Bowel dysfunction following spinal cord injury
11
Scientific Review Bowel dysfunction following spinal cord injury AC Lynch 1,2 , A Antony 1 , BR Dobbs 1 and FA Frizelle* ,1,2 1 Spinal Injuries Unit, Burwood Hospital, Department of Surgery, Christchurch Hospital, Christchurch, New Zealand; 2 Colorectal Unit, Department of Surgery, Christchurch Hospital, Christchurch, New Zealand Study Design: Review. Objectives: To outline the present knowledge of bowel dysfunction following spinal injury, and look at future directions of management and research. Setting: Spinal Unit and Colorectal Unit, Christchurch, New Zealand. Methodology: Review. Results: The underlying physiology of colorectal motility and defecation is reviewed, and consequences of spinal cord injury on defecation are reported. A discussion of present management techniques is undertaken and new directions in management and research are suggested. Conclusion: There is need for more intervention in regard to bowel function that could improve quality of life, but there is also a need for more research in this area. Sponsorship: Dr AC Lynch is a holder of a Royal Australian College of Surgeons Foundation Research Scholarship and the research has been supported by the Canterbury Medical Research Foundation, and the Burwood International Spinal Trust. Spinal Cord (2001) 39, 193 – 203 Keywords: spinal cord injury; bowel function Introduction Bowel dysfunction following spinal cord injury (SCI) is increasingly recognised as an area of major physical and psychological diculty for SCI patients. Following spinal cord injury, changes in bowel motility, sphincter control, and gross motor dexterity interact to make bowel management a major life-style problem limiting quality of life. 1 Once the acute phase is over and patients have adapted to their loss of mobility, surveys have shown that approximately one third of subjects rank colorectal problems as worse than both bladder and sexual dysfunction. 2–6 Colorectal problems can be a significant cause of morbidity immediately after SCI, and chronic gastro- intestinal problems remain common, but may become more frequent with increasing time after injury. 7 Although many SCI patients achieve an adequate bowel frequency with drugs and manual stimulation, the risk and occurrence of faecal incontinence, diculties with evacuation, and need for assistance remain significant problems. In a recent study, questionnaires were sent to 1200 SCI patients, and 1200 age and gender matched controls. The mean faecal incontinence score was higher for SCI patients than controls (P50.0001), and for complete SCI compared with incomplete injury (P=0.0023). 8 Age or time since injury did not aect the faecal incontinence score. Incontinence aected quality of life for 62% of SCI patients, compared with 8% of controls. Faecal urgency and time spent at toilet were also significantly higher for the SCI group. Thirty-nine per cent of SCI patients use laxatives, compared to 4% of controls (P50.0001). Haemorrhoidectomy was more common in the SCI population (9% vs 1.5% (P50.001)), particularly among those requiring manual evacuations. Stone et al. found that improved management of bowel dysfunction led to improved well-being. 9 In order to understand why SCI patients have such problems it is important to review the normal anatomy and physiology, the relationship between the enteric nervous system and autonomic nervous systems. Normal colon anatomy and physiology The human colon is a compliant sac approximately 1.5 m long, closed at one end by the ileocaecal valve and the anal sphincter at the other. It has two layers *Correspondence: FA Frizelle, Professor of Colorectal Surgery, Department of Surgery, Christchurch Hospital, Christchurch, New Zealand Spinal Cord (2001) 39, 193 – 203 ª 2001 International Medical Society of Paraplegia All rights reserved 1362 – 4393/01 $15.00 www.nature.com/sc
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Bowel dysfunction following spinal cord injury

Scienti®c Review
Bowel dysfunction following spinal cord injury
AC Lynch1,2, A Antony1, BR Dobbs1 and FA Frizelle*,1,2
1Spinal Injuries Unit, Burwood Hospital, Department of Surgery, Christchurch Hospital, Christchurch, New Zealand;2Colorectal Unit, Department of Surgery, Christchurch Hospital, Christchurch, New Zealand
Study Design: Review.Objectives: To outline the present knowledge of bowel dysfunction following spinal injury,and look at future directions of management and research.Setting: Spinal Unit and Colorectal Unit, Christchurch, New Zealand.Methodology: Review.Results: The underlying physiology of colorectal motility and defecation is reviewed, andconsequences of spinal cord injury on defecation are reported. A discussion of presentmanagement techniques is undertaken and new directions in management and research aresuggested.Conclusion: There is need for more intervention in regard to bowel function that couldimprove quality of life, but there is also a need for more research in this area.Sponsorship: Dr AC Lynch is a holder of a Royal Australian College of SurgeonsFoundation Research Scholarship and the research has been supported by the CanterburyMedical Research Foundation, and the Burwood International Spinal Trust.Spinal Cord (2001) 39, 193 ± 203
Keywords: spinal cord injury; bowel function
Introduction
Bowel dysfunction following spinal cord injury (SCI) isincreasingly recognised as an area of major physicaland psychological di�culty for SCI patients. Followingspinal cord injury, changes in bowel motility, sphinctercontrol, and gross motor dexterity interact to makebowel management a major life-style problem limitingquality of life.1 Once the acute phase is over andpatients have adapted to their loss of mobility, surveyshave shown that approximately one third of subjectsrank colorectal problems as worse than both bladderand sexual dysfunction.
2 ± 6
Colorectal problems can be a signi®cant cause ofmorbidity immediately after SCI, and chronic gastro-intestinal problems remain common, but may becomemore frequent with increasing time after injury.7
Although many SCI patients achieve an adequatebowel frequency with drugs and manual stimulation,the risk and occurrence of faecal incontinence,di�culties with evacuation, and need for assistanceremain signi®cant problems. In a recent study,questionnaires were sent to 1200 SCI patients, and
1200 age and gender matched controls. The meanfaecal incontinence score was higher for SCI patientsthan controls (P50.0001), and for complete SCIcompared with incomplete injury (P=0.0023).8 Ageor time since injury did not a�ect the faecalincontinence score. Incontinence a�ected quality oflife for 62% of SCI patients, compared with 8% ofcontrols. Faecal urgency and time spent at toilet werealso signi®cantly higher for the SCI group. Thirty-nineper cent of SCI patients use laxatives, compared to 4%of controls (P50.0001). Haemorrhoidectomy wasmore common in the SCI population (9% vs 1.5%(P50.001)), particularly among those requiringmanual evacuations. Stone et al. found that improvedmanagement of bowel dysfunction led to improvedwell-being.9
In order to understand why SCI patients have suchproblems it is important to review the normal anatomyand physiology, the relationship between the entericnervous system and autonomic nervous systems.
Normal colon anatomy and physiology
The human colon is a compliant sac approximately1.5 m long, closed at one end by the ileocaecal valveand the anal sphincter at the other. It has two layers
*Correspondence: FA Frizelle, Professor of Colorectal Surgery,Department of Surgery, Christchurch Hospital, Christchurch, NewZealand
Spinal Cord (2001) 39, 193 ± 203ã 2001 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/01 $15.00
www.nature.com/sc
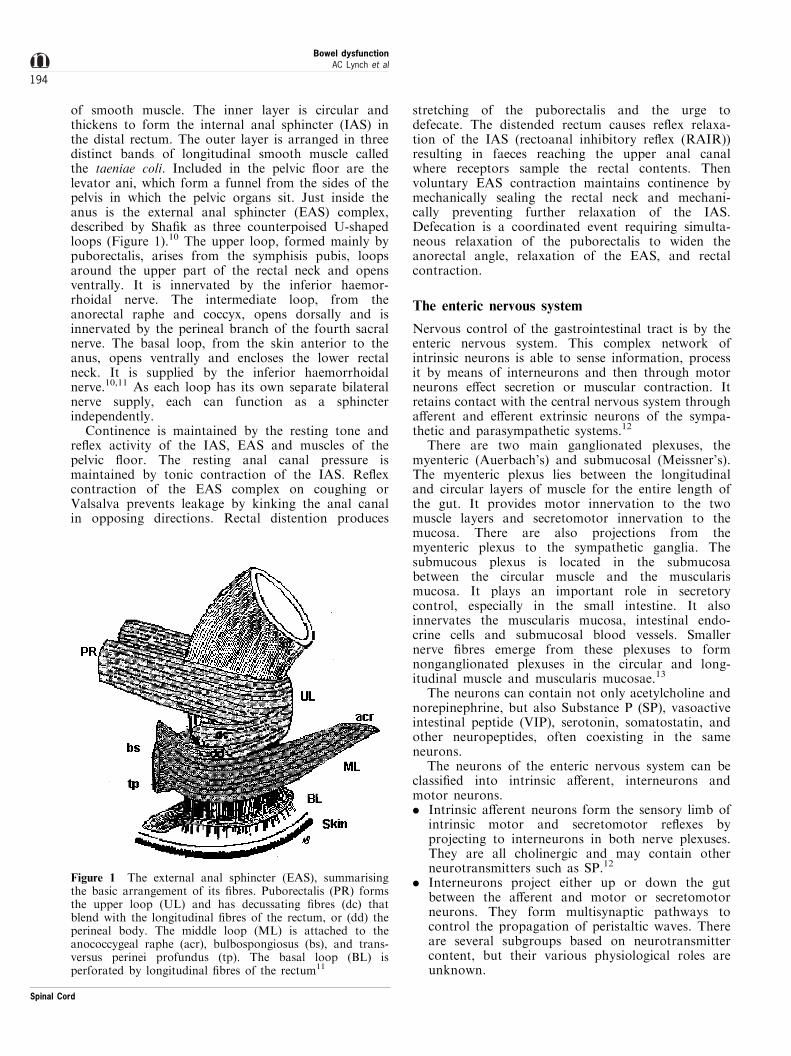
of smooth muscle. The inner layer is circular andthickens to form the internal anal sphincter (IAS) inthe distal rectum. The outer layer is arranged in threedistinct bands of longitudinal smooth muscle calledthe taeniae coli. Included in the pelvic ¯oor are thelevator ani, which form a funnel from the sides of thepelvis in which the pelvic organs sit. Just inside theanus is the external anal sphincter (EAS) complex,described by Sha®k as three counterpoised U-shapedloops (Figure 1).10 The upper loop, formed mainly bypuborectalis, arises from the symphisis pubis, loopsaround the upper part of the rectal neck and opensventrally. It is innervated by the inferior haemor-rhoidal nerve. The intermediate loop, from theanorectal raphe and coccyx, opens dorsally and isinnervated by the perineal branch of the fourth sacralnerve. The basal loop, from the skin anterior to theanus, opens ventrally and encloses the lower rectalneck. It is supplied by the inferior haemorrhoidalnerve.10,11 As each loop has its own separate bilateralnerve supply, each can function as a sphincterindependently.
Continence is maintained by the resting tone andre¯ex activity of the IAS, EAS and muscles of thepelvic ¯oor. The resting anal canal pressure ismaintained by tonic contraction of the IAS. Re¯excontraction of the EAS complex on coughing orValsalva prevents leakage by kinking the anal canalin opposing directions. Rectal distention produces
stretching of the puborectalis and the urge todefecate. The distended rectum causes re¯ex relaxa-tion of the IAS (rectoanal inhibitory re¯ex (RAIR))resulting in faeces reaching the upper anal canalwhere receptors sample the rectal contents. Thenvoluntary EAS contraction maintains continence bymechanically sealing the rectal neck and mechani-cally preventing further relaxation of the IAS.Defecation is a coordinated event requiring simulta-neous relaxation of the puborectalis to widen theanorectal angle, relaxation of the EAS, and rectalcontraction.
The enteric nervous system
Nervous control of the gastrointestinal tract is by theenteric nervous system. This complex network ofintrinsic neurons is able to sense information, processit by means of interneurons and then through motorneurons e�ect secretion or muscular contraction. Itretains contact with the central nervous system througha�erent and e�erent extrinsic neurons of the sympa-thetic and parasympathetic systems.12
There are two main ganglionated plexuses, themyenteric (Auerbach's) and submucosal (Meissner's).The myenteric plexus lies between the longitudinaland circular layers of muscle for the entire length ofthe gut. It provides motor innervation to the twomuscle layers and secretomotor innervation to themucosa. There are also projections from themyenteric plexus to the sympathetic ganglia. Thesubmucous plexus is located in the submucosabetween the circular muscle and the muscularismucosa. It plays an important role in secretorycontrol, especially in the small intestine. It alsoinnervates the muscularis mucosa, intestinal endo-crine cells and submucosal blood vessels. Smallernerve ®bres emerge from these plexuses to formnonganglionated plexuses in the circular and long-itudinal muscle and muscularis mucosae.13
The neurons can contain not only acetylcholine andnorepinephrine, but also Substance P (SP), vasoactiveintestinal peptide (VIP), serotonin, somatostatin, andother neuropeptides, often coexisting in the sameneurons.
The neurons of the enteric nervous system can beclassi®ed into intrinsic a�erent, interneurons andmotor neurons.. Intrinsic a�erent neurons form the sensory limb of
intrinsic motor and secretomotor re¯exes byprojecting to interneurons in both nerve plexuses.They are all cholinergic and may contain otherneurotransmitters such as SP.12
. Interneurons project either up or down the gutbetween the a�erent and motor or secretomotorneurons. They form multisynaptic pathways tocontrol the propagation of peristaltic waves. Thereare several subgroups based on neurotransmittercontent, but their various physiological roles areunknown.
Figure 1 The external anal sphincter (EAS), summarisingthe basic arrangement of its ®bres. Puborectalis (PR) formsthe upper loop (UL) and has decussating ®bres (dc) thatblend with the longitudinal ®bres of the rectum, or (dd) theperineal body. The middle loop (ML) is attached to theanococcygeal raphe (acr), bulbospongiosus (bs), and trans-versus perinei profundus (tp). The basal loop (BL) isperforated by longitudinal ®bres of the rectum11
Bowel dysfunctionAC Lynch et al
194
Spinal Cord

. Motor neurons are either excitatory or inhibitory.The excitatory neurons project either locally ororally to the circular muscle, their main neuro-transmitters being acetylcholine or SP. Theinhibitory motor neurons project to the circularmuscle caudally and contain VIP and nitric oxide(NO).12
Neuropeptides
Peptides destined for secretion by neurons aresynthesised in the cell body then transported intra-axonally to the nerve endings where they are stored insynaptic vesicles until release. There is no evidence fora re-uptake and re-use pathway for neuropeptides.
Substance PSubstance P (SP) was the ®rst gut neuropeptide to bediscovered in 1931. It occurs widely in brain, spinalcord, gut nerves, and mucosal endocrine cells. It is adose-dependent excitatory neurotransmitter actingwithin the myenteric plexus on cholinergic neuronsand directly on smooth muscle to cause contraction inboth longitudinal and circular muscle layers. It isknown to increase gut motility and may promote andmaintain the peristaltic mode of intestinal motility. SPalso increases blood¯ow in gut, binds to speci®creceptors on pancreatic acinar cells associated withenzyme secretion, and inhibits acid secretion andintestinal absorption.14
Evidence for this role includes the observation thatcarcinoid tumors are often associated with increasedgut motility and diarrhoea. These tumours cansynthesise and release large amounts of SP, andserotonin, known to lower the threshold for theperistaltic re¯ex in isolated segments of intestine, intothe portal and systemic circulations.
Vasoactive intestinal peptideVasoactive intestinal peptide (VIP) is present in a widerange of neurons in both gut and elsewhere. It is astrong stimulant of intestinal secretion, and causesgastrointestinal relaxation. Myenteric VIP neuronsproject in an oral to anal direction and are compatiblewith a role in descending inhibition.14
Central and enteric nervous system interaction
The coordination of transport, secretion and blood¯ow requires a high degree of extrinsic and intrinsicneuronal integration. The intrinsic neurons of the gutexhibit a sophisticated pattern of behaviour indepen-dent of, but modulated by the extrinsic parasympa-thetic and sympathetic nervous system.14 The extrinsicsystem acts to modulate intrinsic re¯exes andcoordinate gut activity with that of the wholeorganism. When the gut is disconnected from thecentral nervous system, its function is preserved, but
complex activities requiring both voluntary and re¯exactivity can be impaired.13
The control of colonic movement is largelyautonomous. Intrinsic rhythmic slow waves originat-ing in the submucous plexus occur sequentially alongthe colon. In the right colon slow waves of contractionmay travel in both directions to produce mixing andkneading contractions of the circular muscle layer. Theslow waves in the distal colon are directed towards theanus to produce a propulsive peristaltic force. Normalcolonic transport is between 12 to 30 h from ileocaecalvalve to rectum.15
Peristalsis results in the propulsion of intraluminalcontents over long lengths of small and large intestine.The process requires coordinated contraction of thelongitudinal muscle and inhibition of the circularmuscle ahead of the bolus and simultaneous long-itudinal muscle relaxation and circular muscle con-traction immediately behind the bolus. It can occur inan isolated segment of gut in vitro, implying it isdependent on an intact integrative enteric nervoussystem.16 Activation of the longitudinal muscle aheadof the bolus is produced by acetylcholine released fromthe myenteric plexus. Relaxation of the circular muscleis produced by increased discharge from the intrinsicinhibitory neurons. Contraction of the circular musclebehind the bolus may be a myogenic event followingsynaptic shutdown of continuously active inhibitoryneurons, or it could be produced by cholinergicexcitatory input to the muscle, or both.
The best evidence for intrinsic inhibitory mechan-isms is in Hirschsprung's disease where there is spasmin an aganglionic section of colon. As no re¯exrelaxation is initiated, the aganglionic segmentbehaves like a sphincter, resulting in a functionalobstruction to faceal transit. The failure of relaxationof the diseased segment is accounted for by its lack ofinhibitory neurons containing VIP and NO.
Parasympathetic supply to the colon, rectum andanus
Parasympathetic out¯ow to the colon contains twotypes of preganglionic axons. One leading to intramur-al cholinergic excitatory neurons and one connectingwith intramural noncholinergic nonadrenergic inhibi-tory neurons.
Stimulation of the pelvic nerves elicits a contractionin both colonic muscle layers, but if the cholinergic®bres are blocked with atropine, parasympatheticstimulation results in inhibition of contraction andrelaxation due to muscle cell hyperpolarisation. Inhumans, this can be seen when sectioning of the pelvicnerves may result in impaired defecation.17
Distribution of vagal input is debated;17 it mayproject as far as the rectum, although some authorsfeel only the ascending colon is innervated, and others,up to the transverse colon. It acts to increasecontractile activity by modulating coordinated motorresponses from the enteric nervous system.
Bowel dysfunctionAC Lynch et al
195
Spinal Cord

Sacral input is transmitted by pelvic nerves to thelarge intestine. It issues from spinal roots S2 ± S4 viathe pelvic plexus (Figure 2). It is mediated by nicotiniccholinergic receptors and functions to reinforce masscontraction of the terminal large intestine duringdefecation.18
The parasympathetic supply to the internal analsphincter comes from the sacral spinal cord throughthe pelvic nerves. The parasympathetic e�ect issphincteric relaxation through activation of nonadre-nergic noncholinergic intramural neurons and apresynaptic action of cholinergic intramural neuronson sympathetic nerve endings.
Extrinsic parasympathetic re¯exes
Mechanical stimulation of the colon or rectum elicits acoordinated re¯ex contraction of the rectum that mayresult in defecation. The sacral parasympathetic centreis of major importance in organising colonic motility,especially during defecation.17 It is able to organisedefecation even after upper spinal cord section.19
However the sacral parasympathetic centre is alsoin¯uenced by supraspinal nervous structures. In the
dog, the ®ring of sacral parasympathetic neurons ismodulated by the pontine reticular formation.20
Parasympathetic preganglionic neurons are alsoin¯uenced by a�erents from both the urinary bladderand colon. The ®ring of parasympathetic neurons tothe colon is increased by activatin of colonic a�erentsand decreased by that of vesical a�erents thatreciprocally inhibit colonic parasympathetic neuronsand excite vesical ones.21
Sympathetic supply to the colon, rectum and anus
Sympathetic supply consists of cholinergic preganglio-nic neurons and noradrenergic postganglionic neuronslocated in either the sympathetic chain or prevertebralganglia (coeliac, superior mesenteric, or inferiormesenteric). Preganglionic axons from spinal rootsT9-T10 synapse in the coeliac and superior mesentericganglia. From there, postganglionic nerves innervatethe small intestine and from the superior mesentericganglion to the ascending and transverse colon (Figure2). Sympathetics are inhibitory and function todecrease bloow ¯ow and slow motility by relaxingthe colonic wall to increase compliance. Sympathetic
Figure 2 Autonomic and somatic innervation of the colon, anal sphincters and pelvic ¯oor. Spinal cord segments and nervebranches are illustrated. Dashed lines represent sympathetic pathways with prevertebral ganglia. Solid lines depictparasympathetic pathways that synapse with ganglia in the enteric nervous system within the colonic wall. Dotted linesrepresent mixed nerves supplying somatic musculature of the external anal sphincter (EAS) and pelvic ¯oor15
Bowel dysfunctionAC Lynch et al
196
Spinal Cord

input acts on presynaptic terminals to preventexcitatory transmitter release within the entericnervous system.18
There is evidence that the spinal cord is the sourceof tonic inhibition. In cats, after lumbar ventral rootremoval and spinal cord removal, there was a decreasein e�erent lumbar colonic nerve ®ring and a parallelincrease in colonic motility.22 This suggests e�erentinhibition from between T12-L5. This may not be theonly source of e�erent tra�c in the colonic nerves asthere are tonically discharging neurons in the catinferior mesenteric ganglion.23
Somatovisceral re¯exes have been described suchas inhibition of intestinal motility in response to skinpinching. It appears to have a segmental organisa-tion but its role in spinal patients is unclear althoughdefecation appears enhanced by rubbing armsand abdominal massage. This may indicate thepresence of somatic a�erent pathways connected tovegetative central neurons involved in gut motility,perhaps via the sympathetic chain. However, patientswho have had a complete bilateral sympathectomydo not generally present with change in bowelhabit.24
Postganglionic sympathetic neurons in the prever-tebral ganglia are the sympathetic ®nal common pathfor the integration of information from the peripheryand the CNS. Their function is complicated.Immunocytochemical data indicates that the nerveprocesses contain VIP, encephalin, SP, somatostatin,CCK and bombesin.25,26 Each of the nerve trunksconnected to ganglia contain speci®c peptidergicpathways.25 These substances play a role in synaptictransmission within ganglia or as modulators ofneurotransmitter release.26
SP at low concentration has been shown to increasethe excitability of guinea pig prevertebral ganglionicneurons such that a subthreshold EPSP (excitatorypostsynaptic potential) will generate a spike potentialor give rise to tonic discharge of spike potentials inpostganglionic neurones in the absence of excitatoryinput. Moreover, administering either SP, one of itsanalogs, or a SP-degrading endopeptidase inhibitor torats will result in a signi®cant increase in gastro-intestinal transit.27
Sympathetic innervation of the internal analsphincter
The IAS receives sympathetic innervation from thelumbar spinal cord through the lumbar splanchnicnerves and from the inferior mesenteric ganglionthrough the hypogastric nerves. The sympathetic effectis excitatory, and tonic discharge maintains IASclosure. With rectal distension or digital stimulation,the IAS relaxes probably due to the activation ofintramural inhibitory nonadrenergic noncholinergicneurons. There may be some extrinsic participationsince pelvic nerve stimulation induces sphincterrelaxation.28
Vesicoanal re¯ex
Vesical ®lling increases electromyelographic activity inthe IAS, and after voiding it decreases. The re¯ex isprobably partly from the lumbar spinal cord and partlyfrom the inferior mesenteric ganglion. Sphincterpressure is unchanged after high cord section,implying supraspinal centres have very little in¯uenceon IAS tone. A dual origin for excitation is proposedin the cat as IAS electrical activity remains after sectionof sympathetic excitatory ®bres, but it is desynchro-nised. The implication is that motor activity is bothmyogenic and neurogenic, the latter reinforcing theformer by synchronising electrical activity of smoothmuscle cells.
Sympathetic innervation of the external analsphincter
The EAS is a striated muscle innvervated from thesacral cord via the pudendal nerves (S2-S4). Itsstructure is shown in Figure 1. Some of the EASmotor neurones can be activated by stimulation ofa�erent axons in pudendal nerve branches from theexternal urethral sphincter. Clinical experience withpatients following spinal cord injury does not seem todemonstrate a change in anal tone. This may bebecause supraspinal centres do not in¯uence sphinctertone, the adaptation of remaining structures, or that asingle level sympathectomy is insu�cient to result inchange.29
Chronic changes in colonic function followingspinal cord injury
The extrinsic nervous system acts to modulate theintrinsic system. It is these complex integrated activitiesthat require re¯ex and voluntary muscular control suchas defecation that are a�ected most by spinal cordinjury. Peripheral nerve lesions have been shown toresult in transsynaptic degeneration and Schwann cellproliferation in the colonic wall, but local synapticremodelling after spinal injury has not been demon-strated.17,30
The level of the spinal cord lesion determines thee�ect on colonic motility. A supraconal (Upper MotorNeuron or UMN) SCI results in loss of conscioussphincter control and an inability to signi®cantlyincrease intraabdominal pressure. There is a loss ofvoluntary control of defecation and a degree ofanorectal dyssynergy. This means that straining andrectal contraction result in increased tone in the EAS.Loss of rectal sensation and a spastic EAS requiredefecation to be anticipated. Re¯ex defecation can beinitiated by mucosal stimulation, either digitally orwith a suppository. Stimulation activates the rectoanalinhibitory re¯ex. It can be exploited to causerelaxation of the IAS, re¯ex relaxation of the EASand pelvic nerve mediated peristalsis. If there is nore¯ex relaxation of the EAS complex, re¯ex evacuation
Bowel dysfunctionAC Lynch et al
197
Spinal Cord

will not occur or be incomplete. Manual evacuation orenemata are often required in this situation.
Complete or partial injuries to the cauda equinaresult in a lower motor neuron (LMN) pattern ofinjury. The EAS and pelvic muscle are ¯accid andthere is no re¯ex response to increased intraabdominalpressure. The loss of parasympathetic control andre¯ex innervation of the IAS means a furtherreduction in resting anal tone and leads to faecalincontinence. A person with a LMN lesion followingSCI will have absent EAS tone and decreased re¯experistalsis. Valsalva can result in faecal leakage andthe rectum has to be kept empty to avoid faecalincontinence. Stool has to be removed digitally,assisted by Valsalva and abdominal massage.
Patterns of gut dysmotility have been described fordi�erent levels and degrees of SCI. Lesions above T1result in delayed mouth-to-caecum time, but lesionsbelow this exhibit normal transit times to thecaecum.31 Beyond the ileocaecal valve, transit timesare markedly delayed. A LMN injury from a lesiona�ecting the conus, cauda equina or pelvic nervesresults in interruption of the parasympathetic supplyto the colon and reduced spinal cord-mediated re¯experistalsis. Stool propulsion is by segmental colonicperistalsis only. An UMN lesion results in variablechanges in colonic transit. Marker transit studies andscintigraphy have demonstrated that patients withspinal cord lesions above the lumbar region haveslowed transit throughout the whole colon.32 Onestudy involving 28 SCI patients also demonstrateddistal small bowel dilatation in 10 patients, all ofwhom had abdominal symptoms and nine of whomhad a spinal cord lesion above T5.33 Radioisotopescintigraphy has shown the delay to involve the wholecolon. The velocity of the median position of bowelcontents throughout the colon was signi®cantly slowerin SCI patients (0.63+0.33 cm/h in SCI, 2.58+1.2 cm/h in controls, P50.001).32
The delay in transit may in part be due to loss ofcolonic compliance. The colon of patients with completethoracic injury has been shown to have an abnormalresponse to increasing volume. Distension with water togenerate a volume/pressure curve (colometrogram)produces a hyperre¯exic response similar to thatdescribed in the bladder.34 With a spinal cord lesionabove L1, the left colon is less compliant. Above T5, theright colon is also a�ected. The lack of compliance leadsto functional obstruction, increased transit times, andabdominal distension, bloating and discomfort. Itsuggests that the CNS is necessary to modulate colonicmotility.35 Colonic myoelectric activity has beenrecorded in a group of SCI patients with injuries atvarying levels and controls. This demonstrated asigni®cantly higher level of basal colonic activity inSCI patients (12.6 spikes per 10 min vs 3.3), and nodemonstrable gastrocolic re¯ex.36 This would supportthe assumption that the CNS exerts a tonic inhibitoryin¯uence on basal colonic activity and is consistent withthe hypertonicity seen on colometrograms.34
The conclusion is that the increase in colonicactivity and decrease in compliance may be due toloss of descending inhibitory input from the CNS. Thisis supported by animal studies in the cat wheresympathetic nerve activity via a2-adrenergic receptoractivation resulted in profound inhibition of colonicmotility,37 and sectioning of preganglionic splanchnicsympathetic nerves produced an increase in coloniccontraction.38
E�ects of obstruction on motility and colonicneuropeptides
If the change in colonic motility was due to functionalrectal obstruction secondary to anorectal dyssynergyalone, we should expect changes such as thoseproduced by mechanical obstruction of the colon.Bowel muscle and ganglia hypertrophy, and if theobstruction is not removed, hypertrophy and contrac-tile e�orts continue until enzymatic mediator depletionoccurs.39 Non-constricting obstructive bands in ratsproduces histological changes such as ganglion cellelongation, probably due to bowel distension, but doesnot result in signi®cant changes to the enteric nervoussystem.40
That said, obstruction has been shown to a�ectneurotransmitter levels.41 One study looked at ®vepatients with decompensated ileus due to tumourobstruction of the large bowel. Immediately afterresection, samples were taken 10 cm proximally anddistally to the tumour and SP and VIP levels wereobtained by radioimmunoassay. A signi®cantly de-creased tissue level of both SP and VIP was found inthe prestenotic sample. The mechanisms that lead tothis decrease are unknown. Increased release ofneurotransmitters due to endotoxins may be impor-tant. Decreased SP would impair motility by reducingbowel contractility. VIP may act by causing dysmoti-lity due to loss of descending peristaltic inhibition.While the mechanical obstruction may be the majorcause of obstructive ileus, the ®nal rapid decompensa-tion may be due to alteration of gut neuropeptides.41
Role of neuropeptides in bowel dysfunction
There is a distinction in the intramural distribution ofregulatory neuropeptides within the bowel wall. SP isexclusively localised in nerves. Large quantities of SPand VIP are present in the lamina propria which is inclose contact with the epithelium and muscularismucosae.42 Large numbers of VIP and SP-containingenteric nerves supply the ganglionated plexuses andare especially numerous in the circular muscle layer.They have a role in colon motility while thosesupplying the mucosa are involved with electrolyteand ¯uid transport. SP has been shown to acceleratethe transit of a charcoal meal in rats.27 It increasesintraluminal pressure mainly by circular musclecontraction by direct action on the muscle as well asby simultaneous activation of excitatory cholinergic
Bowel dysfunctionAC Lynch et al
198
Spinal Cord

pathways and inhibitory VIP-independent, NO-regu-lated pathways.43
SP is reduced in the colonic mucosa of patients withchronic constipation and increased in patients withulcerative colitis. In both cases there was a signi®cantcorrelation between mucosal SP levels and the diseasestates.44 The elevated levels in ulcerative colitis may bea reactive e�ect secondary to other in¯ammatoryfactors. The fact that mucosal SP levels are associatedwith two disorders associated with colonic transitsuggests a role in the pathogenesis of intestinal transitdisorders.
A similar scenario exists with diabetic constipationwhere SP in the rectal mucosa of diabetics withconstipation is signi®cantly lower than in diabeticswith normal bowel function.45 Both groups of diabeticpatients exhibited greater SP levels than controls.These abnormalities the mucosal content of SP may bethe result of degenerative changes in the submucosalplexuses of diabetics.46
While mucosal SP may be decreased with chronicconstipation, concentrations in the muscle layers maybe increased. Sjolund et al.47 examined tissue from thecolon of 18 people with slow-transit constipation.Tissue concentrations of VIP and SP were measuredby radioimmunoassay. Signi®cantly increased concen-trations of VIP and SP were found in the ascendingcolon, and in the descending colon, SP was increasedin the myenteric plexus.
Dysfunctional colonic motility in children can resultin severe constipation. A spectrum of dysganglionoseshas been identi®ed of which Hirschsprung's Disease(HD) is a subgroup. There are morphologicaldi�erences between groups but the functional implica-tion of this is unclear. One subgroup has beenidenti®ed from immuno¯uorescence studies of neuro-transmitters in full thickness colonic biopsies inchildren with colonic constipation.48 These childrenhave a markedly reduced number of SP-immunoreac-tive nerve ®bres in the muscularis propria. Thisreduction in excitatory nerve ®bres may be the basisof their functional impairment.49 Intestinal NeuronalDysplasia is a malformation of the enteric plexus thatclinically resembles HD. Its pathogenesis is unknown,but patients appear to have defective innervation ofthe neuromuscular junction that results in chronicconstipation.50
Enteric neurotransmitters such as SP and VIPappear to have a role in disease states a�ectingcolonic transit. If this scenario is applied to colonictransit following SCI, impaired colonic transit may bere¯ected in abnormal concentrations of SP or VIP inthe colonic muscle layers. This may result fromchronic obstruction secondary to anorectal dyssy-nergy, or chronic dysmotility secondary to a changein CNS and sympathetic neuromodulation.
Our recent preliminary work on colonic neurotrans-mitters shows no di�erence in SP, VIP or NSE in SCIpatients and controls.51 In this study, specimens wereobtained from four SCI and seven control patients. No
histological di�erences were found between colonicspecimens from SCI and control patients. The ratio ofSP and VIP to NSE was qualitatively similar for bothSCI patients and controls. There is still considerablymore work to be undertaken in this area and it mayprovide an interesting and possible novel means onintervention.
Relationship of anorectal and bladder function
There are similarities between the bladder and rectumin terms of function and behaviour following spinalcord injury. The dysmotility seen in spinal patients maybe due to decompensation of colorectal smooth musclefollowing chronic colorectal distension, similar todetrusor decompensation seen with chronic bladderoutlet obstruction.29 Colonic compliance is reducedfollowing thoracic SCI, and the uninhibited contractionof the bladder seen following distension produces acystometrogram analogous to the colonic compliancecurves. This perhaps re¯ects a similar interruption ofascending somatosensory and descending visceralpathways.35
We have explored a possible relationship betweenpatterns of anorectal physiology and patterns seenwith cystometrograms. Anorectal manometry wasperformed on 37 SCI volunteers. Patterns of rectaland sphincter function were identi®ed. These patternswere then compared with questionnaire answers onbowel function and cystometrograms to identify arelationship between detrusor dyssynergy and analsphincter tone. Rectal compliance and basal restingsphincter pressures were lower than normal values.Ramp rectal in¯ation demonstrated patterns ofsphincter activity similar to that recorded in thepatients' cystometrograms. There is no de®niterelationship of bowel function to the ®ndings onmanometry in SCI patients. We concluded that SCIpatients have abnormal anorectal function, and thatanorectal manometry results were able to be classi®edinto four patterns relating to rectal pressure andsphincter tone in response to rectal distension. Thepatterns of anorectal manometry seen were similar tothose in cystometrograms, however there is no de®niterelationship to bowel dysfunction.
Mechanisms for bowel dysfunction following spinalcord injury
Colonic dysmotility has been noted, with delayedcolonic transit times and a loss of colonic compli-ance. It is more marked in those with complete cervicalinjuries and can result in constipation, abdominaldistention and discomfort. This may be due to a lossof descending inhibitory modulation from the sympa-thetic nervous system. The observation that transitdelays are more profound in higher injuries supportsthis assumption.
The intrinsic enteric nervous system appears intact.No histological changes have been demonstrated to
Bowel dysfunctionAC Lynch et al
199
Spinal Cord
occur in colonic specimens from long-term SCIpatients.51 Nerve ®bres containing the intrinsicneurotransmitters SP and VIP appear to be presentin qualitatively similar amounts in SCI patients andcontrol specimens.51 The colon may therefore continueto function independently of CNS modulation afterSCI.
The di�culties with defecation following high SCIcould be the result of discoordinate anal sphincterfunction.52 The normal synergistic activity of colonicsmooth muscle and pelvic striated muscle is lost. Theconus-mediated increase in EAS tone with increasingintraabdominal pressure was seen for all groups ofSCI patients. The re¯ex relaxation of the IAS andEAS can be exploited in order to defecate.52 It canalso lead to faecal incontinence as the anal sphinctermay relax at relatively low rectal volume. Lower SCIcan result in faecal incontinence secondary to reducedsphincter tone that is unresponsive to changes inintraabdominal pressure. A loss of rectal tone resultsin a capacious rectum and a reliance on the manualevacuation of stool.
The relationship between colonic dysmotility andanorectal dysfunction is unknown. Does the functionalobstruction caused by dyssynergic EAS contractionduring defecation lead to a change in colonic motility?In constipated non-SCI patients correction of pelvic¯oor abnormality often corrects abnormal transittime.53 Alternatively, does the colon fail to transportfaeces to the rectum at a rate and volume su�cient togenerate sphincter relaxation and defecation? Patternsof bladder and bowel dysfunction following SCI,demonstrate a common loss of coordination in re¯exand voluntary muscle functions.52
Current management strategies
The approach to bowel management in the spinalinjured patient should address speci®c issues such asfaecal incontinence, constipation, and functionalmobility. This must be within the context of thepatient as a whole person and consider their cultural,social, sexual and vocational roles. A bowel careregimen needs to be generated that ®ts the person'slong-term routine. The aim should be e�ective colonicevacuation without faecal incontinence or othercomplications. Regularity of evacuation preventsexcessive buildup of faeces and impaction. Appro-priate equipment, such as commode chairs andwheelchair able toilets, needs to be supplied for anadequate long-term bowel programme.
Dietary manipulation is important. Adequate waterintake promotes transit by keeping the stool soft.Fibre is promoted to give the stool bulk andplasticity.15 This is thought to assist colonic transitin neurologically intact patients, probably by promot-ing propulsive activity secondary to increased colonicwall distention. However, an increase in stool bulkmay mean more time spent with bowel care, andincreasing ®bre intake for SCI patients has not been
shown to result in faster colonic transit time. The mainreason to have a high ®bre intake therefore is toabsorb excess water and keep the stool soft. Forty-three per cent of SCI patients use ®bre sometimes orregularly, compared with only 23.2% of controls.Fibre use didn't change with time after injury andusers were on average younger than controls.
Stool softeners other than ®bre, such as docusatesodium (Coloxyl, [Fawns & McAllan]) increase theamount of water in stool without increasing volumeand have no e�ect on bowel motility. They can alsoa�ect the intestinal absorption of other drugs,resulting in higher plasma levels. The stool is morelikely to be liquid, so continence will not be improved.They are most useful where faecal incontinence is nota risk and straining is to be avoided, such as for thosepatients with haemorrhoids or autonomic dysre¯exia.
Stimulant laxatives act by increasing intestinalmotility resulting in less time for water reabsorption.Senna (Senokot, [Reckitt & Colman]) has a directstimulant e�ect on the myenteric plexus and alsoincreases intraluminal ¯uid. Bisacodyl (Dulcolax,[Boehringer Ingelheim]) has a similar mode of actionand is often used as a suppository to initiate bowelevacuation. Dose dependent side e�ects can occur.These include abdominal cramping, diarrhoea andelectrolyte imbalance. Chronic use of stimulantlaxatives, especially senna, can result in a progressiveunresponsiveness. Osmotic laxatives such as lactulose(Duphalac, [Duphar]) draw ¯uid into the colon. Theycan result in more liquid stool and cause cramping.Laxative use was almost ten times more frequentamong the SCI patients, becoming even more frequentwith increasing time from injury. This may suggest agreater incidence of constipation.
Enemata are often employed when suppositories ordigital stimulation fail. Long term use can result inenema dependence and side e�ects such as rectaltrauma and autonomic dysre¯exia can occur.
Prokinetic agents such as cisapride (Prepulsid,[Janssen-Cilag]) have been employed to reduceconstipation in SCI patients. Transit times areimproved, however, cardiac arrhythmias have beennoted with long-term use.54
SCI patients with UMN lesions can exploit therectocolic re¯ex to e�ect defecation. Digital stimula-tion can result in a re¯ex wave of conus-mediatedrectal peristalsis. The intact rectoanal inhibitory re¯ex(RAIR) then causes IAS relaxation and defecation.Rectal sensation is reduced however, so defecation hasto be anticipated on a regular basis. Based on theanorectal manometry data52 it is possible to identifythose SCI patients who will re¯exly defecate at lowrectal volume. These patients require a bowel manage-ment programme that keeps the rectum empty toreduce the incidence of incontinence. Those patientswith UMN lesions and an obstructed defecatorypattern need a management plan that mimicsanorectal trauma but still allows adequate rectalevacuation to avoid constipation.
Bowel dysfunctionAC Lynch et al
200
Spinal Cord

Patients with LMN lesions have an are¯exic boweland reduced sphincter tone. The increase in sphincterpressure with Valsalva is reduced, leading to increasedrisk of incontinence, especially with liquid stool. Theaim is therefore to keep stool consistency ®rm. Localanorectal re¯exes are often insu�cient to result indefecation, and a compliant rectum acts as a largereservoir, so stool is digitally removed.
A Brindley sacral anterior nerve root stimulator(S2 ± S4) can be used for electromicturition to achieveregular, complete bladder emptying. Often deafferen-tiation of the sacral posterior nerve roots is performedbefore the stimulator is implanted to produce detrusorare¯exia and interim urinary continence. The deaf-ferentation also results in loss of the sacral re¯exesnecessary for defecation. The stimulator can be used toinitiate defecation, not during stimulation, due tosimultaneous rectal and sphincter contraction, butwhen stimulation stops and the EAS relaxes instanta-neously and the rectum relaxes slowly, resulting inspontaneous defecation. This has been shown to resultin quicker, more controllable defecation than the re¯exmethod.55,56
Colostomy may be an alternative for SCI patientswith ongoing bowel management di�culties. It hasbeen shown to result in improved quality of life, it isaccessible for those with poor hand dexterity, ando�ers control of faecal incontinence. Risks andcomplications that are associated with any surgicalprocedure may not make it acceptable to all SCIpatients. A recent study by us has revealed thatpatients with colostomies do not have their quality oflife impaired.57 A standardised previous validatedquestion designed to assess quality of life in spinalinjured patients was sent to 26 spinal cord injuredpatients with colostomies and 26 spinal cord injuredpatients without colostomy. The two groups werematched for level of injury, completeness of injury,length of time with injury, age (+5 years) and gender.There was no signi®cant di�erence (P40.05) in thetwo groups of patients in regard to their generalwellness, emotional, social, or work functioning.Further prospective studies are needed and we haveone underway at present.
The antegrade continence enema (ACE) procedure isnow widely accepted as an option in the treatment offaecal incontinence in children who have not respondedto medical management.58,59 The operation involvesattaching the appendix to the surface of the abdomen asa catheterisable channel to enable regular antegradecolonic washouts. There have been a number ofmodi®cations to the ACE procedure including non-reversal of the appendix,60 various skin ¯ap techni-ques,61 a simpli®ed laparoscopic technique (LACE),62,63
and the use of the procedure in older patients.64 Theprocedure appears to have a low incidence ofcomplications and morbidity. It requires a motivatedpatient with good hand function and is generallyconsidered best in patients with a lax anal sphincter.In a recent study we have undertaken children with
spina bi®da who had the LACE procedure, there was aconsistently high level of functional continence achievedfollowing surgery.65 The use of the procedure in spina-bi®da has shown that this procedure may have an as yetunidenti®ed role in SCI patients.
Future objectives for the investigation andmanagement of bowel dysfunction
The SCI patients with bowel management problems areeasy to identify. Interview and clinical examination cangenerate an impression of their general bowel functionand identify problems such as constipation, faecalimpaction, anal ®ssures, and haemorrhoids. Simpletests of anorectal function are available. These could beperformed on all SCI patients in the same manner thatbladder dysfunction is investigated. Anorectal mano-metry will identify those with dyssynergic sphincterfunction. For those with abdominal bloating andconstipation, abdominal X-ray and colonic motilitystudies give further useful information.
After 12 months from SCI, bowel function does notseem to change either with increasing time after injury,or increasing age. This allows for early identi®cationof what may be ongoing problems.
After the acute phase of spinal cord injury, promptidenti®cation of those with bowel managementproblems would be useful. Anorectal manometrycould then be performed. Speci®c patterns identi®edmay help determine future management.52 Those witha compliant rectum and re¯exly relaxing sphincter canemploy digital stimulation to re¯exly defecate. Patientswith high rectal compliance (pattern 4) may requireregular manual evacuation to ensure their compliantrectum is empty. Patients with increased rectal andsphincter tone (pattern 1) will probably have highinjuries and need to be identi®ed because this patternmay result in inadequate rectal evacuation. Anecdo-tally, these would be the patients where manualevacuation is di�cult and often accompanied byautonomic dysre¯exia.
Following SCI, the colonic nervous system may stillbe intact but functioning in an ummodulated way. Theexistence of SP analogues and inhibitors of SPdegradation that are reactive in vitro and in vivo havealready been used to demonstrate a reduction incolonic transit time in rats.27 These compounds areuseful tools to further investigate the actions ofcolonic neuropeptides. Increasing coordinated colonicperistalsis would be a useful therapeutic modality. Thiscould be done either by direct stimulation of colonicsmooth muscle or by stimulation of SP and VIPimmunoreactive nerve endings.
Although improving colonic motility and appro-priate bowel management may help, there will be someSCI patients with ongoing bowel problems. Colostomyformation has been used to provide the patient withrelief from constipation and anorectal dysfunction andan independent means of managing their own bowelfunction. Further research needs to be done into the
Bowel dysfunctionAC Lynch et al
201
Spinal Cord
di�erences in quality of life and bowel functionfollowing colostomy formation in SCI patients.
Another focus of future investigation is the intrinsiccontrol of colonic motility. The ®ndings of our workon colonic neurotransmitters imply that the intrinsicinnervation of the colonic smooth muscle is intact(with respect to NSE, SP and VIP) following SCI. Theway this muscle functions without spinal cordmodulation may form the basis for some of theseproblems seen clinically, speci®cally, problems withcolonic motility and rectal compliance. Furtherinvestigation may con®rm that the intrinsic colonicnervous system is intact. Such research could involveimmunohistochemical staining for colonic smoothmuscle neurotransmitters to support our initial®ndings, or performing passive and active length-tension curves on isolated colonic smooth muscle tocon®rm its functional similarity to normal muscle.
The bowel problems resulting from SCI are due tothe loss of the complex integrative pathways involvingintrinsic and extrinsic innervation. Investigationtargeted at improving bowel function for these peoplehas been shown to improve quality of life. Pharmaco-logical manipulation of colonic innervation maybecome a therapeutic option. However, improvementin motility requires a coordinated response that maynot be possible following SCI. There is still scope toprovide early assessment of SCI patients in order toinstitute appropriate bowel management, and moreactive surgical intervention (colostomy and ACE) thatmay improve quality of life.
References
1 Longo WE, Ballantyne GH, Modlin IM. The colon,anorectum and spinal cord patient. A review of thefunctional alternations of the denervated hindgut. DisColon Rectum 1989; 32: 261 ± 267.
2 Glickman S, Kamm MA. Bowel dysfunction in spinal-cord-injury patients. Lancet 1996; 347: 1651 ± 1653.
3 Levi R, Hultling C, Nash MS, Seiger AÊ . The Stockholmspinal cord injury study: 1: Medical problems in regionalSCI population. Paraplegia 1995; 33: 308 ± 315.
4 DeLooze D et al. Constipation and other chronicgastrointestinal problems in spinal cord injury patients.Spinal Cord 1998; 36: 63 ± 66.
5 Hanson RW, Franklin MR. Sexual loss in relation toother functional losses for spinal cord injured males.Arch Phys Med Rehabil 1976; 57: 291 ± 293.
6 Han TR, Kim JH, Kwon BS. Chronic gastrointestinalproblems and bowel dysfunction in patients with spinalcord injury. Spinal Cord 1998; 36: 485 ± 490.
7 Stone JM, Nino-Murcia M, Wolfe VA, Perkash I.Chronic gastrointestinal problems in spinal cord injurypatients: a prospective analysis. Am J Gastroenterol 1990;85: 1114 ± 1119.
8 Lynch AC, Antony A, Dobbs BR, Frizelle FA. BowelDysfunction Following Spinal Cord Injury: A Descrip-tion of Bowel Function in a Spinal Cord-InjuredPopulation and Comparison with Age and GenderMatched Controls. Spinal Cord (in press).
9 Stone JM, Wolfe VA, Nino-Murcia M, Perkash I.Colostomy as treatment for complications of spinalcord injury. Arch Phys Med Rehabil 1990; 71: 514 ± 518.
10 Sha®k A. A concept of the anatomy of the anal sphinctermechanism and the physiology of defecation. Dis ColonRectum 1987; 30: 970 ± 982.
11 Bogduk N. Issues in anatomy: The external analsphincter revisited. Aust NZ J Surg 1996; 66: 626 ± 629.
12 Goyal RK, Hirano I. The enteric nervous system. NewEngl J Med 1996; 334: 1106 ± 1115.
13 Costa M, Furness JB, Llewellyn-Smith IJ. Histochem-istry of the enteric nervous system. In Johnson LR (ed).Physiology of the Gastrointestinal Tract, Second Edition,Raven Press, New York, 1987; pp 1 ± 40.
14 Dockray GJ. Physiology of enteric neuropeptides. InJohnson LR (ed). Physiology of the GastrointestinalTract, Second Edition, Raven Press, New York, 1987;pp 41 ± 66.
15 Steins SA, Bergman SB, Goetz LL. Neurogenic boweldysfunction after spinal cord injury: Clinical evaluationand rehabilitative management. Arch Phys Med Rehabil1997; 78: S86 ± S102.
16 Wood JD. Physiology of the enteric nervous system. InJohnson LR (ed). Physiology of the GastrointestinalTract, Second Edition, Raven Press, New York, 1987;pp 67 ± 109.
17 Devrode G, Lamarche J. Functional importance ofextrinsic parasympathetic innervation to the distal colonand rectum in man. Gastroenterology 1974; 66: 273 ± 280.
18 Roman C, Gonella J. Extrinsic control of digestive tractmotility. In Johnson LR (ed). Physiology of theGastrointestinal Tract, Second Edition, Raven Press,New York, 1987; pp 507 ± 553.
19 De Groat WC, Krier J. The sacral parasympathetic re¯expathway regulating colonic motility and defecation in thecat. J Physiol (Lond) 1978; 276: 481 ± 500.
20 Fukuda H, Fukai K, Yamane M, Okada H. Pontinereticular unit responses to pelvic nerve and colonicmechanical stimulation in the dog. Brain Res 1981; 207:9 ± 71.
21 De Groat WC, Booth AM, Milne RJ, Roppolo JR.Parasympathetic preganglionic neurons in the sacralspinal cord. J Auton Nerv Syst 1982; 5: 23 ± 43.
22 De Groat WC, Krier J. The central control of the lumbarsympathetic pathway to the large intestine of the cat. JPhysiol (Lond) 1979; 289: 449 ± 468.
23 Julie Y, Szurszewski JH. Electrophysiology of neuronesof the inferior mesenteric ganglion of the cat. J Physiol(Lond) 1983; 344: 277 ± 292.
24 Pedersen E. Regulation of bladder and colon-rectum inpatients with spinal lesions. J Auton Nerv Syst 1983; 7:329 ± 338.
25 Dalsgaard CJ et al. Origin of peptide-containing ®bres inthe inferior mesenteric ganglion of the guinea-pig:Immunohistochemical studies with antisera to SP,enkephalin, VIP, cholecystokinin and bombesin. Neu-roscience 1983; 9: 191 ± 211.
26 Dun NJ. ``Peptide hormones and transmission insympathetic ganglia.'' In: Elfvin LG (ed). AutonomicGanglia. John Wiley, Chichester, 1983; 345 ± 366.
27 Silko� P et al. E�ect of substance P on rat gastro-intestinal transit. Dig Dis Sci 1988; 33: 74 ± 77.
28 Garrett JR, Howard ER, Jones W. The internal analsphincter in the cat: A study of nervous mechanismsa�ecting anal tone and re¯ex activity. J Physiol (Lond)1974; 243: 153 ± 166.
Bowel dysfunctionAC Lynch et al
202
Spinal Cord
29 Cosman BC, Stone JM, Perkash I. ``The GastrointestinalSystem.'' In Whiteneck GG, Charlifue SW, Gerhart KA,Lammertse DP, Manley S, Menter RR, Seedro� KR(eds). Ageing with Spinal Cord Injury, Demos Publica-tions, New York, 1993; 117 ± 127.
30 Devroede G et al. Traumatic constipation. Gastroenter-ology 1979; 77: 1258 ± 1267.
31 Rajendra SK et al. Gastrointestinal transit after spinalcord injury: E�ect of Cisapride. Am J Gastroenterol 1992;87: 1614 ± 1617.
32 Keshavarzian A et al. Delayed colonic transit in spinalcord-injured patients measured by Indium-111 amberlitescintigraphy. Am J Gastroenterol 1995; 90: 1295 ± 1300.
33 Nino-Murcia M, Stone JM, Chang PJ, Perkash I. Colonictransit in spinal cord-injured patients. Invest Radiol 1990;25: 109 ± 112.
34 Meshkinpour H, Nowroozi F, Glick ME. Coloniccompliance in patients with spinal cord injury. ArchPhys Med Rehabil 1983; 64: 111 ± 112.
35 Glick ME et al. Colonic dysfunction in patients withthoracic spinal cord injury. Gastroenterology 1984; 86:287 ± 294.
36 Aaronson MJ, Freed MM, Burako� R. Colonic myo-electric activity in persons with spinal cord injury. DigDis Sci 1985; 30: 295 ± 300.
37 Gillis RA et al. Inhibitory control of proximal colonicmotility by the sympathetic nervous system. Am J Physiol1987; 253: G531 ±G539.
38 Rostad H. Colonic motility in the cat. II. Extrinsicnervous control. Acta Physiol Scand 1973; 89: 91 ± 103.
39 Pickard LR, Santoro S, Wyllie RG, Haller JA.Histochemical studies of experimental fetal intestinalobstruction. J Pediatr Surg 1981; 16: 256 ± 260.
40 Moore SW, Laing D, Melis J, Cywes S. Secondary e�ectsof prolonged intestinal obstruction on the entericnervous system in the rat. J Pediatr Surg 1993; 28:1196 ± 1199.
41 Prommegger R et al. Obstructive ileus of the large bowelis associated with low tissue levels of neuropeptides inprestenotic bowel segment. Dig Dis Sci 1997; 42: 1513 ±1518.
42 Ferri G-L et al. Tissue localisation and relativedistribution of regulatory peptides in separated layersfrom the human bowel. Gastroenterology 1983; 84: 777 ±786.
43 Scheurer U, Drack E, Halter F. Substance P activates ratcolonic motility via excitatory and inhibitory neuralpathways and direct action on muscles. J Pharmacol ExpTher 1994; 271: 7 ± 13.
44 Goldin E, Karmeli F, Selinger Z, Rachmilewitz D.Colonic substance P levels are increased in ulcerativecolitis and decreased in chronic severe constipation. DigDis Sci 1989; 34: 754 ± 757.
45 Lysy J, Karmeli F, Goldin E. Substance P levels in therectal mucosa of diabetic patients with normal bowelfunction and constipation. Scand J Gastroenterol 1993;28: 49 ± 52.
46 Lysy J, Karmeli F, Sestieri M, Yatzkan Y, Goldin E.Decreased substance P content in the rectal mucosa ofdiabetics with diarrhoea and constipation. Metabolism1997; 46: 730 ± 734.
47 Sjolund K et al. Neuropeptides in idiopathic chronicconstipation (slow transit constipation). Neurogastroen-terol Motil 1997; 9: 143 ± 150.
48 Hutson JM et al. De®ciency of substance p-immunor-eactive nerve ®bres in children with intractable constipa-tion: A form of intestinal neuronal dysplasia. J PaediatrChild Health 1997; 33: 187 ± 189.
49 Hutson JM, Chow CW, Borg J. Intractable constipationwith a decrease in substance P-immunoreactive ®bres: Isit a variation of Intestinal Neuronal Dysplasia? J PediatrSurg 1996; 31: 580 ± 583.
50 Kobayashi H, Hirakawa H, Puri P. Is IntestinalNeuronal Dysplasia a disorder of the neuromuscularjunction. J Pediatr Surg 1996; 4: 575 ± 579.
51 Lynch AC, Anthony A, Dobbs BR, Frizelle FA. ColonicNeurotransmitters Following Spinal Cord Injury. Tech-niques in Coloproctology 2000; 4: 93 ± 97.
52 Lynch AC, Anthony A, Dobbs BR, Frizelle FA.Anorectal physiology following spinal cord injury.Spinal Cord 2000; 38: 573 ± 580.
53 Frizelle FA, Dominguez JM, McCall JL, Santoro GA.Surgical Treatment of Constipation. Int J Surg Sci 1995;2: 100 ± 106.
54 Wysowski DK, Bacsanyi J. Cisapride and fatal arrhyth-mia. N Engl J Med 1996; 335: 290 ± 291.
55 MacDonagh RP et al. Control of defecation in patientswith spinal injuries by stimulation of sacral anteriornerve roots. Br Med J 1990; 300: 1494 ± 1497.
56 Chia YW et al. Microchip implants on the anterior sacralroots in patients with spinal trauma: Does it improvebowel function? Dis Colon Rectum 1996; 39: 690 ± 694.
57 Frizelle FA et al. Does Colostomy Alter Quality of Life inPatients with Spinal Cord Injury? A Controlled Trial.Aust NZ J Surg 2000; 70: A62.
58 Malone PS, Ransley PG, Kiely EM. Preliminary reporton the antegrade continence enema. Lancet 1990; 336:1217 ± 1218.
59 Gri�ths DM, Malone PS. The Malone Antegradecontinence enema. J Pediatr Surg 1995; 30: 68 ± 71.
60 Squire R et al. The clinical application of the Maloneantegrade colonic enema. J Pediatr Surg 1993; 28: 1012 ±1015.
61 Kajbafzedeh AM et al. A review of 100 Mitrofano�stomas and report of the VQZ technique for theprevention of complications at stoma level. PresentationESPU 6th Annual Meeting, Toledo, April 1995.
62 Webb HW, Barraza MA, Crump J. Laparoscopicappendicostomy for management of fecal incontinence.J Pediatr Surg 1997; 32: 457 ± 458.
63 Robertson RW, Lynch AC, Beasley SW, Morreau PN.Early Experience with the Laparoscopic ACE Procedure.Aust NZ J Surg 1999; 69: 308 ± 310.
64 Hill J, Stott S, MacLennan I. Antegrade enemas for thetreatment of severe idiopathic constipation. Br J Surg1994; 81: 1490 ± 1491.
65 Wing NA et al. Does Anorectal manometry predictclinical outcome after laparoscopic procedures inchildren with spina-bi®da. Colorectal Disease (In press).
Bowel dysfunctionAC Lynch et al
203
Spinal Cord