unit Sustained Release Dosage Forms of Captopril - Asian ...
Upload
independentCategory
view
2download
0
Medical and Pediatric Oncology 6:219-228 (1979)
Evaluation of Methotrexate
Overall Toxicity of High-Dosage Regimens
Clara Perez, MD, Wataru W. Sutow, MD, Y.M. Wang, WD, and Jay Herson, P ~ D
Department of Pediatrics (C.P., W. W.S., Y.M. W.) and Department of Biomathematics (J. H.), The University of Texas System Cancer Center-M.D. Anderson Hospital and Tumor Institute, Houston, Texas
The occurrence of overall toxicity was analyzed for 43 patients with osteo- sarcoma who received 349 high-dosage courses of methotrexate (HD-MTX) with citrovorum factor (Leukovorin) “rescue” (CF). The dosages of HD-MTX ranged from 50 to 350 mg/kg. Overall toxicity was assessed on the basis of five manifestations of toxicity: stomatitis, dermatitis, myelosuppression, liver dysfunction, and kidney function abnormalities. The great majority (9 1.4%) of the infusions were well tolerated, but 8.6% were associated with moderate or severe toxicity. Stomatitis and serum glutamic-oxaloacetic transaminase (SCOT) changes were the most frequent postinfusion findings. Three patients died from causes related to MTX toxicity. Dose, age, sex, and number of prior infusions were investigated by logistic regression analysis for prognostic effect on frequency of moderate to severe overall toxicity. Age and number of prior infusions had significant (P < 0.06) effects on overall toxicity. Patients older than 15 years with greater than 10 prior infusions constituted the “high risk” group with a risk of moderate to severe toxicity 6.3 times that of the younger patients with fewer than 10 infusions.
Key words: chemotherapy, toxicity, rnethotrexate, osteosarcoma
INTRODUCTION
Methotrexate has been used in a variety of schedules and routes of administration for the treatment of childhood malignancies [ 1,2] . Known side effects and toxic manifesta- tions include bone marrow depression, mucositis, diarrhea, liver and kidney dysfunction, dermatitis, and neurologic disturbances [ 1,2]. At present, the use of high dosages of methotrexate-citrovorum factor (Leukovorin@) rescue (HD-MTX-CF) regimens has been effective for treating several neoplastic processes. However, severe and fatal reactions have
Address reprint requests to W.W. Sutow, MD, Department of Pediatrics, The University of Texas System Cancer Center, M.D. Anderson Hospital and Tumor Institute, Houston, TX 77030.
0098-1 S32/79/0603-0219$2.00 0 1979 Alan R. Liss, Inc.
220 Perez et a1
also been reported following this method of administration [2,3]. Von Hoff and co-work- ers reviewed the data on 498 patients treated with this regimen and reported 29 drug- related deaths [3] . The unpredictability of the severe side effects makes this regimen hazardous. The following study evaluates the overall toxicity of methotrexate and the possible relationship of this toxicity to dosage, age, sex, and number of prior HD-MTX-CF infusions.
MATERIALS AND METHODS
Patients
with a total of 349 infusions of HD-MTX-CF given as part of adjuvant therapy or for the management of metastatic disease. The ages of the patients ranged from 5 to 22 years (median: 15 years).
Preinfusion Evaluation
of mucosal lesions or infection. To receive HD-MTX-CF, the sequential multianalyzer (SMA) screening battery results had to be w i t h normal limits (BUN < 20 mgldl, creatinine < 1.4 mg/dl, bilirubin < 1 .O mg/dl, SCOT < 50 units/dl). Platelet count was required to be above 150,OOO/cu mm and white cell count above 2,OOO/cu mm, with absolute granulocyte count above 1 ,5OO/cu mm. Creatinine clearance had to be 90 cc/min/1.73 sq. m. or greater.
Infusion Regimen
was started 12 hours prior to infusion concomitant with vincristine (2 mg/sq. m.) Metho- trexate in doses of 50-350 mg/kg was infused over six hours, followed by IV fluids with sodium bicarbonate in doses of 50 mEq/liter for 48 hours. Citrovorum factor rescue was started three hours after completion of infusion in a dose of 15 mg IV every three hours for a total of nine doses, then 15 mg IM every six hours for the next 48 hours. Urinary pH was monitored closely and was kept within a range of 7.0-7.5 for 72 hours postinfusion. The use of concomitant medications that miglit increase renal or hepatic toxicity was avoided.
From December 1975 to January 1978,43 patients with osteosarcoma were treated
Physical examinations were performed on all of the patients to detect the presence
All infusions were given to inpatients. Alkalinization with acetazolamide (Diamox@)
Postinfusion Evaluation
and mucosal and skin examinations. If no abnormalities were detected, the patient was discharged from the hospital at the end of the CF rescue.
Plasma Methotrexate Level
The level of methotrexate was determined at 0,6,24,48, and 72 hours by both kinetic enzymic assay and radioimmunoassay, as described previously [4]. The kinetic enzymic assay was based on inhibition of dihydrofolate reductase. The reproducibility of the results by this method was 9% deviation within one day and 13% during different days. (The enzyme dihydrofolate reductase, isolated from Lactobacillus casei, used in the tests was obtained from the New England Enzyme Center, Tufts Medical School, Boston.)
This included a complete hematologic profile, SMA 12/60 screening test, urinalysis,
Toxicity of High-Dosage Methotrexate 22 1
Evaluation of Toxicity
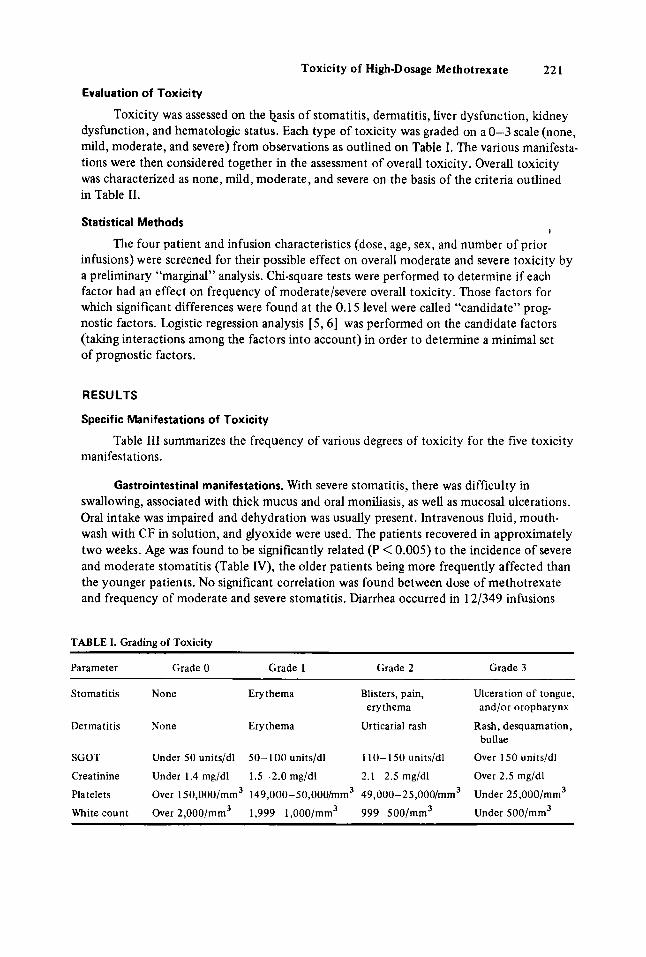
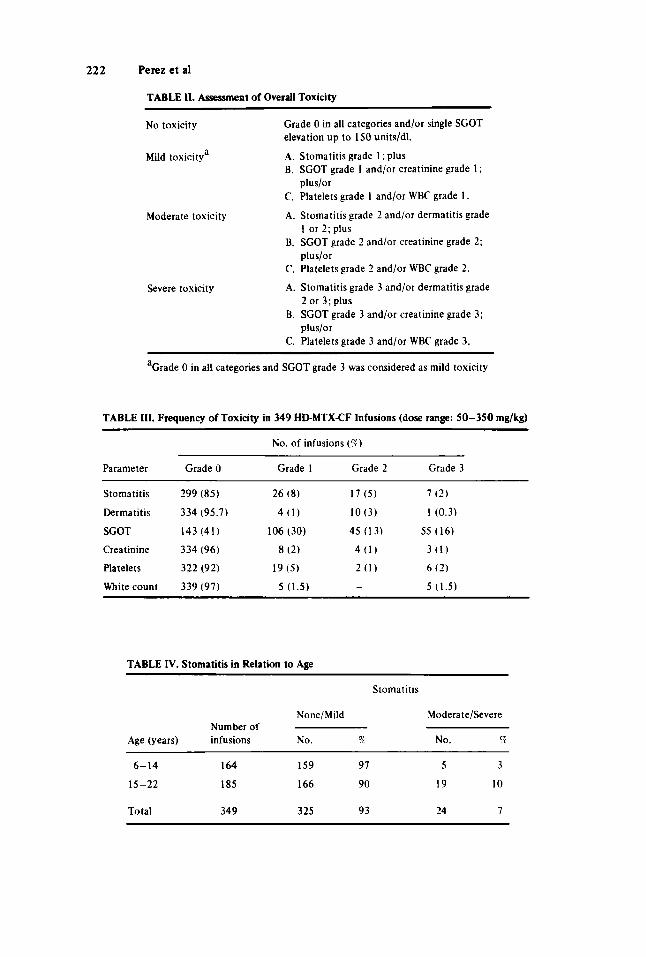
dysfunction, and hematologic status. Each type of toxicity was graded on a 0-3 scale (none, mild, moderate, and severe) from observations as outlined on Table I. The various manifesta- tions were then considered together in the assessment of overall toxicity. Overall toxicity was characterized as none, mild, moderate, and severe on the basis of the criteria outlined in Table 11.
Toxicity was assessed on the basis of stomatitis, dermatitis, liver dysfunction, kidney
Statistical Methods
The four patient and infusion characteristics (dose, age, sex, and number of prior infusions) were screened for their possible effect on overall moderate and severe toxicity by a preliminary “marginal” analysis. Chi-square tests were performed to determine if each factor had an effect on frequency of moderate/severe overall toxicity. Those factors for which significant differences were found at the 0.15 level were called “candidate” prog nostic factors, Logistic regression analysis [5, 61 was performed on the candidate factors (taking interactions among the factors into account) in order to determine a minimal set of prognostic factors.
i
RESULTS
Specific Manifestations of Toxicity
manifestations. Table 111 summarizes the frequency of various degrees of toxicity for the five toxicity
Gastrointestinal manifestations. With severe stomatitis, there was difficulty in swallowing, associated with thick mucus and oral moniliasis, as well as mucosal ulcerations. Oral intake was impaired and dehydration was usually present. Intravenous fluid, mouth- wash with CF in solution, and glyoxide were used. The patients recovered in approximately two weeks. Age was found to be significantly related (P < 0.005) to the incidence of severe and moderate stomatitis (Table IV), the older patients being more frequently affected than the younger patients. No significant correlation was found between dose of methotrexate and frequency of moderate and severe stomatitis. Diarrhea occurred in 12/349 infusions
TABLE I. Grading of Toxicity
Parameter Grade 0 Grade 1 Grade 2 Grade 3
Stomatitis None Erythema Blisters, pain, Ulceration of tongue, erythema and/or oropharynx
Dermatitis None Erythema Urticaria1 rash Rash, desquamation,
SGOT Under 50 units/dl 50-100 units/dl 110-150 units/dl Over 150 units/dl
Creatinine Under 1.4 mg/dl 1.5-2.0 mg/dl 2.1 -2.5 mg/dl Over 2.5 mg/dl
Platelets Over 150,000/mm3 149,000-50,000/mm3 49,000-25,000/mm3 Under 25,000/mm3
White count Over 2,000/mm3 1,999-1 ,000/mm3 999-500/mm3 Under 500/mm3
bullae
222 Perezetal
TABLE 11. Assessment of Overall Toxicity
No toxicity Grade 0 in all categories and/or single SCOT elevation up to 150 units/dl.
Mild toxicitya A. Stomatitis grade 1: plus B. SGOT grade 1 and/or creatinine grade 1 ;
C. Plateletsgrade 1 and/or WBC grade 1.
A. Stomatitis grade 2 and/or dermatitis grade
B. SCOT grade 2 and/or creatinine grade 2;
C. Platelets grade 2 and/or WBC grade 2.
A. Stomatitis grade 3 and/or dermatitis grade
B. SGOT grade 3 and/or creatinine grade 3;
C. Platelets grade 3 and/or WBC grade 3.
plus/or
Moderate toxicity 1 or 2; plus
plus/or
Severe toxicity 2 or 3; plus
plus/or
aCrade 0 in all categories and SGOT grade 3 was considered as mild toxicity
TABLE Ill. Frequency of Toxicity in 349 HDMTX-CF Infusions (dose range: 50-350 mg/kg)
No. of infusions (9)
Parameter Grade 0 Grade 1 Grade 2 Grade 3
Stomatitis 299 (85) 26 ( 8 ) 17 ( 5 ) 7 (2)
Dermatitis 334 (95.7) 4 (1) 10 (3) 1 (0.3)
SCOT 143 (41) 106 (30) 45 (13) 55 (16)
Creatinine 334 (96) 8 (2) 4 (1) 3 ( 1 )
Platelets 322 (92) 19 (5) 2 ( 1 ) 6 (2)
White count 339 (97) 5 (1.5) - 5 (1.5)
TABLE IV. Stomatitis in Relation to Age
Stomatitis
None/Mild Moderate/Severe Number of
Age (years) infusions No. 7% No. ?
6-14 164 159 97 5 3
15-22 185 166 90 19 10
Total 349 325 93 24 I
Toxicity of High-Dosage Methotrexate 223
(3%), usually during the infusion or the following 24 hours; of patients who had diarrhea, 30% developed mild or severe stomatitis.
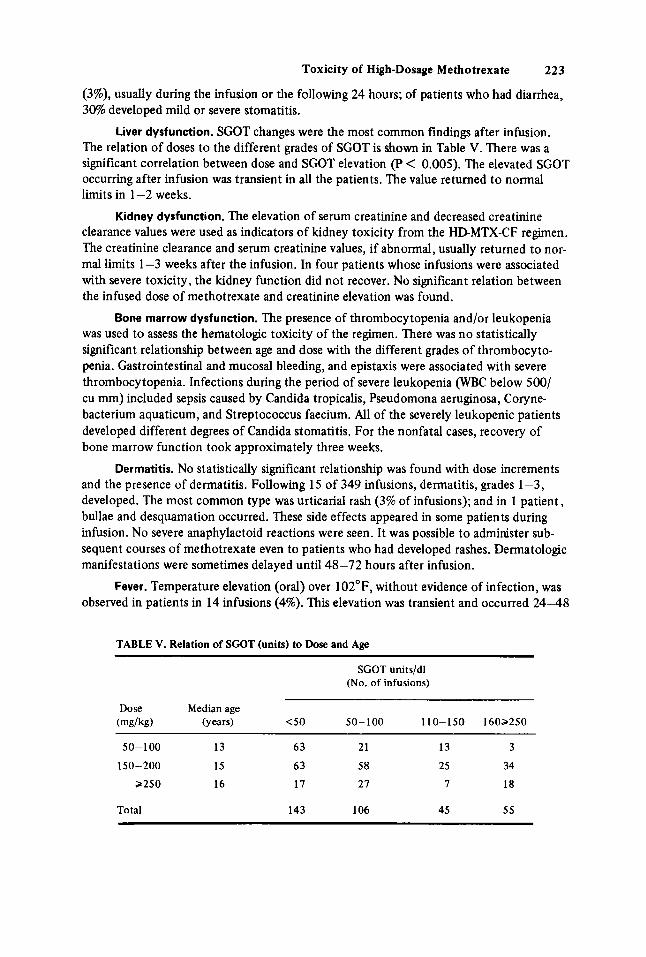
Liver dysfunction. SCOT changes were the most common findings after infusion. The relation of doses to the different grades of SCOT is shown in Table V. There was a significant correlation between dose and SCOT elevation (P < 0.005). The elevated SCOT occurring after infusion was transient in all the patients. The value returned to normal limits in 1-2 weeks.
Kidney dysfunction. The elevation of serum creatinine and decreased creatinine clearance values were used as indicators of kidney toxicity from the HD-MTX-CF regimen. The creatinine clearance and serum creatinine values, if abnormal, usually returned to nor- mal limits 1-3 weeks after the infusion. In four patients whose infusions were associated with severe toxicity, the kidney function did not recover. No significant relation between the infused dose of methotrexate and creatinine elevation was found.
Bone marrow dysfunction. The presence of thrombocytopenia and/or leukopenia was used to assess the hematologic toxicity of the regimen. There was no statistically significant relationship between age and dose with the different grades of thrombocyto- penia. Gastrointestinal and mucosal bleeding, and epistaxis were associated with severe thrombocytopenia. Infections during the period of severe leukopenia (WBC below 500/ cu mm) included sepsis caused by Candida tropicalis, Pseudomona aeruginosa, Coryne- bacterium aquaticum, and Streptococcus faecium. All of the severely leukopenic patients developed different degrees of Candida stomatitis. For the nonfatal cases, recovery of bone marrow function took approximately three weeks.
Dermatitis. No statistically significant relationship was found with dose increments and the presence of dermatitis. Following 15 of 349 infusions, dermatitis, grades 1-3, developed. The most common type was urticaria1 rash (3% of infusions); and in 1 patient, bullae and desquamation occurred. These side effects appeared in some patients during infusion. No severe anaphylactoid reactions were seen. It was possible to administer sub- sequent courses of methotrexate even to patients who had developed rashes. Dermatologic manifestations were sometimes delayed until 48-72 hours after infusion.
observed in patients in 14 infusions (4%). This elevation was transient and occurred 24-48 Fever. Temperature elevation (oral) over 102"F, without evidence of infection, was
TABLE V. Relation of SGOT (units) to Dose and Age
SCOT units/dl (No. of infusions)
Dose Median age (mg/kg) (wars) <50 50-100 110-150 1602250
50-100 13 63 21 13 3
150-200 15 63 58 25 34
>250 16 17 27 7 18
Total 143 106 45 55
224 Perez et a1
hours after infusion. No relation between dose and the presence of temperature elevation was found. One patient developed eight episodes of fever on different occasions; no toxic episodes or other reactions were observed in this patient.
Overall Toxicity
Mild toxicity. When criteria outlined in Table I1 were applied to classify retrospec- tively 349 courses of HD-MTX-CF rescue there was no evidence of toxicity to patients in 69% of the infusions and mild toxicity in 22%. No extension of hospitalization was required for these patients during mild toxicity. They recovered in 1-2 weeks after infusion and continued with their scheduled treatment.
Moderate toxicity.’This was present in 21 of 349 courses (6%). Three patients experienced moderate toxicity on more than two occasions.
Severe toxicity. Nine of 349 infusions (3%) produced clinical and laboratory abnor- malities considered to constitute severe toxicity according to the criteria outlined in Table 11; 50% of these abnormahties occurred at methotrexate doses of 250 mg/kg or higher. Of the nine patients who developed severe toxicity, 3 patients died 10-14 days after infusion, and the rest recovered 12-30 days after infusion. The age range for these patients was 10- 18 years (median: 15 years). All the patients had severe to moderate stomatitis. During the period of severe leukopenia, fever was present. Three patients had bacteriemia and one had fungal (Candida tropicalis) septicemia. For the five surviving patients, abnormal renal func- tion tests persisted in two, and further therapy with HDMTX-CF was discontinued. The autopsy findings for the three patients who died showed hypoplastic bone marrow, mucosal ulcerations, necrotizing enterocolitis, systemic candidiasis, renal tubular necrosis or hydropic degeneration of renal tubular epithelium, and hemorrhagic necrosis of the liver or fatty degeneration.
Factors Affecting Toxicity
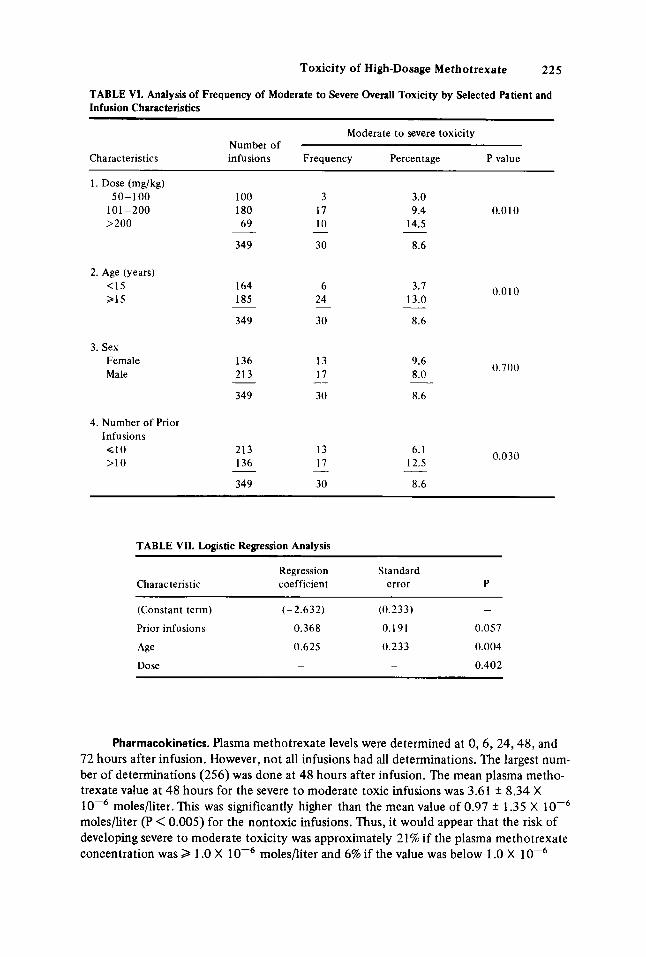
four factors. Dose, age, and number of prior infusions exhibited significant effects at P values < 0.03 and thus qualified as “candidate factors.” The data showed that age and dose were correlated with 61% of the infusions to patients Q 15 years of age in doses under 150 mg/kg as opposed to only 36.8% for patients older than 15 years.
Logistic regression analysis. Table VII presents the results of the logistic regression analysis. Number of prior infusions and age emerged as significant prognostic factors for moderate to severe toxicity with P values 0.057 and 0.004 respectively. After adjustments are made for prior infusions and age, dosage shows no evidence of significance (P = 0.402). mere was no evidence of significant interaction effects among the candidate factors at the probability P = 0.10.
The regression model shows that age is 1.7 times as important as number of prior infusions in its effect on risk of moderate to severe toxicity. The predicted incidence of moderate to severe toxicity in the high-risk group (> 10 infusions and > 15 years of age) is 17.0%. Predicted incidence in the low-risk group (< 10 infusions, < 15 years of age) is 2.7%. The incidence ratio of high- to low-risk patients is thus 6.3 (17.oo/o/2.7%).
Pleural effusion. Six infusions were given to three patients who had radiologic evidences of pleural effusions. Toxic manifestations appeared in these patients; two had severe toxicity and the other patient had three episodes of mild toxicity characterized as mild stomatitis associated with thrombocytopenia and elevation of SCOT.
Marginal analysis. Table VI presents the marginal analysis of overall toxicity for the
Toxic i ty of High-Dosage Methotrexate 225
TABLE VI. Analysis of Frequency of Moderate to Severe Overall Toxicity by Selected Patient and Infusion Characteristics
Moderate to severe toxicity Number of
Characteristics infusions Frequency Percentage P value
1. Dose (mg/kg) 50-100
101-200 >200
100 180 69
2. Age (years) <15 >15
3. Sex Female Male
4. Number of Prior Infusions < l o >10
349
164 185
349
136 213
349
213 136
349 -
3 17 10
30 -
6 24
30 -
13 17
30 -
13 17
30 -
3.0 9.4 0.0 10
14.5
8.6
3.7 13.0
8.6 __
9.6 8.0
8.6
6.1 12.5
8.6 -
0.010
0.700
0.030
TABLE VII. Logistic Regression Analysis
Regression Standard Characteristic coefficient error P
(Constant term) (-2.632) (0.233) -
Prior infusions 0.368 0.191 0.057
Age 0.625 0.233 0.004
Dose - - 0.402
Pharrnacokinetics. Plasma methotrexate levels were determined at 0 , 6 , 24,48, and 72 hours after infusion. However, not all infusions had all determinations. The largest num- ber of determinations (256) was done at 48 hours after infusion. The mean plasma metho- trexate value at 48 hours for the severe to moderate toxic infusions was 3.61 +_ 8.34 X lop6 moles/liter. This was significantly higher than the mean value of 0.97 * 1.35 X moles/liter (P < 0.005) for the nontoxic infusions. Thus, it would appear that the risk of developing severe to moderate toxicity was approximately 21% if the plasma methotrexate concentration was 2 1 .O X 1 0-6 moles/liter and 6% if the value was below 1 .O X lop6
226 Perez et al
moles/liter. The relationship between the 48-hour plasma methotrexate level and severe to moderate overall toxicity has been discussed in greater detail in a separate report [20].
DISCUSSION
Numerous reports describing the toxicity of HD-MTX-CF regimens have been published [ 2 ] . The criteria for the classification and grading of toxicity, however, differ among investigators, and accordingly the results vary among institutions. In our study, the assessment of overall toxicity was based on a combination of five different categories (two clinical and three laboratory parameters): stomatitis, dermatitis, myelosuppression, liver abnormalities, and renal dysfunction.
and that 8.6% were associated with moderate or severe toxicity. These findings were compatible with the results published by Jaffe and Traggis in 1975 [7]. There is an intra- patient as well as an interpatient variation which, in some cases, led to unexpected fatal toxicity. Recently, Von Hoff et al [3] reported a 6% incidence of drug-related mortality with HD-MTX-CF regimens: in the present study, three patients (7%) died from drug related toxicity. The frequency of overall stomatitis was 15%, a rate slightly higher than reported by other investigators [7, 81 but lower than the 93% incidence reported by Rosen et a1 in 1974 [9]. Liver dysfunction, defined as elevation of SCOT above 50 units, was the most frequent postinfusion toxic manifestation and was present in 59% of the courses.
In our study, dermatologic abnormalities of varying grades developed following approximately 4% of the infusions, but there was no apparent relationship to the dose infused. In some patients, this dermatologic manifestation appeared during or shortly after the infusions when the plasma methotrexate levels are high. Dermatologic abnormalities may be related to high methotrexate plasma levels, since the concentration threshold appears to be relatively high (lo-’ moles/liter) for skin effects [ l ] .
depression being 10-14 days after infusion, and the approximate recovery time was three weeks. The recovery pattern for these patients was similar to that reported by Chan et al [ 101 as well as by others [7,8, 11 1 .
Approximately 90% of the methotrexate that is infused is recovered in the urine 24 hours after infusion [4]. With the introduction of alkalinization and intensive hydration for 24-79 hours after infusion, the incidence of nephrotoxicity has decreased significantly [ 12-14]. But despite the use of these preventive measures, 4% of the courses were associ- ated with elevated serum creatinine values. In two patients, low creatinine clearance values persisted and necessitated discontinuance of HD-MTX therapy.
ship of dose, schedule, or the number of previous courses’’ to toxicity; others have reported similar conclusions [ 15). In our study the incidence of moderate to severe toxicity was not found to be related to dosage.
reported by Pitman et al [ 131. Current pharmacokinetic studies suggest that children excrete methotrexate more rapidly than adults [ 161 . The overall incidence of toxicity for patients older than 15 years was 15% and was independent of the dose infused. For patients younger than 15 years, the incidence of severe to moderate toxicity was 4%, and the same dose-independent relationship was observed as for older children.
The overall results of this study show that 91.4% of the infusions were well tolerated,
The overall incidence of myelosuppression was 4%, the nadir of the bone marrow
In 1975, Jaffe and Traggis [7] reported that “there did not appear to be any relation-
The observation that the older patients did not tolerate this regmen well was also
Toxicity of High-Dosage Methotrexate 227
Pharmacokinetic studies are being used to monitor the risk of toxicity with HD- MTX-CF regimen [4, 1 1, 171 , but criteria defining the “safe” levels of plasma metho- trexate following infusion vary among the investigations. The methotrexate plasma level at 6 and 24 hours is dose-dependent, as was demonstrated by Wang et a1 [4]. At 48 hours the plasma methotrexate concentration is independent of the dose infused [4, 171. The significance of the plasma methotrexate level at 48 hours has been examined in depth and will be discussed in a separate report [20].
A “third space,” such as ascites, edema, and pleural effusion, has been shown to “store” methotrexate at levels higher than those in plasma. The slow release from this space has been associated with a prolonged low plasma methotrexate level, which has been implicated in the development of toxicity [18]. Methotrexate determinations in the pleural fluid were obtained for one patient in our series after an infusion of 250 mg/kg. At 72 hours, the plasma level was < 5.5 X lo-’ moles/liter and the pleural fluid had a methotrexate concentration of 5.1 X moles/liter. Approximately nine days after infusion the pleural fluid showed a methotrexate value of 7.0 X lop7 moles/liter and the plasma value at the same time was < 5.5 X lo-’ moles/liter. After the patient recovered from mild toxicity, a smaller dose (100 mg/kg) was infused. The pleural fluid after six days following infusion showed a value of 1 .O X lop6 moles/liter when the plasma value was 5.5 X lo-’ moles/liter. One factor not often considered in toxicity is the nutritional status of the patients. Since 50-70% of methotrexate is bound to albumin [ 191, hypo- albuminemic patients may have an increased risk of developing toxicity.
The technique used to assess overall toxicity took several factors into account. Abnormal values for liver enzyme determinations were so consistently noted that such deviations were considered significant only when accompanied by abnormalities of other parameters, Though arbitrarily chosen, grade 2 (moderate) degrees of toxicity represented those findings that were considered to be clinically suggestive of potential or actual injury to the patient. Grade 3 (severe) degrees of toxicity generally required active supportive care as well as delay of or reduction in subsequent doses of methotrexate. Occasionally life-threatening situations developed.
festations of toxicity were “delayed,” appearing 96 hours or later. For a few patients, with elevated methotrexate levels at 48 hours or with histories of prior toxicity, the citrovorum factor schedule was changed in frequency and/or duration. The degree to which this change ameliorated the appearance of symptoms of toxicity has not been determined. This aspect is being examined currently.
The assessment of clinical toxicity was complicated in a few situations when mani-
ACKNOWLEDGMENTS
This work was supported in part by US Public Health Service grants CA-2501, CA-3713, CA-583 1, and CA-11430 from the National Cancer Institute and by the Beebo Smith Memorial Fund for Bone Cancer Research.
REFERENCES
1. Bleyer AW: The clinical pharmacology of methotrexate. New applications of an old drug. Cancer
2. Chabner BA, Slavik M (eds): Proceedings of the High Dose Methotrexate Therapy Meeting. Cancer 4 1 ~ 3 6 - 5 1 , 1978.
Chemother Rep (pt 3) 6 : l - 7 3 , 1975.
228 Perez et a1
3. Von Hoff DD, Penta JS, Helman LJ, Slavik M: Incidence of drug-related deaths secondary to high- dose methotrexate and citrovorum factor adminstration. Cancer Treat Rep 61:745-478, 1977.
4. Wang Y-M, Lantin E, Sutow WW: Methotrexate in blood, urine and cerebrospinal fluid of children receiving high doses by infusion. Clin Chem 22: 1053-1056, 1976.
5. Fleiss J: “Statistical Methods for Rates and Proportions.” New York: John Wiley, 1973. 6. Lee ET: A computer program for linear logistic regression analysis. Comput Programs Biomed
7. Jaffe N, Traggis D: Tosicity of high-dose methotrexate (NSC-740) and citrovorum factor (NSC-
8. Pratt CB, Roberts DW. Shanks EC, Warmath EL: Clinical trials and pharmacokinetics of intermit-
4:80-92. 1974.
3590) in osteogenic sarcoma. Cancer Treat Rep (pt 3) 6:31-36. 1975.
tent highdose methotrexate-“leucovorin rescue’’ for children with malignant tumors. Cancer Res 34~3326-3331. 1974.
9. Rosen G, Suwansirikul S, Kwon C, Tan C, Wu SJ, Beattie Jr EJ, Murphy ML: High-dose metho- trexate with ci trovorum factor rescue and adriamycin in childhood osteogenic sarcoma. Cancer
10. Chan H, Evans WE, Pratt CB: Recovery from toxicity associated with high-dose methotrexate: Prognostic factors. Cancer Treat Rep 61 :797-804, 1977.
11. Nirenberg A. Mosende C, Mehta BM. Gisolfi AL, Rosen G: High-dose methotrexate with citrovorum factor rescue: Predictive value of scrum methotrexate concentrations and corrective measures to avert toxicity. Cancer Treat Rep 61 :779-783, 1977.
12. Howell BS, Carmody J : Changes in glomerular filtration rate associated with high-dose methotrexate therapy inadults. Cancer Treat Rep61:1389-1391, 1977.
13. Pitman SW, Parker LM. Tattersall MHN, Jaffe N. Frei 111 E: Clinical trials of high-dose methotresate (NSC-740) with citrovorum factor (NSC-3590) - toxicologic and therapeutic observations. Cancer Chemother Rep (pt 3) 6:43-49. 1975.
tresate (NSC-740). Cancer Chemother Rep (pt 3) 6:19-24, 1975.
tion, plasma levels. dose and escretion pattern. Eur J Cancer 8:409-414, 1972.
the pharmacokinetics of methotrexate (MTX) following high-dose methotresate and citrovorum factor (HD-MTXCF) therapy in children. (Abstract) Proc AACR & ASCO 19:381. 1978.
17. Stoller RG, Hande KR, Jacobs SA. Rosenberg SA, Chabner BA: Use of plasma pharmacokinetics to predict and prevent methotresate toxicity. N Engl J Med 297:630-634. 1977.
18. Tattersall MHN, Parker LM. Pitman SW. Frei 111 E: Clinical pharmacology of high-dose methotrexate (NSC-740). Cancer Chemother Rep 6:25-29, 1975.
19. Wan SH, Huffman DH. Azarnoff DL. Stephens R, Hoogstraten B: Effects of route of administration and effusions on methotresate pharmacokinetics. Cancer Res 34:3487-3491. 1974.
20. Perez C, Wang YM, Sutow WW. Herson J : Significance of the 48-hour plasma level in high-dose methotrexate regimens. Cancer Clin Trials 1: 107- 1 11. 1978.
33:1151-1163, 1974.
14. Stoller GR. Jacobs SA, Drake JC, Lutz RJ. Chabner BA: Pharmacokinetics of high-dose metho-
15. Goldie JH, Price LA. Harrap KR: Methotrexate toxicity: Correlation with duration of administra-
16. Wang Y-M, Sutow WW. Sullivan MP. Romsdahl M: Preliminary studies of age and disease effect in
Copyright © 2022 FDOKUMEN