Overall-Mouth Disinfection by Photodynamic Therapy Using ...
Upload
khangminh22Category
view
1download
0
Periodontal Disease and Overall Health: A Clinician’s Guide
EditorsRobert J. GencoRay C. Williams
Supported through an educational grant from
Periodontal Disease and Overall Health: A Clinician’s Guide
Robert J. Genco, DDS, PhDDistinguished Professor of Oral Biology and Microbiology
Schools of Dental Medicine and Medicine and Biomedical SciencesVice Provost, Office of Science,
Technology Transfer and Economic OutreachDirector, Clinical Research Center of the Buffalo Clinical and
Translational Research CenterState University of New York at Buffalo
Buffalo, NY, USA
Ray C. Williams, DMDProfessor and Dean, School of Dental Medicine
Stony Brook UniversityStony Brook, NY, USA
PROFESSIONAL AUDIENCE COMMUNICATIONS, INC.Yardley, Pennsylvania, USA
Periodontal Disease and Overall Health: A Clinician’s Guide
Copyright © 2010 by the Colgate-Palmolive Company. All rights reserved.
No part of this publication may be used or reproduced in any form or by any means, orstored in a database or retrieval system, without prior written permission of the Colgate-Palmolive Company. Making copies of any part of this book for any purpose other thanyour own personal use is a violation of United States copyright laws.
ISBN-13: 978-0-6152-8508-5ISBN-10: 0-6152-8508-2
Published by …
Professional Audience Communications, Inc.PO Box 243Yardley, Pennsylvania 19067 USA
Editorial Quality Control: Teri S. SiegelCopyediting/Proofreading: Michelle RizzoLayout and Design: E. Allen DownsCover Design: Horizons Graphic DesignIndexing: Allegheny Writing & Publishing Services, LLCPublisher: Stephen M. Siegel
Printed in the United States of America
Last digit is the print number: 9 8 7 6 5 4
ii
Silvana P. Barros, DDS, MS, PhD Research Associate ProfessorCenter for Oral and Systemic DiseasesUniversity of North Carolina School of DentistryDepartment of PeriodontologyChapel Hill, NC, USA
Peter Mark Bartold, BDS, DDSc, PhD, FRACDS (Perio)Director, Colgate Australian Clinical DentalResearch CentreProfessor of PeriodonticsUniversity of AdelaideDepartment of DentistryAdelaide, Australia
Yiorgos A. Bobetsis, DDS, PhDLecturer, Department of PeriodontologyUniversity of Athens School of Dentistry Athens, Greece
Wenche Sylling Borgnakke, DDS, MPH, PhDAssistant Research ScientistDepartment of Cariology, Restorative Sciencesand EndodonticsUniversity of Michigan School of DentistryAnn Arbor, MI, USA
Dawn J. Caster, MDNephrology FellowDivision of NephrologyDepartment of Internal MedicineUniversity of Louisville School of MedicineLouisville, KY, USA
Noel M. Claffey BDS, MDent Sc, FDS, FFD, FTCDProfessor of PeriodontologyDental School and HospitalTrinity College DublinDublin, Ireland
Robert J. Genco, DDS, PhDDistinguished Professor of Oral Biologyand MicrobiologySchools of Dental Medicine and Medicineand Biomedical SciencesVice Provost, Office of Science, TechnologyTransfer and Economic OutreachDirector, Clinical Research Center of the BuffaloClinical and Translational Research CenterState University of New York at BuffaloBuffalo, NY, USA
William V. Giannobile, DDS, DMedScNajjar Professor of DentistryMichigan Center for Oral Health ResearchDepartment of Periodontics and Oral MedicineUniversity of Michigan School of DentistryAnn Arbor, MI, USA
Ricardo A. Gómez, MDAssociate ProfessorDepartment of Obstetrics and GynecologyP. Universidad Católica de ChileHospital Sótero del RíoClínica Santa MaríaSantiago, Chile
Dana T. Graves, DDS, DMScProfessor and ChairDepartment of Periodontics New Jersey Dental School (UMDNJ)Newark, NJ, USA
Ying Gu, DDS, PhDAssistant ProfessorDepartment of General DentistryStony Brook University School of DentalMedicineStony Brook, NY, USA
Casey Hein, BSDH, MBAAssistant Professor; Division of PeriodonticsDirector of Education, International Centreon Oral-Systemic HealthFaculty of DentistryUniversity of ManitobaWinnipeg, Manitoba, Canada
William C. Hsu, MDSenior PhysicianMedical Director, Asian ClinicJoslin Diabetes CenterAssistant Professor of MedicineHarvard Medical SchoolBoston, MA, USA
Heather L. Jared, RDH, MS, BSAdjunct Assistant ProfessorUniversity of North Carolina School ofDentistryDepartment of Dental EcologyChapel Hill, NC, USA
CONTRIBUTORSiii
Srividya Kidambi, MDAssistant Professor of MedicineMedical College of WisconsinMilwaukee, WI, USA
Denis F. Kinane, BDS, PhD, FDSRCS, FDSRCPSDean, University of Pennsylvania School ofDental MedicinePhiladelphia, PA, USA
Evanthia Lalla, DDS, MSAssociate Professor of Dental Medicine Columbia University College of Dental MedicineNew York, NY, USA
Ira B. Lamster, DDS, MMScDean and Professor of Dental MedicineColumbia University College of Dental MedicineNew York, NY, USA
Néstor J. López, DDSProfessor of PeriodontologyUniversity of Chile School of DentistrySantiago, Chile
John H. Loughran, MDFellow of Cardiovascular DiseaseUniversity of Louisville School of MedicineLouisville, KY, USA
Phoebus N. Madianos, DDS, PhDProfessorDepartment of PeriodontologyUniversity of Athens School of DentistryAthens, Greece
Angelo J. Mariotti, DDS, PhDProfessor and ChairDivision of PeriodontologyThe Ohio State UniversityCollege of DentistryColumbus, OH, USA
Joseph M. Mylotte, MDProfessor of Medicine EmeritusDepartment of MedicineUniversity at BuffaloSchool of Medicine and Biomedical SciencesBuffalo, NY, USA
Timothy C. Nichols, MDProfessor of Medicine, Pathology, andLaboratory MedicineDirector, Francis Owen Blood Research LaboratoryUniversity of North Carolina at Chapel HillChapel, Hill, NC, USA
Steven Offenbacher, DDS, PhD, MMScOraPharma Distinguished Professor ofPeriodontal MedicineDirector, Center for Oral and Systemic DiseasesUniversity of North Carolina School of DentistryChapel Hill, NC, USA
David W. Paquette, DMD, MPH, DMScProfessor and Associate Dean for Education Stony Brook University School of DentalMedicine Stony Brook, NY, USA
Shailendra B. Patel, BM, ChB, DPhilProfessor of MedicineDivision of Endocrinology, Metabolism andClinical NutritionMedical College of WisconsinMilwaukee, WI, USA
Ioannis Polyzois, DMD, MDentCh, MMedSci Lecturer, Department of Restorative Dentistryand Periodontology Dublin Dental School & HospitalTrinity College Dublin Dublin, Ireland
Hector F. Rios, DDS, PhDAssistant Professor, Department of Periodonticsand Oral MedicineUniversity of Michigan School of DentistryAnn Arbor, MI, USA
Maria Emanuel Ryan, DDS, PhDAssociate Dean for Strategic Planningand External AffairsDirector of Clinical ResearchProfessor, Department of Oral Biologyand PathologyMedical Staff University HospitalStony Brook University School ofDental MedicineStony Brook, NY, USA
Frank A. Scannapieco, DMD, PhDProfessor and ChairDepartment of Oral BiologyUniversity at BuffaloSchool of Dental MedicineBuffalo, NY, USA
George W. Taylor, DMD, MPH, DrPHProfessor, Department of Cariology,Restorative Sciences and EndodonticsUniversity of Michigan School of DentistryAnn Arbor, MI, USA
iv CONTRIBUTORS
Thomas E. Van Dyke, DDS, PhDProfessor, Periodontology and Oral BiologyDirector, Clinical Research CenterBoston University Henry M. Goldman School of Dental MedicineBoston, MA, USA
Stanley S. Wang, MD, JD, MPHClinical Cardiologist and Director ofLegislative Affairs, Austin HeartAdjunct Assistant Professor of MedicineUniversity of North CarolinaChapel Hill, NC, USA
Ray C. Williams, DMDProfessor and Dean, School of Dental MedicineStony Brook UniversityStony Brook, NY, USA
CONTRIBUTORS v
CHAPTER 1From the Editors
Robert J. Genco, Ray C. WilliamsDear Colleagues:
We are very pleased to have had the privilege of assembling and editing this textbook,Periodontal Disease and Overall Health: A Clinician’s Guide.
The relationship of oral disease to overall disease is certainly not a new concept. For centuries,the role of oral infection and inflammation in contributing to diseases elsewhere in the body hasbeen studied and reported. Going back to ancient times in Greece, we learn that Hippocratestreated two patients suffering from joint pain by removal of teeth. Clearly, this was an earlyexample of oral disease being associated with afflictions elsewhere in the body. Then, movingforward in time from 1912 to around 1950, the era of “focal infection” dominated our thinking.Reports by individuals such as WD Miller, William Hunter, and Frank Billings noted that in theiropinion many of the diseases of humans could be traced to specific foci of infection elsewherein the body, such as the teeth and gums, the tonsils, or the sinuses. While these observationswere not supported by sound scientific evidence, and in fact led to largely incorrect practices,they nonetheless brought attention to the effect of the mouth on the rest of the body.
Then in 1989, with a series of intriguing reports from Finland, the current interest in the role oforal health and disease on contributing to general health and systemic conditions was launched.Kimmo Mattila and his coworkers reported that individuals presenting to the emergency roomwith a myocardial infarction were overwhelmingly likely to have periodontal disease. Mightperiodontal disease be a risk factor for cardiovascular disease? Since then, a phenomenal bodyof work has been directed at understanding how periodontal disease might affect distant sitesand organs, and thus have an effect on overall health. Renowned clinicians and scientistsworldwide have studied the relationship of periodontal disease to overall health and disease,and along the way several conferences and workshops have been convened to examine theevidence to date for the relationship between periodontal disease and the risk for systemicconditions. At one of those conferences, in January 2008, we discussed the need for a textbookthat would summarize and put into context the current information on periodontal disease andsystemic disease together for students of dentistry and medicine. Happily for us, Foti Panagakos,Sheila Hopkins, and their team at the Colgate-Palmolive Company agreed to support, throughan educational grant to the publisher, the undertaking of this textbook. We were fortunate tohave assembled a group of respected and scholarly clinicians and scientists who, in eighteenchapters, provide a current and thoughtful perspective on the relationship of periodontal diseaseto systemic conditions.
It is a pleasure to present this textbook. We hope you find it useful and that you enjoy it.
Sincerely,
Robert J. Genco, DDS, PhD Ray C. Williams, DMD
COMPANY

CHAPTER 1Overview 1Robert J. Genco, Ray C. Williams
CHAPTER 2Overview of Periodontal Disease: Causes, Pathogenesis, and Characteristics 5 Ying Gu, Maria E. Ryan
CHAPTER 3Infection and Inflammation 24Phoebus N. Madianos, Yiorgos A. Bobetsis, Thomas E. Van Dyke
CHAPTER 4History of the OralSystemic Relationship 42Noel M. Claffey, Ioannis N. Polyzois, Ray C. Williams
CHAPTER 5Diabetes Mellitus: A Medical Overview 55Srividya Kidambi, Shailendra B. Patel
CHAPTER 6Association Between Periodontal Diseases and Diabetes Mellitus 83George W. Taylor, Wenche S. Borgnakke, Dana T. Graves
CHAPTER 7Atherosclerosis: A Pervasive Disease Affecting Global Populations 105Stanley S. Wang
CHAPTER 8Association Between Periodontal Disease and Atheromatous Diseases 112David W. Paquette, Robert J. Genco
CHAPTER 9Periodontal Disease and Pregnancy Complications 132Silvana P. Barros, Heather L. Jared, Steven Offenbacher
CHAPTER 10Oral Health and Diseases of the Respiratory Tract 147Frank A. Scannapieco, Joseph M. Mylotte
viii
CONTENTS
ix CONTENTS
CHAPTER 11Periodontal Disease and Osteoporosis 162Hector F. Rios, William V. Giannobile
CHAPTER 12Association Between Periodontitis and Rheumatoid Arthritis 179P. Mark Bartold, Angelo J. Mariotti
CHAPTER 13Oral Health, Periodontitis, and Cancer 196P. Mark Bartold, Angelo J. Mariotti
CHAPTER 14Dental and Medical Comanagement of Patients with Diabetes 216Evanthia Lalla, William C. Hsu, Ira B. Lamster
CHAPTER 15Dental and Medical Comanagement of Cardiovascular Disease 237Timothy C. Nichols, David W. Paquette
CHAPTER 16Dental and Medical Comanagement of Pregnancy 250Néstor J. López, Ricardo A. Gómez
CHAPTER 17Dental and Medical Comanagement of Osteoporosis, Kidney Disease, and Cancer 270Dawn J. Caster, John H. Loughran, Denis F. Kinane
CHAPTER 18The Role of the Professional in Educating the Public About the Importance of Oral Health 288Casey Hein
INDEX 305

“A person can’t have good general health without good oral health.”
—Former US Surgeon General C. Everett Koop

INTRODUCTIONPeriodontal disease is one of the most
common diseases of man and is responsiblefor most of the tooth loss in adults. This oraldisease has received considerable attention inthe past several decades and a new under-standing of it is emerging. The microbialcauses of periodontal disease, the mecha-nisms through which periodontal tissues aredestroyed, the effect of the host on perio -dontal disease expression, and the impactperiodontal disease has on overall healthhave been subjects of intense study. Under-standing the complex interaction betweenchronic infections, such as periodontal dis-ease, and systemic conditions such as cardio -vascular disease, has led to a new way ofthinking about the importance of periodon-tal disease in overall health.
Periodontal Disease as anIntegral Link to Systemic DiseaseAccording to the National Center for
Health Statistics, the six leading causes ofdeath in the United States in 2005 were heartdisease (652,091), cancer (559,312), stroke/cerebrovascular diseases (143,579), chroniclower respiratory disease (130,933), unin-tentional accidental injuries (117,809), anddiabetes (75,119).1 Five of these chronic dis-eases are related to periodontal disease. Bysuccessfully meeting the challenge to im-prove oral health and the management of periodontal disease, general health will alsobe advanced through shared approaches targeting common risk factors. To best addressthe common risk factors and interactions
between oral and systemic disease, it is important to understand the extent to whichperiodontal disease is related to certain systemic diseases, the historical foundationsof current therapeutic approaches, the roleof inflammation, and the possibilities for intervention.
THREE HISTORICAL ERAS OF PERIODONTAL DISEASE RESEARCH
In the last 50 years, there has been con-siderable progress in understanding the etiology and pathogenesis of periodontal dis-ease and its interactions with the host. Thestudies and concepts can be described ashaving occurred in three phases or eras: theetiopathologic (or host-parasite) era, the riskfactor era, and most recently, the periodon-tal disease-systemic disease era.
Etiopathologic EraThe etiopathologic era included land-
mark investigations into the microbial etiol-ogy and pathogenesis of periodontal disease.The role of bacteria as a cause of periodontaldisease was demonstrated by a series of seminal studies conducted from the 1960s tothe 1980s. Classic studies by Löe and col-leagues clearly demonstrated that microbialplaque buildup on the teeth was associatedwith the onset of gingivitis, and that the re-moval of microbial plaque resulted in theresolution of gingivitis.2,3 These studies pro-vided unargu able evidence that microbialdental plaque buildup, rather than other sus-pected agents such as calculus, was respon-sible for gingivitis.
CHAPTER 1Overview
Robert J. Genco, Ray C. Williams“A person can’t have good general health without good oral health.”
—Former US Surgeon General C. Everett Koop

In the 1970s and 1980s, Socransky andcoworkers conducted studies showing thatspecific organisms were associated with perio - dontal disease (for review see Socransky andHaffajee, 2005).4 These studies identified several categories of organisms, ranging fromearly colonizers, which are commensal andrelatively nonvirulent, to moderately virulentorganisms, which bridged the early colonizersand interconnected them to specific pathogenssuch as Porphyromonas gingivalis, Tannerellaforsythensis, and Treponema denticola. Re-search from many investigators found that thespecific pathogens, in combination with theearly colonizers and moderately virulent organ -isms, form a complex microflora that exists asa biofilm within the periodontal pocket.
Other investigators began to explainthe pathogenesis of periodontal disease, de-scribing how the host in fact was responsiblefor tissue destruction. We came to under-stand that the initial response to the bacteriaon the tooth and subgingivally is a series ofimmunopathological actions. Antibodies tothese bacteria are formed, which in combi-nation with neutrophils, provide importantprotection.5,6 It was seen that if neutrophilsare suppressed, more severe periodontal dis-ease occurs. Soon thereafter the role of themacrophage was understood. This importantcell invades the gingival tissue and upontriggering by bacterial products such as endo toxin, produces pro-inflammatory cyto -kines and matrix metalloproteinases that destroy the connective tissues of the perio -dontium. Inflammatory mediators such asprostaglandin E2 and interleukin-1 inducealveolar bone resorption. As the role of thehost becomes more understood, it is clearthat inflammation and the inflammatory response can explain much of the tissue destruction caused by periodontal disease.7,8
Risk Factor EraThe second era of discovery brought the
identification of risk factors which influence
or modulate the expression of perio dontal dis-ease. Epidemiologic studies reported that therisk factors in and of themselves were not etiologic, but rather modified or exaggeratedthe etiopathologic processes set into motionby the causative bacteria. These risk factorswere identified in the late 1980s and early1990s and include genetic elements, behav-iors such as smoking, and acquired disor-ders such as diabetes mellitus.9,10 The conceptof modifying risk factors as part of the man-agement of periodontal disease is now wellestablished.
Periodontal Disease-Systemic Disease Era
The understanding of periodontal dis-ease is now focused on the relationship ofperiodontal disease as a risk for certain sys-temic diseases. Robust studies have shownthat periodontal disease is significantly asso -ciated with certain systemic diseases suchas cardiovascular disease,11,12 diabetes andcomplications of diabetes,13-15 adverse preg-nancy outcomes,16 and respiratory infections.17
The periodontal disease-systemic disease concept has amassed enough evidence and support that it is now believed that findingsabout this inter-relationship should be in -corporated into the curriculum in schools forhealth professionals, and should also be madeavailable to enhance the knowledge base ofcurrently practicing healthcare professionals.
The association of periodontal diseasewith several systemic conditions, such as dia betes and atherosclerotic disease, is likelyrelated to the inflammatory response associ-ated with periodontal disease. C-reactive pro- tein is an important marker of the inflam -matory response and is elevated in subjectswith periodontal disease; its levels in periph-eral blood are reduced when periodontal disease is treated. Another indication of the systemic inflammatory response associatedwith periodontal disease is the presence ofcytokines, including tumor necrosis factor
2 Periodontal Disease and Overall Health: A Clinician's Guide

alpha and interleukins 1 and 6, often foundin the circu lation of patients with perio -dontal disease. There are other conditionsthat also contrib ute to a systemic inflamma-tory response including rheumatoid arthritis,psoriasis, and obesity. This chronic systemicinflammatory response in turn increasesthe risk for athero sclerotic disease, diabetesand complications of diabetes, adverse preg-nancy outcomes, and possibly some cancers.The research supporting these associationswill be discussed in detail in the followingchapters.
GOALS FOR THIS TEXTBOOKMuch research is focused on under-
standing how periodontal disease increasesthe risk for systemic diseases. It is not yetclear what impact the biofilm in the oral cav-ity might have on distant sites and organs;likewise the role of the inflammatory re-sponse is not fully understood. Some of thechapters in this textbook will review the bio -logic plausibility for periodontal disease as arisk for systemic conditions. Mechanismsthrough which periodontal disease can con-fer this risk will also be presented.
The overall goal of this textbook is topresent the emerging and compelling evi-dence that periodontal disease is a risk forseveral systemic conditions and to look at therole of oral health in contributing to overallhealth. This book also seeks to provide thereader with a guide to patient management inwhich dentistry and medicine work together.
Textbook OrganizationThe chapters in this book are organized
in the following manner: The initial chaptersfollowing this one outline the basics of un-der standing periodontal disease and its inter-relationship with systemic disease: Chapter2 discusses the causes and pathogenesis ofperiodontal disease; the role of infection andinflammation in periodontal disease is ex-amined in Chapter 3; and the history of the
oral disease-systemic disease relationship isexplained in Chapter 4.
An overview of diabetes (Chapter 5)and atherosclerotic diseases (Chapter 7) arefollowed by chapters that describe the rela-tion ship of periodontal disease to these con-ditions (Chapters 6 and 8, respectively). Thenext chapters examine the evidence for perio -dontal disease as a risk for adverse preg-nancy outcomes (Chapter 9), respiratory dis-eases (Chapter 10), osteoporosis (Chapter11), rheumatoid arthritis (Chapter 12), andcancer (Chapter 13).
The final section of the textbook dis-cusses comanagement of periodontal diseasein diabetes (Chapter 14), cardiovascular dis-ease (Chapter 15), pregnancy (Chapter 16),and other conditions that are associated withperiodontal disease (Chapter 17). Finally,Chapter 18 describes the role of dental pro-fessionals in the education of the public andother health professionals about the oralhealth-general health inter-relationship.
Our Hope for This TextbookIt is the hope of the authors and editors
that this textbook will provide an up-to-dateunderstanding of the information that detailsthe relationship of periodontal disease to sys-temic disease, with each chapter outlining astate-of-the-art understanding of the optimalmanagement of patients. This textbook hasbeen prepared as a resource for dental stu-dents, dental hygiene students, faculty mem-bers of dental educational institutions, andfor dental professionals in general. We alsobelieve this resource will prove valuable tostudents as well as practicing members ofother health professions in the medical com-munity. The integration of medicine and den-tistry grows daily, and a common resourcesuch as this textbook could serve as a con-structive tool to help the two disciplineswork collaboratively.
The editors would like to thank the au-thors and coauthors for their role in preparing
CHAPTER 1 Overview 3

and presenting current information in a com-plete, yet concise and readable manner. Weare hopeful that this textbook will find broadreadership and will be useful to the dental andmedical community.
REFERENCES1. Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek
KD, Tejada-Vera B. Deaths: final data for 2006.Natl Vital Stat Rep 2009;57:1–34.
2. Löe H, Theilade E, Jensen SB. Experimental gin-givitis in man. J Periodontol 1965;36:177–187.
3. Theilade E, Wright WH, Jensen SB, Löe H. Ex-perimental gingivitis in man. II. A longitudinal clin-ical and bacteriological investigation. J Periodon-tal Res 1966;1:1–13.
4. Socransky SS, Haffajee AD. Periodontal microbialecology. Periodontol 2000 2005;38:135–187.
5. Genco RJ, Slots J, Mouton C, Murray P. Systemicimmune responses to oral anaerobic organisms. In:Anaerobic Bacteria: Selected Topics, Lambe DWJr, Genco RJ, Mayberry-Carson KJ, eds., PlenumPublishing Corp., New York, 277, 1980.
6. Ebersole JL, Taubman MA, Smith DJ, Genco RJ,Frey DE. Human immune responses to oral micro-organisms. I. Association of localized juvenile perio dontitis (LJP) with serum antibody responsesto Actinobacillus actinomycetemcomitans. Clin ExpImmunol 1982;47:43–52.
7. Genco RJ. Host responses in periodontal diseases:Current concepts. J Periodontol 1992;63(Suppl):338–355.
8. Page RC, Offenbacher S, Schroeder HE, SeymourGJ, Kornman KS. Advances in the pathogenesis ofperiodontitis: Summary of developments, clinical
implications and future directions. Periodontol2000 1997;14:216 –248.
9. Genco RJ, Löe H. The role of systemic conditionsand disorders in periodontal disease. Periodontol2000 1993;2:98–116.
10. Grossi SG, Genco RJ, Machtei EE, Ho AW, Koch G,Dunford R, Zambon JJ, Hausmann E. As -sessment of risk for periodontal disease. II. Risk indicators for alveolar bone loss. J Periodontol1995;66:23–29.
11. Mattila K, Nieminen M, Valtonen V, Rasi VP,Kesäniemi YA, Syrjälä SL, Jungell PS, Isoluoma M,Hietaniemi K, Jokinen MJ. Association betweendental health and acute myocardial infarction. BMJ1989;298:779–781.
12. DeStefano F, Anda RF, Kahn HS, Williamson DF,Russell CM. Dental disease and risk of coronaryheart disease and mortality. BMJ 1993;306:688 –691.
13. Taylor GW, Burt BA, Becker MP, Genco RJ, Shloss-man M, Knowler WC, Pettitt DJ. Severe periodontitis and risk for poor glycemic control inpatients with non-insulin-dependent diabetes mel-litus. J Periodontol 1996;67:1085–1093.
14. Grossi SG, Genco RJ. Periodontal disease and diabetes mellitus: A two-way relationship. Ann Periodontol 1998;3:52–61.
15. Taylor GW, Borgnakke WS. Periodontal disease:Associations with diabetes, glycemic control andcomplications. Oral Dis 2008;14:191–203.
16. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D,Maynor G, McKaig R, Beck J. Periodontal infec-tion as a possible risk factor for preterm low birthweight. J Periodontol 1996;67:1103–1113.
17. Scannapieco FA. Role of oral bacteria in respiratoryinfection. J Periodontol 1999;70:793–802.
4 Periodontal Disease and Overall Health: A Clinician's Guide
Periodontitis has been defined as the pres-ence of gingival inflammation at sites wherethere has been a pathological detachment ofcollagen fibers from cementum, the junc-tional epithelium has migrated apically, andbone loss can be detected radiographically.The inflammatory events associated withconnective tissue attachment loss lead tothe resorption of coronal portions of toothsupporting alveolar bone.2 The understand-ing of periodontal disease is continuouslychanging as new research evidence emerges.There fore, the classification of periodontaldisease has changed since the system devel-oped at the 1989 World Workshop in Clini-cal Periodontics. The classification presentedin this chapter is based on the results devel-oped at the 1999 International Workshop or-ganized by the American Academy of Perio -dontology (AAP).
The classification of periodontal dis-eases now includes eight general types3:
1. Gingivitis2. Chronic periodontitis3. Aggressive periodontitis4. Periodontitis as a manifestation of
systemic diseases5. Necrotizing periodontal diseases6. Abscesses of the periodontium7. Periodontitis associated with endo -
dontic lesions8. Developmental or acquired deformi-
ties and conditionsThe overall classification system is
presented in Table 1.3 In addition, the aboveclassification is different from case types
INTRODUCTIONPeriodontal diseases are serious chronic
infections that involve destruction of thetooth-supporting apparatus, including thegingiva, the periodontal ligament, and alve-olar bone. These diseases are initiated by alocal accumulation of bacteria adjacent tothe tooth. Periodontal diseases, includinggingivitis and periodontitis, can affect onetooth or many teeth and, if left untreated,can lead to tooth loss, particularly in adults.It is the most common dental condition inadults, and is also one of the most commonchronic inflammatory diseases affecting amajority of the population throughout theworld. Although plaque is essential for theinitiation of periodontal diseases, the major-ity of the destructive processes associatedwith these diseases are due to an excessivehost response to the bacterial challenge.Therefore, periodontal disease is a multifac-torial, complex disease. The purpose of thischapter is to provide a general overview ofthe types of periodontal disease, risk factorsassociated with them, and the etiology,pathogenesis, and management of periodon-tal diseases.
TYPES OF PERIODONTAL DISEASEPeriodontal diseases include two general
categories based on whether there is attach-ment or bone loss: gingivitis and periodon-titis. Gingivitis is considered a reversibleform of the disease, and generally involvesinflammation of the gingival tissues with-out loss of connective tissue attachment.1
CHAPTER 2Overview of Periodontal Disease: Causes, Pathogenesis, andCharacteristics
Ying Gu, Maria E. Ryan

previously developed by the AAP.4,5 The current case types for periodontal diseasesinclude:
• Gingivitis (Case Type I)• Mild periodontitis (Case Type II)• Moderate periodontitis (Case Type III)• Advanced periodontitis (Case Type IV)• Refractory periodontitis (Case Type V)
Gingival DiseasesGingival disease is further characterized
into plaque-induced and nonplaque-inducedcategories.3
Plaque-Induced Gingival DiseasesGingivitis is gingival inflammation as-
so ciated with plaque and calculus accumu-lation. It is the most common form of gin -gival disease. Gingivitis may or may notprogress to periodontitis, in which clinical attachment and alveolar bone loss will
develop. Gingivitis can occur on teeth withno attachment loss; it also occurs in the gin-giva of teeth previously treated for peri-odontitis with no further attachment loss.
Dental Plaque Only: Gingivitis is ini-tiated by local accumulation of bacteria (i.e.,dental plaque) adjacent to the tooth.6 Thebacterial antigens and their metabolic prod-ucts (e.g., endotoxin) stimulate epithelial andconnective tissue cells to produce inflam-matory mediators that result in a localized inflammatory response recruiting polymor-phonuclear leukocytes (PMNLs or neutro -phils) to the site. An antibody response tothese bacterial antigens is also mounted. In-flammatory cells and their products (e.g.,cytokines, enzymes, and antigens) are pres-ent at the site of inflammation. Thus, a hostimmuno-inflammatory response is estab-lished in the gingival tissues and the clinicalsigns of gingivitis develop, including red-ness, swelling, and bleeding. The plaque-host interaction can be altered by the effectsof local factors, systemic factors, or both.
Systemic Factors: Systemic hormonalchanges associated with puberty, menstrualcycle, or pregnancy, as well as with chronicdiseases such as diabetes, can alter the hostresponse to dental plaque.1,7 Hormonalchanges and certain diseases can upregulatesystemic cellular and immunologic functionresulting in local severe gingival inflamma-tion, even in the presence of minimal plaqueor with an equivalent bacterial bioburden toa person who does not have these systemicchallenges. This is commonly seen in preg-nant women who have not had adequate oralhygiene before becoming pregnant. Blooddyscrasias such as leukemia may also alterimmune function by decreasing normal im-munological function. Patients usually pres-ent with gingival enlargement and bleedingassociated with spongy gingival tissues andexcessive vascularity.
Medications: Medications such as an-ticonvulsant drugs (e.g., dilantin), immuno-
6 Periodontal Disease and Overall Health: A Clinician's Guide
Table 1. Periodontal Diseases
VIII. Gingival DiseasesDental plaque-induced gingival diseasesNonplaque-induced gingival lesions
IV.II. Chronic PeriodontitisLocalizedGeneralized
VIII. Aggressive PeriodontitisLocalizedGeneralized
IIIV. Periodontitis as a Manifestation ofIV. Systemic Diseases
IIIV. Necrotizing Periodontal DiseasesNecrotizing ulcerative gingivitisNecrotizing ulcerative periodontitis
IIVI. Abscesses of the PeriodontiumGingival abscessPeriodonal abscessPericoronal abscess
IVII. Periodontitis Associated withEndodontic Lesions
VIII. Developmental or Acquired Deformitiesand Conditions
Adapted from: Ann Periodontol 1999;4:1–6.3

CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 7
suppressive drugs (e.g., cyclosporine), andcalcium channel blockers (e.g., diltiazem)can cause severe gingival enlargement andpseudo-periodontal pocketing (i.e., increasedprobing depths with no associated attach-ment or bone loss).8 Medication-associatedgingival conditions are often reversed afterdiscontinuation of the offending agents.
Malnutrition: The host immune sys-tem can be diminished when malnutritiondevelops, resulting in excessive gingival in-flammation. Severe ascorbic acid (vitamin C)deficiencies (i.e., scurvy) can produce brightred, swollen, and bleeding gingival tissues.1 Inthe case of vitamin C deficiency, gingivitis isassociated with a suppressed synthesis ofboth connective tissue collagens (e.g., TypesI and III) and basement membrane collagen(Type IV). Treatment with vitamin C sup-plements can reverse this condition.
Nonplaque-Induced Gingival LesionsThese types of lesions usually are rare
and mainly due to systemic conditions. Bac-teria, viruses, or fungi can cause these typesof gingival lesions. Sexually transmitted dis-eases such as gonorrhea (Neisseria gonor-rhoeae) and syphilis (Treponema pallidum)can cause lesions in the tissues of the peri-odontium.9 Primary streptococcal gingivitisis an acute inflammation of the oral mucosa.It is associated with pain and fever, as wellas red swollen gingival tissues with bleedingor abscess formation, and can be treated withroutine periodontal scaling and root plan ingin addition to antibiotic therapy. Herpes simplex virus Type I is a common virus thatcan cause gingival lesions.10 In children andyoung adults, herpes infections can be pri-mary and usually without symptoms, but insome cases pain and fever are reported. Inthese cases, the gingival tissues appear redand swollen, and are followed by the for-mation of small blisters, which eventuallybreak down to form shallow, painful ulcers.These lesions are usually self-limiting and
heal within one to two weeks. After a pri-mary infection, the herpes virus becomes la-tent and will be preserved in the ganglion ofthe trigeminal nerve. The virus may be re-activated later in life by reduced immunefunction or stress, resulting in recurrent her-pes labialis, gingivitis, and stomatitis. Gin-gival lesions of fungal origin usually occur inpeople with diabetes or other immunocom-promised states. A shift in the normal oralflora related to the long-term use of system-ically administered antibiotics can also leadto lesions of fungal origin.11 The most com-mon fungal infection is candidiasis, causedby Candida albicans, often seen in patientswearing removable prosthetic devices (e.g.,dentures) and in patients with dry mouthdue to multiple medications or salivary glanddysfunction. Clinical manifestations includewhite patches on the gingiva, tongue, or oralmucous membranes that can be removedwith a cotton swab or gauze, leaving behinda bright red bleeding surface. Treatment withantifungal agents is often necessary to re-solve these conditions.
Gingival lesions can also be caused bygenetic systemic mucocutaneous disorders,allergic reactions, trauma, or foreign-bodyreactions. One of the most common geneticconditions associated with gingival lesionsis autosomal-dominant hereditary gingivalfibromatosis.12 It is a benign condition af-fecting both arches. The gingival tissues areenlarged and asymptomatic. It may be anisolated finding or associated with othersyndromes. Treatment is gingivectomy andrecurrence is possible. Systemic conditionssuch as pemphigoid, pemphigus vulgaris,erythema multiforma, and lupus erythe-matosus can cause desquamative lesions andulceration.10,13 Gingival changes due to al-lergic reactions to certain restorative ma -terials, dentifrices, or mouthrinses are rare,but have been observed.10 Traumatic lesionsare usually produced unintentionally.10 Ag-gressive tooth brushing and flossing can

cause gingival damage. Hot foods and drinkscan cause minor burns of the gingival tissues.Traumatic lesions can also be iatrogenicallyinduced by healthcare professionals duringoral examinations or dental care. Eatingcrunchy foods or foods with small particlesthat can be lodged in the interproximal areasand directly into the gingival tissues cancause these types of lesions as well. Gin- gival tissues can also develop localized in-flammation when exposed to foreign ma -terials. The most common example is theamalgam remaining in gingival tissues dur-ing the placement of restorations or surgicalpro cedures, eventually producing amalgam tattoos.10
PERIODONTITISPeriodontitis is a chronic infection in-
volving destruction of the tooth-supportingapparatus, including the periodontal ligamentand alveolar socket support of the teeth.
Gingivitis may or may not progress toperiodontitis, which is associated with at-tachment and alveolar bone loss. Periodon-tal disease is initiated by a local accumula-tion of bacteria (i.e., dental plaque adjacentto the tooth) and their metabolic products(e.g., endotoxin), that stimulate the junc-tional epithelium to proliferate and producetissue-destructive proteinases that degradethe basement membrane and allow for theapical migration of the junctional epitheliumalong the root surface of the tooth, thus deep-ening the gingival crevice to produce peri-odontal pockets and associated attachmentloss, which is the hallmark lesion of peri-odontal disease. Some of the clinical signsinclude bleeding on probing, deep pockets,recession, and tooth mobility. Often, this de-structive process is silent and continues forlong periods of time without being identified.Eventually, teeth can become loose and maybe lost on their own or deemed hopeless, requiring extraction. There are many formsof periodontitis.
Chronic Periodontitis Chronic periodontitis (CP) is the most
common form of periodontitis and is char-acterized by pockets with associated attach-ment loss and/or recession of the gingival tis-sues. It is common in adults but can occur atany age. Progression of attachment loss usu-ally occurs slowly, but periods of exacerba-tion with rapid progression, or periods of re-mission can occur. Several studies haveaddressed the “episodic” nature of perio -dontitis.14 The rate of disease progressionmay be influenced by local and/or systemicconditions that alter the normal host responseto bacterial plaque. Local factors such assubgingivally placed fillings or crowns thatviolate biological width can promote gingi-val inflammation and clinical attachmentloss. Systemic factors such as diabetes candecrease host defenses to bacterial infection.Environmental factors such as smoking andstress can also decrease host immune func-tion, resulting in increased susceptibility todisease. CP can occur as a localized form inwhich < 30% of the sites are involved, or asa more generalized form in which >30% ofexisting sites demonstrate increased pocketdepth, attachment and bone loss.4 As men-tioned previously, the severity of disease canbe described as slight, moderate, or severe,based on the level of destruction.
Aggressive PeriodontitisThis form of periodontitis was previ-
ously categorized as Juvenile Periodontitis.Common features include rapid attachmentloss and bone destruction in the absence ofsignificant accumulations of plaque and cal-culus.15 These forms of periodontitis usuallyaffect young individuals, often during pu-berty, from 10 to 30 years of age, with a ge-netic predisposition. The bacteria most oftenassociated with aggressive periodontitis areAggregatibacter actinomycetemcomitans(previously Actinobacillus actinomycetem-comitans). Individuals present with hyper-
8 Periodontal Disease and Overall Health: A Clinician's Guide

active inflammatory cells producing highlevels of cytokines and enzymes causingrapid, aggressive destruction of periodontaltissues. Aggressive periodontitis can be fur-ther characterized as localized and general-ized forms. The localized form usually affects first molar and incisor sites. The gen-eralized form usually involves at least threeteeth other than first molars and incisors.
Periodontitis as a Manifestationof Systemic Diseases
Systemic conditions such as diabetesare associated with this form of periodonti-tis.16 Several hematologic and genetic disor-ders have also been associated with the de-velopment of periodontitis such as acquired,familial, and cyclic neutropenias, leukemias,Down’s syndrome, certain types of Ehlers-Danlos syndrome, Papillon-Lefevre syn-drome, Cohen syndrome, and hypophospha -tasia. The mechanisms by which all of thesedisorders affect the health of the periodon-tium are not fully understood and continue tobe investigated by many basic and clinical re-searchers. It is speculated that these diseasescan alter host defense mechanisms and up-regulate inflammatory responses, resultingin progressive periodontal destruction.
Necrotizing Periodontal DiseasesThese lesions are most commonly ob-
served in individuals with systemic condi-tions, such as human immunodeficiency virusinfection, malnutrition, and immunosup-pression. Necrotizing periodontal diseasesare further divided into two forms: necrotiz-ing ulcerative gingivitis (NUG) and necro-tizing ulcerative periodontitis (NUP). Thesetwo diseases have the same etiology andclinical signs, except NUP involves clinicalattachment and alveolar bone loss.17
Abscesses of the PeriodontiumPeriodontal abscess is a localized puru-
lent infection of the periodontal tissues.18
Periodontal abscesses usually develop in periodontitis patients who may have fooddebris lodged in a pocket, or deep depositsof calculus where drainage from a pocketbecomes blocked. Iatrogenic abscess forma-tion can be precipitated after inadequate scal-ing and root planing, leading to a tighteningof the coronal epithelial cuff with continuedsubgingival calculus driving inflammation.Abscesses can also occur in healthy peri-odontal tissues due to the presence of foreignobjects lodged in the gingival crevice, suchas a toothbrush bristle or a popcorn kernelbeing tightly packed into the interproximalspaces or between the tooth and the tissues.A pericoronal abscess is an infection of thegingiva around a partially erupted tooth lead-ing to pericoronitis. A small flap of tissuemay cover a partially erupted tooth surface,serving as a nidus for food and debris to ac-cumulate and become trapped beneath thetissue flap. Patients usually find it very dif-ficult to keep these areas clean, and can de-velop inflammation and infection. In addi-tion, trauma due to constant contact betweenthe tissue flap and a tooth in the opposingarch can also lead to a pericoronal abscess.The areas most commonly affected are as-sociated with mandibular third molars. Pain,swelling, redness, and suppuration are asso-ciated with periodontal abscess. Treatmentmay include incision and drainage, use ofantibiotics, and removal of the offendingsource.
EPIDEMIOLOGY ANDRISK FACTORS
Epidemiology of GingivitisGingivitis can occur in early childhood,
becomes more prevalent during teenageyears, and decreases in older individuals.19 In1986-1987, the National Institute of DentalResearch conducted a nationwide survey oforal health in US school children20 and reported that approximately 60% of chil -dren 14 to 17 years of age were found to
CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 9

10 Periodontal Disease and Overall Health: A Clinician's Guide
have gingivitis. In 1960–1962, the first USnational survey of periodontal disease inadults reported that 85% of men and 79% ofwomen have some degree of gingivitis.21 Inthe most recent National Health and Nutri-tion Examination Survey (NHANES III)conducted from 1988 to 1994,22 more than50% of adults had gingivitis on an average ofthree or four teeth, while 63% of 13- to 17-year-old teenagers had gingival bleeding.Both surveys assessed gingival bleeding bya gingival sweep method.21,22
Epidemiology of PeriodontitisBasic clinical measurements for perio -
dontitis are gingival bleeding on probing,clinical attachment loss, and pocket depthsaccompanied by radiographic bone loss.These types of clinical measurements maybe somewhat subjective. As our knowledgeof the pathogenesis of periodontitis im-proves, new diagnostic markers for the dis-ease may emerge to help better diagnose it.Inflammatory cytokines, enzymes, and bonebreakdown products released into gingivalcrevicular fluid reflect the host response tothe bacterial challenge. These biochemicalmarkers may be good candidates for new diagnostic or prognostic markers of disease.A number of cytokines have been asso ciatedwith active disease, including prostaglandinE2 (PGE2), tumor necrosis factor-alpha(TNF-), interleukin-1 beta (IL-1), andothers.23,24 Enzymes such as matrix metal-loproteinases (MMPs) and breakdown prod-ucts such as the collagen telopeptide havebeen studied as well. To date, these bio-chemical markers in gingival crevicularfluid are still being investigated. It will behelpful to both clinicians and researchersif one or more of these markers can be de-veloped as a more objective chairside tool tomeasure active periodontitis. The devel -opment of these markers will also helpto facilitate screening for periodontaldiseases by medical professionals or even
self- assessment by patients, thereby prompt-ing referrals to the dental office for clinical assessment.
The national data suggest that the milderforms of periodontitis are close to uni -versal.25 The more severe forms are lessprevalent. According to a review of the lit-erature by Brown and Löe26 focused on anumber of epidemiologic studies resultingfrom a 1981 national probability survey, theprevalence of CP is about 36% for the adultUS population as assessed by pocket depthmeasurements. The prevalence of periodon-titis increases with age; 29% in those aged 19to 44 had CP; this rate increased to 50% forpeople 45 years or older. In general, moder-ate periodontitis occurred in 28% of all peo-ple while 8% had advanced disease. How-ever, the prevalence of moderate and severeperiodontitis increased to 44% in the popu-lation older than 45. Based on the presenceof periodontal pockets 4 mm, it was de-termined that 30% of the population has periodontitis on an average of three or fourteeth. Severe pockets of 6 mm were foundin less than 5% of the population.22 Theprevalence of aggressive periodontitis waslow with less than 1%.27 More recently,NHANES III (1988–1994) reported theprevalence of periodontitis for adults 30 to90 years old.28 Attachment loss and probingdepths were assessed at two sites per tooth.When assessed by the level of attachmentloss, 53% of the population was found tohave 3 mm attachment loss. The preva-lence of attachment loss increased with age,from approximately 35% for the 30-year-old participants to 89% for the 80-year-oldparticipants. When assessed by probingdepth, approximately 64% of the populationhad probing depths of 3 mm. The preva-lence of periodontitis increases with age andwas found to be more prevalent in malesthan females, and in African-Americans andMexican-Americans than in non-HispanicCaucasians.

Risk FactorsThere are a number of risk factors asso-
ciated with periodontal diseases.29-34 Deter-mining risk is helpful in developing recom-mendations for prevention and indetermining strategies for the overall man-agement of periodontitis. It has been recog-nized that the severity and progression ofperiodontal disease varies from individualto individual. Bacteria are essential for theinitiation of the disease, but it is the host re-sponse to the bacterial challenge that deter-mines the severity and rate of progression ofthe periodontitis. Therefore, it is the host’simmunologic reaction that determines sus-ceptibility to the disease.
General categories of risk factors asso-ciated with the development of periodontitisinclude genetic, environmental (e.g., tobacco
use), and acquired risk factors (e.g., systemicdisease). Risk factors (Table 2) and risk reduction strategies (Table 3) should be con-sidered when assessing each patient.35 Somerisk factors can be modified to reduce a patient’s susceptibility. Environmental fac-tors such as tobacco use and stress can bemanaged with smoking cessation and stressmanagement; for acquired factors such assystemic diseases, medications usually prescribed by the physician can be used tohelp in the management and control ofchronic disorders (Table 3). The use ofchemotherapeutic agents specifically de-signed to improve the clinical outcomes ofmechanical treatments for periodontal dis-eases may be particularly useful in the man-agement of those individuals with single ormultiple risk factors. Risk assessment can
CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 11
Table 2. Risk Assessment for Periodontitis
1. Heredity as determined by genetic testing and family history
2. Smoking, including frequency, current use, and history
3. Hormonal variations such as those seen in:a. Pregnancy, in which there are increased levels of estradiol and progesterone that may change the
environment and permit virulent organisms to become more destructiveb. Menopause, in which the reduction in estrogen levels leads to osteopenia and eventually osteoporosis
4. Systemic diseases such as:a. Diabetes (the duration and level of control are important)b. Osteoporosisc. Immune system disorders such as HIVd. Hematologic disorders such as neutropeniase. Connective tissue disorders such as Marfan’s and Ehlers-Danlos syndromes
5. Stress as reported by the patient
6. Nutritional deficiencies and obesity that may require a dietary analysis
7. Medications such as:a. Calcium channel blockersb. Immunomodulatory agentsc. Anticonvulsants d. Those known to cause dry mouth or xerostomia
8. Faulty dentistry such as overhangs and subgingival margins
9. Poor oral hygiene resulting in excessive plaque and calculus
10. History of periodontal disease
Sources: J Periodontol 1994;65:260–267.29 J Periodontol 1995;66:23–29.30 J Periodontol 1999;70:711–723.31
J Periodontol 2000;71:1057–1066.32 J Periodontol 2000;71:1215–1223.33 J Periodontol 2000;71:1492–1498.34

12 Periodontal Disease and Overall Health: A Clinician's Guide
help the practitioner to establish an accuratediagnosis, provide an optimal treatment plan,and determine appropriate maintenance pro-grams. In patients with multiple risk factors,the practitioner may aggressively use phar-macologic adjuncts such as antimicrobialsand host-modulatory therapy in addition tomechanical therapy. It is also important toupdate and assess risk factors for each patienton a regular basis as some of these factorsare subject to change throughout life.
ETIOLOGY AND PATHOGENESISOF PERIODONTAL DISEASEInitially, periodontal disease was
thought to be related to aging and was there-fore uniformly distributed in the population,with disease severity being directly corre-lated with plaque levels. Now as a result ofextensive research, it has been shown thatperiodontal disease is initiated by plaque,
but the severity and progression of the dis-ease is determined by the host response tothe bacterial biofilm. People with severeplaque and calculus accumulation will havegingivitis, but not necessarily periodontitis.On the other hand, certain individuals, de-spite maintaining adequate oral hygiene, findthemselves susceptible to aggressive formsof periodontitis, with deep pocketing, toothmobility, and early tooth loss. Clearly, the re-sponse of the periodontal tissues to plaque isdifferent in these two different scenarios. Pe-riodontal disease does not appear to behaveas a classic infection, but more as an oppor-tunistic infection.35 These observations ledresearchers to realize that the host responseto the bacterial challenge, presented by sub-gingival plaque, is the important determinantof disease severity. Although plaque bacteriaare capable of causing direct damage to theperiodontal tissues, it is now recognized that
Table 3. Risk Reduction Strategies
1. More frequent visits for those with a genetic predisposition; use of pharmacotherapeutics for the2.management of periodontitis
2. Smoking cessation using one or more of the six approved regimens; these regimens are rarely2. successful as sole therapies (multiple forms of therapy often are used in combination with2. counseling to achieve success)
3. Hormonal variations such as those seen in:a. Pregnancy, which requires good oral care before conception to prevent complications duringa. pregnancy; treatment during pregnancy may be necessary to prevent adverse pregnancy outcomesb. Menopause, which may require hormonal supplements, calcium, and other medications anda. supplements prescribed by the physician to prevent osteopenia
4. Systemic diseases that require consultation with the physician include:a. Diabetes (for improved glycemic control)b. Osteoporosis (requiring calcium supplements, bisphosphonates)c. Immune system and hematologic disordersd. Connective tissue disorders
5. Stress management; possible referral to a psychologist or psychiatrist
6. Nutritional supplementation and weight reduction; possible referral to a nutritionist
7. Medications can be changed in consultation with the physician
8. Corrective dentistry
9. Improved oral hygiene (brushing, flossing, use of antiseptics)
10. Occlusal adjustments
Source: Dent Clin North Am 2005;49:611–636.35
CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 13
the host immuno-inflammatory response toplaque bacteria produces destructive cy-tokines and enzymes resulting in periodon-tal tissue destruction. The host response is es-sentially protective by intent but can alsoresult in tissue damage, including the break-down of connective tissue fibers in the peri-odontal ligament and the resorption of alve-olar bone. The host response to the plaquebiofilm is modified by genetic factors (help-ing to explain why aggressive periodontitistends to have a familial aggregation), as wellas systemic and environmental factors (e.g., diabetes, stress, smoking).
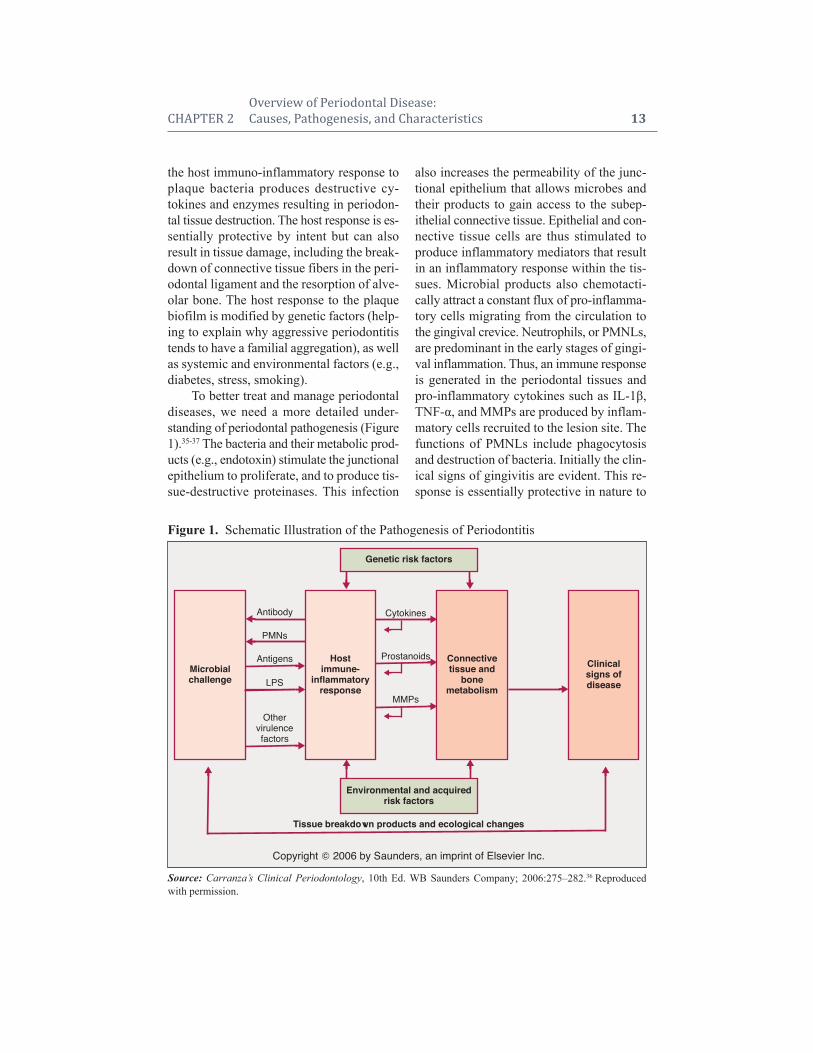
To better treat and manage periodontaldiseases, we need a more detailed under-standing of periodontal pathogenesis (Figure1).35-37 The bacteria and their metabolic prod-ucts (e.g., endotoxin) stimulate the junctionalepithelium to proliferate, and to produce tis-sue-destructive proteinases. This infection
also increases the permeability of the junc-tional epithelium that allows microbes andtheir products to gain access to the subep-ithelial connective tissue. Epithelial and con-nective tissue cells are thus stimulated toproduce inflammatory mediators that resultin an inflammatory response within the tis-sues. Microbial products also chemotacti-cally attract a constant flux of pro-inflamma -tory cells migrating from the circulation tothe gingival crevice. Neutrophils, or PMNLs,are predominant in the early stages of gingi-val inflammation. Thus, an immune responseis generated in the periodontal tissues andpro-inflammatory cytokines such as IL-1,TNF-, and MMPs are produced by inflam-matory cells recruited to the lesion site. Thefunctions of PMNLs include phagocytosisand destruction of bacteria. Initially the clin-ical signs of gingivitis are evident. This re-sponse is essentially protective in nature to
Figure 1. Schematic Illustration of the Pathogenesis of Periodontitis
Source: Carranza’s Clinical Periodontology, 10th Ed. WB Saunders Company; 2006:275–282.36 Reproducedwith permission.
Genetic risk factors
Copyright ! 2006 by Saunders, an imprint of Elsevier Inc.
Tissue breakdown products and ecological changes
Antibody Cytokines
Prostanoids
MMPs
PMNs
Antigens
LPS
Othervirulencefactors
Microbialchallenge
Hostimmune-
inflammatoryresponse
Connectivetissue and
bonemetabolism
Clinicalsigns ofdisease
Environmental and acquiredrisk factors

control bacterial infection. In persons whoare not susceptible to periodontitis, the pri-mary defense mechanisms control the infec-tion, and chronic inflammation (i.e., chronicgingivitis) may persist. However, in indi-viduals susceptible to periodontitis, theabove inflammatory process will eventuallyextend apically and laterally to involvedeeper connective tissues and alveolar bone,recruiting monocytes and lymphocytes tothe site of infection at these later stages.These monocytes and macrophages are activated by the bacterial endotoxins lead-ing to the production of high levels ofprostaglandins (e.g., PGE2), interleukins(e.g., IL-1, IL-1, IL-6), TNF-, and MMPsby the host cells. The MMPs break downcollagen fibers, disrupting the normalanatomy of the gingival tissues, resulting indestruction of the periodontal apparatus. Ifleft untreated, the inflammation continuesto extend apically, and osteoclasts are stim-ulated to resorb alveolar bone triggered by
the high levels of PGs, ILs, and TNF- in thetissues. The elevated levels of pro-inflam-matory mediators and MMPs are counter-balanced by a protective response in the hostwith elevations in anti-inflammatory media-tors such as the cytokines IL-4 and IL-10, aswell as other mediators such as IL-1ra (re-ceptor antagonist) and tissue inhibitors ofMMPs (TIMPs; Figure 2).36,37 Under normal,healthy conditions, the anti-inflammatory mediators are balanced with inflammatorymediators, thereby controlling tissue destruc -tion. If an imbalance is seen, with excessivelevels of the pro-inflammatory mediators,upregulated MMP expression and activity,and insufficient levels of protective anti- inflammatory mediators, loss of periodontalconnective tissue and bone will occur.
Thus, plaque bacteria initiate an in-flammatory response by the host, resulting inexcessive levels of pro-inflammatory medi-ators and enzymes, leading to the destructionof periodontal tissues. If this inflammation
14 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 2. The Periodontal Balance
Source: Carranza’s Clinical Periodontology, 10th Ed. WB Saunders Company; 2006:275–282.36 Reproducedwith permission.
Risk factors (e.g., genetics,smoking, diabetes)
Overproduction of proinflammatory ordestructive mediators and enzymes (e.g.,
IL-1, IL-6, PGE2, TNF-!, MMPs
Underactivity or overactivityof aspects of host response
Poor compliancePoor plaque control
DISEASE
Subgingivalbioburden
Reduction ofrisk factors
Expression of host-derived antiinflammatoryor protective mediators
(e.g., IL-4, IL-10, IL-1ra, TIMPs)
Host modulatorytherapy
Resolution ofinflammation
OHI, SRP, surgery, antiseptics, antibioticsto reduce bacterial challenge
Copyright ! 2006 by Saunders, an imprint of Elsevier Inc.
HEALTH"! !

continues and extends further apically, morebone is resorbed, and more periodontal tissueis broken down, leading to deeper and deeperpockets and associated attachment and boneloss revealed as the clinical and radiographicsigns of periodontitis. In people with peri-odontitis, these inflammatory mediators(e.g., prostanoids and cytokines) and localoral bacteria will eventually enter into thecirculation, stimulating the liver to produceacute-phase proteins (notably C-reactive pro-tein, but also fibrinogen, haptoglobin, etc.)which are “biomarkers” of a systemic in-flammatory response. The ever-expandingdata supporting the fact that this systemicinflammatory response driven by the chronicinfection and inflammation associated withperiodontitis will eventually increase an in-dividual’s risk for developing a number ofsystemic diseases, including cardiovasculardiseases, adverse pregnancy outcomes, anddiabetic complications.
MANAGEMENT OFPERIODONTAL DISEASES
Periodontal management includes acomplete assessment of each individual pa-tient. Medical and dental history, clinical andradiographic examination, as well as an as-sessment of risk factors are all important tomaking an accurate diagnosis, prognosis,and developing an optimal treatment plan.There are many treatment options availablefor the management of periodontal diseases,and review of treatment outcomes or re-eval-uation is key to successful management andlong-term maintenance. In the past, treat-ments that focused on reduction of the mi-crobial load were basically the sole consid-eration for all periodontal therapy. Currently,due to a better understanding of the host re-sponse, host-modulation therapies have beenused as adjunctive approaches to both non-surgical and surgical treatments to aid in reducing probing depths, increasing clinicalattachment levels, and in regeneration of
the lost attachment apparatus. It is likely thatthe most effective therapeutic approacheswill include multiple, synergistic host- modulation therapies combined with treat-ments that target the microbial etiology.
In addition to reducing the bacterialchallenge and modulating the host response,reduction of risk is also a key treatment stra tegy when managing periodontitis. Forexample, it is known that smoking can contribute to the development of periodontaldisease and make management of the dis-ease more difficult;38,39 therefore smoking ces sation would benefit all patients with periodontitis. Smoking cessation can be undertaken in the dental office (if staffis appropriately trained) or in a medical setting. There are a variety of medications toaid with smoking cessation, counseling isimportant as well, and alternative medicinesuch as acupuncture may be used. Systemicdiseases such as diabetes will increase pa-tients’ risk for periodontitis when poorlycontrolled.40 When treating people with dia-betes, knowing the patient’s level of diabeticcontrol is important to assessing risk, andcollaborating with medical colleagues to improve control of diabetes is essential to assure successful periodontal treatment. Perio dontitis is also prevalent in patientswith cardiovascular disease, and periodontaltherapy may have a positive impact on theoverall health status of these individuals.
The management of patients with peri-o dontitis can therefore involve the followingcomplementary treatment strategies:41
• Patient education, including oral hy-giene instruction and explanation ofthe rationale for any adjunctive treat-ments
• Risk factor modification and risk re-duction
• Reduction of bacterial burden withtraditional scaling and root planing
• Intensive periodontal treatment withlocal delivery systems or general
CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 15
antimicrobial therapy with oral ad-ministration of antibiotics
• Host-modulation therapy• Periodontal surgeryIt is the responsibility of the dentist to
provide appropriate treatments on an indi-vidualized basis. A combination of treatmentapproaches (discussed below) for each pa-tient as listed in Figure 3 will provide the ultimate periodontal treatment and result ina better prognosis.41
The Antimicrobial ApproachTraditional periodontal therapy based
on the antimicrobial approach consists ofmechanical nonsurgical and surgical thera-pies that may or may not be supplemented bylocal antiseptics and/or local or systemic antibiotics.
Mechanical TherapyA regimen of brushing and flossing,
combined with the use of dentifrices and/ormouthrinses containing antiseptics is themost basic approach to microbial reductionand control. Good oral hygiene can effec-tively reduce bacterial loads to prevent gin-givitis and aid in the treatment and manage-ment of periodontitis. This simple approachrelies on an individual’s knowledge of thecorrect techniques and compliance with homecare instructions. Unfortunately, many patientsare not compliant, lose motiva tion, and do notspend a sufficient amount of time brushing orflossing on a daily basis.42 It is for this reasonthat dentifrices and mouth rinses containingantiseptics have been devel oped. Antisepticshave been found to improve plaque reduc-tion, as well as reduce gingival inflammation
16 Periodontal Disease and Overall Health: A Clinician's Guide
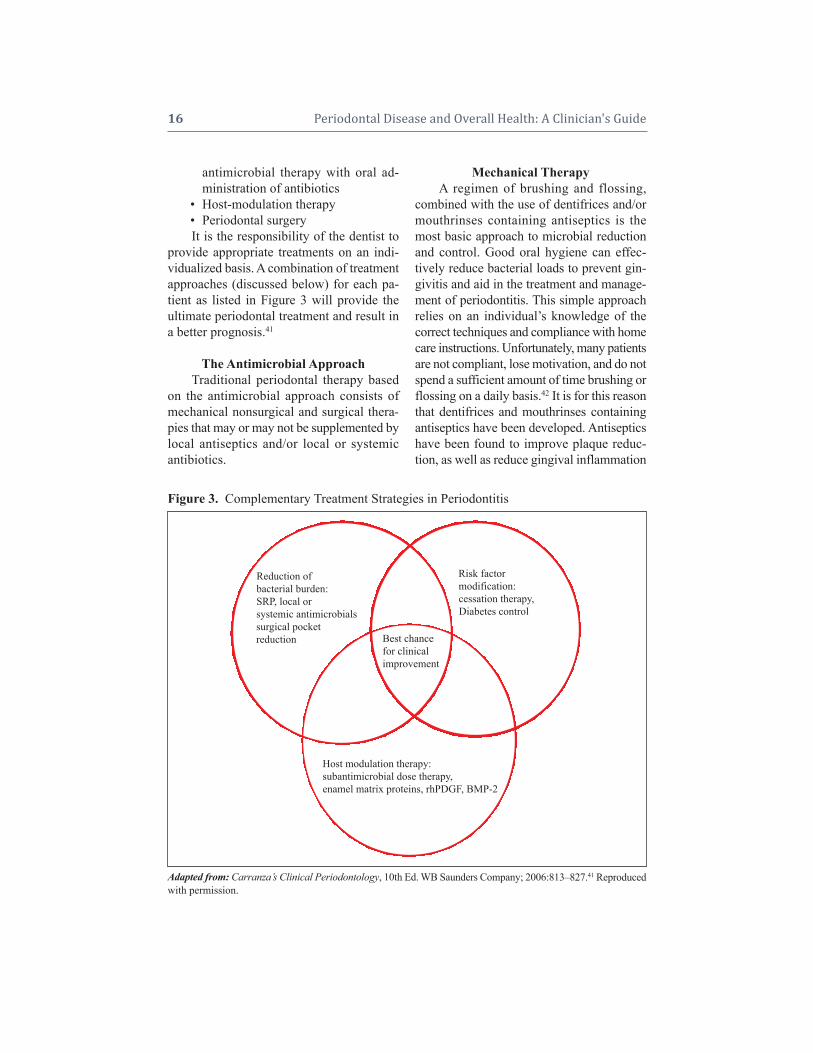
Figure 3. Complementary Treatment Strategies in Periodontitis
Adapted from: Carranza’s Clinical Periodontology, 10th Ed. WB Saunders Company; 2006:813–827.41 Reproducedwith permission.
Reduction ofbacterial burden:SRP, local orsystemic antimicrobialssurgical pocketreduction
Risk factormodification:cessation therapy,Diabetes control
Host modulation therapy:subantimicrobial dose therapy,enamel matrix proteins, rhPDGF, BMP-2
Best chancefor clinicalimprovement

seen with brushing and flossing alone. There-fore, antiseptic-containing dentifrices andmouth rinses have been accepted as adjunctsto the mechanical approach of brushing andflossing.
Routine tooth scaling every six monthsby the dental care provider is also a key com-ponent in treating and preventing gingivitis.Scaling and root planing is the traditionalnonsurgical treatment of periodontitis, withmultiple clinical studies demonstrating thatit effectively reduces the microbial load andleads to reductions in bleeding on probingand probing depths, and allows for gains inclinical attachment.43 However, this proce-dure can be very time-consuming and is op-erator-dependent.44 Surgical procedures canbe used to visualize the remaining subgingivalcalculus, and through resective or regenerativeprocedures will also lead to decreased prob-ing depths that are more manageable for thelong-term maintenance of patients with peri-odontitis. Although nonsurgical and surgicalprocedures aimed at reducing the bacterialload and restoring the attachment apparatuscontinue to be the most widely used methodsof treating periodontitis, these strategies alonemay be insufficient at reducing the bacterialload as significant numbers of micro-organ-isms may be left behind. In addition, many ofthe putative pathogens will remain within theoral cavity at distant sites allowing for re-population in the future. Therefore, the needfor the development of chemotherapeuticagents as adjuncts to mechanical debride-ment was deemed necessary.
Mouthrinses and Dentifrices
Antiseptic MouthrinsesAntiseptic mouthrinses have been used to
reduce plaque levels and gingivitis. Two clin-ically proven American Dental Association-accepted antiseptic mouthrinses are chlorhex-idine gluconate (Peridex®) and the fouressential oils in Listerine®. An association
CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 17
between oral conditions such as periodontaldisease and several respiratory conditionssuch as pneumonia and chronic obstructivepulmonary disease has been noted. Theplaque surrounding the teeth is an excellentharbor for respiratory pathogens. Studies haveshown that using a chlorhexidine oral rinsecan reduce the risk of pneumonia in institu-tionalized patients with poor oral hygiene.45
Locally Applied AntisepticsPeriochip® contains the active ingredi-
ent chlorhexidine gluconate (2.5 mg) that isreleased into the pocket over a period ofseven to 10 days. It has been found to sup-press the bacteria in the pocket for up to 11weeks post-application.46 Periochip is theonly locally applied antiseptic that is ap-proved by the Food and Drug Administration(FDA) for use as an adjunct to scaling androot planing procedures to aid in the reduc-tion of pocket depths. Other locally appliedantimicrobials are antibiotics.
DentifricesMajor improvements in the oral health
of populations in developed countries havebeen seen over the last 50 years. Most of thisresulted from the reduction in the caries rateof about 50%, and the principle reason forthis is thought to be the addition of fluorideto dentifrices. Modern, commercially avail-able dentifrices, in addition to providing anti -caries effects of fluoride, also contribute tothe reduction of plaque, gingivitis, cal culusformation, relief of dentin hypersenitivity,and tooth stain. They also reduce halitosis andresult in a clean, fresh mouth feel. Two den ti-frices available in the US that are approved bythe FDA for their effects on reduction of gin-givitis include a stannous fluoride/sodiumhexametaphosphate den ti frice and a triclosan/copolymer/sodium fluoride dentifrice.
There is a large amount of literature onthese and other dentifrices containing chlor -hexidine and other agents in the control of

gingivitis. A review of the clinical efficacyand safety of a triclosan/copolymer/sodiumfluoride dentifrice was carried out by Blink -horn and colleagues.47 They found about 200articles dating from 1998 to 2008 relating tothis dentifrice and concluded that twice dailyuse of this dentifrice will result in clinicallysignificant improvement in plaque controland gingivitis and slower progression of perio dontal disease. Further long-term stud-ies extending over several years with thesedentifrices are needed to establish whether ornot short-term effects seen will be sustainedover the long term, and indeed result in pre-venting the initiation of perio dontitis andslowing the progression of already existingperiodontitis.
It should be noted that the antiplaqueand antigingivitis effects of dentifrices duringa tooth brushing regimen are mainly on theocclusal and smooth surfaces of the teeth,and that interproximal plaque and gingivitiscontrol is not optimally reduced with toothbrushing alone, with or without a dentifrice.Interproximal aids such as flossing, inter-proximal brushing, and to some extent, flush-ing with effective mouthrinses is often neededfor full plaque control on interproximal sur-faces of the teeth. As periodontal disease isoften initiated and progresses more rapidly ininterproximal spaces, it is clear that inter-proximal cleansing is an important adjunct totoothbrushing with dentifrices.
Locally Delivered Antimicrobials
AtridoxAtridox® is an FDA-approved locally
delivered tetracycline system. It comes witha 10% formulation of doxycycline in a bio -absorbable, “flowable” poly-DL lactide andN-methyl-2-pyrrolidone mixture deliverysystem that allows for controlled release overseven days. This system is applied subgin -givally to the base of the pocket through a cannula. Atridox is a resorbable site-specific
locally delivered antibiotic proven to promoteclinical attachment gains and reduce pocketdepths, bleeding on probing, and levels ofpathogenic bacteria for up to six months post-placement.35 Periodontal disease has beenlinked to systemic diseases such as diabetes.Research has shown that periodontal treat-ment with locally delivered doxycycline 10mg in periodontal pockets produced favor-able clinical results in diabetic patients.48
ArestinArestin® is an FDA-approved minocy-
cline microsphere system that is bioadhesiveand bioresorbable, allowing for sustained re-lease of 1 mg of minocycline up to 19 days.Arestin can be used as an adjunct to scalingand root planing procedures for reduction ofpocket depth in patients with adult perio -dontitis. Arestin is delivered to sites of 5 mmor greater. Periodontitis has been associatedwith increased systemic inflammation, whichis directly linked to diabetes and cardiovas-cular diseases. Recent research has shownthat periodontal therapy with local Arestinadministration resulted in decreased HbA1clevels in diabetic subjects49 and significantreductions in systemic inflammatory bio-markers that are risk factors for cardiovas-cular disease.50
Systemic AntimicrobialsSystemic antimicrobial therapy is usu-
ally reserved for advanced cases of peri-odontitis: 1) for sites that have not respondedto treatment, so-called “refractory periodon-titis,” and 2) for patients demonstrating pro-gressive periodontal destruction.35 Systemicantibiotics can be used as adjuncts to con-ventional mechanical therapy as strong evi-dence for their use as a monotherapy has notbeen developed. For these special situations,randomized double-blinded clinical trials andlongitudinal assessments of patients indicatethat systemic antimicrobials may be usefulin slowing disease progression.51 Metroni -
18 Periodontal Disease and Overall Health: A Clinician's Guide

dazole can be used to treat acute necrotizing ulcerative gingivitis (NUG),52 and metron-idazole/amoxicillin combination therapy canbe used to treat aggressive adolescent peri-odontitis associated with A. actinomycetem-comitans.53 Systemic antibiotic therapy hasthe advantage of simple, easy administrationof drugs to multiple periodontal sites. How-ever, patient compliance needs to be consid-ered, inability to achieve adequate concen-trations at the site of infection, adverse drugreactions, and the develop ment of antibioticresistance can be issues.54 Common antibiotictherapies for the treatment of periodontitisinclude metronidazole, clindamycin, doxy-cycline or minocycline, ciprofloxacin,azithromycin, metronidazole/amoxicillin,and metronidazole/cipro floxacin.55 For adultpatients with acute periodontal abscesses,amoxicillin is used as an adjunct to incisionand drainage. For patients with allergies tobeta-lactam drugs (e.g., amoxicillin), azith -romycin or clindamycin would be the choice.
Researchers have shown that periodon-tal treatment can benefit some systemic dis-eases known to be associated with periodon-titis, such as diabetes and preterm delivery.Grossi and colleagues reported that diabeticpatients receiving scaling and root planingwith systemic doxycycline showed signifi-cant reductions in mean HbA1c.56 Effectivetreatment of periodontal infection and reduc -tion of periodontal inflammation is associ-ated with a reduction in levels of glycated hemo globin. Clothier and colleagues alsoshowed that performing scaling and root plan-ing in pregnant women with periodontitismay reduce preterm delivery.57 However, ad -junc tive metronidazole therapy did not im -prove pregnancy outcomes. Two recent stud-ies have not shown improvements in adverse pregnancy outcomes with scaling and root planing.58 However, the level of perio dontaltreatment provided may have been very inadequate. More studies are needed in thisfield to determine the effect of periodontal
treatment on the outcomes of adverse preg-nancy and the extent of therapy that mayneed to be provided in order to have a sig-nificant impact.
Host-Modulation TherapyBacteria and the host are two essential
factors to the development of periodontitis.Reduction of bacterial load is the con -ventional approach for the management ofperiodontal diseases. More recently, peri-odontal treatment strategies have includedhost-modulation therapy as an adjunctivetreatment option. Host-modulation therapy istreating the host response to either reduce theexcess production of cytokines and destruc-tive enzymes so there is less damage to the periodontal tissues, or to stimulate the re-gen erative process, allowing for the restora-tion of connective tissue attachment andbone formation to occur.
Host modulation was first introduced todentistry by Williams59 and Golub and col-leagues.60 Williams stated: “There are com-pelling data from studies in animals and hu-man trials indicating that pharmacologicagents that modulate the host responses be-lieved to be involved in the pathogenesis ofperiodontal destruction may be efficacious inslowing the progression of periodontitis.”59
Golub and colleagues discussed “host mod-ulation with tetracyclines and their chemi-cally modified analogues.”60 A variety of dif-ferent drug classes have been evaluated ashost-modulation agents, including the non -steroidal anti-inflammatory drugs, bisphos-phonates, tetracyclines (Figure 4),36 enamelmatrix proteins, growth factors, and bonemorphogenetic proteins.
Systemically Administered Agents
Subantimicrobial-Dose DoxycyclineSubantimicrobial-dose doxycycline (SDD)
is the only FDA-approved MMP inhibitorand systemic host-modulation therapy for the
CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 19
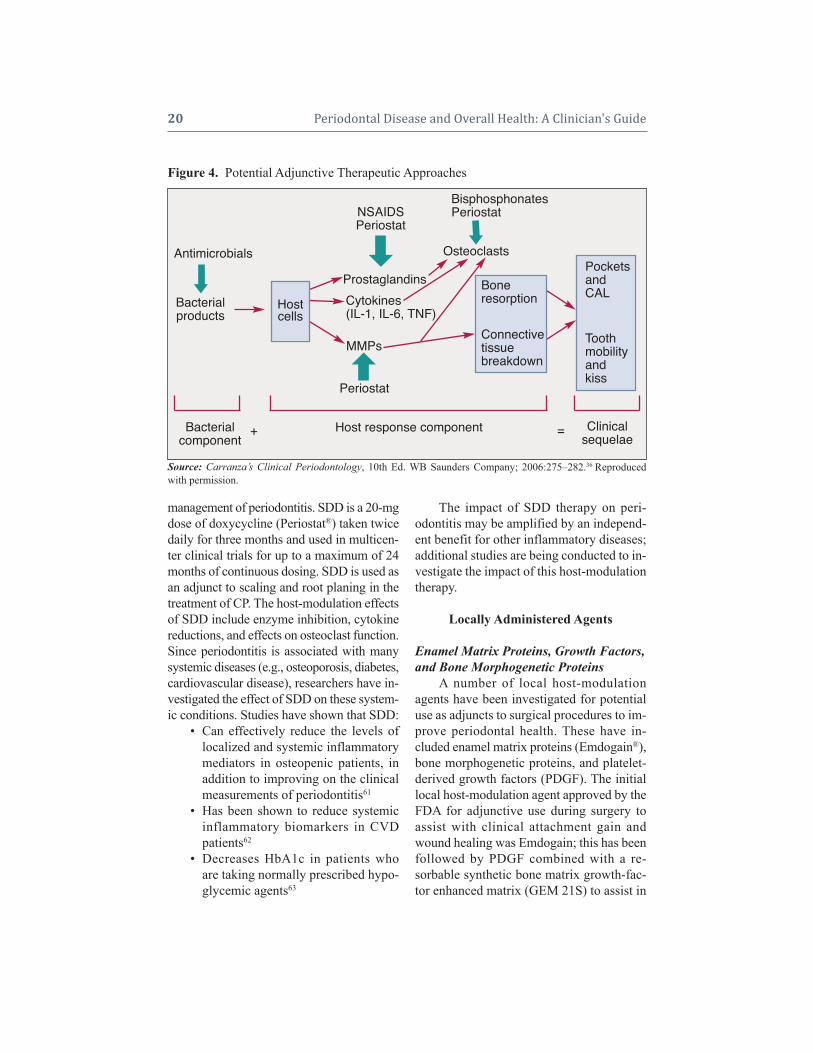
management of periodontitis. SDD is a 20-mgdose of doxycycline (Periostat®) taken twicedaily for three months and used in multicen-ter clinical trials for up to a maximum of 24months of continuous dosing. SDD is used asan adjunct to scaling and root planing in thetreatment of CP. The host-modulation effectsof SDD include enzyme inhibition, cytokinereductions, and effects on osteoclast function.Since perio dontitis is associated with manysystemic diseases (e.g., osteoporosis, diabetes,cardiovascular disease), researchers have in-vestigated the effect of SDD on these system -ic conditions. Studies have shown that SDD:
• Can effectively reduce the levels oflocalized and systemic inflammatorymediators in osteopenic patients, inaddition to improving on the clinicalmeasurements of periodontitis61
• Has been shown to reduce systemicinflammatory biomarkers in CVD patients62
• Decreases HbA1c in patients whoare taking normally prescribed hypo-glycemic agents63
The impact of SDD therapy on peri-odontitis may be amplified by an independ-ent benefit for other inflammatory diseases;additional studies are being conducted to in-vestigate the impact of this host-modulationtherapy.
Locally Administered Agents
Enamel Matrix Proteins, Growth Factors,and Bone Morphogenetic Proteins
A number of local host-modulationagents have been investigated for potentialuse as adjuncts to surgical procedures to im-prove periodontal health. These have in-cluded enamel matrix proteins (Emdogain®),bone morphogenetic proteins, and platelet-derived growth factors (PDGF). The initiallocal host-modulation agent approved by theFDA for adjunctive use during surgery toassist with clinical attachment gain andwound healing was Emdogain; this has beenfollowed by PDGF combined with a re-sorbable synthetic bone matrix growth-fac-tor enhanced matrix (GEM 21S) to assist in
20 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 4. Potential Adjunctive Therapeutic Approaches
Source: Carranza’s Clinical Periodontology, 10th Ed. WB Saunders Company; 2006:275–282.36 Reproducedwith permission.
Antimicrobials
Host response component
Osteoclasts
ProstaglandinsCytokines(IL-1, IL-6, TNF)
Periostat
MMPs
NSAIDSPeriostat
Bacterialproducts
PocketsandCAL
Toothmobilityandkiss
Bacterialcomponent
+ = Clinicalsequelae
BisphosphonatesPeriostat
Hostcells
Boneresorption
Connectivetissuebreakdown

regenerative procedures approved recentlyby the FDA, as well as recombinant humanbone morphogenetic protein-2 (rhBMP-2)contained within an absorbable collagensponge to assist with ridge and sinus aug-mentation. The technology behind GEM 21Shas already been marketed for use in woundhealing, particularly in people with diabetes,and rhBMP-2 has been used for quite sometime by the orthopedic community for thehealing of fractures.
The findings discussed with regard to theuse of host-modulation therapy to better man-age chronic periodontal disease may have ap-plications to other chronic systemic diseasessuch as arthritis, diabetes, osteoporosis, andcardiovascular disease. In addition, studiesutilizing locally delivered antimicrobials aspart of an intensive periodontal therapy reg-imen have shown very promising results.Future studies may demonstrate that in ad-dition to our current standard therapies, in-tensive periodontal therapy with adjunctiveantibiotics and/or host modulation for themanagement of periodontal disease mayhave profound positive effects on the over-all health status of high-risk patients. Theproper management of local infection andinflammation (periodontitis) will have a sig-nificant impact on general overall health ofthe population.
AcknowledgmentsThe authors would like to acknowledge Dr.Hsi-ming Lee, René Martin, and LauraBertolotti for their assistance in the organi-zation of this manuscript.
Supplemental Readings
Williams RC. Periodontal disease. N Engl J Med 1990;322:373-382.
Page RC, Offenbacher S, Schroeder HE, Seymour GJ,Kornman KS. Advances in the pathogenesis of perio -dontitis: summary of developments, clinical implica-tions and future directions. Periodontol 2000 1997;14:216-248.
Brown LJ, Löe H. Prevalence, extent, severity and pro-gression of periodontal disease. Periodontol 2000 1993;2:57-71.
Burt B. Research, Science and Therapy Committee of theAmerican Academy of Periodontology. Position paper:Epidemiology of periodontal diseases. J Periodontol2005;76:1406-1419.
Ryan EM. Nonsurgical approaches for the treatment ofperiodontal diseases. Dent Clin North Am 2005;49:611–636.
Ryan ME, Preshaw PM. Host modulation. In: NewmanMG, Takei HH, Klokkevold PR, Carranza FA, eds.Carranza’s Clinical Periodontology, Edition 10. WBSaunders Co. 2006; pp. 275-282.
Preshaw PM, Ryan ME, Giannobile WV. Host modula-tion agents. In: Newman MG, Takei HH, KlokkevoldPR, Carranza FA, eds. Carranza’s Clinical Periodon-tology, Edition 10. WB Saunders Co. 2006; pp. 813-827.
REFERENCES1. Mariotti A. Dental plaque-induced gingival diseases.
Ann Periodontol 1999;4:7–19.2. Van Dyke TE. The management of inflammation in
periodontal disease. J Periodontol 2008;79(8 Suppl):1601–1608.
3. Armitage GC. Development of a classification sys-tem for periodontal diseases and conditions. AnnPeriodontol 1999;4:1–6.
4. Novak MJ. Classification of diseases and condi-tions affecting the periodontium. In: Newman MG,Takei HH, Carranza FA, eds. Carranza’s ClinicalPeriodontology, 9th Ed. WB Saunders Company;2002:64–73.
5. Flemmig TF. Periodontitis. Ann Periodontol 1999;4:32–38.
6. Armitage GC. Periodontal diseases: diagnosis. AnnPeriodontol 1996;1:37–215.
7. Kinane DF. Blood and lymphoreticular disorders.Periodontol 2000 1999;21:84–93.
8. Rees TD. Drugs and oral disorders. Periodontol2000 1998;18:21–36.
9. Scully C, Monteil R, Sposto MR. Infectious andtropical diseases affecting the human mouth. Peri-odontol 2000 1998;18:47–70.
10. Holmstrup P. Non-plaque induced gingival lesions.Ann Periodontol 1999;4:20–31.
11. Stanford TW, Rivera-Hidalgo F. Oral mucosal le-sions caused by infective microorganisms II. Fungi& parasites. Periodontol 2000 1999;21:125–144.
12. Aldred MJ, Bartold PM. Genetic disorders of thegingivae and periodontium. Periodontol 2000 1998;18:7–20.
CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 21

13. Scully C, Laskaris G. Mucocutaneous disorders.Periodontol 2000 1998;18:81–94.
14. Page RC, Offenbacher S, Schroeder HE, SeymourGJ, Kornman KS. Advances in the pathogenesisof periodontitis: summary of developments, clini-cal implications and future directions. Periodontol2000 1997;14:216–248.
15. Tonetti MS, Mombell A. Early onset periodontitis.Ann Periodontol 1999;4:39–53.
16. Kinane DF. Periodontitis modified by systemic fac-tors. Ann Periodontol 1999; 4:54–64.
17. Novak MJ. Necrotizing ulcerative periodontitis.Ann Periodontol 1999;4:74–78.
18. Meng HX. Periodontal abscess. Ann Periodontol1999;4:79–83.
19. Stamm JW. Epidemiology of gingivitis. J Clin Perio dontol 1986;13:360–370.
20. Bhat M. Periodontal health of 14- to 17-year-oldUS schoolchildren. J Public Health Dent 1991;51:5–11.
21. U.S. Public Health Service, National Center forHealth Statistics. Periodontal Disease in Adults.United States 1960–1962. Washington, DC: Govern -ment Printing Office; 1965.
22. Oliver RC, Brown LJ, Löe H. Periodontal diseasesin the United States population. J Periodontol 1998;69:269–278.
23. Page RC. Host response tests for diagnosing perio -dontal diseases. J Periodontol 1992;63(Suppl.):356–366.
24. Offenbacher S, Collins JG, Yalda B, Haradon G.Role of prostaglandins in high-risk periodontitispatients. In: Genco R, Hamada S, Lehner T,McGhee J. Mergenhagen S, eds. Molecular Patho-genesis of Periodontal Disease. Washington DC:American Society for Microbiology;1994:203–213.
25. Burt B. Research, Science and Therapy Committeeof the American Academy of Periodontology. Po-sition paper: Epidemiology of periodontal diseases.J Periodontol 2005;76:1406–1419.
26. Brown LJ, Löe H. Prevalence, extent, severity andprogression of periodontal disease. Periodontol2000 1993;2:57–71.
27. Löe H, Brown LJ. Early onset periodontitis in theUnited States of America. J Periodontol 1991;62:608–616.
28. Albandar JM, Brunelle JA, Kingman A. Destructiveperiodontal disease in adults 30 years of age andolder in the United States, 1988–1994. J Perio -dontol 1999;70:13–29.
29. Grossi SG, Zambon JJ, Ho AW, Koch G, DunfordRG, Machtei EE, Norderyd OM, Genco RJ. As-sessment of risk for periodontal disease. I. Risk indicators for attachment loss. J Periodontol 1994;
65:260–267.30. Grossi SG, Genco RJ, Machtei EE, How AW, Koch
G, Dunford R, Zambon JJ, Hausmann E. Assess-ment of risk for periodontal disease. II. Risk indi-cators for alveolar bone loss. J Periodontol 1995;66:23–29.
31. Genco RJ, Ho AW, Grossi SG, Dunford RG,Tedesco LA. Relationship of stress, distress andinadequate coping behaviors to periodontal dis-ease. J Periodontol 1999;70:711–723.
32. Nishida M, Grossi SG, Dunford RG, Ho AW, Tre-visan M, Genco RJ. Calcium and the risk for peri-odontal disease. J Periodontol 2000;71:1057–1066.
33. Nishida M, Grossi SG, Dunford RG, Ho AW, Tre-visan M, Genco RJ. Dietary vitamin C and the riskfor periodontal disease. J Periodontol 2000;71:1215–1223.
34. Tezal M, Wactawski-Wende J, Grossi SG, Ho AW,Dunford R, Genco RJ. The relationship betweenbone mineral density and periodontitis in post-menopausal women. J Periodontol 2000;71:1492–1498.
35. Ryan ME. Nonsurgical approaches for the treat-ment of periodontal diseases. Dent Clin North Am2005;49:611–636.
36. Ryan ME, Preshaw PM. Host modulation. In: New-man MG, Takei HH, Klokkevold PR, Carranza FA,eds. Carranza’s Clinical Periodontology, 10th Ed.WB Saunders Company; 2006:275–282.
37. Page RC, Kornman KS. The pathogenesis of hu-man periodontitis: an introduction, Periodontol2000 1997;14:9–11.
38. Grossi SG, Zambon J, Machtei EE, Schifferle R,Andreana S, Genco RJ, Cummins D, Harrap G.Effects of smoking and smoking cessation on heal-ing after mechanical periodontal therapy. J Am DentAssoc 1997;128:599–607.
39. Kinane DF, Chestnutt IG. Smoking and periodontaldisease. Crit Rev Oral Biol Med 2000;11:356–365.
40. Mealey B. Diabetes and periodontal diseases. J Perio dontol 2000;71:664–678.
41. Preshaw PM, Ryan ME, Giannobile WV. Hostmodulation agents. In: Newman MG, Takei HH,Klokkevold PR, Carranza FA, eds. Carranza’s Clin-ical Periodontology, 10th Ed. WB Saunders Com-pany; 2006:813–827.
42. Bader HI. Floss or die: implications for dental pro-fessionals. Dent Today 1998;17:76–82.
43. Cobb CM. Non-surgical pocket therapy: mechani-cal. Ann Periodontol 1996;1:443–490.
44. Greenstein G. Periodontal response to mechanicalnon-surgical therapy: a review. J Periodontol 1992;63:118–130.
45. Nesse W, Spijkervet FK, Abbas F, Vissink A. Linksbetween periodontal disease and general health. 1.
22 Periodontal Disease and Overall Health: A Clinician's Guide

Pneumonia and cardiovascular disease. Ned Tijd-schr Tandheelkd. 2006;113:186–190.
46. Stabholz A, Sela MN, Friedman M, Golomb G,Soskolne A. Clinical and microbiological effects ofsustained release chlorhexidine in periodontal pock-ets. J Clin Periodontol 1986;13:783–788.
47. Blinkhorn A, Bartold PM, Cullinan MP, MaddenTE, Marshall RI, Raphael SL, Seymour GJ. Is therea role for triclosan/copolymer toothpaste in the management of periodontal disease? Br Dent J2009;207:117–125.
48. Martorelli de Lima AF, Cury CC, Palioto DB, DuroAM, da Silva RC, Wolff LF. Therapy with adjunc-tive doxycycline local delivery in patients with type1 diabetes mellitus and periodontitis. J Clin Perio -dontol 2004;31:648–653.
49. Skaleric U, Schara R, Medvescek M, Hanlon A,Doherty F, Lessem J. Periodontal treatment byArestin and its effects on glycemic control in type1 diabetes patients. J Int Acad Periodontol 2004;64(Suppl.):160–165.
50. D’Aiuto F, Nibali L, Parkar M, Suvan J, TonettiMS. Short-term effects of intensive periodontaltherapy on serum inflammatory markers and cho-lesterol. J Dent Res 2005;84:269–273.
51. Haffajee AD, Socransky SS, Dzink JL, TaubmanMA, Ebersole JL. Clinical, microbiological andimmunological features of subjects with refractoryperiodontal diseases. J Clin Periodontol 1988;15:390–398.
52. Duckworth R, Waterhouse JP, Britton DE, Nuki K,Sheiham A, Winter R, Blake GC. Acute ulcerativegingivitis. A double-blind controlled clinical trial ofmetronidazole. Br Dent J 1966;120:599–602.
53. van Winkelhoff AJ, Rodenburg JP, Goene RJ, Ab-bas F, Winkel EG, de Graaff J. Metronidazole plusamoxicillin in the treatment of Actinobacillus actin-omycetemcomitans associated periodontitis. J ClinPeriodontol 1989;16:128–131.
54. Slots J. Research, Science and Therapy Committee.
Systemic antibiotics in periodontics. J Periodontol2004;75:1553–1565.
55. Slots J, van Winkelhoff AJ. Antimicrobial therapyin periodontics. J Calif Dent Assoc 1993;21:51–56.
56. Grossi SG, Skrepcinski FB, DeCaro T, RobertsonDC, Ho AW, Dunford RG, Genco RJ. Treatment ofperiodontal disease in diabetics reduces glycatedhemoglobin. J Periodontol 1997;68:713–719.
57. Clothier B, Stringer M, Jeffcoat MK. Periodontaldisease and pregnancy outcomes: exposure, riskand intervention. Best Pract Res Clin Obstet Gy-naecol 2007;21:451–466.
58. Michalowicz BS, Hodges JS, DiAngelis AJ, LupoVR, Novak MJ, Ferguson JE, Buchanan W, BofillJ, Papapanou PN, Mitchell DA, Matseoane S,Tschida PA. OPT Study. Treatment of periodontaldisease and the risk of preterm birth. N Engl J Med2006;355:1885–1894.
59. Williams RC. Periodontal disease. N Engl J Med1990;322:373–382.
60. Golub LM, Suomalainen K, Sorsa T. Host modu-lation with tetracyclines and their chemically mod-ified analogues. Curr Opin Dent 1992;2:80–90.
61. Golub LM, Lee HM, Stoner JA, Sorsa T, ReinhardtRA, Wolff MS, Ryan ME, Nummikoski PV, PayneJB. Subantimicrobial-dose doxycycline modulatesgingival crevicular fluid biomarkers of periodonti-tis in postmenopausal osteopenic women. J Perio -dontol 2008;79:1409–1418.
62. Brown DL, Desai KK, Vakili BA, Nouneh C, LeeHM, Golub LM. Clinical and biochemical results ofthe metalloproteinase inhibition with subanti -microbial doses of doxycycline to prevent acutecoronary syndromes (MIDAS) pilot trial. Arterio -scler Thromb Vasc Biol 2004;24:733–738.
63. Engebretson SP, Hey-Hadavi J, Celenti R, Lam-ster IB. Low-dose doxycycline treatment reducesglycosylated hemoglobin in patients with type 2diabetes: a randomized controlled trial. J Dent Res2003;82(Spec Iss):Abstract #1445.
CHAPTER 2 Overview of Periodontal Disease:CHAPTER 2 Causes, Pathogenesis, and Characteristics 23
CHAPTER 3Infection and InlammationPhoebus N. Madianos, Yiorgos A. Bobetsis, Thomas E. Van Dyke
INTRODUCTIONPeriodontal diseases (gingivitis and perio-
dontitis) are destructive inflammatory diseasesof the gingiva and the supporting structures ofthe teeth, induced by a microbial biofilmcommonly called dental plaque. The funda-mental principle of the bacterial etiology ofgingivitis was first established in a landmarkstudy by Löe et al. in 1965.1 Using a novel,now classic, experimental design, it wasdemonstrated that when students withhealthy gingiva abstained from oral hygienepractices for 10–21 days, marginal inflam-mation of the gingiva (gingivitis) developedas a result of plaque accumulation. Onceoral hygiene was reinstated, gingival healthreturned. Today, in vitro and in vivo experi-ments, along with histological assessmentsof inflamed and healthy gingiva, have pro-vided a clearer understanding of the nature ofthe interactions between bacteria and hostcells. However, current understanding of theetiology and pathogenesis of the periodontaldiseases is far from complete.
Periodontal bacteria possess a plethoraof virulence factors that, upon interactionwith host cells, induce production of in-flammatory mediators at the gingival level.These mediators are thought to be importantfor the initiation and progression of an in-flammatory response, which although in-tended to eliminate the bacterial challenge,inevitably results in tissue damage when thebacterial challenge persists. It is also impor-tant to note that inflammation is not confinedonly to periodontal tissues. Bacteria and in-flam matory mediators may enter blood circu -lation to induce systemic inflammation. Thereis increasing evidence that cardiovasculardisease,2 adverse pregnancy outcomes,3 and
diabetes mellitus4 are associated with elevatedsystemic inflammation, suggesting a commonpathway in the pathogenesis of a number ofinflammatory diseases.
Depending upon the effectiveness ofthe innate immune response, bacterial infec-tion may persist and lead to perpetuation ofinflammation, which may become chronicwith development of acquired immunity.However, if the infection is cleared, then res-olution of inflammation occurs with the re-turn of tissue homeostasis without perma-nent damage. Recent discoveries have alteredour understanding of inflammation resolu-tion and return of tissue homeostasis. Wenow understand that resolution of inflam-mation is an active process, not the passivedecrease of pro-inflammatory signals as oncethought. The ability to manipulate theseprocesses may provide a new treatment par-adigm for both local and systemic inflam-matory diseases (see Serhan et al.).5
Chapter GoalsThis chapter is structured to: (a) provide
background information regarding the initi-ation and orchestration of inflammation atthe gingival level after the interaction of thebiofilm with host cells; (b) examine the evi-dence for periodontal disease influencingsystemic inflammation and describe the pos-sible biological pathways, as well as the cel-lular and molecular events that may occur;(c) explore the idea that systemic inflamma-tion may be the link that associates peri-odontal with other systemic diseases focus-ing on the potential mechanisms of action;(d) address the role of resolution of inflam-mation in the pathogenesis of inflammatorydiseases; and (e) introduce new strategies

CHAPTER 3 Infection and Inlammation 25
directed at mechanisms of inflammation resolution that may be used in treating in -flammatory diseases.
PART I: INFLAMMATIONAT THE GINGIVAL LEVEL
Periodontal disease is an inflammatorydisorder of the gingiva initiated by bacteriathat leads to the destruction of the supportingtissues of the teeth in a susceptible host. Bac-teria in the oral cavity colonize the teeth, thegingival sulcus, and eventually the perio -dontal pocket, forming an organized biofilm.Depending upon the stage of maturation, thebiofilm may consist of several hundred dif-ferent bacterial species, many of which haveyet to be identified.6 Some of these speciesare associated with health, whereas othersare associated with pathology.7 However,which organisms actually initiate disease re-mains unknown.
Bacterial ComponentsThe formation of organized biofilms
enhances the ability of bacteria to survive.Bacteria have also evolved a variety of viru-lence factors to further enhance their sur-vival, such as toxins, proteases, and glyco -sidases. Virulence factors are presumablyintended to hide the bacteria from host de-tection as well as to provide essential mole-cules for nourishment. Conversely, the hosthas evolved mechanisms for detection ofbacteria through the recognition of structuralcomponents of the bacterial surface, such aslipopolysaccharide (LPS), peptidoglycan(PGN), and other cell surface componentssuch as fimbriae that perform essential phys-iologic functions for the bacteria. Variationsof these bacterial components may be seenbetween various species, or even betweendifferent strains of the same species. Despitetheir structural heterogeneity, most of thesemolecules have conserved motifs known aspathogen-associated molecular patterns(PAMPs) that are recognized by host cell
receptors called pattern recognition receptors(PRRs). These highly conserved innate im-mune receptors evolved for detection of in-vading bacteria. Binding of PAMPs by PRRsactivates specific signaling pathways in hostcells that are important for the initiation of aninflammatory response. Although this re-sponse is intended to eliminate the microbialchallenge, the inflammatory mediators thatare secreted may lead to further tissue damageif bacterial clearance is not achieved.
Today, the most studied bacterial factorsinclude LPS, PGN, lipoteichoic acids (LTAs),fimbriae, proteases, heat-shock proteins(HSPs), formyl-methionyl-leucyl-phenyl -alanine (fMLP) and toxins. Host PRRs in-clude the Toll-like receptors (TLRs) and theG-protein-coupled receptors (GPCRs). Table1 presents a summary of the results by ac-tions of various bacterial factors after inter -action with specific host cells.8
Bacteria and GI EquilibriumThe oral cavity, as part of the gastro -
intestinal tract, is naturally colonized by awide variety of bacteria. This is a physiologicsituation that does not always result inpathology. The tooth-gingival interface is thesite of a variety of natural, innate host defensemechanisms, including the regular sheddingof epithelial cells, the washing effect of thesaliva and the gingival crevicular fluid (GCF),and most importantly, the phagocytic actionof neutrophils that migrate continuouslythrough the junctional epithelium into thegingival sulcus. However, if this equilibriumis disturbed, pathogenic bacteria may over-grow, initiating the pathogenesis of gingivi-tis and possibly periodontitis. Current under -standing of the steps leading to overgrowthof pathogens includes periodontal bacteriaattaching to epithelial cells using their fim-briae and PRR recognition of PAMPs, in-ducing epithelial cell secretion of pro-in-flammatory cytokines (TNF-, IL-1, IL-6)and the chemokine IL-8 in the connective
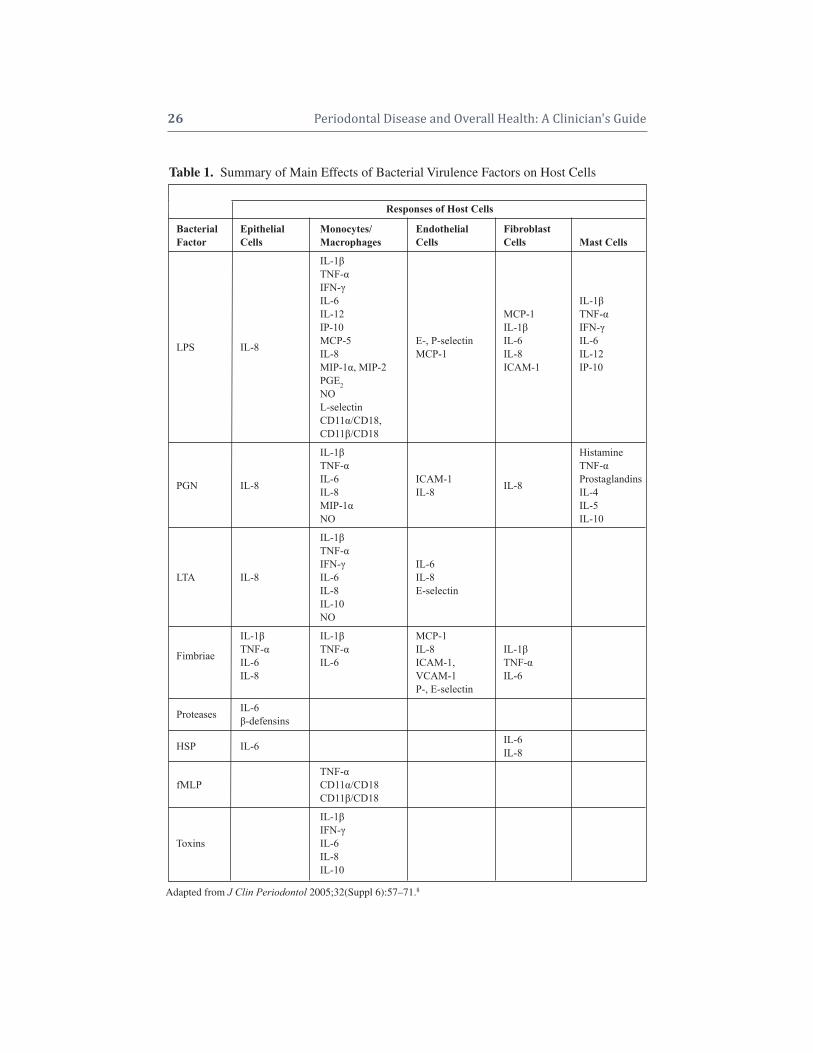
26 Periodontal Disease and Overall Health: A Clinician's Guide
Adapted from J Clin Periodontol 2005;32(Suppl 6):57–71.8
Table 1. Summary of Main Effects of Bacterial Virulence Factors on Host Cells
Responses of Host Cells
Bacterial Epithelial Monocytes/ Endothelial FibroblastFactor Cells Macrophages Cells Cells Mast Cells
IL-1 TNF- IFN- IL-6 IL-1IL-12 MCP-1 TNF-IP-10 IL-1 IFN-MCP-5 E-, P-selectin IL-6 IL-6 LPS IL-8 IL-8 MCP-1 IL-8 IL-12 MIP-1, MIP-2 ICAM-1 IP-10PGE2NO L-selectinCD11/CD18,CD11/CD18
IL-1 HistamineTNF- TNF-
PGN IL-8 IL-6 ICAM-1 IL-8 ProstaglandinsIL-8 IL-8 IL-4MIP-1 IL-5NO IL-10
IL-1TNF-IFN- IL-6
LTA IL-8 IL-6 IL-8IL-8 E-selectinIL-10NO
IL-1 IL-1 MCP-1
Fimbriae TNF- TNF- IL-8 IL-1IL-6 IL-6 ICAM-1, TNF-IL-8 VCAM-1 IL-6
P-, E-selectin
Proteases IL-6-defensins
HSP IL-6 IL-6IL-8
TNF-fMLP CD11/CD18
CD11/CD18
IL-1IFN-
Toxins IL-6IL-8IL-10

CHAPTER 3 Infection and Inlammation 27
tissue. Normally, the intact sulcular and junc-tional epithelium serves as an effective nat-ural barrier that keeps the bacteria from en-tering host tissues. However, severalperiodontopathogens (e.g., P. gingivalis, A.actinomycetemcomitans) have been shownto invade and transverse epithelial cells togain access to the connective tissue. More-over, bacterial components (e.g., LPS, PGN)and products (e.g., proteases, toxins) that areeither shed or secreted can also diffusethrough the epithelial junctions to the con-nective tissue.9
Bacteria in Connective TissueBacteria and/or their virulence factors
found in the connective tissue directly stim-ulate host cells residing in this area, includ-ing leukocytes, fibroblasts, mast cells, endo -thelial cells, dendritic cells and lymphocytes.Neutrophils, macrophages, fibroblasts andmast cells release more proinflammatory cy-tokines (TNF-, IL-1, IL-6, IL-12), chemo-attractants (IL-8, MIP-1- , MIP-2, MCP-1,MCP-5) and PGE2 in the connective tissue.In addition, degranulation of mast cells re-sults in the secretion of histamine andleukotrienes further amplifying the inflam-matory cascade.10,11
Mediators that are secreted from acti-vated host cells (e.g., IL-1, TNF-, PGE2,and histamine) will further assist bacterialvirulence factors in the activation of endo -thelial cells. This leads to secretion of morechemokines (IL-8, MCP-1) and expressionof adhesion molecules on the surface of en-dothelial cells, which are important forleukocyte extravasation (P- and E-selectinsas wells as ICAM-1 and -2).12 Specifically,P- and E-selectins interact with glyco proteinson leukocytes allowing the cells to adhere re-versibly to the vessel wall, causing circulat-ing leukocytes to appear to “roll” along theactivated endothelium. Then, IL-8 and otherchemokines, bound to proteoglycans on thesurface of leukocytes, trigger a conforma-
tional change of integrins (LFA-1, CD11b:CD18). As a result, adhesive properties in-crease dramatically and leukocytes attachfirmly to ICAM-1 expressed on endothelialcells. TNF-, PGE2 and histamine increasevascular permeability, allowing leukocytesto squeeze between the endo thelial cells,thereby entering the connective tissue ina process known as diapedesis. Finally,chemokines, such as IL-8 that are producedat the site of infection and bind to proteo-glycans of the extracellular matrix, alongwith bacterial chemo-attractants (fMLP, fimbriae) form a concentration gradient thatguides the leukocytes to migrate to the focusof infection.
The Inflammatory CascadeNeutrophils are the first leukocytes to
arrive followed by mononuclear phagocytesthat subsequently differentiate into macro -phages. The interaction of these cells withbacterial virulence factors induces further ac-tivation, which enhances their phagocytic ac-tivity by increasing the production of nitricoxide (NO) and the expression of comple-ment receptors (CR3). If the innate immuneresponse is successful, the bacteria are elim-inated and resolution of inflammation fol-lows. However, persistence of bacteria leadsto a chronic response characterized by extra-celluar release of neutrophil granule contents,including degradative enzymes and reactiveoxygen species that spill into the extracellularmilieu, leading to local tissue damage andamplification of acute inflammatory signals.13
Pro-inflammatory cytokines (TNF-,IL-1, IL-6) from the site of inflammationenter the circulation and reach the liverwhere they activate hepatocytes. This leads,among other events, to the synthesis ofplasma proteins known as acute-phase pro-teins, including LPS binding protein (LBP)and CD14, which are important for therecognition of bacterial virulence factors.Complement proteins and C-reactive protein

28 Periodontal Disease and Overall Health: A Clinician's Guide
(CRP), contribute by opsonizing bacteria,thereby aiding in recognition for phagocyto-sis. These products enter the circulation andbecause of increased vascular permeability,diffuse into the inflamed gingival tissues.Figure 1 illustrates the initiation of inflam-mation at the gingiva.
The Immune ResponseIf the infection persists, the acquired
immune response is initiated and the “es- tablished lesion” is created as described by
Page and Schroeder.14 Briefly, dendritic cellswithin the epithelium take up bacterial anti-gens and migrate to the peripheral lymphnodes. The antigens are processed into aform that is recognizable by the immune sys-tem, i.e., the antigenic peptide binds to aClass II major histocompatibility complex(MHC) receptor, and consequently “present”the antigen. As a result, antigen-specific ef-fector T cells and antibody-secreting B cellsare generated by clonal expansion and dif-ferentiation over the course of several days,
Figure 1. Initiation of Inflammation at the Gingival Level
Neutrophils in the GCF and epithelial cells comprise the first line of defense to prevent bacteria from invading thehost. The interaction of the bacterial biofilm with epithelial cells leads to activation and secretion of pro-inflam-matory cytokines (green). Bacteria and their virulence factors (red) may penetrate the epithelial lining and enterthe connective tissue. In this compartment they may interact with host cells, such as macrophages, fibroblasts, andmast cells to stimulate these cells to release more pro-inflammatory mediators such as TNF-, IL-1, IL-8,LTB-4, and histamine. These mediators, along with bacteria/virulence factors, may activate endothelial cells to attractcirculating leukocytes in the connective tissues. In this compartment, phagocytic cells take up bacteria and theirantigenic molecules. This process, if further enhanced by acute-phase response proteins, such as CRP, that are produced from activated hepatocytes, enter the connective tissue via circulation due to increased vascular permeability. If the noxious agents are eliminated, resolution of inflammation follows. However, if the bacterialchallenge persists, the more efficient adaptive immune response takes over. Adapted from J Clin Periodontol 2005;32(Suppl 6):57–71.8

CHAPTER 3 Infection and Inlammation 29
during which time the induced responses ofinnate immunity continue to function. Even-tually, antigen-specific T cells and then an-tibodies are released into the blood to targetthe infection site.15 Macrophages that engulfbacteria at the site of infection express co-stimulatory molecules (MHC-II) and presentbacterial antigens on their surface. Antigen-specific T cells “see” the antigens and acti-vate the macrophages, enabling them to de-stroy intracellular bacteria more efficiently.In addition, secreted antibodies protect thehost from infection by: (a) inhibiting thetoxic effects or infectivity of pathogens bybinding (neutralization); (b) opsonizing thepathogens and promoting phagocytosis; and(c) activating the complement system.Failureto clear the infection at this point leads to fur-ther tissue damage. Activated macrophagesproduce oxygen radicals, NO, and proteasesin the gingival tissues that are toxic to thehost cells. Moreover, recent work on a mousemodel revealed that the induction of an adaptive immune response to colonizingpathogens results in receptor activator of nu-clear factor-kappaB ligand-dependent perio -dontal bone loss.16
Summary of Part IThe trigger that causes the shift from
tissue homeostasis to pathology remains un-clear. The logical extension of Löe’s obser-vation is that this is caused by specific bac-teria and indeed, a large body of evidencesuggests that certain bacteria are associatedwith progressive disease. However, studies ofthe microbiota of the periodontal lesion arecross-sectional and definitive cause/effectrelationships have not been demonstrated.Recently, a longitudinal study of periodontaldisease progression failed to implicate anysingle organism or group of organisms inthe initiation of periodontal attachmentloss.17 In addition, recent animal studies sug-gest that the level of host inflammation hasa major impact on the composition of the
biofilm. Interestingly, inflammation is astronger predictor of periodontal attachmentloss than the composition or quantity of theoral biofilm.17 Clearly, the etiology andpathogenesis of periodontitis requires fur-ther study. It is also apparent that “tradi-tional” periodontal pathogens (Socransky’s“red complex”) contribute to and acceleratedisease when they overgrow in the perio -dontal environment. However, the role of in-flammation and the host immune responsehas taken on a new perspective, potentiallydetermining susceptibility and providing anovel therapeutic target.
PART II: SYSTEMIC INFLAMMATIONDUE TO PERIODONTAL INFECTION
Despite the localized nature of perio -dontal disease, infection of the sulcus/perio -dontal pocket with periodontopathogens maybe responsible for inflammatory responsesthat develop beyond the periodontium. Todate, several biological pathways have beenrecognized that present reasonable hypothe-ses for periodontal disease induction of sys-temic inflammation.
Inflammatory PathwaysIn health, the sulcular epithelium along
with innate immune molecules acts as a nat-ural barrier system that inhibits and elimi-nates penetrating bacteria. Hence, only asmall number of bacteria, mostly facultative,manage to enter the gingival tissues and thebloodstream. However, in cases of perio -dontal disease, the inflamed and ulceratedpocket epithelium is vulnerable to bacterialpenetration and forms an easy port of entryfor the bacteria. This leads to an increase inthe number of periodontopathogens, mainlyanaerobic Gram-negative, in the gingival tis-sues and consequently in the circulation.Bacteremia can be initiated after mechanicalirritation of the inflamed gingiva during toothbrushing, chewing, oral examination, andscaling and root planing.18 The microorgan-

30 Periodontal Disease and Overall Health: A Clinician's Guide
isms that gain access to the blood and circu-late throughout the body are usually elimi-nated by the reticulo-endothelial systemwithin minutes (transient bacteremia) andusually there are no other clinical symptomsother than possibly a slight increase in bodytemperature.19 However, if the disseminatedbacteria find favorable conditions, they maycolonize distant sites and form ectopic foci ofinfection. Similarly, bacterial virulence fac-tors that are secreted or shed in the gingivaltissues may also disseminate via the circula-tion and stimulate remote tissues.20 Bacteriaand bacterial antigens that are systemicallydispersed can trigger significant systemic inflammation. Leukocytes as well as endo -thelial cells and hepatocytes respond to bacteria/virulence factors, producing pro- inflammatory immune mediators. Moreover,soluble antigens may react with circulatingspecific antibodies, forming macromolec ularcomplexes. These immune complexes mayfurther amplify inflammatory reactions atsites of deposition.21
Pro-Inflammatory MediatorsA different biological pathway that may
explain the systemic inflammation inducedby periodontal disease involves pro-inflamma -tory mediators, such as IL-1, IL-6, TNF-and PGE2 that are produced by host cells inthe inflamed gingival tissues. These media-tors are secreted locally in response to bac-terial challenge, but may “spill” into the cir-culation and exert distant or systemic effects.
Specifically, cytokines may reach dis-tant sites and further activate endothelialcells leading, in some cases, to endothelialdysfunction.22 Moreover, the circulating me-diators, due to the increased vascular per-meability at the sites of inflammation, mayenter inflamed tissues and exacerbate the in-flammatory processes. However, the mostimportant impact of these circulating medi-ators is systemic. Pro-inflammatory cyto -kines may induce leukocytosis, which is an
increase in circulating neutrophils. More-over, IL-1, TNF-, and especially IL-6 mayreach the liver and activate hepatocytes toproduce acute-phase proteins. The most im-portant acute-phase reactants include CRP,serum amyloid A (SAA) protein, fibrinogen,plasminogen activator inhibitor 1 (PAI-1),complement proteins, LBP, and solubleCD14. These proteins are released in theplasma and possess a wide variety of func-tions, such as multiple pro-inflammatory ac-tivities and stimulation of tissue repair mech-anisms. The production of these proteins ispart of an acute-phase response that is char-acterized by fever, increased vascular per-meability, and a general elevation of meta-bolic processes. An acute-phase responsestarts within hours or days of most forms ofacute tissue damage or inflammation and de-spite its name, persists with chronic inflam-mation. As acute-phase reactants enter thecirculation, they may return to the inflamedgingival tissues. However, since they circu-late throughout the body they can affect ec-topic sites, causing inflammation or exacer-bation of existing inflammatory processes.This concept takes on new meaning in lightof the recent implication of CRP in thepathogenesis of cardiovascular disease.23
Because there is to date no consensuson the mechanisms that induce systemic in-flammation from periodontal disease, any ofthe above pathways (bacteremia, systemicspilling of cytokines, and activation of theacute-phase response) must be considered acandidate for the generation of systemic in-flammation. It is also possible that depend-ing upon the severity of periodontal disease,any of these mechanisms may occur alone orin combination, leading to variations of in-duced systemic inflammation.
Acute-Phase ProteinsCRP is produced mainly by the liver,
but it may also be synthesized locally at sitesof inflammation. CRP opsonizes different

CHAPTER 3 Infection and Inlammation 31
bacteria by binding to phosphorylcholinefound on the surface, thereby assisting inbacterial uptake by phagocytes.24 Opsoniza-tion and phagocytosis are further enhancedby activation of the complement system byCRP. Other pro-inflammatory activities ofCRP include the up-regulation of the expres -sion of adhesion molecules, such as ICAM-1 and E-selectin on endothelial cells and theinduction of IL-6, IL-1, and TNF-, and ofthe chemokines IL-8 and MCP-1. Otherproperties of CRP that may not be of obviousimportance in periodontal disease but maysignificantly affect other systemic inflam-matory diseases (e.g., atherosclerotic le-sions), include thrombosis due to the pro-coagulant activity and reduction offibrinolysis by inducing an increase in theexpression of PAI-1, the main inhibitor offibrinolysis.25 Finally, CRP mediates prolif-eration and activation of smooth muscle cells(SMCs) and decreases the expression of en-dothelial nitric oxide synthase (eNOS). CRPmay also have anti-inflammatory propertiesand hence its primary role is likely to be theregulation of acute inflammation.
SAASAA proteins are a family of apolipo -
proteins associated with high-densitylipoprotein in plasma. They have several pro-inflammatory functions, such as the recruit-ment of immune cells to inflammatory sitesand the induction of enzymes that degradeextracellular matrix. Also, SAA proteinstransport cholesterol to the liver for secretioninto the bile.
FibrinogenFibrinogen is a soluble plasma glyco-
protein. Processes in the coagulation cascadeactivate prothrombin to thrombin, which isresponsible for converting fibrinogen into fib-rin. Fibrin is then cross-linked by factor XIIIto form a clot. Thus, fibrinogen is involved inblood coagulation and platelet activation.
PAI-1PAI-1 is produced by the liver and en-
dothelial cells. It inhibits the serine proteasestPA and uPA/urokinase, and therefore is aninhibitor of fibrinolysis, the physiologicalprocess that degrades blood clots.
Complement ProteinsThese proteins take part in a triggered-
enzyme cascade that activates the comple-ment system. There are three ways by whichcomplement is involved in inflammatoryprocesses. First, activated complement pro-teins may bind covalently to pathogens asopsonins for engulfment by phagocytes bear-ing receptors for complement. Second, thesmall fragments of some complement pro-teins act as chemo-attractants to recruit moreleukocytes to the site of complement activa-tion. Third, terminal complement compo-nents damage certain bacteria by creatingpores in the bacterial membrane.26
LBP and Soluble CD14 These proteins play an important role in
transferring LPS and PGN to the Toll-like re-ceptors. Hence, their presence is critical forinitiating and organizing an inflammatoryimmune response after bacterial challenge.
Systemic Cellular and Molecular Markers of Inflammation
Periodontal infection may induce an in-flammatory response that is not limited to thetissues surrounding the teeth, but is also ex-tended systemically. The main cellular andmolecular markers of systemic inflamma-tion induced by periodontal disease includethe increased number of peripheral leuko-cytes, the higher concentrations of serumanti bodies against periodontopathogens,and the elevated levels of circulating pro- inflammatory cytokines and acute-phase pro-teins. With the exception of serum antibodiesagainst periodontopathogens, these markersare not specific for periodontal disease, but

32 Periodontal Disease and Overall Health: A Clinician's Guide
could be shared with distant inflammatoryprocesses that have systemic effects. As such,these markers can be affected by other in-flammatory diseases that could occur con-comitantly. The following systemic markershave been associated with the presence of pe-rio dontal disease and are usually affected bythe severity of inflammation in the gingiva.
Peripheral Blood LeukocytesIn periodontitis patients, leukocyte
counts have been shown to be slightly ele-vated compared to healthy subjects, althoughnot always significantly.27 The elevated levelof circulating leukocytes depends largely onthe extent and severity of periodontal dis-ease. Periodontal therapy may lead to a re-duction in the number of peripheral leuko-cytes.28 PMNs are the main leukocytes thatare increased, and it is possible that these cellsare recruited at higher levels during episodesof bacteremia and leakage of bacterial viru-lence factors during periodontal disease.
Serum Antibodies Against Periodontopathogens
In chronic periodontal disease, in whichthe adaptive immune response has been ac-tivated, local and systemic exposure to peri-odontopathogens leads to an increase in thelevels of circulating antibodies against thepathogenic antigens. Treatment of disease isfollowed by a reduction in antibody levels.
Serum Pro-Inflammatory Cytokines In healthy subjects, the levels of circu-
lating pro-inflammatory cytokines are verylow or nondetectable. However, in perio -dontitis patients, several pro-inflammatorycytokines may “spill” into the bloodstreamand increase the concentration in the plasma.Of the pro-inflammatory mediators studied,only the levels of IL-6 have been consistentlyshown to be elevated in the serum. This increase is related to the extent and severityof inflammation in periodontal tissues.29
However, controversial reports have beenpublished on the impact of periodontal ther-apy on IL-6 levels suggesting the need forfurther research on the topic. Finally, most ofthe studies looking at the levels of serumIL-1 and TNF- among healthy and perio -dontitis patients failed to report any differ-ences, and in most cases cytokine levels werenot measurable.30
Acute-Phase ProteinsThe levels of several acute-phase reac-
tants, such as CRP, fibrinogen, LBP and sol-uble CD14 have been studied and have beenshown to be elevated in patients with perio -dontal disease. However, the acute-phaseproteins that have received most attentionand are consistent markers of systemic in-flammation in periodontal disease are CRPand fibrinogen. A large number of studies,both in animal models and humans, have re-vealed a positive association between peri-odontal disease and circulating CRP levels,while a recent meta-analysis limited to hu-man studies has confirmed that plasma CRPis elevated in patients with periodontitis com-pared to healthy individuals.31 Moreover, thisincrease was proportional to the extent andseverity of the disease. Several studies reporta decrease of plasma CRP after periodontalintervention, but there is modest evidencethat periodontal therapy lowers the levels ofthis protein. Finally, in several studies, thelevels of fibrinogen have also been found tobe elevated in periodontitis patients com-pared to healthy individuals.32 However, todate there is no available evidence to supportthat periodontal therapy actually reduces theamount of circulating fibrinogen.
Possible Role of Systemic Inflammationin Various Disorders
During the late nineteenth and earlytwentieth centuries, the “focal infection” the-ory dominated the medical world.33 This the-ory held that foci of sepsis were responsible

CHAPTER 3 Infection and Inlammation 33
for the initiation and progression of a varietyof inflammatory diseases, including arthritis, peptic ulcers, and appendicitis. As a result,therapeutic full-mouth extractions became acommon dental practice. However, many teethwere extracted without evidence of infection.When it was finally realized that there wasno therapeutic benefit, the theory was finallydiscredited and the practice abandoned. Dur-ing the final two decades of the twentiethcentury—as our knowledge concerning theinflammatory component of systemic dis-eases was enriched and our understanding ofthe relationship of periodontal disease to systemic inflammation increased—the ideathat periodontal infection may affect the progression of systemic disorders such as cardiovascular disease, adverse pregnancycomplications, diabetes mellitus, and otherdiseases re-emerged.
In this possible association, systemicinflammation seems to play a key role.Specifically, on one hand, periodontal dis-ease may induce systemic inflammation andon the other, there is increasing evidencesuggesting that elevated levels of the mark-ers of systemic inflammation are associatedwith an increased risk for systemic diseases.
Cardiovascular Disease (CVD)There is now abundant clinical evidence
demonstrating that many biomarkers of in-flammation are elevated years in advance offirst-ever myocardial infarction (MI) orthrombotic stroke, and that these same bio-markers are highly predictive of recurrentMI, recurrent stroke, and death due to CVD.2
Moreover, studies demonstrate that serumIL-6 levels were significantly elevated insubjects who subsequently experienced anMI compared to age-matched controls.34
Similarly, plasma levels of soluble P-selectin,soluble CD40L, and macrophage-inhibitorycytokine-1 were all significantly increased inhealthy subjects who subsequently developedCVD events compared to matched controls.35
Elevated plasma concentrations of TNF-have also been associated with CVD, andspecifically with recurrent nonfatal MI orother CVD events. Moreover, TNF- levelswere persistently higher among post-MI patients at increased risk for recurrent coro-nary events.
Besides these pro-inflammatory cyto -kines, several acute-phase reactants have alsobeen associated with CVD. One of the fac-tors with the strongest evidence as a bio-marker for predicting CVD events is CRP(specifically, high sensitivity CRP, hsCRP).When measured in the blood, hsCRP provedto be a strong, independent predictor of fu-ture MI and stroke among apparently healthyasymptomatic men. Also, the relative riskfor first MI and ischemic stroke increasedsignificantly with each increasing quartileof baseline concentrations of CRP.36 As de-scribed already, CRP may contribute to theinitiation and development of atherothrom-botic lesions not only by up-regulating theexpression of pro-inflammatory cytokines,but also by mediating proliferation and acti-vation of SMCs and by activating the pro- coagulant system. This last property may befurther enhanced by another acute-phase pro-tein, fibrinogen, which is often found to beelevated in CVD patients.
Adverse Pregnancy OutcomesSystemic inflammation has also been
implicated in adverse pregnancy outcomes,since elevated concentrations of CRP in earlypregnancy are associated with an increasedrisk of preterm birth and very-preterm birth.
Diabetes MellitusFinally, systemic inflammation has
been associated with both Type 1 and Type2 diabetes mellitus. Recent studies suggestthat in Type 1 diabetes, the levels of sys-temic markers of inflammation, such as CRP,do not differ between healthy individualsand subjects for which Type 1 diabetes has

34 Periodontal Disease and Overall Health: A Clinician's Guide
been just diagnosed. However, the levels ofcirculating CRP are significantly higher inindividuals with long-term diabetes.37 It isalso believed that inflammatory processesmay have a more pronounced effect on thedevelopment of complications of Type 1 di-abetes. Thus, elevated levels of plasma CRPand of the pro-inflammatory soluble adhe-sion molecule, vascular cell adhesion mole-cule-1 (VCAM-1), have been found in pa-tients with microvascular disease comparedto those without.
In Type 2 diabetes, inflammatoryprocesses are more strongly associated withthe development of the disease. Systemicmarkers of inflammation are found to be in-creased in healthy individuals who developType 2 diabetes later in their lives. AmongPima Indians, a population with a high preva-lence of Type 2 diabetes, subjects with whiteblood cell counts within the highest tertilewere more likely to develop Type 2 diabetesover a period of 20 years compared to those inthe lowest tertile. Moreover, in two other stud-ies, healthy individuals demonstrating serum levels of CRP and IL-6 within the highestquartiles were more likely to develop Type 2diabetes in the next four to seven years com-pared to subjects in the lowest quartile.4 Sim-ilar results were found with increased levelsof another acute-phase protein, PAI-1.
Insulin resistance, which is associatedwith Type 2 diabetes and usually procedesthe development of frank diabetes, may alsobe affected by pre-existing systemic inflam-mation since several pro-inflammatory andacute-phase proteins, such as TNF-, IL-6,MCP-1, PAI-1, and SAA are associated withthe induction of insulin resistance.38
Summary of Part IIBased on available evidence, it is pos-
sible that systemic inflammation may actu-ally be the link that associates periodontaldisease with other systemic diseases. Detailsof the plausible biological mechanisms that
may associate periodontal disease with var-ious systemic diseases are further analyzed inother chapters of this book.
PART III: RESOLUTION OFINFLAMMATION IN PERIODONTITIS AND OTHER SYSTEMIC DISEASES
Inflammation is thought to play a cen-tral role in the progression of periodontaland a number of systemic diseases. Experi-ments in animal models and in man havedemonstrated that periodontal destruction ismediated primarily by the inflammatory re-sponse, although periodontal pathogens area necessary etiologic factor.20,39,40 Geneticpolymorphisms and other factors may alsobe responsible for a “hyperinflammatoryphenotype” that may further affect the sus-ceptibility of the host to periodontal diseaseand tissue destruction. Currently, it is be-lieved that in chronic periodontal disease, de-struction does not follow a linear pattern withtime, but occurs in “random bursts” with pe-riods of remission and exacerbation. How-ever, the reasons behind this random pro-gression are not fully understood. Diseaseprogression becomes even more enigmaticconsidering that it is not always clear why achronic inflammation of the gingiva may re-main as gingivitis in some patients andprogress to periodontitis in others. Irrespec-tive of the nature of periodontal disease pro-gression, the perpetuation of the inflamma-tory process in the gingiva may lead to achronic low-grade systemic inflammatory re-sponse, which in turn potentially contributesto the progression of systemic diseases.
The Process of Inflammatory ResolutionThe landmark events during inflamma-
tion include the accumulation of leukocytesin the infected area and phagocytosis of thebacteria and/or their virulence factors. Aspart of the inflammatory process, activationof neutrophil lysosomal phospholipase re-leases free arachidonic acid from membrane

CHAPTER 3 Infection and Inlammation 35
phospholipids. Once free arachidonic acidis available, two different pathways can beinitiated: (a) the cyclo-oxygenase (COX) pathway that leads to the production ofprostaglandins (e.g., PGE2), and (b) the lipoxy-genase (LO) pathways that lead to the pro-duction of a series of hydroxyl acids charac-terized by the 5-LO products, the leukotrienes(e.g., LTB4). There are three cell type-specificLOs; the 5-LO from myeloid cells, the 12-LOfrom platelets, and the 15-LO of epithelial andendothelial cells. PGE2 is a potent activator ofosteoclast-mediated bone resorption, and withother eicosanoids mediates inflammation andperiodontal tissue destruction. LTB4 attractsneutrophils, stimulates the release of granule-associated enzymes from neutro phils, and con-tributes to pro-inflammatory processes and tofurther tissue damage.
Returning to HomeostasisOnce the bacteria have been removed
by phagocytosis, resolution of inflammationoccurs with the reduction or removal ofleukocytes and debris from inflamed siteswith a return to homeostasis.5 Until recently,resolution of inflammation was considered tobe a passive process in which the lack ofbacterial stimuli decreased the production ofinflammatory mediators, which in turn re-duced the inflammatory response, therebyreturning to normal function. New data sug-gest that resolution of inflammation is an ac-tive biochemical and metabolic process thatis initiated by a newly identified class of re-ceptor agonists that emerge temporally asthe inflammatory lesion matures.5 Althoughprostaglandins and leukotrienes secreted byneutrophils have pro-inflammatory proper-ties, as inflammation proceeds the sameprostaglandins (PGE2 and PGD2) may pro-mote expression of the 15-LO gene, leadingto a switch in the expression of biosyntheticenzymes by infiltrating neutrophils (Figure2). Binding of lipoxin A4 to neutrophils leadsto a phenotypic change, stopping all pro-
inflammatory activity of neutrophils andleading to apoptosis. As a result, they stop secreting the chemo-attractant LTB4 and several cellular pathways are activated, pro-ducing, at a local level, other dual-actinganti- inflammatory and proresolution lipidmediators, including resolvins and protectins.
Mechanisms of Inflammation ResolutionResolvins and protectins provide potent
signals that orchestrate and accelerate mech-anisms that promote resolution of inflam-mation and homeostasis. Specifically, as de-picted in Figure 3, pro-resolution mediatorsstop neutrophil infiltration and drive neu-trophils to apoptosis, while at the same timeattracting monocytes to the lesion.41 Lipoxin-stimulated monocytes/macrophages obtaina nonphlogistic phenotype, which resultsin phagocytosis of apoptotic neutrophilsand enhanced mucosal clearance of bacteriawithout concomitant secretion of pro- inflam -matory mediators that could contribute totissue damage.42 Moreover, pro-resolutionlipid molecules increase the exit of phago-cytes from the inflamed site through the lym-phatics. Finally, some of these moleculesmay also stimulate the uptake and clearanceof local cytokines by apoptotic neutrophils.After neutrophils and debris are removed,homeostasis returns and repair mechanismsare initiated; lipoxins are antifibrotic and allow for complete tissue healing withoutscarring.
Hence, it can be argued that the per-sistence of an inflammatory disease, such asperiodontal disease, may be caused by toomuch pro-inflammatory signal or not enoughproresolution signal. In other words, a “hy-perinflammatory phenotype” due to a par-ticular genetic background of the host mayresult in oversecretion of inflammatory me-diators in response to bacterial stimuli, whichin turn contributes to periodontal disease sus-ceptibility, or a failure of resolution pathways.As high levels of inflammatory cyto kines are
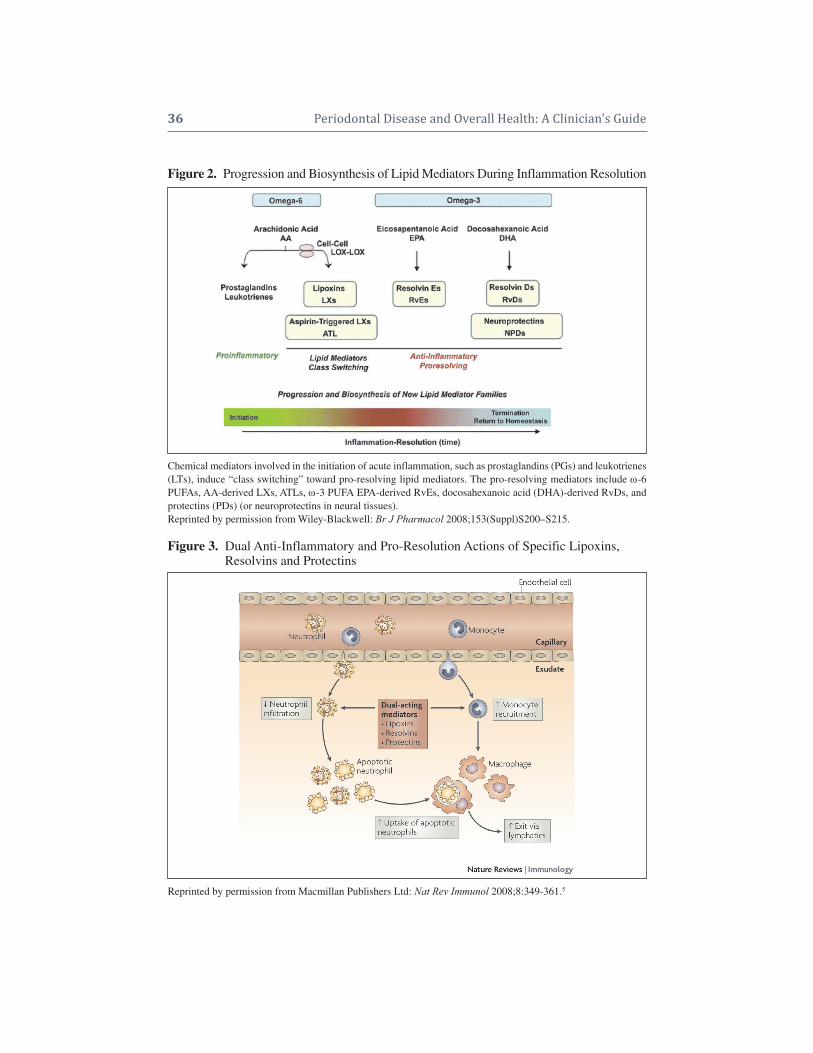
36 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 2. Progression and Biosynthesis of Lipid Mediators During Inflammation Resolution
Chemical mediators involved in the initiation of acute inflammation, such as prostaglandins (PGs) and leukotrienes(LTs), induce “class switching” toward pro-resolving lipid mediators. The pro-resolving mediators include -6PUFAs, AA- derived LXs, ATLs, -3 PUFA EPA-derived RvEs, docosahexanoic acid (DHA)-derived RvDs, andprotectins (PDs) (or neuroprotectins in neural tissues). Reprinted by permission from Wiley-Blackwell: Br J Pharmacol 2008;153(Suppl)S200–S215.
Figure 3. Dual Anti-Inflammatory and Pro-Resolution Actions of Specific Lipoxins, Figure 3. Resolvins and Protectins
Reprinted by permission from Macmillan Publishers Ltd: Nat Rev Immunol 2008;8:349-361.5

CHAPTER 3 Infection and Inlammation 37
maintained, tissue destruction continues andinflammation persists. If pro-resolution sig-nals are weak, neutrophils are not removedand monocytes/macrophages maintain aphlogistic phenotype. This results in furtherproduction of inflammatory cytokines andperpetuation of the inflamed state.
New Treatment ParadigmsIt is reasonable to suggest that the un-
derstanding and ability to manipulate reso-lution of inflammation may provide a newtreatment paradigm for inflammatory dis-eases, local and systemic. Although humandata are not yet available, there is a growingand promising literature from in vitro workand animal models that supports the bene -ficial actions of resolution agonists both onperio dontal and other systemic diseases.5
The Role of Pro-Resolution MediatorsExamples of the actions of therapeutic
pro-resolution mediators in periodontal dis-ease include over-expression of lipoxin A4 intransgenic rabbits protecting against perio -dontitis and atherosclerosis.43 In anotherstudy, topical treatment with resolvins (-3fatty acid derived resolution agonists, vide infra) prevented more than 95% of alveolarbone destruction in rabbits. Moreover, his-tological analysis revealed few, if any, neu-tro phils in the tissue and little tissue damage.At the same time, the numbers of osteoclastswere also found to be reduced. In addition,treatment of periodontitis with resolvins sys-temically reversed the observed increase inCRP and IL-1 levels. Finally, in establishedperiodontal disease, resolvins prevented fur-ther tissue destruction, and both gingival andosseous tissues that were lost during diseasewere regenerated.44
Resolvins, lipoxins, and protectins havealso been shown in animal models to havebeneficial impact on a variety of other in-flammatory diseases. For example, lipoxinsstopped neutrophil recruitment and promoted
lymphatic removal of phagocytes in perio -tonitis.42 Moreover, in cystic fibrosis, lipoxinsdecreased neutrophil inflammation, pulmo -nary bacterial burden, and disease severity.45
Resolvins in a colitis model in mice decreasedneutrophil recruitment and pro-inflammatorygene expression, improved survival, and reduced weight loss.46 In addition, resolvinsprotected against neovascularization inretinopathy.47 Finally, in an asthma model,protectins protected against lung damage,airway inflammation, and airway hyper- responsiveness.48 Table 2 lists the impact oflipoxins, resolvins, and protectins on variousinflammatory disease models.
It is conceivable that the use of pro-resolution mediators in managing periodon-tal and other inflammatory diseases mayprove to be beneficial in humans as well.Mechanical debridement, which aims at thereduction of the bacterial load in the gingivalpocket, may help the host/patient to clearthe infection. In addition, it is possible thatthe use of locally applied pro-resolution me-diators could prevent further tissue damage,enhance the resolution of inflammation(which would lead to healthy gingiva), andideally result in periodontal tissue regenera-tion rather than scarring and repair. More-over, resolution of inflammation at the gingi -val level may minimize systemic inflamma-tion induced by periodontal disease, thereby attenuating the possible negative effects ofperio dontal disease on systemic diseases.
Origins of Pro-Resolution MediatorsIn order to manipulate resolution of
inflammation more effectively, it is imperativeto understand the biological origin of the pro-resolution mediators. Lipoxins (e.g., lipoxinA4) derive from arachidonic acid after acti -vation of the 12-/5-LO or the 15-/5-LO path-ways. Resolvins and protectins are bio synthe-sized from omega-3 essential poly -unsaturatedfatty acids (-3 PUFAs), such as eicosapen-tanoic acid (EPA) and docosahexanoic acid
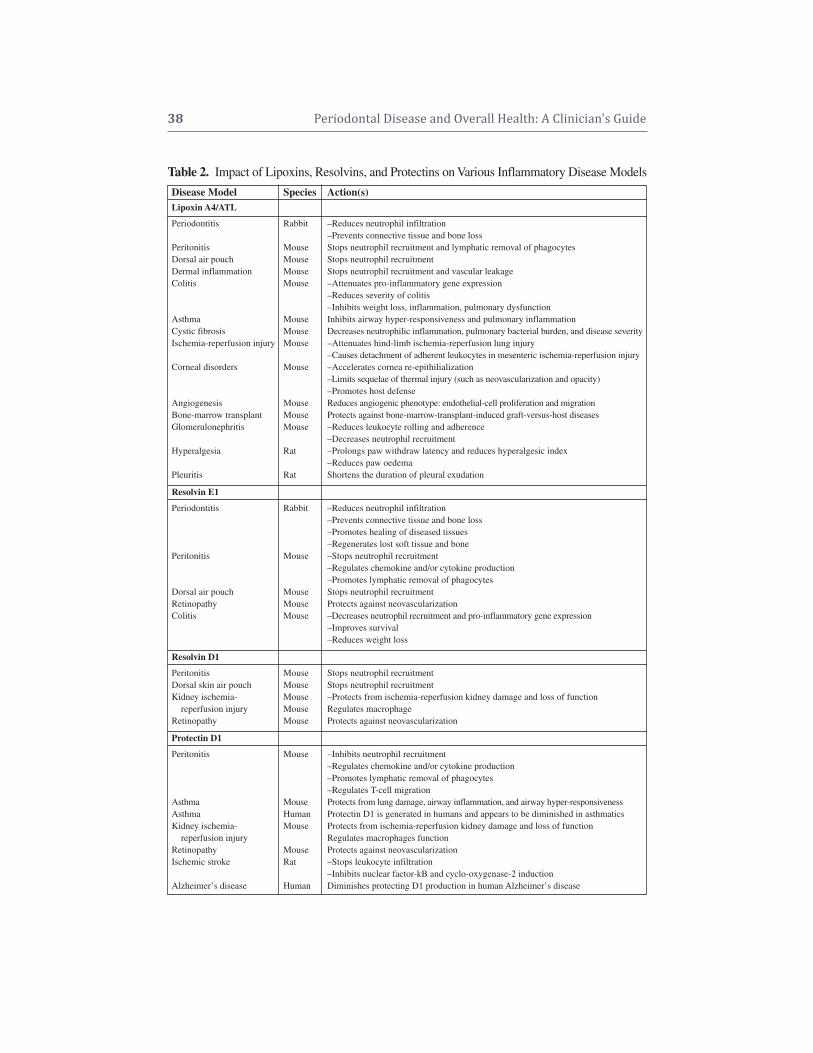
38 Periodontal Disease and Overall Health: A Clinician's Guide
Disease Model Species Action(s)Lipoxin A4/ATL
Periodontitis Rabbit –Reduces neutrophil infiltration–Prevents connective tissue and bone loss
Peritonitis Mouse Stops neutrophil recruitment and lymphatic removal of phagocytesDorsal air pouch Mouse Stops neutrophil recruitmentDermal inflammation Mouse Stops neutrophil recruitment and vascular leakageColitis Mouse –Attenuates pro-inflammatory gene expression
–Reduces severity of colitis–Inhibits weight loss, inflammation, pulmonary dysfunction
Asthma Mouse Inhibits airway hyper-responsiveness and pulmonary inflammationCystic fibrosis Mouse Decreases neutrophilic inflammation, pulmonary bacterial burden, and disease severityIschemia-reperfusion injury Mouse –Attenuates hind-limb ischemia-reperfusion lung injury
–Causes detachment of adherent leukocytes in mesenteric ischemia-reperfusion injuryCorneal disorders Mouse –Accelerates cornea re-epithilialization
–Limits sequelae of thermal injury (such as neovascularization and opacity)–Promotes host defense
Angiogenesis Mouse Reduces angiogenic phenotype: endothelial-cell proliferation and migrationBone-marrow transplant Mouse Protects against bone-marrow-transplant-induced graft-versus-host diseasesGlomerulonephritis Mouse –Reduces leukocyte rolling and adherence
–Decreases neutrophil recruitmentHyperalgesia Rat –Prolongs paw withdraw latency and reduces hyperalgesic index
–Reduces paw oedemaPleuritis Rat Shortens the duration of pleural exudation
Resolvin E1
Periodontitis Rabbit –Reduces neutrophil infiltration–Prevents connective tissue and bone loss–Promotes healing of diseased tissues–Regenerates lost soft tissue and bone
Peritonitis Mouse –Stops neutrophil recruitment–Regulates chemokine and/or cytokine production–Promotes lymphatic removal of phagocytes
Dorsal air pouch Mouse Stops neutrophil recruitmentRetinopathy Mouse Protects against neovascularizationColitis Mouse –Decreases neutrophil recruitment and pro-inflammatory gene expression
–Improves survival–Reduces weight loss
Resolvin D1
Peritonitis Mouse Stops neutrophil recruitmentDorsal skin air pouch Mouse Stops neutrophil recruitmentKidney ischemia- Mouse –Protects from ischemia-reperfusion kidney damage and loss of function
reperfusion injury Mouse Regulates macrophageRetinopathy Mouse Protects against neovascularization
Protectin D1
Peritonitis Mouse –Inhibits neutrophil recruitment–Regulates chemokine and/or cytokine production–Promotes lymphatic removal of phagocytes–Regulates T-cell migration
Asthma Mouse Protects from lung damage, airway inflammation, and airway hyper-responsivenessAsthma Human Protectin D1 is generated in humans and appears to be diminished in asthmatics Kidney ischemia- Mouse Protects from ischemia-reperfusion kidney damage and loss of function
reperfusion injury Regulates macrophages functionRetinopathy Mouse Protects against neovascularizationIschemic stroke Rat –Stops leukocyte infiltration
–Inhibits nuclear factor-kB and cyclo-oxygenase-2 inductionAlzheimer’s disease Human Diminishes protecting D1 production in human Alzheimer’s disease
Table 2. Impact of Lipoxins, Resolvins, and Protectins on Various Inflammatory Disease Models
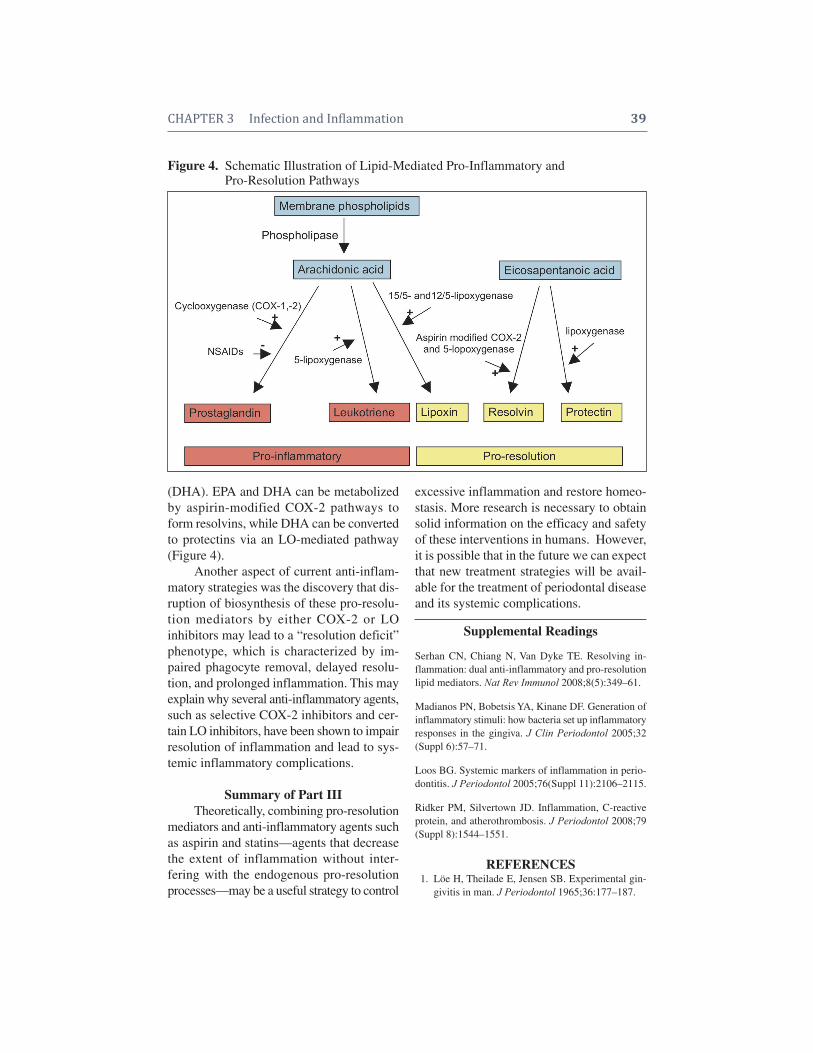
CHAPTER 3 Infection and Inlammation 39
(DHA). EPA and DHA can be metabolizedby aspirin-modified COX-2 pathways toform resolvins, while DHA can be convertedto protectins via an LO-mediated pathway(Figure 4).
Another aspect of current anti-inflam-matory strategies was the discovery that dis-ruption of biosynthesis of these pro-resolu-tion mediators by either COX-2 or LOinhibitors may lead to a “resolution deficit”phenotype, which is characterized by im-paired phagocyte removal, delayed resolu-tion, and prolonged inflammation. This mayexplain why several anti-inflammatory agents,such as selective COX-2 inhibitors and cer-tain LO inhibitors, have been shown to impairresolution of inflammation and lead to sys-temic inflammatory complications.
Summary of Part IIITheoretically, combining pro- resolution
mediators and anti-inflammatory agents suchas aspirin and statins—agents that decreasethe extent of inflammation without inter -fering with the endogenous pro- resolu tionprocesses—may be a useful strategy to control
excessive inflammation and restore homeo -stasis. More research is necessary to obtainsolid information on the efficacy and safetyof these interventions in humans. However,it is possible that in the future we can expectthat new treatment strategies will be avail-able for the treatment of periodontal diseaseand its systemic complications.
Supplemental Readings
Serhan CN, Chiang N, Van Dyke TE. Resolving in-flammation: dual anti-inflammatory and pro-resolutionlipid mediators. Nat Rev Immunol 2008;8(5):349–61.
Madianos PN, Bobetsis YA, Kinane DF. Generation ofinflammatory stimuli: how bacteria set up inflammatoryresponses in the gingiva. J Clin Periodontol 2005;32(Suppl 6):57–71.
Loos BG. Systemic markers of inflammation in perio -dontitis. J Periodontol 2005;76(Suppl 11):2106–2115.
Ridker PM, Silvertown JD. Inflammation, C-reactiveprotein, and atherothrombosis. J Periodontol 2008;79(Suppl 8):1544–1551.
REFERENCES1. Löe H, Theilade E, Jensen SB. Experimental gin-
givitis in man. J Periodontol 1965;36:177–187.
Figure 4. Schematic Illustration of Lipid-Mediated Pro-Inflammatory and Figure 4. Pro-Resolution Pathways

40 Periodontal Disease and Overall Health: A Clinician's Guide
2. Ridker PM, Silvertown JD. Inflammation, C-reac-tive protein, and atherothrombosis. J Periodontol2008;79:1544–1551.
3. Lohsoonthorn V, Qiu C, Williams MA. Maternalserum C-reactive protein concentrations in earlypregnancy and subsequent risk of preterm deliv-ery. Clin Biochem 2007;40:330–335.
4. Pradhan AD, Manson JE, Rifai N, Buring JE, Ridker PM. C-reactive protein, interleukin 6, andrisk of developing type 2 diabetes mellitus. JAMA2001;286:327–334.
5. Serhan CN, Chiang N, Van Dyke TE. Resolving inflammation: dual anti-inflammatory and pro- resolution lipid mediators. Nat Rev Immunol 2008;8:349–361.
6. Paster BJ, Olsen I, Aas JA, Dewhirst FE. Thebreadth of bacterial diversity in the human perio -dontal pocket and other oral sites. Periodontol 20002006;42:80–87.
7. Haffajee AD, Cugini MA, Tanner A, Pollack RP,Smith C, Kent RL Jr, Socransky SS. Subgingivalmicrobiota in healthy, well-maintained elder andperiodontitis subjects. J Clin Periodontol 1998;25:346–353.
8. Madianos PN, Bobetsis YA, Kinane DF. Generationof inflammatory stimuli: How bacteria set up in-flammatory responses in the gingiva. J Clin Perio -dontol 2005;32(Suppl 6):57–71.
9. Sandros J, Papapanou PN, Nannmark U, Dahlén G.Porphyromonas gingivalis invades human pocketepithelium in vitro. J Periodontal Res 1994;29:62–69.
10. Takada H, Mihara J, Morisaki I, Hamada S. Induc-tion of interleukin-1 and -6 in human gingival fibro -blast cultures stimulated with Bacteroides lipopoly -saccharides. Infect Immun 1991;59:295–301.
11. Supajatura V, Ushio H, Nakao A, Akira S, OkumuraK, Ra C, Ogawa H. Differential responses of mastcell Toll-like receptors 2 and 4 in allergy and innateimmunity. J Clin Invest 2002;109:1351–1359.
12. Darveau RP, Cunningham MD, Bailey T, SeachordC, Ratcliffe K, Bainbridge B, Dietsch M, Page RC,Aruffo A. Ability of bacteria associated with chronicinflammatory disease to stimulate E- selectin ex-pression and promote neutrophil adhesion. InfectImmun 1995;63:1311–1317.
13. Weissmann G, Smolen JE, Korchak HM. Release ofinflammatory mediators from stimulated neutro -phils. N Engl J Med 1980;303:27–34.
14. Page RC, Schroeder HE. Pathogenesis of inflam-matory periodontal disease. A summary of currentwork. Lab Invest 1976;34:235–249.
15. Kinane DF, Karim SN, Garioch JJ, al Badri AT,Moughal N, Goudie RB. Heterogeneity and selec-tive localisation of T cell clones in human skin and
gingival mucosa. J Periodontal Res 1993;28:497–499.
16. Kawai T, Paster BJ, Komatsuzawa H, Ernst CW,Goncalves RB, Sasaki H, Ouhara K, Stashenko PP,Sugai M, Taubman MA. Cross-reactive adaptiveimmune response to oral commensal bacteria re-sults in an induction of receptor activator of nuclearfactor-kappaB ligand (RANKL)-dependent perio -dontal bone resorption in a mouse model. Oral Micro biol Immunol 2007;22:208–215.
17. Tanner AC, Kent R Jr, Kanasi E, Lu SC, Paster BJ,Sonis ST, Murray LA, Van Dyke TE. Clinical characteristics and microbiota of progressing slightchronic periodontitis in adults. J Clin Periodontol2007;34:917–930.
18. Kinane DF, Riggio MP, Walker KF, MacKenzie D,Shearer B. Bacteraemia following periodontal pro-cedures. J Clin Periodontol 2005;32:708–713.
19. Li X, Kolltveit KM, Tronstad L, Olsen I. Systemicdiseases caused by oral infection. Clin MicrobiolRev 2000;13:547–558.
20. Jain A, Batista EL Jr, Serhan C, Stahl GL, VanDyke TE. Role for periodontitis in the progressionof lipid deposition in an animal model. Infect Immun 2003;71:6012–6018.
21. Thoden van Velzen SK, Abraham-Inpijn L, MoorerWR. Plaque and systemic disease: A reappraisalof the focal infection concept. J Clin Periodontol1984;11:209–220.
22. Amar S, Gokce N, Morgan S, Loukideli M, VanDyke TE, Vita JA. Periodontal disease is associatedwith brachial artery endothelial dysfunction andsystemic inflammation. Arterioscler Thromb VascBiol 2003;23:1245–1249.
23. Ridker PM, Danielson E, Fonseca FA, Genest J,Gotto AM Jr, Kastelein JJ, Koenig W, Libby P,Lorenzatti AJ, MacFadyen JG, Nordestgaard BG,Shepherd J, Willerson JT, Glynn RJ; JUPITERStudy Group. Rosuvastatin to prevent vascularevents in men and women with elevated C-reactiveprotein. N Engl J Med 2008;359:2195–2207.
24. Casey R, Newcombe J, McFadden J, Bodman-Smith KB. The acute-phase reactant C-reactive protein binds to phosphorylcholine-expressingNeisseria meningitidis and increases uptake by human phagocytes. Infect Immun 2008;76:1298–1304.
25. Nakakuki T, Ito M, Iwasaki H, Kureishi Y, OkamotoR, Moriki N, Kongo M, Kato S, Yamada N, IsakaN, Nakano T. Rho/Rho-kinase pathway contributesto C-reactive protein-induced plasminogen acti -vator inhibitor-1 expression in endothelial cells. Arterioscler Thromb Vasc Biol 2005;25:2088–2093.
26. Janeway C., Travers P., Walport M., Shlomchik M.Immunobiology. The immune system in health and

CHAPTER 3 Infection and Inlammation 41
disease. 5th Edition. Garland Publishing, NewYork; 2001:44.
27. Loos BG. Systemic markers of inflammation in periodontitis. J Periodontol 2005;76:2106–2115.
28. Christan C, Dietrich T, Hägewald S, Kage A, Bern-imoulin JP. White blood cell count in generalizedaggressive periodontitis after non-surgical therapy.J Clin Periodontol 2002;29:201–206.
29. Mengel R, Bacher M, Flores-De-Jacoby L. Inter-actions between stress, interleukin-1beta, inter-leukin-6 and cortisol in periodontally diseased patients. J Clin Periodontol 2002;29:1012–1022.
30. Meyle J. Neutrophil chemotaxis and serum con-centration of tumor-necrosis-factor-alpha (TNF-).J Periodontal Res 1993;28(Pt 2):491–493.
31. Paraskevas S, Huizinga JD, Loos BG. A systematicreview and meta-analyses on C-reactive protein inrelation to periodontitis. J Clin Periodontol 2008;35:277–290.
32. Kweider M, Lowe GD, Murray GD, Kinane DF,McGowan DA. Dental disease, fibrinogen andwhite cell count; links with myocardial infarction?Scott Med J 1993;38:73–74.
33. Scannapieco FA. Position paper of The AmericanAcademy of Periodontology: periodontal disease asa potential risk factor for systemic diseases. J Pe-rio dontol 1998;69:841–850.
34. Ridker PM, Rifai N, Pfeffer M, Sacks F, Lepage S,Braunwald E. Elevation of tumor necrosis factor-alpha and increased risk of recurrent coronaryevents after myocardial infarction. Circulation2000;101:2149–2153.
35. Ridker PM, Buring JE, Rifai N. Soluble P-selectinand the risk of future cardiovascular events. Circu-la tion 2001;103:491–495.
36. Ridker PM, Cushman M, Stampfer MJ, Tracy RP,Hennekens CH. Inflammation, aspirin, and the riskof cardiovascular disease in apparently healthymen. N Engl J Med 1997;336:973–979.
37. Treszl A, Szereday L, Doria A, King GL, Orban T.Elevated C-reactive protein levels do not corre-spond to autoimmunity in type 1 diabetes. Dia-betes Care 2004;27:2769–2770.
38. Shoelson SE, Lee J, Goldfine AB. Inflammationand insulin resistance. J Clin Invest 2006;116:1793–1801.
39. Serhan CN, Jain A, Marleau S, Clish C, Kantarci A,Behbehani B, Colgan SP, Stahl GL, Merched A,Petasis NA, Chan L, Van Dyke TE. Reduced in-
flammation and tissue damage in transgenic rabbitsoverexpressing 15-lipoxygenase and endogenousanti-inflammatory lipid mediators. J Immunol2003;171:6856–6865.
40. Williams RC, Jeffcoat MK, Howell TH, Reddy MS,Johnson HG, Hall CM, Goldhaber P. Topical flur-biprofen treatment of periodontitis in beagles. J Periodontal Res 1988;23:166-169.
41. Ariel A, Fredman G, Sun YP, Kantarci A, Van DykeTE, Luster AD, Serhan CN. Apoptotic neutrophilsand T cells sequester chemokines during immuneresponse resolution through modulation of CCR5expression. Nat Immunol 2006;7:1209–1216.
42. Schwab JM, Chiang N, Arita M, Serhan CN. Re-solvin E1 and protectin D1 activate inflammation-resolution programmes. Nature 2007;447:869–874.
43. Shen J, Herderick E, Cornhill JF, Zsigmond E, KimHS, Kühn H, Guevara NV, Chan L. Macrophage-mediated 15-lipoxygenase expression protectsagainst atherosclerosis development. J Clin Invest1996;98:2201–2208.
44. Hasturk H, Kantarci A, Ohira T, Arita M, EbrahimiN, Chiang N, Petasis NA, Levy BD, Serhan CN,Van Dyke TE. RvE1 protects from local inflam-mation and osteoclast-mediated bone destruction inperiodontitis. FASEB J 2006;20:401–403.
45. Karp CL, Flick LM, Park KW, Softic S, Greer TM,Keledjian R, Yang R, Uddin J, Guggino WB, Ata-bani SF, Belkaid Y, Xu Y, Whitsett JA, Accurso FJ,Wills-Karp M, Petasis NA. Defective lipoxin- mediated anti-inflammatory activity in the cystic fibrosis airway. Nat Immunol 2004;5:388–392.
46. Hudert CA, Weylandt KH, Lu Y, Wang J, Hong S,Dignass A, Serhan CN, Kang JX. Transgenic micerich in endogenous omega-3 fatty acids are pro-tected from colitis. Proc Natl Acad Sci USA 2006;103:11276–11281.
47. Connor KM, SanGiovanni JP, Lofqvist C, Ader-man CM, Chen J, Higuchi A, Hong S, Pravda EA,Majchrzak S, Carper D, Hellstrom A, KangJX, Chew EY, Salem N Jr, Serhan CN, SmithLE. Increased dietary intake of omega-3-poly - un saturated fatty acids reduces pathological retinalangiogenesis. Nat Med 2007;13:868–873.
48. Levy BD, Bonnans C, Silverman ES, Palmer LJ,Marigowda G, Israel E. Severe Asthma ResearchProgram, National Heart, Lung, and Blood Institute.Diminished lipoxin biosynthesis in severe asthma.Am J Respir Crit Care Med 2005;172:824–830.

CHAPTER 4History of the OralSystemic Relationship
Noel M. Claffey, Ioannis N. Polyzois, Ray C. Williams
INTRODUCTIONIn the last decade, the possible association
between oral and systemic health has beenhighlighted in numerous reports. The focus ofattention is mainly periodontitis and its impacton certain conditions. Periodontitis is an infec -tious disease associated with a number of pre -dominantly gram-negative bacteria, and it is nowrecognized that for the initiation and progressionof this disease, a susceptible host is also required.It is also well documented that certain systemicconditions can modify the host’s susceptibility toperiodontitis, but it is only recently that evidencesurfaced about the possi bility of a two-way rela -tionship. Speci fically, perio dontitis has been impli -cated as a potential risk factor for cardio vas culardiseases, respiratory diseases, diabetes mellitus,preterm labor, low birth weight, and renal disease.
Interest in the relationship of oral health/periodontal disease to general health is not new,but more of a resurgence in the old and dis creditedcon cept of focal infection. Focal infec tion theory be came popular in the begin ning of the twentiethcentury because it explained a number of con -ditions for which there was no sci entific explana -tion at the time. It eventually fell in to disreputebecause of a lack of scientific evidence.
This chapter examines the history of thehypothesis that micro-organisms would localizefrom the source focus to the distant, systemicfocus and follows, step by step, concepts of theoral-systemic relationship that have evolvedover the years.
ANCIENT CIVILIZATIONSAND THE MIDDLE AGES
Throughout recorded history, many theories have been put forward to explain
human illness. One area of the body that hasbeen repeatedly implicated in the origin ofhuman diseases is the oral cavity. Writings asfar back as from the ancient Egyptians (2100BC) mention tooth pain associated withwomen’s reproductive system diseases.1 InAssyria, the physician of King Ashurbanipal(669–626 BC) wrote about the troubles ofhis king: “The pains in his head, arms, andfeet are caused by his teeth and must be removed.”2 In ancient Greece, Hippocrates(400 BC) recorded two cases in which erad-ication of the infections of the mouth ap-peared to relieve patients of rheumatic-liketroubles of the joints.3 Aristotle, perhaps thefirst dental anatomist—especially from thestandpoint of comparative anatomy—statedthat “those persons who have the most teethare the longest lived.”4 In his book, On Hy-giene, the Roman physician Galen (166–201AD) emphasized the inter-relationship be-tween the oral cavity and other illnesses.5
From the end of the Roman Empire until the middle ages, all sciences fell intoabeyance, and had it not been for the Arabs(who had access to the learning and sciencecontained in Greek manuscripts brought totheir country by Nestorian exiles from By -zantium and Greeks who settled in southernItaly), the bulk of science and knowledgeaccumulated to that date might have beenlost.4 The next notable advance in dentistryprobably occurred in Italy in the 1400s whena physician named Giovanni d’Arcoli beganfilling decayed teeth with gold leaf; an admirably progressive step for that time. Heis further credited with stating that for casesof severe dental pain, early intervention was

CHAPTER 4 History of the OralSystemic Relationship 43
advisable because “such violent pains arefollowed by syncope or epilepsy, throughinjury communicated to the heart or brain.”6
In 1548, Ryff wrote a monograph thatdealt exclusively with dental afflictions. Inhis pamphlet titled Useful Instructions onthe Way to Keep Healthy, to Strengthen andRe-invigorate the Eyes and the Sight. WithFurther Instructions of the Way of Keepingthe Mouth Fresh, the Teeth Clean and theGums Firm he wrote, “The eyes and teethhave an extraordinary affinity or reciprocalrelation to one another, by which they easilycommunicate to each other their defects anddiseases, so that one cannot be perfectlyhealthy without the other being so too.”5
In 1768, Berdmore in A Treatise on theDisorders and Deformities of the Teeth andGums described the relationship betweenthe teeth and the entire body as one leading tothe most “excruciating pains and dangerousinflammations and sometimes deep seatedabscesses which destroy neighbouring partsand affect the whole system by sympathy, orby infecting the blood with corrupted matter.”7
In 1818, one of the most famous physicians inAmerica, Benjamin Rush, reported the courseof a disease in which a woman who wassuffering from rheumatism of long standinghad an aching tooth extracted and “she re -covered in just a few days.”7
All of these statements over the courseof history were made without sufficient sup-porting evidence, yet they were current be-liefs at the time. These conclusions wereusually drawn by repeated observation of anumber of patients with similar symptomsand outcomes. Today these ancient theories—especially those related to oral systemicconditions—cannot be considered to be any-thing more than guess work based on simpleobservation. However, it is of great interestto see that historically there existed a sus -picion or hunch that an inter-relationship existed between oral disease and systemicconditions.
ORAL SEPSIS AS ACAUSE FOR DISEASE
The importance of oral hygiene in rela-tion to bacteriology was first detailed byDutch scientist Antonie von Leeuwenhoek in1683. However, it was with the discoveriesof the late 1800s that the centuries-old debateabout the influence of the mouth on the restof the body began. One of the main reasonsfor interest in the area was due to stridesmade in the study of microbiology. Majorcontributors to advances in microbiology in-cluded Pasteur, Lister, and Koch. Koch wasa physician working as a District MedicalOfficer in Wöllstein, a small city in what isnow Germany. During the Franco-Prussianwar, he began to study the disease anthrax,which was prevalent among farm animalsin the community. Earlier, the anthrax bacil-lus had been discovered by Pollande, Royer,and Davine. Through a series of experi-ments, Koch demonstrated that pure culturesof the anthrax bacillus could cause the anthrax disease. His work was publishedin 1876 and the “germ theory of disease causation” was introduced to the world.Soon, scientists around the globe became in-terested in bacteria and their role in diseaseetiology.
An American dentist working at Koch’sInstitute for Infectious Diseases, Miller wasconvinced that the bacteria residing in themouth could explain most illnesses. In 1880,to support his theory, Miller published abook with the title The Microorganisms ofthe Human Mouth: The Local and GeneralDiseases Which are Caused by Them. In1891, Miller published a classic article inthe Dental Cosmos journal.8 The title of thearticle was “The Human Mouth as a Focus ofInfection.” This article aimed to “call atten-tion to the various local and general diseaseswhich have been found to result from theaction of microorganisms which have col-lected in the mouth and to various channelsthrough which these microorganisms or their

44 Periodontal Disease and Overall Health: A Clinician's Guide
waste products may obtain entrance to partsof the body adjacent to or remote from themouth.” It also aimed to “establish the greatimportance of thorough understanding onthe part of the physician, no less than of thedentist, of mouth germs as a factor in theproduction of disease.” The article was pre-sented under three headings/sections:
• Diseases of the human body which havebeen traced to the action of mouthbacteria
• The pathogenic mouth bacteria• Prophylactic measuresThe diseases he felt could be traced to
bacteria colonizing the mouth included osti-tis, osteomyelitis, septicemia, pyemia menin-gitis, disturbance of alimentary tract, pneu-monia, gangrene of the lungs, Ludwig’sangina, diseases of the maxillary sinus, actin-omycosis, noma, diphtheria, tuberculosis,syphilis, and thrush. He described 149 cases,many of which he ascribed to a dental origin,such as fistulae that opened on the neck,shoulder, arm, or breast. Thus was devel-oped the concept of focus of infection, withorganisms in the oral cavity being implicatedin diseases of the body remote from themouth. Although he did not mandate re-moval of teeth as a method of eradication offoci of infection, he sometimes suggestedthat the “treatment and filling of root canals”could serve this purpose. In Miller’s opinion,local collection of disease-producing organ-isms could produce “a metastic abscesswherever a point of diminished resistanceexisted.” Moreover, he postulated that teethwere not the only source of aggregation ofsuch bacteria but that foci in other organs, suchas the tonsils and uterus, could be implicated.5,8
The next important figure in the his-tory of oral sepsis as a cause of disease wasthe English physician, Hunter. At the time ofMiller’s paper presentation, which Hunterattended, he was the senior assistant physi-cian at the London Fever Hospital and his at-tention was already drawn to the mouth as a
possible source of infection. In 1900, hewrote an article titled “Oral Sepsis as aCause of Disease,” which was published inthe British Medical Journal.9 Hunter impli-cated poor oral hygiene, together with iatro-genic conservative dentistry, as causes ofthe multitude of diseases attributed to focalinfection. He advocated oral antisepsis meas-ures to diseased teeth or inflamed gums, theremoval of “tooth stumps,” the boiling ofevery “tooth plate” worn, and the avoidanceof restorations such as bridges, which can’tbe cleanly maintained.5,9
In 1900, Godlee described how thesigns and symptoms of other conditions,such as pleurisy, could be attributed to pyorrhea alveolaris, and how all the signsand symptoms disappeared after careful re-moval of all calculus and regular syringingof the pockets with a hydrogen peroxide so-lution.5,10 In 1902, Colyer described the res-olution of irregular heart beat, gastric effectsand “general debility” after the treatment ofany oral sepsis present. He also suggested agood maxim with which a dentist should workwas “better no teeth than septic ones.”5,11
In an article published by Wilcox in1903, antral disease was put forward as animportant sequelae of oral sepsis.12 It wasbelieved that prolonged antral suppurationcould lead to extreme mental depression, of-ten ending in suicidal tendency.5,12 Other re-lationships that were put forward were thosebetween oral sepsis and migraine headaches,laryngeal pain and spasm (which could in-duce cough, loss of voice, and wasting),blindness, and deafness, all of which Wilcoxhypothesized could be cured with treatmentof the oral sepsis.5 As the concept of oralsepsis became more popular, theories wereput forward as to which organs were mostsusceptible to different types of oral sepsis,and how the treatment of oral sepsis couldlead to recovery from tonsillitis, tuberculosis,and diabetes. It was also believed that oralsepsis could be transmitted by the licking of

CHAPTER 4 History of the OralSystemic Relationship 45
envelopes, use of contaminated telephonereceivers, and men with beards.
In 1908, Merritt published an article inDental Cosmos with the title “Mouth Infec-tion: the Cause of Systemic Disease.”13 Inthis article he stated that “there is a generaldisposition on the part of the medical anddental professions to underestimate the relations which exist between an uncleanmouth and many local and systemic disordersof grave nature.” He felt that in many casesof malnutrition, the sole cause was a “filthymouth” and that “no greater good couldcome to humanity than the full recognition ofthe dangers from this insidious, prolific andvirulent infection in the human mouth.” Healso stated that “the adoption of proper oralhygiene practices would result in immediateand marked improvement to general healthand notable increase in the average durationof human life.”
On October 3, 1910, Hunter was invitedto McGill University in Montreal, Canada, togive the keynote address at the dedication ofthe Strathcona Medical Building. The titleof his address was “The Role of Sepsis and Antisepsis in Medicine.” In his address, heblamed “oral sepsis” as the cause of a greatmany diseases, and made an attack on con-servative dentistry, or as he called it “septicdentistry.”5 His address was published inThe Lancet, which was the leading Britishmedical journal at the time, as well as in theDental Register.14,15 Hunter is best remem-bered for the following statement in TheLancet report: “No one has probably hadmore reason than I have had to admire thesheer ingenuity and mechanical skill con-stantly displayed by the dental surgeon. Andno one has had more reason to appreciatethe ghastly tragedies of oral sepsis which hismisplaced ingenuity so often carries in itstrain. Gold fillings, crowns and bridges,fixed dentures, built on and about diseasedtooth roots form a veritable mausoleum ofgold over a mass of sepsis to which there is
no parallel in the whole realm of medicine.”He continued with “The worst cases ofanaemia, gastritis, obscure fever, nervousdisturbances of all kinds from mentaldepression to actual lesions of the cord,chronic rheumatic infections, kidney dis -eases, all those which owe their origin to, orare gravely complicated by the oral sepsisproduced by these gold traps of sepsis. Timeand again I have traced the very first onset ofthe whole trouble to the period within amonth or two of their insertion.” It appearsthat Hunter’s condemnation of conservativedentistry was based primarily on its poorstandard. It was fashionable in London at thetime to mimic complicated Americandentistry. However, in many cases the resultswere often of substandard quality. Some well-respected dentists at the time, such as EdwardCameron Kirk, the editor of Dental Cosmos,recognized the potential systemic effects oforal sepsis, but felt that Hunter’s criticism ofdentistry was unfair as Hunter’s observationswere primarily based on the disastrous effectsof a very low-standard dentistry.5
In 1911, Billings, the long-servingDean of Medicine at the University ofChicago and head of the focal infection re-search team at Rush Medical College andPresbyterian Hospital, replaced the term“oral sepsis” with “focal infection.” Soonafter that, he was honored with being askedto give the annual Lane Memorial Lectureat Stanford University in 1915. There, he defined a focus of infection as a “circum-scribed area of tissue infected with patho-genic organisms” and said that the term focalinfection implied that: (1) such a focus or lesion of infection existed, (2) the infectionwas bacterial in nature, and (3) it was ca pa-ble of dissemination, resulting in systemicinfection of other contiguous or noncon-tiguous parts. The teeth, tonsils, adenoids,and mastoids were thought to be the usualsources of bacteremia, and certain bacteria,such as streptococcus and pneumococcus,

46 Periodontal Disease and Overall Health: A Clinician's Guide
had special affinities for target organs likethe heart and lungs.5,16 Billings advocatedthat chronic infectious arthritis was often as-sociated with remote foci of streptococcus,gonococcus, or tuberculosis organisms, andsuggested the removal of all foci of infectionand the improvement in patients’ immunityby absolute rest and improvement of popu-lation-wide and individual oral hygiene.17,18
One of the first studies measuring the clini-cal benefit of removing focal infection in1917 confirmed his suggestions. The studywas conducted as a retrospective postal sur-vey, and 23% reported a cure for their arthri-tis following removal of infective foci. Anadditional 46% reported experiencing someimprovement in symptoms.5,19
One of Billings’ research associates wasRosenow. He was a graduate of the RushMedical College where he had been a studentof Billings. He utilized special methods forculturing material from various foci ofinfection. He obtained a number of pathogenicbacteria from patients, including streptococciand gonococci, which he injected in animals.He then tested whether these organisms wouldprovoke lesions similar to the secondarymanifestations noted in the patients fromwhom the foci had been removed. He used theterm “elective localization” to note that certainstrains of pathogenic bacteria (mostlystreptococci) isolated from the oral cavity ofthe patients had localized to the joints, cardiacvalves, or other areas of the animals.5
Physicians like Billings and Rosenowwere prominent and convincing. More and morearticles were published and many other physi -cians, such as Barker and Cecil, embraced theconcept of focal infection. Cecil, best knownfor his textbook of medicine, reported in 1933that “the keystone of the modern treatment ofrheumatoid arthritis is the elimination of theinfected foci.”20 In an article in 1938, he quotesRosenow who said “the prevention of oralsepsis in the future, with the view to lessen-ing the incidence of systemic diseases, should
hence forth take precedence in dental practiceover the preservation of the teeth almostwholly for mechanical or cos metic pur -poses.”21 Other leading members of the medicalcommunity, such as Mayo, also advocated thefocal infection theory. He stated that “inchildren the tonsils and mouth probably carryeighty percent of the infective diseases thatcause so much trouble in later life.” He wenton to write “teeth with putrescent pulps mayharbour green-producing streptococci andeven though they show no redness at the gumsthey may be very dangerous to keep in themouth.”3-5
What followed in dentistry as the resultof the “theory of focal infection” was an un-precedented wave of tooth extractions andthe avoidance of conservative dentistry.5,22
All teeth that were endodontically or peri-odontally involved were extracted to avoid apossible focus of infection. This approachcame to be known as the “hundred per-center.” The leading spokesperson for thisradical approach was the physiologist Fisher.He regarded a tooth with a root filling as adead organ that needed to be extracted.5
As biomedical research evolved in theearly 1930s, it also started evaluating con-cepts on a scientific basis. It was then that thestrong belief in the theory of focal infectionbegan to decline. What stimulated this de-cline was the work of Holman, who notedthat Rosenow’s work was fraught with con-tamination and that his data were incon -sistent.22,23 Others noted that Rosenowin oculated animals with such high countsof bacteria that it was inevitable that every organ or joint would be affected.24, 25 Gross-man, in his book Root Canal Therapy, notedthat Rosenow’s technique “so devastates thelaboratory animal that lesions are sometimesproduced in almost every tissue and organ ofthe body.” The fact that Rosenow’s work inanimal models could not be reproduced byother investigators heavily discredited histheories.25

CHAPTER 4 History of the OralSystemic Relationship 47
Cecil, a great proponent of the focal in-fection theory, together with the rest of themedical community, started to re-evaluatehis approach. He and Angevine publishedan article in 1938 that reported a follow-upstudy of 156 patients with rheumatoid arthri-tis who had teeth and/or tonsils removed be-cause of foci of infection. They concludedthat chronic focal infection was relativelyunimportant in rheumatoid arthritis becauseof the 52 patients who had teeth removed, 47did not get any better and three got worse. Intheir own words they concluded that “focalinfection is a splendid example of a plausi-ble medical theory which is in danger of be-ing converted by its enthusiastic supportersinto the status of an accepted fact.”21
In 1940, Reiman and Havens wrote acritical review of the theory of focal infectionin the Journal of the American Medical As-sociation.26 They reviewed the literature indetail and ended the report with the follow-ing paragraph. “It may be said, therefore,that: (a) The theory of focal infection, in thesense of the term used here, has not beenproved, (b) the infectious agents involvedare unknown, (c) large groups of personswhose tonsils are present are no worse thanthose whose tonsils are out, (d) patientswhose teeth or tonsils are removed oftencontinue to suffer from the original diseasefor which they were removed, (e) beneficialeffects can seldom be ascribed to surgicalprocedures alone, (f) measures are often out-weighed by harmful effects or no effect at all,and (g) many suggestive foci of infectionheal after recovery from systemic disease, orwhen the general health is improved withhygienic and dietary measures.”
In 1951, a review by Williams and Burket27 concluded the following “There isno good scientific evidence to support thetheory that removal of these infected teethwould relieve or cure arthritis, rheumaticheart disease, and kidney, eye, sin, or otherdisorders.” The very strongly worded review
by Reiman and Havens, as well as over-whelming new evidence, brought the “eraof focal infection” to an end.26 An editorial inthe Journal of the American Medical Asso-ciation in 195228 stated that this happenedbecause “many patients with diseases pre-sumably caused by foci of infection havenot been relieved of their symptoms by re-moval of the foci. Many patients with thesesame systemic diseases have no evident fo-cus of infection, and also foci of infectionare, according to statistical studies, as com-mon in apparently healthy persons as thosewith disease.” In looking back, the theory offocal infection not only was an easy way toexplain the cause of many diseases, but also advocated treatment that was available tothe patients at the time.5 According to Gib-bons,22 the role of economics in the spread-ing of the focal infection theory should notbe underestimated. It is easy to understandthat as the era of focal infection came to anend the lucrative business of extracting teeth,removing tonsils, and treating sinuses as away of treating human diseases graduallydiminished. In his article “Germs, Dr. Billingsand the Theory of Focal Infection,” Gibbonsquotes one bacteriologist of the focal infec-tion period saying “The age of specializationstimulates surgery. Operations carry thebest fees with them, and without intimatingthat economics play a role in the specialist’s decision, nevertheless it is only reasonable toregard him as human—if he is the proudpossessor of surgical skill, he is more proneto use it.” 22
In dentistry, for almost 50 years (1940–1989), there was little interest in the effectof the mouth on the rest of the body. However,throughout the second half of the twentiethcentury, there were dental scientists whocontinued to question whether oral infection(and inflammation) might in some way contribute to a person’s overall health, butthe reasons given were mostly speculative.They continued to suggest that bacteria and

48 Periodontal Disease and Overall Health: A Clinician's Guide
bacterial products found in the mouth couldenter the bloodstream and could in some waybe harmful to the body as a whole.29 It wasnot until the last decade of the twentieth cen-tury that dentistry and medicine started againto consider the relationship of oral diseases,such as periodontal disease, as a contributorto risk factors for certain systemic diseases.
Oral-Systemic Relationship RevisitedThe late 1980s saw an increasing num-
ber of publications implicating an associationbetween periodontopathogenic bacteria andcertain systemic conditions such as coronaryartery disease, stroke, and preterm/low birthweight babies. Such insinuations had alsobeen made early in the twentieth century, butthis time reports were judged with a more measured response.30 According to Barnett30
this response was a result of several factors:(a) greater analytical and statistical knowl-edge, and a better understanding of the con -strains of epidemiological research in “estab -lishing disease causalty”; (b) increased aware -ness of the etiology and pathogenesis of oraldiseases; (c) increased awareness of the etiology and pathogenesis of associated sys-temic diseases; (d) modern advances in thetreatment of oral conditions; (e) realizationthat bacteria could in some way be impli-cated in the development of diseases that asyet have an undetermined etiology.
In 1989, Mattila and coworkers31 inFinland conducted a case-control study on100 patients who had suffered an acute my-ocardial infarction. They compared these pa-tients to 102 control subjects selected fromthe community. A full dental examinationwas performed on all of the subjects studied.Additionally, a dental index was computed.This index computed the sum of scores fromthe number of missing teeth, carious lesions,peri-apical lesions, probing depths, and thepresence or absence of pericoronitis. It wasfound that dental health was significantlyworse in patients with a history of acute
myocardial infarction than in control sub-jects. This association remained valid evenafter adjustment for age, social class, smok-ing, serum lipid concentrations, and the pres-ence of diabetes. It was mainly this studythat renewed the interest of physicians anddentists in the relationship of oral to sys-temic disease.
In retrospect, it is now clear that theadvent of reports by Mattila and colleagues—followed soon thereafter by DeStefano etal.32 and Offenbacher et al.33—was the be- ginning of a new era of understanding the impact of oral health and disease on overallhealth and disease.25,30 By 1996, the term“periodontal medicine” would emerge as scientists and clinicians in dentistry and medicine began to appreciate the tremen-dous effect that oral disease can have on thebody.34
PERIODONTAL/ORAL DISEASEAS A RISK FACTOR FOR
SYSTEMIC DISEASEDespite many years of history demon-
strating the influence of oral status on generalhealth, recent decades have seen an acceler-ated effort for the prevention and manage-ment of these conditions through ground-breaking advances. Specifically, periodontitis,a chronic infectious and inflammatory dis-ease of the gums and supporting tissues, hasbeen associated with systemic conditionssuch as coronary heart disease and stroke,higher risk for preterm, low-birth-weight babies, and certain cancers. It has also beensuggested that it might pose threats to thosewith chronic disease, e.g., diabetes, respira-tory diseases, and osteoporosis.35-38 Perio -dontal diseases are infections that are causedby micro-organisms that colonize the toothsurface at or below the gingival margin.These infections affect the gingival tissuesand can cause damage to the supportingconnective tissue and bone. Periodontal dis-ease can be caused by specific bacteria (such

CHAPTER 4 History of the OralSystemic Relationship 49
as Porphyromonas gingivalis) from the bio -film within the periodontal pocket. Severaldifferent pathways for the passage of perio -dontal pathogens and their products into thecirculation have been suggested and are cur-rently the subject of intensive research.
The focal infection theory, as proposedand defended the first time around, wasmainly based on anecdotal evidence and theoccasional case report. In order for the hy-pothesis not to fall into disrepute the secondtime around, different levels of evidence mustbe examined in order to establish a relation-ship between the periodontal condition andsystemic health of the patient. Since not allscientific evidence is given the same weight,the stronger the evidence, the more likelyit is that a true relationship exists betweenthese conditions.
Case reports provide us with very weakevidence and can only suggest a link, butnot a relationship. Case-control studies aremainly used to identify factors that may con-tribute to a medical condition by comparingsubjects who have the condition with pa-tients who don’t, but are otherwise similar.These studies may lead to cross-sectionalanalyses. Observational studies are used toexamine associations between exposures anddisease. These are relatively inexpensive andfrequently used for epidemiological studies.However, the fact that they are retrospectiveand not randomized limits their validity.
Cross-sectional analysis studies the rela -tionship between different variables at a pointin time. These type of data can be used to assessthe prevalence of acute or chronic conditionsin a population. However, since exposure anddisease status are measured at the same pointin time, it may not always be possible todistinguish whether the exposure preceded orfollowed the disease. Stronger evidence isprovided with a longitudinal study, in whichsubject populations are examined over time.A longitudinal study is often undertaken toobtain evidence to try to refute the existence
of a suspected association between causeand disease; failure to refute a hypothesisstrengthens confidence in it. Longitudinalstudies with controls are much stronger thanthe ones without. The same applies for inter -vention trials that provide the strongest form ofevidence. Unfortunately, not only are thesedifficult to conduct, they are expensive andinvolve many ethical considerations.
What Is Risk?Risk is the statistical likelihood that cer-
tain factors are associated with the develop-ment of disease. It can be divided into absolute risk, which is the likelihood of ac-quiring a certain disease, and relative risk,which is the likelihood of acquiring a diseaseif certain factors are modified, compared tothe same likelihood if they are not. It is easyto understand that if true risk factors areidentified, then intervention for those at riskcan be planned and implemented.
The strength of association between pu-tative risk factors and a disease state can beexpressed in odds ratios. An odds ratio of oneindicates an equal chance as to whether ornot an association will occur. An odds ratioof two indicates a two-fold chance of an as-sociation being present. Care should be ex-ercised inferring causation from odds ratios.Association does not, in itself, infer causa-tion. In the interpretation of odds ratios, it isimportant that the confidence interval of theodds ratio not traverse one. If it does, theodds ratio—regardless of magnitude—can-not be relied upon.
There has long been an interest in therole of systemic factors as they affect perio -dontal disease. A series of studies were car-ried out looking at systemic risk factors forperio dontal disease and were summarizedby Genco in 1996.39 In this review, it waspointed out that in addition to pre-existingdis eases, sys temic factors have been identified.These in clude reduced neutrophil function,stress and coping behaviors, osteopenia, age,

50 Periodontal Disease and Overall Health: A Clinician's Guide
gender (with more disease seen in males),hereditary factors, infection with periodontalpatho gens, cigarette smoking, and diabetes.It should be noted that these are risk factorscom mon to many chronic, noncommunica-ble diseases, such as heart disease, stroke,and diabetes, all of which are associated withperiodontitis.39
Periodontitis/Oral Healthas a Risk for Specific Diseases:
Evidence for an AssociationCardiovascular
There are at least three possible mech-anisms by which oral infections may con-tribute to cardiovascular disease:40
1. Direct effect of infectious agent inatheroma formation
2. Indirect or host-mediated responses3. Common genetic predisposition Bahekar35 and colleagues recently con-
ducted a systematic review of the literaturein order to evaluate if such an association ex-ists. This review revealed five prospectivecohort studies involving 86,092 patients forat least six years. The authors consideredthat three out of the five prospective studieswere of good quality, and both the incidenceand prevalence of coronary heart diseasewere increased in subjects with periodontaldisease after adjustments for other variablesknown to increase the risk of coronary heartdisease. Furthermore, five case-control stud-ies involving 1,423 patients and five cross-sectional studies involving 17,724 patientswere also evaluated. All supported a sig - nificant relationship between periodontal disease and coronary heart disease. Moreprospective studies are needed, however, toprove the assumption that periodontitis maybe a risk factor for coronary heart disease andto evaluate risk reduction with the treatmentof periodontitis.
In planning prospective studies, it isimportant to remember that patients with pe-riodontal disease share many of the same
risk factors as patients with cardiovasculardisease. These risk factors include age, gen-der, lower socioeconomic status, stress, andsmoking.41 Additionally, a large number ofpatients with periodontal disease also ex-hibit cardiovascular disease; this could bean indication that periodontal disease andatherosclerosis share similar or common eti-ologic pathways.42 The literature also sug-gests that a number of pathogens, antigens,endotoxins, and cytokines of periodontitismight be significant contributing factors.43,44
According to Williams et al.,45 controlling forsuch confounding factors when carrying outepidemiological and observational studies re-quires large numbers of subjects to be en-rolled and these subjects need to be followedover a long period of time. Common perio -don tal pathogens such as Porphyromonas gingi -valis and Streptococcus sanguis have been foundin arterial plaques from carotid en darterec tomysamples. Furthermore, perio dontal disease hasbeen associated with elevated levels of in-flammatory markers, such as C-reactive pro-tein. Although there is growing evidence tosupport a role for C-reactive protein as a pre-dictive, pathogenic factor for vascular risk, itis recognized that more research is needed.35
There is a need for large-scale prospec-tive intervention studies to assess whether ornot periodontitis can be considered an effec -tive modifiable risk factor in the prevention ofcardiovascular disease.
Adverse Pregnancy OutcomesSeveral studies on laboratory animals that
took place in the 1970s and 1980s re vealedthat bacterial endotoxin (a cell wall com ponentisolated from E. coli) is capable of pro ducingspontaneous abortion, low fetal weight, andmalformations.46 Collins and col leagues suc -cessfully demonstrated that oral anaerobessuch as P. gingivalis had similar effects. 47,48
In 1996, Offenbacher and colleaguesconstructed a case-control study with the title “Periodontal Infection as a Possible Risk

CHAPTER 4 History of the OralSystemic Relationship 51
Factor for Preterm Low Birth Weight.”33 Inthis investigation, they sought to determinewhether or not the prevalence of maternalperiodontal infection could be associatedwith preterm low birth weight, while control -ling for known risk factors such as smokingand poor nutrition. Results observed fromthe 124 pregnant or postpartum mothers whotook part in this study indicated that perio -dontal disease represents a clinically signif-icant risk factor for preterm low birth weight.This landmark report by Offenbacher andcolleagues was the first of this kind.
In the last seven years, there has beenan explosion of data released from case- control studies, cohort studies, and clinicaltrials, as well as from systematic reviews.Many studies have reported a positive asso-ciation, but it must be concluded that dueto different study designs, heterogeneity inthe way adverse pregnancy outcomes weremeasured, as well as a lack of adequate analysisfor confounders, there is still no consistent evidence for or against this association.
There is a need for large-scale prospec-tive intervention studies in which adversepregnancy outcomes and the severity of periodontal disease can be clearly defined.
Diabetes: A Two-Way RelationshipIt is clear from epidemiologic studies
that diabetes mellitus increases the risk forperiodontal disease.49,50 The available litera-ture highlights the importance of oral healthin subjects with diabetes, and demonstratesan increased prevalence of periodontitisamong patients with poorly controlled dia-betes.45 Patients with controlled diabetesshow periodontal conditions similar to thoseof the healthy population.
The current literature does not provide uswith conclusive evidence to support a causalrelationship between periodontal disease andrisk for Type 2 diabetes. There is evidencethat there is an increased risk of periodontitisin patients with diabetes, but Taylor and
coworkers also showed that patients with Type2 diabetes who suffer from periodontitis haveworse glycemic control, suggesting that notonly does diabetes affect periodontitis, butonce a diabetic has periodontitis, it leads toworsening diabetes or glycemic control.51 Thiswas followed by a paper by Grossi and Gencoin which periodontal disease and diabetesmellitus was presented as a two-way relation -ship.52 This began a long line of investigationin which treatment of periodontal disease indiabetes was found to contribute to glycemiccontrol, with one of the first studies reportedby Grossi and colleagues.53 Recently, a meta-analysis of nine control studies on the subjectconfirmed that the reduction of glycatedhemoglobin with periodontal therapy can besignificant, comparable to other attempts tocontrol glycated hemoglobin.45 Researcherstried to evaluate the effects of periodontaltherapy on systemic inflammatory markersand on glycemic control.54 Several randomizedcontrol trials and a number of longitudinal andobservational studies pro vided some evidenceto support the concept that periodontitis canadversely affect glycemic man agement.Overall though, it is incon clusive thatperiodontal treatment results in improvementof metabolic control and of markers ofsystemic inflammation.
There is emerging evidence to suggestthat periodontitis predicts the developmentof overt nephropathy and endstage renal dis-ease in patients with Type 2 diabetes.37,55 Aprospective study by Shultis37 and colleagueswas conducted exclusively in individuals withdiabetes. It also included a proportionallylarge number of individuals with kidney dis-ease. Whether or not treatment of periodon-titis will reduce the risk of diabetic kidneydisease has not yet been determined, but thisstudy provides a rationale for further inves-tigation into the connections between perio -dontal disease and diabetic progression.
There is a need for large-scale prospec-tive intervention studies, mainly in specific

52 Periodontal Disease and Overall Health: A Clinician's Guide
high-risk groups because, according toWilliams45 and colleagues, these groupscan provide more immediate answers than studies with a more heterogeneous diabeticpopulation.
Respiratory InfectionsScannapieco56 describes four possible
mechanisms of the presence of oral bacteriain the pathogenesis of respiratory infections:
1. The oral cavity might be a reservoirfor micro-organisms that contaminatesaliva and is then aspirated into thelungs.
2. Periodontal disease-associated en-zymes in saliva may facilitate theadherence of respiratory pathogensin the mucosal surfaces.
3. Periodontal disease-associated en-zymes may destroy protective sali-vary pellicles, resulting in fewernonspecific host defense mecha-nisms in high-risk patients.
4. Cytokines and other molecules orig-inating from untreated periodontaltissues are continuously released insaliva. Aspiration of these may alterrespiratory epithelium and promoterespiratory pathogen colonization.
A systematic review published in 2006by Azarpazhooh and Leake investigated ev-idence for a possible etiological associationbetween oral health and pneumonia or otherrespiratory diseases.57 They concluded thatthere is fair evidence of an association ofpneumonia with oral health, and poor evi-dence of an association of chronic obstruc-tive pulmonary disease with oral health. Additionally, there is good evidence that implementation of high-quality and frequentoral healthcare decreases the occurrence andprogression of respiratory diseases amongelderly hospitalized or institutionalized individuals.57
There is a need for large-scale prospec-tive intervention studies targeting high-risk
people of the community, nursing homes,and intensive care units.
OsteoporosisOver the last decade, it has been specu -
lated that by decreasing the patient’s alveolarbone mass, osteoporosis makes teeth moresusceptible to resorption by the periodontalinflammatory reaction. Human studies haveaddressed this relationship, and several large-scale studies showed there is an associationbetween osteoporosis and reduced alveolarcrestal height in postmenopausal women.58
In another study, osteoporosis and perio -dontal infection were found to be independ-ent risk factors for oral bone loss.59 Otherstudies, especially longitudinal studies, arenecessary to determine the temporal natureof this relationship and to further evaluate it.
Some studies investigated the effect ofhormone replacement therapy or vitamin Dintake on tooth loss.60 In almost all studies,there was a positive correlation between thenumber of teeth retained and medical treat-ment, but it must be kept in mind that con-founding factors such as age, smoking, socio -economic status, and many others may haveaffected the results.40
There is a need for large-scale pro s-pec tive studies with as many confounding factors as possible to be factored into theseinvestigations.
CONCLUSIONSThere is a long-standing and well-
accepted principle that good oral health is anintegral component of good general health.In recent years, there has been an attempt totie oral conditions to systemic diseases in acausal relationship, but existing data supportonly an association. Evidence for this rela-tionship is growing, and a scientifically basedunderstanding of how oral health may posea risk for certain systemic diseases is devel-oping. Certain linkages are stronger than others, but until there are a number of well-

CHAPTER 4 History of the OralSystemic Relationship 53
constructed, controlled intervention studiesproviding “hard” evidence, treatment rec-ommendations need to be guarded.
Supplemental Readings
O’Reilly PG, Claffey NM. A history of oral sepsis as acause of disease. Periodontol 2000 2000;23:13–18.
Gibbons RV. Germs, Dr. Billings and the theory of focalinfection. Clin Infect Dis 1998;27:629–633.
Mattila K, Nieminen M, Valtonen V, Rasi VP, Kesäni-emi YA, Syrjälä SL, Jungell PS, Isoluoma M, Hietani-emi K, Jokinen MJ. Association between dental healthand acute myocardial infarction. Br Med J1989;298:779–782.
Offenbacher S, Katz V, Fertik G, Collins J, Boyd D,Maynor G, McKaig R, Beck J. Periodontal infection asa possible risk factor for preterm low birth weight. J Periodontol 1996;67:1103–1113.
Williams RC, Barnett AH, Claffey N, Davis M, GadsbyR, Kellett M, Lip GY, Thackray S. The potential impactof periodontal disease on general health: A consensusview. Curr Med Res Opin 2008;24:1635–1643.
REFERENCES1. Gold SI. Periodontics. The past. Part (I) Early
sources. J Clin Periodontol 1985;12:79–97.2. Francke OC. William Hunters’ “oral sepsis” and
American odontology. Bull Hist Dent 1973;21:73–79.
3. Mayo CH. Focal infection of dental origin. DentalCosmos 1922; 64:1206–1208.
4. Lindsay LL. A short history of dentistry. London:John Bale, Sons and Danielsson, Ltd; 1933:14–17.
5. O’Reilly PG, Claffey NM. A history of oral sepsisas a cause of disease. Periodontology 2000 2000;23:13–18.
6. Arculani J. Comenteria, Venetiis. Cap. XIViii. DeDolore Dentium 1542:192.
7. Rush ME. An account of the core of several dis-eases by the extraction of decayed teeth.1818:5thed.:197–201.
8. Miller WD. The human mouth as a focus of infec-tion. Dental Cosmos 1891;33:689–706.
9. Hunter WD. Oral sepsis as a cause of disease. BrMed J 1900;2:215–216.
10. Godlee RJ. On some of the medical and surgicalcomplications of pyorrhea alveolaris. Dent Rec1900;20:337–347.
11. Colyer S. Oral sepsis: and some of its effects. DentRec 1902;20:200–206.
12. Wilcox R. Some immediate and remote effects ofsuppuration in the mouth and jaws. Br Dent J1903;24:733–736.
13. Merritt AH. Mouth infection: the cause of systemicdisease. Dental Cosmos 1908;50:344–348.
14. Hunter WD. The role of sepsis and antisepsis inmedicine. Lancet 1911;1:79–86.
15. Hunter W. The role of sepsis and antisepsis in med-icine and the importance of oral sepsis as its chiefcause. Dental Register 1911;44:579–611.
16. Billings FA. Focal infection: its broader applicationin the etiology of general disease. JAMA 1914;63:899–903.
17. Billings FA. Chronic focal infections and their etiologic relations to arthritis and nephritis. Arch IntMed 1912;9:484–498.
18. Billings FA. Chronic focal infection as a causativefactor in chronic arthritis. JAMA 1913;61:819–823.
19. Hughes RA. Focal infection revisited. Br J Rheu -matol 1994;33:370–377.
20. Woods AC. Focal infection. Am J Opthalmol 1942;25:1423–1444.
21. Cecil RL, Angevine DM. Clinical and experimen-tal observations on focal infection with an analysisof 200 cases of rheumatoid arthritis. Ann Int Med1938:12:577–584.
22. Gibbons RV. Germs, Dr. Billings and the theory offocal infection. Clin Infect Diseases 1998;27:627–633.
23. Holman WL. Focal infection and selective localiza -tion: a critical review. Arch Path Lab Med 1928;5:68–136.
24. Beeson PB. Fashions in pathogenetic concepts dur-ing the present century: autointoxication, focal in-fection, psychosomatic disease and autoimmunity.Perspect Biol Med 1992;36:13–23.
25. Pallasch TJ, Wahl MJ. Focal infection: new age orancient history. Endod Topics 2003;4:32–45.
26. Reiman HA, Havens WP. Focal infections andsystemic disease: a critical appraisal. JAMA 1940;114:1–6.
27. Williams NB, Burkett LW. Focal infection—a review. Philadelphia Med 1951;46:1509.
28. Editorial. JAMA 1952;150:490.29. Thoden van Velzen T, Abraham-Inpijn L, Moorer
WR. Plaque and systemic disease: A reappraisal ofthe focal infection concept. J Clin Periodontol1984;11:209–220.
30. Barnett ML. The oral systemic disease connection.An update for the practicing dentist. JADA 2006;137:5S–6S.
31. Mattila K, Nieminen M, Valtonen V, Rasi VP, Ke-säniemi YA, Syrjälä SL, Jungell PS, Isoluoma M,Hietaniemi K, Jokinen MJ. Association betweendental health and acute myocardial infarction. BrMed J 1989;298:779–781.

54 Periodontal Disease and Overall Health: A Clinician's Guide
32. DeStefano F, Anda RF, Kahn HS, Williamson DF,Russell CM. Dental disease and risk of coronaryheart disease and mortality. Br Med J 1993;306:688–691.
33. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D,Maynor G, McKaig R, Beck J. Periodontal infec-tion as a possible risk factor for preterm low birthweight. J Periodontol 1996;67:1103–1113.
34. Rose LF, Genco RJ, Cohen DW, Mealey BL., Eds.,Periodontal Medicine. BC Decker, Inc., Hamilton,Ontario, 2000.
35. Bahekar AA, Singh S, Saha S, Molnar J, Arora R.The prevalence and incidence of coronary heartdisease is significantly increased in periodontitis:a meta-analysis. Am Heart J 2007;154:830–837.
36. Grau AJ, Becher H, Ziegler CM, Lichy C, BuggleF, Kaiser C, Lutz R, Bültmann S, Preusch M, DörferCE. Periodontal disease as a risk factor for ischemicstroke. Stroke 2004;35:496–501.
37. Shultis WA, Weil EJ, Looker HC, Curtis JM, Shloss-man M, Genco RJ, Knowler WC, Nelson RG. Ef-fect of periodontitis on overt nephropathy and endstage renal disease in type 2 diabetes. DiabetesCare 2007;30:306–311.
38. Bobetsis YA, Barros SP, Offenbacher S. Exploringthe relationship between periodontal disease andpregnancy complications. JADA 2006;137:7s–13s.
39. Genco RJ. Current view of the risk factors for perio -dontal diseases. J Periodontol 1996;67:1041-1049.
40. Renvert S. Destructive periodontal disease in rela-tion to diabetes mellitus, cardiovascular diseases,osteoporosis and respiratory diseases. Oral HealthPrev Dent. 2003;1 Suppl:341–357.
41. Beck JD, Offenbacher S, Williams RC, Gibbs P,Garcia R. Periodontitis: A risk factor for coronaryheart disease? Ann Periodontol 1998;3:127–141.
42. Umino M, Nagao M. Systemic diseases in elderlydental patients. Int Dent J 1993;43:213–218.
43. Beck JD, Eke P, Lin D, Madianos P, Couper D,Moss K, Elter J, Heiss G, Offenbacher S. Asso -ciations between IgG antibody to oral organismsand carotid intima-medial thickness in community-dwelling adults Atherosclerosis 2005;183:342–348.
44. Kozarov EV, Dorn BR, Shelburne CE, Dunn WA Jr,Progulske-Fox A. Human atherosclerotic plaquecontains viable invasive Actinobacillus actino-mycetemcomitans and Porphyromonas gingivalis.Arterioscler Thromb Vasc Biol 2005; 25:17–18.
45. Williams RC, Barnett AH, Claffey N, Davis M,Gadsby R, Kellett M, Lip GY, Thackray S. The po-tential impact of periodontal disease on generalhealth: A consensus view. Curr Med Res Opin2008;24:1635–1643.
46. Lanning JC, Hilbelink DR, Chen LT. Teratogenic ef-fects of endotoxin on the golden hamster. Teratog
Carcinog Mutagen 1983;3:145–149.47. Collins JG, Windley HW 3rd, Arnold RR, Offen-
bacher S. Effects of a Porphyromonas gingivalis infection on inflammatory mediator response andpregnancy outcomes in hamsters. Infect Immun1994;62:4356–4361.
48. Collins JG, Smith MA, Arnold RR, Offenbacher S.Effects of Escherichia coli and Porphyromonasgingivalis lipopolysaccharide on pregnancy outcomein the golden hamster. Infect Immun 1994;62:4652–4655.
49. Papapanou PN. Periodontal diseases: epidemiol-ogy. Ann Periodontol;1996:1:1–36.
50. Taylor GW, Manz MC, Borgnakke WS. Diabetes,periodontal diseases, dental caries and tooth loss: Areview of the literature. Compend Contin EducDent 2004;25:179–184.
51. Taylor GW, Burt BA, Becker MP, Genco RJ,Shlossman M, Knowler WC, Pettitt DJ. Severe periodontitis and risk for poor glycemic control inpatients with non-insulin-dependent diabetes mel-litus. J Periodontol 1996;67:1085-1093.
52. Grossi SG, Genco RJ. Periodontal disease and diabetes mellitus: A two-way relationship. Ann Perio dontol 1998;3(1):52–61
53. Grossi SG, Skrepcinski FB, DeCaro T, RobertsonDC, Ho AW, Dunford RG, Genco RJ. Treatment ofperiodontal disease in diabetics reduces glycatedhaemoglobin. J Periodontol 1997;68:713–719.
54. Taylor GW, Borgnakke WS. Periodontal disease:Associations with diabetes, glycemic control andcomplications. Oral Dis 2008;14:191–203.
55. Saremi A, Nelson RG, Tulloch-Reid M, HansonRL, Sievers ML, Taylor GW, Shlossman M, Bennett PH, Genco R, Knowler WC. Periodontaldisease and mortality in type 2 diabetes. DiabetesCare 2005;28:27–32.
56. Scannapieco FA. Role of oral bacteria in respiratoryinfection. J Periodontol 1999;70:793–802.
57. Azarpazhooh A, Leake J. Systematic review ofthe association between respiratory diseases andoral health. J Periodontol 2006;77:1465–1482.
58. Wactawski-Wende J, Hausmann E, Hovey K, Trevisan M, Grossi S, Genco RJ. The associationbetween oteoporosis and alveolar crestal height inpostmenopausal women. J Evid Based Dent Pract2006;6:289–290.
59. Brennan-Calanan RM, Genco RJ, Wilding GE,Hovey KM, Trevisan M, Wactawski-Wende J. Osteoporosis and oral infection: Independent riskfactors for oral bone loss. J Dent Res 2008;87:232–237.
60. Grodstein F, Colditz GA, Stampfer MJ. Post- menopausal hormone use and tooth loss: a pros -pective study. JADA 1996;127:370–377.
CHAPTER 5Diabetes Mellitus: A Medical Overview
Srividya Kidambi, Shailendra B. Patel
INTRODUCTIONDiabetes mellitus (DM) is a quintes-
sential metabolic disease in which the char-acteristic phenotype is loss of control of glu-cose homeostasis, but the pathophysiologyalso affects fat and protein metabolism. Re-sulting hyperglycemia is associated withboth short- and long-term complications,making early diagnosis and treatment of thiscondition essential. The key hormonal dis-turbance causing DM can be either a defectin insulin secretion, insulin action, or both.Several pathogenic mechanisms have beenproposed for the disease, and more than onemechanism may be at play for the disease tobecome clinically evident. This chapter describes the classification, epidemiology,pathogenesis/pathophysiology, clinical pre-sentations, complications, and diagnosis ofthe disease, as well as a brief overview oftreatment options.
Key educational objectives are to under -stand that
• diabetes is a true metabolic disordercaused by disrupting insulin action.
• both genetic and environmental fac-tors are involved in causing diabetes.
• there are two main forms, Type 1 andType 2, distinguished upon abso-lute and relative insulin deficiency,respectively.
• insulin action is intimately tied to manyother counter-regulatory actions.
• long-term complications of diabetesaffect every organ in the body.
• controlling glycemia levels in addi-tion to cardiovascular risk factors isimportant in preventing, delaying, orameliorating disabling or life-threaten -ing complications.
CLASSIFICATION OFDIABETES MELLITUS
DM is classified into several subtypes,based upon etiology, which can help explainclinical manifestations and provide a ration-ale for various treatments (Table 1). The ma-jority of patients with DM have Type 2 dis-ease (85%–90%) marked by defectiveinsulin action as well as relative deficiencyin insulin secretion. Another 5%–10% of pa-tients have Type 1 disease (absolute defect ininsulin secretion). The remaining sub-typesare rare (Table1). This chapter will focus onthe major subgroups: Type 1 DM, Type 2DM, and gestational DM (GDM); the latteraffects fetal and maternal health and is a riskfactor for later development of Type 2 DM.
EPIDEMIOLOGYAccording to 2007 estimates, 23.6 million
people (or 7.8% of the population) in the UnitedStates have DM.1 About 6 million of theseindividuals do not know they have this dis-ease and present to healthcare providers aftera point of no return in preventing compli -cations. Prevalence increases with advancingage, affecting almost 24% of individualsover the age of 60. An epidemic of Type 2DM is underway in both the developed anddeveloping world, but the brunt is being feltsharply in developing countries.2-4 Globally,the number of people with diabetes is ex-pected to rise from the current estimate of150 million to 220 million in 2010 and 300million in 2025, making the cost of treatingDM and its complications a pressing eco-nomic as well as clinical concern.5
Patients with DM are at a two- to four-fold higher risk for developing heart diseaseand stroke compared to people without DM.

In addition, DM s the leading cause of newcases of blindness and kidney failure amongadults ages 20 to 74.1 Gingivitis and perio -dontitis are also more common in peoplewith DM. Almost one-third of people withDM have severe periodontal disease withloss of attachment of gums to teeth measur-ing five millimeters or more.1
In addition to enormous morbidity asso -ciated with DM, this disease was the seventhleading cause of death listed on US deathcertificates in 2006. Overall, the risk fordeath among people with DM is about twicethat of people without DM of similar age.1
PATHOPHYSIOLOGYThe pathophysiology of DM revolves
around impairment of insulin secretion, in-sulin resistance, or both, resulting in reducedutilization of glucose, hyperglycemia, andimpairment of fatty acid metabolism. Symp-toms and complications of DM are due tohyperglycemia as well as lack of adequateinsulin action.
Glucose MetabolismCarbohydrates, broken down mainly into
glucose, are an important source of energy inhumans. Consideration of glucose and insulinmetabolic pathways is crucial to understand-ing the pathophysiology of DM (Figure 1).
Glucose is derived from three sources:in tes tinal absorption following digestion of dietary carbohydrates; glycogenolysis, thebreakdown of glycogen, which is the poly-merized storage form of glucose; and gluco-neogenesis, the formation of glucose fromprecursors including lactate (and pyruvate),amino acids (especially alanine and gluta-mine), and to a lesser extent, glycerol.5 Onlythe liver and kidneys are capable of releasingglucose into circulation by glycogenolysisand gluconeogenesis. All tissues can utilizeglucose as a substrate for energy production,but only the brain is wholly dependent uponglucose as its main energy source. Thus,
56 Periodontal Disease and Overall Health: A Clinician's Guide
Note: Patients with any form of diabetes may re-quire insulin treatment at some stage of their disease.Such use of insulin does not, of itself, classify the patient.Adapted from the American Diabetes Association. Diabetes Care 2009;31(Suppl 1).37
Table 1. Etiologic ClassificationTable 1. of Diabetes MellitusIII. Type 1 diabetes (-cell destruction, usually leading
to absolute insulin deficiency)A.Immune medicatedB.Idiopathic
III. Type 2 diabetes (may range from predominantly insulin resistance with relative insulin deficiencyto a predominantly secretory defect with insulin resistance)
III. Other specific typesA.Genetic defects of -cell function
1.Chromosome 20, HNF-4 (MODY1)2.Chromosome 7, glucokinase (MODY2)3.Chromosome 12, HNF-1 (MODY3)4.Chromosome 13, insulin promoter factor-1
(IPF-1; MODY4)5.Chromosome 17, HNF-1 (MODY5)6.Chromosome 2, NeuroD1 (MODY6)7.Mitochondrial DNA8.Others
B.Genetic defects in insulin action1.Lipodystrophic syndromes2.Type A insulin resistance3.Leprechaunism4.Rabson-Mendenhall syndrome5.Others
C.Diseases of the exocrine pancreas1.Pancreatitis2.Trauma/pancreatectomy3.Neoplasia4.Cystic fibrosis5.Hemochromatosis6.Fibrocalculous pancreatopathy
D.Endocrinopathies1.Cushing’s syndrome 2.Acromegaly3.Glucagonoma4.Pheochromocytoma5.Others
E.Drug- or chemical-induced1.Glucocorticoids2.Atypical Antipsychotics3.Pentamidine4.Diazoxide5.-Interferon6.Others
.F.Infections1.Congenital rubella
G.Uncommon forms of immune-mediated diabetes1. “Stiff-man” syndrome2. Anti-insulin receptor antibodies3.Others
H.Other genetic syndromes sometimes associatedwith diabetes1.Down’s syndrome2.Turner’s syndrome3.Wolfram’s syndrome4.Laurence-Moon-Biedl syndrome5.Prader-Willi syndrome6.Others
.IV. Gestational diabetes mellitus (GDM)
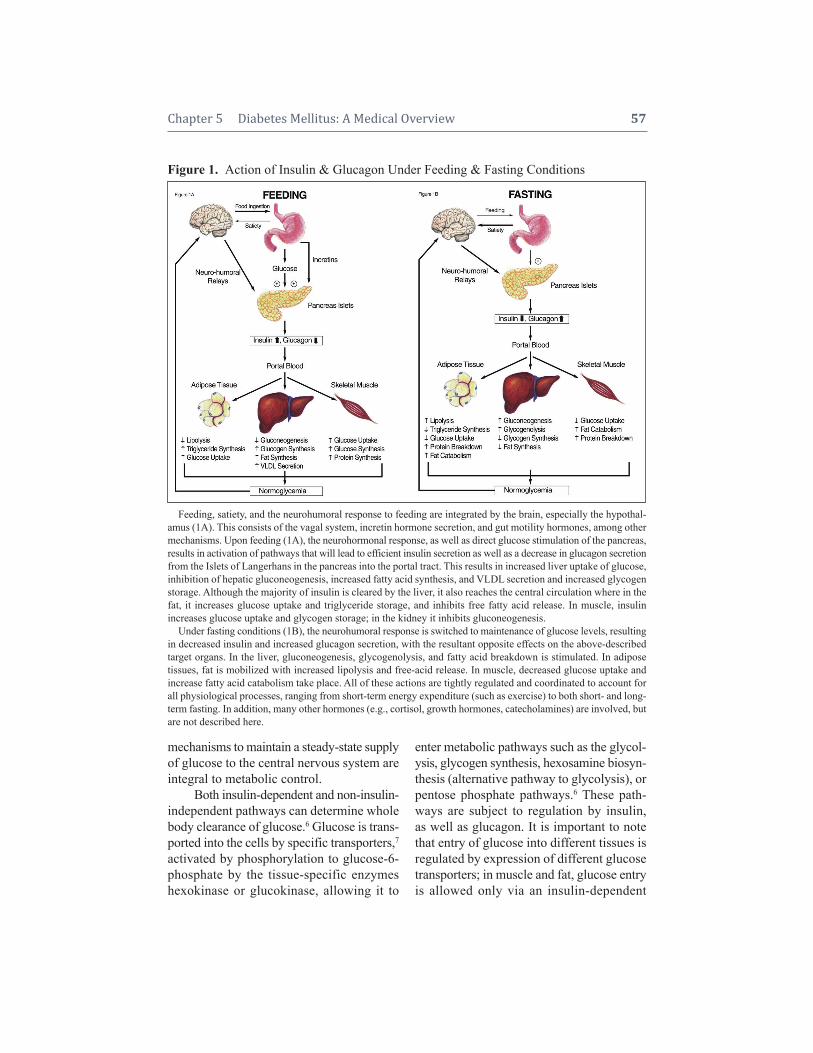
mechanisms to maintain a steady-state supplyof glucose to the central nervous system areintegral to metabolic control.
Both insulin-dependent and non- insulin-independent pathways can determine wholebody clearance of glucose.6 Glucose is trans-ported into the cells by specific transporters,7activated by phosphorylation to glucose-6-phosphate by the tissue-specific enzymeshexokinase or glucokinase, allowing it to
enter metabolic pathways such as the glycol-ysis, glycogen synthesis, hexosamine biosyn- thesis (alternative pathway to glycolysis), orpentose phosphate pathways.6 These path-ways are subject to regulation by insulin,as well as glucagon. It is important to notethat entry of glucose into different tissues is regulated by expression of different glucosetransporters; in muscle and fat, glucose entryis allowed only via an insulin-dependent
Chapter 5 Diabetes Mellitus: A Medical Overview 57
Figure 1.Action of Insulin & Glucagon Under Feeding & Fasting Conditions
Feeding, satiety, and the neurohumoral response to feeding are integrated by the brain, especially the hypothal-amus (1A). This consists of the vagal system, incretin hormone secretion, and gut motility hormones, among othermechanisms. Upon feeding (1A), the neurohormonal response, as well as direct glucose stimulation of the pancreas,results in activation of pathways that will lead to efficient insulin secretion as well as a decrease in glucagon secretionfrom the Islets of Langerhans in the pancreas into the portal tract. This results in increased liver uptake of glucose,inhibition of hepatic gluconeogenesis, increased fatty acid synthesis, and VLDL secretion and increased glycogenstorage. Although the majority of insulin is cleared by the liver, it also reaches the central circulation where in thefat, it increases glucose uptake and triglyceride storage, and inhibits free fatty acid release. In muscle, insulin increases glucose uptake and glycogen storage; in the kidney it inhibits gluconeogenesis.
Under fasting conditions (1B), the neurohumoral response is switched to maintenance of glucose levels, resultingin decreased insulin and increased glucagon secretion, with the resultant opposite effects on the above-describedtarget organs. In the liver, gluconeogenesis, glycogenolysis, and fatty acid breakdown is stimulated. In adipose tissues, fat is mobilized with increased lipolysis and free-acid release. In muscle, decreased glucose uptake and increase fatty acid catabolism take place. All of these actions are tightly regulated and coordinated to account forall physiological processes, ranging from short-term energy expenditure (such as exercise) to both short- and long-term fasting. In addition, many other hormones (e.g., cortisol, growth hormones, catecholamines) are involved, butare not described here.

translocation of the glucose transporter(GLUT)-4, to the cell surface, whereas inthe brain, GLUT-1 is constitutively activeand not dependent upon insulin action. Insulin regulates glucose uptake, inhibitsglycogen breakdown and gluco neogenesis,whereas glucagon has the opposite effects.8Hence, absolute deficiency of insulin (as inType 1 DM), or relative (as in Type 2 DM),is associated with decreased clearance ofblood glucose from the body and leads tohyperglycemia (Figure 1).
Role of Insulin in the BodyInsulin is secreted by -cells of Islets of
Langerhans, an endocrine organ, present inthe pancreas. The pancreatic islet comprisesa group of cells, termed -, -, and -cells,surrounded by exocrine pancreas. Theseislets synthesize and release a number ofhormones, the classic ones being insulin andamylin from the -cell, glucagon from the!-cell, somatostatin from the -cell, as wellas a number of other bioactive polypeptides.Insulin is synthesized as a pro-hormone,transported to granules where it is processedby a pro-protein convertase, resulting in ma-ture insulin, C-peptide (by product of pro- insulin processing), and amylin.9,10 These arestored in these mature granules until releasedupon stimulation of the -cell. Insulin pro-duction usually exceeds the need, so the un-released granules are stored or destroyed inthe lysosomal compartment of the -cell.Glucose is the primary stimulant of insulinsecretion, and oxidative metabolism of glu-cose is required for glucose to stimulategranule exocytosis.11-15 A number of othersecretagogues, including hormones, gut pep-tides, and amino acids also have the abilityto provoke insulin secretion.
Insulin’s primary physiologic functionin the body can be described as anabolic, re-sulting in storage of fuels from ingested car-bo hydrate and fat and regulating catabolismof stored fuel. Its main target tissues are liver,
skeletal muscle, and adipose tissue and itsaction on these tissues (or lack thereof) is re-sponsible for the systemic effects of insulin.16
If insulin is the “Yin,” a group of hormonessuch as glucagon, cortisol, and growth hor-mone comprise the “Yang” to counteract andkeep the metabolism in balance for energyneeds. Under feeding conditions, with entryof nutrients, insulin increases and glucagondecreases, resulting in storage of the incom-ing nutrients. Under fasting conditions, in-sulin decreases, glucagon increases, resultingin increased lipolysis from fat to allow fattyacids to be transported to the liver and other tissues, and increased gluconeogenesis fromthe liver (and kidney) to maintain blood glu-cose, and some glycogenolysis. Under pro-longed starvation, fatty acids are metabo-lized to ketone bodies to supply the centralnervous system with fuel, in addition to theglucose.
Insulin exerts its action by binding to acell-surface receptor, the insulin receptor (IR),which has an extracellular and intracellulardomain.17 Intracellular domain possesses tyrosine-specific protein kinase activity,which activated by insulin binding, phospho-rylates several intra-cellular proteins, specif-ically insulin receptor substrates (IRS) -1, -2,-3, and -4 (Figure 2). These phosphorylatedIRSs lead to activation of multiple down-stream signaling pathways and ultimately toactivation of metabolic pathways, includingincreased uptake of glucose by muscle and fat,activation of glycogen synthesis, and sup-pression of gluco neogenesis by liver andlipolysis by fat.17 In addition to carbohydratemetabolism, insulin has several other actions.Its principle effect on adipose tissue is to sup-press lipolysis, increase uptake of fatty acids,and synthesize triglycerides, thus keepingcirculating free fatty acid levels in check.18,19
Elevated free fatty acids inhibit glucose uti-lization by peripheral tissues20 and also in-crease hepatic gluconeogenesis. Disorderedmetabolism of fatty acids has been proposed
58 Periodontal Disease and Overall Health: A Clinician's Guide
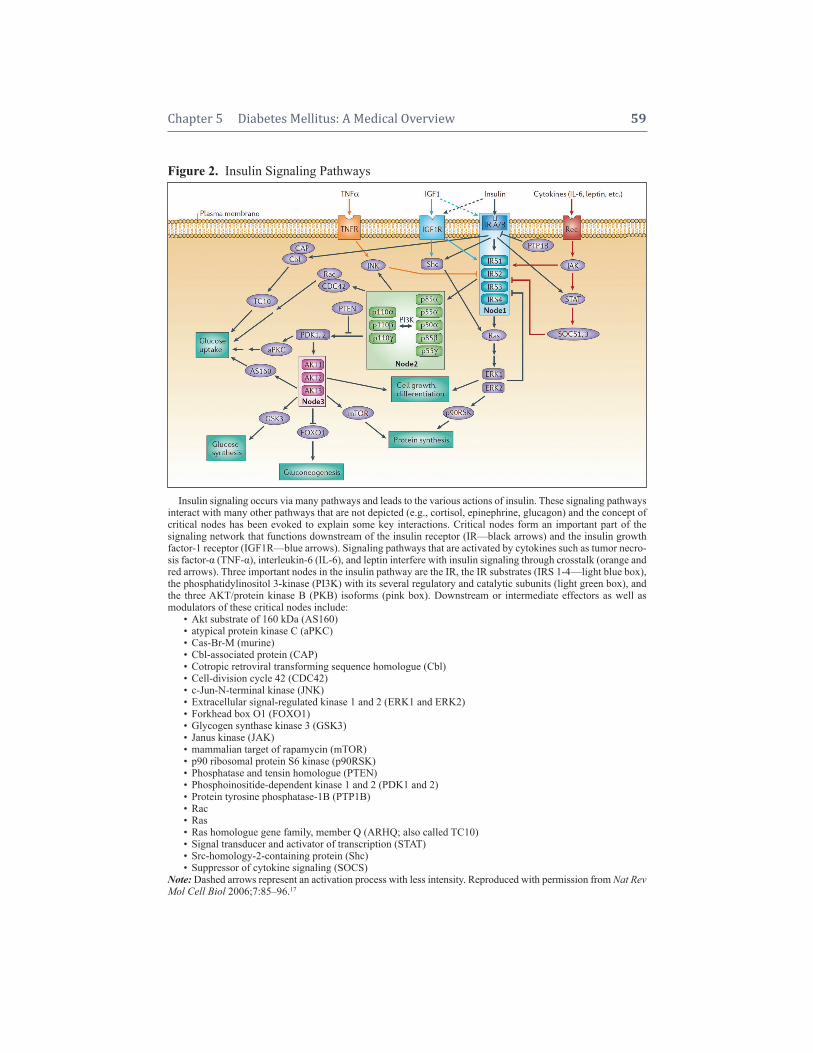
Chapter 5 Diabetes Mellitus: A Medical Overview 59
Figure 2.Insulin Signaling Pathways
Insulin signaling occurs via many pathways and leads to the various actions of insulin. These signaling pathwaysinteract with many other pathways that are not depicted (e.g., cortisol, epinephrine, glucagon) and the concept ofcritical nodes has been evoked to explain some key interactions. Critical nodes form an important part of the signaling network that functions downstream of the insulin receptor (IR—black arrows) and the insulin growth factor-1 receptor (IGF1R—blue arrows). Signaling pathways that are activated by cytokines such as tumor necro-sis factor- (TNF-), interleukin-6 (IL-6), and leptin interfere with insulin signaling through crosstalk (orange andred arrows). Three important nodes in the insulin pathway are the IR, the IR substrates (IRS 1-4—light blue box),the phosphatidylinositol 3-kinase (PI3K) with its several regulatory and catalytic subunits (light green box), andthe three AKT/protein kinase B (PKB) isoforms (pink box). Downstream or intermediate effectors as well as modulators of these critical nodes include:
• Akt substrate of 160 kDa (AS160)• atypical protein kinase C (aPKC)• Cas-Br-M (murine)• Cbl-associated protein (CAP)• Cotropic retroviral transforming sequence homo logue (Cbl)• Cell-division cycle 42 (CDC42)• c-Jun-N-terminal kinase (JNK)• Extracellular signal-regulated kinase 1 and 2 (ERK1 and ERK2)• Forkhead box O1 (FOXO1)• Glycogen synthase kinase 3 (GSK3)• Janus kinase (JAK)• mammalian target of rapamycin (mTOR)• p90 ribosomal protein S6 kinase (p90RSK)• Phosphatase and tensin homologue (PTEN)• Phosphoinositide-dependent kinase 1 and 2 (PDK1 and 2)• Protein tyrosine phosphatase-1B (PTP1B)• Rac• Ras• Ras homologue gene family, member Q (ARHQ; also called TC10)• Signal transducer and activator of transcription (STAT)• Src-homology-2-containing protein (Shc)• Suppressor of cytokine signaling (SOCS)
Note: Dashed arrows represent an activation process with less intensity. Reproduced with permission from Nat RevMol Cell Biol 2006;7:85–96.17

as having a major effect on pathophysiologyin diabetes.21 Insulin’s effect on adipose tis-sue appears to be as important as its effectson carbohydrate metabolism.
The development of DM thus involvesnot only pancreatic -islet cell dysfunc-tion/destruction, but also involves action ofinsulin in the periphery. Although attention isusually focused on insulin, it is important toacknowledge the role counter-regulatory hor-mones (the “Yang”) play to fully understandthe pathophysiology of DM.
Type 1 DMIn the majority of patients, Type 1 DM is
an autoimmune disorder with selective de-struction of the -cells in the pancreatic islets,resulting in absolute insulin deficiency.22-24
Autoantibodies are detected as epiphenomenonin 85%–90% of individuals in the beginningstages of the disease, but the immune dam-age is cell-mediated, involving CD4+ T cell dysfunction. Autoantibodies are directedagainst insulin, glutamic acid decarboxylase(GAD65), and tyrosine phosphatases. In afew patients, autoantibodies may have dissi-pated by the time of diagnosis, or an alternatepathway for destruction of pancreatic cellsis present. Although there are no good mark-ers to predict impending development ofType I DM, the presence of these auto -antibodies have been used to identify high-risk individuals.
Genetics of Type 1Type 1 DM develops in the background
of genetic susceptibility in the context ofpoorly defined environmental factors. Sus-ceptibility to Type 1 DM seems to be deter-mined by multiple genetic loci, and recent ad-vances in genome-wide scanning have begunto elucidate many of these genes.25,26 Althoughthe prevalence of Type 1 DM in Western pop-ulations is approximately 0.3%,27 it increasesto 6% if the father is affected and 3% if themother is affected.28 Although the risk of DM
is greater for the relatives of patients withType 1 DM, > 85% of people who developType 1 DM do not have a first-degree relativewith the disease.29 The risk for an identicaltwin is estimated to be 30%–50%, suggestinga strong environmental effect.30-33 These en-vironmental factors have not been identified.There is a robust association between Type 1DM and the major histocompatibility com-plex on chromosome 6, especially, with poly-morphisms in Class II immune responsegenes (HLA-DR and HLA-DQ).34,35 Specificalleles of both HLA-DR and HLA-DQ can either increase or decrease the risk of Type 1DM. The function of these HLA molecules isto present antigens to the immune cells,specifically T-lymphocytes, thereby sensitiz-ing them to auto-antigens. Patients with Type1 DM are also prone to other autoimmunediseases such as Hashimoto’s thyroiditis (hypo thyroidism), vitiligo (loss of skin pigmentation), Addison’s disease (cortisoland aldosterone deficiency), and perniciousanemia (vitamin B12 deficiency).36
Type 2 DMType 2 DM, also known as non-insulin
dependent DM or adult-onset DM, is associ-ated with impairments in both insulin action(insulin resistance) and insulin secretion.37
Insulin resistance requires elevated levels ofinsulin for glucose and lipid homeostasis; aperson can maintain normoglycemia as longas his or her pancreas can increase the pro-duction of insulin. However, in predisposedindividuals, over time the -cells are unableto increase insulin production to the levels re-quired to compensate for insulin resistance, acondition occasionally called “-cell exhaus-tion,” resulting in increasing hyperglycemiaand finally, diabetes.
Insulin ResistanceIt is likely that several processes, such as
elevations in free fatty acid levels, increases ininflammation of tissues, and rising counter-
60 Periodontal Disease and Overall Health: A Clinician's Guide

regulatory hormones lead to the developmentof insulin resistance.
Obesity can predispose a person to de-velop insulin resistance, and thereby Type 2DM, by causing insulin resistance via severalmechanisms, though many of these mecha-nisms remain to be elucidated.38 One of themechanisms attributed to increased insulinresistance in obesity was decreased insulinreceptor tyrosine kinase activity in the skele-tal muscle39 and possibly other tissues.40,41
Weight loss improves the activity of insulinreceptor tyrosine kinase.42 This and otherstudies provide evidence that insulin resist-ance does not always have to be geneticallydetermined, but can be acquired and reversedto some extent.43,44 Another hypothesis positsthat substances secreted by adipose tissuecause tissues to become insulin resistant.These substances include fatty acids, as wellas pro- and anti-inflammatory adipocyto kinessuch as leptin, tumor necrosis factor-(TNF-), adiponectin, etc.45 Some products,such as free fatty acids, may create a viciouscycle whereby insulin resistance increasesfree fatty acid levels, which in turn increaseinsulin resistance. A break in the cycle of pro-gressively increasing free fatty acids, either bydecrease in weight (thus reducing the insulinresistance) or by treatment with insulin or in-sulin sensitizer, may alleviate the degree of in-sulin resistance. At least some of the defectsrelated to obesity seem to be acquired andpartially reversible.46 Adipose tissue may alsosecrete factors that are beneficial for insulinsensitivity, such as adiponectin, and the fall intheir levels may be contributory.
Glucose toxicity results from chronicexposure of the pancreatic islet cells to sup-raphysiological concentrations of glucose inthe blood leading to cellular dysfunction.-cell toxicity, which is to some extent reversible, may become irreversible overtime.47 In addition, in animals, hyper-glycemia is also associated with insulin resistance by decreasing glucose transport
into the cells.48,49 Thus, high glucose con-centrations can cause secretory defects aswell as increase insulin resistance, but withtimely treatment, this could be reversible.
The relative secretory defect in Type 2DM is not associated with immune-medi-ated destruction of -cells, but amyloid de-posits in the islet that are associated with re-duction in islet cell mass.50-52 The proteincomponent of these deposits was found to bethe -cell secretory product amylin.53,54 How- ever, the mechanism for the initiation of amy-loid formation and deposition in the islets isnot yet clear. It may have both gene tic andenvironmental etiology.55 A number of typesof insulin secretory abnormalities have beendescribed in Type 2 DM, including the timing and intensity of response to glucosechallenge and other secretagogues.56-64
Genetics of Type 2Type 2 DM has a stronger genetic pre-
disposition than Type I DM,26,65 with super-imposed environmental influences.66-69 Sev-eral aspects of development of Type 2 DMare under genetic control, including intra-abdominal obesity, insulin resistance, andinsulin secretory defects.70-78 Studies onmonozygotic twins show an extremely highconcordance rate of close to 90%, which ismuch higher than that of Type 1 DM, sug-gesting higher heritability.79 Although envi-ronmental issues are also important, unlikeType 1 DM, more information about some ofthe environmental influences is available.These include increased centripetal obesity,development of hypertension and dyslipi-demia, and a sedentary lifestyle.
CLINICAL PRESENTATIONIn general, Type 1 DM patients present
in a more acute and dramatic fashion than doType 2 DM patients, which is usually moreinsidious in presentation. In both cases, thecommonest symptoms are polyuria (andnew-onset nocturia), polydypsia, and weight
Chapter 5 Diabetes Mellitus: A Medical Overview 61

loss. However, Type 2 DM is an insidiousdisease and may fester for years before a di-agnosis is made.
Type 1 DMType 1 DM, although commonly known
as juvenile diabetes, can occur at any age, buttypically presents around the age of puberty.There is a short prodromal phase with fatigue,weight loss, polyuria, and polydipsia. Inyoung children, new-onset bedwetting may bea presenting feature. If these symptoms gounrecognized, this could progress to ketoaci-dosis with tachypnea, tachycardia, hypoten-sion—a condition called diabetic ketoacido-sis (DKA)—and may lead to an altered mentalstate and coma. Frequently, an intercurrentillness or infection may be a trigger event.Because there is an absolute deficiency of in-sulin, the presentation is acute (days) andneeds urgent medical attention. In adults whohave autoimmune diseases, or have had dam-age (typically caused by alcohol) or surgery tothe pancreas gland, a diagnosis of diabetesshould be considered for failure to gainweight, or unexplained weight loss.
Type 2 DMType 2 DM has long been considered
an adult-onset disease, although increasingnumbers of children and young adults are be-ing diagnosed with this disease. The diseasecan evolve over several years and the naturalhistory may differ between patients. Manypatients with Type 2 DM are older than 40,overweight or obese, with an increased waistcircumference (a surrogate marker for vis-ceral fat accumulation).80 The presence ofmetabolic syndrome markers (e.g., increasedwaist-to-hip ratio, hypertension, low levelsof high-density lipoprotein [HDL] choles-terol, impaired fasting glucose) is stronglypredictive of development of Type 2 DM.81
Although insulin resistance is the primarycause for Type 2 DM, it is not sufficient tocause DM as long as the pancreas can secrete
enough insulin to compensate. Presentation isusually insidious and goes unrecognized foryears, since mild-to-moderate hyperglycemiamay not cause noticeable symptoms. How-ever, this mild hyperglycemia and associatedlipid and blood pressure abnormalities are notentirely benign as they increase the risk ofmacro- and microvascular complications; upto 20% of newly diagnosed Type 2 DM patients manifest signs of diabetic complica-tions. With worsening hyperglycemia, symp-toms of polyuria, weight loss, etc., may resultin the condition coming to light. It is not un-common for an intercurrent illness, such asstroke, myocardial infarction or infection, toalso uncover diabetes. Rarely, acute severehyperglycemia (over 1–2 days) can lead to ahyperosmolar, hyperglycemic, nonketoticstate (HHS), with altered mental state andcoma as an acute presenting feature. Hence,screening in high-risk individuals is essentialto minimize the risk of these complications.Presentation with ketoacidosis occurs rarelybut may appear in conjunction with other ill-nesses, such as acute myocardial infarction.Type 2 DM could be considered to evolve intwo stages; Stage 1 is development of impairedglucose tolerance or impaired fasting glucose(also called as prediabetes) and Stage 2 is thedevelopment of overt diabetes (Table 2).
Gestational DiabetesGDM is a form of DM that has its ini-
tial onset during the later stage of the secondtrimester of pregnancy and resolves at theend of pregnancy. As many as 4% of preg-nancies in the United States are complicatedby the development of GDM. During preg-nancy, GDM increases both fetal growth(macrosomia) as well as obstetric compli-cations. Although screening guidelines differamong various groups of physicians, mostagree that screening between 24 and 28weeks of pregnancy in women who are obese,have a first-degree relative with diabetes, areolder than 25, and come from a higher-risk
62 Periodontal Disease and Overall Health: A Clinician's Guide

ethnic group (Hispanic, African American,or Native American) should be undertaken.Many of the risk factors and the pathophysi-ological processes for GDM are similar tothose of Type 2 DM.82 With increase in in-sulin resistance during the pregnancy, womenwho are susceptible to develop Type 2 DM dueto a concomitant secretory defect may developType 2 DM. Although the risk of fetal devel-op mental abnormalities is higher in womenwho are diabetic before becoming pregnant,with GDM, the diabetes develops at the endof the second trimester, a time when organo-genesis has already been completed. Mostwomen revert to normal glucose tolerancepostpartum. Approximately 50% of patientswho have had GDM will have a recurrence infuture pregnancies, as well as a 30%–60% riskof developing established diabetes long term.83
GDM provides a unique opportunity to edu-cate women about the need for lifestylechanges (weight loss, exercise, and improveddiet) to prevent overt DM in the future.
Acute ComplicationsDKA and HHS are potentially fatal, but
largely preventable acute complications ofuntreated DM.84 DKA is most common in
patients with Type 1 DM, although it canoccur in patients with Type 2 DM as well;HHS is more common in patients with Type2 DM. Although these conditions are dis-cussed as separate entities, they are part ofthe same spectrum of diseases characterizedby inadequate insulin. DKA results whenthere is absolute insulin deficiency, whileHHS develops with relative insulin defi-ciency. However, they do differ in the degreeof dehydration, ketosis, and metabolic aci-dosis. For both disorders, precipitating fac-tors could be the same, including missed insulin doses, dehydration, infection, certainmedications, or other major illnesses.85,86
However, restricted water intake resultingfrom ill health or immobilization, com-pounded by altered thirst response, may contribute to dehydration and HHS in elderlypatients with Type 2 DM.
Diabetic KetoacidosisDKA is characterized by varying degrees
of hyperglycemia, ketonemia, and metabolicacidosis.87 When combined, these elementsgive rise to the clinical syndrome of DKA,which is associated with dehydration, elec-trolyte abnormalities, and altered sensorium.
Due to severe insulin deficiency, thereis unchecked gluconeogenesis, glycogenol-ysis, and decreased glucose utilization re-sulting in hyperglycemia.88 Gluconeogenesisis also fueled by increased availability ofamino acids that are a result of increased catabolism, again due to decreased insulin.Elevated blood glucose results in increasedplasma osmolality (hyperosmolar state) lev-els causing a shift of water from the intra-cellular space and intracellular dehydration.Increased plasma osmolality promotes os-motic diuresis, resulting in net loss of bodywater, thus initiating a vicious cycle of in-creased plasma osmolality and progressivedehydration. The progressive dehydration alsoleads to reduced tissue perfusion, hypoxia,and thus the generation of lactic acid, which
Chapter 5 Diabetes Mellitus: A Medical Overview 63
a Fasting defined as no caloric intake for 8 hours.b Oral glucose tolerance test involves measurement of
plasma glucose at specified time after consuming a glucose load of 75 or 100 g dissolved in water.
c Random plasma glucose defined as any time of the daywithout any temporal association to caloric intake.
d Symptoms of hyperglycemia include polyuria, poly -phagia, polydypsia, and unexplained weight loss.
Table 2. Diagnostic Criteria forTable 1. Diabetes Mellitus
Pre- OvertDiabetes Diabetes
Test Criteria Mellitus MellitusFasting plasma glucosea 100 mg/dL 126 mg/dLPlasma glucose post 140–199 mg/dL 2 hours: 75 g oral glucose 200 mg/dLtolerance testb
Random plasma glucosec — 200 mg/dLwith symptoms ofhyperglycemiad

will contribute to acidosis. Decreased bloodpH leads to reduced insulin action, setting upa vicious cycle. Osmotic diuresis also pro-motes loss of multiple minerals and elec-trolytes, including sodium, potassium, phos-phate, calcium, magnesium, and chloride,all of which need to be replaced.
Loss of insulin action results in an in-crease in lipolysis and free fatty acid pro-duction; these fatty acids are metabolized bythe liver into ketone bodies (acetone, ace-toacetate, and -hydroxy butyrate, a sourceof energy for the heart and brain used duringstarvation).89 Initially, the ketonemia may bemild as the body tries to metabolize thesefatty acids.90,91 As the acidosis from tissuehypoxia, with further reduced insulin actionoccurs, excessive numbers of ketone bodiesare produced. Acidosis promotes movementof potassium from intracellular to extracel-lular space, from where it can be excreted inurine along with osmotic diuresis, resultingin hypokalemia. Ketones may be detectedclinically in the breath, as these are volatile.Laboratory abnormalities helpful in makingthe diagnosis are hyperglycemia, an in -creased anion gap (indicative of acidosis), alow arterial blood pH(< 7.4 to as low as6.9), a low bicarbonate level, elevated lacticacid levels, and increased ketone bodies.Since ketone body production is part of anormal response to starvation, their detec-tion, per se, is not indicative of DKA.
In addition, DKA may be associatedwith increased levels of proinflammatory cyto kines and procoagulant factors. These,along with dehydration, create a fertileground for a prothrombotic state.92
Hyperglycemic, Hyperosmolar, Nonketotic State
This condition, HHS, is similar toDKA, but differs due to the presence of suf-ficient insulin to prevent lipolysis and thusacidosis is not a major factor. The levels ofinsulin required to inhibit lipolysis are much
lower than required to increase tissue up-take of glucose or inhibit gluconeogenesis.Since patients with Type 2 DM have thisresidual insulin, they are less likely to de-velop DKA but are prone to develop severehyperglycemia and dehydration.93 Other fac-tors such as diuretic use, febrile illness, di-arrhea, nausea, and vomiting can contributeto excessive volume losses. Mortality fromHHS is higher in the presence of older age,comorbid conditions, and the severity of de-hydration. While DKA begins rapidly withina few hours of precipitating events, HHScan be insidious in onset and may not be ap-parent until it is very severe.
Laboratory abnormalities include a significant hyperglycemia (typically > 500mg/dL), but no significant alteration in bloodpH, increased blood osmolality, and eithernormo- or hypernatremia. Hypokalemia maybe less severe and the goals of therapy inthese patients are to restore circulatory vol-ume and tissue perfusion, gradually reduceserum glucose (as rapid reduction may resultin cerebral edema), and correction of elec-trolyte abnormalities. Precipitating causessuch as infection should be identified andtreated. Intravenous fluids and insulin infu-sion are the mainstay of treatment, alongwith frequent monitoring of clinical and laboratory parameters and adjustment oftreatment.
COMPLICATIONS OFDIABETES MELLITUS
Diabetes is a true metabolic disease andcan affect many organ systems over thecourse of the disease. The following com-plications are responsible for considerablemorbidity and mortality. These conditionscan be divided into microvascular, macro -vascular, and nonvascular and are summa-rized in Table 3. The risk of these complicationsincreases as a function of hyper glycemia andduration of DM, and are usually first seen tenyears after diagnosis.
64 Periodontal Disease and Overall Health: A Clinician's Guide
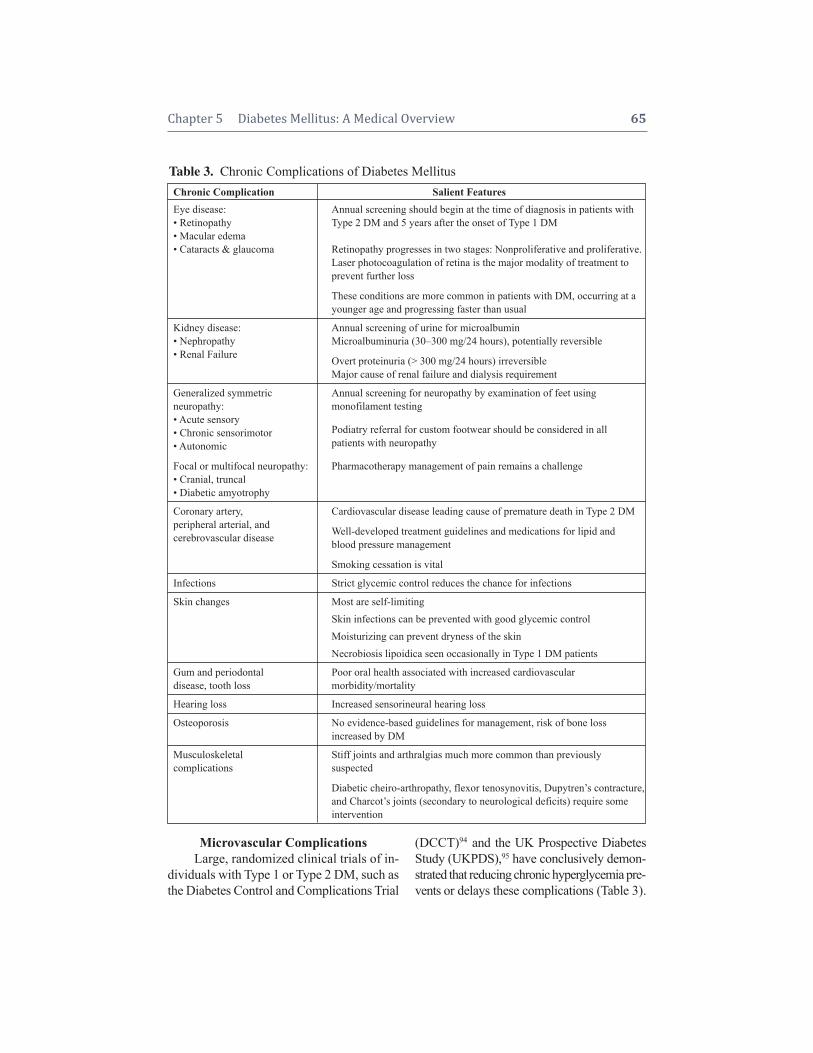
Microvascular ComplicationsLarge, randomized clinical trials of in -
di vid uals with Type 1 or Type 2 DM, such asthe Diabetes Control and Complications Trial
(DCCT)94 and the UK Prospective DiabetesStudy (UKPDS),95 have conclu sively demon-strated that reducing chronic hyperglycemia pre- vents or delays these complications (Table 3).
Chapter 5 Diabetes Mellitus: A Medical Overview 65
Table 3. Chronic Complications of Diabetes MellitusChronic Complication Salient FeaturesEye disease: Annual screening should begin at the time of diagnosis in patients with• Retinopathy Type 2 DM and 5 years after the onset of Type 1 DM• Macular edema• Cataracts & glaucoma Retinopathy progresses in two stages: Nonproliferative and proliferative.
Laser photocoagulation of retina is the major modality of treatment to prevent further loss
These conditions are more common in patients with DM, occurring at a younger age and progressing faster than usual
Kidney disease: Annual screening of urine for microalbumin• Nephropathy Microalbuminuria (30–300 mg/24 hours), potentially reversible• Renal Failure Overt proteinuria (> 300 mg/24 hours) irreversible
Major cause of renal failure and dialysis requirement
Generalized symmetric Annual screening for neuropathy by examination of feet usingneuropathy: monofilament testing• Acute sensory• Chronic sensorimotor Podiatry referral for custom footwear should be considered in all• Autonomic patients with neuropathy
Focal or multifocal neuropathy: Pharmacotherapy management of pain remains a challenge• Cranial, truncal• Diabetic amyotrophy
Coronary artery, Cardiovascular disease leading cause of premature death in Type 2 DMperipheral arterial, and cerebrovascular disease Well-developed treatment guidelines and medications for lipid and
blood pressure management
Smoking cessation is vital
Infections Strict glycemic control reduces the chance for infections
Skin changes Most are self-limitingSkin infections can be prevented with good glycemic controlMoisturizing can prevent dryness of the skinNecrobiosis lipoidica seen occasionally in Type 1 DM patients
Gum and periodontal Poor oral health associated with increased cardiovasculardisease, tooth loss morbidity/mortality
Hearing loss Increased sensorineural hearing loss
Osteoporosis No evidence-based guidelines for management, risk of bone lossincreased by DM
Musculoskeletal Stiff joints and arthralgias much more common than previouslycomplications suspected
Diabetic cheiro-arthropathy, flexor tenosynovitis, Dupytren’s contracture,and Charcot’s joints (secondary to neurological deficits) require someintervention

It must be noted that not all individuals withpoor glycemic control develop these com-plications, suggesting that other factors, suchas genetics or environment, may modulatetheir development.
Ophthalmic ComplicationsDiabetic retinopathy is the leading
cause of blindness in individuals betweenthe ages of 20 and 74. Nonproliferativeretinopathy is characterized by retinal vas-cular microaneurysms, blot hemorrhages, in-traretinal microvascular abnormalities withincreased retinal vascular permeability, andalterations in retinal blood flow, all of whichlead to retinal ischemia. It is present in al-most all individuals who have had DM formore than 20 years. Neovascularization inresponse to retinal hypoxia is characteristicof proliferative retinopathy. These newlyformed blood vessels lack sufficient integ -rity, rupture easily, resulting in intra-vitreoushemorrhage, and subsequently lead to fibro-sis and retinal detachment.
Intensive glucose control from the timeof DM diagnosis is necessary for the pre-vention of onset and progression of retinopa-thy. An annual exam for early detection andlaser photocoagulation (panretinal or focal)can delay or prevent blindness.
Renal ComplicationsDM is the most common cause of renal
failure in United States. The earliest patho-logical changes alter microcirculation, caus-ing structural changes in the glomerular ma-trix, thereby increasing glomerular filtrationrate (GFR). This increases excretion of smallamounts of albumin in the urine (microal-buminuria 30–300 mg/day). Approximately50% of these individuals will progress toovert proteinuria (300 mg to 1 g/day) ornephrotic syndrome (urine protein > 1 g/day).Urinary protein excretion is considerably exacerbated by uncontrolled hypertension,and the combination of diabetes and hyper-
tension is the most frequent predisposingfactor for endstage renal disease.
In addition to nephropathy, Type IV renal tubular acidosis (and resulting hyper-kalemia) and predisposition to radiocontrast-induced nephrotoxicity are also seen in pa-tients with DM. Intensive control of bloodglucose, dyslipidemia, and blood pressure isrecommended to prevent the onset of micro -albuminuria and to prevent progression toovert proteinuria or renal failure.
Neurological ComplicationsApproximately half of patients with
Type 1 or Type 2 DM will develop neurop -athy. It is usually a symmetrical sensory poly -neuropathy but may also be a focal mono -neuropathy and/or an autonomic neuropathy,with loss of both myelinated and unmyeli-nated nerve fibers. Up to 50% of individualswith neuropathy may not be symptomatic.96
Generalized symmetrical polyneuropa-thy is the most common manifestation andcan involve sensorimotor somatic nerves;however, distal nerves of hands and feet aremost commonly affected in a “glove-and-stocking” distribution. Symptoms includepain, tingling, and numbness, and physicalexam reveals loss of fine touch, vibration,and position sense. This may later progressto wasting of small muscles of the hands andfeet, resulting in Charcot’s joints and sensoryataxia. Mononeuropathy is associated withpain and weakness in one nerve distributionthat is self-limiting. Diabetic amyotrophy,seen mainly in elderly Type 2 patients, is associated with pain in the lower limbs followed by muscle weakness in major mus-cles of the buttocks and thighs. It is a self-limiting condition, resolves in 12 to 24months, and treatment is supportive. Auto-nomic neuropathy, though not well diag-nosed, can affect all the major organ sys-tems. Multiple cardiovascular abnormalitiesare noted, including resting tachycardia, di-minished heart rate variability, reduced heart
66 Periodontal Disease and Overall Health: A Clinician's Guide

rate and blood pressure response to exercise,and development of postural hypotension.The typical pain response to cardiac is-chemia is lost, leading to “silent myocardialischemia/infarction.” Altered small- andlarge-bowel motility (constipation or diar-rhea) and gastroparesis (anorexia, nausea,vomiting, and bloating) are frequent mani-festations of gastrointestinal system involve -ment. Genitourinary systems are also in-volved and present with bladder hypotonia(incomplete emptying, dribbling, and over-flow incontinence), erectile dysfunction, andfemale sexual dysfunction. Abnormal sweatproduction may result in xerosis, cracking ofskin, and decreased sweating in response tohypoglycemia. In addition, entrapment syn-dromes (e.g., carpal tunnel syndrome) arealso common among diabetics.
Tight glycemic control from the time ofonset of DM is necessary to prevent diabeticneuropathy. Treatment is difficult once neu-ropathy affects various organ systems. Forsymptomatic treatment of painful neuropa-thy, several therapies have been tried withlimited efficacy and include tricyclic antide-pressants, anticonvulsants, selective sero-tonin and norepinephrine reuptake inhibitors,and topical therapies. Treatment for organ-specific complications of autonomic neu-ropathy is symptomatic.
Macrovascular ComplicationsAssociation of macrovascular compli-
cations with hyperglycemia is less conclu-sive and appears to be related more to co -existing conditions such as dyslipidemia andhypertension.
Cardiovascular disease risk is increasedin individuals with Type 2 DM by two-foldand four-fold in women. It is unclear if pa-tients with Type 1 DM are also at high riskof cardiovascular complications. The pres-ence of Type 2 DM is now counted by theAmerican Heart Association and the Ameri-can Diabetes Association as a major cardio-
vascular risk factor, the equivalent of havinghad a cardiovascular event in the absence ofdiabetes. Additionally, some patients withDM may suffer silent myocardial ischemiaor infarction, which often does not manifestitself by chest pain or other symptoms thatare typical of coronary artery disease. Thepresence of insulin resistance is associatedwith an increased risk of cardiovascularcomplications in individuals both with andwithout DM. Individuals with insulin resist-ance and Type 2 DM have elevated levels ofplasminogen activator and fibrinogen, whichenhance the coagulation process and impairfibrinolysis, thus favoring the developmentof thrombosis. Cardiovascular risk is in-creased when either retinopathy, nephropa-thy, hypertension, or dyslipidemia coexistwith DM.
Dyslipidemia frequently coexists withDM, especially Type 2 DM, with a typicalpattern of increased triglycerides, decreasedHDL cholesterol, and increased small-denselow-density lipoprotein (LDL) cholesterolparticles. The goals of therapy are to reduceLDL cholesterol to < 100 mg/dL and triglyc-erides to < 150 mg/dL.
Hypertension is frequently associatedwith DM and can hasten the onset of com-plications, especially for cardiovascular dis-ease and nephropathy. Management includesaggressive control of blood pressure and mayrequire multiple medications.
As a preventive measure, aspirin shouldbe prescribed for all Type 2 DM patients,unless contraindicated.
Miscellaneous ComplicationsElaborated below are several other
complications of DM.
InfectionsDM is associated with greater fre-
quency and severity of common infections;in addition, some infections are seen exclu-sively in patients with DM. Hyperglycemia
Chapter 5 Diabetes Mellitus: A Medical Overview 67

results in impaired white blood cell functionand enhances the colonization and growth ofvarious bacterial and fungal species. Bacterialinfections such as styes, boils, and carbun-cles are most common. Frequently seen fun-gal infections include intertrigo caused byCandida albicans, and ringworm infections.
Dermatologic ManifestationsDermatologic problems are common in
diabetes, with approximately 30% of patientsexperiencing some cutaneous involvementduring the course of illness. Several skinconditions are more common among patientswith DM, including bacterial infections, fun-gal infections, and itching, but these are notexclusive to patients with DM. Skin mani-festations generally appear during the courseof the disease in patients known to have diabetes but they may also be the first presenting sign of diabetes; they may evenprecede DM diagnosis by several years.97
Some conditions occur exclusively inpatients with DM. Diabetic dermopathy is anasymptomatic, benign condition that arisesdue to small vessel changes and presentsas oval or circular pigmented and scalypatches on the legs. Necrobiosis lipoidica diabeticorum is another disease caused bychanges in blood vessels. This rare disorderbegins in the pretibial region as painful ery-thematous papules that enlarge into glossyplaques with irregular borders and atrophiccenters. These patches are deeper than der-mopathy, can be itchy and painful, and canulcerate. There are no proven treatments, butocclusive steroid dressings have been used toprevent ulceration and breakdown of the skin.Bullous diabeticorum is a condition in whichblisters can occur on the backs of hands andfeet, and are self-limiting. A third of peoplewho have Type 1 DM can develop tight,thick, and waxy skin on the backs of theirhands, known as digital sclerosis. No spe-cific treatment exists for this condition otherthan to achieve adequate glycemic control.
Fungal skin infections, as well as vitiligo,etc., occur more frequently in patients withdiabetes.97
Complications Related to BonesOsteoporosis is the most underappre-
ciated complication of DM.98 The associationof osteoporosis and fracture risk with Type 1DM is relatively noncontroversial.99 For sub-jects with Type 2 DM, general bone densityseems to be preserved. However, there is anincreased risk of fracture that has been at-tributed to several causes, including falls fol-lowing hypoglycemia, poor balance due todiabetic neuropathy, foot ulcers and ampu-tations, poor vision due to cataracts andretinopathy, and orthostatic hypotension.
Periodontal DiseaseOral health is now increasingly recog-
nized as an important part of diabetes man-agement; there is a mutually reciprocal rela-tionship between glycemic control and oralhealth. Periodontal infection worsens meta-bolic control of DM while improving oralhygiene enhances glycemic control.100,101
People with poorly controlled DM are morelikely to develop periodontal disease, drymouth, dental abscess and fungal infections,and slow wound healing.102
The Diabetic FootThe key causes of diabetic foot prob-
lems are neuropathy, vasculopathy, or both,usually on a background of poor glycemiccontrol. Other factors that exacerbate thisare hypertension and smoking. Approxi-mately 15% of diabetic patients may experi-ence foot ulceration in their lifetime. In addition, foot deformities from muscleweakness and visual defects add to the pre-disposing factors for foot injury. Preventivecare is essential and should include not onlyprofessional care (Table 4), but also care bythe individual on a day-to-day basis. Dailyinspection of the feet and wearing clean, soft
68 Periodontal Disease and Overall Health: A Clinician's Guide

socks and properly fitting shoes are amongmany precautions one could take to preventfoot ulceration. Once the ulcer is formed,antibiotics, relief of pressure to the ulcer-ated area, control of blood glucose, and efforts to improve blood flow form the main-stay of treatment.
At present, there is no unifying mech-anism to account for the pathogenesis of di-abetic complications. It seems likely thatseveral different mechanisms are involved.
DIAGNOSIS OFDIABETES MELLITUS
Criteria for diagnosis of DM are basedon plasma glucose levels and symptomatol-ogy. The threshold values for plasma glu-cose were not chosen arbitrarily, but due totheir ability to predict retinopathy.103,104 Thediagnosis of diabetes is met if fasting plasmaglucose level is > 126 mg/dL, 2-hour post-oral glucose tolerance test is 200 mg/dL, orrandom blood glucose is > 200mg/dL withclinical symptoms in an otherwise stable
subject. Although these cutoff values are use-ful for clinical management, it should bepointed out that there is a continuous pro-gression in the level of glucose from nor-mal to impaired glucose to diabetes. Sub-jects with impaired glucose levels have beenshown to have increased cardiovascular risk,thus these biochemical definitions are likelyto undergo revision in the future.
MANAGEMENT OFDIABETES MELLITUS
The goals of managing DM should beto achieve near-normal glucose homeostasis,prevent progression of the disease, and avoidlong-term complications. Treatment goalsare listed in Table 4 and require a multidis-ciplinary approach.
Diabetes EducationEvery patient with DM should be
taught diabetes self-management skills. Education needs to include teaching gooddietary habits and nutrition, weight loss and
Chapter 5 Diabetes Mellitus: A Medical Overview 69
Table 4. Comprehensive Principles for Preventing DM ComplicationsLifestyle changes:• Diet: Sugar-free diet for Type 2 DM; no restrictions for Type 1 DM
Fat 20%–35% of total calorie intake; saturated fat < 7% of calories, < 200 mg/dL dietary cholesterol• Exercise: At least 150 minutes/week of aerobic physical activity• Optimum weight (BMI < 25)• Smoking cessationModifiable risk factors:• Glycemic control:
Glycosylated hemoglobin—measured at least twice a year (HbA1c < 7%) Self-monitoring of blood glucose (SMBG)—no recommended optimal frequency, but probably should be
measured 3–4 times a day in patients who are insulin-treated (pre-prandial plasma glucose 90–130mg/dL, 2-hour postprandia plasma glucose of < 180 mg/dL)
• Lipid management (LDL < 100mg/dL, optimal goal < 70mg/dL; HDL > 45mg/dL in men and > 55 mg/dLin women; triglycerides < 150mg/dL)
• Blood pressure control (< 130/80 mmHg; < 125/75 mmHg preferred in those with nephropathy)• Aspirin prophylaxis (primary prevention in diabetics over the age of 40)
Preventive care:• Annual screening
Screening for microalbuminuria Annual eye exam Podiatric exam
• Annual influenza vaccination• Pneumococcal vaccination

exercise, self-monitoring of blood glucose(SMBG), awareness of acute and chroniccomplications and how to prevent them,treatment options, and insulin administra-tion (if applicable). Patients also need to betaught to recognize and treat hypoglycemiaand modify lifestyle choices, such as smok-ing cessation.
Lifestyle ModificationMedical nutrition therapy (MNT) and
exercise are central components to the man-agement of DM. Patient education regardingthese aspects should be continuous and re-inforced at every healthcare visit. Althoughthe role of diet in managing Type 1 DM isnot as critical as it is for Type 2 DM, atten-tion to calorie intake and a heart-healthy dietis still important.
MNT is important to prevent onset ofType 2 DM by promoting healthy eatinghabits and weight loss in those with obesityand prediabetes (primary prevention), man-aging existing Type 1 and Type 2 DM (sec-ondary prevention), and preventing compli-cations of DM (tertiary prevention). Goals ofMNT should be individualized, and dietsshould be balanced with respect to fat, protein,and carbohydrate content, and should includefruits, vegetables, and fiber. For Type 2 DMpatients, avoidance of dietary sugar is manda-tory, whereas for Type 1, this needs to be tem-pered as well as matched with insulin deliv-ery. Monitoring carbohydrate intake, throughcarbohydrate counting or food exchanges, isessential for achieving glycemic control. Mixedmeals (those with protein/carbohydrate/fatcombination) decrease postprandial excursionof blood glucoses; low-glycemic index foods(associated with lower postprandial rise inblood glucoses) may improve glycemic con-trol. Patients who are on insulin should learnto estimate carbohydrates in their diet andmatch insulin dose to carbohydrates.
In overweight and obese individuals,even modest weight loss of 5%–10% is
associated with improvement in insulin re-sistance, and will prevent development of DMin individuals with prediabetes or improvetreatment requirements in those who alreadyhave DM. Increase in physical activity isalso an essential component, especially tomaintain the weight loss achieved by dietarymodification. Weight loss medications maybe considered as these can help achieveweight loss of 5%–10% as recommended,but the effects may be short-lived, especiallyif lifestyle changes are not implemented. Exercise is essential to maintain weight loss,improve physical fitness, and reduce plasmaglucose concentrations. Bariatric surgery isgrowing as a choice and has some scientificsupport for efficacy.105 Older diabetics start-ing a new exercise program may need to havemedical clearance due to a high prevalenceof asymptomatic cardiovascular disease.
Certain dietary restrictions may be nec -essary once complications set in (e.g., limit-ing protein intake to 0.8 g/kg of body weightper day may be essential in patients with overtdiabetic nephropathy with proteinuria).
Monitoring the Levelof Glycemic Control
Long-term assessment (every threemonths) of glycemic control is made bymeasuring levels of glycosylated hemoglobin(HbA1c) in a clinical setting. Blood glucoseleads to a nonenzymatic glycosylation of hemoglobin. There is a relationship betweenHbA1c and average blood glucose levels thatallows for the overall level of glycemic con-trol to be assessed clinically. Since the meanerythrocyte (and its hemoglobin) life span is120 days, HbA1c levels are taken to representthe mean glycemic control over the past threemonths. In general, target HbA1c should be< 7% (mean blood glucose of ~150 mg/dL),but it may be individualized with both lowerand higher goals being acceptable in somepatients. SMBG with the help of glucometers(long the standard of care for Type 1 DM
70 Periodontal Disease and Overall Health: A Clinician's Guide

patients) is important when insulin is usedas daily treatment to help with insulin dosingand to prevent hypoglycemia. Continuousglucose monitoring systems are a new methodthat can be used to monitor glycemic control.These systems measure glucose in intersti-tial fluid that is in equilibrium with blood glucose.
Pharmacologic TreatmentInsulin is the required treatment for
Type 1 DM (oral agents are not indicatedfor Type 1 DM), whereas patients with Type2 DM can be managed with diet alone ormay require oral hypoglycemic agents and/orinsulin. For the latter, multiple-agent use iscommon and includes pharmacotherapy forcardiovascular risk factor management. Oralagents, summarized in Table 5, can work tostimulate -cells to secrete insulin (sulfo -nylureas, miglinitides); sensitize response toinsulin (thiazolidinediones, biguanides); in-hibit intestinal glucose absorption (alpha-glucosidase inhibitors); or improve incretinfunction that results in increased insulin anddecreased glucagon secretion (gliptins or incretin-mimetics). These agents and theirmajor effects can have other benefits as dis-cussed below. For insulin therapy, there arenow many types of insulins that allow dif-fering onset, peak, and duration-of-actiontimes as well as delivery systems. All ofthe insulins used currently are synthetic with animal-derived insulins being rarely used.
Oral Antidiabetic AgentsSulfonylureas: These time-honored
drugs have been available since the 1950s,and although some older-generation agents(e.g., glyburide) continue to be used, themore common first-line agents are glipizideand glimepiride. Unlike glyburide, which isexcreted primarily via the kidneys, glipizideand glimepiride are metabolized in the liverand are safer for patients with deterioratingrenal function. The sulfonylureas, dosed
once or twice a day, result in increased insulinsecretion from -cells by binding to the sulfonylurea receptor. The major side effectof these agents is hypoglycemia, especiallywhen used in combination with other agents,or if there is extant renal or liver disease.These agents (along with metformin, see below) are the most frequently prescribedagents for Type 2 DM and are now generic.
Miglitinides: These agents (repaglin-ide, nateglinide) also stimulate the sulfo -nylurea receptor, but have very differentpharmacokinetics; they bind, stimulate, andhave a very short action time, allowing theseagents to be used as “real-time” agents.These drugs are particularly useful in theelderly or in subjects for whom inconsistenteating patterns are an issue.
Insulin Sensitizers: These drugs actby improving the action of insulin on targettissues (e.g., liver, skeletal muscle, adiposetissues). This group includes the biguanidemetformin (the action of which is to inhibithepatic gluconeogenesis, along with im-proving skeletal muscle uptake of glucose)as well as the thiazolidinediones pioglita-zone and rosiglitazone (which act primarilyon adipose and skeletal muscle to improveinsulin action). Metformin is one of the mostcommonly used oral agents because it pro-motes weight loss or weight maintenance(an issue for most Type 2 DM patients).However, the major side effect of GI upset(pain and/or diarrhea) can limit its use. Ad-ditionally, a potential side effect is lactic aci-dosis, an effect that can occur in the contextof significant major organ (kidney, liver orheart) failure. These adverse effects, how-ever, are almost negligible when metforminis used per prescribing guidelines. Becausemetformin is excreted via the kidneys, it isnot used in subjects with renal impairment.Its use is suspended when intravenous- contrast agents need to be used for radio-logic purposes as contrast nephropathy canresult.
Chapter 5 Diabetes Mellitus: A Medical Overview 71
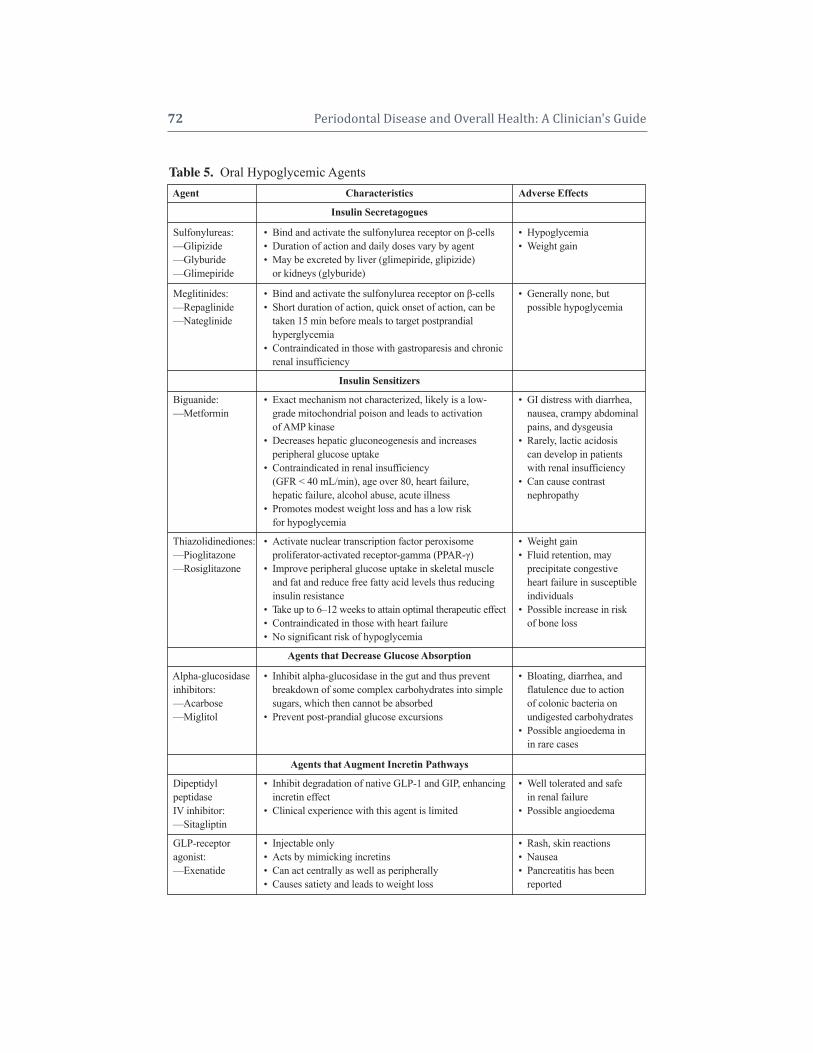
72 Periodontal Disease and Overall Health: A Clinician's Guide
Table 5. Oral Hypoglycemic AgentsAgent Characteristics Adverse Effects
Insulin Secretagogues
Sulfonylureas: • Bind and activate the sulfonylurea receptor on -cells • Hypoglycemia —Glipizide • Duration of action and daily doses vary by agent • Weight gain—Glyburide • May be excreted by liver (glimepiride, glipizide) —Glimepiride • or kidneys (glyburide)
Meglitinides: • Bind and activate the sulfonylurea receptor on -cells • Generally none, but—Repaglinide • Short duration of action, quick onset of action, can be • possible hypoglycemia —Nateglinide • taken 15 min before meals to target postprandial
• hyperglycemia• Contraindicated in those with gastroparesis and chronic • renal insufficiency
Insulin Sensitizers
Biguanide: • Exact mechanism not characterized, likely is a low- • GI distress with diarrhea,—Metformin • grade mitochondrial poison and leads to activation • nausea, crampy abdominal
• of AMP kinase • pains, and dysgeusia• Decreases hepatic gluconeogenesis and increases • Rarely, lactic acidosis• peripheral glucose uptake• • can develop in patients• Contraindicated in renal insufficiency • with renal insufficiency• • (GFR < 40 mL/min), age over 80, heart failure, • Can cause contrast• hepatic failure, alcohol abuse, acute illness • nephropathy• Promotes modest weight loss and has a low risk• for hypoglycemia
Thiazolidinediones: • Activate nuclear transcription factor peroxisome • Weight gain—Pioglitazone • proliferator-activated receptor-gamma (PPAR-) • Fluid retention, may—Rosiglitazone • Improve peripheral glucose uptake in skeletal muscle • precipitate congestive
• and fat and reduce free fatty acid levels thus reducing • heart failure in susceptible• insulin resistance • individuals• Take up to 6–12 weeks to attain optimal therapeutic effect • Possible increase in risk• Contraindicated in those with heart failure • of bone loss• No significant risk of hypoglycemia
Agents that Decrease Glucose Absorption
Alpha-glucosidase • Inhibit alpha-glucosidase in the gut and thus prevent • Bloating, diarrhea, and inhibitors: • breakdown of some complex carbohydrates into simple • flatulence due to action—Acarbose • sugars, which then cannot be absorbed • of colonic bacteria on —Miglitol • Prevent post-prandial glucose excursions • undigested carbohydrates
• Possible angioedema in• in rare cases
Agents that Augment Incretin Pathways
Dipeptidyl • Inhibit degradation of native GLP-1 and GIP, enhancing • Well tolerated and safepeptidase • incretin effect • in renal failureIV inhibitor: • Clinical experience with this agent is limited • Possible angioedema—Sitagliptin
GLP-receptor • Injectable only • Rash, skin reactionsagonist: • Acts by mimicking incretins • Nausea—Exenatide • Can act centrally as well as peripherally • Pancreatitis has been
• Causes satiety and leads to weight loss • reported•

Thiazolidinediones act in adipose andmuscle tissues to sensitize the action of in-sulin. Like metformin, these agents havebeen shown to delay and/or prevent the on-set of diabetes when used in prediabetic sub-jects in clinical trials (thiazolidinediones arenot indicated for this use). The main side ef-fect of these agents is weight gain (due tofluid retention as well as adipose tissue in-crease), and they have been associated withpotential bone loss, limiting widespread use.However, in subjects with considerable in-sulin resistance, they are particularly usefulin limiting the need for insulin therapy.
Alpha-Glucosidase Inhibitors: Theseact by decreasing glucose absorption fromthe intestine. Major side effects include in-testinal upset (e.g., diarrhea and flatulence);high cost also limits their use.
Incretins and Incretin-Mimetics: In-cretins are hormones that upon dietary chal-lenge, amplify glucose-stimulated insulin secretion, decrease glucagon action, and mayimprove islet cell health (the latter has beendemonstrated only in animal models).106
There are two known incretins; glucagon-like-peptide-1 (GLP-1) and gastric- inhibitory-peptide (GIP). Incretins are produced inintestinal L cells (GLP-1) or K cells. In re- sponse to nutrients, these stimulate insulinsecretion in a glucose-dependent fashion,thereby inhibiting glucagon secretion, slow-ing gastric emptying, reducing appetite, andimproving satiety. They act by binding totheir cognate receptors and are inactivatedin the blood stream by dipeptidyl peptidaseIV (DPP-IV). One FDA-approved inhibitorto DDP-IV activity is the drug sitagliptin;others (e.g., vildagliptin, alogliptin) are likelyto be approved in the near future. Becausethe mechanism of action is related, oneinjectable agent, exenatide, is discussed herebecause it also uses the incretin pathway.This drug was identified as the active ingre-dient that causes hypoglycemia in the salivaof the Gila monster. Exenatide binds and
activates the GLP-1 receptor in the hypo-thalamus to suppress feeding and increasesatiety, in addition to action in the periphery.Sitagliptin is generally well tolerated but hasnot been on the market long enough to con-clude it is generally safe. Exenatide is alsogenerally well tolerated; nausea, vomiting,and diarrhea are common but may be transi-tory with continued use. Rarely, pancreatitishas been reported with exenatide.
Combination Therapy: It is common(often necessary) to use combination therapyin the management of Type 2 DM. Usingcombination therapy is predicated on ensur-ing that each of the components acts in adifferent pathway, thereby ensuring syner-gism of action. The most common combi -nations are a sulfonylurea agent and an insulin sensitizer, but triple therapies witha sulfonylurea, insulin sensitizer, and DDP-IV inhibitor are used. Metformin and thiazolidinediones can be used together asthey target different tissues to improve in-sulin sensitivity and act via different path-ways. With all combination therapies, therisk of hypoglycemia is increased and mayrequire appropriate dose titration. In gen-eral, once insulin therapy is initiated, mostoral agents, except for insulin sensitizers,are discontinued.
Insulin TherapyFor Type 1 DM patients, insulin is the
mainstay and in the majority of patients, frequent multiple dosing (basal and bolus) iscommon. Insulin should also be consideredas the initial therapy in certain individualswith Type 2 DM, such as those with renal orhepatic disease, and any acute illness; it canalso be used as the sole therapy for Type 2DM patients. Many patients with Type 2 DMwill need insulin as the disease progressesand the oral hypoglycemic agents fail toachieve good control of blood sugars. Al-though early insulins were extracted frombovine or ovine pancreata, all of the currently
Chapter 5 Diabetes Mellitus: A Medical Overview 73

used insulins are recombinant and rangefrom generic regular and isophane (NPH), tothe more expensive analogs (Table 6). Eachof these insulins has a relatively predictableonset, peak, and duration of action. Thechoice of insulin and method of administra-tion is based on patient characteristics, costs,and health insurance. The type and regimenused is individualized to control blood sugarand minimize hypoglycemia. No currentlyavailable insulin regimen can mimic the waythe endogenous pancreas releases insulin. A favored regimen is a basal insulin, supple-mented with bolus insulin, to cover meals.The newer long-acting insulins, such asonce-daily administered glargine and de-temir, allow for a basal profile, though NPHgiven twice a day can also accomplish thistask. Mealtime insulins are given with eachmeal and typically use the newer analogs(aspart, lispro or glulisine), which are fast-acting and have a short duration of action(< 3 hrs), but regular insulin can also beused. Insulins are self-administered with a
calibrated syringe and ultra-fine needles, al-though devices, such as a pen or continuouspump are available. Continuous subcuta-neous insulin infusion (also known as in-sulin pump therapy) delivers insulin througha tiny, soft tube attached to a cannula that isimplanted under the skin through a needlestick (infusion set). The tubing on the otherend is connected to an external device con-taining a computer chip, an insulin reservoirthat can hold up to 300 units of rapid-actinginsulin, and a pumping system. The infusionset needs to be changed once every threedays. This system is probably the closest ofall available technologies to mimicking thesecretion of insulin by the pancreas. The rateof infusion can be set automatically for several segments throughout the day, andthe pump can be programmed for multiplebasal rates during the 24-hour cycle, basedon exercise and activity level. The pump isan open-loop system, requiring the pump-wearer to decide how much basal or bolusdose to be given. In addition to eliminating
74 Periodontal Disease and Overall Health: A Clinician's Guide
Table 6. Different Types of Insulin and Their ProfilesType of Insulin Characteristics Action in HoursRapid-acting insulin: • Analog insulins Onset of action: < 1 hr —Lispro • Altered amino acid sequence promotes insulin Peak action: 1–2 hrs—Aspart • monomers that are rapidly absorbed Duration of action: 2–3 hrs—Glulisine • Injected shortly before meals
• Shorter duration of action results in fewer• hypoglycemic episodes
Short-acting insulin: • Soluble human insulin, generic Onset of action: 0.50–1 hr—Regular • Injected 30–60 minutes before meals for optimal action, Peak action: 2–4 hrs
• failing to do so results in postprandial hyperglycemia Duration of action: 4–6 hrs• Less convenient than rapid-acting analogs
Intermediate-acting • Formed by adding protamine to human insulin, generic Onset of action: 2– 3 hrsinsulin: • Acts as both basal and bolus insulin due to a peak at Peak action: 4–6 hrs—NPH(isophane • 4–6 hrs Duration of action: 6–8 hrs
suspension • Hypoglycemia a problem due to these peaks • Long-acting insulin: • Insulin analogs Onset of action: 1– 4 hrs—Glargine • Lesser incidence of hypoglycemia than NPH insulin Peak action: none—Detemir • Glargine:Provides consistent level in plasma over Duration of action: up to
• long duration 22 hrs• Detemir:Binds to albumin via fatty acid chain, hence • slower absorption and consistent levels, shorter• duration than glargine

multiple daily injections, it can deliver smallamounts of insulin with great accuracy,thereby reduc ing the risk of hypoglycemia.However, like all regimens, its success isuser-dependent and requires some self- discipline.
Other TherapiesPramlintide: Amylin is a hormone that
is usually cosecreted with insulin in responseto glucose by pancreatic beta cells. Its effectsare mostly on the gut and include suppres-sion of glucagon secretion, slowing of gas-tric emptying, and promotion of satiety, com-plementing insulin’s action in establishingglucose homeostasis. Patients with Type 1and Type 2 DM have been shown to have adeficiency of amylin as well as insulin.Pramlintide, a synthetic amylin analogue, iscurrently approved for use along with in-sulin in patients with Type 1 and Type 2 DM.It is given before meals, usually in conjunc-tion with prandial insulin, but in a separatesubcutaneous injection. Side effects includenausea and vomiting, especially at higherdoses. A frequent dosing schedule (3 timesdaily) also makes it inconvenient for manypatients. Because of its effect on promotingweight loss, pramlintide seems to be most at-tractive for patients who are overweight. In-sulin dose may need to be reduced due to in-creased risk of hypoglycemia.
Exenatide: See Incretins, above. Transplantation: Transplanting the
whole pancreas (common) or isolated isletcells (experimental) is a treatment option forpatients with Type 1 DM. Solid-organ pan-creas transplantation is usually carried out inconjunction with renal transplant (thus mostpatients are those who have renal failure), asthe treatment necessitates taking antirejectionmedications that have potential side effects.Both forms of transplantation eliminate orreduce the need for intensive insulin therapy,which has been associated with severe hy-poglycemia, to attain near normal glycemic
control.107 Whole pancreas transplantation,either performed alone or in combinationwith kidney transplantation, is limited by or-gan availability, graft failure, surgical com-plications, and morbidity associated with im-munosuppressive therapy.108 Improvementsin surgical techniques and immunosuppres-sive therapy regimens have helped reducemorbidity and mortality, making this a viabletherapeutic alternative for treating DM.109
The greatest promise of islet cell trans-plantation is the possibility of immuno -suppression-free transplantation, allowingpatients to avoid the high side effects asso-ciated with antirejection medi cations. Cur-rently, this procedure is experimental. Majorpotential adverse effects from islet cell trans-plantation include failure from rejection, aswell as side effects associated with anti -rejection drugs (e.g., increased risk of long-term immune suppression, steroid-inducedbone and skin changes, certain malignancies,atherosclerotic disease).
Pregnancy and DMMaternal hyperglycemia at the time of
conception from either Type 1 or Type 2 DMgreatly increases the risk of spontaneousmiscarriage and elevates risk or morbidityand mortality to both mother and fetus.110,111
In addition, DM in pregnancy is an inde-pendent risk factor for pregnancy-inducedhypertension and pre-eclampsia.82 Uncon-trolled blood glucose in the last trimester isassociated with fetal macrosomia (due tohigh blood glucoses reaching the fetus andstimulating fetal insulin production, whichincreases fetal growth), polyhydramnios (increased amniotic fluid due to high bloodglucoses), and sudden fetal death. Intensivecontrol of DM from the prepregnancy periodthroughout the pregnancy, along with ag-gressive fetal surveillance and perinatal carecan improve outcomes.82 Control of bloodglucose during this period is now regardedas a standard of care. Insulin is the preferred
Chapter 5 Diabetes Mellitus: A Medical Overview 75

treatment for managing DM during preg-nancy, not only in Type 1 DM, but also inthose with Type 2 DM or GDM in whichdiet therapy alone does not result in goodcontrol. Insulin requirements drop precipi-tously in the immediate postpartum period,so necessary adjustments should be made.Although there is evidence from clinical tri-als that oral hypoglycemic agents may beused under some circumstances in pregnantwomen with Type 2 DM, these are not FDA-approved at this time.
HypoglycemiaThis is the most common daily compli-
cation that can occur in patients with Type 1or Type 2 diabetes. Hypoglycemia resultswhen blood glucose levels fall below 65mg/dL, though the onset of symptoms canvary. Almost all hypoglycemia events in a di-abetic subject are a result of medication; rel-ative nondeliberate insulin overdose is themost frequently cited reason. For example,taking the morning breakfast-time insulinbut not eating enough carbohydrates can re-sult in a falling blood glucose within 1 or 2hours. For Type 2 DM patients, the medica-tions most commonly associated with hypo-glycemia are sulfonylurea agents. In a well-controlled patient, an event such as skip-ping a meal or over-exercising are common reasons. Another iatrogenic cause sometimesoccurs when patients who are on insulin areasked to fast (usually for laboratory tests),but nonetheless take their usual insulindoses.
Other risk factors for hypoglycemia in-clude exercise (causing increased utilizationof glucose), alcoholism (which interfereswith gluconeogenesis), and renal failure (de-creased insulin clearance). All subjects areeducated to recognize these symptoms, con-firm with a glucometer, if available, and totreat promptly with an appropriate snack.
When blood glucose levels reach athreshold of approximately 70–80 mg/dL,
counter-regulatory hormones such as glu -cagon, epinephrine, growth hormone, andcortisol increase. These hormones stimulateglycogenolysis and gluconeogenesis (Figure1). In individuals with DM, these thresholdsmay not be the same as for healthy individ-uals. Blood glucose levels at which counter-regulatory mechanisms get initiated changeto a higher level in those with poorly con-trolled DM (who often have symptoms ofhypoglycemia at normal glucose levels)and to lower levels in people with recurrent hypoglycemia. Hypoglycemia is “sensed” centrally, resulting in activation of the sym-pathetic nervous system, as well as release ofcatecholamines from the adrenal glands.Auto nomic symptoms and signs include pal-pitations, tremors, anxiety, sweating, intensecraving for food, and a rise in blood pressureand pulse rate. With continued glucose,neuro glycopenic symptoms can result inbehavioral changes, confusion, fatigue orweakness, visual changes, seizure, loss ofconsciousness, and rarely—if hypoglycemiais severe and prolonged—permanent neuro-logical damage or death. Once neurogly-copenia (otherwise known as severe hypo-glycemia) develops, patients are no longerable to take care of themselves and need assistance. It is important to minimize thefrequency of hypoglycemic reactions be-cause glucose can drop significantly close tolevels that can compromise mental functionwithout the person being aware. While in-tensive control of DM is recommended toprevent microvascular complications, it isimportant to recognize the limitations ofsuch intensive therapy. Goals of treatmentshould be individualized based on age, co-morbidities, and financial restrictions. Mostepisodes are mild to moderate (with or with-out symptoms) and can be effectively treatedby oral glucose supplementation and par-enteral treatment if necessary in patients whoare unwilling or unable to take oral carbo-hydrates (Table 7).
76 Periodontal Disease and Overall Health: A Clinician's Guide

CONCLUSIONDM is an ancient disease that is be-
coming more prevalent throughout theworld. Although there is a strong geneticpredisposition toward developing Type 1 orType 2 diabetes, environmental factors are acritical component because the rise in inci-dence is occurring at a much faster pace thangenetics alone can produce. The key patho-physiologic disturbance is centered on in-sulin action, which is intimately involvedwith almost every metabolic process and en-do crine pathway. Understanding the patho-physiology necessitates a comprehension ofall disrupted metabolic pathways. For ex-ample, insulin regulates not only glucosemetabolism, but also fatty acid, cholesterol,
and amino acid metabolism in cell growthand cell division, acting as a balance to otherhormones that perform the opposite function.
Long-term disturbances of these path-ways are responsible for devastating com-plications: diabetes is a major cause ofretinopathy and blindness, renal failure anddialysis-requirement, premature cardio -vascular disease (heart attacks, stroke andperiph eral vascular disease), and loss of limbs.Many other organs or systems are also nowrecognized to be affected by diabetes, suchas all aspects of oral health. Although dia-betes is diagnosed with well- defined bio-chemical criteria, it is increasingly appreci-ated that any level of elevated glycemia (anindication of reduced insulin action) leads to
Chapter 5 Diabetes Mellitus: A Medical Overview 77
Table 7. Identification and Treatment of HypoglycemiaSymptoms of Hypoglycemia Signs of Hypoglycemia
• Shakiness • Tremors• Anxiety • Tachycardia• Palpitations • Sweating• Increased sweating • Confusion, inappropriate behavior
General Principles:• Treatment should be initiated as soon as possible• All patients should be given instructions as to how to treat hypoglycemia• When in a healthcare institution, staff should not wait for lab results or wait for response from a physician• If blood glucose is extremely low on the glucometer, e.g., < 40 mg/dL, blood should be drawn and sent to• the lab for accurate blood glucose level as the precision of glucometers is low at extremely low blood• glucose levels
Treating the Conscious Hypoglycemic Patient:• Treat with ~15 gm of simple carbohydrates orally
can of regular soda 4 oz of regular fruit juice, or 3–4 glucose tablets
• Repeat finger stick glucose in 15 minutes• If blood glucose is < 60 mg/dL, repeat 15 gm of simple carbohydrates and check blood glucose in• 15 minutes; continue this protocol until blood glucose is > 60 and then follow with a mixed snack• Ascertain cause and if hypoglycemia not likely to recur, ask patient to discuss the hypoglycemia with his• or her physician
Treating the Unconscious Hypoglycemic Patient or Otherwise Unable to Consume Oral Carbohydrate:• With IV access:
• 25 to 50 gm of 50% dextrose can be given immediately• Without IV access:
• Glucose gel can be applied to the mouth or the rectum in the semi-obtunded patient• Treat with 1 mg of glucagon intramuscularly or subcutaneously; patient should regain consciousness
in 15 to 20 minutes.• Repeat the blood glucose in 15 minutes

greater cardiovascular morbidity and mor-tality. An increasingly sophis ticated groupof therapies are available to manage this dis-order to improve the health of the patient.
Supplemental Readings
Buse JB, Polonsky KS, Burant CF. Type 2 diabetesmellitus. In: Kronenberg HM, Melmed S, Polonsky KS,Larsen RP, eds. Kronenberg: Williams Textbook of Endocrinology, 11th edition. St. Louis: W.B. SaundersCompany; 2008:1329–1330.
Taylor SI. Insulin action, insulin resistance, and type 2diabetes mellitus. In: Valle D, ed. The Online Metabolic& Molecular Bases of Inherited Disease, Part 7; Mc-Graw-Hill, 2006: http://www.ommbid.com/OMMBID/the_online_metabolic_and_molecular_bases_of_inher-ited_disease/b/fulltext/part7/ch68.
McGarry JD. What if Minkowski had been ageusic?An alternative angle on diabetes. Science 1992;258:766–770.
Hales CN, Barker DJ. Type 2 (non-insulin-dependent)diabetes mellitus: The thrifty phenotype hypothesis. Diabetologia 1992;35:595-601.
Kitabachi AE, Fisher JN, Murphy MB, Rumbak MJ. Diabetic ketoacidosis and the hyperglycemic hyper -osmolar nonketotic state. In: Kahn CR, Weir GC, eds.Joslin’s Diabetes Mellitus, 13th edition. Philadelphia;Lea & Febiger; 1994:738–770.
McCabe LR. Understanding the pathology and mecha-nisms of Type I diabetic bone loss. J Biochem 2007;102:1343–1357.
Baggio LL, Drucker DJ. Biology of incretins: GLP-1and GIP. Gastroenterology 2007;132:2131–2157.
REFERENCES1. National Institute of Diabetes, and Digestive and
Kidney Diseases (NIDDK) National Diabetes Statistics, 2007; Vol 2008: National Diabetes In-for mation Clearinghouse. Available at: http://dia-betes.niddk.nih.gov/dm/pubs/statistics/index.htm.Accessed Dec 28, 2008.
2. Boyko EJ, de Courten M, Zimmet PZ, Chitson P,Tuomilehto J, Alberti KG. Features of the meta-bolic syndrome predict higher risk of diabetes and impaired glucose tolerance: a prospective study inMauritius. Diabetes Care 2000;23:1242–1248.
3. Ramachandran A, Snehalatha C, Latha E, Vijay V,Viswanathan M. Rising prevalence of NIDDM inan urban population in India. Diabetologia 1997;40:232–237.
4. O’Dea K. Westernisation, insulin resistance anddiabetes in Australian aborigines. Med J Aust1991;155:258–264.
5. Buse JB, Polonsky KS, Burant CF. Type 2 diabetesmellitus. In: Kronenberg HM, Melmed S, PolonskyKS, Larsen RP, eds. Kronenberg: Williams Text-book of Endocrinology, 11th edition. St. Louis:W.B. Saunders Company; 2008:1329–1330.
6. Cryer P.E. Glucose homeostasis and hypoglycemia.In: Kronenberg HM, Melmed S, Polonsky KS,Larsen RP, eds. Kronenberg: Williams Textbook ofEndocrinology, 11th edition. St. Louis: W.B. Saun-ders Company; 2008:1503–1508.
7. Brown GK. Glucose transporters: Structure, func-tion and consequences of deficiency. J InheritMetab Dis 2000;23:237–246.
8. Bouché C, Serdy S, Kahn CR, Goldfine AB. Thecellular fate of glucose and its relevance in Type 2diabetes. Endocr Rev 2004;25:807–830.
9. Halban PA, Irminger JC. Sorting and processing ofsecretory proteins. Biochem J 1994;299 (Pt 1):1–18.
10. Badman MK, Shennan KI, Jerman JL, Docherty K,Clark A. Processing of pro-islet amyloid polypep-tide (proIAPP) by the prohormone convertase PC2.FEBS Lett 1996;378:227–231.
11. Matschinsky FM. Glucokinase as glucose sensorand metabolic signal generator in pancreatic beta-cells and hepatocytes. Diabetes 1990;39:647–652.
12. Matschinsky F, Liang Y, Kesavan P, Wang L, FroguelP, Velho G, Cohen D, Permutt MA, Tanizawa Y, Jetton TL, et al. Glucokinase as pancreatic betacell glucose sensor and diabetes gene. J Clin Invest1993;92:2092–2098.
13. Cook DL, Hales CN. Intracellular ATP directlyblocks K+ channels in pancreatic B-cells. Nature1984;311:271–273.
14. Yalow RS, Berson SA. Immunoassay of endo -genous plasma insulin in man. J Clin Invest 1960;39:1157–1175.
15. Karam JH, Grodsky GM, Forsham PH. Excessiveinsulin response to glucose in obese subjects asmeasured by immunochemical assay. Diabetes1963;12:197–204.
16. Taylor SI. Insulin action, insulin resistance, andtype 2 diabetes mellitus. In: Valle D, ed. The OnlineMetabolic & Molecular Bases of Inherited Disease,Part 7; McGraw-Hill, 2006: http://www.omm-bid.com/OMMBID/the_online_metabolic_and_molecular_bases_of_inherited_disease/b/fulltext/part7/ch68.
17. Taniguchi CM, Emanuelli B, Kahn CR. Criticalnodes in signaling pathways: insights into insulinaction. Nat Rev Mol Cell Biol 2006;7:85–96.
18. Swislocki AL, Chen YD, Golay A, Chang MO,Reaven GM. Insulin suppression of plasma-free
78 Periodontal Disease and Overall Health: A Clinician's Guide

fatty acid concentration in normal individuals andpatients with type 2 (non-insulin-dependent) dia-betes. Diabetologia 1987;30:622–626.
19. Chen YD, Golay A, Swislocki AL, Reaven GM.Resistance to insulin suppression of plasma freefatty acid concentrations and insulin stimulation ofglucose uptake in noninsulin-dependent diabetesmellitus. J Clin Endocrinol Metab 1987;64:17–21.
20. Randle PJ, Kerbey AL, Espinal J. Mechanisms decreasing glucose oxidation in diabetes and star-vation: Role of lipid fuels and hormones. DiabetesMetab Rev 1988;4:623–638.
21. McGarry JD. What if Minkowski had been ageusic?An alternative angle on diabetes. Science 1992;258:766–770.
22. Pipeleers D, Ling Z. Pancreatic beta cells in insu -lin-dependent diabetes. Diabetes Metab Rev 1992;8:209–227.
23. Doniach I, Morgan AG. Islets of Langerhans in juvenile diabetes mellitus. Clin Endocrinol (Oxf)1973;2:233–248.
24. Gepts W, Lecompte PM. The pancreatic islets in diabetes. Am J Med 1981;70:105–115.
25. Todd JA, Walker NM, Cooper JD, Smyth DJ,Downes K, Plagnol V, Bailey R, Nejentsev S, FieldSF, Payne F, Lowe CE, et al. Robust associations offour new chromosome regions from genome-wideanalyses of type 1 diabetes. Nat Genet 2007;39:857–864.
26. Rich SS, Norris JM, Rotter JI. Genes associatedwith risk of type 2 diabetes identified by a candi-date-wide association scan: As a trickle becomes aflood. Diabetes 2008;57:2915–2917.
27. Rewers M, Norris J, Dabelea D. Epidemiology oftype 1 diabetes mellitus. Adv Exp Med Biol2004;552:219–246.
28. el-Hashimy M, Angelico MC, Martin BC,Krolewski AS, Warram JH. Factors modifying therisk of IDDM in offspring of an IDDM parent. Diabetes 1995;44:295–299.
29. Eisenbarth GS, Polonsky KS, Buse JB. Type 1 di-abetes mellitus. In: Kronenberg HM, Melmed S,Polonsky KS, Larsen RP, eds. Kronenberg: WilliamsTextbook of Endocrinology, 11th edition. St. Louis:W.B. Saunders Company; 2008:1393–1396.
30. Kaprio J, Tuomilehto J, Koskenvuo M, RomanovK, Reunanen A, Eriksson J, Stengård J, KesäniemiYA. Concordance for type 1 (insulin-dependent)and type 2 (non-insulin-dependent) diabetes melli-tus in a population-based cohort of twins in Finland.Diabetologia 1992;35:1060-1067.
31. Leslie RD, Pyke DA. Escaping insulin dependentdiabetes. Br Med J 1991;302:1103–1104.
32. Kumar D, Gemayel NS, Deapen D, Kapadia D,Yamashita PH, Lee M, Dwyer JH, Roy-Burman P,
Bray GA, Mack TM. North-American twins withIDDM. Genetic, etiological, and clinical signifi-cance of disease concordance according to age, zy-gosity, and the interval after diagnosis in first twin.Diabetes 1993;42:1351–1363.
33. Lo SS, Tun RY, Hawa M, Leslie RD. Studies of di-abetic twins. Diabetes Metab Rev 1991;7:223–238.
34. Erlich HA, Zeidler A, Chang J, Shaw S, Raffel LJ,Klitz W, Beshkov Y, Costin G, Pressman S,Bugawan T, et al. HLA class II alleles and suscep-tibility and resistance to insulin dependent diabetesmellitus in Mexican-American families. Nat Genet1993;3:358–364.
35. Noble JA, Valdes AM, Cook M, Klitz W, ThomsonG, Erlich HA. The role of HLA class II genes in insulin-dependent diabetes mellitus: Molecularanalysis of 180 Caucasian, multiplex families. AmJ Hum Genet 1996;59:1134–1148.
36. Thorsby E. Invited anniversary review: HLA asso-ciated diseases. Hum Immunol 1997;53:1–11.
37. American Diabetes Association. Diagnosis andclassification of diabetes mellitus. Diabetes Care2008;31:S55–60.
38. Kolterman OG, Scarlett JA, Olefsky JM. Insulin re-sistance in non-insulin-dependent, type II diabetesmellitus. Clin Endocrinol Metab 1982;11:363–388.
39. Caro JF, Sinha MK, Raju SM, Ittoop O, Pories WJ,Flickinger EG, Meelheim D, Dohm GL. Insulin re-ceptor kinase in human skeletal muscle from obesesubjects with and without noninsulin dependent diabetes. J Clin Invest 1987;79: 1330–1337.
40. Caro JF, Ittoop O, Pories WJ, Meelheim D,Flickinger EG, Thomas F, Jenquin M, Silverman JF,Khazanie PG, Sinha MK. Studies on the mecha-nism of insulin resistance in the liver from humanswith noninsulin-dependent diabetes. Insulin actionand binding in isolated hepatocytes, insulin recep-tor structure, and kinase activity. J Clin Invest1986;78: 249–258.
41. Comi RJ, Grunberger G, Gorden P. Relationship ofinsulin binding and insulin-stimulated tyrosine kinase activity is altered in type II diabetes. J ClinInvest 1987;79:453–462.
42. Freidenberg GR, Reichart D, Olefsky JM, HenryRR. Reversibility of defective adipocyte insulin receptor kinase activity in non-insulin-dependentdiabetes mellitus. Effect of weight loss. J Clin Invest 1988;82:1398–1406.
43. Cama A, Patterson AP, Kadowaki T, Kadowaki H,Siegel G, D’Ambrosio D, Lillioja S, Roth J, TaylorSI. The amino acid sequence of the insulin recep-tor is normal in an insulin-resistant Pima Indian. JClin Endocrinol Metab 1990;70:1155–1161.
44. Moller DE, Yokota A, Flier JS. Normal insulin- receptor cDNA sequence in Pima Indians with
Chapter 5 Diabetes Mellitus: A Medical Overview 79

NIDDM. Diabetes 1989;38:1496–1500.45. Rasouli N, Kern PA. Adipocytokines and the meta-
bolic complications of obesity. J Clin EndocrinolMetab 2008;93:S64–73.
46. Brillon DJ, Freidenberg GR, Henry RR, OlefskyJM. Mechanism of defective insulin-receptor kinaseactivity in NIDDM. Evidence for two receptor pop-ulations. Diabetes 1989;38:397–403.
47. Robertson RP, Harmon J, Tran PO, Tanaka Y, Taka-hashi H. Glucose toxicity in ß-cells: Type 2 dia-betes, good radicals gone bad, and the glutathioneconnection. Diabetes 2003;52:581–587.
48. Kahn BB, Shulman GI, DeFronzo RA, CushmanSW, Rossetti L. Normalization of blood glucosein diabetic rats with phlorizin treatment reverses insulin-resistant glucose transport in adipose cellswithout restoring glucose transporter gene expres-sion. J Clin Invest 1991;87:561–570.
49. Rossetti L, Smith D, Shulman GI, Papachristou D,DeFronzo RA. Correction of hyperglycemia withphlorizin normalizes tissue sensitivity to insulin indiabetic rats. J Clin Invest 1987;79:1510–1515.
50. Westermark P, Wilander E. The influence of amyloiddeposits on the islet volume in maturity onset dia-betes mellitus. Diabetologia 1978;15:417–421.
51. Clark A, Wells CA, Buley ID, Cruickshank JK,Vanhegan RI, Matthews DR, Cooper GJ, HolmanRR, Turner RC. Islet amyloid, increased A-cells, reduced B-cells and exocrine fibrosis: Quantitativechanges in the pancreas in type 2 diabetes. DiabetesRes 1988;9:151–159.
52. Clark A, Saad MF, Nezzer T, Uren C, Knowler WC,Bennett PH, Turner RC. Islet amyloid polypeptidein diabetic and non-diabetic Pima Indians. Dia-betologia 1990:33:285–289.
53. Cooper GJ, Willis AC, Clark A, Turner RC, Sim RB,Reid KB. Purification and characterization of apeptide from amyloid-rich pancreases of type 2 di-abetic patients. Proc Natl Acad Sci USA 1987;84:8628–8632.
54. Bertelli A, Breschi MC, Mazzanti L, Schinetti ML.Protective action of some drugs in amanitin andphalloidin intoxication. Curr Probl Clin Biochem1977;7:75–85.
55. Sakagashira S, Sanke T, Hanabusa T, Shimomura H,Ohagi S, Kumagaye KY, Nakajima K, Nanjo K.Missense mutation of amylin gene (S20G) in Japan-ese NIDDM patients. Diabetes 1996;45:1279–1281.
56. Seltzer HS, Allen EW, Herron AL Jr, Brennan MT.Insulin secretion in response to glycemic stimulus:Relation of delayed initial release to carbohydrateintolerance in mild diabetes mellitus. J Clin Invest1967;46:323–335.
57. Perley MJ, Kipnis DM. Plasma insulin responses to
oral and intravenous glucose: Studies in normaland diabetic subjects. J Clin Invest 1967;46:1954–1962.
58. Cerasi E, Luft R. The plasma insulin response toglucose infusion in healthy subjects and in diabetesmellitus. Acta Endocrinol (Copenh) 1967;55:278–304.
59. Pfeifer MA, Halter JB, Porte D Jr. Insulin secretionin diabetes mellitus. Am J Med 1981;70:579–588.
60. Metz SA, Halter JB, Robertson RP. Paradoxical in-hibition of insulin secretion by glucose in human diabetes mellitus. J Clin Endocrinol Metab 1979;48:827–835.
61. Ferrone JD Jr. Congenital deformities about theknee. Orthop Clin North Am 1976;7:323–330.
62. Ward WK, Bolgiano DC, McKnight B, Halter JB,Porte D Jr. Diminished B cell secretory capacity inpatients with noninsulin-dependent diabetes melli-tus. J Clin Invest 1984;74: 1318–1328.
63. Roder ME, Porte D Jr, Schwartz RS, Kahn SE.Disproportionately elevated proinsulin levels reflectthe degree of impaired B cell secretory capacity inpatients with noninsulin-dependent diabetes mellitus.J Clin Endocrinol Metab 1998;83:604–608.
64. Halter JB, Graf RJ, Porte D Jr. Potentiation of in-sulin secretory responses by plasma glucose levelsin man: Evidence that hyperglycemia in diabetescompensates for impaired glucose potentiation.J Clin Endocrinol Metab 1979;48:946–954.
65. Zeggini E, Scott LJ, Saxena R, Voight BF, MarchiniJL, Hu T, de Bakker PI, Abecasis GR, Almgren P,Andersen G, et al. Meta-analysis of genome-wideassociation data and large-scale replication identifiesadditional susceptibility loci for type 2 diabetes.Nat Genet 2008;40:638–664.
66. Hamman RF. Genetic and environmental determi-nants of non-insulin-dependent diabetes mellitus(NIDDM). Diabetes Metab Rev 1992;8:287–338.
67. Kahn CR. Banting Lecture. Insulin action, diabeto -genes, and the cause of type II diabetes. Diabetes1994;43:1066–1084.
68. Bouchard C. Genetics and the metabolic syndrome.Int J Obes Relat Metab Disord 1995;19:S52–59.
69. Hales CN, Barker DJ. Type 2 (non-insulin-dependent) diabetes mellitus: The thrifty pheno-type hypothesis. Diabetologia 1992;35:595–601.
70. Carey DG, Jenkins AB, Campbell LV, Freund J,Chisholm DJ. Abdominal fat and insulin resistancein normal and overweight women: Direct meas-urements reveal a strong relationship in subjects atboth low and high risk of NIDDM. Diabetes 1996;45:633–638.
71. Lillioja S, Mott DM, Spraul M, Ferraro R, Foley JE,Ravussin E, Knowler WC, Bennett PH, BogardusC. Insulin resistance and insulin secretory dysfunc -
80 Periodontal Disease and Overall Health: A Clinician's Guide

tion as precursors of non-insulin-dependent dia-betes mellitus. Prospective studies of Pima Indians.N Engl J Med 1993;329:1988–1992.
72. Martin BC, Warram JH, Rosner B, Rich SS, Soeld-ner JS, Krolewski AS. Familial clustering of in -sulin sensitivity. Diabetes 1992;41:850–854.
73. DeFronzo RA, Bonadonna RC, Ferrannini E.Pathogenesis of NIDDM. A balanced overview. Diabetes Care 1992;15:318–368.
74. Kissebah AH, Freedman DS, Peiris AN. Healthrisks of obesity. Med Clin North Am 1989;73:111–138.
75. Bogardus C, Lillioja S, Nyomba BL, Zurlo F, Swin-burn B, Esposito-Del Puente A, Knowler WC,Ravussin E, Mott DM, Bennett PH. Distribution ofin vivo insulin action in Pima Indians as mixture ofthree normal distributions. Diabetes 1989;38:1423–1432.
76. Bjorntorp P. Abdominal obesity and the develop-ment of noninsulin-dependent diabetes mellitus.Diabetes Metab Rev 1988;4:615–622.
77. Iselius L, Lindsten J, Morton NE, Efendi S, CerasiE, Haegermark A, Luft R. Genetic regulation ofthe kinetics of glucose-induced insulin release inman. Studies in families with diabetic and non- diabetic probands. Clin Genet 1985;28:8–15.
78. Yki-Jarvinen H. Role of insulin resistance in thepathogenesis of NIDDM. Diabetologia 1995;38:1378–1388.
79. Bowden DW, Sale M, Howard TD, Qadri A, SprayBJ, Rothschild CB, Akots G, Rich SS, FreedmanBI. Linkage of genetic markers on human chromo -somes 20 and 12 to NIDDM in Caucasian sib pairswith a history of diabetic nephropathy. Diabetes1997;46:882–886.
80. Report of the Expert Committee on the Diagnosisand Classification of Diabetes Mellitus. DiabetesCare 1997;20:1183–1197.
81. Sattar N, McConnachie A, Shaper AG, Blauw GJ,Buckley BM, de Craen AJ, Ford I, Forouhi NG,Freeman DJ, Jukema JW, Lennon L, MacfarlanePW, Murphy MB, Packard CJ, Stott DJ, Westen-dorp RG, Whincup PH, Shepherd J, WannametheeSG. Can metabolic syndrome usefully predict cardio -vascular disease and diabetes? Outcome data fromtwo prospective studies. Lancet 2008;371:1927–1935.
82. Miodovnik M, Lavin JP, Knowles HC, Holroyde J,Stys SJ. Spontaneous abortion among insulin- dependent diabetic women. Am J Obstet Gynecol1984;150:372–376.
83. Powers AC. Diabetes Mellitus. In: Fauci AS,Braunwald E, Kasper DL, Hauser SL, Longo DL,Jameson JL, Loscalzo J, eds. Harrison’s Principlesof Internal Medicine, 17th edition. McGraw-Hill,
2006;http://www.accessmedicine.com/content.aspx?aID=2891108.
84. Kitabachi AE, Fisher JN, Murphy MB, RumbakMJ. Diabetic ketoacidosis and the hyperglycemichyperosmolar nonketotic state. In: Kahn CR, WeirGC, eds. Joslin’s Diabetes Mellitus, 13th edition.Philadelphia; Lea & Febiger; 1994:738–770.
85. Wachtel TJ, Silliman RA, Lamberton P. Predispos-ing factors for the diabetic hyperosmolar state. ArchIntern Med 1987;147:499–501.
86. Kitabachi AE, Umipierrez GE, Murphy MB. Dia-betic ketoacidosis and hyperglycemic hyperosmo-lar state. In: DeFronzo RA, Ferrannini E, Keen H,Zimmet P, eds. International Textbook of DiabetesMellitus, 3rd edition. Chichester (UK); John Wiley& Sons; 2004:1101–1119.
87. Kitabachi, AE, Fisher JN. Clinical studies in medical biochemistry. In: Glew RA, Peters SP, eds.Clinical Studies in Medical Biochemistry, 3rd edition. New York; Oxford University Press; 1987:102–117.
88. Exton JH. Mechanisms of hormonal regulation ofhepatic glucose metabolism. Diabetes Metab Rev1987;3:163–183.
89. McGarry JD, Woeltje KF, Kuwajima M, FosterDW. Regulation of ketogenesis and the renaissanceof carnitine palmitoyltransferase. Diabetes MetabRev 1989;5:271–284.
90. Reichard GA Jr, Skutches CL, Hoeldtke RD, OwenOE. Acetone metabolism in humans during dia-betic ketoacidosis. Diabetes 1986;35:668–674.
91. Balasse EO, Féry F. Ketone body production anddisposal: Effects of fasting, diabetes, and exercise.Diabetes Metab Rev 1989;5:247–270.
92. Stentz FB, Umpierrez GE, Cuervo R, Kitabchi AE.Proinflammatory cytokines, markers of cardiovas-cular risks, oxidative stress, and lipid peroxidationin patients with hyperglycemic crises. Diabetes2004;53:2079–2086.
93. Chupin M, Charbonnel B, Chupin F. C-peptideblood levels in keto-acidosis and in hyperosmolarnonketotic diabetic coma. Acta Diabetol Lat 1981;18:123–128.
94. The Diabetes Control and Complications Trial Re-search Group. The effect of intensive treatment ofdiabetes on the development and progression of long-term complications in insulin-dependent diabetesmellitus. N Engl J Med 1993;329:977–986.
95. UK Prospective Diabetes Study (UKPDS) Group.Intensive blood-glucose control with sulphony-lureas or insulin compared with conventional treat-ment and risk of complications in patients with type2 diabetes (UKPDS 33). Lancet 1998;352:837–853.
96. Kles KA, Vinik AI. Pathophysiology and treatmentof diabetic peripheral neuropathy: The case for
Chapter 5 Diabetes Mellitus: A Medical Overview 81

diabetic neurovascular function as an essential component. Curr Diabetes Rev 2006;2:131–145.
97. Van Hattem S, Bootsma AH, Thio HB. Skin mani-festations of diabetes. Cleve Clin J Med 2008;75:772, 774, 776–777.
98. Saller A, Maggi S, Romanato G, Tonin P, CrepaldiG. Diabetes and osteoporosis. Aging Clin Exp Res2008;20:280–289.
99. McCabe LR. Understanding the pathology andmechanisms of type I diabetic bone loss. J CellBiochem 2007;102:1343–1357.
00. Grossi SG, Skrepcinski FB, DeCaro T, RobertsonDC, Ho AW, Dunford RG, Genco RJ. Treatment ofperiodontal disease in diabetics reduces glycatedhemoglobin. J Periodontol 1997;68:713–719.
01. Demmer RT, Jacobs DR Jr, Desvarieux M. Perio -dontal disease and incident type 2 diabetes: Re-sults from the First National Health and NutritionExamination Survey and Its Epidemiologic Follow-Up Study. Diabetes Care 2008;31:1373–1379.
02. Tsai C, Hayes C, Taylor GW. Glycemic control oftype 2 diabetes and severe periodontal disease in theUS adult population. Community Dent Oral Epi-demiol 2002;30:182–192.
03. Engelgau MM, Thompson TJ, Herman WH, BoyleJP, Aubert RE, Kenny SJ, Badran A, Sous ES, AliMA. Comparison of fasting and 2-hour glucoseand HbA1c levels for diagnosing diabetes. Diag-nostic criteria and performance revisited. Diabetes
Care 1997;20:785–791.04. McCance DR, Hanson RL, Charles MA, Jacobsson
LT, Pettitt DJ, Bennett PH, Knowler WC. Com-parison of tests for glycated haemoglobin and fast-ing and two hour plasma glucose concentrations asdiagnostic methods for diabetes. British Med J 1994;308:1323–1328.
05. Pories WJ. Bariatric surgery: Risks and rewards. JClin Endocrinol Metab 2008;93:S89–96.
06. Baggio LL, Drucker DJ. Biology of incretins: GLP-1 and GIP. Gastroenterology 2007;132: 2131–2157.
07. Uwaifo GI, Ratner RE. Novel pharmacologicagents for type 2 diabetes. Endocrinol Metab ClinNorth Am 2005;34:155–197.
08. Meloche RM. Transplantation for the treatment oftype 1 diabetes. World J Gastroenterol 2007;13:6347–6355.
09. Sutherland DE, Gruessner RW, Dunn DL, MatasAJ, Humar A, Kandaswamy R, Mauer SM,Kennedy WR, Goetz FC, Robertson RP, GruessnerAC, Najarian JS. Lessons learned from more than1,000 pancreas transplants at a single institution.Ann Surg 2001;233:463–501.
10. Greene MF. Spontaneous abortions and major mal-formations in women with diabetes mellitus. SeminReprod Endocrinol 1999;17:127–136.
11. Greene MF, Solomon CG. Gestational diabetesmellitus—time to treat. N Engl J Med 2005;352:2544–2546.
82 Periodontal Disease and Overall Health: A Clinician's Guide
1
1
1
1
1
1
1
1
1
1
1
1
CHAPTER 6Association Between PeriodontalDiseases and Diabetes Mellitus
George W. Taylor, Wenche S. Borgnakke, Dana T. Graves
INTRODUCTIONBoth diabetes and periodontal diseases
are common chronic disorders in many partsof the world. This chapter will provide a description of the evidence supporting a bi- directional relationship between diabetes and periodontal disease. This bi-directional rela-tion ship is one in which we recognize that dia - betes adversely affects periodontal health, andperiodontal infection (or periodontal disease) adversely affects diabetes by contributing topoorer glycemic control, increasing the risk forcertain diabetes complications, and possiblyincreasing the risk for the development of dia-betes. It is important for not only dental healthprofessionals, but for all healthcare profes-sionals, to understand the role and importanceof oral health in managing diabetes patients.With a relatively small but concerted effort,a potentially large gain might be obtained inimproving the quality of life for individualswith diabetes, while reducing the immense bur -den of diabetes on the patients, their familiesand employers, and on society as a whole.
The following educational objectivesprovide an overview of the topics in this chapter:
1. Effect of Diabetes on Periodontal Health• Describe in general terms the types
and strength of empirical evidence,e.g., studies conducted on humans,that support the concept that diabeteshas an adverse effect on perio dontalhealth.
• Describe the mechanisms by whichdiabetes is thought to contribute topoor er periodontal health, e.g., tissue,cellular, and molecular dy namics orinteractions.
2. Effect of Periodontal Infection on Gly -cemic Control in Diabetes•Describe the mechanisms by which
periodontal infection is thought tocontribute to poorer glycemic controlin people with diabetes.
•Describe the current state of empiricalevidence derived from observationalstudies regarding perio dontal infectionhaving an adverse effect on glycemiccontrol.
•Describe the current state of empiri calevidence from treatment studies thatshow periodontal therapy has a bene-ficial effect on improving gly cemiccontrol.
3. Periodontal Infection and Developmentof Complications of Diabetes and Possi -bly Diabetes Itself•Describe the role blood glucose con-
trol plays in preventing the occurrenceand/or progression of diabetes com-plications and the definitive evidencefrom clinical trials supporting thisconcept.
•Describe the current state of the evi -dence regarding the effect of se vereperiodontal disease on the risk of diabetes complications and the de -velopment of Type 2 diabetes.
ADVERSE EFFECTS OF DIABETESON PERIODONTAL HEALTH
Evidence from Epidemiologic andOther Clinical Studies
The evidence that diabetes adverselyaffects periodontal health comes from studiesconducted in different parts of the world.
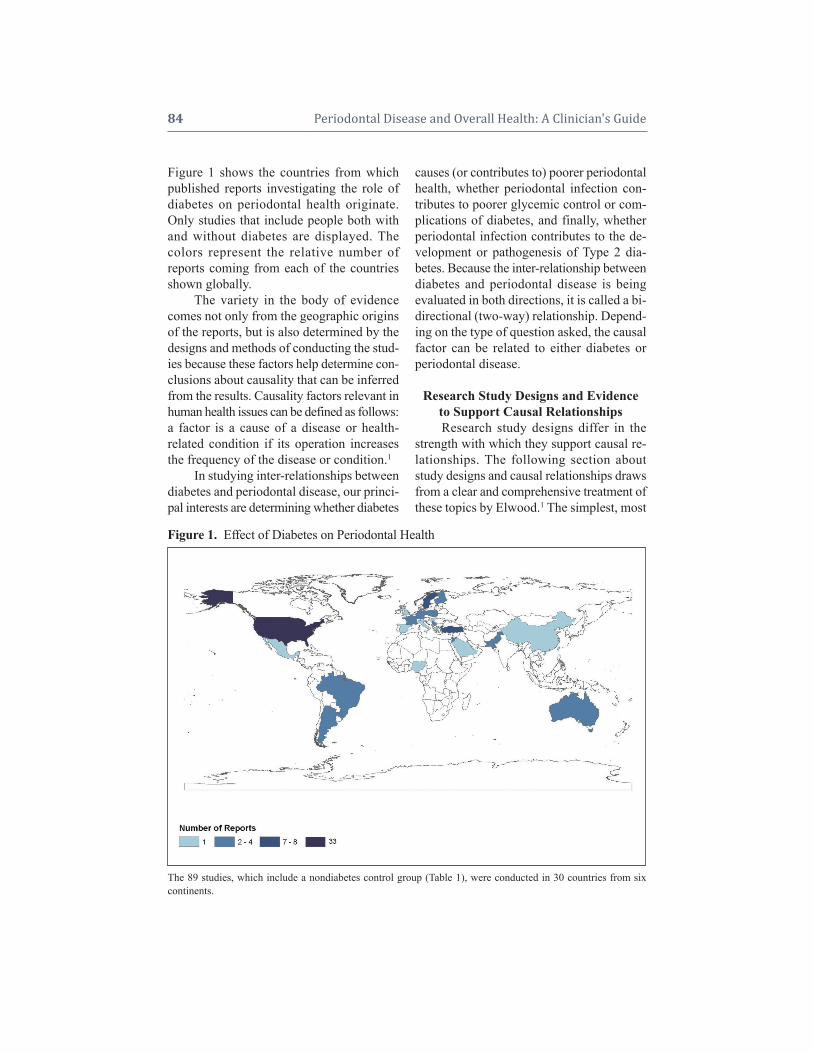
Figure 1 shows the countries from whichpublished reports investigating the role ofdiabetes on periodontal health originate.Only studies that include people both withand without diabetes are displayed. Thecolors represent the relative number ofreports coming from each of the countriesshown globally.
The variety in the body of evidencecomes not only from the geographic originsof the reports, but is also determined by thedesigns and methods of conducting the stud-ies because these factors help determine con-clusions about causality that can be inferredfrom the results. Causality factors relevant inhuman health issues can be defined as follows:a factor is a cause of a disease or health- related condition if its operation increasesthe frequency of the disease or condition.1
In studying inter-relationships betweendiabetes and periodontal disease, our princi-pal interests are determining whether dia betes
causes (or contributes to) poorer perio dontalhealth, whether periodontal infection con-tributes to poorer glycemic control or com-plications of diabetes, and finally, whetherperiodontal infection contributes to the de-velopment or pathogenesis of Type 2 dia-betes. Because the inter-relationship betweendiabetes and periodontal disease is beingevaluated in both directions, it is called a bi-directional (two-way) relationship. Depend-ing on the type of question asked, the causalfactor can be related to either diabetes or periodontal disease.
Research Study Designs and Evidenceto Support Causal RelationshipsResearch study designs differ in the
strength with which they support causal re-lationships. The following section aboutstudy designs and causal relationships drawsfrom a clear and comprehensive treatment ofthese topics by Elwood.1 The simplest, most
84 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 1. Effect of Diabetes on Periodontal Health
The 89 studies, which include a nondiabetes control group (Table 1), were conducted in 30 countries from six continents.

direct test of causation in health is an exper-imental study in which there are two groupsof people who are as similar as possible in allof their relevant characteristics, but the sus-pected (i.e., putative) causal factor is appliedto only one group. Relevant characteristicsare those factors, other than the one beingstudied, that could affect the frequency orseverity of occurrence of the disease or con-dition. In studies of human health, this typeof experiment is called a randomized con-trolled trial (RCT). The RCT has been usedmost extensively in comparing methods oftreatment, in which groups receiving differ-ent treatments are selected by chance as-signment (i.e., random allocation) and, whenpossible, neither the participants nor the in-vestigators are aware of which treatment isgiven (double-blinding or masking). By“blinding” both the investigators and thestudy participants, the observations of theoutcomes can be made the same way for allstudy participants, without knowledge of thetreatment affecting the assessment by the in-vestigators or perception of the effects bythe study participants. The double-blind RCTis the most definitive way to test a causal re-lationship in human health. In appropriatecircumstances, RCTs are considered the“gold standard” or best possible method forcausal evidence.
However, for practical and ethical rea-sons, RCTs are not always appropriate. RCTscan be used only to assess methods of treat-ment that are likely to be beneficial. In studies of human health, many important re-lationships are those in which we are con-cerned about harmful, rather than beneficial,effects or exposures. This is the case in con-ducting studies to establish whether diabeteshas an adverse effect on periodontal health.On the other hand, RCTs involving perio -dontal treat ment are appropriate in providingevidence to demonstrate that treating peri-odontal infection contributes to improvedglycemic control or perhaps reduces the risk
of development of diabetes or its compli -cations. However, in studying the role of periodontal disease in the pathogenesis ofdiabetes or its complications, the RCT mightbe impractical because of the length of timerequired to observe complications or to diagnose diabetes, or the large number ofparticipants required to demonstrate such acausal relationship.
Analytical Observational Study Designs:Cohort, Case-Control, and
Cross-Sectional StudiesBecause of the ethical, methodological,
and practical limitations of experimental stud-ies (i.e., RCTs) for answering questions aboutcausation for many types of health-related is-sues, other study designs are also used. Thethree main types of analytical, nonexperi-mental study designs used to support or ex-plore causal relationships in human health arethe cohort, case-control, and cross-sectionalstudy designs. These three study designs areconsidered “observational” studies that dif-fer in the way study participants are chosenand the relationship in time between the oc-currence of exposure to the putative causalfactor and the occurrence of the disease orcondition, referred to as the “outcome.”
Cohort StudiesThese studies compare groups of peo-
ple exposed to a putative causal factor withthose who are not exposed. The exposuresare identified at a point in time when none ofthe people in either group have the outcomeof interest. The groups are observed over aperiod of time to compare differences be-tween the groups in the occurrence of theoutcome. If a greater number of people in thegroup exposed to the putative causal factordevelop the outcome, and other relevantcharacteristics have been considered, then itcan be inferred that the putative causal fac-tor is likely to be a cause or risk factor for theoutcome.
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 85

Case-Control Studies These studies compare a group of peo-
ple who have already experienced the out-come (cases) with a group of similar peoplewithout the outcome (controls). Investiga-tors then look backward in time, or retro-spectively, to assess the frequency with whichthe cases and controls were exposed to theputative causal factor in the time period priorto the diagnosis of the outcome. If the caseshad a higher frequency of exposure to the pu-tative causal factor, then one can make an in-ference about causality after accounting forother relevant characteristics.
Cross-Sectional StudiesThis study design selects participants
who comprise a population or are consid-ered a sample of people representative of apopulation. All data on the putative causalfactor (or exposure) and the outcome are col-lected at the same point in time, i.e., a cross-section in time. One is able to assess whetherthere is an association between the putativecausal factor and the outcome by comparingdifferences in the frequency of the outcomein those who have the putative causal factorwith people who do not. Although a greaterfrequency of the outcome may be observedin the people exposed to the putative causalfactor, the ability to make causal inferencesabout the relationship is limited because thetime sequence of events cannot be estab-lished. That is to say it cannot be determinedif the exposure to the putative causal factoroccurred before the disease or condition orvice versa. The cross-sectional study designdoes allow testing hypotheses regarding howstrongly associated a putative causal factormay be with an outcome.
To address the question of whether diabetes adversely affects periodontal health,it is not ethical to use an RCT in humans, be-cause doing so would require researchers tocause some individuals to develop diabetes.(However, a section later in this chapter will
describe experimental evidence in rodentmodels). Therefore, the evidence aboutwhether or not diabetes adversely affects pe-riodontal health must come from observa-tional studies.
Adverse Effects of Diabetes on Periodontal Health: Evidence from
Observational StudiesAs might be expected, reports in the
literature provide answers to different kindsof questions and vary in their ability to helpus understand how diabetes can be consid-ered a cause of poorer periodontal healthand establish how strong that relationshipis. The majority of the reports are cross-sec-tional studies that provide information aboutthe association between diabetes and theprevalence of periodontal diseases. Studiesof prevalence allow us to compare the dif-ferences in percentages or proportions of in-dividuals with periodontal disease betweenthose with and without diabetes. The vastmajority of studies reporting on the preva-lence of periodontal disease conclude thatthe prevalence is greater in people who havediabetes.
Some of the studies provide informa-tion about the extent or severity of peri-odontal disease in people with diabetes. Thestudies reporting on the extent of periodon-tal disease assess the number of teeth or sitesaffected, while studies of severity assess theamount of periodontal destruction by con-sidering the extent of pocket depth or at-tachment loss. People with diabetes are morelikely to have deeper periodontal pocketsand greater attachment loss than people whodo not have diabetes.
The strongest type of evidence sup-porting the role of diabetes contributing topoorer periodontal health comes from stud-ies of incidence and progression of perio -dontal disease. These types of studies mustfollow people over time and hence can allowfor conclusions to contribute to establishing
86 Periodontal Disease and Overall Health: A Clinician's Guide

a causal relationship between diabetes andpoorer periodontal health. Incidence is ameasure of the rate of new cases of peri-odontal disease over time. Progression ofperiodontal disease is a measure of the wors-ening of periodontal status over time.
Cross-sectional studies provide infor-mation on the prevalence, extent, and sever-ity of periodontal disease in people with di-abetes at a single point in time. Studiesfollowing individuals with diabetes overtime (i.e., prospective, cohort, or longitudi-nal studies) allow quantification of the de-gree to which diabetes increases the risk forperiodontal disease incidence, severity, orprogression.
Table 1 summarizes the conclusions ofstudies reported in the literature that addressthe question of whether or not diabetes ad-versely affects periodontal health. To inter-pret the contents of Table 1, first look at thecolumn headings and then the row headings.The column headings indicate the type ofdiabetes included in the study and the rowheadings indicate the type of study. Noticethat there are both cohort and cross-sectionalstudies that have addressed the question ofwhether diabetes has an adverse effect onperiodontal health. It is important to keep inmind that RCTs would not be appropriatefor addressing the question summarizedin Table 1, i.e., if diabetes adversely affectsperio dontal health, because it would be unethical to use an intervention in humans
that caused diabetes in an experimentalgroup. Therefore, the highest level of evi-dence useful in addressing this questionwould come from the results of cohort studies.
In each category (group of studies)within Table 1, the numerator is the numberof studies confirming that diabetes adverselyaffects one or more of several measures ofperiodontal health (e.g., gingivitis, probingpocket depth, attachment loss, radiographicbone loss). The denominator represents thetotal number of studies of that particular kind(e.g., cross-sectional studies with participantshaving Type 2 diabetes). For example, allfour of the reports from cohort studies thatincluded people with Type 2 diabetes con-cluded that periodontal health was worse inpeople who had diabetes than in those with-out diabetes. Similarly, all three of the re-ports investigating gestational diabetes mel-litus (GDM) concluded that women withGDM were more likely to have poorer perio -dontal health than pregnant women withoutGDM. In the bottom row there are roughlyequal numbers of studies reporting on Type1 diabetes (26) and Type 2 diabetes (27), exclusively; only three reports addressGDM. From the information presented inTable 1 we can see the vast majority of re-ports, namely 79 of 89 studies as shown inthe extreme bottom right corner, provide evi -dence that diabetes adversely affects perio -dontal health.
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 87
Table 1. Effects of Diabetes on Periodontal Health: Conclusions of the 89 Studies thatTable 1. Include a Nondiabetes Control Group (Figure 1)
Note: The numerator represents the number of studies reporting diabetes having an adverse effect on periodontalhealth; the denominator represents the total number of studies in each group: # Studies with Effect/Total # Studies.
Diabetes Mellitus Type
Type 1 Gestational Type Not Total Number of StudiesStudy Design Type 1 Type 2 or 2 (GDM) Reported (# with Effect /# All Studies)
Cohort 3/3 4/4 0/0 0/0 0/0 7/7Cross-sectional, Descriptive 22/23 20/23 15/18 3/3 11/15 72/83
Total: 25/26 24/27 15/18 3/3 11/15 79/89

Another set of studies in the literatureaddresses the question of whether the de-gree of glycemic control of diabetes is asso-ciated with poorer periodontal health. Thedegree to which diabetes is controlled ormanaged is usually assessed by measuringthe amount of hemoglobin A1c (HbA1c) inthe blood, called glycosylated (or glycated)hemoglobin. HbA1c is a measure of howmuch glucose has been present in the bloodand has bound to the hemoglobin in the redblood cells over the lifetime of those cells.Blood from a simple finger stick can be an-alyzed, and the result indicates the level ofcontrol of glycemia for the previous 60 to90 days, measured as a percent of HbA1c.The current therapeutic target for HbA1c is toachieve a level less than 7%. People withoutdiabetes usually have a level of 4.5%–6%.
Table 2 summarizes the conclusions ofstudies that provided information compar-ing the effects of better or poorer glycemiccontrol on periodontal health in people withdiabetes. Similarly to Table 1, the evidencecomes from both cohort and cross-sectionalstudies, as indicated in the row titles of thetable; the column headings indicate the typeof diabetes of the participants in the studies.The majority of the studies in Table 2 con-cluded that people with poorer glycemic con-trol had worse periodontal health than thosewith better glycemic control (42 of the 61studies). The stronger evidence comes from
the set of cohort studies that followed peopleover time, allowing for more definitive con-clusions regarding causality. Eight of the 10cohort studies supported the conclusion thatpoorer glycemic control leads to poorer pe-riodontal health over time.
Although the majority of studies re-porting on the adverse effects of diabetes arecross-sectional and involve conveniencesamples of patients, principally from hospi-tals and clinics, a smaller subset of longitu-dinal and population-based studies provideadditional support for the association be-tween diabetes and periodontal disease. Thestudies were conducted in different settingsand different countries, with different ethnicpopulations and age mixes, and with a vari-ety of measures of periodontal disease status(e.g., gingival inflammation, pathologicprobing pocket depth, loss of periodontal attachment, or radiographic evidence of alveolar bone loss). The studies used differ-ent parameters to assess periodontal disease occurrence (e.g., prevalence, incidence, ex-tent, severity, or progression). This inevit ablevariation in methodology and study popula-tions limits the possibility that the same biases or confounding factors apply in allthe studies and provides support for con-cluding that diabetes is a risk factor for perio -dontal disease incidence, progression, andseverity. In addition, there is substantial evi -dence to support a “dose-response” relation -
88 Periodontal Disease and Overall Health: A Clinician's Guide
Table 2. Effects of Degree of Glycemic Control on Periodontal Health:Table 1. Conclusions of the Studies
Note: The numerator represents the number of studies reporting increasing degree of glycemic control having decreasing adverse effect on periodontal health; the denominator represents the total number of studies in each group:# Studies with Effect/Total # Studies.
Diabetes Mellitus Type
Type Not Total Number of StudiesStudy Design Type 1 Type 2 Type 1 or 2 Reported (# with Effect /# All Studies)
Cohort 4/4 3/3 1/3 0/0 8/10Cross-sectional, Descriptive 11/18 15/17 7/11 1/5 34/61
Total: 15/22 18/20 8/14 1/5 42/61

ship, i.e., as glycemic control worsens, theadverse effects of diabetes on periodontalhealth become greater. Finally, there are nostudies with superior design features to refutethis conclusion. Examples of comprehensivereviews of the studies in this body of litera-ture are presented in articles by Mealey andOcampo,2 Lamster et al.,3 and Taylor andBorgnakke.4, 5
ADVERSE EFFECTS OF DIABETESON PERIODONTAL HEALTH: EVIDENCE FROM IN VITRO
AND ANIMAL STUDIESThis next section provides insight into
mechanisms of diabetes-enhanced peri-odontal disease from animal and in vitrostudies. Studies in people with diabetesclearly indicate that diabetes causes an in-crease in the inflammatory response. Thishas significant impact on periodontal dis-eases, which largely result from inflamma-tory changes triggered by bacterial invasioninto connective tissue.6 Diabetic rats haveincreased inflammation of the periodontalepithelium and connective tissues, alongwith increased degradation of connective tis-sue and increased bone loss.7,8 Similarly, diabetic mice have been shown to have in-creased inflammation, oxidative stress, andbone loss.9 Furthermore, diabetes may in-crease the systemic response to periodontalbacteria or their products.10
Heightened Inflammatory Response:Cellular and Molecular EventsInsight into mechanisms of diabetes-en-
hanced periodontitis come from in vitro andanimal studies that established cause-and-effect relationships between specific cellu-lar and molecular events that cannot be per-formed easily in human studies.11 Cell culturestudies have demonstrated that lipopolysac-charide (LPS)-stimulated monocytes isolatedfrom individuals with diabetes exhibit greaterproduction of tumor necrosis factor-alpha
(TNF-) than in individuals who do not havediabetes.12 Neutrophils from individuals withdiabetes have increased production of super-oxides, which enhance oxidative stress.13 Inan animal model, injection of Porphyromonasgingivalis, an established periodontal pathogen,into connective tissue was shown to stimulatemore prolonged formation of an inflamma-tory infiltrate with higher levels of inflam-matory cytokines.14 This was linked to higherlevels of TNF- since a specific TNF in-hibitor reversed the increased inflammationin the diabetic mice stimulated by P. gingi-valis.15 In another animal model, Type 2 dia-betes was shown to significantly increase pe-riodontal inflammation induced by the onsetof periodontal disease compared to matchedhealthy rats.16 Diabetic rats had significantlymore prolonged gingival inflammation aswell as greater osteoclast numbers and in-creased bone loss.
Uncoupling of Bone Resorptionand Bone Formation
A second mechanism is proposed tocontribute to greater bone loss in the dia-betic animals, namely an uncoupling of boneresorption and bone formation.16 Once boneis resorbed, it is repaired by new bone for-mation by a process referred to as coupling.17
Thus, the amount of bone lost is equal tothe amount of bone resorption minus theamount of reparative new bone formation.The diabetic animals had significantly lesscoupling so that there was less reparativebone formation following an episode of re-sorption, which contributes to the net boneloss. A potential mechanism was indicatedby decreased numbers of bone-lining andperio dontal ligament cells, which could beexplained by higher levels of cell death(apoptosis).16 This interpretation is supportedby studies in which a cause-and-effect rela-tionship between diabetes-enhanced apop-tosis and the ability to form bone after anepisode of resorption,18 since inhibition of
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 89
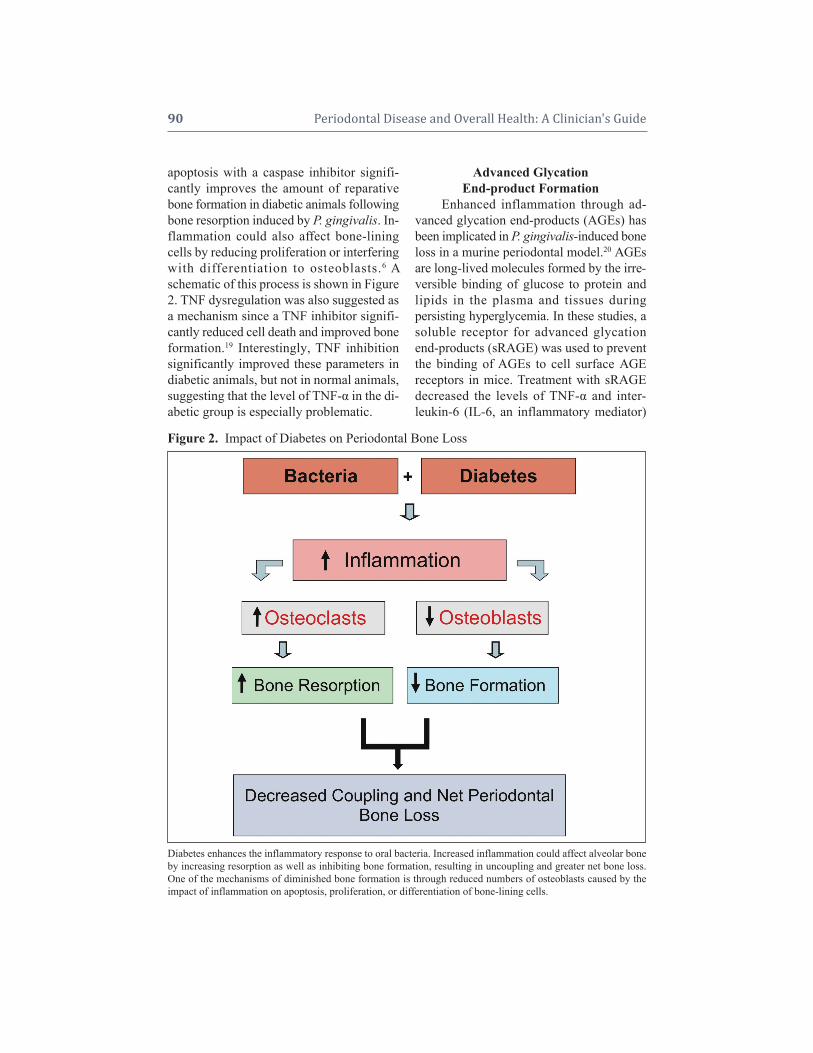
apoptosis with a caspase inhibitor signifi-cantly improves the amount of reparativebone formation in diabetic animals followingbone resorption induced by P. gingivalis. In-flammation could also affect bone-liningcells by reducing proliferation or interferingwith differentiation to osteoblasts.6 Aschematic of this process is shown in Figure2. TNF dysregulation was also suggested asa mechanism since a TNF inhibitor signifi-cantly reduced cell death and improved boneformation.19 Interestingly, TNF inhibitionsignificantly improved these parameters indiabetic animals, but not in normal animals,suggesting that the level of TNF- in the di-abetic group is especially problematic.
Advanced GlycationEnd-product Formation
Enhanced inflammation through ad-vanced glycation end-products (AGEs) hasbeen implicated in P. gingivalis-induced boneloss in a murine periodontal model.20 AGEsare long-lived molecules formed by the ir re-versible binding of glucose to protein andlipids in the plasma and tissues dur ingper sist ing hyperglycemia. In these studies, asoluble receptor for advanced glycationend-products (sRAGE) was used to preventthe binding of AGEs to cell surface AGEreceptors in mice. Treatment with sRAGE decreased the levels of TNF- and inter-leukin-6 (IL-6, an inflammatory mediator)
90 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 2. Impact of Diabetes on Periodontal Bone Loss
Diabetes enhances the inflammatory response to oral bacteria. Increased inflammation could affect alveolar boneby increasing resorption as well as inhibiting bone formation, resulting in uncoupling and greater net bone loss.One of the mechanisms of diminished bone formation is through reduced numbers of osteoblasts caused by the impact of inflammation on apoptosis, proliferation, or differentiation of bone-lining cells.

in gingival tissue and suppressed alveolarbone loss. These findings link AGEs withan exaggerated inflammatory response andincreased bone loss in diabetes-enhanced perio dontal disease.
Other MechanismsSeveral other studies have provided
insight into mechanisms by which diabetesincreases periodontal bone loss in animalmodels. In one example, treatment with N-acetylcysteine significantly inhibited al -veolar bone loss in a murine model.21 SinceN-acetylcysteine reduces inflammation andoxidative stress, these studies suggest that ele -vated levels of inflammation and oxidationin diabetic animals promote greater perio -dontal tissue loss. Mahamed and colleagueshave demonstrated that increased produc-tion of receptor-activator of nuclear factorkappaB (NF-B) ligand (RANKL) occursin the periodontium of diabetic mice.22 Acause-and-effect relationship was shown between diabetes-increased RANKL and accelerated bone loss by successful reduc-tion in bone loss via treatment with a RANKL-inhibitor, osteoprotegerin.
Increased bone loss in diabetic rats hasalso been linked to increased matrix metal-loproteinase (MMP) activity.23 MMPs are agroup of enzymes that can break down pro-teins, such as collagen, that are normallyfound in the spaces between cells in tissues(i.e., extracellular matrix proteins). WhenMMP activity was inhibited, there was sig-nificantly reduced bone loss in diabetic rats.23
Paradoxically, an enhanced inflammatory re-sponse may also be associated with a less ef-fective reaction that results in deficits in bac-terial killing.24 Decreased bacterial killingmay potentially enhance the growth ofpathogens and increase the possibility thatopportunistic bacteria will cause periodontaltissue loss. An altered host response to bac-teria can lead to greater or prolonged ex-pression of cytokines that stimulate bone re-
sorption and may limit bone repair. Similaralterations are noted in other diabetic com-plications, such as retinopathy, nephropathy,and impaired fracture healing.
Lipid Dysregulation andImpaired Wound Healing
Three reviews provide discussion of investigations providing additional per spec-tive on metabolic dysregulation in diabetesand the effects of hyperlipidemia on mono-cyte/macrophage function in wound signal-ing.25-27 The monocyte/macrophage is con-sidered the major mediator of the inflam- matory phase in wound healing, having pri-mary roles in wound signal transduction andin the initiation of the transition of healingfrom the inflammatory to the granulationphase. One hypothesized effect of hyper-lipidemia occurs through fatty acid interac-tion with the monocyte cell membrane, caus-ing impaired function of membrane-boundreceptors and enzyme systems. This leads toimpaired amplification and transduction ofthe wound signal. Another postulated path-way leading to impaired monocyte functionin diabetes and wound signaling is via thenonenzymatic glycosylation of lipids andtriglycerides in addition to proteins. TheseAGEs are thought to affect normal differen-tiation and maturation of specific monocytephenotypes throughout the different stages ofwound healing. The net result of both ofthese pathways is exacerbated host- mediatedinflammatory responses and tissue de -struction. In impairing monocyte function, diabetes-associated lipid dysregulation, lead-ing to high levels of low-density lipopro-teins and triglycerides, may be a major factorin the incidence and severity of perio dontaldisease.
Molecular Dysregulation in Diabetesthat Enhances Inflammation
A number of metabolic pathways areaffected by diabetes. In many cases they
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 91

have been linked to hyperglycemia, althoughthe potential contribution of hypoinsulinemiashould also be considered. One of thechanges that occurs is increased shuntingthrough the polyol pathway that leads to en-hanced aldose reductase activity and greaterproduction of the sugars sorbitol and fruc-tose. As a result, there is increased formationof AGEs and enhanced formation of reactiveoxygen species (ROS) and nitric oxide (NO).AGEs, ROS, and NO are pro-inflammatory.That this pathway is important in diabeteshas been shown by the use of aldose reduc-tase inhibitors. When aldose reductase is inhibited, there is reduced protein kinase C(PKC) activation, less nuclear translocationof NF-B, and reduced expression of mark-ers of inflammation.28,29 Inhibiting aldose reductase also decreases the production ofROS.28,29 In addition, bacterial killing byneutrophils, which is reduced in individualswith diabetes, is improved by use of an aldose reductase inhibitor.30 This may haveimplications for periodontal disease as dia-betes reduces the capacity of neutrophils tokill periodontal pathogens such as P. gingi-valis.24 As indicated above, oxidative stressis significantly increased by diabetes and isassociated with both enhanced formation ofROS and decreased antioxidant capacity.6,7
One of the mechanisms by which this occursis through overloading the electron transportchains in mitochondria, which leads to es-cape of electrons that react with oxygen-pro-ducing superoxides. ROS cause cell dam-age and also stimulate the production ofinflammatory cytokines. The importance ofoxidative stress in diabetic conditions has beendemonstrated by improvements of diabeticcomplications by treatment of diabetic ani-mals with antioxidants.31
Diabetic complications have been linkedto elevated activation of PKC. Diabetes increases glycolysis, which in turn causes in creased levels of dihydroxyacetone phos-phate that may be converted to diacylglyc-
erol. PKC is activated by diacylglycerol andby an increased ratio of nicotinamide ade-nine dinucleotide (reduced form) to nico -tinamide adenine dinucleotide (NADH/NAD+ratio) associated with diabetes.32 IncreasedPKC activity then stimulates formation ofROS and inflammation. PKC-/PKC- inhibitors reverse this increase. Hyperglyce -mia is also linked to increased formation ofadvanced glycation end-products, which arepro-inflammatory.20,39 AGEs also possesspro-apoptotic activity.33-37 Inhibition of oneof the receptors for AGEs, RAGE, reduces in -flammation that is enhanced by diabetes.20,38
The use of a RAGE inhibitor in a periodon talmodel was discussed in a previous section.
ADVERSE EFFECTS OFPERIODONTAL INFECTIONON GLYCEMIC CONTROL
This next section assesses the evidencefor an effect going in the opposite direc-tion, namely periodontal infection adverselyaffect ing glycemic control in people withdiabetes.
In addition to the substantial evidencedemonstrating diabetes as a risk factor forpoorer periodontal health, there is a growingbody of evidence supporting the long-heldclinical observation that periodontal infec-tion adversely affects glycemic control.There is also increasing evidence that peri-odontal infection contributes to greater riskfor diabetes complications. Diabetes compli -cations are the conditions or diseases thatpeople with diabetes often develop due totheir diabetic status, such as increased riskof coronary heart disease (CHD), stroke,myocardial infarction, and other cardio -vascular events; nephropathy (diseases of thekidney, ultimately leading to end-stage renaldisease [ESRD], requiring renal dialysis forthe patient to survive); neuropathy (diseasesof the peripheral and autonomic nerves);retinopathy (diseases of the retina, possiblyleading to blindness); extremely decreased
92 Periodontal Disease and Overall Health: A Clinician's Guide

wound healing; and amputations due to oneor more of the complications mentioned.
Evidence supporting the biologic plau-sibility of periodontal infection contributingto poorer glycemic control, complicationsof diabetes, and perhaps the development ofType 2 diabetes, comes from integrating sev-eral converging perspectives. This biologicplausibility is grounded in periodontitis be-ing a chronic inflammatory response to apredominantly Gram-negative bacterial in-fection and the emerging evidence linkingchronic infection and inflammation, insulinresistance, and the development of diabetesand its complications.39
Periodontal Infection: Contribution to aChronic Systemic Inflammatory Burden
Periodontal infection, if untreated, canlead to extensive destruction of local softconnective tissue and alveolar bone, and is amajor cause of tooth loss.40 Periodontalinfection elicits a local chronic inflammatoryresponse and is considered a contributingsource for the total chronic, systemic,inflammatory burden.41 The highly vascular,inflamed, and ulcerated periodontal pocketepithelium provides a ready portal of entryfor periodontal pathogens from the dentalplaque biofilm, many of which are Gram-negative and obligate anaerobes. Bacteremia,a situation in which bacteria have penetratedinto the blood stream and therefore arecirculated throughout the body, is recognizedto occur in periodontitis. Periodontal patho -gens have been identified in atheromatousplaques and shown to invade aortic andcoronary endothelial cells.42 Bacterial com -ponents (e.g., LPS) are also disseminated intothe systemic circulation. The bacteremia andsubsequent systemic dis persal of periodontalpathogens and bac terial components mayrelocate antigenic stimuli at sites such asendo thelial cells and hepato cytes, elicitingtheir production of pro-inflam matory immunemediators. Additionally, the pro-inflammatory
mediators, such as IL-1, TNF-, IL-6,prostaglandins E2 (PGE2), and thromboxaneB2, produced locally at the periodontal lesion,may also enter the systemic circulation andproduce distant systemic pro-inflammatoryeffects at target tissues and organs.41,42 Hence,the inflamed periodontal tissue behaves as apotential endocrine-like source for increasedchronic systemic inflammatory challenge.
TNF-, IL-6, and IL-1, all mediatorsimportant in periodontal inflammation, havebeen shown to have important effects on glu-cose and lipid metabolism as well as insulinaction, following an acute infectious chal-lenge or trauma.43-47 Additionally, chronic,low-grade inflammation, in which thesesame mediators are involved, has beenshown to be associated with the develop-ment of insulin resistance, diabetes, and itscomplications.39,48
The mechanisms by which periodontalinfection could contribute to insulin resist-ance, poorer glycemic control and compli-cations of diabetes, and possibly the devel-opment of Type 2 diabetes, are perhaps bestunderstood by considering the emerging ev-idence regarding the systemic effects of obe-sity. Adipose tissue is now recognized as im-portant in chronically activating the innateimmune system and contributing to a chronic,low-grade systemic inflammatory burden.The adverse effects of obesity-related acti-vation of systemic inflammation also includedevelopment of insulin resistance, glucoseintolerance, and increased risk for the de-velopment of Type 2 diabetes.49
Adipose tissue secretes several bio - active proteins, known as adipokines, thathave local autocrine/paracrine effects as wellas systemic hormonal effects. Several of theadipokines are pro-inflammatory mediatorsthat can contribute to a state of chronic, low-grade systemic inflammation.50 As previ-ously mentioned, a subset of the adipokinesproduced by the adipose tissue are alsoamong the set of inflammatory mediators
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 93
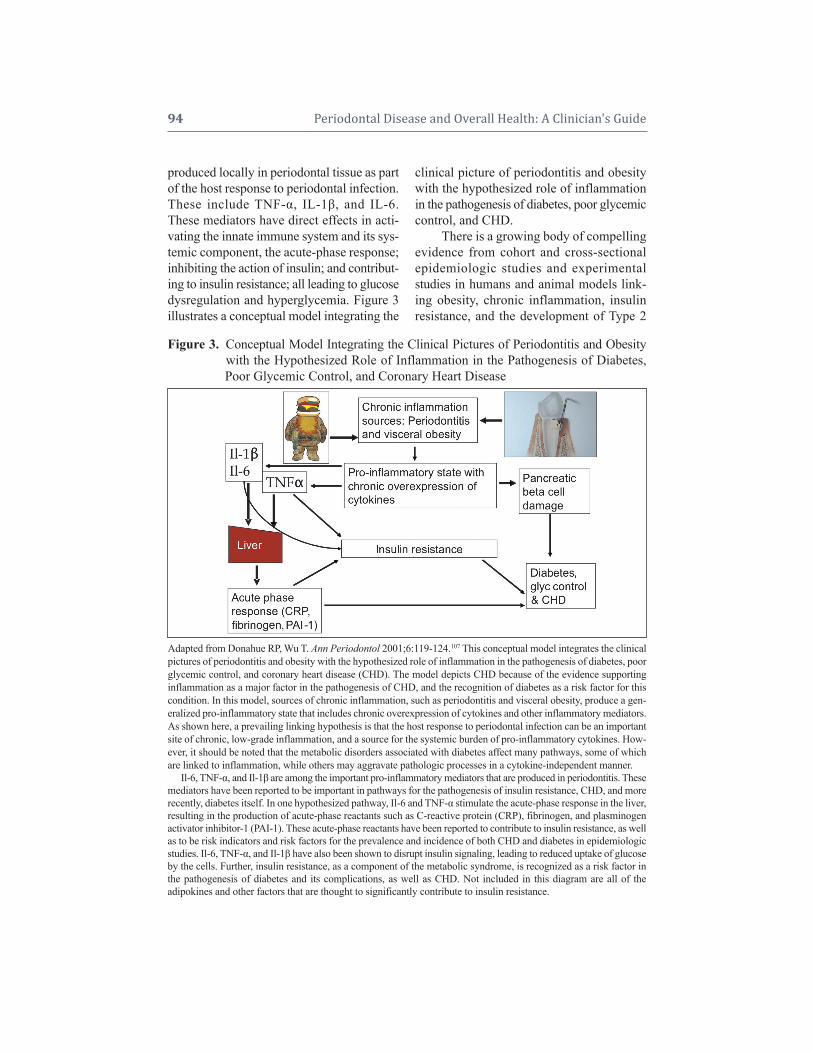
produced locally in periodontal tissue as partof the host response to periodontal infection.These include TNF-, IL-1, and IL-6.These mediators have direct effects in acti-vat ing the innate immune system and its sys-temic component, the acute-phase response;inhibiting the action of insulin; and contribut -ing to insulin resistance; all leading to glucosedysregulation and hyperglycemia. Figure 3illustrates a conceptual model integrating the
clinical picture of periodontitis and obesitywith the hypothesized role of inflammationin the pathogenesis of diabetes, poor glycemiccontrol, and CHD.
There is a growing body of compellingevidence from cohort and cross-sectionalepidemiologic studies and experimentalstudies in humans and animal models link-ing obesity, chronic inflammation, insulin resistance, and the development of Type 2
94 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 3. Conceptual Model Integrating the Clinical Pictures of Periodontitis and ObesityFigure 3. with the Hypothesized Role of Inflammation in the Pathogenesis of Diabetes,Figure 3. Poor Glycemic Control, and Coronary Heart Disease
Adapted from Donahue RP, Wu T. Ann Periodontol 2001;6:119-124.107 This conceptual model integrates the clinicalpictures of periodontitis and obesity with the hypothesized role of inflammation in the pathogenesis of diabetes, poorglycemic control, and coronary heart disease (CHD). The model depicts CHD because of the evidence supporting inflammation as a major factor in the pathogenesis of CHD, and the recognition of diabetes as a risk factor for thiscondition. In this model, sources of chronic inflammation, such as periodontitis and visceral obesity, produce a gen-eralized pro-inflammatory state that includes chronic overexpression of cytokines and other inflammatory mediators.As shown here, a prevailing linking hypothesis is that the host response to periodontal infection can be an importantsite of chronic, low-grade inflammation, and a source for the systemic burden of pro-inflammatory cytokines. How-ever, it should be noted that the metabolic disorders associated with diabetes affect many pathways, some of whichare linked to inflammation, while others may aggravate pathologic processes in a cytokine-independent manner.
Il-6, TNF-, and Il-1 are among the important pro-inflammatory mediators that are produced in periodontitis. Thesemediators have been reported to be important in pathways for the pathogenesis of insulin resistance, CHD, and morerecently, diabetes itself. In one hypothesized pathway, Il-6 and TNF- stimulate the acute-phase response in the liver, resulting in the production of acute-phase reactants such as C-reactive protein (CRP), fibrinogen, and plasminogenactivator inhibitor-1 (PAI-1). These acute-phase reactants have been reported to contribute to insulin resistance, as wellas to be risk indicators and risk factors for the prevalence and incidence of both CHD and diabetes in epidemiologicstudies. Il-6, TNF-, and Il-1 have also been shown to disrupt insulin signaling, leading to reduced uptake of glucoseby the cells. Further, insulin resistance, as a component of the metabolic syndrome, is recognized as a risk factor inthe pathogenesis of diabetes and its complications, as well as CHD. Not included in this diagram are all of theadipokines and other factors that are thought to significantly contribute to insulin resistance.

diabetes. The epidemiologic studies haveshown markers of inflammation are associ-ated with Type 2 diabetes and features ofthe metabolic syndrome in cross-sectional studies of individuals without diabetes orwith impaired glucose tolerance or impairedfasting glucose; markers of inflammationpredict Type 2 diabetes; inflammation is in-volved in the pathogenesis of atherosclerosis,a common feature of Type 2 diabetes; anti-inflammatory agents (e.g., aspirin, statins,glitazones) decrease the acute-phase re-sponse and may reduce the risk of develop-ing Type 2 diabetes and improve glycemiccontrol in established diabetes; and GDN, arisk factor for Type 2 diabetes, is associatedwith an inflammatory response. The experi-mental studies have involved pharmacologic,nutritional, and genetic interventions pro-viding further understanding of the cell-ular and molecular mechanisms throughwhich chronic stressors (e.g., overnutrition, microbial products, hyperglycemia, hyper-lipidemia, oxidative stress, and psycho -logical stress), innate immunity, chronic systemic inflammation, obesity, insulin resistance, and metabolic dysregulation are integrated.49-55 Connecting this evidence tothe potential systemic effects of periodontal infection on chronic inflammation is theemerging body of evidence linking epi-demiologic and intervention studies ofperio dontal infection to markers of systemic inflammation and changes in levels of the inflammatory markers after periodontaltreatment.41,42,56-58
Periodontal Infection Adversely Affecting Glycemic Control:
Empirical Evidence from NonsurgicalPeriodontal Treatment StudiesMore direct, empirical evidence re-
garding the effects of periodontal infectionon glycemic control of diabetes comes fromtreatment studies using nonsurgical perio -dontal therapy and observational studies. The
treatment studies are a heterogeneous set of31 reports that include 10 RCTs and 21 non-randomized clinical treatment studies as dis-played in Table 3. The RCTs used controlgroups that were either nontreated con-trols,59,60 positive controls (i.e., the controlgroup received a relatively less intense formof periodontal treatment),61-66 or controls ad-vised to continue their usual dental care.67 Ofthe 10 RCTs reviewed, six reported a bene-ficial effect of periodontal therapy.60-63,65,66
Among the set of 21 periodontal treat-ment studies that were not RCTs, 12 reporteda beneficial effect on glycemic control68-80
while nine did not.81-89 It is remarkable thatonly two of these 21 studies included controlor comparison groups.68,81 These studies hadmarked variation in the use of adjunctiveanti biotics, with four of the five studies that
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 95
Table 3. Effects of Nonsurgical PeriodontalTable 1. Therapy on Glycemic Control:Table 1. Conclusions of the 31 Studies
*These 10 RTCstudies are further described in Table 4.Note: The numerator represents the number of studiesreporting nonsurgical therapy being associated with in-creasing degrees of glycemic control; the denominatorrepresents the total number of studies in each group: # Studies with Effect/Total # Studies.
Number of Studieswith Significant
Study Design Improvement inGlycemic Control /
All Studies
Randomized Clinical Trials (RCTs):
Nontreated control group 1/3Positive (i.e., less intensely treated) control group 5/6Usual source of care control group 0/1
Total RCTs 6/10
Nonrandomized ClinicalTrials (Non-RCTs):
Nontreated control group 1/2No control group 11/19
Total Non-RCTs 12/21
Total All NonsurgicalTreatment Studies 18/31 (RCTs + Non-RCTs)

used systemic antibiotics reporting a bene -ficial effect on glycemic control71,74,76,79 andone finding a numerical decrease in theHbA1c level that did not reach statisticalsignificance.81
For the body of literature consisting ofboth RCTs and other types of studies, thereis marked hetereogeneity in the studies’ designs, geographic locations, source popu-lations, conduct, length of follow-up forglycemic control assessment, types of par-ticipants and their baseline periodontal dis-ease and glycemic control status, inclusionof control groups, periodontal treatment pro-tocols, sample size and power to detect dif-ferences in periodontal and metabolic re-sponse, and specific hypotheses tested.90 Thedetails of the variation in this body of lit -erature have been extensively described inseveral reviews.43,91,92
Table 4 provides additional informa-tion about the RCTs summarized in Table 3.For each study, information on the number ofparticipants and the type of diabetes included
96 Periodontal Disease and Overall Health: A Clinician's Guide
is given, along with indication of whether antibiotics were used in conjunction with thetreatment. The types of antibiotics used andinformation on their dispensing mode ( local,systemic, rinse) can be seen in the table’s foot -note marked with one asterisk (*). Finally,in the far right column is the outcomeachieved, indicating whether the study treat-ment resulted in improved glycemic controlas measured by a decrease in the level ofHbA1c.
One remarkable observation is the rel-atively small numbers of participants insome of the studies. This is mostly due to theimmense resources required for conductingclinical trials, especially those that have along follow-up period. Also, it is difficult toidentify individuals meeting inclusion crite-ria and those free of exclusion criteria, and torecruit, enroll, and keep participants return-ing for all study visits that typically are oflong duration due to their many components(e.g., interview, clinical examination, blooddraw, radiographic exposure, and initial
Table 4. Effects of Nonsurgical Periodontal Therapy on Glycemic Control (HbA1c):Table 1. Descriptions and Conclusions of the 10 Randomized Clinical Trials (RTCs)Table 1. Summarized in Table 3
*Adjunctive antibiotic types: a) systemic doxycycline, b) amoxicillin and augmentin, c) minocycline, locally delivered.**The group not receiving antibiotic showed greater improvement.
Adjunctive Statistically SignificantClinical Study Design by Sample Diabetes Antibiotics Beneficial EffectType of Control Group Size Type Used* on HbA1c
RCT with Nontreated Control Group:Aldridge et al. study 1 (1995)59 31 1 No NoAldridge et al. study 2 (1995)59 22 1 No NoKiran et al. study 1 (2005)60 44 2 No Yes
RCT with Positive (i.e., LessIntensely Treated) Control Group:Grossi et al. (1997)61
.1130 2 aYesa YesAl-Mubarak et al. (2002)64 78 1,2 No NoRodrigues et al. (2003)62 30 2 aYesb **Yes**Skaleric et al. (2004)63 20 1 aYesc YesYun et al. (2007)66 46 2 aYesa YesO’Connell et al. (2008)65 30 2 aYesa Yes
RCT with Usual Sourceof Care-Control Group:Jones et al. (2007)67 1650 2 aYesa No

therapy and maintenance visits). In addition,clinical studies typically last several monthsor years.
An important source of variation in theRCTs is the use of adjunctive antibiotics withthe nonsurgical periodontal therapy. Amongthe six RCTs that included adjunctive anti -biotics, five used the antibiotics systemi-cally61,62,65-67 and one was locally delivered.63
Five of the six RCTs using antibiotics showedbeneficial effects on glycemic control.61-63,65,66
However, it is important to note the signifi-cant improvement for one study was in thepositive control group that did not receive thesystemic antibiotic.62 Also, one of the sixRCTs reporting a beneficial effect did notuse any antibiotics.60 Hence, to date there issuggestive, but not clear-cut evidence to sup-port the use of antibiotics in combinationwith nonsurgical periodontal treatment inorder to observe an improvement in glycemiccontrol.
Periodontal Infection Adversely Affecting Glycemic Control: Empirical Evidence from Observational Studies
Additional evidence to support the effect of periodontitis on increased risk forpoorer glycemic control comes from a smallnumber of observational studies. A longitu-dinal epidemiologic study of the Pima Indi-ans in Arizona found at baseline that subjectswho had Type 2 diabetes, that was in good tomoderate control, but also had severe perio -dontitis, were approximately six times morelikely to have poor glycemic control at atwo-year follow-up than those who did nothave severe periodontitis at baseline.93 In an-other observational study of 25 adults ages58 to 77 with Type 2 diabetes, Collin et al.also reported an association between ad-vanced periodontal disease and impairedmetabolic control.94
Finally, two cross-sectional studies report findings consistent with poorer peri-odontal health associated with poorer
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 97
glycemic control. One of these studies,which included 127 pregnant women withdiabetes, reported that those with perio -dontitis were more likely to have poorerglycemic control, after controlling for pres-ence of a urinary tract infection and/or cer-vicovaginal infection and a measure of com-pliance to recommended medical treatmentfor the diabetes.95 The other study, analyzingthe association between number of bleed-ing sites and degree of glycemic control(HbA1c), reported a statistically significantassociation, i.e., the HbA1c values increased(poorer control with higher HbA1c) as thenumber of bleeding sites increased. How-ever, the authors determined this resultwould have no clinical significance96 be-cause the measure of association betweenthe number of bleeding sites and glycemiccontrol was very small.
Periodontal Infection as a Potential RiskFactor for Diabetes Complications:
Empirical Evidence fromObservational Studies
It is well recognized that poor glycemiccontrol is a major determinant for the devel-opment of the chronic complications of dia-betes. Results from the landmark DiabetesControl and Complications Trial (involvingType 1 diabetes) and the UK Prospective Di-abetes Study (UKPDS, involving Type 2 di-abetes) demonstrated that attaining andmaintaining good glycemic control could re-duce the risk for and slow the progression ofmicrovascular complications in patients withType 1 and Type 2 diabetes.97-99 Additionally,the UKPDS observed a 16% reduction(p = 0.052) in the risk of combined fatal ornonfatal myocardial infarction and suddendeath. Further epidemiologic analysis fromthe UKPDS showed a continuous associationbetween the risk of cardiovascular compli-cations and glycemia; every percentage pointdecrease in HbAlc (e.g., 9% to 8%) was associated with a 25% reduction in diabetes-

related deaths, 7% reduction in all-causemortality, and 18% reduction in combinedfatal and nonfatal myocardial infarction.100
There is emerging evidence from ob -ser vational studies regarding the association between periodontal disease and the risk for diabetes complications. Thorstensson andcolleagues101 studied 39 case-control pairsof individuals with Type 1 and Type 2 dia-betes for six years’ median follow-up time inJönköping, Sweden. In each pair, the caseshad severe alveolar bone loss and controlshad gingivitis or minor alveolar bone loss.They found that cases were significantlymore likely to have prevalent proteinuriaand cardiovascular complications, includingstroke, transient ischemic attacks, angina,myo cardial infarction, and intermittent clau-dication than controls at their follow-upmedical assessments.
Two reports from the ongoing longitu-dinal study of diabetes and its complicationsin the Gila River Indian Community in Ari-zona, conducted by the National Institute ofDiabetes and Digestive and Kidney Dis-eases, address nephropathy and cardiovas-cular disease. Saremi and colleagues102 stud-ied a cohort of 628 individuals for a medianfollow-up time of 11 years. Individuals with severe periodontal disease had 3.2 timesgreater risk for cardio-renal mortality (i.e., ischemic heart disease and diabetic nephrop -athy combined) than those with no, mild, ormoderate periodontal disease. This estimateof significantly greater risk persisted whilecontrolling for several major risk factors ofcardio-renal mortality, including age, sex, diabetes duration, HbA1c, body mass index,hypertension, blood glucose, cholesterol,electrocardiographic abnormalities, macro -albuminuria, and smoking.
In the second report, Shultis and col-leagues103 investigated the effect of perio -dontitis on risk for development of overtnephropathy (macroalbuminuria) and ESRDin a group of 529 Gila River Indian Com-
munity adults with Type 2 diabetes. Theirproportional hazards model analyses, adjustedfor age, sex, diabetes duration, body mass index, and smoking, indicated periodontitisand edentulism were significantly associatedwith the risk of developing overt nephrop -athy and ESRD. The incidence of macroal-buminuria was 2.0, 2.1, and 2.6 times greaterin individuals with moderate or severe perio -dontitis or in those who were edentulous,respectively, than those with none/mild perio -dontitis. The incidence of ESRD was also2.3, 3.5, and 4.9 times greater for individu-als with moderate or severe periodontitis orfor those who were edentulous, respectively,than those with none/mild periodontitis.
Periodontal Infection as a Potential RiskFactor for Development of Diabetes:
Empirical Evidence fromObservational Studies
In addition to evidence supporting pe-riodontal disease as a potential risk factorfor developing diabetes complications, thereis also evidence emerging that periodontaldisease may be a risk factor for the develop-ment of Type 2 diabetes and possibly GDM.Demmer and colleagues104 investigated theassociation between periodontal disease andthe development (i.e., incidence) of new di-abetes cases in a representative sample ofthe US population, analyzing data from thefirst National Health and Nutrition Exami-nation Survey (NHANES I) and its Epi-demiologic Follow-up Study (NHEFS). Theaverage follow-up period for the 9,296 individuals in the analysis was 17 years, forthe period between 1971 to 1992. Thestudy used a cohort study design because information on the presence or absence ofperio dontal disease (i.e., the hypothesizedcausal factor) was known at the time thestudy began, and the outcome (developmentof diabetes) was assessed subsequently. Thisstudy concluded that having periodontal disease was significantly associated with a
98 Periodontal Disease and Overall Health: A Clinician's Guide

50–100% greater risk for developing Type 2diabetes, after controlling for other estab-lished risk factors for diabetes. The greaterrisk for diabetes was also consistent withprevious research using NHANES I andNHEFS, in which risk factors for diabetesthat did not include perio dontal disease, forexample, measures of adiposity (body massindex and subscapular skinfold thickness),having hypertension, and increased age, werealso statistically significant.105
Finally, Dasanayake and colleagues106
investigated whether or not pregnant womenwho develop GDM, compared to pregnantwomen who do not develop GDM, hadpoorer clinical perio dontal health and/ordemonstrated higher levels of other bio -logical markers of perio dontal disease ap -proximately two months before their GDMdiagnosis. The other biological markersincluded bacterio logical (in dental plaque andcervicovaginal samples), immunological, andperiodontitis-related inflammatory mediatoranalytes. This study found that women whohad higher levels of Tannerella forsythia (T.forsythia), a recognized perio dontal pathogen,in the vaginal flora were statistically signifi -cantly more likely to develop GDM than thosewomen with lower levels. The Dasanayakeet al. study concluded that T. forsythia in thevaginal flora is a potential risk factor for GDM.
SUMMARY AND CONCLUSIONSThe evidence reviewed in this chapter
supports the conclusion that a bi-directionalassociation exists between diabetes mellitusand periodontal health: Diabetes is associ-ated with increased development and pro-gression of periodontitis, and periodontal infection is associated with poorer glycemiccontrol in people with diabetes.
There is also evidence emerging thatgestational diabetes may adversely affect periodontal health.
Additionally, evidence is emerging tosuggest that periodontal disease is asso ciated
with increased risk for diabetes complica-tions, the development of Type 2 diabetes,and perhaps the development of GDM.
While treating periodontal infection inpeople with diabetes is clearly an importantcomponent in maintaining oral health, it mayalso play an important role in establishingand maintaining glycemic control, and pos-sibly in delaying the onset or progression ofdiabetes and its complications.
Therefore, dental health professionalsmight fulfill an important role in maintainingor improving the health, and ultimately thequality of life, of individuals with diabetesand GDM, as well as aiding in lessening theimmense burden of diabetes and periodontaldiseases on our society in general.
Supplemental ReadingsDarre L, Vergnes JN, Gourdy P, Sixou M. Efficacy ofperiodontal treatment on glycaemic control in diabeticpatients: A meta-analysis of interventional studies. Diabetes Metab 2008;34:497-506.
Demmer RT, Jacobs DR Jr, Desvarieux M. Periodontaldisease and incident Type 2 diabetes: results from theFirst National Health and Nutrition Examination Surveyand its epidemiologic follow-up study. Diabetes Care2008;31:1373-1379.
Graves DT, Liu R, Oates TW. Diabetes-enhanced in-flammation and apoptosis: impact on periodontal patho-sis. Periodontology 2000 2007;45:128-137.
King GL. The role of inflammatory cytokines in dia-betes and its complications. J Periodontol 2008;79:1527-1534.
Mealey BL, Ocampo GL. Diabetes mellitus and perio -dontal disease. Periodontol 2000 2007;44:127-153.
Taylor GW, Borgnakke WS. Periodontal disease: asso-ciations with diabetes, glycemic control and complica-tions. Oral Dis 2008;14:191-203.
REFERENCES1. Elwood J. Critical Appraisal of Epidemiological
Studies and Clinical Trials. New York: Oxford Uni-versity Press; 1998.
2. Mealey BL, Ocampo GL. Diabetes mellitus andperiodontal disease. Periodontol 2000 2007;44:127-153.
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 99

3. Lamster IB, Lalla E, Borgnakke WS, Taylor GW.The relationship between oral health and diabetesmellitus. JADA 2008;139(Suppl):19S–24S.
4. Taylor GW, Borgnakke WS. Periodontal disease:associations with diabetes, glycemic control andcomplications. Oral Dis 2008;14:191–203.
5. Taylor GW, Borgnakke WS. Treatment of estab-lished complications: periodontal disease. In: Herman W, Kinmouth AL, Wareham NJ, WilliamsR, eds. The Evidence Base in Diabetes Care, 2ndedition. Chichester, The United Kingdom: JohnWiley & Sons, 2009.
6. Graves DT, Liu R, Alikhani M, Al-Mashat H,Trackman PC. Diabetes-enhanced inflammationand apoptosis—impact on periodontal pathology. JDent Res 2006;85:15–21.
7. Silva JA, Lorencini M, Reis JR, Carvalho HF,Cagnon VH, Stach-Machado DR. The influence oftype I diabetes mellitus in periodontal disease in-duced changes of the gingival epithelium and con-nective tissue. Tissue Cell 2008;40:283–292.
8. Bissada NF, Schaffer EM, Lazarow A. Effect ofalloxan diabetes and local irritating factors on theperiodontal structures of the rat. Periodontics 1966;4:233–240.
9. Gyurko R, Siqueira CC, Caldon N, Gao L, KantarciA, Van Dyke TE. Chronic hyperglycemia predis-poses to exaggerated inflammatory response andleukocyte dysfunction in Akita mice. J Immunol2006;177:7250–7256.
10. Lu H, Raptis M, Black E, Stan M, Amar S, GravesDT. Influence of diabetes on the exacerbation of aninflammatory response in cardiovascular tissue.Endocrinology 2004;145:4934–4939.
11. Graves DT, Fine D, Teng YT, Van Dyke TE, Hajish -engallis G. The use of rodent models to investigatehost-bacteria interactions related to perio dontal dis-eases. J Clin Periodontol 2008;35:89–105.
12. Salvi GE, Collins JG, Yalda B, Arnold RR, LangNP, Offenbacher S. Monocytic TNF alpha secretionpatterns in IDDM patients with periodontal dis-eases. J Clin Periodontol 1997;24:8–16.
13. Omori K, Ohira T, Uchida Y, Ayilavarapu S, BatistaEL Jr, Yagi M, Iwata T, Liu H, Hasturk H, KantarciA, Van Dyke TE. Priming of neutrophil oxidativeburst in diabetes requires preassembly of theNADPH oxidase. J Leukoc Biol 2008;84:292–301.
14. Graves DT, Naguib G, Lu H, Leone C, Hsue H,Krall E. Inflammation is more persistent in type 1diabetic mice. J Dent Res 2005;84:324–328.
15. Naguib G, Al-Mashat H, Desta T, Graves DT. Dia-betes prolongs the inflammatory response to a bac-terial stimulus through cytokine dysregulation. J In-vest Dermatol 2004;123:87–92.
16. Liu R, Bal HS, Desta T, Krothapalli N, Alyassi M,
Luan Q, Graves DT. Diabetes enhances periodon-tal bone loss through enhanced resorption and diminished bone formation. J Dent Res 2006;85:510–514.
17. Parfitt AM. The coupling of bone formation to boneresorption: a critical analysis of the concept and ofits relevance to the pathogenesis of osteoporosis.Metab Bone Dis Relat Res 1982;4:1–6.
18. Al-Mashat HA, Kandru S, Liu R, Behl Y, Desta T,Graves DT. Diabetes enhances mRNA levels ofproapoptotic genes and caspase activity, which con-tribute to impaired healing. Diabetes 2006;55:487–495.
19. Liu R, Bal HS, Desta T, Behl Y, Graves DT. Tumornecrosis factor-alpha mediates diabetes-enhancedapoptosis of matrix-producing cells and impairsdiabetic healing. Am J Pathol 2006;168:757–764.
20. Lalla E, Lamster IB, Feit M, Huang L, Spessot A,Qu W, Kislinger T, Lu Y, Stern DM, Schmidt AM.Blockade of RAGE suppresses periodontitis-asso-ciated bone loss in diabetic mice. J Clin Invest2000;105:1117–1124.
21. Ohnishi T, Bandow K, Kakimoto K, MachigashiraM, Matsuyama T, Matsuguchi T. Oxidative stresscauses alveolar bone loss in metabolic syndromemodel mice with type 2 diabetes. J PeriodontalRes 2009;44:43-51.
22. Mahamed DA, Marleau A, Alnaeeli M, Singh B,Zhang X, Penninger JM, Teng YT. G(-) anaerobes-reactive CD4+ T-cells trigger RANKL-mediatedenhanced alveolar bone loss in diabetic NOD mice.Diabetes 2005;54:1477-1486.
23. Ryan ME, Ramamurthy NS, Sorsa T, Golub LM.MMP-mediated events in diabetes. Ann NY AcadSci 1999;878:311-334.
24. Cutler CW, Eke P, Arnold RR, Van Dyke TE. De-fective neutrophil function in an insulin-dependentdiabetes mellitus patient. A case report. J Perio -dontol 1991;62:394-401.
25. Iacopino AM. Diabetic periodontitis: possible lipid-induced defect in tissue repair through alteration ofmacrophage phenotype and function. Oral Dis1995;1:214–229.
26. Iacopino AM. Periodontitis and diabetes interre -lationships: role of inflammation. Ann Periodontol2001;6:125–137.
27. Cutler CW, Iacopino AM. Periodontal disease: linkswith serum lipid/ triglyceride levels? Review andnew data. J Int Acad Periodontol 2003;5:47–51.
28. Ihm SH, Yoo HJ, Park SW, Park CJ. Effect of tol-restat, an aldose reductase inhibitor, on neutrophilrespiratory burst activity in diabetic patients. Metabolism 1997;46:634-638.
29. Tebbs SE, Lumbwe CM, Tesfaye S, Gonzalez AM,Wilson RM. The influence of aldose reductase on
100 Periodontal Disease and Overall Health: A Clinician's Guide

the oxidative burst in diabetic neutrophils. Dia-betes Res Clin Pract 1992;15:121–129.
30. Boland OM, Blackwell CC, Clarke BF, Ewing DJ.Effects of ponalrestat, an aldose reductase inhibitor,on neutrophil killing of Escherichia coli and auto-nomic function in patients with diabetes mellitus.Diabetes 1993;42:336–340.
31. Stosic-Grujicic SD, Miljkovic DM, Cvetkovic ID,Maksimovic-Ivanic DD, Trajkovic V. Immuno -suppressive and anti-inflammatory action of anti -oxidants in rat autoimmune diabetes. J Autoimmun2004;22:267–276.
32. Koya D, King G. Protein kinase C activation andthe development of diabetic complications. Dia-betes 1998;47:859–866.
33. Hiramatsu Y, Sekiguchi N, Hayashi M, Isshiki K,Yokota T, King GL, Loeken MR. Diacylglycerolproduction and protein kinase C activity are in-creased in a mouse model of diabetic embryopathy.Diabetes 2002;51:2804-2810.
34. Cohen MP, Shea E, Chen S, Shearman CW. Gly-cated albumin increases oxidative stress, activatesNF-kappa B and extracellular signal-regulated kinase (ERK), and stimulates ERK-dependenttransforming growth factor-beta 1 production inmacrophage RAW cells. J Lab Clin Med 2003;141:242–249.
35. Rashid G, Luzon AA, Korzets Z, Klein O, ZeltzerE, Bernheim J. The effect of advanced glycationend-products and aminoguanidine on TNF alphaproduction by rat peritoneal macrophages. PeritDial Int 2001;21:122–129.
36. Alikhani Z, Alikhani M, Boyd CM, Nagao K,Trackman PC, Graves DT. Advanced glycation endproducts enhance expression of pro-apoptotic genesand stimulate fibroblast apoptosis through cyto-plasmic and mitochondrial pathways. J Biol Chem2005;280:12087–12095.
37. Alikhani M, Maclellan CM, Raptis M, Vora S,Trackman PC, Graves DT. Advanced glycation endproducts induce apoptosis in fibroblasts throughactivation of ROS, MAP kinases, and the FOXO1transcription factor. Am J Physiol Cell Physiol2007;292:C850–856.
38. Goova MT, Li J, Kislinger T, Qu W, Lu Y, Buccia-relli LG, Nowygrod S, Wolf BM, Caliste X, Yan SF,Stern DM, Schmidt AM. Blockade of receptor foradvanced glycation end-products restores effectivewound healing in diabetic mice. Am J Pathol2001;159:513–525.
39. King GL. The role of inflammatory cytokines in diabetes and its complications. J Periodontol 2008;79:1527–1534.
40. Phipps KR, Stevens VJ. Relative contribution ofcaries and periodontal disease in adult tooth loss for
an HMO dental population. J Public Health Dent1995;55:250–252.
41. Loos BG. Systemic markers of inflammation inperiodontitis. J Periodontol 2005;76 (Suppl):2106–2115.
42. Kshirsagar AV, Moss KL, Elter JR, Beck JD, Offen -bacher S, Falk RJ. Periodontal disease is associatedwith renal insufficiency in the Atherosclerosis RiskIn Communities (ARIC) study. Am J Kidney Dis2005;45:650–657.
43. Grossi SG, Genco RJ. Periodontal disease and diabetes mellitus: a two-way relationship. Ann Perio dontol 1998;3:51–61.
44. Feingold KR, Soued M, Serio MK, Moser AH,Dinarello CA, Grunfeld C. Multiple cytokines stim-ulate hepatic lipid synthesis in vivo. Endocrinology1989;125:267–274.
45. Ling PR, Istfan NW, Colon E, Bistrian BR. Differ-ential effects of interleukin-1 receptor antagonist incytokine- and endotoxin-treated rats. Am J Physiol1995;268:E255–E261.
46. Feingold KR, Grunfeld C. Role of cytokines in in-ducing hyperlipidemia. Diabetes 1992;41 (Suppl):97–101.
47. Grunfeld C, Soued M, Adi S, Moser AH, DinarelloCA, Feingold KR. Evidence for two classes of cytokines that stimulate hepatic lipogenesis: rela-tionships among tumor necrosis factor, interleukin-1and interferon-alpha. Endocrinology 1990;127:46–54.
48. Shoelson SE, Lee J, Goldfine AB. Inflammationand insulin resistance. J Clin Invest 2006;116:1793–1801.
49. Tataranni PA, Ortega E. A burning question: doesan adipokine-induced activation of the immunesystem mediate the effect of overnutrition on type2 diabetes? Diabetes 2005;54:917–927.
50. Shoelson SE, Herrero L, Naaz A. Obesity, inflam-mation, and insulin resistance. Gastroenterology2007;132:2169–2180.
51. Duncan BB, Schmidt MI. The epidemiology oflow-grade chronic systemic inflammation and type2 diabetes. Diabetes Technol Ther 2006;8:7–17.
52. Pickup JC. Inflammation and activated innate im-munity in the pathogenesis of type 2 diabetes. Diabetes Care 2004;27:813–823.
53. Wellen KE, Hotamisligil GS. Inflammation, stress,and diabetes. J Clin Invest 2005;115:1111–1119.
54. Hotamisligil GS. Inflammation and metabolic dis-orders. Nature 2006;444:860–867.
55. Pradhan A. Obesity, metabolic syndrome, and type2 diabetes: inflammatory basis of glucose meta-bolic disorders. Nutr Rev 2007;65:S152–S156.
56. Beck JD, Offenbacher S. Systemic effects of perio -dontitis: epidemiology of periodontal disease and
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 101

cardiovascular disease. J Periodontol 2005;76(Suppl):2089–2100.
57. Demmer RT, Desvarieux M. Periodontal infectionsand cardiovascular disease: the heart of the matter.JADA 2006;137(Suppl):14S–20S.
58. Tonetti MS, D’Aiuto F, Nibali L, Donald A, StorryC, Parkar M, Suvan J, Hingorani AD, Vallance P,Deanfield J. Treatment of periodontitis and en-dothelial function. New Engl J Med 2007;356:911–920.
59. Aldridge JP, Lester V, Watts TL, Collins A, VibertiG, Wilson RF. Single-blind studies of the effects ofimproved periodontal health on metabolic controlin type 1 diabetes mellitus. J Clin Periodontol1995;22:271–275.
60. Kiran M, Arpak N, Unsal E, Erdoan MF. The ef-fect of improved periodontal health on metaboliccontrol in type 2 diabetes mellitus. J Clin Perio -dontol 2005;32:266–272.
61. Grossi SG, Skrepcinski FB, DeCaro T, RobertsonDC, Ho AW, Dunford RG, Genco RJ. Treatment ofperiodontal disease in diabetics reduces glycatedhemoglobin. J Periodontol 1997;68:713–719.
62. Rodrigues DC, Taba MJ, Novaes AB, Souza SL,Grisi MF. Effect of non-surgical periodontal ther-apy on glycemic control in patients with type 2 dia -betes mellitus. J Periodontol 2003;74:1361–1367.
63. Skaleric U, Schara R, Medvescek M, Hanlon A,Doherty F, Lessem J. Periodontal treatment byArestin and its effects on glycemic control in type1 diabetes patients. J Int Acad Periodontol 2004;6(Suppl):160-165.
64. Al-Mubarak S, Ciancio S, Aljada A, Mohanty P,Ross C, Dandona P. Comparative evaluation of ad-junctive oral irrigation in diabetics. J Clin Perio -dontol 2002;29:295-300.
65. O’Connell PA, Taba M, Nomizo A, Foss FreitasMC, Suaid FA, Uyemura SA, Trevisan GL, No-vaes AB, Souza SL, Palioto DB, Grisi MF. Effectsof periodontal therapy on glycemic control and in-flammatory markers. J Periodontol 2008;79:774–783.
66. Yun F, Firkova EI, Jun-Qi L, Xun H. Effect of non-surgical periodontal therapy on patients with type2 diabetes mellitus. Folia Med (Plovdiv) 2007;49:32–36.
67. Jones JA, Miller DR, Wehler CJ, Rich SE, Krall-Kaye EA, McCoy LC, Christiansen CL, RothendlerJA, Garcia RI. Does periodontal care improveglycemic control? The Department of Veterans Affairs Dental Diabetes Study. J Clin Periodontol2007;34:46–52.
68. Stewart JE, Wager KA, Friedlander AH, ZadehHH. The effect of periodontal treatment on glycemiccontrol in patients with type 2 diabetes mellitus. J
Clin Periodontol 2001;28:306–310.69. Faria-Almeida R, Navarro A, Bascones A. Clinical
and metabolic changes after conventional treat-ment of type 2 diabetic patients with chronic perio -dontitis. J Periodontol 2006;77:591–598.
70. Iwamoto Y, Nishimura F, Nakagawa M, SugimotoH, Shikata K, Makino H, Fukuda T, Tsuji T,Iwamoto M, Murayama Y. The effect of antimi-crobial periodontal treatment on circulating tumornecrosis factor-alpha and glycated hemoglobinlevel in patients with type 2 diabetes. J Periodon-tol 2001;72:774–778.
71. Miller LS, Manwell MA, Newbold D, Reding ME,Rasheed A, Blodgett J, Kornman KS. The rela-tionship between reduction in periodontal inflam-mation and diabetes control: a report of 9 cases. JPeriodontol 1992;63:843–848.
72. Seppälä B, Ainamo J. A site-by-site follow-up studyon the effect of controlled versus poorly controlledinsulin-dependent diabetes mellitus. J Clin Perio -dontol 1994;21:161–165.
73. Seppälä B, Seppälä M, Ainamo J. A longitudinalstudy on insulin-dependent diabetes mellitus andperiodontal disease. J Clin Periodontol 1993;20:161–165.
74. Williams RC, Jr, Mahan CJ. Periodontal diseaseand diabetes in young adults. JAMA 1960;172:776–778.
75. Wolf J. Dental and periodontal conditions in dia-betes mellitus. A clinical and radiographic study.Proc Finn Dent Soc 1977;73 (Suppl):1–56.
76. Fu Y, Ling J, Deng Y. [The effect of non-surgicalperiodontal therapy on blood sugar level of non-in-sulin dependent diabetes mellitus diabetics withperiodontitis]. Zhonghua Kou Qiang Yi Xue Za Zhi2000;35:444–446.
77. Guo YH, Zhu BL. [The effect of initial therapy onperiodontal status and saccharified Hb (HbAIc) ofpatients with type II diabetes mellitus]. ShanghaiKou Qiang Yi Xue 2004;13:150–151.
78. Navarro-Sanchez AB, Faria-Almeida R, Bascones-Martinez A. Effect of non-surgical periodontal ther-apy on clinical and immunological response andglycaemic control in type 2 diabetic patients withmoderate periodontitis. J Clin Periodontol 2007;34:835–843.
79. Yang PS, Wang Y, Qi XM, Ren JM, Ge SH. [Theeffect of periodontal initial therapy on circulatingTNF-alpha and HbA1C in type 2 diabetes patientswith periodontitis]. Zhonghua Kou Qiang Yi Xue ZaZhi 2003;38:364–366.
80. Villa AA. [Clinical, biochemical and histopatho log-ical correlation in diabetic patients with perio dontaldisease]. Rev Fac Cien Med Univ Nac Cordoba 2006;63 (Suppl):50–55.
102 Periodontal Disease and Overall Health: A Clinician's Guide

81. Promsudthi A, Pimapansri S, Deerochanawong C,Kanchanavasita W. The effect of periodontal ther-apy on uncontrolled type 2 diabetes mellitus inolder subjects. Oral Dis 2005;11:293–298.
82. Christgau M, Palitzsch KD, Schmalz G, Kreiner U,Frenzel S. Healing response to non-surgical perio -dontal therapy in patients with diabetes mellitus:clinical, microbiological, and immunologic results.J Clin Periodontol 1998;25:112–124.
83. Smith GT, Greenbaum CJ, Johnson BD, PerssonGR. Short-term responses to periodontal therapy ininsulin-dependent diabetic patients. J Periodontol1996;67:794–802.
84. Talbert J, Elter J, Jared HL, Offenbacher S, Souther-land J, Wilder RS. The effect of periodontal therapyon TNF-alpha, IL-6 and metabolic control in type2 diabetics. J Dent Hyg 2006;80:7.
85. Westfelt E, Rylander H, Blohmé G, Jonasson P,Lindhe J. The effect of periodontal therapy in dia-betics. Results after 5 years. J Clin Periodontol1996;23:92–100.
86. Campus G, Salem A, Sacco G, Maida C, CagettiMG, Tonolo G. Clinical effects of mechanical periodontal therapy in type 2 diabetic patients. Diabetes Res Clin Pract 2007;75:368–369.
87. da Cruz GA, de Toledo S, Sallum EA, Sallum AW,Ambrosano GM, de Cássia Orlandi Sardi J, da CruzSE, Gonçalves RB. Clinical and laboratory evalu-ations of non-surgical periodontal treatment in sub-jects with diabetes mellitus. J Periodontol 2008;79:1150–1157.
88. Makiura N, Ojima M, Kou Y, Furuta N, OkahashiN, Shizukuishi S, Amano A. Relationship of Por-phyromonas gingivalis with glycemic level in pa-tients with type 2 diabetes following periodontaltreatment. Oral Microbiol Immunol 2008;23:348–351.
89. Schara R, Medvescek M, Skaleric U. Periodontaldisease and diabetes metabolic control: a full-mouthdisinfection approach. J Int Acad Periodontol 2006;8:61–66.
90. Taylor GW. The effects of periodontal treatment ondiabetes. JADA 2003;134 (Spec Iss):41S–48S.
91. Darre L, Vergnes JN, Gourdy P, Sixou M. Efficacyof periodontal treatment on glycaemic control in diabetic patients: A meta-analysis of interventionalstudies. Diabetes Metab 2008;34:497–506.
92. Janket SJ, Wightman A, Baird AE, Van Dyke TE,Jones JA. Does periodontal treatment improveglycemic control in diabetic patients? A meta- analysis of intervention studies. J Dent Res 2005;84:1154–1159.
93. Taylor GW, Burt BA, Becker MP, Genco RJ, Shloss-man M, Knowler WC, Pettitt DJ. Severe periodon-titis and risk for poor glycemic control in patients
with non-insulin-dependent diabetes mellitus. J Pe-riodontol 1996;67(Suppl):1085–1093.
94. Collin HL, Uusitupa M, Niskanen L, Kontturi-Närhi V, Markkanen H, Koivisto AM, MeurmanJH. Periodontal findings in elderly patients withnon-insulin dependent diabetes mellitus. J Perio -dontol 1998;69:962–966.
95. Diaz-Romero RM, Casanova-Román G, Beltrán-Zuñiga M, Belmont-Padilla J, Méndez JD, Avila-Rosas H. Oral infections and glycemic control inpregnant type 2 diabetics. Arch Med Res 2005;36:42–48.
96. Lal S, Cheng B, Kaplan S, Softness B, GreenbergE, Goland RS, Lalla E, Lamster IB. Gingival bleed-ing in 6- to 13-year-old children with diabetes mel-litus. Pediatr Dent 2007;29:426–430.
97. Anonymous. The effect of intensive treatment of dia betes on the development and progression oflong-term complications in insulin-dependent dia-betes mellitus. The Diabetes Control and Compli-cations Trial Research Group. N Engl J Med1993;329:977–986.
98. Anonymous. Intensive blood-glucose control withsulphonylureas or insulin compared with con -ventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UKProspective Diabetes Study (UKPDS) Group.Lancet 1998;352:837–853.
99. Anonymous. Effect of intensive blood-glucose con-trol with metformin on complications in overweightpatients with type 2 diabetes (UKPDS 34). UKProspective Diabetes Study (UKPDS) Group.Lancet 1998;352:854–865.
00. Genuth S, Eastman R, Kahn R, Klein R, Lachin J,Lebovitz H, Nathan D, Vinicor F; American Dia-betes Association. Implications of the United King-dom prospective diabetes study. Diabetes Care2003;26 (Suppl):S28–S32.
01. Thorstensson H, Kuylenstierna J, Hugoson A. Med-ical status and complications in relation to perio -dontal disease experience in insulin-dependent diabetics. J Clin Periodontol 1996;23:194–202.
02. Saremi A, Nelson RG, Tulloch-Reid M, HansonRL, Sievers ML, Taylor GW, Shlossman M, Bennett PH, Genco R, Knowler WC. Periodontaldisease and mortality in type 2 diabetes. DiabetesCare 2005;28:27–32.
03. Shultis WA, Weil EJ, Looker HC, Curtis JM,Shlossman M, Genco RJ, Knowler WC, NelsonRG. Effect of periodontitis on overt nephropathyand end-stage renal disease in type 2 diabetes. Dia -betes Care 2007;30:306–311.
04. Demmer RT, Jacobs DR, Jr., Desvarieux M. Perio -dontal disease and incident type 2 diabetes: resultsfrom the First National Health and Nutrition Ex-
Chapter 6 Association Between Periodontal Disease and Diabetes Mellitus 103
1
1
1
1
1

amination Survey and its epidemiologic follow-upstudy. Diabetes Care 2008;31:1373–1379.
05. Lipton RB, Liao Y, Cao G, Cooper RS, McGee D.Determinants of incident non-insulin-dependent diabetes mellitus among blacks and whites in a national sample. The NHANES I EpidemiologicFollow-up Study. Am J Epidemiol 1993;138:826–839.
06. Dasanayake AP, Chhun N, Tanner AC, Craig RG,Lee MJ, Moore AF, Norman RG. Periodontalpathogens and gestational diabetes mellitus. J DentRes 2008;87:328–333.
07. Donahue RP, Wu T. Insulin resistance and perio -dontal disease. An epidemiologic overview of research needs and future directions. Ann Perio -dontol 2001;6:119–124.
104 Periodontal Disease and Overall Health: A Clinician's Guide
1
1
1
coronary atherosclerosis range from stableangina, resulting from ischemia caused bystable coronary arterial plaques that reduceluminal cross-sectional area and restrictblood flow, to acute coronary syndrome(ACS) characterized by unstable, rupturedcoronary atherosclerotic plaques. ACS canbe further subdivided into non-ST elevationACS—such as unstable angina—or ST- elevation and non-ST elevation myocardialinfarction, depending on the degree of luminal occlusion following plaque ruptureand intracoronary thrombosis.
Another location for atherosclerotic disease is in the cerebrovascular bed. As withcoronary atherosclerosis, clinical manifes-tations of cerebrovascular atherosclerosisvary depending on the stability of the arterialplaques. Stable disease may lead to chronicsymptoms of dementia, whereas unstableatherosclerosis may lead to transient ischemicattacks (often called “ministrokes”) andstrokes.
Atherosclerotic disease also occurs inthe aorta, manifesting as aortic atheroscle-rosis and aneurysms, as well as in the periph -eral arteries. In addition, atherosclerosis isthought to contribute to valvular heart dis-eases such as aortic stenosis.2,3
MECHANISMS OFATHEROMA FORMATION
Atherosclerotic disease is thought to pro -gress from microscopic endothelial eventsthat eventually lead to plaque development,growth, and rupture. Multiple complex mech- anisms appear to contribute to the formationof atheromatous plaques. The initiating
INTRODUCTIONAtherosclerotic disease results from the
pathological formation of plaques in arterialwalls. Plaque development, or atherosclero-sis, is a complex process with many under-lying inflammatory molecules participatingin increasingly well-understood pathways.The consequences include a wide varietyof clinical syndromes involving different or-gans with a common underlying deficiency—inadequate blood supply due to reductionof blood flow to the target organ.
This chapter will review the clinicalmanifestations of atherosclerosis and exploreits underlying molecular pathophysiology.Understanding the underpinnings of athero-sclerosis is crucial to appreciating the po-tential interplay between atherosclerosis andperiodontal disease, which is discussed inthe next chapter.
TYPES OFATHEROSCLEROTIC DISEASEAtherosclerosis may occur in any arte-
rial bed with the most clinically relevantones being the coronary, cerebrovascular,and peripheral arterial circulation. Athero-sclerotic plaques may be stable or unstable,based on whether or not the plaque has rup-tured. More recently, studies have shed ad-ditional light on “vulnerable” atheroscleroticplaques, which are stable plaques with apropensity to rupture.
Coronary heart disease is the most clin-ically evident form of atherosclerotic disease,affecting over 17 million Americans accord-ing to the American Heart Association’s2009 statistical update.1 Manifestations of
CHAPTER 7Atherosclerosis: A Pervasive Disease Affecting Global Populations
Stanley S. Wang

process involves endothelial injury, which mayoccur due to mechanical, biochemical, orimmunological factors. At the cellular level,the process begins with the recruitment ofmonocytes into the arterial wall through theeffect of specific molecules, including thechemo -attrac tants interleukin (IL)-1 and tumor necrosis factor-alpha (TNF-).4
Selectins and anti gens on the leukocyte surface induce move ment of the monocytes.5Endothelial cellular adhesion molecules (es-pecially vascular cell adhesion molecule 1and intercellular adhesion molecule 1) in-teract with leukocyte integrins, causing themonocytes to adhere to the endothelium andsubsequently migrate across it.6 After theymove into in a subendo thelial position,monocytes transform into macro phages andbegin to secrete many inflammatory cyto-kines, proteases, and metallo proteinases.
Subsequently, the macrophages accu-mulate and oxidize low-density-lipoproteincholesterol (LDLC), becoming the foamcells that are the precursors of atheroscleroticplaque.7 C-reactive protein (CRP) appearsto stimulate the process of LDLC uptake bymacrophages,5 which may explain why statintreatment of patients with elevated CRP lev-els appears to be clinically beneficial.8 On-going LDLC deposition and inflammationleads to plaque growth, and hemodynamicmechanisms appear to play an important roleas well.9
Plaque rupture may occur at any point inthe process, producing significant clinicalevents. It has been estimated that in abouttwo-thirds of patients with acute coronarysyndromes, the inciting event is rupture of acoronary plaque that had been less than50%–70% occlusive.10 Ruptured plaqueshave distinctive histopathological features,including having a fibrous cap that is defi-cient in collagen and smooth muscle con-tent, a rich lipid core, and an inflammatoryinfiltrate of macrophages and other inflam-matory cells.11
Role of Inflammationin Atherosclerotic Disease
Although the precise mechanisms ofatherosclerosis are not completely under-stood, at the molecular level atherosclerosisappears to arise from an inflammatory reac-tion to cardiovascular risk factors.12,13 Chronicinflammation underlies the processes of plaqueformation and progression, while acute in-flammatory processes are likely involved inplaque rupture.
On a molecular level, many mediatorsof inflammation have been identified andmore than 50 have been classified by struc-ture and function. Some of these cytokines or“protein cell regulators”14 are pro-inflam-matory, including IL-1, IL-12, IL-18, inter-feron gamma, and TNF-. Others are anti- inflammatory, including IL-4, IL-10, IL-13,and transforming growth factor-beta.
In many cellular mediators of athero-sclerosis, including macrophages and en-dothelial cells, pro-inflammatory cytokinesstimulate the nuclear factor-kappa-beta ()pathway, leading to the increased produc-tion of cellular adhesion molecules, chemo -kines, growth factors, and other enzymessuch as cyclo-oxygenases and nitric oxidesynthase.15 Enhanced activity of the nuclearfactor- pathway appears to correlate withan increased risk of developing atheroscle-rotic plaques.
RISK FACTORS FOR CARDIOVASCULAR AND
CEREBROVASCULAR DISEASESTraditional risk factors for athero -
sclerotic disease seem to have an associa-tion with inflammation in common. Theserisk factors include dyslipidemia, hyper-tension, diabetes mellitus, tobacco use, and adiposity.
DyslipidemiaDyslipidemia appears to contribute di-
rectly to atherosclerotic disease, with the risk
106 Periodontal Disease and Overall Health: A Clinician's Guide

CHAPTER 7 Atherosclerosis: A Pervasive Disease Affecting Global Populations 107
of cardiac events rising in direct proportionto plasma cholesterol levels,16 especially cho-lesterol particles containing apolipoprotein (including LDLC).17 The primacy of choles-terol in initiating atherosclerosis has beenshown in many molecular studies, but maybe most evident in studies of fetal aortas, inwhich quantitative and qualitative analysesof fatty streaks have shown that nativeLDLC uptake in the intima precedes LDLCoxidation and subsequent endothelial acti-vation and monocyte recruitment.18 OxidizedLDLC appears to increase endothelial ex-pression of cellular adhesion molecules, at-tracting monocytes and promoting their dif-ferentiation into macrophages. LDLC alsostimulates the release of pro-inflammatorycytokines from macrophages. Apolipopro-tein B particles containing the lipoprotein(a)moiety appear to be particularly athero-genic.19,20 In addition, the ratio of apolipopro-tein B to apolipoprotein A holds promise inthe prognostication of cardiovascular dis-ease across multiple populations.21
HypertensionSystemic hypertension contributes by
enhancing monocyte preactivation, increas-ing production of IL-1 and TNF-,22 and rais-ing circulating levels of cellular adhesionmolecules.23 Studies have shown a clear re-lationship between elevated high-sensitivityCRP levels in normotensive patients and riskof developing incident hypertension, under-scoring its inflammatory nature.24
Diabetes MellitusDiabetes mellitus appears to be associ-
ated with inflammation, which may explainits close relationship to atherosclerosis. Studies have shown that adipose tissue andmacro phages recruited into adipose tissuerelease cytokines, including IL-1, IL-6, andTNF-. These cytokines act on: 1) the liverto promote dyslipidemia and dysfibrinogen-emia, 2) adipose tissue to stimulate leptin
secretion, and 3) the pituitary gland to in-crease secre tion of adrenocorticotropic hor-mone.25 Moreover, serum levels of variousinflammatory markers and mediators (CRP,fibrinogen, IL-6, plasminogen activator in-hibitor 1, and serum amyloid A) correlatewith the degree of hyperglycemia.26 Evi-dence is accruing to suggest that the forma-tion and accumulation of advanced glycationendproducts (AGEs) may be a pathophys -iologic link between diabetes and cardio -vascular disease, mediated in part by the receptor for AGEs (RAGE).27 RAGE, an immunoglobulin that binds multiple ligandsand spurs production of toxic reactive oxygen species, is emerging as a potentialtherapeutic target for antagonists designed to reduce atherosclerosis and ischemia-reperfusion injury.28 Another potential ther-apeutic target that is attracting interest is pro-tein kinase C (PKC) beta, an intracellularsignaling molecule that plays a key role inthe development of diabetic complications.29
Experimental PKC inhibitors have beenshown to delay or even stop the progressionof microvascular complications; one suchagent has been submitted for regulatoryclearance for the treatment of diabeticretinopathy.30
Tobacco UseCigarette smoking contributes to coro-
nary heart disease through at least fourpathophysiological pathways,31 including in-duction of a hypercoagulable state throughincreased plasma levels of factor VII andthromboxane A2, reduction in oxygen deliv-ery as a result of carbon monoxide generation,vasoconstriction of the coronary arteries(which is at least partially mediated by alpha-adrenergic stimulation), and direct hemo -dynamic effects of nicotine. Cigarette usehas gradually declined in the United States inthe past 40 years, but remains a public healthproblem with approximately 20% of the pop-ulation continuing to smoke.32

108 Periodontal Disease and Overall Health: A Clinician's Guide
Of note, cocaine use also causes hemo-dynamic effects as well as significant in-flammation. Studies in mice suggest that cocaine increases the expression of cellularadhesion molecules and promotes greaterneutrophil adhesion to the coronary endo -thelium.33 In human cells, cocaine exposureappears to increase the expression of genecoding for numerous inflammatory markers,including IL-1, IL-6, and TNF-.34
ObesityObesity with visceral adiposity is an-
other emerging atherosclerotic risk factor.Adipose tissue acts as a metabolically ac-tive and dynamic endocrine organ with pro-inflammatory actions. Adipocytes secretemany inflammatory cytokines, includingIL-6 and TNF-.35 Although cytokine levelsvary in proportion to overall adiposity, visceraladipose tissue appears to contribute to inflam -mation to a greater degree than subcutaneousfat.36 There is an inverse relationship betweenvisceral adiposity and plasma levels of theanti-inflammatory adipocyte-derived pro-tein, adiponectin.37 Lower adiponectin levelscorrelate with reduced insulin sensitivityand a higher risk of having diabetes mellitus,38
as well as endothelial dysfunction, increasedinflammation, and clinically significant atherosclerotic events such as myocardialinfarction.39
EPIDEMIOLOGY OFHEART DISEASE AND STROKE
Although the overall death rate fromcardiovascular diseases has declined by29.2% from 1996 to 2006, cardiovasculardiseases remain the number one cause ofmortality in the United States, accountingfor 34.3% of the 2,425,900 deaths (or 1 ofevery 2.9 deaths) in the United States in2006.1 Based on 2004 International Classi-fication of Disease-10 data from the Cen-ters for Disease Control and Prevention,cerebrovascular diseases (including stroke)
account for an additional 5.7% of deaths.40
The American Heart Association esti-mates that 785,000 Americans will suffer anew heart attack in 2010 and another 470,000will experience a recurrent heart attack.1
Furthermore, an additional 195,000 will havea silent first heart attack. Although less lethal,strokes are expected to be highly prevalent in2009, with an anticipated 610,000 new and185,000 recurrent cases.
Despite these numbers, overall choles-terol screening and treatment remain sub -optimal. Data from the 2005–2006 NationalHealth and Nutrition Examination Surveysuggested that 30% or more adults failed toundergo cholesterol screening in the priorfive years, and 16% of adults had total cho-lesterols of 240 mg/dL or greater. Similarly,achieving adequate blood pressure controlhas proven to be challenging. In 2003 and2004, only 44% of blood pressure recordingsin approximately 176 million individualsdemonstrated readings lower than 140/90mmHg.41 Almost two-thirds of the popula-tion in the United States is overweight orobese, and more than one-fourth of the pop-ulation meet diagnostic criteria for metabolicsyndrome, a multiplex cardiovascular riskfactor that arises from the interplay betweenadiposity and inflammation.42
TRENDS IN DISEASE PATTERNSIN DEVELOPED AND
DEVELOPING WORLDSGlobally, cardiovascular disease (pre-
dominantly heart disease and stroke) is theleading chronic disease, accounting for 17million deaths.43 More than one billion in -dividuals meet the medical criteria for being overweight or obese, but the rates of athero -sclerotic disease and risk factors vary betweencountries.44.45 Studies have confirmed the con- sistent impact of established cardiovascularrisk factors (hypertension, dyslipidemia, obesity, smoking) on the risk of athero -sclerotic disease across multiple populations.

The INTERHEART study found that incre-mental changes in these risk factors, such asa 5 mm HG elevation of blood pressure or a10 mg/dL increase in LDLC, raise the risk ofatherosclerotic disease by a similar amountacross people of different nationalities andethnicities.46 The central implication is thatvariations in cardiovascular risk betweenpopulations likely reflect differences in totalexposure to risk factors rather than biologicaldifferences in sensitivity to these risk fac-tors.47 When comparing developed and developing worlds, data indicate that low- income countries have the highest burden ofhigh blood pressure and related sequelae,48
including stroke mortality and morbidity.49
CONCLUSIONIt is clear that more study is needed on
the development, progression, treatment, andexpression of atherosclerotic diseases at alllevels—from molecular to global perspec-tives. Great opportunity remains to reducethe impact of atherosclerosis—a largely pre-ventable disease. Moving forward, interna-tional coalitions such as that initiated by theWorld Heart Federation are likely to play acrucial role in promoting improvements inglobal cardiovascular health.50
Supplemental Readings
Shah PK. Inflammation and plaque vulnerability. Car-dio vasc Drugs Ther. 2009;23(1):31–40.
Ross R. Atherosclerosis—an inflammatory disease. NEngl J Med 1999;340:115–126.
Wang SS, Smith SC Jr. Role of the InflammatoryProcess in Atherosclerosis and Vascular Disease. In:Pollock’s Textbook of Cardiovascular Disease and Re-habilitation, 1st Edition, Durstine JL, Moore GE, La-Monte MJ, Franklin BA, eds. Human Kinetics, 2008.
Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M,Dai S, De Simone G, Ferguson TB, Ford E, Furie K,Gillespie C, Go A, Greenlund K, Haase N, Hailpern S,Ho PM, Howard V, Kissela B, Kittner S, Lackland D,Lisabeth L, Marelli A, McDermott MM, Meigs J,Mozaffarian D, Mussolino M, Nichol G, Roger V, Rosa-mond W, Sacco R, Sorlie P, Stafford R, Thom T,
Wasserthiel-Smoller S, Wong ND, Wylie-Rosett J; onbehalf of the American Heart Association StatisticsCommittee and Stroke Statistics Subcommittee. Heartdisease and stroke statistics—2010 update: a reportfrom the American Heart Association. Circulation 2010;121:e1–e170.
Libby P, Ridker PM, Hansson GK; Leducq Trans atlanticNetwork on Atherothrombosis. Inflammation in athero -sclerosis: from pathophysiology to practice. J Am CollCardiol 2009;54:2129–2138.
REFERENCES1. Lloyd-Jones D, Adams RJ, Brown TM, Carnethon
M, Dai S, De Simone G, Ferguson TB, Ford E,Furie K, Gillespie C, Go A, Greenlund K, HaaseN, Hailpern S, Ho PM, Howard V, Kissela B, Kit-tner S, Lackland D, Lisabeth L, Marelli A, Mc-Dermott MM, Meigs J, Mozaffarian D, MussolinoM, Nichol G, Roger V, Rosamond W, Sacco R,Sorlie P, Stafford R, Thom T, Wasserthiel-SmollerS, Wong ND, Wylie-Rosett J; on behalf of theAmerican Heart Association Statistics Committeeand Stroke Statistics Subcommittee. Heart diseaseand stroke statistics—2010 update: a report fromthe American Heart Association. Circulation 2010;121:e1–e170.
2. Helske S, Kupari M, Lindstedt KA, Kovanen PT.Aortic valve stenosis: an active atheroinflammatoryprocess. Curr Opin Lipidol 2007;18:483–491.
3. Goldbarg SH, Elmariah S, Miller MA, Fuster V. Insights into degenerative aortic valve disease. J AmColl Cardiol 2007;50:1205–1213.
4. Nilsson J. Cytokines and smooth muscle cells inatherosclerosis. Cardiovasc Res 1993;27:1184–1190.
5. Tousoulis D, Charakida M, Stefanadis C. Endo -thelial function and inflammation in coronary arterydisease. Heart 2006;92:441–444.
6. Blankenberg S, Barbaux S, Tiret L. Adhesion mol-ecules and atherosclerosis. Atherosclerosis 2003;170:191–203.
7. Bobryshev YV. Monocyte recruitment and foamcell formation in atherosclerosis. Micron 2006;37:208–222.
8. Ridker PM, Danielson E, Fonseca FA, Genest J,Gotto AM Jr, Kastelein JJ, Koenig W, Libby P,Lorenzatti AJ, MacFadyen JG, Nordestgaard BG,Shepherd J, Willerson JT, Glynn RJ; JUPITERStudy Group. Rosuvastatin to prevent vascularevents in men and women with elevated C-reactiveprotein. N Engl J Med 2008;359:2195–2207.
9. Katritsis DG, Pantos J, Efstathopoulos E. Hemo -dynamic factors and atheromatic plaque rupture inthe coronary arteries: from vulnerable plaque to
CHAPTER 7 Atherosclerosis: A Pervasive Disease Affecting Global Populations 109

110 Periodontal Disease and Overall Health: A Clinician's Guide
vulner able coronary segment. Coron Artery Dis 2007;18:229–237.
10. Hackett D, Davies G, Maseri A. Pre-existing coro-nary stenoses in patients with first myocardial infarction are not necessarily severe. Eur Heart J1988;9:1317–1323.
11. Shah PK. Inflammation and plaque vulnerability.Cardiovasc Drugs Ther. 2009;23(1):31–40.
12. Ross R. Atherosclerosis—an inflammatory disease.N Engl J Med 1999;340:115–126.
13. Lamon BD, Hajjar DP. Inflammation at the molec-ular interface of atherogenesis: an anthropologicaljourney. Am J Pathol 2008;173:1253–1264.
14. Balkwill FR, Burke F. The cytokine network. Im-munol Today 1989;10:299–304.
15. De Martin R, Hoeth M, Hofer-Warbinek R, SchmidJA. The transcription factor NF-kappa B and theregulation of vascular cell function. ArteriosclerThromb Vasc Biol 2000;20:E83–88.
16. Stamler J, Wentworth D, Neaton JD. Is relationshipbetween serum cholesterol and risk of prematuredeath from coronary heart disease continuous andgraded? Findings in 356,222 primary screenees ofthe Multiple Risk Factor Intervention Trial (MR-FIT). JAMA 1986;256:2823–2828.
17. Carmena R, Duriez P, Fruchart JC. Atherogeniclipoprotein particles in atherosclerosis. Circulation2004;109(Suppl 1):1112–1117.
18. Napoli C, D’Armiento FP, Mancini FP, PostiglioneA, Witztum JL, Palumbo G, Palinski W. Fatty streakformation occurs in human fetal aortas and isgreatly enhanced by maternal hypercholes-terolemia. Intimal accumulation of low densitylipoprotein and its oxidation precede monocyte re-cruitment into early atherosclerotic lesions. J ClinInvest 1997;100:2680–2690.
19. Marcovina SM, Koschinsky ML, Albers JJ, Skar-latos S. Report of the National Heart, Lung, andBlood Institute Workshop on Lipoprotein(a) andCardiovascular Disease: recent advances and futuredirections. Clin Chem 2003;49:1785–1796.
20. Anuurad E, Boffa MB, Koschinsky ML, BerglundL. Lipoprotein(a): a unique risk factor for cardio-vascular disease. Clin Lab Med 2006;26:751–772.
21. McQueen MJ, Hawken S, Wang X, Ounpuu S, Sni-derman A, Probstfield J, Steyn K, Sanderson JE,Hasani M, Volkova E, Kazmi K, Yusuf S; INTER-HEART study investigators. Lipids, lipoproteins,and apolipoproteins as risk markers of myocardialinfarction in 52 countries (the INTERHEARTstudy): a case-control study. Lancet 2008;372:224–233.
22. Dörffel Y, Lätsch C, Stuhlmüller B, Schreiber S,Scholze S, Burmester GR, Scholze J. Preactivatedperipheral blood monocytes in patients with essen-
tial hypertension. Hypertension 1999;34:113–117.23. Boulbou MS, Koukoulis GN, Makri ED, Petinaki
EA, Gourgoulianis KI, Germenis AE. Circulatingadhesion molecule levels in type 2 diabetes melli- tus and hypertension. Int J Cardiol 2005;98:39–44.
24. Sesso HD, Buring JE, Rifai N, Blake GJ, GazianoJM, Ridker PM. C-reactive protein and the risk ofdeveloping hypertension. JAMA 2003;290:2945–2951.
25. Pickup JC, Crook MA. Is type II diabetes a diseaseof the innate immune system? Diabetologica 1998;41:1241–1248.
26. Sjöholm A, Nyström T. Inflammation and the eti-ology of type 2 diabetes. Diabetes Metab Res Rev2006;22:4–10.
27. Yan SF, Ramasamy R, Schmidt AM. Mechanisms ofdisease: advanced glycation end-products and theirreceptor in inflammation and diabetes complica-tions. Nat Clin Pract Endocrinol Metab 2008;4:285–293.
28. Yan SF, Ramasamy R, Schmidt AM. The receptorfor advanced glycation endproducts (RAGE) and cardiovascular disease. Expert Rev Mol Med 2009;11:e9.
29. Clarke M, Dodson PM. PKC inhibition and dia-betic microvascular complications. Best Pract ResClin Endocrinol Metab 2007;21:573–586.
30. Budhiraja S, Singh J. Protein kinase C beta in-hibitors: a new therapeutic target for diabeticnephropathy and vascular complications. FundamClin Pharmacol 2008;22:231–240.
31. Ludvig J, Miner B, Eisenberg MJ. Smoking cessa-tion in patients with coronary artery disease. AmHeart J 2005;149:565–572.
32. Centers for Disease Control and Prevention (CDC).Cigarette smoking among adults and trends insmoking cessation—United States, 2008. MMWRWeekly, 2009 Nov 13;54(44):1227–1232.
33. Chen Y, Ke Q, Xiao YF, Wu G, Kaplan E, HamptonTG, Malek S, Min JY, Amende I, Morgan JP. Cocaine and catecholamines enhance inflammatorycell retention in the coronary circulation of mice byupregulation of adhesion molecules. Am J PhysiolHeart Circ Physiol 2005;288:H2323–2331.
34. Crawford FC, Wood ML, Wilson SE, Mathura VS,Hollen TR, Geall F, Kolippakkam DN, Mullan MJ.Cocaine induced inflammatory response in humanneuronal progenitor cells. J Neurochem 2006;97:662–674.
35. Lyon CJ, Law RE, Hsueh WA. Minireview: Adi-posity, inflammation, and atherogenesis. Endo -crinology 2003;144:2195–2200.
36. Dusserre E, Moulin P, Vidal H. Differences inmRNA expression of the proteins secreted by the

CHAPTER 7 Atherosclerosis: A Pervasive Disease Affecting Global Populations 111
adipocytes in human subcutaneous and visceraladipose tissues. Biochim Biophys Acta 2000;1500:88-96.
37. Cnop M, Havel PJ, Utzschneider KM, Carr DB,Sinha MK, Boyko EJ, Retzlaff BM, Knopp RH,Brunzell JD, Kahn SE. Relationship of adiponectinto body fat distribution, insulin sensitivity andplasma lipoproteins: evidence for independent rolesof age and sex. Diabetologia 2003;46:459-469.
38. Bajaj M, Suraamornkul S, Piper P, Hardies LJ,Glass L, Cersosimo E, Pratipanawatr T, Miyazaki Y,DeFronzo RA. Decreased plasma adiponectin con-centrations are closely related to hepatic fat contentand hepatic insulin resistance in pioglitazone-treated type 2 diabetic patients. J Clin Endo crinolMetab 2004;89:200–206.
39. Pischon T, Girman CJ, Hotamisligil GS, Rifai N,Hu FB, Rimm EB. Plasma adiponectin levels andrisk of myocardial infarction in men. JAMA 2004;291:1730–1737.
40. Heron M, Hoyert DL, Murphy SL, Xu J, KochanekKD, Tejada-Vera B. Deaths: final data for 2006.Natl Vital Stat Rep 2009;57:1–80.
41. Fang J, Alderman MH, Keenan NL, Ayala C, CroftJB. Hypertension control at physicians’ offices in theUnited States. Am J Hypertens 2008;21:136–142.
42. Grundy SM. Metabolic syndrome pandemic. Arte-rioscler Thromb Vasc Biol 2008;28:629–636.
43. Beaglehole R, Reddy S, Leeder SR. Poverty and human development: the global implications of cardiovascular disease. Circulation 2007;116:1871–1873.
44. Gaziano TA. Reducing the growing burden of
cardiovascular disease in the developing world.Health Aff (Millwood) 2007;26:13–24.
45. Levi F, Chatenoud L, Bertuccio P, Lucchini F, NegriE, Vecchia CL. Mortality from cardiovascular andcerebrovascular diseases in Europe and other areasof the world: an update. Eur J Cardiovasc PrevRehabil 2009;125:666 –673.
46. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A,Lanas F, McQueen M, Budaj A, Pais P, Varigos J,Lisheng L; INTERHEART Study Investigators. Ef-fect of potentially modifiable risk factors associatedwith myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet2004;364:937-952.
47. Ezzati M. How can cross-country research on healthrisks strengthen interventions? Lessons from IN-TER HEART. Lancet 2004;364:912–914.
48. Lawes CM, Vander Hoorn S, Rodgers A; Interna-tional Society of Hypertension. Global burden ofblood-pressure-related disease, 2001. Lancet 2008;371:1513–1518.
49. Johnston SC, Mendis S, Mathers CD. Global vari-ation in stroke burden and mortality: estimates frommonitoring, surveillance, and modelling. LancetNeurol 2009;8:345-354. (Comments: Lancet Neu-rol 2009;8:306-307; Lancet Neurol 2009;8:308–309; Lancet Neurol 2009;8:700; author reply 700.)
50. Bayés de Luna A, Tse TF, de Figueiredo MB,Maranhão M, Voûte J, Nishtar S, Fuster V, Poole-Wilson P; World Heart Federation. World HeartDay: A World Heart Federation enterprise promot-ing the prevention of heart disease and stroke acrossthe world. Circulation 2003;108:1038–1040.

112 Periodontal Disease and Overall Health: A Clinician's Guide
INTRODUCTIONAtheromatous diseases constitute a broad
set of chronic vascular conditions, includingcardiovascular disease (CVD), which en-compasses coronary artery disease (CAD),cerebrovascular disease (i.e., stroke), and peripheral arterial disease (PAD). These dis-eases are major causes of morbidity and mor-tality in human populations worldwide. Forexample, in the United States, atherosclero-sis affects one in four persons and contri -butes to 39% of deaths annually.1 CVD accounts for 29% of deaths worldwide andranks as the second leading cause of deathafter infectious and parasitic diseases.2
In atherosclerosis, large- to medium-sized muscular arteries and large elastic arteries become occluded with fibro-lipid lesions or “atheromas.” End-stage compli-cations or events associated with athero-sclerosis include coronary thrombosis, acutemyo cardial infarction (MI) and cerebral vas-cular accident or stroke. As presented in thepreceding chapter, traditional risk factors re-lated to behaviors, diet, lifestyle, and familyhistory do not appear to fully account forthe development of atherosclerosis. Further-more, despite continued preventive effortsaddressing modifiable risk factors, mortalityrates from CVD have remained virtually un-changed over the past decade in developedcountries.
The Role of InflammationCurrently, clinicians and investigators
appreciate that inflammation appears to playa pivotal role in the pathogenesis of athero-sclerosis, from the development of the “fatty
streak” to plaque rupture. This appreciationhas intensified the search for chronic expo-sures or infections that potentially cause inflammation in vessels. Putative infectionsthat may at least exacerbate atherosclerosisinclude cytomegalovirus, herpes simplex virus,Chlamydia pneumoniae, Helicobacter pylori,and periodontal disease.3 Over the last twodecades, observational studies in human pop- ulations have consistently shown a modest,but significant association between perio -dontal disease and atheromatous diseases. Inaddition, animal models chronically exposedto periodontal infective agents have demon-strated more rapid progression of athero-sclerosis. Lastly, early intervention studies inhuman subjects suggest that periodontal dis-ease treatment may improve surrogate mark-ers associated with atherosclerosis and CVD.The objective of this chapter is to provide thereader with a strong understanding of theevidence implicating a relationship betweenperiodontal disease and atheromatous diseases.
EVIDENCE FROM HUMAN OBSERVATIONAL STUDIES
Patients with periodontal disease sharemany of the same risk factors as patientswith atheromatous diseases, including age,gender (predominantly male), lower socio -economic status, stress, and smoking.4 Ad-ditionally, a large proportion of patients withperiodontal disease also exhibit atheroscle-rosis or CVD.5 These observations suggestthat periodontal disease and atherosclerosisshare similar or common etiologic pathways.Several recent systematic reviews of the avail- able evidence support an association between
CHAPTER 8Association Between PeriodontalDisease and Atheromatous Diseases
David W. Paquette, Robert J. Genco

CHAPTER 8 Association between Periodontal and Atheromatous Diseases 113
periodontal disease and atheromatous dis-eases. In one systematic review, Scannapiecoand colleagues asked the focused question,“Does periodontal disease influence the initiation/progression of atherosclerosis andtherefore CVD, stroke, and peripheral vas-cular disease?”6 The investigators identified31 human studies. Although the authors didnot perform a meta-analysis due to differ-ences in reported outcomes, they noted relative (not absolute) consistency and con-cluded, “Periodontal disease may be mod-estly associated with atherosclerosis, myo -cardial infarction, and cardiovascular events.”A recent Editors’ Consensus Report pub-lished in the American Journal of Cardiologyand the Journal of Periodontology makesrecommendations for patient information,medical and dental evaluations, and risk fac-tor treatment for patients with periodontitiswho are at risk for atherosclerotic disease.7
Meta-AnalysesIn the interval between this initial review
and the recent consensus report, at least threeother meta-analyses on the atherosclerosis-periodontal disease asso ciation have been con- ducted and published. Meurman and colleaguesreported a 20% increase in the risk for CVDamong patients with periodontal disease (95%CI:1.08– 1.32), and an even higher risk ratiofor cerebrovascular disease or stroke, varyingfrom 2.85 (95% CI:1.78–4.56) to 1.74 (95%CI: 1.08–2.81).8 Similarly, Khader et al. andVettore reported relative risk estimates of1.19 (95% CI:1.08–1.32) and 1.15 (95%CI:1.06–1.25), respectively.9,10 These meta-analyses of the available observational humandata lend credence to the hypothesis that peri-odontal and atheromatous diseases are associ-ated with one another in various populations.
Case-Control StudiesAccordingly, case-control studies, which
select subjects with the dependent diseaseand assess exposure (risk), have consistently
supported a positive association between pe-riodontal disease and atheromatous diseases(Table 1). Matilla et al. first reported thatpoor oral health (including periodontal dis-ease) was a predictor for MI among a Finnishpopulation of 100 cases and 102 control sub-jects.11 Using a Dental Severity Index scoreas a measure of periodontal and endodonticinfections as well as dental caries, the in-vestigators found that individuals with evi-dence of oral infection were 30% more likelyto present with MI compared to subjectswithout oral infections. This association was significant after adjusting for known riskfactors such as age, total cholesterol levels,hypertension, body mass index, and cigarettesmoking. In a follow-up publication in thesame population, these investigators docu-mented a significant and specific associa-tion between dental infections and severecoronary atheromatosis in males.12 More recently, Arbes et al. evaluated availablecross-sectional data from the Third NationalHealth and Nutrition Survey (NHANESIII).13 Accordingly, for cases with severe clin-ical attachment loss and periodontitis, theodds ratio for MI was 3.8 (95% CI:1.5–9.7)compared to periodontally healthy controls.In addition, the probability for a coronaryevent rose with increasing periodontitisseverity. While the discussed case-controlstudies do not provide information on thechronicity of exposure and disease, theydo indicate that the association has relativestrength, is specific, and follows an exposure-response relationship.
Cohort StudiesLongitudinal cohort studies, in contrast,
provide a higher level of evidence since theyproperly document that the periodontitis exposure precedes the CVD (Table 2). Beckand colleagues evaluated 1,147 males ages21–80 who were participants in the NormativeAging Study and who were free of CAD at base- line.14 Periodontal status for this population

114 Periodontal Disease and Overall Health: A Clinician's Guide
ABI = ankle-brachial pressure index; CAL = clinical attachment loss; EKG = electrocardiogram; IMT = intima-media wall thick-ness; MI = myocardial infarction; NHANES = National Health and Nutrition Survey; OR = odds ratio; PAD = peripheral arterialdisease; PD = probing depth
Table 1. Summary of Evidence from Case-Control Studies Investigating an AssociationTable 1. Between Periodontal and Atheromatous Diseases in Human Populations
Periodontal Outcome Cardiovascular Findings andReference Study Design Population or Exposure Outcome Conclusions
Matilla et al. 198911 Case-control 100 cases and Dental Severity Index Evidence of MI Dental health signifi-102 controls (sum of scores for caries, from EKG and cantly worse in patients
periodontal disease, elevated enzyme with MI versus controlsperiapical pathosis, levels (creatinine after adjusting forand pericoronitis) phosphokinase smoking, serum lipids,
isoenzymes) and diabetesMatilla et al. 199312 Case-control 100 cases Dental Severity Index Clinical Significant association
diagnosis or between dentalradiographically infections and severeconfirmed MI coronary atheromatosis
in males (but not females)
Arbes et al. 199913 Case-control 5,564 subjects Percent attachment loss Self-reported MI Positive association(NHANES III) of all teeth (> 3 mm) between periodontal
and categorized disease and CHD according to four levels (OR= 3.8 for severe
attachment loss) and after adjusting for age, gender, race, etc.
Söder et al. 200528 Case-control 82 cases and Clinical periodontitis Carotid IMT Significant association31 controls defined as having values between periodontal
1 site with a pocket disease and carotid depth 5 mm atherosclerosis
(OR = 4.64)Andriankaja et al. 200626 Population- 537 cases and Various including Incident MI Significant association
based case- 800 controls continuous CAL, PD, between periodontalcontrol and missing teeth; also disease and incident
various case definitions MI regardless of measurement or definition of periodontal disease used, after adjusting for multiple potential confounders
Andriankaja et al. 200727 Population- 574 cases and Mean CAL Incident MI Significant associationbased case- 887 controls between periodontalcontrol disease and incident
MI in both genders, and in nonsmokers as well as smokers, after adjusting for multiple potential confounders
Lu et al. 200832 Case-control 3,585 subjects Percent attachment loss PAD defined Significant association(NHANES III) of all teeth (>3 mm) and ABI < 0.9 between periodontal
categorized according to disease and PAD four levels (OR = 2.25 for severe
attachment loss) after adjusting for age, gender, race, poverty, and traditional risk factors for PAD
Chen et al. 200833 Case-control 25 PAD cases Clinical periodontitis PAD diagnosed Significant association32 controls defined as having at via clinical between periodontitis
least one probing site symptoms, ABI, and PAD (OR = 5.45)with PD 4 mm or and angiographic after adjusting for age, CAL 4 mm in each finding gender, diabetes, and quadrant smoking
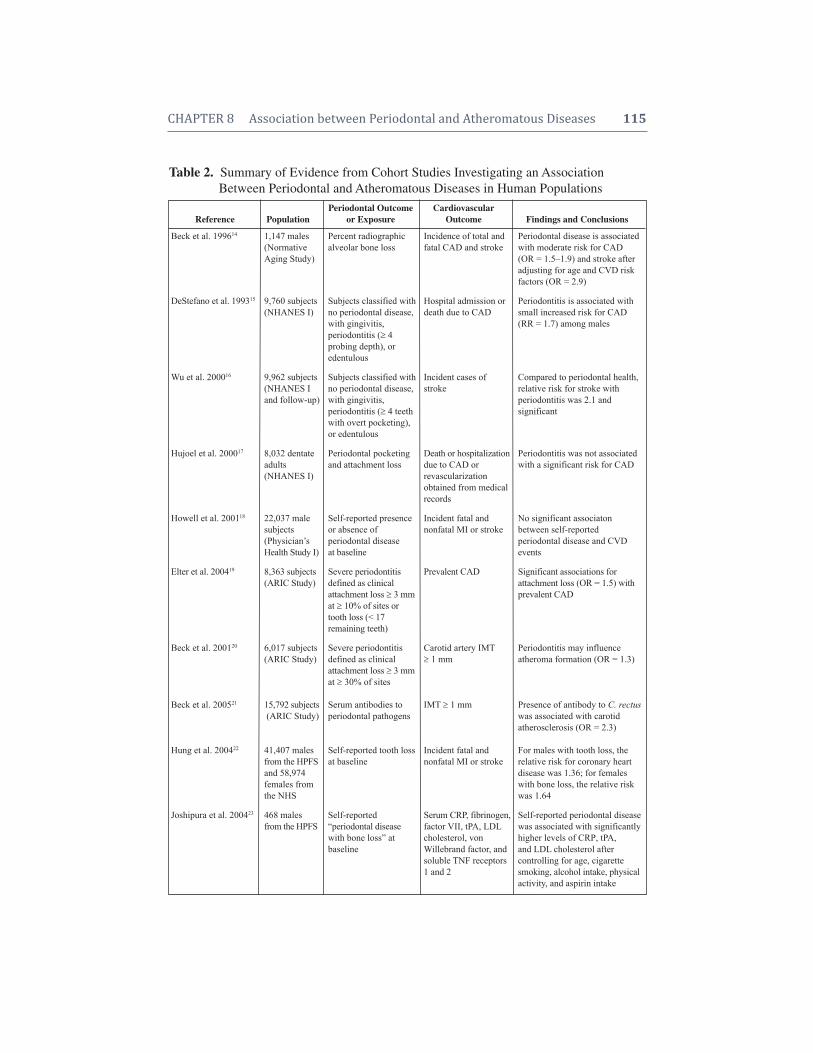
CHAPTER 8 Association between Periodontal and Atheromatous Diseases 115
Table 2. Summary of Evidence from Cohort Studies Investigating an AssociationTable 1. Between Periodontal and Atheromatous Diseases in Human Populations
Periodontal Outcome CardiovascularReference Population or Exposure Outcome Findings and Conclusions
Beck et al. 199614 1,147 males Percent radiographic Incidence of total and Periodontal disease is associated(Normative alveolar bone loss fatal CAD and stroke with moderate risk for CADAging Study) (OR = 1.5–1.9) and stroke after
adjusting for age and CVD riskfactors (OR = 2.9)
DeStefano et al. 199315 9,760 subjects Subjects classified with Hospital admission or Periodontitis is associated with(NHANESI) no periodontal disease, death due to CAD small increased risk for CAD
with gingivitis, (RR = 1.7) among malesperiodontitis ( 4probing depth), oredentulous
Wu et al. 200016 9,962 subjects Subjects classified with Incident cases of Compared to periodontal health,(NHANESI no periodontal disease, stroke relative risk for stroke withand follow-up) with gingivitis, periodontitis was 2.1 and
periodontitis ( 4 teeth significantwith overt pocketing),or edentulous
Hujoel et al. 200017 8,032 dentate Periodontal pocketing Death or hospitalization Periodontitis was not associatedadults and attachment loss due to CAD or with a significant risk for CAD(NHANESI) revascularization
obtained from medicalrecords
Howell et al. 200118 22,037 male Self-reported presence Incident fatal and No significant associatonsubjects or absence of nonfatal MI or stroke between self-reported(Physician’s periodontal disease periodontal disease and CVDHealth Study I) at baseline events
Elter et al. 200419 8,363 subjects Severe periodontitis Prevalent CAD Significant associations for(ARIC Study) defined as clinical attachment loss (OR = 1.5) with
attachment loss 3 mm prevalent CADat 10% of sites ortooth loss (< 17remaining teeth)
Beck et al. 200120 6,017 subjects Severe periodontitis Carotid artery IMT Periodontitis may influence(ARIC Study) defined as clinical 1 mm atheroma formation (OR = 1.3)
attachment loss 3 mmat 30% of sites
Beck et al. 200521 15,792 subjects Serum antibodies to IMT 1 mm Presence of antibody to C. rectus(ARIC Study) periodontal pathogens was associated with carotid
atherosclerosis (OR = 2.3)
Hung et al. 200422 41,407 males Self-reported tooth loss Incident fatal and For males with tooth loss, thefrom the HPFS at baseline nonfatal MI or stroke relative risk for coronary heartand 58,974 disease was 1.36; for females females from with bone loss, the relative risk the NHS was 1.64
Joshipura et al. 200423 468 males Self-reported Serum CRP, fibrinogen, Self-reported periodontal diseasefrom the HPFS “periodontal disease factor VII, tPA, LDL was associated with significantly
with bone loss” at cholesterol, von higher levels of CRP, tPA,baseline Willebrand factor, and and LDL cholesterol after
soluble TNF receptors controlling for age, cigarette1 and 2 smoking, alcohol intake, physical
activity, and aspirin intake

was assessed via percent alveolar bone lossusing dental radiographs. Over an 18-yearfollow-up period, 207 men developed CAD,59 died from CAD, and 40 experiencedstrokes. Odds ratios (OR) adjusted for ageand established cardiovascular risk factorswere 1.5 (95% CI:1.04–2.14), 1.9 (95%CI:1.10–3.43) and 2.8 (95% CI:1.45–5.48)for periodontal bone loss and total coronaryheart disease, fatal coronary heart disease,and stroke, respectively. When Beck and col-leagues graphed the cumulative incidenceof coronary heart disease or events versusbaseline mean alveolar bone loss, they noteda linear relationship such that increasingseverities of periodontitis were accom-panied by increasing occurrences of CVD(Figure 1).14
Another cohort study conducted byDeStefano et al. assessed this risk relation-
ship among 9,760 adults followed for 14years in NHANES I.15 Several potentiallyconfounding variables were also examined,including age, gender, race, education, mar-ital status, systolic blood pressure, total cho-lesterol levels, body mass index, diabetes,physical activity, alcohol consumption,poverty, and cigarette smoking. Accordingly,individuals with pre-existing clinical signs ofperiodontitis were 25% more likely to de-velop CAD relative to those with minimalperiodontal disease after adjusting for otherknown risk factors or confounders. Malesyounger than 50 with periodontitis in thisstudy were 72% more likely to develop CADcompared to their periodontally healthycounterparts. Similarly, Wu et al. evaluatedthe potential contribution of periodontitis tostroke risk within this same NHANES I pop-ulation (n = 9,962 adults).16 The investigators
ARIC: Atherosclerosis Risk in Communities; CAD: coronary artery disease; CRP: C-reactive protein; CVD: cardiovascular disease; HPFS: Health Professional Follow-up Study; IMT: intima-media wall thickness; INVEST: Oral Infections and VascularDisease Epidemiology Study; LDL: low density lipoprotein; MI: myocardial infarction; NHANES: National Health and NutritionExamination Survey; NHS: Nurses Health Study; OR: odds ratio; RR: relative risk; tPA: tissue plasminogen activator
Table 2. Cont’d Summary of Evidence from Cohort Studies Investigating an AssociationTable 1. Between Periodontal and Atheromatous Diseases in Human Populations
Periodontal Outcome CardiovascularReference Population or Exposure Outcome Findings and Conclusions
Engebretson et al. 200524 203 subjects Radiographic alveolar Carotid plaque Severe periodontal bone loss wasfrom INVEST bone loss thickness via independently associated with
ultrasonography carotid atherosclerosis (OR = 3.64)
Desvarieux et al. 200525 1,056 subjects Subgingival bacterial Carotid artery IMT Severe periodontal bone loss wasfrom INVEST burden 1 mm independently associated with
carotid atherosclerosis (OR = 3.64)
Pussinen et al. 200429 6,950 Finnish Serum antibodies to Incident fatal or Seropositive subjects had an ORsubjects in the P. gingivalis or A. nonfatal stroke of 2.6 for stroke Mobile Clinic actinomycetemcomitansHealth Survey
Pussinen et al. 200530 1,023 males Serum antibodies to A. Incident MI or CAD Subjects with the highest tertilein the Kuopio actinomycetemcomitans death of A. actinomycetemcomitansIschemic Heart antibodies were two times moreDisease Study likely to suffer MI or CAD death
(RR = 2.0) compared with those with lowest tertile of antibody levels
Abnet et al. 200531 29,584 rural Tooth loss Incidence of fatal MI Tooth loss was associated with an Chinese or stroke increased odds for death from MIsubjects (RR = 1.29) and stroke (RR = 1.12)
116 Periodontal Disease and Overall Health: A Clinician's Guide
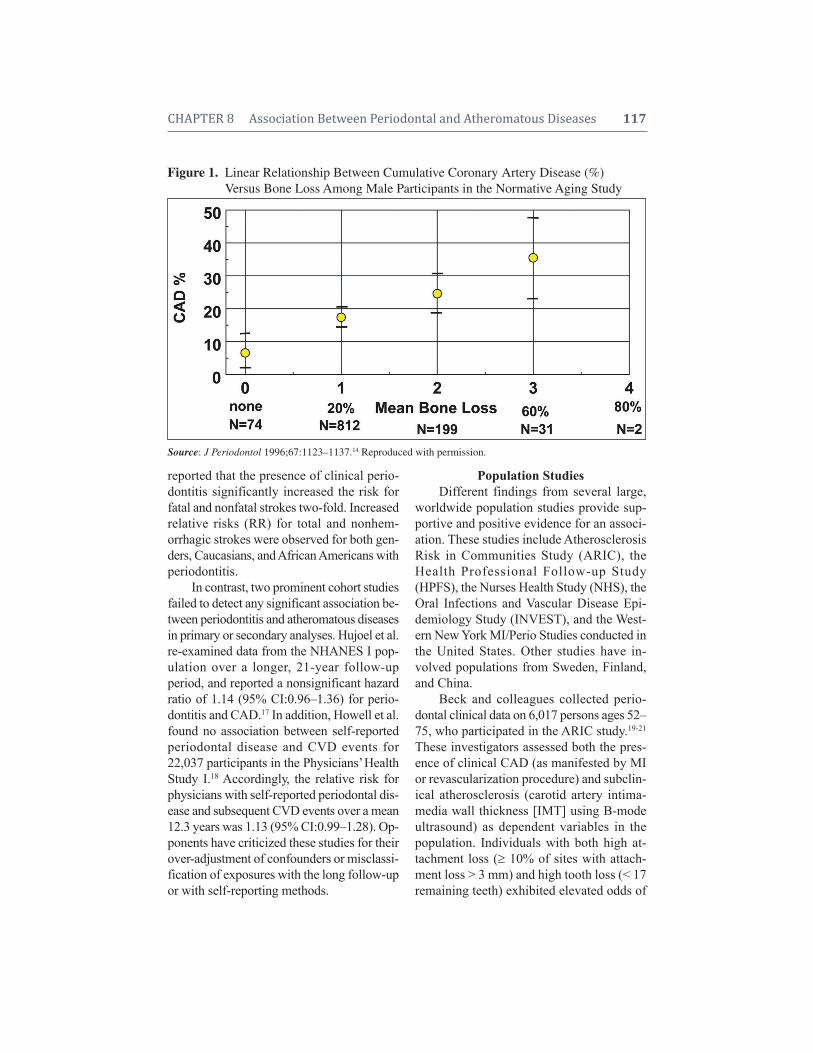
CHAPTER 8 Association Between Periodontal and Atheromatous Diseases 117
Figure 1. Linear Relationship Between Cumulative Coronary Artery Disease (%)Figure 1. Versus Bone Loss Among Male Participants in the Normative Aging Study
Source: J Periodontol 1996;67:1123–1137.14 Reproduced with permission.
Population StudiesDifferent findings from several large,
worldwide population studies provide sup-portive and positive evidence for an associ-ation. These studies include AtherosclerosisRisk in Communities Study (ARIC), theHealth Professional Follow-up Study(HPFS), the Nurses Health Study (NHS), theOral Infections and Vascular Disease Epi-demiology Study (INVEST), and the West-ern New York MI/Perio Studies conducted inthe United States. Other studies have in-volved populations from Sweden, Finland,and China.
Beck and colleagues collected perio -dontal clinical data on 6,017 persons ages 52–75, who participated in the ARIC study.19-21
These investigators assessed both the pres-ence of clinical CAD (as manifested by MIor revascularization procedure) and subclin-ical atherosclerosis (carotid artery intima-media wall thickness [IMT] using B-modeultrasound) as dependent variables in thepopulation. Individuals with both high at-tachment loss ( 10% of sites with attach-ment loss > 3 mm) and high tooth loss (< 17remaining teeth) exhibited elevated odds of
reported that the presence of clinical perio -dontitis significantly increased the risk for fatal and nonfatal strokes two-fold. Increasedrelative risks (RR) for total and nonhem -orrhagic strokes were observed for both gen -ders, Caucasians, and African Americans withperiodontitis.
In contrast, two prominent cohort studiesfailed to detect any significant association be-tween periodontitis and atheromatous diseasesin primary or secondary analyses. Hujoel et al.re-examined data from the NHANES I pop-ulation over a longer, 21-year follow-up period, and reported a nonsignificant hazard ratio of 1.14 (95% CI:0.96–1.36) for perio -dontitis and CAD.17 In addition, Howell et al.found no association between self- reportedperiodontal disease and CVD events for22,037 participants in the Physicians’ HealthStudy I.18 Accordingly, the relative risk forphysicians with self-reported periodontal dis-ease and subsequent CVD events over a mean12.3 years was 1.13 (95% CI:0.99–1.28). Op-ponents have criticized these studies for theirover-adjustment of confounders or misclassi-fication of exposures with the long follow-upor with self-reporting methods.
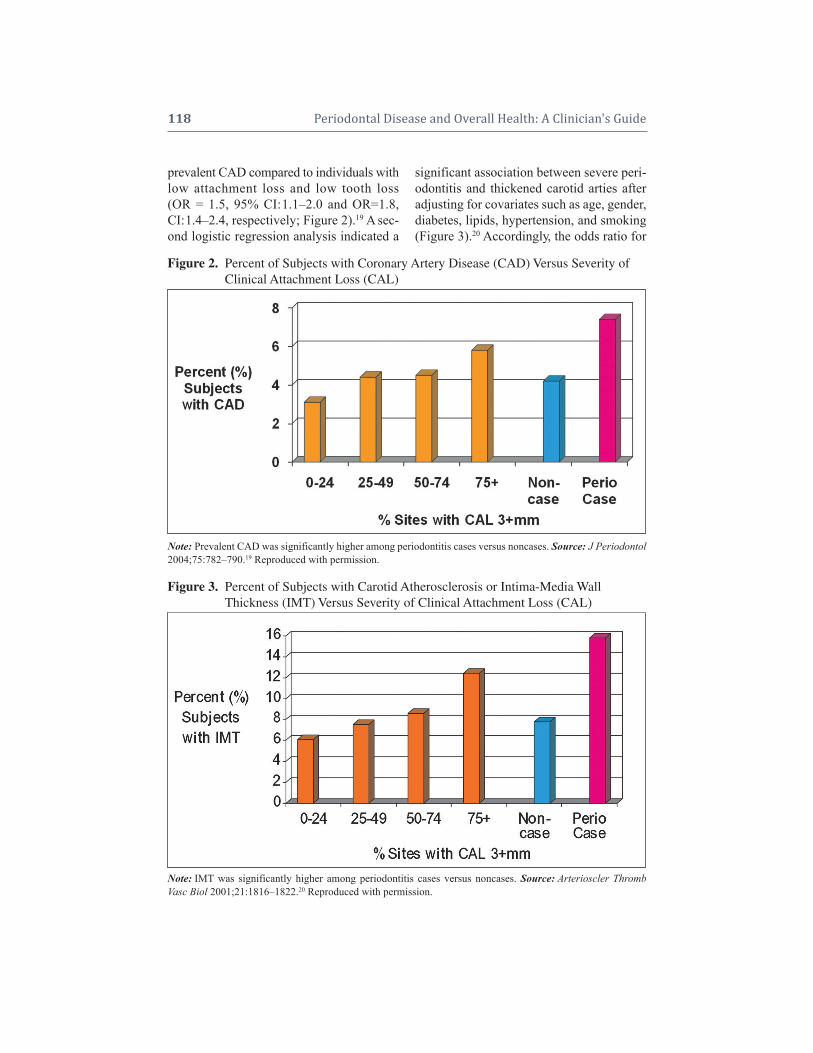
118 Periodontal Disease and Overall Health: A Clinician's Guide
significant association between severe peri-odontitis and thickened carotid arties afteradjusting for covariates such as age, gender,diabetes, lipids, hypertension, and smoking(Figure 3).20 Accordingly, the odds ratio for
prevalent CAD compared to individuals withlow attachment loss and low tooth loss(OR = 1.5, 95% CI:1.1–2.0 and OR=1.8,CI:1.4–2.4, respectively; Figure 2).19 A sec-ond logistic regression analysis indicated a
Note: IMT was significantly higher among periodontitis cases versus noncases. Source: Arterioscler ThrombVasc Biol 2001;21:1816–1822.20 Reproduced with permission.
Figure 3. Percent of Subjects with Carotid Atherosclerosis or Intima-Media Wall Figure 1. Thickness (IMT) Versus Severity of Clinical Attachment Loss (CAL)
Figure 2. Percent of Subjects with Coronary Artery Disease (CAD) Versus Severity of Figure 1. Clinical Attachment Loss (CAL)
Note: Prevalent CAD was significantly higher among periodontitis cases versus noncases. Source: J Periodontol2004;75:782–790.19 Reproduced with permission.

CHAPTER 8 Association Between Periodontal and Atheromatous Diseases 119
severe periodontitis (i.e., 30% or more ofsites with 3 mm clinical attachment loss)and subclinical carotid atherosclerosis was1.31 (95% CI:1.03–1.66). In a third report,these investigators quantified serum IgG antibody levels specific for 17 periodontalorganisms using a whole bacterial checker-board immunoblotting technique.21 Ana lyzingmean carotid IMT ( 1 mm) as the outcomeand serum antibody levels as exposures forthis same population, the investigators notedthe presence of antibody to Campylobacterrectus increased the risk for subclinical ath-erosclerosis two-fold (OR = 2.3, 95% CI:1.83,2.84). In particular, individuals with both highC. rectus and Pepto streptococcus micros anti -body titers had al most twice the prevalence ofcarotid athero sclerosis than did those withonly a high C. rectus antibody (8.3% versus16.3%). Stratification by smoking indicatedthat all microbial models significant for smok-ers were also significant for subjects who hadnever smoked, except for Porphyromonas gin-givalis. Thus, clinical signs of periodontitis areassociated with CAD and subclinical athero-sclerosis in the ARIC population, and expo-sures to specific periodontal pathogens sig-nificantly increase the risk for atherosclerosisin smoking and nonsmoking subjects.
Hung and Joshipura and colleagues as-sessed self-reported periodontal disease out-comes and incident CVD in two extant data-bases, HPFS (n = 41,407 males followed for12 years) and NHS (n = 58,974 females followed for 6 years).22 After controlling forimportant cardiovascular risk factors, maleswith a low number of reported teeth ( 10 atbaseline) had a significantly higher risk ofCAD (RR = 1.36, 95% CI:1.11–1.67) com-pared to males with a high number of teeth(25 or more). For females with the same re-ported extent of tooth loss, the relative riskfor CAD was 1.64 (95% CI:1.31–2.05) com-pared to women with at least 25 teeth. Therelative risks for fatal CAD events increasedto 1.79 (95% CI:1.34, 2.40) for males and
1.65 (95% CI:1.11–2.46) for females withtooth loss, respectively. In a second report,the investigators evaluated the associationbetween self-reported periodontal diseaseand serum elevations in CVD biomarkerscross-sectionally in a subset of HPFS par-ticipants (n = 468 males).23 Serum biomark-ers included C-reactive protein (CRP), fib-rinogen, factor VII, tissue plasminogenactivator (tPA), low density lipoprotein cho-lesterol (LDLC), von Willebrand factor, andsoluble tumor necrosis factor receptors 1 and2. In multivariate regression models con-trolling for age, cigarette smoking, alcoholintake, physical activity, and aspirin intake,self-reported perio dontal disease was as -sociated with significantly higher levels ofCRP (30% higher among periodontal casescompared with noncases), tPA (11% higher),and LDLC (11% higher). These analyses re-veal significant associations between self-reported number of teeth at baseline and riskof CAD, and be tween self-reported perio -dontal disease and serum biomarkers ofendothelial dysfunction and dyslipidemia.
The INVEST StudyThe INVEST population study was
planned a priori and conducted exclusivelyto evaluate the association between CVDand periodontal outcomes in a cohort popu-lation. Engebretson and colleagues reportedthat for a group of 203 stroke-free subjects(ages 54–94) at baseline, mean carotid plaquethickness (measured with B-mode ultrasound)was significantly greater among dentate sub-jects with severe periodontal bone loss ( 50%measured radiographically) than amongthose with less bone loss (< 50%).24 Indeed,the group noted a clear dose-response rela-tionship when they graphed subject tertilesof periodontal bone loss versus carotid plaquethickness. The investigators next collectedsubgingival plaque from 1,056 subjects andtested for the presence of 11 known peri-odontal bacteria using DNA techniques.25
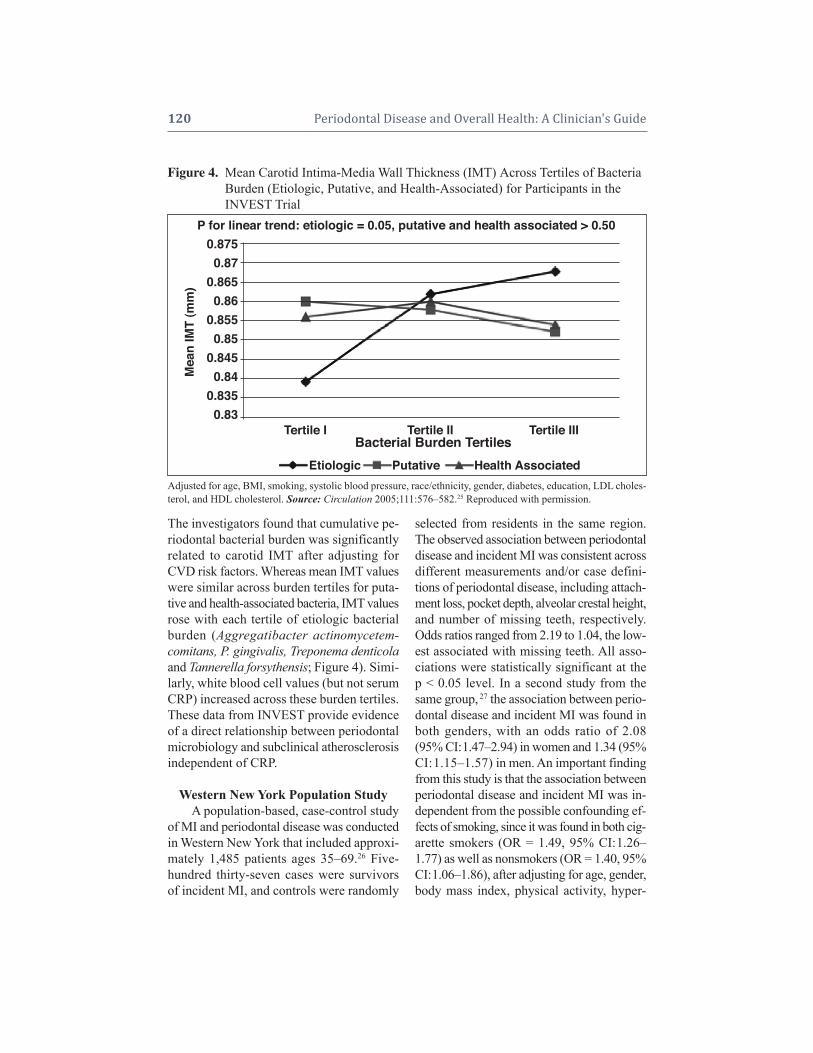
120 Periodontal Disease and Overall Health: A Clinician's Guide
The investigators found that cumulative pe-riodontal bacterial burden was significantlyrelated to carotid IMT after adjusting forCVD risk factors. Whereas mean IMT valueswere similar across burden tertiles for pu ta-tive and health-associated bacteria, IMT valuesrose with each tertile of etiologic bac terialburden (Aggregatibacter actinomy cetem- comitans, P. gingivalis, Treponema denticolaand Tannerella forsythensis; Figure 4). Simi-larly, white blood cell values (but not serumCRP) increased across these burden tertiles.These data from INVEST provide evidenceof a direct relationship between periodontalmicrobiology and subclinical atherosclerosisindependent of CRP.
Western New York Population StudyA population-based, case-control study
of MI and periodontal disease was conductedin Western New York that included approxi -mately 1,485 patients ages 35–69.26 Five-hundred thirty-seven cases were survivorsof incident MI, and controls were randomly
selected from residents in the same region.The observed association between perio dontaldisease and incident MI was consistent acrossdifferent measurements and/or case defini-tions of periodontal disease, including attach-ment loss, pocket depth, alveolar crestal height,and number of missing teeth, respectively.Odds ratios ranged from 2.19 to 1.04, the low-est associated with missing teeth. All asso-ciations were statistically significant at thep < 0.05 level. In a second study from thesame group, 27 the association between perio -dontal disease and incident MI was found inboth genders, with an odds ratio of 2.08(95% CI:1.47–2.94) in women and 1.34 (95%CI:1.15–1.57) in men. An important findingfrom this study is that the association betweenperiodontal disease and incident MI was in-dependent from the possible confounding ef-fects of smoking, since it was found in both cig-a rette smokers (OR = 1.49, 95% CI:1.26–1.77) as well as nonsmokers (OR = 1.40, 95%CI:1.06–1.86), after adjusting for age, gender,body mass index, physical activity, hyper-
Figure 4. Mean Carotid Intima-Media Wall Thickness (IMT) Across Tertiles of BacteriaFigure 4. Burden (Etiologic, Putative, and Health-Associated) for Participants in theFigure 4. INVEST Trial
Adjusted for age, BMI, smoking, systolic blood pressure, race/ethnicity, gender, diabetes, education, LDL choles -terol, and HDL cholesterol. Source: Circulation 2005;111:576–582.25 Reproduced with permission.
P for linear trend: etiologic = 0.05, putative and health associated > 0.50
Etiologic
0.8750.87
0.8650.86
0.8550.85
0.8450.84
0.8350.83
Mea
n IM
T (m
m)
Putative Health Associated
Tertile I Tertile II Tertile IIIBacterial Burden Tertiles

CHAPTER 8 Association Between Periodontal and Atheromatous Diseases 121
tension, cholesterol, diabetes, and total pack-years of cigarette smoking. This is an im-portant finding because there is an active de-bate among authors suggesting smoking is acausal confounding factor between perio -dontal disease and CVD. The positive asso-ciation of periodontal disease and MI in non-smokers provides greater evidence thatperiodontal disease could affect coronaryheart disease independent of smoking.
Population Studies in Europe and AsiaConsistent associations between peri-
odontal outcomes and atherosclerosis havebeen demonstrated among populations inEurope and Asia. For 131 adult Swedes,mean carotid IMT values were significantlyhigher in subjects with clinical and/or radio -graphic evidence of periodontal disease com-pared to periodontally healthy controls.28
Multiple logistic regression analysis identi-fied periodontal disease as a principal inde-pendent predictor of carotid atherosclerosiswith an odds ratio of 4.64 (95% CI:1.64–13.10). Pussinen et al. monitored antibodyresponses for A. actinomycetemcomitans andP. gingivalis among 6,950 Finnish subjectsfor whom CVD outcomes over 13 years wereavailable (Mobile Clinic Health Survey).29
Compared with the subjects who were sero -negative for these pathogens, seropositivesubjects had an odds ratio of 2.6 (95% CI:1.0-7.0) for a secondary stroke. In another report on 1,023 males (Kuopio IschemicHeart Disease Study), Pussinen and col-leagues observed that cases with MI or CADdeath were more often seropositive for A.actinomycetemcomitans than those controlswho remained healthy (15.5% versus 10.2%).30
In the highest tertile of A. actinomycetem-comitans antibodies, the relative risk for MI orCAD death was 2.0 (95% CI:1.2–3.3) com-pared with the lowest tertile. For P. gingivalisantibody responses, the relative risk was2.1 (95% CI:1.3–3.4). Abnet and colleagueshave published findings from a cohort study
of 29,584 healthy, rural Chinese adults mon-itored for up to 15 years.31 Tooth loss was eval-uated as an exposure outcome for perio dontaldisease, and mortality from heart disease orstroke were modeled as dependent variables.Individuals with greater than the age-specificmedian number of teeth lost exhibited a sig-nificantly increased risk of death from MI (RR= 1.28, 95% CI:1.17–1.40) and stroke (RR =1.12, 95% CI:1.02–1.23). These elevated riskswere present in males and females irrespectiveof smoking status. Collectively, these findingsindicate consistent associations for perio dontaldisease and patho genic exposures with CVD.
Observational StudiesTwo recent observational studies have
focused on the relationship between perio -dontal disease and PAD. The study popula-tion for the first of these reports consisted of3,585 participants who were 40 or older inNHANES III during 1999–2002.32 PAD wasdefined as an ankle-brachial pressure indexof < 0.9, and the presence of periodontal dis-ease was based on clinical attachment sever-ity scores (i.e., 0%, 1–15%, 6–33% and morethan 33% of sites with clinical attachmentloss 3 mm). While 4.8% of subjects wererecognized as PAD cases, multiple logisticregression analyses indicated that periodon-tal disease was significantly associated withPAD (OR = 2.25, 95% CI:1.20–4.22) afteradjusting for age, gender, race, poverty, tra-ditional risk factors of PAD, and other po-tential confounding factors. Systemic mark-ers of inflammation (CRP, white blood cellcount, fibrinogen) were also associated withPAD, and were significantly associated withclinical attachment loss or periodontitis. A sec-ond case control study included 25 patientsdiagnosed with PAD (aorto-iliac and/orfemoro-popliteal occlusive disease), and 32generally healthy control subjects.33 Poly-merase chain reaction was used to identify P.gingivalis, T. denticola, A. actinomycetem-comitans, Prevotella intermedia, Cytomegalo -

122 Periodontal Disease and Overall Health: A Clinician's Guide
virus (CMV), Chlamydia pneumoniae, andH. pylori in tissue specimens obtained at thetime of bypass grafting. After adjusting forage, gender, diabetes, and smoking, perio -dontitis increased five-fold the risk of havingPAD (OR = 5.45, 95% CI:1.5718.89). Inaddition, periodontopathic bacteria were detected in approximately half of the ather-osclerotic specimens. In contrast, CMV or C.pneumoniae was detected in only 4% ofspecimens, and H. pylori was detected innone of the specimens. These early observa-tional data suggest a higher likelihood ofPAD among subjects with periodontal dis-ease, and that DNA sequences specific toperiodontal pathogens may be present inPAD lesions.
BIOLOGICAL PLAUSIBILTY ANDEVIDENCE FROM ANIMAL MODELS
Since periodontal infections result inlow-grade bacteremias and endotoxemias inaffected patients,34,35 systemic effects on vas-cular physiology via these exposures appearbiologically plausible. Four specific path-
ways have been proposed to explain theplausibility of a link between CVD and periodontal infection. These pathways (act-ing independently or collectively) include:1) direct bacterial effects on platelets; 2) auto immune responses; 3) invasion and/oruptake of bacteria in endothelial cells andmacrophages; and 4) endocrine-like effectsof pro-inflammatory mediators.36 In sup-port of the first pathway, two oral bacteria, P. gingivalis and Streptococcus sanguis, ex-press virulence factors called “collagen-likeplatelet aggregation-associated proteins” thatinduce platelet aggregation in vitro and invivo.37,38 Secondly, autoimmune mechanismsmay play a role since antibodies that cross-react with periodontal bacteria and humanheat shock proteins have been identified(Figure 5).39,40 Deshpande and colleagueshave thirdly demonstrated that P. gingivaliscan invade aortic and heart endothelial cellsvia fimbriae (Figure 6).41 Several investi -gative groups have independently identi -fied specific oral pathogens in atheromatous tissues.42,43 In addition, macrophages incu-
Figure 5. Infection-Induced Stimulation of Accelerated Atherosclerosis by AutoimmuneFigure 5. Responses or “Molecular Mimicry”
Note: Specific antibodies directed toward bacterial heat shock proteins cross-react with human heat shock proteins,leading to endothelial cell damage, monocyte recruitment, elevated circulating lipids such as oxidized LDL (ox-LDL), and atherogenesis. Source: J Dent Res 2006;85:106–121.36 Reproduced with permission.
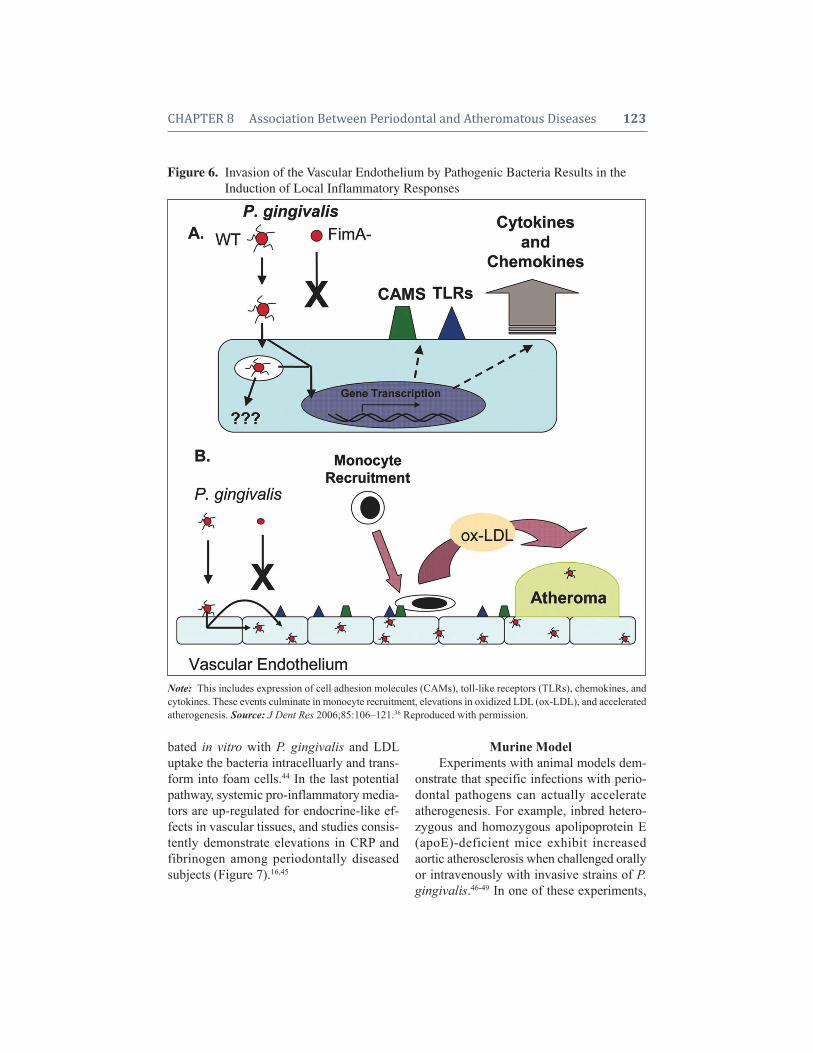
CHAPTER 8 Association Between Periodontal and Atheromatous Diseases 123
bated in vitro with P. gingivalis and LDLuptake the bacteria intracelluarly and trans-form into foam cells.44 In the last potentialpathway, systemic pro-inflammatory media-tors are up-regulated for endocrine-like ef-fects in vascular tissues, and studies consis-tently demonstrate elevations in CRP andfibrinogen among periodontally diseasedsubjects (Figure 7).16,45
Murine ModelExperiments with animal models dem -
onstrate that specific infections with perio -dontal pathogens can actually accelerateatherogenesis. For example, inbred hetero -zygous and homozygous apolipoprotein E(apoE)-deficient mice exhibit increased aortic atherosclerosis when challenged orallyor intravenously with invasive strains of P.gingivalis.46-49 In one of these experiments,
Figure 6. Invasion of the Vascular Endothelium by Pathogenic Bacteria Results in theFigure 6. Induction of Local Inflammatory Responses
Note:This includes expression of cell adhesion molecules (CAMs), toll-like receptors (TLRs), chemokines, andcytokines. These events culminate in monocyte recruitment, elevations in oxidized LDL (ox-LDL), and acceleratedatherogenesis. Source: J Dent Res 2006;85:106–121.36 Reproduced with permission.
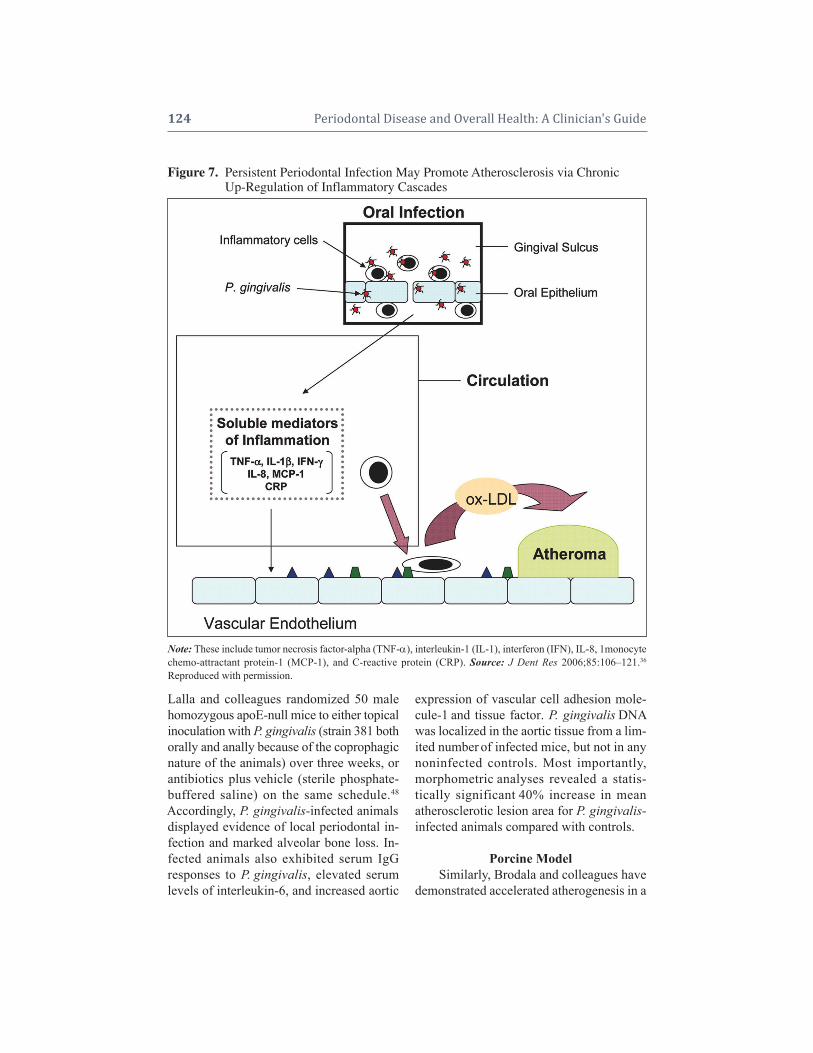
124 Periodontal Disease and Overall Health: A Clinician's Guide
Lalla and colleagues randomized 50 malehomozygous apoE-null mice to either topicalinoculation with P. gingivalis (strain 381 bothorally and anally because of the coprophagicnature of the animals) over three weeks, orantibiotics plus vehicle (sterile phosphate-buffered saline) on the same schedule.48
Accordingly, P. gingivalis-infected animalsdisplayed evidence of local periodontal in-fection and marked alveolar bone loss. In-fected animals also exhibited serum IgG responses to P. gingivalis, elevated serumlevels of interleukin-6, and increased aortic
expression of vascular cell adhesion mole-cule-1 and tissue factor. P. gingivalis DNAwas localized in the aortic tissue from a lim-ited number of infected mice, but not in anynoninfected controls. Most importantly, morphometric analyses revealed a statis -tically significant 40% increase in mean atherosclerotic lesion area for P. gingivalis-infected animals compared with controls.
Porcine ModelSimilarly, Brodala and colleagues have
demonstrated accelerated atherogenesis in a
Figure 7. Persistent Periodontal Infection May Promote Atherosclerosis via ChronicFigure 7. Up-Regulation of Inflammatory Cascades
Note: These include tumor necrosis factor-alpha (TNF-), interleukin-1 (IL-1), interferon (IFN), IL-8, 1monocytechemo-attractant protein-1 (MCP-1), and C-reactive protein (CRP). Source: J Dent Res 2006;85:106–121.36
Reproduced with permission.
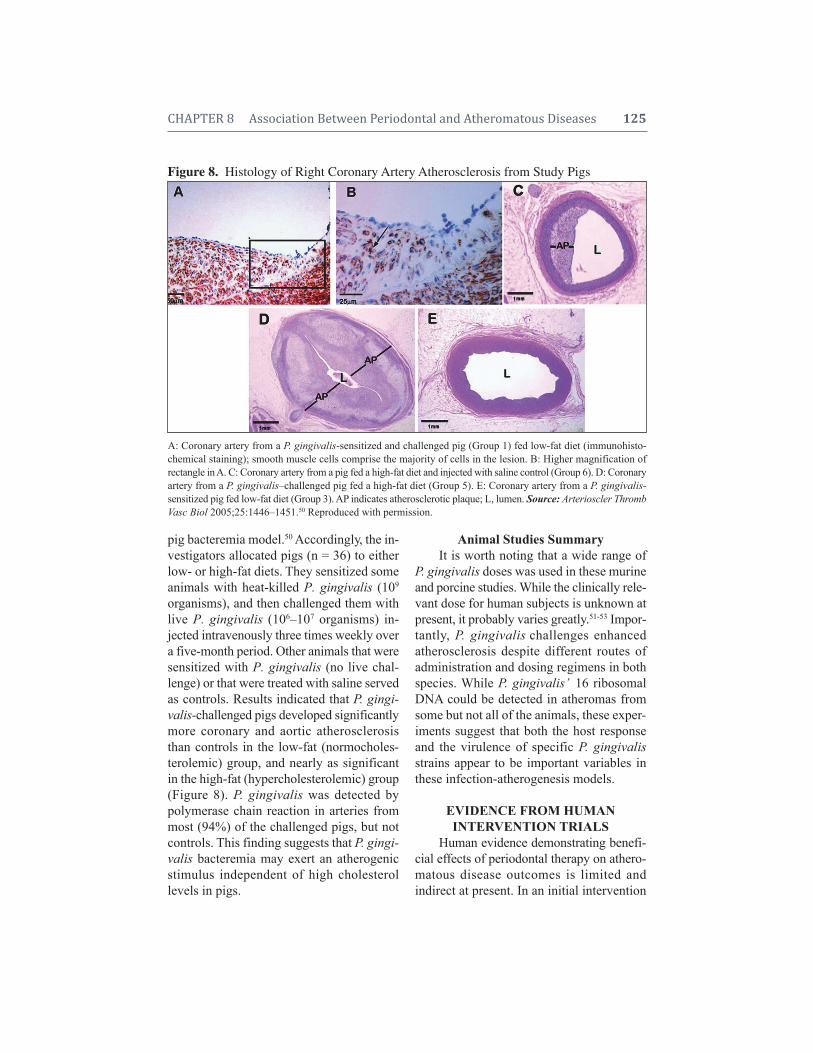
CHAPTER 8 Association Between Periodontal and Atheromatous Diseases 125
pig bacteremia model.50 Accordingly, the in-vestigators allocated pigs (n = 36) to eitherlow- or high-fat diets. They sensitized someanimals with heat-killed P. gingivalis (109
organisms), and then challenged them withlive P. gingivalis (106–107 organisms) in-jected intravenously three times weekly overa five-month period. Other animals that weresensitized with P. gingivalis (no live chal-lenge) or that were treated with saline servedas controls. Results indicated that P. gingi-valis-challenged pigs developed significantlymore coronary and aortic atherosclerosisthan controls in the low-fat (normocholes-terolemic) group, and nearly as significantin the high-fat (hypercholesterolemic) group(Figure 8). P. gingivalis was detected bypolymerase chain reaction in arteries frommost (94%) of the challenged pigs, but notcontrols. This finding suggests that P. gingi-valis bacteremia may exert an atherogenicstimulus independent of high cholesterol levels in pigs.
Animal Studies SummaryIt is worth noting that a wide range of
P. gingivalis doses was used in these murineand porcine studies. While the clinically rele -vant dose for human subjects is unknown atpresent, it probably varies greatly.51-53 Impor -tantly, P. gingivalis challenges enhanced atherosclerosis despite different routes of administration and dosing regimens in bothspecies. While P. gingivalis’ 16 ribosomalDNA could be detected in atheromas fromsome but not all of the animals, these exper-iments suggest that both the host responseand the virulence of specific P. gingivalisstrains appear to be important variables inthese infection-atherogenesis models.
EVIDENCE FROM HUMAN INTERVENTION TRIALS
Human evidence demonstrating benefi-cial effects of periodontal therapy on athero- matous disease outcomes is limited and indirect at present. In an initial intervention
Figure 8. Histology of Right Coronary Artery Atherosclerosis from Study Pigs
A: Coronary artery from a P. gingivalis-sensitized and challenged pig (Group 1) fed low-fat diet (immunohisto-chemical staining); smooth muscle cells comprise the majority of cells in the lesion. B: Higher magnification ofrectangle in A. C: Coronary artery from a pig fed a high-fat diet and injected with saline control (Group 6). D: Coronaryartery from a P. gingivalis–challenged pig fed a high-fat diet (Group 5). E: Coronary artery from a P. gingivalis- sensitized pig fed low-fat diet (Group 3). AP indicates atherosclerotic plaque; L, lumen. Source: Arterioscler ThrombVasc Biol 2005;25:1446–1451.50 Reproduced with permission.

126 Periodontal Disease and Overall Health: A Clinician's Guide
trial, D’Auito and colleagues demonstratedthat periodontitis patients treated with scal-ing and root planing exhibited significantserum reductions in the CVD biomarkers,CRP, and interleukin-6.54 In particular, pa-tients who clinically responded to periodon-tal therapy in terms of pocket depth reduc-tions were four times more likely to exhibitserum decreases in CRP relative to patientswith a poor clinical periodontal response.
The PAVE StudyIn 2009, Offenbacher and collaborators
published results from the Periodontitis andVascular Events (PAVE) pilot study, whichwas conducted to investigate the feasibilityof a randomized secondary-preventiontrial.55 Accordingly, five clinical centers re-cruited participants who had documented CAD( 50% blockage of one coronary artery orprevious coronary event including MI, coro-nary artery bypass graft surgery, or coronarytransluminal angioplasty three to 36 monthsprior to enrollment) and who met study cri-teria for periodontal disease ( 3 teeth withprobing depths 4 mm, 2 teeth with in-terproximal clinical attachment loss 2 mm,and 10% of sites with bleeding on prob-ing). Three-hundred and three eligible par-ticipants were enrolled, and all subjects re-ceived extractions for hopeless teeth. There-after, subjects were randomized to receive either periodontal therapy (“intensive treat-ment” group consisting of scaling and rootplaning at baseline) or community-baseddental care (control). Serum samples ob-tained at baseline (prior to randomization)and at six months were analyzed for levelsof high-sensitivity (hs) CRP. While the in -tensive treatment protocol significantly im-proved periodontal probing parameters oversix months, the treatment did not signifi-cantly improve mean serum hsCRP levels inthe overall population. Interestingly, in sec-ondary analyses it was noted that 48% ofthe community care control group received
some form of preventive or periodontal therapy over the six-month study period(e.g., dental prophylaxis, scaling and rootplaning, and/or periodontal surgery). Whenthe investigators stratified for any treatmentand obesity, they detected a treatment effecton hsCRP levels clustered among the non-obese subjects (Figure 9). Among non-obeseindividuals in the community who receivedno treatment, 43.5% had elevated hsCRP(> 3 mg/L) at six months. In contrast, 18% ofsubjects receiving any treatment exhibitedelevated hsCRP values. Logistical regres-sion modeling indicated that any treatmentamong all subjects resulted in a statisticallysignificant 2.38-fold lower odds for highhsCRP (OR = 0.42, 95% CI:0.18–0.99). Theeffects were even stronger among the non-obese subjects, with a 3.85-fold lower oddsfor having high hsCRP at six months withany treatment (OR = 0.26, 95% CI:0.09–0.72). These data suggest that crossover fromthe control arm may be high within inter-vention studies, and that any periodontal dis-ease treatment effect on hsCRP levels maybe exaggerated among non-obese patients.The data summarized in Figure 9 also sug-gests that even a dental prophylaxis, whichincludes supragingival removal of plaqueand oral hygiene instruction, has an effect onsystemic inflammation. From Figure 9 it canbe seen that those in the Community Screen-ing Group receiving prophylaxis who werenon-obese had a significant reduction inserum CRP levels (p = 0.009). It is reason-able, then, to recommend good oral hygienepractices in cardiovascular patients, includingtooth brushing using a toothpaste containingactive ingredients that have antigingivitis,as well as antiplaque effects.
Studies of Endothelial FunctionAt least three other human intervention
trials have evaluated the effects of perio -dontal disease interventions on endothelialfunction, another surrogate outcome for

CHAPTER 8 Association Between Periodontal and Atheromatous Diseases 127
atherosclerosis. Elter and colleagues treated22 periodontitis patients with “completemouth disinfection” (scaling and root plan-ing, periodontal flap surgery, and extractionof hopeless teeth within a two-week interval)and observed significant improvements inendothelial function (flow-mediated dilationof the brachial artery) and serum biomarkerssuch as interleukin-6.56 Similarly, Seinostand colleagues tested endothelial functionin 30 patients with severe periodontitis ver-sus 31 periodontally healthy control sub-jects.57 Prior to interventions, flow-mediateddilation was significantly lower in patientswith periodontitis than in control subjects.Periodontitis patients with favorable clinicalresponses to nonsurgical periodontal therapy(i.e., scaling and root planing, topical andperoral antimicrobials plus mechanical re-treatment) exhibited concomitant improve -ments in flow-mediated dilation of thebrachial artery and serum hsCRP concentra-tions. In a larger third trial, Tonetti and col-leagues documented endothelial responses
for 120 medically healthy patients with severe perio dontitis.58 Subjects in this trial were randomized to either community-based periodontal care (control) or intensive perio -dontal treatment (extraction of hopelessteeth, scaling and root planing, plus locallyadministered minocycline microspheres). At24 hours post-treatment, intensive flow- mediated dilation was significantly lower inthe intensive-treatment group than in thecontrol-treatment group (Figure 10), and levels of hsCRP, interleukin-6, E-selectinand von Willebrand factor were significantlyhigher. However by 60 and 180 days, subjects receiving the intensive treatment exhibited sig -nificantly improved flow-mediated dilationand the plasma levels of soluble E-selectincompared to control subjects.
While the effects of periodontal therapyon endstage events in patients with athero-matous diseases have yet to be determined,the available evidence suggests that perio -dontal interventions may be associated withthree- to six-month improvements in serum
Figure 9.Percent of Subjects with Elevated Serum High Sensitivity C-Reactive ProteinFigure 9. (hsCRP) > 3 mg/L at Six Months by Treatment Group and Stratified byFigure 9. Obesity for the Periodontitis and Vascular Events (PAVE) Pilot Study
*p = 0.009; †p = 0.03; ‡p = 0.04; §p = 0.006; Tx = treatment; Prophy = prophylaxis; SRP = scaling and root planing.Vertical dashed line designates that “Any Tx” is a composite of the three treatment groups. Source: J Periodontal2009;80:190–2001.55 Reproduced with permission.
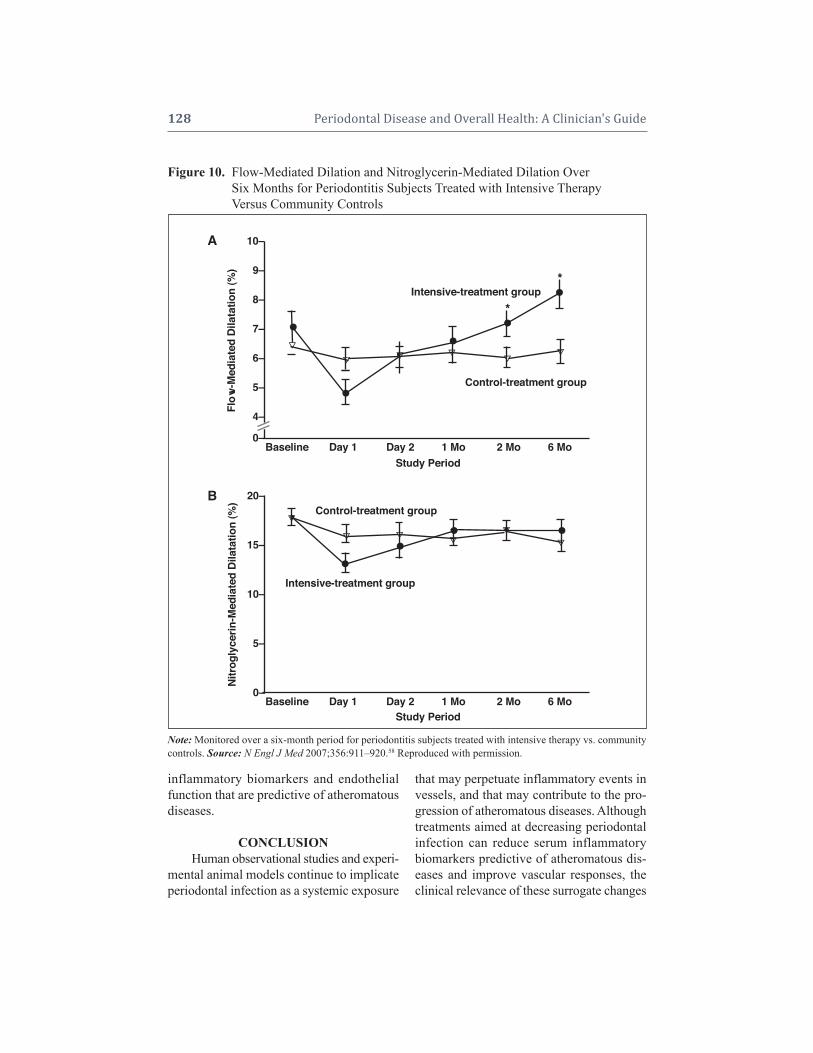
128 Periodontal Disease and Overall Health: A Clinician's Guide
inflammatory biomarkers and endothelialfunction that are predictive of atheromatousdiseases.
CONCLUSIONHuman observational studies and experi -
mental animal models continue to implicateperiodontal infection as a systemic exposure
that may perpetuate inflammatory events invessels, and that may contribute to the pro-gression of atheromatous diseases. Althoughtreatments aimed at decreasing periodontalinfection can reduce serum inflammatorybiomarkers predictive of atheromatous dis-eases and improve vascular responses, theclinical relevance of these surrogate changes
Note: Monitored over a six-month period for periodontitis subjects treated with intensive therapy vs. communitycontrols. Source: N Engl J Med 2007;356:911–920.58 Reproduced with permission.
Figure 10.Flow-Mediated Dilation and Nitroglycerin-Mediated Dilation OverFigure 10. Six Months for Periodontitis Subjects Treated with Intensive TherapyFigure 10. Versus Community Controls
Flow
-Med
iate
d D
ilata
tion
(%)
Study Period
Study Period
B
A
•
• • ••*
*
••••Intensive-treatment group
Intensive-treatment group
Control-treatment group
Control-treatment group
Baseline Day 1 Day 2 1 Mo 2 Mo 6 Mo
Baseline Day 1 Day 2 1 Mo 2 Mo 6 Mo
10–
9–
8–
7–
6–
5–
4–
0–
20–
15–
10–
5–
0–
Nitr
ogly
cerin
-Med
iate
d D
ilata
tion
(%)
• •
•

CHAPTER 8 Association Between Periodontal and Atheromatous Diseases 129
to reduced risk for MI or stroke are notknown at this time. Nevertheless, cliniciansand patients should be knowledgeable aboutthis consistent association and the potential pre-ventive benefits of periodontal interventions.
Supplemental Readings
O’Connor S, Taylor C, Campbell LA, Epstein S, LibbyP. Potential infectious etiologies of atherosclerosis: amultifactorial perspective. Emerg Infect Dis 2001; 7:780–787.
DeStefano F, Anda RF, Kahn HS, Williamson DF, Russell CM. Dental disease and risk of coronary heartdisease and mortality. Br Med J 1993; 306: 688–691.
Wu T, Trevisan M, Genco RJ, Falkner KL, Dorn JP,Sempos CT. An examination of the relation between pe-riodontal health status and cardiovascular risk factors.Serum total and HDL cholesterol, C-reactive protein,and plasma fibrinogen. Am J Epidemiol 2000; 85:180–189.
Andriankaja OM, Genco RJ, Dorn J, Dmochowski J,Hovey K, Falkner KL, Trevisan M. Periodontal diseaseand risk of myocardial infarction: the role of gender andsmoking. Eur J Epidemiol 2007;22(10):699–705. Epub2007 Sep 8.
Haraszthy VI, Zambon JJ, Trevisan M, Zeid M, GencoRJ. Identification of periodontal pathogens in athero-matous plaques. J Periodontol 2000; 71: 1554–1560.
Slade GD. Offenbacher S. Beck JD. Heiss G. PankowJS. Acute-phase inflammatory response to periodontaldisease in the US population. J Dent Res 2000; 79:49–57.
Offenbacher S, Beck JD, Moss K, Mendoza L, PaquetteDW, Barrow DA, Couper DJ, Stewart DD, Falkner KL,Graham SP, Grossi S, Gunsolley JC, Madden T,Maupome G, Trevisan M, Van Dyke TE, Genco RJ.Results from the Periodontitis and Vascular Events(PAVE) Study: a pilot multicentered, randomized, con-trolled trial to study effects of periodontal therapy in asecondary prevention model of cardiovascular disease.J Perio dontol 2009; 80: 190–201.
REFERENCES1. American Heart Association. Heart, Disease and
Stroke Statistics—2004 Update. Dallas, TX: Amer-ican Heart Association; 2003.
2. World Health Organization. The World Health Re-port 1997 Geneva: World Health Organization:1997.
3. O’Connor S, Taylor C, Campbell LA, Epstein S,
Libby P. Potential infectious etiologies of athero-sclerosis: a multifactorial perspective. Emerg InfectDis 2001;7:780–787.
4. Beck JD, Offenbacher S, Williams RC, Gibbs P,Garcia K. Periodontitis: a risk factor for coronaryheart disease? Ann Periodontol 1998;3:127–141.
5. Umino M, Nagao M. Systemic diseases in elderlydental patients. Int Dent J 1993; 43:213–218.
6. Scannapieco FA, Bush RB, Paju S. Associations between periodontal disease and risk for athero-sclerosis, cardiovascular disease, and stroke. A sys-tematic review. Ann Periodontol 2003;8:38–53.
7. Friedewald VE, Kornman KS, Beck JD, Genco R,Goldfine A, Libby P, Offenbacher S, Ridker PM,Van Dyke TE, Roberts WC. The American Journalof Cardiology and Journal of Periodontology Edi-tors’ Consensus: Periodontitis and AtheroscleroticCardiovascular Disease. J Periodontol 2009;80:1021–1032. Published simultaneously in Am J Cardiol 2009;104:59-68.
8. Meurman JH, Sanz M, Janket SJ. Oral health, ath-erosclerosis and cardiovascular disease. Crit RevOral Biol Med 2004;15:403–413.
9. Khader YS, Albashaireh ZS, Alomari MA. Perio -dontal diseases and the risk of coronary heart andcerebrovascular diseases: a meta-analysis. J Perio -dontol 2004;75:1046–1053.
10. Vettore MV. Periodontal disease and cardiovascu-lar disease. Evid Based Dent 2004;5:69.
11. Matilla K, Nieminen M, Valtonen V, Rasi V, Kesaniemi Y, Syrjala S, Jungul P, Isoluoma M, Hietaniemi K, Jokinen M, Huttunen J. Associationbetween dental health and acute myocardial in-farction. Br Med J 1989;298:779–782.
12. Matilla KJ, Valle MS, Nieminen MS, ValtonenVV,Hietaniemi KL. Dental infections and coronary ath-erosclerosis. Atherosclerosis 1993;103:205–211.
13. Arbes SJ, Slade GD, Beck JD. Association betweenextent of periodontal attachment loss and self- reported history of heart attack: An analysis ofNHANES III Data. J Dent Res 1999;78:1777–1782.
14. Beck JD, Garcia R, Heiss G, Vokonas P, Offen-bacher S. Periodontal disease and cardiovasculardisease. J Periodontol 1996;67:1123–1137.
15. DeStefano F, Anda RF, Kahn HS, Williamson DF,Russell CM. Dental disease and risk of coronaryheart disease and mortality. Br Med J 1993;306:688–691.
16. Wu T, Trevisan M, Genco RJ, Falkner KL, Dorn JP,Sempos CT. An examination of the relation be-tween periodontal health status and cardiovascularrisk factors. Serum total and HDL cholesterol, C- reactive protein, and plasma fibrinogen. Am J Epi-demiol 2000;85:180–189.

130 Periodontal Disease and Overall Health: A Clinician's Guide
17. Hujoel PP, Drangsholt M, Spiekerman C, DeRouenTA. Periodontal disease and coronary heart diseaserisk. JAMA 2000;284:1406–1410.
18. Howell TH, Ridker PM, Ajani UA, Hennekens CH,Christen WG. Periodontal disease and risk of sub-sequent cardiovascular disease in U.S. male physi-cians. J Am Coll Cardiol 2001;37:445–450.
19. Elter JR, Champagne CM, Offenbacher S, BeckJD. Relationship of periodontal disease and toothloss to prevalence of coronary heart disease. J Periodontol 2004;75:782–790.
20. Beck J, Elter J, Heiss G, Couper D, Mauriello S,Offenbacher S. Relationship of periodontal diseaseto carotid artery intima–media wall thickness: theAtherosclerosis Risk in Communities (ARIC)Study. Arterioscler Thromb Vasc Biol 2001;21:1816–1822.
21. Beck JD, Eke P, Lin D, Madianos P, Couper D,Moss K, Elter J, Heiss G, Offenbacher S. Associa-tions between IgG antibody to oral organisms andcarotid intima-medial thickness in community-dwelling adults. Atherosclerosis 2005;183:342–348.
22. Hung HC, Joshipura KJ, Colditz G, Manson JE,Rimm EB, Speizer FE, Willet WC. The associationbetween tooth loss and coronary heart disease inmen and women. J Public Health Dent 2004;64:209–215.
23. Joshipura KJ, Wand HC, Merchant AT, Rimm EB.Periodontal disease and biomarkers related to car-diovascular disease. J Dent Res 2004;83:151–155.
24. Engebretson SP, Lamster IB, Elkind MS, Rundek T,Serman NJ, Demmer RT, Sacco RL, PapapanouPN, Desvarieux M. Radiographic measures ofchronic periodontitis and carotid artery plaque.Stroke 2005;36:561–566.
25. Desvarieux M, Demmer RT, Rundek T, Boden- Albala B, Jacobs DR Jr, Sacco RL, Papapanou PN.Periodontal microbiota and carotid intima-mediathickness: the Oral Infections and Vascular Dis-ease Epidemiology Study (INVEST). Circulation2005;111:576–582.
26. Andriankaja OM, Genco RJ, Dorn J, DmochowskiJ, Hovey K, Falkner KL, Scannapieco F, TrevisanM. The use of different measurements and defini-tions of periodontal disease in the study of the association between periodontal disease and riskof myocardial infarction. J Periodontol 2006;77:1067–1073.
27. Andriankaja OM, Genco RJ, Dorn J, DmochowskiJ, Hovey K, Falkner KL, Trevisan M. Periodontaldisease and risk of myocardial infarction: the roleof gender and smoking. Eur J Epidemiol 2007;22:699–705. Epub 2007 Sep 8.
28. Söder PO, Söder B, Nowak J, Jogestrand T. Earlycarotid atherosclerosis in subjects with periodontal
diseases. Stroke 2005;36:1195–1200.29. Pussinen PJ, Alfthan G, Rissanen H, Reunanen A,
Asikainen S, Knekt P. Antibodies to periodontalpathogens and stroke risk. Stroke 2004;35:2020–2023.
30. Pussinen PJ, Nyyssonen K, Alfthan G, Salonen R,Laukkanen JA, Salonen JT. Serum antibody levelsto Actinobacillus actinomycetemcomitans predictthe risk for coronary heart disease. ArteriosclerThromb Vasc Biol 2005;25:833–838.
31. Abnet CC, Qiao YL, Dawsey SM, Dong ZW, Tay-lor PR, Mark SD. Tooth loss is associated with in-creased risk of total death and death from uppergastrointestinal cancer, heart disease, and stroke ina Chinese population-based cohort. Int J Epidemiol2005;34:467–474.
32. Lu B, Parker D, Eaton CB. Relationship of perio -dontal attachment loss to peripheral vascular dis-ease: an analysis of NHANES 1999-2002 data.Atherosclerosis 2008;200:199–205.
33. Chen YW, Umeda M, Nagasawa T, Takeuchi Y,Huang Y, Inoue Y, Iwai T, Izumi Y, Ishikawa I. Periodontitis may increase the risk of peripheralarterial disease. Eur J Vasc Endovasc Surg 2008;35:153–158.
34. Sconyers JR, Crawford JJ, Moriarty JD. Relation-ship of bacteremia to tooth brushing in patientswith periodontitis. J Am Dent Assoc 1973;87:616–622.
35. Silver JG, Martin AW, McBride BC. Experimentaltransient bacteremias in human subjects with vary-ing degrees of plaque accumulation and gingival in-flammation. J Clin Periodontol 1980;4:92–99.
36. Gibson FC 3rd, Yumoto H, Takahashi Y, Chou HH,Genco CA. Innate immune signaling and Porphy-romonas gingivalis-accelerated atherosclerosis. JDent Res 2006;85:106–121.
37. Herzberg MC, Myer MW. Effects of oral flora onplatelets: possible consequences in cardiovasculardisease. J Periodontol 1996;67:1138–1142.
38. Herzberg ME, Meyer MW. Dental plaque, plateletsand cardiovascular diseases. Ann Periodontol 1998;3:152–160.
39. Hinode D, Nakamura R, Grenier D, Mayrand D.Cross-reactivity of specific antibodies directed toheat shock proteins from periodontopathogenicbacteria and of human origin. Oral Microbiol Im-munol 1998;13:55–58.
40. Sims TJ, Lernmark A, Mancl LA, Schifferle RE,Page RC, Persson GR. Serum IgG to heat shockproteins and Porphyromonas gingivalis antigens indiabetic patients with periodontitis. J Clin Perio -dontol 2002;29:551–562.
41. Deshpande RG, Khan MB, Genco CA. Invasion ofaortic and heart endothelial cells by Porphyromonas

CHAPTER 8 Association Between Periodontal and Atheromatous Diseases 131
gingivalis. Infect Immun 1998;66:5337–5343.42. Chiu B. Multiple infections in carotid athero -
sclerotic plaques. Am Heart J 1999; 138:534–536.43. Haraszthy VI, Zambon JJ, Trevisan M, Zeid M,
Genco RJ. Identification of periodontal pathogensin atheromatous plaques. J Periodontol 2000;71:1554–1560.
44. Giacona MB, Pappanou PN, Lamster IB, Rong LL,D’Agati VD, Schmidt AM, Lalla E. Porphyro -monas gingivalis induces uptake by human macro -phages and promotes foam cell formation in vitro.FEMS Microbiol Lett 2004;241:95–101.
45. Slade GD, Offenbacher S, Beck JD, Heiss G,Pankow JS. Acute-phase inflammatory response toperiodontal disease in the US population. J DentRes 2000;79:49–57.
46. Chi H, Messas E, Levine RA, Graves DT, Amar S.Interleukin-1 receptor signaling mediates athero-sclerosis associated with bacterial exposure and/ora high-fat diet in a murine apolipoprotein E hetero -zygote model: pharmacotherapeutic implications.Circulation 2004;110:1678–1685.
47. Gibson FC 3rd, Hong C, Chou HH, Yumoto H,Chen J, Lien E, Wong J, Genco CA. Innate im-mune recognition of invasive bacteria acceleratesatherosclerosis in apolipoprotein E-deficient mice.Circulation 2004;109:2801–2806.
48. Lalla E, Lamster IB, Hofmann MA, Bucciarelli L,Jerud AP, Tucker S, Lu Y, Papapanou PN, SchmidtAM. Oral infection with a periodontal pathogenaccelerates early atherosclerosis in apolipoproteinE-null mice. Arterioscler Thromb Vasc Biol 2003;23:1405–1411.
49. Li L, Messas E, Batista EL, Jr., Levine RA, AmarS. Porphyromonas gingivalis infection acceleratesthe progression of atherosclerosis in a hetero zygousapolipoprotein E-deficient murine model. Circula-tion 2002;105:861–867.
50. Brodala N, Merricks EP, Bellinger DA, DamrongsriD, Offenbacher S, Beck J, Madianos P, Sotres D,Chang YL, Koch G, Nichols TC. Porphyromonasgingivalis bacteremia induces coronary and aortic
atherosclerosis in normocholesterolemic and hyper -cholesterolemic pigs. Arterioscler Thromb Vasc Biol2005;25:1446–1451.
51. Daly CG, Mitchell DH, Highfield JE, GrossbergDE, Stewart D. Bacteremia due to periodontal prob-ing: a clinical and microbiological investigation. JPeriodontol 2001;72:210–214.
52. Haynes WG, Stanford C. Periodontal disease andatherosclerosis: from dental to arterial plaque. Ar-terioscler Thromb Vasc Biol 2003;23:1309–1311.
53. Ide M, Jagdev D, Coward PY, Crook M, BarclayGR, Wilson RF. The short-term effects of treat-ment of chronic periodontitis on circulating levelsof endotoxin, C-reactive protein, tumor necrosisfactor-alpha, and interleukin-6. J Periodontol 2004;75:420–428.
54. D’Aiuto F, Ready D, Tonetti MS. Periodontal dis-ease and C-reactive protein-associated cardiovas-cular risk. J Periodontal Res 2004;39:236–241.
55. Offenbacher S, Beck JD, Moss K, Mendoza L, Paquette DW, Barrow DA, Couper DJ, StewartDD, Falkner KL, Graham SP, Grossi S, GunsolleyJC, Madden T, Maupome G, Trevisan M, Van DykeTE, Genco RJ. Results from the Periodontitis andVascular Events (PAVE) Study: a pilot multicen-tered, randomized, controlled trial to study effectsof periodontal therapy in a secondary preventionmodel of cardiovascular disease. J Periodontol2009;80:190–201.
56. Elter JR, Hinderliter AL, Offenbacher S, Beck JD,Caughey M, Brodala N, Madianos PN. The effectsof periodontal therapy on vascular endothelial func-tion: a pilot trial. Am Heart J 2006;151:47.
57. Seinost G, Wimmer G, Skerget M, Thaller E, Brod-mann M, Gasser R, Bratschko RO, Pilger E. Peri-o dontal treatment improves endothelial dysfunctionin patients with severe periodontitis. Am Heart J2005;149:1050–1054.
58. Tonetti MS, D’Aiuto F, Nibali L, Donald A, StorryC, Parkar M, Suvan J, Hingorani AD, Vallance P,Deanfield J. Treatment of periodontitis and endo -thelial function. N Engl J Med 2007;356:911– 920.
132 Periodontal Disease and Overall Health: A Clinician's Guide
INTRODUCTIONSince the first publication that linked perio -
dontal disease with pregnancy complicationsin 1996, there have been numerous studiesexploring the association.1 These includecase-control, longitudinal, and interventionstudies in humans, as well as models of ex-peri mental periodontal infections in pregnant rodents, rabbits, and monkeys. In the lastdecade, evidence has continued to supportthe concept that periodontal infection canserve as a distant site of infection, affectingprematurity and fetal growth. Although preg-nancy complications are clearly multifactor-ial in nature and involve a complex molecu-lar and biologic interplay of mother and fetus,many studies suggest that periodontal infec-tions may be potentially one of the causes ofadverse pregnancy outcomes.
Furthermore, in women who experiencepreterm delivery, there is direct biologicalevidence that periodontal organisms are as-sociated with amniotic fluid inflammation,intrauterine fetal exposure, and fetal inflam-mation. Despite the evidence supporting anassociation and the biological data suggestingcausality, the evidence supporting the abilityof maternal periodontal treatment to preventprematurity is still equivocal. The associa-tion remains strong between the two condi-tions, but not all treatment studies show re-duction in preterm deliveries. In other words,the findings suggest that managing perio -dontal disease in pregnancy is difficult, andthat treatment to control periodontal diseasemay not disrupt the biological basis of oral infection-mediated pregnancy complications.Some studies suggest that the treatments are
ineffective in reducing prematurity, de pend-ing on the nature and timing of the treatmentprovided. These findings suggests that if perio dontal disease is a bona fide cause ofprematurity, it may be a nonmodifiablecause of disease, or at least our treatmentprotocols are not optimized to yield potentialbenefits.
As researchers begin to better understandthe linkages between periodontal infec tionand systemic health and to examine inter -vention studies, the concept has emerged thatthe treatments used to control oral manifes-tations of periodontal disease may not besufficient to halt the systemic effects of oralinfection. In spite of the tremendous amountof association data gathered from studiesaround the world, as well as the biologicalplausibility and mechanistic incrimina-tion of causality, we have not yet identifiedhow to treat or prevent periodontal infectionfrom having deleterious effects on the fetal- placental unit.
This chapter will discuss the evidencelinking periodontal diseases to pregnancyand neonatal development abnormalities, in-cluding prematurity, fetal growth deviations,and obstetric complications. The condition ofpreeclampsia is quite different in clinicalpresentation and pathogenesis, and is dis-cussed separately. Animal model data as wellas population studies in humans will be high-lighted. The data linking periodontal diseaseto fetal demise and stillbirth are quite limitedand are included under both human and an-imal discussions. Recently published meta-analyses and reviews will be cited as back-ground information to focus on recent trials
CHAPTER 9Periodontal Disease andPregnancy Complications
Silvana P. Barros, Heather L. Jared, Steven Offenbacher

CHAPTER 9 Periodontal Disease and Pregnancy Complications 133
and the interpretation of findings that im-pact clinical practice and healthcare policy.
Key educational objectives include ac-quiring the ability to:
1. understand the types of obstetric com-plications that have been associated withperiodontal disease;
2. learn the evidence linking periodontaldisease to obstetric complications, as itrelates to other risk factors for adversepregnancy outcomes;
3. gain insight into the current models ofpathogenesis that establish biologicalplausibility and the evidence from hu-man and animal models that supportthese mechanisms; and
4. appreciate how this information impactsour thinking regarding the clinical man-agement of the pregnant mother and thepotential implications for maternal-childhealth.
ASSOCIATION OF PREGNANCYWITH PERIODONTAL DISEASE
Epidemiologic and longitudinal studieshave clearly shown that pregnancy is asso-ciated with an increase in gingival inflam-mation and a worsening of periodontal sta-tus. Periodontal diseases, including gingivitisand periodontitis, affect approximately threeout of four pregnant women.1 This increasedsusceptibility during pregnancy is thoughtto be attributable to changes in gingival tis-sue structure, the nature and quality of thehost response, and alterations in the oralbiofilm composition. Pregnancy provides aspecial opportunity for the emergence ofbiofilm pathogens. Increases in serum pro -gesterone serve to amplify gingival crevicu-lar fluid flow rate, altering conditions withinthe subgingival flora, and leading to elevatedlevels of Porphyromonas species. There isan overgrowth of the Socransky Red and Orange complexes. This contributes to anincreased prevalence of gingivitis and sever-ity of periodontal disease during pregnancy.
The gingival tissues themselves are affectedby the hormonal increases that lead to in-creased synthesis of hyaluronic acid and gly-cosaminoglycan aggregates, which osmoti-cally induce tissue edema and gingivalenlargement. These changes lead to greaterclinical inflammation.
The typical inflammatory appearancedemonstrating the changes in gingival tis-sue architecture has been well described andemphasizes that the neovascularizationwithin the gingival tissues increases duringpregnancy, as the gingival changes almostmirror that of the uterus during this hormonalbarrage. Finally, the maternal immune re-sponse changes during pregnancy and can bebest characterized as a relative state of im-munotolerance, which serves to protect thefetus from host versus graft immunorejec-tion. Thus, alteration in the maternal immuneresponse likely contributes to the increasein gingival inflammation that occurs duringpregnancy.
TYPES OF OBSTETRIC ADVERSEEVENTS ASSOCIATED WITH
PERIODONTAL DISEASEMaternal infections have long been rec-
ognized as increasing risk for pregnancycomplications, such as preterm birth, fetalgrowth restriction, preeclampsia, fetal loss(spontaneous abortions and fetal demise),and stillbirths. Although these obstetric com-plications differ in clinical presentation andoutcomes, there are similarities, in terms ofpathogenesis, reflecting common inflamma-tory effector pathways that result in disease.Oral infection in the mother appears to beone potential stimulus for this inflammatoryeffector mechanism, but it is not the onlycause. Rather, it appears that oral infection isjust one factor triggering inflammatoryevents that result in a variety of obstetriccomplications. Furthermore, there is not sufficient evidence to suggest that the ef-fects of periodontal infection are limited to

134 Periodontal Disease and Overall Health: A Clinician's Guide
one particular obstetric complication. Thus,the lack of specificity is likely attributable toa commonality of pathological signals orthe presence of an unknown underlying inflammatory trait that places the mother atrisk for both periodontal disease and obstet-ric complications. It is possible that motherswho have obstetric complications have a genetic trait that creates an abnormal hyper-inflammatory response that can result inpregnancy complications and simultaneouslybe associated with more severe periodontaldisease. Indeed, obstetric complications ex-hibit familial aggregation, suggesting a ge-netic component. However, such “hyper -inflammatory” traits may create the genomicstructure that enables infectious agents todisseminate and cause pathology of the fetal-placental unit. An underlying inflammatoryfactor that places a mother at risk for bothconditions would create the possibility fororal infections, or any infection, to increasethe risk for obstetric complications. Thus,the importance of oral infection is even morerelevant to obstetric risk in the presence of ahyperinflammatory trait.
One might consider that the presence ofa genetic predisposition might diminish theimportance of oral infection as a mitigatingfactor in abnormal pregnancy outcomes, butin fact it increases oral infection’s relevanceto managing maternal-child health outcomes,since the effects of oral infection would beexaggerated in an individual with this trait.More specifically, preeclampsia has beenconceptually characterized as a hyperin-flammatory state, which is linked to the factthat more than 30% of the leukocytic cells inthe placental decidual layer in normal preg-nancy are macrophages. Macrophages at theplacental tissue are important cytokine pro-ducers and may be critical regulatory cellsfor controlling trophoblast cell invasion inthe maternal vascular system. Macrophagesmay have cytolytic effects, presumably bythe production of cytotoxic cytokines, and
the overactivation may be linked to placen-tation defects and pregnancy complications.
PRETERM BIRTH AND FETALGROWTH RESTRICTION
In the United States, preterm birth(PTB), defined as birth of an infant born be-fore 37 weeks completed gestation or before259 days of gestational age,2 is occurring atan increasing rate in the population, with arise of 13% for the period of 1981–1989,and 16% for 1990–2002.3,4 Furthermore, in2004, low birth weight (LBW; < 2,500 gm)affected 8.1% of live births, an increase from7.6% in 1998. Although weight at birth andgestational age are highly correlated, inmany countries the determination of gesta-tional age by date of last menstrual periodand ultrasound are not routinely performed,so LBW becomes a worldwide reportingstandard. The increased rate of prematurity isdue to three factors: an inability to identifyall causal risk factors; the inability to ade-quately control known risk factors; and animproved ability to support survival of thesmallest and most premature babies. As aresult, the incidence of PTB and LBW deliveries has actually increased in most industrialized nations.5-7 With prematurityremaining the leading cause of perinatal mor-bidity and mortality worldwide, and withwidespread recognition that inflammation isresponsible for a substantial fraction ofPTBs,8-10 maternal periodontal disease hasgained prominence as a potentially modifi-able risk factor for adverse pregnancy out-comes. Systemic dissemination of oralpathogens with subsequent maternal, fetal,and/or placental inflammatory responses hasbeen associated with pregnancy complica-tions.11,12 Furthermore, periodontal diseaseand the systemic bacteremias caused by periodontal pathogens are significant con-tributors to a systemic maternal inflamma-tory response during pregnancy, involvingcytokinemia and the release of acute-phase
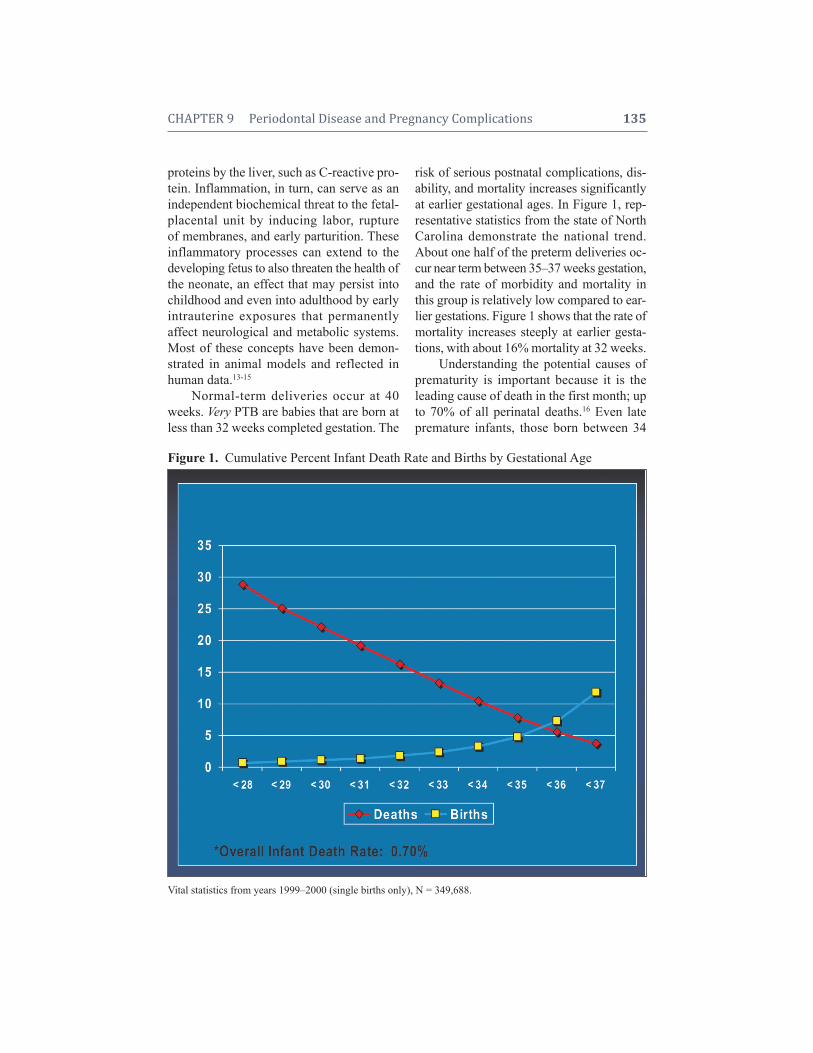
CHAPTER 9 Periodontal Disease and Pregnancy Complications 135
proteins by the liver, such as C-reactive pro-tein. Inflammation, in turn, can serve as anindependent biochemical threat to the fetal-placental unit by inducing labor, ruptureof membranes, and early parturition. These inflammatory processes can extend to the developing fetus to also threaten the health ofthe neonate, an effect that may persist intochildhood and even into adulthood by earlyintrauterine exposures that permanently affect neurological and metabolic systems.Most of these concepts have been demon-strated in animal models and reflected in human data.13-15
Normal-term deliveries occur at 40weeks. Very PTB are babies that are born atless than 32 weeks completed gestation. The
risk of serious postnatal complications, dis-ability, and mortality increases significantlyat earlier gestational ages. In Figure 1, rep-resentative statistics from the state of NorthCarolina demonstrate the national trend.About one half of the preterm deliveries oc-cur near term between 35–37 weeks gestation,and the rate of morbidity and mortality inthis group is relatively low compared to ear-lier gestations. Figure 1 shows that the rate ofmortality increases steeply at earlier gesta-tions, with about 16% mortality at 32 weeks.
Understanding the potential causes ofprematurity is important because it is theleading cause of death in the first month; upto 70% of all perinatal deaths.16 Even latepremature infants, those born between 34
Figure 1. Cumulative Percent Infant Death Rate and Births by Gestational Age
Vital statistics from years 1999–2000 (single births only), N = 349,688.

136 Periodontal Disease and Overall Health: A Clinician's Guide
and 36 weeks,17 have a greater risk of feed-ing difficulties, thermal instability, respira-tory distress syndrome, jaundice, and de-layed brain development.15 Prematurity isresponsible for almost 50% of all neurolog-ical complications in newborns, leading tolifelong complications in health that include,but are not limited to visual problems, devel -opmental delays, gross and fine motor delays,deafness, and poor coping skills. The increasein morbidity among survivors also increasesmarkedly at earlier gestational age.
In many ways, the fetus physiologicallyfunctions as a foreign body with parasiticproperties. The placenta is an invasive fetal-derived tissue and is efficient in its ability totake nutrients from the mother. If the motheris nutritionally deprived, the mother’s reser-voirs are depleted first. All the placental nu-trient exchange molecules have higher bind-ing affinities than those of the mother tofavor a uni-directional nutrient and vitaminexchange from the mother to the fetus. Forexample, if the mother is starving, the ma-ternal liver will shrink to one-third its normalsize during pregnancy and the fetus will con-tinue to grow. Thus, any impairment in fetalgrowth is believed to be attributable to im-pairments in nutrient exchange or impairedgrowth factor secretion via placental damagerather than maternal-based nutrient impair-ments. Prematurity, on the other hand, is dueto maternal responses that involve uterinesmooth muscle contraction and rupture ofthe membranes. This is a maternal tissue response triggered by an inflammatory bio-chemical cascade. Infection can be one important source of inflammation, but fetalstress can be another source of inflam ma -tion that targets the maternal uterine smoothmuscle and/or the membrane integrity.Either or both can be involved in pregnancy complications.
About one-third of preterm delivery occurs as a consequence of preterm pre -mature rupture of membranes, one-third due
to preterm labor, and one third from every-thing else, including preeclampsia, as well asmedical and fetal indications for delivery.Inflammation can extend beyond the mater-nal membranes and uterus to promote pre-maturity, but can also reach the placenta andfetus to impair growth and damage fetal tis-sues. Impaired growth or growth restrictioncan occur at any gestational age, even full-term babies can be small for gestational age(SGA), typically defined as birth weightlower than the 10th percentile of weight forgestational age. Many of the molecular andcellular inflammatory effector pathways thatunderlie the pathogenesis of PTB are also in-volved in growth restriction and develop-mental problems, ranging from respiratorydistress to cognitive and learning disabilities.For example, fetal neurologic tissues are es-pecially susceptible to damage via cyto kines,such as interferon gamma (IFN-), which induce apoptosis and impair development ofsynapse connections among embryologicneurons.18
Although there have been advances intechnology to help save those infants whoare born premature or LBW, the lifelongproblems associated with these conditionshave not declined.
Potential risks to a baby born with fetalgrowth restriction include:
• Increased risk for motor and neuro-logical disabilities
• Chromosomal abnormalities• Hypoglycemia• Increased risk for hypoxia• Decreased oxygen levelsSelected neonatal complications follow -
ing PTB include:• Chronic lung disease• Developmental delay• Growth impairment• Periventricular leukomalacia• Respiratory distress syndrome• Hearing impairment• Intraventricular hemorrhage
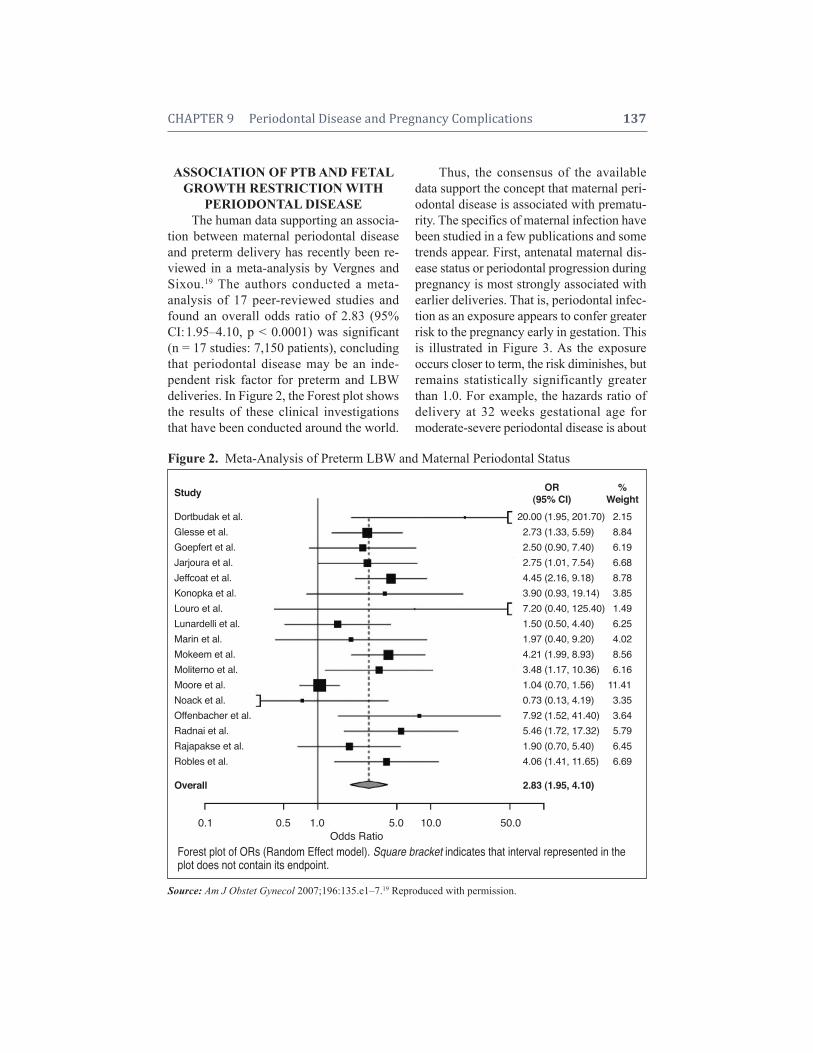
CHAPTER 9 Periodontal Disease and Pregnancy Complications 137
ASSOCIATION OF PTB AND FETALGROWTH RESTRICTION WITH
PERIODONTAL DISEASEThe human data supporting an associa-
tion between maternal periodontal diseaseand preterm delivery has recently been re-viewed in a meta-analysis by Vergnes andSixou.19 The authors conducted a meta-analysis of 17 peer-reviewed studies andfound an overall odds ratio of 2.83 (95%CI:1.95–4.10, p < 0.0001) was significant(n = 17 studies: 7,150 patients), concludingthat periodontal disease may be an inde-pendent risk factor for preterm and LBWdeliveries. In Figure 2, the Forest plot showsthe results of these clinical investigationsthat have been conducted around the world.
Thus, the consensus of the availabledata support the concept that maternal peri-odontal disease is associated with prematu-rity. The specifics of maternal infection havebeen studied in a few publications and sometrends appear. First, antenatal maternal dis-ease status or periodontal progression duringpregnancy is most strongly associated withearlier deliveries. That is, periodontal infec-tion as an exposure appears to confer greaterrisk to the pregnancy early in gestation. Thisis illustrated in Figure 3. As the exposureoccurs closer to term, the risk diminishes, butremains statistically significantly greaterthan 1.0. For example, the hazards ratio ofdelivery at 32 weeks gestational age formoderate-severe periodontal disease is about
Figure 2.Meta-Analysis of Preterm LBW and Maternal Periodontal Status
Source: Am J Obstet Gynecol 2007;196:135.e1–7.19 Reproduced with permission.
Study
Dortbudak et al.Glesse et al.Goepfert et al.Jarjoura et al.Jeffcoat et al.Konopka et al.Louro et al.Lunardelli et al.Marin et al.Mokeem et al.Moliterno et al.Moore et al.Noack et al.Offenbacher et al.Radnai et al.Rajapakse et al.Robles et al.
Overall
OR %(95% CI) Weight
20.00 (1.95, 201.70) 2.152.73 (1.33, 5.59) 8.842.50 (0.90, 7.40) 6.192.75 (1.01, 7.54) 6.684.45 (2.16, 9.18) 8.783.90 (0.93, 19.14) 3.857.20 (0.40, 125.40) 1.491.50 (0.50, 4.40) 6.251.97 (0.40, 9.20) 4.024.21 (1.99, 8.93) 8.563.48 (1.17, 10.36) 6.161.04 (0.70, 1.56) 11.4100.73 (0.13, 4.19) 3.357.92 (1.52, 41.40) 3.645.46 (1.72, 17.32) 5.791.90 (0.70, 5.40) 6.454.06 (1.41, 11.65) 6.69
2.83 (1.95, 4.10)
0.1 0.5 1.0 5.0 10.0 50.0Odds Ratioooooooooooooooooo
Forest plot of ORs (Random Effect model). Square bracket indicates that interval represented in theplot does not contain its endpoint.
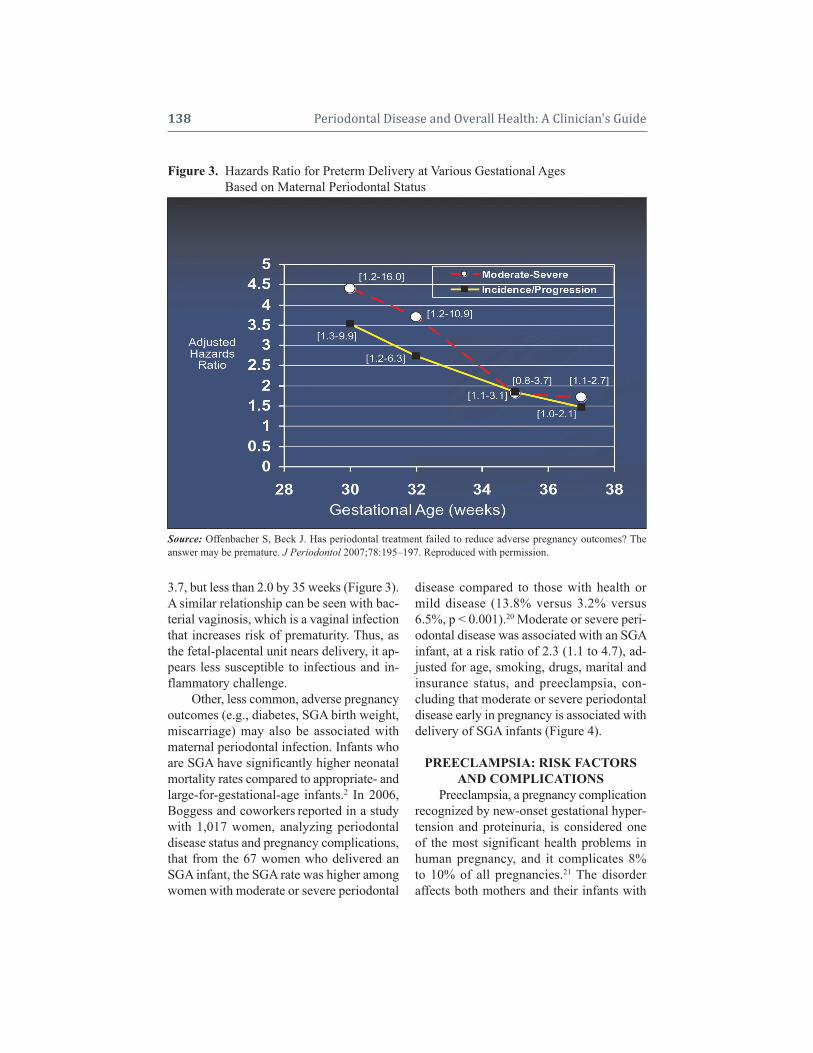
138 Periodontal Disease and Overall Health: A Clinician's Guide
3.7, but less than 2.0 by 35 weeks (Figure 3).A similar relationship can be seen with bac-terial vaginosis, which is a vaginal infectionthat increases risk of prematurity. Thus, asthe fetal-placental unit nears delivery, it ap-pears less susceptible to infectious and in-flammatory challenge.
Other, less common, adverse pregnancyoutcomes (e.g., diabetes, SGA birth weight,miscarriage) may also be associated withmaternal periodontal infection. Infants whoare SGA have significantly higher neonatalmortality rates compared to appropriate- andlarge-for-gestational-age infants.2 In 2006,Boggess and coworkers reported in a studywith 1,017 women, analyzing periodontaldisease status and pregnancy complications,that from the 67 women who delivered anSGA infant, the SGA rate was higher amongwomen with moderate or severe periodontal
disease compared to those with health ormild disease (13.8% versus 3.2% versus6.5%, p < 0.001).20 Moderate or severe peri-odontal disease was associated with an SGAinfant, at a risk ratio of 2.3 (1.1 to 4.7), ad-justed for age, smoking, drugs, marital andinsurance status, and preeclampsia, con-cluding that moderate or severe periodontaldisease early in pregnancy is associated withdelivery of SGA infants (Figure 4).
PREECLAMPSIA: RISK FACTORSAND COMPLICATIONS
Preeclampsia, a pregnancy complicationrecognized by new-onset gestational hyper-tension and proteinuria, is considered oneof the most significant health problems inhuman pregnancy, and it complicates 8%to 10% of all pregnancies.21 The disorder affects both mothers and their infants with
Figure 3. Hazards Ratio for Preterm Delivery at Various Gestational AgesFigure 3. Based on Maternal Periodontal Status
Source: Offenbacher S, Beck J. Has periodontal treatment failed to reduce adverse pregnancy outcomes? The answer may be premature. J Periodontol 2007;78:195–197. Reproduced with permission.
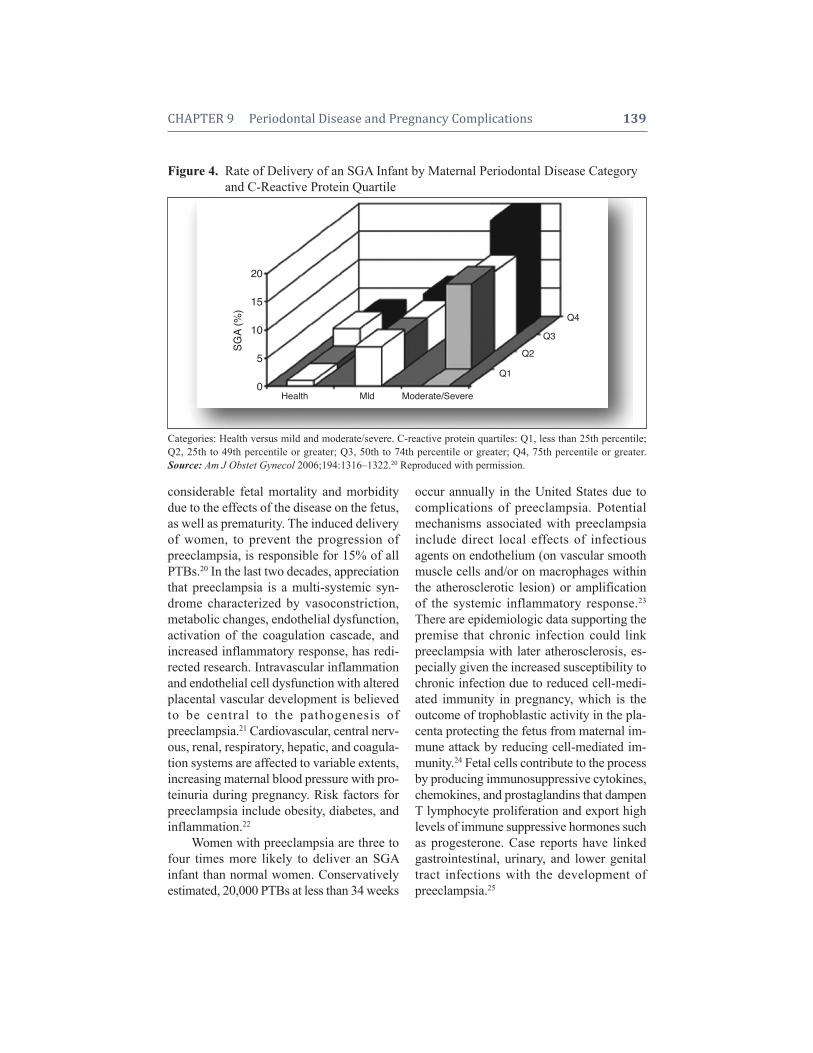
CHAPTER 9 Periodontal Disease and Pregnancy Complications 139
considerable fetal mortality and morbiditydue to the effects of the disease on the fetus,as well as prematurity. The induced deliveryof women, to prevent the progression ofpreeclampsia, is responsible for 15% of allPTBs.20 In the last two decades, appreciationthat preeclampsia is a multi-systemic syn-drome characterized by vasoconstriction,metabolic changes, endothelial dysfunction,activation of the coagulation cascade, andincreased inflammatory response, has redi-rected research. Intravascular inflammationand endothelial cell dysfunction with alteredplacental vascular development is believedto be central to the pathogenesis ofpreeclampsia.21 Cardiovascular, central nerv-ous, renal, respiratory, hepatic, and coagula-tion systems are affected to variable extents,increasing maternal blood pressure with pro-teinuria during pregnancy. Risk factors forpreeclampsia include obesity, diabetes, andinflammation.22
Women with preeclampsia are three tofour times more likely to deliver an SGA infant than normal women. Conservativelyestimated, 20,000 PTBs at less than 34 weeks
occur annually in the United States due tocomplications of preeclampsia. Potentialmechanisms associated with preeclampsiainclude direct local effects of infectiousagents on endothelium (on vascular smoothmuscle cells and/or on macrophages withinthe atherosclerotic lesion) or amplificationof the systemic inflammatory response.23
There are epidemiologic data supporting thepremise that chronic infection could linkpreeclampsia with later atherosclerosis, es-pecially given the increased susceptibility tochronic infection due to reduced cell-medi-ated immunity in pregnancy, which is theoutcome of trophoblastic activity in the pla-centa protecting the fetus from maternal im-mune attack by reducing cell- mediated im-munity.24 Fetal cells contribute to the processby producing immunosuppressive cytokines,chemokines, and prostaglan dins that dampenT lymphocyte proliferation and export highlevels of immune suppressive hormones suchas progesterone. Case reports have linkedgastrointestinal, urinary, and lower genitaltract infections with the development ofpreeclampsia.25
Figure 4. Rate of Delivery of an SGA Infant by Maternal Periodontal Disease CategoryFigure 4. and C-Reactive Protein Quartile
Categories: Health versus mild and moderate/severe. C-reactive protein quartiles: Q1, less than 25th percentile;Q2, 25th to 49th percentile or greater; Q3, 50th to 74th percentile or greater; Q4, 75th percentile or greater.Source: Am J Obstet Gynecol 2006;194:1316–1322.20 Reproduced with permission.
SGA
(%)
20
15
10
5
0Health Mld Moderate/Severe
Q1
Q2
Q3
Q4

140 Periodontal Disease and Overall Health: A Clinician's Guide
Maternal clinical periodontal disease atdelivery has been associated with an in-creased risk for the development ofpreeclampsia, independent of the effects ofmaternal age, race, smoking, gestational ageat delivery, and insurance status. In addition,clinically active disease, as measured by thepresence of periodontal disease progression,was also associated with an increased risk forpreeclampsia.26
ASSOCIATION OF PREECLAMPSIAWITH PERIODONTAL DISEASE
Boggess and colleagues were the firstinvestigators to report an association be-tween maternal clinical periodontal infec-tion and the development of preeclampsia.27
In a longitudinal study of more than 1,000women, the presence of periodontal infectionat delivery, or disease worsening during thecourse of pregnancy, was associated with atwo-fold increased risk for preeclampsiacompared to women without periodontal in-fection or progression. Since that report, sev-eral other investigators have demonstrated anassociation between maternal periodontal in-fection and preeclampsia. Canakci and col-leagues reported that women with preeclamp-sia were three times more likely to haveperiodontal infection than healthy normoten-sive women and that periodontal disease alsoaffects the severity of preeclampsia.26 In an-other case-control study, Barak and cowork-ers also found that women with preeclampsiahad more severe periodontal disease in com-parison to healthy controls, with significantelevation in gingival crevicular fluid levels ofPGE-2, interleukin (IL)-1, and tumor necro-sis factor alpha (TNF-).28 In another study,women with preeclampsia were also found tohave worse periodontal infection than normalhealthy women. In addition, two “red com-plex” micro-organisms, Porphyromonas gin-givalis and Tannerella forsythensis, weremore prevalent in the oral plaque amongpreeclamptic women than among controls.29
All of these studies raise the question as towhether periodontal treatment may be a po-tential preventive intervention therapy forpreeclampsia through periodontal infectioncontrol.
HUMAN STUDIES ON THEASSOCIATIONOF PERIODONTAL DISEASE ANDADVERSE PREGNANCY EVENTS
Several studies suggest a significant as-sociation between maternal periodontal dis-ease and pregnancy complications, includingpremature delivery and preeclampsia.27,28,30
Since the first reported case-control studyin humans published in 1996,1 showing thatmothers with premature LBW babies hadmore severe periodontal disease independentof other traditional obstetric risk factors, manyother studies have explored the potential asso -ciation between maternal periodontal diseaseand prematurity and LBW. These studieshave been generally, but not universally, sup-portive of an association.
Moderate-to-severe periodontal disease(defined as 15 or more sites with five ormore mm of probing depth) is highly preva-lent among pregnant women, with about 15%affected during the first trimester and over-all about 25% showing worsening perio -dontal progression during pregnancy.11,31,32
Both antenatal periodontal disease and pro-gression during pregnancy appear to conferrisk for preterm delivery, and the strength ofthe association increases at earlier gestationaldeliveries. Periodontal disease is twice asprevalent among African-Americans, and ithas been suggested that the difference in perio dontal disease prevalence may, inpart, explain the observed increased risk inpreterm delivery and fetal growth restrictionamong African-Americans.33 Studies explor -ing the connection between maternal in -fection with specific periodontopathogenic organisms and periodontal disease progres-sion in relation to fetal immune responseto oral pathogens have, in general, supported

CHAPTER 9 Periodontal Disease and Pregnancy Complications 141
the notion that periodontitis is independentlyassociated with PTB and LBW.
In 2001, Madianos33 and colleagues an-alyzed clinical data from the first 812 deliv-eries from a cohort study of pregnant moth-ers titled Oral Conditions and Pregnancy.This study demonstrated that both antepar-tum maternal periodontal disease and inci-dence/progression of periodontal disease areassociated with PTB and growth restrictionafter adjusting for traditional obstetric riskfactors. The high prevalence of elevated fe-tal immunoglobulin (Ig)M to Campylobacterrectus among premature infants raised thepossibility that this specific maternal oralpathogen contributed as a primary fetal in-fectious agent eliciting prematurity.
With the objective to determine whetheroral bacteria can be found in the amnioticcavity, Bearfield and colleagues collectedsamples, including dental plaque and am nioticfluid, from 48 women attending for electivecaesarean section.12 Data analysis indicatedthat Streptococcus species and Fuso bacteriumnucleatum in the amniotic fluid may have anoral origin. Han and colleagues also demon-strated that in certain cases of chorioam-nionitis-associated preterm birth, the sameclonal type of organism was found in boththe maternal plaque and the amniotic fluid.34
Later, this same group reported a term still-birth caused by oral Fusobacterium nuclea-tum in a woman with pregnancy-associatedgingivitis and an upper respiratory tract in-fection at term. The linkage was confirmedby examination of different microbial florasfrom the mother identifying the same clonein the placenta, fetus, and subgingival plaque;but not in supragingival plaque, vagina, orrectum. The authors also suggested that thetranslocation of the oral bacteria to placentawas facilitated by the weakened maternalimmune system.35
In 2007, Lin and coworkers explored theunderlying microbial and antibody responsesassociated with oral infection with complexes
most often linked with periodontitis, SocranskyOrange and Red.36 They found that high levelsof periodontal pathogens and low maternal IgGantibody response to periodontal bacteria dur-ing pregnancy are associated with an increasedrisk for preterm delivery, with higher levels ofperiodontal pathogens, measured antepartum,in the preterm compared to the full-term deliv-eries. Overall, the data from meta-analyses thatcombine information from several studies con-tinue to demonstrate a significant associationbetween periodontal disease severity and ab-normal pregnancy outcomes.
ANIMAL STUDIESEarly studies in animal models using
oral organisms as a challenge in the 1980sdemonstrated there is a dose-response re-lated to obstetric outcomes. At low microbialchallenges, there is a mild systemic inflam-matory response which is associated withtransient increases in circulating cytokines,such as TNF-, and increases in the activa-tion of the hepatic acute phase response asevidenced, for example, in mice by increasesin serum amyloid A (SAA). In rodents, themajor acute-phase reactant is SAA, as com-pared to C-reactive protein in humans. Notonly is there a mild systemic inflammatoryresponse at low levels of challenge, there isalso mild inflammation of maternal amni-otic membranes, increase of inflammatorymediators within the amniotic fluid, and uter-ine smooth-muscle irritability. The mem-branes and the uterus are maternal tissuesthat become inflamed at low levels of mi-crobial challenge. In humans, this inflam-mation would be associated with earlier rup-ture of membranes and uterine contraction,leading to preterm delivery. However, thereare no animal models of preterm delivery.For example, in rodents there are changes ininflammatory mediators and histologic evi-dence of inflammation, but only primatesand humans have preterm deliveries. Atmoderate dosages of bacterial challenge

142 Periodontal Disease and Overall Health: A Clinician's Guide
there are enhanced maternal membrane anduterine inflammatory changes compared tothose seen at lower dosages, but now thereare also exposures that reach the fetal tis-sues, beginning with the placenta.
Placental inflammation is associatedwith alterations in placental architecture thatcause the incomplete development of thelabyrinth zone. This is the portion of the pla-centa that exchanges nutrients from the ma-ternal side to the fetal side, and its incompletedevelopment is associated with impaired fetalgrowth. In rodents, one can see there is clearlinkage between placental exposure of theorganisms and fetal outcomes. For exam ple,a pregnant mouse would typically have sevenor eight fetal pups, each with their own pla-centa and membranes. A maternal challengeof 107 colony forming units/mL of P. gingivalisduring pregnancy, as an example, would causethree of the eight fetuses to have impairedgrowth, and these would be runted. Analysisof placentas from all eight fetuses shows thatwhen P. gingivalis is found within the pla-centa the fetus is runted, whereas P. gingi-valis-negative placentas would have normal-sized fetuses. Increasing the concentration to3 ! 10,7 one sees three normal fetuses, fourrunts, and two that have been resorbed. Thatmeans that the fetus is nonviable and is anal-ogous to fetal demise in humans or fetal loss.At even higher bacterial concentrations thereare more resorptions and more runts, withsome runts having congenital anomalies.Thus, the higher the dose of microbial chal-lenge, the more severe the effect on fetal development and the possibility of birth defects among survivors. This suggests thatmany of these infection-mediated complica-tions appear as part of a continuum, begin-ning with prematurity to very preterm togrowth restriction to fetal loss and anom-alies. Thus, when considering the humancondition, the level and the timing of the ex-posure likely have a major influence on thetype of obstetric complication observed.
Early work with pregnant rodent mod-els exploring the role of maternal periodon-titis as a potential maternal-fetal stressordemonstrated that low-grade challenges withoral organisms during pregnancy resulted inimpaired fetal growth that was demonstratedusing a chronic subcutaneous infectionmodel and challenge with P. gingivalis.37
Later, using the same distant chronic infec-tion model in mice and challenging with P.gingivalis and C. rectus, it was also demon-strated that low-grade infections with oralorganisms were associated with disseminationto the fetal unit. These studies have shownthe ability of the oral organisms to translo-cate hematogenously to the placental tissuesto cause growth restriction.37-39 The impor-tance of placental dissemination was con-vincingly demonstrated when it was shownthat placentas that harbored oral organismshad growth-restricted fetuses, whereas pla-centas from normal-sized littermates fromthe same mother had noninfected placentas.Thus, once at the site of the placenta, P. gin-givalis has been shown to modulate both fe-tal growth and the local T helper (TH)-1 andTH-2 immune response.39 Evidence frompregnant murine infection models indicatesthat maternal challenges with P. gingivalisthat resulted in growth restriction were alsoassociated with increases in maternal TNF-and a suppression of IL-10 within the serum.38
This was accompanied by an increase in pla-cental mRNA expression of IFN- and IL-2,as well as a decrease in IL-10, IL-4, and tumor growth factor-. Thus, P. gingivalischallenge was associated with an overall in-crease in the placental TH-1/TH-2 ratio, con-sistent with the observed shifts seen in hu-man growth restriction.
In rodents and humans, there is noblood-brain barrier early in gestation and or-ganisms that cross the placenta can alsoreach the brain. In rodent models, a distantmaternal challenge with C. rectus resulted inC. rectus infecting the fetal brain. This brain

CHAPTER 9 Periodontal Disease and Pregnancy Complications 143
tropism is analogous to that seen during amaternal syphilis infection in humans. In therodent, this challenge was associated withincreasing fetal brain levels of TNF-,mRNA, and attendant growth restriction.This was accompanied by deviations in neuro -development, with altered myelination andwhite matter damage in the hippocampus.38
In 2007, Bobetsis and colleagues re-ported that in addition to the inflammatoryplacental response triggered by maternal in-fections, there were also structural ab -normalities in placental development withimpaired formation of the placental labyrinthzone.40 This zone is the point of maternal- fetal vascular anastomoses that regulate nu-trient and oxygen exchange, and is rich inspongiotrophoblasts which secrete growthfactors such as insulin-like growth factor(IGF) that stimulate fetal growth and devel-opment. In humans, impairment of placentalIGF-2 expression is associated with intra -uterine growth restriction (IUGR). Bobetsiset al. examined whether the alterations inplacental structure seen in the pregnantmouse infection model were related to IGF-2 suppression in murine IUGR.40 Not onlydid the investigators demonstrate that IUGRwas associated with low IGF-2 placental ex-pression, but that this suppression was due toalterations in the placental chromatin struc-ture. This alteration in chromatin structurespecifically involved altered DNA methyla-tion of the IGF-2 promoter, which is termedan “epigenetic modification,” because it doesnot involve a sequence change, but does re-sult in a change in gene expression that canpersist even following gene replication.These investigators reported that the bacterialinfection induced epigenetic modification ofplacental tissues represented by hypermethy-l ation of the IGF-2 gene, with consequentdown-regulation of this gene that plays acritical role in fetal growth and developmentprogramming.41 With these findings, the investigators proposed a new mechanism
linking an environmental infectious and in-flammatory insult to now include epigeneticmodifications.
Epigenetic modifications carry impor-tant consequences for development as theycan be permanently retained in the genome.These potentially permanent alterations mayin part explain the poor prognosis of the in-fant born SGA, since the modifications thatoccur in utero due to alterations in methyla-tion patterns may persist for the entire life ofthe offspring. This was proposed as a new hy-pothesis underlying the linkages found be-tween preterm delivery and diseases of theoffspring that account for a wide spectrum ofadult-onset diseases that include neurologicalimpairments and adult-onset conditions, suchas diabetes and cardiovascular disease.42,43
This concept raises the possibility that in-trauterine exposure to oral organisms of ma-ternal origin may have more permanent ef-fects that extend beyond the perinatal period.
INTERVENTION TRIALSEarly clinical trials that have provided
periodontal treatments with scaling and rootplaning have shown promise for preventingPTB. A landmark study by López et al. sug-gested that periodontal treatment may re-duce the rate of preterm deliveries five-fold.44 However, many additional clinicaltrials are still in progress. The data are encouraging, but not conclusive. A recentmeta-analysis conducted by Polyzos and colleagues summarized the available datafrom seven randomized trials and reportedthat overall treatment reduced prematurity.45
The overall reported odds ratio was 0.48(0.23 – < 1.0, p = 0.049).45 Thus, there ismarked consistency between the two meta-analyses in that periodontal disease increasesthe risk 2.8-fold and treatment potentiallydecreases the risk two-fold. Furthermore, thetreatment provided does not appear to in-crease the rate of adverse events, suggestingthat periodontal treatment during pregnancy

144 Periodontal Disease and Overall Health: A Clinician's Guide
may be safe. Nonetheless, one large, multi-centered study conducted by Michalowiczand colleagues that was included in this treat-ment meta-analysis failed to show any ob-stetric benefits,46 suggesting that additionaltreatment studies need to be conducted tobetter under stand the potential risks and ben-efits of periodontal care. Thus, it remains tobe proven whether periodontal disease is areversible cause of PTB or pregnancy com-plications. Furthermore, the linkage withneonatal health and the recent discovery ofintrauterine epigenetic influences raise im-portant questions for future studies to deter-mine the impact of maternal infection on thehealth of the baby from birth through adulthood.
FUTURE STUDIESClearly, additional research is needed
to understand the effects of periodontal treat-ment on pregnancy outcomes. Many clini-cians and scientists continue to debate whenthe findings from association studies andtreatment studies enable us to infer causality.Some suggest that the Bradford Hill criteriaof causality (strength, consistency, speci-ficity, temporality, biological gradient, bio-logical plausibility) need to be applied beforewe consider public health consequences.However, not all causes of disease are mod-ifiable. For example, bacterial vaginosis isgenerally believed to be a cause of prematu-rity, and yet most intervention trial studiesfail to show any benefits of treatment. Thissuggests that the treatments either confer ad-ditional risk or they fail to modify the com-ponents of the vaginal infection. Importantly,maternal periodontal health is in itself an ex-tremely important outcome irrespective ofthe potential influence on pregnancy. Thus,as long as periodontal care can be providedsafely, it is difficult to imagine a downside toimproving maternal oral health. Ideally, pre-vention would be the public health measureof choice.
Additional studies to understand the bi-ological processes that underlie the associa-tion between maternal periodontal diseaseand pregnancy complications, as well as theeffects of treatments, will provide greaterinsight into pathogenesis. In other words,there needs to be a better understanding ofthe cellular and molecular events that un-derlie the association between periodontalprogression and fetal exposure, and howtreatments, whether successful or not, mod-ify these biological components. For exam-ple, Lin and coworkers reported that al-though periodontal treatments reduced therisk of PTB among treated mothers, therewas a significant persistence of high levels oforal P. gingivalis infection.36 This suggestedthat the treatment provided did not ade-quately control infection in all mothers, andwas therefore insufficient to improve ob-stetric outcomes.
Understanding the mechanism of patho-genesis is the cornerstone of knowledge thatenables us to identify who is at risk, so weunder stand who needs to be treated, and howwe should treat to show maximum benefitand minimized risks. These are critical ques-tions that await further study.
Supplemental Readings
Han YW, Fardini Y, Chen C, Iacampo KG, Peraino VA,Shamonki JM, Redline RW. Term stillbirth caused byoral fusobacterium nucleatum. Obstet Gynecol 2010;115(2, Part 2):442–445.
Hollenbeck AR, Smith RF, Edens ES, Scanlon JW.Early trimester anesthetic exposure: incidence rates inan urban hospital population. Child Psychiatry HumDev 1985;16(2):126–134.
Armitage GC. Periodontal disease and pregnancy: dis-cussion, conclusions, and recommendations. Ann Perio -dontol 2001;6(1):189–192.
Radnai M, Pal A, Novak T, Urban E, Eller J, Gorzo I.Benefits of periodontal therapy when preterm birththreatens. J Dent Res 2009;88:280–284.

CHAPTER 9 Periodontal Disease and Pregnancy Complications 145
REFERENCES1. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D,
Maynor G, McKaig R, Beck J. Periodontal infec-tion as a possible risk factor for preterm low birthweight. J Periodontol 1996;67(10 Suppl):1103–1113.
2. World Health Organization. The prevention of peri-natal mortality and morbidity. WHO technical re-port series (Report 457), 1970. WHO, Geneva.
3. Martin JA. United States vital statistics and themeasurement of gestational age. Paediatr PerinatEpidemiol 2007;21(Suppl 2):13–21.
4. Martin JA, Hamilton BE, Sutton PD, Ventura SJ,Menacker F, Munson ML. 2003 Births: final datafor 2002. National Vital Statistics Reports; 52:1–113. Hyattsville, MD: National Center for HealthStatistics. http://www.cdc.gov/nchs/data/nvsr/nvsr52/nvsr52_10.pdf.
5. US Department of Health and Human Services.Healthy People 2010, 2nd ed. With Understandingand Improving Health and Objectives for Improv-ing Health, 2 Volumes. Washington, DC: US Gov-ernment Printing Office, 2000.
6. Wyatt JS. Mechanisms of brain injury in the new-born. Eye 2007;21:1261–1263.
7. Hack M, Fanaroff AA. Outcomes of extremely im-mature children—a perinatal dilemma. N Engl JMed 1993;329:1649–1650.
8. Goldenberg RL, Hauth JC, Andrews WW. In-trauterine infection and preterm delivery. N Engl JMed 2000;342:1500–1507.
9. Steinborn A, Kühnert M, Halberstadt E. Immun-modulating cytokines induce term and preterm par-turition. J Perinat Med 1996;24:381–390.
10. Romero R, Espinoza J, Goncalves LF, KusanovicJP, Friel LA, Nien JK. Inflammation in pretermand term labour and delivery. Semin Fetal Neona-tal Med 2006;11:317–326.
11. Offenbacher S, Jared HL, O’Reilly PG, Wells SR,Salvi GE, Lawrence HP, Socransky SS, Beck JD.Potential pathogenic mechanisms of periodontitisassociated pregnancy complications. Ann Perio -dontol 1998;3:233–250.
12. Bearfield C, Davenport ES, Sivapathasundaram V,Allaker RP. Possible association between amnioticfluid micro-organism infection and microflora inthe mouth. BJOG 2002;109:527–533.
13. Goncalves LF, Chaiworapongsa T, Romeo R. Intra -uterine infection and prematurity. Ment Retard DevDisabil Res Rev 2002;8:3–13.
14. Adams-Chapman I. Neurodevelopmental outcomeof the late preterm infant. Clin Perinatol 2006;33:947–964.
15. Hagberg H, Mallard C, Jacobsson B. Role of cyto -kines in preterm labour and brain injury. BJOG
2005;112(Suppl 1):16–18.16. D’Aiuto F, Parkar M, Andreou G, Suvan J, Brett
PM, Ready D, Tonetti MS. Periodontitis and sys-temic inflammation: control of the local infection isassociated with a reduction in serum inflammatorymarkers. J Dent Res 2004;83:156–160.
17. Slade GD, Offenbacher S, Beck JD, Heiss G,Pankow JS. Acute-phase inflammatory response toperiodontal disease in the US population. J DentRes 2000;79:49–57.
18. Hagberg H, Mallard C. Effect of inflammation oncentral nervous system development and vulnera-bility.Curr Opin Neurol 2005;18:117–123.
19. Vergnes JN, Sixou M. Preterm low birth weightand maternal periodontal status: a meta-analysis.Am J Obstet Gynecol 2007;196:135.e1–7.
20. Boggess KA, Beck JD, Murtha AP, Moss K, Of-fenbacher S. Maternal periodontal disease in earlypregnancy and risk for a small-for-gestational-ageinfant. Am J Obstet Gynecol 2006;194:1316–1322.
21. Roberts JM, Pearson G, Cutler J, Lindheimer M.Summary of the NHLBI Working Group on Re-search on Hypertension During Pregnancy. Hyper-tension 2003;41:437–445.
22. Roberts JM, Cooper DW. Pathogenesis and genet-ics of preeclampsia. Lancet 2001;357:53–56.
23. Conrad KP, Benyo DF. Placental cytokines and thepathogenesis of preeclampsia. Am J Reprod Im-munol 1997;37:240–249.
24. Petroff MG, Chen L, Phillips TA, Azzola D, Sedl-mayr P, Hunt JS. B7 family molecules are favorablypositioned at the human maternal-fetal interface.Biol Reprod 2003;68:1496–1504.
25. Rustveld LO, Kelsey SF, Sharma R. Association be-tween maternal infections and preeclampsia: a sys-tematic review of epidemiologic studies. MaternChild Health J 2008;12:223–242.
26. Canakci V, Canakci CF, Yildirim A, Ingec M, EltasA, Erturk A. Periodontal disease increases the riskof severe preeclampsia among pregnant women. JClin Periodontol 2007;34:639–645.
27. Boggess KA, Lieff S, Murtha AP, Moss K, Beck J,Offenbacher S. Maternal periodontal disease is as-sociated with an increased risk for preeclampsia.Obstet Gynecol 2003;101:227–231.
28. Barak S, Oettinger-Barak O, Machtei EE, SprecherH, Ohel G. Evidence of periopathogenic microor-ganisms in placentas of women with preeclampsia.J Periodontol 2007;78:670–676.
29. Contreras A, Herrera JA, Soto JE, Arce RM,Jaramillo A, Botero JE. Periodontitis is associatedwith preeclampsia in pregnant women. J Perio -dontol 2006;77:182–188.
30. Gervasi MT, Chaiworapongsa T, Naccasha N, Pacora P, Berman S, Maymon E, Kim JC, Kim

146 Periodontal Disease and Overall Health: A Clinician's Guide
YM, Yoshimatsu J, Espinoza J, Romero R. Mater-nal intravascular inflammation in preterm prema-ture rupture of membranes. J Matern Fetal Neona-tal Med 2002;11:171–175.
31. Offenbacher S, Lieff S, Boggess KA, Murtha AP,Madianos PN, Champagne CM, McKaig RG, JaredHL, Mauriello SM, Auten RL Jr, Herbert WN, BeckJD. Maternal periodontitis and prematurity. Part I:Obstetric outcome of prematurity and growth re-striction. Ann Periodontol 2001;6:164–174.
32. Lieff S, Boggess KA, Murtha AP, Jared H, MadianosPN, Moss K, Beck J, Offenbacher S. The oral con-ditions and pregnancy study: periodontal status ofa cohort of pregnant women. J Periodontol 2004;75:116–126.
33. Madianos PN, Lieff S, Murtha AP, Boggess KA,Auten RL Jr, Beck JD, Offenbacher S. Maternal perio dontitis and prematurity. Part II: Maternal infection and fetal exposure. Ann Periodontol2001;6:175–182.
34. Han YW, Ikegami A, Bissada NF, Herbst M, Red-line RW, Ashmead GG. Transmission of an uncul-tivated Bergeyella strain from the oral cavity toamniotic fluid in a case of preterm birth. J ClinMicrobiol 2006;44:1475–1483.
35. Han YW, Fardini Y, Chen C, Iacampo KG, PerainoVA, Shamonki JM, Redline RW. Term stillbirthcaused by oral fusobacterium nucleatum. ObstetGynecol 2010;115(2, Part 2):442–445.
36. Lin D, Moss K, Beck JD, Hefti A, Offenbacher S.Persistently high levels of periodontal pathogensas sociated with preterm pregnancy outcome. J Pe-riodontol 2007;78:833–841.
37. Lin D, Smith MA, Champagne C, Elter J, Beck J,Offenbacher S. Porphyromonas gingivalis infec-tion during pregnancy increases maternal tumornecrosis factor alpha, suppresses maternal inter-leukin-10, and enhances fetal growth restrictionand resorption in mice. Infect Immun 2003;71:5156–5162.
38. Offenbacher S, Riché EL, Barros SP, Bobetsis YA,
Lin D, Beck JD. Effects of maternal Campylobac-ter rectus infection on murine placenta, fetal andneonatal survival, and brain development. J Perio -dontol 2005;76(11 Suppl):2133–2143.
39. Lin D, Smith MA, Elter J, Champagne C, DowneyCL, Beck J, Offenbacher S. Porphyromonas gingi-valis infection in pregnant mice is associated withplacental dissemination, an increase in the placen-tal Th1/Th2 cytokine ratio, and fetal growth re-striction. Infect Immun 2003;71:5163–5168.
40. Bobetsis YA, Barros SP, Lin DM, Weidman JR,Dolinoy DC, Jirtle RL, Boggess KA, Beck JD, Of-fenbacher S. Bacterial infection promotes DNA hy-permethylation. J Dent Res 2007;86:169–174.
41. Constancia M, Hemberger M, Hughes J, Dean W,Ferguson-Smith A, Fundele R, Stewart F, Kelsey G,Fowden A, Sibley C, Reik W. Placental-specificIGF-II is a major modulator of placental and fetalgrowth. Nature 2002;417:945–948.
42. Allin M, Rooney M, Griffiths T, Cuddy M, WyattJ, Rifkin L, Murray R. Neurological abnormalitiesin young adults born preterm. J Neurol NeurosurgPsychiatry 2006;77:495–499.
43. Mericq V. Prematurity and insulin sensitivity. HormRes 2006;65(Suppl 3):131–136.
44. López NJ, Da Silva I, Ipinza J, Gutiérrez J. Peri-odontal therapy reduces the rate of preterm lowbirth weight in women with pregnancy-associatedgingivitis. J Periodontol 2005;76(11 Suppl):2144–2153.
45. Polyzos NP, Polyzos IP, Mauri D, Tzioras S, TsappiM, Cortinovis I, Casazza G. Effect of periodontaldisease treatment during pregnancy on pretermbirth incidence: a metaanalysis of randomized tri-als. Am J Obstet Gynecol 2009;200:225–232.
46. Michalowicz BS, Hodges JS, DiAngelis AJ, LupoVR, Novak MJ, Ferguson JE, Buchanan W, BofillJ, Papapanou PN, Mitchell DA, Matseoane S,Tschida PA. OPT Study. Treatment of periodontaldisease and the risk of preterm birth. N Engl J Med2006;355:1885–1894.
INTRODUCTIONBecause the surfaces of the oral cavity
are contiguous with those of the trachea andlower airway, pathogenic bacteria that colo-nize the oral cavity can be aspirated into thelower airway to cause infection. These bac-teria could be exogenous pathogens that arenot normal members of the oral flora, or en-do genous, opportunistic commensal organ-isms. In addition, oral inflammation, for example, in the form of periodontal disease,results in the release of biologically active inflam matory mediators and hydrolytic en-zymes into the oral fluids that may also beaspirated into the airway to incite inflamma -tion and increase susceptibility to infection.Recent evidence suggests that oral bacteriaand oral inflammation are associated withrespiratory diseases and conditions that havesignificant morbidity and mortality. Further -more, some respiratory illnesses (such asasthma) may have an effect on orofacialmorphology or even on dentition. This chap-ter discusses several important respiratorydiseases that may be influenced by oral micro flora or oral inflammation. Much ofthe material presented has been previously reviewed and discussed.1-5
PNEUMONIAPneumonia is an infection of the lungs
caused by bacteria, mycoplasma, viruses,fungi, or parasites. Bacterial pneumonia is acommon and significant cause of mortalityand morbidity in human populations. Pneu-monia, together with influenza, is an impor-tant cause of death throughout the world.Pneumonia also contributes to morbidity and
decline in quality of life, as well as increasedmedical costs. Bacterial pneumonia is com–prised of several subtypes: community-acquired pneumonia, aspiration pneumonia,hospital-acquired (nosocomial) pneumonia,ventilator-associated pneumonia, and nurs-ing home-associated pneumonia. In all cases,correlations have been made with oral healthstatus.
Community-Acquired PneumoniaCommunity-acquired pneumonia (CAP)
is an important cause of morbidity and mor-tality. Bacterial pneumonia is often precededby viral infection or Mycoplasma pneumoniaeinfections that diminish the cough reflex, interrupt mucociliary clearance, and enhancepathogenic bacterial adherence to the respi-ratory mucosa to foster the chain of eventsthat may eventually lead to CAP.6
The major etiologic agents of CAP areviruses; for example, respiratory syncytialvirus or rhinovirus. Early in life, bacterialcauses of CAP include group B streptococcior gram-negative enteric bacteria, as well asStreptococcus pneumoniae, while S. pneu-moniae and H. influenzae are often the causeof CAP in adults.
CAP EpidemiologyAbout 4 million CAP cases occur in the
United States each year.7 Most of these pa-tients are treated outside of the hospital. Forexample, a recent large, population-basedcohort study of 46,237 seniors 65 years ofage or older were observed over a three-yearperiod.8 The overall rate of community- acquired pneumonia ranged from 18.2 cases
CHAPTER 10Oral Health andDiseases of the Respiratory Tract
Frank A. Scannapieco, Joseph M. Mylotte

per 1,000 person-years among those whowere 65 to 69 years old, to 52.3 cases per1,000 person-years among those who were85 or older. In this population, 59.3% of allpneumonia episodes were treated on an out-patient basis. Overall, CAP results in morethan 600,000 hospitalizations, 64 milliondays of restricted activity, and 45,000 deathsannually.
CAP Risk FactorsRisk factors for CAP include age, male
sex, chronic obstructive pulmonary disease(COPD), asthma, diabetes mellitus, conges-tive heart failure, and smoking.8 In a study of1,336 patients with CAP and 1,326 controlsfor risk factors, multivariate analysis foundcigarette smoking, usual contact with chil-dren, sudden changes of temperature atwork, inhalation therapy (particularly thosecontaining steroids), oxygen therapy, asthma,and chronic bronchitis to all be independentrisk factors for CAP.9 Interestingly, this studyalso showed that a visit to a dentist in the pre-vious month was an independent protectivefactor for CAP, presumably by encouragingimprovements in oral hygiene, which couldlimit colonization by respiratory pathogens.
CAP Symptoms, Diagnosis, andResistant Strains
Common clinical symptoms of CAP in-clude cough, fever, chills, fatigue, dyspnea,rigors, and pleuritic chest pain.7 Dependingon the pathogen, a patient’s cough may bepersistent and dry, or it may produce sputum.Other presentations may include headacheand myalgia. Certain bacteria, such as Legion -ella may induce gastrointestinal symptoms.
The chest radiography is a critical toolfor the diagnosis of pneumonia. A typicalpositive chest radiograph shows consolida-tion within the lung lobe, or a more diffuseinfiltration.7 However, chest radiographyper formed early in the course of the diseasecould be found to be negative.
A worrisome recent development is theemergence of community-acquired methicil -lin resistant Staphylococcus aureus (MRSA)infections, including CAP.10 While still arare infection, a 2008 analysis of the medicalliterature published in the previous two yearsfound that the median age of MRSA patients,four of whom died, was 21 years, and usuallya short interval occurred between the devel-opment of respiratory symptoms and the detection of disease.10
CAP Treatments and OutcomesAntibiotics are the cornerstone of CAP
treatment. Typical antibiotic regimens includethe use of oral azithromycin (Zithromax®),clarithromycin (Biaxin®), erythromycin (var-ious brand names) or doxycycline (variousbrand names) in otherwise healthy patients,or oral moxifloxacin (Avelox®), gemifloxacin(Factiv®), or levofloxacin (Levaquin®) in patients having other comorbidities.
While the focus for CAP is typically onshort-term outcomes, it is becoming moreapparent that there are sometimes long-termnegative consequences of CAP, particularlyin the elderly.11 For example, a large study ofthe Medicare database used a matched case-control design to evaluate the one-year mor-tality rate of 158,960 older CAP patients to794,333 control subjects hospitalized for reasons other than CAP.12 The single-yearmortality rate for CAP patients exceeded thatof control subjects (40.9% versus 29.1%, respectively); the differences could not beexplained by the types of underlying disease.These findings suggest that the consequencesof CAP in the elderly are important to long-term survival, and thus should be prevented.11
Aspiration PneumoniaAspiration pneumonia is an infectious pro -
cess caused by the inhalation of oropharyn-geal secretions colonized by pathogenic bac-teria.13 This is differentiated from aspirationpneumonitis, which is typically caused by
148 Periodontal Disease and Overall Health: A Clinician's Guide

chemical injury following inhalation of sterilegastric contents. Aspiration pneumonia is oftencaused by anaerobic organisms derived fromthe oral cavity (gingival crevice), and often de-velops in patients with elevated risk of aspira-tion of oral contents into the lung, such as thosewith dysphagia or depressed consciousness, andis very common in the nursing home setting.
Most adults inhale small amounts oforopharyngeal secretions during sleep. How-ever, the small number and typically aviru-lent nature of the commensal microflora, aswell as defense mechanisms such as cough-ing, ciliary action, and normal immune mech -anisms all work together to prevent onset ofinfection. However, circumstances that in-crease the volume of aspirate, especially thenumber of organisms in the aspirate, will in-crease the risk of pneumonia. The risk of as-piration pneumonia is lower in patients with-out teeth as well as in patients who receiveaggressive oral care (explained in further detail below). However, there is little infor-mation available regarding the effect of perio - dontal therapy in the prevention of aspirationpneumonia in vulnerable populations.
Nosocomial PneumoniaHospital-acquired pneumonia (HAP)
was originally defined as pneumonia occur-ring with onset > 48 hours after admission tothe hospital. This classification scheme wasstraightforward and easy to apply. However,over the past decade there has been a shift indelivery of medical care from the hospital tothe outpatient setting for delivery of servicessuch as antibiotic therapy, cancer chemo -therapy, wound management, outpatient dial-ysis centers, and short-term rehabilitation.As a result, the classification scheme for HAPpneumonia has changed. This shift in care fromthe hospital to the outpatient, home setting,or nursing home leads to cases of pneumoniathat occur outside the hospital setting, butclearly within other healthcare delivery set-tings. Thus, such pneumonia has been referred
to as “healthcare-associated pneumonia.”14
Nursing-home associated pneumonia(NHAP) is the most important common in-fection affecting nursing home residents be-cause of its high morbidity and mortality.15
Pneumonia is also a common reason fortransfer of residents from the nursing hometo the hospital.16 HAP is a common infectionin the hospital, often causing considerablemorbidity and mortality, as well as extendingthe length of stay and increasing the cost of hospital care. HAP can be further dividedinto two subtypes: ventilator-associated pneu-monia (VAP) and nonventilator-associatedpneumonia. Pneumonia is the most common infection in the intensive-care unit (ICU) setting, accounting for 10% of infections.17
VAP is the second most common hospi-tal-acquired infection.18,19 It is a leading causeof death in critically-ill patients in the ICU,with estimated prevalence rates of 10%– 65%and mortality rates of 25%–60% depend ingon the study, patient populations, and medical/surgical conditions involved.17,20-25 VAP andother forms of HAP are independent riskfactors for mortality in hospitalized patients,irrespective of the severity and type of un-derlying illness.26 An episode of HAP addsapproximately 5–6 days to the length of hos-pital stay and thousands of dollars in medicalcare costs.20-25 The risk of developing VAP inthe medical and surgical ICU varies from 5–21 per 1,000 ventilator days.27 The onset ofpneumonia easily can double the length ofthe patient’s hospital stay, and the cost ofVAP treatment has been estimated to averageas high as $40,000 per case.28 Pneumonia isalso prevalent in nursing homes, comprising13%–48% of all infections.29 The mortalityrate of nosocomial pneumonia can be as highas 25%.28
The Oral Cavity as a Reservoirof Respiratory Infection
The oral cavity may be an importantsource of bacteria that cause infections of
CHAPTER 10 Oral Health and Diseases of the Respiratory Tract 149

the lungs. Dental plaque, a tooth-bornebiofilm that initiates periodontal disease anddental caries, may host bacterial species aspart of the normal flora that are capable ofcausing respiratory infection, or may becomecolonized by exogenous respiratorypathogens. Oral pathogens may then be shedfrom the oral biofilm and released into theoral secretions, which are then aspirated intothe respiratory tract.
Mechanisms Causing Pulmonary InfectionBacteria causing CAP are species such
as S. pneumoniae, Haemophilus influenzae,and M. pneumonia that normally colonizethe oropharynx. Nosocomial pneumoniais, in contrast, often caused by bacteriathat are not common members of the oro - pharyngeal flora, such as Pseudo monasaeruginosa, S. aureus, and enteric gram- negative bac teria. These organisms colo-nize the oral cavity in certain settings,for example in institutionalized subjectsand in people living in areas served byunsanitary water supplies.1 Respiratorypathogens, such as S. aureus, P. aeruginosa,and Escherichia coli, are found to be presentin substantial numbers on the teeth in bothinstitutionalized elders30 and intensive carepatients.31
One cubic millimeter of dental plaquecontains about 100 million bacteria and mayserve as a persistent reservoir for potentialpathogens, both oral and respiratory bacteria.It is likely that oral and respiratory bacteriain the dental plaque are shed into the salivaand are then aspirated into the lower respi-ratory tract and the lungs to cause infec-tion.1,31 Indeed, the commensal, or normal,microflora of the oral cavity, especially pe-riodontal disease-associated anaerobic bac-teria that reside in the subgingival space, of-ten cause aspiration pneumonia in patientswho have high risk for aspiration, such asthose with dysphagia or neurologic impair-ment affecting the swallowing apparatus.
Cytokines and enzymes induced fromthe periodontally inflamed tissues by the oralbiofilm may also be aspirated into the lungswhere they may stimulate local inflamma-tory processes preceding colonization ofpathogens and the actual lung infection.1,31
Other possible mechanisms to explain pul-monary infection are inhalation of airbornepathogens or translocation of bacteria fromlocal infections via bacteremia.
Patients at Increased RiskIn a healthy subject, the respiratory tract
is able to defend itself against aspirated bac-teria. Patients with diminished salivary flow,decreased cough reflex, swallowing disorders,poor ability to perform good oral hygiene, orother physical disabilities have a high risk forpulmonary infections. Mechanically venti-lated patients in ICUs with no ability to clearoral secretions by swallowing or by coughing,are at particularly high risk for VAP, espe-cially if the ventilation lasts for more than 48hours.32 Oral bacterial load increases duringintubation and higher dental plaque scorespredict risk of pneumonia.33 Anaerobic bac-teria are frequently found to colonize thelower respiratory tract in mechanically venti -lated patients.32 Colonization of bacteria in thedigestive tract has been suggested to be asource for nosocomial pneumonia, but recentlyoral and dental bacterial colonization hasbeen proposed to be the major source of bac-teria implicated in the etiology of VAP.34 It islikely that bacteria that first colonize the den-tal plaque are shed before subsequently at-taching to the tubing that passses throughthe oral cavity into the lung (Figure 1).
In the institutionalized elderly, the aspi -ration of saliva seems to be the main route bywhich bacteria enter the lungs to cause aspi-ration pneumonia. Dysphagia seems to be animportant risk factor, even a predictor, for as-piration pneumonia.35 For example, the ma-jor oral and dental risk factors for aspirationpneumonia in veteran residents of nursing
150 Periodontal Disease and Overall Health: A Clinician's Guide
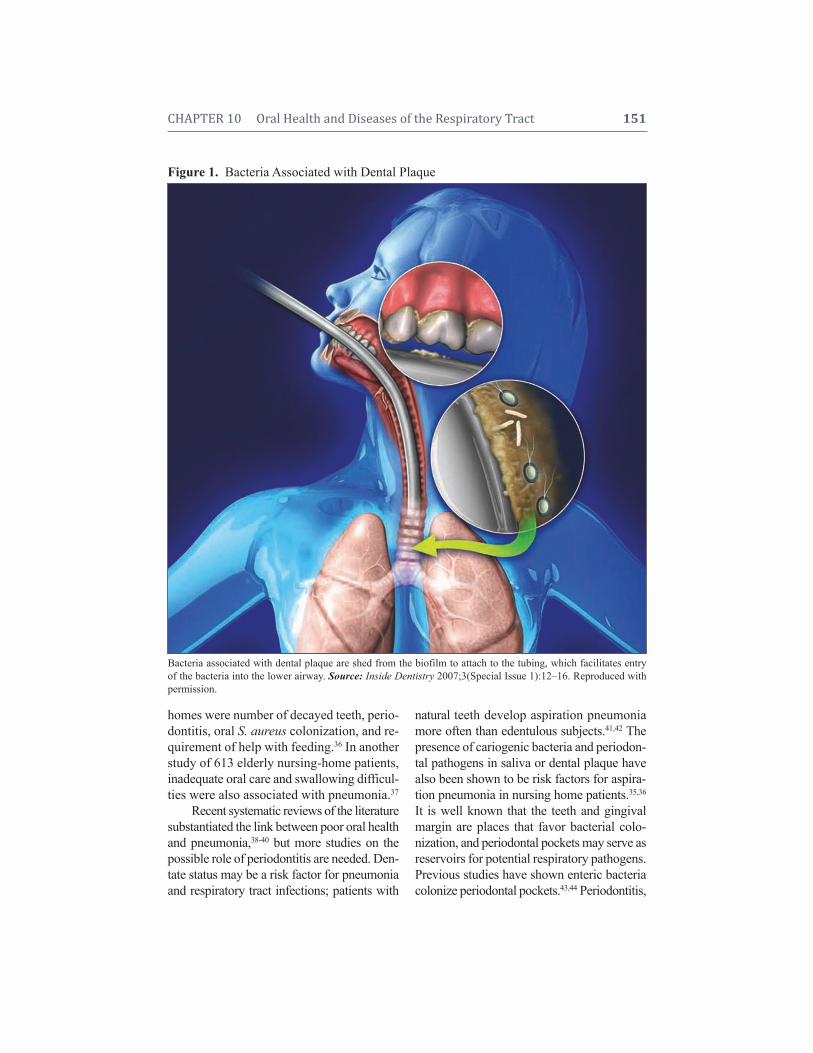
homes were number of decayed teeth, perio -dontitis, oral S. aureus colonization, and re-quirement of help with feeding.36 In anotherstudy of 613 elderly nursing-home patients,inadequate oral care and swallowing difficul -ties were also associated with pneumonia.37
Recent systematic reviews of the literaturesubstantiated the link between poor oral healthand pneumonia,38-40 but more studies on thepossible role of periodontitis are needed. Den -tate status may be a risk factor for pneumoniaand respiratory tract infections; patients with
natural teeth develop aspiration pneu moniamore often than edentulous subjects.41,42 Thepresence of cariogenic bacteria and periodon-tal pathogens in saliva or dental plaque havealso been shown to be risk factors for aspira-tion pneumonia in nursing home patients.35,36
It is well known that the teeth and gingivalmargin are places that favor bacterial colo-nization, and periodontal pockets may serve asreservoirs for potential respiratory pathogens.Previous studies have shown enteric bacteriacolonize periodontal pockets.43,44 Periodontitis,
CHAPTER 10 Oral Health and Diseases of the Respiratory Tract 151
Figure 1. Bacteria Associated with Dental Plaque
Bacteria associated with dental plaque are shed from the biofilm to attach to the tubing, which facilitates entryof the bacteria into the lower airway. Source: Inside Dentistry 2007;3(Special Issue 1):12–16. Reproduced withpermission.
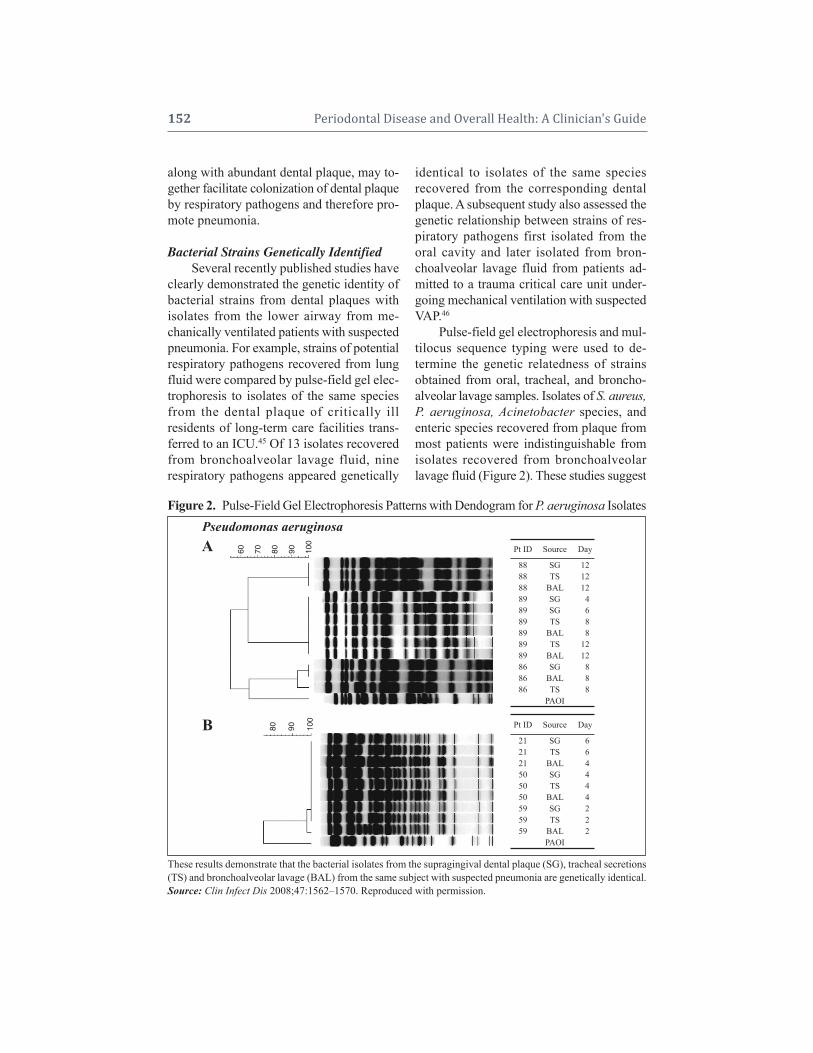
along with abundant dental plaque, may to-gether facilitate colonization of dental plaqueby respiratory pathogens and therefore pro-mote pneumonia.
Bacterial Strains Genetically IdentifiedSeveral recently published studies have
clearly demonstrated the genetic identity ofbacterial strains from dental plaques withisolates from the lower airway from me-chanically ventilated patients with suspectedpneumonia. For example, strains of potentialrespiratory pathogens recovered from lungfluid were compared by pulse-field gel elec-trophoresis to isolates of the same speciesfrom the dental plaque of critically ill residents of long-term care facilities trans-ferred to an ICU.45 Of 13 isolates recoveredfrom bronchoalveolar lavage fluid, nine respiratory pathogens appeared genetically
identical to isolates of the same species recovered from the corresponding dentalplaque. A subsequent study also assessed thegenetic relationship between strains of res-piratory pathogens first isolated from theoral cavity and later isolated from bron-choalveolar lavage fluid from patients ad-mitted to a trauma critical care unit under -going mechanical ventilation with suspectedVAP.46
Pulse-field gel electrophoresis and mul-tilocus sequence typing were used to de -termine the genetic relatedness of strains obtained from oral, tracheal, and broncho -alveolar lavage samples. Isolates of S. aureus,P. aeruginosa, Acinetobacter species, andenteric species recovered from plaque frommost patients were indistinguishable fromisolates recovered from bronchoalveolarlavage fluid (Figure 2). These studies suggest
152 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 2. Pulse-Field Gel Electrophoresis Patterns with Dendogram for P. aeruginosa Isolates
These results demonstrate that the bacterial isolates from the supragingival dental plaque (SG), tracheal secretions(TS) and bronchoalveolar lavage (BAL) from the same subject with suspected pneumonia are genetically identical.Source: Clin Infect Dis 2008;47:1562–1570. Reproduced with permission.
A Pt ID Source Day
88 SG 1288 TS 1288 BAL 1289 SG 489 SG 689 TS 889 BAL 889 TS 1289 BAL 1286 SG 886 BAL 886 TS 8
PAOI
Pt ID Source Day
21 SG 621 TS 621 BAL 450 SG 450 TS 450 BAL 459 SG 259 TS 259 BAL 2
PAOI
B
60 70 80 90 100
80 90 100
Pseudomonas aeruginosa

CHAPTER 10 Oral Health and Diseases of the Respiratory Tract 153
that respiratory pathogens isolated from thelung are often genetically indistinguishablefrom strains of the same species isolatedfrom the oral cavity in patients who receivemechanical ventilation who are admitted tothe hospital from both nursing homes and thecommunity. Thus, dental plaque is an impor -tant reservoir for VAP infection.
Oral Interventions to ReducePulmonary Infections
Oral interventions to reduce pulmonaryinfections have been examined in both me-chanically ventilated ICU patients and non-ventilated elderly patients.38-40 These studiesincluded chemical intervention using topicalantimicrobial agents and traditional oral me-chanical hygiene performed by a profes-sional. The use of oral topical chlorhexidine(CHX) reduces pneumonia in mechanicallyventilated patients, and may even decreasethe need of systemic intravenous antibioticsor shorten the duration of mechanical venti-lation in the ICU.47-50 Also, oral applicationof CHX in the early post-intubation periodlowers the numbers of cultivable oral bacte-ria and may delay the development of VAP.51
Studies validating the effectiveness of oralCHX on reducing pneumonia are not unan-imous. For example, gingival decontamina-tion with CHX gel significantly decreasedthe prevalence of oropharyngeal coloniza-tion by pathogenic bacteria in ventilated pa-tients, but this was not sufficient to reducethe incidence of respiratory infections.52 An-other study reported that a significant re-duction in pneumonia using CHX rinse inICU patients was achieved only after 24hours of intubation.53 However, the efficacyof oral CHX decontamination to reduce VAPneeds further investigation since no clear re-duction in mortality rate has been demon-strated. In addition to CHX, other antiplaqueagents have been investigated. The use ofanti microbial gels, including polymyxin B sulfate, neomycin sulfate, and vancomycin
hydrochloride54 or gentamicin/colistin/van-co mycin55 also reduce VAP. Recently, thefirst study showing that mechanical oral carein combination with povidone iodine signif-icantly decreases pneumonia in ventilatedICU patients was published.56 This suggeststhat tooth brushing combined with a topicalantimicrobial agent is a promising methodfor oral cleansing of mechanically ventilatedpatients.
Institutionalized, but nonventilated pa-tients, mainly elders living in nursing homes,appear to also benefit from improved oralcare by showing lower levels of oral bacte-ria and fewer pneumonia episodes andfebrile days. Daily tooth brushing and topicaloral swabbing with povidone iodine signifi-cantly decreased pneumonia among residentsin long-term care facilities.57-59 However, inan earlier study by the same research group,oral care with both brushing and antimicro-bial gargling had an effect only on febriledays but not on incidence of pneumonia.60
Professional cleaning by a dental hygienistonce a week significantly reduced the preva-lence of fever and fatal pneumonia in 141elderly patients in nursing homes.61 Similaronce-a-week professional oral cleaning sig-nificantly reduced influenza infections in anelderly population.62 Dental plaque is knownto form clearly visible masses on the teeth ina few days, but these studies suggest thatimproved oral care, even without chemicalagents and even if not performed daily, notonly reduces the oral bacterial, viral, andfungal load, but may have an effect on re-ducing the risk of pneumonia. More studiesare needed to find the easiest oral deconta-mination methods to reduce pulmonary in-fections in elderly nursing home patients.
Oral cleansing reduces pneumonia in bothedentulous and dentate subjects, suggestingthat oral colonization of bacteria contributesto nosocomial pneumonia to a greater ex-tent than periodontitis. However, interven-tion studies of the treatment of periodontitis

on the incidence of pneumonia have not beenperformed due to the complexities requiredin investigating ICU or bed-bound nursinghome patients. In edentulous people, den-tures may easily serve as a similar reservoiras natural teeth for oral and respiratory bac-teria if not cleaned properly and daily.
Suggestions for Oral Care of Hospitalized and Nursing Home Residents to Prevent PneumoniaMany studies demonstrate that im-
proved oral hygiene can reduce the risk ofpneumonia in vulnerable patients. This raisesthe question as to what is the present statusof oral hygiene practice in hospitals andnursing homes. Traditional nursing teachingrecommends that toothbrushing be per-formed twice a day together with swabbingof the mouth with glycerine and lemonswabs for comfort. In light of the recent find-ings described above, routine nursing prac-tice needs to include more rigorous oral careprocedures.
A recent survey assessed the type and fre- quency of oral care provided in ICUs in theUnited States, as well as the attitudes, beliefs,and knowledge of healthcare personnel.63
The findings showed that while 512 (92%) of556 respondents perceived oral care to be ahigh priority, primary oral care proceduresinvolved the use of foam swabs, moisturizers,and mouthwash. Interventions thought to re-duce oral colonization by respiratory patho-gens, such as tooth brushing and the use of antiseptic rinses such as CHX, appear to beused infrequently in critical care settings.64
While no official guidelines promul-gated by professional societies or regulatoryagencies have been published to date, a num-ber of prudent actions may be consideredwhen caring for the vulnerable patient:
1. Remove all dental appliances upon ad-mission to the critical care unit.
2. Conduct oral examination initially anddaily by a registered nurse.
3. Brush teeth two or three times per day;also floss if possible.
4. Rinse all oral surfaces with antimicro-bial rinses.
5. Perform frequent deep suction of oraland pharyngeal secretions as needed,as well as prior to repositioning the tubeor deflating the cuff.
6. Remove hard deposits (e.g., tartar/calculus) from the teeth, if possible.
7. Request that teeth be professionallycleaned before admission to the hospi-tal for elective procedures.Several suggestions can also be made to
advise healthcare providers on the properoral hygiene techniques to reduce risk of oralcolonization by respiratory pathogens in ven-tilated patients:
1. Place the patient’s head to the side orplace in semi-fowlers (semi-reclined)body position.
2. Provide deep suction, as needed, in in-tubated patients to remove oropharyn-geal secretions that can migrate downthe tube and settle on top of the cuff.
3. Brush teeth using a wet soft toothbrushfor approximately one to two minutes.
4. Brush tongue and vestibular surfaces.5. Apply mouth moisturizer inside mouth
and lip balm if needed to reduce risk oforal ulceration.
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Patients with COPD have chronic airflowobstruction due to narrowing of the airways,with excess production of sputum resultingfrom chronic bronchitis and/or emphysema.65
Chronic bronchitis is defined as the result ofirritation to the bronchial airway and excessivesecretion of mucus sufficient to cause coughwith expectoration for at least three monthsof the year over two consecutive years.66
Emphysema results from the distention ofthe air spaces distal to the terminal bron -chiole with destruction of the alveolar septa.
154 Periodontal Disease and Overall Health: A Clinician's Guide

CHAPTER 10 Oral Health and Diseases of the Respiratory Tract 155
Although this condition is associated withcertain symptoms, the definitive diagnosis ofemphysema can only be made histologically.
Epidemiology and Costs of COPDChronic bronchitis is quite prevalent,
with 20%–30% of all adults over the age of45 years having some history of this condi-tion,67 typically as a sequela of smoking. Theincidence of emphysema is less well knownsince the main tool for noninvasive diagno-sis (CT scanning) cannot be practically ap-plied in population studies. While it is rare tofind lungs completely free of emphysemapostmortem, the majority of individuals donot show well-defined histologic evidence ofemphysema and do not have clinical symp-toms of the disease.
The most significant risk factor for COPDis prolonged cigarette smoking. Other envi-ronmental risk factors include chronic ex-posure to toxic atmospheric pollutants (e.g.,second-hand smoke). Possible genetic risk fac-tors include a defective alpha-1 antitrypsingene, variant alpha-1 antichymotrypsin, alpha-2 macroglobulin, vitamin D-bindingprotein, and blood group antigen genes.68
These genetic defects account for only asmall percentage of individuals with COPD.
Worldwide, the prevalence of physio -logically defined COPD in adults ages 40 orolder is approximately 9%–10%.69 In 2001,approximately 12.1 million adults older than25 were diagnosed with COPD in the UnitedStates, and another 24 million showed im-paired lung function.70 It is likely that COPDin the community remains underreported dueto difficulties in diagnosing this disorder.COPD is the fourth leading cause of morbid-ity and mortality in the United States, and isprojected to become the fifth most commoncause for morbidity and the third most fre-quent cause of mortality worldwide by theyear 2020. It has been estimated that the meanexcess costs of COPD, after adjustment forsociodemographic factors and smoking status,
is $4,932 per patient.71 Inpatient costs aregreater than outpatient and emergency costs($8.3 versus $7.8 billion) and hospital andmedication costs account for most resourcesspent.72
Pathogenesis of COPDCOPD is the result of chronic airflow
limitation resulting from an inflammatoryresponse to inhaled particles and gasesin the lung, in most cases delivered from tobacco smoking.73 Smoking is related tomacrophage-predominant inflammation andairspace enlargement. High concentrations ofreactive oxygen species in tobacco smokeresults in oxidative stress. Resulting recruit-ment of macrophages leads to release of pro-teases such as macrophage elastase (matrixmetalloproteinase [MMP]-12), which seemsto be a key pathogenic factor in emphysema.For example, an MMP-inhibitor in devel -opment, AZ11557272, prevented smoke- induced increases in lung inflammatory cells,lavage desmosine (a marker of elastin break-down), and serum tumor necrosis factor- alpha (TNF-) in a guinea pig model of cigarette smoke-induced COPD.74
COPD is a complex disease that is in-fluenced by a variety of environmental and genetic factors. Several environmental fac-tors, for example cigarette smoking and airpollution, have been strongly associated withthe initiation and progression of the disease.It is clear that not all smokers develop COPD.Thus other factors, likely genetic, may helpexplain why some people develop COPDwhile others do not.75,76 It is well known thatCOPD is related to alpha-1 anti trypsin defi-ciency,77,78 although severity of disease is af-fected by other risk factors, such as gender,history of asthma, chronic bronchitis, andpneumonia. Some evidence has been pre-sented demonstrating that COPD sometimesclusters in families. Genetic factors may alsoinfluence susceptibility to respiratory infec-tions leading to acute COPD exacer bations.

It appears that, to date, attempts to associateCOPD experience with specific genetic poly-morphisms, for example targeting cytokineor global promoter genes, have proven in-conclusive.76
A major complication of COPD is theoccurrence of periodic “exacerbations” orperiods of aggravation of disease symptoms.Exacerbations have recently been associatedwith bacterial infection,79,80 typically by non-typable H. influenzae, S. pneumonia, and M.catarrhalis. Viral infection has also been im-plicated in initiating this process.81 Acute ex- acerbations of COPD are thus often treatedusing empiric antibiotic therapy. The cost oftherapy for this group of patients is extra -ordinarily high. Treatment failure from rou-tine antimicrobial therapy can lead to hos -pitalization, respiratory failure, and death.Antibiotic therapy for exacerbations ofCOPD can also lead to emergence of bacte-rial antibiotic resistance and increased costs.
Treatment and Management of COPDA mainstay of therapy is the use of
inhaled drug therapy. In severe cases, lungvolume reduction surgery has been shown toreduce mortality, increase exercise capacity,and improve quality of life. Supplementaloxygen during exercise reduces exertionalbreathlessness and improves exercise toler-ance of the hypoxemic patient. Noninvasiveventilation has been used as a palliative treat-ment to reduce dyspnea.
A recent systematic review of the liter-ature concluded that antibiotics effectivelyreduce treatment failure and mortality ratesin COPD patients with severe exacerba-tions.82 However, antibiotics may not be gen-erally indicated for patients with mild-to-moderate exacerbations.
COPD and Oral HealthAssociations between respiratory dis-
eases and oral health in community-dwellingpopulations were initially assessed by analysis
of the National Health and Nutrition Exam-ination Survey (NHANES) I data.83 Thisdatabase contains information on the gen-eral health status of 23,808 people. Of these,365 individuals reported a respiratory con-dition, categorized as confirmed chronic respiratory disease (chronic bronchitis oremphysema), or acute respiratory disease(influenza, pneumonia, acute bronchitis). After controlling for gender, age, and race,subjects with a confirmed chronic respiratorydisease had a significantly greater oral hy-giene index than subjects without respiratorydisease. Further, subjects with acute diseasetended to have more decayed teeth than thosewithout disease. No other statistical associ-ations were noted between any of the othermeasures of oral health and acute respiratorydisease. Also, no associations were notedbetween the periodontal index and eitheracute or chronic diseases.
Another study found that periodontaldisease, measured as alveolar bone loss thatoccurred between baseline and later meas-urements from periapical radiographs, wasan independent risk factor for COPD in adultmales enrolled in the VA Normative Agingstudy.84
These results were supported by a sub -sequent study that measured associations be-tween poor oral health and chronic lung dis-ease, and was able to carefully control for anumber of potentially confounding variables.Data from NHANES III, which documentedthe general health and nutritional status ofrandomly selected US subjects from 1988 to1994, were analyzed.85 This cross-sectional,retrospective study of the NHANES III data-base included a study population of 13,792subjects 20 years of age having at leastsix natural teeth. A history of bronchitisand/or emphysema was recorded from themedical questionnaire. Lung function wasestimated by calculation of the ratio of forcedexpiratory volume after 1 sec/forced vitalcapacity. Oral health status was deduced
156 Periodontal Disease and Overall Health: A Clinician's Guide

from the Decayed Missing Filled System index (summary of cumulative caries ex -perience), gingival bleeding, gingival reces-sion, gingival pocket depth, and periodontalattachment level.
Subjects with COPD had, on average,more clinical attachment loss (CAL;1.48 ±1.35 – mean ± SD) than those without COPD(mean CAL:1.17 ± 1.09). To simultaneouslycontrol for multiple variables that may con-found statistical analysis, gender, age, race,education, income, dental treatment history,alcohol consumption, diabetes status, andsmoking status were considered in a logisticregression model against a history of COPD.The risk for COPD appeared to be signifi-cantly elevated when mean attachment loss(MAL) was found to be severe (MAL 2.0mm) compared to periodontal health (< 2.0mm MAL; odds ratio 1.35, 95% CI:1.07–1.71). Furthermore, the odds ratio was 1.45(95% CI:1.02–2.05) for those who had 3.0mm MAL. A trend was also noted in thatlung function appeared to diminish as theamount of attachment loss increased. Nosuch trend was apparent when gingivalbleeding was considered. No other statisticalassociations were noted between any of themeasures of oral health and acute respiratorydiseases, such as influenza or pneumonia.
Chronic Lung Disease inHospitalized Patients
Dental plaque may serve as a reservoirof respiratory pathogen colonization in hos-pitalized patients with chronic lung dis-eases.86 Using a checkerboard DNA-DNAhybridization technique to determine preva-lence of eight respiratory pathogens and eightoral pathogens, species such as S. aureus,P. aeruginosa, Acinetobacter baumannii, andEnterobacter cloacae were detected in plaquefrom 29 of the 34 (85.3%) hospitalized patients, while only 12 of 31 (38.7%) non-hospitalized subjects were colonized. Theseresults indicate that dental plaque may serve
as a reservoir of infection in hospitalized pa-tients with chronic lung diseases.
Another recent analysis examined the relationship between airway obstructionand periodontal disease in a cohort of 860 community-dwelling elders enrolled in theHealth, Aging, and Body Composition Study.87
Results showed that after stratification bysmoking status and adjustment for age, race,gender, center, and pack-years, those withnormal pulmonary function had significantlybetter gingival index (p = 0.036) and loss ofattachment (p = 0.0003) scores than thosewith airway obstruction. Thus, a significantassociation between periodontal disease andairway obstruction was noted, especially informer smokers.
Finally, an association between chronicperiodontitis and severe COPD was supportedby a recent study that demonstrated a greaterprevalence of chronic periodontitis in 130 patients with very severe COPD than in 50 patients with other very severe respiratorydiseases.88 It was found that prevalence of periodontitis was 44% in the COPD groupversus 7.3% in the non-COPD group, and thisdifference was significant after adjustmentfor age, gender, and pack-years smoked.
CONCLUSIONRecent research points to possible as-
sociations between oral health, especiallydental plaque and periodontal disease, andrespiratory diseases such as community- acquired and nosocomial pneumonia andCOPD. Further research into these associa-tions may allow development and routineimplementation of simple and effectivestrategies to prevent respiratory disease invulnerable populations.
Supplemental ReadingsCoulthwaite L, Verran J. Potential pathogenic aspects ofdenture plaque. Br J Biomed Sci 2007;64:180–189.
Scannapieco FA, Yu J, Raghavendran K, Vacanti A,Owens SI, Wood K, Mylotte JM.A randomized trial
CHAPTER 10 Oral Health and Diseases of the Respiratory Tract 157

of chlorhexidine gluconate on oral bacterial pathogensin mechanically ventilated patients. Crit Care 2009;13:R117.
Sona CS, Zack JE, Schallom ME, McSweeney M, McMullen K, Thomas J, Coopersmith CM, Boyle WA,Buchman TG, Mazuski JE, Schuerer DJ.The impactof a simple, low-cost oral care protocol on ventilator- associated pneumonia rates in a surgical intensive careunit. J Intensive Care Med 2009;24:54–62.
Wang Z, Zhou X, Zhang J, Zhang L, Song Y, Hu FB,Wang C. Periodontal health, oral health behaviours, andchronic obstructive pulmonary disease. J Clin Perio -dontol 2009;36:750-755.
REFERENCES1. Scannapieco FA. Role of oral bacteria in respiratory
infection. J Periodontol 1999;70:793–802.2. Shay K, Scannapieco FA, Terpenning MS, Smith
BJ, Taylor GW. Nosocomial pneumonia and oralhealth. Spec Care Dentist 2005;25:179–187.
3. Scannapieco FA. Pneumonia in nonambulatory pa-tients. The role of oral bacteria and oral hygiene.JADA 2006;137(Suppl):21S–25S.
4. Paju S, Scannapieco FA. Oral biofilms, periodon-titis, and pulmonary infections. Oral Dis 2007;13:508–512.
5. Raghavendran K, Mylotte JM, Scannapieco FA.Nursing home-associated pneumonia, hospital- acquired pneumonia and ventilator-associatedpneumonia: the contribution of dental biofilms andperiodontal inflammation. Periodontol 2000 2007;44:164–177.
6. Stein RT, Marostica PJ. Community-acquired pneu-monia. Paediatr Respir Rev 2006;7 (Suppl 1):S136–S137.
7. Lutfiyya MN, Henley E, Chang LF, Reyburn SW.Diagnosis and treatment of community-acquiredpneumonia. Am Fam Physician 2006;73:442–450.
8. Jackson ML, Neuzil KM, Thompson WW, ShayDK, Yu O, Hanson CA, Jackson LA. The burden ofcommunity-acquired pneumonia in seniors: resultsof a population-based study. Clin Infect Dis 2004;39:1642–1650.
9. Almirall J, Bolibar I, Serra-Prat M, Roig J, Hospi-tal I, Carandell E, Agustí M, Ayuso P, Estela A, Tor-res A; Community-Acquired Pneumonia in CatalanCountries (PACAP) Study Group. New evidence ofrisk factors for community-acquired pneumonia: apopulation-based study. Eur Respir J 2008;31:1274–1284.
10. Durrington HJ, Summers C. Recent changes in themanagement of community acquired pneumoniain adults. BMJ 2008;336:1429–1433.
11. Niederman MS. Recent advances in community-ac-quired pneumonia: inpatient and outpatient. Chest2007;131:1205–1215.
12. Kaplan V, Clermont G, Griffin MF, Kasal J, WatsonRS, Linde-Zwirble WT, Angus DC. Pneumonia:still the old man’s friend? Arch Intern Med 2003;163:317–323.
13. Marik PE. Aspiration pneumonitis and aspirationpneumonia. N Engl J Med 2001;344:665–671.
14. Tablan OC, Anderson LJ, Besser R, Bridges C, Ha-jjeh R; CDE; Healthcare Infection Control PracticesAdvisory Committee. Guidelines for preventinghealth-care-associated pneumonia, 2003: recom-mendations of CDC and the Healthcare InfectionControl Practices Advisory Committee. MMWRRecomm Rep 2004;53(RR-3):1–36.
15. Mylotte JM. Nursing home-acquired pneumonia.Clin Infect Dis 2002;35:1205–1211.
16. Muder RR. Pneumonia in residents of long-termcare facilities: epidemiology, etiology, manage-ment, and prevention. Am J Med 1998;105:319–330.
17. Vincent JL, Bihari DJ, Suter PM, Bruining HA,White J, Nicolas-Chanoin MH, Wolff M, SpencerRC, Hemmer M. The prevalence of nosocomial in-fection in intensive care units in Europe. Results ofthe European Prevalence of Infection in IntensiveCare (EPIC) Study. EPIC International AdvisoryCommittee. JAMA 1995;274:639–644.
18. Richards MJ, Edwards JR, Culver DH, Gaynes RP.Nosocomial infections in medical intensive careunits in the United States. National NosocomialInfections Surveillance System. Crit Care Med 1999;27:887–892.
19. Arozullah AM, Khuri SF, Henderson WG, Daley J.Participants in the National Veterans Affairs Surgi-cal Quality Improvement Program. Developmentand validation of a multifactorial risk index forpredicting postoperative pneumonia after majornoncardiac surgery. Ann Intern Med 2001;135:847–857.
20. Control CFD. National Nosocomial InfectionsStudy Report. Annual Summary. MMWR 1984;35:17SS–29SS.
21. Craven DE, Barber TW, Steger KA, MontecalvoMA. Nosocomial pneumonia in the 1990s: updateof epidemiology and risk factors. Semin Respir In-fect 1990;5:157–172.
22. Craven DE, Steger KA, Barber TW. Preventingnosocomial pneumonia: state of the art and per-spectives for the 1990s. Am J Med 1991;91:44S–53S.
23. Craven DE, Steger KA. Epidemiology of nosoco-mial pneumonia. New perspectives on an old dis-ease. Chest 1995;108(2 Suppl):1S–16S.
158 Periodontal Disease and Overall Health: A Clinician's Guide

24. Kollef MH. The identification of ICU-specific out-come predictors: a comparison of medical, surgical,and cardiothoracic ICUs from a single institution.Heart Lung 1995;24:60–66.
25. Kollef MH. Prevention of hospital-associated pneu-monia and ventilator-associated pneumonia. CritCare Med 2004;32:1396–1405.
26. Fagon JY, Chastre J, Hance AJ, Montravers P, Novara A, Gibert C. Nosocomial pneumonia in venti - lated patients: a cohort study evaluating attri butable mor- tality and hospital stay. Am J Med 1993;94:281–288.
27. Lynch J, Lama V. Diagnosis and therapy of noso-comial ventilator associated pneumonia. AFC 2000;4:19–26.
28. Rello J, Ollendorf DA, Oster G, Vera-Llonch M,Bellm L, Redman R, Kollef MH; VAP OutcomesScientific Advisory Group. Epidemiology and out-comes of ventilator-associated pneumonia in a largeUS database. Chest 2002;122:2115–2121.
29. Crossley KB, Thurn JR. Nursing home-acquiredpneumonia. Semin Respir Infect 1989;4:64–72.
30. Russell SL, Boylan RJ, Kaslick RS, ScannapiecoFA, Katz RV. Respiratory pathogen colonization ofthe dental plaque of institutionalized elders. SpecCare Dent 1999;19:128–134.
31. Scannapieco FA, Wang B, Shiau HJ. Oral bacteriaand respiratory infection: effects on respiratorypathogen adhesion and epithelial cell proinflam-matory cytokine production. Ann Periodontol 2001;6:78–86.
32. Estes RJ, Meduri GU. The pathogenesis of venti-lator-associated pneumonia: Mechanisms of bacte-rial translocation and airway inoculation. IntensiveCare Med 1995;21:365–383.
33. Munro CL, Grap MJ, Elswick RK Jr, McKinney J,Sessler CN, Hummel RS 3rd. Oral health status anddevelopment of ventilator-associated pneumonia: adescriptive study. Am J Crit Care 2006;15:453–460.
34. Garcia R. A review of the possible role of oral anddental colonization on the occurrence of health care-associated pneumonia: underappreciated risk and acall for interventions. Am J Infect Control 2005;33:527–541.
35. Langmore SE, Terpenning MS, Schork A, Chen Y,Murray JT, Lopatin D, Loesche WJ. Predictors ofaspiration pneumonia: how important is dyspha-gia? Dysphagia 1998;13:69–81.
36. Terpenning MS, Taylor GW, Lopatin DE, Kerr CK,Dominguez BL, Loesche WJ. Aspiration pneumo-nia: dental and oral risk factors in an older veteranpopulation. J Am Geriatr Soc 2001;49:557–563.
37. Quagliarello V, Ginter S, Han L, Van Ness P, AlloreH, Tinetti M. Modifiable risk factors for nursinghome-acquired pneumonia. Clin Infect Dis 2005;40:1–6.
38. Scannapieco FA, Bush RB, Paju S. Associations be-tween periodontal disease and risk for nosocomialbacterial pneumonia and chronic obstructive pul-monary disease. A systematic review. Ann Perio -dontol 2003;8:54–69.
39. Azarpazhooh A, Leake JL. Systematic review of theassociation between respiratory diseases and oralhealth. J Periodontol 2006;77:1465–1482.
40. Chan EY, Ruest A, Meade MO, Cook DJ. Oral de-contamination for prevention of pneumonia in me-chanically ventilated adults: systematic review andmeta-analysis. BMJ 2007;334:889.
41. Terpenning M, Bretz W, Lopatin D, Langmore S,Dominguez B, Loesche W. Bacterial colonizationof saliva and plaque in the elderly. Clin Infect Dis1993;16:314–316.
42. Mojon P, Budtz-Jørgensen E, Michel JP, LimebackH. Oral health and history of respiratory tract in-fection in frail institutionalised elders. Gerodon-tology 1997;14:9–16.
43. Rams TE, Babalola OO, Slots J. Subgingival oc-curence of enteric rods, yeasts and staphylococci af-ter systemic doxycycline therapy. Oral MicrobiolImmunol 1990;5:166–168.
44. Slots J, Rams TE, Listgarten MA. Yeasts, entericrods and psuedomonads in the subgingival flora ofsevere adult periodontitis. Oral Microbiol Immunol1988;3:47–52.
45. El-Solh AA, Pietrantoni C, Bhat A, Okada M, Zam-bon J, Aquilina A, Berbary E. Colonization of den-tal plaques: a reservoir of respiratory pathogens forhospital-acquired pneumonia in institutionalizedelders. Chest 2004;126:1575–1582.
46. Heo SM, Haase EM, Lesse AJ, Gill SR, Scanna-pieco FA. Genetic relationships between respiratorypathogens isolated from dental plaque and bron-choalveolar lavage fluid from patients in the inten-sive care unit undergoing mechanical ventilation.Clin Infect Dis 2008;47:1562–1570.
47. DeRiso AJ 2nd, Ladowski JS, Dillon TA, JusticeJW, Peterson AC. Chlorhexidine gluconate 0.12%oral rinse reduces the incidence of total nosocomialrespiratory infection and nonprophylactic systemicantibiotic use in patients undergoing heart surgery.Chest 1996;109:1556–1561.
48. Genuit T, Bochicchio G, Napolitano LM, McCarterRJ, Roghman MC. Prophylactic chlorhexidine oralrinse decreases ventilator-associated pneumonia insurgical ICU patients. Surg Infect 2001;2:5–18.
49. Fourrier F, Cau-Pottier E, Boutigny H, Roussel-Delvallez M, Jourdain M, Chopin C. Effects of den- tal plaque antiseptic decontamination on bacterialcolonization and nosocomial infections in criticallyill patients. Intensive Care Med 2000;26:1239–1247.
CHAPTER 10 Oral Health and Diseases of the Respiratory Tract 159

50. Koeman M, van der Ven AJ, Hak E, Joore HC,Kaasjager K, de Smet AG, Ramsay G, DormansTP, Aarts LP, de Bel EE, Hustinx WN, van derTweel I, Hoepelman AM, Bonten MJ. Oral decon-tamination with chlorhexidine reduces the inci-dence of ventilator-associated pneumonia. Am JRespir Crit Care Med 2006;173:1348–1355.
51. Grap MJ, Munro CL, Elswick RK Jr, Sessler CN,Ward KR. Duration of action of a single, early oralapplication of chlorhexidine on oral microbial florain mechanically ventilated patients: a pilot study.Heart Lung 2004;33:83–91.
52. Fourrier F, Dubois D, Pronnier P, Herbecq P, LeroyO, Desmettre T, Pottier-Cau E, Boutigny H,Di Pompéo C, Durocher A, Roussel-Delvallez M;PIRAD Study Group. Effect of gingival and dentalplaque antiseptic decontamination on nosocomialinfections acquired in the intensive care unit: a double-blind placebo-controlled multicenter study.Crit Care Med 2005;33:1728–1735.
53. Houston S, Hougland P, Anderson JJ, LaRocco M,Kennedy V, Gentry LO. Effectiveness of 0.12%chlorhexidine gluconate oral rinse in reducingprevalence of nosocomial pneumonia in patients un-der going heart surgery. Am J Crit Care 2002;11:567–570.
54. Pugin J, Auckenthaler R, Lew DP, Suter PM.Oropharyngeal decontamination decreases inci-dence of ventilator-associated pneumonia. A ran-domized, placebo-controlled, double-blind clinicaltrial. JAMA 1991;265:2704–2710.
55. Bergmans DC, Bonten MJ, Gaillard CA, PalingJC, van Der Geest S, van Tiel FH, Beysens AJ, deLeeuw PW, Stobberingh EE. Prevention of venti-lator-associated pneumonia by oral decontamina-tion. A prospective, randomized, double-blind,placebo-controlled study. Am J Respir Crit CareMed 2001;164:382–388.
56. Mori H, Hirasawa H, Oda S, Shiga H, Matsuda K,Nakamura M. Oral care reduces incidence of ven-tilator-associated pneumonia in ICU populations.Intensive Care Med 2006;32:230–236.
57. Yoshida M, Yoneyama T, Akagawa Y. [Oral care re-duces pneumonia of elderly patients in nursinghomes, irrespective of dentate or edentate sta-tus].[Article in Japanese]. Nippon Ronen IgakkaiZasshi 2001;38:481–483.
58. Yoneyama T, Yoshida M, Matsui T, Sasaki H. Oralcare and pneumonia. Oral Care Working Group.Lancet 1999;354:515.
59. Yoneyama T, Yoshida M, Ohrui T, Mukaiyama H,Okamoto H, Hoshiba K, Ihara S, Yanagisawa S, Ariumi S, Morita T, Mizuno Y, Ohsawa T, Aka-gawa Y, Hashimoto K, Sasaki H; Oral Care Work-ing Group. Oral care reduces pneumonia in older
patients in nursing homes. J Am Geriatr Soc 2002;50:430–433.
60. Yoneyama T, Hashimoto K, Fukuda H, Ishida M,Arai H, Sekizawa K, Yamaya M, Sasaki H. Oral hy-giene reduces respiratory infections in elderly bed-bound nursing home patients. Arch Gerontol Geri-atr 1996;22:11–19.
61. Adachi M, Ishihara K, Abe S, Okuda K, IshikawaT. Effect of professional oral health care on theelderly living in nursing homes. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2002;94:191–195.
62. Molloy J, Wolff LF, Lopez-Guzman A, Hodges JS.The association of periodontal disease parameterswith systemic medical conditions and tobacco use.J Clin Periodontol 2004;31:625–632.
63. Binkley C, Furr LA, Carrico R, McCurren C. Sur-vey of oral care practices in US intensive care units.Am J Infect Control 2004;32:161–169.
64. Grap MJ, Munro CL, Ashtiani B, Bryant S. Oralcare interventions in critical care: frequency anddocumentation. Am J Crit Care 2003;12:113–118.
65. Ingram RH. Chronic bronchitis, emphysema, andairways obstruction. In: Isselbacher KJ, BraunwaldE, Wilson JD, Martin JB, Fauci AS, Kasper DL,eds. Harrison’s Principles of Internal Medicine.McGraw-Hill: New York 1994:1197–1206.
66. Society AT. Standards for the diagnosis and care ofpatients with chronic obstructive pulmonary dis-ease. Am J Respir Crit Care Med 1995;152:S77–S121.
67. Renwick DS, Connolly MJ. Prevalence and treat-ment of chronic airways obstruction in adults overthe age of 45. Thorax 1996;51:164–168.
68. Sandford AJ, Weir TD, Paré PD. Genetic risk fac-tors for chronic obstructive pulmonary disease. EurRespir J 1997;10:1380–1391.
69. Halbert RJ, Natoli JL, Gano A, Badamgarav E,Buist AS, Mannino DM. Global burden of COPD:systematic review and meta-analysis. Eur Respir J2006;28:523–532.
70. Skrepnek GH, Skrepnek SV. Epidemiology, clini-cal and economic burden, and natural history ofchronic obstructive pulmonary disease and asthma.Am J Manag Care 2004;10 (Suppl):S129–S138.
71. Miller JD, Foster T, Boulanger L, Chace M, RussellMW, Marton JP, Manzin J. Direct costs of COPDin the U.S.: an analysis of Medical ExpenditurePanel Survey (MEPS) data. COPD 2005;2:311–318.
72. Wilson L, Devine EB, So K. Direct medical costsof chronic obstructive pulmonary disease: chronicbronchitis and emphysema. Respir Med 2000;94:204–213.
73. Fujita M, Nakanishi Y. The pathogenesis of COPD:
160 Periodontal Disease and Overall Health: A Clinician's Guide

lessons learned from in vivo animal models. MedSci Monit 2007;13:RA19–24.
74. Churg A, Wang R, Wang X, Onnervik PO, Thim K,Wright JL. Effect of an MMP-9/MMP-12 inhibitoron smoke-induced emphysema and airway remod-el ing in guinea pigs. Thorax 2007;62:706–713.
75. Silverman EK. Genetics of chronic obstructive pul-monary disease. Novartis Found Symp 2001;234:45–58.
76. Molfino NA. Current thinking on genetics ofchronic obstructive pulmonary disease. Curr OpinPulm Med 2007;13:107–113.
77. Snider GL. Two decades of research in the patho-genesis of emphysema. Schweiz Med Wochenschr1984;114:898–906.
78. Demeo DL, Sandhaus RA, Barker AF, Brantly ML,Eden E, McElvaney NG, Rennard S, Burchard E,Stocks JM, Stoller JK, Strange C, Turino GM,Campbell EJ, Silverman EK. Determinants of air-flow obstruction in severe alpha 1-antitrypsin defi-ciency. Thorax 2007;62:706–713.
79. Sethi S, Evans N, Grant BJ, Murphy TF. Newstrains of bacteria and exacerbations of chronic ob-structive pulmonary disease. N Engl J Med 2002;347:465–471.
80. Sethi S, Murphy TF. Acute exacerbations of chronicbronchitis: new developments concerning microbi-ology and pathophysiology—impact on approachesto risk stratification and therapy. Infect Dis ClinNorth Am 2004;18:861–882.
81. Papi A, Bellettato CM, Braccioni F, Romagnoli M,Casolari P, Caramori G, Fabbri LM, Johnston SL.Infections and airway inflammation in chronic ob-
structive pulmonary disease severe exacerbations.Am J Respir Crit Care Med 2006;173:1114–1121.
82. Puhan MA, Vollenweider D, Latshang T, Steurer J,Steurer-Stey C. Exacerbations of chronic obstruc-tive pulmonary disease: when are antibiotics indi-cated? A systematic review. Respir Res 2007;8:30.
83. Scannapieco FA, Papandonatos GD, Dunford RG.Associations between oral conditions and respira-tory disease in a national sample survey population.Ann Periodontol 1998;3:251–256.
84. Hayes C, Sparrow D, Cohen M, Vokonas PS, Gar-cia RI. The association between alveolar bone lossand pulmonary function: the VA Dental Longitudi-nal Study. Ann Periodontol 1998;3:257–261.
85. Scannapieco FA, Ho AW. Potential associationsbetween chronic respiratory disease and periodon-tal disease: analysis of National Health and Nutri-tion Examination Survey III. J Periodontol 2001;72:50–56.
86. Didilescu AC, Skaug N, Marica C, Didilescu C.Respiratory pathogens in dental plaque of hospi-talized patients with chronic lung diseases. ClinOral Investig 2005;9:141–147.
87. Katancik JA, Kritchevsky S, Weyant RJ, Corby P,Bretz W, Crapo RO, Jensen R, Waterer G, RubinSM, Newman AB. Periodontitis and airway obstruction. J Periodontol 2005;76(Suppl):2161–2167.
88. Leuckfeld I, Obregon-Whittle MV, Lund MB,Geiran O, Bjørtuft Ø, Olsen I. Severe chronic ob-structive pulmonary disease: association with mar-ginal bone loss in periodontitis. Respir Med 2008;102:488–494.
CHAPTER 10 Oral Health and Diseases of the Respiratory Tract 161
162 Periodontal Disease and Overall Health: A Clinician's Guide
INTRODUCTIONBone as a tissue represents a highly dy-
namic biologic system that comprises a se-ries of tightly regulated and synergistic ana-bolic and catabolic events that lead to propermetabolic and skeletal structural homeo -stasis. Multiple factors may negatively in-fluence these processes, leading to reducedbone mass, decreased density, altered micro-architecture, and increased bone fragility.The term “osteoporosis” has been collec-tively used to refer to conditions in which theability of the skeletal tissue to respond andadapt to environmental and physiologicalchallenges is compromised. Due to the above-mentioned factors, microdamage accu mu -lation and increased fracture susceptibilitycan occur. Within this context, numerous pro-inflammatory cytokines have been identi-fied as important determinants of bone loss.1-7
A significantly increased production of pro-inflammatory cytokines occurs in conditionssuch as periodontitis, a disease initiated bybacterial plaque biofilms. Understanding theimpact of osteoporosis on host susceptibilityto periodontal breakdown is a developingarea.8-11 This chapter will review and eval -uate the available literature regarding the as-sociation between these two complex multi-factorial conditions, their effect on diseaseextent and severity, and the coexisting mech-anisms by which they may affect overallbone structural integrity and homeostasis.
OSTEOPOROSIS ANDBONE REMODELING
Bone is a highly dynamic tissue that hasthe capacity to adapt based on physiological
needs. Hence, bone adjusts its biologic prop-erties according to metabolic and mechanicalrequirements.12-14 The skeletal adaptation mech- anism is primarily executed by processes ofbone resorption and bone formation, and re-ferred to collectively as “bone remodeling”(Figure 1). Bone is resorbed by osteoclasts,after which new bone is deposited by osteo -blastic cells.15 From the perspective of boneremodeling, it has been proposed that osteo-clasts recognize and target skeletal sites ofcompromised mechanical integrity, therebyinitiating the bone remodeling process forthe purpose of generating new bone that ismechanically competent.16
The remodeling process takes place inbone multicellular units (BMUs; Figure 2).A BMU comprises: 1) a front of osteoclastsresiding on a surface of newly resorbed bonereferred to as the “resorption front;” 2) acompartment containing vessels and peri-cytes; and 3) a layer of osteoblasts present ona newly formed organic matrix known as the“deposition front.” In Figure 2, the resorptionfront is clearly visualized by the cells stainedfor tartrate-resistant acid phosphatase. Thenumber of new and active BMUs is regu-lated by a variety of hormones and cytokines,which dictates the spaciotemporal synchro-nization and coupling of anabolic and cata-bolic remodeling events.
One of the best-studied remodeling cou-pling mechanisms is the receptor activatorfor nuclear factor B ligand (RANKL)- mediated activation of osteoclasts (Figure3). RANKL is a cytokine produced by osteo -blasts and other cells (e.g., lymphocytes); itresides on the surface of osteoblast-like cells.
CHAPTER 11Periodontal Disease andOsteoporosis
Hector F. Rios, William V. Giannobile
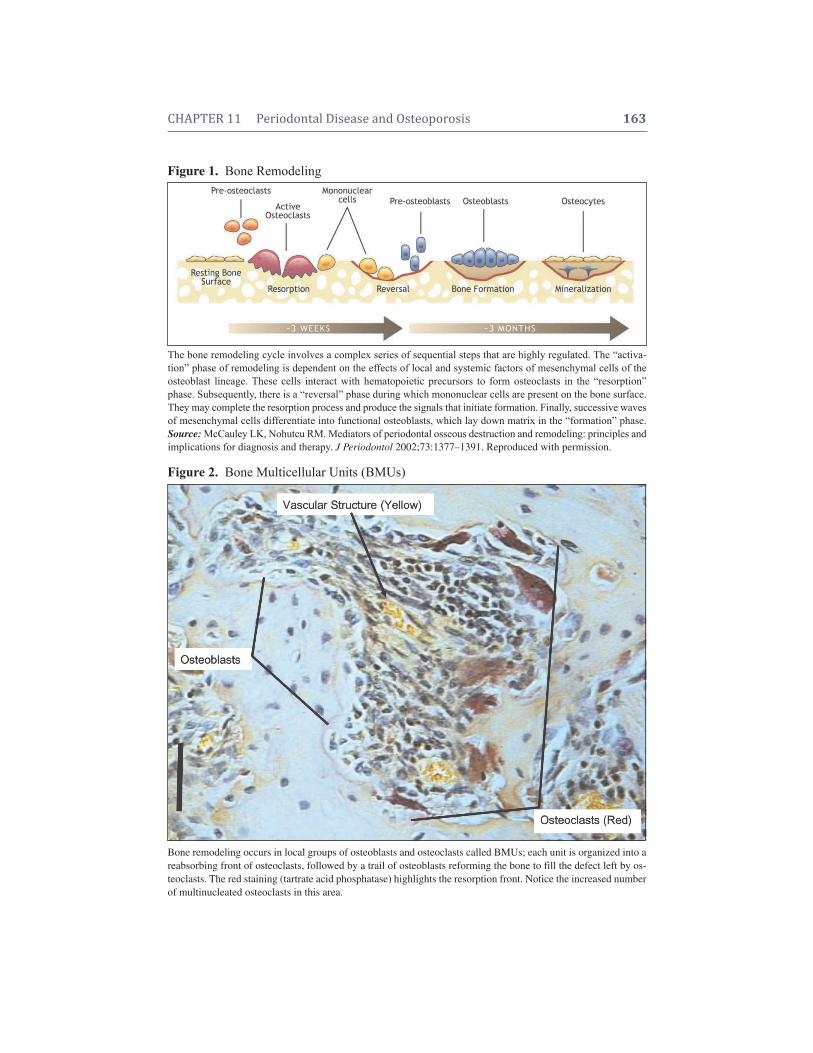
CHAPTER 11 Periodontal Disease and Osteoporosis 163
Figure 1. Bone Remodeling
The bone remodeling cycle involves a complex series of sequential steps that are highly regulated. The “activa-tion” phase of remodeling is dependent on the effects of local and systemic factors of mesenchymal cells of theosteoblast lineage. These cells interact with hematopoietic precursors to form osteoclasts in the “resorption”phase. Subsequently, there is a “reversal” phase during which mononuclear cells are present on the bone surface.They may complete the resorption process and produce the signals that initiate formation. Finally, successive wavesof mesenchymal cells differentiate into functional osteoblasts, which lay down matrix in the “formation” phase.Source: McCauley LK, Nohutcu RM. Mediators of periodontal osseous destruction and remodeling: principles andimplications for diagnosis and therapy. J Periodontol 2002;73:1377–1391. Reproduced with permission.
Figure 2. Bone Multicellular Units (BMUs)
Bone remodeling occurs in local groups of osteoblasts and osteoclasts called BMUs; each unit is organized into areabsorbing front of osteoclasts, followed by a trail of osteoblasts reforming the bone to fill the defect left by os-teoclasts. The red staining (tartrate acid phosphatase) highlights the resorption front. Notice the increased numberof multinucleated osteoclasts in this area.
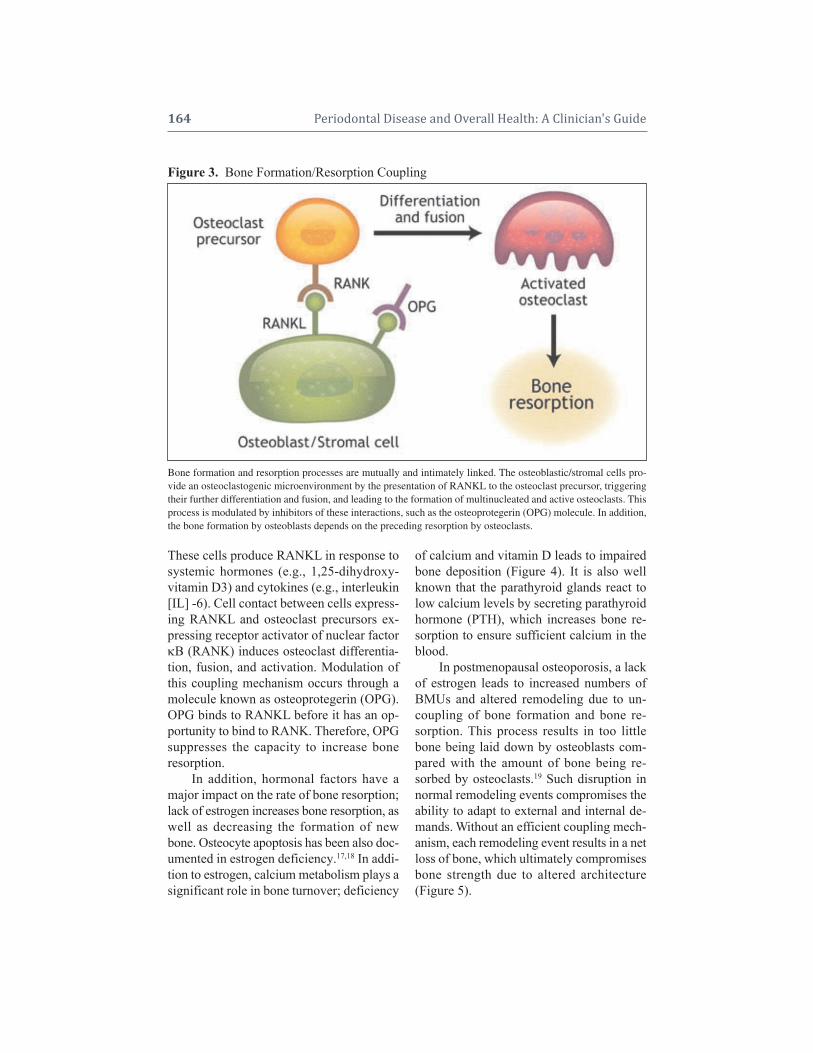
164 Periodontal Disease and Overall Health: A Clinician's Guide
These cells produce RANKL in response tosystemic hormones (e.g., 1,25-dihydroxy -vitamin D3) and cytokines (e.g., interleukin[IL] -6). Cell contact between cells express-ing RANKL and osteoclast precursors ex-pressing receptor activator of nuclear factorB (RANK) induces osteoclast differentia-tion, fusion, and activation. Modulation ofthis coupling mechanism occurs through amolecule known as osteoprotegerin (OPG).OPG binds to RANKL before it has an op-portunity to bind to RANK. Therefore, OPGsuppresses the capacity to increase bone resorption.
In addition, hormonal factors have a major impact on the rate of bone resorption;lack of estrogen increases bone resorption, aswell as decreasing the formation of newbone. Osteocyte apoptosis has been also doc-umented in estrogen deficiency.17,18 In addi-tion to estrogen, calcium metabolism plays asignificant role in bone turnover; deficiency
of calcium and vitamin D leads to impairedbone deposition (Figure 4). It is also wellknown that the parathyroid glands react tolow calcium levels by secreting parathyroidhormone (PTH), which increases bone re-sorption to ensure sufficient calcium in theblood.
In postmenopausal osteoporosis, a lackof estrogen leads to increased numbers ofBMUs and altered remodeling due to un-coupling of bone formation and bone re-sorption. This process results in too littlebone being laid down by osteoblasts com-pared with the amount of bone being re-sorbed by osteoclasts.19 Such disruption innormal remodeling events compromises theability to adapt to external and internal de-mands. Without an efficient coupling mech-anism, each remodeling event results in a netloss of bone, which ultimately compromisesbone strength due to altered architecture(Figure 5).
Figure 3. Bone Formation/Resorption Coupling
Bone formation and resorption processes are mutually and intimately linked. The osteoblastic/stromal cells pro-vide an osteoclastogenic microenvironment by the presentation of RANKL to the osteoclast precursor, triggeringtheir further differentiation and fusion, and leading to the formation of multinucleated and active osteoclasts. Thisprocess is modulated by inhibitors of these interactions, such as the osteoprotegerin (OPG) molecule. In addition,the bone formation by osteoblasts depends on the preceding resorption by osteoclasts.
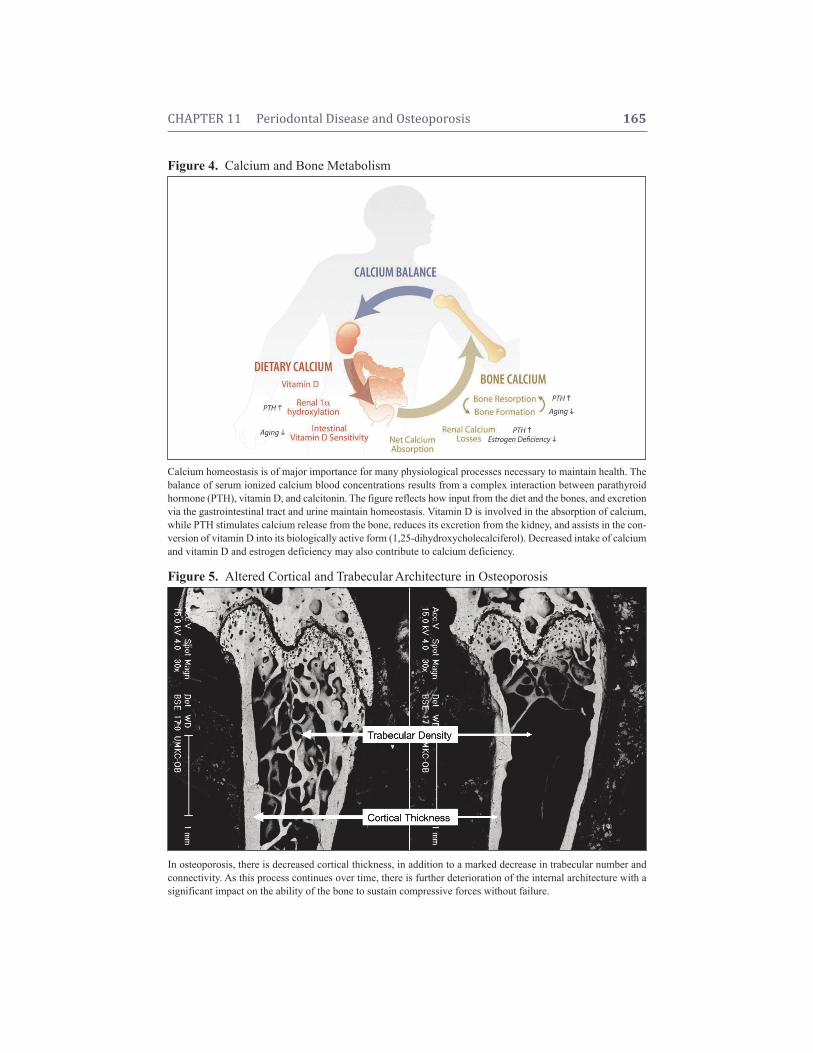
CHAPTER 11 Periodontal Disease and Osteoporosis 165
Figure 4. Calcium and Bone Metabolism
Calcium homeostasis is of major importance for many physiological processes necessary to maintain health. Thebalance of serum ionized calcium blood concentrations results from a complex interaction between parathyroid hormone (PTH), vitamin D, and calcitonin. The figure reflects how input from the diet and the bones, and excretionvia the gastrointestinal tract and urine maintain homeostasis. Vitamin D is involved in the absorption of calcium,while PTH stimulates calcium release from the bone, reduces its excretion from the kidney, and assists in the con-version of vitamin D into its biologically active form (1,25-dihydroxycholecalciferol). Decreased intake of calciumand vitamin D and estrogen deficiency may also contribute to calcium deficiency.
Figure 5. Altered Cortical and Trabecular Architecture in Osteoporosis
In osteoporosis, there is decreased cortical thickness, in addition to a marked decrease in trabecular number andconnectivity. As this process continues over time, there is further deterioration of the internal architecture with asignificant impact on the ability of the bone to sustain compressive forces without failure.

166 Periodontal Disease and Overall Health: A Clinician's Guide
The affected skeletal integrity in osteo-porosis is characterized by cortical and tra-becular thinning, as well as through the lossof trabecular connectivity. In addition, thenumber of osteons per unit volume of bonedecreases, offering less resistance to bone-crack initiation. The diminished bone qual-ity in osteoporosis is also reflected by a de-crease in cell density. The decreased osteo-cytic density in interstitial bone degrades theability to detect damage. If bone formation islessened in the BMU due to decreased num-bers of osteoblasts, then impaired synthesisof osteocytes may contribute to the deficit inthis cell type, which is considered the or-chestrator of bone remodeling. Reduced periosteal bone formation in adulthood con-tributes to skeletal fragility because endo-cortical resorption is not compensated for,creating failure to offset cortical thinningand failure to shift the cortical bone outwardfrom the neutral axis—a change that in-creases resistance to bending.
In summary, the interaction of geneticand environmental factors on bone loss un-derlies the development of fragile bone tis-sue, decreasing the inherent capacity of theskeleton to adapt and respond adequately tostructural needs.
OSTEOPOROSIS ANDBONE MINERAL DENSITY
Osteoporosis severely compromisesskeletal integrity. However, fractures tendto occur late in the disease process. Today, itis generally accepted that bone mineral density (BMD) measurement is the mostvaluable parameter to identify patients whoare more susceptible to, or at greater riskfor, fractures. The widespread availabilityand popularity of bone densitometry has ledto a widely accepted definition proposedby the World Health Organization (WHO)in 1994, based on BMD measurements in standard deviation units called “T-scores”(Figure 6).20
Figure 6. Bone Mineral Density (BMD)
Dual-energy x-ray absorptiometry (DEXA), is considered the preferred technique for measurement of BMD. Thesites most often used for DEXA measurement of BMD are the spine, femoral neck, and forearm. The World HealthOrganization defines osteoporosis based on “T-scores.” T-scores refer to the number of standard deviations aboveor below the mean for a healthy 30-year-old adult of the same sex as the patient.
Young adult standard deviationMeasured BMD – young adult mean BMDT-Score

CHAPTER 11 Periodontal Disease and Osteoporosis 167
Type I osteoporosis (postmenopausalosteoporosis) generally develops in womenafter menopause when the amount of estro-gen in the body greatly decreases. Thisprocess leads to an increase in the resorptionof bone (the bones lose substance). Type Iosteoporosis occurs in 5% to 20% of women,most often between the ages of 50 and 75, because of the sudden postmenopausal de-crease in estrogen levels, which results in arapid depletion of calcium from the skeleton.It is associated with fractures that occurwhen the vertebrae compress together, caus-ing a collapse of the spine, and with fracturesof the hip, wrist, or forearm caused by fallsor minor accidents. Type I accounts for thesignificantly greater risk of osteoporosis inwomen versus men.
Type II osteoporosis (senile osteoporo-sis) typically happens after the age of 70 andaffects women twice as frequently as men.Type II osteoporosis results when the processof resorption and formation of bone are nolonger coordinated, and bone breakdownovercomes bone building. This occurs withage in everyone to some degree. Type II af-fects trabecular and cortical bone, often re-sulting in fractures of the femoral neck, ver-tebrae, proximal humerus, proximal tibia,and pelvis. It may result from age-relatedreduction in vitamin D synthesis or resist-ance to vitamin D activity (possibly medi-ated by decreased or unresponsive vitamin Dreceptors in some patients). In older women,Types I and II often occur together.
Secondary OsteoporosisSecondary osteoporosis is caused by other
conditions, such as hormonal imbalances, cer-tain diseases, or medications (such as corti-co steroids). Secondary osteoporosis accountsfor < 5% of osteoporosis cases. Causes includeendocrine disease (e.g., glucocorticoid excess,hyperparathyroidism, hyper thyroidism, hy-pogonadism, hyperprolacti nemia, diabetesmellitus), drugs (e.g., glucocorticosteroids,
Essentially, the T-score indicates the dif-ference between an individual’s BMD andnormal BMD. As illustrated in Figure 6,WHO defines four main levels of osteo-porosis risk assessment based on t-scores:
• Normal bone mineral density is foundwhen the T-score is –1
• Osteopenia refers to a low BMDT-score between –1.0 and –2.5
• Osteoporosis is diagnosed if the indi-vidual has a T-score –2.5
• Established osteoporosis refers tothose individuals with one or morefragility fractures in addition to aT-score –2.5
Types of OsteoporosisThe clinical presentation of osteoporosis
includes several characteristics that facilitatethe diagnosis. However, the primary etiol-ogy that leads to the appearance of the con-dition may vary considerably. The ability torecognize and classify etiologic differencesamong conditions that may appear clinicallysimilar will impact the ability to successfullytreat these patients. Primary osteoporosis issimply the form seen in older individuals andwomen past menopause in which bone loss isaccelerated over that predicted for age andsex. Secondary osteoporosis results from avariety of identifiable conditions.
Primary OsteoporosisThere are two forms of primary osteo-
porosis: Type I and Type II. The determiningfactor for the actual existence of osteoporo-sis, whether Type I or Type II, is the amountof calcium remaining in the skeleton andwhether it places a person at risk of frac-ture. Someone who has exceptionally densebones to begin with will probably never loseenough calcium to reach the point at whichosteoporosis occurs, whereas a person whohas low bone density could easily developosteoporosis despite losing only a relativelysmall amount of calcium.

168 Periodontal Disease and Overall Health: A Clinician's Guide
and is associated with systemic overproduc-tion of pro-inflammatory mediators, such ascytokines, nitric oxide, and prostaglandins. Inpatients with perio dontal disease and con-comitant postmeno pausal osteoporosis, thepossibility exists that the lack of estrogen in-fluences the activities of bone cells and im-mune cells in such a way that the progressionof alveolar bone loss will be enhanced.
ALVEOLAR BMDVS. SKELETAL BMD
Systemic factors can lead to loss ofBMD throughout the body, including boneloss in the maxilla and the mandible. Theresulting local reduction of BMD in the jawbones could set the stage for more rapid lossof alveolar crestal height because a compa-rable challenge of bacteria-derived bone- resorbing factors could be expected to re-sult in greater alveolar bone destruction thanin an individual with normal bone mass. Inaddition, there are systemic risk factors, suchas smoking, diabetes, diet, and hormone lev-els that affect systemic bone levels that mayalso affect periodontitis.
Oral bone loss has been shown to be as-sociated with osteoporosis and low skeletalBMD. In their search for oral radiographicchanges associated with osteoporosis, mostinvestigators have focused on measures ofjaw bone mass or morphology. The com-monly used assessment of oral bone includesradiographic measures of loss of alveolarcrestal height, measures of resorption of theresidual ridge after tooth loss, and assess-ment of oral BMD. Tools used to measurebone mass include single and dual photonabsorptiometry, dual-energy x-ray absorp-tiometry (DEXA) quantitative computed tomography, and film densitometry.
Mandibular mineral content is reducedin subjects with osteoporotic fractures.21
Further, the BMD of buccal (but not tra becular) mandibular bone correlateswith osteo porosis (low skeletal BMD).22,23
ethanol, dilantin, tobacco, barbiturates, heparin), and other conditions (e.g., immo-bilization, chronic renal failure, liver dis-ease, malabsorption syndromes, chronic ob-structive lung disease, rheumatoid arthritis,sarcoidosis, malignancy, and prolongedweightlessness as found in space flight).
OSTEOPOROSISAND INFLAMMATION
Emerging clinical and molecular evi-dence suggests that inflammation also exertssignificant influence on bone turnover, in-ducing osteoporosis. Numerous pro- inflam -matory cytokines have been implicated in theregulation of osteoblasts and osteoclasts, anda shift toward an activated immune profilehas been hypothesized as an important riskfactor.1 Chronic inflammation and the im-mune system remodeling characteristic of ag-ing, as well as of other pathological conditionscommonly associated with osteoporosis, maybe determinant pathogenetic factors.6
The cellular and molecular pathogeneticmechanisms in inflammation-induced os-teolysis and sclerosis have been explored bydifferent investigators. There is certainlysubstantial evidence that bone remodelingis a tightly regulated, finely balanced processinfluenced by subtle changes in pro-inflam-matory and inhibitory cytokines, as well ashormones and cellular components that actprimarily. but not exclusively, through theRANK/RANKL/osteoprotegerin system.Therefore, an acute or chronic imbalance inthe system due to infection or inflammationcould contribute to systemic (or local) boneloss and increase the risk of fracture.15
Generalized osteoporosis and an in-creased risk of fracture are commonly ob-served in chronic inflammatory diseases, suchas rheumatoid arthritis, ankylosing spondyli-tis, and inflammatory bowel disease. Currentevidence suggests that the osteoporosis de - veloped during chronic inflammation may result from the inhibition of bone formation,

CHAPTER 11 Periodontal Disease and Osteoporosis 169
Mandibular density (measured with a DEXAscan) also correlates with skeletal BMD.24
Using film densitometry, most investi-gators have found that the optical density ofthe mandible is decreased in subjects with osteoporosis compared with controls. Further,mandibular radiographic optical density correlates with vertebral BMD in osteo-porotic women,25 control (nonosteoporotic)women,26 and in women with a history ofvertebral fracture.27,28 Reduction in corticaland subcortical alveolar bone density hasalso been reported to correlate with osteo-porosis in longitudinal studies.29-31 As re-ported by Hildebolt in 1997, the preponder-ance of the evidence indicates that the jawsof subjects with osteoporosis show reducedbone mass.32 Table 1 summarizes the avail-able data regarding the relationship betweensystemic and oral bone loss.
ASSOCIATION BETWEEN OSTEOPENIA AND INCREASED
SEVERITY OF ALVEOLARBONE LOSS AND TOOTH LOSSIt is hypothesized that periodontitis re-
sults from bacteria that produce factors thatcause loss of collagenous support of the teeth,as well as loss of alveolar bone. Systemic factors can lead to loss of BMD throughoutthe body, including bone loss in the maxillaand mandible. The resulting local reductionof BMD in the jawbone could set the stagefor more rapid marginal bone loss becausea comparable challenge of bacterial bone- resorbing factors could be expected to resultin greater alveolar crestal bone resorption. Inaddition to this finding, there are systemicrisk factors, such as smoking, diabetes, diet,and hormone levels, that affect systemicbone level and may also affect periodontitis.Although periodontal disease has historicallybeen thought to be the result of a local in-fectious process, others have suggested thatperiodontal disease may be an early mani-festation of generalized osteo penia.33
Several potential mechanisms by whichosteoporosis or systemic bone loss may beassociated with periodontal attachment loss,reduction of alveolar bone height or density,and tooth loss have been proposed. One ofthese mechanisms states that low BMD orloss of BMD may lead to more rapid resorp -tion of alveolar bone after insult by perio -dontal bacteria. With less dense oral bone tostart, loss of bone surrounding the teeth mayoccur more rapidly. Another mechanism the-ory proposes that systemic factors affectingbone remodeling may also modify the localtissue response to periodontal infection. Per-sons with generalized bone loss are known tohave increased systemic production of cyto -kines (i.e., IL-1 and IL-6) that may have effects on bone throughout the body, includ-ing the bones of the oral cavity. Periodontal infection has been shown to increase local cytokine production that, in turn, increaseslocal osteoclast activity resulting in increasedbone resorption. A third mechanism wouldbe related to genetic factors that predisposean individual to systemic bone loss, and thatwould also influence or predispose an indi-vidual to periodontal destruction. Also, cer-tain lifestyle factors such as cigarette smok-ing and suboptimal calcium intake, amongothers, may put individuals at risk for de-velopment of both systemic osteo penia andoral bone loss.
THE ROLE OFCALCIUM IN
MODERATINGTHE RELATIONSHIPS
BETWEEN OSTEOPOROSISAND PERIODONTAL DISEASEOsteoporosis and osteopenia may in-
fluence periodontal disease and tooth loss.34
Furthermore, it appears that low dietary cal-cium results in more serious periodontal dis-ease.35 Although many studies suggest thatin elderly men and women, maintenance ofnormal bone mineral density is associated

170 Periodontal Disease and Overall Health: A Clinician's Guide
with improved tooth retention, the evidenceis still inconclusive. Hormone replacementtherapy and calcium and vitamin D supple-ments that are used to prevent or treat osteoporosis appear to have beneficial ef-fects on tooth retention as well.36 Futureprospective studies, including randomizedclinical trials, are needed to confirm thesefindings.
THREE CHALLENGES TO PERIODONTAL INTEGRITY
The integrity of the periodontium in os-teoporotic patients faces multiple coexistingchallenges. Local and systemic factors im-pact the ability of the host to maintain thehomeostasis within these tissues. Hypo -thetically, three different challenges may be influencing the periodontal integrity in
BMD = bone mineral density; CAL = clinical attachment loss.a. Earnshaw SA, Keating N, Hosking DJ, Chilvers CE, Ravn P, McClung M, Wasnich RD. Tooth counts do notpredict bone mineral density in early postmenopausal Caucasian women. EPIC study group. Int J Epidemiol1998;27:479–483.b. Elders PJ, Habets LL, Netelenbos JC, van der Linden LW, van der Stelt PF. The relation between periodontitisand systemic bone mass in women between 46 and 55 years of age. J Clin Periodontol 1992;19:492–496.c. Krall EA, Garcia RI, Dawson-Hughes B. Increased risk of tooth loss is related to bone loss at the whole body,hip, and spine. Calcif Tissue Int 1996;59:433–437.d. Jeffcoat MK, Lewis CE, Reddy MS, Wang CY, Redford M. Post-menopausal bone loss and its relationship tooral bone loss. Periodontol 2000 2000;23:94–102.e. Wactawski-Wende J, Hausmann E, Hovey K, Trevisan M, Grossi S, Genco RJ. The association between osteo-porosis and alveolar crestal height in postmenopausal women. J Periodontol 2005;76(11 Suppl):2116–2124.f. Payne JB, Reinhardt RA, Nummikoski PV, Dunning DG, Patil KD. The association of cigarette smoking withalveolar bone loss in postmenopausal females. J Clin Periodontol 2000;27:658–664.g. Yoshihara A, Seida Y, Hanada N, Miyazaki H. A longitudinal study of the relationship between periodontal diseaseand bone mineral density in community-dwelling older adults. J Clin Periodontol 2004;31:680–684.
Table 1. Studies on the Relationship Between Systemic and Oral Bone LossStudy Type
Studies Oral Systemic Cross-Sectional Longitudinal Correlation
Earnshaw et al.a Tooth Count Lumbar BMD NO
Elders et al.b Bone Height/ Lumbar BMDTooth Count NO
Klemetti et al.23 Bone Height/ Skeletal BMDTooth Count YES
Krall et al.c Tooth Loss Skeletal BMD YES
Jeffcoat et al.d Mandibular BMD Femoral Neck BMD YES
Hildebolt32 CAL Lumbar/ YESFemoral Neck BMD
Kribbs25 CAL Normal NOOsteoporosis
Wactawski-Wende et al.e Bone Height Skeletal BMD YES
von Wowern et al.21 CAL Forearm BMD YES
Payne et al.f Bone Height/ NormalBone Density Osteopenia YES
Osteoporosis
Yoshihara et al.g CAL Normal NOOsteopenia
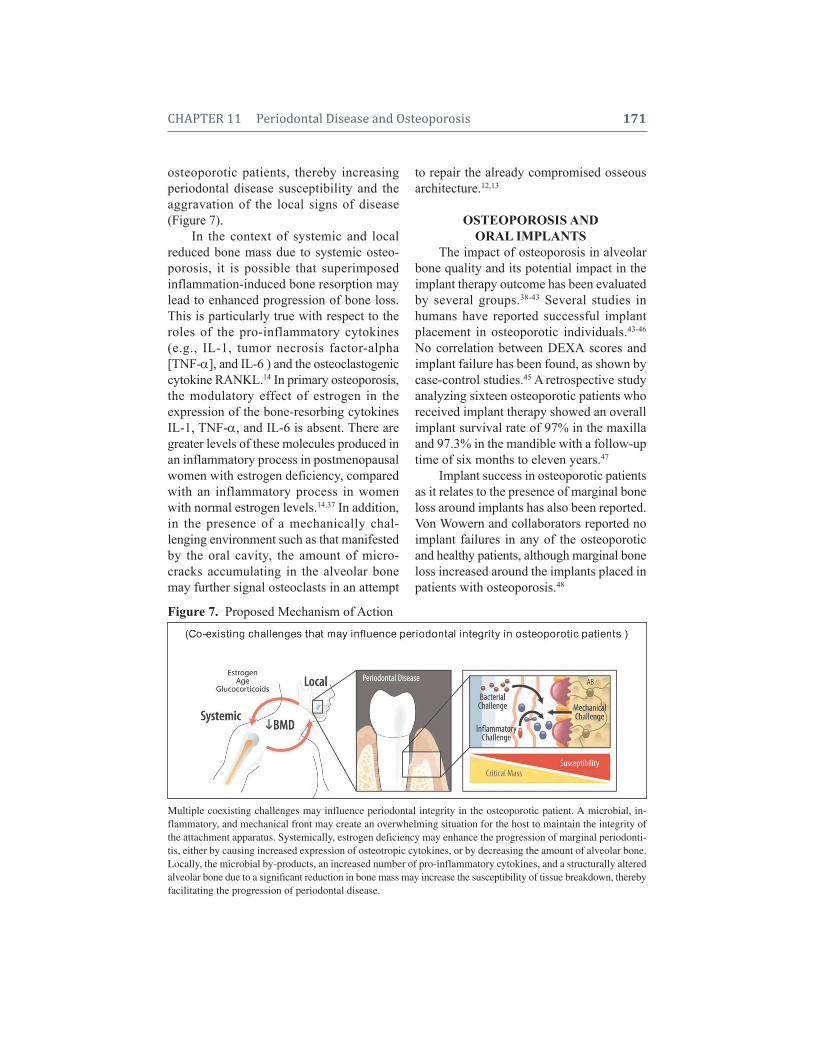
CHAPTER 11 Periodontal Disease and Osteoporosis 171
osteoporotic patients, thereby increasing perio dontal disease susceptibility and the aggravation of the local signs of disease(Figure 7).
In the context of systemic and local reduced bone mass due to systemic osteo-porosis, it is possible that superimposed inflammation-induced bone resorption maylead to enhanced progression of bone loss.This is particularly true with respect to theroles of the pro-inflammatory cytokines(e.g., IL-1, tumor necrosis factor-alpha[TNF-], and IL-6 ) and the osteoclas togeniccytokine RANKL.14 In primary osteoporosis,the modulatory effect of estrogen in the expression of the bone-resorbing cytokinesIL-1, TNF-, and IL-6 is absent. There aregreater levels of these molecules produced inan inflammatory process in postmenopausalwomen with estrogen deficiency, comparedwith an inflammatory process in womenwith normal estrogen levels.14,37 In addition,in the presence of a mechanically chal-lenging environment such as that manifestedby the oral cavity, the amount of micro -cracks accumulating in the alveolar bonemay further signal osteoclasts in an attempt
to repair the already compromised osseousarchitecture.12,13
OSTEOPOROSIS ANDORAL IMPLANTS
The impact of osteoporosis in alveolarbone quality and its potential impact in theimplant therapy outcome has been evaluatedby several groups.38-43 Several studies in humans have reported successful implantplacement in osteoporotic individuals.43-46
No correlation between DEXA scores andimplant failure has been found, as shown bycase-control studies.45 A retrospective studyanalyzing sixteen osteoporotic patients whoreceived implant therapy showed an overallimplant survival rate of 97% in the maxillaand 97.3% in the mandible with a follow-uptime of six months to eleven years.47
Implant success in osteoporotic patientsas it relates to the presence of marginal boneloss around implants has also been reported.Von Wowern and collaborators reported noimplant failures in any of the osteoporoticand healthy patients, although marginal boneloss increased around the implants placed inpatients with osteoporosis.48
Figure 7. Proposed Mechanism of Action
Multiple coexisting challenges may influence periodontal integrity in the osteoporotic patient. A microbial, in-flammatory, and mechanical front may create an overwhelming situation for the host to maintain the integrity ofthe attachment apparatus. Systemically, estrogen deficiency may enhance the progression of marginal periodonti-tis, either by causing increased expression of osteotropic cytokines, or by decreasing the amount of alveolar bone.Locally, the microbial by-products, an increased number of pro-inflammatory cytokines, and a structurally alteredalveolar bone due to a significant reduction in bone mass may increase the susceptibility of tissue breakdown, therebyfacilitating the progression of periodontal disease.
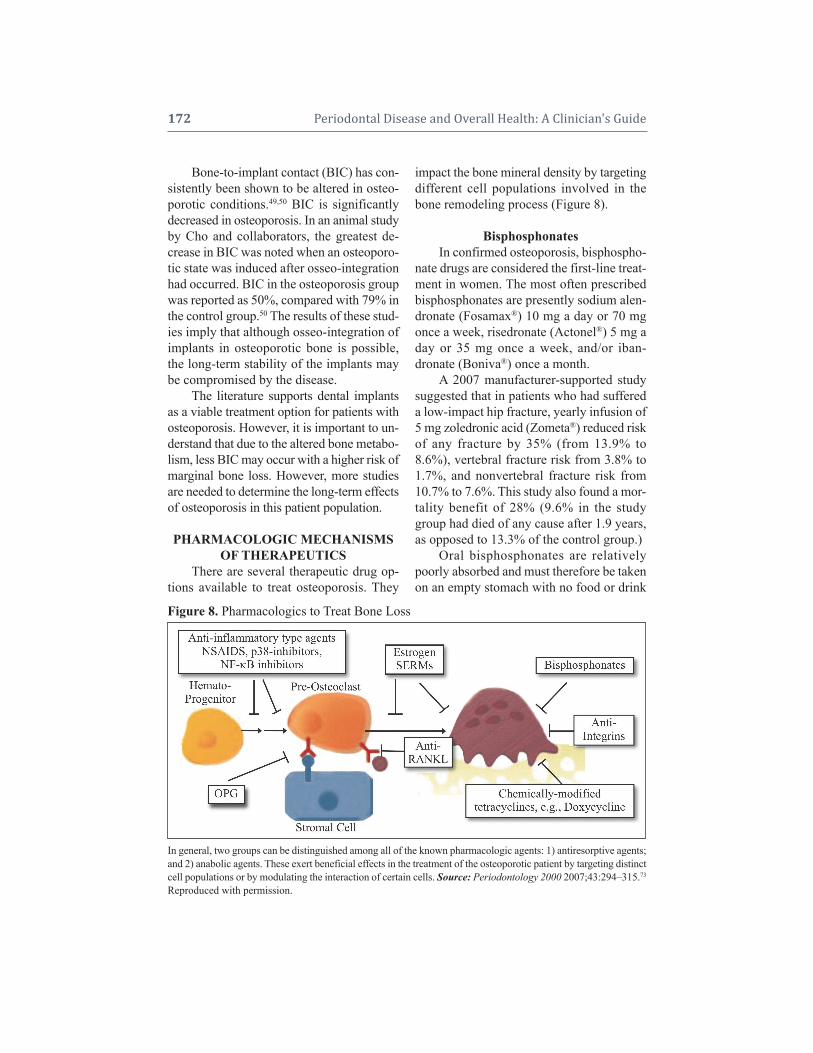
172 Periodontal Disease and Overall Health: A Clinician's Guide
Bone-to-implant contact (BIC) has con-sistently been shown to be altered in osteo-porotic conditions.49,50 BIC is significantlydecreased in osteoporosis. In an animal studyby Cho and collaborators, the greatest de-crease in BIC was noted when an osteoporo -tic state was induced after osseo- integrationhad occurred. BIC in the osteoporosis groupwas reported as 50%, compared with 79% inthe control group.50 The results of these stud-ies imply that although osseo-integration ofimplants in osteoporotic bone is possible,the long-term stability of the implants maybe compromised by the disease.
The literature supports dental implantsas a viable treatment option for patients withosteoporosis. However, it is important to un-derstand that due to the altered bone metabo-lism, less BIC may occur with a higher risk ofmarginal bone loss. However, more studiesare needed to determine the long-term effectsof osteoporosis in this patient population.
PHARMACOLOGIC MECHANISMSOF THERAPEUTICS
There are several therapeutic drug op-tions available to treat osteoporosis. They
impact the bone mineral density by targetingdifferent cell populations involved in thebone remodeling process (Figure 8).
BisphosphonatesIn confirmed osteoporosis, bisphospho-
nate drugs are considered the first-line treat-ment in women. The most often prescribedbisphosphonates are presently sodium alen-dronate (Fosamax®) 10 mg a day or 70 mgonce a week, risedronate (Actonel®) 5 mg aday or 35 mg once a week, and/or iban-dronate (Boniva®) once a month.
A 2007 manufacturer-supported studysuggested that in patients who had suffereda low-impact hip fracture, yearly infusion of5 mg zoledronic acid (Zometa®) reduced riskof any fracture by 35% (from 13.9% to8.6%), vertebral fracture risk from 3.8% to1.7%, and nonvertebral fracture risk from10.7% to 7.6%. This study also found a mor-tality benefit of 28% (9.6% in the studygroup had died of any cause after 1.9 years,as opposed to 13.3% of the control group.)
Oral bisphosphonates are relativelypoorly absorbed and must therefore be takenon an empty stomach with no food or drink
Figure 8. Pharmacologics to Treat Bone Loss
In general, two groups can be distinguished among all of the known pharmacologic agents: 1) antiresorptive agents;and 2) anabolic agents. These exert beneficial effects in the treatment of the osteoporotic patient by targeting distinctcell populations or by modulating the interaction of certain cells. Source: Periodontology 2000 2007;43:294–315.73
Reproduced with permission.

CHAPTER 11 Periodontal Disease and Osteoporosis 173
to follow for the next 30 minutes. They areassociated with esophagitis and are there-fore sometimes poorly tolerated; weekly ormonthly administration (depending on thepreparation) decreases the likelihood ofesophagitis, and is now the standard regi-men. Although intermittent dosing with theintravenous formulations such as zoledronicacid avoids oral tolerance problems, theseagents are implicated at higher rates in a rarebut debilitating oral affliction called osteo -necrosis of the jaw (ONJ). The AmericanSociety of Bone and Mineral Research de-fines ONJ-confirmed lesions as areas of ex-posed bone in the maxillofacial region thathave not healed within 8 weeks after identi-fication by a healthcare provider, in a pa-tient who received bisphosphonate treatmentand was not exposed to radiation therapy inthe craniofacial region.51,52
Based on the review of both publishedand unpublished data, the risk of ONJ asso-ciated with oral bisphosphonate therapy forosteoporosis seems to be low, estimated between 1 in 10,000 patients and < 1 in100,000 patient-treatment years. However,the incidence of ONJ is rapidly evolving andthe true incidence may be higher. The risk ofONJ in patients who have cancer treated withhigh doses of intravenous bisphosphonates isclearly higher, in the range of 1–10 per 100patients (depending on duration of therapy).For this reason, oral bisphosphonate therapyis probably to be preferred, and prescribingadvice now recommends any remedial den-tal work to be carried out prior to com-mencing treatment.
TeriparatidePTH is a potent hormone with catabolic
and anabolic effects in bone. Teriparatide(Forteo®, recombinant human PTH) has beenshown to be effective in osteoporosis man-agement.53,54 It stimulates osteoblasts, thusincreasing their activity. Currently, it is usedmostly for patients with established osteo-
porosis who have particularly low BMD,several risk factors for fracture, or who can-not tolerate oral bisphosphonates. It is givenas a daily injection with the use of a pen-typeinjection device.
The response of the alveolar bone toPTH has been evaluated by several investi-gators.55-57 In an animal study by Miller et al.,PTH significantly increased crestal bone lev-els in the mandibles of ovariectomized rats.56
Furthermore, Barros and collaborators, usinga periodontitis animal model, showed de-creased bone resorption when treating theanimals with PTH.55
PTH is not currently used to treat oralbone loss. However, systemic administrationmay have positive benefits on the oral cavity.
EstrogenEstrogen deficiency in menopause is a
major cause of osteoporosis in women. Itacts to maintain bone mass and its with-drawal leads to accelerated bone resorption.Estrogen protects bone by inducing a para -crine signal originating in osteoblasts andleading to the death of pre-osteoclasts.58 Thisestablishes an appropriate ratio between bone-forming osteoblasts and bone-resorbing osteoclasts, in part through the induction of osteoclast apoptosis.
Estrogen replacement therapy remains agood treatment option for the prevention ofosteoporosis, and is being studied as a wayof preventing oral bone loss. Hormone re-placement therapy, along with calcium andvitamin D supplements, appears to have ben-eficial effects on tooth retention.59
In a cohort of 488 elderly women, Kralland collaborators found an association betweenpostmenopausal hormone replacement ther-apy (HRT) and tooth retention. There was alsoan association between duration of HRT andtooth retention, with the odds of being edentu-lous reduced by 6% for each year of HRT ther-apy. This study suggests that postmenopausalHRT reduces the risk of edentulism.60

174 Periodontal Disease and Overall Health: A Clinician's Guide
Selective Estrogen Receptor ModulatorsSelective estrogen receptor modulators
(SERMs) selectively bind to estrogen re-ceptors and inhibit bone resorption andturnover. This is possible because they lackthe steroid structure of estrogens, but possessa tertiary structure that allows them to bindto the estrogen receptor.61
Unlike estrogens, which are uniformlyagonists, the SERMs exert selective agonist orantagonist effects on various estrogen target tissues. The mechanism of mixed agonism/antagonism may differ depending on thechemical structure of the SERM, but in gen-eral, it appears to be related to the ratio ofcoactivator to corepressor proteins in differ-ent cell types and the conformation of the estrogen receptor induced by drug binding,which in turn determines how strongly thedrug/receptor complex recruits coactivatorsrelative to corepressors.
Clinically, the benefits of SERMs therapy on bone are well-established. In postmenopausal women with osteoporosis,SERMs treatment decreases markers of boneturnover by 30–40% after one year, and in-creases bone density 2–3 % after three years.It also decreased the incidence of vertebralfractures by 30–50%.62-65
Although control studies evaluating oralbone loss are needed, SERMs appear to haveexcellent therapeutic potential for minimiz-ing the local and systemic consequences ofpostmenopausal osteoporosis.
Strontium RanelateOral strontium ranelate (Protelos®) be-
longs to a class of drugs called “dual-actionbone agents.” It stimulates calcium-sensingreceptors and leads to the differentiation ofpre-osteoblasts to osteoblasts which in creasesbone formation. In addition, it en hances thesecretion of osteoprotegerin by osteoblasts,thereby inhibiting osteoclast differentiationin relation to the RANKL system, which leadsto the decrease in bone resorption.66
Strontium ranelate is prescribed for thetreatment of osteoporosis to prevent vertebraland hip fracture. In postmenopausal womenwith osteoporosis, strontium ranelate 2 g/dayincreased BMD.67 This treatment was asso-ciated with vertebral fracture reductions of49% relative to control groups.68 Strontiumranelate has also shown significant efficacyagainst peripheral and hip fractures.69
Although strontium ranelate appears tobe protective against fractures in the osteo-porotic patient and increases BMD values, itis not yet FDA approved for therapeutic usein the United States.
DenosumabDenosumab is a neutralizing human
monoclonal antibody to RANKL, mimickingthe biological function of OPG.70 Using an in-termittent regimen either every three or everysix months, studies of the clinical efficacy ofdenosumab demonstrated a strong inhibi-tion of bone resorption as observed byreductions of up to 88% in the levels ofserum C-telopeptide, an indicator of bone remodeling, with a rapid onset of actionthree days after administration and with a sus -tained, but reversible, antiresorptive effect.71,72
At one year, denosumab treatment signifi-cantly increased bone mineral density, espe-cially in the lumbar spine and, to a lesser extent, in the total hip and distal radius. Theclinical benefits of denosumab were similar toor exceeded those induced by alendronate andrevealed dose-dependency.72 Apart from theestablished increment of dyspepsia duringbisphosphonate treatment, no significant dif-ferences in adverse events were observed be-tween treatment groups. In summary, the re-port by McClung and colleagues introduced apromising and presumably safe anti resorptiveagent to the drug armamentarium for the treat-ment of osteopenia and osteoporosis in post-menopausal women.72 Denosumab has beenin evaluation for consideration of clinical useand may be available in 2010.

CHAPTER 11 Periodontal Disease and Osteoporosis 175
CONCLUSIONAlthough the causality between sys-
temic bone loss and oral bone loss has notbeen fully elucidated, current evidencedemonstrates a plausible association betweenthe two disease entities. Study results implythat individuals with either systemic or oralbone loss should be closely managed with aclinical protocol that minimizes further de-terioration of systemic or oral bony struc-tures. Additional randomized, controlledclinical trials are needed to clarify the causal-ity and/or association between systemic andoral bone loss.
AcknowledgementThis work has been supported by NIH/
NIDCR DE 13397. The authors thank Mr.Chris Jung for his assistance with the figures.
Supplemental Readings
Cohen MM Jr. The new bone biology: pathologic, mo-lecular, and clinical correlates. Am J Med Genet A 2006;140:2646–2706.
Hardy R, Cooper MS. Bone loss in inflammatory dis-orders. J Endocrinol 2009;3:309–320.
Seeman E, Delmas PD (2006). Bone quality–the mate-rial and structural basis of bone strength and fragility.N Engl J Med 2006;354:2250–2261.
Skerry TM. The response of bone to mechanical load-ing and disuse: fundamental principles and influenceson osteoblast/osteocyte homeostasis. Arch Bio chem Bio-phys 2008;473:117-123.
Solomon DH, Rekedal L, Cadarette SM. Osteoporosistreatments and adverse events. Curr Opin Rheumatol2009;21:363–368.
REFERENCES1. Galliera E, Locati M, Mantovani A, Corsi MM.
Chemokines and bone remodeling. Int J Immuno -pathol Pharmacol 2008;21:485–491.
2. Tilg H, Moschen AR, Kaser A, Pines A, Dotan I.Gut, inflammation and osteoporosis: Basic and clin-ical concepts. Gut 2008;57:684–694.
3. Mundy GR. Osteoporosis and inflammation. NutrRev 2007;65:S147–151.
4. Romas E, Gillespie MT. Inflammation-inducedbone loss: Can it be prevented? Rheum Dis ClinNorth Am 2006;32:759–773.
5. De Martinis M, Di Benedetto MC, Mengoli LP, Gi-naldi L. Senile osteoporosis: Is it an immune-me-diated disease? Inflamm Res 2006;55:399–404.
6. Clowes JA, Riggs BL, Khosla S. The role of the im-mune system in the pathophysiology of osteoporo-sis. Immunol Rev 2005;208:207–227.
7. Ginaldi L, Di Benedetto MC, De Martinis M. Os-teoporosis, inflammation and ageing. Immun Age-ing 2005;2:14.
8. Seymour GJ, Ford PJ, Cullinan MP, Leishman S,Yamazaki K. Relationship between periodontal in-fections and systemic disease. Clin Microbiol Infect2007;13(Suppl 4):3–10.
9. Serhan CN. Clues for new therapeutics in osteo-porosis and periodontal disease: New roles forlipoxygenases? Expert Opin Ther Targets 2004;8:643–652.
10. Reinhardt RA, Payne JB, Maze CA, Patil KD, Gal-lagher SJ, Mattson JS. Influence of estrogen and osteopenia/osteoporosis on clinical periodontitis inpostmenopausal women. J Periodontol 1999;70:823–828.
11. Wactawski-Wende J, Grossi SG, Trevisan M, GencoRJ, Tezal M, Dunford RG, Ho AW, Hausmann E,Hreshchyshyn MM. The role of osteopenia in oralbone loss and periodontal disease. J Perio dontol1996;67:1076–1084.
12. Burr DB, Martin RB, Schaffler MB, Radin EL.Bone remodeling in response to in vivo fatigue micro damage. J Biomech 1985;18:189–200.
13. Mori S, Burr DB. Increased intracortical remodel-ing following fatigue damage. Bone 1993;14:103–109.
14. Lerner UH. Inflammation-induced bone remodel-ing in periodontal disease and the influence of post-menopausal osteoporosis. J Dent Res 2006;85:596–607.
15. Raisz LG. Pathogenesis of osteoporosis: Concepts,conflicts, and prospects. J Clin Invest 2005;115:3318–3325.
16. Parfitt AM. Targeted and nontargeted bone remod-eling: Relationship to basic multicellular unit orig-ination and progression. Bone 2002;30:5–7.
17. Tomkinson A, Gevers EF, Wit JM, Reeve J, NobleBS. The role of estrogen in the control of rat os-teocyte apoptosis. J Bone Miner Res 1998;13:1243–1250.
18. Tomkinson A, Reeve J, Shaw RW, Noble BS. Thedeath of osteocytes via apoptosis accompanies estrogen withdrawal in human bone. J Clin Endo -crinol Metab 1997;82:3128–3135.
19. Frost HM. Treatment of osteoporoses by manipu-

176 Periodontal Disease and Overall Health: A Clinician's Guide
lation of coherent bone cell populations. Clin Or-thop Relat Res 1979;143:227–244.
20. Kanis JA. Assessment of fracture risk and its ap-plication to screening for postmenopausal osteo-porosis: Synopsis of a WHO report. WHO StudyGroup. Osteoporos Int 1994;4:368–381.
21. von Wowern N, Klausen B, Kollerup G. Osteo-porosis: A risk factor in periodontal disease. J Pe-riodontol 1994;65:1134–1138.
22. Taguchi A, Tanimoto K, Suei Y, Ohama K, Wada T.Relationship between the mandibular and lumbarvertebral bone mineral density at different post-menopausal stages. Dentomaxillofac Radiol 1996;25:130–135.
23. Klemetti E, Collin HL, Forss H, Markkanen H,Lassila V. Mineral status of skeleton and advancedperiodontal disease. J Clin Periodontol 1994;21:184–188.
24. Horner K, Devlin H, Alsop CW, Hodgkinson IM,Adams JE. Mandibular bone mineral density as apredictor of skeletal osteoporosis. Br J Radiol1996;69:1019–1025.
25. Kribbs PJ. Comparison of mandibular bone in nor-mal and osteoporotic women. J Prosthet Dent 1990;63:218–222.
26. Kribbs PJ, Chesnut CH, 3rd, Ott SM, Kilcoyne RF.Relationships between mandibular and skeletalbone in a population of normal women. J ProsthetDent 1990;63:86–89.
27. Kribbs PJ, Chesnut CH 3rd, Ott SM, Kilcoyne RF.Relationships between mandibular and skeletalbone in an osteoporotic population. J Prosthet Dent1989;62:703–707.
28. Law AN, Bollen AM, Chen SK. Detecting osteo-porosis using dental radiographs: A comparison offour methods. J Am Dent Assoc 1996;127:1734–1742.
29. Civitelli R, Pilgram TK, Dotson M, Muckerman J,Lewandowski N, Armamento-Villareal R,Yokoyama-Crothers N, Kardaris EE, Hauser J, Cohen S, Hildebolt CF. Alveolar and postcranialbone density in postmenopausal women receivinghormone/estrogen replacement therapy: A random-ized, double-blind, placebo-controlled trial. Arch IntMed 2002;162:1409–1415.
30. Payne JB, Reinhardt RA, Nummikoski PV, PatilKD. Longitudinal alveolar bone loss in post-menopausal osteoporotic/osteopenic women. Os-teo poros Int 1999;10:34–40.
31. Payne JB, Zachs NR, Reinhardt RA, NummikoskiPV, Patil K. The association between estrogen sta-tus and alveolar bone density changes in post-menopausal women with a history of periodontitis.J Periodontol 1997;68:24–31.
32. Hildebolt CF. Osteoporosis and oral bone loss. Den-
tomaxillofac Radiol 1997;26:3–15.33. Whalen JP, Krook L. Periodontal disease as the
early manifestation of osteoporosis. Nutrition1996;12:53–54.
34. Kaye EK. Bone health and oral health. J Am DentAssoc 2007;138:616–619.
35. Nishida M, Grossi SG, Dunford RG, Ho AW, Trevisan M, Genco RJ. Calcium and the risk for periodontal disease. J Periodontol 2000;71:1057–1066.
36. Dervis E. Oral implications of osteoporosis. OralSurg Oral Med Oral Pathol Oral Radiol Endod2005;100:349–356.
37. Krejci CB, Bissada NF. Women’s health issues andtheir relationship to periodontitis. J Am Dent Assoc2002;133:323–329.
38. Neukam FW, Flemmig TF. Local and systemic con-ditions potentially compromising osseointegration.Consensus report of Working Group 3. Clin OralImplants Res 2006;17 Suppl 2:160–162.
39. von Wowern N. General and oral aspects of osteo-porosis: A review. Clinical Oral Investig 2001;5:71–82.
40. Weber RL, Wiesen MJ, Iacono VJ, Baer PN. Os-teoporosis: A risk factor for dental implants and inthe prognosis of periodontal therapy. PeriodontalClin Investig 1997;19:5–8.
41. Shibli JA, Aguiar KC, Melo L, Ferrari DS, d’AvilaS, Iezzi G, Piattelli A. Histologic analysis of humanperi-implant bone in type 1 osteoporosis. J Oral Im-plantol 2008;34:12–16.
42. Shibli JA, Grande PA, d’Avila S, Iezzi G, PiattelliA. Evaluation of human bone around a dental im-plant retrieved from a subject with osteoporosis.Gen Dent 2008;56:64–67.
43. Fujimoto T, Niimi A, Nakai H, Ueda M. Osseoin-tegrated implants in a patient with osteoporosis: Acase report. Int J Oral Maxillofac Implants 1996;11:539–542.
44. Degidi M, Piattelli A. Immediately loaded bar-con-nected implants with an anodized surface insertedin the anterior mandible in a patient treated withdiphosphonates for osteoporosis: A case report witha 12-month follow-up. Clin Implant Dent Relat Res2003;5:269–272.
45. Becker W, Hujoel PP, Becker BE, Willingham H.Osteoporosis and implant failure: An exploratorycase-control study. J Periodontol 2000;71:625 –631.
46. Friberg B. Treatment with dental implants in pa-tients with severe osteoporosis: A case report. Int JPeriodontics Restorative Dent 1994;14:348–353.
47. Friberg B, Ekestubbe A, Mellström D, Sennerby L.Brånemark implants and osteoporosis: A clinicalexploratory study. Clin Implant Dent Relat Res2001;3:50–56.

CHAPTER 11 Periodontal Disease and Osteoporosis 177
48. von Wowern N, Gotfredsen K. Implant-supportedoverdentures, a prevention of bone loss in edentu-lous mandibles? A 5-year follow-up study. ClinOral Implants Res 2001;12:19–25.
49. Keller JC, Stewart M, Roehm M, Schneider GB.Osteoporosis-like bone conditions affect osseoin-tegration of implants. Int J Oral Maxillofac Im-plants 2004;19:687–694.
50. Cho P, Schneider GB, Krizan K, Keller JC. Exam-ination of the bone-implant interface in experi-mentally induced osteoporotic bone. Implant Dent2004;13:79–87.
51. Burr DB. Summary of ASBMR Task Force on ONJ.J Musculoskelet Neuronal Interact 2007;7:354–355.
52. Khosla S, Burr D, Cauley J, Dempster DW, Ebel-ing PR, Felsenberg D, Gagel RF, Gilsanz V, GuiseT, Koka S, McCauley LK, McGowan J, McKeeMD, Mohla S, Pendrys DG, Raisz LG, RuggieroSL, Shafer DM, Shum L, Silverman SL, Van PoznakCH, Watts N, Woo SB, Shane E; American Societyfor Bone and Mineral Research. Bisphosphonate-associated osteonecrosis of the jaw: Report of a taskforce of the American Society for Bone and MineralResearch. J Bone Miner Res 2007;22:1479–1491.
53. Neer RM, Arnaud CD, Zanchetta JR, Prince R,Gaich GA, Reginster JY, Hodsman AB, Eriksen EF,Ish-Shalom S, Genant HK, Wang O, Mitlak BH. Ef-fect of parathyroid hormone (1–34) on fracturesand bone mineral density in postmenopausalwomen with osteoporosis. N Engl J Med 2001;344:1434–1441.
54. Misof BM, Roschger P, Cosman F, Kurland ES,Tesch W, Messmer P, Dempster DW, Nieves J,Shane E, Fratzl P, Klaushofer K, Bilezikian J, Lind-say R. Effects of intermittent parathyroid hormoneadministration on bone mineralization density in iliac crest biopsies from patients with osteoporosis:A paired study before and after treatment. J ClinEndocrinol Metab 2003;88:1150–1156.
55. Barros SP, Silva MA, Somerman MJ, Nociti FH Jr.Parathyroid hormone protects against periodontitis-associated bone loss. J Dent Res 2003;82:791–795.
56. Miller SC, Hunziker J, Mecham M, Wronski TJ. Intermittent parathyroid hormone administrationstimulates bone formation in the mandibles of agedovariectomized rats. J Dent Res 1997;76:1471–1476.
57. Padbury AD Jr, Tözüm TF, Taba M Jr, Ealba EL,West BT, Burney RE, Gauger PG, Giannobile WV,McCauley LK. The impact of primary hyperpara -thyroidism on the oral cavity. J Clin EndocrinolMetab 2006;91:3439–3445.
58. Krum SA, Miranda-Carboni GA, Hauschka PV,Carroll JS, Lane TF, Freedman LP, Brown M.
Estrogen protects bone by inducing Fas ligand inosteoblasts to regulate osteoclast survival. EMBOJ 2008;27:535–545.
59. Krall EA. Osteoporosis and the risk of tooth loss.Clin Calcium 2006;16:287–290.
60. Krall EA, Dawson-Hughes B, Hannan MT, KielDP. Postmenopausal estrogen replacement andtooth retention. Compend Contin Educ Dent Suppl1998:S17–22.
61. Riggs BL, Hartmann LC. Selective estrogen- receptor modulators—mechanisms of action andapplication to clinical practice. N Engl J Med 2003;348:618–629.
62. Delmas PD, Bjarnason NH, Mitlak BH, RavouxAC, Shah AS, Huster WJ, Draper M, ChristiansenC. Effects of raloxifene on bone mineral density,serum cholesterol concentrations, and uterine endo -metrium in postmenopausal women. N Engl J Med1997;337:1641–1647.
63. Lufkin EG, Whitaker MD, Nickelsen T, Argueta R,Caplan RH, Knickerbocker RK, Riggs BL. Treat-ment of established postmenopausal osteoporosiswith raloxifene: A randomized trial. J Bone MinerRes 1998;13:1747–1754.
64. Ettinger B, Black DM, Mitlak BH, KnickerbockerRK, Nickelsen T, Genant HK, Christiansen C, Del-mas PD, Zanchetta JR, Stakkestad J, Glüer CC,Krueger K, Cohen FJ, Eckert S, Ensrud KE, AvioliLV, Lips P, Cummings SR. Reduction of vertebralfracture risk in postmenopausal women with os-teoporosis treated with raloxifene: Results from a 3-year randomized clinical trial. Multiple Outcomesof Raloxifene Evaluation (MORE) Investigators.JAMA 1999;282:637–645.
65. Johnston CC Jr, Bjarnason NH, Cohen FJ, Shah A,Lindsay R, Mitlak BH, Huster W, Draper MW,Harper KD, Heath H 3rd, Gennari C, ChristiansenC, Arnaud CD, Delmas PD. Long-term effects ofraloxifene on bone mineral density, bone turnover,and serum lipid levels in early postmenopausalwomen: Three-year data from 2 double-blind, ran-domized, placebo-controlled trials. Arch Int Med2000;160:3444–3450.
66. Meunier PJ, Roux C, Ortolani S, Diaz-Curiel M,Compston J, Marquis P, Cormier C, Isaia G,Badurski J, Wark JD, Collette J, Reginster JY. Effectsof long-term strontium ranelate treatment on verte-bral fracture risk in postmenopausal women with osteoporosis. Osteoporos Int 2009;20:1663–1673.
67. Meunier PJ, Slosman DO, Delmas PD, Sebert JL,Brandi ML, Albanese C, Lorenc R, Pors-Nielsen S,De Vernejoul MC, Roces A, Reginster JY. Strontiumranelate: dose-dependent effects in established post-menopausal vertebral osteoporosis—A 2-year ran-domized placebo controlled trial. J Clin Endo crinol

178 Periodontal Disease and Overall Health: A Clinician's Guide
Metab 2002;87:2060–2066.68. Meunier PJ, Roux C, Seeman E, Ortolani S,
Badurski JE, Spector TD, Cannata J, Balogh A,Lemmel EM, Pors-Nielsen S, Rizzoli R, GenantHK, Reginster JY. The effects of strontium ranelateon the risk of vertebral fracture in women withpostmenopausal osteoporosis. N Engl J Med 2004;350:459–468.
69. Reginster JY, Seeman E, De Vernejoul MC, AdamiS, Compston J, Phenekos C, Devogel/aer JP, CurielMD, Sawicki A, Goemaere S, Sorensen OH,Felsenberg D, Meunier PJ. Strontium ranelate re-duces the risk of nonvertebral fractures in post-menopausal women with osteoporosis: Treatmentof Peripheral Osteoporosis (TROPOS) study. J ClinEndocrinol Metab 2005;90:2816–2822.
70. Lewiecki EM. RANK ligand inhibition with deno-sumab for the management of osteoporosis. ExpertOpin Biol Ther 2006;6:1041–1050.
71. Miller PD, Bolognese MA, Lewiecki EM, Mc-
Clung MR, Ding B, Austin M, Liu Y, San Martin J,Amg Bone Loss Study Group. Effect of denosumabon bone density and turnover in postmenopausalwomen with low bone mass after long-term con-tinued, discontinued, and restarting of therapy: Arandomized blinded phase 2 clinical trial. Bone2008;43:222–229.
72. McClung MR, Lewiecki EM, Cohen SB, Bolog-nese MA, Woodson GC, Moffett AH, Peacock M,Miller PD, Lederman SN, Chesnut CH, Lain D,Kivitz AJ, Holloway DL, Zhang C, Peterson MC,Bekker PJ; AMG 162 Bone Loss Study Group.Denosumab in postmenopausal women with lowbone mineral density. N Engl J Med 2006;354:821-831.
73. Kirkwood KL, Cirelli JA, Rogers JE, GiannobileWV. Novel host response therapeutic approaches totreat periodontal diseases. Periodontol 2000 2007;43:294-315.
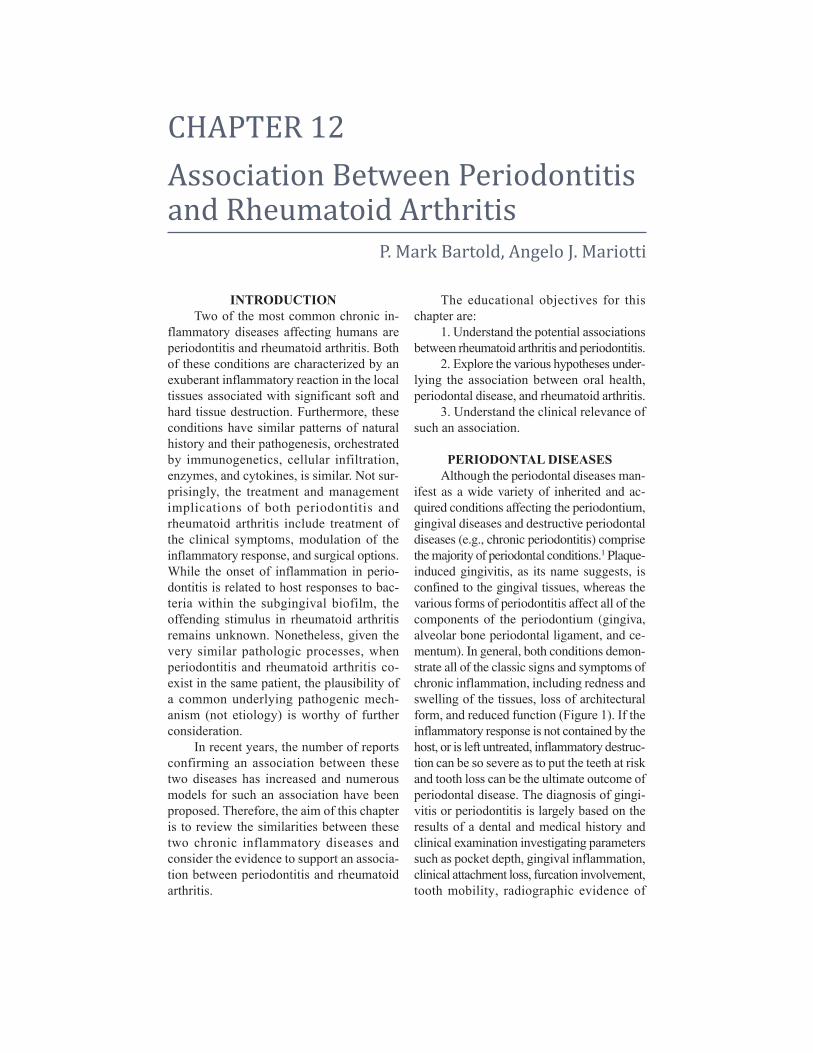
CHAPTER 12Association Between Periodontitisand Rheumatoid Arthritis
P. Mark Bartold, Angelo J. Mariotti
INTRODUCTIONTwo of the most common chronic in-
flammatory diseases affecting humans areperiodontitis and rheumatoid arthritis. Bothof these conditions are characterized by anexuberant inflammatory reaction in the localtissues associated with significant soft andhard tissue destruction. Furthermore, theseconditions have similar patterns of naturalhistory and their pathogenesis, orchestratedby immunogenetics, cellular infiltration, enzymes, and cytokines, is similar. Not sur-prisingly, the treatment and management implications of both periodontitis andrheumatoid arthritis include treatment ofthe clinical symptoms, modulation of the inflammatory response, and surgical options.While the onset of inflammation in perio -dontitis is related to host responses to bac -teria within the subgingival biofilm, the offending stimulus in rheumatoid arthritisremains unknown. Nonetheless, given thevery similar pathologic processes, when periodontitis and rheu ma toid arthritis co- exist in the same patient, the plausibility ofa common under lying pathogenic mech-anism (not etiology) is worthy of furtherconsideration.
In recent years, the number of reportsconfirming an association between thesetwo diseases has increased and numerousmodels for such an association have beenproposed. Therefore, the aim of this chapteris to review the similarities between thesetwo chronic inflammatory diseases and consider the evidence to support an associa -tion between periodontitis and rheumatoidarthritis.
The educational objectives for thischapter are:
1. Understand the potential associationsbetween rheumatoid arthritis and periodontitis.
2. Explore the various hypotheses under -lying the association between oral health,periodontal disease, and rheumatoid arthritis.
3. Understand the clinical relevance ofsuch an association.
PERIODONTAL DISEASESAlthough the periodontal diseases man-
ifest as a wide variety of inherited and ac-quired conditions affecting the periodontium,gingival diseases and destructive periodontaldiseases (e.g., chronic periodontitis) comprisethe majority of periodontal conditions.1 Plaque-induced gingivitis, as its name suggests, is confined to the gingival tissues, whereas the various forms of periodontitis affect all of thecomponents of the periodontium (gingiva,alveolar bone periodontal ligament, and ce-mentum). In general, both conditions demon-strate all of the classic signs and symptoms ofchronic inflammation, including redness andswelling of the tissues, loss of architecturalform, and reduced function (Figure 1). If theinflammatory response is not contained by thehost, or is left untreated, inflammatory destruc -tion can be so severe as to put the teeth at riskand tooth loss can be the ultimate outcome ofperiodontal disease. The diagnosis of gingi -vitis or periodontitis is largely based on theresults of a dental and medical history andclinical examination investigating param eterssuch as pocket depth, gingival inflammation,clinical attachment loss, furcation involvement,tooth mobility, radio graphic evidence of
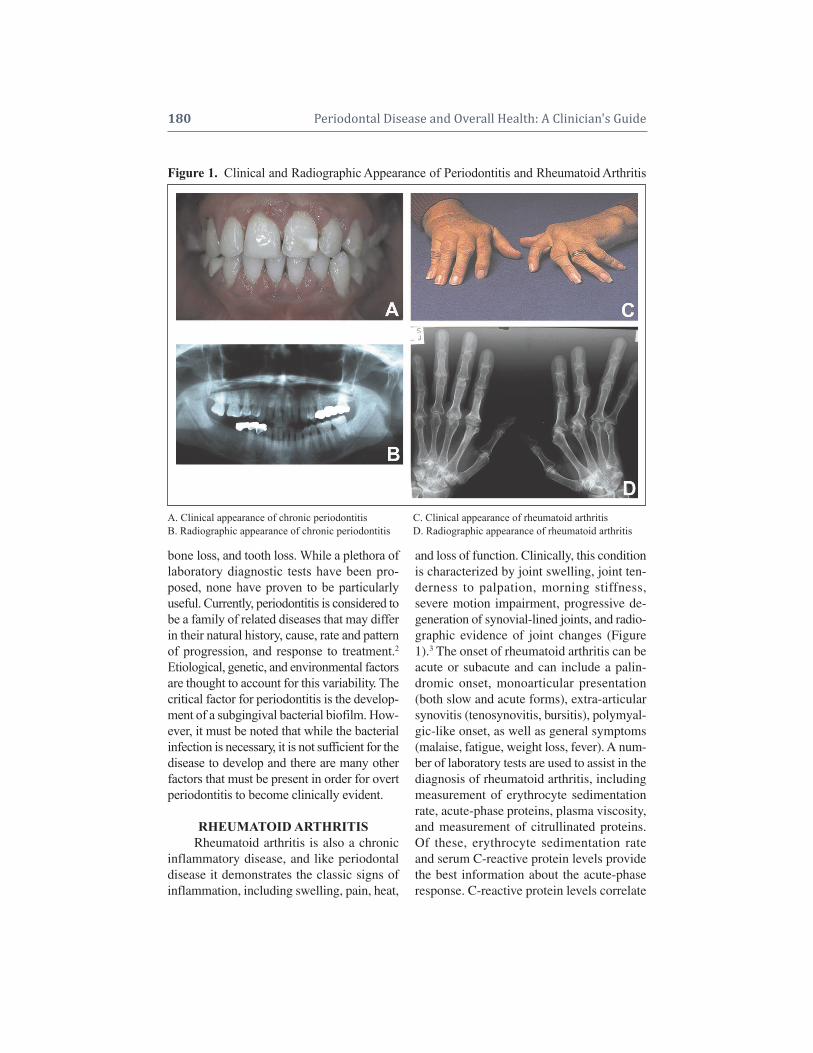
bone loss, and tooth loss. While a plethora oflaboratory diagnostic tests have been pro-posed, none have proven to be particularlyuseful. Currently, periodontitis is considered tobe a family of related diseases that may differin their natural history, cause, rate and patternof progression, and response to treatment.2Etiological, genetic, and environmental factorsare thought to account for this variability. Thecritical factor for periodontitis is the develop-ment of a subgingival bacterial biofilm. How-ever, it must be noted that while the bacterialinfection is necessary, it is not sufficient for thedisease to develop and there are many otherfactors that must be present in order for overtperio dontitis to become clinically evident.
RHEUMATOID ARTHRITISRheumatoid arthritis is also a chronic
inflammatory disease, and like periodontaldisease it demonstrates the classic signs ofinflammation, including swelling, pain, heat,
and loss of function. Clinically, this conditionis characterized by joint swelling, joint ten-derness to palpation, morning stiffness, severe motion impairment, progressive de-generation of synovial-lined joints, and radio -graphic evidence of joint changes (Figure1).3 The onset of rheumatoid arthritis can beacute or subacute and can include a palin-dromic onset, monoarticular presentation(both slow and acute forms), extra-articularsynovitis (tenosynovitis, bursitis), polymyal-gic-like onset, as well as general symptoms(malaise, fatigue, weight loss, fever). A num-ber of laboratory tests are used to assist in thediagnosis of rheumatoid arthritis, includingmeasurement of erythrocyte sedimentationrate, acute-phase proteins, plasma viscosity,and measurement of citrullinated proteins.Of these, erythrocyte sedimentation rateand serum C-reactive protein levels providethe best information about the acute-phaseresponse. C-reactive protein levels correlate
180 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 1. Clinical and Radiographic Appearance of Periodontitis and Rheumatoid Arthritis
A. Clinical appearance of chronic periodontitis C. Clinical appearance of rheumatoid arthritisB. Radiographic appearance of chronic periodontitis D. Radiographic appearance of rheumatoid arthritis

well with clinical assessment and radio -graphic changes. Recently, it has been estab -lished that a positive test for citrullinatedpeptides, with its high sensitivity and speci-ficity, is very close to a diagnostic test forrheumatoid arthritis.4 Historically, the extentof anatomic changes occurring in joints ofrheumatoid arthritis patients has been as-sessed by radiography. More recently, ultra-sonography and magnetic resonance imaginghave gained acceptance for studying joint,tendon, and bursal involvement in rheuma-toid arthritis. The clinical course of rheuma-toid arthritis fluctuates and the prognosis forthis disease is unpredictable. In most situa-tions rheumatoid arthritis is considered amultifactorial disease resulting from a com-bination of host, environmental, and geneticinfluences.
TYPES OF RHEUMATOID ARTHRITIS AND PERIODONTITIS
In general, rheumatoid arthritis can beclassified into three different types depend-ing on its manifestation and response to treat-ment. These are termed self-limited, easilycontrolled, and progressive.5 It seems thatfor the majority of people diagnosed withrheumatoid arthritis, progression is in-
evitable. Even following management withsecond-line medications, only a very smallproportion will undergo remission of longerthan 3 years. Most patients continue to haveprogression of the disease even while takingthese medications.6 In general, these patientshave a number of poor prognostic indica-tors, implying that they have significant sys-temic impairment of the inflammatory andimmune responses that would normally beprotective against such a disease.
Similar to rheumatoid arthritis, perio -dontitis also manifests in three general forms:rapid progression, moderate progression, andno progression of periodontal disease.7 Morerecently, these have been termed aggressiveor chronic, and may exist in either stable oractive forms of the disease.1
PERIODONTITIS ANDRHEUMATOID ARTHRITIS
ARE INFLAMMATORY DISEASESIn both rheumatoid arthritis and peri-
odontitis, inflammation is likely initiated byantigen stimulation (in the form of peptide orvirulence factors), and the subsequent cas-cade of acute and chronic inflammation leadsto a vicious cycle of continuous release ofpro-inflammatory mediators perpetuated by
Chapter 12 Association Between Periodontitis and Rheumatoid Arthritis 181
Table 1. Disease Activity in Periodontitis and Rheumatoid Arthritis
Adapted from J Clin Periodontol 2003;30:761-772.22
Periodontitis Rheumatoid ArthritisWell-Maintained Periodontitis Self-Limiting Rheumatoid ArthritisPeriodontitis commences, but by following simple Following commencement of the disease, it does nottreatment it can be contained and with appropriate progress to more severe formsmaintenance, very little progression occursDownhill Periodontitis Easily Controlled Rheumatoid ArthritisEstablished periodontitis can be largely controlled Once the disease becomes established, its progression with a combination of simple and complex treatments. can largely be controlled through simple treatmentsIn some cases, some further progression may occur including “first line” medicationsbut this is usually only smallExtreme Downhill Periodontitis Progressive Rheumatoid ArthritisOnce established, despite various treatment protocols, Following establishment, the disease continues to the disease progresses over time (not necessarily in a progress causing significant joint damage. Advancedlinear manner) and may even result in tooth loss treatments including “second line” medications and
disease-modifying antirheumatic drugs are of littlehelp in stopping disease progression
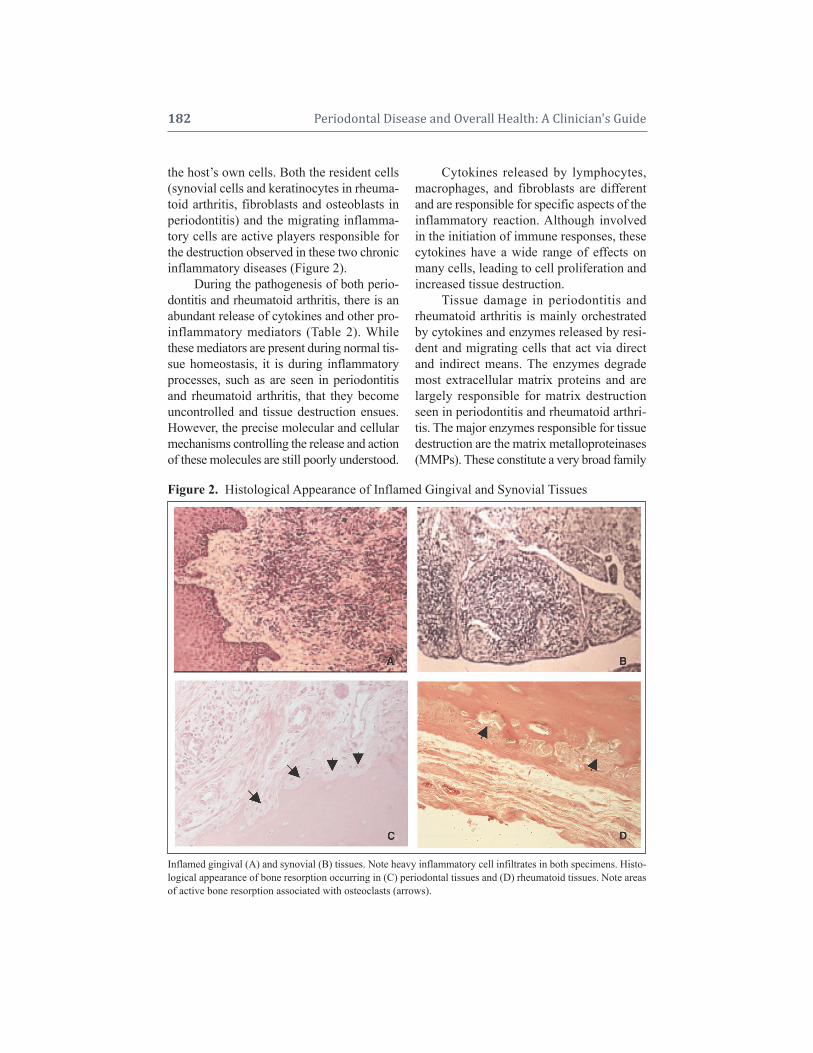
the host’s own cells. Both the resident cells(synovial cells and keratinocytes in rheuma-toid arthritis, fibroblasts and osteoblasts inperiodontitis) and the migrating inflamma-tory cells are active players responsible forthe destruction observed in these two chronicinflammatory diseases (Figure 2).
During the pathogenesis of both perio -dontitis and rheumatoid arthritis, there is anabundant release of cytokines and other pro-inflammatory mediators (Table 2). Whilethese mediators are present during normal tis-sue homeostasis, it is during inflammatoryprocesses, such as are seen in periodontitisand rheumatoid arthritis, that they becomeuncontrolled and tissue destruction ensues.However, the precise molecular and cellularmechanisms controlling the release and actionof these molecules are still poorly understood.
Cytokines released by lymphocytes,macrophages, and fibroblasts are differentand are responsible for specific aspects of theinflammatory reaction. Although involvedin the initiation of immune responses, thesecytokines have a wide range of effects onmany cells, leading to cell proliferation andincreased tissue destruction.
Tissue damage in periodontitis andrheumatoid arthritis is mainly orchestratedby cytokines and enzymes released by resi-dent and migrating cells that act via directand indirect means. The enzymes degrademost extracellular matrix proteins and arelargely responsible for matrix destructionseen in periodontitis and rheumatoid arthri-tis. The major enzymes responsible for tissuedestruction are the matrix metalloproteinases(MMPs). These constitute a very broad family
182 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 2. Histological Appearance of Inflamed Gingival and Synovial Tissues
Inflamed gingival (A) and synovial (B) tissues. Note heavy inflammatory cell infiltrates in both specimens. Histo -logical appearance of bone resorption occurring in (C) periodontal tissues and (D) rheumatoid tissues. Note areasof active bone resorption associated with osteoclasts (arrows).
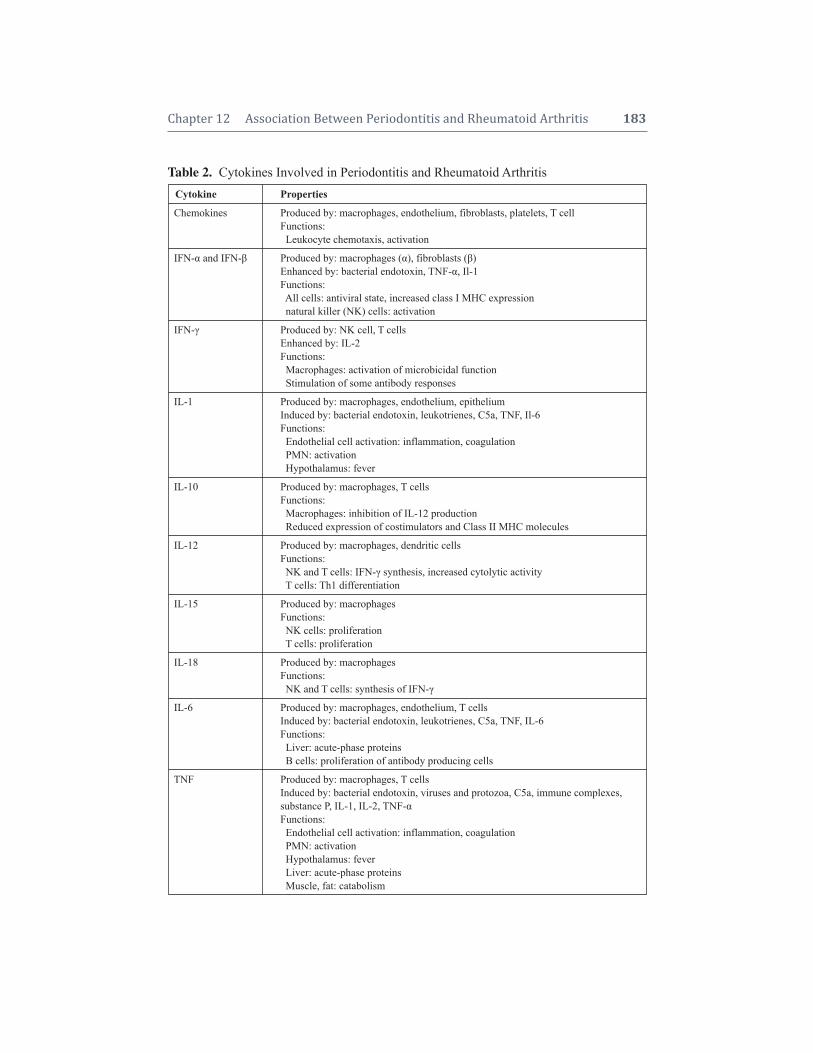
Chapter 12 Association Between Periodontitis and Rheumatoid Arthritis 183
Table 2. Cytokines Involved in Periodontitis and Rheumatoid ArthritisCytokine Properties
Chemokines Produced by: macrophages, endothelium, fibroblasts, platelets, T cellFunctions: Leukocyte chemotaxis, activation
IFN- and IFN- Produced by: macrophages (), fibroblasts ()Enhanced by: bacterial endotoxin, TNF-, Il-1Functions: All cells: antiviral state, increased class I MHC expressionnatural killer (NK) cells: activation
IFN- Produced by: NK cell, T cellsEnhanced by: IL-2Functions:Macrophages: activation of microbicidal functionStimulation of some antibody responses
IL-1 Produced by: macrophages, endothelium, epitheliumInduced by: bacterial endotoxin, leukotrienes, C5a, TNF, Il-6Functions:Endothelial cell activation: inflammation, coagulationPMN: activationHypothalamus: fever
IL-10 Produced by: macrophages, T cellsFunctions:Macrophages: inhibition of IL-12 productionReduced expression of costimulators and Class II MHC molecules
IL-12 Produced by: macrophages, dendritic cellsFunctions:NK and T cells: IFN- synthesis, increased cytolytic activityT cells: Th1 differentiation
IL-15 Produced by: macrophagesFunctions:NK cells: proliferationT cells: proliferation
IL-18 Produced by: macrophagesFunctions:
NK and T cells: synthesis of IFN-
IL-6 Produced by: macrophages, endothelium, T cellsInduced by: bacterial endotoxin, leukotrienes, C5a, TNF, IL-6Functions:Liver: acute-phase proteinsB cells: proliferation of antibody producing cells
TNF Produced by: macrophages, T cellsInduced by: bacterial endotoxin, viruses and protozoa, C5a, immune complexes, substance P, IL-1, IL-2, TNF-Functions:Endothelial cell activation: inflammation, coagulationPMN: activationHypothalamus: feverLiver: acute-phase proteinsMuscle, fat: catabolism

of enzymes with a variety of substrates andfunctions (Table 3). The cells that releaseMMPs in periodontitis and rheumatoidarthritis are polymorphonucleotides (PMNs),monocytic phagocytes, and fibroblasts. BothIL-1 and TNF- may induce the productionof collagenase and other neutral proteasesby most of these cells.
For both rheumatoid arthritis and peri-odontitis, disease progression occurs as a re-sult of very high tissue levels of IL-1 andTNF-, and low levels of cytokines suchas IL-10 and transforming growth Factor ,which suppress the immunoinflammatoryresponse. In addition, an imbalance betweentissue inhibitors of metalloproteinases(TIMPs) and MMPs secreted by macro -phages, fibroblasts, and other resident and inflammatory cells is characteristic of theactive phases of both rheumatoid arthritisand periodontitis.
Bone destruction is a common findingin periodontitis and rheumatoid arthritis.This occurs as a result of disruption to thenormally balanced processes of bone re-sorption and bone formation. The major me-diators of bone resorption are PGE2, IL-1,TNF-, and IL-6.
In both periodontitis and rheumatoidarthritis the immune response is regulatedvia genes that control T cell responses toforeign antigens. In this way the nature of theprotective antibody response, as well as themagnitude of tissue destructive inflamma-tory responses, are determined.
ROLE OF GENETICS IN RHEUMATOID ARTHRITIS
AND PERIODONTITISThe role of genetics in periodontitis and
rheumatoid arthritis is of considerable im-portance. For both chronic periodontitis andrheumatoid arthritis there is considerablevariance in the clinical manifestation of thedisease. Much of this variance can be ac-counted for by genetic factors.8 Many of these
differences in disease manifestation can berelated to the overexpression or underex-pression of numerous cytokines and otherinflammatory mediators. Of these, IL-1,TNF-, and PGE2 have been found to be un-der quite strong genetic control. Numerousstudies have been published concerning theso-called “hyper-responsive monocyte ge-netic traits,” which have common geneticregions that influence the susceptibility toinflammatory diseases. Typical of this trait isthe overproduction of pro-inflammatory me-diators such as IL-1, TNF-, and PGE2, andis typically seen in patients with aggressiveperiodontitis.9 The concept of a monocytichypersecretory state has also been describedfor rheumatoid arthritis patients.10
Many of the genes that regulate the cytokine profiles and responses of mono-cytes have been mapped to the human leuko-cyte antigen D related (HLA-DR) region ofchromosome 5 in the area of the TNF-genes.11 Since both rheumatoid arthritis andperiodontitis have been associated with thisHLA complex, a common genetic basis ex-ists for the observed monocyte trait, linkingrheumatoid arthritis and periodontitis.
ROLE OF ENVIRONMENTAL FACTORS ON PERIODONTITISAND RHEUMATOID ARTHRITIS
It has been recognized for some timethat the clinical manifestation of chronic dis-eases such as periodontitis and rheumatoidarthritis are significantly influenced by en-vironmental or “modifying” factors. Thesefactors are anything that might modify or alter the host inflammatory response, andinclude demographic, socioeconomic, life -style, diet, hormonal, and psychological vari-ables. Since genetic factors may account forup to 50% of the risk for both periodontitisand rheumatoid arthritis,8,12 other factors, in-clud ing environmental influences and gene- environment interactions, must explain therest.
184 Periodontal Disease and Overall Health: A Clinician's Guide
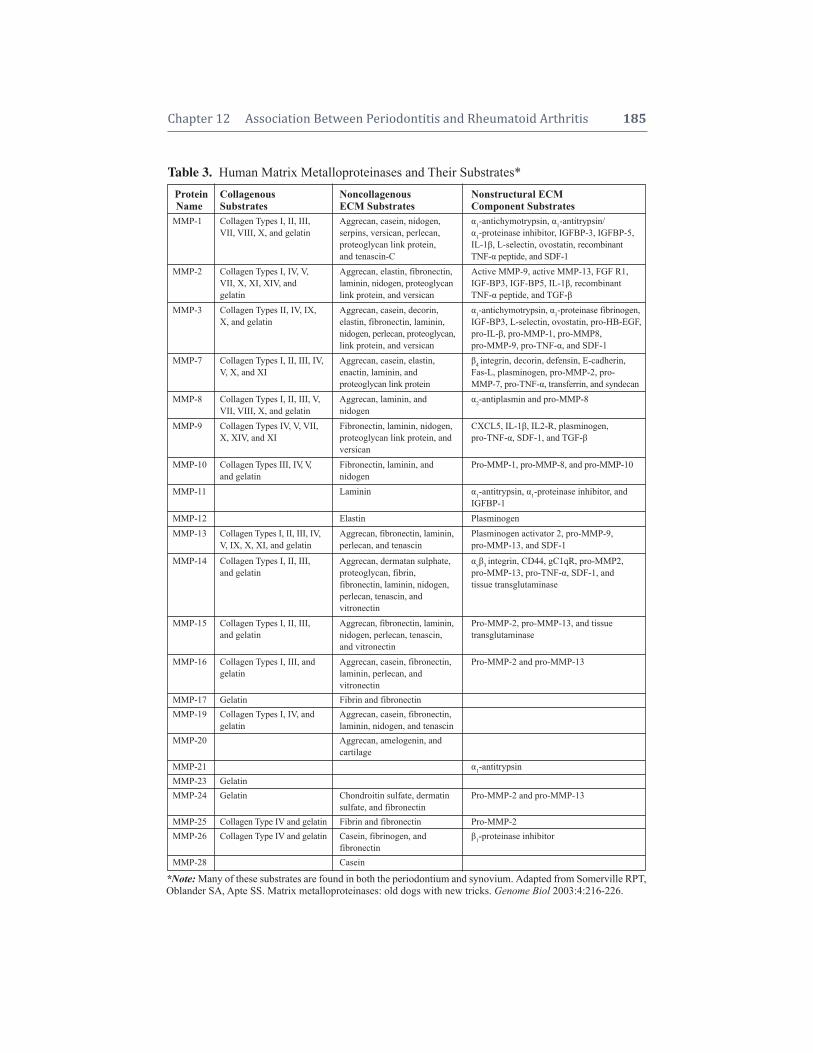
Chapter 12 Association Between Periodontitis and Rheumatoid Arthritis 185
Table 3. Human Matrix Metalloproteinases and Their Substrates*Protein Collagenous Noncollagenous Nonstructural ECMName Substrates ECM Substrates Component Substrates
MMP-1 Collagen Types I, II, III, Aggrecan, casein, nidogen, 1-antichymotrypsin, 1-antitrypsin/VII, VIII, X, and gelatin serpins, versican, perlecan, 1-proteinase inhibitor, IGFBP-3, IGFBP-5,
proteoglycan link protein, IL-1, L-selectin, ovostatin, recombinant and tenascin-C TNF- peptide, and SDF-1
MMP-2 Collagen Types I, IV, V, Aggrecan, elastin, fibronectin, Active MMP-9, active MMP-13, FGF R1,VII, X, XI, XIV, and laminin, nidogen, proteoglycan IGF-BP3, IGF-BP5, IL-1, recombinantgelatin link protein, and versican TNF- peptide, and TGF-
MMP-3 Collagen Types II, IV, IX, Aggrecan, casein, decorin, 1-antichymotrypsin, 1-proteinase fibrinogen,X, and gelatin elastin, fibronectin, laminin, IGF-BP3, L-selectin, ovostatin, pro-HB-EGF,
nidogen, perlecan, proteoglycan, pro-IL-, pro-MMP-1, pro-MMP8,link protein, and versican pro-MMP-9, pro-TNF-, and SDF-1
MMP-7 Collagen Types I, II, III, IV, Aggrecan, casein, elastin, 4 integrin, decorin, defensin, E-cadherin,V, X, and XI enactin, laminin, and Fas-L, plasminogen, pro-MMP-2, pro-
proteoglycan link protein MMP-7, pro-TNF-, transferrin, and syndecan MMP-8 Collagen Types I, II, III, V, Aggrecan, laminin, and 2-antiplasmin and pro-MMP-8
VII, VIII, X, and gelatin nidogenMMP-9 Collagen Types IV, V, VII, Fibronectin, laminin, nidogen, CXCL5, IL-1, IL2-R, plasminogen,
X, XIV, and XI proteoglycan link protein, and pro-TNF-, SDF-1, and TGF-versican
MMP-10 Collagen Types III, IV, V, Fibronectin, laminin, and Pro-MMP-1, pro-MMP-8, and pro-MMP-10and gelatin nidogen
MMP-11 Laminin 1-antitrypsin, 1-proteinase inhibitor, andIGFBP-1
MMP-12 Elastin Plasminogen MMP-13 Collagen Types I, II, III, IV, Aggrecan, fibronectin, laminin, Plasminogen activator 2, pro-MMP-9,
V, IX, X, XI, and gelatin perlecan, and tenascin pro-MMP-13, and SDF-1
MMP-14 Collagen Types I, II, III, Aggrecan, dermatan sulphate, v3 integrin, CD44, gC1qR, pro-MMP2,and gelatin proteoglycan, fibrin, pro-MMP-13, pro-TNF-, SDF-1, and
fibronectin, laminin, nidogen, tissue transglutaminaseperlecan, tenascin, and vitronectin
MMP-15 Collagen Types I, II, III, Aggrecan, fibronectin, laminin, Pro-MMP-2, pro-MMP-13, and tissueand gelatin nidogen, perlecan, tenascin, transglutaminase
and vitronectinMMP-16 Collagen Types I, III, and Aggrecan, casein, fibronectin, Pro-MMP-2 and pro-MMP-13
gelatin laminin, perlecan, and vitronectin
MMP-17 Gelatin Fibrin and fibronectinMMP-19 Collagen Types I, IV, and Aggrecan, casein, fibronectin,
gelatin laminin, nidogen, and tenascinMMP-20 Aggrecan, amelogenin, and
cartilageMMP-21 1-antitrypsinMMP-23 Gelatin MMP-24 Gelatin Chondroitin sulfate, dermatin Pro-MMP-2 and pro-MMP-13
sulfate, and fibronectinMMP-25 Collagen Type IV and gelatin Fibrin and fibronectin Pro-MMP-2MMP-26 Collagen Type IV and gelatin Casein, fibrinogen, and 1-proteinase inhibitor
fibronectin MMP-28 Casein
*Note:Many of these substrates are found in both the periodontium and synovium. Adapted from Somerville RPT,Oblander SA, Apte SS. Matrix metalloproteinases: old dogs with new tricks. Genome Biol 2003:4:216-226.

Of the environmental risk factors iden-tified to date, smoking is probably the singlemost important environmental factor im-pacting many chronic diseases. Through itsadverse effects on the cardiovascular sys-tem, immune cell function, and general tissuephysiology, it is not surprising that smokingis considered a major risk factor for the de-velopment of both rheumatoid arthritis andperiodontitis.13,14
Another environmental factor of inter-est is socioeconomic status. This may be asignificant factor in the outcome of manychronic diseases, including both rheumatoidarthritis and periodontitis.15,16 The reasonsfor this are not entirely clear, although sug-gestions have been made that individualsfrom lower socioeconomic status may beless compliant with regard to their generalhealthcare and have less access to the fullrange of healthcare. However, these expla-nations do not fully explain this relationship.In this regard, allostatic load has also beenproposed to describe dysregulation of phys-iological adaptive processes, including im-mune function, that in health maintain sta-bility to stressors. It has been proposed thatallostatic load may follow a socioeconomicgradient that is, in part, responsible for in-equalities in chronic diseases such as peri-odontitis and rheumatoid arthritis. In thismodel, low socioeconomic status results inincreased exposure to psychosocial stress,which activates primary allostatic mediators,including a wide range of inflammatory me-diators. Under these conditions dysregulationof a range of immunomodulatory functionsoccurs, possibly leading to alterations in theextent and severity of chronic diseases.
PERIODONTITIS AND RHEUMATOIDARTHRITIS CAN BE CLASSED AS“COMPLEX” OR “ECOGENETIC”
DISEASESIn recent times, periodontitis and
rheumatoid arthritis have been considered
“complex” or “ecogenetic” diseases.17,18 Acomplex disease is defined as a disorder witha genetic component but does not follow thesimple single-gene dominant or single-generecessive Mendelian law (Table 4). Since
both inherited genetic variations and envi-ronmental factors, such as smoking, hygiene,and pathogenic bacteria interact to determinean individual’s risk for the development ofperiodontitis and rheumatoid arthritis, thesetwo diseases fit this definition of complexdiseases. Hence in these diseases, in re-sponse to an initiating event, environmentalagents interact with genetic factors to influ-ence disease susceptibility (Figure 3). Suchinteractions initiate and regulate immuno-inflammatory reactions that ultimately man-ifest as the clinical signs of rheumatoidarthritis or periodontitis. While understand-ing the role of dental plaque as being pivotalin the initiating events for periodontal diseaseis well understood, the initiating events forrheumatoid arthritis are less clear.
Interactions between environmental riskfactors and genetics are now providingus with valuable clues as to the nature of complex diseases such as periodontitisand rheumatoid arthritis. One of the best-
186 Periodontal Disease and Overall Health: A Clinician's Guide
Table 4. Features of Complex DiseasesTable 4. or Ecogenetic Diseases
• The diseases interact with ecology, molecular genetics, toxicology, public health medicine, andenvironmental epidemiology.
• These are common chronic diseases with adultonset that show familial aggregation, but do notfollow Mendelian family patterns.
• These diseases appear to be caused by an un-known number of multiple genes, which interactwith environmental factors.
• In these diseases, only a small proportion (1%–7%) of affected individuals show a single mutantgene transmitted by Mendelian inheritance withcharacteristic transmission.
• These genetically exceptional families often havean earlier age of onset and have more severe clinical manifestations.
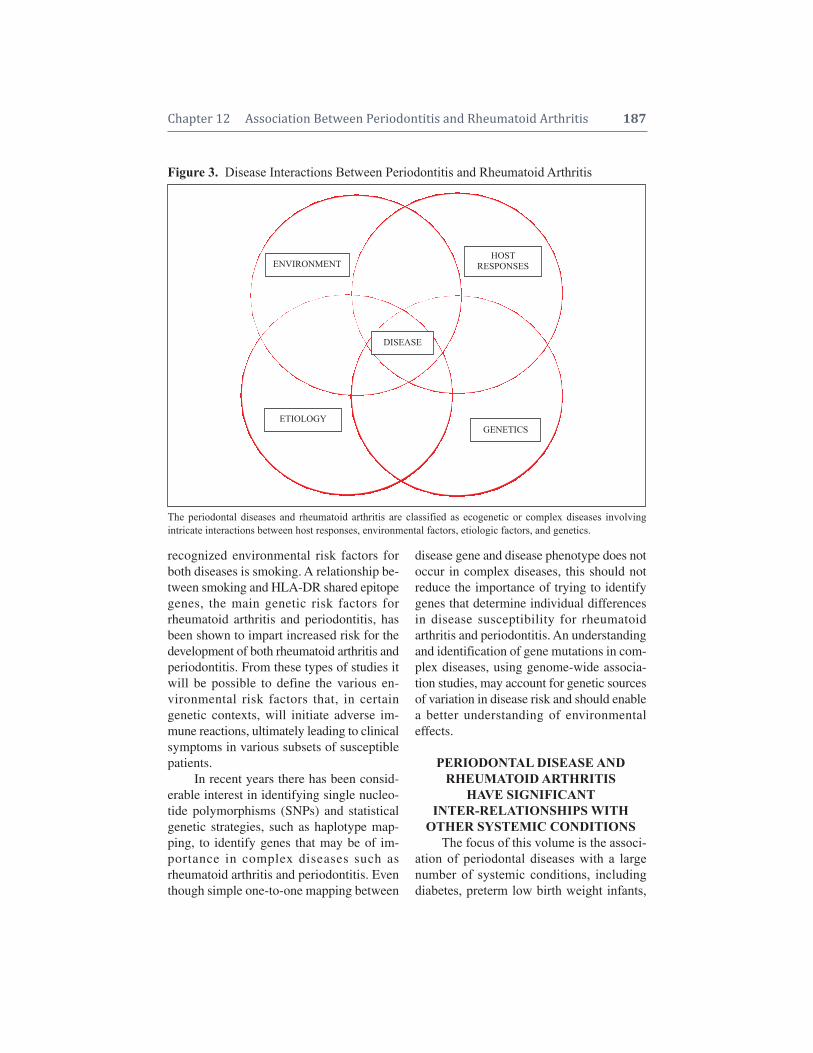
recognized environmental risk factors forboth diseases is smoking. A relationship be-tween smoking and HLA-DR shared epitopegenes, the main genetic risk factors forrheumatoid arthritis and periodontitis, hasbeen shown to impart increased risk for thedevelopment of both rheumatoid arthritis andperiodontitis. From these types of studies itwill be possible to define the various en -vironmental risk factors that, in certain genetic contexts, will initiate adverse im-mune reactions, ultimately leading to clinicalsymptoms in various subsets of susceptible patients.
In recent years there has been consid-erable interest in identifying single nucleo -tide polymorphisms (SNPs) and statisticalgenetic strategies, such as haplotype map-ping, to identify genes that may be of im-portance in complex diseases such asrheumatoid arthritis and periodontitis. Eventhough simple one-to-one mapping between
disease gene and disease phenotype does notoccur in complex diseases, this should not reduce the importance of trying to identifygenes that determine individual differencesin disease susceptibility for rheumatoidarthritis and periodontitis. An understandingand identification of gene mutations in com-plex diseases, using genome-wide associa-tion studies, may account for genetic sourcesof variation in disease risk and should enablea better understanding of environmental effects.
PERIODONTAL DISEASE ANDRHEUMATOID ARTHRITIS
HAVE SIGNIFICANTINTER-RELATIONSHIPS WITH
OTHER SYSTEMIC CONDITIONSThe focus of this volume is the associ-
ation of periodontal diseases with a largenumber of systemic conditions, includingdiabetes, preterm low birth weight infants,
Chapter 12 Association Between Periodontitis and Rheumatoid Arthritis 187
Figure 3. Disease Interactions Between Periodontitis and Rheumatoid Arthritis
The periodontal diseases and rheumatoid arthritis are classified as ecogenetic or complex diseases involving intricate interactions between host responses, environmental factors, etiologic factors, and genetics.
HOSTRESPONSESENVIRONMENT
DISEASE
ETIOLOGYGENETICS

cardiovascular disease, pulmonary disease,obesity, and osteoporosis. In the context ofthis chapter, which considers the potential in-teraction between periodontitis and rheuma-toid arthritis, it is of interest to note that allof these diseases have also been associatedwith individuals suffering from rheumatoidarthritis (Table 5). Even after accounting forvariable confounders, including variousmedications, many studies have been ableto demonstrate significant relationships be-tween rheumatoid arthritis and systemic con-ditions.19 The underlying feature in these re-lationships seems to be dysregulated chronicinflammation in both periodontitis andrheumatoid arthritis.
WHAT IS THE EVIDENCE FORA RELATIONSHIP BETWEEN
PERIODONTITIS AND RHEUMATOID ARTHRITIS?For more than 80 years there have been
reports in the literature concerning a possi-ble relationship between rheumatoid arthritisand periodontitis. A number of reviewsand com mentaries on this topic have beenpublished.20-24
One of the earliest reports concerningthis relationship was written by Sachs, whocommented in 1926 that the relationship between “gelenkrheumatismus and para -dentose” was a question of “a constitutionwith a predisposition to both of these condi-tions” (quoted from Helminen-Pakkala).25
Since then, a number of studies consideredthe relationship between periodontal disease
and rheumatoid arthritis with little agree-ment being reached as to whether this wasindeed possible.
Over the last 30 years, a steady streamof papers that question this relationship havebeen published. For example, an increase inany dental disease, including periodontal dis-ease, was not seen in a group of SouthAfrican patients with advanced joint condi-tions.26 Similarly, a study of Japaneserheumatoid arthritis patients found no evi-dence of elevated levels of serum antibodiesagainst several periodontal pathogens.27 Astudy that considered clinical and immuno-logical features of periodontitis reported thatrheumatoid arthritis patients were not a riskgroup for advanced periodontal conditions.28
Furthermore, a case-control study in a groupof Scandinavian patients (204 cases and 204controls) reported a tendency toward betterperiodontal conditions for the rheumatoidarthritis patients.29 A study of Norwegianrheumatoid arthritis patients between theages of 44 and 56 found no correlation be-tween tooth loss and rheumatoid arthritis.30
In a study using epidemiological data, 523individuals, initially seen during the first National Health and Nutrition ExaminationSurvey (NHANES I) of 1971–75, exhibitedno correlation with self-reported arthritis andthe number of missing teeth.31
Despite the above investigations, whichreported a negative correlation between pe-riodontitis and rheumatoid arthritis, therehave been a larger number of studies thathave supported such a relationship. Whileperhaps the least convincing in terms of sci-entific design, simple pilot studies analyzingdata obtained from self-reported illnesseshave indicated a higher incidence of rheuma-toid arthritis in patients with periodontitis.32-35
A number of case-control studies havealso been carried out. All of these indicatethat rheumatoid arthritis patients have a significantly higher incidence of periodon - tal disease. For these studies, periodontal
188 Periodontal Disease and Overall Health: A Clinician's Guide
Table 5. Systemic Conditions ReportedTable 5. .to be Associated with Both Perio -Table 5. .dontitis and Rheumatoid Arthritis
Cardiovascular DiseaseDiabetesObesityObstetric ProblemsPulmonary ConditionsRenal ConditionsCancer

conditions were variously measured as num-ber of teeth missing, gingival bleeding, at -tachment loss, probing pocket depth, and radiographic bone loss.32,36-44
As a result of these findings, studieshave been carried out to investigate a numberof clinical and laboratory param eters tofurther ascertain if a relationship betweenperiodontitis and rheumatoid arthritis exists.These have included investigations into cyto -kine profiles,45-50 inflammatory mediators,51
HLA-DR antigens,52-54 and hormones.55 Allof these studies have supported the notionthat periodontitis and rheumatoid arthritisare inter-related, and have led variousauthors to conclude that inflammation(and its dys regulation) may be the centrallink between periodontitis and rheuma-toid arthritis.23 At least two studies have concluded that perio dontitis may be a riskfactor or severity factor for rheumatoidarthritis.32,56
As early as 1985, a case report was published describing remission of rheuma-toid arthritis following periodontal treat-ment.57 This study remained largely forgot-ten until the publication of two additionalstudies that indicated periodontal treatmentcould reduce the severity of rheumatoidarthri tis.56,58 While these studies have in-volved relatively low numbers of sub-jects, they highlight the potential for impor-tant clinical ramifications for the relation-ship between periodontitis and rheumatoidarthritis.
Further support for a significant rela-tionship between periodontitis and rheuma-toid arthritis has been highlighted in a re-cent animal study. Moreover, the inductionof adjuvant arthritis in rats resulted in an as-sociated periodontal breakdown evidencedby alveolar bone loss and increased matrixmetalloproteinase activity in adjacent gingi-val tissues.59
Careful assessment of the data reportedfrom many of these studies allows us to
make some important observations. First,few of these studies support the commonlyheld tenet that rheumatoid arthritis patientshave impaired oral hygiene (judged byplaque and bleeding scores) because of their“disability.” It is variously reported that oralhygiene is no different between rheumatoidarthritis patients with periodontitis and non-rheumatoid arthritis patients with periodon-titis.44,60 Another important observation fromrecently published studies is that individualswith severe rheumatoid arthritis are morelikely to suffer from advanced periodontitisand vice versa. However, the associationseems to be in favor of rheumatoid arthritisimpacting periodontitis (Relative Risk 4.1)rather than periodontitis impacting rheuma-toid arthritis (Relative Risk 1.5).60 Also, it isimportant that longitudinal studies be car-ried out from this association to establishthe temporal sequence. Finally, from thestudies published to date, it is interesting toconsider the influence of medications thatrheumatoid arthritis patients may be taking,on periodontitis. Many, if not all, of thesemedications are anti-inflammatory agentsand therefore have the potential to suppressperiodontal inflammation and affect peri-odontal disease progression. Nonetheless,reports indicate that significant periodontaldestruction can still be seen in patients whomay be taking anti-inflammatory medica-tions for rheumatoid arthritis.40,60 It has beenproposed that before development ofrheumatoid arthritis symptoms, the peri-odontitis was most likely also developingand not detected.23 Thus, in the analysis ofthe association between rheumatoid arthritisand periodontitis, consideration of diseaseduration (for both periodontal and rheuma-toid) will be a critical factor. Therefore, fu-ture studies concerning the relationship be-tween periodontitis and rheumatoid arthritisshould address and document the diseasewith regard to severity and duration of bothdiseases.
Chapter 12 Association Between Periodontitis and Rheumatoid Arthritis 189

PROPOSED MECHANISMS FORA RELATIONSHIP BETWEEN
PERIODONTITIS AND RHEUMATOID ARTHRITIS
A number of mechanisms for a rela-tionship between periodontitis and rheuma-toid arthritis have been proposed. The prin-cipal mechanisms may involve changes toblood vessels or infection of host tissues.
Vascular AlterationsRecent investigations into the relation-
ship between osteoclast activation and vas-cular damage have suggested a commonpathway in the development of periodontitisand rheumatoid arthritis. It has been hy-pothesized that both rheumatoid arthritis andperiodontitis share common molecular path-ways within the receptor activator of nuclearfactor Kappa (RANK)/osteoprotegerin(OPG)/tumor necrosis factor-related apop-tosis-inducing ligand (TRAIL) axis, wherebya decrease in OPG leads to reduced vascularprotection.23 In addition, increases in RANKand TRAIL levels within inflamed tissuesmay result in not only the possible develop-ment of vascular damage, but also activationof osteoclasts and subsequent bone resorption.
Another vascular model proposes thatmicrovascular involvement is one of the firststages of a number of chronic diseases, suchas periodontitis and rheumatoid arthritis.61
In this model, reduced caliber of capillaries,along with greater numbers of and elongatedcapillaries, are noted in both periodontal tis-sues and rheumatoid synovium.
Bacterial InfectionData from a number of animal models
demonstrate that arthritis can develop sec-ondarily to several different stimuli andthrough several effector pathways, includ-ing exogenous infections. If the observationsin animal models are also applicable to hu-man rheumatoid arthritis, we might anticipatethat different types of infections, as well as
other environmental exposures with capacityto induce excessive pro-inflammatory cyto -kines in genetically susceptible individuals,may contribute to disease either togetherwith some autoimmune reaction or by them-selves.
Many periodontal pathogens exhibitsimilar characteristics to those micro-organ-isms suspected to induce rheumatoid arthritisin a genetically susceptible host. Periodontalpathogens incite a chronic continuous in-flammation within the periodontal tissuesand also serve as an abundant supply oflipopolysaccharide. Thus, the possibility thatan ongoing periodontitis can trigger or ex-acerbate rheumatoid arthritis in geneticallysusceptible individuals is biologically plau-sible. A number of studies have reported elevated serum antibodies to a number ofperiodontopathic bacteria including Por-phyromonas gingivalis, Prevotella interme-dia, Prevotella melaninogenica, Bacteroidesforsythus, and Aggregatibacter actino-mycetemcomitans.27,62-64 Elevated antibodiesto B. forsythus and P. intermedia have alsobeen found in synovial fluid. Further evi-dence for a role of periodontal pathogens injoint disease have come from a study re-porting DNA for P. gingivalis, T. forsythen-sis and P. intermedia in synovial fluid ofrheumatoid patients.65 No DNA for thesebacteria were found in the synovial fluid ofnonrheumatoid patients.
A novel hypothesis for the developmentof rheumatoid arthritis via the humoral re-sponse to oral bacteria found in periodontitishas been proposed.66 In this model, an auto -immune disease to proteins partially altered bybacterial enzymes in genetically sus ceptibleindividuals may develop (Figure 4). Centralto this hypothesis is the appearance of rheu -matoid factors and anticyclic, citrullinatedpep tide autoantibodies during the develop-ment of rheumatoid arthritis. The productionof deimination enzymes by perio dontal path-ogenic bacteria, such as P. gingivalis, can
190 Periodontal Disease and Overall Health: A Clinician's Guide
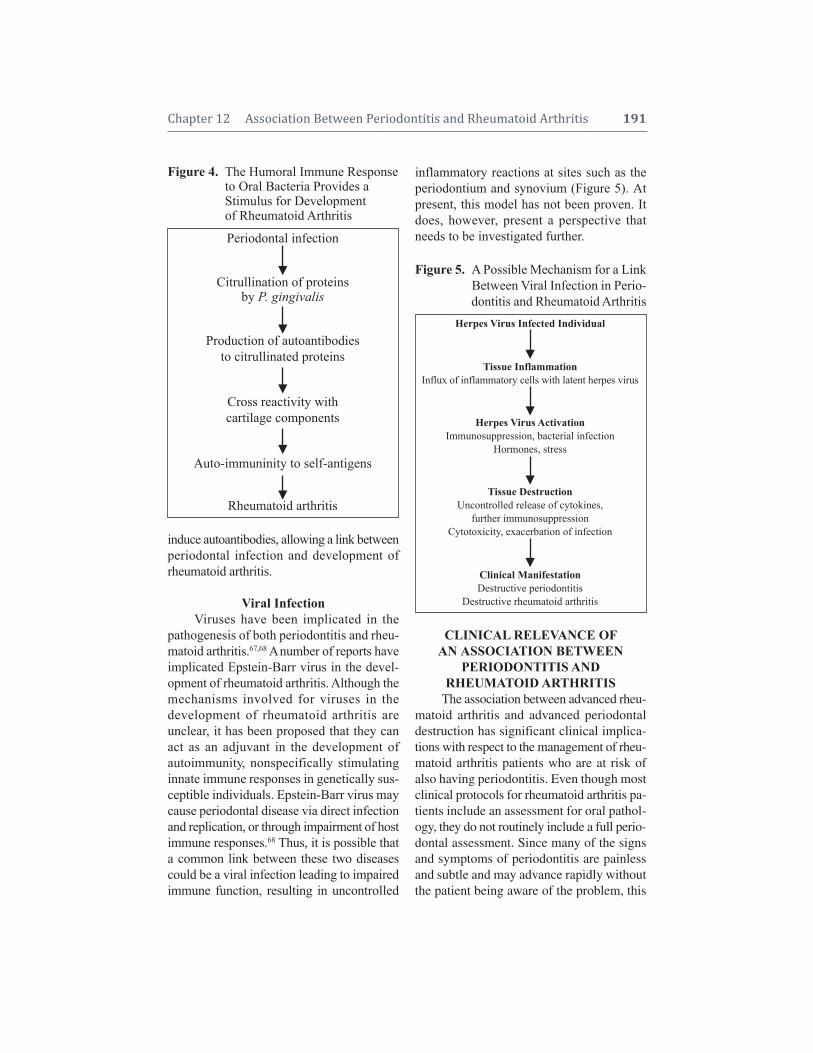
induce autoantibodies, allowing a link betweenperiodontal infection and development ofrheumatoid arthritis.
Viral InfectionViruses have been implicated in the
pathogenesis of both periodontitis and rheu -matoid arthritis.67,68 A number of reports haveimplicated Epstein-Barr virus in the devel-opment of rheumatoid arthritis. Although themechanisms involved for viruses in the development of rheumatoid arthritis are unclear, it has been proposed that they canact as an adjuvant in the development of autoimmunity, nonspecifically stimulatinginnate immune responses in genetically sus-ceptible individuals. Epstein-Barr virus maycause periodontal disease via direct in fectionand replication, or through impairment of hostimmune responses.68 Thus, it is possible thata common link between these two diseasescould be a viral infection leading to impairedimmune function, resulting in uncontrolled
inflammatory reactions at sites such as theperiodontium and synovium (Figure 5). Atpresent, this model has not been proven. Itdoes, however, present a perspective thatneeds to be investigated further.
CLINICAL RELEVANCE OFANASSOCIATION BETWEEN
PERIODONTITIS AND RHEUMATOID ARTHRITIS
The association between advanced rheu -matoid arthritis and advanced perio dontaldestruction has significant clinical implica-tions with respect to the management of rheu -matoid arthritis patients who are at risk ofalso having periodontitis. Even though mostclinical protocols for rheumatoid arthritis pa-tients include an assessment for oral pathol-ogy, they do not routinely include a full perio -dontal assessment. Since many of the signsand symptoms of periodontitis are painlessand subtle and may advance rapidly withoutthe patient being aware of the problem, this
Chapter 12 Association Between Periodontitis and Rheumatoid Arthritis 191
Figure 4.The Humoral Immune ResponseFigure 4.to Oral Bacteria Provides aFigure 4.Stimulus for Development Figure 4. of Rheumatoid Arthritis
Periodontal infection
Citrullination of proteins
by P. gingivalis
Production of autoantibodies
to citrullinated proteins
Cross reactivity withcartilage components
Auto-immuninity to self-antigens
Rheumatoid arthritis
Figure 5. A Possible Mechanism for a LinkFigure 5. Between Viral Infection in Perio -Figure 5. dontitis and Rheumatoid Arthritis
Tissue InflammationInflux of inflammatory cells with latent herpes virus
Herpes Virus Activation
Immunosuppression, bacterial infectionHormones, stress
Tissue Destruction
Uncontrolled release of cytokines,further immunosuppression
Cytotoxicity, exacerbation of infection
Clinical ManifestationDestructive periodontitis
Destructive rheumatoid arthritis
Herpes Virus Infected Individual

aspect of clinical assessment has been over-looked. In light of the current data, individ-uals suffering from rheumatoid arthritis seemto be at higher risk of developing periodon-tal problems. Further, early evidence has sug-gested that treatment of periodontitis can re-duce the clinical symptoms of rheumatoidarthritis. Therefore, early intervention to pre-vent periodontal destruction occurring in in-dividuals with rheumatoid arthritis shouldbe considered to reduce the impact ofrheumatoid arthritis.
CONCLUSIONSFor several decades it has been sus-
pected that because periodontitis and rheuma- toid arthritis share many common pathologicfeatures, they may be clinically related orass ociated diseases. It is now becoming ap-parent, mainly from case-control studies, thatdisease severity and extent may be relatedfor individuals suffering from both rheuma-toid arthritis and periodontitis. While causal-ity between the two diseases is very unlikely,the fact that both diseases can impact eachother is becoming apparent. Thus, it is pro-posed that these two diseases can exist as amanifestation of generalized dysregulationof the immune and inflammatory responses.Hence, both periodontitis and rheumatoidarthritis may be considered clinical mani-festations of the same disease process pre-senting in different parts of the body.69
Supplemental Readings
Mercado FB, Marshall RI, Bartold PM. Inter-relation-ships between rheumatoid arthritis and periodontal dis-ease. A review. J Clin Periodontol 2003;30:761–772.
Bartold PM, Marshall RI, Haynes DR. Periodontitisand rheumatoid arthritis: A review. J Periodontol 2005;76(11 Suppl):2066-2074.
Golub LM, Payne JB, Reinhardt RA, Nieman G. Cansystemic diseases co-induce (not just exacerbate) perio -dontitis? A hypothetical "two-hit" model. J Dent Res2006;85:102-105.
Al-Katma MK, Bissada NF, Bordeaux JM, Sue J, Askari
192 Periodontal Disease and Overall Health: A Clinician's Guide
AD. Control of periodontal infection reduces the severityof active rheumatoid arthritis. J Clin Rheumatol 2007;13:134–137.
Rosenstein ED, Greenwald RA, Kushner LJ, Weiss-mann G. Hypothesis: The humoral immune response tooral bacteria provides a stimulus for the development ofrheumatoid arthritis. Inflammation 2004;28:311–318.
de Pablo P, Chapple IL, Buckley CD, Dietrich T. Perio -d ontitis in systemic rheumatic diseases. Nat RevRheumatol 2009;5:218–224.
REFERENCES1. Armitage GC. Development of a classification sys-
tem for periodontal diseases and conditions. AnnPeriodontol 1999;4:1–6.
2. Pihlstrom BL, Michalowicz BS, Johnson NW. Pe-riodontal diseases. Lancet 2005;366:1809–1820.
3. Persselin JE. Diagnosis of rheumatoid arthritis.Medical and laboratory aspects. Clin Orthop RelRes 1991;265:73–82.
4. Avouac J, Gossec L, Dougados M. Diagnostic andpredictive value of anti-cyclic citrullinated proteinantibodies in rheumatoid arthritis: a systematic lit-erature review. Ann Rheum Dis 2006;65:845–851.
5. Arnett FC, Edworthy SM, Bloch DA, McShaneDJ, Fries JF, Cooper NS, Healey LA, Kaplan SR,Liang MH, Luthra HS, et al. The American Rheu -matism Association 1987 revised criteria for theclassification of rheumatoid arthritis. ArthritisRheum 1988;31:315–324.
6. Wolfe F, Cathey MA. Analysis of methotrexatetreatment effect in a longitudinal observational study:Utility of cluster analysis. J Rheumatol 1991;18:672–677.
7. Hirschfeld L, Wasserman B. A long-term survey oftooth loss in 600 treated periodontal patients. J Perio dontol 1978;49:225–237.
8. Michalowicz BS. Genetic and heritable risk fac-tors in periodontal disease. J Periodontol 1994;65(5 Suppl):479–488.
9. Salvi GE, Yalda B, Collins JG, Jones BH, SmithFW, Arnold RR, Offenbacher S. Inflammatory mediator response as a potential risk marker forperiodontal diseases in insulin-dependent diabetesmellitus patients. J Periodontol 1997;68:127–135.
10. Ollier W, Thomson W. Population genetics ofrheumatoid arthritis. Rheum Dis Clin North Am1992;18:741–759.
11. Bendtzen K, Morling N, Fomsgaard A, SvensonM, Jakobsen B, Odum N, Svejgaard A. Associationbetween HLA-DR2 and production of tumournecrosis factor alpha and interleukin 1 by mononu-clear cells activated by lipopolysaccharide. ScandJ Immunol 1988;28:599–606.

12. MacGregor AJ, Snieder H, Rigby AS, KoskenvuoM, Kaprio J, Aho K, Silman AJ. Characterizing thequantitative genetic contribution to rheumatoidarthritis using data from twins. Arthritis Rheum2000;43:30–37.
13. Wilson K, Goldsmith CH. 1999. Does smoking causerheumatoid arthritis? J Rheumatol 1999;26:1–3.
14. Bergström J, Preber H. Tobacco use as a risk fac-tor. J Periodontol 1994;65(5 Suppl):545–550.
15. Callahan LF, Pincus T. Formal education level as asignificant marker of clinical status in rheumatoidarthritis. Arthritis Rheum 1988;31:1346–1357.
16. Borrell LN, Burt BA, Warren RC, Neighbors HW.The role of individual and neighborhood social fac-tors on periodontitis: The third National Health andNutrition Examination Survey. J Periodontol 2006;77:444–453.
17. Michalowicz BS, Diehl SR, Gunsolley JC, SparksBS, Brooks CN, Koertge TE, Califano JV, Burm-eister JA, Schenkein HA. Evidence of a substantialgenetic basis for risk of adult periodontitis. J Peri-odontol 2000;71:1699–1707.
18. Kobayashi S, Momohara S, Kamatani N, OkamotoH. Molecular aspects of rheumatoid arthritis:role of environmental factors. FEBS J 2008;275:4456–4462.
19. Moreland LW, Curtis JR. Systemic nonarticularmanifestations of rheumatoid arthritis: Focus oninflammatory mechanisms. Semin Arthritis Rheum2008; Epub ahead of print.
20. Snyderman R, McCarty GA. Analogous mecha-nisms of tissue destruction in rheumatoid arthritisand periodontal disease. In: Genco RJ, Mergen-hagen SE eds. Host-Parasite Interactions in Perio -dontal Diseases. American Society for Micro -biology: Washington, DC; 1982:354–362.
21. Okuda K, Ebihara Y. Relationships between chronicoral infectious diseases and systemic diseases. BullTokyo Dent Coll 1998;39:165–174.
22. Mercado FB, Marshall RI, Bartold PM. Inter-rela-tionships between rheumatoid arthritis and perio -dontal disease. A review. J Clin Periodontol2003;30:761–772.
23. Bartold PM, Marshall RI, Haynes DR. Periodonti-tis and rheumatoid arthritis: A review. J Periodon-tol 2005;76(11 Suppl):2066-2074.
24. Golub LM, Payne JB, Reinhardt RA, Nieman G.Can systemic diseases co-induce (not just exacer-bate) periodontitis? A hypothetical “two-hit” model.J Dent Res 2006;85:102–105.
25. Helminen-Pakkala E. Periodontal conditions inrheumatoid arthritis: A clinical and roentgenologi-cal investigation. Part 2: The study in rheumatoidsbased on a hospital material. Suomen hammas -lääkäriseuran toimituksia. Supplementum (Proc
Chapter 12 Association Between Periodontitis and Rheumatoid Arthritis 193
Finnish Dental Assoc Supplement) 1971; Suppl IV;1–108.
26. Blair GS, Chalmers IM. The dental status of achronically disabled section of the community: Astudy of 139 patients suffering from rheumatic dis-eases. J Dent Assoc S Afr 1976;31:329–336.
27. Yusof Z, Porter SR, Greenman J, Scully C. Levelsof serum IgG against Porphyromonas gingivalis inpatients with rapidly progressive periodontitis,rheumatoid arthritis and adult periodontitis. J NihonUniv Sch Dent 1995;37:197–200.
28. Yavuzyilmaz E, Yamalik N, Calgüner M, Ersoy F,Baykara M, Yeniay I. Clinical and immunologicalcharacteristics of patients with rheumatoid arthritisand periodontal disease. J Nihon Univ Sch Dent1992;34:89–95.
29. Sjöström L, Laurell L, Hugoson A, Håkansson JP.Periodontal conditions in adults with rheumatoidarthritis. Comm Dent Oral Epidemiol 1989;17:234–236.
30. Arneberg P, Bjertness E, Storhaug K, Glennås A,Bjerkhoel F. Remaining teeth, oral dryness anddental health habits in middle aged Norwegianrheumatoid arthritis patients. Comm Dent Oral Epi-demiol 1992;20:292–296.
31. Eklund SA, Burt BA. Risk factors for total toothloss in the United States: longitudinal analysis ofnational data. J Public Health Dent 1994;54:5–14.
32. Mercado F, Marshall RI, Klestov AC, Bartold PM.Is there a relationship between rheumatoid arthritisand periodontal disease? J Clin Periodontol 2000;27:267–272.
33. Lagervall M, Jansson L, Bergström J. Systemicdisorders with periodontal disease. J Clin Perio -dontol 2003;30:293–299.
34. Georgiou TO, Marshall RI, Bartold PM. Preva-lence of systemic diseases in Brisbane general andperiodontal practice patients. Aust Dent J 2004;49:177–184.
35. Dumitrescu AL. Occurrence of self-reported sys-temic medical conditions in patients with perio -dontal disease. Rom J Intern Med 2006;44:35–48.
36. Malmström M, Calonius PE. Teeth loss and the in-flammation of teeth-supporting tissues in rheuma-toid disease. Scand J Rheumatol 1975;4:49–55.
37. Albandar JM. Some predictors of radiographicalveolar bone height reduction over 6 years. J Perio -dontal Res 1990;25:186–192.
38. Tolo K, Jorkjend L. Serum antibodies and loss ofperiodontal bone in patients with rheumatoid arthri-tis. J Clin Periodontol 1990;17:288–291.
39. Kässer UR, Gleissner C, Dehne F, Michel A, Wil-lershausen-Zönnchen B, Bolten WW. Risk for pe-riodontal disease in patients with longstandingrheumatoid arthritis. Arthritis Rheum 1997;40:

2248–2251.40. Gleissner C, Willershausen B, Kässer U, Bolten
WW. The role of risk factors for periodontal diseasein patients with rheumatoid arthritis. Eur J MedRes 1998;3:387–392.
41. Novo E, Garcia-MacGregor E, Viera N, ChaparroN, Crozzoli Y. Periodontitis and anti-neutrophil cytoplasmic antibodies in systemic lupus erythe-matosus and rheumatoid arthritis: a comparativestudy. J Periodontol 1999;70:185–188.
42. Zhang DZ, Zhong DY, Deng J, Wang JB. Relati-onship between periodontal disease and rheumatoidarthritis. Hua Xi Kuo Qiang Yi Xue Za Zhi2005;23:498–501.
43. Ishi Ede P, Bertolo MB, Rossa C Jr, Kirkwood KL,Onofre MA. Periodontal condition in patients withrheumatoid arthritis. Braz Oral Res 2008;22:72–77.
44. Pischon N, Pischon T, Kröger J, Gülmez E, KleberBM, Bernimoulin JP, Landau H, Brinkmann PG,Schlattmann P, Zernicke J, Buttgereit F, Detert J.Association among rheumatoid arthritis, oral hy-giene, and periodontitis. J Periodontol 2008;79:979–986.
45. Bozkurt FY, Berker E, Akkus S, Bulut S. Relation-ship between interleukin-6 levels in gingival crevic-ular fluid and periodontal status in patients withrheumatoid arthritis and adult periodontitis. J Perio -dontol 2000;71:1756–1760.
46. Havemose-Poulsen A, Sørensen LK, Stoltze K,Bendtzen K, Holmstrup P. Cytokine profiles in peripheral blood and whole blood cell cultures associated with aggressive periodontitis, juvenileidiopathic arthritis, and rheumatoid arthritis. J Perio -dontol 2005;76:2276–2285.
47. Pers JO, Saraux A, Pierre R, Youinou P. Anti-TNF-alpha immunotherapy is associated with increasedgingival inflammation without clinical attachmentloss in subjects with rheumatoid arthritis. J Perio -dontol 2008;79:1645–1651.
48. Bozkurt FY, Yetkin Ay Z, Berker E, Tepe E, AkkuS. Anti-inflammatory cytokines in gingival crevic-ular fluid in patients with periodontitis and rheuma-toid arthritis: A preliminary report. Cytokine 2006;35:180–185.
49. Havemose-Poulsen A, Westergaard J, Stoltze K,Skjødt H, Danneskiold-Samsøe B, Locht H,Bendtzen K, Holmstrup P. Periodontal and hema -tological characteristics associated with aggressiveperiodontitis, juvenile idiopathic arthritis, andrheumatoid arthritis. J Periodontol 2006;77:280–288.
50. Nilsson M, Kopp S. Gingivitis and periodontitisare related to repeated high levels of circulatingtumor necrosis factor-alpha in patients with rheu -matoid arthritis. J Periodontol 2008;79:1689–1696.
51. Biyikolu B, Buduneli N, Kardeler L, Aksu K,Oder G, Kütükçüler N. Evaluation of t-PA, PAI-2,IL-1beta and PGE(2) in gingival crevicular fluid ofrheumatoid arthritis patients with periodontal dis-ease. J Clin Periodontol 2006;33:605–611.
52. Katz J, Goultschin J, Benoliel R, Brautbar C. Hu-man leukocyte antigen (HLA) DR4. Positive asso-ciation with rapidly progressing periodontitis. JPeriodontol 1987;58:607–610.
53. Bonfil JJ, Dillier FL, Mercier P, Reviron D, Foti B,Sambuc R, Brodeur JM, Sedarat C. A “case control”study on the role of HLA DR4 in severe perio don -titis and rapidly progressive periodontitis. Identifi-ca tion of types and subtypes using molecular biol-ogy (PCR.SSO). J Clin Periodontol 1999;26:77–84.
54. Marotte H, Farge P, Gaudin P, Alexandre C, Mou-gin B, Miossec P. The association between perio -dontal disease and joint destruction in rheumatoidarthritis extends the link between the HLA-DRshared epitope and severity of bone destruction.Ann Rheum Dis 2006;65:905–909.
55. Soory M. Hormone mediation of immune responsesin the progression of diabetes, rheumatoid arthritisand periodontal diseases. Curr Drug Targets Im-mune Endocr Metabol Disord 2002;2:13–25.
56. Ribeiro J, Leão A, Novaes AB. Periodontal infec-tion as a possible severity factor for rheumatoidarthritis. J Clin Periodontol 2005;32:412–416.
57. Iida M, Yamaguchi Y. Remission of rheumatoidarthritis following periodontal treatment. A casereport. Nippon Shishubyo Gakkai Kaishi 1985;27:234–238.
58. Al-Katma MK, Bissada NF, Bordeaux JM, Sue J,Askari AD. Control of periodontal infection re-duces the severity of active rheumatoid arthritis. JClin Rheumatol 2007;13:134–137.
59. Ramamurthy NS, Greenwald RA, Celiker MY, ShiEY. Experimental arthritis in rats induces bio-markers of periodontitis which are ameliorated bygene therapy with tissue inhibitor of matrix metal-loproteinases. J Periodontol 2005;76:229–233.
60. Mercado FB, Marshall RI, Klestov AC, BartoldPM. Relationship between rheumatoid arthritis andperiodontitis. J Periodontol 2001;72:779–787.
61. Scardina GA, Messina P. Microvascular periodon-tal alterations: A possible relationship between perio dontitis and rheumatoid arthritis. Clin Hemor -heol Microcirc 2007;37:229–235.
62. Yoshida A, Nakano Y, Yamashita Y, Oho T, Ito H,Kondo M, Ohishi M, Koga T. Immunodominant re-gion of Actinobacillus actinomycetemcomitans 40-kilodalton heat shock protein in patients withrheumatoid arthritis. J Dent Res 2001;80:346–350.
63. Moen K, Brun JG, Madland TM, Tynning T, Jons-son R. Immunoglobulin G and A antibody responses
194 Periodontal Disease and Overall Health: A Clinician's Guide

to Bacteroides forsythus and Prevotella inter media insera and synovial fluids of arthritis patients. ClinDiagn Lab Immunol 2003;10:1043–1050.
64. Ogrendik M, Kokino S, Ozdemir F, Bird PS, Hamlet S. Serum antibodies to oral anaerobic bac-teria in patients with rheumatoid arthritis. Med-scape Gen Med 2005;7(2):2
65. Moen K, Brun JG, Valen M, Skartveit L, Eribe EK,Olsen I, Jonsson R. Synovial inflammation in activerheumatoid arthritis and psoriatic arthritis facili-tates trapping of a variety of oral bacterial DNAs.Clin Exp Rheumatol 2006;24:656–663.
66. Rosenstein ED, Greenwald RA, Kushner LJ, Weis-
smann G. Hypothesis: The humoral immune re-sponse to oral bacteria provides a stimulus for thedevelopment of rheumatoid arthritis. Inflammation2004;28:311–318.
67. Costenbader KH, Karlson EW. Epstein-Barr virusand rheumatoid arthritis: Is there a link? ArthritisRes Therapy 2006;8(1):204. Epub 2006 Jan 16.
68. Slots J. Herpes viruses in periodontal diseases. Perio dontol 2000 2005;38:33–62.
69. Greenwald RA, Kirkwood K. Adult periodontitis asa model for rheumatoid arthritis (with emphasis ontreatment strategies). J Rheumatol 1999;26:1650–1653.
Chapter 12 Association Between Periodontitis and Rheumatoid Arthritis 195
196 Periodontal Disease and Overall Health: A Clinician's GuideCHAPTER 13Oral Health, Periodontitis, and Cancer
P. Mark Bartold, Angelo J. Mariotti
INTRODUCTIONPeriodontitis is a chronic immuno-
inflammatory reaction to bacteria that residewithin the subgingival plaque biofilm. In ad-dition to pathogenic microorganisms in thebiofilm, genetic and environmental factorscontribute to the pathogenesis of this dis-ease, which results in the destruction of theperiodontal tissues and alveolar bone sup-porting the teeth. During these responsesthere is a potential for complications or otherinfluences to impact systemic health via bac-teremia or dissemination of locally producedinflammatory mediators. Bacteremia has thepotential to result in a general systemic in-flammatory response. Moreover, locally pro-duced inflammatory mediators disseminatedinto the circulation can result in increasedlevels of inflammatory mediators such as tumor necrosis factor alpha (TNF-), inter-leukins 1 beta and 6 (IL-1 and IL-6), andprostaglandin E2 (PGE2), as well as acute-phase proteins such as C-reactive protein.This can result in a chronic inflammatoryburden on distant organ systems.
Recent studies have demonstrated as-sociations between periodontal disease andseveral systemic diseases, including cardio-vascular disease, diabetes mellitus, adversepregnancy outcomes, respiratory diseases,osteoporosis, and rheumatoid arthritis.
With increasing attention being focusedon oral/systemic interactions, studies havesuggested that periodontal disease may be as-sociated with increased cancer risk.1 Interestfor such an association stemmed from earlystudies that investigated the association ofpoor oral health and missing teeth on bothoral cancer and cancer of other systemic or-gans. While tooth loss may be a poor indicator
of periodontal disease, it has been used as amajor surrogate marker for this disease inolder individuals.2 Indeed, there are many rea-sons for tooth loss and while it can be a resultof either dental caries or periodontal diseases,age can also be a major contributing factor forthese two conditions. Thus, in early studies,tooth loss in older individuals was assumed tomore likely be a result of periodontal diseasethan caries. In more recent times, such asser-tions would almost certainly be challenged.Current understanding would indicate thattooth loss in older individuals may be a resultof perio dontal disease, but this associationmay not always be particularly strong. Thisbeing the case, it is surprising that very fewstudies investigating the role of oral healthand cancer have undertaken specific perio -dontal assessments.
The potential interaction between can-cer and periodontal disease is important, andmany studies imply that a specific associa-tion between periodontitis and cancer (bothoral and general) is feasible. However,larger, more defined studies are needed todetermine whether or not the association canbe confirmed and how this might impact ourunderstanding of the etiology of various can-cers, their prevention, and control.
In this review, studies included ad-dressed the association of general oral con-dition (e.g., oral hygiene, restorations, pros-theses, tooth brushing), tooth loss, andperiodontal disease with both oral cancerand cancers of other organs.
The educational objectives for thischap ter are:
1. Understand the potential associationsbetween oral health, periodontal disease, andvarious cancers.
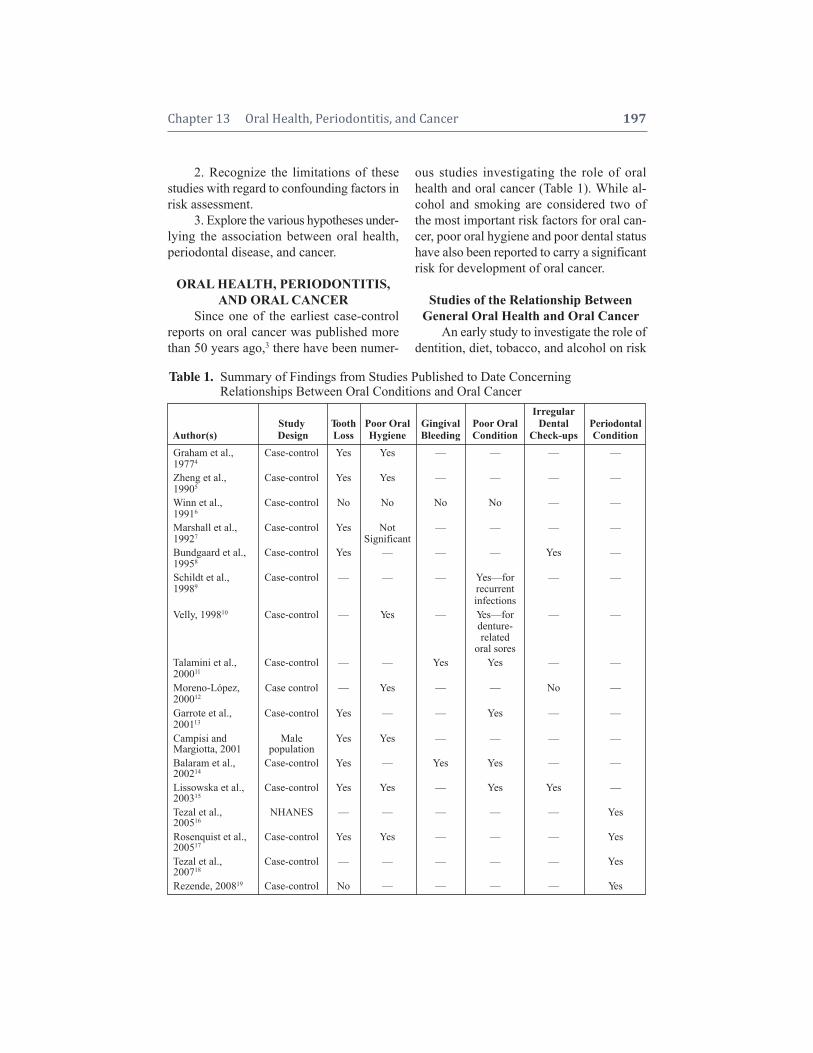
Chapter 13 Oral Health, Periodontitis, and Cancer 197
2. Recognize the limitations of thesestudies with regard to confounding factors inrisk assessment.
3. Explore the various hypotheses under -lying the association between oral health,periodontal disease, and cancer.
ORAL HEALTH, PERIODONTITIS,AND ORAL CANCER
Since one of the earliest case-controlreports on oral cancer was published morethan 50 years ago,3 there have been numer-
ous studies investigating the role of oralhealth and oral cancer (Table 1). While al-cohol and smoking are considered two ofthe most important risk factors for oral can-cer, poor oral hygiene and poor dental statushave also been reported to carry a significantrisk for development of oral cancer.
Studies of the Relationship BetweenGeneral Oral Health and Oral Cancer
An early study to investigate the role ofdentition, diet, tobacco, and alcohol on risk
Table 1. Summary of Findings from Studies Published to Date Concerning Table 1. Relationships Between Oral Conditions and Oral Cancer
IrregularStudy Tooth Poor Oral Gingival Poor Oral Dental Periodontal
Author(s) Design Loss Hygiene Bleeding Condition Check-ups ConditionGraham et al., Case-control Yes Yes — — — —19774
Zheng et al., Case-control Yes Yes — — — —19905
Winn et al., Case-control No No No No — —19916
Marshall et al., Case-control Yes Not — — — —19927 SignificantBundgaard et al., Case-control Yes — — — Yes —19958
Schildt et al., Case-control — — — Yes—for — —19989 recurrent
infectionsVelly, 199810 Case-control — Yes — Yes—for — —
denture-related
oral soresTalamini et al., Case-control — — Yes Yes — —200011
Moreno-López, Case control — Yes — — No —200012
Garrote et al., Case-control Yes — — Yes — —200113
Campisi and Male Yes Yes — — — —Margiotta, 2001 populationBalaram et al., Case-control Yes — Yes Yes — —200214
Lissowska et al., Case-control Yes Yes — Yes Yes —200315
Tezal et al., NHANES — — — — — Yes200516
Rosenquist et al., Case-control Yes Yes — — — Yes200517
Tezal et al., Case-control — — — — — Yes200718
Rezende, 200819 Case-control No — — — — Yes

198 Periodontal Disease and Overall Health: A Clinician's Guide
for oral cancer was a case study by Grahamet al.4 In this study the cases consisted of584 males with cancer of the oral cavityat the Roswell Park Memorial Institute, Buffalo, New York. The controls con-sisted of 1,222 males with no neoplastic dis-eases at the same institute. Interviews werecarried out to obtain information regard-ing dentition, diet, tobacco, and alcoholconsumption.
From this study it was reported that ahigher risk of developing cancer was notedin heavy smokers and heavy drinkers. Poororal hygiene was also associated with in-creased risk for oral cancer. When controlledfor other factors, each of these three factorsdemonstrated a higher risk. When combined,heavy smokers and heavy drinkers with apoor dentition had a risk 7.7 times that ofmen with none of these features.
In another case-control study carriedout in Beijing, Zheng et al.5 investigated thedentition and oral hygiene status for risk oforal cancer. The cases consisted of 404 pa-tients with histologically confirmed oral can-cer and a similar number of control patientswhose hospitalizations were for minor con-ditions. Subjects were interviewed to obtaininformation regarding alcohol, tobacco use,dentition, and oral hygiene. An oral exam -ination included recording the total numberof teeth, jagged teeth, filled teeth, decayedteeth, and presence of gingivitis or perio -dontal disease. After adjustment for tobaccosmoking, alcohol intake, years of education,gender, and age, males who had lost teethhad an increased risk for oral cancer withan odds ratio (OR) of 2.4 (95% confidenceinterval [CI]:1.3–4.5) if they had replace-ment teeth, and an OR of 3.7 (CI: 2.2–6.4)if they had no tooth replacement. The datafor females showed an even stronger ef-fect of tooth loss on increased risk for oralcancer, with an OR of 5.6 (CI:12.2–14.5)if they had replacement teeth and an ORof 8.3 (CI:3.5–19.6) if they had no tooth
replacement. When oral hygiene was as-sessed, according to whether the teeth werebrushed or not, men had an adjusted OR of6.9 (CI: 2.5 –19.4) and women an adjustedOR of 2.5 (CI: 0.9–7.5) for increased risk oforal cancer if they did not brush their teeth.The findings were inter preted to indicate thatmissing teeth and poor oral hygiene were riskfactors for oral cancer independent of theknown risks associated with smoking andalcohol consumption.
In a study aimed primarily at investi-gating the effect of mouthwash use on oralcancer, Winn et al.6 studied 1,114 oral cancerpatients from four population-based registriesin the US. Control subjects (n = 1,268) werenoncancerous individuals selected by ran-dom dialing to select individuals of suitableage and gender-matched status. Interviewswere carried out to obtain information regard -ing tobacco use, alcohol use, diet, occupation,and oral health status. The oral health param -eters included the number of teeth, use ofdentures, tooth brushing frequency, andbleeding gingiva. The presence of other oraldiseases as well as the frequency, intensity,duration, and reason for use of mouthwasheswere recorded. A highly significant relation-ship between mouthwashes of high alcoholcontent and oral cancer was noted for bothmales (OR:1.5; CI:1.1–2.1) and females(OR: 2.0; CI:1.3–3.1). In contrast to mostother studies, this study found no relation-ship between oral/dental conditions and oralcancer.
In another US investigation, Marshall etal.7 carried out a case-control study in threewestern New York counties to investigatethe contribution of alcohol, dentition, anddiet to oral cancer. The cohort consisted of290 pathologically confirmed cases of oralcancer selected from hospital records, whilematched controls were obtained throughneighborhood matching. Cases and controlswere interviewed to gather information con-cerning smoking and tobacco use, alcohol

Chapter 13 Oral Health, Periodontitis, and Cancer 199
consumption, dental history (i.e., tooth loss,tooth replacement, oral hygiene, and dentalcheck-up practices), and diet. Compared toindividuals who had not lost any teeth, an in-creased risk for oral cancer was noted forthose individuals who had lost more than 11teeth (OR: 3.9; CI:1.3–11.3). When furtheranalyzed, individuals who smoked cigarettes,drank alcohol, and had lost teeth without having them replaced had an increased riskfor oral cancer (OR:12.8; CI: 4.9–33.8). Theeffect of oral hygiene in this study was deter-mined to be insignificant.
A population-based case-control studyon a Danish population has examined if therisk of oral squamous cell carcinoma couldbe related to occupation, marital status, den-tal status, and consumption of coffee, tea,alcohol, and tobacco (Bundgaard et al.).8 Inthis study, the cases consisted of 161 con-secutively admitted patients with histologi-cally verified intra-oral squamous cell car-cinoma. Four-hundred age- and gender-matched controls were selected from theneighborhood. Information was gathered byinterview and no clinical dental examinationwas carried out. After correcting for alcoholand tobacco consumption, dental status wasfound to be a significant factor associatedwith oral squamous cell carcinoma manifes-tation. Individuals with fewer than five teethhad an OR of 2.4 (CI:1.3–4.1) compared tothose with 15 or more teeth. Furthermore,those individuals who had irregular dentalcheck-ups had an OR of 2.1 (CI:1.3–3.3)compared to those who had regular dentalcheck-ups. While significant, these findingswere determined to be of less importancethan tobacco or alcohol use with regard torisk for oral squamous cell carcinoma.
In a case-control study of a Swedishpopulation, Schildt et al.9 investigated therelationship of oral infections and other den-tal factors for risk of oral cancer. For thisstudy, 410 cases of oral cancer and 410matched controls were sampled. All subjects
received a mailed questionnaire concerningdifferent exposure factors of interest for oralcancer including oral infections, dental pros-theses, radiographic exposure, restorations,tooth loss, and presence of calculus. Recur-rent oral infection was found to be associatedwith increased risk of oral cancer (OR:3.8;CI:2.1–6.9). Other dental factors such asrestorations, dentures, and dental radiographswere of no significance.
In a study investigating the relationshipbetween dental factors and risk of upper di-gestive tract cancer, Velly et al.10 studied 717patients who had newly diagnosed carcino-mas of the tongue, gingiva, floor of mouth,and other parts of the oral cavity from threecenters in Sao Paulo. Controls (noncancer-ous patients) were selected from the same in-stitutions and data were collected from twocontrols matched to each case on the basis ofgender, five-year age group, trimester of hos-pital admission, and study site. Informationcollected by interview included informationon socio-economic variables, health condi-tions, environmental and occupational ex-posures, tobacco and alcohol consumption,and diet and oral hygiene. The dental healthinformation was obtained only by interviewand included information concerning bro-ken teeth, use of dentures and sores causedby dentures, and frequency of tooth brush-ing. The association between cancer and den-tal factors was assessed using a number ofadjustments for a priori and empirical con-founders, including tobacco and alcohol con-sumption, diet, and socio-economic vari-ables. The risk for all oral cancer in generalwas significantly associated with dentures(OR:0.7; CI:0.52–0.96), history of oral sorescaused by dentures (OR: 0.91; CI: 0.6–1.3), broken teeth (OR:1.42; CI:1.1–1.9) andinfrequent tooth brushing (OR: 2.2; CI:1.6–3.1). Following adjustment of severalconfounders and for all dental factors, onlythe association with tooth brushing fre-quency was significant (OR:1.8; CI:1.2–2.8

200 Periodontal Disease and Overall Health: A Clinician's Guide
and OR:1.7; CI:1.1–2.8, respectively). Whenassessed on a subsite basis, only less-than-daily tooth brushing was a risk for tonguecancer (OR:1.3; CI:0.6–3.0) and other partsof the mouth, including the gingiva (OR:2.4; CI:1.3–4.4). For laryngeal cancer, bro-ken teeth (OR:1.8; CI:1.3–2.7) and infre-quent tooth brushing (OR:1.9; CI:1.2–2.9)were the only significant risk markers. Forpharyngeal cancer, only infrequent toothbrushing (OR:1.5; CI:1.0–2.2) was deter-mined to be a significant risk factor. The au-thors concluded that poor oral hygiene, dueto infrequent tooth brushing and denture- related oral sores, were significant risk fac-tors for cancer of the mouth and upper diges -tive tract, and that these associations werenot due to insufficient controlling for con-founding factors.
Talamini et al.11 carried out a case- control study on an Italian population inves-tigating the effect of oral hygiene and denti-tion status on oral cancer risk. The cohortconsisted of 132 first-incident cases of oralcancer identified in three northern Italy hos-pitals. One-hundred and forty-eight hospital-based control subjects, who had been ad-mitted for acute conditions unrelated tosmoking or drinking habits, were also re-cruited for this study. Cases and controlswere interviewed to obtain information relating to sociodemographic characteristics,smoking and drinking habits, as well as dental information related to oral hygiene,gingival bleeding, mouthwash usage, wear-ing of dentures, and dental check-up history.A visual examination determined number ofmissing teeth, presence of calculus, decayedteeth, and mucosal condition. The presenceof gingival bleeding was found to be sig -nificant (OR:3.9; CI:1.2–12.6) when com-pared to those whose gingiva did not bleed atall. When the general oral condition was assessed as being poor on the basis of cal-culus, decayed teeth, and mucosal irritation,the risk for oral cancer had an OR of 4.5
(CI: 1.8–10.9) compared to those who hadgood oral condition. Interestingly, and incontrast to previous studies, the number ofmissing teeth was not found to be a signifi-cant factor.
The role of tobacco, alcohol, and oralhygiene in the appearance of oral cancerwas investigated in a case-control study byMoreno-López et al.12 For this study, thecases consisted of 75 histologically con-firmed oral squamous cell carcinomas. Thecontrol group consisted of age- and gender-matched individuals in the same healthcarecenter who did not suffer from cancer anddid not have any medical or oral disease ororal manifestation of any systemic disease.An interview was used to obtain informationrelated to demographic variables, tobacco use,alcohol consumption, frequency of dentalcheck-ups, and level of tooth brushing. Nointra-oral examination was carried out.While no statistical significance could befound for dental visits, a significant relation -ship for tooth brushing was found that indi-cated this to be a protective factor (OR: 0.31;CI:0.18–0.56).
In a case-control study on a Cuban pop-ulation, the effect of smoking, alcohol, food,oral hygiene, and sexually transmitted dis-eases on risk for oral cancer was evaluated.Garrote et al.13 compared 200 cases of can-cer of the oral cavity and pharynx with 200frequency-matched age and gender controlsfrom the hospital. Interviews were held toobtain information regarding sociodemo-graphic characteristics, smoking and alcoholuse, prior occurrence of sexually transmittedinfections, family history of cancer, and di-etary information. Indicators of oral hygienewere self-reported via nine specific ques-tions, while the number of missing teeth thathad not been replaced and the general oralcondition with regard to presence of calculus,decayed teeth, and mucosal irritation wereevaluated visually by the interviewing den-tist. After allowance for confounding factors

Chapter 13 Oral Health, Periodontitis, and Cancer 201
such as education, smoking, and drinkinghabits, individuals with greater than 16 miss-ing teeth had a higher risk of having oralcancer (OR: 2.7: CI:1.2–6.1). In addition,poor general oral condition was more fre-quent among cancer cases than controls (OR:2.6: CI:1.2–5.2).
In an Indian population derived fromthree regions (Bangalore, Madras, andTrivandrum), Balaram et al.14 investigatedthe role of smoking, paan chewing, and oralhygiene on risk for oral cancer. In this study,591 incident cases of oral cancer and 582 hos -pital controls that were frequency matchedby age and gender were studied. Informationregarding smoking habits, paan chewing, andoral hygiene habits was obtained by interview.Visual oral inspection allowed assessmentof missing teeth and general oral conditionbased on the presence of calculus, decayedteeth, and mucosal irritation. Regular dentalcheck-ups were found to be protective forwomen but not men (OR: 0.4; CI: 0.19–0.87). Significantly elevated risk for oralcancer for both genders was noted for gin-gival bleeding (men = OR:2.8; CI:1.7–4.7and women = OR:3.4; CI:1.8–6.1), havingsix or more missing teeth (men = OR:3.9;CI: 2,5–6.1 and women = OR:7.6; CI: 3.9–14.9), and interviewer-reported poor generaloral condition (men = OR: 4.9; CI:3.1–7.8and women = OR:6.0; CI:3.00–12.00).
In a European case-control investiga-tion, Lissowska et al.15 studied a Polish pop-ulation to investigate the effect of smoking,alcohol, diet, dentition, and sexual practiceson risk for oral cancer. The study populationconsisted of 122 patients with histologicallyconfirmed cancer of the oral cavity and phar-ynx. The controls consisted of 124 age- andgender-matched patients admitted to the hos-pital for non-neoplastic conditions unrelatedto tobacco and alcohol. The subjects wereinterviewed to obtain information regardingdemographics, smoking, alcohol consump tion,family history of cancer, and oral hygiene.
After adjusting for smoking and alcohol, andpoor dentition as assessed by number of miss-ing teeth (OR: 9.8; CI:2.3–42.8), the fre-quency of dental check-ups (OR:11.9; CI:3.3–42.5) and of tooth brushing (OR: 3.2;CI:1.2–8.5) were found to be the most sig -nificant risk factors for oral cancer. It wascon cluded that poor oral hygiene may bean independent risk factor for oral and oro -pharyngeal cancer.
Studies of the Relationship Between Periodontitis and Oral CancerIn the first study in which the perio -
dontium was assessed, Tezal et al.16 used across-sectional analysis of data extractedfrom the Third National Health and NutritionExamination Survey (NHANES III; NationalCenter for Health Statistics 1994). For thisstudy, individuals who were 20 and olderand had at least six natural teeth were in-cluded. Subjects requiring antibiotics beforea dental examination were excluded. Perio -dontal measurements included assessmentof clinical attachment loss, while other oralassessments included number of missingteeth, caries, restorations, and the presence ofpartial or full prostheses. Following adjust-ment for age, gender, race, ethnicity, educa-tion, tobacco use, alcohol consumption, andoccupational hazard, clinical attachment losswas significantly associated with the pres-ence of oral tumors (OR: 4.6; CI: 2.3–9.3).Additional analyses considering the interac-tions between clinical attachment levels(CAL) and smoking indicated that CALwas a significant risk for tumor (OR: 21.76;CI:3.6–131.63) in current smokers, sug-gesting that it is a risk modifier. This conceptis strengthened by the observation that CALhad no effect on tumor risk for former smokers or people who never smoked andhence, is probably not an independent riskfactor.
Shortly following the Tezal et al.16
study, Rosenquist et al.17 published results

202 Periodontal Disease and Overall Health: A Clinician's Guide
from a study that also used a comprehen-sive periodontal assessment. In this case-control study of a Swedish population, alcohol consumption, tobacco use, oral hy-giene, dental status, and dental radiographicstatus were evaluated for increasing risk fororal cancer. The cases consisted of 132 oraland oropharyngeal cancer patients who wereselected from a population residing in thesouthern healthcare region of Sweden. Age-and gender-matched controls were selectedfrom the same region with no previous can-cer diagnosis (except for skin cancer). Theoral condition was assessed via interviewfor frequency of dental check-ups, visual as-sessment of plaque score, modified gingivalbleeding index, number of missing teeth, defective teeth, tooth mobility, furcation in-volvement, and presence of dentures. A radio - graphic examination of the dentition evalu-ated marginal bone levels, loss of bone alongroot surfaces, angular bony defects, and fur-cation defects. A mucosal assessment wasalso provided. In an unadjusted analysis, individuals with average (OR:3.0; CI:1.7–5.1) or poor (OR:10.0; CI:5.1–20.1) oral hygiene, as assessed by plaque scores, weresignificantly at risk for oral cancer. After ad-justing for smoking and alcohol use, indi-viduals with an average plaque score had anOR of 2.0 (CI:1.1–3.6), while a poor plaquescore had an OR of 5.3 (CI:2.5–11.3). Thenumber of missing teeth was also found to bea significant risk factor, with more than 20missing teeth being statistically significant inunadjusted (OR:6.1; CI:2.7–14.0) and ad-justed analyses (OR:3.4; CI:1.4–8.5). Thosewith more than five missing teeth also hadsignificant risk in both unadjusted (OR: 4.8;CI:2.0–11.4) and adjusted (OR:3.1; CI: 1.2–8.2) analyses. Upon radiographic assess-ment, a high level of marginal bone wasnoted to have an increased risk for oral cancer in unadjusted analyses (OR: 3.00;CI:1.0–8.7); however, this failed to reach significance in adjusted analyses. Regular
dental check-ups were noted to be associatedwith a decreased risk of oral cancer in ad-justed analyses (OR: 0.4; CI:0.2–0.6).
In a subsequent study, Tezal et al.18 car-ried out a case-control study of pre-existingdata for patients seen at the Roswell ParkCancer Center (1999–2005) to assess the roleof periodontitis for risk of tongue cancer.The cases consisted of 54 non-Hispanic Cau-casian males with primary squamous cellcarcinoma of the tongue. Age- and gender-matched non-Hispanic Caucasian men seenin the same hospital department but not diagnosed with any cancer or oral dysplasiaserved as the controls (n = 54). The perio -dontal assessment consisted of evaluation ofalveolar bone loss from panoramic radio -graphs. Other dental information includingcaries, restorations, and endodontic treat-ment was determined from the radiographs.Analyses following adjustments for the con -founders of age, smoking habit, and numberof missing teeth indicated that for every millimeter of alveolar bone loss, there was a5.2-fold increase in the risk of tongue cancer(OR:5.2; CI:2.6–10.4). Other variables stud-ied, including caries, restorations, and rootcanal treatment, failed to show any signifi-cant association with tongue cancer.
The most recent published study as-sessing the association between oral hygiene,periodontal disease, and oropharyngeal andoral cancer was a cross-sectional prospectivecase-control study.19 In this study, 50 caseswith untreated oral and oropharyngeal squa-mous cell carcinoma were compared to5,009 cancer-free subjects matched forage and gender. An oral health questionnairewas used to assess tooth brushing as wellas use of mouthrinses, dental floss, andother oral hygiene aids. An oral examinationwas carried out to determine CommunityPeriodontal Index of Treatment Needs(CPITN) scores, missing teeth, caries,restorations, and prostheses, but there was noconsideration given to smoking status or

Chapter 13 Oral Health, Periodontitis, and Cancer 203
alcohol consumption. Following very sim -plistic statistical analyses, the authors reported that advanced perio dontal diseasewas greater in the subjects with oral andoropharyngeal cancer. Up to 76% of the cancer subjects had periodontal probingpockets greater than 6 mm compared to 20%of the patients without cancer. No statisti-cally significant differences could be foundfor caries, missing teeth, restorations, orprostheses.
Summary of the RelationshipBetween Oral Health and Oral Cancer
It is clear that a number of oral condi-tions, including tooth loss, poor oral hygiene,poor oral condition, and general periodontalcondition are significant risk factors for oralcancer (Table 1). Due to great variability instatistical analyses, it is difficult to deter-mine the real significance of many of thesestudies. Nonetheless, several studies havetried to remove confounding influences andhave been able to demonstrate that many ofthese oral conditions remain significant riskfactors. Perhaps the main confounding fac-tors are smoking and alcohol consumption.When considered together (smoking, alco-hol, and oral conditions), risk for oral cancerseemed to increase significantly. When twoof these confounders (smoking and alcohol)were removed, oral conditions remainedhighly significant risk factors. The interplaybetween oral condition and oral cancer, already induced by recognized risk factorssuch as alcohol and tobacco, needs to be further investigated. It has only been in re-cent years that an evaluation of periodontalcondition has been assessed as a potentialrisk factor. While the early data indicate a putative role for periodontal disease, thereis considerable scope for further studies toinvestigate in more detail specific periodon-tal parameters, as well as types of periodon-titis in the periodontal diseases-oral canceraxis.
ORAL CONDITIONS ANDVARIOUS TYPES OF CANCER
Oral Conditions and Upper Gastrointestinal (GI) Cancer
One of the first reports to suggest an association between oral condition and GIcancer was a case-control study carried outin Germany.20 The cases included stomach cancer patients (n = 257) and healthy, non-cancerous control subjects (n = 766). Infor-mation was obtained from patient interviewsand 20 variables were found to be signifi-cantly associated with gastric cancer. Ofthese, early tooth loss was identified as aprominent variable.
During the 1990s, several case-controlstudies were conducted to investigate the as-sociation of oral health and upper GI cancer.Demirer et al.21 studied a Turkish popula-tion, principally to investigate the relationshipbetween diet and stomach cancer, but usedsome oral measurements as well. The cancercases (n = 100) had histologically provenadenocarcinoma of the stomach, and age,gender, and residential area-matched subjectswith no gastrointestinal disease were usedas controls (n = 100). Information was ob-tained by interview with regard to food andbeverage intake, frequency of tooth brushing,and num ber of missing teeth. In this study,patients with gastric cancer brushed theirteeth less frequently (p < 0.0001) and hadmore missing teeth (p < 0.0001). The relativerisk and confidence intervals for these datawere not reported. A case-control study onChinese populations from three areas inShanxi province (North-Central China) wascarried out to determine the influence of diet,smoking, drinking habits, sociopsychologi-cal factors, and family history on the etiologyof esophageal cancer.22 As part of this study,information concerning dental hygiene habitswas obtained. The cases (n = 326) had beendiagnosed previously with histologicallyconfirmed esophageal cancer and controls

204 Periodontal Disease and Overall Health: A Clinician's Guide
(n = 396) were matched by age, gender, andresidence location. Demographic, social, andmedical information was gathered by inter-view and included dental hygiene habits. Ofthe parameters evaluated, frequency of toothbrushing was found to be associated withreduced risk for esophageal cancer (OR: 0.2;CI:0.1–0.5). In another case-control study,Watabe et al.23 studied a Japanese populationto investigate the etiological relation betweengastric cancer and lifestyle. The cases ofgastric cancer (n = 242) and controls (n = 484)were matched for age, gender, and place ofresidence. Oral condition was determinedaccording to number of teeth present. The re-sults from this study indicated that toothnumber was inversely associated with a highodds ratio for development of gastric cancer.After correcting for some confounders, thenumber of missing teeth was still found to besignificantly associated with gastric cancer.
A number of recent case-control, co-hort, and cross-sectional studies have beencarried out to ascertain the relationship between oral health and gastric cancer. Ina large case-control study of a Chinesepop ulation, Abnet et al.24 investigated there lationship between tooth loss and riskof developing esophageal squamous cell carcinoma, gastric cardiac adenocarcinoma,or gastric noncardiac adenocarcinoma. Thecases had been diagnosed previously throughhistological confirmation of upper gastro -intestinal cancers (n = 2,204). The controls(n = 27,715) were cancer-free, came from theLinxian area of China, and were part of theLinxian General Population Trial cohort in1985. Tooth loss was assessed from subjectinterview and also visual inspection. Toothloss was high in this population with 74% ofparticipants having lost at least one perma-nent tooth. The median number of teeth lostwas six and median age for first tooth lostwas 39. Further analyses indicated that toothloss was significantly (p < 0.01) associatedwith each of the three cancer sites studied.
When assessed for each cancer site, toothloss was associated with a relative risk (RR)of 1.3 (CI:1.1–1.6) in the esophagus, a RR of1.3 (CI:1.0–1.6) for the gastric cardiac, anda RR of 1.8 (CI:1.1–3.0) for the gastric non-cardiac. Additional analyses indicated thatthe increased risk was strongest for the firstteeth lost in younger individuals.
In a similar study, Abnet et al.25 carriedout a prospective cohort study to determinewhether tooth loss was associated with increased risk of gastric noncardiac adeno -carcinoma in a cohort of Finnish smokers.The study population comprised 29,124 sub-jects, which included 49 esophageal squamouscell carcinomas, 66 esophageal/gastric car-diac adenocarcinomas, and 179 gastric non -cardiac adenocarcinomas. Interviews en-abled information to be collected on generalbackground characteristics, smoking, and dietary history. The dentition was assessedby interview and related to number of miss-ing teeth. Tooth loss was found to be signif-icantly associated with an increased hazardratio (HR) for gastric noncardiac cancer,whereby the HR for edentulous people versus those with < 10 teeth lost was 1.65(CI:1.1–2.5). For esophageal squamous cellcarci noma and esophageal/gastric cardiacadeno carcinoma, there were no statisticallysignificant associations with tooth loss.
In another cross-sectional study of a ru-ral Chinese population, Wei et al.26 investi-gated the risk factors for oropharyngealsquamous dysplasia. The study population(Linzhou, formerly Linxian, China) was cho-sen because of a very high prevalence ofesophageal squamous cell carcinoma andgastric cardiac adenocarcinoma. A screeningstudy of 724 adults who were apparentlyhealthy was carried out. An interview wasconducted to obtain general informationon personal characteristics, smoking and al-cohol use, and living conditions. Dental ex-aminations followed the NHANES III pro-tocol and included a tooth count. Of the 720

Chapter 13 Oral Health, Periodontitis, and Cancer 205
subjects, 230 people had a prevalent squa-mous dysplasia. Subjects who had lost be-tween 12 and 31 teeth had higher odds fordysplasia (OR: 1.91; CI: 1.2–3.2). Thesefindings were similar to the earlier report by Abnet and colleagues.25
A cross-sectional study by Dye et al.27
investigated the oral health of a non-representative sample of adult participantsin an esophageal cancer study. In this study,subjects (n = 718) were recruited from three regions within Linzhou, China. They wereexamined by esophageal cytology and inter-viewed to obtain information regardinghealth history and risk behavior. A dentalexamination was also executed according tothe NHANES III protocol, which includedassessment of the number of teeth present.The periodontal examination consisted ofassessing gingival inflammation, clinical at-tachment levels, and bleeding on probing. Asnoted earlier,24 tooth loss was prevalent with17% of the study population being edentu-lous. In an unadjusted model, individualswho had 12–31 teeth had an increased riskfor esophageal cancer (OR:1.7; CI:1.03–2.83). Poor oral health was derived fromboth periodontal status and caries experi-ence and was found to be associated withincreased risk of esophageal cancer (OR:1.58; CI:1.0–6-2.7), and when adjusted fornonsignificant covariates, the OR was 1.59(CI:1.06–2.39). No associations were notedwhen all covariates were considered. Theauthors interpreted this to indicate that theextent and severity of poor oral health couldbe an important contributing factor to theprevalence of esophageal cancer.
Of the previous eight studies mentionedin this section, four have been published bythe same group using essentially similarstudy designs and similar population groups.Nonetheless, from all of the studies pub-lished to date concerning oral conditions andupper GI cancer, evidence has accrued tosuggest that tooth loss may be an important
risk factor for GI cancer. How well toothloss correlates with periodontal conditions isstill open to question. It has, however, beenused as a surrogate marker for periodontaldisease and poor oral health. With only onestudy seriously considering periodontal pa-rameters, it is too early to determine whetherperiodontal health is also a risk factor forthis condition.
Oral Conditions and Lung CancerThere are very few reports in the liter-
ature concerning the relationship betweenoral disease and lung cancer. The most widelyquoted study is population-based and derivedfrom data obtained from the NHANES IEpidemiologic Follow-up Study.28 Data from11,328 adults between the ages of 25–74 un-derwent a medical examination, a standard-ized medical history, and standardized dentalexamination in 1971–1975. The individualswere followed with a 96.2% success rate un-til 1992. Death certificates of deceased indi-viduals were obtained and the analysis con-sidered those who had died from malignantneoplasms including lung and bronchus,pancreas, colon, gingiva, oral cavity, and anyother cancer. The dental examinations in-cluded measuring the extent of gingival in-flammation and the size of perio dontal pock-ets. A periodontal score was obtained usingthe Russell Index. Associations between can-cer types and periodontal status were exam-ined controlling for age and gender. Theseassociations were described using odds ratiosand their 95% confidence intervals. Moredetailed analyses included using Cox pro-portional-hazards models to determinewhether individuals with gingivitis, perio -dontitis, or edentulism at the commencementof the study were at higher risk for develop-ing fatal neoplasms during the study periodto 1992. Following these analyses, it wasdetermined that while periodontitis patientshad an elevated risk of death from cancer,it was significant only for lung cancer

206 Periodontal Disease and Overall Health: A Clinician's Guide
(OR:1.94; CI:1.16–3.26). After a Cox pro-portional hazards analysis adjusting for demo -graphic factors, the hazard ratio was deter -mined to be 2.14 (CI:1.30–3.53). With furtheradjustment for socio-economic status, smok -ing status, alcohol consumption, and the in-take of vitamins A and C, the hazard ratio re-duced to 1.73 (CI:1.01–2.97). No associationbetween periodontitis and lung cancer wasdetected if the analyses were limited to peo-ple who had never smoked. However, if theanalysis was restricted to smokers, then perio -dontitis became significantly associated withlung cancer (HR:1.94; CI:1.14–3.30). Theauthors interpreted these findings to implythat an association between periodontitis andlung cancer, after adjustment for known riskfactors, could be demon strated. However, theycautioned that this periodontitis-cancer asso-ciation could be spurious.
The only other published report inwhich periodontitis and lung cancer wasstudied also does not support a link. In thisstudy, associations between tooth loss andmortality patterns in a cohort from Glasgowwere studied29 in 223 individuals (medianage at baseline was 19) who were followedfor up to 57 years. The cause of death wasrecorded and related to dental data includingmissing teeth, decayed teeth, and restoredteeth. Missing teeth were used as the indexof oral health. Following extensive statisticalanalyses, the authors concluded there wasno association between external causes ofdeath and tooth loss as a continuous (HR:0.97; CI:0.92 –1.03) or categorical variablefor missing five to eight teeth (HR:0.74; CI:0.45–1.21) or missing nine or more teeth(HR:0.89; CI:0.42–1.88). In addition, no evi -dence of an association between lung cancerand tooth loss was found, with or without adjustment for smoking.
While the literature is scant on thistopic, to date it does not seem to support anyassociation between periodontal conditionand lung cancer.
Oral Conditions and Pancreatic CancerIn light of earlier observations that oral
hygiene and tooth loss could be associatedwith increased risk for upper GI cancers,Stolzenberg-Solomon et al.30 hypothesizedthat tooth loss may be associated with pancreatic cancer. This was a cohort studyof Finnish men, ages 50–69, who smokedmore than five cigarettes per day and hadno history of any malignancy apart fromnonmelanoma of the skin or carcinoma insitu. Baseline information obtained by in-terview included medical, dental (number ofteeth), smoking, and dietary history. Out ofthe 29,104 participants, 174 developed pan-creatic cancer. Cox proportional hazard mod-els were used to account for age, smoking, education, urban living, and height. In thisstudy, tooth loss, as accounted for by totaledentulism, was associated with pancreaticcancer when compared to individuals missing10 or fewer teeth (HR:1.63; CI:1.09–2.46).However, for people missing 11–31 teeththis association was not significant (HR:1.23;CI:0.82–1.85). The authors concluded thatfurther studies were needed to fully evaluatethe association between tooth loss and pan-creatic cancer.
Hujoel et al.28 in their study utilizingthe NHANES I data to investigate the asso-ciation between periodontitis and variouscancers found no association for pancreaticcancer.
A subsequent study by Michaud et al.2investigated the association of periodontitisin 216 males diagnosed with pancreatic can-cer from a larger cohort of 48,375 men parti - cipating in the Health Professionals Follow-up Study in the US. The study period was 16years. At baseline, participants reported thenumber of natural teeth and this was updatedevery two years. It was reported that a peri-odontal disease analysis was carried out atbaseline and every two years thereafter.However, no details were provided as to thenature of these analyses. Individuals who

Chapter 13 Oral Health, Periodontitis, and Cancer 207
were assessed to have periodontal diseaseat baseline had an increased risk of having pancreatic cancer (RR:1.83; CI:1.36–2.45).When adjusted for age, smoking, profession,race, geographic location, physical activity,diabetes, body mass index, height, chole-cystectomy, nonsteroidal anti-inflammatorydrug use, multivitamin use, dietary factors,and total calories, the RR was 1.64 (CI:1.19–2.26). Most of this attenuation could beaccounted for by smoking. The number ofteeth present at baseline was not significantlyassociated with pancreatic cancer. However,in a joint analysis, tooth loss in conjunctionwith periodontal disease resulted in a 2.7-foldincrease (RR:2.71; CI:1.70–4.32) in pan-creatic cancer when compared to either noperiodontal disease or no recent tooth loss.Additional analyses indicated that the influ-ence of periodontal disease was stronger inpeople who had never smoked (RR:2.09;CI:1.18–3.71). Furthermore, the influenceof periodontal disease was also stronger inindividuals with a body mass index of lessthan 25 kg/m2 (RR:2.2; CI:1.34–3.61). Theauthors concluded that this indicated thatsmoking and obesity were unlikely to ex-plain the association between periodontaldisease and pancreatic cancer. Nonetheless,they concluded that if the association is to beproven, additional studies are required.
In an interesting follow-up to theMichaud et al.2 publication, Taguchi,31 ina “Letter to the Editor,” commented thatMichaud and colleagues did not adjust forthe effects of passive exposure to cigarettesmoke, which could have negated their find-ings. In addition, Taguchi suggested that tobetter understand the relationship betweenperiodontal disease and pancreatic cancer,it would be helpful to demonstrate an asso-ciation between duration and grade of peri-o dontal disease and pancreatic cancer risk. Inresponse to these comments Michaud et al.2
argued that not withstanding the lack of dataconcerning environmental tobacco smoke,
controlling for passive smoking in theirstudy may have attenuated their findings butnot eliminated the association between peri-odontal disease and pancreatic cancer. It wasnoted that the two-fold increase in risk forpancreatic cancer in people with periodontaldisease who had never smoked is greaterthan the reported association between pas-sive smoking and pancreatic cancer. Fur-thermore, it was pointed out this two-foldincrease in risk for pancreatic cancer amongpatients with periodontal disease who hadnever smoked is of a similar magnitude tothe association between current smoking andpancreatic cancer. With regard to the need forassessment of duration and severity of peri-odontal disease, Michaud was in agreement.Indeed, this should be a requirement for allfuture studies investigating the associationbetween periodontal disease and any cancer.
PERIODONTAL DISEASE,CANCER, AND MORTALITYTo date, very few studies have investi-
gated the association between periodontaldisease and cancer by assessment of the clin-ical parameters of periodontal status. By far,the majority of studies have reported on theassociation between tooth loss and cancerrisk. Such approaches may be flawed sincetooth loss may also result from trauma or,more commonly, caries. However, thesestudies claim that because teeth lost at anolder age are more likely due to periodontaldisease compared to those lost at younger ages(which may be due more to dental caries),tooth loss in older individuals can be a goodsurrogate marker of periodontal disease. Onthe basis of that, it seems assessment of toothloss may provide an insight into the overallrole of oral health and its effect on cancerrisk. The cumulative influence of age ontooth loss and its relationship to periodontaldisease can be seen in the study by Michaud,et al.2 In this study, which ran more than 16years, the number of teeth lost at baseline

208 Periodontal Disease and Overall Health: A Clinician's Guide
was not related to risk of pancreatic cancer.However, by the end of the study, it wasnoted that tooth loss within the previous fouryears was a predictor of pancreatic cancerrisk. When both periodontal disease and re-cent tooth loss were assessed jointly, the riskof pancreatic cancer increased significantlycompared to individuals who did not haveperiodontal disease and had not experiencedany recent tooth loss. These results suggestthat in this population, recent tooth loss maybe a marker for severity of periodontal dis-ease, whereas baseline tooth loss may reflectloss due to factors other than periodontitis.
Another complicating factor in inter-preting many of the published studies is theinfluence of known risk factors which in-clude smoking, alcohol consumption, andsocio-economic status. Smoking is a well-recognized risk factor for oral and lung can-cer but is also a recognized risk factor for periodontal disease and tooth loss. Thus,some authors have questioned any reportedassociation between tooth loss and canceras being due to confounding factors ratherthan a real risk factor.28,29 While this may betrue for lung cancer, other cancers appear tobe less influenced by smoking and indeed,tooth loss persists as a significant risk factorfor both gastric and pancreatic cancer afteradjusting for smoking status.2,27 Similarly,alcohol consumption can be a significantrisk factor for cancer and is also a possiblerisk factor for periodontitis. Thus, alcoholconsumption must be accounted for wheninvestigating the effect of tooth loss on cancer risk. In cancers of the oral cavity, thisis particularly relevant since alcohol is a significant risk factor for oral cancer. A num-ber of studies have adjusted for alcohol intake and found that tooth loss persists as a significant risk factor for this cancer.15-17
Socio-economic status is also considered animportant risk factor for periodontitis andhence there is further potential for socio-economic status to be a confounding issue in
studies considering the effect of tooth loss oncancer. While most studies have includedsocio-economic status in their question-naires, adjustment for this component hasnot always been a prominent feature of thestatistical modeling.
Although smoking, alcohol consump-tion, and socio-economic status may be thethree commonly recognized confounders formany studies concerning cancer risk and perio dontal disease, it is highly likely thatmany other, hitherto unidentified confound-ing factors could be at play and need to beidentified before these associations can beconfidently accepted.
With these caveats in mind, there areseveral scientific reports that attempt to eval-uate the relationship between periodontaldisease, cancer, and mortality. One of thefirst to report that periodontitis was posi-tively associated with cancer was Hujoel etal.28 in 2003. This study has been describedin more detail in the previous section dealingwith lung cancer. Briefly, Hujoel and col-leagues followed 11,328 individuals over a10-year period and compared periodontalstatus to fatal cancer. Associations betweencancer types and periodontal status were ex-amined controlling for age and gender. Ofthe six fatal cancers studied as the main out-come measures, only lung cancer was foundto have a significant association with perio -dontitis. It was noted that the association be-tween periodontitis and lung cancer mortal-ity could be found even after adjusting forknown risk factors for lung cancer such assmoking (OR:1.94; CI:1.16–3.26).
Further prospects for a relationship be-tween oral health and increased risk of totaldeath and death from cancer have been madefrom a cohort study on rural Chinese.32 Thiswas a follow up to the Abnet et al.24 studyon a Chinese population in Linxian, China,in which 29,584 rural Chinese participatedover a 10-year period. Tooth loss was used asthe measure of oral health, and mortality

Chapter 13 Oral Health, Periodontitis, and Cancer 209
outcomes were studied as well as total death,upper GI cancer death, other cancer death,heart disease death, and fatal stroke. It wasfound that individuals with greater than theage-specific median number of teeth lost hadstatistically increased risk of total death (RR:1.13; CI:1.09–1.18) and death from upper GIcancer (RR:1.35; CI:1.14–1.59). After ac-counting for the confounding effect of smok-ing, these associations were generally stillsignificant. Risk from death at other cancersites showed no significant associations withtooth loss. It was concluded that tooth losswas significantly associated with increasedrisk for total death from cancer and from up-per GI cancer.
In contrast to the above findings, Cabreraet al.,33 in a study investigating the relationshipbetween tooth loss and chronic disease, foundno associations between tooth loss and totalcancer mortality after adjusting for knownconfounders (RR:1.16; CI:0.90–1.49). Thiswas a prospective study of females residing inGothenburg, Sweden over 24 years. The dentalexamination consisted of determining toothnumber; mortality outcomes were death fromcardiovascular disease and all-site cancer.Despite no association between tooth numberand all-site cancer mortality, no assessmentof site- specific cancers was made. Similarfindings were noted by Tu et al.29 in thepreviously described Glasgow cohort study.Moreover, after adjusting for a variety of con -founders, no association was found betweenall-cause mortality for each additional missingtooth (HR:1.01; CI:1.00–1.02) or cancermortality (HR:1.00; CI: 0.98–1.02). From thisstudy, it appeared that any relationshipbetween tooth loss and cancer mortality couldbe explained by other causal or confoundingmechanisms.
Tramini et al.34 investigated tooth loss andassociated factors in elderly patients in Francewho had been institutionalized long term. Thiswas a cross-sectional study of 321 elderlypatients in which socio-economic, behavioral,
medical, and oral information was recorded.Multivariate logistic regression analyses werecarried out to test the associations betweenthese covariates and tooth loss. The resultsindicated that “cancerous disease” was themost significant condition associated withpartial tooth loss. The type of “cancerousdisease” was not qualified. From these data,the authors concluded that the number ofremaining teeth has a strong effect on oralhealth-related quality of life.
Söder et al.35 published the results froma 16-year longitudinal study investigatingperiodontitis and premature death. In thisstudy the causes of death for 3,273 individ-uals were recorded and subsequently relatedto dental findings. The dental assessment atbaseline included recording missing teeth,gingival inflammation, oral hygiene status,calculus scores, and periodontal probingpocket depth. An individual was consideredto have periodontitis if he or she had at leastone tooth with a probing pocket depth of 5mm or greater. After logistic relation analy-sis of being dead (dependent variable) andseveral independent variables including age,gender, education, income, smoking, dentalvisits, dental plaque, gingival inflammation,missing teeth, and missing molars, the totalnumber of individuals who died from neo-plasms was significantly higher in the perio -dontitis group who had missing molar teeth(OR:3.62; CI:1.28–10.16). It was concludedthat young periodontitis patients with miss-ing molars were at higher risk for prematuredeath by neoplasm than their more healthycounterparts.
In another case-control study, Hiraki etal.36 examined the relationship between toothloss and the risk of 14 types of cancers ina Japanese population. The cohort consistedof 5,240 cancer subjects and 10,480 non-cancer controls who were age- and gender-matched. Information on lifestyle, smoking,alcohol consumption, diet, exercise, andnumber of teeth present was collected. Of the

210 Periodontal Disease and Overall Health: A Clinician's Guide
14 cancers studied, tooth loss was found tobe associated with esophageal (OR:2.36;CI:1.17–4.75) and lung cancer (OR:1.54;CI:1.05–2.27). After adjusting for age, theseassociations remained significant but weredecreased. These findings are in agreementwith the more focused studies on upper GIcancer and lung cancer.
In a detailed study, Michaud et al.37
analyzed periodontal disease, tooth loss, andcancer risk in a male health professional co-hort. This prospective study was carried outon the same Health Professionals Follow-up Study as described in the above section onpancreatic cancer. Commenced in 1986,51,529 (97% male) participants answered aquestionnaire on lifestyle, smoking history,alcohol consumption, physical activity, diet,and medical history. Follow-up question-naires were completed every two years until2002. Dental assessments were also carriedout and these consisted of self-reported ex-perience of periodontal disease and toothloss. Cancer experience was recorded by theparticipants who were required to report anynew cancer diagnosis on the biennial ques-tionnaires. The data were analyzed and mul-tivariate hazards ratios and 95% confidenceintervals were calculated by Cox propor-tional hazard models for periodontal diseaseexperience and number of missing teeth atthe baseline measurement. From this study,the five main cancers experienced by thiscohort were colorectal, melanoma of theskin, lung, bladder, and prostate. Followingadjustment for known cancer risk factorssuch as smoking history and diet, comparedto individuals with no reported history ofperiodontal disease, individuals with a self-reported history of periodontal diseasedemonstrated an increased risk for total cancer (HR:1.14; CI:1.07–1.22). For specificcancers, a past history of periodontal diseasewas associated with increased risk for lung(HR:1.36; CI:1.15–1.60), kidney (HR:1.49;CI:1.12–1.97), pancreas (HR:1.54; CI:1.16–
2.04) and hematological cancers (HR:1.30;CI:1.11–1.53). These findings for lung andpancreas were in agreement with previouslypublished studies. The findings for kidneyand hematological cancers were new andhave not been reported previously. In con-trast to previous studies, the association foresophageal cancer, while increased, was notsignificant after adjusting for smoking status.Missing teeth, which was also noted to be associated with smoking status, was foundto be associated with increased risk forlung cancer only (HR:1.7; CI:1.37–2.11).The associations were strongest for peri-odontal disease and missing teeth whensmoking was not considered a covariate; thisindicates that smoking was a strong con-founder for these associations. Interestingly,for pancreatic and kidney cancers, the asso-ciations remained strong even after control-ling for smoking. For lung cancer, smokingwas found to be a very strong confounderand was probably largely responsible for riskof this cancer. Removal of confounding fac-tors for kidney and pancreatic cancers suchas diabetes and obesity did not significantlychange the associations, indicating that thesetwo known risk factors were not likely tobe responsible for the noted association of perio dontal disease with pancreatic and kid-ney cancers. Overall, the authors concludedthat periodontal disease appeared to be as-sociated with a small but nonetheless sig-nificant risk for cancer in general. Some in-fluence of smoking was noted in smokersbut the associations persisted in people whohad never smoked. Whether some of theseassociations were due to direct effects of pe-riodontal disease on cancer or the result ofbeing more like a surrogate marker requiresfurther investigation.
PERIODONTITIS, VIRUSES,AND ORAL CANCER
In recent years, several reports havesuggested that viruses may be associated

Chapter 13 Oral Health, Periodontitis, and Cancer 211
with various forms of periodontitis. In par-ticular, Epstein-Barr Virus (EBV) has beenimplicated in the pathogenesis of advancedand aggressive forms of periodontitis.38 Ithas been hypothesized that EBV proteinsmay lead to an up-regulation of growth factors and cytokines involved in celltransformation of EBV-associated oral malig nancies.39 While this is an interesting theory, considerably more research isneeded to determine the exact role, if any,that viruses play in periodontitis and oralmalignancies.
ORAL CONDITIONS, HELICOBACTERPYLORI, AND CANCER
Helicobacter pylori is associated withchronic gastritis, duodenal ulcers, and in-creased risk of developing gastric adenocar-cinoma.40,41 Since H. pylori can be isolated inthe oral cavity, especially in individuals withperiodontitis who have the bacterium in theirgastrointestinal tract,42 it has been proposedthat the oral cavity may act as a reservoir forH. pylori-associated gastric cancer. While ithas been suggested that H. pylori cannot sur-vive in the oral cavity, there are studies thatsupport the notion that H. pylori can be foundin dental plaque and periodontal pockets.43,44
Nonetheless, it is generally accepted that thepresence of H. pylori in the oral cavity maybe independent of infection status of thestomach45 and no good evidence exists forthe presence of periodontal disease, oralH. pylori, and gastric cancer.30
POSSIBLE MECHANISMS FOR THERELATIONSHIP BETWEEN ORAL
CONDITIONS AND CANCERA number of hypotheses have been pro-
posed to explain the observed relationshipsbetween periodontal disease and cancer including poor diet, mechanical irritation,chronic infection, systemic inflammation,and immune suppression, as well as increasedexposure to carcinogens.1,32
Diet and Mechanical IrritationThe role of poor oral condition and
tooth loss with trauma has been well dis-cussed for both oral and upper gastroin -testinal cancer. For decades, an associationbetween poor restorative dentistry and ill-fitting prostheses and oral cancer has beenrecognized.46 However, more recently it hasbeen proposed that tooth loss may alter di-etary patterns and this may be a contributoryfactor to the development of upper GI can-cer.32 In addition, it has been suggested thattooth loss may result in inadequate mastica-tion and the resulting poorly chewed foodbolus could have an irritating effect on theesophagus, leading to increased risk of can-cer through mechanical irritation.47 To datethese hypotheses have not been proven. Inlight of findings that tooth loss and chewingefficiency are not related and that tooth lossis associated with increased risk for GI cancer, the fact that the GI system is a sitethat is unlikely to be affected by food bolussize mitigates against mechanical-trauma hypotheses.32
InflammationInflammation appears to play an im-
portant role in carcinogenesis and the pres-ence of inflammation may enhance cellularproliferation and mutagenesis, reduce adapta -tion to oxidative stress, promote angiogenesis,inhibit apoptosis, and increase secretion ofinflammatory mediators.48 This is demon -strated with chronic pancreatitis being asso-ciated with an increased risk of pancreaticcancer.49 Indeed, inflammation has beenshown, at least in animal studies, to be asso-ciated with the progression of liver and coloncancer.50 Since periodontal disease is an inflammatory disease in which there are elevated levels of circulating inflammatorycytokines, a suggestion has been made thatthis could be a plausible link leading to thebreakdown of normal cell growth controland potential carcinogenesis.1 Thus, the host

212 Periodontal Disease and Overall Health: A Clinician's Guide
response in periodontal disease may lead to asystemic exposure to pro-inflammatory cyto -kines, which in turn may lead to increasedrisk of neoplastic transformation at distantsites. However, the situation may not be assimple as this since most studies investigat-ing the link between cancer and inflamma-tion consider the effect of local inflammationat the site of the cancer rather than systemicelevation of inflammatory mediators. Whileit is possible that elevated systemic levels ofinflammatory cytokines may encourage sub-threshold neoplastic states to become neo-plastic, local inflammation and local releaseof inflammatory mediators at a site of po-tential neoplastic transformation seems morelikely. Alternatively, it has been suggestedthat individuals who suffer from both peri-odontal disease and cancer may share simi-lar gene polymorphisms in genes encodinginflammatory cytokines; thus periodontitismay merely be a marker of an underlying ge-netic predisposing factor rather than a truerisk factor for cancer.
InfectionChronic infections have been associ-
ated with increased cancer risk. For example,bacterial infections such as H. pylori havebeen implicated in gastric cancer as well asHepatitis B and C viral infections implicatedin hepatocellular carcinoma.40,41
Since periodontitis is a chronic infec-tion, it has been postulated that periodontalbacteria within the subgingival plaquebiofilm may be associated with carcinogen-esis through the release of a multitude oftoxic products (endotoxins, enzymes, hy-drogen sulfide, ammonia) leading to cell mu-tations in tumor suppressor genes and proto-oncogenes or alter signaling pathways thataffect cell proliferation or cell survival.18 Inaddition, chronic inflammation induced byperiodontal pathogens results in chronic re-lease of pro-inflammatory cytokines, chemo -kines, prostaglandins, growth factors, and
enzymes that may have indirect effects oncarcinogenesis by deregulating physiologicalcell turnover and cell growth.
In another hypothesis, it has been pro-posed that periodontal pathogens may in-crease the level of certain carcinogens such asnitrosamines.32 The formation of endogenousnitrosamines in the oral cavity by nitrate-reducing bacteria is promoted by poor oralhygiene as well as by tobacco use and certaindietary factors.51 Increased production of car-cinogenic nitrosamines by oral bacteria hasbeen suggested as a possible mechanism foran increased risk of pancreatic cancer in in-dividuals with reported periodontal disease.2
ImmunityPeriodontitis in susceptible patients
may reflect a failure in the interaction be-tween the innate and adaptive immune re-sponse to clear the bacterial challenge withinthe periodontal pocket. Deregulation of theimmune response may also place an indi-vidual at risk of inadequate cellular surveil-lance for tumor growth. In particular, thestable periodontal lesion consists of a pre-dominantly T helper cell 1 (Th l) response52
and is associated with high levels of inter-feron- (IFN-), an important cytokine incell-mediated immunity and tumor surveil-lance.53 The progressive periodontitis lesionconsists predominantly of a Th 2 responsewith lower levels of IFN- and a poor innateimmune response.52 Hence, periodontitis couldmerely be a marker of immune dysfunctionrather than a true risk factor for cancer.
CONCLUSIONTo date, only a limited number of studies
have investigated the association betweenperiodontal disease and cancer risk, althoughmany reports have been published concern-ing the association between cancer risk andoral condition, oral hygiene, and tooth loss.Positive associations have been demonstratedeven after controlling for known risk factors

Chapter 13 Oral Health, Periodontitis, and Cancer 213
alcohol in the epidemiology of oral cancer. J NatlCancer Inst 1977;59:1611–1618.
5. Zheng TZ, Boyle P, Hu HF, Duan J, Jian PJ, Ma DQ,Shui LP, Niu SR, Scully C, MacMahon B. Denti-tion, oral hygiene, and risk of oral cancer: A case-control study in Beijing, People’s Republic ofChina. Cancer Causes Control 1990;1:235–241.
6. Winn DM, Blot WJ, McLaughlin JK, Austin DF,Greenberg RS, Preston-Martin S, Schoenberg JB,Fraumeni JF Jr. Mouthwash use and oral conditionsin the risk of oral and pharyngeal cancer. CancerRes 1991;51:3044–3047.
7. Marshall JR, Graham S, Haughey BP, Shedd D,O’Shea R, Brasure J, Wilkinson GS, West D.Smoking, alcohol, dentition and diet in the epidemi -ology of oral cancer. Eur J Cancer. Part B. OralOncology 1992;28B:9–15.
8. Bundgaard T, Wildt J, Frydenberg M, Elbrønd O,Nielsen JE. Case-control study of squamous cellcancer of the oral cavity in Denmark. CancerCauses Control 1995;6:57–67.
9. Schildt EB, Eriksson M, Hardell L, Magnuson A.Oral infections and dental factors in relation to oralcancer: a Swedish case-control study. Eur J CancerPrev 1998;7:201–206.
10. Velly AM, Franco EL, Schlecht N, Pintos J, Kowalski LP, Oliveira BV, Curado MP. Relation-ship between dental factors and risk of upper aero -digestive tract cancer. Oral Oncol 1998;34:284–291.
11. Talamini R, Vaccarella S, Barbone F, Tavani A, LaVecchia C, Herrero R, Muñoz N, Franceschi S.Oral hygiene, dentition, sexual habits and risk oforal cancer. Br J Cancer 2000;83:1238–1242.
12. Moreno-López LA, Esparza-Gómez GC, González-Navarro A, Cerero-Lapiedra R, González-Hernán-dez MJ, Domínguez-Rojas V. Risk of oral cancer as-sociated with tobacco smoking, alcoholconsumption and oral hygiene: a case-control studyin Madrid, Spain. Oral Oncol 2000;36:170–174.
13. Garrote LF, Herrero R, Reyes RM, Vaccarella S,Anta JL, Ferbeye L, Muñoz, N, Franceschi S. Riskfactors for cancer of the oral cavity and oro-pharynxin Cuba. Br J Cancer 2001;85:46–54.
14. Balaram P, Sridhar H, Rajkumar T, Vaccarella S,Herrero R, Nandakumar A, Ravichandran K, Ram-das K, Sankaranarayanan R, Gajalakshmi V, MuñozN, Franceschi S. Oral cancer in southern India: theinfluence of smoking, drinking, paan-chewing andoral hygiene. Int J Cancer 2002;98:440–445.
15. Lissowska J, Pilarska A, Pilarski P, Samolczyk-Wanyura D, Piekarczyk J, Bardin-Mikollajczak A,Zatonski W, Herrero R, Muñoz N, Franceschi S.Smoking, alcohol, diet, dentition and sexual prac-tices in the epidemiology of oral cancer in Poland.Eur J Cancer Prev 2003;12:25–33.
such as smoking or when analyses are re-stricted to nonsmokers. However, these find-ings need to be interpreted with caution asthere may be additional confounding factorsthat researchers are unaware of and that havenot been included in the analyses for adjust-ment. There is a need for more studies ofappropriate statistical power using appropri-ate markers for periodontal disease, appro-priate consideration of the different types ofperiodontal disease, as well as the appropri-ate consideration of confounding factors.
Supplemental Readings
Meyer MS, Joshipura KJ, Giovannucci E, Michaud DS.A review of the relationship between tooth loss, peri-odontal disease and cancer. Cancer Causes Control2008;19:895–907.
Michaud DS, Joshipura K, Giovannucci E, Fuchs CS. Aprospective studyof periodontal disease and pancreaticcancer in US male health professionals. J Nat CancerInst 2007;17:171–175.
Hujoel PP, Drangsholt M, Spiekerman C, Weiss NS.An exploration of the periodontitis-cancer association.Ann Epidemiol 2003;13:312–316.
Michaud DS, Liu Y, Meyer M, Giovannucci E, Jo-shipura K. Periodontal disease, tooth loss, and cancerrisk in male health professionals: A prospective cohortstudy. Lancet Oncol 2008;9:550–558.
Coussens LM, Werb Z. Inflammation and cancer. Nature2002;420:860-867.
Karin M, Greten FR. NF-KappaÎ: linking inflammationand immunity to cancer development and progression.Nat Rev Immunol 2005;5:749–759.
REFERENCES1. Meyer MS, Joshipura KJ, Giovannucci E, Michaud
DS. A review of the relationship between toothloss, periodontal disease and cancer. Cancer CausesControl 2008;19:895–907.
2. Michaud DS, Joshipura K, Giovannucci E, FuchsCS. A prospective study of periodontal disease andpancreatic cancer in US male health professionals.J Nat Cancer Inst 2007;17:171–175.
3. Wynder EL, Bross IJ, Feldman RM. A study of theetiological factors in cancer of the mouth. Cancer1957;10:1300–1323.
4. Graham S, Dayal H, Rohrer T, Swanson M, Sultz H,Shedd D, Fischman S. Dentition, diet, tobacco, and

214 Periodontal Disease and Overall Health: A Clinician's Guide
16. Tezal M, Grossi SG, Genco RJ. Is periodontitis as-sociated with oral neoplasms? J Periodontol 2005;76:406–410.
17. Rosenquist K, Wennerberg J, Schildt EB, Blad-strom A, Goran Hansson B, Andersson G. Oral status, oral infections and some lifestyle factors asrisk factors for oral and oropharyngeal squamouscell carcinoma. A population-based case-controlstudy in southern Sweden. Acta Otolaryngologica2005;125:1327–1336.
18. Tezal M, Sullivan MA, Reid ME, Marshall JR, Hyland A, Loree T, Lillis C, Hauck L, Wactawski-Wende J, Scannapieco FA. Chronic periodontitisand the risk of tongue cancer. Arch OtolaryngolHead Neck Surg 2007;133:450–454.
19. Rezende CP, Ramos MB, Daguíla CH, DedivitisRA, Rapoport A. Oral health changes in with oraland oropharyngeal cancer. Braz J Otorhinolaryngol2008;74:596–600.
20. Wolff G, Läuter J. On epidemiology of gastric can-cer (author’s transl) Arch Geschwulstforsch 1976;46:1–14.
21. Demirer T, Icli F, Uzunalimoglu O, Kucuk O. Dietand stomach cancer incidence. A case-control studyin Turkey. Cancer 1990;65:2344–2348.
22. Wang YP, Han XY, Su W, Wang YL, Zhu YW,Sasaba T, Nakachi K, Hoshiyama Y, Tagashira Y.Esophageal cancer in Shanxi Province, People’sRepublic of China: a case-control study in high andmoderate risk areas. Cancer Causes Control 1992;3:107–113.
23. Watabe K, Nishi M, Miyake H, Hirata K. Lifestyleand gastric cancer: a case-control study. Oncol Rep1998;5:1191–1194.
24. Abnet CC, Qiao YL, Mark SD, Dong ZW, TaylorPR, Dawsey SM. Prospective study of tooth lossand incident esophageal and gastric cancers inChina. Cancer Causes Control 2001;12:847–854.
25. Abnet CC, Kamangar F, Dawsey SM, Stolzenberg-Solomon RZ, Albanes D, Pietinen P, Virtamo J, Tay-lor PR. Tooth loss is associated with increased riskof gastric non-cardiac adenocarcinoma in a cohortof Finnish smokers. Scand J Gastroenterol2005;40:681–687.
26. Wei WQ, Abnet CC, Lu N, Roth MJ, Wang GQ,Dye BA, Dong ZW, Taylor PR, Albert P, Qiao YL,Dawsey SM. Risk factors for oesophageal squa-mous dysplasia in adult inhabitants of a high risk region of China. Gut 2005;54:759–763.
27. Dye BA, Wang R, Lashley R, Wei W, Abnet CC,Wang G, Dawsey SM, Cong W, Roth MJ, Li X,Qiao Y. Using NHANES oral health examinationprotocols as part of an esophageal cancer screeningstudy conducted in a high-risk region of China.BMC Oral Health 2007;7:10.
28. Hujoel PP, Drangsholt M, Spiekerman C, WeissNS. An exploration of the periodontitis-cancer association. Ann Epidemiol 2003;13:312–316.
29. Tu YK, Galobardes B, Smith GD, McCarron P, Jeffreys M, Gilthorpe MS. Associations betweentooth loss and mortality patterns in the GlasgowAlumni Cohort. Heart 2007;93:1098–1103.
30. Stolzenberg-Solomon RZ, Dodd KW, Blaser MJ,Virtamo J, Taylor PR, Albanes D. Tooth loss, pan-creatic cancer, and Helicobacter pylori. Am J ClinNutr 2003;78:176–181.
31. Taguchi A. Re: A prospective study of periodontaldisease and pancreatic cancer in US male healthprofessionals. J Natl Cancer Inst 2007;99:738–739; author reply 739.
32. Abnet CC, Qiao YL, Dawsey SM, Dong ZW, Tay-lor PR, Mark SD. Tooth loss is associated with increased risk of total death, and death from uppergastrointestinal cancer, heart disease, and stroke ina Chinese population-based cohort. Int J Epidemiol2005;34:467–474.
33. Cabrera C, Hakeberg M, Ahlqwist M, Wedel H,Björkelund C, Bengtsson C, Lissner L. Can the relation between tooth loss and chronic disease beexplained by socio-economic status? A 24-year follow-up from the population study of women inGothenburg, Sweden. Eur J Epidemiol 2005;20:229–236.
34. Tramini P, Montal S, Valcarcel J. Tooth loss and associated factors in long-term institutionalised elderly patients. Gerodontology 2007;24:196–203.
35. Söder B, Jin LJ, Klinge B, Söder PO. Periodontitisand premature death: a 16-year longitudinal studyin a Swedish urban population J Periodontal Res2007;42:361–366.
36. Hiraki A, Matsuo K, Suzuki T, Kawase T, Tajima K.Teeth loss and risk of cancer at 14 common sites inJapanese. Cancer Epidemiol Biomarkers Prev 2008;17:1222–1227.
37. Michaud DS, Liu Y, Meyer M, Giovannucci E, Joshipura K. Periodontal disease, tooth loss, andcancer risk in male health professionals: a prospec-tive cohort study. Lancet Oncol 2008;9:550–558.
38. Rotola A, Cassai E, Farina R, Caselli E, Gentili V,Lazzarotto T, Trombelli L. Human herpesvirus 7,Epstein-Barr virus and human cytomegalovirus inperiodontal tissues of periodontally diseased andhealthy subjects. J Clin Periodontol 2008;35:831–837.
39. Slots J, Saygun I, Sabeti M, Kubar A. Epstein-Barrvirus in oral diseases. J Periodontal Res 2006;41:235–244.
40. Dubois A. Spiral bacteria in the human stomach.The gastric helicobacters. Emerg Infect Dis 1995;1:79–85.

Chapter 13 Oral Health, Periodontitis, and Cancer 215
41. Forman D. Helicobacter pylori infection and can-cer. Br Med Bull 1998;54:71–78.
42. Umeda M, Kobayashi H, Takeuchi Y, Hayashi J,Morotome-Hayashi Y, Yano K, Aoki A, Ohkusa T,Ishikawa I. High prevalence of Helicobacter pyloridetected by PCR in the oral cavities of periodontitispatients. J Periodontol 2003;74:129–134.
43. Anand PS, Nandakumar K, Shenoy KT. Are dentalplaque, poor oral hygiene, and periodontal diseaseassociated with Helicobacter pylori infection? JPeriodontol 2006;77:692–698.
44. Souto R, Colombo AP. Detection of Helicobacterpylori by polymerase chain reaction in the sub -gingival biofilm and saliva of non-dyspeptic perio -dontal patients. J Periodontol 2008;79:97–103.
45. Czenikiewicz-Guzik M, Karczewska E, BielanskiW, Guzik TJ, Kapera P, Targosz A, Konturek SJ,Loster B. Association of the presence of Helico -bacter pylori in the oral cavity and in the stomach.J Physiol Pharmacol 2004;55(Suppl 2):105–115.
46. Budtz-Jørgensen E. Oral mucosal lesions associatedwith the wearing of removable dentures. J OralPathol 1981;10:65–80.
47. Yang CS. Research on esophageal cancer in China:A review. Cancer Res 1980;40:2633–2644.
48. Coussens LM, Werb Z. Inflammation and cancer.Nature 2002;420:860–867.
49. Lowenfels AB, Maisonneuve P, Lankisch PG.Chronic pancreatitis and other risk factors for pan-creatic cancer. Gastroenterol Clin North Am 1999;28:673–685.
50. Karin M, Greten FR. NF-kappa B: linking inflam-mation and immunity to cancer development andprogression. Nat Rev Immunol 2005;5:749–759.
51. Nair J, Ohshima H, Nair UJ, Bartsch H. Endo -genous formation of nitrosamines and oxidativeDNA-damaging agents in tobacco users. Crit RevToxicol 1996;26:149 –161.
52. Seymour GJ, Gemmell E, Reinhardt RA, EastcottJ, Taubman MA. Immunopathogenesis of chronic inflammatory periodontal disease: cellular and mo-lecular mechanisms. J Periodontal Res 1993;28:478–486.
53. Karin M, Lawrence T, Nizet V. Innate immunitygone awry: linking microbial infections to chronic ininflammation and cancer. Cell 2006;124:823–835.
DIABETES AND PERIODONTITIS:PREVALENT AND INTERRELATED
CHRONIC DISEASESDiabetes and periodontitis share many
similar epidemiologic and clinical features.Both are very prevalent, easily screened, andinterconnected by important pathophys -iologic links. The successful treatment for either condition depends heavily on intensiveintervention, active maintenance, and life -style modifications. Managing issues suchas acute hypoglycemia, oral infection, andsmoking cessation in diabetic patients is clin-ically relevant for dental as well as medicalprofessionals. As the incidence of diabetescontinues to rise and the understanding of therelationship between diabetes and perio -dontitis deepens, the comanagement of pa-tients with diabetes is expected to becomethe standard model of care.
DiabetesDiabetes is one of the most common
chronic illnesses, affecting approximately24 million people in the United States and246 million throughout the world.1,2 In thedecade from 1996 to 2006, the prevalence ofdiagnosed diabetes nearly doubled in theUS,1 presenting significant challenges for awide range of healthcare professionals. Theincidence of the disease is rapidly growingacross all age and socio economic strata, butthe highest expansion is seen among the eld-erly and minority populations.1 Despite be-ing the leading cause of blindness, kidneyfailure, and amputations not related to acci-dent or injury in the US, nearly one quarterof those with diabetes are unaware that they
INTRODUCTIONThis chapter discusses the comanage-
ment of diabetic patients by oral and medical healthcare providers. The needfor comanagement of patients becomes evident when one considers the prevalenceand chronic nature of diabetes and perio -dontitis (its major oral complication), andthe link between the two diseases. Bothtopics are briefly reviewed below. Therole of dental and medical professionalsin this setting is then reviewed separatelyand in detail. The chapter concludes by sum marizing the principles related to apatient-centered, team approach to diabetescare.
Educational ObjectivesAfter reading this chapter the reader
should be able to:• Appreciate the importance of dental
and medical comanagement of the patient with diabetes.
• Understand the responsibilities of thedental team towards a patient withknown diabetes and a patient who mayhave diabetes (or prediabetes) but isunaware of it.
• Describe specific procedures requiredto manage such patients in practice.
• Identify ways to prevent and treatemergencies related to diabetes in thedental office.
• Understand the ways medical and den-tal professionals can work togetherto provide better care for their mutualpatients with diabetes.
CHAPTER 14Dental and Medical Comanagement of Patients with Diabetes
Evanthia Lalla, William C. Hsu, Ira B. Lamster

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 217
have this disease.1,3 Because the symptomsare neither specific to the disease nor accu-rately reflective of blood glucose concentra-tion, the diagnosis is frequently not made un-til severe symptoms or complications appear.Once diagnosed, the clinical sequelae of diabetes can be prevented or delayed withstrict metabolic control. Thus, the patientcan play a critical role in how the diseaseprogresses by committing to self-care;healthcare providers (beyond the treatingphysician) can contribute to the better man-agement of affected individuals by reinforc-ing the need for good metabolic control.
PrediabetesAccording to the 2010 Standards of
Medical Care in Diabetes by the AmericanDiabetes Association,4 the term prediabetesapplies to individuals with glycemic levelstoo high to be considered normal, but notmeeting criteria for diabetes. These indi -viduals are identified based on a hemoglobinA1c (HbA1c) result between 5.7% and 6.4%,or a blood glucose level following anovernight fast between 100 and 125 mg/dl(impaired fasting glucose [IFG]), or a bloodglucose level following a two-hour oral glu-cose tolerance test between 140 and 199mg/dl (impaired glucose tolerance [IGT]).Prediabetes is a condition that has receivedlittle medical attention in the past, but hasimportant public health implications. Predi-abetes affects an estimated 57 million Amer-icans ages 20 or older, more than twice thenumber of diabetic cases, and totaling 20%of the adult population. People with predia-betes have a strong risk for developing type2 diabetes and are already at an increased riskfor heart disease, stroke, and microvasculardiseases typical of individuals with fully de-veloped diabetes.5 There is strong evidenceindicating that people with prediabetes wholose weight and increase their physical ac-tivity can prevent or delay diabetes and re-turn their blood glucose levels to normal.6 As
with diabetes, the paramount challenge isearly detection and intervention.
Periodontal DiseasesIn a similar sense, periodontal diseases
are common chronic disorders and arebroadly grouped into gingivitis and perio -dontitis. Gingivitis includes inflammatorydisorders of the nonmineralized tissues sur-rounding the teeth, and there is no evidenceof loss of support around the teeth (referredto as clinical attachment loss or CAL) orloss of alveolar bone surrounding the teeth.Perio dontitis is associated with loss of at-tachment or loss of supporting alveolar boneand loss of teeth. The persistent inflamma-tion and infection associated with periodon-titis has been linked to increased risk formany disorders, including cardiovascularand cerebrovascular diseases, diabetes com-plications, adverse pregnancy outcomes, respiratory disease, and kidney disease. Pe-riodontitis generally takes many years to develop, and more advanced disease is morecommon with advancing age. Once diag-nosed, attendant morbidity (abscess forma-tion, alveolar bone and tooth loss) can bereduced by strict adherence to a rigorousself-administered and professional oral hy-giene regimen.
Defining the prevalence of periodontitishas been challenging because there has notbeen a generally accepted definition of peri-odontitis. When the definition includes anyevidence of periodontal destruction (e.g., twomm of CAL is generally considered the lowerlimit of detection, and this must occur on atleast one tooth surface) the majority of adultswill be identified as affected.7 It is clear, how-ever, that this very mild form of periodon- titis does not affect function or place a toothat risk for being lost. In contrast, advancedforms of periodontitis affect 5% to 15% ofdifferent populations.8 An interesting trendobserved over the last 30 years in developedcountries is increased tooth retention. Data

218 Periodontal Disease and Overall Health: A Clinician's Guide
from Sweden indicate there has been a reduc -tion in the percent of the population that is af- fected by gingivitis and mild-to-moderateperiodontitis, and a cor responding increasein the percent of the population that has ahealthy periodontium.9 As examples, the per-cent of periodontally healthy individuals in1983, 1993, and 2003 was 23%, 22%, and44%, respectively. However, the percentageof individuals with severe disease remainedessentially unchanged during this time (13%,13%, and 11%).
Therefore, both diabetes and periodon-titis are common and present for years beforeclinical symptoms are evident. In addition,proper management of both disorders re-quires affected individuals to be involved intheir own care. For diabetes mellitus, thatmeans careful control of carbohydrate con-sumption, weight control, and followingother aspects of a healthy lifestyle. For perio -dontitis, that means a focus on performanceof proper oral hygiene. Appropriate profes-sional care is also critical, and patients playan active role by keeping to their schedule ofregular visits to their physician or dentist.
Underdiagnosis of Diabetes and Difficulties in Achieving Optimal
Metabolic Control in Diagnosed PatientsA significant percentage of patients with
diabetes remain undiagnosed, indicating theneed for screening at multiple healthcare lo-cations. Fortunately, some progress has beenmade over the past few years in this arena.Increased public attention and enhanced pub-lic health measures have led to a drop in thepercentage of undiagnosed patients with diabetes from 30% in 2005 to 24% in 2007.3Further improvement in the detection of diabetes can be achieved by expanding thenumber of contact points undiagnosed indi-viduals have with a wide range of health-care providers. Currently in the US, thereare only 15,000 certified dia betes educatorsand 4,000 endocrinologists10 whose primary
focus is to provide clinical care, numbersthat pale in comparison to the escalating disease burden. Therefore, the brunt of theresponsibility for diabetes screening andmanagement has fallen on primary carephysicians. A shrinkage in the numbers ofprimary care physicians in the workforce hasgenerated new interest in enlisting morehealthcare providers such as dentists to ex-pand the diabetes screening effort. Nationaldata suggest that approximately 70% ofAmericans have visited a dental office in thepreceding year,11,12 pointing to the potentialfor dental professionals to be involved in theidentification of individuals unaware of theirdiabetic status.
Despite greater understanding of the disease and the ever-expanding options formedical therapy, diabetes remains an incur-able and difficult-to-control disease. Land-mark studies such as the Diabetes Controland Complications Trial (DCCT)13 and theUnited Kingdom Prospective Diabetes Study(UKPDS)14 have convincingly demonstratedthat lowering HbA1c levels was associatedwith significant reductions in risk for com-plications. Although progression to diabetescomplications is not inevitable with intensiveglycemic control, national data from 200415
suggest that only 56.8% of the diabetic pop-ulation in the US achieved glycemic goal,an HbA1c of less than 7% (Figure 1). Con-sequently in 2007, diabetes costs were over$174 billion in the US, most of which wererelated to care for diabetes complications.1
The percentage of diabetic patients achievingthe HbA1c goal of 7% in 2004 appears sig-nificantly increased when compared to ear-lier national data (36.9% in 1999–2000 and49.4% in 2001–2002), but remains an un-satisfactory outcome.15 The underlying rea-sons are not entirely clear, but it is evidentthat the daily challenges of managing dia-betes are inseparable from the complexitiesof life. Managing diabetes often becomes adaily struggle balancing glycemic control

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 219
with quality of life. While the adoption of ad-vanced medical regimens and de vices hasopened up unprecedented possi bilities forimproved diabetes care, successful outcomescan only come about by proficient applica-tion of diabetes self- management skills andconcrete lifestyle changes. Particular areas oflifestyle modification, such as maintaining oralhygiene and smoking cessation, are criticalfor the management of periodontitis and dia-betes, providing strong rationale for membersof the various healthcare disciplines to work together to improve health outcomes for patients.
Moreover, optimal diabetes managementrequires a delicate balance. Theoretically, reach- ing glycemic target should not be difficult aslong as sufficient medications or enough insulin dosages are given. However, the practical challenge is that intensive diabetestherapy potentiates the risk for frequent andserious hypoglycemic events that in turn
limits the intensity of treatment.16 Any in-terruptions such as fasting or stress factorswill have significant impact on glycemic lev-els. All healthcare providers who routinelytake care of diabetic patients should have abasic understanding of diabetic medicationsand the skills to manage acute hypo- and hyper glycemic emergencies.
Underdiagnosis of Periodontitis andComplexities in Achieving Optimal
Oral Hygiene Among Diabetic PatientsUnrecognized oral changes and difficul -
ties by diabetic patients in achiev ing optimaloral hygiene and in receiving professionaldental care highlight the need for support byall healthcare providers.
There are important changes in the oralcavity associated with diabetes mellitus17
that may often go unrecognized and there-fore untreated. Diabetes is an establishedrisk factor for periodontitis, and is the onlydisease that has been shown to independ-ently and significantly increase the risk forperiodontitis.18 Other oral diseases and dis-orders that may be linked to diabetes includeCandida infections, reduced salivary flow,dental caries, and certain oral mucosal dis-orders (e.g., lichen planus, burning mouthsyndrome). Periodontitis does not alwaysmanifest with symptoms that are obvious tothe patient. Further, patients with diabetesare often unaware of their risk for periodon-tal disease, medical professionals may notdiscuss the link between diabetes and perio -dontitis with their patients, and oral care isoften overlooked when trying to controlother problems associated with diabetes.Thus periodontal changes in diabetic patientsmay often go undiagnosed for several years.
Periodontitis is a classic chronic disorderand as such, once a patient is diagnosed,management is dependent upon patient com-pliance for the most successful treatmentoutcomes. Patients are required to performeffective oral hygiene, which requires a daily
Figure 1.Glycemic Control in US Adults Figure 1.with Diabetes (NHANES Data)
Although, levels of glycemic control in individuals withdiagnosed diabetes in the US have improved in recentyears, only 56.8% of diabetic patients are at the treatmentgoal of HbA1c < 7%. Poor control (HbA1c > 9%) wasless prevalent in 2003–2004 compared to earlier years,but remains a significant concern. Further improvementin the glycemic control of diabetic patients can beachieved by expanding the number of contact pointsthese individuals have with a wide range of health careproviders who educate and support them in their effortsto reach glycemic goals and reduce the risk for diabetes-related complications. Source: Diabetes Care 2008;31:81– 86.15
HbA1c < 7%HbA1c > 9%
Perc
enta
ge o
f Pat
ient
s

220 Periodontal Disease and Overall Health: A Clinician's Guide
commitment. Further, maintaining regularappointments with their dentist for oral pro-phylaxis visits and examinations to deter-mine if the periodontal condition is stable requires a continuous decision to scheduleand keep appointments. As is the case for di-abetes, patients with periodontitis are chal-lenged on a daily basis to adhere to theseregimens.19 In both cases, the majority ofpatients are unable to maintain this commit-ment and need the support of all health pro-fessionals involved in their care.
Effect of Periodontal Infectionson the Diabetic State
The relationship of diabetes mellitus andperiodontal disease is bi-directional. In ad-dition to the well-documented increasedprevalence and severity of periodontal dis-ease in patients with diabetes, evidence sug-gests that periodontitis may adversely affectmetabolic control. A recent report20 includeda review of how the presence of periodontaldisease could affect metabolic managementof diabetes, as well as the development ofclinical complications of the disease.
The effect of periodontal disease onboth metabolic control and ultimately oncomplications of diabetes is believed to bedue to the effect of pro-inflammatory cy-tokines and other inflammatory mediatorsproduced in the highly vascular periodontaltissue when periodontitis is present.21 Tumornecrosis factor-alpha as well as interleukins-1 and -6 are three of the many inflammatorymediators produced by the periodontaltissues; if these mediators gain entry to thesystemic circulation, important adverseaffects may result when diabetes is present.Of primary importance, these mediators mayact as insulin antagonists.22,23
Older reports have indicated that thepresence of periodontitis in patients withdiabetes is associated with subsequentdevelopment of clinical complications inthose patients. A number of recent studies
have defined these associations. Saremi andcolleagues24 examined a cohort of 628 mem -bers of the Gila River Indian Community inArizona, a group with a very high prev elanceof type 2 diabetes. Following this cohortfor a minimum of 11 years revealed thatindividuals with severe periodontitis atbaseline (versus a healthy periodontium ormild or moderate periodontitis) were at 3.2times the risk of dying from cardiac or renaldisease. In addition, another report examiningthe same community found that compared tono disease or mild periodontitits, individualswith moderate or severe periodontitis or whowere edentulous were at 2.0 to 2.6 times in -creased risk for the development of nephrop -athy.25 The chance of developing endstagerenal disease was even higher for thoseindividuals with moderate or severe perio -dontitis, or those who were edentulous. Inboth studies, the models were fully adjustedfor potentially confounding variables.
More recently, Demmer and colleagues26
asked an intriguing question: Could thepresence of periodontal disease predict thesubsequent development of diabetesmellitus? Nearly 9,300 individuals wereincluded in this study, specifically thosepeople who were part of the first US Na-tional Health and Nutrition Examination Sur-vey (NHANES I, 1971–1976), had receiveda dental examination, and were seen at leastone other time (1982–1992). Periodontalstatus was determined by the PeriodontalIndex, and patients were graded on a zero tofive scale, with zero being periodontal healthand all others grouped into quintiles byseverity of periodontal disease. Diabetes wasdetermined by evaluation of the deathcertificate (ICD-9 Code for diabetes), use ofdiabetes medication as reported by thepatient, and/or a stay at a healthcare facilitynecesitated by diabetes as determined by thedischarge code. Odds ratios were calculatedto assess the relationship of periodontal dis -ease to subsequent development of dia betes.

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 221
Relative to periodontal health (score of zero),the risk of developing diabetes mellitus wasnot raised for individuals with scores of oneor two. In contrast, the odds ratios ofdeveloping diabetes were elevated in groupswith scores of 3 (2.26, confidence interval[CI] 1.56 to 3.27), 4 (1.71, CI:1.0 to 2.69),and 5 (1.5, CI:0.99 to 2.27). For individualswithout teeth, the odds ratio was 1.3 (CI:1.0to 1.7). Since the investigators used logisticmodeling to account for the effect of othervariables, these data suggest that perio–dontitis is an independent risk factor for thedevelopment of diabetes.
Another approach to examining the effect of periodontitis on the diabetic state isvia studies of the effect of periodontal ther-apy on metabolic control. As reviewed byTaylor and Borgnakke,20 a total of 20 studieswere identified that examined the effect ofnonsurgical periodontal therapy on meta-bolic control. Seven of the studies were ran-domized controlled trials (RCTs) and 13were not (non-RCTs). Of the RCTs, four ofseven studies included the use of adjunctiveantibiotics, and three of those studies demon-strated a positive effect of treatment on meta-bolic control. Of the 13 non-RCTs, eight re-ports were associated with an improvementin metabolic control. Five of the 13 reportsincluded the use of adjunctive antibiotics,and three of these studies demonstrated apositive effect. There is, however, great het-erogeneity in terms of the design of the RCTsand non-RCTs. It was concluded that the useof antibiotics as part of the approach in-volving periodontal therapy to improvemetabolic management in patients with dia-betes has not been proven. Periodontal ther-apy will improve oral health for patients withdiabetes mellitus, and this therapy may alsoresult in improved metabolic control. It isclear that additional clinical research isneeded to better understand this finding.
All the above emphasize the importanceand significant implications of the link
between diabetes mellitus and periodontaldiseases. An emphasis must be placed on in-creasing professional and patient awarenessof this relationship and of the need for medical-dental comanagement of affectedindividuals.
THE ROLE OF DENTAL PROFESSIONALS
The above information strongly sug-gests a greater need for dental professionals(e.g., general dentists, periodontists, and hygienists) to assume a role in the manage-ment of the patient with diabetes.
Diagnosis and treatment of diabetes isclearly within the realm of the physician.However, dental professionals can evaluatesigns and symptoms indicative of poor meta-bolic control in patients with known dia-betes, and seek to identify patients who mayremain undiagnosed and refer such patientsto physicians for proper evaluation and treat-ment. A number of characteristics of dentalpractice are consistent with dentists assum-ing such a role: they treat large numbers ofpatients each year and often provide primaryand preventive care. Dentists frequently seepatients on a regular basis, and most visitsare nonemergent in nature.
Managing the needs of patients with diabetes is not new to dentistry. The associ-ation between diabetes and periodontal dis-ease, the possible other oral manifestationsof this metabolic disorder, treatment guide-lines, and special considerations with regardto the management of these patients in a dental setting have all been discussed in the dental literature, promoted by professional associations, such as the American DentalAssociation and the American Academy ofPeriodontology, and taught in dental anddental hygiene schools for many decades.Similarly to what has been shown withinthe medical profession, however, efforts totranslate research into primary care havebeen met with resistance27 and such a gap

222 Periodontal Disease and Overall Health: A Clinician's Guide
between knowledge and practice appears toexist in the dental profession.
Are Dental Professionals Involved?The first reports to document the extent
of US dentists’ practice activities with re-spect to the management of patients with di-abetes28,29 demonstrated that a clear majorityof general dental practitioners did not feelthey had mastery of the knowledge involved,viewed such activities as peripheral to theirrole as caregivers, and did not believe thatcolleagues or patients expected them to per-form such activities. Although periodontistsgenerally performed risk identification andmanagement for patients with diabetes morefrequently than general practitioners, bothgroups tended to engage in activities that in-quire and discuss, and rates of proactive pa-tient management activities were quite lowfor both groups of clinicians. A subsequentstudy of general dentists in New Zealand30
showed striking similarities in attitudes andorientations compared to those identified inthe US study.
These data suggest there is a need to in-crease dentists’ involvement in the activemanagement of the diabetic patient. Suchactions can be expected to result in improvedperiodontal and general health outcomes.The evidence suggests, however, that ap-proaches to changing dentists’ behaviorshould aim not only at increasing knowl-edge, but also at overcoming attitudes andorientations associated with actively man-aging patients who have diabetes. Basicviews of the dentist’s role as a primary andpreventive care provider need to be changedto facilitate the desired behavioral changes.Interestingly, when looking at predictors ofactive management of the diabetic patient,31
these appear different for general dentistsversus periodontists. For the latter, varia-blesthat reflected feelings of confidence, involvement with colleagues and medicalexperts, and viewing active management of
the diabetic patient as belonging in theirsphere of professional responsibility wereinfluential. Variables pertaining to patientrelations, such as discussion with patients,patient expectations, and the Medicaid statusof their patients were influential predictorsfor general dentists. These findings providethe initial step toward identifying the com-ponents of targeted interventions aimed at in-creasing specialists’ and general dentists’level of involvement in the management ofthe diabetic patient, thereby contributing tothe improvement of the dental patient’s oraland systemic health.
How Can Dental ProfessionalsBe More Involved?
In order for dental professionals to pro-vide safe and effective oral care to patientswith diabetes, to be able to contribute to thepatients’ better overall management, andhelp in the identification of those with pre-diabetes or even those with frank diabeteswho remain undiagnosed, it is essential thatthey have a thorough knowledge of certainaspects of this complex disorder. Dental pro-fessionals need to be aware of and appreci-ate the multiple risk factors involved in thedevelopment of diabetes, the types of treat-ments diabetic patients may be receiving,the risk for emergency episodes, the diffi-culties and everyday challenges that diabeticpatients are faced with, and the constant sup-port and reinforcement these patients need toproperly manage their chronic condition.
Every dental care setting should haveclinical protocols in place to provide for thedental needs of a patient with diabetes. Theseshould include:
• criteria assessed and risk factors con-sidered when screening patients withpotentially unrecognized (pre) diabetes;
• evaluation of every new diabetic patient;
• routine care of a diabetic patient basedon their level of metabolic control;

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 223
and• appropriate equipment, supplies, and
training in order to prevent and/ormanage a diabetic emergency duringor after a dental appointment.
In addition, guidelines should be inplace to determine:
• the need for a medical consultation,referral, or follow up;
• how to perform risk assessment fororal/periodontal diseases;
• the type of dental and/or periodontaltherapy and the frequency of follow-up care; and
• the need to refer to a dental specialist.Taking a complete medical history is
something that all dental practitioners arerequired to do every time they see a new patient, and updates should be performed ateach maintenance/recall visit. However, oncea patient identifies as having diabetes, thedentist should gather and record additionaldetailed information, including:
• time since diagnosis;• type of treatment/medications the pa-
tient is receiving;• level of the patient’s metabolic control,
including recent HbA1c values; • presence of any diabetic complications
or other associated conditions, i.e., hyper tension, hypercholesterol emia,etc.; and
• frequency of prior hypoglycemic epi -sodes and precipitating factors.
One very important next step is thatthe dentist establish communication with thetreating physician. This allows the dentist toconfirm answers to the questions above, es-pecially if the patient is a poor historian. Thedentist can then inform the physician abouthis/her dental treatment plan, discuss anyconcerns, and get advice about potentialchanges in the management of the patient ifthe plan includes any extensive and/or stress-ful procedures. Communication should beongoing, especially if the planned dental
treatment is extensive and the patient ispoorly controlled.
An essential part of the oral disease riskassessment for patients with known diabetesis a detailed clinical evaluation. This shouldinclude:
• a thorough intraoral exam for oral mu-cosal lesions (e.g., lichen planus, apt-hous stomatitis);
• identification of signs and/or symp-toms of opportunistic infections (e.g.,oral Candidiasis);
• evaluation of salivary flow;• assessment of taste disturbances and
signs/symptoms of burning mouthsyndrome;
• dental caries assessment; and• a complete periodontal evaluation with
whole mouth probing depth and at-tachment loss measurements, assess-ment of the level of plaque and gin -gival inflammation, and radio graphicevaluation of bone levels, as needed.
Managing the dental care of diabeticpatients should not be a significant chal-lenge in the large majority of cases. Any ac-tive infection must be immediately treatedas it may also have a significant adverseimpact on the diabetic state, especially onthe level of glycemic control. The patientwith diabetes who is under good medicalcare and maintains good glycemic controlgenerally can receive any indicated dentaltreatment.
Recommendations for proper home careare very important for patients with diabetesand must be discussed in detail prior to anytherapy and reviewed at follow-up visits.The oral hygiene regimen should include theuse of an over-the-counter toothpaste and/ormouthrinse with antibacterial propertiesto help manage supragingival plaque and gingival inflammation. Patients must be en-couraged to brush and floss after each meal,conduct self-examinations regularly, andcontact the dentist or hygienist if they see

224 Periodontal Disease and Overall Health: A Clinician's Guide
signs of infection, such as edematous, bleed-ing gingiva or other oral changes, such as ulcers, burning mouth, or reduced salivaryflow.
In patients with known diabetes, dentistsshould not only aggressively screen for, butalso carefully treat periodontal infections.Important points for consideration follow:
• If periodontal or other oral surgery isneeded, the level of glycemic controlmay determine healing and responseto treatment.
• Elective therapy may be postponeduntil the patient demonstrates im-proved metabolic control.
• The response to initial periodontaltherapy (scaling and root planing)should be closely monitored as it mayhelp the dentist to better assign prog-nosis and predict outcomes of furthertreatment, including response to andhealing capacity following perio dontalsurgery, extractions, implant surgery,or regenerative procedures.
• Following active dental and/or peri-odontal therapy, patients should bescheduled for frequent recall appoint-ments to prevent and monitor bacter-ial recolonization, reinforce properoral hygiene, and treat any disease reactivation.
• There is no need for antibiotic pre-medication, but antibiotics may beconsidered pre-/postoperatively orin conjunction with periodontal ther-apy, especially if an overt infection is apparent.
• Since diabetes affects the host re-sponse to infection, adjunct therapies,such as locally delivered antimicro-bials, systemic antibiotics, or a sub-anti microbial dose of doxycycline maybe considered.
• The patient’s physician should be con-sulted about dietary recommendationsand any modification to the type and
dose of medications both pre- andpostoperatively
• Typically, diabetic patients should receive morning appointments when endogenous corticosteroids are at highlevels (better stress management).
• Vital signs, blood pressure, and glu-cose levels should be assessed preop-eratively and as discussed in detail be-low.
• Appointments should be kept as atrau-matic, short, and stress-free as possi-ble, as endogenous epinephrine re-lease in response to stress and paincan antagonize insulin action and pro-mote hyperglycemia.
• Epinephrine should be used in thedental anesthetics to ensure long last-ing and profound anesthesia.
• Post-operative analgesics should beprovided to ensure that the patient ispain-free following tooth extraction,periodontal surgery, or any other in-vasive procedure.
Prevention and Proper Managementof Diabetes- Related Emergencies
in the Dental OfficeExtreme glycemic variability is one of
the most frequently encountered medicalemergencies in dental offices. All dental professionals should be trained to prevent,recognize, and properly manage both hypo-and hyperglycemic episodes.
Hypoglycemia is defined as plasma glu-cose level below 70 mg/dL and confirmedwhen symptoms are relieved after eating.32 Itis important to note that diabetic patientsmay complain of symptoms suggestive ofhypoglycemia at blood glucose levels higherthan 70 mg/dL, if they have had chronicallyelevated blood glucose. Hypoglycemia iscommonly caused by skipped or delayedmeals while taking medication, alcohol con-sumption, excessive physical activity, or acombination of these factors. Some of the

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 225
important questions to ask patients at the be-ginning of the office visit may include: “Didyou miss or delay your meal?” “Did you exercise without snacking?” or, “Did youadjust your medication and how?”
The classic symptoms of hypoglycemiainclude hunger, shakiness, nervousness,sweating, or weakness.32 However, as the duration of diabetes and the frequency of hypoglycemic events increase, individualswith diabetes gradually lose these obviousadrenergic symptoms. The deficient releaseof counter-regulatory hormones and theblunted autonomic responses eventually re-sult in a state of hypoglycemia unawareness.At this point, the focus for the patient and of-fice staff education should be on identifyinga distinct set of less obvious neuroglycopenicsymptoms, such as slow cognitive response,light-headedness, sleepiness, confusion, dif-ficulty speaking, and anxiety.
The steps for intervention when hypo-glycemia is suspected are outlined in Box 1.The immediate treatment for hypoglycemiais to give glucose or carbohydrates that easilybreak down to glucose, such as glucosetablets, fruit juice, nondiet soda, or honey.Complex carbohydrates or food that con-tains fat may delay the recovery process andare not recommended as first-line treatment.
A commonly recommended treatment algo-rithm for hypoglycemia, also known as the15-15 rule, includes: 1) consume 15 g ofsimple carbohydrates; 2) wait 15 minutes torecheck blood glucose; and 3) repeat 15 g ofcarbohydrates if glucose level is still belowtarget (90 mg/dL). If the initial glucose is below 50 mg/dL, then consumption of 30 gof simple carbohydrates is indicated. Shortlyafter the immediate treatment, the patientshould follow with a meal or snack. In practice, food such as peanut butter sand-wich, 6 saltine crackers, or 3 graham crackersquares provides complex carbohydrates andprotein to prevent further hypoglycemia. Oc-casionally, blood glucose can plunge into thehypoglycemic range again after the return toa normal level. Therefore, further glucosemonitoring may be necessary before leavingthe dental office, especially prior to operatinga motor vehicle. There always exists the temp-tation to overtreat hypogly cemia with a largeamount of carbohydrates due to the urgencyand the discomfort associated with the symp-toms. Yielding to this practice will lead to ex-cessive rebound hyperglycemia, thereby gen-erating vicious cycles of glycemic instability.In the event of severe hypoglycemia wherethe individual is unconscious or too confusedto ingest carbohydrates, trained personnel in
Box 1.Steps for Intervention When Suspecting Hypoglycemia
1. Check blood glucose to confirm hypoglycemia (blood glucose < 70 mg/dL).2. If patient is conscious, give 15 g of simple carbohydrates orally as immediate treatment.
Options include 4 oz of fruit juice, 5–6 oz regular soda, 1 tablespoon of table sugar orhoney, 7–8 Lifesaver candies, 3 tablespoons of jelly, 2 tablespoons of raisins, or 4 –5 glucose tablets. If initial blood glucose is less than 50 mg/dL, give 30 g of simple carbohydrates.
3. Recheck blood glucose after 10–15 minutes. If blood glucose is less than 70 mg/dL repeatthe treatment (step 2) until blood glucose returns to at least 90 mg/dL.
4. Follow with a meal or snack such as 6 saltine crackers, 3 graham cracker squares, or 1⁄2peanut butter sandwich. Further glucose monitoring may be necessary.
5. If patient is unconscious, activate 911. Inject glucagon intramuscularly.6. When patient is alert enough to swallow, give fruit or soda immediately and follow
steps 2 to 4.

226 Periodontal Disease and Overall Health: A Clinician's Guide
addition to activating the emergency medicalservice may intramuscularly inject glucagon,which is packaged as a 1 mg ampoule ofglucagon with diluents and a syringe. Theglucagon injection is expected to restore thepatient to consciousness within 10-15 min-utes, but the effect may be short-lived. Thesecond line of treatment should include in-gestion of juice or soda, followed by a snackof solid food. Every dental office shouldhave staff capable of using a glucose moni-tor and glucagon. In addition, care should betaken to ensure that dental offices areequipped with glucose monitors, unexpiredglucose testing strips, glucagon kits, and ap-propriate food/drink for treatment of a hypo -glycemic episode.
Prevention and early recognition of hypo -glycemia is obviously best and an importantcomponent in the planning for a dental pro ce-dure. Most office-based dental proceduresdo not necessitate an adjustment of diabetic
medications. When fasting or sedation is re-quired, proper medication adjustment shouldbe made in advance to prevent an in-office di-abetic emergency. Close communicationamong the healthcare providers should be apriority. Placing diabetic patients early in the appointment schedule can prevent hypo-glycemic episodes associated with prolongedfasting or delayed/skipped meals.
Not all diabetic medications cause severehypoglycemia. For the purpose of classifyingdrugs according to their risk for hypoglycemia,diabetes medications can be divided into eitherantihyperglycemic or hypoglycemic (Table1). Technically, the antihyperglycemic classof medications includes agents that can lowerglucose from the hyperglycemic range to nearnormal range without the risk of driving theglucose concentration into the hypoglycemicrange. Most of these agents work via mech-anisms distinct from direct stimulation of in-sulin production. For others, the stimulation
Table 1. Classification of Diabetes Agents According to Their Potential toTable 1. Lower Glucose Below Physiologic Range
Hypoglycemic Agents Antihyperglycemic AgentsSulfonylureas Biguanide
Glyburide (Diabeta®, Micronase®) Metformin (Glucophage®)Glipizide (Glucotrol®, Glucotrol XL®) ThiazoladinedionesGlimepiride (Amaryl®) Pioglitazone (Actos®)
Short-acting secretagogues Rosiglitazone (Avandia®)Repaglinide (Prandin®) Alpha-glucosidase inhibitorsNateglinide (Starlix®) Acarbose (Precose®)
Insulin Miglitol (Glyset®)Basal/intermediate to long-acting insulin Incretins
Detemir (Levemir®) Exenatide (Byetta®)Glargine (Lantus®) Sitagliptin (Januvia®)NPH (Novolin N®, Humulin N®)
Amylin analogShort-acting insulinAmylin (Symlin®)Regular human insulin (Novolin R®, Humulin R®)
Bile acid binderUltra-short-acting insulin Colesevelam (Welchol®)Aspart (NovoLog®)
Lispro (Humalog®)Glulisine (Apidra®)
Mixed insulin Aspart 70/30 (NovoLog mix 70/30)Lispro 75/25 (Humalog mix 75/25)Lispro 50/50 (Humalog mix 50/50)Regular human mix 70/30 (Humulin 70/30, Novolin 70/30)Regular human mix 50/50 (Humulin 50/50)

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 227
of insulin release occurs in a glucose-de-pendent manner. In other words, the glu-cose-lowering effect of these drugs moder-ates as glucose levels normalize. These drugsinclude biguanide, thiazoladinediones, al-pha-glucosidase inhibitors, incretins, and bileacid-binders. The hypoglycemic class ofmedications lowers glucose levels either byinsulin replacement or direct insulin stimu-lation. Sulfonylureas, short-acting insulinsecretagogues, and the various insulin for-mulations have the highest hypoglycemicpotential. Insulin-requiring patients are sub -ject to hypoglycemic events and hypogly -cemia unawareness, which can severely disrupt quality of life and compromise theability to tighten glucose control. A commonmisconception is that all patients on insulinhave type 1 diabetes. While it is correct thatindividuals with type 1 diabetes must rely oninsulin for survival, many individuals withtype 2 diabetes also require insulin at laterstages of the disease. It is important to em-phasize that antihyperglycemic agents areassociated with a profound risk of causinghypoglycemia when combined with drugsfrom the hypoglycemic class.
Generally, there is no need for adjust-ment of the medication or insulin regimenprior to or on the day of the dental appoint-ment. If the patient is asked to fast overnightprior to the office visit and basal insulin isused, then either the same dose or no lessthan 75% of its dose should be given thenight before. If neutral protamine hagedorn(NPH) insulin or premix insulin is generallytaken at night, then no dose adjustment is re-quired the night before the procedure. Onthe day of the dental visit, the fasted patientshould be instructed not to take any antidia-betic oral medications or fast-acting insulinin the morning. If basal insulin is usuallytaken in the morning, either the same dose orno less than 75% of its usual dose should begiven. For those who are on NPH or premixinsulin in the morning, they should take only
one third to one half of the usual dose. Afinger stick glucose check should be per-formed prior to the procedure upon arrival inthe office. During a prolonged procedure,periodic glucose monitoring may be neces-sary. The regular medication regimen can beresumed upon returning to normal diet afterthe procedure is finished. In general, and es-pecially for long and stressful procedures,the dentist should consult with the treatingphysician if there is any concern or he/shethinks that a change in the patient’s diabeticregimen may be necessary.
It is well known that chronically ele-vated glucose levels impair wound healingand predispose patients to infections.33 Incontrast, transient hyperglycemia at levelsbelow 300 mg/dL during an office appoint-ment generally does not pose an immediatedanger to most patients with type 2 diabetes,nor does it necessitate cancellation of thedental procedure as long as hyperglycemia iscorrected shortly. Acute hyperglycemia canoccur in the setting of pain, stress, or under-dosing of diabetic medications related to thedental procedure. Reviewing a recent HbA1ctest result can help determine if it reflects theunderlying glycemic trend. However, for pa-tients with type 1 diabetes, significant keto -acidosis (also known as diabetic ketoacidosisor DKA) can occur at glucose concentrationsabove 250 mg/dL in which additional insulinadministration and hydration are urgently in-dicated.34 The telltale signs and symptoms ofDKA include excessive thirst, fatigue, rapidbreathing, fruity breath, nausea, and vomit-ing. While most patients with type 1 diabeteshave the skills to manage hyperglycemia andmild DKA by aggressive rehydration and in-sulin administration, a consultation with theirmedical provider is necessary if the symp-toms become severe. When the patient is se-verely nauseated or unable to keep down flu-ids with blood glucose above 250 mg/dL, thepatient should be transferred to a hospitalEmergency Room for medical intervention.

228 Periodontal Disease and Overall Health: A Clinician's Guide
Screening for Undiagnosed Diabetesin the Dental Office
Early identification of diabetes and, indiagnosed patients, achieving and maintain-ing glycemic levels as close to normal aspossible have been the focus of efforts fromthe American Diabetes Association and themedical and public health communities formany years. With respect to screening forundiagnosed diabetes, the American Dia-betes Association has made recommenda-tions for routine screening in adults 45 orolder, and has defined the high-risk cate-gories in which screening is advisable moreoften or in younger individuals (Box 2). Theincreased risk is associated with certain de-mographic characteristics (minority, race-ethnicity status, family history of diabetes),clinical characteristics (obesity, physical inactivity, hypertension, dyslipidemia), andprior evidence of abnormal glucose values(gestational diabetes, IFG, IGT).4
Historically, the primary method used todiagnose diabetes mellitus has been the fast-ing plasma glucose test. While valuable formaking a diagnosis, this tends to be highlydependent on patient compliance, and ismeaningful only for the immediate time pe-riod prior to when the test is administered.
The HbA1c assay is based on the knowl-edge that blood glucose can bind to hemo-globin molecules. This reaction is not enzy-matically driven and therefore is a measureof the exposure to glucose in the blood.Based on the 2010 revisions of the Standardsof Medical Care in Diabetes by the AmericanDiabetes Association,4 the HbA1c assay isalso now accepted as a test to diagnose dia-betes (with a cut point of 6.5%). In addi-tion, it remains very valuable for monitoringglycemic levels and response to treatment,and can be an excellent screening tool thatdoes not rely on patient compliance, doesnot require fasting, and gives an indication ofglucose levels over an extended period oftime.
The importance of early diagnosis ofdiabetes cannot be overstated and it clearlycannot be the sole responsibility of the med-ical community or of any single group ofhealthcare providers. Survey data from theAmerican Dental Association in 2007 showthat 68.5% of adults had visited a dentist inthe previous year,12 and data from the Be-havioral Risk Factor Surveillance Systemshow an even higher percentage.11 Insuranceutilization patterns indicate that individualstend to seek routine and preventive oral
Box 2.Screening for Diabetes in Asymptomatic Adults
All 45 years of age—if normal, repeat every 3 years. Test at younger ages or more frequently if patient is overweight or obese (body mass index 25 kg/m2 for most, but not allracial/ethnic groups) and having one or more of the following risk factors:
! Family history of diabetes (parent or sibling)! High-risk race/ethnicity (African-American, Hispanic/Latino, Alaska Native, American
Indian, Asian American, or Pacific Islander)! Habitual physical inactivity! Delivery of infant > 9 lbs or history of gestational diabetes! Polycystic ovarian syndrome! Blood pressure 140/90 mm Hg! High-density lipoprotein cholesterol < 35 mg/dL or triclycerides > 250 mg/dL! Impaired glucose tolerance or impaired fasting glucose! History of vascular disease or other diabetes-associated conditions
Adapted from the American Diabetes Association “Standards of Medical Care in Diabetes—2010.” Diabetes Care 2010;33(Suppl1):S11–S61.4

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 229
healthcare on a more frequent basis than rou-tine and preventive medical care.35 Thesefacts allow dentists and dental hygienists tobe at the front line of screening interven-tions and risk-reduction strategies.36 Yet canthis happen in real world practice?
Previous studies have examined the per-formance of predictive models for diabetesscreening in medical settings using a mix ofself-reported and objective characteristics.37
A recent report explored for the first time apredictive model for undiagnosed diabetes38
that included measures of periodontal dis-ease using national data from the third USNHANES study. Findings revealed that, forexample, a 45-year-old person, with self- reported family history of diabetes, self- reported hypertension, high cholesterol levels, and clinical evidence of periodontaldisease bears a probability of having dia-betes (and being unaware of it) between 27%and 53%, with Mexican-American men ex-hibiting the highest and white women thelowest.38 These probabilities increase amongindividuals 60 years of age to between ap-proximately 48% and 74%. These findings,coupled with emerging supportive data byothers,39 demonstrate that simple pieces ofinformation from a patient’s medical historyand an oral examination can be used effec-tively to identify patients at risk for undiag-nosed diabetes in a dental care setting. Theresults of this novel approach are not defin-itive, but afford us the opportunity to testand validate such a model in the clinic.
Participating in the Managementof Patients with Unrecognized
or Known DiabetesBased on the above, the dentist or dental
hygienist should assess the presence of riskfactors for diabetes in their patients (Figure 2).A risk calculator is available from the Amer-ican Diabetes Association and dental profes-sionals can use it to assess (and discuss) lev-els of risk for diabetes in their patients.40 If
they identify a patient at risk, then they can either use a screening blood test in the officeor refer to a physician for diag nostic testing.Irrespective of the strategy used and the resultof any testing, the concerns and findings needto be discussed with the patient and in thecase of a medical referral, the dental profes-sionals need to follow up on the outcome.
Similarly, dental professionals should beinvolved in the ongoing efforts of patientswith known diabetes (or prediabetes) toachieve appropriate glycemic control andmodify behavior and habits, such as smoking,lack of physical activity and unhealthy diet—all risk factors that may exacerbate diabetes-associated complications. Dentists and den-tal hygienists can help their patients by:
• evaluating and managing risks for oralcomplications;
• providing guidance in goal setting;• helping with strategies to achieve
goals and overcome barriers; and• providing continuous education, re -
inforcement, and support.Dental practices should establish a sys-
tem of referrals for routine preventive care aswell as for urgent needs. Dentists and hy-gienists should not just tell the person witha potentially serious problem to consult ahealth specialist right away, they should con-tact primary care and specialty providers todiscuss criteria for referral and ensure thatprocedures are in place for seeing a personwho is referred for care or on an urgent ba-sis. A list of providers, case managers, phonenumbers, and other contact information canbe very useful for quick reference. The den-tal team should also consider giving indi-viduals handouts with referral information,or calling clinics directly. Multidisciplinaryteam care is key to both successful diabetesrecognition and management.
Patient EducationA recent report from the United King-
dom41 assessed the knowledge diabetic
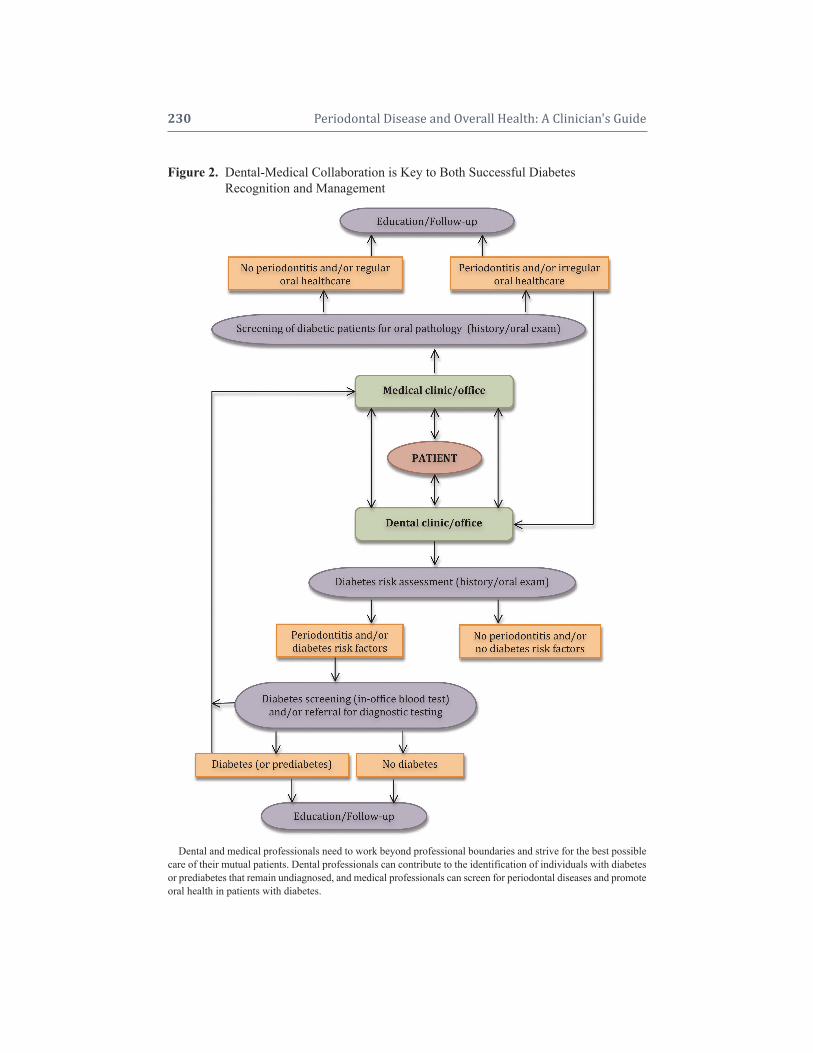
230 Periodontal Disease and Overall Health: A Clinician's Guide
Figure 2.Dental-Medical Collaboration is Key to Both Successful Diabetes Figure 2. Recognition and Management
Dental and medical professionals need to work beyond professional boundaries and strive for the best possiblecare of their mutual patients. Dental professionals can contribute to the identification of individuals with diabetesor prediabetes that remain undiagnosed, and medical professionals can screen for periodontal diseases and promoteoral health in patients with diabetes.

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 231
patients have of their risk for periodontaldisease and their attitudes towards oralhealth. Only a third of the 101 patients whoparticipated in the study were aware of theirincreased risk for periodontitis as opposed totheir knowledge of the risk for other diabeticcomplications, which ranged from 84% to99%. History of prior dental care was spo-radic, with 43% reporting seeing a dentistwithin the past year. An earlier study fromSweden42 had reported that 83% of diabeticpatients were unaware of the link betweendiabetes and oral health, and that 48% be-lieved that their dentist/dental hygienist wereunaware that they even had diabetes. Oralhealth does not appear to be a priority for pa-tients with diabetes.11,43-45 Tomar and Lesterreported that diabetic individuals were lesslikely to visit a dentist than a nondiabeticindividual in the preceding 12 months and,interestingly, the leading reason for not see-ing a dentist was “lack of perceived need.”11
Competing financial and time commitmentsmay explain the inadequacy of routine den-tal care in patients with diabetes.46
Dental professionals have an opportu-nity and the responsibility to educate theirpatients about the diabetes-oral health linkand promote good oral and overall healthbehaviors. They should play a supportingrole in modifying patient behavior and habitsrelated to risk factors that may exacerbate di-abetes-associated complications. Specifi-cally, as part of oral health education, dentalpractitioners and their teams can reinforcethe need for regular dental visits and properoral hygiene, but also the need for propernutrition, exercise, smoking cessation, ad-herence to medication regimens, regularmonitoring of blood glucose levels, and reg-ular medical follow ups, as indicated by thepatient’s physician. Patients should be en-couraged to achieve the best glycemic con-trol possible, as good control can improveoral health and lead to better and more pre-dictable perio dontal treatment outcomes. To
this end, patients need to know that they areat greater risk for increased prevalence,severity, and progression of periodontitis,and that perio dontitis has been recognizedas a condition often found in patients with diabetes. Indeed, the American DiabetesAs sociation Standards of Medical Care in Diabetes recognize that every patient withdiabetes needs to see a dentist for appropri-ate evaluation and treatment of oral dis-eases.4 Patients need to be informed thatproper control of periodontal infections mayeven have a beneficial effect on their level ofmetabolic control and systemic inflamma-tion, as well as the risk for vascular and kid-ney complications.20
Patients must comprehend the overar-ching principle that medical and dental pro-fessionals have common goals: providingthe best possible care to their patients andhelping them avoid complications (Box 3). Multi factorial, complex diseases such as dia -betes and periodontitis interrelate and canam plify one another, creating an imperativefor a comanagement model that has the po-tential to improve patient outcomes.
THE ROLE OF MEDICAL PROFESSIONALS
Members of the medical and dental ac-ademic communities—dentists, hygienists,physicians, nurses, representatives from den-tal and diabetes professional societies—aswell as representatives from dental/medicalinsurance carriers have convened a numberof workshops over the past few years to ad-dress oral-systemic links and discuss issuesrelated to communication among differenthealthcare professionals and patients.
Recently, two such symposia and theirsubsequent reports highlighted these issuesand offered recommendations. Following the“Scottsdale Project” meeting in April 2007,a panel of experts presented a consensus report that stated that “it is appropriateto develop guidelines to assist medical

232 Periodontal Disease and Overall Health: A Clinician's Guide
providers in identifying patients who are atrisk for periodontal disease or screening patients who may have undiagnosed perio -dontal disease.”47 Similarly the report follow - ing the July 2007 “Oral-Systemic Diseases:From Bench to Chair—Putting Informationinto Practice” symposium stated that “thereis a need for coordination and cooperationbetween dental and medical health profes-sionals with regard to screening for and diag nosing diseases or conditions that affectpatients who traditionally have been caredfor by other healthcare providers. Therefore,medical practitioners need to be aware oforal diseases and make appropriate recom-mendations and referrals.”48
The concepts emphasized above are espe -cially important for medical professionalswho treat patients with diabetes (e.g., intern -ists, diabetologists, nurses, diabetes educa-tors) as these patients are more likely to have perio dontal disease and more likely to haveless regular dental care. Medical care pro vid -ers need to discuss with their diabetic pa-tients the importance of oral health and its
relationship to the diabetic state; about thepotential sequelae of long-standing, un-treated oral infections; and to provide edu-cational brochures and other relevant mate-rial. By simply asking patients if they havea dentist and when was the last time theyvisited him/her, physicians can send a power -ful message and play a significant role inpromoting oral health and preventing oralcomplications in patients with diabetes.
Screening for Periodontal Changesand Key Questions to Ask
The guidelines for diagnosis of perio -dontal diseases include a detailed periodon-tal evaluation, including probing depth meas-urements and intraoral radiographs, whichare not feasible in most medical settings.Nevertheless, medical providers can screenfor periodontal diseases (Figure 2) based onpatient history, symptoms (sore, bleedinggums, sensitive teeth, history of abscesses)and a visual assessment of the patient’smouth for relevant signs, such as:
• food debris or plaque around teeth;
Box 3.Key Messages All Healthcare Providers Can Reinforce
! Emphasize the importance of good control (HbA1c, blood pressure, cholesterol) for complication prevention
! Promote a healthy lifestyle! Reinforce self-exams! Explain the benefits of comprehensive multidisciplinary care and emphasize the
importance of regular appointments with medical and oral healthcare providers
How Can a Busy Healthcare Provider Find the Time to Give Key Messages?! Do not give every message at one appointment! Customize and prioritize messages according to the patient’s needs! Provide patient with a computer-generated reminder of key messages discussed! Document what is accomplished at each appointment and the patient’s response! Create pamphlets for office or use materials available through national diabetes or
dental organizations and professional societies! Include key messages in office newsletters
Source: Adapted from the 2007 National Diabetes Education Program publication “Working togetherto manage diabetes: a guide for pharmacists. podiatrists, optometrists, and dental professionals.” Atlanta,GA. USDepartment of Health and Human Services, Public Health Service, Centers for Disease Controland Prevention, National Center for Chronic Disease Prevention and Health Promotion, 2007.51

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 233
• red, swollen, receding, or bleedinggums;
• loose teeth, separation of teeth; • oral abscesses; • missing teeth; or• halitosis. If diabetic patients tell a member of the
medical team that they have not seen a dentistin the last year, they should be immediatelyreferred to one. If a patient has seen a dentistin the past year, but presents with detectablesigns or symptoms of oral/periodontal infec-tions, he or she should again be referred to adentist. Finally, physicians should advise allpoorly controlled diabetic patients to see adentist/periodontist for evaluation and treat-ment on a regular, ongoing basis. Medical careproviders should also facilitate communica-tion with treating dental practitioners by offer -ing information on the patients’ medical back-ground, level of glycemic control, presence ofcomplications, and comorbidities. Further-more, they should be available to offer adviceon medical management modifications thatmay be necessary, and be open to a meaning-ful professional interaction in order to assurethat patients receive the best possible care.
PATIENT-CENTERED TEAM CAREFinally, the concept of a “syndemic
approach to diabetes management” as intro-duced and discussed in the dental literatureby Hein and Small36 deserves some men-tion. “Syndemic” is a term originally used todescribe a set of two or more linked healthproblems, which synergistically contribute toexcess burden in a population.49 A syndemicorientation has the potential to provide aframework that can guide more efficient andeffective initiatives because healthcare pro -viders will not approach diseases like dia-betes and periodontitis as discrete problems,and will be prompted to collaborate acrossand beyond professional boundaries.
The model of “working together” hasbeen discussed in the diabetes literature
extensively. In 2001, the National DiabetesEducation Program (NDEP), a joint programof the National Institutes of Health and the Centers for Disease Control and Prevention,published a report titled “Team Care: Com -prehensive Lifetime Management for Dia-betes.”50 This report was created to help or-ganizational leaders of healthcare systemsand purchasers of healthcare to implementmultidisciplinary team care for people withdiabetes in all clinical settings, and set forthan analysis of the evidence that supportsteam care as an effective method for chronicdisease management.
The executive summary of this reportstated that although primary care physicianscurrently provide 80% to 95% of diabetescare in the US, they cannot do all that is re-quired and often are discouraged that the cur-rent medical system does not function well forpeople with diabetes.50 The challenge is tofind a way to meet the needs of patients withdiabetes by broadening the opportunities fordelivery of care. Team care meets this chal-lenge by integrating the skills of differenthealthcare professionals with those of the pa-tient and family members to create a com-prehensive lifetime diabetes management pro-gram. The report highlights that if diabetescare is to achieve the health benefits that mod-ern science has made possible, it must be:
• continuous, not episodic;• proactive, not reactive;• planned, not sporadic;• patient-centered rather than provider-
centered; and• population-based, as well as individual-
based.
CONCLUSIONAlthough the model of multidiscipli-
nary, patient-centered care presents manychallenges, all healthcare providers shouldstrive to participate in it. There is no doubtthat by changing their thinking and trying toadopt these concepts into everyday practice,

234 Periodontal Disease and Overall Health: A Clinician's Guide
healthcare providers can render better health-care and more predictable therapeutic out-comes, maximize their success in combatingthe diabetes epidemic, and play a significantrole in promoting the oral and overall healthof patients. In the “Working Together toManage Diabetes” 2007 publication by theNDEP, all healthcare providers are calledupon to play a role in diabetes primary pre-vention and in diabetes control.51 Amongothers, dentists and dental hygienists canmake a difference in primary prevention andmanagement because patients are seen on aregular basis by them, patients trust them,and a few words from them can have a ma-jor impact on patients’ healthcare behavior.
Supplemental Readings
American Diabetes Association Position Statement. Di-agnosis and classification of diabetes mellitus. DiabetesCare 2010;33(Suppl 1):S62–S69.
Borrell LN, Kunzel C, Lamster I, Lalla E. Diabetes inthe dental office: using NHANES III to estimate theprobability of undiagnosed disease. J Periodontal Res2007;42:559–565.
Hein C, Small D. Combating diabetes, obesity, peri-odontal disease and interrelated inflammatory condi-tions with a syndemic approach. Grand Rounds in Oral-Systemic Medicine 2006;2:36–47.
Kunzel C, Lalla E, Lamster IB. Management of the pa-tient who smokes and the diabetic patient in the dentaloffice. J Periodontol 2006;77:331–340.
Working together to manage diabetes: a guide for phar-macists, podiatrists, optometrists, and dental profes-sionals. Atlanta, GA: U.S. Department of Health andHuman Services, Public Health Service, Centers forDisease Control and Prevention, National Center forChronic Disease Prevention and Health Promotion,2007.
REFERENCES1. Centers for Disease Control and Prevention. Na-
tional diabetes fact sheet: general information andnational estimates on diabetes in the United States,2007, Atlanta, GA: U.S. Department of Health andHuman Services, Centers for Disease Control andPrevention, 2008.
2. International Diabetes Federation. Diabetes preva-lence. Available at: http://www.idf.org/home. Ac-cessed: January 24, 2010.
3. American Diabetes Association. Diabetes statis-tics. Available at: http://www.diabetes.org/diabetes-statistics. jsp. Accessed: January 24, 2010.
4. American Diabetes Association Position Statement.Standards of medical care in diabetes—2010. Dia-betes Care 2010;33(Suppl 1):S11–S61.
5. Diabetes Prevention Program Research Group. Theprevalence of retinopathy in impaired glucose tol-erance and recent-onset diabetes in the DiabetesPrevention Program. Diabet Med 2007;24:137–144.
6. Knowler WC, Barrett-Connor E, Fowler SE, Ham-man RF, Lachin JM, Walker EA, Nathan DM; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes withlifestyle intervention or metformin. N Engl J Med2002;346:393–403.
7. Albandar JM. Periodontal diseases in North Amer-ica. Periodontol 2000 2002;29:31–69.
8. Papapanou PN. Periodontal diseases: epidemiol-ogy. Ann Periodontol 1996;1:1–36.
9. Hugoson A, Sjodin B, Norderyd O. Trends over30 years, 1973–2003, in the prevalence and sever-ity of periodontal disease. J Clin Periodontol 2008;35:405–414.
10. American Association of Diabetes Educators. Dia betes Education Fact Sheet. Available at:http://www.diabeteseducator.org/export/sites/aade/_resources/pdf/Diabetes_Fact_Sheet.pdf Accessed:January 24, 2010.
11. Tomar SL, Lester A. Dental and other health carevisits among U.S. adults with diabetes. DiabetesCare 2000;23:1505–1510.
12. American Dental Association. 2007 Public OpinionSurvey. American Dental Association Survey Cen-ter, 2008.
13. The Diabetes Control and Complications Trial Re-search Group. The effect of intensive treatment ofdiabetes on the development and progression oflong-term complications in insulin-dependent dia-betes mellitus. N Engl J Med 1993;329:977–986.
14. Turner RC, Cull CA, Frighi V, Holman RR.Glycemic control with diet, sulfonylurea, met-formin, or insulin in patients with type 2 diabetesmellitus: progressive requirement for multiple ther-apies (UKPDS 49). UK Prospective Diabetes Study(UKPDS) Group. JAMA 1999;281:2005–2012.
15. Hoerger TJ, Segel JE, Gregg EW, Saaddine JB. Isglycemic control improving in U.S. adults? Dia-betes Care 2008;31:81–86.
16. Cryer PE. Hypoglycemia: still the limiting factor inthe glycemic management of diabetes. Endocr Pract2008;14:750–756.

CHAPTER 14 Dental and Medical Comanagement of Patients with Diabetes 235
17. Lamster IB, Lalla E, Borgnakke WS, Taylor GW.The relationship between oral health and diabetesmellitus. J Am Dent Assoc 2008;139(Suppl):19S–24S.
18. Mealey BL, Oates TW; American Academy of Periodontology. Diabetes mellitus and periodontaldiseases. J Periodontol 2006;77:1289–1303.
19. Wilson TG Jr. Compliance. A review of the litera-ture with possible applications to periodontics. JPeriodontol 1987;58:706–714.
20. Taylor GW, Borgnakke WS. Periodontal disease:associations with diabetes, glycemic control andcomplications. Oral Dis 2008;14:191–203.
21. Genco RJ, Grossi SG, Ho A, Nishimura F, Mura -yama Y. A proposed model linking inflammationto obesity, diabetes, and periodontal infections. J Perio dontol 2005;76:2075–2084.
22. Grunfeld C, Soued M, Adi S, Moser AH, DinarelloCA, Feingold KR. Evidence for two classes of cyto -kines that stimulate hepatic lipogenesis: relation-ships among tumor necrosis factor, interleukin-1and interferon-alpha. Endocrinology 1990;127:46–54.
23. Pickup JC, Mattock MB, Chusney GD, Burt D.NIDDM as a disease of the innate immune sys-tem: association of acute-phase reactants and inter -leukin-6 with metabolic syndrome X. Diabetologia1997;40:1286–1292.
24. Saremi A, Nelson RG, Tulloch-Reid M, HansonRL, Sievers ML, Taylor GW, Shlossman M, Ben-nett PH, Genco R, Knowler WC. Periodontal dis-ease and mortality in type 2 diabetes. DiabetesCare 2005;28:27–32.
25. Shultis WA, Weil EJ, Looker HC, Curtis JM,Shlossman M, Genco RJ, Knowler WC, NelsonRG. Effect of periodontitis on overt nephropathyand end-stage renal disease in type 2 diabetes. Diabetes Care 2007;30:306–311.
26. Demmer RT, Jacobs DR Jr., Desvarieux M. Perio -dontal disease and incident type 2 diabetes: resultsfrom the First National Health and Nutrition Ex-amination Survey and its epidemiologic followupstudy. Diabetes Care 2008;31:1373–1379.
27. Berwick DM. Disseminating innovations in healthcare. JAMA 2003;289:1969–1975.
28. Kunzel C, Lalla E, Albert DA, Yin H, Lamster IB.On the primary care frontlines: the role of the gen-eral practitioner in smoking-cessation activities anddiabetes management. J Am Dent Assoc 2005;136:1144–1153.
29. Kunzel C, Lalla E, Lamster IB. Management ofthe patient who smokes and the diabetic patient inthe dental office. J Periodontol 2006;77:331–340.
30. Forbes K, Thomson WM, Kunzel C, Lalla E, Lam-ster IB. Management of patients with diabetes by
general dentists in New Zealand. J Periodontol2008;79:1401–1408.
31. Kunzel C, Lalla E, Lamster I. Dentists’ manage-ment of the diabetic patient: contrasting generalistsand specialists. Am J Public Health 2007;97:725–730.
32. National Diabetes Information Clearinghouse, aservice of the National Institute of Diabetes and Di-gestive and Kidney Diseases, NIH. Hypoglycemia.Available at: http://diabetes.niddk.nih.gov/dm/pubs/hypoglycemia/. Accessed: January 24, 2010.
33. Smiley DD, Umpierrez GE. Perioperative glucosecontrol in the diabetic or nondiabetic patient. SouthMed J 2006;99:580–589.
34. Kitabchi AE, Wall BM. Management of diabeticketoacidosis. Am Fam Physician 1999;60:455–464.
35. Glick M, Greenberg BL. The potential role of den-tists in identifying patients’ risk of experiencingcoronary heart disease events. J Am Dent Assoc2005;136:1541–1546.
36. Hein C, Small D. Combating diabetes, obesity, perio dontal disease and interrelated inflammatoryconditions with a syndemic approach. Grand RoundsOral-Systemic Med 2006;2:36–47.
37. Tabaei BP, Herman WH. A multivariate logistic regression equation to screen for diabetes: develop -ment and validation. Diabetes Care 2002;25:1999–2003.
38. Borrell LN, Kunzel C, Lamster I, Lalla E. Diabetesin the dental office: using NHANES III to estimatethe probability of undiagnosed disease. J Perio -dontal Res 2007;42:559–565.
39. Strauss SM, Russell S, Wheeler A, Norman R, Bor-rell LN, Rindskopf D. The dental office visit as apotential opportunity for diabetes screening: ananalysis using NHANES 2003–2004 data. J PublicHealth Dent 2009, Epub ahead of print; doi: 10.1111/j.1752–7325.2009.00157.x.
40. American Diabetes Association. Diabetes Risk Calculator. Available at: http://www.diabetes.org/risktest.jsp. Accessed: January 24, 2010.
41. Allen EM, Ziada HM, O’Halloran D, Clerehugh V,Allen PF. Attitudes, awareness and oral health- related quality of life in patients with diabetes. JOral Rehabil 2008;35:218–223.
42. Sandberg GE, Sundberg HE, Wikblad KF. A con-trolled study of oral self-care and self-perceivedoral health in type 2 diabetic patients. Acta Odon-tol Scand 2001;59:28–33.
43. Karikoski A, Ilanne-Parikka P, Murtomaa H. Oralself-care among adults with diabetes in Finland.Community Dent Oral Epidemiol 2002;30:216–223.
44. Thorstensson H, Falk H, Hugoson A, KuylenstiernaJ. Dental care habits and knowledge of oral health

236 Periodontal Disease and Overall Health: A Clinician's Guide
in insulin-dependent diabetics. Scand J Dent Res1989;97:207–215.
45. Mayfield JA, Rith-Najarian SJ, Acton KJ, SchraerCD, Stahn RM, Johnson MH, Gohdes D. Assess-ment of diabetes care by medical record review.The Indian Health Service model. Diabetes Care1994;17:918–923.
46. Moore PA, Orchard T, Guggenheimer J, WeyantRJ. Diabetes and oral health promotion: a survey ofdisease prevention behaviors. J Am Dent Assoc 2000;131:1333–1341.
47. Hein C, Cobb C, Iacopino A. Report of the inde-pendent panel of experts of the Scottsdale Project.Grand Rounds Oral-Systemic Med 2007;Suppl:6–27.
48. Lamster IB, DePaola DP, Oppermann RV, Papa-panou PN, Wilder RS. The relationship of perio -dontal disease to diseases and disorders at distant
sites: communication to health care professionalsand patients. J Am Dent Assoc 2008;139:1389–1397.
49. Singer M. AIDS and the health crisis of the U.S. urban poor; the perspective of critical medical an-thropology. Soc Sci Med 1994;39:931–948.
50. Team care: Comprehensive lifetime managementfor diabetes. Atlanta, GA: U.S. Department ofHealth and Human Services, Public Health Service,Centers for Disease Control and Prevention, Na-tional Center for Chronic Disease Prevention andHealth Promotion, 2001.
51. Working together to manage diabetes: A guide forpharmacists, podiatrists, optometrists, and dentalprofessionals. Atlanta, GA: U.S. Department ofHealth and Human Services, Public Health Service,Centers for Disease Control and Prevention, Na-tional Center for Chronic Disease Prevention andHealth Promotion, 2007.
1. Define the pathogenesis of coronaryatherosclerosis and recognize its acuteand chronic clinical presentations
2. Comprehend the scientific basis thatidentifies risk factors for CVD
3. Explain the rationale that justifiesintervention by risk factor reduction
4. Describe commonly used medica-tions for patients with CVD andtheir impact on the delivery of oraland dental care
5. Discuss principles of comanagementof patients with cardiovascular dis-ease and periodontal disease
ATHEROSCLEROTIC CARDIOVASCULAR DISEASEAtherosclerosis has been defined as a
progressive disease process that involves thelarge- to medium-sized muscular and largeelastic arteries. Coronary atherosclerosis mayobstruct blood flow and result in ischemia tothe myocardium tissue that is dependenton the blood supply of the diseased artery. Lesions caused by atherosclerosis may alsorupture, and the resulting thrombus may beclinically silent or may cause a fatal myo -cardial infarction (MI, aka “heart attack”).Approximately 40% of deaths in the UnitedStates are attributed to the complications ofatherosclerosis; about half of these sequelaeare represented by coronary atherosclerosiscomplicated by thrombosis and MI.4
PathogenesisAtherosclerosis generally begins in
childhood, and manifests as a flat fatty streakusually detected only as an incidental finding
INTRODUCTIONCardiovascular disease (CVD) accounts
for 29% of deaths worldwide, ranks as theleading cause of death, and poses the great-est threat in low-income and middle-incomecountries.1 Atherosclerosis, which is a majorcomponent of cardiovascular disease, affectsone in four persons and contributes to ~ 40%of deaths annually in the United States.2
The estimated cost of treating CVD in2008 was $448.5 billion, a 20% increase inrecent years (http://www.americanheart.org/presenter.jhtml?identifier=4475, accessed2/20/2010). The pervasiveness of cardio -vascular disease makes it a natural target forprevention by all healthcare professionals. Ifprevention programs could reduce the acute-treatment costs and associated morbidity ofCVD by 20% per year, the savings would beat least $80 billion per year in healthcarecosts. By comparison, the cost of MedicarePart D was estimated to be ~ $70 billion in2008 (http://www.cbo.gov/ftpdoc.cfm?index=6076&type=0#table1, accessed 2/20/2010).Several studies point to the possibility thatperiodontal care in patients with cardio -vascular disease significantly reduced med-ical care costs.3 This chapter reviews theknown risk factors for CVD that are targetsfor disease prevention, and discusses a cur-rent and future rationale for oral, dental, andmedical healthcare practitioners to work together to implement optimal CVD risk fac-tor reduction.
Educational ObjectivesAfter reading this chapter, the reader
should be able to:
CHAPTER 15Dental and Medical Comanagement of Cardiovascular Disease
Timothy C. Nichols, David W. Paquette

at an autopsy that is performed for other rea-sons.5,6 The advanced raised lesion is calledan “atheroma,” which consists of elevatedfocal intimal plaques with a central core con-taining necrotic cells, cholesterol ester crys-tals, lipid-laden foam cells, and plasma pro-teins, including fibrin and fibrinogen. Thiscentral core is also associated with a cellularinfiltrate comprised of hypertrophic smoothmuscle cells, macrophages, and sparse T-lym-phocytes.One theory of atherogenesis is thatthe atherosclerotic plaque develops as a re-sponse to injury to the vascular endothelium,and that the endothelial injury is the primaryevent in atherogenesis. When the endothe-lium is even minimally injured, platelets andmonocytes accumulate and attach to the dam-aged wall. As platelets aggregate around theinjury, they release thromboxane, promotingfurther platelet aggregation and coronaryvasoconstriction. Monocytes invade the in-tima, and scavenge for lipids and other extra -cellular materials. These cells release vari-ous growth factors that attract more smoothmuscle cells from the media of the artery withresultant intima hyperplasia. As the lesionprogresses, fibrosis, lipid deposition, necrosis,and calcification may ensue to yield a com-plicated plaque. Inflammation, oxidative, andmechanical stress through high blood pres-sure can also induce primary injury of the arterial endothelium by which the pathogen-esis of atherosclerosis can be initiated andpropagated.
Risk Factors for the Development ofCoronary Atherosclerosis
Traditional major risk factors for athero -sclerotic cardiovascular disease include:
• Cigarette smoking• Hypertension (> 140/90 mmHg)• High levels of low-density lipo protein
cholesterol (LDLC, defined as > 100mg/dL)
• Low levels of high-density lipo proteincholesterol (HDLC, defined as < 40
mg/dL for men or < 35 mg/dL forwomen)
• Insulin resistance• Diabetes mellitus• Family history of premature coronary
heart disease (occurring in a parent age 45)
• Age (men 45 years, women 55years)
• Obesity (body mass index > 30 kg/m2)• Physical inactivity and an atherogenic
diet (Figure 1)It is also recognized that these factors
can interact with each other to increase therisk of CVD.7 For example, the FraminghamHeart Study involved more than 3,000 pa-tients and showed that for total cholesterollevels between 185 mg/dL and 335 mg/dL,cardiovascular risk was elevated further withthe addition of each of the following risk fac-tors: glucose intolerance; elevated systolicblood pressure; cigarette smoking; and leftventricular hypertrophy on electrocardiogra-phy.8 Data from the Framingham Heart Studyand two other large prospective cohort studies,the Chicago Heart Association DetectionProject in Industry (n = 35,642) and the Multiple Risk Factor Intervention Trial(n = 347,978), indicated that the majority ofpatients with fatal coronary artery athero-sclerosis or nonfatal MI present with at leastone of four risk factors: cigarette smoking; diabetes mellitus; hyperlipidemia; and hyper -tension.9 For fatal MI due to coronary arteryatherosclerosis, exposure to at least one riskfactor ranged from 87% to 100% for all threecohort studies. For nonfatal MI in the Fram-ingham Heart Study, prior exposure to at leastone risk factor was found in 92% of men and87% of women ages 40 to 59 at baseline.Furthermore, another recent analysis involv-ing 14 international randomized clinical trials(n = 122,458) showed that one of these fourconventional risk factors was present in 84.6%of men and 80.6% of women with coronaryartery disease.10
238 Periodontal Disease and Overall Health: A Clinician's Guide
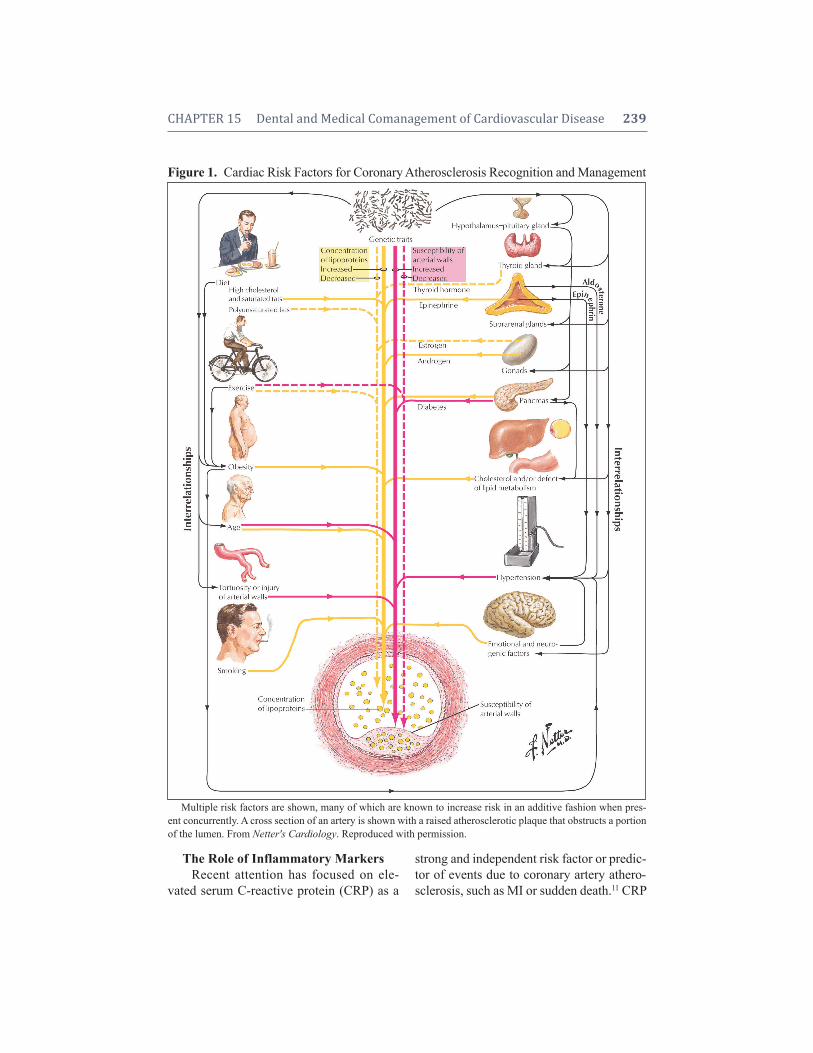
The Role of Inflammatory MarkersRecent attention has focused on ele-
vated serum C-reactive protein (CRP) as a
strong and independent risk factor or predic-tor of events due to coronary artery athero-sclerosis, such as MI or sudden death.11 CRP
CHAPTER 15 Dental and Medical Comanagement of Cardiovascular Disease 239
Figure 1. Cardiac Risk Factors for Coronary Atherosclerosis Recognition and Management
Multiple risk factors are shown, many of which are known to increase risk in an additive fashion when pres-ent concurrently. A cross section of an artery is shown with a raised atherosclerotic plaque that obstructs a portionof the lumen. From Netter's Cardiology. Reproduced with permission.

is an acute-phase reactant primarily producedby the liver in response to infection ortrauma. Other tissues may be involved in itssynthesis including smooth muscle cellsfrom normal coronary arteries and diseasedcoronary artery bypass grafts.12,13 CRP ap-pears to be directly involved in augmentingthe innate inflammatory response via induc-tion of prothrombotic factors (e.g., plas-minogen activator inhibitor-1, pro-inflam-matory adhesion molecules, and monocytechemoattractant protein-1) and interferencewith endothelial nitric oxide synthase.14 Inthe Physicians’ Health Study, an epidemio-logic investigation of more than 22,000healthy middle-aged men with no clinicalevidence of disease, increasing levels ofserum high-sensitivity CRP at study entrywere associated with up to a three-fold in-crease in the risk of incident MI and a two-fold increase in risk of ischemic stroke.15
When compared with other potential serumbiomarkers, such as homocysteine, lipopro-tein(a), interleukin-6, intracellular adhesionmolecule-1, serum amyloid A, and standardlipid measures, CRP proved to be the singlestrongest predictor of cardiovascular risk inapparently healthy participants in theWomen’s Health Study (n = 28,263).16,17 Ac-cordingly, the relative risk ratio for the high-est versus lowest quartile of serum CRP con-centrations was 4.4 (95% CI:1.7–11.3).Moreover, the addition of serum CRP to tra-ditional cholesterol screening enhanced car-diovascular risk prediction and proved to beindependent of LDLC. The poorest event-free survival in women was among thosewith high LDLC and high CRP levels, andthe best event-free survival was among thosewith low LDLC and low CRP levels. No-tably, individuals with low LDLC levels buthigh CRP levels were at higher risk thanthose with high LDLC levels but low CRPlevels.
Very recent data show that treatment withHMG-CoA reductase inhibitors (“statins”)
for asymptomatic individuals with elevatedCRP levels but normal cholesterol levels re-duces risk for future cardiovascular events.11
These provocative findings have triggeredconsiderable debate that may fundamentallyalter our approach to primary prevention ofcoronary atherosclerosis.
Prevention of Coronary Atherosclerosisby Risk Factor Modification
Since atherosclerosis continues to in-crease in prevalence in developed countries,it is counterintuitive that death rates fromcardiovascular diseases overall have de-creased by more than a third in the past twodecades. The explanations most often givenfor this apparent paradox include success ofprimary- and secondary-prevention strate-gies, improvements in patient care, and re-habilitation. These findings underscore theimportance of recognizing risk factors (Fig-ure 1) and optimizing strategies for risk fac-tor reduction (Figure 2). These strategiesconstitute an opportunity for medical anddental professionals to work for a commongoal of continued improvement in cardio-vascular health, but there are formidablechallenges to overcome in order to achievethis goal.18
First is to recognize that we are pro -viding encouragement for lifestyle changesthat patients may find very difficult, includ-ing smoking cessation, weight reduction, dietary changes, regular exercise, and com-pliance with prescribed medications for elevated cholesterol, blood pressure, and diabetes mellitus. While both dental andmedical healthcare providers can fairly encourage all of these, continued patient support over time is essential. Second is toremember that atherosclerosis may be pres-ent but not clinically evident for years,19
underscoring the need for sustained effortsat risk factor reduction even in otherwisehealthy individuals.
240 Periodontal Disease and Overall Health: A Clinician's Guide
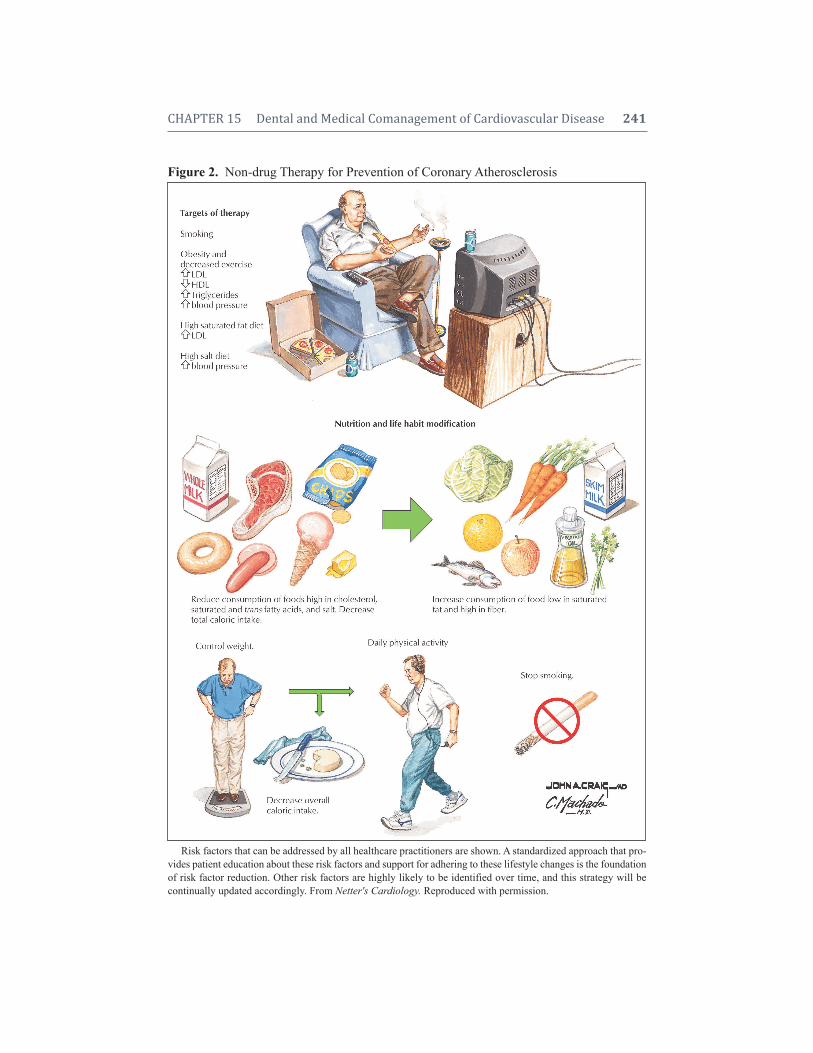
CHAPTER 15 Dental and Medical Comanagement of Cardiovascular Disease 241
Figure 2. Non-drug Therapy for Prevention of Coronary Atherosclerosis
Risk factors that can be addressed by all healthcare practitioners are shown. A standardized approach that pro-vides patient education about these risk factors and support for adhering to these lifestyle changes is the foundationof risk factor reduction. Other risk factors are highly likely to be identified over time, and this strategy will be continually updated accordingly. From Netter's Cardiology. Reproduced with permission.

Clinical Presentation ofCardiovascular Disease
Recognition of the symptoms of coro-nary atherosclerosis is essential and not al-ways straightforward. Three classical clinicalpresentations are possible. Angina pectorisor chest pain is usually retrosternal pressure,tightness, heaviness, or discomfort that radi-ates to the left arm, jaw, or back, and is oftenassociated with dyspnea, diaphoresis, nau-sea, and a feeling of impending doom (Figure3). Angina with exercise or exertion, largemeals, or emotional stress is usually pre-dictable and relieved by rest, a pattern usuallycalled “stable angina.” More ominous is chestpain at rest or a sudden increase in frequencyor ease of onset of angina, a pattern oftentermed “unstable or accelerating angina.”Obtaining a history of angina requires timeand patience and the recognition that there areseveral causes of chest pain.
In addition, women and patients with dia -betes mellitus may have a completely differentpattern to their angina or may have “anginalequivalents,” such as dyspnea alone or ab-dominal discomfort. A high index of clinicalsuspicion in patients with risk factors for coro-nary atherosclerosis is of paramount impor-tance for recognition of anginal equivalents.
The second classic presentation of coro-nary atherosclerosis is MI. Patients experi-encing an MI usually complain of prolongedand sustained (> 5 minutes) chest pain not re-lieved by rest or nitroglycerin. Associatedsymptoms may also be present, such as nau-sea and vomiting, and palpitations signalingirregular heart rhythms. Also alarming is thepresence of heart failure symptoms, includingweakness and dyspnea. The interval betweentreatment and long-term prognosis is directlyproportional; prompt recognition and earlytreatment are associated with marked im-provement in outcomes.
The third manifestation of coronary atherosclerosis is sudden cardiac deathwhen the heart has an irregular rhythm that
is unable to support blood pressure, usuallyventricular fibrillation. Tragically, coronaryatherosclerosis first presents as sudden car-diac death in approximately 25% of patients.The availability of personnel trained to rec-ognize and treat ventricular fibrillation andadminister cardiopulmonary resuscitation isthe primary determinant of outcome. Bothcommunity-based efforts and the presence ofautomatic external defibrillators have beenimportant factors in improved survival forpatients experiencing sudden cardiac death.
MEDICAL MANAGEMENT OFCORONARY ATHEROSCLEROSIS
At present, 80 million Americans arethought to exhibit some form of cardiovas-cular disease.20 Thus, many patients pre-senting to oral and dental healthcareproviders will have coronary atherosclerosisand will be receiving therapy. It will be im-portant, therefore, to understand the basicclasses of drugs that are used in patients withheart disease, especially the ones that mighthave a direct impact on oral health or maycomplicate oral and dental procedures.
Antiplatelet TherapyAll patients with atherosclerosis should
be on some form of antiplatelet therapy. Theminimal cost and relatively profound effec-tiveness of aspirin make it the treatment ofchoice in all patients who can tolerate takingthis medication. Another currently availableantiplatelet drug is the thienopyridine clopi-dogrel, and often patients are on both aspirinand clopidogrel. The primary concern for bothof these drugs is bleeding, especially withprocedures. If the procedure requires tem-porary interruption of use of either of thesetwo drugs, this should be done in consulta-tion with the patient’s regular physician. Thisis especially important for patients who areon clopidogrel to prevent clotting on drug-eluting stents that have been implanted insideone or more coronary arteries to open athero -
242 Periodontal Disease and Overall Health: A Clinician's Guide
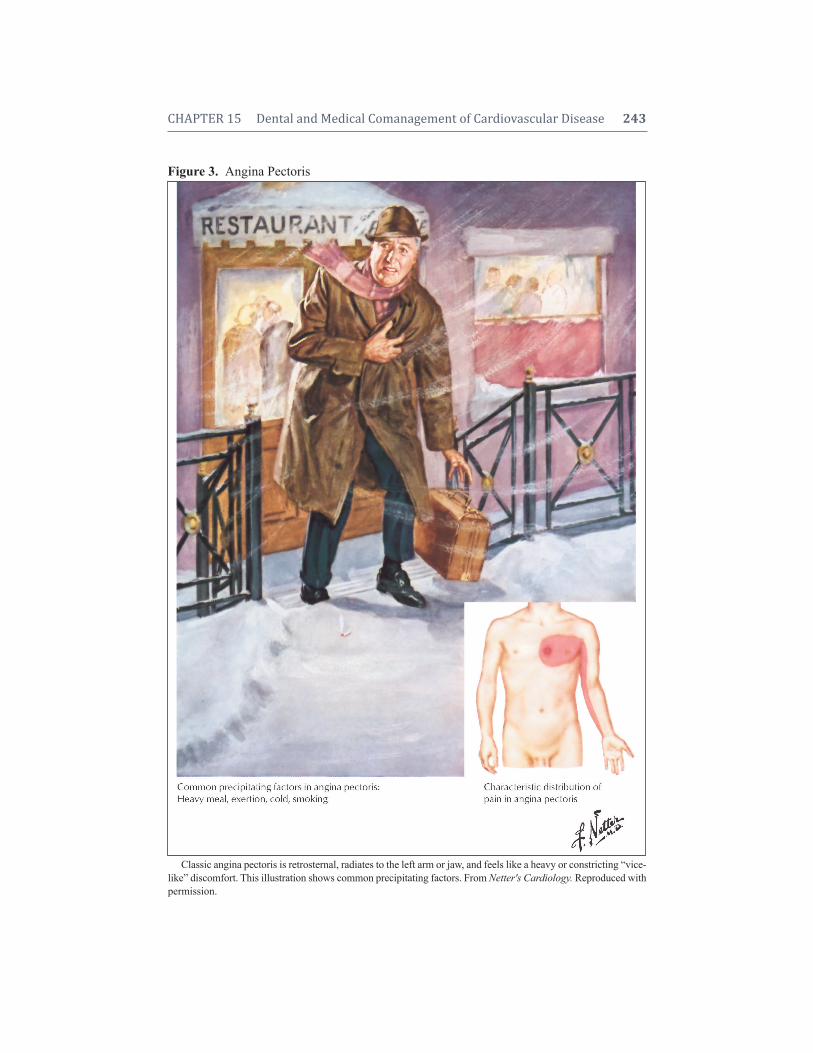
CHAPTER 15 Dental and Medical Comanagement of Cardiovascular Disease 243
Figure 3. Angina Pectoris
Classic angina pectoris is retrosternal, radiates to the left arm or jaw, and feels like a heavy or constricting “vice-like” discomfort. This illustration shows common precipitating factors. From Netter's Cardiology. Reproduced withpermission.

sclerotic obstructions. Abrupt cessation ofclopidogrel during the first year after place-ment of a drug-eluting stent can be associ-ated with acute thrombosis resulting in anotherwise preventable heart attack.
Several investigational antiplatelet drugsare close to FDA approval. Likely, bleedingwill be the major concern for all new anti -platelet drugs. The challenge to all who de-liver healthcare will be to maintain a currentunderstanding of the uses and side effects ofthese novel therapies.
Beta BlockadeAs with aspirin, beta blockade is rec-
ommended for all patients with cardiovas-cular disease unless they have a contraindi-cation, such as untreated conduction diseasein the heart with bradycardia, severe asthma,difficult-to-control diabetes mellitus, and insome cases, severe atherosclerosis in arteriesin the legs. In general, patients already re-ceiving beta blockers should not experienceany complications during oral procedures.In addition, cardiologists may recommendbeta blockers for select patients with heartdisease undergoing general anesthesia fororal or dental procedures. The AmericanHeart Association provides guidelines forsuch situations and these guidelines are con-stantly being revised as new data becomeavailable.21 Considerable planning and dis-cussion between the cardiologist and den-tist would be required in these cases.
ACE Inhibitors and ARBsPatients with coronary atherosclerosis
and depressed heart function are generallyencouraged to take angiotensin-convertingenzyme (ACE) inhibitors. If they are intol-erant to ACE inhibitors due to cough or otherissues, they may be prescribed angiotensin IIrecep tor blockers (ARBs). Mortality rateshave repeatedly been shown to be lower inpost-MI infarction patients who are takingACE inhibitors. Both ACEs and ARBs are
powerful antihypertensive agents. For dentalpatients on stable doses, these drugs are notrecognized to interfere with oral proceduresor dental care.
NitratesBoth short- (less than 10 minutes) and
long- (several hours) acting nitrates are fre-quently used to relieve and prevent, respec-tively, myocardial ischemia. Nitrates mayalso be used to treat heart failure, especiallyin African-Americans, as well as hyper -tension. A “nitrate-free” interval is recom-mended on a daily basis to prevent tachy-phylaxis. For dental patients on stable doses,these drugs are not recognized to interferewith oral procedures or dental care.
Lipid-Lowering TherapyThe current National Cholesterol Edu-
cation Program Guidelines recommend anLDLC level of < 100 mg/dL for patients withknown cardiovascular disease and a total cho-lesterol of < 200 mg/dL. Secondary causes ofhyerlipidemia include diabetes mellitus, liverdisease, and renal failure. Regardless of thecause, all patients who have values abovethese levels should receive dietary counsel-ing, suggestions for weight reduction, andencouragement to increase physical activity.The most commonly used drugs for hyper-lipidemia are the statins, which inhibit cho-lesterol synthesis. Pharmacologic interven-tion with the statin class of drugs is used tofurther reduce serum lipids and the likeli-hood of cardiovascular events, even in thosewith average LDL concentrations.
Numerous clinical trials have consis-tently demonstrated that statin drugs reducecardiovascular events by at least 25%.22 Incontrast, the effect of statins and other lipid-lowering therapies on reducing the size ofatherosclerotic plaques is much smaller.23 Thisfinding has been the basis for seeking alter-native explanations for why statins improveoutcomes so profoundly. For example, statins
244 Periodontal Disease and Overall Health: A Clinician's Guide

may have secondary anti-inflammatory ef-fects. Indeed, CRP concentrations decrease15%–50% with statin therapy.11 Thus, thepleotropic effects of these drugs appear to im-prove outcomes and markers of atheroscle-rotic cardiovascular disease. Fibrates reducelipoprotein lipase activity and nicotinic acidreduces tissue lipase activity, and very-low-density lipoprotein synthesis. Both fibratesand nicotinic acid reduce triglyceride levelseffectively. The cholesterol absorption in-hibitor ezetimibe and bile acid reabsorptioninhibitors (e.g., cholestyramine) are often usedin combination with other drugs to achievetarget goals. Lipid-lowering drugs should notimpact the delivery of oral or dental care.
LDL ApheresisIn rare cases, patients with familial hy-
percholesterolemia do not respond to drugtherapy and require apheresis. In this case, thepatient’s blood is perfused over a column thatbinds and thereby reduces their LDLC levels.Patients with familial hypercholesterolemiafrequently develop coronary atherosclerosisby the second decade of life and should becarefully evaluated for all procedures.
Coronary Angioplasty andBypass Surgery
For patients with severe symptomaticcoronary atherosclerosis, interventions involvephysically expanding stenotic vessels via an-gioplasty (with or without stenting), versusrevascularization via coronarybypass surgery.As discussed above, these patients are likely tobe on medications that could increase the like-lihood of bleeding during dental procedures.
CLINICAL RECOMMENDATIONS FORPATIENTS WITH PERIODONTITIS
AND ATHEROSCLEROTIC CARDIOVASCULAR DISEASECurrent knowledge about the close asso-
ciation between periodontitis and atheroscle-rotic cardiovascular disease is summarized in
Chapter 8. It is clear that although we do nothave ultimate proof, the balance of evidenceis sufficiently strong such that recommen-dations for close cooperation among dentaland medical professionals in the manage-ment of patients with periodontal diseaseand cardiovascular disease are reasonable.Recently there was an Editors’ ConsensusReport published simultaneously in theAmerican Journal of Cardiology and theJournal of Periodontology that makes clini-cal recommendations for patients with peri-odontitis and patients with atheroscleroticcardiovascular disease.18 The potential ben-efits of applying current understanding ofthe association between periodontal diseaseand cardiovascular disease outweighs any neg-ative effects of premature application of thisinformation. Four major recommendations aremade that provide guidance for physicians anddentists who often care for patients either suf-fering from, or at risk for, periodontal diseaseand cardiovascular diseases.
These recommendations include:1. Patients with periodontitis should be
informed that they may be at in-creased risk for atherosclerotic car-diovascular disease. Further, patientswith periodontitis who have one ormore risk factors for cardiovasculardisease should be specifically andclearly referred for medical evalua-tion if they have not been evaluatedin the past 12 months.
2. Patients with periodontitis shouldhave their risk for future cardiovas-cu lar events assessed using validatedtools such as the Reynolds Risk Score(http://www.reynoldsriskscore.org,accessed 2/20/2010) or the NationalCholesterol Education Program RiskCalculator (http://hp2010.nhlbihin.net/atpiii/calculator.asp, accessed2/20/2010). Those patients at highrisk should have a complete physicalexamination by a physician.
CHAPTER 15 Dental and Medical Comanagement of Cardiovascular Disease 245

3. Patients with periodontitis who havecardiovascular risk factors includ-ing abnormal lipids, smoke ciga-rettes, have hypertension, or sufferfrom metabolic syndrome shouldhave their risk factors moderatedand be comanaged by the dentist aswell as the physician. It is especiallyimportant for the dental professionto be involved in cooperating withthe medical team in reducing ciga-rette smoking and controlling diabetesand weight, and modifying diet insuch patients. It is currently well rec-ognized that dentists can play a sig-nificant role in assisting patients insmoking cessation programs. We areproposing that dentists extend theirefforts to include assistance in weightand diet control, and in reinforcingcompliance with blood pressure med-ications in hypertensive patients.
4. Patients with atherosclerotic cardio-vascular disease who do not have aprevious diagnosis of periodontaldisease should be examined for signsof periodontal disease, including lostteeth, gum recession, or inflamedgingivae. They should be referred bythe medical team for a periodontalevaluation. Furthermore, if perio -dontitis is newly diagnosed or existsin patients with atherosclerotic cardio -vascular disease, periodontal therapyshould be carried out and a proactivesecondary prevention and mainte-nance program should be instituted.Physicians and dentists should em-phasize the importance of timelymanagement of periodontal diseasein patients with cardiovascular dis-ease to decrease their inflammatoryburden.
5. Patients with both periodontitis andcardiovascular disease should havemembers of the dental and medical
team work closely together to helpreduce risk factors, especially thosecommon to both diseases, such asuncontrolled diabetes, smoking, andobesity.
The Use of SugarThe dental profession has long been in-
volved in advising patients to reduce theirsugar intake to reduce the risk for dentalcaries. It is reasonable for both dental andmedical professionals to make the recom-mendations of maximum intake of addedsugars, especially in cardiovascular patients,both for reduction of risk for cardiovasculardisease as well as risk for dental caries.
For example, a recent scientific state-ment from the American Heart Associationaddresses dietary sugars and cardiovascularhealth. It is recommended that patients re-duce the intake of sugars added to foods to100 calories per day for women, and 150calories per day for men. This is about 5–6teaspoons of sugar or sugar equivalents perday for the average adult woman, and 9 tea-spoons per day for the average adult man. Itis realized that reduction of dietary carbo-hydrates requires a multifaceted approach,and that one, perhaps, easily implementedapproach is to reduce energy intake fromadded sugars to levels suggested above.
Finally, it should be recognized thatthere is no evidence that suggests that pa-tients with periodontitis and atheroscleroticcardiovascular disease should receive dif-ferent periodontal treatment from other pa-tients with periodontitis. In fact, recent stud-ies suggest that standard treatments ofperiodontitis in patients with cardiovasculardisease are effective and do not lead to ad-verse cardiovascular outcomes.24 As with anypatient, the daily management of plaque andgingival inflammation should be encouraged.Oral hygiene instruction should be provided,and the use of an antibacterial toothpaste andmouthrinse and interproximal cleaning should
246 Periodontal Disease and Overall Health: A Clinician's Guide

be recommended with each patient and re-inforced at each visit.
CONCLUSIONS ANDFUTURE DIRECTIONS
Dental and medical healthcare providersneed to work together closely to provide op-timal care for their patients with establishedcardiovascular disease. A basic understand-ing of the pathogenesis of cardiovasculardisease and commonly used medications willprovide a basis for preventing complicationsduring the delivery of dental and oral health-care in patients with CVD.
The role of the oral and dental healthpractitioner in the prevention of heart diseasehas great potential. Such practitioners areuniquely poised to discuss risk factor reduc-tion with their patients that is paramount forboth oral and cardiovascular health. Preven-tive interventions (primary or secondary) forcoronary atherosclerosis focus on recogni-tion and reduction of modifiable risk factorsin patients (Figures 1 and 2). These ap-proaches include blood pressure screening,weight reduction, exercise, smoking cessa-tion, diet modification, medication compli-ance (especially with treatments for bloodpressure and diabetes), patient counseling,and education. Initiating and maintainingthese lifestyle changes are not easy tasks,but more likely to be adopted by patientswho receive consistent advice and encour-agement from all of their healthcare providers.
For the present, the role of oral health inatherosclerosis remains an association andnot a risk factor. Human trials that directlyaddress the role of periodontitis and athero-sclerosis have been limited to the Periodon-titis and Vascular Events study. This pilotstudy was designed to determine how manypatients with combined symptomatic ather-osclerosis and periodontitis would be neededto document the fact that successful treat-ment of periodontitis reduces sub sequentcoronary and carotid events.24 If perio dontitis
is proven to be a risk factor for cardiovascu-lar disease, cardiologists and oral and dentalhealth practitioners will need to work evenmore closely to provide optimal care for theirpatients.
Supplemental Readings
Tricoci P, Allen JM, Kramer JM, Califf RM, Smith SC,Jr. Scientific evidence underlying the ACC/AHA clini-cal practice guidelines. JAMA 2009;301:831–841.
Fleisher LA, Beckman JA, Brown KA, Calkins H,Chaikof E, Fleischmann KE, Freeman WK, FroehlichJB, Kasper EK, Kersten JR, Riegel B, Robb JF, SmithSC, Jr., Jacobs AK, Adams CD, Anderson JL, AntmanEM, Buller CE, Creager MA, Ettinger SM, Faxon DP,Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW,Nishimura R, Ornato JP, Page RL, Tarkington LG,Yancy CW. ACC/AHA 2007 guidelines on periopera-tive cardiovascular evaluation and care for noncardiacsurgery: executive summary: a report of the AmericanCollege of Cardiology/American Heart AssociationTask Force on Practice Guidelines (Writing Committeeto Revise the 2002 Guidelines on Perioperative Cardio -vascular Evaluation for Noncardiac Surgery). AnesthAnalg 2008;106:685–712.
McFarlane SI, Castro J, Kaur J, Shin JJ, Kelling D, Jr.,Farag A, Simon N, El-Atat F, Sacerdote A, Basta E,Flack J, Bakris G, Sowers JR. Control of blood pres-sure and other cardiovascular risk factors at differentpractice settings: outcomes of care provided to diabeticwomen compared to men. J Clin Hypertens (Greenwich2005;7:73–80.
Fleisher LA, Beckman JA, Brown KA, Calkins H,Chaikof EL, Fleischmann KE, Freeman WK, FroehlichJB, Kasper EK, Kersten JR, Riegel B, Robb JF. 2009ACCF/AHA focused update on perioperative betablockade incorporated into the ACC/AHA 2007 guide-lines on perioperative cardiovascular evaluation andcare for noncardiac surgery. J Am Coll Cardiol 2009;54:e13–e118.
Hunt SA, Abraham WT, Chin MH, Feldman AM, Fran-cis GS, Ganiats TG, Jessup M, Konstam MA, ManciniDM, Michl K, Oates JA, Rahko PS, Silver MA, Steven-son LW, Yancy CW. 2009 focused update incorporatedinto the ACC/AHA 2005 Guidelines for the Diagnosisand Management of Heart Failure in Adults: a report ofthe American College of Cardiology Foundation/Amer-ican Heart Association Task Force on Practice Guide-lines: developed in collaboration with the InternationalSociety for Heart and Lung Transplantation. Circulation2009;119:e391–479.
CHAPTER 15 Dental and Medical Comanagement of Cardiovascular Disease 247

Runge MS, Stouffer G, Patterson C, eds. Netter's Cardiology (Netter Clinical Sciences). Teterboro, NewJersey: Icon Learning Systems LLC; 2010 (Second edition anticipated publication release July 2010).
REFERENCES1. Fuster V, Vedanthan R. Cardiovascular disease and
the UN Millennium Development Goals: Time tomove forward. Nat Clin Pract Cardiovasc Med2008;5:593.
2. Thom T, Haase N, Rosamond W, Howard VJ,Rumsfeld J, Manolio T, Zheng ZJ, Flegal K,O’Donnell C, Kittner S, Lloyd-Jones D, Goff DCJr, Hong Y, Adams R, Friday G, Furie K, GorelickP, Kissela B, Marler J, Meigs J, Roger V, Sidney S,Sorlie P, Steinberger J, Wasserthiel-Smoller S, Wil-son M, Wolf P; American Heart Association Sta-tistics Committee and Stroke Statistics Subcom-mittee. Heart disease and stroke statistics—2006update: A report from the American Heart Associ-ation Statistics Committee and Stroke StatisticsSubcommittee. Circulation 2006;113:e85–151.
3. Albert DA, Sadowsky D, Papapanou P, ConicellaML, Ward A. An examination of periodontal treat-ment and per member per month (PMPM) medicalcosts in an insured population. BMC Health ServRes 2006;6:103.
4. Mackman N. Triggers, targets and treatments forthrombosis. Nature 2008;451:914–918.
5. Rader DJ, Daugherty A. Translating molecular dis-coveries into new therapies for atherosclerosis. Na-ture 2008;451:904–913.
6. Sanz J, Fayad ZA. Imaging of atherosclerotic car-diovascular disease. Nature 2008;451:953–957.
7. Smith SC Jr. Current and future directions of car-diovascular risk prediction. Am J Cardiol 2006;97:28A–32A.
8. Kannel WB. High-density lipoproteins: epidemio-logic profile and risks of coronary artery disease.Am J Cardiol 1983;52:9B–12B.
9. Greenland P, Knoll MD, Stamler J, Neaton JD,Dyer AR, Garside DB, Wilson PW. Major risk fac-tors as antecedents of fatal and nonfatal coronaryheart disease events. JAMA 2003;290:891–897.
10. Khot UN, Khot MB, Bajzer CT, Sapp SK, OhmanEM, Brener SJ, Ellis SG, Lincoff AM, Topol EJ. Preva-lence of conventional risk factors in patients withcoronary heart disease. JAMA 2003;290:898–904.
11. Ridker PM, Danielson E, Fonseca FA, Genest J,Gotto AM Jr, Kastelein JJ, Koenig W, Libby P,Lorenzatti AJ, MacFadyen JG, Nordestgaard BG,Shepherd J, Willerson JT, Glynn RJ; JUPITERStudy Group. Rosuvastatin to prevent vascularevents in men and women with elevated C-reactiveprotein. N Engl J Med 2008;359:2195–2207.
12. Calabro P, Willerson JT, Yeh ET. Inflammatory cy-tokines stimulated C-reactive protein productionby human coronary artery smooth muscle cells.Circulation 2003;108:1930–1932.
13. Jabs WJ, Theissing E, Nitschke M, Bechtel JF,Duchrow M, Mohamed S, Jahrbeck B, Sievers HH,Steinhoff J, Bartels C. Local generation of C-reac-tive protein in diseased coronary artery venous by-pass grafts and normal vascular tissue. Circulation2003;108:1428–1431.
14. Devaraj S, Xu DY, Jialal I. C-reactive protein in-creases plasminogen activator inhibitor-1 expres-sion and activity in human aortic endothelial cells:Implications for the metabolic syndrome andatherothrombosis. Circulation 2003;107:398–404.
15. Ridker PM, Cushman M, Stampfer MJ, Tracy RP,Hennekens CH. Inflammation, aspirin, and the riskof cardiovascular disease in apparently healthymen. N Engl J Med 1997;336:973–979.
16. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and other markers of inflamma-tion in the prediction of cardiovascular disease inwomen. N Engl J Med 2000;342:836–843.
17. Ridker PM, Rifai N, Rose L, Buring JE, Cook NR.Comparison of C-reactive protein and low-densitylipoprotein cholesterol levels in the prediction offirst cardiovascular events. N Engl J Med 2002;347:1557–1565.
18. Friedewald VE, Kornman KS, Beck JD, Genco R,Goldfine A, Libby P, Offenbacher S, Ridker PM,Van Dyke TE, Roberts WC. Editors’ Consensus:Periodontitis and Atherosclerotic CardiovascularDisease. Am J Cardiol 2009;104:59–68.
19. Berry JD, Liu K, Folsom AR, Lewis CE, Carr JJ,Polak JF, Shea S, Sidney S, O’Leary DH, Chan C,Lloyd-Jones DM. Prevalence and progression ofsub clinical atherosclerosis in younger adults withlow short-term but high lifetime estimated risk forcardiovascular disease: the coronary artery risk de-velopment in young adults study and multi-ethnicstudy of atherosclerosis. Circulation 2009;119:382–389.
20. Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E, FurieK, Go A, Greenlund K, Haase N, Hailpern S, HoM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott M, Meigs J,Mozaffarian D, Nichol G, O’Donnell C, Roger V,Rosamond W, Sacco R, Sorlie P, Stafford R, Stein-berger J, Thom T, Wasserthiel-Smoller S, Wong N,Wylie-Rosett J, Hong Y. Heart disease and strokestatistics—2009 update: a report from the AmericanHeart Association Statistics Committee and StrokeStatistics Subcommittee. Circulation 2009;119:480–486.
248 Periodontal Disease and Overall Health: A Clinician's Guide

21. Fleisher LA, Beckman JA, Brown KA, Calkins H,Chaikof E, Fleischmann KE, Freeman WK,Froehlich JB, Kasper EK, Kersten JR, Riegel B,Robb JF, Smith SC Jr, Jacobs AK, Adams CD, An-derson JL, Antman EM, Buller CE, Creager MA,Ettinger SM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R,Ornato JP, Page RL, Riegel B, Tarkington LG,Yancy CW. ACC/AHA 2007 guidelines on periop-erative cardiovascular evaluation and care for non-cardiac surgery: executive summary: a report ofthe American College of Cardiology/AmericanHeart Association Task Force on Practice Guide-lines (Writing Committee to Revise the 2002 Guide- lines on Perioperative Cardiovascular Evaluationfor Noncardiac Surgery). Anesth Analg 2008;106:685–712.
22. Sparrow CP, Burton CA, Hernandez M, Mundt S,Hassing H, Patel S, Rosa R, Hermanowski-VosatkaA, Wang PR, Zhang D, Peterson L, Detmers PA,
Chao YS, Wright SD. Simvastatin has anti-inflam-matory and antiatherosclerotic activities independ-ent of plasma cholesterol lowering. ArteriosclerThromb Vasc Biol 2001;21:115–121.
23. Brown BG, Zhao XQ, Chait A, Fisher LD, CheungMC, Morse JS, Dowdy AA, Marino EK, BolsonEL, Alaupovic P, Frohlich J, Albers JJ. Simvastatinand niacin, antioxidant vitamins, or the combinationfor the prevention of coronary disease. N Engl JMed 2001;345:1583–1592.
24. Offenbacher S, Beck JD, Moss K, Mendoza L, Pa-quette DW, Barrow D, Couper DJ, Stewart DD,Falkner KL, Graham SP, Grossi S, Gunsolley JC,Madden T, Maupone G, Trevisan M, Van Dyke TE,Genco RJ. Results from the Periodontitis and Vas-cular Events (PAVE) Study: a pilot multicentered,randomized, controlled trial to study effects of pe-riodontal therapy in a secondary prevention modelof cardiovascular disease. J Periodontol 2009;80:190–201.
CHAPTER 15 Dental and Medical Comanagement of Cardiovascular Disease 249
2. Identify the effects that pregnancy’sphysiologic changes may have onoral health.
3. Enumerate the most frequent riskfactors for pregnancy complications.
4. Explain the considerations that have tobe applied to provide dental treatmentto women with normal pregnancy.
5. List strategies for the prevention ofmedical and dental complications inpregnant women.
6. Describe the initiatives that can betaken by dentists and obstetricians incomanaging patients with oral dis-eases and who are at risk for adversepregnancy outcomes.
PHYSIOLOGICAL CHANGESIN PREGNANCY AND THEIR
RELATIONSHIP TO ORAL HEALTHPregnancy is characterized by dramatic
endocrine changes. Placental tissues producea significant increase in progesterone andestrogen concentrations, which in turn in-fluence physiological changes in systemicand oral tissues. The most important physi-ological changes associated with pregnancythat have dental relevance are addressed below.
Gingival Hyperplasia and EdemaVasodilatation, increased vascular per-
meability, and cell proliferation elicited bypregnancy hormones result in the swelling ofgingiva and desquamation of cells.1,2
Changes described in the microcircula-tion of pregnant women include swelling ofendothelial cells, adherence of granulocytes
INTRODUCTIONPregnancy involves complex physio-
logic, physical, and psychological changesmediated by female sex hormones that havea profound impact on even healthy women.Physiologic changes during pregnancy canexacerbate already existing oral pathologicconditions, such as gingivitis, periodontitis,and caries lesions. Moreover, oral infectionsduring pregnancy may be associated withadverse pregnancy outcomes. Prenatal careis an essential part of a successful pregnancy,and oral health assessment must be part ofprenatal care. Changes produced by preg-nancy present a number of unique manage-ment problems in dental treatment. The bestapproach to avoid pregnancy complicationsand adverse pregnancy outcomes is to applypreventive strategies. The most importantobjective in planning dental care for thepregnant woman is establishing a healthyoral environment that is free of inflammationand infection.
This chapter reviews the physiologicchanges that occur during normal gestation,and the management of dental treatment inwomen with normal pregnancy, as well aswomen at risk for adverse pregnancy out-comes.
Educational ObjectivesBy the end of this chapter, the reader
should be able to:1. Recognize the most important phys-
iological, physical, and psychologi-cal changes mediated by female sexhormones that have an impact onhealthy pregnant women.
CHAPTER 16Dental and Medical Comanagement of Pregnancy
Néstor J. López, Ricardo A. Gómez

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 251
to vessel walls, generation of microthrombi,disruption of perivascular mast cells, andvascular proliferation.1,2 A concomitant shiftin oral microbiota promotes the growth ofbacteria associated with gingivitis.3 Immuneadaptations that occur during pregnancy mayfurther facilitate infections of oral tissues.For example, gingival fibroblasts exposedto progesterone down-regulate the produc-tion of interleukin-6 and a variety of matrixmetalloproteinases, making the gingiva moresusceptible to inflammatory challengeselicited by bacteria.4,5
Upper Gastrointestinal ChangesBeginning in the first trimester, en-
docrine changes induce a reduction insmooth muscle tissue tone and frequency ofcontractions. This affects gastric emptyingand the functionality of the gastro-esophagicsphincter, facilitating reflux of stomach con-tent towards the esophagus and mouth. Psy-chological changes appear early in preg-nancy and contribute to the nausea andvomiting syndrome called “morning sick-ness.” A small fraction (1% to 3%) of thesepatients progress to hyperemesis gravid -arium, which is associated with weight loss,electrolyte imbalance, dehydration, and,eventually, ketonemia. The persistence ofthese symptoms despite treatment obligatesone to rule out other disorders, such as pan-creatitis, cholecystitis, hepatitis, psychiatricillness, and hyperthyroidism.
Salivary changes during pregnancy in-clude an increase in volume that is dependanton oral-esophagic content delay rather thansalivary flow rate. Rarely, patients may losemore than one liter of saliva per day, a dis-order known as ptyalism. Additional changescomprise a decreased salivary pH and ele-vation of protein and estrogen concentra-tions. Estrogens act locally by increasing theproliferation and desquamation of the oralmucosa, setting the conditions for bacterialgrowth. Recommendations for managing
nausea and vomiting in the dental setting areprovided in the section titled “PregnancyComplications” below.
Cardiovascular Changes and Establishmentof Uteroplacental Circulation
As the placenta and fetus develop, flowthrough the uterine and placental arteries in-creases notably. Changes in the microcir -culation and within the intervillous space(mimicking an arteriovenous shunt) decreasearterial resistance. Elevations in blood vol-ume (especially at the expense of maternalplasma) and heart rate compensate thechanges in vascular resistance. As a conse-quence, cardiac output increases by 30% to40% throughout pregnancy. Maternal bloodpressure tends to lower during the first andsecond trimester, reaching baseline levelsearly in the third trimester. The growinguterus may compress the inferior vena cava,impairing the venous return to the heart andtherefore the stroke volume. Compensatorymechanisms are set in action, leading tosymptoms such as palpitations (due to tachy-cardia) nausea, hypotension, and dizziness.This chain of events is frequently observedduring the second half of pregnancy whenpregnant women are in the supine position.Dentists may reduce the likelihood of thissupine hypotensive syndrome by elevatingthe right hip of the patient with a pillow orfolded sheet, or rolling the patient to the leftin order to alleviate vena cava obstruction.
Respiratory ChangesThe most important physiological adap-
tations at the respiratory level are derived fromthe pressure that the pregnant uterus imposeson the abdominal side of the diaphragm, re-ducing the height and increasing the trans-verse diameter of the thorax. A progesterone-driven hyperventilation compensates for thelessened residual capacity of the lungs. Dys-pnea is not an uncommon sign during thethird trimester, especially in patients with

252 Periodontal Disease and Overall Health: A Clinician's Guide
twin gestation, large fetuses, and/or poli -hydramnios. As stated before, avoiding thesupine position is central to the managementof these patients.
Hematologic ChangesRed blood cells, leukocytes, and most
coagulation factors are increased during preg- nancy. Plasma volume increases above that ofred blood cells, leading to the condition knownas physiologic anemia of pregnancy. Due tothis hematologic adaptation, pregnant womenare diagnosed with anemia only if the hema -tocrit falls below 33%. On the other hand,leukocytosis during pregnancy is established ifthe white blood cell count is above 15,000cells/mm3. This is important when evaluatinglaboratory tests in the setting of oral infec-tions. Clotting factor production by the liver isstimulated by gestational hormones, leading toa “hypercoagulable state” that predisposes tothromboembolism. Several disorders (e.g., an-tiphospholipid syndrome) aggravate this con-dition and may require the utilization of aspirinor heparin. These patients should receive closetreatment surveillance to determine if dentalprocedures may be performed without the riskof excessive bleeding.
Endocrine ChangesMost of the physiological adaptations
described above are the result of primary en-docrine changes during pregnancy. More-over, elevated levels of estrogens, proges-terone, cortisol, and placental lactogenmobilize the patient’s metabolic resourcesin order to secure fetal nutrition. As a result,a “diabetogenic state” develops, especiallyduring the second half of pregnancy, inwhich insulin resistance increases, eventu-ally leading to gestational diabetes in 4% to10% of patients. The resulting glucose avail-ability in oral secretions of patients withpoorly controlled diabetes provides a suit-able environment for the development ofdental infections.
DENTAL MANAGEMENT OF WOMENWITH NORMAL PREGNANCYUtilization of dental care during preg-
nancy is lower than expected. Data from sur-veys indicate that 30% to 50% of women donot receive dental care during pregnancy.6,7
Indeed, only about 10% of dentists providecomplete treatment for conditions consid-ered necessary during the gestation period,delaying most of them for the postpartumperiod.8 Pregnant women are also less likelyto request dental treatment even in the con-text of free health services, such as thoseprovided through the National Health Ser - vice in the United Kingdom.9 Moreover, onlyabout one-quarter of patients are referred toa dental examination by health providersduring pregnancy.9 Collectively, these dataindicate that both health professionals andpatients tend to postpone dental treatmentsuntil after delivery.
Attitudes of Dentists, Physicians, andPatients Towards Dental Treatment
During PregnancyThe reluctance of dental practitioners
to provide dental care to pregnant women10
may explain, among other reasons, the lowpercentage of women who receive dentalcare during pregnancy. Lydon-Rochelle andcolleagues11 found that 58% of pregnantwomen in Seattle, Washington, received nodental treatment during pregnancy. Only22% to 34% of women in the United Statesconsult a dentist during pregnancy. Evenwhen an oral problem occurs, only half ofpregnant women attend to it.12
A common concern of dental practi-tioners is the timing for necessary proce-dures. The evaluation and management ofpregnant women may require special con-sideration, but pregnancy does not precludethem from necessary dental care. There is noevidence that dental or periodontal treatmentis damaging to the pregnant woman or herdeveloping fetus. However, the American

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 253
Dental Association suggests that electivedental care should be avoided, if possible,during the first trimester and the last one-halfof the third trimester.13 The recommenda-tion for not doing procedures during the firsttrimester is because the developing fetus is atgreatest risk of teratogenicity during the em-bryologic development (between the 2nd and8th week after conception) and because thehighest rate of spontaneous abortion occursduring the first trimester. Thus, there is con-cern that the patient may perceive that thecause of an eventual birth defect or sponta-neous abortion is the dental procedure per-formed during that period. The last weeks ofthe third trimester are associated with greaterdiscomfort and risk of supine hypotensionsyndrome, due to the large uterus and itscontent.
Concern about the maternal and fetal ef -fects of pharmacologic agents commonly usedin dentistry offers another reason to explain theattitudes of dentists and women toward den-tal treatment during pregnancy. How ever, mostdrugs used during dental treatment are safeand listed likewise by the Food and DrugAdministration (Table 1). The recommen -dation is based more on fear of litigation thanon evidence of harm. It is there fore remark-able that there is no evidence linking dentaltreatments and adverse pregnancy outcomes.On the contrary, there is a growing body ofevidence, although controversial, that treat-ment of periodontal infection may reduce therate of certain pregnancy complications.14-16
Another factor that prevents dentistsfrom performing treatment in pregnantwomen is the belief that dental proceduresmay initiate an inflammatory cascade lead-ing to uterine response, preterm labor, and/orfetal loss. Although transient bacteremia isrecognized as part of the pathophysiologyfollowing dental invasive procedures, thespecific association between these proce-dures and pregnancy complications has notbeen demonstrated.15-17
Safety of Dental Diagnostic and Therapeutic Procedures During Pregnancy
Dental treatments are preferably per-formed during the second trimester. Emer-gency dental procedures can be performed atany gestational age. During the first and sec-ond trimester, no specific positional require-ment needs to be satisfied. On the contrary,patients with a large uterus (such as those inthe third trimester, twin gestation, or poli-hydramnios) are at risk for supine hypoten-sion due to vena cava compression. There-fore, propping patients to their left side andfrequent repositioning are necessary duringthe dental procedure.
A general principle used for all drugsand diagnostic tests during pregnancy is thatthe period before 12 weeks’ gestation is con-sidered vulnerable for the embryo organo-genesis. Specific drugs and tests may be ad-ministered during the first trimester only ifthe potential benefit surpasses the risks.
RadiographyDental radiographs for acute diagnostic
purposes are associated with minimal fetalexposure to ionizing effects. The examshould be performed using a lead apron andthyroid shield; high-speed film and retakesshould be avoided. Efforts to avoid the periodof embryo organogenesis (up to 12 weeks’gestation) are desirable, but emergency den-tal treatments that rely on radiographic diag-nosis usually incline the risk-benefit balancetowards having the exam performed.
Pharmacologic AgentsDrugs used in dental treatment are fairly
safe during pregnancy (Table 1). Local anes-thetics such as lidocaine and prilocaine areconsidered safe by the Food and Drug Ad-ministration (category B). When possible,co-adjuvant epinephrine should be avoided,since it may impair uterine blood flowthrough the placenta. Epinephrine is contra -indicated in patients with pre-eclampsia and

254 Periodontal Disease and Overall Health: A Clinician's Guide
chronic hypertension. Acetaminophen is ap-propriate to treat dental pain at any gesta-tional age (category B), as well as ibuprofenin the first and second trimesters (categoryB). The latter drug should be avoided duringthe third trimester due to known effects onboth fetal ductus arteriosus and renal function.For severe pain, narcotics such as o xyco donemay be used for a limited time during the firstand second trimester. Avoiding use of thesedrugs during both the third trimester andwomen with impending delivery preventsbreathing/withdrawal complications in thenewborn. If a dental procedure requires seda-tion, a safe choice is premedication with anantihistaminic such as doxylamine (categoryB), which also has an antiemetic effect. Ben-zodiazepines should be avoided throughoutpregnancy unless a specific indication arises(mostly of psychiatric nature). Nitrous oxide
is a sedative-analgesic gas and short-term useis considered safe during the second and thirdtrimesters of gestation. It is contraindicated inpatients with chronic obstructive pulmo narydisease and drug-related dependencies.
AntibioticsAntibiotics used for oral infections are
generally safe for the mother and fetus. Peni-cillin-family agents are frequently used asco- adjuvants in the treatment of periodontaldisease, dental abscesses, and cellulitis.Cephalosporins fall in the same category. Ex-cept for patients with hypersensitivity, both anti -microbial agents are classified as safe by theFood and Drug Administration (category B).Erythromycin (with the exception of the esto-late form, which may produce cholestatic hep-atitis), and clindamycin (category B) are alternatives for penicillin-allergic patients.
Table 1.Drugs Frequently Used by the Dental Professional During PregnancyDrugs FDA Category Comments/Suggestions
Analgesics and anesthetics Acetaminophen B Safe throughout pregnancyAspirin C Avoid after 34 weeksIbuprofen B Do not use after 28 weeksCodeine C Use with caution if benefit outweighs risksOxycodone B Avoid in proximity of laborMorphine B Avoid in proximity of laborMeperidine B Avoid in proximity of laborLidocaine B Safe throughout pregnancyMepivacaine C Use with caution if benefit outweighs risksPrilocaina B Safe throughout pregnancy
Antibiotics/AntifungalsAmpicillin/Amoxicillin B Safe throughout pregnancyCephalosporins B Safe throughout pregnancyChlorhexidine B Safe throughout pregnancyClindamycin B Safe throughout pregnancyClotrimazole B Safe throughout pregnancyErythromycin B Safe throughout pregnancy. Do not use estolateFluconazole C Safe when used in single doseMetronidazole B Avoid before 12 weeksPenicillin B Safe throughout pregnancy
OthersBenzodiazepines D Do not use unless benefit outweighs risksCorticosteroids B Prednisone, betamethasone, and dexamethasone,
safe throughout pregnancyDoxylamine B Safe throughout pregnancyNitrous oxide — Avoid before 12 weeks

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 255
Metronidazole, an alternative for clindamycinin severe infections, may be administered aswell during the second and third trimester (cat-egory B). Tetracyclines are contraindicatedduring pregnancy.
Antibiotic prophylaxis for infective endo -carditis should be administered only to thosewomen with cardiac conditions associatedwith a major risk for endocarditis. A recentcommittee opinion from the American Col-lege of Obstetrics and Gynecology providedup-to-date indications for pregnant womenwith cardiac conditions who require certaindental procedures.18
• Prosthetic cardiac valve or prostheticmaterial used for cardiac valve repair
• Previous infective endocarditis• Specific congenital heart diseases: un-
repaired cyanotic cardiac disease (in-cluding palliative shunts and con-ducts), completely repaired cardiacanomalies with prosthetic material ordevice (whether placed by surgery orcatheter intervention) during the first6 months after procedure, and repairedcardiac disease with residual defects atthe site or adjacent to the site of aprosthetic patch or prosthetic device(which inhibit endothelialization)
Dental procedures eligible for prophy-laxis are those involving manipulation of thegingival tissue or periapical region of theteeth. No prophylaxis is required in cases ofgeneral dental cleaning, cavity filling, takingof radiographs, adjusting orthodontic appli-ances, or when injecting anesthetic into non-infected tissue. Appropriate antibiotics forinfective endocarditis prophylaxis should beadministered 30–60 minutes before the den-tal procedure and include the following:
• Ampicillin 2 g intravenously• Cefazolin or ceftriaxone 1 g intra-
venously• Amoxicillin 2 g oralIn patients allergic to penicillin, clin-
damycin 600 mg intravenously may be used.
It should be noted that drugs other thanampicillin or amoxicillin do not cover ente-rococcus. If enterococcus involvement issuspected, vancomycin 1 g intravenouslyover one hour is the choice. Table 2 summa-rizes the principles guiding dental treatmentduring pregnancy.19
Treatment of Specific Dental ConditionsDuring Pregnancy
During pregnancy, dental or periodontalcare may be modified according to the indi-vidual characteristics of each patient and theconditions of the pregnancy, but there is noneed to withhold treatment for any oral in-fectious condition. Extensive dental treat-ments, such as crowns and reconstructiveprocedures that need long appointments,should not be performed during pregnancy.
The most important objective in plan-ning dental care for the pregnant woman isestablishing previous to pregnancy, or earlyduring pregnancy, a healthy oral environ-ment, free of inflammation and infection.
There is evidence that oral health influ-ences systemic health and well-being.20 Ma-ternal oral health has important implications
Table 2.Principles Guiding Dental Table 2.Treatment During Pregnancy
1. Women should be advised to seek oral healthcareprior to becoming pregnant and throughout gestation.
2. Oral healthcare is safe and effective during pregnancy.3. First trimester diagnosis (including necessary dental
x-rays with adequate shielding) is safe. 4. Acute infection, abscess, and conditions predisposing
to bacteremia and sepsis require prompt interventionregardless of the stage of pregnancy.
5. Necessary treatment can be provided throughoutpregnancy. However, the period between the 12thand 22nd weeks represents the best time to provideoral services, especially scaling and root planing.
6. Elective treatment for conditions considered notprogressive may be deferred until after delivery.
7. Delay in necessary treatment could result in signif -icant risk to the mother and the fetus.

256 Periodontal Disease and Overall Health: A Clinician's Guide
for birth outcomes and infant oral health.The most prevalent oral diseases, dentalcaries and periodontal disease, influence ma-ternal health status and may increase the riskof other diseases. Periodontal disease mayincrease the risk of atherosclerosis,21 dia-betes,22 rheumatoid arthritis,23 and adversepregnancy outcomes.24
Maternal dental caries can also increasethe risk of early development of caries inchildren.25 Dental caries and periodontal dis-ease are both preventable conditions. How-ever, they have a high prevalence in womenof childbearing age, especially among lowsocio-economic level populations. Bothcaries and periodontal disease are chronicdiseases with few or no symptoms, makingit difficult for the patient to be aware of thedisease. The characteristics of both diseases,in addition to their high prevalence and in-sufficient treatment rates, induced the USSurgeon General to characterize dental andoral diseases as a “silent epidemic.”26
Dental Caries and PregnancyOne-fourth of women of reproductive
age in the US have dental caries27 and theprevalence of dental caries may reach 76% inyoung women of low socio-economic statusin developing countries.28 There are no defi-nite data indicating whether the incidence ofdental caries increases during pregnancy. Asdental caries usually takes more than the 40weeks of pregnancy to develop, it is difficultto determine the pregnancy-related incidenceof caries. The main bacteria that producecaries is Streptococcus mutans which is usu-ally acquired by young children through di-rect salivary contact from their mothers.29
Since ma ternal oral flora is the strongest pre-dictor of infant oral flora,30 maternal healthstatus is critical to children’s oral health. Ma-ternal dental educational and behavioral in-terventions that reduce caries activity throughuse of fluorides, control of cariogenic diet,chlorhexidine mouthwashes, and varnishes
can decrease caries activity and the associatedoral flora, thus improving women’s oralhealth and reducing bacterial transmission totheir children.31
Pregnancy-Associated GingivitisPlaque-induced gingivitis is an inflam-
mation of the gingiva resulting from bacter-ial infection, and is one of the most commonoral diseases in pregnant women.32,33 Preg-nant women have more gingivitis than non-pregnant women, with a prevalence rangingfrom 30% to 75%.13,34 During pregnancy, theseverity of gingivitis has been reported tobe elevated, yet unrelated to the amount ofdental plaque present.35,36 Approximately oneof two women with pre-existing gingivitishas significant exacerbation during preg-nancy.37 Gingivitis is usually more evident inthe second month of pregnancy and reachesa maximal level during the eighth month.The severity of gingivitis is correlated withsex steroid hormone levels during preg-nancy.36 The characteristics of pregnancy-associated gingivitis are similar to plaque- induced gingivitis, but there is a tendency tomore severe inflammation.35,36
The factors that have been associatedwith higher gingival inflammation in preg-nancy are increased levels of estrogen andprogesterone,38 changes in oral flora,3 and adecreased immune response.39,40 Aggravationof gingival inflammatory symptoms duringpregnancy is also associated with low con-centrations of plasminogen activator inhibitortype-2 (PAI-2) in gingival fluid. PAI-2, pro-duced by macrophages, is an important in-hibitor of tissue proteolysis, and has multipleother functions. Women showing a low in-flammatory response to plaque have highconcentrations of PAI-2, which probably pro-tects connective tissue from excessive break-down.41 Changes in subgingival flora mayoccur during pregnancy. An increased ratio ofsubgingival anaerobic to aerobic bacteria hasbeen found. The proportion of Prevotella

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 257
intermedia increases during pregnancy,3 butthe relation of P. intermedia to the clinicalsigns of gingivitis has rendered controver-sial results.42
Pregnancy epulis or pregnancy tumoris a pyogenic granuloma that appears in nomore than 5% of pregnant women. It is apedunculated, soft, erythematous lesion thatgrows from an interdental papilla, and is associated with inflammation due to dentalplaque and calculus accumulation. The lesionusually arises during the second trimester,shows rapid growth, bleeds easily, and tendsto diminish after pregnancy. The lesion canbe removed under local anesthesia and some-times there is a risk of excessive hemorrhagedue to its high vascularity.
There is some basis to support the hy-pothesis that gingivitis may be a potentialrisk factor for preterm birth. One of the hy-potheses to explain the association betweenperiodontal disease and preterm birth is thatperiodontal infection is a source of bacteriaand bacterial products that may spread fromthe infected periodontium to the systemiccirculation and, eventually, the amniotic cav-ity, similar to transient bacteremia occurringin patients with periodontitis.43 It has beenshown that bacteremia commonly occurs inpatients with gingivitis,44 and bacteria or theirproducts may conceivably reach the placen-tal tissues, providing an inflammatory settingfor the onset of labor (Figure 1).45 There isevidence that some periodontal pathogenscan cross the placental barrier and produceinfection in the fetal membranes. The preva-lence of P. intermedia has been found to besignificantly higher in preterm than in full-term neonates. The fetal antibody seroposi-tivity for P. intermedia, as indexed by cordblood immunoglobulin M, suggests in uteroexposure of the fetus to this bacterium or itsproducts.43 Fusobacterium nucleatum is oneof the most commonly recovered micro- organisms from sites with gingivitis,46 andis frequently isolated from amniotic fluid
cultures obtained from pregnant women withpremature labor and intact placental mem-branes.47 A study in pregnant mice showedthat F. nucleatum can cross the placenta andspread to the amniotic fluid, producing pre-mature delivery and stillbirths.48 The associ-ation between pregnancy-associated gin-givitis with preterm birth was explored in arandomized controlled trial.49 Women withgingivitis who received periodontal therapybefore 28 weeks of gestation had a signifi-cantly lower incidence of preterm low-birth-weight than women who did not receive perio dontal therapy.
Periodontitis and PregnancyPeriodontitis, the destructive form of
periodontal disease, affects childbearing-aged women, from 15% in developed coun-tries50 to 45% in undeveloped countries.51 Inthe US, up to 40% of pregnant women havesome form of periodontal infection.52 Insome developing countries, such as in Chile,76% of pregnant women of low socio-eco-nomic status have some form of periodontaldisease (López NJ, unpublished data).
Several studies have shown that ma -ternal periodontal infection is associated withadverse pregnancy outcomes, such as pre -term birth,24,53 pre-eclampsia,54 gestationaldiabetes,55 delivery of a small-for-ges -tational-age infant,56 and fetal loss.57 A morecomplete critical review of the studies show-ing association between oral infections andadverse pregnancy outcomes is presented inChapter 9 of this book.
Pre-Conception Oral HealthThe American Academy of Periodontol-
ogy released the recommendation that “allwomen who are pregnant or planning a preg-nancy should undergo periodontal examina-tion, and appropriate preventive or therapeu-tic services, if indicated, should be provided.”58
There is no definitive evidence that the as -sociation between periodontal infection and

258 Periodontal Disease and Overall Health: A Clinician's Guide
adverse pregnancy outcomes is causal or is asurrogate for another maternal factor. How-ever, the strong evidence of an association be-tween periodontal disease and systemic healthmeans that oral healthcare should be the aimof every person. This is especially importantfor pregnant women, since there is evidence tosupport the concept that maternal oral health
influences pregnancy outcome. The obviousand best cost benefits strategy to reduce the effect of periodontal infections on pregnancyoutcome is preconception preventive oralhealthcare to ensure a healthy oral environ-ment throughout pregnancy.
Patient education about the effects oforal health on systemic health and pregnancy
Figure 1. Proposed Mechanisms Involved in Preterm Birth Syndrome,Figure 1. Including Periodontal Disease
Inflammatory mediators and/or bacteria of oral origin may reach the placenta and fetus. Alternatively, pretermlabor and delivery could result from common variations in the inflammatory response to oral and cervicovaginalmicro-organisms.

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 259
outcomes should be given before pregnancyor early in pregnancy. The dentist should inform the pregnant woman of the oralchanges she may expect during pregnancy,and discuss how to prevent dental problemsthat may arise from these changes. Preg-nancy is a good time to obtain modificationsin lifestyle behaviors because women aremore motivated to make healthy changesduring this time.
While there are no oral diseases directlyattributable to pregnancy, the physiologic andbehavioral changes that occur during preg-nancy can aggravate preconceptional existinggingivitis33 or periodontitis.59 Oral hygieneinstructions to control dental plaque must beemphasized in pregnant women, and treat-ment of gingivitis and perio dontitis shouldbe performed if needed.
PREGNANCY COMPLICATIONSNausea and Vomiting
Pregnant patients may experience vary-ing degrees of nausea and vomiting, espe-cially during the first three months of gestation(morning sickness). Changes in the ging ivaltissue elicited by the hormonal profile of gestation, as well as a decreased use of oralhygiene due to nausea, predispose patients togingival inflammation. Therefore, dentaltreatment is warranted for a fraction of thesepatients. Morning appointments should beavoided. When needed, premedication withantihistaminic agents provide significant relief of symptoms along with a sedative ef-fect that is desirable when performing den-tal procedures. Doxylamine 25 mg orally isan approved choice for patients with nauseaand vomiting during gestation, including thefirst trimester.60
Threatened AbortionApproximately 10% of pregnant women
experience uterine bleeding during the firstfive months of gestation. This condition isknown as “threatened abortion” and leads to
spontaneous abortion in 10% to 20% ofcases, with 80% to 90% of women continu-ing with their pregnancies uneventfully. Adefinitive prognostic factor is the presence ofa normal embryo/fetal ultrasound examina-tion.61 Dental treatments may be preferablyperformed after bleeding stops, which usu-ally takes a few days after diagnosis.
Preterm Labor and PretermPremature Rupture of Membranes
Preterm delivery occurs in 3% to 12%of patients worldwide.62 Preterm labor andpreterm premature rupture of membranes arethe predecessors of preterm delivery in twothirds of cases, accounting for most perinatalmortality due to neonatal complications as-sociated with prematurity. Both conditionshave been linked to a hetero geneous group ofetiologies (the preterm delivery syndrome,Figure 1), including perio dontal disease. Intra -uterine infection is asso ciated with both con -ditions, especially preterm premature ruptureof membranes.63-66
Preterm labor is a disorder characterizedby regular uterine contractions and cervicalchanges between 22 and 37 weeks of gestation.Of all patients diagnosed with preterm labor,only 50% will actually deliver before 37weeks. The clinical identification of thisgroup is difficult at the time of admission tothe hospital.67 The most important therapeu-tic measure is the administration of intra-muscular corticosteroids to reduce the risk ofneonatal complications attributable to pre-maturity. Drugs aimed at reducing uterinecontractions (tocolytics such as nifedipine,betamimetics, atosiban) are also utilized inorder to delay delivery for at least 48 hours.Antibiotics are not used routinely in patientswith preterm labor.68
Preterm premature rupture of mem-branes is defined by the bursting of thechorioamniotic membrane containing the fetus and the amniotic fluid, occurring beforelabor begins, prior to 37 weeks of gestation.

260 Periodontal Disease and Overall Health: A Clinician's Guide
Clinical presentation includes fluid leakingfrom the vagina followed by uterine activityin the majority of patients. Management includes the administration of both cortico -steroids and antibiotics to reduce the risk ofneonatal complications, delay delivery, anddecrease the likelihood of maternal and neonatal infections. Antibiotics frequentlyutilized are ampicillin, erythromycin, clin-damycin, and metronidazole.69,70 Delivery isindicated when the pregnancy has reached 32to 34 weeks. Tocolytics are not routinelyused in patients with preterm premature rup-ture of membranes.
For the two conditions described above,essential dental procedures may be performedafter the patient is admitted to the hospital orclinic, treatment is established, and uterinequiescence obtained. Elective treatment maybe postponed until after delivery.
Pre-Eclampsia/EclampsiaThe development of both hyperten-
sion and significant amounts of proteinin urine occurring during the second halfof pregnancy and puerperium is referred toas pre-eclampsia. The progression to seizuresor coma characterizes the presence ofeclampsia. The disorder is multisystemicin nature and affects 3% to 7% of preg -nancies. The etiology of pre-eclampsia isheterogeneous, but a common terminal pathway characterized by endothelial dys-function is the key pathophysiologic land-mark of the disease.71 Patients with pre-eclampsia are at increased risk for maternaland perinatal mortality. Maternal com -plications include persistent hyper tensivecrisis, cerebral hemorrhage, liver/hemato-logic dysfunction, and premature placentalseparation (abruptio placentae). Fetal/neona-tal complications comprise placental insuf-ficiency (chronic fetal hypoxia), fetal growthretardation, and newborn complications derived from medically indicated prematuredelivery.
The progression of the disease is inter-rupted only by delivering the fetus and pla-centa. However, a significant fraction of patients with pre-eclampsia are suitable toexpectant management in order to advance ingestational age and decrease the risk ofneonatal complications derived from earlydelivery.71 Drugs commonly used in womenwith pre-eclampsia are hypotensors such aslabetalol, methyldopa, and hidralazine. Mag-nesium sulphate is used in the prophylaxisand treatment of seizures, especially aroundlabor and delivery. Patients at risk for pre-eclampsia may receive aspirin starting in thesecond trimester of pregnancy in an attemptto reduce the likelihood of developing thedisorder.
Emergency dental treatment should beperformed only after the pre-eclamptic pa-tient is stabilized and goals regarding bloodpressure and neurologic status are reached.The dentist should be aware that patientswith pre-eclampsia suffer from a fragile neu-rologic condition. Informing adequatelyabout the procedure and pre-medication witha sedative agent are to be considered. Epi-nephrine is contraindicated, thus anestheticdrugs with vasoconstrictors must be avoided.If the patient is under aspirin prophylaxis, in-creased bleeding time is expected. Electiveprocedures should be deferred after deliv-ery until complete resolution of the disorder.
Fetal Growth RestrictionFetal growth restriction is a frequent di-
agnosis during the second half of pregnancy.Diagnosis is made by ultrasound fetal biom-etry when the estimated fetal weight fallsbelow the 10th percentile for a specific ges-tational age. The disorder is associated withincreased perinatal morbidity and mortality,although most fetuses diagnosed with thecondition are constitutionally small but oth-erwise healthy.72 This distinction is usuallymade by ultrasound velocimetry of placentalvessels and a detailed examination of fetal

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 261
anatomy. The mother is generally not af-fected, unless there is evidence of maternaldisease predisposing to poor fetal growth(hypertension, diabetes, renal disease, etc.).A significant fraction of fetuses reaches 37weeks of pregnancy under periodic ultra-sound surveillance. Recent investigationshave proposed that fetal growth restrictionis associated with adult disease (diabetes, hypertension, and coronary heart disease).73
There are no specific medications for thetreatment of fetal growth restriction. Intra-muscular corticosteroids may be necessaryif preterm delivery is indicated. In gen-eral, the presence of fetal growth restric-tion does not alter dental treatment during pregnancy.
Fetal DeathFetal demise or stillbirth after 22 weeks
occurs in 5 to 10 per 1,000 births. The condi-tion is diagnosed by establishing the absenceof cardiac activity by ultrasound. The mostfrequent causes of fetal death are maternaldiseases (pre-eclampsia, pre-gestational dia-betes, renal disorders), placental insufficiency(often associated with fetal growth restric-tion), acute fetal hypoxia (due to pla centalabruption, uterine rupture, or cord accidents)congenital anomalies, chromosomal abnor-malities, fetal infection, fetal anemia, and con-ditions specific to multiple gestation. A sig-nificant proportion (30% to 60%) of fetaldeaths have no evident etiology.
Of significance for the dental profes-sional is a rare hematologic condition thatdevelops when the deceased fetus remainsin utero for more than three weeks. In thesecases fibrinogen levels may drop, leadingto a subclinical coagulopathy that couldprogress to disseminated intravascular coag -ulation, characterized by systemic sponta-neous bleeding and multiple organ dysfunc-tion. Any dental procedure should bedeferred until the condition is completely resolved.
DENTAL MANAGEMENT OFWOMEN AT RISK FOR ADVERSE
PREGNANCY OUTCOMESRisk Factors for Preterm Birth
Preterm birth is the most relevant ad-verse outcome for pregnant patients requiringdental treatment. Preterm birth should bethought of as a syndrome caused by multiplemechanisms, including infection, inflam -mation, uteroplacental ischemia, choriode-cidual hemorrhage, uterine overdistension,and stress (Figure 1). A growing number ofrisk factors associated with these etiologicconditions have been described. The mostimportant risk factors for the devel opmentof spontaneous preterm delivery include:62
1. Spontaneous preterm birth occurringin a previous gestation
2. Intrauterine infection3. A short uterine cervical length as
determined by ultrasound in themidtrimester
4. Inflammatory biomarkers in cervico-vaginal fluid or maternal urine (e.g.,fibronectin)
5. Low prepregnancy body mass index6. Systemic inflammation7. Vaginal bleeding of uterine origin
during the second half of pregnancy8. Multiple gestation9. Cigarette smoking
10. Social vulnerability (Afro-Americanrace, adolescent pregnancy, low socio-economic status)
Dental Care in Pregnant Womenat Risk for Preterm Birth
Several review studies74,75 have shownthat it is safe to provide dental care for preg-nant women, although clinical trials support-ing such evidence are scarce.14 The AmericanAcademy of Periodontology recommends thatpregnant women with perio dontal diseaseshould receive periodontal treatment duringpregnancy.58 The notion that periodontal treat-ment and routine dental treatment do not have

262 Periodontal Disease and Overall Health: A Clinician's Guide
special risk for the pregnant patient is basedon indirect observations derived mainly fromclinical trials aimed to determine the effect ofperiodontal treatment on pregnancy out-comes. Six randomized controlled trials ofperiodontal treatment in pregnant womenhave been published. 15-17,49,76,77
Treatment Before and After28 Weeks of Gestation
López and colleagues15 performed arandomized trial with 400 pregnant womenwith moderate-to-severe periodontitis. Thestudy population showed several well-known risk factors for preterm birth. All thewomen were of low socio-economic level,22% were unmarried, 4.7% had a history ofpreterm birth, 15% smoked, 12% were underweight, and 20% had begun prenatalcare after 20 weeks of gestation. In addition,11% had urinary infections and 18% had bacterial vaginosis during pregnancy. Allthese infections were medically treated. Two-hundred women received periodontal treat-ment that consisted of plaque control in-structions, scaling, and root planing underlocal anesthesia without vasoconstrictor be-fore 28 weeks of gestation. A control groupof 200 women received a periodontal ex-amination at the time they were enrolled.Patients were monitored every four to sixweeks during the gestational period, and another complete periodontal examinationwas performed after 28 weeks of gestation.The control group received periodontaltreatment after delivery. Carious lesionswere treated, and all teeth indicated for extraction were extracted from both groups.The incidence of spontaneous abortions andof medically indicated preterm deliverieswere similar in the treatment group and inthe group that had not received treatmentduring pregnancy. No other adverse eventsthat could be ascribed to dental treatmentwere observed among the participants of thestudy.
Treatment with MetronidazoleJeffcoat and colleagues17 did not report
safety outcomes for 366 women randomizedinto a group that received a prophylaxis orscaling and root planing, with or withoutsystemic metronidazole therapy. Unexpect-edly, within this study, the lowest rate ofpreterm birth occurred in women who re-ceived scaling and root planing and placebo,and not in the group that received metron-idazole. Metronidazole has been shown to beeffective in controlling periodontal infectionwhen given as an adjunctive of root planing.However, a later study by Carey and Kle-banoff78 showed that oral metronidazole ther-apy may produce changes in the vaginal floraleading to a heavy growth of Escherichiacoli and Klebsiella pneumonia, which wereassociated with an increased risk of pretermbirth. Thus, oral metronidazole, used as theonly antimicrobial for periodontal infectionin pregnancy should be used with caution.
Treatment of Extensive Pregnancy- Associated Gingivitis
In another randomized trial,49 570 wo -men with extensive pregnancy-associatedgingivitis received periodontal treatment be-fore 28 weeks of gestation. Periodontal treat-ment consisted of plaque-control instruc-tions, subgingival scaling, crown polishing,and mouth rinsing with 0.12% chlorhexidineonce a day. Timing in which women receivedperiodontal treatment is shown in Table 3.
The results of the study showed thattreatment of gingivitis reduced preterm birth
Table 3.Timing in Which Pregnant WomenTable 3.with Gingivitis ReceivedTable 3.Periodontal Treatment
Received Treatment
Week of Gestation n %
Between 7 and 12 weeks 131 23Between 13 and 20 weeks 376 66Between 21 and 28 weeks 63 11Total 470 1000

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 263
and low-birth-weight infant rates by 68%. Noadverse events ascribed to dental treatmentwere identified in the treatment groups duringpregnancy, and no significant differences wereobserved when women of the treatment groupwere compared to the group that did not receive periodontal treatment. The resultsof this study show that periodontal treatmentadministered between 7 and 28 weeks of ges-tation is not associated with an increased riskof serious adverse events in women despitethe presence of other risk factors associatedwith adverse pregnancy outcomes, such aslow socio-economic status, history of pretermbirth, smoking, and genito-urinary infectionsduring pregnancy.
Treatment of PeriodontitisOffenbacher and colleagues76 random-
ized 74 women with mild periodontitis, 40 ofwho received periodontal treatment early inthe second trimester of pregnancy. Perio -dontal treatment consisted of plaque controlinstructions, scaling and root planing, andcrown polishing; 34 women received onlysupragingival debridement. This study pop-ulation represented a high-risk group ofpreterm birth because 60% of the partici-pants were African-American, tending to beeconomically disadvantaged, and 75% hadpreviously experienced pre term births. Thefindings of this study indicate that the inter-vention was successful in treating periodon-tal disease, and no serious adverse eventsoccurred in terms of either obstetric or perio -dontal outcomes that were attributed to pe-riodontal treatment. The authors reportedtwo cases of fetal demise during the study;however, neither the timing nor the groupto which the women with these events be-longed was specified.
Tarannum and Faizuddin77 evaluated theeffect of periodontal therapy on pregnancyoutcome in a randomized trial with 200women with periodontitis. The treatmentgroup received plaque-control instructions
and scaling and root planing under localanesthesia, as well as mouth rinse twice dailywith 0.2% chlorhexidine. The control groupreceived tooth brushing instructions only.A significantly higher incidence of pretermbirth was observed in the control group com-pared to the treatment group (76.4% versus53.5%, p < 0.001). No adverse effects due toperiodontal treatment were reported.
Treatment of Slight-to-Moderate Periodontitis
Michalowicz and colleagues16 con-ducted a multicenter, randomized trial to de-termine if periodontal therapy reduces therisk of preterm delivery. They concluded thattreatment of periodontitis in pregnant womenimproves periodontal disease and is safe, butdoes not significantly alter rates of pretermbirth. The data from this study were alsoused to investigate safety outcomes related tothe provision of dental care in pregnantwomen.14 Participants in the study had gen-eralized, slight-to-moderate periodontitis,and belonged to minority and underservedgroups who were at an elevated risk of ad-verse pregnancy outcomes. The populationstudy consisted of African-American women(45%), Hispanic women (42%), and womenwho had a history of preterm birth deliveries(9.3%). The authors randomized 413 preg-nant women with periodontitis to a groupthat received scaling and root planing be-tween 13 and 21 weeks of gestation. Dentistsprovided periodontal treatment over one tofour visits, and topical or locally injectedanesthetics were administered as needed. Acontrol group of 410 women were monitoredduring pregnancy and treated after delivery.Women of both groups were evaluated foressential dental treatment. The necessity for“essential” dental treatment was defined asthe presence of one or more of the follow-ing: odontogenic abscesses, decayed teethjudged likely to become symptomatic during pregnancy if left untreated, and fractured or

264 Periodontal Disease and Overall Health: A Clinician's Guide
decayed teeth that could adversely affect thehealth of adjacent teeth. Affected teeth weretreated with temporary or permanent restora-tions, endodontic therapy, or extraction at atime between 13 and 21 weeks of gestation.Four-hundred and eighty-three womenneeded essential dental treatment and 72.7%of these women completed all recommendedtreatment. Serious adverse effects wererecorded and included spontaneous abortion,stillbirth, hospitalization for more than 24hours due to labor pains or other reasons,fetal or congenital anomalies, or neonataldeaths. The adjusted odds ratios for all ad-verse outcomes related to essential dentaltreatment were close to one, showing thatthe dental treatments administered were notassociated with any significant increase inrisk for these outcomes.
Nonsignificant differences of adverseevents were found in women who receivedessential dental treatment and who receivedor who did not receive periodontal treatment.The distribution of adverse events was notsignificantly different in women who re-ceived periodontal treatment nor in thosewho did not receive treatment during preg-nancy. Thus, in a population at high risk ofadverse pregnancy outcomes, periodontaland dental treatments administered between13 and 21 weeks of gestation did not in-crease the risk of serious medical adverseevents, preterm deliveries, spontaneousabortion or stillbirths, or fetal anomalies.This study confirms the predominant no-tion in the obstetric community that fewrisks are associated with routine dental careduring pregnancy.79 Some experts recom-mend that it is advisable to defer electivedental treatment during the first 12 weeks ofgestation because of the potential vul -nerability of the fetus.76,80 However, there isno evidence that routine dental treatmentor periodontal treatment may have adverseeffects on fetal development or inducemalformations.
Treatment During Pregnancy ReducesRisk of Preterm Birth
Ideally, women should begin their preg-nancy without periodontal infections, andpreventive oral care services should be pro-vided as early in pregnancy as possible.However, if a periodontal or dental infec-tion is diagnosed at any time during preg-nancy, the treatment should be administeredas soon as possible in order to reduce therisk of preterm birth. In women with perio -dontal disease diagnosed late in the second orin the third trimester of pregnancy, and whohave a high risk of preterm birth or symp-toms of preterm labor, the administration ofsystemic antibiotics to control periodontalinfection is advisable. The combination ofmetronidazole (250 mg) plus amoxicillin(500 mg) three times a day for seven days,used in conjunction with root planing, hasbeen shown to be effective to control peri-odontal infections in patients with chronicperiodontitis.81 The timing of the adminis-tration of antibiotics in relation to the scalingand root planing treatment is controversial,and protocols to determine the best timing toadminister antibiotics have not been tested.Apparently, the results of the administrationof metronidazole and amoxicillin contrastwith those of the administration of metron-idazole alone in relation to changes in thevaginal microflora. This combination of anti -biotics has been widely used to treat peri-odontal infection and no secondary effectson the vaginal flora have been reported.López and colleagues15 gave metronidazoleand amoxicillin to 29 pregnant women withsevere aggressive periodontitis as an adjunctto scaling and root planing. The treatmentwas administered between 16 weeks and 28weeks of gestation; the administration of anti -biotics began the day that scaling and rootplaning was initiated. No adverse effects thatcould have been attributed to antibiotic treat-ment were observed and all the women hadnormal-term parturition.

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 265
Managing Periodontal Infection in thePregnant Adolescent Patient
Maternal age under 18 years is a riskfactor for preterm birth82 and pregnant ado-lescents are at an increased risk for medicalcomplications.83 In the US, more than 6% ofadolescent females become pregnant everyyear. Of these pregnancies, 51% end in livebirths, 35% in induced abortion, and 14% inmiscarriages or stillbirths.84 Poor and low-in-come adolescents make up 38% of allwomen ages 15 to 19 in the US, yet they ac-count for 73% of all pregnancies in that agegroup. It is known that prevalence and sever-ity of periodontal disease are also higher indisadvantaged populations. Teenage mothersare much less likely than older mothers to re-ceive timely prenatal care and are morelikely to smoke during pregnancy. As a resultof these and other factors, babies born toteenagers are more likely to be preterm (< 37weeks’ gestation) and of low birth weight(< 2,500 g) and are at greater risk of seriousand long-term illness, developmental delays,and dying in the first year of life comparedto infants of older mothers.85 There are nostudies about the oral health status in preg-nant adolescents, but extrapolating the in-formation on prevalence of gingivitis andperiodontitis from studies in nonpregnantadolescents, it can be expected that thesediseases have similar prevalence. Gingivi-tis is common in children, reaching a peakat puberty followed by a limited decline in adolescence.
In order to determine the effect of peri-odontal treatment on pregnancy outcomes,a cohort of 164 pregnant adolescents athigh risk of preterm birth was recruited byMitchell-Lewis and colleagues.86 The studypopulation consisted of pregnant adoles-cents, ages 14 to 19. All of them were oflow socio-economic status; 60% were African-American and 39% Hispanic. These socio -demographic characteristics of young age,minority ethnicity, and low socio- economic
status are well-known risk factors for pre -term birth.82 Periodontal examinations wereperformed to assess dental plaque, calculus,bleeding on probing, and pocket depth. Perio -dontal treatment consisted of oral hygiene instructions, scaling, and crown polishing.This treatment was given to 74 women; 90women with no treatment were used as con-trols. Four plaque samples per subject wereobtained during pregnancy and post-partumto study the prevalence of 12 bacterial species.Preterm low birth weight occurred in 13.5%of women who received periodontal treat-ment and 18.9% of women who did not re-ceive treatment. The difference was not sta-tistically significant. However, preterm birthmothers had significantly higher levels ofTannerella forsythia and Campylobacter rectusand consistently higher levels of the otherspecies studied. The reduction of 28.6% inthe incidence of preterm low birth weight,even though not statistically significant,shows that periodontal intervention may reduce adverse outcome in pregnant ado les-cents with periodontal infection. No adverseeffects due to periodontal treatment were reported.
Pregnant adolescents are at high risk foradverse pregnancy outcomes, and for thosewho have gingivitis or periodontitis, the riskmay increase. The principles for medical anddental management of these patients are notvery different from those used for adultwomen, but the higher incidence of complica-tions coupled with more serious social and le-gal issues if they are under the age of 18, maketheir overall management more complex.
CONCLUSIONIn summary, pregnant women with gin-
givitis or periodontitis should receive perio -dontal treatment as soon as the periodontalcondition is diagnosed. In women at risk foradverse pregnancy outcomes and periodontalinfection, collaboration between the obste-trician and dentist is essential to determine

266 Periodontal Disease and Overall Health: A Clinician's Guide
the timing and the characteristics of perio -dontal treatment that should be administered.
Supplemental Readings
Goldenberg RL, Culhane JF, Iams JD, Romero R. Epi-demiology and causes of preterm birth. Lancet 2008;371:75–84.
Gómez R, Romero R, Edwin SS, David C. Pathogene-sis of preterm labor and preterm premature rupture ofmembranes associated with intraamniotic infection. Infect Dis Clin North Am 1997;11:135–176.
Iams JD, Romero R, Culhane JF, Goldenberg RL. Pri-mary, secondary, and tertiary interventions to reducethe morbidity and mortality of preterm birth. Lancet2008;371:164–175.
López NJ, Da Silva I, Ipinza J, Gutierrez J. Periodontaltherapy reduces the rate of preterm low birth weight inwomen with pregnancy-associated gingivitis. J Perio -dontol 2005;76:2144–2153.
López NJ, Smith PC, Gutierrez J. Periodontal therapymay reduce the risk of preterm low birth weight inwomen with periodontal disease: a randomized con-trolled trial. J Periodontol 2002;73:911–924.
Michalowicz BS, DiAngelis AJ, Novak MJ, et al. Ex-amining the safety of dental treatment in pregnantwomen. J Am Dent Assoc 2008;139:685–695.
REFERENCES1. Zachariasen RD. The effect of elevated ovarian
hormones on periodontal health: oral contracep-tives and pregnancy. Women Health 1993;20:21–30.
2. Krejci CB, Bissada NF. Women’s health issues andtheir relationship to periodontitis. J Am Dent Assoc2002;133:323–329.
3. Kornman KS, Loesche WJ. The subgingival mi-crobial flora during pregnancy. J Periodontal Res1980;15:111–122.
4. Lapp CA, Thomas ME, Lewis JB. Modulation byprogesterone of interleukin-6 production by gingi-val fibroblasts. J Periodontol 1995;66:279–284.
5. Lapp CA, Lohse JE, Lewis JB, et al. The effects ofprogesterone on matrix metalloproteinases in cul-tured human gingival fibroblasts. J Periodontol2003;74:277–288.
6. Gaffield ML, Gilbert BJ, Malvitz DM, RomagueraR. Oral health during pregnancy: an analysis of in-formation collected by the pregnancy risk assess-ment monitoring system. J Am Dent Assoc 2001;132:1009–1016.
7. Mangskau KA, Arrindell B. Pregnancy and oralhealth: utilization of the oral health care system bypregnant women in North Dakota. Northwest Dent1996;75:23–28.
8. Pistorius J, Kraft J, Willershausen B. Dental treat-ment concepts for pregnant patients—results of asurvey. Eur J Med Res 2003;8:241–246.
9. Lindow SW, Nixon C, Hill N, Pullan AM. The in-cidence of maternal dental treatment during preg-nancy. J Obstet Gynaecol 1999;19:130–131.
10. Shrout MK, Pooter BJ, Comer RW, Powell BJ.Treatment of the pregnant dental patient: a surveyof general dental practitioners. Gen Dent 1994;42:164–167.
11. Lydon-Rochelle MT, Krakowiak P, Hujoel PP, Peters RM. Dental care use and self -reported den-tal problems in relation to pregnancy. Am J PublicHealth 2004;94:765–771.
12. Gaffield ML, Gilbert BJ, Malvitz DM, RomagueraR. Oral health during pregnancy: an analysis of information collected by the pregnancy risk assess -ment monitoring system. J Am Dent Assoc 2001;132:1009–1016.
13. American Dental Association Council on Access,Prevention and Interprofessional Relations. Wo -men´s oral health issues. American Dental As so -ciation. 2006. http:www.ada.org/sections/profes-sionalResources/pdfs/healthcare_womens.pdf.
14. Michalowicz BS, DiAngelis AJ, Novak MJ, et al.Examining the safety of dental treatment in preg-nant women. J Am Dent Assoc 2008;139:685–695.
15. López NJ, Smith PC, Gutierrez J. Periodontal ther-apy may reduce the risk of preterm low birth weightin women with periodontal disease: a randomizedcontrolled trial. J Periodontol 2002;73:911–924.
16. Michalowicz BS, Hodges JS, DiAngelis AJ, et al.Treatment of periodontal disease and the risk ofpreterm birth. N Engl J Med 2006;355:1885–1894.
17. Jeffcoat MK, Hauth JC, Geurs NC, et al. Perio -dontal disease and preterm birth: results of a pilotintervention study. J Periodontol 2003;74:1214–1218.
18. ACOG. ACOG Committee Opinion No. 421, No-vember 2008: antibiotic prophylaxis for infectiveendocarditis. Obstet Gynecol 2008;112:1193–1194.
19. Brown A. Access to oral health care during theperinatal period: A policy brief. National Maternaland Child Oral Health Resource Center 2008.
20. Editorial. Oral health: prevention is key. Lancet2009;373:1.
21. Beck JD, Pankow J, Tyroler HA, Offenbacher S.Dental infections and atherosclerosis. Am Heart J.1999;138:528–533.
22. Shlossman M, Knowler WC, Pettit DJ, Genco RJ.Type 2 diabetes mellitus and periodontal disease.

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 267
J Am Dent Assoc 1990;121:532–536.23. Mercado, Marshall RI, Klestov AC, Bartold PM. Is
there a relationship between rheumatoid arthritisand periodontal disease? J Clin Periodontol 2000;27:267 –272.
24. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D,Maynor G, et al. Periodontal infection as a possiblerisk factor for preterm low birth weight. J Perio -dontol 1996;67:1103–1113.
25. Köhler B, Andréen I. Influence of caries-preventivemeasures in mothers on cariogenic bacteria andcaries experience in their children. Arch Oral Biol1994;39:907–911.
26. Oral Health in America: A Report of the SurgeonGeneral. In: Services USDoHAH, ed. U.S. De-partment of Health and Human Services, NationalInstitute of Dental and Craniofacial Research, National Institute of Health, Rockville, MD: U.S.Department of Health and Human Services, 2000.
27. U.S. Department of Health and Human Services.National Institute of Dental and Craniofacial Research. Oral Health in America: A report of theSurgeon General. NIH publication no.00-4713.Rockville, Md.: U.S. Public Health Service, Dept.of Health and Human Services;2000.
28. Umesi-Koleoso DC, Ayanbadejo PO, Oremosu OA.Dental caries trend among adolescents in Lagos,South West Nigeria. West Afr J Med 2007;26:201–205.
29. Caufield PW, Cutter GR, Dasanayake AP. Initial acquisition of mutans streptococci by infants: evi-dence for a discrete window of infectivity. J DentRes 1993;72:37–45.
30. Berkowitz RJ. Mutans streptococci: acquisition andtransmission. Pediatr Dent 2006;28:106–109.
31. Kohler B, Bratthall D, Krasse B. Preventive meas-ures in mothers influence the establishment of thebacterium Streptococcus mutans in their infants.Arch Oral Biol 1983;28:225–231.
32. Löe H. Periodontal changes in pregnancy. J Perio -dontol 1965;36:209–217.
33. Arafat AH. Periodontal status during pregnancy. JPeriodontol 1974;45:641–643.
34. Löe H, Sillness J. Periodontal disease in pregnancy.I. Prevalence and severity. Acta Odont Scand 1963;21;533–551.
35. Hugoson A. Gingivitis in pregnant women. A lon-gitudinal clinical study. Odont Revy 1971;22:65–68.
36. Raber-Durlacher JE, Leene W, Palmer-Bouva CC,Raber J, Abraham-Inpijn L. Experimental gingivitisduring pregnancy and postpartum: Immunohisto -chemical aspects. J Periodontol 1993;64:211–218.
37. Hey-Hadavi JH. Women´s oral health issues: sexdifferences and clinical implications. Women´sHealth Prim Care 2002;5:189–199.
38. Mariotti A. Sex steroid hormones and cell dynam-ics in the periodontium. Crit Rev Oral Biol Med1994;5:27–53.
39. Priddy KD. Immunologic adaptations during preg-nancy. J Obstet Gynecol Nursing 1997;263:388–394.
40. Taylor DD, Sullivan SA, Eblen AC, Gercel-TaylorC. Modulation of T-cell CD3-zeta chain expres-sion during normal pregnancy J Reproduct Im-munol 2002;5415–5431.
41. Kunnby B, Matsson L, Astedt B. Aggravation ofgingival inflammatory symptoms during pregnancyassociated with the concentration of plasminogenactivator inhibitor type-2 in gingival fluid. J Peri-o dont Res 1996;31:271–277.
42. Jonsson R, Howland BE, Bowden GHW. Rela-tionships between periodontal health, salivarysteroids, and Bacteroides intermedius in males,pregnant and non-pregnant women. J Dent Res1988;67:1062–1069.
43. Madianos PN, Lieff S, Murtha AP, et al. Maternalperiodontitis and prematurity. Part II: Maternal infection and fetal exposure. Ann Periodontol2001;6:175–182.
44. Ness PM, Perkins HA. Transient bacteremia afterdental procedures and other minor manipulations.Transfusion 1980;20:82–85.
45. Offenbacher S, Jared HL, O´Reilly PG, et al. Potential pathogenic mechanisms of periodontitis-associated pregnancy complications. Ann Peri-odontol 1998;3:233–250.
46. Moore WEC, Moore LVH. The bacteria of peri-odontal diseases. Periodontol 2000 1994;5:66–77.
47. Hill GB. Preterm birth: Associations with genitaland possibly oral microflora. Ann Periodontol1998;3:222–232.
48. Han YW, Redline EW, Li M, Yin L, Hill GB, Mc-Cormick TS. Fusobacterium nucleatum inducespremature and term stillbirths in pregnant mice:Implication of oral bacteria in preterm birth. InfectImmun 2004;74:2272–2279.
49. López NJ, Da Silva I, Ipinza J, Gutierrez J. Perio -dontal therapy reduces the rate of preterm low birthweight in women with pregnancy-associated gin-givitis. J Periodontol 2005;76:2144–2153.
50. Davenport ES, Williams CE, Sterne JA, Sivap-athasundram V, Fearne JM, Curtis MA. The eastLondon study of maternal chronic periodontal dis-ease and preterm low birth weight infants: study de-sign and prevalence data. Ann Periodontol 1998;3:213–221.
51. Baelum V, Scheutz F. Periodontal disease in Africa.Periodontology 2000 2000;29:79–103.
52. Lief S, Boggess KA, Murtha AP, Jared H, Madi-anos PN, Moss K, et al. The oral conditions and

268 Periodontal Disease and Overall Health: A Clinician's Guide
pregnancy study: periodontal status of a cohort ofpregnant women. J Periodontol 2004;75:116–126.
53. Xiong X, Buekens P, Fraser WD, Beck J, Offen-bacher S. Periodontal disease and adverse preg-nancy outcomes: a systematic review. BJOG 2006;113–143.
54. Bogges KA, Lieff S, Murtha AP, Moss K, Beck J,Offenbacher S. Maternal periodontal disease is as-sociated with an increased risk for preeclampsia.Obstet Gynecol 2003;101:227–231.
55. Xiong X, Buekens P, Vastardis S, Pridjian G. Perio -dontal disease and gestational diabetes mellitus.Am J Obstet Gynecol 2006;195:1086–1089.
56. Borgess KA, Beck JD, Murtha AP, Moss K, Of-fenbacher S. Maternal periodontal disease in earlypregnancy and risk for a small-for-gestational-ageinfant. Am J Obstet Gynecol 2006;194:1316–1322.
57. Moore S, Ide M, Coward PY, Randhawa M,Borkowska E, Baylis R, et al. A prospective studyto investigate the relationship between periodontaldisease and adverse pregnancy outcome. Br Dent J2004;197:251–258.
58. Task Force on Periodontal Treatment of PregnantWomen, American Academy of Periodontology.American Academy of Periodontology statementregarding periodontal management of the pregnantpatient. J Periodontol 2004;75:495.
59. Moss KL, Beck JD, Offenbacher S. Clinical riskfactors associated with incidence and progression ofperiodontal conditions in pregnant women. J ClinPeriodontol 2005;32:492–498.
60. Koren G, Maltepe C. Pre-emptive therapy for se-vere nausea and vomiting of pregnancy and hyper-emesis gravidarum. J Obstet Gynaecol 2004;24:530–533.
61. Schauberger CW, Mathiason MA, Rooney BL. Ultrasound assessment of first-trimester bleeding.Obstet Gynecol 2005;105:333–338.
62. Goldenberg RL, Culhane JF, Iams JD, Romero R.Epidemiology and causes of preterm birth. Lancet2008;371:75–84.
63. Gómez R, Ghezzi F, Romero R, Munoz H, TolosaJE, Rojas I. Premature labor and intra-amniotic in-fection. Clinical aspects and role of the cytokines indiagnosis and pathophysiology. Clin Perinatol1995;22:281–342.
64. Gómez R, Romero R, Ghezzi F, Yoon BH, MazorM, Berry SM. The fetal inflammatory responsesyndrome. Am J Obstet Gynecol 1998;179:194–202.
65. Gómez R, Romero R, Edwin SS, David C. Patho-genesis of preterm labor and preterm prematurerupture of membranes associated with intraamnioticinfection. Infect Dis Clin North Am 1997;11:135–176.
66. Romero R, Mazor M, Munoz H, Gómez R, GalassoM, Sherer DM. The preterm labor syndrome. AnnN Y Acad Sci 1994;734:414–429.
67. Gómez R, Romero R, Medina L, et al. Cervico -vaginal fibronectin improves the prediction of pre -term delivery based on sonographic cervical lengthin patients with preterm uterine contractions and intact membranes. Am J Obstet Gynecol 2005;192:350–359.
68. Iams JD, Romero R, Culhane JF, Goldenberg RL.Primary, secondary, and tertiary interventions toreduce the morbidity and mortality of preterm birth.Lancet 2008;371:164–175.
69. Mercer BM. Preterm premature rupture of themembranes: current approaches to evaluation andmanagement. Obstet Gynecol Clin North Am 2005;32:411–428.
70. Ilekis JV, Reddy UM, Roberts JM. Preeclampsia—a pressing problem: an executive summary of aNational Institute of Child Health and Human De-velopment workshop. Reprod Sci 2007;14:508–523.
71. Haddad B, Sibai BM. Expectant management of se-vere preeclampsia: proper candidates and preg-nancy outcome. Clin Obstet Gynecol 2005;48:430–440.
72. Garite TJ, Clark R, Thorp JA. Intrauterine growthrestriction increases morbidity and mortality amongpremature neonates. Am J Obstet Gynecol 2004;191:481–487.
73. Barker DJ. Adult consequences of fetal growth re-striction. Clin Obstet Gynecol 2006;49:270–283.
74. Lakshmanan S, Radfar L. Medical managementupdate: Pregnancy and lactation. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2004;97:672–682.
75. Hilger KK, Douglass J, Mathieu GP. Adolescentpregnancy: a review of dental treatment guidelines.Pediatr Dent 2003;25:459–467.
76. Offenbacher S, Lin D, Strauss R, et al. Effects ofperiodontal therapy during pregnancy on perio -dontal status, biologic parameters, and pregnancyoutcomes: a pilot study. J Periodontol 2006;77:2011–2024.
77. Tarannum F, Faizuddin M. Effect of periodontaltherapy on pregnancy outcome in women affectedby periodontitis. J Periodontol 2007;78:2095–2103.
78. Carey JC, Klebanoff MA. Is a change in the vagi-nal flora associated with an increased risk ofpreterm birth? Am J Obstet Gynecol 2005;192:1341–1347.
79. Shrout MK, Comer RW, Powell BJ. Treatment ofthe pregnant dental patient: four basic rules ad-dressed. J Am Dent Assoc 1992;123:75–80.

CHAPTER 16 Dental and Medical Comanagement of Pregnancy 269
80. Mishkin DJ, Johnson KE, Javed T. Dental diseasesIn: Gleicher N (ed). Principles and Practice ofMedical Therapy in Pregnancy. Stamford, Con-necticut: Appleton / Lange, 1998:1093–1095.
81. Winkel EG, Van Winkelhoff AJ, Timmerman MF,Van der Velden U, Van der Weijden GA. Amoxi-cillin plus metronidazole in the treatment of adultperiodontitis patients. A double-blind placebo-con-trolled study. J Clin Periodontol 2001;28:296–305.
82. Berkowitz GS, Papiernik E. Epidemiology ofpreterm birth. Epidemiol Rev 1993;15:414–444.
83. Fraser AM, Brocker JE, Ward RH. Association ofyoung maternal age with adverse reproductive out-comes. N Eng J Med 1995:332:1113–1117.
84. Committee on Adolescence. Adolescent pregnancy-current trend and issues: 1998. Pediatrics 1999;103:516–520.
85. Ventura SJ, Abma JC, Mosher WD, Henshaw SK.Recent trends in teenage pregnancy in the UnitedStates, 1990–2002. NCHS Health E-Stat. 2006.Available at:http://www.cdc.gov/nchs/products/pubs/pubd/hestat/teenpreg1990–2002/teenpreg1990–2002.htm.
86. Mitchell-Lewis D, Engebretson SP, Chen J, Lam-ster IB, Papapanou PN. Periodontal infections andpre-term birth: early findings from a cohort ofyoung minority women in New York. Eur J OralSci 2001;109:34–39.
Approximately 300,000 hip fractures occureach year requiring hospital admission and,ultimately, surgical correction.2 Consideringthe increasing size of the elderly populationas the “baby boomers” rapidly approach theirsixth and seventh decades of life, it is easy tosee how this disease process can and willaffect the healthcare system of the UnitedStates and worldwide.
Osteoporosis is diagnosed on the basisof a low-impact or fragility fracture or lowbone mineral density (BMD), which is bestassessed by central dual-energy x-ray ab -sorp tiometry (DEXA).3 By World Health Organization guidelines, a diagnosis of os-teoporosis is made by DEXA scan demon-stration of a BMD which is 2.5 standard de-viations below the young adult referencemean based on gender. Classifications forosteoporosis are broken down into primaryand secondary etiologies. Secondary causesof osteoporosis are many, and although theyare less commonly seen in clinical practice,there are a few, such as diabetes mellitus andchronic obstructive pulmonary disease, thatare seen quite often in osteoporosis patients.
Paget’s DiseasePaget’s disease is a disorder character-
ized by excessive resorption of bone. Sub-sequent to this resorption, new bone is de-posited in a haphazard fashion to compensatefor the rapid bone loss. This creates the “mo-saic” pattern commonly associated with thedisease process that describes the disorgan-ized trabecular bone formed instead of the
INTRODUCTIONBefore addressing any therapeutic man-
agement, it needs to be determined whetheror not there are indeed associations, mecha-nistic links, or shared risk factors for dentaldiseases and osteoporosis, kidney disease,and cancer. Fortunately, these are addressedin previous chapters; the goal of this chapteris to consider the management issues thatmay arise in dealing with the comorbid state.Can we modify treatment? Do we need toprescribe the routine drugs or are there al-ternatives? How should the dentist or physi-cian manage these patients presenting withboth oral and systemic conditions? First weneed to consider the diseases and the char-acteristics that might complicate their dualmanagement. Each section concludes withsuggestions for both the physician and den-tist for treating these patients.
OSTEOPOROSIS ANDOTHER BONE DISEASES
OsteoporosisOsteoporosis is the most common bone
disease in humans. Disease prevalence hasbeen reported by some sources as 3% to6% in men and up to 13% to 18% in women(approximately 8 million women and 2 mil-lion men), with a significantly higher preva-lence reported for those meeting diagnosticcriteria for osteopenia.1 The risk of devel -oping osteoporosis increases with age, es -pecially in women, due to loss of ovarianfunction that precipitates rapid bone loss.2
CHAPTER 17Dental and Medical Comanagement of Osteoporosis, Kidney Disease,and Cancer
Dawn J. Caster, John H. Loughran, Denis F. Kinane

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 271
normal pattern of lamellar bone. This disor-dered bone deposition is weak and prone todeformities as well as fracture. Incidence ofPaget’s disease is not well reported, and thecurrent incidence of 3.0% to 3.7% is basedon autopsies and radiographs of patients over40 years of age.4 Etiology of the disease isunknown, although there are several proposedtheories, including viral and genetic factors.Careful evaluation of history and physicalexamination help to delineate Paget’s dis-ease from other possible diagnoses (e.g.,metastatic bone disease). Certain serologi-cal and radiographic tests aid in making thediagnosis. Although there are several clinicalmanifestations of the disease including com-plaints of upper dentures not fitting anymore,it is the skeletal sequelae that are most ger-mane to the current discussion.
Metastatic Bone DiseaseMetastatic bone disease is most com-
monly associated with breast and prostate can-cer, but is frequently seen in many advancedcases of malignancy. Tumor cells express sev-eral chemical and genetic factors that makebone a preferred site for localization andgrowth. There is much discussion in the med-ical literature regarding the propensity of cer-tain malignancies to express osteoblastic ver-sus osteolytic bone lesions. However, mostpatients with bone metastases have evidence ofboth lesions. Clinical manifestations of meta -static bone disease include pain, fracture, andpossibly spinal cord compression. Cord com-pression is a medical emergency requiring im-mediate intervention to avoid permanent neu-rological dysfunction. Although antineoplasticand analgesic therapies are the mainstay oftreatment for most metastatic bone lesions,there are alter native strategies that have beengaining favor, such as bisphosphonate therapy.
Pharmacology of the BisphosphonatesBisphosphonates are synthetic ana-
logues of inorganic pyrophosphate. They
were initially developed in the 1800s andhave industrial uses such as softening waterfor irrigation systems. The compound’s abil-ity to soften water is due to the inhibition ofcalcium carbonate crystal formation, and itwas later found that bisphosphonates canalso inhibit calcium pyrophosphate crystalformation. Bisphosphonates are classifiedinto two groups based on whether or not theycontain an amino group. Mechanism of ac-tion differs between the groups. Aminobis-phosphonates (zolendronate, alendronate,pamidronate, ibandronate, and risedronate)disrupt the pathway involving metabolismof mevalonic acid. They also promote abnormalities in cytoskeleton production, inducing apoptosis of osteoclasts that retardbone resorption. Bisphosphonates thatdo not contain amino groups (etidronate, clodronate, and tiludronate) act by disruptingATP formation after being metabolizedwithin osteoclasts, also promoting apoptosis.There is, unfortunately, a secondary effectthat bisphosphonates exhibit—that is, theirability to inhibit bone mineralization, there-by causing osteomalacia. Once again we seea difference among the classes. Whereasetidronate has been shown to inhibit resorp-tion and mineralization at similar concen-trations, alendronate has been shown tohave a markedly favorable therapeutic in-dex (i.e., better resorption inhibition than defective mineralization) up to 36 monthsfrom the initiation of therapy.5 The overallhigher potency and lower toxicity of amino-bis phosphonates are likely the reasons theyare used more often in clinical practice thanother bisphosphonates.
Although less than 10% of orally in-gested doses of bisphosphonates are ab-sorbed, between 20% and 50% of the ab-sorbed dose accumulates in bone dependingon the rate of bone turnover. The remainderof the dose is excreted in urine. The half-lifeof these drugs varies considerably, but in thecase of alendronate (one of the more common

272 Periodontal Disease and Overall Health: A Clinician's Guide
pharmaceutical agents used in the treatmentof disorders of bone metabolism), it is as longas 10 years. One point of contention is thetimeframe for which the compound persistswithin the bone, which according to somesources can be the lifetime of the patient.6This is an important factor to bear in mindwhen considering interruption of therapyprior to surgical procedures.
Osteonecrosis of the JawOsteonecrosis of the jaw (ONJ) has at-
tracted increased interest for both medicaland dental practitioners in recent years. Inthe early part of the last century, the term“phossy jaw” had been utilized to describethe condition that linked white phosphorusexposure with the disease process of os-teonecrosis. Radiation and chemotherapyhave also been implicated as possible etiolo-gies of ONJ. The most recent debate in thecurrent literature and to be addressed in thischapter is bisphosphonate-associated ONJ.Bisphosphonates have taken on a vital role inthe management of chronic disease processessuch as osteoporosis and Paget’s disease, aswell as the prevention of skeletal complica-tions in patients with bone metastases. Bis-phosphonate-associated ONJ was first re-ported in 2003, and since then many morecases have come to light, propelling theAmerican Society for Bone and Mineral Re-search (ASBMR) to appoint a task force toreview the literature and make recommen-dations for future diagnosis and management.
The case definition of bisphosphonate-associated ONJ is an area of exposed bone inthe maxillofacial region that does not healwithin eight weeks after identification by ahealthcare provider, in a patient who was re-ceiving or had been exposed to a bisphos-phonate and had not had radiation therapy tothe craniofacial region.7 The reporting ofmany cases involving ONJ associated withbisphosphonate use was made prior to the accepted ASBMR task force definition.
Therefore, the quality of evidence regard-ing the true incidence of ONJ is in question,as is the true causal relationship betweenbisphosphonates and ONJ. Information pre-sented here is based on the most current facts,but this is an expanding field and the readershould update regularly on this topic.
The known epidemiologic data for bis-phosphonate-associated ONJ varies greatlybased on the disease processes for which thedrug is utilized (Figures 1-3). Therefore, thischapter will consider the osteoporosis andPaget’s disease patient subsets and those re-ceiving bisphosphonates for skeletal compli -
Figure 1. Clinical Photograph of anFigure 1. Upper Jaw Exhibiting MarkedFigure 1. Osteonecrosis in a Patient onFigure 1. Bisphosphonate Therapy
Courtesy of Dr. George M. Kushner, University ofLouisville Dental School.
Figure 2. Orthopantomograph ofFigure 1. Osteonecrosis in the LowerFigure 1. Border of the Lower Jaw
Courtesy of Dr. George M. Kushner, University ofLouisville Dental School.

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 273
cations of malignancy as separate entities.Patients receiving bisphosphonate therapy forosteoporosis and Paget’s disease are mostlytreated with oral agents, whereas those withmalignancy complications generally receiveintravenous therapy. There is conflicting evidence regarding the incidence of ONJ inpatients receiving bisphosphonates for osteo -porosis. One study estimated the prevalenceto be < 1 in 250,000.8 The incidence of ONJin patients receiving bisphosphonate ther-apy for complications of malignancy rangesbetween 1% and 10%.9 A prospective studyby Bamias and colleagues of cancer patientsreceiving bisphosphonate therapy estimatedthat the risk of developing ONJ increasedwith length of exposure to the drug and wasdependent on the bisphosphonate used. Al-though the data supporting these claims arelimited, it is generally accepted that the riskof developing ONJ is higher in patients re-ceiving treatment for metastatic bone dis-ease. Whether or not these higher incidencerates are secondary to the higher doses re-ceived by patients with malignancy com-pared to those receiving therapy for osteo-porosis or Paget’s disease remains to be seen.
The pathogenesis of ONJ remains un-known. Patients with the aforementioneddisease processes requiring bisphosphonatetherapy have many areas of poor bonehealth. These areas are posited to be at highrisk for developing ONJ. The antiangiogeniceffects attributed to bisphosphonates are pur-ported to leave areas such as these in a rela-tively ischemic condition. Ischemic regionswith infarcted bone will not properly re-model because of the antiresorptive proper-ties of these medications. Areas such as theseare susceptible to further necrosis aftertrauma such as oral surgery. Furthermore,these areas are a perfect nidus for infectionand a wide range of bacterial infections isfound in these situations. Once again, theseare only proposed mechanisms and furtherclinical research is necessary to elicit thepathophysiology of the disorder, particularlyregarding the issue of predisposing factorssuch as corticosteroid use or alcohol abuse.
A currently investigated topic is theearly identification of osteonecrotic boneprior to initiation of bisphosphonate therapyor oral surgery. This is extremely difficult,however, as most readily available radi-ographic techniques cannot identify defectsof cancellous bone until advanced stages.Current recommendations by the task forcecall for development of noninvasive diag-nostic and imaging techniques to furthercharacterize the disorder.
ManagementConditions requiring bisphosphonate
therapy are common and may (especially os-teoporosis) become more prevalent in thenear future. Morbidity secondary to diseaseprogression such as ONJ negatively impactsthe healthcare system financially, and hasconsiderable emotional and physical ramifi-cations for patients. Thus, ongoing preventivemeasures are necessary in the managementof these medical conditions. Until more ef-fective therapies with fewer adverse effects
Figure 3. Computer-Assisted TomographicFigure 1. View of the Same Subject SeenFigure 1. in Figure 2 Demonstrating Figure 1. Extensive Osteonecrosis of theFigure 1. Lower Border of the Lower Jaw
Courtesy of Dr. George M. Kushner, University ofLouisville Dental School.

274 Periodontal Disease and Overall Health: A Clinician's Guide
are available, the use of bisphosphonateswill continue. The heightened awareness ofONJ associated with these medications, com-bined with stronger guidelines outlining casedefinitions and a call to responsible reporting,has already resulted in an increased numberof cases reported over the past two years.Management of bisphosphonate-associatedONJ will require an interdisciplinary ap-proach, with open communication betweenmedical and dental practitioners and patientsalike. Since the incidence and risks of de-veloping this complication are different be-tween patient subsets, this chapter will out-line the recommended management strategiesseparately for patients with osteoporosis/Paget’s disease versus those treated for com-plications of malignancy. These recommen-dations for management are adapted fromthe guidelines of the 2007 ASBMR TaskForce.7
As previously mentioned, free commu-nication between medical and dental practi-tioners is necessary to ensure proper conti-nuity of care. Full disclosure concerning therisks and benefits of medical therapy is theresponsibility of the medical practitioner forany patients initiating treatment with bis-phosphonates. Reducing the risk of devel-oping ONJ includes observing strict mainte-nance of the patient’s oral hygiene andregular follow-ups with a dental practitioner,which should be an integral part of the med-ical care for all patients taking bisphospho-nates. Patients are to be instructed that anyoral problems should be reported to theirphysician and dentist promptly.
As previously discussed, the risk of de-veloping ONJ for patients receiving oraltherapy for osteoporosis or Paget’s disease isfairly low. The risk also seems to be relatedto length of exposure to the medication.Therefore, it is not necessary to have a den-tal evaluation prior to the initiation of bis-phosphonate therapy for these disorders. Forpatients taking these medications longer than
three years, there are more detailed recom-mendations for management. Patients onlong-term therapy should receive appropriatenonsurgical treatment for periodontal dis-ease (unless contraindicated by comorbid ill-ness). Moderate bone recontouring is accep -table if necessary. There is currently nocontraindication to dental implant surgeryin this patient subset. Endodontic treatmentis the preferred mode of therapy over extrac -tion when at all possible. When invasive ther-apy is necessary, it is recommended to tem-porarily discontinue bisphosphonate therapy;however, there is no evidence to support im-proved dental outcomes when discontinuingtherapy. Also as previously mentioned, thelong half-life of certain bisphosphonates andthe even longer retention of the medicationin bone call into question the validity ofsuch strategies. Once again, quality com-munication among practitioners and patientsis of the utmost importance in making thesedecisions.
For patients receiving medical therapyfor complications of malignancy, the risks ofdeveloping ONJ are greater, and thus man-agement strategies are more conservative.Dental evaluation by a qualified specialistshould be completed prior to the initiation oftherapy, with follow-up evaluations at 6- to12-month intervals. If at all possible, inva-sive procedures with appropriate time allot-ted for healing should be performed prior tothe start of medical therapy. If medical ther-apy must be initiated sooner, then concomi-tant surgical treatment is recommended withclose follow-up. Elective procedures suchas implant placement and extraction ofasymptomatic teeth are not recommended.Symptomatic teeth should be treated by non-surgical means when possible, unless thetooth is excessively mobile and presents arisk for aspiration.
Patients with established ONJ shouldbe referred to a qualified dental practitionerfor management. For those with clinical

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 275
evidence of infection, appropriate antimi-crobial therapy is recommended. Surgicalintervention for ONJ should be delayed un-less the necrotic bone has sharp edges thatmay cause continued trauma to adjacent softtissues. Segmental jaw resection may be nec-essary for large areas of necrosis. The decisionto discontinue bisphosphonate therapy forthose with this complication will depend onthe patient’s clinical condition, as this strat-egy has not been established to improve outcome. Recommendations are to ensuremaintenance of a high standard of oral hygiene, and ensure no active disease by employing nonsurgical and surgical therapywhere needed, as well as adjunctive anti -microbial therapy. Anti-inflammatory drugsshould be avoided unless there is evidencefrom research that such medications will notinterfere or interact with medications usedfor osteoporosis. There is a possibility thatany dampening of normal inflammation maypermit the bacteria in an infectious lesion tobecome more virulent, allowing greater de-struction of bone. Alternatively, dampeninginflammation may be helpful in certain casesof periodontal disease, but until there is ev-idence one way or the other, anti-inflamma-tory drugs should be avoided in this comor-bid situation.
KIDNEY DISEASEThe number of patients with chronic
kidney disease (CKD) is growing and is pro-jected to rise in the future. As the incidenceclimbs, patients with CKD, including thosewith end-stage renal disease (ESRD), willrepresent a larger portion of those seek-ing dental treatment. With this in mind, itis important to understand the complex interaction between CKD and periodontal disease.
CKD is associated with many physio-logic changes that might contribute to thedevelopment of periodontal disease. Thereare several documented physiologic changes
in oral tissues that have been associated withCKD. These include xerostomia, decreasedsalivary pH levels, decreased mineralization,and loss of the lamina dura.10 Additionally,some of the medications commonly pre-scribed to CKD patients may increase therisk of developing periodontal disease.
Both CKD and periodontal disease havebeen implicated as sources of chronic in-flammation. Thus, periodontal disease mayrepresent a modifiable contributor to the already high inflammatory burden in pa-tients with CKD, especially in those with diabetes. Treatment of periodontal diseasein these patients could decrease the overallchronic inflammatory burden and its seque-lae. A collaborative effort between dentaland medical professionals is necessary toensure that patients get appropriate adviceand treatment.
Overview of Kidney FunctionThe principle function of the kidneys is
to remove waste products of metabolism, aswell as maintain fluid and electrolyte bal-ance. The kidneys also play a vital role inblood pressure regulation through the releaseof renin. Erythropoietin, a potent stimulatorof red blood cell production, is also madeby the kidneys. Additionally, the kidneysplay an important role in bone health by pro-viding the final step in the conversion of vi-tamin D to its active form. Decreased kidneyfunction can affect each of these areas andhas far-reaching consequences on overallhealth.
The waste products removed by the kid-ney include blood urea nitrogen, a by-productof protein metabolism, and creatinine, a by-product of muscle breakdown. Blood levelsof these compounds are commonly used inlab testing to measure kidney function. Morethan 100 additional uremic solutes have beenidentified, many of which are thought to betoxic. As kidney function deteriorates, thesesolutes can build up, contributing to the

276 Periodontal Disease and Overall Health: A Clinician's Guide
uremic syndrome. The uremic syndrome hasbeen associated with an increase in fatigue,anorexia, and mental status changes, and hasbeen shown to cause leukocyte dysfunction,insulin resistance, and decreased plateletfunction.
Decreased kidney perfusion causes therelease of renin by granular cells in the juxta -glomerular apparatus. This release contrib -utes to the renin-angiotensin-system, leadingto multiple local and systemic effects, in-cluding vasoconstriction, sodium reabsorp-tion, and fluid retention. There are multipleantihypertensive agents targeting this sys-tem, including angiotensin converting en-zyme (ACE) inhibitors, angiotensin II re-ceptor blockers (ARBs), and a new class ofdirect renin inhibitors (DRIs).
Patients with CKD and ESRD are at riskfor developing bone disease secondary tothe electrolyte and endocrine derangementsthat occur with decreased kidney function.
As kidney disease progresses, phosphateexcretion is impaired. Additionally, there isdecreased production of active vitamin D. Vitamin D is either synthesized in the skin af-ter exposure to ultraviolet light or absorbedfrom dietary sources. However, vitamin Dfrom ultra violet light or dietary sources is notactive. It must undergo two hydroxylation re-actions to be activated in the body. The first
hydroxylation reaction occurs in the liverand the final hydroxylation reaction occursin the kidney. Decreased active vitamin Dlevels in combination with decreased phos-phorous excretion leads to hypocalcemia,hyperphosphatemia, and secondary hyper-parathyroidism. Long-standing derangementsin calcium and phosphorus homeo stasiseventually lead to renal osteodystrophy,which is associated with impaired bone min-eralization, increased risk of fractures, andcalcification.
Overview of CKDCKD is a broad term used to encom-
pass patients with evidence of permanentkidney damage and/or progressive decreasein kidney function as defined by glomerularfiltration rate (GFR).11 It is estimated that 31million Americans suffer from CKD and millions of others are at risk (from NationalHealth and Nutrition Examination Surveydata 1999-2006). The most common causesof CKD include diabetes, hypertension, andglomerulonephritis.
The National Kidney Foundation haspublished staging guidelines for adult pa-tients with CKD. These guidelines are basedon estimated GFR, which is calculated us-ing the widely accepted Modification of Dietin Renal Disease (MDRD) equation. The
Table 1. Classification of Chronic Kidney DiseaseGFR Action Required
Disease Stage mL/min/1.73 m2 (Additional to Previous Stage)
Patient with risk factors for CKD 90 Reduce risk factors
1. Kidney damage with normal or increased GFR 90 Diagnose and treatcomorbidities andCVD risk reduction
2. Kidney damage with slight GFR decrease 60–89 Estimate progression
3. Kidney damage with moderate GFR decrease 30–59 Treat complications
4. Kidney damage with severe GFR decrease 15–29 Consider kidney replacement
5. Kidney failure < 15 or Replace kidneydialysis
CKD is defined as either kidney damage (pathological abnormalities in blood, urine, or imaging) or a GFR less than60 for three months or longer. (Table modified from KDOQI 2002.11)

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 277
equation uses serum creatinine level com-bined with the variables of age, sex, and racein the estimation of GFR. (MDRD equation:GFR [mL/min/1.73 m2] = 186 ! [Scr]
-1.154 ![age]-0.203 ! [0.742 if female] ! [1.212 ifAfrican-American] [conventional units]).This equation provides a much better esti-mate of kidney function than creatininealone.11 Creatinine is a byproduct of muscleand thus creatinine levels vary with musclemass. Two individuals with the same creati-nine can have striking differences in GFRbecause of differences in muscle mass. Forexample, an 80-year-old Caucasian femalewith a creatinine of 1 mg/dL has a decreasedestimated GFR of 57 mL/min/1.73 m2, whilea 30-year-old African-American male with acreatinine of 1 mg/dL has a normal estimatedGFR of 123 mL/min/1.73 m2.
Renal Replacement TherapyCKD patients with a GFR of less than
15 mL/min/1.73m2 are considered to be inkidney failure. Most patients at this level ofkidney function present with symptoms ofuremia, and renal replacement therapy mustbe initiated to sustain life. Occasionally, a pa-tient will have symptoms of uremia requiringrenal replacement therapy prior to reachinga calculated GFR of < 15. Any patient witha GFR of < 15 or who is on dialysis is con-sidered Stage V CKD.
Renal replacement therapies include he-modialysis, peritoneal dialysis, and kidneytransplantation. Dialysis provides a mecha-nism for filtration of waste products, removalof excess fluid, and titration of electrolytes.Dialysis does not replace the endocrine func-tions of the kidney. Therefore, many dialysispatients rely on exogenous sources of erythro -poietin and vitamin D as part of their treat-ment regimen. Patients undergoing trans-plantation recover complete kidney function.However, they must remain on lifelongimuno suppressive therapy to prevent allo-graft rejection.
Medications Used for CKDAntihypertensive Agents
Many patients with CKD have hyper-tension and require multiple medications toreach adequate blood pressure control. Fur-thermore, the target blood pressure for pa-tients with CKD, at 130/80, is lower than itis for the general population (according tothe Joint National Committee on Hyperten-sion 7). Major classes of antihypertensiveagents include diuretics, beta blockers, ACEinhibitors, ARBs, and calcium channelblockers. Direct vasodilators, alpha blockers,and centrally acting agents represent less fre-quently used agents. Finally, the newest cat-egory of antihypertensives, DRIs, just be-came available. Of these agents, calciumchannel blockers have been implicated as asource of gingival hyperplasia.
Calcium channel blockers consist of di-hydropyridines and non-dihydropyridines.The dihydropyridines include amlodipine,felodipine, isradipine, nicardipine, nifedip-ine, and nisoldipine. The non-dihydropy-ridines include diltiazem and verapamil. Bothclasses of calcium channel blockers reduceblood pressure by relaxing arteriole smoothmuscle and reducing systemic vascular re-sistance. The non-dihydropyridines also havea significant effect on heart rate through adirect negative chronotropic effect. Calciumchannel blockers have been documented tocause gingival hyperplasia in multiple reports(Figure 4). It is a potential adverse effect withall classes of calcium channel blockers, but isthought to occur more often with the dihy-dropyridine agents.10 Gingival hyperplasiausually occurs within months after the initi-ation of therapy and resolves within monthsof discontinuing therapy.12 Clinicians mayconsider discontinuing these medications inpatients with calcium channel blocker-in-duced gingival hyperplasia. However, careshould be made to find an alternative antihy-pertensive to help maintain adequate bloodpressure control.

278 Periodontal Disease and Overall Health: A Clinician's Guide
Immunosuppressive TherapyPatients who have undergone kidney
transplantation require immunosuppressivetherapy to prevent rejection. There are bothcell-mediated and humeral components totransplant rejection. Transplant medicationstarget both aspects of transplant rejection.Most regimens include calcineurin inhibitorsto decrease the T-cell mediated response.The calcineurin inhibitors include cy-closporine and tacrolimus. Cyclosporine hasbeen documented to cause gingival hyper-plasia in renal transplant patients in multiplestudies.13 Additionally, this effect is thoughtto be augmented when cyclosporine is usedin combination with a calcium channelblocker.14 Tacrolimus has shown muchlower rates of gingival hyperplasia and maybe a safe alternative for a patient experi-encing significant cyclosporine-induced hy-perplasia.14,15 Any change in transplant med-ications should be made by a transplantspecialist to ensure efficacy and safety. An-other approach to treating gingival hyper-plasia might be the combination of a stan-dard oral hygiene program and azithromycintherapy, which has been shown in at leastone study to reduce both symptoms and ob-jective measures of cyclosporine-inducedgingival hyperplasia.16
Inflammatory StateThe relationship of kidney disease to
periodontal disease is a complex one that re-quires further study. Periodontal disease con-tributes to a chronic inflammatory state thathas been linked to multiple systemic ill-nesses. Two recent cross-sectional studiesidentified periodontal disease as an inde-pendent risk factor for chronic kidney dis-ease. However, the temporal relationship be-tween the two is unknown and noconclusions can be made on causality.17-19
Patients with CKD, especially those ondialysis, have exceedingly high mortalityrates. Recent data from the US Renal DataSystem (USRDS) show a mortality rate of84 deaths per 1,000 patient-years among dialysis patients ages 20 to 44, and 174deaths per 1,000 patient-years among those45 to 64 years of age. These rates representan eight-fold increase from the general pop-ulation. The leading cause of morbidity andmortality of CKD patients is cardiovascular disease.
The increased prevalence of cardiovas-cular disease among CKD patients is thoughtto be multifactorial. Many CKD patientshave well-known risk factors associated withcardiovascular disease, such as hypertensionand dyslipidemia. However, chronic inflam-mation is a potential risk factor for cardio-vascular disease in CKD patients. Reduc-tion in kidney function is associated withincreased serum levels of inflammatory cy-tokines and C-reactive protein (CRP) anddecreased levels of albumin. This inflam-matory state appears to accelerate the pro-gression of vascular disease.
Furthermore, periodontal disease mayadd to this inflammatory burden in patientswith CKD. Periodontal disease is commonin CKD patients, often more severe than inthe general population, and is frequentlyoverlooked.20 Death from diabetic nephropa-thy, and ESRD are significantly greater in diabetic patients with periodontal disease
Figure 4. Gross Gingival Hyperplasia inFigure 4. the Upper Anterior Region of aFigure 4. Patient with Hypertension onFigure 4. Treatment with a Calcium Figure 4. Antagonist (Dihydropyridine)

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 279
compared to those with diabetes and little orno periodontal disease.21,22 Multiple studieshave shown the association of inflammatorymarkers to periodontal disease in dialysispatients.23,24 Treatment of periodontal dis-ease has been shown to reduce inflammatorymarkers in non-CKD patients.25 Further-more, in a study of CKD patients, treatmentof periodontal disease was shown to signif-icantly decrease CRP levels.24 Measures thatdecrease periodontal disease in the CKDpopulation may ultimately reduce the in-flammatory burden of the CKD patient, thusdecreasing the mortality from cardiovasculardisease, but no such study has been performed.
Another potential benefit from decreas-ing inflammatory markers in CKD patients isdecreased use of erythropoietin-stimulatingagents. Elevated CRP levels in patients ondialysis are associated with higher doses oferythropoietin.23 Furthermore, the most re-cent information from the USRDS showsthat Medicare spent $1.9 billion on erythro-poietin-stimulating agents in one year alone.Decreasing CRP might result in lower ery-thropoietin doses and thus have a large andpositive financial impact.
Treatment of Periodontal Diseasein the CKD Patient
The management of periodontal diseasefrequently requires significant instrumenta-tion, pharmacotherapy, and sometimes sur-gery. Some clinicians recommend antibioticprophylaxis prior to dental procedures in pa-tients with arterial venous grafts because ofthe risk of infective endocarditis.26 Multipleantibiotic and analgesic regimens exist. Forall antibiotics, it is important to adjust dosebased on GFR and avoid nephrotoxic agentsin patients who are not yet on dialysis. Non-steroidal anti-inflammatory drugs (NSAIDs)can decrease GFR and are best avoided inpatients with CKD. Patients with CKD maybe at increased bleeding risk secondary toplatelet dysfunction, as well as anticoagu-
lants received on hemodialysis. One mighttry to implement a procedure on the day fol-lowing dialysis to decrease the risk.10 Mostrenal transplant protocols include a dentalworkup prior to transplantation to treat anypotential problems once immunosuppressivetherapy is initiated. Extra caution is neces-sary in renal transplant patients as they aremore susceptible to infection.
CANCER ANDPERIODONTAL DISEASE
Almost 11 million people in the US areliving with cancer or have a history of cancer,with approximately 1.4 million new cases oc-curring yearly.27 “Cancer” is a broad termused to describe a group of illnesses definedby uncontrolled growth of abnormal cells thatcan occur anywhere in the body. Many envi-ronmental and intrinsic factors have been im-plicated in the development of various formsof cancer. Environmental factors include to-bacco, chemicals, radiation, and infection. Intrinsic factors include gene mutations, hor-mones, and immune conditions. Many can-cers are likely caused from a combination ofenvironmental and intrinsic factors.27
Patients with cancer represent a uniquesegment of the dental population. Many pa-tients with cancer have pre-existing peri-odontal disease at the time of cancer diag-nosis. Additionally, several cancer treatmentsare toxic to oral tissues and can worsen un-derlying oral disease or result in the devel-opment of new periodontal disease. Cancertreatments include chemotherapy, radiationtherapy, surgery, hormone therapy, biologictherapy, and targeted therapy. Furthermore,some cancers may involve the oral cavityand have a local effect on oral tissues.
In recent years, periodontal disease hasbeen shown to have an association with manychronic diseases, including cardio vasculardisease and diabetes. Much of this associationis thought to be secondary to the chronic in-flammatory state.28 Recent studies have shown

280 Periodontal Disease and Overall Health: A Clinician's Guide
a small but significant increase in cancer riskin patients with periodontal disease.29,30
ChemotherapyChemotherapeutic regimens were de-
veloped to target rapidly dividing cells suchas tumor cells. With that concept in mind, itis logical to draw an association betweenthese therapies and side effects impactingthe gastrointestinal tract. Oral toxicity asso-ciated with chemotherapy in cancer patientsis a common side effect of these medicalregimens, which can affect the entire ali-mentary tract. Symptoms are numerous, in-cluding lesions of the oropharynx, dyspha-gia, gastritis, and diarrhea.
Mucositis is a term used to describe in-flammation of the mucous membranes liningthe oral cavity and digestive tract. Oral mu-cositis is commonly reported and is esti-mated to be found in 35% to 40% of patientsreceiving cytotoxic chemotherapy, and a higherprevalence in those undergoing hemato- poietic stem cell transplantation (HCT).31
Multiple factors contribute to the develop-ment of mucositis. Tissue damage/cell death,stimulation of a pro-inflammatory state, andinterference with normal tissue healing aredirect and indirect effects of the medications.This final chapter section focuses on com-plications of chemotherapeutic regimens andHCT involving the oropharynx, pretreatmentconsiderations, and management of these issues.
Chemotherapeutic EffectsThere are numerous chemotherapy reg-
imens available depending on the type ofcancer being treated. Some of the more com-mon agents associated with oral toxicity in-clude alkylating agents, anthracyclines, anti -metabolites, antitumor antibiotics, taxanes,and topoisomerase inhibitors. There aremany more anticancer drugs associated withoral toxicity and a more comprehensive listcan be seen in Table 2. While the individualmechanism of action of these medications isnot essential to this discussion, it is importantto understand how they exert their effectson tissues. Reactive oxygen species causedamage to the DNA of tumor cells as well ashealthy tissue. Damaged cells undergo apop-tosis, setting into motion the body’s normalresponse to cell death, which includes in-creased activity of the immune system. Ac-tivation of the immune system increases theconcentration of pro-inflammatory mole-cules in the internal milieu, such as cytokinesand biologically active proteins. Normalhealing is compromised by the persistence ofthe offending agent.
Oral MucositisUlcerative oral mucositis is one of the
more common side effects associated withchemotherapy. As previously mentioned,prevalence among cancer patients treatedwith chemotherapeutic regimens can be ashigh as 40% or even higher in patients under -
Table 2. Chemotherapeutic Agents Associated with Oral Toxicity and MucositisDrug Category Chemotherapeutic Drug Names (Generic)Alkylating agents bisulfan, carboplatin, cisplatin, cyclophosphamide, ifofamide,
mechloethamine, melphalan, procarbazine, thiotepaAnthracyclines daunorubicin, doxorubicin, iadarubicin, epirubicin, mitoxantroneAntimetabolites capecitabine, cytarabine, fluorouracil, fludarabine, gemcitabine,
hydroxyurea, methotexate, 6-mercaptopurine, pemetrexed, 6-thioguanine Antitumor antibiotics dactinomycin, bleomycin, mitomycinTaxanes docteaxel, paclitaxelTopoisomerase inhibitors etoposide, topotecan, irinotecan, teniposide
Adapted from UpToDate, 2010.

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 281
going HCT. Intensive chemotherapy cancause ulcerative mucositis that emerges ap-proximately two weeks after initiation ofhigh-dose chemotherapy.32 Risk factors fordevelopment of mucositis include youngerage, quality of dental hygiene, and level ofimmunosuppression prior to the initiation oftherapy. The ulcerations associated with oralmucositis can be extremely painful and mayinterfere with the patient’s capacity for re-quired nutritional intake. Subsequent infec-tion is another noted problem associated withthese lesions. Considering the level of im-munosuppression linked to chemotherapy,these are clinical findings that need to beidentified and addressed in a timely fashionby medical and dental practitioners. If symp-toms are severe, modification of thechemotherapeutic agents as well as dosingmay be necessary. Mucositis is considered tobe self-limited and usually resolves within14 days of cessation of chemotherapy. Thismay coincide with the recovery of granulo-cytes, but has not been shown to have a lin-ear relationship. Other less common side ef-fects include xerostomia, hemorrhage, andneuropathy.
Preventing Oral MucositisThere is limited objective data to sup-
port the concept of dental therapy prior to theinitiation of treatment for cancer. Whilemany feel that aggressive preventive dentalcare limits the extent of oral complicationsassociated with such medical therapy, onestudy proposed that such measures had noimpact on overall outcome.33 Practice guide-lines concerning oral prophylaxis for mu-cositis were published in 2007 by the Mu-cositis Study Section of the MultinationalAssociation of Supportive Care in Cancerand the International Society for Oral On-cology (MSSMA/SCCISO).34 For patientsundergoing standard chemotherapy, evalua-tion by a dental practitioner is encouragedprior to the initiation of therapy. Interval
assessment is recommended to evaluate oralcavity health, including the use of validatedtools such as the National Cancer InstituteCommon Toxicity Criteria or the Universityof Nebraska Oral Assessment Score to as-certain the severity and clinical course ofmucositis.
In those patients undergoing high-dosechemotherapy plus HCT, preventive meas-ures have recently been developed and arecurrently recommended for routine use. Pal-ifermin is a keratinocyte growth factor-1stimulator. It accelerates growth of epidermalcells including those of the gastrointestinaltract. In a double-blinded randomized controltrial, it was shown to reduce the incidence ofsevere mucositis compared with the placebogroup.35 The use of granulocyte-macrophagecolony-stimulating factor mouthwashes arealso recommended for the prevention of mu-cositis in this patient population. Low-levellaser therapy has been recommended in clin-ical guidelines as part of pretreatment forHCT patients. However, this therapy is ex-pensive and not widely available, and thereis limited objective evidence to support itsefficacy. The use of cryotherapy is also rec-ommended for the prevention of oral muco -sitis. It is important to remember that manyof these guidelines are based on expert opin-ion; further clinical research is necessary tovalidate the use of these protocols.
Treating Oral MucositisThe treatment of established oral muco -
sitis is supportive. Soft diets are a good choiceto reduce the incidence of trauma to alreadyfriable tissue. Practitioners need to encour-age sound oral hygiene practice as this will re-duce the incidence of secondary infection andpromote timely healing. Soft toothbrushes,non-irritating oral rinses, and removal of den-tures should all be encouraged as a part of rou-tine care. The use of mucosal coating agentshas been employed, although the data to sup-port the efficacy of such agents are weak.

282 Periodontal Disease and Overall Health: A Clinician's Guide
Oral solutions including lidocaine, diphenhy-dramine, and morphine sulfate have all beenemployed as analgesic control for oral mu-cositis. The MSSMA/SCCISO panel recom-mended systemic morphine as the treatmentof choice for HCT patients with oral painassociated with severe oral mucositis.34
Cautious evaluation of the neutropenicpatient is critical. These patients may presentwith reduced signs and symptoms secondaryto myelosuppression. Antimicrobial therapyearly in the course of infection is required toavert potentially catastrophic complications.Studies have shown that oral and periodon-tal assessment and management reduces therisk of infection and fever associated withoral conditions.36 Studies have also shownthat pretreatment oral care and oral care dur-ing therapy results in reduced oral compli-cations with no increase in risk of fever orbacteremia.36
In summary, the complication of oralmucositis has a very high prevalence amongcancer patients treated with chemotherapy.Clinical guidelines were published in 2007outlining recommendations for the pretreat-ment of cancer patients at risk for develop-ing oral mucositis. While preventive meas-ures such as palifermin and cryotherapy arerecommended for high-dose chemotherapypatients, the basis of care is sound oral hy-giene and regular assessment by a dentalpractitioner. Although oral mucositis is con-sidered to be a self-limiting phenomenon,supportive care is necessary to amelioratethe invasive symptoms associated with thiscomplication. Special attention needs to begiven to the neutropenic patient as infectionin this patient population is potentially life-threatening.
Leukemia and the Oral TissuesLeukemia, a disease of the bone marrow
and blood, is characterized by the malignantproliferation of white blood cells. Leukemiasare further categorized based on the cell type
that is involved; these are divided into myelo -genous and lymphocytic. Futhermore, leuke -mias are categorized as acute or chronic.Chronic leukemias occur more commonlyin older individuals and are characterized bythe excessive proliferation of relatively ma-ture, abnormal white blood cells. Typically,these leukemias progress over a period ofmonths to years. Acute leukemias are char-acterized by a rapid proliferation of im -mature white blood cells. Acute leukemiasare the most common form of leukemia in children, but can also affect adults. The four major classifications of leukemia are acute lympho cytic leukemia, acute myelogenousleukemia, chronic lymphocytic leukemia,and chronic myelogenous leukemia. Withinthese main categories exist several subtypes.Additionally, there are some less-commonforms of leukemia that do not fit well intoany of these categories.
In all forms of leukemia, bone marrowfunction is impaired. Anemia, thrombocy-topenia, and impaired immunity often result.These changes can result in gingival hemor-rhage, oral ulcerations, and increased oralinfections.37,38 The use of chemotherapyand stem cell transplantation can contributefurther to this by causing increased bonemarrow suppression as well as toxic effectson oral tissues.
When evaluating a leukemic patientwith gingival lesions, it is often difficult todistinguish between changes due to the dis-ease process and those brought on by treat-ment. In order to better characterize gingivallesions in patients with leukemia, a classi -fication system has been proposed. This classification system consists of four majorcategories: direct infiltration, direct drug toxicity, graft-versus-host disease, and bonemarrow/lymphoid tissue suppression.39
It is important for dental practitioners torecognize that a patient may present withoral lesions prior to the diagnosis of leuke -mia. Case reports have described gingival

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 283
hyperplasia, rapidly progressive periodon-tal disease, prolonged post-extraction hem-orrhage, and gingival pain as presentingsymptoms that led to various leukemia diagnoses.37,40
Radiation Therapy inHead and Neck Cancer
Head and neck cancers include cancerof the oral cavity, the pharynx, the larynx,salivary glands, nasal cavity, paranasal si-nuses, and neck lymph nodes. The majorityof head and neck cancers are squamous cellcarcinomas. Patients undergoing head andneck radiation treatments are at risk for avariety of oral complications. These com-plications include mucositis, dysgeusia (al-tered sense of taste), xerostomia (dry mouth),dental caries, periodontal disease, and osteo -radionecrosis. Collaboration among physi-cians and dental professionals is necessary toprovide optimal care.
Preradiation oral assessment and inter-vention, followed by the implementation ofan oral care program prior to and during ra-diation, is essential to improve outcomes inpatients undergoing radiation. A recent sur-vey of healthcare professionals reported a75% referral rate for oral and dental assess-ment prior to head and neck radiation. Thesame survey also reported that integrateddental and medical services were available atonly 25% of institutions.41
Mucositis is a common side effect ofradiation therapy and has been reported in upto 80% of patients receiving radiotherapyfor head and neck cancer.42 Radiation dis-rupts DNA replication in the basal layer ofthe oral epithelium. This leads to thinning ofthe epithelium and eventual ulceration oforal tissues. The ulcerative phase is wors-ened by local bacterial colonization.42
As in patients with chemotherapy-in-duced mucositis, the cornerstone of therapyin patients with radiation-induced mucositisincludes adequate pain management and
maintenance of oral hygiene. Recent guide-lines specific to radiation-induced mucositissupport the use of midline radiation blocksand 3-dimensional radiation therapy to min-imize mucosal damage. The guidelines alsorecommend the use of benzydamine, a locallyacting NSAID, for mucositis prevention inpatients exposed to moderate doses of radi-ation. Because of a lack of clinical benefit,the guidelines recommend against routineuse of chlorhexidine rinses and antimicrobiallozenges to prevent radiation-induced oralmucositis. They also recommend against theuse of sucralfate in the treatment of radiation-induced mucositis.34
Dysgeusia and xerostomia are commonside effects of radiation. Radiation therapycan damage taste buds, and in some caseslead to permanent taste loss. Radiation leadsto atrophy, vascular damage, and connectivetissue fibrosis of the salivary glands. The result is both dose- and location-dependent.Higher radiation doses and involvement oflarge areas of salivary tissue will result inmore severe cases of xerostomia. Patientswith significant xerostomia are at muchhigher risk for developing dental caries. Forthese patients, daily fluoride treatment andmeticulous oral hygiene is recommended forthe prevention of dental decay.
Radiation can lead to alterations in vas-cularity of soft tissue and bone, reduced con-nective tissue cellularity, and increased tissuefibrosis. The vascular changes result in de-creased blood flow to tissues, with con-comitant tissue hypoxia and reduction in tis-sue cellularity. This can have a deleteriouseffect on bone and soft tissue in the oral cav-ity. High-dose radiation has been shown tocontribute to tooth loss and greater perio -dontal attachment loss. Furthermore, perio -dontal attachment loss has the potential tolead to osteoradionecrosis.43
Osteoradionecrosis is a less common, butpotentially devastating side effect of radiationthat primarily occurs in the mandible, and

284 Periodontal Disease and Overall Health: A Clinician's Guide
is a condition defined by exposed bone in areas of radiation injury. A recent retrospec-tive study of 207 patients who received radiation therapy showed osteoradio-necrosis in 5.5% of patients.44 This com -plication of radiation therapy occurs as a result of decreased wound healing. It canoccur spon taneously, but more frequentlyoccurs after tissue trauma resulting in exposed bone, especially dental extraction.Preradiation assessment for potential prob-lems and appropriate preradiation extrac-tions can help limit postradiation dental extractions and the potential developmentof osteo radio necrosis.
SurgerySurgical resection is an important treat-
ment modality for head and neck cancers.Unfortunately, these surgeries are frequentlydisfiguring and debilitating. Furthermore,infection of the oral cavity can lead to sig-nificant setbacks in recovery, as well as de-lay adjunctive chemotherapy or radiation.Thorough preoperative oral and dental eval-uation can help improve outcomes. Patientswho undergo significant resections often re-quire removable prostheses to maintain func-tion and may also undergo skin grafting aspart of the surgical procedure. There are in-tra-oral prostheses that can aid in speech andnutrition, while extra-oral prostheses canhelp to reduce disfiguration. Regardless ofthe type of prosthesis, a preoperative meet-ing with the patient and family can help themknow what to anticipate postoperatively.Close postoperative monitoring of the surgi-cal site is essential. When applicable, theskin graft site should be monitored for via-bility. During the initial postoperative eval-uation, the patient can be instructed in anoral care regimen, as well as oral opening exercises to aid in a recovery of function.There are several commercially availablemechanical devices that can aid in oral open-ing exercises.45,46
Periodontal Disease and Cancer RiskThis chapter section has focused on the
effect of cancer treatments on oral tissues. Amultidisciplinary approach, with involve-ment of medical and dental professionals, isnecessary to optimize oral care in cancer pa-tients. However, it must be noted that poororal health may be a risk factor for the de-velopment of cancer. Multiple studies havedemonstrated the inflammatory effects ofperiodontal disease, and this inflammatorystate might have an effect on the develop-ment of cancer. There appears to be a rela-tionship between tooth loss and head andneck cancer that is independent of alcoholand tobacco use. Furthermore, tooth loss hasbeen shown to be a risk factor for the develop -ment of esophageal, gastric, and pancreaticcancers. Additionally, periodontal diseasehas been associated with a small, but signif-icant increase in overall cancer risk.29,30
Recommendations for Cancer and Periodontal Disease ManagementPatients with cancer represent a unique
segment of the dental population. Many can-cer treatments are toxic to oral tissues. Onthe other hand, chronic oral infectious andinflammatory conditions such as periodontaldisease and endodontic lesions may con-tribute to cancer risk, and if they persist orexacerbate during cancer therapy, they couldbe a source of life-threatening infection. Pre-treatment dental evaluation of the cancer patient is highly recommended and can helpidentify potential problems and facilitate themanagement of anticipated side effects oftherapy.
Dentists and physicians need to worktogether to plan care for their patients; inparticular, there should be:
A pretreatment oral evaluation for anyexisting periodontal, carious, or endodonticproblems that may be a future source ofchronic infection or may be exacerbatedby cancer treatment or if cancer therapy

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 285
involves treatments that reduce resistance toinfection.
Treatments that may induce xerostomia,such as radiation therapy, should be per-formed only with the understanding that thereduced salivary flow may result in rampantcaries and oral mucosal problems that needto be regularly checked for and treated.
Supplemental Readings
Khosla S, Burr D, Cauley J, Dempster DW, Ebeling PR,Felsenberg D, Gagel RF, Gilsanz V, Guise T, Koka S,McCauley LK, McGowan J, McKee MD, Mohla S,Pendrys DG, Raisz LG, Ruggiero SL, Shafer DM,Shum L, Silverman SL, Van Poznak CH, Watts N, WooSB, Shane E. Bisphosphonate-associated osteonecrosisof the jaw: report of a task force of the American Soci-ety for Bone and Mineral Research. J Bone Miner Res2007;22:1479 –1491.
Craig RG. Interactions between chronic renal diseaseand periodontal disease. Oral Dis 2008;14:1–7.
Kadiroglu AK, Kadiroglu ET, Sit D, Dag A, YilmazME. Periodontitis is an important and occult source ofinflammation in hemodialysis patients. Blood Purif2006;24:400–404.
Williams RC, Barnett AH, Claffey N, Davis M, GadsbyR, Kellett M, Lip GY, Thackray S. The potential impactof periodontal disease on general health: a consensusview. Curr Med Res Opin 2008;24:1635–1643.
Epstein JB, Stevenson-Moore P. Periodontal diseaseand periodontal management in patients with cancer.Oral Oncol 2001;37:613–619.
Jham BC, Reis PM, Miranda EL, Lopes RC, CarvalhoAL, Scheper MA, Freire AR. Oral health status of 207head and neck cancer patients before, during and afterradiotherapy. Clin Oral Investig 2008;12:19–24.
Toth BB, Chambers MS, Fleming TJ, Lemon JC, Martin JW. Minimizing oral complications of cancertreatment. Oncology (Williston Park) 1995;9:851–858;discussion 858, 863–866
REFERENCES1. Mauck KF, Clarke BL. Diagnosis, screening, pre-
vention, and treatment of osteoporosis. Mayo ClinProc 2006;81:662–672.
2. Ettinger MP. Aging bone and osteoporosis: strate-gies for preventing fractures in the elderly. Arch In-tern Med 2003;163:2237–2246.
3. Qaseem A, Snow V, Shekelle P, Hopkins R Jr, Forciea MA, Owens DK. Screening for osteo -porosis in men: a clinical practice guideline fromthe American College of Physicians. Ann InternMed 2008;148:680–684.
4. Polednak AP. Rates of Paget’s disease of boneamong hospital discharges, by age and sex. J AmGeriatr Soc 1987;35:550–553.
5. Chavassieux PM, Arlot ME, Reda C, Wei L, YatesAJ, Meunier PJ. Histomorphometric assessment ofthe long-term effects of alendronate on bone qual-ity and remodeling in patients with osteoporosis.J Clin Invest 1997;100:1475–1480.
6. Fleisch H. Bisphosphonates: mechanisms of action.Endocr Rev 1998;19:80–100.
7. Khosla S, Burr D, Cauley J, Dempster DW, EbelingPR, Felsenberg D, Gagel RF, Gilsanz V, Guise T,Koka S, McCauley LK, McGowan J, McKee MD,Mohla S, Pendrys DG, Raisz LG, Ruggiero SL,Shafer DM, Shum L, Silverman SL, Van PoznakCH, Watts N, Woo SB, Shane E. Bisphosphonate-associated osteonecrosis of the jaw: report of a taskforce of the American Society for Bone and MineralResearch. J Bone Miner Res 2007;22:1479–1491.
8. Sambrook P, Olver I, Goss A. Bisphosphonates andosteonecrosis of the jaw. Aust Fam Physician 2006;35:801–803.
9. Woo SB, Hellstein JW, Kalmar JR. Narrative [cor-rected] review: bisphosphonates and osteonecrosisof the jaws. Ann Intern Med 2006;144:753–761.
10. Proctor R, Kumar N, Stein A, Moles D, Porter S.Oral and dental aspects of chronic renal failure. JDent Res 2005;84:199–208.
11. National Kidney Foundation. K/DOQI ClinicalPractice Guidelines for Chronic Kidney Disease:Evaluation, classification and stratification. Guide-lines K. Part 4. Definition and classification ofstages of chronic kidney disease Am J Kidney Dis2002;39:S46–S75.
12. Missouris GG, Kalaitzidis RG, Cappuccio FP, Mac-Gregor GA. Gingival hyperplasia caused by cal-cium channel blockers. J Hum Hypertens 2000;14:155–156.
13. Craig RG. Interactions between chronic renal dis-ease and periodontal disease. Oral Dis 2008;14:1–7.
14. Spolidorio LC, Spolidorio DM, Massucato EM,Neppelenbroek KH, Campanha NH, Sanches MH.Oral health in renal transplant recipients adminis-tered cyclosporin A or tacrolimus. Oral Dis 2006;12:309–314.
15. Ellis JS, Seymour RA, Taylor JJ, Thomason JM.Prevalence of gingival overgrowth in transplantpatients immunosuppressed with tacrolimus. J Clin

286 Periodontal Disease and Overall Health: A Clinician's Guide
Periodontol 2004;31:126–131.16. Ramalho VL, Ramalho HJ, Cipullo JP, Azoubel R,
Burdmann EA. Comparison of azithromycin andoral hygiene program in the treatment of cyclo -sporine-induced gingival hyperplasia. Ren Fail2007;29:265–270.
17. Fisher MA, Taylor GW, Papapanou PN, RahmanM, Debanne SM. Clinical and serologic markers ofperiodontal infection and chronic kidney disease.J Periodontol 2008;79:1670–1678.
18. Fisher MA, Taylor GW, Shelton BJ, Jamerson KA,Rahman M, Ojo AO, Sehgal AR. Periodontal dis-ease and other nontraditional risk factors for CKD.Am J Kidney Dis 2008;51:45–52.
19. Kshirsagar AV, Moss KL, Elter JR, Beck JD, Offenbacher S, Falk RJ. Periodontal disease is as-sociated with renal insufficiency in the Athero-sclerosis Risk In Communities (ARIC) study. Am JKidney Dis 2005;45:650–657.
20. Borawski J, Wilczyska-Borawska M, StokowskaW, Myliwiec M. The periodontal status of pre-dialysis chronic kidney disease and maintenancedialysis patients. Nephrol Dial Transplant 2007;22:457–464.
21. Saremi A, Nelson RG, Tulloch-Reid M, HansonRL, Sievers ML, Taylor GW, Shlossman M, Ben-nett PH, Genco R, Knowler WC. Periodontal dis-ease and mortality in type 2 diabetes. DiabetesCare 2005;28:27–32.
22. Shultis WA, Weil EJ, Looker HC, Curtis JM,Shlossman M, Genco RJ, Knowler WC, NelsonRG. Effect of periodontitis on overt nephropathyand end-stage renal disease in type 2 diabetes. Diabetes Care 2007;30:306–311.
23. Rahmati MA, Craig RG, Homel P, Kaysen GA,Levin NW. Serum markers of periodontal diseasestatus and inflammation in hemodialysis patients.Am J Kidney Dis 2002;40:983–989.
24. Kadiroglu AK, Kadiroglu ET, Sit D, Dag A, YilmazME. Periodontitis is an important and occult sourceof inflammation in hemodialysis patients. BloodPurif 2006;24:400–404.
25. Kotanko P. Chronic inflammation in dialysis pa-tients—periodontal disease, the new kid on theblock. Oral Dis 2008;14:8–9.
26. Tong DC, Rothwell BR. Antibiotic prophylaxis indentistry: a review and practice recommendations.J Am Dent Assoc 2000;131:366–374.
27. American Cancer Society. Cancer Facts and Fig-ures. American Cancer Society 2008.
28. Williams RC, Barnett AH, Claffey N, Davis M,Gadsby R, Kellett M, Lip GY, Thackray S. The potential impact of periodontal disease on generalhealth: a consensus view. Curr Med Res Opin 2008;24:1635–1643.
29. Michaud DS, Liu Y, Meyer M, Giovannucci E, Joshipura K. Periodontal disease, tooth loss, andcancer risk in male health professionals: a prospec-tive cohort study. Lancet Oncol 2008;9:550–558.
30. Tezal M, Sullivan MA, Reid ME, Marshall JR, Hy-land A, Loree T, Lillis C, Hauck L, Wactawski-Wende J, Scannapieco FA. Chronic periodontitisand the risk of tongue cancer. Arch OrolaryngolHead Neck Surg 2007;133:450–454.
31. Sonis ST. The pathobiology of mucositis. Nat RevCancer 2004;4:277–284.
32. Anonymous. Oral Complications of Chemother-apy and Head/Neck Radiation. Retrieved 3/14/09from NCI web page: http://www.cancer.gov/can-certopics/pdq/ supportivecare/oralcomplications/HealthProfessional/page3/print 2008.
33. Melkos AB, Massenkeil G, Arnold R, Reichart PA.Dental treatment prior to stem cell transplantationand its influence on the posttransplantation out-come. Clin Oral Investig 2003;7:113–115.
34. Keefe DM, Schubert MM, Elting LS, Sonis ST,Epstein JB, Raber-Durlacher JE, Migliorati CA,McGuire DB, Hutchins RD, Peterson DE. Updatedclinical practice guidelines for the prevention andtreatment of mucositis. Cancer 2007;109:820–831.
35. Spielberger R, Stiff P, Bensinger W, Gentile T,Weisdorf D, Kewalramani T, Shea T, Yanovich S,Hansen K, Noga S, McCarty J, LeMaistre CF, SungEC, Blazar BR, Elhardt D, Chen MG, Em-manouilides C. Palifermin for oral mucositis afterintensive therapy for hematologic cancers. N EnglJ Med 2004;351:2590–2598.
36. Epstein JB, Stevenson-Moore P. Periodontal dis-ease and periodontal management in patients withcancer. Oral Oncol 2001;37:613–619.
37. Cousin GC. Oral manifestations of leukemia. DentUpdate 1997;24:67–70.
38. Lynch MA, Ship II. Initial oral manifestations ofleukemia. J Am Dent Assoc 1967;75:932 –940.
39. Barrett AP. Gingival Lesions in Leukemia: A Clas-sification. J Periodontol 1984;55:585–588.
40. Sydney SB, Serio F. Acute monocytic leukemia di-agnosed in a patient referred because of gingivalpain. J Am Dent Assoc 1981;103:886–887.
41. Barker GJ, Epstein JB, Williams KB, Gorsky M,Raber-Durlacher JE. Current practice and knowl-edge of oral care for cancer patients: a survey ofsupportive health care providers. Support CareCancer 2005;13:32–41.
42. Rubenstein EB, Peterson DE, Schubert M, Keefe D,McGuire D, Epstein J, Elting LS, Fox PC, CooksleyC, Sonis ST. Clinical practice guidelines for theprevention and treatment of cancer therapy-inducedoral and gastrointestinal mucositis. Cancer 2004;100:2026–2046.

CHAPTER 17 Dental and Medical Comanagement of Osteoporosis,CHAPTER 17 Kidney Disease, and Cancer 287
43. Epstein JB, Lunn R, Le N, Stevenson-Moore P. Pe-rio dontal attachment loss in patients after head andneck radiation therapy. Oral Surg Oral Med OralPathol Oral Radiol Endod 1998;86:673–677.
44. Jham BC, Reis PM, Miranda EL, Lopes RC, CarvalhoAL, Scheper MA, Freire AR. Oral health status of 207head and neck cancer patients before, during and af-ter radiotherapy. Clin Oral Investig 2008;12:19–24.
45. Toth BB, Chambers MS, Fleming TJ, Lemon JC,Martin JW. Minimizing oral complications of can-cer treatment. Oncology (Williston Park) 1995;9:851–858; discussion 858, 863–856.
46. Chambers MS, Toth BB, Martin JW, Fleming TJ,Lemon JC. Oral and dental management of the can-cer patient: prevention and treatment of complica-tions. Support Care Cancer 1995;3:168–175.
288 Periodontal Disease and Overall Health: A Clinician's GuideCHAPTER 18The Role of the Professionalin Educating the Public About the Importance of Oral Health
Casey Hein
INTRODUCTIONIt has been recognized for some time
that health outcomes are, in part, a functionof health literacy and education of the public.1The level of health literacy, or level of knowl- edge necessary to guide healthy living withina population, is one of the strongest socialdeterminants of health within a society. Lim-ited healthcare literacy has been implicated inundermining the public’s ability to fully ben-efit from what healthcare systems have to of-fer. Lack of oral health knowledge presentsan obstacle to better oral healthcare in theUnited States;2,3 almost half of all Americanslack adequate oral health skills, which mayaccount for billions of dollars in addedhealthcare costs each year.2,3 It is importantto consider whether or not lack of adequatepractitioner-to-patient communication maybe implicated in the challenges we face re-garding oral health literacy.
Oral diseases are often a source of over-looked infection and systemic inflammationthat has the potential to affect overall health.As such, oral diseases have been termed a“silent epidemic.”4 Given the strength of evidence that supports inter-relationships between oral and overall health, educatingconsumer-patients about the threat that oralinfections may pose to general health canno longer be considered optional. Both den-tal and nondental healthcare practitioners,such as physicians, nurses, and allied health-care providers, share in the responsibility toeducate the public regarding the significanceof oral health in achieving and sustaining
whole-body health. Codes of professionalconduct convey a responsibility of healthcarepractitioners to educate patients. Health out-comes—beyond the oral cavity—may bepositively influenced by effective patient ed-u cation and health literacy campaigns tar-geting oral health.
Information about the relationship be-tween oral and systemic health started to bedisseminated to the public from a number ofsources beginning in the 1990s. Various pub-lic relations campaigns have increased theawareness of the connection between oraland systemic health among a broad audienceof consumer-patients. Information from thelay press, mainstream radio and television,university- and government-sponsored pub-lic health outreach to local communities, in-surance industry campaigns, and commercialadvertising associated with oral care prod-ucts have provided highly visible and effec-tive mechanisms for educating the publicabout the significance of oral health. How-ever, nothing can be as powerful as practi-tioner-to-patient education. The time dentistsand dental hygienists spend with in di vidualpatients presents a valuable opportunity tocommunicate credible findings of researchrelated to systemic inflammation associatedwith oral infections. In addition, as point-of-care providers, dental practitioners maybe uniquely positioned to identify patientswho may be at risk for chronic diseases, suchas diabetes and atherosclerotic diseases,which share risk factors common to oral diseases.

Chapter 18Chapter 18 The Role of the Professional in Educating the Public About the Importance of Oral Health 289
As the depth and breadth of evidence tosupport a relationship between periodontaldiseases and several common systemic in-flammatory diseases continues to expand,the preponderance of evidence suggests thatdental providers have a responsibility to ap-propriately and effectively communicate thisinformation to patients.
In the case of diabetes, evidence frompilot trials shows that treatment of perio -dontal disease may improve metabolic con-trol of diabetes.5-7 However, large-scale, de-finitive trials are still needed to establish theefficacy of periodontal intervention. Simi-larly, in the case of pregnancy outcomes,several pilot trials have shown a reduction ofadverse pregnancy outcomes associated withperiodontal treatment.8,9 However, a largestudy failed to show a reduction in adversepregnancy outcomes associated with treat-ment of periodontal disease.10 Several stud-ies have assessed the effect of periodontaltherapy on cardiovascular outcomes andhave shown improvement in endothelialfunction.11-13 However, large, randomized,controlled trials are needed to look at the ef-fects of perio dontal therapy on cardiovascu-lar outcomes. Even though there are not yetdefinitive data on the effects of periodontaltreatment on several conditions associatedwith perio dontal disease, association dataare strong. Hence, educating patients aboutoral-systemic relationships is appropriate toensure that their treatment decisions are wellinformed.
The medical profession has respondedto emerging evidence of periodontal-sys-temic relationships with a number of arti-cles that call attention to the likelihood thatperiodontal disease is an often overlookedand unrecognized source of infection with thepotential to evoke a systemic inflammatoryresponse.14-16 As these kinds of evidence-based, authoritative statements are circulatedwithin the medical professions, it is reason-able to assume that more and more phy si-
cians and allied healthcare providers will acknowledge the significance of oral healthin achieving and sustaining overall health. Asa result, they will begin to screen for oral dis-eases, educate patients about oral-systemicconnections, and pursue collaborative rela-tionships with dental practitioners in the co-management of inflammatory-driven diseasestates. Already, informally gathered informa-tion from physicians in specialties such as en-docrinology, cardiology, obstetrics, rheuma-tol ogy, pulmonology, and nephrology, amongothers, substantiate that medical practitionersare beginning to incorporate findings of cred-ible research of oral-systemic relationshipsinto their practices. Simultaneously, medicalprotocols that include periodontal evaluation,treatment, and monitoring of clinical out-comes related to the care of patients who maybe at greater risk for cardiovascular disease(CVD) and diabetes may also begin to emerge.
Educational ObjectivesAfter reviewing the information pre-
sented in this chapter, readers should be able to:• Discuss how the limitations in oral
health literacy present a barrier to ef-fective prevention, diagnosis, andtreatment of oral diseases.
• Describe various sources of infor-mation and statistics about the rela-tionship between oral and systemichealth that suggest consumer-patientsare aware of the importance of oralhealth in achieving and maintainingoverall health.
• Identify various hurdles dental prac-titioners face in effectively educatingpatients about oral-systemic healthand describe ways to address these obstacles.
• Describe the responsibility of dentalprofessionals in ensuring that onlyscientifically supported evidence oforal-systemic relationships is com-municated to patients.

290 Periodontal Disease and Overall Health: A Clinician's Guide
• Elaborate upon the professional de-velopment process that will distin-guish individual dentists and dental hy -gienists as authoritative experts in evi -dence of oral-systemic relationships.
• Identify ways in which dentists anddental hygienists can influence thepublic’s perception of the importanceof oral health outside the practice setting.
THE PROCESS OF CHANGEIN INFLUENCING THE
PUBLIC’S PERCEPTION OF THEIMPORTANCE OF ORAL HEALTH
“Because oral diseases in general aretreatable and usually not life threatening,they have been erroneously perceived ashaving little relationship to other aspects ofhealth, often being viewed as of minor im-portance in the social and economic con-text.”17 This opinion reflects the all-too-realdisconnect between oral and overall healthand therefore has far-reaching implications.Segregation of the oral cavity from the restof the body—and consequently the historicalschism between dentistry and medicine—has helped contribute to the disparities thatcurrently exist in oral health among Ameri-cans.4 The failure to recognize oral health asintegral and essential to general health hasalso adversely impacted healthcare policy.18
In 2009, greater appreciation of the signifi-cance of inflammation in prevention andmanagement of chronic diseases and mount-ing evidence in support of oral-systemic inter-relationships at genetic and molecular levelsare changing nondental healthcare providers’perceptions of the importance of oral health.Indeed, the shift from an infection model toan inflammation model relative to the threatthat perio dontal disease poses to overall health,has gar nered the attention of the medical com-munity. Medical journals—including some ofthe most prestigious—are reporting evidenceof oral-systemic relationships with increased
frequency. In addition, governmental reports,4,19
educational institutions,20,21 and professionalassociations22 have called for educational re-form that would increase nondental health-care providers’ knowledge of oral health,and collaborative models of care that wouldbring together dental and nondental health-care providers to focus on interprofessional,comprehensive chronic disease managementthat includes oral care.
The insurance industry has investigatedthe potential cost savings associated withtreatment of periodontal disease, and foundthat medical costs associated with chronicdiseases such as CVD and diabetes may besignificantly reduced when patients aretreated for periodontal disease.23,24 Althoughthese studies do not prove cause and effect,they are sufficient for insurance companiesto be more liberal in their coverage for peri-odontal therapy and maintenance for theirclients with diabetes and CVD. In addition,various guidelines created by health depart-ments of state agencies have begun to ad-dress the importance of oral health in theoverall health of their citizenry.25,26
Changes in public policy, increased in-surance reimbursement, and improved med-ical/dental education undoubtedly will facil-itate interprofessional collaboration betweenthe healthcare professions; however, thismagnitude of change is unlikely to happen inthe short term. In the interim, educating thepublic through commercially supported me-dia campaigns, outreach from professionalorganizations and universities, and individ-ual practitioner-to-patient education are es-sential in helping the public reprioritize theimportance of oral health and its implica-tion to overall health.
The answers to the following four questions provide a reference point to guidepractitioner-to-patient communication and articulate messages that are essential to successful patient education in oral-systemichealth:

Chapter 18Chapter 18 The Role of the Professional in Educating the Public About the Importance of Oral Health 291
1. How much do consumer-patientsknow about the threat inflammationposes to whole body health and oral-systemic relationships?
2. How important do consumer-patientsbelieve oral health is to achievingand sustaining overall health?
3. How well are dental practitioners do-ing regarding educating patientsabout oral-systemic relationships andwhat are the hurdles to effectivelycommunicating this information toconsumer-patients?
4. What research should be credibly com- municated to patients about the rela-tionship between periodontal diseaseand inflammatory-driven diseasestates, such as coronary heart dis-ease, stroke, diabetes, and adversepregnancy outcomes?
5. In addition to individual practitioner-to-patient communication, what typesof activities could dental practitionerspursue to change the perception ofnondental healthcare providers aboutthe importance of oral health, therebyincreasing the public’s awareness oforal-systemic relationships?
CONSUMER-PATIENTS’KNOWLEDGE ABOUT
ORAL-SYSTEMIC LINKS, THESIGNIFICANCE OF ORAL HEALTH,
AND THE THREAT INFLAMMATIONPOSES TO GENERAL HEALTH
Help from Mainstream MediaOver the last decade there have been
numerous sources of information from main-stream media about the relationship betweenoral and systemic health, including lay pub-lications,27,28 television,29 and radio.30 In2004, Time Magazine27 committed an entireissue, “The Secret Killer,” to help readers ex-plore the link between inflammation and var-ious life-threatening conditions such as heart
disease. The article introduced readers tosome fairly sophisticated scientific conceptsthat describe how the body’s efforts to healthe damage produced by infection and in-flammation often end up causing permanentdamage to certain organs and increasing therisk for various systemic diseases. The arti-cle specifically discussed the potential of pe-riodontal disease to elicit such a cascade ofevents: “It appears that some people are moresensitive to plaques and tangles than others.Perhaps they have a genetic predisposition.Or perhaps a long-running, low-grade bac-terial infection, like gum disease, keeps theinternal fires burning and tips the balancetoward chronic infection.”27 If readers cancomprehend such sophisticated information,it is reasonable to assume the public is becom -ing increasingly aware of the relationship be -tween periodontal disease and inflammatory-driven disease states.
CNN News jump-started the year 2009with a segment on “How to Live Longer,”which aired on January 2 and was hosted byDr. Sanjay Gupta, CNN’s Chief Medical Cor-respondent.29 Gupta discussed several simplemodifications to lifestyle that he proposedwould net increased longevity. He cited usingdental floss as the number one recommenda-tion, explaining that oral care could reduce in-flammation, a known contributor to increasedrisk for heart disease. These are only a few ofthe many examples of information on oral-systemic health that have been generatedthrough mainstream media sources.
A Snapshot of What the Public KnowsPiecing together data compiled by vari-
ous professional and nonprofit organizationsand the insurance industry provide a snap-shot of how well the consumer-patient publicunderstands the importance of oral health inachieving and maintaining overall health.Findings of a survey conducted in the year2000 by the American Dental Association indicated that the vast majority of consumer-

292 Periodontal Disease and Overall Health: A Clinician's Guide
patients are aware that there is a link betweenperiodontal disease and systemic conse-quences, and more than 99% recognize thatprevention of periodontal disease is an im-portant step in maintaining oral health.31
Other data indicate that 85% of Amer-icans believe there is a strong connectionbetween oral health and general health.32 Thelarge majority (77%) of Americans believethat personal maintenance of their oral healthis very important to their own overallhealth,33 and 80% of Americans agree thattaking care of one’s mouth, teeth, and gumsis “absolutely needed.”2 When askedwhether “you take dental health into accountwhen rating your overall health,” 78% of re-spondents of a randomly selected nationallyrepresentative survey of US adults indicatedthat they did.34 A correlational analysis ofthe same data showed that the public’s ratingof oral and overall health were strongly re-lated (r = .46, p < .001). These data suggestthat oral health and general health status areclearly connected in the consciousness ofAmericans.34
Patients’ Concerns AboutPeriodontal Disease
Of 1,000 subjects from a randomly selected, nationally representative survey ofUS adults, 85% reported that it was “very im-portant” for dentists to examine their mouthsfor periodontal disease.34 Other data confirmthat patients want to be evaluated for peri-odontal disease because they are concernedabout the systemic implication of periodontaldisease. When briefly educated about the riskof systemic consequences related to peri-odontal disease, and asked what kind of treat-ment they would prefer when they next visitthe dentist, two out of three consumer-pa-tients from a nationally representative sampleopted for periodontal examinations instead ofroutine prophylaxis.35 The survey questionand results of the consumer-patient responsesare included in Figure 1.
The Strength of PatientEducation Campaigns
Various professional organizations suchas the American Academy of Periodontology(http://perio.org/consumer/index.html), theoral care industry (http://www.colgate.com/app/ColgateTotal/US/EN/MBHC.cvsp), andnonprofit organizations such as the AmericanDiabetes Association (http://www.diabetes.org)among others, have mounted impressive web-based patient education campaigns targetingoral-systemic health.
The contribution of medical providersin educating patients about the potential ofperiodontal disease to elicit systemic in-flammation and increased risk for chronicdisease states cannot be overlooked. In aFebruary 2008 issue of the Journal of theAmerican Medical Association,36 a patienteducation page (Figure 2) was dedicated toa discussion of periodontal disease and itspotential association to heart disease, stroke,and premature birth. The article briefly de -fined the causes, signs and symptoms, preven -tion, and treatment of periodontal disease,and offered other resources for additionalinformation.
Summary Points1. Consumer-patients are very aware of
the connection between oral healthand general health.
2. A number of publications from thelay press and mainstream radio andtelevision have done an excellent jobof educating consumer-patients onthe threat that inflammation poses towhole body health and the potentialof periodontal disease to incite an inflammatory response.
3. Consumer-patients seem to be awarethat prevention of periodontal diseaseis important in maintaining overallhealth, and subsequently want to beevaluated for periodontal disease be-cause they are concerned about the

Chapter 18Chapter 18 The Role of the Professional in Educating the Public About the Importance of Oral Health 293
systemic implication of perio dontaldisease.
4. There are numerous sources of infor-mation available for educating pa-tients in oral-systemic health, includ-ing websites designed for direct accessof consumer-patients and printed ma-terials supplied by professional or-gan izations that can be disseminatedby healthcare practitioners.
DEVELOPING EFFECTIVECOMMUNICATION WITH PATIENTSABOUT ORAL-SYSTEMIC HEALTH
The American Dental Association (ADA)Weighs in on Oral Health Literacy
The ADA has defined oral health liter-acy as “the degree to which individuals havethe capacity to obtain, process, and under-
stand basic health information and servicesneeded to make appropriate oral health de-cisions.”3 It is recognized that people withlow oral health literacy are often less likelyto seek preventive care, comply with pre-scribed treatment, and maintain self-care reg-imens; as such, limited oral health literacy isa potential barrier to effective prevention,diagnosis, and treatment of oral disease.3
Addressing Oral Health LiteracyWithin the Dental and Dental
Hygiene ProfessionsIn a 2004 National Institutes of Medi-
cine report, it was estimated that 90 millionadult Americans have difficulty in obtaining,processing, and understanding basic healthinformation and services needed to make ap-propriate health decisions.1 This calls atten-tion to the importance of healthcare providers
Figure 1. Question on Consumer-Patient Survey Conducted in 2005.
Adapted from Hein C et al. Presented at 83rd Annual Session of the American Dental Hygienists’ Association; Orlando, Florida; June 2006.35
The survey question first provided a very brief overview of the risk “gum disease”may pose in increasing the risk for serious systemic diseases. Then consumer-patientswere asked to respond to how important it is to be examined for periodontal disease attheir next check-up visit. Results follow.
It is estimated that 50%–80% of adults have some level of gum disease. More important thoughis that over the last 10 years there has been increasing evidence that periodontal disease may beassociated with serious systemic consequences. This includes the potential for increased risk forheart disease and stroke, and for pregnant women with periodontal disease an increased risk ofdelivering preterm, low birth weight infants. Individuals with impaired immune systems andperiodontal disease may have an increased risk for certain respiratory diseases. In addition,diabetics have an increased risk for developing periodontal disease and periodontal disease indiabetics often makes metabolic control of blood sugar levels very difficult. For this reason, it isvery important that diabetics have thorough periodontal evaluations.
Question: Given the evidence that periodontal disease may be linked to these kinds of seriouswhole body diseases/conditions, at your next visit to the dentist’s office, would you rather beexamined for periodontal disease or have your teeth cleaned?
! Examined for periodontal disease ! Have my teeth cleaned
Results: There were 1,415 responses to this question. 945 (66.78%) of consumer-patients who responded answered that given the evidence that periodontal disease may be linked to seriouswhole body diseases/conditions, they would rather be examined for periodontal disease instead ofhaving their teeth cleaned at their next visit to the dentist’s office.
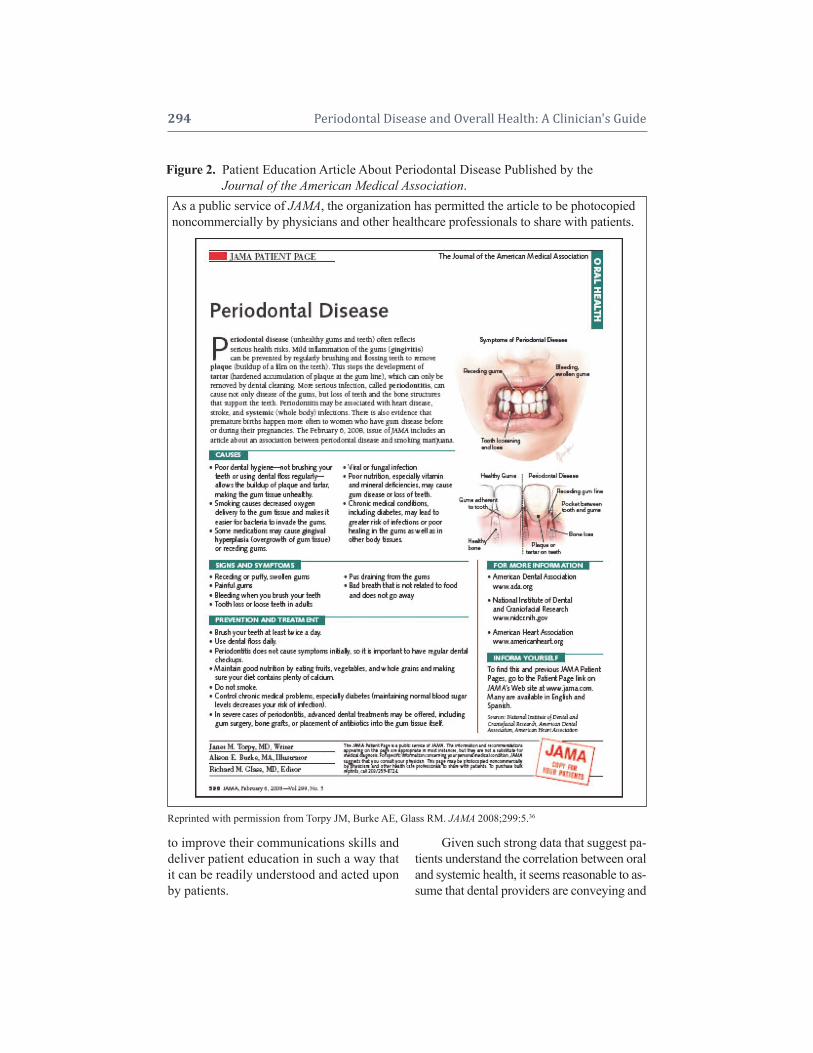
294 Periodontal Disease and Overall Health: A Clinician's Guide
to improve their communications skills anddeliver patient education in such a way thatit can be readily understood and acted uponby patients.
Given such strong data that suggest pa-tients understand the correlation between oraland systemic health, it seems reasonable to as-sume that dental providers are conveying and
Figure 2. Patient Education Article About Periodontal Disease Published by the Figure 2. Journal of the American Medical Association.As a public service of JAMA, the organization has permitted the article to be photocopiednoncommercially by physicians and other healthcare professionals to share with patients.
Reprinted with permission from Torpy JM, Burke AE, Glass RM. JAMA 2008;299:5.36

Chapter 18Chapter 18 The Role of the Professional in Educating the Public About the Importance of Oral Health 295
reinforcing this information. However, evi-dence that dental practitioners are doing anadequate job in educating their patients isnot readily apparent when searching the pro-fessional literature, or reviewing survey datagenerated by professional organizations. Al-though more than 75% of 1,000 subjects ina randomly selected, nationally representa-tive survey of US adults believe oral healthis integral to overall health, it is disconcert-ing to find that in the same survey, only 51%responded that their dentist discussed the re-lationship between oral and overall health.34
It has been estimated that 33% of den-tal patients may not know that periodontaldisease needs to be treated and should not beleft alone;2 another 33% believe that a littlebleeding from brushing is normal.2 While83% of US adults may say their dentist istheir primary source of information on oralcare practices, a significant portion of theseadults also report that they have not dis-cussed their oral health issues with a dentalprofessional.2 This is especially troublingwhen considering that more than half ofthe adults living in the US experience oneor more oral health conditions.2
These types of responses from con-sumer-patients mirror the disturbing find-ings reported by various researchers whenthey studied dental providers’ track recordsin providing smoking cessation counseling.For instance, it has been estimated that only30%–50% of dentists and 25% of dental hygienists in the US ask their patients aboutsmoking,37,38 and the cessation advice pro-vided in dental offices has been described as“rather ad hoc and somewhat superficial.”39
Another study found that when comparingtobacco-use cessation services provided byvarious types of healthcare providers, inter-ventions by dental providers ranked lowest(compared with physicians, mental healthcounselors, and social workers) in terms ofboth quantity and quality of services.40 Lackof training and incentives were most often
cited to explain the reluctance of dentistsand dental hygienists to provide tobacco ces-sation interventions.41
Dismantling the Hurdles toEffectively Educate PatientsAbout Oral-Systemic Health
By virtue of the frequency by whichpeople visit dentists for checkups and routineprophylaxis, dentists and dental hygienistsare in a unique position to deliver a pivotallyimportant message to patients about oral- systemic health. However, this opportunity isoften forfeited. One of the greatest hurdles toeffectively communicating informationabout issues related to oral-systemic health isthat dentists are often reluctant to discuss is-sues that patients may perceive as unpopular.However, evidence that patients are con-cerned about periodontal disease suggeststhat the opposite may be true.34,35 Some den-tists may believe that their involvement ingreater systemic sequelae of oral infectionsand inflammation falls beyond their scope ofpractice. However, data suggest a growingtrend that patients are starting to view den-tists as overall healthcare providers.34 Ac-cordingly, it is crucial that dentists lead thecharge in conveying to patients the impor-tance of maintaining both oral and overallhealth.34 Other hurdles associated with ef-fectively communicating important infor-mation about oral-systemic health includethe barriers listed below.
Lack of Training in Oral-Systemic Science Oral-systemic science may not have
been emphasized during a dentist’s or dentalhygienist’s formal education and training.Many are unclear about the credibility of thescience or strength of evidence; others areuncertain about the etiological mechanismsthat have been implicated in many oral-sys-temic relationships and are uncomfortablewith how these inter-relationships should beexplained to patients.

296 Periodontal Disease and Overall Health: A Clinician's Guide
Organized dentistry has recently takenon the monumental task of planning for edu-cational reform, much of which is related torevision of curricula to include more com-prehensive education in oral-systemic rela-tionships, immunology, genetics, and molec-ular biology.21,42-44 For professionals already inpractice, there exists numerous opportunitiesfor continuing education in oral-systemic science, and a routinely conducted literaturesearch of studies related to oral-systemic re-lationships, that includes both medical anddental journals, will provide practitioners withthe most up-to-date information.
Ineffective Communication SkillsA dentist or dental hygienist may have
inadequate communication skills. Practitioner-to-patient counseling is the
most effective way to increase a consumer-patients’ understanding of the significanceof oral health, assuming practitioners have adequate communication skills. It is unclearwhether or not patients believe their dentistsare as concerned with their overall healthas they are with their oral health.34 As such,dentists and dental hygienists must start toconsider the liability associated with a lim-ited view of their responsibility to ensurepatients’ oral-systemic health, become pro -active in advocating for comprehensive education of patients, and master effective communication skills.
The first step to increasing patients’ un-derstanding of oral-systemic relationships isto provide the right kind of training to ensurethat all the members of the dental team areable to effectively communicate key mes-sages related to oral-systemic health, and beprepared to appropriately answer patients’questions. The ADA has passed a resolutionto seek external funding to support the de-sign and execution of a comprehensive oralhealth literacy awareness and education strat-egy targeting the entire dental team.3 A re-lated resolution encourages the development
of oral health literacy continuing educationprograms to train dentists and allied dentalteam members to communicate effectivelywith patients who have limited literacy skills.3
Scheduling LimitationsScheduling often does not allow for
time to counsel patients; likewise, there areno incentive or reimbursement mechanismsavailable for patient education/counseling.
Regardless of whether or not there is anincentive to educate and counsel patients,dental providers are increasingly expectedto perform these important services. A surveyof the public’s perception of dentistry indi-cates that consumer-patients may see thedentist’s role as much larger than the prac-ticing dentist sees it, and that patients maysee their dentist more as a physician thandentists themselves do.34 Patients expect den-tists to discuss serious health issues they mightbe confronting and not just discuss the tra-ditional expectations of dental services.34
A well-recognized practice management expert45 noted that compared to previousdecades, more dental patients are “shoppingaround” for dental care and changing dentalpractices. More comprehensive service of-ferings was cited as an important factor inpatients’ selection of dentists, and deliveringexceptional customer service, advocating pa-tient education, and developing customizedhome care regimens were cited as key in developing long-term patient retention. Theauthor concluded, “By demonstrating astrong commitment to customer service, ed-ucation, and home care, patients recognizethat oral healthcare pro viders are interested intheir well-being rather than simply treatingproblems.”45 It seems clear that the publicwants a different approach to dental care,and those practitioners who provide effec-tive patient education and risk counselingservices will be well positioned to grow theirpractices, even during economically chal-lenging times.

Chapter 18Chapter 18 The Role of the Professional in Educating the Public About the Importance of Oral Health 297
Summary Points1. Because of a profound limitation in
oral health literacy within the US, alarge portion of the public is not ableto obtain, process, and make appro-priate decisions about their oralhealth. This disparity contributes toavoidable healthcare spending in themagnitude of billions of dollars eachyear. The American Dental Associa-tion recognizes the severity of thelack of oral health literacy in the USand is taking steps to address thisdisparity.
2. It is unclear whether or not the ma-jority of dentists and dental hygien-ists are proactively educating patientsabout the relationship between oraland systemic health; however, this isan important factor to consider in de-termining why oral health literacy isso limited within the US.
3. There are a number of hurdles thatprevent dental practitioners from ef-fectively communicating informationabout issues related to oral-systemichealth. Dentists and dental hygienistsmust address issues related to inade-quate education in oral-systemic re-lationships, philosophies of practicethat may be outdated or preclude pro-viding this level of patient education,and concerns relative to the lack ofcompensation related to providingpatient education. Failure to providepatient education services has bothethical and legal implications.
KEY AND CREDIBLEINFORMATION TO COMMUNICATE
TO PATIENTS ABOUT THE LINKBETWEEN PERIODONTAL DISEASE
AND SYSTEMIC DISEASESInformation about the relationship
between oral and systemic health originatesfrom numerous sources, including consumer
publications, television, radio, continuingeducation programs, and insurance industrycampaigns. Other important sources of in-formation include professional and not-for-profit organizations, such as the AmericanAcademy of Periodontology and the Amer-ican Diabetes Association, as well as fromhealth professionals and industries marketingoral care products. It should be noted that thesource that patients often put the greatestweight on is information coming from theirdentist or dental hygienist. It is therefore ofprime importance that the dental communityand dental paraprofessionals stay currentwith emerging research about oral-systemicconnections. Oral health professionals areresponsible for filtering second-hand sourcesof information on oral-systemic health(sources other than well-respected scientificliterature) to ensure that what is communi-cated to patients is scientifically sound.
The process of professional develop-ment that will prepare individual dentistsand dental hygienists to become authoritativeexperts in the evidence of oral-systemic re-lationships is illustrated in Figure 3. As prac-titioners proceed through this process—fromsurveillance to clinical application and pub-lic outreach—confidence in how to commu-nicate this information to patients becomes anatural by-product of the self-learning thatoccurs throughout the process.
Key and Credible Sound Bitesfor Patient Education
What evidence of oral-systemic rela-tionships should we confidently communi-cate to patients? The following statements,communicated in layman’s terms, are wellsupported by scientific evidence, and easilyunderstood by patients. These statementsprovide an explanation of the potential forperiodontal pathogens and their endotoxinsto gain access to the vasculature and inciteinflammation and a cascade of pathologicalevents in distant organs. This information is
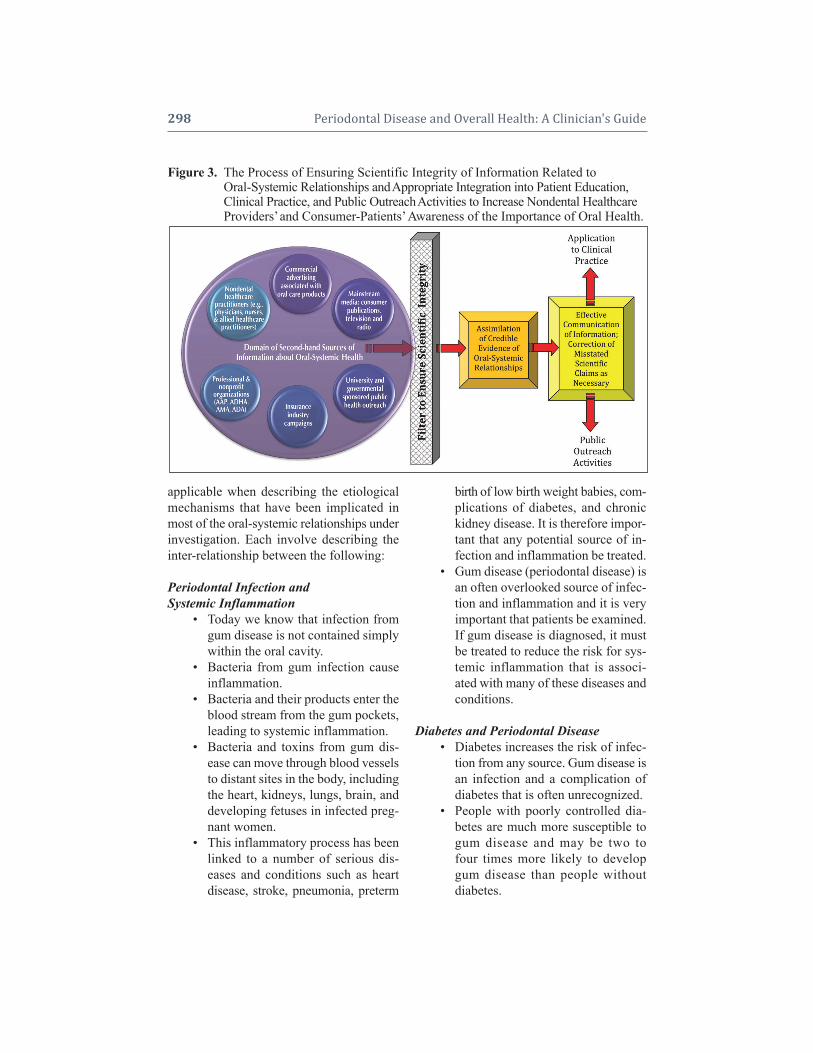
298 Periodontal Disease and Overall Health: A Clinician's Guide
applicable when describing the etiologicalmechanisms that have been implicated inmost of the oral-systemic relationships underinvestigation. Each involve describing theinter-relationship between the following:
Periodontal Infection andSystemic Inflammation
• Today we know that infection fromgum disease is not contained simplywithin the oral cavity.
• Bacteria from gum infection causeinflammation.
• Bacteria and their products enter theblood stream from the gum pockets,leading to systemic inflammation.
• Bacteria and toxins from gum dis-ease can move through blood vesselsto distant sites in the body, includingthe heart, kidneys, lungs, brain, anddeveloping fetuses in infected preg-nant women.
• This inflammatory process has beenlinked to a number of serious dis-eases and conditions such as heartdisease, stroke, pneumonia, preterm
birth of low birth weight babies, com-plications of diabetes, and chronickidney disease. It is therefore impor-tant that any potential source of in-fection and inflammation be treated.
• Gum disease (periodontal disease) isan often overlooked source of infec-tion and inflammation and it is veryimportant that patients be examined.If gum disease is diagnosed, it mustbe treated to reduce the risk for sys-temic inflammation that is associ-ated with many of these diseases andconditions.
Diabetes and Periodontal Disease• Diabetes increases the risk of infec-
tion from any source. Gum disease isan infection and a complication ofdiabetes that is often unrecognized.
• People with poorly controlled dia-betes are much more susceptible togum disease and may be two tofour times more likely to developgum disease than people without diabetes.
Figure 3. The Process of Ensuring Scientific Integrity of Information Related to Figure 3. Oral-Systemic Relationships and Appropriate Integration into Patient Education,Figure 3. Clinical Practice, and Public Outreach Activities to Increase Nondental HealthcareFigure 3. Providers’ and Consumer-Patients’ Awareness of the Importance of Oral Health.

Chapter 18Chapter 18 The Role of the Professional in Educating the Public About the Importance of Oral Health 299
• The presence of gum disease in-creases the risk of worsening glycemiccontrol over time.
• Research suggests gum diseasecauses inflammation throughout thebody, making it more difficult for pa-tients with diabetes to utilize insulin.This may cause hyperglycemia andmake it difficult for patients and theirphysicians to regulate blood sugarlevels. This increases the risk forcoronary heart disease.
• Good glycemic control, an HbA1cvalue of less than 6% for most patients,significantly reduces the risk for theserious complications of diabetes, in-cluding gum disease.
• Although more research needs to beconducted, studies that have meas-ured the difference in HbA1c aftertreatment of gum disease report im-provements in blood glucose controlover time.
• Patients with poor blood sugar controlmay have more rapid recurrence of deeppockets and less favorable long-termresponse to treatment of gum disease.
• When gum disease goes untreated inpatients with diabetes, they are put atgreater risk for developing long-termcomplications associated with diabetes,such as CVD and kidney disease.
• Patients should be counseled to com-ply with their healthcare provider’srecommendations for HbA1c testingat least every three months, and to re-quest that physicians forward copiesof test results to their dentists. Thisallows the dental provider to monitorblood sugar levels and the health oftheir patients’ gums.
Periodontal Disease and Increased Riskfor CVD
• Accumulated evidence suggests thatindividuals with gum disease may
have a moderately increased risk forcoronary heart disease and stroke.
• It is important to identify those indi-viduals who may be at greater riskfor heart disease or stroke and whohave gum disease.
• It is important to understand how gumdisease and increased risk for heartdisease and stroke may be related.
• When there is inflammation withinheart tissues, arteries become lesselastic while the lumen of affectedarteries become narrower and morerestricted.
• When arteries become more nar-rowed, blood clots may form andsmall particles of clots may breakoff, accumulate, and clog arteries,impeding blood flow. This can resultin a heart attack, stroke, or pul-monary embolism, depending on thelocation of the blood clot.
• It is known that damage from infec-tion and inflammation can accumulateover a lifetime, increasing the cumu-lative risk for heart disease and stroke.
• There is some early evidence sug-gesting that treatment of gum dis-ease may improve the flow of bloodto the coronary arteries; however,more research is needed before it isknown for certain how gum treat-ment affects the heart. In the mean-time, the American Academy of Perio dontology has determined thattreatment of gum disease may preventthe onset or progression of athero -sclerosis-induced diseases.
Periodontal Disease and Increased Riskfor Adverse Pregnancy Outcomes
• Infection from any source increasesthe risk of complications during preg-nancy. Gum disease may be one of theinfections that poses a threat to healthypregnancy.

300 Periodontal Disease and Overall Health: A Clinician's Guide
• It is estimated that approximately40% of pregnant women have someform of gum disease.
• Evidence suggests that in some pop-ulations, pregnant women who havegum disease may be at two- to five-times greater risk for various preg-nancy complications, including pre -term birth, pre-eclampsia, gestationaldiabetes, and delivery of low birthweight infants.
• Now that oral healthcare providersand obstetricians recognize theremight be a link between inflamma-tion in the body and problems duringpregnancy, the goal is to eliminateall oral inflammation before and dur-ing pregnancy.
• Oral health before and during preg-nancy may be important for prevent-ing adverse pregnancy events, how-ever, this has yet to be well established.
• Research has confirmed that gumtreatment during pregnancy is safeand improves maternal oral health.
Periodontal Disease and Increased Riskfor Respiratory Infection
• Research suggests that institutional-ized elderly people and patients inintensive care units who have poororal hygiene may be at greater riskfor pneumonia and other respiratoryinfections.
• Oral pharyngeal surfaces, includingthe teeth, can serve as a reservoir forpathogenic bacteria that are known tocause pneumonia. These bacteria canbe aspirated into the lungs wherethey may cause respiratory infections—many of which can be fatal.
• Respiratory infections related to poororal hygiene in institutionalized pa -tients in intensive care units and nurs-ing homes can be reduced by effec-tive oral plaque control measures.
• Cytokines are a type of chemical nor-mally produced by the body to de-fend itself against inflammation.When produced in gum tissue as a re-sult of infection, cytokines may causeinflammation of the lower respira-tory airway following aspiration ofbacteria known to cause pneumonia.This causes the lining of the airwaysto become more vulnerable to in-vading bacteria. Therefore, it is im-portant to identify elderly individualswho may be at greater risk for respi-ratory problems because of undiag-nosed and untreated gum disease.
General Advice to Patients• It has become increasingly clear that
prevention, diagnosis, and treatmentof periodontal disease are very im-portant in maintaining overall healthduring the aging process.
• Patients should be advised to come toeach dental appointment with an up-to-date list of prescribed and over-the-counter medications they are taking sothe dentist or dental hygienist can beaware of any agents that may affectthe oral cavity or be a contraindicationfor certain types of dental treatment.
• Up-to-date information regarding thestatus of the patient’s overall sys-temic health needs to be related tothe oral healthcare provider.
• Patients need to be counseled to pro-vide information about oral health—especially when gum disease has beendiagnosed—to their other medicalproviders.
• Oral healthcare providers should con- tinually reinforce good oral hygieneand home care. Inclusion of an anti-bacterial toothpaste or mouth rinsein the home care regimen can helpreduce dental plaque build-up andgingivitis.

Chapter 18Chapter 18 The Role of the Professional in Educating the Public About the Importance of Oral Health 301
Summary PointsNot only do oral healthcare providers
have an ethical obligation to educate patientson the relationship between oral health andgeneral health, dentists and dental hygienistsare responsible for ensuring that what iscommunicated to patients and the public atlarge is scientifically supported.
1. Given the increasing preponderanceof evidence about oral-systemic rela-tionships generated from second-handsources, the task of ensuring scien-tific integrity of information can bechallenging. If practitioners systemizethe process of updating their knowl-edge base through reading peer- reviewed articles on a routine basis,this will provide an excellent screenthrough which to filter informationfrom the domain of second-hand, of-ten unreliable, sources of information.
2. Although there is much that is still in-conclusive about certain oral-systemicrelationships, there does exist suffi-cient evidence of the relationship be-tween periodontal disease and its rolein amplifying systemic inflammationand increased risk for heart disease,stroke, adverse pregnancy outcomes,complications of diabetes, and in-creased risk for respiratory infectionsin institutionalized patients. Effectivecommunication of this information is
a responsibility of all dentists and dental hygienists.
OUTREACH ACTIVITIES TOINFLUENCE THE PUBLIC’S
PERCEPTION OF THEIMPORTANCE OF ORAL HEALTH
The number of things that dentists anddental hygienists can do to reach out to thecommunity to create greater awareness of oral-systemic health is limited only by individualinitiative and a commitment to change the perceptions of nondental healthcare providersand the public regarding the importance oforal health. Table 1 lists a number of outreach activities that oral healthcare providers have reported as being successful in increasing theawareness of oral-systemic relationships inphysician communities and the public at large.
Beyond the practice setting, dentistsand dental hygienists have the opportunity toengage in novel outreach activities that havethe potential to increase awareness of perio -dontal-systemic relationships. These typesof endeavors are valuable in bringing aboutimprovement in oral health literacy and theyprovide excellent opportunities for practi-tioners to build interpersonal collaborationand enhance their practices.
CONCLUSIONSOral diseases are an often overlooked
source of infection that have the potential to
Table 1. Outreach Activities for Dental Professionals to Influence Nondental Healthcare Providers’Table 1. .and the Public’s Perception of the Importance of Oral Health Outside the Practice Setting
• Volunteer to deliver a presentation at the local hospital’s rounds• Take physicians and nurses to lunch to discuss building a collaborative relationship and systems of triage • Routinely visit physicians’ offices to supply educational materials for patients• Dental hygiene organizations may partner with nursing organizations to conduct a health fair in which
nurses screen for oral diseases/conditions, and hygienists screen for CVD and diabetes• Volunteer to present information at local meetings of civic organizations, hospital programs for the public,
churches, etc.• Volunteer to write a column about oral-systemic relationships in community newspapers• Invite medical colleagues to a study club when information on oral-systemic medicine is being presented• Provide volunteer in-service training in oral healthcare for nursing assistants at nursing home facilities• Use referral letters to simultaneously educate physicians about oral-systemic relationships

302 Periodontal Disease and Overall Health: A Clinician's Guide
compromise overall health, especially in in-dividuals who have an amplified inflamma-tory response to bacterial infections such asperiodontal disease. Evidence to support arelationship between periodontal disease andincreased risk for heart disease, stroke, wors-ened glycemic control in individuals withdiabetes, adverse pregnancy outcomes, res-piratory conditions, chronic kidney disease,and complications of diabetes is emerging asa relatively new body of knowledge that dental and dental hygiene professionals areethically bound to share with their patients.Mainstream media, university- and govern-mental-sponsored public health outreach, insurance industry campaigns, professionaland nonprofit organizations, nondentalhealthcare practitioners and commercial ad-vertising associated with oral care productshave contributed greatly to increasing oralhealthcare literacy. However, it must be rec-ognized that second-hand information aboutoral-systemic health must be filtered by prac-titioners to ensure that what is being com-municated to patients and the public at largeis scientifically supported.
Lack of health literacy has been cited asa significant factor in undermining the effec -tiveness of our current healthcare deliverysystem, and may account for billions of dollars in added healthcare costs each year.There are a number of reasons why dentalproviders may be reluctant to become in-volved with counseling patients about oral-systemic health. However, given the strengthof evidence that supports inter-relationshipsbetween oral diseases and systemic sequelae,providing effective patient education pro-grams is no longer optional.
Beyond practice-based patient educa-tion strategies, forward thinking oral health-care providers must pursue opportunities toincrease the awareness of the importance oforal health within nondental healthcareprovider communities and the consumerpublic. Consumer-patients are increasingly
expecting dental practitioners to reconnectthe mouth to the rest of the body, and are an-ticipating that dentists and dental hygienistswill move beyond a preoccupation with pro-viding traditional dental procedures exclu-sively. Finally, if dentists, dental hygienists,and nondental providers are effective in com- municating how integral oral health is to over-all health, this heightened oral health literacymay prompt changes in public policy.
Supplemental ReadingsAmerican Academy of Periodontology. Parameter onSystemic Conditions Affected by Periodontal Diseases.J Periodontol 2000;71:880–883. http://perio.org/resources-products/pdf/880.pdf.
Mealey BL, Oates TW. Diabetes Mellitus and Perio -dontal Disease. J Periodontol 2006;77:1289–1303.http://perio.org/resources-products/pdf/lr-diabetes.pdf.
Friedewald VE, Kornman KS, Beck JD, et al. TheAmerican Journal of Cardiology and Journal of Perio -dontology Editors’ Consensus: Periodontitis and Athero -sclerotic Cardiovascular Disease. J Periodontol 2009;Vol. 80, No. 7, Pages 1021–1032. http://www.jopon-line.org/doi/pdf/10.1902/jop.2009.097001?cook-ieSet=1.
Hein C, Cobb C, Iacopino A. Report of the Independ-ent Panel of Experts of ‘The Scottsdale Project’. Pub-lished as a Special Supplement to Grand Rounds in Oral-Sys Med 2007;3. Access through www.caseyhein.com.
Hein C. Proceedings and consensus opinion from theglo bal oral and systemic health summit; present evidenceand future directions. Grand Rounds in Oral-Sys Med2007;(Suppl):1. Access through www.caseyhein.com.
REFERENCES1. Nielsen-Bohlman L, Panzer AM, Kindig DA, eds.
Health Literacy: A Prescription to End Confusion.National Institutes of Medicine, Washington, DC,National Academies Press, 2004.
2. American Dental Association. The public speaks upon oral health care. October 2008. Available athttp://ada.org/public/media/presskits/publics-peaks/index.asp. Accessed October 8, 2009.
3. Crozier S. ADA House passes resolutions on oralhealth literacy. Available at http://www.ada.org/prof/resources/pubs/adanews/adanewsarticle.asp?articleid=2236. Accessed October 8, 2009.
4. US Department of Health and Human Services.

Chapter 18Chapter 18 The Role of the Professional in Educating the Public About the Importance of Oral Health 303
Oral Health in America: A Report of the SurgeonGeneral. Rockville, MD: US Department of Healthand Human Services, National Institute of Dentaland Craniofaccial Research, National Institutes ofHealth, 2000.
5. Taylor GW, Burt BA, Becker MP, Genco RJ,Shlossman M, Knowler WC, Pettitt DJ. Severe pe-riodontitis and risk for poor glycemic control inpatients with non-insulin-dependent diabetes mel-litus. J Periodontol 1996;67:1085–1093.
6. Mealey BL, Oates TW. American Academy of Pe-riodontology. Diabetes mellitus and periodontaldiseases. J Periodontol 2006;77:1289–1303.
7. Taylor GW, Borgnakke WS. Periodontal disease:associations with diabetes, glycemic control andcomplications. Oral Dis 2008;14:191–203.
8. López NJ, Smith PC, Gutiérrez J. Periodontal ther-apy may reduce the risk of preterm low birth weightin women with periodontal disease: a randomizedcontrolled trial. J Periodontol 2002;73:911–924.
9. López NJ, DaSilva I, Ipinza J, Gutiérrez J. Perio -dontal therapy reduces the rate of preterm low birthweight in women with pregnancy-associated gin-givitis. J Perio dontol 2005;76(Suppl):2144–2153.
10. Michalowicz BS, Hodges JS, DiAngelis AJ, LupoVR, Novak MJ, Ferguson JE, Buchanan W, BofillJ, Papapanou PN, Mitchell DA, Matseoane S,Tschida PA. Treatment of periodontal disease andthe risk of preterm birth. N Engl J Med 2006;355:1885–1894.
11. Tonetti M, D’Aiuto F, Nibali L, Donald A, StorryC, Parkar M, Suvan J, Hingorani AD, Vallance P,Deanfield J. Treatment of periodontitis and endo -thelial function. N Engl J Med 2007;356:911–920.
12. Elter JR, Hinderliter AL, Offenbacher S, Beck JD,Caughey M, Brodala N, Madianos PN. The effectsof periodontal therapy on vascular endothelial func-tion: a pilot trial. Am Heart J 2006;151:47.
13. D’Aiuto F, Parkar M, Tonetti MS. Acute effects ofperiodontal therapy on bio-markers of vascularhealth. J Clin Periodontol 2007;34:124–129.
14. Hein C, Cobb C, Iacopino A. Report of the inde-pendent panel of experts of the Scottsdale project.Grand Rounds Oral-Sys Med 2007;3(Suppl).
15. Pearson TA, Mensah GA, Alexander RW, AndersonJL, Cannon RO 3rd, Criqui M, Fadl YY, FortmannSP, Hong Y, Myers GL, Rifai N, Smith SC Jr,Taubert K, Tracy RP, Vinicor F; Centers for DiseaseControl and Prevention; American Heart Associa-tion. Markers of inflammation and cardiovasculardisease: Application to clinical and public healthpractice: A statement for healthcare professionalsfrom the Centers for Disease Control and Preven-tion and the American Heart Association. Circula-tion 2003;107:499–511.
16. Friedewald VE, Kornman KS, Beck JD, Genco R,Goldfine A, Libby P, Offenbacher S, Ridker PM,Van Dyke TE, Roberts WC. The American Journalof Cardiology and Journal of Periodontology Edi-tors’ Consensus: Periodontitis and atheroscleroticcardiovascular disease. J Periodontol 2009;80:1021-1032.
17. Barnett ML. Synopsis of oral health, systemichealth, and quality of life; presented by PE Pe-tersen at Coordination Meeting on Oral Health andSystemic Health Periodontal Medicine: Health Policy Implications; Geneva, Switzerland, Dec 5, 6,2002. J Periodontol 2003;74,1081–1086.
18. Nash DA. Oral physician redux: Theses for a (ma-jor) reformation of dental education. The Necessityfor Major Reform in Dental Education; Santa FeGroup Planning Conference; August 29–30, 2004.
19. Hobdell M, Petersen PE, Clarkson J, Johnson N.Global goals for oral health 2020. Int Dent J2003;53:285–288.
20. Report IX; Contemporary Issues in Medicine: OralHealth Education for Medical and Dental Students.Medical School Objectives Project; American As-sociation of Medical Colleges; June 2008.
21. American Dental Education Association. Curricu-lum and Clinical Training in Oral Health for Physi-cians and Dentists: Report of a Panel of the MacyStudy, 2008. Available at http://www.adea.org/pub-lications/Documents/MACY%20RE-PORT%202.pdf. Accessed October 8, 2009.
22. Touger-Decker R, Mobley CC: American DieteticAssociation. Position of the American Dietetic Asso ciation: Oral Health and Nutrition. J Am DietAssoc 2007;107:1418–1428.
23. Albert DA, Sadowsky D, Papapanou P, ConicellaML, Ward A. An examination of periodontal treat-ment and per member per month (PMPM) medicalcosts in an insured population. BMC Health ServRes 2006;6:103–109.
24. Press Release Blue Cross Blue Shield of Michigan.University of Michigan. Blue Care Network studyquantifies health care savings of regular dentalcare for patients with diabetes. Available athttp://bcbsm.com/pr/pr_12-09-2008_11079.shtml.Accessed October 8, 2009.
25. New York State Department of Health. Oralhealth care during pregnancy and early childhood;practice guidelines, August 2006. Available at http://www.health.state.ny.us/publications/0824.pdf. Ac-cessed October 8, 2009.
26. Wisconsin Department of Health Services. Wiscon-sin Diabetes Mellitus Essential Care Guidelines;Section 9: Oral Care. Available at http://dhs.wis-consin.gov/health/diabetes/PDFs/GL09.pdf. Ac-cessed October 8, 2009.

304 Periodontal Disease and Overall Health: A Clinician's Guide
27. Gorman G, Park A. The fires within. Time Maga-zine February 23, 2004;39–46.
28. Rennie J, ed. Oral and whole body health. 2006;Scientific American.
29. Gupta S. How to live longer. CNN broadcast airedon January 2, 2009. Available at http://www.cnn.com/video/#/video/health/2009/01/02/gupta.live.longer.flossing.cnn. Accessed October 8, 2009.
30. Oz M, Levine J. Dental Health. Oprah and FriendsRadio. Available at http://www.oprah.com/arti-cle/oprahandfriends/moz/moz_20070122. AccessedOctober 8, 2009.
31. The American Dental Association. 2000 PublicOpinion Survey. Oral Health of the US Population.2001;15,16.
32. MetLife. MetLife Oral Health Insights Study: Con-sumers Perceive a Strong Link between Oral andMedical Health. 2006 US MetLife.
33. Research! America. Americans Speak Out on OralHealth Research. 2003; US. Research! America.
34. Siperstein GN, Romano N, Glick GC, et al. A national survey of public perceptions of dentistry.2007; University of Massachusetts, Boston.
35. Hein C, Kunselman B, Frese P, Kellar K. Prelimi-nary findings of consumer-patients’ perception ofdental hygienists’ scope of practice/qualificationsand the level of care being rendered. Presented at83rd Annual Session of the American Dental Hy-gienists’ Association; Orlando, Florida; June 2006.
36. Torpy JM, Burke AE, Glass RM. Periodontal dis-ease. JAMA 2008;299:5.
37. Dolan TA, McGorray SP, Grinstead-Skigen CL,Mecklenburg R. Tobacco control activities inU.S. dental practices. J Am Dent Assoc 1997;128:
1669–1679.38. Jones RB, Pomrehn PR, Mecklenburg RE, Lindsay
EA, Manley M, Ockene JK. The COMMIT dentalmodel: tobacco control practices and attitudes. J AmDent Assoc 1993;124:92–104.
39. Hastreiter RJ, Bakdash B, Roesch MH, Walseth J.Use of tobacco prevention and cessation strategiesand techniques in the dental office. J Am Dent As-soc 1994;125:1475–1484.
40. Secker-Walker RH, Solomon LJ, Flynn BS, DanaGS. Comparisons of the smoking cessation coun-seling activities of six types of health professionals.Prev Med 1994;23:800–808.
41. Albert DA, Anluwalia KP, Ward A, Sadowsky D.The use of academic detailing to promote tobacco-use cessation counseling in dental offices. J Am DentAssoc 2004;135:1700–1706.
42. Wilder RS, Thomas KM, Jared H. Periodontal- systemic disease education in United States dentalhygiene programs. J Dent Educ 2008;72:669–679.
43. Wilder RS, O’Donnell JA, Barry JM, Galli DM,Hakim FF, Holyfield LJ, Robbins MR. Is dentistryat risk? A case for interprofessional education. JDent Educ 2008;72:1231–1237.
44. Global News Nexus. Santa Fe Group Salon SpecialReport. The necessity for major reform in dental education. Fall 2004. NYU College of Dentistry.Available at http://www.nyu.edu/dental/nexus/issues/fall2004/santafe.html. Accessed October 8,2009.
45. Levin RP. Developing lifetime relationships withpatients: strategies to improve patient care andbuild your practice. J Contemp Dent Pract 2008;9:105–112.
Tables, figures, and boxes are indicated by an italic t,f, or b.
AA Treatise on the Disorders and Deformities of the
Teeth and Gums (Berdmore), 43abscesses of periodontium, 9Acarbose (alpha-glucosidase inhibitor), 72t, 73ACE. see angiotensin converting enzymeacetaminophen, in pregnancy, 254, 254tAcinetobacter sp., in lung disease, 152, 157acquired neutropenia, 9Actinobacillus actinomycetemcomitans. see
Aggregatibacter actinomycetemcomitansActonel (risedronate), 172acute coronary syndrome (ACS), 105acute leukemia, 282–283acute necrotizing NUG, 18–19acute-phase proteins
activity of, 30–31in atherosclerotic disease, 239–240and cardiovascular disease, 33in inflammatory response, 27in pregnancy, 134–135as systemic cellular markers, 32in systemic inflammation, 30see also C-reactive protein
addiction. see drug-related dependenciesAddison’s disease, in DM, 60adipokines
in insulin resistance, 61role in inflammation, 93–94
adiponectinin DM, 108in insulin resistance, 61
adipose tissuein DM, 58and insulin resistance, 61role in inflammation, 93–94, 107, 108
adolescent patients, pregnancy in, 265adult-onset diabetes mellitus (DM), 60, 62advanced glycation end-products (AGEs), 90, 107African-Americans
adolescent pregnancy, 265DM risk in, 228, 228bgestational diabetes mellitus, 62–63glomerular filtration calculation, 277nitrate treatment, 244periodontal disease, 10preterm birth risk, 140, 263stroke risk, 117
Aggregatibacter actinomycetemcomitansin aggressive periodontitis, 8in connective tissue invasion, 27metronidazole/amoxicillin, 18–19in RA, 190
aggressive periodontitis, 8–9alcohol use, as risk factor for oral cancer, 197–201alendronate, 271–272alkylating agents, 280, 280tallostatic mediators, in RA, 186alpha blockers, in CKD treatment, 277alpha-glucosidase inhibitors, 72t, 73, 227alveolar bone loss
in COPD, 156vs. coronary heart disease, 116, 117tearly research on, 2in osteoporosis, 52in postmenopausal osteoporosis, 168as risk factor for oral cancer, 202vs. skeletal bone loss, 168–169, 170tand teriparatide (PTH) treatment, 173see also bone loss
amalgam tattoos, 8Amaryl (glimepiride), 226tAmerican Academy of Periodontology
patient education campaign, 292preconception recommendations, 257–258pregnancy recommendations, 261
American College of Obstetrics and Gynecology,cardiac conditions guidelines, 255
American Dental Association (ADA)on oral health literacy, 293pregnancy guidelines, 252–253
American Diabetes Association, patient educationcampaign, 292
American Heart Association, statement on dietarysugars, 246
American Journal of Cardiology, Editors’ ConsensusReport, 245
American Society of Bone and Mineral Research(ASBMR)
ONJ lesions defined, 173ONJ task force, 272
ampicillin/amoxicillinin periodontitis, 19in pregnancy, 254t, 255, 264in premature rupture of membranes, 259–260
amylin (Pramlintide), 75amyloid formation, in DM, 61analgesics, in pregnancy, 254, 254tanesthetics, in pre-eclampsia, 260
INDEX305
aneurysms, 105angina pectoris, 105, 242, 243fangioplasty, 245angiotensin converting enzyme (ACE) inhibitors
in atherosclerotic disease, 244in kidney disease, 276, 277
anthracyclines, 280, 280tantibiotic prophylaxis
in DM, 224for Enterococcus sp., 255in kidney disease, 279in pregnancy, 255
antibiotics. see antibiotic prophylaxis; antimicrobialtherapies; pharmacologic treatment; individualnames
antiemetics, in pregnancy, 254antihistamines, in pregnancy, 259antihyperglycemic medications, 226–227, 226tantihypertensive agents, in kidney disease, 277anti-inflammatory drugs
in host-modulation therapy, 19in kidney disease, 279in ONJ, 275
antimetabolites, 280, 280tantimicrobial therapies
antitumor antibiotics, 280, 280tin community-acquired pneumonia, 148for COPD, 156effect on glycemic control, 96teffect on metabolic control, 97, 221in gingival disease, 7in hospital-acquired pneumonia, 149locally applied, 17lozenges in radiation therapy, 283in oral mucositis treatment, 282in osteonecrosis of the jaw, 275in pregnancy, 254–255, 254t, 262in preterm labor, 259–260, 264prophylaxis in DM, 224prophylaxis in kidney disease, 279rinses, 154systemic vs. locally applied, 19in ventilator-associated pneumonia, 153see also pharmacologic treatment
antiplatelet therapy, in atherosclerotic disease, 242–244antitumor antibiotics, 280, 280taortic atherosclerosis, 105Apidra (glulisine), 226tapoptosis
bisphosphonates and, 271in bone remodeling, 89–90, 90f, 164in chemotherapy, 280in estrogen deficiency, 164, 173in inflammation, 35, 211in preterm birth, 136
Arestin (minocycline), 18
arterial plaque. see atheromatous plaquesASBMR. see American Society of Bone and Mineral
Researchaspart (NovoLog), 74, 74t, 226taspiration pneumonia, 148–150aspirin
in atherosclerotic disease, 242in DM, 67, 69, 69t, 95in pre-eclampsia, 260in pregnancy, 252, 254t, 260in treatment of inflammation, 39
asthma, protectins effect on, 37, 38tatherogenesis, theory of, 238atheromatous diseases linked to periodontal disease
animal models, 122–125case-controlled studies, 113, 114tcohort studies, 113–116, 115t–116tendothelial function studies, 126–128meta-analyses of, 113observational studies, 121–122PAVE study, 126, 127fpopulation studies, 117–118, 121role of inflammation in, 112Western New York MI/Perio Studies, 120–121
atheromatous plaquesvs. clinical attachment loss, 118tCRP in, 33formation, 105–106, 238and periodontal disease, 50role of inflammation in, 112and statin treatment, 244–245
atherosclerotic diseaseepidemiology, 108–109mechanisms, 105–106periodontal disease management in, 246–247risk factors, 106–108
Atridox (tetracycline), 18autoantibodies, in DM, 60Avelox (moxifloxacin), in community-acquired
pneumonia, 148azithromycin (Zithromax)
in community-acquired pneumonia, 148in kidney disease, 278in periodontitis, 19
Bbacteremia
animal studies, 124–125following mechanical irritation, 29–30in inflammation, 30, 93in neutropenic patients, 282in pregnancy, 255t, 257, 258fin pulmonary infections, 150sources of, 45transient, 253
bacterial biofilm. see biofilms
306 Periodontal Disease and Overall Health: A Clinician's Guide
bacterial burden, and atherosclerosis, 120bacterial infections, as trigger for RA, 190bacterial virulence
effect on host cells, 26trole in disease etiology, 43
Bacteroides forsythus, in RA, 190-cell exhaustion, in DM, 60benzodiazepines, in pregnancy, 254, 254tbenzydamine, in radiation therapy, 283Berdmore, Thomas, 43beta blockers, 244, 277Biaxin (clarithromycin), in community-acquired
pneumonia, 148BIC. see bone-to-implant contactbi-directional relationship, DM and periodontal
disease, 83, 220–221biguanide, 71–73, 72t, 227bile acid-binders, 227Billings, Frank, 45biofilms
in carcinogenesis, 212composition of, 29early research on, 2in gingival inflammation, 25, 28fhost response to, 12–13impact on systemic health, 3in pregnancy, 133in RA, 179, 180in respiratory tract diseases, 150, 151fin systemic inflammation, 98see also dental plaque
biomarkersin cardiovascular disease, 33, 239–240decreased with Arestin treatment, 18in DM, 34in pregnancy, 261subantimicrobial-dose therapy, 20types of, 15
bisphosphonatesin host-modulation therapy, 19and ONJ, 272–273in osteoporosis, 172–173, 172fpharmacology of, 271–272
blood urea nitrogen (BUN), 275blood-brain barrier, in pregnancy, 142–143BMD. see bone mineral densityBMUs. see bone multicellular unitsbone disease
bone loss, 91metastatic, 271secondary to kidney disease, 276see also alveolar bone loss; osteonecrosis of the
jaw (ONJ)bone mineral density (BMD), 166–169, 166f, 170t, 270bone morphogenetic proteins, 19, 20–21bone multicellular units (BMUs), 162, 163f
bone remodelingin animal studies, 89, 90fprocess of, 162–166, 163f, 164frole of PGE2, 35
bone resorption/formation. see bone remodelingbone-sparing drugs, 172–174bone-to-implant contact (BIC), in osteoporosis, 172Boniva (ibandronate), 172brushing. see mechanical therapyBUN. see blood urea nitrogenbypass surgery, 245
Ccalcineurin inhibitors, in kidney disease, 278calcium
in bone remodeling, 164, 165fin periodontal disease, 169–170
calcium channel blockers, in kidney disease, 277, 278fCampylobacter rectus
in animal studies, 142–143as indicator of atherosclerosis, 119in pregnancy, 141in pregnant adolescents, 265
cancer, 279–285bisphosphonate therapy and ONJ in, 273chemotherapy, 280, 280tcomanagement, 284–285epidemiology, 279metastatic bone disease in, 271oral mucositis, 280–282and osteonecrosis of the jaw, 173radiation therapy, 283–284surgery, 284see also leukemia
cancer and periodontal diseaseHelicobacter pylori, 211, 212lung cancer, 205–206mechanisms of relationship, 211–212mortality in, 207–210pancreatic cancer, 206–207periodontal disease association, 201–203, 284studies showing relationship, 197–201, 197tupper GI cancer, 203–205viruses, 210–211
Candida sp., 7, 68, 219CAP. see community acquired pneumoniacardiac guidelines, American College of Obstetrics
and Gynecology, 255cardiovascular abnormalities
in DM, 66–67in pregnancy, 251
cardiovascular disease (CVD), 237–247biomarker reduction with subantimicrobial-dose
therapy, 20clinical presentation, 242, 243fcomanagement with periodontal disease, 245–247
INDEX 307
in DM, 65tepidemiology, 105–109, 237global trends, 108inflammatory markers, 33, 239–240management, 242–245pathogenesis, 237–238patient education “sound bites,” 299periodontal disease association, 15, 48, 50, 116,
119prevention, 240–241, 240fprognostication, 107related to kidney disease, 278risk factors, 105–109, 238–239, 239fand systemic inflammation, 24Type 2 DM as a risk factor, 67see also atheromatous diseases
causality factorsBradford Hill criteria, 144defined, 84study methods demonstrating relationships, 84–85see also risk factor assessment/reduction
CD14, 27, 30, 31, 32cephalosporins, in pregnancy, 254–255, 254tcerebrovascular disease
in atherosclerotic disease, 105, 108in DM, 65tlinked to periodontal disease, 217risk factors for, 106
Charcot’s joints, 66chemotherapeutic agents
in leukemia, 282–283oral toxicity and, 280–282, 280tin periodontal disease, 11, 17
Chicago Heart Association Detection Project inIndustry, risk factors for atherosclerotic disease, 238
Chlamydia pneumoniae, in atherosclerosis, 112chlorhexidine (CHX), in ventilator-associated
pneumonia, 153chlorhexidine gluconate (Peridex/PerioChip)
in periodontal disease, 17in pregnancy, 254t, 262–263in radiation therapy, 283
chronic kidney disease (CKD). see kidney diseasechronic leukemia, 282–283chronic obstructive pulmonary disease (COPD), 17,
52, 154–157, 254chronic periodontitis (CP), 8ciprofloxacin, in periodontitis, 19citrullinated peptide autoantibodies, in RA, 181–182,
190, 191fCKD (chronic kidney disease). see kidney diseaseclarithromycin (Biaxin), in community-acquired
pneumonia, 148clindamycin
in periodontitis, 19in pregnancy, 254–255, 254t
in premature rupture of membranes, 259–260clinical attachment loss (CAL)
vs. arterial plaque, 118tvs. CAD, 116–117, 118tin COPD, 157in osteoporosis, 170tin radiation therapy, 283as risk factor for oral cancer, 201
clinical protocols for diabetic patients, 222–224, 229clodronate, 271–272clotrimazole, in pregnancy, 254tCNN News, 291cocaine use, hemodynamic effects of, 108codeine, in pregnancy, 254tCohen syndrome, and periodontal disease, 9Colgate-Palmolive Company, patient education, 292colitis, resolvins effect on, 37, 38tColyer, J. F., 44comanagement
of cancer, 270–285of DM, 216–234of kidney disease, 270–285of osteoporosis, 270–285of pregnancy complications, 261–265see also team-care
community acquired pneumonia (CAP), 147–148, 150complement proteins, role in inflammation, 31complex diseases, RA as, 186, 186t, 187fcongenital heart disease, in pregnancy, 255connective tissue, in inflammatory response, 27Consumer-Patient Survey (2005), 292, 293fcoronary artery disease (CAD), vs. clinical
attachment loss, 116–117, 117tcoronary atherosclerosis, 237, 240–241, 240fcoronary heart disease, 105–109corticosteroids
in pregnancy, 254tin premature rupture of membranes, 259–260in secondary osteoporosis, 167
cortisol, in DM, 58coupling process, in bone reformation, 89C-reactive protein (CRP)
in atherosclerotic disease, 239–240as biomarker, 15in hypertension, 107in inflammation, 2–3, 30–31, 32, 33in kidney disease, 278–279in PAVE study, 127fin plaque formation, 106as predictor of cardiovascular disease, 50in pregnancy, 134–135, 139fin RA, 181–182
creatinine, 275, 276–277critical nodes, in insulin signaling pathways, 58–60,
59fcrowns
308 Periodontal Disease and Overall Health: A Clinician's Guide
in chronic periodontitis, 8implicated in systemic disease, 45in pregnancy, 255
cryotherapy, in mucositis prevention, 281, 282CVD. see cardiovascular diseasecyclosporine, in kidney disease, 278cystic fibrosis, lipoxins effect on, 37, 38tcytokines
in bone remodeling, 162–164in chemotherapy, 280in DKA, 64early research on, 2and EBV, 211in inflammatory response, 2–3in insulin signaling pathways, 58–60, 59fin kidney disease, 278–279and neoplastic formation, 211–212in osteoporosis, 168and periodontal disease, 10, 13in plaque formation, 106, 107in pregnancy, 134, 136in RA, 182, 183tin respiratory tract diseases, 150in systemic inflammation, 30, 32
cytomegalovirus, affecting atherosclerosis, 112
Dd’Arcoli, Giovanni, 42–43DCCT. see Diabetes Control and Complications Trialdementia, 105denosumab, 174dental caries
maternal vs. child, 256in pregnancy, 256in radiation therapy, 283–284, 285reduction with fluoride, 17, 256
dental implants, and bisphosphonate therapy, 274dental plaque
compared to respiratory tract pathogens, 152–153composition of, 150, 157in gingivitis, 6as initiator of periodontal disease, 5, 12and ventilator-associated pneumonia, 150, 151f
dental proceduresin pre-eclampsia, 260in pregnancy, 253, 255, 261–265in premature rupture of membranes, 260
dental professionalsattitudes toward treatment in pregnancy, 252–253role in DM management, 221–231
dental prophylaxisin DM, 220in PAVE study, 126, 127tin pregnancy, 262
dental restorationsavoidance for hygiene, 44
Hunter on, 45dentifrices, success of, 17–18dentistry, American vs. English, 45dentition
as risk factor for GI cancer, 203–205as risk factor for oral cancer, 197–201
dermatologic manifestations in DM, 68detemir (Levemir), 74, 74t, 226tDEXA. see dual-energy x-ray absorptiometryDiaBeta/Micronase (glyburide), 226tDiabetes Control and Complications Trial (DCCT),
65, 97–98, 218diabetes mellitus (DM)
and atherosclerotic disease, 107, 238, 239f, 242clinical presentation, 61–64complications, 63, 64–69, 65t, 216–234, 276,
278–279diagnosis, 63t, 64, 69epidemiology, 55–56, 216–217etiology, 55, 56tgenetics of, 60, 61inflammation in, 24, 33–34management of, 69–76, 69t, 72t, 74t, 77tmedications for, 226–227, 226tpathogenesis/pathophysiology, 56–61, 57f, 59fpatient education “sound bites,” 298–299
diabetes mellitus (DM) and periodontal diseasebenefit of periodontal treatment, 18–19effect of periodontal disease on glycemic control,
88t, 92–93effects of DM on periodontal health, 83–84, 84f,
86, 87tperiodontal disease as risk factor for DM, 15, 97,
220–221periodontal disease association, 98–99, 216–234,
217–218periodontal disease in, 56, 65t, 84reciprocal link to periodontal disease, 68studies supporting relationship, 85–86, 89two-way relationship, 51, 83
diabetes mellitus (DM) comanagementemergencies in dental offices, 224–228, 225brole of dental professionals, 221–224, 229, 230frole of medical professionals, 231–234screening in dental offices, 228–229, 228btreatment model, 230funderdiagnosis of DM, 218–219underdiagnosis of periodontitis, 219–220
diabetes self-management skills, 69–70diabetic dermopathy, 68diabetic foot, 68–69diabetic ketoacidosis (DKA)
during dental procedure, 227–228vs. HHS, 63, 64pathogenesis, 63–64in Type 1 DM, 62
INDEX 309
diabetic retinopathy, 66diabetogenic state, in pregnancy, 252diapedesis, in inflammatory response, 27dietary sugar, in DM, 70digital sclerosis, 68dihydropyridines, in kidney disease, 277, 278fdipeptidyl peptidase IV inhibitors, 72t, 73diphenhydramine, in oral mucositis, 282direct renin inhibitors (DRIs), 276disseminated intravascular coagulation (DIC)
in fetal death, 261in pregnancy, 252
diureticsin hyperglycemic/hyperosmolar state, 64in kidney disease, 277
dose-response relationship, of glycemic control andperiodontitis, 88–89
Down’s syndrome, and periodontal disease, 9doxycycline
Atridox (tetracycline), 18in community-acquired pneumonia, 148subantimicrobial-dose therapy, 19–20
doxylamine, in pregnancy, 254, 254t, 259DRIs. see direct renin inhibitorsdrug therapies
causing secondary osteoporosis, 167–168for diabetes mellitus (DM), 71–73, 72tin host-modulation therapy, 19in kidney disease, 279in ONJ, 275
drug-related dependenciescocaine, 108nitrous oxide use in, 254
dual-energy x-ray absorptiometry (DEXA)and dental implants, 171–172interpretation of, 166f, 168–169in osteoporosis, 270
dysgeusia, in radiation therapy, 283–284dyslipidemia
in DM screening, 228genetics of DM, 61in macrovascular complications of DM, 67in renal complications, 66as a risk factor for atherosclerotic disease, 106–
107dyspnea, in pregnancy, 251–252
Eecogenetic diseases, RA as, 186, 186t, 187fedema, in pregnancy, 250–251Ehlers-Danlos syndrome, and periodontal disease, 9emphysema, 154–155enamel matrix proteins (Emdogain), in host-
modulation therapy, 19, 20endocarditis
in kidney disease, 279
in pregnancy, 255endocrine system
changes in pregnancy, 252in secondary osteoporosis, 167
endothelial injury, in atherosclerosis, 238end-stage renal disease (ESRD). see kidney diseaseEnterobacter cloacae, in COPD, 157Enterococcus sp., prophylaxis for, 255environmental risk factors
in DM, 60, 61in RA, 184–187
epigenetic modification, in animal studies, 143epinephrine
as anesthetic in DM, 224contraindicated in pre-eclampsia, 253, 260in hypoglycemia, 76in insulin signaling pathways, 59t
Epstein-Barr virus (EBV)in aggressive periodontitis, 211in RA, 191, 191f
erythema multiforma, in gingival disease, 7erythromycin
in community-acquired pneumonia, 148in pregnancy, 254–255, 254tin premature rupture of membranes, 259–260
erythropoietin, 275, 277, 279Escherichia coli
in nosocomial pneumonia, 150in vaginal flora, 262
ESRD (end-stage renal disease). see kidney diseaseestrogen
in bone remodeling, 164, 165feffect on periodontal health, 250, 251, 256in osteoporosis, 173in primary osteoporosis, 167
etidronate, 271–272etiopathologic era of periodontal disease research, 1–2Exenatide (GLP-receptor agonist), 72t, 73eye disease. see ophthalmic complications
FFactiv (gemifloxacin), in community-acquired
pneumonia, 148fasting, in DM, 227fatty acid metabolism, 58–60, 61, 64fatty streaks, 107, 112, 237–238fibrinogen
in atheromas, 238in DM, 67, 107elevated in cardiovascular disease, 33in fetal death, 261formation of, 31in inflammation, 15, 30, 32in periodontitis, 123
fibroblastscytokines released from, 182, 183t, 184
310 Periodontal Disease and Overall Health: A Clinician's Guide
gingival, 251in pregnancy, 251
fimbriae, in host response, 25, 26tflossing. see mechanical therapyflow-mediated dilation therapy, 127, 128ffluconazole, in pregnancy, 254tfluoride treatment
caries reduction with, 17, 256in radiation therapy, 283
fMLP. see formyl-methionyl-leucyl-phenyl-alaninefocal infection
Billings on, 45concept origins, 44original evidence for, 49theory of, 48
Food and Drug Administration (FDA), pregnancyguidelines, 253–255, 254t
foreign objects, and abscesses, 9formyl-methionyl-leucyl-phenyl-alanine (fMLP), in
host response, 25, 26tForteo (parathyroid hormone), 173Fosamax (sodium alendronate), 172Framingham Heart Study, risk factors for
atherosclerotic disease, 238fungal infections, 7, 68, 219Fusobacterium nucleatum, in pregnancy, 141, 257
Ggastrointestinal (GI) tract
cancer and oral health, 203–205chemotherapeutic toxicity, 280, 280tHelicobacter pylori, 211in pregnancy, 139, 251
GDM. see gestational diabetes mellitusGEM 21S. see growth-factor enhanced matrixgemifloxacin (Factiv), in community-acquired
pneumonia, 148genetic disorders, and periodontal disease, 9genetic predisposition
for COPD, 155–156and periodontal disease, 50in pregnancy, 134
gentamicin/colistin/vancomycin, in ventilator-associated pneumonia, 153
germ theory of disease causation, 43gestational diabetes mellitus (GDM)
effect on oral flora, 252effect on periodontal health, 87epidemiology, 62–63periodontal disease as a risk factor for, 98–99
Gila River Indian Community, DM in, 98, 220gingival diseases
in DM, 56hyperplasia, 277, 277f, 278in leukemia, 282–283in pregnancy, 133, 250–251, 256–257
in pregnant adolescents, 265treatment during pregnancy, 259, 262–263, 262t
glargine (Lantus), 74, 74t, 226tglimepiride (Amaryl), 71, 72t, 226tglipizide (Glucotrol), 71, 72t, 226tglomerular filtration rate (GFR)
in antimicrobial prophylaxis, 279in kidney disease classification, 276–277, 276t
glomerulonephritis, as cause of kidney disease, 276GLP-receptor agonists, 72t, 73glucagon, in glucose metabolism, 57–58, 57fglucagon injections, in hypoglycemic emergencies,
225–226glucose levels, diagnostic of DM, 69glucose metabolism, in DM, 56–58, 57fglucose monitoring
during dental procedure, 227supplies, 226
glucose toxicity, in insulin resistance, 61Glucotrol (glipizide), 226tglulisine (Apidra), 74, 74t, 226tglyburide (DiaBeta/Micronase), 71–73, 72t, 226tglycated hemoglobin. see hemoglobin A1c (HbA1c)glycemic control
affected by periodontal disease, 92–93, 95, 95t, 97,220–221
affected by periodontal treatment, 51, 97assessment of, 70–71difficulty achieving, 218–219, 219fin DM, 69t, 70–71effect on periodontal health, 88, 88tperiodontal disease management and, 51, 95–96, 96tsee also hemoglobin A1c (HbA1c)
glycosylated hemoglobin. see hemoglobin A1c(HbA1c)
Godlee, R. J., 44G-protein-coupled receptors (GPCRs), in host
response, 25, 26tgranulocyte-macrophage colony-stimulating factor
(GM-CSF), in mucositis prevention, 281growth factors, in host-modulation therapy, 19, 20growth hormone, in DM, 58growth-factor enhanced matrix (GEM 21S), in host-
modulation therapy, 20–21gum disease. see periodontal diseaseGupta, Sanjay, 291
HHaemophilus influenzae
in community-acquired pneumonia, 147, 150in COPD, 156
Hashimoto’s thyroiditis, in DM, 60HbA1c. see hemoglobin A1c (HbA1c)HCT. see hematopoietic stem cell transplantationhealthcare-associated pneumonia, 149hearing loss, in DM, 65t
INDEX 311
heart disease, DM as a risk factor, 55heat-shock proteins (HSPs), in host response, 25, 26tHelicobacter pylori
affecting atherosclerosis, 112association with GI cancer, 211, 212
hematologic systemchanges in pregnancy, 252and periodontal disease, 9
hematopoietic stem cell transplantation (HCT), 280,281
hemodialysis, 277, 279hemoglobin A1c (HbA1c)
defined, 88as glycemic control monitor, 70–71in prediabetes, 217reduction with periodontal treatment, 18, 19, 20, 51
heparin therapy, in pregnancy, 252Hepatitis B, in hepatocellular carcinoma, 212hereditary gingival fibromatosis, in gingival disease, 7herpes virus
affecting atherosclerosis, 112in gingival disease, 7in RA, 191, 191f
HHS. see hyperosmolar/hyperglycemic statehigh sensitivity CRP (hsCRP), 33high-density lipoprotein cholesterol (HDLC), 238,
239fHispanics
adolescent pregnancy, 265DM risk in, 228, 228bgestational diabetes mellitus, 62–63preterm birth risk, 263
hormone replacement therapy (HRT)periodontal disease management in, 52and tooth retention, 173
hospital-acquired pneumonia (HAP), 149host response
acute-phase proteins, 30in chronic periodontitis, 8in DM, 224early research on, 2hyperinflammatory phenotype, 34, 91to periodontal bacteria, 24, 25, 26t, 28–29in periodontal disease, 5, 6, 9, 10, 11, 12, 13, 50see also hyperinflammatory phenotype; immuno-
inflammatory responseshost-modulation therapies, 15, 19–21, 20t“How to Live Longer” (CNN News), 291HRT. see hormone replacement therapyHSPs. see heat-shock proteinsHumalog (lispro), 226thuman immunodeficiency virus (HIV), and
periodontal disease, 9human leukocyte antigens
in DM, 60in RA, 184
“Human Mouth as a Focus of Infection, The” (Miller),43–44
Hunter, William, 44, 45hydropyridines, in kidney disease, 278hypercholesterolemia, LDL apheresis in, 245hypercoagulable state
in fetal death, 261in pregnancy, 252
hyperemesis gravidarum, 251hyperglycemia
complications from, 64–67, 65tdiagnosis, 64in DM, 56, 58HHS state, 62HHS vs. DKA, 63and inflammatory markers, 107
hyperinflammatory phenotypecontribution to periodontal disease, 35host response in, 34in RA, 184see also immuno-inflammatory responses
hyperinflammatory traits, in pregnancy, 134hyperlipidemia. see lipid dysregulationhyperosmolar/hyperglycemic state (HHS), 62, 63, 64hyperplasia/edema in pregnancy, 250–251hypertension
as atherosclerotic disease risk factor, 107, 238, 239fcomanagement of, 246in DM, 67, 69tin kidney disease, 276, 277in pregnancy, 253–254
hyperventilation, in pregnancy, 251–252hypoglycemia
in DM, 76emergencies in dental offices, 224–227, 225btreatment, 76
hypoglycemic medications, 71–73, 72t, 226–227, 226thypoinsulinemia, pro-inflammatory mediators, 92hypokalemia, in DKA, 64hypophosphatasia, and periodontal disease, 9hypotension, in pregnancy, 251
Iibandronate (Boniva), 172, 271–272ibuprofen, in pregnancy, 254, 254timmune dysfunction, as risk factor for cancer, 212immuno-inflammatory responses
AGEs role in, 91animal studies in DM, 89in connective tissue, 27in gingivitis, 6and periodontal disease, 9, 11, 12–13, 24in pregnancy, 133, 256see also host-response
immunosuppression, and periodontal disease, 9immunosuppressive therapy, in kidney disease, 278
312 Periodontal Disease and Overall Health: A Clinician's Guide
incretins, 227infant deaths. see pregnancy complications linked to
periodontal diseaseinfections
and cancer, 212in DM, 65t, 67–69ectopic foci, 30
inflammationacute-phase proteins, 30–31adipose tissue, 93–94, 107, 108in atherosclerotic disease, 106and cancer, 211–212, 284cocaine use and, 108gingival, 25–29, 28tin kidney disease, 275, 278–279oral-systemic relationship, 1, 32–34in osteoporosis, 168, 171as predictor of attachment loss, 29in pregnancy, 136, 139, 250–266, 258fin RA, 188, 189resolution, 34–39, 36fsystemic, 15, 29–34
inflammatory markersin atherosclerotic disease, 239in kidney disease, 279
inflammatory response, in oral-systemic relationship,2–3
influenza vaccination, in DM, 69tinsulin
adjustment prior to dental appointment, 227signaling pathways, 58–60, 59ftreatment for DM, 71, 73–75, 74ttypes of, 226t
insulin antagonists, 220–221insulin deficiency, absolute vs. relative, 63insulin resistance/sensitivity
and adiponectin levels, 108in DM, 56, 60–61in pregnancy, 63as a risk factor for atherosclerotic disease, 238, 239fas a risk factor for cardiovascular disease, 67role of inflammation in, 34
interleukinseffect on metabolic control, 220–221in inflammatory response, 2–3in insulin signaling pathways, 58–60, 59fin pregnancy, 251
Islets of Langerhansamyloid formation in, 61insulin secretion, 58transplantation of, 75
isophane suspension (NPH), 74, 74t
JJournal of Periodontology, Editors’ Consensus
Report, 245
Journal of the American Medical Association(JAMA), patient education, 292, 294f
juvenile diabetes, 62
Kketoacidosis, 62, 63, 227kidney disease
classification, 276tcomanagement, 275, 279in DM, 65t, 66, 98ESRD, 275kidney function, 275–277medications, 277–278pathogenesis, 66periodontal disease association, 51, 278–279replacement therapy, 277, 278
Kirk, Edward Cameron, 45Klebsiella pneumoniae, in vaginal flora, 262Koch, Robert, 43
LLantus (glargine), 226tLBP. see LPS binding protein (LBP)LBW (low birth weight). see pregnancy
complications linked to periodontal diseaseLDL apheresis, in atherosclerotic disease, 245Leeuwenhoek, Antonie von, 43Legionella sp., in community-acquired pneumonia, 148leptin
in insulin resistance, 61in insulin signaling pathways, 58–60, 59f
leukemias, 6, 9, 282–283leukocytes, as systemic cellular markers, 32leukocytosis, in pregnancy, 252Levaquin (levofloxacin), in community-acquired
pneumonia, 148Levemir (detemir), 226tlidocaine
in oral mucositis, 282in pregnancy, 253, 253t, 254t
lifestyle modificationin DM, 55–78, 63, 69t, 70inactivity as a risk factor for atherosclerotic
disease, 238, 239fin pregnancy, 258–259
lipid dysregulation, 69t, 91, 244lipid mediators, in inflammation resolution, 36flipid-lowering therapies, 244lipoteichoic acids (LTAs), in host response, 25, 26tlipoxins, 37, 38t, 39flispro (Humalog), 74, 74t, 226tLöe and colleagues, plaque research, 1low birth weight (LBW). see pregnancy
complications linked to periodontal diseaselow-density lipoprotein cholesterol (LDLC), 106,
107, 238, 239f
INDEX 313
LPS binding protein (LBP), 27, 31, 32LTAs. see lipoteichoic acidslung cancer, related to oral health, 205–206lupus erythematosus, in gingival disease, 7lymphocytic leukemia, 282–283
Mmacrophages
in COPD, 155early research on, 2in pregnancy, 134
macrovascular complications, of DM, 67malnutrition, and periodontal disease, 9marginal periodontitis, 257, 263Matilla study, 48matrix metalloproteinases (MMPs)
in COPD, 155defined, 91early research on, 2and periodontal disease, 10in pregnancy, 251in RA, 182–184, 185tsubantimicrobial-dose therapy, 19–20
mechanical irritation, and oral cancer, 211mechanical therapy, in periodontal disease, 12, 16–18medical nutrition therapy (MNT), in DM, 70medical professionals, role in DM comanagement,
231–233meglitinides, 71, 72tmendelian inheritance, 186meperidine, in pregnancy, 254tmepivacaine, in pregnancy, 254tMerrit, Arthur H., 45metabolic control, affected by periodontal disease,
220–221metabolic syndrome, 62metastatic bone disease, 271, 273Metformin (biguanide), 71–73, 72tmethicillin resistant Staphylococcus aureus (MRSA),
148metronidazole
in NUG, 18–19in periodontitis, 19in pregnancy, 19, 254t, 255, 259–260, 262, 264
Microorganisms of the Human Mouth, The (Miller), 43microvascular complications, 65–66, 107Miglitol (alpha-glucosidase inhibitor), 72t, 73Miller, W. D., 43ministrokes, 105minocycline (Arestin), 18, 19MMP inhibitors, periodontal disease management, 91MNT. see medical nutrition therapyModification of Diet in Renal Disease (MDRD),
kidney disease guidelines, 276–277monocyte/macrophage function, lipid dysregulation
effect, 91
Moraxella catarrhalis, in COPD, 156morning sickness, in pregnancy, 251morphine sulfate
in oral mucositis, 282in pregnancy, 254t
mosaic pattern, in Paget’s disease, 270–271“Mouth Infection: The Cause of Systemic Disease”
(Merrit), 45moxifloxacin (Avelox), in community-acquired
pneumonia, 148MRSA. see methicillin resistant Staphylococcus
aureusmucositis
and chemotherapy, 280tmucosal coating agents, 281–282in radiation therapy, 283–284
Mycoplasma pneumoniae, in community-acquiredpneumonia, 147, 150
myelogenous leukemia, 282–283myelosuppression, in oral mucositis, 282myocardial infarction (MI), 48, 67, 105, 108, 242
NN-acetylcysteine, periodontal disease management, 91nateglinide (Starlix), 71–73, 72t, 226tNational Cholesterol Education Program, 244, 245National Kidney Foundation, kidney disease
guidelines, 276–277nausea and vomiting, in pregnancy, 259necrobiosis lipoidica diabeticorum, 68necrotizing periodontal disease, 9, 18–19Neisseria gonorrhoeae, gingival lesions from, 7neomycin sulfate, in ventilator-associated pneumonia,
153neurological complications, 65t, 66–69neutropenia
in oral mucositis, 282and periodontal disease, 9
nitrates, in atherosclerotic disease, 244nitrosamines, as carcinogens, 212nitrous oxide, in pregnancy, 254, 254tNovoLog (aspart), 226tNPH (Novolin/Humulin), 74, 74t, 226t, 227NUG/NUP. see necrotizing periodontal diseasenursing-home associated pneumonia (NHAP), 149nutrition
and GI cancer, 211in gingivitis, 7in oral mucositis, 281in periodontal disease, 9in pregnancy, 136as risk factor for oral cancer, 197–201
Oobesity
and insulin resistance, 61
314 Periodontal Disease and Overall Health: A Clinician's Guide
and periodontal disease, 94, 94fas a risk factor for atherosclerotic disease, 108, 238,
239fOffenbacher, S., 50–51ONJ. see osteonecrosis of the jawOPG. see osteoprotegerinophthalmic complications, 65t, 66opportunistic infections, periodontal disease as, 12oral antiseptic mouthrinses
effect on oral cancer risk, 198in periodontal diseases, 16–17
oral cancer, periodontal disease association, 196–213,201–203
oral floraequilibrium with host, 25, 27humoral immune response to in RA, 190–191,
191fin infants, 256intrauterine exposure to, 141, 143as pathogens in respiratory tract diseases, 52, 147–
157in pregnancy, 251, 256
oral healthin atherosclerotic disease, 247care of institutionalized patients, 154in COPD, 156–157historical improvements in, 17in pregnancy, 250–266relationship to oral cancer, 203sulcular epithelium in, 29
oral health education, 288–302consumer-patients’ knowledge, 291–293, 293finfluencing public perception, 290–291key information, 297–300, 298foral health literacy, 288, 289, 293–295, 301, 302outreach activities, 301, 301tovercoming obstacles, 295–297physicians’ role in, 289responsibility for, 288, 289, 295, 296, 297
oral hygienein DM, 219–220in institutionalized patients, 154in ONJ, 274–275as risk factor for oral cancer, 197–201
oral implants. see dental implantsOral Infections and Vascular Disease Epidemiology
Study (INVEST), 117, 119–120, 120toral mucositis
and chemotherapy, 280–282, 280tand radiation therapy, 283
oral opening exercises, in cancer resection, 284“Oral Sepsis as a Cause of Disease” (Hunter), 44oral sepsis as cause for disease, 44, 48oral toxicity, and chemotherapy, 280, 280toral-systemic relationship
current understanding, 48
dental professionals’ understanding of, 295–296early understanding of, 42–43emerging recognition of importance, 1, 290historical era of research, 2history of, 42–53oral sepsis as cause for disease, 43–48patient education, 288–302
osteoblasts, in bone remodeling, 162–163, 163f, 164fosteoclasts
in bone remodeling, 162, 163fin RA, 190
osteonecrosis of the jaw (ONJ)bisphosphonate associated, 173, 272–273, 272f,
273fcomanagement of, 274–275
osteopeniaand alveolar bone loss, 169defined, 167subantimicrobial-dose therapy, 20
osteoporosisalveolar vs. skeletal bone mineral density, 168–169bisphosphonate pharmacology, 271–272BMD, 166–167bone remodeling and skeletal integrity, 162–166calcium and, 169–170comanagement, 273–275dental implants in, 171–172in DM, 65t, 68etiology and classification, 167–168, 270inflammation, 168linked to periodontal disease, 52, 169and metastatic bone disease, 271Paget’s disease, 270–271periodontal integrity, 170–171, 171ftherapies for, 172–174, 172fsee also osteonecrosis of the jaw
osteoprotegerin (OPG), 164, 164fosteoradionecrosis
in radiation therapy, 283–284see also osteonecrosis of the jaw (ONJ)
oxycodone, in pregnancy, 254, 254t
PPaget’s disease, bisphosphonates and, 272–273PAI. see plasminogen activator inhibitorpalifermin, in mucositis prevention, 281, 282pamidronate, 271–272pancreatic cancer, related to oral health, 206–207Papillon-Lefevre syndrome, and periodontal disease, 9parathyroid hormone, in bone remodeling, 164, 165fparathyroid hormone (Forteo), 173pathogen-associated molecular patterns (PAMPs), in
host response, 25, 26tpatient education
diabetes self-management skills, 69–70, 217in DM, 219–220, 229–231
INDEX 315
key messages for medical professionals, 232, 232bmaternal dental education, 256, 258–259see also oral health education
pattern recognition receptors (PRRs), in hostresponse, 25, 26t
PAVE. see Periodontitis and Vascular Events StudyPDGF. see platelet-derived growth factorspemphigoid, in gingival disease, 7penicillin-family agents, in pregnancy, 254–255, 254tpeptidoglycan (PGN), in host response, 25, 26tPeptostreptococcus micros, in atherosclerosis, 119pericoronal abscess, 9Peridex/PerioChip (chlorhexidine gluconate), 17periodontal disease management
antimicrobial and mechanical therapies, 16–17antimicrobials, 18–19antiseptics/toothpastes, 17–18aspirin in, 39barriers to treatment, 19complimentary strategies, 15–16, 16ffuture therapies, 21host-modulation therapy, 19–21
periodontal diseasesabscesses, 9classification, 5–6, 6tclinical presentation, 6, 7, 8epidemiology/etiology, 9–10, 12, 24gingival diseases, 6–8historical eras of research, 1–3linked to systemic disease, 1, 2–3, 9, 15necrotizing, 9, 18–19pathogenesis, 12–15, 13f, 14fperiodontitis, 8–9risk assessment and reduction, 11–12, 11t, 12t
periodontal health, effects of DM, 86–87“Periodontal Infection as a Possible Risk Factor for
Preterm Low Birth Weight” (Offenbacher), 50–51periodontal-systemic inflammation, 288–302Periodontitis and Vascular Events Study (PAVE), 126,
127f, 247Periostat (doxycycline), 19–20peripheral artery complications, in DM, 65tperitoneal dialysis, 277peritonitis, pro-resolution mediators’ effect on, 37, 38tpernicious anemia, in DM, 60PGN. see peptidoglycanpharmacologic treatment
in periodontal disease, 12in pregnancy, 253, 253–254, 254t
“phossy jaw,” 272physiologic anemia of pregnancy, 252Pioglitazone (thiazolidinedione), 71–73, 72tplaques. see atheromatous plaques; dental plaqueplasminogen activator inhibitor type-2 (PAI-2), in
pregnancy, 256platelet-derived growth factors (PDGF), in host-
modulation therapy, 19, 20pneumococcal vaccination, in DM, 69tpneumonia, 17, 52, 147–149, 153–154polymyxin B sulfate, in ventilator-associated
pneumonia, 153Porphyromonas gingivalis
in animal studies, 89, 142in connective tissue, 27as indicator of atherosclerosis, 119in pregnancy, 133, 140, 144in RA, 190, 191fSocransky’s research on, 2in spontaneous abortion, 50
postmenopausal osteoporosis, 164, 167, 168practitioner-to-patient communication, 288, 296Pramlintide (amylin), 75Prandin (repaglinide), 226tprediabetic state, 62, 63t, 217preeclampsia
clinical presentation, 138as distinct complication, 132epinephrine contraindicated in, 253–254etiology, 260–261as hyperinflammatory state, 134pathogenesis and risk factors, 139periodontal disease association, 140
pregnancycomanagement of adolescent pregnancy, 265comanagement of complications, 258f, 259–265comanagement of DM and GDM, 75–76, 87comanagement of normal pregnancy, 252–255,
255tdental caries, 256gingivitis, 6, 256–257inflammation in, 24, 33marginal periodontitis, 257metronidazole treatment, 19patient education “sound bites,” 299–300periodontal disease management in, 132, 140physiological changes in, 250–252pre-conception recommendations, 257–259pregnancy epulis, 257
pregnancy complications linked to periodontaldisease, 132–144
animal studies supporting, 141–143association with periodontal disease, 137–138, 141clinical presentation, 133future research needs, 144human studies supporting, 140–141infant deaths from, 135–136, 135fintervention trials, 143–144pathogenesis, 133–134periodontal disease connection, 15preeclampsia, 132, 138–140preterm and low birth weight, 134–138, 137f, 138f,
139f
316 Periodontal Disease and Overall Health: A Clinician's Guide
types of complications, 133–134premature rupture of membranes, 259–260preterm birth (PTB)
in adolescents, 265effect of dental care on, 261–265and periodontal disease, 257, 258fperiodontal disease management in, 261–265risk factors for, 261risk from dental procedures, 253
Prevotella intermediain pregnancy, 256–257in RA, 190
prilocaine, in pregnancy, 253, 253t, 254tprocoagulant factors, DKA, 64professional development, and patient education, 297,
297fprogesterone, effect on periodontal health, 250, 256pro-inflammatory mediators
and cardiovascular disease, 33DKA, 64effect on metabolic control, 220–221origins of, 39fin RA, 182, 183t, 184in systemic inflammation, 30
pro-resolution mediators, 35, 36f, 37, 39fprostaglandin E2, early research on, 2prostheses, and oral cancer, 211, 284prosthetic cardiac valves, care during pregnancy, 255protamine hagedorn (NPH) insulin, 227proteases, in host response, 25, 26tprotectins, 35, 36f, 37, 38t, 39fprotein cell regulators, in plaque formation, 106protein kinase C (PKC), 107Protelos (strontium ranelate), 174PRRs. see pattern recognition receptorsPseudomonas aeruginosa
in COPD, 157in nosocomial pneumonia, 150in ventilator-associated pneumonia, 152, 152f
PTB. see preterm birthptyalism, in pregnancy, 251
RRA, periodontal disease management in, 189radiation therapy, in head and neck cancer, 283–284radiography, in pregnancy, 253receptor activator for nuclear factor B ligand
(RANKL), 162–164, 164freceptor agonists, in inflammation resolution, 35receptor for AGEs (RAGE), 107recombinant human bone morphogenetic protein-2
(rhBMP-2), 19, 20–21refractory periodontitis, 18–19renal disease. see kidney diseaserenin, 275, 276repaglinide (Prandin), 71–73, 72t, 226t
“resolution deficit” phenotype, 39resolvins, 35, 36f, 37, 38t, 39frespiratory tract, changes in pregnancy, 251–252respiratory tract diseases, periodontal disease
association, 147–157, 156, 157respiratory tract diseases associated with oral flora
bacterial strains involved, 152–153COPD, 154–157in hospitalized patients, 157mechanisms involved, 52, 150patient education “sound bites,” 300and periodontal disease, 52pneumonia, 147–149prevention of, 153–154risk factors, 150–151, 151f
retinopathyPKC inhibitors, 107predicted by plasma glucose values, 69resolvins effect on, 37, 38t
Reynolds Risk Score, 245rhBMP-2. see recombinant human bone
morphogenetic protein-2rheumatoid arthritis (RA) and periodontal disease
clinical presentation, 179–181, 180f, 181tclinical relevance of association, 191–192cytokines in, 182, 183tas ecogenetic diseases, 186–187, 186t, 187fenvironmental risk factors, 184–186genetic component, 184inflammation in, 181–184, 182fmatrix metalloproteinases in, 182–184, 185tmechanisms of relationship, 190–191similarities, 179studies concerning relationship, 188–189, 188t
risedronate (Actonel), 172, 271–272risk factor assessment/reduction
atherosclerotic disease, 50, 106–108, 240–241,245–246
common to oral and systemic disease, 1defined, 49historical era of research, 2oral cancer, 197, 197–201, 197t, 203periodontal disease, 11, 11–12, 11t, 12t, 49see also causality factors
“Role of Sepsis and Antisepsis in Medicine, The”(Hunter), 45
Rosiglitazone (thiazolidinedione), 71–73, 72tRush, Benjamin, 43Ryff, Walter H., 43
SScottsdale Project (April 2007), 231–233SDD. see subantimicrobial-dose therapy“Secret Killer, The” (Time Magazine), 291sedation, in pregnancy, 254selective estrogen receptor modulators (SERMs), in
INDEX 317
osteoporosis, 174self-monitoring of blood glucose (SMBG), 69–70short-acting insulin secretagogues, 226t, 227“silent epidemic,” 256, 288single nucleotide polymorphisms (SNPs), in RA, 187Sitagliptin (dipeptidyl peptidase IV inhibitor), 72t, 73skeletal integrity
vs. alveolar bone loss, 168–169, 170tin osteoporosis, 166
SMBG. see self-monitoring of blood glucosesmoking. see tobacco usesocioeconomic risk factors
in pregnancy, 256in RA, 186
Socransky’s red/orange complexcontribution to periodontal disease, 2, 29in pregnancy, 133, 140, 141
sodium alendronate (Fosamax), 172sodium fluoride, 17–18soluble receptor for advanced glycation end-products
(sRAGE), in animal studies, 90“sound bites” for patient education, 297–301spontaneous abortion, 259squamous cell carcinomas, 283–284sRAGE, periodontal disease management, 90–91SSA proteins, role in inflammation, 31stannous fluoride/sodium hexametaphosphate, 17–18Staphylococcus aureus
in community-acquired pneumonia, 148, 150in COPD, 157in nosocomial pneumonia, 150in ventilator-associated pneumonia, 151, 152
Starlix (nateglinide), 226tstatins
and CRP, 106, 240in hyperlipidemia, 244–245in inflammation, 39
Streptococcus agalactiae, in community-acquiredpneumonia, 147
Streptococcus mutans, maternal vs. child, 256Streptococcus pneumoniae
in community-acquired pneumonia, 147in COPD, 156
Streptococcus sanguis, 50Streptococcus species, in pregnancy, 141stress, in chronic periodontitis, 8strokes
DM as a risk factor, 55due to atherosclerotic disease, 105
strontium ranelate (Protelos), 174sucralfate, in radiation therapy, 283sudden cardiac death, in atherosclerotic disease, 242sugar intake, in atherosclerotic disease, 246sulfonylureas, 71–73, 72t, 226t, 227supine hypotension syndrome, 251, 253syndemic approach, 233
synovial fluid, periodontopathic bacteria in, 190systemic disease, metastasis from local infections, 44systemic inflammation
biomarkers decreased with Arestin treatment, 18caused by periodontal disease, 24, 27from focal infection, 42patient education “sound bites,” 297reduction with subantimicrobial-dose therapy, 20see also oral-systemic relationship
Ttacrolimus, in kidney disease, 278Tannerella forsythensis
in preeclampsia, 140in pregnant adolescents, 265in RA, 190Socransky’s research on, 2
tartrate acid phosphatase, 162, 163ftaxanes, 280, 280tteam-care
in DM, 233emerging need for, 289see also comanagement
teriparatide (Forteo), 173tetracyclines
contraindication in pregnancy, 255in host-modulation therapy, 19in periodontal disease, 18
thiazolidinediones, 71–73, 72t, 227thienopyridine clopidogrel, 242–244threatened abortion, 259thromboembolism, in pregnancy, 252tiludronate, 271–272Time Magazine, “The Secret Killer,” 291tissue homeostasis
disruption of, 29early research on, 2following inflammation resolution, 24in inflammatory response, 27
TLRs. see Toll-like receptorstobacco use
cessation, 15, 246, 295in chronic periodontitis, 8passive exposure, 207risk factor for atherosclerotic disease, 107–108,
238, 239frisk factor for COPD, 155risk factor for oral cancer, 197–201risk factor for RA, 186
tocolytics, in premature rupture of membranes, 259–260
Toll-like receptors (TLRs)in host response, 25, 26trole in inflammation, 31
tooth lossand GI cancer, 211as indicator of periodontal disease, 207–208
318 Periodontal Disease and Overall Health: A Clinician's Guide
topoisomerase inhibitors, 280, 280ttoxins, in host response, 25, 26ttransient ischemic attacks (TIAs), 105transplantation, 75, 277treatment model, for DM, 230fTreponema denticola, Socransky’s research on, 2Treponema pallidum, gingival lesions from, 7triclosan, 17–18T-scores, 166–167, 166ftumor necrosis factor- (TNF-)
in DM, 89effect on metabolic control, 220–221in inflammatory response, 2–3inhibition of, 90in insulin resistance, 61in insulin signaling pathways, 58–60, 59f
Type 1 vs. Type 2 diabetes mellitus (DM), 55, 60–62
UUnited Kingdom Prospective Diabetes Study
(UKPDS), 65, 97–98, 218upper digestive tract cancer, 199–200uremic syndrome, 275–276Useful Instructions on the Way to Keep Healthy, to
Strengthen and Re-invigorate the Eyes and the Sight(Ryff), 43
uterine bleeding, in pregnancy, 259
Vvaginal flora, metronidazole treatment and, 264vancomycin hydrochloride, in ventilator-associated
pneumonia, 153vascular damage in RA, 190vascular permeability, in pregnancy, 250–251vasoconstrictors, in pre-eclampsia, 260vasodilators, in kidney disease, 277ventilator-associated pneumonia (VAP), 149, 151f,
153–154ventricular fibrillation, in atherosclerotic disease, 242viral infections, in gingival disease, 7virulence factors
effect on host cells, 26tfound in connective tissue, 27of periodontal bacteria, 24, 25in remote tissues, 30
virusescancer and oral health, 210–211in RA, 191, 191f
vitamin Dactivation of, 276in bone remodeling, 164, 165fin kidney disease, 275periodontal disease management in, 52in primary osteoporosis, 167in renal replacement therapy, 277
vitiligo, 60, 68
Wweight control, co-management of, 246weight loss, in DM, 70Western New York MI/Perio Studies, 117, 120–121Wilcox, Robert, 44Women’s Health Study, 240World Health Organization (WHO), T-scores, 166–
167, 166f, 270wound healing, in DM, 227
Xxerostomia, in radiation therapy, 283–284, 285
ZZithromax (azithromycin), in community-acquired
pneumonia, 148Zometa (zoledronic acid), 172, 271–272
INDEX 319

Renowned clinicians and scientists worldwide have studied the
relationship of periodontal disease to overall health and disease.
We are fortunate to have assembled such a respected and scholarly
body of contributors who, in eighteen chapters, provide a current
and thoughtful perspective on this relationship.
—Robert J. Genco, Ray C. Williams
Copyright © 2022 FDOKUMEN