
Immunogenicity and safety of low dose virosomal adjuvanted influenza vaccine administered...
7
Vaccine 27 (2009) 3561–3567 Contents lists available at ScienceDirect Vaccine journal homepage: www.elsevier.com/locate/vaccine Immunogenicity and safety of low dose virosomal adjuvanted influenza vaccine administered intradermally compared to intramuscular full dose administration Valérie Künzi a,∗ , Jaco M. Klap b , Michael K. Seiberling c , Christian Herzog a , Katharina Hartmann a , Oliver Kürsteiner a , Ronald Kompier b , Roberto Grimaldi a , Jaap Goudsmit b a Crucell, Berna Biotech Ltd, 3018 Berne, Switzerland b Crucell Holland BV, Leiden, The Netherlands c Swiss Pharma Contract Ltd, Allschwil, Switzerland article info Article history: Received 12 January 2009 Received in revised form 17 March 2009 Accepted 23 March 2009 Available online 10 April 2009 Keywords: Influenza Intradermal vaccination Virosomes abstract Background: Despite the established benefit of intramuscular (i.m.) influenza vaccination, new adjuvants and delivery methods for comparable or improved immunogenicity are being explored. Intradermal (i.d.) antigen administration is hypothesized to initiate an efficient immune response at reduced antigen doses similar to that observed after i.m. full dose vaccination. Methods: In a randomized, partially blinded phase II study 224, healthy adults aged ≥18 to ≤60 years were randomly assigned to four groups and received trivalent influenza vaccine at single doses of 3.0, 4.5 and 6.0 g hemagglutinin (HA) antigen of each influenza virus strain via i.d. injection or 15.0 g HA of each influenza strain via i.m. delivery. Serum anti-influenza virus antibodies were determined by hemagglutination inhibition (HI) assay before and 3 weeks after vaccination. Safety assessments were made at baseline and at the follow-up visit by the investigators and for a 4-day period post-vaccination by the subjects themselves. Results: The EMEA requirements for re-licensing of influenza vaccines were fulfilled in all groups 3 weeks after vaccination, irrespective of dose and mode of administration. High seroconversion rates were observed in all study groups and for all strains ranging from 50.9 to 85.5% and 70.4 to 87.0% after i.d. and i.m. vaccination, respectively. Seroprotection rates for the A strains A/Solomon Islands and A/Wisconsin were generally higher compared to the B/Malaysia strain and ranged from 89.1 to 98.2% across the i.d. groups. Similar rates of 96.3% for the A/Solomon Islands and 94.4% for the A/Wisconsin strain were observed in the i.m. group. Seroprotection rates for the B/Malaysia strain were 65.5, 83.0 and 72.7% after i.d. admin- istration of 3.0, 4.5, and 6.0 g HA of each strain, respectively, compared to a seroprotection rate of 85.2% in the i.m. group. In addition, marked increases in geometric mean titer (GMT) were observed across the groups for all influenza virus strains ranging from 6.9 to 70.5 for i.d. and from 16.9 to 56.5 for i.m. anti- gen delivery. Both routes of administration were well tolerated. Systemic reactions were broadly similar across the groups. With respect to local reactions the frequency of injection site pain and ecchymosis were significantly lower following i.d. vaccination, while other local reactions such as erythema occurred at higher rates with i.d. than with i.m. vaccine administration, as expected due to the mechanism of action for the i.d. route. Conclusions: The virosomal adjuvanted influenza vaccine (Inflexal ® V) was shown to be overall highly immunogenic and well tolerated when given i.d. at reduced doses to healthy adults, eliciting an immune response similar to that observed with full dose i.m. administration and thus suggesting a promising antigen-sparing strategy for universal influenza vaccination against endemic influenza. Trial registration: ISRCTN registry number: 33950739. © 2009 Elsevier Ltd. All rights reserved. Abbreviations: AE, adverse event; EMEA, European Medicines Agency; GMT, geometric mean titer; HA, hemagglutinin; HI, hemagglutination inhibition; i.d., intradermal; i.m., intramuscular; WHO, World Health Organization. ∗ Corresponding author. Tel.: +41 980 65 26; fax: +41 980 67 72. E-mail address: [email protected] (V. Künzi). 1. Introduction Influenza viruses cause recurrent annual epidemics and can more seriously result in pandemics following an antigenic shift. While healthy adults usually show the mildest disease symptoms, the rate of morbidity and mortality is increased in at risk groups, including elderly, young children and people suffering from chronic disease or immunodeficiency [1–5]. Vaccination against influenza 0264-410X/$ – see front matter © 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.vaccine.2009.03.062
-
Upload
raphygordon -
Category
Documents
-
view
0 -
download
0
Transcript of Immunogenicity and safety of low dose virosomal adjuvanted influenza vaccine administered...

Vaccine 27 (2009) 3561–3567
Contents lists available at ScienceDirect
Vaccine
journa l homepage: www.e lsev ier .com/ locate /vacc ine
Immunogenicity and safety of low dose virosomal adjuvanted influenza vaccineadministered intradermally compared to intramuscular full dose administration
Valérie Künzia,∗, Jaco M. Klapb, Michael K. Seiberlingc, Christian Herzoga, Katharina Hartmanna,Oliver Kürsteinera, Ronald Kompierb, Roberto Grimaldia, Jaap Goudsmitb
a Crucell, Berna Biotech Ltd, 3018 Berne, Switzerlandb Crucell Holland BV, Leiden, The Netherlandsc Swiss Pharma Contract Ltd, Allschwil, Switzerland
a r t i c l e i n f o
Article history:Received 12 January 2009Received in revised form 17 March 2009Accepted 23 March 2009Available online 10 April 2009
Keywords:InfluenzaIntradermal vaccinationVirosomes
a b s t r a c t
Background: Despite the established benefit of intramuscular (i.m.) influenza vaccination, new adjuvantsand delivery methods for comparable or improved immunogenicity are being explored. Intradermal (i.d.)antigen administration is hypothesized to initiate an efficient immune response at reduced antigen dosessimilar to that observed after i.m. full dose vaccination.Methods: In a randomized, partially blinded phase II study 224, healthy adults aged ≥18 to ≤60 yearswere randomly assigned to four groups and received trivalent influenza vaccine at single doses of 3.0,4.5 and 6.0 �g hemagglutinin (HA) antigen of each influenza virus strain via i.d. injection or 15.0 �gHA of each influenza strain via i.m. delivery. Serum anti-influenza virus antibodies were determined byhemagglutination inhibition (HI) assay before and 3 weeks after vaccination. Safety assessments weremade at baseline and at the follow-up visit by the investigators and for a 4-day period post-vaccinationby the subjects themselves.Results: The EMEA requirements for re-licensing of influenza vaccines were fulfilled in all groups 3weeks after vaccination, irrespective of dose and mode of administration. High seroconversion rates wereobserved in all study groups and for all strains ranging from 50.9 to 85.5% and 70.4 to 87.0% after i.d. and i.m.vaccination, respectively. Seroprotection rates for the A strains A/Solomon Islands and A/Wisconsin weregenerally higher compared to the B/Malaysia strain and ranged from 89.1 to 98.2% across the i.d. groups.Similar rates of 96.3% for the A/Solomon Islands and 94.4% for the A/Wisconsin strain were observed inthe i.m. group. Seroprotection rates for the B/Malaysia strain were 65.5, 83.0 and 72.7% after i.d. admin-istration of 3.0, 4.5, and 6.0 �g HA of each strain, respectively, compared to a seroprotection rate of 85.2%in the i.m. group. In addition, marked increases in geometric mean titer (GMT) were observed across thegroups for all influenza virus strains ranging from 6.9 to 70.5 for i.d. and from 16.9 to 56.5 for i.m. anti-gen delivery. Both routes of administration were well tolerated. Systemic reactions were broadly similaracross the groups. With respect to local reactions the frequency of injection site pain and ecchymosiswere significantly lower following i.d. vaccination, while other local reactions such as erythema occurredat higher rates with i.d. than with i.m. vaccine administration, as expected due to the mechanism of actionfor the i.d. route.Conclusions: The virosomal adjuvanted influenza vaccine (Inflexal®V) was shown to be overall highly
immunogenic and well tolerated when given i.d. at reduced doses to healthy adults, eliciting an immuneresponse similar to that observed with full dose i.m. administration and thus suggesting a promisingantigen-sparing strategy for unTrial registration: ISRCTN registAbbreviations: AE, adverse event; EMEA, European Medicines Agency; GMT,geometric mean titer; HA, hemagglutinin; HI, hemagglutination inhibition; i.d.,intradermal; i.m., intramuscular; WHO, World Health Organization.
∗ Corresponding author. Tel.: +41 980 65 26; fax: +41 980 67 72.E-mail address: [email protected] (V. Künzi).
0264-410X/$ – see front matter © 2009 Elsevier Ltd. All rights reserved.doi:10.1016/j.vaccine.2009.03.062
iversal influenza vaccination against endemic influenza.ry number: 33950739.
© 2009 Elsevier Ltd. All rights reserved.
1. Introduction
Influenza viruses cause recurrent annual epidemics and can
more seriously result in pandemics following an antigenic shift.While healthy adults usually show the mildest disease symptoms,the rate of morbidity and mortality is increased in at risk groups,including elderly, young children and people suffering from chronicdisease or immunodeficiency [1–5]. Vaccination against influenza
3 ine 27
rtdaa
tamwfcdaaatt
caircaivb
itDvd
agmv
vsipbt
aiI
iTti
eda
2
2
d
562 V. Künzi et al. / Vacc
emains the cornerstone of prevention. Several studies have shownhat immunization can significantly reduce hospital admission andeath in the elderly [6–8] and that it has substantial health-relatednd economic benefits in children [9–12] and healthy workingdults [13].
Most of the currently available influenza vaccines are adminis-ered intramuscularly (i.m.). Despite the established benefits of thispproach, novel adjuvants and delivery methods such as intrader-al (i.d.) vaccination are being explored, particularly in subjectsith a weakened immune response. Antigen presenting cells are
ound at higher concentrations in the skin compared to the mus-le and efficiently migrate and present antigens to T cells in theraining lymph nodes [14,15]. Therefore a robust immune responset reduced antigen doses is anticipated due to this innate adjuvantction. Sparing of antigen would not only allow to expand the avail-bility of vaccine in case of vaccine shortage but would also supporthe introduction of universal influenza vaccination and would helpo meet the increased antigen demand in case of a pandemic.
I.d. antigen administration has been shown to be safe and effi-acious for several vaccines, e.g. against hepatitis B [16], rabies [17],nd for a virosomal hepatitis A vaccine [18]. In addition, promis-ng results were reported for influenza [14,19–21]. However, withespect to non-adjuvanted vaccine formulations, findings on effi-acy of i.d. administered influenza virus antigens at reduced dosesre conflicting. While some studies showed a similar or bettermmune response in healthy adults [19,20] others found the i.d.accination to be not superior or less immunogenic compared tooth reduced and full dose i.m. vaccination [22,23].
In the elderly it was shown that administration of the standard.m. antigen dose (15 �g of HA per influenza strain) delivered viahe i.d. route with help of the BD Microinjection System (Bectonickinson) highly improved the immunogenicity compared to i.m.accination [14] while reducing the dose for i.d. delivery by hypo-ermic needle was somewhat less effective in this age group [19].
Only very limited data are available for i.d. administration ofdjuvanted influenza vaccines. In a pilot study performed by ourroup in 2006, i.d. administration of a reduced single dose of viroso-al adjuvanted influenza vaccine to healthy young adults revealed
ery promising results in terms of immunogenicity and safety [21].Influenza virosomes are prepared from liposomes containing
iral envelope proteins and represent a versatile antigen deliveringystem inducing both humoral and cellular immunity. The virosomes best described as a structural adjuvant revealing its adjuvantroperties through the function of the HA protein (i.e. receptorinding, fusion and immunostimulation) and its particulate struc-ure [24].
To date, there are three virosomal vaccines registered: a hep-titis A vaccine (Epaxal®, Berna Biotech Ltd., Switzerland) and twonfluenza vaccines (Inflexal®V, Berna Biotech Ltd., Switzerland andnvivac®, Solvay, The Netherlands).
The virosomal adjuvanted influenza vaccine Inflexal®V wasntroduced onto the market in 1997 and is registered in 38 countries.o date more than 41 million doses have been distributed and theolerability, safety and effectiveness of the vaccine were confirmedn numerous pre- and post-marketing trials [25].
In the present study performed in healthy adults, we furtherxplored the immunogenicity and safety of three reduced antigenoses when administered i.d. compared to intramuscular full dosedministration.
. Methods
.1. Clinical study design
Between September and November 2007, a single-centre, ran-omized, partially blinded (i.e. open for the route of vaccination
(2009) 3561–3567
and double blind for the i.d. dose), phase II study was conducted toassess the immunogenicity and safety of three reduced single dosesof the virosomal adjuvanted influenza vaccine Inflexal®V adminis-tered i.d. compared to i.m. full dose administration (ISRCTN registrynumber: 33950739). In addition, subjects were non-randomlyassigned to another experimental arm of i.d. vaccination. These dataare not presented in this publication.
After written informed consent was obtained, subjects werescreened for study entry and randomly assigned to one of the fourstudy arms using a randomization block system prepared by FisherClinical Services, Switzerland.
The primary study objective was to investigate the humoralimmune response of the reduced i.d. formulations compared tothe conventional i.m. dose with respect to the European MedicinesAgency (EMEA) guideline for assessment of influenza vaccines [26].The secondary objective was to compare the safety of both routesof administration, including a set of solicited adverse events (AEs).
Immunogenicity assessments were made before vaccination onDay 1 (baseline) and on Day 22 ± 2 by hemagglutination inhibi-tion (HI) assay. The analysis of the pre- and post-vaccination serasamples were done simultaneously at Berna Biotech Ltd., Switzer-land. The titer assigned to each sample was the geometric mean oftwo independent determinations. In case of a negative baseline titer(<1:10), a value of 5 was used for the calculations. Seroprotectionwas defined as a post-vaccination titer of ≥1:40. Seroconversionwas defined as a ≥4-fold increase in HI antibody titer from baselineand a post-vaccination titer of ≥1:40 [26].
Safety assessments of local and systemic AEs were made by theinvestigators at baseline and at the follow up visit at 3 weeks post-vaccination (Day 22 ± 2), as well as by the participants themselvesfor a 4-day period following immunization. Pain at the injection site,erythema ≥5 mm, ecchymosis ≥5 mm, and induration ≥5 mm weresolicited as local AEs. They were rated as absent (0 to <5 mm), mild(≥5 to <20 mm), moderate (≥20 to <50 mm) or severe (≥50 mm).In addition, induration >50 mm persisting for more than 3 dayswas assessed as a requirement of EMEA [26]. Malaise, shiveringand body temperature were solicited as systemic adverse reac-tions, while only a body temperature of ≥38 ◦C, ≥1 day (fever)fulfilled the criterion of an AE. The local AE pain and all solicitedsystemic AEs were rated on a four-point scale: none (no symp-tom), mild (no inconvenience), moderate (interfering with dailyactivities) and severe (preventing normal daily activities). In addi-tion, unsolicited AEs were reported and rated according to solicitedones.
The study was approved by the independent Ethical Committeeof Both Basels (EKBB), Switzerland and conducted in full compli-ance with the principals of the Declaration of Helsinki (as amendedin Tokyo, Venice, Hong Kong, Somerset and Edinburgh) and GoodClinical Practice. Written informed consent to participate in thestudy was obtained from all subjects prior to any study relatedactivities.
2.2. Study subjects
Medically stable adults aged between 18 and 60 years were eli-gible to participate in the study, provided that they showed none ofthe following characteristics: acute bronchopulmonary infection oranother acute febrile illness (≥38.0 ◦C), prior influenza vaccinationin the past 330 days, known hypersensitivity to any vaccine compo-nent, history of egg protein allergy or severe atopy, serious adversereaction to any influenza vaccine in the past, known blood coagula-
tion disorders or immunodeficiency, simultaneous treatments withsystemic immunosuppressive drugs, recent (≤90 days) receipt of aninvestigational medicinal product and immunoglobulins or bloodtransfusions, pregnancy or lactation, and concomitant participationin another clinical trial.
V. Künzi et al. / Vaccine 27 (2009) 3561–3567 3563
F iffered ffect
2
IvAvifiofont
2
ftosptavTo
imi(mwitbm
TD
AGPE
IT
a
ig. 1. Study design showing tested treatments and contrasts. Model A shows the difference between intramuscular and intradermal vaccination followed by a dose e
.3. Vaccines
The 2007/2008-season virosomal adjuvanted influenza vaccinenflexal®V (Berna Biotech Ltd., Switzerland) contained purifiediral surface antigens of A/Solomon Islands/3/2006 (H1N1)-like,/Wisconsin/67/2005 (H3N2)-like and B/Malaysia/2506/2004-likeirus as recommended by the WHO and EMEA for the 2007/2008nfluenza season [27]. The i.m. formulation was presented as a pre-lled syringe and contained 15.0 �g HA of each strain in a volumef 0.5 mL for i.m. vaccination [28]. The i.d. formulations were takenrom glass vials containing 3.0, 4.5, or 6.0 �g HA per strain per 0.1 mLf vaccine. All subjects were immunized on Day 1 by hypodermiceedle (25 gauge) with a single dose of Inflexal®V either i.m. intohe deltoid region or i.d. over the deltoid region.
.4. Statistical analysis
The HI antibody titers (primary endpoints) of the four vaccineormulations were assessed according to the criteria described inhe EMEA guideline [26]. To confirm immunogenicity at least onef the following criteria had to be met for each strain and in eachtudy group: seroconversion reached in >40% of the vaccinees, sero-rotection achieved in >70% of subjects and a >2.5 geometric meaniter (GMT) fold-increase from baseline. The entire analysis of HIntibodies was performed on log10-transformed data. The meanalues at the log scale converted to GMTs by back-transformation.he AEs (secondary endpoints) were reported descriptively in termsf frequencies and rates.
In a sub-analysis, a between-group comparison was performedn the according-to-protocol (ATP) population. The data were sum-
arized by point estimate (mean or median) and range (95% CI ornterquartile range) for each treatment. In the statistical evaluationFig. 1), all i.d. treatments were compared first with the i.m. for-
ulation (Model A). In the second model (Model B), the contrasts
ere split in a difference between the i.m. treatment and the lowest.d. dose, combined with a linear dose effect towards the other i.d.reatments. The significance of the investigated terms was testedy fitting a model with all contrasts to be tested, not corrected forulti-comparison. The statistical analysis was performed using SAS
able 1emographic and baseline characteristics.
ID 3 �g (n = 56)
ge [years] mean (range)a 39.5 (18.1–59.8)ender [% males] 44.6revious vaccination against influenza [%] 60.7lapsed time since previous influenza vaccination[months], median (quartiles)
24.2 (13.6–50)
nfluenza-like illness in previous influenza season [%] 10.7emperature [◦C] mean (quartiles) 36.7 (36.4–37.0)
Four adults in the study were aged between 60 and 61 years and therefore excluded from
nces between intradermal and intramuscular antigen delivery; Model B shows thewithin the intradermal treatments. ID: intradermal; IM: intramuscular.
software (version 9.1). For all variables the probability distributionwas accounted by using SAS procedures for continuous (normalor log-normal; with left censoring if necessary), dichotomous andordinal variables. The statistical tests are based on t test, F testsor, �2 tests, whenever applicable, and expressed as p values of theinvestigated contrast.
3. Results
3.1. Participants
All 224 vaccinated subjects completed the study to Day 22 ± 2.The ATP population for evaluation of immunogenicity included 217vaccinees. Seven vaccinees deviated from the protocol: four sub-jects were aged between 60 and 61 years, one had a prior influenzavaccination in the past 330 days, one came back for the second visitoutside the defined time window and for one subject no serologicalresult was available for Day 22 ± 2.
The treatment groups were comparable regarding baseline char-acteristics such as age, gender, and medical history. Mean ageranged from 36.1 to 39.6 years and the proportion of males variedbetween 44.6 and 57.1% (Table 1). With respect to previous influenzavaccination between-group differences were observed: 30.4% ofsubjects who were treated i.d. with 6.0 �g HA per strain were pre-viously vaccinated against influenza compared to 60.7, 46.4, and48.2% of subjects vaccinated with 3.0, 4.5, and 15.0 �g HA of eachstrain, respectively. In addition, the time elapsed after the previ-ous influenza vaccination was longer in the group vaccinated i.m.with a median of 37.6 months compared to medians of 24.2–26.7months for the i.d. groups. The experience of influenza-like illnessesin the previous influenza season was similar in all groups and variedbetween 3.6 and 10.7% (Table 1).
3.2. Immunogenicity
Considerable proportions of the ATP population had pre-existingantibodies ≥1:40 against the two influenza A strains. The observedrates ranged from 29.1 to 36.4% for the A/Solomon Islands and from41.8 to 52.7% for the A/Wisconsin strain across the treatment groups
ID 4.5 �g (n = 56) ID 6 �g (n = 56) IM 15 �g (n = 56)
38.4 (18.0–60.9) 39.6 (18.5–58.2) 36.1 (18.8–60.1)57.1 46.4 46.446.4 30.4 48.226.7 (13.6–50) 25.6 (17.7–50) 37.6 (22.6–50)
8.9 5.4 3.636.7 (36.4–37.0) 36.7 (36.5–37.0) 36.7 (36.6–36.9)
the according-to-protocol population; ID: intradermal; IM: intramuscular.

3564 V. Künzi et al. / Vaccine 27 (2009) 3561–3567
Table 2Serological assessments according to EMEA regulations [26].
Vaccine component ID 3 �g (n = 55) ID 4.5 �g (n = 53) ID 6 �g (n = 55) IM 15 �g (n = 54)
Pre-vaccination GMT (quartiles) A/H1N1 27.4 (<5–160) 25.4 (<5–139) 16.4 (<5–80) 20.9 (<5–69)A/H3N2 52.9 (7–453) 45.3 (<5–320) 34.0 (<5–226) 40.9 (<5–277)B 10.5 (<5–17) 9.0 (<5–10) 8.1 (<5–10) 8.5 (<5–10)
Post-vaccination GMT (quartiles) A/H1N1 1034.5 (453–3620) 1788.3 (784–7241) 765.3 (277–4434) 1180.4 (453–3620)A/H3N2 1182.8 (5453–3620) 1293.0 (784–3620) 1324.1 (554–3620) 691.8 (339–2217)B 72.8 (17–160) 149.9 (57–480) 91.4 (35–240) 152.9 (69–453)
Pre-vaccination seroprotection rate [%] A/H1N1 36.4 35.8 29.1 35.2A/H3N2 52.7 50.9 41.8 50.0B 20.0 9.4 9.1 13.0
Post-vaccination seroprotection rate [%] A/H1N1 96.4 96.2 89.1 96.3A/H3N2 96.4 98.1 98.2 94.4B 65.5 83.0 72.7 85.2
Seroconversion rate [%] A/H1N1 85.5 83.0 83.6 87.0A/H3N2 60.0 71.7 78.2 70.4B 50.9 67.9 60.0 79.6
GMT fold-increase (quantiles) A/H1N1 37.8 (6.9–181) 70.5 (8.0–627) 46.6 (9.8–181) 56.5 (11.3–362)A/H3N2 22.4 (2.4–222) 28.6 (4.0–157) 39.0 (4.0–256) 16.9 (2.8–111)B 6.9 (2.0–19.6) 16.7 (4.0–55) 11.4 (3.5–39) 18.0 (6.9–45)
EMEA criterion for seroprotection: achievement of a post-vaccination titer of ≥1:40 in >70% of subjects; seroconversion: ≥4-fold increase in HI antibody titer from baselineand a post-vaccination titer of ≥1:40 in >40% of subjects; GMT fold-increase: >2.5. To confirm immunogenicity at least one of these criteria has to be met for each strain in eachs baseliv consiI
(4tswr
r
cieHmc8assTawutopi(
svsv0napwb
tudy group. GMT: geometric mean titer; pre-vaccination: serological assessment ataccination; A/H1N1: A/Solomon Islands/3/2006 (H1N1)-like virus; A/H3N2: A/WisM: intramuscular.
Table 2). This resulted in an overall seroprotection rate of 34.1 and8.9% for the A/Solomon Islands and A/Wisconsin strain, respec-ively, before vaccination (Fig. 2). In contrast, the pre-vaccinationeroprotection rates for the B/Malaysia strain were relatively lowith an overall value of 12.9%. Across the treatment groups, the
ates varied between 9.1 and 20.0% (Table 2).Table 2 and Fig. 2 provide an overview of the immunogenicity
esults obtained in the four study groups.Three weeks post-vaccination (Day 22 ± 2), the required EMEA
riteria on seroprotection rate, seroconversion rate and GMT fold-ncrease were met in all study groups and all strains with onexception: in the group vaccinated with the lowest i.d. dose (3.0 �gA per strain), the required seroprotection rate of >70% was slightlyissed (65.5%) for the B/Malaysia strain (Fig. 2 and Table 2). The
orresponding seroprotection rates in the other study groups were3.0 and 72.7% after i.d. delivery of 4.5, and 6.0 �g HA, respectively,nd 85.2% after i.m. full dose administration. Sub-analysis of theeroprotection rates achieved for the B/Malaysia strain revealed notatistical differences except for the lowest i.d. dose (p = 0.0158).he seroprotection rates for both A strains were generally higher inll treatment groups compared to the B strain. Rates close to 100%ere achieved across the study groups (Fig. 2) with individual val-es of 89.1–96.4% for the A/Solomon Islands and 94.4–98.2% forhe A/Wisconsin strain (Table 2). Upon comparison of both routesf administration (irrespective of the dose administered), the sero-rotection rate was found to be overall significantly lower following
.d. antigen delivery compared to conventional i.m. vaccinationp = 0.0461).
Very high GMTs were observed in all study groups and for alltrains on Day 22 ± 2. Comparison of the GMTs after i.m. and i.d.accination showed significantly higher titers for the A/Wisconsintrain in all i.d. groups with GMT values between 1182.8 and 1324.1s. 691.8 following i.m. vaccination (Table 2, p values between.0187 and 0.0521). In contrast, for the A/Solomon Islands strain
o significant differences were found. The GMTs following i.d.ntigen administration were lower for the B/Malaysia strain com-ared to conventional i.m. vaccination. However, these differencesere only significant for the lowest i.d. dose (p = 0.0082). Whenoth routes of administration were compared no significant dif-ne (before vaccination); post-vaccination: serological assessment 3 weeks followingn/67/2005 (H3N2)-like virus; B: B/Malaysia/2506/2004-like virus; ID: intradermal;
ferences in GMT fold-increases for both A strains were observed.Following i.d. vaccination, increases ranged from 37.8 to 70.5 forthe A/Solomon Islands and from 22.4 to 39.0 for the A/Wisconsinstrain along the i.d. groups compared to a 56.5-fold increase forthe A/Solomon Islands and a 16.9-fold increase for the A/Wisconsinstrain after i.m. vaccination (Table 2). In contrast, a significantlower GMT fold-increase for the B/Malaysia strain was observedafter i.d. administration of 3.0 �g HA per strain compared to thecorresponding i.m. full dose (6.9 vs. 18.0; p = 0.0019; Table 2). Sub-analysis of the i.d. treatments revealed no compensating dose effect(p = 0.1066).
The seroconversion rates for all strains were comparably high inall study groups at Day 22 ± 2 and exceeded by far the required >40%(Fig. 2). For the A/Wisconsin strain, a significant positive dose effect(p = 0.0367) was observed among the i.d. groups (Fig. 2), althoughnone of the individual i.d. treatments (range 60.0–78.2%; Table 2)differed significantly from the i.m. treatment (70.4%).
3.3. Safety
All subjects completed the 4-day questionnaire and safety dataof all 56 subjects per study group were therefore available. Thevaccine was well tolerated, irrespective of dose and route of admin-istration. No serious adverse event occurred in any study group andmost of the reported symptoms (92.5 and 96.3% of the local andsystemic solicited adverse reactions, respectively) were consideredmild to moderate.
Upon i.d. vaccination with 3.0 �g HA per strain, 69.6% of subjectsreported at least one local adverse reaction compared to 73.2 and78.6% of subjects vaccinated i.d. with 4.5 and 6.0 �g HA per strain,respectively. I.m. vaccination resulted in at least one local adversereaction in 50% of the subjects.
The most frequently reported local reaction was pain at theinjection site after i.m. and erythema after i.d. vaccination. The dif-
ferences of reported vaccine-related AEs were significant betweenthe i.d. treatments and the i.m. vaccination for pain, ecchymosis,erythema, induration and other reactions.Following i.d. vaccination less pain was recorded compared toi.m. vaccination, irrespective of the dose administered (Fig. 3; p

V. Künzi et al. / Vaccine 27 (2009) 3561–3567 3565
F ccinatc preses /Solomv
beiccotiHm
evtrsro
tv
hpti
ig. 2. Serological assessments at baseline (pre-vaccination) and 3 weeks post-vaonversion rates are shown by influenza strain and treatment. The dotted lines reeroprotection, >40% for seroconversion and >2.5-fold in GMT increase. A/H1N1: Airus; B: B/Malaysia/2506/2004-like virus; ID: intradermal; IM: intramuscular.
etween 0.0099 and 0.2062, overall p = 0.0094). The frequency ofcchymosis was overall low (<5%), but still significantly higher after.m. vaccination (p = 0.0336) compared to the i.d. treatments. Inontrast, 62.5–75.0% of subjects vaccinated i.d. reported erythemaompared to 14.3% of subjects in the i.m. group (p ≤0.0001–0.0047;verall p <0.0001). Indurations ≥5 mm occurred in 33.9–50.0% ofhe i.d. vaccinated subjects compared to 17.9% of subjects in the.m. group (p values between 0.0004 and 0.0618; overall p = 0.0760).owever, no vaccinee experienced induration >50 mm lasting forore than 3 days (Fig. 3).No significant differences in elevated body temperature, shiv-
ring or malaise were observed during the 4 days followingaccination (Fig. 3, shivering not shown). After i.d. treatment withhe lowest dose, 35.7% of subjects reported at least one systemiceaction (solicited and unsolicited) compared to 23.2 and 33.9% ofubjects upon i.d. administration of 4.5 and 6.0 �g HA per strain,espectively. I.m. vaccination with the full dose resulted in at leastne systemic adverse reaction in 21.4% of subjects.
None of the vaccinees developed fever (≥38 ◦C, ≥1 day) andhe proportions of participants who reported shivering or malaisearied between 1.8 and 7.1% and between 5.4 and 8.9%, respectively.
The number and intensity of other reactions were significantlyigher (p = 0.0444 vs. p = 0.0244) after i.d. antigen delivery com-ared to i.m. vaccination. Headaches, itching and diarrhea werehe symptoms most often reported and considered related to thenfluenza vaccine in most cases.
ion. Geometric mean titers (GMTs), GMT fold-increases, seroprotection and sero-nt the EMEA requirement set for adults aged between 18 and 60 years: >70% foron Islands/3/2006 (H1N1)-like virus; A/H3N2: A/Wisconsin/67/2005 (H3N2)-like
4. Discussion
Influenza is the oldest and most common disease known to man.Annually 3–5 million cases of severe illness and 0.25–0.5 milliondeaths occur worldwide [29,30]. In addition, an estimated num-ber of one billion people are at high risk of suffering or dyingfrom the disease and its associated complications [30]. Vaccinationagainst influenza remains the most effective means for preven-tion and control of the disease. However, vaccination coverageis low in many countries, despite national vaccination recom-mendations and proven vaccine effectiveness. International effortsare therefore ongoing to improve vaccination rates, particularlyin people at increased risk for severe complications such as theelderly, young children and immunocompromized subjects. Sincethe demographic number of elderly steadily increases and uni-versal influenza vaccination of children is recommended [2] orunder discussion [31,32] future demand for influenza vaccine mayoutgrow the current availability of antigen. In addition, antigensparing would be an attractive option for countries where vaccinedemand is high, yet are unable to afford the full indicated dose.As a consequence, vaccination approaches improving the immune
response at reduced antigen doses are of interest. New adjuvantsand modes of vaccine delivery are under investigation. While adju-vants are known to potentiate the immune response but are alsocommonly associated with increased reactogenicity, changes in theroute of administration are thought to potentially circumvent this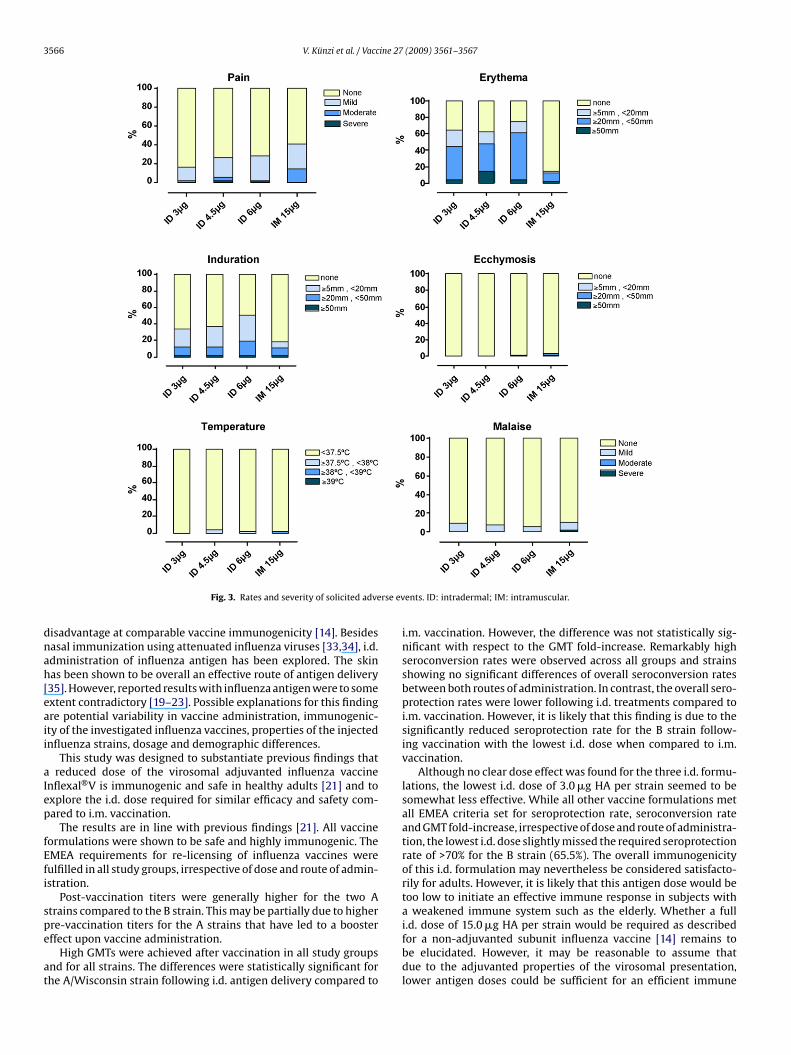
3566 V. Künzi et al. / Vaccine 27 (2009) 3561–3567
rse ev
dnah[eaii
aIep
fEfi
spe
at
Fig. 3. Rates and severity of solicited adve
isadvantage at comparable vaccine immunogenicity [14]. Besidesasal immunization using attenuated influenza viruses [33,34], i.d.dministration of influenza antigen has been explored. The skinas been shown to be overall an effective route of antigen delivery35]. However, reported results with influenza antigen were to somextent contradictory [19–23]. Possible explanations for this findingre potential variability in vaccine administration, immunogenic-ty of the investigated influenza vaccines, properties of the injectednfluenza strains, dosage and demographic differences.
This study was designed to substantiate previous findings thatreduced dose of the virosomal adjuvanted influenza vaccine
nflexal®V is immunogenic and safe in healthy adults [21] and toxplore the i.d. dose required for similar efficacy and safety com-ared to i.m. vaccination.
The results are in line with previous findings [21]. All vaccineormulations were shown to be safe and highly immunogenic. TheMEA requirements for re-licensing of influenza vaccines wereulfilled in all study groups, irrespective of dose and route of admin-stration.
Post-vaccination titers were generally higher for the two Atrains compared to the B strain. This may be partially due to higher
re-vaccination titers for the A strains that have led to a boosterffect upon vaccine administration.High GMTs were achieved after vaccination in all study groupsnd for all strains. The differences were statistically significant forhe A/Wisconsin strain following i.d. antigen delivery compared to
ents. ID: intradermal; IM: intramuscular.
i.m. vaccination. However, the difference was not statistically sig-nificant with respect to the GMT fold-increase. Remarkably highseroconversion rates were observed across all groups and strainsshowing no significant differences of overall seroconversion ratesbetween both routes of administration. In contrast, the overall sero-protection rates were lower following i.d. treatments compared toi.m. vaccination. However, it is likely that this finding is due to thesignificantly reduced seroprotection rate for the B strain follow-ing vaccination with the lowest i.d. dose when compared to i.m.vaccination.
Although no clear dose effect was found for the three i.d. formu-lations, the lowest i.d. dose of 3.0 �g HA per strain seemed to besomewhat less effective. While all other vaccine formulations metall EMEA criteria set for seroprotection rate, seroconversion rateand GMT fold-increase, irrespective of dose and route of administra-tion, the lowest i.d. dose slightly missed the required seroprotectionrate of >70% for the B strain (65.5%). The overall immunogenicityof this i.d. formulation may nevertheless be considered satisfacto-rily for adults. However, it is likely that this antigen dose would betoo low to initiate an effective immune response in subjects witha weakened immune system such as the elderly. Whether a full
i.d. dose of 15.0 �g HA per strain would be required as describedfor a non-adjuvanted subunit influenza vaccine [14] remains tobe elucidated. However, it may be reasonable to assume thatdue to the adjuvanted properties of the virosomal presentation,lower antigen doses could be sufficient for an efficient immune
ine 27
rs
tibrfrtuaw
gtcnmat[dtwa
stsp
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[[
[
[
[
[
V. Künzi et al. / Vacc
esponse in this age group as well as in immunocompromizedubjects.
All vaccine formulations tested in this study were safe and wellolerated. Systemic adverse reactions in the 4-day period follow-ng vaccination were comparable in all study groups. In contrast,etween-group differences were observed for the local adverseeactions, particularly with respect to an increased rate of erythemaollowing i.d. vaccination. However, this is in line with previouseports and was anticipated as a result of this route of administra-ion. Remarkably, pain and ecchymosis were significantly reducedpon i.d. vaccination, irrespective of the dose administered. Overall,dverse reactions were in most cases mild or moderate and resolvedithin few days.
A potential limitation of this study may be that the i.d. anti-en administration was done by hypodermic needle. Despitehe effectiveness of this technique, the successful administrationonsiderably depends on the skill of trained medical person-el. I.d. injection by hypodermic needle may therefore be not asuch appreciated and widely accepted as i.m. vaccination. Recent
pproaches in i.d. administration of antigens therefore explorehe use of patches, electroporation or different types of devices35,36] in order to simplify i.d. antigen delivery and to support stan-ardization of i.d. vaccination. In addition, it cannot be excludedhat reduced i.m. doses of virosomal adjuvanted influenza vaccineould also have elicited satisfactory immunogenicity as shown forsplit influenza vaccine in healthy adults [23].
In conclusion, Inflexal®V proved to be highly immunogenic andafe in healthy adults when given i.d. at reduced doses and fulfilledhe EMEA criteria set for re-licensing of influenza vaccines, irre-pective of dose and route of administration and thus suggests aromising antigen-sparing strategy in this age group.
eferences
[1] Brady MT. Influenza virus infections in children. Seminar Pediatr Infect Dis1998;9:92–102.
[2] Centers for Disease Control and Prevention. Prevention and Control of Influenza.Recommendations of the Advisory Committee on Immunisation Practices(ACIP). MMWR 2008; 57:1–60.
[3] Couch RB, Kasel JA, Glezen WP, Cate TR, Six HR, Taber LH, et al. Influenza: itscontrol in persons and populations. J Infect Dis 1986;153:431–40.
[4] Cox NJ, Subbarao K. Influenza. Lancet 1999;354:1277–82.[5] Glezen WP, Taber LH, Frank AL, Gruber WC, Piedra PA. Influenza virus infections
in infants. Pediatr Infect Dis J 1997;16:1065–8.[6] Gross PA, Quinnan GV, Rodstein M, LaMontagne JR, Kaslow RA, Saah AJ, et al.
Association of influenza immunization with reduction in mortality in an elderlypopulation. A prospective study. Arch Intern Med 1988;148:562–5.
[7] Nichol KL, Margolis KL, Wuorenma J, von Sternberg T. The efficacy and costeffectiveness of vaccination against influenza among elderly persons living inthe community. N Engl J Med 1994;331:778–84.
[8] Patriarca PA, Weber JA, Parker RA, Hall WN, Kendal AP, Bregman DJ, et al. Efficacyof influenza vaccine in nursing homes. Reduction in illness and complicationsduring an influenza A (H3N2) epidemic. JAMA 1985;253:1136–9.
[9] Cohen GM, Nettleman MD. Economic impact of influenza vaccination inpreschool children. Pediatrics 2000;106:973–6.
10] Esposito S, Marchisio P, Bosis S, Lambertini L, Claut L, Faelli N, et al. Clinical and
economic impact of influenza vaccination on healthy children aged 2–5 years.Vaccine 2006;24:629–35.11] Navas E, Salleras L, Dominguez A, Ibanez D, Prat A, Sentis J, et al. Cost-effectiveness analysis of inactivated virosomal subunit influenza vaccination inchildren aged 3–14 years from the provider and societal perspectives. Vaccine2007;25:3233–9.
[
[
(2009) 3561–3567 3567
12] Salleras L, Dominguez A, Pumarola T, Prat A, Marcos MA, Garrido P, et al. Effec-tiveness of virosomal subunit influenza vaccine in preventing influenza-relatedillnesses and its social and economic consequences in children aged 3–14 years:a prospective cohort study. Vaccine 2006;24:6638–42.
13] Nichol KL, Lind A, Margolis KL, Murdoch M, McFadden R, Hauge M, et al. Theeffectiveness of vaccination against influenza in healthy, working adults. N EnglJ Med 1995;333:889–93.
14] Holland D, Booy R, De Looze F, Eizenberg P, McDonald J, Karrasch J, et al.Intradermal influenza vaccine administered using a new microinjection systemproduces superior immunogenicity in elderly adults: a randomized controlledtrial. J Infect Dis 2008;198:650–8.
15] Janeway CAJ, Travers P, Walport M, Capra JD. Immunobiology: the immunesystem in health and disease. 4th ed. New York: Garland Publishing; 1999.
16] Redfield RR, Innis BL, Scott RM, Cannon HG, Bancroft WH. Clinical evaluation oflow-dose intradermally administered hepatitis B virus vaccine. A cost reductionstrategy. JAMA 1985;254:3203–6.
[17] Sabchareon A, Chantavanich P, Pasuralertsakul S, Pojjaroen-Anant C,Prarinyanupharb V, Attanath P, et al. Persistence of antibodies in childrenafter intradermal or intramuscular administration of preexposure primary andbooster immunizations with purified Vero cell rabies vaccine. Pediatr Infect DisJ 1998;17:1001–7.
18] Pancharoen C, Mekmullica J, Thisyakorn U, Kasempimolporn S, Wilde H, Her-zog C. Reduced-dose intradermal vaccination against hepatitis A with analuminum-free vaccine is immunogenic and can lower costs. Clin Infect Dis2005;41:1537–40.
19] Belshe RB, Newman FK, Cannon J, Duane C, Treanor J, Van Hoecke C, et al. Serumantibody responses after intradermal vaccination against influenza. N Engl JMed 2004;351:2286–94.
20] Kenney RT, Frech SA, Muenz LR, Villar CP, Glenn GM. Dose sparing with intra-dermal injection of influenza vaccine. N Engl J Med 2004;351:2295–301.
21] Künzi V, Kürsteiner O, Lazar H, Seiberling M. Intradermal administration of avirosomal influenza vaccine: a promising antigen sparing strategy. Options forthe control of influenza VI. International Medical Press; 2008. p. 380–382.
22] Auewarakul P, Kositanont U, Sornsathapornkul P, Tothong P, Kanyok R,Thongcharoen P. Antibody responses after dose-sparing intradermal influenzavaccination. Vaccine 2007;25:659–63.
23] Belshe RB, Newman FK, Wilkins K, Graham IL, Babusis E, Ewell M, et al. Compara-tive immunogenicity of trivalent influenza vaccine administered by intradermalor intramuscular route in healthy adults. Vaccine 2007;25:6755–63.
24] Moser C, Amacker M, Kammer AR, Rasi S, Westerfeld N, Zurbriggen R. Influenzavirosomes as a combined vaccine carrier and adjuvant system for prophylacticand therapeutic immunizations. Expert Rev Vaccines 2007;6:711–21.
25] Herzog C, Hartmann K, Künzi V, Kürsteiner O, Mischler R, Lazar H. Eleven yearsof Inflexal V. Vaccine; submitted for publication.
26] The European Agency for the Evaluation of Medicinal Products (EMEA).Note for guidance on harmonisation of requirements for influenza vaccines.CPMP/BWP/214/96; 1997.
27] WHO. Recommended composition of influenza virus vaccines for use in the2007–2008 influenza season. Wkly Epidemiol Rec 2007;82:69–74.
28] Mischler R, Metcalfe IC. Inflexal V a trivalent virosome subunit influenza vac-cine: production. Vaccine 2002;20:B17–23.
29] Nicholson KG, Wood JM, Zambon M. Influenza. Lancet 2003;362:1733–45.30] WHO. Influenza: Report by the WHO Secretariat for 111th Session of the WHO
Executive Board, January 2003. Document EB111/10; 2003.31] Heikkinen T, Booy R, Campins M, Finn A, Olcen P, Peltola H, et al. Should healthy
children be vaccinated against influenza? A consensus report of the Summitsof Independent European Vaccination Experts. Eur J Pediatr 2006;165:223–8.
32] McIntosh K, Lieu T. Is it time to give influenza vaccine to healthy infants? N EnglJ Med 2000;342:275–6.
33] Belshe RB, Mendelman PM, Treanor J, King J, Gruber WC, Piedra P, et al. Theefficacy of live attenuated, cold-adapted, trivalent, intranasal influenza virusvaccine in children. N Engl J Med 1998;338:1405–12.
34] Beyer WE, Palache AM, de Jong JC, Osterhaus AD. Cold-adapted live influenzavaccine versus inactivated vaccine: systemic vaccine reactions, local andsystemic antibody response, and vaccine efficacy. A meta-analysis. Vaccine2002;20:1340–53.
35] Glenn GM, Kenney RT. Mass vaccination: solutions in the skin. Curr Top Micro-biol Immunol 2006;304:247–68.
36] Garg S, Hoelscher M, Belser JA, Wang C, Jayashankar L, Guo Z, et al. Needle-free skin patch delivery of a vaccine for a potentially pandemic influenza virusprovides protection against lethal challenge in mice. Clin Vaccine Immunol2007;14:926–8.




















