
the consecutive conference interpreter as intercultural mediator
Upload
independentCategory
view
0download
0
Original Investigations
Mammographic Appearance of Breast Cancer in
African-American Women: Report of 100 Consecut ive Cases 1
Stephanie K. Patterson, MD, Mark A. Helvie, MD, Lynn K. Joynt, MD Marilyn A. Roubidoux, MD, Myla Strawderman, MS
Rationale and Objectives/The authors determined the mammographic appearance of breast carcinoma in Afri- Can-Amaerican women and compared it with that in a white Cohort. i
Materials and Methods. The authors reviewed the mammograms, clinical records, and pathology records of 97 consecutive African-American women with 100 con- firmed breast cancers and 110 white women with 111 confirmed breast cancers.
Results. The mammograms Obtained in African-Ameri- canwomen were positive in 94 cases (94%), and those obtained in white women were positive in 99 cases (89%). Forty-seven percetat of malignancies in African- American women appeared as calcifications, aloneor with a mass, and 41% appeared as a mass only. There Was no statistically significant difference in the Ire= quency of these two findings betweent_he African- American and the white populations. There was no statis- tically significant difference in the breast parenchymal pattern between the two groups. The most common tu- mor location in both races was the upper outer quadrant2
C0uelusion. Breast carcinoma in African-American women is similar to that in white women in terms of
• mam_mographi c appearance, location, and breast density. 'i The matmmograpbic appearance should notbe an impedi- ment to the detection of breast cancer in African-Ameri- can women.
Key Words, Breast neoplasr~s, diagnosis; breast radiog- raphy. ~
Acad Radio11998; 5:2-8
1 From the Departments of Radiology/TC2910 (S,K,P., M.A,H., L.K.J., M.A.R.) and Biostatistics (M,S.), University of Michigan Hospitals, Com- prehensive Cancer Center, 1500 E Medical Center Dr, Ann Arbor, MI 48109-0326. Received April 30, 1996; revision requested June 14; revi- sion received September 18, 1997; accepted September 26. Address reprint requests to S, K.P,
©AUR, 1998
Although the incidence of breast cancer is increasing in both the white and African-American populations, the
mortality rates are higher in African-American women
than in white women (1-6). Whereas breast cancer mor-
tality rates declined 4.7% for American women as a whole between 1989 and 1992, the mortality rate for Af-
rican-American women increased 2.6% in the same pe-
riod (7). Socioeconomic status, stage of disease at diag-
nosis, diagnostic and treatment delays, treatment differ-
ences, and biologic characteristics of breast cancer have
been explored as possible causes of this disparity (1-6).
African-Americans account for 13% of the U.S.-popula-
tion (8). To our knowledge, the utility of mammography in Af-
rican-American women has never been studied in a ran-
domized trial and the mammographic appearance of
breast cancer in these women has not been described. In a recent population-based study, screening mammography
was not beneficial in African-American women for the
protection against advanced disease stage (9). The pur-
pose of our study was to determine the mammographic
appearance of breast cancer in African-American women
and compare it with that in a white cohort.
A search of the computerized database of our multidisciplinary Breast Care Center resulted in finding
143 women who identified themselves as African-Ameri-
can or black and in whom biopsy-proved breast cancer was
diagnosed between June 1986 and March 1995. Patients
with lobular carcinoma in situ were not included. During
the same period and from the same database, 186 of 2,059
women who identified themselves as Caucasian (white) were randomly selected for comparison after matching for
year of diagnosis by using a random numbers table.
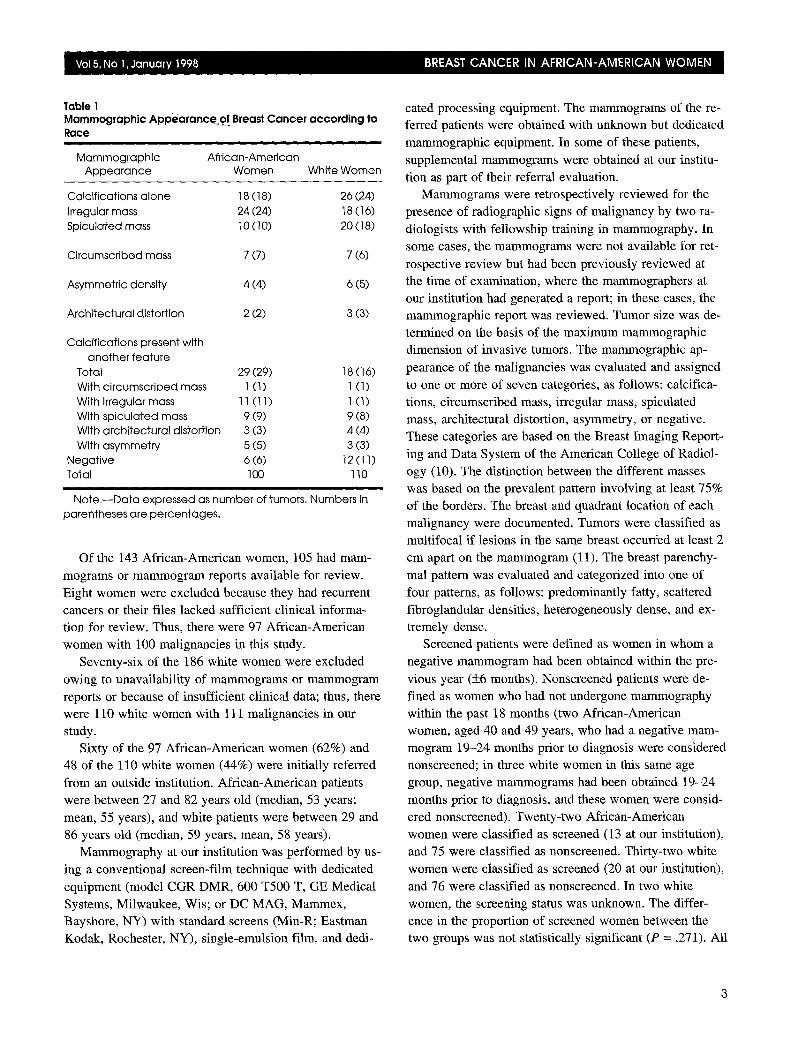
Table 1 Appearance of Breast Cancer according to Mammographic
Race
Mammographic African-American Appearance Women White Women
Calcifications alone 18 (18) 26 (24) irregular mass 24 (24) 18 (16) Spiculated mass 10 (10) 20 (18)
Circumscribed mass 7 (7) 7 (6)
Asymmetric density 4 (4) 6 (5)
Architectural distortion 2 (2) 3 (3)
Calcifications present with another feature
Total 29 (29) 18 (16) With circumscribed mass 1 (1) 1 (1) With irregular mass 11 (11) 1 (1) With spiculated mass 9 (9) 9 (8) With architectural distortion 3 (3) 4 (4) With asymmetry 5 (5) 3 (3)
Negative 6 (6) 12 (11) Total 100 110
i i
Note. - -bata expressed as number of tumors. Numbers in parentheses are percentages.
Of the 143 African-American women, 105 had mam- mograms or mammogram reports available for review.
Eight women were excluded because they had recurrent cancers or their files lacked sufficient clinical informa- tion for review. Thus, there were 97 African-American
women with 100 malignancies in this study. Seventy-six of the 186 white women were excluded
owing to unavailability of mammograms or mammogram reports or because of insufficient clinical data; thus, there were 110 white women with 111 malignancies in our
study. Sixty of the 97 African-American women (62%) and
48 of the 110 white women (44%) were initially referred
from an outside institution. African-American patients were between 27 and 82 years old (median, 53 years;
mean, 55 years), and white patients were between 29 and 86 years old (median, 59 years, mean, 58 years).
Mammography at our institution was performed by us-
ing a conventional screen-film technique with dedicated
equipment (model CGR DMR, 600 T500 T, GE Medical
Systems, Milwaukee, Wis; or DC MAG, Mammex, Bayshore, NY) with standard screens (Min-R; Eastman
Kodak, Rochester, NY), single-emulsion film, and dedi-
cated processing equipment. The mammograms of the re- ferred patients were obtained with unknown but dedicated
mammographic equipment. In some of these patients, supplemental mammograms were obtained at our institu-
tion as part of their referral evaluation. Mammograms were retrospectively reviewed for the
presence of radiographic signs of malignancy by two ra-
diologists with fellowship training in mammography. In some cases, the mammograms were not available for ret-
rospective review but had been previously reviewed at the time of examination, where the mammographers at our institution had generated a report; in these cases, the mammographic report was reviewed. Tumor size was de- termined on the basis of the maximum mammographic dimension of invasive tumors. The mammographic ap-
pearance of the malignancies was evaluated and assigned
to one or more of seven categories, as follows: calcifica- tions, circumscribed mass, irregular mass, spiculated mass, architectural distortion, asymmetry, or negative. These categories are based on the Breast Imaging Report-
ing and Data System of the American College of Radiol- ogy (10). The distinction between the different masses was based on the prevalent pattern involving at least 75% of the borders. The breast and quadrant location of each malignancy were documented. Tumors were classified as multifocal if lesions in the same breast occurred at least 2 cm apart on the mammogram (11). The breast parenchy-
mal pattern was evaluated and categorized into one of four patterns, as follows: predominantly fatty, scattered
fibroglandular densities, heterogeneously dense, and ex- tremely dense.
Screened patients were defined as women in whom a negative mammogram had been obtained within the pre-
vious year (_+6 months). Nonscreened patients were de- fined as women who had not undergone mammography
within the past 18 months (two African-American women, aged 40 and 49 years, who had a negative mam- mogram 19-24 months prior to diagnosis were considered nonscreened; in three white women in this same age group, negative mammograms had been obtained 19-24 months prior to diagnosis, and these women were consid-
ered nonscreened). Twenty-two African-American women were classified as screened (13 at our institution), and 75 were classified as nonscreened. Thirty-two white women were classified as screened (20 at our institution),
and 76 were classified as nonscreened. In two white women, the screening status was unknown. The differ- ence in the proportion of screened women between the two groups was not statistically significant (P = .271). All
patients who underwent screening mammography at our
institution also underwent physical examination of the
breast. Palpable lesions were documented as present if
noted at physical examination by the patient, physician,
or mammography staff. A pathologist at our institution reviewed histologic slides of all outside cases. Histologic
results and axillary lymph node status were recorded. The patients' menstrual status--including whether they were
premenopausal, postmenopausal receiving estrogen re-
placement, or postmenopausal without estrogen replace-
men t - -was also recorded. The proportions of African-American and white pa-
tients with certain characteristics on their mammograms
were compared with the Fisher exact test by using Stat-
Xact software (Cytel Software, Cambridge Mass). The
size of invasive tumors was compared with the Wilcoxon
rank sum test (SAS procedure NPAR1WAY; SAS Insti-
tute, Cary NC). All P values are two-sided.
Mammograms obtained in African-American women
were positive in 94 of the 100 cases (94%), and those ob-
tained in white women were positive in 99 of the 111 cases
(89%). The mammographic appearance of the cancers in
both groups is described in Table 1, and the mammo-
graphic appearance in screened and nonscreened patients is
described in Tables 2 and 3, respectively, and all the data
in the Tables is based on number of malignancies, not number of women. The file of one white woman was miss-
ing information about the mammographic appearance of
her tumor, and she was excluded from this analysis. There
was no statistically significant difference between the two
racial groups overall with regard to malignancies with cal-
cifications, either alone or together with a mass (P = .331), or malignancies that appeared as a dominant mass only (P
> .999) (Table 1). The difference between the proportion of African-American and the proportion of white women
with calcifications and another feature was statistically sig-
nificant (29% vs 16%, P = .031). This finding is probably
due to the fact that a greater proportion of African-Ameri-
can women had tumors described as calcification with an irregular mass (11% vs 1%). In fact, the proportion of Afri-
can-American women with irregular masses--with or
without calcification--was greater than that in white
women (35% vs 17%, P = .0004). There was no significant
difference between the two groups with regard to the pro-
portion of tumors appearing only as calcifications (P =
.397) or appearing as spiculated (P = .116) or circum-
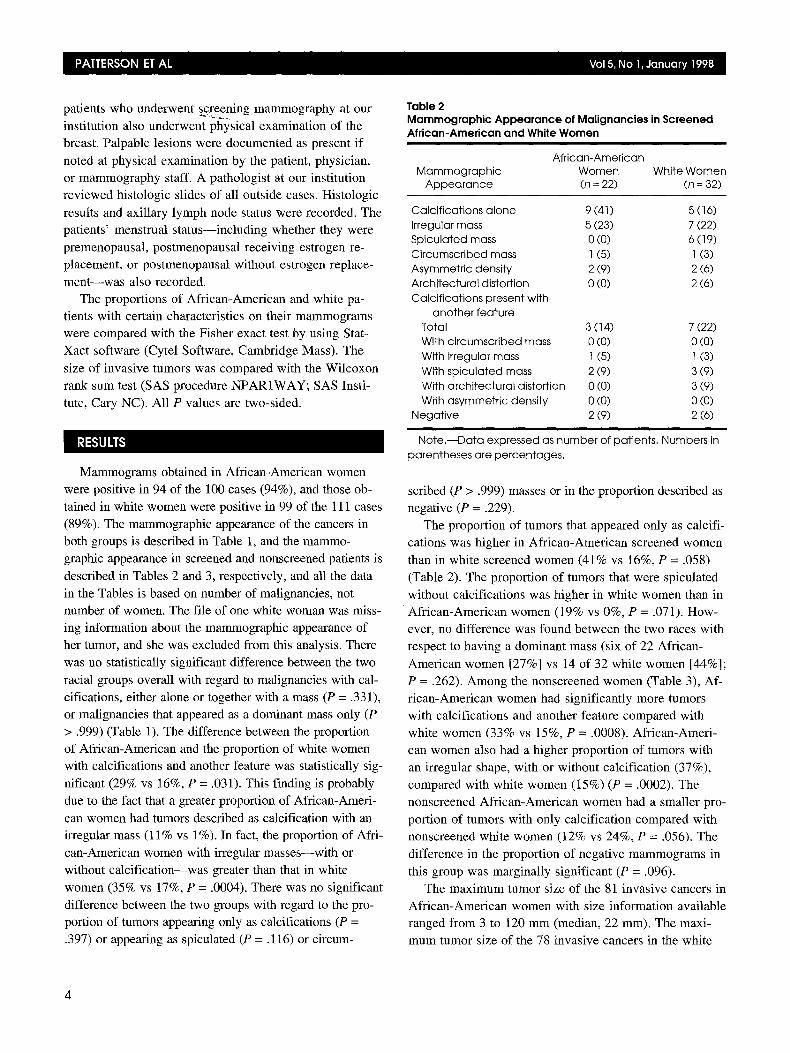
Table 2 Mammographic Appearance of Malignancies in Screened African-American and White Women
African-American Mammographic Women White Women
Appearance (n = 22) (n = 32)
Calcifications alone 9 (41 ) 5 (16) Irregular mass 5 (23) 7 (22) Spiculated mass 0 (0) 6 (19) Circumscribed mass 1 (5) 1 (3) Asymmetric density 2 (9) 2 (6) Architectural distortion 0 (0) 2 (6) Calcifications present with
another feature Total 3 (14) 7 (22) With circumscribed mass 0 (0) 0 (0) With irregular mass 1 (5) 1 (3) With spiculated mass 2 (9) 3 (9) With architectural distortion 0 (0) 3 (9) With asymmetric density 0 (0) 0 (0)
Negative 2 (9) 2 (6)
Note.--Data expressed as number of patients. Numbers in parentheses are percentages.
scribed (P > .999) masses or in the proportion described as
negative (P = .229).
The proportion of tumors that appeared only as calcifi-
cations was higher in African-American screened women
than in white screened women (41% vs 16%, P = .058)
(Table 2). The proportion of tumors that were spiculated
without calcifications was higher in white women than in African-American women (19% vs 0%, P = .071). How-
ever, no difference was found between the two races with
respect to having a dominant mass (six of 22 African-
American women [27%] vs 14 of 32 white women [44%];
P = .262). Among the nonscreened women (Table 3), Af-
rican-American women had significantly more tumors with calcifications and another feature compared with
white women (33% vs 15%, P = .0008). African-Ameri- can women also had a higher proportion of tumors with
an irregular shape, with or without calcification (37%),
compared with white women (15%) (P = .0002). The
nonscreened African-American women had a smaller pro-
portion of tumors with only calcification compared with nonscreened white women (12% vs 24%, P = .056). The
difference in the proportion of negative mammograms in
this group was marginally significant (P = .096).
The maximum tumor size of the 81 invasive cancers in
African-American women with size information available ranged from 3 to 120 mm (median, 22 mm). The maxi-
mum tumor size of the 78 invasive cancers in the white
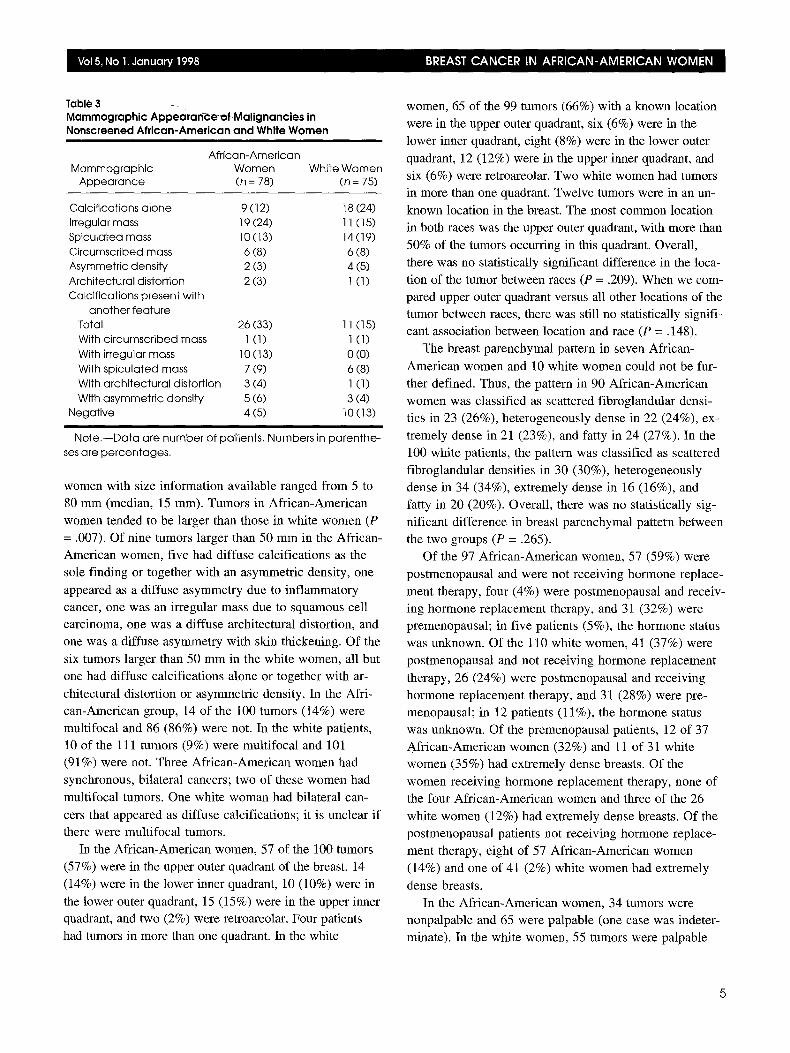
Table 3 -. Mammographic Appearar~e 'o fMal ignancies in Nonscreened African-American and White Women
i
African-American Mammographic Women White Women
Appearance (n = 78) (n : 75)
Calcifications alone 9 (12) 18 (24) Irregular mass 19 (24) 11 (15) Spiculated mass 10 (13) 14 (19) Circumscribed mass 6 (8) 6 (8) Asymmetric density 2 (3) 4 (5) Architectural distortion 2 (3) 1 (1) Calcifications present with
another feature Total 26 (33) 11 (15) With circumscribed mass 1 (1) 1 (1) With irregular mass 10 (13) 0 (0) With spiculated mass 7 (9) 6 (8) With architectural distortion 3 (4) 1 (1) With asymmetric density 5 (6) 3 (4)
Negative 4 (5) 10 (13)
Note.--Data are number of patients. ses are percentages.
Numbers in parenthe-
women with size information available ranged from 5 to
80 mm (median, 15 mm). Tumors in African-American
women tended to be larger than those in white women (P
= .007). Of nine tumors larger than 50 mm in the African-
American women, five had diffuse calcifications as the
sole finding or together with an asymmetric density, one
appeared as a diffuse asymmetry due to inflammatory cancer, one was an irregular mass due to squamous cell
carcinoma, one was a diffuse architectural distortion, and
One was a diffuse asymmetry with skin thickening. Of the
six tumors larger than 50 mm in the white women, all but
one had diffuse calcifications alone or together with ar-
chitectural distortion or asymmetric density. In the Afri-
can-American group, 14 of the 100 tumors (14%) were
multifocal and 86 (86%) were not. In the white patients, 10 of the 111 tumors (9%) were multifocal and 101
(91%) were not. Three African-American women had
synchronous, bilateral cancers; two of these women had
multifocal tumors. One white woman had bilateral can-
cers that appeared as diffuse calcifications; it is unclear if there were multifocal tumors.
In the African-American women, 57 of the 100 tumors
(57%) were in the upper outer quadrant of the breast, 14
(14%) were in the lower inner quadrant, 10 (10%) were in
the lower outer quadrant, 15 (15%) were in the upper inner quadrant, and two (2%) were retroareolar. Four patients
had tumors in more than one quadrant. In the white
women, 65 of the 99 tumors (66%) with a known location
were in the upper outer quadrant, six (6%) were in the
lower inner quadrant, eight (8%) were in the lower outer
quadrant, 12 (12%) were in the upper inner quadrant, and
six (6%) were retroareolar. Two white women had tumors in more than one quadrant. Twelve tumors were in an un-
known location in the breast. The most common location in both races was the upper outer quadrant, with more than
50% of the tumors occurring in this quadrant. Overall,
there was no statistically significant difference in the loca-
tion of the tumor between races (P = .209). When we com-
pared upper outer quadrant versus all other locations of the tumor between races, there was still no statistically signifi-
cant association between location and race (P = .148).
The breast parenchymal pattern in seven African-
American women and 10 white women could not be fur-
ther defined. Thus, the pattern in 90 African-American
women was classified as scattered fibroglandular densi-
ties in 23 (26%), heterogeneously dense in 22 (24%), ex-
tremely dense in 21 (23%), and fatty in 24 (27%). In the
100 white patients, the pattern was classified as scattered
fibroglandular densities in 30 (30%), heterogeneously
dense in 34 (34%), extremely dense in 16 (16%), and
fatty in 20 (20%). Overall, there was no statistically sig-
nificant difference in breast parenchymal pattern between
the two groups (P = .265).
Of the 97 African-American women, 57 (59%) were
postmenopausal and were not receiving hormone replace-
ment therapy, four (4%) were postmenopausal and receiv- ing hormone replacement therapy, and 31 (32%) were
premenopausal; in five patients (5%), the hormone status
was unknown. Of the 110 white women, 41 (37%) were
postmenopansal and not receiving hormone replacement
therapy, 26 (24%) were postmenopausal and receiving
hormone replacement therapy, and 31 (28%) were pre- menopausal; in 12 patients (11%), the hormone status
was unknown. Of the premenopausal patients, 12 of 37
African-American women (32%) and 11 of 31 white
women (35%) had extremely dense breasts. Of the
women receiving hormone replacement therapy, none of
the four African-American women and three of the 26
white women (12%) had extremely dense breasts. Of the
postmenopausal patients not receiving hormone replace-
ment therapy, eight of 57 African-American women
(14%) and one of 41 (2%) white women had extremely
dense breasts.
In the African-American women, 34 tumors were nonpalpable and 65 were palpable (one case was indeter-
minate). In the white women, 55 tumors were palpable
5
and 53 were nonpalpable(three cases were unknown).
More women in both race groups with nonpalpable tu-
mors had undergone screening. The median tumor size of
the palpable tumors in the African-American group was 25 mm (range, 8-120 mm). The median tumor size of the
palpable tumors in the white group was 20 mm (range, 5-
80 ram). The palpable tumors in African-American women tended to be larger than the palpable tumors in
white women (P = .053). Tumor sizes were unavailable
for five tumors in the African-American cohort and nine
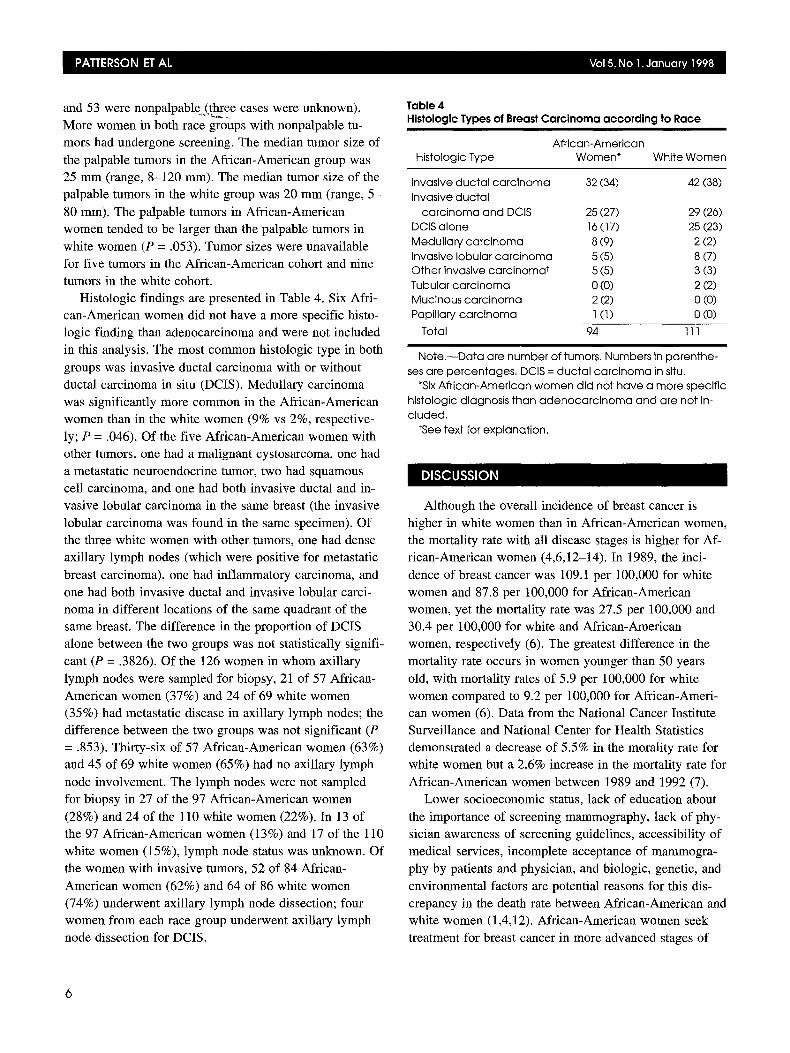
tumors in the white cohort. Histologic findings are presented in Table 4. Six Afri-
can-American women did not have a more specific histo-
logic finding than adenocarcinoma and were not included
in this analysis. The most common histologic type in both
groups was invasive ductal carcinoma with or without
ductal carcinoma in situ (DCIS). Medullary carcinoma
was significantly more common in the African-American
women than in the white women (9% vs 2%, respective-
ly; P = .046). Of the five African-American women with other tumors, one had a malignant cystosarcoma, one had
a metastatic neuroendocrine tumor, two had squamous
cell carcinoma, and one had both invasive ductal and in- vasive lobular carcinoma in the same breast (the invasive
lobular carcinoma was found in the same specimen). Of
the three white women with other tumors, one had dense
axillary lymph nodes (which were positive for metastatic
breast carcinoma), one had inflammatory carcinoma, and
one had both invasive ductal and invasive lobular carci-
noma in different locations of the same quadrant of the same breast. The difference in the proportion of DCIS
alone between the two groups was not statistically signifi-
cant (P = .3826). Of the 126 women in whom axillary
lymph nodes were sampled for biopsy, 21 of 57 African-
American women (37%) and 24 of 69 white women (35%) had metastatic disease in axillary lymph nodes; the
difference between the two groups was not significant (P
= .853). Thirty-six of 57 African-American women (63%) and 45 of 69 white women (65%) had no axillary lymph
node involvement. The lymph nodes were not sampled for biopsy in 27 of the 97 African-American women
(28%) and 24 of the 110 white women (22%). In 13 of the 97 African-American women (13%) and 17 of the 110
white women (15%), lymph node status was unknown. Of
the women with invasive tumors, 52 of 84 African-
American women (62%) and 64 of 86 white women
(74%) underwent axillary lymph node dissection; four
women from each race group underwent axillary lymph
node dissection for DCIS.
Table 4 Histologic Types of Breast Carcinoma according to Race
African-American Histologic Type Women* White Women
Invasive ducta l carc inoma 32 (34) 42 (38) Invasive ducta l
carc inoma and DCIS 25 (27) 29 (26) DCIS alone 16 (17) 25 (23) Medullary carc inoma 8 (9) 2 (2) Invasive Iobular carc inoma 5 (5) 8 (7) Other invasive carc inoma t 5 (5) 3 (3) Tubular carc inoma 0 (0) 2 (2) Mucinous carc inoma 2 (2) 0 (0) Papillary carc inoma 1 (1) 0 (0)
Total 94 111
Note. - -Data are number of tumors. Numbers in parenthe- ses are percentages. DCIS = ducta l carc inoma in situ.
*Six Afr ican-American women did not have a more specific histologic diagnosis than adenoca rc inoma and are not in- c luded.
tSee text for explanation.
Although the overall incidence of breast cancer is
higher in white women than in African-American women,
the mortality rate with all disease stages is higher for Af-
rican-American women (4,6,12-14). In 1989, the inci-
dence of breast cancer was 109.1 per 100,000 for white
women and 87.8 per 100,000 for African-American
women, yet the mortality rate was 27.5 per 100,000 and 30.4 per t00,000 for white and African-American
women, respectively (6). The greatest difference in the
mortality rate occurs in women younger than 50 years
old, with mortality rates of 5.9 per 100,000 for white
women compared to 9.2 per 100,000 for African-Ameri-
can women (6). Data from the National Cancer Institute
Surveillance and National Center for Health Statistics demonstrated a decrease of 5.5% in the morality rate for
white women but a 2.6% increase in the mortality rate for
African-American women between 1989 and 1992 (7).
Lower socioeconomic status, lack of education about
the importance of screening mammography, lack of phy- sician awareness of screening guidelines, accessibility of
medical services, incomplete acceptance of mammogra-
phy by patients and physician, and biologic, genetic, and
environmental factors are potential reasons for this dis-
crepancy in the death rate between African-American and white women (1,4,12). African-American women seek
treatment for breast cancer in more advanced stages of
6

disease, even when age and~s0cioeconomic levels are controlled for (1,4,13,14). They are also more likely to delay treatment after diagnosis (4,13). Some studies sug-
gest treatment differences as a cause for increased mortal- ity. Other studies, however, have shown little difference
in the natural history of breast cancer between African- American women and white women if appropriate treat- ment is given (4,15).
Other reports indicate several histologic differences. Breast carcinomas in African-American women have less frequent estrogen receptor positivity, poorer differentia- tion, and less fibrosis (16). A recent report suggests dif- ferences in the tumor suppressor gene P-53 (17). An ex- cess of A:T---~G:C transitions in P-53 were found in Afri-
can-American women with breast cancer compared with
white women with breast cancer from the United States and Scotland (17). Regardless of the stage of diagnosis, poorer survival has been found in African-American women compared with white or Hispanic women (18).
Also, African-American women are more likely to have axillary lymph node involvement and a greater number of
positive lymph nodes than white women (18). Lower so- cioeconomic status was not associated with less favorable histologic findings (16). These studies suggest the possi- bility of more aggressive tumor characteristics, which could be acquired or inherited.
Herein, we reported on the mammographic findings of
breast cancer in African-American women and compared them with those in a white cohort. To our knowledge, the mammographic appearance of breast cancer in African- American women has not been described in the radiology literature. The location of breast carcinoma and breast
density were found to be the same in our two groups and
similar to those seen in previous studies based primarily on non-African-American women. Overall, no statisti- cally significant difference was found between our Afri- can-American and white groups, in whom calcification and masses were found in most cases--similar to the findings of other series based primarily on non-African-
American women (11,19). The frequency of calcifications found alone in our screened African-American population
(41%) was higher than that in our screened white group (16%). However, the frequency of calcifications found alone in our African-American population with nonpalp- able malignancies (44%, 15 of 34 patients) is similar to
that reported in studies of nonpalpable malignancies in predominantly non-African-American women (36% and 41%) (11,19). The screened white patients had more spiculated tumors without calcifications than did our
screened African-American patients (19% vs 0%, P =
.071). These differences in our two race groups are likely related to our small sample size of screened women: 22
and 32, respectively. The frequency of a mass found alone in our screened African-American population, how- ever, was not significantly different from that in our
screened white population (27% vs 44%, P = .292). Also, the frequency of a mass found alone in our African- American population with nonpalpable malignancies
(26%, nine of 34 patients) is similar to that reported in a study of predominantly non-African-American women (26%) (11). Because the mammographic appearance of breast carcinoma in our study is similar between our two race groups and to that reported in predominantly non-
African-American women (11,19), this factor does not
appear to impede mammographic detection. Most malignancies were located in the upper outer
quadrant of the breast, with no differences between the two race groups and similar to the 52% reported in a pri-
marily non-African-American population and the 50% reported in the pathology literature (11,20). The distribu-
tion of malignancies among breast parenchymal patterns in African-American women was also similar among our two groups and to that of other non-African-American populations. Sickles (11) described 40% of nonpalpable malignancies in P1 and P2 patterns, 31% in an N1 pat- tern, and 29% in a DY pattern. Therefore, the density of
the breast and the mammographic location of carcinoma do not appear to represent impediments to mammo- graphic detection.
Invasive ductal carcinoma was the most common his- tologic tumor type. However, there was a statistically sig- nificantly greater percentage of medullary carcinoma in
African-American women than in white women (8% vs 2%, P = .046). This finding has been noted in previous reports of poor African-American women (5). This greater percentage of medullary carcinoma may indicate different tumor characteristics.
In a recent study, mammographic screening was not
found to be protective against later-stage diagnosis in Af- rican-American women (as was found in white women)
(9). The lack of a protective effect of mammography in that study was unexpected because underutilization of
screening mammography and physical examination has frequently been proposed to explain the increased diagno-
sis at late-stage disease in African-American women. The lack of a protective effect of mammography persisted when adjusted for multiple factors, including socioeco- nomic status, access to health care, age, obesity, insur-

ance coverage, menstrual history, and family history (9). Differences in the quality of mammography or mammog- raphy reporting were postulated as possible explanations, as were biologic factors. Delay in diagnosis was not ob- served in our study because women were informed of re- sults at mammography, and all were compliant with the recommended surgical management.
In summary, breast cancer in African-American women was found to be similar to that in a white popula- tion and to that reported in previous studies of primarily white populations with regard to mammographic tumor appearance, location, and breast density. Mammographic differences do not explain the reported lack of benefit of mammography to overcome late-stage diagnosis in Afri- can-American women. The efficacy of mammography in this group has not been completely documented.
kCKNOWLEDGMEN"
We thank Shelley McCarthy for data entry and manu- script preparation.
REFERENCE
1. Coates R J, Gransfield DD, Wesley M, et al. Differences between black and white women with breast cancers in t ime from symp- tom recognit ion to medical consultation: b lack/whi te cancer survival study group. J Natl Cancer Inst 1992; 84:938-950.
2. Elias EG, Suter CM, Brown SD, Buda BS, Vachon DA. Survival dif- ferences between black and white women with breast cancer, J Surg Onco11994; 55:37-41.
3. Caplan LS, Wells BL, Haynes S. Breast cancer screening among older racial /ethnic minorities and whites: barriers to early detec- tion. J C-eronto11992; 47:101-110.
4. Long E. Breast cancer in Afr ican-American women: review of the literature. Cancer Nursing 1993; 16:1-24.
5. Freeman HP, Wasfie TJ. Cancer of the breast in poor black women. Cancer 1989; 63:2562-2569.
6. Sondik EJ. Breast cancer trends: incidence, mortality, and sur- vival. Cancer 1994; 74:995-999.
7. Smigel K. Breast cancer death rates decline for white women. J Natl Cancer Inst 1995; 87:173.
8. U.S. Bureau of the Census. 1990 and 1980 U.S. race and Hispanic origin summary. Washington, DC: U.S, Department of Com- merce, 1990.
9, Jones BA, Stanislav VK, Curnen MC-M, Owens PH, Dubrow R. Can mammography screening explain the race di f ference in stage at diagnosis of breast cancer? Cancer 1995; 75:2103-2113.
10. American Col lege of Radiology. Breast imaging reporting and da ta system (BI-RADS). 2nd ed. Reston, Va: American Col lege of Radiology, 1995.
11. Sickles EA. Mammograph ic features of 300 consecut ive non- palpable breast cancers. A JR 1986; 146:661-663.
12. Burack RC, Gimotty PA, Stengle W, Eckert D, Warbasse L, Moncrease A. Detroit's avoidable mortality project: breast can- cer control for inner city women. Public Health Rep 1989; 104:527-535.
13. Satariano WA, Belle SH, Swanson GM. The severity of breast can- cer at diagnosis: a comparison of age and extent of disease in black and white women. Am J Public Health 1986; 76:779-782.
14. Vernon SW, Tiliey BC, Neale AV, Steinfeldt L. Ethnicity, survival, and delay in seeking t reatment for symptoms of breast cancer. Cancer 1985; 55:1563-1571.
15. Briele HA Jr, Walker M J, Wild L, et al. Results of t reatment of stage I-III breast cancer in black Americans: the Cook County Hospital experience, 1973-1987. Cancer 1990; 65:1062-1067.
16. Chen VW, Correa P, Kurman R J, et al, Histological characteristics of breast carc inoma in blacks and whites. Cancer Epidemiol Biomarkers Prev 1994; 3:127-135.
17. Blaszyk H, Vaughn CB, Hartmann A, et al. Novel pattern of P53 gene mutations in an American black cohort with _high mortality from breast cancer. Lancet 1994; 343:1195-1197.
18. Elledge RM, Clark GM, Chamness GC, Osborne CK. Tumor bio- logic factors and breast cancer prognosis among white, His- panic, and black women in the United States. J Natl Cancer Inst 1994; 86:705-712+
19. Ciaffo S, Cataliott i L, Distante V. Nonpalpable lesions de tec ted with mammography: review of 512 consecut ive cases. Radiol- ogy 1987; 165:99-102.
20. Rosai J. Breast. In: Stamathus G, ed. Ackerman's surgical pathol- ogy. 7th ed. St Louis, Mo: Mosby, 1989; 1216.
Copyright © 2022 FDOKUMEN




















