
Planmeca Ultra Low Dose - cimm-icmm.org
84
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Planmeca Ultra Low Dose - cimm-icmm.org

Planmeca Ultra Low Dose™
High image quality at a low dose
•Acquire a maxillofacial CBCT image at a
lower dose than panoramic imaging
•An average dose reduction of 77%
See scientific evidence on the effect
of Low Dose imaging!
www.planmeca.com/uld-poster
Planmeca ProMax® 3D
Planmeca Oy Asentajankatu 6, 00880 Helsinki, Finland Tel. +358 20 7795 500, fax +358 20 7795 555, [email protected]
Find more info and your local dealer www.planmeca.com

International Review of the
ARMED FORCES MEDICAL SERVICESInternational Review of the
ARMED FORCES MEDICAL SERVICESRevue Internationale des Services de Santé des Forces Armées
ww
w.c
imm
-icm
m.o
rg
EDITION / REDACTION
Director / DirecteurMaj. Gen. (ret.) R. VAN HOOF (MD)[email protected]
Editor-in-Chief / Rédacteur en chefMaj. Gen. Prof. (ret.) M. MORILLON (MD)[email protected]
Assistant Chief-Editor / Rédacteur en chef adjointCol. Prof. X. DEPARIS (MD)[email protected]
Secretary of the Editorial BoardSecrétaire du Comité de rédactionAdjt. Maj. I. [email protected]
Editor’s office / Bureau de la rédactionInternational Committee of Military MedicineComité International de Médecine MilitaireHôpital Militaire Reine AstridBE-1120 Brussels (Belgium)& : +32 2264 43 48 - 6 : +32 2264 43 [email protected]
ADVERTISING / PUBLICITÉ
Négociations & Editions Publicitaires13, rue Portefoin - FR-75003 Paris (France)& : +33 1 40278888 - 6 : +33 1 [email protected]
SCIENTIFIC COMMITTEE / COMITÉ SCIENTIFIQUE
Brig. Gen. J. ALSINA (MD)(Spain / Espagne)
Col. Prof. H. BAER (MD)(Switzerland / Suisse)
Col. JJ BRAU (Dent.)(France / France)
Col. T. S. GONZALES (Dent.)(U.S.A. / Etats-Unis)
Maj. Gen. KHALID A. ABU-AZAMAH AL-SAEDI (MD)(Saudi Arabia / Arabie Saoudite)
Col. I. KHOLIKOV (MC)(Russian Federation / Fédération de Russie)
Sen. Col. Dr C. M. LOMMER (Pharm.)(Germany / Allemagne)
Maj. V. ROUS (Vet.)(France / France)
Col. P. VAN DER MERWE (Vet.)(South Africa / Afrique du Sud)
Sen. Col. Prof. L. ZHANG(China / Chine)
VOL.82/1
3International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
Official organ of theInternational Committee of Military Medicine
Organe officiel duComité International de Médecine Militaire
VOL.89/1
01-Sommaire.qxp_Mise en page 1 16/03/2016 14:43 Page1
Planmeca Ultra Low Dose™
High image quality at a low dose
•Acquire a maxillofacial CBCT image at a
lower dose than panoramic imaging
•An average dose reduction of 77%
See scientific evidence on the effect
of Low Dose imaging!
www.planmeca.com/uld-poster
Planmeca ProMax® 3D
Planmeca Oy Asentajankatu 6, 00880 Helsinki, Finland Tel. +358 20 7795 500, fax +358 20 7795 555, [email protected]
Find more info and your local dealer www.planmeca.com
International Review of the
ARMED FORCES MEDICAL SERVICESInternational Review of the
ARMED FORCES MEDICAL SERVICESRevue Internationale des Services de Santé des Forces Armées
ww
w.c
imm
-icm
m.o
rg
EDITION / REDACTION
Director / DirecteurMaj. Gen. (ret.) R. VAN HOOF (MD)[email protected]
Editor-in-Chief / Rédacteur en chefMaj. Gen. Prof. (ret.) M. MORILLON (MD)[email protected]
Assistant Chief-Editor / Rédacteur en chef adjointCol. Prof. X. DEPARIS (MD)[email protected]
Secretary of the Editorial BoardSecrétaire du Comité de rédactionAdjt. Maj. I. [email protected]
Editor’s office / Bureau de la rédactionInternational Committee of Military MedicineComité International de Médecine MilitaireHôpital Militaire Reine AstridBE-1120 Brussels (Belgium)& : +32 2264 43 48 - 6 : +32 2264 43 [email protected]
ADVERTISING / PUBLICITÉ
Négociations & Editions Publicitaires13, rue Portefoin - FR-75003 Paris (France)& : +33 1 40278888 - 6 : +33 1 [email protected]
SCIENTIFIC COMMITTEE / COMITÉ SCIENTIFIQUE
Brig. Gen. J. ALSINA (MD)(Spain / Espagne)
Col. Prof. H. BAER (MD)(Switzerland / Suisse)
Col. JJ BRAU (Dent.)(France / France)
Col. T. S. GONZALES (Dent.)(U.S.A. / Etats-Unis)
Maj. Gen. KHALID A. ABU-AZAMAH AL-SAEDI (MD)(Saudi Arabia / Arabie Saoudite)
Col. I. KHOLIKOV (MC)(Russian Federation / Fédération de Russie)
Sen. Col. Dr C. M. LOMMER (Pharm.)(Germany / Allemagne)
Maj. V. ROUS (Vet.)(France / France)
Col. P. VAN DER MERWE (Vet.)(South Africa / Afrique du Sud)
Sen. Col. Prof. L. ZHANG(China / Chine)
VOL.82/1
3International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
Official organ of theInternational Committee of Military Medicine
Organe officiel duComité International de Médecine Militaire
VOL.89/1
01-Sommaire.qxp_Mise en page 1 16/03/2016 14:43 Page1

CONTENTS Sommaire
CONTENTSSommaire
Equipement médicaux du personnel santé enopérations : du besoin à la satisfaction du besoin.Par P. FAVARO, B. CONTE et R. LE BARS. France
Individual Psychological Debriefing does notPrevent Post-Traumatic Stress Disorder: a ProspectiveComparative Study.By A. OUMAYA, M.W. KRIR, C. BEN CHEIKH, Y. GUETARI,H. ELKEFI and S. EDHIF. Tunisia
A New Reality: Critical Skills Retention andReadiness for Military Trauma Surgery.By J. L. ANTEVIL, J. A. BAILEY, M. W. BOWYER, E. M. RITTERand E. A. ELSTER. U.S.A.
Application Features for External andSequential Osteosynthesis in Patients with GunshotFractures of Long-Bones of the Extremities.By V.V. KHOMINETS, V.M. SHAPOVALOV, S.V. MIKHAILOV,D.A. SHAKUN, A.V. SHCHUKIN, M.V. TKACHENKO andA.L. KUDIASHEV. Russian Federation
Infectious Diseases after Floods in AsianCountries: A Literature Review.By Y. JUNG, M. LEE and M. KIM. Republic of Korea
53
50
63
42
73
ORIGINAL ARTICLES / ARTICLES ORIGINAUX
Are Military Hospitals Prepared to Deal with CBRNCasualties in Urban Environment?By I. GALATAS. Greece
Aerodontalgia Case Series: Dental Complications Causedby Changes in Air Pressure.By K. KISMANTO. Indonesia
Activité dentaire de l’hôpital militaire togolais deniveau 2 déployé au Mali dans le cadre de missions desNations Unis.Par K.M. BOUASSALO, S. ADAM, H.D. SAMA, B.E. KEBINA,H. BISSA et M. GUNEPIN. Togo
Multiple Casualties: Regulation of a Non-SaturatedMass Casualties by French Medical Teams during SANGARISOperation in Centrafrican Republic.By L. AIGLE, C. GAILLARD, G. DOUILLARD, D. SCHLIENGER,O. BRUNEAU, F. THIEN and V. BEYLOT. France
Assessment of Medical Relief Capability for MassCasualty Events in ChinaBy Z. ZONG, S. CHEN, Q. BAO, Q. HAO, D. LIU, H. LIU, L. ZHANG,Y. SHEN and J. HUANG. China
5
11
16
25
34
Views and opinions expressed in this Review are those of the authorsand imply no relationship to author’s official authorities policy, presentor future.
Les idées et opinions exprimées dans cette Revue sont celles des auteurs etne reflètent pas nécessairement la politique officielle, présente ou futuredes autorités dont relèvent les auteurs.
VOL.89/1
4International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
Photo on the cover: Multiple Casualties: Regulation of a Non-Saturated Mass Casualties by French Medical Teams during SANGARIS Operation inCentrafrican Republic. - by Luc AIGLE.
01-Sommaire.qxp_Mise en page 1 18/03/2016 12:38 Page2

By I. GALATAS. Greece
Ioannis GALATAS
Are Military Hospitals Prepared to Deal with CBRNCasualties in Urban Environment?*
Brigadier General (ret’d) Ioannis GALATAS, MD, MA (Army MC), is a retiredmilitary physician with 35 years military industry experience. His is specialized
in Allergy and Clinical Immunology (Board certified) and for more than twodecades he served as Head of the Department of Allergy & Clinical Immunology at
Army General Hospital of Athens, Greece.Since 2001 he has been involved in CBRNE operations as planner and instructor trained (including liveagent training) in a number of countries abroad. His main passion is «Hospitals’ CBRN Defense &Preparedness in Megapolis Environment», «CBRNE Design/Hardening of Critical Infrastructure» [airports,shopping malls, hotels etc] and «CBRN Forensics & Management of Contaminated Corps». During the 2004Athens’ Olympic Games, he served as Commandant of the Olympic Hospital CBRN Response Unit – the onlyhospital-based specialized unit (70 people) deployed for the Olympic & Paralympic Games.He holds a M.A. degree (with merits) on «International Terrorism, Organized Crime and Global Security»from Coventry University, UK (2010) and he is a PhD candidate since May 2012 (Athens MedicalSchool/Dept of Forensics & Toxicology).His last appointment (as of August 2010), was as Head of the Department of Asymmetric Threats at theIntelligence Analysis Branch, Joint Military Intelligence Service of the Hellenic National Defense GeneralStaff in Athens, Greece.After retirement he conducted CBRNE classes for Abu Dhabi Police Authority and continues to participateas invited speaker in many CBRNE/security conferences, congresses and workshops around the globe.Currently he is the Editor-in-Chief of the monthly on-line «CBRNE Terrorism Newsletter» (www.cbrne-terrorism-news-letter.com) initiated in November 2005 and delivered freely to CBRNE-CT First Responders of more than 80countries around the globe. He is also a CBRNE Research Associate at «Center for Security Studies»(KEMEA), Athens, Greece (under the Ministry of Public Order & Civil Protection) and a Research Associateat National Nuclear Research Center «Demokritos». As of January 2015, he is member of Didactical Bardof University of Rome «Tor Vergata» delivering classes for their «International CBRNe Masters» programs.
5International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Les hôpitaux militaires sont-ils préparés à prendre en charge des victimes d’événements NRBC en milieuurbain ?
En dépit du fait que, 14 ans après l’effroi causé par les lettres à l’anthrax aux Etats-Unis et 19 ans après l’attaque au sarin dans lemétro de Tokyo, aucune autre attaque NRBC n’ait été observée en milieu urbain, il reste toujours probable qu’un tel incident sur-vienne demain ! Dans une telle situation, ce seraient les hôpitaux qui auraient à faire face à un probable afflux massif de victimes.Les hôpitaux sont-ils prêts à faire face à un scénario aussi préoccupant ? A l’exception de quelques pays à travers le monde, la plupartne sont pas prêts à faire face à ce problème spécifique. Cet article développe quelques idées mais la défense NRBC et l’entraînementdes équipes hospitalières demande une approche multi-disciplinaire, du dévouement et de la continuité pour être applicable et durable.
VOL.89/1
KEYWORDS: Hospitals, Military, CBRN, Preparedness, Urban.MOTS-CLÉS : Hôpitaux, Militaire, NRBC, Préparation, Plan.
The question posed in the title of this article is easy toanswer in a generic way: "No! Hospitals are not pre-pared to deal with CBRN casualties". Both state andmilitary hospitals are not prepared for such extreme
emergencies and it is interesting to investigate whyand what can be done to fortify hospitals' defensesjust in case a real asymmetric incident evolves in urbanenvironment.
CBRNE_GALATAS.qxp_Mise en page 1 16/03/2016 15:20 Page1
WHY WE ARE NOT PREPARED?
The easy answer might be cost and budget. We live intodifficult financial times and money allocated to hospi-tals aim to cover functional needs and daily consuma-bles and services. The hidden answer is the inherentbelief that "it will never happen to us" or that "eventerrorists will not use weapons of mass destructionagainst other human beings". This attitude is based onthe fact that besides the 1995 Tokyo subway sarin inci-dent, the 2001 anthrax letters' scare and threeOlympiads' apart (2004-2008-2012) there was no rele-vant urban release of CBRN agents in the last 20 yearsworldwide. Putting the above two together one has asolid attitude against spending money for a situationthat almost does not exist.
But is this a good excuse to claim in public if such anincidence happens one day somewhere in the world?Surely it is not! And this is the main reason why shouldall hospitals be prepared for the unexpected thatunfortunately almost always happens.
WHAT COSTS MONEY AND WHAT DOES NOT?
This article will address these two categories in aneffort to put down to earth the needs of what shouldbe done and how to do it in order to achieve a baseline CBRN hospital defense:
1. Perimeter fencing
In modern hospital design the outdoor environment isusually composed by vast gardens and green spaces thatsoothe the sick and support their fast recovery. But howcan the hospital control the incoming contaminated flowof victims rushing to the nearest hospital without a solidhard fence and a strong gate? Ground floor has tens ofdoors and windows that can provide entry to hospital ifunguarded, unlock or easy to brake by frustrated incomersin need. Their uncontrolled entry will lead to overall hos-pital’s contamination and make things worse. Conclusion:hard perimeter fence; main gate; secure/locked grounddoors and windows are mandatory precautions to pre-serve hospital’s integrity and working personnel’s safety.Addition of a fence is costly and hardening of doors andwindows with special films might be expensive as well.Most military hospitals are considered military camps anddo have perimeter fence and main gate with a post.
2. Security personnel
All hospitals have them and they are very important forthe daily function of the hospital (incoming vehiclesand visitors, wards' security, following the visitinghours' program, etc.). But can the hospital count onthem for controlling the incoming flow of contamina-ted victims without specialized training, specializedequipment and hands-on experience? Surely not! Mostprobably they will either lock themselves inside hospi-tal or leave premises. Situation might be better in themilitary hospitals but even there training and equip-ment needs to be available and know how to use them.Specialized equipment and training cost money.
3. Planning
Plan is nothing; planning is everything! In that respecthospital needs to have a small, flexible, realistic, upda-ted and anthropocentric plan readily available to allthose involved. Planners' worldwide need to answer avery simple question: "What would be my reaction, if Iwas involved in a real CBRN incident?" Planners' shouldplan based on what people will actually do; not onideal responses and academic expectations that usuallyhave no place in actual mass emergency situations.Thus the anthropocentric (from Greek: anthropos[man] + kentro [center]) element should be prominentand the most important pylon in planning process.Plans do not cost a lot but require a lot of brain workand hands-on operational experience!
4. Exercises and drills
The best way to test plans and preparedness is byconducting exercises and drills. Although all know thisis true we either do not do it or do it wrong! One bigCBRN drill every two years equals nothing! One pre-scheduled drill is best for policy reasons but operatio-nally equals nothing as well! Because in real life an inci-dent will happen right here, right now! Usually badthings happen during off-working hours, vacations andholidays or weekends or during the night. In that res-pect exercises and drills within the hospital or withneighboring hospitals both at local and national levelsshould take these elements into account in order togenerate drills that will stimulate personnel and simu-late reality as close as possible. Exercises and drills donot stop at the entrance of the hospital or when casual-ties are safe inside ambulances. Ask your ambulancecrews to proceed to the nearest hospital and delivertheir casualties to the Emergency Department (ED)without a notice. This might change your preparednessmindset completely. Continuous acclimatization to per-sonal protective equipment (PPE) is mandatory andshould be included in each department’s routine activi-ties. Wearing PPE once or twice a year, it is like the firsttime!
5. Hospital’s personnel
This is the key player in all response plans. Withoutthem no plan is effective or applicable. All should beinvolved at various levels of engagement. All should beeducated and trained depending on their speciality andduties assigned with special emphasis to ED’s personnelbut also to certain medical specialities closely related toCBRN agents. If they are not very enthusiastic abouttheir involvement, speak with them to dig out why andimprovise ways to motivate them. CBRN medicine iskind of a medical speciality requiring a lot of studying,
6International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
Correspondence:Brigadier General Dr. Ioannis GALATAS, MA, MC, MD, PhDCenter of Securities Studies KEMEA4, P. Kanellopoulou StreetGR-101 77 AthensGreeceE-mail: [email protected]
* Presented at the 41st ICMM World Congress on Military Medicine,Bali, Indonesia, 17-22 May 2015.
VOL.89/1
CBRNE_GALATAS.qxp_Mise en page 1 16/03/2016 15:20 Page2

training in difficult environments, performing dutieswhile wearing uncomfortable PPE compromisingsenses and dexterities – and all that for what? Just foran incident once in a life time; if ever? At the sametime, they have to face their daily emergencies, to takecare of their patients, to improvise based on their deepmedical knowledge and lots more. On top of these, weask them to add another speciality as described above?These are only few of the questions and doubts posedto and by medical personnel. Think of intelligentapproaches for intelligent people, fight their fearsgenerated by ignorance and infuse interest throughmodern educational methodologies – you might besurprised by their reactions and change of overall atti-tude. If we ever manage to introduce "CBRNEMedicine" into the curricula of the medical and nursinguniversity schools this would be the first step towardsbetter educated future front-line health professionalsthat one day might confront with the real enemy. Andthis does not cost a lot!
6. Infrastructure
a. Decontamination facilities look expensive but arethey? Depending on the hospital’s budget and strate-gic mission there are many commercial solutions avai-lable in two forms: deployable and fixed. The firstchoice is usually a trailer containing deflated tents andrelated decontamination equipment. The later is aseparate/adjacent infrastructure (usually one or tworooms) that serves the purpose. The ideal setting is tohave an ED with two separate entrances: one is lea-ding to "regular" ED for daily emergencies and theother (CBRN/HAZMAT) leading to a decontaminationstation first and then to regular ED. In case of an emer-gency – especially if the incident’s scene is in closeproximity to the hospital and response time is almostzero – hospital seals the one door, opens theCBRN/HAZMAT entrance and is ready for acceptingcontaminated casualties. All the above raise an impor-tant issue that usually is not taken into account. It ischeaper if we incorporate decontamination facilities and
capabilities during the hospital’s design phase instead ofhardening premises later on under the pressure ofchange of threat estimate. A good solution for this is toput the civil engineers/architects' community intocontact with medical/health community. Collaborationwill surely provide clever and affordable solutions. Inthe bottom line, what is the difference of a fixed ordeployable decontamination system with the showerswe have at home? Improvisation will save money andwill come up with custom-made solutions that fit speci-fic needs. Imagine placing a big number of showers onthe perimeter ground walls of your hospital; thenconnect them with the main water supply system, installa waste water collection tank underneath, add a num-ber of privacy panels and you are set to go with a frac-tion of money. Use pipes, nuzzles and hoses and you canconstruct your own decontamination systems for yourfirst responders!
If the above are still expensive for you then close colla-boration with your local fire station is a one-way solu-tion. Firemen are very good in providing "water cur-tains" (high volume/low pressure [60psi]) at no time. Butyou have to test this solution and solve the small pro-blems that come with it by working together with themand let them know what you want them to do.
Other issues of concern are the isolation rooms (withpositive/negative pressure) and radiation rooms (forinner contaminated casualties especially following adetonation of a radiological dispersion device [RDD]).
b. Existing laboratories pose a second problem. Are theyat least of BSL-2 quality? Do they have any BSL-3 capa-bilities or do you have to transfer samples to an autho-rized bio-safety lab (BSL-3 or BSL-4)? Is the reference labin the country or need to send samples abroad? Do youhave proper protocols and means for transferringhighly contagious samples? Do you have the equipmentfor fast verification of exposure to chemical warfareagents (i.e. organophosphates)?
c. Field hospitals : Hospitals can easily handle big numbersof "clean" chemical casualties. But can they equally
7International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 1: Olympic Hospital CBRNE Response Unit(Army General Hospital, Athens, Greece),
Non-ambulatory victims’ decontamination station,First Responder in Level B PPE.
Figure 2: Olympic Hospital CBRNE Response Uni(Army General Hospital, Athens, Greece),Decontamination station in a container.
CBRNE_GALATAS.qxp_Mise en page 1 16/03/2016 15:20 Page3
perform when confronting biological or radiologicalcasualties? Do you have quarantine hospitals includedin your plans? A field hospital (tents or containers) is agood solution and can be transported near to the infec-ted area fulfilling the basic rule indicating that in biolo-gical attacks we do not transfer casualties to hospitals;instead we transfer hospitals to casualties. Armed Forcesworldwide do have field hospitals for their own opera-tional purposes – are these hospitals suitable to performin a contaminated environment as well?
7. Equipment
Most of the equipment that hospital’s personnel willneed is already available and used on routine basis (e.g.IV fluids, intubation sets, suction pumps, haemostatictourniquets, consumables etc.). In addition to these,specialized items need to be purchased.
8. Specialized equipment
a. PPEs: Best choice for ED’s personnel is the powered air-purifying respirator (PAPR) ensemble that is comfortableand provides wide view helmet without restrictions onfacial hair, glasses etc. In combination with a splash proof(water resistant) suit, makes an ideal ensample serving allpurposes including decontamination procedures.
Biological threats (e.g. Ebola virus) need different PPEsfor the protection of personnel involved. So far therelated technical document produced by the EuropeanCenter for Disease Control (ECDC – October 2014) ishighly recommended1 and so is the new PPE prototypeMKVI proposed by John Hopkins University2. Sameapplies for another ECDC technical report addressingthe issue of aerial medical transportation of bio-conta-minated patients3. There are many related solutions inthe market – choose one that can be folded (to savespace) and can provide both positive and negative pres-sure inside the transportation capsule (it can be usedfor both biological and chemical/radiological agents'exposures).
Radiological casualties represent another category weshould also focus on mainly because our medical know-ledge on management issues is very limited. Even specia-lists in nuclear medicine and medical physics are not veryfamiliar with triage and management protocols in case ofmass casualties following a RDD’s detonation in urbanenvironment. An excellent source of related informationis the REMM website4 that is highly recommended forfurther exploitation and study.
b. AMBU and respirators: Since the area outside the EDis considered a "warm zone" (contaminated) it is bestto use equipment connected with gas filters (like thoseused in gas masks).
c. Field consumables: There are only three medicalinterventions that can be performed under PPE in acontaminated environment: provide auto-injectableantidotes (for nerve gases and cyanide); support respi-ration (chest seals would be beneficial in case of anexplosion) and control hemorrhage (with modern hae-mostatic sponges or gauges). Remember: it is importantto keep contaminated casualties alive until they are"clean" (decontaminated) and ready to undergo a pro-per triage at the ED where all means would be availableto support their survival.
9. Interoperability
This is the term that the military love the most but civi-lian counterparts usually forget its importance.Imagine two hospitals having two different decontami-nation systems – one has it in deflated tents and theother in a container: what will actually happen whenone hospital will be asked to support the other? Uponarrival, personnel of the first hospital will found them-selves in an unfamiliar working environment and in themiddle of havoc you do not ask questions or read theoperational manual! Imagine now that these two hos-pitals had the same field equipment: upon arrival, thenew crews will immediately start providing services byusing their "own" systems. Sounds simple and logic butthese are two qualities often forgotten or neglectedduring planning phases!
10. Morgues and contaminated corps' management
Hospitals are not equipped to handle big numbers ofcorps nor contaminated corps. In that respect you needto have solutions ready and applicable that will provideyou time for further adequate management of this pro-blem. Cemeteries might have big refrigerated roomsthat can be used; commercial refrigerated trucks can bedeployed provided that you remove the identificationmarkings from outside surfaces; ice-skating halls mightprovide more space for storing the dead as well. Thehuge morgue facility deployed within 72 hours afte r the7/7 London bombings (2005) represent a fine exampleof an holistic solution with excellent working environ-ment and consideration of many ethical issues derivedfrom the multiculturalism of the victims. Take also intoconsideration the burial processes to be used for thevarious types of CBRN contamination. This is one of the
8International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
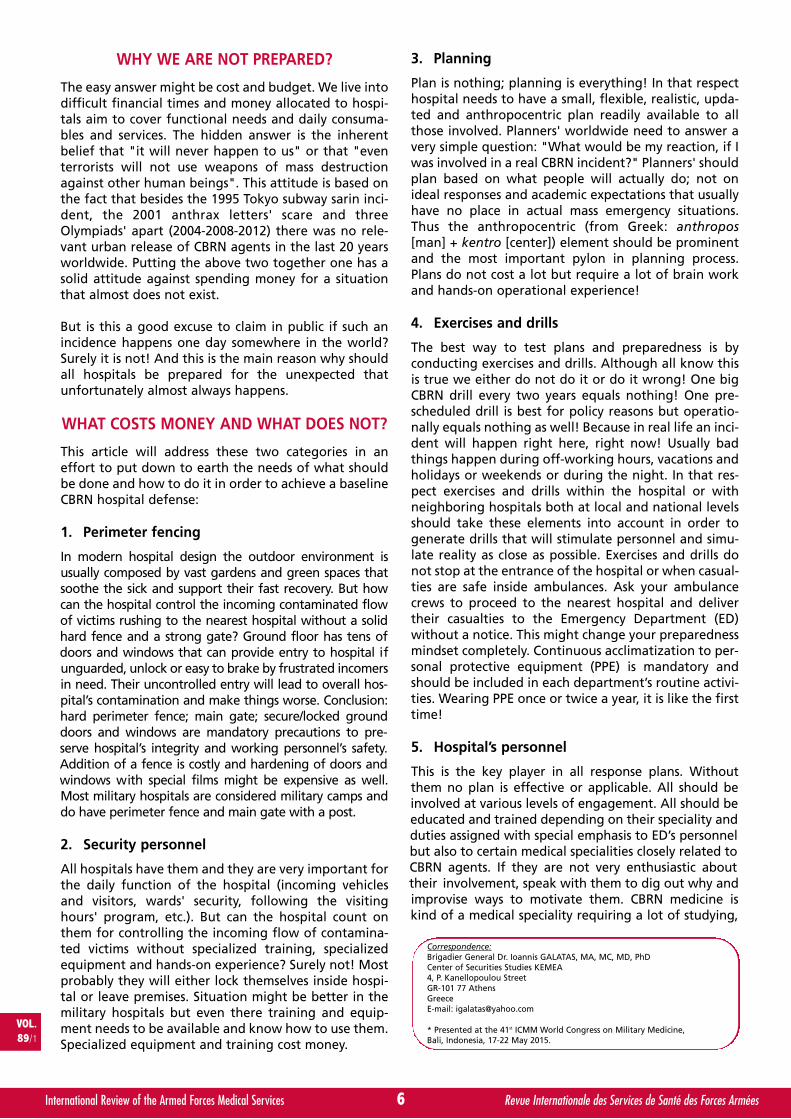
Figure 3: Olympic Hospital CBRNE Response Uni,(Army General Hospital, Athens, Greece),
Field CBRNE First Aid StationLeft: Cutter - Middle: Physician - Right: Nurse
Notice the field respirator with NBC filter (next to the physician).
CBRNE_GALATAS.qxp_Mise en page 1 16/03/2016 15:20 Page4

MightySat™ Rx Fingertip Pulse OximeterFeaturing Masimo SET® (Signal Extraction Technology®)
STG
-012
6A/C
O-0
2469
6Designed for Performance
> High-resolution display> Plethysmographic waveform
> Durable and lightweight > Enhanced comfort
SpO2
PR
PI
PVI®
Measurements
Oxygen Saturation
Pulse Rate
Perfusion Index
Pleth Variability IndexFree Downloadable Masimo Professional Health App*> View, trend, and share
up to 12 hours of data iPhone not included
www.masimoprofessionalhealth.comCaution: Federal (USA) law restricts this device to sale by or on the order of a physician. See instructions for use for full prescribing information, including indications, contraindications, warnings, and precautions.© 2016 Masimo. All rights reserved.
Apple is a registered trademark of Apple Inc. registered in the U.S. and other countries.
*The Masimo Professional Health app is downloadable from the App storeSM for iOS devices or Google Play™ store for select Android devices. For an up-to-date list of compatible smart devices, see: www.masimoprofessionalhealth.com. Only available for Bluetooth® LE enabled models.
XXXXA, STG-0126A, Ad, MightySat Rx, International Committee of Military Medicine, March 2016, 210x297mm.indd 1 3/1/16 7:28 AM

major problems communities affected by the ongoingEbola outbreak in certain African countries: superficialburial led to secondary infection of stray sarcobores(carnivores) digging into the shallow graves looking forfood5, 6.
CONCLUSIONS
The topic presented at the 41st World ICMM Congresson Military Medicine Congress, Bali, Indonesia (17-22May, 2015) is complex and multi-dimensional andaddressed only the headlines of hospitals' CBRNdefense and preparedness. Deeper study and thoroughevaluation is needed for a successful outcome. But eventhe summarized information provided herein shouldbe enough to alert hospitals' military and civilian offi-cials on their potential to deal with asymmetric threatsproducing mass casualties in urban environment whileproviding two alternatives: to pray nothing that horri-ble ever happens in their city or to do something toprotect both their hospital and people working the-rein. It is their choice and so are the consequences oftheir decisions! Open source intelligence reveals thatthe Islamic State has chemical and radiological terroristambitions and their - so far – immoral behavioralmodus operandi reveals that they are capable of releasingCBRN agents against «Western infidels».
In conclusion there are some key points that need to betaken into serious account in case authorized personneldecides to step up and take actions:
a. Anthropocentric planning is mandatory;
b. Save the savers to save the hospital;
c. Continuous exercising and acclimatization to PPE isthe antidote against fear and ignorance;
d. HAZMAT/CBRNE treatment is mostly empirical andrequires a lot of studying and field improvisation;
e. All medical specialities will be involved;
f. Medical decisions might contradict ordinary medicalethics and regulations;
g. Introduce HAZMAT/CBRNE Medicine to medicalschools’ curricula – invest in the future!
ABSTRACT
Despite the fact that 14 years after the anthrax letters' scarein the United States and 19 years after the unique Tokyosubway sarin incident, no CBRN attacks has been recordedin urban environment there is always a chance that thismight happen tomorrow! And if it happens it would behospitals that would have to deal with the mass conse-quences expected. Are hospitals prepared enough for sucha worrisome scenario? With some exceptions in certaincountries around the globe, hospitals are not prepared todeal with this specific problem. Some insights are providedherein but hospital’s CBRN defense and preparednessrequires multi-level approach, dedication and continuity inorder to be effective, applicable and long lasting.
Potential Conflict of Interest: None.
REFERENCES
1. ECDC: Critical aspects of the safe use of personal protectiveequipment. Version 2: December 2, 2014. Retrieved from:http://ecdc.europa.eu/en/publications/Publications/safe-use-of-ppe.pdf [accessed: 12/6/15].
2. Johns personal protective equipment prototype for Ebola.Retrieved from: https://www.youtube.com/watch?v=kRab2bGahCE[accessed: 12/6/15].
3. ECDC: Assessing and planning medical evacuation flightsto Europe for patients with Ebola virus disease and peo-ple exposed to Ebola. October 21, 2014. Retrieved from:http://ecdc.europa.eu/en/publications/Publications/ebola-guidance-air-transport-update-decontamination.pdf[accessed: 12/6/15].
4. Radiation Emergency Medical Management (REMM).Retrieved from: http://www.remm.nlm.gov [accessed: 12/6/15].
5. New WHO safe and dignified burial protocol - key to redu-cing Ebola transmission. November 7, 2014. Retrieved from:(http://www.who.int/mediacentre/news/notes/2014/ebola-burial-protocol/en/) [accessed: 12/6/15].
6. WHO: How to conduct safe and dignified burial of a patientwho has died from suspected or confirmed Ebola virusdisease. October 2014. Retrieved from:http://apps.who.int/iris/bitstream/10665/137379/1/WHO_EVD_GUIDANCE_Burials_14.2_eng.pdf?ua=1 [accessed: 12/6/15].
10International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Health consequences of using weapons of mass destruction have usually an impactboth on individuals and teams. It is not only about the armed forces, but also civilians.Hence, the importance of active prevention and protection intensifies due to thepossibility of its abuse, especially in the field of international terrorism. Last yearwe also had to face the problem of a highly contagious disease Ebola and thussolve its spreading and endangering people on several continents. All such situationsare forcing us to look into possible countermeasures in the field of antidotes,
modern pharmaceuticals, or improve the first aid methods on the battlefield.
The aim of the World CBRN & Medical Congress is to contribute prevention against State and non-State actorsby taking part in development and the harmonizing of protection & defence capabilities.
This congress will also foster the development of specific capabilities to support impeding the trafficking of WMD,related materials and means of delivery and will support the CBRN Defence interdependence with other sectors suchas logistics, healthcare, ... and especially necessity to apply civil - military cooperation.
CONTACT FOR PARTNERS AND PARTICIPANTSMAJ (Ret.) Pavel ZELENKA, Director of Foreign Relations
E-mail: [email protected]
CBRNE_GALATAS.qxp_Mise en page 1 16/03/2016 15:20 Page5

By KISMANTO. Indonesia
KISMANTO
Aerodontalgia Case Series: Dental ComplicationsCaused by Changes in Air Pressure.*
Lt.-Colonel/Air Force drg. KISMANTO Sp.BM, born in Yoyakarta, Indonesia, 18September 1966, graduated as Dentist with specialization in Oral Surgery.
Currently, he is Secretary Institute at the Dental and Oral Health institute of theAir Force Health Department in Jakarta, Indonesia.
11International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Quelques cas d’aérodontalgies : complications dentaires dues aux changements de pression atmosphérique.
Nous présentons trois cas d’aérodontalgies chez des membres de l’armée de l’air indonésienne et leur traitement.L’aérodontalgie a été décrite pour la première fois pendant la deuxième guerre mondiale lorsque des équipages eurent souffertde douleurs dentaires au cours de leurs missions. On identifia le phénomène de douleur dentaire au cours du vol comme lié àdes différences de pression atmosphérique. Dans la mesure où l’atmosphère entourant la terre a une masse et un poids, ellegénère une pression appelée pression atmosphérique. Lorsque l’on se trouve à haute altitude cette pression diminue. La loi deBoyle Law établit que le volume d’un gaz est inversement proportionnel à sa pression et chaque individu doit s’accommoder deces différences. L’aérodontalgie est la douleur dentaire causée lorsque le volume d’air emprisonné dans l’espace clos d’une dentest incapable de se dilater ou de se contracter pour s’aligner sur la pression atmosphérique ambiante. L’aérodontalgie survientplus fréquemment sur des dents en mauvaise santé, atteintes d’infections de caries ou de fractures. Un traitement convenabledes maladies dentaires est la meilleure stratégie de prévention.
INTRODUCTION
The air surrounding the Earth is called atmosphere andextends from the earth surface to 3000 km skyward1.The air encircling the earth have a mass and weight sothat will generate pressure so that is called air pressure.The higher altitudes have less mass of air so this willresult in a lower air pressure. As a result, the edge ofatmosphere or beyond the highest altitude of theatmosphere is “space” or empty space.
Certainly, pressure changes around human body willaffect its physiology. The type and size of alteration inhuman’s body physiology will be determined by theamount of air pressure changes with larger adjust-ments required for significant pressure changes. If thebody is unable to accommodate these changes thenthe individual may experience physiological changes orpain due to the pressure differences.
Individuals serving in aviation will experience altitudechanges regularly when aircrafts ascend and descend.
These air pressure changes can cause medical complica-tions. H.F. Adler referred to this as dysbarism which hedivided into two types:
1. Trapped gas2. Evolved gas
This article will discuss dysbarism caused by trapped gas.
According to the definition, dysbarism is caused by trap-ped gas in the body which cannot adjust to the changingair pressure of the outside environment. This can occurin different body cavities such as: cavum tympani, sinus
VOL.89/1
KEYWORDS: Aerodontalgia, Airforce.MOTS-CLÉS : Aérodontalgies, Armée de l’air.
Correspondence:Lieutenant Colonel drg. KISMANTO. Sp.BMDental and Oral Health instituteAir Force Health DepartmentLembaga Kesehatan Gigi & Mulut TNI AUJL. Puntodewo, No. 1, Komp. Dirgantara IIHalim Perdanakusumah, Makasar,Jakarta Utara, 13610, [email protected]
* Presented at the 41st ICMM World Congress on Military Medicine,Bali, Indonesia, 17-22 May 2015.
Aerodontalgia_KISMANTO.qxp_Mise en page 1 16/03/2016 14:33 Page1

paranasalis, teeth with cavities, tractus digestivus andtractus respiratorius. In air transportation, Boyle’s law isprevailing, which state that inversely proportional gasvolume with its pressure. Hence as the air pressurearound body increases or decreases, the differences ofair pressure between the trapped air inside the bodycavity and the external environment causes pressurewithin the body cavity.
In this article the FDI classification (Fédération dentaireinternationale) is used.
AERODONTALGIA
Aerodontalgia is a painful feeling in the teeth resultingfrom atmospheric pressure changes such as that experien-ced at high-altitudes. The more general diagnosis of baron-dontalgia applies to any condition that is a result of air pres-sure differences which would include air crew and seadivers. Aerodontalgia incidence was 0.7 - 9.5%8. This painwas first identified during military conflicts where militaryaviation was utilized. This finding resulted in researchregarding barodontalgia. It was discovered that predispo-sing factors such as dental caries, defective restorations, andfractured teeth often initiated a pulpal response of painwith changes in air pressure.
The altitude of 5.000 ft – 15.000 ft, is the most commonrange at a constant altitude in which barodontalgiaoccurs, but the pain is variable depending on the indi-vidual and tooth related complications. The pain willusually cease at ground level.
Aerodontalgia occurs when decayed teeth or defectivetreatment exists, for example:
1. Caries or damage toothCaries or decayed teeth with a narrow orifice creates anenclosed space subject to air pressure differences. Researchshows that an asymptomatic tooth pain can become symp-tomatic during flight due to an exacerbation of a pre-exi-ting tooth fracture or decayed tooth1. Real tooth pain canappear as a result from barometric pressure changes. Dentaltreatment not completed on caries teeth, fractured teeth, orteeth with incomplete root canal treatment are the mostcommon clinical situations that result in pain experienced athigh altitudes. In those cases, etiologies of pain are dividedinto two types. The first type of pain is caused by a vital pulpreaction of a caries tooth as a result of increased atmosphe-ric pressure. The second type is pain caused by a non-vitalpulp reaction where the surrounding tissue or a pre-existinginfection is affected by the atmospheric pressure causingpatient pain.
2. Defective tooth restorationA defective tooth restoration can result in an enclosedspace or cavity between the tooth and the restoration.
Previous restorations placed to treat extensive cariescan create this situation resulting in aerodontalgiaexperienced weeks after dental treatment.
3. Periapical abscessThe periapical abscess is an infection of the pulp of thetooth which results in a localized infection encompas-sing the tissue around the roots of a tooth. That locali-zed infection can create an air space that is influencedby changes in air pressure.
In many places in the world, public awareness of den-tal health is still relatively low; therefore, they do notseek treatment for existing dental problems6. The phy-siological changes of air travel alters the oral environ-ment resulting in asymptomatic dental problems beco-ming symptomatic with pain.
The degree of aerodontalgia can be influenced by thefollowing environmental changes and result in moredental pain:
1. TemperatureHigher altitude results in colder temperatures whichresults in a trigger factor, to isothermal layer placed whereconstant relatively temperature is -55 Celsius degree7.
2. Air PressureAir/gas exploitation causes pressure in dental pulp andpain symptoms will occur7.
3. G. ForceBoth G positive or G negative may affect pre-existingdental conditions. When G positive, blood fluid collectsto the end of body part, so that the top of body part,including teeth will experience a deficiency of bloodcirculation. Inversely if G negative, blood collecting tothe top of body part may include teeth. Deficient bloodcirculation caused by G force may trigger pre-existingdental conditions resulting in pain7.
4. Air emboliIf an air emboli occurs around the apical area of a toothwhich encompasses the pulpal or nerve tissue, this pres-sure change may cause tooth pain as air planes ascendsor descends. This typically occurs when a plane ascends,because of the exploitation effect more spontaneousthan emphasis effect1.
CASE SERIES
The following three cases reports describe cases ofaerodontalgia experienced by Suswatud andSuskesbangan’s students after their experiences in ahyperbaric chamber. A hyperbaric chamber is a roomthat is pressurized three times higher than normal airpressure and delivers pure oxygen. It used to simulateair travel and treat a variety of conditions includingserious infections and decompression sickness. In thesecases, two of the students experience pain in theirteeth resulting from atmospheric pressure changes,while a third student has his pre-existing tooth painrelieved with altitude (pressure) change.
12International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
QUADRANT 1 QUADRANT 2
QUADRANT 4 QUADRANT 3
FDI (Fédération dentaire internationale) classification.
Aerodontalgia_KISMANTO.qxp_Mise en page 1 16/03/2016 14:33 Page2
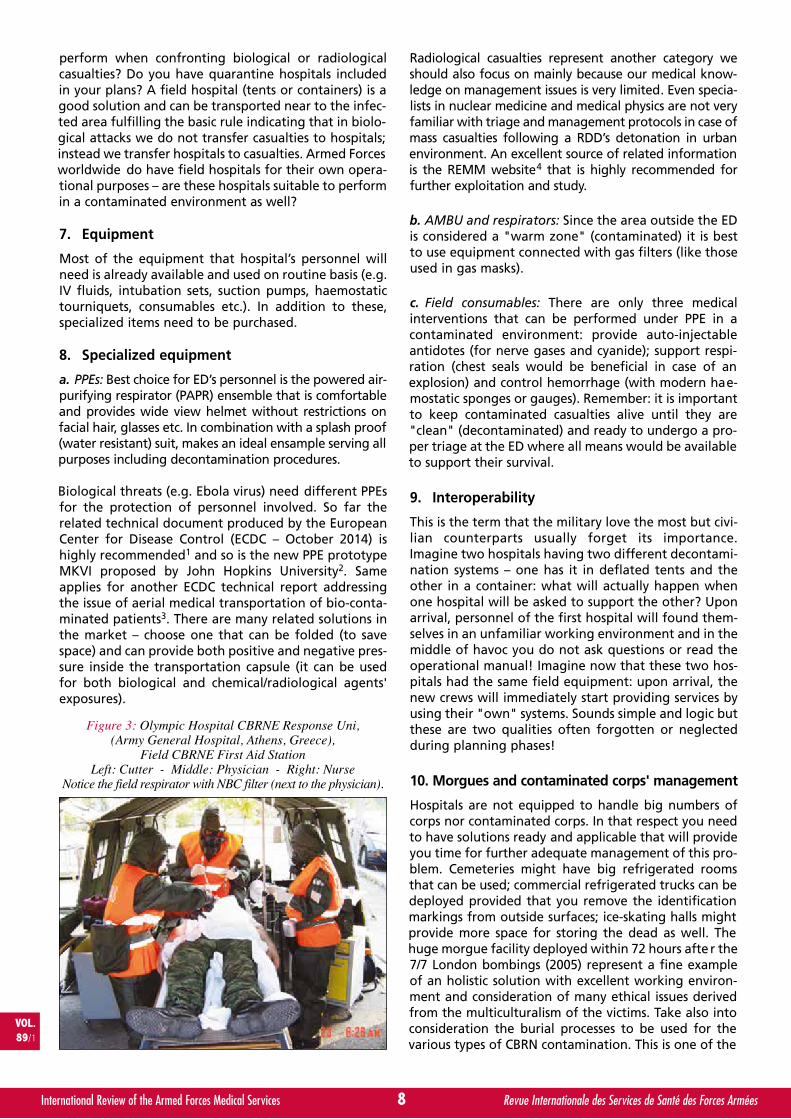
Case I
29 year-old male experiences toothache in lower leftposterior tooth when reaching an altitude of 5000 ft.Dental history of having restoration replaced on lowerleft posterior tooth two years prior. Since the second res-toration, patient’s tooth was asymptomatic with no otherdental conditions such as an abscess, tooth fracture, ortemporal-mandibular pain.
Case II
29 year old female complains of pain in maxillary leftmolar within altitude range of 8000 to 25000 ft. After alti-tude was normalized, tooth pain was alleviated. Extensivedental history with several extractions and restorations intooth number 12, 21, 22, 26, 36 and 35. Tooth restorationin 26 was restored by non-dentist. No history of dentalabscess, tooth fractures or temporal-mandibular pain.
For these cases, the diagnosis is aerodontalgia or baro-dontalgia which is dental pain experienced in teethresulting from pressure differences in entrapped gaswithin the tooth.
Case I, aerodontalgia derived from space below dentalfillings due to incomplete root canal treatment. Case IIaerodontagia derived from tooth #26, with caries inthe distal part. At ground level, both patients did notexperience dental pain so they did not seek treatment.After patients were educated on etiology of paintreatment was completed which included root canaltreatment and replacement of restorations.
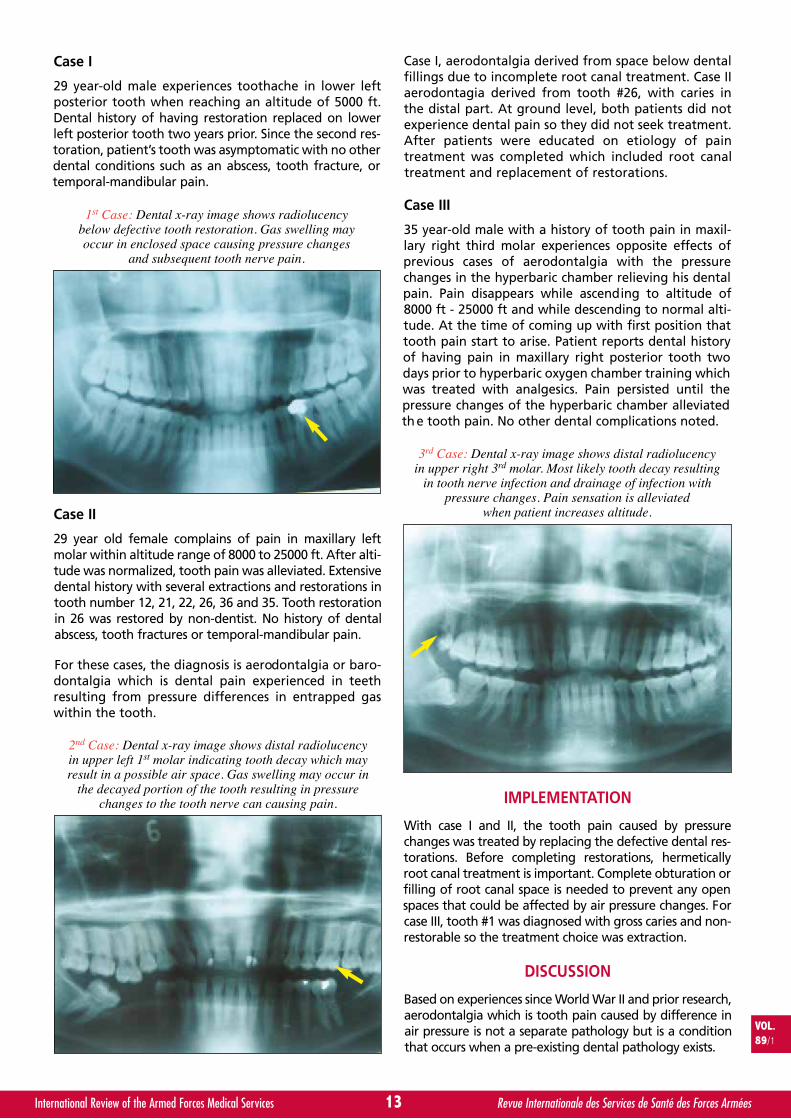
Case III
35 year-old male with a history of tooth pain in maxil-lary right third molar experiences opposite effects ofprevious cases of aerodontalgia with the pressurechanges in the hyperbaric chamber relieving his dentalpain. Pain disappears while ascending to altitude of8000 ft - 25000 ft and while descending to normal alti-tude. At the time of coming up with first position thattooth pain start to arise. Patient reports dental historyof having pain in maxillary right posterior tooth twodays prior to hyperbaric oxygen chamber training whichwas treated with analgesics. Pain persisted until thepressure changes of the hyperbaric chamber alleviatedth e tooth pain. No other dental complications noted.
IMPLEMENTATION
With case I and II, the tooth pain caused by pressurechanges was treated by replacing the defective dental res-torations. Before completing restorations, hermeticallyroot canal treatment is important. Complete obturation orfilling of root canal space is needed to prevent any openspaces that could be affected by air pressure changes. Forcase III, tooth #1 was diagnosed with gross caries and non-restorable so the treatment choice was extraction.
DISCUSSION
Based on experiences since World War II and prior research,aerodontalgia which is tooth pain caused by difference inair pressure is not a separate pathology but is a conditionthat occurs when a pre-existing dental pathology exists.
13International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
1st Case: Dental x-ray image shows radiolucencybelow defective tooth restoration. Gas swelling mayoccur in enclosed space causing pressure changes
and subsequent tooth nerve pain.
2nd Case: Dental x-ray image shows distal radiolucencyin upper left 1st molar indicating tooth decay which mayresult in a possible air space. Gas swelling may occur in
the decayed portion of the tooth resulting in pressurechanges to the tooth nerve can causing pain.
3rd Case: Dental x-ray image shows distal radiolucencyin upper right 3rd molar. Most likely tooth decay resulting
in tooth nerve infection and drainage of infection withpressure changes. Pain sensation is alleviated
when patient increases altitude.
Aerodontalgia_KISMANTO.qxp_Mise en page 1 16/03/2016 14:33 Page3

The influence of barometric pressure causes changesthat results in either gas expansion or contraction inthe human body. While in-flight, air pressure increasesinside the body cavities which can cause an expansion.If either an anatomical or physiological barrier existsthat prevents equalization of the gas pressure, then apressure will be created that can cause pain within thebody.
Pathologic gas expansion in aerodontalgia is relatedwith Boyle’s law, which states that volume of a gas isdirectly proportional to the pressure on it, when tem-perature is constant (P1 x V1 = P2 x V2). As a result, thepressure changes in a tooth affect the nerve tissueknown as the pulp within the tooth and that results inthe pain sensation experienced by the patient5. Theability to adapt to pressure changes in high-altitude isdifferent with for each individual. It can depend onoverall health and physical condition, previous high-altitude experience, and individual response to velocityand pressure changes. Rudge’s reports that decompres-sion sickness happens at an altitude of 8.000 ft, Allan’sat 14.000 ft, Rayman and Mc. Naugtan’s 11.000 ft, andVoge’s at 14.000 ft4.
Aerodontalgia usually occurs at altitudes between5.000–15.000 ft after the aircraft reaches a constantaltitude. This pain may become more severe with anincrease in altitude but will usually dissipate at groundlevel.
In the first case, the x-ray revealed that a radiolucencyexisted under the dental restoration. That non-filledspace resulted in trapped gas which exerted a pressureon the pulpal and apical nerve tissue resulting in patientpain. A similar situation also existed in the second case.The treatment in both of these cases was removal ofdefective restoration, root canal therapy, and placementof new restorations. The root canal treatment will sealthe pulpal space and prevent any trapped gas associatedwith symptoms of aerodontalgia.
The third case was characterized by tooth pain thatoccurred during increasing elevation or air pressurewhile in the hyperbaric chamber. Dental x-ray imagedemonstrated a radiolucency on distal portion tooth#18 signifying gross dental caries. In situations of grossdental caries, gas may be trapped within the decayedportion of the tooth. The increase in air pressure duringflight will result in pressure changes within a carioustooth and can result in symptoms of aerodontalgia.Once normal air pressure is reestablished, those pres-sure differences in the carious tooth normalize so thepatient will no longer experience pain.
Treatment for the third case is extraction, because thetooth is a 3rd molar (wisdom) tooth that does not func-tion in mastication or occlude with the opposing tooth.This tooth is also difficult to treat due to its location.
Predisposing factors of aerodontalgia include toothdecay, irreversible pulpitis, pulpal necrosis, and partial ordefective previous root canal treatment. Other etiologies
include crown-tooth fracture, tooth erosion, acute abs-cess periapical, odontogenic infections and barophysicphenomena, also imperfect tooth restoration “3”.
Main etiologies of aerodontalgia are also related tonon-hermetic endodontic treatment and subsequentpulpitis which is caused by bacterial contaminationsecondary to a defective tooth restoration. One of themost painful responses that often occurs while in-flightor in a decompression chamber is due to defective amal-gam restorations which are undercondensed or incom-pletely filled within the preparation. In cases of aero-dontalgia, replacement of defective restoration willoften alleviate symptoms of tooth pain immediately.
La rge tooth restorations in close proximity to the pulpcan induce tissues changes so that symptoms may occurweeks after its insertion and may mimic aerodontalgiaduring flight. In these situations, no treatment shouldbe completed because the hypersensitive pulp or rever-sible pulpitis due to the large restoration will oftennormalize. If the symptoms continue after a few weeksand the tooth is diagnosed with an irreversible pulpitis,then root canal treatment should be completed.
Carious or decayed teeth where the pulp has been com-promised will often become symptomatic with altitudechanges. In those cases, the etiologies of the pain canbe divided into two categories. First category is paincaused by vital pulp reaction of decayed tooth as aresult from atmospheric pressure. Second category ispain caused by non-vital pulp reaction or pulpal necro-sis as a result of atmospheric pressure changes. Dentaltreatment will be unique for each clinical case withroot canal therapy preferred versus extraction.
In each case of aerodontalgia, the symptoms are oftenunique to the individual patient. In some instances, apatient may experience pain on ground level and thenexperience no pain during flight at a higher altitude. Inmost cases, the common presentation of aerodontalgiais for the patient to be asymptomatic at ground leveland then to experience pain at higher altitudes. In eithercase, the aviator should seek immediate treatment toaddress the underlying dental disease that is responsiblefor the symptom of pain.
CONCLUSION
The best treatment to avoid cases of aerodontalgia isto maintain optimal dental health and readiness for allmilitary members. This includes proper prevention,diagnosis and treatment of dental disease. When apatient experiences aerodontalgia, dental pain relatedto changes in altitude, then the underlying dentalabnormality should be diagnosed and treated.
SUMMARY
We presented three cases of aerodontalgia inIndonesian airforce personnel and their treatment.Aerodontalgia was first described in World War II whenair crew experienced tooth related pain during military
14International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Aerodontalgia_KISMANTO.qxp_Mise en page 1 16/03/2016 14:33 Page4

missions. They identified the phenomena of tooth rela-ted pain during flight that is caused by differences inair pressure. Air encircling earth has mass and weight,so that will generate a pressure which is called air pres-sure. As you proceed to higher altitudes, the outsidepressure decreases. Boyle Law states that gas volume isinversely proportional with its pressure, hence as theair pressure increases or decreases, the individual needsto physically accommodate these differences.Aerodontalgia is tooth related pain that is causedwhen the air pressure in the enclosed space of a toothis unable to expand or contract to adjust to the outsideair pressure. Aerodontalgia more frequently occurswhen dental health is compromised due to a complica-tions such as infection, caries, or tooth fracture. Thecorrect treatment of dental disease is the best strategyin avoiding aerodontalgia.
REFERENCES
1. ADLER HF. 1964 Aeromedical Reviews Dysbarism. USAFSchool of Aerospace, Medicine Aerospace Medical
Division, Brooks Air Force Bace, Texas.
2. Air Force Pamphlet, 1968 Effect of Altitude on Ears, Sinusesand Teeth Department of The Air Force; Washington, 161-16.
3. Anonim, 1995, Dasar-Dasar Ilmu Kesehatan Penerbangan,Direktorat Kesehatan TNI AU, Jakarta.
4. FABIAN B.G 1998 Case Report: Inflight Decompressionsickness Affecting the Temporomandibular Joint,Aviation, Space and Environmental Vol. 69. No. 5.
5. LARSEN A.S, BUCHWALD C, VESTERHAUGE S 2003 SinusBarotrauma-Late Dignosisi and treatment with Computer-Aided Endoscopi Surgery, Aviation, Space andEnvironmental Vol. 74. No. 2.
6. SRIYONO W.N, 2009 Pencegahan Penyakit Gigi dan MulutGuna Meningkatkan Kualitas hidup, UGM Yogyakarta
7. SUKOCO D, 2008 Aspek Aerofisiologi dalamPenerbangan, Perkespra Pusat, Jakarta.
8. ZADIK Y, 2009 Aviation Dentistry: Current Concepts andPractice, British Dental Journal 206 (11-16).
15International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Aerodontalgia_KISMANTO.qxp_Mise en page 1 16/03/2016 14:33 Page5
frasaco – Modelling reality.
www.frasaco.com
There’s only one thing closer to reality than frasaco’s phantom heads, jaw and teeth models and strip crowns, and that’s the real thing itself. That’s what has made frasaco the world’s premier choice for universities and dental students. After studying with models, students will have to treat real patients, which is why the simulation must be as realistic as possible. The success of the renowned frasaco brand is based upon this fundamental approach.
frasaco GmbH • P.O. Box 1244 • D-88061 Tettnang / Germany • Tel.: +49 (0) 75 42 93 15-23 • Fax: +49 (0) 75 42 93 15-15 • E-Mail: [email protected]

Komlan Mawabah BOUASSALO
Activité dentaire de l’hôpital militaire Togolaisde niveau 2 déployé au Mali dans le cadre demissions des Nations Unies.
Le chirurgien-dentiste Komlan Mawabah BOUASSALO est né le 5 mars 1985 àDadja (Togo). Il est de nationalité togolaise.
Diplôme obtenu :2010 : Doctorat d’Etat en Chirurgie dentaire à l’Université Cheick Anta Diop de
Dakar au SénégalExpérience professionnelle :- 2011 : Chirurgien-dentiste, chef service du service d’odonto-stomatologie du Centre hospitalier régionalde Dapaong.- de février 2013 à avril 2014 puis de décembre 2014 à août 2015 : chirurgien-dentiste à l’Hôpital niveau 2Togolais de la MINUSMA (Mission Multidimensionnelle Intégrée des Nations Unies pour la Stabilisation auMali).
16International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
SUMMARY
Dental Activity of the Togolese Military Hospital Level 2 Deployed in Mali as part of United NationsMissions.
Introduction: Since 2012, the security context in Mali led the United Nations Organisation (UN) to establish the InternationalSupport Mission in Mali (AFISMA) then the United Nations Multidimensional Integrated Stabilization Mission in Mali(MINUSMA). To provide dental support of UN personnel (UN patients) and a dental assistance to population (AMP) (AMPpatients), the Togolese military health service deployed a dental office located in the Togolese military hospital of level 2 (HN2-Togo).Methods: Data on the dental emergencies of patients treated at the dental office of the HN2-Togo were collected from the 22nd
of February 2013 to the 30th of October 2014.Results: 929 dental emergencies (among them 415 soldiers of eight different nationalities) and 894 treatments were recordedduring the period covered by the study. Caries is the main reason for consultation for UN patients (22,9% of reasons for consultation)except for Togolese soldiers who consult less for caries other than UN patients (OR = 0,4; 95% IC, 0,24-0,66). Main dental treatmentsfor UN patients are tooth extractions (34,3%) and dental fillings (31,7%). Among AMP patients, tooth extractions are more frequent(60,6%) than for UN patients (OR = 2,95; 95%IC, 2,24-3,88) due to a poor oral health (higher frequency in AMP than UN patientsof residual roots (respectively 37,6% and 18%; OR = 2,03; 95%IC, 1,52-2,71) and cellulitis (respectively 7,8% and 1,2%; OR = 7,13;95%IC, 2,78-18,29).Conclusion: The inhomogeneity of the reasons for dental consultation between different UN contingents could be due to theuneven quality of dental preparedness of forces (with a better preparedness of Togolese forces). The poor oral health of AMPpatients could be due to a lack of local care structures aggravated by the war and to the precariousness of population. This poor oralhealth involves a high frequency of surgical treatments which have to be taken in account in the training of deployed dentists. Moregenerally, the number of UN patients treated and the diversity of their nationality highlight the importance of dental support to
INTRODUCTION
Le coup d’état survenu au Mali en 2012 a conduit lesautorités transitoires maliennes à solliciter l’assistance
de l’Organisation des Nations Unies (ONU) qui arépondu par la création, en décembre 2012, de laMission Internationale de Soutien au MAli (MISMA)1.La dégradation de la situation sécuritaire début 2013 a
VOL.89/1
MOTS-CLÉS : Dentisterie militaire, Opération extérieure, Pathologie bucco-dentaire, Aide médicale auxpopulations, Soutien dentaire.KEYWORDS: Military dentistry, Dental support, Oral pathology, Medical aid to population.
Par K.M. BOUASSALO∑, S. ADAM∏, H.D. SAMAπ, B.E. KEBINA∫, H. BISSAª et M. GUNEPINº. Togo
ARTIC
LES
ARTIC
LES
Activite Dentaire_BOUASSALO.qxp_Mise en page 1 18/03/2016 13:43 Page1

entraîné, à la demande des autorités maliennes, ledéclenchement par la France de l’opération Serval le11 janvier 2013. Puis, du fait de l’amélioration de la situa-tion sécuritaire suite aux opérations militaires françaiseset africaines, le Conseil de sécurité de l’ONU a décidé detransformer la MISMA en une opération de stabilisationet de maintien de la paix (Mission multidimensionnelleIntégrée des Nations Unies pour la Stabilisation au Mali(MINUSMA)). La MINUSMA a été créée par la résolution2100 du 25 avril 20131. Afin de garantir le succès de cesmissions (MISMA et MINUSMA), le soutien dentaire dupersonnel de l’ONU déployé (que nous appelleronspatients ONU) mais aussi celui des populations locales(que nous appellerons patients AMP (Aide Médicale auxPopulations)) sont essentiels. C’est pourquoi l’arméeTogolaise a déployé à Sévaré (Mali), dès le 17 janvier2013, un hôpital de niveau 2 (HN2-Togo) incluant un ser-vice dentaire. Ce travail a pour objectif de présenter lebilan de 20 mois d’activité au sein de ce service dentaire(du 22 février 2013 au 30 octobre 2014).
LE SOUTIEN MEDICAL ET DENTAIREDU PERSONNEL DE L’ONU DEPLOYE
AU MALI ET DES POPULATIONS LOCALES
Afin d’assurer le soutien médical de son contingent, maiségalement de l’ensemble du personnel civil et militaire del’ONU déployé dans le cadre de la MISMA puis de laMINUSMA, le Togo a projeté au Mali un hôpital de cam-pagne de niveau 2 (HN2-Togo). Initialement implanté àSévaré (de février 2013 à octobre 2014), l’HN2-Togo a ététransféré à Kidal en décembre 2014. En fonction ducontexte sécuritaire et de l’activité réalisée au profit dupersonnel de l’ONU, les populations locales peuvent éga-lement bénéficier d’une prise en charge médicale et den-taire à l’HN2-Togo dans le cadre de l’AMP et des ActionsCivilo-Militaires (ACM). L’AMP et les ACM font partie desmissions confiées par l’ONU à toutes les unités déployéessur le théâtre Malien dans le cadre de la MISMA et de laMINUSMA2. L’objectif de l’AMP et des ACM est d’apporterune aide humanitaire aux populations et d’améliorer l’ac-ceptation du personnel de la MISMA et de la MINUSMApar les populations locales2.
L’HN2-Togo permet de dispenser des soins urgents desauvetage et de stabilisation (diagnostic et prise encharge des urgences médicales et chirurgicales, réanima-tion et stabilisation des blessés ou autres patients graves)et des soins dentaires et d’assurer les évacuations aéro-médicales de l’HN2-Togo vers un hôpital de niveau supé-rieur. L’HN2-Togo dispose de deux salles de consultation,d’un bloc opératoire, d’une unité de déchoquage, d’unesalle de réveil, d’une salle de stérilisation et d’un cabinetdentaire. Le service de soins dentaires de l’HN2-Togo estarmé par un chirurgien-dentiste et un assistant dentaire.Il est installé sous tente modulaire militaire F1 et équipéd’un fauteuil dentaire hydraulique avec un compresseursilencieux de 10 litres, d’un appareil de radiographie por-tatif, d’un autoclave et des instruments et consomma-bles nécessaires à la réalisation de soins dentaires (cf.figure 1). Le service dentaire a une capacité de prise encharge de 10 patients par jour. La gestion des déchetsd’activité de soins a été réalisée initialement par l’hôpital
civil Sominé Dolo de Mopti avant que l’HN2-Togo ne sedote de son propre incinérateur. Les deux principalescontraintes auxquelles fait face le cabinet dentaire del’HN2-Togo sont :
- l’exposition du matériel dentaire à un environne-ment contraignant (chaleur, poussière) qui impose unemaintenance plus suivie et plus poussée que cellerecommandée par le fabricant de l’équipement.
- le ravitaillement sanitaire du cabinet réalisé unique-ment une fois par trimestre par voie routière depuisLomé (Togo) (distant d’environ 1 700 km de Sévaré) quiimpose une gestion précise des consommables demanière à prévenir toute rupture de stock.
MATERIEL ET METHODE
Echantillon et méthode
Les données médico-administratives relatives aux patientsse présentant à la consultation au service dentaire de l’HN2-Togo ont été recueillies du 22 février 2013 au 30 octobre2014. Le recueil s’est fait à partir du registre d’activité duservice dentaire de l’HN2-Togo. Une fiche d’enquête préa-lablement établie a servi de support pour la collecte desdonnées. Les paramètres étudiés étaient l’origine despatients (militaire, civil de l’ONU ou patient pris en chargedans le cadre de l’AMP), la nationalité pour les militaires, lemotif de la consultation et le ou les traitements réalisés.L’analyse des données a été faite à l’aide du logiciel EPIINFO 7.1.5.0.
17International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 1 : Fauteuil du cabinet dentairede l’HN2-Togo à Sévaré.
∑ Chirurgien-dentisteService d’odontostomatologie CHR-Dapaong, BP 57, Dapaong (Togo).
∏ Médecin,Service d’ORL et de chirurgie cervico-maxillo-faciale, Service d’odontostoma-tologie, CHU Sylvanus Olympio, BP 75 Lomé (Togo).
π Médecin,Service d’anesthésie réanimation, CHU Sylvanus Olympio, BP 75 Lomé (Togo).
∫ Chirurgien-dentiste,Service de stomatologie CHU Campus, 03 BP 30284 Lomé (Togo).
ª Médecin,Service d’ORL et de chirurgie cervico-maxillo-faciale, Serviced’odontostomatologie, CHU Sylvanus Olympio, BP 57 Lomé (Togo).
º Chirurgien-dentiste,Equipe Résidente de Recherche Subaquatique Opérationnelle de l’Institut deRecherche Biomédicale des Armées - BP 600 83800 Toulon Cedex 9 (France).
Activite Dentaire_BOUASSALO.qxp_Mise en page 1 18/03/2016 13:43 Page2

Analyse statistique
Les analyses uni variées sont effectuées avec le logicielR (version 2.2.0.) et avec le package Meta (version 0.5).Les tests statistiques réalisés sont des Chi-2 de Wald etles Odds Ratios (ORs) correspondants sont présentésavec leur intervalle de confiance à 95 %. Les résultatsavec p < 0,01 sont considérés comme significatifs.
RESULTATS
Du 22 février 2013 au 30 octobre 2014, 6 630 patientsont été pris en charge au sein de l’HN2-Togo dont 929pour une consultation dentaire (14 % de l’activité del’HN2-Togo) (cf. tableau I). Parmi les 1 928 consultantsde l’ONU (1 691 militaires et 237 civils), 439 (soit22,8 %) ont consulté pour des problèmes dentaires(415 militaires et 24 civils). Les militaires ayant consultépour des problèmes dentaires étaient issus de huitpays, majoritairement du Togo (43,1 %) et du Sénégal(32,0 %) (cf. tableau II). L’analyse des motifs de consul-tation dentaire des patients pris en charge par le ser-vice dentaire et des thérapeutiques odontologiquesque leur état bucco-dentaire a nécessité, a permis demettre en évidence que :
- chez les patients ONU :* Les caries dentaires sont le motif de consultation
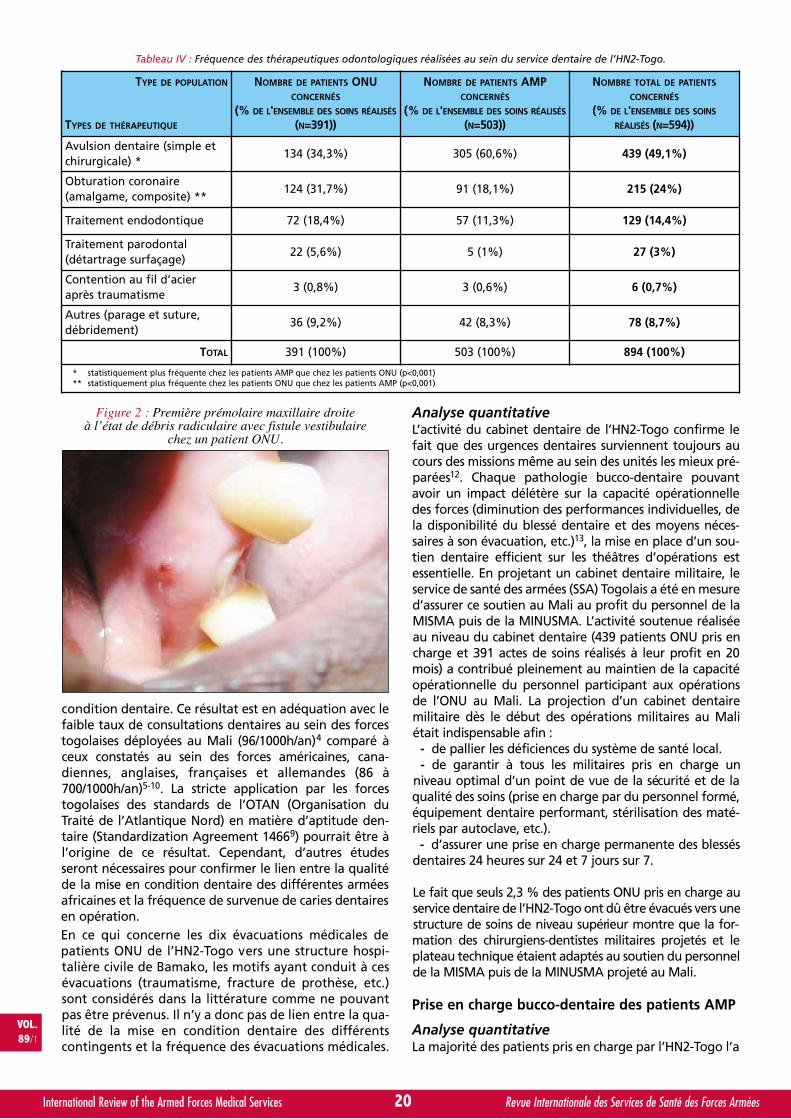
dentaire le plus fréquent (22,8 % des cas), devant lesdébris radiculaires (18,8 %) (cf. figure 2) et les paro-dontites apicales (16,5 %) (cf. tableau III).
* Les avulsions dentaires sont les traitementsodontologiques les plus fréquents (35,9 % des traite-ments) devant les obturations coronaires (30,4 %) et lestraitements endodontiques (19,3 %) (cf. tableau IV).
- chez les patients AMP :* Les débris radiculaires sont le motif de consulta-
tion dentaire le plus fréquent (37,6 % des cas), devantles caries dentaires (14,7 %) et les parodontites apicales(10,2 %) (cf. tableau III).
* Les avulsions dentaires sont les traitementsodontologiques les plus fréquents (60,6 % des traite-ments) devant les obturations coronaires (18,1 %) et lestraitements endodontiques (11,3 %) (cf. tableau IV).
Du fait de l’état bucco-dentaire de certains patients etdes limites du plateau technique du service dentaire del’HN2-Togo, dix patients ONU (neuf militaires et uncivil) (2,3 % des consultants dentaires) ont dû être éva-cués de l’HN2-Togo vers une structure hospitalière civilede Bamako. Ces évacuations ont été effectuées lorsquedes travaux de prothèse se sont avérés nécessaires(réparation de prothèse adjointe partielle, réhabilita-tion prothétique après luxation totale de plusieursdents consécutive à un traumatisme).
18International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
TYPE DE CONSULTATIONS
POPULATIONS
NOMBRE DE CONSULTATIONS
MÉDICALES
(% DE L'ENSEMBLE DES
CONSULTATIONS MÉDICALES)
NOMBRE DE CONSULTATIONS
CHIRURGICALES
(% DE L'ENSEMBLE DES
CONSULTATIONS
CHIRURGICALES)
NOMBRE DE CONSULTATIONS
DENTAIRES
(% DE L'ENSEMBLE DES
CONSULTATIONS DENTAIRES)
NOMBRE TOTAL
DE CONSULTATIONS
(% DE L'ENSEMBLE DES
CONSULTATIONS)
Militaires
Togolais1009
(19,3%)
742(14,2%) 267
(58,5%)
125(27,4%) 415
(44,7%)
179(19,3%) 1691
(25,5%)
1046(15,8%)
Autres 267 (5,1%)142
(31,1%)236
(25,4%)645 (9,7%)
Personnel civil de l'ONU 200 (3,8%) 13 (2,9%) 24 (2,6%) 237 (3,6%)
Patients AMP 4036 (77,0%) 176 (38,6%) 490 (52,8%) 4702 (70,9%)
TOTAL
5245 (79,1% DE L'ACTIVITÉ DE
L'HN2-TOGO)
456 (6,9% DE L'ACTIVITÉ DE
L'HN2-TOGO)
929 (14% DE L'ACTIVITÉ DE
L'HN2-TOGO)6630
Tableau I : Activités médicale et dentaire de l’HN2-Togo du 22 février 2013 au 30 octobre 2014.
NATIONALITÉ DES PATIENTS MILITAIRES NOMBRE DE PATIENTS MILITAIRESPOURCENTAGE DE L'ENSEMBLE
DES PATIENTS MILITAIRES
Togolais 179 43,1%
Sénégalais 133 32,0%
Burkinabé 67 16,1%
Tchadien 21 5,1%
Guinéen 11 2,7%
Libérien 2 0,5%
Rwandais 1 0,2%
Nigérian 1 0,2%
TOTAL 415 100%
Tableau II : Répartition des patients militaires par nationalité.
Activite Dentaire_BOUASSALO.qxp_Mise en page 1 18/03/2016 13:43 Page3

DISCUSSION
Soutien dentaire des patients ONU
Analyse qualitativeLa diversité des nationalités des consultants dentairesmilitaires (huit nationalités différentes) montre que lesproblèmes bucco-dentaires ne sont pas spécifiques à uncontingent mais concernent l’ensemble des forcesdéployées sur le théâtre d’opérations. Cependant, lacomparaison des motifs de consultation dentaire entreles différents contingents (cf. tableau III) permet demettre en évidence que les militaires togolais consultentstatistiquement significativement moins pour des caries
dentaires que le personnel des autres contingents afri-cains (Chi² = 13,58; OR = 0,4, 95 % IC [0,24-0,66], p= 0,0002) notamment que les militaires sénégalais (Chi²= 8,7; OR = 0,43, 95 % IC [0,24-0,76], p = 0,003),deuxième contingent en nombre de consultants den-taires à l’HN2-Togo. Concernant les autres motifs deconsultation dentaire en urgence, il n’existe pas de dif-férence statistiquement significative entre les différentscontingents. Les urgences dentaires pour cause de cariesont considérées comme évitables par la réalisation d’undépistage et de soins adéquats avant projection3. La fré-quence moins élevée des caries dentaires chez les mili-taires togolais par rapport aux autres contingents pour-rait donc être liée à la meilleure qualité de leur mise en
19International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
POPULATION
MOTIFS DE
CONSULTATION
DENTAIRE
PATIENTS ONU PATIENTS AMP
NOMBRE DE PATIENTS
TOGOLAIS
(% DE L'ENSEMBLE DES
MOTIFS DE CONSULTATION
(N=171))
NOMBRE DE PATIENTS
SÉNÉGALAIS
(% DE L'ENSEMBLE DES
MOTIFS DE CONSULTATION
(N=126))
NOMBRE DE PATIENTS
BURKINABÉ
(% DE L'ENSEMBLE DES
MOTIFS DE CONSULTATION
(N=62))
NOMBRE TOTAL DE
PATIENTS AMP (% DE
L'ENSEMBLE DES MOTIFS
DE CONSULTATION
(N=428))
NOMBRE DE PATIENTS
CONCERNÉS AMP(% DE L'ENSEMBLE DES
MOTIFS DE CONSULTATION
(N=490))
Carie de la dentine * 26 (15,2%) 37 (29,4%) 15 (24,2%) 98 (22,9%) 72 (14,7%)
Débris radiculaire ** 35 (20,5%) 23 (18,2%) 7 (11,3%) 77 (18%) 184 (37,6%)
Parodontite apicale 22 (12,9%) 24 (19,0%) 15 (24,2%) 68 (15,9%) 50 (10,2%)
Pulpite 16 (9,4%) 18 (14,3%) 6 (9,7%) 47 (11%) 41 (8,4%)
Parodontopathie 12 (7,0%) 4 (3,2%) 3 (4,8%) 24 (5,6%) 21 (4,3%)
Restaurationdéfectueuse+
7 (4,1%) 6 (4,8%) 4 (6,5%) 21 (4,9%) 16 (3,3%)
Syndrome duseptum
8 (4,7%) 5 (4%) 3 (4,8%) 19 (4,4%) 16 (3,3%)
Lésions de lamuqueuse buccale
7 (4,1%) 2 (1,6%) 1 (1,6%) 12 (2,8%) 11 (2,2%)
Hyperesthésiedentinaire
5 (2,9%) 3 (2,4%) 2 (3,2%) 11 (2,6%) 4 (0,8%)
Fracture coronaired’origine nontraumatique
7 (4,7%) 2 (1,6%) 0 (0%) 9 (2,1%) 1 (0,2%)
Péricoronarite de ladent de sagesse
4 (2,3%) 0 (0%) 2 (3,2%) 8 (1,9%) 6 (1,2%)
Traumatismebuccodentaire
6 (3,5%) 0 (0%) 0 (0%) 7 (1,6%) 2 (0,4%)
Lésion cervicalenon carieuse
2 (1,2%) 1 (0,8%) 1 (1,6%) 6 (1,4%) 5 (1%)
Cellulites circons-crites d’origine
dentaire **2 (1,2%) 1 (0,8%) 0 (0%) 5 (1,2%) 38 (7,8%)
Prothèse partielleamovible en résine
défectueuse5 (2,9%) 0 (0%) 0 (0%) 5 (1,2%) 10 (2%)
Tumeurs 0 (0%) 0 (0%) 0 (0%) 0 (0%) 8 (1,6%)
Fracture mandibu-laire par trauma
balistique0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (0,2%)
Autres 7 (4,7%) 0 (0%) 3 (4,8%) 0 (0%) 3 (0,6%)
* statistiquement plus fréquente chez les patients ONU que chez les patients AMP (p<0,001)** statistiquement plus fréquent chez les patients AMP que chez les patients ONU (p<0,001)
Tableau III : Répartition des motifs de consultation au service dentaire de l’HN2-Togo par catégorie de population.
Activite Dentaire_BOUASSALO.qxp_Mise en page 1 18/03/2016 13:43 Page4
condition dentaire. Ce résultat est en adéquation avec lefaible taux de consultations dentaires au sein des forcestogolaises déployées au Mali (96/1000h/an)4 comparé àceux constatés au sein des forces américaines, cana-diennes, anglaises, françaises et allemandes (86 à700/1000h/an)5-10. La stricte application par les forcestogolaises des standards de l’OTAN (Organisation duTraité de l’Atlantique Nord) en matière d’aptitude den-taire (Standardization Agreement 14669) pourrait être àl’origine de ce résultat. Cependant, d’autres étudesseront nécessaires pour confirmer le lien entre la qualitéde la mise en condition dentaire des différentes arméesafricaines et la fréquence de survenue de caries dentairesen opération.En ce qui concerne les dix évacuations médicales depatients ONU de l’HN2-Togo vers une structure hospi-talière civile de Bamako, les motifs ayant conduit à cesévacuations (traumatisme, fracture de prothèse, etc.)sont considérés dans la littérature comme ne pouvantpas être prévenus. Il n’y a donc pas de lien entre la qua-lité de la mise en condition dentaire des différentscontingents et la fréquence des évacuations médicales.
Analyse quantitativeL’activité du cabinet dentaire de l’HN2-Togo confirme lefait que des urgences dentaires surviennent toujours aucours des missions même au sein des unités les mieux pré-parées12. Chaque pathologie bucco-dentaire pouvantavoir un impact délétère sur la capacité opérationnelledes forces (diminution des performances individuelles, dela disponibilité du blessé dentaire et des moyens néces-saires à son évacuation, etc.)13, la mise en place d’un sou-tien dentaire efficient sur les théâtres d’opérations estessentielle. En projetant un cabinet dentaire militaire, leservice de santé des armées (SSA) Togolais a été en mesured’assurer ce soutien au Mali au profit du personnel de laMISMA puis de la MINUSMA. L’activité soutenue réaliséeau niveau du cabinet dentaire (439 patients ONU pris encharge et 391 actes de soins réalisés à leur profit en 20mois) a contribué pleinement au maintien de la capacitéopérationnelle du personnel participant aux opérationsde l’ONU au Mali. La projection d’un cabinet dentairemilitaire dès le début des opérations militaires au Maliétait indispensable afin :
- de pallier les déficiences du système de santé local.- de garantir à tous les militaires pris en charge un
niveau optimal d’un point de vue de la sécurité et de laqualité des soins (prise en charge par du personnel formé,équipement dentaire performant, stérilisation des maté-riels par autoclave, etc.).
- d’assurer une prise en charge permanente des blessésdentaires 24 heures sur 24 et 7 jours sur 7.
Le fait que seuls 2,3 % des patients ONU pris en charge auservice dentaire de l’HN2-Togo ont dû être évacués vers unestructure de soins de niveau supérieur montre que la for-mation des chirurgiens-dentistes militaires projetés et leplateau technique étaient adaptés au soutien du personnelde la MISMA puis de la MINUSMA projeté au Mali.
Prise en charge bucco-dentaire des patients AMP
Analyse quantitativeLa majorité des patients pris en charge par l’HN2-Togo l’a
20International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
TYPE DE POPULATION
TYPES DE THÉRAPEUTIQUE
NOMBRE DE PATIENTS ONUCONCERNÉS
(% DE L'ENSEMBLE DES SOINS RÉALISÉS
(N=391))
NOMBRE DE PATIENTS AMPCONCERNÉS
(% DE L'ENSEMBLE DES SOINS RÉALISÉS
(N=503))
NOMBRE TOTAL DE PATIENTS
CONCERNÉS
(% DE L'ENSEMBLE DES SOINS
RÉALISÉS (N=594))
Avulsion dentaire (simple etchirurgicale) *
134 (34,3%) 305 (60,6%) 439 (49,1%)
Obturation coronaire(amalgame, composite) **
124 (31,7%) 91 (18,1%) 215 (24%)
Traitement endodontique 72 (18,4%) 57 (11,3%) 129 (14,4%)
Traitement parodontal(détartrage surfaçage)
22 (5,6%) 5 (1%) 27 (3%)
Contention au fil d’acieraprès traumatisme
3 (0,8%) 3 (0,6%) 6 (0,7%)
Autres (parage et suture,débridement)
36 (9,2%) 42 (8,3%) 78 (8,7%)
TOTAL 391 (100%) 503 (100%) 894 (100%)
* statistiquement plus fréquente chez les patients AMP que chez les patients ONU (p<0,001)** statistiquement plus fréquente chez les patients ONU que chez les patients AMP (p<0,001)
Tableau IV : Fréquence des thérapeutiques odontologiques réalisées au sein du service dentaire de l’HN2-Togo.
Figure 2 : Première prémolaire maxillaire droiteà l’état de débris radiculaire avec fistule vestibulaire
chez un patient ONU.
Activite Dentaire_BOUASSALO.qxp_Mise en page 1 18/03/2016 13:43 Page5
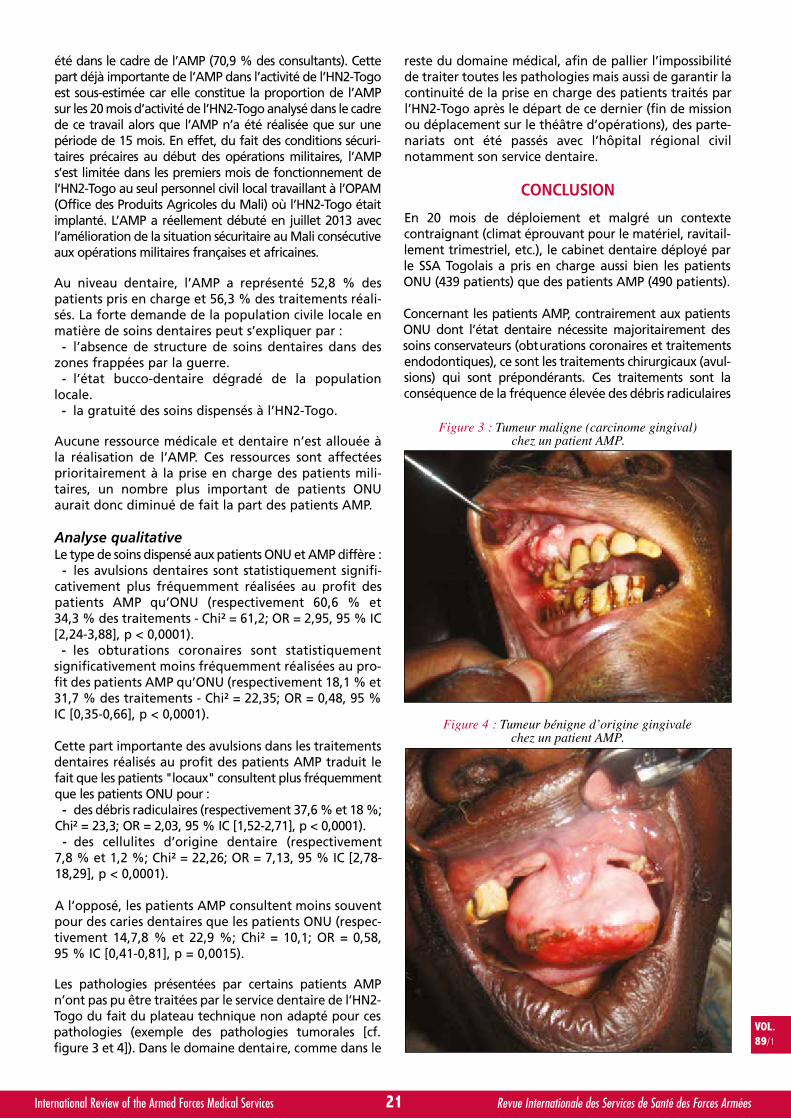
été dans le cadre de l’AMP (70,9 % des consultants). Cettepart déjà importante de l’AMP dans l’activité de l’HN2-Togoest sous-estimée car elle constitue la proportion de l’AMPsur les 20 mois d’activité de l’HN2-Togo analysé dans le cadrede ce travail alors que l’AMP n’a été réalisée que sur unepériode de 15 mois. En effet, du fait des conditions sécuri-taires précaires au début des opérations militaires, l’AMPs’est limitée dans les premiers mois de fonctionnement del’HN2-Togo au seul personnel civil local travaillant à l’OPAM(Office des Produits Agricoles du Mali) où l’HN2-Togo étaitimplanté. L’AMP a réellement débuté en juillet 2013 avecl’amélioration de la situation sécuritaire au Mali consécutiveaux opérations militaires françaises et africaines.
Au niveau dentaire, l’AMP a représenté 52,8 % despatients pris en charge et 56,3 % des traitements réali-sés. La forte demande de la population civile locale enmatière de soins dentaires peut s’expliquer par :
- l’absence de structure de soins dentaires dans deszones frappées par la guerre.
- l’état bucco-dentaire dégradé de la populationlocale.
- la gratuité des soins dispensés à l’HN2-Togo.
Aucune ressource médicale et dentaire n’est allouée àla réalisation de l’AMP. Ces ressources sont affectéesprioritairement à la prise en charge des patients mili-taires, un nombre plus important de patients ONUaurait donc diminué de fait la part des patients AMP.
Analyse qualitativeLe type de soins dispensé aux patients ONU et AMP diffère :
- les avulsions dentaires sont statistiquement signifi-cativement plus fréquemment réalisées au profit despatients AMP qu’ONU (respectivement 60,6 % et34,3 % des traitements - Chi² = 61,2; OR = 2,95, 95 % IC[2,24-3,88], p < 0,0001).
- les obturations coronaires sont statistiquementsignificativement moins fréquemment réalisées au pro-fit des patients AMP qu’ONU (respectivement 18,1 % et31,7 % des traitements - Chi² = 22,35; OR = 0,48, 95 %IC [0,35-0,66], p < 0,0001).
Cette part importante des avulsions dans les traitementsdentaires réalisés au profit des patients AMP traduit lefait que les patients "locaux" consultent plus fréquemmentque les patients ONU pour :
- des débris radiculaires (respectivement 37,6 % et 18 %;Chi² = 23,3; OR = 2,03, 95 % IC [1,52-2,71], p < 0,0001).
- des cellulites d’origine dentaire (respectivement7,8 % et 1,2 %; Chi² = 22,26; OR = 7,13, 95 % IC [2,78-18,29], p < 0,0001).
A l’opposé, les patients AMP consultent moins souventpour des caries dentaires que les patients ONU (respec-tivement 14,7,8 % et 22,9 %; Chi² = 10,1; OR = 0,58,95 % IC [0,41-0,81], p = 0,0015).
Les pathologies présentées par certains patients AMPn’ont pas pu être traitées par le service dentaire de l’HN2-Togo du fait du plateau technique non adapté pour cespathologies (exemple des pathologies tumorales [cf.figure 3 et 4]). Dans le domaine dentaire, comme dans le
reste du domaine médical, afin de pallier l’impossibilitéde traiter toutes les pathologies mais aussi de garantir lacontinuité de la prise en charge des patients traités parl’HN2-Togo après le départ de ce dernier (fin de missionou déplacement sur le théâtre d’opérations), des parte-nariats ont été passés avec l’hôpital régional civilnotamment son service dentaire.
CONCLUSION
En 20 mois de déploiement et malgré un contextecontraignant (climat éprouvant pour le matériel, ravitail-lement trimestriel, etc.), le cabinet dentaire déployé parle SSA Togolais a pris en charge aussi bien les patientsONU (439 patients) que des patients AMP (490 patients).
Concernant les patients AMP, contrairement aux patientsONU dont l’état dentaire nécessite majoritairement dessoins conservateurs (obturations coronaires et traitementsendodontiques), ce sont les traitements chirurgicaux (avul-sions) qui sont prépondérants. Ces traitements sont laconséquence de la fréquence élevée des débris radiculaires
21International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 4 : Tumeur bénigne d’origine gingivalechez un patient AMP.
Figure 3 : Tumeur maligne (carcinome gingival)chez un patient AMP.
Activite Dentaire_BOUASSALO.qxp_Mise en page 1 18/03/2016 13:43 Page6

et des cellulites parmi les motifs de consultation traduisantun défaut de suivi des patients en raison du manque destructures de soins, aggravé par la guerre, et de la préca-rité de la population. Cette fréquence élevée du besoin ensoins chirurgicaux doit être prise en compte dans la for-mation des chirurgiens-dentistes appelés à être projetéssur les théâtres d’opérations.
Concernant les patients ONU, l’analyse des motifs deconsultation dentaire montre que la fréquence des cariesest moins élevée chez les militaires Togolais qu’au sein desautres contingents. Les caries étant des pathologies pou-vant être dépistées et traitées avant la projection, ce résul-tat pourrait traduire une meilleure mise en condition den-taire des forces Togolaises par rapport aux autres contin-gents. D’autres études sont nécessaires pour préciser le lienentre la qualité de la mise en condition dentaire et les fré-quences et les motifs de consultation dentaire en urgenceau sein des forces africaines.
Plus généralement, le nombre de patients ONU ayantnécessité une prise en charge odontologique montre unenouvelle fois l’importance du soutien dentaire dans lemaintien de la capacité opérationnelle des forces proje-tées. Au Mali, ce soutien dentaire été rendu possible par lamontée en puissance de l’odontologie militaire au sein desforces togolaises. Le Togo participe ainsi à l’autonomie desforces africaines lors des opérations de l’ONU.
RESUME
Introduction : Dès 2012, le contexte sécuritaire au Mali aconduit l’Organisation des Nations Unies (ONU) à créer deuxmissions internationales. Afin d’assurer le soutien dentairedu personnel de ces missions (patients ONU) et l’aide médi-cale aux populations (patients AMP), le service de santé desarmées Togolais a projeté au Mali un cabinet dentaireimplanté au sein de l’hôpital de niveau 2 (HN2-Togo).Méthode : Les données médico-administratives despatients consultant au service dentaire de l’HN2-Togo ontété recueillies du 22 février 2013 au 30 octobre 2014.Résultats : Au cours de l’étude, 929 patients ont été pris encharge (dont 415 militaires de huit nationalités différentes)et 894 traitements ont été réalisés. Les caries sont le pre-mier motif de consultation des patients ONU (22,9 % desmotifs de consultation) hormis pour les militaires togolaischez qui les caries sont moins fréquentes que pour le restedes patients ONU (OR = 0,4; 95 % IC, 0,24-0,66). Les traite-ments les plus fréquents chez les patients ONU sont lesavulsions (34,3 %) et les obturations coronaires (31,7 %).Chez les patients AMP les avulsions sont plus fréquentes(30,6 %) que chez les patients ONU (OR = 2,95; 95 % IC,2,24-3,88) du fait d’un état bucco-dentaire plus dégradé(fréquence plus importante de débris radiculaires (respecti-vement 37,6 % et 18 %; OR = 2,03; 95 % IC, 1,52-2,71) et decellulites d’origine dentaire (respectivement 7,8 % et 1,2 %;OR = 7,13; 95 % IC, 2,78-18,29).Conclusion : L’inhomogénéité des motifs de consultationentre les différents contingents de l’ONU pourrait être liéà des qualités inégales de mise en condition dentaire(meilleure mise en condition dentaire chez les militairestogolais). L’état bucco-dentaire dégradé des patients AMPpourrait être lié au manque de structures locales de soins
dentaires aggravé par la guerre et à la précarité de lapopulation. Cet état dentaire implique une fréquence éle-vée du besoin en soins chirurgicaux qui doit être prise encompte dans la formation des chirurgiens-dentistes proje-tés. Plus généralement, le nombre de patients ONU prisen charge et la diversité de leur nationalité montrent l’im-portance du soutien dentaire dans le maintien de la capa-cité opérationnelle des forces et la capacité du service desanté des armées togolais à assurer ce soutien.
REFERENCES
11. Organisation des nations unies. MINUSMA -Mission multidi-mensionnelle intégrée des Nations Unies pour la stabilisationau Mali. Historique. Accessible le 30 juillet 2015 surhttp://www.un.org/fr/peacekeeping/missions/minusma/back-ground.shtml
12. De BRITO M. The relationship between peacekeepers, hostgovernments and the local population. Monograph no 10 :conflict management, peacekeeping and peace building.Maputo : United Nations Institute for Research Development.
13. GUNEPIN M, BENMANSOUR A, DERACHE F, MARESCA S,BLATTEAU JE, RISSO JJ. Motifs de consultation en urgenceau cabinet dentaire du groupement médico-chirurgical deGao : quelles leçons en tirer ? Médecine et Armées 2015;43 (4) : 345-51.
14. BOUASSALO KM, ADAM S, SAMA HD, KEBINA BE, BISSAH, GUNEPIN M. Problèmes dentaires rencontrés par lesforces Togolaises déployées au Mali. Médecine et armées2015. Soumis pour publication.
15. GUNEPIN M, DERACHE F, AUSSET I, BERLIZOT P, SIMECEK J.The rate of dental emergencies in French Armed Forcesdeployed to Afghanistan. Mil. Med. 2011; 176 (7) : 828-325.
16. DUNN WJ. Dental emergency rates at an expeditionarymedical support facility supporting Operation EnduringFreedom. Mil Med. 2004 May; 169 (5) : 349-53.
17. MAHONEY G, COOMBS M. A literature review of dentalcasualty rates. Mil Med 2000; 165 : 751-756.
18. MAHONEY D. The operational dental officer in the ADF.ADF Health 2003; 4: 40-44.
19. MOSS D. Dental Emergencies during Stabilization Force 8in Bosnia, Mil Med. 2002; 167 (11) : 904-6.
10. SIMECEK JW, COLTHIRST P, WOJCIK BE, EIKENBERG S,GUERRERO AC, FEDOROWICZ A, SZESZEL-FEDOROWICZW, DeNICOLO P. The incidence of dental disease nonbat-tle injuries in deployed U.S. Army personnel. Mil Med.2014; 179 (6) : 666-73.
11. Organisation du Traité de l’Atlantique Nord (OTAN). Stanag 2466.Normes d’aptitude dentaire pour le personnel militaire et classifi-cation OTAN des aptitudes dentaires. Edition 3. 10 octobre 2014.NSO (MED) 1203 (2014) MEDSTD/2466. Accessible le 16 novembre2015 sur http://nso.nato.int/nso/zPublic/stanags/CURRENT/2466EFed03.pdf
12. GUNEPIN M, DERACHE F. Impact opérationnel et prise encharge des pathologies bucco-dentaires dans le cadre desopérations extérieures. Médecine et Armées 2009; 37 : 313-8.
13. Organisation du Traité de l’Atlantique Nord (OTAN). Stanag2466. Normes d’aptitude dentaire pour le personnel militaire etclassification OTAN des aptitudes dentaires. Edition 3. 10 octo-bre 2014. NSO (MED) 1203 (2014) MEDSTD/2466. Accessible le4 juillet 2015 sur http://nso.nato.int/nso/zPublic/stanags/CUR-RENT/2466EFed03.pdf
22International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Activite Dentaire_BOUASSALO.qxp_Mise en page 1 18/03/2016 13:43 Page7

et des cellulites parmi les motifs de consultation traduisantun défaut de suivi des patients en raison du manque destructures de soins, aggravé par la guerre, et de la préca-rité de la population. Cette fréquence élevée du besoin ensoins chirurgicaux doit être prise en compte dans la for-mation des chirurgiens-dentistes appelés à être projetéssur les théâtres d’opérations.
Concernant les patients ONU, l’analyse des motifs deconsultation dentaire montre que la fréquence des cariesest moins élevée chez les militaires Togolais qu’au sein desautres contingents. Les caries étant des pathologies pou-vant être dépistées et traitées avant la projection, ce résul-tat pourrait traduire une meilleure mise en condition den-taire des forces Togolaises par rapport aux autres contin-gents. D’autres études sont nécessaires pour préciser le lienentre la qualité de la mise en condition dentaire et les fré-quences et les motifs de consultation dentaire en urgenceau sein des forces africaines.
Plus généralement, le nombre de patients ONU ayantnécessité une prise en charge odontologique montre unenouvelle fois l’importance du soutien dentaire dans lemaintien de la capacité opérationnelle des forces proje-tées. Au Mali, ce soutien dentaire été rendu possible par lamontée en puissance de l’odontologie militaire au sein desforces togolaises. Le Togo participe ainsi à l’autonomie desforces africaines lors des opérations de l’ONU.
RESUME
Introduction : Dès 2012, le contexte sécuritaire au Mali aconduit l’Organisation des Nations Unies (ONU) à créer deuxmissions internationales. Afin d’assurer le soutien dentairedu personnel de ces missions (patients ONU) et l’aide médi-cale aux populations (patients AMP), le service de santé desarmées Togolais a projeté au Mali un cabinet dentaireimplanté au sein de l’hôpital de niveau 2 (HN2-Togo).Méthode : Les données médico-administratives despatients consultant au service dentaire de l’HN2-Togo ontété recueillies du 22 février 2013 au 30 octobre 2014.Résultats : Au cours de l’étude, 929 patients ont été pris encharge (dont 415 militaires de huit nationalités différentes)et 894 traitements ont été réalisés. Les caries sont le pre-mier motif de consultation des patients ONU (22,9 % desmotifs de consultation) hormis pour les militaires togolaischez qui les caries sont moins fréquentes que pour le restedes patients ONU (OR = 0,4; 95 % IC, 0,24-0,66). Les traite-ments les plus fréquents chez les patients ONU sont lesavulsions (34,3 %) et les obturations coronaires (31,7 %).Chez les patients AMP les avulsions sont plus fréquentes(30,6 %) que chez les patients ONU (OR = 2,95; 95 % IC,2,24-3,88) du fait d’un état bucco-dentaire plus dégradé(fréquence plus importante de débris radiculaires (respecti-vement 37,6 % et 18 %; OR = 2,03; 95 % IC, 1,52-2,71) et decellulites d’origine dentaire (respectivement 7,8 % et 1,2 %;OR = 7,13; 95 % IC, 2,78-18,29).Conclusion : L’inhomogénéité des motifs de consultationentre les différents contingents de l’ONU pourrait être liéà des qualités inégales de mise en condition dentaire(meilleure mise en condition dentaire chez les militairestogolais). L’état bucco-dentaire dégradé des patients AMPpourrait être lié au manque de structures locales de soins
dentaires aggravé par la guerre et à la précarité de lapopulation. Cet état dentaire implique une fréquence éle-vée du besoin en soins chirurgicaux qui doit être prise encompte dans la formation des chirurgiens-dentistes proje-tés. Plus généralement, le nombre de patients ONU prisen charge et la diversité de leur nationalité montrent l’im-portance du soutien dentaire dans le maintien de la capa-cité opérationnelle des forces et la capacité du service desanté des armées togolais à assurer ce soutien.
REFERENCES
11. Organisation des nations unies. MINUSMA -Mission multidi-mensionnelle intégrée des Nations Unies pour la stabilisationau Mali. Historique. Accessible le 30 juillet 2015 surhttp://www.un.org/fr/peacekeeping/missions/minusma/back-ground.shtml
12. De BRITO M. The relationship between peacekeepers, hostgovernments and the local population. Monograph no 10 :conflict management, peacekeeping and peace building.Maputo : United Nations Institute for Research Development.
13. GUNEPIN M, BENMANSOUR A, DERACHE F, MARESCA S,BLATTEAU JE, RISSO JJ. Motifs de consultation en urgenceau cabinet dentaire du groupement médico-chirurgical deGao : quelles leçons en tirer ? Médecine et Armées 2015;43 (4) : 345-51.
14. BOUASSALO KM, ADAM S, SAMA HD, KEBINA BE, BISSAH, GUNEPIN M. Problèmes dentaires rencontrés par lesforces Togolaises déployées au Mali. Médecine et armées2015. Soumis pour publication.
15. GUNEPIN M, DERACHE F, AUSSET I, BERLIZOT P, SIMECEK J.The rate of dental emergencies in French Armed Forcesdeployed to Afghanistan. Mil. Med. 2011; 176 (7) : 828-325.
16. DUNN WJ. Dental emergency rates at an expeditionarymedical support facility supporting Operation EnduringFreedom. Mil Med. 2004 May; 169 (5) : 349-53.
17. MAHONEY G, COOMBS M. A literature review of dentalcasualty rates. Mil Med 2000; 165 : 751-756.
18. MAHONEY D. The operational dental officer in the ADF.ADF Health 2003; 4: 40-44.
19. MOSS D. Dental Emergencies during Stabilization Force 8in Bosnia, Mil Med. 2002; 167 (11) : 904-6.
10. SIMECEK JW, COLTHIRST P, WOJCIK BE, EIKENBERG S,GUERRERO AC, FEDOROWICZ A, SZESZEL-FEDOROWICZW, DeNICOLO P. The incidence of dental disease nonbat-tle injuries in deployed U.S. Army personnel. Mil Med.2014; 179 (6) : 666-73.
11. Organisation du Traité de l’Atlantique Nord (OTAN). Stanag 2466.Normes d’aptitude dentaire pour le personnel militaire et classifi-cation OTAN des aptitudes dentaires. Edition 3. 10 octobre 2014.NSO (MED) 1203 (2014) MEDSTD/2466. Accessible le 16 novembre2015 sur http://nso.nato.int/nso/zPublic/stanags/CURRENT/2466EFed03.pdf
12. GUNEPIN M, DERACHE F. Impact opérationnel et prise encharge des pathologies bucco-dentaires dans le cadre desopérations extérieures. Médecine et Armées 2009; 37 : 313-8.
13. Organisation du Traité de l’Atlantique Nord (OTAN). Stanag2466. Normes d’aptitude dentaire pour le personnel militaire etclassification OTAN des aptitudes dentaires. Edition 3. 10 octo-bre 2014. NSO (MED) 1203 (2014) MEDSTD/2466. Accessible le4 juillet 2015 sur http://nso.nato.int/nso/zPublic/stanags/CUR-RENT/2466EFed03.pdf
22International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Activite Dentaire_BOUASSALO.qxp_Mise en page 1 18/03/2016 13:43 Page7
advancingsepsis
managementEarly identification of sepsis is crucial to improving patient outcomes. Yet sepsis can be difficult
to differentiate from nonbacterial infections. Procalcitonin (PCT) is a biomarker that exhibits a
rapid, clinically significant response to severe bacterial infection. In patients with sepsis, PCT
levels increase in correlation to the severity of the infection. Adding the PCT biomarker assay
can help improve the accuracy of risk assessment in sepsis1 and guide therapeutic decisions.2,3
Procalcitonin (PCT)

www.cimm-icmm.org
4 th
Pan European Congress ICMM
23 24 25 26May
Mai
May
Mai
May
Mai
May
Mai
Monday
Lundi
Tuesday
Mardi
Wednesday
Mercredi
Thursday
Jeudi
Travel dayJour de voyage
---14.00 - 18.00
Welcome of attendeesRegistration
Accueil des déléguéset inscriptions
---19.00 - 21.00
Icebreakercocktail de bienvenue
9.00 - 12.35Scientifi c session
Session scientifi que---
12.30 - 13.30 Lunch - buffet Déjeuner - buffet
---14.00 - 16.00
Carousel show by the Cavalry Regiment of the French
Republican GuardCarrousel de la Garde Républicaine à cheval
---19.30 - 23.00
Gala Dinner Dîner de gala
9.30 - 12.15Welcome Accueil
Opening CeremonyCérémonie d’ouverture
Offi cial speechesDiscours des autoritésAdministrative remarksInformations logistiques
Scientifi c sessionSession scientifi que
Group photo Photo de groupe---
12.30 - 14.00Lunch - buffet Déjeuner - buffet
---14.00 - 19.00
Scientifi c sessionSession scientifi que
---Free evening Soirée libre
9.00 - 11.50 Scientifi c session &
ICMM Regional Assembly Backbrief of scientifi c sessionsClosing remarks of the Regional
AssemblyClosing ceremony
Session scientifi queet assemblée régionale Restitution des sessions
scientifi ques et conclusionsde l’assemblée régionale
Cérémonie de clôture---
12.15 - 13.30 Lunch - buffet Déjeuner - buffet
---Travel day
Jour de voyage
23-26 May 2016PARIS V
Ecole du Val-de-GracePA
RIS
• Éco le du Va l-de-Grâce • 23rd -
26th
May
201
6 Pan European Congresson Military Medicine
4th ICMM
International Congresson Military Medicine
War wounded • Epidemics and disasters• International law • Exhibition of systemsand medical devices • In a prestigious sitein the heart of Paris
Congrès internationalde médecine militaire
Blessés de guerre • Épidémie et catastrophes • Droit international
• Exposition technique autour dela médecine en opérations
• Sur un site historique au cœur de Paris
© P
hoto
s : E
CPA
D -
Sirp
a Te
rre

By L. AIGLE∑, C. GAILLARD∏, G. DOUILLARDπ, D. SCHLIENGER∫, O. BRUNEAUª, F. THIENº and V. BEYLOTΩ. France
Luc AIGLE
Multiple Casualties: Regulation of a Non-SaturatedMass Casualties by French Medical Teams duringSANGARIS Operation in Centrafrican Republic.
After entering the School of Health Services at Bordeaux in 1992, Colonel Dr. LucAIGLE served successively in the 1st Paratroopers Regiment (1 RCP), the 2nd Foreign
Paratroopers Regiment (2 REP), the 13th Foreign Legion Demi-Brigade (13 DBLE)and the 1st Marine Infantry Paratroopers Regiment (1 RPIMa). He took command of
the Army Medical Center (CMA) of Calvi (2nd REP) in summer 2013. Being an experienced"operational skydiver" since 2002 and trained to jump on Very High Altitude, he is the author of a medicalthesis on "Stress during the operational skydiving at great heights: contribution of ECG Holtering".
Colonel AIGLE is also at the foundation of the development in medical aid in combat situations within theCommando Parachute Group (GCP), since 2004 and within the units of the 11th Paratroopers Battalion.
Cited several times, he participated in many foreign operations, especially in Africa and Afghanistan.
25International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Blessés multiples : gestion d’un afflux limité non saturant par les équipes médicales de l’opérationSANGARIS en République Centrafricaine.
Le 3 juillet 2014 dans la soirée, alors que la force SANGARIS patrouille dans une ville de province, la tension monte avec desrebelles,… une grenade explose au milieu d’un groupe de combat français. Le lendemain matin, un autre mouvement de foulehostile survient sur Bangui provoquant une nouvelle poussée de tension et le jet d’une autre grenade… ainsi que d’autres blessésfrançais.L’ensemble du dispositif médical de la force française est alors mis en œuvre pour gérer ces afflux limités non saturants successifs.Au total, trois équipes médicales de l’avant, deux équipes AMET, les Rôle 1 et Rôle 2 de Bangui, le tout régulé par le DIRMED etle PECC pour la gestion des évacuations intra théâtre puis vers la France, auront pris en charge 14 blessés en moins de 20 heures.Après un bref rappel sur le dispositif en présence et les événements militaires survenus les 3 et 4 juillet, nous reviendrons sur lagestion de cet afflux limité non saturant pendant près de 19 heures afin d’en tirer des enseignements sur l’optimisation du tempset la gestion au « fil de l’eau » des évacuations afin de ne pas compromettre les capacités de relevage à l’avant ni de saturer leRôle 2.
INTRODUCTION
We report the medical management, by ROLE 1 and 2 of theSANGARIS force II, of 14 French combat casualties in a conti-nuous and non-saturating influx during the night of 3 and 4July 2014 in Bambari and also Bangui in the Central AfricanRepublic (CAR).
Looking at the context in which the elements were engagedin and the organisation of the medical support, we will firstlyhave a look at the chain of events, then analyse the results ofmedical care of the front line casualties and also the TACT-AE,
the triage, front line surgery, and STRAT-AE. Finally we willgive an insight of the various problems encountered facingthis continuous influx of combat casualties as seen by theDIRMED and as seen by the PECC.
CONTEXT
Rules of SANGARIS forces engagement
On 5 December 2013 the operation was put into actionafter voting of Resolution N° 2127 of the United Nation inorder to cease intercommunity hostilities in the CAR. With
VOL.89/1
KEYWORDS: Role 2, Multiple casualties, Forward Field Medical Card, Forward medicine, Triage.MOTS-CLÉS : Antenne chirurgicale, Afflux non saturant, Fiche Médicale de l’Avant, Médecine de l’avant, Triage.
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page1
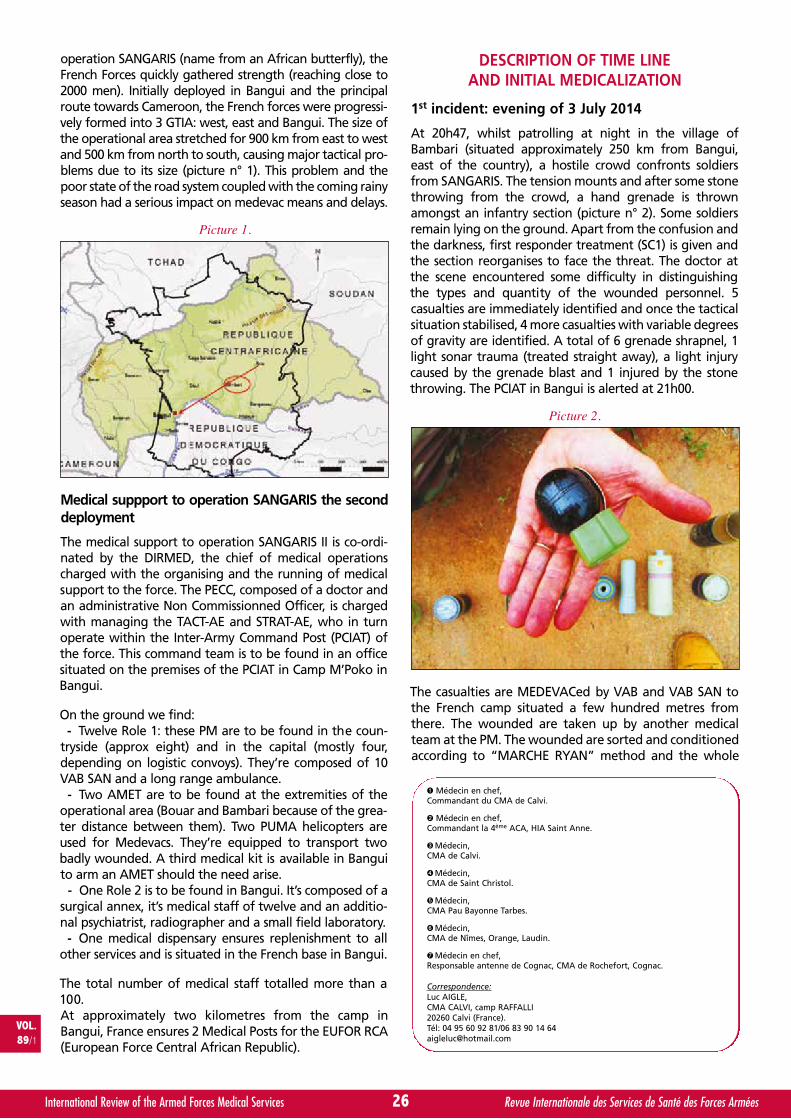
operation SANGARIS (name from an African butterfly), theFrench Forces quickly gathered strength (reaching close to2000 men). Initially deployed in Bangui and the principalroute towards Cameroon, the French forces were progressi-vely formed into 3 GTIA: west, east and Bangui. The size ofthe operational area stretched for 900 km from east to westand 500 km from north to south, causing major tactical pro-blems due to its size (picture n° 1). This problem and thepoor state of the road system coupled with the coming rainyseason had a serious impact on medevac means and delays.
Medical suppport to operation SANGARIS the seconddeployment
The medical support to operation SANGARIS II is co-ordi-nated by the DIRMED, the chief of medical operationscharged with the organising and the running of medicalsupport to the force. The PECC, composed of a doctor andan administrative Non Commissionned Officer, is chargedwith managing the TACT-AE and STRAT-AE, who in turnoperate within the Inter-Army Command Post (PCIAT) ofthe force. This command team is to be found in an officesituated on the premises of the PCIAT in Camp M’Poko inBangui.
On the ground we find:- Twelve Role 1: these PM are to be found in the coun-
tryside (approx eight) and in the capital (mostly four,depending on logistic convoys). They’re composed of 10VAB SAN and a long range ambulance.
- Two AMET are to be found at the extremities of theoperational area (Bouar and Bambari because of the grea-ter distance between them). Two PUMA helicopters areused for Medevacs. They’re equipped to transport twobadly wounded. A third medical kit is available in Banguito arm an AMET should the need arise.
- One Role 2 is to be found in Bangui. It’s composed of asurgical annex, it’s medical staff of twelve and an additio-nal psychiatrist, radiographer and a small field laboratory.
- One medical dispensary ensures replenishment to allother services and is situated in the French base in Bangui.
The total number of medical staff totalled more than a100.At approximately two kilometres from the camp inBangui, France ensures 2 Medical Posts for the EUFOR RCA(European Force Central African Republic).
DESCRIPTION OF TIME LINEAND INITIAL MEDICALIZATION
1st incident: evening of 3 July 2014
At 20h47, whilst patrolling at night in the village ofBambari (situated approximately 250 km from Bangui,east of the country), a hostile crowd confronts soldiersfrom SANGARIS. The tension mounts and after some stonethrowing from the crowd, a hand grenade is thrownamongst an infantry section (picture n° 2). Some soldiersremain lying on the ground. Apart from the confusion andthe darkness, first responder treatment (SC1) is given andthe section reorganises to face the threat. The doctor atthe scene encountered some difficulty in distinguishingthe types and quantity of the wounded personnel. 5casualties are immediately identified and once the tacticalsituation stabilised, 4 more casualties with variable degreesof gravity are identified. A total of 6 grenade shrapnel, 1light sonar trauma (treated straight away), a light injurycaused by the grenade blast and 1 injured by the stonethrowing. The PCIAT in Bangui is alerted at 21h00.
The casualties are MEDEVACed by VAB and VAB SAN tothe French camp situated a few hundred metres fromthere. The wounded are taken up by another medicalteam at the PM. The wounded are sorted and conditionedaccording to “MARCHE RYAN” method and the whole
26International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
∑ Médecin en chef,Commandant du CMA de Calvi.
∏ Médecin en chef,Commandant la 4ème ACA, HIA Saint Anne.
π Médecin,CMA de Calvi.
∫ Médecin,CMA de Saint Christol.
ª Médecin,CMA Pau Bayonne Tarbes.
º Médecin,CMA de Nîmes, Orange, Laudin.
Ω Médecin en chef,Responsable antenne de Cognac, CMA de Rochefort, Cognac.
Correspondence:Luc AIGLE,CMA CALVI, camp RAFFALLI20260 Calvi (France).Tél: 04 95 60 92 81/06 83 90 14 [email protected]
VOL.89/1
Picture 1.
Picture 2.
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page2

second responder treatment (SC2) methodology isapplied. The first assess of the situation are reported tothe PECC in order to establish evacuation priorities. At thesame instant, a soldier on guard is bitten by a scorpion onthe lower leg, he is taken to the PM for treatment.
Following this first phase, we account for:- Two “Alpha” casualties, (vascular leg wounds),- Four “Bravo” casualties (flesh wounds by grenade
shrapnel)- Four “Charlie” casualties (light sonar trauma, a
lightly blasted, an injured by stone throwing, a scorpionbite), according to the 9-lines medical request classifica-tion used (evacuation delay for a patient classed A < 1h30,B < 4h, C < 24h, routine).
2nd incident: morning of 4 July 2014
In the early morning, hostile barricades are rised in thecapital city against the international presence. Several ele-ments of SANGARIS and EUFOR are attacked 2km from theFrench camp of M’Poko on the road leading to the airport.Here too the situation deteriorates. Stone throwing andMolotov cocktails are followed by a grenade thrown at theFrench soldiers at 10h15. A first soldier is injured by thestone throwing whilst two others are injured by grenadeshrapnel. At 11h05 a fourth EUFOR soldier is wounded bygrenade shrapnel. They all receive initial SC1 treatmentand are evacuated to the Role 1 of the EUFOR not far fromthere. After having their wounds re-evaluated, theyreceive additional SC2 treatment and are evacuated to theRole 2. The DIRMED follows the events in real time as he ispresent at the PCIAT because of the day’s events.
The assessment give through is:- Two initial “Bravo” patients (articulation of the finger
and shrapnel in the groin, shrapnel in the buttock).- Two “Charlie” (shrapnel in the thigh and stone
throw in the face and elbow).
In total, the assessment of the soldiers taken into careat Role 1 level in the field following the two clashes isfourteen wounded and are set out as follows:At BAMBARI:
Six wounded by grenade shrapnelOne light sonar traumatismOne blasted by the grenade explosionOne light stone throwing casualtyOne scorpion bite at the FOB
At BANGUI:One stone throwing casualtyThree wounded by grenade shrapnel
TACT-AE MANAGEMENT
Let us take a look at the management of the two inci-dents separately. The rundown of the events can beseen in the time line of the table n° 1.Evening of 3 July 2014
The evacuation management was co-ordinated by thePECC who was inserted in the OC of the PCIAT. Becauseof its geographical distance from Bambari, the onlyevacuation route available was by air.
The means available were: one AMET team stationed inBambari. A second medical team present in the campof Bria, was positioned there and made use of theopportunity to medically equipe a tactical helicopterfor use in another operation. Finally, tactical air trans-port planes were used to ensure rotations betweenBambari and Bangui during the day of 4 July.
The first two casualties, initially classified “Alpha” wereflown out on a first rotation by the AMET who werealready in place, this allowed decluttering casualties atthe MP of Bambari. At the same time an AMET was cal-led in from Bria, making use of the presence of a doc-tor, a nurse and an available helicopter to evacuate 4other casualties that evening.
One of the wounded by shrapnel, who at first remai-ned in his combat platoon, was finally flown out on arotation by ATT late in the morning on next day, due tothe severity of his injury (open fracture of the ulna).
All of these casualty evacuations were activated follo-wing the standard procedure of a 9-line message sentand taking into account the problems due to distanceand the refuelling of the planes.
Morning of 4 July 2014
After a quick taking into care of the casualties by theRole 1 of the EUFOR, the problem soon arose as to thebarricades that blocked access to the camp. They sepa-rated the Role 1 from the Role 2. The doctor at the MPwas asked to prepare the evacuations by VAB SAN inorder to eventually force the barricades once the ordergiven.
The primary objective of the DIRMED was to preventthe saturation of the Role 1 and to ensure it more free-dom of movement as the tension remained high in thetown all day. The first evacuation of 2 casualties tookplace around 10h30 and a second at 11h30. The 9-linemedevac was equally used and sent over the commandnetwork for these evacuations.
TRIAGE AND SURGERY’S CONCLUSIONON BANGUI
Overall after the initial management on the ground byteams of Role 1 and the TACT-AE, 11 casualties werefinally received, sored and processed on the Role 2 ofBangui (picture n° 3): six grenade shrapnel’s injuredand a scorpion bite from Bambari and three grenadefragments wounded and a jet of stone on Bangui.Patients were numbered as follows:
• Patient 1: schrapnel right leg, left ankle, vascularwound (femoral vein).
• Patient 2: schrapnel left thigh.• Patient 3: schrapnel left elbow, left thigh, left leg,
arterial section and tibial lesion of left tibias.• Patient 4: schrapnel left thigh, right arm, right hip.• Patient 5: schrapnel left thigh.• Patient 6: calf scorpion sting.• Patient 7: schrapnel left elbow, open fracture ulnar.
27International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page3

• Patient 8: fracture by splinters of a finger, schrapnelleft hip.
• Patient 9: schrapnel wound to the buttock.• Patient 10: elbow contusion seen in Role 1 and Role
2 radiography.• Patient 11: schrapnel wound of the thigh.
The surgical care took place in two times: between00h10 and 7h00 AM for the first influx, then between12h10 and 16h10 pm for the second round of casualties.
It consisted in a stabilization of vital functions beforeoperating for trimming and wound debridement.Vascular lesions were controlled by vascular and thoracicsurgeon. Joints and soft parts were washed. Schrapnelwere removed if possible (picture n° 4), but without riskof aggravating the injury and without slowing down therhythm of procedures. We have not closed lesionswithout drainage and members have all been fixed. Thewar-surgery antibiotic prophylaxis protocol associatedgentamicin and amoxicillin + clavulanic acid.
MANAGEMENT OF STRAT-AE
Upon receipt of the first results and due to the numberand type of injuries, it was asked at the medical EMO totake off a first type of FALCON’s aircraft (picture 5) inorder to quickly evacuate the most serious patients andto alert a second aircraft able to take off depending onthe evolution of the clinical situation of the wounded.
The choice of patients to be evacuated was made aftersorting, integrating the severity of some wounds and
the results of the first surgeries in a tripartite dialogueinvolving the PECC, the DIRMED and the head of thefield hospital. The first FALCON evacuated two woundedlying, from the early morning of July 4.
Medical information was transmitted in real time byPECC at the medical EMO throughout the night inorder to adapt the configuration of the second planecarrying three casualties (two long and one sitting). OnJuly 4th in the late morning consideration of four newconsecutive casualties in a clash, which occurred inBangui, obliged us to change the evacuation order ofpatients.
Filling of both aircraft was optimized (Table 1) in order toextract the maximum patients from the theater due to theunpredictable situation, typical of the CAR intervention.
Once again, we aimed to decongest the antenna asquickly as possible in view of the highly unstable situa-tion in Bangui and the provinces.
The last patients were secondarily evacuated by a sche-duled flight. Finally, three patients treated for gunshotand scorpion’s sting were kept in the theatre becauseof the favourable evolution of their lesions.
DISCUSSION
Total management other 19 hours is sum up in a "timeline". It allows understanding the management by theDIRMED, PECC of all health chain components (Table 1).It will serve as a basis for discussion at to follow.
28International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Picture 3.
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page4
1. Special feature of this support
It has been a limited non saturating influx taking placein two stages. These events had a total duration of 19h,from initial management until take off of the secondFALCON. It required a perfect coordination among allhealth actors of the field.
Medical facilities were sufficient and had never beenoverwhelmed or saturated, all the casualties have beentreated. Triage performed on the antenna allowed stag-gering surgeries and conditioning before evacuation. Thefirst STRAT-AE to France has helped to keep or restore asufficient capacity at all levels of the health chain.
Two patients have returned to the national territory bymilitary airplane on the 6th and 9th July. The last threeheld in the territory have return on duty after 15 daysof treatment on average.
2. Forward medicalization
All casualties were taken over following the "MARCHERYAN" Combat Rescue method1. The set of actions wasachieved without problem: first dressings, tourniquetsthat were subsequently revaluated considering patho-logy, then morphine analgesia by auto injection syringeand titration, immobilization, injection of 1g of tra-nexamic acid2 for the two most seriously wounded the,
29International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
NUMBER
NAME
HOUR OF
ARRIVAL
DIAGNOSTICBLOOD
PRESURE
HEART
RATE
HEMO-GLOBIN
OXYGEN
SATURATION
GLASGOW
SCOREXRAY
EMERGENCY
CLASSIFICATION
SURGERY
RANKBECOMING
1 23h33MultipleWounds
110/70 66 10 100% 15Pulmonary
2 Legs2 2 Falcon 1
2 23h33
LeftThigh and
KneeSchrapnel
140/78 101 11 and 9 100% 14Left
Thigh2 1 Falcon 2
3 01h45SchrapnelLeft Leg
124/70 64 12 98% 15Thigh andLeft Leg
2 3 Falcon 1
4 01h45SchrapnelLeft ThighRigh Hip
110/55 78 11 100% 15Thigh
HumerusPelvis
2 4 Falcon 2
5 01h45SchrapnelLeft Leg
123/11 60 13 97% 15 Left Leg 3 5R1 and
R2
6 01h45Scorpion
Sting129/73 83 11 100% 15 - 3 - R1
7 10h35Buttock
Schrapnel117/88 87 13 100% 15
HipPelvis
2 7 R2
8Finger
and HipSchrapnel
121/76 76 10 98% 15Finger
Hip2 6 Falcon 2
9Elbow
Contusion109/69 81 13 100% 15 Elbow 3 - R1
10 11h30Elbow
Schrapnel125/75 69 12 97% 15
RightElbow
2 8 Falcon 2
11 10h35Thigh
Schrapnel124/88 74 13 100% 15
RightThigh
3 9 Role 2
Picture 4.
Picture 5.
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page5
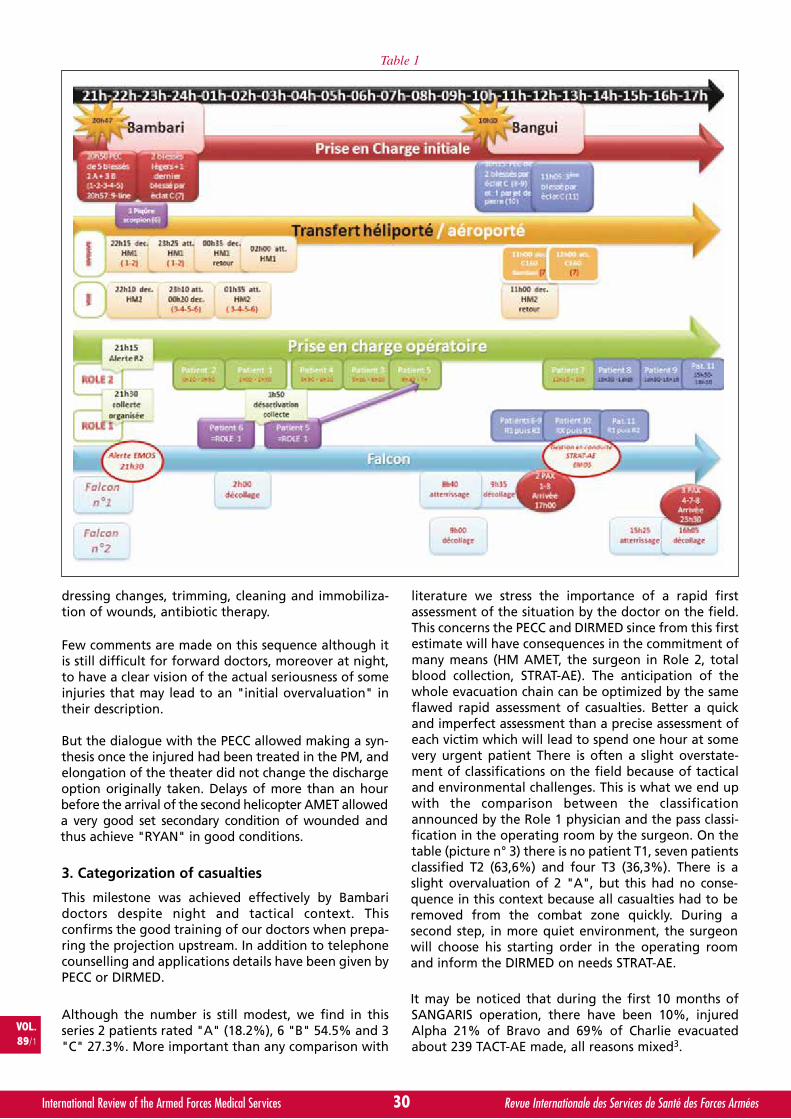
dressing changes, trimming, cleaning and immobiliza-tion of wounds, antibiotic therapy.
Few comments are made on this sequence although itis still difficult for forward doctors, moreover at night,to have a clear vision of the actual seriousness of someinjuries that may lead to an "initial overvaluation" intheir description.
But the dialogue with the PECC allowed making a syn-thesis once the injured had been treated in the PM, andelongation of the theater did not change the dischargeoption originally taken. Delays of more than an hourbefore the arrival of the second helicopter AMET alloweda very good set secondary condition of wounded andthus achieve "RYAN" in good conditions.
3. Categorization of casualties
This milestone was achieved effectively by Bambaridoctors despite night and tactical context. Thisconfirms the good training of our doctors when prepa-ring the projection upstream. In addition to telephonecounselling and applications details have been given byPECC or DIRMED.
Although the number is still modest, we find in thisseries 2 patients rated "A" (18.2%), 6 "B" 54.5% and 3"C" 27.3%. More important than any comparison with
literature we stress the importance of a rapid firstassessment of the situation by the doctor on the field.This concerns the PECC and DIRMED since from this firstestimate will have consequences in the commitment ofmany means (HM AMET, the surgeon in Role 2, totalblood collection, STRAT-AE). The anticipation of thewhole evacuation chain can be optimized by the sameflawed rapid assessment of casualties. Better a quickand imperfect assessment than a precise assessment ofeach victim which will lead to spend one hour at somevery urgent patient There is often a slight overstate-ment of classifications on the field because of tacticaland environmental challenges. This is what we end upwith the comparison between the classificationannounced by the Role 1 physician and the pass classi-fication in the operating room by the surgeon. On thetable (picture n° 3) there is no patient T1, seven patientsclassified T2 (63,6%) and four T3 (36,3%). There is aslight overvaluation of 2 "A", but this had no conse-quence in this context because all casualties had to beremoved from the combat zone quickly. During asecond step, in more quiet environment, the surgeonwill choose his starting order in the operating roomand inform the DIRMED on needs STRAT-AE.
It may be noticed that during the first 10 months ofSANGARIS operation, there have been 10%, injuredAlpha 21% of Bravo and 69% of Charlie evacuatedabout 239 TACT-AE made, all reasons mixed3.
30International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Table 1
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page6

4. FMA and identification
Casualty management by serial number is the only rule(left column on the picture n° 3). It has once more permit-ted to speak on the radio and call simply and reliably4. Thenew FMA is well suited except missing of a box dedicatedto the registration of the injured’s number5. We can alsoregret the too poor room devoted to follow constants.Proposals for improvement were made in this direction.
The exact casualties’ identification of is paramount forthe DIRMED in the frame of official reports, and thehealth chain is initially more responsive to confirmthese data requested to decide.
Nevertheless the main challenge for the health systemis set in the nature and severity of the injuries, in orderto anticipate the arrival of injured (preparation of ope-ration room sequences, sterilization management, aler-ting the whole blood collection system, consideringresupply). In the initial precipitation may occur harmfulidentity’s errors (bad identity and/or bad informationtransmitted which could have significant consequencesfor relatives in France). The media coverage of conflictand the quick transmission of information requiregreat vigilance in this area.
The communication advisor of the commander of theforce participate in the control of information.
5. Time
The expected time scheduled in our rules of engagement6
have been respected in terms of elongation: 2h30 wereneeded to arrive to Bangui for the first two casualties and3h40 for the following 4. Anticipation and availability ofvectors have reduced the trigger delay.
We had an average engagement time of helicopter veryshort due to the rapid drafting of "9-lines" (it was madeby the PECC at PCIAT, with locations of helicoptersalready known).
In some theaters such as middle Africa or Mali, categori-zation of our casualties, which was relevant forAfghanistan (very short evacuation time to the surgeon)was no longer adapted and became obsolete due tolong distance evacuation7, 8. Casualties are often eva-cuated not because they are serious, but because theyare far from the Role 2 and they may deteriorateSecondarily. This requirement related to the fieldconstraints explains the choice made to quickly evacuatethe Bambari scorpion sting. Indeed, in case of worseningit was no longer possible to pick up the patient for manyhours. The experience of engagement in Afghanistan9
and especially in Mali showed an upsurge of such biteswith sometimes highly complex clinical cases to manage,especially in the absence of Scorpifav® in CAR10, 11.
6. Transmissions
That night, military communication networks, as well aslocal telephony were of good quality. If the use of localmobile phone can be discussed during some missions, in
the context of engagement in CAR, patient’s safety hasbeen a priority over any other tactical consideration.
The "mood balance sheet" obtained from the firstminutes allowed the PECC to make quick choices, butalso to give advices to doctors deployed on the field.
Nevertheless, it appears that the military medical serviceshould provide each PM a satellite phone to give moreautonomy and safety in the crucial phase of initialassessment and regulation of discharges from the front4.
Moreover the quality of the chain alert of the medical EMOallowed rapid mobilization of resources12. This responsive-ness and confidence that was placed in us has enabled theprovision of 2 FALCON including a "blind" starting and thenext driving. It was possible to change a patient during theday for the second FALCON (communication possibleduring the flight) depending on the evolution of the triageand surgeries related to the second collision.
7. Role 1 in Bangui
Some personal was first appointed in reception and trans-fer of all casualties in yard area in front of the antenna, andin a second time welcomed some patients who had alreadybenefited from the triage (scorpion sting, people waitingto the operating room). Similarly when the transferring offour injured on July 4th, they received a first evaluation inRole 1 before switching to some at Role 2.
The other part of the personal has been able to raise veryquickly a whole blood collection chain within the infra-structure of Role 1 (from 9h30 pm). It should be empha-sized the high reactivity of the militaries who massivelyattended and remained there until the lifting of the alertdecided by the resuscitator at 1h50 on July 4 (Table 1).
8. Role 2
A total of nine surgeries have followed in two stages: 6during the night then 3 during the next day, with 11hours of actual surgery on a total of 16 hours. The ste-rilization was performed to allow continuous flow andseamless surgical sequence.
A team composed by an anaesthetist nurse (IADE), anurse (IDE) and a paramedic (AS) was kept in reserveafter triage has been done. It took over the block in themorning allowing the first team to reach the airport forthe first STRAT-AE. There was almost no loss of time bet-ween operations because awakening of patients wasmade in resuscitation area by nurses previously trainedin their respective hospitals. The principles of "damagecontrol" have been applied: quick surgical care, stabili-zation, without attempt to be comprehensive, enablingeffective resuscitation and sometimes requiring a"second look" after 48 hours to complete treatment.There was no saturation of the surgical unit despite thelimited number of hospital beds (six) as the first eva-cuations to France liberated some place. Tiredness wasbearable for the personal, thanks to operations, whichdid not lasted beyond 16 hours.
31International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page7

9. Composition of teams
Role 1: the dispersion of medical teams on the groundimposed by splitting of the force nevertheless alloweda quality medical network, sometimes split into twoteams (physician and AS, nurses and AS on two diffe-rent sites).
AMET: The format has proven to be suitable and well-sized. Their positioning on the field was a major gainfor reducing evacuation times. We have always had theability to generate a third opportunity to team Banguiby taking off a doctor and a nurse from the Role 1Bangui.
Role 2: "enhanced" format is particularly suitable, thepresence of a manipulator and a radiological labora-tory being real efficient. Having an IDE in addition allo-wed also to create a working team to manage theinflux of wounded and waking but also the hospitalseveral days later.
10. DIRMED and PECC
It should be emphasized the very good coordinationwith PCIAT but also with medical EMO and doctors onthe field which prevailed throughout that sequence13.This is the consequence of a good knowledge of thetheater, of the teams and of well-established procedures(9-Lines, official messages).
Contact with medical EMO has always been easy andconstituted a good support for the team DIRMED/PECC which was deployed for the first time in thesefunctions.
The co-location of Role 1, Role 2 and DIRMED/PECC inthe same place (M’poko) and a good mutual know-ledge were assets for the wounded in the managementof this influx14. Fortunately, a MASCAL exercise and atotal blood collection exercise had been performedsome days before, again emphasizing the importanceof this type of preparation.
The policy of the binomial DIRMED/PECC was to quicklyretrieve all the casualties on the field for several reasons:restore flexibility of action at 2 PM (EUFOR and Bambari)because of ongoing problems, allowing them to regene-rate their means "Health"(teams and equipment includingequipment for the fighters SC1) by the return on theBambari position of the first AMET (at 2h00 am) based onthe expected consumption of "consumables" health.
Regarding the STRAT-AE, the will of the PECC to quicklyevacuate patients from the theater was of course lin-ked to the need not to overload the Role 2 in view ofthe volatile situation in Bangui.
Furthermore, the complexity of any night landing onM’poko airport (absence of markup, risk of flooding ofthe track by the population of CAR refugees from slee-ping on the hot tar at nightfall) was taken into accountin the planning of arrivals of both Falcon.
CONCLUSION
These intense and almost 19 hours of continuous medicalcare and evacuation management have been marked bymajor fluidity of the sequence and the satisfaction of seeingthe most serious injuries repatriated in France so quickly.There is little time to win over the whole of the sequence.This must be credited to the quality of training of any healthsystem and the need to train upstream. The French commit-ment in Afghanistan has raised awareness among comba-tants blood donation: the number and spontaneity soldierswho volunteered are there to remind us.
The quality of the training of Role 1, the right positioningof the AMET, the Role 2 enhanced and the binomial DIR-MED/PECC have contributed to the success of this sequencewar medicine.
The management of this influx of wounded had a verypositive impact on the moral of the SANGARIS force butalso of EUFOR troops.
ABSTRACT
In the evening of 2014 July the 4, during a SANGARIS ope-ration ground patrol in a provincial town tension increasesuddenly with the rebels… a grenade exploded in a Frenchcombat team. The next day in the morning in the capital,another hostile crowd induced a new climax of tension andone more grenade was thrown… and some more Frenchcasualties.
All the French medical teams are involved in the manage-ment of this non saturated mass casualties. For this, 3 for-ward medical teams, 2 aero medical evacuation team, allRole one and Role two teams at Bangui managed by themedical director and the patient evacuation and coordina-tion cell for the regulation of the forward evacuations andstrategic evacuations to France, were involved and managednot less than 14 French casualties.
After a short brief for the medical deployment and the mili-tary context of the 3 and 4 of July, we came back to themanagement of this non saturation mass casualties during19 hours to extract some learnings of optimization of timesand the management of the evacuation in order toimprove role 1 capabilities and not to saturate the role 2.
Glossaries:ROLE 1: first medical outpost.ROLE 2: forward surgical team.TACT AE: tactical aero evacuation.STRAT AE: strategic aero evacuation.DIRMED: medical director.PECC: patient evacuation and coordination cell.GTIA: joint tactical group.PCIAT: joint tactical command post.PM: medical outpost.VAB: armoured personal carrier.VAB SAN: medical armoured personal carrier.AMET: aeromedical evacuation team.ATT: tactical combat plane.EUFOR: European force in CAR.
32International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page8
9. Composition of teams
Role 1: the dispersion of medical teams on the groundimposed by splitting of the force nevertheless alloweda quality medical network, sometimes split into twoteams (physician and AS, nurses and AS on two diffe-rent sites).
AMET: The format has proven to be suitable and well-sized. Their positioning on the field was a major gainfor reducing evacuation times. We have always had theability to generate a third opportunity to team Banguiby taking off a doctor and a nurse from the Role 1Bangui.
Role 2: "enhanced" format is particularly suitable, thepresence of a manipulator and a radiological labora-tory being real efficient. Having an IDE in addition allo-wed also to create a working team to manage theinflux of wounded and waking but also the hospitalseveral days later.
10. DIRMED and PECC
It should be emphasized the very good coordinationwith PCIAT but also with medical EMO and doctors onthe field which prevailed throughout that sequence13.This is the consequence of a good knowledge of thetheater, of the teams and of well-established procedures(9-Lines, official messages).
Contact with medical EMO has always been easy andconstituted a good support for the team DIRMED/PECC which was deployed for the first time in thesefunctions.
The co-location of Role 1, Role 2 and DIRMED/PECC inthe same place (M’poko) and a good mutual know-ledge were assets for the wounded in the managementof this influx14. Fortunately, a MASCAL exercise and atotal blood collection exercise had been performedsome days before, again emphasizing the importanceof this type of preparation.
The policy of the binomial DIRMED/PECC was to quicklyretrieve all the casualties on the field for several reasons:restore flexibility of action at 2 PM (EUFOR and Bambari)because of ongoing problems, allowing them to regene-rate their means "Health"(teams and equipment includingequipment for the fighters SC1) by the return on theBambari position of the first AMET (at 2h00 am) based onthe expected consumption of "consumables" health.
Regarding the STRAT-AE, the will of the PECC to quicklyevacuate patients from the theater was of course lin-ked to the need not to overload the Role 2 in view ofthe volatile situation in Bangui.
Furthermore, the complexity of any night landing onM’poko airport (absence of markup, risk of flooding ofthe track by the population of CAR refugees from slee-ping on the hot tar at nightfall) was taken into accountin the planning of arrivals of both Falcon.
CONCLUSION
These intense and almost 19 hours of continuous medicalcare and evacuation management have been marked bymajor fluidity of the sequence and the satisfaction of seeingthe most serious injuries repatriated in France so quickly.There is little time to win over the whole of the sequence.This must be credited to the quality of training of any healthsystem and the need to train upstream. The French commit-ment in Afghanistan has raised awareness among comba-tants blood donation: the number and spontaneity soldierswho volunteered are there to remind us.
The quality of the training of Role 1, the right positioningof the AMET, the Role 2 enhanced and the binomial DIR-MED/PECC have contributed to the success of this sequencewar medicine.
The management of this influx of wounded had a verypositive impact on the moral of the SANGARIS force butalso of EUFOR troops.
ABSTRACT
In the evening of 2014 July the 4, during a SANGARIS ope-ration ground patrol in a provincial town tension increasesuddenly with the rebels… a grenade exploded in a Frenchcombat team. The next day in the morning in the capital,another hostile crowd induced a new climax of tension andone more grenade was thrown… and some more Frenchcasualties.
All the French medical teams are involved in the manage-ment of this non saturated mass casualties. For this, 3 for-ward medical teams, 2 aero medical evacuation team, allRole one and Role two teams at Bangui managed by themedical director and the patient evacuation and coordina-tion cell for the regulation of the forward evacuations andstrategic evacuations to France, were involved and managednot less than 14 French casualties.
After a short brief for the medical deployment and the mili-tary context of the 3 and 4 of July, we came back to themanagement of this non saturation mass casualties during19 hours to extract some learnings of optimization of timesand the management of the evacuation in order toimprove role 1 capabilities and not to saturate the role 2.
Glossaries:ROLE 1: first medical outpost.ROLE 2: forward surgical team.TACT AE: tactical aero evacuation.STRAT AE: strategic aero evacuation.DIRMED: medical director.PECC: patient evacuation and coordination cell.GTIA: joint tactical group.PCIAT: joint tactical command post.PM: medical outpost.VAB: armoured personal carrier.VAB SAN: medical armoured personal carrier.AMET: aeromedical evacuation team.ATT: tactical combat plane.EUFOR: European force in CAR.
32International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page8
SC1/2: combat casualties care level 1/2.FOB: forward operational base.OC: operation center.EMO: operational medical command center.FMA: forward field medical card.IADE: anesthesit nurse.IDE: nurse.AS: paramedic.
BIBLIOGRAPHY
11. Enseignement Sauvetage au combat. Référentiel de for-mation validé sous le numéro d’enregistrement:0309/EVDG/DPMO du 30 mars 2012.
12. ANDREW P, DAVID G, et al. Tranexamic Acid for traumapatients: a critical review of the literature. J Trauma. 2011;71 (1): S9 – S14.
13. BEYLOT V, AIGLE L, GRAS D. Synthèse des TACTICAL AEROEVACUATION au cours de l’opération SANGARIS. Retourd’expérience sur 10 mois d’opération. Médecine aéronau-tique et spatiale. 2015; 56 (209): 28. (French).
14. AIGLE L, Le GOFF A. Prise en charge d’un afflux massif deblessés de guerre Djiboutiens par deux équipes médicalesd’unité en situation d’isolement. Médecine et Armées.2010; 38 (1): 55-62. (French).
15. Note n° 511288/DEF/DCSSA/PC/CCO du 02/06/2015 relativeà la fiche médicale de l’avant. (French).
16. MED 3.001. Délais Cliniques et catégorisation pour la relève et
le triage des blessés de guerre. 913/DEF/DCSSA/EMO du15/11/2010. (French).
17. FREIERMUTH J-P, BOISSIER J, GONZALES S, TAVEAU A,NEEL F, DE MARTENE H. Analyse de l’activité de la ForwardMEDEVAC française en Afghanistan de janvier 2010 à juin2012. Médecine et Armées. 2014; 42 (5): 421-38. (French).
18. CZERNIAK E, REGARD M, BOISSIER J, GONZALEZ S, POWELLB, BAY C. Le Patient Evacuation Coordination Center de laTask Force “La Fayette”: maillon incontournable du supportmedical des forces terrestres françaises en Afghanistan.Médecine et Armées. 2011; 39 (4): 311-6. (French).
19. DONAT N, MASSON Y, VILLEVIELLE TH, PELLETIER CH,ROUSSEAU JM, PLANCADE D et al. Envenimation scorpio-nique au Combat. Reanoxyo 2010; 26 (2): 51-2. (French).
10. Réunion annuelle du CTE dans les armées. Note n° 511705DEF/DCSSA/PC/ERS/EPID du 04/06/2015. (French).
11. Note n° 521957/DEF/DCSSA/PC/ERS/EPID du 21 octobre 2014.Modalités de prescription et de délivrance du SCORPIFAV®pour les forces de présence/en opérations en Afrique. (French).
12. MED 3.003. Procédure de demande d’évacuation médicalestratégique. 458/DEF/DCSSA/EMO du 20 avril 2011. (French).
13. Doctrine du soutien médical aux engagements opération-nels. DIA-4.0.10_SOUTMED-OPS (2014). n° 176/DEF/CICDE/NP du 31 juillet 2014. (French).
14. BOMBERT C, CHAUFER M, BOISSIER J, RICHECOEUR L. Opération« Serval » : intérêt du « patient evacuation coordination cell ».Médecine et armées. 2015 ; 43(4) : 325-29. (French).
33International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Multiple casualties_AIGLE.qxp_Mise en page 1 16/03/2016 14:59 Page9
Losberger Rapid Deployment Systems SAS58 A rue du Dessous des Berges
75013 PARIS Phone : + 33 1 46 72 42 69
Fax : + 33 1 45 85 48 46
E-mai l : [email protected]
LOSBERGER RDS
From decades, international leader in fast deployable, re-locatable and modular shel-ters systems, for civilian and military organizations.
Turnkey solutions The largest range of shel-ters and temporary/perma-nent structures :
Field Hospitals Decontamination systems
Field campsHeadquaters
Command Posts Workshops & storage hangars
COLPRO systems (CBRN) Special applications
(camouflage, missiles & radar protections).
w w w . l o s b e r g e r - r d s . c o m
Revue internationale des services de santé des forces armées.indd 1 12/03/2015 11:31:12

By Z. ZONG, S. CHEN, Q. BAO, Q. HAO, D. LIU, H. LIU, L. ZHANG, Y. SHEN and J. HUANG. China
Zhaowen ZONG
Assessment of Medical Relief Capability for MassCasualty Events in China.*
Lieutenant Colonel Zhaowen ZONG, MD and PhD,Vice Director of Department of Trauma Surgery, Daping Hospital, Third Military
Medical University, Traumatic Orthopaedics Surgeon.Major field: basic research and clinical treatment of severely injured traumatic
patients.
34International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Evaluation des capacités de prise en charge médicale d’un afflux massif de blessés en Chine;
La Chine est un pays régulièrement touché par des accidents avec pertes massives (MCEs) et cette étude a pour but d’évaluer lescapacités de prise en charge de ces MCEs. Une enquête par questionnaire a été effectuée dans 67 hôpitaux à travers tout le pays.Elle a révélé que tous les hôpitaux examinés avaient incorporé des scénarii d’inondations, de tremblements de terre et de pandémiesdans leurs plans de préparation mais que seulement une partie d’entre eux avaient prévu des accidents de circulation, des incendiesou des accidents dans les mines de charbon. Seulement 25 des 67 hôpitaux organisaient régulièrement des exercices et des misesà jour. En ce qui concerne les savoir-faire, les participants au test se sont révélés aptes pour la prise en charge des patients trau-matisés ou brûlés mais insuffisamment préparés en ce qui concerne les pandémies et les victimes d’accidents NRBC.
Nous en concluons que la capacité globale des secours médicaux en cas de MCE s’est beaucoup améliorée en Chine. Néanmoins,il persiste des lacunes comme le manque d’entraînement et la méconnaissance de certains savoir-faire. Cette constatation appelled’autres améliorations pour une prise en charge meilleure encore.
INTRODUCTION
Disaster is a difficult concept to define; existing definitionstend to be either too broad or too narrow. The WorldHealth Organization/Emergency and HumanitarianAction Department defines disasters as, «Any occurrencethat causes damage, ecological disruption, loss of humanlife or deterioration of health and health services on ascale sufficient to warrant an extraordinary response fromoutside the affected community area». An essential fea-ture of a disaster involves a major disruption of the infra-structure of a community, and always results in masscasualty. Under the circumstance of mass casualty events(MCEs), the magnitude of destruction exceeds that of rou-tine emergency situations to such an extent that the res-ponse to it must be entirely different in order to restoresome semblance of order and normalcy1. Proper triagestrategy should be used to ensure the greatest good forthe greatest number2. In addition, powerful command
and control is essential to make the MCEs medical reliefwork orderly and in high efficiency1, 3, 4.
China is one of the countries constantly affected bynatural and man-made MCEs. According to the annualreport of State Administration of Work Safety, the mostoften MCEs caused by man-made disasters in China weretraffic accidents, coalmine accidents, fire accidents andterrorist attacks, while that caused by natural disasters
VOL.89/1
KEYWORDS: Mass casualty event, China, Hospitals, Skills, Preparedness.MOTS-CLÉS : Afflux massif de blessés, Chine, Hôpitaux, Savoir-faire, Préparation.
Correspondence:Lieutenant Colonel ZhaoWen ZONGState Key Laboratory of Trauma, Burn and Combined injury,Department of Trauma Surgery, Daping Hospital,Third Military Medical University,PRC-400042 ChongQing, China,Tel: +86-23-68757996.Fax number: +86-23-68757995.E-Mail: [email protected]
* Presented at the 41st ICMM World Congress on Military Medicine,Bali, Indonesia, 17-22 May 2015.
Assessment of Medical Relief_ZONG.qxp_Mise en page 1 18/03/2016 14:02 Page1
.

were pandemics, flood, and earthquake5. Although themedical relief work for different kinds of mass casualtymight differs at various degrees due to different extentand intrinsic property of the disaster, there are some keyfactors in common to make a successful rescue occur.These factors include effective legislation, smooth com-mand and control, well-oriented and workable prepa-redness plans, sophisticated equipment and skilled medi-cal personnel6-10. Understanding the current state of themedical relief capacity for MCEs is the first step toimprove it, so the present study aimed to evaluate themain progress and existing pitfalls of the MCEs medicalrelief capability in China. The authors hope that thismanuscript could provide valuable information forpolicy-makers and medical practitioners to improvemanagement of MCEs in China.
METHODS
The protocol was reviewed and approved by the EthicalCommittee of the Daping Hospital, Third MilitaryMedical University, P.R. China.
Literature review
Extensive literature reviews were performed by sear-ching PubMed, EMBASE, Web of Science, Cochrane data-bases and the Chinese biomedical literature databasewith the terms «mass casualty», «disaster», «legislation»,«command and control», «preparedness plan», and«medical relief». Then, from the search results, we revie-wed all abstracts to find content related to the keyaspects of medical relief in China including legislation,preparedness plan, medical equipment, and medicalcare skills. Government documents and bulletins that areessential to demonstrate the topics were also included.
Hospital visit, survey and test
Hospitals play a key role in the medical relief for MCEs10,so the capacity of hospital’s medical relief for MCEs wasassessed. From June 2012 to April 2014, totally 25 civilianhospitals and 42 military hospitals were visited. The visitedhospitals are all designated trauma centers or emergencyhospitals at the corresponding cities. All of them are ter-tiary hospitals. In China a tertiary hospital is defined as ahealth facility covering a large administrative area andcapable of providing comprehensive and specialized
medical care. The cities where the hospital locatedinclude Beijing, Shanghai, Tianjing, Chongqing, et al,distributing evenly in China (Fig. 1A). There were 20university teaching hospitals, and 13 hospitals hadnational medical rescue teams (Fig. 1B).
In every hospital, written survey addressing variousaspects of preparedness plans and the equipment was car-ried out, and the detailed items were shown in Table 1.Each answered item in written survey was scored 1 for«yes» and 0 for «no» or «unknown». Item scores were cal-culated by adding together «yes» or «no» answers andused for statistics.
35International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 1: A. Geographic characteristics of the investigatedhospitals. B. Demographic characteristics of the surveyed
hospitals. In the figure, NMRT stand for hospitals havenational medical rescue team.
60
50
40
30
20
10
0
Civilian
hospital
(25)
Military
hospital
(42)Teaching
hospital
(20)
Non-
Teaching
hospital
(47)
No
NMRT
(13)
NMRT
(13)
A
B
Photography of Visiting 1.
Photography of Visiting 2.
Assessment of Medical Relief_ZONG.qxp_Mise en page 1 18/03/2016 14:02 Page2

A written test based on «Guidelines for the test ofnational medical rescue team» was made. The examincluded 5 parts: triage, treatment of trauma patients,treatment of burned patients, treatment of pandemicdiseases, and treatment of CBRN affected patients. Thefull score for each part was 20, and the total score was100. Three surgeons, 3 physicians and 3 nurses wereselected from each hospital to take the exam to testthe skills for treatment of MCEs patients. The averagescores were obtained and used for statistics.
All the participants provided their written informedconsent.
Statistics analysis
Data were summarized and analyzed using SPSS 13.0 forWindows. A P value of less than 0.05 was consideredsignificant.
RESULTS
Initially, 1583 citations were retrieved from the abovenamed search engines. Screening by titles narrowed the
focus to 325 articles and a further screening by abstractled to 125 articles. And only 25 articles are selected even-tually and the contents of these selected articles wereembedded in the following part of results and discussion.
Legislation, command and control
At the national level, there are totally 5 laws related tomedical relief of MCEs11-15. «National natural disasterrelief emergency plan» and «Emergency Response Lawof the People’s Republic of China» are laws to directthe organization of medical relief in natural and man-made MCEs respectively. According to the law, theState Council is the highest leadership responsible forthe organization of medical relief for MCEs. Dependedon the extent and degree of disaster, local or nationalentities will be activated. One major shortcoming ofthese laws is that principles but not details are given bythese legislations. For example, according to the laws,hospital should be prepared for MCEs medical reliefwork, but it did not give the details how to prepareand the standard of preparedness. So many local lawsand regulations were made by local governments,further describing the details.
36International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
PREPAREDNESS PLAN
OrganizationIs there an office to cope with MCEs?Are there designated personnel in the office?
Types of preparedness planIs there preparedness plan for medical relief of MCEs caused by traffic accidents, coalmine accidents, fire accidents,terrorist attacks, pandemics, flood, and earthquake, respectively?
Is the plan regularly updated?Are there any regulation for:
Mobilization of extra personnel?Mobilization of extra supplies, including ventilators?Creation of extra bed?
Training and DrillIs there a training program?Is the training program regularly updated?Did the hospital drill regularly?
EQUIPMENT, STOCK AND SUPPLIES
Did the hospital have the facilities to deploy a field hospital include:Shelter?Trucks and ambulance?Field operation room?Mobile X-ray machine?Mobile Ultra-sound machine?Mobile Lab examination machine?Mobile ICU?Full logistic self-sufficiency?Sufficient stock?
Did the hospital have the facilities to carry out medical relief in a regional area which include:Ambulance equipped with necessary facilities for a finite MCEs?Sufficient drug stock?
Do the hospital have aeroevacuation ability?Did the hospital have decontamination facilities? Are there personnel trained to use it?Does the hospital have regular protective equipment such as gown, gloves, goggles, and N95 respirators, and personal
protective equipment?Dose the hospital have antidotes such as atropine, naloxone, et al?Is there radiation detector?Is there sufficient blood supply?
Table 1: Surveyed questions in each hospital.
Assessment of Medical Relief_ZONG.qxp_Mise en page 1 18/03/2016 14:02 Page3
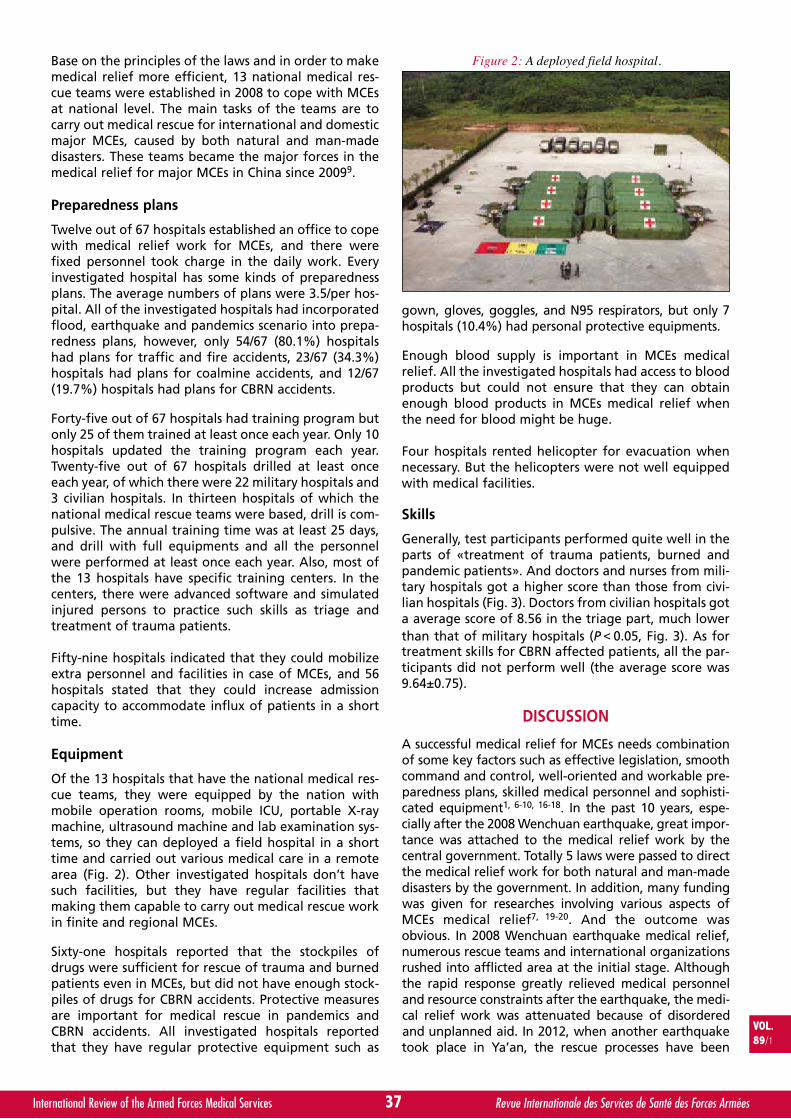
Base on the principles of the laws and in order to makemedical relief more efficient, 13 national medical res-cue teams were established in 2008 to cope with MCEsat national level. The main tasks of the teams are tocarry out medical rescue for international and domesticmajor MCEs, caused by both natural and man-madedisasters. These teams became the major forces in themedical relief for major MCEs in China since 20099.
Preparedness plans
Twelve out of 67 hospitals established an office to copewith medical relief work for MCEs, and there werefixed personnel took charge in the daily work. Everyinvestigated hospital has some kinds of preparednessplans. The average numbers of plans were 3.5/per hos-pital. All of the investigated hospitals had incorporatedflood, earthquake and pandemics scenario into prepa-redness plans, however, only 54/67 (80.1%) hospitalshad plans for traffic and fire accidents, 23/67 (34.3%)hospitals had plans for coalmine accidents, and 12/67(19.7%) hospitals had plans for CBRN accidents.
Forty-five out of 67 hospitals had training program butonly 25 of them trained at least once each year. Only 10hospitals updated the training program each year.Twenty-five out of 67 hospitals drilled at least onceeach year, of which there were 22 military hospitals and3 civilian hospitals. In thirteen hospitals of which thenational medical rescue teams were based, drill is com-pulsive. The annual training time was at least 25 days,and drill with full equipments and all the personnelwere performed at least once each year. Also, most ofthe 13 hospitals have specific training centers. In thecenters, there were advanced software and simulatedinjured persons to practice such skills as triage andtreatment of trauma patients.
Fifty-nine hospitals indicated that they could mobilizeextra personnel and facilities in case of MCEs, and 56hospitals stated that they could increase admissioncapacity to accommodate influx of patients in a shorttime.
Equipment
Of the 13 hospitals that have the national medical res-cue teams, they were equipped by the nation withmobile operation rooms, mobile ICU, portable X-raymachine, ultrasound machine and lab examination sys-tems, so they can deployed a field hospital in a shorttime and carried out various medical care in a remotearea (Fig. 2). Other investigated hospitals don’t havesuch facilities, but they have regular facilities thatmaking them capable to carry out medical rescue workin finite and regional MCEs.
Sixty-one hospitals reported that the stockpiles ofdrugs were sufficient for rescue of trauma and burnedpatients even in MCEs, but did not have enough stock-piles of drugs for CBRN accidents. Protective measuresare important for medical rescue in pandemics andCBRN accidents. All investigated hospitals reportedthat they have regular protective equipment such as
gown, gloves, goggles, and N95 respirators, but only 7hospitals (10.4%) had personal protective equipments.
Enough blood supply is important in MCEs medicalrelief. All the investigated hospitals had access to bloodproducts but could not ensure that they can obtainenough blood products in MCEs medical relief whenthe need for blood might be huge.
Four hospitals rented helicopter for evacuation whennecessary. But the helicopters were not well equippedwith medical facilities.
Skills
Generally, test participants performed quite well in theparts of «treatment of trauma patients, burned andpandemic patients». And doctors and nurses from mili-tary hospitals got a higher score than those from civi-lian hospitals (Fig. 3). Doctors from civilian hospitals gota average score of 8.56 in the triage part, much lowerthan that of military hospitals (P<0.05, Fig. 3). As fortreatment skills for CBRN affected patients, all the par-ticipants did not perform well (the average score was9.64±0.75).
DISCUSSION
A successful medical relief for MCEs needs combinationof some key factors such as effective legislation, smoothcommand and control, well-oriented and workable pre-paredness plans, skilled medical personnel and sophisti-cated equipment1, 6-10, 16-18. In the past 10 years, espe-cially after the 2008 Wenchuan earthquake, great impor-tance was attached to the medical relief work by thecentral government. Totally 5 laws were passed to directthe medical relief work for both natural and man-madedisasters by the government. In addition, many fundingwas given for researches involving various aspects ofMCEs medical relief7, 19-20. And the outcome wasobvious. In 2008 Wenchuan earthquake medical relief,numerous rescue teams and international organizationsrushed into afflicted area at the initial stage. Althoughthe rapid response greatly relieved medical personneland resource constraints after the earthquake, the medi-cal relief work was attenuated because of disorderedand unplanned aid. In 2012, when another earthquaketook place in Ya’an, the rescue processes have been
37International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 2: A deployed field hospital.
Assessment of Medical Relief_ZONG.qxp_Mise en page 1 18/03/2016 14:02 Page4

much more ordered21 ,22. When Pu’dian earthquake tookplace in August 2014, the need for medical relief wasassessed shortly after the quake, and then a well-plan-ned rescue work was carried out. This time, the medicalrescue was well-organized with high efficiency. A limitedbut sufficient medical rescue teams was sent to theaffected area to make sure that smooth rescue work becarried out without causing chaos. These indicated thatgreat progresses had been made in China as for thelegislation, organization, command and control ofmedical relief work.
The unpredictability of MCEs makes advance prepara-tions essential for a successful response at the time ofthe event1, 23-25. The formulation of a plan should beginwith an assessment of the most likely threats that maygive rise to a MCEs in any given community, which isknown as a hazards vulnerability analysis. Once formu-lated, disaster plans must be tested regularly throughboth hospital drills of a single facility and community-wide exercises1, 16, 26, 27. In China, the most often MCEsare traffic accidents, coalmine accidents, fire accidents,terrorist attacks, pandemics, flood, and earthquakeaccording to a government bulletin5. Thus, prepared-ness plans should aim at these MCEs. However, the pre-sent study found that only a small portion of hospitalshad preparedness plans for coalmine accidents, andCBRN accidents. Shortage of drill and training is ano-ther problem. We found that although some kinds ofplans were made in all the hospitals, most of the plansdrilled poorly. Two recent surveys further showed thatcontinual education focusing on disaster medicine wasin urgent need in China28-30. Disaster medicine has nowbecome mandatory course for bachelor in China, butnot mandatory for higher education and continualeducation like that in developed countries and some
developing countries such as Iran26. This needed to beaddressed to obtain a better outcome.
The current study found that all the investigated hos-pitals have necessary equipment to carry out medicalrescue work for finite MCEs, and some of hospitals(13/67) are capable of carrying out medical relief workfor large-scale MCEs, thanking to the sustained effortsmade by the governments. The issues most needed tobe improved include dependable communication sys-tem, sufficient and effective aeromedical evacuationsystem and various kinds of portable facilities whichcould make on-site rescue work easier and more effi-cient7, 31-33.
As for the skills, it was found that the test participantsare good at treatment of trauma and burned patients,but not good at the management of CBRN affectedpatients. When we put the preparedness plan, equip-ment and skill together, it was found that hospitals arepoor prepared in medical rescue work for CBRN acci-dents. On 3 March 2014, a terrorist attack took place inKunming train station, resulting in 29 dead and 143injured. This attack raised the Chinese’s awareness thatlarge scale terrorist attack could happen in China. Asresult, many fear that terror attacks involving CBRNdevices could take place. Thus we should be ready forthis threat both at the national and hospital level.
Based on the above-mentioned pitfalls, we offer oursuggestions. Firstly, legislation with more details shouldbe made. We suggest that details such as the standardof preparedness be established. Secondly, financial sup-port should be guaranteed so that the hospital couldimprove their facilities and skills. Thirdly, we proposethat the government should construct a sophisticated
38International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 3: The performance of participants in the section of written test for skill. In the figure, triage, trauma, burn,pandemics and CBRN stand for triage, treatment of trauma patients, treatment of burned patients,
treatment of pandemic diseases, and treatment of CBRN affected patients respectively.* p < 0.05, compared with civilian hospitals.
20
16
12
8
4
0TRIAGE TRAUMA BURN PANDEMICS
MILITARY HOSPITALS
CIVILIAN HOSPITALS
ALL HOSPITALS
CBRN
**
Assessment of Medical Relief_ZONG.qxp_Mise en page 1 18/03/2016 14:02 Page5

trauma care system34. It was suggested that traumacenters and trauma systems should be the foundationof all disaster response systems, as they have the per-sonnel, equipment, liaisons, and daily experience withmanaging large numbers of injured patients and rapiddecision making that are so necessary in MCEs1, 35.
There are several limitations of the current study. Onelimitation is that some gray evidence obtained fromwebsite was included in the present manuscript.Another limitation is that although the investigatedhospitals distributed all over China, they are all des-ignated trauma centers or emergence centers of thecorresponding cities. Hospitals of lower levels were notincluded. These make our results can not represent allaspects of the medical relief capacity for MCEs in China.
CONCLUSIONS
The current study found comprehensive capacity ofmedical relief for MCEs had improved greatly in China.However, pitfalls do exist such as shortage of drill andunfamiliarity of certain skills. These asked for furtherimprovement in order to obtain a more successfulmedical relief for MCEs in China.
ABSTRACT
China is one of the countries constantly affected byvarious mass casualty events (MCEs), and the presentstudy aimed to assess medical relief capability for MCEsin China. Written surveys and tests were carried out in67 hospitals nationwide. It was found that all of theinvestigated hospitals had incorporated flood, earth-quake and pandemics scenario into preparedness plans,however, only part of the investigated hospitals hadplans for traffic, fire accidents, coalmine accident. Only25/67 hospi tals drilled and updated the plans regularly.As far as skills as concerned, the test participants weregood at treatment of trauma and burned patients, butnot good at the management of pandemics and CBRNaffected patients. In conclusion, comprehensive capa-city of medical relief for MCEs had improved greatly inChina. However, pitfalls do exist such as shortage of drilland unfamiliarity of certain sk ills. These asked for fur-ther improvement in order to obtain a more successfulmedical relief for MCEs in China.
Potential Conflict of Interest
This work was supported by The Military MedicalResearch Foundation of China (AWS11J008 andAWS14L012). The authors have no other financialconflict to disclose.
REFERENCES
11. ERIC R. FRYKBERG ER and SCHECTER WP (2013) Disasterand mass casualty. In: Mttox KL, Moore EE, Feliciano DV,editors. Trauma. The McGraw Companies. PP.315-352.
12. NIE H, TANG SY, LAU WB, ZHANG JC, JIANG YW, et al.(2011) Triage during the week of the Sichuan earthquake:a review of utilized patient triage, care, and dispositionprocedures. Injury 42: 515-520.
13. MURRAY V1, GOODFELLOW F. m (2002) Mass casualtychemical incidents--towards guidance for public healthmanagement. Public Health 116: 2-14.
14. GOFIN R. (2005) Preparedness and response to terrorism:a framework for public health action. Eur J Public Health15: 100-104.
15. State Administration of Work Safety. 2013 annual reporton the safety development and production in China.Available at http://www.chinasafety.gov.cn/newpage/ajmj_gg/ajmj_gg.htm [accessed 8.16.2014].
16. KALANTAR MOTAMEDI MH, SAGAFINIA M, EBRAHIMI A,SHAMS E, KALANTAR MOTAMEDI M. (2012) Major earth-quakes of the past decade (2000-2010): a comparativereview of various aspects of management. Trauma Mon17: 219-229.
17. SHEN J, KANG J, SHI Y, LI Y, LI Y, et al. (2012) Lessons lear-ned from the Wenchuan earthquake. J Evid Based Med 5:75-88.
18. CRAIG AT1, KASAI T, LI A, OTSU S, KHUT QY. (2010)Getting back to basics during a public health emergency:a framework to prepare and respond to infectious diseasepublic health emergencies. Public Health 124: 10-13.
19. ZHANG L, LIU X, LI Y, LIU Y, LIU Z, et al. (2012) Emergencymedical rescue efforts after a major earthquake: lessonsfrom the 2008 Wenchuan earthquake. Lancet 379: 853-861.
10. ZHONG S, CLARK M, HOU XY, ZANG Y, FITZGERALD G.(2014) Validation of a framework for measuring hospitaldisaster resilience using factor analysis. Int J Environ ResPublic Health 11: 6335-6653.
11. The central people’s government of People’s Republic ofChina. Flood control law of the People’s Republic ofChina, Available at http://www.gov.cn/ztzl/2006-07/27/content_347485.htm [accessed 8.16.2014].
12. The central people’s government of People’s Republic ofChina. Emergency Response Law of the People’s Republicof China, Available at athttp://politics.people.com.cn/GB/1026/6195721.html [accessed 8.16.2014].
13. China Earthquake Administration. Earthquake disastermitigation law of the People’s Republic of China.Available at http://www.cea.gov.cn/manage/html/8a8587881632fa5c0116674a018300cf/_content/09_03/03/1236062289677.html [accessed 8.16.2014].
14. Ministry of Civil Affairs of the People’s Republic of China.Regulation of natural disaster relief. Available athttp://www.mca.gov.cn/article/zwgk/fvfg/jzjj/201008/20100800095101.shtml [accessed 8.16.2014].
15. The central people’s government of People’s Republic ofChina. National natural disaster relief emergency plan.Available at http://www.gov.cn/gongbao/content/2011/content_1992570.htm [accessed 8.16.2014].
16. BIDDINGER PD, BAGGISH A, HARRINGTON L,D’HEMECOURT P, HOOLEY J, et al. (2013) Be prepared--the Boston Marathon and mass-casualty events. N Engl JMed 368: 1958-1960.
17. HUNTER JC1, YANG JE, CRAWLEY AW, BIESIADECKI L,ARAGÓN TJ. (2013) Public health response systems in-
39International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Assessment of Medical Relief_ZONG.qxp_Mise en page 1 18/03/2016 14:02 Page6
action: learning from local health departments' expe-riences with acute and emergency incidents. PLoS One 8:e79457.
18. BITTNER MI, MATTHIES EF, DALBOKOVA D, MENNE B.(2014) Are European countries prepared for the next bigheat-wave? Eur J Public Health 24: 615-619.
19. LI X, TAN Q. (2013) Vehicle scheduling schemes for com-mercial and emergency logistics integration. PLoS One 8:e82866.
20. HAN YL, LIANG Z, YAO TM, SUN JY, LIANG M, et al. (2012)Novel miniature mobile cardiac catheterization laboratoryfor critical cardiovascular disease following natural disas-ters: a feasibility study. Chin Med J (Engl) 125: 995-999.
21. ZHANG L, LIU X, LI Y, LIU Y, LIU Z, et al. (2012) Emergencymedical rescue efforts after a major earthquake: lessonsfrom the 2008 Wenchuan earthquake. Lancet 379: 853-861.
22. TANG B, ZHANG L. (2013) Ya’an earthquake. Lancet 381:1984-1985.
23. MORTELMANS LJ, VAN BOXSTAEL S, De CAUWER HG,SABBE MB; Belgian Society of Emergency and DisasterMedicine (BeSEDiM) study. (2014) Preparedness of Belgiancivil hospitals for chemical, biological, radiation, andnuclear incidents: are we there yet? Eur J Emerg Med 21:296-300.
24. De CAUWER HG, MORTELMANS LJ, D’ORIO V. (2007) AreBelgian hospitals prepared for an H5N1-pandemic? Eur JEmerg Med 14: 204-206.
25. WANG C, XIANG H, XU Y, HU D, ZHANG W, et al. (2010)Improving emergency preparedness capability of ruralpublic health personnel in China. Public Health 124: 339-344.
26. ARDALAN A, MESDAGHINIA A, MASOUMI G,HOLAKOUIE NAIENI K, AHMADNEZHAD E. (2013) Higher
education initiatives for disaster and emergency healthin iran. Iran J Public Health 42: 635-638.
27. ADINI B1, GOLDBERG A, COHEN R, BAR-DAYAN Y. (2012)Impact of pandemic flu training on ability of medical per-sonnel to recognize an index case of avian influenza. EurJ Public Health 22: 169-173.
28. HUANG B, LI J, LI Y, ZHANG W, PAN F, et al. (2011) Needfor continual education about disaster medicine forhealth professionals in China--a pilot study. BMC PublicHealth 11: 89. doi: 10.1186/1471-2458-11-89.
29. SU T, HAN X, CHEN F, DU Y, ZHANG H, et al. (2013)Knowledge levels and training needs of disaster medicineamong health professionals, medical students, and localresidents in Shanghai, China. PLoS One 8: e67041.
30. ZHANG L, ZHAO M, FU W, GAO X, SHEN J, et al. (2014)Epidemiological analysis of trauma patients following theLushan earthquake. PLoS One 9: e97416.
31. GUO Y, SU XM. (2012) Mobile device-based reporting sys-tem for Sichuan earthquake-affected areas infectiousdisease reporting in China. Biomed Environ Sci 25: 724-729.
32. HE P, ZHOU C, LI H, YU Y, DONG Z, et al. (2012) A portablecontinuous blood purification machine for emergencyrescue in disasters. Blood Purif 33: 227-237.
33. LIU X, LIU Y, ZHANG L, LIANG W, ZHU Z, et al. (2013) Massaeromedical evacuation of patients in an emergency:experience following the 2010 Yushu earthquake. JEmerg Med 45: 865-871.
34. ZONG ZW, LI N, CHENG TM, RAN XZ, SHEN Y, et al. (2011)Current state and future perspectives of trauma care sys-tem in mainland China. Injury. 42: 874-878.
35. LENNQUIST S. (2007) Management of major accidentsand disasters: an important responsibility for the traumasurgeons. J Trauma 62: 1321–1329.
40International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
The 2016 AMSUS Annual Continuing Education Meeting will take place from 29 November to 2 December 2016at the Gaylord National, MD. Pre-con sessions will take place on 28 November.
The Gaylord National is located in the National Harbor, MD, just minutes from Washington, DC and is accessiblefrom the three local airports and public transportation.
For more information:
www.amsusmeetings.org
Assessment of Medical Relief_ZONG.qxp_Mise en page 1 18/03/2016 14:02 Page7

Headquarters: SCHILLER AG, Altgasse 68, CH-6341 BaarPhone +41 41 766 42 42, Fax +41 41 761 08 [email protected], www.schiller.ch
ARGUS PRO LIFECARE 2
Defi brillator, pacemaker, patient monitor and 12-channel ECG in a compact design.
DEFIGARD TOUCH 7
Specially designed for fi rst aiders: a compact combination of state-of-the-art defi brillation technology and comprehensive monitoring functions.
SCHILLER: the partner of all rescue teams
Latest member of the family
Int_Rev_AFMS_2016-03_APLC2-DGT7_A4_210x297plus5bleed_EN.indd 1 29.02.2016 15:01:55

Par P. FAVARO∑, B. CONTE∏ et R. LE BARSπ. France
Pascal FAVARO
Equipement médicaux du personnel santé enopérations : du besoin à la satisfaction du besoin.
Le Pharmacien en chef Pascal FAVARO est né le 8 octobre 1962 à Limoges (France).Il a intégré le Service de Santé des Armées français en 1986.
Il est titulaire du diplôme d’études spécialisées de pharmacie hospitalière et descollectivités et du diplôme d’études approfondies de systèmes de soins hospitaliers.
Il est spécialiste des techniques médico-militaires: « techniques d’organisation de la logistique santé » et titulairedu brevet d’études militaires supérieures de défense (Collège interarmées de défense. IXème promotion 2002). Ildétient également la qualification logistique interarmées du 3ème degré.
Il est le représentant français au sein du groupe de travail « Matériel médical et pharmacie militaire » duComité des chefs de services de santé militaires de l’OTAN (Medical materiel and military pharmacy - panel -Commitee of the chiefs of military medical services in NATO) et président du groupe utilisateurs médicauxde l’agence OTAN de soutien (Medical & pharmaceutical user group - NATO support agency).
Depuis 2010, il est le chef du bureau « Politique des approvisionnements en produits de santé, à la sous-direction -Appui à l’activité » au sein de la direction centrale du service de santé des armées, à Paris.
42International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
SUMMARY
Medical needs on operation: from request to its achievement.
Over the past thirty years, the French military medical service has been deployed on many theaters of operations. Therefore itacquired an excellent reputation on its expertise among all nations who stood alongside in multinational operations. This couldbe done thanks to the skill level of technicality of its staff and the quality of materials it uses, allowing it to provide optimal carefor wounded and sick soldiers. Requiring the same criteria of technical performance as those applicable on the national terri-tory, the modernity of the projected material responds to a coherent process for its acquisition using all qualifications of the per-sonal of the Service. The purpose of this article is to present the development of this process from the request of the operationalneed to its achievement.
INTRODUCTION
Le savoir-faire du service de santé des armées (SSA) fran-çais, reconnu notamment pour sa composante opéra-tionnelle, est dû à la haute technicité de ses praticiensqui disposent de matériels de qualité pouvant être utili-sés dans des conditions d’environnement dégradées. Cesarticles vont du médicament et dispositif médicalconsommable à l’équipement lourd en passant par lepetit matériel biomédical. Ils sont réalisés grâce à la coor-dination d’une chaîne d’acteurs œuvrant au sein du SSA:spécialistes hospitaliers, médecins des forces, pharmaciens,ingénieurs biomédicaux, commissaires et officiers du corps
technique et administratif, techniciens des « matérielssanté », infirmiers, etc... L’exercice quotidien en métro-pole, associé à l’expérience sur les théâtres d’opérations,va contribuer à définir et réaliser une gamme d’articlespermettant la prise en charge optimale du blessé enopérations avec le maximum de chances de survie et leminimum de séquelles. Le système recherche une homo-généité des matériels pour les besoins opérationnels etpour le temps de paix, une efficience dans la gestion desstocks et des gains économiques, tout en évitant lesdélais d’adaptation des personnels.
Nous présenterons les grandes lignes du processus
VOL.89/1
MOTS-CLÉS : Approvisionnement, Equipements médicaux, Opérations militaires, Ravitaillement sanitaire.KEYWORDS: Procurement, Medical equipments, Military operations, Supply chain.
Equipement Médicaux_FAVARO.qxp_Mise en page 1 18/03/2016 14:04 Page1

d’acquisition des équipements médicaux pour les OPEX,allant de l’expression initiale du besoin à sa réalisationcomplète.
L’EXPRESSION INITIALE DU BESOIN
L’efficience des soins en OPEX est directement condition-née par la qualité de la gamme thérapeutique (équipe-ments, dispositifs médicaux, médicaments) mise à disposi-tion du personnel « santé ». Cette gamme thérapeutiquedoit être adaptée et nécessairement limitée pour permet-tre un système de gestion centralisée. Son actualisation,pour rester aux standards de la médecine moderne, se faitpar différents modes d’expression: l’identification « iso-lée » d’un nouveau produit, la révision périodique desdotations des unités médicales opérationnelles, les retoursd’expérience et l’évolution du contrat opérationnel.
IDENTIFICATION ISOLÉE
Le personnel du Service est confronté à l’évolution despratiques médicales avec l’utilisation de nouveauxmatériels ou la mise en œuvre de thérapeutiques nova-trices. Ces progrès sont présentés par des visiteurs médi-caux qui proposent des échantillons, ou identifiés lorsde congrès ou séminaires propices aux échanges entrespécialistes au même titre que par la veille techniqueeffectuée dans la littérature scientifiqu e.
Souvent limitée au départ, l’utilisation d’un nouvel arti-cle au sein d’un établissement ou dans un contexteproche des conditions opérationnelles permet de validerl’amélioration de la pratique médicale. Tous les testseffectués font l’objet d’un rapport de l’utilisateur per-mettant de proposer un référencement au sein duService. Ce rapport est soumis à la validation du consul-tant national de la spécialité qui analyse le bien-fondéde l’expérimentation, les bénéfices attendus et étudieson intégration au sein des articles déjà mis à disposition.Une fois la pertinence confirmée, le besoin peut suivreles cycles d’intégration par les commissions ou comitésad hoc existant au sein du Service qui aboutiront à sonréférencement et à son acquisition.
Le principal comité permettant le référencement aubénéfice des forces en opérations est le comité du médi-cament et des dispositifs médicaux stériles1 (COMEDIMS).Placé sous la tutelle de l’inspection des services médicauxdu SSA, il rassemble annuellement un collège d’expertset d’acteurs du SSA qui décide des intégrations et sup-pressions d’articles dans le catalogue des droits ouvertspour la médecine de soutien des forces. Ainsi, desdizaines d’articles d’abord mis en place en opérationsextérieures sont devenus disponibles pour la pratiquequotidienne. C’est le cas par exemple, des pansementshémostatiques, des manchettes à perfusion ou desattelles CT-6 (photo n° 1) mais également de médicamentscomme l’acide tranexamique (Exacyl®).
Si des évolutions sont nécessaires pour répondre auxexigences de la réglementation, le circuit est identique.
Si le besoin n’est initialement qu’un concept ou une idée,il faut définir précisément les modalités et les conditions
d’emploi puis identifier un fournisseur potentiel prêt àaccompagner son développement pour passer à un proto-type testé puis validé. Ce type de collaboration est souventformalisé par un partenariat au moment de la réalisation.Ces dernières années, les contenants de toutes tailles à desfins médicales, comme la trousse individuelle du combat-tant (photo n° 2) ou les sacs d’intervention pour les per-sonnels de santé ont ainsi vu leurs modèles évoluer plu-sieurs fois. Des partenariats ont également été menés pourretenir des moyens d’extraction comme le brancard filettype Golanis® ou un matelas gonflable Aerazur®.
LES DOTATIONS TECHNIQUES DES UNITÉSMÉDICALES OPÉRATIONNELLES (UMO)2
Afin de disposer d’une chaîne complète de prise encharge de blessés sur les théâtres, le SSA a développédes dotations techniques adaptées aux trois niveauxdéfinis par l’organisation du traité de l’Atlantique nord(OTAN), appelés « rôles ».
43International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
∑ Pharmacien en chef,Direction centrale du service de santé des armées,Sous-direction appui à l’activité,Bureau politique des approvisionnements en produits de santé.
∏ Pharmacien en chef,Direction centrale du service de santé des armées,Sous-direction appui à l’activité,Bureau politique des approvisionnements en produits de santé.
π Pharmacien en chef,Direction des approvisionnements en produits de santé des armées,Division du ravitaillement sanitaire opérationnel,Bureau cohérence capacitaire.
Correspondance:Pharmacien en chef Pascal FavaroDirection Centrale du Service de Santé des ArméesSous-direction appui à l’activitéBureau politique des approvisionnements en produits de santé,Fort neuf de Vincennes, Cours des Maréchaux75614 Paris Cedex 12Téléphone : 0141932584E-Mail : [email protected]
VOL.89/1
Photo n° 1 : Attelle CT-6 Traction unit.
Photo n° 2 : Evolution de la trousse individuelle du combattant(ancien modèle II/93 à droite et nouveau modèle II/08 à gauche).
Equipement Médicaux_FAVARO.qxp_Mise en page 1 18/03/2016 14:04 Page2
- les UMO de rôle 1 assurent la médicalisation del’avant;- les UMO de rôle 2 réalisent le traitement chirurgicalde l’avant et la mise en condition d’évacuation;- les UMO de rôle 3 permettent le traitement intra-théâtre et possèdent des capacités d’hospitalisation enattente d’une évacuation vers la métropole ou lareprise d’activité du blessé.
L’adaptation de ces dotations répond à plusieurs impé-ratifs : ergonomie, encombrement limité, tout enconservant des qualités techniques satisfaisantes. A ceteffet, la direction centrale du service de santé desarmées (DCSSA) constitue des groupes de travail ras-semblant des professionnels dont l’expérience opéra-tionnelle est reconnue, pour créer ou moderniser lesdotations par un assemblage d’articles cohérent. Lesrapports de ces groupes de travail identifient desbesoins spécifiques à intégrer dans les dotations.
La modernisation des dotations de rôle 1 a permisrécemment l’acquisition de matériels biomédicauxminiaturisés, dont la mise à disposition a pu être géné-ralisée (moniteur de surveillance cardiaque de typePropaq LT, micro pousse-seringue…).
LES RETOURS D’EXPÉRIENCE (RETEX)
Les engagements des forces armées françaises au coursdes dernières décennies ont permis au Service d’éprouverses capacités dans des conditions d’emploi difficiles.
Ainsi, sur les théâtres d’opérations, les professionnels duSSA formalisent leurs retours d’expérience, soit par desfiches dédiées à une question spécifique, soit par l’inter-médiaire du rapport de fin de mission adressé à la DCSSA.
Le problème est décrit et des solutions sont proposées.L’exploitation systématique de ces RETEX par la DCSSApermet donc de prendre en compte le besoin et d’initiersa réalisation.
L’opération Pamir en Afghanistan a été un pourvoyeurmajeur de RETEX compte tenu des conditions d’enga-gement. L’intégration dans une opération multinatio-nale a permis au SSA, d’identifier des matériels auprèsde nos alliés et d’en proposer certains en référence-ment (comme le Combat ready clamp ou CRoC, moyende compression arrêtant une hémorragie profonde).
Une partie de ces RETEX est consacrée aux dotationstechniques des UMO, qui peuvent évoluer à la suite deces rapports.
LE CONTRAT OPÉRATIONNEL
En complément des UMO, le SSA doit détenir des capacitésparticulières afin d’optimiser les moyens mis à dispositionlors des déploiements des forces armées. Ces matériels sou-vent spécifiques, non disponibles sur le marché civil, répon-dent alors à la fois à des exigences techniques précises et àdes caractéristiques permettant de supporter des conditionsdégradées. Cela se traduit, par exemple, par la définition de
matériels intégrés dans des conteneurs (module deproduction d’oxygène, scanner sheltérisé).
Ainsi, les critères généraux suivants seront toujours prisen compte pour répondre à un besoin opérationnel :
- qualité;- disponibilité opérationnelle (utilisable sur le terrain
et destiné à une mission spécifique : poste médical,antenne chirurgicale, hôpital médico-chirurgical…);
- adaptation à l’emploi, éventuellement par la milita-risation d’appareils médico-chirurgicaux et par la réali-sation de médicaments sous une forme galéniqueappropriée.
LA RÉALISATION DU BESOIN
Le processus d’acquisition a pour objectif de mettre àdisposition du professionnel de santé ciblé un produitde qualité, efficace, économiquement performant etdans les délais prévus.
En plus de ces fondamentaux d’évidence, descontraintes législatives et réglementaires doivent êtreprises en compte avec notamment, dans le domaine dela santé, le code de la santé publique et dans celui desachats, le code des marchés publics3 (CMP). Sur le plantechnique, le SSA ne pourra qu’exceptionnellements’affranchir des règles élaborées dans le secteur civilpour la sécurité du patient (autorisation de mise sur lemarché pour les médicaments, marquage CE médicalpour les dispositifs médicaux4, 5, etc.).
Toute procédure d’achat doit respecter les règles com-plexes et contraignantes édictées par le CMP aux-quelles ne peut échapper la réalisation d’un besoinopérationnel. Les trois grands principes de la com-mande publique (transparence, libre accès à la com-mande publique et égalité de traitement des candi-dats) doivent être respectés. La professionnalisation del’achat au sein du SSA, par la centralisation à la direc-tion des approvisionnements en produits de santé desarmées (DAPSA), permet d’utiliser au mieux les possibi-lités offertes par le CMP pour mettre à disposition desutilisateurs le produit répondant au besoin identifié etselon l’objectif souhaité. Cet objectif n’est pas forcé-ment l’urgence de l’acquisition - opérationnel ne veutpas forcément dire urgent – mais, par exemple, l’adap-tation d’un matériel existant aux contraintes du ter-rain. Par exemple, les panneaux modulaires permettantle déploiement du lot de chirurgie vitale ont évolué parrapport au modèle standard afin de répondre auxattentes des équipes le mettant en œuvre (photo n° 3).
Au sein de la DAPSA, la division achats finances santé disposeau sein de son bureau achats de trois sections spécialisées:
- une section produits de santé et laboratoires;- une section équipements médicaux – matériels d’ex-
ploitation;- une section services et maintenances des structures
médicales.
La professionnalisation du personnel spécialisé dans ledomaine de l’achat public et dans un domaine technique
44International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Equipement Médicaux_FAVARO.qxp_Mise en page 1 18/03/2016 14:04 Page3

doit permettre de sécuriser juridiquement l’acte admi-nistratif, d’optimiser l’aspect économique et de garantirla réalisation du besoin exprimé conformément auxattentes de l’utilisateur final.
Quel que soit le produit, trois grandes étapes peuventêtre identifiées dans la réalisation du besoin :
- l’étude de la faisabilité technique, budgétaire et desdélais;
- la préparation du marché proprement dite: choix de laprocédure, rédaction du cahier des charges – notammentle cahier des clauses techniques particulières –, définitiondes critères d’attribution;
- le déroulement de la procédure administrative etl’analyse des offres.
Enfin, une dernière étape qui ne sera pas abordée danscet article consiste dans le retour d’expérience de la miseen œuvre du matériel validant la poursuite de son appro-visionnement ou entraînant des mesures correctives lorsdes procédures ultérieures ou des avenants.
ETUDE DE FAISABILITÉ TECHNIQUE,BUDGÉTAIRE ET DES DÉLAIS
L’expression d’un besoin se traduit par une premièreétape destinée à appréhender la faisabilité :
- le produit existe-t-il « sur étagère » (besoin simple)?- s’il n’existe pas, est-il envisageable de demander un
développement (besoin complexe)?- est-ce un besoin quantitativement limité (matériel
d’équipement) ou récurrent (consommables) ?- quelles sont les contraintes de délais pour la réalisation?- quel est le budget disponible et peut-il couvrir
l’opération qualitativement et quantitativement ?
Pour la division achats finances santé, cette étape néces-site des allers-retours entre le demandeur (DCSSA, groupede travail…), les experts du SSA (praticiens spécialistes,ingénieurs biomédicaux…) et les fournisseurs. Ceséchanges permettront d’analyser et d’affiner le besoin,d’estimer la disponibilité ou non du produit sur le marchéprivé et l’enveloppe financière qui devra être mobilisée.
La veille technique au sein de la DAPSA par domainepermet de connaître le marché, les innovations, lesprincipaux acteurs, les fourchettes de prix, les délais deréalisation.
L’évaluation de la faisabilité budgétaire est un élémentdéterminant du ressort de la DCSSA. Après une pre-mière évaluation, la DAPSA estime l’enveloppe finan-cière devant être consacrée à l’achat. Une mauvaiseévaluation financière initiale, notamment par sous-éva-luation, peut conduire à un marché déclaré infructueuxsi ce dernier ne peut être notifié faute de financement.
Les besoins opérationnels et particulièrement les délaisinterviennent également à ce stade. Outre la nécessitéimposée par les conditions de terrain (théâtre afghanpar exemple au moment des menaces majeures subiespar nos forces) de disposer très rapidement d’un articlecomme le garrot tactique SOFTT ou tactical tourniquet(photo n° 4), le calendrier de mise en place du nouveléquipement doit être défini dès ce stade (acquisitionunique, échelonnée sur un exercice annuel ou de façonpluriannuelle). Ce calendrier conditionne le choix de laprocédure de marché mais doit tenir compte des délais,notamment pour sa partie administrative (délais depublicité, de convocation de commissions…).
LA PRÉPARATION DU MARCHÉ
Elle comprend le choix de la procédure, la rédaction ducahier des charges et notamment du cahier des clausestechniques particulières, enfin la définition des critèresd’attribution.
Le cahier des clauses techniques particulières(CCTP)
Le CCTP est le fondement de la demande adressée auxfournisseurs. Selon la procédure choisie et le nombre
45International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Photo n°3 : Panneau modulaire du lot de chirurgie vitale.
Photo n° 4 : Garrot tactique SOFTT.
Equipement Médicaux_FAVARO.qxp_Mise en page 1 18/03/2016 14:04 Page4
de fournisseurs potentiels, il pourra aller d’un descriptifsommaire à une rédaction très élaborée. Pour un produitsimple disponible immédiatement chez des industriels, leCCTP se résumera à quelques lignes génériques décri-vant l’article souhaité. En revanche, si le produit à acqué-rir est complexe et de surcroît, s’il n’est pas disponible telquel dans le secteur civil, le CCTP pourra devenir undocument de plusieurs dizaines de pages. Dans ce der-nier cas, il fera l’objet d’étapes itératives entre deman-deur, experts du Service et rédacteurs des marchés pourtraduire la demande de la façon la plus précise possible,ce qui permettra aux fournisseurs de proposer le produitle plus conforme aux attentes du SSA.
LE CHOIX DE LA PROCÉDURE
Les seuils financiers sont un des critères qui vont orien-ter le type de procédure et les obligations en matièrede publicité.
Ces procédures peuvent être :- formalisées, parmi lesquelles on retrouve l’appel
d’offres ouvert ou restreint, le dialogue compétitif, laprocédure négociée, le système d’acquisition dynamiqueou le concours;
- adaptées (MAPA), si le seuil est inférieur à207000 euros hors taxes, ce qui permet de laisser uneplus grande place au dialogue entre l’acheteur publicet les prestataires, pourvu que les trois principes debase soient respectés : liberté d’accès à la commandepublique, transparence et égalité de traitement entrecandidats;
- très simplifiées, sous le seuil de 15000 euros horstaxes sans obligation de procédure écrite, si ce n’estune demande de devis effectuée auprès d’au moinsdeux fournisseurs avec une fiche de traçabilité.
Le besoin de certains équipements très spécifiques auxOPEX amène à recourir régulièrement à une procédureformalisée dite de dialogue compétitif. Les caractéris-tiques de la prestation seront élaborées lors de la phasede dialogue avec les prestataires sélectionnés sur appel àcandidature. Les candidats seront départagés de lamême manière que pour une procédure d’appel d’offresclassique.
Les critères d’attribution
Le prix est évidemment important, mais il ne doit pasocculter la qualité du produit car le risque est de dispo-ser d’un article de qualité inférieure et non satisfaisant.A ces deux critères peuvent s’ajouter les délais de réali-sation, la maintenance ou d’autres critères discrimi-nants, ce qui amène à des compromis faisant l’objet dela définition des critères de choix avec leur pondération.
LE DÉROULEMENT DE LA PROCÉDUREADMINISTRATIVE ET L’ANALYSE DES OFFRES.
Les délais avant réception et analyse des offres sontvariables : de quelques jours à environ 6 mois pour uneprocédure d’appel d’offres, voire des années pour ledialogue compétitif. Le choix du prestataire mobilise
des experts du SSA pour tester les équipements propo-sés. Cette étape, même si elle se déroule en Francemétropolitaine, donc hors contexte d’opérations, estimpérative. Une grille d’évaluation est généralementétablie entre la DAPSA et l’expert qui peut provenir detous les établissements du SSA. L’établissement centraldes matériels du SSA, subordonné à la DAPSA, est parti-culièrement sollicité en matière d’acquisition d’appa-reils biomédicaux. Il est important de mobiliser un paneld’experts pour qu’il reflète la diversité de s utilisateurs etles attentes du plus grand nombre.
In fine, le pouvoir adjudicateur, grâce aux différents aviset au rapport de présentation fournis par la divisionachats finances santé mettant en regard les qualités del’offre présentée et les critères de choix annoncés,retiendra le prestataire auquel le marché sera notifié.
ANALYSE DES AUTRES POSSIBILITÉSD’ACHAT HORS PROCÉDURES CONDUITES
INTÉGRALEMENT PAR LA DAPSA
Avec la centralisation des achats au sein de la DAPSA, leSSA a diversifié ses modes d’achats pour une plusgrande efficience économique avec de nouvelles voies :
- l’union des groupements d’achat public (UGAP) estune centrale d’achat publique française, accessible auxpersonnes publiques. L’UGAP propose un catalogued’articles immédiatement disponibles pour la plupart.L’offre est assez diversifiée dans le domaine de la santé,même si elle ne cible pas particulièrement les besoinsopérationnels.
- la centrale d’achat de l’OTAN, NATO support agency(NSPA) : le SSA y a adhéré en 2010. La NSPA propose uncatalogue d’articles ou la réalisation d’une procédure demarché dont elle assure la mise en œuvre à partir d’uncahier des charges techniques que fournit le demandeur.L’intérêt de la NSPA est qu’elle est destinée à fournir lesarmées de l’OTAN et leurs services de santé avec des arti-cles et des équipements en cohérence avec les besoinsopérationnels. Des rencontres annuelles entre les ser-vices de santé militaires des pays membres fédèrent lesbesoins et synchronisent les achats, ce qui facilite lesinterventions multinationales et l’interopérabilité.
Le recours à la NSPA est concrétisé depuis quatre anspar l’acquisition aussi bien de matériels simples qued’équipements lourds :
• nombreux petits articles référencés grâce aux RETEXdu théâtre afghan et destinés au sauvetage au combat,y compris pour l’instruction dans ce domaine soit auCentre de Formation Opérationnelle Santé ou dans lescentres médicaux des armées;
• tentes pour unités médicales opérationnelles;• équipements lourds comme un scanographe de
campagne intégré en conteneur (photo n° 5).
Dans le cas du scanographe, le matériel souhaité n’étaitpas disponible sur le marché. La NSPA, sur la base du cahierdes charges présenté par le SSA, a « généré » l’associationde deux industriels, l’un fabricant de scanographes, l’autreintégrateur militaire (pour la partie shelter). Cette procé-dure a mis quatre ans pour aboutir. Cet exemple illustre la
46International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Equipement Médicaux_FAVARO.qxp_Mise en page 1 18/03/2016 14:04 Page5

complexité de certaines acquisitions, nécessitant desadaptations pour répondre aux exigences opérationnelles.
Le recours à la NSPA et à l’UGAP n’est, par contre, pasadapté à l’achat en urgence de produits non référencés.
Enfin, les autres centrales d’achats du monde de lasanté sont également utilisées (UniHA, Résa-Idf),constituées à partir de réseaux d’acheteurs regroupantplusieurs dizaines d’hôpitaux, d’établissements médico-sociaux ou d’établissements d’intérêt collectif de santé.Néanmoins, ces centrales d’achats sont plutôt tournéesvers le monde hospitalier civil et les produits offertsrépondent peu aux besoins opérationnels du SSA.
CONCLUSION
Le service de santé des armées français a acquis unerenommée en opérations extérieures, en raison de lahaute qualité de sa pratique médicale. Cette dernièrecherche à offrir sur un théâtre de crise une qualité de soinsquasi équivalente au territoire national. Cette qualité nepeut se satisfaire de l’immobilisme, aussi le SSA doit-ilconserver sa capacité d’adaptation au progrès médicaldans le domaine des produits de santé ravitaillés. Tous lespersonnels du Service sont ainsi mobilisés pour leurs com-pétences techniques et administratives afin d’analyser enpermanence le besoin de modernisation des pratiques etdes matériels et d’assurer sa concrétisation dans un cadrejuridique et économique de plus en plus contraignant.
RÉSUMÉ
Le service de santé des armées français est intervenudepuis plus de trente ans sur de nombreux théâtresd’opérations. Il en a acquis une excellente réputationauprès des nations qui l’ont côtoyé dans les interven-tions multinationales. Cela n’a pu se faire que grâce àla haute technicité de son personnel et à la qualité desmatériels qu’il utilise, qui lui permettent une prise encharge optimale des militaires blessés et malades.Cherchant à répondre aux mêmes critères de perfor-mance technique que sur le territoire national, lamodernité des matériels projetés est le résultat d’unprocessus parfaitement cohérent qui associe pour sonacquisition toutes les qualifications du personnel duService. L’objet de cet article est de présenter le dérou-lement de ce processus, de l’expression d’un besoinopérationnel à sa réalisation.
BIBLIOGRAPHIE
1. Décision n° 5719/DEF/DCSSA/CAB du 15/12/2003 portantcréation du comité de coordination du médicament et desdispositifs médicaux stériles et des commissions associées.
2. Instruction n° 3557/DEF/DCSSA/OSP/ORG du 18/06/2007relative au processus de conception, de mise en place, derévision et de réforme des dotations du service de santédes armées.
3. Code des marchés publics - édition 2006 (version consoli-dée au 22/03/2015).
4. Règlement (CE) No 765/2008 du Parlement européen etdu Conseil du 9 juillet 2008 fixant les prescriptions rela-tives à l’accréditation et à la surveillance du marché pourla commercialisation des produits.
5. Décision n° 768/2008/CE du Parlement européen et duConseil du 9 juillet 2008 relative à un cadre commun pourla commercialisation des produits.
47International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Photo n°5 : Abri modulaire pour scanographe.
Equipement Médicaux_FAVARO.qxp_Mise en page 1 18/03/2016 14:04 Page6
Order DEF/ 1670/2015, 24th July, announcing the ninth edition of the international Prize“FIDEL PAGÉS MIRAVÉ”
In accordance with the Order DEF/1760/2007, of 11th June, that creates the Prize “Fidel Pagés Miravé”, the GeneralInspection of the Medical Service announces its ninth edition, establishing the conditions and requirements in thisMinisterial Order.
First. Denomination.Given the possibility of non-Spanish authors it is renamed as International Prize “Fidel Pagés Miravé” since 2011.
Second. Contestants.Physical persons, Spanish or not, may opt to the Prize, individually or in groups.
Third. Manuscripts.The papers presented to this Prize have to be unpublished. Those papers which are a PhD thesis, or a significant partof it, defended in any University, public or private, will not be accepted. The papers will be written in Spanish orEnglish, with numbered pages, double-spaced and printed on only one side of the page, in DIN A-4, Arial font, size12 and a maximum length of 50 pages. The papers will be sent printed (five copies) and in digital format. An abstractin Spanish and English, and no longer than one page, will be included. The subject will be an original work in theHealth Sciences, in accordance with the scientific research methodology, its utility or relationship to the MilitaryMedical Service will be evaluated; or an original paper on Historical Science of the Military Medical Service withthe same methodological demands and based essentially on primary sources.
Fourth. Identification.The papers will be presented with a title and signed with a pseudonym or motto, not including data that identifydirectly its authors. The package will include a sealed envelope on which appears the title of the paper, motto orpseudonym, and containing a document with the following data: Title, Motto or Pseudonym, Author or authors (ifmilitary, rank and appointment), full address, telephone, fax or email and authorization for publication in the Journal“Sanidad Militar” signed by the author/authors. The papers will be sent to Inspección General de Sanidad de la Defensa,Hospital Central de la Defensa "Gómez Ulla", Glorieta del Ejército 1. 28047 Madrid, España.
Fifth. Deadline.The deadline for the reception of papers is the 15th May 2016. Papers received after the deadline or not fulfillingthe established requirements will not be accepted.
Sixth. Prize.Only one prize will be awarded: Prize “Comandante médico Fidel Pagés Miravé” worth 6000 €. Should the winnerbe a multi-authored paper the award will be given to the first author.
Seventh. Jury.The composition of the jury will be in accordance with the provisions of article sixth of the Order Def/1760/2007,11th June. (Official State Gazette, BOE n. 144, date 16th June 2007). The decision of the jury will be final; it will benotified to the winners and published in the Official Defense Gazette (BOD), in the Journal “Sanidad Militar” andin all centers of the General Inspection of the Medical Service. The jury may consider the prize void.
Eighth. Decision and advertising.The Prize will be awarded by order of the Minister of Defense at the proposal of the jury and published in theOfficial State Gazette (BOE).
Ninth. Publication of the papers.All papers will be considered as submitted for publication in the Journal “Sanidad Militar”. The prize-winning paperwill be accepted for publication, in their entirety, or as a summary that would be requested from the authors, in anormal or special issue of the Journal “Sanidad Militar”, or another format to be determined by the General Inspectionof the Military Medical Service and the Defense Documentation and Publications Center.
Tenth. Award Ceremony.The award ceremony will take place publicly on a date near the 23rd September, date of demise of the Major FidelPagés Miravé.
Eleventh.The participation implies the acceptance of each and every one of these conditions and the renunciation of anyclaim.
Annonce_Prix Pagès Miravé 2016_Annonce Pan American 2012 16/12/15 19:21 Page1

€€

By A. OUMAYA∑, M.W. KRIR∑, C. BEN CHEIKH∑, Y. GUETARI∑, H. ELKEFI∑ and S. EDHIF∑. Tunisia
Abdelaziz OUMAYA
Individual Psychological Debriefing does not PreventPost-Traumatic Stress Disorder: a Prospective ComparativeStudy.*
Le médecin colonel Major Abdelaziz OUMAYA est né le 25 juin 1959 à Béni-khalleden Tunisie.
Il est marié et père de 4 enfants.
TITRES et DIPLOMES UNIVERSITAIRES1. Docteur en Médecine.2. Professeur en Psychiatrie3. Diplôme de criminologie appliquée à l’expertise mentale avec mémoire soutenue en juin 1994 Sujet :« Schizophrénie : Agression inaugurale et problème médico-légaux », Institut Médico-légal de Paris,Université de René DECARTES : Paris V.4. Formation en criminalistique Institut médico-légal de Paris, Université de René DECARTES : Paris V.5. Formation en Pédopsychiatrie dans le cadre d’un diplôme universitaire, du Professeur Bernard GOLSE.
FONCTIONS ET ACTIVITES6. Chef de Service de psychiatrie de l’Hôpital Militaire Principal d’Instruction de Tunis.7. Médecin expert auprès du ministère de l’intérieur.8. Médecin expert auprès du ministère de la justice.9. Médecin expert auprès des tribunaux militaires et civils.
50International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Le débriefing psychologique individuel ne prévient pas le trouble de stress post-traumatique : une étudeprospective comparative
Introduction : Afin de prévenir l’état de stress post-traumatique (ESPT), le débriefing psychologique individuel en séance unique(DPISU) est largement utilisé en Tunisie. L’objectif de cette étude était d’évaluer l’efficacité de cette intervention dans la préventionde l’ESPT.Méthodes : 48 heures après l’explosion d’une mine, les 23 personnes exposées ont été évaluées et assignées au hasard soit à ungroupe débriefing (DPISU) soit à un groupe contrôle. Trois mois plus tard, tous les participants ont été évalués par l’échelle PCL-M.Résultats : le score PCL-M moyen était de 46.58 ± 2.13 dans le groupe débriefing et de 45.55 ± 2.32 dans le groupe contrôle (p = 0.74).Un tiers des participants dans le groupe débriefing et 27.3 % des sujets contrôles avaient un ESPT (p = 1).Conclusion : Cette étude ne fournit pas de preuve en faveur de l’intérêt du DPISU dans la prévention de l’ESPT. D’autres stratégiesthérapeutiques devraient être considérées.
INTRODUCTION
Traumatic events have increased dramatically after therevolution in Tunisia especially in relation to terrorism.Military personnel is particularly exposed to these eventsand the number of Tunisian traumatized soldiers is highand increasing. Traumatized people in general are at riskof developing post-traumatic stress disorder (PTSD) and at
least a third of the individuals who initially develop PTSDstay symptomatic for 3 years or longer1. This can lead tosecondary problems such as job loss, separation and subs-tance abuse and may thus create a vicious circle. In orderto prevent such an evolution, Tunisian psychologists andpsychiatrists usually offer individual single-session psycho-logical debriefing (ISSPD) as an immediate psychologicalassistance to survivors of all kinds of traumatic events. On
VOL.89/1
KEYWORDS: Psychological debriefing, Post-traumatic stress disorder, Military, Tunisia.MOTS-CLÉS : Débriefing psychologique, Etat de stress post-traumatique, Militaire, Tunisie.
Psychological Debriefing_OUMAYA.qxp_Mise en page 1 16/03/2016 10:09 Page1
.

the other hand, it is known that a substantial proportionof traumatized individuals recover without treatment inthe following years, with a steep decline in PTSD ratesoccurring in the first year2. In addition, empirical evi-dence for the efficacy of ISSPD is noticeably lacking andits preventive effects are controversial3, 4.
In this Tunisian new and challenging context and sincethe national ISSPD interventions have never been eva-luated, the aim of this study was to assess the efficacyof ISSPD in preventing symptoms of PTSD.
METHODS
A military psychiatrist was deployed in Châambi area inJuly 2013. During his deployment, a mine exploded ona tank causing 2 deaths and physical injuries for adozen of military personnel. All persons exposed to thisincident were included in the study. Exclusion criteriawere: agitation; psychotic reactions and suicidal idea-tion. Participants were recruited only after obtainingtheir free and informed consent. Their anonymity andthe confidentiality of data were respected.
Participants were evaluated 48 hours after the incidentby the deployed military psychiatrist. They were ran-domly assigned to either a debriefing group (these par-ticipants had ISSPD) or to a control group (no debrie-fing). Three months after the incident, all participantswere evaluated using the PTSD Checklist – Military ver-sion (PCL-M)5 translated into Tunisian dialect. The PTSDChecklist (PCL) is a 17-item self-report measure reflec-ting DSM-IV symptoms of PTSD. It has a variety of clini-cal and research purposes, including screening indivi-duals for PTSD and monitoring change in PTSD symp-toms. The military version used in this study is aimed toask about symptoms in response to "stressful militaryexperiences." It is often used with active service mem-bers and Veterans. A high cutoff score of 50 for a PTSDdiagnosis was considered since a high rate of PTSD wasexpected.
RESULTS
The number of people directly exposed to the incidentwas 23. All of them were included in the study. Twelveof them were randomized to the debriefing group and11 to the control group.
All participants were male and their mean age was25.76 ± 4.49. The mean number of study years was10.57 ± 2.44 with most of participants having a secon-dary education (69.6%). Three participants had primaryeducation (13%) and 4 of them went to the university(17.4%). Nineteen participants were celibate (82.6%)while the other were married (17.4%). Tobacco andalcohol consumption were observed in 60.9% and26.1% of participants respectively. No participant hadany personal psychiatric history.
The evaluation after three months revealed mean PCL-M scores as follow: 46.09 ± 7.38 for all participants;46.58 ± 2.13 in the debriefing group and 45.55 ± 2.32 in
the control group with no significant difference betweenthe last two groups (p = 0.74).
Considering a PCL-M cutoff score of 50 as mentioned above,one third of participants in the debriefing group and 27.3%of controls had PTSD with no significant difference betweenthe groups (p = 1).
DISCUSSION
This study was motivated by the increasing number oftraumatized people in the Tunisian army and aimed toassess the efficacy of ISSPD, which is widely used butnever evaluated in Tunisia, in preventing symptoms ofPTSD. The major two limitations of this study were thesmall sample size and the absence of a baseline evalua-tion with the PCL-M. Despite the intuitive appeal of thetechnique, we found that ISSPD had no efficacy inreducing symptoms of PTSD and did not prevent itsonset.
These results are in line with the findings of previousstudies examining different types of traumatic events6-
10. In fact, all these studies found that debriefing had noeffect on symptoms of PTSD. A meta-analysis of sevenstudies has even suggested that debriefing would havea detrimental effect3 and advanced several explanationsfor this lack of efficacy as follow: First, the natural pro-cessing of a traumatic event is characterized by analternation of intrusion and avoidance and leads inmany cases to recovery. Debriefing might interferewith this natural processing and can therefore beharmful11. ISSPD can also constitute a premature expo-sure to trauma-related stimuli in a non-structured waywhich might not allow victims adequate time for habi-tuation, thereby further sensitizing them to these sti-muli. It might also inadvertently lead victims to bypassthe support of family, friends, or other sources of socialsupport, while this support is assumed to be one of thebest resilience-recovery factors in PTSD12. In addition,people having ISSPD are informed about reactions fol-lowing a traumatic event while normalizing these reac-tions. However, this might inadvertently increase awa-reness of normal manifestations of distress aftertrauma which can once again be harmful.
Besides, despite the fact that risk factors for PTSD arewidely investigated13, 14, they were not explored in thisstudy and both victims at risk and those not at risk forPTSD were included in the study. This factor might obs-cure a true beneficial effect of debriefing on the deve-lopment of chronic symptoms for individuals at risk and
51International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
∑ Service de PsychiatrieHôpital Militaire Principal d’Instruction de Tunis.
Correspondence:Médecin Colonel Major Abdelaziz OUMAYAService de Psychiatrie,Hôpital Militaire Principal d’Instruction de TunisTN-1008 Montfleury, Tunis (TUNISIE).E-Mail : [email protected]éléphone : +216 98.326 206
* Presented at the 41st ICMM World Congress on Military Medicine,Bali, Indonesia, 17-22 May 2015.
VOL.89/1
Psychological Debriefing_OUMAYA.qxp_Mise en page 1 16/03/2016 10:09 Page2

studies should be done to assess whether targetingdebriefing to at-risk individuals is warranted3. Finally,we did not investigate and did not take into considera-tion the other aspects of management which is a verylarger concept than ISSPD (gratitude, indemnity, phar-macological treatment etc.).
In conclusion, despite the limitations of the study, itdoes provide some evidence for the uselessness ofISSPD in preventing PTSD, which is in line, to our know-ledge, with all previous studies evaluating this tech-nique on different types of trauma. Therefore, alterna-tive therapeutic strategies for people exposed to trau-matic events should be used. According to a recent sys-tematic review, evidence is very limited regarding bestpractices to treat trauma-exposed individuals15 but atleast, on the basis of current evidence, more benefitsare expected from early treatment of patients withacute stress disorder or acute PTSD with brief cognitivebehavioral therapy15-17. This kind of interventionshould be used and evaluated in further studies.
SUMMARY
Introduction: In order to prevent onset of post-trauma-tic stress disorder (PTSD), individual single-session psy-chological debriefing (ISSPD) for traumatized people iswidely used in Tunisia. The aim of this study was toassess the efficacy of this intervention in preventingsymptoms of PTSD.Methods: 48 hours after a mine explosion, 23 exposedpersons were evaluated and randomly assigned toeither a debriefing group (ISSPD) or to a control group.Three months later, all participants were evaluatedusing the PTSD Checklist – Military version (PCL-M).Results: The mean PCL-M score was 46.58 ± 2.13 in thedebriefing group and 45.55 ± 2.32 in the control group(p = 0.74). One third of participants in the debriefinggroup and 27.3% of controls had PTSD (p = 1).Conclusion: This study does not provide any evidencefor the usefulness of ISSPD in preventing PTSD.Alternative therapeutic strategies for people exposedto traumatic events should be used.
Conflict of interest
None of the authors have any conflict of interests todeclare.
REFERENCES
11. KESSLER RC, SONNEGA A, BROMET E, HUGHES M, NELSONCB. Posttraumatic stress disorder in the NationalComorbidity Survey. Archives of general psychiatry. 1995;52 (12): 1048-60.
12. BRESLAU N, DAVIS GC, ANDRESKI P, PETERSON E.Traumatic events and posttraumatic stress disorder in anurban population of young adults. Archives of generalpsychiatry. 1991; 48 (3): 216-22.
13. VAN EMMERIK AA, KAMPHUIS JH, HULSBOSCH AM,EMMELKAMP PM. Single session debriefing after psycho-logical trauma: a meta-analysis. The Lancet. 2002; 360(9335): 766-71.
14. ROSE S, BISSON J, CHURCHILL R, WESSELY S. Psychologicaldebriefing for preventing post traumatic stress disorder(PTSD). Cochrane Database Syst Rev. 2002; 2 (2).
15. WEATHERS F, HUSKA J, KEANE T. The PTSD checklist mili-tary version (PCL-M). Boston, MA: National Center forPTSD. 1991.
16. CONLON L, FAHY T, CONROY R. PTSD in ambulant RTA vic-tims: a randomized controlled trial of debriefing. Journalof psychosomatic research. 1999; 46 (1): 37-44.
17. ROSE S, BREWIN CR, ANDREWS B, KIRK M. A randomizedcontrolled trial of individual psychological debriefing forvictims of violent crime. Psychological Medicine. 1999; 29(04): 793-9.
18. HOBBS M, MAYOU R, HARRISON B, WORLOCK P. A ran-domised controlled trial of psychological debriefing forvictims of road traffic accidents. Bmj. 1996; 313 (7070):1438-9.
19. BISSON JI, JENKINS PL, ALEXANDER J, BANNISTER C.Randomised controlled trial of psychological debriefingfor victims of acute burn trauma. The British journal ofpsychiatry. 1997; 171 (1): 78-81.
10. SIJBRANDIJ M, OLFF M, REITSMA JB, CARLIER IV, GERSONSBP. Emotional or educational debriefing after psychologi-cal trauma. The British Journal of Psychiatry. 2006; 189 (2):150-5.
11. HOROWITZ MJ. Stress-response syndromes. Internationalhandbook of traumatic stress syndromes: Springer; 1993.p. 49-60.
12. KING LA, KING DW, FAIRBANK JA, KEANE TM, ADAMS GA.Resilience – recovery factors in post-traumatic stress disor-der among female and male Vietnam veterans: Hardiness,postwar social support, and additional stressful lifeevents. Journal of personality and social psychology. 1998;74 (2): 420.
13. BREWIN CR, ANDREWS B, VALENTINE JD. Meta-analysis ofrisk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of consulting and clinical psycho-logy. 2000; 68 (5): 748.
14. PERKONIGG A, KESSLER RC, STORZ S, WITTCHEN HU.Traumatic events and post§traumatic stress disorder in thecommunity: prevalence, risk factors and comorbidity. Actapsychiatrica scandinavica. 2000; 101 (1): 46-59.
15. FORNERIS CA, GARTLEHNER G, BROWNLEY KA, GAYNESBN, SONIS J, COKER-SCHWIMMER E, et al. Interventions toprevent post-traumatic stress disorder: a systematicreview. American journal of preventive medicine. 2013; 44(6): 635-50.
16. SIJBRANDIJ M, OLFF M, REITSMA JB, CARLIER IV, DE VRIESMH, GERSONS BP. Treatment of acute posttraumatic stressdisorder with brief cognitive behavioral therapy: a rando-mized controlled trial. The American journal of psychia-try. 2007; 164 (1): 82-90.
17. BISSON JI, SHEPHERD JP, JOY D, PROBERT R, NEWCOMBERG. Early cognitive – behavioural therapy for post-trau-matic stress symptoms after physical injury Randomisedcontrolled trial. The British journal of psychiatry. 2004;184 (1): 63-9.
52International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Psychological Debriefing_OUMAYA.qxp_Mise en page 1 16/03/2016 10:09 Page3
studies should be done to assess whether targetingdebriefing to at-risk individuals is warranted3. Finally,we did not investigate and did not take into considera-tion the other aspects of management which is a verylarger concept than ISSPD (gratitude, indemnity, phar-macological treatment etc.).
In conclusion, despite the limitations of the study, itdoes provide some evidence for the uselessness ofISSPD in preventing PTSD, which is in line, to our know-ledge, with all previous studies evaluating this tech-nique on different types of trauma. Therefore, alterna-tive therapeutic strategies for people exposed to trau-matic events should be used. According to a recent sys-tematic review, evidence is very limited regarding bestpractices to treat trauma-exposed individuals15 but atleast, on the basis of current evidence, more benefitsare expected from early treatment of patients withacute stress disorder or acute PTSD with brief cognitivebehavioral therapy15-17. This kind of interventionshould be used and evaluated in further studies.
SUMMARY
Introduction: In order to prevent onset of post-trauma-tic stress disorder (PTSD), individual single-session psy-chological debriefing (ISSPD) for traumatized people iswidely used in Tunisia. The aim of this study was toassess the efficacy of this intervention in preventingsymptoms of PTSD.Methods: 48 hours after a mine explosion, 23 exposedpersons were evaluated and randomly assigned toeither a debriefing group (ISSPD) or to a control group.Three months later, all participants were evaluatedusing the PTSD Checklist – Military version (PCL-M).Results: The mean PCL-M score was 46.58 ± 2.13 in thedebriefing group and 45.55 ± 2.32 in the control group(p = 0.74). One third of participants in the debriefinggroup and 27.3% of controls had PTSD (p = 1).Conclusion: This study does not provide any evidencefor the usefulness of ISSPD in preventing PTSD.Alternative therapeutic strategies for people exposedto traumatic events should be used.
Conflict of interest
None of the authors have any conflict of interests todeclare.
REFERENCES
11. KESSLER RC, SONNEGA A, BROMET E, HUGHES M, NELSONCB. Posttraumatic stress disorder in the NationalComorbidity Survey. Archives of general psychiatry. 1995;52 (12): 1048-60.
12. BRESLAU N, DAVIS GC, ANDRESKI P, PETERSON E.Traumatic events and posttraumatic stress disorder in anurban population of young adults. Archives of generalpsychiatry. 1991; 48 (3): 216-22.
13. VAN EMMERIK AA, KAMPHUIS JH, HULSBOSCH AM,EMMELKAMP PM. Single session debriefing after psycho-logical trauma: a meta-analysis. The Lancet. 2002; 360(9335): 766-71.
14. ROSE S, BISSON J, CHURCHILL R, WESSELY S. Psychologicaldebriefing for preventing post traumatic stress disorder(PTSD). Cochrane Database Syst Rev. 2002; 2 (2).
15. WEATHERS F, HUSKA J, KEANE T. The PTSD checklist mili-tary version (PCL-M). Boston, MA: National Center forPTSD. 1991.
16. CONLON L, FAHY T, CONROY R. PTSD in ambulant RTA vic-tims: a randomized controlled trial of debriefing. Journalof psychosomatic research. 1999; 46 (1): 37-44.
17. ROSE S, BREWIN CR, ANDREWS B, KIRK M. A randomizedcontrolled trial of individual psychological debriefing forvictims of violent crime. Psychological Medicine. 1999; 29(04): 793-9.
18. HOBBS M, MAYOU R, HARRISON B, WORLOCK P. A ran-domised controlled trial of psychological debriefing forvictims of road traffic accidents. Bmj. 1996; 313 (7070):1438-9.
19. BISSON JI, JENKINS PL, ALEXANDER J, BANNISTER C.Randomised controlled trial of psychological debriefingfor victims of acute burn trauma. The British journal ofpsychiatry. 1997; 171 (1): 78-81.
10. SIJBRANDIJ M, OLFF M, REITSMA JB, CARLIER IV, GERSONSBP. Emotional or educational debriefing after psychologi-cal trauma. The British Journal of Psychiatry. 2006; 189 (2):150-5.
11. HOROWITZ MJ. Stress-response syndromes. Internationalhandbook of traumatic stress syndromes: Springer; 1993.p. 49-60.
12. KING LA, KING DW, FAIRBANK JA, KEANE TM, ADAMS GA.Resilience – recovery factors in post-traumatic stress disor-der among female and male Vietnam veterans: Hardiness,postwar social support, and additional stressful lifeevents. Journal of personality and social psychology. 1998;74 (2): 420.
13. BREWIN CR, ANDREWS B, VALENTINE JD. Meta-analysis ofrisk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of consulting and clinical psycho-logy. 2000; 68 (5): 748.
14. PERKONIGG A, KESSLER RC, STORZ S, WITTCHEN HU.Traumatic events and post§traumatic stress disorder in thecommunity: prevalence, risk factors and comorbidity. Actapsychiatrica scandinavica. 2000; 101 (1): 46-59.
15. FORNERIS CA, GARTLEHNER G, BROWNLEY KA, GAYNESBN, SONIS J, COKER-SCHWIMMER E, et al. Interventions toprevent post-traumatic stress disorder: a systematicreview. American journal of preventive medicine. 2013; 44(6): 635-50.
16. SIJBRANDIJ M, OLFF M, REITSMA JB, CARLIER IV, DE VRIESMH, GERSONS BP. Treatment of acute posttraumatic stressdisorder with brief cognitive behavioral therapy: a rando-mized controlled trial. The American journal of psychia-try. 2007; 164 (1): 82-90.
17. BISSON JI, SHEPHERD JP, JOY D, PROBERT R, NEWCOMBERG. Early cognitive – behavioural therapy for post-trau-matic stress symptoms after physical injury Randomisedcontrolled trial. The British journal of psychiatry. 2004;184 (1): 63-9.
52International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Psychological Debriefing_OUMAYA.qxp_Mise en page 1 16/03/2016 10:09 Page3
By J. L. ANTEVIL∑, J. A. BAILEY∏, M. W. BOWYERπ, E. M. RITTER∫ and E. A. ELSTERª. U.S.A.
Jared L. ANTEVIL
A New Reality: Critical Skills Retention and Readinessfor Military Trauma Surgery.*
Commander ANTEVIL was originally commissioned a Naval Officer in 1994, andbegan his surgical training at Naval Medical Center San Diego, California in 1998.
He completed his training as a Cardiothoracic Surgeon in 2009. CommanderANTEVIL currently serves as the Chief of Cardiothoracic Surgery in the Walter Reed
National Military Medical Center in Bethesda, MD, and as the U.S. Navy’s SpecialtyLeader for Cardiothoracic Surgery.
He is board certified in General and Thoracic Surgery, and holds a current academic appointment in TheDepartment of Surgery at Uniformed Services University of the Health Sciences & the Walter ReedNational Military Medical Center.
He has completed operational deployments with the U.S. Marines, aboard a U.S. Navy amphibious warship,and in support of Operation Enduring Freedom in Afghanistan.
53International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Un nouveau défi : la conservation des compétences critiques et du niveau de préparation en chirurgietraumatologique militaire.
Bien que les Etats-Unis et leurs alliés aient réalisé des progrès sans précédents en termes d’efficacité et de succès dans la prise encharge chirurgicale des blessés au cours des conflits les plus récents, la baisse du nombre de déploiements et les évolutions de lachirurgie du temps de paix sont de nature à dégrader l’aptitude des chirurgiens devant mettre en œuvre ces progrès remarquableslors des opérations à venir. Le maintien du savoir faire chirurgical adapté aux opérations de guerre est une priorité absolue qui vanécessiter de définir une liste de compétences indispensables et de s’appliquer à maintenir ces compétences tant dans l’entraînementque dans la pratique quotidienne du temps de paix tout en s’assurant que les chirurgiens militaires participent tous de façon régulièreà la prise en charge des traumatisés. De plus, les chirurgiens destinés aux opérations extérieures devraient participer à intervallesréguliers à des cycles d’Entraînement spécifiques et intégrés de prise en charge de la traumatologie de guerre.
INTRODUCTION
The US and its global partners have achieved unprece-dented success in forward casualty care through recentconflicts in the Middle East. The establishment and matu-ration of a US military trauma system, the use of evidence-based decisions to drive practice, and the cumulativeexperience of deployed military medical personnel haveall contributed to a new benchmark for survival aftercombat injury. The sustainment of these successes duringfuture combat operations depends on ensuring that sur-geons and other trauma team members maintain the skilland experience needed to implement best practice withinexisting combat trauma support systems.
SUCCESSES
Recent conflicts in Iraq and Afghanistan have spanneda period of greater than 11 years, and involved injuriesto over 50,000 United States (US) and coalition war-fighters. Over the course of these conflicts, evolutionsin injury prevention, battlefield care, casualty evacua-tion with robust en route care, and forward surgicalcare drove a 72% reduction in the combat injury case-fatality rate1. This improvement in trauma patient out-comes occurred in spite of advancements in improvisedexplosive device design, progressively increasing injuryseverity, and a rising incidence of multiple amputationsand other complex injury patterns2.
VOL.89/1
KEYWORDS: Military Medicine, Hospitals, Military, Trauma Centers, Clinical Competence.MOTS-CLÉS : Médecine Militaire, Hôpitaux Militaires, Centres de Traumatologie, Compétence Clinique.
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:07 Page1

The vast majority of combat-related mortality in recentconflicts occurred prior to a casualty reaching a militarytreatment facility3. Improvements in outcome afterinjury for coalition casualties are therefore attributablein large part to «pre-hospital» factors, including theadaptation of battlefield tactics, the routine use of per-sonal protective equipment, improvements in the medi-cal evacuation system, and evidence-based advances inbattlefield care3, 4. Tactical Combat Casualty Care (TCCC)guidelines for battlefield care were established in theUS in 1996, are regularly updated and revised, and arenow part of standard pre-deployment and sustainmenttraining across all three US military services4, 5. TCCCstandardized and formalized evidence-based improve-ments including the aggressive use of tourniquets, theoptimal use of topical hemostatic agents, and recom-mendations for the initial treatment of tension pneumo-thorax, airway obstruction, shock, and pain in a tacticalenvironment.
Many service member deaths in Iraq and Afghanistanwere likely not survivable even under optimal circums-tances, and over 70% of US combat fatalities had aninjury severity score of at least 252, 3. Studies estimatethat 17 to 28% of combat fatalities were potentiallysurvivable, the most common etiology for which wasjunctional and torso, or «non-compressible,» hemor-rhage on the battlefield3. However, if a US or coalitioncasualty was evacuated to a surgically capable facilitylate in the Afghanistan conflict with a salvageableinjury, his or her likelihood of survival exceeded 98%6,establishing a new standard for success in the forwardhospital care of combat casualties.
The recent, unprecedented success in the comprehen-sive forward care of combat casualties was largely dri-ven by efforts within the US Joint Theater TraumaSystem (JTTS). Building on civilian trauma models, theJTTS was established as a formal, systematic, and inte-grated approach to organize and coordinate combatcasualty care, with the intent of optimizing the chanceof survival and functional recovery for every US or coali-tion casualty7. With a clinically oriented leadershipstructure both in the US and within the combat theater,the JTTS successfully executed a relentless and scientificapproach to optimizing outcomes. A robust set of clini-cal practice guidelines (CPGs), evidence-based recom-mendations for combat trauma care, were developed,distributed and refined. A weekly teleconference revie-wed all combat casualties with the intent of continualprocess improvement. The JTTS was later broadened inscope to the Joint Trauma System (JTS), which extendedits influence across the entire continuum of militaryoperations. The Joint Theater Trauma Registry (JTTR)was established in 2005. The JTTR captured injury demo-graphics , anatomic and physiologic parameters, andtrauma care and outcomes across the continuum ofcombat casualty care. This registry data was used toeffect improvements in clinical care, drive medicallyrelated doctrine and policy, and support advancementsthrough scientific research. The JTTR was later expandedto a Department of Defense Trauma Registry (DoDTR),which now has over 23,000 individual US military
casualty data entries and is the world’s largest combatdata set4, 7, 8. Evidence-based investigation within theJTS has defined new worldwide best practice standardsin the use of resuscitative fluids, damage control sur-gery, tourniquet use and hemostasis9, 10.
In addition to the creation and evolution of the UScombat trauma system, US Critical Care Air Transport(CCAT) teams were battle-tested and refined over thecourse of recent conflicts. CCAT teams developed signi-ficant experience in the dynamic care of critically inju-red or ill patients along the chain of evacuation.Patients often needed to be transported distances wellover 6,000 miles, and undergo multiple operations bydifferent surgical teams in a span of several days. Likethe JTTS, CCAT program leaders met regularly throu-ghout combat operations to assess the state of the pro-gram, address challenges, and recommend futurecourse for development11. By the end of the conflict inAfghanistan, CCAT teams had achieved unprecedentedsafety in aeromedical evacuation, with an en routemortality of less than 0.2% in spite of a mean injuryseverity score of 2412.
The cumulative experience of deployed military sur-geons and other providers through recent conflicts hasled to a large pool of physicians with both remote andrecent deployment experience. In a recent survey ofactive duty surgeons across all three US services with atleast one combat deployment, 68% had two or moredeployments13. Although the success of the US militarytrauma system, military trauma registry and air trans-port program will be enduring legacies for future com-bat operations, the single greatest threat to long termsuccess in care for the combat injured is the potentialloss of the personnel skill and experience necessary tosuccessfully implement trauma care within these sys-tems. Sustainment of the critical skills necessary for for-ward combat trauma care is a formidable challenge,which will require a thoughtful and comprehensiveapproach.
54International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
∑ Commander, MC, USNThe Department of Surgery at Uniformed Services Universityof the Health Sciences & the Walter Reed National Military Medical Center.
∏ Colonel, MC, USAF,The Department of Surgery at Uniformed Services Universityof the Health Sciences & the Walter Reed National Military Medical Center.
π Colonel (ret), MC, USAF,The Department of Surgery at Uniformed Services Universityof the Health Sciences & the Walter Reed National Military Medical Center.
∫ Lt-Colonel, MC, USAF,The Department of Surgery at Uniformed Services Universityof the Health Sciences & the Walter Reed National Military Medical Center.
ª Captain, MC, USN,The Department of Surgery at Uniformed Services Universityof the Health Sciences & the Walter Reed National Military Medical Center.
Correspondence:Commander Jared ANTEVIL, MC, USNThe Department of Surgery at Uniformed Services Universityof the Health Sciences & the Walter Reed National Military Medical Center4301 Jones Bridge RoadBethesda, Maryland 20814, USAPhone: (301) 295-3155Fax: (301) 295-3627E-mail: [email protected]
* Presented at the 41st ICMM World Congress on Military Medicine,Bali, Indonesia, 17-22 May 2015.
VOL.89/1
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:07 Page2

CURRENT STATE
As the pace of US engagement in active global conflicthas waned, deployment requirements for US surgeons,emergency medicine physicians, anesthesia providersand others have declined significantly. Parallel to thisdecline, the US military health system has renewed itsfocus on the «recapture» of beneficiary care into mili-tary hospitals within the US, in an effort to contain theincreasing cost of beneficiary care in the civilian medi-cal network, ensure quality care, and to ensure readi-ness of military medical personnel in support of a«medically ready force and ready medical force»14. Inaddition to fiscal considerations, the US military healthsystem has faced increasing public scrutiny with regardto hospital and patient outcomes, and has redoubledits commitment to ensuring high quality care within itswalls15.
As a result of the decline in recent combat deploy-ments, and despite the goals of bolstering patientvolumes within US military hospitals and ensuring qua-lity care, maintaining clinical readiness for combatcasualty care is a significant challenge. Although some«peacetime» surgical skills within military hospitalsmay translate to combat trauma practice, there is anational trend towards less invasive procedures andcare delivery13. There has been a steady decline inopen vascular procedures13, 16, and current US resi-dency training programs for military surgeons empha-size skills such as advanced laparoscopy and otherminimally invasive techniques rather than skills thatmay translate into effective combat casualty care17. In arecent survey of US military surgeons, less than 50% feltthat residency training prepared them well for deploy-ment, in spite of the fact that nearly 70% graduatedfrom military programs13.
Although all US military surgical residents receive expe-rience in trauma, most of this experience is achieved atcivilian institutions. The majority of trauma patientstreated at the few US military facilities that care foracute trauma are not military care beneficiaries, havelow rates of injury severity, and have a high proportionof isolated orthopedic injury relative to battlefieldinjury patterns18. Although collaboration with civiliantrauma centers to provide real world trauma expe-rience for military surgeons has great value19, theinjury patterns, available resources and treatment algo-rithms differ significantly between most civilian traumaand modern combat trauma surgery16, 20, 21. Althoughthere is a small subset of US urban trauma centers witha robust volume of penetrating traumatic injuries, pro-cedures such as laparotomy or thoracotomy are uncom-monly performed in the vast majority of US civiliantrauma centers, and there is a heavy emphasis onadvanced imaging and non-operative management22-24.There is minimal exposure to multiple amputees orhigh-energy explosive injury3. A review of a busy civilianUS trauma center surgical experience revealed that over50% of patients admitted to the trauma service had nosignificant injury to the abdomen, chest or neck, andonly 11% had a surgical procedure performed by a
trauma surgeon25. Operative trauma case volumes forUS surgical trainees have declined by nearly 50% overthe past two decades26. Furthermore, while civiliantrauma experience may benefit military surgeons, themultidisciplinary nature of modern trauma care man-dates the clinical readiness of the entire operationaltrauma care team.
Unlike civilian trauma, trauma care in the deployedmilitary setting is administered by a diverse group ofhealthcare providers, for whom trauma training highlyvariable in extent and quality. Even surgeons withsignificant prior experience in trauma care are vulnera-ble to clinical skill erosion if they do not care fortrauma patients on a regular basis17. A number of «pre-deployment» courses have been developed to bridgethe gap between peacetime surgical experience andcombat trauma care. However, pre-deployment courseattendance is highly variable within the US military,including at least six different courses with widely dif-fering curricula13, 16. A significant proportion of currentpre-deployment training for US medical personnelfocuses on tactical skills and general military trainingrather than medical care16. Although the completion ofsome form of combat trauma training immediatelyprior to deployment is now largely standard across allthree US military services, to date there has been littleformal emphasis on the continual sustainment of surgi-cal skills16. In spite of their being curricula available forthe training of surgeons prior to deployment, this trai-ning is not universally attended. Dubose and col-leagues reported in 2012 a survey of 137 active duty USmilitary surgeons from all three branches, revealingthat only 44% had attended any form of combat-rela-ted trauma pre-deployment training16. A survey of 62US Army surgeons conducted in 2014 (unpublisheddata) found that 64% of the respondents stated thatthey did not attend any surgery-specific pre-deploy-ment training prior to their first deployment. Theseresults reflect the lack of a standardized approach tosurgery-specific pre-deployment training. The failure toprovide or mandate such training is contrary to thebest interests and care of our wounded warriors, aswell as the surgeons who are deployed with incom-plete skill sets.
SURGICAL COMPETENCY AND CURRENCY
Surgical competency is defined as having the requiredtraining and qualification for an acceptable level ofperformance, or as being «qualified» for a given pro-cedure or skill. In contrast, surgical currency reflectsactual performance in practice, which is a product ofcompetence and cumulative experience27. A fellows-hip-trained surgical subspecialist may be qualified toperform a trauma laparotomy based on training andcertification, but his or her currency to skillfully per-form this operation will degenerate over time withoutongoing experience. There is some evidence to suggesta volume-outcome relationship for surgeons practicingacute trauma care, although the lower limit of surgicalvolume to maintain acceptable currency in this specialtyhas not been clearly defined28-30.
55International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:07 Page3

Operational requirements for modern military sur-geons are not confined to combat trauma. Surgeonsmust also be able to care for disease-non-battle surgi-cal conditions, and may be called upon to participate inHumanitarian Assistance/Disaster Relief (HA/DR) mis-sions. Such missions require proficiency in skills largelypracticed during daily peacetime care, in the field ofacute care surgery.
SKILL SETS FOR SURGICAL CURRENCY
There have been several proposals over the years todefine a «board-certified» military physician, but theprecise skill set, training, and certification for safe andeffective combat trauma practice is currently not welldefined9. Previous efforts to describe standards for theattainment and sustainment of combat trauma surgicalcurrency have often incorporated comprehensive listsof procedures and skills that encompass the entire spec-trum of operational surgical care31. Recognizing thattime and resources for deployment-related surgicaltraining are finite, and that efforts to build traumaskills must not impede high quality elective surgicalcare, it is useful to prioritize surgical procedures in thecontext of combat trauma management. A surgeon’sclinical readiness for combat deployment may be defi-ned by his or her ability to safely and independentlyperform procedures that are required frequently in thecombat trauma environment, require early interven-tion for the salvage of life, limb or eyesight, and/orrequire significant technical expertise and experiencebeyond the skills typically exercised in peacetime practice(figure 1).
Studies from recent conflicts have consistently demons-trated that extremity injuries are the most frequentpattern, with an incidence of over 50% in combatcasualties31, 32. Based on a recent survey of US surgeons
with combat deployment experience, more than onequarter applied an external fixator without the assis-tance of an orthopedic surgeon, 70% did at least onefasciotomy, and over 50% placed at least one vascularshunt and performed at least one primary vascularrepair13. Deploying surgeons must therefore be compe-tent in independent temporary fracture fixation, fas-ciotomy, and the initial management of peripheral vas-cular injuries. Five of the top six survey areas where res-pondents felt the greatest need for additional expe-rience were related to vascular injury, and most sur-geons reported that their skills had lapsed eitherbecause they were not exposed to vascular trauma inclinical practice, or because of a significant time lapsesince their last exposure13. Although much less com-monly encountered, significant truncal injuries (thorax,abdomen, pelvis) and head injuries are nearly alwayspotentially life-threatening. The critical nature of theseinjuries and complexity of their surgical care man-date their emphasis in any deployment-related skillsprogram.
The creation of a «surgical skills set» for deployablemilitary surgeons will require additional investigationand review by military subject matter experts, as theexpectation that every surgeon will maintain currencyfor all potentially relevant combat trauma proceduresis simply not viable in the current environment. Skillsets should likely be customized for different deploy-ment roles, with different expectations for surgeonspracticing at different levels of care, surgeons deployedin a remote care setting, and those assigned to HA/DRmissions. Additionally, mechanisms for «just in timetraining» and rapid skill refreshment for low-fre-quency, high-criticality skill should be developed toenhance currency.
SURGICAL CURRENCY SUSTAINMENT
Developing surgical currency programs that will alwaysremain relevant for future conflicts is a formidablechallenge. Regardless of the format of such a program,the associated training must be dynamic - it mustreflect wounds and injury patterns seen in current ope-rations, and must be revised to incorporate real-timedata and real world scenarios33. Because operationalassignments for surgeons are rarely service-specific,combat trauma training should be standardized for allmilitary surgeons across all services. Although there is acore set of procedures, skills, and knowledge applicablefor all operational missions, certain skill sets must bespecified based on anticipated mission. Skill sets shouldbe developed from the current, battle-tested jointtrauma guidelines for surgeons deploying to a Role 2setting, a Role 3 setting, anticipated remote care sur-gery, and for HA/DR missions. These skill sets should beorganized in the educational framework of the sixAccreditation Council for Graduate Medical Educationcore competencies (patient care, medical knowledge,practice based learning, systems based practice, profes-sionalism, and interpersonal skills) and should be mea-sured with robust assessment tools. Finally, effectivecombat trauma surgical currency must not rely on «just
56International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 1: Depiction of several combat trauma procedureswithin a model to prioritize pre-deployment and
sustainment surgical training skills based on1) «frequency» of utilization in a combat trauma setting,
2) «criticality» (defined as need for intervention on an emer-gent or urgent basis to preserve life, limb, or eyesight), and3) «complexity» (defined as the degree to which a procedurerequires skills beyond those typically practiced by a generalsurgeon or surgical sub-specialist in a peacetime practice).
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:07 Page4

Operational requirements for modern military sur-geons are not confined to combat trauma. Surgeonsmust also be able to care for disease-non-battle surgi-cal conditions, and may be called upon to participate inHumanitarian Assistance/Disaster Relief (HA/DR) mis-sions. Such missions require proficiency in skills largelypracticed during daily peacetime care, in the field ofacute care surgery.
SKILL SETS FOR SURGICAL CURRENCY
There have been several proposals over the years todefine a «board-certified» military physician, but theprecise skill set, training, and certification for safe andeffective combat trauma practice is currently not welldefined9. Previous efforts to describe standards for theattainment and sustainment of combat trauma surgicalcurrency have often incorporated comprehensive listsof procedures and skills that encompass the entire spec-trum of operational surgical care31. Recognizing thattime and resources for deployment-related surgicaltraining are finite, and that efforts to build traumaskills must not impede high quality elective surgicalcare, it is useful to prioritize surgical procedures in thecontext of combat trauma management. A surgeon’sclinical readiness for combat deployment may be defi-ned by his or her ability to safely and independentlyperform procedures that are required frequently in thecombat trauma environment, require early interven-tion for the salvage of life, limb or eyesight, and/orrequire significant technical expertise and experiencebeyond the skills typically exercised in peacetime practice(figure 1).
Studies from recent conflicts have consistently demons-trated that extremity injuries are the most frequentpattern, with an incidence of over 50% in combatcasualties31, 32. Based on a recent survey of US surgeons
with combat deployment experience, more than onequarter applied an external fixator without the assis-tance of an orthopedic surgeon, 70% did at least onefasciotomy, and over 50% placed at least one vascularshunt and performed at least one primary vascularrepair13. Deploying surgeons must therefore be compe-tent in independent temporary fracture fixation, fas-ciotomy, and the initial management of peripheral vas-cular injuries. Five of the top six survey areas where res-pondents felt the greatest need for additional expe-rience were related to vascular injury, and most sur-geons reported that their skills had lapsed eitherbecause they were not exposed to vascular trauma inclinical practice, or because of a significant time lapsesince their last exposure13. Although much less com-monly encountered, significant truncal injuries (thorax,abdomen, pelvis) and head injuries are nearly alwayspotentially life-threatening. The critical nature of theseinjuries and complexity of their surgical care man-date their emphasis in any deployment-related skillsprogram.
The creation of a «surgical skills set» for deployablemilitary surgeons will require additional investigationand review by military subject matter experts, as theexpectation that every surgeon will maintain currencyfor all potentially relevant combat trauma proceduresis simply not viable in the current environment. Skillsets should likely be customized for different deploy-ment roles, with different expectations for surgeonspracticing at different levels of care, surgeons deployedin a remote care setting, and those assigned to HA/DRmissions. Additionally, mechanisms for «just in timetraining» and rapid skill refreshment for low-fre-quency, high-criticality skill should be developed toenhance currency.
SURGICAL CURRENCY SUSTAINMENT
Developing surgical currency programs that will alwaysremain relevant for future conflicts is a formidablechallenge. Regardless of the format of such a program,the associated training must be dynamic - it mustreflect wounds and injury patterns seen in current ope-rations, and must be revised to incorporate real-timedata and real world scenarios33. Because operationalassignments for surgeons are rarely service-specific,combat trauma training should be standardized for allmilitary surgeons across all services. Although there is acore set of procedures, skills, and knowledge applicablefor all operational missions, certain skill sets must bespecified based on anticipated mission. Skill sets shouldbe developed from the current, battle-tested jointtrauma guidelines for surgeons deploying to a Role 2setting, a Role 3 setting, anticipated remote care sur-gery, and for HA/DR missions. These skill sets should beorganized in the educational framework of the sixAccreditation Council for Graduate Medical Educationcore competencies (patient care, medical knowledge,practice based learning, systems based practice, profes-sionalism, and interpersonal skills) and should be mea-sured with robust assessment tools. Finally, effectivecombat trauma surgical currency must not rely on «just
56International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 1: Depiction of several combat trauma procedureswithin a model to prioritize pre-deployment and
sustainment surgical training skills based on1) «frequency» of utilization in a combat trauma setting,
2) «criticality» (defined as need for intervention on an emer-gent or urgent basis to preserve life, limb, or eyesight), and3) «complexity» (defined as the degree to which a procedurerequires skills beyond those typically practiced by a generalsurgeon or surgical sub-specialist in a peacetime practice).
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:07 Page4
in time» pre-deployment training – it must be rooted ineveryday practice. Surgeons not exposed to traumacare and associated surgical procedures in peacetimepractice must exercise this skill set at regular, prescribedintervals.
The optimal combat trauma training and sustainmentplan for military surgeons would incorporate exposureto real-world trauma under the guidance of experien-ced military trauma surgeons (at either a military hos-pital or a partnered civilian center). Because effectivecombat trauma management relies heavily on multidis-ciplinary coordination, training should incorporatenon-surgical specialists, nursing staff, and enlisted per-sonnel, in addition to surgeons. Training should opti-mally occur in platform-based teams to facilitate teamcohesiveness. In the current state, this model for com-bat trauma surgical currency would be most readilyachieved through partnerships with civilian facilities.Because of the gap between civilian trauma practiceand the skills required for effective combat trauma sur-gical management, additional training utilizing simula-tion equipment, vivarium exercises, and cadaversshould focus on wartime injuries/patterns and combattrauma surgical skill requirements not routinelyencountered in the civilian trauma setting. Key fea-tures of a combat trauma surgical currency programare outlined in Table 1.
A recently released report from the US Defense HealthBoard (DHB) entitled «Combat Trauma Lessons Learnedfor Military Operations of 2001-2013» cited in Lesson 8that «the lack of comprehensive, standardized trainingfor military health care providers created an operationalgap that affects unit-level training as well as effectiveutilization of the military system to reduce combat mor-tality.» The DHB report recommended that multi-modaleducational strategies be used in trauma training, toinclude an «appropriate balance» of didactics, practical,
application, scenario-based learning, distance learning,cadavers, live tissue training, human role models, clini-cal experience, virtual reality, serious games, and high-fidelity simulation34.
RESOURCES FOR COMBAT TRAUMA SURGICALCURRENCY ATTAINMENT AND SUSTAINMENT
Graduate Medical Education (GME)
Combat trauma management should be an area ofgreater emphasis within military surgical training pro-grams. Residents must graduate with a foundation ofknowledge and skill in this arena that is above andbeyond the minimal competencies defined by the civi-lian accreditation council, and current military hospitalswith surgical training programs need to formalize a«military-unique» surgical curriculum. For military phy-sicians that complete surgical training at a civilian pro-gram, similar expectations must be achieved throughsupplemental training after the completion of civilianresidency training. Given the increasing requirementsbeing placed on US surgical residency programs byregulatory agencies, this curriculum may need to beadministered outside of the current confines of the USResidency Review Committee for Surgery and theAmerican Board of Surgery. Developing a method toassess the desired skills will help ensure that GME gra-duates are as well prepared as possible for the chal-lenges of deployed surgical care.
Complex Military Hospital Surgical Care
Increasing the volumes of complex elective surgicalcases at US military hospitals would not only drive costcontainment and support quality outcomes, but wouldsupplement the surgical skills needed for combattrauma management. Open vascular procedures, openabdominal procedures, solid organ transplantation,complex oncologic resections and procedures requiring
57International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
ATTRIBUTE DESCRIPTION
Dynamic Structure- Emphasize wounds and injury patterns seen in current/recent operations.- Continually revise program to incorporate real world scenarios.
Standardized Format - Ensure consistent content foor all military surgeons across all services.
Team-Based Organization- Incorporate non-surgical specialists, nursing staff and enlisted personnel.- Train in groups based on anticipated deployment platforms.
Continual Emphasis- Create resources available for surgeons to train on recurring basis, ensuring that surgeonsnot exposed to trauma care and associated surgical procedures exercise this skill set at regular,prescribed intervals.
Real World Experience- Include real-world trauma experience, either in military hospital or partnered civiliantrauma center.
Simulation Training- Utilize simulation, vivarium/cadaveric training to emphasize skills not exercised in peace-time practice, those required frequently during operational medical care, and those most cri-tical for salvage of life/limb/eyesight.
Assessment- Evaluate impact of program on individual knowledge base and surgical capability, andidentify areas for additional emphasis.
Table 1: Key Features of a Combat Surgical Currency Program.
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:07 Page5

thoracotomy are all associated with exposure to ana-tomy and basic techniques relevant for trauma surgery.Military surgeons with elective practices that offer lit-tle exposure to these procedures (e.g. those practicingprimarily minimally invasive surgery or breast surgery)likely represent a group that is especially vulnerable tothe erosion of combat trauma management skills.Global health partnerships with international allieswhose standard of peacetime care includes more tradi-tional open procedures should be considered as apotentially beneficial resource for skills sustainment.
Military Hospital Trauma Care and Civilian TraumaPartnerships
The creation of robust trauma systems within additio-nal existing military medical facilities would allow forsurgical trauma skill acquisition and sustainmentwithout requirements for civilian partnerships or lossof personnel resources from military hospitals. It wouldsupport surgical training programs and would allowfor clinical currency in trauma care across the conti-nuum of trauma care, including non-surgical physiciansinvolved in trauma management, nursing and enlistedpersonnel, and ancillary services (e.g. blood banking,
pharmacy). Unfortunately, there are numerous geogra-phic, financial, and political obstacles to the establish-ment of acute trauma care programs at most US militaryhospitals in the near term35. There are active US militarytraining and sustainment programs that combine real-world civilian trauma experience with military traumasurgery team guidance and mentorship. However thetraining capacity of these programs is limited. Whilethere is presently no system-wide mechanism for themajority of US military surgeons to continually care fortrauma patients, there are multiple options being explo-red21. Such efforts should continue to build additionalcollaborative programs between military hospitals andlocal or regional civilian trauma centers.
Trauma Surgery Training Courses
Existing courses for surgical trauma skills sustainmentinclude those with primarily a didactic format, and pro-grams with combined didactic education and hands-onexperience (Table 2). Training that is learner-focusedand includes active learning components (i.e. combinesinteractive didactics with hands-on experience) hasbeen shown to be far more effective than traditionalpassive, instructor-focused training modalities17.
58International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
COURSE NAME SPONSORING ORGANIZATION FORMAT LENGTH CONTENT
ADVANCED SURGICAL SKILLS
EXPOSURE FOR TRAUMA
(ASSET)
American Collegeof Surgeons
Case Scenarios,Cadaveric Exercises
One Day
- Overview of surgical exposuresin key areas: neck, chest,
abdomen and pelvis, and upperand lower extremities
ADVANCED TRAUMA LIFE
SUPPORT (ATLS)American College
of SurgeonsDidactic Lectures, Skill
Stations, Case ScenariosTwo Days
- Simplified and standardizedapproach to initial civilian
trauma care
ADVANCED TRAUMA
OPERATIVE MANAGEMENT
(ATOM)
American Collegeof Surgeons
Didactic Lectures,Vivarium Exercises
One Day- Review of operative management
of penetrating injuries tothe chest and abdomen
EMERGENCY WAR SURGERY
COURSE (EWSC)US Department
of Defense
Didactic Lectures,Cadaveric and
Vivarium Exercises,Case Scenarios
Three Days
- Broad overview of initialmanagement of combat trauma
and basic trauma skills- Intended for general and
orthopedic surgeons- Incoporates content from
ASSET course
JOINT FORCES COMBAT
TRAUMA MANAGEMENT
COURSE (JFCTMC)
US Departmentof Defense
Didactic Lectures,Cadaveric and
Vivarium Exercises,Case Scenarios
Five Days
- Review of battlefield medicineand advanced traumamanagement for third
echelon providers- Breakout speciality-specific
instruction sections- Includes content from ATOM
and ASSET courses
TACTICAL COMBAT MEDICAL
CARE (TCMC)US Department
of Defense
Didactic Lectures,Skill Stations,
Case Scenarios,Vivarium Exercises
Five Days
- Advanced life-saving interventionsand live tissue training forsecond echelon providers
- Includes first responder combattrauma training (e.g. propertourniquet use, evacuation
under fire)
Table 2: Current Trauma Courses Available for United States (US) Military Surgeons.
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:07 Page6
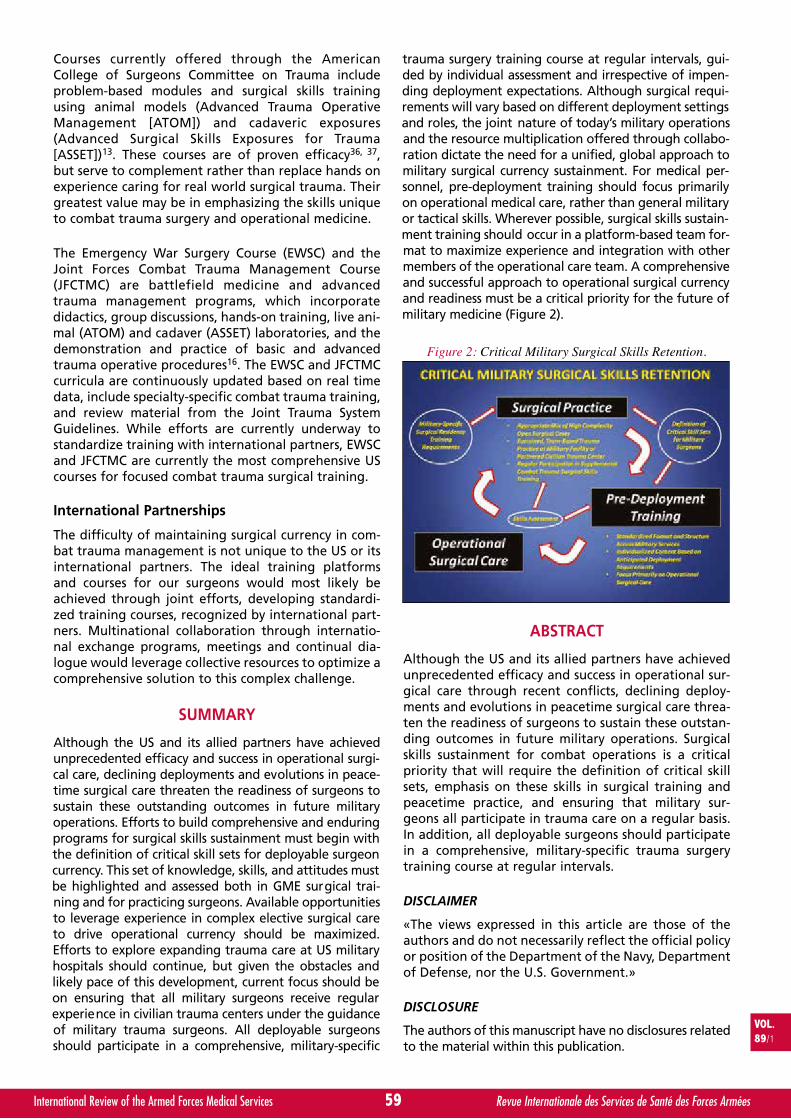
Courses currently offered through the AmericanCollege of Surgeons Committee on Trauma includeproblem-based modules and surgical skills trainingusing animal models (Advanced Trauma OperativeManagement [ATOM]) and cadaveric exposures(Advanced Surgical Skills Exposures for Trauma[ASSET])13. These courses are of proven efficacy36, 37,but serve to complement rather than replace hands onexperience caring for real world surgical trauma. Theirgreatest value may be in emphasizing the skills uniqueto combat trauma surgery and operational medicine.
The Emergency War Surgery Course (EWSC) and theJoint Forces Combat Trauma Management Course(JFCTMC) are battlefield medicine and advancedtrauma management programs, which incorporatedidactics, group discussions, hands-on training, live ani-mal (ATOM) and cadaver (ASSET) laboratories, and thedemonstration and practice of basic and advancedtrauma operative procedures16. The EWSC and JFCTMCcurricula are continuously updated based on real timedata, include specialty-specific combat trauma training,and review material from the Joint Trauma SystemGuidelines. While efforts are currently underway tostandardize training with international partners, EWSCand JFCTMC are currently the most comprehensive UScourses for focused combat trauma surgical training.
International Partnerships
The difficulty of maintaining surgical currency in com-bat trauma management is not unique to the US or itsinternational partners. The ideal training platformsand courses for our surgeons would most likely beachieved through joint efforts, developing standardi-zed training courses, recognized by international part-ners. Multinational collaboration through internatio-nal exchange programs, meetings and continual dia-logue would leverage collective resources to optimize acomprehensive solution to this complex challenge.
SUMMARY
Although the US and its allied partners have achievedunprecedented efficacy and success in operational surgi-cal care, declining deployments and evolutions in peace-time surgical care threaten the readiness of surgeons tosustain these outstanding outcomes in future militaryoperations. Efforts to build comprehensive and enduringprograms for surgical skills sustainment must begin withthe definition of critical skill sets for deployable surgeoncurrency. This set of knowledge, skills, and attitudes mustbe highlighted and assessed both in GME surgical trai-ning and for practicing surgeons. Available opportunitiesto leverage experience in complex elective surgical careto drive operational currency should be maximized.Efforts to explore expanding trauma care at US militaryhospitals should continue, but given the obstacles andlikely pace of this development, current focus should beon ensuring that all military surgeons receive regularexperience in civilian trauma centers under the guidanceof military trauma surgeons. All deployable surgeonsshould participate in a comprehensive, military-specific
trauma surgery training course at regular intervals, gui-ded by individual assessment and irrespective of impen-ding deployment expectations. Although surgical requi-rements will vary based on different deployment settingsand roles, the joint nature of today’s military operationsand the resource multiplication offered through collabo-ration dictate the need for a unified, global approach tomilitary surgical currency sustainment. For medical per-sonnel, pre-deployment training should focus primarilyon operational medical care, rather than general militaryor tactical skills. Wherever possible, surgical skills sustain-ment training should occur in a platform-based team for-mat to maximize experience and integration with othermembers of the operational care team. A comprehensiveand successful approach to operational surgical currencyand readiness must be a critical priority for the future ofmilitary medicine (Figure 2).
ABSTRACT
Although the US and its allied partners have achievedunprecedented efficacy and success in operational sur-gical care through recent conflicts, declining deploy-ments and evolutions in peacetime surgical care threa-ten the readiness of surgeons to sustain these outstan-ding outcomes in future military operations. Surgicalskills sustainment for combat operations is a criticalpriority that will require the definition of critical skillsets, emphasis on these skills in surgical training andpeacetime practice, and ensuring that military sur-geons all participate in trauma care on a regular basis.In addition, all deployable surgeons should participatein a comprehensive, military-specific trauma surgerytraining course at regular intervals.
DISCLAIMER
«The views expressed in this article are those of theauthors and do not necessarily reflect the official policyor position of the Department of the Navy, Departmentof Defense, nor the U.S. Government.»
DISCLOSURE
The authors of this manuscript have no disclosures relatedto the material within this publication.
59International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Figure 2: Critical Military Surgical Skills Retention.
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:08 Page7

REFERENCES
11. ELSTER EA, BUTLER FK, RASMUSSEN TE. Implications ofCombat Casualty Care for Mass Casualty Events, CombatCasualty Care and Mass Casualty Events. JAMA. 2013; 310(5): 475-476.
12. KELLY JF, RITENOUR AE, MCLAUGHLIN DF, et al. Injuryseverity and causes of death from Operation IraqiFreedom and Operation Enduring Freedom: 2003-2004versus 2006. J Trauma. 2008; 64 (suppl 2): S21-S26.
13. EASTRIDGE BJ, MABRY RL, SEGUIN P, et al. Death on theBattlefield (2001-2011): Implications for the future ofcombat casualty care. J Trauma. 2012; 73: S431-7.
14. BUTLER FK, BLACKBOURNE LH. Battlefield trauma carethen and now: a decade of tactical combat casualty care.J Trauma Acute Care Surg. 2012; 73: S395-402.
15. BUTLER FK, HOLCOMB JB, GIEBNER SD, et al. TacticalCombat Casualty Care 2007: Evolving concepts and bat-tlefield experience. Mil Med. 2007; 172: 1-19.
16. KOTWAL RS, BUTLER FK, EDGAR EP, et al. Saving Lives onthe Battlefield: A Joint Trauma System Review of Pre-Hospital Trauma Care in Combined Joint Operating Area– Afghanistan. (CJOA-A). FINAL REPORT, 30 January 2013,U.S. Central Command Pre-Hospital Trauma CareAssessment Team. Accessed at http://rdcr.org/wp-content/uploads/2013/02/CENTCOM-Prehospital-Final-Report-130130.pdf.
17. BLACKBOURNE LH, BAER DG, EASTRIDGE BJ. Militarymedical revolution: military trauma system. J TraumaAcute Care Surg. 2012; 73: S388-S394.
18. EASTRIDGE BJ, MABRY R, BLACKBOURNE LH, BUTLER FK.We don’t know what we don’t know: prehospital data incombat casualty care. US Army Med Dep J. 2011; Apr-Jun:11-14.
19. MABRY RL, DELORENZO RA. Improving Role I battlefieldcasualty care from point of injury to surgery. US ArmyMed Dep J. 2011; Apr-Jun: 87-91.
10. HOLCOMB JB. Optimal use of blood products in severelyinjured trauma patients. Hematology Am Soc HematolEduc Program. 2010; 2010: 465-469.
11. BENINATI W, MEYER MT, CARTER TE. The critical care airtransport program. Crit Care Med. 2008; 36: S370-376.
12. INGALLS N, ZONIES D, BAILEY JA, et al. A review of thefirst 10 years of critical care aeromedical transport duringoperation Iraqi freedom and operation enduring free-dom: the importance of evacuation timing. JAMA Surg.2014; 149: 807-13.
13. TYLER JA, RITCHIE JD, LEAS ML, et al. Combat readinessfor the modern military surgeon: data from a decade ofcombat operations. J Trauma Acute Care Surg. 2012; 73:S64-70.
14. Congressional Budget Office report: Approaches to redu-cing federal spending on military healthcare, January 2014.Accessed at http://www.cbo.gov/sites/default/files/44993-MilitaryHealthcare.pdf.
15. Military Health System Review, U.S. Department of
Defense. Accessed at http://www.defense.gov/home/fea-tures/2014/0614_healthreview/.
16. DUBOSE J, RODRIGUEZ C, MARTIN M, et al. Preparing thesurgeon for war: present practices of US, UK, andCanadian militaries and future directions for the US mili-tary. J Trauma Acute Care Surg. 2012; 73: S423-S430.
17. SOHN VY, RUNSER LA, PUNTEL RA, et al. Training physi-cians for combat casualty care on the modern battlefield.J Surg Educ. 2007; 64: 199-203.
18. WOJCIK BE, STEIN CR, DEVORE RB, et al. Status of traumacare in U.S. Army hospitals. Mil Med. 2005; 170: 141-148.
19. THORSON CM, DUBOSE JJ, RHEE P, et al. Military traumatraining at civilian centers: A decade of advancements. JTrauma. 2012; 73: S483-489.
20. STARNES BW, BEEKLEY AC, SEBESTA JA, et al. Extremityvascular injuries on the battlefield: Tips for surgeonsdeploying to war. J Trauma. 2006; 60: 432-442.
21. HIGHT RA, SALCEDO ES, MARTIN SP, et al. Level I academictrauma center integration as a model for sustaining combatsurgical skills: the right surgeon in the right place for theright time. J Trauma Acute Care Surg. 2015; 78: 1176-1181.
22. SCHWAB CW. Selection of nonoperative managementcandidates. World J Surg. 2001; 25: 1389-1392.
23. STAWICKI SP. Trends in non-operative management of trau-matic injuries: A synopsis. OPUS 12 Scientist. 2007; 1: 19-35.
24. FRAGA GP, RIZOLI S. Chapter 1, Trauma Laparotomy, In:DiSaverio S, Tugnoli G, Catena F, Ansaloni L, Naidoo N eds.Trauma Surgery, Volume 2: Thoracic and AbdominalTrauma. Milan: Springer, 2014; 1-20.
25. CIESLA DJ, MOORE EE, COTHREN CC, et al. Has the TraumaSurgeon Become House Staff for the SurgicalSubspecialist? Am J Surg. 2006; 192: 732-737.
26. DRAKE FT, VAN EATON EG, HUNTINGTON CR, et al.ACGME case logs: Surgery resident experience in opera-tive trauma for two decades. J Trauma Acute Care Surg.2012; 73: 1500-1506.
27. RETHANS JJ, NORCINI JJ, BARON-MALDONADO M, et al.The relationship between competence and performance:implications for assessing practice performance. MedicalEduc. 2002; 36: 901-9.
28. KONVOLINKA CW, COPES WS, SACCO WL. Institution andper-surgeon volume versus survival outcome inPennsylvania’s trauma centers. Am J Surg. 1995; 170: 333-40.
29. PELLETIER SJ. Surgical Critical Care Privileges, In: CorePrivileges for Physicians: A practical approach to develo-ping and implementing criteria-based privileges, 5th ed.Danvers, MA: HCPro, Inc, 2010; 634-5.
30. RICHARDSON JD, SCHMEIG R, BOAZ P, et al. Impact oftrauma attending surgeon case volume: Is more better? JTrauma. 1998; 44: 266-272.
31. RAMASAMAY A, HINSLEY DE, EDWARDS DS, et al. Skillsets and competencies for the modern military surgeon:Lessons from UK military operations in SouthernAfghanistan. Injury. 2009; 41: 453-9.
60International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:08 Page8

32. KEARNEY SP, BLUMAN EM, LONERGAN KT, et al.Preparedness of orthopaedic surgeons for modern battle-field surgery. Mil Med. 2012; 177: 1058-1064.
33. RIGNAULT DP. How to train war surgery specialist: part II.Mil Med. 1990; 155: 143-147.
34. JENKINS D (Committee Chair). Defense Health BoardTrauma and Injury Subcommittee Report: Combat TraumaLessons Learned from Military Operations of 2001-2013.Released March 9, 2015.
35. GRASER JC, BLUM D, BRANCATO K, et al. The economicsof Air Force medical service readiness. Project Air Force,RAND Corporation 2010. Accessed athttp://www.rand.org/content/dam/rand/pubs/technical_reports/2010/RAND_TR859.pdf.
36. ABOUD ET, KRISHT AF, O’KEEFE T, et al. Novel simulation fortraining trauma surgeons. J Trauma. 2011; 71: 1484-1490.
37. KUHLS DA, RISUCCI DA, BOWYER MW, LUCHETE FA.ASSET: An effective educational experience for practicingsurgeons. Bull Am Coll Surg. 2012; 97: 31-35.
61International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Critical Skill_ANTEVIL.qxp_Mise en page 1 16/03/2016 10:08 Page9
Stop Bleeding. Save Lives
Contact us at www.celoxmedical.com/ICMM
1. Testing a new gauze hemostat with reduced treatment time. A Hoggarth et al. Poster ATACCC 2011, FL.2. Chitosan based advanced hemostatic dressing is associated with decreased blood loss in swine uncontrolled hemorrhage model.
Kunio et al. Am J Surg 2013. TM Trademark of Medtrade Products Ltd. Image UK MOD Crown Copyright 2013
Medtrade Products Ltd.Electra House, Crewe Business Park, Crewe, Cheshire, UK. CW1 6GL
Telephone: +44 (0) 1270 500019 Fax: +44 (0) 1270 500045 [email protected]
Please quote reference ICMM when replying
RAPID
Works with just 60 seconds compression1
Stops life-threatening bleeding – fast
Reduces blood loss in an independent study2
CeloxTM Rapid the fastest acting battlefield haemostatic
Come and see us at 4th ICMM Pan European Congress Paris
Celox Half Page Advert AW.indd 1 15/03/2016 11:54


By V.V. KHOMINETS∑, V.M. SHAPOVALOV∏, S.V. MIKHAILOVπ, D.A. SHAKUN∫, A.V. SHCHUKINª, M.V. TKACHENKOº
and A.L. KUDIASHEVΩ. Russian Federation
Vladimir V. KHOMINETS
Application Features for External and SequentialOsteosynthesis in Patients with Gunshot Fracturesof Long-Bones of the Extremities.*
Vladimir V. KHOMINETS, MD, PhD
GENERAL INFORMATION
Date of Birth: September 28, 1962Home address: Saint Petersburg, Russia
EDUCATION
Graduated from Military Medical Academy (Saint Petersburg, Russia) in 1989Military Medical Academy postgraduate training in 1994-1997
PROFESSIONAL EXPERIENCE
Military service: 1989-1994Department of Military Traumatology and Orthopedics: 1997- present
CURRENT POSITION
The chief of the Military Traumatology and Orthopedics Department of the Military Medical Academy(Saint Petersburg, Russia), the colonel of Medical Service of Russian Army.
PROFESSIONAL MEMBERSHIP
AO Trauma from 2007SICOT from 2001AAOS from 2013Russian National Faculty of AO Trauma, SICOT member and Aesculap Academy
SCIENTIFIC ACHIEVEMENTS
PhD, professor of Traumatology and OrthopedicsOver 100 of scientific publicationsAuthor of 3 monographs and 5 textbooks on Traumatology and Orthopedics5 patents.
63International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Indications de fixateur externe ou d’ostéosynthèse en deux temps chez les blessés souffrant de fracturespar balles des os longs des extrémités.
Cet article analyse les résultats du traitement de deux groupes de patients présentant des fractures par balles des os longs desextrémités, traités par ostéosynthèse par fixateur externe (Groupe I, 206 cas) et par ostéosynthèse séquentielle en deux temps(Groupe II, 79 cas) au moment de leur évacuation sanitaire. Dans la plupart des cas l’ostéosynthèse séquentielle permet d’obtenirune bonne consolidation et réduit l’incidence du retard de consolidation ou de pseudarthrose lorsqu’on la compare à l’ostéosynthèsepar fixateur externe. L’incidence de la contracture des grosses articulations est diminuée de 3 à 5,5 fois moins (en fonction du sitede la blessure) lorsque l’ostéosynthèse en deux temps est pratiquée.
INTRODUCTION
One of the important tendencies of the modern surgicaltrauma is a significant increase of its severity, number of
cases with multiple or combined injuries, extent ofvarious tissue damage5, 6, 11, 14, 15, 22, 23. These factorsdefine the complexity and labor intensity of the medicalcare in patients with gunshot fractures at the medical
VOL.89/1
KEYWORDS: Gunshot fractures, Sequential osteosynthesis, External osteosynthesis, Wounded casualty.MOTS-CLÉS : Fracture par balle, Ostéosynthèse séquentielle, Ostéosynthèse par fixateur externe, Blessure.
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page1

evacuation stages, as well as high rate of non-satisfac-tory results of anatomical and, in particular, functionaltreatment outcomes1, 4, 6, 15, 17, 20, 22. Analysis of the spe-cialized scientific literature of the last decade showsthat authors have no consolidated opinion concerningthe osteosynthesis techniques, that should be used forthe treatment of the above mentioned category ofpatients in different levels of specialized traumatologiccare.
The theoretical justification of a through-bone osteo-synthesis using external fixators in cases of extremitywar injuries was obtained in the experimental and cli-nical studies, conducted at the Military Traumatologyand Orthopaedics Department of the Military MedicalAcademy1, 4, 6, 9, 10, 14. The advantages of this fixationmethod of the gunshot fractures consist not only in thereliable immobilization, correction of bone fragment’sposition and ensuring more favorable conditions fordynamic control of the wound process, but also in pos-sibility to apply elements of the reconstructive andplastic surgery at the early stages after the gunshotwounds15, 18.
Many military traumotologists and surgeons considerapplication of early internal osteosynthesis in the treat-ment of gunshot wounds to be unacceptable4, 5, 6, 11, 14.There are only a few publications providing an evidencefor possibility of application of this technique withappropriate duration of massive antibiotic therapy orafter the dermal wound healing2, 3, 7, 8, 12, 13, 16, 17, 19, 21, 22.Moreover, there are no data on publications, devoted tothorough comparative studies of the effectiveness ofdifferent osteosynthesis techniques in the treatment ofpatients with gunshot fractures of long-bones of theextremities at the stages of medical evacuation.
The actual significance of the above mentioned unsol-ved issues has determined the goal of our study - tocompare the effectiveness of through-bone andsequential osteosynthesis in the treatment of patientswith gunshot fractures of long bones at the stages ofspecialized trauma care.
MATERIAL AND METHODS
The comparative analysis of stage treatment of militarymen with gunshot fractures of humerus (84 cases),forearm (21 cases), femur (39 cases) and shin (62 cases),who underwent throughbone (1 group - 206 cases) orsequential two-step osteosynthesis (2 group - 79 cases)at the stages of the medical evacuation, was held.Segmental division was as following: humerus (17 cases– 21.5%), forearm (11 cases – 13.9%), femur (32 cases –40.5%), shin (19 cases – 24.1%). The methods of two-step sequential osteosynthesis included a primary bonereposition and external fixation, following by the remo-val of these fixation devices and repeated extramedul-lary osteosynthesis using plates or intramedullary osteo-synthesis with locking nails, performed after the soft tis-sues healing (up to 14 days) and stabilization of thegeneral patient’s condition. Minimally-invasive surge-ries and biological osteosynthesis were used. The main
tasks of the sequential two-step osteosynthesis werethe early movement in the adjacent joints of the injuredsegment and prevention of the pin-track osteomyelitis.
In view of the above, the comparative analysis of thefeatures and treatment outcomes in two groups ofpatients was held taking into the consideration thenature and severity of the gunshot wounds, fracturetypes and existence of bone defects. Special attentionwas paid to the procedures and manipulations perfor-med at the stages of specialised trauma care.Treatment time, complications occurred, the nature ofgunshot fractures union as well as achieved anatomicaland functional outcomes were also examined in details.
RESULTS AND DISCUSSIONS
The comparative analysis of the effectiveness andapplication features of two osteosynthesis techniquesin patients with gunshot long-bone fractures of theextremities at the stages of the specialized trauma careprovides new data and enables to make some practi-cally important generalizations. Among them it isworth to mention the identified differences in treat-ment outcomes in patients, who underwent through-bone or sequential two-step osteosynthesis.
In our point of view, one of the most important identi-fied fact is a proved decrease of an overall treatmenttime and improvement of functional outcomes, achievedby the application of the active surgical approach, whenexternal fixation devices are substituted with the extra-medullary plates. In particular, overall treatment time inpatients with sequential two-step osteosynthesis wereshorter by 25-35% in comparison with external fixationdevices, depending on the injured extremity segmentand severity of the gunshot wound (Table 1). With that,in most cases the identified results were statisticallysignificant (≤ 0.05 or ≤ 0.01).
64International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
∑ MD, PhD, Associate Professor,Head of the Military Traumatology and Orthopedics Department of theMilitary Medical Academy.
∏ MD, PhD,Professor of the Military Traumatology and Orthopedics Department of theMilitary Medical Academy.
π MD, PhD,Senior Professor of the Military Traumatology and Orthopedics Departmentof the Military Medical Academy.
∫ Professor of the Military Traumatology and Orthopedics Department of theMilitary Medical Academy.
ª Head of the Traumatology and Orthopedics Clinic’s Unit of the MilitaryMedical Academy.
º Senior Professor of the Military Traumatology and Orthopedics Departmentof the Military Medical Academy, Candidate of Medical Sciences.
Ω Deputy Head of the Military Traumatology and Orthopedics Department ofthe Military Medical Academy, Candidate of Medical Sciences.
Correspondence:Colonel Vladimir V. KHOMINETS, MD, PhDHead of the Military Traumatology and Orthopedics Department of theMilitary Medical AcademyMilitary Medical Academy n.a. S. M. Kirov6 Lebeva Str.RUS-194017 Saint PetersburgRussian Federation
* Presented at the 41st ICMM World Congress on Military Medicine,Bali, Indonesia, 17-22 May 2015.
VOL.89/1
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page2
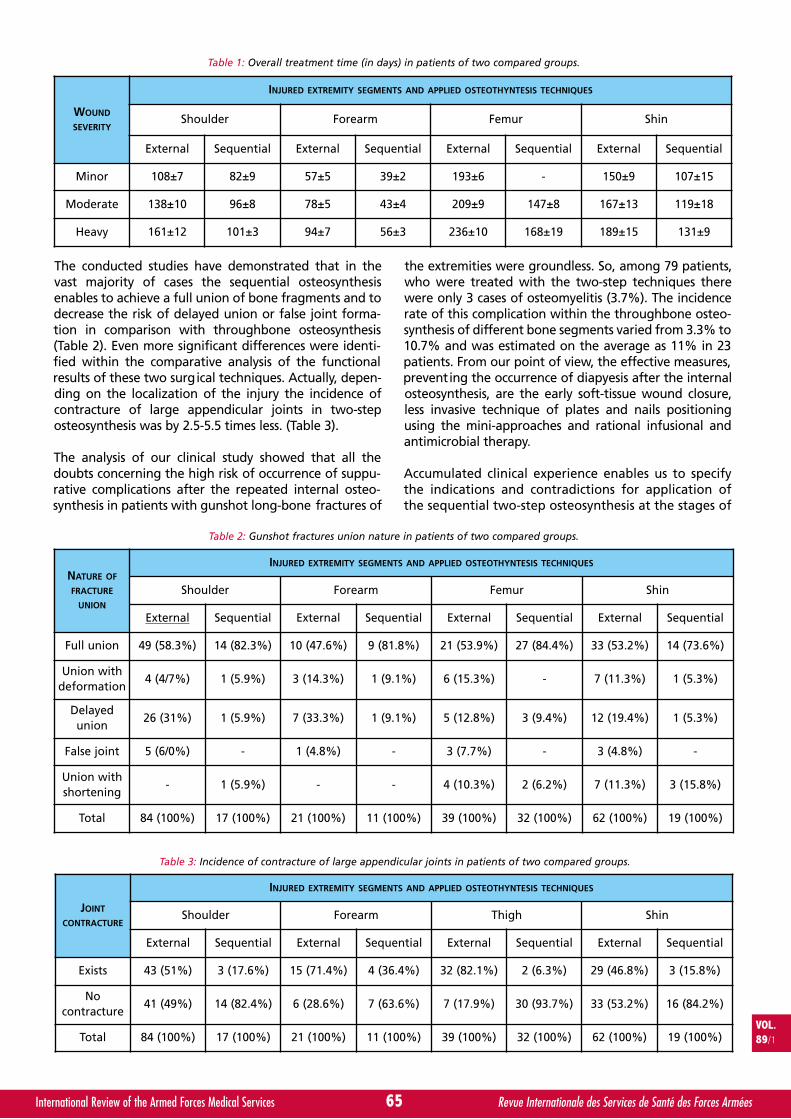
The conducted studies have demonstrated that in thevast majority of cases the sequential osteosynthesisenables to achieve a full union of bone fragments and todecrease the risk of delayed union or false joint forma-tion in comparison with throughbone osteosynthesis(Table 2). Even more significant differences were identi-fied within the comparative analysis of the functionalresults of these two surgical techniques. Actually, depen-ding on the localization of the injury the incidence ofcontracture of large appendicular joints in two-steposteosynthesis was by 2.5-5.5 times less. (Table 3).
The analysis of our clinical study showed that all thedoubts concerning the high risk of occurrence of suppu-rative complications after the repeated internal osteo-synthesis in patients with gunshot long-bone fractures of
the extremities were groundless. So, among 79 patients,who were treated with the two-step techniques therewere only 3 cases of osteomyelitis (3.7%). The incidencerate of this complication within the throughbone osteo-synthesis of different bone segments varied from 3.3% to10.7% and was estimated on the average as 11% in 23patients. From our point of view, the effective measures,preventing the occurrence of diapyesis after the internalosteosynthesis, are the early soft-tissue wound closure,less invasive technique of plates and nails positioningusing the mini-approaches and rational infusional andantimicrobial therapy.
Accumulated clinical experience enables us to specifythe indications and contradictions for application ofthe sequential two-step osteosynthesis at the stages of
65International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
WOUND
SEVERITY
INJURED EXTREMITY SEGMENTS AND APPLIED OSTEOTHYNTESIS TECHNIQUES
Shoulder Forearm Femur Shin
External Sequential External Sequential External Sequential External Sequential
Minor 108±7 82±9 57±5 39±2 193±6 - 150±9 107±15
Moderate 138±10 96±8 78±5 43±4 209±9 147±8 167±13 119±18
Heavy 161±12 101±3 94±7 56±3 236±10 168±19 189±15 131±9
Table 1: Overall treatment time (in days) in patients of two compared groups.
NATURE OF
FRACTURE
UNION
INJURED EXTREMITY SEGMENTS AND APPLIED OSTEOTHYNTESIS TECHNIQUES
Shoulder Forearm Femur Shin
External Sequential External Sequential External Sequential External Sequential
Full union 49 (58.3%) 14 (82.3%) 10 (47.6%) 9 (81.8%) 21 (53.9%) 27 (84.4%) 33 (53.2%) 14 (73.6%)
Union withdeformation
4 (4/7%) 1 (5.9%) 3 (14.3%) 1 (9.1%) 6 (15.3%) - 7 (11.3%) 1 (5.3%)
Delayedunion
26 (31%) 1 (5.9%) 7 (33.3%) 1 (9.1%) 5 (12.8%) 3 (9.4%) 12 (19.4%) 1 (5.3%)
False joint 5 (6/0%) - 1 (4.8%) - 3 (7.7%) - 3 (4.8%) -
Union withshortening
- 1 (5.9%) - - 4 (10.3%) 2 (6.2%) 7 (11.3%) 3 (15.8%)
Total 84 (100%) 17 (100%) 21 (100%) 11 (100%) 39 (100%) 32 (100%) 62 (100%) 19 (100%)
Table 2: Gunshot fractures union nature in patients of two compared groups.
JOINT
CONTRACTURE
INJURED EXTREMITY SEGMENTS AND APPLIED OSTEOTHYNTESIS TECHNIQUES
Shoulder Forearm Thigh Shin
External Sequential External Sequential External Sequential External Sequential
Exists 43 (51%) 3 (17.6%) 15 (71.4%) 4 (36.4%) 32 (82.1%) 2 (6.3%) 29 (46.8%) 3 (15.8%)
Nocontracture
41 (49%) 14 (82.4%) 6 (28.6%) 7 (63.6%) 7 (17.9%) 30 (93.7%) 33 (53.2%) 16 (84.2%)
Total 84 (100%) 17 (100%) 21 (100%) 11 (100%) 39 (100%) 32 (100%) 62 (100%) 19 (100%)
Table 3: Incidence of contracture of large appendicular joints in patients of two compared groups.
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page3

specialized trauma care. We believe, that discussed activesurgical approach, assuming the following removal of theexternal fixation devices and repeated internal osteosyn-thesis, can be successfully used in the treatment of guns-hot wounds of humerus, forearm, femur and shin,accompanied with simple or complicated (comminutedor multifragmental) fractures of the bone segmentswithout bone defects or with localized bone defects.Wherein, the severity of wound is not of a crucial impor-tance. For instance, the above mentioned technique wassuccessfully applied in the treatment of patients withminor or moderate injuries of humerus, forearm andshin; and for femur - even in case of severe injuries.However, it is quite important to achieve the stabilizationof the general patient’s condition and to ensure thatgunshot wounds of the soft tissues are healed up by thetime of the repeated internal osteosynthesis.
A clinical case is used as an illustration:Wounded patient Ya., 23 years old, accociated woundof head, upper and lower extremities and scrotal.Acubarotrauma. Gunshot communited tangentialwound of the left auricle. Gunshot missile perforatingwound of scrotal combined with the crush injury of lefttestis. Gunshot missile perforating wound of the left
shoulder and forearm combined with the gunshot frac-ture of lateral condyle of humerus, gunshot fracture ofboth forearm bones and posttraumatic neuropathy of theleft radial nerve. Gunshot missile wound of the left shincombined with the gunshot fracture of tibia and post-traumatic neuropathy of the left fibular nerve.Gunshot missile perforating wound of the soft tissuesof the left femur.
At the previous stages of the medical evacuation a left-sided orchiectomy, fixation of the left shoulder andforearm by using of pin-rod external fixation device(EFD), fixation of the left shin with rod-type externalfixation device (EFD) were performed (Fig. 1).
The following treatment was conducted at the MilitaryTraumatology and Orthopedics Department: plastics ofskin defects of the left upper extremity and both lowerextremities (Fig. 2); removal of the external fixationdevice, closed reduction, osteosynthesis of the left shinby using of intramedular locking nail; removal of EFD,plate osteosynthesis of the left humerus and plateosteosynthesis of left forearms (Fig. 3).
During the post-operative period the patient received
66International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Fig. 1: Appearance and the radiographs of wounded patient Ya. on admission to hospital.
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page4

the following treatment: physical therapy, rehabilitationexercises, hyperbaric oxygenation, anticoagulant, anti-microbial, neurophilic, vascular and sympthomatic the-rapy, the wounds healed by primary intention. Apatient was discharged in satisfactory condition (Fig. 4).
We suppose, that the contradictions for application ofthe sequential osteosynthesis in patients with theextremities wounds are injuries of major neurovascularfascicles, a deep wound infection as well as generalheavy condition of the patients, preventing from therepeated internal osteosynthesis.
An issue concerning the application of active surgicalapproach, assuming the repeated internal osteosynthe-sis at the stages of the specialized trauma care shouldbe separately discussed. We think, that such a compli-cated interventions, for which the qualified specialistsand special equipment is required, could be recom-mended at the third echelon of the specialized care.
The performed comparative analysis of the clinicalapplication of two osteosynthesis techniques enablesnot only to make general comparison, but also to provesome conclusions and to develop practically importantrecommendations for treatment of patients with guns-hot fractures of different extremity segments. In parti-cular, the repeated osteosynthesis using plates andnails in that very extremity segment has demonstratedthe most positive differences in comparison with the
throughbone osteosynthesis taking into account suchimportant aspects as an overall treatment time(decrease by 25%) and decrease of patients withcontracture of large appendicular joints (decrease by5.5 times). Moreover, based on our experience, only incase of the sequential osteosynthesis of femur all thepatients were fully rehabilitated (32 cases). Extra-corti-cal osteosynthesis was used in the treatment of the dis-tal femur fractures (12 cases), in all other cases an intra-medullar osteosynthesis was used.
The second perspective segment for application of thesequential osteosynthesis is a humerus. In the group of17 patients with the shoulder wound, the full bonefragments union was achieved in 8 patients (10.1%),who underwent the two-step surgery with externalextramedullary fixation and in 9 patients (11.4%), whounderwent the intramedullary osteosynthesis. Also, theincidence of shoulder and (or) elbow joint contracturein this group was three times less (17.6%) in compari-son with patients treated by using of external fixationdevices (51%).
Application of the sequential two-step osteosynthesis inthe treatment of forearm and shin gunshot fractureswas not so advantageous in comparison with thethroughbone osteosynthesis technique. However, anactive two-step surgery approach has demonstrated bet-ter results even at these extremity segments, comparingwith osteosynthesis by the external fixation devices.
67International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Fig. 2: Outcome of flap coverage of the soft-tissue wound of the left forearm and shin.
Fig. 3: Radiograps of wounded patient Ya. after the removal of external fixation device, closed reduction, osteosynthesisof the left tibia by using of intramedular locking nail; removal of EFD, plate osteosynthesis of the left humerus
and plate osteosynthesis of left forearms.
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page5

In comparison, complications incidence (Table 4) wassignificantly less in the group of patients with sequen-tial osteosynthesis (6 cases (7.71%)), whereas in thegroup of patients with external osteosynthesis therewere 47 cases (23%).
As an example we introduce the following clinicalobservation:Wounded patient Z., 29 years old, multiple gunshotextremity wounds, bullet perforating wound of theright forearm combined with gunshot comminutedforearm fracture and radial bone defect, post-trauma-tic neuropathy of the right radial, medius and ulnarnerves, gunshot comminuted ulnar bone fracture, bul-let perforating wound of the left shin combined withthe gunshot comminuted fracture of shin bone andtibia defect.
At the previous stages of the medical evacuation theIlizarov fixation of bones of the right forearm and theleft shin was performed. (Fig. 5).
The following treatment was conducted at the MilitaryTraumatology and Orthopedics Department: remounting ofIlizarov apparatus on the left shin; removal of apparatus(right forearm), osteosynthesis of the right ulnar bone usingan Ilizarov apparatus, revision of radial bone defect zone,placement of antibiotic-impregnated cement spacer; repea-ted surgical debridement, removal of cement spacer,debride (fragment), pin re-passage in the Ilizarov apparatus;removal of EFD (right forearm), plate osteosynthesis of theright ulnar bone; free flap plasty using iliac crest bone graft;free vascularized dermic-fascial-bone grafting using rightfibular bone graft, osteosynthesis of the right radial bone byusing of locking nail; removal of EFD, osteotomy at thelower third level, osteosynthesis of the left tibia by using ofintramedullar locking shifts, Ilizarov fixation (Fig. 6, 7).
During the post-operative period the patient received thefollowing treatment: physical therapy, rehabilitation exer-cises, hyperbaric oxygenation, anticoagulant, antimicrobial,neurophilic, vascular and sympthomatic therapy, thewounds healed by primary intention. (Fig. 8).
68International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Fig. 4: Radiograps and functional outcomes of wounded patient Ya. in 3 months after the removal of external fixation device,closed reduction, osteosynthesis of the left tibia by using of intramedular locking nail; removal of EFD,
plate osteosynthesis of the left humerus and plate osteosynthesis of left forearms.
COMPLICATIONS (NUMBER OF CASES,%)
EXTERNAL OSTEOSYNTHESIS (47 CASES, 23%) SEQUENTIAL OSTEOSYNTHESIS (6 CASES, 7.7%)
12 (6%) Venous thrombosis 2 (3%)
4 (2%) Artery injury 0 (0%)
8 (4%) Nerve injury 1 (1%)
23 (11%) Infection 3 (3.7%)
Table 4
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page6

In comparison, complications incidence (Table 4) wassignificantly less in the group of patients with sequen-tial osteosynthesis (6 cases (7.71%)), whereas in thegroup of patients with external osteosynthesis therewere 47 cases (23%).
As an example we introduce the following clinicalobservation:Wounded patient Z., 29 years old, multiple gunshotextremity wounds, bullet perforating wound of theright forearm combined with gunshot comminutedforearm fracture and radial bone defect, post-trauma-tic neuropathy of the right radial, medius and ulnarnerves, gunshot comminuted ulnar bone fracture, bul-let perforating wound of the left shin combined withthe gunshot comminuted fracture of shin bone andtibia defect.
At the previous stages of the medical evacuation theIlizarov fixation of bones of the right forearm and theleft shin was performed. (Fig. 5).
The following treatment was conducted at the MilitaryTraumatology and Orthopedics Department: remounting ofIlizarov apparatus on the left shin; removal of apparatus(right forearm), osteosynthesis of the right ulnar bone usingan Ilizarov apparatus, revision of radial bone defect zone,placement of antibiotic-impregnated cement spacer; repea-ted surgical debridement, removal of cement spacer,debride (fragment), pin re-passage in the Ilizarov apparatus;removal of EFD (right forearm), plate osteosynthesis of theright ulnar bone; free flap plasty using iliac crest bone graft;free vascularized dermic-fascial-bone grafting using rightfibular bone graft, osteosynthesis of the right radial bone byusing of locking nail; removal of EFD, osteotomy at thelower third level, osteosynthesis of the left tibia by using ofintramedullar locking shifts, Ilizarov fixation (Fig. 6, 7).
During the post-operative period the patient received thefollowing treatment: physical therapy, rehabilitation exer-cises, hyperbaric oxygenation, anticoagulant, antimicrobial,neurophilic, vascular and sympthomatic therapy, thewounds healed by primary intention. (Fig. 8).
68International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Fig. 4: Radiograps and functional outcomes of wounded patient Ya. in 3 months after the removal of external fixation device,closed reduction, osteosynthesis of the left tibia by using of intramedular locking nail; removal of EFD,
plate osteosynthesis of the left humerus and plate osteosynthesis of left forearms.
COMPLICATIONS (NUMBER OF CASES,%)
EXTERNAL OSTEOSYNTHESIS (47 CASES, 23%) SEQUENTIAL OSTEOSYNTHESIS (6 CASES, 7.7%)
12 (6%) Venous thrombosis 2 (3%)
4 (2%) Artery injury 0 (0%)
8 (4%) Nerve injury 1 (1%)
23 (11%) Infection 3 (3.7%)
Table 4
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page6
69International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Fig. 5: Radiographs of wounded patient Z. on admission.
Fig. 6: Preparation of the bone graft.
Fig. 7: Functional result and the radiographs of wounded patient Z. after removal of the apparatus from the right forearm,osteosynthesis of the right ulnar bone (with the Ilizarov apparatus), revision of the radial bone defect area, placement
of antibiotic-impregnated cement spacer; repeated surgical debridement, removal of cement spacer, debride (fragment),pin re-passage in the Ilizarov apparatus; removal of EFD from the right forearm, plate osteosynthesis of right ulnar bone;free flap plasty using iliac crest bone graft, free vascularized dermic-fascial-bone grafting using right fibular bone graft,
osteosynthesis of the right radial bone by using of locking nail.
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page7
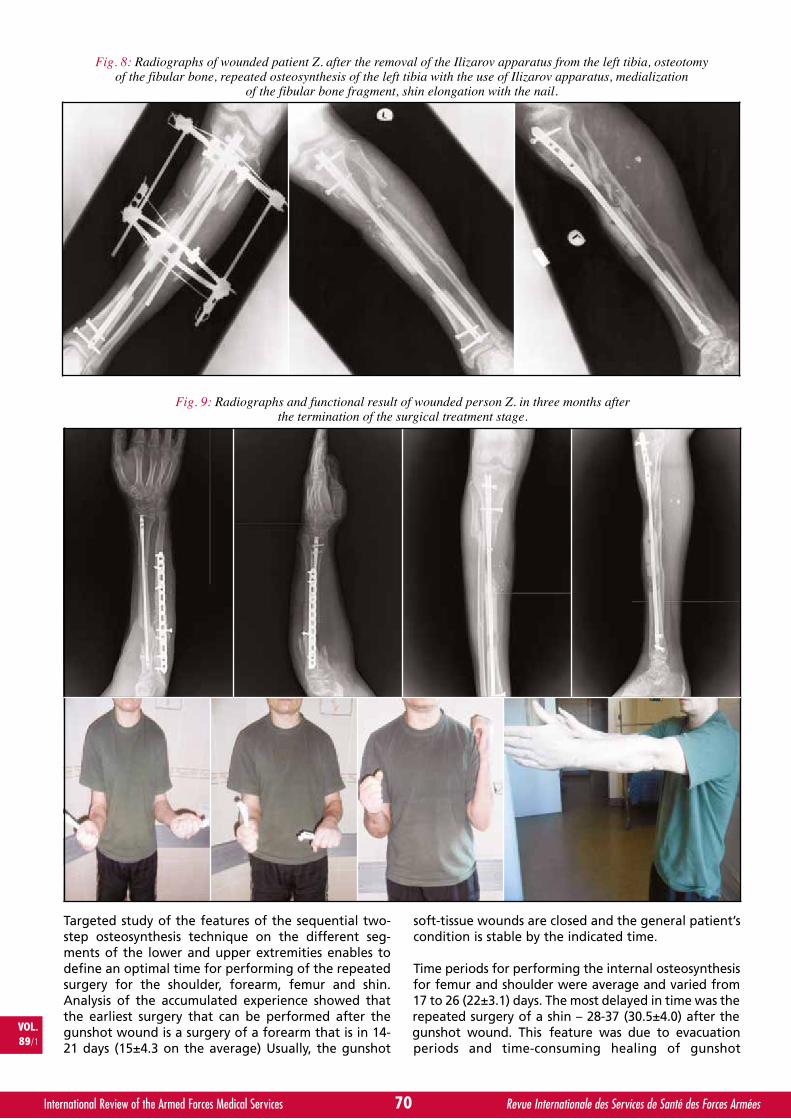
Targeted study of the features of the sequential two-step osteosynthesis technique on the different seg-ments of the lower and upper extremities enables todefine an optimal time for performing of the repeatedsurgery for the shoulder, forearm, femur and shin.Analysis of the accumulated experience showed thatthe earliest surgery that can be performed after thegunshot wound is a surgery of a forearm that is in 14-21 days (15±4.3 on the average) Usually, the gunshot
soft-tissue wounds are closed and the general patient’scondition is stable by the indicated time.
Time periods for performing the internal osteosynthesisfor femur and shoulder were average and varied from17 to 26 (22±3.1) days. The most delayed in time was therepeated surgery of a shin – 28-37 (30.5±4.0) after thegunshot wound. This feature was due to evacuationperiods and time-consuming healing of gunshot
70International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Fig. 8: Radiographs of wounded patient Z. after the removal of the Ilizarov apparatus from the left tibia, osteotomyof the fibular bone, repeated osteosynthesis of the left tibia with the use of Ilizarov apparatus, medialization
of the fibular bone fragment, shin elongation with the nail.
Fig. 9: Radiographs and functional result of wounded person Z. in three months afterthe termination of the surgical treatment stage.
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page8
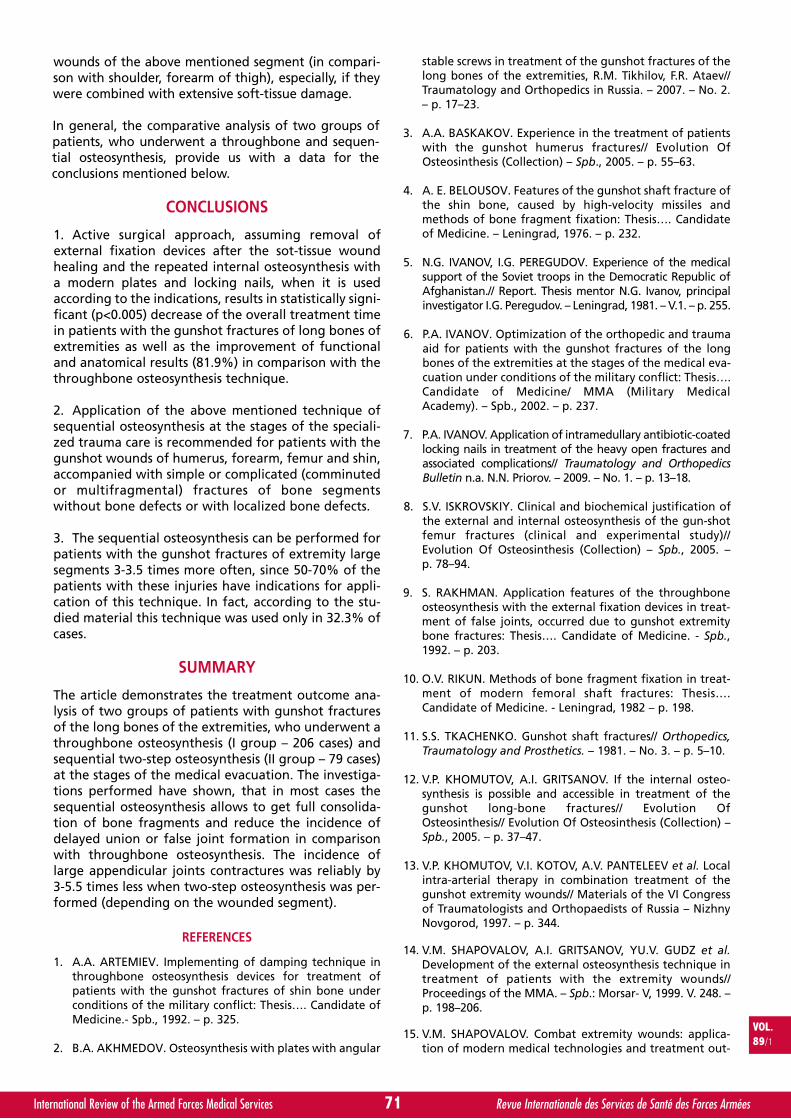
Targeted study of the features of the sequential two-step osteosynthesis technique on the different seg-ments of the lower and upper extremities enables todefine an optimal time for performing of the repeatedsurgery for the shoulder, forearm, femur and shin.Analysis of the accumulated experience showed thatthe earliest surgery that can be performed after thegunshot wound is a surgery of a forearm that is in 14-21 days (15±4.3 on the average) Usually, the gunshot
soft-tissue wounds are closed and the general patient’scondition is stable by the indicated time.
Time periods for performing the internal osteosynthesisfor femur and shoulder were average and varied from17 to 26 (22±3.1) days. The most delayed in time was therepeated surgery of a shin – 28-37 (30.5±4.0) after thegunshot wound. This feature was due to evacuationperiods and time-consuming healing of gunshot
70International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Fig. 8: Radiographs of wounded patient Z. after the removal of the Ilizarov apparatus from the left tibia, osteotomyof the fibular bone, repeated osteosynthesis of the left tibia with the use of Ilizarov apparatus, medialization
of the fibular bone fragment, shin elongation with the nail.
Fig. 9: Radiographs and functional result of wounded person Z. in three months afterthe termination of the surgical treatment stage.
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page8
wounds of the above mentioned segment (in compari-son with shoulder, forearm of thigh), especially, if theywere combined with extensive soft-tissue damage.
In general, the comparative analysis of two groups ofpatients, who underwent a throughbone and sequen-tial osteosynthesis, provide us with a data for theconclusions mentioned below.
CONCLUSIONS
1. Active surgical approach, assuming removal ofexternal fixation devices after the sot-tissue woundhealing and the repeated internal osteosynthesis witha modern plates and locking nails, when it is usedaccording to the indications, results in statistically signi-ficant (p<0.005) decrease of the overall treatment timein patients with the gunshot fractures of long bones ofextremities as well as the improvement of functionaland anatomical results (81.9%) in comparison with thethroughbone osteosynthesis technique.
2. Application of the above mentioned technique ofsequential osteosynthesis at the stages of the speciali-zed trauma care is recommended for patients with thegunshot wounds of humerus, forearm, femur and shin,accompanied with simple or complicated (comminutedor multifragmental) fractures of bone segmentswithout bone defects or with localized bone defects.
3. The sequential osteosynthesis can be performed forpatients with the gunshot fractures of extremity largesegments 3-3.5 times more often, since 50-70% of thepatients with these injuries have indications for appli-cation of this technique. In fact, according to the stu-died material this technique was used only in 32.3% ofcases.
SUMMARY
The article demonstrates the treatment outcome ana-lysis of two groups of patients with gunshot fracturesof the long bones of the extremities, who underwent athroughbone osteosynthesis (I group – 206 cases) andsequential two-step osteosynthesis (II group – 79 cases)at the stages of the medical evacuation. The investiga-tions performed have shown, that in most cases thesequential osteosynthesis allows to get full consolida-tion of bone fragments and reduce the incidence ofdelayed union or false joint formation in comparisonwith throughbone osteosynthesis. The incidence oflarge appendicular joints contractures was reliably by3-5.5 times less when two-step osteosynthesis was per-formed (depending on the wounded segment).
REFERENCES
1. A.A. ARTEMIEV. Implementing of damping technique inthroughbone osteosynthesis devices for treatment ofpatients with the gunshot fractures of shin bone underconditions of the military conflict: Thesis…. Candidate ofMedicine.- Spb., 1992. – p. 325.
2. B.A. AKHMEDOV. Osteosynthesis with plates with angular
stable screws in treatment of the gunshot fractures of thelong bones of the extremities, R.M. Tikhilov, F.R. Ataev//Traumatology and Orthopedics in Russia. – 2007. – No. 2.– p. 17–23.
3. A.A. BASKAKOV. Experience in the treatment of patientswith the gunshot humerus fractures// Evolution OfOsteosinthesis (Collection) – Spb., 2005. – p. 55–63.
4. A. E. BELOUSOV. Features of the gunshot shaft fracture ofthe shin bone, caused by high-velocity missiles andmethods of bone fragment fixation: Thesis…. Candidateof Medicine. – Leningrad, 1976. – p. 232.
5. N.G. IVANOV, I.G. PEREGUDOV. Experience of the medicalsupport of the Soviet troops in the Democratic Republic ofAfghanistan.// Report. Thesis mentor N.G. Ivanov, principalinvestigator I.G. Peregudov. – Leningrad, 1981. – V.1. – p. 255.
6. P.A. IVANOV. Optimization of the orthopedic and traumaaid for patients with the gunshot fractures of the longbones of the extremities at the stages of the medical eva-cuation under conditions of the military conflict: Thesis….Candidate of Medicine/ MMA (Military MedicalAcademy). – Spb., 2002. – p. 237.
7. P.A. IVANOV. Application of intramedullary antibiotic-coatedlocking nails in treatment of the heavy open fractures andassociated complications// Traumatology and OrthopedicsBulletin n.a. N.N. Priorov. – 2009. – No. 1. – p. 13–18.
8. S.V. ISKROVSKIY. Clinical and biochemical justification ofthe external and internal osteosynthesis of the gun-shotfemur fractures (clinical and experimental study)//Evolution Of Osteosinthesis (Collection) – Spb., 2005. –p. 78–94.
9. S. RAKHMAN. Application features of the throughboneosteosynthesis with the external fixation devices in treat-ment of false joints, occurred due to gunshot extremitybone fractures: Thesis…. Candidate of Medicine. - Spb.,1992. – p. 203.
10. O.V. RIKUN. Methods of bone fragment fixation in treat-ment of modern femoral shaft fractures: Thesis….Candidate of Medicine. - Leningrad, 1982 – p. 198.
11. S.S. TKACHENKO. Gunshot shaft fractures// Orthopedics,Traumatology and Prosthetics. – 1981. – No. 3. – p. 5–10.
12. V.P. KHOMUTOV, A.I. GRITSANOV. If the internal osteo-synthesis is possible and accessible in treatment of thegunshot long-bone fractures// Evolution OfOsteosinthesis// Evolution Of Osteosinthesis (Collection) –Spb., 2005. – p. 37–47.
13. V.P. KHOMUTOV, V.I. KOTOV, A.V. PANTELEEV et al. Localintra-arterial therapy in combination treatment of thegunshot extremity wounds// Materials of the VI Congressof Traumatologists and Orthopaedists of Russia – NizhnyNovgorod, 1997. – p. 344.
14. V.M. SHAPOVALOV, A.I. GRITSANOV, YU.V. GUDZ et al.Development of the external osteosynthesis technique intreatment of patients with the extremity wounds//Proceedings of the MMA. – Spb.: Morsar-V, 1999. V. 248. –p. 198–206.
15. V.M. SHAPOVALOV. Combat extremity wounds: applica-tion of modern medical technologies and treatment out-
71International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page9
comes/V.M. Shapovalov// Traumatology and Orthopedicsin Russia. – 2006. – No. 2. – p. 307–308.
16. BERGMAN M., TORNETTA P., KERINA M. et al. Femur frac-tures caused by the gunshots: Treatment by immediate rea-med intramedullary nailing. J Trauma. 1993 Jun; 34 (6): 783-5.
17. BOWYER G., RYAN J., KAUFMANN C. et al. General princi-ples of wound management. In: Ryan JM, Rich NM, DaleRF, Morgans BT, Cooper CJ, eds. Ballistic trauma. London:Edward Arnold, 1997.
18. COULL J. War Injuries. In: Coombs R, Green S, SarmientoA, eds. External fixation and functional bracing. London:Orthotext 1979: 239-43.
19. DOUGHERTY P., GHEREBEH P., ZEKAJ M. et al. Retrograde ver-sus antegrade intramedullary nailing of gunshot diaphyseal
femur fractures Clin Orthop Relat Res. 2013 Dec; 471 (12):3974-80.
20. DOUGHERTY P., VAIDYA R., SILVERTON C. et al. Joint andlong-bone gunshot injuries. J Bone Joint Surg Am. 2009;91: 980–997.
21. NICHOLAS R., McCOY G. Immediate intramedullary nai-ling of femoral shaft fractures due to gunshots. Injury.1995 May; 26 (4): 257-9.
22. PAUL A., DICPINIGAITIS M., KENNETH J. et al. GunshotWounds to the Extremities Bulletin of the NYU Hospitalfor Joint Diseases, Volume 64, Numbers 3 & 4, 2006.
23. RYAN J., COOPER G., HAYWOOD I. et al. Field surgery ona future conventional battlefield: strategy and woundmanagement. Ann R Coll Surg Engl 1991; 73: 13-20.
72International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
External Osteosynthesis_KHOMINETS.qxp_Mise en page 1 16/03/2016 10:03 Page10
Titanium Pin & K-Wire
Gex-Foot
Gexfix external fixation orthopaedics
Easy-clip Connectors
Gex-Finger
New D.O.S. System
MiniBone
Gexfix SAAvenue de la Praille 50 - CH – 1227 CarougeT + 41(0)22 308 16 70 - F + 41(0)22 308 16 [email protected] - www.gexfix.ch
By Y. JUNG∑, M. LEE∏ and M. KIMπ. Republic of Korea
Yoomi JUNG
Infectious Diseases after Floods in Asian Countries:A Literature Review.* #
Major Yoomi JUNG graduated from Korea Armed Forces Nursing Academy inDaejeon, Korea and was commissioned as 2nd Lieutenant in the Army Nurse
Corps in 1997. After five years of clinical experience in several Korean militaryhospitals. She earned her master’s degree in women’s health and her doctoral
degree in nursing management from Seoul National University, Seoul, Korea in 2004and 2011, respectively.
Currently appointed as Head of Military Health Policy Research Center of Korea Armed Forces NursingAcademy, she is the editor-in-chief of Korean Military Nursing Research, the journal published by theresearch center. She has been teaching nursing cadets in the academy for 8 years.
Major JUNG also has experience in teaching and program design in disaster healthcare education and trainingprograms. Her research interests include infectious disease after natural disasters, disaster healthcare ethicalissues, women’s health, organizational efficiency, and organizational culture.
73International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Infections faisant suite aux inondations en Asie : revue de la littérature.
Objectif : Cette étude donne un aperçu à travers une revue de la littérature des maladies infectieuses pouvant survenir après desinondations.
Méthodes : Il s’agit d’une revue systématique de la littérature. Un total de 209 articles a été retrouvé en appliquant les mots indicateurs.Après l’application des critères d’inclusion et d’exclusion, il restait finalement 9 articles.
Résultats : Sept pays d’Asie ont rapporté douze épisodes d’inondations dans la période étudiée. La région la plus fréquemmenttouchée était Dhaka au Bangladesh. La principale cause des inondations était des pluies intenses entre juillet et septembre. Lesdiarrhées infectieuses étaient les maladies les plus fréquentes, suivies par les leptospiroses et les cellulites. Le principal agentpathogène des diarrhées était Vibrio cholerae.
Conclusion : les maladies infectieuses faisant site à des catastrophes naturelles peuvent être différentes selon les types de catastropheet les régions. C’est pourquoi les personnels de santé doivent avoir une bonne compréhension des maladies endémiques et des typesde catastrophes les plus fréquentes dans la région où ils servent de façon à apporter une réponse efficace.
INTRODUCTION
Background
We are living in an era of disaster. In 2012 alone, therewere 357 natural disasters worldwide, claiming 9,655lives; and among the top 10 natural disasters of theyear, by number of victims, six were floods1. Asia is themost vulnerable region to floods2. In 2012, out of 13natural disasters reported in Asia, eight were floods1.
An average of 82 hydrological disasters, includingfloods, per year occurred between 2002 and 2011, cau-sing an average of 111 million victims, and over 13 bil-lion dollars damage1. This is a huge number comparedto less than 29 hydrological disasters on average in therest of the world during the same period.
Given that water- or vector-borne diseases prevail especiallyin areas with poor sanitation, and many parts of Asian
VOL.89/1
KEYWORDS: Disaster, Flood, Infection, Diarrhea, Leptospirosis, Cellulitis, Asia.MOTS-CLÉS : Catastrophe, Inondation, Infection, Diarrhée, Leptospirose, Cellulite, Asie.
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page1
countries still remain underdeveloped, floods could bea critical cause of epidemics in the region. In addition,infectious diseases observed after natural disasters areknown to be caused by infectious agents which com-monly exist in the local area3. Thus, as healthcare pro-fessionals living in an Asian country, if we can predictinfectious diseases which could break out in the wakeof floods in neighboring countries as well as our own,we would be able to deal with them better and evenprevent them. To that end, we need to incorporateresearch findings into practice as a way to prepare our-selves against flooding events which have more frequentlyaffected the region than other types of disaster.
Many authors have been reporting infectious diseaseswhich were faced after floods in their countries.However, research putting such studies together from aregion-specific perspective to give us an insight intowhat to expect in terms of disease in the aftermath offloods can hardly be found. Therefore, the authors car-ried out a literature review to figure out what kinds ofoutbreaks were reported post flooding in Asian coun-tries in order to help healthcare professionals to beable to better respond to natural disasters.
Purpose
The purpose of this study was to provide an insight,with a literature review, into infectious diseases whichcould break out after floods. The aims were as follows:
A. to identify flooding events reported over the pastten years in Asia, and their features and impacts,
B. to see if there were outbreaks of infectious diseasesafter floods,
C. to investigate diagnostic tests and treatments usedfor those epidemics,
D. to suggest further studies.
METHOD
Study Design
This study was a systematic literature review, followingthe steps used in the study of Cann, Thomas, Salmon,Wyn-Jones, and Kay (2013)4.
Search Strategy
The authors searched Pubmed, a medical article data-base, between 16 and 17 January, 2014 to identify stu-dies reporting infectious diseases which broke out afterflooding. The search words used included: infection,infectious disease, communicable disease, flood, andflooding, and their combinations: flooding and commu-nicable disease, flooding and infectious disease, floodingand infection, flood and communicable disease, floodand infectious disease, and flood and infection.Additional search conditions were; 'to be published overthe past 10 years,' and 'provide full text and abstract'.
Selection Criteria
As a result of the search strategy, the authors found 209full-text articles. Among them, 102 articles emergedafter removing duplicates and those wrongly having
come out due to the name of its author, Flood. Aftertwo reviewers separately read all of the abstracts andremoved inappropriate ones, 45 articles remained. Thereviewers selected 10 studies by applying the inclusioncriteria. The inclusion criteria used to choose literaturesuitable for the purpose of this study included:
1. Literature type: not a review article,2. Subject: human,3. Region: Asia,4. Disaster type: flood,5. Data: primary data from affected population, sur-
veillance report, and so on,6. Language: English.
In the final selection, there were two articles whichreported the same flood in different years. After dis-cussion, the authors decided to exclude one of them.Since it used data collected through a literature review,the authors considered the data secondary eventhough it was mentioned as primary data in the report.
Therefore, 9 articles remained to be analyzed.
Among the 12 review articles which were excluded, noreview article with focus on infectious diseases afterflooding in Asia was identified. The details were asseen below. The number of articles is presented in thebracket.
1. Infectious diseases following natural disasters (1),2. One disease focused: Leptospirosis (5),3) Health impact of climate change (2),4. Extreme water-related weather events and water-
borne disease (1),5. Microbiology: Enteric Protozoa (1); pathogenic
bacteria (1); Schistosomiasis Japonica (1),
The process of article selection is presented in Figure 1.During the whole selection process, the agreement ratebetween the two authors was 95.1%. The third revie-wer intervened with five studies over which the tworeviewers disagreed.
Data extraction and analysis
With a thorough review of the chosen articles, the
74International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
∑ Major, Assistant Professor,Korea Armed Forces Nursing Academy.
∏ Assistant Professor,Korea Armed Forces Nursing Academy.
π Assistant Professor,College of Nursing and Health Science, Dong-Eui University.
Correspondence:Major Yoomi JUNG, RN, PhD.Assistant Professor,Korea Armed Forces Nursing AcademyHead of Military Health Policy Research CenterP.O.Box 78-502Jaun-ro 90, Yuseong-guDaejeon 305-878Republic of [email protected]
* Presented at the 1st Conference Asia Pacific Military Health Exchange (APMHE),Da Nang, Vietnam, 14-18 September 2015.
# With the courtesy of the Editor of Korean Journal of Military NursingResearch.This article is not the original article appeared in the issue 33 (1) of the Journalin 2015.
VOL.89/1
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page2

authors extracted various data and analyzed them. Thedata collected from the articles were: flood event coun-tries and cities; flood year and size; types of disease andtheir pathogens; morbidity and mortality rates; anddiagnostic methods and treatments.
RESULTS
Main features of the floods
An overview of the findings is presented in Table 1.Since one of the 9 articles covered four flooding caseswhich broke out in Bangladesh from 1988 to 20045, atotal of 12 floods were analyzed here in this study. Themost frequently affected country was Bangladesh.Among the 12 flooding disasters analyzed, five(41.7%), in 1988, 1998, July 2004 and September 2004,and 2007, happened in this country5, 6. Remarkably, allthe five floods were reported from just one city, Dhaka,and 2004 saw two floods. Other countries included ThePhilippines, Vietnam, China, Malaysia, India, andTaiwan with one case each. The flooding years rangedfrom 1988 to 2010. When taking the beginning monthof those floods as the basis, 75% of them happenedbetween July and September. The details were shownin Figure 2 and Figure 3.
Seven (58.3%) out of 12 floods were presented withthe cause. The heavy rainfall (57.1%) identified as themain cause of flooding, followed by typhoon (28.6%)
75International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
209 articles identifiedwith search words and
search conditions
102 articles remainded
45 articles remainded
10 articles selected
9 articles finally selected
1st removal of 107 articles- 89 duplicates- 18 by authors named Flood
2nd removal of 57 articles- 54 with no relevance to the topic- 3 with other languages
3rd removal of 35 articles- 12 review articles- 4 little focus on flood- 2 commentories- 1 guide book- 1 using second data- 14 of other regions- 1 of pseudofungemia- 1 with pathogen subject
Final removal of 1 article- using secondary data from a
literature review
Figure 1: The records selection process.
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0Jun Jul Aug Sep Oct
MONTH
FREQ
UEN
CY
Figure 3: Seasonal distribution of floods.
Figure 2: Regional distribution of floods.
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page3

and unusual heavy monsoon rain (14.3%). The authorsmeasured the size of flooding with precipitation, eitherof height of water or flooding days reported in eachstudy. Two studies stated that the precipitation wasranging from 87.6 mm in China in 2013 to 2,748 mm inTaiwan in 20097, 8. The average water height in Hanoï,Vietnam in 2011 was between 0.3 m and 0.8 m9.Bangladesh suffered an average over 26 flood days infour flooding cases between 1988 and 20045.
Only three (25%) of the 12 cases presented one ormore factors which were used here to estimate theimpact of the floods: the death toll, the number of theinjured, or the population affected3, 9. A total of 33.1million people were affected, 1,722 died, and threewere injured through the three flooding disasters.Other two studies reported the size of patients: 2,999patients visited 15 hospitals after the flood inPhilippines, and among them, 178 were recorded asdeceased10, and there was a total of 20,395 patientsenrolled in a surveillance system in the wake of fourfloods in Bangladesh5. Even though CDC report (2012)did not present the impact of the flood of Pakistan in2010, the authors of this study were able to measurethe impact as 1,985 deaths, 2,946 injuries, and 20.2 mil-lion people affected via another study which reportedthe same flood, but was excluded from this studybecause it used data from a literature review11.
Infectious diseases
Diarrhea was the most common disease in the after-math of flooding. Four (44.4%) out of nine studies,with seven (58%) of 12 flooding events in total, repor-ted diarrhea3, 5, 6, 7, and two (17%) of 12 floods repor-ted leptospirosis10, 12. Others involved cellulitis,Hantavirus infection, skin diseases, respiratory infec-tions, Dengue fever, pink eye, and dermatitis. When itcomes to the number of patients, skin disease toppedthe list with 1,029,942 patients, followed by respiratoryinfection (850,292), diarrhea (787,430), and leptospiro-sis (517)3. The details of the three most frequentlyreported diseases; diarrhea, leptospirosis, cellulitis,directly related to the flood water, are presentedbelow.
A. Diarrhea787,430 diarrhea cases, as mentioned above, werereported in seven floods from Bangladesh, Pakistan,and China between 1988 and 20103, 5, 6, 7. There were
130 outbreak alerts after flooding in Pakistan in 2010,and, among them, 115 (88.5%) were reported as forAcute Watery Diarrhea (AWD)3.
Vibrio cholerae was found as the most common patho-gen of diarrhea after floods3, 5, 6. The proportion of V.cholerae infection during the flood period was fourtimes higher than that of non-flood period, and infec-tion caused especially by O1 serogroup and El Tor bio-type of V. cholerae prevailed while V. cholerae O 139decreased5. Schwartz et al. (2006) reported, through aninvestigation of four floods between 1988 and 2004,that Rota virus following V. cholerae was the secondmost common cause, and Shigella, Salmonella, E. hito-lytica/dispar, G. lamblia, Enterotoxigenic Escherichiacoli (ETEC), and C. jejuni were found responsible forepidemic diarrhea too while, interestingly, 23%~51%of the cases were caused by no identifiable organism5.The flooding in China in 2007 was accompanied by aninfectious diarrhea outbreak, and among 102 cases tes-ted by the local laboratories, 66 cases (64.7%) wereidentified as dysentery diarrhea7. The study also saidthat the average number of diarrheal patients per dayincreased twice compared to that of before the flood.Alam et al. (2011) described the diagnostic test imple-mented, the rectal swab. The treatment of choice fordiarrhea was re-hydration, including oral re-hydrationand intravenous fluid, and antibiotics5, 6.
B. LeptospirosisLeptospirosis patients were observed after floods; 471 inPhilippines in 200910 and 46 in Malaysia in 199912. The res-pective case fatality rate (CFR) was 10.8% and 2.2%, and10.1% combined. The main cause of death was pulmonaryhemorrhage in both studies, and acute respiratory distresssyndrome and acute renal failure also contributed to death.
Diagnostic tests revealed that L. borgpetersenii serovarTarassovi was the most prevalent organism, followed by sero-vars Poi and Sejroe and L. interrogans serovars Losbanos andManilae10. As seen in Table 1, Leptospira Serology Kit, PanBioIgM ELISA, plasma collection, and microscopic agglutinationtest (MAT) were used for diagnostic tests.
Antibiotic agents were used as the standard treatment.In more than 90% of the cases, Penicillin G was admi-nistered10, and Ceftriaxone, Doxycycline, Amoxycillin,IV C-Penicilline, and others were also used10, 12.
76International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
https://en.wikipedia.org
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page4
and unusual heavy monsoon rain (14.3%). The authorsmeasured the size of flooding with precipitation, eitherof height of water or flooding days reported in eachstudy. Two studies stated that the precipitation wasranging from 87.6 mm in China in 2013 to 2,748 mm inTaiwan in 20097, 8. The average water height in Hanoï,Vietnam in 2011 was between 0.3 m and 0.8 m9.Bangladesh suffered an average over 26 flood days infour flooding cases between 1988 and 20045.
Only three (25%) of the 12 cases presented one ormore factors which were used here to estimate theimpact of the floods: the death toll, the number of theinjured, or the population affected3, 9. A total of 33.1million people were affected, 1,722 died, and threewere injured through the three flooding disasters.Other two studies reported the size of patients: 2,999patients visited 15 hospitals after the flood inPhilippines, and among them, 178 were recorded asdeceased10, and there was a total of 20,395 patientsenrolled in a surveillance system in the wake of fourfloods in Bangladesh5. Even though CDC report (2012)did not present the impact of the flood of Pakistan in2010, the authors of this study were able to measurethe impact as 1,985 deaths, 2,946 injuries, and 20.2 mil-lion people affected via another study which reportedthe same flood, but was excluded from this studybecause it used data from a literature review11.
Infectious diseases
Diarrhea was the most common disease in the after-math of flooding. Four (44.4%) out of nine studies,with seven (58%) of 12 flooding events in total, repor-ted diarrhea3, 5, 6, 7, and two (17%) of 12 floods repor-ted leptospirosis10, 12. Others involved cellulitis,Hantavirus infection, skin diseases, respiratory infec-tions, Dengue fever, pink eye, and dermatitis. When itcomes to the number of patients, skin disease toppedthe list with 1,029,942 patients, followed by respiratoryinfection (850,292), diarrhea (787,430), and leptospiro-sis (517)3. The details of the three most frequentlyreported diseases; diarrhea, leptospirosis, cellulitis,directly related to the flood water, are presentedbelow.
A. Diarrhea787,430 diarrhea cases, as mentioned above, werereported in seven floods from Bangladesh, Pakistan,and China between 1988 and 20103, 5, 6, 7. There were
130 outbreak alerts after flooding in Pakistan in 2010,and, among them, 115 (88.5%) were reported as forAcute Watery Diarrhea (AWD)3.
Vibrio cholerae was found as the most common patho-gen of diarrhea after floods3, 5, 6. The proportion of V.cholerae infection during the flood period was fourtimes higher than that of non-flood period, and infec-tion caused especially by O1 serogroup and El Tor bio-type of V. cholerae prevailed while V. cholerae O 139decreased5. Schwartz et al. (2006) reported, through aninvestigation of four floods between 1988 and 2004,that Rota virus following V. cholerae was the secondmost common cause, and Shigella, Salmonella, E. hito-lytica/dispar, G. lamblia, Enterotoxigenic Escherichiacoli (ETEC), and C. jejuni were found responsible forepidemic diarrhea too while, interestingly, 23%~51%of the cases were caused by no identifiable organism5.The flooding in China in 2007 was accompanied by aninfectious diarrhea outbreak, and among 102 cases tes-ted by the local laboratories, 66 cases (64.7%) wereidentified as dysentery diarrhea7. The study also saidthat the average number of diarrheal patients per dayincreased twice compared to that of before the flood.Alam et al. (2011) described the diagnostic test imple-mented, the rectal swab. The treatment of choice fordiarrhea was re-hydration, including oral re-hydrationand intravenous fluid, and antibiotics5, 6.
B. LeptospirosisLeptospirosis patients were observed after floods; 471 inPhilippines in 200910 and 46 in Malaysia in 199912. The res-pective case fatality rate (CFR) was 10.8% and 2.2%, and10.1% combined. The main cause of death was pulmonaryhemorrhage in both studies, and acute respiratory distresssyndrome and acute renal failure also contributed to death.
Diagnostic tests revealed that L. borgpetersenii serovarTarassovi was the most prevalent organism, followed by sero-vars Poi and Sejroe and L. interrogans serovars Losbanos andManilae10. As seen in Table 1, Leptospira Serology Kit, PanBioIgM ELISA, plasma collection, and microscopic agglutinationtest (MAT) were used for diagnostic tests.
Antibiotic agents were used as the standard treatment.In more than 90% of the cases, Penicillin G was admi-nistered10, and Ceftriaxone, Doxycycline, Amoxycillin,IV C-Penicilline, and others were also used10, 12.
76International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
https://en.wikipedia.org
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page4
C. CellulitisOnly one study identified cellulitis as an infectiousdisease which prevailed in the aftermath of flooding8.There was an 88% increase in the number of lowerextremity cellulitis patients after flooding, comparedto that of before it, 344 and 183 respectively, in Taiwanin 2009. The average number of patients who hadimmersed their affected limbs in flood waters, labeledas W +, were over 10 times higher than that of beforeflooding, 31 and 3 per week, respectively.
Wound or pus specimen culture identified more Gram-negative bacilli (GNB) in W + patients group than in theW- group, 86% and 34% respectively. W + group alsodemonstrated a higher Entrococcus spp. infection rate,16%, than W- group, 3%. Among others, Aeromonashydrophilia and Enterobacteriaceae, includingEscherichia coli, Klebsiella pneumoniae, Enterobactercloacae, and Proteus mirabilis, were predominant. Incontrast, the W- group showed more Gram-positive cocci(GPC) and Staphylococcus aureus infection than the W+ group, 80% vs. 43% and 51% vs. 16% respectively.Treatment used was not mentioned in the study.
DISCUSSION
Since water sources are easily contaminated by floodwaters, and contaminated water sources cause fecal-oral transmission to be increased5, 6, 13, 14, diarrhea isreported as one of the most common infectiousdiseases after floods. Due to this fact, underdevelopedcountries are most vulnerable to the disease since theyhave poor water supply and sewage system, and a rela-tively small number of well-designed latrines comparedto their populations. Earthquakes, which destroy infra-structure, can also increase diarrheal diseases.Therefore, when a natural disaster hits a region, safedrinking water supply is top priority. Also healthcareworkers should educate people to wash their handsafter using latrines, and not to share water containersand cooking pots with others13. If healthcare workerscan beforehand know and reserve antibiotics provedeffective to dominant strains of diarrheal diseases afterflooding, they would be able to better control such afecal-oral transmitted disease.
The authors found two interesting facts in leptospirosiscases. First, both studies reviewed reported that the
patients were dominantly young males. When conside-ring that leptospirosis is a direct zoonosis, and thus themain source of infection is animal urine15, boys can beconsidered the most vulnerable population to thedisease in the aftermath of flooding. It is because theyare far more active than girls or adult males, easily sus-tain skin wounds from outdoor activities, throughwhich leptospires can invade into their body, and highlylikely to have more contacts with contaminated envi-ronments or infected animals. Additionally Koay et al.(2004) reported the patients were infected after swim-ming in a creek. It implies that flood waters sweep thepathogen away from the environment, such as soil orbushes, and move it to other places like creeks or lakes.The WHO recommends that the treatment should startwithin five days after the disease developed10. Thus,healthcare workers need to be aware of the possibilitiesof the disease so that they can identify the symptoms,and quickly start antimicrobial therapy. Otherwise, theCFR will increase, and so does death rate.
Cellulitis was also reported after tsunami, and Proteusspp., Klebsiella spp., Enterobacter spp., and E. coli werethe main organisms16, 17 just as found in this study. Theyare commonly found in nature including soil, plants,animal feces, and sewage system. Subsequently, wheninundated, they flow in water so people with skinwounds can readily be infected and develop into cellu-litis. Therefore, it is important to educate people toavoid immersing their limbs into flood waters whenthey do not have skin integrity.
Flood waters can cause critical health problems becauseit easily grows, passes, and spreads various pathogens inthe affected area7, 12. It also hinders the supply of cleandrinking water and destructs sewage systems, causingan increase in fecal-oral transmission of pathogens, andthus the rate of infection7, 17, 18. Accordingly, epidemicscan be triggered by floods. Epidemics caused by naturaldisasters, including floods, reflect endemic diseases orthe pathogens which were prevalent in the area beforethe disaster3, 13. Healthcare providers shall better pre-pare for natural disasters by foreseeing possiblediseases with the awareness of predominant infectiousagents of the local area where they serve.
For that matter, vaccination is also important in infec-tion control after a natural disaster. There are threemost useful vaccines post disasters; tetanus toxoid,hepatitis A, and cholerae19. Healthcare workers canprevent people from suffering certain infections byeffectively using the vaccines.
The underprivileged should be considered one of the mostvulnerable populations when a natural disaster breaksout. They already have less access to clean water sourcesand other infrastructures than others, so they naturally fallinto the worst situation when hit by a disaster. In addition,healthcare professionals should define each vulnerablepopulation according to the main infectious diseaseswhich can break out in their region, so that they can focustheir investigative efforts on them to prevent and identifyany epidemics after a disaster strikes the region.
77International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page5

78International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1 A
UTH
OR*
COU
NTR
Y(A
REA)
- FL
OO
DIN
GY
EAR
- CA
USE
- SI
ZE
IMPA
CT†
- D
ISEA
SE
- M
ORB
IDIT
YO
RM
ORT
ALI
TYRA
TEPA
THO
GEN
- D
IAG
NO
STIC
TEST
- TR
EATM
ENT
Ala
m e
t al
.(2
011)
Ban
gla
des
h(D
hak
a)
- A
ug
200
7-
un
usu
al h
eavy
mo
nso
on
rai
ns
- n
ot
men
tio
ned
No
t m
enti
on
ed
·Cho
lera
·21,
401
diar
rhea
pat
ien
ts w
ere
trea
ted
in t
he
Inte
rnat
ion
alC
ente
r fo
r D
iarr
hea
l Dis
ease
Res
earc
h, B
ang
lad
esh
(IC
DD
R,B
)h
osp
ital
in A
ug
200
7
Vib
rio
ch
ole
rae
O1
[TES
T]·R
ecta
l sw
ab
[TRE
ATM
ENT]
·Ag
gre
ssiv
e re
-hyd
rati
on
CD
C (
2012
)Pa
kist
an(u
ncl
ear)
·Ju
l-A
ug
201
0·n
ot
men
tio
ned
·n
ot
men
tio
ned
1,70
0 p
lus
dea
ths,
18 m
il af
fect
ed
·2,1
74,3
68 r
epo
rted
co
nd
itio
ns
a.sk
in d
isea
se1,
029,
942
(18.
3%)
b. r
espi
rato
ry in
fect
ion
850,
292
(15
.1%
)c.
acu
te d
iarr
hea
745,
532
(13
.3%
)·1
30 o
utb
reak
ale
rts
a. 1
15 A
WD
‡ (s
usp
ecte
dch
ole
rae)
(88
.5%
)b
. 1 b
loo
dy
dia
rrh
ea (
susp
ecte
dm
alar
ia)
(0.8
%)
c. 7
su
spec
ted
mea
sles
(5.
4%)
d. 2
su
spec
ted
men
ing
itis
(1.5
%)
e. 2
acu
te f
lacc
id p
aral
ysis
(su
spec
ted
po
liom
yelit
is)
(1.5
%)
f. 1
acu
te h
emo
rrh
agic
fev
ersy
nd
rom
e (0
.8%
)
-Ou
t o
f 82
wit
h la
bsa
mp
les,
of
115
AW
Dal
erts
, 55
(67.
1%)
test
edp
osi
tive
fo
r V
ibri
och
ole
rae
-No
co
nfi
rmat
ion
on
mea
sles
, po
lio, o
rb
acte
rial
men
ing
itis
[TES
T]·N
ot
men
tio
ned
[Tre
atm
ent]
·No
t m
enti
on
ed
Din
g e
t al
.(2
013)
Ch
ina
(Fu
yan
g a
nd
Bo
zho
u,
An
hu
i)
·Ju
n-J
ul 2
007
·sev
ere
hea
vy r
ain
fall
·th
e to
tal p
reci
pit
atio
no
f 42
5.9
mm
in F
uya
ng
and
87.
6-29
7.6
mm
inB
ozh
ou
15.1
mil
affe
cted
·Infe
ctio
us d
iarr
hea
of
102
case
s a.
66
dys
ente
ry d
iarr
hea
(64.
7%)
b. 3
6 o
ther
infe
ctio
us
dia
rrh
ea(3
5.3%
)c.
Inci
den
t ra
tes
of
2.04
8/10
5in
Fuya
ng
an
d 4
.609
/105
in
No
t m
enti
on
ed
[TES
T]·N
ot
men
tio
ned
[Tre
atm
ent]
·No
t m
enti
on
ed
Sch
war
tz e
t al
.(2
006)
Ban
gla
des
h(D
hak
a)
·Sep
-Oct
198
8, J
uly
-Oct
1998
, an
d J
uly
-Au
g &
Sep
-Oct
200
4·n
ot
men
tio
ned
No
t m
enti
on
ed
·Dia
rrhe
al e
pide
mic
s·a
to
tal o
f 20
,395
pat
ien
tsen
rolle
d in
to t
he
surv
eilla
nce
syst
em
·V. c
ho
lera
(mo
st c
om
mo
n)
a. O
1 se
rog
rou
p: O
gaw
asy
roty
pe
[TES
T]·N
ot
men
tio
ned
Tabl
e1:
Sum
mar
y of
revi
ewed
lite
ratu
re.
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page6

79International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1A
UTH
OR*
COU
NTR
Y(A
REA)
- FL
OO
DIN
GY
EAR
- CA
USE
- SI
ZE
IMPA
CT†
- D
ISEA
SE
- M
ORB
IDIT
YO
RM
ORT
ALI
TYRA
TEPA
THO
GEN
- D
IAG
NO
STIC
TEST
- TR
EATM
ENT
·29
flo
od
day
s in
198
8,39
in 1
998,
31
in t
he
firs
tfl
oo
d a
nd
6 in
th
ese
con
d in
200
4
·3 f
atal
itie
s p
er 1
,000
vis
its
(no
sig
nif
ican
t d
iffe
ren
ce f
rom
2 fa
talit
ies
in n
on
-flo
od
per
iod
s)
b. E
1 To
r b
ioty
pe
·Ro
tavi
rus
(2n
dm
ost
co
mm
on
)·S
hig
ella
& S
alm
on
ella
spec
ies
a. S
hig
ella
fle
xner
i·O
ther
sa.
E. h
isto
lyti
ca/ d
isp
arb
. G. l
amb
li (1
998)
c. E
TEC
d. C
.jeju
ni
·no
iden
tifi
able
org
anis
m(2
3%~
51%
/ yea
r)
[Tre
atm
ent]
·OR
S (o
ral r
e-h
ydra
tio
nso
luti
on
s), i
ntr
aven
ou
sfl
uid
an
d a
nti
bio
tics
Am
ilasa
n e
t al
.(2
012)
Phili
pp
ines
(Met
ro M
anila
)
·Sep
200
9·t
yph
oo
n·n
ot
men
tio
ned
2,29
9 p
atie
nts
wit
h 1
78d
eath
s in
15
ho
spit
als
·Lep
tosp
iros
is·O
ut
of
471
case
s, 5
1 d
ied
(C
FR§
10.8
%),
an
d 7
(1.
5%)
wer
etr
ansf
erre
d t
o o
ther
ho
spit
als
for
hem
orr
hag
e
-L. b
org
pet
erse
nii
sero
var
Tara
sso
vi(m
ost
co
mm
on
)-L
. bo
rgp
eter
sen
iise
rova
rs P
oi
-L. b
org
pet
erse
nii
sero
vars
Sej
roe
-L. i
nte
rro
gan
s se
rova
rsLo
sban
os
-L. i
nte
rro
gan
s se
rova
rsM
anila
e
[Tes
t]·R
apid
dia
gn
ost
ic t
ests
a. L
epto
spir
a Se
rolo
gy
(Bio
-Rad
, Mar
nes
-la-
coq
uet
te, F
ran
ce)
b. P
anB
io Ig
M E
LISA
(Pan
bio
Dia
gn
ost
ics,
Bri
sban
e, Q
uee
nsl
and
,A
ust
ralia
)
[Tre
atm
ent]
·An
tim
icro
bia
l dru
gs
a. P
enic
illin
(92
.5%
)b
. Cef
tria
xon
e (2
.1%
)c.
Do
xycy
clin
e (1
.9%
)d
. Oth
ers
(3.4
%)
Ko
ay e
t al
.(2
004)
Mal
aysi
a(B
eau
fort
)
·Fir
st w
eek
Oct
, 199
9·h
eavy
rai
nfa
ll·N
ot
men
tio
ned
No
t m
enti
on
ed
·Lep
tosp
iros
is·4
6 ca
ses
·on
e d
eath
fro
m h
aem
orr
hag
icsh
ock
sec
on
dar
y to
pu
lmo
nar
yh
aem
orr
hag
e
Lep
tosp
ira
[Tes
t]·S
ero
log
ical
tes
ta.
mic
rosc
op
icag
glu
tin
atio
n t
est
(MA
T)
[Tre
atm
ent]
·An
tib
ioti
c tr
eatm
ent
a. D
oxy
cycl
ine
b. A
mo
xyci
llin
c. IV
D-P
enic
illin
Tabl
e1:
Sum
mar
y of
revi
ewed
lite
ratu
re (c
ontin
uatio
n).
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page7
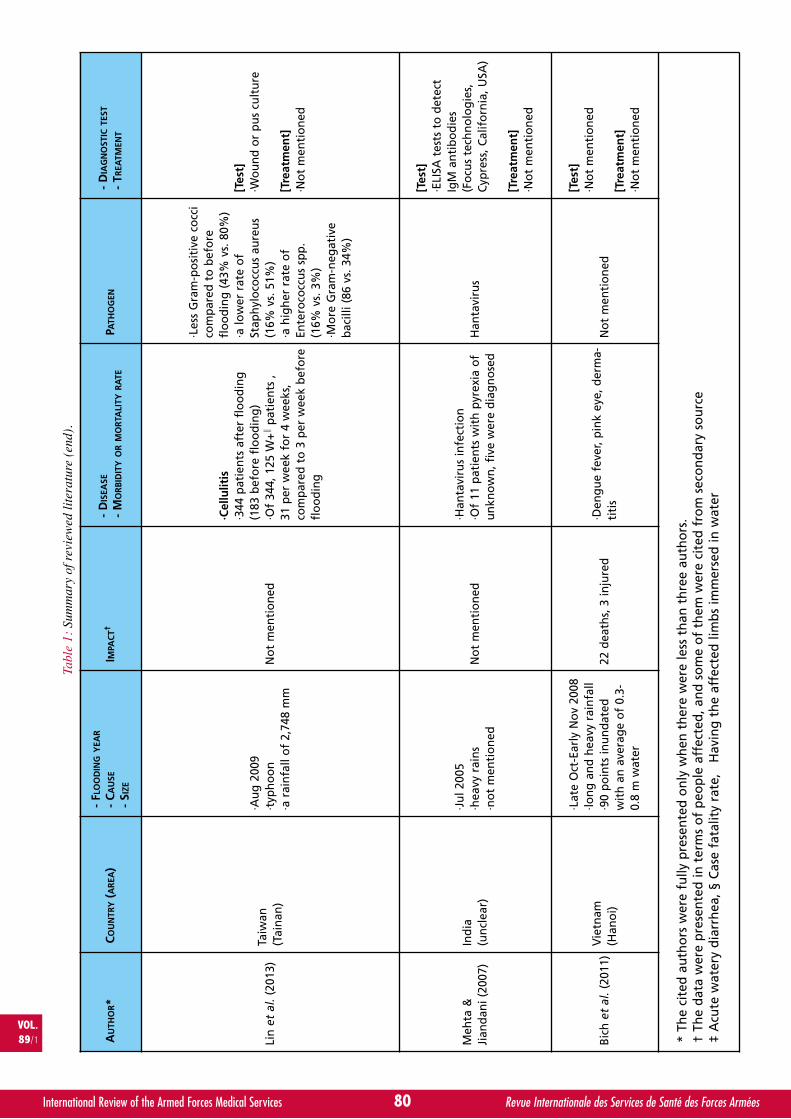
80International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1 A
UTH
OR*
COU
NTR
Y(A
REA)
- FL
OO
DIN
GY
EAR
- CA
USE
- SI
ZE
IMPA
CT†
- D
ISEA
SE
- M
ORB
IDIT
YO
RM
ORT
ALI
TYRA
TEPA
THO
GEN
- D
IAG
NO
STIC
TEST
- TR
EATM
ENT
Lin
et
al.(
2013
)Ta
iwan
(Tai
nan
)
·Au
g 2
009
·typ
ho
on
·a r
ain
fall
of
2,74
8 m
mN
ot
men
tio
ned
·Cel
lulit
is·3
44 p
atie
nts
aft
er f
loo
din
g(1
83 b
efo
re f
loo
din
g)
·Of
344,
125
W+∥
pat
ien
ts ,
31 p
er w
eek
for
4 w
eeks
,co
mp
ared
to
3 p
er w
eek
bef
ore
flo
od
ing
·Les
s G
ram
-po
siti
ve c
occ
ico
mp
ared
to
bef
ore
flo
od
ing
(43
% v
s. 8
0%)
·a lo
wer
rat
e o
fSt
aph
ylo
cocc
us
aure
us
(16%
vs.
51%
)·a
hig
her
rat
e o
fEn
tero
cocc
us
spp
.(1
6% v
s. 3
%)
·Mo
re G
ram
-neg
ativ
eb
acill
i (86
vs.
34%
)
[Tes
t]·W
ou
nd
or
pu
s cu
ltu
re
[Tre
atm
ent]
·No
t m
enti
on
ed
Meh
ta &
Jian
dan
i (20
07)
Ind
ia(u
ncl
ear)
·Ju
l 200
5·h
eavy
rai
ns
·no
t m
enti
on
edN
ot
men
tio
ned
·Han
tavi
rus
infe
ctio
n·O
f 11
pat
ien
ts w
ith
pyr
exia
of
un
kno
wn
, fiv
e w
ere
dia
gn
ose
dH
anta
viru
s
[Tes
t]·E
LISA
tes
ts t
o d
etec
tIg
M a
nti
bo
die
s(F
ocu
s te
chn
olo
gie
s,C
ypre
ss, C
alif
orn
ia, U
SA)
[Tre
atm
ent]
·No
t m
enti
on
ed
Bic
h e
t al
.(20
11)
Vie
tnam
(Han
oi)
·Lat
e O
ct-E
arly
No
v 20
08·lo
ng
an
d h
eavy
rai
nfa
ll·9
0 p
oin
ts in
un
dat
edw
ith
an
ave
rag
e o
f 0.
3-0.
8 m
wat
er
22 d
eath
s, 3
inju
red
·Den
gu
e fe
ver,
pin
k ey
e, d
erm
a-ti
tis
No
t m
enti
on
ed
[Tes
t]·N
ot
men
tio
ned
[Tre
atm
ent]
·No
t m
enti
on
ed
* Th
e ci
ted
au
tho
rs w
ere
fully
pre
sen
ted
on
ly w
hen
th
ere
wer
e le
ss t
han
th
ree
auth
ors
.†
The
dat
a w
ere
pre
sen
ted
in t
erm
s o
f p
eop
le a
ffec
ted
, an
d s
om
e o
f th
em w
ere
cite
d f
rom
sec
on
dar
y so
urc
e‡
Acu
te w
ater
y d
iarr
hea
, § C
ase
fata
lity
rate
, ¢ H
avin
g t
he
affe
cted
lim
bs
imm
erse
d in
wat
er
Tabl
e1:
Sum
mar
y of
revi
ewed
lite
ratu
re (e
nd).
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page8
CONCLUSION
The authors found that diarrhea, leptospirosis, and cel-lulitis were reported in the aftermath of flooding inAsian countries. However, the types of infectiousdiseases can vary depending on the types of naturaldisasters, the regions where the disasters hit, climate ofthe regions, and others. Therefore, in order for health-care providers to improve the preparedness and res-ponse efficiency of natural disasters, they should conti-nue to keep updated with infectious diseases and theirpathogens that are common in the areas they are wor-king, and prevention measures and treatment of them.The authors suggest that future research should inves-tigate the relation between the types of disaster andthe infectious diseases.
ABSTRACT
Purpose: this study provides an insight, with a litera-ture review, into infectious diseases which could breakout after floods.Methods: The study systematically reviewed literature.A total of 209 articles emerged with search words andconditions. After applying the inclusion and exclusioncriteria, nine studies finally remained for review.Results: Seven Asian countries reported twelve floo-ding cases during the given time frame. The most fre-quently hit area was Dhaka in Bangladesh. The maincause of flood was heavy rainfall between July andSeptember. Diarrhea was the most common infectiousdisease after the incidents, followed by Leptospirosisand cellulitis. Vibrio cholerae was the major pathogencausing diarrhea.Conclusion: Types of infectious disease in the aftermathof natural disasters may be different upon types of disas-ters and regional characteristics. Therefore, healthcareprofessionals need to understand well endemic diseasesand the dominant types of disaster in the area that theyserve in order to effectively respond to disasters.
REFERENCES
11. GUHA-SAPIR, D., HOYOIS, P., BELOW, R. (2013). Annual disasterstatistical review 2012: The numbers and trends. Brussels: CRED.http://www.cred.be/sites/default/files/ADSR_2012.pdf. Retrieved26th January, 2014.
12. United Nations University (2004). via EurekAlert!; NASA’s EarthObservatory. http://radio-weblogs.com/0105910/2004/06/15.html.Retrieved 26 January, 2013.
13. Centers for Disease Control and Prevention (CDC). (2012). Earlywarning disease surveillance after a flood emergency-Parkistan,2010. Morbidity and Mortality Weekly Report. 61 (49).
14. CANN, K. F., THOMAS, D. RH, SALMON, R. L., WYN-JONES, A. P.,& KAY, D. (2013). Systematic review: Extreme water-related wea-ther events and waterborne disease. Epidemiology & Infection.141 (4), 671-686. http://dx.doi.org/10.1017/S0950268812001653.Epub 2012 Aug 9.
15. SCHWARTZ BS, HARRIS JB, KHAN AI, LAROCQUE RC, SACK DA,MALEK MA, et al. (2006). Diarrheal epidemics in Dhaka,Bangladesh, during three consecutive floods: 1988, 1998, and2004. American Journal of Tropical Medicine and Hygiene. 74(6), 1067-1073.
16. ALAM M., ISLAM, A., BHUIYAN, N. A., RAHIM, N., HOSSAIN,A., KHAN G. Y., et al. (2011). Clonal transmission, dual peak,and off-season cholera in Bangladesh. Infection Ecologyand Epidemiology, 1. http://dx.doi.org/10.3402/iee.v1i0.7273. Epub 2011 Aug 8.
17. DING, G., ZHANG, Y., GAO, L., MA, W., LI, X., LIU, J. et al.(2013). Quantitative analysis of burden of infectious diar-rhea associated with floods in northwest of Anhui Province,China: A mixed method evaluation. PLoS ONE 8 (6): e65112.http://dx.doi.org/10.1371/journal.pone.0065112.
18. LIN, P. C., LIN, H. J., GUO, H. R., & CHEN, K. T. (2013).Epidemiological characteristics of lower extremity cellulitisafter a typhoon flood. PLoS One. 8 (6): e65655.http://dx.doi.org/ 10.1371/journal.pone.0065655. Print 2013.
19. BICH, T. H., QUANG, L. N., HA LE, T. T., HANH, T. T., & GUHA-SAPIR, D. (2011). Impacts of flood on health: epidemiologicevidence from Hanoi, Vietnam. Global Health Action. 4(6356), 1-11. http://dx.doi.org/ 10.3402/gha.v4i0.6356. Epub2011 Aug 23.
10. AMILASAN, A. S., UJIIE, M., SUZUKI, M., SALVA, E., BELO,M. C., KOIZUMI, N., et al. (2012). Outbreak of leptospirosisafter flood, the Philippines, 2009. Emerging InfectiousDisease. 18 (1), 91-94. http://dx.doi.org/10.3201/eid1801.101892.
11. SHABIR, O. (2013). A summary case report on the healthimpacts and response to the pakistan floods of 2010. PLoSCurrents. 5, http://dx.doi.org/ 10.1371/currents.dis.-cc7bd532ce252c1b740c39a2a827993.
12. KOAY, T. K., NIRMAL, S., NOITIE, L., & TAN, E. (2004). An epi-demiological investigation of an outbreak of leptospirosisassociated with swimming, Beaufort, Sabah. MedicalJournal of Malaysia. 59 (4), 455-459.
13. KOUADIO, I. K., ALJUNID, S., KAMIGAKI, T., HAMMAD, K., &OSHITANI, H. (2012). Infectious diseases following naturaldisasters: prevention and control measures. Expert ReviewAnti-Infective Therapy. 10 (1), 95-104. http://dx.doi.org/10.1586/eri.11.155. Review.
14. SINGH, P. K. & DHIMAN, R. C. (2012). Climate change andhuman health: Indian context. Journal of Vector BorneDisease. 49 (2), 55-60.
15. VIJAYACHARI, P., SUGUNAN, A. P., & SHRIRAM, A. N. (2008).Leptospirosis: an emerging global public health problem.Journal of Bioscience. 33 (4), 557-569.
16. MAEGELE, M., GREGOR, S., YUECEL, N., SIMANSKI, C.,PAFFRATH, T., RIXEN, D., HEISS, M.M., RUDROFF, C., SAAD,S., PERBIX, W., WAPPLER, F., HARZHEIM, A., SCHWARZ, R., &BOUILLON, B. (2006). One year ago not business as usual:Wound management, infection and psychoemotionalcontrol during tertiary medical care following the 2004Tsunami disaster in Southeast Asia. Critical Care, 10 (R50).
17. UNAHLEKHAKA, A. & MEHTA, G. (2006). The tsunami disasterin Asia. International Journal of Infection Control, 2 (1), 1-5.
18. MEHTA, S., & JIANDANI, P. (2007). Ocular features of hanta-virus infection. Indian Journal of Ophthalmology. 55 (5),378-380.
19. WIWANITKIT, V. (2010). Vaccination in post-earthquakecrisis. Human Vaccines, 6 (7), 595-596.
VOL.89/1
81International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
Flood in Asia_JUNG.qxp_Mise en page 1 16/03/2016 15:13 Page9

82International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
INSTRUCTIONS TO AUTHORS
• All material intended for publication in the International Review of the Armed ForcesMedical Services (IRAFMS) should be submitted to the Editor’s office:
International Committee of Military MedicineHôpital Militaire Reine AstridBE - 1120 Brussels, Belgium.
• Scientific articles, analyses or reviews of books and articles related to military medicine,symposia or congress proceedings, scientific events and announcements written in Frenchand English will be considered for review.
• In its editorial policy, IRAFMS follows the guidelines of the International Committee ofMedical Journal Editors (http://www.icmje.org/index.html). Authors are encouraged toadhere to these guidelines when writing their article, both in methodology and in thestructure of the manuscript. Authors will be informed of the progress of the review process.Manuscripts under review are considered confidential. By submitting the manuscript, theauthor agrees to transfer the ownership to ICMM.
• The submitted article must be accompanied by the full name (s) and by the address(es)of all authors as well as a short curriculum vitæ and a photograph (high resolution) of themain author.
• The authors implicitly recognize that the submitted article has not been sent simultaneouslyto other journals or has not recently been published under the same title.
• The Editor of the IRAFMS may require authors to justify the assignment of authorship.
• Partial or total reproduction of an article which has been published in the IRAFMS issubject to the prior consent of the editor of the IRAFMS.
• Potential Conflict of Interest. To ensure that authors are not influenced in any way intheir writing by third parties for financial or other reasons and to ensure the credibility of thepublication, the author and science itself, the Editor may request for this purpose a ‘declaration ofconflict of interests. This declaration will entail financial support arrangements, possibleimpairment of freedom of writing and free access to relevant data due to regulations fromsuperiors and peers and/or other competing interests. Authors of a manuscript will mentionall contributors to their work.
• Privacy and confidentiality. Authors will ensure the right to privacy and confidentialityof all human subjects involved in their manuscript. They will not disclose any personal information,including photographs of subjects unless they possess and are able to show a statement ofinformed consent.
• Protection of human subjects and animals in research. In manuscripts which report experimentson human subjects, authors should indicate whether the procedures followed were in accordancewith the ethical standards of the responsible committee and with the Helsinki Declaration. Foranimal experimentation, the authors should indicate whether the institutional, national andother legal guides for the care and use of laboratory animals were followed.
• Other stipulations. Articles accepted for publication in the IRAFMS should not to be publishedelsewhere without the explicit consent of the Editor-in-Chief. Articles based on presentationsduring congresses and/or workshops of the ICMM should with priority be published in theIRAFMS. The ICMM will not pay for any article. However, every two years, however, a paper ofhigh quality may be awarded with the Jules Voncken prize, which includes a modest amountof money.
• Manuscripts should be typed on one side only, double-spaced throughout, with a 3 cmmargin at the left hand side and a maximum of 35 lines per page. The text should notexceed 25 typewritten pages, including bibliographic references. It should be submitted asan A4 paper size Word document (format Arial 12) by e-mail to [email protected] orby postal service on a CD Rom accompanied by a hard copy (also on A4 paper size).
• A summary of no more than 150 words should be included. It is desirable to submit thesummary in both in French and in English.
• Three to five keywords both in French and in English should be provided in order tofacilitate indexing the article.
• Abbreviations should be avoided in the text except those relating to accepted scientificunits of measurements (SI units). If other abbreviations are used, they should be spelt outin full when first mentioned in the text.
• When sending their manuscripts, the authors are invited to include the necessary tables,graphs, photos and illustrations, along with their legends. Drawings and legends shouldbe carefully printed so as to be directly reproduced. Each illustration should be identifiedby a reference in order to be properly included in the text.
• References should be numbered in the order in which they appear in the text and referredto by Arabic numerals in brackets. They will be listed as follows:1. For a journal: the names and initials of all authors, full title of the article (in the originallanguage), name of the journal, year, volume, first and last page of the article.
2. For a book: name(s) and initials of the author(s), title of the book, name of the publisherand city, year of publication, pages corresponding to the quotation.
RECOMMANDATIONS AUX AUTEURS
• Tout travail destiné à la publication dans la Revue Internationale des Services de Santédes Forces Armées (RISSFA) doit être envoyé au Bureau de la rédaction :
Comité International de Médecine MilitaireHôpital Militaire Reine AstridBE - 1120 Bruxelles (Belgique)
• Sont pris en considération les articles scientifiques, les analyses d’ouvrages ou d’articlesmédico-militaires, les comptes rendus de réunions, de congrès, d’événements scientifiqueset les annonces, rédigés en français et en anglais.
• Pour sa politique éditoriale, la RISSFA suit les directives de l’International Committee of MedicalJournal Editors (http://www.icmje.org/index.html). Les auteurs sont encouragés à adhérer à ces lignesdirectrices lors de la préparation et de la rédaction de leur article, aussi bien dans la méthodologieque dans la structure du manuscrit. Les auteurs seront informés des progrès de l’évaluation de leurmanuscrit. Les manuscrits en cours d’évaluation sont considérés comme confidentiels. En soumettantle manuscrit, l’auteur s’engage à accepter leur transfert de propriété au CIMM.
• Tous ces travaux doivent être accompagnés des noms, prénoms et adresses de tous lesauteurs, ainsi qu’un bref curriculum vitæ et photo (en haute résolution) de l’auteur principal.
• Les auteurs reconnaissent implicitement que l’article proposé n’a pas été envoyé enmême temps à d’autres journaux, ou qu’il n’a pas été publié récemment sous le même titre.
• La Direction de la RISSFA se réserve le droit de demander au signataire d’un article lajustification de sa qualité d’auteur.
• Toute reproduction partielle ou totale d’un article paru dans la RISSFA doit être soumiseà l’accord préalable de l’Editeur de cette dernière.
• Conflit d’intérêts potentiel. Pour s’assurer que les auteurs ne sont pas influencés par des tiersdans l’écriture de l’article, pour des raisons financières ou autres, et pour garantir la crédibilité dela publication, de l’auteur et de la science elle-même, la Direction de la RISSFA peut demander àcet effet, une « déclaration de conflit d’intérêts ». Cette déclaration devra faire mention dessoutiens financiers ayant pu influencer la liberté d’écriture ainsi que la possibilité d’accès auxdonnées utilisées pour la rédaction de l’article, les conflits d’intérêts avec les pairs ou laconcurrence. Les auteurs d'un manuscrit révéleront tous les contributeurs à leur travail.
• Vie privée et confidentialité. Les auteurs préserveront le droit à la vie privée et à la confidentialitéde tous les sujets humains impliqués dans leur manuscrit. Ils ne divulgueront pas d’informationspersonnelles, y compris des photographies de sujets à moins qu’ils ne possèdent et puissentmontrer une déclaration de consentement éclairé.
• Protection des sujets humains et animaux dans la recherche. Dans les manuscrits qui rapportentdes expériences sur des sujets humains, les auteurs devront indiquer si les procédures suiviesétaient conformes aux normes éthiques du comité responsable et avec la Déclarationd’Helsinki. Pour l’expérimentation animale, les auteurs devront indiquer si les règles légalesinstitutionnelles, nationales et autres pour l’utilisation d’animaux de laboratoire, ont été suivies.
• Autres dispositions. Les articles acceptés pour publication dans la RISSFA ne doivent pasêtre publiés ailleurs sans le consentement explicite du Rédacteur en chef. Les articles issusdes présentations lors des congrès et/ou des ateliers du CIMM devront en priorité êtrepubliés dans la RISSFA. Le CIMM ne paiera pour aucun article. Cependant, tous les deuxans, un article de haute qualité peut être récompensé par le prix « Jules Voncken », quicomprend une modeste somme d’argent.
• Le manuscrit sera dactylographié en double interligne, marge gauche de 3 cm, 35 lignes parpage, sur le recto seulement et n’excédera pas 25 pages, références bibliographiques comprises.Il sera envoyé, soit par e-mail à l’adresse suivante: [email protected], soit par voie postalesur CD-Rom accompagné d’une épreuve papier en format A4 (texte en Word, Arial 12).
• Un résumé ne dépassant pas 150 mots y sera incorporé. Il est souhaitable que ce résumé,y compris le titre de l’article, soit traduit en français et en anglais.
• Il est indispensable de fournir 3 à 5 mots-clés en français et en anglais afin de faciliterl’indexation de l’article.
• Les abréviations doivent être évitées dans le texte, sauf celles se rapportant aux unitésscientifiques de mesure, dûment acceptées (unités SI). Si d’autres abréviations sont utilisées,elles doivent être précédées de la terminologie complète à laquelle elles se rapportent,lorsqu’elles sont mentionnées dans le texte pour la première fois.
• Les auteurs sont invités à inclure, dans l’envoi de leur manuscrit, les tableaux, graphiques,photos et illustrations indispensables, accompagnés de leurs légendes. Les dessins etlégendes, soigneusement exécutés, devront pouvoir être reproduits directement. Chaquefigure sera identifiée par une mention permettant de l’inclure correctement dans le texte.
• Les références seront inscrites dans l’ordre dans lequel elles paraissent dans le texte etindiquées par des chiffres arabes, entre parenthèses. Elles seront mentionnées comme suit :1. Pour un périodique: nom et initiales des prénoms de tous les auteurs, titre de l’article (dans lalangue originale), nom du périodique, année, volume, page initiale et page finale de l’article.
2. Pour un livre : nom et initiales des prénoms du ou des auteurs, titre du livre, nom de lamaison d’édition, ville et année de publication, pages correspondant à la citation.
ADDRESS FOR SUBSCRIPTION
SUBSCRIPTIONS 2016International Review of the Armed Forces Medical Services
N.E.P.13, rue Portefoin - FR-75003 Paris, France
Tel. : +33 (0)1 40 27 88 88 - Fax : +33 (0)1 40 27 89 43E-mail : nep@wanadoo. fr
Credit Lyonnais : 7828 H - Paris Haxo (N.E.P.)
Subscription for one year : € 60Cost for a single copy : € 20
ADRESSE POUR LES ABONNEMENTS
ABONNEMENTS 2016Revue Internationale des Services de Santé des Forces Armées
N.E.P.13, rue Portefoin - FR-75003 Paris (France)
Tél. : +33 (0)1 40 27 88 88 - Fax : +33 (0)1 40 27 89 43E-mail : nep@wanadoo. fr
Crédit Lyonnais : 7828 H - Paris Haxo (N.E.P.)
Abonnement pour 1 an : € 60Prix du numéro ordinaire : € 20
I.S.S.N. : 0259-8582 Imprimerie dans l’Union européenne
Recommandations aux Auteurs_Mise en page 1 16/03/2016 09:55 Page1
82International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
INSTRUCTIONS TO AUTHORS
• All material intended for publication in the International Review of the Armed ForcesMedical Services (IRAFMS) should be submitted to the Editor’s office:
International Committee of Military MedicineHôpital Militaire Reine AstridBE - 1120 Brussels, Belgium.
• Scientific articles, analyses or reviews of books and articles related to military medicine,symposia or congress proceedings, scientific events and announcements written in Frenchand English will be considered for review.
• In its editorial policy, IRAFMS follows the guidelines of the International Committee ofMedical Journal Editors (http://www.icmje.org/index.html). Authors are encouraged toadhere to these guidelines when writing their article, both in methodology and in thestructure of the manuscript. Authors will be informed of the progress of the review process.Manuscripts under review are considered confidential. By submitting the manuscript, theauthor agrees to transfer the ownership to ICMM.
• The submitted article must be accompanied by the full name (s) and by the address(es)of all authors as well as a short curriculum vitæ and a photograph (high resolution) of themain author.
• The authors implicitly recognize that the submitted article has not been sent simultaneouslyto other journals or has not recently been published under the same title.
• The Editor of the IRAFMS may require authors to justify the assignment of authorship.
• Partial or total reproduction of an article which has been published in the IRAFMS issubject to the prior consent of the editor of the IRAFMS.
• Potential Conflict of Interest. To ensure that authors are not influenced in any way intheir writing by third parties for financial or other reasons and to ensure the credibility of thepublication, the author and science itself, the Editor may request for this purpose a ‘declaration ofconflict of interests. This declaration will entail financial support arrangements, possibleimpairment of freedom of writing and free access to relevant data due to regulations fromsuperiors and peers and/or other competing interests. Authors of a manuscript will mentionall contributors to their work.
• Privacy and confidentiality. Authors will ensure the right to privacy and confidentialityof all human subjects involved in their manuscript. They will not disclose any personal information,including photographs of subjects unless they possess and are able to show a statement ofinformed consent.
• Protection of human subjects and animals in research. In manuscripts which report experimentson human subjects, authors should indicate whether the procedures followed were in accordancewith the ethical standards of the responsible committee and with the Helsinki Declaration. Foranimal experimentation, the authors should indicate whether the institutional, national andother legal guides for the care and use of laboratory animals were followed.
• Other stipulations. Articles accepted for publication in the IRAFMS should not to be publishedelsewhere without the explicit consent of the Editor-in-Chief. Articles based on presentationsduring congresses and/or workshops of the ICMM should with priority be published in theIRAFMS. The ICMM will not pay for any article. However, every two years, however, a paper ofhigh quality may be awarded with the Jules Voncken prize, which includes a modest amountof money.
• Manuscripts should be typed on one side only, double-spaced throughout, with a 3 cmmargin at the left hand side and a maximum of 35 lines per page. The text should notexceed 25 typewritten pages, including bibliographic references. It should be submitted asan A4 paper size Word document (format Arial 12) by e-mail to [email protected] orby postal service on a CD Rom accompanied by a hard copy (also on A4 paper size).
• A summary of no more than 150 words should be included. It is desirable to submit thesummary in both in French and in English.
• Three to five keywords both in French and in English should be provided in order tofacilitate indexing the article.
• Abbreviations should be avoided in the text except those relating to accepted scientificunits of measurements (SI units). If other abbreviations are used, they should be spelt outin full when first mentioned in the text.
• When sending their manuscripts, the authors are invited to include the necessary tables,graphs, photos and illustrations, along with their legends. Drawings and legends shouldbe carefully printed so as to be directly reproduced. Each illustration should be identifiedby a reference in order to be properly included in the text.
• References should be numbered in the order in which they appear in the text and referredto by Arabic numerals in brackets. They will be listed as follows:1. For a journal: the names and initials of all authors, full title of the article (in the originallanguage), name of the journal, year, volume, first and last page of the article.
2. For a book: name(s) and initials of the author(s), title of the book, name of the publisherand city, year of publication, pages corresponding to the quotation.
RECOMMANDATIONS AUX AUTEURS
• Tout travail destiné à la publication dans la Revue Internationale des Services de Santédes Forces Armées (RISSFA) doit être envoyé au Bureau de la rédaction :
Comité International de Médecine MilitaireHôpital Militaire Reine AstridBE - 1 120 Bruxelles (Belgique)
• Sont pris en considération les articles scientifiques, les analyses d’ouvrages ou d’articlesmédico-militaires, les comptes rendus de réunions, de congrès, d’événements scientifiqueset les annonces, rédigés en français et en anglais.
• Pour sa politique éditoriale, la RISSFA suit les directives de l’International Committee of MedicalJournal Editors (http://www.icmje.org/index.html). Les auteurs sont encouragés à adhérer à ces lignesdirectrices lors de la préparation et de la rédaction de leur article, aussi bien dans la méthodologieque dans la structure du manuscrit. Les auteurs seront informés des progrès de l’évaluation de leurmanuscrit. Les manuscrits en cours d’évaluation sont considérés comme confidentiels. En soumettantle manuscrit, l’auteur s’engage à accepter leur transfert de propriété au CIMM.
• Tous ces travaux doivent être accompagnés des noms, prénoms et adresses de tous lesauteurs, ainsi qu’un bref curriculum vitæ et photo (en haute résolution) de l’auteur principal.
• Les auteurs reconnaissent implicitement que l’article proposé n’a pas été envoyé enmême temps à d’autres journaux, ou qu’il n’a pas été publié récemment sous le même titre.
• La Direction de la RISSFA se réserve le droit de demander au signataire d’un article lajustification de sa qualité d’auteur.
• Toute reproduction partielle ou totale d’un article paru dans la RISSFA doit être soumiseà l’accord préalable de l’Editeur de cette dernière.
• Conflit d’intérêts potentiel. Pour s’assurer que les auteurs ne sont pas influencés par des tiersdans l’écriture de l’article, pour des raisons financières ou autres, et pour garantir la crédibilité dela publication, de l’auteur et de la science elle-même, la Direction de la RISSFA peut demander àcet effet, une « déclaration de conflit d’intérêts ». Cette déclaration devra faire mention dessoutiens financiers ayant pu influencer la liberté d’écriture ainsi que la possibilité d’accès auxdonnées utilisées pour la rédaction de l’article, les conflits d’intérêts avec les pairs ou laconcurrence. Les auteurs d'un manuscrit révéleront tous les contributeurs à leur travail.
• Vie privée et confidentialité. Les auteurs préserveront le droit à la vie privée et à la confidentialitéde tous les sujets humains impliqués dans leur manuscrit. Ils ne divulgueront pas d’informationspersonnelles, y compris des photographies de sujets à moins qu’ils ne possèdent et puissentmontrer une déclaration de consentement éclairé.
• Protection des sujets humains et animaux dans la recherche. Dans les manuscrits qui rapportentdes expériences sur des sujets humains, les auteurs devront indiquer si les procédures suiviesétaient conformes aux normes éthiques du comité responsable et avec la Déclarationd’Helsinki. Pour l’expérimentation animale, les auteurs devront indiquer si les règles légalesinstitutionnelles, nationales et autres pour l’utilisation d’animaux de laboratoire, ont été suivies.
• Autres dispositions. Les articles acceptés pour publication dans la RISSFA ne doivent pasêtre publiés ailleurs sans le consentement explicite du Rédacteur en chef. Les articles issusdes présentations lors des congrès et/ou des ateliers du CIMM devront en priorité êtrepubliés dans la RISSFA. Le CIMM ne paiera pour aucun article. Cependant, tous les deuxans, un article de haute qualité peut être récompensé par le prix « Jules Voncken », quicomprend une modeste somme d’argent.
• Le manuscrit sera dactylographié en double interligne, marge gauche de 3 cm, 35 lignes parpage, sur le recto seulement et n’excédera pas 25 pages, références bibliographiques comprises.Il sera envoyé, soit par e-mail à l’adresse suivante: [email protected], soit par voie postalesur CD-Rom accompagné d’une épreuve papier en format A4 (texte en Word, Arial 12).
• Un résumé ne dépassant pas 150 mots y sera incorporé. Il est souhaitable que ce résumé,y compris le titre de l’article, soit traduit en français et en anglais.
• Il est indispensable de fournir 3 à 5 mots-clés en français et en anglais afin de faciliterl’indexation de l’article.
• Les abréviations doivent être évitées dans le texte, sauf celles se rapportant aux unitésscientifiques de mesure, dûment acceptées (unités SI). Si d’autres abréviations sont utilisées,elles doivent être précédées de la terminologie complète à laquelle elles se rapportent,lorsqu’elles sont mentionnées dans le texte pour la première fois.
• Les auteurs sont invités à inclure, dans l’envoi de leur manuscrit, les tableaux, graphiques,photos et illustrations indispensables, accompagnés de leurs légendes. Les dessins etlégendes, soigneusement exécutés, devront pouvoir être reproduits directement. Chaquefigure sera identifiée par une mention permettant de l’inclure correctement dans le texte.
• Les références seront inscrites dans l’ordre dans lequel elles paraissent dans le texte etindiquées par des chiffres arabes, entre parenthèses. Elles seront mentionnées comme suit :1. Pour un périodique: nom et initiales des prénoms de tous les auteurs, titre de l’article (dans lalangue originale), nom du périodique, année, volume, page initiale et page finale de l’article.
2. Pour un livre : nom et initiales des prénoms du ou des auteurs, titre du livre, nom de lamaison d’édition, ville et année de publication, pages correspondant à la citation.
ADDRESS FOR SUBSCRIPTION
SUBSCRIPTIONS 2016International Review of the Armed Forces Medical Services
N.E.P.13, rue Portefoin - FR-75003 Paris, France
Tel. : +33 (0)1 40 27 88 88 - Fax : +33 (0)1 40 27 89 43E-mail : nep@wanadoo. fr
Credit Lyonnais : 7828 H - Paris Haxo (N.E.P.)
Subscription for one year : € 60Cost for a single copy : € 20
ADRESSE POUR LES ABONNEMENTS
ABONNEMENTS 2016Revue Internationale des Services de Santé des Forces Armées
N.E.P.13, rue Portefoin - FR-75003 Paris (France)
Tél. : +33 (0)1 40 27 88 88 - Fax : +33 (0)1 40 27 89 43E-mail : nep@wanadoo. fr
Crédit Lyonnais : 7828 H - Paris Haxo (N.E.P.)
Abonnement pour 1 an : € 60Prix du numéro ordinaire : € 20
I.S.S.N. : 0259-8582 Imprimerie dans l’Union européenne
Recommandations aux Auteurs_Mise en page 1 16/03/2016 09:55 Page1
82International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.89/1
INSTRUCTIONS TO AUTHORS
• All material intended for publication in the International Review of the Armed ForcesMedical Services (IRAFMS) should be submitted to the Editor’s office:
International Committee of Military MedicineHôpital Militaire Reine AstridBE - 1120 Brussels, Belgium.
• Scientific articles, analyses or reviews of books and articles related to military medicine,symposia or congress proceedings, scientific events and announcements written in Frenchand English will be considered for review.
• In its editorial policy, IRAFMS follows the guidelines of the International Committee ofMedical Journal Editors (http://www.icmje.org/index.html). Authors are encouraged toadhere to these guidelines when writing their article, both in methodology and in thestructure of the manuscript. Authors will be informed of the progress of the review process.Manuscripts under review are considered confidential. By submitting the manuscript, theauthor agrees to transfer the ownership to ICMM.
• The submitted article must be accompanied by the full name (s) and by the address(es)of all authors as well as a short curriculum vitæ and a photograph (high resolution) of themain author.
• The authors implicitly recognize that the submitted article has not been sent simultaneouslyto other journals or has not recently been published under the same title.
• The Editor of the IRAFMS may require authors to justify the assignment of authorship.
• Partial or total reproduction of an article which has been published in the IRAFMS issubject to the prior consent of the editor of the IRAFMS.
• Potential Conflict of Interest. To ensure that authors are not influenced in any way intheir writing by third parties for financial or other reasons and to ensure the credibility of thepublication, the author and science itself, the Editor may request for this purpose a ‘declaration ofconflict of interests. This declaration will entail financial support arrangements, possibleimpairment of freedom of writing and free access to relevant data due to regulations fromsuperiors and peers and/or other competing interests. Authors of a manuscript will mentionall contributors to their work.
• Privacy and confidentiality. Authors will ensure the right to privacy and confidentialityof all human subjects involved in their manuscript. They will not disclose any personal information,including photographs of subjects unless they possess and are able to show a statement ofinformed consent.
• Protection of human subjects and animals in research. In manuscripts which report experimentson human subjects, authors should indicate whether the procedures followed were in accordancewith the ethical standards of the responsible committee and with the Helsinki Declaration. Foranimal experimentation, the authors should indicate whether the institutional, national andother legal guides for the care and use of laboratory animals were followed.
• Other stipulations. Articles accepted for publication in the IRAFMS should not to be publishedelsewhere without the explicit consent of the Editor-in-Chief. Articles based on presentationsduring congresses and/or workshops of the ICMM should with priority be published in theIRAFMS. The ICMM will not pay for any article. However, every two years, however, a paper ofhigh quality may be awarded with the Jules Voncken prize, which includes a modest amountof money.
• Manuscripts should be typed on one side only, double-spaced throughout, with a 3 cmmargin at the left hand side and a maximum of 35 lines per page. The text should notexceed 25 typewritten pages, including bibliographic references. It should be submitted asan A4 paper size Word document (format Arial 12) by e-mail to [email protected] orby postal service on a CD Rom accompanied by a hard copy (also on A4 paper size).
• A summary of no more than 150 words should be included. It is desirable to submit thesummary in both in French and in English.
• Three to five keywords both in French and in English should be provided in order tofacilitate indexing the article.
• Abbreviations should be avoided in the text except those relating to accepted scientificunits of measurements (SI units). If other abbreviations are used, they should be spelt outin full when first mentioned in the text.
• When sending their manuscripts, the authors are invited to include the necessary tables,graphs, photos and illustrations, along with their legends. Drawings and legends shouldbe carefully printed so as to be directly reproduced. Each illustration should be identifiedby a reference in order to be properly included in the text.
• References should be numbered in the order in which they appear in the text and referredto by Arabic numerals in brackets. They will be listed as follows:1. For a journal: the names and initials of all authors, full title of the article (in the originallanguage), name of the journal, year, volume, first and last page of the article.
2. For a book: name(s) and initials of the author(s), title of the book, name of the publisherand city, year of publication, pages corresponding to the quotation.
RECOMMANDATIONS AUX AUTEURS
• Tout travail destiné à la publication dans la Revue Internationale des Services de Santédes Forces Armées (RISSFA) doit être envoyé au Bureau de la rédaction :
Comité International de Médecine MilitaireHôpital Militaire Reine AstridBE - 1 120 Bruxelles (Belgique)
• Sont pris en considération les articles scientifiques, les analyses d’ouvrages ou d’articlesmédico-militaires, les comptes rendus de réunions, de congrès, d’événements scientifiqueset les annonces, rédigés en français et en anglais.
• Pour sa politique éditoriale, la RISSFA suit les directives de l’International Committee of MedicalJournal Editors (http://www.icmje.org/index.html). Les auteurs sont encouragés à adhérer à ces lignesdirectrices lors de la préparation et de la rédaction de leur article, aussi bien dans la méthodologieque dans la structure du manuscrit. Les auteurs seront informés des progrès de l’évaluation de leurmanuscrit. Les manuscrits en cours d’évaluation sont considérés comme confidentiels. En soumettantle manuscrit, l’auteur s’engage à accepter leur transfert de propriété au CIMM.
• Tous ces travaux doivent être accompagnés des noms, prénoms et adresses de tous lesauteurs, ainsi qu’un bref curriculum vitæ et photo (en haute résolution) de l’auteur principal.
• Les auteurs reconnaissent implicitement que l’article proposé n’a pas été envoyé enmême temps à d’autres journaux, ou qu’il n’a pas été publié récemment sous le même titre.
• La Direction de la RISSFA se réserve le droit de demander au signataire d’un article lajustification de sa qualité d’auteur.
• Toute reproduction partielle ou totale d’un article paru dans la RISSFA doit être soumiseà l’accord préalable de l’Editeur de cette dernière.
• Conflit d’intérêts potentiel. Pour s’assurer que les auteurs ne sont pas influencés par des tiersdans l’écriture de l’article, pour des raisons financières ou autres, et pour garantir la crédibilité dela publication, de l’auteur et de la science elle-même, la Direction de la RISSFA peut demander àcet effet, une « déclaration de conflit d’intérêts ». Cette déclaration devra faire mention dessoutiens financiers ayant pu influencer la liberté d’écriture ainsi que la possibilité d’accès auxdonnées utilisées pour la rédaction de l’article, les conflits d’intérêts avec les pairs ou laconcurrence. Les auteurs d'un manuscrit révéleront tous les contributeurs à leur travail.
• Vie privée et confidentialité. Les auteurs préserveront le droit à la vie privée et à la confidentialitéde tous les sujets humains impliqués dans leur manuscrit. Ils ne divulgueront pas d’informationspersonnelles, y compris des photographies de sujets à moins qu’ils ne possèdent et puissentmontrer une déclaration de consentement éclairé.
• Protection des sujets humains et animaux dans la recherche. Dans les manuscrits qui rapportentdes expériences sur des sujets humains, les auteurs devront indiquer si les procédures suiviesétaient conformes aux normes éthiques du comité responsable et avec la Déclarationd’Helsinki. Pour l’expérimentation animale, les auteurs devront indiquer si les règles légalesinstitutionnelles, nationales et autres pour l’utilisation d’animaux de laboratoire, ont été suivies.
• Autres dispositions. Les articles acceptés pour publication dans la RISSFA ne doivent pasêtre publiés ailleurs sans le consentement explicite du Rédacteur en chef. Les articles issusdes présentations lors des congrès et/ou des ateliers du CIMM devront en priorité êtrepubliés dans la RISSFA. Le CIMM ne paiera pour aucun article. Cependant, tous les deuxans, un article de haute qualité peut être récompensé par le prix « Jules Voncken », quicomprend une modeste somme d’argent.
• Le manuscrit sera dactylographié en double interligne, marge gauche de 3 cm, 35 lignes parpage, sur le recto seulement et n’excédera pas 25 pages, références bibliographiques comprises.Il sera envoyé, soit par e-mail à l’adresse suivante: [email protected], soit par voie postalesur CD-Rom accompagné d’une épreuve papier en format A4 (texte en Word, Arial 12).
• Un résumé ne dépassant pas 150 mots y sera incorporé. Il est souhaitable que ce résumé,y compris le titre de l’article, soit traduit en français et en anglais.
• Il est indispensable de fournir 3 à 5 mots-clés en français et en anglais afin de faciliterl’indexation de l’article.
• Les abréviations doivent être évitées dans le texte, sauf celles se rapportant aux unitésscientifiques de mesure, dûment acceptées (unités SI). Si d’autres abréviations sont utilisées,elles doivent être précédées de la terminologie complète à laquelle elles se rapportent,lorsqu’elles sont mentionnées dans le texte pour la première fois.
• Les auteurs sont invités à inclure, dans l’envoi de leur manuscrit, les tableaux, graphiques,photos et illustrations indispensables, accompagnés de leurs légendes. Les dessins etlégendes, soigneusement exécutés, devront pouvoir être reproduits directement. Chaquefigure sera identifiée par une mention permettant de l’inclure correctement dans le texte.
• Les références seront inscrites dans l’ordre dans lequel elles paraissent dans le texte etindiquées par des chiffres arabes, entre parenthèses. Elles seront mentionnées comme suit :1. Pour un périodique: nom et initiales des prénoms de tous les auteurs, titre de l’article (dans lalangue originale), nom du périodique, année, volume, page initiale et page finale de l’article.
2. Pour un livre : nom et initiales des prénoms du ou des auteurs, titre du livre, nom de lamaison d’édition, ville et année de publication, pages correspondant à la citation.
ADDRESS FOR SUBSCRIPTION
SUBSCRIPTIONS 2016International Review of the Armed Forces Medical Services
N.E.P.13, rue Portefoin - FR-75003 Paris, France
Tel. : +33 (0)1 40 27 88 88 - Fax : +33 (0)1 40 27 89 43E-mail : nep@wanadoo. fr
Credit Lyonnais : 7828 H - Paris Haxo (N.E.P.)
Subscription for one year : € 60Cost for a single copy : € 20
ADRESSE POUR LES ABONNEMENTS
ABONNEMENTS 2016Revue Internationale des Services de Santé des Forces Armées
N.E.P.13, rue Portefoin - FR-75003 Paris (France)
Tél. : +33 (0)1 40 27 88 88 - Fax : +33 (0)1 40 27 89 43E-mail : nep@wanadoo. fr
Crédit Lyonnais : 7828 H - Paris Haxo (N.E.P.)
Abonnement pour 1 an : € 60Prix du numéro ordinaire : € 20
I.S.S.N. : 0259-8582 Imprimerie dans l’Union européenne
Recommandations aux Auteurs_Mise en page 1 16/03/2016 09:55 Page1

OR
For Minimally Invasive
Open Abdominal Surgery
ImproveYour
Exposure732-602-7717 (USA) • [email protected] • www.ironintern.com

ZOLL continues its commitment to broadening its portfolio for the military. With the addition of new products via recent acquisitions, ZOLL has the most comprehensive solutions for military critical care. From monitoring and airway management to enhanced perfusion, ZOLL is focused on providing you with lifesaving technologies that are portable and effective throughout all echelons of care.
Propaq® M Monitor
The standard in vital signs monitoring, with optional defibrillation, pacing,
and Real CPR Help®
ResQPOD® ITD ResQGARD® ITD
Noninvasive impedance threshold devices (ITDs) that improve blood flow and reduce
intracranial pressure1,2
EMV+® 731 Series Ventilator
A rugged, lightweight ventilator with real altitude compensation for
all levels of care.
© 2015 ZOLL Medical Corporation, Chelmsford MA, USA. EMV +, ResQGARD, ResQPOD, and ZOLL are trademarks or registered trademarks of ZOLL Medical Corporation in the U.S.
and/or other countries. Propaq is a registered trademark of Welch Allyn. All other trademarks are the property of their respective owners. MCN MP 1506 0016-05
1Lurie KG, et al. J Med Soc Toho. 2012;59(6):304-315.2Convertino VA, et al. Resp Care. 2011;56(6):846-857.
Learn more about ZOLL’s resuscitation solutions at www.zoll.com/military
EXPANDING YOUR HORIZONS FOR ENROUTE CASUALTY CARE




















