
Beta-specificity: The turnover of host species in space and another way to measure host specificity
Upload
independentCategory
view
1download
0
10ournal of Epidemiology and Community Health 1997;51:180-186
Quantitative estimates of the impact ofsensitivity and specificity in mammographicscreening in Germany
Peter G Warmerdam, Harry J de Koning, Rob Boer, Petra M M Beemsterboer,Marie-Luise Dierks, Enno Swart, Bernt-Peter Robra
AbstractStudy objective - To estimate quant-itatively the impact of the quality ofmammographic screening (in terms ofsensitivity and specificity) on the effectsand costs of nationwide breast cancerscreening.Design - Three plausible "quality" scen-arios for a biennial breast cancer screeningprogramme for women aged 50-69 in Ger-many were analysed in terms of costs andeffects using the Microsimulation Screen-ing Analysis model on breast cancerscreening and the natural history ofbreastcancer. Firstly, sensitivity and specificityin the expected situation (or "baseline"scenario) were estimated from a modelbased analysis of empirical data from35 000 screening examinations in two Ger-man pilot projects. In the second "highquality" scenario, these properties werebased on the more favourable diagnosticresults from breast cancer screening pro-jects and the nationwide programme inThe Netherlands. Thirdly, a worst case,"low quality" hypothetical scenario witha 25% lower sensitivity than that ex-perienced in The Netherlands was ana-lysed.Setting - The epidemiological and socialsituation in Germany in relation to massscreening for breast cancer.Results - In the "baseline" scenario, an11% reduction in breast cancer mortalitywas expected in the total German femalepopulation, ie 2100 breast cancer deathswould be prevented per year. It was es-timated that the "high quality" scenario,based on Dutch experience, would lead tothe prevention of an additional 200 deathsper year and would also cut the numberoffalse positive biopsy results by half. Thecost per life year gained varied from De-utsche mark (DM) 15 000 in the "high qual-ity" scenario to DM 21000 in the "lowquality" setting.Conclusions - Up to 20% of the total costsofa screening programme can be spent onquality improvement in order to achieve asubstantially higher reduction in mortalityand reduce undesirable side effects whileretainiing the same cost effectiveness ratioas that estimated from the German data.
(J7 Epidemiol Community Health 1997;51: 180-186)
Breast cancer screening for women aged 50 andover is being implemented in a large number ofEuropean countries. These programmes aimto achieve a relatively high level of qualityby means of strict organisation, training, andevaluation.'2 The definition of screening qual-ity is often narrowed down to two properties -sensitivity (ie the capability of accurately de-tecting cancer at a screening examination andspecificity (the ability to pinpoint accuratelythose women without breast cancer). Highsensitivity can be assumed to be one of the keyelements in achieving a reduction in breastcancer mortality, while high specificity will re-duce the negative side effects of screening.3The nationwide programmes in the United
Kingdom and The Netherlands have made agood start in providing facilities which ensurehigh standards. It is not certain, however, thatthese high standards can be achieved in allcountries or programmes, especially where theorganisation of screening is not centralised.Where screening is carried out in the privatepractices of gynaecologists or radiologists itmay be of poorer quality than that undertakenin specialist screening units. The reasons forthis are that in a decentralised screening settingquality control is less easily achieved, radi-ologists who are not specialists in this areamay be less skilled in screening mammography,and the mammography equipment may be ofan inferior quality.The decentralised health care setting in Ger-
many has occasioned discussion about the in-troduction of a nationwide breast cancerscreening programme.45 In 1990, a pilot studywas set up in the Aurich and Braunschweigregions to investigate quality and to test thequality assurance necessary for the im-plementation of a nationwide programme (theDeutsche Mammographie Studie, DMS) .6Data from this DMS study support the hypo-thesis of less than optimal quality: relativelyold equipment, poorer image quality, and arelatively low number of mammograms perradiologist. Although it has been possible toestimate the effects and costs of breast cancerscreening in other countries with different back-grounds on the basis of incidence and mortalitylevels,7 the consequences of lower quality onthe expected results of a screening programmehave not yet been quantified in detail. It ispossible that a decentralised screening setting,such as the one in Germany, might affect thequality of screening so adversely that a breast
Department of PublicHealth, ErasmusUniversity Rotterdam,PO Box 1738, 3000 DR,Rotterdam, TheNetherlandsP G WarmerdamH J de KoningR BoerP M M Beemsterboer
AbteilungEpidemiologie undSozialmedizin,MedizinischeHochschule Hannover,GermanyM-L Dierks
Institut fiirSozialmedizin, Otto-von-GuerickeUniversitat,Magdeburg, GermanyE SwartB-P Robra
Correspondence to:Mr P G Warmerdam.Accepted for publicationJuly 1996
180

Impact of quality in mammographic screening
cancer screening programme is not worth im-plementing.
In this study we have estimated the expectedsensitivity and specificity for a nationwide Ger-man programme, based on the results fromthe Aurich and Braunschweig pilot projects.Screening performance results predicted by theMicrosimulation Screening Analysis (MISCAN)model8 were compared with the observed datain these projects to estimate sensitivity. Sincethe true extent of the future quality in a de-centralised system is ofcourse difficult to assess,we have defined two other sets of plausiblequality assumptions as follows:
1 A "high quality" scenario based on the situ-ation in the Dutch nationwide programme;and
2 A hypothetical "low quality" scenario witha 25% lower sensitivity than that experiencedin The Netherlands.
The impact of these various quality as-sumptions (sensitivity and specificity) on theoutcomes of a screening programme was evalu-ated and quantified in terms of a reduction inbreast cancer mortality and costs and in neg-ative side effects. The results from this studygive indications for the cost effectiveness ofquality assurance and evaluation.
MethodsTHE MISCAN APPROACHIn this study the MISCAN model for screeninganalysis and evaluation was used.89 The naturalhistory of breast cancer was reflected in thismodel in four states - one ductal carcinomain situ DCIS) and three invasive states withincreasing tumour size. By incorporating demo-graphic aspects, individual life histories can begenerated to simulate a "real life" dynamicpopulation with breast cancer incidence andmortality, and death from other causes. Ascreening programme can be applied to thispopulation to determine what changes wouldoccur. Various characteristics of screening pol-icies or programmes can be defined, such asscreening ages, interval, and attendance. Im-portant screening parameters embedded in themodel were the sensitivity and specificity ofthe screening test and the improvement inprognosis after screen detection.The sensitivity of a screening examination is
an age and state dependent model parameter,defined as the probability of a positive screenresult when screening a woman with preclinicalbreast cancer. Preclinical cancer is defined hereas a lesion that has not yet been clinicallydiagnosed. Specificity is defined as the prob-ability of a negative test result in a womanwithout preclinical cancer. Given the preclinicalprevalences and detection rates as model out-comes, specificity of screening can be modifiedin the model by adjusting the positive predictivevalues (PPVs) of the subsequent additionaldiagnostic steps. In this way, the numbers ofdiagnostic assessments without breast cancerbeing diagnosed (false positives) can be de-termined.
Improvement in prognosis due to early de-tection was defined in the model as the re-duction in risk of dying from breast cancer forscreen detected cases, and was dependent onage and cancer stage. The estimate of thisimprovement in prognosis after screening de-tection was based on the breast cancer mortalityreduction reported in the overview ofthe Swed-ish randomised trials.910The design ofthe analysis on effects and costs
of breast cancer screening has been describedbefore.1'12 In short, the effects and costs ofdifferent policies are compared to the situationin which mass screening is not applied, basedon national data on assessment and treatment.Adjustments have been made for the Germansituation if data were available. This methodhas been shown to be useful for predicting theeffects and costs of screening in Australia" andItaly. 4
THE GERMAN MODEL: DEMOGRAPHY ANDEPIDEMIOLOGYThe demography was based on the 1989 agespecific distribution ofthe total German femalepopulation; death rates from causes other thanbreast cancer were based on 1990 data fromthe former West Germany, combined with lessdetailed data from the former German Demo-cratic Republic (GDR). Breast cancer mortalityrates were calculated on the basis of 1990 datafrom the former West Germany, incorporating25% lower rates for the former GDR. 16 Theclinical stage distribution of breast cancer wasbased on published series'718 and assumed notto be different from The Netherlands.'9 Datafrom the Saarland cancer registry were usedto determine the breast cancer incidence atnational level.20 Regional differences in in-cidence were assumed to be negligible on thebasis of the regional mortality data for breastcancer.2' Relative survival rates in the modelhad to be adjusted slightly downwards for allages, and specifically for the younger age group,to make the simulated breast cancer mortalityfit the observed data.
THE GERMAN MODEL: PRECLINICAL DURATIONOF BREAST CANCER AND SENSITIVITYAge specific assumptions on the mean dur-ations of preclinical states in The Netherlandswere based on data from the Dutch screeningprojects in Utrecht and Nijmegen and havebeen published before.8' The mean durationof preclinical disease was estimated to rangefrom 2.7 (age 50) to 6.2 (age 70) years. Dur-ations for the preclinical stages ofbreast cancerin Germany were assumed not to be differentfrom those estimated for The Netherlands.The expected sensitivity of a screening pro-
gramme in Germany has been assessed fromthe results oftwo German pilot projects, Aurichand Braunschweig, in the Deutsche Mam-mographie Studie.6 In these regions, breastcancer screening has been carried out since1990. Data from 35 000 screening ex-aminations (27 000 ofwhich were first screens)in the first two years (1990.III-1992.III) were
181

Warmerdam, de Koning, Boer, et al
Table I Sensitivity in relation to tumour stage, and referral rates (for additional examinations and biopsy) and positivepredictive values (PPV) (of a referral for biopsy), for first and subsequent screens as proxy indicators for specificity inthree quality scenarios - baseline, high quality and low quality
Sensitivity* per tumour stage (size) Baseline High Low
Ductal carcinoma in situ 0.350 0.400 0.300Invasive <1Omm 0.620 0.700 0.525Invasive 10-19 mm 0.840 0.950 0.713Invasive . 20 mm 0.840 0.950 0.713
Referral rates (%o)t and PPV Baseline High Lowfor 1st and subsequent (Subs)screenst 1st Subs Ist Subs Ist Subs
Referred for additional examination 3.9 2.1 0.9 0.5 3.3 1.9Referred for biopsy after additional 24 24 76 79 24 24examinationPPV (biopsy) 34 53 52 73 34 53
* In the MISCAN screening model sensitivity is defined as the stage specific probability of a positive screen result when screeninga woman with preclinical screen detectable breast cancer.tWomen with a positive screen result are referred for additional cxamination; women with a positive result for additionalexamination are referred for biopsy.t Mean values for a screening programme in Germany for women aged 50-69 (2 year interval) starting in 1994 and running for27 years.
analysed for specific age distribution andscreening interval. To simulate these pilot pro-
jects a MISCAN analysis model was con-
structed using this information together withthe assumptions on German breast cancer in-cidence, clinical stage distribution, and mean
durations of preclinical disease. Observed de-tection rates and stage distribution of screen
detected cancers were compared with the val-ues predicted by the model for different as-
sumptions on sensitivity. Calibration in thismodel based analysis lead to an approximately12% lower sensitivity for the DMS pilot pro-
jects than had been experienced in The Neth-erlands (see Results section).
THREE SCENARIOSFor the "baseline" scenario (the expected situ-ation) of a screening programme in Germany,the results from the DMS pilot projects were
used, ie sensitivity 12% lower than estimatedfor the Netherlands. Specificity in this scenariowas based on PPVs of referrals for additionalexamination and biopsy as observed in thesepilot projects.The "high quality" scenario was based on
the more favourable diagnostic results in theDutch screening projects and the nationwideprogramme. The specificity of the Dutch pro-
gramme was estimated with the use of the agespecific referral and detection rates (all rounds)in the Utrecht and Nijmegen projects.'" Thenew results in the nationwide programme were
consistent with these earlier assumptions.2 Inthe high quality scenario Dutch sensitivity andPPVs were used.
Thirdly, a "low quality" variant was analysed,incorporating a hypothetical 25% lower sensi-tivity than in the Dutch model. Positive pre-dictive values, however, were assumed to bethe same as in the baseline scenario.
Values for sensitivity as well as referral rates
and predictive values of the three scenarios are
shown in table 1.For all scenarios the German population
and epidemiology are considered. All results/computations were made for a screening pro-gramme starting in 1994, with a build up periodof five years, and running for 27 years. Effects
and costs which occurred during, as well as
after, this period were included. From a publichealth perspective we have chosen to considerthe effects in the total German female popu-
lation (all ages). Attendance rates, steeplydecreasing from 65% to under 30% in theage group 50-69, were based on the experiencein the general screening programme inGermany,'222 and on rates obtained from a
recent telephone survey, since data on at-tendance rates in the DMS study were notavailable.
All costs due to screening, diagnosis, andtreatment of breast cancer were considered," 12
and are presented in Deutsche mark (DM).Because the structure of care was based on theDutch situation, all costs were corrected forthe purchasing power parities (PPP) of the costof health care.23 This PPP was 1.19, whichmeans that health care in Germany is 19%more expensive.
ResultsMODEL BASED ANALYSIS OF EMPIRICAL
SCREENING DATA: ASSESSMENT OF EXPECTED
SENSITIVITY FOR A SCREENING PROGRAMME IN
GERMANY
This first part of the Results section describesthe model based analysis of the pilot projectsin Aurich and Braunschweig, with which theexpected sensitivity for a screening programmein Germany (baseline scenario) has been es-
timated.In table 2, the observed numbers of detected
breast cancers and detection rates of the DMS
Table 2 Number of observed and model expected breastcancers detected in the DMS study* (and detection ratesper 1000 screens)
No of detected tumoursNo ofscreens Observed Expectedt Expectedt
1st screen 27099 91 (3.4) 104 (3.8) 93 (3.4)2nd screen 8 188 14 (1.7) 14 (1.7) 14 (1.7)Total 35287 105 (3.0) 118 (3.3) 107 (3.0)* Women screened aged 35-84, average interval 1.1 year.tjAssuming sensitivity as experienced in The Netherlands (scctable 1).4:Sensitivitv for all stages lowered by approximately 12% (seetable 1).
182
Impact of quality in mammographic screening
pilot projects are displayed. In the age group35-84, a total of 105 tumours was detected (ofwhich 11 were after a six months early recall).The MISCAN model, adapted for Germanunderlying breast cancer incidence and as-suming sensitivity as experienced in The Neth-erlands, predicted 118 tumours (given thespecific ages of the women screened and anobserved average screening interval of 1.1 yearin these projects). Hence, the observed de-tection rates in the DMS study were lower thanexpected, although not statistically significant.The same analysis was carried out assuming
an approximately 12% lower sensitivity (allstages) than experienced in The Netherlands,leading to a better fit (107 tumours predicted)with the observed data. These results wereconsistent in the major age categories (under50, 50-69, and over 70). In the age group50-69, a total of 70 screen detected tumourswas observed. The model with Dutch sensi-tivity resulted in 78 predicted tumours, whereasthe 12% lower sensitivity variant predicted 71tumours, which came closer to the observednumber. It seems that the detection rates inthe second round have hardly been influencedby assuming a lower sensitivity in the model,presumably since some of the extra number ofmissed cancers at the prevalence screens willbe detected at the subsequent screens now,and probably also due to the short re-screeninterval.Based on these results, together with the
present discussion on quality of screening inGermany and DMS data,6 the expected sensi-tivity in the baseline scenario was assumed tobe 12% less than that experienced in TheNetherlands.
In the following parts of the Results section,this scenario will be evaluated and comparedwith the other two scenarios.
diagnosed breast cancer cases, especially in thebeginning of the programme when the pre-valence of screen detectable cases is relativelyhigh.24 A five year build up period in the pro-gramme will cause this increase in annual in-cidence to be spread more evenly over time.
In the baseline scenario, biennial screeningofwomen aged 50 to 69 in Germany is expectedto lead to increases in the total annual in-cidences (all ages) of 6%, 10%, 6%, and 3.%in the 2nd, 4th, 6th, and 8th years of theprogramme respectively. The maximum in-crease is to be expected in the 4th year, when3900 more women will be diagnosed withbreast cancer than in a situation without screen-ing. Different levels of sensitivity are expectedto result in similar sequences of increases inannual incidence, with a maximum of 9% inthe low quality scenario compared with 11% inthe high quality scenario. The present screeningprogramme in The Netherlands is expected tolead to a maximum increase of 15%, mainlybecause of a higher screening attendance.
In all three scenarios the stage distributionof screen detected breast cancers is far morefavourable than that of clinically diagnosedbreast cancers in the same age group. Theimpact on the overall stage distribution (allages), however, is relatively small, since only17% of all breast cancers are expected to bedetected by screening. In the present (noscreening) situation, 62% of the breast cancersare invasive and larger than 20 mm in size. Witha screening programme (baseline scenario) onlyabout 23% of the screen detected cancers willbe larger than 20 mm, while among all diag-nosed cancers this stage is still expected tocomprise 5 5%.
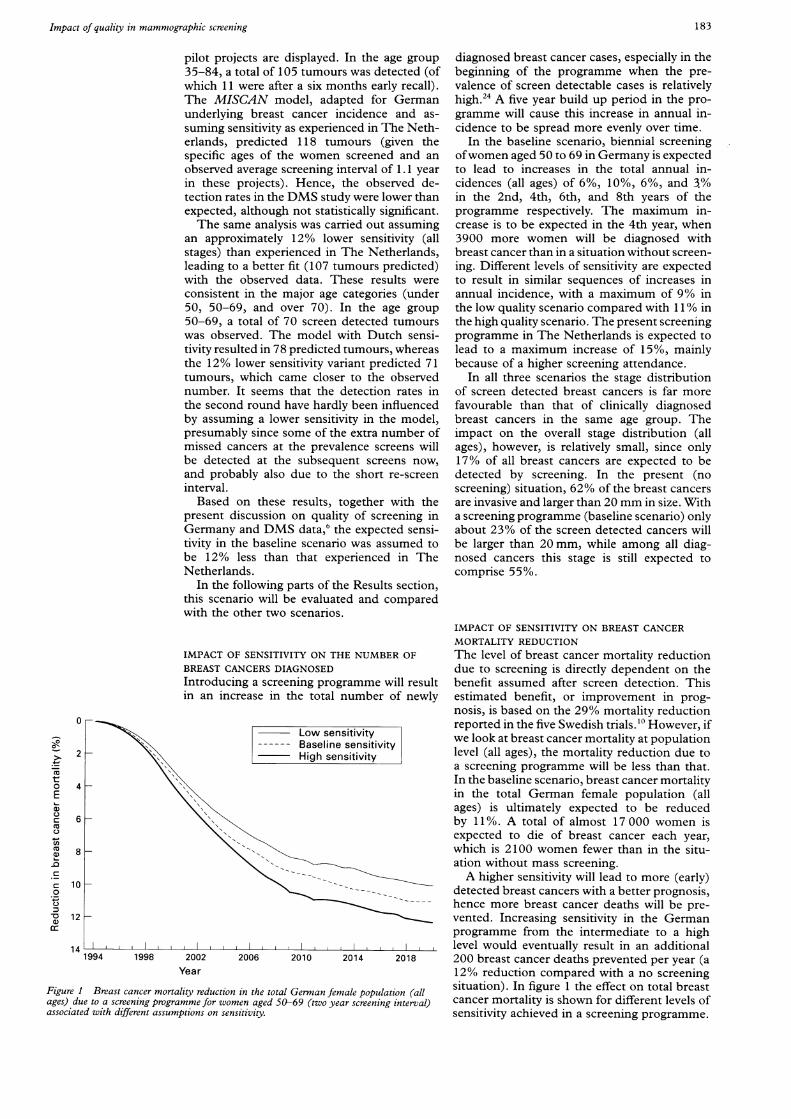
IMPACT OF SENSITIVITY ON BREAST CANCERMORTALITY REDUCTION
IMPACT OF SENSITIVITY ON THE NUMBER OF The level of breast cancer mortality reductionBREAST CANCERS DIAGNOSED due to screening is directly dependent on theIntroducing a screening programme will result benefit assumed after screen detection. Thisin an increase in the total number of newly estimated benefit, or improvement in prog-
nosis, is based on the 29% mortality reduction-_
o n
reported in the five Swedish trials.0 However, if------ Baseline sensitivity we look at breast cancer mortality at population
-BaseHigh sensitivity level (all ages), the mortality reduction due toa screening programme will be less than that.In the baseline scenario, breast cancer mortalityin the total German female population (allages) is ultimately expected to be reducedby 11%. A total of almost 17 000 women isexpected to die of breast cancer each year,which is 2100 women fewer than in the situ-ation without mass screening.A higher sensitivity will lead to more (early)
detected breast cancers with a better prognosis,hence more breast cancer deaths will be pre-vented. Increasing sensitivity in the Germanprogramme from the intermediate to a high
I,,, I I, I,, I level would eventually result in an additional1994 1998 2002 2006 2010 2014 2018 200 breast cancer deaths prevented per year (a
Year 12% reduction compared with a no screeningBreast cancer mortality reduction in the total German female population (all situation). In figure 1 the effect on total breast
te to a screening programme for women aged 50-69 (two year screening interval) cancer mortality is shown for different levels ofwd with different assumptions on sensitivity. sensitivity achieved in a screening programme.
0
2
4
6
8
-
:LI
t0Ea)
n
a,)ccnC
pC
cJ0
-as
10
12
14
Figure Iages) duassociate
183

Warmerdam, de Koning, Boer, et al
Table 3 Referrals and positive predictive values (PPV) in a screening programme inGermany for women aged 50-69 (2 year interval) in relation to two differentassumptions on quality* - baseline and high quality scenarios
Baseline High
1998t 2008j 1998-i 2008t
No of screens ( x 1000) 2 212 2 421 2 212 2 428No of positive screen results 73 974 58 931 17 063 13 702No of women referred for biopsy 17 531 13 977 13 090 10 676Biopsy diagnosis:
Malignant 6 966 6 481 7 714 7 075Benign 10 565 7 496 5 376 3 601
PPV of positive screen result (%) 9.4 11.0 45.2 51.6PPV of referral for biopsy (%) 39.7 46.4 58.9 66.3
* As defined in table 1; referral rates and predictive values in a screening programme are resultsof a mixture of 1st and subsequent screens.
t End of build up phase.t Steady state.
IMPACT OF SENSITIVITY AND SPECIFICITY ON
CONSEQUENCES FOR THE WOMENA screening programme will lead to a decreasein the number of advanced breast cancers.
Consequently, women who, in a no screeningsituation, would have undergone mastectomy,have a chance of being treated less radicallybecause of earlier detection. Screening willtherefore cause a shift from mastectomies tobreast conserving therapies. In the steady statesituation of a screening programme, almost2000 (14%) more breast conserving therapiesare expected to be performed each year thanin the situation without mass screening. Partof this favourable increase, however, is due to
the extra incidence caused by screening, iecases that are detected earlier as well as latentcases that otherwise would not have been diag-nosed.24 This extra annual incidence in Ger-many is estimated to be 1.8%, or 750 cases eachyear (of which approximately 40% otherwisewould not have been diagnosed). Increasingsensitivity in the programme is expected toresult in 40 additional detected breast cancers;
the number of breast conserving therapies isexpected to increase by 160 each year.A higher specificity will have favourable con-
sequences for the women, since fewer womenwill be exposed to the anxiety of undergoingadditional examination or even being referredfor biopsy without breast cancer being diag-nosed (table 3). In the baseline scenario almost74 000 women will be subjected to additionalexaminations after a positive screen (3.3% ofall screened women) in the year 1998, at theend of the build up phase. With a high speci-ficity only 0.8% would have to be referred thatyear, which is 57 000 fewer women. Ten yearslater these figures will be more favourable since,by then, only a small portion of the screeningexaminations will be first screens, which haverelatively high referral rates compared with sub-sequent screens (table 1). The increase ofspeci-ficity is expected to cause the yearly numberof women referred for biopsy without breastcancer being diagnosed to be halved: 10 600compared with 5400 in 1998; 7500 comparedwith 3600 in a steady state situation.
EXTRA COSTS AND COST EFFECTIVENESS
Costs and effects of the three scenarios for an
age 50-69 years screening programme with a
Table 4 Costs* (x 1O6 DM) and effects of a screeningprogramme in Germany for women aged 50-69 (2 yearinterval) in relation to three different assumptions onquality - baseline, high, and low quality scenarionst (5%discount rate)
Baseline High Low
Breast cancer deathsprevented 19 627 21 843 17 510
Life years gained 206525 230079 182919Costs of screening 4 005 4 002 4 008Costs of false positive
biopsies 576 232 500Costs of advanced disease -889 -989 -793Other costs 199 215 175Total extra costs 3 891 3 460 3 890Costs (DM) per life year
gained 18 842 15 037 21264
* Cost amounts are expected differences between situation withand without screening.t Values as in table 1.
two year interval are displayed in table 4 (at a5% discount rate to establish a time pref-erence). The bulk of the costs (about DM 4.0billion) is directly attributable to the screeningprogramme as such (overhead costs, mam-mography). The main costs incurred by a pro-gramme are due to biopsies performed onwomen who are apparently without breast can-cer (DM 576 million in the baseline scenario).The main cost savings are due to treating fewerwomen with advanced disease (DM 889 mil-lion)25. The entry "Other costs" (DM 199 mil-lion) includes costs of diagnostic assessment inthe programme, costs due to the increase inprimary treatments and follow up, savings ondiagnostic assessment outside the programmeand savings on adjuvant therapies.Hence, in the baseline scenario almost DM
3.9 billion (discounted) needs to be spent togain 207 000 life years (discounted): a costeffectiveness ratio of DM 19 000 per life yeargained. A screening programme with highsensitivity and specificity is expected to be lessexpensive (DM 3.5 billion). The direct screen-ing costs are about the same, but many fewerbiopsies are performed on women without,breast cancer, and more money is saved ontreatment of advanced disease. A high qualityprogramme is also more effective (230 000 lifeyears gained), resulting in a cost effectivenessratio ofDM 15 000 per life year gained. A lowsensitivity screening programme leads to a ratioof more than DM 21 000 per life year gained.
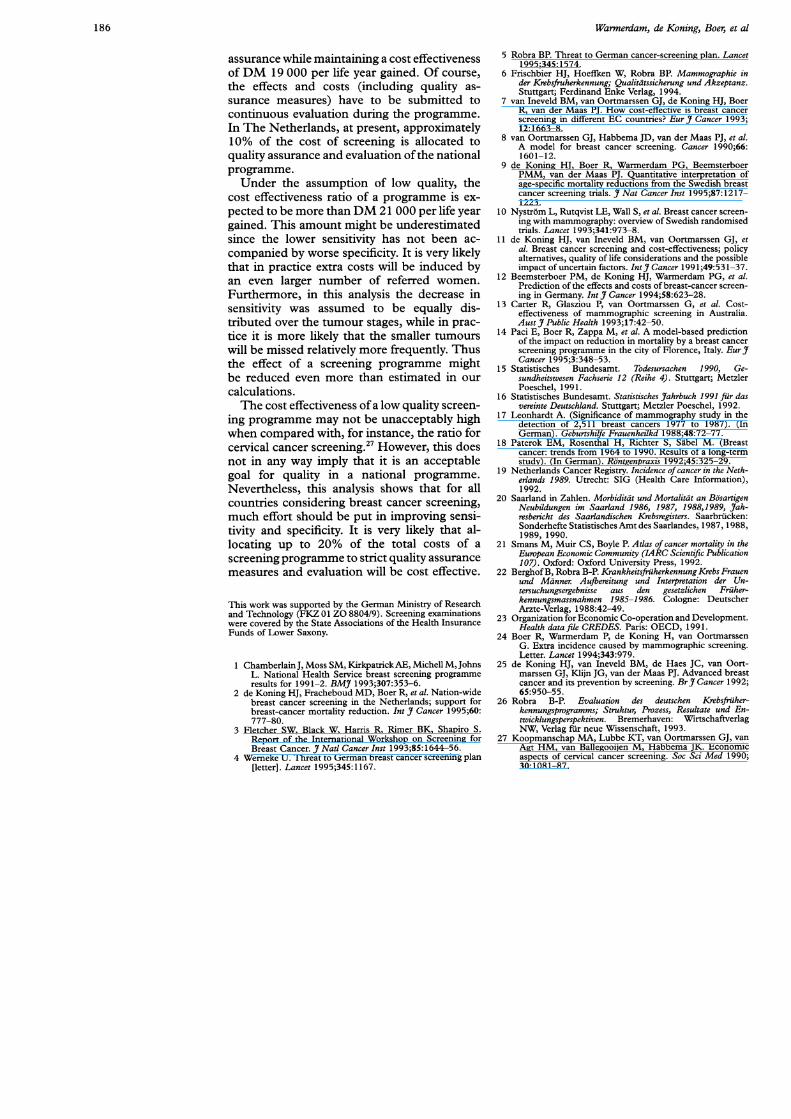
In figure 2 it can be seen that varying thesensitivity has a large impact on the effects, butalmost no impact on the total difference incosts. A higher sensitivity, while maintainingthe level of positive predictive values, leads tomore savings in terms of treatment of advanceddisease, but also to extra costs incurred by alarger number of women referred, treated, andfollowed up. Consequently, a higher specificitycan have a strong impact on costs, but will notincrease the number of life years gained.
DiscussionIt is of course difficult to make assumptionson the quality of a future population basedscreening programme in Germany that arebased only on the available screening data fromthe German pilot projects. Using the MISCAN
184

Impact of quality in mammographic screening
Increasing sensitivity The attendance rates used in the analyses areIncreasing specifity low compared to attendance in other European
countries. It is not unlikely that attendance in aGerman screening programme with a personalinvitation system would be higher than es-
High quality timated here. However, it is impossible to pre-scenario dict attendance in this situation since the health
care system is different. Since the attendancerate has a large impact on reducing breastcancer mortality, more attention to this aspect
Baseline is needed.scenario The assumption that the clinical stage dis-
tribution in Germany is equal to that in TheNetherlands is rather fragile. Diversity of datasources makes it hard to compare accurately,but the scarce German data give no reason toassume a different stage distribution. There arelimited data on the baseline level of screening,
Low quality and the extent to which this has caused ascenario shift in the clinical stage distribution prior to
I I I I I screening can be assumed to be negligible.26 A3500 3600 3700 3800 3900 4000 4100 screening programme may have an eliciting
Difference in costs (in million DM) effect on spontaneous screening in women not(yet) eligible for screening. We have not con-
Impact of changes in sensitivity and specificity of a screening programme in sidered this effect, since it is difficult to estimatefor women aged 50-69 (two year interval) on the total number of life years the extent of this spontaneous screening, asidonthe total extra costs; (5% discount rate).
well as what effect this has on mortality.It is clear that the importance of sensitivity
and specificity in a mass screening programmefor breast cancer should not be underestimated.
model we can analyse screening data by making The favourable and unfavourable effects forestimates for age specific detection rates, while the women involved are highly dependent ontaking into account the underlying incidence the levels of sensitivity and specificity achieved.and clinical stage distribution of breast cancer Increasing sensitivity will lead to more detectedand by comparing these with the observed rates. cases in an early stage, and thus to a moreBecause ofthe decentralised health care system effective programme with a higher number ofin Germany, there is reason to believe that prevented breast cancer deaths. Also, with athe screening quality in Germany could be higher sensitivity more mastectomies can beimproved. The results of the model, an ex- prevented in favour of breast conserving ther-pected 12% sensitivity difference compared apies. However, if specificity in the screeningwith The Netherlands, support this opinion, programme is low, these favourable effects arealthough there were no data on interval cancers. only achieved by referring a considerable num-To account for the uncertainty in assessing the ber of women for additional examinations andextent of this loss in quality, we have defined biopsies, thereby making the programme moretwo other sets of quality assumptions. The expensive.range of differences in sensitivity assumed for In Germany, introducing a programme withthe three German scenarios in this study was the baseline sensitivity and specificity as-somewhat arbitrary, based on expert opinion, sumptions is expected to result in a total differ-but seems plausible, considering the outcomes ence in costs of DM 3.9 billion (5% discountof the model. However, larger differences in rate). A high quality programme is expectedquality between European countries might to lead to only DM 3.5 billion (discounted).exist. Therefore, 11% of the total costs of a pro-The various assumptions made about several gramme can be invested in quality assurance
factors are, of course, open to discussion. For (in technique and interpretation), provided thatinstance, one could question how rep- the higher levels ofsensitivity and specificity canresentative the Saarland registry data on breast be achieved. In this way, an equally expensivecancer incidence rates are. National data on programme will gain an additional 24 000 lifethese incidence rates are lacking, but national years (5% discounted) and will prevent anbreast cancer mortality rates closely resemble additional 200 cases of breast cancer death perthose of the Saarland region. Furthermore,regional differences in incidence were assumedto be negligible on the basis of the regionalmortality data for breast cancer.2' Therefore,it is likely that breast cancer incidences are
comparable, unless major differences exist insurvival between Saarland and all of Germany.Because of an absence of data, this questioncannot be addressed. The extrapolation is notlikely to have significantly influenced the res-ults.
year.If DM 19 000 per life year gained is con-
sidered to be cost effective, then in order togain as many life years as in a high qualityprogramme an amount ofDM 4.3 billion (DM18842 x 230 079 life years, table 4) is con-sidered good value for money. Since the costsof a high quality programme is estimated to beonly DM 3.5 billion, an amount of almostDM 0.9 billion (20% of the total costs ofthe programme) can be invested in quality
240
230
-aC.
00
C.C'Ua)
01)L-
220
210
200
190
180
Figure 2Germanygained an
185
Warmerdam, de Koning, Boer, et al
assurance while maintaining a cost effectivenessof DM 19 000 per life year gained. Of course,
the effects and costs (including quality as-
surance measures) have to be submitted to
continuous evaluation during the programme.
In The Netherlands, at present, approximately10% of the cost of screening is allocated to
quality assurance and evaluation of the nationalprogramme.
Under the assumption of low quality, thecost effectiveness ratio of a programme is ex-
pected to be more than DM 21 000 per life yeargained. This amount might be underestimatedsince the lower sensitivity has not been ac-
companied by worse specificity. It is very likelythat in practice extra costs will be induced byan even larger number of referred women.
Furthermore, in this analysis the decrease insensitivity was assumed to be equally dis-tributed over the tumour stages, while in prac-
tice it is more likely that the smaller tumours
will be missed relatively more frequently. Thusthe effect of a screening programme mightbe reduced even more than estimated in our
calculations.The cost effectiveness of a low quality screen-
ing programme may not be unacceptably highwhen compared with, for instance, the ratio forcervical cancer screening.27 However, this doesnot in any way imply that it is an acceptablegoal for quality in a national programme.
Nevertheless, this analysis shows that for allcountries considering breast cancer screening,much effort should be put in improving sensi-tivity and specificity. It is very likely that al-locating up to 20% of the total costs of a
screening programme to strict quality assurance
measures and evaluation will be cost effective.
This work was supported by the German Ministry of Researchand Technology (FKZ 01 ZO 8804/9). Screening examinationswere covered by the State Associations of the Health InsuranceFunds of Lower Saxony.
1 ChamberlainJ, Moss SM, Kirkpatrick AE, Michell M, JohnsL. National Health Service breast screening programme
results for 1991-2. BMJ 1993;307:353-6.2 de Koning HJ, Fracheboud MD, Boer R, et al. Nation-wide
breast cancer screening in the Netherlands; support forbreast-cancer mortality reduction. Int I Cancer 1995;60:777-80.
3 Fletcher SW, Black W, Harris R, Rimer BK, Shapiro S.Report of the International Workshop on Screening forBreast Cancer. _7 Natl Cancer Inst 1993;85:1644-56.
4 Wemeke U. Threat to German breast cancer screening plan[letter]. Lancet 1995;345:1167.
5 Robra BP. Threat to German cancer-screening plan. Lancet1995;345:1574.
6 Frischbier HJ, Hoeffken W, Robra BP. Mammographie inder Krebsfruherkennung; Qualitatssicherung und Akzeptanz.Stuttgart; Ferdinand Enke Verlag, 1994.
7 van Ineveld BM, van Oortmarssen GJ, de Koning HJ, BoerR, van der Maas PJ. How cost-effective is breast cancerscreening in different EC countries? Eur 7 Cancer 1993;12:1663-8.
8 van Oortmarssen GJ, Habbema JD, van der Maas PJ, et al.A model for breast cancer screening. Cancer 1990;66:1601-12.
9 de Koning HJ, Boer R, Warmerdam PG, BeemsterboerPMM, van der Maas PJ. Quantitative interpretation ofage-specific mortality reductions from the Swedish breastcancer screening trials. _7 Nat Cancer Inst 1995;87:12171223.
10 Nystrom L, Rutqvist LE, Wall S, et al. Breast cancer screen-ing with mammography: overview of Swedish randomisedtrials. Lancet 1993;341:973-8.
11 de Koning HJ, van Ineveld BM, van Oortmarssen GJ, etal. Breast cancer screening and cost-effectiveness; policyalternatives, quality of life considerations and the possibleimpact of uncertain factors. Intr Cancer 1991;49:531-37.
12 Beemsterboer PM, de Koning HJ, Warmerdam PG, et al.Prediction of the effects and costs of breast-cancer screen-ing in Germany. IntrJ Cancer 1994;58:623-28.
13 Carter R, Glasziou P, van Oortmarssen G, et al. Cost-effectiveness of mammographic screening in Australia.Aust _j Public Health 1993;17:42-50.
14 Paci E, Boer R, Zappa M, et al. A model-based predictionof the impact on reduction in mortality by a breast cancerscreening programme in the city of Florence, Italy. Eur_7Cancer 1995;3:348-53.
15 Statistisches Bundesamt. Todesursachen 1990, Ge-sundheitswesen Fachserie 12 (Reihe 4). Stuttgart; MetzlerPoeschel, 1991.
16 Statistisches Bundesamt. Statistisches3rahrbuch 1991 fur dasvereinte Deutschland. Stuttgart; Metzler Poeschel, 1992.
17 Leonhardt A. (Significance of mammography study in thedetection of 2,511 breast cancers 1977 to 1987). (InGerman). Geburtshilfe Frauenheilkd 1988;48:72-77.
18 Paterok EM, Rosenthal H, Richter S, Sabel M. (Breastcancer: trends from 1964 to 1990. Results of a long-termstudy). (In German). Rontgenpraxis 1992;45:325-29.
19 Netherlands Cancer Registry. Incidence of cancer in the Neth-erlands 1989. Utrecht: SIG (Health Care Information),1992.
20 Saarland in Zahlen. Morbiditdt und Mortalitdt an BosartigenNeubildungen im Saarland 1986, 1987, 1988,1989, J7ah-resbericht des Saarlandischen Krebsregisters. Saarbrucken:Sonderhefte Statistisches Amt des Saarlandes, 1987, 1988,1989, 1990.
21 Smans M, Muir CS, Boyle P. Atlas of cancer mortality in theEuropean Economic Community, (IARC Scientific Publication107). Oxford: Oxford University Press, 1992.
22 Berghof B, Robra B-P. Krankheitsfruherkennung Krebs Frauenund Mdnner Aujbereitung und Interpretation der Un-tersuchungsergebnisse aus den gesetzlichen Friiher-kennungsmassnahmen 1985-1986. Cologne: DeutscherArzte-Verlag, 1988:42-49.
23 Organization for Economic Co-operation and Development.Health data file CREDES. Paris: OECD, 199 1.
24 Boer R, Warmerdam P, de Koning H, van OortmarssenG. Extra incidence caused by mammographic screening.Letter. Lancet 1994;343:979.
25 de Koning HJ, van Ineveld BM, de HaesJC, van Oort-marssen GJ, Klijn JG, van der Maas PJ. Advanced breastcancer and its prevention by screening. BrJ_ Cancer 1992;65:950-55.
26 Robra B-P. Evaluation des deutschen Krebsfriiher-kennungsprogramms; Struktur, Prozess, Resultate und En-twicklungsperspektiven. Bremerhaven: WirtschaftverlagNW, Verlagfur neue Wissenschaft, 1993.
27 Koopmanschap MA, Lubbe KT, van Oortmarssen GJ, vanAgt HM, van Ballegooijen M, HabbemaJK. Economicaspects of cervical cancer screening. Soc Sci Med 1990;30:1081-87.
186
Copyright © 2022 FDOKUMEN




















