EEG AND MEMORY EFFECTS OF LOW-DOSE INFUSIONS OF PROPOFOL
11
British Journal of Anaesthesia 1992; 69: 246-254 EEG AND MEMORY EFFECTS OF LOW-DOSE INFUSIONS OF PROPOFOLf R. A. VESELIS, R. A. REINSEL, M. WRONSKI, P. MARINO, W. P. TONG AND R. F. BEDFORD SUMMARY The purpose of this study was to identify EEG changes associated with low-dose propofol in- fusion producing only sedative effects, and to describe the memory effects of low-dose propofol infusion. Ten healthy volunteers underwent EEG monitoring (at F p C p P z and O z electrode sites) before, during and after propofol 0.5mg kg' 1 i.v. bolus and 75 fig kg~' min~'- as an infusion. Mean serum concentration of propofol during infusion was 0.86 (so 0.14) fig mt'. The EEG changed significantly during infusion, with increased power in the beta, (15-20 Hz). beta 2 (20.5-30 Hz) and delta (1-3.5 Hz) frequencies. Beta, and beta 2 power changes were most marked at the F z and C z electrodes. Subjects were sedated, but able to complete cognitive tasks. Visual analogue scales of attention and sleepiness were obtained throughout the study and demonstrated a sedative effect during propofol infusion, but were not a significant factor in memory performance or EEG changes. A verbal learning task (Rey Auditory-Verbal Learning Task) administered before, during and after infusion showed a marked reduction in short-term memory capacity and dramatically impaired free recall and recognition during infusion. Nine of 10 subjects had partial amnesia for complex visual scenes presented during infusion, recalling less than 50% of the mater/a/. Stronger cueing was required to retrieve information presented during propofol in- fusion, with an increase in mean retrieval time from 95.4 (41.2) s to 426.8 (83.1) s. EEG and memory effects resolved quickly after the end of infusion. We conclude that anterior, high frequency EEG activity increases significantly during low-dose propofol infusion and that propofol produces significant memory impairment which has charac- teristics of true amnesia, concurrent with changes in beta, power in the EEG. The fact that low-dose propofol produces significant changes in both cognitive and EEG measures warrants further in- vestigation into the utility of the EEG power spectrum as a useful monitor of amnesia during conscious sedation with propofol. KEY WORDS Anaesthetics, intravenous: propofol. Anaesthetic techniques: sedation. Memory: drug effects. Monitoring: electroencephal- ography. Propofol is used frequently for conscious sedation [1]. Schwilden, Stoeckel and Schuttler used the EEG to regulate administration of propofol at anaesthetic concentrations [2]. The EEG may be useful also as a monitor when propofol is admin- istered to produce sedation. Although several studies have investigated the EEG effects of propofol at anaesthetic concentrations [1-5], to our knowledge there have been no reports of the EEG effects of propofol at plasma concentrations associated with continued consciousness. Memory impairment, which may be either a true amnesic effect of propofol, or simply related to its sedative properties, has been described both during and shortly after administration of propofol [6-9]. Accordingly, the present investigation in volunteers was performed to assess the EEG and memory effects, if any, of low-dose propofol infusion. The EEG power spectrum was monitored using anterior to posterior midline electrodes to assess both the time and topographic effects of propofol on the EEG. To elucidate the memory effects of propofol, and to demonstrate that the infusion resulted in a clinically relevant degree of sedation, memory im- pairment was assessed using timed, cued recall of complex visual scenes and recall on a standardized word memorization task—the Rey Auditory-Verbal Learning Test. Visual analogue scales were used to assess the degree of sedation, and blood samples were analysed for plasma concentrations of propofol. METHODS EEG data and other measurements were obtained before (baseline), and during, and 8 and 50-60 min after infusion of propofol. The EEG was recorded continuously during the infusion. A timetable of tests and measurements made during the study is shown in table I. ROBERT A. VESELIS, M.D., RUTH A. REINSEL, PH.D., MAREK WRONSJU, M.D., PAOLA MARINO, M.D. (Department of Anes- thcsiology & Critical Care Medicine); WILLIAM P. TONG, PH.D. (Pharmacology Analytical Core Laboratory); Memorial Sloan- Kettering Cancer Center, 1275 York Avenue, New York, NY 10021, U.S.A. ROBERT F. BEDFORD, M.D., Department of Anes- thesiology, University of Virginia Medical School, P.O. Box 1321, Charlottesville, VA 22902, U.S.A. Accepted for Publi- cation: March 23, 1992. t Parts of this paper were presented to the American Society of Anesthesiologists, San Francisco, October 28-30, 1991. by guest on October 20, 2016 http://bja.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of EEG AND MEMORY EFFECTS OF LOW-DOSE INFUSIONS OF PROPOFOL
British Journal of Anaesthesia 1992; 69: 246-254
EEG AND MEMORY EFFECTS OF LOW-DOSE INFUSIONS OFPROPOFOLf
R. A. VESELIS, R. A. REINSEL, M. WRONSKI, P. MARINO, W. P. TONG ANDR. F. BEDFORD
SUMMARY
The purpose of this study was to identify EEGchanges associated with low-dose propofol in-fusion producing only sedative effects, and todescribe the memory effects of low-dose propofolinfusion. Ten healthy volunteers underwent EEGmonitoring (at Fp Cp Pz and Oz electrode sites)before, during and after propofol 0.5mg kg'1 i.v.bolus and 75 fig kg~' min~'- as an infusion. Meanserum concentration of propofol during infusionwas 0.86 (so 0.14) fig mt'. The EEG changedsignificantly during infusion, with increased powerin the beta, (15-20 Hz). beta2 (20.5-30 Hz) anddelta (1-3.5 Hz) frequencies. Beta, and beta2
power changes were most marked at the Fz andCz electrodes. Subjects were sedated, but able tocomplete cognitive tasks. Visual analogue scales ofattention and sleepiness were obtained throughoutthe study and demonstrated a sedative effect duringpropofol infusion, but were not a significant factorin memory performance or EEG changes. A verballearning task (Rey Auditory-Verbal Learning Task)administered before, during and after infusionshowed a marked reduction in short-term memorycapacity and dramatically impaired free recall andrecognition during infusion. Nine of 10 subjectshad partial amnesia for complex visual scenespresented during infusion, recalling less than 50%of the mater/a/. Stronger cueing was required toretrieve information presented during propofol in-fusion, with an increase in mean retrieval time from95.4 (41.2) s to 426.8 (83.1) s. EEG and memoryeffects resolved quickly after the end of infusion.We conclude that anterior, high frequency EEGactivity increases significantly during low-dosepropofol infusion and that propofol producessignificant memory impairment which has charac-teristics of true amnesia, concurrent with changesin beta, power in the EEG. The fact that low-dosepropofol produces significant changes in bothcognitive and EEG measures warrants further in-vestigation into the utility of the EEG powerspectrum as a useful monitor of amnesia duringconscious sedation with propofol.
KEY WORDS
Anaesthetics, intravenous: propofol. Anaesthetic techniques:sedation. Memory: drug effects. Monitoring: electroencephal-ography.
Propofol is used frequently for conscious sedation[1]. Schwilden, Stoeckel and Schuttler used theEEG to regulate administration of propofol atanaesthetic concentrations [2]. The EEG may beuseful also as a monitor when propofol is admin-istered to produce sedation. Although several studieshave investigated the EEG effects of propofol atanaesthetic concentrations [1-5], to our knowledgethere have been no reports of the EEG effects ofpropofol at plasma concentrations associated withcontinued consciousness.
Memory impairment, which may be either a trueamnesic effect of propofol, or simply related to itssedative properties, has been described both duringand shortly after administration of propofol [6-9].Accordingly, the present investigation in volunteerswas performed to assess the EEG and memoryeffects, if any, of low-dose propofol infusion. TheEEG power spectrum was monitored using anteriorto posterior midline electrodes to assess both thetime and topographic effects of propofol on theEEG. To elucidate the memory effects of propofol,and to demonstrate that the infusion resulted in aclinically relevant degree of sedation, memory im-pairment was assessed using timed, cued recall ofcomplex visual scenes and recall on a standardizedword memorization task—the Rey Auditory-VerbalLearning Test. Visual analogue scales were used toassess the degree of sedation, and blood sampleswere analysed for plasma concentrations of propofol.
METHODS
EEG data and other measurements were obtainedbefore (baseline), and during, and 8 and 50-60 minafter infusion of propofol. The EEG was recordedcontinuously during the infusion. A timetable oftests and measurements made during the study isshown in table I.
ROBERT A. VESELIS, M.D., RUTH A. REINSEL, PH.D., MAREKWRONSJU, M.D., PAOLA MARINO, M.D. (Department of Anes-thcsiology & Critical Care Medicine); WILLIAM P. TONG, PH.D.(Pharmacology Analytical Core Laboratory); Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY10021, U.S.A. ROBERT F. BEDFORD, M.D., Department of Anes-thesiology, University of Virginia Medical School, P.O. Box1321, Charlottesville, VA 22902, U.S.A. Accepted for Publi-cation: March 23, 1992.
t Parts of this paper were presented to the American Society ofAnesthesiologists, San Francisco, October 28-30, 1991.
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from
PROPOFOL, EEG AND MEMORY 247
TABLE I. Timetable of experimental procedures in the baseline,infusion and recovery conditions. Times are calculated from thebeginning of the propofol infusion (time = 0). The average duration ofinfusion was 42.5 (SD 3.9) min. During the infusion, EEG wasrecorded continuously for 18—30 min. Times given for the Rey AVLTare the onset of testing; the test takes approximately 12 min to
administer
Condition
Baseline
Infusion
After infusion
Procedure
Rey AVLT, No. 1EEG, No. 1.Visual memory, No. 1Delayed recall, No. 1Rey AVLT, No. 2Visual memory, No. 2Delayed recall, No. 2EEG, No. 2Visual memory, No. 3Rey AVLT, No. 3EEG, No. 3Delayed recall, No. 3Questioning for recall ofvisual memory pictures
EEG, No. 4Recognition of all word lists
Time relativeto infusion start
(min)
- 6 844
- 1 7- 1 1+ 7
+ 38+ 45+ 50+ 70+ 72+ 96
+ 156+ 160
+ 205+ 240
SubjectsAfter obtaining local Ethics Committee approval
and informed consent, we studied 10 paid adultvolunteers (seven male) of mean age 34.4 yr (range21—41 yr). Subjects were screened for medical andneurological abnormalities and had nothing bymouth for at least 6 h before the study. Subjects werenot allowed any caffeine on the day of the study.
InfusionAfter an initial bolus of 0.5 mg kg"1, propofol was
infused i.v. at 75 ug kg"1 min"1 until a total dose of3.5 mg kg"1 was administered. The period of infusionlasted 40-45 min. During the infusion, subjectsexperienced a state of drowsiness, but were readilyresponsive to verbal commands and easily able tofollow directions for cognitive tests.
EEG recording and analysisEEG monitoring was performed with a Tracor-
Northern Nomad 3400 EEG monitor (Middleton,WI, U.S.A.). Following the International 10-20electrode system [10], Grass gold cup electrodessecured with collodion were placed at F r, C,, Px andOz, referenced to linked mastoids (A1-A2). The skinwas prepared using Omni-Prep; electrode impedancewas less than 5000 Q during the study. Subjects weregiven specific instructions not to open their eyes, talkor move during EEG recording in order to avoidartefacts. Subjects were monitored visually by theinvestigators at all times to ensure compliance withthese instructions. All EEG recordings were per-formed while subjects had their eyes closed, whetherthey were sedated or not; this was intended to reducethe artefactual contribution of eye movements topower in the delta band. The analogue EEG signalwas acquired using a sensitivity of ± 50 uV, withon-line artefact rejection of signals exceeding 99 %of the full scale deflection of 100 uV. High- and low-
pass niters were set for 1 and 30 Hz, respectively(filter roll-off of 12 db/octave for activity at greaterthan 30 Hz) and a notch filter (58-62 Hz) was used toeliminate extraneous 60-Hz electrical noise.Additionally, the analogue EEG signal was inspectedfrequently to check for the presence of artefact. TheEEG power spectrum was computed on each 2-sepoch using a Fast Fourier Transform algorithm.
Segments of the EEG power spectrum lasting4.26 min (128 epochs), representing baseline, in-fusion and early (+ 8 min) and late (+ 50 to+ 60 min) post-infusion periods were chosen foranalysis. The continuous EEG record obtainedduring infusion was inspected visually and artefact-free segments were chosen from the beginning(5 min) and end (20 min) of the propofol infusion.These two EEG segments were compared by pairedt test on all EEG variables at all electrode positions.As no significant differences were found, the twoinfusion segments were averaged for statisticalcomparison with the other experimental conditions.
The power spectrum of these EEG segments wasanalysed using software developed by one of us(R.A.V.) and verified against the data analysisprovided by Tracor-Northern with the Nomad EEGmonitor. (Comparison between 29272 EEG datapoints was performed between values produced byour software and software provided by Tracor-Northern with the Nomad EEG monitor. Overallcorrelation was 0.990 (P < 0.00001). Correlations ofdata values in specific EEG bands were as follows:delta r = 0.992, theta r = 0.974, alpha r = 0.983,beta! r = 0.99, beta2 r = 0.998.) The following EEGvariables were analysed: absolute power in thefrequency bands delta (1-3.5 Hz), theta (4-7.5 Hz),alpha (8-12 Hz), betax (15-20 Hz) and beta2 (20.5-30 Hz); total power in the 1-30 Hz range, and thefrequencies marking the 50th percentile (medianfrequency) and the 95th percentile (spectral edge) ofthe total EEG power distribution. With the ex-ception of the percentile measures, the data were log-transformed before statistical analysis to producenormality and satisfy the assumptions of the analysisof variance [11].
Measurement of memory impairmentAdministration of word lists. The Rey Auditory-
Verbal Learning Test (Rey AVLT) is a standardizedverbal learning task [12]. It consists of a list of 15common words (the primary list) presented fivetimes in sequence, to assess learning over trials (trialsL1-L5). After each presentation of the word list, thesubject is given 1 min to recall as many of the wordsas possible. Without warning, a new list is presentednext, and the subject is asked to recall as many of thenew words as possible (trial INT). This new list,which is presented only once, assesses short-termmemory capacity for a new word list, and interfereswith recall of the previously learned words. Withoutpresenting the stimulus words again, immediate anddelayed recall of the primary word list is elicitedfrom the subject (trials IR and DR). Performanceon these latter trials reflects long-term memoryfunction.
Three semantically equivalent versions of the Rey
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from
248
AVLT were administered. Lists were given incounterbalanced order, so that the list given duringinfusion was different from those given at baseline orrecovery. Recognition of all words presented duringthe study was tested approximately 3.5 h after theend of the infusion.
Visual stimuli. Subjects were shown three differentgroups of five pictures each before, during and25 min after the infusion. Pictures consisted of full-colour 20 x 28-cm magazine photographs and adver-tisements. Subjects were shown each picture for 30 sand asked to describe it aloud, to ensure that anadequate stimulus for memory had been given.Notes were made of the subject's comments on eachpicture. About 2 h after the end of infusion, subjectswere asked to recall each of the three sets of pictures.Two minutes was allowed for spontaneous recall foreach group of five pictures. If the subject failed torecall any picture spontaneously (spont.), a standard-ized hint (hint) was given and a further 20 s wasallowed for recall for each picture. If recall againfailed, a hint drawn from the subject's own commentson originally viewing the picture was given (assoc),and a further 20 s allowed for recall. If this did notprompt recall, the picture in question was presentedfor recognition, with four distractor pictures (recog.).
The total time (in seconds) before the picture wasrecalled or recognized by the subject was measuredusing a stopwatch, which was stopped while theinvestigators gave verbal cues to the subject. Recallwas scored on an all or none basis, and the total timeto recall or recognize each picture (retrieval latencytime) was recorded. The maximal retrieval latencytime possible was 480 s if the subject could not recallor recognize any picture in a five-picture group. Thecue level needed for recall was recorded for eachpicture.
Blood samples
Eleven samples of venous blood were taken from
4.0 -,
3.0 -
IIoQ.CDO
2.0 -
1.0 -
0.0 -
BRITISH JOURNAL OF ANAESTHESIA
the antecubital vein in the arm contralateral to thesite of propofol infusion. Each 8-ml sample wascollected in a heparinized tube and centrifuged at3900 g for 7 min. Plasma was separated and stored at— 20 °C. Plasma concentrations of propofol weremeasured using high pressure liquid chromat-ography (HPLC).
Plasma propofol assay
Equipment. The modular HPLC system consistedof a SP8810 isocratic pump with a SP8775 auto-sampler and a SP4290 integrator with a WINnerchromatography station (Spectra-Physics, San Jose,CA). The eluent was monitored using a fluorescencedetector, model RF535 by Shimadzu (Columbia,MD).
Procedure. The concentration of propofol inplasma was measured by HPLC based on the methodof Vree, Barrs and DeGrood [13]. Briefly, to onevolume of plasma, two volumes of acetonitrile wereadded and allowed to stand in refrigerator overnight.The precipitant was removed by centrifugation and50 |il of the supernatant was analysed by HPLCusing an Econosphere C-18, 5-um, 4.6x250-mmcolumn by Alltech Associates (Deerfield, IL) with amobile phase of 70% acetonitrile-potassium di-hydrogenphosphate 50 mmol litre"1 with 0.02% v/vtriethylamine (HPLC grade, Fisher Scientific). Theflow rate was 1 ml min"1 and the eluent was moni-tored by a fluorescence detector with excitationwavelength 275 nm and emission wavelength of310 nm [14]. The standard curve was prepared byusing spiked plasma, which gave good recovery. Forexample, on the same day the spiked plasma standardcurve was jy = 269*+ 0.25 (r2 = 0.999), while thespiked mobile phase standard curve was y =257x-4.6 (r2 = 0.999). The limit of detection was2.5 ng. Plasma drug concentration was calculatedusing a standard curve generated by the linearregression function of Lotus 123.
•3 .0
2.0 —co
1.0
cIDUcoO
• 0.0
50 100 150
Time (min)
200
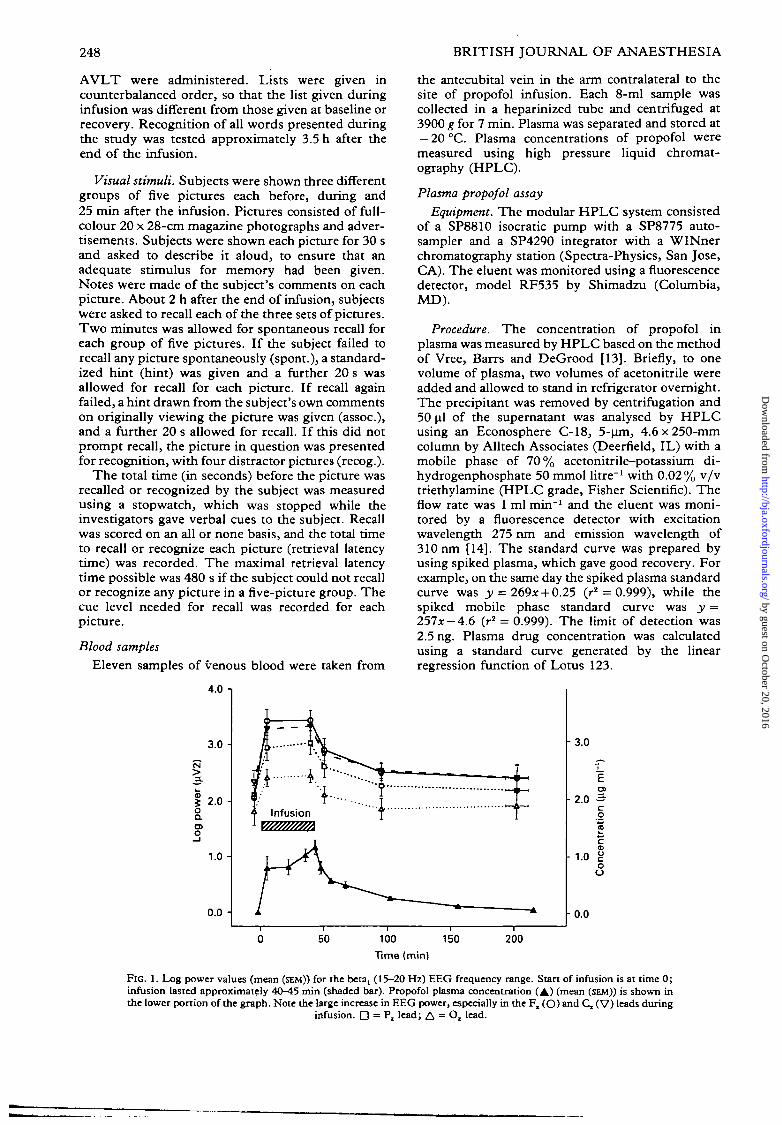
FIG. 1. Log power values (mean (SEM)) for the beta, (15—20 Hz) EEG frequency range. Start of infusion is at time 0;infusion lasted approximately 40-45 min (shaded bar). Propofol plasma concentration (A) (mean (SEM)) is shown inthe lower portion of the graph. Note the large increase in EEG power, especially in the F. (O) and C, (V) leads during
infusion. D = P, lead; A = O, lead.
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from
PROPOFOL, EEG AND MEMORY 249
Visual analogue scalesVisual analogue scales (VAS) of sleepiness and
attention were obtained throughout the study.Subjects indicated their current state with a verticalmark on a 15-cm line between two anchored end-points (very wide awake...very sleepy; cannotconcentrate at all...can concentrate fully). Thedistance between the low end of the scale and thesubject's mark was measured in centimetre. Thethree ratings taken during baseline were averaged.VAS measures taken concomitantly with the EEGsamples were compared using repeated measuresanalysis of variance (ANOVA).
Statistical analysisData from the four experimental conditions were
analysed using the SAS software package (Release6.03, SAS Institute Inc., SAS Circle, Box 8000,Cary N.C. 27512-8000). Average values are ex-pressed as mean (SD). Simple (Pearson) and partialcorrelations were computed between VAS self-ratings, memory scores and plasma concentrations ofpropofol.
A 4 x 4 (four conditions, four channels) repeatedmeasures analysis of variance (ANOVA) was per-formed for each EEG variable (across experimentalcondition, electrode site and the condition x siteinteraction) at baseline, during infusion and at thetwo post-infusion times. Planned orthogonal con-trasts (a priori, statistically independent compari-sons) were computed between adjacent electrodesites and between the following data pairs: baselineand infusion, infusion and 8 min after infusion,infusion and 60 min after infusion. Because of thesmall sample size, P values < 0.01 were taken assignificant. Post-hoc paired t tests were computedbetween baseline and 8 and 60 min after infusion todetermine if the EEG variables had returned tobaseline at these times. P < 0.001 was consideredsignificant for post-hoc paired t tests, using theBonferroni correction for multiple comparisons.
RESULTS
EEG changes during propofol infusion
During infusion, significant increases in power inthe beta! (P = 0.01) (fig. 1), beta2 (P = 0.002) anddelta (P = 0.004) bandwidths occurred (table II).Alpha, theta and total power (1-30 Hz) did notchange significantly. Spectral edge and medianfrequencies at F,, both increased by about 3 Hz frombaseline (P < 0.0001) (table II). There were nosignificant differences for any EEG variable betweenbaseline values and those obtained 8 and 60 min afterinfusion.
Effects of electrode location
There were significant differences in EEG powerand frequency values between the four electrodesites, except for F, and Q (table II). The changes inbeta! and beta2 power were greatest in the frontal andcentral areas (fig. 1). The changes in delta powerwere greatest in the occipital area. Median andspectral edge frequencies snowed a trend similar tothe changes in high frequency EEG power (P =0.05), but did not meet the Bonferroni criterion forsignificance.
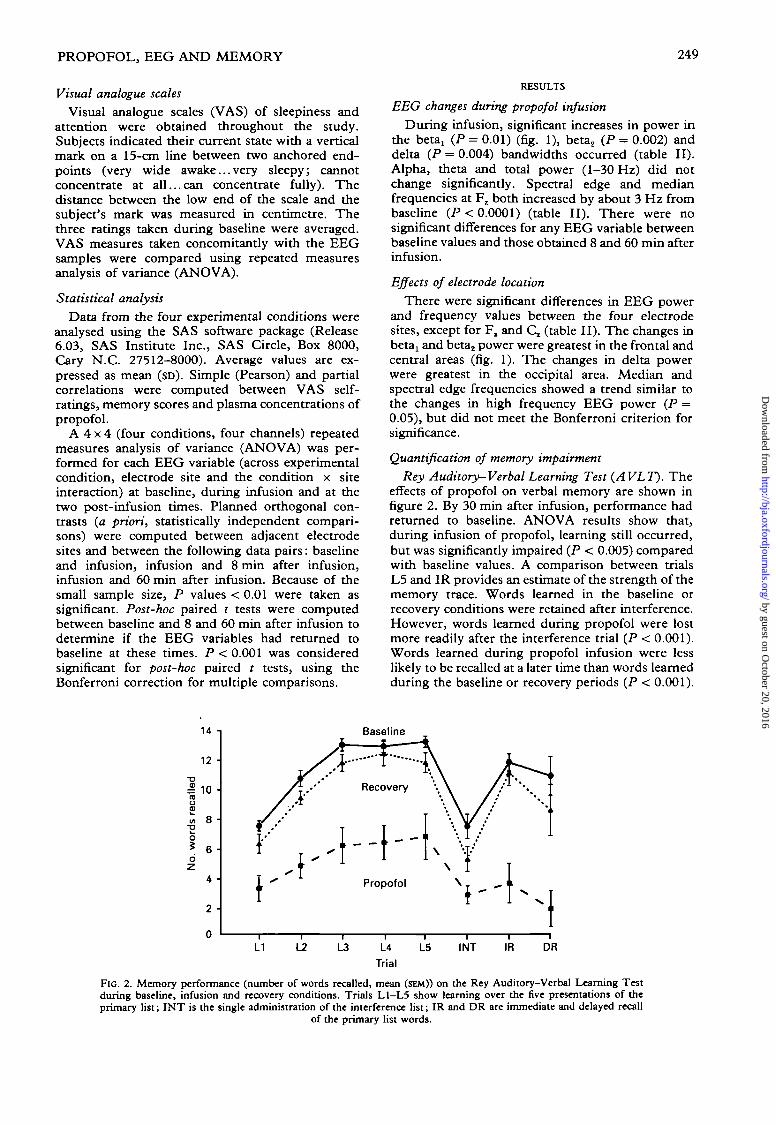
Quantification of memory impairmentRey Auditory-Verbal Learning Test (AVLT). The
effects of propofol on verbal memory are shown infigure 2. By 30 min after infusion, performance hadreturned to baseline. ANOVA results show that,during infusion of propofol, learning still occurred,but was significantly impaired (P < 0.005) comparedwith baseline values. A comparison between trialsL5 and IR provides an estimate of the strength of thememory trace. Words learned in the baseline orrecovery conditions were retained after interference.However, words learned during propofol were lostmore readily after the interference trial (P < 0.001).Words learned during propofol infusion were lesslikely to be recalled at a later time than words learnedduring the baseline or recovery periods (P < 0.001).
1 4 -i
1 2 •
rou£to
•p
o5
8 •
4 •
2 -
Baseline
¥
L1 L2 L3 L4
Trial
L5 INT IR DR
FIG. 2. Memory performance (number of words recalled, mean (SEM)) on the Rey Auditory-Verbal Learning Testduring baseline, infusion and recovery conditions. Trials L1-L5 show learning over the five presentations of theprimary list; INT is the single administration of the interference list; IR and DR are immediate and delayed recall
of the primary list words.
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from

250 BRITISH JOURNAL OF ANAESTHESIA
TABLE II. EEG power (log (jiVTj) spectral edge and median frequency (Hz) by experimental condition and electrode (mean(SD)). CN = ANOVA P value across condition; EL <= ANOVA P value across electrode; CxE = ANOVA P valuecondition by electrode interaction. P values for orthogonal contrast vs infusion condition (inf.) and post-hoc paired t testsvs baseline (B) are given below each column. * EEG power different (P < 0.01) from adjacent electrode (F, vsC,;C, vs P,;
/>, vs Ot)
Beta, (log (nV2))F ,
*c.*P,o,CN = 0.0092EL = 0.0001C x E = 0.0002
Beta, Gog (uV2))F ,
*c.*P,orCN = 0.0002EL = 0.0001C x E — ns
Delta (log 0iV2))F r
c.P,oxCN = 0.0013EL = 0.0001C x E = 0.0003
Theta Gog (nV2))F%
c.*P,o,CN = nsEL = 0.0001CxE = ns
Alpha (log (uV2))F ,
c,*Pr
o,CN = nsEL = < 0.05CxE = ns
Total power (log(MV2))
F,c,*P.o,CN = nsEL = 0.0002CxE = ns
Spectra] edge(95%) (Hz)
F ,
*c,P,
o.CN = 0.0001EL = < 0.05C x E = < 0.05
Median freq.(50%) (Hz)
F ,
c.P,
o,CN = 0.0001EL = nsC x E = 0.0076
Baseline
2.28 (0.70)2.35 (0.72)2.17(0.75)1.78(0.84)
0.0141 vsinf.
1.98(0.72)2.17(0.66)1.74(0.78)1.24(1.00)
0.0021 vs inf.
3.97 (0.69)3.58 (0.49)3.30 (0.42)2.68 (0.45)
0.0037 vs inf.
3.43 (0.53)3.36 (0.54)3.10(0.54)2.47 (0.50)
ns vs inf.
3.67 (0.76)3.82 (0.79)3.98 (0.84)3.60(0.88)
ns vs inf.
5.08 (0.55)4.99 (0.54)4.88 (0.60)4.44(0.61)
ns vs inf.
20.0 (2.82)20.9 (2.96)19.4(2.95)19.3(3.23)
0.0001 vs inf.
6.41 (1.83)7.61 (1.44)8.27(1.32)8.75(2.18)
0.0001 vs inf.
Infusion
3.48 (0.63)3.40 (0.55)3.11(0.67)2.47 (0.46)
3.21 (0.53)3.07 (0.46)2.55(0.61)1.95(0.51)
4.23 (0.46)3.84 (0.40)3.63 (0.52)3.59 (0.44)
3.26 (0.50)3.09 (0.33)2.96 (0.40)2.44 (0.27)
3.50(0.42)3.56(0.46)3.53 (0.49)3.16(0.64)
5.38(0.35)5.19(0.29)5.02 (0.38)4.67 (0.28)
23.1(1.41)23.4(1.37)22.0(1.83)21.0(1.76)
9.26(2.81)10.0(2.17)9.59 (2.30)8.98(1.50)
After infusion (min)
8
2.93 (0.69)2.89 (0.59)2.69 (0.63)2.09 (0.50)
0.006 lw inf.ns vs B
2.42 (0.82)2.42 (0.58)1.94(0.70)1.19(0.54)
0.0005 vs inf.ns vs B
3.65 (0.64)3.44 (0.62)3.27 (0.55)3.03 (0.74)
• 0.0042 vs inf.nstiiB
2.94 (0.48)2.90 (0.47)2.80(0.51)2.22(0.51)
ns vs inf.nstuB
3.56 (0.65)3.76 (0.69)3.86 (0.85)3.38 (0.83)
ns vs inf.ns vs B
4.96 (0.48)4.94 (0.42)4.90 (0.53)4.48 (0.47)
ns vs inf.n s w B
21.7(2.89)21.7(2.01)19.8(2.50)19.3(2.33)
0.0001 vs inf.n s m B
8.74 (2.91)8.86(1.67)9.09(1.47)8.96(1.35)
0.0001 vs inf.ns TO B
60
2.49(0.51)2.56 (0.52)2.34 (0.60)1.84(0.65)
0.0054 vs inf.ns vs B
1.96(0.49)2.11(0.40)1.61 (0.47)1.03(0.50)
0.0001 vs inf.ns m B
3.90(0.62)3.69 (0.46)3.37 (0.47)2.85 (0.32)
0.0027 vs inf.n i w B
3.39 (0.52)3.41 (0.48)3.19(0.48)2.57(0.42)
ns vs inf.ns vs B
3.67(0.73)3.82(0.77)3.97 (0.87)3.52 (0.95)
ns vs inf.ns vs B
5.06 (0.48)5.05(0.41)4.93 (0.55)4.43 (0.57)
ns vs inf.ns vs B
20.0 (3.00)20.3 (2.48)19.1 (2.33)19.0(2.73)
0.0001 vs inf.n s w B
6.92(1.83)7.53(1.23)8.23(1.30)8.59(1.38)
0.0001 vs inf.ns vs B
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from
PROPOFOL, EEG AND MEMORY 251
TABLE III. Number of words recognized (mean (SD)) on delayedrecognition trial of Rey AVLT, by word list within experimental
condition
Primary list Interference list
BaselineInfusionRecovery
13.5(1.4)2.8(3.7)
13.7(1.2)
5.7(3.2)0.6(1.6)4.5(3.2)
Results of the recognition test are shown in tableIII. Nearly all (90%) of the 15 words presented onthe primary list in the baseline and recoveryconditions were recognized by the subjects. Wordspresented only once were less likely to be recognized(38 % of the interference list words). However, only18.7% of the primary list words and 4% of theinterference list words presented during propofolcould be recognized. These differences betweenlists and experimental conditions are significant(P < 0.001) by repeated measures ANOVA.
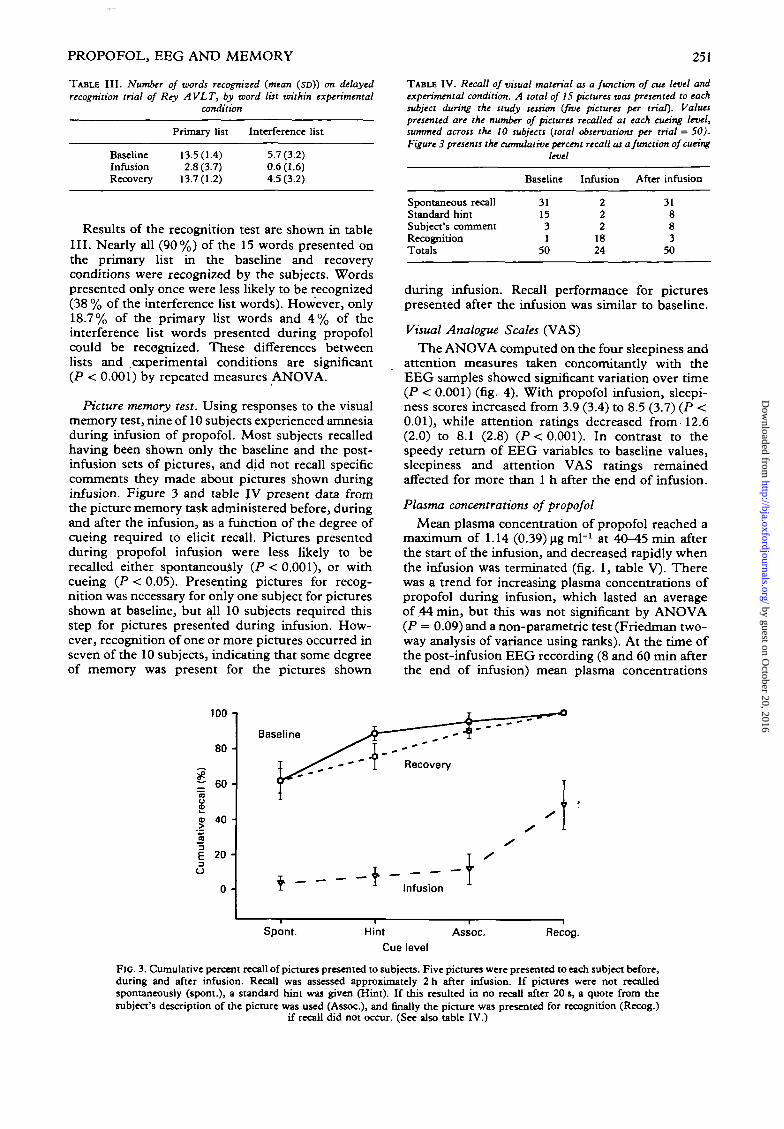
Picture memory test. Using responses to the visualmemory test, nine of 10 subjects experienced amnesiaduring infusion of propofol. Most subjects recalledhaving been shown only the baseline and the post-infusion sets of pictures, and did not recall specificcomments they made about pictures shown duringinfusion. Figure 3 and table JV present data fromthe picture memory task administered before, duringand after the infusion, as a function of the degree ofcueing required to elicit recall. Pictures presentedduring propofol infusion were less likely to berecalled either spontaneously (P < 0.001), or withcueing (P < 0.05). Presenting pictures for recog-nition was necessary for only one subject for picturesshown at baseline, but all 10 subjects required thisstep for pictures presented during infusion. How-ever, recognition of one or more pictures occurred inseven of the 10 subjects, indicating that some degreeof memory was present for the pictures shown
TABLE IV. Recall of visual material as a function of cue level andexperimental condition. A total of 15 pictures was presented to eachsubject during the study session (five pictures per trial). Valuespresented are the number of pictures recalled at each cueing level,summed across the 10 subjects (total observations per trial = 50).Figure 3 presents the cumulative percent recall as a function of cueing
level
Baseline Infusion After infusion
Spontaneous recallStandard hintSubject's commentRecognitionTotals
311531
50
222
1824
31883
50
during infusion. Recall performance for picturespresented after the infusion was similar to baseline.
Visual Analogue Scales (VAS)
The ANOVA computed on the four sleepiness andattention measures taken concomitantly with theEEG samples showed significant variation over time(P < 0.001) (fig. 4). With propofol infusion, sleepi-ness scores increased from 3.9 (3.4) to 8.5 (3.7) (P <0.01), while attention ratings decreased from 12.6(2.0) to 8.1 (2.8) (P< 0.001). In contrast to thespeedy return of EEG variables to baseline values,sleepiness and attention VAS ratings remainedaffected for more than 1 h after the end of infusion.
Plasma concentrations of propofol
Mean plasma concentration of propofol reached amaximum of 1.14 (0.39) ug ml"1 at 40-45 min afterthe start of the infusion, and decreased rapidly whenthe infusion was terminated (fig. 1, table V). Therewas a trend for increasing plasma concentrations ofpropofol during infusion, which lasted an averageof ,44 min, but this was not significant by ANOVA(P = 0.09) and a non-parametric test (Friedman two-way analysis of variance using ranks). At the time ofthe post-infusion EEG recording (8 and 60 min afterthe end of infusion) mean plasma concentrations
100 -i
80 -
l e oCD
2£D 4 0
I 20o
0 -
Baseline
Recovery
Spont. Hint Assoc. Recog.Cue level
FIG. 3. Cumulative percent recall of pictures presented to subjects. Five pictures were presented to each subject before,during and after infusion. Recall was assessed approximately 2 h after infusion. If pictures were not recalledspontaneously (spont.), a standard hint was given (Hint). If this resulted in no recall after 20 s, a quote from thesubject's description of the picture was used (Assoc.), and finally the picture was presented for recognition (Recog.)
if recall did not occur. (See also table IV.)
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from

252 BRITISH JOURNAL OF ANAESTHESIA
15 -
14
13 -
12 -
11 -
10 -
9 -
8 -
7 -
6 -
5 -
4 -
3 -
2 -
1 -
0
W////////A
-50 50 150 200 250100Time (min) "
FIG. 4. Sleepiness (# ) increased and attention (A) decreased significantly during infusion (time 0 = start of infusion),but returned to baseline values within 1 h of the end of infusion. These scores lagged behind the return to baseline
of the cognitive and EEG changes.
had decreased to 0.67 (0.23) |ig ml"1 and 0.26(0.08) ug ml"1, respectively. Two subjects had sub-stantially greater plasma concentrations than others,and this skewed the distribution of drug concentra-tions. The mean plasma concentration of propofolduring the infusion EEG recordings was 0.86(0.45) ng ml"1 (median 0.66 ug ml"1).
Relationships among EEG beta! power, memoryperformance, sedation ratings dnd plasma propofolconcentration
Linear regressions were computed to predictmemory scores on the Rey AVLT from plasmapropofol concentrations, sleepiness ratings and vari-ous EEG measures. Log betax power was thestrongest predictor of final learning (P < 0.05),immediate (P < 0.01) and delayed (P < 0.01) recalland delayed recognition (P < 0.01). Plasma propofolconcentrations at the time of learning predictedimmediate recall (P < 0.05) and delayed recognition(P < 0.05). Sleepiness ratings were ineffective aspredictors of memory performance.
Pearson correlations were computed between EEGpower at Fz and the recall and recognition
scores on the Rey AVLT. In the infusion condi-
TABLE V. Plasma concentrations ofpropofol (mean (SEM)). Samplingtime is relative to the start of infusion. The infusion lasted an average
of 42.5 min
ConditionSample
No.Time(min)
Propofol cone,(ug ml"1)
tion, correlations approach significance (r = —0.6,P < 0.10), with increasing betax power being associ-ated with decreasing memory. Lack of statisticalsignificance was most probably attributable to thesmall sample size. The correlation between log betajpower at Fz and plasma propofol concentrations was0.36 (ns) during infusion, and 0.17 (ns) during thepost-infusion memory test, indicating a variableindividual response of EEG betat power to a givenplasma concentration of propofol. Subjects' VASratings of sleepiness and concentration were nega-tively related (r = — 0.52, P < 0.05). Correlationsbetween subjects' VAS ratings of sleepiness andconcentration and the memory scores from the ReyAVLT were low and non-significant (0.0 < r < 0.2).The correlations of memory scores with plasmaconcentration of propofol were higher, about r =-0.5 (P < 0.05) for overall learning and r = -0.4(P = 0.07) for immediate recall. To determine if therelationship between memory and plasma concentra-tions was mediated by a sedation effect, we used the
TABLE VI. Simple (Pearson) and partial correlations (r) betweenlearning (LS) and recall (IR, DR) scores on the Rey AVLT, VASself-ratings of sleepiness, and plasma concentration ofpropofol. VASself-ratings taken immediately before and after the Rey A VL T wereaveraged to yield a single data point for the computation. Correlationsare computed over the full range of plasma concentrations for drugand recovery conditions combined. The partial correlation removesthe overlapping or shared variance between sleepiness and drugconcentrations, and expresses the independent relationship of plasmaconcentration with memory scores. Note that the strength of thecorrelation between plasma concentration and memory is not changed
by the removal of the sleepiness variance. fP < 0.10; *P < 0.05
BaselineInfusion
After infusion
1234
D6789
1011
-376
2336AA
485668
103156216
00.77(0.20)0.80(0.14)1.01 (0.11)1 1 A fC\ 1 "W1.1** ^U. 1 j)0.78(0.11)0.55 (0.05)0.48 (0.06)0.25 (0.03)0.12 (0.02)0.07 (0.01)
SimpleSleepinessPlasma concn.
PartialPlasma concn.(sleepiness removed)
Rey
L5
0.11-0.49*
-0.49*
AVLT trial
IR
0.02-0.41t
-0.41f
W
DR
0.04-0.27
-0.27
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from
PROPOFOL, EEG AND MEMORY 253
technique of partial correlation to obtain an in-dependent estimate of the relation between memoryperformance and plasma concentrations after stat-istically removing the influence of sedation scores.Even when the sleepiness rating is thus statistically"partialled out", the correlation of learning withplasma concentration is not changed (partial r =-0.49, P < 0.05) (table VI). This finding indicatesthat the memory impairment seen with propofol isstatistically independent of sedation effects.
DISCUSSION
Propofol administered in sedative doses had asignificant effect on the EEG which was not onlystatistically significant, but was readily appreciatedby visual inspection of the density spectral array(DSA) display. We found that propofol infusion inthese doses caused a significant increase in highfrequency beta power, most notably in the anteriorleads, and a less evident increase in low frequencydelta power. The changes in high frequency EEGpower are reflected in both the spectral edge andmedian frequencies. Both values changed equally,but the change in median frequency was pro-portionally much larger with respect to baselinevalues. The changes in median frequency may bemore readily appreciated than those in the spectraledge frequency; however, variability between sub-jects also tended to be greater for the medianfrequency measure. The EEG changes associatedwith propofol infusion resolved quickly after theinfusion was stopped, and 8 min after the end ofinfusion the EEG had returned to baseline.
The increase in delta power, which may representa sedative effect, is consistent with the previouslyreported EEG effects during propofol anaesthesia,which report onset of slow wave activity in the deltafrequency range. Kearse and Fahmy report a markedslowing of the EEG, characterized by 1-2 Hz high-amplitude waves, within 1 min of a bolus of propofol2.5 mg kg"1 i.v. [3]. Many agents in anaestheticconcentrations cause increased delta activity, andthis effect is unlikely to be specific for propofol atanaesthetic blood concentrations [15]. However, wefound this effect occurred with doses of propofol thatresulted in sedation only, when the plasma concen-tration was of the order of 0.5-1 ug ml"1. Highfrequency elements in the alpha and beta frequencyrange have been described during induction andmaintenance of anaesthesia with propofol. Kearseand Fahmy described an alpha spindle-like patternduring infusion of propofol 100-200 ug kg"1 min"1.However, nitrous oxide, which itself can cause highfrequency EEG activity, was used with the propofol[16]. Borgeat and co-workers found that 5-10 s aftera bolus dose of propofol 3 mg kg"1 i.v., beta wavesappeared transiently and were followed by lowfrequency delta waves [5]. During subsequent in-fusion of propofol 100 ug kg"1 min"1, the beta wavesreappeared and a mixture of beta and delta activitypersisted. However, that study was performed in apaediatric population, and may not be comparable tothat in our adult volunteers.
The change in high frequency power was not
uniform across the cortex. We found the largestincrease occurred in the frontal and central areas.Similarly, Kearse and Fahmy reported that the alphaspindle pattern was predominant in the fronto-central regions [3] and coincided with the areas ofgreatest EEG changes observed in this study.Changes in anterior high frequency EEG activityhave been reported with several i.v. sedative agents[17-20] and low doses of inhalation agents [21,22].This distribution may be explained by the normalpredominance of beta activity over anterior cortex,or may reflect some common electrophysiologicalmechanism occurring during sedation with differentanaesthetic agents.
The dose of propofol used in this study resulted ina significant degree of sedation, as assessed by theVAS scores, and the occurrence of a significantdegree of amnesia, as demonstrated by the results oftesting for visual and verbal recall tasks. The resultsof this study seem to indicate that propofol, duringlow-dose infusion, produced amnesia independent ofits sedative effects. All subjects were able to followcomplex commands in order to complete the cog-nitive tasks, yet had impaired recall of visual andauditory stimuli. Several subjects seemed to be wideawake during the infusion period, yet subsequentlydemonstrated significant amnesia. A similar ob-servation was reported by Rupreht when a patientwas able to follow commands during operation,during a propofol infusion, yet was not able to recallthis event subsequently [23]. In our study, the lackof correlation of memory impairment with sedationindicates that the effect of propofol on memoryperformance was not dependent on sedation.
The results of the Rey AVLT indicate that, whilesome learning did take place during propofol in-fusion, the memory trace formed under the influenceof propofol was fragile, vulnerable to interferencefrom new material, and showed enhanced decay overtime. Recognition performance for words shownduring propofol infusion was very poor. The poorrecall coupled with the poor recognition indicatedfailure to consolidate short-term memory under theinfluence of propofol [24]. This was confirmed bythe visual tests, where 52 % of the material could notbe recognized. We demonstrated anterograde am-nesia in this study, as words and pictures presentedduring the baseline condition could be both recalledand recognized well after the infusion of propofol.Any memory traces that were retained under theinfluence of propofol were more difficult to retrieve,as shown by the results of the visual recognition test.Initial free recall of pictures was very poor (4 %), butup to 48 % of the material was recalled eventuallyusing progressively stronger cueing stimuli.
Often, intraoperative recall is assessed by non-specific questioning. Our data indicate that cueingfor specific intraoperative stimuli may be necessaryto ensure that memories are not present. Kestin,Harvey and Nixon reported a similar discrepancy infree recall compared with recognition in a picturetest following an infusion of propofol, when othercognitive effects were minimal [6]. Thus our dataindicate that, when propofol is used as a sole agentfor anaesthesia, there is a possibility of recall
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from

254 BRITISH JOURNAL OF ANAESTHESIA
occurring when the infusion rate is of the order of75 ng kg"1 mkr1, and that specific prompting shouldbe used to assess the degree of this recall.
One subject did not experience significant am-nesia, but we noted that his plasma concentrations ofpropofol during infusion were smaller than average(0.4-0.8 ug ml"1). However, there were three othersubjects who experienced amnesia with even smallerplasma concentrations. The first subject had the leastbeta! power of any subject during infusion. Twoother subjects had beta! power values during in-fusion close to those of this subject, and these threesubjects were the only ones able to recall byrecognition all five pictures presented during in-fusion. This finding, and the fact that changes inbeta! power were related to performance on the ReyAVLT test, lead us to postulate that increased beta!power may be related to the presence of amnesia. Astudy of more subjects who do not experienceamnesia at these concentrations of propofol would berequired to make a more definitive statement.
EEG changes associated with propofol seem to berelated to plasma concentration [25]. Using variousEEG indices such as burst suppression or medianfrequency, it has been possible to titrate propofol inanaesthetic doses [2,26,27]. Our data demonstratethat the EEG may similarly be a useful monitorduring propofol sedation, as significant memoryimpairment occurred at a time when increases inhigh frequency EEG activity were evident.
ACKNOWLEDGEMENT
The authors acknowledge the support of Tracor NorthernMedical Instrument Co., Middleton, WI., (now Noran Instru-ments) who provided the Tracor Nomad 3400 EEG acquisitioninstrument.
REFERENCES1. Langley MS, Heel RC. Propofol—a review of its pharmaco-
dynamic and pharmacokinetic properties and use as anintravenous anaesthetic. Drugs 1988; 35: 334-372.
2. Schwilden H, Stoeckel H, Schuttler J. Closed-loop feedbackcontrol of propofol anaesthesia by quantitative EEG analysisin humans. British Journal of Anaesthesia 1989; 62: 290-296.
3. Kearse LA, Fahmy NR. The electroencephalographic effectsof propofol anesthesia in humans: a comparison withthiopental/cnflurane anesthesia. Anesthesiology 1989; 71:A121.
4. Romano R, DeFeo MR, Favaro R, Arcioni R, Cavaliere G,Mecarelli O, Rina MG, Gattorini F. EEG aspects ofanaesthesia with ICI 35,868 (propofol) in man—preliminarynotes. In: Proceedings of the 42nd Congresso NazionaleSiaarti, Sorrento, October 20-23, 1988; 183-186.
5. Borgeat A, Dessibourg C, Popovic V, Meier D, Blanchard M,Schwander D. Propofol and spontaneous movements: anEEG study. Anesthesiology 1991; 74: 24-27.
6. Kestin IG, Harvey PB, Nixon C. Psychomotor recovery afterthree methods of sedation during spinal anaesthesia. BritishJournal of Anaesthesia 1990; 64: 675-681.
7. Dubois A, Balatoni E, Peeters JP, Baudoux M. Use ofpropofol for sedation during gastrointestinal endoscopies.Anaesthesia 1988; 43: 75-80.
8. Wilson E, Mackenzie N, Grant IS. A comparison of propofol' and midazolam by infusion to provide sedation in patients
who receive spinal anaesthesia. Anaesthesia 1988; 43: 91-94.9. Rodrigo MRC, Jonsson E. Conscious sedation with propofol.
British Dental Journal 1989; 166: 75-80.10. Jasper HH and the Committee on Clinical Examination in
EEG. The ten-twenty electrode system of the internationalfederation. Electroencephalography and Clinical Neurophys-lology 1958; 10: 371-375.
11. Gasser T, Backer P, Mocks J. Transformations towards thenormal distribution of broad band spectral parameters of theEEG. Electroencephalography and Clinical Neurophysiology1982; 53: 119-124.
12. Lezak MD. In: Neuropsychological Assessment. New York:Oxford University Press, 1976; 352-356.
13. Vree TB, Barrs AM, DeGrood PMRM. High performanceliquid chromatographic determination and preliminarypharmacokinetics of propofol and its metabolite in humanplasma and urine. Journal of Chromatography 1987; 417:458-^64.
14. Plummer GF. Improved method for the determination ofpropofol in blood by high performance liquid chromatographywith fluorescence detection. Journal of Chromatography 1987;421: 171-176.
15. Bart AJ, Homi J, Linde HW. Changes in power spectra ofelectroencephalograms during anesthesia with fluoroxene,methoxyflurane and ethrane. Anesthesia and Analgesia 1971;50: 53-63.
16. Yamamura T, Fukuda M, Takeya H, Goto Y, Furukawa K.Fast oscillatory activity induced by analgesic concentrationsof nitrous oxide in man. Anesthesia and Analgesia 1981; 60:283-288.
17. Veselis RA, Reinsel R, Alagesan R, Heino R, Bedford RF.The EEG as a monitor of midazolam amnesia: changes inpower and topography as a function of amnesic state.Anesthesiology 1991; 74: 866-874.
18. Dzwonczyk RR, Howie MB. Comparison of a set of powerdistribution parameters for intraoperativc EEG monitoring.IEEE Transactions on Biomedical Engineering 1986; 33:792-795.
19. Schwartz J, Feldstein S, Fink M, Shapiro DM, Itil TM.Evidence for a characteristic EEG frequency response tothiopental. Electroencephalography and Clinical Neurophys-iology 1971; 31: 149-153.
20. Domino EF, French J, Pohorecki R, Pandit SK, Galus C.Further observations on the effects of subhypnotic doses ofmidazolam in normal volunteers. Psychopharmacology Bull-etin 1989; 25:460-465.
21. Tinker JH, Sharbrough FW, Michenfelder JD. Anterior shiftof the dominant EEG rhythm during anesthesia in the Javamonkey: correlation with anesthetic potency. Anesthesiology1977; 46: 252-259.
22. Levy WJ. Power spectrum correlates of changes in con-sciousness during anesthetic induction with enflurane. Anes-thesiology 1986; 64: 688-693.
23. Rupreht J. Awareness with amnesia during total intravenousanaesthesia with propofol. Anaesthesia 1989; 44: 1005.
24. Mandler G. Recognising: The judgment of previous oc-currence. Psychology Review 1980; 87: 252-271.
25. Bendriss P, Stoiber HP, Bendriss-Brusset AC, Dabaide P,Erny P. Propofol effects on EEG and relationship withplasma concentration during ncurosurgery. Anesthesiology1990; 73: A203.
26. van Hemelrijck J, Teropelhoff R, Jellish WS, White PF. Useof EEG for determining propofol requirement during neuro-anesthesia. Anesthesiology 1990; 73: A2O2.
27. Suttman H, Juhl G, Morgenstern W, Doenicke A. VisuelleEEG-analyse zur Steuerung intravenoser Narkosen mitPropofol (Visual analysis of EEG for regulation of intravenousanesthesia with propofol). (Abstract in English). Anaesthesist1989; 38: 180-188.
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from
Department of Anesthesiologyand
Continuing Medical EducationJefferson Medical College
Philadelphia, Pennsylvania
present
Bermuda Shorts for ClinicalAnesthesiologists
March 29, to April 2,1993
at
Marriott Castle HarbourBermuda
Program Director: Joseph L. Seltzer, M.D.
An early morning/late afternoon lecture schedule isarranged with ample time for you and your party
to partake of the pleasures of Bermuda:pink sand beaches, championship golf courses,
tennis and a wide variety of shopping.
For Further InformationCall: 215-955-6992Fax: 215-923-6939
HAHNEMANN UNIVERSITYDepartment of Anesthesiology
Faculty positions available at Instructor andAssistant Professor level. Hahnemann is atertiary care medical center located in CenterCity Philadelphia with a fully approved residencyprogram, a very active cardiac program (about1400 open heart procedures/year), trauma andkidney transplant programs. Obstetric, neuro-surgical orthopedic and ambulatory surgeryservices round our caseload to 14,000 procedures/year.
Active research programs exist in malignanthyperthermia, cardiac anesthesia, neuromuscularpharmacology and a variety of other areas.
For further information, please contact:
Henry Rosenberg, M.D.Professor and Chairman
Department of AnesthesiologyHahnemann University
Broad & VinePhiladelphia, Pa. 19102-1192
* *
THE UNIVERSITY
[OF HONG KONGjChair of Anaesthesiology
(Ref. 91/92-105)
Applications are Invited for the Chair of Anaesthesiology from assoon as possible. Applicants should have strong academicqualifications and a substantial record of research and publications.Appointees to Chairs may be called upon to become Head ofDepartment.
The University would prefer to make a permanent appointment butconsideration may also be given to applications for appointment for afixed-term or on secondment for a period of preferably not less thanthree academic years.
Trie University reserves the right not to fill the Chair or to fill the Chairby Invitabon or to make an appointment at a lower level.
Annual salary (superannuate) will be within the clinical professorialrange, of which the minimum is HK$1,030,200 (approx. £72,040)and the average is HK$1,215,060 (approx. £84,970; sterlingequivalent as at 16 June 1992). At current rates, salaries tax will notexceed 15% of gross income. Housing at a charge of 7.5% ofsalary, children's education allowances, leave and medical benefitsare provided.
Further particulars and application torms may be obtained fromAppointments (40788), Association of Commonwealth Universities,36 Gordon Square, London WC1H OPR UK; or from theAppointments Unit, Registry, The University of Hong Kong, HongKong,(Fax(852)5592058;E-maa:APPTUNrr<MHKUVM1.HKU.HK)
Closes: 30 September, 1992.
ANAESTHETISTSMONTREAL
- FFARCS/ Board certified/FRCPC.
Pediatric academic teaching hospital
with all major subspecialties.
Guaranteed research time. Interest
in pain management and/or cardio-
vascular anaesthesia an advantage.
In accordance with Canadian imm-
igration requirements this is directed
to Canadian Citizens and permanent
residents of Canada. McGill Univer-
sity is committed to equity in
employment.
CV to: Dr. DG Spence, Director,
Montreal Children's Hospital,
2300 Tupper St., Rm. C-1118,
Montreal, QC, H3H 1P3.
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from
ThoraxThe Journal of the British Thoracic Society
EXECUTIVE EDITOR: STEPHEN G. SPIRO
THORAX, a leading journal inrespiratory medicine, is the officialjournal of the British Thoracic Society.It enjoys an enviable and longstandingreputation for publishing clinical andexperimental research articlescovering many disciplines, includingpathology, immunology and surgery.In addition it provides coverage of therecent developments in basicbiomedical sciences, including cellularbiochemistry and molecular biology,enabling the thoracic specialist toremain abreast of advances.All papers are subject to peer review7
and this, together with emphasis onclarity and rapid publication, hasenabled Thorax to maintain itsposition as one of the leadinginternational journals in its specialty.As well as original papers, Thoraxpublishes editorials, reviews, shortreports, book reviews, andcorrespondence; series of articles area new feature.
REVIEW SERIESThe journal publishes highlysuccessful, up to date review series.
RECENT EXAMPLES:• Aids and the Lung
edited by D.M. Mitchell andA.A. Woodcock
• Molecular Biology andRespiratory Diseaseedited by R.A. Stockley
• Assisted Ventilationedited by John Moxham
• Cystic Fibroslsedited by D.J. Shale
• Statistics In Respiratory Medicineby Susan Chinn
• New Perspectives in Lung Canceredited by S. Spiro
1992 Subscription Rate: £146USA Only: $255To Order Your Subscription or Sample CopyPlease Complete the Order Form Below:
THORAXISSN: 0040-6376PUBLICATION: Monthly1992 SUBSCRIPTION RATE: £146USA ONLY: $255Please tickC3 Please enter my subscription, start dateCI Please send me a sample copyD Please send me Instructions to Authors• I enclose a cheque for
Order FormCard Number
MasterCard users should add the numbers appearing above their name
Expiry date :
Signature ., (Your signature Is essential, especially when paying by credit card)
N a m e (Capitals) .
Address •
(Payable to British Medical journal)
• I wish to pay by credit card. /
American Express/Visa(Barclaycard)/Mastercard(Delete as appropriate) Date
BMJSend orders to: BM| Publishing Croup, BMA House, Tavlstock Square, London. WC1H 9JR.
by guest on October 20, 2016
http://bja.oxfordjournals.org/D
ownloaded from