
Histoplasma capsulatum proteome response to decreased iron availability
Upload
uni-duesseldorfCategory
view
0download
0
PDCPSA
Addedltp
smaa
RACMssgco
a
Journal of the American College of Cardiology Vol. 47, No. 3, 2006© 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00P
lasma Nitroso Compounds Areecreased in Patients With Endothelial Dysfunction
hristian Heiss, MD,* Thomas Lauer, MD,† André Dejam, MD,*etra Kleinbongard, PHD,* Sandra Hamada, MS,* Tienush Rassaf, MD,*imone Matern, BS,* Martin Feelisch, PHD,‡ Malte Kelm, MD*achen and Duesseldorf, Germany; and Boston, Massachusetts
OBJECTIVES We investigated whether plasma nitros(yl)ated species (RXNOs) that mediate systemic nitricoxide (NO) bioactivity are depleted in individuals with cardiovascular risk factors andendothelial dysfunction.
BACKGROUND Endothelium-derived NO acts not only as a regional messenger but exerts significant systemiceffects via formation of circulating RXNOs delivering NO to sites of impaired production.
METHODS Endothelial function was assessed in 68 patients with one to four major cardiovascular riskfactors (RF) and 39 healthy control subjects (C) by measurement of flow-mediated dilation(FMD) of the brachial artery using high-resolution ultrasound. In parallel, plasma RXNOswere determined by reductive gas phase chemiluminescence.
RESULTS Increasing numbers of risk factors were accompanied by a progressive decrease in FMD: 6.5 �0.4% (C); 4.7 � 0.5% (one RF); 2.8 � 0.4% (two RF); 2.2 � 0.4% (three RF); and 1.0 � 0.3%(four RF). Progressively impaired vascular function was associated with a concomitant decreasein plasma RXNOs (p � 0.01): 39 � 2 nmol/l (C); 30 � 2 nmol/l (one RF); 24 � 3 nmol/l(two RF); 22 � 3 nmol/l (three RF); and 15 � 2 nmol/l (four RF), with univariate correlationbetween FMD and RXNO (r � 0.41, p � 0.001). In a multivariate regression model, RXNOwas an independent predictor of endothelial function.
CONCLUSIONS Endothelial dysfunction in patients with cardiovascular risk factors is associated withdecreased levels of circulating RXNOs. Plasma RXNOs may be diagnostically useful markersof NO bioavailability and a surrogate index of endothelial function. Whether the observeddecrease in concentration reflects impaired NO formation, accelerated decomposition, and/orconsumption of RXNOs and whether these processes play a causal role in the pathophysi-ology of arteriosclerosis remain to be investigated. (J Am Coll Cardiol 2006;47:573–9)
ublished by Elsevier Inc. doi:10.1016/j.jacc.2005.06.089
© 2006 by the American College of Cardiology Foundation
padvfcravc“tuc(SwSp(Mnpt
rteriosclerosis is the major cause for chronic vasculariseases such as coronary artery disease, cerebrovascularisease, and peripheral arterial occlusive disease. The keyvent in the pathogenesis of arteriosclerosis is believed to beysfunction of the endothelium and disruption of endothe-
ial homeostasis, predisposing blood vessels to vasoconstric-ion, inflammation, leukocyte adhesion, thrombosis, androliferation of vascular smooth muscle cells.
See page 580
Endothelium-derived nitric oxide (NO) is an essentialhort-lived signaling molecule important for vascular ho-eostasis. Decreased NO bioactivity leads to accelerated
therogenesis. Until recently, it was believed that the bio-ctivity of NO is limited to close temporal and spatial
From the *Department of Cardiology, Pneumology, and Vascular Medicine,WTH Aachen, Aachen, Germany; †Department of Cardiology, Pneumology, andngiology, Heinrich-Heine University, Duesseldorf, Germany; and the ‡Whitakerardiovascular Institute, Boston University School of Medicine, Boston,assachusetts. Dr. Kelm received a grant from the Deutsche Forschungsgemein-
chaft (SFB 612); Dr. Lauer received a grant from Klinische Forschungskommis-ion of the Heinrich-Heine University Duesseldorf; and Dr. Feelisch received arant from the National Institutes of Health (HL69029). Drs. Heiss and Lauerontributed equally to this work. Dr. Heiss is currently affiliated with the Divisionf Cardiology, UCSF, San Francisco, California.
tManuscript received May 5, 2005; revised manuscript received June 3, 2005,
ccepted June 27, 2005.
roximity of the endothelium and that NO is a mereutocrine/paracrine effector (i.e., that it can only travel shortistances in the bloodstream (1) before it becomes inacti-ated). Recent studies challenge this concept by suggesting thatree NO is in equilibrium with a pool of various NO-ontaining compounds in blood that have a bioactivity thatesembles that of authentic NO. Inhaled and intravenouslypplied exogenous NO is transported and delivered along theascular tree to dilate distal conduit arteries and the microvas-ulature (2,3). While we have recently reported that thiscirculating NO pool” can be modulated by dietary interven-ion (4), the chemical identity of those species is currentlynclear. Initially, the circulating pool was believed to be mainlyomprised of nitrosothiols, in particular S-nitrosoalbumin�80%), and to a lesser extent S-nitrosohemoglobin,-nitrosoglutathione, and S-nitrosocysteine (5). Consistentith this view, intravenous application of authentic-nitrosothiols leads to vasodilation (2), inhibition oflatelet activation (6), abolition of carotid embolization7), and protection from ischemia/reperfusion injury (8).
ore recently, however, N-nitroso proteins and iron-itrosyl complexes (9,10), as well as nitrite (11,12) andotentially nitrated lipids (13), have also been implicatedo serve as plasma NO stores.
The measurement of flow-mediated dilation (FMD) of
he brachial artery (BA) as a noninvasive endothelial func-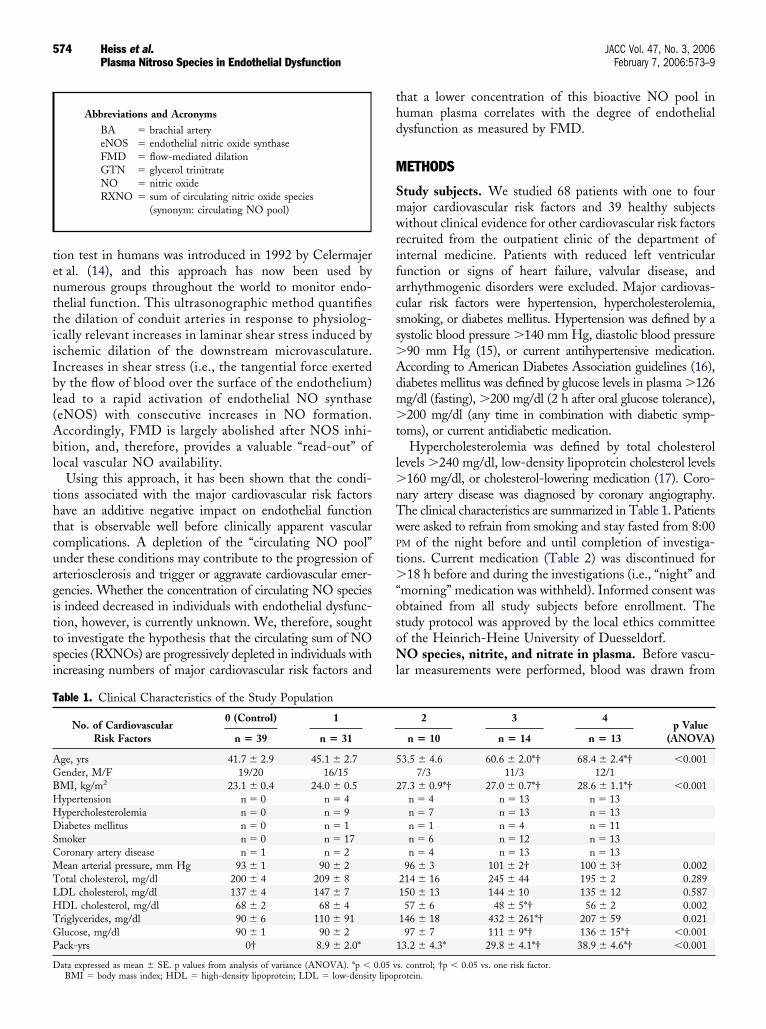
tenttiiIbl(Abl
thtcuagittsi
thd
M
Smwrifacss�Adm�t
l�nTwP
t�“osoNl
T
AGBHHDSCMTLHTGP
D
574 Heiss et al. JACC Vol. 47, No. 3, 2006Plasma Nitroso Species in Endothelial Dysfunction February 7, 2006:573–9
ion test in humans was introduced in 1992 by Celermajert al. (14), and this approach has now been used byumerous groups throughout the world to monitor endo-helial function. This ultrasonographic method quantifieshe dilation of conduit arteries in response to physiolog-cally relevant increases in laminar shear stress induced byschemic dilation of the downstream microvasculature.ncreases in shear stress (i.e., the tangential force exertedy the flow of blood over the surface of the endothelium)ead to a rapid activation of endothelial NO synthaseeNOS) with consecutive increases in NO formation.ccordingly, FMD is largely abolished after NOS inhi-ition, and, therefore, provides a valuable “read-out” ofocal vascular NO availability.
Using this approach, it has been shown that the condi-ions associated with the major cardiovascular risk factorsave an additive negative impact on endothelial functionhat is observable well before clinically apparent vascularomplications. A depletion of the “circulating NO pool”nder these conditions may contribute to the progression ofrteriosclerosis and trigger or aggravate cardiovascular emer-encies. Whether the concentration of circulating NO speciess indeed decreased in individuals with endothelial dysfunc-ion, however, is currently unknown. We, therefore, soughto investigate the hypothesis that the circulating sum of NOpecies (RXNOs) are progressively depleted in individuals withncreasing numbers of major cardiovascular risk factors and
Abbreviations and AcronymsBA � brachial arteryeNOS � endothelial nitric oxide synthaseFMD � flow-mediated dilationGTN � glycerol trinitrateNO � nitric oxideRXNO � sum of circulating nitric oxide species
(synonym: circulating NO pool)
able 1. Clinical Characteristics of the Study Population
No. of CardiovascularRisk Factors
0 (Control) 1
n � 39 n � 31
ge, yrs 41.7 � 2.9 45.1 � 2.7ender, M/F 19/20 16/15MI, kg/m2 23.1 � 0.4 24.0 � 0.5ypertension n � 0 n � 4ypercholesterolemia n � 0 n � 9iabetes mellitus n � 0 n � 1
moker n � 0 n � 17oronary artery disease n � 1 n � 2ean arterial pressure, mm Hg 93 � 1 90 � 2
otal cholesterol, mg/dl 200 � 4 209 � 8DL cholesterol, mg/dl 137 � 4 147 � 7DL cholesterol, mg/dl 68 � 2 68 � 4riglycerides, mg/dl 90 � 6 110 � 91lucose, mg/dl 90 � 1 90 � 2ack-yrs 0† 8.9 � 2.0*
ata expressed as mean � SE. p values from analysis of variance (ANOVA). *p � 0.05 vBMI � body mass index; HDL � high-density lipoprotein; LDL � low-density lipop
hat a lower concentration of this bioactive NO pool inuman plasma correlates with the degree of endothelialysfunction as measured by FMD.
ETHODS
tudy subjects. We studied 68 patients with one to fourajor cardiovascular risk factors and 39 healthy subjectsithout clinical evidence for other cardiovascular risk factors
ecruited from the outpatient clinic of the department ofnternal medicine. Patients with reduced left ventricularunction or signs of heart failure, valvular disease, andrrhythmogenic disorders were excluded. Major cardiovas-ular risk factors were hypertension, hypercholesterolemia,moking, or diabetes mellitus. Hypertension was defined by aystolic blood pressure �140 mm Hg, diastolic blood pressure90 mm Hg (15), or current antihypertensive medication.ccording to American Diabetes Association guidelines (16),iabetes mellitus was defined by glucose levels in plasma �126g/dl (fasting), �200 mg/dl (2 h after oral glucose tolerance),200 mg/dl (any time in combination with diabetic symp-
oms), or current antidiabetic medication.Hypercholesterolemia was defined by total cholesterol
evels �240 mg/dl, low-density lipoprotein cholesterol levels160 mg/dl, or cholesterol-lowering medication (17). Coro-
ary artery disease was diagnosed by coronary angiography.he clinical characteristics are summarized in Table 1. Patientsere asked to refrain from smoking and stay fasted from 8:00
M of the night before and until completion of investiga-ions. Current medication (Table 2) was discontinued for
18 h before and during the investigations (i.e., “night” andmorning” medication was withheld). Informed consent wasbtained from all study subjects before enrollment. Thetudy protocol was approved by the local ethics committeef the Heinrich-Heine University of Duesseldorf.O species, nitrite, and nitrate in plasma. Before vascu-
ar measurements were performed, blood was drawn from
2 3 4p Value
(ANOVA)n � 10 n � 14 n � 13
3.5 � 4.6 60.6 � 2.0*† 68.4 � 2.4*† �0.0017/3 11/3 12/1
7.3 � 0.9*† 27.0 � 0.7*† 28.6 � 1.1*† �0.001n � 4 n � 13 n � 13n � 7 n � 13 n � 13n � 1 n � 4 n � 11n � 6 n � 12 n � 13n � 4 n � 13 n � 13
96 � 3 101 � 2† 100 � 3† 0.002214 � 16 245 � 44 195 � 2 0.289150 � 13 144 � 10 135 � 12 0.58757 � 6 48 � 5*† 56 � 2 0.002
146 � 18 432 � 261*† 207 � 59 0.02197 � 7 111 � 9*† 136 � 15*† �0.0013.2 � 4.3* 29.8 � 4.1*† 38.9 � 4.6*† �0.001
5
2
1
s. control; †p � 0.05 vs. one risk factor.rotein.

toPoachspthv1t(gEvw(ntboaatflt1pdtmba(Cdfp
ifctpmeSCvtwsPfcakStaAC
R
Eeicrr0ndg0rr(
nsin I
575JACC Vol. 47, No. 3, 2006 Heiss et al.February 7, 2006:573–9 Plasma Nitroso Species in Endothelial Dysfunction
he antecubital vein. All measurements were performed aftervernight fasting of more than 12 h between 8:00 and 9:00 AM.lasma levels of nitros(yl)ated NO species (RXNO: the sumf S-nitrosothiols, N-nitrosamines, iron-nitrosyl species)nd nitrite were determined using a triiodide/ozone-basedhemiluminescence assay, essentially as described (18,19). Aigh reproducibility of RXNO measurements has beenhown previously for standards (19). In addition, we haveerformed repeated measurements of plasma RXNOs onwo separate days at the same time of the day in fastedealthy volunteers (n � 20) and found an intrasubjectariation (i.e., averaged deviation between measurements of.8 � 9%). Nitrate was quantified after enzymatic reductiono nitrite by nitrate reductase using flow-injection analysis20). All analyses were performed by independent investi-ators blinded to the clinical history of study subjects.ndothelium-dependent and endothelium-independent
asodilation. Endothelium-dependent dilation of the BAas measured noninvasively by high-resolution ultrasound
SONOS 5500, Agilent Technologies, Palo Alto, Califor-ia, with a 15-MHz linear-array transducer) using standardechniques (21). Briefly, baseline data for diameter andlood-flow velocity of the BA were quantified after 10 minf supine rest in an air-conditioned room (21°C) 1 to 2 cmbove the elbow. Then a blood pressure cuff was placedround the forearm distal to the cubital fossae and inflatedo 200 mm Hg for a period of 5 min. Diameter and bloodow velocity were measured immediately after deflation ofhe cuff (hyperemic blood flow) as well as 60, 75, 90, and20 s later. Maximal BA diameter observed during this timeeriod was used to calculate FMD. Endothelium-independentilation of BA was quantified 4 min after sublingual adminis-ration of 400 �g glycerol trinitrate (GTN) (Nitrolingualite, Pohl, Germany). All ultrasound scans were performed
y the same operator using the same equipment. Anutomated analysis system was used to measure diametersBrachial Analyzer, Medical Imaging Applications, Iowaity, Iowa) yielding low variabilities of our methodologyescribed elsewhere (21). Internal quality control was per-ormed by an independent investigator blinded to the
Table 2. Current Medication of the Study Pop
No. of CardiovascularRisk Factors
0 (Control)
n � 39
ACE inhibitors 0ATII receptor antagonists 0Beta-blockers 0Diuretics 0Calcium-channel antagonists 0Nitrates 0Acetylsalicylic acid 1 (5)Statins 0Oral antidiabetics 0Insulin 0
Data expressed as n (% of group).ACE � angiotensin-converting enzyme; ATII � angiote
rotocol (96% approved); FMD and endothelium- 1
ndependent dilation were expressed as a percentage changerom baseline. To estimate the relative proportion of FMDompared to the maximally achievable diameter after GTN,he FMD/GTN ratio was calculated and expressed asercentage for each individual. Blood flow was calculated byultiplication of cross-sectional area and mean velocity at
ach time point.tatistical analysis. Results are expressed as means � SE.omparisons between groups were analyzed by analysis of
ariance (ANOVA) and, if significant, consecutive post-hocest (Bonferroni). P values from Bonferroni post-hoc testsere corrected for 10 pairwise comparisons. Linear relation-
hips between continuous variables were calculated usingearson’s r. A multivariate regression analysis was per-
ormed, to estimate the predictive value of plasma RXNOoncentrations to explain the variability of vascular functions a surrogate for cardiovascular risk. Established parametersnown to affect FMD were also included in the model.tandardized coefficients were calculated as a measure forhe relative predictive value. Statistical significance wasssumed if a null hypothesis could be rejected at p � 0.05.ll analyses were performed with SPSS 11.0.1 (SPSS Inc.,hicago, Illinois).
ESULTS
ffect of cardiovascular risk factors on vascular param-ters. Endothelial function measured by FMD was signif-cantly impaired in individuals with increasing numbers ofardiovascular risk factors (one risk factor: 4.7 � 0.4%; twoisk factors: 2.8 � 0.4%; three risk factors: 2.2 � 0.4%; fourisk factors: 1.0 � 0.3%) compared to control subjects (6.5 �.4%; p � 0.005 Bonferroni; Fig. 1A), irrespective of theature of risk for cardiovascular disease. Flow-mediatedilation in individuals with one risk factor was significantlyreater than in those with three and four risk factors (p �.003, Bonferroni). Endothelium-independent dilation inesponse to GTN was similarly impaired: 14.5 � 1.0% (zeroisk factors); 12.3 � 1.0% (one risk factor); 10.6 � 1.3%two risk factors); 9.1 � 1.9% (three risk factors); 6.8 �
on
1 2 3 4
� 31 n � 10 n � 14 n � 13
(7) 4 (40) 10 (71) 10 (77)0 2 (20) 1 (7) 1 (8)0 4 (40) 10 (71) 12 (92)(7) 2 (20) 2 (14) 5 (38)(13) 1 (10) 2 (14) 3 (23)(3) 2 (20) 4 (29) 4 (31)(7) 3 (30) 12 (86) 13 (100)(7) 3 (30) 8 (57) 9 (67)0 1 (10) 1 (7) 3 (23)(3) 0 1 (7) 1 (8)
I.
ulati
n
2
24122
1
.0% (four risk factors) (ANOVA: p � 0.05). However, the

sesawrpiDEtRIs(nfsfts1a0d3f�EpF0dRfifb(
gBc3gcRcrv
D
Tp
F(roB
Foflt
576 Heiss et al. JACC Vol. 47, No. 3, 2006Plasma Nitroso Species in Endothelial Dysfunction February 7, 2006:573–9
ignificantly lowered FMD/GTN ratio indicates preferentialndothelial dysfunction (Fig. 1B). The baseline diameter wasignificantly increased in the groups with three (5.1 � 0.2 mm)nd four risk factors (5.1 � 0.2 mm) compared to subjectsith zero to two risk factors (control: 4.0 � 0.1 mm; one
isk factor: 4.3 � 0.1 mm; two risk factors: 4.7 � 0.3 mm;� 0.001 Bonferroni). No significant differences were seen
n terms of blood flow at baseline, during hyperemia, oroppler flow reserve (data not shown).ffect of cardiovascular risk factors on NO-related me-
abolites in plasma. In individuals without risk factors,XNO plasma concentration amounted to 39 � 2 nmol/l.
ncreasing numbers of risk factors were associated with aignificant reduction in plasma RXNO levels: 30 � 2 nmol/lone risk factor); 24 � 3 nmol/l (two risk factors); 22 � 3mol/l (three risk factors); and 16 � 2 nmol/l (four riskactors) (p � 0.001 Bonferroni; Fig. 1C). Also, RXNO wasignificantly different in the groups with one and four riskactors (p � 0.003 Bonferroni). Plasma nitrite concentra-ions followed a similar trend without reaching statisticalignificance: 142 � 13 (control); 125 � 13 (one risk factor);31 � 23 (two risk factors); 118 � 17 (three risk factors);nd 106 � 19 (four risk factors) nmol/l (ANOVA: p �.821). Nitrate concentrations were not significantlyifferent between groups: 21 � 3 �mol/l (control); 23 �
�mol/l (one risk factor); 26 � 5 �mol/l (two riskactors); 32 � 7 �mol/l (three risk factors); and 23 � 4mol/l (four risk factors) (ANOVA: p � 0.800).ndothelial function correlates with circulating NOool. There was a highly significant correlation betweenMD and plasma RXNO concentration (r � 0.41; p �.001; Fig. 2) suggesting an association between endothelialysfunction and circulating NO pool.XNOs as an independent predictor of endothelial dys-
unction. In order to establish RXNO concentration as anndependent predictor of endothelial function, we per-ormed a multivariate linear regression analysis includingaseline characteristics known to affect vascular function
igure 1. Endothelial function and plasma nitric oxide species are decA) Flow-mediated dilation (FMD) and (B) percentage of FMD compareatio) are significantly lower in individuals with cardiovascular risk factors.f bioactive nitric oxide, are also significantly attenuated with increasing nonferroni-corrected for 10 pairwise comparisons.
age, gender, body mass index, total cholesterol, plasmapc
lucose, mean arterial blood pressure, pack years, diameter ofA, nitrite) and current medication with angiotensin-
onverting enzyme inhibitors and statins. As shown in Table, the independent predictor variables for FMD wereender, age, RXNO concentration, and BA diameter ac-ounting for 53% of the total variability of FMD (adjusted2 � 0.526; p � 0.001). The magnitudes of standardized
oefficients for the independent predictors were in the sameange as gender and age suggesting a comparable predictivealue.
ISCUSSION
he key findings of the present study are that: 1) the plasmaool of RXNOs is depleted in patients with cardiovascular
in individuals with increasing numbers of cardiovascular risk factors.lycerol trinitrate (GTN)-induced dilation of brachial artery (FMD/GTNitros(yl)ated species (RXNO) in plasma, representing the circulating pool
rs of risk factors. Columns � mean values; error bars � SE. P values are
igure 2. Vascular endothelial function correlates with circulating nitricxide (NO) pool. Endothelial function, measured as NO-dependentow-mediated dilation of the brachial artery, correlates with the concen-ration of circulating nitroso/nitrosyl species (RXNO) in plasma (r � 0.41,
reasedd to g(C) Numbe
� 0.001). Circles � individual values; filling � number of majorardiovascular risk factors (RF).

ro
umshsPdsuvdl
batdhfavrpwbid
bdref
posfcsabpnciitvfifj
icpaiesvovhtfecbif
tdSh(oodsolpfnc
T
GABMPTPRNBASAS
Abo
577JACC Vol. 47, No. 3, 2006 Heiss et al.February 7, 2006:573–9 Plasma Nitroso Species in Endothelial Dysfunction
isk factors; and that 2) RXNO is an independent predictorf endothelial function in a multivariate regression model.The earliest studies of endothelial control of vasomotion
sed quantitative coronary angiography to examine the vaso-otor response of the epicardial coronary artery during infu-
ion of acetylcholine (22) or increased blood flow (23). Inealthy individuals, the endothelium responds to thesetimuli by releasing vasodilator factors, in particular NO.atients with angiographically documented coronary arteryisease display impaired FMD and a vasoconstrictor re-ponse to acetylcholine, which likely reflects loss of NO andnopposed muscarinic receptor activation at the level of theascular smooth muscle. Notably, studies suggest that en-othelial function detected noninvasively in the BA corre-
ates with function in conduit coronary arteries (24).As in the coronary circulation, endothelial function in the
rachial circulation is impaired in the setting of traditionalnd novel risk factors and responds to interventions knowno reduce cardiovascular disease risk (25). Traditional car-iovascular risk factors as diverse as smoking, aging (26),ypercholesterolemia, hypertension, hyperglycemia, and aamily history of premature atherosclerotic disease are allssociated with attenuation/loss of endothelium-dependentasodilation in both adults and children. More recentlyecognized risk factors such as obesity, elevated C-reactiverotein, and chronic systemic infection are also associatedith endothelial dysfunction. Corroborating several studiesy Celermajer et al. (14) and other groups, we observed annverse association between the cumulative number of car-iovascular risk factors and FMD of the BA.Although case-control studies indicate an association
etween endothelial dysfunction and acute coronary syn-romes (27), more convincing evidence for a pathogenicole of the former is provided by studies demonstrating thatndothelial function identifies patients at increased risk for
able 3. Multivariate Linear Regression Analysis
FMD
StandardizedCoefficient p Value
ender 0.224 0.029ge �0.189 0.045MI �0.039 0.706ean arterial blood pressure 0.091 0.267
ack-yrs �0.010 0.920otal cholesterol �0.048 0.552lasma glucose �0.161 0.052XNO 0.163 0.044itrite 0.093 0.212rachial artery diameter �0.377 0.001CE inhibitors �0.189 0.077tatins �0.066 0.527djusted R2 0.526ignificance (ANOVA) �0.001
CE � angiotensin-converting enzyme; ANOVA � analysis of variance; BMI �ody mass index; FMD � flow-mediated dilation; RXNO � sum of circulating nitricxide species.
uture events. Numerous published studies involving �2,000 c
atients with atherosclerosis have proven the prognostic valuef endothelial vasomotor dysfunction (25). These studiestrongly and consistently demonstrate that endothelial dys-unction identifies patients who have increased risk forardiovascular events in the short and long run. Primary andecondary preventive therapies (e.g., exercise therapy,ngiotensin-converting enzyme inhibitors, and statins) areelieved to mediate their positive prognostic effect in largeart by increasing endothelial function. In our study, we didot observe significant contributions of body mass index orurrent medication with angiotensin-converting enzymenhibitors or statins to the variability of endothelial functionn our multivariate regression model. This may either be dueo the small n-number or the significantly greater predictivealue of other included parameters. Thus, endothelial dys-unction appears to be a systemic process that can bedentified in different vascular beds, including those remoterom the coronary and cerebral circulation where the ma-ority of actual events occur.
The present study is the first to report that RXNO levelsn plasma are lower in individuals with one or moreardiovascular risk factors compared to controls. The im-ortance of RXNOs results from the very similar biologicalctions exhibited by both NO and RXNOs in vivo as well asn vitro (28). Cannon et al. (3) have provided the firstvidence for the intravascular delivery of bioactive NOpecies in humans. Inhaled NO restored blood flow andascular resistance of the forearm during regional inhibitionf NO synthesis. Intravenous infusion of NO in healthyolunteers increased plasma RXNOs and induced systemicemodynamic effects at the level of both conduit and resis-ance vessels, as reflected by dilator responses in the BA andorearm microvasculature. Infusion of S-nitrosoglutathionexerted similar effects, and the observed changes in RXNOoncentrations correlated with the vasodilator effects exertedy NO and S-nitrosoglutathione (2). Furthermore, RXNOsnhibit platelet aggregation (29) and abolish embolizationrom carotid plaques (30).
The RXNO levels reported in the literature range fromhe low nanomolar up to the micromolar range. This may beue to differences in the methodology applied to measure-nitrosothiols and N-nitrosamines, sample preparation andandling, choice of standards, and detection methods5,9,10,19,31,32). In view of the fact that the chemical identityf most of these species is currently unknown, we intentionallypted to measure the sum of all nitroso and nitrosyl speciesetectable under these conditions attempting a group-pecific analysis as opposed to quantification of select speciesf unclear physiological role (19). Regardless of the absoluteevels of RXNOs, the significant difference between theatient groups in relation to the impairment of endothelialunction remains (31). Nevertheless, future studies areeeded to identify relevant individual bioactive compoundsomprising RXNOs.
The decreased pool of circulating NO with increasing
ardiovascular risk load may be secondary to endothelial
dscRogswislsdcdcplNbaNasasdboeccdps
mfsa(cswabnibbbit(mi
fcrpadmebnsvpbCtcteifmwpa
ATa
RmAE
R
578 Heiss et al. JACC Vol. 47, No. 3, 2006Plasma Nitroso Species in Endothelial Dysfunction February 7, 2006:573–9
ysfunction reflected by the impaired FMD. This is under-cored by the univariate correlation between FMD and theirculating NO pool and the multivariate analysis withXNO being a significant predictor for FMD independentf age, gender, body mass index, blood pressure, cholesterol,lucose, baseline diameter of the BA, pack years, currenttatin and angiotensin-converting enzyme inhibitor therapyith comparable magnitude as gender and age. Corroborat-
ng our previous findings, the baseline diameter was also aignificant predictor (33). Also, cigarette smoke containsarge amounts of nitrogen oxides (34); the subgroup ofmokers without other cardiovascular risk factors showedecreased RXNOs and FMD. Potentially, the reducedirculating NO pool may accelerate atherogenesis and pre-ispose individuals to clinical arteriosclerotic syndromesharacterized by impaired regional NO production, such aseripheral and coronary artery disease. Whether decreased
evels of RXNO are a consequence of reduced endogenousO synthesis and/or bioavailability or that of an accelerated
reakdown and/or NO consumption is currently unclear. Inddition to a diminished NO production, alterations inOS expression, co-factor, and/or substrate availability may
lso contribute directly to oxidative stress by producinguperoxide as a consequence of uncoupling of NOS. Thus,lthough the sources of oxidative stress may differ andeveral different enzymatic and biochemical mechanisms canisrupt normal NO signaling, a central problem appears toe a shift in NO/nitroso-redox balance away from “physi-logic” heme nitrosylation and S-nitrosation to one ofnhanced nitrosation/nitration of protein targets underonditions of oxidative stress. Whether plasma RXNOoncentration represents a valid surrogate marker for car-iovascular risk burden or oxidative stress and qualifies as arognostic factor cannot be concluded from the presenttudy and remains to be investigated.
In newer publications, nitrite, one of the major oxidativeetabolites of NO, was implicated to be both an indicator
or NOS activity (35) and a circulating NO donor that mayelectively donate NO to hypoxic vascular beds (11). Thus,part from RXNOs, nitrite within the blood and tissues11,36,37) may evolve as an important contributor to theirculating pool of bioactive NO. Although in the presenttudy no significant differences in mean plasma nitrite levelsere observed between individual groups, there was clearly
n inverse relationship between nitrite levels and the num-er of cardiovascular risk factors. The fact that RXNOs, butot nitrite, predicts endothelial dysfunction in the multivar-
ate regression model in this relatively small sample size maye explained by several differences in biochemical features ofoth compounds. The short half-life of plasma nitrite inlood, which is a consequence of its rapid transition (38)nto red blood cells and surrounding tissues (19), contributeso its usefulness to index acute changes in eNOS activity35). Although the absolute levels are conserved throughoutany mammalian species (36), the intraindividual variabil-
ty still poses a problem because diet, NO donor drugs, renal
unction, gut bacteria (39), and other NOS-independentonfounders may influence baseline levels and thus requireelatively large n-values to detect clear differences betweenatient populations. Because of its longer half-life andpparent robustness against influence by NOS-independentietary confounders such as nitrate (40), RXNOs may be aore suitable diagnostic marker for long-term changes in
NOS activity. Nevertheless, new analytical methods capa-le of differentiating between individual RXNO compo-ents and an identification of the physiological roles of thesepecies are necessary. Despite these obstacles, a compositeiew and analysis of the constituents of the circulating NOool is a promising first step toward the development of newiochemical approaches to assess endothelial dysfunction.onclusions. From the data presented herein, we conclude
hat endothelial dysfunction is associated with a depletion ofirculating nitroso/nitrosyl species in plasma, which is likelyo contribute to the increased risk for major cardiovascularvents in individuals with endothelial dysfunction. Measur-ng circulating nitroso/nitrosyl species may help in identi-ying individuals at risk and serve as a therapeutic surrogatearker in the future. Further studies are needed to establishhether the plasmatic RXNO pool represents a valuablearameter that allows optimal dose titration of therapeuticgents aimed at targeting endothelial dysfunction.
cknowledgmenthe authors wish to thank Gabi Schoder for her technical
ssistance.
eprint requests and correspondence: Dr. Malte Kelm, Depart-ent of Cardiology, Pneumology, and Vascular Medicine, RWTHachen, Pauwelsstraße 30, 52074 Aachen, Germany.-mail: [email protected].
EFERENCES
1. Liao JC, Hein TW, Vaughn MW, Huang KT, Kuo L. Intravascularflow decreases erythrocyte consumption of nitric oxide. Proc Natl AcadSci U S A 1999;96:8757–61.
2. Rassaf T, Kleinbongard P, Preik M, et al. Plasma nitrosothiolscontribute to the systemic vasodilator effects of intravenously appliedNO: experimental and clinical study on the fate of NO in humanblood. Circ Res 2002;91:470–7.
3. Cannon RO, Schechter AN, Panza JA, et al. Effects of inhaled nitricoxide on regional blood flow are consistent with intravascular nitricoxide delivery. J Clin Invest 2001;108:279–87.
4. Heiss C, Dejam A, Kleinbongard P, Schewe T, Sies H, Kelm M.Vascular effects of cocoa rich in flavan-3-ols. JAMA 2003;290:1030–1.
5. Stamler JS, Jaraki O, Osborne J, et al. Nitric oxide circulates inmammalian plasma primarily as an S-nitrose adduct of serum albumin.Proc Natl Acad Sci U S A 1992;89:7674–7.
6. Langford EJ, Brown AS, Wainwright RJ, et al. Inhibition of plateletactivity by S-nitrosoglutathione during coronary angioplasty. Lancet1994;344:1458–60.
7. Kaposzta Z, Martin JF, Markus HS. Switching off embolization fromsymptomatic carotid plaque using S-nitrosoglutathione. Circulation2002;105:1480–4.
8. Hallström S, Gasser H, Neumayer C, et al. S-Nitroso human serum
albumin treatment reduces ischemia/reperfusion injury in skeletalmuscle via nitric oxide release. Circulation 2002;105:3032–8.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
579JACC Vol. 47, No. 3, 2006 Heiss et al.February 7, 2006:573–9 Plasma Nitroso Species in Endothelial Dysfunction
9. Rassaf T, Bryan NS, Kelm M, Feelisch M. Concomitant presence ofN-nitroso and S-nitroso proteins in human plasma. Free Radic BiolMed 2002;33:1590–6.
0. Wang X, Tanus-Santos JE, Reiter CD, et al. Biological activity ofnitric oxide in the plasmatic compartment. Proc Natl Acad Sci U S A2004;101:11477–82.
1. Dejam A, Hunter CJ, Schechter AN, Gladwin MT. Emerging role ofnitrite in human biology. Blood Cells Mol Dis 2004;32:423–9.
2. Lundberg JO, Weitzberg E. NO generation from nitrite and its role invascular control. Arterioscler Thromb Vasc Biol 2005;25:915–22.
3. Baker PR, Schopfer FJ, Sweeney S, Freeman BA. Red cell membrane andplasma linoleic acid nitration products: synthesis, clinical identification,and quantitation. Proc Natl Acad Sci U S A 2004;101:11577–82.
4. Celermajer DS, Sorensen KE, Gooch VM, et al. Non-invasivedetection of endothelial dysfunction in children and adults at risk ofatherosclerosis. Lancet 1992;340:1111–5.
5. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of theJoint National Committee on Prevention, Detection, Evaluation, andTreatment of High Blood Pressure. Hypertension 2003;42:1206–52.
6. The Expert Committee on the Diagnosis and Classification ofDiabetes Mellitus. Report of the Expert Committee on the Diagnosisand Classification of Diabetes Mellitus. Diabetes Care 2003;23 Suppl1:S5–20.
7. The National Cholesterol Education Program (NCEP) Expert Panelon Detection, Evaluation, And Treatment of High Blood CholesterolIn Adults (Adult Treatment Panel III). Executive summary of thethird report of the National Cholesterol Education Program (NCEP)Expert Panel on Detection, Evaluation, and Treatment of High BloodCholesterol In Adults (Adult Treatment Panel III). JAMA 2001;285:2486–97.
8. Rassaf T, Preik M, Kleinbongard P, et al. Evidence for in vivotransport of bioactive nitric oxide in human plasma. J Clin Invest2002;109:1241–8.
9. Feelisch M, Rassaf T, Mnaimneh S, et al. Concomitant S-, N-, andheme-nitros(yl)ation in biological tissues and fluids: implications forthe fate of NO in vivo. FASEB J 2002;16:1775–85.
0. Schulz K, Kerber S, Kelm M. Reevaluation of the Griess method fordetermining NO/NO2- in aqueous and protein-containing samples.Nitric Oxide 1999;3:225–34.
1. Preik M, Lauer T, Heiss C, Tabery S, Strauer BE, Kelm M.Automated ultrasonic measurement of human arteries for the deter-mination of endothelial function. Ultraschall Med 2000;21:195–8.
2. Ludmer PL, Selwyn AP, Shook TL, Wayne RR, Mudge GH,Alexander RW. Paradoxical vasoconstriction induced by acetylcholinein atherosclerotic coronary arteries. N Engl J Med 1986;315:1046–51.
3. Cox DA, Vita JA, Treasure CB, et al. Atherosclerosis impairsflow-mediated dilation of coronary arteries in humans. Circulation1989;80:458–65.
4. Anderson TJ, Uehata A, Gerhard MD, et al. Close relation ofendothelial function in the human coronary and peripheral circulation.
J Am Coll Cardiol 1995;26:1235–41.5. Widlansky ME, Gokce N, Keaney JF Jr., Vita JA. The clinicalimplications of endothelial dysfunction. J Am Coll Cardiol 2003;42:1149–60.
6. Heiss C, Keymel S, Niesler U, Ziemann J, Kelm M, Kalka C.Impaired progenitor cell activity in age-related endothelial dysfunc-tion. J Am Coll Cardiol 2005;45:1441–8.
7. Okumura K, Yasue H, Matsuyama K, et al. Effect of acetylcholine onthe highly stenotic coronary artery: difference between the constrictorresponse of the infarct-related coronary artery and that of thenoninfarct-related artery. J Am Coll Cardiol 1992;19:752–8.
8. Rossi R, Giustarini D, Milzani A, Colombo R, Dalle-Donne I, DiSimplicio P. Physiological levels of S-nitrosothiols in human plasma.Circ Res 2001;89:E47.
9. de Belder AJ, MacAllister R, Radomski MW, Moncada S, VallancePJ. Effects of S-nitroso-glutathione in the human forearm circulation:evidence for selective inhibition of platelet activation. Cardiovasc Res1994;28:691–4.
0. Kaposzta Z, Baskerville PA, Madge D, Fraser S, Martin JF, MarkusHS. L-arginine and S-nitrosoglutathione reduce embolization inhumans. Circulation 2001;103:2371–5.
1. Gandley RE, Tyurin VA, Huang W, et al. S-nitrosoalbumin-mediated relaxation is enhanced by ascorbate and copper: effects inpregnancy and preeclampsia plasma. Hypertension 2005;45:21–7.
2. Foster MW, Pawloski JR, Singel DJ, Stamler JS. Role of circulatings-nitrosothiols in control of blood pressure. Hypertension 2005;45:15–7.
3. Lauer T, Heiss C, Preik M, et al. Reduction of peripheral flow reserveimpairs endothelial function in conduit arteries of patients withessential hypertension. J Hypertens 2005;23:563–9.
4. Ambrose JA, Barua RS. The pathophysiology of cigarette smoking andcardiovascular disease: an update. J Am Coll Cardiol 2004;43:1731–7.
5. Lauer T, Preik M, Rassaf T, et al. Plasma nitrite rather than nitratereflects regional endothelial nitric oxide synthase activity but lacksintrinsic vasodilator action. Proc Natl Acad Sci U S A 2001;98:12814–9.
6. Kleinbongard P, Dejam A, Lauer T, et al. Plasma nitrite reflectsconstitutive nitric oxide synthase activity in mammals. Free Radic BiolMed 2003;35:790–6.
7. Bryan NS, Rassaf T, Maloney RE, et al. Cellular targets andmechanisms of nitros(yl)ation: an insight into their nature and kineticsin vivo. Proc Natl Acad Sci U S A 2004;101:4308–13.
8. Dejam A, Pelletier MM, Saijo F, et al. Erythrocytes are the majorintravascular storage sites of nitrite in human blood. Blood 2005;106:734–9.
9. Janero DR, Bryan NS, Saijo F, et al. Differential nitros(yl)ation ofblood and tissue constituents during glyceryl trinitrate biotransforma-tion in vivo. Proc Natl Acad Sci U S A 2004;101:16958–63.
0. Lundberg JO, Govoni M. Inorganic nitrate is a possible source forsystemic generation of nitric oxide. Free Radic Biol Med 2004;37:
395– 400.Copyright © 2022 FDOKUMEN




















