
Effects of Blood Flow Restriction Exercise on Muscular ...
19
Page 1/19 Effects of Blood Flow Restriction Exercise on Muscular Endurance and Cardiopulmonary Endurance: A Systematic Review and Meta-Analysis Feng Xiong Chengdu University of TCM Jie Feng Chengdu University of TCM Panyun Mu Chengdu University of TCM Qiulin Deng Beijing Sport University Hairui Guo Chengdu University of TCM Wenbin Zhang Chengdu University of TCM Haoran Sun Chengdu University of TCM Yimei Hu ( [email protected] ) Chengdu University of TCM Article Keywords: Posted Date: June 6th, 2022 DOI: https://doi.org/10.21203/rs.3.rs-1664011/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Effects of Blood Flow Restriction Exercise on Muscular ...

Page 1/19
Effects of Blood Flow Restriction Exercise on Muscular Endurance andCardiopulmonary Endurance: A Systematic Review and Meta-AnalysisFeng Xiong
Chengdu University of TCMJie Feng
Chengdu University of TCMPanyun Mu
Chengdu University of TCMQiulin Deng
Beijing Sport UniversityHairui Guo
Chengdu University of TCMWenbin Zhang
Chengdu University of TCMHaoran Sun
Chengdu University of TCMYimei Hu ( [email protected] )
Chengdu University of TCM
Article
Keywords:
Posted Date: June 6th, 2022
DOI: https://doi.org/10.21203/rs.3.rs-1664011/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 2/19
Abstract
BackgroundIn recent years, blood �ow restriction (BFR) training, which can improve body function with lower intensity exercise, has attracted more and moreattention. However, there are inadequate systematic evaluation and high-quality evidence to search the impact of BFR on muscular endurance andcardiopulmonary endurance, so the target of the study is to evaluate whether BFR training can promote physical endurance.
MethodsA systematic review and meta-analysis had been conducted. Literature was retrieved from original to 2022-01-18 in the following electronicdatabases: PubMed, Web of Science, the Cochrane Library databases, Embase, CNKI (China National Knowledge Internet), CBM (China BiologyMedicine disc).
ResultsThe results showed that aerobic exercise combined with BFR (AE-BFR) and moderate to low intensity exercise with BFR (ML-BFR) signi�cantlyimproved participants' aerobic endurance, compared with non-BFR exercise. However, low-load resistance training with BFR (LBFR-RT) didn’t havesigni�cant difference compared with low-load resistance training (LL-RT) or high-load resistance training (HL-RT) on muscle endurance, and thesame with between anaerobic exercise with BFR (ANA-BFR) and anaerobic exercise (ANA-E).
ConclusionBased on current data, the results need to be interpreted cautiously and conservatively. BFR training is a very promising method to improveendurance for the elderly, patients with chronic diseases, musculoskeletal injury or postoperative rehabilitation, and athletes looking to improveexercise ability. For people who cannot tolerate high-intensity exercise, in order to improve the aerobic endurance, using moderate to low intensityexercise with BFR may be a better choice than only moderate to low intensity exercise. The bene�ts of BFR for muscular endurance and the valueof using high-intensity BFR training still need further study.
IntroductionEndurance is an important indicator of human health and athletic ability. There is no doubt that cardiopulmonary endurance is of great importanceto health, to predict the occurrence and development of disease and the risk of death[1, 2]. There is a close relationship between muscle enduranceand cardiopulmonary endurance. Lacking muscle endurance will reduce people's ability to adapt to environmental changes and hard work andlearning tasks, and make people vulnerable to chronic diseases related to skeletal muscle system. In the �eld of sports, endurance is an importantindex to measure the athletic level of an athlete, and one of the key physical functions of athletes to improve in daily training. Patients with sportsinjuries, in postoperative rehabilitation and elderly patients, due to long-term braking or disease restrictions, not only vulnerable to muscle atrophyand strength decline, but easily get lower physical endurance. In clinical work, we found that the decline of muscular endurance orcardiopulmonary endurance is not isolated, but often occurs with each other, which is the comprehensive impact of the patient's impaired health.
Moderate to high intensity resistance training and endurance training are the most common and also effective ways to enhance muscle enduranceand cardiopulmonary endurance. But many patients who are affected by poor physical conditions or diseases have di�culty in tolerating mediumand high intensity exercise, and there may be risks when they do high-intensity exercise. Therefore, blood �ow restriction (BFR) training, which canimprove body function with lower intensity exercise, is an option. In recent years, BFR has received increasing attention in medical and athletic�elds. Current studies held the view that BFR training has a signi�cant advantage in promoting muscle mass and strength [3–7]. Althoughresearchers have also studied the effect of BFR on endurance, which is often their secondary research objective, no one high quality evidence hasbeen conducted on the effects of BFR training on both muscular endurance and cardiopulmonary endurance.
Current studies couldn’t provide de�nitive answers to the mechanism of how BFR training improves physical endurance. BFR training has beenshown to enhance muscle endurance by increasing muscle microvascular function and oxygenation[8–11]. one study showed that BFR trainingincreases the percentage of VO2max sustained throughout exercise by increasing convective oxygen delivery to the legs and reducing lactic acidrelease[12]. Increased cell proliferation and capillarization contribute to improved endurance performance of local muscles[13, 14]. Furtherresearch has shown that the higher metabolic/cardiopulmonary adaptive response of ET-BFR (endurance training-BFR) seems to be associatedwith the activation of key genes that drive angiogenesis (VEGF and COXIV)[15, 16].

Page 3/19
So far, researchers had some understandings about the effect of BFR on endurance, but high-quality evidence, to support BFR to improve muscularendurance and cardiopulmonary endurance, was scarce. Therefore, evaluating the effect of the BFR training on endurance is the aim of this study,which may be helpful to improve the understanding of this training mode, or provide more su�cient evidence for the further application of BFRtraining in the �eld of medicine and sports.
MethodOur study was based on the Cochrane Handbook 5.3 and PRISMA checklist, and GRADEfpro�le software was used to evaluate the quality of theresearch.
Search Strategy and Study SelectionCurrent evidence was searched in the PubMed, Web of Science, the Cochrane Library, Embase, CNKI (China National Knowledge Infrastructure),and CBM (China Biology Medicine ). All databases were searched from their establishment to 2022-01-18. The search hasn’t had restrictions ontime, geography or language.
The search strategy combined the following keywords: "BFR", "blood �ow-restricted", "vascular restriction", "blood �ow strength training", "blood�ow restriction", "ischaemia training", "KAATSU", "vascular occlusion training", "vascular occlusion", "BFR training", "occlusion training", "exercise","training". Research information were exported from the database and stored in a citation manager. All duplicate studies were deleted beforefurther process. Titles and abstracts of the retrieved articles were evaluated by two reviewers (Jie Feng Panyun Mu) to assess their eligibility forthe meta-analysis. In case of disagreement, a third reviewer (Feng Xiong) evaluated the article again. If the abstract lacked su�cient informationto determine whether it met the inclusion criteria, the reviewers need to read the full text.
Inclusion and exclusion criteria
1. Study Design: only randomized controlled trials (RCT) were included. Systematic reviews, narrative reviews, editorials, conference abstracts,letters or publications not-inclusive of original data were not adopted.
2. Patients: include healthy people, athletes, and patients with skeletal or cardiopulmonary diseases.3. Intervention: the study must have one type of exercise combined with BFR, and the training should go on several weeks at least.4. Controls: control groups in the study must have the same training method, but without BFR.5. Outcomes: must have included at least one objective indicator of muscle endurance or cardiopulmonary endurance.
Examples of objective indicators: times of repetition, duration, amount of exercise, etc. (the ability to perform an exercise repeatedly); maximaloxygen uptake(VO2max), peak oxygen uptake (VO2peak), 30s Wingate test, etc. (measures of cardiopulmonary endurance).
Data ExtractionAll articles were evaluated by two reviewers (Qiulin Deng Hairui Guo and) independently, and then extracted data. Data to be extracted: (1)participant information (i.e., age, sex and weight), (2) study information (i.e., training program, exercise intensity, occlusion pressure, cuff type andintervention period), (3) muscle endurance, aerobic endurance (i.e., VO2max, VO2peak, anaerobic threshold (AT), ventilatory threshold (VT)) andanaerobic endurance were extracted. Finally, in order to ensure accuracy, all articles were cross-checked. In case of disagreement, a third reviewer(Wenbin Zhang) would check again and made sure that a consensus was adopted.
Assessment of Risk BiasThe risk of bias was assessed with the Cochrane risk of bias tool. We illustrated the potential biases of each study by making a table, graph andsummary of the risk of bias.
The risk of bias for each study was independently assessed and cross checked by two researchers(Jie Feng and Haoran Sun) using the methodsrecommended by the Cochrane Collaboration Handbook: (1) random sequence generation (2) allocation concealment (3) blind method (4)incomplete result data (5) selective result reporting (6) other biases. In these six areas, we made " low risk", "high risk" and "unclear risk" judgmentsto assess the risk of bias in each study.
Statistical AnalysesRevMan (Review Manager Version 5.4, The Cochrane Collaboration, 2014) was used to conduct statistical analyses and GRADEfpro�le softwarewas used to evaluate the quality of the research. We used the difference in pre- and post-intervention mean and standard deviation (SD) values ofmuscle endurance and cardiopulmonary endurance for all groups in each study to calculate the standardized mean difference (SMD). To presentthe 95% con�dence intervals (CIs) and SMD of muscle endurance and cardiopulmonary endurance for all comparisons, we created forest plots.When I2 > 50%, there was heterogeneity, and random effects model was used. When I2 < = 50%, the �xed-effect model was used. Pooled effectssizes (ES) of each comparison were calculated. ES were set at < 0.10:trivial effect, 0.10–0.34:small effect, 0.35–0.64:medium effect, 0.65–

Page 4/19
1.19:large effect, ≥ 1.20:very large effect[17]. Alpha level was set to p < 0.05. To measure the stability of the results, we performed a sensitivityanalysis. Thus, one study at a time was deleted and the effect of comparison between groups was examined.
Results
Search resultThe database search yielded 4443 articles. After removing duplicates, 1177 studies have been remained, which couldn’t be excluded according totitle and abstract. Finally, 59 studies met our criteria previously set. 40 articles didn’t contain detailed data or comparable studies, and outcomemeasures of one study didn’t accurately re�ect muscular endurance[18]. Finally, 18 studies and 35 comparisons with a total population of N = 398(829 pieces of data) were included. The selection process is detailed in Fig. 1.
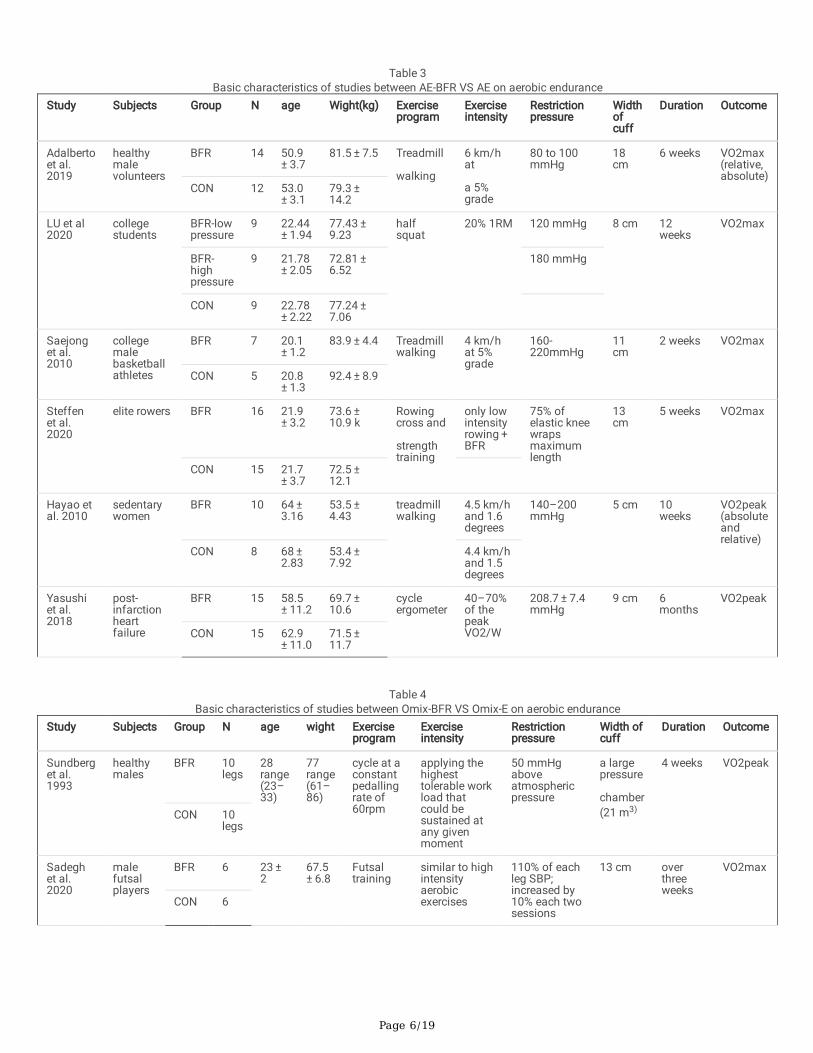
Basic characteristicsIn the literature retrieved, physical endurance was measured including muscular endurance and cardiopulmonary endurance. After excludingstudies that lacked speci�c data and su�cient number, muscular endurance was measured by the number of repetitions of exercise (the numberof exercise repetitions or change in performance of repetitions)in the literature that was eventually included. VO2max and VO2peak were used tomeasure cardiopulmonary endurance. Other indicators in the researches included muscle strength, muscle thickness, pain scores, maximalvoluntary contraction, etc. No serious adverse event was recorded in 20 studies, and muscle soreness was the common discomfort. Only onepatient in the intervention group became disoriented during a training session[19], but was not triggered by the BFR training. An overview of thestudies was summarized in Table 1–5.

Page 5/19
Table 1Basic characteristics of studies between LBFR-RT VS LL-RT on muscle endurance
Study Subjects Group N age wight Exerciseprogram
Exerciseintensity
Restrictionpressure
Widthofcuff
Duration Outcomeload(repetitions)
Christopheret al. 2014
Middle-agedpeople
BFR 17 55 ± 7
82.7 ± 16.5
kneeextension
30%1RM
80% ofAOP butno higherthan 240mmHg
5 cm 6 weeks 30% 1RM
CON
Gabriel etal. 2019
Activeyoungpeople
CBFR 9 26.1 ± 5.0
67.5 ± 9.7
low-loadexercises,benchpress, frontpull-down,tricepspulley andpulleybiceps curl
20%1RM
80% ofAOP
6 cm 6 weeks 40% 1RM
IBFR 8 23.8 ± 5.6
79.2 ± 9.3
CON 8 22.2 ± 3.5
78.0 ± 10.9
Matthew etal. 2018
healthyyoungparticipants
BFR-lowpressure
20legs
21 ± 2
68.37 ± 11.49
kneeextensions
15%1RM
40% ofAOP
10cm
8 weeks 42.5% 1RM
BFR-highpressure
20legs
80% ofAOP
CON 20legs
Apiwan etal. 2012
femalenetballers
BFR 10 20.2 ± 3.3
65.2 ± 6.5
kneeextensions;knee�exions
20%1RM
160mmHg to230mmHg
5 cm 5 weeks 20%1RM
CON 10
Apiwan etal. 2013
femalenetballers
BFR 10 20.2 ± 3.3
65.2 ± 6.5
Kneeextensions;knee�exions
20%1RM
160mmHg to230mmHg
5 cm 5 weeks 20%1RM
CON 10
Eric et al.2019
recreational-levelathletes
BFR 16legs
27 ± 3.4
? Lower limbtraining
30% of1RM
80% ofAOP
4inch
6 weeks 30%1RM
No-BFR 16legs
CON 16legs
Table 2
Basic characteristics of studies between LBFR-RT VS HL-RT on muscle enduranceStudy Subjects Group N age wight Exercise
programExerciseintensity
Restrictionpressure
Widthofcuff
Duration Outcomeload(repetitions)
Matthewet al.2018
healthyyoungparticipants
BFR-lowpressure
20legs
21 ± 2 68.37 ± 11.49
kneeextensions
15%1RM
40% of AOP 10 cm 8 weeks 42.5% 1RM
BFR-highpressure
20legs
15%1RM
80% of AOP
CON 20legs
70%1RM
Thiagoet al.2020
healthy,physicallyactiveparticipants
BFR 15 23.53 ± 2.77
76.26 ± 12.76
elbow�exors andkneeextensors
30%1RM
Arm:20 mmHg belowsystolicbloodpressure
Thigh:40mm Hgabove thearm value
arm:14 cmthigh:16cm?
8 weeks 60%1RM
CON 13 24.46 ± 2.56
79.36 ± 11.3
80%1RM
Page 6/19
Table 3
Basic characteristics of studies between AE-BFR VS AE on aerobic enduranceStudy Subjects Group N age Wight(kg) Exercise
programExerciseintensity
Restrictionpressure
Widthofcuff
Duration Outcome
Adalbertoet al.2019
healthymalevolunteers
BFR 14 50.9 ± 3.7
81.5 ± 7.5 Treadmill
walking
6 km/hat
a 5%grade
80 to 100mmHg
18cm
6 weeks VO2max(relative,absolute)
CON 12 53.0 ± 3.1
79.3 ± 14.2
LU et al2020
collegestudents
BFR-lowpressure
9 22.44 ± 1.94
77.43 ± 9.23
halfsquat
20% 1RM 120 mmHg 8 cm 12weeks
VO2max
BFR-highpressure
9 21.78 ± 2.05
72.81 ± 6.52
180 mmHg
CON 9 22.78 ± 2.22
77.24 ± 7.06
Saejonget al.2010
collegemalebasketballathletes
BFR 7 20.1 ± 1.2
83.9 ± 4.4 Treadmillwalking
4 km/hat 5%grade
160-220mmHg
11cm
2 weeks VO2max
CON 5 20.8 ± 1.3
92.4 ± 8.9
Steffenet al.2020
elite rowers BFR 16 21.9 ± 3.2
73.6 ± 10.9 k
Rowingcross and
strengthtraining
only lowintensityrowing + BFR
75% ofelastic kneewrapsmaximumlength
13cm
5 weeks VO2max
CON 15 21.7 ± 3.7
72.5 ± 12.1
Hayao etal. 2010
sedentarywomen
BFR 10 64 ± 3.16
53.5 ± 4.43
treadmillwalking
4.5 km/hand 1.6degrees
140–200mmHg
5 cm 10weeks
VO2peak(absoluteandrelative)
CON 8 68 ± 2.83
53.4 ± 7.92
4.4 km/hand 1.5degrees
Yasushiet al.2018
post-infarctionheartfailure
BFR 15 58.5 ± 11.2
69.7 ± 10.6
cycleergometer
40–70%of thepeakVO2/W
208.7 ± 7.4mmHg
9 cm 6months
VO2peak
CON 15 62.9 ± 11.0
71.5 ± 11.7
Table 4
Basic characteristics of studies between Omix-BFR VS Omix-E on aerobic enduranceStudy Subjects Group N age wight Exercise
programExerciseintensity
Restrictionpressure
Width ofcuff
Duration Outcome
Sundberget al.1993
healthymales
BFR 10legs
28range(23–33)
77range(61–86)
cycle at aconstantpedallingrate of60rpm
applying thehighesttolerable workload thatcould besustained atany givenmoment
50 mmHgaboveatmosphericpressure
a largepressure
chamber(21 m3)
4 weeks VO2peak
CON 10legs
Sadeghet al.2020
malefutsalplayers
BFR 6 23 ± 2
67.5 ± 6.8
Futsaltraining
similar to highintensityaerobicexercises
110% of eachleg SBP;increased by10% each twosessions
13 cm overthreeweeks
VO2max
CON 6

Page 7/19
Table 5Basic characteristics of studies between ANA-BFR VS ANA-E on aerobic endurance
Study Subjects Group N age wight Exerciseprogram
Exerciseintensity
Restrictionpressure
Widthofcuff
Duration Outcomeload(repetitions)
Carl etal.2017
young,healthy,activeparticipants
BFR 8 25 ± 7
75 ± 14 Run onthetreadmill
treadmill speedat 80% of eachindividual PRV(peak runningvelocity)
aperceivedpressureof 7 out of10
7.5cm
4 weeks VO2max
CON 8
Michailet al.2012
healthy,younguntrainedsubjects
BFR 10 23.3 ± 3.9
60.9 ± 10.0
trainedon aMonarkcycleergomet
2 min work,2min activerecovery boutsat 90% ofVO2maxPRESS(with cuff) and50% ofVO2max
90mmHg ? 6 weeks VO2max
CON 10 22.7 ± 4.7
67.6 ± 18.7
XU etal.2021
healthyyoungpeople
BFR 10 24.3 ± 3.8
BMI:20.63 ± 2.48
limblinkagetraining
the loading ofanaerobicthreshold (AT)
250mmHg
? 2 weeks VO2peak
CON 10 24.1 ± 3.35
BMI:20.81 ± 2.56
VO2max and VO2peak can represent aerobic endurance. Although VO2max was the gold standard for measuring aerobic endurance, usingVO2peak also accurately re�ected changes in endurance levels[20–22]. While it is possible that measurements of VO2peak in professionalathletes were unstable and couldn’t truly re�ect aerobic endurance levels, VO2peak was used in our systematic evaluation by the non-athletepopulation, middle-aged and elderly population[23–26]. Therefore, a meta-analysis evaluated the aerobic endurance of blood �ow restrictionexercise.
In this study, young people aged about 20 to 30 are the main subjects, in which women accounted for about 35%(n = 140). The study mainlyincluded healthy people and athletes, one study recruited patients with heart failure[25]. Some studies used absolute load pressure to occlusiveblood vessels, ranging from 90mmHg to 250mmHg, while some selected a certain ratio of pressure according to different individual bloodpressure or atmospheric pressure, or a perceived pressure [27]. The lower limb cuff varied in width from 4cm to 18cm and the upper limb cuff was6 or 14 cm wide, which was selected for the proximal limb. Very wide cuffs were chosen in Ramis et al [28](upper limb 14cm, lower limb 16cm)and in Ferreira et al [26] (18cm). Held et al [29]used elastic knee wraps (200*13cm) instead of pneumatic wraps. Sundberg et al [23]used a largepressure chamber (21 m3), which reduced leg blood �ow during exercise by about 20%. Two studies didn’t specify the cuff width to be used[30,31].
The studies on searching aerobic endurance and muscular endurance used different exercise methods, and the literature on searching muscularendurance used resistance exercise. The literature on measuring aerobic endurance mainly made participants on the bike, treadmill for training,exercise intensity includes aerobic exercise, mixed oxygen exercise and anaerobic exercise. Considering its applicability to healthy and sick people,we believed that the intensity of low intensity resistance training is about 30% of the one-repetition maximum (1RM), and the high intensityresistance training is over 70%1RM. According to the American Heart Association(AHA),exercises below 70% VO2max are aerobic exercise, thoseabove 85% VO2max are anaerobic exercise, and those in the middle are mixed oxygen exercise, during which anaerobic metabolism and aerobicmetabolism coexist. Blood lactate concentration, which doesn’t exceed the �rst lactate threshold (about 2mmol/L), is considered aerobic exercise,and blood lactate concentration, which exceed the second lactate threshold (4-6mmol/L), is considered anaerobic exercise.
Seven researches studied the effect of LBFR-RT on muscular endurance. Six articles studied the effect of AE-BFR on aerobic endurance, twoarticles studied the effect of mixed oxygen exercise combined with BFR and three researches studied the effect of anaerobic training combinedwith BFR. Studies on muscle endurance mainly focused on lower limb endurance training, with loads ranging from 15% 1RM (one repetitionmaximum) to 80% 1RM and training duration ranging from 5 weeks to 8 weeks. Muscle endurance tests were performed using loads ranging from20% 1RM to 42.5% 1RM, but one paper used 60% 1RM for the test[28]. Articles on aerobic endurance had participants mainly train on a treadmill,bike. Experiments were conducted from aerobic exercise to anaerobic exercise, with training duration varying widely from two weeks to six months.But there was one article[30] that did 20%1RM weight squat training to promote aerobic endurance, since the subjects were all healthy youngpeople with low load and low amount of exercise, we classi�ed this study into the aerobic exercise group for analysis.
Risk of bias and research qualityThe main �nding of the bias risk assessment was that many studies did not clearly explain the implementation of randomization, allocationconcealment, and blinding (Fig. 2 3). Although randomized controlled trials could be determined based on the full text information, the lack ofdetailed information about random methods might lead to the neglect of possible selection bias. BFR training was di�cult to blind due to

Page 8/19
signi�cant implementation differences, but it might affect the quality of our evaluation. In blinding of participants and personnel assessment, dueto the obvious difference between BFR training and traditional training, we believed that failure to implement blinding might impact the real effectof BFR training, so we rated the studies without explanation whether to implement blinding as “high risk”. The blind method was explained or thecontrol group using a non-in�atable cuff was rated “low risk”. Only four of the studies included were rated “low risk” in this category.
The quality of the research by GRADEfpro�le software showed all meta-analyses were “low quality” (Supplementary material 2). According to thescoring rules, all groups were "-2" in risk of bias and “-1” in imprecision. It was caused by the lack of detailed explanation of blind method, randommethod, allocation hiding in the included literature and small sample size.
Muscle Endurance
Low-load resistance training with BFR (LBFR-RT) VS Low-load resistance training(LL-RT)6 studies[32–37] and 16 comparisons which measured muscular endurance following LL-RT and LBFR-RT training were included in this meta-analysis, which were divided to two groups according to different outcome measures (Repetitions of number; Change in performance ofrepetitions: Fig. 4). Quantitative analysis showed that LBFR-RT and LL-RT had the same ability to increase muscular endurance(Z = 1.47, p = 0.14)in Number group, but LBFR-RT improved muscle endurance more than LL-RT in Change group (Z = 5.24, p < 0.05).The pooled ES was 0.18(95%CI -0.06–0.42) in Number group and 1.11(95%CI 0.70–1.53) in Change group. Heterogeneity was low for Number group with I2 = 12% (p = 0.33) and Change group with I2 = 27% (p = 0.25). Sensitivity analysis showed that none of the articles had a signi�cant impact on the results.
Low-load resistance training with BFR (LBFR-RT) VS high-load resistance training(HL-RT)Two studies[34, 38] with four comparisons investigated the effects of LBFR-RT and HL-RT training on muscle endurance (see Fig. 5). The weightedaverage ES was 0.28 (95%CI − 0.06–0.62), supporting LBFR-RT training. However, there was not statistical signi�cance (Z = 1.60, p = 0.11). Thecalculation of I2 showed a heterogeneity of 0% (p = 0.57). Sensitivity analysis showed that muscle endurance results were not affected by anysingle study.
Aerobic Endurance
Aerobic exercise with BFR (AE-BFR) VS aerobic exercise (AE)Six studies[24–26, 29, 30, 39] and nine comparisons were incorporated in this meta-analysis (Fig. 6 7). The overall result showed a moderateeffect in support of AE-BFR (Z = 4.20, p < 0.05), heterogeneity was not signi�cant with an I2 of 1% (p = 0.42). The subgroup analysis of VO2maxgroup showed a large effect supporting AE-BFR, which the pooled ES was 0.75 (95%CI 0.39–1.11). However, the advantage of BFR training of theVO2peak group was not statistically signi�cant(p = 0.40). Sensitivity analysis showed that Ozaki et al[40], in which traditional aerobic trainingshowed a slight advantage, led to signi�cant effect value and heterogeneity changes in this group. After removing the study, a largely signi�cant(Z = 4.81, p < 0.05) pooled ES of 0.80(95%Cl 0.47 to 1.13; I2 = 0%, p = 0.86) showed up which supported the AE-BFR in the overall meta-analysis.Only this study showed that AE was slightly superior to AE-BFR. Heterogeneity analysis and comparison between groups were conducted in thestudy, we took into account the likelihood of gender, age, health, exercise content, pressure level, training duration, but no obvious source ofheterogeneity and reason for the obvious difference was found.
Mixed oxygen exercise with BFR (Omix-BFR) VS mixed oxygen exercise (Omix-E)Only two studies[23, 41] (three comparisons) assessed aerobic endurance changes following Omix-BFR and Omix-E (Fig. 8). The weighted averageES was 0.46 (95% CI -0.09 to 1.02) in favour of Omix-BFR, no statistical signi�cance of the effect was reached (Z = 1.63, p = 0.10). I2 for this meat-analysis was 0% (p = 0.61). Sensitivity analysis showed that the result was not affected by any research in aerobic endurance.
Moderate to low intensity exercise with BFR(ML-BFR) VS moderate to low intensityexercise (ML)In actual exercise, it was di�cult to distinguish aerobic exercise from mixed oxygen exercise completely, and both exercises often existsimultaneously in the training process. In essence, both aerobic exercise and mixed oxygen exercise can be regarded as moderate to low intensityexercise. Therefore, in order to be closer to the clinical scene, we conducted an analysis of moderate to low intensity exercise. the meta-analysisincluded eight studies[23–26, 29, 30, 39, 41] and 12 comparisons comparing the effects of ML-BFR and ML on aerobic endurance (Fig. 9). Thecalculation of the meta-analysis was the favour of ML-BFR showing a moderately signi�cant (Z = 4.47, p < 0.05) pooled ES of 0.59(95% CI 0.33 to0.85). Heterogeneity was not signi�cant with an I2 of 0% (p = 0.59). Subgroup analysis of VO2max and VO2peak was performed, the results

Page 9/19
showed that the BFR group still had better effect(ES 0.71, p < 0.05; ES 0.44,p < 0.05).The heterogeneity between studies was small(I2 = 0%;I2 = 30%).The sensitivity analysis was similar to that of aerobic exercise, Ozaki et al[40] led to signi�cant effect value and heterogeneity changes in thegroup. After removing the study, the subgroup showed a largely signi�cant (Z = 2.89, p < 0.05) pooled ES of 0.72 in favor of ML-BFR. Similarchanges were observed in the overall meta-analysis (ES = 0.71,95%Cl 0.43 to 0.99; I2 = 0%, p < 0.00001).
Anaerobic exercise with BFR (ANA-BFR) VS anaerobic exercise (ANA-E)Three studies including three comparisons measured the changes of aerobic endurance after training with ANA-BFR or ANA-E (Fig. 10). Theweighted average ES was 0.07 (95% CI -0.46 to 0.59) in favour of ANA-BFR. However, no statistical signi�cance of the effect was reached (Z = 0.25,p = 0.80). I2 for this analysis was 0% (p = 0.88). Sensitivity analysis revealed that the aerobic endurance results were not affected by any study.
DiscussionAssessing the effects of BFR training on muscle endurance and cardiopulmonary endurance was the main aim of this study, compared withconventional exercise. In this article, our analyses demonstrated that AE-BFR got moderately better aerobic endurance performance than AE, ML-BFR training was the same. In muscle endurance, the results of LBFR-RT were different in Change and Number group comparing with and LL-RT.LBFR-RT had similar effects to HL-RT, the same as ANA-BFR VS ANA-E. However, the current evidence is not su�cient to draw �rm conclusions,and more high-quality studies are needed to explore this.
Muscle EnduranceIn the retrieved searches, four comparisons of Neto et al[33] and Fahs et al[42] showed that the effect of LL-RT was better than equivalent LBFR-RT. In Fahs et al, the comparison between PRE1 (pre-training) and PRE2 (three weeks after the interval) showed that LBFR-RT was superior, but thecomparison between PRE1 and the post-training was opposite. Neto et al showed that LBFR-RT in muscle endurance of bench press and front pull-down in continuous BFR group was less effective than LL-RT, as muscle endurance of bench press in intermittent BFR group. We didn't know whatcaused the discrepancy. Few articles supported that the effect of LBFR-RT was similar to equivalent non-BFR exercise[33, 43–47]. Most currentstudies supported that LBFR-RT could improve muscle endurance better than the same volume of LL-RT[10, 18, 19, 28, 33, 37, 42, 48–60]. Wefound that BFR training showed a greater reduction in muscular endurance during the follow-up period than equivalent training in Ampomah etal[46]. Meanwhile, there was a signi�cant increase of control group in time to task failure (45.5% ± 17.0%, P = 0.01). The authors did not elaboratefurther, and it was hard to speculate because of the lack of information about post-training participants. Although there were some differencesamong participants' selection, exercise methods and measurement methods in the meta-study, all exercise methods were low-load resistancetraining, and the measurement methods of muscular endurance were relatively reliable.
The comparison of whole body vibration (WBV) training and the same WBV training combined with BFR in Cai et al[61] also showed theadvantages of WBV + BFR group. All of the articles we retrieved showed signi�cantly better improvement in muscle endurance with LBFR-RT thanwithout training[18, 37, 55, 62], which at least demonstrated that BFR training was not detrimental to muscle endurance. This meta-analysisshowed that LBFR-RT achieved increase of muscular endurance similar to HL-RT. Sousa et al[51] and Groennebaek et al[62] supported this view.Even three researchers thought that LBFR-RT improved muscle endurance more[63–65]. Zinner et al[66] compared high load resistance trainingcombined with vibration (VIBRA) with the same training added BFR (VIBRA1 + COMP), after both VIBRA1 + COMP and VIBRA, the number ofrepetitions during the muscular endurance test increased by 55% and 34% respectively (P < 0.05; best d = 1.1).
In the research, we conducted a subgroup analysis of LL-RT on continuous BFR and intermittent BFR (Supplementary material 3), and both groupsshowed that BFR training improved muscle endurance more than non-BFR training, but neither was statistically signi�cant (continuous BFR: SMD0.19 [-0.08, 0.46], P = 0.18; intermittent BFR: SMD 0.15 [-0.35, 0.65], P = 0.55). More researches may be needed to investigate the differencesbetween the two types of BFR. Davids et al[60] showed that exercise with continuous BFR produced higher perceptions of pain (p = 0.026) andeffort (p = 0.033), both intermittent BFR training and LL-RT might be more tolerable for participants. Intermittent BFR may have some advantagesin patient tolerance and compliance, but we need to further clarify the effects of both BFR trainings.
The results of the meta-analysis were not stable, obvious differences between the two subgroups were shown. Subjects' baseline and trainingprogram was not signi�cantly different between the two groups. Although BFR in the Chang group showed great bene�ts, the small number ofstudies and small sample size couldn’t provide reliable results. Meanwhile, current researches, which we retrieved, showed the more support for theBFR training. Therefore, we cannot draw a de�nite conclusion, which needs to be clari�ed by subsequent studies.
Cardiopulmonary enduranceIn the included literatures, only Ozaki et al[40] showed that AE-BFR improved aerobic endurance worse than AE, though both got signi�cantimprovement. At present, most of the relevant studies believed that AE-BFR was better than AE in improving aerobic endurance [25, 26, 29, 30, 39,49, 67, 68]. Amano et al[69] showed both AE-BFR and AE had signi�cant improvement in VO2max (13.2% and 10.8% for AE and AE-BFR groups,respectively; P < 0.05), and no signi�cant difference in improvement of VO2max between groups was found (P < 0.05). An uncontrolled trial[70]

Page 10/19
showed no improvement in aerobic endurance after blood �ow restriction training. BFR training didn’t make a statistically signi�cant change inVO2peak or VT (P > 0.05). The authors thought that improvements were limited because their participants were so healthy. But some studies thatshowed signi�cant effects of BFR training also recruited healthy people and even professional athletes[23, 29, 30, 39, 49, 67]. We thought too lowblood pressure may be the reason. In the whole training process, the pressure of the cuff remained between 60 and 80 mmHg in this research. Thiswas signi�cantly lower than the set point of other studies. Abe et al[71] compared AE-BFR with no training, and there was no change in theestimated V̇O2peak for either group. Besides, the data showed a decrease in aerobic capacity in both groups after the intervention. During theactual training, the researchers found that calculated target HR (more than 50% of HR maximum reserve) was not reached by the participants.
The meta-analysis showed that ANA-BFR improved aerobic endurance similar to ANA-E. Libardi et al[72] and Thiago et al[73] showed thatendurance exercise combined with HL-RT and equal intensity endurance training combined with LL-RT achieved similar aerobic enduranceimprovement. Oliveira et al[67] and Kim et al[74] supported ANA-E was superior to ANA-BFR after training. However, VO2peak decreased slightly inthe BFR group and was opposite in the high load group three weeks after the training in Kim et al. Mueller et al[75] showed that the combination ofvibration training and high load training with BFR did not improve aerobic endurance trainer after training. Sadegh et al[76] tried to observe thein�uence of change in exercise intensity and limited blood pressure on VO2max. The result showed that participants with complete occlusion(240mmHg) and increasing exercise intensity experienced the greatest improvements in aerobic parameters.
Current literature has studied the effects of different intensities and different types of exercise combined with BFR on anaerobic endurance. Wesearched for literature ranging from healthy young adults to older adults with chronic diseases, using anaerobic threshold (AT), metabolicequivalent (METs) and 30S Wingate test to measure anaerobic endurance. Several studies have shown that BFR training signi�cantly increasedthe subjects' anaerobic endurance[25, 30, 31, 41, 76–78].This is a promising training method for athletes, but it needs to be con�rmed in morespeci�c trials with athletes. The six-minute walking test is often used to measure cardiopulmonary function in patients with cardiopulmonarydiseases. Several studies have looked at people with poor cardiopulmonary function, the results showed that aerobic exercise combined with BFRhad a longer walking distance than only aerobic exercise[79–83]. This result was consistent with the e�cacy of BFR on cardiorespiratoryendurance shown in the meta-analysis.
In the articles we retrieved, we found that the effect of BFR training decreased signi�cantly after a period of rest[46, 74], and even the enduranceperformance of the BFR training group was lower than the baseline, but the control group was maintained. This led us to question whether theeffects of BFR training could be sustained, but Lamberti et al[84] showed the endurance effect of BFR training group and control group wasmaintained for 6 weeks after the end of the training program in patients with multiple sclerosis and severe gait disabilities. There are not enoughdata to analyze this, and future research may focus on the effect of BFR after training. This will be of great help for the better promotion of BFRtraining in clinic and the development of more individualized treatment plan.
Besides, we found that few trials studied on the effects of BFR training on muscular endurance and cardiopulmonary endurance at the same time.In two studies[49, 81], the LBFR-RT signi�cantly improved aerobic and muscular endurance, and was superior to non-BFR training. Although theoptimum training program to improve muscular endurance and cardiopulmonary endurance is often different, the appropriate amount of exerciseshould have some effect on both. In practical work, for patients suffering from chronic illness, muscular endurance and cardiopulmonaryendurance are often reduced simultaneously, and simple and effective training programs are more easily accepted by trainees. Therefore, in futurestudies of BFR, muscular endurance and cardiopulmonary endurance should be evaluated simultaneously. This will be helpful to summarize ane�cient training program of BFR, making it possible to signi�cantly improve both muscle endurance and cardiopulmonary endurance by lowintensity exercise.
Practical ImplicationsThe safety of blood �ow restriction has been studied and discussed by researchers, and current studies showed that the risk of blood �owrestriction training was low. Hughes et al[3] believed that extra damage from BFR training would be very few. Pope et al[14] and Manini et al[85]thought proper use was considered to pose no greater risk than traditional exercise patterns. Muscle injury is the most common adverse effect ofBFR training, Wernbom et al[86] reviewed several studies on rhabdomyolysis and muscle injury, it disputed the contention of Loenneke et al[87]that BFR training caused little or no muscle damage. The author believed that mechanical damage and ATP depletion were the two mainmechanisms of muscle injury and rhabdomyolysis. Strenuous BFR training could cause some signs and symptoms of muscle damage, and undersome circumstances could even lead to rhabdomyolysis in subjects. For patients with heart failure, the change of BNP levels was signi�cantlynegatively correlated with exercise capacity[25]. A randomized controlled study[88] showed that vascular endothelial growth factor (VEGF) andsoluble VEGFR expression increased after BFR low-intensity resistance training (65% systolic pressure of the upper arm) for 8 weeks, which mightbe more effective in protecting the vascular endothelium. But one review[89] supported that BFR training could enhance and continuously activatemuscle metabolic re�exes, which might cause elevated blood pressure, and make other abnormal cardiovascular responses. Seriouscardiovascular events in populations with high cardiovascular risks might be triggered by increased blood pressure responses. In one meta-analysis[90], higher systolic and/or diastolic BP values were observed during exercise with BFR too, especially in hypertensive individuals. Bond etal[91] discussed the risk of VTE in the use of BRF during orthopedic postoperative rehabilitation training. It should be low risk that restrictedlyusing a wide, partially occluding cuff during resistance exercise, and BFR directly lead to the possibility of VTE is small

Page 11/19
Current studies have shown that BFR training can cause greater PRE and discomfort than the same amount of non-BFR training[92]. Somestudies[93–96] supported the low-intensity exercise with BFR could increase similar or higher perceived exertion parameters with high-intensityexercise. A pilot study[97] examined perceptual psychological parameters, and showed that affect and task motivation in BFR walking group wassigni�cantly lower than those in NBFR walking group. Regarding the discomfort caused by BFR training, Loenneke et al[98] supported that thematerial of the cuff didn’t affect the discomfort. But it seemed that people preferred to use a narrow cuff, even though it required more pressure toprovide the same blocking effect[99]. A recent trial[99] also con�rmed this view and higher pressure of BFR tended to increase discomfort[100–103]. A meta-analysis[104] examined the effects of continuous BFR training versus intermittent BFR training on training tolerance ,and showedthat intermittent BFR training did not improve exercise tolerance (SMD 0.06,p = 0.73, I 2 = 80%),which was different with Davids et al[60].
Meanwhile some evidence demonstrated that BFR exercise has therapeutic effect on chronic pain. Hughes et al[105] con�rmed a hypoalgesiaresponse was elicited by BFR at a low aerobic exercise intensity, which didn’t happen without BFR. The review[106] and meta-analysis[107] haveshown that BFR training could reduce pain of patients with knee injuries, but Ivan et al[108] came to the opposite conclusion in their meta-analysis:more effectively reducing pain didn’t happened to patients with knee pain who conducted resistance exercise with BFR (SMD: -0.37, P = 0.19)
At present, the research design of RPE and discomfort in BFR training is very different. The selected load, cuff pressure, whether exhaustingtraining was performed or not, and whether the exercise amount was controlled between different groups would affect the patients' feeling afterexercise. In order to better select the training mode that patients are more tolerant to and get great endurance bene�ts, we need a more rigorousexperimental design to reduce differences between groups and control variables. It would be helpful to get a clearer answer.
There's no consensus on how to set the right limiting pressure. A systematic review[109] showed that the selection of a non-individualized,arbitrary pressure was the most common approach to determining restriction pressure (56.6% of the 129 studies). Some researchers[110–112]have suggested that pressure could be set according to arterial occlusion pressure (AOP), and applying a percentage of pressure during exercise torestrict blood �ow. However, the restriction pressure used in some studies is beyond this range, and many studies set individualized restrictionpressures without clear reasoning[113]. One review[114], considering the damage that excessive vascular constriction can do to endothelial cellsand even endothelial function, suggested that setting the pressure to a percentage of AOP per subject (40–60%) is one feasible way to ensure thatno subject achieve complete arterial occlusion due to unnecessary high pressure. A cross-sectional study[115] showed that leg circumference hadgreat in�uence on the AOP, AOP was quite different between men and women, the same as between dominant and non-dominant legs (maximum80 mmHg). Therefore, it was necessary to measure the AOP of each leg when setting the occlusion pressure. Considering the different restrictionpressure in terms of its effect on endurance, the difference between high and low BFR is not clear, there is not enough exploration in this �eld, andthe results of previous studies were not consistent[30, 34, 101, 116].
LimitationsThe main problem with this systematic evaluation was the diversity of data in the literature. Among the included studies, training content, trainingduration, selected cuff width, occlusion pressure, measures of outcome indicators and measurement site differ in varying degrees. There is nogeneral consensus on the current BFR training mode, which is objectively existing and unavoidable. In the comparative analysis, only studies withsimilar outcome indicators were compared. However, the difference of objective data may affect the quality of our system evaluation. Secondly,some of the included literatures failed to double blind or did not mention relevant information, which was mainly due to the signi�cant differencebetween BFR training and non-BFR training, making it di�cult to double blind researchers and experimental subjects in practical work. However,this can be avoided to some extent. For example, participants in different experimental groups are separated for training and measurement,different professionals are selected to guide the training and measure the outcome indicators, and the speci�ed training program is strictlyimplemented. Non-BFR participants can tie cuff without in�ating, or be given extremely low pressure. In addition, some of the included researchesdidn’t give detailed descriptions of random sequence generation and allocation concealment. We attempted to �nd registration information andcontact the authors for more detailed information, but only a few authors responded to our request[29, 37, 38, 41]. The total sample size weincluded was 398, but it was scattered in various groups and the sample size was not su�cient. We included 18 articles, but the number of articlesin each group was small, and the lack of literature prevented us from conducting the test of publication bias. Considering the actual applicationscenarios, the subjects included in the study were mainly healthy people, which was different with patients who truly need endurance training inclinic, so our results should be used more carefully in recommendation.
ConclusionBased on current data, the results need to be interpreted cautiously and conservatively. BFR training is a very promising method to improveendurance for the elderly with decreased endurance and low exercise ability, patients with chronic diseases, musculoskeletal injury orpostoperative rehabilitation, and athletes looking to improve exercise ability. For people who cannot tolerate high-intensity exercise, in order toimprove the aerobic endurance, using moderate to low intensity exercise with BFR may be a better choice than only moderate to low intensityexercise. Since the results of the LBFR-RT on muscle endurance were not stable, considering the potential risks brought by BFR training, more trialsare needed to study the in�uence of BFR training on muscle endurance. For people who can tolerate high-intensity training, it's hard to say whetherlow-intensity training combined with BFR is an alternative. Bene�ts and possible risks of high-load training combined with BFR is unclear. Future

Page 12/19
trails should measure both muscular endurance and cardiopulmonary endurance, so as to explore a possibility of a simple program of BFRtraining to comprehensively improve the participants' muscle endurance and cardiopulmonary endurance. More importantly, studies with morerigorous design, large sample size, targeting at patients, are needed to improve the quality of evidence that BFR training promotes physicalendurance.
DeclarationsThanks to the authors of the cited literature for providing detailed information. Medical writers, proofreaders and editors are also greatlyappreciated for their help.
Data availability statements
The data that support the �ndings of this study are available from the corresponding author upon reasonable request.
Con�ict of interest
Feng Xiong, Jie Feng, Panyun Mu, Hairui Guo, Wenbing Zhang, Haoran Sun, Yimei Hu declare that they have no con�icts of interest relevant to thecontent of this review.
Funding
The author(s) received no �nancial support for the research, authorship, and/or publication of this article.
References1. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N
Engl J Med. 2002 Mar 14;346(11):793-801.https://doi.org/10.1056/NEJMoa011858
2. Lee DC, Artero EG, Sui X, Blair SN. Mortality trends in the general population: the importance of cardiorespiratory �tness.J Psychopharmacol.2010 Nov;24(4 Suppl):27-35.https://doi.org/10.1177/1359786810382057
3. Hughes L, Paton B, Rosenblatt B, Gissane C, Patterson SD. Blood �ow restriction training in clinical musculoskeletal rehabilitation: asystematic review and meta-analysis. British journal of sports medicine. 2017;51(13):1003-11.https://doi.org/10.1136/bjsports-2016-097071
4. Centner C, Wiegel P, Gollhofer A, König D. Effects of Blood Flow Restriction Training on Muscular Strength and Hypertrophy in OlderIndividuals: A Systematic Review and Meta-Analysis. Sports medicine (Auckland, NZ). 2019;49(1):95-108.https://doi.org/10.1007/s40279-018-0994-1
5. Dankel SJ, Jessee MB, Abe T, Loenneke JP. The Effects of Blood Flow Restriction on Upper-Body Musculature Located Distal and Proximal toApplied Pressure. Sports medicine (Auckland, NZ). 2016;46(1):23-33.https://doi.org/10.1007/s40279-015-0407-7
�. Grønfeldt BM, Lindberg Nielsen J, Mieritz RM, Lund H, Aagaard P. Effect of blood-�ow restricted vs heavy-load strength training on musclestrength: Systematic review and meta-analysis. Scandinavian journal of medicine & science in sports. 2020;30(5):837-48.https://doi.org/10.1111/sms.13632
7. Lixandrão ME, Ugrinowitsch C, Berton R, Vechin FC, Conceição MS, Damas F, et al. Magnitude of Muscle Strength and Mass AdaptationsBetween High-Load Resistance Training Versus Low-Load Resistance Training Associated with Blood-Flow Restriction: A Systematic Reviewand Meta-Analysis. Sports medicine (Auckland, NZ). 2018;48(2):361-78.https://doi.org/10.1007/s40279-017-0795-y
�. Bjørnsen T, Wernbom M, Kirketeig A, Paulsen G, Samnøy L, Bækken L, et al. Type 1 Muscle Fiber Hypertrophy after Blood Flow-restrictedTraining in Powerlifters. Medicine and science in sports and exercise. 2019 Feb;51(2):288-98.https://doi.org/10.1249/mss.0000000000001775
9. Ferguson RA, Hunt JEA, Lewis MP, Martin NRW, Player DJ, Stangier C, et al. The acute angiogenic signalling response to low-load resistanceexercise with blood �ow restriction. European journal of sport science. 2018;18(3):397-406.https://doi.org/10.1080/17461391.2017.1422281
10. Kacin A, Strazar K. Frequent low-load ischemic resistance exercise to failure enhances muscle oxygen delivery and endurance capacity.Scandinavian Journal of Medicine and Science in Sports. 2011;21(6):e231-e41.https://doi.org/10.1111/j.1600-0838.2010.01260.x
11. Nielsen JL, Frandsen U, Jensen KY, Prokhorova TA, Dalgaard LB, Bech RD, et al. Skeletal Muscle Microvascular Changes in Response to Short-Term Blood Flow Restricted Training-Exercise-Induced Adaptations and Signs of Perivascular Stress. Frontiers in Physiology. 2020 Jun12;11.https://doi.org/10.3389/fphys.2020.00556
12. Christiansen D, Eibye K, Hostrup M, Bangsbo J. Training with blood �ow restriction increases femoral artery diameter and thigh oxygendelivery during knee-extensor exercise in recreationally trained men. Journal of Physiology. 2020;598(12):2337-53.https://doi.org/10.1113/JP279554

Page 13/19
13. Jensen L, Bangsbo J, Hellsten Y. Effect of high intensity training on capillarization and presence of angiogenic factors in human skeletalmuscle. J Physiol. 2004 Jun 1;557(Pt 2):571-82.https://doi.org/10.1113/jphysiol.2003.057711
14. Pope ZK, Willardson JM, Schoenfeld BJ. Exercise and blood �ow restriction. Journal of strength and conditioning research. 2013;27(10):2914-26.https://doi.org/10.1519/JSC.0b013e3182874721
15. Conceição MS, Junior EMM, Telles GD, Libardi CA, Castro A, Andrade ALL, et al. Augmented Anabolic Responses after 8-wk Cycling with BloodFlow Restriction. Medicine and science in sports and exercise. 2019 Jan;51(1):84-93.https://doi.org/10.1249/mss.0000000000001755
1�. Larkin KA, Macneil RG, Dirain M, Sandesara B, Manini TM, Buford TW. Blood �ow restriction enhances post-resistance exercise angiogenicgene expression. Medicine and science in sports and exercise. 2012 Nov;44(11):2077-83.https://doi.org/10.1249/MSS.0b013e3182625928
17. Schober P, Mascha EJ, Vetter TR. Statistics From A (Agreement) to Z (z Score): A Guide to Interpreting Common Measures of Association,Agreement, Diagnostic Accuracy, Effect Size, Heterogeneity, and Reliability in Medical Research. Anesth Analg. 2021 Dec 1;133(6):1633-41.https://doi.org/10.1213/ane.0000000000005773
1�. Early KS, Rockhill M, Bryan A, Tyo B, Buuck D, McGinty J. EFFECT OF BLOOD FLOW RESTRICTION TRAINING ON MUSCULAR PERFORMANCE,PAIN AND VASCULAR FUNCTION. International journal of sports physical therapy. 2020;15(6):892‐900.https://doi.org/10.26603/ijspt20200892
19. Jønsson AB, Johansen CV, Rolving N, Pfeiffer-Jensen M. Feasibility and estimated e�cacy of blood �ow restricted training in female patientswith rheumatoid arthritis: a randomized controlled pilot study. Scandinavian journal of rheumatology. 2021 May;50(3):169-77.https://doi.org/10.1080/03009742.2020.1829701
20. Loftin M, Sothern M, Abe T, Bonis M. Expression of VO2peak in Children and Youth, with Special Reference to Allometric Scaling. Sports Med.2016 Oct;46(10):1451-60.https://doi.org/10.1007/s40279-016-0536-7
21. Engel FA, Ackermann A, Chtourou H, Sperlich B. High-Intensity Interval Training Performed by Young Athletes: A Systematic Review and Meta-Analysis. Front Physiol. 2018;9:1012.https://doi.org/10.3389/fphys.2018.01012
22. Lin YN, Tseng TT, Knuiman P, Chan WP, Wu SH, Tsai CL, et al. Protein supplementation increases adaptations to endurance training: Asystematic review and meta-analysis. Clin Nutr. 2021 May;40(5):3123-32.https://doi.org/10.1016/j.clnu.2020.12.012
23. Sundberg CJ, Eiken O, Nygren A, Kaijser L. Effects of ischaemic training on local aerobic muscle performance in man. Acta physiologicaScandinavica. 1993 May;148(1):13-9.https://doi.org/10.1111/j.1748-1716.1993.tb09526.x
24. Ozaki H, Sakamaki M, Yasuda T, Fujita S, Ogasawara R, Sugaya M, et al. Increases in thigh muscle volume and strength by walk training withleg blood �ow reduction in older participants. The journals of gerontology Series A, Biological sciences and medical sciences. 2011;66(3):257-63. https://doi.org/10.1093/gerona/glq182
25. Tanaka Y, Takarada Y. The impact of aerobic exercise training with vascular occlusion in patients with chronic heart failure. ESC heart failure.2018 Aug;5(4):586-91.https://doi.org/10.1002/ehf2.12285
2�. Ferreira Jr A, de Araujo AC, Chimin P, Okuno NM. Effect of walk training with blood �ow restriction on oxygen uptake kinetics, maximumoxygen uptake and muscle strength in middle-aged adults. Medicina Dello Sport. 2019 Dec;72(4):616-27.https://doi.org/10.23736/s0025-7826.19.03402-1
27. Paton CD, Addis SM, Taylor LA. The effects of muscle blood �ow restriction during running training on measures of aerobic capacity and runtime to exhaustion. European journal of applied physiology. 2017 Dec;117(12):2579-85.https://doi.org/10.1007/s00421-017-3745-3
2�. Ramis TR, Muller CHdL, Boeno FP, Teixeira BC, Rech A, Pompermayer MG, et al. Effects of Traditional and Vascular Restricted StrengthTraining Program With Equalized Volume on Isometric and Dynamic Strength, Muscle Thickness, Electromyographic Activity, and EndothelialFunction Adaptations in Young Adults. Journal of strength and conditioning research. 2020 Mar;34(3):689-98.https://doi.org/10.1519/jsc.0000000000002717
29. Held S, Behringer M, Donath L. Low intensity rowing with blood �ow restriction over 5 weeks increases V(O)over dot(2) max in elite rowers: Arandomized controlled trial. Journal of science and medicine in sport. 2020 Mar;23(3):304-8.https://doi.org/10.1016/j.jsams.2019.10.002
30. Lu JM, Liu SY, Sun P, Li WL, Lian ZQ. [Effects of low intensity resistance training of blood �ow restriction with different occlusion pressure onlower limb muscle and cardiopulmonary function of college students]. Zhongguo ying yong sheng li xue za zhi = Zhongguo yingyongshenglixue zazhi = Chinese journal of applied physiology. 2020 Nov;36(6):595-9.https://doi.org/10.12047/j.cjap.6032.2020.125
31. Keramidas ME, Kounalakis SN, Geladas ND. The effect of interval training combined with thigh cuffs pressure on maximal and submaximalexercise performance. Clinical physiology and functional imaging. 2012 May;32(3):205-13.https://doi.org/10.1111/j.1475-097X.2011.01078.x
32. Fahs CA, Loenneke JP, Thiebaud RS, Rossow LM, Kim D, Abe T, et al. Muscular adaptations to fatiguing exercise with and without blood �owrestriction. Clinical physiology and functional imaging. 2015 May;35(3):167-76.https://doi.org/10.1111/cpf.12141
33. Neto GR, da Silva JCG, Freitas L, da Silva HG, Caldas D, Novaes JS, et al. Effects of strength training with continuous or intermittent blood�ow restriction on the hypertrophy, muscular strength and endurance of men. Acta Scientiarum - Health Sciences.2019;41(1).https://doi.org/10.4025/actascihealthsci.v41i1.42273

Page 14/19
34. Jessee MB, Buckner SL, Grant Mouser J, Mattocks KT, Dankel SJ, Abe T, et al. Muscle adaptations to high-load training and very low-loadtraining with and without blood �ow restriction. Frontiers in Physiology. 2018;9(OCT).https://doi.org/10.3389/fphys.2018.01448
35. Manimmanakorn A, Hamlin MJ, Ross JJ, Taylor R, Manimmanakorn N. Effects of low-load resistance training combined with blood �owrestriction or hypoxia on muscle function and performance in netball athletes. Journal of science and medicine in sport. 2013 Jul;16(4):337-42.https://doi.org/10.1016/j.jsams.2012.08.009
3�. Manimmanakorn A, Manimmanakorn N, Taylor R, Draper N, Billaut F, Shearman JP, et al. Effects of resistance training combined with vascularocclusion or hypoxia on neuromuscular function in athletes. European journal of applied physiology. 2013;113(7):1767-74.https://doi.org/10.1007/s00421-013-2605-z
37. Bowman EN, Elshaar R, Milligan H, Jue G, Mohr K, Brown P, et al. Proximal, Distal, and Contralateral Effects of Blood Flow Restriction Trainingon the Lower Extremities: A Randomized Controlled Trial. Sports health. 2019 Mar/Apr;11(2):149-56.https://doi.org/10.1177/1941738118821929
3�. Ramis TR, Muller CHL, Boeno FP, Teixeira BC, Rech A, Pompermayer MG, et al. Effects of Traditional and Vascular Restricted Strength TrainingProgram With Equalized Volume on Isometric and Dynamic Strength, Muscle Thickness, Electromyographic Activity, and Endothelial FunctionAdaptations in Young Adults. Journal of strength and conditioning research. 2020 Mar;34(3):689-98.https://doi.org/10.1519/jsc.0000000000002717
39. Park S, Kim JK, Choi HM, Kim HG, Beekley MD, Nho H. Increase in maximal oxygen uptake following 2-week walk training with blood �owocclusion in athletes. European journal of applied physiology. 2010 Jul;109(4):591-600.https://doi.org/10.1007/s00421-010-1377-y
40. Ozaki H, Sakamaki M, Yasuda T, Fujita S, Ogasawara R, Sugaya M, et al. Increases in thigh muscle volume and strength by walk training withleg blood �ow reduction in older participants. J Gerontol A Biol Sci Med Sci. 2011 Mar;66(3):257-63.https://doi.org/10.1093/gerona/glq182
41. Amani-Shalamzari S, Sarikhani A, Paton C, Rajabi H, Bayati M, Nikolaidis PT, et al. Occlusion Training During Speci�c Futsal TrainingImproves Aspects of Physiological and Physical Performance. Journal of sports science & medicine. 2020 Jun;19(2):374-82
42. Fahs CA, Loenneke JP, Thiebaud RS, Rossow LM, Kim D, Abe T, et al. Muscular adaptations to fatiguing exercise with and without blood �owrestriction. Clin Physiol Funct Imaging. 2014 May;35(3):167-76.https://doi.org/10.1111/cpf.12141
43. Teramoto M, Golding LA. Low-intensity exercise, vascular occlusion, and muscular adaptations. Res Sports Med. 2006 Oct-Dec;14(4):259-71.https://doi.org/10.1080/15438620600985860
44. Buckner SL, Jessee MB, Dankel SJ, Mattocks KT, Mouser JG, Bell ZW, et al. Blood �ow restriction does not augment low force contractionstaken to or near task failure. Eur J Sport Sci. 2020 Jun;20(5):650-9.https://doi.org/10.1080/17461391.2019.1664640
45. Scott BR, Peiffer JJ, Goods PSR. The Effects of Supplementary Low-Load Blood Flow Restriction Training on Morphological andPerformance-Based Adaptations in Team Sport Athletes. J Strength Cond Res. 2017 Aug;31(8):2147-54.https://doi.org/10.1519/jsc.0000000000001671
4�. Ampomah K, Amano S, Wages NP, Volz L, Clift R, Ludin AFM, et al. Blood Flow-restricted Exercise Does Not Induce a Cross-Transfer of Effect:A Randomized Controlled Trial. Medicine and science in sports and exercise. 2019 Sep;51(9):1817-27.https://doi.org/10.1249/mss.0000000000001984
47. Jessee MB, Buckner SL, Mouser JG, Mattocks KT, Dankel SJ, Abe T, et al. Muscle Adaptations to High-Load Training and Very Low-LoadTraining With and Without Blood Flow Restriction. Front Physiol. 2018;9:1448.https://doi.org/10.3389/fphys.2018.01448
4�. Hosseini Kakhak SA, Kianigul M, Haghighi AH, Nooghabi MJ, Scott BR. Performing Soccer-Speci�c Training With Blood Flow RestrictionEnhances Physical Capacities in Youth Soccer Players. J Strength Cond Res. 2020 Jul 23.https://doi.org/10.1519/jsc.0000000000003737
49. Manimmanakorn A, Hamlin MJ, Ross JJ, Taylor R, Manimmanakorn N. Effects of low-load resistance training combined with blood �owrestriction or hypoxia on muscle function and performance in netball athletes. J Sci Med Sport. 2012 Jul;16(4):337-42.https://doi.org/10.1016/j.jsams.2012.08.009
50. Manimmanakorn A, Manimmanakorn N, Taylor R, Draper N, Billaut F, Shearman JP, et al. Effects of resistance training combined with vascularocclusion or hypoxia on neuromuscular function in athletes. Eur J Appl Physiol. 2013 Jul;113(7):1767-74.https://doi.org/10.1007/s00421-013-2605-z
51. Sousa J, Neto GR, Santos HH, Araújo JP, Silva HG, Cirilo-Sousa MS. Effects of strength training with blood �ow restriction on torque, muscleactivation and local muscular endurance in healthy subjects. Biol Sport. 2017 Mar;34(1):83-90.https://doi.org/10.5114/biolsport.2017.63738
52. Žargi T, Drobnič M, Stražar K, Kacin A. Short-Term Preconditioning With Blood Flow Restricted Exercise Preserves Quadriceps MuscleEndurance in Patients After Anterior Cruciate Ligament Reconstruction. Front Physiol. 2018;9:1150.https://doi.org/10.3389/fphys.2018.01150
53. Christiansen D, Eibye KH, Hostrup M, Bangsbo J. Blood �ow-restricted training enhances thigh glucose uptake during exercise and muscleantioxidant function in humans. Metabolism-Clinical and Experimental. 2019 Sep;98:1-15.https://doi.org/10.1016/j.metabol.2019.06.003
54. Pignanelli C, Petrick HL, Keyvani F, Heigenhauser GJF, Quadrilatero J, Holloway GP, et al. Low-load resistance training to task failure with andwithout blood �ow restriction: muscular functional and structural adaptations. American journal of physiology Regulatory, integrative andcomparative physiology. 2020 Feb 1;318(2):R284-r95.https://doi.org/10.1152/ajpregu.00243.2019

Page 15/19
55. Takarada Y, Sato Y, Ishii N. Effects of resistance exercise combined with vascular occlusion on muscle function in athletes. Eur J Appl Physiol.2002 Feb;86(4):308-14.https://doi.org/10.1007/s00421-001-0561-5
5�. Corvino RB, Oliveira MFMd, Santos RPd, Denadai BS, Caputo F. Four weeks of blood �ow restricted training increases time to exhaustion atsevere intensity cycling exercise. Revista Brasileira de Cineantropometria & Desempenho Humano. 2014 2014-09;16(5):570-8.https://doi.org/10.5007/1980-0037.2014v16n5p570
57. Kacin A, Drobnic M, Mars T, Mis K, Petric M, Weber D, et al. Functional and molecular adaptations of quadriceps and hamstring muscles toblood �ow restricted training in patients with ACL rupture. Scandinavian journal of medicine & science in sports. 2021 Aug;31(8):1636-46.https://doi.org/10.1111/sms.13968
5�. Lambert B, Hedt C, Daum J, Taft C, Chaliki K, Epner E, et al. Blood Flow Restriction Training for the Shoulder: A Case for Proximal Bene�t. TheAmerican journal of sports medicine. 2021;49(10):2716-28.https://doi.org/10.1177/03635465211017524
59. Park J-C, Ju MD, . Effect of Lumbar Stabilization Exercise using Blood Flow Restriction on Muscle Strength, Muscular Endurance, and Gaitin Patients with Chronic Back Pain. Journal of Korea Society for Neurotherapy. 2021 2021;25(3):71-6.https://doi.org/10.17817/2021.10.06.1111674
�0. Davids CJ, Raastad T, James LP, Gajanand T, Smith E, Connick M, et al. Similar Morphological and Functional Training Adaptations OccurBetween Continuous and Intermittent Blood Flow Restriction. Journal of strength and conditioning research. 2021;35(7):1784-93.https://doi.org/10.1519/JSC.0000000000004034
�1. Cai ZY, Wang WY, Lin JD, Wu CM. Effects of whole body vibration training combined with blood �ow restriction on muscle adaptation. Eur JSport Sci. 2020 Feb 28:1-9.https://doi.org/10.1080/17461391.2020.1728389
�2. Groennebaek T, Jespersen NR, Jakobsgaard JE, Sieljacks P, Wang J, Rindom E, et al. Skeletal Muscle Mitochondrial Protein Synthesis andRespiration Increase With Low-Load Blood Flow Restricted as Well as High-Load Resistance Training. Frontiers in Physiology. 2018Dec;9.https://doi.org/10.3389/fphys.2018.01796
�3. Hackney KJ, Downs ME, Ploutz-Snyder L. Blood Flow Restricted Exercise Compared to High Load Resistance Exercise During Unloading.Aerospace medicine and human performance. 2016;87(8):688-96.https://doi.org/10.3357/AMHP.4566.2016
�4. Ladlow P, Coppack RJ, Dharm-Datta S, Conway D, Sellon E, Patterson SD, et al. Low-Load Resistance Training With Blood Flow RestrictionImproves Clinical Outcomes in Musculoskeletal Rehabilitation: A Single-Blind Randomized Controlled Trial. Frontiers in Physiology. 2018Sep;9.https://doi.org/10.3389/fphys.2018.01269
�5. Morley WN, Ferth S, Debenham MIB, Boston M, Power GA, Burr JF. Training response to 8 weeks of blood �ow restricted training is notimproved by preferentially altering tissue hypoxia or lactate accumulation when training to repetition failure. Applied physiology, nutrition, andmetabolism = Physiologie appliquee, nutrition et metabolisme. 2021;46(10):1257-64.https://doi.org/10.1139/apnm-2020-1056
��. Zinner C, Baessler B, Weiss K, Ruf J, Michels G, Holmberg HC, et al. Effect of resistance training with vibration and compression on theformation of muscle and bone. Muscle & Nerve. 2017 Dec;56(6):1137-42.https://doi.org/10.1002/mus.25560
�7. de Oliveira MFM, Caputo F, Corvino RB, Denadai BS. Short-term low-intensity blood �ow restricted interval training improves both aerobic�tness and muscle strength. Scandinavian journal of medicine & science in sports. 2016 Sep;26(9):1017-25.https://doi.org/10.1111/sms.12540
��. Karabulut M, Esparza B, Dowllah IM, Karabulut U. The impact of low-intensity blood �ow restriction endurance training on aerobic capacity,hemodynamics, and arterial stiffness. The Journal of sports medicine and physical �tness. 2021;61(7):877-84.https://doi.org/10.23736/S0022-4707.20.11526-3
�9. Amano T, Inoue Y, Koga S, Nishiyasu T, Kondo N. In�uence of exercise training with thigh compression on heat-loss responses. Scandinavianjournal of medicine & science in sports. 2015 Jun;25 Suppl 1:173-82.https://doi.org/10.1111/sms.12365
70. Jensen AE, Palombo LJ, Niederberger B, Turcotte LP, Kelly KR. Exercise training with blood �ow restriction has little effect on muscularstrength and does not change IGF-1 in �t military war�ghters. Growth Horm IGF Res. 2016 Apr;27:33-40.https://doi.org/10.1016/j.ghir.2016.02.003
71. Abe T, Sakamaki M, Fujita S, Ozaki H, Sugaya M, Sato Y, et al. Effects of low-intensity walk training with restricted leg blood �ow on musclestrength and aerobic capacity in older adults. Journal of geriatric physical therapy (2001). 2010 Jan-Mar;33(1):34-40
72. Libardi CA, Chacon-Mikahil MP, Cavaglieri CR, Tricoli V, Roschel H, Vechin FC, et al. Effect of concurrent training with blood �ow restriction inthe elderly. International journal of sports medicine. 2015 May;36(5):395-9.https://doi.org/10.1055/s-0034-1390496
73. de Souza TMF, Libardi CA, Cavaglieri CR, Gáspari AF, Brunelli DT, de Souza GV, et al. Concurrent Training with Blood Flow Restriction does notDecrease In�ammatory Markers. Int J Sports Med. 2018 Jan;39(1):29-36.https://doi.org/10.1055/s-0043-119222
74. Kim D, Singh H, Loenneke JP, Thiebaud RS, Fahs CA, Rossow LM, et al. Comparative Effects of Vigorous-Intensity and Low-Intensity BloodFlow Restricted Cycle Training and Detraining on Muscle Mass, Strength, and Aerobic Capacity. Journal of strength and conditioning research.2016 May;30(5):1453-61.https://doi.org/10.1519/jsc.0000000000001218

Page 16/19
75. Mueller SM, Aguayo D, Lunardi F, Ruoss S, Boutellier U, Frese S, et al. High-load resistance exercise with superimposed vibration and vascularocclusion increases critical power, capillaries and lean mass in endurance-trained men. European journal of applied physiology. 2014Jan;114(1):123-33.https://doi.org/10.1007/s00421-013-2752-2
7�. Amani-Shalamzari S, Rajabi S, Rajabi H, Gahreman DE, Paton C, Bayati M, et al. Effects of Blood Flow Restriction and Exercise Intensity onAerobic, Anaerobic, and Muscle Strength Adaptations in Physically Active Collegiate Women. Frontiers in Physiology. 2019Jun;10.https://doi.org/10.3389/fphys.2019.00810
77. Kargaran A, Abedinpour A, Saadatmehr Z, Yaali R, Amani-Shalamzari S, Gahreman D. Effects of dual-task training with blood �ow restrictionon cognitive functions, muscle quality, and circulatory biomarkers in elderly women. Physiology and Behavior.2021;239.https://doi.org/10.1016/j.physbeh.2021.113500
7�. Nakajima T, Kurano M, Sakagami F, Iida H, Fukumura K, Fukuda T, et al. Effects of low-intensity KAATSU resistance training on skeletal musclesize/strength and endurance capacity in patients with ischemic heart disease. International Journal of KAATSU Training Research.2010;6(1):1-7.https://doi.org/10.3806/ijktr.6.1
79. Cardoso RK, Araujo AM, Del Vechio FB, Bohlke M, Barcellos FC, Oses JP, et al. Intradialytic exercise with blood �ow restriction is more effectivethan conventional exercise in improving walking endurance in hemodialysis patients: a randomized controlled trial. Clinical rehabilitation.2020 Jan;34(1):91-8.https://doi.org/10.1177/0269215519880235
�0. Clarkson MJ, Conway L, Warmington SA. Blood �ow restriction walking and physical function in older adults: A randomized control trial.Journal of science and medicine in sport. 2017 Dec;20(12):1041-6.https://doi.org/10.1016/j.jsams.2017.04.012
�1. Groennebaek T, Sieljacks P, Nielsen R, Pryds K, Jespersen NR, Wang J, et al. Effect of Blood Flow Restricted Resistance Exercise and RemoteIschemic Conditioning on Functional Capacity and Myocellular Adaptations in Patients With Heart Failure. Circulation Heart failure. 2019Dec;12(12):e006427.https://doi.org/10.1161/circheartfailure.119.006427
�2. Kargaran A, Abedinpour A, Saadatmehr Z, Yaali R, Amani-Shalamzari S, Gahreman D. Effects of dual-task training with blood �ow restrictionon cognitive functions, muscle quality, and circulatory biomarkers in elderly women. Physiology & behavior. 2021 Oct1;239:113500.https://doi.org/10.1016/j.physbeh.2021.113500
�3. Wooten SV, Fleming RYD, Wolf JS, Stray-Gundersen S, Bartholomew JB, Mendoza D, et al. Prehabilitation program composed of blood �owrestriction training and sports nutrition improves physical functions in abdominal cancer patients awaiting surgery. European Journal ofSurgical Oncology. 2021;47(11):2952-8.https://doi.org/10.1016/j.ejso.2021.05.038
�4. Lamberti N, Straudi S, Donadi M, Tanaka H, Basaglia N, Manfredini F. Effectiveness of blood �ow-restricted slow walking on mobility in severemultiple sclerosis: A pilot randomized trial. Scandinavian journal of medicine & science in sports. 2020 Oct;30(10):1999-2009.https://doi.org/10.1111/sms.13764
�5. Manini TM, Clark BC. Blood �ow restricted exercise and skeletal muscle health. Exercise and Sport Sciences Reviews. 2009;37(2):78-85.https://doi.org/10.1097/JES.0b013e31819c2e5c
��. Wernbom M, Paulsen G, Bjørnsen T, Cumming K, Raastad T. Risk of Muscle Damage With Blood Flow-Restricted Exercise Should Not BeOverlooked. Clinical journal of sport medicine : o�cial journal of the Canadian Academy of Sport Medicine. 2021;31(3):223-4.https://doi.org/10.1097/JSM.0000000000000755
�7. Loenneke JP, Thiebaud RS, Abe T. Does blood �ow restriction result in skeletal muscle damage? A critical review of available evidence.Scandinavian journal of medicine & science in sports. 2014;24(6):e415-e22.https://doi.org/10.1111/sms.12210
��. Zhao Y, Lin A, Jiao L. Eight weeks of resistance training with blood �ow restriction improve cardiac function and vascular endothelial functionin healthy young Asian males. International health. 2021 Sep 3;13(5):471-9.https://doi.org/10.1093/inthealth/ihaa089
�9. Cristina-Oliveira M, Meireles K, Spranger MD, O'Leary DS, Roschel H, Pecanha T. Clinical safety of blood �ow-restricted training? Acomprehensive review of altered muscle metabore�ex in cardiovascular disease during ischemic exercise. American Journal of Physiology-Heart and Circulatory Physiology. 2020 Jan;318(1):H90-H109.https://doi.org/10.1152/ajpheart.00468.2019
90. Domingos E, Polito MD. Blood pressure response between resistance exercise with and without blood �ow restriction: A systematic review andmeta-analysis. Life Sciences. 2018;209:122-31.https://doi.org/10.1016/j.lfs.2018.08.006
91. Bond CW, Hackney KJ, Brown SL, Noonan BC. Blood Flow Restriction Resistance Exercise as a Rehabilitation Modality Following OrthopaedicSurgery: A Review of Venous Thromboembolism Risk. The Journal of orthopaedic and sports physical therapy. 2019;49(1):17-27.https://doi.org/10.2519/jospt.2019.8375
92. Spitz RW, Wong V, Bell ZW, Viana RB, Chatakondi RN, Abe T, et al. Blood Flow Restricted Exercise and Discomfort: A Review. Journal ofstrength and conditioning research. 2020.https://doi.org/10.1519/JSC.0000000000003525
93. Bell ZW, Buckner SL, Jessee MB, Mouser JG, Mattocks KT, Dankel SJ, et al. Moderately heavy exercise produces lower cardiovascular, RPE,and discomfort compared to lower load exercise with and without blood �ow restriction. European journal of applied physiology. 2018Jul;118(7):1473-80.https://doi.org/10.1007/s00421-018-3877-0

Page 17/19
94. Hughes L, Patterson SD. The effect of blood �ow restriction exercise on exercise-induced hypoalgesia and endogenous opioid andendocannabinoid mechanisms of pain modulation. Journal of applied physiology (Bethesda, Md : 1985). 2020;128(4):914-24.https://doi.org/10.1152/japplphysiol.00768.2019
95. Loenneke JP, Kim D, Fahs CA, Thiebaud RS, Abe T, Larson RD, et al. The effects of resistance exercise with and without different degrees ofblood-�ow restriction on perceptual responses. Journal of sports sciences. 2015;33(14):1472-9.https://doi.org/10.1080/02640414.2014.992036
9�. Silva JCG, Domingos-Gomes JR, Freitas EDS, Neto GR, Aniceto RR, Bemben MG, et al. Physiological and Perceptual Responses to AerobicExercise With and Without Blood Flow Restriction. Journal of strength and conditioning research. 2021 Sep 1;35(9):2479-85.https://doi.org/10.1519/jsc.0000000000003178
97. Mok E, Suga T, Sugimoto T, Tomoo K, Dora K, Takada S, et al. Negative effects of blood �ow restriction on perceptual responses to walking inhealthy young adults: A pilot study. Heliyon. 2020 Aug;6(8).https://doi.org/10.1016/j.heliyon.2020.e04745
9�. Loenneke JP, Thiebaud RS, Fahs CA, Rossow LM, Abe T, Bemben MG. Blood �ow restriction: effects of cuff type on fatigue and perceptualresponses to resistance exercise. Acta physiologica Hungarica. 2014 Jun;101(2):158-66.https://doi.org/10.1556/APhysiol.101.2014.2.4
99. Fallon NE, Urbina E, Whitener DV, Patel MH, Exner RJ, Dankel SJ. The impact of cuff width on perceptual responses during and followingblood �ow restricted walking exercise. Clinical physiology and functional imaging. 2022;42(1):29-34.https://doi.org/10.1111/cpf.12732
100. Cerqueira MS, Costa EC, Santos Oliveira R, Pereira R, Brito Vieira WH. Blood Flow Restriction Training: To Adjust or Not Adjust the CuffPressure Over an Intervention Period? Frontiers in Physiology. 2021;12.https://doi.org/10.3389/fphys.2021.678407
101. Counts BR, Dankel SJ, Barnett BE, Kim D, Mouser JG, Allen KM, et al. In�uence of relative blood �ow restriction pressure on muscle activationand muscle adaptation. Muscle and Nerve. 2016;53(3):438-45.https://doi.org/10.1002/mus.24756
102. Yasuda T, Abe T, Brechue WF, Iida H, Takano H, Meguro K, et al. Venous blood gas and metabolite response to low-intensity musclecontractions with external limb compression. Metabolism: clinical and experimental. 2010 Oct;59(10):1510-9.https://doi.org/10.1016/j.metabol.2010.01.016
103. Mattocks KT, Jessee MB, Counts BR, Buckner SL, Grant Mouser J, Dankel SJ, et al. The effects of upper body exercise across different levelsof blood �ow restriction on arterial occlusion pressure and perceptual responses. Physiology and Behavior. 2017;171:181-6.https://doi.org/10.1016/j.physbeh.2017.01.015
104. Sinclair P, Kadhum M, Paton B. Tolerance to Intermittent vs. Continuous Blood Flow Restriction Training: A Meta-Analysis. International journalof sports medicine. 2021.https://doi.org/10.1055/a-1537-9886
105. Hughes L, Grant I, Patterson SD. Aerobic exercise with blood �ow restriction causes local and systemic hypoalgesia and increases circulatingopioid and endocannabinoid levels. Journal of applied physiology (Bethesda, Md : 1985). 2021 Nov 1;131(5):1460-8.https://doi.org/10.1152/japplphysiol.00543.2021
10�. Zaremba M, Martin J, Fyock-Martin M. Does Blood Flow Restriction Resistance Training Improve Knee-Extensor Strength, Function, andReduce Patient-Reported Pain? A Critically Appraised Topic. Journal of sport rehabilitation. 2021:1-6.https://doi.org/10.1123/jsr.2021-0081
107. Li S, Shaharudin S, Abdul Kadir MR. Effects of Blood Flow Restriction Training on Muscle Strength and Pain in Patients With Knee Injuries: AMeta-Analysis. American journal of physical medicine & rehabilitation. 2021 Apr 1;100(4):337-44.https://doi.org/10.1097/phm.0000000000001567
10�. Cuyul-Vásquez I, Leiva-Sepúlveda A, Catalán-Medalla O, Araya-Quintanilla F, Gutiérrez-Espinoza H. The addition of blood �ow restriction toresistance exercise in individuals with knee pain: a systematic review and meta-analysis. Brazilian journal of physical therapy.2020;24(6):465-78.https://doi.org/10.1016/j.bjpt.2020.03.001
109. Murray J, Bennett H, Boyle T, Williams M, Davison K. Approaches to determining occlusion pressure for blood �ow restricted exercise training:Systematic review. Journal of sports sciences. 2021;39(6):663-72.https://doi.org/10.1080/02640414.2020.1840734
110. Lixandrão ME, Ugrinowitsch C, Laurentino G, Libardi CA, Aihara AY, Cardoso FN, et al. Effects of exercise intensity and occlusion pressure after12 weeks of resistance training with blood-�ow restriction. European journal of applied physiology. 2015;115(12):2471-80.https://doi.org/10.1007/s00421-015-3253-2
111. Patterson SD, Hughes L, Head P, Warmington S, Brandner C. Blood �ow restriction training: a novel approach to augment clinicalrehabilitation: how to do it. British journal of sports medicine. 2017;51(23):1648-9.https://doi.org/10.1136/bjsports-2017-097738
112. McEwen JA, Owens JG, Jeyasurya J. Why is it Crucial to Use Personalized Occlusion Pressures in Blood Flow Restriction (BFR)Rehabilitation? Journal of Medical and Biological Engineering. 2019;39(2):173-7.https://doi.org/10.1007/s40846-018-0397-7
113. Clarkson MJ, May AK, Warmington SA. Is there rationale for the cuff pressures prescribed for blood �ow restriction exercise? A systematicreview. Scandinavian journal of medicine & science in sports. 2020;30(8):1318-36.https://doi.org/10.1111/sms.13676
114. Nascimento DdC, Schoenfeld BJ, Prestes J. Potential Implications of Blood Flow Restriction Exercise on Vascular Health: A Brief Review.Sports Medicine. 2020 Jan;50(1):73-81.https://doi.org/10.1007/s40279-019-01196-5

Page 18/19
115. Tafuna'i ND, Hunter I, Johnson AW, Fellingham GW, Vehrs PR. Differences in Femoral Artery Occlusion Pressure between Sexes and Dominantand Non-Dominant Legs. Medicina (Kaunas, Lithuania). 2021;57(9).https://doi.org/10.3390/medicina57090863
11�. Buckner SL, Jessee MB, Dankel SJ, Mattocks KT, Mouser JG, Bell ZW, et al. Blood �ow restriction does not augment low force contractionstaken to or near task failure. European journal of sport science. 2020;20(5):650-9.https://doi.org/10.1080/17461391.2019.1664640
Figures
Figure 1
The search process of the system review
Figure 2
The assessment of risk bias about included studies
Figure 3
The assessment of risk bias about included studies
Figure 4
Low-load resistance training with BFR (LBFR-RT) VS low-load resistance training (LL-RT) on muscle endurance
Figure 5
Low-load resistance training with BFR (LBFR-RT) VS high-load resistance training (HL-RT) on muscle endurance
Figure 6
Aerobic exercise with BFR (AE-BFR) VS aerobic exercise (AE) on aerobic endurance (a)
Figure 7
Aerobic exercise with BFR (AE-BFR) VS aerobic exercise (AE) on aerobic endurance (b)
Figure 8
Mixed oxygen exercise with BFR (Omix-BFR) VS mixed oxygen exercise (Omix-E) on aerobic endurance
Figure 9
Moderate to low intensity exercise with BFR(ML-BFR) VS moderate to low intensity exercise (ML) on aerobic endurance

Page 19/19
Figure 10
Anaerobic exercise with BFR (ANA-BFR) VS anaerobic exercise (ANA-E) on aerobic endurance
Supplementary Files
This is a list of supplementary �les associated with this preprint. Click to download.
SupplementaryMaterial1SearchstrategysampleofPubMed.docx
SupplementaryMaterial2.docx
SupplementaryMaterial3.pdf




















