Intrauterine Fetal Demise After Uncomplicated COVID-19 - MDPI

lable at ScienceDirect
Placenta 35 (2014) 431e436
Contents lists avai
Placenta
journal homepage: www.elsevier .com/locate/placenta
Reduction of maternal circulating endothelial progenitor cells inhuman pregnancies with intrauterine growth restriction
F. Calcaterra a,b, A. Taddeo a,1, E. Colombo a,b, M. Cappelletti a,b, A. Martinelli c, S. Calabrese c,D. Mavilio a,b, I. Cetin c, S. Della Bella a,b,*
aDepartment of Medical Biotechnologies and Translational Medicine, University of Milan, Italyb Lab of Clinical and Experimental Immunology, Humanitas Clinical and Research Center, Rozzano, MI, ItalycCenter for Fetal Research “Giorgio Pardi”, Department of Biomedical and Clinical Sciences Luigi Sacco, University of Milan, Italy
a r t i c l e i n f o
Article history:Accepted 15 April 2014
Keywords:Endothelial progenitor cellsHuman pregnancyIntrauterine growth restrictionPlacental growth factor
Abbreviations: EPC, endothelial progenitor cell; Kceptor; IUGR, intrauterine growth restriction; PlGF, plstromal-derived factor-1; VEGF, vascular endothelial g* Corresponding author. Lab of Clinical and
Department of Medical Biotechnologies and TranslatMilan e IRCCS Istituto Clinico Humanitas, Via ManzItaly. Tel.: þ39 (0)2 82245144; fax: þ39 (0)2 8224510
E-mail address: [email protected] (S. Della1 Present address: Autoimmunity Group/Cell
Rheumaforschungszentrum, Berlin, Germany.
http://dx.doi.org/10.1016/j.placenta.2014.04.0030143-4004/� 2014 Elsevier Ltd. All rights reserved.
a b s t r a c t
Introduction: Circulating endothelial progenitor cells (EPCs) may play a crucial role during pregnancyby sustaining adequate placentation and fetal growth. Unambiguous demonstration of EPC increaseduring pregnancy has been hampered so far by lack of standardized methods for EPC quantification.In this study we used the currently most accepted phenotype for EPC detection forinvestigating whether maternal circulating EPCs might increase during normal pregnancy andwhether they may fail to increase in pregnancy complicated by idiopathic intrauterine growth re-striction (IUGR), a leading cause of perinatal mortality and morbidity characterized by insufficientplacental perfusion.Methods: Twenty-one non-pregnant women, 44 women during healthy pregnancy progression (9, 13and 22 women in the first, second and third trimester, respectively) and 11 with pregnancy complicatedby idiopathic IUGR were recruited in a cross-sectional study. EPCs in maternal blood were identified asCD45dim/CD34þ/KDRþ cells by flow cytometry. Plasmatic cytokines were measured by ELISA.Results: We observed a significant and progressive increase of EPCs in normal pregnancy, yet detectablein early pregnancy but even more pronounced in the third trimester. The increase of EPCs was impairedin IUGR-complicated pregnancies at comparable gestational age. The circulating levels of placentalgrowth-factor and stromal-derived-factor-1 were significantly lower in IUGR than normal pregnancies,possibly contributing to EPC impairment.Conclusions: EPC count in maternal circulation may have a great potential as a novel biomarker forpregnancy monitoring and may represent the target of novel therapeutic strategies designed to preventadverse pregnancy outcomes often occurring in IUGR.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Endothelial progenitor cells (EPCs) are circulating cells that playa critical role in adult vasculogenesis and endothelial homeostasis.They originate from the bone marrow, circulate in the peripheral
DR, kinase insert domain re-acental growth factor; SDF-1,rowth factor.Experimental Immunology,ional Medicine, University ofoni 113, 20089 Rozzano, MI,1.Bella).Biology Group, Deutsches
blood and are recruited to sites of endothelial injury and new bloodvessel formation. In those sites, EPCs contribute to both vasculo-genesis and angiogenesis by direct integration into the endothe-lium and by paracrine stimulation of the endothelial cells liningexisting vessels [1].
Since their first description in 1997, EPCs have been largelyinvestigated, and variations in their number and function havebeen demonstrated in many different human physiological andpathological conditions. In cardiovascular diseases, the number ofcirculating EPCs is reduced and, according to the role played byEPCs in maintaining endothelial integrity and promoting endoge-nous vascular repair, low EPC levels independently predictatherosclerotic disease progression and confer increased risk ofadverse cardiovascular outcome [2]. On the other hand, in patientswith various types of cancer, in whom EPCs are thought to

Table 1Age and gestational age of the study population.
Characteristic Non-pregnant controls Normal pregnancy IUGR pregnancy
I trimester II trimester III trimester III trimester
Number of cases 21 9 13 22 11Age, years 27.8 � 1.8 28.1 � 2.3 28.8 � 1.4 32.9 � 1.2 34.2 � 1.8Gestational age at blood collection, weeks n.a. 10.9 � 1.0 21.3 � 1.0 34.5 � 0.6 33.1 � 1.0
IUGR: intrauterine growth restriction; n.a.: not applicable. Data are presented as mean � s.e.
F. Calcaterra et al. / Placenta 35 (2014) 431e436432
contribute significantly to tumor angiogenesis, the levels of circu-lating EPCs are increased [3].
In healthy pregnancy, EPCs may actively contribute to thedevelopment and maintenance of the vascular network needed toensure successful placentation and fetal growth. Indeed, data on thelevels of EPCs circulating in the maternal peripheral blood duringhumanpregnancy are conflicting, the few studies addressing this cuereporting either increased or reduced or unchanged numbers of EPCsin the blood of healthy pregnant compared with nonpregnantwomen [4e7]. The reasons for these discrepancies may be explainedat least inpartwithmethodological differences among the studies. Infact, although in all cases EPCs were quantified by flow cytometricenumeration, which is the most quantitative method to measureEPCs [8], the above studies differed from each other in the samplematerial used for EPC counting (whole blood vs. peripheral bloodmononuclear cells) and in the markers used to define EPCs. Actually,flow cytometric quantification of EPCs relies on a combination ofprogenitor antigens (CD34 or CD133, or both) and endothelialmarkers (mainly kinase insert domain receptor: KDR) that stillawaits standardization. The inclusion in the analysis of the pan-leukocyte marker CD45 has recently gained higher precision, and ithas been suggested that the CD45dim/CD34þ/KDRþ phenotype mayrepresent the best combination to quantify EPCs in the clinicalsetting [8,9]. Notably, CD45 staining was missing in three of the fourabove studies assessing EPCs during human pregnancy.
Therefore, in this study we applied a flow cytometric methodwhich uses CD45 gating and that we had previously used to suc-cessfully demonstrate EPC changes in response to various physio-logical and pathological conditions [10e13], for investigatingwhether the number of EPCs might increase in the maternal cir-culation during normal pregnancy. We also investigated whetherthe levels of EPCs may fail to increase in the blood of women withpregnancy complicated by idiopathic intrauterine growth restric-tion (IUGR), a leading cause of perinatal mortality and morbiditycharacterized by insufficient placental perfusion [14,15]. The plas-matic levels of the main angiogenic factors known to affect thecirculating levels of EPCs were evaluated, as well.
We observed, indeed, that EPCs increase in maternal circulationduring healthy pregnancy and that such an increase is impaired inpregnancies complicated by IUGR, switching on the possibility thatEPCsmay represent the target of novel strategies for themonitoringand treatment of this severe pregnancy complication. Because ofthe known beneficial effects of statins on EPCs [9], our study mayprovide the theoretical basis for using statins in the prevention ofIUGR-related adverse pregnancy outcomes, thus joining the currentat-large animated debate on the therapeutic indication of statin usein pregnancy.
2. Methods
2.1. Patients and controls
The study population consisted of 21 non-pregnant women in the follicular phaseof themenstrual cycle, 44 healthy pregnantwomen (9 in the first,13 in the second and22 in the third trimester) and 11 women with pregnancy complicated by idiopathicIUGR. Their age and gestational age at blood collection are reported in Table 1. None ofthe subjects included in the study were cigarette smokers or were suffering from anymedical conditions that may affect EPC count (i.e. diabetes, hypertension,
hypercholesterolemia, cardiovascular or respiratory diseases, cancer). Non-pregnantcontrols had regular menstrual cycles and were not using hormonal contraceptives.All enrolled pregnancies were singleton followed-up at the Unit of Obstetrics andGynecology of the University Hospital Luigi Sacco of Milan. Gestational diabetes,abnormal fetal karyotype, fetal malformations, preeclampsia and infections wereconsidered exclusion criteria. Normal pregnancies were characterized by absence ofmaternal or fetal pathologies, no history of obstetric complications during pregnan-cies, and no pharmacologic treatment that could influence pregnancy outcome andfetal growth. Normal intrauterine fetal growth was confirmed by routine ultrasoundscans performed at 20 and 32 weeks of gestation, according to Italian guidelines. Allnormal pregnant women delivered at term, between 37 and 42 weeks of gestation, anappropriate-for-gestational-age newborn according to birth weight references [16].IUGR were characterized by abdominal circumference measurements <10th percen-tile of reference values for fetuses of similar ages, together with a shift of theabdominal growth of >40th percentiles diagnosed by ultrasound in utero [17].
Peripheral blood samples (1.8 ml) were obtained by venipuncture and collectedinto sodium citrate Vacutainer tubes (Becton Dickinson, San Jose, CA, USA). Ethicsapproval was obtained from the local Institutional Review Committee and a signedinformed consent was obtained from all participants.
2.2. Quantification of circulating EPCs
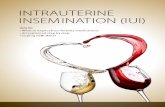
Whole peripheral blood samples were analyzed by flow cytometry as previouslydescribed [11]. Briefly, 200 ml of anticoagulated whole blood were incubated for20minwith biotin-conjugated anti-human KDR (SigmaeAldrich, St Louis, MO, USA),phycoerythrin (PE)-conjugated anti-human CD133 (Miltenyi-Biotec, GmbH, Ber-gisch Gladbach, Germany), allophycocyanin (APC)-conjugated anti-human CD34(BeckmaneCoulter Immunotech, Marsille, France) and peridininechlorophylleprotein complex (PerCP)-Cy5.5-conjugated anti-human CD45 (e-Bioscience, SanDiego, CA, USA) monoclonal antibodies. After incubation, erythrocytes were lysedand the remaining cells were further incubated in the dark for 20 min with fluo-rescein isothiocyanate (FITC)-conjugated streptavidin (SigmaeAldrich) to revealbiotin-conjugated anti-human KDR. Fluorescence minus one samples were used asnegative controls. Samples were analyzed using a FACSCanto2 flow cytometer andFACSDiva Software (Becton Dickinson). A representative flow cytometric analysis isshown in Fig. 1. An acquisition gate was established based on forward scatter (FSC)and side scatter (SSC) that included mononuclear cells but excluded most gran-ulocytes and debris. 300,000 eventswere routinely collected to visualize and gate onthis population. EPCs were identified as either CD45dim/CD34þ/KDRþ or CD45dim/CD34þ/KDRþ/CD133þ. Estimates of the absolute numbers of peripheral blood pro-genitor cells were calculated from the proportion of cells recorded by flow cytom-etry in the mononuclear gate multiplied by absolute mononuclear cell countmeasured using a standard hematology analyzer.
2.3. Measurement of plasmatic cytokines
All ELISA kits were purchased from R&D Systems (Minneapolis, MN, USA). Theamounts of free vascular endothelial growth factor (VEGF) and free placental growthfactor (PlGF) were determined by Quantikine ELISA kits (catalog number DVE00 andDPG00, respectively). The amounts of stromal-derived factor-1 (SDF-1) weredetermined by DuoSet ELISA kits (catalog number DY350). All individual steps wereperformed according to the manufacturer’s instructions.
2.4. Statistical analysis
Statistical analyses were performed using Openstat3 software. All statisticalanalyses assumed a two-sided significance level of p < 0.05. The ManneWhitney Utest was used for comparisons between groups. The Spearman rank test was used toinvestigate for possible correlations.
3. Results
3.1. Low birth weight due to IUGR
Growth restriction was confirmed at birth by a neonatal weight<10th percentile according to Italian standards for birth weight andgestational age [16] (fetal birth weight IUGR vs. healthy
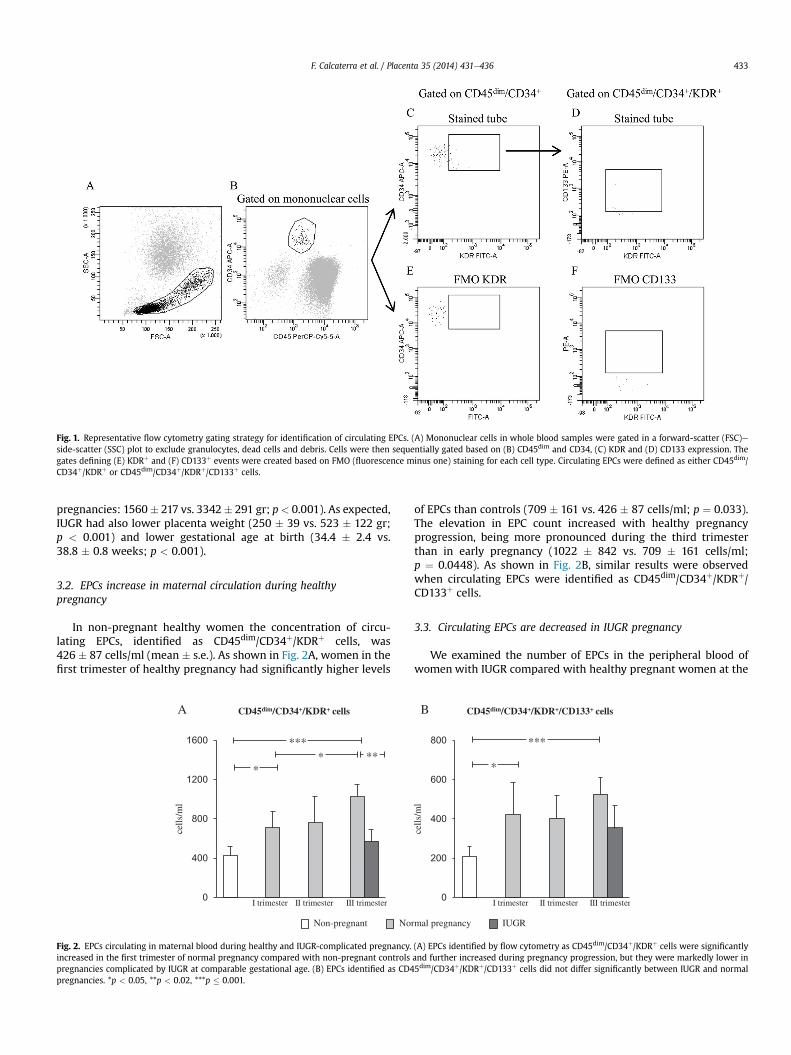
Fig. 1. Representative flow cytometry gating strategy for identification of circulating EPCs. (A) Mononuclear cells in whole blood samples were gated in a forward-scatter (FSC)eside-scatter (SSC) plot to exclude granulocytes, dead cells and debris. Cells were then sequentially gated based on (B) CD45dim and CD34, (C) KDR and (D) CD133 expression. Thegates defining (E) KDRþ and (F) CD133þ events were created based on FMO (fluorescence minus one) staining for each cell type. Circulating EPCs were defined as either CD45dim/CD34þ/KDRþ or CD45dim/CD34þ/KDRþ/CD133þ cells.
F. Calcaterra et al. / Placenta 35 (2014) 431e436 433
pregnancies: 1560� 217 vs. 3342� 291 gr; p< 0.001). As expected,IUGR had also lower placenta weight (250 � 39 vs. 523 � 122 gr;p < 0.001) and lower gestational age at birth (34.4 � 2.4 vs.38.8 � 0.8 weeks; p < 0.001).
3.2. EPCs increase in maternal circulation during healthypregnancy
In non-pregnant healthy women the concentration of circu-lating EPCs, identified as CD45dim/CD34þ/KDRþ cells, was426 � 87 cells/ml (mean � s.e.). As shown in Fig. 2A, women in thefirst trimester of healthy pregnancy had significantly higher levels
0
400
800
1200
1600
I trimester II trimester III trimester
cells
/ml
****
***
NoNon-pregnant
A CD45dim/CD34+/KDR+ cells
Fig. 2. EPCs circulating in maternal blood during healthy and IUGR-complicated pregnancy.increased in the first trimester of normal pregnancy compared with non-pregnant controlspregnancies complicated by IUGR at comparable gestational age. (B) EPCs identified as CD4pregnancies. *p < 0.05, **p < 0.02, ***p � 0.001.
of EPCs than controls (709 � 161 vs. 426 � 87 cells/ml; p ¼ 0.033).The elevation in EPC count increased with healthy pregnancyprogression, being more pronounced during the third trimesterthan in early pregnancy (1022 � 842 vs. 709 � 161 cells/ml;p ¼ 0.0448). As shown in Fig. 2B, similar results were observedwhen circulating EPCs were identified as CD45dim/CD34þ/KDRþ/CD133þ cells.
3.3. Circulating EPCs are decreased in IUGR pregnancy
We examined the number of EPCs in the peripheral blood ofwomen with IUGR compared with healthy pregnant women at the
0
200
400
600
800
rmal pregnancy IUGR
***
*
cells
/ml
B CD45dim/CD34+/KDR+/CD133+ cells
I trimester II trimester III trimester
(A) EPCs identified by flow cytometry as CD45dim/CD34þ/KDRþ cells were significantlyand further increased during pregnancy progression, but they were markedly lower in5dim/CD34þ/KDRþ/CD133þ cells did not differ significantly between IUGR and normal

0
200
400
600
pg/m
l
A
I trimester II trimester III trimester 0
200
400
600
800
1000
1200
1400
pg/m
l
I trimester II trimester III trimester
B
***
**** ***
** *
Normal pregnancyNon-pregnant IUGR
PlGF SDF-1
Fig. 3. Plasmatic levels of the angiogenic factors PlGF and SDF-1 in healthy and IUGR-complicated pregnancy. (A) The levels of PlGF increased progressively along healthy pregnancy,and they were significantly lower in IUGR than normal pregnancy at the same gestational age. (B) The levels of SDF-1 increased during normal pregnancy, with an early increaseobserved in the first trimester that progressively mitigated during pregnancy progression, but they were lower in IUGR than normal pregnancy. *p < 0.05, **p < 0.02, ***p � 0.001.
F. Calcaterra et al. / Placenta 35 (2014) 431e436434
same gestational age. As shown in Fig. 2A, the number of circulatingCD45dim/CD34þ/KDRþ EPCs was significantly lower in IUGR than innormal pregnancy (570 � 123 vs. 1022 � 842 cells/ml; p ¼ 0.020),showing values that were similar to those observed in non-pregnant controls (570 � 123 vs. 426 � 87 cells/ml; p ¼ n.s.).Similar results were observed when circulating EPCs were identi-fied as CD45dim/CD34þ/KDRþ/CD133þ cells, though in this case thedifference between IUGR and normal pregnancies did not reach thestatistical significance (353 � 20 vs. 525 � 17 cells/ml; p ¼ 0.082)(Fig. 2B).
3.4. Plasmatic PlGF levels are markedly reduced in IUGR pregnancy
In order to investigate whether the changes in EPC numbersoccurring during healthy pregnancy and IUGR may be related to thelevels of circulating soluble factors, wemeasured the plasmatic levelsof angiogenic cytokines known to affect the number of circulatingEPCs. As shown in Fig. 3A, the levels of PlGF increased progressivelyalong healthy pregnancy, and they were significantly lower in IUGRthan normal pregnancy, showing a course that roughly recapitulatedthe course of circulating EPCs. As shown in Fig. 3B, the levels of SDF-1were also increased during normal pregnancy, with an early increaseobserved in the first trimester that progressively mitigated duringpregnancy progression. Plasmatic SDF-1 was lower in IUGR thannormal pregnancy, as well. The plasmatic levels of free VEGF werebelow the detection limit of 9 pg/ml in all trimesters of normalpregnancy, as well as in IUGR pregnancy. No correlation wasobserved between the levels of CD45dim/CD34þ/KDRþ or CD45dim/CD34þ/KDRþ/CD133þ EPCs and any of the measured plasmatic fac-tors (namely PlGF, SDF-1 or VEGF).
4. Discussion
In this study we demonstrated that in normal human pregnancyEPCs undergo a progressive increase in the maternal blood. Thisresult was not surprising, as an increased availability of EPCsstarting from the early stages of pregnancy might reasonably beexpected in order to ensure the formation of a placental vascularnetwork adequate to sustain placentation and fetal growth.Nevertheless, an unambiguous demonstration of EPC increase innormal pregnancy has been hampered so far by the lack of stan-dardized methods employed for EPC quantification and analysis.Indeed, previous studies assessing EPC number in normal
pregnancy either by in vitro cell culture assays or by flow cyto-metric detection reported contradictory results [4e7,18e20]. In thisstudy, we investigated the course of maternal EPCs during preg-nancy by applying a flow cytometric method, already publishedelsewhere [11], which identifies EPCs directly in blood samples asCD45dim/CD34þ/KDRþ cells. Notably, it is possible that these cellsdo not directly contribute to vasculogenesis [21,22], yet they arethought to greatly contribute to endothelial homeostasis andangiogenesis [23]. Although a definitive consensus on the pheno-type of EPCs is still lacking, current literature supports the idea thatCD45dim/CD34þ/KDRþ represents the best antigenic combination todefine EPCs in terms of detection accuracy, biological meaning andclinical usefulness [2,9,24,25]. With this method, we observed thatEPCs are increased in the blood of pregnant women starting fromthe first trimester and they further increase with pregnancy pro-gression. We further demonstrated that EPCs were markedlyreduced in the blood of women with pregnancies complicated byidiopathic IUGR, a late pregnancy complication associated withplacental vascular insufficiency [14,15]. Notably, roughly similar butnot significant results were obtained when the stem cell antigenCD133 was used as an additional marker to restrict EPCs, thussupporting the opinion that CD45dim/CD34þ/KDRþmay be themostappropriate phenotype to identify EPCs. This conclusion is inaccordance with the demonstration that endothelial outgrowthcells do not derive from CD133þ cells [21].
VEGF, PlGF and SDF-1 are the main angiogenic cytokinesinvolved in EPCmobilization and recruitment [1,26e28]. In order toinvestigate their possible involvement in IUGR-associated EPCreduction, we measured their plasmatic levels. According to pre-vious studies [29,30], free plasmatic VEGFwas undetectable in bothnormal and IUGR pregnancies. Free PlGF and SDF-1 wereconversely detected in all samples and were significantly reducedin IUGR compared with normal pregnancies. PlGF is a potentangiogenic factor acting by several mechanisms including EPCmobilization and recruitment; it is highly expressed in the placentathroughout all stages of gestation and it plays a key role in placentalvascularization and fetal growth [27,28,31]. Therefore, reducedlevels of PlGF levels in maternal circulation may be particularlyrelevant to IUGR pathogenesis, as previously suggested by otherAuthors [29,32]. SDF-1 is primarily involved in mobilizing EPCsfrom the bone marrow and stimulating EPC traffic from the circu-lation into the vessel wall in conditions of tissue hypoxia andvascular damage [26]. It is also involved in key aspects of placental

F. Calcaterra et al. / Placenta 35 (2014) 431e436 435
development [33,34]. To our knowledge, SDF-1 levels in maternalcirculation of IUGR pregnancy have never been investigated so far,and our novel finding of markedly reduced SDF-1 levels may beworthy to the comprehension of IUGR pathogenesis. In this respect,although we did not observe a significant correlation betweeneither PlGF or SDF-1 levels and EPC count, our results may overallsuggest that impaired availability of both cytokines may likelycontribute to EPC impairment in IUGR.
Our demonstration that maternal EPCs are markedly reduced inIUGR-complicated pregnancies may suggest that EPCs may partic-ipate in the defective placental development which characterizesIUGR. This hypothesis may be strengthened by the recent demon-stration that endothelial colony forming cells cultured from thecord blood of IUGR pregnancies are rarefied and functionallyimpaired [35,36]. These cells represent a relevant population ofEPCs endowed with proven clonal proliferative potential andin vivo vasculogenic activity [37]. According to these findings, it hasalso been reported that circulating angiogenic cells cultured fromthe blood of IUGR pregnancies after delivery are reduced andimpaired in their migratory function [38], and that EPCs counted byflow cytometry are decreased in IUGR cord blood, as well [39].Compared with the other approaches, flow cytometric count ofEPCs in maternal blood performed in our study has key advantagesconsisting in need for very small blood samples, rapidity ofexecution, easy accessibility of blood. These properties may renderflow cytometric analysis of circulating maternal EPCs a convenientprocedure that can be serially repeated during pregnancy follow-up, suggesting that the circulating levels of EPCs could probablybe developed as key biomarkers in IUGR pregnancies.
All together, the demonstration of numerical reduction andfunctional impairment of EPCs occurring during IUGR pregnanciesmay suggest that EPCs may represent the target of novel therapeuticstrategies for this condition, aimed to prevent IUGR-related adversepregnancyoutcomes. Inparticular,womenwith IUGRpregnancymaybenefit from treatment with statins that are known to increase thenumber of circulating EPCs, to improve their mobilization, migratorycapacity and survival, and to induce PlGF [9,40e42]. Indeed, ananimated debate is currently ongoing on the feasibility of statinuse inpregnancy. In fact, statins are contraindicated inpregnancymainly onthe basis of isolated retrospective case reports raising teratogenicpotential, and their safety remained then unquestioned primarilybecause there was no therapeutic indication of their use in pregnantwomen [43]. With the more recent demonstration that statins havebeneficial pleiotropic effects that go far beyond their cholesterol-reducing activity, the possible therapeutic applications of statins inpregnancy, including inherited hyperlipidemia and preeclampsia, areincreasing [44,45]. Indeed, growing evidence seems to support thesafety of statins in pregnancy, and a pilot trial evaluating the safetyand pharmacokinetics of pravastatin in high-risk pregnant women isrunning [43]. In this scenario, wewould suggest that, once the safetyof statins in pregnancy will be established, IUGRmay be counted as acandidate pregnancy condition that may benefit from statin therapy.
In conclusion, in this study we demonstrated that EPCs increasein maternal circulation during healthy pregnancy and that such anincrease is impaired in pregnancies complicated by IUGR, sug-gesting that flow cytometric count of EPCs in the maternal bloodmight be developed as a valuable biomarker useful in the diagnosisand monitoring of IUGR pregnancies also in the perspective offuture EPC-targeted therapeutic approaches for this severe preg-nancy complication.
Conflict of interest
We wish to confirm that there are no conflicts of interest asso-ciated with this publication and there has been no significant
financial support for this work that could have influenced itsoutcome.
Acknowledgments
This study was supported by grants from the Italian MInistry ofEducation, University and Research (MIUR) (PRIN 2008A3E9WM-003) and Università degli Studi di Milano (2009-ATE-0573) to SDB;Fondazione Cariplo (1055/104878-2005) to IC. AT, EC and MC weresupported by a fellowship of the Doctorate School of MolecularMedicine, University of Milan, Italy. FC is a recipient of a fellowshipawarded by the Fondazione Italiana per la Ricerca sul Cancro.
References
[1] Raval Z, Losordo DW. Cell therapy of peripheral artery disease: from experi-mental findings to clinical trials. Circ Res 2013;112:1288e302.
[2] Schmidt-Lucke C, Rossig L, Fichtlscherer S, Vasa M, Britten M, Kämper U, et al.Reduced number of circulating endothelial progenitor cells predicts futurecardiovascular events. Circulation 2005;111:2981e7.
[3] De la Puente P, Muz B, Azab F, Azab AK. Cell trafficking of endothelial pro-genitor cells in tumor progression. Clin Cancer Res 2013;19:3360e8.
[4] Buemi M, Allegra A, D’Anna R, Coppolino G, Crasci
E, Giordano D, et al. Con-centration of circulating endothelial progenitor cells (EPC) in normal preg-nancy and in pregnant women with diabetes and hypertension. Am J ObstetGynecol 2007;196:68.e1e6.
[5] Luppi P, Powers RW, Verma V, Edmunds L, Plymire D, Hubel CA. Maternalcirculating CD34þVEGFR-2þ and CD133þVEGFR-2þ progenitor cells increaseduring normal pregnancy but are reduced in women with preeclampsia.Reprod Sci 2010;17:643e52.
[6] Matsubara K, Abe E, Matsubara Y, Kameda K, Ito M. Circulating endothelialprogenitor cells during normal pregnancy and pre-eclampsia. Am J ReprodImmunol 2006;56:79e85.
[7] Karthikeyan VJ, Blann AD, Baghdadi S, Lane DA, Beevers DG, Lip GYH. Endo-thelial dysfunction in hypertension in pregnancy: associations betweencirculating endothelial cells, circulating progenitor cells and plasma vonWillebrand factor. Clin Res Cardiol 2011;100:531e7.
[8] Van Craenenbroeck EM, Van Craenenbroeck AH, van Ierssel S, Bruyndonckx L,Hoymans VY, Vrints CJ, et al. Quantification of circulating CD34þ/KDRþ/CD45dim endothelial progenitor cells: analytical considerations. Int J Cardiol2013;167:1688e95.
[9] Schmidt-Lucke C, Fichtlscherer S, Aicher A, Tschope C, Schultheiss HP,Zeiher AM, et al. Quantification of circulating endothelial progenitor cellsusing the Modified ISHAGE protocol. PLoS ONE 2010;5(11):e13790.
[10] Cobellis G, Botti C, Taddeo A, Silvestroni A, Lillo S, Da Ponte A, et al. Successfulbone marrow transplantation reveals the lack of endothelial progenitor cellsmobilization in a patient with critical limb ischemia: a case report. TransplantProc 2010;42:2816e20.
[11] Colombo E, Marconi C, Taddeo A, Cappelletti M, Villa ML, Marzorati M, et al.Fast reduction of peripheral blood endothelial progenitor cells in healthyhumans exposed to acute systemic hypoxia. J Physiol 2012;590:519e31.
[12] Mezzani A, Grassi B, Jones AM, Giordano A, Corrà U, Porcelli S, et al. Speedingof pulmonary VO2 on-kinetics by light-to-moderate-intensity aerobic exercisetraining in chronic heart failure: clinical and pathophysiological correlates. IntJ Cardiol 2013;167:2189e95.
[13] Eleuteri E, Mezzani A, Di Stefano A, Vallese D, Gnemmi I, Delle Donne L, et al.Aerobic training and angiogenesis activation in patients with stable chronicheart failure: a preliminary report. Biomarkers 2013;18:418e24.
[14] Cetin I, Alvino G. Intrauterine growth restriction: implications for placentalmetabolism and transport. A review. Placenta 2009;30:S77e82.
[15] Cerdeira AS, Karumanchi SA. Angiogenic factors in preeclampsia and relateddisorders. Cold Spring Harb Perspect Med 2012;2:a006585.
[16] Parazzini F, Cortinovis I, Bortolus R, Fedele L. Standard di peso alla nascita inItalia. Ann Ostet Ginecol Med Perinat 1991;112:203e46.
[17] Todros T, Ferrazzi E, Groli C, Nicolini U, Parodi L, Pavoni M, et al. Fittinggrowth curves to head and abdomen measurements of the fetus: a multi-centric study. J Clin Ultrasound 1987;15:95e105.
[18] Savvidou MD, Xiao Q, Kaihura C, Anderson JM, Nicolaides H. Maternal circu-lating endothelial progenitor cells in normal singleton and twin pregnancy.Am J Obstet Gynecol 2008;198:414e1e5.
[19] Sugawara J, Mitsui-Saito M, Hoshiai T, Hayashi C, Kimura Y, Okamura K.Circulating endothelial progenitor cells during human pregnancy. J ClinEndocrinol Metab 2005;90:1845e8.
[20] Sipos PI, Crocker IP, Hubel CA, Baker PN. Endotheial progenitor cells: theirpotential in the placental vasculature and related complications. Placenta2010;31:1e10.
[21] Timmermans F, Van Hauwermeiren F, De Smedt M, Raedt R, Plasschaert F, DeBuyzere ML, et al. Endothelial outgrowth cells re not derived from CD133þcells or CD45þ hematopoietic precursors. Arterioscler Thromb Vasc Biol2007;27:1572e9.

F. Calcaterra et al. / Placenta 35 (2014) 431e436436
[22] Estes ML, Mund JA, Ingram DA, Case J. Identification of endothelial cells andprogenitor cell subsets in human peripheral blood. Curr Protoc Cytom2010;9(9.33):1e11.
[23] Estes ML, Mund JA, Mead L, Prater DN, Cai S, Wang H, et al. Application ofpolychromatic flow cytometry to identify novel subsets of circulating cellswith angiogenic potential. Cytom A 2010;77:831e9.
[24] Fadini GP, Baesso I, Albiero M, Sartore S, Agostini C, Avogaro A. Technicalnotes on endothelial prognitor cells: ways to escape from the knowledgeplateau. Atherosclerosis 2008;197:496e503.
[25] Fadini GP, Losordo D, Dimmeler S. Crtical reevaluation of endothelial pro-genitor cell phenotypes for therapeutic and diagnostic use. Circ Res 2012;110:624e37.
[26] Ceradini DJ, Gurtner GC. Homing to hypoxia: HIF-1 as a mediator of progen-itor cell recruitment to injured tissue. Trends Cardiovasc Med 2005;15:57e63.
[27] Li B, Sharpe EE, Maupin AB, Teleron AA, Pyle AL, Carmeliet P, et al. VEGF andPlGF promote adult vasculogenesis by enhancing EPC recruitment and vesselformation at the site of tumor neovascularization. FASEB J 2006;20:E664e76.
[28] Fischer C, Mazzone M, Jonckx, Carmeliet P. FLT1 and its ligands VEGFBand PlGF: drug targets for anti-angiogenic therapy? Nat Rev Cancer 2008;8:942e56.
[29] Wallner W, Sengenberger R, Strick R, Strissel PL, Meurer B, Beckmann MW,et al. Angiogenic growth factors in maternal and fetal serum in pregnanciescomplicated by intrauterine growth restriction. Clin Sci 2007;112:51e7.
[30] Banks RE, Forbes MA, Searles J, Pappin D, Canas B, Rahman D, et al. Evidence ofthe existence of a novel pregnancy-associated soluble variant of the vascularendothelial growth factor receptor Flt-1. Mol Hum Reprod 1998;4:377e86.
[31] Clark D, Smith S, Licence D, Evans A, Charnok-Jones D. Comparison ofexpression patterns for placental growth factor, vascular endothelial growthfactor (VEGF),VEGF-B and VEGF-C in the human placenta throughout gesta-tion. J Endocrinol 1998;159:459e67.
[32] Benton SJ, Hu Y, Xie F, Kupfer K, Lee SW, Magee LA, et al. Can placental growthfactor in maternal circulation identify fetuses with placental intrauterinegrowth restriction? Am J Obstet Gynecol 2012;206:163.e1e7.
[33] Wu X, Li DJ, Yuan MM, Zhu Y, Wang MY. The expression of CXCR4/CXCL12 infirst-trimester human trophoblast cells. Biol Reprod 2004;70:1877e85.
[34] Red-Horse K, Drake PM, Gunn MD, Fisher SJ. Chemokine ligand and receptorexpression in the pregnant uterus: reciprocal patterns in complementary cellsubsets suggest functional roles. Am J Pathol 2001;159:2199e213.
[35] Sipos PI, Bourque SL, Hubel CA, Baker PN, Sibley CP, Davidge ST, et al. Endo-thelial colony forming cells derived from pregnancies complicated by intra-uterine growth restriction are fewer and have reduced vasculogenic capacity.J Clin Endocrinol Metabol 2013;98:4953e60.
[36] Crocker IP, Sipos PI. Endothelial progenitor cells in pregnancy and obstetricpathologies. Placenta 2013;34:S62e7.
[37] Yoder MC, Mead LE, Prater D, Krier TR, Mroueh KN, Li F, et al. Redefiningendothelial progenitor cells via clonal analysis and hematopoietic stem/pro-genitor cell principals. Blood 2007;109:1801e9.
[38] King TF, Bergin DA, Kent EM, Manning F, Reeves EP, Dicker P, et al. Endothelialprogenitor cells in mothers of low-birthweight infants: a link betweendefective placental vascularization and increased cardiovascular risk? J ClinEndocrinol Metab 2013;98:E33e9.
[39] Monga R, Buck S, Sharma P, Thomas R, Chouthai NS. Effect of preeclampsiaand intrauterine growth restriction on endothelial progenitor cells in humanumbilical cord blood. J Matern Fetal Neonatal Med 2012;25:2385e9.
[40] Everarert BR, van Craenenbroeck EM, Hoymans VY, Haine SE, Nasauw LV,Conraads VM, et al. Current perspective of pathophysiological and interven-tional effects on endothelial progenitor biology: focus on Pi3K/AKT/eNOSpathway. Int J Cardiol 2010;144:350e66.
[41] Huang CY, Lin FY, Shih CM, Au HK, Chang YJ, Nakagami H, et al. Moderate tohigh concentrations of high-density lipoprotein from healthy subjects para-doxically impair human endothelial progenitor cells and related angiogenesisby activating Rho-associated kinase pathways. Arterioscler Thromb Vasc Biol2012;32:2404e17.
[42] Kumasawa K, Ikawa M, Kidoya H, Hasuwa H, Saito-Fujita T, Morioka Y, et al.Pravastatin induces placental growth factor (PGF) and ameliorates pre-eclampsia in a mouse model. Proc Natl Acad Sci USA 2011;108:1451e5.
[43] Vlachadis N, Tsamadias V, Economou E. Statins in pregnancy: safety andperspectives of therapeutic applications. BJOG 2013;120:1439e40.
[44] Lecarpentier E, Morel O, Fournier T, Elefant E, Chavatte-Palmer P, Tsatsaris V.Statins and pregnancy between supposed risks and theoretical benefits. Drugs2012;72:773e88.
[45] Leiva A, de Medina CD, Salsoso R, Saez T, San Martin S, Abarzua F, et al.Maternal hypercholesterolemia in pregnancy associates with umbilicalvein endothelial dysfunction. Arterioscler Thromb Vasc Biol 2013;33:2444e53.
Copyright © 2022 FDOKUMEN