
p28 Bap31, a Bcl2/BclXL- and Procaspase-8-associated Protein in the Endoplasmic Reticulum

Available online at www.sciencedirect.com
gy 13 (2009) 313–321
Annals of Diagnostic PatholoPredictive value of cyclooxygenase 2 and Bcl-2 for cervical lymph nodemetastasis in mucoepidermoid carcinoma
Manal M. Zyada, PhD a,⁎, Mohammed E. Grawish, PhDb, Heba M. Elsabaa, PhDb
aOral Pathology Department, Faculty of Dentistry, Mansoura University, 35516 EgyptbOral Biology Department, Faculty of Dentistry, Mansoura University, 35516 Egypt
Abstract The expression of cyclooxygenase 2 (COX-2) is induced by growth factors, tumor promoters, and
⁎ Corresponding aE-mail address: zy
1092-9134/$ – see frodoi:10.1016/j.anndiag
cytokines. It is correlated with carcinogenesis and apoptosis inhibition. This study was designed toinvestigate the expression of COX-2 and BCl-2 and to correlate their expressions with theclinicopathologic features in the mucoepidermoid carcinoma (MEC). The expression of COX-2 andBCl-2 proteins was investigated in 16 archival tumor tissues of MEC using the streptavidin-biotincomplex technique. Clinical information was obtained through the computerized retrospectivedatabase from the tumor registry between 2001 and 2007. It revealed that grading system of MECdid not correlate with the presence or absence of node metastasis. The expression of COX-2 andBCl-2 was variably expressed in all the examined specimens. COX-2 and BCl-2 immunoreactivitywas observed mainly in the cytoplasm of neoplastic cells. As regard the clinicopathologicparameters, there was no significant difference in expression rates of COX-2 in patients among age,sex, and MEC grades (P N .05). However, the expression of COX-2 in node-positive tumors wassignificantly higher than that of node-negative tumors (P = .001). For BCL-2 expression, there wasno significant difference in expression rates of BCl-2 in patients among age, sex, site, clinical stage,and lymph node metastasis (P N .05), whereas a high significant difference was observed betweenBCl-2 staining index and MEC grades (P = .027). Moreover, there is a positive correlation betweenCOX-2 expression and BCL-2 staining index (P = .000). COX-2 is a good predictor for lymph nodemetastasis as well as ideal therapeutic target for the prevention or treatment of MEC. BCl-2 andCOX-2 are potentially useful prognostic markers for MEC.
© 2009 Elsevier Inc. All rights reserved.Keywords: COX-2; Bcl-2; Mucoepidermoid carcinoma; Salivary gland
1. Introduction
Salivary gland tumors represent 6% of head and neckcancers and 0.3% of all cancer in the United States.Mucoepidermoid carcinoma (MEC) is a malignant locallyinvasive neoplasm of the salivary glands. The incidence ratefor MEC has been reported at 0.44 per 100,000 [1]. It is themost common malignant neoplasm of the salivary glands,especially in the parotid gland, but MEC also can occur insubmandibular and minor salivary glands [2-4]. Based on thehistologic finding, MEC is usually characterized by 3 typesof cells: mucous-producing, epidermoid, and intermediate
[email protected] (M.M. Zyada).
nt matter © 2009 Elsevier Inc. All rights reserved.path.2009.06.003
cells that have the ability to differentiate into either mucous-producing or epidermoid cells. Because of the relative rarityof MECs and the variability in their biologic behavior, therehas been considerable debate regarding their classification,grading, and treatment. Current opinion still divergesbetween a 2-tier system that classifies MEC into low andhigh grade and a 3-tier grading system that incorporates anintermediate level [5,6].
Metastasis is the most dreadful biologic hallmark ofmalignant tumors and the primary cause of death in cancerpatients. Salivary gland malignancies are slow-growingtumors, which eventually will develop metastasis if leftuntreated. However, the timing of metastasis of thesemalignancies varies from patient to patient. It is importantto determine the metastatic potential of these tumors at the

314 M.M. Zyada et al. / Annals of Diagnostic Pathology 13 (2009) 313–321
time of diagnosis because of the nature of these slow-growing tumors. Histologic grading was considered a usefulparameter to predict the metastatic potential of malignancies[7-9]. However; current parameters may not be completelyreliable. It is necessary to search for new biomarker(s)capable of providing a better prediction of the metastaticpotential of MEC.
Cyclooxygenases are the rate-limiting key enzymes forthe metabolism of arachidonic acid and the production ofeicosanoids such as prostaglandins and thromboxanes [10].Two isoforms of cyclooxygenase (COX), COX-1 and COX-2, have been identified. COX-1 is constitutively expressed inmost tissues and aids homeostatic function. COX-2 isnormally undetectable in most tissues and is induced inresponse to a number of stimuli [11,12]. The importance ofCOX-2 in the tumorigenesis of solid tumors has beenemphasized in numerous studies [13-15]. In vitro, theoverexpression of COX-2 has been shown to have a numberof cellular effects, including a reduction in apoptosis, anincrease in proliferation, promotion of angiogenesis, adecrease in E-cadherin expression, and an increase in theinvasive/metastatic potential [14,16,17].
The BCL-2 gene encodes a 26-kDa protein located in themitochondrial inner membrane and cell cytosol that prolongscell survival by blocking apoptosis and may promote tumordevelopment [18]. Overexpression of BCL-2 protein hasbeen shown to be correlated with poor prognosis in severalsolid tumor types such as ovarian and prostate cancer [19].However, in follicular B-cell lymphomas, the expression ofBCL-2 was found to suppress the growth of developing Blymphocytes and leukemia cells by a cell cycle inhibitoryfunction; thus, the overexpression of BCL-2 gene mightdelay the growth of cancer cells [20].
A reduction in apoptosis is thought to be the mostimportant factor affecting the malignant potential of tumors.The importance of COX-2 in tumorigenesis in vivo has beenemphasized in numerous studies, but few studies have beenconducted to investigate coexpression of COX-2 and BCL-2protein in MECs of salivary gland tissues [21].
Thus, the aim of the current study was to investigate theexpression of COX-2 and BCl-2 and to correlate theirexpressions with the clinicopathologic features in the MEC.
2. Materials and methods
2.1. Tissue specimens
Sixteen samples of MEC of salivary gland were collectedfrom the archives of the Oral and General PathologyDepartments, Faculty of Dentistry and Faculty of Medicine,Mansoura University (Egypt), between 2001 and 2007. Theclinical data were collected retrospectively through thecomputerized retrospective database from the tumor registry,regarding age, sex, site, tumor size, and lymph nodemetastasis. All of the cases were reviewed and categorized
according to the World Health Organization classification ofsalivary gland tumors [22].
For the purpose of this study, we used the 3-tier gradingsystem that incorporates an intermediate level [5,6]. Stagingof tumors was done according to the TMN classification ofthe American Joint Committee on Cancer [23]. For analyticpurposes, 2 groups were delineated according to theobserved biologic behavior of the lesions. These 2 groupsare MEC cases with no evidence of lymph node metastasis (n= 11) and MEC cases with evidence of lymph nodemetastasis (n = 5).
2.2. Immunohistochemical analysis
Tissue specimens were fixed in 10% formalin, embeddedin paraffin, and cut into 4 μm thick sections. Primaryantibodies against human COX-2 and BCL-2 were ready touse. For the immunohistochemical study, a modifiedstreptavidin-biotin-peroxidase complex method [24] wasperformed. The tissue sections were deparaffinized andrehydrated in a graded series of alcohols. The sections weremicrowaved 3 times for 5 minutes each in citrate phosphatebuffer (pH 6.0) for antigen retrieval. Endogenous peroxidaseactivity was blocked with 0.3% H2O2 for 15 minutes.
The sections were incubated with 10% normal bovineserum albumin in phosphate-buffered saline for 10 minutes toblock nonspecific background staining. Monoclonal antibo-dies against COX-2 (clone 294; Dako, Glostrup, Denmark)and BCL-2 (clone 124; Dako) were then applied as a primaryantibody at 4°C overnight. Normal rabbit and mouse sera wereused as a negative control. Biotinylated goat antirabbitimmunoglobulin (IgG) (Vector, Burlingame, Calif) wasapplied as secondary antibody to the sections, which werethen incubated for 30 minutes at room temperature.
After washing with phosphate-buffered saline, thestreptavidin-biotin complex (LSAB-2, Dakopatts, Copenha-gen, Denmark) immunoperoxidase reaction was carried outfor 1 hour at 4°C. Peroxidase reactivity was detected with theuse of 3, 3′-diaminobenzidine tetrahydrochloride containing0.03% H2O2. Sections were lightly counterstained withhematoxylin, dehydrated, and mounted with glycerol gelatin.
2.3. Immunohistochemical evaluation
The immunoreactivity of each specimen was evaluatedby light microscopy to assess the intensity of COX-2expression, graded according to a 5-grade scale, and thestaining index of BCL-2. The percentage of COX-2–positive tumor cells showing cytoplasmic staining wasdetermined by counting a total of 2000 cells in 10randomly selected fields of each section examined at 400magnification. COX-2 expression was then classified asgrade 0 (negative expression); grade 1 (low expression),1% to 25% of tumor cells positive; grade 2 (intermediateexpression), 26% to 50% positive; grade 3 (high expres-sion), 51% to 75% positive; or grade 4 (high expression),76% or more positive [25].

Table 1Clinical features, histopathologic condition, and COX-2 and BCL-2immunostaining indices of the MECs with and without evidence of lymphnode metastasis investigated in the present study
Case Age Sex Primarysite
Tumorsize
Lymphnodemetastasis
TNMstaging
Grading
1 65 Female Palate T1 N0 I Low2 30 Female Parotid T2 N0 II Low3 35 Female Parotid T1 N0 I Low4 70 Male Palate T1 N0 I Low5 72 Female Tongue T1 N0 I Low6 62 Female Parotid T2 N0 II Low7 33 Female Palate T1 N0 I Low8 40 Male Parotid T3 N1 III Low9 40 Female Tongue T2 N1 III Low10 6 Female Parotid T4a N0 IVA Intermediate11 75 Male Parotid T2 N0 II Intermediate12 75 Male Parotid T3 N0 III Intermediate13 16 Female Parotid T2 N0 II High14 63 Male Parotid T1 N2 IVA High15 50 Female Parotid T2 N1 III High16 52 Male Parotid T4a N1 IVA High
ig. 1. Photomicrograph shows strong cytoplasmic BCL-2 immunostainingas observed in the basal ductal cells and in some serous acini.
315M.M. Zyada et al. / Annals of Diagnostic Pathology 13 (2009) 313–321
The staining index of BCL-2 was evaluated by calculatingthe percentage of stained malignant cells in all 10 fields in asimilar manner as described for COX-2 expression. Thepercentage of BCL-2–positive tumor cells showed cytoplas-mic staining.
2.4. Statistical analysis
It was performed using SPSS program version 11 (SPSSInc, Chicago, Ill). One-way analysis of variance test, Studentt test, χ2 test, Fisher exact test, and Spearman rankcorrelation test were used for statistical analysis. P b .05was regarded as statistically significant.
3. Results
3.1. Clinicopathologic results
Table 1 shows the clinical and pathologic characteristicsof the 16 MEC specimens used in the study. The mean age ofthe patients was 49.3 years (range, 6-75 years). There were10 women and 6 men. Eleven tumors were located in theparotid gland and 5 in minor salivary glands (base of tongueand hard palate). Nine MEC specimens were low grade; 3,intermediate grade; and 4, high grade. The tumor size variedaccording to the site of the lesions. Twelve patients (75%)had stage T1 or T2 disease, and 5 patients (31.2%) had
Table 2Distribution of node-negative and node-positive in the studied cases
Total Node-positive Node-negative Grades
7 3 4 Intermediate and high-grade9 2 7 Low-grade16 5 11 Total
χ2 = 0.780; P = .377.
Fw
regional metastasis. Final TNM staging revealed that 56.3%of the patients had stage I or stage II disease (Table 1).
Regarding the grading of MEC, there were 9 low-gradecases, 3 intermediate-grade cases, and 4 high-grade cases(Figs. 2-8A). Results of Fisher exact test (Table 2)revealed that the grading system of MEC was not relatedto the presence or absence of node metastasis (χ2 = 0.780;P = .377).
3.2. Immunohistochemical results
3.2.1. COX-2 expression and BCL-2 staining index innormal salivary gland tissues and MEC
The expression of BCL-2 and COX-2 appeared as diffusebrown cytoplasmic reaction. In normal salivary glandtissues, the acinar cells showed variable reactivity. Strongcytoplasmic BCL-2 immunostaining was observed in thebasal ductal cells and in some serous acini (Fig. 1). Somemucous acini showed restricted positivity outlining theseacini. Also, COX-2 protein was seen in the cytoplasm of theserous acini. The stromal lymphocytes and normal lymphoidfollicles surrounding the tumors stained positive for BCL-2and COX-2 and thus were used as internal controls.
Positive expression of BCL-2 was detected in 12specimens of MEC (75%). In all the studied MEC cases,the distribution and proportion of BCL-2–positive cellsvaried considerably between different histologic grades(Figs. 2-4B).
In low-grade cases, some mucous cells showed moderateto strong reaction, whereas in intermediate- and high-gradecases, a weak reaction was observed in the few positivemucous cells present.
In most of the cases, positive BCL-2 epidermoid cellswere found in the form of small clusters or lining cysticspaces with varying degrees of intensity (Fig. 2B). However,most of the intermediate cells showed moderate to strong

Fig. 2. Low-grade MEC shows numerous cystic spaces formed of an admixture of mucous, intermediate, and epidermoid cells. A strong positive cytoplasmicimmunoreactivity in variety of cell types ([A] hematoxylin and eosin, original magnification ×100; [B] anti–BCL-2, original magnification ×100).
316 M.M. Zyada et al. / Annals of Diagnostic Pathology 13 (2009) 313–321
positive immunoreactivity and were distributed all over thelesion in the form of solid sheets or clusters or amalgamatedwith other cell types (Fig. 3B). Positive BCL-2 columnarcells were found lining cystic spaces and surrounded byepidermoid and intermediate cells while showing moderateto strong positivity. The clear cells failed to show anyreactivity for BCL-2 (Fig. 4B).
Positive expression of COX-2 was detected in all16 specimens of MEC (100%). Scores for COX-2 immunor-eactivity were as follows: 1 (4/16), 2 (2/16), 3 (5/16), and4 (5/16), respectively. Variation of cytoplasmic COX-2staining intensity was also noted from case to case. Theintensity varied from weak to strong (Figs. 5-8B).
Fig. 3. Intermediate-grade MEC shows sheets of neoplastic glandular cells. A diffuseosin, original magnification ×100; [B] anti–BCL-2, original magnification ×400)
In MEC, a strong COX-2 immunostaining was seen in theintermediate and luminal cells of the cystic and solid areas.The mucous and clear cells were negative.
3.2.2. Relation of COX-2 expression and BCL-2 stainingindex with clinicopathologic variables
The expression of COX-2 in low grade was notsignificantly different from that of intermediate- and high-grade MEC, whereas there was a significant difference(P = .027) between the MEC grades and BCL-2staining index.
Regarding the 1-way analysis of variance test, there wasa highly significant difference (P = .005) between the
e moderate positive staining reaction in neoplastic cells ([A] hematoxylin and.

Fig. 4. High-grade MEC shows numerous islands and cords of neoplastic glandular cells. A heterogeneous positive staining reaction of epidermoid and mucouscells. Positive and negative cells are also evident ([A] hematoxylin and eosin, original magnification ×100; [B] anti–BCL-2, original magnification ×400).
317M.M. Zyada et al. / Annals of Diagnostic Pathology 13 (2009) 313–321
MEC grades and BCL-2 staining index. Also, a highlysignificant difference was found between the BCL-2staining index of low- and intermediate-grade MEC cases(P = .000).
Spearman rank correlation test was performed todetermine the relation between BCL-2 staining index andMEC grades. A tendency toward an inverse correlationbetween BCL-2 staining index and MEC grades (P = .011)was observed.
However, no other clinicopathologic factors correlatedwith BCL-2 staining index, whereas there was a significantdifference in expression rates of COX-2 in patients among
Fig. 5. Low-grade MEC of minor salivary gland shows a mixture of intermedicytoplasmic reaction with variation in the intensity in some neoplastic cells. Notecase. Stromal lymphocytes are strongly positive ([A] hematoxylin and eosin, orig
lymph node metastasis and TNM staging (P = .001 and .043,respectively) (Table 3).
3.2.3. Relationship between COX-2 expression and BCL-2staining index
There is a positive correlation between COX-2 expressionand BCL-2 staining index (P = .000) (Table 4).
4. Discussion
Mucoepidermoid carcinoma remains one of the com-monest malignant tumors arising from salivary glands,
ate, epidermoid, and mucous cells with lymphocytic infiltration. Positivethe nests of strong reactive cells and nests of moderate intensity in the sameinal magnification ×100; [B] anti–COX-2, original magnification ×100).
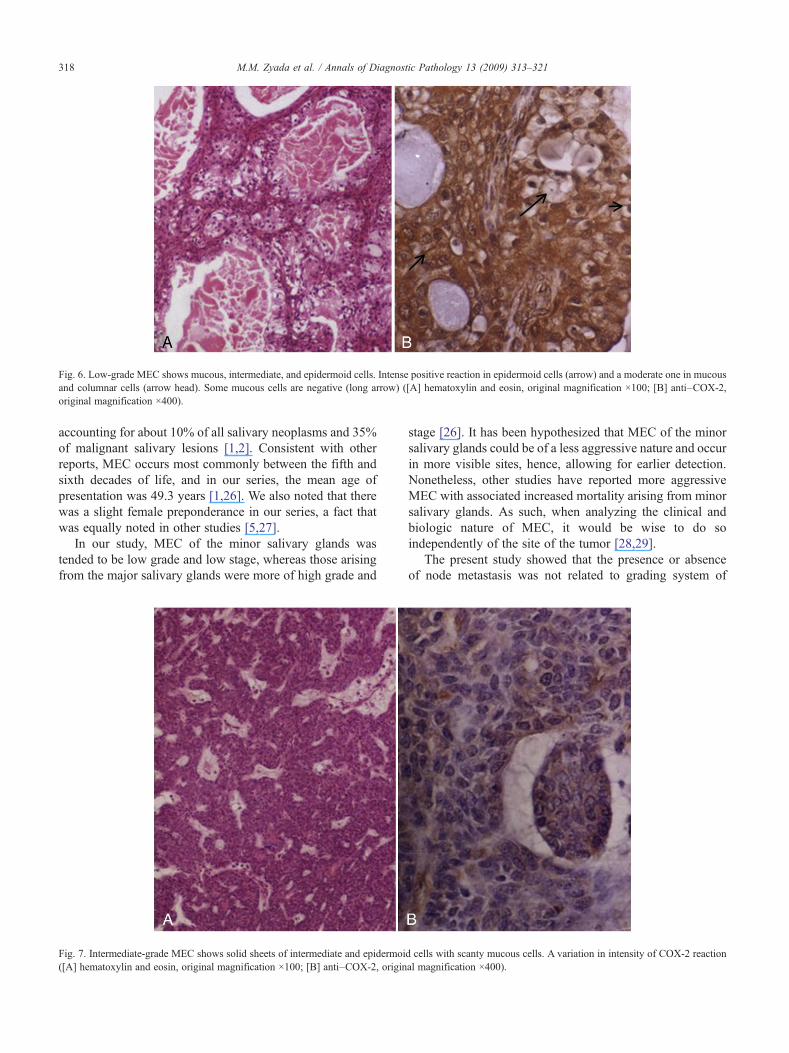
Fig. 6. Low-grade MEC shows mucous, intermediate, and epidermoid cells. Intense positive reaction in epidermoid cells (arrow) and a moderate one in mucousand columnar cells (arrow head). Some mucous cells are negative (long arrow) ([A] hematoxylin and eosin, original magnification ×100; [B] anti–COX-2,original magnification ×400).
318 M.M. Zyada et al. / Annals of Diagnostic Pathology 13 (2009) 313–321
accounting for about 10% of all salivary neoplasms and 35%of malignant salivary lesions [1,2]. Consistent with otherreports, MEC occurs most commonly between the fifth andsixth decades of life, and in our series, the mean age ofpresentation was 49.3 years [1,26]. We also noted that therewas a slight female preponderance in our series, a fact thatwas equally noted in other studies [5,27].
In our study, MEC of the minor salivary glands wastended to be low grade and low stage, whereas those arisingfrom the major salivary glands were more of high grade and
Fig. 7. Intermediate-grade MEC shows solid sheets of intermediate and epidermoi([A] hematoxylin and eosin, original magnification ×100; [B] anti–COX-2, origin
stage [26]. It has been hypothesized that MEC of the minorsalivary glands could be of a less aggressive nature and occurin more visible sites, hence, allowing for earlier detection.Nonetheless, other studies have reported more aggressiveMEC with associated increased mortality arising from minorsalivary glands. As such, when analyzing the clinical andbiologic nature of MEC, it would be wise to do soindependently of the site of the tumor [28,29].
The present study showed that the presence or absenceof node metastasis was not related to grading system of
d cells with scanty mucous cells. A variation in intensity of COX-2 reactional magnification ×400).

Fig. 8. High-grade MEC shows epidermoid cells displaying considerable variation in nuclear size and shape. An intense positive staining reaction among theepidermoid islands ([A] hematoxylin and eosin, original magnification ×100; [B] anti–COX-2, original magnification ×250).
319M.M. Zyada et al. / Annals of Diagnostic Pathology 13 (2009) 313–321
MEC. This finding signifies that the current gradingsystem is highly subjective and cannot be used as areliable prognostic factor.
The expression of BCL-2 in a variety of epithelial and ofepithelial tissues triggered intense researches directed towardthe role of this molecule in the pathogenesis [30].
Table 3Relation between clinicopathologic features of the studied cases and bothCOX-2 and BCL-2 immunoreactivity
Variable n COX-2expression (%)
P BCL-2 stainingindex (%)
P
Ageb40 7 45. ± 17.44 NS 46.76 ± 21.52 NS≥40 9 56.94 ± 17.28 43.41 ± 26.54SexMale 6 61.15 ± 14.06 NS 45.85 ± 25.71 NSFemale 10 46.10 ± 18.04 44.29 ± 23.92SiteParotid 11 52.98. ± 16.79 NS 40.38 ± 27.77 NSMinor salivarygland
5 49.02 ± 21.75 54.76 ± 4.19
Tumor sizeT1-T2 12 49.53 ± 18.12 NS 46.48 ± 22.65 NST3-T4 A 4 58.38 ± 17.52 40.08 ± 29.69Lymph node metastasisPositive 5 68.82 ± 6.93 .001 39.44 ± 36.37 NSNegative 11 43.98 ± 15.67 47.35 ± 17.19TNM stageI-II 9 44.14 ± 17.51 .043 48.12 ± 19.12 NSIII-VI 7 1.51 ± 13.716 40.70 ± 29.78GradesLow 9 51.46 ± 17.43 NS 58.06 ± 6.83 .027Intermediateand high
7 52.11 ± 19.73 27.93 ± 27.43
NS indicates not significant.
In the present results, the normal salivary gland tissuesshowed positive strong immunoreactivity for BCL-2 amongthe cells of the ducts. However, some serous acini showedstrong cytoplasmic staining, whereas some mucous acinishowed restricted positivity outlining these acini. The currentresults parallel those of other studies on normal adult tissues,which revealed that BCL-2 protein is regularly present inductal epithelial cells of all exocrine glands [31].
Absence of COX-2 in some acinar cells may be related tothe rapid turnover of these cells (high apoptosis). On theother hand, acinar cells could be filled with secretorygranules, thus, resulting in potentially lesser volume for thedistribution of the gene product.
In the present study, BCL-2 and COX-2–positiveimmunostaining were found in infiltrating lymphocytesthat serve as internal positive control. Similar results werereported by other studies as the work of Eid et al [32,33] ontesticular carcinoma, Rochaix et al [34] on breast carcinoma,and Itoh et al [35] on oral squamous cell carcinoma. Thesefindings suggest that the immunoreactivity for COX-2 maybe modulated by interaction of the stromal cells with cancercells in the process of destructive invasion.
able 4orrelation between BCL-2 staining index and expression of COX-2 inEC cases
OX-2 BCL-2
otal Positive Negative
3 (18.7%) 3 (18.7%) 0 (100%) Negative13 (81.3%) 13 (81.3%) 0 (100%) Positive16 (100%) 16 (100%) 0 (100%) Total
2 test, P = .000.
TCM
C
T
χ

320 M.M. Zyada et al. / Annals of Diagnostic Pathology 13 (2009) 313–321
The results of the present study revealed that BCL-2 wasfrequently expressed in epidermoid, intermediate, andcolumnar cells, whereas mucous cells were infrequentlypositive. However, clear cells failed to reveal any reactivityfor BCL-2. The present results are in agreement with Yanezet al [36] who found BCL-2 expression only in theepidermoid areas of MEC of salivary glands. Variabledistribution of BCL-2 staining observed in the present studymay be due to variation of the amount of organellesnecessary for linkage and storage of BCL-2 (mitochondriaand endoplasmic reticulum).
COX-2 has been paid an attention to study because itcould play an important role in the initiation and progressionof carcinomas of the various organs [37,38]. Enhancedsynthesis of prostaglandins because of up-regulation ofCOX-2 increase proliferative activity of neoplastic cells,promote angiogenesis, and inhibit immune surveillance[14,39,40]. In addition, immunohistochemical overexpres-sion of COX-2 inhibits apoptosis and enhances invasiveness[14,17].
The finding of this study comes with Sakamoto et al [21]who reported that in most of COX-2–positive cases, thestaining intensity was homogenous, but in a few cases, itvaried greatly between tumor cells in the same section.
The results of the present study showed that theexpression of COX-2 in low grade was not significantlydifferent from that of intermediate- and high-grade MEC.This finding reconfirms the pitfalls of the grading system ofMEC. However, the low-grade cases showed significantlyhigher BCL-2 staining indices than those of intermediate andhigh grades. These findings parallel recent reports by Yin etal [41] who found that low-grade MEC showed higherexpression of BCL-2 than higher grades. Our results are inaccordance with many studies on breast carcinoma thatrevealed that BCL-2 immunostaining was inversely corre-lated with increasing histologic grades [42,43]. Shibata et al[44] found similar results in oral squamous cell carcinoma asthey found no association between COX-2 expression andhistopathologic phenotype. However, low levels of COX-2expression were associated with an improved prognosis.COX-2 expression correlated with clinical stage andmetastasis to lymph nodes [45].
From the results of the current study, it was revealed thatCOX-2 was present in all cases of MEC; the expression ofCOX-2 was significantly higher in node-positive tumorscompared to that of node-negative tumors. Similar resultshave been also reported in other tumor types [42,45]. Thisfinding might account for the aggressiveness of the tumorsexhibiting node metastasis. COX-2 overexpression wasfound to correlate with tumors associated with highproliferative potential and aggressiveness [25,42].
In addition, the results of the present study revealed thatCOX-2 expression correlated significantly with BCL-2staining index. These findings appear to be expected becauseCOX-2 may regulate apoptosis in MEC through over-expression of BCL-2 protein. The regulation of apoptosis is
cell type-specific and dependent on the balance between pro-and antiapoptotic factors. A few experimental studies havedemonstrated a clear positive correlation between COX-2expression and resistance to apoptosis in human cells[46,47].
5. Conclusions
From the present study, it can be concluded that COX-2and BCL-2 are potentially useful prognostic markers forMEC. The coexpression between COX-2 and BCL-2 is acritical factor affecting the biologic behavior of MECcarcinogenesis and metastasis. In addition, the immunor-eactivity of COX-2 and BCL-2 can be used to evaluate thenature of a borderline malignancy in the MEC. Theseretrospective results need to be confirmed by prospectiverandomized and larger studies.
References
[1] Speight PM, Barrett AW. Salivary gland tumors. Oral Dis2002;8:229-40.
[2] Kusafuka K, Takizawa Y, Iida Y, Ebihara M, Onitsuka T, Kameya T.Primary nasopharyngeal mucoepidermoid carcinoma in Japanesepatients: two case reports with histochemical and immunohistochem-ical analysis and a review of the literature. Virchows Arch2007;450:343-8.
[3] Kuo TT, Chan JKC, Wenig BM, Eveson JW. Nasopharyngealadenocarcinoma and salivary gland-type carcinoma. In: Barnes L,Eveson JW, Reichart P, Sidransky D (eds). World Health Organizationclassification tumours: pathology & genetics head and neck tumours.WHO Publications Center, Albany, NY, USA, IARC Press, Lyon,2005;p 98.
[4] Shaheel Chummun S, McLean NR, Howlett PC, Kelly CG, Welsh AR,Soames JV. Mucoepidermoid carcinoma of the head and neck: a 13-year review. Eur J Plast Surg 2008;30:277-82.
[5] Goode RK, Auclair PL, Ellis GL. Mucoepidermoid carcinoma of themajor salivary glands: clinical and histopathologic analysis of 234cases with evaluation of grading criteria. Cancer 1998;82(7):1217-24.
[6] Brandwein MS, Ivanov K, Wallace DI, Hille JJ, Wang B, Fahmy A, etal. Mucoepidermoid carcinoma: a clinicopathologic study of 80patients with special reference to histological grading. Am J SurgPathol 2001;25(7):835-45.
[7] Bevilacqua G, Sobel ME, Liotta LA, Steeg PS. Association of lownm23 RNA levels in human primary infiltrating ductal breastcarcinomas with lymph node involvement and other histopathologicalindicators of high metastatic potential. Cancer 1989;49:5185-90.
[8] Bradley PJ. Distant metastases from salivary glands cancer. ORL JOtorhinolaryngol Relat Spec 2001;63:233-42.
[9] Ellis GL, Auclair P. Tumors of the salivary glands. Atlas of tumorpathology, series 3, fascicle 17. Washington: Armed Forces Institute ofPathology; 1996. p. 155-75.
[10] Kase S, Osaki M, Honjo S, Adachi H, Tsujitani S, Kaibara N, et al.Expression of cyclo-oxygenase-2 is correlated with high intratumoralmicrovessel density and low apoptotic index in human esophagealsquamous cell carcinomas. Virchows Arch 2003;442:129-35.
[11] Fosslien E. Biochemistry of cyclooxygenase (COX)-2 inhibitors andmolecular pathology of COX-2 in neoplasia. Crit Rev Clin Lab Sci2000;37:431-502.
[12] Farrow DC, Vaughan TL, Hansten Stanford JL, Risch HA, GammonMD, Chow WH, et al. Use of aspirin and other nonsteroidal anti-

321M.M. Zyada et al. / Annals of Diagnostic Pathology 13 (2009) 313–321
inflammatory drugs and risk of esophageal and gastric cancer. CancerEpidemiol Biomarkers Prev 1998;7:97-102.
[13] Reddy BS, Maruyama H, Kelloff G. Dose-related inhibition of coloncarcinogenesis by dietarypiroxicam, a nonsteroidal anti-inflammatorydrug during different stages of rat colon tumor development. CancerRes 1987;47:5340-6.
[14] Tsujii M, Kawano S, Tsuji S, Sawaoka H, Hori M, DuBois RN.Cyclooxygenase regulates angiogenesis induced by colon cancer cells.Cell 1998;93:705-16.
[15] Attiga FA, Fernandez PM, Weeraratna AT, Manyak MJ, Patierno SR.Inhibitors of prostaglandin synthesis inhibit human prostate tumor cellinvasiveness and reduce the release of matrix metalloproteinases.Cancer Res 2000;60:4629-37.
[16] Tsujii M, DuBois RN. Alterations in cellular adhesion and apoptosis inepithelial cells overexpressing prostaglandin endoperoxide synthase 2.Cell 1995;83:493-501.
[17] Tsujii M, Kawano S, DuBois RN. Cyclooxygenase-2 expression inhuman colon cancer cells increases metastatic potential. Proc NatlAcad Sci U S A 1997;94:3336-40.
[18] Wang Y, Szekely L, Okan J, et al. Wild type p53 triggered apoptosis isinhibited by bcl-2 in v-myc induced T-cell lymphoma lines. Oncogene1993;8:3427-31.
[19] JohnsonMI, Hamdy FC. Apoptosis regulating genes in prostate cancer.[review]Oncol Rep 1998;5:553-7.
[20] Vairo G, Innes KM, Adems JM. BCL-2 has a cycle inhibitory functionseparable from its enhancement of cell survival. Oncogene1996;13:1511.
[21] Sakamoto T, Uozaki H, Kondo K, Imauchi Y, Yamasoba T, SugasawaM, et al. Cyclooxygenase-2 regulates the degree of apoptosis bymodulating bcl-2 protein in pleomorphic adenoma and mucoepider-moid carcinoma of the parotid gland. Act Oto-Laryngologica2005;125:191-5.
[22] Barnes L, Eveson JW, Reichart P, Sindransky D, editors. Pathology andgenetics of head and neck tumors. World Health Organizationclassification of tumours. Lyon: IARC Press; 2005. p. 313.
[23] Wittenkind C, Greene FL, Hutter RVP, Klimpfinger M, Sobin LH.TNM Atlas. 5th ed. Berlin: Springer; 2004. p. 5-65.
[24] Hsu SM, Raine L, Fanger H. Use of avidin-biotin-peroxidase complex(ABC) in immunoperoxidase techniques a comparison between ABCand unlabeled antibody PAP procedures. J Histochem Cytochem1981;29:577-80.
[25] Segawa E, Sakurai K, Kishimoto H, Takaoka K, Noguchi K, HashitaniS, et al. Expression of cyclooxygenase-2 and DNA topoisomerase II inprecancerous and cancerous lesions of the oral mucosa. Oral Oncol2008;44:664-71.
[26] Ozawa H, Tomita T, Sakamoto K, Tagawa T, Fujii R, Kanzaki S, et al.Mucoepidermoid carcinoma of the head and neck: clinical analysis of43 patients. Jpn J Clin Oncol 2008;38(6):414-8.
[27] Spiro RH, Huvos AG, Berk R, Strong EW. Mucoepidermoidcarcinoma of salivary glands: a clinicopathologic study of 367 cases.Am J Surg 1978;136:461-8.
[28] Suzuki M, Ichimiya I, Matsushita F, Mogi G. Histological features andprognosis of patients with mucoepidermoid carcinoma of the parotidgland. J Laryngol Otol 1998;112:944-7.
[29] Evans HL. Mucoepidermoid carcinoma of salivary glands. a study of69 cases with special attention to histologic grading. Am J Clin Pathol1984;81(6):696-701.
[30] Kaklamanis L, Savage A, Mortensen N, Tsiotos P, AnagnostopoulouID, Biddolph S, et al. Early expression of BCL-2 protein in theadenoma-carcinoma sequence of colorectal neoplasia. J Pathol1996;179:10.
[31] Friess H, Lu Z, Graber HU, Zimmermann A, Alder G, Korc M, et al.Bax, but not bcl-2, influences the prognosis of human pancreaticcancer. Gut 1998;43:414-21.
[32] Hu YX, Watanabe H, Ohisubo K, et al. BCL-2 expression related toaltered p53 protein and its impact on the progression of humanpancreatic carcinoma. Br J Cancer 1999;80:1075-9.
[33] Eid H, Gulyas M, Geczi L, Bodrogi I, Institoris E, Bak M. Expressionof BCL-2 in testicular carcinoma. Cancer 1998;83:331-6.
[34] Rochaix P, Krajewski S, Reed JC, Bonnet F, Voigt JJ, Brousset F. Invivo patterns of BCL-2 family protein expression in breast carcinomain relation to apoptosis. J Pathol 1999;187:410-5.
[35] Itoh S, Matsui K, Furuta I, Takano Y. Immunohistochemical study onoverexpression of cyclooxgenase-2 in squamous cell carcinoma of theoral cavity: its importance as a prognostic predictor. Oral Oncol2003;39:829-35.
[36] Yanez M, Roa T, Garcia M, Ibacache G, Villaseca M. BCL-2 geneprotein expression in salivary gland tumors. Rev Med Chil 1999;127(2):139-42.
[37] Yoshikawa R, Sano H, Masuda C, Tsubouchi Y, Chargui J, YoshimuraN, et al. Expression of cyclooxygenase-2 in prostate carcinoma. Cancer2000;89:589-96.
[38] Peng J, Su C, Chang H, Chai C, Hung W. Overexpression ofcyclooxygenase 2 in squamous cell carcinoma of the hypopharynx.Hum Pathol 2002;33:101-4.
[39] Zimmermann KC, Sarbia M, Weber A, Borchard F, Gabbert HE,Schror K. Cyclooxygenase-2 expression in human esophagealcarcinoma. Cancer Res 1999;59:198-204.
[40] Huang M, Stolina M, Sharma S, Mao JT, Zhu L, Miller PW, et al. Non-small cell lung cancer cyclooxygenase-2 dependent regulation ofcytokine balance in lymphocytes and macrophage: up-regulation ofinterleukin 10 and down-regulation of interleukin 12 production.Cancer Res 1998;58:1208-16.
[41] Yin HF, Okada N, Takagi M. Apoptosis and apoptotic-related factors inmucoepidermoid carcinoma of the minor salivary glands. Pathol Int2000;50(8):603.
[42] Siziopikou KP, Prioleau JE, Harris JR, Schnit SJ. BCL-2 expression inthe spectrum of preinvasive breast lesions. Cancer 1996;77:499-506.
[43] Yang E, et al. Prognostic value of BCL-2 in invasive breast cancerreceiving chemotherapy and endocrine therapy. Oncol Rep 2003;10(1):121-5.
[44] Shibata M, Kodani I, Osaki M, Araki K, Adachi H, Ryoke K, et al.Cyclo-oxygenase-1 and 2-expression in human oral mucosa, dysplasiaand squamous cell carcinomas and their pathological significance. OralOncol 2005;41:304-12.
[45] Tsubochi H, Sato N, Hiyama M, Kaimori M, Endo S, Sohara Y, et al.Combined analysis of cyclooxygenase-2 expression with p35 and ki-67 in non small cell lung cancer. Ann Thorac Surg 2006;82:1198-204.
[46] Smith ML, Hawcroft G, Hull MA. The effect of nonsteroidal anti-inflammatory drugs on human colorectal cancer cells: evidence ofdifferent mechanisms of action. Eur J Cancer 2000;36:664-74.
[47] Watson AJ. Chemopreventive effects of NSAIDs against colorectalcancer: regulation of apoptosis and mitosis by COX-1 and -2. HistolHistopathol 1998;13:591-7.
Copyright © 2022 FDOKUMEN




















