Perspectives in Multiphasic Osteochondral Tissue Engineering
10
Perspectives in Multiphasic Osteochondral Tissue Engineering JUNE E. JEON, 1 CEDRYCK VAQUETTE, 1 TRAVIS J. KLEIN, 1 AND DIETMAR W. HUTMACHER 1,2 * 1 Institute of Health and Biomedical Innovation, Queensland University of Technology 60 Musk Ave., Kelvin Grove, QLD, 4059, Australia 2 George W. Woodruff School of Mechanical Engineering, Georgia Institute of Technology, 315 Ferst Drive Atlanta, GA 30332, USA ABSTRACT Critical-sized osteochondral defects are clinically challenging, with limited treatment options available. By engineering osteochondral grafts using a patient’s own cells and osteochondral scaffolds designed to facili- tate cartilage and bone regeneration, osteochondral defects may be treated with less complications and better long-term clinical outcomes. Scaffolds can influence the development and structure of the engineered tissue, and there is an increased awareness that osteochondral tissue engineering concepts need to take the in vivo complexities into account in order to increase the likelihood of successful osteochondral tissue repair. The developing trend in osteochondral tissue engineering is the utiliza- tion of multiphasic scaffolds to recapitulate the multiphasic nature of the native tissue. Cartilage and bone have different structural, mechanical, and biochemical microenvironments. By designing osteochondral scaffolds with tissue-specific architecture, it may be possible to enhance osteochon- dral repair within shorter timeframe. While there are promising in vivo outcomes using multiphasic approaches, functional regeneration of osteo- chondral constructs still remains a challenge. In this review, we provide an overview of in vivo osteochondral repair studies that have taken place in the past three years, and define areas which needs improvement in future studies. Anat Rec, 297:26–35, 2014. V C 2013 Wiley Periodicals, Inc. Key words: tissue engineering; stem cell; osteochondral INTRODUCTION Patients affected with traumatic osteochondral lesions, osteochondritis dissecans, and osteochondroses have osteochondral defects with limited spontaneous healing. When left untreated, these lesions cause pain and limited mobility, and eventually lead to degenerative conditions such as osteoarthritis. Current treatment strategies such as osteochondral autograft transplantation (OATS)/ mosaicplasty and osteochondral allograft transplant have resulted in good cartilage/bone repair. However, these techniques can result in further complications such as donor site morbidity and graft rejections (Paul et al., 2009), and further degenerative changes in some patients (Hangody et al., 2010). By engineering osteochondral grafts using a patient’s own cells and osteochondral scaf- folds designed to facilitate cartilage and bone regenera- tion, osteochondral defects may be treated with less complications and better long-term clinical outcomes. Over the last decade, there have been many new developments in various aspects of scaffold manufactur- ing. Computer-aided designs and manufacturing technol- ogies are being used to fabricate personalized scaffolds *Correspondence to: Prof. Dietmar W. Hutmacher, PhD, MBA, Institute of Health and Biomedical Innovation, Queens- land University of Technology, 60 Musk Ave., Kelvin Grove, QLD 4059, Australia. Fax: 161-7-3138-6030. E-mail: [email protected] Received 13 September 2013; Accepted 13 September 2013. DOI 10.1002/ar.22795 Published online 2 December 2013 in Wiley Online Library (wileyonlinelibrary.com). THE ANATOMICAL RECORD 297:26–35 (2014) V V C 2013 WILEY PERIODICALS, INC.
Transcript of Perspectives in Multiphasic Osteochondral Tissue Engineering

Perspectives in MultiphasicOsteochondral Tissue Engineering
JUNE E. JEON,1 CEDRYCK VAQUETTE,1 TRAVIS J. KLEIN,1 AND
DIETMAR W. HUTMACHER1,2*1Institute of Health and Biomedical Innovation, Queensland University of Technology 60
Musk Ave., Kelvin Grove, QLD, 4059, Australia2George W. Woodruff School of Mechanical Engineering, Georgia Institute of Technology,
315 Ferst Drive Atlanta, GA 30332, USA
ABSTRACTCritical-sized osteochondral defects are clinically challenging, with
limited treatment options available. By engineering osteochondral graftsusing a patient’s own cells and osteochondral scaffolds designed to facili-tate cartilage and bone regeneration, osteochondral defects may betreated with less complications and better long-term clinical outcomes.Scaffolds can influence the development and structure of the engineeredtissue, and there is an increased awareness that osteochondral tissueengineering concepts need to take the in vivo complexities into account inorder to increase the likelihood of successful osteochondral tissue repair.The developing trend in osteochondral tissue engineering is the utiliza-tion of multiphasic scaffolds to recapitulate the multiphasic nature of thenative tissue. Cartilage and bone have different structural, mechanical,and biochemical microenvironments. By designing osteochondral scaffoldswith tissue-specific architecture, it may be possible to enhance osteochon-dral repair within shorter timeframe. While there are promising in vivooutcomes using multiphasic approaches, functional regeneration of osteo-chondral constructs still remains a challenge. In this review, we providean overview of in vivo osteochondral repair studies that have taken placein the past three years, and define areas which needs improvement infuture studies. Anat Rec, 297:26–35, 2014. VC 2013 Wiley Periodicals,Inc.
Key words: tissue engineering; stem cell; osteochondral
INTRODUCTION
Patients affected with traumatic osteochondral lesions,osteochondritis dissecans, and osteochondroses haveosteochondral defects with limited spontaneous healing.When left untreated, these lesions cause pain and limitedmobility, and eventually lead to degenerative conditionssuch as osteoarthritis. Current treatment strategies suchas osteochondral autograft transplantation (OATS)/mosaicplasty and osteochondral allograft transplant haveresulted in good cartilage/bone repair. However, thesetechniques can result in further complications such asdonor site morbidity and graft rejections (Paul et al.,2009), and further degenerative changes in some patients(Hangody et al., 2010). By engineering osteochondralgrafts using a patient’s own cells and osteochondral scaf-folds designed to facilitate cartilage and bone regenera-
tion, osteochondral defects may be treated with lesscomplications and better long-term clinical outcomes.
Over the last decade, there have been many newdevelopments in various aspects of scaffold manufactur-ing. Computer-aided designs and manufacturing technol-ogies are being used to fabricate personalized scaffolds
*Correspondence to: Prof. Dietmar W. Hutmacher, PhD,MBA, Institute of Health and Biomedical Innovation, Queens-land University of Technology, 60 Musk Ave., Kelvin Grove,QLD 4059, Australia. Fax: 161-7-3138-6030.E-mail: [email protected]
Received 13 September 2013; Accepted 13 September 2013.
DOI 10.1002/ar.22795Published online 2 December 2013 in Wiley Online Library(wileyonlinelibrary.com).
THE ANATOMICAL RECORD 297:26–35 (2014)
VVC 2013 WILEY PERIODICALS, INC.

for irregularly shaped defects (Hung et al., 2003; Swiesz-kowski et al., 2007). Materials used for scaffolds and mat-rices are becoming smarter and more versatile, and canbe modified to incorporate bioactive peptides (Grafahrendet al., 2011). Even though scaffold manufacturing technol-ogies are advancing at a rapid pace, no engineering strat-egies used to date can fully recapitulate the biochemicaland physical characteristics of the native osteochondraltissue. While it is usually helpful to simplify the approachto in vivo repair from an engineering point of view, for asuccessful in vivo outcome, the biological complexitiesthat take place within the joint must also be accounted forin the design. Furthermore, it is important to evaluateand analyze in vivo successes and failures to improve thedesign of future implants.
Osteochondral tissue has a heterogeneous, multilay-ered structure comprised of non-calcified cartilage(superficial, middle, deep zone), calcified cartilage, andsubchondral bone. The developing trend in osteochondraltissue engineering is the utilization of multiphasic scaf-folds to recapitulate the multiphasic nature of the nativetissue (Keeney and Pandit, 2009). There are a number ofdifferent multiphasic approaches which involve differentmaterials, cells, and bioactive molecules. In this review,we will discuss the emergence of multiphasic osteochon-dral tissue engineering concepts, then shift our focustoward in vivo successes and failures of multiphasic scaf-folds to date and highlight future trends that are gearedtoward more clinically relevant osteochondral tissueengineering strategies.
PREVALENCE OF MULTIPHASIC APPROACH
Different types of biomaterials can be used to fabricateosteochondral scaffolds, and both hydrogels/matrices andpolymeric scaffolds have been used in the past. Hydrogelsare synthetic or natural polymeric matrices with an excel-lent ability to attract and retain water. Mechanical prop-erties of hydrogels can be influenced by the polymercontent and crosslink density. Hydrogels are used exten-sively in many different medical applications, includingtissue engineering, and there is a good review on this
topic (Drury and Mooney, 2003). Polymeric scaffolds cantake on a variety of shapes and porosity, and they can bemanufactured into woven/non-woven fabrics, meshes,sponges, and porous scaffolds with defined three-dimensional structures. Different types of polymers havebeen used for cartilage and bone tissue engineering scaf-folds, and has been reviewed by Hutmacher et al (Hut-macher, 2000). The cartilage compartment is generallycomposed of hydrogels (collagen type I or II, hyaluronan,chitosan, alginate, gelatin, agarose) although biodegrad-able synthetic polymers such as polylactic acid (PLA), pol-y(lactic-co-glycolic acid) (PLGA), and polycaprolactone(PCL) have also been used for this application. The bonecomportment is usually made from synthetic polymers orstiff materials (e.g., hydroxyapatite, tri-calcium phos-phate, calcium polyphosphate, bioglass). There are goodreviews available on commonly used biomaterials for scaf-folds used in osteochondral tissue engineering (Martinet al., 2007; O’Shea and Miao, 2008; Keeney and Pandit,2009), and they will not be covered in detail in this review.
Scaffolds can influence the development and structureof the engineered tissue, and there is an increased aware-ness that osteochondral tissue engineering concepts needto take the in vivo complexities into account in order toincrease the likelihood of a successful osteochondral tis-sue repair. Tissue structure is often linked to tissue func-tion, and from a tissue engineering perspectives, theability to recapitulate the structural aspects of the tissuecan be important in order to restore function. Osteochon-dral scaffold designs can be generally categorized asmonophasic, biphasic, or triphasic (Fig. 2). Monophasicapproaches feature constructs fabricated from one mate-rial or one type of composite material with no spatial var-iations. In cellular or biological perspective, monophasicscaffolds do not have more than one cell type throughoutthe construct, and have no variation in the distribution ofbioactive molecules. On the other hand, biphasic or tri-phasic approaches utilize two or three different materials,composites, or architecture to create a multilayered struc-ture. One material can also be used to create biphasic ortriphasic scaffolds if significant depth-dependent varia-tions in physical properties exist between the differentlayers. Seeding different types of cells in the differentscaffold layers or having more than one biological envi-ronment through incorporation of bioactive molecules canalso result in biphasic/triphasic scaffolds. While mono-phasic approaches are still being used in some osteochon-dral regeneration studies, research focus is currentlyshifting toward multiphasic designs. The major advant-age of multiphasic approaches is the ability to providephysical or biochemical cues which specifically targetscartilage or bone development. Cartilage and bone havedifferent structural, mechanical, and biochemical micro-environments, and there are obvious limitations whenosteochondral scaffold designs do not address such differ-ences. Although scaffolds do not necessarily have to repli-cate all such parameters, tailoring osteochondral scaffoldswith tissue-specific architecture may aid in generatingfunctional osteochondral constructs within a shortertimeframe.
BENCH-TO-BEDSIDE
Implantation of tissue-engineered osteochondral con-structs in vivo presents various challenges that are
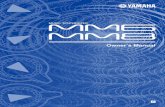
Fig. 1. Osteochondral tissue has a heterogeneous, multilayeredstructure comprised of non-calcified cartilage (superficial, middle,deep zone), calcified cartilage, and subchondral bone. Osteochondraltissue stained with Safranin-O shows depth-dependent distribution ofglycosaminoglycans (GAG).
PERSPECTIVES IN MULTIPHASIC OSTEOCHONDRAL TISSUE ENGINEERING 27

absent in an in vitro environment. The implanted con-struct is exposed to many different biological, chemical,and physical constraints which greatly influence neo-tissue survival, development, and functionality. Cellswithin the implanted construct will be exposed to vari-ous soluble factors secreted by the other cells (e.g., chon-drocytes, osteoblasts, and synovial cells), oxygen andnutrient gradient within the joint tissues, and thedynamic mechanical environment within the joint cannot only contribute to the development of the osteochon-dral grafts, but also their failures. Therefore, it is impor-tant that follow-up and evaluation studies are performedon the scaffold designs that were particularly promisingin vivo, and in case of failures, discuss how they can beimproved for future success. This point also leads us tothe fact that while extensive in vitro studies on scaffoldproperties and cell-culture work can provide some keyimplications about the scaffold, research efforts mustcontinue toward in vivo studies in order to gauge itspotential impact on osteochondral tissue regeneration.
Promising Approaches
Growth factors. Cartilage and bone have differ-ent healing timeframe and growth factors that directlyinfluence tissue morphogenesis. By targeting them sepa-rately with biphasic distribution of growth factors, it is
possible to accelerate and enhance the overall repair ofthe osteochondral defect. Integrating bioactive compo-nents into the scaffold designs have become one of themost interesting developments, and there is a recentreview on this topic (Santo et al., 2013a, 2013b). Biomate-rials can be synthesized or manufactured to provide notonly the structural support, but also biological cues toinfluence cellular activity and tissue development. Incor-poration of transforming growth factor beta (TGF-b1) andbone morphogenic protein-2 (BMP-2) in scaffolds usingPLGA microspheres have shown sustained growth factorrelease over 3–6 weeks (Dormer et al., 2010; Reyes et al.,2012), and have resulted in bone development as early asweek 6 post implantation in rabbit osteochondral defects(Dormer et al., 2012). A slightly different approachinvolves altering the biomaterials themselves to facilitatestronger affinity to bioactive peptides and growth factorsto improve their retention (Grafahrend et al., 2011).Recently, chemically modified alginate hydrogels withincreased affinity toward growth factors have been usedto create biphasic osteochondral constructs with good invivo outcomes (Re’em et al., 2012). This group reportedthat their bilayer constructs with affinity bound TGF-b1and BMP-4 resulted in rapid cartilage and bone formationin as little as 4 weeks post-implantation, with good colla-gen type II distribution in the cartilage compartment.Another interesting and successful approach in this
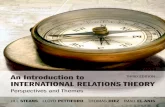
Fig. 2. Various osteochondral scaffold design approaches. Osteochondral tissue engineering strategiescan be categorized into monophasic, biphasic, and triphasic based on the physical/chemical or cellular/biological characteristics of the scaffold.
28 JEON ET AL.

regard is to integrate biphasic scaffolds with growth fac-tor plasmids to alter cellular activity. Chen et al. (2011)have used TGF-b1 and BMP-2 plasmids to influence carti-lage and bone regeneration, respectively, in biphasic scaf-folds made of gelatine, chitosan, and hydroxyapatite, andfound that biphasic scaffolds with the plasmids had excel-lent osteochondral regeneration by week 4 in rabbit osteo-chondral defect model. With the current trend ofcombining biological functionality with multiphasic scaf-folds, it is likely that osteochondral tissue engineeringapproaches will become much more comprehensive andmultifaceted to augment the osteochondral repair in vivo.
Pre-culture. Reports show that allowing osteo-chondral grafts to develop in vitro prior to in vivoimplantation can have a positive influence in improvingthe quality of the repair following implantation in vivo.Miot et al. (2012) have reported that chondrocyte-seededbiphasic scaffolds that were pre-cultured for at least 2weeks had significantly improved tissue morphologycompared to those that were implanted without pre-culture following 8 months of in vivo implantation in acaprine model. Pre-culture in differentiation media mayespecially be beneficial when using multipotent progeni-tor cells or dedifferentiated chondrocytes or osteoblasts.In vitro culture in the presence of specific growth factors(e.g., TGF-b1/BMP-2) allows the progenitor cells to com-mit to either the chondrogenic or osteogenic pathway,inducing tissue-specific developments. This approachhas been adopted by Sheehy, et al., and they havereported that pre-differentiation of agarose-encapsulatedbone marrow stromal cells (BMSCs) in either chondro-genic or osteogenic medium (3 weeks) prior to biphasicassembly enhanced the accumulation of glycosaminogly-cans (GAG) and calcium in vivo (Sheehy et al., 2013).The maturation of tissue engineered constructs in vitroallows them to gain matrix molecules such as GAG andcollagen, which play important roles in withstanding thephysiological mechanical load. Some modeling studieshave shown that the maturity of tissue at the time ofimplantation has a large influence not only on theimplanted construct itself, but on the surrounding carti-lage, and affects collagen remodeling of the tissue (Nageland Kelly, 2013). While culturing osteochondral grafts invitro prior to in vivo implantation can be labor-intensiveand time consuming, they can potentially influence thelong-term repair, making them an important considera-tion in an in vivo study.
Need for Future Improvement
Analysis of mechanical properties. Clinically,an osteochondral injury from trauma usually occurs onthe load-bearing part of the joint. As a result, in mostanimal models, osteochondral defects are created on thefemoral condyles, which are subjected to various types ofmechanical loading such as compression, shear, andhydrostatic pressure. It is commonly accepted thatcritical-sized osteochondral defects can induce significantdegenerative changes to the surrounding cartilage andbone, possibly due to mechanical destabilization origi-nating from from the defect region not being able tocarry the load (Schinhan et al., 2012). In this regard, anewly developing osteochondral construct with inferiormechanical properties can also contribute to the
mechanical imbalance near the defect region until theirmechanical properties have matured (Khoshgoftar et al.,2013). Mayr, et al., have reported that the cartilage com-ponent of the osteochondral graft had only half the stiff-ness of the surrounding cartilage 6 months postimplantation Mayr et al. (2013). The longer the osteo-chondral graft takes to fully mature in mechanical prop-erties, the longer the surrounding cartilage is exposed toexcessive load, which can contribute to degenerativeprocesses. Unfortunately, few in vivo studies investigatethe mechanical stiffness of the repaired tissue or thesurrounding tissue. Considering the effort and cost of anin vivo experiment, it should be emphasized that thor-ough evaluation of the in vivo explants, above andbeyond the histological means, could provide importantdata sets that can be used to improve osteochondral tis-sue engineering designs used in future studies.
Integration. Integration between the host tissueand the osteochondral graft is critical in the long-termsurvival of the implant. However, incomplete integrationis frequently observed, especially in the cartilage com-partment. There are a number of potential factors whichcan impede integration. PRG4, a lubricating moleculeabundantly present in synovial fluid, has been shown toinhibit cartilage integration (Englert et al., 2005). Inaddition, studies show that cell death around the edge ofthe tissue has been found to hamper tissue integration(Gilbert et al., 2009). In order to facilitate cell-mediatedbridging between the host cartilage and the engineeredgraft, chondrocyte-seeded collagen gel can be used toseal the gap between the host cartilage and the engi-neered graft (Pabbruwe et al., 2009).
It can also be postulated that the typical lack of colla-gen fiber orientation in the repaired cartilage also has arole in preventing strong integration at the cartilagelevel. The superficial zone of the cartilage in normal car-tilage is aligned horizontally, parallel to the direction ofjoint articulation. However, within the repaired carti-lage, this arrangement is often missing, hence the edgeadjoining the native and engineered cartilage tissue isprone to breakage. Vertical orientation of collagens nearthe subchondral bone has been attributed to anchoringthe cartilage tissue against large strains (Shirazi et al.,2008). Lack of collagen orientation in a dynamic loadingenvironment of the joint is likely to have a role in invivo failure of implanted constructs and diminished inte-gration. Additionally, it is well-documented that carti-lage stiffness is depth-dependent, and that superficialcartilage layer deforms much more than the deeperlayers (Schinagl et al., 1997). In this regard, when thecartilaginous component of the osteochondral scaffoldslack the depth-varying deformation patterns, mis-matched compressive strain levels between the cartilageand the implant is likely to result in increased shearstress at the interface region, causing a tear. Tissueengineering cartilage grafts with depth-varying compres-sive properties have also been proposed in the past(Klein et al., 2009), and can be incorporated in futureosteochondral construct designs. Scaffold architectureand the presence of migratory cells within or immedi-ately surrounding the osteochondral tissue graft willlikely to play a key role in integration and tissue repair,
PERSPECTIVES IN MULTIPHASIC OSTEOCHONDRAL TISSUE ENGINEERING 29

and have important implications for future osteochon-dral tissue engineering approaches.
Sinking scaffolds. One of the problems oftenobserved in vivo is that the implanted scaffold sinks intothe bone (Fig. 3). This has been reported in studiesusing stiff scaffold materials (e.g., tantalum metal (Mro-sek et al., 2010), PCL (Ho et al., 2010)) as well thoseusing soft materials (e.g., alginate (Heiligenstein et al.,2011)) for their in vivo implants. Reasons behindscaffold-sinking most likely come from a few differentfactors. Some of the likely contributing factors includeincreased macrophage activity (Pei et al., 2009) as wellas the resorption of bone on the bottom of the osteochon-dral defect through increased osteoclast activity relatedto mechanical stress (Duda et al., 2005). The types ofcells seeded in the implanted osteochondral constructmay also affect tissue development by attracting macro-phages. One study which used xenogenic synovium-derived cells to seed the osteochondral implant reportedpositive staining of macrophages around the osteochon-dral graft which are likely to have caused scaffold sink-ing and ultimately implant failure (Pei et al., 2010). Inorder to improve the integration and functionality of theimplanted osteochondral constructs, further investiga-tion is needed to determine the exact causes of scaffoldsinking.
Fibrocartilage formation. Tissue-engineeredosteochondral grafts do not always result in hyaline car-tilage, and fibrocartilage developments have beenreported in the past. Fibrocartilage refers to cartilagetissues that contain high percentage of collagen type I,which is not normally found in healthy hyaline cartilage.This type of cartilage has inferior mechanical properties,
and has limited longevity in the demanding mechanicalenvironment within the joint. It is one of the causes oftreatment failures in patients that receive autologouscell implantations or subchondral drilling/microfracture,as a large percentage of such treatments result in theformation of fibrocartilage (Bentley et al., 2003; Williamsand Harnly, 2007). While most investigators stain theirtissue explants with Safranin-O (GAG) and hemotoxy-lene/eosin (nucleus, cytoplasm), it is important to alsoroutinely stain or analyze for collagen type I and II (Fig.4). Many of the in vivo osteochondral tissue engineeringstudies induce subchondral bone bleeding as they createfull-thickness osteochondral defects, and with theimplantation of the new scaffold, whether with or with-out the previous cell-seeding, the scaffolds may becomeinfused with the blood from the subchondral bone. Whilethere are advantages to this, mainly the recruitment ofthe progenitor cells, this could also lead to fibrocartilageformation and therefore it is important to perform sys-tematic analysis to detect collagen type I in the repairedcartilage, and compare them to the untreated emptydefect, which is most likely to be similar to the clinicallyused treatments such as subchondral drilling. It hasbeen seen in the past that even when the repaired carti-lage has good macroscopic morphology and GAG levels,it is possible to have high levels of collagen type I (Peiet al., 2010). Unfortunately, the majority of the recent invivo studies do not report on collagen type I content intheir repaired cartilage. Unless the newly implantedscaffolds can reduce fibrocartilage formation whileimproving overall tissue quality, it will be difficult to jus-tify the efficacy of such treatment.
Furthermore, it is also important to investigate thestructural organization of the collagen fibrils within thecartilage. While the cartilage may have decent GAG con-tent, without the zone-specific collagen organization, the
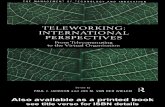
Fig. 3. Scaffold sinking in vivo. PCL (A) and tantalum metals (B) have been reported to sink furtherbelow the site of initial defect (Bal et al., 2010; Ho et al., 2010).
30 JEON ET AL.

repaired cartilage grafts will not have similar mechani-cal properties as the native cartilage (Laasanen et al.,2003). Zone-dependent organization of collagen fibrilswithin the healthy articular cartilage is well docu-mented, and such organization has a large influence onthe mechanical properties of the cartilage and how itbehaves under joint loading (Halonen et al., 2013).Polarized light microscopy can be used to visualize thebirefringence from depth-dependent collagen fiber orien-tations within the cartilage tissue (Kiraly et al., 1997).More recently, small angle X-ray scattering (Mogeret al., 2007), Fourier transform infrared spectroscopy(Boskey and Pleshko Camacho, 2007) and second har-monic generation multiphoton microscopy (Brown et al.,2003) have also been used to this end. It has proven dif-ficult, however, to control how the collagen fibers arearranged and remodeled within the repaired cartilage,but its importance in the functionality of the repairedcartilage tissue is clear, and collagen fiber alignmentneeds to be examined when in vivo explants are eval-uated. Apart from the role that collagen fibrils play indetermining the mechanical properties of the cartilage,collagen fibers also help control proteoglycan (PG) swel-ling and retention within its framework (Poole et al.,2001). Lack of collagen network and its unique architec-ture may result in PG loss and tissue swelling (Khosh-goftar et al., 2013). One study in particular has reportedthat tissue engineered cartilage in minipigs begin toshow depth-dependent collagen orientation at 26 weeks,and continues to develop until they reach native-cartilage like collagen orientation after 52 weeks (Paet-zold et al., 2012). Since typical in vivo studies last for up
to 6 months (26 weeks), it is likely that some collagenalignment is present within the tissue, and will offeradditional information on the functionality of therepaired osteochondral tissue.
Natural healing of immature animals:Deciphering scaffold benefits. Immature ani-mals have naturally excellent regenerative abilities, andthere are a number of differences in the way osteochon-dral defects in immature animals heal compared to thoseof an adult animal. A study has shown that when anosteochondral defect was left untreated in an immaturerabbit, it showed an excellent repair, comparable to nor-mal cartilage, while the same untreated defect in maturerabbits did not heal (Mrosek et al., 2010). In this respect,it is important to state whether the animal used in the invivo study is skeletally fully mature, as this may haveeven greater influence on the outcomes compared to thetreatment groups that was being studied. In addition, it isalso important to determine whether the osteochondraldefect created is of critical size, that is, a defect that willnot heal on its own without further treatment. This willserve as an important factor in deciphering the benefits ofthe newly implanted osteochondral construct, and it willmake it more feasible to compare between other studiesthat have used similarly mature animal.
FUTURE DIRECTIONS
Scaling-Up Animal Models
Many different animal species have been used in thepast for in vivo implantation of osteochondral constructs.
Fig. 4. Osteochondral repair in vivo. Rabbit osteochondral defects filled with porous hydroxyapatite/col-lagen biphasic constructs were stained with toluidine blue (A, B), collagen type II (C), and collagen type I(D) (Maehara et al., 2009).
PERSPECTIVES IN MULTIPHASIC OSTEOCHONDRAL TISSUE ENGINEERING 31

TABLE 1. In Vivo Osteochondral Repair Evaluation in Studies Conducted Between 2009 and 2012
Species
Defectdiameter
(mm)
Defectdepth(mm)
Emptydefect
control?Cell freecontrol?
Col IIstaining?
Col Istaining?
Mechanicaldata? References
Canine 4.2 6 No Yes Yes No No Yang et al. (2011)Canine 4 6 Yes No No No No Ng et al. (2010)Equine 10 10 No All cell free No No No Kon et al. (2010b)Goat 6 5 Yes Yes Yes
(ELISA)Yes
(ELISA)No Miot et al. (2012)
Goat 3 5 Yes Yes Yes No No Zhu et al. (2011)Human Variable 9 No All cell free Yes Yes No Kon et al. (2011)Minipigs 6 1 Yes All cell free Yes Yes No Hui et al. (2012)Minipigs 6 7 Yes Yes Yes Yes Yes (Stress relaxation) Im et al. (2010)Ovine 7 25 Yes No Yes No Yes (Stiffness) Mayr et al. (2013)Ovine 7 9 Yes All cell free Yes Yes No Kon et al. (2010a)Ovine 3.2 4 No Yes No No No Heiligenstein et al. (2011)Ovine 6.4 12 No No No No Yes (Indentation) Marquass et al. (2010)Ovine 7 2 Yes Yes Yes No No Zscharnack et al. (2010)Pigs 6.5 3 Yes Yes No No Yes (Stiffness) Chang et al. (2011)Pigs 8 8 Yes No Yes No Yes (Stiffness) Cui et al. (2011)Pigs 8 8 No Yes Yes Yes Yes (Stiffness) Ho et al. (2010)Pigs 8 8 Yes Yes Yes No Yes (Stress relaxation) Chiang et al. (2010)Rabbits 3 3 Yes All cell free Yes No No Re’em et al. (2012)Rabbits 4 5 Yes All cell free No No No Abarrategi et al. (2010)Rabbits 3 3 Yes All cell free Yes No No Chang et al. (2012)Rabbits 4 5 Yes No Yes No No Chen et al. (2011)Rabbits 4 5 Yes Yes No No No Cao et al. (2012)Rabbits 5 3 No No Yes Yes No Chen et al. (2009)Rabbits 3.2 4 Yes Yes Yes Yes No Bal et al. (2010)Rabbits 3 3 Yes No No No No Dormer et al. (2012)Rabbits 4.5 3 No Yes No No No Chen et al. (2011b)Rabbits 3 Variable Yes No No No No Emans et al. (2010)Rabbits 3 3 No Yes No No No Guo et al. (2010)Rabbits 4 5 Yes No Yes Yes No Pei et al. (2010)Rabbits 5 3 Yes No Yes No No Jin et al. (2011)Rabbits 5 6 Yes No No No No Mrosek et al. (2010)Rabbits 2 3 No Yes Yes No No Jung et al. (2012)Rabbits 4.5 4 Yes All cell free Yes Yes No Reyes et al. (2012)Rabbits 10, 15 5 Yes Yes Yes Yes No Deng et al. (2012)Rabbits 4 4 Yes No No No No Emans et al. (2012)Rabbits 4 2 Yes Yes Yes No No Lee et al. (2012)Rabbits 5 5 Yes All cell free Yes Yes No Maehara et al. (2010)Rabbits 3 2 Yes Yes No No No Miller et al. (2010)Rabbits 3.7 3 Yes Yes Yes No No Oshima et al. (2009)Rabbits 4 5 Yes Yes Yes Yes No Pei et al. (2009)Rabbits 4 4 No No Yes No No Wang et al. (2010)Rabbits 4.5 5 Yes Yes Yes No No Xie et al. (2010)Rabbits 3.5 3 Yes All cell free No No No Mohan et al. (2011)Rabbits 6 5 Yes Yes Yes Yes No Ahn et al. (2009)Rat 1 1 Yes All cell free Yes No No Unterman et al. (2012)Rat 1.5 3 Yes No Yes Yes No Xue et al. (2010)
TABLE 2. Average Osteochondral Defect Area and Depth in Animal Models and Human Clinical Trials
In vivo osteochondral defect studiesNumber of
studiesAverage defect
area (cm2)Average defect
depth (cm)
Rabbits 28 0.14 6 0.02 0.39 6 0.11Sheeps 5 0.29 6 0.02 1.00 6 0.91Pigs 4 0.46 6 0.00 0.68 6 0.25Rats 2 0.01 6 0.00 0.20 6 0.14Dogs 2 0.13 6 0.00 0.60 6 0.00Goats 2 0.16 6 0.04 0.50 6 0.00Minipigs 2 0.28 6 0.00 0.40 6 0.42Horses 1 0.79 6 0.00 1.00 6 0.00Human (knee; N 5 34; Average
age 5 35.3 6 10.2 years)1 1.5–6 0.9
32 JEON ET AL.

Rabbits, pigs, sheeps, horses, dogs, minipigs, and evenrats have been used for osteochondral defect models inthe past (Table 1). The defect size is often limited by thesize of the animal’s joint, and while cost-effective, thereare obvious limitations in extrapolating results fromsmaller animals to plan human clinical trials. As anexample, average size of osteochondral defects made inrabbits and dogs were about 0.14 cm2 and 0.13 cm2,respectively (Table 2), while osteochondral defects inhuman patients were more than 10 times larger, rangingfrom 1.5–6 cm2 (Kon et al., 2011). While in vivo experi-ments using small animal models bring innovative osteo-chondral tissue engineering concepts one step closer tohuman clinical trials, it is important to follow up suc-cessful small animal experiments by scaling up andusing animal models that have comparable joint dimen-sions and joint load. Animals such as sheeps, pigs, andhorses have surgically created defect sizes which rangefrom 0.29–0.79 cm2 and have average defect depths simi-lar to humans at around 0.68–1 cm. Body weights ofthese animals are also either comparable or much heav-ier than humans, making them a better suited models topredict the outcomes in clinical trials.
Multiphasic Designs
The emergence of biphasic scaffold designs hasenabled researchers to develop strategies to regenerateboth cartilage and bone simultaneously, and there aremany promising results to date. In the future, it is pro-jected that increasing number of triphasic designs willemerge. Kon, et al., have already carried this concept tohuman clinical trials Kon et al. (2011), but it is stilllargely a novel approach. Triphasic constructs may tar-get cartilage, calcified cartilage, and bone simultane-ously, allowing the transitional layer to tie in cartilageand bone compartment smoothly. Additionally, triphasicconcepts may also be interpreted as further developingthe idea of stratified cartilage and incorporating theminto osteochondral models. There are a number of groupsthat have developed multilayered cartilage constructseither with different chondrocyte subpopulations (Kimet al., 2003) or by using hydrogels with varying degreeof stiffness to mimic the stratified nature of the cartilage(Nguyen et al., 2011). And it will be interesting to seewhether osteochondral constructs with stratified carti-lage design produce tissue grafts with similar propertiesas the natural cartilage.
CONCLUSIONS
Osteochondral tissue engineering is continuing toevolve, as are osteochondral scaffolds, at a fast rate.Active research is being carried out in order to fabricatesmarter scaffolds. Osteochondral scaffolds are beingdesigned to facilitate tissue-specific growth-factor deliv-ery, mimic connective tissue ECM, be chondro- or osteo-inductive, and recapitulate the stratified nature of theosteochondral tissue through multiphasic designs. Whilethere are considerable efforts in finding new ways toimprove osteochondral scaffolds, evaluating their poten-tial in a long-term in vivo study is equally important. Inorder to expedite our progress in developing successfultissue engineering strategies, our standards for in vivoexperiments should be set higher. The scope of implant
evaluation should not be limited to evaluating generalmorphologies and macroscopic/histological scores, butalso include the assessment of collagen types, matrixorganization, and mechanical properties, since theirfunctionality is as important as their gross morphology.It is also highly encouraged that studies include appro-priate controls (empty defects, cell-free group) or providecomparisons to current clinical treatment strategies(subchondral drilling, OATS, ACI) to highlight the bene-fits and novelty. While it is difficult to directly comparedifferent tissue engineering strategies, standardized andsystematic evaluation of in vivo experiments will surelybenefit current efforts in osteochondral regeneration andpromote efficiency in future bench-to-bedside concepts.
LITERATURE CITED
Abarrategi A, Lopiz-Morales Y, Ramos V, Civantos A, Lopez-DuranL, Marco F, Lopez-Lacomba JL. 2010. Chitosan scaffolds for osteo-chondral tissue regeneration. J Biomed Mater Res A 95:1132–1141.
Ahn JH, Lee TH, Oh JS, Kim SY, Kim HJ, Park IK, Choi BS, ImGI. 2009. Novel hyaluronate-atelocollagen/beta-TCP-hydroxyapa-tite biphasic scaffold for the repair of osteochondral defects inrabbits. Tissue Eng Part A 15:2595–2604.
Bal BS, Rahaman MN, Jayabalan P, Kuroki K, Cockrell MK, YaoJQ, Cook JL. 2010. In vivo outcomes of tissue-engineered osteo-chondral grafts. J Biomed Mater Res B Appl Biomater 93:164–174.
Bentley G, Biant LC, Carrington RW, Akmal M, Goldberg A,Williams AM, Skinner JA, Pringle J. 2003. A prospective, rando-mised comparison of autologous chondrocyte implantation versusmosaicplasty for osteochondral defects in the knee. J Bone JointSurg Br 85:223–230.
Boskey A, Pleshko Camacho N. 2007. FT-IR imaging of native andtissue-engineered bone and cartilage. Biomaterials 28:2465–2478.
Buckwalter JA, Mankin HJ. 1998. Articular cartilage: tissue designand chondrocyte-matrix interactions. Instr Course Lect 47:477–486.
Cao Z, Hou S, Sun D, Wang X, Tang J. 2012. Osteochondral regen-eration by a bilayered construct in a cell-free or cell-basedapproach. Biotechnol Lett 34:1151–1157.
Chang CH, Kuo TF, Lin FH, Wang JH, Hsu YM, Huang HT, LooST, Fang HW, Liu HC, Wang WC. 2011. Tissue engineering-basedcartilage repair with mesenchymal stem cells in a porcine model.J Orthop Res 29:1874–1880.
Chang N-J, Lin C-C, Li C-F, Wang D-A, Issariyaku N, Yeh M-L.2012. The combined effects of continuous passive motion treat-ment and acellular PLGA implants on osteochondral regenerationin the rabbit. Biomaterials 33:3153–3163.
Chen HC, Chang YH, Chuang CK, Lin CY, Sung LY, Wang YH, HuYC. 2009. The repair of osteochondral defects using baculovirus-mediated gene transfer with de-differentiated chondrocytes in bio-reactor culture. Biomaterials 30:674–681.
Chen J, Chen H, Li P, Diao H, Zhu S, Dong L, Wang R, Guo T,Zhao J, Zhang J. 2011. Simultaneous regeneration of articularcartilage and subchondral bone in vivo using MSCs induced by aspatially controlled gene delivery system in bilayered integratedscaffolds. Biomaterials 32:4793–4805.
Chen W-C, Yao C-L, Wei Y-H, Chu I-M. 2011b. Evaluating osteo-chondral defect repair potential of autologous rabbit bone marrowcells on type II collagen scaffold. Cytotechnology 63:13–23.
Chiang H, Liao C-J, Wang Y-H, Huang H-Y, Chen C-N, Hsieh C-H,et al. 2010. Comparison of articular cartilage repair by autologouschondrocytes with and without in vitro cultivation. Tissue EngPart C 16:291–300.
Cui W, Wang Q, Chen G, Zhou S, Chang Q, Zuo Q, Ren K, Fan W.2011. Repair of articular cartilage defects with tissue-engineeredosteochondral composites in pigs. J Biosci Bioeng 111:493–500.
PERSPECTIVES IN MULTIPHASIC OSTEOCHONDRAL TISSUE ENGINEERING 33

Deng T, Lv J, Pang J, Liu B, Ke J. Construction of tissue-engi-neered osteochondral composites and repair of large joint defectsin rabbit. J Tissue Eng Regen Med, in press.
Dormer NH, Singh M, Wang L, Berkland CJ, Detamore MS. 2010.Osteochondral interface tissue engineering using macroscopic gra-dients of bioactive signals. Ann Biomed Eng 38:2167–2182.
Dormer NH, Singh M, Zhao L, Mohan N, Berkland CJ, DetamoreMS. 2012. Osteochondral interface regeneration of the rabbitknee with macroscopic gradients of bioactive signals. J BiomedMater Res Part A 100:162–170.
Drury JL, Mooney DJ. 2003. Hydrogels for tissue engineering: scaf-fold design variables and applications. Biomaterials 24:4337–4351.
Duda GN, Maldonado ZM, Klein P, Heller MO, Burns J, Bail H.2005. On the influence of mechanical conditions in osteochondraldefect healing. J Biomech 38:843–851.
Emans PJ, Jansen EJ, van Iersel D, Welting TJ, Woodfield TB,Bulstra SK, Riesle J, van Rhijn LW, Kuijer R. 2013. Tissue-engi-neered constructs: the effect of scaffold architecture in osteochon-dral repair. J Tissue Eng Regen Med 7:751–756.
Emans PJ, van Rhijn LW, Welting TJ, Cremers A, Wijnands N,Spaapen F, Voncken JW, Shastri VP. 2010. Autologous engineer-ing of cartilage. Proc Natl Acad Sci U S A 107:3418–3423.
Englert C, McGowan KB, Klein TJ, Giurea A, Schumacher BL, SahRL. 2005. Inhibition of integrative cartilage repair by proteogly-can 4 in synovial fluid. Arthritis Rheum 52:1091–1099.
Gilbert SJ, Singhrao SK, Khan IM, Gonzalez LG, Thomson BM,Burdon D, Duance VC, Archer CW. 2009. Enhanced tissue inte-gration during cartilage repair in vitro can be achieved by inhibi-ting chondrocyte death at the wound edge. Tissue Eng Part A 15:1739–1749.
Grafahrend D, Heffels KH, Beer MV, Gasteier P, Moller M, BoehmG, Dalton PD, Groll J. 2011. Degradable polyester scaffolds withcontrolled surface chemistry combining minimal protein adsorp-tion with specific bioactivation. Nat Mater 10:67–73.
Guo X, Park H, Young S, Kretlow JD, van den Beucken JJ, BaggettLS, Tabata Y, Kasper FK, Mikos AG, Jansen JA. 2010. Repair ofosteochondral defects with biodegradable hydrogel compositesencapsulating marrow mesenchymal stem cells in a rabbit model.Acta Biomater 6:39–47.
Halonen KS, Mononen ME, Jurvelin JS, Toyras J, Korhonen RK.2013. Importance of depth-wise distribution of collagen and pro-teoglycans in articular cartilage–a 3D finite element study ofstresses and strains in human knee joint. J Biomech 46:1184–1192.
Hangody L, Dobos J, Balo E, Panics G, Hangody LR, Berkes I.2010. Clinical experiences with autologous osteochondral mosaic-plasty in an athletic population: a 17-year prospective multicenterstudy. Am J Sports Med 38:1125–1133.
He W, Ma Z, Yong T, Teo WE, Ramakrishna S. 2005. Fabrication ofcollagen-coated biodegradable polymer nanofiber mesh andits potential for endothelial cells growth. Biomaterials 26:7606–7615.
Heiligenstein S, Cucchiarini M, Laschke MW, Bohle RM, Kohn D,Menger MD, Madry H. 2011. In vitro and in vivo characterizationof nonbiomedical- and biomedical-grade alginates for articularchondrocyte transplantation. Tissue Eng Part C Methods 17:829–842.
Ho ST, Hutmacher DW, Ekaputra AK, Hitendra D, Hui JH. 2010.The evaluation of a biphasic osteochondral implant coupled withan electrospun membrane in a large animal model. Tissue EngPart A 16:1123–1141.
Hui JH, Ren X, Afizah MH, Chian KS, Mikos AG. 2013. Oligo[poly(-ethylene glycol)fumarate] hydrogel enhances osteochondral repairin porcine femoral condyle defects. Clin Orthop Relat Res 471:1174–1185.
Hung CT, Lima EG, Mauck RL, Takai E, LeRoux MA, Lu HH,Stark RG, Guo XE, Ateshian GA. 2003. Anatomically shapedosteochondral constructs for articular cartilage repair. J Biomech36:1853–1864.
Hutmacher DW. 2000. Scaffolds in tissue engineering bone and car-tilage. Biomaterials 21:2529–2543.
Im GI, Ahn JH, Kim SY, Choi BS, Lee SW. 2010. A hyaluronate-ate-locollagen/beta-tricalcium phosphate-hydroxyapatite biphasic scaf-fold for the repair of osteochondral defects: a porcine study.Tissue Eng Part A 16:1189–1200.
Jin CZ, Cho JH, Choi BH, Wang LM, Kim MS, Park SR, Yoon JH,Oh HJ, Min BH. 2011. The maturity of tissue-engineered carti-lage in vitro affects the repairability for osteochondral defect. Tis-sue Eng Part A 17:3057–3065.
Julkunen P, Iivarinen J, Brama PA, Arokoski J, Jurvelin JS,Helminen HJ. 2010. Maturation of collagen fibril network struc-ture in tibial and femoral cartilage of rabbits. Osteoarthritis Car-tilage 18:406–415.
Jung MR, Shim IK, Chung HJ, Lee HR, Park YJ, Lee MC, Yang YI,Do SH, Lee SJ. 2012. Local BMP-7 release from a PLGA scaffold-ing-matrix for the repair of osteochondral defects in rabbits. JControl Release 162:485–491.
Keeney M, Pandit A. 2009. The osteochondral junction and itsrepair via bi-phasic tissue engineering scaffolds. Tissue Eng PartB Rev 15:55–73.
Khoshgoftar M, Wilson W, Ito K, van Donkelaar CC. 2013. Theeffect of tissue-engineered cartilage biomechanical and biochemi-cal properties on its post-implantation mechanical behavior. Bio-mech Model Mechanobiol 12:43–54.
Kim TK, Sharma B, Williams CG, Ruffner MA, Malik A, McFarlandEG, Elisseeff JH. 2003. Experimental model for cartilage tissueengineering to regenerate the zonal organization of articular car-tilage. Osteoarthritis Cartilage 11:653–664.
Kiraly K, Hyttinen MM, Lapvetelainen T, Elo M, Kiviranta I, DobaiJ, Modis L, Helminen HJ, Arokoski JP. 1997. Specimen prepara-tion and quantification of collagen birefringence in unstained sec-tions of articular cartilage using image analysis and polarizinglight microscopy. Histochem J 29:317–327.
Klein TJ, Malda J, Sah RL, Hutmacher DW. 2009. Tissue engineer-ing of articular cartilage with biomimetic zones. Tissue Eng PartB 15:143–157.
Kon E, Delcogliano M, Filardo G, Busacca M, Di Martino A,Marcacci M. 2011. Novel nano-composite multilayered biomaterialfor osteochondral regeneration: a pilot clinical trial. Am J SportsMed 39:1180–1190.
Kon E, Filardo G, Delcogliano M, Fini M, Salamanna F, GiavaresiG, Martin I, Marcacci M. 2010a. Platelet autologous growthfactors decrease the osteochondral regeneration capability of acollagen-hydroxyapatite scaffold in a sheep model. BMC Muscu-loskelet Disord 11:220.
Kon E, Mutini A, Arcangeli E, Delcogliano M, Filardo G,Nicoli Aldini N, Pressato D, Quarto R, Zaffagnini S,Marcacci M. 2010b. Novel nanostructured scaffold for osteochon-dral regeneration: pilot study in horses. J Tissue Eng Regen Med4:300–308.
Laasanen MS, Toyras J, Korhonen RK, Rieppo J, Saarakkala S,Nieminen MT, Hirvonen J, Jurvelin JS. 2003. Biomechanicalproperties of knee articular cartilage. Biorheology 40:133–140.
Lee H-R, Park KM, Joung YK, Park KD, Do SH. 2012. Platelet-richplasma loaded hydrogel scaffold enhances chondrogenic differen-tiation and maturation with up-regulation of CB1 and CB2. JControl Release 159:332–337.
Marquass B, Somerson JS, Hepp P, Aigner T, Schwan S, Bader A,Josten C, Zscharnack M, Schulz RM. 2010. A novel MSC-seededtriphasic construct for the repair of osteochondral defects. JOrthop Res 28:1586–1599.
Martin I, Miot S, Barbero A, Jakob M, Wendt D. 2007. Osteochon-dral tissue engineering. J Biomech 40:750–765.
Maehara H, Sotome S, Yoshii T, Torigoe I, Kawasaki Y, Sugata Y,Yuasa M, Hirano M, Mochizuki N, Kikuchi M, Shinomiya K,Okawa A. 2010. Repair of large osteochondral defects in rabbitsusing porous hydroxyapatite/collagen (HAp/Col) and fibroblastgrowth factor-2 (FGF-2). J Orthop Res 28:677–686.
Mayr HO, Klehm J, Schwan S, Hube R, Sudkamp NP, Niemeyer P,Salzmann G, von Eisenhardt-Rothe R, Heilmann A, Bohner M,Bernstein A. 2013. Microporous calcium phosphate ceramics astissue engineering scaffolds for the repair of osteochondraldefects: biomechanical results. Acta Biomater 9:4845–4855.
34 JEON ET AL.

Miller RE, Grodzinsky AJ, Vanderploeg EJ, Lee C, Ferris DJ, BarrettMF, Kisiday JD, Frisbie DD. 2010. Effect of self-assembling pep-tide, chondrogenic factors, and bone marrow-derived stromal cellson osteochondral repair. Osteoarthr Cartil 18:1608–1619.
Miot S, Brehm W, Dickinson S, Sims T, Wixmerten a, Longinotti C,Hollander aP, Mainil-Varlet P, Martin I. 2012. Influence of invitro maturation of engineered cartilage on the outcome of osteo-chondral repair in a goat model. Eur Cell Mater 23:222–236.
Moger CJ, Barrett R, Bleuet P, Bradley DA, Ellis RE, Green EM,Knapp KM, Muthuvelu P, Winlove CP. 2007. Regional variationsof collagen orientation in normal and diseased articular cartilageand subchondral bone determined using small angle X-ray scat-tering (SAXS). Osteoarthr Cartil 15:682–687.
Mohan N, Dormer NH, Caldwell KL, Key VH, Berkland CJ,Detamore MS. 2011. Continuous gradients of material composi-tion and growth factors for effective regeneration of the osteo-chondral interface. Tissue Eng Part A 17:2845–2855.
Mrosek EH, Schagemann JC, Chung HW, Fitzsimmons JS,Yaszemski MJ, Mardones RM, O’Driscoll SW, Reinholz GG. 2010.Porous tantalum and poly-epsilon-caprolactone biocomposites forosteochondral defect repair: preliminary studies in rabbits. JOrthop Res 28:141–148.
Nagel T, Kelly DJ. 2013. The composition of engineered cartilage atthe time of implantation determines the likelihood of regeneratingtissue with a normal collagen architecture. Tissue Eng Part A 19:824–833.
Ng KW, Lima EG, Bian L, O’Conor CJ, Jayabalan PS, Stoker AM,Kuroki K, Cook CR, Ateshian GA, Cook JL, Hung CT. 2010. Pas-saged adult chondrocytes can form engineered cartilage withfunctional mechanical properties: a canine model. Tissue EngPart A 16:1041–1051.
Nguyen LH, Kudva AK, Saxena NS, Roy K. 2011. Engineeringarticular cartilage with spatially-varying matrix composition andmechanical properties from a single stem cell population using amulti-layered hydrogel. Biomaterials 32:6946–6952.
O’Shea TM, Miao X. 2008. Bilayered scaffolds for osteochondral tis-sue engineering. Tissue Eng Part B 14:447–464.
Oshima Y, Harwood FL, Coutts RD, Kubo T, Amiel D. 2009. Varia-tion of mesenchymal cells in polylactic acid scaffold in an osteo-chondral repair model. Tissue Eng Part C 15:595–604.
Pabbruwe MB, Esfandiari E, Kafienah W, Tarlton JF, Hollander AP.2009. Induction of cartilage integration by a chondrocyte/collagen-scaffold implant. Biomaterials 30:4277–4286.
Paetzold H, Goepfert C, Huber G, Hoenig E, Portner R, SchillingAF, Meenen NM, Morlock MM. 2012. The development of the col-lagen fibre network in tissue-engineered cartilage constructs invivo. Engineered cartilage reorganises fibre network. Eur CellMater 23:209–221.
Paul J, Sagstetter A, Kriner M, Imhoff AB, Spang J, HinterwimmerS. 2009. Donor-site morbidity after osteochondral autologoustransplantation for lesions of the talus. J Bone Joint Surg Am Vol91:1683–1688.
Pei M, He F, Boyce BM, Kish VL. 2009. Repair of full-thicknessfemoral condyle cartilage defects using allogeneic synovial cell-engineered tissue constructs. Osteoarthritis Cartilage 17:714–722.
Pei M, Yan Z, Shoukry M, Boyce BM. 2010. Failure of xenoimplan-tation using porcine synovium-derived stem cell-based cartilagetissue constructs for the repair of rabbit osteochondral defects. JOrthop Res 28:1064–1070.
Poole AR, Kojima T, Yasuda T, Mwale F, Kobayashi M, Laverty S.2001. Composition and structure of articular cartilage: a templatefor tissue repair. Clin Orthop Relat Res 391:S26–33.
Re’em T, Witte F, Willbold E, Ruvinov E, Cohen S. 2012. Simultane-ous regeneration of articular cartilage and subchondral bone
induced by spatially presented TGF-beta and BMP-4 in a bilayeraffinity binding system. Acta Biomater 8:3283–3293.
Reyes R, Delgado A, Sanchez E, Fernandez A, Hernandez A, EvoraC. Repair of an osteochondral defect by sustained delivery ofBMP-2 or TGFbeta1 from a bilayered alginate-PLGA scaffold. JTissue Eng Regen Med, in press.
Santo VE, Gomes ME, Mano JF, Reis RL. 2013a. Controlledrelease strategies for bone, cartilage, and osteochondral engineer-ing--Part I: recapitulation of native tissue healing and variablesfor the design of delivery systems. Tissue Eng Part B Rev 19:308–326.
Santo VE, Gomes ME, Mano JF, Reis RL. 2013b. Controlled releasestrategies for bone, cartilage, and osteochondral engineering–PartII: challenges on the evolution from single to multiple bioactivefactor delivery. Tissue Eng Part B Rev 19:327–352.
Schinhan M, Gruber M, Vavken P, Dorotka R, Samouh L, Chiari C,Gruebl-Barabas R, Nehrer S. 2012. Critical-size defect inducesunicompartmental osteoarthritis in a stable ovine knee. J OrthopRes 30:214–220.
Schinagl RM, Gurskis D, Chen AC, Sah RL. 1997. Depth-dependentconfined compression modulus of full-thickness bovine articularcartilage. J Orthop Res 15:499–506.
Sheehy EJ, Vinardell T, Buckley CT, Kelly DJ. 2013. Engineeringosteochondral constructs through spatial regulation of endochon-dral ossification. Acta Biomater 9:5484–5492.
Shirazi R, Shirazi-Adl A, Hurtig M. 2008. Role of cartilage collagenfibrils networks in knee joint biomechanics under compression. JBiomech 41:3340–3348.
Swieszkowski W, Tuan BH, Kurzydlowski KJ, Hutmacher DW.2007. Repair and regeneration of osteochondral defects in thearticular joints. Biomol Eng 24:489–495.
Unterman SA, Gibson M, Lee JH, Crist J, Chansakul T, Yang EC,Elisseeff JH. 2012. Hyaluronic acid-binding scaffold for articularcartilage repair. Tissue Eng Part A 18:2497–2506.
Wang W, Li B, Yang J, Xin L, Li Y, Yin H, Qi Y, Jiang Y, Ouyang H,Gao C. 2010. The restoration of full-thickness cartilage defectswith BMSCs and TGF-beta 1 loaded PLGA/fibrin gel constructs.Biomaterials 31:8964–8973.
Williams RJ, III Harnly HW. 2007 Microfracture: indications, tech-nique, and results. Instr Course Lect 56:419–428.
Xie J, Han Z, Naito M, Maeyama A, Kim SH, Kim YH, Matsuda T.2010. Articular cartilage tissue engineering based on a mechano-active scaffold made of poly(L-lactide-co-epsilon-caprolactone): invivo performance in adult rabbits. J Biomed Mater Res Part BAppl Biomater 94:80–88.
Xue D, Zheng Q, Zong C, Li Q, Li H, Qian S, Zhang B, Yu L, Pan Z.2010. Osteochondral repair using porous poly(lactide-co-glycolide)/nano-hydroxyapatite hybrid scaffolds with undifferentiated mes-enchymal stem cells in a rat model. J Biomed Mater Res Part A94:259–270.
Yang Q, Peng J, Lu SB, Guo QY, Zhao B, Zhang L, Wang AY, XuWJ, Xia Q, Ma XL, Hu YC, Xu BS. 2011. Evaluation of an extrac-ellular matrix-derived acellular biphasic scaffold/cell construct inthe repair of a large articular high-load-bearing osteochondraldefect in a canine model. Chin Med J 124:3930–3938.
Zhu S, Zhang B, Man C, Ma Y, Hu J. 2011. NEL-like molecule-1-modified bone marrow mesenchymal stem cells/poly lactic-co-glycolic acid composite improves repair of large osteochondraldefects in mandibular condyle. Osteoarthritis Cartilage 19:743–750.
Zscharnack M, Hepp P, Richter R, Aigner T, Schulz R, Somerson J,Josten C, Bader A, Marquass B. 2010. Repair of chronic osteo-chondral defects using predifferentiated mesenchymal stem cellsin an ovine model. Am J Sports Med 38:1857–1869.
PERSPECTIVES IN MULTIPHASIC OSTEOCHONDRAL TISSUE ENGINEERING 35