
Postpartum Spinal Cord, Root, Plexus and Peripheral Nerve ...
The Biopsychosocial Experience of Chronic Neuropathic Pain after Spinal Cord Injury: An Interpretative Phenomenological AnalysisJasmine Hearn
•Jasmine HearnDPhil Psychology (Research) StudentUniversity of [email protected]
•Dr Katherine FinlayLecturer in Psychology, Health PsychologistUniversity of Buckingham
•Dr Philip FineSenior Lecturer in PsychologyUniversity of Buckingham
•Dr Imogen CotterClinical PsychologistNational Spinal Injuries Centre
Background•Neuropathic pain arises from nerve damage.•Over 60% of those with a spinal cord injury (SCI) suffer with chronic neuropathic pain (Kennedy et al, 1997; Modirian et al, 2010; Ulrich et al, 2007).
•This pain is debilitating, persistent over time, and resistant to treatment (Modirian et al, 2010; Siddall et al, 2003; Warms et al, 2002).
•Pain reduces quality of life (Donnelly & Eng, 2005), and increases risk of depression and anxiety (Nicholson Perry et al, 2009).
•Pain management programmes developed for general chronic pain populations deliver limited effectiveness for SCI patients (Nicholson Perry et al, 2009).
Current State of the Literature Base•Accepted view of pain from biopsychosocial model.
•Majority of neuropathic pain in SCI research is quantitative.
•Lack of understanding of the lived experience.
•Is there an aspect that isn’t being studied and treated?
This Study•Aim▫To understand the experience of chronic neuropathic pain after SCI from a patient perspective, using a qualitative methodology.
•Design▫Qualitative, single interview study
•Analysis▫Interpretative Phenomenological Analysis (IPA)

Method•Participants▫8 outpatient participants were included in the analysis▫All had diagnosed neuropathic pain as a result of SCI
•Interviews▫Semi-structured, open-ended questions▫Audio recorded▫At time, day and location most convenient for the participants.
•Ethics▫NHS REC Ref: 13/LO/0558▫R&D▫The University of Buckingham School of Science Ethics Committee▫National Spinal Injuries Centre, Stoke Mandeville Hospital, UK
Interview Questions• Tell me about your experience of pain since your spinal cord injury.
• Describe your pain.▫ How long have you had it? How does it feel?
• Tell me about your pain at its best.• Tell me about your pain at its worst.▫ How often is it best/worst? ▫ How often does it present itself?
• How does your pain affect you physically?• How does your pain affect you psychologically?
• How do you deal with your pain?▫ Coping strategies?
• How does the pain affect your everyday life and relationships?
Analysis•Interpretative Phenomenological Analysis (IPA, Smith, 1996)▫Relatively new method of qualitative analysis
▫Uses broad, open questions about the lived experience
▫Themes emerge from data to identify most important aspects of an experience
The Contributions of IPA•Open to flexibility▫Not limited to rigidly defined variables
•Openness•Rich, deep knowledge and meaning that contribute to the understanding of an individual and group phenomena
•Attempts to avoid pre-judgement•Explore new areas •Generate ideas, theories▫Theoretical generalisability
Results•3 Superordinate Themes:▫The Chasm Between Biomedical Perspectives and Patient Beliefs and Needs
▫The Battle for Ultimate Agency of Life
▫The Coexistence of Social Cohesion and Social Alienation
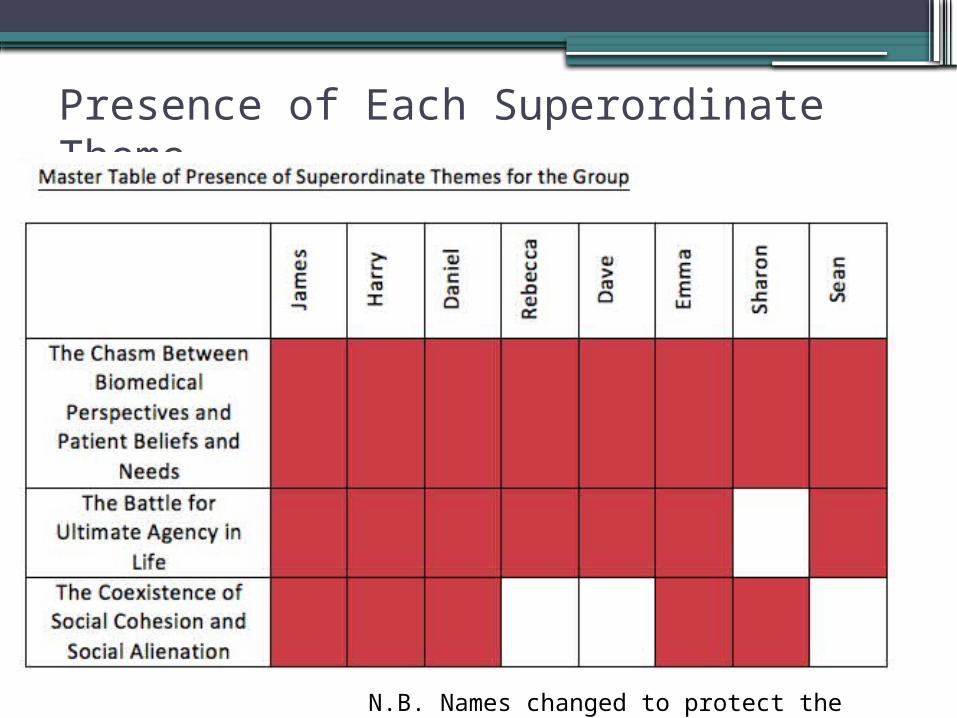
Presence of Each Superordinate Theme
N.B. Names changed to protect the patients’ identity
Superordinate Theme Breakdown•The Chasm Between Biomedical and Patient Beliefs and Needs ▫Excessive Reliance on Insufficient Medication ▫Relationships with HCPs: Losing Faith▫Lack of Input into own Care
•The Battle for Ultimate Agency in Life▫Pain is Winning▫I am Winning
•The Coexistence of Social Cohesion and Social Alienation▫SCI Population are United but Alone in Experience
▫Painful Self as an Affliction on Able-Bodied

The Chasm Between Biomedical and Patient Beliefs and Needs •Excessive Reliance on Insufficient Medication ▫… all these kinds of drugs, but, I’ve tried them, and I’ve
rejected them. Because it makes no difference whether I have them and I’m not prepared to take high doses constantly, and be a zombie, and I’d rather put up with a bit of pain than take those drugs and have a blank mind. Because that’s how they make you feel. It’s like your thoughts are trying to fight their way through a thick lump of fog.
▫Harry: page 6, lines 135-139
The Chasm Between Biomedical and Patient Beliefs and Needs •Relationships with HCPs: Losing Faith
▫ Like I’ve said to my doctors … it’s taken this long to get an appointment sorted out. As soon as I went to [local hospital] they were like couldn’t believe that I wasn’t with a pain team … they said “your doctor should have done it”. But my doctor said to ring them, when I said “I haven’t got a number”, he looked at a bit of paper and said “well I haven’t got the number either”. So I was like, alright well that’s a load of good then.
▫Daniel: page 18, lines 427-432
The Chasm Between Biomedical and Patient Beliefs and Needs •Lack of Input into own Care▫ I felt I went to my GP and I felt so frustrated that
my whole life was being judged by someone else in order to say “no well we know better than you”. As much as it’s my [said with emphasis] experience, it’s my pain, I’m telling you my experience, you don’t seem to be listening because you’re not giving me what works for me.
▫Emma: page 21, lines 492-496

The Battle for Ultimate Agency of Life•Pain is Winning• Just like horrible and low. I feel depressed …
Because there’s no little light at the end any more, it’s just like a big black hole. Because it it, it’s it’s just like [. .] it’s never going to end.
▫Daniel: page 15, lines 348-350
The Battle for Ultimate Agency in Life•I am Winning• … it [pain] hasn’t held me back so far … just like
carrying around another bag I suppose. Don’t think about it ... something I can deal with that I’m not too fussed about, you know, doesn’t get in the way … I can’t see it holding me back at all really.
▫Sean: page 13, lines 301-305
The Coexistence of Social Cohesion and Social Alienation•SCI Population are United but Alone in Experience▫ I think being around people in wheelchairs more
might give me … [unfinished sentence] I’m looking forward to that … that’s why they call [specialised spinal unit] bubble world, because everyone’s the same, you don’t feel like an outcast, do you know what I mean?
▫Daniel: page 20, lines 480-482

The Coexistence of Social Cohesion and Social Alienation•Painful Self as an Affliction on Able-Bodied▫… my wife, she retreats into her shell when I’m in agony, she’s
seen it so many times [. . .] and because it impacts on her so much, she could even … enter a sort of phase of to get on with it you know. “For God’s sakes”, you know? Become irritable with me …
▫Harry: page 14, lines 319-322▫… it makes me feel as if my pain is responsible for her emotional
pain … it makes me feel uncomfortable … because she loves me she doesn’t want me to be so distressed and knowing that I am distressed with all the pain and there’s nothing she can do.
▫Harry: page 14, lines 328-332
Discussion•Confirms of biopsychosocial model in experience of SCI-neuropathic pain. •Identifying discrepancies between support currently offered and the support that patients want/need:▫HCPs should offer more than just medication.▫Need to teach SCI patients how to regain control over their lives.▫Support for pain education for able-bodied family and friends.
•Knowing which aspects of the pain experience influence an outpatient’s well-being. •Enhanced outpatient support from healthcare professionals.
Next Steps•Questions:▫Are these experiences specific to outpatients? ▫How do inpatients experience neuropathic pain?
•Inpatient Phase (Ethics approved)▫Match current study for comparison▫Potential to map the ‘journey’ of pain from inpatient to outpatient.
▫Does pain change from in- to outpatient?
•Room for future research:▫Why is medication ineffective? ▫Interventions for teaching life control and acceptance.▫Potential for mindfulness interventions.▫How does pain education for friends and family affect outcomes?

References• Cardenas, D. D., Turner, J. A., Warms, C. A., & Marshall, H. M. (2002).
Classification of chronic pain associated with spinal cord injuries. Archives of Physical Medicine and Rehabilitation. 83(12), pp. 1708-1714.
• Donnelly, C., & Eng, J. J. (2005). Pain following spinal cord injury: the impact on community reintegration. Spinal Cord. 43(5) pp. 278-282.
• Kennedy, P., Frankel, H., Gardner, B., & Nuseibeh, I. (1997). Factors associated with acute and chronic pain following traumatic spinal cord injuries. Spinal Cord. 35 pp. 814-817.
• Modirian E., Pirouzi P., Soroush M., Karbalaei-Esmaeili S., Shojaei H., & Zamani H. (2010). Chronic pain after spinal cord injury:results of a long-term study. Pain Medicine. 11(7) pp. 1037-1043.
• Perry, K. N., Nicholas, M. K., & Middleton, J. (2009). Spinal cord injury-related pain in rehabilitation: A cross-sectional study of relationships with cognitions, mood and physical function. European Journal of Pain. 13(5) pp. 511-517.
• Siddall, P. J., McClelland, J. M., Rutkowski, S. B., & Cousins, M. J. (2003). A longitudinal study of the prevalence and characteristics of pain in the first 5 years following spinal cord injury. Pain. 103 pp. 249-257.
• Smith, J. A. (1996). “Beyond the divide between cognition and discourse: Using interpretative phenomenological analysis in health psychology”. Psychology and Health, 11, pp. 261-271.
• Ullrich, P., Jensen, M., Loeser, J., & Cardenas, D. (2007). Catastrophising mediates associations between pain severity, psychological distress, and functional disability among persons with spinal cord injury. RehabilitationPsychology, 52, (4), pp. 390-398
• Warms, C. A., Turner, J. A., Marshall, H. M., & Cardenas, D. D. (2002). Treatments for chronic pain associated with spinal cord injuries: Many are tried, few are helpful. Clinical Journal of Pain. 18, pp. 154.
• Werhagen, L., Budh, C. N., Hultling, C., & Molander,. C. (2004). Neuropathic pain after traumatic spinal cord injury – relations to gender, spinal level, completeness, and age at the time of injury. Spinal Cord. 42, pp. 665-673.
Thank you!•Attendance and presentation at the ASCIP Conference has been supported and funded by The University of Buckingham.
Copyright © 2022 FDOKUMEN




















