmosphere , bu t the chart does no t show that. At 2 a tm ads it says 9.93 msw. It can ' t be that! 2 a tm abs is 1.01325 bars or 10.1325 msw. (This depends on point of reference at sea level; see my earlier note).
It probably won ' t bu rn any patients to death if this is no t corrected, b u t i t will embarrass me, the-committee, and the NFPA. Tables have errors because people mh~ke mistakes, bu t to pr int it wrong when we know it is wrong is a travesty.
O n e o ther small ~,oint. T he table shou ld say "a tmospheres absolute" and no t 'ATA" at the head of the a tmosphere column. The term "ata" is used differently elsewhere so is no t specific and therefore no t r e c o m m e n d e d .
NOTE: Suppor t ing material is available for review at NFPA Headquarters . WORKMAN: Concur with Bill Hami l ton ' s rationale.
(Log #CP1) Commit tee: I-lEA-DIS
99-421 - (Annex 1): Correlat ing Commit tee Note: The Technica l Correlating Commit-
tee (TCC) notes that this material is "general" in content, an d thus belongs with general r equ i rements o f Chapters 1 to 10. As a result, the TCC places this material as Chapter 11.
The TCC also directs the TG on Dmaster P lanning to review the applicability s ta tement in theproposa l , a n d to deve lopment commit tee commen t s for e ac f i o fChap t e r s 12 to 19 as to what is applicable f rom this proposal in each of these chapters. ° SUBMITrER: Subcomrhit tee on Disaster P lann ing RECOMMENDATION: Comple te revision and upda te of A n n e x 1 f rom a "guide" to a "stmadard by creating new Ghapter 20 in NFPA 99, and rifling it "Health Care Emergency Preparedness."
NOTE: In accompl ish ing this, new terms have been added to Chapter 2, and material no t revised to requ i rements have been placbd in Appendices A and C.
1. Add the following three te rms and defini t ions to 2-2, including appendix material
]31~saster. * Within the context of this document , a disaster is def ined as any un fo reseen si tuation that seriously overtaxes or threa tens to seriously overtax the rout ine capabilities of a hea l th care facility. . ~,
NOTE 1: A disaster may be ei ther an event tha t causes or mrea t ens to cause physical damage and i_njury to facility personne l or p, atients within the facility;, or an event tha t requires expans ion of facilities to receive and care for a large n u m b e r ot ~ casualties result ing f rom a disaster tha t p roduces no damage or injury to the heal th care facility a n d staff; or a combina t ion thereof.
NOTE 2: Such a si tuation creates the need for emergency expansion of.facilities, as well as operat ion of this expanded facility in an unfamil iar envi ronment . U n d e r this definition, the recognitaon of a disaster si tuation will vary greatly f r om one facility to ano the r and f rom t ime to t ime in any ~ v e n facility. Such recogni t ion and concomi tan t activation of t h e H e a l t h Care Disaster Plan is depen- den t u p o n mutua l aid agreements , facility type, geographic location, bed capacity, bed occupancy at a given t ime, staff size, staff experi- ence w~th disaster situations, and other factors. For example, the rout ine workload o f the emergency depa r tmen t of a large metropoli- t an general hospital would consti tute a disaster, requi r ing activa~aon of tt~e Heal th Care Disaster Plan, were this same workloa(t to be suddenly applied to a small commun i ty hospital.
A-2-2 Dis,Yas-ter: Causes. Disasters have a variety of causes, all of which mus t be considered in effective emergency preparedness planning. A m o n g the mos t c o m m o n a re natural dt'sasters such as earthquakes, hur-ricanes, tornadoes, and floods; mass food poison- ing; industrial accidents involving explosion or envi ronmenta l release of toxic chemicals; t ransportat ion accidents involving crashes of trains, planes, or automobiles-with result ing mass casualties; civil dlsturban~:es; bui lding fires; extensive or p ro longed utility failure; collapse of buildings or o ther occupied structures; a n d toxic smogs in u rban areas. Arson a t tempts a n d b o m b threats have been m ad e on hea l th care facilities and mus t therefore be considered. Potential admission to the facility of h igh profile persons shou ld be addressed. While the last does no t involve rna~ casualties or the potential of mass casualties, the degree o f d is rupt ion o f no rma l rout ine will be sufficient to qualify it as a disasterlike situation.
NOTE: Disaster plans shou ld reflect a facility's location f rom internal a n d external disasters. As an example, areas subject to f r equen t wildiand fires should invoke coun te rmeasures for smoke m a n a g e m e n t and air quality main tenance .
Incident C o m m a n d System. (See defini t ion of "Incident Manage- m e n t System.")
Inc ident M a n a g e m e n t System. The m a n a g e m e n t system an d c o m m a n d structure used du r ing emergency operat ions to identify clearly who is in c o m m a n d of the i n d d e n t a n d what roles and responsibilities are assigned to various members . [from NFPA 600, Fire Brigades.]
2. Delete A n n e x 1, and add the following new Chapter 20, Heal th Care Emergency Preparedness, in NFPA 9~ (Draft as of Ju ly 22, 1994)
Chapter 20 Heal th Care Emergency Preparedness 20-1 Scope. This chapter establishes m i n i m u m criteria for heal th
care facility disaster m a n a g e m e n t in the deve lopment o f a p rog ram for effective disaster preparedness, mitigation, response a n d recovery.
NOTE : Since no single mode l of a disaster p l an is feasible for every heal th care facility, this chapter is i n t ended toprov ide criteria in the preparat ion and implementa t ion of an individual plan. The principles involved are universally applicable; the implem- entat ion needs to be tailored to the specific facility.
106
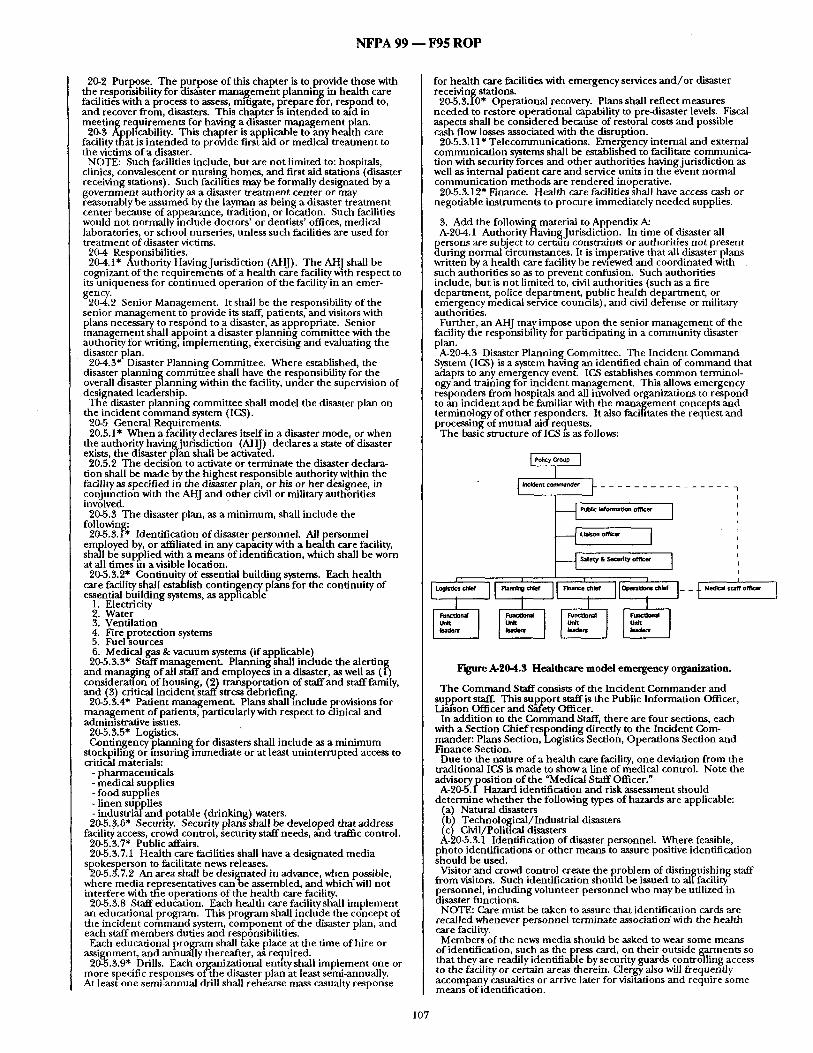
N F P A 9 9 - - F 9 5 R O P
20-2 Purpose. The purpose of this chapter is to provide those with the responsibility for ~isa~ter management planning in health care facilitie-s with a process to assess, mii.igate, pi 'epare for, respond to, and recover froin, disasters. This ch~/pter is iritended to aid in meet ing requirements for having a disaster mal~agement plan.
20-3 Applicability. This chapter is applicable'to any health care facility thfit is in tended to provide first aid or medical t rea tment to the victims of a disaster.
NOTE: Such facilities include, but are no t limited to: hospitals, clinics, convalescent or nursing homes, and first aid stations (disaster receiving stations). Such facilities may be formally designated by a government authority as a disaster t reatment center or may (easonably be assumed by the layman as being a disaster t reatment center because of appearance, tradition, or Idcation. Such facilities would not normall)/include doctors ' or dentists' offices, medical laboratories, or school nurseries, unless such facilities are used for t reatment of disaster victims.
20-4 Responsibilities. 20-4.1" Authority Having Jurisdiction (AHJ). The AH.] shall be
cognizant of the requirements of a health care facility with respect to its uniqueness for cont inued operation of the facility in an emer-
g20-~.'2on~' Senior Management. It shall be the responsibility of the senior management to provide its staff, patients, and visitors with plans necessary to respond to a disaster/as appropriate. Senior management shall appoint a disaster p lann ing committee with the authority for wri t ing, implementing, exercisin-g and evaluating the
• disaster plan. 20-4.3* Disaster Planning Committee. Where established, the
disaster p lanning committee shall have the responsibility for the overall disaster planning within the facility, under the supervision of designated leadership.
The disaster planning committee shall model the disaster plan on the incident c o m m a n d system (IGS).
20-5 General Requirements. 20.5.1" When a facility declares itself in a disaster mode, or when
the authori.ty having jurisdiction (AHJ) declares a state of disaster exists, the disaster plan shall be activated.
20.5.2 The decision to activate or terminate the disaster declara- tion shall be made by the highest responsible authority within the facility as specified in the dis-aster plah, or his or her designee, in conjunction with the AHJ and other civil or military autho- rifles involved.
20-5.3 The disaster plan, as a minimum, shall include the followinl~:
20-5.3.iV* Identification of disaster personnel. All personnel employed by, or affiliated in any capacity with a health care facility, shall be supplied with a means of identification, which shall be worn at all times in a visible location.
20-5.3.2* Continuity of essential building systems. Each health care facility shall establish contingency plans for the continuity of essential building systems, as applicable-
1. Electricity 2. Water 3. Ventilation 4. Fire protect ion systems 5. Fuel sources 6. Medical gas & vacuum systems (if applicable)
20-5.3.3" Staff management . Planning shall include the alerting and managing of all stuff and employees in a disaster, as well as (1-) considerauon of housing, (2) t ransportat ion of staff and staff family, and (3) critical incident staff stress itebriefing.
20-5.3.4* Patient management . Plans shal l include provisions f o r management of patients,-particularly with respect to clinical and administrative issues.
20-5.3.5* Logistics. Contingency p lanning for disasters shall include as a minimum
stockpiling or insuring immediate or at least uninterrupted access to critical materials:
- pharmaceuticals - medical supplies - food supplles - l inen supplies - indust r ia iand potable (drinking) waters. 20-5.&6" Security. Security plans shall be developed that address
facility access, crowd control, security staff needs, and traffic control. 20-5.3.7* Public affairs. 20-5.3.7.1 Health care facilities shall have a designated media
spokesperson to facilitate news releases. "20-5.5.7.2 An area shall be designated in advance, when possible,
where media representatives c a n b e assembled, and which will n o t interfere with tile operations of the health care facility.
20-5.3.8 Staff education. Each health care facility shall implement an educational program. This program shall include the concept of the incident command system, componen t of the disaster plan, and each staff members duties and respo-nsibilities.
Each educational program shall fake place at the time of hire or assignment, and annually thereafter, as required.
20-5.3.9* Drills. Each organizational entttyshali implement one or more specific responses of-the disaster plan at least semi-annually. At least one semi-annual drill shall rehearse mass casualty response
for health care facilities with emergency services a n d / o r disaster receiving stations.
20-5.3.I0" Operational recovery. Plans shall reflect measures needed to restore operational capability to pre-disaster levels. Fiscal aspects shall be considered because of restoYal costs and possible cash flow losses associated with the disruption.
20-5.3.11" Telecommunications. Emergency internal and external communicat ion systems shall be established to facilitate communica- tion with security forces and other authorities having jurisdiction as well as internal patient care and service units in the event normal communica t iof fmethods are rendered inoperative.
20-5.3.12" Finance. Health care facilities shall have access cash or negotiable instruments to procure immediately needed supplies.
3. Add the following material to Appendix A: A-20-4.1 Authority Having Jurisdiction. In time of disaster all
persons are subject to cereaqn constraints or authorities not present ;:luring normal ~ircumstances. It is imperative that all disaster plans written by a health care facility be rewewed and coordinated with such authorities so as to prevent confusion. Such authorities include, but is not limited to, civil authorities (such as a fire department , police department , public health department , or eniergency rdedicai se~'ice countils), and civil defense or military authorities.
Further, an AHJ may impose upon the senior management of the facility the responsibility for pariJcipating in a commfinity disaster plan. A-20-4.3 Disaster Planning Committee. The Incident Command
System (1CS) is a system having an identified chain of command that adapts to any..emerg, cyen event. ICS establishes.common terminol- ogy and training for mc:dent management . This allows emergency responders from hospitals and all involved organizations to respond to ~n incident and be familiar with the management concepts and terminology of other responders. It also facifitates the requ-est and processing of mutual aldrequests .
The basic structure of IGSis as follows:
Log~cs chief
I.~ ~,on oNicer I
~__~' "Safety & ,~¢ufit:y officer ]
F ' g u r e A - 2 0 a l . $ H e a l t h c a r e m o d e l e m e r g e n c y o ~ r a n i z a t i o n .
T h e Command Staff consists of the Incident Commander and support state This support staff is the Public Information Officer, Li~Yson Officer and ~t 'e ty Officer.
In addit ion to the Command Staff, there are four sections, each with a Section Chief responding directly to the Incident Com- mander: Plans Section, Logistic~ Section, Operations Section and Finance Section.
Due to the nature of a health care facility, one deviation from the traditional ICS is made to show a line of medical control. Note the advisoryposition of the "Medical Staff Officer."
A-20-5.I Hazard identification and risk assessment should determine whether the following types of hazards are applicable:
(a) Natural disasters (b) Technological/Industrial disasters (c) Civil/Political disasters A-20-5.3.1 Identification of disaster personnel. Where feasible,
photo identifications or other means to assure positive identification should be used.
Visitor and crowd control create the problem of distinguishing staff from visitors. Such identification should be issued to allfacility- personnel, including volunteer personnel who may be utilized in disaster functions.
NOTE: Care most be taken to assure that identification cards are recalled whenever personnel terminate association with the health care facility.
Members of the news media should be asked to wear some means of identification, such as the press card, on their outside garments so that they are readily identifiable by security guards controlling access to the facility or certain areas therein. Clergy also will frequently accompany casualties or arrive later for visitations and require some means of identification.
107
N F P A 99 - - F95 R O P
A-20-5.3.2 Continuity of Essential Buildinl~ Systems. For essential building systems, consideration should be Knven to the installation of exterior building connectors to allow for die attachment of portable emergency utility modules. Water storage systems should be inventoried and protected to the
greatest extent ossible A-20-5.3.3 S~d~ Management. Management of staff and employees
allow for the best and effective use of the entity's human resources during disaster operations. Consideration should be given to both persofinei on-hand and those that can be alerted. Sp&ifically staff management includes:.
a- assignment of roles and responsibilities b. me{hod for identifying human resource needs to include status
of families c. method for recalling personnel and augmenting staff d. management of space (housing, day care, etc.) e. management ofsiafftransl?ortation f. critica/incident stress debriefing (Much case history shows that
not only victims but also rescuers and treatment/handler staff bear serious emotional or even mental scars from their traumatic experiences. Emergency room and ambulance staff can also benefit f r tm such help when stress has been acute.) A-20-5.~.4 Patient Management. The plans should focus also on
modification or discontinuation of non-essential patient services, control of patient information and admission/diScharge and transfer of patients. Emergency transfer plans need to consider the proper handling of patient personal property and medical records that WIU accompany the patient as well as assurance of continuity of quality care. E~aJuatlon-ofspace, ~atient transport resources and a process to ensure patient location information should be included. A-20-5.3.5 Logistics. It will be essential to assess these kinds of
resources currently available within the health care facility itself, and within the local community as a whole. Community sources identification can be effectively performed by the local disaster council, through the cooperation of local hospitals individually or collectively through local hospital associations, nursing homes, clinics, and other outpatient facilities, retail pharmacies, wholesale dru g.su pp liers, ambulance, services, and local medical/sur g icai supphers and their warehouses.
Knowing the location and amount of in-house and locally available medical and other supply sources, a given health care facility might then desire to stockpfl6 such additional critical material and supplies as might be needed to effectively cope with the disaster situation. A-20-5.3.6 Security and Traffic Control. Facilities should formally
coordinate their security needs during a disaster with local law enforcement agencies.This action may be necessary as a means to supplement the facility security capabilities, or to provide all security needs when the facility lacks its own internal security forces. The health care institution will find it necessary, to share their
disaster plans with local law enforcement agencies, or better stall involve them in the process of planning for security support during disasters. The information should at least include availability of parking for both staff, patients and visitors, normal vehicular,
merg~ncy vehicular., ahd pedestrian traffic flow. patterns in and around the facihty. The extent of the securtty and traffic control problems for any given health care facility will depend upon its geographical location, physical arrangement, availability of visitor parKinl~ areas, number of entrances, etc. A-20-5.3.6.1 Crowd Control. Visitors can he expected to increase
in number with the severity of the disaster. The)~ should not be allowed to disrupt the disaster functioning of the facility. Ideally, a visitor's receptio-n center should be established away from the main
d fadlity itself, particularly in major disasters. Volunteer personnel such as Red Cross, Explorer Scouts or other helpers can be utilized as liaisons between the visitors and the health care facility itself. Normal visiting hours on nursing units should be suspended where
ossible p • , .
A-20-5.3.6.2 Vehtcular Traffic Control. Arrangement for vehicular traffic control into and on the facility premises s-hould be made in the disaster planning period. It will b~necessary to direct ambu- lances and other emergency vehicles carrying casualties to triage areas or the emergency room entrance, and to direct incominlg and outgoing vehicles carrying people, supplies and equipment. T(affic- flo,d chairs indicating ent~ance-s to be u-sed, evacuatio-n routes to be followed, etc., should be prepared and included in the Health Care Disaster Plan. Parking arrangements must not be overlooked. A-20-5.3.6.3 InternairSecunty and Traffic Control. Internal
security and traffic control are best conducted by facility trained personnel, i.e., regular health care facility security forces, with reinforcements as necessary. Additional assistance from the local law enforcement agencies should be coordinated in the disaster planning phase. Upon activation of the Health Care Disaster Plan, security guards should be stationed at all unlocked entrances and exits. Eritrance to the facility should be restricted to personnel be .aring staff identification cards and to casualties. Iri the case of major access corridors between key areas of the facility, pedestrian traffic should be restricted to one side of the corridor k-eeping one side of the corridor free for movement of casualties. Traffii: flow charts for internal traffic should also be prepared in the planning phase, as is the case with external traffic control.
A-20-5.3.7 News Media. Because of the intense public interest in disaster casualties, news media representatives must be given as much consideration as the situation will permit. Ideally, news media personnel should be provided with a reception area, with access to telephone communicttion and, if possible, an expediter who, thofigh not perrnittedl*to act as spokesman for nei~s releases, may provi-de other assistance to thes~ individuals. News media personnel should not be allowed into the health care facility without-proper identification. To alerting off-duty health care staff, and for reassuring the public use of broadcast media should be planned. Media represefitatives should have access to telephone 6ornmunica- tions. Media representatives should be requested to wear some means ~f identification for security purposes. A-20-5.3.9 Drills. Experiences show die importance of drills to
rehearse the implementation of all elements of a specific response including the entity's role in the community, space management, staff management and patient management activities. A-20-5.3.10 Ol?eration-al Recovery. -Recovery measures mayinvolve
a simple reposiuoning of staff, equipment, supplies and information services; or it may demand extensive cleanup and repair. It may, under certain circumstances, present an opportunity to evaluate long-range ideas concerning modifications to the facility. Filing of loss-claims may be require special approaches. A-20-5.3.11 Telecommunication Systems. The basi'c form of
communication in a disaster is the telephone system. As part of the contingency plan to maintain communqcation, a plan for restoring telephhne systems or the use of alternate systems-is necessary. Typtcally, the first line of internal defense for a system out,age are strategically placed power-failure stations that are designed to contiriue to function in the event of system failure. Plans for external outages and load control should include the use of Bell System pay phones that have first priority status in external system restoration.
Contingency plans should also contain strategies for the use of radio-frequency communications to supplement land-line usage. The plan should include a means to distihbute and use two-way radio comhlunication throughout the facility. A plan for the incorpora- tion and use of amateur radio operators should also be considered.
It must recognized that single-channel radio communication is less desirable than telephone system restoration due to the limited number of messages that can be managed. Cellular telephones, although useful in some disaster situau~ons, should not be consid- ered ai:ontingency having high reliability due to its vulnerability to load control schemes of telephone companies.
4. Add the following new references in Appendix B: Appendix B-4 Addresses of organizations, agencies, etc. that
prowde health care emergency preparedness educational material ~written, audio-visual, etc.) (Ref.: Chapter 20)
Publications National Fire Protection Association, 1 Batterymarch Park, P.O.
Box 9101, Quincy, MA 02269-9101. American Health Care Association, 1200 Fifteenth Street NW,
Washington, DC 20005. American Hospital Association, 840 North Lake Shore Drive,
Chicago, IL 606"11. American Medical Association, 535 North Dearborn Street,
Chicago, IL 60610. American National Red Cross, National Headquarters, 17th & D
Streets, NW, Washington, DG 20006. American Nurses' .~ssociation, 10 Columbus Circle, NewYork, NY
10019. Association of American Railroads, 1920 L Street NW, Washington,
DC 20036. Charles C. Thomas Publisher, 301-327 East Lawrence Avenue,
Springfield, IL 60611. Dun-Donnelley Publishing Corp., 666 Fifth Avenue, NewYork, NY
10019. Federal Emergency Management Agency, Washington, DC 20472. Florida Health Care Assodation, P.O. Box 1459, Tallahassee, FL
32302 Helicopter Association Intematlonal, 1635 Prince Street, Alexan-
dria, VA- 22314-2818 International Association of Fire Chiefs, 4025 Fair Ridge Drive,
Fairfax, VA 22035-2868 Jo in t Commission on Accreditation of Healthcare Organizations (ICAHO), One Renaissance Blvd., Oakbrook Terrace, IL 6018I P a n American Health Organization, 525 23rd Street NW, Washing- ton, DC 20036 (Attn.: Editor, Disaster Preparedness in the Americas).
University of Delaware, Disaster Research Center (Publications), Newark, DE 19716.
U.S. Department of Transportation (available from Superintendent of Documents, U.S. Government Printing Office, Washington, DC 204O2). Audio-visual material National Fire Protection Association, 1 Batte~'ymarch Park, P.O.
Box 9101, _Quincy, MA 02269-9101. Abbott LaBoratories, Audio/Visual Services, 565 Fifth Avenue, New
York, NY 10017.
108

N F P A 99 - - 1¢95 R O P
#
Brose Productions, Inc., 10850 Riverside Drive, N. Hollywood, CA 91602.
Federal Emergency Management Agency, Office of Public Affairs, Washington, DC 20472.
Fire Prevention Through Films, Inc., P.O. Box 11, Newton Hi~hnlands , MA 02161.
eral Services Administration, National Audiovisual Center, Reference Section, Washington, DC 20409.
Helicopter Association International, 1635 Prince Street, Alexan- dria, VP/ 22514-2818
~ s d, P.O. Box 1048, Santa Monica, CA 90406. ity of llllnois Medical Center, Circle Campus, Chicago, IL
6O612.
5. Add the following material in Appendix C: C-20 Additional Information on Oaapter 20. C-20-1 General Considerations. G20-2 Personnel Notification and Recall. C~20~ Special Considerations and'Protocols. C,20-I Generai Considerations. The basic plan should be written
broadly, providinggenerai but concise cove .r.age of disaster . responsibilities affd-procedures for each facili6/ctepartment and prdviding detailed responsibilities and procedures for those functions not normally a part of regular routines, e.g., operation of the disaster control center. Keyed to the basic plan, the departmen- tal annexes of the plan then outline individual-department responsibilities in greater detail. Finally, the disaster procedures for each function withha each department are described]n terms of actual instructions for individual staff members and employees. Individuals should never be mentioned by name in the plan; rather, responsibilities and procedures should be written in terms of job flue. The health care occupancy chapters of NFPA 101, Life Safety Code, are relevant for review and rehearsal~
C-20-2 Personnel Notification and Recall, Medical gtafl~ key personnel, and other personnel needed will be notified and recalled as required. In order to relieve switchboard congestion, it is desir '~le to utilize a pyrami'dal system to recall individualswho are off duty or omerwise out of the facility. Under the pyramicta~ s~tem, an individual who has been notified will notify two other individuals, who in turn will each notify two other individuals, and so on. A current copy of the notflication and recall roster, with current home and on-call telephone numbers, will be m .aintainect at the h. ospital switchboard at gll times. In case the pyramicua system is to be utilized, each individual involved in the system must maintain a current copy of the roster at all times, in order that each may know whom they are to notify and the telephone numbers concerned. It is essential that key personnel rosters fie kept current.
C-20-3 Special Considerations and Protocols. C-20-3.1 Irlre and Explosion. In the event that the health care
facilityneed not be completely evaomted immediately, the actions staff should take when they are alerted to a fire are detailed in Chapter 51 of NFPA 101, Life Safety Code.
Gg0-5.2 Severe Storm. The warmngsystem operated by the National Oceanic and Atmospheric AcTministrafion will, in most cases, provide adequate time to permit the health care facility to take certain precautions, and if disaster appears Inevitable, to activate the Health Care Disaster Plan in advance -of the d~saster event. A~um. ing evacuation is not feasible, some precau0ons indude the following:
(a) Draw all shades and dose all drapes as protection against shattering glass;
(b) Lower all patient beds to the low position, wherever possible; (c) Place blankets on patients/residents; (d) Close all doors an/l windows. (e) Bring indoors those lawn obiects that could become missiles. (f) Remove all articles fi'om wini~ow ledges. (g) Relocate pa0ents/residents to windowless hallways or rooms. G20-3.3 Evacuation. Evacuation maybe partial or total. It may
involve moving from one story to another, one lateral section or wing to another, or moving out of the structure. Even partial evacuations may involve all categories of L~atients; where these are people who would not routinely be moved, extraordinary measures may be required to support life. It is also necessary to ensure movement of supplies in conjunction with any evacuation. Decisions to evacuate maybe made as a result of internal problems or under menace of engulfing external threats. In all cases, the following considerations govern;
(a) Move to pre-designated areas, whether in the facility, nearby, or in remote zones. Evacuation directives will normally indicate destinations.
NOTE: It is recommended topredesign a mutual aid evacuation plan with other health care facinties in the community.
(b) Ensure movement of equipment, supplies and medical records to accompany or meet patients gnd staffin the new location.
(c) Execute predeter/nlned staffing plans. Some staffwill accompany patients; others will rendezvous in the new location. Maintenance of shifts is more complex than normal, especially when (1) some hard-to-move patients stay behind in the threateneo location, and (2) staffmay be sepa/ated from their own relocated families.
(d) Protection of l~Qflents and staff (during and after movement) against the threatening environment must be provided.
{e) Planning must consider wansportaflon arrangements ana patient tracking.
C-20-5.4 Higti Profile Person Admission.. Admission of a high profile person to a health care facility in an emergency creates two sets of problems, which may require partial acflvaiion of the Health Care Du~ster Plan. These problems are:
C.20-3.4.1 Security. Provtsion of security forces in this s i t , on will normally be a responsibility of the U.S. Secret ~ervice or o m ~ governmental agency. However, activation of facility securitytorces may be required to prevent hordel of curious onlookers from entering fgctllty wor~ ~eas and interferingwith routine facility funcflofiing. Routine visifln$ privileges anii routine visiting hours may neeo to be suspended m _parts of the facility.
G20-3.4.2 Recepuon of News Media. The news media ~cept ion plans will need to be activated. In this instance, additional co.mmu- /~ications to the news reception center will be required. Additional telephones ano telephone lines can be installed on an emergency barn on request to the local telephone corn .pany. Such requests for additional telephone connections in the facility should, however, first be coordifiated with the senior Secret Service officer or governmental representative accompanyin$ the dignitary.
G-20-3.50ther~Protocols as Deemed Desti~He. In addition to the above, there should follow a number of additional protocols for , internal disasters, to be determined by the geogvaphical location of the individual health care facility, e.g., nam/al i]ls~sters, civil disturbance protocol, bomb threat protocol, hazardous material protocol, loss of central services (power, water and gas) .
G-20-3.6 Activation of Emergency Utility Resources. In the planning phase, backup utility resources will have been s to~pi led " and arrangements made for mutual aid when required. Such utilities in~ude electrical power, water, and fuel. 'Through prior coordinaflon with the local office of emergency preparedness or fire oepartment, mobile generators and auxUiarypumps can be obtained in the internal disaster situation. Through these same sources arrangements could be made to supply water tank trucks. Obviously, such I~lanning is in addition to routine planning, in which all health care facilities maintain emergency elect/ical power plants and, in those areas requiring central-heating in winter, backup supplies of oil, coal, or gas. Priorities for use of available power (e.g.,/~r circulation Out not air conditioning) must be determined. Sanitation re quirements, can become. .°verriding in p rolon g ed disasters,, and. even an ordinary strike by garbage collectors can cause difficulties.
G20-5.7 Civil Disturbance. La/ge-scale civil disturbances in recent years have shown that health care facilities and their personnel are not immune to the direct effects of human violence in such disturbances. Hospitals in large urban areas must make special pro~sious in theft disaster plans to ensure the physical sgfety of their employees, particularly ferdale employees, in transit from the hospital exit to and from a sfcure means of transportation to their homes. In extreme cases it may be necessary to house employees within the health care facility itself during such civil disturbances. Examples of direct attacks or sniping are extremely rare. Another aspect of civil disturbahces not to be overlooked in facility
security plafinin~ is the possibility that a given health care facility may have to adnfit and treat large numbers of prisoners during such emergencies; however,, security ~ for such patt'ents will norm~dly be provided by the locai police d e ~ e n t .
C-20-3.8 Bomb Threats. The dis~r~r potential inherent in the telephoned~bomb threat warrants inclusion of this disaster confln- ~[aency in the Health Care Disaster Plan. Experience has shown that
cility personnel must accompany police or military bomb demolifionpersonnel in searching ~or the suspected bomb, sinte speed is of the essence and only individuals ~ with a given area can rapidly spot unfamiliar or suspicious objects or condition in the area. This is particularly true in health care facilities. The f a c i l i t y " switchboard operator must be provided with a checklist to be kept available at alrtimes, in order to obtain as much information as - possible from the caller concerning location of the supposed bomb, time of detonation, and other esse/ltial data, which must be considered in deciding whether or not to evacuate all or part of the facility_.
G-20-5.9 Radioactive Contamination. Disaster planning must consider the possibility that radioactive material/may be released from nuclear reactors or Uansportation accidents, as well as from internal spills. These incidents may require that health chre staffand patients I~e sheltered. Shelter areas can be selected in existing structures and should be planned for durin~ design of new facilities or additions. Similarly, plans must.also consider rgdiation dose control and deconmmifiation of viddms or staff personnel and public safety in connection with nuclear accidents or incidems such as reactor excursions.
C-20-5.10 H~wdous Material. There are at least three major sources of concelxl with regard to non-radioactive hazardous materials. The first is the pbssibility of a large spill or venting of " hazardous materials near the facility;, this is especially likely near major rail or truck shipping routes, near pipefines, or near heavy mahufacturing plants. Second, every facifit~ containa~.~thin its boundaries varying amounts of such materials; .espeaally in the laboratory and custodial areas. A spill of a highly volatile chemical
109

N F P A 99/99B - - 1¢95 R O P
can quickly contaminate an entire structure byway of the air ducts. Finally, contaminated patients can pose a risk to staff, though on a more localized basis. Usually remox:'al of their clothing will ~educe the risk materially. In any case, staff must be preparedto seek advice on unknown hazards. This.type of advice is not usuall~ available from poison centers, but rather from a central referral, such as CHEMTREC, and its toll-free emergency information service number (800-424-9500).
C-20-3.11 Volcanic Eruptions. While most of the direct effects of a volcanic eruption are covered in other protocols for disasters (fire, explosion, et-c.), it is necessary to make s- pecial provisions for functioning in areas of heavy to moderate ash fall. This hazard can exist huncl~eds of miles downwind from the eruption. Volcanic "ash" is actually finely pulverized rocl~ blown out of the
volcano. Outside the area of direct damage, the ash varies from a . fine powder to a coarse sand. General housekeeping measures can exclu-de much ash. It should be noted, however, tha-t people move about freely during and after ash fall. Ash fall presents four problems for health care facilities: (1) People require cleanup (brushing, vacuuming) before
entering ~ e building. (2) El~ctromechanical and automotive equipment and air-filtering
systems require special care because of the highly abrasive and fine penetratiofi nature of the ash.
(5) Increased flow of patients with respiratory complaints can be expected.
(4) Eye protection is required for people who must be out in the dust. (No contact lenses should be worn; goggles are suggested.) Dust masks are available. They are approved-by the National Institute for Occupational Safety and'Health (NIOSH), and are marked TC-21 plus other digits. SUBSTANTIATION: This codifies existing practices widely referenced by governmental authorities and nongovernmental bodies with regard to health care facilities, notably the incorporation of incident command system (IC, S). This effort also supports the efforts of the T/C on Disaster Management, which is preparing a general standard addressing the subject of disaster management. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 8 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 8
P ~ T H
(Log #1) 9913-1 - (1-4): Accept SUBMITYER: John F. Greear, III, Orlando, FL RECOMMENDATION: Revise the 3rd sentence of the paragraph to read as follows:
"Existing construction or equipment shall be permitted to be continued in use when use does not constitute a distinct hazard to life as determined by the authority having jurisdiction." SUBSTANTIATION: The 3rd sentence of the paragraph ends with the four words- "administration of the institution." The phrase "administration of the institution" is not defined in Chapter 2 Definitions. However, paragraph 2-1 .Official NFPADefinifions does define the term ~Authority Having Jurisdiction." Substitution of the phrase "Authority Having Jurisdiction" for "administration of the restitution" will assure a defined phrase is included in paragraph 1-4. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 12 NOT RETURNED: Murray
(Log #5) 99B- 2 - (1-4): Accept SUBMITTER: John F. Greear, I11, Orlando, FL RECOMMENDATION: Revise the 1st sentence to read as follows:
"This standard shall be applied only to the following: new construc- tion; new ecjuip.ment added to new facilities; new equipment added to existing facilities." SUBSTANTIATION: The existing wording, by error of omission, implies that when new equipment is added to existing facilities, or hypobaric chambers are upgraded, it does not need to meet codes. This creates a potentially dangerous situation. Per the Cognizant Field Activities TSA and POA&M reports, there are many hypobaric altitude training chambers between 22 and 51 years old. Many are in critical need of an aggressive engineering cognizance program to prevent additional electrical and oxygen system fires. For the
rOtection of occupants, when new equipment is added to existing cilities, or hypobaric chambers are upl#aded , the code should
require compliance. This will provide the assurance of protection intended by the National Fire Protection Association. COMMITrEE ACTION: Accept.
NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 12 NOT RETURNED: Murray
(Log #CP2) 99B- 3 - (1-5.2(c)): Accept SUBMITTER: Technical Committee on Hyperbaric & Hypobaric Facilities, RECOMMENDATION: Delete 1-5.2(c). SUBSTANTIATION: Committee is unaware of any current hypobaric techniques involving atmospheres other than those used in Class D and E chambers. COMMITI~E ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13" VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 12 NOT RETURNED: Murray
(Log #2) D9B- 4 - (2-1): Reject SUBMITTERa John F. Greear, III, Orlando, FL RECOMMENDATION: Revise the last sentence of the note to the definition of the term 'Authority Having Jurisdiction' to read as follows:
"at government installations, the Systems Command, Cognizant Field Activity (CFA), Commanding Officer, or Department Official may be the 'au~ority havingjurisdictign'." SUBSTANTIATION: Pressure Vessels for Human Occupancy (PVHOs) used within the Department of Defense normally come under one Central Authority. This is typically a Systems command, or Cognizant Field Activity (CFA). Rarely does an individual Commanding Officer or Local Department Official have the resources, expertise or authority to assure code compliance. The current wording is confusing and has resulted in administrative and bureaucratic conflicts between Government agencies. The result is there are 50+ years aged PVHOs in use with potentially lethal failure nodes. Addition of the two terms, i.e., "Systems Command" and "Cognizant Field Activity," will clarify the confusion and help establish proper accountability and responsibility to assure hazards are recognized and protective procedures are in place. COMMIT1T.E ACTION: Reject. COMMITTEE STATEMENT: Not within scope of committee to revise an NFPA definition. Submitter should send recommendation to NFPA Standards Council. NUMBER OF COMMITIT~ MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 12 NOT RETURNED: Murray
(Log #CP1) OgB- 5 - (2-2 Atmosphere): Accept SUBMIIq'ER: Technical Committee on Hyperbaric and Hypobaric Facilities, RECOMMENDATION: In definition of"AUnosphere," make sentences 2 and 3 a NOTE. SUBSTANTIATION: Editorial. Conform to NFPAStyle Manual. COMMITrEE ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMrI'FEE ACTION:
AFFIRMATIVE: 12 NOT RETURNED: Murray
(Log #CP3) 99B- 6 - (4-7.5.1): Accept SUBMITIXR: Technical Committee on Hyperbaric & Hypobaric Facilities,
I RECOMMENDATION: Make sentence 1 in 4-7.5.1 a NOTE. SUBSTANTIATION: Conform to NFPA Style Manual. COMMIaq~E ACTION: Accept. NUMBER OF COMMITTEE MEMBERS ELIGIBLE TO VOTE: 13 VOTE ON COMMITTEE ACTION:
AFFIRMATIVE: 12 NOT RETURNED: Murray
110

![Second Revision No. 3-NFPA 53-2020 [ Detail ]](https://static.fdokumen.com/doc/165x107/631ed16a1aedb9cd850fee3c/second-revision-no-3-nfpa-53-2020-detail-.jpg)