
To the question of the heart rate fluctuations during submaximal workload (In Ukrainian)
Upload
khangminh22Category
view
3download
0
Submaximal Exercise Testing:Clinical Application andInterpretation
Compared with maximal exercise testing, submaximal exercise testingappears to have greater applicability to physical therapists in their roleas clinical exercise specialists. This review contrasts maximal andsubmaximal exercise testing. Two major categories of submaximal tests(ie, predictive and performance tests) and their relative merits aredescribed. Predictive tests are submaximal tests that are used to predictmaximal aerobic capacity. Performance tests involve measuring theresponses to standardized physical activities that are typically encoun-tered in everyday life. To maximize the validity and reliability of dataobtained from submaximal tests, physical therapists are cautioned toapply the tests selectively based on their indications; to adhere tomethods, including the requisite number of practice sessions; and touse measurements such as heart rate, blood pressure, exertion, andpain to evaluate test performance and to safely monitor patients.[Noonan V, Dean E. Submaximal exercise testing: clinical applicationand interpretation. Phys Ther. 2000;80:782–807.]
Key Words: Functional limitation, Maximal exercise test, Outcome measures, Oxygen transport,
Performance, Prediction, Rehabilitation, Submaximal exercise test.
782 Physical Therapy . Volume 80 . Number 8 . August 2000
Pers
pect
ive
Vanessa Noonan
Elizabeth Dean
v
IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
III
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

Although maximal exercise testing is consid-ered the gold standard for assessing maximalaerobic capacity, the role of such testing islimited in people whose performance may be
limited because of pain or fatigue rather than exertionand in cases where maximal exercise testing is contrain-dicated. Submaximal exercise testing overcomes many ofthe limitations of maximal exercise testing, and it is themethod of choice for the majority of individuals seen byphysical therapists in that these individuals are likely tobe limited physically by pain and fatigue or have abnor-mal gait or impaired balance. This article contrastsmaximal and submaximal exercise testing and describesthe clinical application of submaximal testing. Thestrengths and limitations of both predictive and perfor-mance submaximal tests and the means of maximizingvalidity and reliability of data are presented. Predictivetests are submaximal tests that are used to predictmaximal aerobic capacity. Typically, heart rate (HR) oroxygen consumption (V̇o2) at 2 or more workloads ismeasured.1,2 A predicted V̇o2 value is obtained by extrap-olating the relationship between HR and V̇o2 to age-predicted maximal heart rate (HRmax). Performancetests involve measuring the responses to standardizedphysical activities that are typically encountered in every-day life. Finally, we discuss the use of submaximalexercise testing in clinical decision making and theimplications for professional education and research.
Maximal Versus Submaximal Exercise TestsMaximal exercise tests either measure or predict maxi-mum oxygen consumption (V̇o2max) and have beenaccepted as the basis for determining fitness.3–7 They
have served as a stan-dard against which tocompare other mea-sures.8 Maximum oxy-gen consumption isdependent on the abil-ity of the oxygen trans-port system to deliverblood and the ability ofcells to take up and uti-
lize oxygen in energy production.9 Theoretically, a max-imal test is defined by the plateau of V̇o2 with furtherincreases in workload.10,11 Other indexes used to assessmaximal effort include obtaining HRmax within 15beats per minute (bpm) of age-predicted HRmax(ie, 2202age) and a respiratory exchange ratio .1.10(ratio of metabolic gas exchange calculated by carbondioxide production divided by V̇o2).12 Maximum oxygenconsumption is typically expressed relative to bodyweight (ie, mLzkg21zmin21),13 which enables individualsof different body masses to be compared. When amaximal test is performed but the criteria for V̇o2maxare not met, the maximal V̇o2 achieved is termed a“V̇o2peak.”14 Few individuals reach a true V̇o2max, andV̇o2peak values are often incorrectly reported as maxi-mal values.14 The intraindividual day-to-day variation inmeasuring V̇o2max is between 4% to 6% in individualswith no known cardiopulmonary pathology or impair-ment.15,16 In people with various diagnoses, such as thosewith chronic obstructive pulmonary disease (COPD),this variation is between 6% and 10%.17
V Noonan, PT, MSc, is Research Coordinator, Orthopaedic Spine Program, Vancouver Hospital, Vancouver, British Columbia, Canada.
E Dean, PT, PhD, is Professor, School of Rehabilitation Sciences, University of British Columbia, T325-2211 Wesbrook Mall, Vancouver, BritishColumbia, Canada V6T 1Z3 ([email protected]). Address all correspondence to Dr Dean.
Both authors provided concept/idea, writing, literature collection and analysis, project management, and consultation (including review ofmanuscript before submission). Dr Dean also provided clerical support.
Submaximal
exercise testing
overcomes many of
the limitations of
maximal exercise
testing.
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 783
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIIII
IIIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

There are several limitations to assessing maximal per-formance with a V̇o2max test. Unless an individual isable to attain a V̇o2max without fatiguing first or beinglimited by musculoskeletal impairments or other prob-lems, the results of the test are invalid. In addition,higher levels of motivation are required by the individ-ual, and maximal tests require additional monitoringequipment (eg, electrocardiograph machine) andtrained staff and are labor intensive.1,13,18
In comparison with maximal tests, submaximal exercisetests and their applications have been less well devel-oped, which we find surprising given the large numberof patient types and individuals who should be able tobenefit from nonmaximal exercise tests. For the purposeof this review, submaximal tests are classified as eitherpredictive tests or performance tests.
Clinical Application of Submaximal ExerciseTesting
SafetyExercise constitutes a physiologic stress that may pose agreater risk to people with various diagnoses than topeople without pathology or impairment. The space fortesting must be sufficient to minimize injury should thepatient fall or have an arrest. All physical therapistsshould have current certification in cardiopulmonaryresuscitation. Emergency procedures and basic equip-ment need to be in place to ensure that the individualhas immediate care until paramedical or medical assis-tance arrives. There are other critical needs for exercisetesting. Basic emergency supplies, including a sugarsource for people with diabetes, should be on hand. Aportable oxygen source and suction device should beaccessible. People who are stable and who have a historyof angina should have their antianginal medication, andthe physical therapist should have access to this medica-tion. Monitoring equipment should be maintained andregularly calibrated.
Indications for testing and any contraindications fortesting should be determined before testing.19 In thepresence of relative contraindications, the person mayrequire additional monitoring (eg, 12-lead electrocardi-ography) or be cleared for such testing by an appropri-ate medical practitioner. A high proportion of peopleover the age of 65 years without known cardiac diseasehave a high incidence of cardiac dysrhythmias,20,21 whichmay necessitate greater attention to monitoring cardiacstatus during exercise. Individuals requiring additionalmonitoring or considered to be at hemodynamic riskshould be tested in a setting with medical personnelpresent.
IndicationsMaximal exercise testing has a role in the assessment ofmaximal aerobic capacity or functional work capacity.Because people are frequently limited by cardiopulmo-nary, musculoskeletal, and neuromuscular impairmentsand complaints such as exertion, dyspnea, fatigue, weak-ness, and pain during their activities of daily living,maximal testing is often contraindicated or of limitedvalue. In people without cardiopulmonary or musculo-skeletal impairments, the reserve capacity of the cardio-pulmonary and musculoskeletal systems is thought to bebarely tapped during daily activities.22 In people withpathology, this reserve can be greatly reduced, and agreater than usual proportion of a person’s maximalcapacity may be needed to perform routine activities.23
Exercise constitutes a major physiological stress that canlead to untoward responses in patients as well as inindividuals without known pathology. In addition, suchtesting is resource intensive and thus should be appliedand performed judiciously. The purposes of maximaltests include determination of V̇o2max and use as diag-nostic or treatment outcome tools. Submaximal exercisetests can be used to predict V̇o2max, to make diagnosesand assess functional limitations, to assess the outcomeof interventions such as exercise programs, to measurethe effects of pharmacological agents, and to examinethe effect of recovery strategies on exerciseperformance.13,19,23–25
Guidelines for Test SelectionThere are numerous submaximal tests from which tochoose. These tests have been developed to meet theneeds of people with various functional limitations anddisabilities and the needs of older adults. In our opinion,however, inappropriate selection may lead to eitherunderstressing or overstressing the individual. Suchunderstressing or overstressing of the person, in ourview, can lead to invalid conclusions because of ceilingor floor effects, and the testing may be hazardous. Thegoal of testing should be to produce a sufficient level ofexercise stress without physiologic or biomechanicalstrain. Factors that we believe should be considered inselecting the appropriate test include the person’s pri-mary and secondary pathologies and how these pathol-ogies physically affect the person’s daily life. Otherfactors include cognitive status, age, weight, nutritionalstatus, mobility, use of walking aids or orthotic orprosthetic devices, independence, work situation, homesituation, and the person’s needs and wants. People whomay be medically unstable and at risk for an arrest mayneed to be tested in the presence of a cardiologist orpulmonary specialist or by a physical therapist in aspecialized setting where emergency services are onhand. The population for which a given test was devel-oped, the degree of validity and reliability of measure-
784 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

ments obtained with each test, and test sensitivity alsoshould be considered (Appendix). Reports in the liter-ature on the common submaximal tests described in thisarticle vary with respect to the adequacy of establishingvalidity, reliability, and sensitivity; thus, test interpreta-tion may be limited. These limitations should be consid-ered in the selection of each test. Physical therapistsshould determine what information will be added byperforming an exercise test and how that informationwill alter clinical decision making.
Pretest WorkupA detailed medical and surgical history is needed toidentify the indications for an exercise test and to alertthe physical therapist about any underlying conditions(eg, cardiovascular, pulmonary, musculoskeletal, or neu-rological dysfunction or the presence of diabetes, hyper-tension or heart block requiring a pacemaker, anemia,thyroid dysfunction, obesity, deformity, vertigo, orimpaired cognitive function). The therapist should beaware of medications (indications, response, and sideeffects) that can influence the test procedures and theresponse to the exercise. Laboratory tests and investiga-tions that may be relevant include electrocardiograms,echocardiograms, pulmonary function tests, investiga-tions of peripheral vascular function, blood chemistrytests, bone density measures, radiographs, scans, thyroidfunction tests, glucose tolerance tests, autonomic ner-vous system function tests, sleep studies, nutritionalassessment, and tests for level of hydration.
The effect of each medication on exercise response andthe medication’s side effects should be known to theperson administering the test. Beta blockers, for exam-ple, attenuate normal HR and blood pressure (BP)responses to exercise and contribute to fatigue in somepeople. The purpose of the test must be clear so that theperson can be appropriately premedicated (eg, withantidysrhythmic drugs, inotropic drugs, anticoagulants,antithrombolytics, bronchodilators, vasodilators, diuret-ics, and analgesics). For example, medications such asbronchodilators and analgesics have peak effect times;thus, it is important to ensure that these medications areat peak effect during the test and that this effect isreplicated on subsequent tests.
People with a history of angina should be screenedcarefully. The objective of submaximal testing is to testthe individual below the work rate that induces angina.The person’s anginal history will divulge the range ofactivities and the activities that are not associated withsymptoms. Labile angina, angina at rest, and frequentpremature ventricular contractions (PVCs) at rest are, inour opinion, absolute contraindications to exercise test-ing in the absence of a cardiologist unless in a special-ized setting where physical therapists are qualified to
perform such testing. Premature ventricular contrac-tions can be detected reliably only with electrocardio-grams and not by palpation or verbal report. A detailedanginal history, including what triggers episodes ofangina and the frequency of self-medication with anti-anginal medication and its effect, should be recorded.Any history of chest discomfort or pain from any causeshould be noted by the tester. We also believe that anymedication should be checked for its expiration dateand should be available in the event it is needed duringor after the test. A person with a history of angina and forwhom antianginal medication is prescribed, in our opin-ion, should be considered at risk even if the medicationhas not been required for a prolonged period. We advisethat a risk assessment should be conducted for everyindividual, regardless of whether a maximal exercise testor a submaximal exercise test is being performed. Thisassessment will help to determine which test is appropri-ate, predict an adverse response to testing, identify thelevel of monitoring needed, and whether there are anycontraindications to submaximal exercise testing.
Standardization of ProceduresA primary concern about submaximal exercise testing isthe lack of standardization of the procedures. We believethat general procedures should include informing theperson about the type and purpose of the test andinstructing the person to avoid any strenuous activity for24 hours prior to testing and to avoid a heavy meal,caffeine, or nicotine within 2 to 3 hours of testing.19
Medications taken prior to testing should be noted bythe examiner, and, if appropriate, their use should beconsistent from one test to the next. The individualshould become familiar with the equipment and testprocedures to minimize anxiety. Many tests require oneor more practice sessions. If time and resources do notpermit these practice sessions, we argue that the testshould not be performed because the results, in ourview, will not be valid. Appropriate rest periods, in ouropinion, need to be scheduled between practices andbetween the last practice and the actual test. We havepreviously shown that performance of a submaximaltreadmill walking test requires at least one practicesession, even in young subjects without functionalimpairments, in order for the measurements to bevalid.26 For some individuals, more practice sessions arejustified. The number of practice sessions required tomake the results valid, in our opinion, is dependent onthe test and on the experience and functional capacity ofthe person being tested. Verbal encouragement in sub-maximal testing should be standardized to ensure thatthis does not affect the person’s performance.27 Failureto calibrate both exercise devices and monitoring equip-ment can lead to erroneous results.
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 785
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

MeasurementsBasic measures of exercise responses include HR, BP,respiratory rate (RR), rating of perceived exertion(RPE), and breathlessness. Depending on the person’shistory and other variables, the examiner may find othermeasures to be useful (eg, a 3-lead electrocardiogram,arterial saturation assessed using a pulse oximeter,cadence, ratings of fatigue and discomfort or pain).Because tests are performed over a wide area or circuit,monitoring equipment should be portable. Repeatedmeasurements of each variable of interest, in our opin-ion, should be taken prior to the exercise test to ensurea stable baseline, at various points during the test(depending on the type of test), and during the cool-down period, if applicable, and these measurementsshould be repeated during recovery to ensure that themeasures have returned to baseline levels. As a precau-tion, we recommend that the person should not leavethe testing area until all measures have returned towithin 10% of resting values.19 Based on the history ofthe person being tested, additional monitoring may beindicated to maximize the safety of the test.
Because the measurement of BP is an important part ofexercise testing, the validity of these measurementsshould be maximized with an appropriately sized cuff, itsposition on the midshaft of the humerus, its tightness,the cuff deflation rate, and the position of the stetho-scope over the brachial artery as it courses over theantecubital fossa.28 Skill in recording BP is essential,given that many people have undiagnosed or poorlycontrolled hypertension.
Measures of exertion, breathlessness, fatigue, discomfortor pain, and well being in response to physical activity orexercise are important exercise responses reported bythe person being examined. Many people, particularlyolder people, more readily and reliably monitor and acton their complaints, rather than using measures such asHR to guide their activities or exercise intensity.
InterpretationThe interpretation of the submaximal exercise testresults is based primarily on the type of test conducted,its indications (eg, assessment, diagnostic, exercise pre-scription), specified outcomes, and, in some instances,norms (Appendix). Submaximal exercise tests can beused to predict aerobic capacity or to assess the ability toperform a standardized exercise or task. In addition,measurements taken before, during (where applicable),and after the test can yield valuable information regard-ing the person’s exercise response. These values can becompared across subsequent tests. They can alert thephysical therapist to undue pretest arousal (a measure ofthe adequacy of the pretest standardization), exagger-ated exercise responses, and delayed recovery, which are
consistent with deconditioning or pathology, or both.Comparison of the responses with pretest and posttestmeasurements is particularly useful for assessing theeffect of an intervention such as an exercise program. Inthis case, a reduction in submaximal exercise responsessuch as HR, RR, and BP can be consistent with improvedaerobic conditioning or movement economy, or both.Movement economy refers to the efficient use of energyduring movement (ie, not excessive V̇o2 for a givenactivity or work rate).
Predictive Submaximal Exercise Tests
Modified Bruce Treadmill Test
Description. The Bruce Treadmill Test5 is a maximaltest that was designed to diagnose coronary heart dis-ease. Some preliminary stages have been added to theoriginal test, which has given rise to the use of theModified Bruce Treadmill Test in people with otherconditions.29,30 Compared with the original test, whichstarts at 1.7 mph at a grade of 10%, the modified test hasa zero stage (1.7 mph at 0% grade) and a one-half-stage(1.7 mph at 5% grade) (Tab. 1). Predictive equations forestimating V̇o2max have been developed and can beused with the original and modified tests. Bruce et al5developed the first predictive equations, which arepopulation-specific for active and sedentary adults withand without cardiac conditions. Individuals must becorrectly classified to determine which equation isappropriate. Foster et al30 later developed a regressionequation applicable to all men based on a sample of 230men of various ages with a variety of clinical conditions(symptomatic angina, n514; postmyocardial revascular-ization surgery, n536; outpatient cardiac rehabilitationsurgery, n563; preventative medicine program, n590,and athletes, n527) and activity levels. The details of the
Table 1.Modified Bruce Treadmill Test: Protocola
Stage Speed (mph) Grade (%) Duration (min)
0 1.7 0 30.5 1.7 5 31 1.7 10 32 2.5 12 33 3.4 14 34 4.2 16 35 5.0 18 36 5.5 20 37 6.0 22 3
a Adapted from Bruce RA. Exercise testing of patients with coronary arterydisease: principles and normal standards for evaluation. Ann Clin Res. 1971;3:323–332 and Bruce RA, Kusumi F, Hosmer D. Maximal oxygen intake andnomographic assessment of functional aerobic impairment in cardiovasculardisease. Am Heart J. 1973;85:564–562. The standard Bruce protocol begins atstage 1; stages 0 and 0.5 are used for individuals with reduced exercisecapacity.
786 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

Modified Bruce Treadmill Test are provided in theAppendix.
Reliability and validity. Bruce et al5 reported Pearsonproduct moment correlation coefficients (r) betweenpredicted V̇o2max and measured V̇o2max of .94 forwithout cardiac conditions (n5292), .93 for womenwithout cardiac conditions (n5509), and .87 for menwith cardiac disease (n5153). Foster et al30 comparedpredicted V̇o2max and measured V̇o2max for the gen-eral equation and the population-specific equationsintroduced by Bruce et al.5 The average predicted errorwas 20.6 mLzkg21zmin21 for the general equation versus22.0 mLzkg21zmin21 for the population-specific equa-tions. The correlation between measured V̇o2max andpredicted V̇o2max for the general equation was high(r 5.96), with a multiple correlation coefficient (R)of .98 and a standard error of the estimate (SEE) of3.5 mLzkg21zmin21.30
Strengths and weaknesses. The Bruce Treadmill Testand the Modified Bruce Treadmill Test are widely used,especially for the diagnosis of coronary heart disease,and, as a result, normative data are available. Comparedwith the original protocol, which starts with a largeworkload, the modified protocol has a more gradualinitial workload. Thus, we contend that the modifiedprotocol is more applicable for individuals with lowfunctional capacity. The large increases in workload inthe original protocol, however, allowed the test to becompleted within 6 to 9 minutes.23
Single-Stage Submaximal Treadmill Walking Test
Description. Ebbeling et al12 developed the Single-Stage Submaximal Treadmill Walking Test (SSTWT),which can be used by individuals of various ages andfitness levels. The test was developed on a sample of 139volunteers with no health problems (67 men and 72women) aged 20 to 59 years. The subjects were randomlyassigned to either an estimation group (n5117) or across-validation group (n522). Subjects walked on atreadmill at a constant speed, ranging from 2.0 to 4.5mph at grades of 0%, 5%, and 10%, with each stagelasting 4 minutes. A maximal test was then performed.The regression equation used to estimate V̇o2max wasbased on data obtained from the estimation group fromthe 4-minute stage at a grade of 5%. The details of theSSTWT are given in the Appendix.
Reliability and validity. The SSTWT was validated bycorrelating the estimated V̇o2max and the measuredV̇o2max in the cross-validation group. A correlation (r)of .96 was obtained, with a multiple correlation (R) of.86 (SEE54.85 mLzkg21zmin21).
Strengths and weaknesses. This test is suitable for test-ing people with various diagnoses in clinical andresearch settings. It consists of only a warm-up sessionand a single stage on the treadmill. This test, in our view,is useful for assessing people who are prone to fatigue.
Further research is needed to validate this test in peoplewith various diagnoses, in individuals over 60 years ofage, and in both unfit and highly trained individuals.Further studies are needed to establish its sensitivity todetect change. Finally, because this test is based on HR,factors that affect HR must be controlled; otherwise, thetest results will be invalidated.
Astrand and Ryhming Cycle Ergometer Test
Description. The Astrand and Ryhming (A-R) CycleErgometer Test, which is used to predict V̇o2max by useof a cycle ergometer, is based on the linear relationshipbetween V̇o2 and HR.31 Astrand and Ryhming31 notedthat, in subjects aged 18 to 30 years, the men had anaverage HR of 128 bpm at 50% of V̇o2max and anaverage HR of 154 bpm at 70% of V̇o2max, and thewomen had an average HR of 138 bpm at 50% ofV̇o2max and an average HR of 164 bpm at 70% ofV̇o2max. A nomogram was developed by Astrand andRyhming31 to estimate V̇o2max (Fig. 1), and later anage-correction factor was incorporated to account forthe decrease in HRmax with age (Tab. 2).32 Modificationof the A-R nomogram were proposed by Legge andBanister33 and by Hartung and colleagues9,34 to improvethe accuracy of the equation. A revision to the A-Rnomogram was also proposed by Siconolfi et al.35 Thedetails of the A-R Cycle Ergometer Test are presented inthe Appendix.
Reliability and validity. Astrand32 reported a correlation(r) of .71 between the measured V̇o2max and theestimated V̇o2max in the original A-R Cycle ErgometerTest and a correlation (r) of .78 between the measuredV̇o2max and the A-R Cycle Ergometer Test using theage-correction factor. Teraslinna et al36 reported a cor-relation (r) of .69 between the original A-R Cycle Ergome-ter Test and the measured V̇o2max and a correlation (r) of.92 using the age-correction factor in a sample of 31sedentary men. Kasch37 reported that the A-R CycleErgometer Test predicted a V̇o2max that was too low (by21%) in 83 men aged 30 to 66 years. Other research-ers38,39 have reported similar findings. Hartung et al,34 ina study of women aged 19 to 70 years, found that the A-Rmethod overestimated V̇o2max by 3% to 21%. In addi-tion, an overestimation of V̇o2max by the A-R methodhas been documented in women who were pregnant.40
Legge and Banister33 reported a correlation (r) betweentheir revised nomogram and the measured V̇o2max of
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 787
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

.98. Hartung and colleagues9,34 reported a correlation(r) of .95 between the measured V̇o2max and theestimated V̇o2max using their revised nomogram. How-ever, the revised nomogram still predicted a V̇o2maxthat was too low (by 8.1 mLzkg21zmin21) in a sample ofsedentary and trained men.9 In a sample of women(n538) aged 19 to 47 years, the revised nomogramoverestimated V̇o2max by 18.5%.34
Strength and weaknesses. The A-R Cycle ErgometerTest is one of the most frequently used submaximal cycleergometer tests.41,42 This test has been a standard usedby fitness facilities as part of fitness evaluations and todevelop a training plan and evaluate the results.43 Theprotocol uses HR, which is easy to measure. Limitationsof the test include the margin of error in the predictedV̇o2max values. The protocol can elicit lower-extremitydiscomfort in some people, which may invalidate theresults.
Canadian Aerobic Fitness Test
Description. The Canadian Aerobic Fitness Test(CAFT), formerly known as the Canadian Home FitnessTest, is unique in that it was designed to promote fitnesstesting at home. The CAFT was developed on a sampleof 1,544 individuals (699 men and 845 women) aged 15to 69 years.44 The CAFT is a measure of fitness and isbased on the duration of the step test and a 10-secondrecovery of HR (Tabs. 3 and 4). Norms for the recoveryHR in men and women have been reported,44 and a“Physical Fitness Evaluation Chart” for various agegroups is available (Tab. 5). In addition, Jette et al45
developed a regression equation for the CAFT to predictV̇o2max. A sample of 59 individuals, aged 15 to 74 years,completed the CAFT and then underwent a progressivetreadmill test to evaluate V̇o2max.
The CAFT was modified (mCAFT)46,47 following reportsthat it predicted a V̇o2max that was too low in womenaged 20 to 30 years and in heavy, older, and well-trainedindividuals.48–50 Use of too few stages can produce aceiling effect, and, if the target HR is not attained, theV̇o2max prediction may be too low.46 The modificationallows an individual to complete the number of stagesnecessary to reach a target HR within 85% of theage-predicted maximum. Weller et al46 developed 2additional stages for the original CAFT for individualswho exceed stage 6. A new regression equation was alsodeveloped.51 The details of the CAFT52 are shown in theAppendix.
Reliability and validity. The reliability of measurementsof recovery time for HR for the CAFT was determinedusing a sample of 102 individuals (r 5.79).44 In terms ofvalidity, the regression equation developed by Jette
Figure 1.The Astrand and Ryhming nomogram. Estimated maximum oxygenconsumption (V̇O2max) can be determined by reading horizontally fromthe body weight scale (step test) or workload scale (cycle test) to theoxygen uptake (V̇O2) scale. The predicted V̇O2max value is obtained byconnecting the point on the V̇O2 scale (V̇O2 , liters per minute) with thecorresponding point on the pulse rate scale (in beats per minute). Thehorizontal line extends from the workload and V̇O2 scales to the pulserate scale. Where the line intersects the max V̇O2 scale (liters per minute)is the estimate of the individual’s V̇O2max. Reprinted with permissionfrom Astrand I. Aerobic capacity in men and women with specialreference to age. Acta Physiol Scand. 1960;49(suppl 169):2–92.
788 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

et al45 had a multiple correlation (R) of .905(SEmeas54.08 mLzkg21zmin21). The regression equationfor the mCAFT demonstrated the same strengthbetween the predicted V̇o2max and the measuredV̇o2max as the original equation for the CAFT (mCAFT,r 5.88; CAFT, r 5.99), but there was a lower meansquare error (mCAFT537.0 and CAFT563.3).
Strengths and weaknesses. The CAFT is a step test and,therefore, is inexpensive to administer and requires noelectricity or calibration. A person’s power output can becalculated within 6% to 7% if the individual steps in timewith the beat, stands erect on the top step, and placesboth feet flat on the ground at the end of each steppingcycle.11
This test may not be suitable for people whose ability tobalance is diminished because no handrail is used. It isalso difficult to monitor individuals while they are step-ping. Because we believe there is a ceiling effect, wecontend that the original protocol appears to be moresuited for assessing individuals who are unfit. Furtherresearch is needed to validate both the CAFT and themCAFT with people with various diagnoses.
12-Minute Run Test
Description. The 12-Minute Run Test (12-MRT) wasdeveloped by Cooper53 in 1968. This test is based on thework of Balke,54 which indicated that various run-walktests could relate V̇o2 to either the distance covered in agiven period of time or the time taken to cover a givendistance. A sample of 115 men with no health problemsaged 17 to 52 years completed two 12-MRTs and aV̇o2max test on a treadmill, and a regression equation
was developed. The details of the 12-MRT are shown inthe Appendix.
Reliability and validity. Test-retest reliability (r) of mea-surements obtained with the 12-MRT was reported byCooper53 to be .90. In terms of validity, Cooper53
reported a correlation (r) of .90 between the 12-MRTdistance and V̇o2max. Jessup et al55 reported a lowercorrelation (r) of only .13 between the 12-MRT andV̇o2max in a sample of male subjects with no healthproblems aged 18 to 23 years. Safrit et al56 reportedfindings similar to those of Jessup et al.55
Strengths and weaknesses. The 12-MRT requires nospecialized equipment and allows more than one indi-vidual to be tested at a time. We suggest that this test isappropriate for assessing the cardiopulmonary fitness ofindividuals with high levels of function. The 12-MRT hasbeen modified as a 12-Minute Walk Test (12-MWT),which we believe is more appropriate for the rehabilita-tion setting.
This test was developed using a male population. Nocross-validation group was used to validate the equation.The 12-MRT requires a constant level of motivation, and
Table 2.Astrand and Ryhming Cycle Ergometer Test: Correction Factor forAge-Predicted Maximal Heart Ratea
Age (y) FactorMaximal HeartRate (bpm) Factor
15 1.10 210 1.1225 1.00 200 1.0035 0.87 190 0.9340 0.83 180 0.8345 0.78 170 0.7550 0.75 160 0.6955 0.71 150 0.6460 0.6865 0.65
a Use the correction factor if the individual is over 30 to 35 years of age or ifthe maximal heart rate is known. The actual factor should be multiplied bythe value in Table 2. Note: one correction factor is multiplied by age, and theother correction factor is multiplied by maximal heart rate. Reprinted withpermission from Astrand PO, Rodahl K. Textbook of Work Physiology. 2nd ed.New York, NY: McGraw-Hill Book Co; 1977:279.
Table 3.Canadian Aerobic Fitness Test: Starting Tempo of the SteppingExercise Based on Age and Sexa
Age (y)
Starting Exerciseb
Males Females
60 and over 1 (66) 1 (66)50–59 2 (84) 1 (66)40–49 3 (102) 2 (84)30–39 4 (114) 3 (102)20–29 5 (132) 3 (102)15–19 5 (132) 4 (114)
a Reprinted with permission from Operations Manual: Canadian Home FitnessTest, 2nd ed, Health Canada. © Minister of Public Works and GovernmentServices Canada, 2000.b Stepping tempo (in parentheses) in steps per minute.
Table 4.Canadian Aerobic Fitness Test: Ceiling Postexercise Heart Ratesa
Age (y)
Heart Rate
10 s After1st Stage
10 s After2nd Stage
60 and over 24 2350–59 25 2340–49 26 2430–39 28 2520–29 29 2615–19 30 27
a Reprinted with permission from Operations Manual: Canadian Home FitnessTest, 2nd ed, Health Canada. © Minister of Public Works and GovernmentServices Canada, 2000.
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 789
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

Table 5.Canadian Aerobic Fitness Test: Physical Fitness Evaluation Charta
AgeGroup
Start at SteppingExercise No.
Your pulse rate after first exerciseMales Females
60s 1 1 Stop if 24 or more If 24 or more, you have anundesirable (below average)personal fitness level
Go only if 23 or less Everybody stop
50s 2 1 Stop if 25 or more If 25 or more, you have anundesirable personal fitnesslevel
Go only if 24 or less Stop if 23 or more
40s 3 2 Stop if 26 or more If 26 or more, you have anundesirable personal fitnesslevel
Go only if 25 or less Stop if 24 or more
30s 4 3 Stop if 28 or more If 28 or more, you have anundesirable personal fitnesslevel
Go only if 27 or less Stop if 25 or more
20s 5 3 Stop if 29 or more If 29 or more, you have anundesirable personal fitnesslevel
Go only if 28 or less Stop if 26 or more
15–19 5 4 Stop if 30 or more If 30 or more, you have anundesirable personal fitnesslevel
Go only if 29 or less Stop if 27 or more
Your pulse rate after second exercise Your pulse rate after third exercise* Caution: The advanced version of the Canadian Home Fitness Test is
intended for use only by those individuals who have attained therecommended fitness level.
If 23 or more, you havethe minimum personalfitness level
If 22 or less, you havethe recommendedpersonal fitnesslevel
Advanced ONLY
If 23 or more, you havethe minimum personalfitness level
Go only if 22 or less Everybodystop
If 23 or more, you havethe recommendedpersonal fitness level
GOOD
If 21–22, you havethe recommendedpersonal fitnesslevel
VERY GOOD
If 20 or less, you havethe recommendedpersonal fitnesslevel
EXCELLENT
If 24 or more, you havethe minimum personalfitness level
Go only if 23 or less Everybodystop
If 24 or more, you havethe recommendedpersonal fitness level
GOOD
If 22–23, you havethe recommendedpersonal fitnesslevel
VERY GOOD
If 21 or less, you havethe recommendedpersonal fitnesslevel
EXCELLENT
If 25 or more, you havethe minimum personalfitness level
Go only if 24 or less Everybodystop
If 25 or more, you havethe recommendedpersonal fitness level
GOOD
If 23–24, you haveto recommendedpersonal fitnesslevel
VERY GOOD
If 22 or less, you havethe recommendedpersonal fitnesslevel
EXCELLENT
If 26 or more, you havethe minimum personalfitness level
Go only if 25 or less Everybodystop
If 26 or more, you havethe recommendedpersonal fitness level
GOOD
If 24–25, you havethe recommendedpersonal fitnesslevel
VERY GOOD
If 23 or less, you havethe recommendedpersonal fitnesslevel
EXCELLENT
If 27 or more, you havethe minimum personalfitness level
Go only if 26 or less Everybodystop
If 27 or more, you havethe recommendedpersonal fitness level
GOOD
If 25–26, you havethe recommendedpersonal fitnesslevel
VERY GOOD
If 24 or less, you havethe recommendedpersonal fitnesslevel
EXCELLENTa Reprinted with permission from Operations Manual: Canadian Home Fitness Test, 2nd ed, Health Canada. © Minister of Public Works and Government ServicesCanada, 2000.
790 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022
the individual must pace herself or himself. The wordingof the instructions makes this a potentially maximalexercise test, so well-defined testing criteria are neededto ensure that it is a submaximal exercise test. Finally,this test fails to account for age or body weight, whichcan influence exercise responses.18
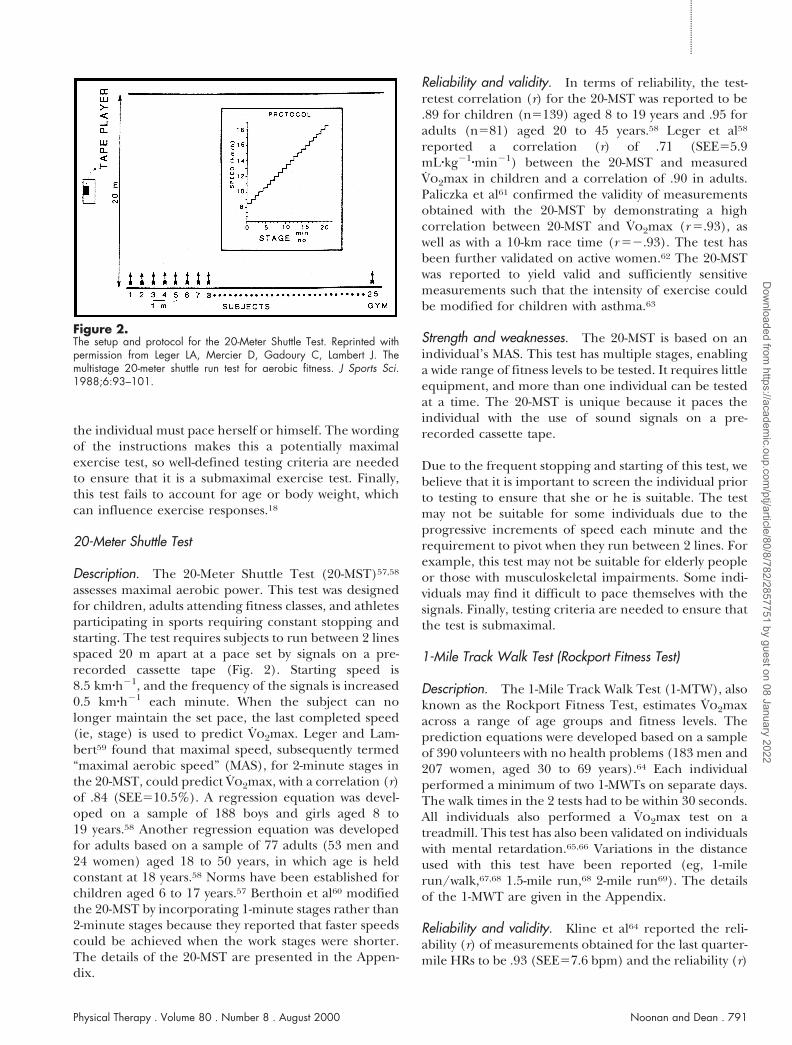
20-Meter Shuttle Test
Description. The 20-Meter Shuttle Test (20-MST)57,58
assesses maximal aerobic power. This test was designedfor children, adults attending fitness classes, and athletesparticipating in sports requiring constant stopping andstarting. The test requires subjects to run between 2 linesspaced 20 m apart at a pace set by signals on a pre-recorded cassette tape (Fig. 2). Starting speed is8.5 kmzh21, and the frequency of the signals is increased0.5 kmzh21 each minute. When the subject can nolonger maintain the set pace, the last completed speed(ie, stage) is used to predict V̇o2max. Leger and Lam-bert59 found that maximal speed, subsequently termed“maximal aerobic speed” (MAS), for 2-minute stages inthe 20-MST, could predict V̇o2max, with a correlation (r)of .84 (SEE510.5%). A regression equation was devel-oped on a sample of 188 boys and girls aged 8 to19 years.58 Another regression equation was developedfor adults based on a sample of 77 adults (53 men and24 women) aged 18 to 50 years, in which age is heldconstant at 18 years.58 Norms have been established forchildren aged 6 to 17 years.57 Berthoin et al60 modifiedthe 20-MST by incorporating 1-minute stages rather than2-minute stages because they reported that faster speedscould be achieved when the work stages were shorter.The details of the 20-MST are presented in the Appen-dix.
Reliability and validity. In terms of reliability, the test-retest correlation (r) for the 20-MST was reported to be.89 for children (n5139) aged 8 to 19 years and .95 foradults (n581) aged 20 to 45 years.58 Leger et al58
reported a correlation (r) of .71 (SEE55.9mLzkg21zmin21) between the 20-MST and measuredV̇o2max in children and a correlation of .90 in adults.Paliczka et al61 confirmed the validity of measurementsobtained with the 20-MST by demonstrating a highcorrelation between 20-MST and V̇o2max (r 5.93), aswell as with a 10-km race time (r 52.93). The test hasbeen further validated on active women.62 The 20-MSTwas reported to yield valid and sufficiently sensitivemeasurements such that the intensity of exercise couldbe modified for children with asthma.63
Strength and weaknesses. The 20-MST is based on anindividual’s MAS. This test has multiple stages, enablinga wide range of fitness levels to be tested. It requires littleequipment, and more than one individual can be testedat a time. The 20-MST is unique because it paces theindividual with the use of sound signals on a pre-recorded cassette tape.
Due to the frequent stopping and starting of this test, webelieve that it is important to screen the individual priorto testing to ensure that she or he is suitable. The testmay not be suitable for some individuals due to theprogressive increments of speed each minute and therequirement to pivot when they run between 2 lines. Forexample, this test may not be suitable for elderly peopleor those with musculoskeletal impairments. Some indi-viduals may find it difficult to pace themselves with thesignals. Finally, testing criteria are needed to ensure thatthe test is submaximal.
1-Mile Track Walk Test (Rockport Fitness Test)
Description. The 1-Mile Track Walk Test (1-MTW), alsoknown as the Rockport Fitness Test, estimates V̇o2maxacross a range of age groups and fitness levels. Theprediction equations were developed based on a sampleof 390 volunteers with no health problems (183 men and207 women, aged 30 to 69 years).64 Each individualperformed a minimum of two 1-MWTs on separate days.The walk times in the 2 tests had to be within 30 seconds.All individuals also performed a V̇o2max test on atreadmill. This test has also been validated on individualswith mental retardation.65,66 Variations in the distanceused with this test have been reported (eg, 1-milerun/walk,67,68 1.5-mile run,68 2-mile run69). The detailsof the 1-MWT are given in the Appendix.
Reliability and validity. Kline et al64 reported the reli-ability (r) of measurements obtained for the last quarter-mile HRs to be .93 (SEE57.6 bpm) and the reliability (r)
Figure 2.The setup and protocol for the 20-Meter Shuttle Test. Reprinted withpermission from Leger LA, Mercier D, Gadoury C, Lambert J. Themultistage 20-meter shuttle run test for aerobic fitness. J Sports Sci.1988;6:93–101.
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 791
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

of measurements obtained for the total time for the 2trials of the track walk to be .93 (SEE50.26 minute). Thevalidity of the regression equation was established byhaving a validation group (n5174) and a cross-validation group (n5169). The sample of 390 volunteerswere assigned to the validation and cross-validationgroups based on alternate case assignment (ie, odd-evencase selection). Descriptive statistics revealed no differ-ence between the 2 groups. The correlation (r) betweenthe predicted V̇o2max and the actual V̇o2max was .93(SEE50.325 Lzmin21) for the validation group and .92(SEE50.355 Lzmin21) for the cross-validation group.
Strengths and weaknesses. This test, in our view, isapplicable to a wide range of individuals. It requires littlespecialized equipment and uses the familiar activity offast walking. Thus, we contend that it is suitable for usein the rehabilitation setting. The test was cross-validated,which confirms the accuracy of prediction.
The test and regression equations need to be validatedin patient groups. Finally, research is needed to deter-mine whether a practice test improves the prediction.
Performance Submaximal Tests
Self-Paced Walking Test
Description. The Self-Paced Walking Test (SPWT)70 isan exercise test developed for elderly and frail individu-als. It consists of free walking at 3 speeds down an indoorcorridor (ie, 250 m). Various exercise responses can beassessed such as speed, time, stride frequency, stridelength, HR, and predicted V̇o2max. The test was devel-oped on 24 individuals aged 64 to 66 years. Ten activestudents aged 19 to 21 years served as a comparisongroup. Each subject performed the SPWT and a progres-sive cycle ergometer test. Only 17 elderly individualscould complete the cycle ergometery test, whereas all ofthem completed the SPWT.
Performance of the SPWT is correlated with V̇o2max andis independent of age.71 Following an exercise program,the speed of walking was reported to increase, whereasHR remained unchanged.72 A predicted V̇o2max can beobtained from estimating V̇o2 from an aerobic demandcurve and then extrapolating a predicted V̇o2max fromV̇o2 and HR. To date, this test has been used primarilywith older individuals.71–73 The details of the SPWT arepresented in the Appendix.
Reliability and validity. The test-retest reliability formeasurements obtained with the SPWT when it wasrepeated a few days later for the older group was 65.2%,64.7%, and 611% for the fast, normal, and slow paces,respectively.70 The younger group varied by 67%, but
no difference was found between the 2 tests on separatedays. In terms of validity, the assessments (ie, standard-ized HR from the SPWT and a progressive cycle test)were correlated (r 5.79).70
Strengths and weaknesses. The SPWT assesses cardio-pulmonary fitness as well as walking efficiency, both ofwhich are beneficial in daily activities.70 This test issuitable for individuals requiring mobility devices orwhen a treadmill or cycle ergometer is not indicated.This test may also be suitable for monitoring an olderperson’s mobility status over time, including the effectsof aging and the effect of using mobility aids anddevices.70 The information obtained from this test canprovide safety guidelines (eg, for crossing an intersec-tion safely requires a speed of 3.5 ft/s).24 Individuals whoare at risk for injury while crossing an intersection maybe identified. Individuals who are not able to walk at thisspeed should be identified as being not safe, and alter-native means of mobility or mobility aids need to berecommended.
This test is limited because it does not provide a measureof endurance and may not be sufficiently sensitive to testindividuals with higher levels of function. For someindividuals with diminished function, it may be toodifficult to complete the 3 selected walks with only 5minutes of rest.
Modified Shuttle Walking Test
Description. The Modified Shuttle Walking Test(MSWT) was modified from the 20-MST to provide astandardized progressive test for obtaining a symptom-limited maximum performance in individuals withchronic airway obstruction (CAO).74,75 The individualwalks up and down a 10-m course at incremental speeds
Table 6.Modified Shuttle Walking Test: Protocola
LevelSpeed(m/s)
Speed(mph)
No. ofShuttles
1 0.50 1.12 32 0.67 1.50 43 0.84 1.88 54 1.01 2.26 65 1.18 2.64 76 1.35 3.02 87 1.52 3.40 98 1.69 3.78 109 1.86 4.16 11
10 2.03 4.54 1211 2.20 4.92 1312 2.37 5.30 14
a Reprinted with permission of the BMJ Publishing Group from Payne GE,Skehan JD. Shuttle walking test: a new approach for evaluating patients withpacemakers. Heart. 1996;75:414–418.
792 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

of 0.17 m/s each minute dictated by a prerecordedaudio signal on a cassette deck74 (Tab. 6), whereas theoriginal 20-MST required the individual to run a 20-mdistance at a starting speed of 8.5 km/h with incrementsof 0.5 km/h each minute.58
A sample of 35 individuals with CAO aged 45 to 74 yearswas used to develop the test.74 This test has been furthervalidated on individuals with pacemakers.76 Singh andcolleagues74,75 have recommended the MSWT for use asan assessment tool for individuals with a wide range ofcardiac and respiratory disabilities. The details of theMSWT are shown in the Appendix.
Reliability and validity. The measurements obtainedwith this test were replicable in a sample of 10 individu-als after one practice trial.74 The mean differencebetween trials 2 and 3 was 22.0 m (95% confidenceinterval of 221.9 to 17.9 m). The validity of measure-ments obtained with the test, which was established bycomparing the distance completed during the MSWTwith the distance completed during the 6-Minute WalkTest (6-MWT), was moderate (rho5.68).74 The HRs,however, were higher on the MSWT, indicating a greatercardiovascular response. A strong relationship (r 5.81and r 5.88) was observed on comparing the V̇o2maxrecorded in 2 tests using treadmill walking with theV̇o2max recorded during the MSWT.75
Strengths and weaknesses. The MSWT requires littleequipment and is easy to administer. The audio signalstandardizes the increments in walking speed and moti-vates the individual. We believe that the initial speed issufficiently slow to be used with most types of patients.No individual in the studies attained the highest level(ie, level 12).74,75 This test can be used to prescribe anappropriate walking speed for an exercise program byevaluating the individual’s HR and RPE responses at thevarious stages.74
This test, however, requires a near-maximal effort byhaving the speeds continue to increase. We believe,therefore, that it is essential to monitor the individualduring the test to ensure that she or he is respondingappropriately. Familiarizing the individual with the pac-ing required for the test may require some time.
Bag and Carry Test
Description. The Bag and Carry Test (BCT)77 is used toassess a task that evaluates both endurance and muscleforce. The BCT involves walking a circuit carrying a0.9-kg package for 7.5 m, up and down a 4-step flight ofstairs, and back 7.5 m. On the completion of eachcircuit, 0.9 kg is added to the package until the individ-ual can no longer complete the circuit. It requires 10
minutes to complete. A sample of 61 women aged 48 to93 years was recruited from the community and aresidential home. Fifty-six subjects completed the test.The maximal weight they could carry up and down thestairs ranged between 3 and 26 kg. The test developersconcluded that this test was easy to administer andsuitable for testing individuals with higher levels offunction. The details of the BCT are presented in theAppendix.
Reliability and validity. The test-retest reliability of mea-surements obtained with the BCT was established byadministering the BCT 3 days later (r 5.89). MaximalHR was 90%610% of the HR achieved during theV̇o2peak test on a cycle ergometer. The BCT correlatedwith force of the quadriceps femoris muscle (r 5.43),hamstring muscle (r 5.54), gastrocnemius muscle(r 5.52), and soleus muscle (r 5.62).77
Strength and weaknesses. The BCT is designed to inte-grate endurance, muscle force, and balance capabilityand is based on an everyday activity. This test, in ourview, is easy to administer and can be used in researchand clinical settings. However, it may be difficult toreplicate the test with 4 steps. A platform or landingshould be at the top of the stairs to allow the individualto turn around safely.
The guidelines for administering this test are not welldescribed in the literature. There are no specificationsregarding the height of the steps, whether the individualis allowed to use a handrail for support, or whether apractice trial is required. In the absence of criteria foradministering the test, this test could become a maximaltest if the individual is not properly monitored duringthe test. We argue that this test has the potential to be avery useful submaximal exercise test if the individual istimed as opposed to being scored by only the weight heor she carried. The number of circuits completed in aspecified time could be measured, or the time to com-plete the circuit while carrying a specified weight andwalking at a safe and comfortable pace could be scored.
Timed Up & Go Test
Description. The Timed Up & Go Test (TUGT)78 wasmodified from the Get-up & Go Test.79 Both tests arebased on a functional task of rising from a standardarmchair, walking 3 m, turning, and returning to thechair. Podsiadlo and Richardson,78 however, changedthe scoring system from an observer rating of 1 to 5 to atimed version. The test was modified using a sample of60 frail, community-dwelling, elderly individuals (23men and 37 women, aged 60 to 90 years) and 10volunteers with no health problems (6 men and 4women, aged 70 to 84 years). Medical diagnoses of thestudy population included cerebrovascular accident
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 793
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

(n523), Parkinson disease (n510), rheumatoid arthritisor osteoarthritis (n59), and miscellaneous conditions(eg, postsurgical hip fractures, general deconditioning)(n58).78 The TUGT has been used as a test of mobilityto assess change following an exercise program forelderly individuals aged 79 to 86 years80 and aged 75 to96 years.81 No improvement in mobility based on this testfollowing an exercise programs was reported.80,81 Thedetails of the TUGT are given in the Appendix.
Reliability and validity. The interrater reliability fortimes obtained on the same day and the intraraterreliability tested 3 days to 5 weeks apart were good(intraclass correlation coefficient5.99 for both).78 Valid-ity was assessed by correlating the time (in seconds) onthe TUGT with the log-transformed scores on the BergBalance Scale (r 52.72), gait speed (r 52.55), andBarthel Index of Activities of Daily Living (r 52.51). Thecorrelations were negative, indicating that those individ-uals who took longer with the TUGT had lower scores onthe Berg Balance Scale, with gait speed, and on theBarthel Index.
Strengths and weaknesses. The TUGT is easy to admin-ister, and no training is required. This test is easy toperform in research and clinical settings. The resultsfrom this test provide information related to mobility.Based on the time taken to complete the test, the level ofassistance required in mobility tasks can bedetermined.78
A limitation of this test is that it may not detect a changefollowing an exercise program because of the lack ofsensitivity of the measure.81 Further studies are war-ranted to examine its sensitivity, using a larger sample,and to investigate its predictive capacity. Sensitivity couldpossibly be improved by increasing the distance walkedor having subjects sit down and get up again at each endof the 3-m walkway, but research is needed to determinewhether this is true.
12- and 6-Minute Walk Tests
Description. The 12-MWT was introduced by McGavinand colleagues82,83 to assess the distance covered in 12minutes in individuals with chronic bronchitis. The totaldistance covered in 12 minutes is recorded, and theindividual is allowed to stop and rest. This test wasmodified from the 12-MRT described by Cooper53 forindividuals without health problems. The 12-MWT hasbeen used primarily for people with COPD,82–91 but ithas also been used with college-aged students.92
Butland et al93 reported that similar results could beobtained in 6 minutes. Guyatt et al94 applied the 6-MWTin individuals with heart failure. The 6-MWT has been
used with individuals with end-stage lung disease,95 peo-ple with chronic heart failure,96,97 people with COPD,98–100
children who are severely ill,101 people with chronicrenal failure,102 and older adults between the ages of 65and 89 years.103 Two practice tests appear to be requiredto obtain reproducible results,93,94 the walking circuitneeds to be identical,92 and encouragement needs to bestandardized.27 Walk tests with durations of 4 minutes104
and 2 minutes93 have also been reported. The details ofthe 6-MWT and the 12-MWT are presented in theAppendix.
Reliability and validity. Reliability has been assessed formeasurements obtained with the 12-MWT. Mungall andHainsworth89 reported a coefficient of variation of68.2% over 6 tests. This statistic, however, is not aprobabilistic measure, which is normally used to assessreliability. If the results of the first 2 tests were elimi-nated, however, the coefficient of variation was reducedto 64.2%. Guyatt et al94 also reported that 2 practicetests are required. Other researchers95,96 have reportedintraclass correlation coefficients of .96 to .99 betweenthe second and third administrations of the 6-MWT,suggesting that only one practice test is required.
The concurrent validity of measurements obtained withthe 6-MWT and the 12-MWT based on measurements ofV̇o2max or V̇o2peak is not clear. Some investigators havereported a correlation between the distance covered inthe 6-MWT and V̇o2peak (r 5.6496 and r 5.70101) as wellas between the distance covered in the 12-MWT andV̇o2max (r 5.4985 and r 5.5282). Other researchers havereported no correlation between V̇o2max and either thedistance covered in the 6-MWT94 or the distance coveredin the 12-MWT.82 The physiologic demand of the walktest appears to be distinct from that of cycle ergometertests and, therefore, may be a better indicator of func-tion in normal daily activities.102,105 The correlationbetween lung function and the distance covered in the6-MWT and the 12-MWT has also shown conflictingresults.85,99,100
Strengths and weaknesses. The 6-MWT and the12-MWT are simple tests that are inexpensive to admin-ister. Walking for a given time seems, in our opinion, tocorrespond to functional activities used in daily activities.These tests, therefore, can be administered to individu-als without health problems and to patients with a varietyof diagnoses. The use of a standard time rather than apredetermined distance provides a better test of endur-ance.82 The tests allow the individual to set her or hisown pace and stop if necessary. The 12-MWT can beused to detect a change following an exercise program.86
In the literature in which these tests are described, thenumber of practice trials varies. Often only one practice
794 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

test was given,99–102 and there was considerable variationin the rest periods between tests. Some investiga-tors95,96,100,102 reported having the subjects perform thetest on the same day as the practice, whereas otherinvestigators94,99,105 reported having the test and practiceon separate days. In addition, different versions of theinstructions have been used for both the 6-MWT and the12-MWT. Some investigators101 stated in their instruc-tions that the individual was allowed to stop if necessary,whereas other investigators85 instructed the individual topace herself or himself so that she or he would not haveto stop. The scoring of the test has also varied. Mostinvestigators83,94,105 used the final distance (ie, that ofthe last test trial), whereas some investigators99 reportedthe longest distance of all test trials. We believe thatother limitations of the timed walk tests include lack ofmonitoring of physiological variables while the individ-ual is completing the test and the lack of specificperformance criteria to ensure that a maximal effort isnot performed.
Other Performance TestsPerformance tests are frequently incorporated as a mea-sure of mobility in global physical assessments used forelderly people. The most common performance test is ameasure of walking speed, which is similar to the 3walking speeds (ie, slow, normal, and fast) used with theSPWT. Typically, a 10-ft walk106–108 is used for assessingindividuals who are confined indoors and a 50-ftwalk107,109–111 is used for all others. A 30-m walk has alsobeen used, as this is the usual distance for pedestriancrossings.112 The instructions are for the individual towalk from a standing start at his or her regular pace andto use any mobility devices that he or she normally uses.106
The individual is timed, and the walking speed (in metersper second or feet per second) is calculated. Reports ofaverage walking speed range from 0.7460.29 mzs21 forindividuals aged 60 to 99 years113 to 1.1 and 1.2 mzs21 for70-year-old women and men with no health problems,respectively.112
The assessment of walking speed is very important forassessing independent mobility in the community.Pedestrian intersection crossing times are calculatedbased on a walking speed of 1.22 mzs21.114 A walkingspeed of 11.5 mzmin21 is a threshold value for predictingnursing home status,107 with a normal walking speedbeing 70 mzmin21.107 Two factors, quadriceps femorismuscle weakness and joint impairment, are thought tobe critical variables in determining walking speed,which, in turn, determines some aspect of dependencyin elderly people. Variations in walking speed are due toa change in stride length rather than an alteration infrequency or cadence.113 The onset of pathology short-ens the stride length and influences speed of walking.113
Chronologic age is not thought to be a primary factor indetermining gait speed.113
Researchers have assessed a maximum walking speed fora given distance (eg, 30 m). In a sample of 70-year-oldsubjects (n5602), the maximum walking speed was themost reliable predictor of dependence in activities ofdaily living.112 The critical levels for the threshold ofbeing dependent in activities of daily living was found tobe a maximum walking speed of 1.7 mzs21 in men and1.5 mzs21 in women. It is not entirely clear whether adecline in cardiopulmonary fitness affects walkingspeeds for short distances; it is more likely to be acontributing rather than a primary factor.112
Other performance tests cited in the literature include astep test. This test requires 3 boxes combined to formsteps of 10, 20, 30, 40, and 50 cm in height and ahandrail on the wall.112 The highest possible step heightthat the individual is able to climb up and down witheither leg and without a rail is recorded. There are alsovariations of this step test.115,116 Correlations have beenreported between the maximum step height up anddown with a comfortable walking speed in 70-year-oldmen (r 5.39) and women (r 5.37).112
An obstacle course described by Imms and Edholm113 isused in a test that is similar to the BCT. In this test, theindividual rises from a chair, walks across the room,climbs 3 stairs (rails on either side), turns around,descends the stairs, and returns to the chair. The indi-vidual is allowed to go at her or his own speed and to usea mobility aid. Two practice trials are given, and the time(in seconds) taken to complete the course is recorded.In a sample of 71 subjects (28 men and 43 women) aged60 to 99 years, the time to complete the course was notcorrelated with age but was correlated with walkingspeed (r 52.80).113
Examples of Test Selection
1. The patient is a 65-year-old man with severe chronicairflow limitation and right atrial enlargement. He hasno history of angina but does have hypertension, whichis controlled with medication. He is 18.1 kg (40 lb)overweight and is unaccustomed to physical activity. Hisactivity is normally terminated by shortness of breath.
Indications: to establish an exercise profile to ensure thathe is safe to undertake an exercise program and todefine the parameters for such a program.
Test: 6-MWT or SPWT.
Clinical Decision-Making Process: The 6-MWT and theSPWT are both suited for older patients with chroniclung disease. This patient is deconditioned, overweight,and hypertensive. These tests enable him to perform an
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 795
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

activity (ie, walking) that is useful to him on a daily basis.In addition, with portable equipment, including HRmonitor, BP measurement apparatus, and pulse oxime-ter, he can be readily monitored. Furthermore, the scaleof breathlessness can be used to assess his symptoms.The physical therapist can correlate the rating of breath-lessness and physiologic parameters to prescribe theparameters of an exercise program, including type ofexercise, intensity, frequency, duration, continuous ver-sus discontinuous program, and its course. These testscan be repeated at various intervals to evaluate theoutcome of the training program.
2. The patient is a 52-year-old man who had bypasssurgery 10 years ago. He had one recurrence of angina.He has intermittent claudication in the left calf at amoderate walking speed.
Indications: to establish safe exercise intensity (no angi-nal symptoms) and a training program for his peripheralvascular disease as well as heart disease.
Test: Modified Bruce Treadmill Test, SPWT, or 6-MWT.
Clinical Decision-Making Process: This patient is showingsigns and symptoms of reocclusion of his coronaryarteries and stenosis of a lower-extremity artery, whichresults in claudication. He could be a candidate formaximal exercise testing; however, if he stops because ofleg pain, the test results will be limited. Alternatively, hecould undergo submaximal exercise testing (eg, Modi-fied Bruce Treadmill Test, SPWT, 6-MWT). Because ofhis cardiac history, precautions must be taken. Having acardiologist present is recommended, and the treadmilltest is preferable for monitoring electrocardiographicactivity. If the electrocardiogram is normal, the SPWT orthe 6-MWT can be performed, and one of these tests canbe used to assess training response, if preferred. Theparameters of the training program are set to keep thepatient below his anginal threshold and his leg paintolerable.
Summary and ConclusionsPhysical therapists are clinical exercise specialists whoapply exercise as an assessment and diagnostic tool andin treatment. We believe that they should have a thor-ough knowledge of exercise testing, including submaxi-mal exercise testing. Physical therapists, in our opinion,need to assume a role in refining existing exercise testsand measures and to assume a leadership role in devel-oping new tests and measures. Refinement of submaxi-mal exercise tests is needed to increase their sensitivity asassessment, diagnostic, and treatment outcome toolsand to provide valid indexes of a person’s capacity toassume a given type of employment, homemaking activ-ities, and activities of daily living. They also need to serveas a basis for exercise prescription.
We believe that there is a need for standardized submaxi-mal ergometer tests for people with musculoskeletallimitations, people who have impaired balance, peoplewho are overweight, people who are unable to walk on atreadmill for other reasons, and for people who requireclose monitoring during exercise. There is also, in ouropinion, a need for the development of upper-extremitysubmaximal exercise tests for people with lower-extremity paresis or severe deformity.
We contend that stringent monitoring of exerciseresponses is essential both for test validity and for safety.When testing people with a wide range of conditions,including cardiovascular and cardiopulmonary condi-tions that can be life threatening, even people withoutknown health problems can exhibit unexpectedresponses. People without known health problems, forexample, can have cardiac dysrhythmias; and this inci-dence increases with advancing age.20 Safety and mini-mizing undue strain, in our view, are essential in plan-ning and implementing submaximal exercise testing.
Research is also needed for the development and re-finement of scales used to assess exercise response(eg, exertion, breathlessness, fatigue, discomfort orpain, and even well being associated with physical activ-ity). Given that people are limited by their symptomsthat correlate to physiologic measures, assessment oftheir symptoms can provide critical information abouttheir exercise responses as well as a basis for setting theintensity of tolerable physical activity or an exerciseprogram.
References1 Montoye HJ, Ayen T, Washburn RA. The estimation of V̇o2max frommaximal and submaximal measurements in males, age 10–39. Res Q.1986;57:250–253.
2 Wyndham CH. Submaximal tests for estimating maximum oxygenintake. Can Med Assoc J. 1967;96:736–745.
3 Balke B, Ware R. An experimental study of Air Force personnel. USArmed Forces Med J. 1959;10:675–688.
4 Brouha L, Fradd NW, Savage BM. Studies in physical efficiency ofcollege students. Res Q. 1944;15:211–224.
5 Bruce RA, Kusumi F, Hosmer D. Maximal oxygen intake andnomographic assessment of functional aerobic impairment in cardio-vascular disease. Am Heart J. 1973;85:546–562.
6 Ellestad MH. Stress Testing. 2nd ed. Philadelphia, Pa: FA Davis Co;1980.
7 Patterson JA, Naughton J, Pietras RJ, Gunnar RM. Treadmill exercisein assessment of patients with cardiac disease. Am J Cardiol. 1972;30:757–762.
8 Shephard RJ, Allen C, Benade AJS, et al. The maximum oxygenintake: an international reference standard of cardiorespiratory fitness.Bull World Health Org. 1968;38:757–764.
9 Hartung GH, Krock LP, Crandall CG, et al. Prediction of maximaloxygen uptake from submaximal exercise testing in aerobically fit andnonfit men. Aviat Space Environ Med. 1993;64:735–740.
796 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

10 McArdle WD, Katch FI, Katch VL. Exercise Physiology: Energy, Nutri-tion, and Human Performance. 2nd ed. Philadelphia, Pa: Lea & Febiger;1990.
11 Shephard RJ. Exercise Physiology. Toronto, Ontario, Canada: BCDecker Inc; 1987.
12 Ebbeling CB, Ward A, Puleo EM, et al. Development of a single-stage submaximal walking test. Med Sci Sports Exerc. 1991;23:966–973.
13 American College of Sports Medicine. Guidelines for Exercise Testingand Prescription. 5th ed. Philadelphia, Pa: Lea & Febiger; 1995.
14 Zeballos RJ, Weisman IM. Behind the scenes of cardiopulmonaryexercise testing. Clin Chest Med. 1994;15:193–213.
15 Jones NL. Clinical Exercise Testing. Philadelphia, Pa: WB SaundersCo; 1988.
16 Shephard RJ. Tests of maximal oxygen intake: a critical review.Sports Med. 1984;1:99–124.
17 Brown SE, Fischer CE, Stansbury DW, Light RW. Reproducibility ofV̇o2max in patients with chronic air-flow obstruction. Am Rev Respir Dis.1985;131:435–438.
18 Ward A, Ebbeling CB, Ahlquist LE. Indirect methods for estimationof aerobic power. In: Maud PJ, Foster C, eds. Physiological Assessment ofHuman Fitness. Champaign, Ill: Human Kinetics; 1995:37–56.
19 Dean E. Mobilization and exercise. In: Frownfelter D, Dean E, eds.Principles and Practice of Cardiopulmonary Physical Therapy. 3rd ed. StLouis, Mo: Mosby; 1996:265–298.
20 Aronow WS. Usefulness of the resting electrocardiogram in theelderly. Compr Ther. 1992;18:11–16.
21 Mihalick MJ, Fisch C. Electorcardiographic findings in the aged. AmHeart J. 1974;87:1117–1128.
22 Fletcher GF, Froelicher VF, Hartley LH, et al. Exercise standards: astatement for health professionals from the American Heart Associa-tion. Circulation. 1990;82:2286–2322.
23 Hagberg JM. Exercise assessment of arthritic and elderly individu-als. Clin Rheumatol. 1994;8:29–52.
24 Questead KA, Alquist A. Exercise assessment in clinical practice.Phys Med Rehab Clin North Am. 1994;5:243–253.
25 Marciniuk DD, Gallagher CG. Clinical exercise testing in interstitiallung disease. Clin Chest Med. 1994;15:287–303.
26 Dean E, Ross J, Bartz J, Purves S. Improving the validity of clinicalexercise testing: the relationship between practice and performance.Arch Phys Med Rehabil. 1989;70:599–604.
27 Guyatt GH, Pugsley SO, Sullivan MJ, et al. Effect of encouragementon walking test performance. Thorax. 1984;39:818–822.
28 Dean E. Assessment of peripheral circulation: an update for prac-titioners. Australian Journal of Physiotherapy. 1987;33:164–172.
29 Bruce RA. Exercise testing of patients with coronary heart disease:principles and normal standards for evaluation. Ann Clin Res. 1971;3:323–332.
30 Foster C, Jackson AS, Pollock ML, et al. Generalized equations forpredicting functional capacity from treadmill performance. Am Heart J.1984;107:1229–1234.
31 Astrand PO, Ryhming I. A nomogram for calculation of aerobiccapacity from pulse rate during submaximal work. J Appl Physiol.1954;7:218–221.
32 Astrand I. Aerobic capacity in men and women with special refer-ence to age. Acta Physiol Scand. 1960;49(suppl 169):2–92.
33 Legge BJ, Banister EW. The Astrand-Ryhming nomogram revisited.J Appl Physiol. 1986;61:1203–1209.
34 Hartung GH, Blancq RJ, Lally DA, Krock LP. Estimation of aerobiccapacity from submaximal cycle ergometry in women. Med Sci SportsExerc. 1995;27:452–457.
35 Siconolfi SF, Cullinane EM, Carleton RA, Thompson PD. AssessingV̇o2max in epidemiological studies: modification of the Astrand-Ryhming test. Med Sci Sports Exerc. 1982;14:335–338.
36 Teraslinna P, Ismail AH, MacLeod DF. Nomogram by Astrand andRyhming as a predictor of maximum oxygen intake. J Appl Physiol.1966;21:513–515.
37 Kasch FW. The validity of the Astrand and Sjostrand submaximaltests. Physician & Sportsmedicine. 1984;12:47–52.
38 Glassford RG, Baycroft GHY, Sedgwick AW, Macnab RBJ. Compar-ison of maximal oxygen uptake values determined by predicted andactual methods. J Appl Physiol. 1965;20:509–513.
39 Rowell LB, Taylor HL, Wang Y. Limitations to prediction ofmaximal oxygen intake. J Appl Physiol. 1964;19:919–927.
40 Lotering FK, Struijk PC, Van Doorn MB, Wallenburg HCS. Errors inpredicting maximal oxygen consumption in pregnant women. J ApplPhysiol. 1992;72:562–567.
41 Jessup GT, Riggs CE, Lambert J, Miller WD. The effect of pedallingspeed on the validity of the Astrand Ryhming aerobic work capacitytest. J Sports Med Phys Fitness. 1977;17:367–371.
42 Terry JW, Tolson H, Johnson DJ, Jessup GT. A workload selectionprocedure for the Astrand-Ryhming test. J Sports Med Phys Fitness.1977;17:361–366.
43 Wisen AGM, Wohlfart B. A comparison between two exercise testson cycle: a computerized test versus the Astrand test. Clin Physiol.1995;15:91–102.
44 Bailey DA, Shephard RJ, Mirwald RL. Validation of a self-adminis-tered home test of cardiorespiratory fitness. Can J Appl Sport Sci.1976;1:67–78.
45 Jette M, Campbell J, Mongeon J, Routhier R. The Canadian HomeFitness Test as a predictor for aerobic capacity. Can Med Assoc J.1976;114:680–682.
46 Weller IMR, Thomas SG, Corey PN, Cox MH. Selection of amaximal test protocol to validate the Canadian Aerobic Fitness Test.Can J Sport Sci. 1992;17:114–119.
47 Weller IMR, Thomas SG, Cox MH, Corey PN. A study to validate theCanadian Aerobic Fitness Test. Can J Public Health. 1992;83:120–124.
48 Jette M. A comparison between predicted V̇o2max from the Astrandprocedure and the Canadian Home Fitness Test. Can J Appl Sport Sci.1979;4:214–218.
49 Shephard RJ. The current status of the Canadian Home FitnessTest. Br J Sports Med. 1980;14:114–125.
50 Shephard RJ, Cox M, Corey P, Smyth R. Some factors affectingaccuracy of Canadian Home Fitness Test scores. Can J Appl Sport Sci.1979;4:205–209.
51 Weller IMR, Thomas SG, Gledhill N, et al. A study to validate themodified Canadian Aerobic Fitness Test. Can J Appl Physiol. 1995;20:211–221.
52 Canadian Standardized Test of Fitness Operations Manual. 3rd ed.Ottawa, Ontario, Canada: Government of Canada Fitness & AmateurSport; 1986.
53 Cooper KH. A means of assessing maximal oxygen intake: correla-tion between field and treadmill testing. JAMA. 1968;203:201–204.
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 797
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

54 Balke B. A Simple Test for the Assessment of Physical Fitness. OklahomaCity, Okla: Civil Aeromedical Research Institute, Federal AviationAgency; 1963. CARI Rep. No. 63-18.
55 Jessup GT, Tolson H, Terry JW. Prediction of maximal oxygenintake from the Astrand Ryhming test, 12-minute run, and anthropo-metric variables using stepwise multiple regression. Am J Phys Med.1974;53:200–207.
56 Safrit MJ, Costa MG, Hooper LM, et al. The validity and generali-zation of distance run tests. Can J Sport Sci. 1988;13:188–196.
57 Leger LA, Lambert J, Mercier D. Predicted V̇o2max and maximalspeed for a multistage 20-m shuttle run in 7000 Quebec children aged6–17. Med Sci Sports Exerc. 1982;15:142–143.
58 Leger LA, Mercier D, Gadoury C, Lambert J. The multistage 20meter shuttle run for aerobic fitness. J Sports Sci. 1988;6:93–101.
59 Leger LA, Lambert J. A maximal multistage 20-m shuttle run test topredict V̇o2max. Eur J Appl Physiol. 1982;49:1–12.
60 Berthoin S, Gerbeaux M, Turpin E, et al. Comparison of two fieldtests to estimate maximum aerobic speed. J Sports Sci. 1994;12:355–362.
61 Paliczka VJ, Nichols AK, Boreham CAG. A multi-stage shuttle run asa predictor of running performance and maximal oxygen uptake inadults. Br J Sports Med. 1987;21:163–165.
62 Ramsbottom R, Brewer J, Williams C. An examination of themaximal multistage shuttle run test as a predictor of V̇o2max in activefemale subjects [abstract]. J Sports Sci. 1988;6:165A.
63 Ahmaidi SB, Varray AL, Savy-Pacaux AM, Prefaut CG. Cardiorespi-ratory fitness evaluation by the shuttle test in asthmatic subjects duringaerobic training. Chest. 1993;103:1135–1141.
64 Kline GM, Porcari JP, Hintermeister R, et al. Estimation of V̇o2maxfrom a one-mile track walk, gender, age, and body weight. Med SciSports Exerc. 1987;19:253–259.
65 Kittredge JM, Rimmer JH, Looney MA. Validation of the RockportFitness Walking Test for adults with mental retardation. Med Sci SportsExerc. 1994;26:95–102.
66 Rintala P, Dunn JM, McCubbin JA, Quinn C. Validity of a cardio-respiratory fitness test for men with mental retardation. Med Sci SportsExerc. 1992;24:941–945.
67 Cureton KJ, Sloniger MA, O’Bannon JP, et al. A generalized equa-tion for prediction of V̇o2peak from 1-mile run walk performance. MedSci Sports Exerc. 1995;27:445–451.
68 George JD, Vehrs PR, Allsen PE, et al. Development of a submaxi-mal treadmill jogging test for fit college-aged individuals. Med Sci SportsExerc. 1993;25:643–647.
69 Ribisl PM, Kachadorian WA. Maximal oxygen intake prediction inyoung and middle-aged males. J Sports Med Phys Fitness. 1969;9:17–22.
70 Bassey EJ, Fentem PH, MacDonald IC, Scriven PM. Self-pacedwalking as a method for exercise testing in elderly and young men. ClinSci Mol Med Suppl. 1976;51:609–612.
71 Cunningham DA, Rechnitzer PA, Pearce ME, Donner AP. Determi-nants of self-selected walking pace across ages 19 to 66. J Gerontol.1982;37:560–564.
72 Cunningham DA, Rechnitzer PA, Donner AP. Exercise training andthe speed of self-selected walking pace in men at retirement. Can JAging. 1986;5:19–26.
73 Mattsson E, Brostrom LA. The physical and psychosocial effect ofmoderate osteoarthritis of the knee. Scand J Rehabil Med. 1991;23:215–218.
74 Singh SJ, Morgan MDL, Scott S, et al. Development of a shuttlewalking test of disability in patients with chronic airways obstruction.Thorax. 1992;47:1019–1024.
75 Singh SJ, Morgan MDL, Hardman AE, et al. Comparison of oxygenuptake during a conventional treadmill test and the shuttle walking testin chronic airflow limitation. Eur Respir J. 1994;7:2016–2020.
76 Payne GE, Skehan JD. Shuttle walking test: a new approach forevaluation of patients with pacemakers. Heart. 1996;75:414–418.
77 Posner JD, McCully KK, Landsberg LA, et al. Physical determinantsof independence in mature women. Arch Phys Med Rehabil. 1995;76:373–380.
78 Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basicfunctional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39:142–148.
79 Mathias S, Nayak USL, Isaccs B. Balance in elderly patients: the“get-up and go” test. Arch Phys Med Rehabil. 1986;67:387–389.
80 Connelly DM, Vandervoort AA. Improvement in knee extensorstrength of institutionalized elderly women after exercise with ankleweights. Physiotherapy Canada. 1995;47:15–23.
81 McMurdo ME, Johnstone R. A randomized controlled trial of ahome exercise programme for elderly people with poor mobility. AgeAgeing. 1995;24:425–428.
82 McGavin CR, Gupta SP, McHardy GJR. Twelve-minute walking testfor assessing disability in chronic bronchitis. Br Med J. 1976;1:822–823.
83 McGavin CR, Artvinli M, McHardy GJR. Dyspnea, disability, anddistance walked: comparison of estimates of exercise performance inrespiratory disease. Br Med J. 1978;2:241–243.
84 Alison JA, Anderson SD. Comparison of two methods of assessingphysical performance in patients with chronic airway obstruction. PhysTher. 1981;61:1278–1280.
85 Bernstein ML, Despars JA, Singh NP, et al. Reanalysis of the12-minute walk in patients with chronic obstructive pulmonary disease.Chest. 1994;105:163–167.
86 Cockcroft AE, Saunders MJ, Berry G. Randomised controlled trial ofrehabilitation in chronic respiratory disease. Thorax. 1981;36:200–203.
87 Jones PW, Baveystock CM, Littlejohns P. Relationships betweengeneral health measured with the Sickness Impact Profile and respira-tory symptoms, physiological measures, and mood in patients withchronic airflow limitation. Am Rev Respir Dis. 1989;140:1538–1543.
88 Leidy NK, Traver GA. Psychophysiologic factors contributing tofunctional performance in people with COPD: are there genderdifferences? Res Nurs Health. 1995;18:535–546.
89 Mungall PF, Hainsworth R. Assessments of respiratory function inpatients with chronic obstructive airway disease. Thorax. 1979;34:254–258.
90 Swinburn CR, Wakefield JM, Jones PW. Performance, ventilation,and oxygen consumption in three different types of exercise tests inpatients with chronic obstructive lung disease. Thorax. 1985;40:581–586.
91 Weaver TE, Narsavage GL. Physiological and psychological variablesrelated to functional status in chronic obstructive pulmonary disease.Nurs Res. 1992;41:286–291.
92 Siler WL, Koch NQ, Frese EM. The path utilized affects the distancewalked in the 12 minute walk test. Cardiopulmonary Physical Therapy.1999;10:80–83.
93 Butland RJ, Pang J, Gross ER, et al. Two-, six-, and 12-minutewalking tests in respiratory disease. Br Med J. 1982;284:1607–1608.
798 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

94 Guyatt GH, Sullivan MJ, Thompson PJ, et al. The 6-minute walk: anew measure of exercise capacity in patients with chronic heart failure.Can Med Assoc J. 1985;132:919–923.
95 Cahalin LP, Pappagianopoulos P, Prevost S, et al. The relationshipof the 6-minute walk test to maximal oxygen consumption in trans-plant candidates with end-stage lung disease. Chest. 1995;108:452–459.
96 Cahalin LP, Mathier MA, Semigran MJ, et al. The six-minute walktest predicts peak oxygen uptake and survival in patients with advancedheart failure. Chest. 1996;110:325–332.
97 Peeters P, Mets T. The 6-minute walk as an appropriate exercise testin elderly patients with chronic heart failure. J Gerontol. 1996;51:M147–M151.
98 Andersen KL. The effect of pulmonary disease on quality of life. ResNurs Health. 1995;18:547–556.
99 Gosselink R, Troosters T, Decramer M. Peripheral muscle weaknesscontributes to exercise limitation in COPD. Am J Respir Crit Care Med.1996;153:976–980.
100 Mak VHF, Bugler JR, Roberts CM, Spiro SG. Effect of arterialoxygen desaturation on six minute walk distance, perceived effort, andperceived breathlessness in patients with airflow limitation. Thorax.1993;48:33–38.
101 Nixon PA, Joswiak ML, Fricker FJ. A six-minute walk test forassessing exercise tolerance in severely ill children. J Pediatr. 1996;129:362–366.
102 Fitts SS, Guthrie MR. Six-minute walk by people with chronic renalfailure: assessment of effort by perceived exertion. Am J Phys MedRehabil. 1995;74:54–58.
103 Harada ND, Chiu V, Stewart AL. Mobility-related function in olderadults: assessment with a 6-minute walk test. Arch Phys Med Rehabil.1999;80:837–841.
104 Flavell HA, Carrafa GP, Thomas CH, Disler PB. Managing low backpain: impact of an interdisciplinary team approach. Med J Aust.1966;165:253–255.
105 Guyatt GH, Thompson PJ, Berman LB, et al. How should wemeasure lung function in patients with chronic heart and lung disease?J Chronic Dis. 1985;38:517–524.
106 Chang RW, Dunlop D, Gibbs J, Hughes S. The determinants ofwalking velocity in the elderly: an evaluation using regression trees.Arthritis Rheum. 1995;38:343–350.
107 Gibbs J, Hughes S, Dunlop D, et al. Predictors of change inwalking velocity in older adults. J Am Geriatr Soc. 1996;44:126–132.
108 Gill TM, Williams CS, Tinetti ME. Assessing risk for the onset offunctional dependence among older adults: the role of physicalperformance. J Am Geriatr Soc. 1995;43:603–609.
109 Gerety MB, Mulrow CD, Tuley MR, et al. Development andvalidation of a physical performance instrument for the functionallyimpaired elderly: the Physical Disability Index (PDI). J Gerontol. 1993;48:M33–M38.
110 Reuben DB, Siu AL. An objective measure of physical function ofelderly outpatients: the Physical Performance Test. J Am Geriatr Soc.1990;38:1105–1112.
111 Siu AL, Ouslander JG, Osterweil D, et al. Change in self-reportedfunctioning in older persons entering a residential care facility. J ClinEpidemiol. 1993;46:1093–1101.
112 Aniansson A, Rundgren A, Sperling L. Evaluation of functionalcapacity in activities of daily living in 70-year-old men and women.Scand J Rehabil Med. 1980;12:145–154.
113 Imms FJ, Edholm OG. Studies of gait and mobility in the elderly.Age Ageing. 1981;10:147–156.
114 Hoxie RE, Rubenstein LZ. Are older pedestrians allowed enoughtime to cross intersections safely? J Am Geriatr Soc. 1994;42:241–244.
115 Skelton DA, Young A, Greig CA, Malbut KE. Effects of resistancetraining on strength, power, and selected functional abilities of womenaged 75 and older. J Am Geriatr Soc. 1995;43:1081–1087.
116 Winograd CH, Lemsky CM, Nevitt MC, et al. Development of aphysical performance and mobility examination. J Am Geriatr Soc.1994;42:743–749.
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 799
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

Appen
dix
.Pr
edic
tive
and
Perfo
rman
ceSu
bmax
imal
Exer
cise
Tests
a
Pre
dic
tive
Subm
ax
imalE
xer
cise
Test
s
Test
Set-
up
and
Supplie
sPra
ctic
ePro
toco
lO
utc
om
eReg
ress
ion
Equations
Popula
tion
Studie
d
Mod
ified
Bruc
eTr
eadm
illTe
st5,2
9,3
0
Clin
ic/l
abor
ator
y
●M
otor
-driv
entre
adm
ill●
HR
mon
itor
●St
opw
atch
●El
ectro
card
iogr
am(o
ptio
nal)
Fam
iliar
ize
the
indi
vidu
alw
ithtre
adm
illw
alki
ng
●Th
ein
divi
dual
uses
1to
2fin
gers
for
hand
rail
supp
ort
●Fo
llow
the
Mod
ified
Bruc
eTr
eadm
illTe
stpr
otoc
ol(T
ab.1
)and
the
indi
vidu
alco
ntin
ues
until
heor
she
deve
lops
pred
eter
min
edsi
gns
orsy
mpt
oms3
0
●Re
duce
the
grad
eto
0%,
redu
cesp
eed,
and
cont
inue
wal
king
slow
lyto
cool
dow
n
Apr
edic
ted
V̇O2m
axva
lue
(mLzk
g21zm
in2
1)
isob
tain
edus
ing
the
appr
opria
tere
gres
sion
equa
tion
1.Br
uce
and
colle
ague
s5,3
0;
War
det
al1
8
(a)
Act
ive
men
,esti
mat
edV̇O
2m
ax(m
Lzkg2
1zm
in2
1)5
3.77
83tim
e(m
in)1
0.19
(b)
Sede
ntar
ym
en,e
stim
ated
V̇O2m
ax5
3.29
83tim
e(m
in)
14.
07(c
)Pa
tient
sw
ithca
rdia
cdi
seas
e,es
timat
edV̇O
2m
ax5
2.32
73tim
e(m
in)1
9.48
(d)
Adu
ltsin
good
heal
th,
estim
ated
V̇O2m
ax5
6.70
22.
823
sex
(15
men
and
25w
omen
)10.
0563
time
(s)
2.Fo
ster
etal
30
V̇O2m
ax(m
Lzkg2
1zm
in2
1)5
14.7
621.
383
time
(min
)1
0.45
13tim
e(m
in)2
20.
0123
time
(min
)3
●M
enan
dw
omen
ingo
odhe
alth
●Pa
tient
sw
ithca
rdia
cdi
seas
e●
Endu
ranc
eat
hlet
es●
Sede
ntar
yin
divi
dual
s(s
eeBr
uce
etal
5)
Sing
le-S
tage
Subm
axim
alTr
eadm
illW
alki
ngTe
st(S
STW
T)1
2
Clin
ic/l
abor
ator
y
●M
otor
-driv
entre
adm
ill●
HR
mon
itor
●St
opw
atch
●Ra
ting
ofpe
rcei
ved
exer
tion
(RPE
)sca
le
Fam
iliar
ize
the
indi
vidu
alw
ithtre
adm
illw
alki
ng
●Es
tabl
ish
asa
fe,b
utco
mfo
rtabl
e,w
alki
ngsp
eed
betw
een
2.0
and
4.5
mph
,at
a0%
grad
efo
r4
min
;an
HR
betw
een
50%
and
70%
ofag
e-pr
edic
ted
HRm
axsh
ould
beob
tain
ed●
Incr
ease
the
grad
eto
5%an
dw
alk
atth
ees
tabl
ishe
dsp
eed
for
4m
in●
Reco
rdth
eH
Ran
dRP
Eat
the
end
ofth
ew
arm
-up
sess
ion
and
the
first
stage
●Re
duce
the
grad
eto
0%an
dco
ntin
uew
alki
ngslo
wly
toco
oldo
wn
Apr
edic
ted
V̇O2m
axva
lue
(mLzk
g21zm
in2
1)
isob
tain
edus
ing
the
regr
essi
oneq
uatio
n
Estim
ated
V̇O2m
ax(m
Lzkg2
1zm
in2
1)5
15.1
121
.83
spee
d(m
ph)
20.
3273
HR
(bpm
)2
0.26
33sp
eed3
age
(y)
10.
0050
43H
R3ag
e15.
983
sex
(05
wom
en,1
5m
en)
●M
enan
dw
omen
ingo
odhe
alth
aged
20–5
9y
800 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022
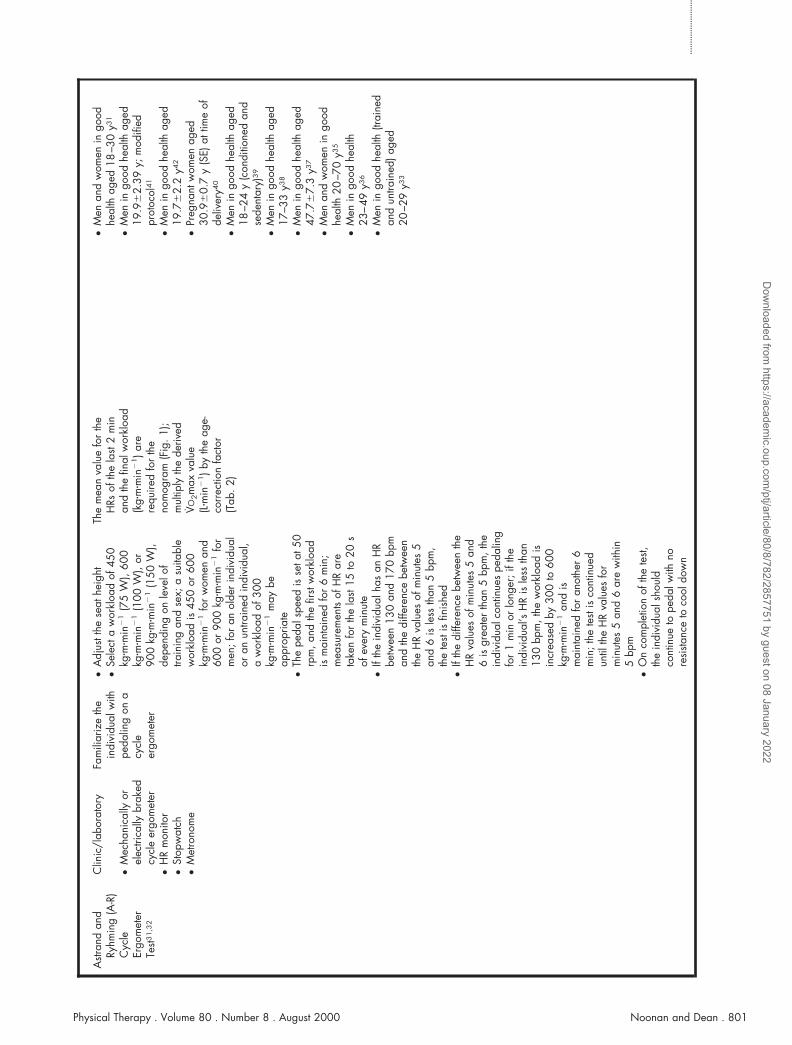
Astr
and
and
Ryhm
ing
(A-R
)C
ycle
Ergo
met
erTe
st31
,32
Clin
ic/l
abor
ator
y
●M
echa
nica
llyor
elec
trica
llybr
aked
cycl
eer
gom
eter
●H
Rm
onito
r●
Stop
wat
ch●
Met
rono
me
Fam
iliar
ize
the
indi
vidu
alw
ithpe
dalin
gon
acy
cle
ergo
met
er
●A
djus
tthe
seat
heig
ht●
Sele
cta
wor
kloa
dof
450
kgzm
zmin
21
(75
W),
600
kgzm
zmin
21
(100
W),
or90
0kg
zmzm
in2
1(1
50W
),de
pend
ing
onle
velo
ftra
inin
gan
dse
x;a
suita
ble
wor
kloa
dis
450
or60
0kg
zmzm
in2
1fo
rw
omen
and
600
or90
0kg
zmzm
in2
1fo
rm
en;f
oran
olde
rin
divi
dual
oran
untra
ined
indi
vidu
al,
aw
orkl
oad
of30
0kg
zmzm
in2
1m
aybe
appr
opria
te●
The
peda
lspe
edis
seta
t50
rpm
,and
the
first
wor
kloa
dis
mai
ntai
ned
for
6m
in;
mea
sure
men
tsof
HR
are
take
nfo
rth
ela
st15
to20
sof
ever
ym
inut
e●
Ifth
ein
divi
dual
has
anH
Rbe
twee
n13
0an
d17
0bp
man
dth
edi
ffere
nce
betw
een
the
HR
valu
esof
min
utes
5an
d6
isle
ssth
an5
bpm
,th
ete
stis
finis
hed
●If
the
diffe
renc
ebe
twee
nth
eH
Rva
lues
ofm
inut
es5
and
6is
grea
ter
than
5bp
m,t
hein
divi
dual
cont
inue
spe
dalin
gfo
r1
min
orlo
nger
;ift
hein
divi
dual
’sH
Ris
less
than
130
bpm
,the
wor
kloa
dis
incr
ease
dby
300
to60
0kg
zmzm
in2
1an
dis
mai
ntai
ned
for
anot
her
6m
in;t
hete
stis
cont
inue
dun
tilth
eH
Rva
lues
for
min
utes
5an
d6
are
with
in5
bpm
●O
nco
mpl
etio
nof
the
test,
the
indi
vidu
alsh
ould
cont
inue
tope
dalw
ithno
resi
stanc
eto
cool
dow
n
The
mea
nva
lue
for
the
HRs
ofth
ela
st2
min
and
the
final
wor
kloa
d(k
gzm
zmin
21)a
rere
quire
dfo
rth
eno
mog
ram
(Fig
.1);
mul
tiply
the
deriv
edV̇O
2m
axva
lue
(Lzm
in2
1)b
yth
eag
e-co
rrec
tion
fact
or(T
ab.2
)
●M
enan
dw
omen
ingo
odhe
alth
aged
18–3
0y3
1
●M
enin
good
heal
thag
ed19
.96
2.39
y;m
odifi
edpr
otoc
ol4
1
●M
enin
good
heal
thag
ed19
.76
2.2
y42
●Pr
egna
ntw
omen
aged
30.9
60.
7y
(SE)
attim
eof
deliv
ery4
0
●M
enin
good
heal
thag
ed18
–24
y(c
ondi
tione
dan
dse
dent
ary)
39
●M
enin
good
heal
thag
ed17
–33
y38
●M
enin
good
heal
thag
ed47
.76
7.3
y37
●M
enan
dw
omen
ingo
odhe
alth
20–7
0y3
5
●M
enin
good
heal
th23
–49
y36
●M
enin
good
heal
th(tr
aine
dan
dun
train
ed)a
ged
20–2
9y3
3
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 801
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

Appen
dix
.C
ontin
ued
Pre
dic
tive
Subm
ax
imalE
xer
cise
test
s
Test
Set-
up
and
Supplie
sPra
ctic
ePro
toco
lO
utc
om
eReg
ress
ion
Equations
Popula
tion
Studie
d
Can
adia
nA
erob
icFi
tnes
sTe
st(C
AFT
)44,4
5,5
2
and
mod
ified
CA
FT(m
CA
FT)4
6,4
7,5
1
Ath
ome
orcl
inic
/la
bora
tory
●A
doub
le8-
in(2
0.3-
cm)s
tep
●H
Rm
onito
r●
Prer
ecor
ded
audi
otap
e●
Cas
sette
reco
rder
●Sp
hygm
oman
omet
er●
Stet
hosc
ope
●St
opw
atch
Dem
onstr
ate
the
stepp
ing
cycl
ean
dal
low
the
indi
vidu
alto
prac
tice
●C
AFT
44
,52
●M
easu
res
ofre
sting
BPan
dH
Rar
eop
tiona
l●
Follo
win
ga
war
ning
sign
alon
anau
diot
ape,
the
indi
vidu
alis
instr
ucte
dto
clim
ba
doub
le8-
inste
pfo
ra
3-m
in“w
arm
-up
”at
aste
ppin
gte
mpo
base
don
his
orhe
rage
(see
Tab.
3)52;t
heSt
anda
rdiz
edTe
stof
Fitn
ess
pack
age5
2co
ntai
nsth
eca
sset
tes
with
the
vario
uste
mpo
s;fo
llow
ing
the
first
stage
,th
ein
struc
tions
onth
eca
sset
tein
dica
tew
hen
toob
tain
a10
-sm
easu
rem
ento
fHR
●C
onsu
ltth
eta
ble
“Cei
ling
Poste
xerc
iseH
eart
Rate
s”(se
eTa
b.4)
52
tode
term
ine
whe
ther
the
indi
vidu
alco
ntin
ues
fora
seco
ndsta
geor
whe
ther
the
test
iste
rmin
ated
●If
the
indi
vidu
alha
san
HR
belo
wth
ece
iling
HR
indi
cate
din
the
tabl
e,he
orsh
epr
ocee
dsto
the
seco
ndsta
ge;H
Ris
mea
sure
dag
ain
follo
win
gth
ese
cond
stage
tode
term
ine
whe
ther
heor
she
proc
eeds
toth
eth
irdan
dfin
alsta
ge;a
mea
sure
ofH
Ris
take
nfo
r10
sfo
llow
ing
the
third
stage
●In
the
poste
xerc
isepe
riod,
mea
sure
men
tsof
BPca
nbe
take
nin
the
first
2m
inan
dm
easu
rem
ents
ofre
sting
HR
can
beta
ken
inth
eth
irdm
inut
e●
Follo
win
gth
ete
st,th
ein
divi
dual
shou
ldco
ntin
ueste
ppin
gor
wal
king
slow
lyto
cool
dow
n●
Fort
hepr
otoc
olof
the
CA
FT,
see
Wel
lera
ndco
lleag
ues4
6,4
7
Con
sult
the
“Phy
sica
lFi
tnes
sEv
alua
tion
Cha
rt”(s
eeTa
b.5)
tode
term
ine
leve
lof
fitne
ssba
sed
onth
efin
alex
erci
seH
Rre
adin
g52;a
pred
icte
dV̇O
2m
axva
lue
(mLzk
g21zm
in2
1)
isob
tain
edus
ing
the
regr
essi
oneq
uatio
n
1.C
AFT
(Jette
etal
45)
estim
ated
V̇O2m
ax(m
Lzkg2
1zm
in2
1)5
42.5
116
.63
V̇O2
(Lzm
in2
1)*
20.
123
body
wei
ght(
kg)2
0.12
3H
Rfo
llow
ing
last
stage
(bpm
)20.
243
age
(y)
*V̇O
2is
the
aver
age
oxyg
enco
stof
the
last
com
plet
edsta
ge(L
zmin
21);
obta
inva
lue
from
the
tabl
e“E
nerg
yRe
quire
men
tsfo
rth
eVa
rious
Stag
esof
the
CA
FT”4
5
2.m
CA
FT(W
elle
ret
al5
1)
estim
ated
V̇O2m
ax(m
Lzkg2
1zm
in2
1)5
32.0
116
.03
V̇O2
for
final
stage
(Lzm
in2
1)2
0.17
3bo
dyw
eigh
t(kg
)20.
243
age
(y)
●M
enan
dw
omen
ingo
odhe
alth
aged
15–6
9y4
4,4
5
●M
enan
dw
omen
ingo
odhe
alth
aged
15–7
4y,
mod
ified
prot
ocol
47
●M
enan
dw
omen
ingo
odhe
alth
aged
15–6
9y4
6,4
7
●M
enan
dw
omen
ingo
odhe
alth
aged
15–6
9y5
1
802 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

12-M
inut
eRu
nTe
st(1
2-M
RT)5
3M
easu
red
track
●St
opw
atch
●Ta
pem
easu
re
Fam
iliar
ize
the
indi
vidu
alw
ithth
etra
ckan
dth
eco
ncep
tof
paci
ng
●Th
ein
divi
dual
isin
struc
ted
to“c
over
the
long
est
poss
ible
dista
nce
in12
min
,ru
nnin
gpr
efer
ably
but
wal
king
whe
neve
rne
cess
ary
topr
even
tbec
omin
gex
cess
ivel
yex
haus
ted”
53
●Re
cord
the
dista
nce
inm
iles
com
plet
edin
12m
in●
On
com
plet
ion
ofth
ete
st,th
ein
divi
dual
shou
ldco
ntin
uew
alki
ngto
cool
dow
n
Apr
edic
ted
V̇O2m
axva
lue
(mLzk
g21zm
in2
1)i
sob
tain
edus
ing
the
regr
essi
oneq
uatio
ns
1.C
oope
r53
wal
k/ru
ndi
stanc
e50.
3138
10.
0278
3V̇O
2(m
Lzkg2
1zm
in2
1)
2.W
ard
etal
18
estim
ated
V̇O2m
ax(m
Lzkg2
1zm
in2
1)5
35.9
73di
stanc
e(m
ile)
211
.29
●M
enin
good
heal
thag
ed17
–52
y53
●M
enin
good
heal
thag
ed18
–235
5
20-M
eter
Shut
tleTe
st(2
0-M
ST)5
7–5
9
Mea
sure
dco
rrid
or
●H
Rm
onito
r●
Prer
ecor
ded
audi
otap
e●
Cas
sette
reco
rder
●Py
lons
●Ta
pem
easu
re
Fam
iliar
ize
the
indi
vidu
alw
ithth
eco
urse
●Th
ein
divi
dual
runs
betw
een
2lin
es20
map
art;
whe
nth
ein
divi
dual
hear
sa
shor
tso
und,
heor
she
has
tobe
on1
ofth
ese
2lin
es,a
ndw
hen
alo
ngso
und
ishe
ard,
itin
dica
tes
ach
ange
insta
ge●
The
first
stage
is8.
5km
zh2
1
for
wom
enan
d10
kmzh
21
for
men
;the
spee
dis
incr
ease
dby
0.5
kmzh
21
per
1-m
insta
ges
(see
Fig.
2)●
The
indi
vidu
alco
ntin
ues
until
she
orhe
isun
able
tom
aint
ain
the
rhyt
hmof
runn
ing
●Th
esp
eed
atth
ela
stco
mpl
eted
runn
ing
stage
iste
rmed
the
“max
imal
aero
bic
spee
d”(M
AS)
●O
nco
mpl
etio
nof
the
test,
the
indi
vidu
alsh
ould
cont
inue
wal
king
toco
oldo
wn
Apr
edic
ted
V̇O2m
axva
lue
(mLzk
g21zm
in2
1)i
sob
tain
edus
ing
the
regr
essi
oneq
uatio
ns
1.G
ener
aleq
uatio
n(L
eger
etal
58)e
stim
ated
V̇O2m
ax(m
Lzkg2
1zm
in2
1)5
31.0
251
3.23
83sp
eed
(km
zh2
1)
23.
2483
age
(y)
10.
1536
3(a
ge3
spee
d)
2.A
dults
(Leg
eret
al5
8)
estim
ated
V̇O2m
ax(m
Lzkg2
1zm
in2
1)5
224
.41
6.03
spee
d(k
mzh
21)
●M
enan
dw
omen
ingo
odhe
alth
aged
20–4
5y5
8
●Bo
ysan
dgi
rlsin
good
heal
thag
ed6
–19
y58
,62
●Bo
ysan
dgi
rlsin
good
heal
thag
ed8
–19
y58
●A
ctiv
em
enin
good
heal
thag
ed18
–42
y(m
odifi
edpr
otoc
ol)6
0
●M
enan
dw
omen
with
asth
ma
aged
12–1
7y6
3
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 803
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

Per
form
ance
Subm
ax
imalE
xer
cise
Test
s
Test
Set-
up
and
Supplie
sPra
ctic
ePro
toco
lO
utc
om
ePopula
tion
Studie
d
Self-
Pace
dW
alki
ngTe
st(S
PWT)
70
Mea
sure
dco
rrid
or
●H
Rm
onito
r●
Stop
wat
ch●
Tape
mea
sure
●Py
lons
Fam
iliar
ize
the
indi
vidu
alw
ithth
eco
urse
●Th
ein
divi
dual
isin
struc
ted
tow
alk
am
easu
red
dista
nce
(ie,2
50m
)at3
diffe
rent
spee
ds,w
itha
5-m
inre
stbe
twee
ntri
als:
(a)r
athe
rslo
wly
(ie,s
low
pace
),(b
)ata
norm
alpa
ce,n
eith
erfa
stno
rslo
w,a
nd(c
)ra
ther
fast,
butw
ithou
tove
rexe
rting
your
self
(ie,f
astp
ace)
●Re
cord
the
time
inse
cond
sfo
rea
chof
the
3tri
als
●Fo
llow
ing
the
3tri
als,
the
indi
vidu
alsh
ould
cont
inue
wal
king
slow
lyto
cool
dow
n
For
each
wal
king
trial
,the
spee
d,tim
eto
com
plet
eth
edi
stanc
e,an
dstr
ide
frequ
ency
are
calc
ulat
ed;i
nad
ditio
n,av
erag
eH
R,str
ide
leng
th,a
nda
pred
icte
dV̇O
2m
axva
lue
can
bede
term
ined
●M
enin
good
heal
thag
ed64
–66
y●
Act
ive
men
ingo
odhe
alth
aged
19–2
1y7
0
●M
enin
good
heal
thag
ed19
–66
y71
,72
Appen
dix
.C
ontin
ued
Pre
dic
tive
Subm
ax
imalE
xer
cise
test
s
Test
Set-
up
and
Supplie
sPra
ctic
ePro
toco
lO
utc
om
eReg
ress
ion
Equations
Popula
tion
Studie
d
1-M
ileTr
ack
Wal
kTe
st(R
ockp
ort
Fitn
ess
Test)
(1-M
TW)6
4
Mea
sure
dtra
ck
●St
opw
atch
●H
Rm
onito
r●
Tape
mea
sure
●A
min
imum
of2
tests
are
requ
ired;
the
times
ofbo
thte
stssh
ould
bew
ithin
30s
ofea
chot
her;
othe
rwis
e,su
bseq
uent
tests
are
perfo
rmed
until
this
isac
hiev
ed
●Th
ein
divi
dual
isin
struc
ted
“to
wal
kas
fast
aspo
ssib
lear
ound
the
cour
se”6
4
●Re
cord
HR
atth
een
dof
ever
yqu
arte
rm
ile●
Reco
rdth
etim
eto
com
plet
eth
ete
st(in
min
utes
)●
On
com
plet
ion
ofth
ete
st,th
ein
divi
dual
shou
ldco
ntin
uew
alki
ngto
cool
dow
n
The
HR
atth
een
dof
the
four
thqu
arte
rof
the
test
isus
edfo
rth
ere
gres
sion
equa
tion;
apr
edic
ted
V̇O2m
axva
lue
(Lzm
in2
1)i
sob
tain
edus
ing
the
regr
essi
oneq
uatio
n
Klin
eet
al6
4es
timat
edV̇O
2m
ax(L
zmin
21)5
6.96
521
0.00
913
body
wei
ght(
lb)
20.
0257
3ag
e(y
)1
0.59
553
sex
(men
51,
wom
en5
0)2
0.22
403
T 1(tr
ack
wal
ktim
e)2
0.01
153
HR 1
–4
(four
thqu
arte
rH
Rfo
rtra
ckw
alk)
●M
enan
dw
omen
ingo
odhe
alth
aged
30–6
9y6
4
●M
enan
dw
omen
with
men
talr
etar
datio
nag
ed26
–40
y65
804 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

Mod
ified
Shut
tleW
alki
ngTe
st(M
SWT)
74
,75
Mea
sure
dco
rrid
or10
min
leng
thw
ith2
pylo
nspl
aced
0.5
mfro
mea
chen
d
One
prac
tice
trial
isre
quire
d
●Th
ete
ststa
rtsw
itha
tripl
ebe
ep;
afte
rth
at,a
sing
lebe
epin
dica
tes
whe
nth
ein
divi
dual
shou
ldbe
wal
king
arou
ndth
eco
ne;a
tripl
ebe
epal
sosi
gnifi
esa
chan
gein
stage
Tota
lnum
ber
ofsh
uttle
sat
each
leve
l;re
port
tota
ldis
tanc
e(in
met
ers)
●M
enan
dw
omen
with
chro
nic
airw
ayob
struc
tion
aged
45–7
4y7
4,7
5
●M
enan
dw
omen
with
pace
mak
ers
aged
27–7
4y7
6
●H
Rm
onito
r●
Prer
ecor
ded
audi
otap
e●
Cas
sette
reco
rder
●Py
lons
●Ta
pem
easu
re
●Th
ein
divi
dual
isin
struc
ted:
“Wal
kat
aste
ady
pace
,aim
ing
totu
rnar
ound
whe
nyo
uhe
arth
esi
gnal
,yo
ush
ould
cont
inue
tow
alk
until
you
feel
that
you
are
unab
leto
mai
ntai
nth
ere
quire
dsp
eed
with
out
beco
min
gun
duly
brea
thle
ss”7
4
●RP
Esc
ale
●Th
eM
SWT
starts
at0.
50m
zs21
(1.1
2m
ph)f
orle
vel1
;eac
hle
vel
lasts
1m
in,a
ndth
esp
eed
isin
crea
sed
by0.
17m
zs21
for
12m
in;t
hefin
alsp
eed
is2.
37m
zs21
(see
Tab.
6)●
The
indi
vidu
alco
ntin
ues
until
:(a)
heor
she
isto
obr
eath
less
tom
aint
ain
the
requ
ired
spee
d,(b
)he
orsh
eis
mor
eth
an0.
5m
away
from
the
cone
whe
nth
ebe
epis
soun
ded,
or(c
)atta
inm
ento
f85%
ofag
e-pr
edic
ted
HRm
ax●
The
tota
lnum
ber
ofco
mpl
eted
shut
tles
(10-
mle
ngth
s)at
each
leve
lis
reco
rded
(inm
eter
s)●
On
com
plet
ion
ofth
ete
st,th
ein
divi
dual
shou
ldco
ntin
uew
alki
ngslo
wly
toco
oldo
wn
Bag
and
Car
ryTe
st(B
CT)
77
Mea
sure
dco
urse
7.5
min
leng
th,
inad
ditio
nto
a4-
step
fligh
tof
stairs
●H
Rm
onito
r●
Pack
age
toca
rry
wei
ghts
●W
eigh
tsof
0.9
kgea
ch●
Stop
wat
ch●
Tape
mea
sure
●Th
ein
divi
dual
isin
struc
ted
tow
alk
the
circ
uitc
arry
ing
apa
ckag
ew
eigh
ing
0.9
kg,w
ithbo
thar
ms,
7.5
m,u
pan
ddo
wn
a4-
step
fligh
tof
stairs
,and
back
7.5
m●
On
com
plet
ion
ofea
chci
rcui
t,0.
9kg
ofw
eigh
tis
adde
dto
the
pack
age,
the
indi
vidu
alco
ntin
ues
until
heor
she
isno
long
erab
leto
com
plet
eth
eci
rcui
tcar
ryin
gth
epa
ckag
e,re
cord
the
heav
iest
wei
ght
the
indi
vidu
alca
rrie
d
The
heav
iest
wei
ght(
inki
logr
ams)
carr
ied
byth
ein
divi
dual
●W
omen
aged
48–9
3y
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 805
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

Appen
dix
.C
ontin
ued
Per
form
ance
Subm
ax
imalE
xer
cise
Test
s
Test
Set-
up
and
Supplie
sPra
ctic
ePro
toco
lO
utc
om
ePopula
tion
Studie
d
Tim
eU
p&
Go
Test
(TU
GT)
78
Clin
ic/c
orrid
orth
atha
sat
leas
ta
3-m
floor
spac
e
●A
rmch
air
(sea
the
ight
of46
cm)
●St
opw
atch
●Ta
pe●
Tape
mea
sure
One
prac
tice
trial
isre
quire
d
●Th
ein
divi
dual
starts
with
his
orhe
rba
ckag
ains
tthe
chai
r,ar
ms
resti
ngon
the
arm
rests
,and
mob
ility
aid
inha
nd,i
fnee
ded;
noph
ysic
alas
sista
nce
isgi
ven
●In
struc
tions
are
“On
the
wor
d‘G
o,’
you
are
toge
tup
and
wal
kat
aco
mfo
rtabl
ean
dsa
fepa
ceto
alin
eon
the
floor
3m
eter
saw
ay,t
urn,
retu
rnto
the
chai
r,an
dsi
tdow
nag
ain”
74;r
ecor
dth
etim
e(in
seco
nds)
Repo
rtth
etim
e(in
seco
nds)
●O
lder
inpa
tient
san
dou
tpat
ient
s;m
ale
and
fem
ale
geria
tric
patie
nts
aged
52–7
4y7
9
●El
derly
men
and
wom
enin
good
heal
thag
ed70
–84
y●
Men
and
wom
en,a
ged
60–9
0y,
with
Park
inso
nsy
ndro
me,
strok
e,rh
eum
atoi
dar
thrit
isan
dos
teoa
rthrit
is,po
stsur
gica
lhip
fract
ures
,ge
nera
ldec
ondi
tioni
ng78
●El
derly
men
and
wom
enw
ithlim
ited
mob
ility
aged
75–9
6y8
1
12-M
inut
eW
alk
Test
(12-
MW
T)8
2,8
3
6-M
inut
eW
alk
Test
(6-M
WT)
27
,94
Mea
sure
dco
rrid
or,
appr
oxim
atel
y33
min
leng
th
●H
Rm
onito
r●
Stop
wat
ch●
Tape
mea
sure
Two
prac
tice
trial
sar
ere
quire
d
●Th
ein
divi
dual
wal
ksa
mea
sure
ddi
stanc
e(e
g,33
m)
●Fo
rth
e12
-MW
T,th
ein
divi
dual
isin
struc
ted
“to
cove
ras
muc
hgr
ound
aspo
ssib
leon
foot
in12
min
utes
and
toke
epgo
ing
cont
inuo
usly
ifpo
ssib
lebu
tnot
tobe
conc
erne
dif
you
have
toslo
wdo
wn
orre
st”8
2,8
3;
atth
een
dof
the
test,
subj
ects
shou
ldfe
elth
eyco
uld
noth
ave
cove
red
mor
egr
ound
inth
etim
e●
For
the
6-M
WT,
the
indi
vidu
alis
instr
ucte
d“t
ow
alk
from
end
toen
d,co
verin
gas
muc
hgr
ound
aspo
ssib
lein
6m
inut
es”9
4;a
tthe
end
ofth
e6
or12
min
,the
indi
vidu
alis
instr
ucte
dto
stop;
the
tota
ldis
tanc
eis
reco
rded
●If
enco
urag
emen
tis
give
n,pr
edet
erm
ined
phra
ses
shou
ldbe
deliv
ered
ever
y30
sw
hile
faci
ngth
ein
divi
dual
Repo
rtth
eto
tald
ista
nce
cove
red
(inm
eter
s)●
12-M
WT;
men
with
chro
nic
bron
chiti
sag
ed40
–70
y82
●12
-MW
T;m
enan
dw
omen
with
chro
nic
bron
chiti
sag
ed22
–75
y83
●6-
MW
T;pa
tient
sw
ithch
roni
che
artf
ailu
re(re
spira
tory
and
card
iac
cond
ition
s)ag
ed64
.76
8.3
y27
,94
●6-
MW
T;m
enan
dw
omen
with
CO
PDag
ed40
–84
y92
●12
-MW
T,m
odifi
edpr
otoc
ol;
men
with
CO
PDag
ed67
64
y85
●12
-MW
T;m
enan
dw
omen
with
CO
PDag
ed31
–75
y87
●12
-MW
T;m
enan
dw
omen
with
CO
PDag
ed68
.46
9.6
y88
●6-
MW
T;m
enan
dw
omen
with
CO
PDag
ed48
–85
y98
●4-
MW
T;m
enan
dw
omen
with
low
back
pain
(no
age
rang
ere
porte
d)104
●O
nco
mpl
etio
nof
the
test,
the
indi
vidu
alsh
ould
cont
inue
wal
king
toco
oldo
wn
●12
-MW
T;m
enw
ithch
roni
cre
spira
tory
disa
bilit
yag
ed61
.26
5.0
y86
●6-
MW
T;m
enan
dw
omen
with
adva
nced
hear
tfai
lure
aged
496
8y9
6
806 . Noonan and Dean Physical Therapy . Volume 80 . Number 8 . August 2000
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022

●6-
MW
T;m
enan
dw
omen
with
chro
nic
rena
lfai
lure
aged
22–6
7y1
02
●6-
MW
T;m
enan
dw
omen
with
end-
stage
lung
dise
ase
aged
43.5
611
y95
●6-
MW
T;m
enan
dw
omen
with
chro
nic
lung
dise
ase
and
asth
ma
aged
57.4
612
.9y
and
62.3
69.
1y1
00
●6-
MW
T;bo
ysan
dgi
rlsw
ithcy
stic
fibro
sis,
pulm
onar
yhy
perte
nsio
n,an
dob
struc
tive
lung
dise
ase
aged
9–1
9y1
01
●12
-MW
T;m
enan
dw
omen
with
chro
nic
airw
ayob
struc
tion
aged
38–7
5y8
4
●12
-MW
T;m
enan
dw
omen
with
chro
nic
obstr
uctiv
elu
ngdi
seas
eag
ed49
–73
y90
●6-
MW
T;m
enan
dw
omen
with
CO
PDag
ed58
610
y99
●6-
MW
T;el
derly
peop
lean
dm
enan
dw
omen
with
chro
nic
hear
tfai
lure
aged
70–9
0y9
7
●12
-MW
T;m
enw
ithch
roni
cob
struc
tive
airw
aydi
seas
eag
ed47
–64
y89
aH
R5
hea
rtra
te,
V̇o
2m
ax5
max
imum
oxyg
enco
nsu
mpt
ion
,H
Rm
ax5
max
imal
hea
rtra
te,
CO
PD5
chro
nic
obst
ruct
ive
pulm
onar
ydi
seas
e,B
P5bl
ood
pres
sure
,V̇
o25
oxyg
enco
nsu
mpt
ion
.
Physical Therapy . Volume 80 . Number 8 . August 2000 Noonan and Dean . 807
IIIIII
IIIIII
IIIIII
IIIIII
IIII
Dow
nloaded from https://academ
ic.oup.com/ptj/article/80/8/782/2857751 by guest on 08 January 2022
Copyright © 2022 FDOKUMEN




















