Assessment of Autonomic Dysfunction in Childhood Guillain ...
51
Assessment of Autonomic Dysfunction in Childhood Guillain-Barré Syndrome Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 81-85 doi: 10.5681/jcvtr.2013.018 http://journals.tbzmed.ac.ir/JCVTR *Corresponding author: Babak Kazemi, E-mail: [email protected] Copyright © 2013 by Tabriz University of Medical Sciences Introduction: Autonomic dysfunction (AD) is a common and important complication in Guillain-Barré syndrome (GBS) and may be the cause of significant morbidity or death. Limited studies have evaluated this complication in childhood GBS. Our objectives were to show the prevalence of AD in children with GBS and investigate its association with the severity of the disease. Methods: Study included 28 children admitted with a diagnosis of GBS. Heart rate variability (HRV), motor function disability of the upper limbs and GBS disability scores were measured at admission and the results were compared with 20 healthy age/gender matched subjects (2-13 years; 43% male). GBS subtypes were defined by electromyography: acute inflammatory demyelinating polyneuropathy (AIDP) or acute motor axonal neuropathy (AMAN). Results: The mean age was 5.5±3.4 years (range 1.5-14 years; 50% male). AIDP and AMAN subtypes comprised 57.1% and 42.9% of cases, respectively. In the upper limbs, 85.7% and in the GBS disability grading, 50% of patients had ≤ 3 scores, implying less severe motor dysfunction. There was no difference in the mean heart rate between patients vs. controls (103.9 vs. 98.2 bpm; P= 0.16), but half of patients showed AD and HRV was significantly reduced in patients compared to controls. Of the 16 patients with AIDP, 11 (68.8%) showed reduced HRV compared to 3 (25%) out of 12 AMAN cases (P= 0.02). There was no significant relation between HRV and motor disability scores. Conclusion: AD was present in half of children with mild GBS and it showed no significant association with disease severity. . A B S T R A C T A R T I C L E I N F O Article Type: Original Article Article History: Received: 12 August 2013 Accepted: 8 September 2013 Keywords: Guillain-Barré Syndrome Autonomic Dysfunction Heart Rate Variability Mahmood Samadi, Babak Kazemi * , Sona Golzari Oskoui, Mohammad Barzegar Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran Introduction The term Guillain-Barré syndrome (GBS), first described in 1916 in two soldiers by French neurologists Georges Guillain, Jean-Alexandre Barré and Andre Strohl, defines a recognizable clinical entity that is characterized by rapidly evolving symmetrical limb weakness, loss of tendon reflexes, absent or mild sensory signs, and variable autonomic dysfunction (AD). Since the virtual elimination of poliomyelitis, GBS has become the leading cause of acute flaccid paralysis in western countries. 1 The condition, however, is known to occur at all ages, though it is rare in infancy, affecting approximately 0.3 to 2 per 100,000 children per year. 2-4 Weakness can develop acutely (within days) or subacutely (up to 4 weeks) and reaches a plateau, with subsequent spontaneous resolution of paralysis. Although the pathogenesis of GBS remains incompletely defined, there is increasing support for the concept that GBS results from an aberrant organ specific immune response. 5 GBS is now classified into two major demyelinating [acute inflammatory demyelinating polyneuropathy (AIDP)] and axonal [acute motor axonal neuropathy (AMAN)] categories according to clinical, electrophysiological, and pathological criteria. 6-8 Rare subtypes are acute motor sensory axonal neuropathy, accompanied by the variant of the Fisher syndrome presenting with ophthalmoplegia, ataxia, and areflexia. Very rare pure autonomic variants of GBS, defined as pandysautonomia were also reported. 9 The most frequent subtype of GBS in North America and Europe is AIDP, which accounts for 90% of GBS cases, while in Asia, South and Central America, the axonal form of GBS constitutes 30% to 47% of cases. 10 Only about 5% to 10% of patients in North America and Europe have an axonal subtype. AD is a common and important complication in GBS and occurs in approximately two- thirds of patients and is often associated with a variety of derangements including cardiovascular, vasomotor, or dysfunctions in both the sympathetic and parasympathetic systems 11 . The analysis of variations in the heart rate (HRV) has
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Assessment of Autonomic Dysfunction in Childhood Guillain ...

Assessment of Autonomic Dysfunction in Childhood Guillain-BarréSyndrome
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 81-85doi: 10.5681/jcvtr.2013.018http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Babak Kazemi, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Introduction: Autonomic dysfunction (AD) is a common and important complication in Guillain-Barré syndrome (GBS) and may be the cause of significant morbidity or death. Limited studies have evaluated this complication in childhood GBS. Our objectives were to show the prevalence of AD in children with GBS and investigate its association with the severity of the disease.Methods: Study included 28 children admitted with a diagnosis of GBS. Heart rate variability (HRV), motor function disability of the upper limbs and GBS disability scores were measured at admission and the results were compared with 20 healthy age/gender matched subjects (2-13 years; 43% male). GBS subtypes were defined by electromyography: acute inflammatory demyelinating polyneuropathy (AIDP) or acute motor axonal neuropathy (AMAN).Results: The mean age was 5.5±3.4 years (range 1.5-14 years; 50% male). AIDP and AMAN subtypes comprised 57.1% and 42.9% of cases, respectively. In the upper limbs, 85.7% and in the GBS disability grading, 50% of patients had ≤ 3 scores, implying less severe motor dysfunction. There was no difference in the mean heart rate between patients vs. controls (103.9 vs. 98.2 bpm; P= 0.16), but half of patients showed AD and HRV was significantly reduced in patients compared to controls. Of the 16 patients with AIDP, 11 (68.8%) showed reduced HRV compared to 3 (25%) out of 12 AMAN cases (P= 0.02). There was no significant relation between HRV and motor disability scores.Conclusion: AD was present in half of children with mild GBS and it showed no significant association with disease severity..
A B S T R A C TA R T I C L E I N F O
Article Type:Original Article
Article History:Received: 12 August 2013Accepted: 8 September 2013
Keywords:Guillain-Barré Syndrome Autonomic DysfunctionHeart Rate Variability
Mahmood Samadi, Babak Kazemi*, Sona Golzari Oskoui, Mohammad Barzegar
Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
IntroductionThe term Guillain-Barré syndrome (GBS), first described in 1916 in two soldiers by French neurologists Georges Guillain, Jean-Alexandre Barré and Andre Strohl, defines a recognizable clinical entity that is characterized by rapidly evolving symmetrical limb weakness, loss of tendon reflexes, absent or mild sensory signs, and variable autonomic dysfunction (AD). Since the virtual elimination of poliomyelitis, GBS has become the leading cause of acute flaccid paralysis in western countries.1 The condition, however, is known to occur at all ages, though it is rare in infancy, affecting approximately 0.3 to 2 per 100,000 children per year.2-4 Weakness can develop acutely (within days) or subacutely (up to 4 weeks) and reaches a plateau, with subsequent spontaneous resolution of paralysis. Although the pathogenesis of GBS remains incompletely defined, there is increasing support for the concept that GBS results from an aberrant organ specific immune response.5
GBS is now classified into two major demyelinating [acute
inflammatory demyelinating polyneuropathy (AIDP)] and axonal [acute motor axonal neuropathy (AMAN)] categories according to clinical, electrophysiological, and pathological criteria.6-8 Rare subtypes are acute motor sensory axonal neuropathy, accompanied by the variant of the Fisher syndrome presenting with ophthalmoplegia, ataxia, and areflexia. Very rare pure autonomic variants of GBS, defined as pandysautonomia were also reported.9 The most frequent subtype of GBS in North America and Europe is AIDP, which accounts for 90% of GBS cases, while in Asia, South and Central America, the axonal form of GBS constitutes 30% to 47% of cases.10 Only about 5% to 10% of patients in North America and Europe have an axonal subtype. AD is a common and important complication in GBS and occurs in approximately two-thirds of patients and is often associated with a variety of derangements including cardiovascular, vasomotor, or dysfunctions in both the sympathetic and parasympathetic systems11. The analysis of variations in the heart rate (HRV) has

Samadi et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 81-85 Copyright © 2013 by Tabriz University of Medical Sciences82
been used to determine the balance between cardiac sympathetic and vagal nerve activities.12 There have been only a few studies which used this technique for evaluation of AD in GBS. Flachenecker et al. indicated that 24-h heart rate power spectrum is a powerful predictor of serious autonomic complications in patients with GBS, and may help to identify patients at risk of potentially life-threatening arrhythmias.13,14 The natural course of GBS is characterized by the onset of symmetric weakness with an initial rapid progressive phase, a second plateau phase at the maximum disability level, and a third phase of recovery. Disability level in GBS is often measured using the Hughes clinical grading scale (Motor Disability Grading Scale) scored from 1 to 7, with 1 being normal, 6 being the point where patients require mechanical ventilation, and 7 equating with death (Table 1).15
The AIDP and AMAN may have different immunopathogeneses and target molecules, which could be the cause of the difference in patterns of involvement of the autonomic nervous system. While many authors report these findings in adult GBS patient series, studies on affected children with AD are sparse.16,17 On the other hand, many reports suggest that AD is present more often in those with severe motor deficits and with respiratory failure,18-20 while others found no relationship between the severity of AD and the degree of motor disturbances.17,21-23 Therefore, there still is debate whether there is any relationship between AD and the degree of motor disturbances. Thus, we undertook the present prospective study to examine the prevalence of AD in childhood GBS and whether there is any association between AD and the severity of illness in these patients.
Materials and MethodsPatients Twenty eight GBS patients and 20 normal subjects were studied. All patients fulfilled the clinical criteria for GBS.2 Motor function was evaluated according to the GBS disability grading system (Table 1). Weakness of arms was graded according to Table 2. Subtypes of GBS were determined from electromyograms and nerve conduction studies, which were obtained from all patients.
Evaluation of autonomic function The parameters of HRV were gathered from a 24-h Holter Monitoring. All recordings were analyzed using the AB-180R Holter monitoring software system (Advanced Biosensor, USA) with DL800 Holter Recorder (Norav Medical Ltd., USA) and manual correction of artifacts. HRV was assessed in two ways: (1) time domain analysis and (2) frequency domain analysis. The following time domain indexes were obtained: (1) the standard deviation (SD) of all R–R intervals (SDNN; which estimates overall HRV), (2) the SD of the averages of R–R intervals during all 5-min periods that constitute the 24-h day (SDANN; which reflects circadian rhythmicity of autonomic function), (3) the root mean square of successive differences (RMSSD; which estimates the short-term components of HRV and provides a vagal index), and (5) The integral of the density distribution (i.e. number of all NN intervals plotted in a histogram) divided by the maximum of the density distribution (HRV-triangular index; which estimates the overall HRV). In the frequency domain analysis: (1) low frequency (LF) power, the power between the 0.04 to 0.15 Hz, and (2) high frequency (HF) power, the
Table 1. Motor disability grading scale in Guillain-Barré Syndrome
0 Healthy
1 Minor signs or symptoms
2 Able to walk 5 m without walker or support
3 Able to walk 5 m with walker or support
4 Bed- or chair-bound: unable to walk 5 m with walker or support; can rise the leg
5 Bed- or chair-bound: unable to walk 5 m with walker or support; cannot rise the leg
6 Requires assisted ventilation
7 Dead
Table 2. Upper limb disability grading scale
0 Normal
1 Can move his arm vertically above his head while the elbow is extended
2 Can move his arm vertically above his head only while the elbow is flexed
3 Cannot move the arm above the head but can bring the glass of water to the mouth
4 Cannot bring the glass of water to the mouth but can bring the hand to the mouth
5 Cannot bring the hand to the mouth but can touch small objects
6 Cannot use the hands
7 Complete paralysis

Autonomic dysfunction and Guillain-Barré syndrome
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 81-85Copyright © 2013 by Tabriz University of Medical Sciences 83
power between the 0.15 and 0.40 Hz were measured. Measurement of LF and HF power components were presented in absolute values of power (ms2). HF generally represents parasympathetic activity and is therefore generally considered to be a marker of vagal activity. LF is influenced by both sympathetic and parasympathetic activity. Statistical analysisContinuous variables were expressed as mean±standard deviation. All continuous variables were checked with the Kolmogorov-Smirnov normality test to show their distributions. Continuous variables with normal distributions were compared using the unpaired Student t-test. Continuous variables with abnormal distributions were compared using the Mann-Whitney U-test. For categorical variables, the chi-square test was used. Values for P<0.05 were considered statistically significant. SPSS 13.0 (SPSS Inc., Chicago, IL, USA) was used for data storage and analysis.
ResultsThe mean age was 5.5±3.4 years (range 1.5-14 years; 50% male). The control group had an age range between 2-13 years and 43% were male. AIDP and AMAN subtypes comprised 57.1% and 42.9% of cases, respectively. According to the upper limb motor function, 13 patients (46.4%) were in stage 1, 7 patients (25%) in stage 2, 4 ones (14.3%) in stage 3, 2 patients (7.1%) in stage 4, and 2 patients (7.1%) were in stage 5. Based on GBS disability score, 5 patients (17.9%) were in stage 2, 9 (32.1%) in stage 3, 7 (25%) in stage 4, 6 (21.4%) in stage 5, and 1 (3.6%) in stage 6. Altogether, in the upper limbs, 85.7% and in the GBS disability grading, 50% of patients had ≤ 3 scores, implying less severe motor dysfunction. As stated earlier, there was no death during the study and only one patient needed mechanical ventilation. There was no difference in the mean heart rate between patients and controls (103.9 vs. 98.2 bpm; P= 0.16), but half of patients showed AD and HRV was significantly reduced in some time domains (SDNN and HRV-triangular index; P= 0.001 in both; Table 3) in patients compared to controls. The LF domain was significantly increased in patients vs. controls (P= 0.01; Table 3). Of the 16 patients with AIDP, 11 (68.8%) showed reduced HRV in the SDNN of the time domain category (Table 4) compared to 3 (25%) out of 12 AMAN cases (P= 0.02). There was no significant association between the presence of AD and the grades of upper or total GBS disability scores.
DiscussionOur study had three major findings. First, there was a 50% prevalence of AD in mild childhood GBS. Second, the prevalence of AD was much more common in the AIDP subtype than the AMAN subtype. Third, there was no association between the presence of AD and the severity
Table 3. HRV in patients vs. controls in both time and frequency domains
HRV domains Patients Control P
SDNN (ms) 101.62 ± 29.01 138.6 ± 35 0.001
SDANN (ms) 78.02 ± 68.42 97.3 ± 25 0.96
RMSSD (m/s) 76.38 ± 39.25 85 ± 30 0.36
HRV-TI (ms) 20.96 ± 96 33.34 ± 11 0.001
LF (ms2) 187.37 ± 49.25 158.39 ± 33 0.01
HF (ms2) 153.68 ± 41.94 169.5 ± 38 0.14
SDNN= SD of all R–R intervals; SDANN= SD of the averages of R–R intervals during all 5-min periods that constitute the 24-h day; RMSSD= the root mean square of successive differences; HRV-TI= The integral of the density distribution (ie number of all NN intervals plotted in a histogram) divided by the maximum of the density distribution; LF= Low Frequency power; HF= High Frequency power.
Table 4. Comparison between GBS subtypes according to the number (%) of patients showing reduced HRV in both time and frequency domains
Abnormal HRV domain
GBS subtype
AIDP AMAN P
SDNN n(%) 11 (68.8%) 3 (25%) 0.02
SDANN n(%) 10 (62.5%) 8 (66.7%) 0.82
RMS-SD n(%) 5 (31.3%) 4 (33.3%) 0.90
HRV-TI n(%) 10 (62.5%) 8 (66.7%) 0.82
LF powern(%) 1 (6.3%) 1 (8.3%) 0.83
HF power n(%) 8 (50%) 4 (33.3%) 0.37
SDNN= SD of all R–R intervals; SDANN= SD of the averages of R–R intervals during all 5-min periods that constitute the 24-h day; RMSSD= the root mean square of successive differences; HRV-TI= The integral of the density distribution (ie number of all NN intervals plotted in a histogram) divided by the maximum of the density distribution; LF= Low Frequency power; HF= High Frequency power.
of motor dysfunction in this subset of patients.The use of the GBS Motor Disability Scale of 7 grades of impairment, which was initially used in the study of adult patients with severe GBS to compared plasmapheresis with conventional therapy,24 has enabled an integrated method for analyzing motor disability and predicting outcome. Currently, scores ≥3 usually need medical support. In the present study, upper limb motor function and GBS disability grading showed ≤ 3 scores, in 85.7% and 50% of patients, respectively. This implies that motor dysfunction

Samadi et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 81-85 Copyright © 2013 by Tabriz University of Medical Sciences84
in our cohort was mild with no death and only one patient with respiratory failure.Cardiovascular autonomic neuropathy is a common and potentially grave complication in GBS, however, quantitative tests to assess such patients have rarely been used. The main reason for this shortcoming is that patients with severe motor disability are usually unable to perform standardized tests of autonomic function appropriately.19 HRV analysis is non-invasive and easily applicable, requiring no active motor tasks, and is therefore feasible, even in severely affected patients.13,14 Normal HRV depends on the balance between the sympathetic and parasympathetic systems. A high variability in heart rate is a sign of a healthy functioning autonomic control mechanism, especially the parasympathetic nervous system. The loss of this HRV due to an imbalance in sympathovagal system can predispose to various tachy- and bradyarrhythmias in both in-vivo and in-vitro conditions.25 Mild autonomic disturbance is reported to occur in 65% of patients with GBS.20 Sinus tachycardia is one of the most frequent manifestations and hypertension and postural hypotension are common.22 Some reports suggested a worse prognosis in the presence of AD, but others have refuted this26. Furthermore, many reports suggest that AD is present more often in those with severe motor deficits and with respiratory failure,18-20 while others found no relationship between the severity of AD and the degree of motor disturbances.17,21-23 Our findings are more in accordance with the latter studies with no relation between the presence of AD and the stage of motor disability. It seems that the consequences of involvement of the autonomic nervous system in GBS are negligible in many patients but on occasion they can be life threatening. Severe GBS is associated with progressive motor disability leading to respiratory failure. About a third of children with GBS experience severe motor disability and approximately 15% to 24% require mechanical ventilation due to respiratory failure (8% of the current series).2,27-31 AD has been reported in up to 90% of patients with moderate to severe GBS.19,21-23
There are very few studies which have specifically evaluated AD in childhood GBS.16,17,32 Cooper et al.16 retrospectively studied 30 children with GBS and found a 66.7% prevalence of AD. Similarly, DiMario et al.17 studied 26 patients retrospectively with a mean age of 11.3 years (range 6-17 years) with about half having mild GBS and showed AD in up to 77% of them. Only one small study of 5 patients has evaluated AD in mild adulthood GBS with various noninvasive tests, not including Holter monitoring and HRV testing.32 This study had no control group for comparison, nonetheless, no patient showed tachycardia or bradycardia during hospitalization. All patients in this study initially showed moderate AD according to the calculated composite autonomic score, described by Flachenecker et al.19 We used HRV measured
during Holter monitoring in 28 children with mild GBS and showed a 50% prevalence of AD, mostly in the AIDP subtype. SDNN, and HRV-triangular index, which estimate the overall HRV in the time domain, were significantly reduced in our patients compared to controls. In the frequency domain analysis, the HF domain was decreased in patients vs. controls but it did not reach statistical significance, again due to a small sample size. On the other hand, the LF power was significantly increased, implying sympathovagal imbalance with the tendency for increased sympathetic drive in affected patients. This confirms the previous study that AD not only occurs in moderate to severe GBS but also in mild forms of the disease with rather high prevalence. The mean heart rate was higher in our patients vs. controls but it did not reach statistical significance probably due to a small patient population. In our patients AD was significantly more prevalent in AIDP vs. AMAN cases. This is in accordance with a previous report that showed the patterns of AD are different for the two subtypes of GBS.33 This is the only report that has evaluated differences of autonomic manifestations between AIDP and AMAN subtypes.33 Our results suggest that HRV parameters may be used for early detection of any AD in patients with GBS. Cardiovascular response may be different in AMAN and AIDP patients, and this difference may play a role in the underlying pathogenesis, the clinical outcome, and in determining appropriate care for these patients. More conclusive results may be gained with larger study groups comprised of different subtypes of GBS. In addition, evaluating the impact of AD in the course of treatment or its interaction with the type of delivered treatment (plasmapheresis or intravenous immunoglobulin) would be valuable in future studies. ConclusionAD was prevalent in mild childhood GBS, more so in the AIDP subtype, and showed no significant association with the severity of motor dysfunction in this subset of patients.
AcknowledgmentsThis article was written based on a dataset of a thesis submitted for specialty degree in pediatrics, registered in Tabriz University of Medical Sciences.
Ethical issues: All patients gave written informed consents and the study was approved by our local Ethics Committee.Conflict of interests: The authors declare no conflicts of interest.
References1. Olivé J-M, Castillo C, Garcia Castro R, de Quadros CA. Epidemiologic study of Guillain-Barré syndrome in children <15 years of age in Latin America. J Infect Dis 1997;175:S160–64. 2. Asbury AK, Cornblath DR. Assessment of current diagnostic criteria for Guillain-Barré syndrome. Ann Neurol 1990;27:S21-4.3. Bradshaw DY, Jones HR Jr. Guillain-Barré syndrome in

Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 81-85Copyright © 2013 by Tabriz University of Medical Sciences 85
Autonomic dysfunction and Guillain-Barré syndrome
children: clinical course, electrodiagnosis, and prognosis. Muscle Nerve1992;15:500-6.4. Hartung HP, Kieseier BC, Kiefer R. Progress in Guillain-Barré syndrome. Curr Opin Neurol 2001;14:597-604.5. Giovannoni G, Hartung HP. The immunopathogenesis of multiple sclerosis and Guillain-Barré syndrome. Curr Opin Neurol 1996;9:165-77.6. Griffin JW, Li CY, Ho TW, Xue P, Macko C, Gao CY, et al. Guillain-Barré syndrome in northern China: the spectrum of neuropathological changes in clinically defined cases. Brain 1995;118:577-95. 7. Ho TW, Li CY, Cornblath DR, Gao CY, Asbury AK, Griffin JW, et al. Patterns of recovery in the Guillain-Barre syndromes. Neurology 1997;48:695-700. 8. Kuwabara S, Asahina M, Koga M, Mori M, Yuki N, Hattori T. Two patterns of clinical recovery in Guillain-Barré syndrome with immunoglobulin G anti-GM1 anti-body. Neurology 1998;51:1656-60.9. Kuwabara S. Guillain-Barré syndrome: epidemiology, pathophysiology and management. Drugs 2004;64:597-610.10. Hughes RA, Cornblath DR. Guillain-Barré syndrome. Lancet 2005;366:1653-66.11. Hartung HP, Pollard JD, Harvey GK, Toyka KV. Immunopathogenesis and treatment of the Guillain-Barré syndrome--Part I. Muscle Nevre 1995;18:137-53.12. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur Heart J 1996;17:354-81.13. Flachenecker P, Reiners K. Twenty-four-hour heart rate power spectrum for evaluation of autonomic dysfunction in Guillain-Barré syndrome. J Neurol Sci 1999;165:144-53.14. Flachenecker P, Lem K, Müllges W, Reiners K. Detection of serious bradyarrhythmias in Guillain-Barré syndrome: sensitivity and specificity of the 24-hour heart rate power spectrum. Clin Auton Res 2000;10:185-91.15. Hughes RAC, Newsome-Davies JM, Perkin GD, Pierce JM. Controlled trial of prednisolone in acute polyneuropathy. Lancet 1978;312:750-3.16. Cooper WO, Daniels SR, Loggie JMH. Prevalence and correlates of blood pressure elevation in children with Guillain-Barré syndrome. Clin Pediatr 1998;37:621-5.17. Dimario FJ Jr, Edwards C. Autonomic dysfunction in childhood
Guillain-Barré syndrome. J Child Neurol 2012;27:581-6.18. de Jager AE, Sluiter HJ. Clinical signs in severe Guillain-Barré syndrome: analysis of 63 patients. J Neurol Sci 1991;104:143-150.19. Flachenecker P, Wermuth P, Hartung HP, Reiners K. Quantitative assessment of cardiovascular autonomic function in Guillain-Barré syndrome. Ann Neurol 1997;42:171-9.20. Truax BT. Autonomic disturbances in the Guillain-Barré syndrome. Semin Neurol 1984;4:462-8.21. Tuck RR, McLeod JG. Autonomic dysfunction in Guillain-Barré syndrome. J Neurol Neurosurg Psychiatry 1981;44:983-90.22. Singh NK, Jaiswal AK, Misra S, Srivastava PK. Assessment of autonomic dysfunction in Guillain-Barré syndrome and its prognostic implications. Acta Neurol Scand 1987;75:101-5.23. Bansal BC, Sood AK, Jain SK. Dysautonomia in Guillain-Barré syndrome. J Assoc Physicians India 1987;35:417-9.24. Guillain-Barré Study Group. Plasmapheresis and acute Guillain-Barré syndrome. Neurology 1985;35:1096-104.25. Stein PK, Bosner MS, Kleiger RE, Conger BM. Heart rate variability: a measure of cardiac autonomic tone. Am Heart J 1994;127:420-4.26. Lichtenfeld P. Autonomic dysfunction in the Guillain-Barré syndrome. Am J Med 1971;50:772-80. 27. Kanra G, Ozon A, Vajsar J, Castagna L, Secmeer G, Topaloglu H. Intravenous immunoglobulin treatment in children with Guillain-Barré syndrome. Eur J Paediatr Neurol 1997;1:7-12.28. Rantala H, Uhari M, Niemela M. Occurrence, clinical manifestations, and prognosis of Guillain-Barré syndrome. Arch Dis Child 1991;66:706-8.29. Rantala H, Cherry JD, Shields WD, Uhari M. Epidemiology of Guillain-Barré syndrome in children: relationship of oral polio vaccine administration to occurrence. J Pediatr 1994;124:220-3.30. Rantala H, Uhari M, Cherry JD, Shields WD. Risk factors of respiratory failure in children with Guillain-Barré syndrome. Pediatr Neurol 1995;13:289-92.31. Paulson GW. The Landry-Guillain-Barré-Strohl syndrome in childhood. Dev Med Child Neurol 1970;12:604-7.32. Lyu RK, Tang LM, Hsu WC, Chen ST, Chang HS, Wu YR. A longitudinal cardiovascular autonomic function study in mild Guillain-Barré syndrome. Eur Neurol 2002;47:79-84. 33. Asahina M, Kuwabara S, Suzuki A, Hattori T. Autonomic function in demyelinating and axonal subtypes of Guillain-Barré syndrome. Acta Neurol Scand 2002;105:44-50.


Video Assisted Rigid Thoracoscopy in the Diagnosis of UnexplainedExudative Pleural Effusion
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 87-90doi: 10.5681/jcvtr.2013.019http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Farzad Kakaei, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Introduction: An undiagnosed exudative pleural effusion is often a difficult diagnostic dilemma that needs further histological study for a definitive etiological diagnosis. Video assisted rigid thoracoscopy is a minimally invasive procedure with a minor morbidity and mortality risk that could resolve this problem.Methods: Between January 2010 and December 2011, we performed thoracoscopy in 26 patients for diagnosis of undiagnosed exudative pleural effusion. Clinical and paraclinical data of patients were collected prospectively and analyzed.Results: Sole pleural effusion was the most common CT scan finding seen in 17 (65.4%) patients. Thoracoscopy was diagnostic in 24 patients (92.3%). The pathologic findings were carcinoma (46.2%), tuberculosis (30.8%) and chronic inflammation without a definitive microbiologic culture (15.4%). Surprisingly mean ADA level in the tuberculosis group was in normal range. No mortality or complication related to our operation was observed. Conclusion: Video assisted thoracoscopy is a minimally invasive procedure with a high definitive diagnostic accuracy in the evaluation of tuberculosis and malignant pleural effusions. Pulmonologist should refer these patients sooner to decrease the waiting period of diagnosis and treatment of such conditions.
A B S T R A C TA R T I C L E I N F O
Article Type:Original Article
Article History:Received: 21 June 2013Accepted: 2 September 2013
Keywords:ThoracoscopyPleural EffusionTuberculosisMalignancy
Samad Beheshtirouy1, Farzad Kakaei2*, Mohammad Mirzaaghazadeh3
1Department of Thoracic Surgery, Tabriz University of Medical Sciences, Tabriz, Iran2Department of General Surgery, Tabriz University of Medical Sciences, Tabriz, Iran3Faculty of Medicne, Ardabil University of Medical Sciences, Ardabil, Iran
IntroductionDiagnosis and treatment of the diseases has always been a major concern throughout the medicine history.1 An undiagnosed exudative pleural effusion is often a difficult diagnostic dilemma that needs further histological study for a definitive etiological diagnosis. Approximately 20% of exudative pleural effusions remain without an established etiology even after simple pleural aspiration and percutaneous biopsy.2 Complicated situations could alter the definite diagnosis in the diseases affecting thoracic cavity.3,4 When conditions such as neoplasia, tuberculosis or other granulomatous disorders are suspected, thoracoscopy should be considered; as this procedure provides larger biopsy specimens and more accurate sampling of abnormal pleura under direct vision.5
Numerous invasive and non-invasive methods have been introduced for diagnosis of the thoracic diseases.6 Video assisted rigid thoracoscopy is a minimally invasive procedure with a minor morbidity and mortality risk for the evaluation of the pleural space by direct vision through small incisions. Direct visual inspection of the pleural space, drainage of pleural fluid, and taking a large amount of pleural tissue for pathologic evaluation are the
commonly performed procedures during video assisted thoracoscopy which may be performed under general or even local anesthesia in special situations. At the same time pleurodesis and decortications may be done during this procedure for preventing recurrence of the pleural effusion and palliation of dyspnea.7
Material and MethodsIn a prospective study conducted in the department of general thoracic surgery, Imam Reza hospital, Tabriz University of medical sciences, Tabriz, Iran between January 2010 and December 2011, we performed thoracoscopy for diagnosis of undiagnosed exudative pleural effusions referred to our institute by pulmonologists. Undiagnosed exudative pleural effusion was defined as failure to achieve an etiologic diagnosis by initial pleural fluid microscopic and biochemical analysis including sugar, protein, triglyceride (TG), lactate dehydrogenase (LDH), cell count, cytology, Gram stain, Acid fast bacilli (AFB) smear and culture, pleural fluid adenosine deaminase (ADA) levels and at least two pleural percutaneous needle biopsies negative for malignancy or other definite causes. All patients underwent detailed

Beheshtirouy et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 87-90 Copyright © 2013 by Tabriz University of Medical Sciences88
clinical evaluation with history and clinical examination. Computed tomography (CT) of the chest was performed to assess feasibility of thoracoscopy. Patients unable to tolerate general anesthesia and one lung ventilation were excluded from study. Other exclusion criteria were: patients with excess rib crowding with narrow intercostal space, loculated pleural effusion, bleeding diathesis, hemodynamic instability and dysrhythmias. All the patients underwent general anesthesia and intubated by a suitable double lumen endotracheal tube. The patients were first placed in the lateral decubitus position with the affected side up. First a ten-millimeter port was placed in the fifth intercostal space at the mid-axillary line. The second port was placed in the forth intercostal space at the anterior axillary line.Keeping the lung deflated and allowing adequate visualization of the pleural surfaces, all of the pleural fluid was aspirated and sent for cytology and culture. Biopsies were taken from the parietal pleura where macroscopic abnormalities were obvious. Hemostasis was controlled by electrocautery or other devices. After the procedure was completed, thoracoscope and the other port(s) were removed and a 28 to 32 Fr chest tube was inserted through the same incision. Chest drain was connected to water-sealed drainage bottle. Chest X-ray was taken the next day. Once the lung had expanded and drain output decreased to less than 50mL per 24 hours, chest drain was removed.
ResultsDuring this period, 26 patients who underwent thoracoscopy for diagnosis of undiagnosed pleural effusion were included in this study. There were 11 (42.3%) males and 15 (57.7%) females, with a mean age of 51.96 ± 19.79 years (range, 18 to 85 years). The most common chief complaint was chest p ain in 8 (30.8%) patients. Other complaints include dyspnea in 6 (23.1%) patients, cough in 5 (19.2%) patients, cough and dyspnea in 3 (11.5%) patients, chest pain and dyspnea in 3 (11.5%) patients and incidental finding in 1 (3.8%) patient. The mean time prior to the patient referral for thoracoscopy was 4.85 months (range: 0-16 months). Eleven patients had a history of medical illness (Table 1). Only 4 patients had history of smoking.
Mean LDH level of pleural fluid was 831 (range: 160-4018). Mean ADA level was 29.43 (range: 1-123). The most common CT scan finding was sole pleural effusion that was observed in 17 (65.4%) patients (Table 2). Five of the patients had a distinct pleural or pulmonary lesion amenable to CT or ultrasound guided pleural biopsy; however, the biopsy specimen was not enough for accurate diagnosis. All of the patients had previously undergone percutaneous blunt pleural biopsy but in all of them the reported pathologic diagnosis was nonspecific inflammation without any accurate diagnosis.
Table 1. Underlying co-morbidities of the patients
Past medical history No. Percent
Hypertension 5 19.2
Previous cancer history 2 7.7
Previous tuberculosis 1 3.8
Ischemic heart disease + hypertension + diabetes mellitus 1 3.8
Diabetes mellitus + hypertension 2 7.7
Negative 15 57.7
Table 2. CT scan findings of the patients
CT finding No. Percent
Pleural effusion 17 65.4
Pleural effusion +lung mass 2 7.7
Massive pleural effusion 4 15.4
Pleural effusion +pleural mass 3 11.5
Right hemi-thorax was the most common affected side by pleural effusion (61.5%). Mean hospital stay was 5.35 days (range: 2-17). No mortality or complication related to our operation was observed.Thoracoscopy was diagnostic in 24 patients (92.3%). The most common pathologic finding was carcinoma [12 (46.2%) patients]. Tuberculosis was the second common pathologic finding seen in 8 (30.8%) patients. Surprisingly, mean ADA level in these group was in normal range (25.00±11.16) except for 1 case (123). Chronic inflammation was seen in four (15.4%) patients without a definitive microbiologic culture. In these 4 patients, pathologic evaluation was highly suggestive of TB diagnosis. PCR for tuberculosis was positive in 2 of them and their pleural effusion was resolved by a 6 month period of treatment by Anti-TB drugs. In the next 2 patients, the pleural effusion was treated by only broad spectrum antibiotics for 2 weeks. Two of the patients with cancer pathology had a previous history of treated breast cancer and treated ovarian cancer. We performed removal of loculated pleural effusion in 15 cases, decortication in 14 patients, and chemical pleurodesis in 11 patients in conjunction with pleural biopsy during thoracoscopic evaluation of them.
DiscussionOne of the most common chest problems in terms of diagnosis and effective management is pleural effusion. There is a long list of differential diagnosis and treatment options, and in general, its management largely relies on effective therapy of the underlying cause. The differential diagnosis can be narrowed based on dividing the effusion in exudative or transudative effusion based on the Light’s criteria.5 If one or more of Light’s criteria are met, the patient has an exudative effusion. Evaluation of

Video assisted rigid thoracoscopy
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 87-90Copyright © 2013 by Tabriz University of Medical Sciences 89
Light’s criteria demonstrates 97.5% sensitivity and 80% specificity for identifying pleural exudates.8 Based on the patients’ presentation, there are many algorithms for investigation of patients presented by pleural effusion that include thoracocentesis (aspirate for pH, protein, amylase, lactate dehydrogenase, glucose, Gram stain and culture, and acid-fast bacilli stains and culture, cell count and differential, cytopathologic studies and other specific tests as suggested by the clinical condition—lipids, fungal culture, viral culture, immunoglobulins), imaging modalities and percutaneous biopsy, open biopsy by thoracoscopy or thoracotomy. Collins and Sahn estimated that up to 75% of diseases presenting with pleural effusion can be diagnosed by analyzing the fluid tapped by simple thoracocentesis, if used in conjunction with the patient presentation.9 It has been suggested that a positive diagnosis is more likely with diseases such as parapneumonic effusions, empyema thoracis, chylothoraces, and hemothoraces which do not require a precise cytologic diagnosis. However, for diseases that require cytopathologic for diagnosis, such as malignant pleural disease, the results are much lower. Positive cytologic diagnosis rates from thoracocentesis of 45% to 80%, with rates for malignant mesothelioma as low as 20 %.10 In these cases other diagnostic modalities should be tried.Traditional (non-CT or ultrasound guided) percutaneous pleural biopsy using an Abrams needle has a positive diagnosis rates of only 38% to 67% for malignant diseases.11,12 Adding CT scan or ultrasonography for localizing the lesions improve the accuracy of sampling and reduce its complications but again the sample is a small tissue fragment.13 Tomlinson and Sahn, reported only 54% to 75% positive diagnosis rates for tuberculosis14
but others using combination of histology (80% percent sensitivity) and culture (56% sensitivity) of pleural biopsy tissue establishes the diagnosis of tuberculosis in up to 90% of patients.15 Real time PCR or adenosine deaminase evaluation will increase the accuracy of this technique in diagnosis of tuberculosis.16,17 In our 7 from 8 cases of tuberculosis-induced pleural effusion ADA level was in normal range. The cause of this difference is not known but this finding suggests that we could not rely on ADA level in the diagnosis of TB pleural effusion in our patients and again thoracoscopy would be the main diagnostic tool in such cases. The problem, therefore, is that at least 15% to 25% of pleural effusions may remain undiagnosed using the aforementioned nonsurgical techniques. Boutin and coworkers reported that 215 in a series of 1,000 pleural effusions remained undiagnosed. However, in the same 215 patients, thoracoscopy gave 96% diagnostic accuracy, suggesting that thoracoscopy and VATS may indeed be the ideal investigative tools for such situations.18 In our study thoracoscopy was diagnostic in 92.3% of the cases.Janssen, in a review of efficacy of three different methods
of pleural biopsy (old technique using Abrams needle closed pleural biopsy, thoracoscopic biopsy, computed tomography-guided biopsy and ultrasound-guided biopsy), showed that thoracoscopy was of a sensitivity of 90-95% compared with other methods (40% to 85%). They commented that although thoracoscopy is a more invasive procedure compared with image-guided pleural biopsy, the major advantage of thoracoscopy is its possibility to perform a simultaneous therapeutic intervention.19 The possible therapeutic procedures during thoracoscopy are: 1) removal of (septated) pleural effusions; 2) talc instillation (under visual control if preferred) 3) pulmonary decortication (if needed); and 4) drain positioning under visual control. In our study, this additional procedure was performed in all of the patients (as indicated) including: removal of loculated pleural effusion (58%), decortication (54%), and chemical pleurodesis (42%). Thoracoscopy is the preferred procedure if no clear target lesion is visible on the CT scan, and in patients with large or recurrent effusions in whom drainage and pleurodesis is indicated.19
The 2000 American Thoracic Society statement on management of malignant pleural effusions states that indications for performing thoracoscopy include “the evaluation of exudative effusions of unknown cause,” among others, and that “in cases of undiagnosed exudative effusions with a high clinical suspicion for malignancy, some clinicians may proceed directly to thoracoscopy”.20
As in our study, thoracoscopy is a safe method with a very low risk of mortality and mortality and in suspected cases it is more appropriate to directly refer such patients for video-assisted thoracoscopy. This would decrease the delay in diagnosis; it also, by its therapeutic effects, could decrease the patients’ morbidity. For more critical patients unable to tolerate general anesthesia this procedure can be performed by local or regional anesthesia or even by a single port.21 Ethical issues: The study was approved by the ethics committee of the
University.
Competing interests: The authors had no competing interests to declare
in relation to this article.
References1. Golzari SE, Khan ZH, Ghabili K, Hosseinzadeh H, Soleimanpour H, Azarfarin R, et al. Contributions of medieval Islamic physicians to the history of tracheostomy. Anesth Analg 2013;116:1123-32. 2. Light RW. Clinical practice. Pleural effusion. N Engl J Med 2002;346:1971-7.3. Sokouti M. Golzari S. A giant bulla of the lung mimicking tension pnemothorax (a case report). J Cardiovasc Thorac Res 2010;2:41-4. 4. Sokouti M, Halimi M, Golzari SE. Squamous cell carcinoma on the remaining sequel of tuberculosis, presented as pancoast tumor 8 years later. Tanaffos 2012;11:49-51.5. Loddenkemper R, Boutin C. Thoracoscopy: Present diagnostic and therapeutic indications. Eur Respir J 1993; 6: 1544-55.

Beheshtirouy et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 87-90 Copyright © 2013 by Tabriz University of Medical Sciences90
6. Golzari SE, Sokouti M, Ghaffari A, Bazzazi AM, Ghabili K. Ultrasonography in diagnosis of pulmonary hydatid cysts. Lancet Infect Dis 2013;13:294. 7. Hashemzadeh S, Hashemzadeh K, Mamaghani K, Ansari E, Aligholipour R, Golzari SE, et al. Pleurodesis by erythromycin, tetracycline, AerosilTM 200, and erythromycin plus AerosilTM 200 in a rat model: a preliminary study. Daru 2012, 20:79.8. Romero S, Martinez A, Hernandez L, Fernandez C, Espasa A, Candela A, et al. Light’s criteria revisited: consistency and comparison with new proposed alternative criteria for separating pleural transudates from exudates. Respiration 2000: 67:18–23. 9. Collins TR, Sahn SA. Thoracocentesis. Clinical value, complications, technical problems, and patient experience. Chest 1987;91:817-22.10. Menzies R, Charbonneau M. Thoracoscopy for the diagnosis of pleural disease. Ann Intern Med 1991;114:271.11. Rao NV, Jones PO, Greenberg SD, Bahar D, Daysog AO, Schweppe HI, et al. Needle biopsy of parietal pleura in 124 cases. Arch Intern Med 1965;115:34 12. Cantó A, Blasco E, Casillas M, Zarza AG, Padilla J, Pastor J, et al. Thoracoscopy in the diagnosis of pleural effusion. Thorax 1977;32:55013. Sconfienza LM, Mauri G, Grossi F, Truini M, Serafini G, Sardanelli
F, et al. Pleural and Peripheral Lung Lesions: Comparison of US- and CT-guided Biopsy. Radiology 2013;266:930-5.14. Tomlinson JR, Sahn SA. Invasive procedures in the diagnosis of pleural disease. Semin Respir Med 1987;9:3015. Porcel JM, Light RW. Diagnostic approach to pleural effusion in adults. Am Fam Physician 2006;73:1211-20.16. Garcia-Zamalloa A, Taboada-Gomez J. Diagnostic Accuracy of Adenosine Deaminase and Lymphocyte Proportion in Pleural Fluid for Tuberculous Pleurisy in Different Prevalence Scenarios. PLoS One 2012; 7: e38729. 17. Rosso F, Michelon CT, Sperhacke RD, Verza M, Olival L, Conde MB, et al. Evaluation of real-time PCR of patient pleural effusion for diagnosis of tuberculosis. BMC Res Notes 2011; 4:279. 18. Boutin C, Viallat JR, Cargnino P, Farisse P. Thoracoscopy in malignant pleural effusions. Am Rev Respir Dis 1981;124:588. 19. Janssen JP. Why you do or do not need thoracoscopy. Eur Respir Rev 2010;19:213-6.20. American Thoracic Society. Management of malignant pleural effusions. Am J Respir Crit Care Med 2000;162:1987-2001.21. Yalcinkaya S, Vural AH, Ozyazicioglu AF. Single port videothoracoscopy under epidural anesthesia for undiagnosed pleural effusions. An alternative approach. Saudi Med J 2011;32:1082-4.

Correlation between Aortic Wall Thickness and Coronary ArteryDisease by 64 Slice Multidetector Computed Tomography
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 91-95doi: 10.5681/jcvtr.2013.020http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Bassir Abolghassemi Fakhree, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Introduction: Atherosclerotic cardiovascular disease is a dispersed pathology involving the coronary arteries, carotid arteries, aorta and peripheral arteries. It has been previously suggested that coronary and aortic atherosclerosis may be associated. Imaging of the aorta and the aortic wall can be performed by various imaging modalities including state-of-the-art multidetector computer tomography (MDCT). This study aimed to investigate a possible association between the MDCT-measured thickness of the thoracic aorta and the presence of coronary artery disease (CAD) as well as its severity. Methods: Three hundred and fifty candidates of coronary computer tomography angiography (CTA) with signs and symptoms suggestive of CAD were recruited in Tabriz Parsian and Iran CTA Centers. Contrast-enhanced MDCT examinations were performed using a 64 detector scanner. Maximum aortic wall thickness in the mid-portion of descending thoracic aorta (region of pulmonary trunk to diaphragm) was measured perpendicular to the center of the vessel. Results: CAD was confirmed in 189 cases (54%) and the remaining 161 cases served as controls. The mean age of the cases, as well as the percentage of male subjects was significantly higher in the CAD group. The mean aortic wall thickness was also significantly higher in the patient group (2.21±0.63 mm vs. 1.88±0.58 mm; P<0.001). In multivariate analysis, however, the two groups turned up comparable as to the aortic wall thickness (P=0.31). The optimal cut-off point of aortic wall thickness was ≥2 mm in discriminating between CAD+ and CAD- groups, with a corresponding sensitivity and specificity of 65% and 57%, respectively. There was no significant association between aortic wall thickness and the severity of CAD (the number of significantly occluded coronary arteries). Conclusion: Aortic wall thickness is apparently neither an independent predictor of CAD nor is it associated with the severity of CAD in candidates of CTA.
A B S T R A C TA R T I C L E I N F O
Article Type:Original Article
Article History:Received: 17 May 2013Accepted: 14 September 2013
Keywords:Coronary Artery Disease Multidetector Computer TomographyAortic Wall Thickness
Abolhassan Shakeri1, Farnaz Hafez Quran2, Reza Javadrashid2, Mohammad Hossein Abdekarimi3, Morteza Ghojazadeh4, Mohammad Bassir Abolghassemi Fakhree5*
1Tuberculosis and Pulmonary Disease Research Center, Tabriz University of Medical Sciences, Tabriz, Iran2Department of Radiology, Imam Reza Hospital, Tabriz University of Medical Sciences, Tabriz, Iran3Iran Imaging Center, Tabriz, Iran4RDCC Center, Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran5Department of General & Vascular Surgery, Imam Reza Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
IntroductionThe importance of coronary artery disease (CAD) is obvious concerning the epidemiologic figures in general population. Based on Framingham study, risk of developing symptomatic CAD after 40 years of age is 49% for men and 32% for women.1 Current data have shown association of presence of CAD and peripheral atherosclerosis. It has been reported that CAD is associated with carotid intima-media thickness, presence of atherosclerotic plaques in aorta, presence of calcifications in mitral ring,
and lower limb atherosclerosis.2 In addition, there is a strong association between presence and burden of aortic plaques, and presence and extent of CAD.3,4 Usefulness of measurement of arterial wall thickness has been shown for prediction of cardiovascular disease risk.5,6 Takasu et al demonstrated that aortic plaque detected by enhanced CT scan is a better predictor of CAD compared to other non-dependent aortic parameters. They also concluded that aortic calcification seen in non-enhanced CT scan images is very specific for CAD.7 Sensitivity of 64 slice

Shakeri et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 91-95 Copyright © 2013 by Tabriz University of Medical Sciences92
multi-detector CT (64-MDCT) to detect coronary artery occlusion is estimated to be 83 to 99%, with specificity of 93 to 99% and negative predictive value (NPV) of 95 to 100%.8 In a study by Belhassen et al, carotid intima-media thickness (CIMT) < 0.55 mm and aortic intima-media thickness (AoIMT) < 3 were good predictors of absence of CAD. CIMT had sensitivity of 100%, specificity of 50%, and NPV of 100%. For AoIMT, sensitivity was found to be 98%, specificity 65%, and NPV 99%.2 Jeltsch et al demonstrated that aortic wall thickness of 3 mm can predict CAD with specificity of 96.6%, sensitivity of 27.5%, and positive predictive value of 93.3%. Aortic wall thickness of 2.4 mm was associated with specificity of 81%, sensitivity of 55%, and positive predictive value of 83.5%.9 The aim of this study is to evaluate descending thoracic aorta wall thickness as a potential predictor of CAD by 64-MDCT. If this association is found to be strong, one can suggest additional coronary artery evaluations in cases of incidental finding of increased aortic wall thickness, to prevent and early diagnose coronary artery complications.
Materials and Methods380 patients with age over 40, referred to coronary CTA were included in this analytical prospective study. The study was done in Tabriz Parsian and Iran CT angiography centers over a 17 month period. Exclusion criteria were history of coronary stent (17 patients), sever calcification of coronary arteries that interferes with CTA diagnosis (12 patients), and presence of thoracic aortic aneurysm (1 patient). Based on this criteria 350 patients finally entered the study. MDCT evaluations were done using Siemens Somatom Sensation 64 (Siemens Healthcare, Malvern PA). Axial 0.6 mm images synchronized with patient ECG were acquired and reconstructed as sagital and coronal images using MIP and MPR techniques and Curved Multiplanar Reformat. Additional 3D reconstructions were done using VRT, Inspace and vessel view. Reconstructed imaged were reviewed for presence of CAD. Coronary artery occlusion was considered as greater than 50% narrowing in the artery (significant involvement). Maximum wall thickness in mid-portion of descending thoracic aorta (between pulmonary trunk and diaphragm) was measured perpendicular to the center of the aorta. Window of 1000 with center of 250 was used for this measurement. Concerning that differentiating aortic wall layers is not possible in images acquired by MDCT, maximal wall thickness (and not intima-media thickness) was used. Data acquired from the study were reviewed using descriptive statistical methods (prevalence, percentage, mean ± SD), and analyzed by t-test for quantitative data, or chi-square for qualitative data. Correlation between parameters was evaluated using Pearson’s r Correlation. Multivariate logistic regression model was used to predict continuous variables. Receiver operating characteristic (ROC) curve was used to determine the cutting point for best specificity and sensitivity. Statistical analysis was
done using SPSS 16. P less than 0.05 was considered significant.
ResultsBased on coronary CTA findings, CAD was diagnosed in 189 patients (54%) and 161 patients (46%) were considered negative for CAD. 69 patients (36.5%) had no coronary artery with significant involvement (0VD). In 59 patients (31.2%) one coronary artery (1VD), in 35 patients (18.5%) 2 arteries (2VD), and in 26 patients (13.8%) 3 arteries (3VD) were significantly involved. In age group of 40-49, 70 cases (43.5%) had CAD and 28 cases (14.8%) were disease free. In age group of 50-59, 51 cases (31.7%) had CAD and 57 cases (30.2%) were diagnosed with no CAD. In age group of 60-69, 29 cases (18%) had CAD and 61 cases (32.3%) were disease free. In age group of ≥70, 11 cases (6.8%) were diagnosed with CAD and 43 cases (22.8%) were disease free. Mean age of group with CAD was 60.9 ± 10.58 (min 40, max 85) years, and mean age of non-diseased group was 52.61±9.74 (min 40, max 79) years. Using t-test for independent groups, mean age of CAD group was significantly greater than non-diseased group (P<0.001). 99 males (52.4%) and 90 females (47.6%) were studied in the CAD group, and there were 59 males (36.6%) and 102 females (63.4%) in non-diseased group. Based on the results of chi-square test, percentage of males was significantly higher in the CAD group compared to non-diseased group (P=0.003). Mean aortic wall thickness in CAD group was 2.21±0.63 mm (min 1, max 4.6 mm), and mean aortic wall thickness in non-diseased group was 1.88 ± 0.58 mm (min 1, max 4 mm). Using t-test for independent groups, mean aortic wall thickness in CAD group was significantly higher than mean aortic wall thickness in non-diseased group (P<0.001; Figure 1). ROC curve for age and aortic wall thickness to discriminate CAD and non-diseased group is shown in Figure 2. Area under age curve was 0.72 (P<0.001), and area under aortic wall thickness curve was 0.65 (P<0.001). The best age cutting point to discriminate CAD and non-diseased group was 56.5 years with sensitivity of 66% and specificity of 68%. The best aortic wall thickness cutting point to discriminate CAD and non-diseased group was 2 mm with sensitivity of 65% and specificity of 57%. In logistic regression model percentage of males (Exp (B)=0.32, P<0.001), and mean of age (Exp (B)=1.09, P<0.001) were higher in CAD group compared to non-diseased group. In this model mean aortic wall thickness was not significantly different in two groups (Exp (B)=1.26, P=0.31). There was a positive and significant correlation between age and aortic wall thickness in CAD group (Pearson’s r=0.42, P<0.001) (Figure 3A). Also a positive and significant correlation between age and aortic wall thickness was found in non-diseased group (Pearson’s r=0.56, P<0.001; Figure 3B). Mean age of 0VD group was 58.74±9.92 years (min 40, max 82), for 1VD group 60.69±11.35 years (min 40, max 82), in 2VD group 61.91±10.19 years (min 46, max 85),

Correlation between aortic wall thickness and CAD
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 91-95Copyright © 2013 by Tabriz University of Medical Sciences 93
and mean age for 3VD group was 65.77±9.76 years (min 49, max 85). In one-way analysis of variance, mean age of the patients in these groups was significantly different (P=0.03). In Tukey’s HSD post-hoc test, this difference remained significant only between 0VD and 3VD groups (P=0.02). In 0VD group we had 28 males (40.6%) and 41 females (59.4%), in 1VD group 33 males (55.9%) and 26 females (44.1%), in 2VD group 22 males (62.9%) and 13 females (37.1%), and in 3VD group 16 males (61.5%) and 10 females (38.5%). Based on chi-square test there was no significant difference between these groups (P=0.09). Mean aortic wall thickness was 2.15±0.58 mm (min 1 max 3.7 mm) in 0VD group, it was 2.20±0.61 mm (min 1 max 3.9 mm) for 1VD group, 2.18±0.79 mm (min 1.1, max 4.6 mm) for 2VD group, and 2.40±0.57 mm (min 1.4, max 3.8) for 3VD group. In on-way analysis of variance mean aortic wall thickness was not significantly different in these groups (P=0.38; Figure 4). Mean aortic wall thickness for CAD and non-diseased cases in age groups is
Figure 1. Mean aortic wall thickness (mm) in CAD and non-diseased group
Figure 2. ROC curve for age and aortic wall thickness to discriminate CAD and non-diseased group
shown in Table 1. Based on t-test for independent groups, mean aortic wall thickness was not significantly different in any of these age groups.
DiscussionIn this research correlation of maximal wall thickness of descending thoracic aorta with presence and severity of CAD was studied. Previously it has been shown that atherosclerotic cardiovascular disease is a disseminated condition in which aorta, coronary, carotid, and peripheral
Figure 3. Correlation between age and aortic wall thickness (mm) in CAD group (A), and non-diseased group (B)
Figure 4. Mean aortic wall thickness (mm) based on number of diseased coronary vessels

Shakeri et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 91-95 Copyright © 2013 by Tabriz University of Medical Sciences94
Table 1. Mean aortic wall thickness (mm) in CAD and non-diseased groups based on age groups
Age group CAD Group (n=189)
Non-diseased Group (n=161) P
40-49 years 1.71±0.55 1.56±0.43 0.1450-59 years 2.14±0.58 1.97±0.51 0.1060-69 years 2.29±0.55 2.33±0.47 0.72≥70 years 2.49±0.67 2.37±0.73 0.60Data are in Mean±SD format
arteries are involved.10,11 In two studies by Rohani et al and Couturier et al it has been demonstrated that thoracic aortic wall thickness, measured through trans-esophageal echocardiography, is positively correlated to severity of angiographic involvement of coronary vessels in CAD patients.12,13 Meenakshisundaram et al, in a study on 40 patients with CAD and 30 normal cases, showed that thoracic aortic intima-media thickness measured by trans-esophageal echocardiography is correlated to CAD.14
Also in other similar studies it has been concluded that atherosclerosis of thoracic aorta and CAD is associated with each other.15-20 Tarzamni et al showed that histopathologic severity of atherosclerosis in ascending aorta/aortic arch is correlated o severity of CAD.21 In our study maximal wall thickness of mid-portion descending thoracic aorta was significantly greater in CAD group compared to non-diseased group (2.21±0.63 mm vs. 1.88±0.58, P<0.001). In this study aortic wall thickness measurement was done using MDCT, and presence or absence of CAD was diagnosed by CT angiography. Jeltsch et al in a similar study determined thoracic aortic wall thickness in 160 cases with probable CAD using MDCT. In their study mean aortic wall thickness was significantly higher in the CAD group (2.72 mm compared to 1.88 mm).9 Jang et al measured maximal thoracic aortic wall thickness using MDCT in 120 cases with suspected CAD. Mean of aortic wall thickness was significantly higher in the diseased group (4.13 mm compared to 3.40 mm).22 Our results were in par with results of these two studies. Using ROC curve it was shown that the best cutting point to discriminate CAD from non-diseased cases is the aortic wall thickness of ≥2 mm (sensitivity of 65% and specificity of 57%). In the study of Jeltsch et al this cutting point was considered to be ≥3 mm (sensitivity of 27.5% and specificity of 96.6%).9
Although the cutting points in studies are different, it must be remembered that in our study we balanced sensitivity and specificity to find the cutting point, but in the other study sensitivity was sacrificed for better specificity. In univariate analysis mean aortic wall thickness was significantly higher in CAD group, but after controlling the effect of age and sex (which were both significantly different between two groups), this difference proved to be non-significant in multivariate analysis. On the other hand, positive and significant correlation was found between aortic wall thickness and age of cases. Besides, there was no significant difference for mean aortic wall thickness among age groups. Thus it seems that
increased aortic wall thickness in CAD patients is mainly due to higher ages of the patients. Jeltsch et al demonstrated that there is a direct and significant correlation between age and aortic wall thickness.9 A similar association of aortic wall thickness and age or sex of patients with CAD has been shown in other studies.23-27 Using MDCT, Mao et al demonstrated that ascending aortic wall thickness is significantly related to age and male sex of patients with CAD. They suggested that for the study of atherosclerotic changes in CAD patients, the effect of age and sex must be controlled.28 Results of current study confirm these conclusions. In This study there was no significant correlation between aortic wall thickness and severity of CAD (based on number of involved vessels). Also in the study of Jeltsch et al mean aortic wall thickness was not significantly different between patients with obstructive or non-obstructive CAD.9 It must be mentioned that atherosclerosis process is very complex and is related to many factors in different vessels. Various arteries in different points are under different hydrostatic pressures, and vessel wall thickening patterns are different among them. It has also been shown that other factors (besides ages, sex, and race) can have effect on aortic wall thickness including hypertension, lipid profile, diabetes mellitus, anthropometric parameters such as height, BMI, and history of smoking.29-31
This study has had some limitations. Cases were included from patients that were referred to coronary CT angiography with some symptoms, so the non-diseased group was not completely normal. Also, as mentioned above, other factors besides age and sex can have effect on aortic wall thickness. Controlling possible effects of these factors can solidify results of the study. Measurement of other parts of aorta, including ascending part, aortic arch and abdominal aorta were not included in this study and could have had better results compared to this study.21 It has also been shown that atherosclerotic aortic plaques are more correlated to CAD.7 In addition using CT angiography as a gold standard to detect CAD status has its own limitations.In conclusion, although aortic wall thickness after controlling age and sex parameters was not significantly correlated with the presence of CAD, its mean was higher in CAD patients for most age groups. Concerning that evaluating aortic pathologies, coronary arteries, and pulmonary emoli (Triple Rule-out protocol) in chest CT scans is easy with little extra expenses, it can be

Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 91-95Copyright © 2013 by Tabriz University of Medical Sciences 95
Correlation between aortic wall thickness and CAD
recommended based on the findings of the current study.
Ethical issues: This study was reviewed and confirmed by the ethics
committee of Tabriz University of Medical Sciences.
Conflict of interests: The authors declare no conflicts of interest.
References1. Morrow DA, Gersh BJ. Chronic Coronary Artery Disease. 3rd ed. Saunders: Philadelphia; 2008. p.1353.2. Belhassen L, Carville C, Pelle G, Monin JL, Teiger E, Duval-Moulin AM, et al. Evaluation of carotid artery and aortic intima-media thickness measurements for exclusion of significant coronary atherosclerosis in patients scheduled for heart valve surgery. J Am Coll Cardiol 2002; 39:1139-44.3. Fazio GP, Redberg RF, Winslow T, Schiller NB. Transesophageal echocardiographically detected atherosclerotic aortic plaque is a marker for coronary artery disease. J Am Coll Cardiol 1993; 21:144-50.4. Khoury Z, Gottlieb S, Stern S, Keren A. Frequency and distribution of atherosclerotic plaques in the thoracic aorta as determined by transesophageal echocardiography in patients with coronary artery disease. Am J Cardiol 1997; 79:23-7.5. Hodis HN, Mack WJ, LaBree L, Selzer RH, Liu CR, et al. The role of carotid arterial intima-media thickness in predicting clinical coronary events. Ann Intern Med 1998; 128:262-9.6. O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, et al. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study Collaborative Research Group. N Engl J Med 1999; 340:14-22.7. Takasu J, Mao S, Budoff MJ. Aortic atherosclerosis detected with electron-beam CT as a predictor of obstructive coronary artery disease. Acad Radiol 2003; 10:631-7.8. Haaga JR. CT and MRI of the whole body. 2nd ed. Mosby; Philadelphia; 2000. p. 1191.9. Jeltsch M, Klass O, Klein S, Feuerlein S, Aschoff AJ, Brambs HJ, et al. Aortic wall thickness assessed by multidetector computed tomography as a predictor of coronary atherosclerosis. Int J Cardiovasc Imaging 2009; 25:209-17.10. Budoff MJ. Atherosclerosis imaging and calcified plaque: coronary artery disease risk assessment. Prog Cardiovasc Dis 2003; 46:135-48.11. Fuster V, Fayad ZA, Moreno PR, Poon M, Corti R, Badimon JJ. Atherothrombosis and high-risk plaque: Part II: approaches by noninvasive computed tomographic/magnetic resonance imaging. J Am Coll Cardiol 2005; 46:1209-18.12. Rohani M, Jogestrand T, Ekberg M, van der Linden J, Källner G, Jussila R, et al. Interrelation between the extent of atherosclerosis in the thoracic aorta, carotid intima-media thickness and the extent of coronary artery disease. Atherosclerosis 2005; 179:311-6. 13. Couturier G, Voustaniouk A, Weinberger J, Fuster V. Correlation between coronary artery disease and aortic arch plaque thickness measured by non-invasive B-mode ultrasonography. Atherosclerosis 2006; 185:159-64.14. Meenakshisundaram R, Devidutta S, Michaels AD, Senthilkumaran S, Rajendiran C, Thirumalaikolundusubramanian P. Significance of the intima-media thickness of carotid and thoracic aorta in coronary artery disease in the South Indian population. Heart Views 2011; 12:150-6.15. Takasu J, Takanashi K, Naito S, Onishi M, Miyazaki A, Aoyagi Y, et al. Evaluation of morphological changes of the atherosclerotic aorta by enhanced computed tomography. Atherosclerosis 1992; 97:107-21.16. Agmon Y, Khandheria BK, Meissner I, Schwartz GL, Petterson
TM, O’Fallon WM, et al. Relation of coronary artery disease and cerebrovascular disease with atherosclerosis of the thoracic aorta in the general population. Am J Cardiol 2002; 89:262-7.17. Belhassen L, Carville C, Pelle G, Monin JL, Teiger E, Duval-Moulin AM, et al. Evaluation of carotid artery and aortic intima-media thickness measurements for exclusion of significant coronary atherosclerosis in patients scheduled for heart valve surgery. J Am Coll Cardiol 2002; 39:1139-44.18. Tribouilloy C, Shen WF, Peltier M, Lesbre JP. Noninvasive prediction of coronary artery disease by transesophageal echocardiographic detection of thoracic aortic plaque in valvular heart disease. Am J Cardiol 1994; 74:258-60.19. Zegers ES, Gehlmann HR, Verheugt FW. Acute myocardial infarction due to an acute type A aortic dissection involving the left main coronary artery. Neth Heart J 2007; 15:263-4.20. de Leeuw JG, Wardeh A, Sramek A, van der Wall EE. Pseudo-aortic dissection after primary PCI. Neth Heart J 2007; 15:265-6.21. Tarzamni MK, Eshraghi N, Fouladi RF, Afrasiabi A, Halimi M, Azarvan A. Atherosclerotic changes in common carotid artery, common femoral artery, and ascending aorta/aortic arch in candidates for coronary artery bypass graft surgery. Angiology 2012; 63:622-9.22. Jang S, Yong HS, Doo KW, Kang EY, Woo OH, Choi EJ. Relation of aortic calcification, wall thickness, and distensibility with severity of coronary artery disease: evaluation with coronary CT angiography. Acta Radiol 2012; 53:839-44.23. Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common carotid intima-media thickness and risk of stroke and myocardial infarction: the Rotterdam Study. Circulation 1997; 96:1432-7.24. Stary HC, Chandler AB, Dinsmore RE, Fuster V, Glagov S, Insull W Jr, et al. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Arterioscler Thromb Vasc Biol 1995; 15:1512-31.25. Jaffer FA, O’Donnell CJ, Larson MG, Chan SK, Kissinger KV, Kupka MJ, et al. Age and sex distribution of subclinical aortic atherosclerosis: a magnetic resonance imaging examination of the Framingham Heart Study. Arterioscler Thromb Vasc Biol 2002; 22:849-54.26. Anonymous. The French Study of Aortic Plaques in Stroke Group. Atherosclerotic disease of the aortic arch as a risk factor for recurrent ischemic stroke. N Engl J Med 1996; 334:1216-21.27. Haberl R, Becker A, Leber A, Knez A, Becker C, Lang C, et al. Correlation of coronary calcification and angiographically documented stenoses in patients with suspected coronary artery disease: results of 1,764 patients. J Am Coll Cardiol 2001; 37:451-7.28. Mao SS, Ahmadi N, Shah B, Beckmann D, Chen A, Ngo L, et al. Normal thoracic aorta diameter on cardiac computed tomography in healthy asymptomatic adults: impact of age and gender. Acad Radiol 2008; 15:827-34.29. Dawson JD, Sonka M, Blecha MB, Lin W, Davis PH. Risk factors associated with aortic and carotid intima-media thickness in adolescents and young adults: the Muscatine Offspring Study. J Am Coll Cardiol 2009; 53:2273-9.30. Bural GG, Torigian DA, Chamroonrat W, Alkhawaldeh K, Houseni M, El-Haddad G, et al. Quantitative assessment of the atherosclerotic burden of the aorta by combined FDG-PET and CT image analysis: a new concept. Nucl Med Biol 2006; 33:1037-43. 31. Malayeri AA, Natori S, Bahrami H, Bertoni AG, Kronmal R, Lima JA, et al. Relation of aortic wall thickness and distensibility to cardiovascular risk factors (from the Multi-Ethnic Study of Atherosclerosis [MESA]). Am J Cardiol 2008; 102:491-6.


Prevalence and Risk Factors of Postoperative Delirium in PatientsUndergoing Open Heart Surgery in Northwest of Iran
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 97-99doi: 10.5681/jcvtr.2013.021http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Ahmadreza Jodati, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Introduction: Delirium as a relatively common complication following cardiac surgery remains a contributory factor in postoperative mortality and an obstacle to early discharge of patients.Methods: In the present study 329 patients who underwent open heart surgery between 1st January 2008 to 1st January 2009 in Shahid Madani Heart Center, Tabriz, Iran were enrolled.Results: Overall 4.9% of patients developed delirium after cardiac surgery. We found atrial fibrillation (P = 0.005), lung diseases (P = 0.04) and hypertension (P = 0.02) to be more common in patients who develop delirium postoperatively. Furthermore, the length of intensive care unit (ICU) stay, cardiopulmonary bypass (CPB) time, and ventilation period were also significantly increased. Also a statistically meaningful relationship between the female gender and development of delirium was also noted (P = 0.02). On the other hand no meaningful relationship was detected between diabetes, history of cerebral vascular diseases, peripheral vascular diseases, myocardial infarction, development of pneumonia following surgery, and laboratory levels of sodium, potassium, glucose, and complete blood cell count (CBC) including white blood cells, red blood cells, platelets in the blood-hemoglobin and hematocrits. Also environmental factors like presence of other patients or companion with the patient, and objects like clock, window and calendar in the patient’s room did not affect prevention of delirium.Conclusion: Based on this and other investigations, it can be suggested to use MMPI test to recognize pathologic elements to prevented delirium after surgery and complementary treatment for coping with delirium.
A B S T R A C TA R T I C L E I N F O
Article Type:Original Article
Article History:Received: 11 May 2013Accepted: 10 September 2013
Keywords:DeliriumPrevalenceRisk FactorsOpen HeartSurgeryPatients
Ahmadreza Jodati1*, Nasser Safaie1, Mohammadbagher Raoofi2, Ladan Ghorbani1, Fatemeh Ranjbar3, Golamreza Noorazar3, Majid Mosharkesh1
1Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran2Department of Guidance and Consultation, Tabriz University of Medical Sciences, Tabriz, Iran3Department of Psychiatry, Tabriz University of Medical Sciences, Tabriz, Iran
Introduction Delirium is a frequently encountered problem in hospitalized patients that could even be life threatening.1 Virtually any medical condition can potentially cause delirium. For example, delirium may be the first sign of a serious, life—threatening illness such as a heart attack. The efficacy of costly medical interventions mandating prolonged hospitalizations which may contribute to delirium development should be carefully considered.2
This issue has been addressed in some studies.3
Thus the aim of the present study is to evaluate the prevalence and risk factors for development of delirium in patients undergoing open heart surgery in Shahid Madani Heart Center, Tabriz, Iran.
Literature reviewDelirium as an underdiagnosed disorder is classified as a
syndrome rather than a disease.4 Delirium is frequently encountered in patients undergoing heart surgery and in some studies has been reported with a frequency of up to 90% in these patients.5
In a study it was shown that 5.23% of cases after thorax Surgery experienced delirium from second day to 12th day after the operation. Older age, abnormal levels of sodium or glucose levels, insomnia, duration of surgery and diabetes are considered as risk factors.6
In another study a percentage of about 80 of cases with risk factors of diabetes, duration of surgery etc. was reported to have developed delirium after surgery.7 A report from San Diego Veterans Administration medical center shows delirium occurred in 77% of patients with a peak incidence around 72 hours post operatively.8 In similar studies, it was also shown that there are further risk factors including cognitive, visual and auditory impairment, immobility,

Jodati et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 97-99 Copyright © 2013 by Tabriz University of Medical Sciences98
dehydration, sleep deprivation9 age 65 years old or higher10, being jobless, unmarried, prolonged operation11, impaired behavior12, levels of albumin13, post-surgery vs. post-trauma14, head/neck cancer surgery15, alcoholism and laryngeal cancer16 major depression, peripheral arterial disease history and cognitive impairments.17
Most of the aforementioned studies indicated older age as the most important risk factor.18
Materials and MethodsSubjects who underwent open heart surgery between 1st January 2008 to 1st January 2009 in Shahid Madani Heart Center, Tabriz, Iran were enrolled in this study. The obtained data were analyzed by t- test statistical procedure, average value, standard derivation and ANOVA. ResultsA close correlation was observed between hypertension (P=0.02), atrial fibrillation (P=0.005), carotid bruit (P=0.005) and lung disease (P=0.04) and developing delirium. However, there was no significant relationship between diabetes, cerebrovascular diseases history, environmental- vascular diseases, myocardial infarction, postoperative pneumonia, dementia, epilepsy, congenital diseases, sodium levels, potassium levels, creatinine, glucose and CBC. Furthermore, between interferences of environmental factors such as presence of patient companion, clock, window, night light, and calendar no significant relationship was observed.The frequency of delirium intensity and the frequency of delirium itself have been presented in Table 1.Thus, totally about 4.9% of patients undergoing heart surgery developed delirium. The present study indicates the incidence of delirium to be 4.2% for coronary surgery, 5.9% for valve aortic surgery and 3.4% for other operations of delirium. The above percentage based on the standards was χ2=4.28 and the level was P=0.033. Delirium was not reported in congenital surgery cases.Between gender and delirium, a significant relationship was present (P=0.02). It can be said that the number was higher between and especially between female patients (P=0.005). The marginal findings supported the use of MMPI- test (in Persian) as a tool. Other findings were
Table 1. Degree of delirium for patients
Degree Frequency Percent Valid Percent
0.00 312 95.1 95.1
5.00 1 0.3 0.3
13.00 10 3.0 3.0
27.00 2 0.6 0.6
29.00 1 0.3 0.3
33.00 2 0.6 0.6
Total 328 100.0 100.0
successful to show in delirious patients, the scales such as MA scale (P=0.000), PT scale (P=0.01), PD scale (P=0.01), SC Scale (P=0.02) and PA scale (P=0.02) as significant.Table 2 represents the significant relationship between staying in ICU, CPB, ventilator time and delirium development.
DiscussionIt was observed that the severity of delirium in 95.1% of the cases in the present study was the least, and 4.9% of patients undergoing heart surgery developed delirium. The research demonstrated that 4.8% with risk factors such as older age, longer ICU stay, longer CPB time, and longer mechanical ventilation time developed delirium. These findings confirm the previous studies.Comparison of the average CPB time among individuals who developed delirium and who did not develop delirium was significant (P=0.03). This was in accordance with the findings of San Diego University in which delirium risk factors were studied among Cardiac Pulmonary Bypass surgery cases. As figured out in our study, more than 14% of surgeries had psychological disorders that required psychotherapy. The consequences of our study confirm the Shelly’s study19
in which they demonstrated that cardiac patients generally have psychological-neurotic profiles.Kampman studies in Finland showed the constructive impact of psychological conditions during heart surgery upon their physical recovery.20
The various studies in Finland on heart surgery cases indicated that neurotic diseases such as hypochondriacs and anxiety accompanied mitral value malfunction patients.21
Similarly in our study; depression, hypochondriasis and hysteria were seen in 14% of the subjects in the present investigations.The obtained tests by MMPI demonstrated that 48 people completed questionnaires rated by numbers above 70 (14%) based on the procedure of scaling by one or two or probably several MMPI tests. It seems that regarding the presence of psychological disorders, the cases should be treated with pharmacotherapy or pathological treatments. Collectively the studies which were carried out by Universities of Kerman, Gilan, Vancouver, and University of Brigham in Boston (United States) are in line with the present study in defining age as a principle factor to cause delirium. None of the cases undergoing surgery for congenital heart disease developed delirium. Semi-literacy was a prevalent characteristic in most of the delirious patients. It can be pointed that cognitive disorders are less frequent when somebody is educated and have enough familiarity with environment and surrounding vicinity.
AcknowledgmentsWe would like to express our sincere gratitude and appreciation to our patients and research participants and

Risk factors of delirium open heart patients
we are also indebted to our colleagues.
Ethical issues: This study was reviewed and confirmed by the ethics committee of Tabriz University of Medical Sciences.Conflict of interests: The authors declare no conflicts of interest.
References 1. Bonacchi M, Prifti E, Maiani M, Bartolozzi F, Di Eusanio M, Leacche M. Does off-pump coronary revascularization reduce the release of the cerebral markers, S-100beta and NSE? Heart Lung Circ 2006;15:314-9.2. Siddiqi N, Stockdale R, Britton AM, Holmes J. Interventions for preventing delirium in hospitalized patients. Cochrane Database Syst Rev 2007;18:CD005563.3. Levkoff S, Cleary P, Liptzin B, Evans DA. Epidemiology of delirium: an overview of research issues and findings. Int Psychogeriatr 1991; 3:149-67.4. Rafee R. An introduction to behavioral sciences, clinical psychiatry. Tehran: Arjmand publication; 2003. p. 3375. Sadock BJ, Sadock VA. Kaplan& Sadock’s Synopsis of Psychiatry. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2003. p. 552 6. Yildizeli M, Özyurtkan O, Batirel HF, Kuscu K, Bekiroglu N, Yüksel M. Factors associated with postoperative delirium after thoracic surgery. Ann Thorac Surg 2005;79:1004-9.7. Bucerius J, Gummert JF, Borger MA, Walther T, Doll N, Falk V, et al. Predictors of delirium after cardiac surgery delirium: Effect of beating-heart (off-pump) surgery. J Thorac Cardiovasc Surg 2004;127:57-64.8. Wrage RE, Dims dole JE. Operative predictors of delirium after Pulmonary thromboendor ferectomy. A model for post craniotomy delirium ? J Thorac Cardiovasc Surg 1988; 96: 524-9. 9. Tashakori A, Shanehsaz A, Khajeh Moughahi N. Comparison of incidence rate of post operative Delirium between patients with open-heart surgery and general surgery, Ahwaz Golestan Hospital. Scientific Medical Journal 2004;41:37-43.10. Modirnya M, Khalkhali M. Delirium In CCU patients. Gilan University Journal 2002;1:1-7.11. Baghaei Vaji M, Dehghan A, Ostovar Sirjani F, Parvaresh N. A
study on the incidence of postoperative Delirium in the operated patients in Kerman medical sciences university hospitals in 1999. Journal of Kerman University of Medical Sciences 2001; 8:74-80.12. Rogers MP, Liang MH, Daltroy LH, Eaton H, Peteet J, Wright E, et al. Delirium after elective orthopedic surgery: risk factors and natural history. Int J Psychiatry Med 1989;19:109-21.13. Manos PJ, Wu R. The Duration of Delirium in medical and Post operative Patients Reffered for psychiatric consultation. Ann Clin Psychiatry 1997;9:219-26.14. Pandharipande P, Cotton BA, Shintani A, Thompson J, Pun BT, Morris JA Jr, et al. Prevalence and risk factors for development of delirium in surgical and trauma intensive care unit patients. J Trauma 2008;65:34-41.15. Yamagata K, Onizawa K, Yusa H, Wakatsuki T, Yanagawa T, Yoshida H. Risk factors for postoperative delirium in patients undergoing head and neck cancer surgery. Int J Oral Maxillofac Surg 2005;34:33-6.16. Penel N, Amela EY, Mallet Y, Lefebvre D, Clisant S, Kara A, et al. A simple predictive model for postoperative mortality after head and neck cancer surgery with opening of mucosa. Oral Oncol 2007;43:174-80. 17. Kazmierski J, Kowman M, Banach M, Pawelczyk T, Okonski P, Iwaszkiewicz A, et al. Preoperative predictors of delirium after cardiac surgery: a preliminary study. Gen Hosp Psychiatry 2006;28:536-8.18. de Jonghe JF, Kalisvaart KJ, Dijkstra M, van Dis H, Vreeswijk R, Kat MG, et al. Early symptoms in the prodromal phase of delirium: a prospective cohort study in elderly patients undergoing hip surgery. Am J Geriatr Psychiatry 2007;15:112-21.19. Shealy AE, Walker DR. Minnesota Multiphasic Personality Inventory prediction of intellectual changes following cardiac surgery. J Nerv Ment Dis 1978;166:263-7.20. Kampman R, Tienari P, Outakoski J, Hirvenoja R, Juolasmaa A. Psychic Complication following open heart surgery: A review article. Psychiatria Fennica 1977;484-95. 21. Juolasmaa A, Outakoski J, Hirvenoja R, Tienari P, Sotaniemi K, Takkunen J. Effect of open-heart surgery on intellectual performance. J Clin Neuropsych 1981;3:181-97.
Table 2. Significant findings between ICU staying, CPB, ventilator time and delirium developing
Not delirious patients Delirious Patients P
Age 55.37± 14.11 59.50 ± 13.44 NS
ICU stay 4.14 ± 3.10 7.16 ± 3.90 0.001
Anesthesia Time (hours) 5.76 ± 2.46 4.91 ± 1.68 NS
CPB time (minutes) 103.71 ± 75.73 155.90 ± 77.02 0.03
Hospital Stay (days) 5.25 ± 3.38 6.00 ± 4.51 NS
Ventilation Time (hours) 13.13 ± 13.66 25.96 ± 21.94 0.006
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 97-99Copyright © 2013 by Tabriz University of Medical Sciences 99


Postoperative Atrial Fibrillation following Open Cardiac Surgery:Predisposing Factors and Complications
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 101-107doi: 10.5681/jcvtr.2013.022http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Marjan Dehdilani, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Introduction: New-onset postoperative atrial fibrillation (POAF) is a common complication of cardiac surgery that has substantial effects on outcomes. The aim of this study is to analyze the risk factors in the pre, intra, and postoperative periods, and evaluate its impact on patients’ outcome. Methods: In this prospective study, between March 2007 and February 2011, a total of 1254 patients with preoperative sinus rhythm who underwent open cardiac surgery were included of which 177 (13.6%) had developed POAF. Many clinical variables that are associated with the development of POAF, were evaluated.Results: The study population consisted of 1254 patients that 864 (68.9%) were male and 390 (31.1%) female, and average age was 55.1±15.7 years. POAF occurred in 171 (13.6%) of patients and most of them (68.4%) developed within the first two days after surgery. Multivariate logistic regression analysis was used to identify the following risk factors of POAF: Preoperative risk factors: age>50, smoking, Left ventricular hypertrophy, renal dysfunction, intraoperative risk factors: intraoperative inotrope use, valve surgery, atrial septal defect (ASD) surgery, bicaval cannulation, concomitant cardiac venting of pulmonary and aorta, longer cardiopulmonary time, longer cross-clamp time, postoperative use of inotropic agent after termination of cardiopulmonary bypass. Conclusion: POAF is the most common arrhythmia after cardiac surgery and not only concerted effort should be performed to identify and to reduce the risk factors, but also effective treatment is necessary to prevent mortality and morbidity.
A B S T R A C TA R T I C L E I N F O
Article Type:Original Article
Article History:Received: 2 July 2013Accepted: 9 September 2013
Keywords:Atrial FibrillationCardiac SurgeryRisk Factor
Khosrow Hashemzadeh1, Mahnaz Dehdilani2, Marjan Dehdilani1*
1Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran2Department of Cardiovascular Surgery, Tabriz University of Medical Sciences, Tabriz, Iran
IntroductionPostoperative atrial fibrillation (POAF) is the most common arrhythmia after cardiac surgery. The true incidence of POAF following cardiac surgery is unclear. Reported incidences range from 10-65%, depending on patient profile, type of surgery, method of arrhythmia surveillance, and definition of arrhythmia.1-4 POAF normally develops between days 2 and 4 after surgery. The maximum incidence of POAF was usually seen on postoperative day 2. Ninety percent of the patients who develop POAF do so by day 4 after surgery; and 94%, by the end of day 6.5,6
The precise pathophysiology of POAF is unknown; however, most of the evidence suggests that it is multifactorial. A common underlying factor associated with POAF induced by mechanical, metabolic or pharmacologic stimuli is the redox changes in atrial tissue associated with tachyarrhythmia.7 POAF is often a short-lived and self-limiting condition. Around 25%-80% of patients convert within 24 hours through correction of
electrolyte imbalances only.8,9 POAF adversely affects the mortality and morbidity and consequently leads to a longer hospital stay, and more use of resources, driving up the cost of care.10,11
This prospective study was conducted to determine the incidence of postoperative AF in patients undergoing a variety of open cardiac surgery procedures and identify preoperative, intraoperative and postoperative factors which have significant association with the development of postoperative AF, and to evaluate its impacts on patients, outcome, and to compare the in-hospital outcome of patients who remain in sinus rhythm postoperatively.
Materials and MethodsIn this prospective study, a total of 1254 patients entered the study between March 2007 and February 2011 in Shahid Madani Heart center, Tabriz, Iran. Patients with any history of preoperative AF or any other arrhythmias were excluded. POAF was defined by the documentation of AF rhythm with at least 5 minutes duration within 96 hours at

Hashemzadeh et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 101-107 Copyright © 2013 by Tabriz University of Medical Sciences102
postoperative period. Patients with POAF are diagnosed using continuous electrocardiogram (ECG) monitoring and ECG and finally analyzed by a cardiologist. Patients with POAF were treated by Amiodarone and replacement of potassium and magnesium. First for intravenous loading, Amiodarone (150 mg) was given over 10 minutes for acute therapy in adults, followed by a secondary loading infusion of 60 mg/h for 6 hours and then by a maintenance infusion of 30 mg/h to achieve a 1000 mg/d dosing, then oral administration of Amiodarone was continued 600-800 mg/d for 4-6 weeks and finally decided according to the response of treatment. Anticoagulation was instituted in only those patients who have persistent AF more than 48 hours or valve surgery. A total of 1254 patients were included of which 171 (13.6%) developed POAF. Patients’ details, medical records were surveyed. Many clinical variables that are associated with the development of PAOF were shown in Table 1. Preoperative, intraoperative and postoperative risk factors were analyzed for their association with POAF. In addition, other complications that associated with POAF were surveyed too.
StatisticsIn the statistical analysis, numerical variables were presented as mean (SD). The t-test was used to compare values of continuous variables between patients in whom AF developed versus those in whom AF did not develop whereas categorical variables were compared with the χ2 test. For all analyses, a P< 0.05 was considered significant. Multivariate logistic regression analysis was used to identify the following risk factors of POAF. The odds ratio (OR) and 95% confidence interval (CI) for each independent variable in the final regression model presented. For the statistical analysis, the statistical software SPSS 19.0 (SPSS Inc., Chicago, IL, USA) was used.
ResultsThe demographic characteristics of the patients included in this study are shown on Table 2.A total of 1254 patients were included in the study. Of these patients 864 (68.9%) were male and 390 (31.1%) female, and average age was 55.1±15.7 years (range, 1 to 85). Patients younger than 50 years constituted only approximately 29.6% of the total population. Postoperative AF occurred in 171 (13.6%) of patients. The incidence of AF by type of operative procedure was listed in Table 3. Coronary artery bypass grafting (CABG) as the sole operative procedure was performed in 1007 (80.3%) of patients, CABG + valve in 48 (3.8%), and isolated valve surgery were done in 132 (10.5%) patients. In nearly 68.4% AF occurred within the first 2 days of surgical ICU hospitalization, with a mean delay of 2.1 ± 1.5 (median, 2 days). Preoperative, intraoperative, and postoperative risk factors were presented in Table 1. POAF
was more frequent in patient’s > 50 years old (81.3%). POAF were characterized by higher incidence of smoking, left ventricular hypertrophy and renal dysfunction. Preoperative use of beta-blocker was not associated with a lesser incidence of AF (P=0.364). Intraoperatively, patients who have valve surgery, atrial septal defect (ASD) closure, use of introptic agents, longer CPB time, longer aortic cross- clamp time, concomitant venting of pulmonary vein and aorta, and bicaval cannulation increased frequency of AF. Multivariant analysis identified 12 independent factors as predictors of POAF (Table 4). From preoperative variables left ventricular hypertrophy was the strongest predictor of AF (OR=2.373; P=0.009). Age, smoking and renal dysfunction were independent predictors of AF (OR=0.505, P=0.000, OR=0.629, P=0.005 & OR=1.661, P=0.042; respectively). From intraoperative variables, type of surgery (valve surgery, OR=0.573, P=0.017, ASD surgery, OR=0.171; P=0.028), bicaval cannulation (OR=1.833; P=0.020), concomitant pulmonary vein and aortic root venting (OR=0.272; P=0.001), aortic cross-clamp time (OR=1.012; P=0.040), CPB time (OR=0.984; P=0.000) were associated with AF. Postoperative variables associated with AF was postoperative inotrope use (OR=1.622; P=0.007). Inotropic requirement postoperatively was significantly higher in the AF group (P=0.007). The reintubation rate (4.7% AF vs 1.1% no AF), was also higher in the AF group (P=0.003). In addition, length of ICU stay (6.16±7.36 AF vs 3.79±3.71 no AF), as well as hospital stay were significantly higher in the AF patients compared to those remaining in sinus rhythm (P=0.000). In this study, the rate of stroke was higher in the AF group (4.7% AF vs 2.0% no AF; P=0.041). This finding also showed that about 85.4% of POAF converted to sinus rhythm through correction of electrolyte imbalances and administration of amiodarone. In-hospital mortality was significantly greater in patients who developed AF (8.2% AF vs 2.1% no AF) compared to group in sinus rhythm before and after matching for patients and operative characteristics (P=0.000).
DiscussionPOAF remains the most frequent postoperative complication of cardiac surgery.12 Despite all the modern anti-arrhythmic drugs, the incidence of POAF remains unchanged. Patients who develop POAF show significantly worse outcome compare to those without AF. The incidence of AF in general populations and general surgical procedures are approximately 1.8% and 5% respectively.13-15 For patients undergoing open cardiac procedures, the incidence of POAF is clearly much higher and it has been reported to be between 10 and 65%4,16, with most large series reporting an incidence around 30%.6,10,17-23 The current study shows an average incidence of 13.6% for POAF. Although in this study group, mean

Cardiac surgery and atrial fibrillation
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 101-107Copyright © 2013 by Tabriz University of Medical Sciences 103
Table 1. Pre-, intra-, and post-operative variables according to atrial fibrillation following cardiac surgery
Characteristics Total AF No-AF P
Preoperative risk factorsAge(year) 0.000
≤50 371/1253(29.6%) 32/171(18.7%) 339/1082(31.3%)>50 882/1253(70.4%) 139/171(81.3%) 743/1082(68.7%)
Smoking 504/1254(40.2%) 53/171(31.0%) 451/1083(41.6%) 0.005History of cardiac surgery 27/1254(2.2%) 2/171(1.2%) 25/1083(2.3%) 0.265Diabetes 257/1254(20.5%) 34/171(19.9%) 223/1083(20.6%) 0.462COPD 155/1254(12.4%) 19/171(11.1%) 136/1083(12.6%) 0.348CVA 37/1252(3.0%) 7/171(4.1%) 30/1081(2.8%) 0.232Peripheral vascular disease 10/1254(0.8%) 3/171(1.8%) 7/1083(0.6%) 0.145Renal failure (cr≥2.5) 12/1243(1.0%) 1/170(0.6%) 11/1073(1.0%) 0.496Beta-blocker consumption 965/1254(77.0%) 133/171(77.8%) 832/1083(76.8%) 0.434
Hypertension≥140/90 100/1254(8.0%) 19/171(11.1%) 81/1083(7.5%) 0.074Pulse≤70(min) 374/1254(29.8%) 47/171(27.5%) 327/1083(30.2%) 0.266CCS>III 49/1219(4%) 5/165(3%) 44/1054(4.2%) 0.329NYHA Function Class≥III 601/1213(49.5%) 89/163(54.6%) 512/1050(48.8%) 0.096Cardiomegaly 230/1248(18.4%) 29/171(17%) 201/1077(18.7%) 0.339Left ventricular hypertrophy 53/1248(4.2%) 14/171(8.2) 39/1077(3.6%) 0.009Creatinine=1.4-2.5(mg/dl) 67/1243(5.4%) 14/170(8.2%) 53/1073(4.9%) 0.042Hemoglobin<12 (g/dl) 178/1239(14.4%) 30/170(17.6%) 148/1069(13.8%) 0.117
Intraoperative risk factors
Aortic cross-clamp time(min) 64.7±22.5 67.9±25.2 64.2±22.0 0.040CPB time(min) 107.7±31.8 116.8±40.6 106.2±29.9 0.000Cold blood cardioplegia 0.421
Antegrade 621/1254(49.5%) 80/171(46.8%) 541/1083(50.0%)Both(antegrade+retrograde) 630/1254(50.2%) 91/171(53.2%) 539/1083(49.8%)Retrograde 3/1254(0.2%) 0/171(0%) 3/1083(0.3%)
Aortic root reperfusion 460/796(57.8%) 78/129(60.5%) 382/667(57.3%) 0.284Topical ice slush 662/763(86.8%) 106/119(89.1%) 556/644(86.3%) 0.258Cardiac venting techniques 0.003
Aorta 1193/1254(95.1%) 156/171(91.2%) 1037/1083(95.8%)Pulmonary vein 33/1254(2.6%) 5/171(2.9%) 28/1083(2.6%)Both 28/1254(2.2%) 10/171(5.8%) 18/1083(1.7%)
Bicaval cannulation 93/1254(7.4%) 20/171(21.5%) 73/1083(78.5%) 0.020Need of perioperative IABP 32/1254(2.6%) 5/171(2.9%) 27/1083(2.5%) 0.447Type of surgery 0.014
CABG 1007/1254(80.3%) 128/171(74.9%) 879/1083(81.2%)CABG+Valve 48/1254(3.8%) 10/171(5.8%) 38/1083(3.5%)Valve 132/1254(10.5%) 27/171(15.8%) 105/1083(9.7%)Congenital 55/1254(4.4%) 3/171(1.8%) 52/1083(4.8%)Other 12/1254(1.0%) 3/171(1.8%) 9/1083(0.8%)
Inotropic agents 350/1254(27.9%) 71/171(41.5%) 279/1083(25.8%) 0.000Dopamine 48/1254(3.8%) 12/171(7.0%) 36/1083(3.3%) 0.023Dobutamine 297/1254(23.7%) 58/171(33.9%) 239/1083(22.1%) 0.001Epinephrine 31/1254(2.5%) 12/171(7.0%) 19/1083(1.8%) 0.000Norepinephrine 18/1254(1.4%) 5/171(2.9%) 13/1083(1.2%) 0.086Amrinone 19/1254(1.5%) 8/171(4.7%) 11/1083(1.0%) 0.002
Postoperative (ICU) risk factors
Inotropic agents 258/1254(20.6%) 48/171(28.1%) 210/1083(19.4%) 0.007Beta blocker use 1005/1254(80.1%) 132/171(77.2%) 873/1083(8.06%) 0.174Red blood cell transfusion 178/1239(14.4%) 30/170(16.9%) 148/1069(83.1%) 0.117
CVA: Cerebrovascular Accident; CCS: Canadian Cardiovascular Society Angina Score; CPB: Cardiopulmonary Bypass; IABP: Intra Aortic Balloon Pump; COPD: Chronic Obstructive Pulmonary Disease; NYHA: New York Heart Association
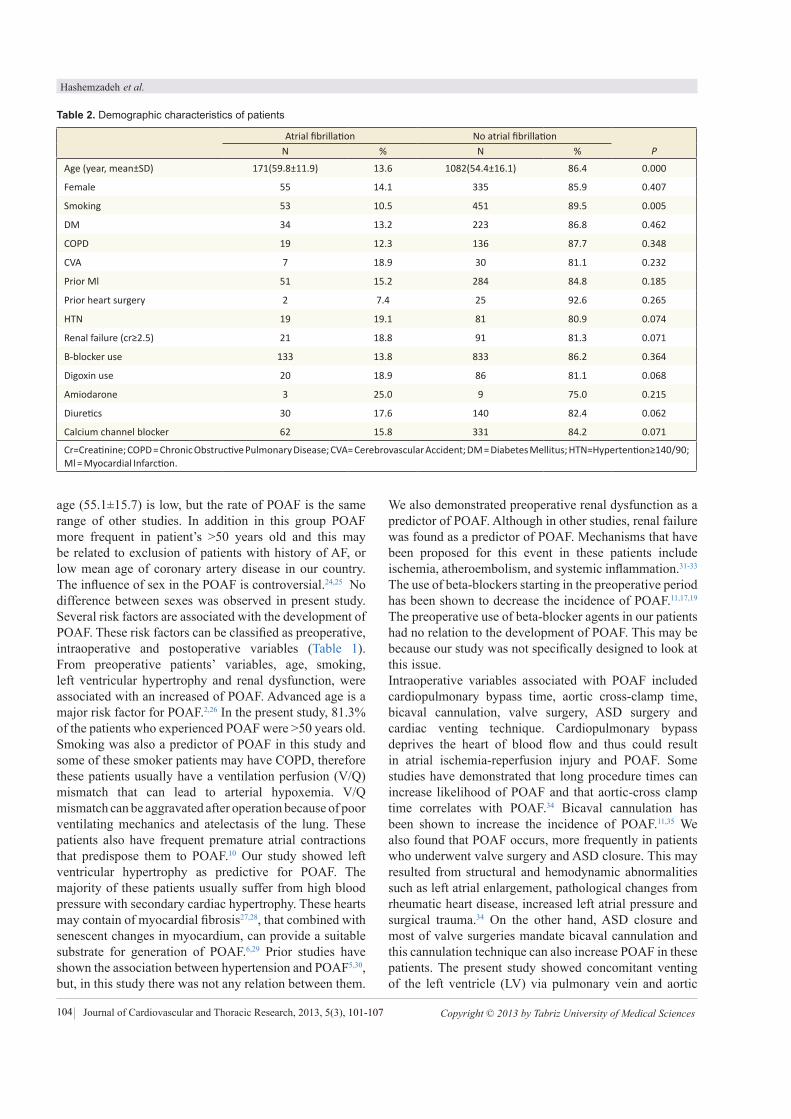
Hashemzadeh et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 101-107 Copyright © 2013 by Tabriz University of Medical Sciences104
age (55.1±15.7) is low, but the rate of POAF is the same range of other studies. In addition in this group POAF more frequent in patient’s >50 years old and this may be related to exclusion of patients with history of AF, or low mean age of coronary artery disease in our country. The influence of sex in the POAF is controversial.24,25 No difference between sexes was observed in present study.Several risk factors are associated with the development of POAF. These risk factors can be classified as preoperative, intraoperative and postoperative variables (Table 1). From preoperative patients’ variables, age, smoking, left ventricular hypertrophy and renal dysfunction, were associated with an increased of POAF. Advanced age is a major risk factor for POAF.2,26 In the present study, 81.3% of the patients who experienced POAF were >50 years old. Smoking was also a predictor of POAF in this study and some of these smoker patients may have COPD, therefore these patients usually have a ventilation perfusion (V/Q) mismatch that can lead to arterial hypoxemia. V/Q mismatch can be aggravated after operation because of poor ventilating mechanics and atelectasis of the lung. These patients also have frequent premature atrial contractions that predispose them to POAF.10 Our study showed left ventricular hypertrophy as predictive for POAF. The majority of these patients usually suffer from high blood pressure with secondary cardiac hypertrophy. These hearts may contain of myocardial fibrosis27,28, that combined with senescent changes in myocardium, can provide a suitable substrate for generation of POAF.6,29 Prior studies have shown the association between hypertension and POAF5,30, but, in this study there was not any relation between them.
We also demonstrated preoperative renal dysfunction as a predictor of POAF. Although in other studies, renal failure was found as a predictor of POAF. Mechanisms that have been proposed for this event in these patients include ischemia, atheroembolism, and systemic inflammation.31-33
The use of beta-blockers starting in the preoperative period has been shown to decrease the incidence of POAF.11,17,19
The preoperative use of beta-blocker agents in our patients had no relation to the development of POAF. This may be because our study was not specifically designed to look at this issue. Intraoperative variables associated with POAF included cardiopulmonary bypass time, aortic cross-clamp time, bicaval cannulation, valve surgery, ASD surgery and cardiac venting technique. Cardiopulmonary bypass deprives the heart of blood flow and thus could result in atrial ischemia-reperfusion injury and POAF. Some studies have demonstrated that long procedure times can increase likelihood of POAF and that aortic-cross clamp time correlates with POAF.34 Bicaval cannulation has been shown to increase the incidence of POAF.11,35 We also found that POAF occurs, more frequently in patients who underwent valve surgery and ASD closure. This may resulted from structural and hemodynamic abnormalities such as left atrial enlargement, pathological changes from rheumatic heart disease, increased left atrial pressure and surgical trauma.34 On the other hand, ASD closure and most of valve surgeries mandate bicaval cannulation and this cannulation technique can also increase POAF in these patients. The present study showed concomitant venting of the left ventricle (LV) via pulmonary vein and aortic
Table 2. Demographic characteristics of patients
Atrial fibrillation No atrial fibrillationN % N % P
Age (year, mean±SD) 171(59.8±11.9) 13.6 1082(54.4±16.1) 86.4 0.000
Female 55 14.1 335 85.9 0.407
Smoking 53 10.5 451 89.5 0.005
DM 34 13.2 223 86.8 0.462
COPD 19 12.3 136 87.7 0.348
CVA 7 18.9 30 81.1 0.232
Prior Ml 51 15.2 284 84.8 0.185
Prior heart surgery 2 7.4 25 92.6 0.265
HTN 19 19.1 81 80.9 0.074
Renal failure (cr≥2.5) 21 18.8 91 81.3 0.071
B-blocker use 133 13.8 833 86.2 0.364
Digoxin use 20 18.9 86 81.1 0.068
Amiodarone 3 25.0 9 75.0 0.215
Diuretics 30 17.6 140 82.4 0.062
Calcium channel blocker 62 15.8 331 84.2 0.071
Cr=Creatinine; COPD = Chronic Obstructive Pulmonary Disease; CVA= Cerebrovascular Accident; DM = Diabetes Mellitus; HTN=Hypertention≥140/90; Ml = Myocardial Infarction.

Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 101-107Copyright © 2013 by Tabriz University of Medical Sciences 105
Cardiac surgery and atrial fibrillationTa
ble
3. p
reop
erat
ive
char
acte
ristic
s Isol
ated
CAB
GCA
BG +
Val
ve su
rger
yIs
olat
ed V
alve
surg
ery
Oth
er c
ardi
ac o
pera
tions
AF(n
=128
)N
o AF
(n=8
79)
PAF
(n=1
0)N
o AF
(n=3
8)P
AF(n
=27)
No
AF(n
=105
)P
AF (n=6
)N
o AF
(n=6
1)P
Age
(mea
n+SD
)63
.1±8
.958
.7±1
0.5
0.00
058
.8±8
.758
.9±9
.90.
966
49.8
±12.
335
.9±1
8.7
0.00
037
.3±2
1.2
20.6
±19.
00.
831
Fem
ale
gend
er
37(2
8.9)
229(
26.1
)0.
279
3(30
.0)
14(3
6.8)
0.49
712
(44.
4)55
(52.
4)0.
302
3(50
.0)
37(6
1.7)
0.44
3
Angi
na c
lass
>III
3(2.
4)35
(3.8
)0.
264
03(
7.9)
0.48
80
6(6.
0)0.
281
2(33
.3)
00.
009
NYH
A≥III
69(5
5.6)
427(
49.6
)0.
122
6(60
)27
(71.
1)0.
377
11(4
7.8)
49(4
9.5)
0.53
53(
50.0
)9(
17.3
)0.
096
Rece
nt M
I47
(36.
7)27
4(31
.2)
0.12
44(
40.0
)8(
21.1
)0.
202
01(
1.0)
0.79
50
1(1.
6)0.
910
Curr
ent s
mok
er45
(35.
2)40
3(45
.8)
0.01
43(
30.0
)17
(44.
7)0.
320
5(18
.5)
26(2
4.8)
0.34
30
5(8.
2)0.
616
Diab
etes
32(2
5.0)
212(
24.1
)0.
452
1(10
.0)
4(10
.5)
0.72
41(
3.7)
4(3.
8)0.
729
03(
4.9)
0.75
1
HTN
15(1
1.7)
74(8
.4)
0.14
50
1(2.
6)0.
792
3(11
.1)
5(4.
8)0.
208
1(16
.7)
1(1.
6)0.
172
COPD
15(1
1.7)
119(
13.5
)0.
343
3(30
.0)
00.
007
1(3.
7)14
(13.
3)0.
141
03(
4.9)
0.75
1
CVA
6(4.
7)22
(2.5
)0.
134
03(
7.9)
0.48
81(
3.7)
5(4.
8)0.
644
00
-
PVD
2(1.
6)4(
0.5)
0.17
10
1(
2.6)
0.79
20
2(1.
9)0.
632
1(16
.7)
00.
090
Rena
l dys
func
tion
13(1
0.2)
78(9
.0)
0.36
94(
40.0
)3(
7.9)
0.02
73(
11.1
)8(
7.7)
0.40
41(
16.7
)4(
6.6)
0.25
2
Prio
r sur
gery
010
(1.1
)0.
255
02(
5.3)
0.62
31(
3.7)
9(8.
6)0.
352
1(16
.7)
1(11
.1)
0.38
4
Drug
hist
ory
115(
89.8
)79
3(90
.2)
0.49
810
(100
)36
(94.
7)0.
623
21(7
7.8)
69(6
5.7)
0.16
72(
33.3
)20
(32.
8)0.
649
MI:
Myo
card
ial I
nfar
ction
; PVD
: Per
iphe
ral V
ascu
lar D
iseas
e; A
F: A
tria
l Fib
rilla
tion;
CVA
: Cer
ebro
vasc
ular
Acc
iden
t; HT
N:H
yper
tens
ion≥
140/
90; O
ther
car
diac
ope
ratio
ns c
onsis
t sur
gery
for
cong
enita
l hea
rt d
iseas
e (n
=55)
, Per
icar
dial
Cys
t (n=
2),
Aneu
rysm
(n=4
), Ao
rtic
Diss
ectio
n (n
=3).

Journal of Cardiovascular and Thoracic Research, 2014, 5(3), 101-107 Copyright © 2013 by Tabriz University of Medical Sciences106
root has also been associated with POAF, whereas, in some studies LV venting through the pulmonary vein had been associated with increased risk of POAF.11,35 Therefore it appears that the cause of POAF with pulmonary vein venting is related to other factors. Our data imply that the use of inotropic agent in the postoperative period is related to POAF. Several studies have suggested that a heightened sympathetic response predisposes a patient to developing POAF.22,36,37 In this study, the postoperative morbid events were also increased with POAF. The need for reintubation was almost tripled in patients with POAF. In addition, the median length of ICU stay was significantly higher in the POAF patients (6 days) compared to these remaining in sinus rhythm (4 days). The POAF also increased the median postoperative hospital stay from 7 days to 11 days. Some other studies have found similar associations.6,10,30,38 The POAF also increases the risk of stroke by fivefold39 and several reports39-41 show a significantly high stroke rate in patients developing POAF. This is largely due to circulatory stasis in the left atrum resulting in the formation of an embolus.40
In the current study, the rate of stroke in patients with POAF (4.7%) was almost double the rate of stroke in patients without AF (2.0%) This results also revealed higher in-hospital mortality rate in patients with POAF than without AF (8.2% AF vs 2.1% no AF). Similar results were also observed by other investigators.16,29,31 It is clear that a longer hospital stay and more use of resources will have significantly driven up the cost of hospitalization.
ConclusionPOAF is the most common arrhythmia after cardiac surgery and can affect the outcome and survival of the patients. We concluded that not only concerted effort
should be performed to identify the risk factors, but also preventive measures should be done to reduce POAF. In addition, POAF should be treated effectively to prevent mortality and morbidity.
Ethical issues: This study was reviewed and confirmed by the ethics
committee of Tabriz University of Medical Sciences.
Conflict of interests: The authors declare no conflicts of interest.
References 1. Bradley D, Creswell L, Hogue C. Pharmacologic prophylaxis. Chest 2005;128:39S–47S.2. Maisel WH, Rawn JD, Stevenson WG. Atrial fibrillation after cardiac surgery. Ann Intern Med 2001;135:1061–1073. 3. Martinez E, Bass E, Zimetbaum P. Pharmacologic control of rhythm. Chest 2005;128:48S–55S. 4. Alqahtani AA. Atrial fibrillation post cardiac surgery trends toward management. Heart Views 2010;11:57-63.5. Nair SG. Atrial fibrillation after cardiac surgery. Ann Card Anaesth 2010;13:196-205.6. Aranki SF, Shaw DP, Adams DH, Rizzo RJ, Couper GS, VanderVliet M, et al. Predictors of atrial fibrillation after coronary artery surgery. Current trends and impact on hospital resources. Circulation 1996;94:390-7. 7. Hogue CW Jr, Creswell LL, Gutterman DD, Fleisher LA. Epidemiology, Mechanisms and Risks. American College of Chest Physicians Guidelines for the Prevention and Management of Postoperative Atrial Fibrillation after cardiac Surgery. Chest 2005;128:9S-16S.8. Cochrane AD, Siddins M, Rosenfeldt FL, Salamonsen R, McConaghy L, Marasco S, et al. A comparison of amiodarone and digoxin for treatment of supraventricular arrhythmias after cardiac surgery. Eur J Cardiothorac Surg 1994;8:194–8. 9. Gavaghan TP, Feneley MP, Campbell TJ, Morgan JJ. Atrial tachy-arrhythmias after cardiac surgery: results of disopyramide therapy. Aust NZ J Med 1985;15:27–32.10. Creswell LL, Schuessler RB, Rosenbloom M, Cox JL. Hazards of post-operative atrial arrhythmias. Ann Thorac Surg 1993; 56:539-49.11. Mathew JP, Parks R, Savino JS, Friedman AS, Koch C,
Table 4. Significant variables associated with atrial fibrillation
Variable Odds ratio 95% confidence interval P
PreoperativeAge>50 0.505 0.336-0.757 0.000Smoking 0.629 0.445-0.890 0.005LVH 2.373 1.260-4.471 0.009Renal dysfunction 1.661 0.988-2.790 0.042
Intraoperative
Type of surgeryValve surgery 0.573 0.362-0.905 0.017ASD closure 0.171 0.023-1.256 0.028
Intraoperative inotrope use 2.046 1.466-2.855 0.000Aortic cross-clamp time 1.012 1.001-1.024 0.040Cardiopulmonary bypass time 0.984 0.976-0.992 0.000Bicaval cannulation 1.833 1.086-3.093 0.020Concomitant venting of PV&Aorta 0.272 0.123-0.600 0.001
Postoperative(ICU) Inotrope use 1.622 1.125-2.339 0.007
ASD= Atrial Septal Defect; LVH= Left Ventricular Hypertrophy; PV=Pulmonary Vein; Renal Dysfunction: cr=1.4-2.5
Hashemzadeh et al.

Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 101-107Copyright © 2013 by Tabriz University of Medical Sciences 107
Mangano DT, et al. Atrial fibrillation following coronary artery bypass graft surgery. JAMA 1996;276:300-6.12. Lauer MS, Eagle KA, Buckley MJ. Atrial fibrillation following coronary artery bypass surgery. Prog Cardiovasc Dis 1989;31:367–78.13. Kannel WB, Abbott RD, Savage DD, McNamara PM. Epidemiologic features of chronic atrial fibrillation: The Framingham Study. N Engl J Med 1982;306:1018–22.14. Goldman L. Supraventricular tachyarrhythmia in hospitalized adults after surgery. Clinical correlates in patients over 40 years of age after major non cardiac surgery. Chest 1978;73:450–4.15. Johnston KW. Multicenter prospective study of nonruptured abdominal aortic aneurysm. Part II. Variables predicting morbidity and mortality. J Vasc Surg 1989;9:437–47.16. Attaran S, Shaw M, Bond L, Pullan MD, Fabri BM. Atrial fibrillation postcardiac surgery: a common but a morbid complication. Interact Cardiovasc Thorac Surg 2011;12:772–7. 17. Rubin DA, Nieminski KE, Reed GE, Herman MV. Predictors, prevention, and long-term prognosis of atrial fibrillation after coronary artery bypass graft operations. J Thorac Cardiovasc Surg 1987;94:331–5.18. Chung MK, Asher CR, Dykstra D. Does post-operative atrial fibrillation predispose to stroke, embolic events, or death after coronary artery bypass grafting? Circulation 1995; 92:1-644.19. Fuller JA, Adams GG, Buxton B. Atrial fibrillation after coronary artery bypass grafting: is it a disorder of the elderly? J Thorac Cardiovasc Surg 1989;97:821–5.20. Lauer MS, Eagle KA, Buckley MJ. Atrial fibrillation following coronary artery bypass surgery. Prog Cardiovasc Dis 1989; 31:367-78.21. Mendes LA, Connelly GP, McKenney PA, Podrid PJ, Cupples LA, Shemin RJ, et al. Right coronary artery stenosis: an independent predictor of atrial fibrillation after coronary artery bypass surgery. J Am Coll Cardiol 1995;25:198–202.22. Kalman JM, Munawar M, Howes LG, Louis WJ, Buxton BF, Gutteridge G, et al. Atrial fibrillation after coronary artery bypass grafting is associated with sympathetic activation. Ann Thorac Surg 1995;60:1709–15.23. Klemperer JD, Klein IL, Ojamaa K, Helm RE, Gomez M, Isom OW, et al. Triiodothyronine therapy lowers the incidence of atrial fibrillation after cardiac operations. Ann Thorac Surg 1996;61:1323–9.24. Bender JS. Supraventricular tachyarrhythmias in the surgical intensive care unit: an under-recognized event. Am Surg 1996;62:73–5.25. Reinelt P, Karth GD, Geppert A, Heinz G.. Incidence and type of cardiac arrhythmias in critically ill patients: a single center experience in a medical-cardiological ICU. Intensive Care Med 2001;27:1466–73. 26. Fuster V, Rydén LE, Asinger RW, Cannom DS, Crijns HJ, Frye RL, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. A Report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences
(Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation): developed in Collaboration With the North American Society of Pacing and Electrophysiology. J Am Coll Cardiol 2001;38:1231–66. 27. Lie JT, Hammond PI. Pathology of the senescent heart: anatomic observations on 237 autopsy studies of patients 90 to 105 years old. Mayo Clin Proc 1988;63:552–64.28. Toyoshima H, Park YD, Ishikawa Y, Nagata S, Hirata Y, Sakakibara H, et al. Effect of ventricular hypertrophy on conduction velocity of activation front in the ventricular myocardium. Am J Cardiol 1982;49:1938–48.29. Patel D, Gillinov MA, Natale A. Atrial fibrillation after cardiac surgery: where are we now? Indian Pacing Electrophysiol J 2008;8:281–91. 30. Almassi GH, Schowalter T, Nicolosi AC, Aggarwal A, Moritz TE, Henderson WG, et al. Atrial fibrillation after cardiac surgery: a major morbid event? Ann Surg 1997;226:501–13.31. Shirzad M, Karimi A, Tazik M, Aramin H, Hossein Ahmadi S, Davoodi S, et al. Determinants of postoperative atrial fibrillation and associated resource utilization in cardiac surgery. Rev Esp Cardiol 2010;63:1054–60. 32. Royston D. Systemic inflammatory responses to surgery with cardiopulmonary bypass. Perfusion 1996;11:177–89.33. Dernellis J, Panaretou M. C-reactive protein and paroxysmal atrial fibrillation: evidence of the implication of an inflammatory process in paroxysmal atrial fibrillation. Acta Cardiol 2001;56:375–80.34. Creswell LL, Alexander JC Jr, Ferguson TB Jr, Lisbon A, Fleisher LA. Intraoperative Interventions: American College of Chest Physicians Guidelines for the prevention and management of postoperative atrial fibrillation after cardiac surgery. Chest 2005;128:28S–35S. 35. Rousou JA, Meeran MK, Engelman RM, Breyer RH, Lemeshow S. Does the type of venous drainage or cardioplegia affect postoperative conduction and atrial arrhythmis? Circulation 1985;72:II259–II263. 36. Mathew JP, Fontes ML, Tudor IC, Ramsay J, Duke P, Mazer CD, et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA 2004;291:1720–9. 37. Workman J. Mechanisms of post-cardiac surgery atrial fibrillation: more pieces in a difficult puzzle. Heart Rhythm 2009; 6:1423–4. 38. Borzak S, Tisdale JE, Amin NB, Goldberg AD, Frank D, Padhi ID, et al. Atrial fibrillation after bypass surgery: does the arrhythmia or the characteristics of the patient prolong hospital stay? Chest 1998;113:1489–91.39. Wolf PA, Kannel WB, McGee DL, Meeks SL, Bharucha NE, McNamara PM. Duration of atrial fibrillation and imminence of stroke: The Framingham Study. Stroke 1983;14:664–7.40. Mariscalco G, Engström KG. Postoperative atrial fibrillation is associated with late mortality after coronary surgery, but not after valvular surgery. Ann Thorac Surg 2009;88:1871–6. 41. Villareal RP, Hariharan R, Liu BC, Kar B, Lee VV, Elayda M, et al. Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. J Am Coll Cardiol 2004;43:742–8.
Cardiac surgery and atrial fibrillation


Hemodynamic Changes following Anesthesia Induction and LMA Insertion with Propofol, Etomidate, and Propofol + Etomidate
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 109-112doi: 10.5681/jcvtr.2013.023http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Samad EJ Golzari, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Introduction: LMA is a simple supra-laryngeal device which is used to establish and maintain airway. Despite the common use of the LMA, there are no optimal methods for induction of anesthesia that can guarantee a proper insertion. The purpose of this study is comparing three methods of induction of anesthesia (Propofol, Etomidate, Propofol+Etomidate) in the hemodynamic stability after LMA insertion in elective surgeries. Methods: A total of 90 patients with ASA classes I and II undergoing elective surgeries were randomly allocated into one of the following three groups. Before anesthesia induction, all patients were premedicated. Anesthesia induction methods included: Group P (propofol 2.5 mg/kg), Group E (etomidate 0.3 mg/kg) and Group P+E (propofol 1 mg/kg plus etomidate 0.2 mg/kg). Heart rate, systolic blood pressure, diastolic blood pressure, and mean arterial pressure were measured before induction and 30 seconds after induction. Apnea time is recorded in all patients. Number of attempts to laryngeal mask insertion, ease of placement, were compared in three groups. Results: There was no significant difference between demographic data and BIS, SaO2, Etco2 associated diseases, in three group (P>0.5). There is significant difference in hemodynamic (Systolic, diastolic and mean blood pressures) changes between group 1 in comparison with group 2 and group 3. HR was significantly lower in group 1 than group 2 (P=0.16). There was significant difference in the number of attempts and ease of LMA insertion between group 2 in comparison with group 3 and group 1. The duration of apnea in group 2 was a (8.67± 6) min, where as it was (18.10±6.25) min in group 1 and (12.03±6.4) min group 3.Conclusion: Etomidate plus propofol is an effective and alternative to propofol and etomidate for facilitating LMA insertion with the added advantage of lack of cardio-vascular depression.
A B S T R A C TA R T I C L E I N F O
Article Type:Original Article
Article History:Received: 12 August 2013Accepted: 8 September 2013
Keywords:InductionPropofolEtomidate-Laryngeal Mask
Hamzeh Hosseinzadeh1, Samad EJ Golzari2*, Effat Torabi1, Marjan Dehdilani1
1Department of Anesthesiology, Tabriz University of Medical Sciences, Tabriz, Iran2Cardiovascular Research Center,Tabriz University of Medical Sciences, Tabriz, Iran
IntroductionAirway management and patient safety have always been of great importance for physicians of both modern and ancient medicine while numerous devices and methods have been devised to fulfill this goal.1,2 Laryngeal Mask Airway (LMA) is a simple supraglottic device which is placed without requiring direct laryngoscopy. It is an appropriate device for maintaining airway in both elective and emergency surgeries either in adults or in children. Several methods have been introduced for LMA insertion while no standard anesthesia induction method has been proposed to guarantee a proper placement of the device.3,4 LMA is a very safe device with the least complications.5 The most frequent anesthetic used for LMA placement is propofol which is widely used in out-patient surgeries due to its associated low postoperative nausea and vomiting
rate.6,7 The recommended dose of propofol for induction is 1-2.5 mg/kg which not only is associated with desired jaw relaxation but also prohibits reflexes such as coughing or bucking following LMA insertion. On the other hand, it is of some unwanted complications such as hypotension, bradycardia and prolonged apnea. With an elimination half-life of 4-7 hours, propofol is distributed rapidly in the circulation and enter central nervous system. Some of the complications of the propofol include pain on injection site, cardiovascular depression and probability of the infection due to its combination. When administered alone for LMA insertion, propofol could be associated with undesirable complications including coughing, gag reflex and laryngospasm.8 Numerous pharmacological agents and combinations have been introduced to decrease the hemodynamic instability throughout anesthesia.9,10

Hosseinzadeh et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 109-112 Copyright © 2013 by Tabriz University of Medical Sciences110
Etomidate is one of the IV anesthetics which are used alone or in combination with other anesthetics for anesthesia induction; it also has been used for anesthesia maintenance in different contexts.11 However, it is mostly used in the cardiac patients in whom the risk of cardiovascular instability following the administration of other IV anesthetics such as propofol or thiopental cannot be underestimated. Etomidate is of a rapid onset and emergence from anesthesia and it is not associated with histamine release.12 In addition, it has sedative and hypnotic characteristics with no analgesic effects.13,14 It provides a proper condition for LMA insertion in combination with fentanyl and mini-doses of succinylcholine; however, single administration of etomidate can cause nausea, vomiting, agitation and cortisol suppression. The main objective of this study was to compare the efficacy of three different anesthesia induction approaches [propofol (P), etomidate (E), propofol + etomidate (P+E)] in maintaining cardiovascular stability following LMA insertion in elective surgeries.
Materials and MethodsIn a double-blind randomized clinical trial, 90 patients (18-70 years old; ASA class I and II) scheduled to undergo elective surgeries were studied in three equal groups (n=30). The study was conducted in Imam Reza Hospital, Tabriz, Iran in a period of 12 months from Jan 2011 to Jan 2012. Based on the literature, to discover a 10 unit change in HR/BP (α=0.05, β=0.2 and power=0.8) sample size of 90 was considered. Patients were randomly divided into three groups using Randomly Permuted Blocks and an online software (http://www.randomization.com). Inclusion criteria were patients with ASA class I or II. Exclusion criteria were existence of a considerable pathology in the larynx or pharynx, mouth opening less than 2.5 cm, bronchial asthma, cardiovascular diseases and Mallampati scores of 3-4. Prior to anesthesia induction, all patients received 6 mL/kg of normal saline 0.9%. The anesthesiologists administering the medications and inserting the LMAs were unaware of the content and quantity of the used medications as they were prepared by the third anesthesiologist. All patients received fentanyl 2 microgram/kg IV, midazolam 0.025 mg/kg IV and lidocaine 1 mg/kg IV. Later, group P received propofol 2.5 mg/kg IV, group E received etomidate 0.3 mg/kg IV and group P+E received propofol 1 mg/kg IV and etomidate battle which was mixed in a 10 mL syringe. The volume of the medications and the speed of the injection (10 seconds) were equal in all three groups. Prior to induction and 30 seconds after induction hemodynamic variables were recorded. Later, 60 seconds after loss of consciousness, which was confirmed by inability to reply to verbal commands and loss of eyelash reflex, LMA was inserted by the second anesthesiologist. Proper placement of the LMA was approved by chest expansion and capnography. Following successful LMA insertion, anesthesia was
maintained by isoflurane 1-1.5% and an equal mixture of O2-N2O (6 L/min). In cases with apnea, manual ventilation was continued. In all three groups, blood pressure, heart rate, pulsoxymetry and capnography values were recorded and compared. The obtained data were compared and presented as Mean±SD, frequency and percentage. Categorical variables were evaluated using contingency tables and Chi-square or Fisher’s Exact test. To compare the quantitative variables, repeated measures analysis was used. P≤0.05 was considered statistically significant.
ResultsDemographic characteristics of the patients in three groups have been presented in Table 1. No significant difference could be observed regarding demographic characteristics of the patients in three groups. Hemodynamic changes (SBP, DMP, MAP and HR) at different stages of anesthesia in all groups have been presented in Table 2.
Discussion The current study has been conducted on the hemodynamic stability in elective surgeries. In our study, decease in systolic blood pressure, diastolic blood pressure, and mean arterial pressure were significantly more frequent in group P compared with other groups. Hemodynamic stability was more visible in groups E and P+E.Etomidate is a hypnotic of choice in most cardiac diseases and also an excellent option to be used in combination with other anesthetics.11 Uzun et al., in a study on 50 patients, compared etomidate and remifentanil with propofol in LMA insertion.15 They reported decrease in MAP in 25 patients having received propofol 2.5 mg/kg and remifentanil 0.05 mg/kg in comparison with the patients having received etomidate 0.3 mg/kg and remifentanil 0.05 mg/kg. They later concluded that etomidate would provide a better hemodynamic stability. Propofol with the dose of 2.5 mg/kg is accompanied by appropriate relaxation and avoidance of complications such as coughing and bucking following LMA insertion. This, however, could be associated with undesirable decreased blood pressure, bradycardia, and prolonged apnea. Combination of etomidate with propofol would not only decrease the required dose of both medications but also provide us with the benefits of both agents including more
Table 1. Demographic characteristics of the patients in three groups
Group P Group E Group P+E PSex
0.282Male 24 26 21Female 6 4 9ASA
0.585Male 27 29 28Female 3 1 2Age 40 ± 16 38.5 ± 12.5 40.4 ± 16.5 0.865Weight 71.5 ± 13 74 ± 9.9 73.5 ± 12.3 0.608

Propofol, Etomidate, and Propofol+Etomidate
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 109-112Copyright © 2013 by Tabriz University of Medical Sciences 111
Table 2. Hemodynamic changes (SBP, DMP, MAP and HR) at different stages of anesthesia in all groups
Groups Before anesthesia After anesthesia P Before LMA After LMA P
SBPP 122.7 ± 19.2 104.6± 22.9 0.000 102.5 ± 14.4 99.4 ± 12.9 0.07E 131 ±18.2 121.7 ± 14.9 0.326 111.1 ± 23.8 109.4 ± 15.8 0.231
P+E 129.1 ± 16/5 117.4± 18.5 0.023 110.2 ± 14.5 110.8 ± 19.2 0.723
DBPP 76.2 ± 10.1 64.7 ± 12.3 0.000 63.5 ± 14.1 59.4 ± 12.8 0.002E 80.5 ± 9.3 74.1 ± 9.2 0.010 69.7 ± 10.2 65.9 ± 11.3 0.000
P+E 78 ± 11.1 72.2 ± 12.5 0.001 66 ± 12.7 65.8 ± 17 0.022
MAPP 90 ± 10.89 77.4 ± 12.3 – 75.2 ± 15.1 73.3 ± 17.6 0.307E 97.6 ± 9.7 89.6 ± 11.4 – 84.3 ± 10.7 78.7 ± 8.6 0.020
P+E 95.4 ± 12.8 86.5 ± 12 – 80.3 ± 12.2 80.7 ± 17.6 0.015
HRP 78.2 ± 13.9 73.2 ± 13.3 0.019 70.9 ± 11.3 69.6 ± 11.5 0.000E 80.4 ± 18.7 82.4 ± 15.3 0.035 73.6 ± 14.6 66.8 ± 10.7 0.000
P+E 82.9 ± 18.9 81 ± 17.2 0.563 71.8 ± 15.9 73.7 ± 12.1 0.007Data are presented as Mean ± SD.
stable hemodynamic, enough muscle relaxation required for LMA insertion and better airway quality. Etomidate administration could lead to agitation and postoperative nausea and vomiting which could be eliminated by adding propofol. In our study, heart rate decreased significantly in group P compared with group E. However, no difference could be observed comparing groups P and P+E. MAP was more stable in groups E and P+E compared with group P while the difference between groups E and P+E was not significant highlighting the hemodynamic stability in these groups following decreasing the required propofol dose and addition of etomidate as an adjuvant. In a study, the effect of P, E and P+E were studied on 90 patients concluding that most hemodynamic variable were more stable in P+E and MAP was decreased more significantly in group P compared with other groups.16 The findings of this study are in line with ours; the most frequent decrease in blood pressure occurs in the group P while groups E and P+E are associated with the least changes in blood pressure. However, the combination ratio of 1:1 was used in their study; unlike our study in which the combinations were used on dose-basis.The major finding of the present study is that P+E provides a more stable hemodynamic in comparison with either P or E. Hemodynamic stability is considered a prominent characteristic of a proper anesthetic; propofol reduces blood pressure and heart rate but P+E provides a desirable stable hemodynamic.
ConclusionQuality of the maintained airway and LMA insertion was different in all groups. P+E is superior to E regarding the number of the attempts and insertion ease and considering the fact that it provides appropriate condition for LMA insertion, it could replace other agents.
Ethical issues: This study was reviewed and confirmed by the ethics
committee of Tabriz University of Medical Sciences.
Conflict of interests: The authors declare no conflicts of interest.
References1. Khodadoust K, Ardalan M, Ghabili K, Golzari SE, Eknoyan G. Discourse on pulse in medieval Persia—the Hidayat of Al-Akhawayni (?–983AD). Int J Cardiol 2013;166:289-93. 2. Golzari SE, Khan ZH, Ghabili K, Hosseinzadeh H, Soleimanpour H, Azarfarin R, et al. Contributions of medieval Islamic physicians to the history of tracheostomy. Anesth Analg 2013;116:1123-32. 3. Mahmoodpoor A, Golzari SE, Hamidi M, Hamidi M, Parish M, Soleimanpour H, et al. Comparison of Three Methods for Laryngeal Mask Airway Insertion in Adults: Standard, Lateral and Rotational. J Clin Anal Med 2013. (In Press)4. Aghamohammadi D, Eydi M, Hosseinzadeh H, Rahimi MA, Golzari SE. Assessment of Mini-dose Succinylcholine Effect on Facilitating Laryngeal Mask Airway Insertion. J Cardiovasc Thorac Res 2013;5:17-21. 5. Peirovifar A, Eydi M, Mirinejhad MM, Mahmoodpoor A, Mohammadi A, Golzari SE. Comparison of postoperative complication between Laryngeal Mask Airway and endotracheal tube during low-flow anesthesia with controlled ventilation. Pak J Med Sci 2013;29:601-5. 6. Hosseinzadeh H, Eidy M, Golzari SE, Vasebi M. Hemodynamic Stability during Induction of Anesthesia in Elderly Patients: Propofol + Ketamine versus Propofol + Etomidate. J Cardiovasc Thorac Res 2013;5:51-4.7. Seyedhejazi M, Eydi M, Ghojazadeh M, Nejati A, Ghabili K, Golzari SE, et al. Propofol for laryngeal mask airway insertion in children: Effect of two different doses. Saudi J Anaesth 2013;7:266-9.8. Jamil SN, Singhal V, Habib SK. The effect of mini-dose suxamethonium to facilitate laryngeal mask airway insertion under propofol anesthesia. Rawal Medical Journal 2010; 35:2-5.9. Hosseinzadeh H, Eidi M, Ghaffarlou M, Torabi E, Ghabili K, Golzari SE. Comparison of remifentanil with esmolol to blunt the cardiovascular response to tracheal extubation in patients undergoing neurosurgical procedures for intracranial masses. J Pak Med Assoc 2013;63;8:950-410. Hosseinzadeh H, Eydi M, Ghaffarlou M, Ghabili K, Golzari SE. Esmolol: a unique beta-blocker in maintaining cardiovascular stability following neurosurgical procedures. Advanced Pharmaceutical Bulletin 2012;2:249-52.11. Morgan M, Lumley J, Whitwam JG. Respiratory effects of etomidate. Br J Anaesth 1977;49:233-6.12. Bergen JM, Smith DC. A review of etomidate for rapid

Hosseinzadeh et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 109-112 Copyright © 2013 by Tabriz University of Medical Sciences112
sequence intubation in the emergency department. J Emerg Med 1997; 15:221-30.13. Van Hamme MJ, Ghoneim MM, Ambre JJ. Pharmacokinetics of etomidate, a new intravenous anesthetic. Anesthesiology 1978;49:274-7.14. Meuldermans WE, Heykants JJ. The plasma protein binding and distribution of etomidate in dog, rat and human blood. Arch Int Pharmacodyn Ther 1976; 221:150-62.15. Uzun S, Gozacan A, Canbay O, Ozgen S. Remifentanil and etomidate for laryngeal mask airway insertion. J Int Med Res 2007;35:878-85.16. Saricaoglu F, Uzun S, Arun O, Arun F, Aypar U. A clinical comparison of etomidate-lipuro, propofol and admixture at induction. Saudi J Anaesth 2011;5:62-6.17. Khan P, Afridi Y. Comparison between propofol and thiopentone sodium for laryngeal mask airway insertion in day case surgery. Journal of Postgraduate Medical Institute 2008;22:238-42.18. Monem A, Chohan U. Comparison of low dose succinylocholine with low dose atracurium to evaluate LMA insertion during thiopentone induction. J Anaesth Clin Pharmacol 2004;20:39-44.

Patient’s Perception of Stressors Associated with CoronaryArtery Bypass Surgery
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 113-117doi: 10.5681/jcvtr.2013.024http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Mitra Mousavi Shabestari, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Introduction: Cardiac surgery, due to being associated with stressors, has many physiological, psychological, emotional, growths, and spiritual potential consequences. However, few studies have been conducted about identifying the stressors. Therefore, the objective of the study was to determine patients’ perceptions of stressors associated with coronary artery bypass surgery.Methods: In this descriptive study during the two-month investigation, qualified patients for participation in the study (68 persons) undergoing coronary artery bypass graft surgery on the third to fifth postoperative day were selected and with using of Revised Cardiac Surgery Stressors Scale (RCSSS), interpersonal, intrapersonal, and extra personal stressors were determined. Results: The findings showed that intrapersonal stressors are perceived more than interpersonal and extra personal stressors by patients. In the analysis of data, the highest stressors were “pain and discomfort”, “the need to have heart surgery”, “death due to illness or surgery”, “being away from home and work”, “having chest tube”.Conclusion: In this study the intrapersonal stressors were perceived more than interpersonal and extra personal stressors by patients, which nurses should put emphasis on identification and elimination of intrapersonal stressors based on the needs of patients.
A B S T R A C TA R T I C L E I N F O
Article Type:Original Article
Article History:Received: 9 July 2013Accepted: 21 August 2013
Keywords:PerceptionPatientStressorsCoronary Artery Bypass Surgery
Kobra Parvan1, Vahid Zamanzadeh1, Sima Lak Dizaji2, Mitra Mousavi Shabestari3*, Nasser Safaie3
1Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran2Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran3Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
IntroductionNowadays, coronary artery bypass graft surgery is one of the coronary artery disease (CAD) treatments.1 Coronary artery bypass graft surgery (CABG) is a major incident with a main psychological and emotional impact on patients and their families.2 In Iran, 60% of the total open heart surgery is coronary artery bypass surgery.3 Identified concerns in CABG surgery are known as stressors.4,5 CABG is a physical and psychological stress and the surgery is as a life-threatening incident for patients which is along with adapting problems and hospital schedules, they feel suffering and lack of control, and hospitalization separates them from their relatives, friends and everyday life situation.6 Patients concerns related to coronary artery bypass graft surgery are chances of successful surgery, length of the waiting period before operation, fear of death, previous negative hospital experience, fear about the recovery process, fear of pain and discomfort, fear about loss of appetite, weakness, sleep disturbances, resumption of normal life activities after surgery, cardiac monitoring, drug addiction, length of hospitalization and
hospital costs.7 However, few studies in relation to CABG surgery stressors level is available.4 It is believed nursing is a profession that provides comprehensive caring based on organized system and using nursing science. Nurses evaluate and take care of a patient along with health care team on the base of their knowledge, integrated presence planning, programming, and management. Health is understandable by a patient’s perspective, therefore, patients’ perception of health and stressors is crucial for meaningful nursing and care programs.8 In patients who have undergone CABG surgery, stress leads to the feeling of life control loss also increasing sensitivity to pain and cause to feel weakness. The apparent loss of control prevents the patients who have undergone CABG surgery from proper care of themselves, thus renders nursing care more complex and possibly prolongs the improvement process.9 It is important to determine the stress levels of patients and patient’s concerns related to CABG surgery. Studies show that education given to patients improves them to feel better after surgery.10 This study is based on the Neuman Systems Model. Neuman system model states

Parvan et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 113-117 Copyright © 2013 by Tabriz University of Medical Sciences114
that patients are an open system constantly interacting with their environment. To ensure that the special needs of the patient are identified, this open system needs to have two-way communication at any time and a thorough assessment of the patient includes looking at all patient’s psychological, social, cultural, emotional, developmental, and religious variables.11 Internal and external factors that interact with the client system are part of the environment. The intrapersonal environment is the internal environment that includes influences within the system. The external environment includes interpersonal and extra personal factors.12 Stressors in the intrapersonal, interpersonal, and extra personal environment can influence the potential or actual reaction in system, therefore, the main purpose of nursing is assessing the client to gain system stability through the attainment, retention, and maintenance optimal health and it is the nurse that creates a link among the client, environment, and health and leads to the stability of the system.12 Nursing researchers have been increasingly interested in understanding the effects of stressors associated with disease and treatment in the patient’s recovery process. It is known that stressors associated with hospitalization have an adverse effect on patient recovery although specific stressors experienced by patients are often not clearly specified but nurses can identify them and help the patients to deal with the hospital stressors.13 Detection of stressors for patients undergoing CABG surgery is vital for nurses, because it helps them prioritize and extend effective interventions.4 Therefore, there is a need to evaluate the patient’s own perceptions of CABG surgery stressors. Advances in health care knowledge and changes in health care providing created new questions and new stressors in the hospital units. These changes have led researchers to identify the new stressors that can affect on patients. Despite the importance of identifying patient needs and psychological stressors in developing strategies of coping and effectively managing stress by nurses, few studies have been done in this connection. According to recent studies in Iran, depression and anxiety in patients awaiting heart surgery were more and on the other hand the training of health professionals can be effective in reducing anxiety in patients.14 When the stressors are identified by nurses, they can deal with the stressors affecting the patient by manipulating the environment and provide the appropriate care. Therefore, this study is performed to determine patients’ perceptions of stressors in recovery period after coronary artery bypass surgery.
Materials and MethodsIn a descriptive study conducted in cardiac surgical wards of Madani hospital, Tabriz, Iran between June and August 2011, identification of the patient population meeting the criteria was performed by reviewing the daily CABG surgery census log kept in the cardiovascular intensive care unit, the unit to which all post-operative CABG patients are sent immediately after surgery. Patients undergoing
CABG for the first time, 40-75 years old, alert and aware of time, place, person, and situation, and confined to bed about 3 to 5 days after operation were selected. After a pilot study on 10 patients, using descriptive statistics the number of the patients participating in this study was 68 people. Reliability for the RCSSS was determined using Cronbach Alpha (r=0.81) method in a pilot study of 10 patients. Cardiac Surgery Stressors Scale (CSSS) was developed by Carr and Powers in 1986.15 White in 1998, adding six items to the Cardiac Surgery Stressors Scale (CSSS) introduced Revised Cardiac Surgery Stressors Scale (RCSSS) consisting of 37 questions which has been used in this study. In this study, with the permission of the author, the (RCSSS) were used.16 The questionnaire consisted of two parts, the first part includes individual and social data and the second part includes RCSSS that is divided into intrapersonal, interpersonal, and extra personal subsystems. Items are scaled in terms of the participant’s current level of concern, from 0 (not at all) to 4 (a great deal). In this study, patients were asked to complete questionnaires on the third to fifth postoperative days and it took approximately 25-35 minutes for the patients to complete RCSSS. Some patients had to be assisted with the completion of the data sheet and survey, for various reasons including poor eyesight, weakness, and illiteracy.
Statistical analysisAll statistical analysis was performed using SPSS 13 (SPSS Inc., IL, Chicago, USA). With the descriptive statistics, we presented numbers and Mean ± SD. The overall score on the RCSSS was calculated by summing each individual’s responses to the 37 items. We determined the most stressful and least stressful items. We considered the value P<0.05 to be statistically significant.
ResultsMost patients were male (69.1%), married (92.6%) with no formal education (36.8%) and participated on the fifth post-operation day (50%). In this study, RCSSS scores range was from 0 to 4, and higher scores indicated a greater understanding of the stressors by patient. The mean RCSSS was 1.63 ± 0.36 indicating that the general perception of artery bypass graft surgery stressors is “least concern”. According to subsystems mean score, interpersonal stressors perception is “a little”, extra personal stressors perception is “more than a little” and intrapersonal stressors perception is “average”. The most important top six stressors were ranked according to their mean score. This stressors include “pain or discomfort”, “having to have cardiac surgery”, “dying because of patients’ illness or surgery” from intrapersonal stressors and “being away from home or/and business” and “having chest tube” from extra personal stressors. The lowest stressors perceived by patients are “call light being answered”, “The number of doctors involves patients’

Patient’s Perception of Stressors Associated with CABG
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 113-117Copyright © 2013 by Tabriz University of Medical Sciences 115
care”, “having doctors and nurses discuss about patient or patients” from interpersonal stressors and “explanation of hospital routines and procedures” from extra personal. According to the results obtained it can be seen that intrapersonal stressors perceived more than other stressors and extra personal factors are the second stressors and interpersonal stressors are the lowest stressors perceived by patients (Tables 1,2,3 and 4).
Table 1. Top 6 stressors (ranked by mean scores) in patients undergoing CABG surgery
Patient stressors Rank Mean ±SD
Pain or discomfort 1 2.86 ± 1.23
Being away from home or/and business 2 2.77 ± 1.30
Having to have cardiac surgery 3 2.61 ± 1.50
Having chest tube 4 2.61 ± 1.41
Dying because of patients’ illness or surgery 5 2.51 ± 1.38
Time lapse before actual surgery 6 2.39 ± 1.45
Table 2. Intrapersonal stressors
Stressors Rank Mean ± SDPain or discomfort 1 2.86 ± 1.23Having to have cardiac surgery 2 2.61 ± 1.50Dying because of patients’ illness or surgery 3 2.51 ± 1.38
Time lapse before actual surgery 4 2.39 ± 1.45Needing pain medications 5 2.35 ± 1.32Change in diet and eating habit 6 2.22 ± 1.36Increasing activity 7 2.10 ± 1.18Resuming previous lifestyle 8 1.89 ± 1.31Being thirty 9 1.47 ± 1.48Resuming sexual activity 10 1.38 ± 1.14The progress she/he making 11 1.35 ± 1.12Total intra personal stressors 2.10 ± 0.65
Table 3. Interpersonal stressors
Stressors Rank Mean ± SD
Needing assistance with various activities eg. bathing, getting out of bed, using bedpan or urinal
1 2.22 ± 1.18
Sharing the room with one or more patients 2 1.43 ± 1.11Different nurses caring for patient 3 1.33 ± 1.00Taking medications 4 1.30 ± 1.21Discussing patient concerns about surgery with doctors and nurses 5 1.29 ±1.35
Explanation of hospital routines and procedures 6 0.94 ± 0.84
Having doctors and nurses discuss about patient or patients 7 0.94 ± 1.19
The number of doctors involves patients’ care 8 0.72 ± 1.00
Call light being answered 9 0.55 ± 1.15Total interpersonal stressors 1.20 ± 0.66
Table 4. Extra personal stressors
Stressors Rank Mean ± SD
Being away from home or/and business 1 2.77 ± 1.30
Having chest tube 2 2.61 ± 1.41
Having visitors only certain hours 3 2.0 ± 1.41
Sleeping in strange and uncomfortable 4 1.85 ± 1.18
Having patients’ sleep interrupted 5 1.85 ± 1.18
Having tubes in patients’ nose and mouth 6 1.76 ± 1.58
Problems that other patients are having 7 1.72 ± 1.24
Being stuck with needles 8 1.67 ± 1.32
Payment of hospital and medical bills 9 1.54 ± 1.45
Being restrained 10 1.51 ± 1.35Being transferred from intensive care unite 11 1.26 ± 1.31
Loss of income because of disease 12 1.23 ± 1.63
Not having thing within easy reach eg. call light, phone, drinks 13 1.16 ± 1.16
Following hospital schedule rather than own 14 1.08 ± 1.01
Having the monitoring equipment discontinued
15 1.07 ± 1.24
Having a foley catheter (urine drainage tube) 16 1.07 ± 1.24
Cardiac monitors and other equipment 17 0.66 ± 0.82
Total extra personal stressors 1.60 ± 0.49
DiscussionSurgery is a major stressor for patients that with reduced functional reserves cause the deduction of muscle mass, and is associated with hypoxemia, sleep and mental disorders. Anxiety, depression and stress, is associated with more complications after heart surgery.17,18 In this study perception of post-operative patients from intrapersonal, interpersonal and extra personal stressors were determined and according to the Likert were classified as “a little” rate. But intrapersonal stressors were perceived more than interpersonal and extra personal stressors by patients, in this regard; nurses can help through individual assessing and training according to individual needs in patient’s compliance with these factors. Also cultural beliefs in different forms can be underlying or resonator factor for stressors. Understanding and explanation of these beliefs to provide effective education to patient is essential. It seems the chronical interventions are most effective when they appropriate with each individual coping style.19 In our study “pain and discomfort” (mean=2.86) is the first stressor among the other intrapersonal stressors perceived by patients; it is also the first among the other stressors of coronary artery bypass graft surgery perceived by patients. In 2007 a study by Gallagher and Mckinley related to stressors a n d anxiety in patients undergoing coronary artery bypass surgery was performed. 172 patients before surgery, before discharge 143 patients and 130 people after discharge participated in this study. King et al. stressors

Parvan et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 113-117 Copyright © 2013 by Tabriz University of Medical Sciences116
scale was used and five items were added to this scale. This study showed that “pain and discomfort” stressor (mean=1.45) among operative patients before discharge was the third stressor, that is not congruent with our study, in our study, patients perceiving stress reported more pain and discomfort and it may be due to low number of nurses caring of more patients, and as nurses’ perception of patient pain is an important factor in the strategy of decision making about pain relief, therefore, in our study it is important for the nurses to pay more attention to patient’s pain. Postoperative pain is a common experience for patients in the surgical ward.20 Extensive clinical observations suggest that usually pain is caused after surgery and lack to comfort the post operation pain in patients especially patients undergoing coronary artery bypass graft surgery, cause death and complications from it. Therefore, effective management of pain is the most common topics of today’s society, especially the medical community and health professionals.21
In our study, “being away from home and work” stressor (mean= 2.77) is the first factor in extra-personal stressors, and the second stressor among all coronary artery bypass surgery stressors perceived by patients. Also in 1998, a study by White related to the patient - the nurse perception of the stressors in coronary artery bypass surgery conducted with 35 patients, showed that “being away from home and work” (mean = 2.86) as the seventh rate stressors perceived by patients16, despite different ranking in two studies, the mean scores are the same, so that White study is congruent with our study. In our study, although “ being away from home and work” is the second stressor among the patients, the average score is less than White’s study; again, in our study most patients wanted to be nearby their family during the convalescence period before they return home. To reduce this concern, the proper way is for patient to spend recovery period of surgery with family away from stress in the hospital at particular hours. Similar to pain concern, being away from home and work is also serious for patients and most patients come from a long distance to reach the hospital traveling long distance is not only uncomfortable for patients, It also has consequences for the patient’s family. So it is not surprising that the patients report extra primary concern that disease impact on their families. Again it is not surprising that this concern to continue after discharge.4
In our study, “having to have cardiac surgery” (mean= 2.61) is the second factor in intrapersonal stressors and the third factor in the all coronary artery bypass surgery stressors. White study in 1998 showed, “having to have cardiac surgery” stressor (mean= 3.37) as the first stressor perceived by patients, that with our study is not congruent. This difference in patients’ understanding of stressors is because of education and psychological support from nurses. Nurses can somewhat reduce the patient’s concerns with appropriate training about coronary artery
bypass surgery, risk factors of heart disorders and pre-operative education and establish a relationship among with confidence.In our study, “fear of death” (mean= 2.51) is the third stressor among intrapersonal stressors and fifth stressor between all CABG surgery stressors. Gallagher and McKinley in 2007 found that, “fear of death” (mean = 1.63) was the fifth stressor among operative patients before discharging4, that is not congruent with our study. It is better for the nurses to encourage the patients and help them by expressing and repeating their anxiety. The assessing of patient perception like their fear and anxiety may help to detect patients at risk of progressing psychological stress.22 In addition, it can help the nurses to encourage patients to tell their feelings of anxiety and to deal with fear as a source of stress.23 In this study, “Time lapse before actual surgery” (mean = 2.39) is the fourth factor of stressors within the intrapersonal stressors and the sixth among all stressors perceived by patients. In Gallagher and McKinley study “Time lapse before actual surgery” (mean = 2.02) was the first stressor among patients4 that is congruent with our study, in our study, this stress factor can be minimized by proper hospital management. Any pre-operation intervention refers to the stress of waiting for surgery. Because the waiting for surgery is a major concern for patients and strongly associated with anxiety. Waiting for surgery is very stressful.24 In addition, often long period of waiting for heart surgery can exacerbate the stress and anxiety.25 And adversely affects on the physical and social functioning.26 Therefore current cardiac surgical patients may benefit from preoperative interventions to speed healing and reduce surgical complications.
ConclusionThe main emphasis of this study was to determine patients’ perceptions of stressors associated with recovery process during coronary artery bypass surgery. The present study showed that CABG surgery intrapersonal stressors are perceived more than interpersonal and extra-personal stressors by patients and “pain and discomfort” from intrapersonal stressors is the most important stressor perceived by patients. It is necessary for the nurses to assess the patients individually, do proper nursing activities, and create an open relationship among patients and themselves, and nurses should not assume that the patient understands everything in a certain way without validating this with the patient. It is necessary to ask patients questions to know how they perceive stressors.
SuggestionConsidering the research results it is suggested that nurses should assess and recognize properly the nature of stressors, know the prior needs of patients, plan training and care taking programs according to individual needs of every

Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 113-117Copyright © 2013 by Tabriz University of Medical Sciences 117
Patient’s Perception of Stressors Associated with CABG
patient in order to eliminate and adjust the stress factors so that the interventions could ultimately lead to prevention of complications, improvement of physiological function and provide physical, mental and emotional comfort of patients. Planning and implementing nursing care help to achieve maximum performance and affect on the health and well-being of a patient. It is important to consider a patient as an individual character and while reviewing his needs, all aspects of his personality like physical, psychological, social, cultural, intellectual, and environmental aspects should be taken in to consideration.
LimitationsOne of the limitations of our study was small sample size and sampling was restricted to the cardiac surgery wards.
AcknowledgementsThe authors would like to offer their thanks to the deputy of Tabriz University of Medical Sciences, respected authorities of the hospital under study and Madani Hospital Research Center for their financial support. We would like to thank all of our colleagues who helped us in this study.
Ethical issues: The study was performed after receiving approval from the
university research council and obtaining ethical license, furthermore, the
investigator explained the logical reason of the study to each patient and
insured them that their decision to participate in the study would have no
affect on the care that they received.
Conflict of interests: The authors declare no conflicts of interest.
References1. Alexiou K, Kappert U, Staroske A, Joskowiak D, Wilbring M, Matschke K, et al. Coronary surgery for acute coronary syndrome: which determinants of outcome remain? Clin Res Cardiol 2008;97:601-8.2. Stroobant N, Vingerhoets G. Depression, anxiety, and neuropsychological performance in coronary artery bypass graft patients: a follow-up study. Psychosomatics 2008;49:326-331. 3. Babaee G, Keshavarz M, Heidarnia A. Evaluation of quality of life inpatients with coronary artery bypass surgery using controlled clinical trial. Acta Med Iranica 2007;1:69-74.4. Gallagher R, Mckinley S. Stressors and anxiety in patients undergoing coronary artery Bypass Surgery. Am J Crit Care 2007;16:248-257.5. Mccormick KM, Naimark BJ, Tate RB. Uncertainty, symptom distress, anxiety, and functional status in patients awaiting coronary artery bypass surgery. Heart Lung 2006; 35:34-45.6. Bergvik S, Wynn R, Sørlie T. Nurse training of a patient-centred information procedure for CABG patients. Patient Educ Couns 2008;70:227–33.7. Yarcheski A, Knapp-Spooner C. Stressors associated with coronary artery bypass surgery. Clin Nurs Res 1994; 3:57-68.
8. Chitty KK. Professional nursing: concepts & challenges. 4th ed. St. Louis: Elsevier,Saunders:2005.9. Sarpy NL, Galbraith M, Jones PS. Factors related to recovery in coronary artery bypass graft surgery patients. Dimens Crit Care Nurs 2000;19:40-5.10. Ozer N, Akyil R, Yurttas A. The effect of education on the stress levels in patients undergoing coronary artery bypass graft surgery. Pak J Med Sci 2010; 26:282-7.11. Reed KS, Betty N. The Neuman systems model. California: Sage publication;1993.12. Neuman B. The Neuman Systems Model. In Neuman B & Fawcett J (Eds). The Neuman Systems Model. 4th ed. p. 3-33. Upper Saddle River, NJ: Prentice Hall;2002.13. Ross S, MacKay R. Postoperative stress: Do nurses accurately assess their patients? J Psychosoc Nurs Ment Health Serv 1986 Apr;24:16-22.14. Mousavi SS, Sabzevari S, Abbaszade A, Hosseinnakhaie F. [The Effect of Preparatory Face to Face Education to Reduce Depression and Anxiety in Open Heart Surgery Adult Patient in Shafa Hospital in Kerman]. Nursing Research 2011; 21:29-38. 15. Carr JA, Powers MJ. Stressors associated with coronary bypass surgery. Nurs Res 1986;35:243-6.16. White RM. Nurse-Patient Perception of Stressors Associated with Coronary Artery Bypass Surgery[Thesis]. Las Vagas: University of Nevada;1998. 17. Tully P, Baker R, Knight J. Anxiety and depression as risk factors for mortality after coronary artery bypass surgery. J Psychosom Res 2008;64:285-90.18. Tully P, Baker R, Turnbull D, Winefield H, Knight J. Negative emotions and quality of life six months after cardiac surgery: the dominant role of depression not anxiety symptoms. J Behav Med 2009;32:510-22.19. Martelli MF, Auerbach SM, Alexander J, Mercuri LG. Stress management in the health care setting: matching interventions with patient coping styles. J Consult Clin Psychol 1987;55: 201–7.20. Ger L, Chang C, Ho S, Lee M, Chiang H, Chao C, et al. Effects of a continuing education program on nurses’ practices of cancer pain assessment and their acceptance of patients’ pain reports. J Pain Symptom Manage 2004; 27:61e71.21. Mohamedi M. [Comparison of relation to analgesics between nurses and patients perception in pain]. Journal of Esfehan University of Nursing & Miduifery 2001;15:36.22. Samuelson KAM, Lundberg D, Fridlund B. Stressful memories and psychological distress in adult mechanically ventilated intensive care patients - a 2-month follow-up study. Acta Anaesthesiologica Scandinavica 2007; 671-8.23. Yava A, Tosun N, Ünver V, Çiçak H. Patient and Nurse Perceptions of Stressors in the Intensive Care Unit. Stress Health 2011;27:e36-e47.24. Voss JA, Good M, Yates B, Baun MM, Thompson A, Hertzog M. Sedative music reduces anxiety and pain during chair rest after open-heart surgery. Pain 2004;112:197-203. 25. Carli F, Zavorsky G. Optimizing functional exercise capacity in the elderly surgical population. Curr Opin Clin Nutr Metab Care 2005;8:23-32.26. Sampalis J, Boukas S, Liberman M, Reid T, Dupuis G. Impact of waiting time on the quality of life of patients awaiting coronary artery bypass grafting. CMAJ 2001;165:429-33.


Home and Clinical Cardiovascular Care Center (H4C): a Framework for Integrating Body Sensor Networks andQTRU Cryptography System
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 119-124doi: 10.5681/jcvtr.2013.025http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Massoud Sokouti, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Quick responds to heart attack patients before arriving to hospital is a very important factor. In this paper, a combined model of Body Sensor Network and Personal Digital Access using QTRU cipher algorithm in Wifi networks is presented to efficiently overcome these life threatening attacks. The algorithm for optimizing the routing paths between sensor nodes and an algorithm for reducing the power consumption are also applied for achieving the best performance by this model. This system is consumes low power and has encrypting and decrypting processes. It also has an efficient routing path in a fast manner.
A B S T R A C TA R T I C L E I N F O
Article Type:Original Article
Article History:Received: 17 July 2013Accepted: 2 Sep 2013
Keywords:QTRU CryptographyBody Sensor NetworkPersonal Digital AccessHeart AttackWireless Networks
Ali Zakerolhosseini1, Massoud Sokouti1*, Massoud Pezeshkian2
1Faculty of Electrical & Computer Engineering, Shahid Beheshti University, Tehran, Iran2Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
IntroductionRecent reports show that coronary artery disease (CAD) risk factors have been increased among Iranian people.1
Moreover, cardiovascular diseases are one of the important results of these risk factors which lead to high rate of mortality and disability according to WHO reports on worldwide people.2-4 Both the Heart rhythmic disorders and the arrhythmia are popular alarm signs in patients who are suffering from heart disease. Although, ECG (Electrocardiogram) can detect myocardial infarctions, however exercising and Holter monitoring tests are more accurate for medical diagnosing than a simple experimental diagnosis. Analysis of ECG with or without exercising tests is being done by a medical doctor and there are challenges over these clinical cases.5
These days, Wireless Sensor Network (WSN) system is being used for cardiac monitoring which transfers ECG signals to Personal Digital Assistant (PDA) by using a cellular network. As a result, the combination of WSN and computer electronic infrastructures can assist the healthcare monitoring era efficiently.6-9
Some examples of WSN hardware designs are as follows: (i) Berkeley’s Mica2, (ii) ETH’s (iii) BTNodes, (iv) Intel’s iMote, (v) UCC’s DSYS25, (vi) SmartITs, and (vii) MITes.9-12 The Body Sensor Network (BSN) is a hardware platform that it uses a wide range of bandwidth because of using the IEEE 802.15.4 standard. In the design of this
platform, a lot of sensors are used to detect signals easily; the most of them are those which can detect Physiologic signals whereas stress and nervous tensions signals are omitted from the main signals.13
The security of data among medical doctor, patient, and ICU is an important issue which should be well addressed in the implementation of this system. The cryptographic algorithms such as RSA (i.e., stands for Ron Rivest, Adi Shamir and Leonard Adleman) and ECC (i.e. Elliptic Curve Cryptography) have a great security for transferring data through an unsecured channel but they are slow in encrypting and decrypting processes. The NTRU encryption system has a hard and unbreakable core which is standardized by IEEE with the most acceptable cryptography algorithm and because of its high speed and promising security, it can be implemented in WSNs. The most advantage of NTRU system over RSA and ECC is based on its lattice-based architecture which has the complexity of O(n2). This means it is the cheapest, fastest and the most effective cipher algorithm.14,15
In this article, we present a combination of Quaternion algebra with NTRU in WSN for healthcare and cardiovascular disease in order to increase the security of data transferred in WSNs environments. The new system is known as QTRU with the ability of parallel processing and encrypting four vectors at the same time. The complexity orders of encrypting and decrypting in QTRU system is

Zakerolhosseini et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 119-124 Copyright © 2013 by Tabriz University of Medical Sciences120
O(4n2) and the dimension of lattice matrix which is needed to attack this cipher is 8N×8N. Having the high speed property in encrypting and decrypting is an advantage of QTRU over NTRU with degree of four, at the same security level. Also, we represent algorithms for energy optimization between WSN nodes and for reducing hops between modes in order to reduce the possible distance rate between WSN nodes.
NTRUThe first version of NTRU cipher algorithm was proposed by Silverman et al. in 1998.14 This system is based on lattice using Multi sentences ring complexity which uses matrices. It uses Shortest Vector Problem (SVP) to reduce its lattices. The basis of NTRU is the ring of Z[x]/(xN-1) and is described by the complexity of the ring, while N is a primitive number. In these rings, complexity order of adding operation is ( )nO and the complexity order of multiplying is O(n2).16 Using this ring in the NTRU structure provides high speed and efficiency. According to16,17, we define three following rings: R= Z[x]/(xN-1), Rp=Z/Zp[x]/xN-1, Rq=Z/Zq[x]/xN-1.
Key GenerationLet df, dg, dᵠ and dm be constant integer numbers less than N which are known as public parameters, N is a prime number, p and q are two co-prime numbers which are relatively prime and q is a number more greater than p. To create an NTRU key, at first two small polynomials g and f are generated randomly. The polynomial f must be invertible in Rp and Rq. The inverse of f over Rp and Rq are computed using the extended Euclidian algorithm. The two inverses are denoted by f p
−1 and fq−1 , respectively.
Hence, we have f f p f f qp q− −≡ ≡1 11 1* (mod ), * (mod ) .
While 1 1, , ,p qf g f f− − are kept private, the public key h is computed based on formula (1):
h f g qq= −1 * (mod )
(1)
Encrypting processBy considering as ephemeral key and converting the input message to a polynomial m, the cipher text is computed as below [i.e., formula (2)]:
e p h m q= +. * (mod )ϕ (2)
In this step, the number of total multiplications is N2 where that of additions is N mod q.
Decrypting processAfter receiving polynomial e , the encrypted message can be decrypted by using the private key f and the formula (3) is used for this calculation:
f e q f p h m qp f h f m qp f f gq
* (mod ) *( . * ) (mod ). * * * (mod ). * * *
= += +
= −
ϕϕ
ϕ1 ++
= +
f m qp q f m q
* (mod )
. * * (mod )ϕ
(3)
QTRUThe QTRU cipher system18 uses the Quaternion algebra, so a little information about this algebra is needed to be described. The real quaternion, denoted by H is a vector space of dimension 4 over R. The two lattice spaces denoted by Lp, Lq are being described in quaternion algebra as below:
L a bi cj dk a b c d GF pp : { | , , , ( )}.= + + + ∈ (4)
L a bi cj dk a b c d GF qq : { | , , , ( )}= + + + ∈ (5)
In quaternion algebra, two polynomials Zp[x]/(xN-1), Zq[x]/(xN-1) are described as follows:
AZ x x
f x f x i f x j f x kp
N0 0 1 2 31 1
1=
− −−
= + + +
,[ ] ( )
{ ( ) ( ). ( ). ( ). || , , , [ ] ( ),
, , }
f f f f Z x x
i j ij ji k
pN
0 1 2 3
2 2
1
1 1
∈ −
= − = − = − =
(6)
AZ x x
g x g x i g x j g x kq
N1 0 1 2 31 1
1=
− −−
= + + +
,[ ] ( )
{ ( ) ( ). ( ). ( ). || , , , [ ] ( ),
, , }
g g g g Z x x
i j ij ji k
qN
0 1 2 3
2 2
1
1 1
∈ −
= − = − = − =
(7)
For generating public keys and private keys, two quaternion polynomials are generated randomly based on formula (8):
F f f i f j f k such that f f f f Lf→
= + + + ∈0 1 2 3 0 1 2 3. . . , , , (8)
(9)G g g i g j g k such that g g g g Lg→
= + + + ∈0 1 2 3 0 1 2 3. . . , , ,
Where is used for multiplying in quaternion algebra and is computed as follows:
F G f f i f j f k g g i g j g kf g f g
→ →
= + + + + + += −
( . . . ) ( . . . )( * *
0 1 2 3 0 1 2 3
0 0 1 1 −− −f g f g3 3 2 2* * )
+ + − +
+ + + −+
( * * * * ).( * * * * ).(
f g f g f g f g if g f g f g f g j0 1 1 0 3 2 2 3
3 1 2 0 0 2 1 3
ff g f g f g f g k1 2 0 3 2 1 3 0* * * * ). .+ − + (10)
Where F→
must be invertible in AZ x xp
N01 1
1=
− −−
,[ ] ( )
and AZ x xq
N11 1
1=
− −−
,[ ] ( )
.
F Fp q
→ →
, are computed as follows:

Home and clinical cardiovascular care center
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 119-124Copyright © 2013 by Tabriz University of Medical Sciences 121
F f f f f over Z x x F i jp pN
→−
→
= ⟨ + + + − ⟩ = + + +( ) [ ] ( ) . .*02
12
22
32 1
0 1 21 µ µ µ µµ3.k
(11)
F f f f f over Z x x F i jq qN
→−
→
= ⟨ + + + − ⟩ = + + +( ) [ ] ( ) . .*02
12
22
32 1
0 1 21 η η η ηη3.k
(12)
The public key will be calculated according to formula (13):
H F Gg g g gg g g
q
→ → →
= =
− − − ++ + − +
( * * * * )( * * *η η η ηη η η η0 0 1 1 3 3 2 2
0 1 1 0 3 2 2 ** ).( * * * * ).( * * * *
g ig g g g jg g g
3
3 1 2 0 0 2 1 3
1 2 0 3 2 1 3
+ + + −+ + − +η η η ηη η η η gg k0 ). .
(13)
Where are private and can be used in decrypting process. Although, the QTRU cipher system is 16 times slower than NTRU cipher system, however QTRU can work on small dimensions without reducing the system’s security. The message and Blinding Quaternions are shown as below: M m m i m j m k
m m x m m x m m x m m x
→
= + + +
= = = =
0 1 2 3
0 0 1 1 2 2 3 3
. . .
( ), ( ), ( ), (∆ ∆ ∆ ∆
)){ }∈Lm (14)
ϕ ϕ ϕ ϕ ϕ
ϕ ϕ ϕ ϕ ϕ ϕ ϕ ϕ
→
= + + +
= = = =
0 1 2 3
0 0 1 1 2 2 3 3
. . .
( ), ( ), ( ), (
i j k
x x x x∆ ∆ ∆ ∆
)){ }∈Lϕ
(15)
The cipher text can be calculated by the following equation and we can decrypt the cipher text by formula (17):
E p H M→ → →
= +. ϕ (16)
F E F p H M q
F p H F M q
p F
→ → → → → →
→ → → → →
= +
= +
=
( ( . ) (mod )
( . ) (mod )
( .
ϕ
ϕ→→ → → → → →
→ → → →
+
= +
F G F M q
p G F M
q ϕ
ϕ
(mod )
( . ).
(17)
The new system has a parallel processing feature which can encrypt 4 vectors at the same time. The complexity order of encrypting and decrypting of QTRU system is O(4n2) and the dimension of lattice matrix which is needed to attack this cipher is 8N×8N. As mentioned before, the high speed in encrypting and decrypting processes is counted as an advantage of QTRU over NTRU with degree 4, at the same security level.
BSN and its architecture designBSN13 is a WSN hardware platform which works on a
Figure 1. Body Sensor Network
Figure 2. Architecture design of BSN
wide range bandwidth using the IEEE 802.15.4 standard. It incorporates the wireless physiological sensors for measuring the status of the patient. In Figure 1 we can see a simple BSN on the human body. To minimize the usage of bandwidth, a BSN and a PDA is used before sending the data to the server. The architecture design of BSN is illustrated in Figure 2.This node uses Texas Instrument (TI) MSP40 16-bit ultra low power RISC processor accompanied by a flash memory 60 KB+256 B, 2 KB RAM, 12-bit ADC and 6 analog channels. The throughput bandwidth is 250 kbps with a range of over fifty meters. The flash memory is used for either storing or buffering the data. The operating system (OS) which is used in BSN is TinyOS by U.C Berkeley. Being small, open source and efficient power usage sensors are the advantages of this OS. It has small files designers that can choose the components they need. Also, the OS manages the hardware and the wireless network, takes sensor measurements, makes sensor routing decisions, and finally reduces the usage of power. Since the TI microcontroller is used, the BSN node only needs 0.01 mA in active mode and 1.3 mA in calculating mode. In the BSN architecture, a lot of wireless biosensors such as 3-lead ECG, 2-lead ECG strip, and context sensors such as accelerometers and also temperature and humidity sensors are being used. The compact flash BSN card in the PDA can gather the sensor signals. Furthermore, the PDA can display, analyze and process the sensor signals as

Zakerolhosseini et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 119-124 Copyright © 2013 by Tabriz University of Medical Sciences122
well as working as a router too. The transmission of sensor networks is being done through a Wifi or GPRS network.
Probabilistic distance vector for sensor networksThe probabilistic distance distributions are used for random sensor networks that can calculate the distance and send data with high accuracy.19 The two nodes (X1, Y1) and (X2, Y2) are supposed, the distribution of node distance P(D≤d) is needed to be calculated, where D X X Y Y= − + −( ) ( )1 2
21 2
2 In grid-based clustering scheme, there are two cases of cluster head communications: between cluster heads in diagonal adjacent grids or parallel grids, such as PQ and RS in Figure 3.We will suppose non-uniform griding with a fixed ratio q is a special case of variable-size griding.
Two random nodes in diagonal neighbor gridsBy normalizing the A × A sensing field to a unit-size square as shown in Figure 3. The grids 1 and 3 are diagonal squares with size of (1-q2) and q2(1-q2) respectively. By using the Heaviside Step Function H(x) we can formulate the coordinate distributions for P and Q as follows:
f x f x H x H x qq
f x f x H x q q
X Y
Y Y
1 1
2 2
111
( ) ( ) ( ) [ ( )]
( ) ( ) [ ( )]
= =− − −
−
= =+ − −HH xq q
( )( )1−
(18)
Where
H xxx
( ) =<≥
0 01 0
Figure 3. Non-uniform griding with size ratio q
X1, Y1 ≈ U [0, 1-q] and X2, Y2≈ U[-q(1-q),0]
Two random nodes in parallel neighbor gridsThe grids 2 and 4 shown in Figure 2 are parallel rectangles with size of (1-q)×q and q(1-q)×q2 respectively. For the nodes in these parallel rectangles, the coordinate distribution is formulated as below:
f x H x q H xq
f x H x H x qq
X
Y
1
11
1
( ) ( ) ( )
( ) ( ) [ ( )]( )
=+ −
=− − −
−
(19)
f x H x q H x q qq
f x H x q q H xq q
X
Y
2 2
2
1
11
( ) ( ) ( ( ))
( ) [( ( )] ( )( )
=+ − + −
=+ − −
−
(20)
Now let V=X1–X2 or V=Y1–Y2, S=V2, Z= SX+SY and D Z=so we can obtain fD(d). According to BT node Platform we can easily find the Distance distribution.9
Probabilistic energy optimizationIt is very important to reduce the usage of energy in wireless sensor networks.19 According to Barroso et al. study10 the energy which is consumed by the radio transmitter is calculated by equation (21):
E x f x dxTxaD= ∫λε ( ) (21)
λ is a data transmitter rate, ε is a constant related to the environment, and a is known as the path loss exponent. The traffic pattern of “many to one” in WSNs is also illustrated in Figure 3.Let Ei be the energy consumed in the i-th ring:
Ei = λi(ERe + ETe) + λiETx (22)
λi is the data rate going through the i-th ring. The parameters ERE and ETE are the energies consumed by the receiver and transmitter circuitry, and ETX is used by the transmitter power amplifier. According to Pentland et al. study7 we have ERe=ETe=Ee. so,
Ei = λi(2Ee + ETx) (23)
The aggregated data can be divided into two parts: between parallel rectangles λip, and between diagonal squares λid, i.e., λi = 2λip + λid and ρ is the node density. The λip and λid parameters can be calculated as follows:
λ ρλ
λ ρλ
ipi
idi
A qq
q
A qq
q
=+
−
=−+
−
22
22
11
11
1
( )
( ) ( )
(24)
Therefore,
E E x f x dx E x f x dxi ip e
aD id e
aDPar Diag
= + + +∫ ∫2 2 2λ ε λ ε( ( ) ) ( ( ) ) (25)
For minimizing the total network energy consumption we have the following equation:
min
. .
E
s t Aq rAq r
ii
K
K
k
=
−
∑>
≤
11
0
0

Home and clinical cardiovascular care center
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 119-124Copyright © 2013 by Tabriz University of Medical Sciences 123
Where r0 is the minimal distance between wireless transceivers, and K is the maximum number of hops from the source node to the sink.
Implementation of framework Initially assume the patient is stationed in his/her house. The patient is relaxed and the ECG and the body temperature and the blood pressure sensors do not detect any suspicious. Suddenly, the sensors detect heart rhythmic disorders, arrhythmia, and a change in the body temperature and the blood pressure. The alert signals are accordingly sent to the PDA (i.e., mostly ECG signals). The BSN which is located inside the PDA does a processes these signals and makes a decision on whether the occurred condition is life threatening or not. If the condition is life threatening, an appropriate signal is generated and routed to the PDA. As previously indicated, the PDA also performs as a router as initially encrypts the alert data signals. The importance of encrypting these signals lie on protecting patients information. These information regarding patient health is secret and except the doctor no other persons would have access to these information’s Also other hospitals can’t decrypt other patients’ data which do not belong to their hospital. The encryption is being done by the QTRU algorithm. We used this cipher system since it is faster in comparison to NTRU in 4 dimensions. In this way, the speed of transferring data will increase. On the other hand, there is a Wifi or GPRS network between the server of the hospital and patient’s PDA which includes lots of sensor networks for receiving data signals and transferring them to the others just as a router. In this part, the best and closest path to the server should be chosen which consumes small amount of power. When the data signal has arrived at the server of the hospital, the server immediately decrypts the data and alerts the emergency. Also, it sends the encrypted data to the doctor who decrypts the data by his PDA and checks the condition of the patient and as a result may make the doctor become ready for the operation if necessary. The implementation of this scenario is shown in Figure 4. Also, this system can work inside the hospitals
Figure 4. Implementation of proposed framework
so the Wifi or GPRS Sensor Network is not needed and transfer of data is done directly between the server of the hospital and the patient’s PDA and doctor’s PDA.
DiscussionCardiovascular disease is one of the most important reasons of sudden death in Iran. In this study we present a low consuming power and high speed cryptographic Body Sensor Network architecture which is used to detect arrhythmias in cardiovascular disease patients. Wifi or GPRS Sensor networks are the main related networks that are mainly addressed to BSNs and PDAs and server of hospital by using QTRU cipher system in this paper. It can also be used by patients for self-monitoring or alerting the doctors and ICU healthcare personnel. Generally, usual health care systems perform monitoring and analysis for a variety of cardiac care functions but our presented system can detect arrhythmias in cardiovascular patients with high speed and security. The QTRU cryptosystem can encrypt and decrypt 4 vectors at the same time with the complexity order of O(4n2) while NTRU cryptosystem with 4 dimensions can encrypt and decrypt with the complexity order of O(16n2). Although, they are at the same security level, however QTRU cryptosystem is faster than NTRU cryptosystem in 4 dimensions. Also we used probabilistic distance vector for Sensor Networks in order to reduce the hops between WSN node and increasing the speed of transferring and routing process. For reducing the usage of power, the Probabilistic Energy optimization is used. Energy optimization is very important since most of WSNs use rechargeable batteries.
ConclusionIn this paper a new H4C system is proposed by which the number of human deaths resulted by cardiovascular disease can be reduced. This system is a very fast and low power consumption system that uses the cheap chips in comparison to other healthcare chips. The encryption and decryption algorithm used for securing the insecure channel of communication reduces the calculations.

Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 119-124 Copyright © 2013 by Tabriz University of Medical Sciences124
Additionally, the methods used for reducing distances and energy make the overall operations and functions faster.
Ethical issues: The study was approved by the ethics committee of the
University.
Competing interests: The authors had no competing interests to declare in
relation to this article.
References1. Hatmi ZN, Tahvildari S, Gafarzadeh Motlag A, Sabouri Kashani A. Prevalence of coronary artery disease risk factors in Iran: a population based survey. BMC Cardiovasc Disord 2007;7:32.2. Braunwald S. Heart disease: a textbook of cardiovascular medicines. 7th ed. Philadelphia: WB Saunders; 2005.3. Campbell RL, Banner R, Konick-McMahan J, Naylor MD. Discharge planning and home follow-up of the elderly patient with heart failure. Nurs Clin North Am 1998;33:497-513. 4. WHO. Cardiovascular diseases. [cited 2012 Dec]. Available from: http://www.who.int/cardiovascular_diseases/en/5. Standing P, Dent M, Craig A, Glenville B. Changes in referral patterns to cardiac out-patient clinics with ambulatory ECG monitoring in general practice. Br J Cardiol 2001;8:396-8. 6. Liszka KJ, Mackin MA, Lichter MJ, York DW, Pillai D, Rosenbaum DS. Keeping a beat on the Heart. IEEE Pervasive Computing 2004; 3:42-9.7. Pentland A. Healthwear: Medical Technology Becomes Wearable. IEEE Computer 2004;37:42-9.8. Ross PE. Managing care through the air. IEEE Spectrum 2004;41;14-9.
9. BTnode Platform. [cited 2013 Feb]. Available from: http://www.btnode.ethz.ch10. Barroso A, Benson J, Murphy T, Roedig U, Sreenan C, Barton J, et al. The DSYS25 Sensor Platform. Proceedings of the 2nd international conference on Embedded networked sensor systems. New York: ACM, 2004. p. 314-314.11. Intel Labs. [cited 2013 Feb]. Available from: http://www.intel.com/research/exploratory/motes.htm12. TinyOS. [cited 2013 Feb]. Available from: http://www.tinyos.net13. Lo BPL, Thiemjarus S, Panousopoulou A, Yang GZ. Bioinspired Design for Body Sensor Networks [Life Sciences]. IEEE Signal Processing Magazine 2013; 30:165-70.14. Hoffstein J, Pipher J, Silverman J. NTRU: A new high speed public key cryptosystem. Algorithmic Mumber Theory (ANTS III). Lecture Notes in Computer Science 1998;143:267-88.15. Bailey DV, Coffin D, Elbirt A, Silverman JH, Woodbury AD. NTRU in Constrained Devices, Cryptographic Hardware and Embeded Systems, CHES 2001 Lecture Notes in Computer Science, Third International Workshop, Proceedings, Springer-Verlag, Paris, France, 2001; 2162: 262-272.16. Pipher J. NTRU Cryptosystems. Lectures on the NTRU encryption algorithm and digital signature, 2005.17. Kouzmenko R. Generalizations of the NTRU cryptosystem. [Master’s thesis]. Polytechnique, Montreal, Canada, 2006.18. Malekian E, Zakerolhosseini A, Mashatan A. Qtru: Quaternionic Version of the NTRU Public-Key Cryprosystems. ISeCure 2011;3:2919. Zhuang Y, Pan J, Cai L. Minimizing energy consumption with probabilistic distance models in wireless sensor networks. INFOCOM, 2010 Proceedings IEEE, 14-19 March 2010, p. 1-9.
Zakerolhosseini et al.

Coronary Heart Disease: Pandemic in a True Sense
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 125-126doi: 10.5681/jcvtr.2013.026http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Saurabh RamBihariLal Shrivastava , E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Cardiovascular diseases are caused because of abnormalities in the heart and blood vessels. Recent trends reveal that the incidence of coronary heart disease (CHD) has gradually decreased in many developed countries, but the situation remains quite challenging in developing nations that account for more than 60% of the global burden. Multiple socio-demographic, personal, physician related and healthcare delivery system related factors have been identified which act in variable combinations to either influence the incidence of CHD or affect the short/long-term outcome of the disease. Of all CHD cases who succumb within 28 days of onset of symptoms, almost 67% fail to reach even a hospital. This clearly signifies the importance of primary prevention and early recognition of the warning signs in averting cause-specific mortality. The main priority is to develop cost-effective equitable health care innovations in CHD prevention and to monitor the trend of CHD so that evidence-based interventions can be formulated. To conclude, inculcating health-promoting behaviors in school children and the general population by means of community-based health screening and education interventions could avert many more deaths attributed to CHDs.
A B S T R A C TA R T I C L E I N F O
Article Type:Short Communication
Article History:Received: 29 May 2013Accepted: 4 September 2013
Keywords:Coronary Heart Disease PreventionPublic HealthLifestyleTobacco
Saurabh RamBihariLal Shrivastava*, Prateek Saurabh Shrivastava, Jegadeesh Ramasamy Department of Community Medicine, Shri Sathya Sai Medical College & Research Institute, Kancheepuram, India
Cardiovascular diseases are caused because of abnormalities in the heart and blood vessels, and mainly include coronary heart disease, stroke,
hypertension, peripheral vascular disease, rheumatic heart disease, and heart failure.1 Recent trends reveal that the incidence of coronary heart disease (CHD) has gradually decreased in many developed countries, but the situation remains quite challenging in developing nations that account for more than 60% of global burden.2 CHDs have contributed significantly towards loss of disability-adjusted life years and are the leading cause of mortality worldwide resulting in 3.8 million deaths in men & 3.4 million in women annually.2
Multiple socio-demographic, personal, physician related and healthcare delivery system related factors such as globalization;1,2 urbanization;2,3 increased life expectancy;1 age-gender-ethnicity;1 poor educational status;4 adoption of harmful lifestyles;1,3 socioeconomic status;5 stressful working conditions and job characteristics;3 migration;1 poor awareness among general population about risk factors;3,6 poor treatment compliance;3 depression;7 lack of social/family support and biopsychosocial parameters;7,8 tobacco use;8 obesity with high waist-hip ratio;8,9 post-menopause;3 deranged lipid profile with high cholesterol level;8,9 presence of chronic diseases like hypertension/diabetes/metabolic syndrome;3,5,10 dietary habits and food fads;3 low consumption of fruits and vegetables;3,10 physician related-poor awareness about early warning
signs/low index of suspicion/poor awareness about risk assessment in asymptomatic patients;10 and accessibility and availability of medical/surgical treatment options or healthcare professionals;1,3 have been identified which act in variable combinations to either influence the incidence of CHD or affect the short/long-term outcome of the disease.Of all CHD cases who succumb within 28 days of onset of symptoms, almost 67% fail to reach even a hospital. This clearly signifies the importance of primary prevention and early recognition of the warning signs in averting cause-specific mortality.2 The main priority is to develop cost-effective equitable health care innovations in CHD prevention and to monitor the trend of CHD so that evidence-based interventions can be formulated.1,3 Considering the magnitude of CHD, a comprehensive and integrated approach is required to minimize the risks in high-risk as well as in general population.3,11 Implementation of other measures such as improvement in the socio-economic/literacy status;4,5 creation of an enabling environment for increasing awareness of community members about risk factors;3,6,9 strategic implementation of primordial and primary prevention strategies targeted towards school children encouraging them to adopt healthy lifestyles;1,8,9,11 secondary prevention and targeted interventions towards high-risk group patients;11 training sessions for private practitioners;10 facilitation of early detection of clinical cases and cost-effective secondary prevention measures to

Shrivastava et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 125-126 Copyright © 2013 by Tabriz University of Medical Sciences126
prevent long-term complications;9,10 legislative measures to stop tobacco production/sale/advertising;9 promotion of research work to establish guidelines pertaining to dietary modifications/weight loss in different age-groups and for surveillance of CHD trends/associated risk factors;3,8 and universal adoption of WHO cardiovascular risk prediction charts;11 can be strategically planned according to the particular setting and prevailing cultural perceptions. To conclude, inculcating health-promoting behaviors in school children and general population by means of community-based health screening and education interventions could avert many more deaths attributed to CHDs.
Ethical issues: This study was confirmed by the ethics committee of
University.
Conflict of interests: The authors declare no conflicts of interest.
References1. World Health Organization. Cardiovascular diseases - Fact sheet N°317. [updated 2013 Mar; cited 2013 Jun 22]. Available from: http://www.who.int/mediacentre/factsheets/fs317/en/2. Mackay J, Mensah GA. The atlas of heart disease and stroke. World Health Organization & Center for Disease Control and Prevention. [cited 2013 Jun 22]. Available from: http://www.who.int/cardiovascular_diseases/resources/atlas/en/3. Saidi O, Ben Mansour N, O’Flaherty M, Capewell S, Critchley
JA, Ben Romdhane H. Analyzing recent coronary heart disease mortality trends in Tunisia between 1997 and 2009. PLoS One 2013;8:e63202.4. Chandola T, Plewis I, Morris JM, Mishra G, Blane D. Is adult education associated with reduced coronary heart disease risk? Int J Epidemiol 2011;40:1499-509. 5. Kim JY, Kim SH, Cho YJ. Socioeconomic status in association with metabolic syndrome and coronary heart disease risk. Korean J Fam Med 2013;34:131-8.6. Mooney LA, Franks AM. Impact of health screening and education on knowledge of coronary heart disease risk factors. J Am Pharm Assoc (2003) 2011;51:713-8.7. Ferris PA, Kline TJ, Bourdage JS. He said, she said: work, biopsychosocial, and lifestyle contributions to coronary heart disease risk. Health Psychol 2012;31:503-11. 8. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. on behalf of the interheart Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the interheart study): Case-control study. Lancet 2004;364:937-53.9. Prabhakaran D, Singh K. Premature coronary heart disease risk factors & reducing the CHD burden in India. Indian J Med Res 2011;134:8-9.10. Shillinglaw B, Viera AJ, Edwards T, Simpson R, Sheridan SL. Use of global coronary heart disease risk assessment in practice: a cross-sectional survey of a sample of U.S. physicians. BMC Health Serv Res 2012;12:20. 11. World Health Organization. Prevention of cardiovascular disease: Guidelines for assessment and management of cardiovascular risk. WHO Press: Geneva; 2007.

Simultaneous Operation of Hydatid Cyst of the Heart and Liver:A Case Report
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 127-128doi: 10.5681/jcvtr.2013.027http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Rezayat Parvizi, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Primary echinococcosis of the heart is exceptionally uncommon and is reported 0.5% to 2% of all hydatid cyst sites in comparison with liver (70%) or lung (20%) involvement. Hydatid disease of the heart is caused by the cestode tapeworm echinococcosis granulosis or alveolaris. We present a 29-year-old female with hydatid disease of the liver and heart. She only complained of abdominal pain and palpitation. Echocardiography and multi-slice computed tomography (MSCT) showed a 120×101 mm cyst in the liver and 64 mm in the right ventricular free wall. Both cysts were excised within one procedure successfully.
A B S T R A C TA R T I C L E I N F O
Article Type:Case Report
Article History:Received: 1 August 2013Accepted: 4 September 2013
Keywords:Hydatid CystLiverHeart
Rezayat Parvizi1*, Hossein Namdar1, Eissa Bilehjani1, Amrollah Bayat2, Mohammad ali sheikhalizadeh1
1Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran2Department of General Surgery, Tabriz University of Medical Sciences, Tabriz, Iran
Case ReportA 29-year-old woman was admitted to the cardiology unit with a progressive abdominal pain and occasional brief episodes of palpitations. Multi-Slice computed tomography (MSCT) showed a 120×101 mm hydatid cyst in the left lobe of the liver and a 64 mm cyst in the free wall of the right ventricle; later, TEE study confirmed diagnosis. Further surgical consultation suggested a simultaneous operation on both cysts. Initially, general surgeon team made a sub costal incision to approach the liver. A huge cyst was found at the left lobe that was punctured and its content aspirated. Then warm hypertonic saline (5%) was instilled into the cyst and after 3-4 minutes it was opened and containers (daughter cysts) were evacuated. Subsequently, open heart surgery was performed via median sternotomy.The cyst area was distinguished from surrounding to prevent rupture. Cold hypertonic saline (5%) was instilled into the cyst and after 3-4 minutes, infected cyst was opened and evacuated which produced a large cavity (60 ml) at site which was sutured afterward.
DiscussionCardiac involvement of hydatid cyst is rare and usually with minimal symptoms always overlooked by the patient as well as physicians.Human echinococcosis is caused most commonly by echinococcus granulosus.1 The reported prevalence is about 0.5-2%. Human beings are only incidental hosts by contamination from contact with animals.2 Chitinous eggs are lysed in the proximal digestive tract releasing six
larvae which would ultimately reach the liver via portal venous system and rarely the heart via thoracic lymphatic duct.3 In the liver, larvae can pass through sinusoids, suprahepatic veins and right chambers of the heart and eventually reside the lungs.4 In the parenchyma of the liver and the lungs, the larvae could growth and produce hydatid cysts.5 After infection, the embryo usually reaches the myocardium via coronary circulation from the left side of the heart.6 The cyst is then formed within a period of 1 to 5 years.7 Myocardial reaction consists of a fibrous adventitial pericyst layer surrounding the laminated membrane.8 The left ventricular and interventricular septum free walls are the most common locations of the cysts in the myocardial region right-sided cysts have a tendency to expand intracavitarily and subendocardially, whereas the left-sided cysts tend to grow sub-epicardially.9 This may be due to the thicker and denser myocardium of the left than the right heart.10 It has been reported that most of the cysts locate in the left ventricular wall because of the rich vascular supply of the left ventricle.10 Cardiac hydatid cysts produce a large variety of symptoms via any of four mechanisms.11 They can obstruct blood flow or cause valve dysfunction. They can lead to arrhythmias or pericardial effusion with tamponade by local invasion. Rupture of the cyst causes embolization leading to systemic reaction when the cysts are on the left side of the heart, or pulmonary embolism when the cysts are on the right side.12 Moreover, some cardiac hydatid cysts may stay asymptomatic for many years so that the diagnosis of cardiac echinococcosis can be difficult and must be suspected in any patient from endemic or sheep

Parvizi et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 127-128 Copyright © 2013 by Tabriz University of Medical Sciences128
Figure 1. Multi-slice computed tomography
Figure 2. Removed cyst from left lobe of liver
Figure 3. Hydatid cyst at free wall of right ventricle
farming areas especially with a cystic tumor of other infected organs such as liver.13 2D echocardiography, computed tomography scan or MRI may be helpful but trans-esophageal echocardiography is the gold standard in detecting intracardiac echinococcosis.10 In conclusion, the treatment of hydatid cyst is surgical and should not be delayed. Extirpation of the lesion is recommended under cardiopulmonary bypass. Serologic and echocardiographic controls are recommended for 5 years after extirpation to detect recurrences after surgical manipulation or cysts that were not discovered at operation (Figures 1-3).
Ethical issues: This study was reviewed and confirmed by the ethics
committee of Tabriz University of Medical Sciences.
Conflict of interests: The authors declare no conflicts of interest.
References1. Sokouti M, Golzari S, Aghdam BA. Surgery of uncomplicated pulmonary hydatid cysts: capitonnage or uncapitonnage? Int J Surg 2011;9:221-4. 2. Sokouti M, Pezeshkian M, Ghabili K, Golzari SE. Surgical Procedures and Postoperative Complications in Patients with Giant and Non-giant Pulmonary Hydatid Cysts. Life Sci J 2013;10: 138-42. 3. Golzari SE, Sokouti M, Ghaffari A, Bazzazi AM, Ghabili K. Ultrasonography in diagnosis of pulmonary hydatid cysts. Lancet Infect Dis 2013;13:294. 4. Sokouti M, Golzari SE, Tizro P, Khanli HM, Ghabili K. Genitourinary hydatid disease. Int Urol Nephrol 2013;45:759.5. Golzari SE, Sokouti M, Bazzazi AM, Khanli HM, Ghabili K. Serodiagnostic tests in musculoskeletal hydatid disease. Spine (Phila Pa 1976) 2013;15;38:1797. 6. Nazyrov FG, Abdumadzhidov KhA, Buranov KhD, Akbarov MM, Aliev ShM, Mukaddirov MM. Surgical treatment of the combined heart, lung and liver hydatid disease. Khirurgiia (Mosk) 2009;5:23-67. Onursal E, Elmaci TT, Tireli E, Dindar A, Atilgan D, Ozcan M. Surgical treatment of cardiac echinococcosis: report of eight cases. Surg Today 2001;31:325–30. 8. Calamai G, Perna AM, Venturini A. Hydatid disease of the heart report of five cases and review of the literature. Thorax 1974;29: 451-8.9. Erentuğ V, Bozbuğa N, Kirali K, Mataraci I, Kaymaz C, Balkanay M, et al. Cardiac hydatid cysts: surgical treatment and results. J Card Surg 2004;19:358-60.10. Kojundzic SL, Dolic K, Buca A, Jankovic S, Besenski N. Hydatid disease with multiple organ involvement: a case report. Macedonian Journal of Medical Sciences 2010;3:154-8.11. Saad RA, Amer KM, Migliore M, Aziz T, Azzu A. Right intraventricular hydatid cyst of the heart. Asian Cardiovasc Thorac Ann 2003;11:160-62.12. Shehatha J, Alward M, Saxena P, Konstantinov IE. Surgical management of cardiac hydatidosis. Tex Heart Inst J 2009; 36:72–3.13. Parvizi R, Joudati AR, Montazeri V, Susan Hassanzadeh Salmasi S, Varshouchi M. Cardiac Echinococcosis: Surgical Treatment and Results in 10 Cases. Iranian Heart Journal 2006;7:67-71.

Total Pulmonary Artery Atresia Associated with Abnormal PulmonaryVenous Drainage as a Rare Presentation of Scimitar Syndrome
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 129-131doi: 10.5681/jcvtr.2013.028http://journals.tbzmed.ac.ir/JCVTR
*Corresponding author: Homa Akbari, E-mail: [email protected] © 2013 by Tabriz University of Medical Sciences
Scimitar syndrome or pulmonary venolobar syndrome is a rare, complex, and variable malformation of the right lung characterized by an abnormal right sided pulmonary drainage into the inferior vena cava, malformation of the right lung, abnormal arterial supply, and sometimes cardiac malformation. Despite the varying degrees of pulmonary hypoplasia and pulmonary artery hypertension, about half of the patients with scimitar syndrome are asymptomatic or mildly symptomatic when the diagnosis is made. Neonates have severe symptoms and worse prognosis while older children come to light because of recurrent respiratory infections, heart murmur, or an abnormal chest radiograph.
A B S T R A C TA R T I C L E I N F O
Article Type:Case Report
Article History:Received: 19 May 2013Accepted: 1 August 2013
Keywords:Pulmonary Artery Atresia Scimitar SyndromeCT Angiography
Reza Javadrashid1, Mahmood Samadi2, Homa Akbari1*
1Department of Radiology, Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran2Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
IntroductionScimitar syndrome is a congenital cardiac malformation in which pulmonary flow from the right lung is partially or totally drained via a venous channel that joins the inferior vena cava (IVC). Dupuis et al. identified two types of scimitar syndrome: the infantile and adult forms. The infantile form has a severe presentation with major associated cardiac lesions, varying degrees of hypoplasia of the right pulmonary artery and right lung bronchial anomalies, dextroposition of the heart, pulmonary hypertension, and anomalous systemic supply to the right lung.1 This syndrome has varied presentations, from an asymptomatic state2 to severe pulmonary hypertension and/or heart failure.3 Those who present early in life usually have associated congenital heart disease4 also hemoptysis5 and pulmonary arterial hypertension (PAH) 6,7 both are uncommon presenting complaints of this rare syndrome beyond infancy.
Case HistoryA 15-year-old boy referred to our center with the complaint of hemoptysis and cough from 1.5 years ago. He suffered from chronic cough without fever from 3 years old. On examination, the patient was comfortable and weak. Her pulse was 72 beats/minute and regular, blood pressure 110/70 mm Hg, and respiratory rate 27 breaths/minute. Respiratory system examination revealed reduced intensity of breath sounds on the right side. P2 sound was dominant. He had received a period of empiric therapy for tuberculosis infection without response to it.Chest PA x-ray showed cardiac dextroposition associated
with several costal and vertebral anomalies as fusion of posterior arches of second and third right and left ribs and bifid anterior arch of left third rib and butterfly appearance at third thoracic vertebrae (Figure 1).CT angiography was performed by 64 multidetector CT (MDCT) and then reconstructed via MIP and VRT techniques, and showing dilated main pulmonary artery with normal-looking left pulmonary artery and hypoplastic right pulmonary artery, a curved linear (scimitar shape) opacity running from the middle of the lung toward diaphragm. Left pulmonary vein ending into left atrium is well visualized; corresponding pulmonary vein on the right side was absent. Therefore, CT angiogram showed hypoplasia of right lung and anomalous drainage of right pulmonary veins by scimitar vein in to IVC below the diaphragm. Thickening of peribronchovascular and peripheral interstitium in favor of interstitial edema was noted (Figure 2).
DiscussionScimitar syndrome is a rare congenital abnormality that occurs in approximately 2 of every 100 000 live births.7 Dupuis and associates collected data from 22 university centers and demonstrated differences in patients whose diagnosis was made during the first year of life—dubbed the “infantile” form—compared with patients whose diagnosis was made after 1 year of age—called the “adult” form.8 In contrast to more than 90% survival of those with the adult form, there was a considerably poorer prognosis for patients with the infantile form. Pulmonary hypertension is frequent in this subset of patients and is

Javadrashid et al.
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 129-131 Copyright © 2013 by Tabriz University of Medical Sciences130
attributed to multiple factors 8,9: 1) stenosis of the scimitar vein; 2) presence of systemic arterial supply to the right lung; 3) reduction of the pulmonary vascular bed on the right side; 4) increased pulmonary blood flow resulting from anomalous drainage or from the presence of some associated intracardiac defect. Hemoptysis as a presenting symptom is exceptionally rare in patients with scimitar syndrome.10
Among the five large series of patients with this syndrome comprising of total 39 subjects aged one year and above, only four has hemoptysis during their course of illness.11,12 Possible mechanisms of hemoptysis in scimitar syndrome include rupture of hypertrophied systemic pulmonary anastomosis13 or bleeding from some of the bronchiectatic segment in the hypoplastic lung. Clinical symptomatology
Figure 1. A) 15-year-old boy with hemoptysis and cough; A, scout view depicts cardiac dextroposition ; B, C, D) CT angiography im-ages demanestrate hypoplastic right pulmonary artery, a curved linear (scimitar shape) opacity running from the middle of the lung toward diaphragm.
Figure 2. VRT images: Left pulmonary vein ending into left atri-um is well visualized; corresponding pulmonary vein on the right side is absent.
of the scimitar syndrome is governed by the age at which the patient presents. Infants having scimitar syndrome present with cyanosis, poor growth, PAH and often complex cardiac defects, many of them need surgical intervention having a high mortality.14,15 Disease in older children and adults commonly presents with recurrent pulmonary infections and/or exertional dyspnea. This group of the patients usually has a benign course.5 Diagnosis of this syndrome is straightforward in presence of characteristic radiological sign (scimitar sign) on conventional chest radiography. However, when scimitar vein is masked by cardiac shadow, diagnosis can be documented by one or more traditional modalities, for example angiography16, CT scan17 and echocardiography.18 Currently available MR technology also provides excellent visualization of vascular anatomy of this complex congenital defect noninvasively.Ethical issues: This study was reviewed and confirmed by the ethics
committee of Tabriz University of Medical Sciences.
Conflict of interests: The authors declare no conflicts of interest.
References1. Canter CE, Martin TC, Spray TL, Weldon CS, Strauss AW. Scimitar syndrome in childhood. Am J Cardiol 1986; 58: 652-4.2. Oakley D, Naik D, Verel D, Rajan S. Scimitar vein syndrome: report of nine new cases. Am Heart J 1984; 107: 596-8.3. Gikonyo DK, Tandon R, Lucas RV Jr, Edwards JE. Scimitar syndrome in neonates: Report of four cases and review of the literature. Pediatr Cardiol 1986; 6:193-74. Gikonyo DK, Tandon R, Lucas RV Jr, Edwards JE. Scimitar syndrome in neonates: Report of four cases and review of the literature. Pediatr Cardiol 1986; 6:193-7.5. Canter CE, Martin TC, Spray TL, Weldon CS, Strauss AW. Scimitar syndrome in childhood. Am J Cardiol 1986; 58:652-54.6. Seaton D, Seaton A. Developmental disorders of the lungs. In: Seaton A, Seaton D, Leitcha G, eds. Crofton and Douglas’s respiratory diseases. 5th ed. Oxford: Blackwell Science; 2000. pp. 1309-29.7. Brown JW, Ruzmetov M, Minnich DJ, Vijay P, Edwards CA, Uhlig PN, et al. Surgical management of scimitar syndrome: an alternative approach. J Thorac Cardiovasc Surg 2003; 125:238-45.8. Dupuis C, Charaf LA, Breviere G, Abou P. Infantile form of the scimitar syndrome with pulmonary hypertension. Am J Cardiol 1993; 71:1326-30.9. Najam HK, Williams WG, Coles JG, Rebeyka IM, Freedom RM. Scimitar syndrome: twenty years’ experience and results of repair. J Thorac Cardiovasc Surg 1996; 112:1161-9.10. Reddy R, Shah R, Thorpe JA, John G. Scimitar syndrome: A rare cause of hemoptysis. Eur J Cardiothorac Surg 2002;22:821.11. Najm HK, William WG, Coles JG, Rebeyka IM, Freedom RM. Scimitar syndrome: Twenty years’ experience and results of repair. J Thorac Cardiovasc Surg 1996; 112 :1161-8.12. Canter CE, Martin TC, Spray TL, Weldon CS, Strauss AW. Scimitar syndrome in childhood. Am J Cardiol 1986; 58:652-54.13. Haroutunian LM, Neill CA. Pulmonary complications of congenital heart disease: Hemoptysis. Am Heart J 1972; 84:540-59.14. Huddleston CB, Exil V, Canter CE, Mendeloff EN. Scimitar syndrome presenting in infancy. Ann Thorac Surg 1999; 67:154-9.15. Saha K, Iyer KS. Intracardiac repair of obstructed right sided Scimitar syndrome. Indian Heart J 1995; 47:378-9.

Pulmonary artery atresia associated with abnormal pulmonary venous drainage
Journal of Cardiovascular and Thoracic Research, 2013, 5(3), 129-131Copyright © 2013 by Tabriz University of Medical Sciences 131
16. Schramel FM, Westermann CJ, Knaepen PJ, van den Bosch JM. The scimitar syndrome: Clinical spectrum and surgical treatment. Eur Respir J 1995; 8:196-201.17. Wang CC, Wu ET, Chen SJ, Lu F, Huang SC, Wang JK, et al. Scimitar syndrome: Incidence, treatment and prognosis. Eur J Pediatr 2008; 167:155-60.18. Mordue BC. A case series of five infants with scimitar syndrome. Adv Neonatal Care 2003; 3:121-32.