Evaluation of overall toxicity of high-dosage methotrexate regimens
Upload
khangminh22Category
view
4download
0
The Access to Health Fund’s Overall Strategy
2
Sections
I. Contents and Overview 3 II. Overall Strategy 8
III. Programme Intervention Logic and Theory of Change 40 IV. M&E Strategy 67
Acronyms: ● EHO and ECBHOs: Ethnic Health Organizations and Community-based Health Organizations in
Ethnic areas, serving populations who are not (or not entirely) served by the Ministry of Health and Sports
● HMIS: Health management Information System ● IPs: Implementing Partners ● MNCH: Maternal, Newborn and Child Health ● MOHS: Ministry of Health and Sports ● SRHR: Sexual Reproductive Health and Rights
3
Contents
Contents 3 Overview 6
The Access to Health Fund’s Strategy 9 I. Myanmar and the Access to Health Fund 9
Health in Myanmar 9 The Access to Health Fund 10
II. The Access to Health Fund’s Strategy 111 III. A focus on vulnerable populations in conflict-affected areas: definitions 133 IV. Service-delivery 177 V. Demand-side and alleviation of barriers to access 199 VI. Health System Strengthening 20 VII. Strategic considerations for the Fund’s work in ethnic and contested areas 211
Increased opportunities for joint MOHS/EHO dialogue and initiatives 244 Increased decision making for ethnic groups and women 244
VIII. Strategic considerations for the Fund’s work in Rakhine 245 IX. Strategic considerations for the Fund’s work in the Development/Humanitarian nexus 26 X. Monitoring and Evaluation 277 XI. Key Principles 30 XII. Annexes 31 Programme Intervention Logic and Theory of Change 411 I. Purpose 411 II. An evidence-based approach 411 III. Guiding Principles 433 IV. Maternal and Child Health: reducing Maternal, Neonatal, and Under-5 Mortality 444
4.1. Global Evidence 444 4.2. Myanmar-specific obstacles 455 4.3. Intervention logic 466
Maternal Health 466 Sexual and Reproductive Health and Rights 477 Child Health 499
4.4. Interventions and desired outcomes 50 4.5. Assumptions 511 4.6. Alternative or additional interventions 522
V. HIV: Work on Harm Reduction 533 5.1. Global Evidence 533 5.2. Myanmar-specific obstacles 544 5.3. Intervention Logic 555 5.4. Interventions 555 5.5. Assumptions 566 5.6. Alternative interventions 577
4
VI. Tuberculosis 577 6.1. Global Evidence 577 6.2. Myanmar-specific obstacles 578 6.3. Intervention Logic 588 6.4. Assumptions 60 6.5. Alternative interventions 60
VII. Malaria 60 7.1. Global Evidence 60 7.2. Myanmar-specific obstacles 6161 7.3. Intervention Logic 612 7.4. Assumptions 622 7.5. Alternative interventions 622
VIII. Health Systems Strengthening 622 8.1. Global Evidence 622 8.2. Myanmar-specific obstacles 633 8.3. Intervention Logic 655 8.4. Assumptions 677 8.5. Alternative interventions 677
IX. Social Cohesion 677 Monitoring and Evaluation Strategy 688
1.1. Programme Context 688 1.2. Programme Strategy 69 1.3. Monitoring and Evaluation Strategy Development Process 69
1. Monitoring, Evaluation and Learning 70 2.1. Spheres of Control, Influence and Interest 70
Sphere of Control 711 Sphere of Influence 722 Sphere of Interest 733
2.2. Monitoring and Evaluation on Two Levels 744 Level 1: Implementing Partners 744 Level 2: The Fund Management Office 766
2.3. Units of Intervention and Units of Monitoring 777 2.4. Learning 788
2. The Fund’s Monitoring Plan 79 3.1. Monitoring Grant Outputs 79 3.2. Monitoring Grant Outcomes 79 3.3. Monitoring Programme Outcomes 844 3.4. Additional Elements of the Monitoring Plan 889
Population-Based Surveys 890 Monitoring Social Equity and Gender Equality 900 Monitoring Programme Quality 911
5
3. The Access Evaluation Plan 911 4.1. Evaluations of Access Grants 912 4.2. Programme Evaluation 922
The Mid-Term Evaluation 922 The Final Evaluation 933 Value For Money Analysis 944
Annex 1 – Initial list of Grant Output indicators for reporting under Access 955 Annex 2 – Unit of Implementation and Unit of Monitoring in Integrated Grants (2021-23) 977
6
Overview
The purpose of this document is to present a number of papers which, taken together, make up the Access to Health Fund’s Overall Strategy. The documents are in two categories: constitutive documents and core documents.
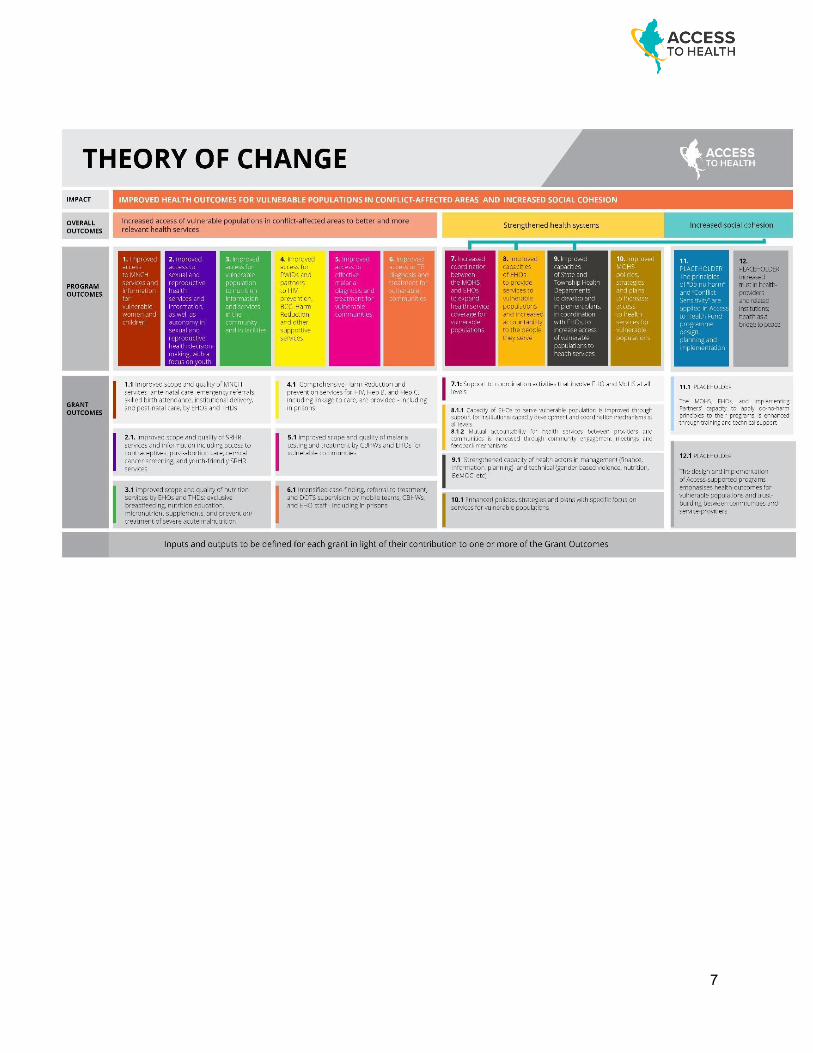
The Fund Management Office will be guided by this Strategy in all of its actions and decisions (and will ensure the Fund’s Partners are equally guided by this Strategy) - not deviating from approaches, service packages, partnerships, or any other agreements described herein without formal Board approval. The Fund’s Strategy however is flexible and adaptive - adapting to changing contexts, to lessons learned, to the Fund’s evolving understanding of its mission and best practices, to priorities voiced by key partners, to risks and opportunities... As a direct consequence, this Overall Strategy once approved by the Board will remain a living document, updated from time to time at the Access to Health Fund Board’s discretion - and when relevant, the Fund Management Office will be expected to bring to the Board requests for flexibility and adaptation. 1. Constitutive documents 1.1. The Joint Collaboration Arrangement, signed by Donors on the 20th November 2018 determines that the Fund, formerly known as the Three Millennium Development Goal Fund (3MDG), will adopt a new phase of programme and be known as the Access to Health Fund from 01 January 2019 for five years. The JCA notes the overarching goal of the Access to Health Fund: to contribute to progress towards the health Sustainable Development Goals (SDGs). Specifically to improve the health status of the population by reducing the maternal, neonatal, and child mortality; increasing sexual and reproductive health and rights; reducing HIV and malaria prevalence; and reducing tuberculosis incidence. The Fund will further the Myanmar Government’s commitment to achieve Universal Health Coverage by 2030 and focus on serving the most vulnerable populations: people living in hard-to-reach and conflict-affected areas, and other populations that the government cannot easily reach or support. 1.2. The Description of Actions describes the operating context and level of intervention of the Access to Health Fund. It also presents the program’s goal, purpose and outputs, as well as the Fund’s Theory of Change. The DOA notes that the Fund builds on a number of core priorities: a focus on conflict-affected areas and on work with both the MOHS and Ethnic Health Organizations; a conflict-sensitive Programme Management approach; a gender and a Human Rights Based Approach, ensuring service-provision understands and alleviates barriers to women’s (and other vulnerable groups’) access to health; and strengthening the health system to ensure sustainable essential services. 2. Core documents 2.1. The Access to Health Fund Strategy lays out the Fund’s vision, goals, objectives, and approaches, summarized in the diagramme on the following page.
7
8
2.2. The Fund’s approach to engaging with Ethnic Health Organizations and Ethnic Community Based Health Organizations (EHO and ECBHOs) is summarized in the overall strategy (as well as being captured in a more detailed working paper). It outlines ways in which the Fund strives to strengthen EHO and ECBHO capacity, improve service-delivery in areas where they are active, increase collaboration between EHO and ECBHOs and the Ministry of Health and Sports where possible, increase coordination among ethnic health organizations, and support improved health outcomes for populations covered by EHO and ECBHOs. Given its focus on conflict-affected areas, the Fund’s approach to EHO and ECBHOs is an integral part of its overall strategy. 2.3. The Theory of Change Narrative provides a logical path linking the Fund’s expected impact with interventions, outputs, and outcomes. It also outlines assumptions and provides justification for the Fund’s proposed approaches, based on global evidence and an analysis of Myanmar-specific gaps. 2.4. The Monitoring and Evaluation Strategy sets out the Fund’s approach to monitoring changes brought about at all levels - from individual grants all the way to overall programme impact - and its approach to mid-term and final evaluations. This is summarized in the strategy, as well as attached in its entirety.
9
The Access to Health Fund’s Strategy I. Myanmar and the Access to Health Fund
Health in Myanmar
1. Over the last half a century of isolation, Myanmar has seen very low levels of basic health services, poor infrastructure, shortage of trained medical and paramedical staff, a chronic shortage of essential drugs and supplies, and high levels of out-of-pocket payments for health. Discrepancies in health services between central and peripheral areas mean that the health situation is notably worse in remote and hard-to-reach geographical areas, which often overlap with areas of conflict.
2. Myanmar is the site of the world’s longest running civil war. Large swaths of the country are not accessible to government health providers because they lie outside of government control, or are under mixed (government and ethnic) control. In these places, communities are reliant on Ethnic Health Organizations and Community-Based Health Organizations (EHOs and ECBHOs) for care and prevention services; these organizations may be severely under-resourced, and support provided to them operates within the interim arrangements framework. As the peace process continues, the term ‘interim arrangements’ is used to describe governance and service-delivery arrangements in conflict-affected areas between the times of an initial ceasefire to comprehensive peace agreement; these include work in support to EHOs and ECBHOs, and the relationship between these organizations and government systems.
3. Country background: a. Based on the 2014 Census, Myanmar’s Maternal Mortality Ratio is at 282 per 100,000 live
births1; under-five mortality rate is at 71, and Infant mortality rate (IMR) at 622. All three rates are more than double those observed in the rest of South-East Asia.
b. According to the 2015-16 Myanmar Demographic Health Survey, 27% of under-five children are stunted (especially in rural areas), 7% are wasted, and 19% are underweight3.
c. The contraceptive prevalence rate among married women aged 15-49 is 52%, which puts Myanmar on track for meeting its “FP 2020”4 commitment; nonetheless, 16% of married women in the country have an unmet need for family planning5.
d. HIV/AIDS, with 11,000 new infections each year, is a major public health problem. More than a quarter of new infections (28%) are among people who inject drugs. There are approximately 93,000 people who inject drugs in Myanmar,6 and HIV prevalence among them has increased from 28.5%7 in 2014 to 34.9% in 2017.8
e. A national Tuberculosis prevalence survey conducted in 2017-2018 found that Tuberculosis prevalence declined from 613 per 100,000 people in 2009 to 466 per 100,000, but with high
1 Census 2014 2 Census 2014 3 MDHS 2015-16 4 MDHS 2015-16 5 MDHS 2015-16 6 IBBS; Integrated HIV Bio-Behavioral Surveillance 2017 7 IBBS; Integrated HIV Bio-Behavioral Surveillance 2014 8 IBBS; Integrated HIV Bio-Behavioral Surveillance 2017
10
pockets of Tuberculosis and drug-resistant Tuberculosis in Yangon and other geographies.
4. Health indicators in conflict-affected States fare lower than national indicators. In the Access to Health Fund’s focus States, for example (based on MDHS 2015-2016): a. Institutional deliveries in Kachin (30%), Kayah (29%) Rakhine (19%) and Shan (28% are
considerably lower than the Union result of 37%. b. Basic vaccination coverage rates among children under 2 year of age are similarly much lower
in Rakhine (41%) and Shan (46%) compared to the Union average of 55%. c. Stunting among children under 5 is significantly higher in Kachin (36%), Kayah (40%), Rakhine
(38%) and Shan (37%) than the Union average of 29%.
5. The Government of Myanmar’s commitment to Universal Health Coverage by 2030 prioritizes questions of equity and access to health for the most marginalized populations. The Ministry of Health and Sports (MOHS) launched the 2017-2021 National Health Plan (NHP) identifying the country’s priorities, needs, and gaps. The National Health Plan provides a roadmap to the Access to Health Fund, including: a. Phased access to an ‘Essential Package of Health Services’ for the entire population; b. An emphasis on primary health care delivered at township level and below; c. A defined role for health providers outside the Ministry of Health and Sports, including EHOs
and ECBHOs, non-government organizations, and private providers; d. A shift away from top-down planning and towards a more inclusive approach; e. Recognition of the critical role of health systems strengthening in creating a health system
that is self-reliant and supports universal access.
The Access to Health Fund
6. The Access to Health Fund (Access) is a multi-donor fund that began operation in January 2019. The Fund is driven by the conviction that pooling donor resources enables programme coherence and leads to greater impact. At the writing of this Strategy, Access has received funding from four Donors – the UK, Sweden, USAID, and Switzerland. The United Nations Office for Project Services (UNOPS) is contracted as the Fund Manager, to administer the funds and provide monitoring and oversight.
7. Access (2019-2023) is the third round of multi-donor financing for health in Myanmar – and builds on the work of the Three Diseases Fund (2007-2012) and the 3MDG Fund (2013-2018). The purpose of the present strategy is to ensure that Access maximizes its impact and delivers on its commitments as captured in this document.
8. The Fund will focus its interventions in Rakhine, Kachin, Shan, Kayin, Kayah and Mon States – all States affected by latent or active conflict. The Fund will also be active in Yangon, Sagaing, and
11
Chin State.
9. The Access to Health Fund works with the Ministry of Health and Sports, Implementing Partners, Community-based Organizations, EHOs and ECBHOs and the private sector, including in places that the government is not able to reach and support, and where EHOs and ECBHOs provide primary health care (non-government controlled areas and mixed areas). The Fund targets some of Myanmar’s least equitable access-to-health situations by bringing health services to vulnerable populations in conflict-affected areas, and supports the strengthening of Health and Community Systems for immediate and long-term improvement of Myanmar’s health response.
10. With its focus on vulnerable populations in conflict-affected areas, the Access to Health Fund works in the ‘nexus’ of (or intersection between) development and humanitarian work, funding programmes which address the health needs of the most vulnerable people in conflict affected areas, as well as improved and sustainable health outcomes, contributing to reduced humanitarian dependency. The Fund also touches on the third component of the ‘nexus’ – peace – by supporting social cohesion through the promotion of dialogue and collaboration between the Ministry of Health and Sports and EHOs and ECBHOs.
II. The Access to Health Fund’s Strategy 11. The Access to Health Fund aims to provide long-term systemic improvements to Myanmar’s
Health response, beyond the life of its individual interventions and activities. 12. The Fund is driven by the vision of vulnerable populations in conflict-affected areas having full
access to healthcare and improved health outcomes, under Myanmar’s commitment to Universal Health Coverage. In the Fund’s vision, access is ensured through joint efforts by EHOs and ECBHOs, the Ministry of Health and Sports and civil society, thus contributing to dialogue, social cohesion, and peace.
13. To deliver on this vision, the Fund’s goals are to increase access of vulnerable populations in conflict-affected areas to quality essential health services, increase populations’ health-seeking behaviour, ensure that health systems serve these populations’ needs, and increase coordination/collaboration between the Ministry of Health and Sports, EHOs and ECBHOs, and other actors to reach vulnerable people in conflict-affected areas with quality essential health services.
14. Access will achieve its goal by focusing on the following program objectives, which themselves are
focused on vulnerable populations in conflict-affected areas: 1. More and better quality health services delivered by government and ethnic/non-government
actors 2. More and more informed demand for health services 3. Alleviate barriers to access to services
12
4. Improved accountability of Ministry of Health and Sports and EHOs and ECBHOs to vulnerable populations
5. Improved capacity of institutional systems to deliver quality services 6. Increased decision making for ethnic groups and women 7. Increased opportunities for joint dialogue and initiatives between the Ministry of Health and
Sports and EHOs and ECBHOs. 15. Partnerships and Collaboration. The Access to Health Fund coordinates with Partners to ensure
complementarity of interventions and the avoidance of inefficiencies and duplicated efforts. The Fund will be meeting key actors (the Humanitarian Health Cluster, the Global Fund, UN agencies, the World Bank) on a regular basis to ensure mutual information about programmes and plans, and conduct joint planning. In addition to the Ministry of Health and Sports, the Fund collaborates with the Ministry of Home Affairs (e.g. on prison health), the Ministry of Social Welfare (e.g. discussions about nutrition behavior-change communication alongside Maternal Cash-Transfers) and is always open to collaboration with other Ministries and institutions.
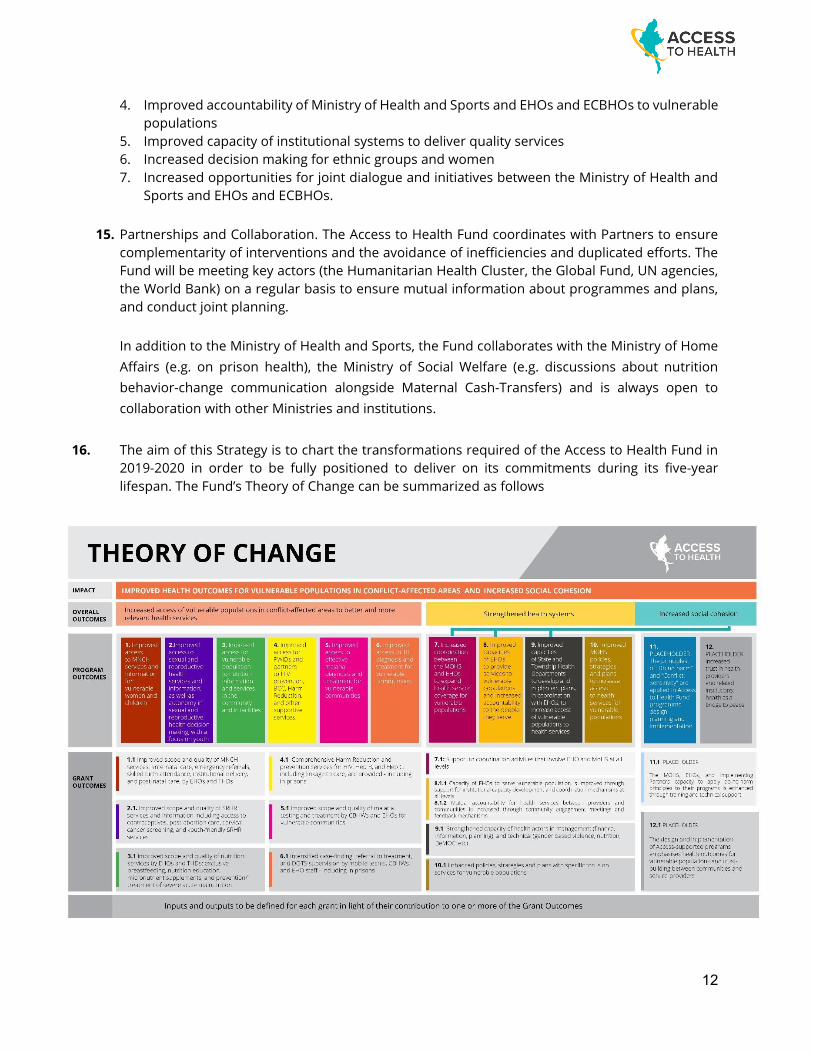
16. The aim of this Strategy is to chart the transformations required of the Access to Health Fund in
2019-2020 in order to be fully positioned to deliver on its commitments during its five-year lifespan. The Fund’s Theory of Change can be summarized as follows
13
III. A focus on vulnerable populations in conflict-affected areas: definitions 17. Under this Strategy, investments by the Access to Health Fund will only be made if they
predominantly serve to improve access to health for vulnerable populations in conflict-affected areas. Investment analyses will start from an understanding of barriers to access, and a clear link between proposed services (or Health System Strengthening activities) and the alleviation of these barriers.
18. The Fund applies three consecutive filters to identify target populations: a. A geographic filter, applied to select conflict-affected areas; b. A programming filter, applied to select program townships; c. A vulnerability filter, applied to select vulnerable populations eligible to Access support.
19. Conflict-affected areas in this Strategy are defined as Townships with latent or active armed
clashes9 or widespread violence over the last five years that resulted in fatalities and displacement. The definition also includes populations who are victims of protracted crises – for example Internally Displaced Populations displaced by past/ongoing conflicts and experiencing situations of vulnerability and limited access to health
20. Conflict-affected Townships (for 2021-2023 programming) are identified on the basis of the above
definition and a number of recent reports on conflict and vulnerability in Myanmar10, which use different pointers to classify subnational conflicts.
21. The Fund expects to identify – and prioritize for programming – between 50 and 100 conflict-
affected Townships (as compared with 82 Townships covered in Years 1 and 2 of the Fund), taking into account the balance between breadth (number of townships covered by the Fund) and depth (namely the nature and scope of interventions made possible by different levels of investment). The Fund will work with relevant Partners to determine which programmes can already start moving out of non-conflict Townships and into conflict-affected Townships in 2019-2020 – but the expectation remains that the shift will take place after the current contracts (signed for 2019-2020) are renewed for 2021-2023. This work will specifically involve the humanitarian Health Cluster to ensure complementarity.
22. The Fund upholds the principle of flexibility, and has allowed three exceptions to its focus on
conflict-affected areas: a. Access will be funding Tuberculosis and multidrug resistant Tuberculosis interventions in
Yangon; b. The Fund will pursue activities in Chin State, due to significant health needs, remoteness and
underserved populations, and taking into account also the need to consolidate gains from 3MDG-funded programs in a very challenging context;
9 Armed clashes may take a variety of forms, such as a clash between state security forces and non-state actors, two or more non-state actors, security forces and civilians, or non-state actors and civilians. 10 “Contested Areas of Myanmar: Subnational Conflict, Aid, and Development”, Asia Foundation “Vulnerability in Myanmar: a Secondary Data Review of Needs, Coverage and Gaps”, MIMU/HARP “Annual Peace and Security Review 2018”, Myanmar Institute for Peace and Security “Deciphering Myanmar Peace Process 2017-2018 (Myanmar Version)”, Myanmar Peace Monitor
14
c. The Fund Board has allowed funding of Harm Reduction interventions in Sagaing, across the State-border from Kachin, due to significant health needs, remoteness and underserved populations and in order to ensure continuity and coherence in the Fund’s response.
23. The third filter aims to identify vulnerable populations eligible for Access to Health Fund support.
The following describes the Fund’s approach to defining these populations under different types of interventions:
a. Integrated grants
Integrated grants comprise MNCH interventions, community-based TB care, and diagnosis and treatment of malaria through Community-based Health Workers. Geographic vulnerability Area Populations eligible for support
Non-Government controlled areas
All populations whose health needs are covered by EHOs and ECBHOs
Areas of mixed control
All populations whose health needs are covered by EHOs and ECBHOs and the MOHS
Government- controlled areas
Population of hard-to-reach villages in ACCESS-supported townships. ‘Hard-to-reach’ villages will be defined jointly by the THD and IP, based on specific criteria (e.g. distance to the health facility). Note: Rakhine is an exception, for conflict-sensitivity considerations. ACCESS will continue supporting township-wide approach
IDP camps All populations residing in Internally Displaced Population (IDP) camps
b. Sexual and Reproductive Health and Rights grants
Populations running a distinct health risk with no alternative access to information or services. This category may include women and girls in need of post abortion care, contraceptive commodities,11 and SRHR services; young people who are out of school, working, migrating, living in remote rural areas, using drugs or at-risk of drug use, orphaned, discriminated against, or mentally or physically disabled.
c. Harm Reduction and Prison-health grants
In addition to HIV and STI services, this comprises Hepatitis B and C testing, vaccination, and small-scale treatment programme;12 mental health counselling and therapy; TB screening/referral; and malaria testing/ treatment activities.
11 Commodities are available nationwide, for greater coverage 12 The Hepatitis C treatment programme is only supported in prisons - this is currently under discussion.
15
Vulnerable populations under these grants are defined as (i) all people who inject/use drugs and their intimate partners, and (ii) people detained in prisons where ACCESS supports interventions.
d. Tuberculosis Active Case Finding grants
Vulnerable populations under these grants are defined as all people with presumptive TB in ACCESS-supported townships.
e. Emergency Referrals
Under the Access strategy, emergency-referral support in conflict-affected townships is extended to all pregnant women with danger signs who need to be referred to a health facility and under-five children under 5 who need emergency care13. Support is extended throughout the township, but will be limited to the cost of transportation and meals.
24. The Fund’s Strategy for the next five years requires that the Fund and its Partners be able to define
and identify vulnerable populations, identify gaps in their access to health, work to improve their access through services, Community Systems Strengthening, and Health Systems Strengthening, and be able to measure the difference the Fund makes to these populations’ health outcomes:
a. The identification of vulnerable populations in each geography will build on the definitions
above as well as on consultations with Partners (including the Humanitarian Health Cluster), available data (census, Demographic Health Survey, other surveys), Township mapping and situation-analysis exercises, local knowledge and understanding of populations’ socio-economic status, and other available knowledge (studies, publications…)
b. Identifying gaps in people’s access will require consultations and the development of an
overview of barriers to access. This will be based on community feedback mechanisms, follow-on studies commissioned by the Fund as needed, and existing knowledge – including information and analysis developed by the Humanitarian Health Cluster and Humanitarian Response Plan.
c. Improving populations’ access will require investing in services and Health System Strengthening activities which predominantly serve the needs of vulnerable populations. However, the Fund’s ability to report on population subsets in some Townships14 is limited by the national Health Management Information System, which does not identify vulnerable populations, and the multitude of EHOs and ECBHOs information systems which may or may
13 This inclusive approach is in recognition of two township-level realities:
- In many of the townships supported by the Fund, a large number of women and children fall in the “vulnerable” category;
- Some would be in that category because of poverty, but a proactive identification of poor beneficiaries would require a significant investment, which the Fund’s implementing partners would not be able to make.
14 Townships in which the Fund is supporting integrated programmes, namely programmes covering more than one disease and funding more than one intervention
16
not track vulnerabilities (this will be further explored)"; the Fund, weary of creating parallel reporting systems, has been relying on national systems for its reporting. Improving reporting on vulnerable populations’ access requires that: - The Access to Health Fund commission program-level survey, special studies, and adaptive
monitoring approaches – which the Fund will do - The HMIS improve its capacity to report on services to vulnerable populations; while this
is outside of the Fund’s mandate, Access will seek opportunities to advocate the MOHS in that direction.
- As far as routine-reporting goes, when it comes to integrated grants in conflict-affected Townships, Access will explore with NGO Implementing Partners and EHOs and ECBHOs the feasibility of approximating the proportion of vulnerable beneficiaries. This will be done by making an assumption on the percentage of vulnerable people in a given area, and applying this percentage to the Fund’s spend, services delivered, people reached, and achievements.
d. Whenever possible, the Fund will be guided by the following considerations:
- Health services supported by the Fund will aim to serve a majority of beneficiaries who can be defined as ‘vulnerable’; the Fund will set targets of vulnerable people reached at 60%, 80% or more. Exceptions to this principle will only touch on interventions which (by definition) serve all populations – for example when supporting infrastructure construction, immunization activities, or providing prevention messages which will reach vulnerable and non-vulnerable populations alike.
- When funding Health System Strengthening activities, the Fund will ensure that each activity either (i) has a direct benefit to vulnerable populations (e.g. reinforcing the Township’s capacity to reach vulnerable people) or (ii) can demonstrate an indirect benefit (e.g. support to a national policy which benefits all populations but is particularly relevant to vulnerable people)
- The Fund will only support Community Systems Strengthening activities in vulnerable communities15
- By focusing on understanding and addressing barriers to access (e.g. language, trust, physical access, traditional and cultural taboos…), the Access to Health Fund will aim to ensure that services are as accessible as possible to vulnerable populations.
e. (Please refer to the M&E Strategy, below, for more detailed explanations on this point)
Measuring the difference the Fund makes to vulnerable populations’ access and health is challenging, as the Fund relies to a large extent on national data systems and standardized indicators and as Myanmar at the moment does not have measures focused on vulnerable populations. As routine reporting does not include measurements specific to health outcomes among vulnerable populations, program-level surveys, special studies, and adaptive monitoring approaches will be required. The following dependencies, which will be considered and addressed during the development of the M&E Strategy, need to be noted: - In order to undertake a program-level survey, the FMO will need to (i) seek permissions
from the MoHS and relevant ethnic authorities, (ii) overcome issues related to the feasibility of studies in areas of limited security, and (iii) explore funding options.
15 The only caveat to that consideration being the need for a context-sensitive approach, to ensure the Fund does not harm social cohesion by providing one-sided support
17
- Monitoring of the new approaches focused on vulnerable groups will require adequate resourcing both by Implementing Partners and the FMO. The FMO will work to secure a pool of specialized technical experts available ‘on call’.
- As the focus on vulnerable populations increases, original result-projections are likely to decrease, while intervention unit-costs increase. When results projected in the original Business Case cannot be decreased (e.g. because of Donor commitments to global targets), the Fund will discuss alternative approaches with the Board.
25. The Access to Health Fund’s Logframe will be developed based on the Fund’s Overall Strategy and
annexed to it once approved by the Board. IV. Service-delivery 26. Thematically, the Access to Health Fund invests in three areas: quality essential services, Health
System Strengthening, and the Demand-side.
27. The Fund invests to bring quality essential health services to vulnerable populations in conflict-affected areas and achieve improvements in health outcomes along several themes:
a. Maternal, Newborn and Child Health:
- The Fund supports capacity-building for health staff (Ministry, EHOs and ECBHOs), outreach activities for the provision of essential MNCH services (antenatal and postnatal care, immunization, nutrition, referrals), and planning and coordination support (EHOs and ECBHOs, Township Health Departments, Township Health Working Groups)
- The Fund also supports EHO health-posts with medicines and equipment, mobile visits conducted by EHO health staff, capacity building, and coordination with MOHS for services such as immunization
- Interventions focus on vulnerable populations as defined above. - Examples of expected outputs16 include:
▪ Number and percentage of births attended by skilled health personnel (doctor, nurse, lady health visitor or midwife)
▪ Number and percentage of children under one immunized with Penta3
b. Nutrition: - The Fund strengthens the delivery of quality nutrition services to pregnant and lactating
women, and to children under five years of age, including micronutrient supplementation and nutrition promotion activities.
- A focus on vulnerable populations is ensured through the implementation of the Access-supported Multi-sectoral State/Regional Nutrition Action Plan, coupled with supportive supervision by State/Regional Nutrition Teams of work implemented by EHOs and ECBHOs, Implementing Partners, Basic Health Staff, and volunteers.
- Examples of expected outputs include: ▪ Number of newborns initiating breastfeeding within one hour of birth
16 Specific indicators (all areas) will be developed and proposed in the Logframe, once the programmatic service delivery approaches and data system capacities have been clarified
18
▪ Number of under 5 children screened for malnutrition ▪ Number of pregnant mothers receiving Infant and Young Child Feeding counselling
c. Sexual Reproductive Health and Rights
- The Fund supports improved access for young people (age 15-24) to sexual and reproductive health and rights information, knowledge, goods and services.
- The Fund promotes young people’s knowledge and skills on SRHR, including comprehensive sexuality education and capacity building on life-skills and gender-based violence;
- The Fund promotes access to youth-friendly SRHR services through training of general practitioners;
- The Fund provides SRHR services, family planning contraceptives for women aged 15-49, cervical cancer screening and post-abortion care.
- The Fund supports the prevention of gender-based violence and care activities - SRHR activities focus on vulnerable populations as defined above – including migrants, IDPs,
out-of-school youth, disabled persons (mental and/or physical), and other vulnerable populations in conflict-affected areas.
- Examples of expected outputs include: Modern contraceptive prevalence rate among married women
d. HIV/Harm Reduction:
- The Fund supports comprehensive harm-reduction services focused on HIV prevention, including needle and syringe exchange programs, HIV testing, Hepatitis B testing and vaccination, Hepatitis C testing, TB screening and referral, overdose management, condom distribution, referrals for antiretroviral therapy, opioid substitution therapy, and sexual and reproductive health services.
- A focus on vulnerable populations is ensured through peer-based outreach, centre-based primary health care, and mobile HIV testing. The overlap between the most vulnerable and at-risk populations for HIV (and other Sexually Transmitted Infections, TB and Hepatitis C) and those most in need of SRHR services is significant, including sex workers, men who have sex with men, people who inject drugs, and prison/camp populations.
- Services are made available for people who use drugs but also for their intimate partners and family members, who are able to access prevention and treatment services in one place.
- Examples of expected outputs include: Number and percentage of people who inject drugs testing positive for HIV, who enrol on ART treatment
e. Tuberculosis and MDR TB: - The Fund aims to accelerate TB case-finding through mobile teams and community
volunteers, coordinate with EHO health staff for Active Case Finding, referral, and improved case holding, and ensure treatment compliance through DOTS supervision.
- The program will target vulnerable populations likely to comprise of undetected TB cases. - Examples of expected outputs include:
▪ Number of notified cases of all forms of tuberculosis ▪ Number of MDR TB patients detected and treated (Yangon only)
f. Malaria: - The Fund supports the Ministry's Malaria Elimination strategy and Integrated Community
19
Malaria Volunteer (ICMV) strategy - The programme will be recruiting ICMVs and training EHO and ECBHO health staff in hard-to-
reach areas, where vulnerable groups are located. - Examples of expected outputs include: Number of confirmed malaria cases treated in
accordance with national malaria treatment guidelines.
g. Health in Prisons: - The Fund helps operationalize Standard Operating Procedures for Health Care in prisons,
including capacity building of prison health staff - The Fund supports HIV testing and referral for treatment, provision of Hepatitis C screening
and treatment to prisoners (and in particular people who inject drugs), pre-entry screening of syphilis, health education, screening/referral for sexually transmitted infection and (in some prisons) hepatitis B testing and vaccination.
- Prisons are selected based on disease prevalence and estimated numbers of drug users. - Examples of expected outputs include: Number of HIV positive prisoners who received
treatment for HIV. V. Demand-side and alleviation of barriers to access 28. The Fund pays special attention to the Demand-side of Health, exploring barriers to healthcare
access, and supporting coordination between public health providers and local organizations (EHOs and ECBHOs, Faith Based Organizations…) to alleviate obstacles, maximize resources, and serve vulnerable populations.
29. The Fund will focus on: a. Demand generation. Supporting demand-generation activities: increased community
Health awareness and literacy, increased Health-seeking behavior by vulnerable populations, increased mutual accountability between communities and providers
b. Health information sharing, promotion and education sessions in local languages in collaboration with local partners
c. Voices of communities. Mechanisms to bring out the voices of communities, build trust, and create strong linkages between health and community systems
d. Community engagement meetings/events between healthcare providers and community representatives at township and RHC levels, to exchange information, build trust, and improve a linkage between health system and community system.
e. Working to increase women’s representation in decision-making f. Greater community engagement by the MOHS and Implementing Partners g. Capacity building. Building capacity of community-systems (including community-based
emergency-referral support) and reinforcing community-level health structures and health-governance (Community-based Health Workers, village health committees, self-help groups…)
h. Partnership with EHOs and ECBHOs and local organizations to help build their capacity i. strengthening capacity of village health committees/peer groups/self-help groups
including increasing women representation to overcome gender related constraints j. Recruitment of (and skills-development for) local staff k. Support to community volunteers for basic essential services
20
l. Financial protection. Increased financial protection, including through strategic purchasing: conducting strategic purchasing pilots to contribute to the broader health financing agenda
m. Improved services. Context-appropriate community feedback mechanisms to address issues raised by communities in order to enhance the responsiveness of health systems
30. Access will continue to work with Implementing Partners and EHOs and ECBHOs to overcome any additional barriers that come up in project implementation.
31. To enhance health-service accountability and responsiveness to vulnerable populations, the Fund will provide needs-based capacity development support to target communities, the MoHS, EHOs and ECBHOs, and implementing partners.
32. Context-appropriate community feedback mechanisms and community engagement approaches, supported by the Fund, will provide space for vulnerable people to share their views, be heard, and be empowered to own their health outcomes, which in turn will enhance the responsiveness of the health systems. Listening to community voices in relation to the Fund’s activities is an important way of ensuring that health-service providers are accountable, responsive, address issues, and adjust their programs in a timely manner. This allows them to meet the health needs of vulnerable populations.
VI. Health System Strengthening 33. To ensure the sustainability of Myanmar’s Health response and its capacity to serve vulnerable
populations, the Fund invests in Health System Strengthening, with the aim of improving service-provision and quality, and increasing health equity. Through its funding to EHOs and ECBHOs and the MOHS (operational support for capacity building, improved leadership and management, improved coordination of health services, development of policies, strategies, and plans), the Fund will be constantly seeking opportunities to invest in systems that better identify and serve vulnerable populations. This includes support to strengthening forecasting, coordination and joint planning with implementing partners and EHOs and ECBHOs, and building administrative and logistic capacities. Access to Health Fund has been supporting the development of long-term costed plans (for example, the National Strategic Plans and MSNPAN) which the Ministry of Health and Sports will use to budget for future years.
34. The Fund’s investments in Health System Strengthening need to answer three questions: a. What prevents the current Health System from delivering and sustaining more quality services
to vulnerable people in conflict-affected areas? b. What additional concrete steps can Access take to close existing gaps? c. How does the Fund need to transform in order to make the biggest possible impact?
35. The Fund’s investments in Health System Strengthening will be tailored to assessed gaps and needs, as identified by the Fund and key Partners (e.g. the Humanitarian Health Cluster, the Global Fund, LIFT, UNFPA, WHO, UNICEF, the World Bank, and others); they are likely to fall into the following categories:
a. Strengthen EHOs and ECBHOs’ capacity to serve vulnerable populations: improved
21
organizational capacity; better evidence-basis; financial management; human Resources Production; guidelines development; support to inter-EHO coordination; support coordination with MOHS and Basic Health Staff at local level.
b. Strengthen MOHS capacity to serve vulnerable populations: improved financial protection; support the National Health Plan’s equity agenda; support Strategic Purchasing pilots; promote pro-vulnerable Policies. The Fund’s support will also aim to strengthen Health Systems which indirectly contribute to vulnerable populations, as long as a clear link can be established between the intervention and the health of vulnerable populations (e.g. national policies, HRH, HIS, etc.)
c. Strengthen State Health Departments’ focus on equity, and their capacity to identify and address barriers to vulnerable populations’ access to health: pro-vulnerable planning, coordination, supervision, and training…; improved quality of care; better use of evidence in decision-making and approaches.
d. Strengthen Township Health Departments’ focus on equity: strengthen their capacity to identify and address barriers to vulnerable populations’ access; focus on areas which impact vulnerable populations (introduction of the Inclusive Township Health Plan; improved Human Resources for Health; improved capacity to manage funds; reliance on functioning Township Health Working Groups; etc.)
e. Strengthen Implementing Partners’ focus on equity: consult with IPs on how they propose increasing identification and services to vulnerable populations; get IPs to play a proactive role in focusing Partners on defining and identifying vulnerable populations, identifying gaps, improving access, and measuring improvements.
f. The Fund will strive to collaborate with the Private Sector, as an important provider of health services – as recognized by the National Health Plan 2017-2021 – through commodity supply and social marketing: contraception and micronutrient powders, livelihoods activities, public private partnerships for cash transfer programmes, and mass media and health education activities.
VII. Strategic considerations for the Fund’s work in ethnic and contested areas Vision
The Fund’s vision is that of a continuous engagement with Ethnic Health Organizations and Ethnic Community-Based Health Organizations in Ethnic Areas (EHOs and ECBHOs) in Myanmar. By the end of 2023, EHOs and ECBHOs will have demonstrably improved capacity to sustainably improve health service use by poor, underserved, marginalized and vulnerable people in their areas to reduce maternal and child mortality, and to reduce the prevalence of HIV, malaria and TB. They will have expanded networks with other EHOs and ECBHOs and increased technical, financial and advocacy capacity, and increased access to technical, financial and advocacy support. EHOs and ECBHOs will have increased voice to coordinate with one another and engage individually and collectively with the Ministry of Health and Sports (MOHS). Ministry policies and practices at central and State-level will be more inclusive, allowing for more meaningful collaboration with EHOs and ECBHOs.
22
Background Large areas of Myanmar remain outside of government control, making it difficult or impossible for government health providers to access these areas and deliver health services. Ethnic Health Organizations and Ethnic Community-Based Health Organizations in Ethnic Areas (EHOs and ECBHOs) have emerged as a critical health-service provider for people living in these areas, but they often face significant challenges related to resources, security, legitimacy, and geographic coverage. Positive trends point to opportunities in bringing more and better services into ethnic areas: some EHOs and ECBHOs have seen a definite increase in their cooperation and communication with the Ministry of Health and Sports and local authorities. Several EHOs and ECBHOs across the country have seen their capacity increase significantly, allowing them to deliver health services at scale. EHOs and ECBHOs, however, have widely differing levels of maturity in their capacity, their coordination with the MOHS, their legitimacy in the eyes of the Myanmar government, and their ability to receive and manage external support.
The Fund’s work with EHOs and ECBHOs: The Access to Health Fund‘s focus on vulnerable populations in conflict-affected areas has called for enhanced engagement with EHOs and ECBHOs. Building on the work of the 3MDG Fund, who began working with EHOs and ECBHOs in September 2013, starting in January 2019, the Access to Health Fund has been supporting a number of implementing partners working with EHOs and ECBHOs. Together, these organizations cover service-delivery in Southeast Myanmar, Kachin and Shan including Special Regions of Kachin and Shan.
36. The Fund and its implementing partners are working with EHOs and ECBHOs as equals, co-
defining approaches (including capacity building) and ensuring that ownership for improvements and strengthening activities is held within the EHO/ECBHO, together with the commitment to improve themselves. The Fund will continue to pay special attention to this point and to the long-term dividends/sustainability of its capacity-building approach. In the last three years of the Fund (2021-2023) the amount of Access to Health funding to IPs working with EHOs and ECBHOs will increase. The Fund is committed to including EHO and ECBHO representation on the Board and to supporting such representation on a number of other forums such as the MHSCC and State and Township/State level meetings.
Aims of this EHO and ECBHO Strategy
37. Achieving the right engagement with EHOs and ECBHOs is vital to the Fund’s achievement of its overall strategy. Funding to EHOs and ECBHOs aims to support improved service delivery in areas where EHOs and ECBHOs are active, predominantly conflict-affected, which in turn would support improved health outcomes for populations covered by EHOs and ECBHOs. As detailed in the Fund’s Theory of Change, social cohesion will be served through the application of Do No Harm principles, greater collaboration between EHOs and ECBHOs and the Ministry of Health and Sports, and the ‘peace dividends’ experienced by populations served by EHOs and ECBHOs or jointly by them and the Ministry of Health and Sports. The Access to Health Fund aims to support
23
EHOs and ECBHOs along five lines: a. Better organizational capacity: Working with EHOs and ECBHOs to increase their capacity
to lead and manage health systems for people in their geographic areas, through strategic and operational health planning, advocacy, managing participation, general management capacity, project management and implementation capacity, accountability for results, financial management, and capacity to manage direct funding.
b. Ability to deliver more and better services: Working with EHOs and ECBHOs to increase their capacity to plan, finance and deliver more and better services to their target populations, including improved service readiness and quality, and demand creation. Measures for improved service readiness include recruitment and training of health staff, renovation of labour rooms, and technical support in assessment and supervision. On the demand side, the Fund’s Theory of Change (Section III) and Strategy (Section II) have outlined some of the efforts the Fund supports both in EHO and ECBHO areas - including community feedback mechanisms, raised awareness of available services, and mutual accountability.
c. Effective Networking: First steps have been taken by the Fund to support better networking among EHOs and ECBHOs to build common understanding, supports learning lessons from others’ experiences and challenges, and allows exploration of mechanisms such as institutionalized communication channels and the development of representative bodies.
d. Strengthened collaboration with the Ministry of Health and Sports: The Fund, as an ‘honest broker’ trusted by both the MOHS and EHO and ECBHO partners, can play a role in bringing partners together when possible, to explore ways in which two parallel health systems can increase collaboration and reach. To further such collaboration, the Fund is providing the Ministry of Health and Sports with direct grants, including grants to State Health Departments aimed in particular at a stronger work with EHOs and ECBHOs. The Fund also builds on joint mobile clinic visits, township coordination meetings, and trainings at township/state levels for increased collaboration.
e. Safeguarding: Mirroring the work it conducts with its Implementing Partners, the Fund will work with EHOs and ECBHOs to put in place better systems and processes to ensure the safeguarding of the communities EHOs and ECBHOs work with – including the prevention of sexual exploitation and abuse. Within the next three years, all supported EHOs and ECBHOs will have solid safeguarding policies and practices in place.
Principles of the EHOs and ECBHOs Engagement Strategy
38. Principles of the EHOs and ECBHOs Engagement Strategy
I.The Fund as a listener to EHOs and ECBHOs voices and needs II.Conflict Sensitivity
III.EHO and ECBHO System Strengthening IV.Contribution to social cohesion in Myanmar V.Adapting to context: one-size does not fit all
For more, please refer to the Fund’s Approach to Engaging with Ethnic Health Organizations and Ethnic Community-Based Health Organizations in Ethnic Areas.
24
Increased opportunities for joint MOHS/EHO dialogue and initiatives
39. Under this Strategy, the Fund has defined people served by EHOs and ECBHOs as one of its key target-populations, and support to EHOs and ECBHOs as one of its key objectives. In 2021-2023 (Years 3-5 of the Fund) Access will aim to significantly increase the amount and percentage of funds supporting EHOs and ECBHOs.
40. The Fund aims to provide EHOs and ECBHOs with support that is gap-filling, strategic, and based on an in-depth understanding of their needs. Listening to the voices of EHOs and ECBHOs, and understanding their situation in their own terms, is central to the Fund’s approach.
41. In its work in ethnic areas, the Fund will adopt a conflict-sensitive, ‘do no harm’ approach
42. The Fund will uphold the highest standards of transparency in its support to ethnic and contested
areas, openly disclosing and discussing plans with EHOs and ECBHOs, the MOHS, and other relevant Partners.
43. The Fund will work to support coordination between EHOs and ECBHOs as they deem it relevant,
both regionally and across the Union.
44. As part of its commitment to (i) supporting the Health Response in ethnic areas and (ii) promoting social cohesion, the Fund will seek opportunities to bring together EHOs and ECBHOs, the MOHS, and other relevant partners, to create platforms for discussion, build trust and collaboration and (when relevant and agreed) foster joint initiatives.
Increased decision making for ethnic groups and women
45. The Fund will support organizational capacity development interventions for EHOs and ECBHOs
– enhancing their leadership, governance, skills, structure, and systems. Ethnic-group representatives will be included in oversight committees and given decision-making roles. Additional support will be provided to improve EHO coordination mechanisms, and their participation in Township Health Working Groups.
46. Women in the community often have insufficient decision-making power or influence over the organization and delivery of health services, yet are an important resource in ensuring that the design and implementation of services is adapted and response. Participation, including voice and representation, empowers women and helps ensure that health services address their needs. The Fund will work with Implementing Partners to strengthen equal engagement of women and men, focusing on information sharing, participation, and community feedback mechanisms. This will enhance women’s role in personal and family health decisions, and increase their representation in decision-making forums such as Village Health Committees and self-help groups.
VIII. Strategic considerations for the Fund’s work in Rakhine 47. In the Fund’s portfolio, Rakhine poses unique challenges given institutional and informal barriers
25
to movement (and therefore to health access) for Muslim populations, and poverty-levels which hinder health-seeking behaviors for all communities.
48. While the Fund’s approach to Rakhine programming is ‘conflict-sensitive’ and concerned with
mitigating perceptions of inequity in the provision of services, the Fund needs to go one step further and be clear about its added-value for increased access to health for all communities; in the absence of a clear understanding of that added-value, the Fund runs the risk of itself contributing to inequity.
49. The Fund will build from the principles established by the Annan report from the Advisory Commission on Rakhine State as well as principles agreed within the international community, for example the Strategic Framework for International Engagement in Rakhine.
50. The presence of the MoHS on the Fund Board presents a unique opportunity for transparent discussions on the most appropriate modalities to support Health outcomes across Rakhine State. The commitment of the Access to Health Fund to full transparency with all actors involved, helps build a trusting relationship in which situations can be openly discussed and approaches agreed to and tested.
51. In Rakhine, the Fund will closely collaborate with relevant stakeholders in the international
communities, such as the HOMs Rakhine Group, Humanitarian Country Team, and Cooperation Partners Group
52. Through Implementing Partners, the Fund aims to strengthen the community volunteer network
(capacity building and supplies); improve outreach (package-tours and mobile clinics) in areas of poor health-coverage; introduce and promote community-based nutrition activities; and support emergency maternal and young child referrals from vulnerable and conflict-affected communities to facilities that will accept them.
53. An important part of the Fund’s aim in Rakhine is to table difficult discussions with the State Health
Department, other local authorities, and the central MOHS, to extend the limits of possible interventions: expand Muslim access to health facilities, bring community-based services to remote or closed settings, and increase vulnerable populations’ demand for and access to services.
54. True to its conflict-sensitive approach, the Fund’s engagement approach aims to support all
townships – recognizing that all populations in the State need support, and that the State’s overall development, including through better health services, contributes to reconciliation. The Fund is nonetheless guided by a number of principles for its operations in Rakhine: a. The Fund only supports programmes in mixed-community areas if activities support all
communities (equity, whole-township approach) b. In its support to health and nutrition interventions, the Fund follows the Rakhine Advisory
Commission recommendations c. The Fund aims to provide populations, in order of priority, with access to the nearest existing
health facility or health volunteer, access to outreach care (e.g. mobile clinics), or referral services for care in other facilities
26
IX. Strategic considerations for the Fund’s work in the Development/Humanitarian nexus 55. The Access to Health Fund works at the intersection of development and humanitarian situations
– often covering the needs of populations in protracted humanitarian crises. With its focus on vulnerable populations in conflict-affected areas, the Fund is highly sensitive to coordinating and finding synergies with humanitarian response in Myanmar, aiming to complement humanitarian health response and finding sustainable solutions for vulnerable people and reducing humanitarian dependency.
56. In order to play its role in full, the Access to Health Fund engages in constant dialogue and
coordination with Humanitarian actors, including sharing analyses and planning, and seeking areas of complementarity. The Fund is reporting to the Myanmar Health Sector Coordinating Committee through the Health Cluster, which will allow greater complementarity with humanitarian partners, and a reduction in communities’ dependence on humanitarian support.
57. The Fund also aims at increasing its Partners’ emergency preparedness and response and through
them that of their downstream partners (Ethnic Health Organizations, Community-based Organizations…). Such response will be aligned with Myanmar’s Humanitarian Response Plan. The Fund has the flexibility to work with partners to quickly respond to emergency and disaster situations (contingency budgets and reprogramming)
I. Working with the Private Sector The Access to Health Fund’s strategy in relation to working with the private sector will seek to establish strong relationships with key stakeholders and leverage the expertise, reach and resources of companies, associations, and individuals in areas of common interest. This will be built on partnerships established since the 3MDG Fund in areas such as sexual and reproductive health and rights, primary health care through private health providers, innovation, technology and communications, cash transfer and improved incentive and payment systems, and commodities procurement and distribution. The Fund will invest in initiatives that aim to improve the quality and responsiveness of the private health sector in recognition of its role in the provision of health care in Myanmar. For example, the Fund supports training for general practitioners in the provision of youth friendly services, particularly in sexual and reproductive health and rights in order to create a safe and welcoming environment for young people to access care. Taking advantage of their significant reach, the Access to Health Fund also utilizes private clinics and pharmacies to distribute family planning and nutrition commodities. This can also reduce the cost and availability of products for the end-user. In addition, the Access to Health Fund has been supporting a pilot on strategic purchasing of basic health services provided by private general practitioners to targeted beneficiaries to test the effectiveness of innovative payment solutions for health. These initiatives all aim to take advantage of the capacities of the private sector and/or test new methods of delivering more health care per dollar.
27
X. Monitoring and Evaluation Executive Summary of M&E Strategy 58. The M&E Strategy for Access to Health (ACCESS) was developed iteratively, using the draft ACCESS
strategy, the initial Theory of Change (ToC) framework and recommendations of the final 3MDG evaluation. The M&E Strategy is a product of consultations with FMO staff from all relevant Units, IPs working in EHO areas and donors. It has benefited from support by a senior M&E expert from Hera consultancy.
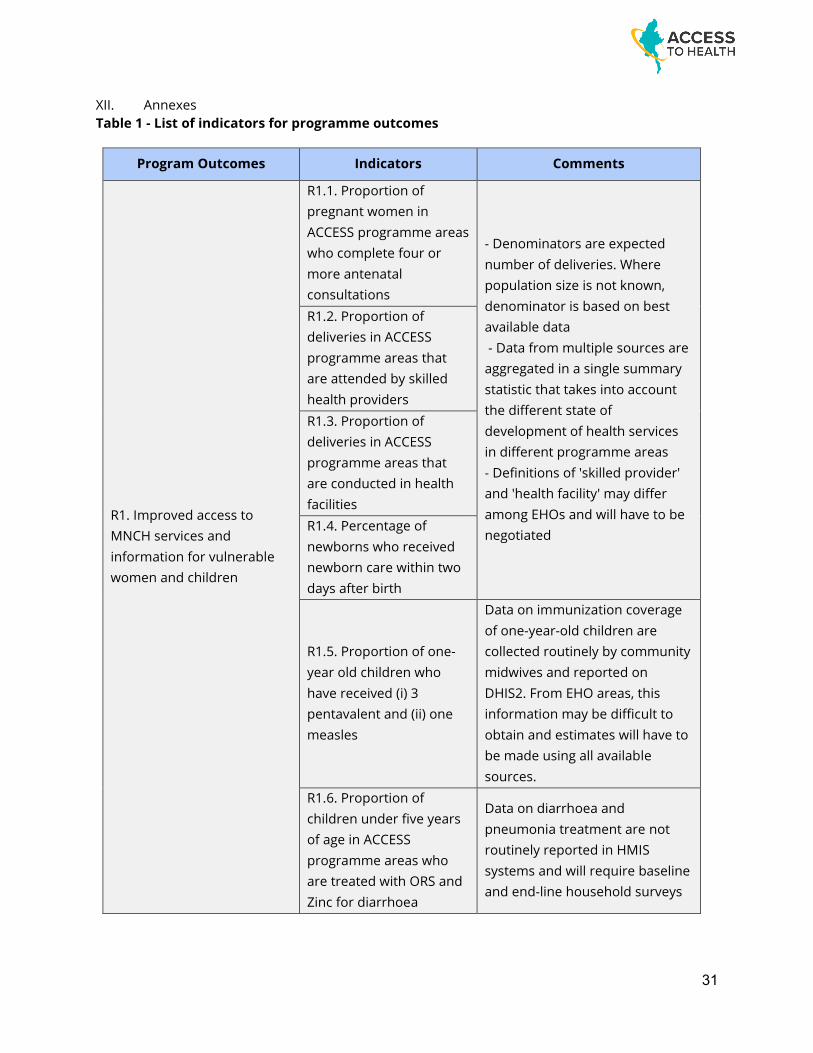
Monitoring of programme outcomes 59. The 12 programme outcome results in the Theory of Change are the highest level results that are
within scope of routine monitoring. This unusually high number of high-level outcomes reflects the broad scope of objectives of the ACCESS Strategy. Table 1 reflects indicators to track achievement on the programme-level outcomes.
60. Monitoring and reporting programme outcomes is a responsibility of the FMO M&E unit. Data collection for many of the programme-level indicators will require a close collaboration with IP M&E staff.
61. Data for the majority of indicators at programme level are captured in the MOHS and EHO HMIS systems, including monitoring systems for national programmes for malaria and tuberculosis. The indicators are therefore defined by these systems. Definitions used in national HMIS and in the systems established by EHOs may differ. Therefore a major ‘indicator mapping’ exercise will be required with participation of IPs and EHOs. In all cases, real-time access of the FMO and of IPs to HMIS data, for instance to the national DHIS2 database, will have to be assured, as well as participation of the FMO and the relevant IPs in data quality audits.
Monitoring of grant outcomes
62. Each grant is expected to contribute to one or more of the 12 results (see Table 2). None of these results will be directly attributable to grant inputs because all of them are contingent on contextual factors and on the contribution of others. A total of 26 proxy indicators to monitor progress towards the outcomes were developed. IPs will integrate those that are relevant to their activities into their grant-level M&E framework and report on them in their biannual progress reports.
63. All grant-level outcomes are specific to IPs’ scope of implementation. The intervention sites may be health facilities or villages in government-controlled and EHO areas, prisons with ACCESS-supported health programmes, harm reduction centres and other. The monitoring systems of IPs are therefore sources of data for all indicators in this category
28
Monitoring of grant outputs 64. Monitoring grant outputs (e.g. the number of health workers trained, the number of syringes and
needles distributed) will continue. The indicators and targets are defined in the grant agreements with IPs, and partners are required to report performance against targets biannually and to explain variances. Specific donor requirements will be integrated in the definition of output indicators of the grant agreements.
65. A performance monitoring matrix for grant outputs will be developed, reviewed annually and submitted for approval by the Fund Board.
66. A change from the 3MDG M&E practice will be that the quantities of outputs generated will no longer be the main focus of analysis and reporting of ACCESS performance. The annual programme reports will place a stronger focus on progress towards programme outcomes and on lessons learnt in the process.
Evaluation plan 67. Similarly to monitoring, evaluation will be conducted on two levels, on the level of grants to IPs
funded by ACCESS and on the level of the ACCESS programme
68. Grant Evaluations: Most ACCESS grants under the new programme strategy will start implementation in 2021 with a smaller number already starting in the transition-year of 2020. The timeline for grant implementation will therefore be short and for most grants no longer than three years. Scheduling both mid-term and final evaluations in such a short implementation period is not practical.
69. Instead of a mid-term grant evaluation, the formative input into grant implementation will be provided through outcome monitoring and thematic expert reviews that will cover groups of grants working in the same thematic area.
70. Final evaluations that focus on the effectiveness and efficiency of contributions to the grant outcome results will provide important information to the IPs, to MOHS and EHOs, and to the overall ACCESS programme. These will be conducted for a sample of grants across different thematic areas. The selection of grants and the type of evaluation will be determined during the development of a detailed evaluation plan.
71. Programme evaluation: The usual approach to evaluating a five-year programme is to schedule a formative mid-term evaluation towards the end of the second year and a summative final evaluation in the last year of the programme. ACCESS will schedule a mid-term evaluation in 2021 at the beginning of the new strategy implementation and a final evaluation in 2023, in the last programme year. The two evaluations will be timed in tandem with the baseline and end-line household surveys (described further).
72. Mid-term evaluation (MTE): As full implementation of the ACCESS Strategy will only start in 2021 and the implementation period will be three years, the mid-term evaluation will not focus on the
29
progress towards the achievement of outcomes but rather on the critical process of transition from 3MDG to the new ACCESS strategy.
73. The MTE will assess the efficiency with which the transition was implemented, assess the relevance and alignment of programming with the ACCESS strategy, the extent to which key principles of the ACCESS Fund were respected during this process, and gauge the level of commitment of partners, most of all of the MOHS and the EHOs, to the implementation of the strategy.
74. The objective of the MTE is to provide assurance to the Fund Board that ACCESS is on course towards the achievement of agreed outcomes, and to provide independent recommendations to the FMO for possible strategic adjustments and measures to strengthen systems in order to increase the relevance, feasibility and effectiveness of implementation arrangements.
75. Final evaluation: The final evaluation will serve primarily for accountability and to generate lessons that will contribute to international and national health sector development policies and programmes. It is envisaged to schedule it when at least preliminary results of the end-line household survey are available i.e. not earlier than the second half of 2023.
76. As for any summative evaluation, the evaluation parameters will be to assess the efficiency, effectiveness, equity, impact and sustainability of ACCESS. It will also include a value for money analysis.
Other elements of the M&E plan 77. Population-based surveys: The accountability and the learning generated by routine data
collection and analysis will be much enhanced with population-based data that are linked more directly to the programme interventions in timing and geography.
78. The M&E strategy therefore includes a baseline and an end-line survey to collect and analyze data on the effects of ACCESS at the level of beneficiary populations. The surveys will focus mainly on the availability, access, utilization and outcomes of health services for maternity, child and adolescent health in geographic areas where the majority of services are provided by EHOs. The end-line survey results will have to be available around Quarter 3 2023, in time to inform the final evaluation.
79. Data quality audits (DQAs) by an external contractor serve as an additional independent assurance of the validity of reported monitoring data, in addition to the DQAs performed routinely by the IPs and the FMO, including the participation of IPs and the FMO in joint DQAs of HMIS data with the MOHS and the EHOs. External DQAs are planned annually in 2020-2022.
80. Thematic expert reviews are mainly planned towards the end of the first year and throughout the second year of new strategy implementation to provide guidance to IPs and FMO on the highest technical standards of programming in their area as well as on the implementation of key ACCESS principles in their grants.
81. Technical assistance is external expert assistance to the FMO M&E unit to IPs for the development of harmonized monitoring instruments and methodologies. There will be a strong
30
requirement for this type of assistance during the transition year, with decreasing need as implementation of the strategy evolves.
82. Finally, as accountability and learning are the overriding goals of M&E, learning is not identified as a distinct activity of the M&E Strategy but rather as an objective pursued under all activities.
See the Annexes for the List of Indicators.
XI. Key Principles 83. The Fund will be driven by the following principles as it works to deliver on its mission: 84. Human Rights-Based Approach: The Access to Health Fund promotes accountability, equity,
inclusion, non-discrimination, participation; and is committed to the AAAQ Framework (Availability, Accessibility, Acceptability and Quality). The Fund upholds people’s free, active and meaningful participation in health-related decisions, their right to access information, their ability to hold decision-makers to account through demand generation activities, project information sharing, community engagement activities, and community feedback mechanisms; and that health-service providers listen to the voices of people and are accountable in their delivery of quality services.
85. Promoting Gender Equality: The Access to Health Fund is committed to accelerating efforts to promote gender equality and ensure equal access to health services for people of all genders, by better understanding context and needs, overcoming barriers to healthcare access, and increasing women’s voice and representation.
86. Sustainability: The Access to Health Fund builds long-term capacity in Myanmar’s health response
87. Conflict Sensitivity and Social Cohesion: The Access to Health Fund upholds at all times the principle of “do no harm” and seeks avenues – through its work – to promote social cohesion without challenging or threatening ethnic, cultural, or religious identity.
88. Flexibility: The Access to Health Fund is open to change and adapts its approach to best deliver on the mission. The Fund is a learning organization, focused on creating knowledge and acting upon it to transform approaches and adapt.17
17 More detail on the Access to Health Fund’s approach to learning can be found in the Access to Health Fund paper Learning, evidence, and research at the Access to Health Fund (the Access to Health Fund as a Learning Organization):
31
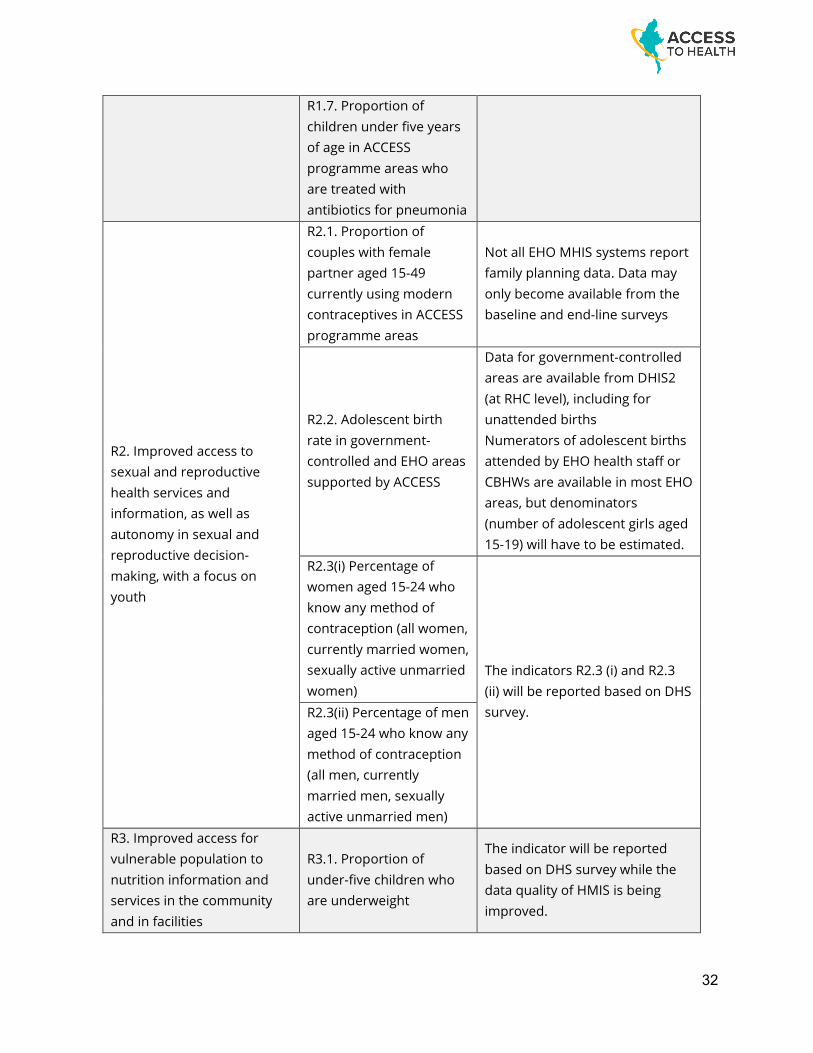
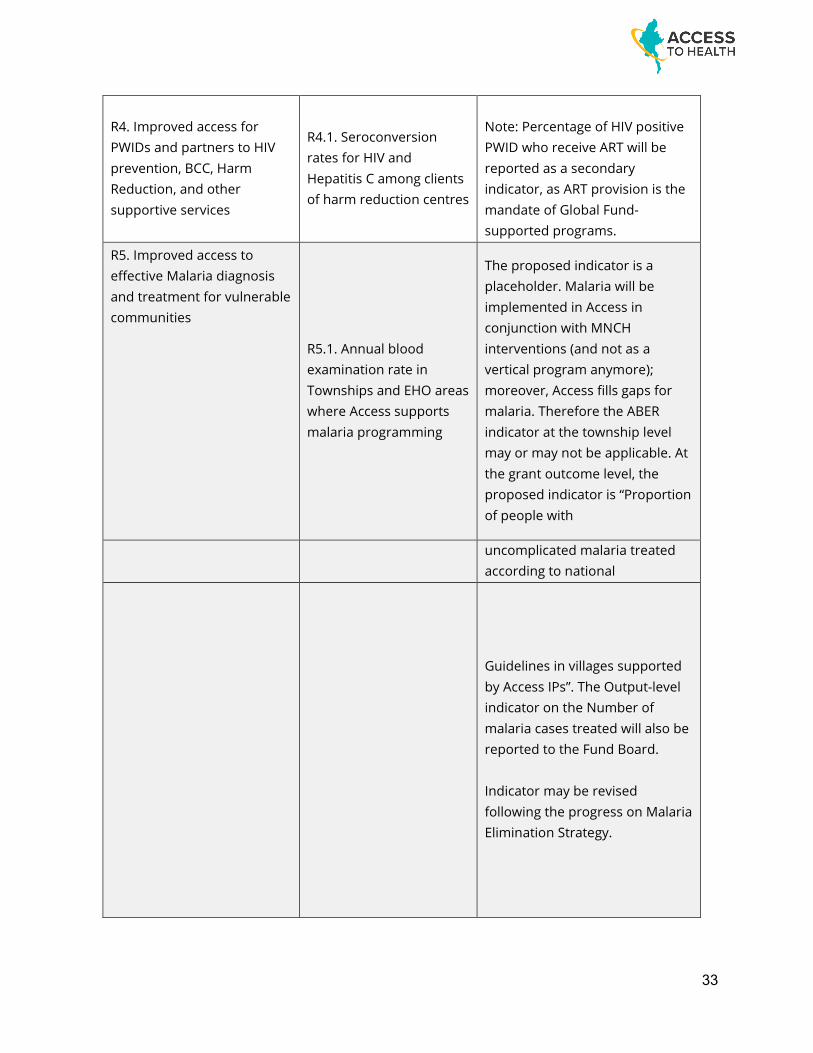
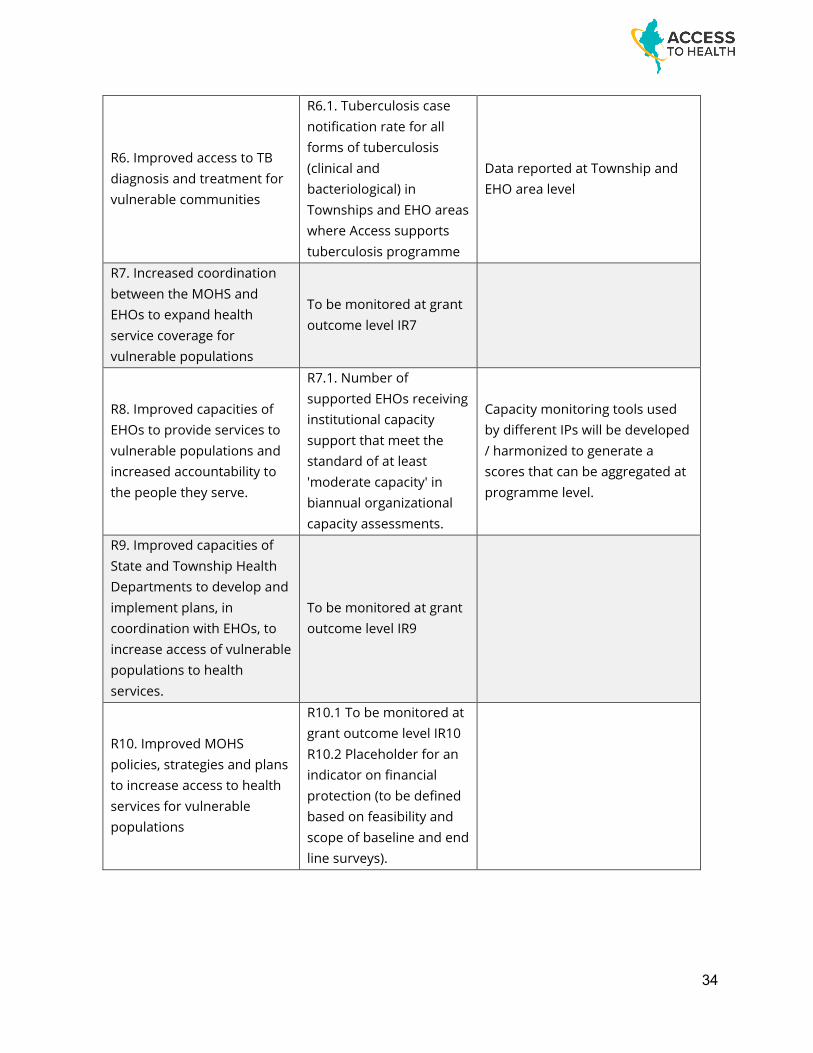
XII. Annexes Table 1 - List of indicators for programme outcomes
Program Outcomes Indicators Comments
R1. Improved access to MNCH services and information for vulnerable women and children
R1.1. Proportion of pregnant women in ACCESS programme areas who complete four or more antenatal consultations
- Denominators are expected number of deliveries. Where population size is not known, denominator is based on best available data - Data from multiple sources are aggregated in a single summary statistic that takes into account the different state of development of health services in different programme areas - Definitions of 'skilled provider' and 'health facility' may differ among EHOs and will have to be negotiated
R1.2. Proportion of deliveries in ACCESS programme areas that are attended by skilled health providers R1.3. Proportion of deliveries in ACCESS programme areas that are conducted in health facilities R1.4. Percentage of newborns who received newborn care within two days after birth
R1.5. Proportion of one-year old children who have received (i) 3 pentavalent and (ii) one measles
Data on immunization coverage of one-year-old children are collected routinely by community midwives and reported on DHIS2. From EHO areas, this information may be difficult to obtain and estimates will have to be made using all available sources.
R1.6. Proportion of children under five years of age in ACCESS programme areas who are treated with ORS and Zinc for diarrhoea
Data on diarrhoea and pneumonia treatment are not routinely reported in HMIS systems and will require baseline and end-line household surveys
32
R1.7. Proportion of children under five years of age in ACCESS programme areas who are treated with antibiotics for pneumonia
R2. Improved access to sexual and reproductive health services and information, as well as autonomy in sexual and reproductive decision-making, with a focus on youth
R2.1. Proportion of couples with female partner aged 15-49 currently using modern contraceptives in ACCESS programme areas
Not all EHO MHIS systems report family planning data. Data may only become available from the baseline and end-line surveys
R2.2. Adolescent birth rate in government-controlled and EHO areas supported by ACCESS
Data for government-controlled areas are available from DHIS2 (at RHC level), including for unattended births Numerators of adolescent births attended by EHO health staff or CBHWs are available in most EHO areas, but denominators (number of adolescent girls aged 15-19) will have to be estimated.
R2.3(i) Percentage of women aged 15-24 who know any method of contraception (all women, currently married women, sexually active unmarried women)
The indicators R2.3 (i) and R2.3 (ii) will be reported based on DHS survey. R2.3(ii) Percentage of men
aged 15-24 who know any method of contraception (all men, currently married men, sexually active unmarried men)
R3. Improved access for vulnerable population to nutrition information and services in the community and in facilities
R3.1. Proportion of under-five children who are underweight
The indicator will be reported based on DHS survey while the data quality of HMIS is being improved.
33
R4. Improved access for PWIDs and partners to HIV prevention, BCC, Harm Reduction, and other supportive services
R4.1. Seroconversion rates for HIV and Hepatitis C among clients of harm reduction centres
Note: Percentage of HIV positive PWID who receive ART will be reported as a secondary indicator, as ART provision is the mandate of Global Fund-supported programs.
R5. Improved access to effective Malaria diagnosis and treatment for vulnerable communities
R5.1. Annual blood examination rate in Townships and EHO areas where Access supports malaria programming
The proposed indicator is a placeholder. Malaria will be implemented in Access in conjunction with MNCH interventions (and not as a vertical program anymore); moreover, Access fills gaps for malaria. Therefore the ABER indicator at the township level may or may not be applicable. At the grant outcome level, the proposed indicator is “Proportion of people with
uncomplicated malaria treated according to national
Guidelines in villages supported by Access IPs”. The Output-level indicator on the Number of malaria cases treated will also be reported to the Fund Board. Indicator may be revised following the progress on Malaria Elimination Strategy.
34
R6. Improved access to TB diagnosis and treatment for vulnerable communities
R6.1. Tuberculosis case notification rate for all forms of tuberculosis (clinical and bacteriological) in Townships and EHO areas where Access supports tuberculosis programme
Data reported at Township and EHO area level
R7. Increased coordination between the MOHS and EHOs to expand health service coverage for vulnerable populations
To be monitored at grant outcome level IR7
R8. Improved capacities of EHOs to provide services to vulnerable populations and increased accountability to the people they serve.
R7.1. Number of supported EHOs receiving institutional capacity support that meet the standard of at least 'moderate capacity' in biannual organizational capacity assessments.
Capacity monitoring tools used by different IPs will be developed / harmonized to generate a scores that can be aggregated at programme level.
R9. Improved capacities of State and Township Health Departments to develop and implement plans, in coordination with EHOs, to increase access of vulnerable populations to health services.
To be monitored at grant outcome level IR9
R10. Improved MOHS policies, strategies and plans to increase access to health services for vulnerable populations
R10.1 To be monitored at grant outcome level IR10 R10.2 Placeholder for an indicator on financial protection (to be defined based on feasibility and scope of baseline and end line surveys).
35
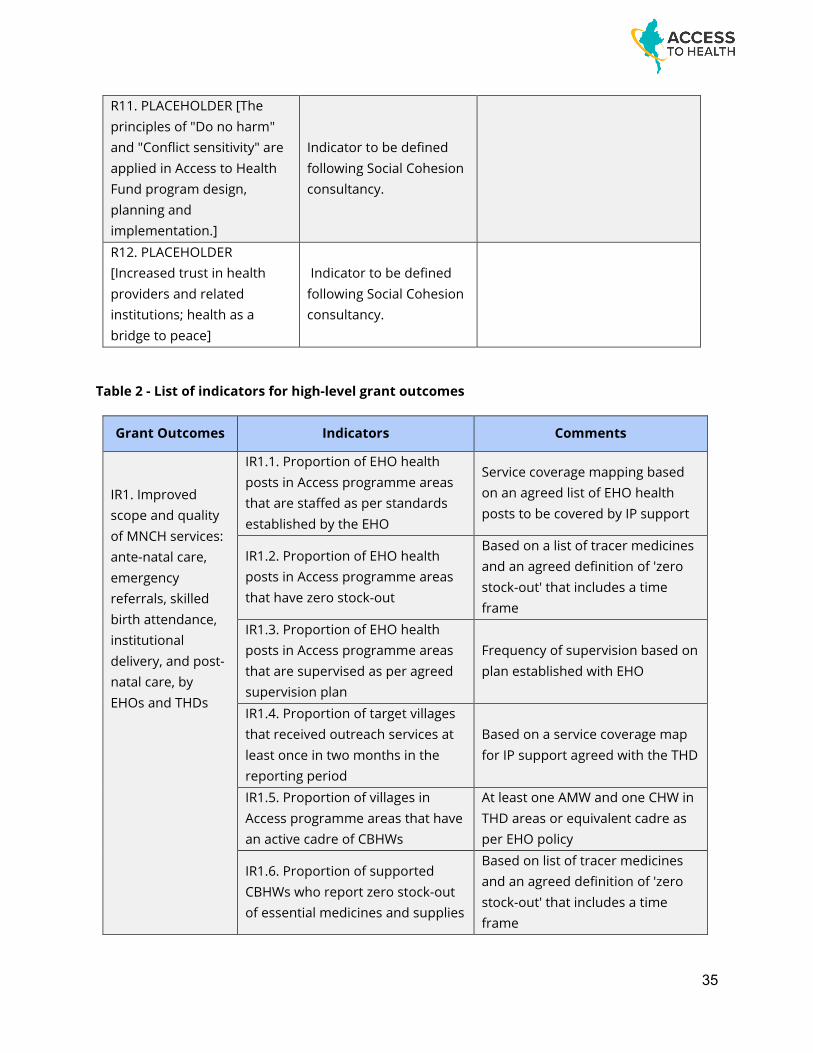
R11. PLACEHOLDER [The principles of "Do no harm" and "Conflict sensitivity" are applied in Access to Health Fund program design, planning and implementation.]
Indicator to be defined following Social Cohesion consultancy.
R12. PLACEHOLDER [Increased trust in health providers and related institutions; health as a bridge to peace]
Indicator to be defined following Social Cohesion consultancy.
Table 2 - List of indicators for high-level grant outcomes
Grant Outcomes Indicators Comments
IR1. Improved scope and quality of MNCH services: ante-natal care, emergency referrals, skilled birth attendance, institutional delivery, and post-natal care, by EHOs and THDs
IR1.1. Proportion of EHO health posts in Access programme areas that are staffed as per standards established by the EHO
Service coverage mapping based on an agreed list of EHO health posts to be covered by IP support
IR1.2. Proportion of EHO health posts in Access programme areas that have zero stock-out
Based on a list of tracer medicines and an agreed definition of 'zero stock-out' that includes a time frame
IR1.3. Proportion of EHO health posts in Access programme areas that are supervised as per agreed supervision plan
Frequency of supervision based on plan established with EHO
IR1.4. Proportion of target villages that received outreach services at least once in two months in the reporting period
Based on a service coverage map for IP support agreed with the THD
IR1.5. Proportion of villages in Access programme areas that have an active cadre of CBHWs
At least one AMW and one CHW in THD areas or equivalent cadre as per EHO policy
IR1.6. Proportion of supported CBHWs who report zero stock-out of essential medicines and supplies
Based on list of tracer medicines and an agreed definition of 'zero stock-out' that includes a time frame
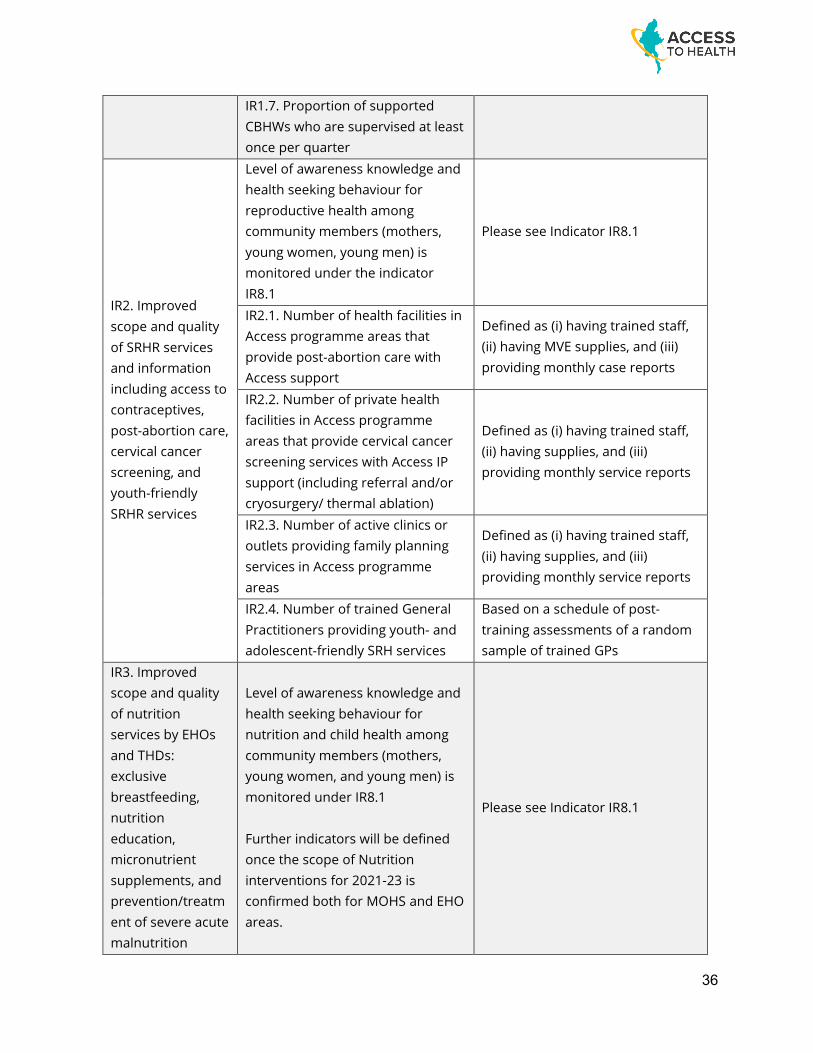
36
IR1.7. Proportion of supported CBHWs who are supervised at least once per quarter
IR2. Improved scope and quality of SRHR services and information including access to contraceptives, post-abortion care, cervical cancer screening, and youth-friendly SRHR services
Level of awareness knowledge and health seeking behaviour for reproductive health among community members (mothers, young women, young men) is monitored under the indicator IR8.1
Please see Indicator IR8.1
IR2.1. Number of health facilities in Access programme areas that provide post-abortion care with Access support
Defined as (i) having trained staff, (ii) having MVE supplies, and (iii) providing monthly case reports
IR2.2. Number of private health facilities in Access programme areas that provide cervical cancer screening services with Access IP support (including referral and/or cryosurgery/ thermal ablation)
Defined as (i) having trained staff, (ii) having supplies, and (iii) providing monthly service reports
IR2.3. Number of active clinics or outlets providing family planning services in Access programme areas
Defined as (i) having trained staff, (ii) having supplies, and (iii) providing monthly service reports
IR2.4. Number of trained General Practitioners providing youth- and adolescent-friendly SRH services
Based on a schedule of post-training assessments of a random sample of trained GPs
IR3. Improved scope and quality of nutrition services by EHOs and THDs: exclusive breastfeeding, nutrition education, micronutrient supplements, and prevention/treatment of severe acute malnutrition
Level of awareness knowledge and health seeking behaviour for nutrition and child health among community members (mothers, young women, and young men) is monitored under IR8.1 Further indicators will be defined once the scope of Nutrition interventions for 2021-23 is confirmed both for MOHS and EHO areas.
Please see Indicator IR8.1
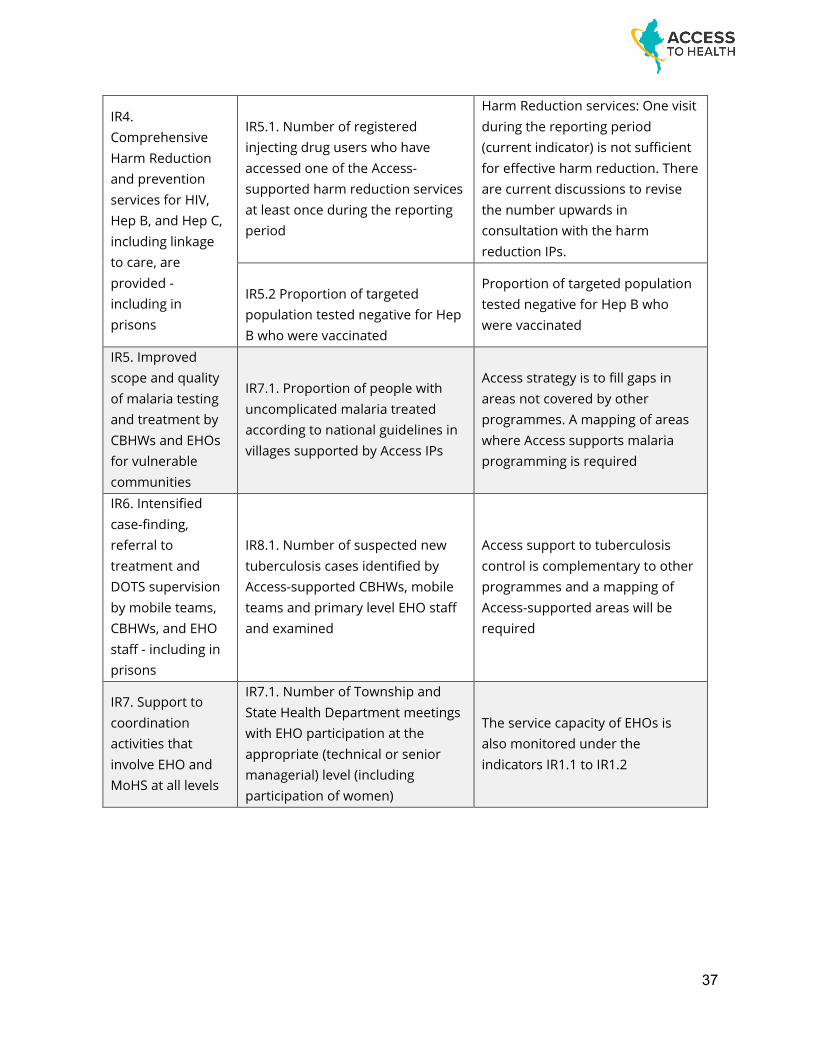
37
IR4. Comprehensive Harm Reduction and prevention services for HIV, Hep B, and Hep C, including linkage to care, are provided - including in prisons
IR5.1. Number of registered injecting drug users who have accessed one of the Access-supported harm reduction services at least once during the reporting period
Harm Reduction services: One visit during the reporting period (current indicator) is not sufficient for effective harm reduction. There are current discussions to revise the number upwards in consultation with the harm reduction IPs.
IR5.2 Proportion of targeted population tested negative for Hep B who were vaccinated
Proportion of targeted population tested negative for Hep B who were vaccinated
IR5. Improved scope and quality of malaria testing and treatment by CBHWs and EHOs for vulnerable communities
IR7.1. Proportion of people with uncomplicated malaria treated according to national guidelines in villages supported by Access IPs
Access strategy is to fill gaps in areas not covered by other programmes. A mapping of areas where Access supports malaria programming is required
IR6. Intensified case-finding, referral to treatment and DOTS supervision by mobile teams, CBHWs, and EHO staff - including in prisons
IR8.1. Number of suspected new tuberculosis cases identified by Access-supported CBHWs, mobile teams and primary level EHO staff and examined
Access support to tuberculosis control is complementary to other programmes and a mapping of Access-supported areas will be required
IR7. Support to coordination activities that involve EHO and MoHS at all levels
IR7.1. Number of Township and State Health Department meetings with EHO participation at the appropriate (technical or senior managerial) level (including participation of women)
The service capacity of EHOs is also monitored under the indicators IR1.1 to IR1.2
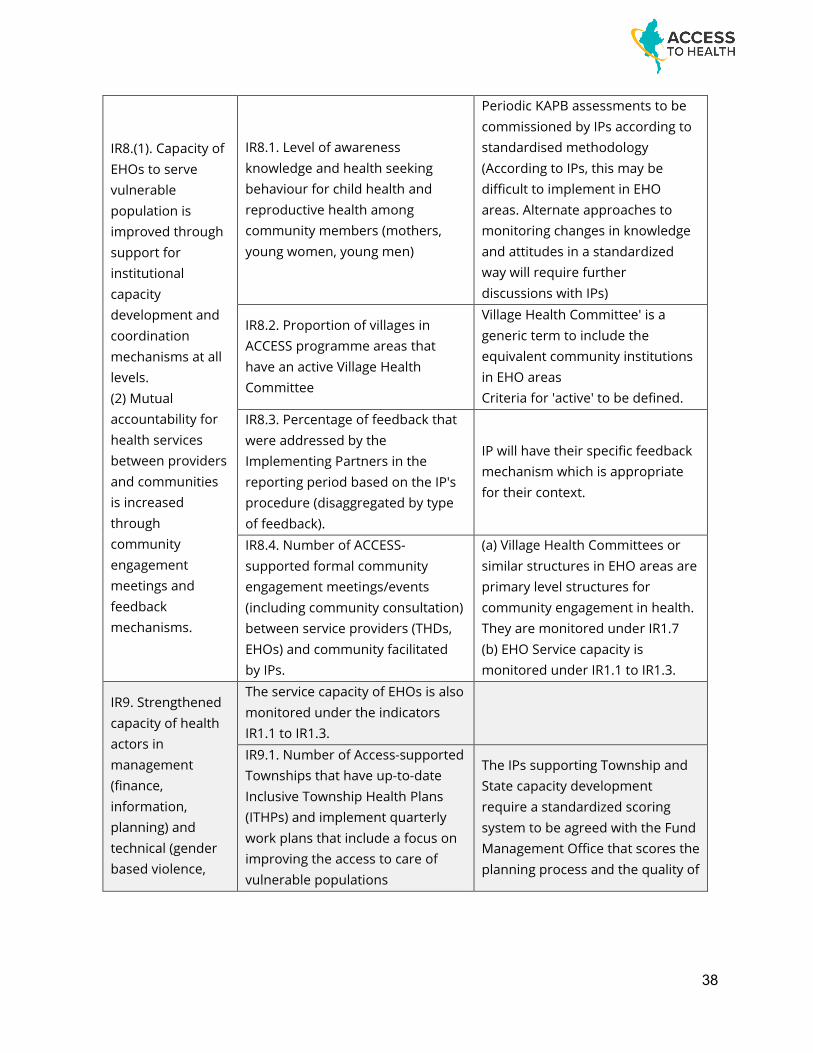
38
IR8.(1). Capacity of EHOs to serve vulnerable population is improved through support for institutional capacity development and coordination mechanisms at all levels. (2) Mutual accountability for health services between providers and communities is increased through community engagement meetings and feedback mechanisms.
IR8.1. Level of awareness knowledge and health seeking behaviour for child health and reproductive health among community members (mothers, young women, young men)
Periodic KAPB assessments to be commissioned by IPs according to standardised methodology (According to IPs, this may be difficult to implement in EHO areas. Alternate approaches to monitoring changes in knowledge and attitudes in a standardized way will require further discussions with IPs)
IR8.2. Proportion of villages in ACCESS programme areas that have an active Village Health Committee
Village Health Committee' is a generic term to include the equivalent community institutions in EHO areas Criteria for 'active' to be defined.
IR8.3. Percentage of feedback that were addressed by the Implementing Partners in the reporting period based on the IP's procedure (disaggregated by type of feedback).
IP will have their specific feedback mechanism which is appropriate for their context.
IR8.4. Number of ACCESS-supported formal community engagement meetings/events (including community consultation) between service providers (THDs, EHOs) and community facilitated by IPs.
(a) Village Health Committees or similar structures in EHO areas are primary level structures for community engagement in health. They are monitored under IR1.7 (b) EHO Service capacity is monitored under IR1.1 to IR1.3.
IR9. Strengthened capacity of health actors in management (finance, information, planning) and technical (gender based violence,
The service capacity of EHOs is also monitored under the indicators IR1.1 to IR1.3.
IR9.1. Number of Access-supported Townships that have up-to-date Inclusive Township Health Plans (ITHPs) and implement quarterly work plans that include a focus on improving the access to care of vulnerable populations
The IPs supporting Township and State capacity development require a standardized scoring system to be agreed with the Fund Management Office that scores the planning process and the quality of
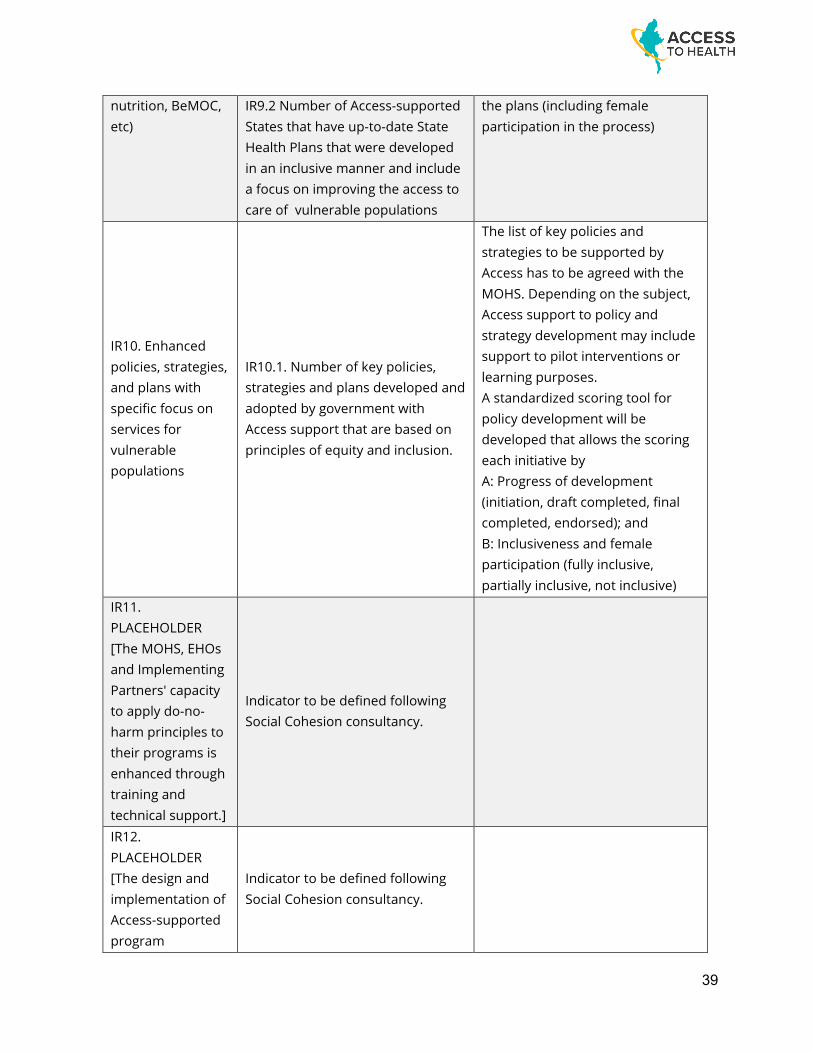
39
nutrition, BeMOC, etc)
IR9.2 Number of Access-supported States that have up-to-date State Health Plans that were developed in an inclusive manner and include a focus on improving the access to care of vulnerable populations
the plans (including female participation in the process)
IR10. Enhanced policies, strategies, and plans with specific focus on services for vulnerable populations
IR10.1. Number of key policies, strategies and plans developed and adopted by government with Access support that are based on principles of equity and inclusion.
The list of key policies and strategies to be supported by Access has to be agreed with the MOHS. Depending on the subject, Access support to policy and strategy development may include support to pilot interventions or learning purposes. A standardized scoring tool for policy development will be developed that allows the scoring each initiative by A: Progress of development (initiation, draft completed, final completed, endorsed); and B: Inclusiveness and female participation (fully inclusive, partially inclusive, not inclusive)
IR11. PLACEHOLDER [The MOHS, EHOs and Implementing Partners' capacity to apply do-no-harm principles to their programs is enhanced through training and technical support.]
Indicator to be defined following Social Cohesion consultancy.
IR12. PLACEHOLDER [The design and implementation of Access-supported program
Indicator to be defined following Social Cohesion consultancy.
40
emphasizes health-outcomes for vulnerable population and trust building between communities and service-providers]
41
Programme Intervention Logic and Theory of Change
I. Purpose The purpose of this note is to elaborate on the Access to Health Fund’s Theory of Change, global evidence underpinning the high-level impact pursued by the Fund, linkages between outputs, outcomes, and impact, and underlying assumptions in the programme design and interventions. II. An evidence-based approach The Fund’s Theory of Change was developed through a dialogue between the Fund Management Office and the Fund Board, with input from key Partners. The result of that dialogue is captured in Diagram 1 overleaf.
The Fund’s vision is improved health outcomes for vulnerable populations in conflict affected areas - thus reducing health inequalities - and increased social cohesion.
High-level outcomes are expected at three levels: - Increased access of vulnerable populations in conflict-affected areas to better and more
relevant health-services - Improved Health Services and functions essential to improving health outcomes for vulnerable
people in conflict-affected areas, through a number of targeted health system strengthening interventions spanning policy, management information systems and workforce - with both the Ministry of Health and Sports, Ethnic Health Organizations and Ethnic Community Based Health Organizations (EHO and ECBHO)
- Increased social cohesion: in a country strife with internal conflicts and ethnic tensions, Access is in the process of commissioning a study of this area of work to better define the Fund’s ambition and options in pursuing its social cohesion related objectives.
Program outcomes are expected on maternal and child Health (contributing to reduction of maternal mortality, newborn mortality, and Under-5 mortality); improved nutrition; improved sexual and reproductive health among vulnerable communities, and these communities’ improved ability to exercise their sexual and reproductive rights; increased prevention of new HIV infections among drug users through harm reduction interventions; reduction in TB prevalence; and a reduction of malaria morbidity.
The Fund will be measuring progress based on key indicators selected on the basis of global evidence and examined by Donors and the Ministry of Health through the approval, in 2017, of the Fund’s Programme Description, Description of Actions, and Call for Proposals - as well as the Fund’s approved18 Monitoring and Evaluation Strategy and logframe. (Please refer to larger document on page 8)
18 The M&E Strategy is submitted for Board approval on 15 November, together with the Theory of Change.
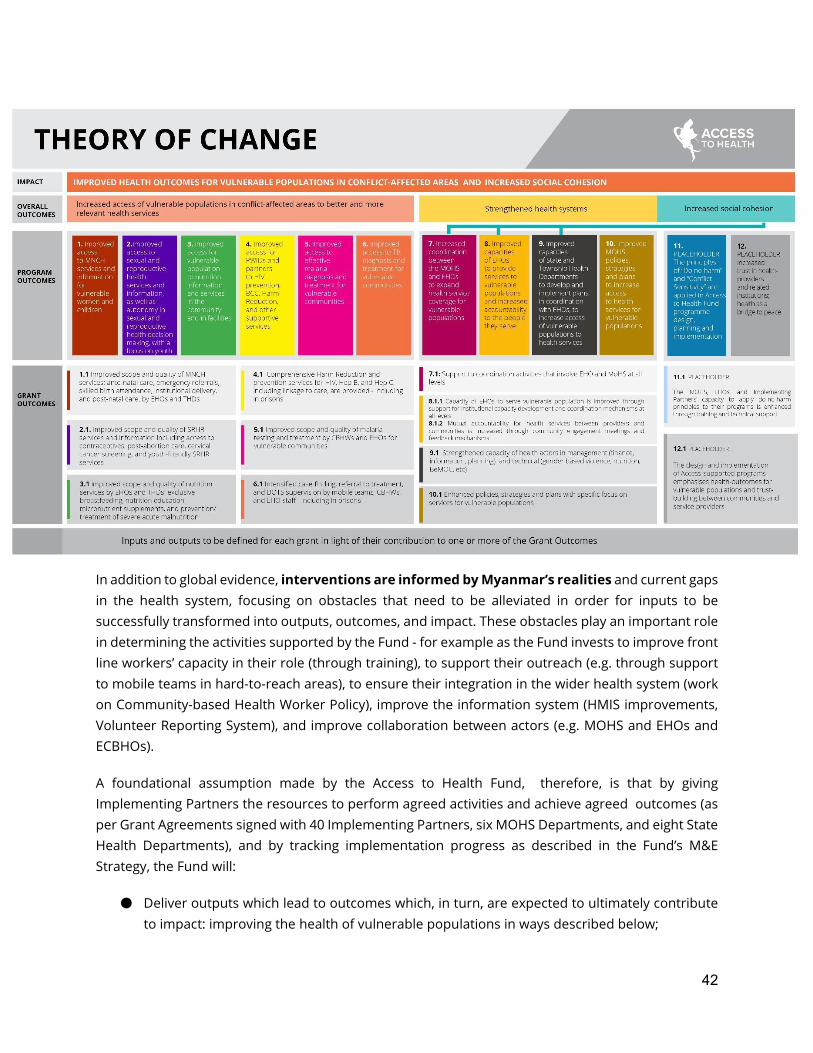
42
In addition to global evidence, interventions are informed by Myanmar’s realities and current gaps in the health system, focusing on obstacles that need to be alleviated in order for inputs to be successfully transformed into outputs, outcomes, and impact. These obstacles play an important role in determining the activities supported by the Fund - for example as the Fund invests to improve front line workers’ capacity in their role (through training), to support their outreach (e.g. through support to mobile teams in hard-to-reach areas), to ensure their integration in the wider health system (work on Community-based Health Worker Policy), improve the information system (HMIS improvements, Volunteer Reporting System), and improve collaboration between actors (e.g. MOHS and EHOs and ECBHOs).
A foundational assumption made by the Access to Health Fund, therefore, is that by giving Implementing Partners the resources to perform agreed activities and achieve agreed outcomes (as per Grant Agreements signed with 40 Implementing Partners, six MOHS Departments, and eight State Health Departments), and by tracking implementation progress as described in the Fund’s M&E Strategy, the Fund will:
● Deliver outputs which lead to outcomes which, in turn, are expected to ultimately contribute to impact: improving the health of vulnerable populations in ways described below;
43
● Contribute to building sustainable capacity for outcomes to be delivered in the long-term through selected support to (i) community systems and (ii) the wider Health system.
III. Guiding Principles
The Access to Health Fund Guiding Principles are: ● Human Rights-Based Approach: The Access to Health Fund promotes accountability, equity,
inclusion, non-discrimination, participation; and is committed to the AAAQ Framework (Availability, Accessibility, Acceptability and Quality). The Fund upholds people’s free, active and meaningful participation in health-related decisions, their right to access information, their ability to hold decision-makers to account through demand-generation activities, project information sharing, community engagement activities, and community feedback mechanisms; and that health-service providers listen to the voices of people and are accountable in their delivery of quality services.
● Promoting Gender Equality: The Access to Health Fund is committed to accelerating efforts to promote gender equality and ensure equal access to health services for people of all genders, by better understanding context and needs, overcoming barriers to healthcare access, and increasing women’s voice and representation.
● Sustainability: The Access to Health Fund builds long-term capacity in Myanmar’s health response.
● Conflict Sensitivity and Social Cohesion: The Access to Health Fund upholds at all times the principle of “do no harm” and seeks avenues – through its work – to promote social cohesion without challenging or threatening ethnic, cultural, or religious identity.
● Flexibility: The Access to Health Fund is open to change and adapts its approach to best deliver on the mission.
Integration is also a key principle of the Fund’s interventions. In line with the Ministry of Health and Sports’ goal to deliver an essential package of health services, the 3MDG Fund transitioned from a vertical, disease-specific implementation model to a geographic, service-integrated approach in 2018. This is continued in the Access to Health Fund, fostering better value for money and service coverage, as well as bring fully aligned with Ministry of Health and Sports efforts towards universal health coverage. There are two main types of integrated grants in the Access to Health Fund:
● Maternal, newborn and child health (MNCH) integrated grants, where MNCH activities are implemented together with activities for nutrition, sexual and reproductive health and rights, tuberculosis, malaria and disability inclusion through the township health department or EHOs and ECBHOs.
● Drug Use and its Health Consequences (also known as Harm Reduction grants) are being integrated with malaria, tuberculosis, overdose prevention and management, SRHR, mental health, and disability inclusion.
44
Furthermore, all service delivery grants under the Access to Health Fund are required to mainstream and integrate the six cross cutting themes identified in the Cross Cutting Themes Manual. IV. Maternal and Child Health: reducing Maternal, Neonatal, and Under-5 Mortality
4.1. Global Evidence
Globally in 2015, an estimated 526,000 episodes of diarrhea and 922,000 cases of pneumonia in children under age five years led to death19. Undernutrition is a primary underlying cause of 3.5 million maternal and child deaths each year20; stunting, wasting, and micronutrient deficiencies are responsible for approximately 35% of the disease burden in children under the age of five years and 11% of the total global disease burden21.
Although maternal mortality is caused chiefly by postpartum hemorrhage, preeclampsia and eclampsia, and sepsis, a large proportion of maternal deaths can be attributed to limited access to skilled care during childbirth and the postnatal period22 as well as to limited access to sexual and reproductive health services and safe abortions23. Global evidence supports high-impact intervention on the continuum of care through skilled health personnel and community based health volunteers24 - which is the approach adopted by the Fund.
An appropriate mix of interventions can significantly reduce the burden of maternal and child mortality and morbidity. However, these interventions often do not reach those who need them most. An integrated approach that includes community-based care as an essential component has the potential to substantially improve maternal, newborn, and child health outcomes.25 Based on global evidence26, community-based management of common childhood diseases is associated with a (up to) 160% increase in the use of oral rehydration solution, 80% increase in the use of zinc for management of diarrhea, and an over 30% reduction in pneumonia-related mortality27. Nutrition education specifically is associated with an increase in under-five nutritional status and increased exclusive breastfeeding practices28.
Almost two thirds of maternal deaths occur during the 48-hour period immediately before delivery. Ensuring that women plan for and deliver their babies in health facilities, attended by skilled health
19 Liu and others 2016 20 Black and others 2013 21 Lozano and others 2011 22 Lozano and others 2011 23 UNFPA and Guttmacher Institute 2010 24 World Health Organisation, 2006 25 Bayer 2001; Sines, Tinker, and Ruben 2006 26 Das and others 2013 27 https://www.unicef.org/sowc08/docs/sowc08_panels.pdf 28 Bhutta and others 2013; Lassi and others 2013
45
professionals, is critical to saving both maternal and newborn lives. If all deliveries occurred in health facilities, as many as 65% of maternal deaths could be averted29.
As noted in the Access to Health Fund’s Programme Description, sexual and reproductive health rights – including access to sexual and reproductive health care and information, as well as autonomy in sexual and reproductive decision-making – are universal human rights that apply to both men and women. There is a clear connection between sexual and reproductive health, human rights and sustainable development. When sexual and reproductive health needs are not met, individuals are deprived of the right to make crucial choices about their own bodies and futures, with a cascading impact on their families’ welfare and future generations. And because women bear children, and also often bear the responsibility for nurturing them, sexual and reproductive health and rights issues cannot be separated from gender equality. Cumulatively, the denial of these rights exacerbates poverty and gender inequality.
4.2. Myanmar-specific obstacles
In Myanmar, a series of obstacles makes reaching remote, conflict-affected, and vulnerable populations into a major challenge for the Ministry of Health, EHOs and ECBHOs, and other providers. Supply-side obstacles include:
- Inadequate staffing, especially in very remote areas: in 2016, Myanmar had 1.33 health workers per 1,000 population, compared with WHO’s recommended threshold of 4.45 required for Universal Health Coverage30
- Infrastructure challenges in remote areas include insufficient facilities, the location of some existing health facilities in zones of active conflict, and the lack/inadequacy of critical amenities such as water and sanitation31
- Health workers incur out-of-pocket expenditures when conducting outreach visits; their remuneration package magnifies the challenge to rural retention.32
- EHOs and ECBHOs face significant challenges to their ability to deliver health services which meet the health needs of their populations. Two of the most significant challenges are the limited availability of funding and lack of skilled workers. In many ethnic minority areas (like for example the Southeast33) infant, child and maternal mortality are two to three times as high as the national averages.
29 Ending Preventable Maternal Mortality: USAID Maternal Health Vision for Action, June 2014 30 Myanmar National Health Plan 2017-2021 31 Myanmar National Health Plan 2017-2021 32 Myanmar Human Resources for Health Strategy (2018-2021); it is noted in particular that the remuneration should be consistent with the standards of the Union Civil Service Board 33 Back Pack Health Worker Team, “Chronic emergency: Health and human rights in eastern Burma,” ReliefWeb, Aug. 22, 2006, http://reliefweb.int/report/myanmar/chronic-emergency-health-andhuman-rights-eastern-burma; Burma Medical Association, et al., “Diagnosis Critical: Health and Human Rights in Eastern Burma” (2010), http://www.jhsph.edu/research/centers-and-institutes/ center-for-public-health-and-human-rights/_pdf/Burma_DiagCritical_19Oct10.pdf; HISWG, “Long Road to Recovery”
46
- Despite international non-government organizations’ long-term efforts on maternal and child health in ethnic areas, levels of institutional delivery are low. For example in Northeastern Myanmar3, only 14.28% of all inpatient services for women had to do with hospital-facilitated child delivery, as compared to Myanmar’s national average of 36.2%.
- Review of the available literature also identifies language and cultural barriers to accessing health services in ethnic areas with signs, written resources, and staff often using Burmese. MOHS staff are often unable to converse in local languages.34
Demand-side obstacles include:
- Financial barriers: only 7% of the rural population belong to the wealthiest quintile, compared with 56% of the urban population35
- Transportation difficulties in hard to reach areas: 12% of the total population lives in moderate to very hard-to-reach areas in Myanmar36
- Limited health knowledge: for example, the Myanmar Demographic and Health Survey 2015-16 mentions that only 65% of women and 57% of men in rural areas know that TB spreads through cough, compared with 84% and 77% in urban areas respectively.
4.3. Intervention logic
Maternal Health
In the maternal health domain, the Fund contributes to a reduction in maternal mortality through desirable health outcomes - increased coverage of antenatal care, postnatal care, and skilled birth attendance, increased contraceptive prevalence, increased institutional deliveries and reduced unwanted pregnancies. In order to reach these health outcomes, the Fund supports township health departments, basic health staff, and community-based health workers through specific activities. To improve coverage of antenatal care, skilled birth attendance and postnatal care, ACCESS supports outreach visits (especially hard to reach and ethnic areas) by basic health staff by funding transportation allowances. The Fund supports community-based health workers through new trainings, refresher trainings, drug supplies, and supervision support; on the demand side, it works to ensure that the community is informed of danger signs, receives support for emergency referrals37, and is mobilized to receive consultations by basic health staff in outreach sessions and in health facilities. These interventions
34 “Achieving health equity contested area of South East Myanmar, Bill Davis and Kim Jolliffe, June 2016, the Asia Foundation
35 MDHS 2015-16. This is corroborated by 2017 Myanmar Living Conditions Survey (MLCS) estimates that the number of poor people is 6.7 times higher in rural than in urban areas. 36 MIMU (2019), https://themimu.info/sites/themimu.info/files/documents/Hazard_Map_Socially_Hard_To_Reach_Area_MIMU1648v01_23Aug2019_A3_0.pdf 37 ACCESS provides emergency maternal-referral support to women who require emergency obstetric care; the support includes transportation and meal allowance.

47
aim at getting more women to consult38 before delivery, and to deliver at a facility attended by a skilled health-professional. On the supply side, ACCESS supports training for basic health staff in the provision of Basic Emergency Management of Obstetric Care (BeMOC). In addition, ACCESS provides BEmOC kits for basic health staff and EHO and ECBHO staff. The Fund has set aside some funding to support renovation of health facilities, especially in conflict-affected areas39.
Sexual and Reproductive Health and Rights
The Guttmacher–Lancet Commission40 defines Sexual and reproductive health as a state of physical, emotional, mental, and social well-being in relation to all aspects of sexuality and reproduction, not merely the absence of disease, dysfunction, or infirmity.
The Commission adds that
Therefore, a positive approach to sexuality and reproduction should recognize the part played by pleasurable sexual relationships, trust, and communication in the promotion of self-esteem and overall well-being. All individuals have a right to make decisions governing their bodies and to access services that support that right. Achievement of sexual and reproductive health relies on the realization of sexual and reproductive rights, which are based on the human rights of all individuals to: have their bodily integrity, privacy, and personal autonomy respected; freely define their own sexuality, including sexual orientation and gender identity and expression; decide whether and when to be sexually active; choose their sexual partners; have safe and pleasurable sexual experiences; decide whether, when, and whom to marry; decide whether, when, and by what means to have a child or children, and how many children to have; have access over their lifetimes to the information, resources, services, and support necessary to achieve all the above, free from discrimination, coercion, exploitation, and violence.
Essential sexual and reproductive health services must meet public health and human rights standards, including the “Availability, Accessibility, Acceptability, and Quality” framework of the right to health.28 The services should include: accurate information and counselling on sexual and reproductive health, including evidence-based, comprehensive sexuality education; information, counselling, and care related to sexual function and satisfaction; prevention, detection, and management of sexual and gender-based violence and coercion; a choice of safe and effective contraceptive methods; safe and effective antenatal, childbirth, and postnatal care; safe and effective
38 Monica Okuga, Margaret Kemigisa, Sarah Namutamba, Gertrude Namazzi, Peter Waiswa Glob Health Action. 2015; 8: 10.3402/gha.v8.23968. Published online 2015 Mar 31. doi: 10.3402/gha.v8.23968 PMCID: PMC4385211 39 While construction and renovation of Health facilities was an important activity under the 3MDG Fund, Access to Health has a limited amount dedicated to this activity; assumptions around infrastructure improvement mostly rely on Government or other sources of funding. 40 https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(18)30293-9.pdf

48
abortion services and care41; prevention, management, and treatment of infertility; prevention, detection, and treatment of sexually transmitted infections, including HIV, and of reproductive tract infections; and prevention, detection, and treatment of reproductive cancers. As noted in the Access to Health Fund’s Description of Actions, women’s health interventions in Myanmar are overwhelmingly focused on maternal and reproductive health, with little attention to women’s and girls’ sexual health issues beyond maternity and child bearing years. Little attention is paid to emotional health and violence-related health concerns. Sexual and Reproductive Health and Rights services have been reported to be insufficiently sensitive to the needs of adolescents, and youth often fall outside of available interventions. Sexual and reproductive health is a lifetime concern for both women and men, and rights include access to comprehensive sexuality education and information, family planning, antenatal and safe delivery care, postnatal care, prevention and treatment of sexually transmitted infections (including HIV). ACCESS focuses its resources on supporting Sexual and Reproductive health services as well as sexual and reproductive health rights (right to the highest attainable standard of sexual health, including access to sexual and reproductive health care services, right to sexuality education, right to autonomy and bodily integrity, the right to decide whether and when to be sexually active, right to freely define one’s own sexuality including sexual orientation and gender identity and expression, the right to choose their sexual partners, right to decide whether, when and by what means to have a child or children, and how many children to have, and right to privacy and confidentiality - among others) as one of the Fund’s priority areas. ACCESS supports sexual and reproductive health commodity-distribution to end-users through different modalities (mobile/fixed clinics, community-based health workers and social marketing). These efforts will contribute to increased contraceptive prevalence rate. SRHR awareness-raising in target populations (e.g. youth, women and men in hard-to-reach and conflict-affected areas) is an important intervention in ACCESS-supported townships. Increased SRHR awareness aims at reducing unwanted pregnancies and transmission of sexually transmitted infections, including HIV, especially among adolescents and youth. ACCESS has defined vulnerable youth based on national youth policy (e.g. out of school youth, disable youth, youth in EHO and ECBHO areas, orphanages, youth in drug affected community, etc.). Since 2019, ACCESS is making the transition from general youth to vulnerable populations, and is generating relevant evidence for programming. One ACCESS implementing partner will move to an exclusive focus on vulnerable populations in one township in Southern Shan in 2020; based on learning from this township, approaches will be adopted for reaching the most vulnerable youth.
41 Note that these services are not available in Myanmar nor included in the package of services supported by the Access to Health Fund
49
Provision of quality post-abortion care services by manual vacuum aspiration is now recommended to replace the dilation and curettage method42. ACCESS supports training on manual vacuum aspiration techniques to public sector and EHO and ECBHO providers, and supports quality post-abortion care services to clients.
As part of reducing reproductive morbidity, ACCESS supports cervical cancer awareness-raising and screening (as per the Description of Actions, in Annex) of women through fixed clinics and mobile outreach, to detect cervical cancer at early stages and provide treatment for positive cases (cryotherapy and thermal ablation method). Where needed, ACCESS covers referral costs for those who need the intervention of a local obstetrician-gynecologist.
Child Health
Child health interventions aim to reduce leading causes of under-five mortality in Myanmar: Services are provided through township health departments, basic health staff, and community-based health workers, with system-support through Implementing Partners. ACCESS supports increased capacity for basic health staff and community-based health workers through (i) technical trainings on infant and young child feeding, community case management of pneumonia and diarrhea, and integrated management of acute malnutrition; (ii) drug and equipment support; (iii) support to growth monitoring activities; (iv) referral of malnourished children for further treatment at a facility; (v) support to “newborn care corners” in selected health facilities, so that newborn babies receive appropriate care after delivery. This combined support allows community-based health workers and basic health staff to diagnose and treat under-five pneumonia and diarrhea cases, and ensure timely referral when required; outreach visits by basic health staff are strengthened and supported, increasing the number of under-five children in target areas who get immunized. The Fund’s support to the procurement of micronutrient powder and ready-to-use supplementary food (RUSF), and to their distribution to end-users, reduces childhood diseases and contributes to reducing child mortality. Micronutrient powder will be procured and distributed to 6-35 months old children in both government-controlled and non-government controlled areas, including camps and emergency settings. To tackle acute malnutrition among under-5 children, the Fund supports ‘integrated management of acute malnutrition’ (IMAM), including procurement of ready-to-use supplementary food sachets, while UNICEF supports other nutrition commodities to severely malnourished children. For demand generation, behaviour change communication activities are supported in collaboration with the National Nutrition Program. These activities include counseling on community-based infant
42 Safe abortion: technical and policy guidance for health systems, Second Edition, WHO 2012
50
and young child feeding, cooking demonstration in the community, and community mobilization through health workers. These activities increase appropriate feeding practices and prevent child malnutrition.
4.4. Interventions and desired outcomes
The Access to Health Fund supports the following interventions (and pursues some of the following outcomes) related to SRHR:
- Improved access for young people to sexual and reproductive health information, knowledge and services (including information about the opposite gender, to reduce stigma and discrimination)
- Promotion of young people’s knowledge and skills on SRHR, including comprehensive sexuality education and capacity building on life-skills and gender-based violence
- Promotion of access to youth-friendly SRHR services through training of general practitioners - Access to contraceptives to allow women to choose if and when to become pregnant, allow
spacing, and prevent unintended pregnancies thus reducing maternal death43 - Post abortion care services with misoprostol and manual vacuum aspiration, as
recommended by the Ministry of Health and Sports44 - Advocacy to MOHS to include into the Essential Package of Health Services cryotherapy
treatment services for cervical cancer, by showing that a ‘one-stop shop’ approach through private sector providers will increase the early detection and treatment of cervical cancer
The Fund supports the following interventions (and pursues some of the following outcomes) in relation to Maternal, Newborn, and Child Health:
- Antenatal coverage at least four times to identify high-risk pregnancies and provide care and support throughout pregnancy45
- Midwife outreach - Facility-based delivery and/or with a skilled birth attendant, ensuring quality of care and
access to emergency treatment46 - First postpartum visit taking place within the first two days to ensure early detection and
treatment of complications and preventive care for both mother and baby47 - Improving vaccination coverage through outreach visits (in townships not supported by GAVI)
to prevent most deadly childhood diseases such as measles, pneumonia, diphtheria, and tetanus48
- Community-based management of common childhood diseases
43 https://www.who.int/news-room/fact-sheets/detail/family-planning-contraception 44 Guideline on Postabortion Care for Public Sector Health Facilities, 2014, MRH division, MoHS 45 https://www.who.int/reproductivehealth/news/antenatal-care/en/ 46 https://www.thelancet.com/action/showPdf?pii=S0140-6736%2806%2969853-X 47 WHO, 1998a; WHO, 2001b 48 https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality
51
- Assessment of the nutritional status of children followed by interventions building on people’s own resources to prevent malnutrition (growth monitoring, timely referral)49
- Nutrition education including individual and group counseling, in both food-secure and food-insecure populations
- Distribution of micronutrient powder to young children aged 6-23 months to prevent micronutrient deficiencies50
4.5. Assumptions
In listing assumptions, we are not repeating risks in the Access to Health Fund’s Risk Matrix. For example, the risk of active conflict breaking out in areas supported by the Fund is the mirror image of the assumption that, in order for work to proceed, there needs to be no active-conflict situation.
1. As MNCH interventions facilitate service-delivery by basic health staff, they rely on functioning Township Health Departments and health facilities that are adequately staffed (number of staff, skills) and resourced (equipment, commodities…); when this assumption is not met and gaps are identified, the Fund steps in to fill them - through training, supportive supervision, and supplies.
2. Trust between service-providers and the community is essential to the successful delivery of services, as is a working relationship between Township Health Departments and Ethnic and Community-based Organizations.
3. The second major assumption is that the MOHS takes steps to increase and formalize the recognition of Community Based Health Workers and support their functioning and retention through supervision and standardized incentives. The Fund has been working upstream on this issue, supporting the Ministry of Health and Sports to develop a policy on Community-based Health Workers, currently under Minister’s review. A related assumption is that this policy will be endorsed in the near future and its operationalization supported not only by ACCESS but also by other major development partners.
4. To maintain the functionality of community-based health workers, midwives need to be able to provide adequate supervision.
5. Another assumption (linked to assumption 1 above) relates to the continued process of procurement and distribution of drugs (amoxicillin, paracetamol, ORS, Micronutrient powders51) and contraceptives, so that supplies are not interrupted and allow community-based health workers to deliver on their role.
6. The assumption that infrastructure is (i) in place and (ii) functional is an important one. While the Fund is not in a position to create new infrastructure at scale, it can work to influence and support the Ministry of Health and Sports’ approach to establishing/improving, staffing, and
49 Getachew 2011; World Bank 2012 50 https://www.who.int/elena/titles/micronutrientpowder_infants/en/ 51 The Access to Health Fund is the only external source of funding supporting procurement of Ready-to-use supplemental food
52
resourcing facilities. A joint assessment of Health infrastructure will be undertaken jointly with relevant actors, such as the World Bank.
The following assumptions are specific to EHO and ECBHOs; they are true for this section (MNCH) as they are true for other sections below but - for purposes of brevity - will not be repeated:
1. EHO and ECBHOs; have secured funding to deploy adequate human workforce; 2. EHO and ECBHOs; have sufficient technical capacity to provide relevant health services; 3. Good coordination between EHO and ECBHOs; and MoHS at different levels: collaborative
health services are provided when relevant 4. No outbreak of armed conflict which would prevent provision of services 5. Access to Health Fund is not subjected to pressure which prevents meaningful interaction
with EHO and ECBHO providers.
4.6. Alternative or additional interventions
Note: at the request of the Board, this document includes ‘alternative interventions’ - namely interventions not currently supported by the Access to Health Fund but which could possibly be explored and considered as either (i) alternatives to current approaches or (ii) complementary interventions to be supported by the Fund in the future. Interventions listed here are (by definition) not supported - and any decision to support them would be the result of a Board request to the FMO.
The 3MDG’s final evaluation was critical of the Fund’s confining its EmOC (Emergency Management of Obstetric Care) referral-focus to (i) providing cash-support to pregnant women and (ii) training basic health staff in BeMOC (Basic Emergency Management of Obstetric Care) - without investing more comprehensively in the improvement of facilities to provide (Basic or Comprehensive) Emergency Management of Obstetric Care services. ACCESS concurs with this finding and will need to explore enhancing its support to strengthening service-readiness in health facilities (beyond the currently planned training and kits). In line with the "Ending Preventable Maternal Mortality" Strategy for Myanmar (2017-2021), the Fund will explore the following interventions:
● Quality improvements such as clinical audits at Stations and Township hospitals ● Support to the implementation in health facilities of WHO’s global standards on Quality of
Care ● Equipment support for labour-room facilities (Rural Health Centres and EHO and ECBHO
health posts)
53
● Setting up maternity waiting homes (note: these are areas for exploration, not current activities)
● On the demand side, the Fund will explore further advocacy for institutional delivery and pilot incentive-schemes to promote institutional delivery for vulnerable populations.
In relation to Child Health, the Fund’s support to PMTCT52 was discussed in the past; the main reason for not supporting this intervention has been the division of roles between the 3MDG/Access Fund and the Global Fund, with the latter supporting the procurement of ARVs in Myanmar. The Fund could also tackle non-communicable diseases in children such as congenital disorders; however, a choice has been made to focus investments on interventions that reduce the diseases that cause high mortality. (Again, this is a possible area for exploration to be potentially discussed by the Board; it is not an area in which the Fund has decided to invest, and is only presented here as a possible additional/alternative intervention, as requested by the Board). Lastly, mobile-clinic support in hard to reach areas, which the Fund is implementing in Northern Rakhine and areas covered by EHOs and ECBHOs could be expanded; such support would be a complementary approach to the Fund’s current interventions, especially in very remote areas with limited government access or resources. V. HIV: Work on Harm Reduction
5.1. Global Evidence
Technical agencies have developed a clear set of recommended interventions in relation to harm reduction:
- WHO53 recommends interventions on HIV testing and counselling, outreach, Syringe exchange, drug-dependence treatment, mental health care for people who inject drugs and live with HIV, as well as people who inject drugs in prisons.
- WHO’s department of HIV/AIDS established that sufficient evidence exists for the effectiveness of needle and syringe programmes for the protection of people who inject drugs against HIV.54
- UNAIDS, UNODC and WHO endorsed a package of nine core interventions for the prevention and treatment of HIV/AIDS among Injecting drug users.55
52 Prevention of Mother to Child Transmission of HIV 53 Department of Mental Health and Substance Abuse Management: “Treatment of injecting drug users with HIV/ AIDS: promoting access and optimized service delivery” https://www.who.int/substance_abuse/publications/treatment_idus_hiv_aids.pdf 54 WHO, “Effectiveness of Sterile Needle and Syringe Programming in Reducing HIV/ AIDS among Injecting Drug Users”, 2014 https://www.who.int/hiv/pub/prev_care/effectivenesssterileneedle.pdf 55 https://www.who.int/hiv/pub/idu/targets_universal_access/en/
54
5.2. Myanmar-specific obstacles
Based on the latest estimates56 there are 93,000 injecting drug users in Myanmar. The highest proportion of new infections (28%) is among males who inject drugs with contaminated injecting equipment57. HIV prevalence among people who inject drugs has been increasing, from 28.5% in 2014 to nearly 35% in 201758. 56% of injecting drug users have Hepatitis C, while 27% show an HIV/Hepatitis C coinfection.59 According to UNAIDS and the National Strategic Plan for HIV/AIDS, 60 to 90 million additional needles/syringes are required per year60.
There are both supply-side and demand-side obstacles to applying best-practices based on global evidence. Supply-side:
● Limited number of qualified implementers in harm reduction resulting in inadequate number of service delivery facilities61
● Community resistance which impedes delivery of services (UNAIDS, 2015)62. ● Limited number of facilities and human resourcing difficulties in MOHS to provide opioid
substitution therapy. Currently, less than 20% of 93,000 people who inject drugs (17%)63 are on methadone maintenance therapy, far less than WHO-recommended range of 40% (WHO, UNODC, UNAIDS technical guide, 2012)64
Demand-side: ● Limited knowledge about risk factors and hazards of needle-sharing combined with fatalist
attitudes (IBBS 2017) ● Distance from work-sites and homes to service-delivery facilities, especially in hard-to-reach
areas, resulting in high cost of travel and significant time commitment (Source: 3MDG programme data)
● Community pressure and stigmatization of people who inject drugs (UNAIDS, 2015)65.
56 IBBS, 2017 57 HIV NSP 2016-2020 https://www.aidsdatahub.org/sites/default/files/highlight-reference/document/Myanmar_National_Strategic_Plan_on_HIV_and_AIDS_2016-2020.pdf 58 IBBS, 2014 and 2017 59 Myanmar Integrated Biological and Behavioural Surveillance Survey & Population Size Estimates among People Who inject Drugs (PWID) 2017-2018, National AIDS Program, Ministry of Health and Sports, Myanmar
60 https://www.avert.org/professionals/hiv-around-world/asia-pacific/myanmar 61 Source: 3MDG programme data 62 Situational Analysis on Drug Use, HIV and the response in Myanmar (UNAIDS, 2015) https://themimu.info/sites/themimu.info/files/assessment_file_attachments/situational_analysis_on_drug_use_and_hiv-_final.pdf 63 https://pr-myanmar.org/en/disease/hiv 64 WHO, UNODC, UNAIDS technical guide (2012) https://www.who.int/hiv/pub/idu/targets_universal_access/en/ 65 Situational Analysis on Drug Use, HIV and the response in Myanmar (UNAIDS, 2015) https://themimu.info/sites/themimu.info/files/assessment_file_attachments/situational_analysis_on_drug_use_and_hiv-_final.pdf
55
5.3. Intervention Logic
The Fund aims at reducing new HIV infections among people who inject drugs; outcomes include a higher utilization of sterile injecting equipment, higher coverage of receiving HIV testing services and linkage to care and treatment. Through outreach services and drop-in-centres, ACCESS delivers a comprehensive service packages for people who inject drugs (including in hard-to-reach areas), their regular sexual partners, people who use drugs, and people in prisons and other closed settings - as prescribed in the National Strategic Plan for HIV/AIDS. To ensure the package is indeed comprehensive, ACCESS partners support the nine core interventions for injecting drug users programs66 endorsed by UNAIDS, UNODC and WHO that collectively maximize impact for HIV prevention and treatment. Increased knowledge from HIV prevention and education sessions will encourage beneficiaries to get tested for HIV and, when relevant, start the cascade of care with antiretroviral therapy and opioid-substitution therapy (with ACCESS providing referral support). For the expansion of service delivery and filling the manpower gaps in station hospitals and rural health centers in hard-to-reach areas, ACCESS will support secondment of staff67 in methadone clinics and expansion to new sites under the grant of National AIDS program and Drug Treatment Unit.
5.4. Interventions
Service-delivery interventions include: 1. Needle and syringe programmes (NSPs) 2. Opioid substitution therapy and referral support for other evidence-based drug dependence
treatment 3. Renovation of methadone maintenance therapy centres 4. HIV testing and counseling 5. Referral support to antiretroviral therapy (funded by the Global Fund) so that HIV-positive
cases are systematically linked to care, as well as tracking follow-up to support adherence 6. Prevention and treatment of sexually transmitted infections (STIs) 7. Condom distribution to people who inject drugs and their sexual partners 8. Sexual Reproductive Health and Rights awareness and service provision 9. Targeted information, education and communication for people who inject drugs and their
sexual partners 10. Prevention, vaccination, diagnosis and treatment for viral hepatitis 11. Prevention, diagnosis and systematic referral support for treatment of Tuberculosis
In addition, ACCESS harm reduction service delivery now integrates mental health interventions for people who inject drugs and people who use drugs especially for methamphetamine users. Interventions include capacity building for medical doctors working at drop-in centres, mental health assessments, and psychosocial/pharmacological treatment.
66 WHO U. U., 2012 Revision
67 Medical doctor for the facilitation of methadone induction and Nurse for methadone dispensing, testing and counseling service
56
Once the national operational guidelines are approved, ACCESS will expand the service-package to include community-based HIV screening and index testing activities, in order to increase effectiveness of HIV prevention and harm reduction68. These two new testing strategies are among the key recommendations made in the 2019 National HIV Prevention Strategy. Thus, HIV testing will be offered to sexual and needle sharing partners of index clients (i.e. HIV-positive people who inject or use drugs); for females who inject drugs, this will also include their biological children." Health in Prisons: Myanmar has 85,000-90,000 prisoners (a breakdown by gender is not available) in 46 overcrowded prisons; half the inmates are in prison or labour camps for drug-related offences. Those people in prisons also need health support69. ACCESS interventions in prisons and labour camps include TB case-finding with mobile teams from the National TB Programme, testing for syphilis (with National AIDS Programme), HIV testing70, referral to NAP team, hepatitis B screening and vaccination (by partners in selected prisons). Hepatitis C screening and treatment with National Hepatitis Control Programme will be provided in four prisons (Insein, Mandalay, Lashio and Myitkyina). Supporting an enabling environment Through UNODC, Access supports creation of an enabling environment for improved community acceptance and participation, community advocacy and mobilization, and demand generation. The Fund also supports policy reform activities with community involvement, and expansion of services with community advocacy for increased inclusion.
5.5. Assumptions
Harm reduction interventions necessitate adequate human and technical resources, and a social and political environment that is, at best, supportive - or at a minimum not hostile. The Fund supports advocacy activities within the community and among faith-based organization, aimed at increasing their acceptance of harm reduction interventions and lowering their resistance to the provision of services Effective collaboration with the Ministry of Home Affairs and the Ministry of Health and Sports is essential for the success of our harm reduction and prison health interventions.
68 The model, ‘community-based screening for HIV’ (CBS), aims to identify more hidden people who inject drugs in the community. It is based on HIV screening by lay-testers, with positive cases linked to nearby facilities where confirmatory tests are available. CBS will increase HIV testing uptake by PWID. 69 See a paper submitted to the 4 October 2019 Board: Healthcare in Prisons and Human Rights: Considerations for the Access to Health Fund, which outlines in particular how Access’ work in prisons contributes to the improvement of the system. (Side note: there are 502 women identified as HIV positive in prisons, and among them 384 are on ART) 70 Access Partners (AHRN, MANA) are providing HIV testing services in Bhamo, Kale, Hsipaw, Monywa, Khamtee, Nyaung Shwe prisons and in collaboration with respective NAP teams. Positive cases are referred to NAP teams for care. After years of resistance, the Prison department now agrees to Methadone Maintenance Treatment in prisons, and first steps are being taken. The next National Strategic Plan will be a platform to launch one pilot MMT project on prison.
57
5.6. Alternative interventions
Further establishment of ART initiation centres at the sub-township level (by the Global Fund and/or other ARV-providers) should be considered for treatment expansion at community-level for high-risk populations. VI. Tuberculosis
6.1. Global Evidence
In 2017 alone, globally, 10 million people fell ill with TB and 1.6 million people died from the disease. It was one of the top-ten causes of death worldwide, and was responsible for more deaths than HIV71. More than 3.5 million cases are estimated to be “missed” annually because they are not diagnosed, or not treated, or treated but not officially notified by the national TB programmes72. TB progression can be controlled and mitigated by the early diagnosis and treatment through a patient-initiated pathway and/or a population-based screening pathway73.
In “A world free of tuberculosis”,74 WHO outlines plans for integrated, patient-centered care and prevention including activities to achieve “zero TB deaths”. These interventions are reflected under the Global Fund’s summary of high-impact TB interventions.75 They include a focus on active case-finding contributing to (i) the early diagnosis of tuberculosis, including universal drug-susceptibility testing, and systematic screening of contacts and high-risk groups; and (ii) treatment of all people with tuberculosis, including drug-resistant tuberculosis, and patient support.
Globally, the total cost of TB care (diagnosis and treatment) has been estimated on average to represent nearly 40% of annual household income76 - namely double the accepted 20%-threshold qualifying “catastrophic” health expenditures. According to the existing evidence, cases diagnosed early (through active-case funding) tend to incur catastrophic costs less frequently compared to cases found through passive case finding.77
6.2. Myanmar-specific obstacles
Background
In Myanmar, the National Tuberculosis Programme is aligned to the WHO End-TB strategy:
71 https://www.who.int/tb/post2015_TBstrategy.pdf?ua=1 72 https://www.theglobalfund.org/media/4762/core_tuberculosis_infonote_en.pdf?u=637001819990000000 73 https://www.who.int/tb/areas-of-work/laboratory/early-detection/en/ 74 https://www.who.int/tb/post2015_TBstrategy.pdf 75 https://www.theglobalfund.org/media/4762/core_tuberculosis_infonote_en.pdf?u=637001819990000000 76https://www.theunion.org/news-centre/news/new-operational-research-finds-tb-patients-diagnosed-through-active-case-finding-suffer-less-financial-costs 77 Global Health Action, 2018 https://www.tandfonline.com/doi/full/10.1080/16549716.2018.1494897
58
1. Conducive policies and supportive systems 2. Intensified research and innovation 3. Integrated patient-centered care and prevention
● Early diagnosis of tuberculosis including universal drug-susceptibility testing, and systematic screening of contacts and high-risk groups
● Treatment of all people with TB (including drug-resistant TB) and patient support ● Collaborative tuberculosis/HIV activities, and management of comorbidities ● Preventive treatment of persons at high risk, and vaccination against tuberculosis
The result of the recent Tuberculosis prevalence survey demonstrated a decreasing TB prevalence trend (613 per 100,000 population in 2009 to 466 per 100,000 population in 2018), indicating that the case-notification gap is lower than prior estimates. However, a gap still exists, and is particularly high among people in some hard-to-reach areas (Kachin, Sagaing) and specific population groups (e.g. migrant workers). Supply-side barriers include:
● Limited human resources and facilities for diagnosis (laboratory facilities for sputum examination, chest X-ray machines) resulting in lengthy diagnosis processes
● Lack of reporting from private sector health facilities contributes to the gap in TB notification ● Insufficient risk-based targeting of testing, outreach, and service capacity
Demand-side barriers include:
● Access to TB diagnosis facilities in hard to reach areas is an obstacle for early diagnosis of TB for vulnerable populations.
● Limited health knowledge: as noted earlier, only 65% of women and 57% of men in rural areas know TB spreads through cough compared, with 84% and 77% in urban areas respectively78
6.3. Intervention Logic
In line with the Tuberculosis National Strategic Plan (2016-2020), ACCESS supports accelerated (or active) case finding and treatment-adherence to narrow the notification gap, reduce TB incidence, and reduce TB mortality. Interventions prioritize populations in conflict-affected States, high TB-incidence areas such as Yangon, and ethnic and hard-to-reach areas. ACCESS intervenes through mobile teams and community-based health workers (through implementing partners). Early case notification prevents further case transmission, fills the TB notification gap, and reduces catastrophic costs due to TB among vulnerable populations.
1. Active Case Finding includes: ● TB case finding with mobile teams in urban poor and hard-to-reach areas ● TB screening through diabetes clinics
78 MDHS 2015-16
59
● TB case finding integrated with Maternal Newborn and Child Health Clinics ● TB case finding in prisons and worksites
2. Community-based TB care through community-based health workers
3. Chest X-Ray trainings to the ‘Yangon TB consortium mobile team’ and National TB Program’s mobile team assure quality of chest X-ray diagnosis. Diagnosis quality assurance (second reading) within the consortium is ensured by the Myanmar Anti-TB Association’s TB specialist, who is part of the consortium.
In all above interventions, ACCESS works to cover the following: - Increased access to diagnosis and immediate linkage to care - Travel allowance to patients for diagnosis - Training to community-based health workers - Information, Education and Communications to raise awareness of TB risks and increase
demand for testing and treatment - Support to mobile-teams’ operation-costs - MDR-TB patient support (Yangon) - Provision of Directly Observed Treatment(DOT)
Additional support: - The Fund and the National TB Program have devised a new approach to serving vulnerable
communities through night-time and Sunday clinics, facilitating the screening of (and services to) urban poor populations who cannot visit township TB care facilities during weekdays.
- ACCESS also supports TB case-finding through integrated approaches (integration of TB activities with MNCH and Harm Reduction service-delivery), especially in remote/uncovered areas.
- Community-based health workers provide health education on TB and refer TB suspected cases for examination and further treatment, as necessary.
- ACCESS continues to support Multi-drug resistant TB interventions complementary to the Global Fund’s activities, aimed to promote adherence: provision of Directly Observed Treatment and monitoring of side effects for Multi-drug resistant TB patients, infection control measures, health education, and counselling services, contact-tracing. While the National TB Program (NTP) focused its resources on responding to the MDR-TB crisis in Yangon region, the major gap remains in human resources. Without the additional HR support, delays in early initiation of MDR-TB treatment and challenges in continuum of care for the long MDR-TB treatment cannot be avoided. To fill this gap, the Fund supports seconded staff to the National Tuberculosis Programme through implementing partners for the MDR-TB crisis response in Yangon (medical officers, nurses, and data assistants based at MDR-TB decentralized sites and providing immediate MDR-TB care and support.)
60
6.4. Assumptions
Key assumptions related to the Fund’s TB work are broadly outside of the Fund’s control: X-ray machines’ functioning status in mobile teams, township TB facilities for tuberculosis diagnosis, township TB team functioning for treatment, community-based health workers’ motivation in conducting integrated activities. However, these areas are not outside of the Fund’s sphere of influence, and the Fund is working with all relevant stakeholders to try to ensure optimal conditions for the implementation of TB-related activities. As per the Fund’s overall Risk Matrix, an assumption is made that mobile-team visits to EHO and ECBHO catchment areas and hard-to-reach villages in Government-controlled areas will remain possible and that expansion of coverage will be feasible.
6.5. Alternative interventions
Several alternative or experimental interventions to combat TB are being piloted in parts of the country – such as expansion of TB case finding through contact-tracing, establishment of sputum collection centers, public-private-mix DOT centres79, pharmacy channels for TB diagnosis and treatment expansion, etc. Many of these interventions are carried out by the Global Fund; ACCESS, is not considering taking on these activities as that would duplicate efforts. VII. Malaria
7.1. Global Evidence
With 219 million cases of malaria in 2017 worldwide, malaria is a global health priority.80 The WHO Global Technical Strategy for Malaria 2016-2030 sets ambitious but not unrealistic global targets,81 including:
● Reducing malaria case-incidence and mortality rates by at least 90% by 2030 ● Eliminating malaria in at least 35 countries by 2030 ● Preventing a resurgence of malaria in all countries that are malaria-free.
The Global Malaria Strategic Framework82 outlines: ● Pillar 1: ensure universal access to malaria prevention, diagnosis and treatment ● Pillar 2: accelerate efforts towards elimination and attainment of malaria-free status ● Pillar 3: transform malaria surveillance into a core intervention ● Supporting element 1: harnessing innovation and expanding research ● Supporting element 2: strengthening the enabling environment
79 Please note that public-private mix DOT, in private sector hospitals and GP clinics, is still part of the Yangon TB consortium, but not offered in other States. 80 World Malaria Report 2018 (WHO) 81 https://www.who.int/news-room/fact-sheets/detail/malaria 82 The Global Technical Strategy for Malaria 2016–2030 http://apps.who.int/iris/bitstream/10665/176712/1/9789241564991_eng.pdf?ua=1&ua=1
61
7.2. Myanmar-specific obstacles
Malaria morbidity declined considerably over the past few years, with over 500,000 reported cases in 201283 versus just over 75,000 cases in 201784. Malaria mortality also declined steadily - from 1,707 in 2005 to just 37 in 2015 (98% reduction over 10 years85). Despite an overall decline in malaria positivity, the disease remains a key health problem in forest and forest fringe communities, particularly in hard-to-reach and remote border-areas - including some conflict affected areas where ethnic communities reside.
The National Malaria Strategic Plan (2016-2020) prioritizes the following: 1. Reduce malaria burden in the most endemic areas 2. Eliminate falciparum malaria in areas of multidrug resistance, including artemisinin resistance 3. Strengthen the existing surveillance system 4. Strengthen the capacity of healthcare providers and programme staff in elimination activities
and prevention of malaria resurgence.
The National Malaria Control Programme establishes three key interventions86: 1. Case detection and effective management 2. Malaria prevention 3. Malaria case and entomological surveillance
Supply-side barriers include:
● Insufficient qualified workforce to implement the ambitious elimination agenda ● With a significant decline in morbidity, the workload for malaria-specific community-based
health workers is often too low to justify their role. ● As the country gets closer to elimination, another barrier is the need for customized
approaches to specific sites.
Demand-side barriers include: ● Limited accessibility to health facilities in hard-to-reach areas ● Knowledge on malaria transmission and service availability ● Financial limitations and socio cultural obstacles in getting prevention, testing and treatment
7.3. Intervention Logic
The Fund’s malaria interventions aim at reducing malaria mortality rates in Myanmar by ensuring that malaria cases are identified and receive antimalarial treatment according to national policy. With
83 World Malaria Report, 2018 84 NMCP program data, 2018 85 http://www.searo.who.int/myanmar/documents/malarianationalstrategicplan2016-2020.pdf 86 Myanmar National Malaria Strategic Plan (2016-2020)
62
declining morbidity country-wide, retaining vertical malaria intervention programmes is no longer efficient, and integration of malaria services with other services was adopted by the Ministry of Health and Sports. This is done through the “Integrated Community Malaria Volunteer” approach (ICMV) whereby community-based health workers are equipped with knowledge on dengue, filariasis, leprosy, TB and HIV. The integration approach substantially complements and extends the reach of services particularly in rural and remote areas, where health infrastructure is weak or absent and malaria transmission tends to be highest. It will help to monitor population movement and support real time reporting in the areas of malaria elimination phase. The National Malaria Control Program is also planning to strengthen needs-based training as per National guidelines to be able to apply the customized approaches in specific areas. In the case of the Access to Health Fund, further integration has taken place with maternal and child health activities, as well as harm-reduction activities.
7.4. Assumptions
Malaria interventions at community-level require human resources (trained volunteers, mobile team staff), drugs and RDT test kits, standardized incentive scheme, supportive supervision, stable operational situation and endorsement of the Community-based Health Worker Policy. Meanwhile, comprehensive coverage of malaria interventions is mainly funded by the Global Fund.
7.5. Alternative interventions
As Myanmar is moving toward Malaria Elimination by 2030, elimination-specific activities (such as case investigation, foci investigation, etc.) will be implemented mainly with Global Fund support. For the support of addressing malaria elimination, ACCESS will consider supporting selected townships that are included in the National Malaria Elimination plan, however, it may face funding gaps. Malaria prevention activities such as bednet distribution and insecticide-spraying are covered by the Global Fund and the President's Malaria Initiative. VIII. Health Systems Strengthening
8.1. Global Evidence
The inclusion of Universal Health Coverage in the Sustainable Development Goals presents an opportunity to promote a comprehensive and coherent approach to health. While the ultimate goal is service coverage and universal access, the means to that end is stronger health care systems - through a focus on health systems strengthening. Global evidence points to a number of essential ingredients that a resilient system needs to develop in order to “provide all people with access to needed health services of quality without experiencing financial hardship”87:
87 Myanmar National Health Plan 2017-2021
63
Primary Health Care. In most settings, coverage, efficiency and equity in the delivery of health services require an increased emphasis on frontline services, particularly primary health care.88 Evidence points in particular to the importance of skilled and motivated health workers being deployed to the right places (and in the right quantity)89. Governments’ capacity to provide and enforce fair, transparent and effective regulatory frameworks and accreditation systems is critical.90 Governance arrangements determine key institutional attributes such as transparency, accountability, participation, integrity and capacity, and therefore have far-reaching consequences for system performance91. Improving the use of funds and system efficiency is essential.92 Innovation and new service delivery models are needed to meet the health needs of vulnerable and marginalized groups and overcome challenges, in particular in contexts of fragility and conflict;93 this is also true of innovative partnerships with non-state providers.
8.2. Myanmar-specific obstacles
“The Myanmar health system currently faces many challenges. These relate to the availability and distribution of inputs (e.g. human resources, physical infrastructure, essential medicines and supplies, financial resources) and to weaknesses in key functions such as supportive supervision, referral, supply chain, health management information system, and public financial management. Limited oversight, leadership and accountability further exacerbate these challenges.”94
The National Health Plan (2017-2021) aims to strengthen the country’s health system and pave the way towards UHC, choosing a path that is explicitly pro-poor. The main goal of NHP 2017-2021 is to extend access to a Basic Essential Package of Health Services (EPHS) to the entire population by 2020 while increasing financial protection. One of the key obstacles to Universal Health Coverage in Myanmar, and therefore one of the key roles of health system strengthening in the coming years, is the highly inequitable access to health afforded to different populations. Disparities affect in particular conflict-affected areas and populations living in hard-to-reach locations.95 EHOs and ECBHOs, which may be under resourced, are often the only health provider in some remote or conflict-affected areas, and government health staff may have no access.
88 WHO (2008) Primary Health Care – Now More Than Ever, World Health Report 2008 89 Jha, P., and A. Mills. 2002. Improving Health Outcomes of the Poor: Report on Working Group 5 of the Commission of Macroeconomics and Health. Geneva: World Health Organization 90 Clarke, D.; Rajan, D. and Schmets, G. (2016) ‘Creating a Supportive Legal Environment for Universal Health Coverage’, Bulletin of the World Health Organization 91 Greer, L.; Wismar, M. and Figueras, J. (2016) Strengthening Health System Governance: Better Policies, Stronger Performance 92 OECD (2017) Tackling Wasteful Spending on Health, Paris: OECD 93 Fragility, Conflict and Violence – Overview, World Bank 94 Myanmar National Health Plan - op. cit. 95 For example, the MMR in Chin State is 357, compared to 213 in Yangon. Children from poorer households are more than twice as likely to be undernourished than those from better-off households. The 2014 Myanmar Population and Housing Census
64
Despite its role in reducing inequity and affording access to all, primary care takes second place to hospital services. The current public sector health services provision focuses on tertiary care, with station hospitals and below receiving less attention over the past few decades. This underinvestment has led to various shortcomings in service availability, readiness and coverage. Furthermore, there is limited public sector service-delivery in both conflict-affected and post- conflict affected areas96. Deployment, distribution and retention of health staff has been a major challenge, including shortage of human resources, inappropriate balance and mix of skills, inequitable distribution, and difficulties in rural retention - especially when it comes to placing and retaining health workers in less-secure and in hard-to-reach areas97. High out of Pocket Expenditures for Health: Myanmar currently allocates only 3.65% of its total budget to health, which is extremely low by global and regional standards. Household out-of-pocket payments make up 74% of total health expenditure, the predominant source of health service financing. As a result, utilization of services depends more on people’s capacity to pay for medical care and transport costs than on health needs.98 Public Financial Management is weak, with a disconnect between planning and budgeting functions, little to no consultation with implementers at lower levels, and little evidence that information from the paper-based financial reports is being used in decision-making.99 Despite recent promising initiatives, standardization of services among EHOs and ECBHOs and between them and the public sector faces many challenges. Health workers employed by EHOs and ECBHOs are trained through parallel systems, with limited or no recognition from the MOHS. Service provision by EHOs and ECBHOs relies heavily on donor support, without focusing much on strengthening their systems, which puts their sustainability at risk100. Leadership and Governance – Successful implementation of the National Health Plan towards Universal Health Coverage will require strong policies, strengthened MOHS leadership and oversight and enhanced accountability at all levels to operationalize these policies. Strong coordination with EHOs and ECBHOs and government is critical to achieving equitable health coverage for the whole population. Central MoHS takes the functions of setting rules and standards as included in the provisions of respective health laws. In addition, it retains the authority of placing and transferring doctors and staff, although the regional health directors were allowed to take temporary measures for filling vacant posts when the need arose. Decentralization is still limited in all three different dimensions: political, administrative and fiscal dimensions
96 Myanmar National Health Plan 2017-2021 97 WHO Asia Pacific Observatory on Health Systems and Policies: What are the challenges facing Myanmar in progressing towards Universal Health Coverage? 98 Myanmar National Health Accounts (2014-2015) 99 Myanmar National Health Plan 2017-2021 100 Myanmar National Health Plan 2017-2021
65
8.3. Intervention Logic
The Fund’s investment in Health Systems Strengthening aims to increase access of vulnerable populations in conflict-affected areas to better and more relevant health services, and to increase coordination of health-service coverage for vulnerable populations between the MOHS and EHO and ECBHO. Interventions are summarized below in categories:
● Central MoHS level for development and implementation of policies, strategies and plans; ● Building of EHO and ECBHO systems ● State and Township Health Departments for planning and implementation of health
services, with a focus on vulnerable populations ● Increased coordination between EHO and ECBHO and the MOHS
1. The Access to Health Fund supports the development and implementation of equity-focused health policies, strategies and plans that are related to both the health system and technical areas.
Key policies and plans include: - The community-based health workers policy - Rural health workforce retention strategy - Annual operational plans of the National Health Plan - Accreditation system for pre-service education - Sexual and reproductive health and rights policy - Sub-national plans for Myanmar Multi-sectoral National Plan of Action on Nutrition (MS-NPAN) - National strategic plan for prison health - National strategic framework for health and drugs - National strategic plan for reproductive, maternal, newborn, child and adolescent health
(RMNCAH) In addition, the fund also supports key guidelines and manuals related to system strengthening such as referral guidelines and Rural Health Center manual. The Fund also supports the development of guidelines for state/regional health plan and inclusive township health plan. In order to generate evidence that inform planning, decision making and policy development, Access supports interventions such as:
- The strengthening of human resources for health information management system - Strategic purchasing pilots (including coordination meetings to discuss lessons learned and
way forward for these pilots) - The Nationwide health facility assessment (to assess supply-side readiness of public health
facilities to provide basic essential package of health services) - The development of a National Research Agenda for Health Systems Strengthening in
Myanmar, to bring coherence and unity to research, so that it is more relevant to (and better informs ) policy and practice.
66
2. In order to improve EHOs and ECBHOs’ institutional capacity to provide services to vulnerable populations and increase accountability to the populations they serve, the following interventions will be conducted:
- Strengthening coordination (Inter EHOs and ECBHOs, EHOs and ECBHOs with MoHS) through National, State and local level forum and meetings
- Promotion of Service Quality through regular Continuous Medical Education sessions - Strengthening service availability and readiness capacity through renovation of health facilities,
Primary Health Care Workers Production, and medicines and supplies for ECBHO clinics. These interventions aim to fill the gaps in the short-term while system-building efforts are underway
- Strengthening EHOs and ECBHOs’ institutional capacity in evidence-based planning, analysis, budgeting, programming, leadership, human resource management, logistics and supply chain management and financial management through trainings and workshops
- Fostering involvement of EHOs and ECBHOs in the national health system, for example consultation for the National Health Plan, EHO and ECBHO representation in technical working groups at Central and State Level, Health Financing Pilot in EHO and ECBHO areas, and readiness on delivery of the Essential Package of Health Services by strengthening technical capacity and medical supplies
- Bringing two health systems closer and strengthening technical capacity of EHOs and ECBHOs through joint training, joint monitoring visit and exchange visits at different levels.
3. The Fund is also strengthening the capacity of State and Township health departments to develop and implement plans to increase access of marginalized and vulnerable populations to health services:
- Development of State Health Plans and Inclusive Township Health Plans - Strengthening/establishment of State and Township Health Working Groups to jointly plan
and cost actions that need to be taken to fill coverage gaps to meet the needs of underserved populations
- Strengthening State and Township Health Department's capacity in evidence-based planning, budgeting, analysis, programming, leadership and management, and financial management through trainings and workshops
- Community-based Health Workers registry/mapping workshops to identify gaps, especially among the communities in conflict-affected and hard-to-reach areas.
- Improving technical capacity and emergency-response capacity of Health staff through training
4. As noted above, increased coordination between EHOs and ECBHOs and the MOHS is a key component of an efficient Health System in Myanmar in the long-term. This point is discussed in more detail in the enclosed ECBHO Engagement paper. Through these interventions, Fund supports the NHP goals of responsiveness, capacity of health systems at local levels and link to deconcentration/decentralization.
67
8.4. Assumptions
The strengthening of Myanmar’s Health System (or systems, as they currently stand) depends on the continued commitments of key stakeholders, especially the MOHS, to pursue the implementation of the National Health Plan; it also requires clear governance and coordination mechanisms within the Ministry and EHOs and ECBHOs to develop and execute policies, and effective collaboration mechanisms between the MoHS and other key stakeholders, especially EHOs and ECBHOs. Myanmar is approaching its next Government election in 2020. Politics shapes the social, economic, and environmental conditions that, in turn, shape the health of populations. It is important that the new Government’s political agenda brings a promising future to the National Health Plan and the promise of Universal Health Coverage. At the same time, Myanmar is home to an array of armed and intercommunal conflicts; Access’ capacity to deliver on its commitments depends on the evolution of peace and conflict in the country.
8.5. Alternative interventions
Strengthening the Logistics Management Information System (LMIS) of the public sector has been carried out at the central level by different partners. A few States and Regions are implementing the system for reproductive health commodities. Access could explore support in this area, and in particular strengthening the capacity of State and Township level health departments to manage the system. Strengthening the public financial management system and MOHS’ capacity to manage the system is supported by the World Bank and Access in a coordinated way. The fund could also explore the possibility of providing mentoring support at the State level, especially during budget-preparation and budget-revision periods. Accreditation of EHO and ECBHO providers through a licensing examination can also be considered, given that the fund is supporting the professional councils to roll out the accreditation system for pre-service education. IX. Social Cohesion The promotion of social cohesion is part of the Access to Health Fund’s vision, and one of its explicit goals. The Fund is currently exploring opportunities to promote social cohesion through its health-related work. As noted at the outset of this Overall Strategy, Terms of Reference for that exercise are in Annex, and the Strategy will be updated on the basis of findings in this space.
68
Monitoring and Evaluation Strategy
1.1. Programme Context
Programme plans and grant agreements for the first two years of the Access to Health Fund (2019-2020) were largely developed in the third quarter of 2018 - prior to the finalization of the Access Strategy - to assure a seamless transition from the 3MDG. Monitoring and Evaluation frameworks and systems for 2019-2020 were carried forward from the 3MDG. The transition to the new M&E strategy will start in 2020 in selected programme areas (known as Early Strategy Adopters) and will be fully implemented from 2021. The Monitoring and Evaluation Strategy also incorporates the following recommendations of the Final 3MDG Evaluation:
Recommendation 5: Impact indicators should indicate reduced disparities in health between remote and conflict-affected populations and the general population, as well as indicating overall improvement. Recommendation 6: It should be clear whether indicators relate to a programme area or population group, and where they are reporting national or whole population data. Recommendation 7: Whatever indicators are selected, Access should confirm that they are feasible, i.e. whether reliable, comparable and timely data will be available or not. Annual reporting is not required for impact figures, but there may be a need to supplement them with proxy outcome indicators. Recommendation 8: Outcome indicators should provide achievable targets for improved access by the target populations – remote and conflict-affected populations – as well as reduced disparity between target populations and the general population. Recommendation 9: Target populations should be clearly defined, in order to design qualitative, quantitative and proxy indicators that demonstrate health outcomes. Recommendation 11: Access should obtain and report baseline and end-line data where possible, as these are essential for both monitoring and evaluation – even though such data will necessarily be imperfect. Recommendation 12: Where possible, data from local health assessments, plans and routine data should be used for local monitoring, and aggregated as sources for baseline and end-line data. If relevant and feasible, Access could additionally incorporate data from 3MDG baseline health needs assessments. Recommendation 13: In order for outcome indicators to include ethnic minority and conflict-affected populations, there may be need for proxy indicators or special activities, such as an EHO-supported survey of health conditions and needs in conflict-affected areas. Recommendation 14: Facility-level data, from HMIS, IPs and from Rural and Sub-Rural Health Centers RHCs/SRHCs may provide targeted indicators and proxy indicators of outcomes, particularly where there is uneven access across the township, or particular population groups (e.g. according to age or location) are underutilizing services. We note that Access is currently developing indicators showing more vulnerable categories of women, for targeting purposes. Recommendation 15: Outcome indicators should be timely. 3MDG’s support may have made it possible to start to use and aggregate in-year child death surveillance reports. DHS and similar survey reports of child mortality rates are too late, infrequent, and lacking in detail for use as outcome indicators.
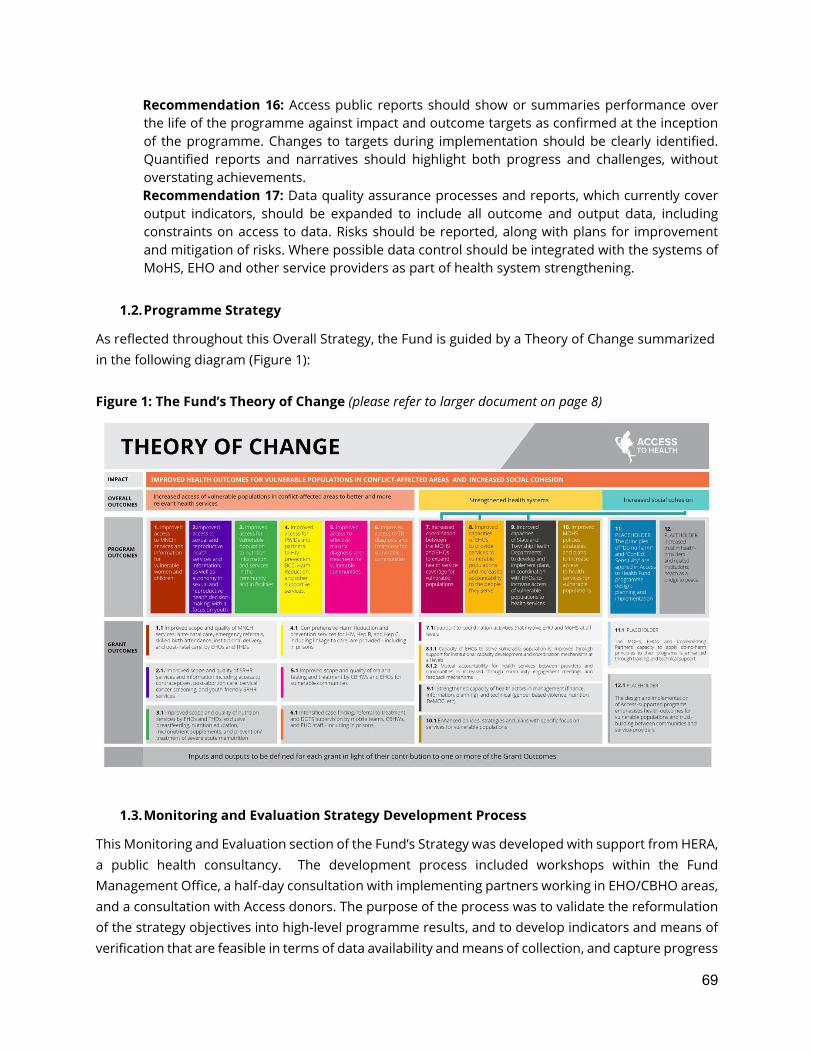
69
Recommendation 16: Access public reports should show or summaries performance over the life of the programme against impact and outcome targets as confirmed at the inception of the programme. Changes to targets during implementation should be clearly identified. Quantified reports and narratives should highlight both progress and challenges, without overstating achievements. Recommendation 17: Data quality assurance processes and reports, which currently cover output indicators, should be expanded to include all outcome and output data, including constraints on access to data. Risks should be reported, along with plans for improvement and mitigation of risks. Where possible data control should be integrated with the systems of MoHS, EHO and other service providers as part of health system strengthening.
1.2. Programme Strategy
As reflected throughout this Overall Strategy, the Fund is guided by a Theory of Change summarized in the following diagram (Figure 1): Figure 1: The Fund’s Theory of Change (please refer to larger document on page 8)
1.3. Monitoring and Evaluation Strategy Development Process
This Monitoring and Evaluation section of the Fund’s Strategy was developed with support from HERA, a public health consultancy. The development process included workshops within the Fund Management Office, a half-day consultation with implementing partners working in EHO/CBHO areas, and a consultation with Access donors. The purpose of the process was to validate the reformulation of the strategy objectives into high-level programme results, and to develop indicators and means of verification that are feasible in terms of data availability and means of collection, and capture progress
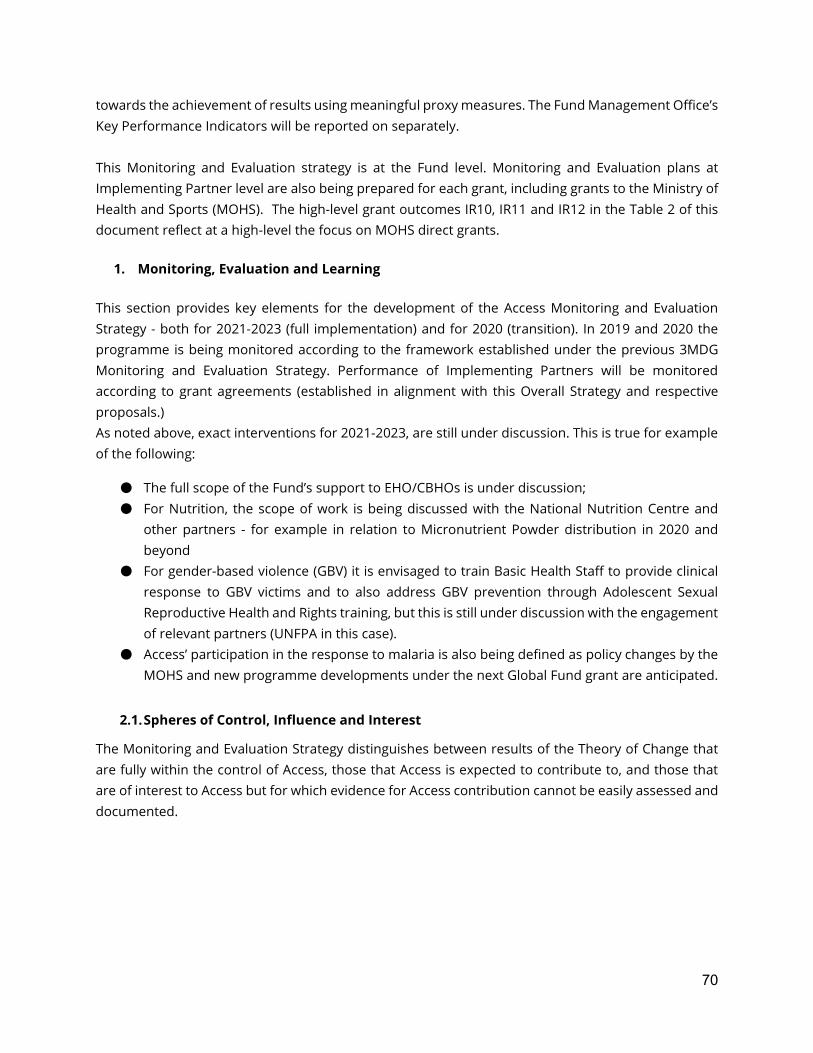
70
towards the achievement of results using meaningful proxy measures. The Fund Management Office’s Key Performance Indicators will be reported on separately. This Monitoring and Evaluation strategy is at the Fund level. Monitoring and Evaluation plans at Implementing Partner level are also being prepared for each grant, including grants to the Ministry of Health and Sports (MOHS). The high-level grant outcomes IR10, IR11 and IR12 in the Table 2 of this document reflect at a high-level the focus on MOHS direct grants.
1. Monitoring, Evaluation and Learning This section provides key elements for the development of the Access Monitoring and Evaluation Strategy - both for 2021-2023 (full implementation) and for 2020 (transition). In 2019 and 2020 the programme is being monitored according to the framework established under the previous 3MDG Monitoring and Evaluation Strategy. Performance of Implementing Partners will be monitored according to grant agreements (established in alignment with this Overall Strategy and respective proposals.) As noted above, exact interventions for 2021-2023, are still under discussion. This is true for example of the following:
● The full scope of the Fund’s support to EHO/CBHOs is under discussion; ● For Nutrition, the scope of work is being discussed with the National Nutrition Centre and
other partners - for example in relation to Micronutrient Powder distribution in 2020 and beyond
● For gender-based violence (GBV) it is envisaged to train Basic Health Staff to provide clinical response to GBV victims and to also address GBV prevention through Adolescent Sexual Reproductive Health and Rights training, but this is still under discussion with the engagement of relevant partners (UNFPA in this case).
● Access’ participation in the response to malaria is also being defined as policy changes by the MOHS and new programme developments under the next Global Fund grant are anticipated.
2.1. Spheres of Control, Influence and Interest
The Monitoring and Evaluation Strategy distinguishes between results of the Theory of Change that are fully within the control of Access, those that Access is expected to contribute to, and those that are of interest to Access but for which evidence for Access contribution cannot be easily assessed and documented.
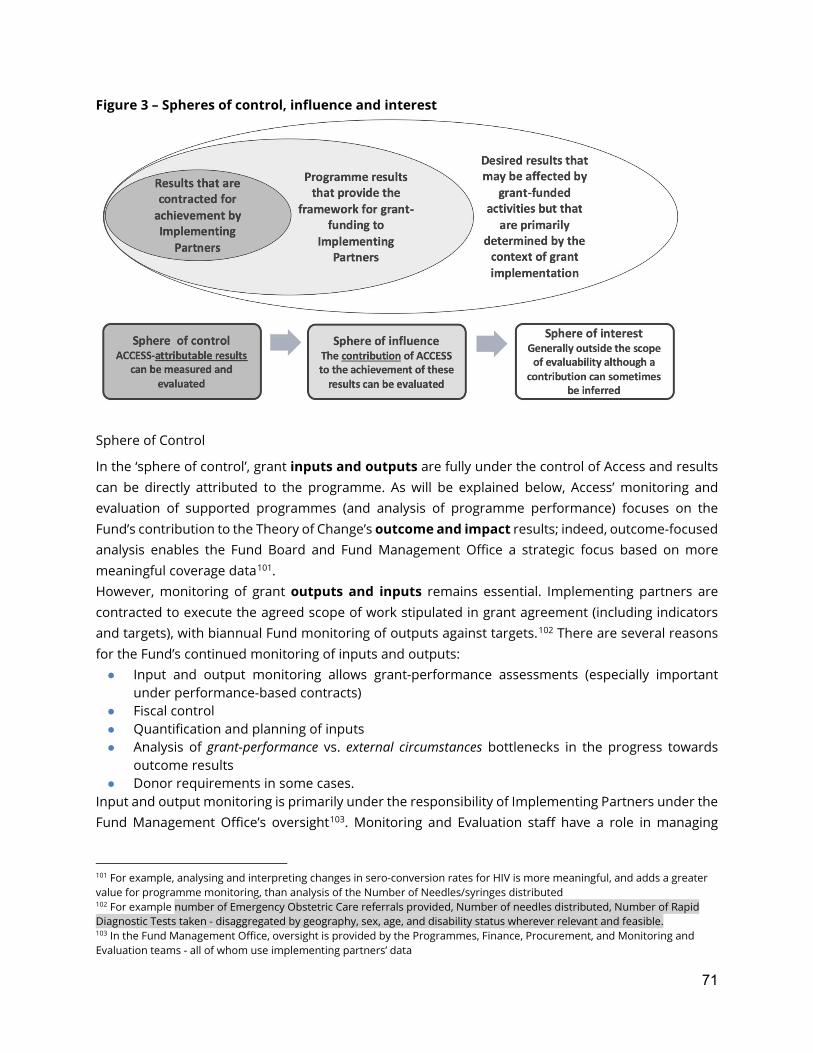
71
Figure 3 – Spheres of control, influence and interest
Sphere of Control
In the ‘sphere of control’, grant inputs and outputs are fully under the control of Access and results can be directly attributed to the programme. As will be explained below, Access’ monitoring and evaluation of supported programmes (and analysis of programme performance) focuses on the Fund’s contribution to the Theory of Change’s outcome and impact results; indeed, outcome-focused analysis enables the Fund Board and Fund Management Office a strategic focus based on more meaningful coverage data101. However, monitoring of grant outputs and inputs remains essential. Implementing partners are contracted to execute the agreed scope of work stipulated in grant agreement (including indicators and targets), with biannual Fund monitoring of outputs against targets.102 There are several reasons for the Fund’s continued monitoring of inputs and outputs: ● Input and output monitoring allows grant-performance assessments (especially important
under performance-based contracts) ● Fiscal control ● Quantification and planning of inputs ● Analysis of grant-performance vs. external circumstances bottlenecks in the progress towards
outcome results ● Donor requirements in some cases.
Input and output monitoring is primarily under the responsibility of Implementing Partners under the Fund Management Office’s oversight103. Monitoring and Evaluation staff have a role in managing
101 For example, analysing and interpreting changes in sero-conversion rates for HIV is more meaningful, and adds a greater value for programme monitoring, than analysis of the Number of Needles/syringes distributed 102 For example number of Emergency Obstetric Care referrals provided, Number of needles distributed, Number of Rapid Diagnostic Tests taken - disaggregated by geography, sex, age, and disability status wherever relevant and feasible. 103 In the Fund Management Office, oversight is provided by the Programmes, Finance, Procurement, and Monitoring and Evaluation teams - all of whom use implementing partners’ data

72
routine data collation systems and frameworks. The accuracy of the reported data is assessed during supervision and data quality audit exercises led by the Fund Management Office’s Monitoring and Evaluation team, in line with data-quality assessment procedures covered in a dedicated Standard Operating Procedure.
Sphere of Influence
Access’ contribution to results that are within its sphere of influence can be assessed, but attribution is more difficult to establish:
Impact: Inferences can be made on Access’ contribution to improved health of vulnerable populations based on available national survey and research data. The contribution will be small, given that the Fund is expected to contribute less than 0.8%104 of the per-person total health expenditure in Myanmar. For specific sub-populations (e.g. people in prisons) the contribution may be easier to assess, but the scope of the programme is also limited in these areas, for instance targeting only a limited number of prisons and supporting only a small number of interventions that will have an impact on the health of prisoners.
An assessment of Access’ contribution to the programme’s impact will therefore be based primarily on qualitative data that will also capture the leveraging effects of policy and systems support.
Overall Outcomes:
There are three overall outcomes, one of them defined at the end-user level (vulnerable populations), the other two are defined at the health systems level (increased coordination and focus on vulnerability) and social cohesion. Quantification of the contribution of the programme to improved access of vulnerable populations to better health services is possible if population-level baseline and end-line data on equity, utilization and outcome of health services are available for Access programme areas (or among groups that are specifically targeted by Access). These can be compared to national trends, and inferences can be made on the basis of positive deviations of trends in programme areas, taking other factors (such as other targeted programmes) into consideration. Major deviations are not likely to be achieved in the relatively short timeframe of the programme. Such an analysis would therefore require a large sampling frame and sample size.
Access contributions at the policy and systems level to increased coordination and coverage for vulnerable populations cannot be quantified, but can be assessed qualitatively through policy analyses and structured interviews with key informants.
The mechanisms for assessing Access contributions in terms of social cohesion will be defined following the completion of specialized technical support in this area.
104 Based on WHO estimates of annual per person total health expenditure of $103 in 2014

73
Programme Outcomes
In the Theory of Change, six Program Outcomes are results at the end-beneficiary (or population) level, while fours are at the systems and policy level, with further two envisaged outcomes on social cohesion. As these results are specific to the Access programme, they define the main level at which the Fund’s performance and contribution to change will be monitored, in order to provide assurance to the Fund Board that the logic of the Programme’s Theory of Change continues to hold.
Monitoring indicators for this level were identified in the workshop with programme staff and are listed in Tables 1 and 2. The majority of these indicators are from the national Health Management Information System (for Government-controlled areas) and EHO systems (for non-Government controlled and mixed-controlled areas), with a smaller number of survey-based indicators.
End-beneficiary level results require data at the level of targeted beneficiaries. For these data, Access has to largely rely on the timely availability and quality of data collected by the Health Management Information Systems of the MOHS and EHO/CBHOs. Real-time access to these systems and participation in data quality audits is therefore an essential requirement.
Monitoring indicators also cover five policy and system outcomes (IR7, IR8.1, IR8.2, IR9 and IR10) in Table 1, and R7, R8, R9 and R10in Table 2. These indicators rely on qualitative or semi-quantitative data, such as structured scoring systems for capacity development that are comparable among all Access systems and policy partners. The development and agreement on standardized tools for these assessments will be a focus of the Fund’s Monitoring and Evaluation activities during the transition period.
Program and grant outcomes on social cohesion will be defined following the completion of specialized technical support in this area
Grant Outcomes
As noted, the 13 results identified in the Theory of Change framework at the Grant Outcome level are the high-level results that define the objectives of each grant. Each grant is expected to contribute to the achievement of one or more of these results. Measurement of progress towards the achievement of Grant Outcomes will take into account the baseline situation, the contribution of other (non-grant) interventions, and contextual factors (especially in programme-areas affected by conflict).105
An important consideration in this process is a clear definition of the unit of intervention and the unit of monitoring - discussed under a separate heading.
Sphere of Interest
The overall outcome of ‘increased social cohesion’ is an important part of the Fund’s mandate. While the Fund’s contribution to this vision will be difficult to evaluate (weak linkage to programme results,
105 For two of the four policy and systems-level outcomes, no specific indicators were identified at grant outcome level as these policy and systems-level outcomes can be monitored by applying the higher-level (Programme) outcome indicators to the relevant grant agreements.

74
importance of external factors…) the Fund is currently commissioning more work on its possible contribution to social cohesion - see Terms of Reference in Annex. This Overall Fund Strategy will be updated in the near future with a more developed approach to social cohesion and proposed measurement of progress.
2.2. Monitoring and Evaluation on Two Levels
Level 1: Implementing Partners
Grant outputs. Implementing Partners’ monitoring and reporting on Grant Outputs is done through standardized Access templates which allow data aggregation per thematic area;106 targets are set at grant-level (e.g. people reached, deliveries attended by skilled provider...) based on the context and scope of the grant. Grant Outputs are the basis of monitoring IP performance, with variances in outputs against targets explained by IPs. The Fund Management Office analyses reported outputs biannually, and verifies (on a case-by-case basis during monitoring visits) ‘red flags’ raised by variances between targets and reported outputs. Proposed indicators will be measured at the portfolio level from 2021. In 2020, measurement will be piloted in Early Strategy Adopter townships and adjustments may be made based on the learning. Unit costs. Access also requires information on unit costs of outputs to facilitate the evaluation of the programme’s value for money. A limited number of tracer outputs will be defined by the Fund Management Office, with IPs reporting on the unit costs of these outputs in a standardized format (to calculate, for instance, the cost of training days for selected types of trainees. Tracer outputs will be selected among outputs for which IPs have complete costing information,107 and used during programme implementation to assess grant-performance and reach funding decisions. Large unit-cost variation within a grant will need to be explained by the implementing partners; large between-grant differences that cannot be explained by contextual factors will be scrutinized by the Fund Management Office before aggregating these data to generate an average unit cost estimate for selected Access interventions. These data will provide information on the economy and efficiency of the programme, the first two elements of DFID’s ‘4E’ value for money framework108. Further Value for Money indicators will be proposed once the Value for Money framework is developed - and the Final Programme Evaluation will relate these data to achieved outcomes and impact for an overall value for money analysis of the programme.
106 Reporting forms from IPs will be received in Word (narrative) and Excel formats (quantitative programmatic and financial data). The Fund is setting up a database to facilitate compilation of IP data and reporting 107 For example, while assisted delivery costs could be useful output to monitor, these costs cannot be derived from routine data – they will comprise Government- and EHO/CBHO-supported components (e.g. health staff salary, facilities) on which data is not easily available. 108 A comprehensive Value for Money framework will be developed by Fund Management Office in early 2020. For more on this, please refer to the Terms of Reference for a Value for Money framework, in annex to this Overall Strategy.

75
Grant outcomes. IPs are also contractually obligated to report progress against the standardized Grant Outcome indicators, to which their outputs contribute109. Data on these indicators will be collected in collaboration with EHO/CBHOs and Township Health Departments. Targets for grant outcomes will be set only at the Access portfolio level - not at the level of townships and Rural Health Centers, and while IPs will not be held accountable for achievement against these outcomes, they will be expected to report progress and provide justification of Rural health Centre-level trends.110 Programme Outcomes. Finally, IPs are expected to collect and report data on progress towards Programme Outcome (e.g. tuberculosis case notification rate, adolescent birth rate…) The sources for the majority of these data are the health information systems of the MOHS and EHO/CBHOs, but for some indicators and in some townships, data from these sources will have to be complemented or corrected with data collected directly by IPs. Final Evaluations will be conducted for some grants that are of high value or of strategic importance to Access. These grants will be sampled at a later stage, a few months before the Final Evaluation of the Fund is conducted. Criteria for sampling will be defined in the Final Evaluation Terms of Reference rather than in advance, to minimize bias (e.g. IPs unduly focusing on those grants that would be evaluated). Mid-term evaluations. As the grant periods under the new strategy will only be three years (2021-2023), mid-term evaluations of grant-funded projects are not foreseen. However, thematic expert-reviews covering technical areas such as tuberculosis, malaria, harm reduction, maternal health, or cross-cutting themes such as gender and human rights mainstreaming will be commissioned at about mid-term of the new strategy period, covering all grants that are active in a particular theme. These reviews will, by and large, provide the mid-term guidance that would be generated by mid-term project evaluations. Research. IPs are encouraged to include research proposals in their grant applications. These may range from qualitative case-studies to documentation of project interventions and achievements that are of value for external communications about the Fund’s work. They could also include implementation research to generate evidence and build knowledge about the effectiveness of innovative interventions. Research proposals will be reviewed by the Fund Management office, and funding decisions will be based on an assessment of the likelihood that the research will generate new evidence as well as on the strength of the knowledge-translation strategy111.
109 For example, proportion of EHO health posts supported by Access that are fully functional (staff, medicines, supervision) or number of people who inject drugs (PWID) who accessed a programme-supported harm reduction centre with an agreed frequency during the reporting period 110 Unlike in 3MDG Fund, in integrated grants target-setting will no longer be done at township level due to the move away from comprehensive township approach. The unit of implementation will be village and the unit of reporting RHC. RHC-level outcome data will be reported by IPs (without target-setting which is not done at RHC level). 111 For more on this, please see a paper on Fund as a Learning Organization.
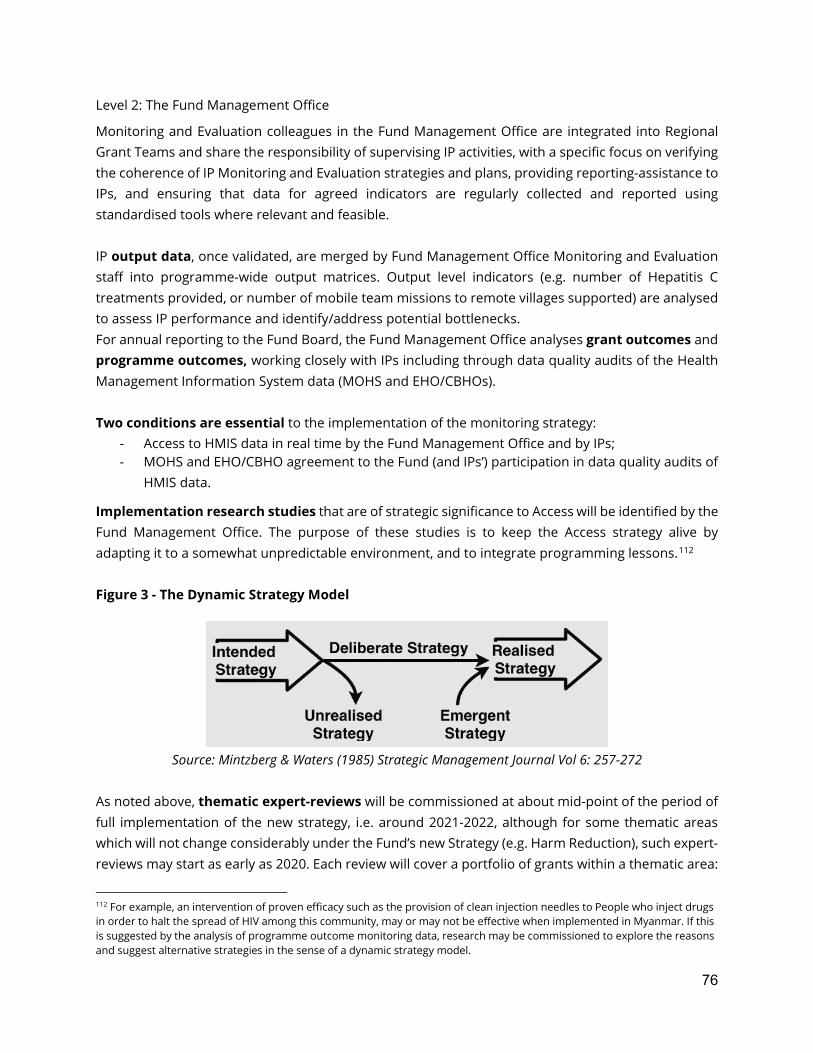
76
Level 2: The Fund Management Office
Monitoring and Evaluation colleagues in the Fund Management Office are integrated into Regional Grant Teams and share the responsibility of supervising IP activities, with a specific focus on verifying the coherence of IP Monitoring and Evaluation strategies and plans, providing reporting-assistance to IPs, and ensuring that data for agreed indicators are regularly collected and reported using standardised tools where relevant and feasible. IP output data, once validated, are merged by Fund Management Office Monitoring and Evaluation staff into programme-wide output matrices. Output level indicators (e.g. number of Hepatitis C treatments provided, or number of mobile team missions to remote villages supported) are analysed to assess IP performance and identify/address potential bottlenecks. For annual reporting to the Fund Board, the Fund Management Office analyses grant outcomes and programme outcomes, working closely with IPs including through data quality audits of the Health Management Information System data (MOHS and EHO/CBHOs). Two conditions are essential to the implementation of the monitoring strategy:
- Access to HMIS data in real time by the Fund Management Office and by IPs; - MOHS and EHO/CBHO agreement to the Fund (and IPs’) participation in data quality audits of
HMIS data.
Implementation research studies that are of strategic significance to Access will be identified by the Fund Management Office. The purpose of these studies is to keep the Access strategy alive by adapting it to a somewhat unpredictable environment, and to integrate programming lessons.112 Figure 3 - The Dynamic Strategy Model
Source: Mintzberg & Waters (1985) Strategic Management Journal Vol 6: 257-272
As noted above, thematic expert-reviews will be commissioned at about mid-point of the period of full implementation of the new strategy, i.e. around 2021-2022, although for some thematic areas which will not change considerably under the Fund’s new Strategy (e.g. Harm Reduction), such expert-reviews may start as early as 2020. Each review will cover a portfolio of grants within a thematic area:
112 For example, an intervention of proven efficacy such as the provision of clean injection needles to People who inject drugs in order to halt the spread of HIV among this community, may or may not be effective when implemented in Myanmar. If this is suggested by the analysis of programme outcome monitoring data, research may be commissioned to explore the reasons and suggest alternative strategies in the sense of a dynamic strategy model.
77
malaria, tuberculosis, harm reduction, child health, sexual and reproductive health, maternal and neonatal health. Additional thematic reviews of cross-cutting themes such as gender mainstreaming, disability, or rights-based programming may also be included. The focus will be on providing assurance and advice to the Fund Management Office and IPs for the implementation of their project according to the highest technical standards and the Fund’s principles. Programme evaluations are external evaluations commissioned by the Fund Management Office and conducted according to guidelines issued by the United Nations Evaluation Group (UNEG). They focus on the Fund’s relevance, efficiency, effectiveness, equity, sustainability, and impact:113
- Evaluations of the Fund’s efficiency require access to the database of institutional performance indicators monitored by the Fund Manager’s office (not included in the Monitoring and Evaluation Strategy)
- Evaluation of effectiveness, equity and impact, requires evidence-based inferences on results at the overall outcome level, which is beyond the scope of monitoring and requires end-beneficiary data through representative population-based surveys. While such surveys are not feasible for some programme outcomes (e.g. surveys of all prisoners or of all injecting drug users) they are potentially feasible - and would be essential - for integrated community health projects, primarily in the areas of MNCH and nutrition. For malaria and tuberculosis, strong national programme monitoring and reporting systems that can supply the required information.
Population-based surveys are included in the Fund’s evaluation plan - please see section 3.4. below.
2.3. Units of Intervention and Units of Monitoring
The question of approximating the unit of monitoring to the unit of intervention does not arise at the output level. Condoms, malaria tests, or Hepatitis C treatments can be counted at the end-user point. At the programme outcome and grant outcome levels, the issues are more complex, particularly in areas where services are provided by MoHS:
- Township Health Departments collect and report HMIS data monthly on the national DHIS2 platform, down to the level of the Rural Health Centre;
- Remote and hard-to reach villages targeted by Access may be located under several Rural Health Centers and may represent a large or a small proportion of villages under any given Rural Health Centre.
- Programme interventions that target only a small proportion of villages in an RHC area cannot be expected to have a measurable impact on changes in the entire reporting area. In other words, the Fund should only claim outcomes when its interventions are sufficiently important to influence such outcomes.
113 The degree to which these parameters are addressed will differ at mid-term - when the primary purpose of the evaluation is formative and serves to provide assurance and guidance to the strategy under implementation - and at end-term when the primary purpose will be summative, to provide accountability for the implemented strategy.

78
- Through selective sampling, the Fund should therefore only monitor the service and outcome indicators (derived from HMIS reports) in those Rural Health Centres where the programme supports a significant proportion of villages114.
- The level of ‘significance’ will have to be defined and may differ among townships. This reporting of proxy indicators will make the monitoring data more relevant in terms of measuring programme contributions; it will also greatly reduce the effort of monitoring, and thereby increase its efficiency.
Annex 2 elaborates further on monitoring outcomes in integrated grants and provides an illustration. For EHO/CBHO areas, this issue should not arise as all populations served by EHO/CBHOs are - by definition - eligible.
2.4. Learning
Learning is not identified as an activity of the Monitoring and Evaluation Strategy, it is an objective pursued under all activities. Please refer to the paper on the Access to Health Fund as a Learning Organization, in annex. The Access programme is being implemented in a dynamic context of political change and rapid social and economic development. The information required to keep the Access programme strategy relevant is generated by the activities implemented under the Monitoring and Evaluation strategy and through the transformation of experience into knowledge - and the application of that knowledge into more effective policies, strategies and programmes By tracking progress towards the achievement of programme outcomes, the Fund is in a privileged position to generate lessons on ‘what works’ and transform them into action. Research activities are planned at the IP (grant) level and at the Fund Management Office (programme) level. Defining research themes will start at the time of negotiation of grants under the new Access strategy, and implementation can already start in the transition year of 2020. Operational research and implementation research can fill important evidence gaps, in particular regarding the effectiveness and cost-effectiveness of interventions focused on vulnerable populations115. The Fund will be conducting both qualitative and quantitative research on topics to be defined as the Fund advances. The strength of research proposals will be assessed based on the likelihood that it will generate evidence to improve implementation, as well as technical dimensions. IPs are encouraged to include research proposals in their grant application. These may range from qualitative case studies to documenting project interventions and achievements that are of value for
114 In other words: When the Fund (for example) supports only one remote village out of 15 villages under a given RHC, the results of this RHC at outcome level should not be reported by the Fund. 115 Operational research provides information to programme managers on how to do things better, i.e. what they can do to improve progress towards defined programme objectives. Implementation research takes the lessons generated at project level and tests them for wider programme application. Hirschhorn LR1, Ojikutu B, Rodriguez W. (2007) Research for change: using implementation research to strengthen HIV care and treatment scale-up in resource-limited settings. Clin Infect Dis 2007;196(S3):S516
79
external communications of the work of Access, to implementation research to generate evidence and build knowledge about the effectiveness of innovative interventions.
2. The Fund’s Monitoring Plan
3.1. Monitoring Grant Outputs
Information on grant outputs116 will continue to be collected throughout the lifetime of the Fund. As already noted:
- Indicators and targets are defined in IPs’ grant agreements - The Fund will make sure it meets Donors’ corporate requirements on the delivery of outputs - For a selected number of outputs delivered at high volume under several grants, IPs will be
contractually required to calculate and report unit costs per output - Large within-grant variances in unit costs between reporting periods will have to be explained.
These data will facilitate the VfM evaluation of Access - Standardized/digitalized data reporting forms will be developed and used by all IPs to allow
easy aggregation of reported outputs. - A performance monitoring matrix for grant outputs will be developed, reviewed annually and
submitted for approval by the Fund Board. The selection of cost indicators for a later VFM evaluation will be made in consultation with the Fund Board and IPs.
Also as noted, in a shift from the 3MDG Fund, quantities of outputs generated will no longer be the main focus of analysis and reporting of Access performance and annual programme reports will place a stronger focus on progress towards programme outcomes and on lessons learnt in the process. The proposed list of Grant Output indicators for reporting under ACCESS is included in Annex 1.
3.2. Monitoring Grant Outcomes
As already noted, each grant is expected to contribute to one or more of the 12 grant outcome results included in the Theory of Change. None of these results will be directly attributable to grant inputs because all of them are contingent on contextual factors and on the contribution of others. Depending on the case, the Access contribution to the result will be more or less important. A total of 26 proxy indicators to monitor progress towards outcomes were developed. IPs will integrate those relevant to their grant-funded activities into their grant-level Monitoring and Evaluation frameworks, and report on them in their biannual progress reports. The focus of MoHS direct grants is reflected in grant outcomes IR7, IR9 and IR10 of the Table 1. A Fund-level logframe including these indicators will be prepared annually from 2021; will include baseline data, targets and essential assumptions /clarifications. Based on evolving priorities of the
116 e.g. number of health workers trained, number of clean syringes and needles distributed, number of women screened for cervical dysplasia
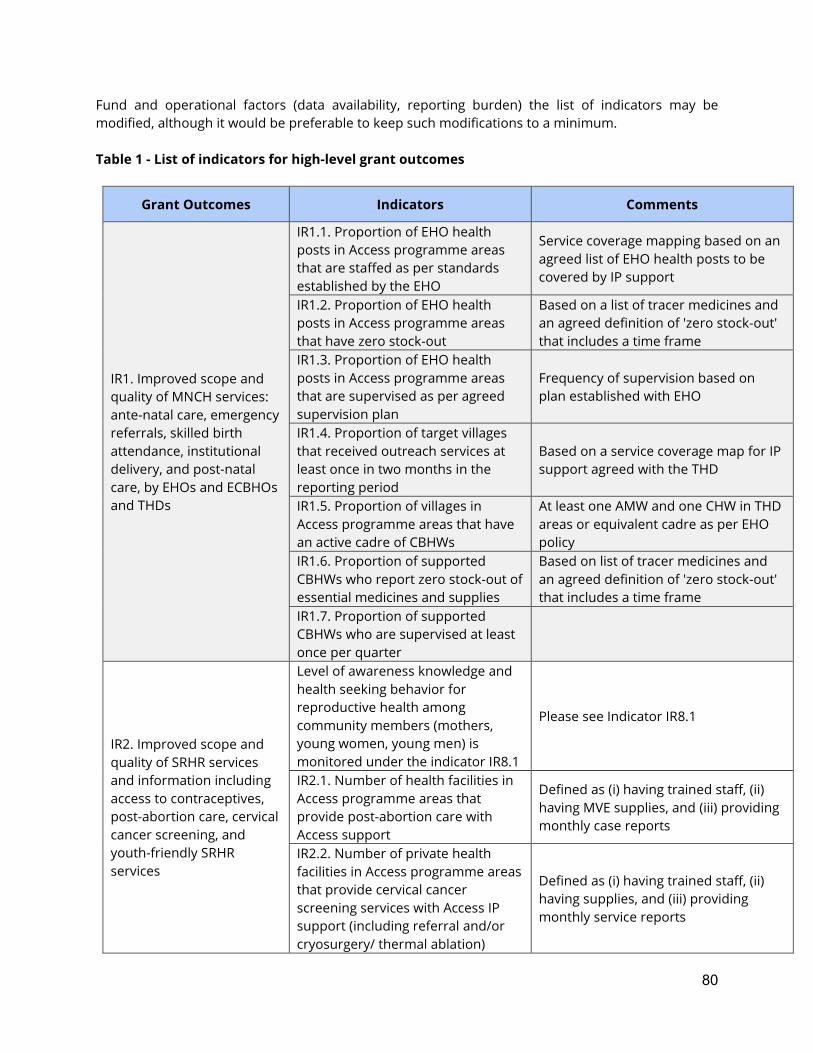
80
Fund and operational factors (data availability, reporting burden) the list of indicators may be modified, although it would be preferable to keep such modifications to a minimum. Table 1 - List of indicators for high-level grant outcomes
Grant Outcomes Indicators Comments
IR1. Improved scope and quality of MNCH services: ante-natal care, emergency referrals, skilled birth attendance, institutional delivery, and post-natal care, by EHOs and ECBHOs and THDs
IR1.1. Proportion of EHO health posts in Access programme areas that are staffed as per standards established by the EHO
Service coverage mapping based on an agreed list of EHO health posts to be covered by IP support
IR1.2. Proportion of EHO health posts in Access programme areas that have zero stock-out
Based on a list of tracer medicines and an agreed definition of 'zero stock-out' that includes a time frame
IR1.3. Proportion of EHO health posts in Access programme areas that are supervised as per agreed supervision plan
Frequency of supervision based on plan established with EHO
IR1.4. Proportion of target villages that received outreach services at least once in two months in the reporting period
Based on a service coverage map for IP support agreed with the THD
IR1.5. Proportion of villages in Access programme areas that have an active cadre of CBHWs
At least one AMW and one CHW in THD areas or equivalent cadre as per EHO policy
IR1.6. Proportion of supported CBHWs who report zero stock-out of essential medicines and supplies
Based on list of tracer medicines and an agreed definition of 'zero stock-out' that includes a time frame
IR1.7. Proportion of supported CBHWs who are supervised at least once per quarter
IR2. Improved scope and quality of SRHR services and information including access to contraceptives, post-abortion care, cervical cancer screening, and youth-friendly SRHR services
Level of awareness knowledge and health seeking behavior for reproductive health among community members (mothers, young women, young men) is monitored under the indicator IR8.1
Please see Indicator IR8.1
IR2.1. Number of health facilities in Access programme areas that provide post-abortion care with Access support
Defined as (i) having trained staff, (ii) having MVE supplies, and (iii) providing monthly case reports
IR2.2. Number of private health facilities in Access programme areas that provide cervical cancer screening services with Access IP support (including referral and/or cryosurgery/ thermal ablation)
Defined as (i) having trained staff, (ii) having supplies, and (iii) providing monthly service reports
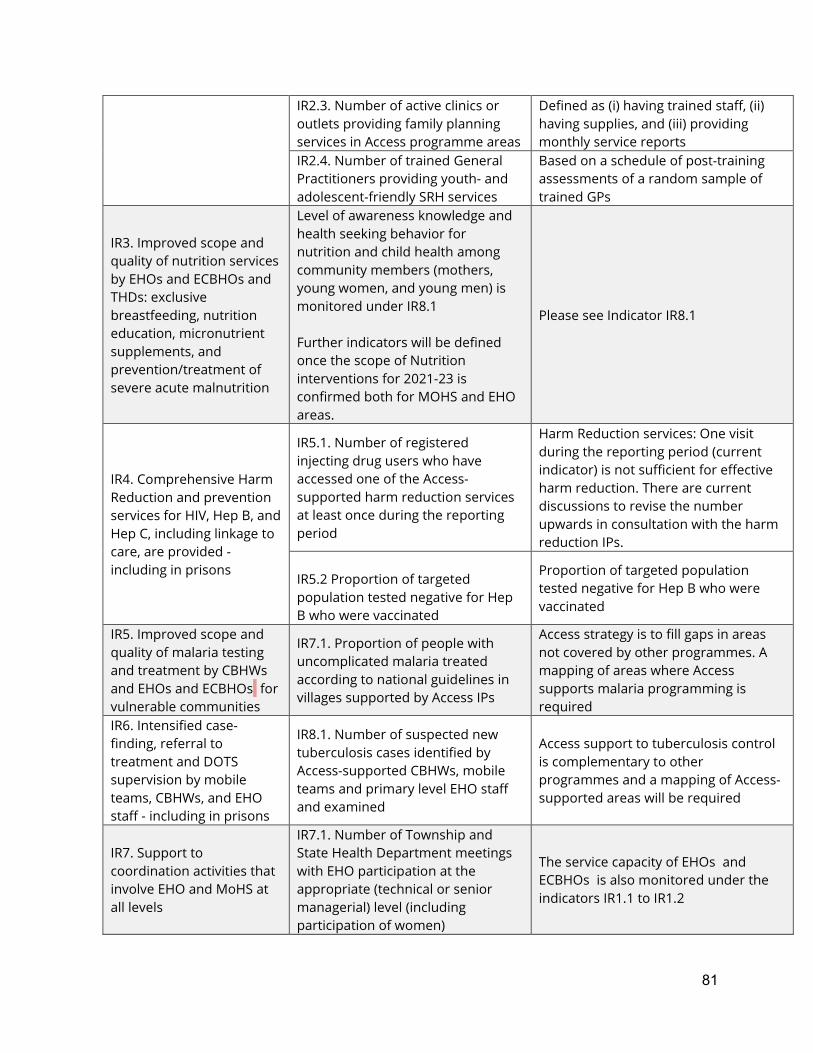
81
IR2.3. Number of active clinics or outlets providing family planning services in Access programme areas
Defined as (i) having trained staff, (ii) having supplies, and (iii) providing monthly service reports
IR2.4. Number of trained General Practitioners providing youth- and adolescent-friendly SRH services
Based on a schedule of post-training assessments of a random sample of trained GPs
IR3. Improved scope and quality of nutrition services by EHOs and ECBHOs and THDs: exclusive breastfeeding, nutrition education, micronutrient supplements, and prevention/treatment of severe acute malnutrition
Level of awareness knowledge and health seeking behavior for nutrition and child health among community members (mothers, young women, and young men) is monitored under IR8.1 Further indicators will be defined once the scope of Nutrition interventions for 2021-23 is confirmed both for MOHS and EHO areas.
Please see Indicator IR8.1
IR4. Comprehensive Harm Reduction and prevention services for HIV, Hep B, and Hep C, including linkage to care, are provided - including in prisons
IR5.1. Number of registered injecting drug users who have accessed one of the Access-supported harm reduction services at least once during the reporting period
Harm Reduction services: One visit during the reporting period (current indicator) is not sufficient for effective harm reduction. There are current discussions to revise the number upwards in consultation with the harm reduction IPs.
IR5.2 Proportion of targeted population tested negative for Hep B who were vaccinated
Proportion of targeted population tested negative for Hep B who were vaccinated
IR5. Improved scope and quality of malaria testing and treatment by CBHWs and EHOs and ECBHOs for vulnerable communities
IR7.1. Proportion of people with uncomplicated malaria treated according to national guidelines in villages supported by Access IPs
Access strategy is to fill gaps in areas not covered by other programmes. A mapping of areas where Access supports malaria programming is required
IR6. Intensified case-finding, referral to treatment and DOTS supervision by mobile teams, CBHWs, and EHO staff - including in prisons
IR8.1. Number of suspected new tuberculosis cases identified by Access-supported CBHWs, mobile teams and primary level EHO staff and examined
Access support to tuberculosis control is complementary to other programmes and a mapping of Access-supported areas will be required
IR7. Support to coordination activities that involve EHO and MoHS at all levels
IR7.1. Number of Township and State Health Department meetings with EHO participation at the appropriate (technical or senior managerial) level (including participation of women)
The service capacity of EHOs and ECBHOs is also monitored under the indicators IR1.1 to IR1.2
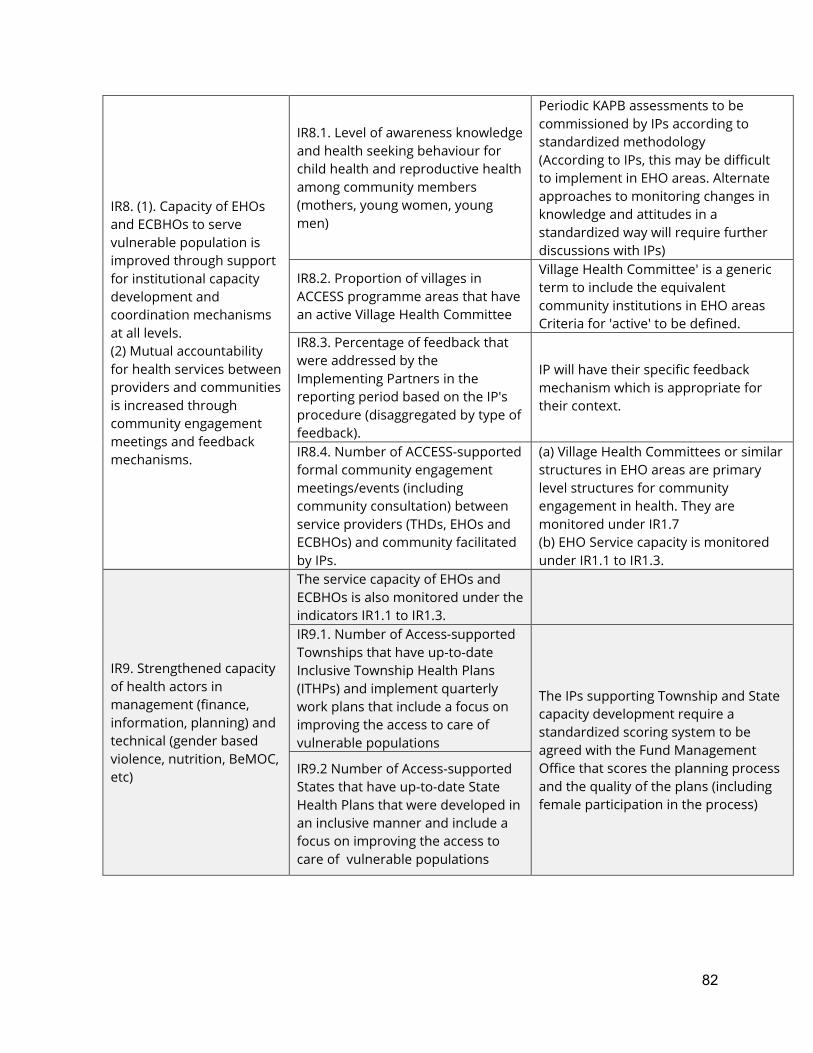
82
IR8. (1). Capacity of EHOs and ECBHOs to serve vulnerable population is improved through support for institutional capacity development and coordination mechanisms at all levels. (2) Mutual accountability for health services between providers and communities is increased through community engagement meetings and feedback mechanisms.
IR8.1. Level of awareness knowledge and health seeking behaviour for child health and reproductive health among community members (mothers, young women, young men)
Periodic KAPB assessments to be commissioned by IPs according to standardized methodology (According to IPs, this may be difficult to implement in EHO areas. Alternate approaches to monitoring changes in knowledge and attitudes in a standardized way will require further discussions with IPs)
IR8.2. Proportion of villages in ACCESS programme areas that have an active Village Health Committee
Village Health Committee' is a generic term to include the equivalent community institutions in EHO areas Criteria for 'active' to be defined.
IR8.3. Percentage of feedback that were addressed by the Implementing Partners in the reporting period based on the IP's procedure (disaggregated by type of feedback).
IP will have their specific feedback mechanism which is appropriate for their context.
IR8.4. Number of ACCESS-supported formal community engagement meetings/events (including community consultation) between service providers (THDs, EHOs and ECBHOs) and community facilitated by IPs.
(a) Village Health Committees or similar structures in EHO areas are primary level structures for community engagement in health. They are monitored under IR1.7 (b) EHO Service capacity is monitored under IR1.1 to IR1.3.
IR9. Strengthened capacity of health actors in management (finance, information, planning) and technical (gender based violence, nutrition, BeMOC, etc)
The service capacity of EHOs and ECBHOs is also monitored under the indicators IR1.1 to IR1.3.
IR9.1. Number of Access-supported Townships that have up-to-date Inclusive Township Health Plans (ITHPs) and implement quarterly work plans that include a focus on improving the access to care of vulnerable populations
The IPs supporting Township and State capacity development require a standardized scoring system to be agreed with the Fund Management Office that scores the planning process and the quality of the plans (including female participation in the process)
IR9.2 Number of Access-supported States that have up-to-date State Health Plans that were developed in an inclusive manner and include a focus on improving the access to care of vulnerable populations
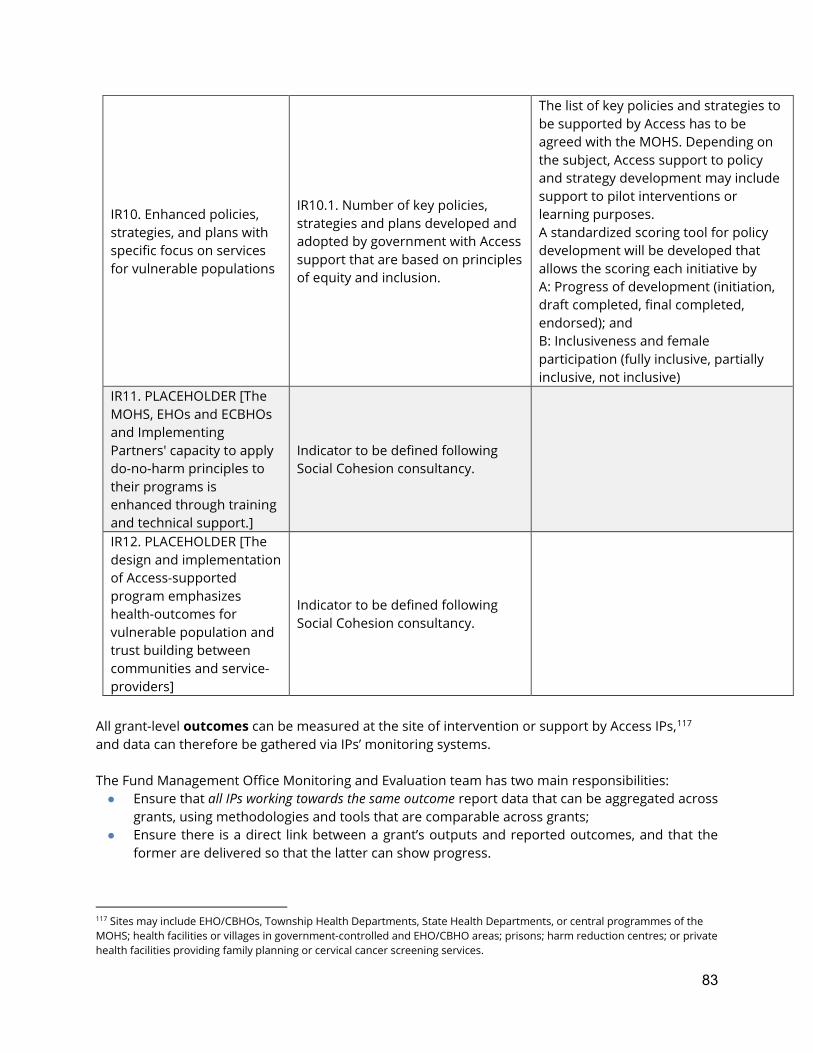
83
IR10. Enhanced policies, strategies, and plans with specific focus on services for vulnerable populations
IR10.1. Number of key policies, strategies and plans developed and adopted by government with Access support that are based on principles of equity and inclusion.
The list of key policies and strategies to be supported by Access has to be agreed with the MOHS. Depending on the subject, Access support to policy and strategy development may include support to pilot interventions or learning purposes. A standardized scoring tool for policy development will be developed that allows the scoring each initiative by A: Progress of development (initiation, draft completed, final completed, endorsed); and B: Inclusiveness and female participation (fully inclusive, partially inclusive, not inclusive)
IR11. PLACEHOLDER [The MOHS, EHOs and ECBHOs and Implementing Partners' capacity to apply do-no-harm principles to their programs is enhanced through training and technical support.]
Indicator to be defined following Social Cohesion consultancy.
IR12. PLACEHOLDER [The design and implementation of Access-supported program emphasizes health-outcomes for vulnerable population and trust building between communities and service-providers]
Indicator to be defined following Social Cohesion consultancy.
All grant-level outcomes can be measured at the site of intervention or support by Access IPs,117 and data can therefore be gathered via IPs’ monitoring systems. The Fund Management Office Monitoring and Evaluation team has two main responsibilities: ● Ensure that all IPs working towards the same outcome report data that can be aggregated across
grants, using methodologies and tools that are comparable across grants; ● Ensure there is a direct link between a grant’s outputs and reported outcomes, and that the
former are delivered so that the latter can show progress.
117 Sites may include EHO/CBHOs, Township Health Departments, State Health Departments, or central programmes of the MOHS; health facilities or villages in government-controlled and EHO/CBHO areas; prisons; harm reduction centres; or private health facilities providing family planning or cervical cancer screening services.
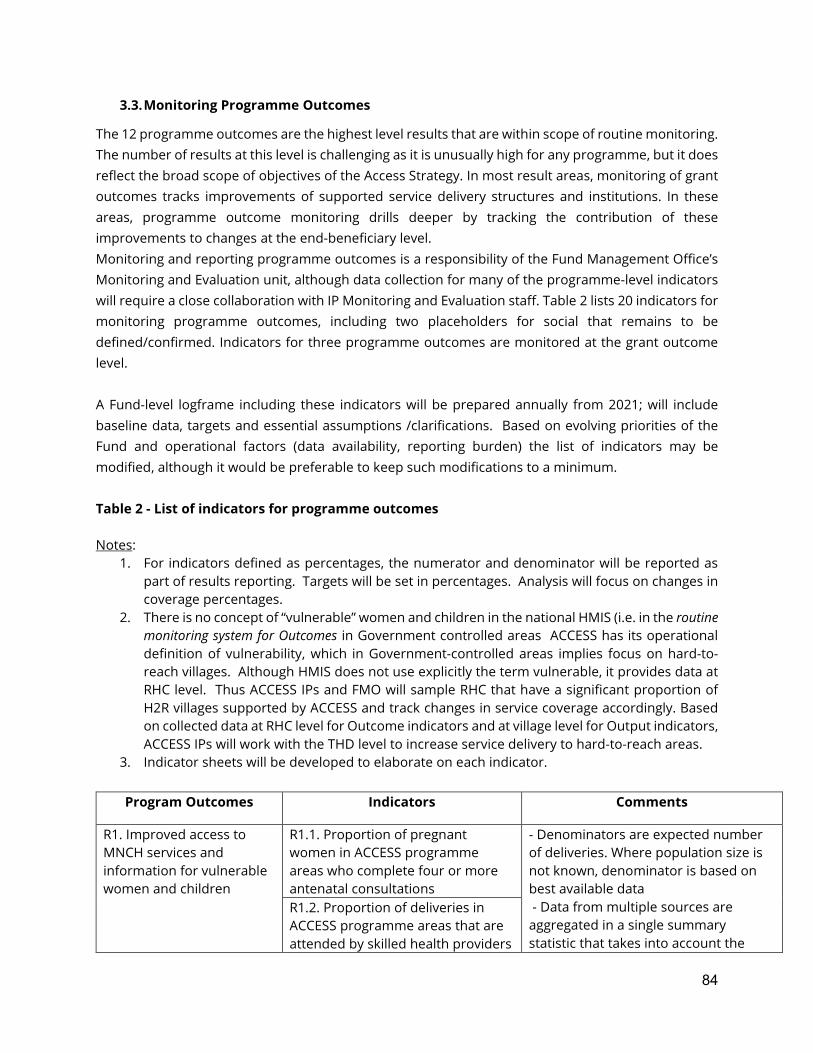
84
3.3. Monitoring Programme Outcomes
The 12 programme outcomes are the highest level results that are within scope of routine monitoring. The number of results at this level is challenging as it is unusually high for any programme, but it does reflect the broad scope of objectives of the Access Strategy. In most result areas, monitoring of grant outcomes tracks improvements of supported service delivery structures and institutions. In these areas, programme outcome monitoring drills deeper by tracking the contribution of these improvements to changes at the end-beneficiary level. Monitoring and reporting programme outcomes is a responsibility of the Fund Management Office’s Monitoring and Evaluation unit, although data collection for many of the programme-level indicators will require a close collaboration with IP Monitoring and Evaluation staff. Table 2 lists 20 indicators for monitoring programme outcomes, including two placeholders for social that remains to be defined/confirmed. Indicators for three programme outcomes are monitored at the grant outcome level. A Fund-level logframe including these indicators will be prepared annually from 2021; will include baseline data, targets and essential assumptions /clarifications. Based on evolving priorities of the Fund and operational factors (data availability, reporting burden) the list of indicators may be modified, although it would be preferable to keep such modifications to a minimum. Table 2 - List of indicators for programme outcomes Notes:
1. For indicators defined as percentages, the numerator and denominator will be reported as part of results reporting. Targets will be set in percentages. Analysis will focus on changes in coverage percentages.
2. There is no concept of “vulnerable” women and children in the national HMIS (i.e. in the routine monitoring system for Outcomes in Government controlled areas ACCESS has its operational definition of vulnerability, which in Government-controlled areas implies focus on hard-to-reach villages. Although HMIS does not use explicitly the term vulnerable, it provides data at RHC level. Thus ACCESS IPs and FMO will sample RHC that have a significant proportion of H2R villages supported by ACCESS and track changes in service coverage accordingly. Based on collected data at RHC level for Outcome indicators and at village level for Output indicators, ACCESS IPs will work with the THD level to increase service delivery to hard-to-reach areas.
3. Indicator sheets will be developed to elaborate on each indicator.
Program Outcomes Indicators Comments
R1. Improved access to MNCH services and information for vulnerable women and children
R1.1. Proportion of pregnant women in ACCESS programme areas who complete four or more antenatal consultations
- Denominators are expected number of deliveries. Where population size is not known, denominator is based on best available data - Data from multiple sources are aggregated in a single summary statistic that takes into account the
R1.2. Proportion of deliveries in ACCESS programme areas that are attended by skilled health providers
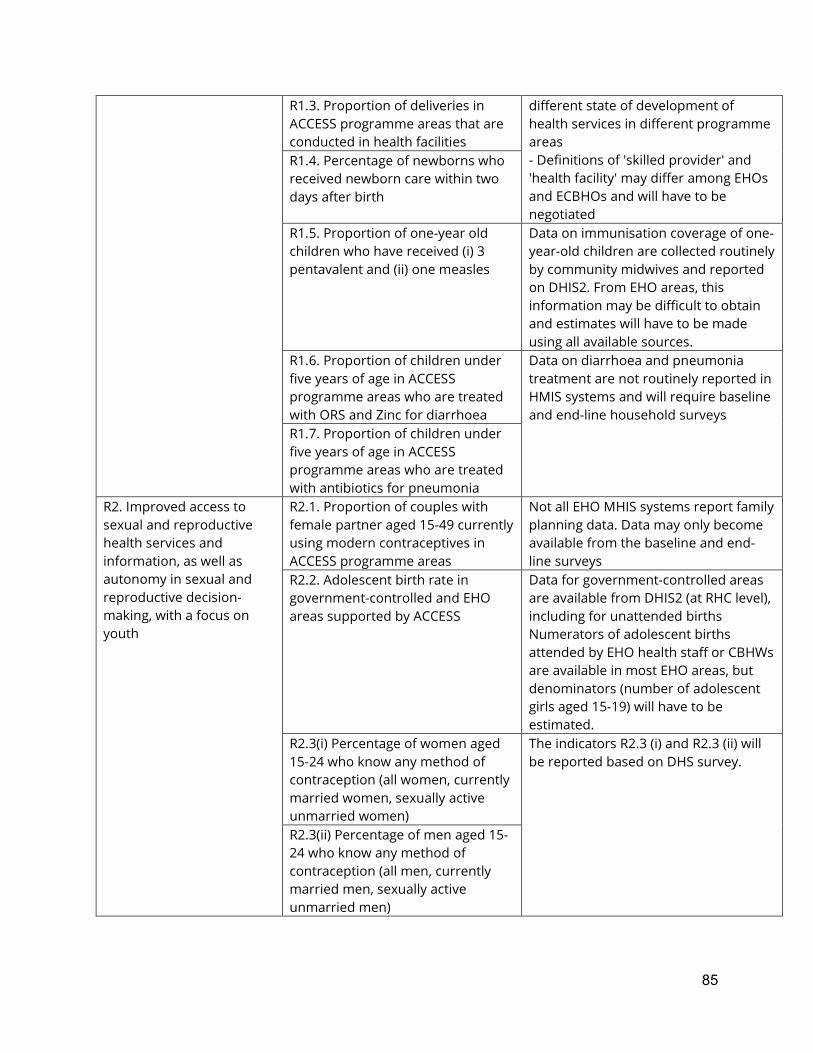
85
R1.3. Proportion of deliveries in ACCESS programme areas that are conducted in health facilities
different state of development of health services in different programme areas - Definitions of 'skilled provider' and 'health facility' may differ among EHOs and ECBHOs and will have to be negotiated
R1.4. Percentage of newborns who received newborn care within two days after birth
R1.5. Proportion of one-year old children who have received (i) 3 pentavalent and (ii) one measles
Data on immunisation coverage of one-year-old children are collected routinely by community midwives and reported on DHIS2. From EHO areas, this information may be difficult to obtain and estimates will have to be made using all available sources.
R1.6. Proportion of children under five years of age in ACCESS programme areas who are treated with ORS and Zinc for diarrhoea
Data on diarrhoea and pneumonia treatment are not routinely reported in HMIS systems and will require baseline and end-line household surveys
R1.7. Proportion of children under five years of age in ACCESS programme areas who are treated with antibiotics for pneumonia
R2. Improved access to sexual and reproductive health services and information, as well as autonomy in sexual and reproductive decision-making, with a focus on youth
R2.1. Proportion of couples with female partner aged 15-49 currently using modern contraceptives in ACCESS programme areas
Not all EHO MHIS systems report family planning data. Data may only become available from the baseline and end-line surveys
R2.2. Adolescent birth rate in government-controlled and EHO areas supported by ACCESS
Data for government-controlled areas are available from DHIS2 (at RHC level), including for unattended births Numerators of adolescent births attended by EHO health staff or CBHWs are available in most EHO areas, but denominators (number of adolescent girls aged 15-19) will have to be estimated.
R2.3(i) Percentage of women aged 15-24 who know any method of contraception (all women, currently married women, sexually active unmarried women)
The indicators R2.3 (i) and R2.3 (ii) will be reported based on DHS survey.
R2.3(ii) Percentage of men aged 15-24 who know any method of contraception (all men, currently married men, sexually active unmarried men)
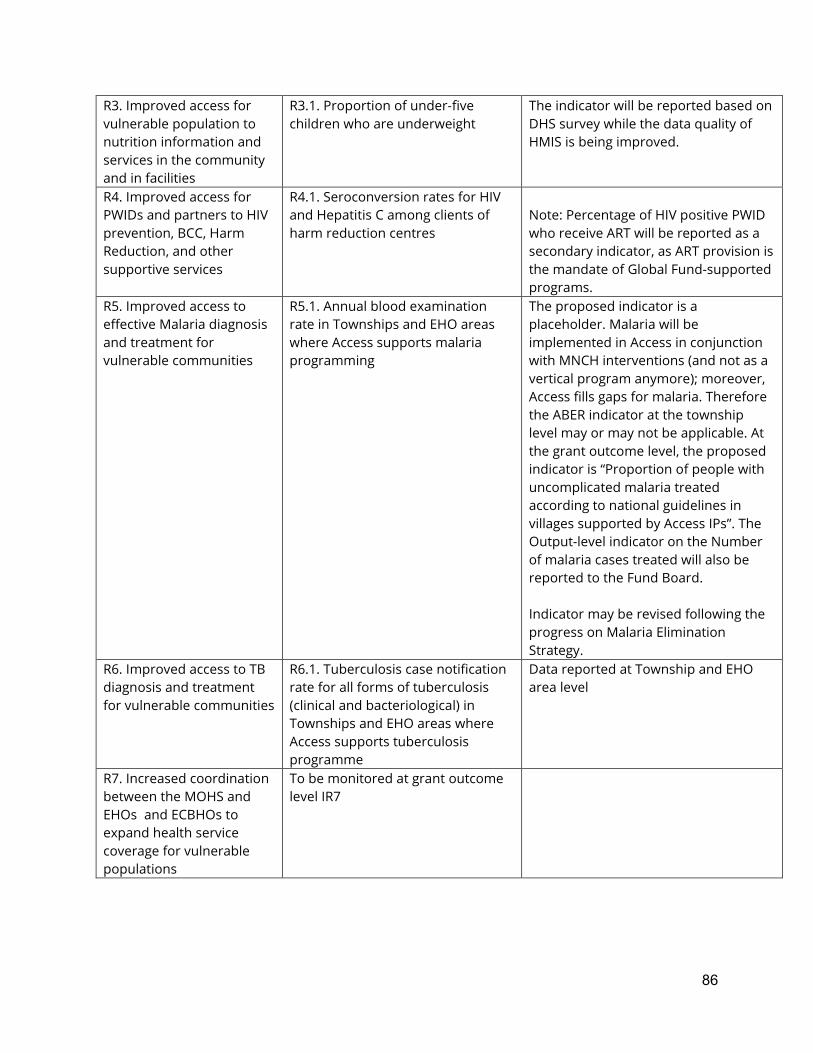
86
R3. Improved access for vulnerable population to nutrition information and services in the community and in facilities
R3.1. Proportion of under-five children who are underweight
The indicator will be reported based on DHS survey while the data quality of HMIS is being improved.
R4. Improved access for PWIDs and partners to HIV prevention, BCC, Harm Reduction, and other supportive services
R4.1. Seroconversion rates for HIV and Hepatitis C among clients of harm reduction centres
Note: Percentage of HIV positive PWID who receive ART will be reported as a secondary indicator, as ART provision is the mandate of Global Fund-supported programs.
R5. Improved access to effective Malaria diagnosis and treatment for vulnerable communities
R5.1. Annual blood examination rate in Townships and EHO areas where Access supports malaria programming
The proposed indicator is a placeholder. Malaria will be implemented in Access in conjunction with MNCH interventions (and not as a vertical program anymore); moreover, Access fills gaps for malaria. Therefore the ABER indicator at the township level may or may not be applicable. At the grant outcome level, the proposed indicator is “Proportion of people with uncomplicated malaria treated according to national guidelines in villages supported by Access IPs”. The Output-level indicator on the Number of malaria cases treated will also be reported to the Fund Board. Indicator may be revised following the progress on Malaria Elimination Strategy.
R6. Improved access to TB diagnosis and treatment for vulnerable communities
R6.1. Tuberculosis case notification rate for all forms of tuberculosis (clinical and bacteriological) in Townships and EHO areas where Access supports tuberculosis programme
Data reported at Township and EHO area level
R7. Increased coordination between the MOHS and EHOs and ECBHOs to expand health service coverage for vulnerable populations
To be monitored at grant outcome level IR7
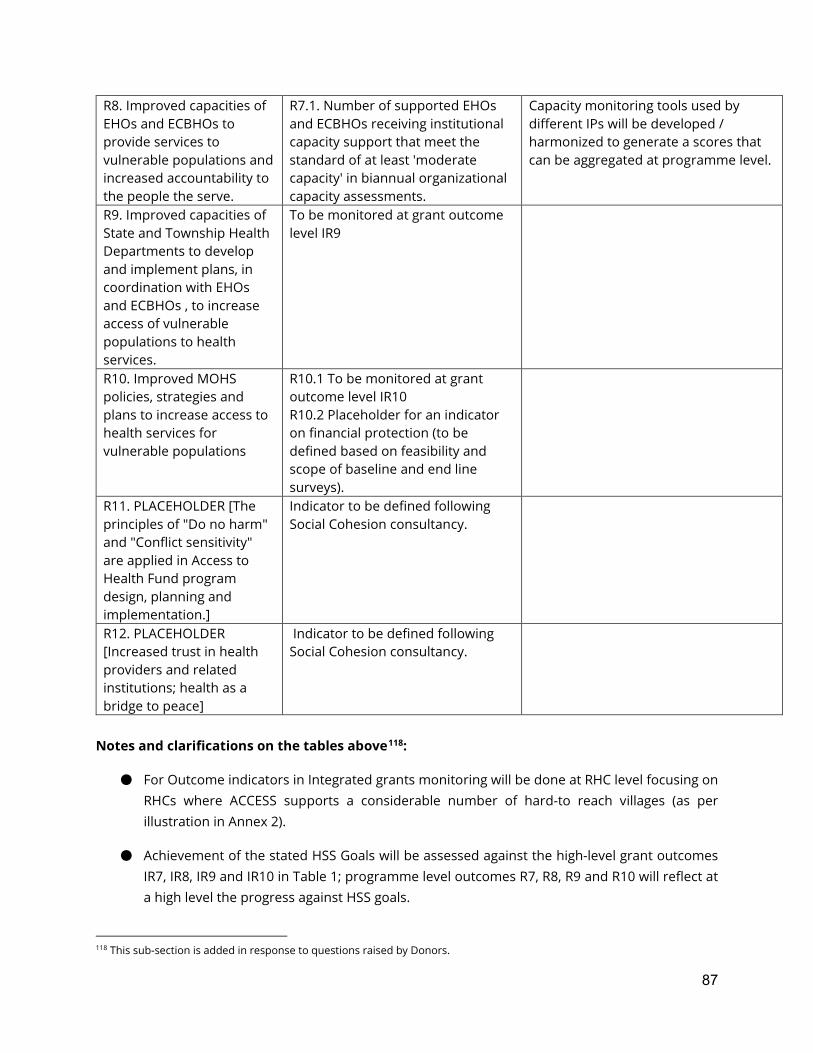
87
R8. Improved capacities of EHOs and ECBHOs to provide services to vulnerable populations and increased accountability to the people the serve.
R7.1. Number of supported EHOs and ECBHOs receiving institutional capacity support that meet the standard of at least 'moderate capacity' in biannual organizational capacity assessments.
Capacity monitoring tools used by different IPs will be developed / harmonized to generate a scores that can be aggregated at programme level.
R9. Improved capacities of State and Township Health Departments to develop and implement plans, in coordination with EHOs and ECBHOs , to increase access of vulnerable populations to health services.
To be monitored at grant outcome level IR9
R10. Improved MOHS policies, strategies and plans to increase access to health services for vulnerable populations
R10.1 To be monitored at grant outcome level IR10 R10.2 Placeholder for an indicator on financial protection (to be defined based on feasibility and scope of baseline and end line surveys).
R11. PLACEHOLDER [The principles of "Do no harm" and "Conflict sensitivity" are applied in Access to Health Fund program design, planning and implementation.]
Indicator to be defined following Social Cohesion consultancy.
R12. PLACEHOLDER [Increased trust in health providers and related institutions; health as a bridge to peace]
Indicator to be defined following Social Cohesion consultancy.
Notes and clarifications on the tables above118:
● For Outcome indicators in Integrated grants monitoring will be done at RHC level focusing on RHCs where ACCESS supports a considerable number of hard-to reach villages (as per illustration in Annex 2).
● Achievement of the stated HSS Goals will be assessed against the high-level grant outcomes IR7, IR8, IR9 and IR10 in Table 1; programme level outcomes R7, R8, R9 and R10 will reflect at a high level the progress against HSS goals.
118 This sub-section is added in response to questions raised by Donors.
88
● In the area of Financial protection and reduced out-of-pocket (OoP) health spending by vulnerable people in conflict-affected areas, in addition to supporting greater accessibility of services, Access will support advocacy in favour of a health financing strategy, development of a legal framework for that strategy, law-making processes, and more generally support the country’s early steps towards putting in place Financial Protection. However, the outputs of these activities will only result in reduced out-of-pocket expenditures if the framework development is successful and its implementation succeeds in the long-run. OoP can be measured only through a survey. Under MDHS 2020-21, inclusion of OoP Health Expenditure Module is being considered. ACCESS is actively participating in these discussions. Once the decision is made on whether MDHS will be used as a baseline, specific indicators can be proposed. For the time-being a placeholder will be included (Program outcome 10.2).
● Increased availability and quality of essential services for vulnerable people in conflict-affected areas, and among prisoners, will be monitored based on programme and grant outcome indicators as per tables 1 and 2.
● Increased and more equitable coverage of essential services for vulnerable people in conflict-affected areas, and among prisoners, will be monitored based on programme and grant outcome indicators as per table 1 and 2.
● Results on specified outcomes will be reported in the Access Result Matrix both at portfolio level and at State level.
● A major ‘indicator mapping’ exercise will be required to align key terms and definitions between the national HMIS and in the systems used by EHO/CBHOs.
● Malaria and tuberculosis programme data are generally only disaggregated to the Township level. Township data will therefore be used as proxy indicators for Access programme outcomes.
● Use of qualitative data: qualitative data and indicators will be collected through different channels: routine monitoring and reporting (e.g. field mission findings using structured checklists, IP reporting of Most Significant Change), KAPB surveys, Operational research by IPs, and special studies commissioned by the Fund Management Office (e.g. policy analyses or case-studies focused on specific topic). Some qualitative indicators monitored through routine monitoring systems are included already, even if they are translated into numbers, proportions or scores to allows progress monitoring119 and be useful as a management instrument. More qualitative indicators to measure changes in behaviours, social norms and rights could be useful, and Fund Management Office will work on this in due course. Two examples of qualitative indicators are provided in the text-box below for reference:
Example 1: Targeted outcome: The capacity of the MOHS is increased for the development and adoption of policies, strategies and plans focusing on services for vulnerable populations in areas such as nutrition, gender-based violence, social protection and CBHWs in an open and participatory manner (including meaningful participation of women).
119 One example is indicator IR2.1 “Level of awareness knowledge and health seeking behaviour for child health and reproductive health among community members (mothers, young women, young men)” in Table 1.

89
Indicator - IR10.1. Number of key policies and strategies developed and adopted by government with Access support that are based on principles of equity and inclusion. A standardized scoring tool for policy development will be put in place to allow the scoring of each initiative by (i) Progress of development (initiation, draft completed, final completed, endorsed); and (ii) inclusiveness and female participation. Example 2: Targeted outcome: The capacities of State and Township Health Departments are increased for planning and implementation of initiatives to decrease barriers of vulnerable people to health services Indicators: IR12.1. Number of Access-supported Townships that have up-to-date ITHPs and implement quarterly work plans that include a focus on improving the access to care of marginalized or hard-to-reach populations; IR12.2. Number of Access-supported States that have up-to-date State Health Plans that were developed in an inclusive manner and include a focus on improving the access to care of marginalized or hard-to-reach population; IPs supporting Township and State capacity development require a standardized scoring system to be agreed with the Fund Management Office that scores the planning process and the quality of the plans. The above demonstrates that even qualitative outputs need to be quantified to some extent to be measurable.
3.4. Additional Elements of the Monitoring Plan
Population-Based Surveys
Population-based health surveys include Demographic and Health Surveys (DHS), Multiple Indicator Cluster Surveys (MICS), malaria, tuberculosis and HIV surveys, retrospective morbidity and mortality surveys among IDPs and in EHO areas, as well as other surveys that collect health-related data. None of these surveys are aligned with the Access programme in terms of timing or geography, but most of them are likely to include data that can be triangulated with Access monitoring data to validate and enrich the monitoring reports. They also provide information for the Access performance monitoring framework, required for the establishment of baseline data and the setting of feasible targets; and they provide baseline and end-line data which will allow the evaluation of the Fund’s impact. Surveys will focus mainly on collecting information on the demand and supply sides to understand the availability, access, utilization and outcomes of health services for maternity, child and adolescent health in geographic areas where the majority of services are provided by EHO/CBHOs. The Monitoring and Evaluation plan therefore includes baseline and an end-line population-based surveys to collect and analyze data on Access’ effects on beneficiary populations120. The implementation of these surveys have to overcome a number of challenges:
120 This applies, for instance, to coverage rates for the treatment of children with diarrhoea or pneumonia, as well as to reliable statistics on immunisation coverage, contraceptive prevalence and adolescent birth rate. In these cases, data will only be available when surveys are conducted.
90
● The diversity of Access programme interventions; ● The geographic targeting of Access programmes on remote and hard-to reach villages in
government-controlled areas, in conflict-affected townships and on areas served by EHO health services.
● Political tensions and conflicts between government and ethnic political organizations in conflict-affected areas which, in some cases, give rise to mutual suspicion and reluctance authorize surveys, and publish or share data that may be considered of strategic importance. The Fund will strive to secure such authorizations from all of Access’ 19 EHO/CBHO partners (as of December 2019) and from the MOHS.
For the baseline survey, there are two options: ● Implementation of an Access baseline household survey in 2020 in programme areas that
primarily receive health services from the EHO/CBHO systems. ● The baseline survey could be conducted as part of the Demographic Household Survey (DHS)
which is planned for 2020/21. This would require an increase in the DHS’ sampling clusters in EHO/CBHO areas. The advantages of this option would be cost-savings, as well as avoiding the need for separate negotiations of survey authorisations and ethics review. It would also avoid any over-surveying of some populations. DHS questionnaire modules are extensive, but a limited application of only relevant modules in these areas could possibly be negotiated.
For the end-line survey which will be required to provide data for the final programme evaluation in 2023, there are no alternative options to conducting a household survey in a sample of Access programme areas. On-going EHO-led surveys (e.g. Eastern Burma Retrospective Mortality Survey including EHO areas in Kayin, Mon, Shan and other) will be considered in planning the baseline survey by Access.
Monitoring Social Equity and Gender Equality
Social equity and gender equality are core principles of the Access to Health Fund, as is the focus on vulnerable populations in conflict affected areas. The administration of a baseline and endline survey will respectively help stratify target communities by wealth and access to infrastructure, and then verify that programme benefits were applied equitably. Many of the Fund’s proposed outcome indicators (monitoring end-beneficiary results) call for disaggregated data, and yet many of the data sources are non-disaggregated national or EHO/CBHO HMIS reports. As long as Access works with these data sources (as part of the Fund Donors’ commitment to effective development cooperation), it can only report at the level of disaggregation that these systems have adopted - and advocate for more disaggregated data within them. For data collected through parallel systems (for instance for People who inject drugs or prisoners) the Fund can ask IPs to disaggregate, including for sex, age and disability. Indicators to monitor institutional and policy support, on the other hand, include gender equality as one of the scoring parameters. It is expected that the IPs providing institutional, policy and planning support to the MOHS, State Health Departments, Township Health Departments, and EHO/CBHOs include the promotion of gender equality in their objectives. Wherever possible, this should also

91
include advocacy for the collection and reporting of sex-disaggregated data in HMIS. Baseline and end-line surveys will of course disaggregate all relevant data by sex.
Monitoring Programme Quality
The Fund collects and analyses quantitative data in order to track the effectiveness and efficiency of programme dlivery, and qualitative data in the form of narrative reports - for example to explain variations, obstacles, and other phenomena. Qualitative information (e.g. to explain a high HIV seroconversion rate harm reduction centre clients despite an active needle exchange programme) and will lead to programmatic adjustments. Equally, counting the number of General Practitioners who were trained and are providing youth-friendly SRHR services is not enough. The quality of the services, and most importantly the views of young people using the services, will also have to be documented. This will be done in operational research studies that relevant IPs will include in their Monitoring and Evaluation plans. There is no unified way to capture the many activities of IPs and of the Fund Management Office for the collection and reporting of qualitative monitoring data in a single programme-wide Monitoring and Evaluation plan, but there are substantive budgetary provisions to support these activities. One of them is the provision for thematic expert reviews in 2021 and 2022. The intention of these Fund Management Office-managed reviews is to provide feedback to programme staff, IPs and implementing partners on the technical quality of their work, both in their specific thematic area and in the application of cross-cutting Access principles such as rights-based programming, promotion of gender equality or conflict sensibility and social cohesion. The results of the reviews will enrich the annual assessment of programme performance.
3. The Access Evaluation Plan Developing and presenting a detailed evaluation plan, including the terms of reference and evaluation questions for evaluations conducted between 2020 and 2023, would be premature as there are still open questions about the geographic and thematic scope of the Access Strategy. The geographic scope of the programme in 2021-23 under the new Strategy will be finalized in early 2020. At this time, a framework is provided to allow setting milestones for evaluations and estimating the programme evaluation costs. Evaluation, just like monitoring, will be conducted on two levels: on the level of grants to IPs funded by Access and on the level of the Access programme.
4.1. Evaluations of Access Grants
Most Access grants under the new programme strategy will start implementation in 2021, with a smaller number already starting in the transition year of 2020. The timeline for grant implementation will therefore span three years. As noted in Section 3.4, scheduling both mid-term and final evaluations in a short 3-year implementation period may be counterproductive, and the formative
92
input into grant implementation will instead be provided through outcome monitoring, including thematic expert reviews. Final evaluations that focus on the effectiveness and efficiency of contributions to grant outcome results will, however, provide important information to Access programme. These will not be required for all grants - but rather for those expected to deliver important contributions to a programme outcome. For malaria control/elimination and for tuberculosis control (and possibly other areas), evaluations should be conducted as part of scheduled national programme evaluations. The selection of grants requiring final evaluations, and the type of evaluation to be conducted, will be negotiated in due course as part of the grant application and approval processes.
4.2. Programme Evaluation
Access will schedule a mid-term evaluation in 2021 at the beginning of the new strategy implementation period and a final evaluation in 2023, in the last programme year. The two evaluations will be timed in tandem with the baseline and end-line household surveys (see Section 3.4). The surveys are expected to provide critical information for the assessment of the relevance, effectiveness, equity and impact of the Access programme.
The Mid-Term Evaluation
As the mid-term evaluation is scheduled in the first year of the strategy implementation period, it will not focus on the progress towards the achievement of outcomes. Instead, its main focus will be on the critical process of transition from the previous 3MDG strategy to the new Access strategy. The transition process will be complex as new types of working partnerships between IPs, MOHS, EHOs and ECBHOs and private sector health partners will have to be developed with mutual engagement and commitment to the Access goal of improving the health of (and health services for) vulnerable populations in conflict-affected areas. In light of data, or at least preliminary data, collected in the baseline survey, the evaluation will be able to test the relevance of the 2021 to 2023 work plan in contributing to this goal. It will assess the efficiency with which the transition was implemented, assess the extent to which key principles of the Access Fund, such as a rights-based approach and the promotion of gender equality, were respected during this process, and gauge partners’ level of commitment to the implementation of the strategy. This is summarized in a preliminary list of five main evaluation questions:
1. Does the Access Programme Strategy, in view of baseline information and of the outcomes of consultations with communities and partners conducted during the transition period, offer feasible and relevant solutions for the improvement of health, health services, and health systems for vulnerable populations in conflict affected areas?
2. Are key principles such as the promotion of human rights and of gender equality sufficiently reflected in the implementation arrangements and plans of the contracted IPs?
93
3. Are all partners in the new Access Strategy aware of its goals and objectives and committed to its implementation?
4. How efficient and participatory was the management of the transition from the 3MDG to the Access strategy by the Fund Management Office?
5. Are efficient and effective systems in place to guide and monitor programming under the Access Strategy and to generate practical lessons in real time for dynamic strategic adjustments?
The objective of the mid-term evaluation is to provide assurance to the Fund Board that Access is on course towards the achievement of agreed outcomes, and to provide independent recommendations to the Fund Management Office for possible strategic adjustments and measures to strengthen systems in order to increase the relevance and feasibility of implementation plans and arrangements. More detailed evaluation questions will be defined and agreed with the Fund Board in due course. If, towards the end of Access, a follow-up multi-donor health sector programme were to be considered, the mid-term evaluation would provide important lessons about relevance, feasibility and processes to guide future strategy development - even if it does not include information on programme outcomes.
The Final Evaluation
The final evaluation of the Access programme serves primarily for accountability and to generate lessons that, in a larger frame, will contribute to international and national health sector development policies and programmes. It will have to be timed to have access to at least preliminary results of the end-line household survey, which means that it cannot be scheduled earlier than the second half of 2023. Although the evaluation report will then be too late to inform the strategy of a possible follow-up programme to Access, it will still provide additional recommendation to those already formulated in the mid-term evaluation. As for any summative evaluation, the evaluation parameters will be to assess the efficiency, effectiveness, equity, impact and sustainability of Access. It will also include a VfM analysis by relating the cost and unit cost data that were collected throughout implementation in the monitoring framework to programme effectiveness as determined by the contribution of the programme to progress towards programme outcomes. The five main evaluation questions of the final evaluation are:
1. To what extent has the design of the Access programme responded to the health needs and priorities of vulnerable populations and communities in conflict-affected regions of Myanmar in the context of national, state, township and ethnic health organization systems and strategies?
2. To what extent have the Access-funded programmes, including through operational and implementation research, contributed to enhancing the access of vulnerable populations in conflict-affected areas to better and more relevant health services? (including an assessment of the value for money of the contribution)

94
3. To what extent have policy and institutional capacity-building interventions of Access-funded programmes contributed to improved coordination and a stronger focus on vulnerable populations among MOHS and EHO partners?
4. To what extent has the Access programme contributed to the achievement of greater social equity and gender equality in governance of and access to health services in conflict-affected areas?
5. What are the lessons for health programming at the intersection of humanitarian aid and development cooperation that were learnt by the implementation of the Access programme in conflict-affected areas of Myanmar?
Value for Money Analysis
Please see in Annex the Terms of Reference for a consultancy on the Fund’s Value for Money proposition and framework. Among other things, the Fund’s Value for Money analysis will be based on average unit cost data collected throughout programme implementation in the monitoring framework. It can be expected that the monitoring of unit costs will already have generated information about the economy and efficiency of expenditures on items such as medicines, training or supervision. The final evaluation will be expected to benchmark them against costs in comparable programmes and relate them to the assessed contribution of Access to the relevant outcomes. Some components of the Access programme, such as comprehensive support to primary health services in EHO/CBHO areas, may also allow the application of a cost model using the WHO OneHealth Tool,121 relating actual expenditures to modelled total costs and comparing assessed outcome contributions to the proportion of modelled total costs that were covered by financial contributions from Access.
121 www.who.int/choice/onehealthtool/en/
95
Annex 1 – Initial list of Grant Output indicators for reporting under Access NB: This list will be amended based on donor requirements and taking into consideration operational factors feasibility of measurement, relevance, data availability). Maternal Health Number of Emergency maternal referral supported - Total & HtR (disaggregated by sex and type of disability) Number of HtR outreach sessions conducted according to the established schedule Child Health Number of Under-five child referral supported - Total & HtR (disaggregated by sex) Number of under-five diarrhoea cases treated with ORS+Zinc at community by CBHW Number of under-five suspected pneumonia cases treated with antibiotics at community by CBHW Nutrition Number of pregnant and lactating mothers in HtR and EHO areas who received iYCF counseling Number of under-five children in HtR and EHO areas who were weighted through Growth Monitoring activities (disaggregated by sex) Sexual and Reproductive Health and Rights Number of Couple Year Protection (CYP) delivered in the ACCESS programme areas Number of peer educators for sexual and reproductive health & rights trained and supported (disaggregated by sex) Number of young people who received awareness session on SRHR through interpersonal communication (disaggregated by sex) Number of post-abortion care services with appropriate technology provided to women through public sector service providers Number of women 30-49 who have been screened at least once for cervical cancer Number of women who received family planning service with SRHR information Township Health System and EHO System Strengthening Number of Basic Health Staff who received at least one technical training Number of new CHW trained (disaggregated by sex) Number of new AMW trained (disaggregated by sex) Number of new EHO health volunteers trained Number of ACCESS-supported community engagement meetings/events (including community consultation) between service providers (THDs, EHOs and ECBHOs) and community Number of Township and State Health Department meetings with EHO participation at the appropriate (technical or senior managerial) level with adequate participation of women Number of ITHPs completed in the Access supported townships
96
Support to service delivery and community demand generation Number of patient visits /consultations in EHO health posts supported by Access (disaggregated by sex) Number of mobile clinic sessions conducted according to the established schedule Number of Village health committee formed and revitalized HIV/ Harm Reduction and Prison Health Number of people who inject drugs (PWID) reached with HIV prevention programmes Number of People who inject drug (PWID) who received an HIV test and known the result (Disaggregate by sex) Number of newly diagnosed PWID who initiated ART within a calendar year (Cumulative annually) Malaria and TB Number of people with confirmed malaria treated according to national treatment guidelines (disaggregated by sex and age group) Number of RDTs taken and read (Do not count invalid RDTs) Number of suspected cases examined (for TB) Number of notified cases of bacteriologically confirmed TB Number of notified TB cases all forms of TB (bacteriologically confirmed plus clinically diagnosed)
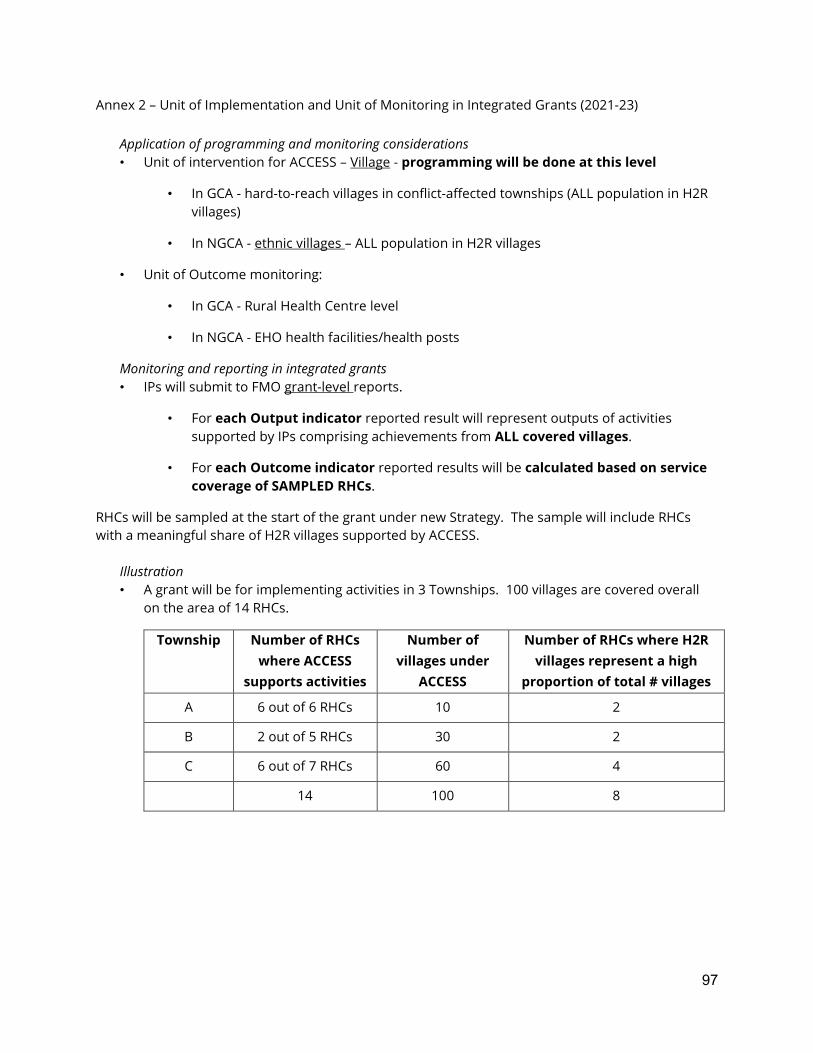
97
Annex 2 – Unit of Implementation and Unit of Monitoring in Integrated Grants (2021-23)
Application of programming and monitoring considerations • Unit of intervention for ACCESS – Village - programming will be done at this level
• In GCA - hard-to-reach villages in conflict-affected townships (ALL population in H2R villages)
• In NGCA - ethnic villages – ALL population in H2R villages
• Unit of Outcome monitoring:
• In GCA - Rural Health Centre level
• In NGCA - EHO health facilities/health posts
Monitoring and reporting in integrated grants • IPs will submit to FMO grant-level reports.
• For each Output indicator reported result will represent outputs of activities supported by IPs comprising achievements from ALL covered villages.
• For each Outcome indicator reported results will be calculated based on service coverage of SAMPLED RHCs.
RHCs will be sampled at the start of the grant under new Strategy. The sample will include RHCs with a meaningful share of H2R villages supported by ACCESS.
Illustration • A grant will be for implementing activities in 3 Townships. 100 villages are covered overall
on the area of 14 RHCs.
Township Number of RHCs where ACCESS
supports activities
Number of villages under
ACCESS
Number of RHCs where H2R villages represent a high
proportion of total # villages
A 6 out of 6 RHCs 10 2
B 2 out of 5 RHCs 30 2
C 6 out of 7 RHCs 60 4
14 100 8
98
(Continued) • IP project outputs will be reported for 100 villages (based on IP data collection systems)
• Programme outcomes will be reported for 8 RHC (based on DHIS2)
• The level of disaggregation of programme outcomes (Township or RHC) – to be explored further.
• FMO will report to the Fund Board Programme outcomes and analysis at the programme level, and provide disaggregated State-level result.
• Dependencies / assumptions:
• Access to DHIS2 data
• EHO data systems adapted for reporting on the agreed indicators.
END
Copyright © 2022 FDOKUMEN