
Proteomic analysis of purified protein derivative of Mycobacterium tuberculosis

Purified Collagen I Oriented Membrane for Tendon Repair:An Ex Vivo Morphological Study
Antonio Gigante,1 Alberto Busilacchi,1 Barbara Lonzi,2 Stefano Cecconi,1 Sandra Manzotti,1 Chiara Renghini,3
Alessandra Giuliani,4 Monica Mattioli-Belmonte1
1Department of Clinical and Molecular Sciences, School of Medicine, Universita Politecnica delle Marche, Via Tronto 10/60126, Ancona, Italy,2Department of Industrial Engineering and Mathematical Sciences, Universita Politecnica delle Marche, via Brecce Bianche, 60131 Ancona, Italy,3SOMACIS SpA, R&D Department, Castelfidardo, Italy, 4Department of Clinical Sciences and Stomatology, Universita Politecnica delle Marche,via Brecce Bianche, Istituto Nazionale Biostrutture e Biosistemi, CNISM—MATEC, 60131 Ancona, Italy
Received 2 June 2012; accepted 25 October 2012
Published online 17 January 2013 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/jor.22270
ABSTRACT: Injured tendons have limited repair ability after full-thickness lesions. Tendon regeneration properties and adverse reac-tions were assessed ex vivo in an experimental animal model using a new collagen I membrane. The multilamellar membrane obtainedfrom purified equine Achilles tendon is characterized by oriented collagen I fibers and has been shown to sustain cell growth andorientation in vitro. The central third of the patellar tendon (PT) of 10 New Zealand White rabbits was sectioned and grafted with thecollagen membrane; the contralateral PT was cut longitudinally (sham-operated controls). Animals were euthanized 1 or 6 monthsafter surgery, and tendons were subjected to histological and Synchrotron Radiation-based Computed Microtomography (SRmCT)examination and 3D structure analysis. Histological and SRmCT findings showed satisfactory graft integration with native tendon.Histological examination also showed ongoing angiogenesis. Adverse side-effects (inflammation, rejection, calcification) were notobserved. The multilamellar collagen I membrane can be considered as an effective tool for tendon defect repair and tendon augmenta-tion. � 2013 Orthopaedic Research Society. Published by Wiley Periodicals, Inc. J Orthop Res 31:738–745, 2013
Keywords: tendon repair; tendon augmentation; collagen; SRmCT; bioscaffold
Tendons and ligaments have poor spontaneous regen-eration ability and never completely recover from full-thickness lesions, be they treated conservatively orsurgically.1 Several common approaches to tendon rup-ture involve surgical repair; this entails working ondegenerative, frayed, atrophic or metaplastic tendontissue2 that is unable to sustain the mechanical stressof normal activities, leading to a high risk of re-fail-ure.3 Research has been conducted for decades to findsuitable materials to reinforce or even substitute dam-aged tendons. A range of autografts, allografts, xeno-grafts, and synthetic prostheses have been tried fortendon augmentation.4 Autografts remain the goldstandard of tendon and ligament reconstruction, sinceautologous tissue is endowed with excellent compati-bility and possesses high mechanical strength and thepropensity to revascularize and remodel when trans-planted.5 Although autografts have been advocated asideal substitutes, the substantial donor site morbidityinvolved has encouraged the search for alternativesolutions.4
As far back as 1903, Lange used silk to augmentthe semitendinosus, albeit without success.6 In 1914,Corner employed silver wires.7 More recently, synthet-ic tissues such as carbon fibers,8 Gore-Tex1,9 andLARS110 have been introduced. All were described assuitable tendon replacement materials; however, hun-dreds of surgical procedures eventually highlightedendurance and durability problems related to frictional
characteristics11 and a number of side-effects rangingfrom immunogenic reactions to necrotic phenomena,12
decreeing the failure of artificial substitutes. At thesame time cadaveric allografts, mainly employed intendon revision procedures, were seen to give rise tocomplications due to incomplete decellularization anddeantigenation, besides being limited in supply.
Improved outcomes were achieved in the early1990s with the introduction of collagen membranes,among which porcine small intestinal submucosa (SIS)is considered the forerunner of biological products.13
Current biological scaffolds are obtained by processingmammalian (human, porcine, bovine, and equine) tis-sues like SIS, dermis, pericardium, and equine tendon.Their properties have gradually been improved as aresult of in vitro and in vivo studies.3,14 Tendon substi-tutes must be devoid of any factor that could inducerejection or inflammatory responses and must possessintrinsic resistance to cyclic mechanical stress or atleast help the residual healthy tissue to bear part ofthe load. Scaffolds must be resorbable and capable ofdriving and correctly modulating tenocyte behavior.Fiber shape and alignment, which confer mechanicalproperties, are therefore critical in engineering re-placement constructs.
This ex vivo study assesses the tendon regenerationability of a new oriented collagen I membrane in anexperimental animal model using histological and Syn-chrotron Radiation-based Computed Microtomography(SRmCT) examination and 3D structure analysis.
MATERIALSCollagen MembranesOriented collagen I membranes were manufactured by OpocrinSpA (Corlo di Formigine, Italy) according to a proprietary
Additional supporting information may be found in the onlineversion of this article.Correspondence to: Antonio Gigante (T: þ39-071-220-6069;F: þ39-071-220-6066; E-mail: [email protected])
� 2013 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
738 JOURNAL OF ORTHOPAEDIC RESEARCH MAY 2013

method (EU Pat. No. WO/2007/115974). The production pro-cess15 uses purified equine Achilles tendon collagen to pro-vide a biocompatible, non-immunogenic, non-cytotoxic, andnon-sensitizing membrane.15,16 In brief, oriented multilamel-lar membranes were prepared by pouring successive collagengel layers onto electrostatically charged trays, and partiallydrying each layer before pouring the next. The gel was deaer-ated under vacuum to remove air microbubbles, subjected toplanetary agitation, and then left under vacuum without agi-tation.10 Membranes were sterilized with gamma irradiation(25 kGy), dipped in sterile saline buffer for 5 min before im-plantation for easier handling (Fig. 1), and finally cut to le-sion size.
Surgical ProcedureTwelve male New Zealand rabbits (Harlan Laboratories,Udine, Italy) weighing 3 � 0.5 kg, selected for the similaritybetween the rodent and human knee extensor system,17 wereused. The experimental protocol was approved by the ItalianHealth Ministry; the policies and procedures used agreedwith those detailed in directive 86/609/EEC. Antibiotic pro-phylaxis with intramuscular (i.m.) enrofloxacin (20 mg/kg)was started prior to surgery and administered for 7 days.Animals were anesthetized with an i.m. injection of ketamine(20 mg/kg), medetomidine (0.3 mg/kg), and diazepam (0.75–1.5 mg/kg). The shaved cutis overlying both knees wasdissected under sterile conditions; the central third of thepatellar tendon (PT) was explanted without removing anybony part of the patella or of the tibial tubercle (Fig. 2), care-fully avoiding vessels and fat pads, whose lesion is associatedwith postoperative pain, bleeding, and formation of
adhesions. The size of the tendon lesion was 3 cm � 0.5 cmaccording to Karaglou.18 In each animal, one tendon wasgrafted with the collagen membrane, which was sutured(Ethilon 4:0, Ethicon, Inc., Johnson & Johnson, Somerville,NJ) to the upper (one suture) and lower (one suture) patellarpole and at the paramedian level (one or two sutures) to en-sure correct adhesion to tendon tissue. The contralateral ten-don was only cut longitudinally (sham-operated control). Thehole left by the suture was used as a landmark for postopera-tive discrimination of native from newly formed tendon(Fig. 3a).
Each procedure was rated using a 3-point scale, that wecalled Surgical Quality Score (SQS), to describe the quality/accuracy/amount of the surgical access, anesthesia, PT exci-sion, bleeding, and surgical wound (see Supplementary Mate-rial SI). Subjects were returned to their individual cages(155 cm width � 840 cm length � 184 cm height), fed ad libi-tum, and allowed unrestricted activity; wounds were medi-cated every 2 days. Animals were euthanized after 1 or6 months (4 and 8 rabbits, respectively), and the entire PT,including the lower patellar pole and the tibial tubercle, washarvested. Four animals per time point were used for histo-logical investigations and two for SRmCT examination.
Histological EvaluationPT specimens were fixed in 4% paraformaldehyde overnight.After washes in PBS they were paraffin-embedded. Serialdecalcified paraffin sections 6 mm in thickness were stainedwith hematoxylin–eosin, Alcian Blue, Gomori’s trichrome, andHalmi’s aldehyde fuchsin trichrome and examined with aDMRBE Leitz light microscope (Leica Microsystem, Wetzlar,
Figure 1. Collagen I membrane before (b) and after (a) 30 minhydration in sterile saline. Figure 2. (a) Intraoperative image of the treated tendon. (b)
Gross appearance of the entire patellar tendon harvested at6 months. The nylon suture to native tendon is still visible (!).
COLLAGEN I MEMBRANE FOR TENDON AUGMENTATION 739
JOURNAL OF ORTHOPAEDIC RESEARCH MAY 2013

Germany). Histological changes in tendon structure were ratedby two blinded observers in 5 fields/section (3 sections/lesion)using the Movin scale.19 This 4-point scale (0 ¼ normal;1 ¼ slightly abnormal; 2 ¼ abnormal; 3 ¼ markedly abnor-mal), originally developed to assess tendinopathic changes,was applied to describe the repair process in healing tendonsrather than degenerative tissue changes.
Synchrotron Radiation-Based mCT EvaluationTreated and control samples from the rabbits euthanized6 months after surgery were fixed and embedded in paraffin.
Non-destructive imaging and quantification of 3D micro-structural morphology of samples was obtained using anSRmCT system, available at the SYRMEP beamline of theELETTRA Synchrotron Radiation Facility (Trieste, Italy).Morphometric parameters and tendon density were deter-mined in regions of interest (ROI) having a volume of315 mm � 360 mm � 360 mm selected in treated (22 sub-vol-umes in native tissue and 22 sub-volumes at the level of theimplant) and control tendons (11 in native tissue and 11 atthe level of the lesion). Quantitative analysis included extrac-tion of the parameters listed in Table I. The thickness distri-bution of treated and sham-operated tendon fibers wascompared in another SRmCT experiment performed at theID19 beamline of the European Synchrotron Radiation Facil-ity (ESRF, Grenoble, France).
The acquisition setup of the two experiments, based onpreviously described 3D parallel tomography studies,20,21 isdetailed in the supplementary material (SII). Since both mCTexperiments were performed in absorption conditions, thegray levels in the 3D images, which represent samples’ linearabsorption coefficient (expressed in cm�1), are not uniform inthe tissue. Only areas strictly ascribable to the tissue weretherefore considered, whereas those close to the tissue bor-ders were not investigated, to exclude peripheral voxels. Thereconstructed gray levels of the X-ray mCT images wererelated to the tissue physical density (gColI/cm3) using a the-oretical relationship validated with experimental data.22
Statistical AnalysesAnalyses were performed with the SigmaStat 3.5 software(Systat Software, San Jose, CA). The four fiber groups,Treated Tendon@Native tissue (Trt-Nt); Treated Tendon@-Membrane site (Trt-Ms); Control Tendon@Native tissue(Ctr-Nt); and Control Tendon@Lesion site (Ctr-Ls), werecross-compared using ANOVA followed by multiple compari-son tests. Significance was set at p < 0.05.
RESULTS
Gross ExaminationThe mean SQS was 8.6. Gross examination at 6 monthsdisclosed good implant integration with native tendon(Fig. 2b).
HistologyOne month after implantation, fibroblast-like cellswere detected both on the surface and in the deeplayers of the collagen membrane. At 6 months, theydisplayed a better orientation along the collagen scaf-fold, with a reduction in cell density. Satisfactory
Figure 3. Histological micrographs of treated tendon at 6months: (a) integration of the collagen membrane (�) to nativetendon is visible at low magnification; the hole (H) was previous-ly occupied by the nylon suture; (b) detail of the previous imageshowing the tendon-membrane interface at 6 months. Implantintegration is demonstrated by the superimposition (!) of themembrane (blue/green) on native tissue. Scale bars ¼ 100 mm
Table I. 3D Parameters Included in mCT Quantitative Analysis
Parameter Abbreviation Unit
Tendon volume TdV mm3
Total volume of interest TotV mm3
Tendon volume to total volume ratio TdV/TotV %Tendon surface to tendon volume ratio TdS/TdV mm�1
Tendon thickness TdTh mmTendon number TdN mm�1
Tendon separation TdSp mmTendon (physical) density TdD mgColI/cm3
740 GIGANTE ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH MAY 2013
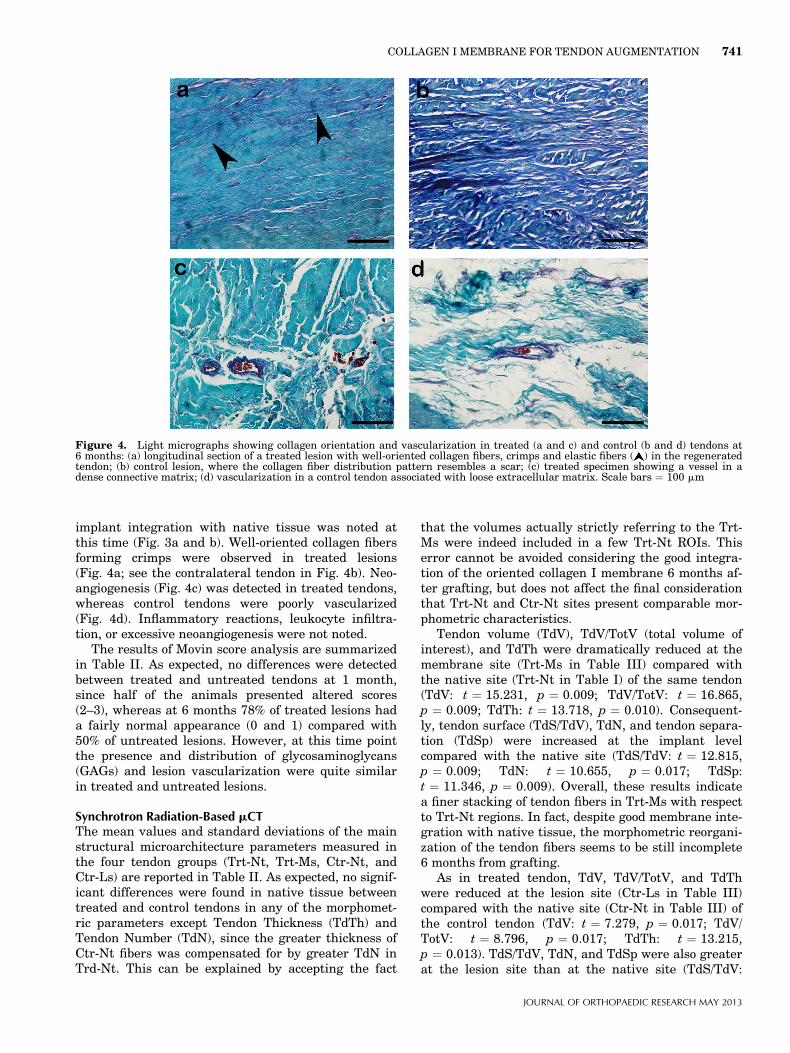
implant integration with native tissue was noted atthis time (Fig. 3a and b). Well-oriented collagen fibersforming crimps were observed in treated lesions(Fig. 4a; see the contralateral tendon in Fig. 4b). Neo-angiogenesis (Fig. 4c) was detected in treated tendons,whereas control tendons were poorly vascularized(Fig. 4d). Inflammatory reactions, leukocyte infiltra-tion, or excessive neoangiogenesis were not noted.
The results of Movin score analysis are summarizedin Table II. As expected, no differences were detectedbetween treated and untreated tendons at 1 month,since half of the animals presented altered scores(2–3), whereas at 6 months 78% of treated lesions hada fairly normal appearance (0 and 1) compared with50% of untreated lesions. However, at this time pointthe presence and distribution of glycosaminoglycans(GAGs) and lesion vascularization were quite similarin treated and untreated lesions.
Synchrotron Radiation-Based mCTThe mean values and standard deviations of the mainstructural microarchitecture parameters measured inthe four tendon groups (Trt-Nt, Trt-Ms, Ctr-Nt, andCtr-Ls) are reported in Table II. As expected, no signif-icant differences were found in native tissue betweentreated and control tendons in any of the morphomet-ric parameters except Tendon Thickness (TdTh) andTendon Number (TdN), since the greater thickness ofCtr-Nt fibers was compensated for by greater TdN inTrd-Nt. This can be explained by accepting the fact
that the volumes actually strictly referring to the Trt-Ms were indeed included in a few Trt-Nt ROIs. Thiserror cannot be avoided considering the good integra-tion of the oriented collagen I membrane 6 months af-ter grafting, but does not affect the final considerationthat Trt-Nt and Ctr-Nt sites present comparable mor-phometric characteristics.
Tendon volume (TdV), TdV/TotV (total volume ofinterest), and TdTh were dramatically reduced at themembrane site (Trt-Ms in Table III) compared withthe native site (Trt-Nt in Table I) of the same tendon(TdV: t ¼ 15.231, p ¼ 0.009; TdV/TotV: t ¼ 16.865,p ¼ 0.009; TdTh: t ¼ 13.718, p ¼ 0.010). Consequent-ly, tendon surface (TdS/TdV), TdN, and tendon separa-tion (TdSp) were increased at the implant levelcompared with the native site (TdS/TdV: t ¼ 12.815,p ¼ 0.009; TdN: t ¼ 10.655, p ¼ 0.017; TdSp:t ¼ 11.346, p ¼ 0.009). Overall, these results indicatea finer stacking of tendon fibers in Trt-Ms with respectto Trt-Nt regions. In fact, despite good membrane inte-gration with native tissue, the morphometric reorgani-zation of the tendon fibers seems to be still incomplete6 months from grafting.
As in treated tendon, TdV, TdV/TotV, and TdThwere reduced at the lesion site (Ctr-Ls in Table III)compared with the native site (Ctr-Nt in Table III) ofthe control tendon (TdV: t ¼ 7.279, p ¼ 0.017; TdV/TotV: t ¼ 8.796, p ¼ 0.017; TdTh: t ¼ 13.215,p ¼ 0.013). TdS/TdV, TdN, and TdSp were also greaterat the lesion site than at the native site (TdS/TdV:
Figure 4. Light micrographs showing collagen orientation and vascularization in treated (a and c) and control (b and d) tendons at6 months: (a) longitudinal section of a treated lesion with well-oriented collagen fibers, crimps and elastic fibers ( ) in the regeneratedtendon; (b) control lesion, where the collagen fiber distribution pattern resembles a scar; (c) treated specimen showing a vessel in adense connective matrix; (d) vascularization in a control tendon associated with loose extracellular matrix. Scale bars ¼ 100 mm
COLLAGEN I MEMBRANE FOR TENDON AUGMENTATION 741
JOURNAL OF ORTHOPAEDIC RESEARCH MAY 2013

t ¼ 8.547, p ¼ 0.017; TdN: t ¼ 12.072, p ¼ 0.009;TdSp: t ¼ 3.776, p ¼ 0.017). Altogether, these datapoint to incomplete morphometric reorganization ofthe tendon fibers 6 months from lesion, as seen intreated tendons.
Finally, comparison of the implant site of thetreated tendon with the lesion area of the control ten-don showed lower TdV and TdV/TotV in Trt-Ms thanin Ctr-Ls (TdV: t ¼ 3.050, p ¼ 0.025; TdV/TotV:
t ¼ 4.768, p ¼ 0.025). Similarly TdS/TdV, TdN, andTdSp were greater at the implant level than at thelesion site (TdS/TdV: t ¼ 1.584, p ¼ 0.025; TdN:t ¼ 2.645, p ¼ 0.025; TdSp: t ¼ 5.609, p ¼ 0.013).These data indicate finer fiber stacking in the treatedtendon compared to the lesion site of the control ten-don but, interestingly, the morphometric parameterTdTh was not significantly different between treatedand control tendons either at the implant site or at the
Table II. Movin Score Distribution
Variable
Tendon Sections (1 Month; N ¼ 12)
Treated Control
t p Power (%)Mean � SD Mean � SD
Fiber structure 1.50 � 1.17 2.75 � 0.45 3.46 0.005 89Fiber arrangement 1.50 � 0.52 2.25 � 0.45 3.76 0.003 95Rounding of the nuclei 0.25 � 0.45 1.25 � 0.87 3.55 0.005 92Regional changes in cellularity 2.75 � 0.45 1.50 � 0.52 6.27 0.000 99Increased vascularity 2.50 � 0.52 1.25 � 0.45 6.27 0.000 99Decreased collagen stainability 0 � 0 2.00 � 0.74 9.38 0.000 100Hyalinization 0.75 � 0.45 1.75 � 0.45 5.42 0.000 99GAGs 2.75 � 0.45 1.25 � 0.45 8.12 0.000 100
Variable
Tendon Sections (6 Months; N ¼ 24)
Treated Control
t p Power (%)Mean � SD Mean � SD
Fiber structure 0.37 � 0.49 2.85 � 0.34 20.45 0.000 100Fiber arrangement 0.25 � 0.44 2.65 � 0.49 17.54 0.000 100Rounding of the nuclei 0.37 � 0.71 1.50 � 0.72 5.44 0.000 99Regional changes in cellularity 1.37 � 0.88 1.50 � 0.52 0 1.000 /Increased vascularity 1.25 � 0.85 0.87 � 0.61 1.76 0.092 33Decreased collagen stainability 0 � 0 1.50 � 0.72 10.17 0.000 100Hyalinization 0.62 � 0.71 1.50 � 0.51 4.90 0.000 99GAGs 1.37 � 0.49 1.50 � 0.51 0.86 0.398 14
0 ¼ normal; 1 ¼ slightly abnormal; 2 ¼ abnormal; and 3 ¼ markedly abnormal. The total semiquantitative histological score for a givenslide can range from 0 (normal tendon) to 24 (the most severe abnormality detectable). GAGs, glycosaminoglycans.
Table III. Morphometric Parameters of Tendon Microarchitecture
Treated Tendon Control Tendon
Native Tissue (Trt-Nt) Membrane Site (Trt-Ms) Native Tissue (Ctr-Nt) Lesion Site (Ctr-Ls)
Mean SD Mean SD Mean SD Mean SD
TdV 0 (mm3) 3.66Eþ07 0.33Eþ07 1.85Eþ07 0.39Eþ07 3.51Eþ07 0.15Eþ07 2.29Eþ07 0.67Eþ07TdV/TotV (%) 88.2 4.7 43.8 8.4 92.0 4.2 59.2 16.1TdTh (mm) 83.57 12.94 23.99 5.07 112.06 25.27 30.88 15.58TdS/TdV (mm�1) 2.45E�02 0.39E�02 8.70E�02 1.86E�02 1.86E�02 0.39E�02 7.75E�02 2.90E�02TdN (mm�1) 1.08E�02 0.13E�02 2.09E�02 0.25E�02 0.84E�02 0.17E�02 1.85E�02 0.40E�02TdSp (mm) 10.75 3.61 31.27 8.25 9.19 4.66 18.85 5.58
SD, standard deviation; TdV, tendon volume; TotV, total volume of interest; TdV/TotV, tendon volume to total volume ratio; TdS/TdV,tendon surface to tendon volume ratio; TdTh, tendon thickness; TdN, tendon number; TdSp, tendon separation.
742 GIGANTE ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH MAY 2013
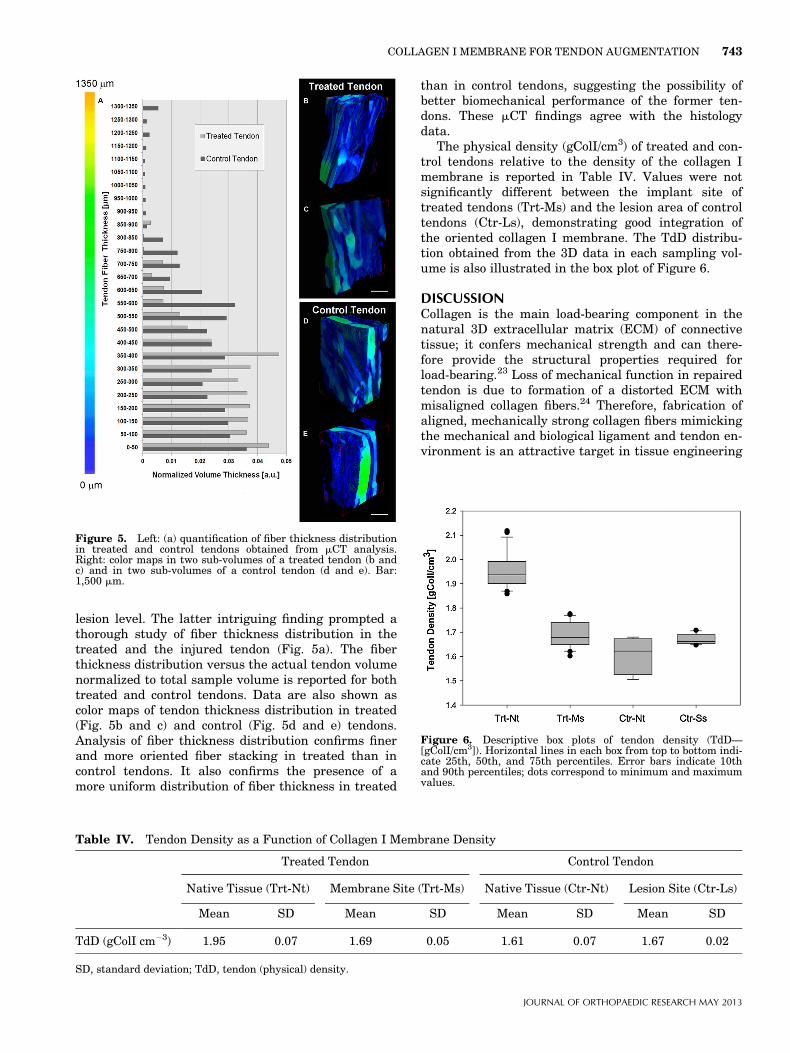
lesion level. The latter intriguing finding prompted athorough study of fiber thickness distribution in thetreated and the injured tendon (Fig. 5a). The fiberthickness distribution versus the actual tendon volumenormalized to total sample volume is reported for bothtreated and control tendons. Data are also shown ascolor maps of tendon thickness distribution in treated(Fig. 5b and c) and control (Fig. 5d and e) tendons.Analysis of fiber thickness distribution confirms finerand more oriented fiber stacking in treated than incontrol tendons. It also confirms the presence of amore uniform distribution of fiber thickness in treated
than in control tendons, suggesting the possibility ofbetter biomechanical performance of the former ten-dons. These mCT findings agree with the histologydata.
The physical density (gColI/cm3) of treated and con-trol tendons relative to the density of the collagen Imembrane is reported in Table IV. Values were notsignificantly different between the implant site oftreated tendons (Trt-Ms) and the lesion area of controltendons (Ctr-Ls), demonstrating good integration ofthe oriented collagen I membrane. The TdD distribu-tion obtained from the 3D data in each sampling vol-ume is also illustrated in the box plot of Figure 6.
DISCUSSIONCollagen is the main load-bearing component in thenatural 3D extracellular matrix (ECM) of connectivetissue; it confers mechanical strength and can there-fore provide the structural properties required forload-bearing.23 Loss of mechanical function in repairedtendon is due to formation of a distorted ECM withmisaligned collagen fibers.24 Therefore, fabrication ofaligned, mechanically strong collagen fibers mimickingthe mechanical and biological ligament and tendon en-vironment is an attractive target in tissue engineering
Figure 5. Left: (a) quantification of fiber thickness distributionin treated and control tendons obtained from mCT analysis.Right: color maps in two sub-volumes of a treated tendon (b andc) and in two sub-volumes of a control tendon (d and e). Bar:1,500 mm.
Table IV. Tendon Density as a Function of Collagen I Membrane Density
Treated Tendon Control Tendon
Native Tissue (Trt-Nt) Membrane Site (Trt-Ms) Native Tissue (Ctr-Nt) Lesion Site (Ctr-Ls)
Mean SD Mean SD Mean SD Mean SD
TdD (gColI cm�3) 1.95 0.07 1.69 0.05 1.61 0.07 1.67 0.02
SD, standard deviation; TdD, tendon (physical) density.
Figure 6. Descriptive box plots of tendon density (TdD—[gColI/cm3]). Horizontal lines in each box from top to bottom indi-cate 25th, 50th, and 75th percentiles. Error bars indicate 10thand 90th percentiles; dots correspond to minimum and maximumvalues.
COLLAGEN I MEMBRANE FOR TENDON AUGMENTATION 743
JOURNAL OF ORTHOPAEDIC RESEARCH MAY 2013

products for tendon healing. Aligned collagen fiberscaffolds based on self-assembled collagen were firstdescribed by Kato et al.25 More recently, Baker et al.26
showed on the nano and the microscale how fibrousconstruct alignment is capable of guiding tissue align-ment, providing a useful scaffold. The collagen I mem-brane tested in this study has an oriented fiberscaffold both on the microscale (as shown by mCT mor-phometric analysis) and on the nanoscale.16 Previousin vitro studies16 showed its ability to sustain cell via-bility and proliferation; its correct fiber orientationprovides an instructive pattern for cell growth anddrives cell alignment mimicking that seen in normaltendon. Our experiments showed that it also promotestendon healing. Histological and mCT examination dis-closed properly arranged collagen fibers and the lackof inflammatory cell infiltration in treated lesions,even though it demonstrated incomplete tendonremodeling at 6 months. Fibroblasts and capillariesgradually increased, and collagen became more dense-ly and regularly packed as healing progressed. Withregard to vascularization, an adequate blood supply isneeded to bring nutrients and growth factors to thehealing site, since blood-derived mesenchymal cellsand fibroblasts are critical in the early healingphase.26,27 The role of collagen orientation in tendonhealing is emphasized by studies showing how the par-allel fiber arrangement is to a large extent responsiblefor normal tensile strength.28 Disorganized collagenfibrils are generally indicative of poor healing and con-tribute to poor tendon biomechanics.29,30
A major concern in biological and synthetic scaffoldsis biocompatibility and the inflammatory response as-sociated with foreign body reaction.31 Even though bio-logical scaffolds are increasingly used, data fromwell-conducted clinical human studies describing com-plications or adverse events are insufficient. Malcar-ney32 observed a chronic inflammatory pattern aroundthe implant in 25% of cases treated with collagenmembranes, and Iannotti et al.33 described high re-rupture rates in treated tendons reinforced with bio-logical scaffolds. Depending on the product, processingmay involve acellularization, chemical cross-linking,and lamination of multiple layers or lyophilization.34
The present membrane is acellular, not chemicallycross-linked, and contains no proinflammatory mole-cules such as free DNA or elastin.15 Elastin, despiteits useful tissue restoration properties, like its chemo-tactic action on leukocytes, stimulation of fibroblastand smooth muscle cell proliferation, and proangio-genic activity, can contribute to creating a chronicinflammatory state.35 Such features increase thebiocompatibility and resorbability of the collagen mem-brane and reduce the scope for adverse reactions.
In conclusion, this experimental ex vivo study sup-ports the notion that the multilamellar collagen Imembrane tested here facilitates tendon healingwithout adverse side-effects, thus proving to be auseful tool for tendon augmentation. The term
‘‘augmentation’’ is commonly used in the literature toindicate scaffolds devised to reinforce weak or torntendons; therefore, none of the scaffolds currentlyavailable on the market can be defined as ‘‘substi-tutes’’, because biological restoration has never beenreported. The encouraging findings of this study haveprompted a new, extensive experimental study, nowbeing designed, directed at gaining further insightsinto the functional and biomechanical aspects of thismultilamellar collagen I membrane.
ACKNOWLEDGMENTSNo external funding was received apart from support by theauthors’ Institutions. No benefits in any form have been orwill be received from a commercial party directly or indirect-ly related to the subject of this article. The authors thankDr. Bruna Parma (Opocrin SpA, Corlo di Formigine, Italy)for providing the collagen I membranes, Dr. FiorenzaOrlando for veterinary controls, and Dr. Silvia Modena forlanguage revision. The authors are grateful to ELETTRA(Trieste, Italy) and ESRF (Grenoble, France) User Offices forproviding beam-time, to Dr. Giuliana Tromba for technicalsupport during the ELETTRA mCT experiments, and toDr. Paul Tafforeau for technical support during the ESRFmCT experiments.
REFERENCES1. Lin TW, Cardenas L, Soslowsky LJ. 2004. Biomechanics of
tendon injury and repair. J Biomech 37:865–877.2. Gigante A, Marinelli M, Chillemi C, et al. 2004. Fibrous
cartilage in the rotator cuff: a pathogenetic mechanism oftendon tear? J Shoulder Elbow Surg 13:328–332.
3. Longo UG, Lamberti A, Petrillo S, et al. 2012. Scaffoldsin tendon tissue engineering. Stem Cells Int 2012:517165.
4. Longo UG, Lamberti A, Maffulli N, et al. 2010. Tendon aug-mentation grafts: a systematic review. Br Med Bull 94:165–188.
5. Janssen RP, van der Wijk J, Fiedler A, et al. 2011. Remodel-ling of human hamstring autografts after anterior cruciateligament reconstruction. Knee Surg Sports TraumatolArthrosc 19:1299–1306.
6. Lange F. 1903. Uber die Sehnenplastik. Verh Dtsch OrthopGes 2:10–12.
7. Corner EM. 1914. Notes of a case illustrative of an artificialanterior crucial ligament, demonstrating the action of thatligament. Proc R Soc Med 7:120–121.
8. Jenkins DH, McKibbin B. 1980. The role of flexible carbon-fibre implants as tendon and ligament substitutes in clinicalpractice. A preliminary report. J Bone Joint Surg Br 62-B:497–499.
9. Bolton CW, Bruchman WC. 1985. The GORE-TEX expandedpolytetrafluoroethylene prosthetic ligament. An in vitroand in vivo evaluation. Clin Orthop Relat Res 196:202–213.
10. Naim S, Gougoulias N, Griffiths D. 2011. Patellar tendon re-construction using LARS ligament: surgical technique andcase report. Strategies Trauma Limb Reconstr 6:39–41.
11. Thomas JM, Beevers D, Dowson D, et al. 2011. The bio-tri-bological characteristics of synthetic tissue grafts. Proc InstMech Eng H 225:141–148.
12. McKibbin B. 1984. Carbon fibre as a surgical implant. JBone Joint Surg Br 66:157–158.
13. Badylak SF, Lantz GC, Coffey A, et al. 1989. Small intesti-nal submucosa as a large diameter vascular graft in the dog.J Surg Res 47:74–80.
744 GIGANTE ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH MAY 2013

14. Badylak SF, Record R, Lindberg K, et al. 1998. Small intesti-nal submucosa: a substrate for in vitro cell growth. J Bio-mater Sci Polym Ed 9:863–878.
15. Bianchini P, Parma B. 2001. Immunological safety evalua-tion of a horse collagen haemostatic pad. Arzneimittelfor-schung 51:414–419.
16. Gigante A, Cesari E, Busilacchi A, et al. 2009. Collagen Imembranes for tendon repair: effect of collagen fiber orienta-tion on cell behavior. J Orthop Res 27:826–832.
17. Gomes-Barrena E, Fernandes-Baillo N. 2001. La rodila en elanimal de experimentacion. Morfologia y cinematica compa-radas y su applicacion a los modelos esperimentales derodila. Rev Ortop Trauma 35:100–112.
18. Karaoglu S, BF M, Woo SL, et al. 2008. Use of a bioscaffoldto improve healing of a patellar tendon defect after graftharvest for ACL reconstruction: a study in rabbits. J OrthopRes 26:255–263.
19. Maffulli N, Longo UG, Franceschi F, et al. 2008. Movin andbonar scores assess the same characteristics of tendon histol-ogy. Clin Orthop Relat Res 466:1605–1611.
20. Salome M, Peyrin F, Cloetens P, et al. 1999. A synchrotronradiation microtomography system for the analysis of trabec-ular bone samples. Med Phys 26:2194–2204.
21. Tavella S, Ruggiu A, Giuliani A, et al. 2012. Bone turnoverin wild type and pleiotrophin-transgenic mice housed forthree months in the International Space Station (ISS). PLoSONE 7:e33179.
22. Nuzzo S, Peyrin F, Cloetens P, et al. 2002. Quantification ofthe degree of mineralization of bone in three dimensionsusing synchrotron radiation microtomography. Med Phys29:2672–2681.
23. Buehler MJ. 2006. Nature designs tough collagen: explain-ing the nanostructure of collagen fibrils. Proc Natl Acad SciUSA 103:12285–12290.
24. Bi Y, Ehirchiou D, Kilts TM, et al. 2007. Identification oftendon stem/progenitor cells and the role of the extracellularmatrix in their niche. Nat Med 13:1219–1227.
25. Kato YP, Christiansen DL, Hahn RA, et al. 1989. Mechani-cal properties of collagen fibres: a comparison of reconsti-tuted and rat tail tendon fibres. Biomaterials 10:38–42.
26. Baker BM, Mauck RL. 2007. The effect of nanofiber align-ment on the maturation of engineered meniscus constructs.Biomaterials 28:1967–1977.
27. Kajikawa Y, Morihara T, Watanabe N, et al. 2007. GFP chi-meric models exhibited a biphasic pattern of mesenchymalcell invasion in tendon healing. J Cell Physiol 210:684–691.
28. Thomopoulos S, Marquez JP, Weinberger B, et al. 2006. Col-lagen fiber orientation at the tendon to bone insertion andits influence on stress concentrations. J Biomech 39:1842–1851.
29. Galatz LM, Sandell LJ, Rothermich SY, et al. 2006. Charac-teristics of the rat supraspinatus tendon during tendon-to-bone healing after acute injury. J Orthop Res 24:541–550.
30. Rosenbaum AJ, Wicker JF, Dines JS, et al. 2010. Histologicstages of healing correlate with restoration of tensilestrength in a model of experimental tendon repair. HSS J6:164–170.
31. Barber FA, Herbert MA, Coons DA, et al. 2006. Suturesand suture anchors—update 200. Arthroscopy 22:1063 e1–1063 e9.
32. Malcarney HL, Bonar F, Murrell GA. 2005. Early inflamma-tory reaction after rotator cuff repair with a porcine smallintestine submucosal implant: a report of 4 cases. Am JSports Med 33:907–911.
33. Iannotti JP, Codsi MJ, Kwon YW, et al. 2006. Porcine smallintestine submucosa augmentation of surgical repair ofchronic two-tendon rotator cuff tears. A randomized, con-trolled trial. J Bone Joint Surg Am 88:1238–1244.
34. Aurora A, McCarron J, Iannotti JP, et al. 2007. Commercial-ly available extracellular matrix materials for rotator cuffrepairs: state of the art and future trends. J Shoulder ElbowSurg 16:S171–S178.
35. Antonicelli F, Bellon G, Debelle L, et al. 2007. Elastin-elastases and inflamm-aging. Curr Top Dev Biol 79:99–155.
COLLAGEN I MEMBRANE FOR TENDON AUGMENTATION 745
JOURNAL OF ORTHOPAEDIC RESEARCH MAY 2013
Copyright © 2022 FDOKUMEN




















