Has Clinical and Epidemiological Varicella Burden ... - MDPI
Upload
khangminh22Category
view
0download
0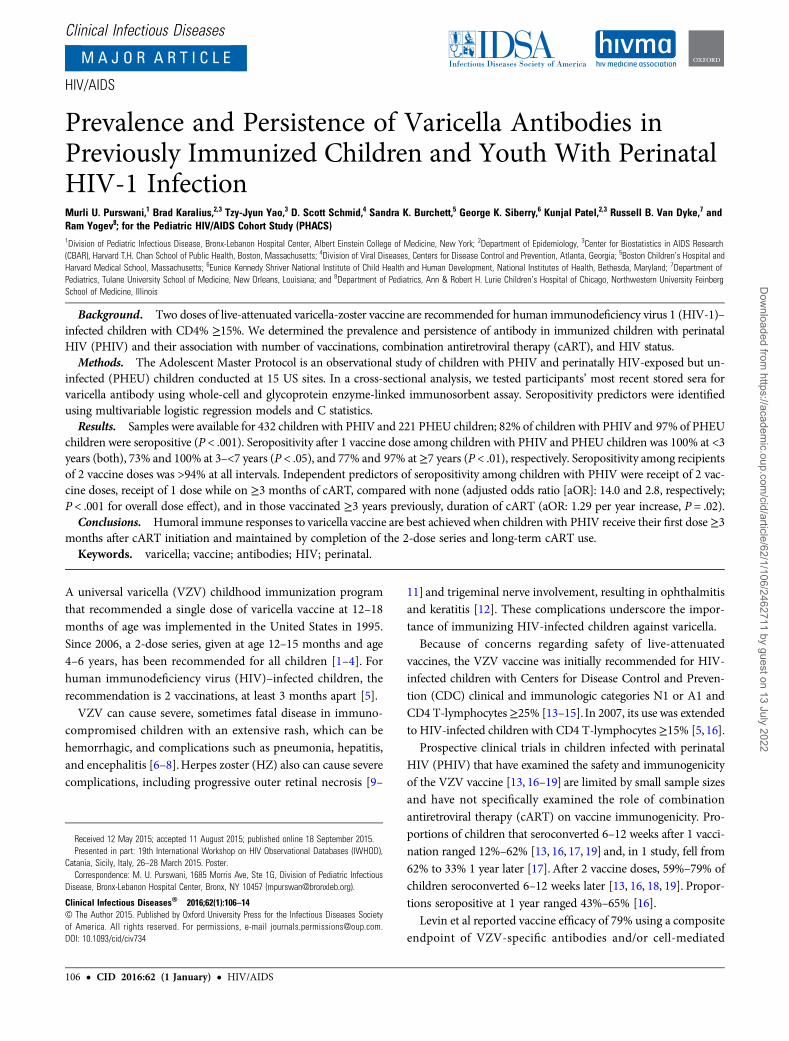
Clinical Infectious Diseases
M A J O R A R T I C L E
HIV/AIDS
Prevalence and Persistence of Varicella Antibodies inPreviously Immunized Children and Youth With PerinatalHIV-1 InfectionMurli U. Purswani,1 Brad Karalius,2,3 Tzy-Jyun Yao,3 D. Scott Schmid,4 Sandra K. Burchett,5 George K. Siberry,6 Kunjal Patel,2,3 Russell B. Van Dyke,7 andRam Yogev8; for the Pediatric HIV/AIDS Cohort Study (PHACS)1Division of Pediatric Infectious Disease, Bronx-Lebanon Hospital Center, Albert Einstein College of Medicine, New York; 2Department of Epidemiology, 3Center for Biostatistics in AIDS Research(CBAR), Harvard T.H. Chan School of Public Health, Boston, Massachusetts; 4Division of Viral Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia; 5Boston Children’s Hospital andHarvard Medical School, Massachusetts; 6Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, Bethesda, Maryland; 7Department ofPediatrics, Tulane University School of Medicine, New Orleans, Louisiana; and 8Department of Pediatrics, Ann & Robert H. Lurie Children’s Hospital of Chicago, Northwestern University FeinbergSchool of Medicine, Illinois
Background. Two doses of live-attenuated varicella-zoster vaccine are recommended for human immunodeficiency virus 1 (HIV-1)–infected children with CD4% ≥15%. We determined the prevalence and persistence of antibody in immunized children with perinatalHIV (PHIV) and their association with number of vaccinations, combination antiretroviral therapy (cART), and HIV status.
Methods. The Adolescent Master Protocol is an observational study of children with PHIV and perinatally HIV-exposed but un-infected (PHEU) children conducted at 15 US sites. In a cross-sectional analysis, we tested participants’ most recent stored sera forvaricella antibody using whole-cell and glycoprotein enzyme-linked immunosorbent assay. Seropositivity predictors were identifiedusing multivariable logistic regression models and C statistics.
Results. Samples were available for 432 children with PHIV and 221 PHEU children; 82% of children with PHIV and 97% of PHEUchildren were seropositive (P < .001). Seropositivity after 1 vaccine dose among children with PHIV and PHEU children was 100% at <3years (both), 73% and 100% at 3–<7 years (P < .05), and 77% and 97% at ≥7 years (P < .01), respectively. Seropositivity among recipientsof 2 vaccine doses was >94% at all intervals. Independent predictors of seropositivity among children with PHIV were receipt of 2 vac-cine doses, receipt of 1 dose while on ≥3 months of cART, compared with none (adjusted odds ratio [aOR]: 14.0 and 2.8, respectively;P < .001 for overall dose effect), and in those vaccinated ≥3 years previously, duration of cART (aOR: 1.29 per year increase, P = .02).
Conclusions. Humoral immune responses to varicella vaccine are best achieved when children with PHIV receive their first dose ≥3months after cART initiation and maintained by completion of the 2-dose series and long-term cART use.
Keywords. varicella; vaccine; antibodies; HIV; perinatal.
A universal varicella (VZV) childhood immunization programthat recommended a single dose of varicella vaccine at 12–18months of age was implemented in the United States in 1995.Since 2006, a 2-dose series, given at age 12–15 months and age4–6 years, has been recommended for all children [1–4]. Forhuman immunodeficiency virus (HIV)–infected children, therecommendation is 2 vaccinations, at least 3 months apart [5].
VZV can cause severe, sometimes fatal disease in immuno-compromised children with an extensive rash, which can behemorrhagic, and complications such as pneumonia, hepatitis,and encephalitis [6–8].Herpes zoster (HZ) also can cause severecomplications, including progressive outer retinal necrosis [9–
11] and trigeminal nerve involvement, resulting in ophthalmitisand keratitis [12]. These complications underscore the impor-tance of immunizing HIV-infected children against varicella.
Because of concerns regarding safety of live-attenuatedvaccines, the VZV vaccine was initially recommended for HIV-infected children with Centers for Disease Control and Preven-tion (CDC) clinical and immunologic categories N1 or A1 andCD4 T-lymphocytes≥25% [13–15]. In 2007, its use was extendedto HIV-infected children with CD4 T-lymphocytes ≥15% [5, 16].
Prospective clinical trials in children infected with perinatalHIV (PHIV) that have examined the safety and immunogenicityof the VZV vaccine [13, 16–19] are limited by small sample sizesand have not specifically examined the role of combinationantiretroviral therapy (cART) on vaccine immunogenicity. Pro-portions of children that seroconverted 6–12 weeks after 1 vacci-nation ranged 12%–62% [13, 16, 17, 19] and, in 1 study, fell from62% to 33% 1 year later [17]. After 2 vaccine doses, 59%–79% ofchildren seroconverted 6–12 weeks later [13, 16, 18, 19]. Propor-tions seropositive at 1 year ranged 43%–65% [16].
Levin et al reported vaccine efficacy of 79% using a compositeendpoint of VZV-specific antibodies and/or cell-mediated
Received 12 May 2015; accepted 11 August 2015; published online 18 September 2015.Presented in part: 19th International Workshop on HIV Observational Databases (IWHOD),
Catania, Sicily, Italy, 26–28 March 2015. Poster.Correspondence: M. U. Purswani, 1685 Morris Ave, Ste 1G, Division of Pediatric Infectious
Disease, Bronx-Lebanon Hospital Center, Bronx, NY 10457 ([email protected]).
Clinical Infectious Diseases® 2016;62(1):106–14© The Author 2015. Published by Oxford University Press for the Infectious Diseases Societyof America. All rights reserved. For permissions, e-mail [email protected]: 10.1093/cid/civ734
106 • CID 2016:62 (1 January) • HIV/AIDS
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022

immunity [16]. A subsequent retrospective study of childrenwith PHIV at 2 centers in the United States reported an efficacyof 82% based on a clinical diagnosis of varicella [20].
These data suggest that a substantial proportion of childrenwith PHIV may remain at risk of breakthrough varicella despitevaccination. A better understanding of the optimal manner inwhich to immunize this population is needed, particularly inthe cART era.
The aim of this study was to evaluate persistence of VZV-specific antibodies after vaccination with 1 or 2 doses of VZVvaccine and to identify determinants of varicella seropositivityin a large cohort of children and adolescents with PHIV and alsoin perinatally HIV-exposed but uninfected (PHEU) children.
METHODS
Study PopulationThe Adolescent Master Protocol (AMP), a component of thePediatric HIV/AIDS Cohort Study, is an ongoing prospectivecohort study designed to evaluate long-term effects of HIV in-fection and antiretroviral therapy (ART) among children withPHIV. It enrolled 451 children with PHIV and 227 PHEU chil-dren aged 7–16 years from March 2007 to November 2009 at 15sites in the United States, including Puerto Rico. Participantswere required to have complete medical history of ART use,plasma HIV RNA concentrations, and lymphocyte subset mea-surements since birth. Repository sera were frozen at −70°C.The protocol was approved by the institutional review boardat each site and at the Harvard T.H. Chan School of PublicHealth. Informed consent was obtained from the parent orlegal guardian, and assent was obtained from child participants,per local institutional review board guidelines.
Eligibility CriteriaEligible participants were those with repository serum speci-mens available for varicella antibody testing as of 31 October2012. Their last VZV vaccination had to be >21 days beforethe date the specimen was obtained.
Data ElementsDemographic and clinical characteristics of interest includedage, sex, race, ethnicity, body mass index (BMI), vaccinationhistory, plasma HIV RNA, CD4%, CDC clinical classificationfor HIV disease [14, 15], and prescribed ART. BMI was calcu-lated as weight divided by height squared (kg/m2) and expressedas z scores for age and sex [21]. The area-under-the-curve(AUC) viral load from the last vaccine dose to serologic testing,expressed as log10 copy-years, was calculated using the trapezoidalmethod [22].To calculate a time-averaged version of this measure,the AUC was subsequently divided by the years of follow-up time.cART was defined as a regimen consisting of at least 3 antiretro-viral drugs from at least 2 different drug classes, and the era ofcART was defined as the period from 1998 on [23].
Serologic TestingSerum specimens were analyzed by the National VZV Labora-tory at the CDC using a 2-step testing algorithm. All sampleswere first tested using an immunoglobulin G whole-infectedcell enzyme-linked immunosorbent assay (wcELISA). Samplestesting negative/equivocal were retested using glycoproteinenzyme-linked immunosorbent assay (gpELISA), a highly sensitiveand specific method developed at the CDC using highly purifiedVZV glycoproteins obtained through amaterial transfer agreementwith Merck and Co (Valley Forge, Pennsylvania) [24, 25]. Partici-pants were seropositive if they had a positive result from either test.
Statistical AnalysisProportions of seropositive subjects were estimated with 95%exact binomial confidence intervals (CIs) and compared betweensubjects with PHIV and PHEU subjects using Fisher’s exact test.Estimates were further stratified by number of vaccine doses andthe time from last vaccination to serologic testing and comparedusing Fisher’s exact test. Demographic and clinical characteristics,HIV severity measures, and ART at the time of last varicella vac-cine dose and date of specimen were compared among subjectswith PHIV by varicella antibody status using Wilcoxon ranksum and Fisher’s exact tests as appropriate. We hypothesizedthat the relationship between varicella seropositivity and yearsfrom last dose to specimen date may be modified by the numberof vaccine doses and timing of cART. We therefore compared theeffect on varicella seropositivity of the interval from last vaccinedose to specimen date in 3 vaccine dose–cART groups: receiptof 1 vaccination after≥3months of cART; receipt of 1 vaccinationwith <3 months of cART; and receipt of 2 vaccinations regardlessof cART. Ninety-five percent exact binomial CIs and Fisher’sexact test were used for statistical inference in these comparisons.
To identify independent predictors of varicella seropositivityamong subjects with PHIV, univariable and multivariable logis-tic regression models that included all covariables were per-formed to generate C statistics. To further identify a key set ofcovariables that would be most predictive of varicella seroposi-tivity among subjects with PHIV who received 1 or 2 vaccinedoses and had at least 3 years between their last dose and speci-men date, univariable logistic regression models were perfor-med using this subgroup. A multivariable predictive logisticregression model was then built by first including the vaccinedose–cART grouping variable and subsequently including allother covariables significant at α = .10 with a C statistic ≥0.60from univariable models. To avoid possible collinearity issues,only the strongest predictor within each set of CD4% and viralload parameters meeting the above selection criteria was includ-ed in the multivariable model. This multivariable model build-ing process was also repeated for subjects with PHIV who hadonly 1 vaccine dose and at least 3 years between their vaccina-tion and specimen date. All analyses were conducted using SASversion 9.4 (SAS Institute, Cary, North Carolina).
HIV/AIDS • CID 2016:62 (1 January) • 107
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022
RESULTS
Characteristics of the CohortThere were 653 subjects (432 PHIV and 221 PHEU) whosebirth years ranged from 1991 to 2002 (Supplementary Table 1).Compared with PHEU subjects, more subjects with PHIV wereblack, fewer were Hispanic, and more were living in poverty. Atthe time their specimens were obtained for testing, subjects withPHIV were older and had a lower BMI z score than PHEU sub-jects. Overall, fewer subjects with PHIV compared with PHEUsubjects received the VZV vaccine, with 38% vs 18% unvacci-nated, 26% vs 25% having received 1 dose, and 34% vs 55% hav-ing received 2 doses, respectively (P < .001). Subjects with PHIVwere older than PHEU subjects at the time of their first vaccine(median: 4.7 vs 1.5 years; P < .001), had a shorter interval be-tween first and second vaccinations (median: 3.9 vs 6.1 years;P < .001), and had more documented HZ episodes (10% vs0%; P < .001). The median interval from last vaccine dose tosample collection was longer for subjects with PHIV than PHEUsubjects (4.2 vs 3.5 years; P < .05).
Varicella Seroprevalence Among PHIV and PHEU SubjectsOf the 653 subjects tested, 491 (75.2%) tested positive by wcE-LISA. Among those testing negative, 78 (11.9% of all subjects)then tested positive by gpELISA. Overall, 87% of the cohort wasseropositive to varicella, with a seroprevalence among subjectswith PHIV of 82% (95% CI, 78%–86%), significantly lower thanamong PHEU subjects (97%; 95% CI, 94%–99%). For subjects
who had not received the vaccine, seroprevalence was again sig-nificantly lower among subjects with PHIV (71%; 95% CI, 63%–77%) than PHEU subjects (88%; 95% CI, 73%–96%) (Figure 1).Seroprevalence among those who received 1 vaccination was80% (95% CI, 71%–87%) for subjects with PHIV and 98%(95% CI, 90%–100%) for PHEU subjects. Seroprevalenceamong those who received 2 vaccinations was 97% (95% CI,93%–99%) for subjects with PHIV and 100% (95% CI, 97%–
100%) for PHEU subjects.
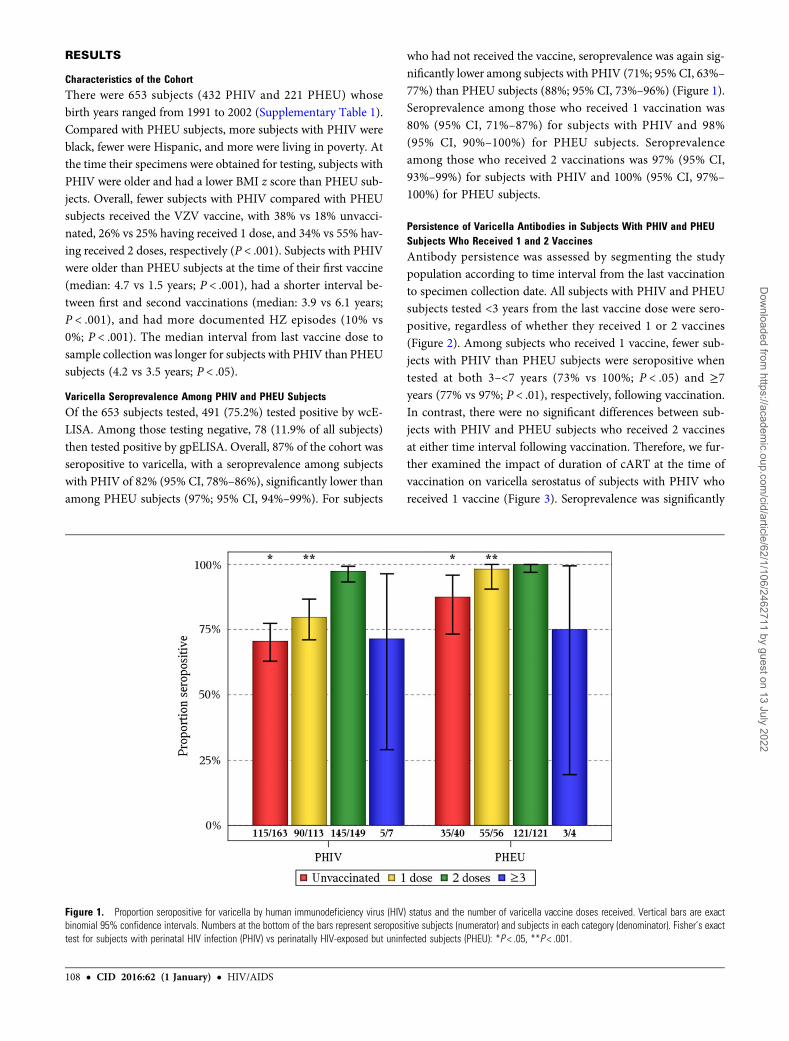
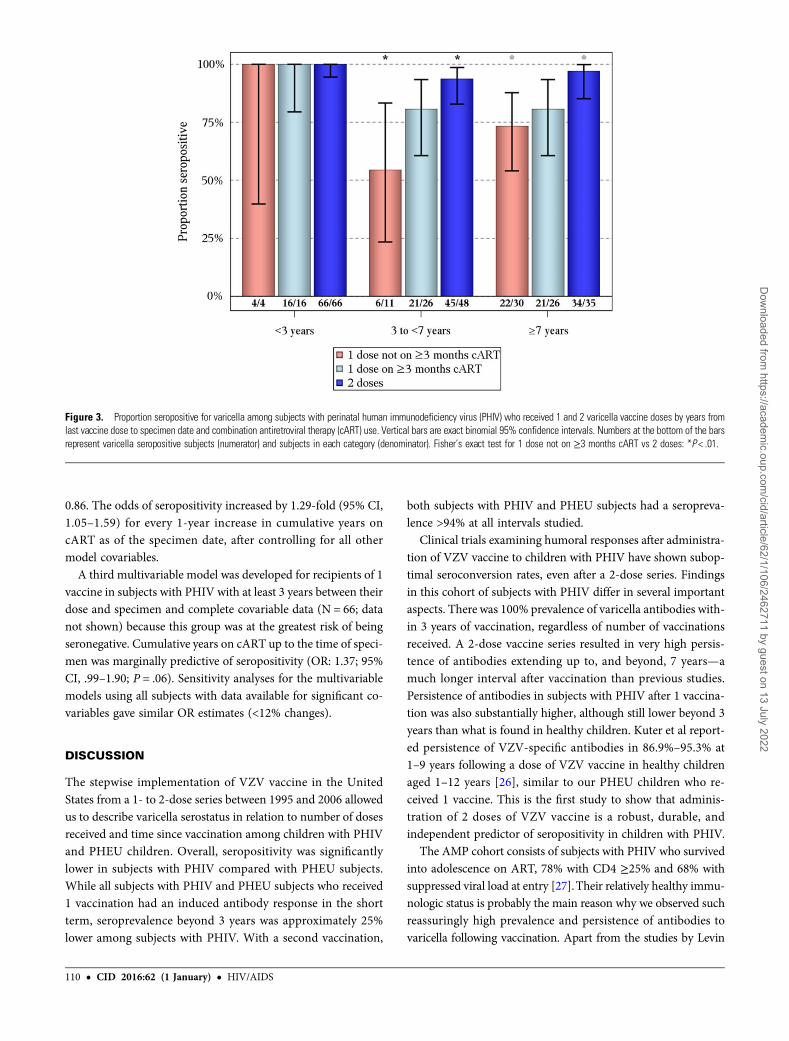
Persistence of Varicella Antibodies in Subjects With PHIV and PHEUSubjects Who Received 1 and 2 VaccinesAntibody persistence was assessed by segmenting the studypopulation according to time interval from the last vaccinationto specimen collection date. All subjects with PHIV and PHEUsubjects tested <3 years from the last vaccine dose were sero-positive, regardless of whether they received 1 or 2 vaccines(Figure 2). Among subjects who received 1 vaccine, fewer sub-jects with PHIV than PHEU subjects were seropositive whentested at both 3–<7 years (73% vs 100%; P < .05) and ≥7years (77% vs 97%; P < .01), respectively, following vaccination.In contrast, there were no significant differences between sub-jects with PHIV and PHEU subjects who received 2 vaccinesat either time interval following vaccination. Therefore, we fur-ther examined the impact of duration of cART at the time ofvaccination on varicella serostatus of subjects with PHIV whoreceived 1 vaccine (Figure 3). Seroprevalence was significantly
Figure 1. Proportion seropositive for varicella by human immunodeficiency virus (HIV) status and the number of varicella vaccine doses received. Vertical bars are exactbinomial 95% confidence intervals. Numbers at the bottom of the bars represent seropositive subjects (numerator) and subjects in each category (denominator). Fisher’s exacttest for subjects with perinatal HIV infection (PHIV) vs perinatally HIV-exposed but uninfected subjects (PHEU): *P < .05, **P < .001.
108 • CID 2016:62 (1 January) • HIV/AIDS
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022
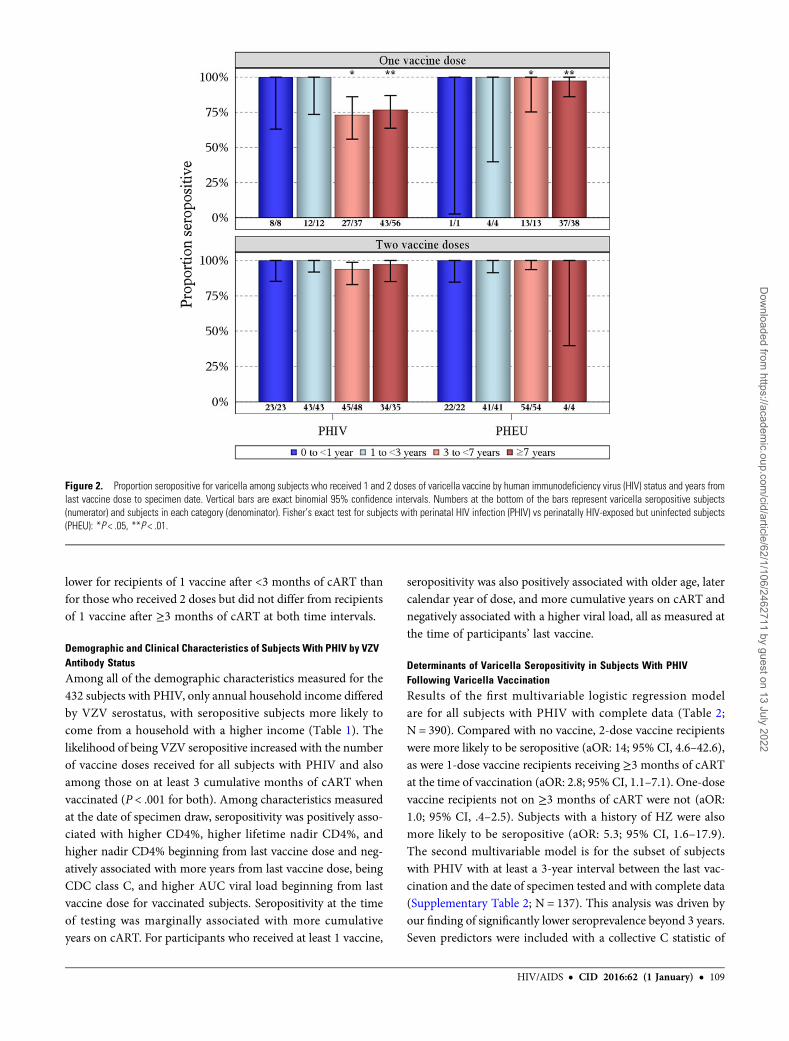
lower for recipients of 1 vaccine after <3 months of cART thanfor those who received 2 doses but did not differ from recipientsof 1 vaccine after ≥3 months of cART at both time intervals.
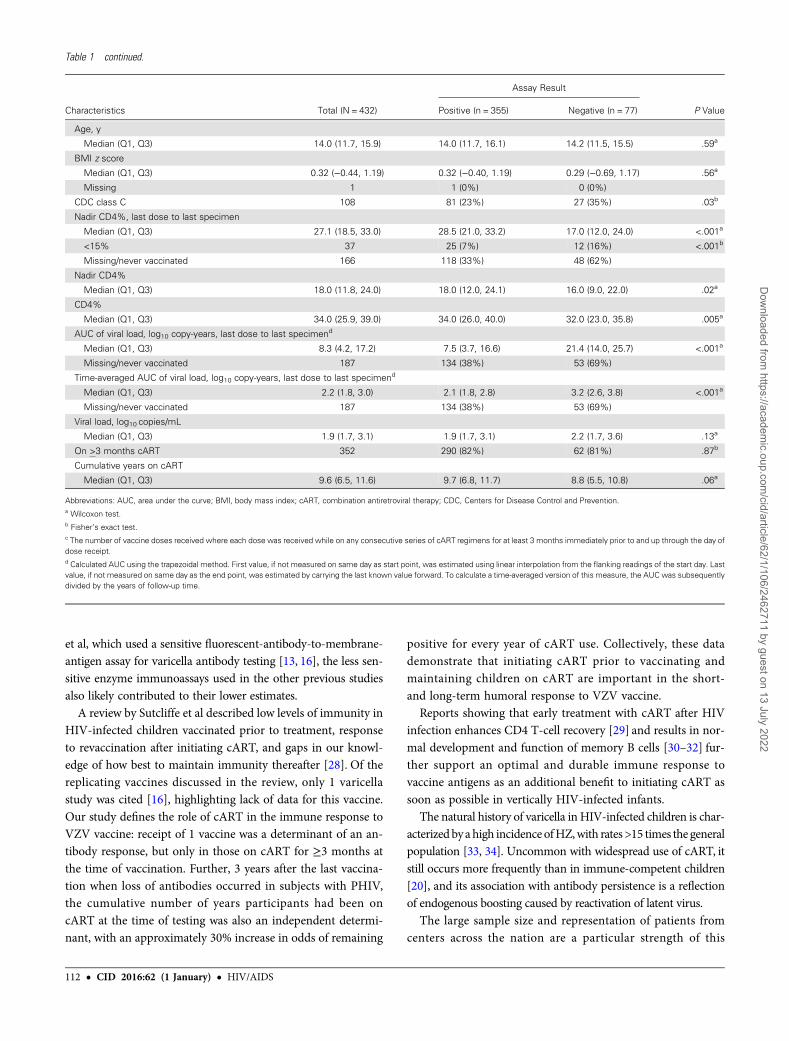
Demographic and Clinical Characteristics of Subjects With PHIV by VZVAntibody StatusAmong all of the demographic characteristics measured for the432 subjects with PHIV, only annual household income differedby VZV serostatus, with seropositive subjects more likely tocome from a household with a higher income (Table 1). Thelikelihood of being VZV seropositive increased with the numberof vaccine doses received for all subjects with PHIV and alsoamong those on at least 3 cumulative months of cART whenvaccinated (P < .001 for both). Among characteristics measuredat the date of specimen draw, seropositivity was positively asso-ciated with higher CD4%, higher lifetime nadir CD4%, andhigher nadir CD4% beginning from last vaccine dose and neg-atively associated with more years from last vaccine dose, beingCDC class C, and higher AUC viral load beginning from lastvaccine dose for vaccinated subjects. Seropositivity at the timeof testing was marginally associated with more cumulativeyears on cART. For participants who received at least 1 vaccine,
seropositivity was also positively associated with older age, latercalendar year of dose, and more cumulative years on cART andnegatively associated with a higher viral load, all as measured atthe time of participants’ last vaccine.
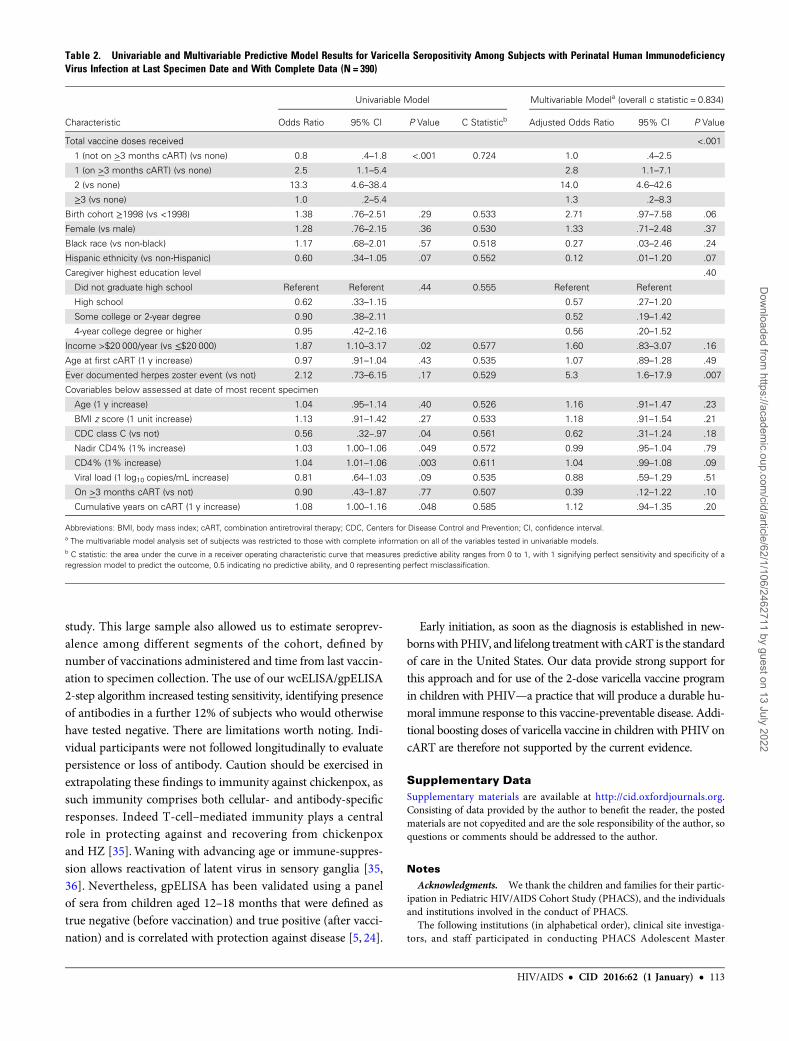
Determinants of Varicella Seropositivity in Subjects With PHIVFollowing Varicella VaccinationResults of the first multivariable logistic regression modelare for all subjects with PHIV with complete data (Table 2;N = 390). Compared with no vaccine, 2-dose vaccine recipientswere more likely to be seropositive (aOR: 14; 95% CI, 4.6–42.6),as were 1-dose vaccine recipients receiving ≥3 months of cARTat the time of vaccination (aOR: 2.8; 95% CI, 1.1–7.1). One-dosevaccine recipients not on ≥3 months of cART were not (aOR:1.0; 95% CI, .4–2.5). Subjects with a history of HZ were alsomore likely to be seropositive (aOR: 5.3; 95% CI, 1.6–17.9).The second multivariable model is for the subset of subjectswith PHIV with at least a 3-year interval between the last vac-cination and the date of specimen tested and with complete data(Supplementary Table 2; N = 137). This analysis was driven byour finding of significantly lower seroprevalence beyond 3 years.Seven predictors were included with a collective C statistic of
Figure 2. Proportion seropositive for varicella among subjects who received 1 and 2 doses of varicella vaccine by human immunodeficiency virus (HIV) status and years fromlast vaccine dose to specimen date. Vertical bars are exact binomial 95% confidence intervals. Numbers at the bottom of the bars represent varicella seropositive subjects(numerator) and subjects in each category (denominator). Fisher’s exact test for subjects with perinatal HIV infection (PHIV) vs perinatally HIV-exposed but uninfected subjects(PHEU): *P < .05, **P < .01.
HIV/AIDS • CID 2016:62 (1 January) • 109
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022
0.86. The odds of seropositivity increased by 1.29-fold (95% CI,1.05–1.59) for every 1-year increase in cumulative years oncART as of the specimen date, after controlling for all othermodel covariables.
A third multivariable model was developed for recipients of 1vaccine in subjects with PHIV with at least 3 years between theirdose and specimen and complete covariable data (N = 66; datanot shown) because this group was at the greatest risk of beingseronegative. Cumulative years on cART up to the time of speci-men was marginally predictive of seropositivity (OR: 1.37; 95%CI, .99–1.90; P = .06). Sensitivity analyses for the multivariablemodels using all subjects with data available for significant co-variables gave similar OR estimates (<12% changes).
DISCUSSION
The stepwise implementation of VZV vaccine in the UnitedStates from a 1- to 2-dose series between 1995 and 2006 allowedus to describe varicella serostatus in relation to number of dosesreceived and time since vaccination among children with PHIVand PHEU children. Overall, seropositivity was significantlylower in subjects with PHIV compared with PHEU subjects.While all subjects with PHIV and PHEU subjects who received1 vaccination had an induced antibody response in the shortterm, seroprevalence beyond 3 years was approximately 25%lower among subjects with PHIV. With a second vaccination,
both subjects with PHIV and PHEU subjects had a seropreva-lence >94% at all intervals studied.
Clinical trials examining humoral responses after administra-tion of VZV vaccine to children with PHIV have shown subop-timal seroconversion rates, even after a 2-dose series. Findingsin this cohort of subjects with PHIV differ in several importantaspects. There was 100% prevalence of varicella antibodies with-in 3 years of vaccination, regardless of number of vaccinationsreceived. A 2-dose vaccine series resulted in very high persis-tence of antibodies extending up to, and beyond, 7 years—amuch longer interval after vaccination than previous studies.Persistence of antibodies in subjects with PHIV after 1 vaccina-tion was also substantially higher, although still lower beyond 3years than what is found in healthy children. Kuter et al report-ed persistence of VZV-specific antibodies in 86.9%–95.3% at1–9 years following a dose of VZV vaccine in healthy childrenaged 1–12 years [26], similar to our PHEU children who re-ceived 1 vaccine. This is the first study to show that adminis-tration of 2 doses of VZV vaccine is a robust, durable, andindependent predictor of seropositivity in children with PHIV.
The AMP cohort consists of subjects with PHIV who survivedinto adolescence on ART, 78% with CD4 ≥25% and 68% withsuppressed viral load at entry [27].Their relatively healthy immu-nologic status is probably the main reason why we observed suchreassuringly high prevalence and persistence of antibodies tovaricella following vaccination. Apart from the studies by Levin
Figure 3. Proportion seropositive for varicella among subjects with perinatal human immunodeficiency virus (PHIV) who received 1 and 2 varicella vaccine doses by years fromlast vaccine dose to specimen date and combination antiretroviral therapy (cART) use. Vertical bars are exact binomial 95% confidence intervals. Numbers at the bottom of the barsrepresent varicella seropositive subjects (numerator) and subjects in each category (denominator). Fisher’s exact test for 1 dose not on ≥3 months cART vs 2 doses: *P < .01.
110 • CID 2016:62 (1 January) • HIV/AIDS
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022
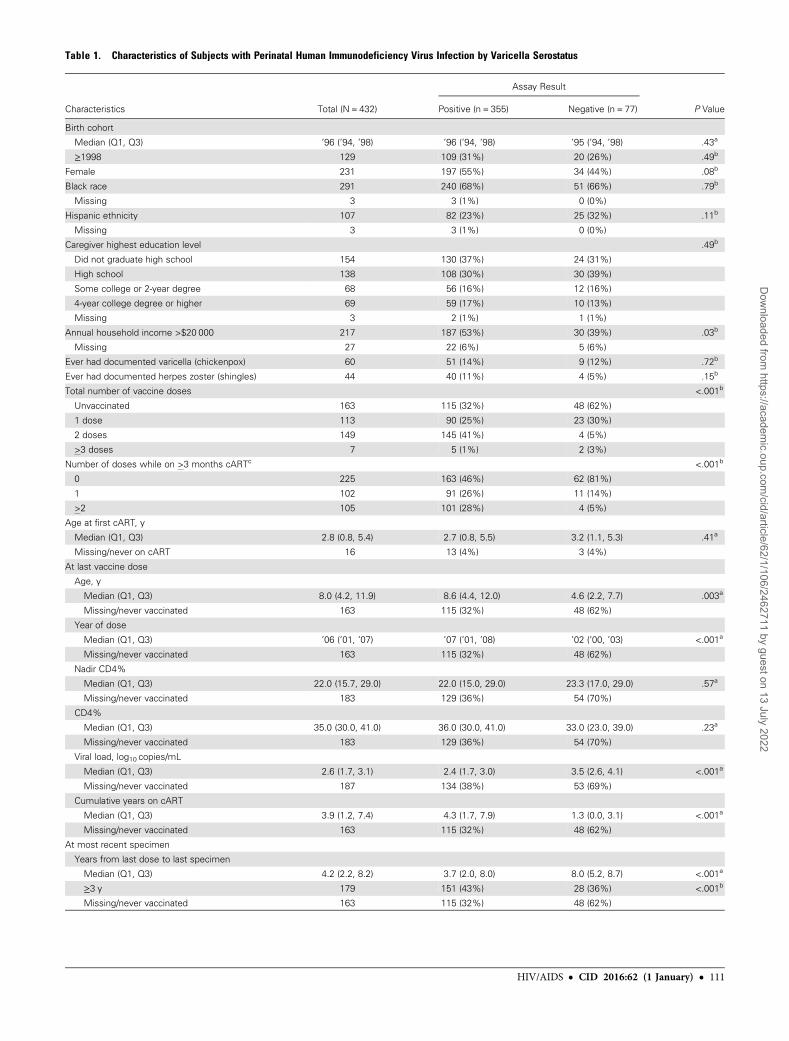
Table 1. Characteristics of Subjects with Perinatal Human Immunodeficiency Virus Infection by Varicella Serostatus
Characteristics Total (N = 432)
Assay Result
P ValuePositive (n = 355) Negative (n = 77)
Birth cohort
Median (Q1, Q3) ’96 (’94, ’98) ’96 (’94, ’98) ’95 (’94, ’98) .43a
≥1998 129 109 (31%) 20 (26%) .49b
Female 231 197 (55%) 34 (44%) .08b
Black race 291 240 (68%) 51 (66%) .79b
Missing 3 3 (1%) 0 (0%)
Hispanic ethnicity 107 82 (23%) 25 (32%) .11b
Missing 3 3 (1%) 0 (0%)
Caregiver highest education level .49b
Did not graduate high school 154 130 (37%) 24 (31%)
High school 138 108 (30%) 30 (39%)
Some college or 2-year degree 68 56 (16%) 12 (16%)
4-year college degree or higher 69 59 (17%) 10 (13%)
Missing 3 2 (1%) 1 (1%)
Annual household income >$20 000 217 187 (53%) 30 (39%) .03b
Missing 27 22 (6%) 5 (6%)
Ever had documented varicella (chickenpox) 60 51 (14%) 9 (12%) .72b
Ever had documented herpes zoster (shingles) 44 40 (11%) 4 (5%) .15b
Total number of vaccine doses <.001b
Unvaccinated 163 115 (32%) 48 (62%)
1 dose 113 90 (25%) 23 (30%)
2 doses 149 145 (41%) 4 (5%)
>3 doses 7 5 (1%) 2 (3%)
Number of doses while on >3 months cARTc <.001b
0 225 163 (46%) 62 (81%)
1 102 91 (26%) 11 (14%)
>2 105 101 (28%) 4 (5%)
Age at first cART, y
Median (Q1, Q3) 2.8 (0.8, 5.4) 2.7 (0.8, 5.5) 3.2 (1.1, 5.3) .41a
Missing/never on cART 16 13 (4%) 3 (4%)
At last vaccine dose
Age, y
Median (Q1, Q3) 8.0 (4.2, 11.9) 8.6 (4.4, 12.0) 4.6 (2.2, 7.7) .003a
Missing/never vaccinated 163 115 (32%) 48 (62%)
Year of dose
Median (Q1, Q3) ’06 (’01, ’07) ’07 (’01, ’08) ’02 (’00, ’03) <.001a
Missing/never vaccinated 163 115 (32%) 48 (62%)
Nadir CD4%
Median (Q1, Q3) 22.0 (15.7, 29.0) 22.0 (15.0, 29.0) 23.3 (17.0, 29.0) .57a
Missing/never vaccinated 183 129 (36%) 54 (70%)
CD4%
Median (Q1, Q3) 35.0 (30.0, 41.0) 36.0 (30.0, 41.0) 33.0 (23.0, 39.0) .23a
Missing/never vaccinated 183 129 (36%) 54 (70%)
Viral load, log10 copies/mL
Median (Q1, Q3) 2.6 (1.7, 3.1) 2.4 (1.7, 3.0) 3.5 (2.6, 4.1) <.001a
Missing/never vaccinated 187 134 (38%) 53 (69%)
Cumulative years on cART
Median (Q1, Q3) 3.9 (1.2, 7.4) 4.3 (1.7, 7.9) 1.3 (0.0, 3.1) <.001a
Missing/never vaccinated 163 115 (32%) 48 (62%)
At most recent specimen
Years from last dose to last specimen
Median (Q1, Q3) 4.2 (2.2, 8.2) 3.7 (2.0, 8.0) 8.0 (5.2, 8.7) <.001a
≥3 y 179 151 (43%) 28 (36%) <.001b
Missing/never vaccinated 163 115 (32%) 48 (62%)
HIV/AIDS • CID 2016:62 (1 January) • 111
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022
et al, which used a sensitive fluorescent-antibody-to-membrane-antigen assay for varicella antibody testing [13, 16], the less sen-sitive enzyme immunoassays used in the other previous studiesalso likely contributed to their lower estimates.
A review by Sutcliffe et al described low levels of immunity inHIV-infected children vaccinated prior to treatment, responseto revaccination after initiating cART, and gaps in our knowl-edge of how best to maintain immunity thereafter [28]. Of thereplicating vaccines discussed in the review, only 1 varicellastudy was cited [16], highlighting lack of data for this vaccine.Our study defines the role of cART in the immune response toVZV vaccine: receipt of 1 vaccine was a determinant of an an-tibody response, but only in those on cART for ≥3 months atthe time of vaccination. Further, 3 years after the last vaccina-tion when loss of antibodies occurred in subjects with PHIV,the cumulative number of years participants had been oncART at the time of testing was also an independent determi-nant, with an approximately 30% increase in odds of remaining
positive for every year of cART use. Collectively, these datademonstrate that initiating cART prior to vaccinating andmaintaining children on cART are important in the short-and long-term humoral response to VZV vaccine.
Reports showing that early treatment with cART after HIVinfection enhances CD4 T-cell recovery [29] and results in nor-mal development and function of memory B cells [30–32] fur-ther support an optimal and durable immune response tovaccine antigens as an additional benefit to initiating cART assoon as possible in vertically HIV-infected infants.
The natural history of varicella in HIV-infected children is char-acterized bya high incidence ofHZ,with rates >15 times the generalpopulation [33, 34]. Uncommon with widespread use of cART, itstill occurs more frequently than in immune-competent children[20], and its association with antibody persistence is a reflectionof endogenous boosting caused by reactivation of latent virus.
The large sample size and representation of patients fromcenters across the nation are a particular strength of this
Table 1 continued.
Characteristics Total (N = 432)
Assay Result
P ValuePositive (n = 355) Negative (n = 77)
Age, y
Median (Q1, Q3) 14.0 (11.7, 15.9) 14.0 (11.7, 16.1) 14.2 (11.5, 15.5) .59a
BMI z score
Median (Q1, Q3) 0.32 (−0.44, 1.19) 0.32 (−0.40, 1.19) 0.29 (−0.69, 1.17) .56a
Missing 1 1 (0%) 0 (0%)
CDC class C 108 81 (23%) 27 (35%) .03b
Nadir CD4%, last dose to last specimen
Median (Q1, Q3) 27.1 (18.5, 33.0) 28.5 (21.0, 33.2) 17.0 (12.0, 24.0) <.001a
<15% 37 25 (7%) 12 (16%) <.001b
Missing/never vaccinated 166 118 (33%) 48 (62%)
Nadir CD4%
Median (Q1, Q3) 18.0 (11.8, 24.0) 18.0 (12.0, 24.1) 16.0 (9.0, 22.0) .02a
CD4%
Median (Q1, Q3) 34.0 (25.9, 39.0) 34.0 (26.0, 40.0) 32.0 (23.0, 35.8) .005a
AUC of viral load, log10 copy-years, last dose to last specimend
Median (Q1, Q3) 8.3 (4.2, 17.2) 7.5 (3.7, 16.6) 21.4 (14.0, 25.7) <.001a
Missing/never vaccinated 187 134 (38%) 53 (69%)
Time-averaged AUC of viral load, log10 copy-years, last dose to last specimend
Median (Q1, Q3) 2.2 (1.8, 3.0) 2.1 (1.8, 2.8) 3.2 (2.6, 3.8) <.001a
Missing/never vaccinated 187 134 (38%) 53 (69%)
Viral load, log10 copies/mL
Median (Q1, Q3) 1.9 (1.7, 3.1) 1.9 (1.7, 3.1) 2.2 (1.7, 3.6) .13a
On >3 months cART 352 290 (82%) 62 (81%) .87b
Cumulative years on cART
Median (Q1, Q3) 9.6 (6.5, 11.6) 9.7 (6.8, 11.7) 8.8 (5.5, 10.8) .06a
Abbreviations: AUC, area under the curve; BMI, body mass index; cART, combination antiretroviral therapy; CDC, Centers for Disease Control and Prevention.a Wilcoxon test.b Fisher’s exact test.c The number of vaccine doses received where each dose was received while on any consecutive series of cART regimens for at least 3 months immediately prior to and up through the day ofdose receipt.d Calculated AUC using the trapezoidal method. First value, if not measured on same day as start point, was estimated using linear interpolation from the flanking readings of the start day. Lastvalue, if not measured on same day as the end point, was estimated by carrying the last known value forward. To calculate a time-averaged version of this measure, the AUC was subsequentlydivided by the years of follow-up time.
112 • CID 2016:62 (1 January) • HIV/AIDS
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022
study. This large sample also allowed us to estimate seroprev-alence among different segments of the cohort, defined bynumber of vaccinations administered and time from last vaccin-ation to specimen collection. The use of our wcELISA/gpELISA2-step algorithm increased testing sensitivity, identifying presenceof antibodies in a further 12% of subjects who would otherwisehave tested negative. There are limitations worth noting. Indi-vidual participants were not followed longitudinally to evaluatepersistence or loss of antibody. Caution should be exercised inextrapolating these findings to immunity against chickenpox, assuch immunity comprises both cellular- and antibody-specificresponses. Indeed T-cell–mediated immunity plays a centralrole in protecting against and recovering from chickenpoxand HZ [35].Waning with advancing age or immune-suppres-sion allows reactivation of latent virus in sensory ganglia [35,36]. Nevertheless, gpELISA has been validated using a panelof sera from children aged 12–18 months that were defined astrue negative (before vaccination) and true positive (after vacci-nation) and is correlated with protection against disease [5, 24].
Early initiation, as soon as the diagnosis is established in new-borns with PHIV, and lifelong treatment with cART is the standardof care in the United States. Our data provide strong support forthis approach and for use of the 2-dose varicella vaccine programin children with PHIV—a practice that will produce a durable hu-moral immune response to this vaccine-preventable disease. Addi-tional boosting doses of varicella vaccine in children with PHIV oncART are therefore not supported by the current evidence.
Supplementary DataSupplementary materials are available at http://cid.oxfordjournals.org.Consisting of data provided by the author to benefit the reader, the postedmaterials are not copyedited and are the sole responsibility of the author, soquestions or comments should be addressed to the author.
NotesAcknowledgments. We thank the children and families for their partic-
ipation in Pediatric HIV/AIDS Cohort Study (PHACS), and the individualsand institutions involved in the conduct of PHACS.The following institutions (in alphabetical order), clinical site investiga-
tors, and staff participated in conducting PHACS Adolescent Master
Table 2. Univariable and Multivariable Predictive Model Results for Varicella Seropositivity Among Subjects with Perinatal Human ImmunodeficiencyVirus Infection at Last Specimen Date and With Complete Data (N = 390)
Characteristic
Univariable Model Multivariable Modela (overall c statistic = 0.834)
Odds Ratio 95% CI P Value C Statisticb Adjusted Odds Ratio 95% CI P Value
Total vaccine doses received <.001
1 (not on >3 months cART) (vs none) 0.8 .4–1.8 <.001 0.724 1.0 .4–2.5
1 (on >3 months cART) (vs none) 2.5 1.1–5.4 2.8 1.1–7.1
2 (vs none) 13.3 4.6–38.4 14.0 4.6–42.6
≥3 (vs none) 1.0 .2–5.4 1.3 .2–8.3
Birth cohort ≥1998 (vs <1998) 1.38 .76–2.51 .29 0.533 2.71 .97–7.58 .06
Female (vs male) 1.28 .76–2.15 .36 0.530 1.33 .71–2.48 .37
Black race (vs non-black) 1.17 .68–2.01 .57 0.518 0.27 .03–2.46 .24
Hispanic ethnicity (vs non-Hispanic) 0.60 .34–1.05 .07 0.552 0.12 .01–1.20 .07
Caregiver highest education level .40
Did not graduate high school Referent Referent .44 0.555 Referent Referent
High school 0.62 .33–1.15 0.57 .27–1.20
Some college or 2-year degree 0.90 .38–2.11 0.52 .19–1.42
4-year college degree or higher 0.95 .42–2.16 0.56 .20–1.52
Income >$20 000/year (vs ≤$20 000) 1.87 1.10–3.17 .02 0.577 1.60 .83–3.07 .16
Age at first cART (1 y increase) 0.97 .91–1.04 .43 0.535 1.07 .89–1.28 .49
Ever documented herpes zoster event (vs not) 2.12 .73–6.15 .17 0.529 5.3 1.6–17.9 .007
Covariables below assessed at date of most recent specimen
Age (1 y increase) 1.04 .95–1.14 .40 0.526 1.16 .91–1.47 .23
BMI z score (1 unit increase) 1.13 .91–1.42 .27 0.533 1.18 .91–1.54 .21
CDC class C (vs not) 0.56 .32–.97 .04 0.561 0.62 .31–1.24 .18
Nadir CD4% (1% increase) 1.03 1.00–1.06 .049 0.572 0.99 .95–1.04 .79
CD4% (1% increase) 1.04 1.01–1.06 .003 0.611 1.04 .99–1.08 .09
Viral load (1 log10 copies/mL increase) 0.81 .64–1.03 .09 0.535 0.88 .59–1.29 .51
On >3 months cART (vs not) 0.90 .43–1.87 .77 0.507 0.39 .12–1.22 .10
Cumulative years on cART (1 y increase) 1.08 1.00–1.16 .048 0.585 1.12 .94–1.35 .20
Abbreviations: BMI, body mass index; cART, combination antiretroviral therapy; CDC, Centers for Disease Control and Prevention; CI, confidence interval.a The multivariable model analysis set of subjects was restricted to those with complete information on all of the variables tested in univariable models.b C statistic: the area under the curve in a receiver operating characteristic curve that measures predictive ability ranges from 0 to 1, with 1 signifying perfect sensitivity and specificity of aregression model to predict the outcome, 0.5 indicating no predictive ability, and 0 representing perfect misclassification.
HIV/AIDS • CID 2016:62 (1 January) • 113
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022

Protocol in 2014: Ann & Robert H. Lurie Children’s Hospital of Chicago:Ram Yogev, Margaret Ann Sanders, Kathleen Malee, Scott Hunter; BaylorCollege of Medicine: William Shearer, Mary Paul, Norma Cooper, LynnetteHarris; Bronx Lebanon Hospital Center: Murli Purswani, MahboobullahBaig, Anna Cintron; Children’s Diagnostic & Treatment Center: AnaPuga, Sandra Navarro, Patricia Garvie, James Blood; Children’s Hospital,Boston: Sandra Burchett, Nancy Karthas, Betsy Kammerer; Jacobi MedicalCenter: AndrewWiznia, Marlene Burey, Molly Nozyce; Rutgers–New JerseyMedical School: Arry Dieudonne, Linda Bettica, Susan Adubato;St. Christopher’s Hospital for Children: Janet Chen, Maria Garcia Bulkley,Latreaca Ivey, Mitzie Grant; St. Jude Children’s Research Hospital: KatherineKnapp, Kim Allison, Megan Wilkins; San Juan Hospital/Department of Pe-diatrics: Midnela Acevedo-Flores, Heida Rios, Vivian Olivera; Tulane Uni-versity Health Sciences Center: Margarita Silio, Medea Jones, Patricia Sirois;University of California, San Diego: Stephen Spector, Kim Norris, SharonNichols; University of Colorado Denver Health Sciences Center: ElizabethMcFarland, Alisa Katai, Jennifer Dunn, Suzanne Paul; University ofMiami: Gwendolyn Scott, Patricia Bryan, Elizabeth Willen.B. K. and T.-J. Y. had full access to all of the data in the study and take
responsibility for the integrity of the data and the accuracy of the data analysis.Conception and design of the study: M. U. P., B. K., T.-J. Y., and R. Y. Acqui-sition, analysis, and interpretation of data: All authors. Drafting of manuscript:M. U. P., B. K., T.-J. Y., and R. Y. Revision of manuscript: All authors. Statisticalanalysis: B. K., and T.-J. Y. Administrative, technical, or material support: Allauthors. Supervision of the study: M. U. P., D. S. S., R. Y., and R. B. V. D.Disclaimer. The conclusions and opinions expressed in this article are
those of the authors and do not necessarily reflect those of the National In-stitutes of Health or US Department of Health and Human Services.Financial support. The PHACS was supported by the Eunice Kennedy
Shriver National Institute of Child Health and Human Development withco-funding from the National Institute on Drug Abuse, the National Insti-tute of Allergy and Infectious Diseases, the Office of AIDS Research, theNational Institute of Mental Health, the National Institute of NeurologicalDisorders and Stroke, the National Institute on Deafness and Other Com-munication Disorders, the National Heart Lung and Blood Institute, theNational Institute of Dental and Craniofacial Research, and the NationalInstitute on Alcohol Abuse and Alcoholism, through cooperative agree-ments with the Harvard T.H. Chan School of Public Health (HD052102;Principal Investigator: George Seage; Project Director: Julie Alperen) andthe Tulane University School of Medicine (HD052104; Principal Investiga-tor: Russell Van Dyke; Co-Principal Investigator: Kenneth Rich; Project Di-rector: Patrick Davis). Data management services were provided by FrontierScience and Technology Research Foundation (Principal Investigator:Suzanne Siminski), and regulatory services and logistical support were pro-vided by Westat, Inc (Principal Investigator: Julie Davidson).Potential conflicts of interest. All authors: No reported conflicts. All
authors have submitted the ICMJE Form for Disclosure of Potential Con-flicts of Interest. Conflicts that the editors consider relevant to the contentof the manuscript have been disclosed.
References1. Prevention of varicella. Update recommendations of the Advisory Committee on
Immunization Practices (ACIP). MMWR Recomm Rep 1999; 48(RR-6):1–5.2. Varicella surveillance practices—United States, 2004. MMWR Morb Mortal Wkly
Rep 2006; 55:1126–9.3. Marin M, Meissner HC, Seward JF. Varicella prevention in the United States: a
review of successes and challenges. Pediatrics 2008; 122:e744–51.4. Guris D, Jumaan AO, Mascola L, et al. Changing varicella epidemiology in active
surveillance sites—United States, 1995–2005. J Infect Dis 2008; 197(suppl 2):S71–5.5. Marin M, Guris D, Chaves SS, Schmid S, Seward JF. Prevention of varicella: rec-
ommendations of the Advisory Committee on Immunization Practices (ACIP).MMWR Recomm Rep 2007; 56(RR-4):1–40.
6. Corti M, Trione N, Villafane MF, Risso D, Yampolsky C, Mamanna L. Acute me-ningoencephalomyelitis due to varicella-zoster virus in an AIDS patient: report ofa case and review of the literature. Rev Soc Bras Med Trop 2011; 44:784–6.
7. Lechiche C, Le Moing V, Francois Perrigault P, Reynes J. Fulminant varicella hep-atitis in a human immunodeficiency virus infected patient: case report and reviewof the literature. Scand J Infect Dis 2006; 38:929–31.
8. Popara M, Pendle S, Sacks L, Smego RA Jr, Mer M. Varicella pneumonia in pa-tients with HIV/AIDS. Int J Infect Dis 2002; 6:6–8.
9. Gore DM, Gore SK, Visser L. Progressive outer retinal necrosis: outcomes in theintravitreal era. Arch Ophthalmol 2012; 130:700–6.
10. Yin PD, Kurup SK, Fischer SH, et al. Progressive outer retinal necrosis in the era ofhighly active antiretroviral therapy: successful management with intravitreal injec-tions and monitoring with quantitative PCR. J Clin Virol 2007; 38:254–9.
11. Purdy KW, Heckenlively JR, Church JA, Keller MA. Progressive outer retinal necro-sis caused by varicella-zoster virus in children with acquired immunodeficiency syn-drome. Pediatr Infect Dis J 2003; 22:384–6.
12. Wilhelmus KR, Hamill MB, Jones DB. Varicella disciform stromal keratitis. Am JOphthalmol 1991; 111:575–80.
13. Levin MJ, Gershon AA,Weinberg A, et al. Immunization of HIV-infected childrenwith varicella vaccine. J Pediatr 2001; 139:305–10.
14. 1993 revised classification system for HIV infection and expanded surveillancecase definition for AIDS among adolescents and adults. MMWR Recomm Rep1992; 41(RR-17):1–19.
15. Centers for Disease Control and Prevention. 1994 revised guidelines for the per-formance of CD4+ T-cell determinations in persons with human immunodefi-ciency virus (HIV) infections. MMWR Recomm Rep 1994; 43(RR-3):1–21.
16. Levin MJ, Gershon AA, Weinberg A, Song LY, Fentin T, Nowak B. Administrationof live varicella vaccine to HIV-infected children with current or past significantdepression of CD4(+) T cells. J Infect Dis 2006; 194:247–55.
17. Armenian SH, Han JY, Dunaway TM, Church JA. Safety and immunogenicity oflive varicella virus vaccine in children with human immunodeficiency virus type 1.Pediatr Infect Dis J 2006; 25:368–70.
18. Bekker V, Westerlaken GH, Scherpbier H, et al. Varicella vaccination in HIV-1-infected children after immune reconstitution. AIDS 2006; 20:2321–9.
19. Taweesith W, Puthanakit T, Kowitdamrong E, et al. The immunogenicity and safe-ty of live attenuated varicella-zoster virus vaccine in human immunodeficiencyvirus-infected children. Pediatr Infect Dis J 2011; 30:320–4.
20. Son M, Shapiro ED, LaRussa P, et al. Effectiveness of varicella vaccine in childreninfected with HIV. J Infect Dis 2010; 201:1806–10.
21. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. CDC growth charts: Unit-ed States. Adv Data 2000; 314:1–27.
22. Cole SR, Napravnik S, Mugavero MJ, Lau B, Eron JJ Jr, Saag MS. Copy-years vi-remia as a measure of cumulative human immunodeficiency virus viral burden.Am J Epidemiol 2010; 171:198–205.
23. Brogly S, Williams P, Seage GR III, Oleske JM, Van Dyke R, McIntosh K. Antire-troviral treatment in pediatric HIV infection in the United States: from clinical tri-als to clinical practice. JAMA 2005; 293:2213–20.
24. Behrman A, Lopez AS, Chaves SS, Watson BM, Schmid DS. Varicella immunity invaccinated healthcare workers. J Clin Virol 2013; 57:109–14.
25. Reynolds MA, Kruszon-Moran D, Jumaan A, Schmid DS, McQuillan GM. Vari-cella seroprevalence in the U.S.: data from the National Health and Nutrition Ex-amination Survey, 1999–2004. Public Health Rep 2010; 125:860–9.
26. Kuter B, Matthews H, Shinefield H, et al. Ten year follow-up of healthy children whoreceived one or two injections of varicella vaccine. Pediatr Infect Dis J 2004; 23:132–7.
27. Van Dyke RB, Patel K, Siberry GK, et al. Antiretroviral treatment of US childrenwith perinatally acquired HIV infection: temporal changes in therapy between1991 and 2009 and predictors of immunologic and virologic outcomes. J AcquirImmune Defic Syndr 2011; 57:165–73.
28. Sutcliffe CG, Moss WJ. Do children infected with HIV receiving HAART need tobe revaccinated? Lancet Infect Dis 2010; 10:630–42.
29. Le T, Wright EJ, Smith DM, et al. Enhanced CD4+ T-cell recovery with earlierHIV-1 antiretroviral therapy. N Engl J Med 2013; 368:218–30.
30. Pensieroso S, Cagigi A, Palma P, et al. Timing of HAART defines the integrity ofmemory B cells and the longevity of humoral responses in HIV-1 vertically-infect-ed children. Proc Natl Acad Sci U S A 2009; 106:7939–44.
31. Cagigi A, Rinaldi S, Cotugno N, et al. Early highly active antiretroviral therapy en-hances B-cell longevity: a 5 year follow up. Pediatr Infect Dis J 2014; 33:e126–31.
32. Cotugno N, Douagi I, Rossi P, Palma P. Suboptimal immune reconstitution in ver-tically HIV infected children: a view on how HIV replication and timing ofHAART initiation can impact on T and B-cell compartment. Clin Dev Immunol2012; doi:10.1155/2012/805151.
33. Gershon AA, Gershon MD. Pathogenesis and current approaches to control ofvaricella-zoster virus infections. Clin Microbiol Rev 2013; 26:728–43.
34. Gershon AA, Mervish N, LaRussa P, et al. Varicella-zoster virus infection in chil-dren with underlying human immunodeficiency virus infection. J Infect Dis 1997;176:1496–500.
35. Duncan CJ, Hambleton S. Varicella zoster virus immunity: a primer. J Infect 2015;71(suppl 1):S47–53.
36. Weinberg A, Levin MJ. VZV T cell-mediated immunity. Curr Top Microbiol Im-munol 2010; 342:341–57.
114 • CID 2016:62 (1 January) • HIV/AIDS
Dow
nloaded from https://academ
ic.oup.com/cid/article/62/1/106/2462711 by guest on 13 July 2022
academic.oup.com/cid of 1 4
Please excuse the presence of this and the following test pages, which have been
added to a small number of article PDFs for a limited time as part of our process of
continual development and improvement.
academic.oup.com/cid
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do academic.oup.com/cid of 2 4
eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. academic.oup.com/cid of 3 4
Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum.
academic.oup.com/cid of 4 4
Copyright © 2022 FDOKUMEN